By Most Reverend Shelton J. Fabre
Archbishop of Louisville
Although fathers do not physically carry their children from conception, fathers can still be overwhelmed by an unexpected pregnancy. We Christians must support men who, in following the example of St. Joseph, choose to embrace their role as a father in all circumstances, but especially in challenging situations. St. Joseph was unexpectedly called to fatherhood amid extremely confusing and difficult circumstances. However, despite many obstacles, St. Joseph chose to be faithful. St. Joseph chose life by listening to God’s will and consciously deciding to be a father to Jesus, the Son of God. Pope Saint John Paul II said that fathers are called to exhibit “generous responsibility for the life conceived under the heart of the mother” (Familiaris Consortio 25). Like St. Joseph, all fathers are uniquely entrusted with the protection and defense of both mother and child and, in this way, safeguard the sanctity of human life. But biological fathers, because they do not physically carry the child, sometimes fail to truly father their children.
Our society increasingly tells fathers that they should have no say in the lives of their unborn children, no opportunity to choose to father their children. Our society seems to restrict the decisions regarding an unborn child solely to the discretion of the mother. In the face of false messages about fatherhood, we must respond with the truth that the role of a father “is of unique and irreplaceable importance” (FC 25). We know that the assistance and support of the father of a child, or lack thereof, can often be a deciding factor in a woman’s decision to choose life. Tragically, there are men who sometimes pressure mothers to make the decision to abort the child, sinning grievously and making the cowardly choice. These men are not following the example of St. Joseph and are not exercising true, spiritual fatherhood.
In all circumstances, but especially in difficult circumstances, a father needs to be encouraged to faithfully accept the role entrusted to him by God and support the mother of his child. Through our prayers and through the intercession of St. Joseph, patron of fathers, may fathers come to know the irreplaceable role they hold in the lives of their children, and the responsibility they share in welcoming God’s gift of new life!
A study published online Oct. 30 in the journal JAMA Oncology found that hormonal contraception is an important risk factor for the development of breast cancer in younger women.
Researchers from the Department of Immunology, Genetics, and Pathology at the University of Uppsala, Sweden, followed more than 2 million adolescent and premenopausal women for about 13 years. The study design was a population-based cohort study conducted using the Swedish, national registers.
The goal of the study was to determine if breast cancer risk differs by the content of hormonal contraceptives. The authors of the study analyzed the use of hormonal contraceptives, categorized by hormone formulations and route of administration.
In the population of adolescents and women younger than 50 years studied, 16,385 breast cancer cases occurred. Ever use of any hormonal contraceptive was associated with an increased breast cancer risk 24%. Higher risk was associated with oral desogestrel-only contraceptives as well as implants containing etonogestrel and desogestrel. Medroxyprogesterone acetate injection, etonogestrel vaginal ring, or combined oral drospirenone, did not have a statistically significant increased risk.
The findings of this cohort study are significant, considering that breast cancer incidence is rising around the globe in premenopausal women.
The authors of the study concluded that “findings of this cohort study highlight that breast cancer risk varies substantially by progestin content in hormonal contraceptives”. The authors support informed consent in the prescription of contraception. It is crucial to ensure that every woman is fully aware of the risks and benefits associated with the use of potent hormonal contraceptive methods.
Today’s post is from Fr. Eric Nielsen, a priest in Wisconsin.
As a young man I went on a motorcycle trip through Corsica at the same time that the Italians were on their school break. The beautiful winding roads of this Mediterranean island were filled with young Italian men on motorcycles with their lovely Italian girlfriends gracefully sitting behind them. At night they would enjoy the night life of the island and in the morning I would see them at the campgrounds we shared.
It was not a pretty sight. While their boyfriends slept in I watched the girls coming out of their tents, hair in a mess, tight clothes that looked not quite put on right, and long faces as they prepared something for breakfast. I didn’t speak Italian, but the short words spoken back into the tent did not seem like gentle wake-up calls.
On the third morning of the trip I noticed a young woman in front of her tent looked different. Her hair was neatly combed and held back by a headband, she was comfortably dressed, and she looked happy as she started to collect the things necessary for breakfast. What made her so different, I wondered? Like the rest she had crawled out of the same little tent pitched next to a motorbike.
What made her so unusual, I noticed, was her wedding ring. Unlike the other girls who were traveling and sleeping with boys who had given them little commitment this young woman had a man who loved her enough to make a permanent commitment to her. It was a vivid visual symbol of the difference between a relationship built on pleasure and one built on a lifelong promise of love.
One of the results of a contraceptive society is that young people can easily pursue a sexual relationship without the responsibility of commitment. Rare is the young man or woman who does not desire a relationship with someone of the opposite sex, and what seems equally rare is the young person in such a relationship who is ready to be married.
This is a very bad mix for it leads to relationships built more on a selfish desire for instant physical and superficial emotional pleasures rather than on a wise and authentic pursuit for genuine and comprehensive marital love. With couples habitually forging their intimate relationships with such mutually selfish practices, it is no wonder so many marriages end in failure.
Furthermore, it is our fault that young people lead this type of destructive lifestyle because we do little to stop it. It seems we would rather see them graduate from college, pursue a good career, develop some wealth, and keep their options open, than mary too young and be “burdened” with children. Thus we condone things such as vacations together on un-chaperoned trips with the only stipulation that no one gets pregnant. And we give them such sage advice as, “don’t get married too early.”
Let’s be honest, very few people will have the skills and opportunity to find a great measure of satisfaction in their careers, while most people, by simply following God’s plan for them, can find great happiness in their marriages.
We need to rethink our principles. Open-ended youthful relationships may look intriguing, but in the end they mostly bring about misery. The sacrificial love of marriage is what brings true lasting joy, and only those serious about getting married have the necessary intentions and dispositions to form a serious dating relationship.
Our expectations for our children should be clear and firm. For their own long-term happiness we expect nothing short of complete chastity prior to marriage and long-term relationships only when the intention for marriage is clear and foreseen.
Breast cancer is the most prevalent cancer around the world. According to the WHO, 2.26 million new cases of breast cancer were reported in the year 2020. A combination of genetic, hormonal, and environmental factors likely causes breast cancer.
In this article, Dr Susan Caldwell explains the link between low progesterone, contraceptives, infertility and breast cancer and provides prevention tips.
How Charting Your Cycles Could Help Prevent Breast Cancer
Dr. Susan Caldwell
During the month of October, we see an abundance of pink ribbons intended to make us more aware of the reality of breast cancer. Women are reminded to have their annual mammogram to detect cancer early so that it can be treated or even cured in the early stages. Breast cancer is very common. In fact, in America, it is the leading cause of cancer in women. One out of every eight women will be diagnosed with breast cancer. Our modern health care system focuses on the detection and treatment of breast cancer, but rarely do you hear about what women can do to prevent breast cancer. This is unfortunate because now we have much more understanding of the environmental factors that can increase a woman’s risk of being diagnosed with breast cancer. When women understand their own individual risks, they can work to lower their risk of breast cancer long before their first mammogram at age 40.
Marco Tejeda, marriage coach and father of six, joins the One More Soul podcast in the first of our Fivefold Fathers series to discuss his experiences as the father of many children with One More Soul Board Chair David Stiennon. In this series, we are interviewing fifty-five fathers of five or more children to share the joys and challenges of fatherhood from those who have chosen to welcome many children.
A recent study published in the journal Human Brain Mapping reported that the use of hormonal oral contraceptives may alter how the brain is functionally organized.
According to the United Nations, oral contraceptive pills (OCPs) were used by approximately 150 million women in the year 2020. OCPs contain synthetic estrogen and synthetic progestins, hormones that impair the endogenous healthy progesterone and estradiol production. These potent steroids suppress the hypothalamic–pituitary axis from secreting luteinizing hormone (LH) and follicle-stimulating hormone (FSH), altering an ovulatory event. Also, OCPs affect the uterine cervix, thickening cervical mucus, and altering the uterine lining, impeding implantation.
Although OCPs are promoted as safe and effective birth control method, they negatively affect not only the reproductive system but every cell in the woman’s body. Synthetic estrogen and progestins have effects in the brain. The brain is an endocrine organ, sensitive to the rhythmic changes in sex hormone production that occur in women after puberty.
In clinical practice, the use of OCPs has been associated with emotional lability, irritability, or depressive symptoms, and research studies using neuroimaging studies have reported that oral contraceptive pills (OCPs) alter brain connectivity.
Researchers from the Department of Psychiatry and Biobehavioral Sciences from UCLA, and the University of Cambridge conducted a randomized, double-blind, placebo-controlled crossover trial to investigate the changes in brain network activity and mood in OCPs users.
The researchers recruited 26 women from a community in Los Angeles, CA, between the ages of 20 and 33 who reported past negative effects with the use of OCPs. The participants were randomly assigned to the intervention groups, Group A (took oral contraceptive pills for 18–21 days) or Group B (took a placebo). The women rested for one cycle to eliminate the effects of OCPs. Each participant in the study was evaluated with functional MRI scans, mood-related questionnaires, and hormonal analyses. Functional connectome fingerprinting, a method to identify the individual brain connectivity pattern and determine individual uniqueness, was used.
The results reported that the use of OCPs suppressed the normal hormonal production of estrogen and progesterone and altered the brain connectivity in some areas of the brain, specifically the subcortical, executive, and somatomotor circuits. Interestingly, when using OCPs, functional MRI profiles became similar between participants of the study, reducing variability between the participants. The mood-related questionnaires revealed that the changes in functional connectivity were significantly associated with increases in negative effect in mood.
The authors of the study concluded that, “These findings suggest that OCPs induce widespread and individually meaningful alterations to brain network organization, which may underlie mood-related side effects and should be considered in future neuroimaging research involving hormonal contraceptive users.”
The study has some limitations due to the small sample size. Also, only one type of OCP was used during a short period of time. More research using a larger population is needed to determine the long-term effects of the use of OCPs on brain function.
Understanding the effects of OCPs on the brain is crucial in research and in clinical practice. Women need to know that OCPs not only prevent pregnancy but also alter brain function. This is important for informed consent.
Posted in News & Commentary | Comments Off on Oral Contraceptives and Brain Organization
A recent study published in the journalNutrients found that some types of oral contraceptives may impair the sugar metabolism in healthy women.
The study included 21 healthy and non-obese women between the ages 18-40. The women were using combined monophasic OCP for more than three months. The OCPs contained ethinylestradiol (EE) and the progestin component varied in the androgenic characteristics, some androgenic and others antiandrogenic.
The authors of the study reported markers of blood sugar (glucose, insulin and C-peptide). The markers were evaluated in participants of the study before 60 g glucose drink (fasting) and for 4 hours after drinking the sugar. The measurements were done during the “active” pill phase and once during the “inactive” (hormone-free) pill phase.
Although the fasting blood sugar levels were not affected in androgenic pill users, glucose, insulin, and C peptide responses to an oral glucose bolus were ~100% ~50%, ~44% greater. This intolerance to the sugar was noticeable during the active pill phase compared to the hormonal free or inactive pill phase.
The authors of the study concluded that that androgenic component of the combined oral contraceptive pills formulations may impair glucose tolerance and increase insulin resistance. This rising incidence of these adverse effects on glucose tolerance and insulin resistance contribute to detrimental of metabolic health and is linked to an increased prevalence of cardiometabolic diseases in women. Young women need to be informed of the metabolic risk associated to the use of combined hormonal contraceptives.
Fertility awareness methods and fertility appreciation can help young women to monitor health biomarkers of hormonal and metabolic activity and are healthier and safer alternatives to oral contraceptive pills.
According to the World Health Organization, 248 million women use hormonal contraception worldwide. In the United States, almost a million women use the vaginal ring and the contraceptive patch.
A recent study published in the BMJ analyzed the association between hormonal contraceptive use and the risk of myocardial infarction and stroke.
The authors included data from two million women aged 15 to 49 living in Denmark. They compared medical records of women who had been prescribed hormonal contraception, including combined oral contraceptives, progestogen-only pills, hormonal intrauterine devices, contraceptive implants, injections, patches, and vaginal rings with non-users of hormonal contraception
In the results, they reported 4730 ischemic strokes and 2072 myocardial infarctions that occurred between 1996 and 2021.
The users of combined oral contraceptive pills had a two-fold increased risk of heart attack and stroke compared to non-users. Users of progestin-only contraceptives such as the intrauterine device and implants had an increased risk but lower than the risk of users of combined hormonal contraceptive pills.
A higher risk of arterial thrombotic events was also observed with the use of the vaginal ring. Compared to non-users of contraception, vaginal ring users had a rate ratio of 2.4 for ischemic stroke and 3.8 for myocardial infarction. Additionally, the contraceptive patch, which contains synthetic estrogen and progestins, appeared to carry a 3.4-fold increased risk of stroke.
The use of the levonorgestrel-releasing intrauterine device was not associated with stroke or myocardial infarction.
The authors of the study concluded that users of hormonal contraception that contain synthetic estrogen-progestin and progestin-only contraceptives experienced an increased risk of ischemic stroke and, in some cases, myocardial infarction. The absolute risks were low but informed consent is necessary to alert women of these serious side effects that can result in increased mobility and mortality of women in reproductive age.
The potential risk of arterial thrombosis can be avoided by the screening of risk factors for cardiovascular disease and the use of natural family planning a non-hormonal method morally acceptable and healthier than hormonal contraception.
Managing a couple’s fertility to regulate their family size does not require removing said fertility from the woman’s or the man’s body. This is not primarily a religious issue. Some years ago a psychologist from the National Institutes of Health (NIH) who had no religious affiliation came to me for instruction in the Billings Ovulation Method of natural family planning. She had already used mechanical and hormonal contraceptives, but, responding to a comment I had made at an NIH meeting, she decided to seek a natural method. After using the method for three months she told me, “This method is so different—now I can be all there, now I am not holding anything back.” The contrast between contraception and fertility acceptance methods has never been explained more simply.
The blood of Christ, while it reveals the grandeur of the Father’s love, shows how precious man is in God’s eyes and how priceless the value of his life. The Apostle Peter reminds us of this: “You know that you were ransomed from the futile ways inherited from your fathers, not with perishable things such as silver or gold, but with the precious blood of Christ, like that of a lamb without blemish or spot” (1 Pt 1:18-19). Precisely by contemplating the precious blood of Christ, the sign of his self-giving love (cf. Jn 13:1), the believer learns to recognize and appreciate the almost divine dignity of every human being and can exclaim with ever renewed and grateful wonder: “How precious must man be in the eyes of the Creator, if he gained so great a Redeemer’ (Exsultet of the Easter Vigil), and if God gave his only Son’ in order that man should not perish but have eternal life’ (cf. Jn 3:16)!”.
Furthermore, Christ’s blood reveals to man that his greatness, and therefore his vocation, consists in the sincere gift of self. Precisely because it is poured out as the gift of life, the blood of Christ is no longer a sign of death, of definitive separation from the brethren, but the instrument of a communion which is richness of life for all. Whoever in the Sacrament of the Eucharist drinks this blood and abides in Jesus (cf. Jn 6:56) is drawn into the dynamism of his love and gift of life, in order to bring to its fullness the original vocation to love which belongs to everyone (cf. Gen 1:27; 2:18-24).
It is from the blood of Christ that all draw the strength to commit themselves to promoting life. It is precisely this blood that is the most powerful source of hope, indeed it is the foundation of the absolute certitude that in God’s plan life will be victorious. “And death shall be no more”, exclaims the powerful voice which comes from the throne of God in the Heavenly Jerusalem (Rev 21:4). And Saint Paul assures us that the present victory over sin is a sign and anticipation of the definitive victory over death, when there “shall come to pass the saying that is written: Death is swallowed up in victory’. O death, where is your victory? O death, where is your sting?’ ” (1 Cor 15:54-55).
Dr. Chris Kahlenborn sent a letter to the editor almost 15 years ago to raise awareness of an epidemic of breast cancer and a risk factor that is not emphasized in Breast Cancer Campaigns. His Mayo Clinic Proceedings peer-reviewed meta-analysis report had been buried since its publication. He had been told to expect a LOT of calls from the media when his work came out. Crickets! NO ONE CALLED! Then came the 50th anniversary of the Food and Drug Administration’s approval of the Pill, which prompted Dr. Kahlenborn to write his letter to the editor, and to beg for help in getting the word out.
We believe that the time is NOW to step up and help Dr. Kahlenborn. Women deserve to know that contraceptive steroids (in pills, patches, vaginal rings, IUDs, or injectable forms) increase estrogen exposure and increase the risk of breast cancer. See current research: Contemporary Hormonal Contraception and the Risk of Breast Cancer – PubMed
Last week was the 50th anniversary of the Food and Drug Administration’s approval of the birth control pill in the United States. Newspapers and magazines around the country ran stories on this, mostly extolling the social and medical benefits of the pill. This theme was bolstered by a recent communiqué from the American College of Obstetricians and Gynecologists (ACOG) which noted: “The pill remains one of the safest and most popular forms of contraception in the U.S.” (Office of Communications, ACOG, May 6, 2010)
I find it disturbing that after nearly 50 years, both the media and the medical establishment have failed to give a true airing to one of the pill’s most dangerous side effects; namely, that “dirty little secret.” What’s that? One need only check the Mayo Clinic Proceedings-the major medical publication of the Mayo Clinic-to find our little-known study, which showed that the pill increases the risk of premenopausal breast cancer substantially when taken at a young age (see Mayo Clinic Proceedings: October, 2006: available to the public on line). In October, 2006, we reviewed the medical literature and combined data in an analysis (referred to as a meta-analysis): we found that 21 out of 23 studies showed that using oral contraceptives prior to a woman’s first birth resulted in a 44% increased risk in premenopausal breast cancer. Our meta-analysis remains the most recent study in this area and updates the previously analysis (the Oxford-analysis published in 1996) which relied on older data with older women (two-thirds of whom were over age 45); unfortunately, the Oxford study continues to be quoted by ACOG, textbooks, the National Cancer Institute, the American Cancer Society and most researchers and obstetricians, claiming that oral contraceptives carry little breast cancer risk especially ten years after last use.
I continue to be amazed at the discordance between the medical literature and public/medical awareness. To my dismay, after our meta-analysis was published, the Mayo Clinic sent out a press release to all major media in the country. The response?: ( ). The blank space between the parentheses is purposeful. Although our meta-analysis received scant internet coverage, almost no major media covered this study, which is shocking, given the fact that about 40,000 women in the U.S. get premenopausal breast cancer annually, oral contraceptives are an elective risk factor and our study is the most recent meta-analysis to date on the oral contraceptive-breast cancer link.
In addition to our meta-analysis, it’s important to note that the World Health Organization classified oral contraceptives as a Class I carcinogen in 2005 (ie, the most dangerous classification). Even more data has come forth recently in a paper by several researchers-one of whom is a major researcher of the National Cancer Institute-which not only cited our meta-analysis, but found that oral contraceptives increase the risk of triple-negative breast cancer in women under forty by 320 percent (triple-negative breast cancers are extremely aggressive) . (Cancer Epidemiology, Biomarkers & Prevention; April, 2009)
Few in the medical establishment or the public are aware of these data, or if they are, young women almost never hear about them. It’s been almost four years since the publication of our study in the Mayo Clinic Proceedings; I am beginning to think that our study has been effectively “buried.” Breast cancer and the pill-that dirty little secret? Some day perhaps someone in the media and/or medical establishment will dust a little dirt off those pink ribbons and let young women hear all the facts so they can finally make truly informed decisions.
Chris Kahlenborn, MD
Dr. Chris Kahlenborn is a medical doctor, specializing in internal medicine. Dr. Kahlenborn graduated from Penn State Medical University in 1988 and has been researching the effects of oral contraceptives on women’s health for well over twenty years. He is the author of our best-selling pamphlets, What a Woman Should Know about Birth Control, The Pill and Breast Cancer, and Breast Cancer Risk from Abortion
Dr. Kahlenborn is the lead author of the Mayo Clinic Proceeding’s article cited above. He testified before the FDA in June, 2000 regarding the link between oral contraceptives and breast cancer
The Polycarp Research Institute Box 105 Enola, PA 17025 717-732-4904 Drchrisk@polycarp.org
A recent study on dermatologic effects of the Levonorgestrel IUD was published online in the Journal of the American Academy of Dermatology.
Researchers from the Cleveland Clinic Lerner College of Medicine, Cleveland, Ohio, reviewed the US Food and Drug Administration (FDA) Adverse Events Reporting System (FAERS) through December 2023 for dermatological adverse events associated with IUDs that release hormones.
They compared users of copper IUDs with users of levonorgestrel IUDs where IUDs were the only suspected cause of acne, alopecia, and hirsutism. The research included 139,348 reports related to Levonorgestrel IUDs (including Kyleena, Liletta, Mirena, and Skyla), and 50,450 reports of copper IUD users ( paragard).
Findings
In general Levonorgestrel IUD users showed higher odds of reporting acne (odds ratio [OR], 3.21), alopecia (OR, 5.96), and hirsutism (OR, 15.48; all P < .0001) than copper IUD users.
The Kyleena 19.5 mg levonorgestrel IUD was associated with the highest odds of acne reports (OR, 3.42), followed by the Mirena 52 mg (OR, 3.40) and Skyla 13.5 mg (OR, 2.30) levonorgestrel IUDs (all P < .0001).
The Mirena IUD was associated with the highest odds of alopecia and hirsutism reports (OR, 6.62 and 17.43, respectively), followed by the Kyleena (ORs, 2.90 and 8.17, respectively) and Skyla (ORs, 2.69 and 1.48, respectively) IUDs (all P < .0001).
Levonorgestrel is a synthetic progestin with androgenic properties that stimulates male characteristics. The use of androgenic compounds increases the risk of acne or sexual hair growth in some women.
The authors of the study concluded “Overall, we identified significant associations between levonorgestrel IUDs and androgenic cutaneous adverse events,” They added, “Counseling before initiation of levonorgestrel IUDs should include information on possible cutaneous adverse effects including acne, alopecia, and hirsutism to guide contraceptive shared decision making.”
A recent study investigated the association between the use of Hormonal Contraception (HC) and inflammatory responses to an ecological stressor (namely, public speaking). The article was published in the Journal of Brain, Behavior, and Immunity and coauthored by Sarah E. Hill, author of the book This Is Your Brain on birth control.
The participants of the study were 153 young women. Among the participants, 75 women reported being non-users of contraception for more than a year, and 78 women reported using at least three months (first, second, or third generation combined oral contraceptive pills). The women participated in the luteal phase of the cycle because past research demonstrated a difference between the stress response of naturally cycling women and women using birth control. The women were given 5 minutes to give a speech about their dream job in front of a researcher. The participants provided saliva samples to measure cortisol and cytokines (proteins that regulate inflammation) before and after the test and a subjective assessment of their mood and stress levels.
The authors of the study reported that women on birth control had higher cortisol levels in response to acute stress compared to the response to the same stressor of naturally cycling women. Also, increases in cortisol levels following the stressful situation were associated with more negative moods for HC users. In contrast, women not using contraception reported a better mood. Thus, HC users reported higher stress levels than NC women.
Women using HC experienced an increase in cytokines, suggesting more inflammation compared to naturally cycling women. Women using HCs exhibited a significant decrease in IL-1β levels and an increase in TNF-α (tumor necrosis factor that induces inflammation). Non-contraceptive women experience the opposite. The authors reported that “these differences could be explained by the androgenic effects of HCs on the inflammatory response, with HC users having an inflammatory stress response that is biased toward a more male-typical response.” Consistent with this interpretation, research finds that women generally exhibit a larger but more delayed IL-6 response and a smaller TNF-α response to stress than men.
The results of this study suggest that hormonal contraception use impacts corticoid, inflammatory, and psychological responses to psychosocial stress.
The authors mentioned that HC users are at elevated risk of developing some autoimmune disorders when compared to NC women. This increased risk may be mediated through the increase in inflammatory cytokines such as TNF-α. in response to stress.
Future research is needed to examine this possibility and to better understand the mechanisms by which HC use impacts women’s inflammatory reactivity to stress and women’s mental and physical health.
Hormonal birth control methods, have multiple mechanisms for how to prevent pregnancy.
According to The American College of Obstetricians and Gynecologists:
The mucus in the cervix thickens, making it difficult for sperm to enter the uterus and fertilize an egg.
Progestin stops ovulation, but it does not do so consistently. About 4 in 10 women who use progestin-only pills will continue to ovulate.
Progestin thins the lining of the uterus.
Hormonal birth control pill that contains progestin also works to thin the endometrium, making it more difficult for an new conceived human being to implant into the uterus.
Informative video about the truth About Oral Contraceptives. As the author concludes “it’s not just the millions of women who are on contraceptives or HRT who are at risk. Today, an ever-growing number of young boys who feel like girls are also being placed on estrogen therapy under the guise of “gender-affirming care.” The future of these boys may be grimmer than we dare conceive at the moment”.
A recent study published in the British Medical Journal found that prolonged use of hormones used in some contraceptives may be associated to the increased risk intracranial meningioma. Meningiomas are tumors that grow from the membranes that surround the brain and the spinal cord. They are slow-growing and mostly benign, but it can cause symptoms requiring surgery. The median age of diagnosis of meningiomas is 65 years.
The authors of the paper conducted a national case-control study involving 108,366 women in France. The purpose of the study was to examine the risk for a common brain tumor with use of progestogens. Women who had intracranial surgery were include in the cases and matched with five controls by age.
The researchers found that the use for one year or more of 150 mg medroxyprogesterone acetate was associated with a 5.6-fold increased risk of intracranial meningioma requiring surgery. The use of cyproterone acetate, medrogestone, and promegestone was also associated with an excess risk of meningioma.
Medroxyprogesterone acetate known as Depo Provera, is used for contraception approximately by 74 million women worldwide. The authors of the study reported that 3 out of 9 meningiomas diagnosed in women who used medroxyprogesterone were younger than 45 and one was observed before the age of 35. The number of attributable meningiomas in young women who use Depro provera may potentially be high.
The researchers reported that “no excess risk of meningioma was associated with the use of progesterone, dydrogesterone, or spironolactone, or the hormonal intrauterine systems”.
“Further studies are also needed to assess the meningioma risk with the use of medroxyprogesterone acetate, which, in this study, was considered at a dose of 150 mg and corresponded to a second line injectable contraceptive that is rarely used in France. Studies from countries with a broader use of this product, which, furthermore, is often administered to vulnerable populations, are urgently needed to gain a better understanding of its dose-response association.”
The Feast of the Annunciation was moved from March 25th to April 8, 2024, due to Holy Week.
Dr. Robert Walley, Executive Director of MaterCare International (Canada) wrote this article for the Feast of the Annunciation in 2018.
The Feast of the Annunciation (of the Incarnation) has been transferred this Year to April 9th as the usual day of March 25th occurred on Palm Sunday. This commemorates the visit when “the Angel Gabriel declared unto Mary, and she conceived by the Holy Spirit” and became the mother of the Son of God. The Incarnation began when the divine nature of the Son was united but not mixed with human nature in one divine Person, Jesus Christ, Who was both “truly God and truly man”. Thus began the most intimate relationship between God and a human being, when the Divine embryo was implanted into the womb of a young women and was nourished and nurtured through the zygotic and foetal stages of his first 266 days of earthly life. Pope St John Paul II in his millennium letter, reminded us that we were to celebrate the most important motherhood in human history, “The Father chose a woman for a unique mission in the history of salvation: that of being the Mother of the long awaited Saviour. The Virgin Mother responded with complete openness”. His mother was with him through many early trials and tribulations, the flight into Egypt when the Holy Family became refugees, the finding in the Temple and was close to Him at their home for 30 years. His mother followed him during his public ministry from Canna, to be with him at His crucifixion and finally to hold His body in her arms.
God wonderfully decided that all human beings, should be conceived by the union of a woman and a man, and should also be nourished and nurtured in their mother’s wombs. Therefore, all our mothers surely have a special share in the mystery of the Incarnation, through their own intimate relationship with God and with all of us. They also have a special understanding with Jesus Mother, when they too lose their baby, through complications of pregnancy, childbirth or die from disease or malnutrition or are killed during war.
Motherhood has special significance for all Christians but its value however in our modern world has been reduced to a matter of choice. Each year on March 8th, organizations from around the world come together to celebrate, acknowledge and address issues affecting women. We hear words such as equality, inclusiveness and justice. But mothers are the missing women from the women’s movement for they are women too. They are not trained, paid, nor pensioned for what they do. They are in many ways the heart and soul of their families and thus are the most important contributors in the support of healthy societies and therefore the environment. Mothers who have special needs too are dismissed as failures are undervalued by the women’s movement and now it seems in the opinion of one senior Vatican cleric, they pose a threat to the environment.
Last Year the Vatican’s Pontifical Academy of Sciences commented on an article in the New York Times about people using birth control to stop having children because of “climate change” fear. The Academy suggested that being “pro-life” includes environmentalism. “You cannot call yourself [a] ‘pro-life advocate’ unless you take a stand against ALL threats to life – the catastrophe of climate change, war and the arms trade, an economic system with vast amounts of exclusion and inequality,” the tweet, written by an International Monetary Fund (IMF) employee, said. “You must stand with Pope Francis.”
Archbishop Marcelo Sánchez Sorondo, the Chancellor for the Pontifical Academy for Sciences, at a recent Vatican conference titled “Biological Extinction,” which included world-famous, pro-abortion and pro-contraception population control advocates in attendance stated that the Church’s teaching on reproduction is unclear. Seemingly wanting to be politically correct he went on to say the following “We know some part but not all of the doctrine of the Church” about fertility and procreation,” “Many times, we don’t know exactly what is the doctrine of the Church – we know some part but not all the doctrine of the Church about the question of the fecundity,” The Archbishop then added that “education” will help women have fewer children, “When you have education, we don’t have children ” “We don’t have seven children. Maybe we have one children. two children. No more.” (LifeSiteNews March 9th 2018)
It would seem that the Chancellor, who holds important offices of the Church needs to improve his knowledge of Church teaching starting with Blessed (Saint to be) Pope Paul VI, then Pope St John Paul II and Pope Benedict and indeed Pope Francis, before causing further offence and confusion among Catholic mothers. Having offended mothers directly he indirectly insulted fathers as well, especially this writer whose wife had seven children, who nourished and nurtured them into adulthood and still does as they have their children.
We are told in the book of Genesis by God “Be fruitful and multiply”, and this is the responsibility of parents not population controllers, The Chancellor seems unaware that the population in the western world is falling rapidly e.g. Italy is dying and newborns are not replacing those who die. He should know that over 300,000 mothers die annually in the developing world, in particular in sub-Saharan Africa and 2.6 million children died in the first month of life in 2016 – approximately 7,000 newborn deaths every day as well all because they do not have necessary health care. Fortunately, many governments are trying very hard to reverse these trends, realizing the serious consequences.
On this Feast Day let us pray for all mothers to Our Great Mother, Mary Mother of God and Mary Mother of the Church.
Dr R. L Walley
Emeritus Professor of Obstetrics and Gynecology,
Founder and Executive Director of MaterCare International
Elon Musk, the billionaire founder of Tesla and SpaceX, has made comments on the past about how abortion and birth control will lead to the “collapse of the civilization”.
In a recent tweet Musk commented that birth control will make you fat, depressed and lead to suicide.
The conversation got started when Ashley St. Clair tweeted:
“Doctors hardly, if ever, advise women that it may be their birth control making them depressed or even suicidal, despite documented risk of both on the pill. Instead, doctors prescribe an anti-depressant and tell them this pharmaceutical cocktail will solve their problems.”
Elon Musk, quickly replied:
“Wow, I just searched medical research papers and it turns out that birth control meds triple the risk of suicide!! I never heard that before you posted.”
According to the CDC in the United States almost 30 million women use hormonal contraception. Many young girls are put on potent hormonal steroids pills and patches for painful periods, heavy bleeding, and even for acne.
Mr. Musk tweet got multiple responses including women sharing their own stories. Abby Johnson, a prolife leader and former Planned Parenthood clinic director responded: “Hormonal birth control gave me pseudotumor cerebri, which causes debilitating headaches and if untreated, blindness,” she wrote. “I will have to be on medication for my entire life or otherwise lose my sight.”
In our brochure Health Problems Associated with Hormonal Birth Control four doctors explain how birth control increases the risk of suicide, causes changes in healthy body metabolism, cause heart issues, and increase the risk of breast and other types of cancer.
Our goal is to educate many women, men, and even Musk about the risks of hormonal birth control and safe, healthy, and morally acceptable alternatives. It will be awesome to get Mr. Musk on our list of donors. Do you agree?
According to the American Cancer Society, each year about 13,000 new cases of invasive cervical cancer are diagnosed and more than 4,000 women will die from cervical cancer.
Cervical cancer originates in the lower part of the uterus, the cervix, and can cause abnormal vaginal discharge, pelvic pain, vaginal bleeding, and painful sex.
The World Health Organization states that 99% of cervical cancers are linked to infection with HPV, (human papillomavirus) transmitted through sexual contact. Other risk factors for cervical cancer include smoking, immunodeficiency, and hormonal contraception.
A recent study published in the International Journal of Cancer analyzed the connection between the use of hormonal contraception and the diagnosis of cervical cancer. The cohort study included >20 million person-years, and 3643 incident cervical cancers that occurred in women aged 15 to 49 living in Denmark from 1995 to 2014.
The authors of the study found that the relative risk of ever-users of hormonal birth control was 1.19 compared to women who did not use contraception. Cervical cancer was diagnosed about 19% more often in women who had used birth control at any point compared to women who had never used birth control. In the women who were current or recent users of any hormonal the risk increased to 30%. Longer duration of use was associated with an increased risk of cervical cancer and the risk declined after stopping the use of the artificial hormones.
The use of combined contraceptives( artificial estrogen and progestins) increased the risk of cervical cancer by 40%. Recent use of progestin-only contraceptives was not associated with an increase in cervical cancer.
The authors of the study concluded that their “results indicate that currently available combined contraceptives continue to be positively associated with the risk of cervical cancer, at least among women not vaccinated against HPV. Women wishing to use this method of contraception need to be informed of this risk and encouraged to participate in a cervical screening program, if available. They should also be alert to any symptoms indicative of cervical cancer, and report these promptly to their health care provider. Our findings also reinforce the urgent public health need for global interventions to prevent cervical cancer.”
Iversen L, Fielding S, Lidegaard Ø, Hannaford PC. Contemporary hormonal contraception and cervical cancer in women of reproductive age. Int J Cancer. 2021 Apr 5. doi: 10.1002/ijc.33585. Epub ahead of print. PMID: 33818778.
Church Has Always Condemned Abortion By Fr. William Saunders
The Roman Catholic Church has consistently condemned abortion — the direct and purposeful taking of the life of the unborn child. In principle, Catholic Christians believe that all life is sacred from conception until natural death, and the taking of innocent human life, whether born or unborn, is morally wrong. The Church teaches, “Human life is sacred because from its beginning it involves the creative action of God and it remains for ever in a special relationship with the Creator, who is its sole end. God alone is the Lord of life from its beginning until its end: no one can under any circumstance claim for himself the right directly to destroy an innocent human being” (“Donum vitae,” 5).
The respect for the sacredness of life in the womb originates in Christianity’s Jewish roots. The ancient Jewish world was much different from the surrounding cultures of Palestine where infanticide, infant sacrifice and abortion were not uncommon, and in some cases prevalent. For the Jewish people of those times and orthodox Jews to this day, all human life has as its author the one God whose creative power produces the child in the mother’s womb and brings it step-by-step to full life. The Old Testament revelation, which the Church inherited and accepted, gives clear evidence that life in the womb was considered as sacred. Moses proclaimed, “When you hearken to the voice of the Lord, your God, all these blessings will come upon you and overwhelm you: May you be blessed in the city, and blessed in the country! Blessed be the fruit of your womb, the produce of your soil and the offspring of your livestock, the issue of your herds and the young of your flocks! Blessed be your grain bin and your kneading bowl! May you be blessed in your coming in and blessed in your going out!” (Dt 28:2-6). The angel told the mother of Sampson, “As for the son you will conceive and bear, no razor shall touch his head, for this boy is to be consecrated to God from the womb” (Jgs 13:5). Job stated, “Did not he who made me in the womb make him? Did not the same one fashion us before our birth?” (Jb 31:15). In Psalm 139:13, we pray, “Truly you have formed my inmost being; you knit me in my mother’s womb.”
The Old Testament also testifies how God had specially marked individuals for an important role of leadership from the very first moment of their lives: “Beloved of his people, dear to his Maker, dedicated from his mother’s womb, consecrated to the Lord as a prophet, was Samuel, the judge and priest” (Sir 46:13). The prophet Isaiah proclaimed, “Hear me, O coastlands, listen, o distant peoples. The Lord called me from birth, from my mother’s womb He gave me my name. He made of me sharp-edged sword and concealed me in the shadow of His arms. He made me a polished arrow; in His quiver He hid me. You are my servant, He said to me, Israel, through whom I show my glory. Though I thought I had toiled in vain, and for nothing, uselessly spent my strength, yet my reward is with the Lord, my recompense is with my God. For now the Lord has spoken who formed me as His servant from the womb, that Jacob may be brought back to Him and Israel gathered to Him, and I am made glorious in the sight of the Lord, and my God is now my strength!” (Is 49:1-5). Likewise, the prophet Jeremiah recalled, “The word of the Lord came to me thus: Before I formed you in the womb I knew you, before you were born I dedicated you, a prophet to the nations I appointed you” (Jer 1:4-5).
Granted, some later rabbinic interpretations allowed exceptions for abortion, but there was no consistent or prevailing justification. The overriding Jewish teaching upheld the sanctity of the life of the unborn child.
The Greco-Roman world at the time of our Lord and in which Christianity grew permitted abortion and infanticide. In Roman law, the two acts were really not distinguished because an infant did not have legal status until accepted by the pater familias, the head of the family; until accepted, the infant was a non-person who could be destroyed. In some parts of the Roman Empire, abortion and infanticide were so prevalent that reproduction rates were below the zero-growth level. (Sad to say, most European countries face a similar plight today due to contraception and abortion.)
Nevertheless, the Christians upheld the sanctity of the life of the unborn child, not only because of the Old Testament revelation as cited but also because of the mystery of the incarnation. The early Christians, as we still do, believed that Mary had conceived by the power of the Holy Spirit, and through her, Jesus Christ — second person of the Holy Trinity, consubstantial with the Father, and true God — became also true man. No faithful Christian would ever deny that Jesus was a true person whose life was sacred from the first moment of His conception in the womb of His blessed Mother Mary.
The story of the visitation further attests to the sanctity of life in the womb and the personhood of the unborn child: “Thereupon Mary set out, proceeding in haste into the hill country to a town of Judah, where she entered Zechariah’s house and greeted Elizabeth. When Elizabeth heard Mary’s greeting, the baby leapt in her womb. Elizabeth was filled with the Holy Spirit, and cried out in a loud voice: ‘Blest are you among women and blest is the fruit of your womb. But who am I that the mother of my Lord should come to me? The moment your greeting sounded in my ears, the baby leapt in my womb for joy. Blest is she who trusted that the Lord’s words to her would be fulfilled’” (Lk 1:39-45).
Given the revelation of the Old and New Testaments, with special emphasis on the mystery of the incarnation, the Roman Catholic Church has condemned the practice of abortion. Several examples of teaching which span the first three hundred years of our Church include the following: The “Didache” (“The Teachings of the Twelve Apostles,” c. 80 A.D.) asserted, “You shall not procure abortion. You shall not destroy the newborn child.” The “Epistle of Barnabas” (138) also condemned abortion. Athenagoras (177) in his “A Plea on Behalf of Christians” (a defense against paganism) emphasized that Christians consider as murderers those women who take medicines to procure an abortion; he condemns the killer of children, including those still living in their mother’s womb, “where they are already the object of the care of divine providence.” Tertullian, (197) in his “Apologeticum” likewise asserted, “To prevent birth is anticipated murder; it makes little difference whether one destroys a life already born or does away with it in its nascent stage. The one who will be man is already one.” In the year 300, the Council of Elvira, a local church council in Spain, passed specific legislation condemning abortion (Canon 63).
After the legalization of Christianity in 313, the condemnation against abortion remained. For instance, St. Basil in a letter to Bishop Amphilochius (374) clearly pronounces the Church’s teaching: “A woman who has deliberately destroyed a fetus must pay the penalty for murder” and “Those also who give drugs causing abortions are murderers themselves, as well as those who receive the poison which kills the fetus.”
While many other examples could be offered, the key point is that the Roman Catholic Church from the beginning has consistently upheld the sanctity of the life of the unborn child and condemned the act of direct abortion. To oppose this teaching contradicts the revelation of Sacred Scripture and Christian tradition. As our nation marks the anniversary of the tragic Supreme Court decision, Roe v. Wade, we as Catholic Christians must pray for a change of heart in all citizens and courageously teach and defend the sanctity of human life, particularly that of the defenseless, innocent unborn children.
Source: Rev. William Saunders, “Church Has Always Condemned Abortion.” Arlington Catholic Herald (www.catholicherald.com/).
A recent study published in the journal Frontiers in Endocrinology studied the effect of the use of hormonal oral contraceptives and fear responses in the brain.
Deborah Pirchner, from Frontiers wrote:
“Fluctuations in sex hormones influence brain activity of the fear circuitry. A team of researchers in Canada has now examined the effects of oral contraceptive (OC) use on women’s brains.Their findings showed that ventromedial prefrontal cortex (vmPFC) thickness of women who were using OCs was reduced compared to men, suggesting a mechanism on how OC use could impair emotion regulation in women. Based on this study, this effect appears to be reversible after discontinuing use. More studies on impact and reversibility are needed, the researchers cautioned.“
More than 150 million women worldwide use oral contraceptives. Combined OCs (COCs), made up of synthetic hormones, are the most common type. Sex hormones are known to modulate the brain network involved in fear processes.
Now a team of researchers in Canada has investigated current and lasting effects of COC use, as well as the role of body-produced and synthetic sex hormones on fear-related brain regions, the neural circuitry via which fear is processed in the brain.
“In our study, we show that healthy women currently using COCs had a thinner ventromedial prefrontal cortex than men,” said Alexandra Brouillard, a researcher at Université du Québec à Montréal and first author of the study published in Frontiers in Endocrinology. “This part of the prefrontal cortex is thought to sustain emotion regulation, such as decreasing fear signals in the context of a safe situation. Our result may represent a mechanism by which COCs could impair emotion regulation in women.”
Emotion regulation and contraceptives
“When prescribed COCs, girls and women are informed of various physical side effects, for example that the hormones they will be taking will abolish their menstrual cycle and prevent ovulation,” Brouillard explained. However, the effects of sex hormones on brain development, which continues into early adulthood, are rarely addressed. Considering how widespread COC use is, it is important to better understand its current and long-term effects on brain anatomy and emotional regulation, the researchers said.
The team recruited women who were currently using COCs; women who used COCs previously but did not at the time of the study; women who never used any form of hormonal contraception; and men. Comparing these groups allowed the researchers to see if COC use was associate with current or long-term morphologic alterations as well as to detect sex differences, since it is established that women are more susceptible to experience anxiety and stress-related disorders than men.
“As we report reduced cortical thickness of the ventromedial prefrontal cortex in COC users compared to men, our result suggests that COCs may confer a risk factor for emotion regulation deficits during their current use,” Brouillard said.
The impacts of COC use, however, may be reversible once intake is discontinued, the researchers said. Given that the vmPFC effect found in current users was not observed in past users, the findings did not support lasting anatomical effects of COC use. This, the researchers wrote, will need to be confirmed in further studies.
There is still much to learn when it comes to women’s brains and how they are impacted by COC use. For example, Brouillard and team are currently investigating the impact of age of onset and duration of use to delve further into the potential lasting effects of COCs. Given that many teenage girls start using COCs during adolescence, a sensitive period in brain development, user age might also impact reversibility.
Pointing to limitations in their study, the scientists said that no causal relationship can be implied between COC use and brain morphology and that generalization of their results to a general population may be limited. The researchers also cautioned that drawing conclusion from anatomical findings to behavioral and psychological impact is not possible at this point.
“The objective of our work is not to counter the use of COCs, but it is important to be aware that the pill can have an effect on the brain. Our aim is to increase scientific interest in women’s health and raise awareness about early prescription of COCs and brain development, a highly unknown topic,” concluded Brouillard.
The following excerpt is from Fr. Lovasik book “Clean love and Courtship”. Every Catholic young lady and young man should read in their formative years.
THE SIXTH AND NINTH COMMANDMENTS
Soul-death
True happiness comes from God. It fills your heart if you live according to God’s plan and His commandments. Unhappiness comes from breaking those commandments by sin. Disobedience is the spirit of Lucifer: “I will not serve”;
“God can’t tell me what to do.”
Since mortal sin is a grievous offense against the law of God, it is the greatest tragedy in the world. The emphasis is on God.
You were made His child and friend in baptism. He gives you His life, the supernatural life through the sacraments, and then in a moment of selfishness you turn your back on Him.
Do not try to make yourself believe that hurting those around you is the only possible evil. God does not agree with that view. When you break God’s law, you hurt God—and yourself!
Sin is called mortal because it causes death to your soul. It is a complete turning from God. If you do not want God in your heart, He will get out. He will not force Himself on you.
And if He leaves you, He takes with Him the supernatural life—which means spiritual death for you, because without God there can be no spiritual life, no happiness either.
The apostle says: “The wages of sin is death.” (Rom.6, 23.) Breaking God’s law by impurity in company-keeping spells death: death of the soul through the loss of sanctifying grace; death of the peace of conscience through the crushing remorse for sin; death of the delightful consciousness of the possession of unsoiled purity; death of high ideals; death of the lofty esteem and sacred reverence two people formerly had for one another.
Spiritual death of mortal sin brings misery and unhappiness in this world and eternal damnation in the next. Sin and damnation seem to be out of tune with the spirit of our time.
Just because people have stopped talking about sin, do not let yourself be fooled into thinking it must not be so bad. Sin is just as nasty and just as harmful today as it ever was.
Do not excuse your shortcomings on the plea that everybody is doing it. Evil may never be done even if everybody is doing it. Because it is too much trouble to behave yourself, you cannot say it is all right to misbehave.
It is God, not people, who declares what is right and what is wrong; and He is right, and His Church with Him, even though the whole world may call Him wrong.
The misery of the world is due to that selfishness which puts our own pleasure ahead of God’s will.
It is important to remember that three things are necessary for a sin to be mortal:
I. The thing must be very bad, e.g. any deliberate thought, word or deed against the sixth and ninth commandments.
II. It must be done with the full knowledge that it is against God. You must KNOW what you are doing.
III. The wrong must have the full consent of our will. You must really WANT to do it. When one of these three conditions is missing, there is no mortal sin.
The Sixth Commandment
The sixth commandment is: “Thou shalt not commit adultery.” It forbids not only adultery, but also all actions which are contrary to the orderly propagation of the human race.
The faculty of sex has been bestowed upon man primarily for the propagation of the race. It is to be used only in the family and not for the benefit of the individual; otherwise it is a grievous crime against nature and a violation of God’s law.
General Principle
All sexual pleasure outside marriage, alone or with others, that is directly willed or desired, intentionally procured or permitted, is a MORTAL SIN.
Therefore, it is grievously sinful in the unmarried to think, say or do anything with the intention of arousing even the smallest degree of sensual pleasure.
If, however, this pleasure has arisen and (a) there was no intention of arousing it, (b) and no danger of consenting to it when aroused, it is a VENIAL SIN only if there was at least semi-deliberate consent, otherwise there is NO SIN at all.
MORTAL SIN:
All impure actions that are directly willed, procured or permitted. (Sexual intercourse, intimate, passionate kissing and embracing which form the natural preliminary to intercourse; unnatural acts, such as self-abuse or sexual intimacies with a person of the same sex.)
All other actions performed for the purpose of arousing sexual pleasure. (To kiss improperly or to read a book, to look at pictures, to attend plays or see movies in order to arouse passion.)
All actions which are a near danger of performing an impure action or of consenting to illicit pleasure. (Kissing, reading of a particular type of magazine which generally leads you to lose control of yourself.)
In performing these actions you are practically certain to sin. If you knowingly court such a danger, you are already showing a will to sin. Ordinarily you are obliged under pain of serious sin to avoid such occasions.
If the occasion cannot be avoided, then you must find some means which will strengthen you against the danger.
Some things are practically always near occasions of sin; e.g., the modern burlesque show, obscene literature that portrays adultery or fornication in an attractive manner.
VENIAL SIN:
Impure actions performed without a good and sufficient reason. (Curious and imprudent looks and reading; pondering on dangerous thoughts through idle curiosity unduly prolonged; repeated kisses by lovers, even though they intend no passion; kissing from frivolous motives.)
No SIN:
Sexual actions performed with a good and sufficient reason. Your thoughts and actions are sinless when you have a good reason for them; you may ignore the sexual stimulation that may accidentally result. (Medical examination, dancing, slightly suggestive motion pictures, generally decent picture magazines, personal cleanliness.)
But sometimes sexual disturbances arising from physical causes, such as fatigue, from some local irritation, from nervousness, are apt to be pro longed and to be a source of very severe temptation.
They become mortally sinful only when you make them perfectly voluntary by deliberately promoting, approving of and enjoying them.
They are not sinful at all if you do what you reasonably can to yourself of any temptation involved in them.
This can be done by a brief, calm act of the will, “I don’t want it”; by saying a little aspiration for grace of a “Hail Mary”; by trying to divert the mind to something else that is interesting or humorous; by making a brief change in external occupation.
IN REGARD TO OTHERS:
In regard to others, you must always remember the great law of charity by which you are bound not to induce others to sin or to help them to sin, and you must also take reasonable means to prevent their sinning when you can do so.
In such things as kissing, conversation, and choice of entertainment, you cannot simply settle the matter by saying: “It doesn’t bother me; therefore it’s all right.”
For instance, in kissing, a girl should keep in mind that a boy is more responsive physically than she; but if there is some good reason for a decent manifestation of affection, she may presume that he has the proper control of himself, unless he attempts or suggests immodesty.
The Ninth Commandment
The ninth commandment is: “Thou shalt not covet thy neighbor’s wife.” It forbids all lustful thoughts and desires.
MORTAL SIN:
To entertain a bad thought willfully for the purpose of enjoying it or to entertain it willfully so that it becomes a near occasion of performing an unchaste action.
VENIAL SIN:
To think about sexually-stimulating things without a sufficient reason.
No SIN:
To think about sexually-stimulating things with a sufficient reason. He who wishes to keep his body clean must begin by keeping his mind clean. Indulging in morbid erotic thoughts will lead to evil deeds, and may also cause mental disturbances.
Temptation is Not a Sin
Temptation is not a sin; it is an invitation to sin. It is a fight between your duty to obey God’s law and your evil desires. As soon as you decide to give in to your evil desires and you want to disobey God’s commandment, the temptation is over and you have committed a sin. You must know what you are doing and you must want to break a serious commandment of God before a mortal sin can be committed.
The most violent emotional desires and the most pursuing evil imaginations do not constitute sin until your will gives consent. No temptation can harm you as long as you are sincerely seeking to retain the friendship and the love of God.
By turning your will resolutely to God and prudently avoiding occasions of sin, you can enjoy a good conscience peace of mind even in time of temptation.
If doubts should come as to whether you have consented to a temptation or not, remember that if you have the habitual will and determination to resist evil thoughts and if you have prayed, you may elude that deliberate consent was lacking.
Allay scruple or doubt to keep you from receiving Holy Communion.
Abstain only when you can put your hand on the Bible and swear that you are absolutely certain you are guilty of deliberate mortal sin.
Dependent upon the nature of the temptation, your disposition, and the circumstances, all temptation against purity in thought, desire, or act, must be met decisively either by directly opposing them or directly ignoring them. Be prepared to meet temptation:
I. By regular confession and frequent Holy Communion
II. By prayer
III. By self-denial, so that when temptation comes, your will may be strong enough to want good instead of evil
IV. By turning your mind away from bad thoughts becoming busy with other things; By avoiding whatever may lead you into temptation (the suggestive story, the smutty joke, the lewd picture, the suggestive movie or novel, bad companions, questionable places)
V. By fighting against temptations from the very first moment they come up
VI. By loving Jesus and the Blessed Virgin sincerely
Whether married, single, religious, or priests, all Saints Day feast reminds us that we are all called to be saints.
1. Bl. Luigi Beltrame Quattrochi and Maria Corsini Quattrochi (d. 1951 and 1965, Italy)
Luigi was a banker, and she was a homemaker, speaker, and writer.
They raised four children, volunteered generously in their community for Catholic and social causes, and lived their faith fervently.
In discernment with guidance from a spiritual director, they decided to take a special vow of abstinence from marital relations after 20 years of marriage. Still, they remained emotionally close, loving, and affectionate to one another.
“they made their family an authentic domestic church, open to life, prayer, witness of the Gospel, the social apostolate, solidarity with the poor, and friendship… Intimately united in love and Christian ideals, they walked together on the path of holiness.”
Cardinal Martin
2. Sts. Louis and Zelie Martin
This quiet watchmaker and energetic lacemaker raised St. Therese of Lisieux and her four other sisters who lived to adulthood (including Servant of God Leonie Martin). Four other children, two sons and two daughters, died in early childhood or infancy.
Guidance from their confessor convinced them to give up the idea of an abstinent, Josephite marriage that Louis had convinced Zelie to adopt for the first nine months of their marriage.
Their devotion to their faith and prayer life, to their family, and to charitable outreach in various forms did not take away from their tenderness and care for each other.
3.Servants of God Cyprien and Daphrose Rugamba (d. 1994, Rwanda)
Daphrose’s prayers for her unfaithful husband’s conversion bore amazing fruit.
As he was healed from a mysterious, life-threatening disease, her composer and government officer husband received the gift of faith. He turned wholeheartedly back to his wife, asking her forgiveness.
They lived the remaining years of their life together in great affection, serving together in evangelization and charity, until dying along with most of their children on the first night of the Rwandan genocide.
Source: Nathan and Sarah headsteward@canafeast.com
A group of researchers from Oxford University confirmed that progestin-only birth control, which is promoted as a “safer” and “lower-risk” alternative to combined hormonal contraception, is associated with an increased risk of breast cancer.
More than nine thousand premenopausal women with incident invasive breast cancer diagnosed were compared with eighteen thousand healthy controls. The study aimed to assess the relationship between a woman’s recent use of hormonal contraceptives and her subsequent risk of breast cancer.
The authors of the study reported a relative increase of around 20% to 30% in breast cancer risk associated with the current or recent use of either combined oral or progestagen-only contraceptives.
It is important to note that 44% of women with breast cancer and 39% of women without breast cancer had a prescription for a hormonal contraceptive an average of three years before diagnosis. Half of the hormonal contraceptive prescriptions were for progestagen-only contraceptives.
The researchers found that the increased risk of breast cancer was similar regardless of whether the preparation last used was oral combined, oral progestagen-only, injectable progestagen, progestagen implant, or progestagen intrauterine device.
The researchers examined if the increased breast cancer risk remained elevated for women even after they stopped using birth control. They compared results from previous studies including women in a wider age range. They found that in young women aged 16-20, the 15-year absolute excess risk of breast cancer associated with the use of oral contraceptives was 8 per 100,000 users. In older women, from age 35 to 39, the risk was 265 per 100,000 users.
The authors concluded that the current or recent use of progestagen-only contraceptives is associated with a slight increase in breast cancer risk, similar to the risk associated with the use of combined hormonal contraceptives. The risk is estimated to be smaller in women who use it at younger age rather than at older ages.
The first OTC contraceptive, Opill, is on the way to shelves near you without age restrictions.
On July 13, 2023, the Federal Drug Administration approved the first over-the-counter hormonal birth control. The decision will allow American women and girls to obtain potent hormonal contraceptives/abortifacients as quickly as they buy vitamins and aspirin.
Here’s why it matters:
Opill also known as the “mini-pill” is manufactured by the Irish company Perrigo.
The mini-pill contains a synthetic form of the hormone progesterone called progestin. According to the prescription label, progestin-only oral contraceptives such as Opill tablets, prevent conception by various mechanisms of action. The mini-pill may suppress ovulation in approximately half of the cycles. Some users may experience thickening of the cervical mucus to inhibit sperm penetration. Also, the mini-pill lowers the midcycle LH and FSH peaks, slowing the movement of the ovum through the fallopian tubes, and altering the endometrium. If fertilization occurs and an egg is fertilized, the mini-pill will prevent the newly conceived human being from implanting within the endometrium.
“Opill over the counter may prevent conception or implantation.”
Opill use can be associated with ectopic pregnancy. “The incidence of ectopic pregnancies for progestin-only oral contraceptive users is 5 per 1000 woman-years. Up to 10% of pregnancies reported in clinical studies of progestin-only oral contraceptive users are extrauterine.”
The FDA emphasizes that Opill contains a single synthetic hormone and generally carries fewer side effects than combination hormone pills that contain progestin and synthetic estrogen. What women probably do not know is that the mini-pill still comes with many side effects, including headache, dizziness, nausea, increased appetite, abdominal pain, cramps and bloating, fatigue, vaginal discharge, dysmenorrhea (painful menstruation), nervousness, backache, breast discomfort, and acne. The use of progestin has been associated with an increased risk of depression, breast cancer, cervical cancer, and brain cancer.
Making Opill over the counter put women at unnecessary health risks. Opill causes changes in menstrual bleeding, including bleeding and spotting between menstrual periods, and ovarian cysts. Sometimes surgery is needed to remove a cyst on the ovary. Opill also contains FD&C Yellow No. 5 (tartrazine) which may cause allergic reactions (including bronchial asthma). Although the overall incidence of FD&C Yellow No. 5 (tartrazine) sensitivity in the general population is low, it is frequently seen in patients who also have aspirin sensitivity.
The label of Opill states, “These are not all the possible side effects of Opill.Call your doctor for medical advice about side effects.” Women deserve better than easy access to a potent steroid with many dangerous side effects. Women need more education and guidance from doctors, NP, nurses, and health advocates no less.
It is interesting that the manufacturer Perrigo says Opill could be an “important new option for the estimated 15 million U.S. women who currently use no birth control or less effective methods, such as condoms. They are a fifth of women who are child-bearing age.” A big lucrative business!
A recent study published in the Journal for Divorce and Remarriage examined the connection between the use of birth control and marriage dissolution. Also, the authors of the study analyzed the influence of the use of methods of Natural Family Planning on divorce. The sample size was a total of 5,403 ever-married women from the National Survey of Family Growth in the years 2015 to 2019. Statistic analysis of divorce was calculated for the family planning variables (ever-use vs. never-use). The study also examined the influence of family planning methods relative to other known factors involved with divorce such as income, education level, etc.
The results of the study indicated that the use of contraception was associated with increased odds of divorce, from 30% to 200%, whereas ever-use of NFP was associated with a 31% lower probability. Users of hormonal oral contraceptives (the combined pill or mini pill) divorced at a rate 54% above the study average. Sterilization was the birth control method that had the highest probability of divorce. Women who had a tubal ligation divorced at a rate 78% above the study average and the probability of divorce doubled in men with vasectomies. Condom use was associated with 67% above the average divorce rate.
In contrast, users of methods of Natural Family Planning were 31% less likely to divorce than the study average. Other risk factors such as poverty level and education levels did not meaningfully influence the probability of divorce.
The authors of the study concluded that “ever-married women who have ever used NFP have lower odds of divorce, whereas those who have ever used most the common contraceptives have higher odds of divorce. More research is needed to understand how and why choices in family planning affect the stability of marriage.”
In an article published by Linacre Quarterly in February 2021, the authors analyzed the differences between the terms natural family planning (NFP) and fertility awareness-based methods (FABM) in the scientific terminology and in the practical language of health policy. The article mostly concentrates on the World Health Organization’s definition of FAMB which includes recognizing the fertility cycle and using barrier methods to avoid a pregnancy.
Anthropological and methodological differences between NFP and FABM are presented. The authors of the article concluded that NFP can be used to avoid or achieve a pregnancy and it respects fertility. NFP users are open to the possibility of maternity. NFP is open to life and love.
In contrast, the use of contraception and FAMB does not require self-control, fertility may be suppressed, and the dignity of the individual may not be taken into account as the other person may be used for sexual gratification.
According to the World Health Organization birth control is used by more than 800 million women around the globe. Beyond contraception, hormonal birth control is used for the treatment of many gynecological and medical conditions. The Guttmacher Institute reports that the average U.S. woman uses contraceptives for 30 years to attain her family planning goal of two children. But what happens when a couple starts efforts to have children or expand their family? Does birth control affect the women’s body’s ability to conceive and carry to full term?
The World Health Organization (WHO) recently reported that about one in six persons in adulthood has experienced infertility at least once in their life. Infertility is defined as the inability to conceive within one year, or not being able to carry a pregnancy to term. Infertility may occur in a couple’s first attempts to bring a child into the world, or as secondary infertility when they have successfully given birth before, but are not able to carry to term again.
Does the use of hormonal contraception contribute to the burden of infertility? Popular sources throughout the internet give assurance that most birth control does not affect future fertility. However, sources have indicated otherwise. Why do some couples struggle to get pregnant after stopping birth control? We have more questions than answers.
Pregnancy depends on many factors. A hormonal balance of estrogen and progesterone are among the most important factors. Oral contraceptive pills are a combination of synthetic estrogen or progestin. In a woman using hormonal contraception, her pituitary gland is unable to release follicle-stimulating hormone and luteinizing hormone affecting the development of the uterine lining, cervical mucus production, and the development of healthy eggs. Prolonged use of birth control pills is associated with temporary impairment to the ovulatory event. This negative impact on hormonal balance could prevent future pregnancies. It will take time to heal. Once a woman stops taking the pill, regularizing the menstrual cycle may take almost three to six months, depending on the age and the woman’s individual response to artificial hormones.
Some negative effects of the use of hormonal birth control are related to menstrual bleeding. After a woman stops the pill she can experience extremely heavy blood flow, significantly less blood flow, or no flow at all. This irregularity of the menstrual cycle can cause temporary difficulty in conception. One explanation for menstrual irregularity is the fact that long-term use of combined oral contraceptive pills is associated with adverse endometrial growth. Embryo implantation depends on endometrial thickness. A thinner endometrium after using the pill for more than five years can make it difficult to achieve and carry a pregnancy to term.
The use of oral contraceptives also impairs the production of cervical mucus. The presence of cervical mucus is essential to achieve pregnancy, indeed pregnancy cannot occur without the presence of healthy cervical mucus. A study published in the Journal of Women’s Health reported that the women who had recently stopped oral contraceptives had lower mucus quality for the first two cycles.
Another issue after stopping birth control is the nutritional deficiencies caused by artificial hormones. Birth control causes nutritional deficiencies due to its impact on liver function. The low nutrient status after contraception has been associated not only with fertility problems but also with low nutrient status in the fetus. The pill has been associated with a number of nutrient deficiencies including vitamin B6, magnesium, vitamin b12, folic acid, vitamin C, and zinc. After stopping the use of hormonal birth control the level of vitamin D drops. Also, a recent review reported that birth control pills may exacerbate Insulin Resistance. This condition increases inflammation and contributes to infertility experienced by women, especially if they suffer from PCOS. Insulin resistance can lead to pregnancy loss due to inadequate nutrition and support of the growing embryo.
In sporadic cases, infertility is permanent which may be due to some pre-existing conditions as well. Therefore, women who stop using contraception need to give time to the body to heal and get adequate nutrition. A consultation with health care provider is recommended to evaluate the status of the hormonal imbalance, nutritional deficiencies, and restoration of the fertility cycle.
Pop culture, schools, and the media all tell you that artificial birth control is a wonderful development of modernity. Explaining why they’re wrong and the official Church teaching is correct can be a painful matter. The teaching itself is a difficult one, but if you support contraception, I invite you to rethink your position.
Some find Church arguments against contraception confusing. Simply put, artificial birth control separates two aspects of sex that God wished never to be separated: the unitive, which brings two people together; and the procreative, which brings new life into the world (see Pope Paul VI’s encyclical Humanae Vitae).
Of course, that won’t satisfy those of a less philosophical and more pragmatic bent. Happily, there are plenty of practical reasons why the Church’s teaching is preferable.
First, some studies suggest that couples who choose natural methods of spacing births (natural family planning, or NFP) instead of artificial means experience a divorce rate as low as 2 percent, compared to 50 percent for the general population. NFP, in which husband and wife cooperate, actually has the effect of strengthening the marital bond.
Additionally, sexual intimacy within the sacrament of marriage is improved with NFP. Devices such as condoms block that perfect union between a husband and wife, while the pill actually changes the wife’s body chemistry and can reduce her desire for sexual intimacy. Neither of these outcomes falls within God’s plan for husband and wife.
Pontiffs throughout the 20th century have endorsed NFP as a moral method of spacing births. The Couple to Couple League is a wonderful place to start for those preparing for marriage, or for those who may want to “start over” and need guidance on the method.
Of course, the real problems with artificial birth control are hidden and emerge from a single fact: Contraceptives eliminate from sex the “risk” of pregnancy. This is a dramatic technological shift, and it has had terrible consequences for our society.
Perhaps the most obvious effect has been an increase in promiscuity. Adults and teenagers, freed from the “consequences” of sex, began having casual sexual encounters in numbers unseen before. Once sex was detached from pregnancy, it moved into the realm of a leisure activity, a cultural pastime to enjoy whether married or not.
Not only that, but contraceptives put pregnancy in the same category as a disease to be prevented (as recently noted by Sen. Barack Obama). Within a few years, this view became so prevalent that when women were “stricken” with pregnancy, they needed a cure. Welcome to 1973 and abortion on demand, thanks to Roe v. Wade.
The social connection between public acceptance of birth control and public acceptance of abortion is inescapable; it’s virtually impossible to find a group that supports abortion that doesn’t also support artificial birth control. If birth control is an issue of privacy, so is abortion; if birth control is a way for the poor to have fewer children, so is abortion. Abortion advocates use the same arguments to favor abortion as they do for contraceptives. That alone should give pause.
But there’s another grave side-effect of the contraception revolution: Since pregnancy was considered a “disease,” and children were the result of pregnancy, they came to be seen considered undesirable and inconvenient — an impediment to life’s goals. After all, if children were so wonderful, why were so many people going out of their way to avoid having them? While life goals used to center around raising a family, the introduction of artificial birth control shifted the focus to the career as the summit of satisfaction. Money, material goods, and comfort became more important than the family. (On a purely pragmatic level, one can see this mentality’s economic fruit — or, rather, lack of fruit — in Japan and other industrialized nations.)
And so, the divorce rate rose. The argument that one can have actions without consequences — that careers and personal satisfaction came before families — led to such legislation as “no-fault” divorce, first signed into law in the mid-1970s.
The Church has herself paid the price for contraception, as a final and often neglected result of the decline of families has been the parallel collapse in religious vocations. Once people started having fewer children, it became more important for each child to marry and produce grandchildren. As this went on, of course, fewer families encouraged religious vocations, and fewer children felt called to them. Thus, America encounters a tragic shortage of priests, sisters, and brothers at a time when we need them most.
Promiscuity, abortion, the destruction of the family, the decline in religious vocations — these are the rotten fruits of artificial contraception. If one supports contraception, these are the effects he or she is promoting, whether intentionally or not.
——————————————————————————–
Eric Pavlat is a board member of Democrats for Life of Maryland, Inc., and a columnist and blogger for InsideCatholic.com.
The Holy Family, c. 1660-70 (detail), Bartolomé Esteban Murillo / Bridgeman Images
JESUS TELLS of a nobleman who entrusts his servants with gold, or talents, before leaving on a journey. When the man returns and sees what two of his servants have gained with the riches, he says to each, “Well done, my good and faithful servant. Since you were faithful in small matters, I will give you great responsibilities. Come, share your master’s joy” (Mt 25:21, 23).
While considering this parable, we can think of St. Joseph. He was entrusted with much, and God rewarded his faithfulness by entrusting him with even more. Because St. Joseph was faithful as the spouse of the Blessed Virgin, the earthly father to the Son of God, and the head of the Holy Family, he has been entrusted by God with the protection of the whole Church.
The names, titles and honors recited in the Litany of St. Joseph help us discover the good and faithful servant whom God the Father entrusted with his own Son. As “husband of the Mother of God” and “faithful guardian of Christ,” he stands as a “pillar of family life” and shines as an “example to parents.” He is invoked as the “hope of the sick,” “patron of the dying” and “comfort of the troubled.” He offers guidance as “model of workers” and power as “terror of evil spirits.” Born with our own weak and sinful nature, Joseph is the man who practices giving himself to God as “obedient and loyal,” “prudent and brave.”
The Litany of St. Joseph leads us down a path of contemplation. To contemplate Joseph requires that we contemplate the mysteries of God, because Joseph, who utters not a word in Scripture, is directed by and responsive to the Word who tells of our salvation. Joseph not only displays for us what obedience to God’s Word looks like, but also reflects to us the wisdom of God’s ways. In this way, Joseph is a gift to all Christians who call upon him.
The task, of course, is to actually call upon him. St. Joseph never cries out for attention; rather, he waits patiently for those who need him to seek his aid. This is who Joseph has been from the beginning: the man who waits — attentive and ready. He hears what is needed, heeds the complexities of all circumstances, and acts in accordance with the Lord’s will. As St. Teresa of Á;vila confessed: “To other saints, our Lord seems to have given grace to succor men in some special necessity; but to this glorious saint, I know by experience, he has given the power to help us in all.”
For what do we need help? As husbands we need help to honor and reverence the wives to whom we have vowed ourselves. Fathers need help to guard, teach and strengthen the children entrusted to us. Workers need help to labor with dignity, care and purpose. The Son of God himself experienced a father’s love in Joseph, witnessed a husband’s devotion in Joseph’s love for Mary, and grew in skill and competence in Joseph’s own workshop. The servant who helped raise the Son of God to manhood is the same one whom Jesus gives to us to help us become who we are called to be.
In order to grow as disciples and become ever more capable of God’s call in our lives, we would do well to turn to the intercession of St. Joseph, especially through his litany. As a concrete commitment, consider setting aside time each day for a month to pray the Litany of St. Joseph and to reflect on one of his names, titles or honors. Keep a journal in which to write a short thought or insight at the end of your periods of prayer. By praying in this way — and by developing this habit of prayer and reflection — we stand to grow as Joseph himself grew in obedience to the Lord, becoming a man after God’s own heart.
*****
LEONARD J. DELORENZO, Ph.D. , works in the McGrath Institute for Church Life and teaches theology at the University of Notre Dame in South Bend, Ind., where he is a member of the Knights of Columbus. He is the author of Model of Faith: Praying the Litany of Saint Joseph (OSV, 2021).
A new article published in the journal Trens in Cognitive Sciences analyzed brain changes in mothers and the long-term effects of motherhood on cognitive reserve.
Mothers experience long-lasting cognitive adaptations that can be present throughout their lives. The ongoing environmental complexity of motherhood, with new responsibilities and increased cognitive load increases and adapts as the child grows.
The authors of the study summarize that exposure to a more complex environment during long periods of time is beneficial for the brains of mothers in humans and animals. These findings suggest that the surge in complex environments in motherhood may result in increased cognitive reserve in late life.
The authors of the study conclude that the neurodevelopmental period of “matrescence” (becoming a mother) is associated with better cognitive performance and “younger-looking” brains later in life.
(IFN) A new study on the effects of abortion on women’s health finds, among other things, that there is no scientific evidence that abortion protects or improves women’s mental health. The study thus questions in part the current German legislation on abortion.
For more than 12 months, the interdisciplinary team of researchers examined 13 internationally frequently cited studies on abortion and women’s health for their validity and messages.
They concluded that a substantial proportion of methodologically well-done international studies agree that abortion is associated with an increased risk of mental health problems or exacerbates preexisting problems. For example, abortion is statistically associated with an increased risk of suicide and suicide attempts, addiction, alcohol and drug abuse, depression, and anxiety. Multiple abortions increase the risk.
Nevertheless, the study notes that, due to methodological problems, there is no scientifically valid method to reliably exclude or prove a direct causal link between an abortion and later psychological consequences:
“One would have to assign, as for example in a drug trial, a group of women with completely equal preconditions and randomly assigned them either to an ‘abortion group’ or to a ‘birth group’ after an unplanned/unwanted pregnancy, without the woman or the physician knowing who was assigned to which group. In this case, the design of this randomized controlled double-blind study is completely unusable and must also be rejected on ethical grounds,” explains ethicist and co-author of the study Susanne Kummer.
However, no scientific evidence could be provided for the hypothesis that abortion has a positive effect on a woman’s psyche. The study also found that abortion has no therapeutic effect in reducing psychological risks compared to women who give birth after an unwanted or unplanned pregnancy.
This in part calls into question the medical indication for abortion in Germany and Austria, among other countries. In these countries, abortion has been exempt from punishment for almost 50 years now in order to avert a supposed “serious harm to the mental health of the pregnant woman.” But if “abortion has been shown to have no positive effect on a woman’s psyche and thus offers no protective factor for mental health–something that reputable studies agree on–the scientific basis for this legal construct is lacking,” the researchers conclude.
Instead, they call for better education of women about adoption options and protection of special at-risk groups, such as women with pre-existing mental health conditions or women who have had multiple abortions.
The study will be published in “IMABE Studies” series of the Institute of Medical Anthropology and Bioethics (IMABE) in spring 2023.
Editor’s note:This article was published by International Family News and is reprinted with permission.
WASHINGTON, D.C., February 10 (C-Fam) Since the U.S. Supreme Court overturned a federal right to abortion, activists have been looking for ways to ensure abortion remains available, even if illegal in some states. One strategy—“missed period pills”—is unfamiliar to many in the U.S. but is widely used in Bangladesh as the result of a legal loophole.
“Menstrual regulation,” as it is known in Bangladesh, employs the same procedures as a surgical or chemical first-trimester abortion. While abortion is legally restricted, “menstrual regulation” has been part of Bangladesh’s family planning program since 1979, and was later expanded to include the use of pills. The stated intention is to restore a woman’s menstrual cycle, ensuring that she is not pregnant. If she was pregnant, the child is aborted, but it is not legally considered an abortion as no pregnancy test was done first.
In the U.S., there are already efforts by the government to ensure that abortion pills can be obtained in local pharmacies, and overseas groups advertise illegal abortion pills to U.S. women by mail. In many ways, those selling “period pills” are no different, as the drugs are the same, and the legal peculiarities of Bangladesh and other countries that allow “menstrual regulation,” like Cuba, do not apply in the U.S.
However, proponents of so-called “period pills” are trying to appeal to an audience that is uncomfortable with abortion for moral reasons. A website promoting the pills quotes women’s reasons to prefer this method to a standard abortion following a pregnancy test. “It would be easier on my emotional well-being to not know I was actually pregnant,” one woman said. Another said, “I wouldn’t feel I am a bad person.”
In an interview on U.S. public radio, promoters of “period pills” waved away modern medical knowledge about fertilization and pregnancy and talked about ancient concepts like quickening, the point at which a pregnant woman can first feel the unborn child move. “A lot of people that I talked with talked about how pregnancy isn’t just a bodily reality, it’s a state of mind,” said Abby Wendle, who produces a podcast for National Public Radio. “It’s a desire to have a baby and be a parent.”
While a missed period does not always mean a pregnancy, “period pills” are marketed for one purpose: the intentional destruction of an unborn life, if one is present. The website promoting the pills warns that if they fail to work and the pregnancy continues, “there may be a risk to the developing embryo.” They warn that women should only use them if they “would have an abortion if the period pills did not work.” While the website claims that “serious side effects are rare” for women using the pills, they are not nonexistent, and the expected results include cramping and bleeding.
From a legal perspective, using pills to induce a period in the absence of a confirmed pregnancy test may not meet some definitions of abortion, although pro-life lawmakers will need to take these issues into account when writing legislation to protect unborn life. For people on both sides of the abortion issue in the U.S., “period pills” represent a relatively new area within the larger debate, and an important example of how practices developed internationally are increasingly relevant in the U.S. since the overturning of Roe v. Wade.
Yet the percentage of women who sacrifice their own children to maintain a lifestyle shocked even me.
An analysis of state abortion statistics by Charlotte Lozier Institute revealed an appalling, widespread practice of women using abortion as a means of birth control.
Not all states keep current statistics on abortion, so they looked at the eight states that do. These states account for approximately 13% of all abortions done.
Charlotte Lozier’s research looked at the reasons why women have abortions. What we normally call the “hard case exceptions” have been broken down like this:
Rape and incest, 0.3%
Risk to the woman’s life or a major bodily function, 0.2%
Other physical health concerns, 2.5%
Abnormality in the unborn baby, 1.3%
The total percentage of abortions involving the “hard cases” or “common exceptions” made up only 4.3% of all abortions done.
The remaining 95.7% fell under the category of “elective and unspecified reasons.”
Charlotte Lozier Institute concluded that over 95% of all abortions committed are done for birth control.
When the vast majority of women use abortion as a means of birth control, it is logical that they would experience more than one abortion during their reproductive years. Let’s look at the number of repeat abortions – that is, women having more than one abortion.
Pew Research released data from the Centers for Disease Control and Prevention (CDC) on abortions done in 2020, the latest data available. The information shows:
58% of women had their first abortion
24% had their second abortion
10% experienced their third abortion
8% had their fourth or more abortion
Human carnage is likely to worsen. Both New York and California have passed legislation mandating free abortions. And there’s more.
Recently New York City’s mayor Eric Adams announced the city would give free chemical abortion pills to accommodate the deaths of 10,000 unborn babies each year. Distribution sites include the Bronx, Brooklyn, Harlem and Queens.
The Department of Justice recently determined that it would allow the US Postal Service to mail the dangerous abortion pills into any state regardless of whether or not they prohibit the use of the pills.
We’re battling an organized, well-funded effort to use abortion as birth control and erase all stigma associated with the killing of our most vulnerable citizens.
An evil was unleashed on America with the reversal of Roe v. Wade. The forces against us are strong, but we will NOT give up. We will NOT back down. In the immediate wake of the Roe ruling in 1973, they told us to give up, that we couldn’t win – BUT WE DID!
Now our opponents are using that same tired old attempt of intimidation and fear. But as long as babies are brutally killed by abortion, as long as their parents are left in the devastating emotional wake of grief and shame, we will be there to help and restore, to turn back the culture of death and nurture a culture of life.
Editor’s note: Bradley Mattes is president of the Life Issues Institute. This article first appeared on the Life Issues Institute website.
A recent Sweeden study shows that teens and young adults with ADHD (attention-deficit/hyperactivity disorder) may have an even higher risk of developing depression when using hormonal contraception. The study was published in the Journal of the American Academy of Child and Adolescent Psychiatry and used a large-scale population record. It compared 29,767 girls and young women with ADHD aged 15 to 24 years and 763,146 peers without an ADHD diagnosis. The authors of the study determined if those women used hormonal birth control (HBC).
The results reported by the authors of the study showed that women with ADHD who used HBC had a 5 times higher risk of depression compared with non-ADHD women who were not using birth control. Also, it is significant that the risk was 6 times higher risk in comparison with non-ADHD women who were on oral combined HBC. The risk of developing depression when using non-oral HC was similarly moderately increased in both groups.
More research is needed to determine the exact mechanism behind the increased risk of depression in HBC users with a diagnosis of ADHD. The authors suggest that “hypothetically, the increased sensitivity to oral HBC in women with ADHD may be due to fluctuating hormonal levels following oral intake or during the pill-free interval. There is a considerable lack of studies on how women with ADHD respond to hormonal fluctuations, but there are several reports on how progesterone (or synthetic progestogen) fluctuations affect mood in women.”
The authors of the study concluded that “information on risks with HCs as well as potential benefits with user-independent long-acting reversible contraception needs to be an integrated part of the shared decision making and contraception counseling for young women with ADHD”. A large prospective cohort study already demonstrated that adolescent users of LARC such as the patch and the levonorgestrel intrauterine system had a higher risk of subsequent use of antidepressants and a first diagnosis of depression.
Young ladies deserve better and safer alternatives to hormonal birth control and LARCs. The fertility cycle is part of a young lady’s development and should not be suppressed by dangerous artificial hormones. Teaching adolescents and young ladies to chart their cycles can protect them not only from depression but also from a host of side effects. Fertility education gives young women tools to learn more about their developing bodies, and monitor symptoms to look for real solutions in health care. Fertility education programs that foster chastity and purity can prevent many unwanted pregnancies.
Matt Fradd is the creator and host of the Pints With Aquinas. He talks with Jason Evers about potentially underselling the difficulty of Natural Family Planning in Marriage, and the clear difference between NFP and Contraceptives, in principle and intent.
Ectopic pregnancy is defined as a pregnancy that occurs outside of the uterus. The most common site of ectopic pregnancy is the fallopian tube. In the United States, it’s estimated that one in every 50 pregnancies is tubal pregnancy,
Levonorgestrel (LNG), is advertised as emergency contraception (EC). It has been available over the counter in the United States since 2006 and without an age limit since 2013.
Levonorgestrel a type of progestin. works by several mechanisms, including delayed tubal transport of the ovum. A study published in the Journal of Pathology revealed the increased risk of tubal pregnancy following the failure of levonorgestrel (LNG)-induced emergency contraception. The occurrence of tubal pregnancy was attributed to reduced ciliary motility in the fallopian tubes in response to Levonorgestrel.
Most tubal ectopic pregnancies can be detected and treated but in some cases, an unstable patient is a medical emergency that requires prompt surgical intervention. Women need to know about the risk involved in over-the-counter hormonal emergency contraception since tubal pregnancy is the leading cause of maternal mortality in the first trimester of pregnancy and accounts for almost 5% of maternal deaths.
I had an extraordinary experience a few weeks ago while attending Mass at Sacred Heart Parish in Winchester, Virginia. No, it wasn’t a mystical experience, but it struck me with almost the force of one. For the first time in 31 years as a Catholic, I heard a priest preach—clearly and confidently—against contraception at Sunday Mass.
Now over the decades I have known many pro-life priests, chief among them Father Paul Marx, OSB, speak forthrightly about the truth and beauty of human sexuality. They defended Humanae Vitae, Pope Paul VI’s prophetic encyclical of 1968, that was widely criticized by the modernists within the Church. They vigorously taught, following Saint Pope John Paul himself, the perennial teaching of the church that preventing conception through artificial means was a sin.
But these talks were all given at Catholic pro-life meetings and conferences, where the vast majority of those present were already predisposed to listen. The choir, in other words. I had never before heard—at an ordinary Sunday Mass attended by ordinary Catholics—a clear and definitive exposition of the Church’s teaching in this area. Occasional homilies against abortion, yes. Homilies contra contraception, never.
But there I was, sitting in the second pew on the right at Sacred Heart, when Father Stephen Vaccaro, the young Parochial Vicar of Sacred Heart Parish in Winchester, Virginia, strode to the ambo. The day’s reading concerned the Parable of the “Fool” who sought to store up his treasure on earth and died that very night. On this “seemingly harsh, often overlooked, but crucially important teaching about the Christian life” Fr. Vaccaro promised a “two-point meditation … First, how this should drive us to an examination of our own lives. Second, a very practical suggestion for married couples.
Neither I, nor anyone in the congregation, had any idea what this “practical suggestion for married couples” would turn out to be.
“In our Gospel,” Father Vaccaro began, “our Lord tells the parable of the rich man who, after achieving worldly success and comfort, settles back to enjoy his labor, only to be reprimanded by God and then dying. I’m sure many of us don’t see anything wrong with what this man did, as some here are retired and many hope one day to be retired. What’s wrong with enjoying the fruits of your labor, resting after a life of work?
“But Jesus’ shows harshness in how He speaks of the man, with the words, ‘You fool!’ What is He rebuking here? That the rich man, and so many of us, are practical atheists. That may sound harsh. But notice what the man does not do. Never does he thank God, consider using his bounty to help the poor, or dedicate his newfound free time for prayer that God was so good and generous to him. Rather, he says he will commit his life to comfort. No thought is given to God, just to this world.
“Whether we like to admit it, so many of us, for so much of our lives, and in so many parts of our lives, live as if this world is all there is. … We store up treasure in this world. We live as if our choices don’t really matter to God, because He’s merciful whether we repent or not. We don’t live as if we will render an account for how we live. To put it another way: we live to retire well in this world, we don’t live every day as if we want to be in Heaven.
“How do I know this? Well, look around the world. We check the stock market every day, our retirement accounts every day, but don’t visit the Blessed Sacrament every day, don’t pray every day. … We don’t live for Heaven.
“This is what Jesus was pointing out, as a loving warning. Basically, if we don’t remember where we are going, the journey always becomes confused and the things necessary to get there get ignored. In short, we are fools!
“But Jesus goes on to point out an amazing irony: it is only by remembering our Home of Heaven that we will ever truly value this world, live a truly awesome life. If this world is all there is, nothing really matters, so do what you want because everything is ultimately meaningless. But if Heaven is real, is waiting for us, and is tied to how we live now, each moment in this life is infused with eternal meaning. We have every reason to bring God into every moment.
“This is why Jesus spoke so starkly. If we, Christians, are no different from unbelievers, then we are fools. We have squandered our lives calling things treasure that are trash and ignored the things that matter to God. So, here’s the examination: the things that keep you up at night, the way you spend your time, the motivation of why you work or study, what occupies your schedule? That will show you your treasure. Is it the treasure of earth? If so, Jesus invites you to repent and convert, to live differently. If Heaven and the things of God are not our only motivation and end, our joy and inspiration, and clearly so, then we are fools. “Second, related to this first point that our lives must be focused on what matters to God, I present a thought for married couples. I preface by saying this one might sting or make people uncomfortable. But I am following Christ.
“This week is Natural Family Planning Awareness week, where the Church calls all married couples to remember what is stated in Scripture, defined by the Church, inspired by the Holy Spirit: any use of artificial contraception within sexual intimacy is a grave sin, and that authentic marital love requires avoiding all such means in order to remain in the state of Grace. Maybe this is not a widely known truth, but if known, it is not widely followed.
“We tell ourselves that the world knows more about sexual morality than the Church. Well, today Christ lovingly says to this idea: ‘You fools!’ Marital intimacy is meant to be a total gift of self, an incarnation of your wedding vows. Contraception is a conscious choice to follow earthly wisdom, reject God’s plan, and hold something back in expressing love, thus rotting marital love from within.
“If you have ever contracepted or willfully been sterilized, and have not Confessed this, you must do so. If you are now contracepting, the Lord is calling you to stop, repent, and trust in Him.
“Yes, this will be a sacrifice. But remember Jesus said every part of marriage, even marital intimacy, is to be modeled on the Cross. It is to be focused on Heaven, holiness, and sacrifice. If married couples want to build treasure in Heaven and abandon foolishness, then embrace Natural Family Planning.
“I end with this quote from Pope Saint John Paul II: ‘What really matters in life is that we are loved by Christ and that we love Him in return. In comparison to the love of Jesus, everything else is secondary. And, without the love of Jesus, everything is useless.’”
As I listened to this young priest, clearly and without hesitation, state the perennial teaching of the Church, I was deeply touched. God created humanity in a great act of love, and he expects us to love him in return, in part by following the first commandment given to our first parents, to be fruitful and multiply.”
Or as I said to Father Vaccaro himself after Mass, “Souls will be created and babies will live because of your words today, Father. Thank you for your courage in speaking the Truth.”
This article first appeared in Steven’s blog on LifeSiteNews.com on Monday, August 29.
Steven W. Mosher is the President of the Population Research Institute and the author, most recently, of The Politically Incorrect Guide to Pandemics (Regnery Press).
A paper published in the journal ESC Heart Failure reported that obese women who use combined oral contraceptives have a 24-fold increased risk of venous thromboembolism (VTE) compared to non-obese women who do not use the drugs.
The authors of the study reported in the abstract of the paper: “Obesity and estrogen-containing contraceptive products are well-known independent cardiovascular risk factors. However, a significant number of obese women continue to receive prescriptions of hormonal products that contain estrogens for their contraception.”
Obese women already had an increased risk of VTE compared to non-obese women. Using combined hormonal contraception presents a greater risk (between 12 and 24 times) to develop VTE. VTE is defined as a blood clot in a vein. There are two potentially fatal conditions: deep venous thrombosis and pulmonary embolism.
The author of the study Professor Giuseppe Rosano concluded, “Obese women taking contraceptives should be viewed as an ‘at risk’ population, and as such, they should receive advice to change their lifestyle, avoiding other cardiovascular risk factors, as a form of primary prevention. This indication should be extended to young women, as data show that combined oral contraceptives should be avoided in obese women of any age”.
(Homily delivered at St. Paul Parish – Cambridge, MA, October 14th, 2018)
Today the Church honors a man whom many consider to be a modern-day prophet. Fifty years ago, just as the sexual revolution was in full swing, he predicted that four things would happen in society if the Church’s teachings on marital love were not embraced:
1. A general lowering of moral standards.
2. A rise in marital infidelity.
3. A lessening of respect for women by men.
4. A coercive use of reproductive technologies by governments.
This man is Pope Paul VI, and he was canonized a saint earlier today in Rome by Pope Francis. These four predictions, which Paul VI made in his famous encyclical Humanae vitae, have not only come true, but they came true sooner and to a far greater extent than anyone, including Paul VI himself, would have ever imagined. If you find yourself skeptical of the claim that these predications have come true, look no further than the $12 billion pornography industry, which is based primarily on the objectification and exploitation of women.
At Humanae vitae’s release in 1968, it was met with scorn and ridicule. Today it seems pathetically antiquated to most people and laughable to the world that the Church actually still maintains her teaching against the use of artificial contraception. So what relevance, if any, do the teachings of Humanae vitae have for us today – 50 years later – on its author’s canonization?
The encyclical’s fundamental goal is not to impose a moral norm, but rather to provide a total vision of the human person and an answer to the question, “What do certain actions mean?” By asking that very question, we have already delved into controversial philosophical territory. The dominant philosophy in our present culture is nominalism, which maintains that things do not carry an objective, intrinsic existence; the meaning of things only comes from what our minds assign to them. To the nominalist, I am free to assign meaning to things as I please, because nothing carries an objective existence or meaning outside of my mind.
But this doesn’t work in Catholic theology. We believe in a God who, though invisible, really exists. And through divine revelation, we can know objective truths about God in such a way that our knowledge of him is not simply a product of my thoughts or feelings, or imagination. A Christian must be rooted in a metaphysical understanding of reality. In the Aristotelian tradition of realism inherited and perfected by Saint Thomas Aquinas, things have real existence in themselves and carry objective meaning that I am not free to assign on my own.
Therefore, marital love carries a specific meaning that is discoverable by philosophy and confirmed by revelation. Marital love is the exclusive and total giving of self between husband and wife. The marital act is a particular physical expression of that, through which spouses speak their wedding vows to each other with their body. This is why we say that a couple consummates their vows; instead of verbalizing the words they first declared to one another at the altar on their wedding day, the spouses speak those words to one another through their bodies. This is completely distinct from animals. Human love is a free act, proceeding from the intellect and the will, involving both body and soul. It would therefore be contradictory to the very inner meaning of marital love if a couple were to say to one another, “I give myself to you totally and freely: everything that I have and all that I am… except my fertility, except my potential to be a parent with you.” Spousal love, which by its very nature involves total self-giving, admits of no exceptions.
The Church does not teach that couples must have as many children as physically possible, nor is the Church interested in imposing arbitrary restrictions on people’s private lives. The teachings of the Church, reiterated in Humanae vitae, exist to give spouses the freedom to give of themselves fully to each other so that they can experience the full depths of marital love. The sexual revolution promised freedom and liberation. But it was a radicalization of the good feminist movement of the earlier 20th century. So instead of new freedom, it has brought about the enslavement of men and women to their passions and the further degradation of women. Again, if you question that claim, look no further than the $12 billion pornography industry.
I recommend Humanae vitae for everyone to read because we are all suffering the effects of a culture that has rejected its teachings outright. While it is the most controversial encyclical of modern times, it is also one of the shortest encyclicals. The beauty of its simple and succinct message is that it applies to everyone, both married and unmarried. Humanae vitae teaches everyone that because we are made out of love we are made for love: love that is free – not simply acting upon passions but fully human and intelligent; we are made for love that is total – that seeks the good of the other and holds nothing back; love that is faithful and love that bears fruit in the lives of others. These are Paul VI’s four characteristics of authentic human love. It’s the only love that satisfies: free, total, faithful, and fruitful.
All of what I’ve said thus far belongs to natural law and does not require Christian faith to believe. Nonetheless, it is affirmed and deepened by divine revelation. We only need to look at the person of Jesus Christ, who is love incarnate. Jesus Christ is mystically married to the Church. And this mystical marriage was consummated on the cross; it was at that moment when Christ gave himself freely, totally, faithfully, and fruitfully for his beloved bride, holding nothing back. That is perfect love. That is the love we are called to imitate.
Sound impossible? Well, it is – on merely human terms. Like the rich young man in today’s Gospel, we too can be tempted to walk away from Jesus’s invitation to enter upon the path of perfection. It is certainly discouraging when most people around us see this path as impossible and unreasonable. But Jesus’s invitation is not an invitation to impose new rules on one’s life. It is an invitation to respond to grace that is freely offered to us, to follow Christ in faith and hope, and to entrust every little part of our lives to his plan of loving goodness.
On November 18, 2022, the FDA advisers will meet to review the application for making available the hormonal contraceptive “Opill” over-the-counter (OTC).
Opill is a progestin-only oral contraceptive, with the active ingredient norgestrel. It has been available with a prescription in the U.S. since 1973.
A partner at the law firm Goodwin who specializes in the FDA’s regulation of drugs and biologics said that two advisory committees will consider switching the drug from prescription to over-the-counter and weigh how the drug itself is used.
If the application to make Opill OTC is approved, all women in the United States will be able to purchase Opill without health provider oversight. This includes teenagers, who will be able to purchase this drug without parental knowledge.
According to the American College of Obstetricians and Gynecologists ACOG, “the potential toxicity of the medication and whether the medication can benefit consumers without endangering their safety” is the principal factor the FDA considers to make OTC a medication. Progestin-only contraceptives are often advertised as being “safer” than contraceptives that contain estrogen, but they are associated with many health risks. Total synthetic progestins have been associated with an increased risk of breast cancer, increased risk of clinical depression, and increased risk of ectopic pregnancy
Four months ago, the world was stunned by the U.S. Supreme Court’s landmark decision in Dobbs v. Jackson Women’s Health Organization. The decision overturned Roe vs. Wade, the 1973 ruling that had effectively legalized the horrific procedure of abortion throughout the land. The Dobbs decision now makes it possible to save thousands of lives – lives of babies and mothers alike – as efforts on the state and local level gain momentum to put it into practice.
Already, numerous States are crafting legislation to make it more difficult to get an abortion, or even to outlaw the procedure altogether. And while at least 66 clinics across 15 states have closed down or stopped offering abortions, not everyone is happy.
That’s right – today the sexual and reproductive health and rights (SRHR) “activists” are not happy, and they’re working 24/7 to engineer ways to bypass these new “restrictions.” In fact, the same activists are working worldwide to prevent any influence that Dobbs might have in Europe and beyond.
Previous chapters in the elites’ worldwide effort to eliminate the “excess population” have always begun with efforts to increase access to contraception and abortion. These efforts always bear the same shopworn banner of “women’s rights,” “women’s health” and “climate activism.”
Close up of a girl hands buying contraceptive pills and pharmacist explaining in a pharmacy
Money certainly talks, and it is no secret that money plays a central role in attempts to eliminate the “overflow” population as well – one innocent life at a time. Not surprisingly funding is a primary component in their next strategy, too.
And what is that, you may ask?
Meet The Killer Calculator
Introducing the next chapter in the population control agenda: the Family Planning Investment Impact Calculator. This project, or, better yet, this tool, has been created by the Guttmacher Institute, and it is designed to have a powerful impact worldwide.
According to Dr. Herminia Palacio, President and CEO of the Guttmacher Institute, this interactive, web-based tool “will provide stakeholders with evidence-based estimates of the health benefits they can expect from investments in family planning services.”
The Family Planning Investment Impact Calculator produces data and graphs presenting the following information:
The number of women and couples who would receive modern contraceptive care
The number of unintended pregnancies, unplanned births, and unsafe abortions averted by increased contraceptive use
The number of women’s and girls’ lives that would be saved
Cost savings that would be achieved
“Investment Calculator”? That’s right. It all boils down to dollars and cents. Capitalizing on the self-indulgent culture spawned by the sexual revolution sixty years ago, The Guttmacher Institute is pandering to “instant gratification” when it comes to sex – and selling it as “transparency.”
Here’s how it works: when prospective stakeholders (another euphemism; that means “donors”) can directly and transparently see the impact that their donation will produce based on the program’s calculations, they are more likely to donate. The success of the Guttmacher “calculator” rests on the assumption that donations from stakeholders will cover the full cost of contraceptive care—both service delivery costs, and associated programs and systems costs.
The main goal of this “tool” is clear. It is designed to generate worldwide funding for international access to contraceptives because such funding is indispensable to the effort to control the sexual and reproductive health for women and girls by medicinally sterilizing them.
Realizing that they face increasing opposition in their battle to provide legal abortions, the SRHR activists have realized that contraception is their primary weapon in their campaign to “empower” women and girls.
“Fewer Babies Means Better Weather – May Start Trend!”
“Funding sexual and reproductive health care is not only the right and sensible thing to do for the health of women and girls—it’s also a smart investment that leads to significant savings in the long run,” Palacio said.
“Savings” only for the survivors, of course. “There’s just enough of me, but waaaay too many of you,” as P.J. O’Rourke once put it.
P.J. was a satirist, but, for the Guttmacher Institute, the campaign for fewer humans is grim.
Indeed, the notion goes hand in hand with the United Nations’ Sustainable Development Goals (SDGs). These goals include Family Planning as a critical component of the SDG agenda, which promises to “end poverty, hunger, AIDS, and discrimination against women and girls.”
In commenting about the tool, Rachel Murro, Senior Research Assistant for the Guttmacher Institute, says “[it] is an important resource to equip advocates, policymakers, and donors with a strong business case for investing in these essential services.”
We should not confuse this idea of “family planning” with any desire to protect and prosper families and children. For the Guttmacher Institute, its Family Planning Investment Impact Calculator is designed for “stakeholders” – that is, donors. It’s a business, and it’s about finance, not families.
That’s right. Financiers, including governments as well as businesses, can use the calculator to see how much their investments will aid in “health benefits” in the countries or regions of their choice. The Guttmacher Institute makes no effort to hide what they mean by “health benefits.” These “benefits” essentially come down to increased use of contraceptives and fewer babies.
So the phrase “family planning” is but a euphemism for “contraception,” which even the notorious secular Internet resource Wikipedia makes clear.
Abortion activists always complain that there are not enough abortions per year to meet “full equity” in each country per year, so they have to sell their contraception campaign as the next best tool to “invest in family planning.” This moves them closer to the cynical and destructive national “development goals” as described by global organizations such as the United Nations and the World Health Organization.
Do not let warm words like “family planning” lead you to believe otherwise, because “family planning” programs are not always what they seem.
The thyroid gland is part of the endocrine system and has a crucial role in women’s health. The gland located in the lower part of the neck produces triiodothyronine (T3) and thyroxine (T4). These hormones are critical for normal metabolism, growth, brain development, energy production, temperature control, and reproduction. When the gland is underactive, it does not produce enough thyroid hormones. This condition is known as Hypothyroidism.
A large epidemiological study published in the British Medical Journal evaluated the association between the use of birth control pills and thyroid abnormal function.
The team of investigators analyzed data from the National Health and Nutrition Examination Survey conducted in the USA from 2007 to 2012. More than 7000 health records were analyzed. The authors of the study included women who reported the use of birth control pills in a reproductive health questionnaire, and also reported thyroid medication use or had thyroid function laboratory test values.
Women who had ever taken birth control pills had a higher prevalence of hypothyroidism, compared to women who never used hormonal oral contraceptives. Further statistical analysis of confounding variables (such as age, race, education, body mass index, smoking status, alcohol use, history of thyroid disease, current thyroid disease, first menstrual age, pregnancy history, menopause status, and history of hormone replacement use) was performed using multivariate logistic regression. The analysis demonstrated a significant association between hypothyroidism and a history of taking birth control pills for more than 10 years.
The authors of the study concluded that a “long history of using birth control pills was strongly associated with hypothyroidism, especially for more than 10 years.”
A recent article published in the Linacre Quarterly describes how seven years of working as an embryologist revealed IVF’s disordered approach to patient care. It articulates the social, legal, ethical, and medical issues with artificial reproductive technologies.
Abstract
This article is a case study illuminating the experience of a cradle Catholic who pursued a career in the field of Assisted Reproductive Technology (ART) as a laboratory director and embryologist. Twenty years after leaving the field, the observations leading to the crisis of conscience are further amplified by the reports of social, legal, ethical, and medical consequences of the technology. These consequences are explored in detail and can serve as a mini-review of the published scientific literature describing the obstetrical complications, peri-natal outcomes, and the long-term health effects on the offspring. This paper provides the documented evidence that can be used by the religious and medical community for shepherding the flock. The disordered approach to patient care is evidenced by five serious consequences resulting from the use of the technology. These include multiple pregnancy and selective reduction, abandoned and discarded embryos, adverse health effects to the women and children, legal and ethical problems, and human experimentation. An explanation for the adverse consequences can be found by exploring and applying the principles of Natural Law. Natural Law, as embraced by the Catholic Church, can be used as a starting point for conversion of heart for many who struggle with the immorality of ART. Deterring use of the technology coupled with increased motivation by scientist and health professionals to pursue restorative approaches within a moral framework offer our best solution to the treatment of infertility. Natural Law and the consequences of violating it provide evidence that science and medicine should not be practiced in a vacuum void of ethical and moral boundaries grounded in divine Wisdom.
Hanna Klaus, Nora Dennehy, and Jean Turnbull Presented at Teen Pregnancy Prevention Conference Pennsylvania State University, State College, PA October 21, 2001 Reproduced with Permission
The efficacy of the Teen STAR Program, a proactive educational program in human sexuality to undergird virginity andÚor facilitate a return to chastity has been reported previously. The 1999-2001 cohorts are similar to previously reported cohorts. The 8-month program joins experiential learning of fertility signs to a developmental didactic curriculum plus regular teacher-student interaction. Our U.S. study population from 5 sites consisted of 822 males aged 12-17 years; 71 were sexually active, 42 virgins (5.5%) transitioned to sexual activity, while 39 (35%) discontinued activity. Of 496 females aged 12-16 years 16 (3.2%) were sexually active, before the program, 14 (2.9%) transitioned while 16 (53%) discontinued activity. The rate of discontinuation was approximately double of that among the general population: 53 vs. 26 % for females, 49 vs. 27% for males.
Responses were stratified by early, middle and late adolescence and tabulated by virginÚnon-virgin status. Both virgins and non-virgins identified chastity, the consequences of sex: unwanted pregnancy and STD’s, and selfÐknowledge as the most important thing(s) they learned and remembered about the program. A previously validated Likert scale measured behavioral parameters: speaking about the program with parents, with friends, greater control of emotions, greater empathy with others, overall helpfulness of the program and reasons for maintaining or returning to chastity. In middle and late adolescence non-virgins generally presented at the lower end of the scale in all parameters, lending support to Erikson’s theory of identity foreclosure or at least delay as a result of participation in adult tasks before emotional maturity has been reached, while early adolescents were equally enthusiastic, and predominantly returned to chastity. The fact that at least half of locus of control responses indicated an internal locus may indicate progress toward growing up. Failure to discontinue intercourse was associated with contraceptive use by 72% of the males and 43% of the females.
Conclusion: Tracking of fertility patterns joined to discussion of their meaning correlates positively with maintaining virginity as well as a return to chastity. The overall 50% discontinuation rate exceeds that of the general population and can be an important tool for prevention of STD and premarital pregnancy.
This must seem like a strange title, “Contraception: Fatal to the faith.” What does the title mean? Does it mean that to believe in contraception is contrary to the faith? Or does it mean that-Christian believers may not practice contraception? Or does it mean that those who practice contraception are in danger of losing their faith?
Please be more clear on just what we mean when we say, “contraception, fatal to the faith?”
What do we mean by the title and what is the thesis of this presentation? We mean that professed Catholics who practice contraception either give up the practice of contraception or they give up their Catholic faith.
Needless to say, this is a startling statement that many would violently disagree with. They will point out the widespread practice of contraception among many–some would say the majority of professed Catholics in a country like the United States. They will quote from numerous professedly Catholic moral theologians openly defending contraception. They will give you the pronouncements of whole conferences of bishops who claim that contraception is really a matter of conscience. Those who sincerely believe that contraception is morally permissible may not be told they are doing wrong; they may not be debarred from receiving Holy Communion; in fact, they need not even have to confess the practice of contraception when they go to confession.
We return to where we began, to make clear what we are saying. We affirm in this conference that the deliberate practice of contraception between husband and wife is objectively a mortal sin. Those who persist in its practice are acting contrary to the explicit teaching of the Roman Catholic Church. They may protest that they are Catholic. They may profess to be Catholics. But their conduct belies their profession.
Someone may object that we are living in a contraceptive society. Moreover, the silence of so many bishops and the overt teaching of so many nominally Catholic moralists defending contraception forbids our saying that contraception and the Catholic faith are incompatible.
In the light of all the foregoing, let me address myself to the following topics which collectively prove the underlying thesis of this lecture.
The Catholic Church teaches infallible doctrine, both in faith and morals. This infallible teaching is done by the Church’s extraordinary and by her ordinary universal authority or magisterium.
The grave sinfulness of contraception is taught infallibly by the Church’s ordinary universal teaching authority.
Therefore, those who defend contraception forfeit their claim to being professed Catholics. Consequently, those who persist in their defense of contraception, deprive themselves of the divine graces which are reserved to bona fide members of the Roman Catholic Church. The church teaches infallibly on faith and morals.
There is some value in explaining that the Church’s infallibility covers not only doctrines that are to be believed, like Christ’s divinity or His Real Presence in the Eucharist. No, the Church also, and with emphasis, also teaches infallibly what the followers of Christ are to do.
In His final commission to the Apostles, Jesus told them to teach all nations, “to observe all that I have commanded you.”
To mention just one infallible teaching in the moral order: the permanence of the marriage bond. Emphatically, the Church’s irreversible doctrines include truths that we are obliged to believe. But they also include precepts that we are universally bound to obey.
This deserves to be emphasized. Why? Because there are nominally Catholic writers who are claiming that the Church’s gift of infallibility extends only to her teaching of the faith. It does not, so the claim goes, include grave moral obligations like the prohibition of adultery, sodomy or contraception. That is not true.
Two forms of infallible teaching
What are the two ways in which the Church teaches infallibly? She does so whenever the Pope solemnly defines a dogma of the faith, as when in 1950 Pope Pius XII declared that Our Lady was assumed body and soul into heavenly glory.
But the Church also teaches infallibly whenever her bishops, united with the Pope, proclaim that something is to be accepted by all the faithful. Thus abortion was condemned as murder by the Catholic hierarchy, under the Pope, already in the first century of the Christian era–and ever since.
It is therefore infallibly true that abortion is a crime of willful homicide. So, too, the grave sinfulness of homosexuality is infallible Catholic teaching.
Infallibly true that contraception is a mortal sin
We return to where we began, to the subject of contraception. It is infallible Catholic doctrine that contraception is a mortal sin? Yes!
How do we know? We know this from the twenty centuries of the Catholic Church’s teaching. Already in the first century, those who professed the Catholic Faith did not practice either contraception or abortion, which were commonly linked together.
The people of the pagan Roman Empire into which they were born universally practiced
Abortion Contraception Infanticide Cohabitation of one man with either several legal wives or with a plurality of concubines.
In contrast with this moral promiscuity, Christians practiced monogamy, one man with one woman; they did not use drugs to prevent conception; they did not kill the newborn children whom they did not want to live; they did not practice sodomy or prostitution; and for the Christian, adultery and fornication were grave sins that might require several years of penitential expiation.
What do we call the Church’s unbroken tradition in forbidding contraception? We call it her ordinary universal magisterium or teaching authority. This has always been considered a proof of infallibility, or from another perspective, irreversibility.
What do these two terms mean?
Infallibility means that God protects the Church from error in her 2000 years of teaching that contraception is a grave sin against God. Irreversibility means that this teaching will never be reversed. Contraception will remain a grave sin until the end of time.
To defend contraception forfeits the catholic faith. As Christianity expanded, the inevitable happened. Once professed Christians lapsed into their former paganism.
We read in the first three centuries about the thousands of Christians who chose to be thrown to the lions, or beheaded, or crucified–rather than conform to the pagan immorality that was so prevalent in the culture in which they lived.
It is possible to misunderstand the Age of Martyrs of the first three centuries of the Christian era. We are liable to associate professing the Christian faith by refusing to drop a grain of incense before a statue of one of the pagan gods. No, the issue was much deeper and more serious. To be a Christian meant to refuse to conform to the pagan morality of those who did not believe in Christ. To be a Christian meant to reject the pagan immorality of the contemporary world–at the heart of which was the practice of contraception.
The situation in the modern world
Contraception as a general practice is a recent innovation in the western nominally Christian world.
Its rise is partly explained by the medical discovery of drugs which either prevent conception, or which destroy the unborn child in its mother’s womb.
But the rise of contraception is mainly the result of widespread propaganda by women like Margaret Sanger and the powerful forces of population control.
What have been the consequences of this return to pre-Christian paganism which is now “the law of the land” in once-Christian nations like the United States? The consequences are inevitable.
The once solitary defender of the sanctity of marital relations is now on trial for the profession of its Catholic faith.
In 1968, when Pope Paul VI published Humanae Vitae, the episcopal conferences of one country after another met in solemn sessions to pass judgment on the teachings of the Vicar of Christ.
Bishops in what we call the “Third World Countries” stood firmly behind the Pope’s teaching. But the bishops of so-called developed countries, like the United States, Canada, France, Germany, Austria, or Scandinavia issued long documents that, to put it mildly, compromised the teachings of the Vicar of Christ.
What followed was as inevitable as night follows day. Once firmly believing Catholics became confused, or bewildered, or simply uncertain about the grave moral evil of contraception.
The spectacle of broken families, broken homes, divorce and annulments, abortion and the mania of homosexuality–all of this has its roots in the acceptance of contraception on a wide scale in what only two generations ago was a professed Catholic population.
Contraception fatal to the faith
We come back to where we started–by claiming that contraception is fatal to the Catholic Faith.
By divine ordinance, those who call themselves Catholic must subscribe to the moral teachings of the Catholic Church of which the Bishop of Rome is the visible head.
This Catholic Church now stands alone in the world as the one universal authority which condemns contraception as contrary to the will of God.
Within the Catholic ranks has arisen an army of dissidents who speak and write in defense of contraception. The sex-preoccupied Andrew Greeley of Chicago recently devoted a whole chapter of a book entitled, “That damned encyclical,” referring to Humanae Vitae. This priest remains in good standing in ecclesiastical circles.
When the present Holy Father made his first pilgrimage as Pope to the United States, he pleaded in Chicago with the American bishops to do something over the scandal of so many Catholics on Sundays going to Holy Communion and so few going to confession.
All the evidence indicates that the core issue at stake is contraception. If contraception is not a grave sin, well then what is? And why go to confession if I am still in God’s friendship although practicing contraception.
What is the new conclusion? That the single, principal cause for the breakdown of the Catholic faith in materially overdeveloped countries like ours has been contraception.
St. James tells us that faith with out good works is dead. What good is it to give verbal profession of the Catholic faith, and then behave like a pagan in marital morality?
Recommendations
The single most crucial need to stem this hemorrhage from the Catholic faith is for the Church’s leaders to stand behind the Vicar of Christ in proclaiming the Church’s two millennia of teaching that no marital act can be separated from its God-given purpose to conceive and procreate a child.
I make bold to say that the Catholic Church, the real Roman Catholic Church, will survive only where its bishops are courageous enough to proclaim what the followers of Christ have believed since apostolic times. But the bishops are frail human beings. They need, Lord how they need the backing and support of the faithful under their care. So I would like to close with a prayer:
“Lord Jesus, you ordained your Apostles as Bishops at the Last Supper on Holy Thursday night. We beg You to give our bishops the wisdom to see that contraception is fatal to Catholic Christians. Above all, give them the courage of Thomas a Becket and John Fisher, to stand firm against the demonic pressure to destroy the human family by contraception. Amen.”
Scripture Readings for 26th Sunday in Ordinary Time: Amos 6:1a, 4-7, 1 Timothy 6:11-16, Luke 16:19-31
By Deacon Rusty Baldwin
The readings today are about the sin of indifference; two kinds of indifference as a matter of fact. The first kind is indifference to the bodily and material needs of others which is depicted in the rich man’s indifference to Lazarus in the Gospel. This kind of suffering is alleviated by practicing the corporal works of mercy in a spirit of love, which includes feeding the hungry and binding up their wounds.
The second kind of indifference is indifference to the moral suffering of others which the “complacent in Zion” were guilty of in the first reading. Zion, that is, God’s chosen people were not made ill by the collapse of Joseph. The prophet Amos was writing in the 8th century B.C., right after the tribe of Joseph had been conquered by the Assyrians. For decades the people of the tribe of Joseph had become weaker and weaker due to their sins of commission, which included apostasy, turning from God to idols, and their abandonment of the rest of the 10 Commandments as well. Finally in their weakness, they were conquered by the Assyrians. During the many years of their decline, however, their fellow Israelites didn’t seem the least bit concerned about their sorry moral and spiritual state, according to Amos. Moral and spiritual suffering is alleviated by practicing the spiritual works of mercy in a spirit of love, which includes instructing the ignorant, admonishing the sinner, and praying for the living and the dead.
And even though sin is not a popular topic, it is the one thing Jesus himself told us to fear, because sin brings death to our souls. That’s why although God loves sinners like you and me, God hates sin! God hates sin like a doctor hates cancer. Doctors do everything in their power to kill cancer because cancer kills us!
In just the same way, sin kills if we deliberately choose to commit a mortal sin and remain unrepentant; if, in an act of rebellion, we decide we’re going to sin, knowing full well what we are about to do is seriously wrong. But it would be a mistake to think such an act of rebellion has to be the in your face, shaking your fist at God kind that says, “God, I don’t care what you say or what your Church says; I don’t care what the Bible says, I’m doing this anyway!” Just as deadly is a passive rebellion, a kind that sadly and quietly with eyes cast down says, “God, I know what I’m about to do is seriously wrong, but I’m going to do it anyway. I’m really sorry it hurts you – I hope you understand.” Either way, I still chose to sin, didn’t I? But what constitutes a mortal sin? Well, beyond obvious things like theft and murder, you can pick just about anything our culture praises in the name of freedom for an example of mortal sin. Things like pornography, premarital sex or homosexual acts, using contraception, or abortion – these are a societal cancer. But what happens when you tell people such things are wrong? They accuse you of being hateful, when actually it is precisely because you love them that you are warning them that such things are so very harmful to them; when you say that if they but ask, God is longing to forgive and heal them. We need to understand that our modern culture has perverted the truth about sin and we should be heartsick our society has reached such a state that it calls evil good and good evil.
And that’s what the prophet Amos is asking us today. Are we heartsick over what America has become or are we complacent? Do we have the attitude: well, our society is what it is, what can be done? Well, perhaps the first thing to be done is to realize Amos was talking to us today as well. And let’s do that by bringing the reading from Amos a little closer to home: from Zion to America; from 800 B.C. to 2022 A.D. Here’s an updated version of the reading for today.
“Thus says the Lord God of hosts. Woe to the complacent in America, stretched out in front of their big screen TVs, eating their fill, lying comfortably on their couches. They spend hours on social media, talk endlessly on their smartphones, drink their lattes and Frappuccino’s and yet are not made ill by the collapse of their culture.”
The plain fact is our culture has made freedom its idol and god. Not the kind of freedom God intended; a noble freedom to choose to do any number of good things for love of God or neighbor. That is, a freedom for doing good for others. No, our culture has corrupted freedom in the same way it tries to corrupt our consciences – by equating freedom with license. By saying freedom is all about doing anything you want to as long as, we all know how this ends, you don’t hurt anybody. That, my friends, is a lie on a couple of levels. First, as I said previously, that’s not what true freedom is. Second, there is no such thing as a sin that doesn’t hurt anybody. There is no such thing as a private sin. Any sin I commit may not affect you immediately, but unless I repent, it will eventually. Why? Because my conscience will be weakened and injured by that sin and eventually, the sin I commit in private, I’ll want to justify committing in public, and I will also want to convince you that it is not a sin but rather just a choice, just a choice…maybe a choice you wouldn’t make, maybe one you would – but in any case, who are you to interfere with my freedom to choose? And then I will try to convince you that interfering with my freedom to choose is the real evil.
OK, you might be saying, but what do you expect me to do? Singlehandedly root out all the evil in the world? No, we need to do something much harder than that. Something none of us are exempt from, no matter what our state in life, no matter what our age, no matter what our position in the parish or even in the universal Church. It’s something you need to do no matter how corrupt the culture becomes, whether you are the Pope or the newest member of the Church. It’s what St. Paul said so plainly in his letter to Timothy and the bottom line is this: however much sin there is in the world, you’re still responsible for rooting out the sin in you.
“But you man of God, but you woman of God, pursue righteousness, pursue devotion, faith and love. Compete well for the faith by keeping the commandments without stain or reproach.” You see, no matter what else God calls you to do in life, you are to be holy, to love God and neighbor. And that’s hard work, much harder than many other tasks God may call us to because it means dying to ourselves every day, it means giving up our selfish will, our sinful thoughts and desires every day of our lives and replacing them with his perfect will instead.
And that’s hard. And Satan knows it’s hard and so rather than getting us to commit serious sins, sometimes he tries to convince us that God will be satisfied as long as we are nice, as long as we are a so-called good person. Satan tries to deceive us by saying, you don’t have to be holy, just be nice. Be a nice Catholic whose goal is to be liked by everybody. Why does Satan do that? Because he knows the opposite of being holy is not being evil, the opposite of being holy is being complacent. When we don’t do the good we should, when we are complacent, when our goal is to be nice, rather than holy, we commit a sin of omission. When you get home, reread the Gospel passage for today. You’ll find the rich man wasn’t a murderer or a thief, he wasn’t sexually immoral or mean to his mother. He didn’t kick puppies. He was simply a bit self-centered. He didn’t pursue righteousness. Today we would probably say he was a nice person.
The 1993 movie “Schindler’s List” provides a poignant example of the sin of omission. Schindler’s List is a true story of a rather mediocre Catholic businessman, Oskar Schindler, who lived in Poland during World War II. When the war started, he saw an opportunity to make money. He became friends with German officials and worked out a deal with them to use Jewish prisoners as free labor for his munitions factory. Since he didn’t have to pay his workers, he made enormous profits. But little by little he realized the horrors of the Nazi regime. His heart changed, and he started using his factories and his connections with German officers to save his Jewish workers from the Holocaust. He used the money he made early in the war to “buy” more and more Jewish workers, just so he could save their lives. By the end of the war, he was as broke as he had been at the beginning, but he managed to save hundreds of Jews from being massacred.
In the last scene of the movie, the Germans are fleeing as allied troops approach the town where the factory is located. We see Schindler surrounded by the workers whom he had saved; they were thanking him. But then Schindler starts to cry. He looked around at the faces of the people he saved and told them, “I could have done so much more.” He held up his gold watch, and said, “This could have bought someone’s freedom.” “If I had started sooner,” he sobbed, “I could have saved twice as many.” Every face Schindler saw made him think of another person he could have saved if he had been less self-centered. Schindler was completely distraught. He had come to understand firsthand the destructive power of the sin of omission.
Today, you and I have been given a chance to correct any sin-of-omission mentality we may have … to stop being complacent about seeking holiness by loving God and our neighbor whole-heartedly. God gave us the means to be holy by giving us abundant graces through the sacraments, especially the Eucharist and Reconciliation. And He rightly expects us to follow the example of Our Lord and spend our lives building up the Kingdom of Heaven – not merely seeking our own comfort. Our Lord gives himself entirely to us in Holy Communion. If in turn we give ourselves entirely to him, if we seek righteousness and put all we have and all we are at his service, there’s one thing we can be sure of: when eternity rolls around, we will have absolutely no regrets.
A recent article published by Contemporary OBGYN presented an update on Emergency Contraception. The authors mentioned the need for accurateinformation about emergency contraception pills anticipating legal changes in reproductive health after Roe and Wade reversal. Following the high court’s decision pharmacies have reported an increase of up to 3000% in the sales of emergency contraception.
The FDA has approved two types of oral emergency contraception pills: levonorgestrel 1.5 mg (Plan B One-Step or generic equivalents) and ulipristal acetate 30 mg as a single dose (Ella). We will focus here on the mechanism of action of Plan B.
The principal mechanism of action of Levonorgestrel (a synthetic progestin ) is believed to be the inhibition of ovulation. The Contemporary OBGYN article mentioned that Levonorgestrel “does not harm or disrupt an existing pregnancy” but later affirms that “The drug may also alter the endometrium to inhibit implantation“.
In order to understand what is an existing pregnancy, we need to review what is needed for a new human being to enter into existence. Fertilization (the union of the ovum and sperm to form a zygote) normally occurs in the fallopian tube after ovulation. The new human being (blastocyst) moves from the fallopian tube to the uterus where it implants 5-7 days after conception. A receptive endometrium provides the embryo with the opportunity to attach and develop in the woman’s womb. Research has demonstrated that Levonorgestrel given in high doses caused obvious alteration of the endometrium (loss of ciliated cells, and pinopodes disappeared). Another study found that Levonorgestrel altered endometrial glycodelin-A levels, which could affect implantation. A drug or device that alters the endometrium will disrupt the implantation and cause an early abortion. Following this logic Levonorgestrel can harm and disrupt an existing pregnancy by inhibiting implantation.
In summary labeling Plan B as emergency contraception, or non-abortifacient drug is not accurate information. Emergency Contraception Plan B is available for purchase without any restrictions due to age, gender, or insurance status. It is imperative that accurate information is given, and people receive fully informed consent about the probable abortifacient mechanism of action of emergency contraception pills.
Research published in the journal of Adaptive Human Behavior and Psychology looked at how hormonal contraception affects a woman’s competitive drive. Women who do not use hormonal contraception experience a surge in motivation during the days leading to ovulation. This is caused by the high levels of estrogen and testosterone before ovulation. Women who use artificial hormones or don’t ovulate don’t experience that surge.
Lead researcher, Lindsie Arthur-Hulme, reported that 75% of the population of the study who were on hormonal contraceptives took the contraceptive pill. Other participants on contraceptives used the contraceptive implant, the vaginal ring, or the contraceptive patch. She said: “It’s crazy, it blows my mind” about the fact that, for more than 61 years, no one has studied the psychological impact of the pill on the more than 100 million women who take it each day.
The authors of the study conclude that this “research contributes to the growing body of literature suggesting that hormonal contraceptives may influence psychology and behavior by disrupting evolved hormonal mechanisms”.
Most people in the Western World today, including Catholics, approve of contraception and practice it as a way of controlling birth. Young persons growing up in our culture for the most part consider contraception an intelligent way of coping with difficult problems; it is the “natural,” “responsible” way to act. They find the Catholic Church’s opposition to contraception a relic of a bygone age, unrealistic, and impracticable.
During his pontificate, John Paul II sought valiantly to show that contraception violates the “language of the body” and the love that spouses are to have for one another. Thus in Familiaris Consortio 32, he wrote: “When couples, by means of recourse to contraception, separate these two meanings that God the Creator has inscribed in the being of man and woman and in the dynamism of their sexual communion, they act as ‘arbiters’ of the divine plan and they ‘manipulate’ and degrade human sexuality – and with it themselves and their married partner – by altering its value of ‘total’ self-giving. Thus the innate language that expresses the total reciprocal self-giving of husband and wife is overlaid, through contraception, by an objectively contradictory language, namely, that of not giving oneself totally to the other. This leads not only to a positive refusal to be open to life but also to a falsification of inner truth of conjugal love, which is called upon to give itself in personal totality.”
He also frequently noted that contraception is “anti-life” (e.g., in his Homily to youth in Kenya 17 Aug 85) and in Familiaris Consortio 32 he also wrote: “the difference, both anthropological and moral, between contraception and recourse to the rhythm of the cycle, is much wider and deeper than is usually thought. It is a difference which, in the final analysis, is based on irreconcilable concepts of the human person and of human sexuality.”
Here he had in mind the mentality rooted in a dualistic understanding of the human person that regards the “person: as the subject conscious of himself or herself and capable of relating to other conscious selves, and the human body as an “instrument” of the person. This understanding of human persons and of human sexuality considers our biological fertility part of the sub-personal world over which the “person” has been given dominion, and as “persons” we have the right to suppress this fertility by using contraceptives should its continued flourishing inhibit our participation in the “personal” values of human sexuality.
This mentality, as John Paul pointed out in Evangelium Vitae 19, is one of the bases for the “culture of death.” On this view not all living members of the human species are “persons,” but only those who are capable of conscious awareness; the unborn, the severely mentally crippled, and those in the “vegetative” state thus do not count as persons, who alone are the subjects of rights that must be recognized by the state.
From this it can be seen that contraception is the “gateway” to abortion and other grave offenses against the goodness of human life. Contraception paved the way for abortion, which is frequently considered a backup to failed contraception. All this explains why the Catholic Church is so opposed to contraception.
When God made man, He did not make a subject aware of itself as a self and capable of relating to other selves to which He then added a body as an afterthought. Rather, when He created man, “male and female He created them” (Gen 1:27), i.e., he created them as bodily, sexual beings, whose fertility is a blessing, not a curse.
Moreover, when the eternally begotten Son of God, His “Word,” became man to show us God’s love for us and to redeem us, He became living flesh: “the Word became flesh” (Jn 1:14). He became incarnate.
Thus the Church’s teaching on contraception goes hand-in-hand with the great truth that human persons are bodily persons and that every living member of the human species, the unborn as well as the born, the severely mentally impaired as well as the mentally gifted, is a person, a being of moral worth, a living image of the one and triune God.
William E. May is the Michael J. McGivney Professor of Moral Theology at the John Paul II Institute for Studies on Marriage and Family. In 2009 Pauline Books & Media will publish his book, Pope John Paul II’s Teaching on the Person, Marriage and Family. He and his wife, Patricia, are the parents of seven, and grandparents of f fourteen.
The postpartum or postnatal period, by definition, begins immediately after the birth of a baby. During this time, the mother’s body, including hormone levels and uterus size, returns to a non-pregnant state. It is exciting but at the same time challenging for couples to navigate this period with new responsibilities, little spleep, and fertility uncertainty. Couples need to be aware of some facts about the postpartum period regarding the return of fertility. The first ovulation postpartum varies from woman to woman and even from one postpartum experience to another for the same woman. Ovulation can resume as early as 4 weeks postpartum or even years after the baby’s birth. Ovulation always precedes menstruation in a postpartum mother.
Natural family planning is a good option for couples. The specific method depends on the possibility to breastfeed the baby, experience with NFP before pregnancy, and professional support to navigate the challenges.
The following article was published by FACTS, a group of health care professionals educating on fertility awareness. The author, Johanna Longrenn, presents an interview with a fellow midwife to explore the role of midwives in educating women and couples about the option of fertility awareness-based methods (FABMs) throughout a woman’s reproductive lifetime, especially during the postpartum period.
According to a new report out from American Life League (ALL), the nation’s largest abortion provider is becoming increasingly reliant on chemical abortion, as evidenced by an 82% increase in affiliates offering the abortion pill regimen between 2005 and 2021. As of 2021, 391 of Planned Parenthood’s 567 active locations (69%) offered either chemical or surgical abortions, with a majority committing chemical abortions only, and the remainder offering both chemical and surgical options.
All 567 locations dispense or administer potentially abortifacient contraceptive drugs and devices.
The report was compiled by ALL’s STOPP International project, which “exposes the true nature of Planned Parenthood and documents its anti-life, anti-family programs,” according to its website, utilizing research done by Operation Rescue and Planned Parenthood’s own data.
“Planned Parenthood now runs 55% of all surgical and/or pill abortion facilities in the United States,” STOPP International interim director Rita Diller noted. “This includes a whopping 82% of pill-only and 39% of all surgical locations.”
The report also included statistics on Planned Parenthood abortion facility openings and closures. Of the 18 facilities temporarily closed in 2020 due to the COVID-19 pandemic, eight reopened in 2021. On the whole, Planned Parenthood closed more facilities than it opened, opening six new abortion facilities last year but closing eleven.
Yet the emphasis of the report is on the dangers of the abortion pill regimen.
“These unsupervised procedures — self-administered and without medical oversight — are incredibly dangerous [to women],” Diller said. “In addition to the risk of hemorrhaging and possible serious complications without any medical supervision, there is an increased incidence of uterine infection, pelvic inflammatory disease, and infertility, not the mention the mental anxiety that can be induced by the trauma of expelling your dead baby’s body by yourself [and possibly] in secret.”
Previous reports from Live Action News note that in both the United States and the United Kingdom, approximately 5-6% of women using the abortion pill have visited hospital emergency rooms for resulting complications. And yet, in the U.S., only 28 states even require the reporting of abortion complications to state agencies, and abortion industry mouthpieces are encouraging medical personnel to falsify records if women do visit emergency rooms as a result of the abortion pill regimen. If accuracy in reporting is not a priority, women may never know the true risks of the abortion pill.
In its conclusion, the report referenced the significant impact of the Supreme Court’s June 2022 overturning of Roe v. Wade on Planned Parenthood’s abortion business.
“While this report reflects Planned Parenthood facility numbers for 2021, we note that many Planned Parenthood affiliates across the nation closed and/or halted abortions immediately following the announcement of the Dobbs decision on June 22, 2022,” the report read. “[A]ffiliates located in states where abortion is now or will soon be highly restricted began announcing immediately that they will stop operations or cease abortions. In the same breath, they provided links to get abortions at [Planned Parenthood] facilities in other states, some offering links to funding.”
Following the supreme court’s decision, overthrowing of Roe v. Wade and Planned Parenthood v. Casey, more men are taking charge of their reproductive health, to permanent ends. “There is a definitive uptick in men exploring vasectomies,” reported Dr Alex Shteynshlyuger, a New York City urologist.
“The supreme court decision has prompted a lot of conversation about contraception in general, as well as raising the awareness about vasectomy as an effective, low cost, safe, and permanent method of contraception that gives men control over their procreation.”
Jonathon Van Maren, public speaker, writer, and pro-life activist said “The assumption here, keep in mind, is that those men made use of legal abortion to terminate any children resulting from coital encounters they intended to be strictly casual. It’s no surprise that many men are upset by Roe’s overturn—in front of the U.S. Supreme Court this weekend, I saw men holding signs reading: “Men for Choice!” and one fellow with a sign that stated: “I will aid and abet abortion!” These men need abortion access because it gives them access to women’s bodies without commitment to any children they might conceive.
What is male sterilization?
Male sterilization is any procedure or treatment that intends to make it impossible for a man to fertilize a woman’s egg (ovum). Men can be sterilized by removal of the testicles, by treatment with chemicals that shut down the activity of the testicles, or by a vasectomy. Vasectomy is a surgical procedure to block sperm transport from the testicles to the male urethra/penis. Vasectomy usually involves the removal of a small piece of each vas deferens.
How is vasectomy performed?
To perform a vasectomy requires three steps. First, the vas deferens is found by a single or double incision in the scrotum (skin that surrounds the testicles) with a scalpel, or without scalpel using special instruments. Second, the vas deferens on each side is disrupted by cutting, burning, or clipping, with the edges sewn or not. Finally, the scrotal tissue is closed.3
Is vasectomy 100% effective in preventing pregnancies?
Recent research indicates that one or two women per 1,000 per year become pregnant when using vasectomy as a means of birth control.4 Pregnancy may result from natural healing, or failure in the surgical procedure.
Are there short-term complications?
Vasectomy causes damage to a healthy part of the body. As a consequence, males can suffer anatomical, hormonal, immunological, psychological, and social changes that are undesirable. Early complications include local hematoma, bleeding, swelling of the scrotum (range 2-29% of cases), and infection of the skin, urinary tract, testicles, or epididimus (range 12-38% of cases).5 Inflammation of the testicles and epididymus may require antibiotics and anti-inflammatories to resolve.
An additional potential early complication is the formation of a sperm granuloma. After vasectomy sperm production continues at the same rate as before since the testes do not “know” that the outlet system has been obstructed. Pressure builds in the entire tubular network proximal to the vasectomy and the testes eventually respond to this feedback by slowing production and shutting down entire areas of sperm production. In the meantime, however, the pressure may cause sperm to leak out the end of the obstructed vas. Because sperm contain only half the chromosomes of the body’s cells the immune system thinks they are foreign invaders and quickly walls them off, creating a firm nodule of tissue at the end of the vas. This so-called sperm granuloma may become quite tender to the touch and require removal for resolution of the pain.
Are there long-term complications?
Because vasectomy blocks the natural way to evacuate sperm, a buildup in pressure breaks down the natural barrier that exists between the teticles and blood, enabling sperm to enter the blood.This is important because sperm contain antigens (substances that can trigger the body’s immune system). About sixty percent of males who elect to have vasectomies develop anti-sperm antibodies.6 These can cause a number of local and full body reactions. Although no final conclusion has been reached about the cause-and-effect relationship between vasectomy and long-term disease, principally due to lack of long- term medical studies, many diseases have been reported in males post-vasectomy. In the book, Is Vasectomy Worth the Risks? the author states that in his medical practice he has encountered many young males who had undergone a vasectomy, and have diseases with unexplained causes. The following diseases have been reported in men after vasectomy: atherosclerosis, psychogenic impotence, rheumatoid arthritis, multiple sclerosis, migraine, hypoglycemia, narcolepsy, thromboflebitis, pulmonary embolism, infection, allergic reactions, kidney stones, and angina pectoris.7
What is Post-vasectomy Pain Syndrome (PVPS)?
PVPS is another complication after vasectomy. It can occur up to ten years after the procedure.8 Some males suffering from PVPS report a sharp testicular pain during certain activities such as sitting, sexual intercourse, or during exercise. Others report dull, constant pain or pain radiating to the scrotal area or the back. Unfortunately, many cases of PVPS are misdiagnosed due to lack of association of their symptoms with vasectomy. The incidence rate for this condition is 1:10 9. Although the cause for the pain is still the object of research, it is believed that distention of the tissues due to pressure, inflammation, sperm granulomas, fibrosis and nerve entrapment may explain the pain. Removal of granulomas, vasectomy reversal 10, and removal of nerves, and in extremes cases, removal of the testicles, are treatment options for PVPS.
Is vasectomy associated with cancer?
According to the American Cancer Society, prostate cancer is the most common cancer for males in America. In the year 2011, 238,467 new cases of prostate cancer were identified and more than 33,000 men died from prostate cancer or its complications.11 Although mortality rates from prostate cancer have decreased, more than two million men are living with this disease.
Risk factors for prostate cancer include non-modifiable risk factors such as family history of prostate cancer and ethnicity (African-American males have a high incidence of prostate cancer), and modifiable risk factors such as diet, alcohol consumption, and smoking. Even though medical and government organizations do not regard vasectomy as a risk factor for prostate cancer,12 several studies have noted that men who undergo a vasectomy have a higher incidence of developing prostate cancer, especially 15-20 years after their vasectomy. 13,14,15 A large study looking for a link between prostate cancer and vasectomy was done in the 1990’s. The author of this study found a significant increase in the risk of cancer in males who had undergone vasectomy at a young age (less than 35 years).16 After the publication of these studies, the National Cancer Institute and other organizations sponsored a conference in 1993 to debate the association between prostate cancer and vasectomy. Experts concluded that the risk was very small and just due to chance. However statistical analysis of recent studies claiming no link indicates a significant link between vasectomy and prostate cancer.17,18 Also, research has demonstrated that hormonal alterations due to vasectomy (such as high testosterone levels) could coincide with increases in prostate cancer.19,20
Is vasectomy associated with psychiatric problems?
Researchers from Northwestern University in Illinois published a study that looked into one patient’s belief that his dementia resulted from his vasectomy.21 His was not a common dementia; it was a relatively new kind of dementia called Primary Progressive Aphasia (PPA). Its onset is characterized by language impairment (aphasia) rather than the forgetfulness characteristic of Alzheimer’s Disease. Another reason for the study was the interesting fact that the testicles and the brain have similar molecular substances. Vasectomy may have a role in the development of PPA based on the immune reactions to sperm after vasectomy and on the similarity of brain and sperm proteins. New antibodies produced after vasectomy may attack brain cells and cause PPA. The authors found that 40% of the men in their study who suffered from PPA also had undergone vasectomies. The study involved a control group of males who did not have PPA, and 16% of that group had vasectomies. The study revealed that PPA subjects had their vasectomy at a younger age—36 years old on average. In contrast, the control group had their vasectomies performed at an average age of 44 years. It appears that longer exposure to this sort of immune attack increases the probability of developing PPA. A recent case report analyzed whether or not the use of steroids (drugs that inhibit the immune system) could modify the symptoms of PPA. The authors of this study found improvement in one patient suffering from PPA after the steroid treatment. Although more research with large populations is needed, the improvement in this particular case supports the hypothesis that PPA in men may be a treatable autoimmune disease related to vasectomy.22
Are there emotional disorders related to vasectomy?
Emotional disorders such as anxiety, depression and changes in personality have been reported after vasectomy.23 Men who had undergone vasectomy have reported regret, resentment, and feelings that their masculine image has been threatened.
Are there social consequences associated with vasectomy?
More research is needed to determine the social consequences from sterilization. It has been suggested that vasectomy can open the door to infidelity and marital instability. Looking to the divorce rate in the USA and other developed countries where vasectomy is a widely used method of birth control, we come to the hypothesis that vasectomy may have contributed to the increase in divorce rates.
Many authors tried to warn about the powerful negative social consequences that would result from the widespread use and acceptance of artificial methods of birth control and voluntary sterilization-such as the potential for abuse by governments which might institute programs of forced abortion and sterilization for population control.24 We can now verify the accuracy of those predictions and see that the voluntary use of artificial methods of birth control and sterilization did indeed open the door to forced abortions and forced sterilizations for population control.
Are there alternatives to vasectomy?
Natural Family Planning (NFP) is a safe, healthy, and effective alternative to sterilization. NFP is morally acceptable. Studies have demonstrated that couples who use NFP are more satisfied with their marriage, and these couples have lower divorce rates compared to couples who use contraception or sterilization.25 For males who have undergone vasectomy, the reversal procedure is an alternative to alleviate some secondary effects and to restore fertility. The reversal procedure is not 100% effective in restoring fertility. Microsurgery is highly recommended. Our web site, www.OneMoreSoul.com includes a list of NFP-only physicians (some offer sterilization reversal in the United States), NFP teachers, and NFP Centers.
As we mark National NFP Week, there have been confusing ideas coming from the Pontifical Academy of Life that seem to imply that the Church’s teaching on contraception can “develop” to allow the use of artificial contraception.
This week, 54 years ago, on July 25, 1968, Pope St. Paul VI released the encyclical Humanae Vitae, confirming the Church’s teaching that contraception, whether through sterilization of the man or woman in any act before, during, or after the conjugal act to prevent procreation is morally evil and violates the “unitive and procreative” goods “inherent to the marriage act.” Further, he allowed for couples who have reasonable motives for avoiding having another child to exclusively use the infertile periods of the wife’s cycle, what is now commonly called natural family planning or NFP. This teaching was received in varying ways, with many laypeople and priests choosing to ignore this in favor of the world’s acceptance of birth control. Those obedient to the truth worked hard to defend it, such as philosopher Dietrich von Hildebrand, who explained:
“Every true Catholic must rejoice also when he is allowed to see clearly that the Church does not conform to the ‘majority opinion’ but to the Word of God, and that the Holy Father [Paul VI] must proclaim the truth even when it goes against the current of the times. […] The encyclical Humanae Vitae, in which the Holy Father teaches us clearly the true moral nature of artificial birth control, enables the individual to know exactly what God expects of him and appeals to our conscience not to offend God” (The Encyclical Humanae Vitae: A Sign of Contradiction).
As we mark National NFP Week, there have been confusing ideas coming from the Pontifical Academy of Life that seem to imply that the Church’s teaching on contraception can “develop” to allow the use of artificial contraception. This idea flies in the face of the most basic principles of what is legitimate development of doctrine — for never in Scripture or in the history of the Church has it been moral for married couples to interfere with the procreative end of the marital act. The very moral truths on which marriage is based necessitate that every sexual act must be done within marriage and be a consensual act of self-gift and union of the couple which is open to the procreation of a new human life.
Continuity of Principles and Natural Law
St. John Henry Newman, in An Essay on the Development of Christian Doctrine, lays down six guidelines with which to measure the development of doctrine. While I do not have space here to go into all of them, the Church’s teaching on the two ends of marriage and the sexual act as procreation and union and teaching against the use of artificial contraception fits with all six of his guidelines. Here, I want to show how the Church’s teaching cannot legitimately develop to say that is it moral to interfere with the procreative end of marriage because it violates what Newman calls the necessary “continuity of principles” required for development of doctrine.
The Church has always held the principle that it is wrong to interfere with the bringing about of a new human life in the sexual act. Further, the principle of the two ends of marriage, while first stated and understood by the Church in the 20th and 21st century, is rooted in natural law and the whole history of the Church’s understanding of marriage. This is why the condemnation of contraceptive acts as “intrinsically evil” (see Catechism of the Catholic Church, 2370) is a true part of Tradition.
First of all, this principle of the two ends of marriage can be seen in natural law, which is the law implanted in us by God that says we ought to use our natural abilities to pursue the goods for the sake of which our abilities naturally exist and ought not perform acts in which we use a natural ability but simultaneously actively prevent its natural goal from coming about. Our sexual abilities naturally exist for the sake of bringing new persons into existence and for the sake of a complete gift of self between persons. To use this ability but simultaneously prevent either of these goals from coming about, as is done when one uses contraception, violates the natural goal-directedness of this ability, and so violates the natural law, and so ought not be done. (I owe this formulation to my husband, Mark Spencer.)
Pope St. John Paul II explained in Familiaris Consortio, in 1981, that, “when couples, by means of recourse to contraception, separate these two meanings that God the Creator has inscribed in the being of man and woman and in the dynamism of their sexual communion,” they interfere with the divine plan and “manipulate and degrade human-sexuality … by altering its value of ‘total’ self-giving.” The evil is not just in contraception’s severing of procreation from the unitive end but also in the couple’s denial of the gift of fertility to each other. A couple using contraception in the conjugal act makes themselves incapable of a total self-gift and complete union.
It further violates the gift of cooperating with God’s creative act of bringing each person’s soul into existence. Hildebrand explained two levels of sinfulness in using artificial contraception:
“We thus see that artificial birth control is sinful not only because it severs the mysterious link between the most intimate love-union and the coming into existence of a new human being, but also because in a certain way it artificially cuts off the creative intervention of God, or better still, it artificially separates an act which is ordained toward cooperation with the creative act of God from this its destiny” (The Encyclical Humanae Vitae: A Sign of Contradiction).”
In Scripture and Tradition
Secondly, we can see these principles in Scripture and Tradition. Scripture shows us that procreation and union are intrinsic to marriage, beginning in Genesis 1-2, when man and woman were created by God, the Author of Life, and were meant to become “one flesh” and to be “fruitful and multiply.” In the New Testament, the unitive aspect is highlighted in St. Paul’s comparison of the man to Christ and of the woman to the Church in Ephesians 5. In the liturgy, Christ and the Church come into union through the consummation of the people of the Church receiving the Body of Christ into their bodies, and this love of Christ for the Church is deep and personal. If one compares marriage to this analogy, one can see that the physical union of the husband and wife is meant to be deep and personal and a sign of their unity of hearts.
The early tradition of the Church emphasized the procreative aspect of marriage and the conjugal act. St. Augustine of Hippo wrote against the Manicheans, who saw procreation as evil and sex as something for pleasure. He explained that the “union … of male and female for the purpose of procreation” was “the natural good of marriage,” and he saw any other use of the sexual act as sinful (On Marriage and Concupiscence). In the Middle Ages, St. Thomas Aquinas explained the conjugal act in terms of nature, such as what semen is for, condemning unnatural uses of the sexual organs. He also saw how, in nature, not every conjugal act ended in procreation. This is an example of the continuity of the principle based in the need to follow the natural order God created. Also, there is a beginning of the development of thought viewing an end of the conjugal act as being more than just procreation, as Aquinas explained that it was not sinful for naturally sterile couples to have intercourse (Summa Contra Gentiles, 3.122.4-5). This view is an anticipation of the clear acknowledging by the Church of the unitive end of marriage and a couple’s recourse to using infertile periods of the women’s cycle for serious reasons to avoid conception.
In 1880, Pope Leo XIII continued this development by explaining that “marriage was instituted for the propagation of the human race” and “also that the lives of husbands and wives might be made better and happier” (Arcanum, 26). Pope Pius XI developed this view further in Casti Connubii,written in 1930, describing procreation as the primary end of marriage and “mutual aid, cultivating mutual love, and the quieting of concupiscence” as secondary and subordinate to this natural end. Venerable Pope Pius XII further developed the idea of two ends of marriage in his “Allocution to Midwives”in 1951, emphasizing that procreation is not the only end of marriage:
“To reduce the common life of husband and wife and the conjugal act to a mere organic function for the transmission of seed would be but to convert the domestic hearth, the family sanctuary, into a biological laboratory. […] The conjugal act, in its natural structure, is a personal action, a simultaneous and immediate cooperation of husband and wife, which by the very nature of the agents and the propriety of the act, is the expression of the reciprocal gift, which, according to Holy Writ, effects the union ‘in one flesh.’”
From there was the proclamation of Pope Paul VI’s win Humanae Vitae, which we remember and promote during this National NFP Week.
Continuing in the Truth
During his pontificate, Pope John Paul II upheld the teaching in Humanae Vitae in his encyclical Evangelium Vitae, explaining that in the culture of death “the original import of human sexuality is distorted and falsified, and the two meanings, unitive and procreative, inherent in the very nature of the conjugal act, are artificially separated.” He says further that, with this attitude:
“[T]he marriage union is betrayed and its fruitfulness is subjected to the caprice of the couple. Procreation then becomes the ‘enemy’ to be avoided in sexual activity: If it is welcomed, this is only because it expresses a desire, or indeed the intention, to have a child ‘at all costs,’ and not because it signifies the complete acceptance of the other and therefore an openness to the richness of life which the child represents.”
In one way, this view hearkens back to the Manichean view that sex was for pleasure and procreation is evil — except that it is not consistent, as people want to have children at their convenience. They follow “one rule,” which is what Dietrich von Hildebrand would call the desire to fulfill what is “subjectively satisfying.” One has sex when one desires without consequences. One has a child on demand, reducing the child to a commodity.
The Church must not give into the world’s push to claim that “union” in the sexual act can be morally separated from procreation through artificial means. In the 20th century, the crisis of widespread acceptance of contraception in the world caused the Church to examine the goods of marriage to the extent that it saw the need to emphasize procreation in relation to the good of the union in marriage. Contraception divides procreation, the physical fruit of union, from union; and because it violates the complete self-gift of one person to another, by limiting the physical union, it violates the union itself. In the 21st century, the Church must not lose sight of these ends. An emphasis on the unitive end that makes the procreative end optional is a false understanding on the nature of the sexual act.
The first reading from last Thursday (of the 16th Week of Ordinary Time, Year II) is a clear reminder of the importance of not straying from the truths preserved by Tradition and those given to us by God in natural law:
Be appalled, O heavens, at this, be shocked, be utterly desolate, says the Lord, for my people have committed two evils: They have forsaken me, the fountain of living waters, and hewed out cisterns for themselves, broken cisterns, that can hold no water. (Jeremiah 2:12-13)
Claiming that the Church can “develop” her teaching so that it is moral to use contraception would be nothing more than “hewing out broken cisterns that can hold no water.” The Church would be forsaking the fountain of living waters. Let us pray for our shepherds, that they do not forsake the truth preserved by Tradition. And let us pray for married couples, that they may see the beauty of the Church’s teaching on sexuality and marriage and always be open to the gift of life.
Note: Natural Family Planning Awareness Week is a national educational campaign. This year is celebrated July 24-30. The following testimony was originally published by the Natural Family Planning Program of the United States Conference of Catholic Bishops at usccb.org.
Michael and Alysha Chambers
Many will tell you that the responsibility of being permanently faithful to one person is too great and that being open to life is too much of a burden. They say contraception brings with it freedom and life; however, we have found that it is in openness to God, to each other, and to new life that true freedom is obtained. This is what living Natural Family Planning (NFP) can help couples to experience.
Alysha was in college when she first heard NFP mentioned. All she knew then was that it existed and the Catholic Church considered it a good thing. Michael, a convert to Catholicism, grew up believing that contraception was good and that all couples should use it. Our first real understanding of what NFP is, and what the Church teaches came during our marriage preparation program. We learned that NFP at its core is simply knowledge of the physical changes one can observe in the woman’s fertility cycle. It gives couples a way to measure and chart their fertility signs. We also learned how responsible parenthood is and the virtuous application of this fertility knowledge.
One unexpected aspect of NFP that impressed us was how it fosters communication between spouses. Couples practicing NFP discuss the future of their family with every cycle. Knowing how to discuss such important matters has proven a great blessing to many marriages. Michael decided that blessing, by itself, was enough of a reason to learn NFP.
God’s love is a total gift of self.
God’s love is life-giving.
As husband and wife one way we
love like God is through our sexuality.
Another theme we discussed in marriage preparation was the Theology of the Body. It helped us understand who we are and how God created us. It is through our bodies that we express who we are spiritually. Also, because we were made in the image and likeness of God, our bodies are supposed to reflect who God is which means we are to act as He acts. How does God act? He loves. God’s love is a total gift of self. God’s love is life-giving. As husband and wife one way we love like God is through our sexuality. If NFP is studied in this context, our appreciation of each other as man and woman increases because the uniqueness and dignity that God has imprinted in our bodies is revealed. It was at this point that Michael realized NFP was not moral birth control; rather, it is a complete way of life honoring one’s spouse’s sexuality and fertility. It is loving naturally – the way God designed it.
In studying NFP in the context of the Theology of the Body, both of us have become more open to each other, to God, and to children. We truly believe that “children are the crown of marriage” and we pray that God will bless us with children someday. Until then, we will “make our plans but hold them lightly.” For us, that means planning to use NFP both when we are attempting or delaying pregnancy, all the while striving to hear and do God’s will!
Michael and Alysha Chambers, Diocese of Arlington, Va., were married on September 24, 2005. This article first appeared in the Couple to Couple League’s Family Foundations (Jan/Feb. 2006). It has been edited to fit this publication and is printed with permission. Microsoft Word – Witness-Chambers.doc (usccb.org)
The study published in the Linacre Quarterly evaluated the effects of periodic abstinence on marital relationships. According to the authors, “this study showed that ever-use of natural family planning (NFP) among ever-married women was associated with 58 percent lower odds of divorce than among women who never-used NFP. Ever-use of contraceptive methods was associated with two times the odds of divorce and four times for cohabitation compared to those women who never-used those methods. The use of periodic abstinence with NFP is the practice of marital chastity and is thought to strengthen the marital relationship”.
The pill could be blurring your social judgment – but perhaps not enough so you’d notice. By challenging women to identify complex emotional expressions like pride or contempt, rather than basic ones like happiness or fear, scientists have revealed subtle changes in emotion recognition associated with oral contraceptive pill (OCP) use. Published in Frontiers in Neuroscience, their study found that OCP users were nearly 10% worse on average than non-users in deciphering the most enigmatic emotional expressions, raising questions over the possible impact of OCPs on social interactions in intimate relationships.
What are the risks and benefits of OCP use?
Women deciding whether to take an oral contraceptive have access to a lot of reliable information about the potential physical effects.
Besides birth control, hormonal contraceptives can help control acne, heavy periods, and endometriosis – as well as reducing the risk of ovarian, uterine and colon cancers. On the downside, the pill can increase slightly the risk of breast and cervical cancer, blood clots and high blood pressure.
But the psychological effects of OCP use are less well documented.
“More than 100 million women worldwide use oral contraceptives, but remarkably little is known about their effects on emotion, cognition and behavior,” says study senior author Dr Alexander Lischke of the University of Greifswald, Germany.
“However, coincidental findings suggest that oral contraceptives impair the ability to recognize emotional expressions of others, which could affect the way users initiate and maintain intimate relationships.”
OCP users are worse at recognizing subtle expressions of complex emotions
To further investigate the effects of OCPs on women’s emotion recognition, the researchers administered a special emotion recognition task to two similar groups of healthy women: 42 OCP users, and 53 non-users.
“If oral contraceptives caused dramatic impairments in women’s emotion recognition, we would have probably noticed this in our everyday interactions with our partners,” suggests Lischke. “We assumed that these impairments would be very subtle, indicating that we had to test women’s emotion recognition with a task that was sensitive enough to detect such impairments. We, thus, used a very challenging emotion recognition task that required the recognition of complex emotional expressions from the eye region of faces”
The results were, as expected, subtle – but very clear: OCP users were less accurate in the recognition of the most subtle complex expressions than non-users – by nearly 10%, on average.
“Whereas the groups were equally good at recognizing easy expressions, the OCP users were less likely to correctly identify difficult expressions.”
The effect held for both positive and negative expressions, and regardless of the type of OCP or the menstrual cycle phase of non-users.
Should clinical guidelines change?
According to Lischke, the findings are consistent with previous research.
“Cyclic variations of estrogen and progesterone levels are known to affect women’s emotion recognition, and influence activity and connections in associated brain regions. Since oral contraceptives work by suppressing estrogen and progesterone levels, it makes sense that oral contraceptives also affect women’s emotion recognition However, the exact mechanism underlying oral contraceptive induced changes in women’s emotion recognition remains to be elucidated.”
He stresses the need for further studies that replicate and extend the findings of the present study before thinking about changing current guidelines regarding the prescription of OCPs.
“Further studies are needed to investigate whether oral contraceptive-induced impairments in emotion recognition depend on the type, duration or timing of use. These studies should also investigate whether these impairments actually alter women’s ability to initiate and maintain intimate relationships. If this turns out to be true, we should provide women with more detailed information about the consequences of oral contraceptive use.”
In 1998 Pope John Paul II wrote a letter to Dr. Anna Cappella, director of the Center for Research and Study on the Natural Regulation of Fertility at Rome’s Catholic University of the Sacred Heart. The occasion was a convention commemorating Humanae Vitae, Pope Paul VI’s 1968 encyclical. Excerpts are reprinted below.
I hope that everyone will benefit from a closer study of the Church’s teaching on the truth of the act of love in which spouses become sharersin God’s creative action.
The truth of this act stems from its being an expression of the spouses’ reciprocal personal giving, a giving that can only be total since the person is one and indivisible. In the act that expresses their love, spouses are called to make a reciprocal gift of themselves to each other in the totality of their person: nothing that is part of their being can be excluded from this gift. This is the reason for the intrinsic unlawfulness of contraception: it introduces a substantial limitation into this reciprocal giving, breaking that “inseparable connection” between the two meanings of the conjugal act, the unitive and the procreative, which, as Pope Paul VI pointed out, are written by God himself into the nature of the human being (HV, no. 12).
Continuing in this vein, the great pontiff rightly emphasized the “essential difference” between contraception and the use of natural methods in exercising “responsible procreation.” It is an anthropological difference because in the final analysis, it involves two irreconcilable concepts of the person and of human sexuality (cf. Familiaris Consortio, no. 32).
It is not uncommon in current thinking for the natural methods of fertility regulation to be separated from their proper ethical dimension and to be considered in their merely functional aspect. It is not surprising then that people no longer perceive the profound difference between these and the artificial methods. As a result, they go so far as to speak of them as if they were another form of contraception. But this is certainly not the way they should be viewed or applied.
On the contrary, it is only in the logic of the reciprocal gift between man and woman that the natural regulation of fertility can be correctly understood and authentically lived as the proper expression of a real and mutual communion of love and life. It is worth repeating here that “the person can never be considered as a means to an end, above all never a means of ‘pleasure.’ The person is and must be nothing other than the end of every act. Only then does the action correspond to the true dignity of the person.” (cf. Letter to Families, no. 12).
The Church is aware of the various difficulties married couples can encounter, especially in the present social context, not only in following but also in the very understanding of the moral norm that concerns them. Like a mother, the Church draws close to couples in difficulty to help them; but she does so by reminding them that the way to finding a solution to their problems must come through full respect for the truth of their love. “It is an outstanding manifestation of charity toward souls to omit nothing from the saving doctrine of Christ,” Paul VI admonished (HV, no. 29).
The Church makes available to spouses the means of grace which Christ offers in redemption and invites them to have recourse to them with ever renewed confidence. She exhorts them in particular to pray for the gift of the Holy Spirit, which is poured out in their hearts through the efficacy of their distinctive sacrament: this grace is the source of the interior energy they need to fulfill the many duties of their state, starting with that of being consistent with the truth of conjugal love. At the same time, the Church urgently requests the commitment of scientists, doctors, health-care personnel and pastoral workers to make available to married couples all those aids which prove an effective support for helping them fully to live their vocation (cf. HV, no. 23-27).
A dangerous lie is circulating on social media again, planting the notion in women’s and girls’ minds that pro-life laws ban life-saving treatment for ectopic pregnancies and miscarriages.
But it resurfaced again this week after the U.S. Supreme Court overturned Roe v. Wade in a historic ruling and states began protecting unborn babies from abortion again.
This week, millions of impressionable women and girls heard from celebrities like Halle Berry and Meghan Markle that pro-life laws will put their lives in jeopardy and ban life-saving pregnancy care, according to The Federalist.
“The treatment for an ectopic pregnancy is abortion,” Berry wrote in a tweet that amassed hundreds of thousands of responses. “… The treatment for a miscarriage that your body won’t release is abortion. If you can’t get those abortions, you die. You. Die.”
Politicians like Hillary Clinton and the mayor of San Francisco, writers at ABC News, NBC News, the Daily Beast and others spouted similar claims, The Federalist reports.
But they are not true, and the lie could put women’s lives at risk. Women suffering from life-threatening complications could delay seeking medical treatment because of the lie and put their lives at even greater risk.
“My heart is breaking that women are being made to feel fearful by the misinformation that’s out there,” said Dr. Christina Francis, a leading pro-life OB-GYN. “As a pro-life OB/GYN who’s practiced my entire career in hospitals that do not allow abortions, I have never been prevented from safely treating an ectopic pregnancy.”
Pro-life doctors and hospitals have and will continue to treat women suffering from miscarriages and ectopic pregnancies, too, said Francis, of the American Association of Pro-Life OB-GYNs.
She said treating ectopic pregnancies, miscarriages or other life-threatening conditions in pregnancy are not the same as elective abortions, which is what pro-life laws prohibit. Even the U.S. Food and Drug Administration states that chemical abortions, or abortion drugs, cannot treat an ectopic pregnancy, Francis continued.
“I’ve never needed to perform an elective abortion, and yet I’ve been able to take care of women with ectopic pregnancies and miscarriages throughout my career,” she said.
Treatments for miscarriages and ectopic pregnancies are not the same as abortions because the purpose is to save the mother’s life, not to kill an unborn baby. Even Planned Parenthood admits this on its website, lawyer Mary FioRito with the de Nicola Center for Ethics and Culture pointed out on Twitter this week.
Sharing an image from the abortion group’s website, FioRito wrote: “Catholic hospitals treat women with ectopic pregnancies every day. Abortion clinics don’t. Most abortion practitioners aren’t even ON/GYNs, much less surgeons. Planned Parenthood recommends women go to a local ER to be treated. Not to an abortion clinic.”
The Charlotte Lozier Institute also published a fact sheet this week that explains the facts about miscarriages, ectopic pregnancies and abortion laws.
Legally, most laws that restrict or ban abortions specifically state that treatments for miscarriages and ectopic pregnancies are not abortions, and all pro-life laws allow exceptions if the mother’s life is at risk, which includes such situations.
The truth is women’s lives matter to the pro-life movement, too. Many pro-life leaders have suffered miscarriages, ectopic pregnancies and abortions themselves, and they know the heartache of losing a child. The pro-life movement is based on the fundamental belief that every human life is valuable and deserving of human rights, and that includes every mother and every child.
Martin and I decided to use Natural Family Planning (NFP) because it’s what is best for our marriage (even though the world tells us otherwise) we knew NFP would lead us to the most fruitful marriage, but not without its cross. Understanding NFP and its purpose in our life showed us God’s never-ending love and how we can, with Him, create new life. Once we understood sacrificial love and the deeper love it brings forth our cross seemed a little lighter. Leaning on God’s will and wisdom led us to true happiness.
Couples who use NFP have a less than 4% divorce rate, and when those couples pray together and attend mass every Sunday the divorce rate is less than 1%.
Times Review, La Crosse, WI, February 15, 2000
We wanted to give ourselves the best chance at a healthy and happy marriage. Not only do the statistics speak loud and clear, but NFP is also in line with the Church’s teaching on marriage and sexuality, it’s the only approved method for spacing children. NFP still allows the couple to grow in love for each other and God by inviting Him into our marriage.
Using NFP (CRMS) has helped us experience faithfulness. Having had some ups and downs with understanding all that comes with Natural Family Planning, I have grown closer to Jesus and the Church’s teachings on marriage and family. It is only when we are faced with challenges that we seek to find the truth and understanding. Reading books about Natural Family Planning, Theology of the Body, and what it means to be a Godly wife and mother has improved my understanding of God’s plan for me.
My husband and I have improved our communication and how we work together. My husband’s faithfulness has grown also, and he, too, understands God’s plan for him as the spiritual leader of our family. Keep the invitation into your marriage always open to Him and he will make everything fruitful.
“Sweeter even than to have had the joy of children of my own has it been for me to help bring about a better state of things for mothers generally, so that their unborn little ones could not be willed away from them.”
The two words most often abused today are “freedom” and “sex.” Freedom is often used to mean absence of law, and sex is used to justify absence from restraint. Sometimes the two words fuse into the one, “license.” Reason, which should be used to justify God’s law, is thus invoked to justify human lawlessness and carnality with two spurious arguments. The first is that every person must be self-expressive, that purity is self-negation; therefore, it is destructive of freedom and personality.
The second argument is that nature has given to every person certain impulses and instincts, and that principal among them is sex. Therefore, one ought to follow these instincts without the taboos and restrictions which religion and custom impose. Consequently, purity is looked upon as negative and cold, or as a remnant of Puritanism, monasticism, and Victorian strait-lacedness, despite the fact that the Lord of the Universe in the first of the Beatitudes said: “Blessed are the clean of heart; they shall see God.” (Matt. 5:8)
Purity is as self-expressive as impurity, though in a different way. There are two ways in which a locomotive can be self-expressive: either by keeping its pressure within the limits imposed by the designer and the engineer, or by blowing up and jumping the tracks. The first self-expression is the perfection of the locomotive; the second is its destruction. In like manner, a person may be self-expressive either by obeying the laws of his nature, or by rebelling against them, which rebellion ends in slavery and frustration. Suppose the same argument of self-expression were used in war as is used to justify carnal license. In that case, a soldier at the front who, on hearing screaming shells, dropped his gun and ran to the rear line, would be greeted by a captain full of modern self-expression and told: “I commend you for throwing off Victorian convention and moral scruples. The trouble with the rest of the army is that they are not self-expressive; they overcome their fear and fight. I shall recommend a medal of honor for asserting your personality.”
There is no quarreling with those who say, “Be yourself.” The point is, which is your true self: is it to be a beast, or to be a child of God? Those who get over the wickedness of licentiousness say: “Thank God, I am myself again.” This is real self-expression.
A provisional report published Tuesday by the Centers for Disease Control (CDC) indicates that a total of 3,659,289 babies were born in 2021, which marks a one percent increase in the birth rate from 2020. This is the first rise in births the United States has seen since 2014.
While the overall birth rate rose, births for teens aged 15-19 declined six percent, which ABC News said is a record low. Women in their 30s saw the highest rise in fertility rates. Additionally, the birthrate rose two percent for white and Hispanic women but declined by two percent to three percent for Black, Asian, and Native American women.
Analysts predict that the slight rise was due to people overcoming their initial fears about the Covid-19 pandemic.
“That sort of suggests [that] when we saw the decline in births from 2019 to 2020, probably a lot of births were postponed,” Dr. Brady Hamilton, the lead author of the report and works with the NCHS Division of Vital Statistics, told ABC News. “People were waiting to see what happened [with the pandemic] and rates rose in older women as they may have proceeded to have that child.”
Despite the marginal rise in births, the country still faces an uphill battle when it comes to achieving a replaceable birth rate. In order to be demographically solvent, the average woman needs to have 2.1 children over the course of her childbearing years — the current rate stands at 1.7 children per woman.
“I’m not going to get too excited about this,” Kenneth Johnson, a demographer at the University of New Hampshire, told the New York Times. “It’s really a very modest increase.”
Notwithstanding the current rise, the U.S. has faced a steady decline in birth rates for years. As the New York Times points out, the current year’s slight rise is still less than the overall births in 2019. As Live Action News has previously reported, abortion undoubtedly contributes to the declining birth rates, as does the use of birth control, rising childcare costs, and the lack of support for mothers and families. Many people still buy into the lie that the world is on the brink of overpopulation, despite the data suggesting otherwise. Yet, instead of pushing policies that encourage and support families — which would, in turn, lead to a robust nation and economy — many in the government today still push for abortion as the only way to boost an ailing economy.
Some 14 percent of women between the ages of 15 and 49 are currently taking hormonal birth control pills in America, according to government data. That’s more than 10 million people, about the equivalent of the entire population of Portugal.
According to a 2019 United Nations report, about 151 million women take the pill worldwide.
Kristin, a mom of two, was one of them. She was prescribed birth control pills when she was still in high school. While her doctor told her the pills would help with her headaches and irregular and heavy periods, no one talked to her about the risks associated with taking them.
However, when she was 20 years old, she had an elective surgery. Although Kristin had no complications from the surgery itself, a few days later, she was unable to take a full deep breath and she felt a pain in her arm. She knew something was seriously wrong, but she had no idea that she was having a pulmonary embolism.
A pulmonary embolism, which can be lethal, happens when a blood clot gets logged in an artery in the lungs.
This medical crisis, which kept her hospitalized for six days and on medication for six months afterward, was from taking hormonal birth control pills as a teen, Kristin told me.
“Everyone has been in agreement that it was from the birth control,” said Kristin, who asked not to use her last name because she’s currently part of a class-action lawsuit.
Oral Contraceptives Increase Risk of Death
Indeed, in 2018 a team of researchers, led by Dr. Lynn Keenan, M.D., at the University of California–San Francisco’s Fresno campus, found that women who use oral contraceptive are between three and nine times more likely to have of blood clots in the lungs, legs, and brain than women who don’t take oral contraceptives.
They also face a much higher risk of death because of blood clots. The same study found that between 300 and 400 healthy young women die unnecessarily every year due to hormonal birth control.
“Women should be informed of these risks,” the researchers concluded.
Pill Linked to Depression, Bloating
Taking hormonal birth control is also associated with a host of other negative health outcomes.
For example, a 2016 study of a million women in Denmark found that taking hormonal contraception was associated with depression, especially in teenagers.
Oral contraceptives have also been linked to lower levels of the steroid hormone DHEA in the blood and a decreased ability to gain muscle during exercise, according to a 2009 study.
Another older study, from 2008, found that these pills can cause bloating, while an earlier study found that oral contraceptives lead to women having more subcutaneous fat and other changes in the way the body stores fat.
Though many women report gaining weight while taking the pill, the peer-reviewed literature on this seems to be inconclusive, according to a 2014 Cochrane review.
It’s clear from the scientific literature, however, that oral birth control use also increases a woman’s risk of developing breast cancer and cervical cancer.
“Neither of my daughters can menstruate on their own,” a mom of two young adults, ages 21 and 23, told me recently. “They’ve both been on the pill since they were teens.”
While girls in the United States usually begin menstruating around age 11 or 12, the onset of menses is widely variable and precocious puberty (before age 8) is becoming more common. Recent research from Italy has found that precocious puberty has increased during COVID-19. One team of researchers hypothesized that this may be due to stress, lack of sunlight, lack of exercise, and exposure to a higher number of environmental toxins, especially endocrine disruptors.
Doctors routinely prescribe birth control pills to tweens, teens, and young adults who are menstruating but not sexually active to treat the following conditions:
Acne
Amenorrhea (lack of menstruation)
Cramps and other menstrual pain
Endometriosis
Heavy periods
Headaches
Migraines
PMS and mood swings
I found this out when my oldest daughter, who is 22 now, was still in middle school.
“Mom,” she said to me one day, “I think I should take the pill to help me with my acne. That’s what my friends are doing and they say it works.”
Harms of Hormonal Birth Control Pills
Birth control pills disrupt the endocrine system, essentially fooling the body into believing it is pregnant, in order to stop ovulation.
We know we should try to avoid disrupting children’s hormones. As Joseph Braun, Ph.D., an associate professor of epidemiology at Brown University, explained in a 2017 peer-reviewed article, endocrine-disrupting chemicals increase the risk of childhood diseases “by disrupting hormonally mediated processes critical for growth and development,” and may be contributing to obesity and neurodevelopmental problems.
“In residency, you learn to use birth control like you learn to wash your hands,” said Nathan Riley, M.D., who is unabashedly critical of the practice of prescribing contraceptives to young woman to treat menstrual problems.
“You bring it out anytime that anyone has an issue,” Riley said. “We use it for everything. You’ve got a quote ‘lady problem’? Let’s put you on birth control.”
Then, he said, if the birth control pills themselves cause side effects, doctors add more prescription medications to the mix.
“Synthetic hormones lead to mood disorders, depression, anxiety, and sleep disorders, among other things, all of this is well documented,” Riley said. “Women have complained about everything under the sun. But their doctors say it’s not the birth control. And instead of stopping the medication that started the problem, their doctor gives them an antidepressant.”
He believes this is harmful, arguing that the practice of rushing patients through appointments and writing prescriptions for the pill makes the pharmaceutical industry richer, while making female patients sicker.
Hormonal birth control alleviates symptoms without treating the underlying problems, he said. The key, he insisted when we spoke, is to treat the root cause of the menstrual irregularities.
For instance, a woman’s periods may be irregular because she’s severely anemic, either because she is not eating iron-rich foods or suffering from malabsorption.
All of these health problems are treatable, he said. While prescription medications can help for the short-term, the goal is to get the body back in balance. To do so, he talks to his patients about making lifestyle changes, including dietary improvements, engaging in daily movement and exercise, getting adequate and high quality hydration, improving sleep, limiting exposure to electromagnetic fields, learning to do breathwork, and improving both your attitude and your emotional intelligence.
“Sometimes you do need a temporizing measure like birth control,” Riley said. “But it shouldn’t be used for long.”
Marie (her middle name) is a 32-year-old lawyer based on the East Coast. She was first prescribed birth control pills for endometriosis when she was 15, and it seemed to help.
Besides, she really liked taking the pill: It made her breasts bigger and cleared up her acne. So when her periods suddenly became more painful, even on the pill, and her doctor told her to start taking it continuously (so she would not menstruate at all), she didn’t think to question it.
Her doctors said taking the pill would help her avoid surgery for endometriosis. But she ended up having surgery anyway, in 2018, to cauterize tissue in her pelvic cavity.
It wasn’t until Marie had a miscarriage at age 27 and it took 15 months to get pregnant again—and only with the help of fertility drugs—that she started to regret taking hormonal birth control for so many years.
The science is inconclusive about whether the pill negatively affects fertility. In fact, some studies, such as one published in 2002 in Human Reproduction, show it may increase the odds of getting pregnant after quitting the pill.
But when I interviewed the late science writer Barbara Seaman, who had written several books about women and hormones, several years ago, she insisted that hormonal birth control is a causative factor in infertility and that it can take women as long as 12 to 24 months after taking the pill to become pregnant without assistance.
Marie, like many other women, is convinced her long-term use of birth control for endometriosis contributed to some of her continuing health challenges, including fertility issues.
“I was just not healthy as a teenager,” she confessed.
For Kristin, the decision to go on birth control as a teenager and subsequent pulmonary embolism made her two pregnancies more dangerous. She was considered high-risk and had to inject herself with anticoagulants during the pregnancy and for one month afterward.
“I will never be on any hormones ever again,” Kristin told me. “I really wish I knew of alternate, more natural ways to have treated my adolescent issues. The psychological damage it’s caused is irreversible. I hate how doctors are so quick to take out that pen and pad and throw meds at teenagers.”
The 25-year-old model Hailey Bieber was hospitalized last month. Her face started drooping, and she found herself unable to speak. At the hospital, she learned that she had suffered a blood clot that caused a transient ischemic attack or ministroke. Bieber released a video explaining what caused what she called “the scariest moment of my life.”
Birth control was a factor that led to a blood clot in her brain. “I had just recently started birth control pills, which I should have never been on because I am somebody who suffered from migraines anyway. And I just did not talk to my doctor about this,” she said. “So ladies, if you suffer from bad migraines and you plan on being on birth control pills, make sure you tell your doctor because having a stroke is a potential side effect from birth control pills.”
Some types of birth control methods are linked to clotting problems. The pill, the patch, and the ring contain the hormone estrogen which increases the risk of dangerous blood clots. Although estrogen is known to affect multiple variables in the coagulation system, the exact molecular mechanism of estrogen-induced thrombosis is not totally understood. Estrogens in the pill, the patch, or the ring cause the body to hormonally imitate pregnancy. In doing so, they not only prevent pregnancy but program the woman’s body to produce more clotting factor proteins. Their bodies actually produce clotting to protect them from any bleeding challenge that might occur with a miscarriage or during childbirth. These same changes caused by hormonal contraception put women at an increased risk for blood clots.
How common is the risk to develop a blood clot?
According to the FDA if 10,000 women who are not pregnant and do not use birth control pills are followed for one year, between 1 and 5 of these women will develop a blood clot. The chance of clots is 2 to 6 times greater among women taking the pill vs. women who don’t use birth control and the risk increases 6.5 times for women using the ring. One reason patches and rings are more dangerous is because the amount of estrogen absorbed from them is reported to be 60 percent higher than the amount of estrogen delivered by pills. The risk is greater for a woman who has a clotting disorder, a family history of blood clots, or who previously experienced a blood clot.
How can you reduce your risk?
It is projected that 300- 400 healthy women will die from blot clots associated with the use of contraception. There are healthier and safer options for women to avoid the risk of blood clots associated with hormonal birth control use. Natural Family Planning (NFP), doesn’t have the side effects of hormonal birth control, is based on the understanding of the woman’s body, and can help women to monitor their reproductive health.
Women who suffer blot clot disorders can experience heavy menstrual bleeding or bleeding at the time of ovulation each month. Heavy menstrual bleeding can be monitored with an NFP method and can be managed without the use of dangerous hormonal birth control.
Research published in the American Journal of Obstetrics and Gynecology regarding selective reduction abortions suggests that “reducing” triplet pregnancies to singletons versus “reducing” to twins creates a better chance of seeing the surviving babies born at an older gestational age and a greater birth weight. But there are many ethical issues to unpack with regard to this research.
Selective reduction means that certain children are targeted for death in the womb as they grow alongside their siblings. given the fact that the majority of twins and triplets in the United States are created using fertility assistance such as IVF, this means they are being created only to be destroyed through selective reduction despite little proof that selective reduction abortion will save the lives of the other babies.
Kamran Hessami, MD, a postdoctoral research fellow in the department of obstetrics and gynecology at Baylor College of Medicine said that it is “not completely clear” from the research whether reducing to singletons instead of to twins actually improves outcomes for the surviving babies. While the surviving singletons were born later and heavier than the surviving twins, there was “no substantial difference for the rates of early pregnancy loss and neonatal death,” according to the study.
This means that the twins had a greater chance of preterm birth but not of dying.
Additional research shows that the rate of loss is similar in triplet pregnancies that have been reduced compared to triplet pregnancies that have not been reduced. In this study of 132 triplet pregnancies, 30 sets of parents decided to abort one of the babies. 102 opted to manage the pregnancy with all three babies. While the women who aborted one of their babies delivered at a later average gestational age (32.52 weeks vs 34 weeks), there were no neonatal deaths for any of the babies. Four of the pregnancies in the non-abortion group were lost, compared to one in the selective reduction group, which researchers noted as “no difference.”
This begs the question: Why are doctors killing a triplet or two triplets with no proof that it will make a significant difference in the survival rates for the non-aborted sibling or siblings?
The answer seems to be that selective reduction may reduce some of the risks to the mother’s health associated with a triplet pregnancy. The non-abortion group experienced greater rates of preterm labor, preeclampsia, and gestational diabetes, and spent more days in the hospital after birth. No mothers died in either group.
Creating babies to kill them
What isn’t mentioned in the research published in the American Journal of Obstetrics and Gynecology is how these babies came to be in the first place. The researchers identified 10 studies published between 2012 and 2020 involving 2,392 triplet pregnancies.
The natural twin pregnancy rate is about 2% while the twin pregnancy rate with fertility assistance is as high as 40%. More than one-third of the twins and more than three-quarters of the triplets and higher-order multiples born in the U.S. resulted from fertility treatments, signaling that many of the triplets in the study were created using IVF or other fertility assistance methods. In other words, these babies were purposefully created to meet adults’ desire to have a baby, but then, any “extra” babies were killed through selective reduction abortion.
Take Calli and Ashley, for example. They used a sperm donor and stimulated ovulation even though Calli knew she produced more follicles than the average woman. When she became pregnant, there were five babies — babies that she and her partner Ashley paid to create in order to fill their own desires. But five was too many, they decided, because they didn’t want Calli to have to go on bed rest or have one of them quit their jobs to take care of five babies. So they decided to kill three of the babies by injecting feticide into their beating hearts at 12 weeks.
Children are not products to be bought, sold, or returned. Yet that’s what is happening with selective reduction abortions. Children are being purposefully created by adults who know there is a risk of multiples, and then those adults are killing the extra children they created.
IVF increases pregnancy complication risk
While the health and life of the mother should be considered with the utmost respect and care, doctors know what the risks are and should therefore be prepared to handle them. There is a known increased risk to the mother’s health during pregnancies created using IVF — meaning that these parents and fertility specialists are not only creating “extra” babies that they later abort, but they also know that these mothers will be at an increased risk for complications.
Women who have had fertility treatments — especially IVF — are likely at a higher risk for serious pregnancy complications compared to women who become pregnant naturally. According to a study that looked at 814,000 births and stillbirths in Ontario between 2006 and 2012, rates of severe pregnancy complications were about 31 per 1,000 IVF-assisted pregnancies and 22 per 1,000 for natural pregnancies.
Overall, “[W]e found that the women who received infertility treatment, especially in vitro fertilization, were about 40 percent more likely to experience a severe pregnancy complication compared with women who gave birth without any treatment,” said Dr. Natalie Dayan, director of obstetrical medicine at McGill University Health Center, in a journal news release.
Killing instead of healing
Of the 2,392 triplet pregnancies the researchers analyzed, 1,903 were reduced to twins and 489 were reduced to singletons. The majority were killed through the use of potassium chloride injections to cause cardiac arrest, while 68 were killed through aspiration abortion.
One of the risks of selective reduction abortion is the miscarriage of the other babies. In the process of killing these “selectively reduced” human beings, no health conditions or illnesses were healed; they were killed in the hopes of preventing future complications for their mothers.
For many parents, it is fear alone that drives their decision to kill some of their babies in hopes that the others will thrive or that the mother’s health remains stable. But rather than instill fear in patients, it is important that those in the medical community offer hope. Doctors should be studying and learning how to best help all of the babies survive, and then implementing what they have learned.
Killing doesn’t advance medicine. Searching for ways to help does. Today, babies born at 21 weeks have a chance of surviving when given medical care. If certain doctors had never tried to save these babies, then progress would never have been made, and micro-preemies born today would still have no chance.
Meanwhile, preventable maternal deaths have been increasing in the United States despite wide access to abortion. There is a shortage of doctors offering maternity care, and what’s worse is that many doctors largely dismiss women’s symptoms until it’s too late.
It’s a horrific cycle. Fertility doctors allow the creation of ‘multiples’ pregnancies knowing the increased risk to women from both IVF and the number of children in the womb. Then they kill the babies they created and successfully implanted in an attempt to lessen those risks.
Doctors are meant to heal patients and help them thrive — all of them, not just the select few. Killing must never be a solution to health concerns that may arise. Mothers and babies deserve better.
Eccentric billionaire and tech entrepreneur Elon Musk has once again issued a warning about the risk posed by low birth rates, rejecting the assessments of global “experts” who continue to insist that there are too many people occupying the planet.
“Most people in the world are operating under the false impression that there are too many people,” Elon Musk told Mathias Döpfner, the CEO of German publishing company Axel Springer last week.
“This is not true,” the 50-year-old Tesla and SpaceX founder said. “Earth could maintain a population many times the current level. And the birth rate has been dropping like crazy.”
"Most people in the world are operating under the false impression that we've got too many people. This is not true. Earth could maintain a population many times the current level. The birth rate has been dropping like crazy." — @elonmuskpic.twitter.com/5BpOYThLRM
A study published in the journal The Linacre Quarterly involved ten sites across the United States and Canada to demonstrate the effectiveness of the Marquette Method of Natural Family Planning (NFP).
The Marquette Model of NFP uses urine fertility biomarkers collected at home that measure hormone levels. These biomarkers can be used in conjunction with other biomarkers such as cervical mucus or basal body temperature and an algorithm to determine the woman’s fertility cycle.
The multisite study used Statistical Data Analysis to determine typical unintended pregnancy rates for a total of 1,221 women.
The authors of the study reported there were forty-two unintended pregnancies which provided a typical use unintended pregnancy rate of 6.7 per 100 women over twelve months of use. According to the Centers for Disease Control and Prevention, the Marquette Method is as effective as the Pill, patch, ring, or injectable birth control methods.
Further analysis revealed that eleven of the forty-two unintended pregnancies were associated with the correct use of the method. The total unintended pregnancy rate over twelve months of use was 2.8 per 100 for women with regular cycles, 8.0 per 100 women for postpartum and breastfeeding women, and 4.3 per 100 for women with irregular menstrual cycles.
It was reported that The Marquette Model was effective when provided by health professionals who completed the Marquette Model NFP teacher training program.
The use of NFP includes the identification of important biomarkers during the fertility cycle. These signs can be used to identify not only fertile and infertile phases of the cycle but also potential health problems. The American Academy of Pediatrics and the American Academy of Obstetrics and Gynecology have recommended adolescents and young women monitor the menstrual cycle as a vital sign. Women of all reproductive ages benefit from monitoring their menstrual cycle to identify and monitor health problems such as unusual uterine bleeding, polycystic ovary syndrome (PCOS), endometriosis, metabolic syndrome, eating disorders, and sub-fertility.
Healthcare providers can successfully incorporate NFP services into their practice with appropriate training. They will assist their patients to choose healthy and effective family planning methods. NFP programs can contribute to the promotion of health and prevention of disease.
Many young women who exercise regularly and use oral contraceptives (OCs) are not aware of the effects of hormones on their body composition. High-intensity workouts and weight-lifting exercises usually result in muscle gain. Taking potent hormones such as birth control pills could impair muscle response to standardized exercise.
A study published in The Journal of Strength and Conditioning Research compared the muscle growth of women on hormonal birth control and those who were not using hormonal contraception. The women were between the ages of 18-and 29 years and completed a 10-week total-body resistance training program designed to build muscle.
The authors of the study used hydrostatic weighing to determine body composition, and blood samples were taken before and after training to measure the hormones, dehydroepiandrosterone (DHEA), DHEA sulfate (DHEAS), IGF-1, and cortisol levels.
The authors reported that the group of women who were on hormonal birth control developed 40% less lean muscle mass than the women who were not taking hormonal birth control. Additionally, there were significant differences in lean mass gains depending on the type of progestin in hormonal contraceptives users. The more androgenic progestin used less muscle gain was found. Hormonal profiles at rest and post-workout showed that the women taking birth control had lower levels of anabolic hormones (DHEA, DHEAS, and IGF-1), but higher levels of cortisol.
Muscle growth is influenced by several hormones in the woman’s body. Testosterone and growth hormone cause muscle gain. In contrast, cortisol is a catabolic hormone, meaning it breaks muscle tissue down.
The authors of the study concluded that the diminished lean mass may be related to the effect of hormonal contraceptives on anabolic and catabolic hormone levels. Also, progestin present in hormonal contraceptives may bind to androgen receptors and inhibit its function.
Young women need to be informed of the side effects and hormonal changes caused by birth control. Although more research needs to be done in this area, safer alternatives to birth control need to be considered to achieve not only muscle-focused fitness goals but general health and wellbeing.
Given that one in eight women receive a devastating breast cancer diagnosis in their lifetime, virtually all women—myself included—want to know their personal risk factors for developing breast cancer and how to reduce their risk. You may have heard that one common personal risk factor, hormonal birth control use, increases your risk for breast cancer only slightly—around 20%—and that this effect eventually goes away. A closer look at the evidence, however, shows the risk may be much higher for a particular group of women: namely, young women who use hormonal birth control before their first full-term pregnancy. They are at increased risk for developing breast cancer because their breast tissue is not fully developed, and is thereby especially susceptible to carcinogens (substances that can cause cancer) like the synthetic estrogen and progestin in hormonal birth control.
Women Breast Cancer Support Charity Concept
Your breast cancer risk may be relative to childbearing and hormonal birth control use
In a recent Natural Womanhood article, “Does birth control prevent—or cause—cancer?” I discussed the increased breast cancer risk experienced by women on hormonal birth control, and the theory that birth control may increase breast cancer risk by overstimulating a woman’s breast cells. But research suggests that a woman’s breast cancer risk may also be related to when she begins using hormonal birth control.
A 2007 meta-analysis of 34 studies showed that the risk of developing breast cancer before menopause was 19% higher for women who used birth control—which aligns with the often cited 20% increased risk for breast cancer [1]. But that risk rose to 44% when birth control was started before women had their first full-term pregnancy, and rose to 52% when birth control was used at least four years before their first full-term pregnancy.
Young women who began birth control before age 20 had nearly double the risk of developing breast cancer by age 30 when compared with their peers who started birth control after age 20.
In a 2010 meta-analysis of 54 studies, young women who began birth control before age 20 had nearly double the risk of developing breast cancer by age 30 when compared with their peers who started birth control after age 20 [2]. That risk decreased as the group of women aged, but suggests that starting birth control at such a young age, when most women have not yet had children, could greatly affect breast cancer risk.
Pregnancy and breast cancer risk
Angela Lanfranchi, MD, co-founder of the Breast Cancer Prevention Institute and Clinical Assistant Professor of Surgery at Robert Wood Johnson Medical School, has written an extensive peer-reviewed article as well as brochures about how breast tissue develops before and during pregnancy, and much of what follows is based on her writings and insights shared during an interview with Natural Womanhood.
Birth control-induced changes to breast tissue make-up and why they matter
As Dr. Lanfranchi explains, the breast is made up of milk-producing structures called lobules, of which there are four types: 1, 2, 3, and 4. Each type represents a different stage of development, with type 1 being the least mature and type 4 being the most mature. Women who have never been pregnant and carried a child to term have breasts that are primarily made up of immature type 1 and 2 lobules. This makes their breasts more susceptible to carcinogens, because immature lobules have far more estrogen and progesterone receptors present than more mature type 3 and 4 lobules.
When type 1 or 2 lobules are exposed to estrogen and progesterone (including the synthetic versions found in hormonal birth control), their cells begin multiplying—and each time a cell splits into two, it runs the risk of making an error in the DNA, also known as a mutation. Mutations can lead to cancer. “That’s why breast cancer will only start in immature lobules,” said Dr. Lanfranchi. She added that cancer simply “doesn’t happen” in type 3 or 4 lobules.
Breast tissue make-up in women who have carried full-term pregnancies
In contrast, the breast cancer risk for women who have already carried a child to term may be less affected by hormonal birth control, precisely because their breast tissue has fully matured to type 4 lobules during pregnancy.
By week 32 of pregnancy, or midway through the third trimester, 70% of the lobules have become type 4, and that proportion rises to 85% by the end of the third trimester. At delivery, the breast is made up of mostly mature, type 4 lobules—and, for the most part, once breast tissue has matured, it stays that way. And while the appearance of the breast lobules does transition to type 3 after a child stops breastfeeding, the protective benefits of a full-term pregnancy against breast cancer development are largely permanent.
How breast tissue make-up is connected to the type of breast cancer diagnosis
Breast cancer that forms in type 1 lobules, known as ductal cancer, makes up about 85% of breast cancer diagnoses (type 1 lobules are mostly made up of ductal cells, hence why cancer in this area is named ductal cancer). Nearly the rest of breast cancer is found in type 2 lobules, and termed lobular cancer. Only rarely does breast cancer form elsewhere in the breast, such as in the muscle, fat, or blood vessels.
When pregnancy ends prematurely, your breast cancer risk goes up
Another important aspect of breast development is what happens to a woman’s breast tissue when she gets pregnant, but the pregnancy ends before full-term. Evidence suggests that when pregnancy is interrupted, either through an induced abortion, spontaneous miscarriage, or delivery before 32 weeks, the risk for breast cancer temporarily rises, because the types 1 and 2 lobules have multiplied but not yet matured into types 3 and then 4 lobules [3]. In essence, Dr. Lanfranchi explained, “Abortion [and, likewise, miscarriage and preterm delivery] increases your risk of breast cancer because it leaves your breasts with more places for cancers to start.”
To complicate matters, abortion can also increase breast cancer risk by hindering future full-term pregnancies. Abortion procedures can permanently weaken the cervix, a structure critical for carrying a baby to term. Research shows that pregnant women who previously had an abortion go on to have a higher risk of delivering their subsequent baby or babies early [4]. As with any woman who delivers prematurely, if a woman who has had a prior abortion goes on to have a subsequent pregnancy where she delivers before her type 1 and type 2 lobules mature around 32 weeks, she may not develop fully mature, cancer-resistant breast tissue–and therefore have a heightened risk for developing breast cancer.
[1] Kahlenborn C, et al. Oral contraceptive use as a risk factor for premenopausal breast cancer: a meta-analysis. Mayo Clin Proc. 2006 Oct;81(10):1290-302. doi: 10.4065/81.10.1290. PMID: 17036554.
[2] Bjelic-Radisic, V., Petru, E. Hormonelle Kontrazeption und Brustkrebsrisiko. Wien Med Wochenschr160, 483–486 (2010). https://doi.org/10.1007/s10354-010-0807-0
[3] Melbye, M., Wohlfahrt, J., Andersen, AM. et al. Preterm delivery and risk of breast cancer. Br J Cancer80, 609–613 (1999). https://doi.org/10.1038/sj.bjc.6690399
[4] Shah PS, Zao J; Knowledge Synthesis Group of Determinants of preterm/LBW births. Induced termination of pregnancy and low birth weight and preterm birth: a systematic review and meta-analyses. BJOG. 2009 Oct;116(11):1425-42. doi: 10.1111/j.1471-0528.2009.02278.x. PMID: 19769749.
The following article about Depoprovera and HIV transmission guidelines was published in DifferenTakes. It is a publication of the Population and Development Program PopDev (hampshire.edu)
Editor’s note
Concerns about Depo-Provera and increased rates of HIV transmission are of vital importance to women’s health, especially to those at high risk of HIV acquisition. Despite compelling evidence of a Depo-Provera-HIV link and regulatory bodies’ unclear guidance around the method’s use,1 distribution of the injectable contraceptive has been on the rise. For instance, in 2017 the Indian government began offering free Depo injections through its public health system, despite opposition from women and health groups in India.2 Since 2008, a public-private partnership has tested and distributed the Sayana Press, which delivers a lower dosage formulation of Depo-Provera, in countries including Uganda, Senegal, and Niger.3
In this DifferenTakes, scholar C. Sathyamala critically examines the ECHO trial, which aimed to conclusively answer the Depo-Provera-HIV question. It ended in spring 2019. The author argues that the trial results add to the existing evidence that Depo-Provera increases the risk of HIV transmission. She challenges the World Health Organization’s June 13 statement reporting “no link.” This stance, she argues, dangerously misrepresents the study’s findings and, further, disregards key critical challenges, including those from AIDS and reproductive justice activists. As the author argues, the World Health Organization guidance fails to appropriately warn users of the potential risk associated with Depo-Provera use and wrongly concludes that it is “safe.” — Anne Hendrixson
World Health Organization (WHO) guidelines recommend: “Women at a high risk of HIV infection are eligible to use all progestogen-only contraceptive methods without restriction(MEC Category 1), including progestogen-only pills (POPs), intramuscular and subcutaneous depot medroxyprogesterone acetate (DMPA-IM and DMPA-SC), norethisterone enanthate (NET-EN), levonorgestrel (LNG) implants and etonogestrel (ETG) implants.”
See for instance Marion Stevens, “Elevated Risk: Injectable Contraceptives and HIV—a Reproductive Justice Perspective from the Global South,” DifferenTakes, no. 90, Summer 2017, https://sites.hampshire.edu/popdev/ elevated-risk-injectable-contraceptives-and-hiv-a-reproductive-justice-perspective-from-south-africa/;
Shaifali Agrawal, “Risking Health Of Its Women, India Uses Controversial Contraceptive In Family Planning Programme,” IndiaSpend, October 18, 2017, https://archive.indiaspend.com/cover-story/ risking-health-of-its-women-india-uses-controversial-contraceptive-in-family-planning-programme-36857
See Daniel Bendix, Ellen E. Foley, Anne Hendrixson and Susanne Schultz, “Targets and Technologies: Sayana Press and Jadelle in Contemporary Population Policies,” Gender, Place & Culture, https://doi.org/10.1080/0966369X.2018.1555145
Evidence for Contraceptive Options and HIV Outcomes (ECHO) Trial Consortium, “HIV Incidence Among Women Using Intramuscular Depotmedroxyprogesterone Acetate, a Copper Intrauterine Device or a Levonorgestrel Implant for Contraception: A Randomised, Multicentre, Open-label Trial,” The Lancet, (June 13, 2019) http://dx.doi.org/10.1016/S0140-6736(19)31288-7
See for instance, World Health Organization, “Hormonal Contraceptive and HIV: Science and Policy,” Geneva: World Health Organization, 2005, (https://www.who.int/reproductivehealth/topics/family_planning/nairobi_statement.pdf)
Renee Heffron, Deborah Donnell, Helen Rees, et al., “Use of Hormonal Contraceptives and Risk of HIV-1 Transmission: A Prospective Cohort Study” Lancet Infectious Diseases, vol. 12, (February 2012): 19–26.
Paula Donovan, “The UN’s Gag Order on Reproductive Health,” AIDS-Free World, February 13, 2012, http://pharmpdf.com/a/ aids-freeworld.org1.html
World Health Organization, “Hormonal Contraception and HIV: Technical Statement. WHO/RHR/12.08.” Geneva: WHO, 2012, https://www.who.int/reproductivehealth/topics/family_planning/Hormonal_contraception_and_HIV.pdf
G. Justus Hofmeyr, Charles S. Morrison, Jared Baeten, et al., “Rationale and Design of a Multi-center, Open-label, Randomised Clinical Trial Comparing HIV Incidence and Contraceptive Benefits in Women Using Three Commonly-used Contraceptive Methods (the ECHO study), [version2; referees 2 approved],” Gates Open Research (2018), 1, 17. https://doi.org/10.12688/ gatesopenres.12775.2
Gianni Di Perri, “How Does Contraceptive Use Increase the Risk of HIV Acquisition?” 15th European AIDS conference, October 21- 24, 2015, https://www.eacsociety.org/files/giovanni_di_perri.pdf
Lauren J. Ralph, Sandra I. McCoy, Timothy Hallet and Nancy Padian, “Next Steps for Research on Hormonal Contraception and HIV,” The Lancet, vol. 382, no.9903 (June 28, 2013): 1467–1469. https://doi.org/10.1016/S0140-6736(13)61420-8
World Health Organization. “Hormonal Contraceptive Methods for Women at High Risk of HIV and Living with HIV, 2014 Guidance statement,” (2014), http://apps.who.int/iris/bitstream/10665/128537/1/WHO_RHR_14.24_eng.pdf?ua=1
Lillian Mworeko and Mitchell Warren, “Women’s Response to new WHO statement on DMPA,” Letter to Dr. Margaret Chan, Director General of the World Health Organization and Dr. James Kiarie, Coordinator, Human Reproduction Team, World Health Organization. Undated. https://www.avac.org/sites/default/files/u3/CivilSocietyWHOresponse.pdf
Billboards have begun to pop up throughout Portland with a surprisingly personal message:stop having kids. While the idea itself is a bad one, as I’ll discuss later, one interesting question to ask is, where did this sentiment come from?
I’m not interested in diving into the history of the particular organization behind this campaign. Instead, a more interesting question is where and when did this sentiment in the United States originate?
To understand the roots of this misanthropic movement, we need to meet the advertising expert who used his fortune and expertise for the primary purpose of decreasing the number of humans: Hugh Moore (1887–1972).
Hugh Moore starts his campaign
Although not all roads lead to Moore, a significant portion of anti-population activities are connected to him. Moore’s most well-known claim to fame is his founding of the Dixie Cup Company, but he was aided by years of working in advertising.
Moore worked as an advertising solicitor for various publications including The Reform in Kansas City and then for The Packer where he was promoted to ad manager while in his second year of attendance at Harvard. Moore left the advertising business to run the Dixie cup company, but he never gave up on his interest in advertising. In fact, he channeled it elsewhere: anti-population propaganda.
Moore was inspired by William Vogt’s book Road to Survival which convinced him population growth would lead to the spread of wars and communism, among other calamities. So Moore got to work using his money and power to influence population discourse and policy.
Moore convinces the national security apparatus
Arguably, Moore’s most important influence was over Maj. General William Henry Draper Jr. General Draper’s influence on President Nixon was particularly important. Draper, a friend of Moore’s, was convinced of the dangers of population in part by Moore.
Moore’s influence through Draper began with the Draper Committee formed by then President Eisenhower. The committee itself was noted for being “top heavy with military men,” in the words of Senator William Fulbright.
The day after the committee was assembled, Hugh Moore sent his friend a lengthy wire which concluded, “If your committee does not look into the impact and implications of the population explosion, you will be derelict in your duty.”
The Draper committee made three recommendations:
assistance to “developing” countries in establishing programs to check population growth
increased assistance to maternal and child health programs
support for research programs on population, including research by other countries and the United Nations.
According to the United Nations Fund for Population Activities (UNFPA), this report and the conclusions were central to USAID (the international aid branch of the US government) establishing an Office of Population under President Richard Nixon.
Nixon wasn’t the first president to be influenced by the newly forming population lobby. His predecessor, Lyndon Johnson, was also influenced by Draper. In 1965, Draper and other members of the population establishment began to work on changes to the “Food for Peace” law which would give additional funding to countries that utilized population policies.
Outside of government, Moore worked diligently to tie aid success to population control. In 1969 he sponsored newspaper advertisements with the heading, “Latin American Aid Nullified by Population Explosion.”
And throughout his presidency, LBJ was thoroughly convinced of the relevance of population to aid. In a call with an advisor on famine in India, Johnson argued the country should be withheld aid because of their population.
“I’m not going to piss away foreign aid in nations where they refuse to deal with their own population problems,” Johnson said.
Over the next decade, India would take on one of the largest forced sterilization campaigns in history. The UNFPA went on to give India (and China) an Award for the population program in 1983.
The national security state mobilizes
As previously mentioned, Draper’s report was extremely influential on Richard Nixon as well. During Nixon’s administration, a new report was commissioned which would become one of the most infamous pieces of US population policy history.
In the early 1970s Nixon commissioned a report later made national policy by President Ford—National Security Study Memorandum 200. The report is surprisingly candid. NSSM 200 states,
“The U.S. economy will require large and increasing amounts of minerals from abroad, especially from less developed countries… That fact gives the U.S. enhanced interest in the political, economic, and social stability of the supplying countries. Wherever a lessening ofpopulation pressures through reduced birth rates can increase the prospects for such stability, population policy becomes relevant to resource supplies and to the economic interests of the United States.”
In other words, the US government was interested in lowering foreign populations in order to increase US access to raw materials. The report recognizes this sort of policy sounds bad. The solution? Don’t get caught.
“We must take care that our activities should not give the appearance to the LDCs of an industrialized country policy directed against the LDCs. Caution must be taken that in any approaches in this field we support in the LDCs are ones we can support within this country. ‘Third World’ leaders should be in the forefront and obtain the credit for successful programs. In this context it is important to demonstrate to LDC leaders that such family planning programs have worked and can work within a reasonable period of time” (NSSM 200).
The report discusses in detail how non-government organizations and foreign organizations can be used to provide cover. Lastly, and most chillingly, the report offers no clear condemnation of involuntary programs.
“In these sensitive relations, however, it is important in style as well as substance to avoid the appearance of coercion” (Emphasis added).
The report recommends influencing external actors to create, “improved world-wide support for population-related efforts” through “increased emphasis on mass media and other population education and motivation programs.”
Population explosion propaganda
Moore’s influence wasn’t limited to his influence on Draper. Moore’s public propaganda campaign began with his 1954 publication of the proactively titled pamphlet, “The Population Bomb.”
Demographers concerned about population were initially surprised by his colorful tactics, but Moore trusted his own marketing savvy. He told one demographer, “[y]ou’ve been raised in academic halls. I’ve been raised in the market place. I’m used to presenting facts dramatically. Students of demography have talked for years and nobody listened.”
The population bomb propaganda was a hit. The New York Times ran an article echoing the propaganda calledThe Population Explosion in May, 1961.
Moore’s phrase was also adopted by someone whose popularity overshadowed his own. Ecologist Paul Ehrlich asked if he could borrow the title for his 1968 book. Moore was happy to support Ehrlich’s book, which gained widespread popularity and even led to Ehrlich appearing on the TV show at the center of American television: Johnny Carson Tonight.
Hugh Moore paid for a slew of advertisements through his self-financed organization The Hugh Moore Fund. In a letter to Draper, Moore admitted to his intentional strategy of using mass marketing gimmicks.
“[W]e must gather the best and most clever public relations people, motivation experts, advertising specialists, sociologists…who can contribute to a no-fail campaign…There are geniuses in communications and selling who have sold the American public every gee-gaw and gimmick conceivable.”
The vehicle of paid space in newspapers was chosen. In his notes he wrote,
“[t]he Hugh Moore Fund has tried within its slender resources to meet this need by using paid space, for in paid space you can tell people what they should do, when they should do it and where.”
In 1967, Moore’s fund created “The Campaign to Check the Population Explosion” with Emerson Foote, the famous ex Tobacco advertising mogul, as the chair. The campaign created several advertisements. Here are two examples:
Many of these ads were published in paid space in the New York Times. This uses a favorite propaganda phrase: “the population bomb”. pic.twitter.com/oxzwJYkbdc— Peter Jacobsen (@PeterPashute) March 29, 2022
The first ad, particularly heavy handed, suggests if population growth continues unchecked, youmay be mugged! These are just two examples, but the ads targeted society, politicians, and even the Catholic church.
The population establishment, established
Along with the Hugh Moore fund and the Campaign to Check the Population Explosion, Moore supported, headed, and founded several other anti-population organizations. Notably, Moore became the president of The Human Betterment Association and renamed the organization The Association for Voluntary Sterilization, to more boldly articulate its mission.
Moore also founded the Population Crisis Committee (with Draper), which later changed its name to what it is today—Population Action International. Moore was also Chairman of the Population Reference Bureau, a think tank dedicated to supporting “evidence-based policies” related to demography and health. He also served as VP of the International Planned Parenthood Federation.
Many of these organizations continue to exist today and attempt to influence public policy and public opinion in the same way Moore did during his lifetime. So although the billboard in Portland couldn’t be Moore’s personal handiwork seeing as he died in 1972, it’s likely that the legacy of Moore’s money, advertising strategy, and influence on ideas is somewhere at the root.
Less is not more
In a recent Atlantic article, Derek Thompson explores why US population has cratered. The author concludes, “U.S. has too few births, too many deaths, and not enough immigrants” (emphasis added). One can’t help but wonder if the millions of dollars spent on anti-population activity is to blame.
Unfortunately for the world, Moore spent the last years of his life promoting an idea that’s simply wrong. This ideology, which persists today (as seen in Portland) is an overly simplistic view of population.
Moore, Draper, Ehrlich, and the modern anti-natalists share an incomplete view of humanity. Anti-natalists generally share a modified version of the thesis of Thomas Malthus in his Essay on the Principle of Population.
The thesis is simple: human beings are consumers, and their consumption grows faster than their ability to produce with their laborer. Malthus argued that food growth is linear but population growth is exponential.
Another way to understand Malthus’ fear of population is with the law of diminishing marginal returns (which Malthus originated). The law says that, beyond some point, the more of a homogeneous input (like labor) you add to the production process, the less productive each additional unit will become.
Since the addition is decreasing while consumption needs remain the same, eventually the population will outpace productive powers. Malthus’s concern was about food, although the same argument is occasionally made with reference to the environment, for example.
The problem with this argument is that humans are, in fact, not homogeneous blobs of labor. People are creative and entrepreneurial, and they use those talents to create new products and institutional systems which allow “finite” resources to effectively multiply.
This does not mean the law of returns isn’t true, only that it requires everything else to be held constant. But, in the real world, things are rarely held constant. Advances in technology and production processes can cause returns to increase.
For example, with the invention of more fuel efficient vehicles, a fixed supply of oil is able to produce more services than before. Likewise, anti-pollution technologies can actually cause environments to improve as countries grow richer. This logic has been confirmed empirically by Nobel Prize winner Simon Kuznets’ environmental Kuznets curve.
Not everyone was fooled during Moore’s campaign. Economist Julian Simon noticed that the data simply didn’t reflect the doom and gloom of these anti-natalists. Simon challenged and beat Ehrlich in a bet on improving resource availability, and poked fun at Moore’s “HAVE YOU EVER BEEN MUGGED?” propaganda in the first edition of his book, The Ultimate Resource.
The only source of solutions to the environmental problems we face today exist in the human mind. Future generations will be at the forefront of solving today’s problems, and more minds are better than fewer.
So don’t let a billboard in Portland based on decades-old propaganda made by advertising moguls deter you. Don’t stop having kids. If you want kids—have kids. The world will be better off for it.
This article was originally published on FEE.org. Read the original article.
To know how contraception damages relationships call for taking a good look at the way human relationships come about. It all starts with the relationship between a mother and a child. The mother needs a solid, healthy relationship with the father, and the relationship between mother, father, and child becomes the nucleus of a vast array of relationships. It works like this:
Bearing and rearing a child means freely accepting the immense burdens of
• pregnancy
• infant care
• training the child (or children)
• supporting them for many years while they cannot support themselves, and
• providing occasional support and guidance for many years after that.
For this to work well, it requires a strongly bonded couple who will devote a great deal of time, energy, and resources to this process. Needs that they cannot cover will require help from other members of their community, which causes a large network of support persons to grow around them.
How can two free human beings willingly involve themselves in such a challenging process? It seems impossible. But reproduction is so important to our genes that we can say confidently that biology strongly supports this choice. We know a lot about how this happens because we have all seen it happen or experienced it ourselves. It comes in two stages: A) formation of the pair bond, and B) the biological consequences of living as a bonded pair.
A) Pair bonding
We all know bonded pairs. They are pervasive in all societies all over the world. The steps by which the bond forms are very familiar:
1) After puberty we find ourselves attracted to members of the opposite sex
2) One such person begins to have a stronger attraction for us.
3) The attraction strengthens and that person becomes the center of our universe, the most wonderful person we have ever met, the summation of all our hopes and dreams. Lots of songs and poems have been written about this phase. It is intense. This is called “infatuation.” It is driven by a fairly well-known set of hormones that remain in effect for about two years.
4) We spend as much of our time as possible with that one.
5) After much time and much communication, we formalize that bond in a way that involves the wider community.
6) We make a home together and begin having children.
Of course, life is hardly ever this neat and tidy, but these are the basics. We can see the driving force of our genes in every step. For example, people don’t choose to go through puberty, their genes do that for them. Similarly, people don’t choose to fall madly in love with someone, it “just happens.” These are the steps biology decrees for the beginning of the human pair bond, which is the core of the human reproductive strategy.
B) Life as a bonded pair.
After the infatuation, hormones are reduced, and IF the couple has been able to find some common ground, a set of maintenance hormones develops that can keep the bond going indefinitely, but the experience is very different. If, however, they discover that they have nothing in common, the relationship often fails. When they have children, this helps greatly. If they don’t, they still have their freedom. They can find another basis for the relationship, but might not. A significant portion of our married couples divorce after one and a half to two years, and then try to find someone else they can “love.”
Sexual relations, before or after the infatuation period, also produce bonding hormones, but, sooner or later, the effect wears thin. This is a harsh reality, but, like anything real, we can’t ignore it or just wish it away. It forces us to give the relationship a foundation stronger than sensations or emotions or else quit the relationship. We all know people who have gone through this crisis, and we know that some choose one way and some the other.
When children come into an established relationship, another whole set of hormones steps into action. We find child-rearing/family building pleasurable in ways we never would have expected, many of them obviously driven by our biology.
Couples with children will always encounter needs that they cannot meet themselves, so they become the nucleus of a larger community that contributes to the care of the children. Thus clans, tribes, nations, and whole world systems arise.
What can go wrong?
The bonding process can be derailed at almost any point:
In steps 1) or 2) some males find easy pleasure in various experiences of uncommitted sex, and some females may find something satisfying in that also. We all know or have heard of people who, “never grow up.” This forming and breaking of multiple partial bonds becomes unsatisfying, or even miserable, so some wind up looking for something better and may move on.
In steps 3) and 4) the couple find each other intensely attractive and sometimes become sexually involved. When this happens, one of the harsher aspects of biology tends to step in: We are genetically programmed to seek a reproductive partner. For the male, that means finding a mate who will dependably produce only his offspring. An “easy” girl isn’t that. This sort of relationship has no future. Similarly, the female is “programmed” to seek a dependable helper and provider. She really needs an extended period of communication so that she can have confidence in this person. The male also needs to have confidence that this woman is worth sacrificing his freedom and his whole future. Sex at this stage leaves them with unanswered questions and unresolved anxieties which will certainly burden the relationship and may terminate it.
Steps 5 and 6: Once the couple’s relationship is formally and publicly recognized, the beginning of the bonding process is complete. With the arrival of children, the couple’s biology introduces them to many satisfactions they likely never expected. Working together, they acquire a common perspective on many issues. Maturity “happens.” Sexual contact becomes deeply meaningful since they now know by experience that it opens their lives to massive unpredictable changes.
Marriage without children presents different challenges, but if they have done a good job of communicating during the infatuation stages, they still have the strong beginnings of a relationship and can find something that they can share and find mutually fulfilling. They will likely do many small and large things for each other, not based on wanting something in return. They will also find ways to benefit the larger community together “just because”. This is practical, effective love.
Heterosexual contact not dominated by contraception can also have a relationship-building effect. Each member of the pair is risking his or her entire future in every sexual connection. This has a unifying force that defies description. Conversely, sex that seeks only momentary pleasure has a brutally divisive effect, because, in fact, his sensations and emotions can never be her sensations and emotions, and vice-versa.
Contraception
In all of these phases, the effect of contraception can be, and likely will be, devastating:
The culture of contraception leads people to assume that sex is an intense, but meaningless, pleasure. After puberty, this can lead to many short, painful relationships that make it harder to form meaningful relationships later on.
Contraceptive use during infatuation is likely to lead to premature sexual involvement. The extremely important communication phase is short-circuited, leaving them no way to move forward once the infatuation hormones wear off.
If a married couple uses contraception, they will experience sexual contact devoid of meaning. After repeated sexual encounters with someone who, “just doesn’t care about me,” their relationship becomes more and more abrasive. Sooner or later their reasons for staying together become unconvincing. We see these things happening all around us.
What to do
Humans have an amazing ability to shape their behavior toward satisfying outcomes. Practically speaking, this means that when we know that some behavior will make us happy, we will likely choose that way. The opposite is also true. Note that this is not absolute. We all have experienced making disastrous choices even when we “knew” that trouble would arise. The overall pattern, however, is that we can learn from our mistakes and the mistakes of others.
To help ourselves and those we care for, then, means taking three basic steps: 1) know the truth, 2) tell the truth, and 3) live the truth. None of these steps is easy or simple, but if we want satisfying outcomes, we MUST put in the necessary effort. God bless you!!
The practice of decency and modesty in speech, action and dress is very important for creating an atmosphere suitable for the growth of chastity, but this must be well motivated by respect for one’s own body and the dignity of others. Parents, as we have said, should be watchful so that certain immoral fashions and attitudes do not violate the integrity of the home, especially through misuse of the mass media.
Progressives and LGBT activists are in an uproar over a bill that was just passed in Florida, which they have dubbed – rather disingenuously – the “don’t say gay” bill.
The actual title of the legislation is the Parental Rights in Education bill. As the title suggests, the bill aims to ensure that parents hold the cards in terms of what their children are taught about sex at the earliest ages.
In brief, the bill states that children in kindergarten through grade three are not given classroom instruction on topics such as sexual orientation or gender identity. The bill also requires that parents be informed about changes in services related to their child’s physical or psychological health.
As the bill’s co-sponsor, Rep. Joe Harding, made clear, this latter provision is designed to prevent the growing number of cases where school staff are introducing or asking children about such topics as sexual orientation or gender identity, and then encouraging the children to keep those conversations secret from their parents. As I have written recently, there have been cases where parents have only found out that their child now identifies as “transgender” long after school staff knew, in some cases because a staff member had actively encouraged the child.
“We have a choice to empower parents in Florida or we have a choice to empower school districts. I’m asking you to side with the side of parents in Florida,” Rep. Harding said.
Early in the debate, opponents of the bill hit upon the strategy of labeling it the “don’t say gay” bill, arguing (falsely) that the bill would ban the word “gay” from the classroom. Practically every mainstream news outlet in the country cynically ran with this hysterical propaganda. In recent days liberal legislators and activists have engaged in truly childish antics, such as chanting “We say gay!” during legislative hearings.
Fortunately, their efforts have not paid off. Last Tuesday the bill passed the Florida Senate in a 22-17 vote. As the bill had already handily passed the state House in late February in a 69-47 vote, it will now be sent to Gov. Ron DeSantis for his signature. Given that Gov. DeSantis has signaled his support for the legislation, its passage into law seems to be a fait accompli.
Graphic Sex-Ed Camps
If there is any doubt that such legislation is very much needed, it should be put to rest by news recently making the rounds about the growing trend of sex-ed camps aimed at kids.
As Live Action reports, one online camp that was aimed at teens included explicit “education” about masturbation, BDSM, transgenderism, abortion, and even (it boggles the mind) having sex while using illegal drugs.
Here are the titles of some of the presentations from this camp: “Sex with ME — Self pleasure,” “Sexy Trans Sex Ed,” “Self-Managed Abortion Info Share,” “Reproductive Health: The Basics,” “Sex on Drugs,” “The 3 P’s: Pee, Poop, and Pleasure,” and “Contraceptive Options.”
Perhaps unsurprisingly, one of the individuals leading the camp, Tanya Turner, calls herself a witch. Her passion seems to be for encouraging children, starting with toddlers, to masturbate. “Masturbation is really healthy and I recommend it to people of all ages,” she said. “All ages. As soon as my nephews could talk, they were doing that.”
Among information provided to teens during the camp was info from the World Health Organization (WHO) about how to perform a self-abortion by ordering abortion drugs and administering them at home. Besides the horrific fact that teens are being taught how to go about killing their unborn children, also troubling is the heedlessness towards the health of the teens themselves, given everything we know about the dangers and trauma involved in DIY medical abortions.
Another sex-ed camp, the “Spring Break Sex-Ed Camp,” was supposed to be held March 14-17 at libraries in the city of Austin. Organizers of this camp planned to pay teenagers $100 to attend (why on earth, one wonders, are adults luring teens to hear about sex with cash payments?). That camp, however, has now been cancelled after a backlash.
Meanwhile, Not the Bee reports on another sex-ed summer camp in Indianapolis, this one aimed at children in grades 3-5. Children in those grades are only eight to ten years old.
After showing disturbing screenshots from the organizer’s social media feed, Not the Bee notes, “This is being hosted by an individual who thinks that kids should be learning ‘non-binary’ vocabulary, taught how to wear a condom, and be ‘responsibly’ introduced to pornography.”
The site adds, “This lady is a literal groomer.”
Comprehensive Sex-Ed As Grooming
That last remark is worth focusing on.
Perhaps the strangest thing about these camps is that apparently there are parents who think it a good idea to use spring break or summer vacation for a camp that’s all about having adult strangers talk to their children in graphic detail about sex. Whatever happened to good old-fashioned camps, where kids learned to canoe, fish, play sports, and generally enjoy their friends and their childhood?
It’s bad enough that these children are being robbed of the opportunity to enjoy the sort of innocent fun that we all had as children, and instead are being dragged into the dark and complicated world of a very disturbed brand of adult sexuality. However, what’s worse is that there are very real concerns that these kids are being used to fuel the sexual kicks and fantasies of disturbed adults.
Imagine for an instant if the Catholic Church was offering such camps. It would make the national headlines with people accusing the Church of being “perverted,” “sick,” or “disgusting.” Many of the same LGBT activists running these camps, or the journalists that defend them, would be wringing their hands about how the Church is “grooming” children for sexual abuse.
Well, why is it any different when other adults who seem to have a bizarre fixation on sex spend all day talking to young kids, in graphic detail, about sex? It isn’t!
“Grooming” involves breaking down a person’s normal and healthy sexual boundaries, in order to get them to engage in sexual behaviors that benefit the exploiter. Adults who sexually abuse children, for instance, will often first introduce them to pornography. The goal is to pique the curiosity of their victims and to convince them that engaging in sexual behaviors is perfectly “normal.” Then the abuse begins in earnest.
There is simply no conceivable reason why children and teenagers need to know all the details about having sex while using drugs, BDSM, bizarre transgender practices, and all the minute ins-and-outs of contraception, abortion, and pornography. However, there are clearly adults who feel a curiously strong urge to teach them about these things. That should set off every alarm bell in the head of any loving parent, as well as any rational adult with a moral compass.
Parents, Take Charge of Sex-Ed
Unfortunately, parents who are striving to raise their children to have a healthy understanding of sexuality face enormous challenges in today’s culture.
As the Pontifical Council for the Family noted in the opening section of The Truth and Meaning of Human Sexuality, it used to be the case that “the general culture was permeated by respect for fundamental values and hence served to protect and maintain them” (no. 1). Even if the family failed to provide sex education, in many cases children still naturally absorbed positive and healthy ideas about family and sexuality. Such ideas – e.g., that sex should be kept for marriage, or that children are a positive good – were simply in the cultural water.
Now, however, everything is different. Not only are movies, music, and social media aimed at children often filled with sexual innuendo and subtle or not-so-subtle jabs at marriage and the family, but also there are activists who have learned that they can practically get away with murder, so long as they claim to be engaged in “sex education.”
There is absolutely no excuse, as parents, for allowing these people within a hundred miles of your children. As the Vatican has stated, there is nothing intrinsically wrong with sex-ed in school, so long as it is grounded in a true moral worldview, is presented in an age-appropriate way, and parents are proactively kept in the loop and given the choice to opt their children out if preferred.
However, it is a grave mistake simply to outsource sex-ed to third parties, even if that third party is the most faithful Catholic teacher in the world. Education – including sex education – begins in the home. Whatever happens in school (with your knowledge and permission) should be, at most, intended to augment, not replace, an ongoing conversation between parents and child.
As the Vatican laments in The Truth and Meaning of Human Sexuality, “In many cases parents have given up their duty in this field or agreed to delegate it to others, because of the difficulty and their own lack of preparation” (no. 1).
No matter how well you might control the flow of media into your house, we live in an age where your children are bound, one way or another, to encounter ideas or content that would have shocked our parents and grandparents. Rather than waiting for that to happen, get out ahead and start open, age-appropriate conversations with your children, arming them with the tools they need to detect problematic materials, and the confidence and trust to approach you with questions and concerns when they do.
“The Church has always affirmed that parents have the duty and the right to be the first and the principal educators of their children,” note the authors of The Truth and Meaning of Human Sexuality, and this because “having given and welcomed life in an atmosphere of love, parents are rich in an educative potential which no one else possesses” (no. 5).
They add: “The normal and fundamental method [of sex education] … is personal dialogue between parents and their children, that is, individual formation within the family circle. In fact there is no substitute for a dialogue of trust and openness between parents and their children, a dialogue which respects not only their stages of development but also the young persons as individuals” (no. 129).
It is encouraging to see Florida taking proactive measures to protect parental rights and to defend our children from ideologues who would steal their innocence. Let us pray that other states follow their example.
Mike Gaskins is a women’s health advocate, independent researcher, and author who spent much of the past decade exploring the dubious history and science of birth control. In a recent interview, Epoch Times contributor Martha Rosenberg asked him about his 2019 book, “In the Name of the Pill,” the culmination of his investigation, which was recently updated in its audiobook release.
Individuals with Down syndrome and their families were shocked and disheartened by a recent social media post from The World Health Organization (WHO) last week that listed Down syndrome as a birth defect that can be prevented. However, there is no way to prevent Down syndrome itself. “Eliminating” Down syndrome really means eliminating those who have the condition through abortion.
“Today is World Birth Defects Day,” WHO originally wrote on March 3, according to the screenshot below. “Most birth defects can be prevented and treated with access to quality maternal and newborn care. Yet, every year, they cause the deaths of close to 250,000 babies within just 1 month of birth.”
Down syndrome was then listed as one of the “most common severe birth defects.” After receiving backlash, the WHO edited the Facebook post to remove Down syndrome from the list, and deleted the paragraph of information. However, it appears a separate post on Twitter also included Down syndrome as a birth defect.
WHO Screenshot
News host Rachel Campos-Duffy, a mother of nine children — including one with Down syndrome, replied to the WHO tweet with a tweet of her own saying, “[…]#WHO. Down syndrome is NOT a birth defect. It’s a chromosomal variation. My baby w/ Downs is as human & valuable as any of my other kids. These comments lead to discrimination & abortion. Celebrate, don’t eliminate differences.”
Likewise, Kurt Kondrich, an author, advocate, and father of Chloe who has Down syndrome, tweeted, “The World Health Organization recently posted that Down syndrome is a ‘severe birth defect’! My amazing daughter Chloe who has changed the world has a response!” The tweet included a photo of Chloe, who is the inspiration behind Pennsylvania’s “Chloe’s Law” ensuring that parents who receive a prenatal diagnosis of Down syndrome receive resources and support. The photo states, “I am Chloe Emmanuelle Kondrich and I am NOT a ‘severe birth defect.’”
The Facebook page, Raising Josee Hope, also commented on the WHO’s classification of Down syndrome, stating in part, “The only way Down syndrome is prevented is through abortion, is this what they’re advocating for?! An apology to the community rather than an edited post would be appreciated. And you wonder why we are left with NO CHOICE but to tirelessly advocate?!! Imagine if this was your child being spoken about. It wrecks our day. It takes time away from our kids. It breaks our heart to advocate. We don’t want to be ‘strong warrior mums’ we just want to enjoy life with our kids knowing they’re safe. When the global peak body for health refers to your child as a birth defect that can be prevented what Hope do we have?”
People who have Down syndrome are human beings with intrinsic value, yet they are consistently targeted for abortion. The abortion rate for children diagnosed prenatally with Down syndrome in the United States is nearly 70%.
Parents are fighting back against pressure to abort their babies, but as was made evident by the WHO’s social media posts, there is much more work to be done.
Dr. Kahlenborn discusses current controversies regarding Plan B, including its’ overrated efficacy, its’ possible link to breast cancer and its’ controversial mechanism of action.
In an attempt to normalize abortion by using deceptive euphemisms, the abortion industry is now referring to the use of mifepristone and/or misoprostol (the same drugs as are used in the abortion pill regimen) as “missed period pills” or “later period pills.” The drugs are being sold to women without a confirmation of pregnancy, and they are led to believe the drugs will merely “bring down a period,” allowing them to escape the knowledge of whether or not they killed their own preborn children.
This unapproved process also flouts important safety regulations put in place by the Food and Drug Administration (FDA) under a program called REMS, which requires prescribers of the abortion pill mifepristone to properly date a pregnancy. While abortion enthusiasts are calling their latest scheme “creative,” pro-life advocates accurately refer to it as “abortion in disguise.”
A COLLABORATION OF GROUPS WITH THE GOAL OF KEEPING WOMEN IN IGNORANCE
“Period pills bring on your period when it is late, even by just a few days. If you are pregnant, these pills will end your very early pregnancy,” the website claims. “But you do not have to take a pregnancy test or confirm you are pregnant before using period pills. Yes! Period Pills are real… Sometimes this is referred to as menstrual regulation, or pushing a period, or bringing down a period.”
The site actually admits that the whole point of “missed period pills” is to remain in ignorance, noting (emphasis added), “If someone is pregnant, taking these medications will end their pregnancy. This can be referred to as an abortion. But since pregnancy is not verified before taking the pills, a person will never know if they were or weren’t starting a pregnancy when they took the pills. Late period pills will bring down a person’s menses even if they aren’t pregnant, and can provide reassurance and peace of mind if someone doesn’t want to be pregnant. A person does not need to take a pregnancy test or confirm a pregnancy to use missed period pills.”
The site adds, “Late period pills let us choose to get our periods or have chemical pregnancies when we don’t want a pregnancy to become established. Instead of waiting and worrying, we can take pills and bring on our periods.”
GYNUITY: IF PREGNANT, IT CAUSES ABORTION; IF NOT, WOMEN ‘PROBABLY DON’T NEED’ IT
Gynuity also wrote about its intention to partner with abortion chain Carafem to “study the acceptability and use of mifepristone plus misoprostol for menses induction in the US.”
A 2021 archived page from Carafem’s website shows how the abortion chain deceptively marketed so-called missed period pills as a new medication option. “If you don’t want to be pregnant, you may be eligible to use a new medication option as soon as 28 days from when your last period started… with no requirement to wait several weeks for treatment,” they wrote. A more current page at Carafem’s website states the abortion business is “conducting a study that uses Mifepristone and Misoprostol within as little as 28 days from your last period.”
Carafem archived 2021 website Missed Period Pill uses the abortion pill regimen
Melissa Grant, chief operations officer of Carafem, recently acknowledged to Ms. Magazine, “We actually were doing a Gynuity study in D.C. last year on missed period pills that temporarily paused during the pandemic….We let them know clearly, if you do this and you’re pregnant, it’s an abortion, and if you do this and you’re not pregnant, you’re taking medication that you probably don’t need…” (emphasis added).
Wendy Sheldon, a senior associate at Gynuity, suggested to Rewire News Group that this deception is “liberating” and carries “benefits” so women can “take control over their reproduction without being constrained by other people’s definitions of pregnancy, abortion, or other terms that may not reflect their beliefs or lived experiences….”
Sheldon added, “Missed period pills can also provide the psychological space for people to define what’s happening to their bodies on their own terms, consistent with their beliefs. For me, this is one of the most liberating and appealing aspects of this idea…”
UCSF Missed Period Pill Study (MPP)
The University of California San Francisco (UCSF) calls its missed period pill study a “more creative method” to support abortion goals. UCSF’s study began recruiting in June of 2021 and will utilize just the second pill in the abortion pill regimen — misoprostol, originally approved as an ulcer drug under the brand name Cytotec. The drug’s label warns that misoprostol can cause uterine rupture and will not impact a dangerous ectopic pregnancy. It will induce heavy bleeding and cramping if a woman is pregnant, and cause contractions strong enough to kill and then expel the child. By using misoprostol alone without mifepristone to first block progesterone and deprive the preborn child of nutrients, the abortion industry knows women will be unable to reverse the effects of the drug.
“As the number of state laws restricting access to abortion increases across the country, more creative methods are needed to support individuals in achieving their reproductive goals. Misoprostol alone for people who suspect, but have not confirmed pregnancy, has the potential to fulfill this growing need,” UCSF’s Missed Period Pill study (MPPS) states.
“The goal of this research study is to test a traditional but underutilized framework of menstrual regulation for pregnancy loss, to ‘bring back’ a period when it is missed,” the study, whose principle investigator is Dr. Ushma Upadhyay, also states.
“The participant will not know the results of the first visit’s pregnancy test at any point. The clinic staff member administering the participant’s care will not know of the pregnancy test result while the participant is at the clinic,” the study, which will require one study visit and one telehealth visit, points out.
Missed Period Pills or Late Period Pill abortion study at UCSF (Image: PeriodPillStudy.org)
Eliminating guilt and interfering with informed consent
In September of 2020, Gynuity published findings from a study analyzing potential interest in the concept. “In the study… researchers surveyed women seeking pregnancy tests at nine reproductive health centers in two states. They asked women if they would be happy or unhappy about becoming pregnant and if, instead of a pregnancy test, they would be interested in a hypothetical service offering what they called ‘missed-period pills,’” wrote the New York Times (NYT) about the study published in the pro-abortion Journal Contraception.
“Doing so, many said, would allow them to avoid the burden of that knowledge and the pain of self-flagellation, providing them with a psychological benefit at a time of great stress,” NYT wrote.
“It would be easier on my emotional well-being to not know I was actually pregnant but to alleviate the issue which is my missed period,” one of the study participants stated.
“I wouldn’t feel I am a bad person,” another said.
Equal Rights Institute editor Andrew Kaake pointed out how the deceptive name interferes with informed consent, writing in part, “The use of a euphemistic name… does not change the pill into anything other than an abortion pill, and an attempt to use such marketing to fool women or induce them to fool themselves interferes with informed consent. More troubling, though, is the idea that it’s better for the woman if she thinks, by taking the “missed period pill,” she only maybe had an abortion.”
“Why is intentionally muddying the moral waters and getting women to act a certain way despite their beliefs a positive thing?” writer Petra asked at Pregnancy Help News. “In reality, it’s just a way for abortion advocates to try to further the idea that abortion is a morally good and normal choice to increase their sales; there is no real concern for these conflicted women. MPPs are a marketing scheme to directly influence ambivalent women or women who outright do not agree with abortion to go ahead and do something which may go against their beliefs,” she stated.
Women can report suspected adverse reactions or complications of any drug including the abortion pill to the FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
“A 2011 survey of 123 skiers and biathletes by FasterSkier found that 71 percent had used hormonal birth control. Of those, almost half believed that it had negatively impacted their performances via weight gain, reduced strength and endurance, mood swings, loss of competitive drive, and other factors. Two standout high school skiers told FasterSkier that after starting hormonal birth control just before going to college, their performances either stagnated or declined – that is until each decided to stop taking contraceptives.“
Athletes face enormous pressure over whether to take hormonal contraceptives (HC). There are many questions surrounding the decision to use HC. “Does it increase the risk of breast cancer? Lead to infertility? Cause increased mortality? While the answers to these questions appear to be “no,” the effects of added hormones on the human body still aren’t fully understood – and the impact on athletic performance has barely been examined”. HC use is common among elite athletes, and the continuation of HC is used to manipulate the menstrual cycle in sports competitions. Although HC use is common in elite athletes knowledge surrounding the menstrual cycle and oral contraceptives is low
HC not only affects performance in athletes but it affects every cell and system in their bodies. A recent study found that Combined Oral Contraceptive use markedly elevated chronic low-grade inflammation in athletes, which could predispose to a higher inflammatory response to physical stress and elevate cardiovascular risk. Also, the use of oral, transdermal, and vaginal contraceptives impairs glucose tolerance. The use of the potent synthetic steroids has been associated with low bone mineral density and increased fracture risk in some studies.
Athletes who use the oral contraceptive pill may be exposed to long-term problems from low values of “unbound” testosterone. Synthetic hormones decrease the levels of androgens by two mechanisms. First, the direct inhibition of androgen production in the ovaries. Second the lower levels of androgens stimulates an increase in the hepatic synthesis of sex-hormone binding globulin, the major binding protein for androgens and other steroids. The combination of these two mechanisms leads to low circulating levels of “unbound” or “free” testosterone potentially leading to continuing sexual, metabolic, and mental health consequences.
Instead of compromise their performance and wellbeing with the use of Hormonal Contraception, female athletes have a safe, natural, and smart alternative. Learning a fertility awareness method, athletes can track the biomarkers of their fertility cycle and tailor their training and nutrition. The knowledge of the cyclical hormonal changes in their bodies can empower athletes to make wise decisions, avoid injury, and improve performance. Tracking the fertility cycle can help athletes to identify abnormalities caused by underlying medical conditions, nutrition deficiencies, and over training. Hormonal contraception can mask the underlying problem delaying appropriate medical intervention and adding more health issues. The challenge for athletes is to work with their natural hormones not against them.
A new report from the National Women’s Law Center (NWLC) has revealed that instead of being a decades-old obsolete horror left to the past, forced sterilization is still legal in over 30 states.
According to the report, 31 states plus Washington, D.C., allow for people to be forcibly sterilized. Most often, sterilization is used against people with disabilities, especially those who are also people of color. Sometimes, parents or guardians are complicit, but not always. And the person being sterilized isn’t always told what has been done to them until they find out on their own later.
“Linda Kay Sparkman was a 15-year-old with an intellectual disability,” the report reads. “Linda’s mother asked a judge for permission to get Linda sterilized. The judge agreed that sterilization was a good idea. No one told Linda she was going to be sterilized. The doctors told her she was getting a different operation. Linda tried to have a baby a few years later. That is when she found out that she was sterilized.”
Another story featured is that of Ashley X. Horrifyingly, Ashley’s parents successfully sought her sterilization at the age of six, through hysterectomy. As Ashley’s parents also did not want her to grow breasts or get taller, doctors also performed an operation to ensure her breasts did not grow and put her on hormones so she would remain small, like a child. Stunningly, Ashley is not the only child to have suffered through this; other children have undergone the same treatment, which is now called the Ashley Treatment.
Not Dead Yet, a disability rights advocacy group, condemned the Ashley Treatment in a statement, pointing out that despite pushback from disability groups, the Ashley Treatment has largely been received positively. “We are saddened but not surprised by the fact that this was publicized and met with a great deal of public approval,” Diane Coleman, founder of Not Dead Yet, said at the time. “The public is willing to sanction the murders of disabled children by their parents, so it’s hardly surprising they would rush to the support of parents and their medical partners in a matter like this.”
Coleman further added, “Ethics Committees often say they strive for diversity in their membership, but they have historically excluded representation from the disability community about whom they are making life and death decisions.”
It isn’t just people with disabilities who have been forcibly sterilized. Prison inmates have suffered this inhumanity as well, as recently as 2021, in states like California and Tennessee. In California alone, over 1,000 female inmates were sterilized, most of them Black, and many of the women were not told they were being sterilized. Instead, prison officials told them they had other medical conditions. It was only later that the women learned what had been done to them. The doctors reportedly believed it was better to sterilize the inmates while in prison than for them to leave jail, have children, and possibly be on welfare.
“Forced sterilization laws are not an aberration – they are part of a larger, horrifying system that prevents disabled people from making basic decisions about their lives, their families, and their futures,” Ma’ayan Anafi, the author of the report, said in a statement. “These laws are part of a long history of state-sanctioned sterilizations and are rooted in false, paternalistic assumptions about disabled people. No judge, guardian, or politician should have the right to take away anyone’s fundamental right to decide whether to have children. It’s long overdue to fully transform this ruthless system.”
On Feb. 23, the Catholic Church remembers the life and martyrdom of St. Polycarp, a disciple of the apostle and evangelist St. John.
This is a nice story of St Polycarp intersection for a pro-life cause.
“When Marilyn Szewczyk was about to launch a network of pro-life pregnancy centers in Maryland, she turned to St. Polycarp for help. Reasoning that the obscure early Christian martyr didn’t have many people asking for his intercession, Szewczyk figured she’d have easy access to his ear. Lynn Anne Sukeena, one of Szewczyk’s daughters, told me that her late mom put St. Polycarp to the test before selecting him. When a pro-life lobbying group was looking for office space in Annapolis, Szewczyk prayed to St. Polycarp. Sure enough, a prime spot was located in the State House. That was enough for Szewczyk, who officially named him the patron saint of her outreach network, Pregnancy Center, Inc.” More than thirty years later, the network is thriving.
St Polycarp is the patron of another pro-life organization, The Polycarp Research Institute a non-profit organization (501 C3) dedicated to the promotion and dissemination of high-quality research designed to enhance the physical, psychological and spiritual condition of mankind.
It’s Time to put St. Polycarp on our list of intercessors!
IUDs work against pregnancy in several ways. Some of these effects take place before fertilization, and others take place after the sperm and egg have united to form a new human being.
Although IUDs are marketed as the most effective form of reversible contraception women who use IUD can become pregnant. Many of those pregnant women continue using the IUD because it is difficult to remove. There is a possibility of miscarriage after IUD removal.
The authors reported that the study focused on the measurement of the changes in human leucocyte antigen-G (HLA-G) and insulin-like growth factor II (IGF-II) levels in the decidua and villi to explore the effect of a copper IUD on embryonic development. The human leucocyte antigen-G (HLA-G) is a molecule found in trophoblast membranes, reflecting the immune tolerance of the mother to the embryo. Insulin-like growth factor II (IGF-II) is a protein hormone similar to insulin. The protein is an important regulator of early embryonic development, particularly placental development.
A total of 54 samples of decidual and villus tissue (the maternal and fetal portion of the placenta) was collected from pregnant women with IUDs (27 samples) or without IUDs (27 samples). The morphological characteristics and protein expression levels were evaluated.
The authors found that Copper IUDs may reduce IGF-II expression in villus tissue, which could compromise the development of an embryo. They conclude, “Thus, use of an IUD during pregnancy may be risky.” Women need to be informed about the possibility of pregnancy when using IUDs and the negative effects on the development of the fetus.
The possible explanation for the increased risk of glaucoma in hormonal contraception users is the estrogen deficiency created by synthetic estrogen. The natural hormonal rise and fall in a specific pattern are suppressed by the constant levels of artificial estrogen, affecting the intraocular pressure. Also, estrogen deficiency causes premature aging of the optic nerve.
The author also explored evidence of other eye problems in hormonal contraceptive users. A study from 1997 showed that women 35 years and younger who took oral contraceptives had an increased risk of Retinal Vascular Occlusion.
The article concludes that women who use hormonal birth control should have a comprehensive eye evaluation with routine imagen exams. How many health care providers are considering a patient’s ocular personal history before prescribing hormonal birth control for contraception or other reasons?
“Kelly knows she isn’t going to get a guy if she sticks with that, right?”
Those were the words spoken by the boyfriend of one of my friends in college. He had just learned that I was one of those religious “oddities” who not only went to Mass, but also believed the Church’s teachings that sex was intended only for within the confines of marriage, and then with an openness to life.
Fortunately, I knew enough young couples who had also chosen to follow this apparently unthinkable path, so I was unconcerned by his incredulous proclamation. However, I was struck by the sincerity with which he declared it. There was no doubt in his mind, and clearly not in the minds of many of my girlfriends, though they halfheartedly assured me otherwise, that the Church was condemning me to a life alone by forcing this antiquated worldview upon me. The irony, of course, was that in the name of my freedom, they thought I should compromise my principles in order to snag myself a man who would not have wanted me had I stayed true to my faith. I was unconvinced by this logic, but my heart broke for them for believing it.
Like so much in our culture, sex has become entirely self-focused. No longer aimed toward the higher goods of bonding within marriage and bringing about new life, it has been reduced in importance, such that women — and men — are mocked for reserving it for after the wedding. But in a perverse twist, it has been simultaneously magnified in necessity, such that a dating relationship without it is nearly unheard of in most circles.
Kate Bryan, the author of Living the Feminist Dream and the founder of 1 Girl Revolution, was committed to the virtue of chastity in high school, but her view of it at the time was more one-dimensional. She saw it as a good thing, but, to her, it was a system built upon the notion of what not to do. Over time, this evolved as her understanding of the theology behind chastity further developed during her college and young professional years.
“I’ve learned that chastity is a perfection of love. It’s not just a list of dos and don’ts,” she told the Register.
Threaded throughout all of Church teachings is the truth that every man and woman is created in the image and likeness of God, and thus imbued with a dignity that is meant to be protected and valued, not degraded. Therefore, every element of the Catechism is designed not to be a ledger of rules to get us to heaven, but as a holistic and divinely revealed set of teachings grounded in the natural law and intended to uphold and defend the dignity of every man, woman, and child, born and unborn. Church teachings on chastity are no different. The Catechism of the Catholic Church defines chastity as “the successful integration of sexuality within the person and thus the inner unity of man in his bodily and spiritual being” (2331-2334).
In her years working in both Washington, D.C., and Detroit, Bryan has seen how the desire for love often leads to lowered expectations in relationships, especially for the young women she knows. “[Women] want love so desperately, and we lower our expectations, and, honestly, we often put up with bad behavior. We have a responsibility to stand up and demand better.”
For a generation of young men and women, coming of age in the “hook-up culture,” the highest standard for sex in this view is that it be “consensual.” But it’s difficult to demand fidelity and love from a girl you just met or from the guy that refuses to commit to a relationship, and it’s often even impossible to know that is what you are owed if you live immersed in a world where sex is depicted as an act intended merely for pleasure, not as an unconditional gift of self, to say nothing of the creation of a child.
Yet despite the incessant cultural messaging that both trivializes sex and makes it the pinnacle of the human experience, Bryan notes that the message of chastity, as taught by the Church, will always resonate with young men and women seeking true relationship. “No matter who you are, everyone is looking for love. We’re made to love and be loved.”
“[Love and Responsibility] held an event near UCLA to attract more college students, and it was heartbreaking,” Bodenhammer recalled. “We got girls sharing in Q&A about their struggles with unhealthy relationships, and we want to help women to see their own value and worth and know they do not need to seek it out in a man and instead should find it in God.”
These discussions were a driving force behind Love and Responsibility, named after the great work by Karol Wojtyla (St. John Paul II). The mission is to spread the message of dignity and cherishing of the other that is enshrined within the Church’s teachings on sexuality and chastity. And it’s a message that men and women are responding to. Bodenhammer recalled one young man who was thrilled by the primacy of relationship and communication in chaste relationships. He shared that he loved having wonderful conversations with the women he went on dates with and how he enjoyed making them laugh. When asked if she could pick one takeaway for the men and women who participate in the group’s events, Bodenhammer responded: “All people are created with value, and we’re not meant to be used. There is so much utilitarianism in this culture, and we want to make sure both men and women know that they are meant to be cherished and valued on a deeper level in a relationship, where they are hopefully led closer to God. as well.”
For Tasha Tormey, a young woman living in Los Angeles, her faith and a strong community have been sources of strength in her commitment to chastity while dating. She encourages other young men and women on the same path. “Get as involved in Catholic community as soon as you can, and make friends with other Catholics and Christians who are striving to live chastely,” she advised.
Tormey also recognizes that far from being an optional guideline to follow, as too many young men and women raised in Catholicism have come to think, chastity is a prerequisite both for true love and for full communion with the Church.
“Because I am Catholic, I strive to accept all the Church teachings. I also know that God wants us to love, and only the chaste can love truly, without confusing lust or sentimentality with real love. It is definitely a hard teaching to accept, but if I were to live without chastity, I would not be able to receive the greatest gift there is: the Eucharist. When we have God present with us on earth, we must do all we can to be in a state of grace to receive him.”
In my own work with young women and high-school girls, the questions I am most frequently asked circle around how to enjoy dating and pursue good relationships while remaining confident in their principles (and these struggles are shared by young men, as well). They are bombarded on all sides by a culture that encourages “sex positivity” and tells them that any messages of chastity and sexual restraint they hear are from nefarious forces determined to hamper their freedom, not nurture their souls. The answer lies not just in explaining the Church’s teaching to them. Though that is a critical step, it is not sufficient. They must be taught not merely the “what” of the rules, but the why behind them. To quote St. Paul, that most bold author of epistles, “… the letter brings death, but the Spirit gives life” (2 Corinthians 3:7). Young men and women must be taught not just what not to do, but also to whom they belong and how they are called to honor and defend the dignity of everyone they encounter.
New evidence is demonstrating there’s a strong correlation between happiness and large families, and the link between both is religious faith. In tonight’s In-Depth Report, Church Militant’s Paul Murano examines the social science, which lends further proof of the Church’s divine wisdom.
A new survey from the National Opinion Research Center reveals two basic things: A happy population is one that flourishes with procreation, and Americans are now less happy than they’ve been in over 50 years.
Nastasia Grace, YouTube personality: “Something just pounds on my brain saying, ‘You’re not happy!'”
The data shows an epidemic of loneliness and depression — exacerbated by COVID lockdowns — has taken its toll. Only 19% of Americans say they’re very happy while 24% admit they’re not too happy.
Boiled down, the survey shows two primary causes: a lack of faith and a breakdown of the family.
Steve Hilton, host, The Next Revolution, Fox News: “And we see the disaster all around us — the kids without fathers, the broken homes, the impact on their lives.”
With regard to faith, psychologist, professor and author Dr. Lisa Miller found religious people are much less likely to suffer major depression and that religiosity actually thickens the cerebral cortex.
Sadly, a recent Pew Research poll shows almost a third of American adults have no religious affiliation. And a lack of faith is linked to a lack of children.
America’s annual birth rate fell six straight years, reaching its lowest point ever in 2020. It’s now half of what it was in the early 1960s — before the sexual revolution began with the birth control pill.
Kent Niebuhr, Catholic father of seven and former stay-at-home dad: “It makes sense that having more children would make you happier because it really pulls away the disillusions of pursuing happiness in material things.”
And fewer people are getting married. According to a 2020 report from the Institute for Family Studies or IFS, never-married adults increased over 100% since 1970. And it’s no surprise since the divorce rate hovered at around 50%.
It’s also no surprise that sins of lust are primary factors in divorce. A 2019 Florida State study found attitudes toward premarital sex are a major factor. This was confirmed in a 2019 IFS survey showing married couples who’ve had sexual relations only with their spouses were markedly happier than those who had other intimate partners before marriage. Further, couples using artificial contraception are much more likely to divorce.
These studies prove what has always been true: People who live contrary to Catholic doctrine cannot be happy.
The average fertility rate in America has been decreasing since the industrial revolution from seven children per family in 1800 to around four in 1960, to less than two in recent times. More technology doesn’t always mean more flourishing and happiness.
In the 1400s the printing press revolutionized Europe, enabling mass distribution of printed material fast. The Reformation roiled Europe in the 1500s, in no small measure due to Gutenberg’s invention. In the wake of Martin Luther and Ulrich Zwingli came a variety of sects, including the radical Anabaptists, who believed in adult baptism and strict separation of church and state. In 1693 the Anabaptists splintered into three sects, including the followers of one Jakob Ammann. They called themselves Amish.
About the Amish
Amish organize into districts governed by an Ordnung (set of rules) that governs personal attire, domestic life, and work. Today the Ordnung forbids use of electricity, automobiles, telephones and a range of modern labor-saving devices. The Ordnung must be strictly obeyed under penalty of shunning or even excommunication. Implementation of the Ordnung may vary in different communities. It is intended to promote the virtues of hard work, humility, rural life, and separation from the world. Their inspiration comes from James 1:27: “To keep oneself from being polluted by the world” (NIV).
Weary of persecution and the world around them, in the mid-1700s about 500 Amish arrived in the New World, settling mostly in Pennsylvania. In the 1800s about 1500 more came, settling in the Midwest. Most Amish are descended from about 200 families who crossed the Atlantic.
Population and fertility
“Over the last century the Amish population has doubled on average every 19.63 years,” according to the Young Center for Anabaptist and Pietist Studies at Pennsylvania’s Elizabethtown College, which further states:
“The North American Amish population grew by an estimated 183,565 since 2000, increasing from approximately 177,910 in 2000 to 361,475 in 2021, an increase of 103.2 percent.”
In 1992 there were 125,000 Amish in the US. By 2020 there were 350,000, an almost 180 percent increase. The US population increased approximately 29 percent during that period, thus the Amish population growth rate was six times that of the US (including immigration). That is exponential population growth, though it begins from a very low base.
Today there are 375,000 Amish in America.
Amish live in districts, each comprising roughly 30 families. When a district surpasses that, a new district is formed. A new district is founded every 3.5 weeks. Associated districts form settlements. From 2000 to 2021, the Amish gained 290 new settlements. Present in 31 US states, they have recently established districts in four Canadian provinces and single districts in Argentina and Bolivia.
At home the Amish speak a form of German known as Pennsylvania Dutch. Due to their rural customs, personal privacy (Amish do not keep photographs as they are believed to cultivate vanity) and lack of technology, surveys of the Amish are an inexact science. Several groups may be considered a variant of Amish, but with fertility research the accepted criteria for Amish is that they speak Pennsylvania Dutch and have no household phones. That group consistently averages close to seven births per female.
Were the Amish a separate country, they would be right up there with Niger (6.9) contending for the world’s highest fertility rate. Amish fertility was the basis for demographer Lyman Stone’s 2018 paper “How Long Until We’re All Amish?”
I occasionally encounter Amish in my travels, and once visited a workshop where a father and his four sons made buggy wheels. They were back-ordered for months.
Reasons for population growth
Like other Christians, Amish see children as a gift from God.
Their lifestyle incentivizes having children. Without the efficiency and productivity of technology, children are essential to work the farm, do the chores and look after their parents in old age. (Amish do not participate in Social Security.) Simply put, they value familial cooperation through labour over efficiency and productivity. Requiring more labour (children) engenders cooperation and close familial bonds without the worldly distractions of university, cinema, social media, bars, etc. There is no social atomization among the Amish. They believe that labour-saving technology would breed idleness. Amish are exempt from schooling past the eighth grade by the US Supreme Court’s ruling in Wisconsin v. Jonas Yoder, 406 U.S. 205 (1972).
Another growth factor is that Amish have the highest retention rate of any religion or denomination in America at almost 90 percent. In adolescence Amish youth are allowed to leave their communities virtually free of constraints in a rite of passage called Rumspringa (jumping or hopping about). Baptism comes after they return.
Conclusion
There is evidence of some very slight decline in Amish fertility, though similar declines have been previously observed. Provided the current Amish growth rate holds, in 215 years their population is projected to be larger than the current US population of 327 million. It would be interesting to stick around and see if that pans out.
Amish farms and businesses are usually quite profitable. They pay cash for farms. Amish have the lowest rates of depression, anxiety, and schizophrenia of any American demographic.
The Amish are not without critics. Some regard them as a cult. Like any population, they are not immune from occasional criminal or deviant behavior. Conformity is expected or demanded, depending on your point of view. Those who stray from the Ordnung are shunned (a traumatic ordeal) or even excommunicated. They keep to themselves and do not proselytize or encourage outsiders to join. They are pacifist and do not serve in the military. A small number leave Amish communities as adults.
After observing life among the Amish, Business Insider published an article headlined, “If you want to be happier, should you be a billionaire or be Amish?”
The Amish are obviously doing something right. Their faith and largely pre-modern lifestyle works for them.
What works for the rest of us?
Louis T. March
Louis T. March has a background in government, business and philanthropy. A former talk show host, author and public speaker, he is a dedicated student of history and genealogy. Louis lives with his family… More by Louis T. March
In a recent article published in the Institute of Family Studies, the author showed that marriage and especially parenthood reduce the suicide risk. Jason Manning, Associate Professor of Sociology at West Virginia University, and author of Suicide: The Social Causes of Self-Destruction wrote: “For over a century, at least since the pioneering work of French sociologist Emile Durkheim, we have known that social bonds—or their absence—plays a crucial role in suicide.”
Some highlights of the article:
In the US, the risk of suicide for separated or divorced people is near twice that for married
people.’
A study of a birth cohort of 1.5 million Swedes found that parenthood lowered suicide risk for
both men and women, and that having two children lowered the risk more.
While abusive or dysfunctional relationships are dangerous, the evidence shows that the
bonds of marriage and parenthood generally reduce the risk of suicide.
Pregnancy. An injury? Run-of-the-mill event? Special circumstance? Choice? A recent report in the National Post highlighted the indignation of Olympic athletes in learning that pregnancy is often categorized by the I-word — “injury” — in their contracts.
“It’s not an injury, it’s a decision that’s made,” Canadian field hockey player Kate Gillis said.
Fair enough. As a decidedly non-elite sports enthusiast, I’d still hate to see my various sports injuries made equal with gestating a new soul. Yet the article reveals a bigger problem we have with the basics of addressing pregnancy and childbearing in the policy.
Overlooked
We don’t have a category for it. We struggle with how to make special arrangements around it, and frankly, whether to do so at all. Pregnancy and childbearing are confusing propositions today.
This becomes clear in many different corners. An opposing view to pregnancy-as-injury is pregnancy-as-invisible. Whether it’s a dear friend who sang opera on stage two days after giving birth, or New Zealand’s Prime Minister Jacinda Ardern, who was back to work in weeks, not months, these Super Women lead the rest of us to believe pregnancy is easy peasy lemon squeezy. For some women, it is, of course. I wasn’t one of them. In the latter stages of pregnancy, I found it difficult to shuffle to the bus stop. This alone quickly ruled out the possibility of running my own household, let alone a country.
Working mums
If I were running a country (which clearly I’m not) I’d aim to tackle maternity benefits delivered via unemployment insurance, as if giving birth were a routine part of losing a job. Ironically, benefits delivered in this way also cement ideas about a return to work in the government’s chosen timeframe, not yours. Why is a year-long maternity leave standard? Because the government made it so.
Is there no middle ground? In an earlier era, women who got pregnant were immediately let go. Now we have “golden handcuffs” and we return to routine waged work quickly. Pumping breast milk in a closet is sometimes not possible, sometimes not desirable. There are reasons why some European countries offer three years’ leave.
Career first
It is harder and harder for adolescents to move into adulthood, including the formation of families of their own. The average age at first marriage is rising, now 31 for men, almost 30 for women. Difficulties getting married delay childbearing too, which means women by default, not necessarily a choice, cannot have as many children as they might like. When you have your first child at 43, the likelihood of having more is slim to none.
This hints at another problem we have with pregnancy and children, treating it as something that inhibits real life rather than contributes to it. So many young people are waiting to start a family until they have solidified other aspects of working life.
This makes it little surprise that Canada’s fertility rate fell in 2020 to an all-time low of 1.4. (Replacement fertility for a country is 2.1 births per woman.) Having fewer children normalizes never seeing children and not knowing what to do with pregnancy and childbirth. It’s a vicious cycle.
Furbabies vs human babies
I could go on and on about the problems — after all, I haven’t even mentioned feminism, the Pill or abortion yet. Yet for better or worse, it’s into this messy, confusing environment that we hear Pope Francis say having a pet is selfish. Except he didn’t quite say that at all.
Rather, he said that all too often we claim to not have room in our homes for orphans, whilst simultaneously having two dogs and two cats. It was a bit more of a lighthearted remark in a homily dedicated to highlighting that no child should grow up parentless.
The problem I have with the pontiff’s remarks is not that he is incorrect, but that there is virtually no audience for his words. The media response, replete with a newly created pet owners guild defensively arguing that having a pet is very meaningful indeed, may only prove this point.
For calls to defend orphans to fall on fertile ground, pardon the pun, we need to have a media that actually value marriage, family, and children in the context of an ongoing robust discussion of what it means to normalize marriage, family, kids, and their care.
And that, ultimately, is what I view as the real and, unfortunately, far bigger conundrum than how to treat Olympic female athletes who get pregnant. Until we gain a shared vocabulary for understanding mothers, fathers, marriage, and families, until children are so ubiquitous that finding workable solutions is unavoidable, we will continue to find tired administrators filing pregnancy under “I” for Injury, much to our dismay.
Pope Francis caused a great deal of consternation among population control activists when he recently called out the growing trend of replacing human babies with what are sometimes – somewhat nauseatingly – referred to as “fur babies” – i.e. pets.
“Today we see a form of selfishness,” said the Pope at a public audience in early January. “We see that people do not want to have children, or just one and no more. And many, many couples do not have children because they do not want to, or they have just one — but they have two dogs, two cats … Yes, dogs and cats take the place of children.”
“[T]his denial of fatherhood or motherhood diminishes us, it takes away our humanity,” he added.
The remarks caused quite the media furor. In an op-ed published on CNN, Alistair Currie, the head of campaigns and communications at Population Matters, declared pompously that the Pope’s comments “are wholly wrong.”
According to Currie, choosing to have few or no children is always and everywhere the selfless choice. “[T]he choice to have a small family, or no human family at all, is one that helps everyone,” he wrote, “particularly children, whose future depends on a more sustainable planet.” He adds that “showing love for animals is surely something that enhances and demonstrates our humanity – rather than diminishing it.”
Let me see if I have this right: On the one hand, choosing to have children is an inhumane choice, particularly towards children (who will suffer if we beget them). But, on the other hand, choosing to have non-human pets is a humane choice that demonstrates our humanity.
Now, I don’t disagree that a rightly ordered love for animals can indeed enhance our humanity. However, the idea that loving animals enhances our humanity, while loving human children enough to bring them into existence is somehow inherently selfish and inhumane, betrays some remarkably muddy thinking.
It is particularly puzzling when you consider that animals, too, consume resources. There are hundreds of millions of dogs and cats globally. And as one article put it, “What cats and dogs eat annually generates the same amount of carbon emissions as a year’s worth of driving 13.6 million cars.” It seems to me that if we are as deadly serious about reducing our carbon footprint as Currie wishes us to be, we should not be raising animals that serve no practical purpose.
I’m not serious, of course. But if we are going to endorse such an extreme position as that every human child threatens the planet, then we ought to be consistent, and acknowledge the environmental harms of pet ownership as well.
The Risk of Childlessness
In his remarks during that audience, the Holy Father put in a plug for adoption. “How many children in the world are waiting for someone to take care of them,” Pope Francis said. “Having a child is always a risk, either naturally or by adoption. But it is riskier not to have them. It is riskier to deny fatherhood, or to deny motherhood, be it real or spiritual.”
What a wonderful way to think about “risk” in conjunction with parenthood!
As I wrote a few weeks ago, when thinking about welcoming children many young couples can only see the innumerable “risks”: of financial hardship, of lifestyle changes, missed vacations, sleepless nights, and a lifetime of worry about that child’s welfare.
One the one hand, this is understandable. There is something about the idea of co-creating a whole new human being that is so inconceivably mysterious and consequential that it causes the head to spin. A couple, by uniting together in a fleeting physical union, can bring into being an immortal human being: one with his or her own personality, desires, ambitions, talents; a whole new life that will impact the lives of countless people in potentially life-changing ways, beginning with the parents. Looked at this way, the risks do seem enormous.
However, we can also turn this whole idea on its head. If the risks of welcoming a child are too huge to take, then what about the risks of not welcoming a child?
Decision theorists often point out that every choice comes with an “opportunity cost.” That is, when you choose one thing, you necessarily forego everything entailed by the alternatives. There are no “riskless” decisions. To choose to avoid the “risk” of parenthood, is to assume the “risks” involved in sterility.
And what are the risks of sterility? Well, the non-existence of a potential child who could have been, and all that that entails: the non-existence of the experience of parenthood for the parents; the non-existence of a brother or sister, nephew, or niece; the non-existence of countless experiences and memories; the non-existence of a potential carpenter, engineer, artist, mother or father; the non-existence of grandchildren and great grandchildren.
And on and on. An inexhaustible list of potential losses.
The Unanticipated Rewards of Parenthood
This does not mean, of course, that there are not sometimes very good reasons to postpone welcoming a child. The Church has always encouraged “responsible parenthood.” But it does mean that we must be honest and clear-sighted in weighing the risks: if welcoming a new life into the world seems too risky to venture, that also implies that it might be too risky not to venture! We only live one life, and the choice not to welcome children means to forego one of the most meaningful of life’s experiences.
In my line of work, I often have the chance to speak with parents who, at some point, either aborted a child, or avoided welcoming children by contracepting. I also have the opportunity to speak with many parents who unexpectedly became pregnant at a time when they were trying to postpone pregnancy, but who faced the challenge and welcomed the child.
It is heartbreaking to hear the deep regret from those first parents, who later realized that they desperately wanted the child they aborted, or who realized they wanted children, but only when it was too late. On the other hand, it is deeply moving to hear the stories of parents who found themselves with an unplanned pregnancy, and yet who accepted the great adventure of new life.
Their stories are not always easy. Children can come at times of great hardship: in the midst of serious illness, or severe financial difficulties. And yet, in the end, there is the child: a whole other human being, to know and to love; a whole other person who brings a new life and light to the family, contributing a personality and gifts that no other person could. A child that, in time, learns to give back to his or her parents; to love them as they age; to give them grandchildren.
“Children are really the supreme gift of marriage and contribute very substantially to the welfare of their parents,” wrote the Second Vatican Council Fathers in Gaudium et spes. “Hence, while not making the other purposes of matrimony of less account, the true practice of conjugal love, and the whole meaning of the family life which results from it, have this aim: that the couple be ready with stout hearts to cooperate with the love of the Creator and the Savior. Who through them will enlarge and enrich His own family day by day.” (no. 50)
Many couples who nearly aborted a child, later say that that child turned out to be the “greatest gift” of their lives, the gift that brought unanticipated joy, who in some cases got them to turn their lives around in dramatic ways.
Embrace the Adventure
G.K. Chesterton once wrote that an adventure is simply “an inconvenience rightly considered.”
There is no doubt that there are many “inconveniences” involved in parenthood. It is even true that a human being does consume resources, and that the number of humans on the planet can present an environmental challenge. However, this is not a challenge that is best avoided by deliberately getting rid of the humans that present the challenge. It is, rather, a challenge to be solved by the humans who are welcomed into the world by parents who have discerned, in a spirit of adventure, that welcoming a child is a risk worth taking.
As Pope St. Paul VI put it in Humanae vitae: “The transmission of human life is a most serious role in which married people collaborate freely and responsibly with God the Creator. It has always been a source of great joy to them, even though it sometimes entails many difficulties and hardships.” (no. 1)
From the very beginning of Genesis, with God’s command to “be fruitful and multiply,” the Scriptures and Tradition have always cultivated a radical belief in the goodness of human life. To be parents is essentially to receive a gift that gives a new prospect of love, understood from the lens of reciprocal generosity and gift of self.
Rather than discouraging couples with the doom and gloom anti-natalism of eco-extremism, we should be encouraging in our young this spirit of “adventuresomeness,” encouraging them to be open to welcoming the unfathomable gift of new life, should God so bless them with so great a gift.
It is undeniable that marriage and family in contemporary society are under constant attack from a poor, limiting, and unsatisfying understanding of the truth about the sexual life and conjugal love. Only by “pricking” the consciences of persons and society – as Pope Francis did – can we hope to awaken the desire for what is good, true, and beautiful about marriage, family, and children.
I conclude with an appeal made by Pope Benedict XVI to European government leaders in 2007. The Holy Father’s challenging words remain valid today, not only for European leaders but also for all countries and government leaders, especially those that promote secular ideologies which assault the dignity of marriage and family life and the sanctity of human life. Let us pray Benedict’s petition to build a Culture of Life will not fall upon deaf ears and hardened hearts but, instead, be welcomed and realized.
[Do] not allow children to be considered as a form of illness … do everything possible to make European countries once again open to welcoming children … to favor conditions enabling young couples to raise children … All this will be pointless, unless we can succeed in creating once again in our countries a climate of joy and confidence in life, a climate in which children are not seen as a burden, but rather as a gift for all.
Nearly 70,000 chemical abortions are committed annually in California (50% of all abortions committed in the state), according to a study sponsored by the University of California San Francisco (UCSF), which trains abortion providers through its Bixby Center for Global Reproductive Health. The information comes from a clinical trial sponsored by UCSF called the CHAT Study, which stands for California Home Abortion by Telehealth.
“CHAT is the first study of its kind in the U.S. that will evaluate abortion medication by mail without the need for a doctor’s visit or ultrasound,” a fundraising page for the study states.
UCSF wrote about the trial, “The study will aim to reach a diverse sample of medication abortion patients across the country in states where care is provided including California, New York, and Washington, thus far. In California alone, an estimated 50% of all abortions are medication abortions resulting in >66,000 medication abortions per year. California accounts for 20% of the nation’s medication abortions.” (emphasis added)
California is not required to report abortions in the state and these numbers are therefore not factored into data published by the Centers for Disease Control and Prevention (CDC), which recently noted that chemical abortions comprised nearly 44% (43.7%, to be exact) of abortions reported to the CDC in 2019.
UCSF abortion pill study 66K chemical abortions in California a year recruits girls as young as 13
California has vowed to be a sanctuary for abortion and recently formed the California Future of Abortion Council initiative. In 2019, Live Action News reviewed reports published by Medi-Cal, a California state taxpayer-funded program for low-income children and adults, and found that in just the state’s Fee for Service (FFS) Program, taxpayers paid nearly $700 million for abortions over 25 years, from 1989 to 2014.
California Home Abortion by Telehealth (CHAT) Study
The CHAT study, which it is expected to be completed in October of this year, aims to “assess efficacy and safety outcomes of a telehealth model of abortion care,” and “will compare efficacy of this model to usual in-clinic care based on published rates. It will also investigate participant acceptability and feasibility of this model of care.”
The CHAT study is sponsored by UCSF and is being overseen by Ushma Upadhyay and Jennifer Ko. It is recruiting “females ages 13 years and up.” Upadhyay is an Associate Professor at UCSF’s Advancing New Standards in Reproductive Health (ANSIRH). ANSIRH is part of UCSF’s Bixby Center for Global Reproductive Health. In 2019, well before the COVID-19 pandemic, Upadhyay advocated a “no test/no touch” approach where she and her colleagues suggested that abortion providers should simply “believe the woman” about the exact dating of her pregnancy.
“We will examine medical chart data on all patients from partnered telehealth providers to analyze efficacy and safety outcomes for medication abortion. These medical chart data will include medical/pregnancy history and abortion outcome and de-identified apart from date of birth, zip code, and dates of service,” the sponsors wrote on the trial website.
Then, each telabortion client will receive an optional survey “following completion of the telehealth provider’s standard medical screening.”
The study sponsor claims, “Among those who complete the study surveys, we will investigate the feasibility, time to abortion, efficacy, safety, and acceptability of telehealth provision of mifepristone, measured using a 4-week follow-up though open-ended and closed-ended survey questions. Individuals who opted not to take the medications will be asked a separate set of follow-up questions to collect data related to diversion, to better understand potential risks.”
“With the recent announcement that the FDA is planning to review the REMS requirement, we are at a pivotal moment for the future of abortion care and reproductive autonomy…” Upadhyay previously wrote. “On May 1st 2021, clinical data collection to assess the safety and efficacy of telehealth abortion care commenced. This is the data that the FDA is interested in. We’ll be able to get it in front of them.”
UCSF partners with virtual chemical abortion pill Choix
UCSF is partnering with multiple virtual abortion pill dispensaries to recruit teens and women for their CHAT study, including Choix Inc., HeyJane, and virtual abortion pill website Abortion on Demand (AOD).
A Satanic cult leader and well-known abortion activist shocked Michigan news watchers over the weekend when she took an abortion pill on live TV during an interview with Fox 2 Detroit.
Blackmore appeared on the station’s “Let It Rip” program to debate pro-life advocate Rebecca Kiessling on the anniversary of Roe v. Wade, the U.S. Supreme Court ruling that forces states to legalize abortion up to viability.
In the midst of their debate, Blackmore held up a pill that she said was mifepristone, the first of two abortion drugs taken to abort unborn babies up to 10 weeks, and swallowed it on-air with a smile, according to the blog.
“I want to show you how easy it is, how safe it is, by taking it myself,” she told host Charlie Langton.
“You’re taking it? Are you-?” an obviously shocked Langton responded. “You’re not pregnant, are you?”
So many of us have the deep desire to have biological children of our own. It’s what drives hundreds of thousands of couples to use IVF to create their children. Still others, despite their wishes for a biological child, turn to adoption. Both options can be incredibly expensive, but from an ethical standpoint, the human toll of IVF makes adoption the morally sound option.
The death toll from IVF
The most glaringly obvious issue with IVF is the death toll that accompanies it. IVF is used by couples to create life, and those who turn to IVF may have good intentions. But its failure rate and the (often required) destruction of certain embryos means more human beings are destroyed in their embryonic life stage than are born.
Each round of IVF only carries a 20-30% chance of successful birth and couples can create up to 20 embryos to increase their odds — but most couples don’t want 20 children. As a result, while an estimated one million valuable and worthy people have been born thanks to IVF, 1.7 million have died, and another one million are said to be currently frozen in the United States while their parents decide if they still want them.
Some embryos simply don’t survive the IVF process on their own. Others are killed for having certain genetic traits such as cystic fibrosis or other genetic conditions the parents are trying to weed out by using IVF. Others meet death after being donated to scientific research. Others have died when the storage containers they were in malfunctioned. In some instances, when more than the desired number of embryos implant and grow, parents will abort the “extras” through selective abortion. These embryos and fetuses are human beings created to fulfill the desires of adults, and whose lives are lost, destroyed, or abandoned in the process.
The physical toll of IVF on children
The children who do survive the IVF process do not always escape its physical effects. Children created through IVF have increased risk of low birth weight, premature birth, hospital admission, perinatal mortality, cerebral palsy, and “significantly” increased risk of birth defects compared to children conceived naturally. They are also at risk for high blood pressure, and girls conceived through IVF sometimes have advanced bone age and hormonal imbalances during puberty.
Some studies have also shown an increased risk of childhood illnesses for all children born through IVF, including an elevated risk of cardiovascular problems, early-onset acute lymphoblastic leukemia, an increased risk of cancer in general, epigenetic disorders, cognitive impairment, and possible infertility of their own.
The emotional toll of IVF
The IVF process is often spoken about as emotionally and physically taxing for the adults involved, but the pain is considered to be worth it because they (sometimes) get to have their baby. But there are psychological and emotional issues for children created through IVF that few parents know about or consider. Claire, who was conceived through IVF, explained that she always knew her parents loved her and wanted her, but that learning about her conception caused her emotional pain. She said:
Somehow, somewhere, my parents developed the idea that they deserved to have a baby, and it didn’t matter how much it cost, how many times it took, or how many died in the process. They deserved a child. And with an attitude like that, by the time I was born they thought they deserved to have the perfect child… as Dad defined a perfect child. And since they deserved a child, I was their property to be controlled, not a person or a gift to be treasured.
In addition to feeling like a consumer product, children conceived through IVF have an increased risk of ADHD, autism, and depression.
IVF is seeking to fulfill the wants and desires of adults who feel they deserve a baby and because of this, IVF creates wounds. It harms children both physically and emotionally, but it continues to happen because creating children has become a billion-dollar industry.
Adoption, on the other hand, attempts to heal wounds that were already created. Katy Faust, founder of Them Before Us and author of the book by the same name, explained, “Adoption should be sought only when all avenues to keep the child with their family of origin have been exhausted. The trauma a child faces when they’ve lost a relationship with their biological parents should not be minimized or ignored.” She states that adoption, when it is “properly understood” is “child-centric” not simply a way for adults to become parents. The prospective adoptive parents are not the true client in adoption as in IVF. The children are. This is why prospective adoptive parents go through a screening process and home visits and training. Parents using IVF don’t.
“For the child, adoption begins with great loss,” Faust continued. “Adoption is society’s attempt to mend that wound. However, while adoption is the best case scenario for a child in need, adoptive parents — no matter how loving — cannot fully compensate for the loss of the child’s first family.”
With this knowledge, adoption agencies and the foster care system evaluate which parents are best for which child — to find a family that can help heal the child’s wounds from the loss of her biological family. If a couple struggling with infertility is choosing between adoption and IVF, adoption is the more ethical path, but that does not mean it comes without challenges.
Ultimately, while a person’s desire to have a biological child is as understandable as a child’s right to know their biological parents, the IVF process causes far too much damage for the ends to justify the means. There are thousands of children in the foster care system waiting to be adopted. Life after adoption will not be miraculously perfect, but when adoptive parents acknowledge the trauma these children have suffered, the future can be bright — and no innocent lives had to be destroyed in the process.
Modern forms of non-invasive prenatal tests (called NIPT, for short) are growing in popularity, being used by hundreds of thousands, if not millions, of women every year in the United States alone. These highly profitable tests, which promise parents a glimpse into the future of an unborn child by detecting some type of malformation or genetic abnormality, are aggressively marketed to pregnant women, and in many OB/GYN practices are now routine.
However, a devastating new investigation by The New York Times has found that many of those tests, which are completely unregulated by the FDA, are not remotely as accurate as the biomedical companies behind them would like parents to believe. Marketing materials put out by the testing companies suggest that the tests are “reliable” and “highly accurate.” In reality, however, some of the most common tests return false positives as much as 85-90% of the time, according to the Times’ analysis.
The tests that the Times looked at are blood tests, using blood drawn from the mother in the first trimester of pregnancy. Their allure is that they are significantly less invasive than other forms of testing, such as amniocentesis, which requires drawing a sample of amniotic fluid, and which carries a risk of miscarriage.
One marketing brochure from a testing company promises that the tests can provide “peace of mind” for the parents. However, as the Times notes, parents who receive a positive result often find anything but peace of mind:
In interviews, 14 patients who got false positives said the experience was agonizing. They recalled frantically researching conditions they’d never heard of, followed by sleepless nights and days hiding their bulging bellies from friends. Eight said they never received any information about the possibility of a false positive, and five recalled that their doctor treated the test results as definitive.
Unfortunately, much of this mental suffering is not precipitated simply by the knowledge that their child may be suffering from a serious malformation or genetic disorder. Much of it is due to the feeling of pressure that the parents must do something about it, i.e., they must quickly make a decision whether or not they will abort their child.
In theory, women whose unborn children return a positive result from one of the blood tests are supposed to go on to get more reliable – but still far from perfect – tests, such as those done through amniocentesis: i.e., the removal of a sample of the amniotic fluid. However, one 2014 study found that over 6% of women simply aborted their children without pursuing follow-up testing. No doubt, some of those children were healthy.
This, in turn, leads to a further trauma for the parents – that of discovering that they aborted a healthy child. One Irish couple was described, after aborting their child who was wrongly diagnosed with Trisomy 18, as “utterly, utterly mentally and physically devastated.”
Jeanne Mancini, president of the March for Life, reacted to the Times’ investigation, noting in remarks to the Catholic News Agency that children diagnosed with health problems are “disproportionately targeted for abortion.”
“Parents who receive such a prognosis while their baby is in utero should be given the medical and other supports necessary to allow them to cherish the gift of life, but most often they are not supported in this way,” Mancini lamented. “That prenatal tests are consistently erroneous adds an even deeper level of tragedy to the wrongful pressure on parents to abort. In the end, every life is a gift and deserves protection — regardless of disability.”
Catholic Teaching on Prenatal Testing
Catholic teaching does not necessarily oppose the practice of prenatal testing, acknowledging that it does have its valid uses and applications. However, the temptation to misuse prenatal testing is a serious one, which requires that the decision to carry out such testing be made very carefully and within a limited set of circumstances.
This concern about the potential misuse and abuse of prenatal testing was raised by the Vatican’s Congregation for the Doctrine of the Faith (CDF), in its 1987 document Donum vitae, which urged significant caution. The document noted that prenatal diagnosis can make it possible “to anticipate earlier and more effectively, certain therapeutic, medical or surgical procedures.” In such a case prenatal diagnosis “is permissible,” albeit only “if the methods employed safeguard the life and integrity of the embryo and the mother, without subjecting them to disproportionate risks.” (DV, I, 2)
Donum vitae adds that such testing “is gravely opposed to the moral law when it is done with the thought of possibly inducing an abortion depending upon the results.”
Thus, a woman would be committing a gravely illicit act if she were to request such a diagnosis with the deliberate intention of having an abortion should the results confirm the existence of a malformation or abnormality. The spouse or relatives or anyone else would similarly be acting in a manner contrary to the moral law if they were to counsel or impose such a diagnostic procedure on the expectant mother with the same intention of possibly proceeding to an abortion. So too the specialist would be guilty of illicit collaboration if, in conducting the diagnosis and in communicating its results, he were deliberately to contribute to establishing or favouring a link between prenatal diagnosis and abortion. (DV, I, 2)
Prenatal diagnosis is permitted when the procedure does not threaten the life or physical integrity of the unborn child or the mother and does not subject them to disproportionate risks; when the diagnosis can provide information to guide preventative care for the mother or pre- or postnatal care for the child; and when the parents, or at least the mother, give free and informed consent. Prenatal diagnosis is not permitted when undertaken with the intention of aborting an unborn child with a serious defect. (2018, no. 50)
The New Eugenics
As Donum vitae and the Ethical and Religious Directives suggest, prenatal testing is not inherently problematic. In a truly tolerant and humane society, such testing could be used to develop or administer treatments to those children that are diagnosed with medical problems, or to help prepare the parents to face the challenges of caring for a child with a disability.
Therefore, a “diagnosis which shows the existence of a malformation or a hereditary illness must not be the equivalent of a death-sentence.” (Donum vitae, I, 2) However, this is not what many parents experience who receive a serious prenatal diagnosis. Instead, they are often told that their child’s disabilities are “incompatible with life” or that the child has a “fatal anomaly.” In many cases, the label “incompatible with life” reflects a judgment of quality of life, not an actual medical diagnosis, and children whose diagnoses are labeled “incompatible with life” are also at risk for being denied basic life-saving treatment.
Unfortunately, in our anti-life society astonishing advances of medical science are being used not to protect, but to attack human life.
Moreover, the financial and legal incentives in our highly litigious culture actually favor the aggressive identification of prenatal abnormalities, and the proactive presentation of abortion as a possible reaction to a positive test. If testing companies fail to detect a disorder, or if an OB/GYN fails to present abortion as a “solution,” there is always the risk of a so-called “wrongful birth” lawsuit. In some cases, doctors have had to pay huge sums in damages, because they did not give a woman the option to abort a child that she later realized she would have aborted.
As I have often warned, the rise of routine prenatal screening for health problems and genetic disorders has ushered in a new age of eugenics – a eugenic movement hidden behind a soothing veneer of lab coats and sterile clinics. In some cases, prenatal testing has given rise to what can only be called a “genocide.”
I do not use that term lightly. A genocide is defined as the attempted destruction of a particular group of people. What else are we to call the systematic elimination of as many as 90% of children diagnosed in utero with Down Syndrome? In some Western countries, such as Iceland, children with Down Syndrome have all but disappeared.
However, our modern technocratic eugenicists do not want to stop at Down Syndrome. They hope to eliminate all genetic disease, not by eliminating the disease itself, but rather unborn children diagnosed with that disease. And their primary tool for accomplishing this is widespread prenatal testing.
Offering Hope
Although I am grateful that The New York Times has shed the light of truth on the shoddy prenatal testing industry, I also acknowledge that prenatal testing likely isn’t going anywhere anytime soon. The technology exists, and though it is currently wildly inaccurate, it will likely be improved over time.
As a movement, we must do everything in our power to shift the conversation on prenatal testing, ensuring that every prenatal diagnosis is received within a culture that champions the right to life of every child, including those with disabilities.
More specifically, we in the pro-life movement must find ways to give hope to those parents who receive difficult news. One pro-life organization already doing just that is Be Not Afraid, which calls themselves a non-profit “supporting parents carrying to term following a prenatal diagnosis.”
“We believe that every baby is a gift,” they state on their website, “and we support parents not only in advocating for basic care, but also in obtaining the treatment they deem appropriate for their child after birth no matter the diagnosis.”
If you aren’t familiar with Be Not Afraid, go check out their work. Their website contains a wealth of information about prenatal testing, and about the many genetic disorders that children may suffer in the womb. Sadly, many parents who receive a prenatal diagnosis are left to navigate the aftermath without any support – indeed, often while being pressured by their doctors to do the “right thing” and abort the child.
The existence of Be Not Afraid is further evidence of the remarkable ingenuity of this great “movement for life,” as Pope St. John Paul II called the pro-life movement, with so many brilliant pro-life minds responding to so many different forms of attack on human life by offering their unique gifts.
Let us work and pray that one day we may live in a culture in which the only response to a prenatal diagnosis is renewed resolve to do everything possible to assist and accompany parents in the care of their child, welcoming him or her joyfully and with hope, no matter how short or physically limited his or her life might be.
breastfeed, motherhood, Mothers day, family love. mom breastfeeding her little son. breast feeding, lactation, maternity and healthy lifestyle
Type in the phrase “milk supply” on Pinterest or Google, and you’re likely to find oodles of recipes, baked goods, herbs, and over-the-counter compounds that claim to “boost milk supply.” If I’m being frank, in my work as a Lactation Consultant, most of my clients are struggling with milk supply because of ineffective or inefficient milk removal. Prioritizing sufficient milk removal is the best way to “boost milk supply.”
Butoccasionally, I see a mom struggling with low milk supply because of IGT (Insufficient Glandular Tissue). This means that even with efficient suckling or pumping, they will not be able to make a full supply and will need to supplement with formula or donor milk. Contrary to what people often think, a diagnosis of IGT does not mean that a mom can’t breastfeed, but it does mean breastfeeding might look a little different than anticipated.
IGT is not due to “small breasts.” Size is not indicative of the quantity of glands. IGT breasts can be big, small, medium, round, flat, high or low—the only thing they all have in common is that the glandular tissue is simply not sufficient to make a full milk supply.1
The biggest red flags for potential IGT are widely spaced breasts, and particularly those that don’t grow during pregnancy. The exact root cause of IGT is still being studied, but some of the coinciding factors are a pre-pregnant body mass index (BMI) greater than 30, BMI greater than 26 or 30 during puberty, hormonal disorders (such as insulin resistance, diabetes, or hyperandrogenism), and use of hormonal birth control during puberty.2
Did you catch that last one? If you, your daughter, or a loved one was put on the pill as a teenager, there is an increased likelihood that you will experience impaired lactation. Did the doctor explain that to you? No? Didn’t think so.
How breast tissue matures
Breast maturation begins in the womb. “As early as 4 to 6 weeks of gestation, mammary-specific progenitor cells may be seen.”1 Around day 35 of gestation, proliferation of paired areas of epithelial cells in the epidermis of the thoracic region occurs.”3 Up until age 2, breast tissue goes through a process of “epithelial differentiation”—in other words, when cells prepare for lactation. This is also why endocrine disruptors should especially be avoided during pregnancy. Exposure to toxins like dioxin in utero can predispose a woman to have insufficient breast growth. Breast tissue then remains dormant until puberty.4
Alveoli—these are the small sacs that fill with milk—are laid during each menstrual cycle, through the exposure of cyclical estrogen and progesterone. Estrogen is responsible for elongation of milk ducts (the branches that hold the alveoli) while progesterone works on ductal side branching. As ductal elongation continues, the rest of the breast tissue fills in with adipose tissue, blood vessels, immune cells, and fibroblasts. After puberty, breast tissue remains relatively stable until the final stage of maturation during pregnancy.3
That’s right—breasts are not considered fully developed until they’ve gone through a full pregnancy. During this time of intense estrogen and progesterone exposure, as well as human placental lactogen, the ductal system expands and branches out into the adipose tissue for its final stage of growth in preparation for lactation.3
So what does the pill have to do with it?
Hormonal birth control and IGT are correlated for two reasons. The first is that hormonal birth control is often given to teens to “cure” period problems. These period problems likely stem from hormonal disorders that affect breast tissue maturation and, therefore, future lactation. These hormonal conditions include, but are not limited to: PCOS, luteal phase defects, thyroid issues, and insulin resistance.
Restorative care—not suppression of symptoms—should be prioritized for teen’s reproductive and general health. Restorative care will protect not only her future fertility and lactation but also her future bone, heart, and immune health.
The second reason is that a teen on hormonal birth control doesn’t have monthly, cyclical exposure to their own hormones that are necessary for proper ductal growth. The artificial hormones in birth control do not have the same effect as endogenous ones.
A 2021 research study found that “[different] progestins have distinct biological activities in the human breast epithelium depending on their androgenic properties.” They also found that “progestins routinely included in contraceptives have properties that overlap with testosterone, androgenic progestins, which induce expression of important mediators of progesterone receptor signaling and consistently elicit proliferation of human breast epithelial cells.”5
This means the hormones in modern contraceptives cause breast tissue growth—but not in the same way that endogenous hormones would.
For many, increased breast size is a common side effect of hormonal contraception. It’s been touted that since the pill (and any of its formulations) “trick the body into thinking it’s pregnant,” the breast growth women experience while taking hormonal contraceptives is akin to breast growth in early pregnancy. But we now know differently.
Exposure to androgenic progestins causes hyperproliferation with cellular changes. Breast tissue growth during pregnancy is biologically normal, while growth during hormonal contraceptive use is not normal. This is also probably why full-term pregnancy (particularly during a woman’s twenties) has a protective factor against breast cancer while hormonal contraceptive use does the opposite.6
It’s important to note that just because you were on hormonal contraception as a teen doesn’t automatically mean you will struggle with IGT. Conversely, some women struggling with IGT have never used a hormonal contraceptive. Rather, hormonal contraceptive use during teenage years just seems to be one of the pieces in unlocking the IGT puzzle. And it’s certainly one more reason to steer clear of hormonal birth control for the teens in your life.
What if I think I have IGT?
If you are having lactation problems, you should schedule a full consultation with an International Board Certified Lactation Consultant, who can confirm the source of potential low milk supply, rule out baby-stemmed issues, and work toward a care plan that will suit both the mom and baby. You don’t have to throw the baby out with the bathwater—breastfeeding in some capacity is still possible.
If you are expecting and hoping to breastfeed, but are worried you could end up with IGT, you can have your breast tissue examined by your health practitioner or a lactation consultant. But, this is likely premature. You don’t really know how lactation will unfold until it does. That’s why it’s so important to have lactation support lined up for when you need it.
In conclusion, the association between hormonal birth control use in the adolescent years and IGT, is one worthy of your consideration. Teenagers may not be thinking about breastfeeding, but one day down the line, they may—and we want to give them every chance to succeed when that time comes.
The Church, “expert in humanity” (as Pope Paul VI put it), knows that the mystery of Christmas (like that of Easter) is so great that it cannot be adequately plumbed – let alone celebrated – in a single day. And so, taking a page out of our Jewish liturgical heritage, the Church gives us an octave observance – eight full days to consider the central doctrine of the Incarnation, enabling us to reflect on it from a variety of perspectives, not unlike holding a diamond up to the sun in an attempt to appreciate its beauty from many different angles.
Oddly, it might seem, however, throughout the Christmas Octave, we encounter a number of saints’ feasts. Don’t these commemorations serve as distractions from the central mystery of the Octave on which we are meant to focus our attention? Not at all – because, as St. Paul teaches us, “God is glorious in His saints” (2 Thess 1:10). Indeed, we can say that the very first fruits of the Incarnation are saints, the comites Christi (the companions of Christ), and in this week, the majority of them are martyrs – privileged “witnesses” to Christ: Stephen, the so-called “proto-martyr” (Dec. 27); Thomas à Becket, the medieval defender of the freedom of the Church (Dec. 29); and today, the Holy Innocents, really the first to shed their blood for Christ.
We are introduced to the “Holy Innocents” by St. Matthew (2:16-18) after he has told us of the visit of the Magi, whom Herod wanted to use as “reconnaissance” men to determine the identity of this “new-born King of the Jews.” Not obtaining the information he desired, Herod resorts to mass murder to ensure his competition is dead, ordering the execution of all male babies under the age of two in Bethlehem.
As children in our Bible history books in school and through Cecil B. DeMille-like productions, we were led to believe that hundreds or even thousands of baby boys were the victims of Herod’s treachery. Such poignant and dramatic scenes would certainly leave an impression on impressionable children. Unfortunately (or perhaps, fortunately), the real number was probably much smaller, maybe no more than a dozen since Bethlehem was a tiny, backwater town with a tiny population as Matthew himself suggests by citing the Prophet Micah’s description of the “little town of Bethlehem,” as we sing in the carol.
No, the horror of Herod’s deed resides not in the number of infants killed but in the fact that even one would be killed. The historicity of the event gains considerable credibility since we know that the crazed and paranoid king even killed his own sons, so terrified was he of a usurper.
The Collect for the day’s liturgy notes that these little ones confessed the true faith, “not by speaking but by dying.” Indeed, the very word “infant” in Latin means one who cannot yet speak! The prayer goes on to ask the Lord for the great grace “that the faith in you which we confess with our lips we may also speak through the manner of our life.” Talking the talk must be matched by walking the walk. How can this feast help us do that?
Today’s Office of Readings treats us to a reflection of Quodvultdeus, a fifth-century bishop of Carthage in North Africa and a spiritual son of the great Augustine. His name means “what God wants.” The North Africans had a knack for names. Another bishop was called “Deogratias” (Thanks be to God), and Augustine named his illegitimate son “Adeodatus” (Given by God) – a reminder that all human life is sacred, even when conceived under less than optimal circumstances. These North African theologians stand as testimonies to the vitality of the Church in that region in the early centuries but a reality that was almost totally eradicated by the Muslim invasions of the seventh century, which brought death to many and, sadly, apostasy from not a few. Another reminder and warning: While the Church Universal has divine assurance of remaining until the end of time, particular churches (dioceses) do not.
But back to the contribution of Quodvultdeus. Using the literary device known as “apostrophe,” the author addresses a question to the absent Herod:
Why are you afraid, Herod, when you hear of the birth of a king? He does not come to drive you out, but to conquer the devil. But because you do not understand this you are disturbed and in a rage, and to destroy one child whom you seek, you show your cruelty in the death of so many children.
Of course, for decades now, the Church in the United States has seen in the Holy Innocents the forerunners of the millions of babies slaughtered through legalized abortion in this country since 1973. As we have protested against this monstrosity and blight on our national character, have we not all witnessed the fear and rage of those ensnared in the culture of death? But why such rage? The vast majority of pro-lifers offer a kindly protest. The rage is born of insecurity, no doubt, because – deep-down – everyone knows the truth of what is happening in the abortion clinics and everyone knows – deep-down – that Our Lord was right in asserting that “the truth will set you free” (Jn 8:32). Dr. Bernard Nathanson came to the right conclusion, after years of aborting thousands of children, bringing him to produce the very appropriately-titled film, The Silent Scream.
The Church in our country – especially the hierarchy – have made numerous mistakes in the post-Vatican II era, however, the one area in which the Church shines is in her unrelenting pro-life witness and action. People forget that ours was a lone voice in the immediate wake of Roe v. Wade. In fact, the pro-abortionists used our solitary witness to press the anti-Catholic button, hoping to make the issue appear as a uniquely Catholic issue, as documented by Dr. Nathanson. While we rejoice in Evangelicals getting onboard with us, truth compels us to note that they were late arrivals.
This counter-cultural stance has been powerfully aided by our Catholic school system, which has provided strength and youthfulness to the pro-life movement. A few days after the 2010 March for Life in Washington, D. C., a journalist in favor of “abortion rights” wrote an article in the Washington Post (also strongly pro-abortion) noting that he was “expecting to write about [the March’s] irrelevance,” however, he indicated: “I was especially struck by the large number of young people among the tens of thousands at the march.” He highlighted the fact that the vast majority came from Catholic schools who “were taught from an early age to oppose abortion.” The piece ended up being remarkably fair and even positive.
The Shrine and Parish of the Holy Innocents (where I have happily provided assistance for nearly a quarter of a century) in Midtown Manhattan is home to the Shrine of the Unborn. Quodvultdeus reproached Herod:
You are not restrained by the love of weeping mothers or fathers mourning the deaths of their sons, nor by the cries and sobs of the children. You destroy those who are tiny in body because fear is destroying your heart. You imagine that if you accomplish your desire you can prolong your own life, though you are seeking to kill Life himself.
This shrine allows parents to mourn the loss of their unborn children (whether through abortion or miscarriage), entering the names of their children into a Book of Life.
Europeans are stunned by the vitality of the pro-life movement in America; most of them have given up on the cause a long time ago. Statistics tell us that abortion is still a lively and hotly contested dimension of American politics, as was on clear display in the shameful confirmation hearings of Judge Brett Kavanaugh. Most interesting of all is that young people, perhaps realizing that they themselves could have been aborted or impressed by what science tells us about life in the womb, are among the most pro-life of all.
The innocent unborn, then, have not died in vain. Quodvultdeus ends his homily thus:
To what merits of their own do the children owe this kind of victory? They cannot speak, yet they bear witness to Christ. They cannot use their limbs to engage in battle, yet already they bear off the palm of victory.
All you Holy Innocents, pray that the witness of our lives will always match the words of lips.
(Editor’s note: This essay was first posted at CWR on December 28, 2018.)
Governor Mike DeWine signed a bill protecting abortion survivors. Ohio Bill 157 will (1) require medical professionals to provide life-sustaining care to children who survive a botched abortion, and (2) prohibit medical professionals who receive taxpayer-funded salaries from working for or contracting with abortion facilities. This bill will cut tax dollars from funding abortions and potentially close down two abortion facilities in Ohio.
Time Magazine has just named Tesla CEO Elon Musk as their “Man of the Year.” The Time feature on Musk, the richest man in the world, naturally focuses on Musk’s extraordinary career as the founder and CEO of world-changing corporations like Paypal, Neuralink, SpaceX, and, of course, Tesla.
However, Musk has been in the news recently for another reason: warning the world of the danger posed by collapsing global birth rates. “I can’t emphasize this enough: There are not enough people,” Musk stated during The Wall Street Journal’s CEO Council Summit a couple of weeks ago. “One of the biggest risks to civilization is the low birth rate and the rapidly declining birth rate.”
To say that this is an unusual message coming from a billionaire is an understatement. Since the late 1960s, most of the world’s wealthy elite have more or less bought into the population control ideology, convinced by the doomsday theorizing of the likes of Paul Ehrlich, author of the best-seller The Population Bomb.
Fellow billionaire Bill Gates and his now-ex-wife Melinda Gates, for instance, have committed an enormous amount of their wealth to the cause of reducing the global population. Gates’ recent $1.7 million donation to a research team working on male contraception is the merest tip of the iceberg. In 2017, the Gates Foundation announced that they were giving over $375 million in support of “family planning” over the space of four years, which was only the latest installment of many financial gifts aimed at reducing the population.
Musk, however, is known for an independent streak, with many of his views defying easy categorization. This is not the first time that he has raised the alarm about the detrimental long-term effects of collapsing population numbers. Earlier this year he tweeted, “Population collapse is potentially the greatest risk to the future of civilization,” linking to a Wall Street Journal article on falling U.S. birth rates.
In fact, he has repeatedly addressed the issue since at least 2017. In some 2019 remarks, he noted that “most people think we have too many people on the planet, but actually, this is an outdated view.”
People are Valuable
Musk is right. Although he may be the most high-profile person raising the alarm about depopulation, more and more political figures and economists are starting to wake up to the reality that a world without babies poses enormous challenges and risks.
A study published last year in The Lancet, one of the world’s most prestigious medical journals, predicted a “jaw-dropping” crash in global fertility by 2100. As the BBC reported, “the researchers expect the number of people on the planet to peak at 9.7 billion around 2064, before falling down to 8.8 billion by the end of the century.”
“That’s a pretty big thing; most of the world is transitioning into natural population decline,” says researcher Prof. Christopher Murray. “I think it’s incredibly hard to think this through and recognise how big a thing this is; it’s extraordinary, we’ll have to reorganise societies.”
Whereas the overpopulation doomsayers view people as a liability, what Musk recognizes is that even from a purely practical perspective people are also (and predominantly) an asset. That is, people are not merely biological beings that consume resources. They are also intelligent beings who use their ingenuity and creativity to produce good things, and to change the world for the better.
This is not to say that it is completely unreasonable to be concerned about the pragmatic challenges posed by rapid population growth. In Evangelium Vitae, even Pope St. John Paul II acknowledged that some poorer countries “generally have a high rate of population growth, difficult to sustain in the context of low economic and social development, and especially where there is extreme underdevelopment.” However, in the face of these challenges, the Holy Father noted, creative politicians must work hard to implement “programmes of cultural development and of fair production and distribution of resources” instead of “anti-birth policies.” (no. 16)
Indeed, despite the consistent fear-mongering that has accompanied population growth ever since Thomas Malthus published his “Essay on the Principle of Population” in 1798, a growing population has not ushered in the apocalyptic disease and starvation that Malthus predicted. Instead, the past few centuries have seen unprecedented advances in human health and well-being, with the widespread eradication of childhood disease, enormous increases in longevity, and reductions in global hunger that have defied the predictions of even the sunniest optimists.
Even someone like Musk can see that human beings are something truly special, and that any temptation to view humans as resource-consuming “parasites” – one thinks of Agent Smith’s rant in the film The Matrix – is based upon a catastrophic misunderstanding not only of the intrinsic dignity of every human being, but also of the practical facts of how humans consume resources: not with the uncontrolled rapacity of a horde of locusts, but with intelligence and foresight.
A Catholic View of Population Issues
If even a non-Christian like Musk can see that the overpopulation ideology is catastrophically mistaken, we must go deeper still. Within the Christian worldview, not only are individual human persons potential practical assets, but they are also something much, much greater: beings made in the image and likeness of God.
As the Catechism teaches, “[Man] alone is called to share, by knowledge and love, in God’s own life… This is the fundamental reason for his dignity… Being in the image of God, the human individual possesses the dignity of a person, who is not just something, but someone.” (paragraphs 356-357)
Rooted in a rich understanding of the inexpressible dignity of every individual human person, the Catholic Church has repeatedly warned against a simplistic approach to addressing complex problems that assumes that eliminating the human beings who suffer from those problems is the answer. In even the best-case scenario, this view inevitably leads to a cynical paternalism that robs developing nations of their freedom, and in the worst case, to horrific human rights abuses, such as the forced abortion and sterilization policies we have seen in places like China and India.
‘‘We must renounce the sophist view which holds that ‘to be many is to condemn ourselves to be poor,’” Pope St. John Paul II said in remarks at the opening of the World Food Summit in 1996. ‘‘It would be illusory to believe that an arbitrary stabilization of the world population, or even its reduction, could solve the problem of hunger directly.”
In Evangelium Vitae, the saintly pope compared globalist leaders who push population control on developing nations to the Pharaoh who ordered the first-born sons of the enslaved Israelites to be killed at birth. He wrote:
Today not a few of the powerful of the earth act in the same way. They too are haunted by the current demographic growth, and fear that the most prolific and poorest peoples represent a threat for the well-being and peace of their own countries. Consequently, rather than wishing to face and solve these serious problems with respect for the dignity of individuals and families and for every person’s inviolable right to life, they prefer to promote and impose by whatever means a massive programme of birth control. Even the economic help which they would be ready to give is unjustly made conditional on the acceptance of an anti-birth policy. (no. 16)
The Holy Father added that any effort to address population questions must “take into account and respect the primary and inalienable responsibility of married couples and families.” Certainly, political leaders can never “employ methods which fail to respect the person and fundamental human rights, beginning with the right to life of every innocent human being.” (no. 91)
“It is therefore morally unacceptable to encourage, let alone impose, the use of methods such as contraception, sterilization and abortion in order to regulate births,” he added. (no. 91)
Musk is on the Right Track
It goes without saying that Musk’s views are no approximation of the richness of the Catholic view. At the end of the day, Musk is only looking at the problem from a purely practical point of view, drawing our attention to the fact that falling birth rates portend a rapidly diminishing work force, an aging population, reduced economic output, reduced tax revenue, huge demographic shifts, etc.
However, he is on the right track. In acknowledging that humans are a resource more than a liability, he is at least partway towards a deeper understanding of the human person than the likes of Bill Gates, who has dedicated his life to ensuring that there are no more humans than he deems ideal.
“Be fruitful and multiply,” God told Adam and Eve in Genesis. This comes immediately after the passage which reads: “And God said, let us make man in our image, after our likeness … So, God created man in his own image, in the image of God he created him; male and female he created them.” (Genesis 1:28; 26-27)
Every human born is not just another mouth to feed but is an image of God Himself, a spark of the divine on earth, endowed with rationality, and a spiritual soul capable of intimate union with God Himself. At an earthier level, every human being is another potential mother, father, daughter, son, friend, another employee, taxpayer, inventor, and creator. Every human life is a life of inexpressible richness: of triumphs, sorrows, joys, accomplishments. Every human born has the ability to give something to the world that no other person can give.
When a society moves towards the denial or suppression of life, it ends up no longer finding the necessary motivation and energy to strive for man’s true good. If personal and social sensitivity towards the acceptance of new life is lost, then other forms of acceptance that are valuable for society also wither away. The acceptance of life strengthens moral fiber and makes people capable of mutual help. By cultivating openness to life, wealthy peoples can better understand the needs of poor ones, they can avoid employing huge economic and intellectual resources to satisfy the selfish desires of their own citizens, and instead, they can promote virtuous action within the perspective of production that is morally sound and marked by solidarity, respecting the fundamental right to life of every people and every individual. (no. 28)
And so, rather than reacting to human life with fear, as the population controlling elite have done for so long, we ought, as a civilization, to rejoice in every new life, and to reject the technocratic temptation that says we can build a better world by violently yoking nature to our narrow purposes. For, as Musk has rightly warned, we may learn all too soon that there are unpleasant consequences to our short-sighted hubris.
This fall the film Business of Birth Control was released at the Doc NYC fest and now is available for streaming nationwide. Abby Epstein and Ricki Lake, authors of the film, also produced “The Business of Being Born“
The film does a critical review of the effects of birth control. “In the 1960’s the pill was revolutionary, giving women the ability to control their fertility and advancing their equality in the workplace and in society. But when the pill came onto the market, women were not fully informed of the side effects and risks. Sixty years later, any conversation around the drawbacks of hormonal birth control remains politicized and suppressed.”
The filmmakers highlighted testimonies of two families who have lost their daughters to fatal side effects of hormonal birth control. “Today, over 35% of hormonal birth control prescriptions are for non-contraceptive reasons like acne, irregular or painful periods, PCOS and endometriosis. Hormonal birth control has been linked to depression, autoimmune disease, cervical cancer, fatal blood clots and other chronic conditions; yet it is still prescribed to healthy women as a panacea for every hormonal and reproductive issue.”
The film does a good job talking about the dangerous physical and mental sideeffects of the pill, but it is missingmentioning other methods of birth control such theLARC, very popular and producing many sideeffects. Moral and ethical aspects are an important piece missed for not secular audiences. People needs to know about the mechanism of action of hormonal birth control preventing implantation of a recently conceived embryo.
A recent article published online Patients, doctors are clashing about side effects of hormonal birth control (statnews.com) discuss the lack information about artificial birth control side effects. The article describes how women suffer side effects that are caused by the artificial hormones and how the issue may not be properly addressed by the health care professionals.
I offer an analogy for the pro-life mission. The doctrine of the Immaculate Conception of the Blessed Virgin Mary did for the understanding of Christian doctrine what the pro-life movement does for the understanding of human dignity. The Immaculate Conception endows Mary with Redemption, salvation and holiness, her eternal worth, rights and personhood “from the first moment of… conception.”
HARRISBURG, PA. (Catholic online) – The Catechism of the Catholic Church explains the Feast we celebrate on December 8th in this way: “To become the mother of the Savior, Mary “was enriched by God with gifts appropriate to such a role.” The angel Gabriel at the moment of the annunciation salutes her as “full of grace”. In fact, in order for Mary to be able to give the free assent of her faith to the announcement of her vocation, it was necessary that she be wholly borne by God’s grace.
“Through the centuries the Church has become ever more aware that Mary, “full of grace” through God, was redeemed from the moment of her conception. That is what the dogma of the Immaculate Conception confesses, as Pope Pius IX proclaimed in 1854: “The most Blessed Virgin Mary was, from the first moment of her conception, by a singular grace and privilege of almighty God and by virtue of the merits of Jesus Christ, Savior of the human race, preserved immune from all stain of original sin.”“The “splendor of an entirely unique holiness” by which Mary is “enriched from the first instant of her conception” comes wholly from Christ: she is “redeemed, in a more exalted fashion, by reason of the merits of her Son”.
The Father blessed Mary more than any other created person “in Christ with every spiritual blessing in the heavenly places” and chose her “in Christ before the foundation of the world, to be holy and blameless before him in love”. (Eph. 1:3,4) “The Fathers of the Eastern tradition call the Mother of God “the All-Holy” (Panagia), and celebrate her as “free from any stain of sin, as though fashioned by the Holy Spirit and formed as a new creature”. By the grace of God Mary remained free of every personal sin her whole life long.” (CCC #490-493)
What comes to mind as I reflect on this beautiful Feast is a vital analogy I offer to the Pro-Life movement to help in the mission. The doctrine of the Immaculate Conception of the Blessed Virgin Mary did for the understanding of Christian doctrine what the pro-life movement does for the understanding of human dignity.
The Immaculate Conception endows Mary with Redemption, salvation and holiness, her eternal worth, rights and personhood ” from the first moment of conception.” Let me explain the analogy. By withholding the recognition of personhood from the unborn child, the Supreme Court in Roe V Wade, made the human child in the womb a worthless blob waiting for value and meaning to be conferred upon her at some later time. That judgment would be made by others, all of whom would be less noble, certainly more sinful than she.
The personhood of the unborn child is the most compelling moral issue of our time. It is so precisely because it defines who is a human being – and who a human being is. We all know that we must treat each and every human being with the ultimate respect and never deem any person “disposable.”
Genocide, homicide, and murder must never be condoned because it unjustifiably destroys a human being. The reason the unborn child is at the very essence of the question of human dignity, human rights and protection is that, if it is unknown who is a human being, then how can human rights be defined and protected? If any human being can be deprived of the right to life, then all human beings can be deprived of life. It is no longer possible to avoid the question of when a human begins – too much is at stake. We must end the debate and resolve that each and every human being is a person – and that person begins in their first moment of conception.
The doctrine of the Immaculate Conception teaches that “the most Blessed Virgin Mary, in the first instant of her Conception, by a singular grace and privilege granted by Almighty God, in view of the merits of Jesus Christ, the Savior of the human race, was preserved free from all stain of original sin.” The Encyclopedia of the Blessed Virgin Mary lists three Scripture passages that imply the Immaculate Conception: Genesis 3:15, Luke 1:28 and Luke 1:42. The Genesis passage points to Mary as the Mother of the Redeemer who bears and brings to birth the one who will reverse the curse of Adam and Eve.
In this respect, she was the New Eve. The first Eve’s disobedience brought death, the Second Eve’s fiat brought life. Luke tells us that Mary was full of Grace. For the Church throughout the ages this meant that she possesses every aspect of God’s Grace, all the moral and theological virtues, all the extraordinary gifts and fruits of the Holy Spirit. And Luke says that she was blessed among women. The Church embraces Mary as unique and unrepeatable. Among women she is singular. As daughter, virgin, wife and mother, she is the supreme example of woman and the fulfillment of every woman’s aspirations.
The Immaculate Conception teaches us that everything that Mary would become she already was in the first moment of her conception.” Mary was not less than Mary before her birth. She possessed, albeit, in a hidden way, all the Grace and spiritual attributes granted her by the merits of Jesus Christ the Redeemer, from the first moment of her conception. What does this teach us about ourselves? That we possess our full potential – our full personhood – from the first moment of our conception. There is no one reading this article today who was not who you are now ever since the very first moment of your conception.
Let me try that again: Every one of you has always been who you are today. You have grown in knowledge, experience, and even faith – but you have never been anyone but yourself, you have never been anyone other than you, you have never, ever been anything less than a unique, unrepeatable, human person. The Immaculate Conception demonstrates that God created each one of us with a unique purpose and plan for our lives, and that plan began the first moment of our conception.
+ Hail Mary, full of Grace. —– Fr. Paul Schenck, a Priest of the Diocese of Harrisburg, PA., is the founding Director of the National Pro-Life Center (NPLC) on Capitol Hill in Washington, DC. The Center gives the Justices of the Supreme Court, their high-level staff, members of the federal judiciary, members of the US Senate and other public policymakers the information, education, and inspiration they need to better form their consciences so they will make better decisions. He is a Champion of the Pro-Life movement.
Roe v. Wade’s days are numbered. That, remarkably, seems to be the consensus after the U.S. Supreme Court heard oral arguments (transcript here) last Wednesday in Dobbs v. Jackson Women’s Health Organization.
This blockbuster case involves a challenge by Mississippi’s last abortion facility against the state’s 15-week abortion ban. That law, passed in 2018, has been blocked from going into effect by lower courts, based upon arguments that it violates Roe v. Wade, the infamous Supreme Court case that legalized abortion in 1973.
Roe and subsequent cases, including Planned Parenthood v. Casey (1992), state that there is a Constitutional “right” to abortion up to the point of viability – that is, the point when the baby can survive outside the womb. The Mississippi law, banning abortion after 15-weeks, was framed in part as a direct challenge to Roe, in the hopes the Supreme Court could finally overturn Roe, giving far more latitude to states to outlaw the killing of unborn children.
Hope was kindled in May, when enough of the SCOTUS justices agreed to hear the challenge against the Mississippi law. As legal scholars noted at the time, there was no conceivable reason for the Court to hear the case, unless enough of the justices are open to overturning Roe outright, or (at the very least) charting some new compromise that would allow states to ban abortions earlier than Roe and Casey allow.
However, while acknowledging that things looked positive, many experienced pro-life leaders have viewed the case with only cautious optimism, knowing that previous opportunities to overturn Roe at the Supreme Court have ended with bitter disappointment.
A Sea Change at the Court?
Wednesday’s oral hearings have markedly changed the mood. Almost every commentator – both pro-abortion and pro-life – who watched the arguments agreed that the Court’s six conservative justices all more or less strongly signaled an openness to rejecting Roe.
In a feature article for The Atlantic entitled “The End of Roe,” legal scholar Mary Ziegler wrote, “Anyone listening to today’s oral argument on abortion could not miss that something historic was happening. … Today’s oral argument signaled that the Court is poised to reverse Roe outright when it decides Dobbs, probably sometime in June or early July.”
The editors of the National Review gave a nod to the delicacy of predicting outcomes at the Court, but concurred that something massively positive seemed to unfold in the courtroom. “Veterans of Supreme Court cases past know that it is risky to read the tea leaves from questions at argument,” they wrote, “but it is hard to see how the argument could have gone much better for the pro-life cause.”
There were many instances in which the more conservative justices appeared to play their hand in a way that suggests that Roe is on the brink. Of course, we shouldn’t be surprised that as strongly a pro-life justice as Justice Alito would suggest (as he did) that Roe’s viability line “really doesn’t make any sense,” and that it seems “arbitrary” (which it is).
More encouraging, however, is that Justices Gorsuch, Kavanaugh, and Barrett – Trump’s three recent SCOTUS appointees, whose positions are less known – also seemed skeptical that Roe and Casey withstand close scrutiny.
For instance, at one point Justice Kavanaugh expressed skepticism that – contra Roe – the Constitution has anything at all to say about abortion. Echoing pro-life arguments, Justice Kavanaugh noted that “the core problem here is that the Court has been forced…to pick sides on the most contentious social debate in American life and to do so in a situation where…the Constitution is neutral on the question of abortion.” As such, he concluded, pro-life legal analysts “would say, therefore, it should be left to the people, to the states, or to Congress.”
Importantly, many of the Justices appeared to question the idea that stare decisis – i.e., the legal doctrine that says that judges should, in general, follow court precedent – provides an ironclad reason to resist rejecting Roe.
Much of the debate about the fate of Roe has centered on the question of stare decisis, with pro-abortion legal scholars and justices arguing that overturning Roe would hurt the “reputation” or “legitimacy” of the Court. However, as Mississippi State Solicitor General Scott Stewart astutely argued in the courtroom on Wednesday, the legitimacy of the Court is protected not by blindly upholding precedent, but in having the courage “to stand strong and stand firm” and to follow “constitutional principle” in overruling erroneous precedent when the errors become manifest.
In other words, the reputation of the Court is not protected by doubling down on egregious errors, but in choosing to stand for truth, at all costs.
Amen to that.
Our Work is Just Beginning
It is crucial to note, however, that even if Roe is overturned or modified, it will not be the end of the pro-life movement. Not by a long shot.
It is true that overturning Roe is something that pro-lifers have worked towards, and prayed for, for decades. When we have gathered at the March for Life, we have chanted and held signs urging the Court to “overturn Roe.” But getting rid of Roe has never been the end goal. Ending abortion is.
As Tom McClusky, president of March for Life Action, noted to the New York Times, there will be some pro-life activists who will “claim victory and walk away” once Roe is overturned. However, he added, “We want to build a culture where abortion is unthinkable. So even if by some miracle next spring Roe is overturned, there is still going to be a ton of work to do.”
Overturning Roe does not immediately make abortion illegal. It only returns the issue to the individual states. Fortunately, brilliant pro-life legal activists and legislators have presciently focused on state-level legislation for decades now, working to pass strong pro-life legislation, even when that legislation can’t go into effect until Roe is overturned.
According to the pro-abortion Guttmacher Institute, if Roe is overturned, twenty-six states will mostly or completely ban abortion. In a detailed breakdown, pro-abortion Democratic activist Jessica Post notes that nine states have never repealed pre-Roe abortion bans. With Roe overturned, they would immediately go back into effect. Meanwhile, twelve states (including four with pre-Roe bans on the books) have passed so-called “trigger laws,” that will automatically ban abortion once Roe is overturned.
On the other hand, however, fourteen states and D.C. have passed laws strongly defending abortion. In those states, the killing of unborn children would go on as before. Indeed, likely at a higher level than before, with some women traveling to those states to have their children killed.
In her analysis, however, Jessica Post unintentionally gave high praise to the grit and genius of the pro-life strategy, noting that “Republicans worked for decades to win state legislatures so they could pass extreme abortion bans that rile up their far-right base with the hope of overturning Roe. We can no longer rely on SCOTUS to protect this fundamental right. That time is up.” She added, “We need Dems to throw themselves into state legislative elections just like Republicans have been doing.”
What a testimony to pro-life prescience! However, Post is right: once (or if) Roe is overturned, all attention will turn to the state level. At that point, there will be a greater need than ever for pro-life activists to get involved at the local and state level. There can be no passing the buck: at that point, the issue lands right at our doorsteps.
And our efforts can’t only be aimed at passing (and protecting) pro-life laws! With abortion becoming illegal in many states, there will be a rise in the number of women needing practical help to bring their children safely into the world. We will need a movement like none other to provide concrete resources to families, ensuring that no couple need face the uncertainties and hardship of a difficult pregnancy alone. True, pro-lifers have already done yeoman’s labor in building a social safety net by founding thousands of pro-life pregnancy centers. With Roe gone, however, that net will have to expand even further.
Pray for Courage for Our Justices
There are many variations of the proverb “don’t count your chickens until they hatch.” Indications at the Court last Wednesday were extraordinarily promising. However, as the editors of National Review wrote, “A majority of the Court appears to understand that Roe is bad law. What remains to be seen is whether they have the courage to act on that.”
That must be our prayer today: Pray ardently, and fast, for our Supreme Court justices. They have heard the arguments. Enough of them appear to be sympathetic to the truth. But there is a difference between knowing the truth and acting on it. Most of us cannot understand the level of pressure – psychological, social, and spiritual – that is being placed upon them. If they overturn Roe, all the ire of the powerful abortion lobby, and the dark spirits that revel in the slaughter of abortion, will be aimed in their direction.
Let us cover them with prayer. May we all yet live to see not only the end of Roe, but also the end of the violence and scourge of abortion, in the United States and around the world.
This week, a new study about the systemic effects of IUDs will be presented at the annual meeting of the Radiological Society of North America (RSNA). The author of the study used Breast MRI to show that (LNG-IUS) has effects not only in the uterus but also systemic effects.
Levonorgestrel-releasing (LNG-IUS) is used by millions of women worldwide and appears to have systemic effects on the body like those of hormone replacement therapy. “It has been claimed that IUDs have a purely local effect on the uterus,” said Luisa Huck, M.D., a radiology resident in the Department of Diagnostic and Interventional Radiology at RWTH Aachen University in Aachen, Germany. “Our study results suggest that this is not true.”
LNG-IUS works by releasing a small amount of progestins into the uterus. It was believed that any side effects would be confined to the reproductive system. However, this study suggests that LNG-IUS can be associated with systemic side effects similar to those of systemic hormonal contraception.
The author of the study concluded that “IUDs appear to be a very safe means of contraception and are generally well-tolerated,” she said. “However, if women with an IUD in place experience unexplainable side effects, they should talk to their doctor and consider using other types of contraception.”
A recent study has found that women who currently or recently used the LNG-IUS had an increase of 21% in the risk of breast cancer compared to women who had never used hormonal contraceptives.
In 1992, the British Medical Journal published a disturbing study which suggested that human semen quality had declined by approximately 50% from 1930 to 1991 (1). Subsequent research has confirmed that male fertility seems to be declining—and a whole host of man-made chemicals appears to be a possible cause.
These chemicals, known as endocrine disruptors or endocrine-disrupting chemicals (EDCs), are used in plastic, food packaging, pesticides, cosmetics, cleaning products, paint, toys, personal care products, and household products. The amount of these chemicals produced annually around the globe is measured in the millions of tons!
Many of these man-made chemicals affect our endocrine system by interfering with our hormones’ normal functions, directly affecting our reproductive functioning.
We’ve discussed endocrine disruptors before and this time we’re focusing specifically on how they affect males and their fertility. We’ll also look at ways to reduce exposure to endocrine-disrupting chemicals, and how protect the men in our lives.
It’s important to note that these chemicals seem to have the most significant impact on babies and children as their bodies are developing, which is all the more reason for women who are looking to get pregnant anytime soon to limit their exposure to EDCs—including hormonal contraception—as much as possible.
Androgens are key for healthy male development
A category of hormones called androgens are essential for the development of the male reproductive system. Androgens—testosterone being the most well known—are usually thought of as the male reproductive hormones, though smaller amounts are necessary in women’s bodies as well. The masculinization of a boy’s internal and external male reproductive organs are dependent mostly on testosterone and one of its metabolites, dihydrotestosterone (DHT), which are produced in the testicles. Thus, normal male development requires a balanced hormonal environment.
The period of time when the male reproductive system is developing is incredibly sensitive to chemicals that have an anti-androgen effect. At about eight weeks gestation, the cells of the forming testes begin to produce testosterone, which drives the differentiation and development of the internal and external genitalia. The ability of endocrine-disrupting chemicals to suppress androgen synthesis during fetal and neonatal life can cause a series of male reproductive disturbances, such as cryptorchidism (the failure of one or both testicles to descend into the scrotal sac), hypospadias (a condition in which the opening of the urethra is somewhere other than at the tip of the penis), impaired fertility (especially due to poor semen quality), and an elevated incidence of testicular cancer. (2, 3, 4, 5) The abnormal development of testes in an infant boy can have long-term consequences for sperm production, and therefore his future ability to conceive children.
The perinatal period is a particularly sensitive window of development in which minor hormonal disturbances may have a long-lasting impact on fertility.
Other less talked about effects of endocrine-disrupting chemicals include alterations of genetic systems and gene expression. These effects are particularly troubling since alterations in genetic programming during early stages of development can have profound effects years later and may also lead to transgenerational inheritance of disease. (6,7)
Worst endocrine disruptors for males
Bisphenol A
BPA is an endocrine-disrupting chemical used in the manufacturing of plastics and epoxy resins used in food and drink containers, plastic water bottles, baby bottles, dental sealants, and a variety of household products. It is widespread in the environment and every year 2.2–4.7 million tons of BPA are released into the environment. Humans are mainly exposed to BPA as it leaches from the inner lining of canned food and microwave containers during heating of food or through beverages in plastic bottles. BPA can be detected in several human body samples, such as serum, urine, amniotic fluid of pregnant women, breast milk, and even in semen. It has been estimated that urinary BPA is detected in more than 90% of Americans. Several studies have shown that increased urine BPA levels may be associated with decreased sperm concentrations and decreased semen quality. (8)
Alkylphenols
Alkylphenols are used industrially in the production of detergents, latex paint, adhesives, and plastics as the stabilizers to package food, detergents, disinfectants, surface cleaners, cosmetic products, herbicides, and pesticides. Unlike most chemicals, which usually become less toxic with biodegradation, alkylphenols become more toxic when they break down. Humans are primarily exposed to alkylphenols through contaminated food and water. Alkylphenols have been shown to affect testicular development and testosterone production.
Phthalates
Phthalates are industrial chemicals used as plasticizers in the manufacture of plastics, solvents, sealants, paints, varnishes, detergents, cosmetics, personal care products, toys, and household products.
Phthalates easily leach from plastics into foods, beverages and body fluids. Factors such as product age, use, and ultraviolet light exposure cause phthalates to leach even more. Humans can be exposed to them through ingestion, absorption, inhalation, and skin contact. Around 6 million tons of phthalates are produced worldwide every year.
Phthalates are considered to be one of the major groups of anti-androgenic substances causing disorders of male reproductive development, such as hypospadias, cryptorchidism, smaller testes and penis size, alterations of the vas deferens and epididymis, poor sperm production, testicular germ cell tumors and reduced semen quality. In humans, maternal exposure to phthalates also results in fetal exposure to these toxins.
Start by filtering what you bring into your home
Avoiding every product with these chemicals may seem daunting, but you can dramatically reduce your family’s exposure by making one small change at a time. You have a lot of control over what you bring into your home, so begin making some simple swaps when it comes to what you put in and on your body.
Pregnant and breastfeeding women, or any woman planning to conceive, should take extra care to avoid endocrine disrupting-chemicals for the future hormonal health of their offspring.
Avoid endocrine disruptors in your food:
Thoroughly wash fruits and vegetables before consuming them,
Replace food storage containers with glass, especially when storing hot food or drinks.
Find reusable glass or stainless steel drink containers and metal straws for your coffee, tea, and water.
Reduce consumption of canned and processed foods (or at least check the label that items are in BPA free packaging).
Never microwave food in plastic containers.
Avoid plastic containers designated #3, #6, and #7.
Consider using a water filter (we know that women on the synthetic estrogens found in hormonal contraception excrete it through their urine, where it ultimately ends up in our water supply).
If possible, purchase organic produce, meat, and dairy products.
Replace older, non-stick pans with newer, ceramic-coated pans.
Avoid endocrine disruptors in your body products:
Each time you need to buy a new bottle of something, look for a new natural brand to try.
Avoid anything that has “fragrance” or “parfum” in the ingredient list.
Use washing balls (Google “washing balls” or “laundry balls”).
Do not use fabric softener—use wool dryer balls instead.
Use the apps ThinkDirty or SkinSafe to see how safe your products are.
Though endocrine-disrupting chemicals can seem unavoidable, the good news is that their dangers are becoming more well-known and many companies are voluntarily offering safer product options. If you begin to read labels, you’ll find lots of packages that say “BPA free” or “No phthalates.”
It has taken me years to make healthy product swaps, and some of the easiest changes I’ve made to avoid the extra chemicals for my family is to replace all our food and drink containers with glass or stainless steel. I also steer away from using canned food. Whenever we run out of a lotion, soap or detergent, I look for a healthier product to replace it. Yes, these products can be pricey, but there have been many products I’ve found we don’t really need, like dryer sheets. The extra time and money it has taken to make these changes is well worth the peace of mind knowing my husband, children (and especially my two boys) have healthy bodies and healthy hormones.
References:
Carlsen E., Giwercman A., Keiding N. and Skakkebaek N.E. 1992 Evidence for decreasing quality of semen during past 50 years. British Medical Journal 305 609–613.
McLachlan, J. A., Newbold, R. R., and Bullock, B. (1975). Reproductive tract lesions in male mice exposed prenatally to diethylstilbestrol. Science 190, 991–992. doi: 10.1126/science.242076
Gill, W. B., Schumacher, G. F., Bibbo, M., Straus, F. H. II, and Schoenberg, H. W. (1979). Association of diethylstilbestrol exposure in utero with cryptorchidism, testicular hypoplasia and semen abnormalities. J. Urol. 122, 36–39.
Jensen, T. K., Toppari, J., Keiding, N., and Skakkebaek, N. E. (1995). Do environmental estrogens contribute to the decline in male reproductive health? Clin. Chem. 41, 1896–1901.
Zhang, L., Dong, L., Ding, S., Qiao, P., Wang, C., Zhang, M., et al. (2014). Effects of n-butylparaben on steroidogenesis and spermatogenesis through changed E2 levels in male rat offspring. Environ. Toxicol. Pharmacol. 37, 705–717. doi: 10.1016/j.etap.2014.01.016
Schug, T. T., Janesick, A., Blumberg, B., and Heindel, J. J. (2011). Endocrine disrupting chemicals and disease susceptibility. J. Steroid Bichem. 127, 204–215. doi: 10.1016/j.jsbmb.2011.08.007
Skinner, M. K. (2011). Role of epigenetics in developmental biology and transgenerational inheritance. Birth Defects Res. C Embryo Today 93, 51–55. doi: 10.1002/bdrc.20199
Li, D. K., Zhou, Z., Miao, M., He, Y., Wang, J., Ferber, J., et al. (2011). Urine bisphenol-A (BPA) level in relation to semen quality. Fertil. Steril. 95, 625–630. doi: 10.1016/j.fertnstert.2010.09.026
A recent study published in The American Journal of Reproductive Immunology evaluated the possible cross-reactivity of antibodies against Spike proteins and proteins related to human fertility. The authors belong to research centers in Israel, Italy, France and Russia. They conducted a systematic study to understand the immunological potential of peptides shared between SARS-CoV-2 Spike glycoprotein and human proteins involved in reproduction and the possible effects that molecular mimicry may have on female fertility.
Molecular mimicry is the resemblance that exists between antigens; in this case, between the Spike glycoprotein of SARS-CoV-2 and the proteins of human tissues. It is a mechanism that can contribute to female and male infertility, by generating autoantibodies that react against the organs of human reproduction.
The authors of the study did a search in a library of 82 human proteins linked to the process of differentiation of the ovum (oogenesis). They compared immunological potential of the peptides shared between SARS-CoV-2 spike glycoprotein and oogenesis-related proteins. SARS-CoV-2 spike glycoprotein was found to share 41 minimal immune determinants, with 27 human proteins that relates to oogenesis, placentation and/or decidualization.
These findings suggest potential cross-reactivity between the homologous peptides that may result in the development of autoantibodies and new-onset of related autoimmune manifestations.
The authors of the study emphasized that the molecular mimicry found in the study does not indicate female reproductive dysfunction in people who suffer COVID-19 infection. They suggest potential cross-reactivity between the homologous peptides that may result in the development of autoantibodies and new-onset of related autoimmune manifestations.
These scientific discoveries about the similarity between Spike glycoprotein and human tissues are very important. All the approved COVID 19 vaccines used the Spike protein. Clinicians should monitor patients vaccinated against COVID-19, due to the problems of cross-reactivity between the homologous peptides and possible autoimmune diseases, cancer, and infertility that may appear among the vaccinated population.
Editor’s Note: This week, we publish a review of important research[i] published in the Journal of Women’s Health in 2011. Dr. Grace Strella summarized the research while on the FACTS elective. The study by Nassaralla et al is titled, “Characteristics of the menstrual cycle after discontinuation of oral contraceptives.” Before this research was published in 2011, no studies had assessed cervical mucus quality upon discontinuation of oral contraceptives (OCPs). Although a 2002 study[ii] by Gnoth et al had assessed basal body temperature and ovulation, cycle lengths, luteal lengths, and cervical mucus peak, it did not evaluate cervical mucus quality. More research is still needed like this groundbreaking 2011 study to understand the full impact of OCPs on fertility and other important aspects of women’s health.
Why This Matters
A woman came into my clinic to discuss fertility and wanted counseling on how to prepare to become pregnant. She had just gotten married and they decided to start a family, so she wanted to stop her birth control pills. She asked me how long it would take for things to “go back to normal,” as she wanted to have children as soon as possible. I told her it could be a few months, but that her fertility would eventually return to normal.
Thankfully, she did not ask any further questions because honestly, I don’t think I would have had many answers for her. This experience showed me I lack knowledge on this important topic, and need to fill in these gaps before another patient comes in seeking my help with such an important aspect of her life.
According to the CDC website, approximately 14% of women ages 15 to 49 were using the pill between 2017 and 2019.[iii] It would make sense intuitively that many of these women would eventually decide to discontinue oral contraceptives to achieve pregnancy. When it comes time for them to attempt to conceive, it would also make sense for women to use fertility awareness-based methods (FABMs) to increase their chances of conception. For this reason, it is important to know what biomarkers will be affected after stopping their oral contraceptives, and for how long these changes will affect their menstrual cycle charting.
Although a few studies have looked at the effects of discontinuing oral contraceptives on a woman’s hormones and return of fertility, this 2011 article by Nassaralla et al was the first to integrate charting, cervical mucus, and specific characteristics of menstrual flow.
Study Design
This was a retrospective matched cohort study that evaluated the biomarkers of the menstrual cycle after stopping OCPs. A total of 140 women were involved in the study. The researchers randomly matched 70 women who had just stopped taking oral contraceptives by age and parity with 70 women who had not used oral contraceptives for more than a year. For six months, they recorded daily observations including menstrual flow (intensity, duration) and mucus characteristics. With this information recorded, they calculated the cycle mucus score, luteal phase length, and the estimated day of ovulation, and assessed overall cycle length.
Biomarkers Altered by OCPs
The study found that the women who had recently stopped oral contraceptives had lower mucus quality scores for the first two cycles. They also noted a later estimated day of ovulation in the second cycle, and an overall decreased menstrual flow intensity in the first four cycles. These results were all statistically significant. In summary, multiple biomarkers were altered for at least two months after stopping oral contraceptives.
Unfortunately, this study has a few limitations that could be addressed in future studies. The study only looked at the first 6 months after discontinuation of oral contraceptives. It might be helpful to see if more patterns are observed a full year after stopping, although the study did show the differences had already minimized by six months. Future research could also assess hormonal levels and biomarkers in the same group of women and assess the impact of potential treatment with hormones such as cyclic progesterone.
The theory behind the delayed normalization of these menstrual cycle biomarkers is that it takes time for the hypothalamic-pituitary-ovarian (HPO) axis to normalize after being affected by exogenous estrogen from OCPs. In patient care, it would be helpful to be able to provide a woman with specific examples of how certain biomarkers will be affected as she begins to chart her cycles in an attempt to increase her chances of conception after stopping OCPs. Information from studies like this one can be applied clinically as physicians and other medical professionals counsel patients on their return to normal fertility after stopping oral contraceptives.
Editor’s Note: Dr. Joe Stanford, one of the study authors, was kind enough to review this summary of their research. Reflecting back, he thinks perhaps the main limitation of this study is that “it’s old enough that the oral contraceptives studied are somewhat different than the ones in use today.” Still, the study design and important data collected can both inspire and inform future research.
Dr. Stanford also shared how their study was strengthened through a timely collaboration:
“Some may be interested in the back story on this publication. Diane Daly and I recognized the need for more data on the impact of recent use of oral contraceptives on women charting their cycles, with the Creighton Model specifically. We started working on collecting data for this study as early as 1992. A few years later, we had completed some preliminary data and analyses.
“Subsequently, I became aware that Claudia Nassaralla and Richard Fehring were working on the same question with a nearly identically designed study (matched retrospective cohort study). Great minds think alike! We communicated and decided to combine our data for better sample size and analysis. After our first submission to the journal, the reviewers requested a more sophisticated statistical analysis appropriate to matched data with variable numbers of cycles per woman. Peer review with added value! Karen Schliep joined the team to do the final statistical analysis, and the manuscript was then accepted for publication, nearly 20 years later!”
References
[i] Nassaralla CL, Stanford JB, Daly KD, Schneider M, Schliep KC, Fehring RJ. Characteristics of the menstrual cycle after discontinuation of oral contraceptives. J Womens Health (Larchmt). 2011;20(2):169-177. doi:10.1089/jwh.2010.2001.
[ii] Gnoth C, Frank-Herrmann P, Schmoll A, Godehardt E, Freundl G. Cycle characteristics after discontinuation of oral contraceptives. Gynecological endocrinology : the official journal of the International Society of Gynecological Endocrinology 2002;16:307-17.
Grace Strella, MD is a family medicine resident at Via Christi Family Medicine Residency in Wichita, KS. She participated in the FACTS elective during residency.
I am a French mother whose teenage daughter recently announced to me that she was gender dysphoric and wanted hormones. Being left-wing politically oriented, a feminist, and sensitive to the rights of minorities, I first thought my daughter had to be supported in the difficult path to transition.
I find this is a common first thought. But after researching the issue, I discovered a completely different—and terrifying indeed—perspective— that my distressed daughter was being rushed down a highly dangerous path. I found also, that, as girls like my daughter hurtle down this road, they are encouraged at all turns by LGBT activists who sincerely believe they are fighting for freedom and against discrimination, while, at the same time, being secretly funded by companies with dubious ethics.
This happens in a context where the media, the educational sphere and the medical world are largely and woefully misinformed, and generally sympathetic to trans claims of marginalization to the exclusion of all other perspectives.
Great Britain, Sweden and Finland are ahead of France on this path of gender ideology—and in terms of resistance to the trend. For years, in these countries, as well as in North America, parents and health professionals have kept their doubts alive and have challenged the ideology behind medical transition of minors. Today medical studies abound showing the ineptitude and danger of early transitions before age 25.
You may not feel concerned by this story. Maybe you are more interested in classical politics, social inequalities and the climate change. But… the trans wave is now in France, just four or five years after Great Britain, and we need to be vigilant and aware.
Today, it is my daughter. Maybe your daughter will be next? Or her childhood friend? Or the neighbour’s daughter? Your niece? One of your students? One of your patients? Your granddaughter? Your sister or cousin? And this contagion is not limited to girls. Boys too are increasingly under threat from trans ideology.
More than anything else, I researched and wrote this to protect my daughter and help her question this dangerous path before rushing headlong into it. For this reason, I must keep my name secret, and I cannot activate my usual professional, friendly, feminist, political networks.
My hope is that my research, written in French and translated into English, will help others. Most of the resources linked in this article are in French, some in English. This is a world-wide phenomenon and resources should be available, eventually, in all languages.
I thank you for disseminating this text as widely as possible, by all the means at your disposal, including social networks used by young people: Tiktok, Instagram, Facebook, and your friendly, educational, medical, lesbian, feminist, media, political networks… All ideas are welcome to support our girls and boys!
1. What is this about ?
Gender dysphoria is a kind of suffering related to the feeling that one belongs to the other gender, in relation to one’s birth sex. Until recently, this was a rather rare diagnosis. However, in the last decade, this phenomenon has increased exponentially, by + 1500% to + 4000%, especially among young girls in Western countries.
The documentaries The Trans Train1and Dysphoricare excellent resources to discover a phenomenon which has swept through the USA, Canada, Great Britain, Sweden, Finland, and is now arriving in France, Spain and the rest of Europe. The video “Gender or Sex?” (in French) is also very educational and family-friendly.
Some studies suggest a kind of social contagion is going on, a phenomenon related to a form of expression of adolescent suffering in young girls similar to adolescent anorexia. Clusters—groups of young girls wishing to transition—are frequently seen appearing.
2. Sex and gender, vocabulary and ideologies
Gender ideology is rife with new and reinterpreted terms, and it’s important to learn how trans-activists use them in untraditional ways.
The sex of a person is biological data linked to our DNA (XX or XY in 99.8% of cases, intersexin rare cases). This genetic heritage determines (except intersex exceptions, in 1 to 2% of cases) the primary sexual characteristics: ovaries, uterus / penis, testes as well as secondary sexual characteristics, after puberty (chest, hair, etc).
By widely shared convention, we call female a human female (XX) and man a human male (XY). Genderusually refers to the set of socially constructed differences and stereotypes associated, in a given culture, with each biological sex. So, today, pink is said to be the colour of girls and blue that of boys, although the opposite convention prevailed in the past.
Thus, from a classical feminist perspective, sex is a physiological datum that cannot be changed, but stereotypes and gender norms can be questioned and challenged. This is the spirit underlying texts such as the Woman’s Declaration, an international declaration of women rights based on biological sex. Many lesbianand homosexualmovements are also part of this classical feminist tradition.
The trans movement uses very different terminology.
Harry Potter’s author J.K. Rowling’s alleged transphobia recent controversystems from the fact that she joked about the disappearance of the word “woman” to describe a person having their period—a factual statement that would have been uncontroversial up until the very recent past.
The video “Gender or Sex?”(in French) provides a very educational scientific reminder on the terminological confusion between sex and gender. The video “An honest discussion on Gender”, with Dr Debrah Soh also covers this issue well.
3. Psychotherapeutic follow-up or medical transition?
Moreover, regardless of any transphobia, it is an undeniable fact that medical transition (hormones and surgery) is largely irreversibleand dangerousfor bone density, heart4 and fertility. Moreover it hasn’t been demonstrated to even improve mental health.
Our purpose here is not to deny the possibility of medically transition for adults who have thought at length about this issue. What we do aim is to question:
the permanence or desistance of gender dysphoria in children and adolescents
the usefulness of an irreversible medical transition, potentially dangerous and often unsuited to their suffering
the influence that social networks and LGBT activism can have on young people experiencing doubt and suffering, while being very much mobilized against discrimination
Detransition is a growing phenomenon related to the explosion of gender dysphoria and the transition of young minors. Discussion of detransition has been taboo within the trans community, as it counters the narrative about the immutability of gender identity. Nonetheless, more and more young people are detransitioning. Medically speaking, the transition pathway is delicate.
Studies on this phenomenon remain scarce because showing interest in detransition is considered by activists as transphobia, and those looking into it have been shunned and vilified.
5. International situation. Legislative developments
In Sweden, Finlandand the United Kingdom, legislation has changed very recently to the effect that puberty blockers and transition hormones are now prohibited for minors.
In England, the Keira Bell case (a young woman who transitioned at age 16 and sued the clinic a few years later) resulted in a chilling in support for the medical transition of minors. An article in Medscape(translated in French here) was published in April 2021 under the title“Transgender adolescents: Are the winds starting to turn?”. In the United States, Arkansas has just adopted legislation similar to that of Finland. In Canada the recently passed “Bill C6” law aroused oppositionbecause of the ambiguous wording comparing the psychotherapeutic treatment of young dysphoric patients to conversion therapy.
The trans movementdemandsthe withdrawal of trans identity questions from the psychiatric sphere (depsychiatrization) and the right to self-determination of one’s gender and to medical treatment (hormones, sex reassignment surgery), fully reimbursed by social security without prior psychotherapeutic follow-up.
The main oppositions come from the conservative movements, which the present text does not study further, and from various movements already mentioned above:
These movements, irrespective of their political opinions on other subjects, are all very worried about this trend towards the rapid medical transition of young minors, and their medicalization for life, without serious psychotherapeutic follow-up.
The LGB Alliance in the UK goes so far as to call trans medicine conversion therapy for young gay men.
7. The weight of lobbies
Very large companies linked to the medical world massively subsidize the Trans movement, or certain political parties with positions favourable to the positions of the trans community. For example Ferring Pharmaceuticals has regularly subsidizedthe Liberal Democrats in the United Kingdom.
The very educational Australian video, “The business model of youth transitioning”highlights the huge markets behind the potential life-long medicalization of hundreds of thousands of young Westerners.
In France, information offering an alternative to the medical transition for minors is difficult to find. As this text shows, the (most certainly sincere) speech of many trans activists calling for the transition on simple request, without psychiatric follow-up, including for minors, meets very little institutional opposition, and disqualifies all oppositions as transphobic.
What is more, Family Planning institutions, the Mediator of Rights, and many doctors, are trained by transactivist groups pushing them to accept young people’s transition desires without questioning them. Parents that question the trans affirmative narrative have very few resources, although a parent group in France will be created soon.
The usual difficulty faced by parents of dysphoric children is a kind of suicide blackmail: either you accept your child’s medical transition, for his or her good, or your child will commit suicide (and in addition you are transphobic). From a scientific standpoint, this threat is a myth and has been thoroughly discredited.
1 “The Trans Train” is a 2019 three-part Swedish documentary that rocked Sweden very quickly and ditched medical transitions on minor. Part 2 and Part 3 are also available on YouTube with English subtitles.
This summer, the Marvel movie Black Widow featuring Scarlet Johannson finally offered some backstory into the life of the much-neglected superheroine, Natasha Romanoff. As one of the Avengers without superhuman strength, Romanoff is known for her expert interrogation and investigatory skills gained from her time as a Russian operative. Films reveal tidbits from her past over the Marvel Comic Universe cannon. We know her training was something of a forced trial by fire, and in Avengers: Age of Ultron, it’s revealed that a part of the training includes sterilization. “It’s efficient,” she tells Bruce Banner.
In Black Widow, Romanoff, reconnected with her sister Yelena, vows to combat the system that led to her oppression. It is revealed that the two sisters do not have menstrual cycles as a result of their exploitative training program.
“They rip out all of your reproductive organs,” Yelena explains. “They chop them all away . . . so you can’t have babies.”
The system Yelena and Natasha Romanoff end up fighting in the culmination of Black Widow reveals a network of trafficked women treated as disposable pawns in the battles of more powerful actors. The women were kidnapped as girls or otherwise lured into the “Red Room,” before being enslaved and forced into an aggressive militia training program, wherein their free will is stripped from them, requiring them to comply with everything commanded of them. Some escape, as Natasha and Yelena did, but these are the exceptions.
The film Black Widow is not making a subtle comparison to human trafficking and other exploitations of girls and women in its plot. While it’s a comic book story, the plot contains clear allusions to real-life abuses of girls and women, and not by accident. Black Widow director Cate Shortland told USA Today her goal was to “have the Marvel universe intersect with reality. So we talked about trafficking. We talk about women’s reproductive rights in the film because they’re things we care about.”
Reproductive harm and sex trafficking
Human trafficking takes place in the forms of labor trafficking (when people perform labor through the use of force, fraud, or coercion) and sex trafficking (when people are sold in commercial sex acts through the use of force, fraud, or coercion, or when any minor is sold in commercial sex acts). Trafficking is a modern-day slavery that takes place all over the world, including the United States. And, as I discovered completing a yearlong journalism fellowship on the topic, sex trafficking takes place in all areas of the sex industry, from prostitution and strip clubs to pornography.
Sex traffickers most often come in the form of a “pimp,” a person who grooms, recruits, and profits from selling people in sex. Young women, men, girls, and boys, can become caught up in sex trafficking in a number of ways, from being kidnapped, to being manipulated by a charming boyfriend into helping him make money to get out of a bind. However it begins, sex trafficking involves significant sexual abuse and trauma, often a Stockholm Syndrome-type bonding to the trafficker making it hard to escape, and harder for law enforcement to detect. For many girls and young women, it involves significant reproductive abuse as well.
The role of birth control in sex trafficking
Survivors of sex trafficking have told me that pimps will take advantage of any opportunity to make a buck by selling sex. Since much of sex trafficking involves selling sex in prostitution, maximizing profit for traffickers requires that trafficked women not get pregnant. In other words, birth control is essential to be “efficient” in the sale of sex. Whether a trafficked woman attempts to use condoms, is on hormonal contraceptives, is sterilized, uses Plan B, or has an abortion when pregnant, birth control is an essential part of making money for traffickers.
“Commercial sex has a wide range of negative effects on the reproductive health of prostituted women and trafficked girls,” Dr. Michael Shively, senior advisor on research and data analysis for the National Center on Sexual Exploitation, told me in an email. “The consent and welfare of prostituted women is of little concern to pimps, traffickers, and brothel owners, and maximizing income is always the objective.” As a result of pressure to please and earn money, Dr. Shively explains, condom use is largely ineffective as a means of protecting from STIs or preventing pregnancy for trafficked women. As he told me:
Sexually exploited people often try to protect themselves through condom use but are usually forced or pressured into unprotected sex. Unprotected sex is regarded as an occupational hazard. Those who insist on condoms are frequently forced to engage in sex without them, and those who succeed in consistent condom use earn far less money than those who don’t. . . . Women insisting to protect themselves are substandard earners, and often pay the consequences of beatings and coercion until they become compliant and accommodating about allowing sex buyers unprotected sex.
Connie Rose, a sex trafficking survivor who helps other trafficked people with the organization Victims 2 Survivors, shared with me how she has known many women who have suffered reproductive harm from menstruation control methods as well as birth control methods. “I have known other survivors who were forced to use vagina cups so that your flow was not a part of the sexual experience. They are also a form of birth control,” she told me in a phone call, but used during prostitution, she says, “they created irritation in the lining of the uterus, and a lot of my friends who used them ended up having hysterectomies and incredible health problems.”
Rose told me that in the past when helping trafficked women, it was hard to set up a well women’s visit to the doctor without fear, “when there’s a warrant out for your arrest.” Rose is now a survivor trainer at Global Strategic Operatives, an organization that trains healthcare professionals how to identify and support trafficking survivors, stating “88% of victims seek medical care or treatment while being trafficked.” And since many girls and women who have been trafficked into prostitution are treated as criminals by law enforcement, advocacy organizations like Shared Hope International aim to train law enforcement officials how to recognize the signs and work with survivor-led groups to help women recognize cycles of abuse and leave their traffickers.
Shared Hope and NCOSE and other anti-trafficking organizations insist that the most effective way to reduce trafficking of persons is to follow the Nordic Model—to decriminalize prostituted people and focus law enforcement efforts on reducing demand for prostitution by criminalizing sex buyers, in addition to targeting traffickers.
While traction is being made to recognize signs of trafficking and help victims get the health and recovery services they need, there is a lot of work still left to be done, including in the area of women’s health. Often those seeking women’s health services are not identified as victims of trafficking, and are therefore given incomplete care.
According to Amanda De Jesus, a FertilityCare Practitioner Intern (FCPI) and a member of the Northwest Indiana Anti-Trafficking Coalition, “Unfortunately, there are many women and girls who are being evaluated by medical professionals while they are still being trafficked. Because a lot of these doctors aren’t trained to recognize the signs of trafficking, often they are just being treated for UTIs, STIs, etc., given birth control, and sent out the door.”
While some might still view this as a net good for the trafficked women coming in to receive birth control services, viewed another way, it is overlooking the larger problem and applying an insufficient treatment—one that might even cover up or further the abuse. “Birth control, in many ways, is another tool that a trafficker can use to take control away from a survivor,” De Jesus told me in an email. “When birth control is forced upon women (or they are coerced into taking it), I believe it shows these girls that their natural bodies are something to be hated and suppressed while they are used as an object for another’s pleasure. Not to mention the myriad of negative side effects that often accompany taking hormonal contraceptives.”
“Birth control, in many ways, is another tool that a trafficker can use to take control away from a survivor.”
This is born out in survivors’ testimonies. A 2015 report by Laura Lederer and Christopher Wetzel, published in the legal journal Annals of Health Law, was the first of its kind “to examine many of the reproductive health issues experienced by sex trafficking victims, including birth control usage, pregnancies, miscarriages, and forced and elective abortions.” Of the surveyed women, “a large majority (80.9%) of those who answered the question indicated that they had used some form of birth control for some portion of their time being trafficked. Of those who specified where they obtained the birth control, approximately half (51.7%) said they had obtained it from a doctor or clinic.”
As one survivor shared in Lederer’s report:
During the time I was on the street, I went to hospitals, urgent care clinics, women’s health clinics, and private doctors. No one ever asked me anything anytime I ever went to a clinic. . . . I was on birth control during the 10 years I was on the streets—mostly Depo-Provera shots which I got at the Planned Parenthood and other neighborhood clinics. I also got the morning-after pill from them.
Among the report’s recommendations to medical professions are to urgently “be made aware of critical signals for identifying trafficking victims.” Healthcare professionals need to be trained to “understand the coercive dynamic of trafficking, especially the extreme degree of control exercised by traffickers, and the prevalence of this criminal exploitation of women and girls.”
Abortion and sex trafficking
When trafficked women do get pregnant, many suffer forced abortions as a vicious follow-up measure of birth control. “Part of my story is that I was forced to have an abortion at 16,” Connie Rose told me. “It was a late-term abortion” at eight months gestation, and “a lot of my friends also had abortions, too,” she said, “as a means of birth control.”
“Some of it was controlled by their trafficker; some was by choice [of the trafficked woman] because the last thing they were going to do was let a trafficker have their child.” She added that the fallout of abortion is “not just mental side of it, but what it is doing to your body physically.”
Later in her advocacy work, Rose also helped a trafficked woman whose trafficker “beat her up” when she was pregnant, “so she would just naturally abort. I’m sure she’s not the only one,” she told me.
Sadly, forced abortion, and abortion under the oppressive context of sex trafficking, are very common for women and girls trafficked into prostitution. Lederer’s 2015 report found “more than half (55.2%) of the sixty-seven respondents who answered reported at least one abortion, with twenty respondents (29.9%) reporting multiple abortions.”
The report further explains, “While only thirty-four respondents answered the question whether their abortions were of their own volition or forced upon them, more than half (eighteen) of that group indicated that one or more of their abortions was at least partly forced upon them.”
Numbers like this make it unsurprising that the anti-abortion group Live Action revealed in undercover investigative videos of Planned Parenthood that abortion providers were ready to offer no-questions-asked abortion services to girls and women who identified as minors with pimp-like figures in their clinics. While protocol insists that people who appear trafficked should be connected with authorities and abuse-recovery services, these videos echo what many survivors say in their testimonies—that abortion clinics often provide the requested services without question, and then send them on their way.
Better ways forward for the reproductive health, empowerment, and protection of girls and women
While abuses against women are not entirely due to birth control, birth control is a constant that makes these sexual abuses easier to take place, and easier to keep under wraps. When a 14-year-old gets pregnant, for instance, that can be an obvious sign that statutory rape has happened (and may, in fact, be continuing to happen). When a 14-year-old is on birth control, that kind of abuse can go on much longer before people see the signs.
While abuses against women are not entirely due to birth control, birth control is a constant that makes these sexual abuses easier to take place, and easier to keep under wraps.
Even from women who are not sex trafficked, I hear echoes in social media groups of the pressure many women today feel to be “constantly available sexually” for their partners in order to have relationship security. Nonstop sexual activity separated from procreation isn’t sustainable without birth control, and this outlook is creating sex drives that are not naturally sustainable. It can foster difficulty down the road in maintaining self-control when sex is not available for completely human reasons, such as when a partner isn’t well, has surgery, is bereaved, or is postpartum—times when love should be expressed in different ways. And it gives women the impression they are not valuable for simply being themselves, but for their utility to be used by others for pleasure, which is to reduce their value to that of an object.
To use women as objects dehumanizes them, and a part of what makes women human is our reproductive capabilities. As a result, we should consider no-questions-asked birth control services for women and girls with some amount of skepticism and apprehension. If we don’t work harder as a society to identify the controlling of women and girls in sex trafficking, we may ignorantly participate in the perpetuation of abuse, and birth control can be just another form of exploitative control.
Women who use modern fertility awareness methods instead of birth control say they feel more in the driver’s seat of their reproductive health, and they are more able to read their body’s signs and understand their health and fertility. As a result, women who have switched from birth control to fertility awareness methods express feelings of being more in tune with their bodies, greater self-agency in sexual relations, and a greater sense of equality between partners.
When teen girls are taught fertility awareness, there is evidence that it helps reduce at-risk behavior. As Anna Migeon shared in her impactful article on “Cycle Mindfulness:”
In the 1980s, Leslie Carol Botha taught basic fertility awareness charting to teen girls (13-17 year-olds) at eight different restorative care homes for at-risk girls. A typical girl in the program had been a victim of sexual assault, ran away from home, used drugs and alcohol, and ended up in jail. In working with these girls, Ms. Botha made an amazing discovery: teens who are taught fertility awareness and how to chart their cycles can regain control of their lives.
Here is what she found out: for 90% of the girls in the program who had ended up in jail, it happened during the premenstrual phase of her cycle, that monthly darkness that Ms. Botha calls “falling down the rabbit hole:” increased anger, disruptive and self-destructive behaviors, suicidal ideation, and drug and alcohol cravings.
While fertility awareness is not a quick fixfor the exploitation and complex problems caused by sex trafficking, educating girls and women about their bodies and reproductive health can assist them in achieving greater self-knowledge, agency, and healing, no matter where they are on their journeys.
The document“Called to the Joy of Love: National Pastoral Framework for Marriage and Family Life Ministry” was developed by the Committee on Laity, Marriage, Family Life and Youth of the United States Conference of Catholic Bishops (USCCB). It was approved by the USCCB at its June 2021 Plenary Assembly. The framework is intended to assist dioceses as local pastoral planning and implementation continue to take place since the publication of the 2016 apostolic exhortation on the family, Amoris Laetitia. It provides guidelines for the pastoral accompaniment of married couples and families in every phase of life, drawing upon the teachings and recommendations contained in the apostolic exhortation.
See the digital edition of the pastoral framework here
A new bill introduced by Ohio State Rep. Jena Powell aims to reduce the number of abortions in the United States from 2,363 each day to zero. The 2363 Act would ban abortion in Ohio, except in the rare situation where a mother’s life is at grave risk (see more here on why abortion is never truly medically necessary). Like the Heartbeat Act in Texas, citizens would be able to sue an abortionist for violating the law by committing an abortion, while the bill would exempt women undergoing abortions from legal repercussions.
Powell spoke with Live Action News in an exclusive interview about the legislation.
“The 2363 Act is… based off of the Arkansas Unborn Child Protection Act, which was signed into law earlier this year, but we’ve made a couple of changes,” explained Powell. “This bill uses the enforcement language by the Texas Heartbeat Act, which has been upheld by the 5th Circuit Court. We stated Alabama, Louisiana, Arkansas, and Utah as having recently passed similar pieces of legislation.”
The 2363 Act is one in which Powell has a personal investment, due to her upbringing and her passionately held pro-life beliefs.
“As a woman legislator in our state, I believe it is crucial that we move forward on pro-life issues,” she said. “I’m very, very passionate; I’m actually one of seven children. I’ve grown up in a household that protects life, and understands that abortion is wrong. And so for me, being in the legislature, it was exciting to start working on crucial pieces of legislation. We already passed the heartbeat bill in my first term, and that said that at the time we can see a heartbeat, that child deserves life, and to be protected; that’s currently being held up in the courts, but what I realized was, if we believe life begins at fertilization, then we have to continue moving the ball forward in protecting every life.”
Powell is also doing more than just passing legislation to defend life. She’s founded the Ohio Pro-Life Caucus, which aims to take pro-life activism even further. Powell and the Pro-Life Caucus believe in taking a dual approach to ending abortion, both through enacting pro-life legislation and offering increased support to women, children, and families.
“We have a lot of pro-life members in our state,” she said. “In Ohio, we’re trying to pull together as many conservative Republicans that believe in life, or members [who] holistically believe in the pro-life movement. We’ve sent out a co-sponsorship request, and we’re really moving forward on the bill. The goal of the pro-life caucus is to inform and educate members, as well as help them move forward the narrative and policies to protect every single life in the state of Ohio. We have bills that we’re working towards in the caucus between members — everything from eradicating abortion holistically, to protecting and preserving life, to helping pregnancy resource centers, to helping hurting mothers and families in our state. So, we’re kind of looking at a two-pronged approach, and saying, all right, let’s end abortion in our state, and let’s also move forward and help women, help children, and take steps to eradicate abortion as well.”
Despite support for pro-life bills across the country, the abortion industry continues to go on the attack against them. One common argument is that pro-life legislators are only concerned with protecting children before birth, which Powell said was “categorically untrue.”
“The state of Ohio gives tons of money to women, families, and children in our state. We continue to support pregnancy resource centers, we provide a lot of opportunities, whether it’s struggling mothers or young children, in our state,” she said. “Data would show us that those claims are untrue. And I understand why the pro-abortion movement wants to say that. But at the end of the day, the stats, the data, the knowledge, is on our side.”
Powell currently has 33 co-sponsors and one joint sponsor for the 2363 Act, noting that she believes there is “an appetite to protect and support life in our state, specifically with everything that’s going on in the Supreme Court. Ohio is a pro-life state. My first general assembly, we passed the Heartbeat Bill, and our voters — there’s over 11 million Ohioans — were in huge support of that bill, and were very thrilled that we moved forward on it. Ohio is a more conservative state for sure, and Ohioans see that we not only support mothers and children, but also we’re looking to protect life in the process.”
Live Action president and founder Lila Rose noted in a press release:
Abortion is our nation’s leading cause of death, killing more people than heart disease, cancer, or COVID-19. This gruesome truth echoes throughout the 2363 campaign, pleading with our national conscience that action must be taken on behalf of the most vulnerable. The science is crystal clear – human life begins at the moment of fertilization – not at birth, not at 15 weeks gestation, not even at 6 weeks when a preborn child’s heartbeat can be first detected. Every single preborn child deserves protection and no child should be discriminated against based on race, gender, medical diagnosis, or age.
The 2363 Act ensures that no child will be left behind to face the abandonment and violence of abortion. We must be absolutely fearless in our efforts to protect these children as well as their mothers and families from the predatory abortion industry. The 2363 Act is the beginning of the end of legally sanctioned abortions in America.
Altogether, Powell expects great things in the future for the pro-life movement in Ohio, which will have a positive effect for residents throughout the state.
“We’re just really excited,” she said. “Ohio did not have a pro-life caucus, and so we’re excited to move forward holistically on helping women and children in the state of Ohio. We know abortion does not help women. There are so many resources for women and children, and men, because we know abortion harms everyone. It’s not just a female issue.”
Once he has established some fundamental principles, St. Paul VI proceeds to evaluate, from the moral perspective, the problem of contraception within the context of conjugal love and the transmission of human life. First, he affirms this moral norm in its positive sense or its prescriptive dimension, i.e., what must be done. The term “prescriptive” simply means “to prescribe,” to command the performance of a certain action (like “feed the poor” or “clothe the naked”).
Later, the Pope affirms the moral norm in its negative sense or its prohibitive dimension, i.e., what must be avoided. The term “prohibitive” simply means to prohibit, to forbid the commission of some evil action (like abortion or contraception).
In the positive sense, Humanae Vitae commands that in the conjugal act, husband and wife remain open to the possibility of transmitting human life: “The Church, nevertheless, in urging men to the observance of the precepts of the natural law, which it interprets by its constant doctrine, teaches that each and every marital act must of necessity retain its intrinsic relationship to the procreation of human life” (11).
Must new life come from every conjugal act?
This norm does not at all mean that a new life must ensue from every conjugal act. As a matter of fact, such an occurrence is biologically impossible, as St. Paul VI himself recognizes. In addition, the Pope teaches that the spouses do not commit any sin when they engage in a conjugal act that they foresee to be infertile through no fault of their own. Even in such cases, the Holy Father calls the conjugal act itself “chaste, noble and worthy” when husband and wife truly love each other and are not closed to the possibility of transmitting a new human life:
The sexual activity, in which husband and wife are intimately and chastely united with one another, through which human life is transmitted, is, as the recent II Vatican Council recalled, “noble and worthy.” It does not, moreover, cease to be legitimate even when, for reasons independent of their will, it is foreseen to be infertile. For its natural adaptation to the expression and strengthening of the union of husband and wife is not thereby suppressed. The fact is, as experience shows, that new life is not the result of each and every act of sexual intercourse. God has wisely ordered laws of nature and the incidence of fertility in such a way that successive births are already naturally spaced through the inherent operation of these laws. (11, emphasis added)
What Then Does Humanae Vitae Command?
The positive norm of Humanae Vitae consists in commanding the spouses to always respect the inseparable connection between the unitive meaning and the procreative meaning of the conjugal act:
This particular doctrine, often expounded by the magisterium of the Church, is based on the inseparable connection, established by God, which man on his own initiative may not break, between the unitive meaning and the procreative meaning which are both inherent to the marriage act. (12)
However, respect for the inseparable connection between the unitive and procreative meanings implies a lot more than just abstaining from contraception. Recall that in Humanae Vitae 9 St. Paul VI explained the four characteristics of conjugal love: fully human, total, faithful and exclusive, and fecund. The spouses are called to grow in all of these values and in their love for each other. Each spouse is called to always see his beloved as a gift from God, as end in himself or herself, as a person, and not as an object for selfish pleasure. True conjugal love requires that the husband sees himself as a gift from God to his wife and at the same time to welcome his wife as a gift from God. Likewise, the wife must see herself as a gift from God to her husband and at the same time to welcome her husband as a gift from God. In the words of the Holy Father himself: “Whoever really loves his spouse loves not only for what he receives, but loves that spouse for the spouse’s own sake, content to be able to enrich the other with the gift of himself” (9, emphasis added).
The Wedding Register – Edmund Blair
This dynamic of love as self-gift, together with the practice of self-control, enables the spouses to acquire and practice those virtues that enrich conjugal life and the conjugal act itself: sincerity, honesty, tenderness, affection, and solicitude, among many others.
Openness to Life
Recall that one of the characteristics of true conjugal love is its inherent openness to the transmission of new life. If the spouses truly love each other and avoid contraception, they will be able to develop a deep love for the transmission of life and for their children when God decides to give them this precious gift. Pope Paul VI teaches us that the value of self-control or self-discipline also enables the spouses to
fully recognize and value the true blessings of family life…and confers upon them as parents a deeper and more effective influence in the education of their children. As their children grow up, they develop a right sense of values and achieve a serene and harmonious use of their mental and physical powers. (21).
Why must the spouses always respect this inseparable connection between the unitive and procreative meanings of marriage?
The answer to this question is astonishing simple: because the nature of true conjugal love demands it. Recall that one of the characteristics of conjugal love is its fertility. The Holy Father explains that true conjugal is inherently open to the possibility of transmitting human life. A conjugal love that deliberately closes itself to life is no love at all; it is a lifeless “love.” As the Holy Father writes of true conjugal love:
This love is fecund. It is not confined wholly to the loving interchange of husband and wife; it also contrives to go beyond this to bring new life into being. Marriage and conjugal love are by their nature ordained toward the procreation and education of children. Children are really the supreme gift of marriage and contribute in the highest degree to their parents’ welfare.
If the spouses, through contraception, destroy their sexual act’s capacity to transmit life, they are not only violating the procreative meaning of the conjugal act, but also its unitive meaning. Contraception is not only anti-life; it is also anti-love.
Let us also recall that another characteristic of conjugal love is that conjugal love is total. It encompasses the whole person. Husband and wife give themselves to each other completely in their conjugal act, leaving nothing out. But if they contracept, then they are leaving out their fertility and not giving themselves completely. Therefore, once again, contraception is contrary to conjugal love and not only to procreation.
The Prohibitive Norm of Humanae Vitae
The prohibitive norm of Humanae Vitae is that nobody may ever deliberately break the inseparable connection between the procreative and unitive meanings of the conjugal act by means of contraception, anti-natural uses of the sexual act (such as sodomy or coitus interruptus), sterilization, or abortion. In the words of St. Paul VI:
Therefore We base Our words on the first principles of a human and Christian doctrine of marriage when We are obliged once more to declare that the direct interruption of the generative process already begun and, above all, all direct abortion, even for therapeutic reasons, are to be absolutely excluded as lawful means of regulating the number of children. Equally to be condemned, as the magisterium of the Church has affirmed on many occasions, is direct sterilization, whether of the man or of the woman, whether permanent or temporary. Similarly excluded is any action which either before, at the moment of, or after sexual intercourse, is specifically intended to prevent procreation—whether as an end or as a means (14).
It is clear from this passage that not only direct abortion and direct sterilization are absolutely prohibited, but also all kinds of contraceptives, whether barrier contraceptives, hormonal contraceptives (which are also abortifacients), or mechanical contraceptives (such IUDs, which are also abortifacients).
Why Is Contraception “Intrinsically and Gravely Evil”?
The act of contraception always violates the intrinsic goods of marriage and of the conjugal act: the unitive and the procreative. Therefore, it is intrinsically evil. Since the goods that contraception violates are at the same time values of great importance (love and life), contraception is also gravely evil. This means that no circumstance or motive can ever justify it. The norm that prohibits contraception in all its forms is an absolute norm, i.e., it admits of no exception.
In addition, if we consider the teachings of St. John Paul II on the theology of the body, we will discover that contraception is also anti-sacrament. The sign of the sacrament of marriage is comprised of (1) the vows that bride and groom exchange during their wedding, and (2) the conjugal act that expresses those vows through the language of the body. The true language of the body, in the case of marriage, includes the conjugal acts that physically express the sign expressed in the words (the marital vows) of the sacrament of marriage. Furthermore, it is clear that the sign of the sacrament of marriage includes the unitive and procreative meanings that God has inscribed in the souls and bodies of husbands and wives, because those meanings are included in the marital vows in one way or another.
But contraception goes against both of those meanings, the unitive and procreative. Therefore, it is a counter-sign, an anti-sacrament.
Wedding of Mary and Joseph – Artist Unknown
Is Contraception a Mortal Sin?
When the spouses possess full knowledge that contraception is an intrinsically and gravely evil act but nevertheless freely and fully will it, they commit a mortal sin. They cannot receive Holy Communion nor enter Heaven upon their deaths.
But if they put their trust in our all-merciful God, repent, promise to amend their lives, go to confession and fulfill the penance imposed by the confessor, they will be filled with God’s infinite mercy and love. They can and should receive Holy Communion and the strength it provides to live righteously and to love God and neighbor. God will heal their lives and lead them to a life of holiness and happiness.
An Objective or Subjective Argument?
It may seem that this whole discussion against contraception is based on subjective arguments because the Holy Father appeals to the subjective characteristics of conjugal love: fully human, total, faithful and exclusive, and fecund.
But we must clarify that we are discussing marriage morality not only from a subjective perspective on the values of conjugal love. We are also discussing marriage morality from an objective perspective. The same values that characterize true conjugal love are at the same time objective goods that God has inscribe in the very beings of the spouses and that they must respect and develop. The spouses who truly love each other and are faithful to God through His Church internalize these objective goods, making them their own. Once the spouses have accepted these goods in their hearts, the goods become values that the spouses cherish and develop so that their love for each other and for their children grows and flourishes.
A value is the internal experience of an objective good. The principal objective goods of marriage (conjugal love, the procreation and education of children, and the sacramental sign) ought to be interiorized and personalized by the spouses, and so become values.
In this way, spouses render justice to the objective and subjective dimensions of conjugal morality and of the whole spectrum of Catholic morality. The objective goods that God’s commandments protect become the interior values that propel good Catholics to act. God’s commandments are no longer seen as “external rules” but as guarantors of that happy life (here and beyond) that the goods protected by the commandments make possible.
Finally, it should be clear that by “subjective” we do not mean at all subjectivism. These two are completely different. In fact, they are opposites of each other. Subjective values correspond to the interiorization of objective goods, while subjectivism is an ideology whose adherents believe that their inner feelings, no matter how wicked, are true for them, even if they are not true for others. Subjectivism leads to relativism and relativism destroys morality completely, because relativism leads to the erroneous belief that morality is subjective and individualistic, and that objective and universal moral norms do not exist.
The medical device company Contraline has invented a new male contraceptive. Using advancements in hydrogel technology the company developed a device called ADAM™ .
The device is implanted into the vas deferens through an outpatient procedure. The hydrogel works by blocking the vas deferens preventing sperm from traveling through.
This device is similar to intrauterine devices (IUDs) for women, and it is designed to last for years and be reversible. Contraline initiates its first-in-human clinical trial in 2021.
Although, the company emphasizes that the hydrogel is easily injectable, safe, and long-lasting, the moral aspects and problems to the conscience of married people are ignored.
Humane Vitae tell us “Consequently, unless we are willing that the responsibility of procreating life should be left to the arbitrary decision of men, we must accept that there are certain limits, beyond which it is wrong to go, to the power of man over his own body and its natural functions—limits, let it be said, which no one, whether as a private individual or as a public authority, can lawfully exceed.”
“The question of human procreation, like every other question which touches human life, involves more than the limited aspects specific to such disciplines as biology, psychology, demography or sociology. It is the whole man and the whole mission to which he is called that must be considered: both its natural, earthly aspects and its supernatural, eternal aspects. ”
On Monday, the City of Mason, Ohio (pop. 35,450), became the 41st city in the nation and the second city in Ohio to pass an enforceable ordinance outlawing abortion within its city limits. The second and final reading vote passed 4-3 in the packed city council chambers.
Mayor Kathy Grossmann was joined by council members T.J. Honerlaw, Mike Gilb, and Tony Bradburn in favor of the ordinance outlawing abortion, while council members Ashley Chance, Diana Nelson, and Josh Styrcula voted against the measure. While the ordinance passed by a majority vote, the ordinance did not receive the five votes required to go into immediate effect. This means that the ordinance will go into effect on November 24th, which will be 30 days after Monday’s vote.
Mark Harrington, president of Created Equal, was one of the many pro-life leaders present for the historic meeting. Harrington shared, “Joe Biden has stated he wants abortion in every zip code in America. Hence, citizens across America are acting by preventing abortion from being committed in their communities. Ohio is once again taking the lead to protect children and more cities are joining this movement every week!”
Mason is the 24th city to pass an ordinance outlawing abortion since the Biden Administration stated their commitment to see abortion access in every zip code in January of this year.
The first to introduce the ordinance to be placed on the agenda was Councilman T.J. Honerlaw. Upon the passage of the ordinance, Honerlaw shared, “Passing the sanctuary city for the unborn ordinance is my greatest accomplishment while serving my first term on Mason City Council. It’s been an honor to work with my pro-life colleagues to keep abortion out of Mason, Ohio.”
Vice-Mayor Mike Gilb also stood confident in his decision, knowing that it was what his constituents placed him there to do. “I’m here to protect life. For me it’s a fundamental issue . . . I’m not just here to decide how bright the street lights should be or where the next roundabout goes. Those things are certainly important issues, but they’re not as fundamental as protecting life.”
For the four outspoken and passionate members on the council who were for the ordinance, there were three outspoken and passionate members on the council who were against the ordinance. The most outspoken on the council against the ordinance was Councilwoman Diana Nelson, who appeared to affirm that women had a constitutional right to an abortion.
Nelson shared, “The Supreme Court has made a ruling on abortion, regardless of one’s opinion on abortion; creating local laws that contradict with federal laws is illegal and unconstitutional.” Nelson continued, “When local leaders begin enacting laws which are in violation of our resident’s constitutional rights we have a much larger problem.”
Mayor Kathy Grossmann pushed back on Councilwoman Diana Nelson’s claim that they, as elected officials, were entertaining a piece of legislation which contradicted the Constitution, any federal laws, or any Supreme Court ruling. Grossman shared that based on statements from attorneys, the ordinance is consistent with the Constitution, all state and federal laws, and worked within Supreme Court rulings. Grossman asked Vice Mayor Mike Gilb, who is a local attorney, his assessment on the matter. Vice Mayor Gilb shared, “From my review of the ordinance I certainly understand it to be not in conflict with Roe v. Wade and constitutional in the way it is presented.”
Mason, Ohio (Photo: Mark Lee Dickson)
The Mason Ordinance Outlawing Abortion states, “The Supreme Court’s decision in Roe v. Wade, 410 U.S. 113 (1973), which invented a constitutional right for pregnant women to kill their unborn children through abortion, is a lawless and unconstitutional act of judicial usurpation, as there is no language anywhere in the Constitution that even remotely suggests that abortion is a constitutional right.” The ordinance goes on to say, “Constitutional scholars have excoriated Roe v. Wade, 410 U.S. 113 (1973), for its lack of reasoning and its decision to concoct a constitutional right to abortion that has no textual foundation in the Constitution or any source of law.”
Even though these strong statements are made in the findings section of the ordinance, the Mason Ohio Ordinance does not go against Roe v. Wade (1973), Planned Parenthood v. Casey (1992) or any Supreme Court ruling, but works within those rulings and current federal and state laws to go as far it can go to prohibit and restrict abortion access under the confines of the undue burden standard which was set by the United States Supreme Court in Planned Parenthood v. Casey (1992).
The Sanctuary City for the Unborn Ordinance for Mason, Ohio, does not prevent pregnant mothers in Mason from getting an abortion outside of the city limits. All the ordinance does is prevent a pregnant mother from obtaining an abortion within the city limits. Mayor Grossmann argued this point repeatedly throughout the council meetings, stressing that the ordinance simply preserves the status quo by keeping abortion out of the city limits of Mason.
While Councilwoman Nelson raised concern that the passage of the ordinance would open the City of Mason up for lawsuits, no lawsuit has been successful against the Sanctuary Cities for the Unborn movement. In February of 2020, the ACLU sued seven cities in East Texas which had outlawed abortion. After three months, the ACLU withdrew their lawsuit and, to this day, abortion remains banned in each city which was sued. In May 2021, Planned Parenthood and the ACLU filed a lawsuit against the City of Lubbock for outlawing abortion within the city. Before the month was up, Planned Parenthood lost their lawsuit. Due to the ordinance going into effect, Planned Parenthood stopped performing abortions in Lubbock on June 1, and is currently not performing abortions in Lubbock.
If the City of Mason is sued, attorney Jonathan F. Mitchell, the former Solicitor General of the State of Texas and the legal mind behind the enforcement mechanism of the Texas Heartbeat Law, has agreed to represent the city at no cost to the city and taxpayers.
The Mason Ordinance states, “It shall be unlawful for any person to procure or perform an abortion of any type and at any stage of pregnancy in the city of Mason, Ohio,” and “It shall be unlawful for any person to knowingly aid or abet an abortion that occurs in the city of Mason, Ohio.” Abortion is defined by the ordinance as “the act of using or prescribing an instrument, a drug, a medicine, or any other substance, device, or means with the intent to cause the death of an unborn child of a woman known to be pregnant.” The Ordinance is also clear that the act is not an abortion if the act is done with the intent to “save the life or preserve the health of an unborn child” or to “remove a dead, unborn child whose death was caused by accidental miscarriage” or to “remove an ectopic pregnancy.”
There is one other exception listed in the ordinance and that is a very narrow exception for cases where the mother’s life is at risk. This is listed as an affirmative defense and falls upon the one performing the abortion to provide that defense if necessary. This is outlined by the ordinance as abortions in cases where the abortion is “in response to a life-threatening physical condition aggravated by, caused by, or arising from a pregnancy that, as certified by a physician, places the woman in danger of death or a serious risk of substantial impairment of a major bodily function unless an abortion is performed.”
Besides outlawing abortion, the Mason Ordinance declares abortion-inducing drugs to be contraband, stating, “It shall be unlawful for any person to possess or distribute abortion-inducing drugs in the Mason, Ohio, and it shall be unlawful for any person to mail or ship abortion-inducing drugs into the city of Mason, Ohio.” Abortion-inducing drugs are defined as “mifepristone, misoprostol, and any drug or medication that is used to terminate the life of an unborn child.”
Many of the opposition in attendance attempted to attack the ordinance for this section, arguing that these drugs had other uses. However, the ordinance is clear that “the term also does not include drugs or medication that are possessed or distributed for a purpose that does not include the termination of a pregnancy.”
According to the ordinance, those who are found in violation are guilty of a misdemeanor in the first degree and, under Ohio law, are not to serve more than six months in jail or pay more than $1,000 in fines. This prosecution or penalty contains only one exception: “Under no circumstance may the penalty be imposed on the mother of the unborn child that has been aborted, or the pregnant woman who seeks to abort her unborn child, be subject to prosecution or penalty under this section.” The implementation of these penalties are not dependent upon the overturning of Roe v. Wade or any other court ruling, but are immediately enforceable.
It is not likely that Mason, Ohio, will be the last city in Ohio to outlaw abortion. On the same night of Mason’s vote, the City of Celina (population 10,687) also discussed an ordinance outlawing abortion. The City of London, Ohio (pop. 10,436), is also considering a similar ordinance.
Ohio State Representative Jena Powell shared, “What a great day in Mason! Thrilled to see that Mason is now a sanctuary city for the unborn. I’m excited to see more cities across our state and nation fight to protect the unborn. It’s crucial that every child is protected in the state of Ohio, and this is a huge step in the right direction.”
The Sanctuary Cities for the Unborn Initiative encourages all who wish to see abortion outlawed in their city, regardless of what city or state they live in, to sign the online petition on the Sanctuary Cities for the Unborn website.
Mark Lee Dickson is a Director with Right to Life of East Texas, a Pastor of SovereignLOVE Church in Longview, Texas, and the founder of the Sanctuary Cities for the Unborn initiative.
(C-Fam – New York) UNICEF’s Executive Board has approved a strategic plan that endorses sexual autonomy for children and school-based access to abortion and contraception.
The new strategic plan, which will guide the agency through 2025, added “sexual and reproductive health and rights” and “sexual orientation and gender identity” to the agency’s mandate for the first time. The Biden administration endorsed the new plan.
UNICEF already promoted the ability of adolescents to make autonomous decisions about their sexuality and the presence of sexuality education and sexual health services for children in schools. But this was the first time these had appeared in UNICEF’s internal strategic documents with the approval of UN member states, as the Friday Fax reported in August.
Thirty-six nations that sit on the UNICEF Executive Board endorsed the new plan with the disclaimer that it was not negotiated by UN Member States and that it “includes some terms that have not been intergovernmentally endorsed in the United Nations system.” The decision does not identify the terms in the strategic plan covered by the disclaimer.
The plan further protects Member States by directing the agency to implement the strategic plan “in accordance with the principles of national ownership of programme countries, taking into account their national priorities and needs, recognizing their different contexts and particular characteristics, guided by international human rights treaties and humanitarian principles for humanitarian assistance.”
“Sexual and reproductive health and rights” is a term of art coined by countries and groups to promote abortion….
A recent article published in the journal Frontiers in Behavioral Neurosciences evaluated the effects of the use of hormonal contraceptives upon the behaviors of intimate partners. The study of the physiology of women using hormonal contraceptives has provided insight into the possible basis for the resulting increase in violent death. The author of this review investigated the changes that are potential contributors to the reported increase in violent death by suicide, accident, or homicide.
It has been demonstrated that hormonal contraceptive use affects the behaviors of both female and male partners which can cause changes in mate retention behaviors. These changes in mate retention behaviors could lead to intimate partner violence and death. The review also analyzed how hormonal contraception modify brain structure and function.
The authors conclude: “there is a great need for further research concerning brain function and structure relating to exposure to hormonal contraceptives, especially since these drugs are often given to young women whose brains are not fully matured. Through the use of physician screening and patient education, the incidence of violent death can potentially be mitigated. It cannot be denied that millions of women are potentially affected adversely by hormonal contraception and its potential link to increased suicide, intimate partner violence, induced abortion, and worsening of BPD traits, such as substance abuse and risk- taking”.
Editor’s Note: This year, October 13th is World Thrombosis Day, which provides an opportunity to raise awareness about this potentially life-threatening medical condition or complication. The 2018 research summarized below is titled, “Systematic Review of Hormonal Contraception and Risk of Venous Thrombosis.” The study was published by Keenan et al in 2018 and won the 2019 Linacre Award for outstanding research paper of the year. The researchers reviewed the literature assessing the risk of venous thrombotic events in women who choose hormonal contraception. Dr. Natalie Gould’s summary of this important study ends by discussing fertility awareness-based methods (FABMs) as a reasonable, safe, and effective option for women who need or prefer a different approach for pregnancy prevention, health monitoring, and/or to diagnose and manage a variety of women’s health conditions.
A Personal Story
It was just a few days after Christmas and we were sitting outside, sharing our shock in silence. Reunited with our college friends, we should have been happy — happy to see one another, enjoying the joyful nature of the season, and sharing adventure stories from our young lives. Instead, most of us were quiet and tearful, having just attended our friend’s memorial service. Despite her youth, she collapsed suddenly due to massive pulmonary emboli — blood clots within her lungs.
She had been on hormonal contraception … and many of us had been or were on hormonal contraception too… While grieving, we wondered, could this happen to me too? Why had our doctors never discussed this possible deadly side effect with any of us?
Years later, I am in medical school, where the risk of venous thromboembolism (VT) has hardly been mentioned as a potential side effect of hormonal contraception. If it is mentioned, it is touted as a rare occurrence. While this may be so, it is in our best interest as medical professionals to discuss all potential side effects with our patients so they have true informed consent and the highest sovereignty over choices affecting their bodies. Hormonal contraception is often used as a first line therapy for women’s health issues beyond pregnancy prevention. Women have the right to know all the evidence about these medications before choosing to take them.
In the 2018 study titled, “Systematic Review of Hormonal Contraception and Risk of Venous Thrombosis,” Keenan et al reported the significant increased risk of venous thromboembolism in healthy young women using hormonal birth control. This is a review of their findings.
Introduction
Hormonal contraception (HC) continues to have high prevalence use worldwide, with over 80 percent of women in the U.S. alone reporting use of some form of HC at some point during their reproductive years. Despite the widespread use, the safety of HC is primarily determined through observation and case control trials due to ethical concerns of having women who are trying to avoid pregnancy take a placebo. Hormone replacement therapy (HRT) practices have changed drastically in the last twenty years, since data surfaced showing increased cardiovascular risks with HRT, so that their benefit does not outweigh the potential harm. Despite these findings, HC doses are often given in five to ten times the dose of HRT.
In medicine and bioethics, informed consent is paramount. The intent of the research by Keenan et al was to look at broad safety data of hormonal contraception and evaluate for potential increased risk for venous thromboembolism, including deep vein thrombosis (DVT), pulmonary embolism (PE), and central venous thrombosis (CVT) in healthy female populations of reproductive age.
Methods
A PubMed search was performed for all relevant publications from inception through April 2018. The following inclusion criteria were used: all articles evaluating risk of any form of HC for first VT in healthy women. Articles had to have a nonuser comparison group and VT confirmed with either imaging study or strong clinical diagnosis with minimum four weeks anticoagulation. Studies had to report relative risk (RR) or odds ratios (OR) with 95% confidence interval (CI). Type of HC used must have been identified, including the generation of oral contraceptives.
Results
Of the studies reviewed (n=15), 12 were case control studies ranging in size from 36 to 1,524 cases, and 3 were cohort studies ranging in size from 8 to 17.2 million-women-years of observation. All the studies showed an increased risk of VT in women using HC compared to their controls, with the exception of users of the levonorgestrel-releasing IUD. Interestingly, a few studies showed that risk generally decreased with longer use time, with the first year of use demonstrating the greatest risk.
Obesity was also shown to be associated with higher risk of VT in patients using HC. In one study, women taking second generation HC had significantly higher risk, with a sixfold increase in risk if body mass index (BMI) was greater than 30.
This review demonstrated that users of second and third generation HC have significantly increased risk of death due to a fatal pulmonary embolus. A Swedish study demonstrated significant risk of death in women aged 15 to 24 when reviewing the death registry.
Overall, risk was increased for users of all generations of HC, with use of fourth generation HC being greater than third, and third generation greater than second. Use of transdermal patch and hormonal vaginal rings was associated with significant increased risk of VT. Finally, the progestin-only implant was not shown to increase risk, and the levonorgestrel IUD showed decreased risk.
Discussion
This review article set out to explore whether users of HC have a significantly increased risk of confirmed venous thrombotic events when compared to nonusers. The studies reviewed demonstrate that, indeed, users of HC have a three- to ninefold increased risk of confirmed VT. The study reports that HC can therefore be estimated to cause 300-400 young healthy women to die each year because of their contraceptive choices.
The authors go on to say that this risk is often justified in the studies reviewed by noting the risks of pregnancy. Yet, the reviewers point out that the absence of HC use is not equivalent to pregnancy, and the studies fail to discuss options that would not expose these healthy women to the potential harmful side effects to which HC exposes them.
This raises an important issue: are women being adequately informed of the potential risks of their contraceptive choices? Birth control has long been viewed as a positive development for women, and while the benefits are shouted from the rooftops, should we not also be willing to explore their potential harm?
The possibility of venous thrombotic events due to HC use is often under-reported and appears to be overlooked by the general public. Although medication safety is usually determined through the gold standard of randomized controlled trials (RCTs), it is not possible to study HC with RCTs, as giving women placebo could lead to unintended pregnancy. Thus, it is imperative to consider studies such as this review to understand the risks of HC and to properly counsel patients on their contraceptive choices so they have full informed consent.
A Reasonable, Safe Alternative
The study authors point out that several fertility awareness-based methods (FABMs) of family planning demonstrate typical use rates comparable to those of oral contraceptives. These FABMs have no medical side effects, making the potential harm of VT avoidable if these options are presented to women alongside HC options. They go on to suggest further research to follow a large cohort of women using FABMs compared to a cohort of women using HC to evaluate health outcomes of each choice.
Many women do not think of HC choices as potentially harmful, and many are not counseled on the increased risk of VT. As it relates to HC, for women to have full sovereignty over their bodies and provide true informed consent, physicians must be aware of these risks and personalize counseling.
Death due to VT may seem like a rare possibility, but when it is your best friend, your wife, your daughter, or you, it matters. It’s no longer rare; it’s real.
FABMs are often not presented to women as a viable option for pregnancy prevention. If more physicians were educated about these options, perhaps we would not have to ignore or accept the risk of losing 300-400 healthy young women — women like my friend — each year.
FABMs empower women with knowledge of whether or not their bodies are healthy. They can also help identify the root causes of women’s health problems that are often merely masked by HC use. This would decrease medical use of HC for reasons other than contraception.
This brings up the painful, yet important question we must consider: what would have happened if, years ago, my friend’s doctor presented an FABM as an option to her?
References
Keenan L, Kerr T, Duane M, Van Gundy K. Systematic Review of Hormonal Contraception and Risk of Venous Thrombosis. Linacre Q. 2018;85(4):470-477. doi:10.1177/0024363918816683.
ABOUT THE AUTHOR
Natalie Gould, DO
Natalie Gould, DO is a first-year resident at Peak Vista Family Medicine Residency in Colorado Springs, CO. She wrote this review as a fourth-year medical student at Rocky Vista University College of Osteopathic Medicine. She participated in an FABM elective and is excited to continue her education regarding these important options for women for her future practice as a family physician. She believes all women should have access to FABMs and is excited to do her part to share this important information
Prophetic words of Pope Saint Paul VI in his most famous encyclical, Humanae Vitae.
“The danger of this power passing into the hands of those public authorities who care little for the precepts of the moral law…. Who will prevent public authorities from favoring those contraceptive methods which they consider more effective? Should they regard this as necessary, they may even impose their use on everyone.”
According to C-Fam, abortionists are claiming that climate change negatively impacts the ability of a woman to access abortion. As a result, they’re vying to use funding meant for climate change to help boost access to abortion — in other words, to boost their own financial profit.
A coalition of more than 60 pro-abortion organizations penned a letter to Alok Sharma, president of the UN Cop26 climate conference requesting that the United Kingdom change its funding eligibility rules to allow reproductive healthcare programs to receive funds meant for combating climate change.
“Billions are allocated now to climate financing, adaptation and resilience. We’re hearing loud and clear from communities and women and our clients who are most affected by climate crisis that what they really want is access to reproductive healthcare, so that they can make choices about when or whether they have children,” said Bethan Cobley, a director of abortion giant MSI Reproductive Choices, formerly Marie Stopes International.
MSI Reproductive Choices has been caught committing illegal abortions in Africa. In addition, according to the Right to Life UK, all 70 Marie Stopes clinics had a policy in place that included sales tactics to convince women to have abortions, calling those who had chosen life to try to persuade them to come in for another appointment to discuss abortion. Another report discovered nearly 400 botched abortions had taken place at Marie Stopes clinics in just two months.
Women in African nations do not include contraception and abortion at the top of their priority list, as has been pointed out numerous times by Obianuju Ekeocha, founder and president of Culture of Life Africa. She has called contraception a “Western solution” to African poverty, and considers the Western push for abortion in Africa to be a form of colonization.
“If we’re talking about abortion, well, I don’t think that any Western country has a right to pay for abortions in an African country, especially when the majority of people don’t want abortion… That then becomes a form of ideological colonization,” said Ekeocha. She has also argued that population control programs send about two billion donated condoms to Africa each year at a cost of about $17 million — money that could be used to solve actual problems such as access to affordable food, clean water, health care, and education.
Yet, the UN continues to promote abortion around the world, and it appears its new move is to aid the abortion industry under the guise of addressing climate change. The United Nations Population Fund (UNFPA) published “Five ways climate change hurts women and girls,” listing a disruption to “sexual and reproductive health” and limited access to contraception as two of the effects of climate change.
“As COVID-19 has shown, emergencies divert health-care resources toward fighting the latest threat and away from services deemed less essential,” said UNFPA. “Emergencies due to climate change will become more frequent, meaning sexual and reproductive health and rights services may be among the first to be curtailed.”
The organization went on to say that after Cyclone Idai hit Malawi in 2019, many areas were underwater and health providers were forced to use a helicopter to provide condoms to people — people who were suffering the devastation of a cyclone and likely needed access to clean drinking water, food, and shelter rather than condoms. There is a reason that abortion and contraception are not included on the “essentials” list when a crisis occurs — because they are not “essential” to anyone’s survival.
The UNFPA also argued that when crops fail due to climate change, women turn to sex work and therefore need contraception and abortion. Rather than helping these women recover their crops or income to remain in their homes as they wish, the UNFPA wants to give them condoms so they can earn money through sexual exploitation which leaves them at high risk of STDs, human trafficking, and physical abuse. Instead of helping them to avoid this horrific fate, the UNFPA helps them dive deeper into it.
Prostitution, sex trafficking, and abortion are all businesses that go hand in hand, and when condoms fail and women become pregnant or get STDs, abortion businesses like MSI Reproductive Choices profit from their misfortune.
The UN has an agenda to reduce certain populations by 2030, and expanding abortion is part of that agenda. The issue is not one of climate, but of a worldview that sees human beings as disposable, and as conduits of profit for an unaccountable worldwide abortion industry.
“Riccardo, you are a gift for us.” These are the words a 26-year-old Italian mother wrote to her newborn 26 years ago. They were words she was willing to live by – and die for.
On Aug. 30, Pope Francis advanced the sainthood cause of Maria Cristina Cella Mocellin, who sacrificed her life for the sake of her baby. Catholics already are comparing her to another saint, St. Gianna Beretta Molla, because both women refused medical treatment that would have endangered their unborn babies, according to EWTN Pro-Life Weekly. After close examination, the Church now recognizes Maria Cristina as a “venerable” for leading a heroically virtuous life.
This is the story of that life.
Maria Cristina was born in 1969 in a town called Cinisello Balsamo, located in Milan. According to La Stampa, she grew up next to the Sisters of Charity of Saint Joan Antida Thouret, and served as a catechist and youth leader. She strongly considered religious life while still a young teenager.
“Lord, show me the way: it doesn’t matter if you want me as a mother or a nun, what really matters is that I always do your will,” she wrote in her spiritual diary in 1985.
Her vocation became clear when, at 16 years old, she met Carlo Moccellin. She was called to marriage – a marriage with him. She never wavered from that conviction, even when doctors discovered a sarcoma in her left leg, Vatican News reported.
“I realized that everything is a gift, even a disease, because if lived in the best way it can really help to grow,” she wrote to Carlo in 1988.
She was successfully treated, and finished her high-school education before marrying Carlo in 1991. They soon welcomed two children into their home, Francesco and Lucia. They were expecting a third – Riccardo – when they found out that her cancer had returned.
Her first thought was of her unborn baby boy.
“My reaction was to say over and over: ‘I am pregnant! I am pregnant! But doctor I am pregnant,’” she wrote in a 1995 letter to her little Riccardo. “I fought with all my power and did not give up on the idea of giving birth to you, so much so that the doctor understood everything and said no more.”
Maria Cristina refused the chemotherapy treatments that would have threatened her unborn baby’s life. Instead, she waited until after Riccardo was born, in 1994. But at that point, the cancer had already spread to her lungs and caused her tremendous suffering.
“I believe that God would not allow pain if he did not want to obtain a secret and mysterious but [a] real good,” she wrote. “I believe that one day I will understand the meaning of my suffering and I will thank God for it.”
On Oct. 22, 1995, she died at 26 years old.
But her story – and her baby – live on. In her letter to Riccardo, which she penned a month before she died, she stressed the beauty of his life.
“Dear Riccardo, you need to know that you are not in the world by chance,” she began.
“The Lord wanted your birth despite all the problems there were… when we found out about you, we loved you and wanted you with all our heart.”
“It was that evening, in the car on the way back from the hospital, that you moved for the first time. It seemed as if you were saying, ‘Thank you mamma for loving me!’ And how could we not love you?” she added. “You are precious, and when I look at you and see you so beautiful, lively, friendly, I think that there is no suffering in the world that is not worth bearing for a child.”
Maria Cristina wrote regularly, and kept a spiritual journal, according to The Associazione Amici di Cristina (Friends of Cristina Association), which promotes the dignity of human life in honor of its namesake. The association’s website includes excerpts from her diary and from her letters.
“Lord I only want You! I only love you! I’m just looking for you!” the organization quotes her as saying. “What does it matter to suffer in life if you are around the corner waiting for me to give me immense joy?”
Joy appears repeatedly in her writings.
“It is my motto: ‘Do everything with joy!’” she stressed in a 1985 letter to Carlo. “Even if sometimes it costs me a lot, especially when my morale is low or when … ‘it seems to you that all things are against you …’ as you say, in your beautiful letter. But, as light comes after darkness, so, after despair, rediscover joy.”
This joy shaped her love of God and her love for Carlo.
“Don‘t you think it’s extraordinary?” Maria Cristina asked Carlo in 1987. “If it weren’t for you and I who love each other, the world would lack that something that no one else in our place could give.”
She also wrote of God’s love – and the call to perfection.
“I become holy to the extent that I empty myself of everything, I remove every impediment from my mind, heart and life to allow myself to be completely penetrated by the love of God,” she stressed to Carlo in 1990. “More concretely, it means living everyday life with great simplicity, in the family, in the study, in the relationship with you, Carlo. My place is in the simple and ‘routine.’”
In the simple, she found the miraculous. In the ordinary, she discovered the extraordinary.
The year that she died, she wrote in another letter that “Although my health is precarious… I AM HAPPY!” She concluded, “I am ashamed to ask the Lord for anything else, for us the miracle is already there: if He loves us and we love each other, nothing else matters.”
“The encyclical of Pope Paul VI on birth control is true and must be followed by mankind. There shall be no rationalization of sin.” – Our Lady of the Roses, October 2, 1976
Dietrich von Hildebrand, called by Pope Pius XII “the 20th Century Doctor of the Church,” was one of the world’s most eminent Catholic philosophers. Cardinal Ratzinger (Pope Benedict) wrote about Dietrich von Hildebrand in the year 2000: “I am firmly convinced that, when at some time in the future, the intellectual history of the Catholic Church in the 20th century is written, the name of Dietrich von Hildebrand will be most prominent among the figures of our time.” No other Catholic writer has so thoroughly echoed the message of Our Lady of the Roses than Dietrich von Hildebrand. The following is an excerpt from his essay,
The Encyclical Humanae Vitae: A Sign of Contradiction:
We can now see more clearly the difference between natural and artificial birth control. The sinfulness of artificial birth control is rooted in the arrogation of the right to separate the actualized love union in marriage from a possible conception, to sever the wonderful, deeply mysterious connection instituted by God. This mystery is approached in an irreverent attitude. We are here confronted with the fundamental sin of irreverence toward God, the denial of our creaturehood, the acting as if we were our own lords. This is a basic denial of the religio, of our being bound to God; it is a disrespect for the mysteries of God’s creation, and its sinfulness increases with the rank of the mystery in question. It is the same sinfulness that lies in suicide or in euthanasia, in both of which we act as if we were masters of life.
Every active intervention of the spouses that eliminates the possibility of conception through the conjugal act is incompatible with the holy mystery of the superabundant relation in this incredible gift of God. And this irreverence also affects the purity of the conjugal act, because the union can be the real fulfillment of love only when it is approached with reverence and when it is embedded in the religio, the consciousness of our basic bond to God.
To the sublime link between marriage and procreation Christ’s words on the marriage bond also apply: “What God has joined together, let no man put asunder.” This becomes still clearer when we consider that the mystery of the birth of a man not only should be essentially linked to wedded love (through the conjugal act, which is destined to be the expression and fulfillment of this love), but is always linked to a creative intervention of God. Neither wedded love nor, still less, the physiological process of conception is itself capable of creating a human being with an immortal soul. On this point Pope Paul VI quotes the encyclical Mater et Magistra: ” ‘Human life is holy,’ Pope John XXIII reminds us, ‘and from conception on it demands the immediate intervention of God!'” (Humanae Vitae,13). Man always comes forth directly from the hand of God, and therefore there is a unique and intimate relation between God and the spouses in the act of procreation. In a fruitful conjugal act we can say that the spouses participate in God’s act of creation; the conjugal act of the spouses is incorporated into the creative act of God and acquires a serving function in relation to His act.
We thus see that artificial birth control is sinful not only because it severs the mysterious link between the most intimate love union and the coming into existence of a new human being, but also because in a certain way it artificially cuts off the creative intervention of God, or better still, it artificially separates an act which is ordained toward co-operation with the creative act of God from this its destiny. For, as Paul VI says, this is to consider oneself not a servant of God, but the “Lord over the origin of human life” (Humanae Vitae, 13).
This irreverence, however, is exclusively limited to active intervention severing the conjugal act from its possible link with procreation.
The conjugal act does not in any way lose its full meaning and value when one knows that a conception is out of the question, as when age, or an operation for the sake of health, or pregnancy excludes it. The knowledge that a conception is not possible does not in the least taint the conjugal act with irreverence. In such cases, if the act is an expression of a deep love, anchored in Christ, it will rank even higher in its quality and purity than one that leads to a conception in a marriage in which the love is less deep and not formed by Christ. And even when for good and valid reasons conception should be avoided, the marital act in no way loses its raison d’être, because its meaning and value is the actualization of the mutual self-donation of the spouses. The intention of avoiding conception does not imply irreverence as long as one does not actively interfere in order to cut the link between the conjugal act and a possible conception.
Nor is the practice of rhythm to avoid conception in any way irreverent, because the existence of rhythm—that is to say, the fact that conception is limited to a short period—is itself a God-given institution. In Section 6 we shall show in greater detail why the use of rhythm implies not the slightest irreverence or rebellion against God’s institution of the wonderful link between the love union and procreation; it is in no way a subterfuge, as some Catholics tend to believe. On the contrary, it is a grateful acceptance of the possibility God has granted of avoiding conception—if this is legitimately desirable—without preventing the expression and fulfillment of spousal love in the bodily union.
PARIS (LifeSiteNews) — Earlier this month, French health minister Olivier Véran proudly proclaimed that as of January 1, 2022, contraception will be 100 percent “free” for all women up to age 25, as well as pregnancy tests, medical appointments and bio-analyses in connection with birth control. Less than 24 hours later, France’s move was enthusiastically commended by the World Economic Forum in a short video published on its official Twitter account.
Véran made his announcement on the nationwide taxpayer-funded television station France 2, explaining that the main reason a number of young women do not use contraception is because of its cost. This statement was contradicted by the news center of the Fondation Jérome-Lejeune, Généthique.
TACOMA, Washington, June 30, 2021 (LifeSiteNews) — An eighth-grade teacher in a Tacoma public school distributed a flyer detailing Washington state laws allowing minors to get abortions and contraceptives without parental consent. The flyer, produced by abortion giant Planned Parenthood, was given to Stewart Middle School students as part of their science curriculum.
The flyer said:
ABORTION: You do not need to get permission from your parents or guardians at any age.
BIRTH CONTROL: You are allowed to get a prescription for birth control without your parent or guardian’s permission.
CONDOMS: You can buy condoms at any age.
EMERGENCY CONTRACEPTION: You can buy Plan B Emergency Contraception at a local pharmacy without a prescription at any age.
The flyer also mentions that there are exceptions to state law that says the age of consent is 16, assuring children they can lawfully have sexual intercourse “with somebody two years older or less” at the age of 11.
The flyer caused controversy after a concerned parent posted a picture of it on social media and confronted the school about it. After an investigation, the assistant director of education in the district, Eric Hogan, responded in an email to parents that was obtained by the Jason Rantz Show.
“The flyer is not part of our curriculum and should not have been sent home with students,” Hogan argued. “Previously, Planned Parenthood taught within our schools and supplied the flyer that was distributed to students. We discovered a binder of curriculum materials was left behind for an incoming teacher to use this year, and this flyer was in the binder. Not realizing the flyer wasn’t approved material, the teacher sent it home with students. Corrective action has been taken with this employee.”
Planned Parenthood, in addition to providing hundreds of thousands of abortions each year, is a big player in the field of sex education in schools. The organization and its allies have taught things like BDSM, including using whips, chains and gagging; have informed 11-year-olds about anal and oral sex; and introduced a chatbot that allows kids to go behind their parents’ back to ask about sex and abortion.
The enactment of the Texas Heartbeat Act has exposed the pseudoscience undergirding the worldview of abortion-rights supporters.
Heartbeat bills such as the one in Texas are predicated on the fact that an unborn child’s heartbeat can be detected via ultrasound at about six weeks’ gestation. For a movement that defends abortion on the grounds that the unborn child is not human — or has no claim to rights — this scientific reality poses some difficulties.
An enormous number of the justifications for legal abortion are detached from science, declaring the fetus inhuman or not a rights-bearing person on account of its as-yet-undeveloped or underdeveloped mental or physical functions.
The argument for legal abortion prior to “viability,” for instance, rationalizes abortion before about 20 weeks’ gestation on the grounds that the unborn child’s lungs are insufficiently developed to allow for survival outside the womb. Therefore, on this view, that child can be killed prior to such development because it remains dependent on its mother. (Why this logic doesn’t allow for the killing of newborns or adults who are on ventilators typically remains unexplained.)
Philosophical justifications for abortion follow a similar pattern. In her famous 1973 essay arguing that abortion is morally acceptable, philosopher Mary Anne Warren asserted that it is wrong to kill persons, but that not all human beings count as persons. Under her criteria for personhood — consciousness and capacity to feel pain, an ability to reason, self-motivated activity, capacity to communicate, and self-awareness — unborn human beings do not count and therefore can be killed. (Critics have noted that Warren’s criteria exclude additional categories of human beings, too, not just the unborn.)
Many rationalizations for abortion are far less sophisticated. Take one, for example, that suggests that a fetus isn’t human until it is born — as if the birth canal magically confers humanity on an organism that, mere seconds earlier, possessed the exact same qualities as the crying newborn. This is the case for abortion at its most illogical.
This last phrase, which sounds a bit like something out of a horror movie, became so popular among abortion activists that actress Alyssa Milano demanded that the press refer to all heartbeat bills as “fetal pole cardiac activity” bills.
Time magazine obliged Milano with “fetal cardiac activity.” The Guardian updated its style guide on the advice of the American College of Obstetricians and Gynecologists — a powerful abortion lobby disguised as a medical group — citing the group’s statement that “ACOG does not use the term ‘heartbeat’ to describe these legislative bans on abortion because it is misleading language, out of step with the anatomical and clinical realities of that stage of pregnancy.”
The New York Times chose “the pulsing of what becomes the fetus’s heart” and “embryonic pulsing.” New York magazine’s The Cut ran a piece called “Embryos Don’t Have Hearts,” referring to the heartbeat as “pulsing cells” and dedicated to debunking the “unscientific” notion of a fetal heartbeat:
What is detectable at or around six weeks can more accurately be called “cardiac activity,” says Robyn Schickler, OB/GYN and fellow with Physicians for Reproductive Health. The difference between “cardiac activity” and “heartbeat” may seem linguistically minimal, but Schickler and others argue otherwise. At this stage, she says, what doctors can detect is essentially communication between a group of what will eventually become cardiac cells.
The Washington Post quoted unnamed “doctors who oppose the legislation” to assert that “what appears to be a heartbeat . . . is simply a vibration of developing tissues that could not exist without the mother. This vibration is a medical term called ‘embryonic cardiac activity.’”
The Post offered a similar notion in an article yesterday, again quoting anonymous “doctors opposed to the bills” who say that “the fluttering [i.e., the heartbeat] that is detected cannot exist outside the womb.” The Post appears to think it revelatory that removing an unborn child from the womb at six weeks’ gestation will result in its death.
In a piece yesterday, the New York Times insisted that the Texas heartbeat bill is misdescribed because “there is no heart at this stage of development, only electrical activity in developing cells. The heart is not fully formed until later in pregnancy.”
None of this has to do with real science or real medicine, both of which confirm the humanity of the unborn child at every stage of development. It is rather a game, designed to do one thing and one thing only: justify, by any means necessary, the ongoing killing of inconvenient human beings before birth.
Far from being champions of science, defenders of abortion twist the facts of biology and push the limits of language to justify dehumanization.
Editor’s Note: This article was originally published at National Review and is reprinted here with permission.
The National Institutes of Health (NIH) has awarded one-year supplemental grants totaling $1.67 million to five institutions to explore potential links between COVID vaccines and menstrual changes, after thousands of women reported menstrual irregularities after vaccination.
According to the NIH website, some women have reported experiencing irregular or missing menstrual periods, heavier-than-usual bleeding and other menstrual changes after receiving COVID vaccines.
The new funding will go toward research to determine whether the changes may be linked to COVID vaccination itself, and how long the changes last. Researchers will also seek to clarify the mechanisms underlying potential vaccine-related menstrual changes.
The year-long study will initially follow unvaccinated participants to observe changes that occur following each dose. Some groups will exclude participants on birth control or gender-affirming hormones, which may have their own impact on periods.
Researchers will assess the prevalence and severity of post-vaccination changes to menstrual characteristics, including flow, cycle length, pain and other symptoms. These analyses will account for other factors that can affect menstruation — such as stress, medications and exercise — to determine whether the changes are attributable to vaccination.
The five NIH-funded studies will be conducted by researchers at Boston University, Harvard Medical School, Johns Hopkins University, Michigan State University and Oregon Health and Science University.
The studies will likely incorporate between 400,000 and 500,000 participants –– including adolescents and transgender and nonbinary people, according to Dr. Diana Bianchi, director of the agency’s Institute of Child Health and Human Development, which is funding the research along with NIH’s Office of Research on Women’s Health.
“Nobody expected it [vaccination] to affect the menstrual system, because the information wasn’t being collected in the early vaccine studies,” said Bianchi, who credited The Washington Post’s early coverage of the issue, in April, with first making her and her staff aware of it.
These “rigorous scientific studies will improve our understanding of the potential effects of COVID-19 vaccines on menstruation, giving people who menstruate more information about what to expect after vaccination and potentially reducing vaccine hesitancy,” Bianchi added.
So far, no published studies have examined — or offered conclusive evidence — of possible links between the vaccines and menstruation.
The COVID vaccine trials did not specifically ask participants whether they saw adverse side effects in their menstrual cycles or volumes — an omission Bianchi attributes to the fact “the Emergency Use Authorization was really focused on critical safety issues” and “changes to your menstrual cycle is really not a life and death issue.”
But the lack of formal research on the potential link between the two “points out the fact that safety studies for vaccines … are not necessarily thinking about the reproductive health of women,” Bianchi said. “We hope one of the things that’s going to come out of this is that questions will be added to clinical trial studies to include any changes in menstrual health.”
According to the NIH, numerous factors can cause temporary changes in the menstrual cycle, which is regulated by complex interactions between the body’s tissues, cells and hormones.
Immune responses to a COVID vaccine could affect the interplay between immune cells and signals in the uterus, leading to temporary changes in the menstrual cycle.
Menstrual changes after COVID vaccination also could be attributed to immune responses to the vaccines and their impacts on the uterus, as well as to pandemic-related stress, lifestyle changes and the virus itself.
The new studies will build on existing research and leverage data from menstrual tracking applications to evaluate the potential impacts of COVID vaccination on menstrual health among geographically and racially and ethnically diverse populations.
The researchers hope that, following a peer-review process, findings will be published by the end of 2022 or soon after.
As The Defender reported, researchers have called for clinical trials since April to track and document menstrual changes in vaccinated women after some women reported hemorrhagic bleeding with clots, delayed or absent periods, sudden pre-menopausal symptoms, month-long periods and heavy irregular bleeding after being vaccinated with one or both doses of a COVID vaccine.
If you recently stopped taking the pill and find that your digestive system is in disarray (or, if you’re like I was, and struggling with both PCOS and poor gut health), you’re not alone. As I shared in this article, a number of recent studies suggest that oral birth control may negatively impact gut health, decreasing microbial diversity and leading to intestinal permeability. Eventually, these imbalances in your microbiome can lead to symptoms like bloating, food sensitivities and cravings, nausea after eating, and even inflammatory bowel disease (IBD). In fact, a 2017 meta-analysis suggested that those exposed to oral birth control had a 30 percent increased risk for developing an inflammatory bowel disease like Crohn’s disease or ulcerative colitis.
Learning all this can be overwhelming when you’re already feeling unwell. The good news, though, is that these unpleasant symptoms can often be reversed by using natural remedies and forming new habits. Below, you’ll find five strategies based on the latest scientific research to intentionally heal your gut after being on birth control.
Tip #1: Replenish key nutrients for gut health that were depleted by birth control
Studies dating back to the late 1960s have shown that the birth control pill depletes key B vitamins (B2, B6, B12, and folate), along with vitamins C and E and the minerals magnesium, selenium, and zinc. Although it’s unclear how these depletions occur, it’s been suggested that the pill causes either malabsorption or increased excretion of these nutrients. Since a number of these nutrients are important in gut function and detoxification, it’s important to get your levels back up to normal. Zinc enhances the gut lining, for example, while selenium has been shown to improve gut microbial diversity.
To replenish your nutrient stores, look for a high quality prenatal or multivitamin from a reputable source. It’s a good idea to choose brands that are third-party tested, such as Pure Encapsulations or Thorne. When looking for a prenatal containing folate, consider brands like Designs for Health that use the bioavailable form of folate, L-methylfolate. Many brands opt for cheaper, synthetic folic acid, but studies have shown that 40 – 60% of the population has a genetic mutation that inhibits the conversion of folic acid to its active form. You may also wish to have your doctor run bloodwork, which can help determine if you should supplement your multivitamin with a higher daily dose of any particular vitamin.
Tip #2: Incorporate probiotic and prebiotic foods into your diet
Moving forward, you’ll want to focus on eating foods that will support your microbiome in the long-term. This advice isn’t limited to those coming off the pill. Many of us would do well to incorporate prebiotic and probiotic foods into our diet, as these foods work together to promote a healthy gut.
Because probiotic foods have been fermented by good bacteria, eating them introduces these beneficial bugs into your gut lining. Some common (and delicious) fermented foods include yogurt, raw sauerkraut, kimchi and other pickled vegetables, kefir, and kombucha. Just be sure to select a yogurt, kefir, or kombucha brand that is low in sugar, as eating too much sugar promotes inflammation and alters our microbiome. One word of caution, though, is that if you have SIBO (small intestinal bacterial overgrowth), which has been associated with using oral birth control, it’s recommended that you avoid fermented foods until the infection has healed.
Prebiotic foods, on the other hand, contain fiber and resistant starch that “feed” your good gut bugs to maintain the health of your microbiome. We’ve already touched on fiber-rich vegetables in tip #1. Resistant starch, however, is a complex carbohydrate that ferments in your large intestine, feeding good gut bacteria in the process. Try incorporating sweet potatoes and yams into your diet or making tortillas and pancakes out of plantains and green bananas. There is even a gluten-free flour made from green bananas that is becoming increasingly popular! Since these foods are high in carbs, just be sure to round out your plate with plenty of non-starchy vegetables to help balance your blood sugar.
Tip #3: Support your birth control detox through diet
Dr. Jolene Brighten, a functional medicine physician and pioneer in treating post-birth control syndrome, emphasizes in her popular book Beyond the Pill that those coming off the pill should focus on foods that assist natural detoxification pathways. These foods should support the liver in processing the excess synthetic estrogen that forms a key component of the pill.
Dr. Brighten recommends eating a minimum of 25 grams of fiber a day from 3 to 6 cups of organic vegetables, especially leafy greens and cruciferous vegetables. If this constitutes a huge change in your diet, though, you’ll want to build up your fiber consumption slowly so that you don’t encourage further digestive distress. She also stresses the importance of finding a high-quality protein source. In practice, this means eating the best meat and eggs that fit your grocery budget. Ideally, you’ll be focusing on grass-fed, organic meats and pasture-raised eggs, but don’t let “perfect” be the enemy of the good.
Tip #4: Find a probiotic that specifically addresses birth control pill-related gut imbalances
In addition to eating the right foods, supplementing with a probiotic pill can help balance your gut bacteria. This daily, concentrated dose will help re-introduce the “good gut bugs” that have been crowded out by the bad. Dr. Brighten suggests that the organisms that have proved most helpful for her post-birth control patients are “high-dose, high-strain Lactobacillus and Bifidobacterium species, Saccharomyces boulardii, and spore-forming probiotics” (126). What constitutes a high dose? Dr. Hyman at the Cleveland Clinic Center for Functional Medicine recommends seeking out a probiotic with at least 25 – 50 billion living CFUs (colony-forming unity).
Tip #5: Avoid inflammatory foods
Knowing which foods to avoid is just as important as knowing which foods to incorporate. Many experts recommend avoiding the top inflammatory foods for 30 days to give your gut time to heal. Then, you can reintroduce them one at a time to determine if they give you a reaction. I have personal experience with the Autoimmune Protocol (AIP), which eliminates all potentially inflammatory foods for 30 days, and it had a powerful effect on my own gut health. Many women have also had great success with the Whole30, which focuses on “whole foods” rather than processed foods. The big three offenders are gluten, dairy, and refined sugar, but both of these food protocols also recommend avoiding grains, soy, caffeine, alcohol, and inflammatory fats from vegetable and seed oils like canola and safflower.
If you’d like to dive deeper into current research on post-birth control syndrome, I wholeheartedly recommend reading Dr. Brighten’s Beyond the Pill in full. It’s chock full of information and is written in an accessible, conversational style. As Dr. Brighten reminds us, healing your gut is the first step toward reclaiming your health after being on the pill. And, when you’re ready, learning to chart your cycle with a fertility awareness method (FAM) is another excellent way to truly take charge of your reproductive health.
As of midnight on September 1, 2021, the U.S. Supreme Court had not yet responded to an emergency appeal from abortion proponents to stop the Texas Heartbeat Act from going into effect, which protects preborn children from the first detectable heartbeat (around five to six weeks gestation). According to the Associated Press, at least 12 other states had previously passed legislation to protect children at the same point in gestation, none had been allowed to go into effect until now, making Texas the first state to successfully enforce such a law.
News outlets reported that abortion facilities in the state had stopped scheduling abortions past six weeks days in advance of the September 1 effective date. The AP noted, “Planned Parenthood is among the abortion providers that have stopped scheduling abortions beyond six weeks from conception.”
According to the emergency appeal, the law will “immediately and catastrophically reduce abortion access in Texas, barring care for at least 85 percent of Texas abortion patients (those who are six weeks pregnant or greater) and likely forcing many abortion clinics ultimately to close.” The University of Texas at Austin’s Texas Policy Evaluation Project estimates that about 80% of in-state abortions will be prevented. However, these estimates are not verifiable because Texas abortion data lumps abortions at eight weeks or earlier together. Data from Texas Health and Human Services shows that in 2020 there were 53,922 total abortions committed in Texas on Texas residents. Of those, 45,458 (about 84%) occurred eight weeks or less into the pregnancy. The Texas Heartbeat Act does not restrict abortion based on gestational age but on the detection of a fetal heartbeat using whatever method the abortionist deems appropriate — likely either an ultrasound or Doppler fetal heartbeat monitor. According to the law, “A physician does not violate this section if the physician performed a test for a fetal heartbeat as required […] and did not detect a fetal heartbeat.” This makes it difficult to determine how many abortions will be prevented, but it will likely be a large percentage, perhaps even greater than 85%.
“Right now in the great state of Texas, every single child with a detectable heartbeat is legally protected from being killed by the violence of abortion. This is a historic step forward for basic human rights,” said Lila Rose, founder and president of Live Action. “I applaud the brave advocates and lawmakers in Texas for passing this innovative law designed to withstand the tidal wave of attacks from abortionists and their apologists. Citizens and lawmakers must be vigilant in their defense of this law because we know that the abortion industry is determined to profit from the deaths of as many children as they can. No matter what happens going forward, today is a day for celebration and a vital reprieve for the precious children scheduled for death behind the doors of a Texas abortion business. Dozens of life affirming pregnancy centers all around the state stand by with the resources and compassion to ensure every mother and father are equipped to care for their children and families. The pro-life movement will continue fighting until every single child is protected in law and supported to live out her full potential.”
The Texas Heartbeat Act is unique in that it allows for civil penalties against those who commit or “aid and abet” an abortion once a heartbeat is detectable. As Live Action News reported in May following the signing of the law, “Though the law does not include punishments for women who undergo abortions after a heartbeat is detected in their child, it does allow private citizens to file lawsuits against a doctor that commits an abortion on such a child” as well as those who are involved in helping a woman to procure that abortion. The abortion industry responded by labeling the civil action portion of the law as an “abortion bounty.”
A preborn child’s heart begins to beat between 16 and 22 days after fertilization, but a unique human life begins at the moment of fertilization.
Editor’s Note: This article has been updated from its original publication.
Over the last year, I was diagnosed with polycystic ovary syndrome (PCOS) and began working to balance my hormones through diet and lifestyle changes. My personal experience with the Autoimmune Protocol (AIP) diet aligned with recent studies suggesting that an anti-inflammatory diet can mitigate the symptoms of both PCOS and gut dysbiosis—an imbalance in the microorganisms living in your digestive system that can cause a host of GI symptoms.
By all accounts, I am not alone in my gut-related symptoms. While my digestive complaints were not severe enough to warrant a clinical diagnosis, studies show that cases of inflammatory bowel diseases (IBD), an umbrella term for disorders involving chronic inflammation of the gastrointestinal tract, are rising rapidly worldwide. Symptoms of IBD can include nausea, vomiting, diarrhea, cramping, bloating, and abdominal pain, among others.
While researching the risk factors for IBD, I was surprised to learn that a genetic predisposition can account for less than 25% of cases. Scientists now believe that external, environmental factors may account for much of the remaining 75%. What shocked me most was learning that oral contraceptives have been clearly and consistently associated with an increased risk for IBD since at least 2008, with case reports stretching back to the 1960s.
The connection between the pill and IBD
In fact, the number of studies suggesting that oral contraceptives negatively impact gut health grows each year, and known side effects of hormonal birth control include GI issues like nausea and upset stomach. The association was first suggested through case reports that appeared in the 1960s and 1970s. Then, in 1984, one study showed that oral birth control use was common in 100 consecutive women attending follow-up clinics for IBD. Other studies demonstrated that symptoms of IBD often resolved when patients discontinued oral contraceptive use.
A 2008 meta-analysis published in Gastroenterology, which combined the results of 14 different studies including a total of 75,815 patients, found that those using oral contraceptives had a nearly 50% increased risk of developing IBD. Dr. Hamed Khalili, a Harvard-trained gastroenterologist at Massachusetts General Hospital, headed a sweeping 2013 prospective study involving over 200,000 women that suggested that “oral contraceptive use was associated with risk of Crohn’s disease [a type of IBD].” Shockingly, the study specified that oral contraceptive use could triple the risk of Crohn’s disease in women with a family history of the condition.
More recently, a 2017 meta-analysis of twenty studies and multiple databases reported that those exposed to oral birth control had a 30 percent increased risk for the development of IBD. Specifically, the studies showed that those exposed to birth control had a 24 percent higher risk for developing Crohn’s disease and a 30 percent higher risk for developing ulcerative colitis.
Why a “leaky” gut is an unhealthy gut
At this point, you might be wondering what birth control pills and the hormones they contain could possibly have to do with your digestive system—and if you yourself might be at risk for IBD if you are on or have ever taken birth control.
First, it’s important to understand that the gut microbiome is composed of the “flora” or microbes lining your digestive tract, and that these bacteria and viruses have a large impact on our overall health. For example, we rely on our intestines to form a tight barrier and keep harmful microbes out of our bloodstream. Sometimes, however, gaps form. When this intestinal permeability develops, a phenomenon sometimes called “leaky gut,” invaders may squeeze between the cracks. These harmful microbes may trigger inflammation and changes in our gut flora.
In a 2016 article, Dr. Khalili points to two biological mechanisms through which birth control might harm gut health. First, he notes that oral estrogen is known to negatively impact gut flora. Oral estrogen, of course, is one of two main hormones found in birth control pills. When a woman is prescribed oral contraceptives, she is usually given a combination of the synthetic versions of two key female sex hormones: estrogen (estradiol) and progestin. The two hormones work together to hinder ovulation, thereby preventing conception. In addition, they make cervical mucus inhospitable to sperm, and change the uterine lining so that an embryo would be unable to implant should breakthrough ovulation occur and fertilization happen.
Intestinal permeability appears to be another, unintended consequence of the hormonal changes wrought by birth control. Dr. Khalili cites experimental data from two studies suggesting that estrogen helps maintain the function of the intestinal barrier. He also writes, in no uncertain terms, that oral estrogen “has been shown to modify intestinal permeability,” and that intestinal permeability is “a critical step in the pathophysiology of inflammatory bowel disease.” In other words, oral birth control may lead to leaky gut, and a leaky gut may lead to IBD. If this is the case, then we have a clear indication of how oral birth control is detrimental to gut health.
Similarly, Dr. Jolene Brighten, a naturopathic physician and leader in alerting women to the realities of post-birth control syndrome, emphasizes in one article that birth control can lead not only to leaky gut, but to “yeast overgrowth (candida), decreased microbial diversity and altered gut motility.” In fact, the problems birth control causes in the gut are the subject of an entire chapter in Dr. Brighten’s popular book about hormones, Beyond the Pill.
Strategies for improving gut health
If you’re suffering from IBD or compromised gut health, there is hope. The five strategies I outline in this article have been shown to help restore the gut microbiome, no matter how that dysbiosis occurred. Those approaches include incorporating probiotic and prebiotic foods into your diet, reducing your intake of sugar and processed foods, and switching out make-up and household products that contain potentially harmful ingredients. In a future article, I will offer more in-depth suggestions for how women exposed to oral birth control can intentionally heal their gut and restore healthy flora. If you’d like to learn more about the documented side effects of birth control, you can find a wealth of information here. It’s time to pay attention to the growing body of scientific literature showing that birth control is harming our health.
The Hyde Amendment is one of the most important pro-life achievements in U.S. history. But right now, it is under serious threat.
For those who are unaware, the Hyde Amendment, named after pro-life Rep. Henry Hyde, is an amendment that has been appended to every appropriations (i.e., spending) bill since 1976. The amendment clearly states that taxpayer dollars cannot be used to fund abortions.
Last year, pro-life scholar Michael New analyzed the impact of the Hyde Amendment. According to his analysis, from 1976 to 2020, the Hyde Amendment stopped some 2.4 million abortions.
How? Simple. Research consistently shows that reducing funding for abortion also reduces abortions. By ensuring that our hard-earned tax dollars do not get used by pro-abortion politicians to abort innocent unborn babies, the Hyde Amendment has saved countless lives.
“Don’t let anybody tell you that pro-life political involvement has been for naught,” Dr. New said in an interview last year. “There are 2.4 million women out there who have been spared a lifetime of regret because of the Hyde amendment and there are 2.4 million people walking around today who owe their lives to the Hyde Amendment.”
One of the most important facts about the Hyde Amendment is that it has been passed every year regardless of who was in power – Democrats or Republicans. That is, it has been a truly bipartisan amendment. While there have always been some extremist pro-abortion Democrats who have wanted to get rid of the amendment, there has always been enough consensus to ensure that spending bills were protected by it.
Until now.
Democrats Ditch the Hyde Amendment
One of President Biden’s campaign promises was to scrap the Hyde Amendment. And now it appears that Democrats in Congress are working to make that happen.
A few weeks ago, the House Appropriations Committee advanced an appropriations bill that conspicuously lacked the Hyde Amendment. Pro-life Republican Rep. Tom Cole attempted to introduce the amendment, but to no avail.
In a speech, Rep. Cole noted that President Biden had consistently supported the Hyde Amendment throughout his time in the U.S. Senate, but only flip-flopped on the issue while running for President. “There is no moral equivalent to life and death,” Rep. Cole noted in his speech. “The preservation of one of our nation’s most enduring compromises to protect life and respect religious beliefs goes back to our founding principles. Any other issue falls far short of that standard. That is why we offer this amendment first. That is why this amendment has unanimous support on our side. And that is why we will vigorously fight to ensure this amendment is included in any final agreement.”
The appropriations committee voted 32-27 against Cole’s amendment. Shortly thereafter, the appropriations bill was approved in a 219-208 party line vote by the full House, which is controlled by the Democrats. This marks the first time in some 45 years that the House has passed a spending bill without the life-protecting amendment.
One prominent pro-abortion Democrat, House Appropriations Committee Chairwoman Rosa DeLauro, D-Connecticut, attempted to defend the removal of the Hyde Amendment, decrying it as “discriminatory.”
“I am proud that this bill promotes equal treatment for women through increased funding for Title X and by repealing the discriminatory Hyde Amendment,” she said. “But I do believe repealing the Hyde Amendment is the best thing we can do to support our mothers and families and help prevent, rather than penalize unwanted pregnancies and later, riskier and more costly abortions.”
This is the kind of double-speak that abortion supporters have to use to defend using our money to kill unborn children! Somehow preventing taxpayer dollars from paying for abortions is “discriminatory,” while paying for the killing of unborn children somehow supports “families.”
Infuriatingly, the two most prominent figures pushing for the end to the Hyde Amendment are also the two politicians who most conspicuously tout their alleged “devout” Catholic faith – President Joe Biden, and House Speaker Nancy Pelosi.
In response to this attack on the unborn, Cardinal Timothy M. Dolan of New York, chairman of the U.S. Conference of Catholic Bishops’ (USCCB) Committee for Religious Liberty, and Archbishop Joseph F. Naumann of Kansas City in Kansas, chairman of the USCCB’s Committee on Pro-Life Activities, issued a statement strongly decrying the effort to scrap the amendment.
“The House has voted in a way that is completely out of step with the will of the American people who overwhelmingly oppose taxpayer-funded abortion,” they noted. “The Hyde Amendment has saved at least 2.4 million lives since its enactment. Without it, millions of poor women in desperate circumstances will make the irrevocable decision to take the government up on its offer to end the life of their child.”
They added, “Funding the destruction of innocent unborn human lives, and forcing people to kill in violation of their consciences, are grave abuses of human rights. We call on the Senate to redress this evil in H.R. 4502, and for Congress to ultimately pass appropriations bills that fully support and protect human dignity, and the most vulnerable among us.”
Hope Remains
Fortunately, the passage of the appropriations bill by the House is not the end of the story. The bill still needs to pass the Senate, and while Democrats hold a narrow majority there, it appears that there is yet hope that it will not pass.
Democrat Senator Bob Casey, D-Pennsylvania, told Chad Pergram of Fox News that he suspects the bill may not pass without the Hyde Amendment.
Pergram reported: “It’s probable the House and Senate will have to do some sort of interim spending bill to avoid a government shutdown at the end of September. Such a Band-Aid bill simply renews all spending at old levels and restores old policy on a temporary basis. That means the Hyde Amendment remains in place. Congress will likely pass an amalgamated spending package for all of the measures later in the fall or winter. Stripping the Hyde Amendment on that mega-bill could be enough to spark a government shutdown on its own. So, pro-choice Democrats are unlikely to go to the mat the over the Hyde Amendment.”
In other words, if the Democrats stick to their intent to get rid of the Hyde Amendment, they would be in for a fight that they would likely lose, and that would come with significant political costs. As Pergram notes, that includes the risk of galvanizing pro-life activists into pushing back and perhaps even strengthening the bipartisan commitment to the Hyde Amendment.
However, even if this attempt to gut the Hyde Amendment fails, it stands as proof of just how deadly serious President Biden and the Democrats are about rejecting even the most commonsense and widely supported compromise measures on abortion.
Indeed, in addition to removing the Hyde Amendment, the Democrat-controlled Appropriations Committee also stripped the appropriations bill of the Weldon amendment – an amendment included in spending bills since 2005 that prohibits government funds from going to programs that discriminate against health care workers who object to abortion.
As I was concluding this article for publication, I learned that that the Senate voted for a budget amendment to its multi-trillion-dollar spending bill that bans taxpayer-funding of abortions for any federal funds authorized under the bill.
The amendment, if adopted by Congress in the final budget resolution, would ensure that the budget will comply with the long-standing Hyde amendment, which bars the use of federal tax dollars to pay for abortion, and the Weldon amendment, which protects health care providers who refuse to participate in abortion from discrimination.
The House of Representatives returns from recess the week of August 23rd where they will reconcile the Senate’s budget with their own. So, please join me in praying that the budget amendment by the Senate will be adopted by Congress. Also, let us call our representatives in Congress, asking them to defend human life and protect freedom of conscience.
By the way, the next time you hear the Democrats proclaim that they want abortion to be “safe, legal and rare,” just remember that they are trying to make you pay for abortions with your taxpayer dollars, and they are actively seeking to undermine the rights of pro-life health care workers to follow their consciences.
While some have attempted to claim that pregnancy risks are greater than hormonal birth control risks, this is not an apples to apples comparison. A far better comparison is to assess the risks of someone using hormonal birth control (HBC) to someone who is not — as in the case of women who use fertility awareness methods (FAM) as natural birth control or to address reproductive health issues. In the final analysis, FAMs are the clear winner for promoting true women’s health rather than merely masking symptoms.
Hormonal birth control
Taking hormonal birth control involves a true risk vs. benefit analysis, as the risks are many. Hormonal birth control impacts far more than “just” the reproductive system and the parts of the brain that control it. In her book, “This is Your Brain on Birth Control,” evolutionary psychologist Sarah Hill, who is not opposed to contraception, said on p. 90, “The brain and the rest of the body are too flush with hormone receptors for the pill not to change women.” Also impacted are the areas of the brain responsible for “things like emotional processing, social interactions, attention, learning, memory, facial recognition, self-control, eating behavior, and language processing. And we’re also talking about non-brain body parts like the immune system, the stress response, and your gut hormones.”
Accordingly, the Mayo Clinic notes that the Pill is not recommended for women who:
have recently given birth
are older than age 35 and smoke, have high blood pressure, a blood clotting disorder, or a history of deep vein thrombosis or pulmonary embolism
have a history of breast cancer, stroke or heart disease, diabetes-related complications, liver or gallbladder disease, migraines with aura, or unexplained uterine bleeding
will be immobilized for a prolonged period due to major surgery
are taking St. John’s wort or anticonvulsant or anti-tuberculous agents
While the Cleveland Clinic cites stoppage of unwanted hair growth as a potential benefit of taking HBC, multiple versions of the Pill can actually cause male-pattern hair growth in women because the synthetic form of progesterone used in HBC is actually derived from testosterone. Testosterone-derived progestins are also linked to acne, weight gain, and decreases in good cholesterol (HDL). Additionally, HBC worsens migraines for some women.
The Cleveland Clinic cites potential for “irritability and moodiness” in HBC users, but the Mayo Clinic is more straightforward, noting that some women experience depression. In reality, both statements give an inadequate picture of the emotional distress many women, especially young women, experience on HBC. Hill shares on p. 174 of her book, “mood-related issues like anxiety and depression are super-common among women who go on the pill.”
Disturbing research from Denmark gave a framework for quantifying the risk, finding that women on hormonal contraception “were 50% more likely to be diagnosed with depression six months later” vs. non-HBC users, and that “women who were on hormonal contraceptives were 40% more likely to be prescribed an antidepressant” than non-HBC users. Worst of all, women taking HBC “were twice as likely to have attempted suicide” than non-HBC users during the eight-year study, and were three times more likely than non-HBC users to have been successful in taking their own lives, according to Hill’s book, on pages 179-180.
In addition, most forms of HBC can act as abortifacients, killing preborn children without a woman knowing she was even pregnant. Both the Cleveland Clinic and the Mayo Clinic acknowledge endometrial thinning due to HBC use.
Despite all of the risks, some women take birth control to prevent pregnancy, lighten periods, and lessen menstrual pain. Others take it to alleviate the symptoms of polycystic ovary syndrome (PCOS), endometriosis, and uterine fibroids, and more — though these conditions are actually masked by the birth control rather than addressed.
Fertility awareness methods
The truth is that the steady stream of tiny synthetic hormonal spikes in HBC merely band-aid the symptoms of the variety of reproductive issues it is prescribed to treat. FAMs help women to get to the bottom of their fertility health concerns, rather than masking the symptoms of irregular periods with “faux” regular periods that are actually withdrawal bleeds, for example. FAMs actually promote truly comprehensive pro-women’s health, body literacy, and women’s ability to advocate for themselves.
Additionally, there are no physical side effects of using FAM, and ovulating normally each cycle has health benefits. Trained medical professionals can use a woman’s FAM chart data to help diagnose and treat the root causes of her problems, including endometriosis, PCOS, PMS, irregular bleeding, and more.
Women can expect to improve their health by using FAMs, though the same cannot be said for HBC users. Importantly as well, modern FAMs have similar pregnancy prevention effectiveness rates to HBC when taught by a trained instructor and used properly.
Comparing apples to apples, women who utilize fertility awareness methods for pregnancy prevention or to address reproductive health issues can expect to improve their health whereas women who utilize HBCs are automatically accepting certain physical trade-offs with varying degrees of seriousness.
Scientists have developed tiny magnetic particles that could one day be used by men for birth control.
The nanoscopic particles are injected into the bloodstream and would then be guided to the testes with a magnetic field, which also generates heat for contraception.
Heat is a natural contraceptive. Male mammals often have a suspended scrotal sac to keep their testes cool. By wearing tight pants or underwear, some male humans also raise the temperature of their scrotums, which can lower sperm counts.
Led by Fei Sun and Weihua Ding from the Institute of Reproductive Medicine at Nantong University in China, a team of researchers has been studying artificial ways to heat the testes — using nanoscopic particles as contraceptives.
In a previous study, the team tested gold nanorods that control contraception by using beams of light to heat the metal pills and create a ‘photothermal effect’.
But as they note in their new study, gold nanorods have “associated limitations, such as testicular administration and infrared laser inflicting severe pain.”
Besides the fact that jabbing your balls and heating them with lasers may not be ideal before lovemaking, the gold nanorods were just 90% effective at reducing fertility, as well as being non-biodegradable and potentially toxic.
Any fair analysis of how well the Catholic Church has done in educating Catholics about – let alone convincing them of – the Church’s teaching on contraception, would have to conclude that the Church’s ministers have failed quite spectacularly.
One much-cited poll from 2016 found that only 13% of weekly Mass-going Catholics agreed with the Church’s teaching that contraception is “morally wrong.” The number was even lower for those Catholics who do not attend Mass weekly – around six percent.
To say those numbers are dismal is an understatement. So, what went wrong?
Answering that question would take several volumes. Certainly, there is the blunt fact of the unforeseen cultural revolution of the 1960s, which swept and radically transformed practically every nation, class, institution, religion, and denomination, with few exceptions. In the face of the tidal wave of revolutionary moral teaching, the Church was in many ways caught unaware and unprepared.
Then of course, there is that little object, that small round pill, that made that revolutionary tidal wave possible: the birth-control pill. With the invention of the Pill (so monumental was this discovery that we tend to capitalize the “P”), for the first time in history it looked as if it might be possible for human beings to engage in the one activity that for many represents the height of physical pleasure, but without any thought for the enormous consequences that sex naturally carries with it.
Hidden Consequences
“Looked,” I say. Because as Pope St. Paul VI so prophetically warned in Humanae Vitae, behind that great, glistening promise of a new age of unfettered sexuality lay a whole world of pain. As Paul VI anticipated, the Pill unleashed abortion on a scale never seen before; caused men, allured by the promise of “consequence-free” sex, to objectify and abuse women as a matter of course; coarsened public morals beyond recognition, undermining marriage and elevating hedonism; and led to grave threats to human dignity and freedom, with totalitarian nations imposing coercive population control measures on their populace.
But there have been other consequences, too.
A friend of mine, a father of a large family, was describing how, on one occasion, he mentioned to two non-Catholic female friends that he and his wife used Natural Family Planning (NFP). He mentioned to them that not only does the method work, but that, among many reasons, he appreciates it because it is healthier for his wife and respects the love-giving and life-giving natures of marriage. Contraception, on the other hand, he added, not only distorts the ends of marriage but many women who take large doses of artificial hormones suffer from several physical side effects. “Yeah,” one of the women agreed wryly, “like reducing a woman’s libido.”
Of course, this is hardly the most important reason to oppose hormonal contraception, but it is a very telling reason. Modern human beings, in their drive to conquer nature, have also attempted to conquer sex, taming it, and making it do our bidding on our terms. And yet, while progressives have a great deal to say about how subjecting nature to violence inevitably leads to unforeseen consequences, for some reason they never seem to consider how our technological violence against sex has had unintended side effects.
The fact that many women do experience reductions in libido while on the birth control pill is perhaps the most ironic of these side effects. In the effort to unleash sex from all limits and to maximize pleasure, our technocratic solution has sometimes had precisely the opposite effect!
However, there are other, graver side effects associated with the Pill: increased risks of stroke, certain types of cancer, and even heart attack; weight gain; headaches; high blood pressure, and others. Which should hardly come as a surprise. What, after all, could possibly be “healthy” about using the blunt instrument of huge doses of synthetic chemicals to interrupt the delicate and complex processes of a woman’s reproductive cycle?
A Better Way
All of which brings me to the central point of this column, and a possible answer to the question I raised above. One possible reason that the Church has not been successful in convincing Catholics of Catholic teaching, is that we have done a very poor job of preaching the beauty of Church teaching regarding the dignity of marriage and the conjugal act and its openness to life. We have not preached an attractive alternative to the contraceptive mentality.
Last week, the U.S. Catholic Church marked Natural Family Planning (NFP) Awareness Week. Let me begin by saying that I don’t want you to misunderstand me: It would be a grave mistake to think of NFP simply as an “alternative” to the Pill. While it is true that NFP is a method (or rather, a collection of methods) that can be used by married couples to postpone having another child for legitimate reasons, it is certainly not a method of contraception. For starters, unlike contraception, NFP is a method that is equally successful in helping married couples who are having difficulty conceiving to do so. I’d like to see the Pill do that!
What I mean by an “attractive alternative” is that NFP is a collection of methods that translate into action the totality of the Catholic Church’s teaching on marriage and sexuality in a way that offers a compelling response to the many unforeseen side effects and sources of pain brought about by the sexual revolution.
In his encyclical Evangelium Vitae, Pope St. John Paul II beautifully expressed the truth about NFP in a single paragraph, writing:
The work of educating in the service of life involves the training of married couples in responsible procreation. In its true meaning, responsible procreation requires couples to be obedient to the Lord’s call and to act as faithful interpreters of his plan. This happens when the family is generously open to new lives, and when couples maintain an attitude of openness and service to life, even if, for serious reasons and in respect for the moral law, they choose to avoid a new birth for the time being or indefinitely. The moral law obliges them in every case to control the impulse of instinct and passion, and to respect the biological laws inscribed in their person. It is precisely this respect which makes legitimate, at the service of responsible procreation, the use of natural methods of regulating fertility. From the scientific point of view, these methods are becoming more and more accurate and make it possible in practice to make choices in harmony with moral values. An honest appraisal of their effectiveness should dispel certain prejudices which are still widely held, and should convince married couples, as well as health-care and social workers, of the importance of proper training in this area. (no. 97)
Unpacking that paragraph, we can note a few key characteristics of NFP:
1) It’s scientific. The Church has always acknowledged that married couples may have legitimate reasons for postponing having another child, and that there is no intrinsic moral impediment to timing sexual relations to coincide with the infertile period of the woman’s cycle. However, while a rudimentary understanding of the female reproductive cycle has existed for a long time, until relatively recently we lacked sufficiently detailed scientific information to formulate clear principles.
That all changed beginning in the early 20th century. Now, the science of fertility is a highly developed science, and there are several different methods of NFP that, if carefully followed, will help married couples either to postpone having a child, or to conceive a child, with a remarkable degree of reliability. With the recent explosion in, and popularity of, fertility apps, it is rarer to hear people denigrate “the rhythm method.” But even still a huge number of people remain unaware of just how scientifically advanced NFP has become, and how much easier to practice, due to a huge growth in resources and training materials.
2) It is embedded in a basic stance of “openness to life.” Unlike the case of artificial contraception, married couples who practice NFP always have fertility and children on their mind. Whereas the contracepting couple can simply take the Pill and go on “autopilot,” never giving a moment’s thought to children for years and years, the couple practicing NFP is prodded to re-evaluate their reasons for postponing having a child on a monthly basis. It is very difficult for the couple practicing NFP to lose sight of the fact that their reproductive systems are naturally designed for procreation. In this sense, NFP is simply more biologically and philosophically “truthful” than artificial contraception.
3) It demands personal virtue. Unlike artificial contraception, NFP demands personal sacrifice from the married couple, and often, in a special way, from the man, who must gain control over his sexual desires and channel them in a healthy way out of respect for his wife. At first glance this may not seem like a particularly “attractive” feature of NFP, and it is certainly the one that scares many couples away from it. However, those who have achieved any level of personal maturity have learned the truth that true satisfaction in this life is closely linked to the willingness to do difficult things and to delay gratification for good reasons. Married couples who use NFP consistently report all sorts of positive benefits, including better communication; a deepening of the couple’s love; a growth in spiritual and personal maturity; a sense that the woman is not being “used” by her husband for sex; more fulfilling sexual intimacy.
In an age where we prioritize and value “holistic” lifestyles, NFP is the ultimate holistic approach to sexuality: embracing body, mind, and soul. The Church has every reason to be proud of the fact that, long before Silicon Valley app designers discovered the benefits of “fertility awareness” (which is an often flawed ideology that relies on some of the same biological principles) we have preached a holistic approach to sex that emphasizes profound respect for natural processes.
But more than that, we should be proud that the Church’s prophetic vision saw clearly the spiritual, social, and physical dangers of the sexual revolution and the contraceptive mentality. In championing NFP, the Church highlights a far better response to our modern culture of sexual exploitation, or what Pope Francis calls the “throwaway culture,” a culture of discarding the fruit of our sexual unions as well as our exploited sexual partners.
Sexuality must be integrated into a holistic vision of the human person, that considers our fundamental dignity, deepest needs and moral responsibilities. Sexual pleasure is a good, but only when integrated into a loving, permanent union that is open to life. This is the vision of human sexuality embodied in Natural Family Planning. It is worth celebrating, and it is worth telling others about.
As Pope St. John Paul II wrote in Evangelium Vitae, “The Church is grateful to those who, with personal sacrifice and often unacknowledged dedication, devote themselves to the study and spread of these methods, as well to the promotion of education in the moral values which they presuppose.” (no. 97)
In its teachings on sexuality, the Church has a great light to share with the world. It is time to stop hiding that light under a bushel basket. For this reason, I am grateful to the USCCB for organizing this NFP Awareness Week.
President of Planned Parenthood Leana Wen speaks during a protest against abortion bans, Tuesday, May 21, 2019, outside the Supreme Court in Washington. A coalition of dozens of groups held a National Day of Action to Stop the Bans, with other events planned throughout the week. (AP Photo/Jacquelyn Martin)
A new peer-reviewed examination of almost eight million pregnancies over a 15-year period debunks the abortion industry’s fictional narrative that abortion is a normal experience for mothers who already have children.
Below is one example of the abortion industry’s myth from Planned Parenthood’s own website:
“Deciding to have an abortion doesn’t mean you don’t want or love children. In fact, 6 out of 10 people who get abortions already have kids — and many of them decide to end their pregnancies so they can focus on the children they already have.”
The researchers also found that women in the study population almost never used abortion as a tool to space their children, proving another abortion industry myth is also false.
The institute’s researchers conducted a retrospective, cross-sectional, and longitudinal analysis of the pregnancy outcomes experienced by 4.9 million Medicaid-enrolled women who had 7.8 million pregnancies between 1999 and 2014. These women were at least 13 years old, had at least one identifiable pregnancy outcome, and were from the 17 states whose official policies use state taxpayer funds to pay for abortions.
“After studying the largest universe of actual pregnancy outcomes ever analyzed, our team found that abortion is in no way typical of motherhood,” Dr. James Studnicki, CLI vice president and director of data analytics, and one of the paper’s authors said.
“We didn’t sample or conduct surveys – we analyzed all recorded events. We followed the data. It is quite uncommon, if not rare, to have both births and abortions. The overwhelming number of children are born to mothers who never have an abortion,” Studnicki noted.
Other key findings from the CLI study include:
Women with both births and abortions have more abortions than births. Women in the study who had both births and state-funded abortions averaged 3.2 pregnancies or more than twice the average number of pregnancies for women with “only births” or “only state-funded abortions.”
Abortion was rarely used to support healthy families or space out children. Abortions that could have been performed to delay a first birth (2.2%), space two births (1.0%), or end childbearing (3.0%) were rare.
This latest study expands on ongoing CLI research led by Studnicki analyzing Medicaid claims data to shed light on pregnancy outcome patterns.
As CBN News reported last month, another CLI study published online in the peer-reviewed Medical Science Monitor found 2,162,600 Medicaid beneficiaries in 17 states with state taxpayer-funded abortion reveals that “rapid repeat pregnancy” (defined as a second pregnancy within 2 years) is most common among women who have abortions.
Contrary to the narrative pushed by the abortion industry that abortion eases financial or personal problems for pregnant women, the study authored by CLI researchers suggests that a high number of women are pressured into having unwanted first-time abortions.
Data Doesn’t Lie – Most Mothers Not Undergoing Abortions
CLI President Charles A. “Chuck” Donovan said the new study reveals the abortion industry’s narrative isn’t true.
“They want to make it acceptable to target vulnerable women and children by citing estimates and surveys conducted at abortion centers to support the narrative that ‘everybody is doing it,’” he said.
“What Dr. Studnicki and his team have done is truly remarkable. This peer-reviewed research is based on nearly five million women who had nearly eight million pregnancies. By comparison, the frequently cited ‘Turnaway Study’ from the abortion industry is based on interviews with just 813 women,” Donovan continued.
“Most mothers are not undergoing abortions. We know that instinctively. We know that based on logic. Now, we know it based on data,” he added.
The Charlotte Lozier Institute was launched in 2011 as the education and research arm of Susan B. Anthony List. CLI is a hub for research and public policy analysis on some of the most pressing issues facing the United States and nations around the world.
John and Sheila Kippley
(World NFP Congress, Milan, Italy, June 13, 2015))
Abstract
Background: Breastfeeding mothers experience widely different durations of breastfeeding amenorrhea. Some have a first menses by three months; others one or two years later. Research studies, both prospective and retrospective, were reviewed to determine if breastfeeding patterns affect the duration of breastfeeding amenorrhea. Studies from the 1940s up to the 21stth century show that only frequent suckling provides a significant delay of fertility.
The type called ecological breastfeeding provides, on average, 14 to 15 months of breastfeeding amenorrhea.
Conclusion: Breastfeeding types need to be defined. The Church should promote and teach ecological breastfeeding as a desirable option for natural family planning. Eco-breastfeeding involves no abstinence, offers many benefits to mother and baby, is ecologically sound, and provides extended natural infertility. God does have a natural plan for spacing babies.
Continue reading document “Talk at Natural Family Planning Conference, Milan, June 13, 2015;Delivered by David F. Prentis” here
In a study published in the journal The Linacre Quarterly, Dr. Lynn Keenan and collaborators did a systematic review the literature to determine the risk of objectively confirmed Venous Thrombosis with the use of Hormonal contraceptives in healthy women compared to nonusers.
The authors searched 1962 publications and identified 15 publications that fit the criteria and were included.
The researchers found the following results.
1.Users of oral contraception with levonorgesterol had increased risk of VT by a range of 2.79–4.07.
2. The first-generation oral contraceptives had an increased risk of VT of 3.37–8.7. The second-generation oral contraceptives had an OR range of 2.79–4.07. Most studies of Third-generation oral contraceptives were in the range of 4–9. Of those that separated gestodene from desogestrel, the gestodene range was 5.2–9.1, and the desogestrel was 4.9–9.1. Oral contraceptives with drospirinone had a risk of 6.3 (2.9–13.7).
3. The nonoral forms showed that depot-medroxyprogesterone carried an RR of 3.6 (1.8–7.1).
4. Levonorgestrel intrauterine devices did not increase risk.
5. Etonogestrel/ethinyl estradiol vaginal rings increased the risk of VT by 6.5. Norelgestromin/ethinyl estradiol patches increased risk of VT by 7.9. Etonogestrel subcutaneous implants by 1.4 and depot-medroxyprogesterone by 3.6.
6. The risk of fatal VT was increased in women aged fifteen to twenty-four by 18.8-fold.
The authors of the study concluded “current hormonal contraceptives carry a three- to nine fold risk of VT compared to nonusers. Third-generation contraceptives are about twice the risk of the other generations. Combined HC vaginal rings and transdermal patches carry a six- to eightfold risk. Obesity can double the risk compared to normal weight. Use during the first year carries the greatest risk, especially in women under age thirty, where the risk increases thirteenfold.”
Informed consent is needed to provide women with information on the medical risks of oral contraceptives. Women should be made aware of these risks when choosing family planning. Abstinence or fertility awareness-based methods are licit, safe, and effective options for women.
“The Martian Chronicles” author Ray Bradbury once said, “I define science fiction as the art of the possible.” And sometimes, science fiction provides us with a picture of possibilities in the form of pro-life themes found in unexpected places.
Unlikely sources
“The Pre-Persons” is a little-known science fiction short story published in 1974 in the wake of the Roe v. Wade Supreme Court case that made abortion legal in all 50 states. The story takes place in a dystopian United States where abortion is legal not just for preborn children, but also for children under the age of 12 who are unable to comprehend algebra.
As the plot goes, when one adult male sees a group of children about to be taken to the abortion facility, he insists on being taken with the children, claiming he has forgotten how to do algebra. Naturally, this creates quite a stir when he arrives, forcing the administrator and the staff into a quandary as the man insists that he, too, meets the qualifications to be aborted. Soon, the administration decides to let the man and the children go, in an acknowledgement of the humanity of the entire group.
The pro-life themes are quite prevalent throughout the story, showing the humanity of all the characters involved with the plot. Anyone who reads a copy is likely to think that a pro-life advocate penned it — but they would be wrong.
Philip K. Dick was the writer for many groundbreaking science-fiction stories. His novella, “Do Androids Dream Of Electric Sheep,” would go on to become the basis for the hit film “Blade Runner” and its sequel “Blade Runner 2049.” Likewise, his writings such as “Total Recall,” “The Minority Report,” and “The Adjustment Bureau” have all gone on to become major motion pictures. Dick helped to define cyberpunk and is considered one of the best sci-fi writers in the United States.
Philip K. Dick (Screenshot: YouTube)
What readers might not know is that he also is the author of “The Pre-Persons,” which first appeared in the pages of “The Magazine of Fantasy and Science Fiction” and would go on to be reprinted in anthologies of Dick’s works. However, as his stories gained more notoriety, “The Pre-Persons” slowly vanished from the collections with the last major U.S. reprint being in 2014.
It is no secret that pop culture is plagued with pro-abortion content. From dystopian tales like ‘The Handmaid’s Tale’ to comedies like ‘Shrill,’ the pendulum tends to swing away from the pro-life message. However, “The Pre-Persons” is no outlier. I would make the case that science fiction, even accidentally, is predisposed to being pro-life.
Exploring the possibilities of life
Science fiction is all about the unknown. Even subgenres like steampunk, time-travel, and cyberpunk explore the unknown world to find new adventures. They show the potential and the possibilities that humanity has in making new discoveries. The pro-life message is all about giving preborn children the chance to live — the result being to find their own life adventures, so to speak.
In the episode “Evolution” in season three of “Star Trek: The Next Generation,” Acting Ensign Wesley Crusher accidentally creates a form of sentient microscopic robots after they are exposed to the Enterprise’s computer core. At first, a guest on the starship insists they be destroyed, likening them to “insects,” but the crew decides to defend the new life forms and eventually allows them to speak through the android crew member, Data. Their request is simple: “let us live.” In the end, the Enterprise crew leaves the robotic beings on an uninhabited planet that they can make their own.
Star Trek: The Next Generation “Evolution” (Screenshot: YouTube)
It is unknown whether Star Trek creator Gene Roddenberry or any of his successors writing Star Trek episodes were at all pro-life. That being said, the analogy is clearly there. The microscopic robots have no voice to speak for themselves, one person insists they be “aborted,” but the crew gives them a chance at life — and they flourish.
Another example of a pro-life ethic displayed in sci-fi is the Netflix thriller “I Am Mother,” in which a robot raises a young girl to eventually take her place and restore humanity after it was wiped out in a catastrophic event. The girl soon realizes that the robot has other sinister motives, but it is the undertones that are important. When we see tubes of preborn human beings gathered in the robot’s lair, it is made clear that these children are alive and that they will eventually become a new population for Earth.
While, again, there is no evidence that the filmmakers are closeted pro-life advocates, it is hard to miss such a clear message that these children are not mere “clumps of cells,” — they are humanity’s future.
Netflix’s “I Am Mother” (Screenshot: YouTube)
This perspective on the pro-life themes found in science fiction is, of course, up for debate. Yet, the reasoning is there. When we approach science fiction, we see new galaxies, advanced technology, intrepid explorers, and brave men and women pushing past their limits into futuristic adventures. You cannot see a galaxy, build equipment, or map new worlds without first recognizing that life, from its beginning moments, is the greatest adventure.
A child in the womb is a human being who is simply growing and being prepared for all of the adventures and possibilities to come.
The class of hormonal methods of birth control include birth control pills; implants such as Norplant, Jadelle and Implanon; injectables such as Depo-Provera and Lunelle; intrauterine devices (IUDs), patches and rings, and, of course, the class of abortion pills and so-called emergency “contraception,” which includes Cytotec, ellaOne, Mifegyne, Mifeprix, Plan B and Misoprostol.
All of these contain either one or a combination of artificial progestins and artificial estrogens.1
Health Issues Caused Hormonal Contraception
Though feminist groups and the mainstream media typically present hormonal contraceptives as a boon for women, they overlook the serious side effects reported in mainstream scientific literature, either through deliberate intent or negligence. Women who regularly ingest the powerful steroids in all modern hormonal methods of birth control will find that they usually suffer a wide range of side effects.
This should come as no surprise since hormonal birth control methods such as “the Pill” are listed as carcinogens (causes of cancer) by their own manufacturers.2
The patient information pamphlets for hormonal birth control methods list a long range of side effects, including:3
Heart attacks
Cancers
Anaphylaxis
Sudden total or partial blindness
Pulmonary embolisms
Early unintended abortion
High blood pressure
Dizziness and fainting
Abdominal discomfort, bloating, and pain
Gall bladder problems, including gallstones
Inflammation of the pancreas
Nausea and vomiting
Fluid accumulation
Long-term hormonal regulation problems
Ectopic pregnancies
Insulin sensitivity
Elevated potassium levels
Migraines or severe headaches
Depression and mood swings
Breast pain and swelling
Changes in menstruation patterns, e.g., PMS and dysmenorrhea
Acne
Rashes
Stroke
Hair loss
Loss of libido
Fatigue
Significant weight gain
Fatal blood clots
One of the most serious negative effects of the Pill and other hormonal methods of birth control is the increased risk of deep vein thrombosis, or blood clots that can potentially be fatal.
According to the Journal of Pharmacology and Pharmaco-therapeutics, some versions of the Pill increase the risk of deep vein thrombosis up to eight-fold:4
Among the other various negative effects of the hormonal methods is difficulty regulating a woman’s testosterone levels even when she no longer uses the method. Researchers have found that abnormally low amounts of unbound testosterone caused by the use of the Pill (or other methods of hormonal birth control) persist after women cease using it. Women’s bodies use testosterone, as men’s do, to regulate sexual function, though in far lower amounts. Report coauthor Dr. Irwin Goldstein clarified: “This work is the culmination of 7 years of observational research in which we noted in our practice many women with sexual dysfunction who had used the oral contraceptive but whose sexual and hormonal problems persisted despite stopping the birth control pill.”5
Primary Concern: Cancer
The hormonal methods of birth control increase the risk of cancer in women of childbearing age.
When taking hormonal contraceptives, “teenagers are especially vulnerable to breast cancer risk because their breasts are growing,” reports the Breast Cancer Prevention Institute. The Institute also says that although the Pill lowers the risk of ovarian and endometrial cancers, “according to the American Cancer Society, out of [a random selection of] 100 women with cancer, 31 have breast cancer, 6 have endometrial cancer and only 3 have ovarian cancer, so it is not a good ‘trade-off’ in risk.”
The National Cancer Institute confirms this view by stating that “studies have provided consistent evidence that the risks of breast and cervical cancers are increased in women who use oral contraceptives, whereas the risks of endometrial, ovarian, and colorectal cancers are reduced.”6
Psychological Impacts
Elizabeth Lee Vliet, MD, a women’s health specialist and the author of It’s My Ovaries, Stupid!, has studied the birth control pill’s negative impacts on women’s moods, with a particular emphasis on high-progesterone formulations. She found that they “might even bring about the need for antidepressants: The Pill screws up a woman’s mood and libido, and then she ends up on Prozac.”7
Dr. Vliet’s opinion is reinforced by the manufacturers of the hormonal methods themselves. Their patient information pamphlets list depression and nervousness as psychiatric disorders caused by their methods.8
These methods directly influence the hormonal cycle in women, but their impacts go far beyond mood swings. One of the most interesting studies done on the health impacts of the hormonal methods found that they may cause women to begin a relationship with the wrong men.
A study published in the August 2008 edition of the Proceedings of the Royal Society B found that when women smelled the T-shirts worn by men, they were attracted to more genetically dissimilar men before going on the Pill, and more genetically similar men after going on it.
As evolutionary psychologist Craig Roberts, one of the researchers, explains, “Not only could [genetic] similarity in couples lead to fertility problems but it could ultimately lead to the breakdown of relationships when women stop using the contraceptive pill, as odor perception plays a significant role in maintaining attraction to partners.”9
This fascinating study has thus found that the negative effects of the Pill are not just physical, but social as well, and may subtly influence a woman into being attracted to “Mr. Wrong.”
Environmental Poisoning
Much of the female hormonal content in these birth control methods is excreted via urine and ends up in rivers and lakes. Scientists are finding ever-greater numbers of “intersex” animals in aquatic environments that could lead to a collapse in fish and other populations, followed by a collapse in the populations of animals dependent upon them.
In 2004, The Washington Post reported that 79% of the male smallmouth bass in the Potomac River are growing eggs.10 In certain places, said the Post, “100% of the male fish had some female characteristics.”
Environmental Effects of the Pill: 79% of Male Smallmouth Bass in the Potomac Growing Eggs
A later Washington Post article described how scientists said the cause “is probably some pollutant created by humans — perhaps a farm chemical, or treated sewage, which can contain human hormones or residue from birth-control pills.” The later Post article reported that scientists think the problem is caused by a mixture of hormone and hormone-mimicking pollutants and have found negative effects on female fish as well.11
Iain Murray, author of The Really Inconvenient Truths, wrote on National Review Online, “By any standard typically used by environmentalists, the pill is a pollutant. It does the same thing, just worse, as other chemicals they call pollution.”
Early Abortion
Though the hormonal methods of contraception, including the Pill, appear to act the great majority of the time in preventing conception by suppressing ovulation and inhibiting sperm transport through the woman’s body, at other times they cause abortion by preventing or disrupting the implantation of an already-conceived child.
In some women, the Pill suppresses ovulation completely. But if the method fails, conception may follow and the user may feel that because she intended not to have a child, and because “technology failed her,” that she is entitled to a surgical or medical abortion.
Conclusion
The negative effects of the hormonal methods range from headaches and hair loss to fatal diseases such as cancer and deep-vein thrombosis. They also impact other people and society in general through psychological problems of the users and the environmental pollution they cause. In summary, these methods not only harm women, they harm the rest of us as well.
Want to know more? Try this video:
HLI’s Brian Clowes contributed substantially to this article.
Endnotes
[1] The chemicals used in hormonal methods of birth control commonly include one of about a dozen different artificial progestins — cyproterone acetate, dienogest, desogestrel, drospirenone, ethynodiol diacetate, etonogestrel, gestodene, levonorgestrel, medroxyprogesterone acetate (DMPA), norelgestromin, norethindrone, norethindrone acetate and norgestrel. All of the methods (except for the progestin-only minipill and some other methods such as IUDs, implants and abortion pills) also include the artificial estrogens ethinyl estradiol or estradiol cypionate. See the patient information pamphlets for each method to determine the exact combination of hormones they contain.
[2] Review of 1,346 patient information pamphlets on various hormonal methods of birth control distributed by the manufacturers. The National Cancer Institute (NIC) states, “The risks of breast and cervical cancers are increased in women who use oral contraceptives, whereas the risks of endometrial, ovarian, and colorectal cancers are reduced.”
[3] This example is Janssen Pharmaceuticals, “Micronor®” Oral Contraceptive Tablets, May 2020. Bayer HealthCare Pharmaceuticals, “Highlights of Prescribing Information: Yasmin,” April 2012.
To see the patient information pamphlet for any hormonal birth control method, visit the National Institute for Health’s DailyMed website.
[5] Claudia Panzer, M.D., et.al. “Impact of Oral Contraceptives on Sex Hormone‐Binding Globulin and Androgen Levels: A Retrospective Study in Women with Sexual Dysfunction.” The Journal of Sexual Medicine, Volume 3, Issue 1 [January 1, 2006], pages 104 to 113.
Recently, Live Action News reported that as part of a broader national conversation about population control, the Indian state of Uttar Pradesh is considering implementing coercive population control measures that would strongly incentivize couples who have just one child, and directly penalize couples who have more than two children.
While the case for a need for population control in India as a country is very weak due to a total fertility rate that is already below replacement level, critics of coercive measures correctly noted that in areas where women are more educated, the fertility rate drops naturally. Teaching women in poverty about fertility awareness is a form of education that helps them plan their families without the bodily harms that many experience from hormonal birth control, and which can be particularly dangerous for poor women unable to access follow-up care.
Mother Teresa on “throwaway culture”
The Missionaries of Charity, an order of religious sisters founded by the late Mother Teresa of Calcutta, have for decades successfully taught women in Calcutta and throughout India to chart their cycles for pregnancy achievement or avoidance through the symptothermal method of natural family planning (NFP). Mother Teresa saw natural family planning as the antidote to a “throwaway culture” that views children and people in general as problems rather than as unique and unrepeatable gifts.
She commented in a 1994 address to U.S. legislators at the National Prayer Breakfast, “I know that couples have to plan their family and for that there is natural family planning. The way to plan the family is natural family planning, not contraception.”
She also drew a connection between contraception and abortion, saying, “In destroying the power of giving life, through contraception, a husband or wife is doing something to self. This turns the attention to self and so it destroys the gift of love in him or her. In loving, the husband and wife must turn the attention to each other as happens in natural family planning, and not to self, as happens in contraception. Once that living love is destroyed by contraception, abortion follows very easily.”
Every woman can learn
Mother Teresa’s Missionaries of Charity first embraced the Billings Ovulation Method in 1969, a form of the symptothermal method of NFP that utilizes both cervical mucus and temperature observations, after a woman trained in the method applied to join the religious order. An undated handbook put out by the Missionaries of Charity in Calcutta sometime during the 1990s entitled “Natural Family Planning and Family Life Education” reported that “12,000 couples are successfully receiving instruction and have been able to rear their families in dignity and happiness.”
While pregnancy avoidance effectiveness statistics for the various methods of NFP can be notoriously hard to come by because many women use barrier methods such as condoms during their fertile time, a 1993 study in the British Medical Journal found that 19,843 women practicing the symptothermal method with abstinence during the fertile time (as taught by the Missionaries of Charity) “had a pregnancy rate approaching zero.” The official website about Mother Teresa maintained by the Missionaries of Charity reports that natural family planning is taught to this day.
The success of the Missionaries of Charity in teaching poor women to use NFP is a reminder that women of every socioeconomic status can learn the natural patterns of fertility and infertility within their own bodies, and they can utilize that information to plan their families in a manner that respects the dignity of all human life.
A recent review article published in the journal The Linacre Quarterly evaluated “whether there is evidence that ovulation can occur in women using hormonal contraceptives and whether these drugs might inhibit implantation”.
The authors reviewed “English-language research articles that focused on how hormonal birth control, such as the birth control pill, may affect very early human embryos. The authors found that abnormal ovulation, or release of an egg followed by abnormal hormone levels, may often occur in women using hormonal birth control.
This may increase the number of very early human embryos who are lost before a pregnancy test becomes positive.
For women who are thinking about using hormonal birth control, this is important information to consider”.
“Grandparents are the ring linking generations, to transmit to young people the experience of life and faith.”
Pope Francis (2021)
In January 2021, after praying the Angelus, Pope Francis declared the fourth Sunday in July as World Day for Grandparents. The date has been chosen to be near the liturgical memorial (July 26) of Saints Anne and Joachim, grandparents of Jesus. Since the date of the memorial falls within the week devoted to raising awareness of Natural Family Planning and Church teaching which support its use in marriage due to the anniversary of Humanae vitae (July 25), it is appropriate for all NFP Week celebrations to include reflection upon the vital role that grandparents play in the lives of their grandchildren.
July 20, 2021 (LifeSiteNews) – A recent article in the Washington Post’s women’s newspaper The Lily provides several accounts of women enduring agonizing pain after having intrauterine devices (IUDs) inserted, most of whom were dismissed by their doctors.
The IUD is a contraceptive tool. According to IUD manufacturer Mirena, IUDs prevent pregnancy by “thickening cervical mucus, preventing sperm from entering the uterus, inhibiting sperm movement so it’s more difficult to reach and fertilize an egg.”
It can also work as an abortifacient by thinning the lining of the uterus and preventing the embryo from attaching to the uterus. The copper IUD causes an inflammatory reaction which is toxic to sperm and eggs as well as to the fertilized embryo, thereby causing abortions.
Many obstetricians warn their patients of potential discomfort after the IUD insertion procedure, including irregular cramping. However, many women reported extreme pain which forced them to take medication and use other non-pharmaceutical methods to deal with the pain.
The Lily asked women to share their testimonies. One hundred thirty-one women responded, most of whom recounted severe pain either during the procedure or after they received their IUD.
The article cites gynecologist and Planned Parenthood associate medical director Stacy De-Lin. Planned Parenthood is the nation’s largest abortion chain. De-Lin claimed the “vast majority of her patients who use the IUD are thrilled with their experience,” but many said that they felt ignored or overlooked by doctors who refused to adequately address their pain and were unwilling to remove the IUDs to relieve it.
Danielle Petermann, a 48-year-old woman who has had an IUD since 2013, said, “There are enough tales of discomfort that go beyond just taking an Advil or Tylenol that I think there should be more information available.”
After receiving her IUD, another woman, Tiffany Washington, returned to her doctor because of intense pain that forced her to spend two days in bed. The nurse in the office reportedly rolled her eyes at Washington, asking, “Back so soon?”
This caused Washington to reconsider her decision and to determine to attempt to endure the pain. However, after a few more weeks, she visited a local Planned Parenthood abortuary and had the device removed.
Many other women recounted stories of doctors dismissing their complaints and instead telling them to continue with the IUDs. One doctor advised her patient to remove the IUD herself.
Another woman, Valerie Johnson, recounted her doctor dismissing her extreme pain, only to realize weeks later that the IUD had perforated her uterus and lodged itself in a fat deposit.
She went into surgery a few days later. “I tend to defer to the experts,” Johnson said. “I wish I had been a stronger advocate for myself when my pain was dismissed.”
Pro-lifers have long noted that most gynecologists prioritize contraception over solving women’s underlying health concerns, and that most forms of contraception – including “the pill” and IUDs – have the capacity to induce very early abortions.
July 19, 2021 (LifeSiteNews) – Many women choosing a medical abortion (Mifegymiso in Canada) change their minds having taken the first pill.
Abortion Pill Reversal has been developed to assist these women who want to save their children from the effects of the first pill in this protocol (Mifepristone).
Records indicate that so far, 112 Canadian women have contacted the Abortion Pill Rescue Network for information on stopping an ongoing chemical abortion, with 57 choosing to undergo the abortion pill reversal procedure. Nine of these women have reported successful interventions with one mother agreeing to provide her testimony.
Abortion Pill Rescue believes there are many more Canadian babies alive whose mothers have not yet reported back their success stories.
The message that AllianceforLife Ontario is conveying to Canadian women is that there is a safe, effective (64% to 68%) method that may save their children if they have second thoughts after starting the Mifegymiso process.
It seems Canadian abortion advocates do not want women to know that this second chance at “choice” exists, as they are currently engaged in a campaign to silence the message that AllianceforLife Ontario is providing for these women.
In April 2021, MP Pam Damoff called our facts “dangerous misinformation” in Parliament. This is an outrageous lie, but parliamentary privilege protects her from the consequences of that lie. Our Facebook page has been taken down after erroneous complaints, our Google ad campaign has been limited, and now our website abortionpillreversal.ca is being attacked with complaints being made to Health Canada. Since this Health Canada avenue did not work, we are awaiting possible complaints to the Ontario Ministry of Health and the College of Physicians of Ontario from the so-called “pro-choicers.”
Abortion Pill Reversal is being offered around the world with 2,000 little ones saved to-date. Women deserve to know the truth about this second chance at choice and that there are physicians trained and willing to help them try to save their children using similar methods to those used for the last 50 years to assist in the prevention of miscarriage.
However, the politicization of abortion and medical science has world medical bodies, including those in Canada, expressing opposition to the use of progesterone protocols to save these tiny children from the effects of abortion drugs. Physicians are being hauled up before kangaroo courts to explain why they are using drugs “off-label” to save a life – and yet these same medical bodies appear to have no problem with the use of drugs “off-label” to kill a child in the womb.
The Ontario Ministry of Health has reported to AllianceforLife Ontario that a total of 45,363 prescription claims from Canadian pharmacies for Mifegymiso were made between August 10, 2017 and December 31, 2020. Yet we found no sign of these in the official abortion statistics for Ontario released from the Canadian Institute for Health Information (CIHI).
And the 45,363 does not include women receiving Mifegymiso in hospitals or prescriptions paid in cash or by another insurance rather than OHIP.
A final and outrageous fact is that a small study, ostensibly undertaken to prove Abortion Pill Reversal does not work ended up proving that it does and yet the authors had the audacity to claim the opposite of their results.
The study was abandoned because the Mifepristone caused extremely heavy bleeding in three participants, two of whom were in the placebo group and had not been given progesterone. The woman who had the progesterone did not experience such traumatic bleeding.
This study also proved that the progesterone protocol actually had an 80% success rate in maintaining the pregnancy in women who received progesterone without the second abortion drug and a 40% success rate in those who received both abortion-inducing drugs.
We believe that women who decide to have an abortion do not give up their right to the truth. Why does “choice” always have to mean abortion?
Below is Alliance for Life Ontario’s petition to Health Ministeer Patty Hajdu (click HERE to sign it):
To Health Minister Patty Hajdu:
Whereas: Women deserve a second chance at choice, and
Whereas A 2018 peer reviewed study showed positive results for Abortion Pill Reversal, establishing its effectiveness 64%-68% of the time, its safety for women; no increase in birth defects, and a lower preterm delivery rate than the general population, and
Whereas 2,000 pre-born children’s lives were saved in 2020 by Abortion Pill Reversal, and
Whereas Women who decide to have an induced abortion do not give up their right to the truth, and
Whereas, we know of at least 9 Canadian babies who are living today because of the abortion pill reversal procedure, and
Be it resolved that, any Canadian woman requesting Mifegymiso, must be provided Abortion Pill Reversal Procedure contact information, should she wish a second chance at choice after beginning the Mifegymiso abortion procedure.
A recent study published in the journal Human Fertility looked into the effectiveness of a fertility-awareness method in achieving pregnancy. The study particularly observed factors associated with the achievement of pregnancy and the usefulness of the mucus pattern, in the context of infertility.
The authors of the study identified 384 eligible women who attended 17 Australian Billings Ovulation Method® and were achieving a pregnancy. Pregnancy was achieved by 240 couples (62.5%) who received instruction to identify mucus symptom observations after a follow-up of two years maximum.
The participants kept a diary record of observations of vulvar sensation and vaginal discharge following the Billings Ovulation Method® criteria. A changing pattern of vulvar wetness or slippery sensation indicated hormonal activity and potential fertility. The authors stratified “low pregnancy potential” and “high pregnancy potential” according to mucus symptom observations. Pregnancy rates were ∼30% higher in the high pregnancy potential” group (44.4% versus 72.3%). Also the “high pregnancy potential” group achieved pregnancy in a shorter period of time (4.2 versus 6.4 months).
In conclusion, these findings indicate that the use of fertility awareness methods helps women to identify critical biomarkers of fertility that may be used to achieve a pregnancy. These methods “provide a rapid, reliable and cost-effective approach to stratifying fertility potential, including directing timely and targeted investigations/management, and is accessible for women who may be remote from primary or specialist care”.
According to a prospective observational study of more than 17,000 women that evaluated fecundability after stopping contraception the answer is YES.
The authors found hormonal intrauterine device (IUD) users had slightly increased fecundability compared with users of barrier methods.
There was no difference in fecundability for users of copper IUDs, implant, oral contraception, patches, rings, or natural methods compared with barrier methods.
Users of injectable contraceptives experienced the longest delay in return of normal fertility, about 5 to 8 menstrual cycles.
In an often-quoted and often-misunderstood section of the letter to the Ephesians, St. Paul begins a passage about wives and husbands with these words: Be subordinate to one another out of reverence for Christ. (Eph 5:21ff)
In the late fourth century, St. John Chrysostom suggested that young husbands should say
to their wives:
I have taken you in my arms, and I love you, and I prefer you to my life itself. For the present life is nothing, and my most ardent dream is to spend it with you in such a way that we may be assured of not being separated in the life reserved for us . . . I place your love above all things, and nothing would be more bitter or painful to me than to be of a different mind than you. (Homily on Ephesians 20,8).
John captured well Paul’s teaching that wives and husbands are to be subordinate to one another–in other words, they are to consider the other’s good as of greatest importance, they are to sacrifice for one another as Christ himself has done, and as a couple they are to see themselves as subject to Christ. The concept of mutual subordination is a way of expressing the particular kind of love which characterizes Christian marriage, which is a union of loves so complete that the two become one.
In the Roman Catholic Church, it is ordinarily understood that husband and wife are ministers of God’s grace and confer on one another the sacrament of matrimony by declaring their consent before the Church. They are chosen instruments of God in one another’s lives–and not just the day of the wedding, but until death do us part. They are literally to help one another get to heaven! Moreover, their vocation entails not only being one in love for each other but also 2 being God’s instruments as a couple, most especially instruments of his creative power in giving life to children. Their love looks beyond itself and seeks to raise up new lives.
These two meanings or values of Christian marriage–the unitive and procreative–are intimately, inseparably linked; they cannot be divided without affecting the couple’s spiritual life and compromising their marriage and the future of their family. In fact, if a person enters marriage with the deliberate intention to exclude children from the marriage, the consent is invalid. Just as the persons of the Trinity are fruitful in love for one another and in creation, so the love of husband and wife is intended to be fruitful in love and offspring. Married couples are cooperators in the love of God the creator and are, in a certain sense, its interpreters.
Being cooperators and interpreters of the creative love of God carries both extraordinary joys and extraordinary responsibilities. An especially intimate and personal responsibility of every couple is making decisions about the regulation of births. Just as the crown of creation was human life, so the supreme gift of marriage is a human person, and the vocation of husband and wife entails honoring this capacity of their love with special care.
The Church does not teach that couples should have a certain number of children, but it does offer teaching about responsible parenthood, which can be summarized in these five points:
1. Husbands and wives have a responsibility to understand and honor the wisdom of the body, including its biological processes.
2. Humans share certain instincts and passions, and Christians are to guard and control them through reason and will.
3. Taking into consideration the physical, economic, psychological and social conditions of their marriage, couples exercise responsible parenthood by a prudent and generous 3 decision to raise a large family, or by a decision (for serious reasons and made according to the moral law) to avoid a new birth for the time being, or even for an indefinite period.
4. Responsible parenthood has its roots in the truth about right and wrong established by God, and spouses have a duty to inform their consciences and make decisions according to this truth. Husbands and wives recognize their duties toward God, themselves, their family and society, and are called to maintain a proper set of priorities.
5. Offering their marriage in discipleship to the Lord Jesus, couples do not make purely arbitrary or subjective decisions regarding becoming parents but use the wisdom of God as their guide. As in every other aspect of their lives, Christian couples always remain open to God’s wisdom and providence regarding family life, including the size of their particular family. Since God brought them together and shares his love with them, he will always guide them along paths that are best for them.
Interwoven among these aspects of responsible parenthood is the understanding that the two great meanings or values of marriage–the unitive and procreative–are never separated. A love that is complete and faithful, a love which holds nothing back from the other, will remain open to Gods creative plan. After all, it is God’s love in the first place.
_________________________
Most Rev. J. Peter Sartain is the Archbishop of Seattle. This article is part of a six-part series
first published for the Arkansas Catholic, a publication of the Diocese of Little Rock. It is
reprinted here with permission.
Over the last decade, United States population growth was at its lowest rate since the 1930s, according to a report released by the US Census Bureau in April. Population was up by 7.4 percent over the previous decade, the slowest growth rate the US has seen since the Great Depression. (These findings are a bit surprising since 93 percent of American adults either would like children or already have them, and only 5 percent do not want children, according to a 2013 Gallup poll.)
The Nobel Prize-winning economist and New York Times columnist Paul Krugman had positive words to say about the census news. He wrote in a Times article recently, “Is stagnant or declining population a big economic problem? It doesn’t have to be. In fact, in a world of limited resources and major environmental problems there’s something to be said for a reduction in population pressure.”
By expressing a rosy attitude toward the waning of humankind’s proliferation on Earth, Krugman is joining a dubious tradition that has been ascendant since the 18th century.
“Paul Krugman at The Commonwealth Club” by commonwealth.club is licensed under CC BY 2.0
From Malthus to Krugman
The idea that a smaller human population is desirable on environmental grounds has been popular ever since the economist Thomas Malthus published his highly influential 1798 work, An Essay on the Principle of Population. Arguing that each plot of land could only yield so much produce, Malthus surmised that if population growth were to continue without drastic reduction, the vast majority of humanity would inevitably starve within a century of his writing.
Throughout the 19th century, Malthus’s predictions were conclusively disproved by widespread reductions in both poverty and food prices as the population continued to increase. But in the 1960s and 1970s, when the global population was roughly half what it is today, Malthusian ideas once again rose to global prominence. Stanford biologist Paul Ehrlich, for example, became a celebrity by inciting an international hysteria over population growth. His 1968 book The Population Bomb became a worldwide bestseller, and he got plentiful mainstream media exposure for his ideas, including over twenty appearances on NBC’s “Tonight Show” with Johnny Carson. Ehrlich claimed that not just food, but virtually all natural resource supplies were at the brink of collapse.
His predictions included death by starvation for hundreds of millions before the end of the 1970s (including 65 million Americans), the essential doom of India in its entirety, and even the non-existence of England by the year 2000. Perhaps his grandest forecast, made in 1970, was that “an utter breakdown of the capacity of the planet to support humanity” would arrive by 1985.
In the 21st century, population panic has shifted focus mostly to climate change. Environmentalists can now often be heard advocating smaller family sizes, or avoiding child conception altogether, in an effort to limit carbon emissions.
An article in The Guardian is titled, “Want to fight climate change? Have fewer children.” According to an NPR piece, “A recent study from Lund University in Sweden shows that the biggest way to reduce climate change is to have fewer children.” And the Bulletin of the Atomic Scientists published an essay titled, “Stabilize global population and tax carbon to reduce per-capita emissions,” in which it is argued that, “Tax and other economic incentives should be continuously reconsidered to make population stabilization more likely”.
Given the apocalyptic terms in which some of our most esteemed politicians and news outlets speak about the risks of climate change, these contemporary population doomsayers can hardly be considered less alarmist than Malthus and Ehrlich.
Hunger Versus Science
As you may have noticed, the predictions of Malthus and Ehrlich turned out to be epically off.
Food prices have been falling rapidly since Malthus made his predictions in 1798, and the share of the population living in absolute poverty has fallen even faster.
And according to research by Oxford University economist Max Roser, global per capita calorie intake increased nearly every year during the period about which Ehrlich made his predictions. Data show that between 1961 and 2013, per capita calorie intake increased from 2,196 kcal to 2,884 kcal—even while the world’s population nearly doubled.
What accounts for the radical improvements in global nutrition? The New York Times ran an article about the progress against world hunger since Ehrlich’s predictions. The author stated:
No small measure of thanks belonged to Norman E. Borlaug, an American plant scientist whose breeding of high-yielding, disease-resistant crops led to the agricultural savior known as the Green Revolution. While shortages persisted in some regions, they were often more a function of government incompetence, corruption or civil strife than of an absolute lack of food.
But Borlaug’s innovation was just one in a long trend of improvements to agricultural technology. Early that century, in 1909-1910, the Haber-Bosch process was invented, for which Haber and Bosch each earned a Nobel Prize in chemistry. Their process facilitated the creation of synthetic fertilisers, which revolutionised the capabilities of farmers worldwide and made it possible to feed a much larger population from the same amount of farmland.
Even throughout the nineteenth century, industrialisation was radically improving farmland efficiency. The political economist and historian Peter Kropotkin wrote in his 1892 book The Conquest of Bread about the game-changing impact greenhouses were having on agriculture:
And yet the market-gardeners of Paris and Rouen labour three times as hard to obtain the same results as their fellow-workers in Guernsey or in England. Applying industry to agriculture these last make their climate in addition to their soil, by means of the greenhouse.
Kropotkin noted,
Fifty years ago the greenhouse was the luxury of the rich. It was kept to grow exotic plants for pleasure. But nowadays its use begins to be generalized. A tremendous industry has grown up lately in Guernsey and Jersey, where hundreds of acres are already covered with glass — to say nothing of the countless small greenhouses kept in every little farm garden.
These are just a few of countless such examples of scientific and technological innovations revolutionising the ability of humankind to more resourcefully subsist within its environment.
The Ultimate Resource
Every new human will consume resources, produce carbon emissions, and pollute their environment to some degree. But every new human also comes with a human mind, the source of potential solutions to these problems and many others. Each new able body also contributes precious labour to the economy, contributing to the rearrangement of the world’s atoms into more useful configurations.
The people whose future existence Malthus feared would lead to mass starvation, in some cases, turned out to be the very people who would revolutionise agriculture and virtually every other productive industry.
Likewise, when Krugman’s fear of “limited resources and major environmental problems” leads him to speak positively of “a reduction in population pressure,” he assumes that the destructive capacities of future people are likely to outweigh their creative capacities. But as we have seen, the history of such predictions suggests precisely the opposite. The above-mentioned Lund University study accounts for the carbon emissions of future people, but it does not account for the creative visions of those people, nor can any study before the people exist.
Paul Ehrlich’s archnemesis, the economist Julian Simon, understood this fundamental flaw in Malthusian thinking. As he argued in the second edition of his 1980 book The Ultimate Resource,
Adding more people to any community causes problems, but people are also the means to solve these problems. The main fuel to speed the world’s progress is our stock of knowledge, and the brake is our lack of imagination. The ultimate resource is people – skilled, spirited, and hopeful people – who will exert their wills and imaginations for their own benefit as well as in a spirit of faith and social concern. Inevitably they will benefit not only themselves but the poor and the rest of us as well.
If you want to increase resource abundance and have the climate engineered to your liking, perhaps consider having more children. Your future descendants may be the ones to grow up and create the knowledge required to usher in levels of prosperity that we have seldom dared to imagine.
In 1998 Pope John Paul II wrote a letter to Dr. Anna Cappella, director of the Center for Research and Study on the Natural Regulation of Fertility at Rome’s Catholic University of the Sacred Heart. The occasion was a convention commemorating Humanae Vitae, Pope Paul VI’s 1968 encyclical. Excerpts are reprinted below.
I hope that everyone will benefit from a closer study of the Church’s teaching on the truth of the act of love in which spouses become sharers in God’s creative action.
The truth of this act stems from its being an expression of the spouses’ reciprocal personal giving, a giving that can only be total since the person is one and indivisible. In the act that expresses their love, spouses are called to make a reciprocal gift of themselves to each other in the totality of their person: nothing that is part of their being can be excluded from this gift. This is the reason for the intrinsic unlawfulness of contraception: it introduces a substantial limitation into this reciprocal giving, breaking that “inseparable connection” between the two meanings of the conjugal act, the unitive and the procreative, which, as Pope Paul VI pointed out, are written by God himself into the nature of the human being (HV, no. 12).
Continuing in this vein, the great pontiff rightly emphasized the “essential difference” between contraception and the use of natural methods in exercising “responsible procreation.” It is an anthropological difference because in the final analysis it involves two irreconcilable concepts of the person and of human sexuality (cf. Familiaris Consortio, no. 32).
It is not uncommon in current thinking for the natural methods of fertility regulation to be separated from their proper ethical dimension and to be considered in their merely functional aspect. It is not surprising then that people no longer perceive the profound difference between these and the artificial methods. As a result, they go so far as to speak of them as if they were another form of contraception. But this is certainly not the way they should be viewed or applied.
On the contrary, it is only in the logic of the reciprocal gift between man and woman that the natural regulation of fertility can be correctly understood and authentically lived as the proper expression of a real and mutual communion of love and life. It is worth repeating here that “the person can never be considered as a means to an end, above all never a means of ‘pleasure.’ The person is and must be nothing other than the end of every act. Only then does the action correspond to the true dignity of the person.” (cf. Letter to Families, no. 12).
The Church is aware of the various difficulties married couples can encounter, especially in the present social context, not only in following but also in the very understanding of the moral norm that concerns them. Like a mother, the Church draws close to couples in difficulty to help them; but she does so by reminding them that the
way to finding a solution to their problems must come through full respect for the truth of their love. “It is an outstanding manifestation of charity toward souls to omit nothing from the saving doctrine of Christ,” Paul VI admonished (HV, no. 29).
The Church makes available to spouses the means of grace which Christ offers in redemption and invites them to have recourse to them with ever renewed confidence. She exhorts them in particular to pray for the gift of the Holy Spirit, which is poured out in their hearts through the efficacy of their distinctive sacrament: this grace is the source of the interior energy they need to fulfill the many duties of their state, starting with that of being consistent with the truth of conjugal love. At the same time, the Church urgently requests the commitment of scientists, doctors, health-care personnel and pastoral workers to make available to married couples all those aids which prove an effective
support for helping them fully to live their vocation (cf. HV, no. 23-27).
Doctors for Life, a pro-life lobby group, spoke out against the recent vote by the European Union Parliament in favor of the Matić Report, which defends abortion as a human right and puts pressure on pro-life member states to legalize abortion. The group called the report “another step in the efforts of the pro-abortion lobby to normalize this abhorrent practice in Europe and force it on member states.”
The Matić Report on the situation of sexual and reproductive health and rights in the EU, in the frame of women’s health, pressures pro-life member states of the EU to enact pro-abortion laws. Introduced by S&D MEP Fred Matić, it calls for guaranteed access to sexual and reproductive health. This includes not only abortion, but fertility treatments that often result in the destruction of human lives. The report also aims to end conscience protections for pro-life doctors and medical workers, forcing them to commit or participate in abortions.
“The report utilizes the same shrewd and misleading approach to force politicians and the public to acquiesce and submit to its conclusions by repeatedly conflating gender equality and basic human rights with abortion,” Doctors for Life said in a statement, according to the Times Malta.
“This rationale makes the rejection of abortion equivalent to an unwillingness to grant equality or essential human rights and is a strategy employed repeatedly to compel others to accept such proposals,” the group continued. “Of course, such a strategy necessitates the continued employment of euphemisms like reproductive rights and healthcare to sanitize the brutal reality of the intervention.”
That brutal reality is that abortion “unequivocally involves the intentional killing of a human life,” Doctors for Life said. Each abortion procedure uses violence to end the life of a living, growing, preborn human being. Abortion is not health care.
Just 16 weeks in the womb
Doctors for Life was also critical of the report’s efforts to end conscience objections, stating that in countries in which abortion is legal, there are a significant number of physicians who are unwilling to partake in abortions. In parts of Italy, 90% of doctors refuse to carry out abortions, and in Ireland, 68% of doctors have said they would not commit abortions.
Deliberately killing human beings in the womb is not health care, and does not make women equal to men. All human beings, regardless of age or gender, are intrinsically equal. Forcing pro-life nations in the EU, or anywhere else in the world, to decriminalize abortion will not decrease poverty or child abuse, and it will not save women from oppression. Abortion is simply oppression redistributed to the most innocent.
Should you have children? And if so, how many? Asking and answering these questions is not only deeply anguishing for many individuals but also bears on national and global well-being. Contemporary discussions of childbearing range from the writer who got a vasectomy due to climate change to the regular reports of declining fertility across the world, including the 4% decline in 2020 in the US.
Amid this discussion, The New York Times opinion writer Elisabeth Bruenig penned a moving essay about her personal experience as an outlier among her high-status, educated peers— she gave birth to her first child at 25 and, what’s more, she’s “not sorry she didn’t wait.” This simple notion, timed to coincide with Mother’s Day of all days, caused pandemonium. Among the various critiques of Bruenig’s lived experience were those who suggested that if we have to hear from women who love their children, we should also read more essays from women and men “who regret having children,” as writer Jill Filipovic suggested. Among the many replies were those like this, from @MAStirling, who wrote:
I have daughters so I’ve been pretty honest with them. I’ve encouraged them not to have children. They know I love them, but they also know that motherhood in our country is a prison sentence.
While the commentary focused on whether we should regret the decisions we make about having or not having children, no one presented the facts about how many of us actually do regret these decisions. Each person may have their own individual story to tell, but it turns out that the vast majority of people want to have children and, as we’ll show, more than a third wish they had more children than they currently have.
This is according to the second wave of the “U.S. Adult Sexual Behaviors and Attitudes Study,” a survey of 1,518 adults I designed and fielded in March 2021. Among the respondents, ranging in age from 18 to 74, 68% have at least one child. Another 19% have not had children nor want to have children, while the remaining 13% do not have children but still hope to. The fact that more than three-fourths of adults already have or want to have children should itself be evidence that something very fundamental is at work, likely the same biological predisposition that motivates all life on the planet.
But that fact could open the door to even more regret. If we’re physiologically bent on having children, perhaps we later regret the outcome, encumbering as it is upon our personal freedoms. Though some commenters on the Bruenig essay feel this way, it is not common. While the present study did not explicitly ask whether people regretted having children, it did approach a topic that is similar, asking those with children to agree or disagree with the statement, “I wish I had had fewer children.”
Just 14% of people with children (10% of all adults) agreed with the statement. And even with these, we don’t know whether they regret ever having children or just wish that they had fewer children. Either way, the maximum share of people who are not inclined toward joy in children is 29%, including those who don’t currently have children and those who don’t want to, as well as those who wish they’d had fewer. This is not close to a majority, but it is also not a trivial number.
Conversely, when asked if they wished for the opposite, if they agree that, “I wish I had or would still like to have more children,” 24% fall into the category of already having but still wanting more children. This is consistent with research shared on IFS in 2018 using Gallup data showing that women regularly wish to have more children than they do.
The final score? As shown in the figure below, 29% of U.S. adults either do not want to have children or wish they had fewer. A third (34%) have children and are happy with the number they have and another third—the largest group—wish they had more (37%), whether currently parents or not. In other words, those with no apparent regret or reluctance outnumber the rest by more than 2 to 1.
Of course, none of the aggregate statistics tell us what we should feel individually, nor should they compel someone’s personal choices. But this should give us pause as we consider whether we can so easily tell people that personal choices related to procreation are merely that, just personal choices, some of which we will regret and others we will not. For some reason, most of us really want to have kids. And for those that do, an astonishing 88% agree that “having children is one of the most important things I have done.” This suggests the joy far outweighs the regret.
This all suggests that our bodies are doing what they seem designed to do: motivating us to bond with mates and procreate. As I’ve previously written, people who want marriage and family are happier than those who do not. This includes singles who do not currently have a partner—their life satisfaction is predicted by their desire to bond and procreate independent of their current life situation.
Borrowing from the old Sinatra hit: “Regrets? I’ve had a few.” But having children is not one of them for the majority of Americans.
In March, 2021, the survey of US Adult Sexual Behaviors and Attitudes was fielded to a U.S. representative sample of adults ranging in age from 18 to 74. The outgoing sample was balanced by sex, age cohort, and U.S. Census region. Sample sourced from and data collection provided by Dynata, a global leader in first-party data and data services. The respondents were weighted back to the outgoing sample parameters for sex, age, marital status and region. Data were validated for internal consistency and compared for population representation to U.S. / Census data and GSS data for income, rates of marriage, and childbearing. The project was conceived, designed, executed, and paid for entirely by Dr. James McQuivey.
After the copper IUD caused Tamara Wilder physical symptoms like sore tailbone and heavy bleeding, followed by more severe symptoms of debilitating anxiety, she founded IUD Awareness, a website with resources for women who have experienced adverse reactions to the IUD. Tamara now also serves on an online IUD support group and says it was finding other women’s stories that helped her find the cause of her health problems. Here is Tamara’s story.
I didn’t recognize the early warning signs when they started happening. Like so many of us, things were going on in my life, and so when I started feeling weird, which when I look back, was right away. Within days of having it inserted I was having a really sore tailbone. I couldn’t sit down for about three or four months without having pain. And I didn’t even identify that as an early warning sign until way later when I got on support groups and I started seeing other people mention it; but it was way at the very beginning.
And then I had a lot of heavy bleeding. I was warned that I would bleed more than usual for several months, and I was bleeding pretty heavily, so I told myself, “I just have to get through this.” And like many doctors, my naturopath said, “your body’s going to do weird things for a few months but you just gotta bear through it, but then it’s all going to calm down and this thing’s going to be great for you.”
But it wasn’t great for me.
This was the first time I’d put anything in my body or altered my body for birth control. And since I’ve joined the support groups and hear other women’s stories, and hear how many birth control types they’ve gone through and how many problems they’ve gone through, I feel incredibly lucky.
The copper IUD did not work for me. It was something that my body responded to negatively from the very, very beginning. And I still was trying to give it a try because my naturopath said it was great. I’d actually had it inserted at Planned Parenthood and they were so pro-IUD. And I remember in the first couple months I would call and say, “I’m bleeding a lot; I’ve sort of bled all month, and it hasn’t stopped.” (I bled about three weeks of every month that I had the IUD, and I would spot every week that I wasn’t heavy bleeding, so I really was constantly bleeding.)
And I was in a new relationship, which was very problematic; this was a bloody, bloody existence. That’s one of the things they tell you [with contraceptive devices]: you can have trouble-free sex, without worrying about getting pregnant. But if you’re bleeding all the time on the copper IUD, that doesn’t make sex very fun.
Ultimately, I had a very negative experience with the IUD, but it took me ten months to figure out what was going on. Even though my body reacted so negatively from the very beginning, looking back I can see the early warning signs. And for that reason, when I did finally make the connection and figured it out, I felt really driven.
From fog to clarity
I was very fortunate that I had a lot of support in my recovery. I was very fortunate that financially, my family helped me out and allowed me to not have to worry about finances for a year; they told me to just take care of my health. And so part of my healing process was getting the word out and telling people my story. Because when I was first trying to figure it out, five months in, I searched like crazy but could not find the information I needed; in fact, I found information that diverted me from what was going on.
So I just wanted to make that information available to people and make a place where stories could be told and people could find them. And so I founded IUD Awareness as a part of my healing process. On the support groups I was seeing so many people having to recover while they had children, while they were still working, while they were struggling on a daily basis—and all of us struggle on a daily basis to recover. So many of us have hard recoveries, but I was being so supported in my recovery and in my financial existence for my first year. So I felt what I needed to do was to put my time and energy into creating an entity that could help people.
The freedom found in IUD support groups
When I found the IUD Side Effects support group it was almost six years ago, and there were 1800 members. At the time there were three admins, and I became the fourth admin. Because it was growing so fast, that it was really overwhelming…
We get about 100 member requests a week, which is our average. When a film comes out, or like when The Bleeding Edgecame out all of a sudden, that went to 200 or 300 a week. And we lose a certain amount, so we’re gaining a net of about 50 members a week as a really constant growth rate, and we’re almost at 25,000 now, which is incredible.
Not everybody on the group has IUD side effects; many women are on the group because they’re looking for side effects. They feel like the IUD is working for them, but they’re trying to empower and educate themselves. And I am very supportive of that because if I had had that information, I would have been able to see the side effects that were plaguing me. Some women don’t see a problem, and they feel like it’s fine. But the majority of the women on the group have seen side effects, have had their lives devastated, have already removed the IUD, and/or are in recovery. We also have some women on the group who are considering getting the IUD, and they’re doing their own research and finding women’s real-life experiences instead of what I call propaganda, hearing all the good things instead of being told what can go wrong.
And we’re not saying on the support groups and on IUD Awareness that an IUD will always go wrong, but we’re saying that it’s going wrong more often than people realize. Because the stories aren’t being reported.
Personally, after my experience and after reading all the stories, I do not think that IUDs are safe; I would never recommend them to anybody, but everybody needs to be able to make their own decisions. So by sharing our stories and real-life experiences, people can choose to take the risk, and realize that getting an IUD is actually a risky choice, despite being told it’s totally safe by the doctors who are promoting it to you. And if you do your research you realize it is not totally safe, that there are chances that it will go wrong—and when it goes wrong, it usually goes really wrong. Some people have minor problems, but the majority of people on the support group have huge problems… We’re trying to find people before they’re in that severe state so they don’t have to go through the depth of the health crisis that so many of us have.
Common threads in IUD side effects
One of the trends I see on the support group is people say “the doctor told me to keep it.”… They say, “it’s a foreign object in your body, your body’s going to react to it, but it will get used to it.” And my response to that is: our bodies will adapt to most anything, but that does not mean that the state that we end up in is a healthy, balanced state.
In the training that doctors are receiving, they’re being told don’t take it out too soon; if someone’s having problems with it, get them to hang in there; get them to have it for at least six to eight months before you will take it out. And so that’s why, so many of us, if our bodies are telling us from the very beginning that it’s not working for us, we go to the doctor, and the doctor, if they’re experienced with IUDs, they’ll say “you just have to hang in there.” And if they’re not experienced with IUDs, like my general practitioner, they’ll say, “there’s no way what is happening to you could be related to the IUD, it must be something else.”
My IUD and severe anxiety
In my case, I had worsening symptoms for five months that were taking me down in so many ways. My mental state was degrading really quickly and I didn’t realize what was going on because I never suffered from anxiety before. I’ve always been a very balanced person; I never had any depression or any anxiety. And so I just thought I was feeling tired; I just thought I was feeling stressed. But I was actually falling and running over the cliff and one day I just went over the cliff into the big pit of massive anxiety. And I had a breakdown.
I got diagnosed with sudden anxiety disorder and put on Ativan and then Paxil. My doctor kept increasing the doses of Paxil, and I was completely dysfunctional. Within five months of getting an IUD I went from running my own business, being a super independent person (I’m admired for my independence and my ability to handle anything, because I teach ancient living skills! I teach people how to survive in the woods!) and within five months, I collapsed completely into an agoraphobic, hiding person in a room in my parents’ house, and taking these anti-anxiety meds that were not doing anything. Totally suicidal. Totally not understanding, feeling disconnected, feeling like I was living on a different planet, like a foreign world. And it was a devastating thing. And that started five months after my IUD was inserted.
And for the next five months, I would try to figure it out; I would go online and search and I would try to find answers, and I wouldn’t find anything. Everything would say the copper IUD couldn’t cause these kinds of things. Everything was saying, “oh, it’s totally healthy” which is the propaganda I was finding in my searches. And my mind wasn’t together enough to go deep enough to find all the stories; everything I was finding at the time was pro-IUD. And so I kept saying “well the doctors are saying it can’t be related; I’m not finding anything on the Internet.” I’d find a few little things and then the doctor would say “well that’s just a hack.” And then he told my parents, “don’t let her use the Internet anymore because it’s increasing her anxiety.” And so I actually stopped searching.
About six or seven months in, I had just given up. My doctor just kept saying, “you just have to accept that this happens to women sometimes and you just need to adjust. There’s something you need to change in your life and you just need to adjust to this.”
Funnily enough he was right; the thing I needed to change in my life was I needed to get a foreign object that was poisoning me out of my body, and that made everything get better. But that wasn’t what he was talking about; he was talking about something in my brain.
And that is one of the trends that we on the support groups. And I don’t really see any changing trends; what I see on the support groups is everybody has different clusters of symptomatology. And so we have common clusters, and everybody’s clusters are slightly different, but we have common things that everybody sees. And to me, anxiety disorders and depression—either starting anew, or if you already have it, it getting worse and the things that used to work for you not working anymore—is the predominant thing. Almost everybody experiences some level of that, altering their body.
And I think it is something from what’s in the IUDs; a little bit probably toxicity issues of things that could be causing the anxiety, but I feel that for me, because it went away so quickly after removal—my debilitating anxiety was gone within twenty minutes of the IUD being removed from my body.
So for me it was a foreign object inside my body; I call it a body invasion issue. Our bodies respond to foreign objects being put into them, and the anxiety is the way that they respond in trying to tell you that something’s wrong. But what happened with me was I was being told that something was wrong, but I wasn’t looking in my body for the source, I was looking outside in my world for the source but I couldn’t find it. And the side effects almost keep us from seeing it.
Watch Natural Womanhood’s full interview with Tamara below.
To learn about safe and effective nonhormonal methods of fam
Parents in Tacoma, Washington, are reportedly furious after a Planned Parenthood flyer promoting sex among pre-teen children was distributed at Stewart Middle School. Yet in a statement provided by Tacoma Public Schools to the Post Millennial, the flyer was not part of the curriculum and should never have been sent home with students.
Eric Hogan, assistant director of secondary education at Tacoma Public Schools, told the Post Millennial that the flyer was only distributed to students at Stewart Middle School, and apologized for the mistake. “Previously, Planned Parenthood taught within our schools and supplied the flyer which was distributed to students,” his statement read. “We discovered a binder of curriculum materials was left behind for an incoming teacher to use for this year, and the flyer was in the binder. Not realizing the flyer wasn’t approved material, the teacher sent it home with students. Corrective action has been taken with this employee.”
Hogan added, “Planned Parenthood is no longer giving presentations within our schools.”
Copies of the flyer were posted on social media, and the information was beyond disturbing. Under the title, “Age of minority & consent for sex,” students were told “it is not a crime” if they have sex as young as 11 years old, as long as their sex partners are no more than two years older than they are.
Photo shared publicly on Diego Lopez’ Facebook page.
The flyer reads:
It is not a crime if you are…
11 and have sex with somebody 2 years older or less.
12 to 13 and have sex with somebody who is 3 years older or less.
14 or 15 ad have sex with somebody who is 4 years older or less.
… If you are 14 years and older, you do not need permission from your parent or guardian to get treated for STDs or HIV, or to get treatment…
You are allowed to get a prescription for birth control without your parent or guardian’s permission…
ABORTION – You do not need to get permission from your parent or guardian AT ANY AGE…
The flyer also explained how students could obtain condoms “at any age” and Plan B, explaining that they didn’t need their parents’ permission for that, either. The only sexual behavior discouraged on the flyer was sexting, which Planned Parenthood noted is illegal in Washington.
Letter from Tacoma Public Schools
Meanwhile, the flyer failed to point out that the consent laws in Washington merely mean the state will not prosecute; as the state points out, “[a]ge is just one of many factors involved in consent.” Emotional and psychological development should be considered as another factor of consent, which for an 11-year-old, raises many red flags. The preteen stage is a time when children are experiencing a lot of hormonal changes, and begin to not only desperately seek independence from their family, but begin to strongly rely on their peer groups instead. This, while perfectly normal, can easily cause pressure and coercion to have sex, with a child feeling that they must have sex in order to be accepted. Adding Planned Parenthood’s propaganda doesn’t help.
But Planned Parenthood’s brand of sex education has been known to go far beyond even what this flyer promotes, as Live Action’s Sex Ed investigation revealed. Planned Parenthood employees were secretly recorded promoting pornography, BDSM, whips, handcuffs, and other violent sexual behaviors and torture devices to teens, encouraging them to experiment and “Google whatever is in your head.”
Encouraging students to use birth control without their parents’ knowledge is also deeply problematic; an 11-year-old is unlikely to know if they have a pre-existing condition which could make hormonal birth control in particular more dangerous. But even more disturbing is the possibility of Planned Parenthood using birth control as a way to get secure pre-teens as future customers, for services other than just contraception.
Former Planned Parenthood manager Ramona Treviño told 40 Days for Life that “contraception and abortion are two sides of the same coin,” and that selling promiscuity to young people creates a market for abortion.
“The more people use birth control and adopt a contraceptive mentality, the higher the odds that they’ll seek an abortion,” she explained. “Because, let’s face it, if they’re using birth control, a child is not part of the ‘plan.’ Abortion is the backup, so to speak, for contraceptive failure, misuse, or lack of self-control.”
Monica Kline, a former Planned Parenthood sex educator, agreed that Planned Parenthood intentionally sells sex to children, knowing that it will create future abortion clients.
This blatant effort to promote sex to children, who are too young to truly understand or consent, should never be permitted. Yet too often, Planned Parenthood is still welcomed in schools across the country, grooming them to become future paying clients who will learn to rely on the abortion corporation.
One of the most prominent features of the culture of death is its short-sightedness. It puts grand plans into action and makes sweeping promises about how many lives will be saved or improved by its initiatives. And then its architects are invariably shocked and surprised when a galaxy of negative unintended consequences quickly emerge, usually making the situation much worse than it was before. To put it simply, the culture of death is entirely ignorant of sinful human nature.
The classic example of this absolute lack of foresight is the birth control pill.
From the very first day it was introduced, “family planning” experts hailed the Pill as the conclusive solution to “unwanted pregnancies.” But continued promises of high efficiency, combined with the easy availability of abortion as a “backup,” inevitably led to widespread careless use and abuse of the Pill. When the Pill failed to prevent pregnancy, many women felt entitled to an abortion because they believed that medical technology had failed them and that another type of medical technology was the “answer” to their problem.
Failure Rate of the Pill
Use of the Pill requires care and consistent attention. Each cycle of pills must be taken in the proper order every day at about the same time. So women often forget to take pills, take them at the wrong time, or lose them. This is the major contributor to an incredible number of unintended pregnancies, especially among younger women. U.S. women who are on the Pill experience nearly a million unintended pregnancies annually, and more than 40% of these occur among girls and women 15 to 24 years old.1
The method effectiveness of the Pill is 99.7% per year. This percentage is extremely high, but it refers to the efficiency of the Pill when a woman is in excellent health and uses the Pill without error. When user error and illness are factored in, the result is the actual, or “real world” user effectiveness rate. In the case of the Pill, this is only 91% per year.2 This means that 9% of women on the Pill will become pregnant in any given year of use. In other words, the Pill itself is responsible for only about 3% of all failures, and the users are responsible for the remainder.
The 91% “real world” effectiveness rate for the Pill still sounds high until we calculate the probability of a woman becoming pregnant over an extended period of time when using it. She has a:
9% probability of becoming pregnant in the first year
One in four (25%) probability in three years
38% in five years
61% in ten years.3
In summary, if a sexually active girl of 15 starts using the Pill continuously, there is a nearly 50% chance that she will become pregnant by the time she is 22!
This statistic is verified by pro‑abortionists, including Dr. Christopher Tietze, who said, “Within 10 years, 20 to 50 percent of Pill users and a substantial majority of users of other methods may be expected to experience at least one repeat abortion.”4 Note that Tietze is speaking about repeat (second or more) abortions here. These statistics are significant when one considers that one of the primary goals of school‑based clinics (SBCs) is to distribute contraceptives and abortifacients to teenagers without parental consent or knowledge.
These rates are in line with Alan Guttmacher Institute figures which show that half of all abortion patients thirty years ago were practicing contraception during the month in which they conceived. Additionally, the majority of abortion patients who had stopped using a method prior to becoming pregnant said they had most recently used the Pill.4
The situation has not improved, despite decades of saturation propaganda campaigns by everyone from big pharma to Neofeminist groups. A 2007 Marie Stopes International study found that 43% of aborting women were using the Pill when they got pregnant, and another 27% were using condoms. And in 2014, the British Pregnancy Advisory Service, the largest chain of abortion mills in the United Kingdom, found that 27% of women obtaining abortions were on the Pill when they got pregnant, while 35% were using condoms. BPAS Executive Director Ann Furedi confirmed what pro-lifers have always claimed when she acknowledged, “Ultimately women cannot control their fertility through contraception alone, and need accessible abortion services as a back-up for when their contraception lets them down.”
Dangers of Birth Control Pills
Even after the shift from high-dose to low-dose pills, United States federal courts classified the birth control as “unavoidably unsafe.”5 This means that implicit in a woman’s consent to use the Pill is an acknowledgement of physical risk ― even if she is not entirely informed of all (or any) of its dangers.
This legal classification means that women injured by the Pill have a much harder time recovering damages. Dr. John Hildebrand, an expert in the field of human reproduction, estimated that more than 500 women die every year because of pill‑induced effects. This startling number is confirmed by figures provided by the Alan Guttmacher Institute (the world’s foremost abortions statistics analyzer) and one of the foremost abortionists in the United States, Warren Hern. His textbook Abortion Practice contains figures that lead to the conclusion that more than 30,000 American women have died due to direct side effects of the Pill since it was adopted in the United States ― with a current average of 600 to 700 deaths per year.6
It is ironic indeed that the same pill that the radical feminists pushed so hard as part of their solution to illegal abortion deaths now kills five to seven times as many women per year as illegal abortions themselves did before Roe v. Wade. And, with a few minor exceptions, these feminists do not breathe a word about it.
In 2010, major magazines, newspapers and pro‑abortion organizations celebrated fifty years of “The Pill” and trumpeted how it has freed women from “unwanted childbearing” and drudgery. Perhaps they should tell that to the loved ones of the more than thirty thousand women who have died from the fatal side effects of the Pill.
The manufacturers of each of the more than 125 brands of birth control pill issue patient information pamphlets (PIPs) which give detailed information on each one. These standardized forms each have sections entitled “Warnings and Precautions” and “Adverse Reactions,” which list anywhere from 50 to 67 side effects of the Pill. The most serious of these include cardiovascular and breast problems.
The most dangerous and well‑documented side effects commonly associated with the Pill are heart attacks and strokes. The eight‑year Nurse’s Health Study at Harvard Medical School found that Pill users are 250% as likely to have heart attacks and strokes than those who don’t use the Pill, probably because the Pill greatly increases blood clotting ability. One of the major findings of the study was that women who get off the Pill have rates of cardiovascular disease equal to that of the general population after a period of one year.7 All of the patient information pamphlets produced by the manufacturers of the Pill confirm that the drug increases these risks.
Soon after the high-dose pills were phased out in favor of the low-dose regimen, the Pill came under intense scrutiny by researchers. In 1988, scientists at the Boston University School of Medicine, the University of Pennsylvania, and New York’s Memorial Sloan‑Kettering Cancer Center showed that the longer women took the Pill, the greater were their chances of contracting breast cancer. The risk of developing breast cancer was found to be twice as great by age 45 for women who had used the Pill for less than ten years and four times as great for women who had used the Pill for greater than ten years.
After a decade of accumulating evidence, the International Agency for Research on Cancer (IARC) classified combined oral contraceptives as “carcinogenic to humans” (Group 1). In 2005, the IARC confirmed this classification and has not changed it since.8
Researchers at the Mayo Clinic followed up this classification with the most comprehensive review of studies on the Pill-breast cancer link ever performed. They found that 21 of 23 large, well-conducted studies found that there was an average of a 44% increased risk of breast cancer in women who were taking the Pill prior to their first pregnancy.
Indirect Dangers of Birth Control
We have seen that the birth control pill is so ineffective that it fails hundreds of thousands of times annually in the United States, leading to hundreds of thousands of surgical abortions. We have also covered some of the more serious physical side effects inflicted upon women by the Pill, including more than 30,000 deaths and tens of thousands seriously injured since its introduction.
The indirect impacts of the Pill are much more diffuse, but are terribly damaging to society in general. The Pill impacts not only women, but men and children.
Since its introduction, the Pill has contributed heavily towards sexual promiscuity, the increase of illegitimate births, and the degradation of marriage and the family.
1. Increased Promiscuity
Immediately after the Pill was introduced in the mid‑1960s, pre‑marital sex and cohabitation both almost doubled in only five years. Currently, 48% of all couples living together are not married. People of all ages (but especially teenagers) are having premarital sex more than ever before.
Wife‑swapping clubs, organized orgies, membership in sex addiction treatment organizations like Sexaholics Anonymous, hard‑core pornography, and “fantasy [sex] tours” to Far East nations have increased tremendously.
After witnessing two decades of this social carnage, the developers of the Pill admitted that its wide availability appeals strongly to those persons with little regard for sexual ethics. Dr. Robert Kirstner of Harvard Medical School said, “About ten years ago, I declared that the Pill would not lead to promiscuity. Well, I was wrong. The birth control pill has been a major causal factor in the rapid increase in both V.D. and cervical cancer among adolescents by stimulating higher levels of promiscuity.”9 And Dr. Min‑Chueh Chang acknowledged, “[Young people] indulge in too much sexual activity … I personally feel the Pill has rather spoiled young people. It’s made them more permissive.”10
Dr. Alan Guttmacher, former Medical Director of the International Planned Parenthood Federation, also drew a clear picture of the link between abortion and contraception within the context of increased promiscuity nearly fifty years ago: “When an abortion is easily obtainable, contraception is neither actively nor diligently used. If we had abortion on demand, there would be no reward for the woman who practiced effective contraception. Abortion on demand relieves the husband of all possible responsibility; he simply becomes a coital animal.”11
Finally, psychologists Eugene Sandburg and Ralph Jacobs noted the obvious connection between contraception and abortion as birth control: “As legal abortion has become increasingly available, it has become evident that some women are now intentionally using abortion as a substitute for contraception.”12
Drs. Kirstner and Min‑Chueh were certainly correct in their assessment of the situation. In 1970, only 4.6% of all 15‑year‑old girls had experienced premarital sex. By 2000, this rate had increased more than eightfold to 40%. Of all unmarried girls in the 15 to 19 age bracket, 28.6% had had premarital sex in 1970. This rate had more than doubled to 61.4% by 199013 and reached about 80% by 2000.14
2. Illegitimate Births
The inevitable result of the combination of increases in premarital sex and of ‘unwanted pregnancy’ is an increase in illegitimate births and abortion. This principle is so obvious that leading “family planners” recognized it in the early 1970s.
Professor Kingsley Davis of the United States Commission on Population Growth and the American Future stated:
The current belief that illegitimacy will be reduced if teenage girls are given an effective contraceptive is an extension of the same reasoning that created the problem in the first place. It reflects an unwillingness to face problems of social control and social discipline, while trusting some technological device to extricate society from its difficulties. The irony is that the illegitimacy rise occurred precisely while contraceptive use was becoming more, rather than less, widespread and respectable.15
The illegitimacy rate for births among teenaged girls hovered around 5 – 7% for decades until about 1960. Between 1960 and 1970, it doubled as the birth control pill ushered in the “Sexual Revolution.” After 1970, the teenage illegitimacy rate exploded with the introduction of comprehensive sex education programs and school‑based clinics.
The overall illegitimacy rate for all children born in the United States was 5% in 1960. This rate had increased by 700% to 40.7% by 2008.16
This phenomenon is not just an ethical or religious concern, it is a profoundly practical one. Social workers know that children born into one‑parent families are much more likely to be abused and abusive, to be undereducated, to be under‑ or unemployed, to have illegitimate children themselves, and to be far more likely to become involved in criminal activity.
3. Degradation of Marriage and Family
In 1965, before the Pill became widely available, about 15% of all couples lived together before marriage. The major reason for the relatively low incidence of this arrangement was simple: Living together meant more sex, and more sex meant a greater chance of a pregnancy in a nation where abortion was still illegal.
Today, many young unmarried women are on the Pill and abortion is readily available as a backup. They feel that they have no reason not to be sexually active and “shack up” before marriage.
As a result, nearly half of all couples in the United States now live together before marriage. This in turn causes great problems because more than 75% of all couples who lived together before marriage eventually divorce.17 The Pill has also contributed greatly to our country’s exploding divorce rate, which was about 18% in 1965 and now stands at about 50%.
Predictably, the innocent children of divorced couples are always those who suffer the most. But the gender feminists and sexologists simply write them off as a sort of necessary “collateral damage,” inevitable victims of the Sexual Revolution and the war against one’s own sexuality.
Implications for Pro‑Lifers
Millions of women in the USA and all over the world use the Pill. Many women who would never consider a surgical abortion now use low‑dose pills that cause them to abort a new life an average of once or twice every year. A large number of women who claim to be pro‑life use these pills, many at the urging of their husbands. These are usually women who are ignorant of the Pill’s abortifacient mode of action, those who think that their way of life requires that they use the Pill, or those who cannot mentally make the connection between contraception and abortion.
Pro-abortionists play upon this theme constantly. For example, “Catholic” House Minority Leader Nancy Pelosi claimed, “98 percent of Catholic women use birth control to determine the size and timing of their families.” The reality is that 83% of Catholic women use artificial birth control (32% have been sterilized), and only 31% of Catholic women use the Pill.
Researchers have calculated that the birth control pill directly causes between 1.53 and 4.15 million chemical abortions per year in the United States ― up to four times the total number of surgical and medical abortions committed every year! We can calculate that about 750 million “silent abortions” have occurred in the United States since the birth control pill began to come into wide use in 1965.18
To put this into perspective, for every surgical and RU-486 abortion that has been performed in this country, a dozen “silent abortions” have taken place.
This means that otherwise pro‑life women who are using the Pill or some other means of abortifacient birth control are committing abortions themselves on a frequent basis. These abortions are “silent” and unseen, but they are no less abortions than are gruesome third‑trimester D&X abortions. There are many pro‑lifers who are using these pills and who are involved in their promotion and distribution. These people must consider whether they can, in good conscience, criticize women whose action differs from their own only in that they have to drive to an abortion mill to commit it.
Conclusion
When Pope Paul VI overrode the recommendations of his Birth Control Commission and wrote Humanae Vitae in 1968, he was exposed to widespread criticism, dissent and ridicule. But the four predictions he made in his great encyclical have undeniably come true. These are:
Infidelity and moral decline
Loss of respect for women
Abuse of power by public authorities
A false sense of unlimited dominion over one’s body.
Today, most women (and men) see contraception as essential to their lives, and what was once mortal sin has “evolved” in the minds of most Catholics into an absolute necessity of life, something they simply cannot do without.
The great irony in all of this is that those who follow Church teachings regarding sexual morality are not only happier, they find their lives less difficult and complicated in the long run.
This is how Our Lord planned it, and this is the way we should live.
Endnotes
[1] See Chapter 21 of The Facts of Life, “Contraception.”
[2] Robert A. Hatcher, et. al.Contraceptive Technology (20th Revised Edition) [New York: Ardent Media, Inc.], 2011. Table 26‑1, “Percentage of Women Experiencing an Unintended Pregnancy During the First Year of Typical Use and the First Year of Perfect Use of Contraception and the Percentage Continuing Use at the End of the First Year. United States,” page 791.
[3] For references and calculations, e-mail Brian Clowes at bclowes@hli.org and ask for Excel spreadsheet F-02-05.XLS, “Probability of Pregnancy over Time for Fertile Women Who Use Various Methods of Birth Regulation, Ranked by User Effectiveness Rates.”
[4] Christopher Tietze, quoted in the National Abortion Rights Action League’s A Speaker’s and Debater’s Guidebook. June 1978, page 24.
[5] Thomas P. Monaghan, Co‑Chairman, Free Speech Advocates. “Unavoidably Unsafe.” Fidelity Magazine, October 1987, pages 14 and 15.
[6] For references and calculations, e-mail Brian Clowes at bclowes@hli.org and ask for Excel spreadsheet F-02-06.XLS, “Estimate of Annual Deaths Attributable to Use of the Birth Control Pill in the USA, 1960-2014.”
[7] Dr. Meir J. Stampfer. New England Journal of Medicine, November 24, 1988. This study was based on an eight‑year follow-up of 119,061 female nurses, ranging in age from 30 to 55 in 1980. 7,074 were current pill users and 49,269 were previous users. Overall, there were 380 heart attacks, 205 strokes, and 230 cardiovascular deaths among pill users.
[8] UNDP/UNFPA/WHO/World Bank Special Program of Research, Development and Research Training in Human Reproduction (HRP). “Carcinogenicity of Combined Hormonal Contraceptives and Combined Menopausal Treatment,” September 2005, page 1.
[9] Dr. Robert Kirstner, Harvard Medical School, one of the original developers of the birth control pill. Quoted in Barret L. Mosbacker. Special Report: Teenage Pregnancy and School‑Based Clinics [Washington, D.C.: Family Research Council], 1986, and in ALL About Issues, June 1981, page 5 [emphasis in the original].
[10] Dr. Min‑Chueh Chang, one of the inventors of the birth control pill. Quoted by Charles E. Rice. “Nature’s Intolerance of Abuse.” ALL About Issues, August 1981, page 6.
[11] Dr. Alan Guttmacher in a discussion at the Law, Morality and Abortion Symposium, held at Rutgers University Law School, March 27, 1968. Rutgers Law Review, 1968(22):415‑443.
[12] Eugene C. Sandburg, M.D. and Ralph I. Jacobs, M.D. “Psychology of the Misuse and Rejection of Contraception.” American Journal of Obstetrics and Gynecology, May 15, 1971, pages 227 to 237.
[13] “The US Family Staggers into the Sexy Secular Future.” Family Research Newsletter, January‑March 1991, page 1, Table 1, “Percentage of Women Aged 15‑19 Who Reported Having Had Premarital Sexual Intercourse, By Race and Age ― United States, 1970‑1988.” Numbers from 1988 to 1992 are linearly extrapolated using 1985‑1988 rates.
[14] United Nations Children’s Fund (UNICEF). “A League Table of Teenage Births in Rich Nations.” July 2001, page 2.
[15] Professor Kingsley Davis. “The American Family, Relation to Demographic Change.” Research Reports, United States Commission on Population Growth and the American Future. Volume I, Demographic and Social Aspects of Population Growth, edited by Robert Parke, Jr., and Charles F. Westoff [Washington, D.C.: United States Government Printing Office], 1972, page 253.
[16] United States Department of Commerce, Bureau of the Census. Reference Data Book and Guide to Sources, Statistical Abstract of the United States [Washington, DC: United States Government Printing Office], 2012 (132nd Edition). Table 78, “Live Births, Deaths, Marriages and Divorces: 1960 to 2008,” shows 4,248,000 total births for the year 2008, and Table 85, “Births to Unmarried Women by Race, Hispanic Origin, and Age of Mother: 1990 to 2008” shows 1,727,000 births to unmarried mothers in 2008, for a percentage rate of 40.7%. The entire Statistical Abstract for the current year in PDF format is available on the Census Bureau website.
[17] In 1989, James Bumpass, James Sweet, and Andrew Cherlin of the University of Wisconsin completed a long‑term study to determine the effect of prenuptial cohabitation on marriage. Described in Dale Vree. “Hey, it Sounds Plausible.” National Catholic Register, May 7, 1989, page 5.
[18] For references and calculations, e-mail Brian Clowes at bclowes@hli.org and ask for Excel spreadsheet F-02-A.XLS, “Birth Control Methods Used by United States Women, and Overall Estimated Number of “Silent Abortions,” 1965-2013.”
June 16, 2021 (LifeSiteNews) — In 2011, a ground-breaking film titled Anonymous Father’s Day was released, detailing the struggles of thousands of people seeking to discover their genetic origins. Conceived through artificial insemination with donor semen from sperm banks, the documentary traces the stories of men and women attempting to identify their biological fathers. It is based largely on a study on the subject called “My Daddy’s Name is Donor.”
In recent years, there has been an increase in stories about fertility doctors who have artificially inseminated women with their own sperm. USA Today, for example, reported this month on the story of Dr. Martin Greenberg, who worked in New York City in the 1980s and secretly used his own semen while artificially inseminating women. As people increasingly seek out their origins using DNA tests such as 23andMe and AncestryDNA, they are making unexpected discoveries.
In response, the biological children of these fertility doctors are demanding regulation and reform. Some doctors have been sued. Six states, including Indiana, Colorado, California, Texas, Arizona, and Florida have passed laws against “fertility fraud.” Other states are contemplating doing the same. The reproductive technology industry sprung up quickly and spread fast — and not until DNA tests became affordable and widely available did it become clear how many physicians were acting unethically, and with bizarre results.
Some, like Greenberg, took the opportunity presented to them by this industry to artificially inseminate women with their own sperm when they believed they were using semen that had been frozen in sperm banks.
But as USA Today revealed in its report, not all of these women were. Dr. Cecil Jacobson of Virginia was revealed to have fathered a minimum of 15 children in this fashion, and was convicted of 52 instances of fraud and perjury in 1992. Ten other doctors have thus far been accused, in court, of “fertility fraud,” according to the research of Jody Madeira of Indiana University. Dr. Donald Cline of Indiana conceived at least 60 children through his fertility clinic to date and was discovered — and convicted — after a DNA test. Attorneys say there are dozens of such cases that have been litigated.
Many other bizarre situations have arisen as the result of the artificial reproduction industry. As the New York Times explained in its 2011 investigative report titled “One sperm donor, 150 offspring,” artificial insemination often has unintended consequences:
Cynthia Daily and her partner used a sperm donor to conceive a baby seven years ago, and they hoped that one day their son would get to know some of his half siblings — an extended family of sorts for modern times.
So Ms. Daily searched a Web-based registry for other children fathered by the same donor and helped to create an online group to track them. Over the years, she watched the number of children in her son’s group grow. And grow.
Today there are 150 children, all conceived with sperm from one donor, in this group of half siblings, and more are on the way. “It’s wild when we see them all together — they all look alike,” said Ms. Daily, 48, a social worker in the Washington area who sometimes vacations with other families in her son’s group …
Now, there is growing concern among parents, donors and medical experts about potential negative consequences of having so many children fathered by the same donors, including the possibility that genes for rare diseases could be spread more widely through the population. Some experts are even calling attention to the increased odds of accidental incest between half sisters and half brothers, who often live close to one another.
“My daughter knows her donor’s number for this very reason,” said the mother of a teenager conceived via sperm donation in California who asked that her name be withheld to protect her daughter’s privacy. “She’s been in school with numerous kids who were born through donors. She’s had crushes on boys who are donor children. It’s become part of sex education for her.
Critics say that fertility clinics and sperm banks are earning huge profits by allowing too many children to be conceived with sperm from popular donors, and that families should be given more information on the health of donors and the children conceived with their sperm. They are also calling for legal limits on the number of children conceived using the same donor’s sperm and a re-examination of the anonymity that cloaks many donors.
As it turns out, the cost of defying nature can be a high one. The reproductive technology industry is in the business of giving people babies, no matter the cost. As one donor-conceived man muses in Anonymous Father’s Day, those babies grow up — and they want to know where they came from. Many of them are not happy with the answers they find.
Have you ever stopped for gas and watched a giant ten-wheel fuel tanker rumble up to refill the gas station’s tanks? These trucks are enormous, forty feet long, and each carries enough gasoline to fill a small backyard swimming pool.
The powerful hormones in abortifacient methods of birth control dictate their modes of operation. Every year, women in the United States ingest enough of these hormones to fill one of these tanker trucks ― 3,290 gallons (12,500 liters) worth.1 Now imagine a long line of tanker trucks parked bumper to bumper and stretching half a mile. If they were all filled to the brim, they would represent the amount of powerful birth control hormones women have ingested since 1960 in the United States alone.
Environmental Effects of Birth Control
The serious physical side effects inflicted upon women by the Pill, the patch, injectables, implants, and hormone-loaded IUDs are well documented. But the harmful impacts of birth control extend far beyond the boundaries of women’s bodies.
Environmentalists tell us that our ecosystem depends upon an extremely delicate balance of a large number of factors, and that even the most apparently insignificant activities of man are enough to have major impacts upon it.
Yet they are dead silent on the ecological effects of some of the most powerful chemicals on earth.
Twenty years ago, the United Kingdom’s Environmental Agency stated: “Estrogenic steroids ― natural and synthetic hormones in sewage effluent ― have been shown to be more potent than previously thought, with the synthetic steroid 17a ethinyl estradiol showing effects in fish at concentrations below 1 nanogram [one billionth of a gram] per liter.”2 These findings were confirmed in a 2020 study which also found that some streams had an ethinyl estradiol concentration of more than 60 nanograms per liter, far beyond the limit that causes grave harm to fish populations.3 This means that the problem of hormonal pollution is longstanding and causing ever more severe environmental impacts with each generation of fish.
Another 2020 study conducted in a laboratory in order to precisely control all inputs found that a few picograms [one trillionth of a gram] per liter of water caused malformations, decreased egg production and DNA methylation, which represses gene transcription.4
To visualize the scales we are talking about, a single drop of one of these steroids pollutes 66,500 gallons of water severely enough to cause significant health problems in fish at a concentration of one part per billion. This is equivalent to ten drops in a standard Olympic-sized swimming pool of 660,000 gallons. A single thimbleful would have major impacts on fish living in a lake 300 yards in diameter.5
This is because excreted birth control pill hormones are a pollutant, just like trenbolone (a synthetic steroid that “bulks up” cattle) and the pesticide bifenthrin. Gord Miller, Ontario’s environmental commissioner, said, “If you were designing the perfect pollutant, it would probably look like a pill.”6
Estrogens which are excreted into the environment are classed as endocrine-disrupting chemicals (EDCs) because they interfere with the endocrine systems of both humans and animals. Other EDCs, such as those that find their way into the environment from vehicle exhaust, paints, plastics and adhesives, can be filtered out in wastewater treatment plants, but estrogen-based EDCs cannot, and thus pose a greater threat.7 While municipalities that operate water filtration plants insist that there is no threat to the environment, they cannot explain why the reproductive lives of multiple fish species are being dangerously altered.
The top environmental agencies in the United States, Canada and England have all found that exposure to unmetabolized birth control hormones has caused feminization of male fish, delayed reproduction in female fish, and damaged the kidneys and livers of fish of both sexes.8 Studies have found that female fish outnumber male fish in streams by a ratio of ten to one in areas where there is a high incidence of birth control pill usage. Biologist John Wooding said about this finding, “It’s the first thing that I’ve seen as a scientist that really scared me.”9
One study in New Brunswick by the Canadian Rivers Institute found that entire species of fish were exterminated in a large lake because all of the male fish had become feminized. Study leader Dr. Karen Kidd said, “What we demonstrated is that estrogen can wipe out entire populations of small fish ― a key food source for larger fish whose survival could in turn be threatened over the longer term.”10
These effects of birth control are not limited to fish ― they happen to large mammals as well. A study by the University of Aberdeen found that sheep that grazed on land fertilized with sewage sludge had a high rate of abnormalities in the testes, ovaries, uteri, brains, and thyroid and adrenal glands. These problems were attributed to the high levels of artificial hormones found in birth control pills that cannot be removed by wastewater treatment processes. The study authors warned:
These chemicals are in our air, soil and water. Some are fat soluble and may accumulate in our bodies while others are water soluble and end up passing through us and being flushed down our toilets, entering our environment where they may affect other animals or enter our food chain re-exposing humans.
Many of the changes we see are very subtle and not apparent in the living animal; nevertheless, they may be associated with disruptions of many different physiological systems and increased incidences of diseases and reproductive deficiencies such as those that have been reported in a variety of species, including humans. Embryos, fetuses and young animals appear to be particularly vulnerable.
It’s notable that incidences of breast and testicular cancer and of fertility problems in humans are increasing, while populations of animal groups as diverse as amphibians and honeybees are in decline.11
Why Don’t We Hear of The Effects of Birth Control?
The environmental effects of hormonal birth control have been suspected for more than two decades, yet environmentalists are completely silent on this issue.
If there is the slightest theoretical chance bird eggs might be damaged or thinned by pesticides, the environmentalists’ outcry is immediate and forceful (recall the propaganda campaign regarding DDT). But let the top environmental agencies from several nations definitively document the link between birth control pills and ecological damage, and all we hear from “progressive” groups is … silence.
This is because “progressives” hold “reproductive rights” above all other considerations ― the right to life, free speech, and even our environment. As Betty Ball of the Rocky Mountain Peace and Justice Center said, asking people to stop polluting water with hormones “gets into the bedroom.” She said, “I’m not going there. This involves people’s personal lives, childbearing issues, sex lives and personal choices.”12
And Curt Cunningham, water quality issues chairman for the Rocky Mountain Chapter of Sierra Club International, said that people “would not take kindly” to the suggestion of banning or restricting hormonal contraceptives. He added, “For many people it’s an economic necessity. It’s also a personal freedom issue.”13
In other words, “progressive” activists consider their birth control pills, morning-after pills and abortion pills to be so important that even the environment must take second place to “sexual freedom.” Such is the self-centered and hypocritical nature of the culture of death.
The attempts by pro-lifers like Jill Stanek to sound an environmental alarm have been met with silence, denial, and accusations of hypocrisy. The Left employs its usual tactic of suppressing the point so vigorously that anyone who brings it up will be so ruthlessly stigmatized that people will learn that it is unacceptable to bring up the issue in polite [“progressive”] company. Another topic we are commanded to avoid is the spectacle of top global warming alarmists (John Travolta, Al Gore, Leonard DiCaprio, Harrison Ford and many others) zipping all around the world in their private jets to attend lavish environmental conferences that are always held in only the poshest cities.
We also dare not mention the Birkenstock-wearing, fair-source, granola-munching, strictly vegan activists who vigorously protest genetically modified foods and hormonal beef additives ― and then, at the same time every day, pop a powerful steroid pill.
We Drink Estrogen-Polluted Water
Although birth control hormones in the water are not as dangerous to human beings as they are to fish, we must note again that sewage and water treatment filtration cannot remove all of them from the water we drink.
Studies in the United States, the United Kingdom, New Zealand and Canada have shown that breast development in young girls has rapidly accelerated since the 1960s, probably due to the estrogens in drinking water. Now young girls are developing breasts as early as six or seven years of age, and spokesmen for the medical societies are, for the most part, silent. Marcia Herman-Giddens, adjunct professor at the School of Public Health at the University of North Carolina, said, “My fear is that medical groups could take the data and say ‘This is normal. We don’t have to worry about it.’ My feeling is that it is not normal. It’s a response to an abnormal environment.”14
Dr. Michelle Bellingham of the University of Glasgow is among the growing number of scientists who believe that male fertility is declining because of the estrogens in our water supplies, leading to an increased use of in-vitro fertilization (IVF) and other assisted reproductive technologies.15
Another study by the University of Pittsburgh Center for Environmental Oncology found that chemicals extracted from randomly sampled fish in the Allegheny, Monongahela and Ohio rivers caused growth of estrogen-sensitive breast cancer cells cultured in a laboratory, eleven of which “produced very aggressive cancer growth.”16
One British study found that the incidence of prostate cancer in men is highest in areas where the use of oral contraceptives is the greatest.17 Several such studies are widely varied in their geographical locations and objectives and, as a whole, are not yet conclusive, but their results should concern conscientious scientists and sociologists.
The University of Aberdeen scientists who performed the sheep study darkly warned:
If we do nothing, endocrine disruptors may not only impact human health but all the ecosystems including those on which we depend ― if we compromise soil productivity and sustainability of our agricultural systems or cause imbalance in marine and freshwater ecosystems through damage to populations of top predators, ultimately, we threaten our own survival.18
Final Thoughts
Virtually every environmentalist group and celebrity is caught up in the cause du jour of global warming. It would be ironic indeed if the end of the human race came about because of the widespread use and effects of birth control pills.
“Fish are really a sentinel, just like canaries in the coal mine 100 years ago,” says Conrad Volz, co-director of exposure assessment at the University of Pittsburgh Cancer Institute’s Center for Environmental Ecology. “We need to pay attention to chemicals that are estrogenic in nature, because they find their way back into the water we all use.”19
“Progressives” push for all kinds of compensation for damage to the environment, the best-known being carbon offsets. Perhaps if a heavy surcharge on the use of birth control pills were levied, people would begin to wake up.
But don’t hold your breath. That idea would actually help the situation — and we can’t have that! After all, if we solved enough of the major crises facing humanity, what would “progressives” have to virtue-signal about?
Endnotes
[1] “Fact Sheet: Contraceptive Use in the United States.” Guttmacher Institute, April 2014. According to this source, 9,572,477 women in the United States use the birth control pill, 965,539 use the implant, 1,481,902 use the injectables, 905,896 use the Nuva Ring, 4,452,344 use intrauterine devices (IUDs), 69,106 use the patch, 69,967 use emergency “contraception,” and 375,700 use the abortion pill.
Thus, the total amount of hormones absorbed annually by American women on these birth control methods would be 11,636 kilograms or 3,290 gallons. (The Facts of Life, Excel spreadsheet F-21-06.XLXS)
[2] March 26, 2002 statement by the UK’s Environmental Agency. Described in “Contraceptive Pill Confirmed as Pollutant, Says UK Environment Agency.” LifeSite Daily News, April 11, 2002.
[5] “Pill-Popping Society Fouling Our Water, Official Says.” CBC News, March 27, 2006; E. Vulliet, C. Cren-Olive and M.F. Grenier-Loustalot.
“Occurrence of Pharmaceuticals and Hormones in Drinking Water Treated from Surface Waters.” Environmental Chemistry Letters, September 2011, pages 103 to 114.
There are about 15,040 drops of water in a gallon. There are 660,000 gallons of water in an Olympic-sized swimming pool. There are about 20 drops in a milliliter and about ten milliliters in a thimble (See? Your math teacher told you this kind of thing would be fun)! The total amount of 17a ethinyl estradiol in a woman is about 300 parts per trillion of body weight (telephone discussion with Dr. Joel Brind on March 25, 2015).
[6] “Pill-Popping Society Fouling Our Water, Official Says.” CBC News, March 27, 2006.
[7] Thaddeus Baklinski. “Scientists: Harmful Hormones from Birth Control Pill Can’t be Filtered out in Sewage Treatment.” LifeSite Daily News, September 12, 2012.
See also “Can Birth Control Hormones Be Filtered from the Water Supply?” Scientific American, July 28, 2009.
Studies are ongoing, and developments regarding various types of reverse osmosis filtering may remove these hormones from the water we drink. Whether it is economically possible to treat the water that goes into areas where wild fish live is a different story.
[8] “Pill-Popping Society Fouling Our Water, Official Says.” CBC News, March 27, 2006.
[9] “Birth-Control Pills Poison Everyone?: Environmentalists Silent on Threat from Water Tainted with Estrogen.” WorldNetDaily, July 12, 2007.
[10] Canadian Natural Sciences and Engineering Research Council. “Fish Devastated by Sex-changing Chemicals in Municipal Wastewater.” Science Daily, February 20, 2008. Described in Hilary White. “Study Confirms Estrogen in Water from the Pill Devastating to Fish Populations.” LifeSite Daily News, February 18, 2008.
[11] Professor Paul Fowler, University of Aberdeen, Chair of Translational Medical Sciences, and Dr. Stewart Rhind, James Hutton Institute. “Sex and Sewage.” University of Aberdeen, Café Scientifique talk of June 13, 2012. Described in Thaddeus Baklinski. “Scientists: Harmful Hormones from Birth Control Pill Can’t be Filtered out in Sewage Treatment.” LifeSite Daily News, September 12, 2012.
[12] “Birth-Control Pills Poison Everyone?: Environmentalists Silent on Threat from Water Tainted with Estrogen.” WorldNetDaily, July 12, 2007.
[13] Iain Murray. The Really Inconvenient Truths: Seven Environmental Catastrophes Liberals Don’t Want You to Know About — Because They Helped Cause Them (Simon and Schuster, 2008).
Hilary White. “Hormonal Contraceptives Pollute Drinking Water ― Environmentalists Turn a Blind Eye.” LifeSite Daily News, July 11, 2007.
[14] Marcia E. Herman-Giddens, et.al. “Secondary Sexual Characteristics and Menses in Young Girls Seen in Office Practice: A Study from the Pediatric Research in Office Settings Network.” Pediatrics, April 1997 (Volume 99, Number 4), pages 505 to 512.
Described in Hilary White. “Study Confirms Estrogen in Water from the Pill Devastating to Fish Populations.” LifeSite Daily News, February 18, 2008.
[15] Professor Paul Fowler, University of Aberdeen, Chair of Translational Medical Sciences, and Dr. Stewart Rhind, James Hutton Institute. “Sex and Sewage.”
Described in Thaddeus Baklinski. “Scientists: Harmful Hormones from Birth Control Pill Can’t be Filtered out in Sewage Treatment.” LifeSite Daily News, September 12, 2012.
[16] Hilary White. “Hormonal Contraceptives Pollute Drinking Water ― Environmentalists Turn a Blind Eye.” LifeSite Daily News, July 11, 2007.
[17] D. Margel and N.E. Fleshner. “Oral Contraceptive Use is Associated with Prostate Cancer: An Ecological Study.” British Medical Journal, November 2011.
[18] Thaddeus Baklinski. “Scientists: Harmful Hormones from Birth Control Pill Can’t be Filtered out in Sewage Treatment.” LifeSite Daily News, September 12, 2012.
[19] David Biello. “Bringing Cancer to the Dinner Table: Breast Cancer Cells Grow Under Influence of Fish Flesh.” Scientific American, April 17, 2007.
Birth rates are decreasing worldwide. In all European countries, they’re even dropping below population replacement levels, which refers to the number of children needed per woman to keep a population stable.
While these decreases might be due to many adults intentionally postponing when they have their first child — or actively choosing not to have children — an increasing number of studies suggest these don’t fully explain decreasing birth rates. Some research also indicates that decreasing fertility is a major contributing factor in this decline.
One factor linked to decreased fertility is the presence of industrial chemicals found in our environment. Much is known about the impact of these chemicals on male fertility, but little research has looked into how they affect women. This is what our recent study sought to do.
We found that exposure to common chemical contaminants was associated with reduced egg counts in the ovaries of reproductive-aged women. Though these chemicals have since been banned, they were once used in household products like flame retardants and mosquito sprays, and are still present in the environment and in foods like fatty fish.
Fewer eggs
We measured the levels of 31 common industrial chemicals, such as HCB (an agricultural fungicide) and DDT (an insecticide), in the blood of 60 women. To gauge their fertility, we measured the number of immature eggs they had in their ovaries by counting them in ovarian tissue samples using a microscope. Because ovaries are located inside the body and would require surgery to access, we chose pregnant women who were having a caesarean section, as this made it possible to access tissue samples without additional surgery.
We found that women with higher levels of chemicals in their blood sample also had fewer immature eggs left in their ovaries. We found significant connections between reduced egg numbers and certain chemicals, including PCB (used in coolants), DDE (a by-product of DDT) and PBDE (a flame retardant). As female fertility is age-dependent, we made sure to adjust our calculations accordingly depending on the age of the woman in question. This showed us that exposure to these chemicals resulted in fewer eggs for women of all ages.
We also found that women with higher chemical levels in their blood had to try for longer to get pregnant. For the women with the highest levels of chemicals in their blood, it took more than a year.
Unlike men, women are only born with a fixed set of immature eggs in their ovaries, and cannot produce new ones after birth. A woman’s “reserve” (the number of eggs in her ovaries) naturally diminishes through monthly ovulations, as well as by normal follicle death. When depleted below a critical level, natural fertility ends and menopause begins. Our findings imply that toxic chemicals may speed up the disappearance of ovarian follicles, which could lead to reduced fertility and earlier menopause.
Chemical soup
We’re exposed to industrial chemicals through our food, the products we put on our skin and even through our mothers while developing in the womb.
The number of industrial chemicals, as well as their abundance in the environment, has steadily increased since the 1940s — with devastating effects on ecosystems, wildlife and even human fertility. Many chemicals were introduced to the market with little testing for safety. This has led to a situation where humans and the environment are exposed to an extensive “soup” of industrial chemicals.
So far, multiple chemicals have been found to be harmful to reproduction after only decades of consumer use. These include PFAS (the chemical used in Teflon, Scotch Guard and firefighting foam), phthalates (used in plastic packaging, medical equipment and soaps and shampoos), as well as pesticides and other industrial chemicals like PCBs.
The negative effects include reduced sperm counts in men, and potentially the ability of women to become pregnant. Our study is the first to investigate the link between chemical exposure and the number of eggs a woman has.
The chemicals we studied were all “persistent”, meaning they build up in the body over time. Strikingly, the chemicals that we found to be associated with lower egg counts were restricted by an international treaty decades ago. Yet because of their persistence, they still contaminate the ecosystem and our food.
Interestingly, PCBs (one of the chemicals we studied) have also been connected to decreased sperm counts and infertility in men. Simultaneous decreases in male and female fertility could make it more difficult for couples to get pregnant.
In future, researchers should investigate whether the fertility of all women — as opposed to pregnant women — is similarly affected by these chemicals. But these findings may encourage us to rethink chemical safety to take fertility into consideration during safety assessments.
Avoiding certain foods (such as seafood) and certain products (such as those we put on our skin and hair) may also help minimize the negative effects of chemicals on our chances of having a baby
By Nancy Flanders | Becoming critically ill while pregnant can be devastating. While high-risk conditions associated with pregnancy often don’t occur until later in the pregnancy — allowing the preborn child to be delivered prematurely so the mother’s life can be saved — conditions unrelated to pregnancy, such as cancer or ALS, can be diagnosed at any time.
Some cancer treatments are safe during pregnancy, but some are not, and these mothers chose to forgo their own life-saving care to allow their babies a chance at life.
St. Gianna
St. Gianna Beretta Molla was an Italian pediatrician who suffered from chronic illness. During her pregnancy with her fourth baby, Gianna began to suffer immense pain. Doctors found a tumor in her uterus and gave her three choices: an abortion, a complete hysterectomy, which would also mean the death of her child, or attempted removal of just the tumor in an attempt to save both lives.
Gianna chose the third option and the surgery was a success, but complications continued through the rest of the pregnancy. When it came time to deliver the baby, Gianna told her family, “If you must decide between me and the child, do not hesitate. Choose the child. I insist on it. Save the baby.”
In April 1962, Gianna Emanuela Molla was delivered by C-section, and though doctors worked hard to save her, her mother Gianna died just a week later from septic peritonitis. She was 39 years old.
In 2004, Gianna was canonized as a saint. She is known as the patron saint of mothers, physicians, and preborn children, and is the inspiration behind the first pro-life Catholic healthcare center for women in New York: the Gianna Center.
Blessed Chiara
Chiara Corbella Petrillo was just 28 years old when she died. She and her husband Enrico had already lost two babies at birth, Maria and David, choosing to carry them each to term knowing that they would likely die. Pregnant with her third child, the couple discovered he was healthy, but that Chiara was not.
Diagnosed with aggressive cancer, doctors advised her to begin treatments, but those treatments would have risked her baby’s life. She decided to forgo the treatments to protect her preborn son, Francisco. After he was born in May 2011, Chiara began treatments, but the cancer progressed, and she lost sight in one eye. On June 13, 2012, Chiara passed away. In a letter she wrote to Francisco a few days before her death, she told her son, “I am going to heaven to take care of Maria and David, you stay here with Dad. I will pray for you.”
In an interview with Vatican Radio, Enrico said that he and Chiara had learned from their three children that there is no difference in a life that lasts 30 minutes or 100 years. As her cancer progressed, love grew even stronger.
“I said, ‘But Chiara, my love, is this cross really sweet, like the Lord says?’ She looked at me and she smiled, and in a soft voice she said, ‘Yes, Enrico, it is very sweet,’” he explained. “In this sense, the entire family didn’t see Chiara die peacefully, but happily, which is totally different.”
Ashley Caughey
In 2012, already a mother to a young son, Ashley Caughey began to suffer pain in her knee that doctors wrote off as arthritis. But a year later, the pain began increasing, and walking becoming difficult. An X-ray revealed the news that she had osteosarcoma, a bone cancer. She also learned she was 10 weeks pregnant. The chemotherapy she needed posed a threat to her preborn child, Paisley. Ashley told CNN:
They told me what would likely happen to Paisley, that you know, she most likely wouldn’t make it and I just knew. It wasn’t a choice to me. It was like this is what needs to be done. She’s first. I’m not going to kill a healthy baby because I’m sick. There’s nothing wrong with her. Her life is just as important as mine if not more important. I mean as a mother my job is to protect my kids.
After Paisley’s birth, the cancer spread throughout her body and to her brain, and Ashley was given just months to live. She hoped to make it to her daughter’s first birthday, but Ashley passed away in 2014, a month shy of Paisley’s birthday.
Ellie Whittaker
Two months after suffering the miscarriage of her first baby, Ellie Whittaker found a lump in her neck, and then learned she was pregnant. She was diagnosed with stage two Hodgkin’s Lymphoma. Doctors advised her to abort her baby and begin chemotherapy.
“The doctor advised I have an abortion because cancer treatment could cause problems for the baby,” she explained. “There was no way I was going to give her up so I chose to delay it.”
Doctors planned to begin chemotherapy at 27 weeks, when it was less likely to harm the baby. But Ellie did so well, doctors held off on treatments until after her c-section at 37 weeks in March 2020. The cancer had progressed to stage three, but after 12 rounds of chemotherapy, in October 2020, Ellie learned she was cancer-free.
Amanda Bernier
Two weeks after she and her husband learned they were having their first baby, Amanda Bernier learned she had ALS, also known as Lou Gehrig’s disease. Doctors advised her to abort her baby, but Amanda refused.
Arabella was born in November 2014, and by that time, Amanda was unable to walk, and had lost over 50% of her lung function. She lived for two more years, breastfed her baby, and worked from her bed. She died in 2016.
Having lost both her mother and grandmother to ALS, Amanda asked everyone prior to her death to help find a cure for ALS for her own daughter, “and all of the unborn future ALS patients.”
Angela Bianco
During the first trimester of her pregnancy, Angela Bianco learned she had a malignant brain tumor. She was at her grandfather’s birthday party when suddenly, she fainted after feeling horrific pain in her head. After a few days in a coma, she was told she could have cancer treatments if she had an abortion. She thought it was the end of her and her baby.
“I didn’t want to abort and think about saving myself,” Angela said. “My duty was to give birth.”
She added, “I thought about my life, but also about the baby that was inside me. I told the doctors I did not want to abort, that I wanted my daughter to be born and that she was a great gift, at whatever the price.”
She was found to be a candidate for robotic radiation treatment in Italy, but bureaucratic delays stalled the trip until the fifth month of pregnancy. The cancer had progressed, but she was able to receive the treatment.
Angela gave birth to her daughter Francesca Pia in 2014, and the two are reportedly doing well.
Paula Cawte
Paula Cawte was told by doctors that her pregnancy was ectopic, and her preborn baby was developing outside of the uterus — but not in the Fallopian tubes. The baby was in Cawte’s abdomen, and doctors said she could have an abortion, or risk her own life to save a baby whom they said would likely be disabled or stillborn.
“We had been trying for over a year to have a baby and there was no way I could terminate when I knew she was healthy,” Cawte said. “We knew it was dangerous. The doctors said I could bleed to death if she ruptured an organ or an artery.”
Cawte had moments of intense pain, but she made it to 30 weeks when she delivered baby Eva. Doctors said the baby survived because the membrane of Paula’s abdomen had created a sac containing amniotic fluid that helped the baby’s lungs develop. Paula, however, nearly bled to death as doctors gave her eight pints of blood.
Today, mother and daughter are doing well.
“Now we can’t believe we have such a beautiful, healthy and happy little girl,” said Paula. “It’s a miracle.’
Mothers are constantly giving of themselves to care for their children, even to the point of death. But abortion advocates have long-pitted mother against child for any reason — financial, social, or physical. Sacrificing one’s life for the life of another is the ultimate gift a person can give.
May 28, 2021 (LifeSiteNews) – Human Life International is calling for May 31, the Feast of the Visitation, to be a day of prayer in reparation for the babies murdered by abortion.
Human Life International, the largest global pro-life apostolate, is inaugurating the “Prayer of Reparation for the Murder and Abuse of Unborn Children” to be said on annually on May 31. The prayer is available in English, Spanish, Italian, French, Germany, and Portuguese.
“To defeat evil and counteract the culture of death, we need to bend our knees in prayer, do penance, and offer reparation,” Father Shenan J. Boquet, president of Human Life International, wrote in a column. The prayer is to be recited on the Feast of the Visitation, which has much “significance” according to Boquet.
“Mary is a powerful pro-life figure and model,” he told LifeSiteNews. “After learning that she is to be the mother of the Messiah and that her cousin Elizabeth is also with child, Mary goes in haste to the home of St. Elizabeth to assist her.”
“Her example reminds us of how we too are to respect the beauty of human dignity and the sacredness of human life by generously giving of ourselves in their service,” he continued.
“The encounter between the two holy women is in fact a meeting of four people, even if St. John and the Divine Child are hidden beneath the protruding bellies of their mothers,” Fr. Boquet said. “While worldly powers strive to deny the humanity of the unborn child, the Visitation reminds us of the fundamental truth of the dignity of all human life and affirms the immense value of life from its very conception.”
The pro-life priest praised the ever-growing pro-life movement across America, saying, “Despite the Biden administration’s aggressive anti-life and family tactics and current positions of authority and influence, various states have courageously passed pro-life laws, protecting mothers and their unborn children from the violence of abortion.”
“Of course, these pro-life actions have not gone announced by abortion-minded enthusiasts, who see this as a direct assault upon their beloved industry,” Boquet continued. “The Guttmacher Institute recently voiced its grave concern over the number of pro-life legislation being introduced and signed into law.”
“According to Guttmacher, ‘the number of abortion restrictions – and specifically bans on abortion designed to directly challenge Roe v. Wade and the U.S. constitutional right to abortion [sic] – that have swiftly been enacted over the past four months is unprecedented,’” he added. “If this trend continues, 2021 will end up as the most damaging antiabortion state legislative session in a decade – and perhaps ever.’”
“We could not ask for a better endorsement,” Boquet said, “testifying that pro-lifers are making a tremendous impact. I pray we will keep this momentum.”
LEBANON, Ohio, May 26, 2021 (LifeSiteNews) – The city of Lebanon, Ohio, unanimously voted to outlaw abortion in order to protect both mothers and their babies.
According to Lebanon mayor Amy Brewer, the decision, made on Tuesday evening, will be enforced immediately, The Cincinnati Enquirer reported. While there are currently no abortion facilities in the city, the ordinance aims at stopping all abortions, including mail abortions.
Mark Lee Dickson, founder of Sanctuary Cities for the Unborn, said, “Cities must be prepared. The future of the abortion industry is not necessarily brick and mortar but abortion by mail or abortion by vending machine at a school or outside of a grocery store.”
“We are clearly saying in our community we do not think it is in our best interest to open a clinic or a hospital that does abortions,” Brewer said. “We are elected to make decisions based on what’s good for our community today.”
The newly passed law forbids providing an abortion, aiding in an abortion, providing money or transportation for an abortion, or offering instructions to procure an abortion.
Violations are punishable by up to six months in jail and a $1,000 fine. However, pregnant women are exempt from prosecution.
Mark Harrington, president of Created Equal and director for the Ohio initiative, said, “Joe Biden has stated he wants abortion in every zip code in America. Hence, citizens across the country are preventing abortion from being committed in their communities. Ohio is once again taking the lead to protect children, and more cities are joining this movement every week!”
This decision brought an uproar of responses from abortion activist groups. City Council member Krista Wyatt resigned in protest before the meeting took place. She claimed that “as a respectable, decent human being, I can no longer allow my name to be associated with the Lebanon City Council.”
Similarly, Planned Parenthood and the ACLU of Ohio have condemned the ordinance, with the ACLU threatening a legal challenge.
“This hyper-local strategy is another attempt by anti-abortion extremists to stigmatize and ban abortion in Ohio, by whatever means necessary,” said Freda Levenson, the legal director for the ACLU of Ohio.
With the ordinance, Lebanon is joining the ever-growing pro-life movement across America. Recently, cities are seeing an increasing number of pro-life bills either limiting or outlawing abortions. Approximately 20 other cities, all in Texas, have declared themselves “Sanctuary Cities for the Unborn.”
For the first time in years, pro-lifers have serious reason to hope that the aim towards which they have worked for so many decades – the end of Roe v. Wade – will finally come about, and as soon as next year.
A few days ago, the United States Supreme Court agreed to hear Dobbs v. Jackson Women’s Health Organization. This case – called a “blockbuster dispute” by CBSNews – involves a challenge against a Mississippi law (The Gestational Age Act) that bans abortion after fifteen weeks, except in cases of medical emergency and severe fetal abnormality. The challenge was filed by the state’s only surviving abortion facility.
So far, lower court judges have blocked the Mississippi law from going into effect, citing the 1973 Roe v. Wade case, which legalized abortion-on-demand in the United States. Roe v. Wade, and subsequent SCOTUS decisions, have consistently upheld the “right” to abortion pre-viability – that is, before the time when the child can survive on his own outside his mother’s womb. So long as Roe stands, states are prohibited from enforcing any restrictions on abortions pre-viability.
That hasn’t stopped states from passing such laws anyway. In fact, almost a dozen states have so-called “trigger laws” on the books, which would completely ban abortion the moment Roe v. Wade is overturned. Others have passed “heartbeat” laws (including Texas, just last week), which would ban abortion from the moment an unborn child’s heartbeat can be detected. However, to date, none of these laws have been allowed to go into effect, because of Roe.
The Mississippi law, by banning abortion after 15 weeks, clearly challenges the viability requirement. And that’s the point. Mississippi’s own attorney general has urged the high court to review the challenge against the law, arguing that the viability requirement, “is increasingly out of step with other areas of the law, rejects science and common sense, and is shaky precedent at best.”
According to the Alliance Defending Freedom (ADF), whose lawyers are involved in the case, the state will argue that “‘viability’ is an arbitrary standard for determining when a state’s interests are sufficient to regulate” abortion.
“Thanks to amazing progress in scientific research and medical technology, the concept of ‘viability’ is an ever-moving target as younger children have survived and thrived after preterm birth,” said ADF Senior Counsel and Vice President of Appellate Advocacy John Bursch last week. “But ‘viability’ has never been a legitimate way to determine a developing infant’s dignity or to decide anybody’s legal existence. The high court should take this important opportunity to resolve the conflicts between its previous rulings and affirm the constitutionality of Mississippi’s law.”
The ‘Best Opportunity’ to Overturn Roe
Pro-abortion advocates are already expressing outrage and outright terror over the Court’s decision to hear the case. In a statement last week reacting to this decision, Nancy Northup, President & CEO of the Center for Reproductive Rights, said that overturning Roe would be “devastating.” Northup noted that with Roe overturned, “Over 20 states would prohibit abortion outright.”
As legal experts are already pointing out, the mere fact that enough of the justices agreed to hear the case (at least four have to do so, in order for the case to move forward) shows that a sizable number of the justices are at least sympathetic to arguments that Roe must be revisited.
Over at The Dispatch, lawyer David French writes that “the most compelling reason for the emotional reaction is simply this—if the court didn’t want to do something dramatic with abortion jurisprudence, it could have simply left the case alone. It could have denied cert and let the case die.”
They didn’t. And with President Trump having appointed three justices to the court, there is reason to hope that among the six at least-moderately conservative justices now on the court, there are enough with the courage and conviction to revisit and overturn the absurd and flagrantly unconstitutional reasoning that underpins Roe.
However, while the court’s decision to hear this case is enormously encouraging news, it is far too early to celebrate.
Legal abortion is one of the most ferociously defended planks of the left’s political platform. The Biden-Harris administration is easily one of the most – if not the most – radically pro-abortion administrations in U.S. history, and will no doubt do everything in their power to promote their preferred outcome at the court.
Furthermore, this is not the first time that conservatives have hoped that GOP-appointed justices would overturn Roe. On previous occasions – e.g., Planned Parenthood v. Casey – our hopes have been cruelly dashed.
Over at National Review, Ed Whelan has argued that this case may be the “best opportunity the Supreme Court will ever have to overturn Roe.” Matt Purple, writing at The American Conservative, agrees. Dobbs v. Jackson Women’s Health Organization is, he writes, “the big one.” However, adds Purple, this case may also mark the Court’s last chance to overturn Roe.
As Purple notes, if the current Court, with its six conservative justices, many of them still quite young, still upholds Roe, further cementing decades-old judicial precedent, it is difficult to imagine any future justices having the courage to revisit the case, and to do the right thing. At least, not any time soon.
In other words, the stakes could not be higher.
The US Supreme Court in Washington DC with dark storm clouds
Roe Must Go!
According to many news articles, the case will be heard sometime this fall, and a decision is likely to be handed down next spring or summer.
The court’s decision to accept this case has given pro-lifers reason for hope, but also a great deal to fast and pray about. For decades now, Roe v. Wade has been the law of the land, removing all human rights protections for unborn children pre-viability, and in many cases all the way up to birth. The result has been untold millions of aborted children, and wounded mothers and fathers.Legal abortion contradicts everything that the U.S. founders aimed to protect and defend. “We hold these truths to be self-evident,” they wrote in the Declaration of Independence, “that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness.” (emphasis added)
Of these three unalienable rights, the right to life is the most fundamental. Without the right to life, there can be no right to liberty or the pursuit of happiness. The justices who discovered a “right” to abortion in the U.S. Constitution were guilty of an act of naked judicial activism. The consequences of this tyrannical decision have been incomprehensibly destructive.
As Pope St. John Paul II wrote in Evangelium Vitae:
“The moral gravity of procured abortion is apparent in all its truth if we recognize that we are dealing with murder and, in particular, when we consider the specific elements involved. The one eliminated is a human being at the very beginning of life. No one more absolutely innocent could be imagined. In no way could this human being ever be considered an aggressor, much less an unjust aggressor! He or she is weak, defenceless, even to the point of lacking that minimal form of defence consisting in the poignant power of a newborn baby’s cries and tears. The unborn child is totally entrusted to the protection and care of the woman carrying him or her in the womb. And yet sometimes it is precisely the mother herself who makes the decision and asks for the child to be eliminated, and who then goes about having it done.” (no. 58)
However, responsibility for this great crime also “falls on the legislators [and judges!] who have promoted and approved abortion laws, and, to the extent that they have a say in the matter, on the administrators of the health-care centers where abortions are performed.” (EV, no. 59)
For governments and legislative bodies to make intrinsically evil actions legal is unconscionable. Thus, those who have the duty to formulate law have an obligation in conscience to work toward correcting morally defective laws, as Pope Benedict XVI emphasized in 2005 during a meeting with the Presidents of the Episcopal Commissions for Family and Life of Latin America: “In attacking human life in its very first stages, it [abortion] is also an aggression against society itself. Politicians and legislators, therefore, as servants of the common good, are duty bound to defend the fundamental right to life, the fruit of God’s love.” Failing to safeguard the lives of innocent and defenseless unborn children and ignoring their duty to correct such an injustice, politicians and legislators are, thus, guilty of cooperating in evil and in sinning against the common good.
In their document, Living the Gospel of Life, the U.S. bishops remind us of the unique and irreplaceable role Catholics play in defending and serving human life, especially those holding public office:
“Catholics who are privileged to serve in public leadership positions have an obligation to place their faith at the heart of their public service, particularly on issues regarding the sanctity and dignity of human life.” (no. 30)
They also offer a word of warning and fraternal correction:
“We urge those Catholic officials who choose to depart from Church teaching on the inviolability of human life in their public life to consider the consequences for their own spiritual well being, as well as the scandal they risk by leading others into serious sin.” (no. 31)
“We call on them to reflect on the grave contradiction of assuming public roles and presenting themselves as credible Catholics when their actions on fundamental issues of human life are not in agreement with Church teaching. No public official, especially one claiming to be a faithful and serious Catholic, can responsibly advocate for or actively support direct attacks on innocent human life…no appeal to policy, procedure, majority will or pluralism ever excuses a public official from defending life to the greatest extent possible. As is true of leaders in all walks of life, no political leader can evade accountability for his or her exercise of power (Evangelium Vitae, 73-4). Those who justify their inaction on the grounds that abortion is the law of the land need to recognize that there is a higher law, the law of God. No human law can validly contradict the Commandment: ‘Thou shalt not kill.’” (no. 31)
In 1976 during the Eucharistic Congress held in Pennsylvania, Pope St. John Paul II, then Cardinal Karol Wojtyla, prophetically stated that “we are now standing in the face of the greatest historical confrontation humanity has gone through.” The would-be pope and saint further stressed that we are “facing the final confrontation between the Church and the anti-Church, of the Gospel versus the anti-Gospel.”
It is undeniable. We are engaged in a confrontation between two diametrically opposed forces. As Wojtyla emphasized, “it is a trial of not only our nation and the Church, but, in a sense, a test of 2,000 years of culture and Christian civilization with all of its consequences for human dignity, individual rights, human rights and the rights of nations.”
In the months ahead, we must keep our eye on the truth, firmly committing to speak out and defend the right to life of all persons, no matter their age or any other characteristics, and no matter how fierce the opposition. We must also ardently fast and pray for those serving in public office and for the right outcome to this once-in-a-lifetime court case, which could alter the future of the United States for the better, contributing to creating a true Culture of Life.
May we live to see the United States finally become a pro-life nation, setting an example for the whole world of how it is possible to reverse course and right the great wrong of legal abortion.
AUSTIN, May 19, 2021 (LifeSiteNews) – Texas Gov. Greg Abbott signed a law Wednesday attempting to ban the abortion of babies with detectable heartbeats through an unusual enforcement mechanism supporters hope will get around the legal obstacles pro-life laws normally face.
House Bill 1515, titled the Texas Heartbeat Act, requires abortionists to screen for a preborn baby’s heartbeat and prohibits abortion if a heartbeat can be heard (generally as early as six months), with exceptions only for medical emergencies.
Notably, however, the state would not be prosecuting violators of the new law, which actually forbids any enforcement action “by this state, a political subdivision, a district or county attorney, or an executive or administrative officer or employee of this state or a political subdivision.”
Instead, it “exclusively” empowers private citizens to bring civil suits against the abortionists, punishable by a minimum of $10,000 in statutory relief per abortion plus whatever additional injunctive relief is deemed “sufficient to prevent the defendant from violating this chapter or engaging in acts that aid or abet violations of this chapter.”
“It’s a very unique law and it’s a very clever law,” South Texas College of Law Houston professor Josh Blackman toldThe Texas Tribune. “Planned Parenthood can’t go to court and sue Attorney General [Ken] Paxton like they usually would because he has no role in enforcing the statute. They have to basically sit and wait to be sued.”
Notably, these private citizens do not need to have any connection to anyone involved in a specific abortion. “Every citizen is now a private attorney general,” Blackman said. “You can have random people who are against abortion start suing tomorrow.”
Whether this new strategy will prevail remains to be seen, but such experimentation with legal strategies has been provoked by national judicial precedent that forbids states from directly banning abortion. Full bans take effect well before the Supreme Court’s “fetal viability” threshold, and so are consistently enjoined by lawsuits from the abortion industry.
Instead, states typically enact them in hopes of provoking a legal battle that would hopefully reach the nation’s highest court and instigate a review of Roe v. Wade, thereby potentially overturning decades of pro-abortion legal precedent and freeing the states to set their own abortion laws.
Pro-lifers are cautiously hopeful that the Supreme Court’s upcoming hearing of Dobbs v. Jackson Women’s Health Organization, which concerns a 15-week abortion ban in Mississippi, will provide such an opportunity.
May 10, 2021 (LifeSiteNews) — Vogue recently ran an article entitled, “Is Having A Baby In 2021 Pure Environmental Vandalism?” The uproar from conservatives was swift. Many commentators blasted the article, with one major media outlet saying the piece was “ripped as completely insane for calling childbearing environmental vandalism.”
Fox News contributor Rachel Campos-Duffy called the article “hysterical,” and one Twitter user said, “These people are completely insane.”
Indeed, Nell Frizzell’s article reveals that she was irrationally fearful at one point about the planetary consequences of having a child. “Before I got pregnant, I worried feverishly about the strain on the earth’s resources that another Western child would add,” she wrote.
Frizzell appears to have simmered down a bit after she conceived the child that she — as revealed elsewhere — had longed for so much. But concerns remained: “While gestating my son, and probably every day since, I have wondered whether having children is, in itself, an ecologically sound or unsound decision.”
“Well, spoiler!” She continues. “Like so much in this life, it’s not a simple binary.”
While her thought process is cause for concern, throwing the javelin of the pen at Frizzell like she’s a crazy woman misses the mark. This is not only because, to her credit, she refuses to treat “overpopulation” as a specter to be avoided, but because doing so ignores her piece’s greater context.
More precisely, what is outrageous about the piece is that Frizzell feels compelled to ask the question that she does.
It signals that we have reached a disturbing point in our society, when a sizable number of couples are staying childless — or perhaps worrying “feverishly,” like Frizzell once did — because of concerns about their children’s effects on the planet, or fears that their child will meet with a disastrous planetary future. The likes of a woman who writes for Vogue is swimming in the sea of “climate crisis” hysteria, and without an intellectual anchor, she will easily be caught up in its currents.
In fact, Frizzell’s piece comes close on the heels of another Vogue piece from March, Emma Harding’s “Fear Over the Climate Crisis Has Made Me Reconsider Having Children,” in which she reveals that she has, tragically and truly insanely, abstained from having children in order to help “save” the planet.
“Our own prevailing rationale for not having children stems from the crisis and the limited time we now have to address the climate emergency. I feel privileged to be in a position to be able to make this choice,” wrote Harding. She continues, saying “it is what feels right for us.”
“Even though up until now (I can’t promise an overriding maternal urge won’t consume my body one day) we have decided not to have children of our own, I hope we leave the world a little bit better for the children I so love — my nieces, nephews and goddaughter — so that they, too, can experience, love and protect the wonder of this Earth, for themselves and the generations beyond,” she concluded.
In fact, these worries are common enough — or at least, politically expedient enough — to prompt several mainstream news pieces in recent years featuring couples who’ve decided not to have children due to the climate “crisis.”
These fears generally revolve around both the worldwide environmental impact on others of a new human being’s resource consumption/carbon footprint, and the perceived likelihood that their child will meet with an inhospitable earth.
In 2019, the BBC featured a movement called anti-natalism, which is “based around the tenet that it’s cruel to bring sentient lives, doomed to suffering and to causing suffering, into the world.” The article revealed that anti-natalists had created an online petition, “Overpopulation root of the climate catastrophe — worldwide birth stop now,” which had garnered at least 27,000 signatures, and which they hoped to send to the United Nations.
The Guardian ran a piece in 2018 featuring people who gave up having children to “save” the planet, including a 26-year-old woman who sterilized herself, as well as members and patrons of the group Population Matters, which campaigns for population reduction. One of the group’s board members, Emma Olif, told the Guardian that having children, “from a biological point of view, is probably one of the most selfish things you can do.”
Then there’s the BBC interview with the “[w]omen too scared of climate change to have children,” who are part of the U.K. movement Birthstrike, “a voluntary organisation for women and men who have decided not to have children in response to the coming “climate breakdown and civilisation collapse.”
“I’m so depressed, I feel so hopeless over what I’m reading, just the last couple of months even,” Alice Brown told the BBC. “Insect numbers are plummeting so fast. We’re destroying Biodiversity so quickly that that threatens our food, and the UN have said that that can lead to the risk of our own extinction. My decision for being on Birthstrike mostly has come from not wanting to pass that fear onto someone else.”
The Founder of “Birthstrike,” Blythe Pepino, in an interview with The YEARS Project explained why she founded the movement, despite her own strong desire to have a family. She cited food and water shortages, rising seas, rising carbon emissions, and fear of future instability because of these factors.
“All of those things blew my mind. My life changed. I effectively took the blue pill from the Matrix and I couldn’t go back with what I had learned,” said Pepino.
“Red-pilled” is a term commonly used in reference to a famous scene from the movie The Matrix in which the main character, Neo, reaches a crossroads: He is given the option to become awakened to the true nature of reality (red-pilled), or remain ignorant and accepting of an illusion (blue-pilled).
Neo is told by Morpheus, “You take the blue pill: The story ends, you wake up in your bed and believe whatever you want to believe. You take the red pill: You stay in Wonderland, and I show you how deep the rabbit hole goes.”
Her reference to taking the “blue pill” is perhaps a telling slip of the tongue.
A new mentality that has been in the works for years
This mentality has been in the works for years. Janet Smith, in a revised transcription of her lecture Contraception, Why Not?, given in 2005, shares a sad story that reveals how the “overpopulation” hysteria even affects the minds of children:
Your children are being taught from kindergarten through college that there are simply too many people on the face of the earth. Every child that is being born is being treated as though it’s a little environmental hazard, someone who’s going to “take a bite of my piece of the pie.” Some children think that they are one of those too many people on the face of the earth. I read about one little girl, nine years old, who came home and threw out all of her dolls. Her mother asked her: “Why are you doing that?” She replied: “Because there are too many people on the face of the earth. I’m never going to be a mother.” She got the message: she’s been taught that it is irresponsible to have children.
The idea that we shouldn’t have children — or even that we need to significantly reduce consumption, that is, learn “to live within our environmental means,” as Frizzell argues — is directly challenged by research from an initiative of the Cato Institute.
HumanProgress.org tweeted in response to Frizzell’s article, “@NellFrizzell should read our #SimonAbundanceIndex. Children do not strain the world’s resources. In fact, the opposite is true: each new child is correlated with an increase in resource abundance.”
The Simon Abundance Index, which “measures the relationship between population growth and the abundance of 50 basic commodities,” including food and energy, found that the average person’s “personal resource abundance rose by 303 percent” between 1980 and 2020.
In the United States, farmers continue to be paid by the government to leave land unfarmed.
Even if this were not documented to be the case, it’s strange that many so-called “progressives” — supposedly firm believers in the power of men’s ingenuity to solve the problems of mankind — essentially suppress their imagination about sustainability solutions. That is, if they don’t conclude we must give up children altogether, they conclude that we must live in poverty, or “own nothing,” as the World Economic Forum has told us will be our fate (the original video has since been removed due to backlash).
If human beings can learn to communicate wirelessly from thousands of miles apart, to make 400-ton hunks of metal fly, to make electricity from wind or sunlight … Then why must we resign ourselves to giving up children or living like a third-world country to save the planet?
Frizzell noted that despite her concerns that the world “now is dangerous for children” — because of, for example, the dangers of pollution — she had a baby “anyway,” adding, “Is that because I am selfish, myopic or greedy?… Perhaps.”
But who really suffers from myopia?
A materialist worldview
Those who decide not to have children to “help” the planet are really saying that the world would be worse off, not better off, if they brought a child into it.
There is nothing more cynical, more anti-”progressive,” more self-denigrating, more dense, more senseless, more anti-human, more tragic.
What such a stance really does is expose the frightening and pitiably two-dimensional worldview of the pure materialist, which reduces human beings to their material productivity. If your child consumes more resources than they expend, well, they are a mathematical liability, a useless eater.
Whether or not it is articulated or realized as such, the mentality is that if one human being inconveniences or materially reduces the “quality of life” of another, it is better if the human being didn’t exist. Hence: contraception as the norm, euthanasia for the elderly, abortion of the disabled — abortion, period.
Frizzell’s “feverish” worry before pregnancy about “strain” on the earth’s resources, and her expressed hope that her son doesn’t “destroy” “future humanity,” suggest that she buys into this materialist philosophy.
I imagine that many, many parents have concerns or worries about bringing children into what is — and what has always been — a dangerous world.
But I fear that anxiety about purely material concerns — which do have their place — overshadows concerns about what has a much more profound impact on our posterity’s well-being:
Whether our children can establish whole and meaningful relationships in a forever “socially distanced” and masked world; whether our children will grow up in a loving household with both a mother and a father; whether our children can retain their innocence, or even have an idea of what innocence is; whether our children will live a life of character and principles, even when it is not politically correct or popular; whether they will have a firm reason for and source of those principles; whether our children will grow up knowing they have a loving Father in Heaven, their unshakable Rock and reason for hope.
The greatest miseries of our world are not the physical sufferings. They are the miseries of abuse, mental illness, addiction, neglect, hatred, apathy, loneliness, nihilism … And no amount of “saving the planet” can cure and heal these blights — nor will technological progress, and, it is true, nor will material wealth.
Along with a societal return to God, the opportunity to raise and form strong, principled, and loving children — if possible, many children — is a bright and promising, and beautiful antidote.
By now many Americans have read a glowing news article about the latest celebrity to have a child via surrogacy or watched a human-interest piece about a woman carrying a child for a loved one.
From New York, which just quietly legalized commercial surrogacy, to California, which remains a hotspot for individuals and couples from across the country and around the world seeking such services, surrogacy is often positioned only as a positive good. No equivocation or mention of the harms it poses to women and children is even mentioned.
Avoiding the other side of the conversation does a disservice to us all, however. It’s time to talk about the dangers of surrogacy.
Just ask some of the children themselves. “There are a lot of days …where I feel adrift, kind of like a tumbleweed… It’s days like today where my heart hurts a bit more over a surrogacy agency, doctors, lawyers, and the rest of the adults involved not successfully making sure that this product they were creating would be o.k.,” writes “jkiam83” an anonymous surrogate-born woman on her blog. “Where are the resources and communities for us products of surrogacy? [I]s this really what is in the best interest of a child?”
From the perspective of Brian, a surrogate-born man, it’s not; he writes, “It looks to me like I was bought and sold.”
In a surrogacy arrangement, a woman carries a child for an individual or couple who is unable to do so themselves. Sometimes the child is genetically related to the commissioning parents, but often donor gametes are used, and the child is related to only one, or in some cases neither, of the commissioning parents.
Please follow LifeNews.com on Gab for the latest pro-life news and info, free from social media censorship.
Sometimes the surrogate mother is genetically related to the child she carries, but often she is not. Some surrogacy arrangements are domestic, but many commissioning parents pursue international surrogacy arrangements, which adds an additional layer of logistical and legal difficulties.
Surrogacy is fraught with ethical and moral considerations. It is a process that can exploit vulnerable women. It carries significant health and psychological risks for the women whose wombs have been “rented,” the women whose eggs have been harvested to create an embryo, and the children who are born from these arrangements. All too often, the desires of adults—namely, the commissioning parent(s)—supersede the interests of children. Unfortunately, discussions of surrogacy in media—and culture more broadly—rarely focus on the latter.
At the recent United Nations Commission on the Status of Women, The Heritage Foundation and the Center for Family and Human Rights drew attention to surrogacy and the dangers it poses to women at an event that highlighted several instances of women who had been trafficked, rendered infertile, or even died as a result of surrogacy. Michelle Reaves was one such surrogate mother from California. She lost her life last year while delivering a baby for someone else, leaving her own son and daughter motherless and her husband a widower.
By its very nature, surrogacy commodifies both a woman’s body as well as that of the child. The women targeted to become a surrogate by the multi-billion-dollar fertility industry are often wooed by the opportunity to make tens of thousands of dollars in exchange for renting their body. In some cases, a surrogate arrangement is altruistic—perhaps the surrogate mother may want to help a friend or family member who desperately wants a baby, and she does not profit financially from the exchange.
Nevertheless, regardless of the circumstances or motivation, in a surrogacy arrangement a woman’s body is used as a conduit for a transaction that provides a baby for someone else—and the risks for both her, and the baby, are significant.
Whether a surrogate mother is compensated or not, serious concerns involving health risks to mothers and babies remain, and the rights of children must not be ignored.
Children who are born as the result of a surrogacy arrangement are more likely to have low birth weights and are at an increased risk for stillbirth. When a woman carries a child conceived from an egg that is not her own—a traditional gestational surrogate arrangement—she is at a three-fold risk of developing hypertension and pre-eclampsia.
Egg donors have spoken up about experiencing conditions such as loss of fertility, blood clots, kidney disease, premature menopause, and cancer, and the lack of data and studies on both short and long term health outcomes for egg donors makes true informed consent unattainable.
While scientists do not fully understand the scope of these health considerations, it is clear that for both short and long-term outcomes, surrogacy is a frontier of unknowns; children, egg donors, and surrogate mothers may pay a physical or psychological price nobody yet fully knows or understands.
Children’s Rights Matter
Surrogacy gives little consideration to the rights of a resulting child, who in many cases will be intentionally separated from at least one biological parent, as well as potential half-siblings in cases where the commissioning parents are using egg or sperm donors in conjunction with the surrogacy arrangement. In cases of anonymous egg and/or sperm donation, children have been denied part, or in some cases all, of the details of their biological origins. “Genealogical bewilderment” and adjustment difficulties among surrogate-born children are well documented.
Even in cases where a child is raised by his or her biological parents, children’s rights advocate Katy Faustnotes that many surrogate-born children in these circumstances experience the primal wound of losing their birth mother, an experience well-documented among adopted children. She argues that “surrogacy is, by its very nature, an injustice to the child. Birth is intended to be a continuation of the mother/child bond, not the moment at which the child suffers an intentional, primal wound. It’s the day when a baby should see the mother she already loves for the first time… not the last.”
Sometimes parallels are drawn between adoption and surrogacy. But this is a false comparison. In many cases surrogacy intentionally creates a situation in which a child will be denied his or her biological parent-child relationship. In every circumstance, the children of surrogacy arrangements are deliberately separated from the only mother they have ever known the moment they are born. Adoption, in contrast, responds to this separation rather than creates it.
Surrogacy Knows No Borders
International surrogacy arrangements can be even more complicated than domestic surrogacy arrangements because issues of citizenship and nation-specific determinations of legal parentage come into play. While there are no exact numbers available of how many children have been born from surrogacy worldwide, it is currently a global industry that is projected to grow to over $20 billion within the next few years.
As Professor David Smolin, a leading legal expert on surrogacy and author of “The One Hundred Thousand Dollar Baby: The Ideological Roots of a New American Export,” explains, “The United States is attractive to foreigners seeking surrogacy services because it is one of the few nations that offers stable legal systems explicitly supportive of commercial surrogacy.”
While America is a popular destination for surrogacy for those who can afford it, some commissioning parents engage in international surrogacy arrangements in countries with even less regulation such as Ukraine and Russia, which raises additional concerns about maternal and postpartum health care for surrogate mothers and babies.
Heartbreaking stories at the height of the coronavirus pandemic exposed the uglier side of international surrogacy as travel restrictions separated surrogates and babies from commissioning parents across the globe.
With such international variation in the legal status of surrogacy, as well as the establishment of parentage and citizenship, commissioning parents and surrogate mothers can find themselves navigating a minefield of unanticipated practical and legal issues.
Internationally, women’s rights groups are split on the issue of surrogacy—much as they are in the debates over prostitution or “sex work”—about whether it exemplifies a woman’s autonomy and choice over what to do with her body or whether it constitutes commodification of a woman’s reproductive and life-giving capabilities.
Sadly, the international surrogacy market appears to have significant and growing overlap with human trafficking. Given the amount of money involved, traffickers stand to profit substantially from selling women and girls into surrogacy arrangements.
As Dr. Sheela Saravanan, author of “A Transnational Feminist View of Surrogacy Biomarkets in India,” wrote in a submission to the UN Special Rapporteur on the sale and sexual exploitation of children, “The surrogacy trafficking trade used the same network that was used for domestic work and sex trade from the poor regions of India into urban areas. These unmarried girls [were] impregnated with embryos without their consent. Others were confined in homes and when some girls tried to run away, they [were] caught, brought back and beaten.”
How Are Governments Responding?
The international community is currently debating a new protocol on international surrogacy arrangements. A group of experts—including one representing the U.S. Government, convened by the Hague Conference on Private International Law—is discussing how to address legal parentage, jurisdictional, and ethical questions about surrogacy, particularly from the perspective of protecting children.
In response to various injustices and exploitation, several countries have closed their borders to international surrogacy arrangements in recent years, including India and Thailand.
Regrettably, the current official position of the United States with respect to international surrogacy is that surrogacy does not involve the exploitation or commodification of children. The U.S. signed and ratified the optional protocol to the Convention on the Rights of the Child that prohibits the sale of children, but holds that “surrogacy arrangements fall outside the scope” of the protocol.
The UN Special Rapporteur on the sale and sexual exploitation of children recommends that surrogacy agreements be regulated in order to prevent exploitation of women and sale of children. But she has not called for a global ban on surrogacy, although an increasing number of voices do, including hundreds of organizations from eighteen countries that signed an International Statement for a Global Ban on Womb Rental in 2018.
Within the United States, a patchwork of laws makes for a Wild West situation. Some states allow commercial surrogacy, some limit surrogacy to altruistic arrangements, and some do not recognize surrogacy contracts. But most states do not specifically address the issue.
Proposals to more tightly regulate surrogacy, clarify contract legalities, or in the case of the state of New York, provide a full-fledged stamp of approval, don’t resolve the full scope of surrogacy’s challenges and harms.
Time to Reframe the Conversation
Beyond the debates in state houses and international bodies, it’s time to reframe the conversation. Infertility and other health conditions that render a person unable to have a child of his and her own can be a painful and isolating experience, and our society should have compassion for people who walk the road of infertility and loss.
But we should approach the matter of surrogacy from an understanding that the desires of adults to raise a child do not supersede the rights and needs of children.
Listening to the women and children who have suffered deeply because of surrogacy is critically important. Organizations like Them Before Us and the Center for Bioethics and Culture are leading the important work to elevate these voices and tell the stories of women and children that are too often ignored or dismissed.
Clarifying legalities and increasing regulations does not address fully the ethical problems with surrogacy and its harms to women and children. Opposition to surrogacy is not a simple left versus right issue, and people across the political spectrum can agree that American laws and society need to prioritize the dignity and health of women, the needs of children, and the fundamental human rights of all individuals when addressing the matter of surrogacy.
LifeNews Note: Grace Melton is The Heritage Foundation’s associate for social issues at the United Nations. She is part of the think tank’s DeVos Center for Religion and Civil Society. This originally appeared at Daily Signal.
Portrait of lonely teenage girl sitting alone with depressed expression and showing a paper with a help text. Sad and lonely girl crying with a hand covering her face with help sign
“I had severe depression with suicidal thoughts. I had no libido and I got severe fatigue. I took on weight and was not able to lose it…. After stopping with the birth control pill these symptoms vanished.” —Ursula, public commenter on the FDA Citizen’s Petition for greater transparency of birth control side effects.
It’s not all in your head: the Pill definitely affects mental health
I cannot count the number of times I’ve heard women share that they didn’t feel themselves—and worse, experienced severe mental health affects like depression, anxiety, or suicidal thoughts—on the Pill, patch, shot, vaginal ring, hormonal IUD, or even the copper IUD. It is so common you might think it’d be common knowledge. Yet, week after week I still see women asking about their mental health symptoms on Facebook groups, “is it the Pill or just me?”
Unfortunately, many women don’t find answers from their doctors or even mental health professionals if their depressive or anxious symptoms are due to hormonal contraceptives. Perhaps because contraception is seen as a “given” for all young women of reproductive age, there seems to be a major blind spot in recognizing and addressing the problematic mental health side effects of birth control.
A woman named Rachael left a telling comment at the FDA Citizen’s Petition filed in 2019, which is still open for comment. Immediately after being prescribed the Pill at age 18, she said, she experienced multiple side effects, including depression.
“When I discussed these symptoms with my doctors, I was told that I wasn’t drinking enough water, I was simply underweight or that there was something wrong with me—not the medication … In fact, every Gynecologist I’ve ever seen pushes the pill or another form of hormonal birth control with me even after I discuss with them all of my concerns regarding the bad side effects I’ve had in the past. I find this strange, because whenever I discuss side effects with doctors about other medications, they do their best to avoid it if at all possible, or switch to ones that work differently. Hormonal birth control is the only medication I’ve ever been not just prescribed, but actively encouraged to take despite having an adverse reaction to every single brand I’ve ever taken.”
Why your doctor ignores the mental health side effects of birth control
In an interview with Natural Womanhood this year, Lisa Hendrickson-Jack, founder of the Fertility Friday podcast and author of The Fifth Vital Sign, explained: “We already know women are considered more emotional… all of the stereotypes… so when you as a woman go to a doctor and say that you have anxiety, depression, or panic attacks, there’s this inherent issue with ‘well that’s a part of being a woman.’ So, there’s an inherent barrier to proper diagnosis and care in general and I think we can all recognize those stereotypes.”
Hendrickson-Jack noted that, although every hormonal contraceptive product insert discloses that mental health effects like depression and mood change are among the most common side effects, many doctors dismiss the severity when patients bring them up.
“What I learned when I interviewed a number of doctors over the years on the [Fertility Friday] podcast,” Hendrickson-Jack said, “is that in medical school it seems as though doctors are taught about the life-threatening side effects and how to mitigate those risks, almost to the exclusion of the non-life-threatening risks.”
“When it comes to anxiety and depression,” she said, “many doctors don’t seem to know or aren’t necessarily familiar with those [birth control] side effects.”
Teens are at the greatest risk
Hendrickson-Jack continued:
“A scary stat to illustrate this is that teenage girls who are on hormonal contraceptives are much more likely to also be on antidepressants. There’s research and studies that show this correlation. If you knew that hormonal contraceptives increase your chance of depression, anxiety, then if a 16-year-old comes into your office and says she’s depressed you could say, ‘Are you on hormonal contraceptives? There’s a link there, so maybe we come off it for some months and see if there’s an improvement, and if there isn’t, then we can look at some other prescription or some other treatment for that.’ That’s not what happens.
“So for adult women that are facing these side effects and symptoms, the hard truth is it’s kind of up to you to educate yourself on those most common [birth control] side effects because it’s not every time that you go into your doctor’s office that those links are going to be made, and you’re maybe more likely to come out with another prescription for an antidepressant than you are for someone to make the link that it could be related to the birth control.…”
All of this is especially troubling when we consider how in 2017, The American Journal of Psychiatry published a study of nearly a half million Danish girls, which found that girls and women using hormonal contraception were 97% more likely to attempt suicide than those not taking the drugs, and were 200% more likely to succeed in their suicide attempt. There have also been accounts of women experiencing symptoms of psychosis—symptoms which disappeared as soon as these women stopped taking their contraceptive drugs. All this has begun making more sense as new studies discover the effects that hormonal contraceptives have on the brain.
A better way to plan your family, get help for infertility, or heal painful and irregular cycles
What’s more, fertility awareness methods can assist teen girls in greater understanding of their bodies, and assist them in documenting and receiving treatment for irregularities in their cycles. There are now so many excellent resources for teaching teens fertility awareness, and, as teen FAM educator Cassie Moriarty shared in a Natural Womanhood article, many teens prefer fertility awareness to birth control drugs: “I’ve found that when teens understand what hormonal contraception is, how it operates, and what their alternatives are, they are much more likely to choose a Fertility Awareness-Based Method where they can work with, not against, their body’s natural processes.” Further, Cassie says, teen girls “want to know how it works and what the heck is going on with their emotions. This is a crucial step in creating a positive relationship with their bodies.”
Want to hear more about the mental health effects of birth control? Watch this five-minute interview with Lisa Hendrickson-Jack (below) on the truth about mental health and birth control.
Interested in hearing more about what fertility awareness has to offer teens? Watch this three-minute video (below) where Lisa Hendrickson-Jack explains how FAMs can be transformative for teen girls.
Reuters reports the birth rate has been falling steadily for decades in the United States, and, in 2020, it reached a 42-year low.
Many linked anxieties and financial troubles from the COVID-19 pandemic to the drop, though the Centers for Disease Control did not mention this as a possible factor in its new report.
According to the CDC National Center for Health Statistics, the birth rate fell 4 percent in 2020 in the U.S. – the lowest rate since 1979. The birth rate is calculated by the number of births per 1,000 women of childbearing age.
Approximately 3.6 million babies were born in 2020, the CDC found.
Another sign of the decline, companies that sell baby formula and other baby products, including Reckitt, Nestle and Danone, saw a drop in sales last year, Reuters noted.
The CDC did not attribute the overall decline to the pandemic, but experts have predicted that pandemic-led reasons including anxiety will hit the country’s birth rate.
In general, US fertility rates have continued to fall over the years as women marry late and delay motherhood especially in years when the economy has slowed.
The report did not mention abortion, though it could be another reason for the declining birth rate.
A recent study by Japanese health ministry researchers suggests the pandemic may have led to an increase in abortions in 2020. They found that about 8 percent of the women who had abortions in Japan between October and November 2020 did so because of the pandemic.
However, the study and others also have found that women often mention multiple reasons for an abortion, including relationship problems, future goals, other children and even just “bad timing.”
“Women have cited ‘social reasons,’ not mother’s health or rape/incest, as their motivation in approximately 93% of all abortions,” according to National Right to Life.
Pro-lifers work hard to make sure women never have to feel that they need an abortion because they are financially unstable. Thousand of pregnancy resource centers, maternity homes, adoption agencies and other charities provide material and financial support to help families in need.
April 30, 2021 (LifeSiteNews) — In this episode of The John-Henry Westen Show, I speak with Dr. Michelle Cretella, the executive director of the pro-life and pro-family American College of Pediatricians. She recounts an incredible miracle story she underwent when she had brain cancer, and how her health struggles changed her perspective on contraception.
Dr. Cretella tells me that even though she always maintained her Catholic faith throughout, she did disagree with the Church’s teaching on contraception. Despite this, she was still very “dedicated to doing all I could to save babies from abortion and … to help women have alternatives to abortion.”
Dr. Cretella describes how in 2001, after waking up from sleep at night with terribly painful headaches, she was diagnosed with a tumor in her brain. The cancer was glioblastoma multiforme, a common and deadly brain tumor. Her husband immediately informed their church prayer group about this.
Throughout her experience, Dr. Cretella and her family continued to pray and rely on God for help. Between the diagnosis and the surgery, she was able to go to a parish mission where they were holding confessions. She says that the priest who headed the mission reminded and spoke about how “mortal sins … need to be confessed.”
Cretella mentions that when the priest spoke the words “artificial contraception,” she began to believe in the Church’s stance on the issue without fully understanding it. She states that “every argument in favor of contraception” she had heard and trusted in was all lies. She then promised God she would never use and promote it again.
gery, medical doctors discovered that the tumor was in fact a juvenile parasitic astrocytoma that’s “typically present in children.” It was therefore cured through surgey alone, and she was discharged a few days later cancer-free.
Ever since that experience, Dr. Cretella has refused to prescribe any contraception, and says that “fertility is not a disease.” Lastly, in our interview, she calls on doctors and scientists to put a Christian worldview in science and medicine. “Sometimes you must first believe in order to understand, and that’s what I have learned in my life.”
The John-Henry Westen Show is available by video on the show’s YouTube channel and right here on my LifeSite blog.
April 29, 2021 (LifeSiteNews) – It was hardly a fast track, but 14th century St. Margaret of Castello – who was beatified in 1609 – was elevated to sainthood by Pope Francis on April 24 using a process called “equipollent canonization.”
The Arlington Catholic Heraldexplained exactly what that means:
“The decree is what the Vatican terms an ‘equipollent’ or equivalent canonization; when there is evidence of strong devotion among the faithful to a holy man or woman, the pope can waive a lengthy formal canonical investigation and can authorize the person’s veneration as a saint.”
I’m not sure why the Vatican chose to do it this way, since her intercession is said to have prompted many miracles, but I’m very happy for St. Margaret of Castello, patron saint of the unwanted. For decades, we at Priests for Life have certainly promoted devotion to her and spread the story of her life everywhere.
That story is almost too hard to contemplate. Born around 1287 blind, lame and apparently with dwarfism, her socially prominent parents, who had wanted a boy, were horrified thinking word would get out that their baby was less than perfect. They spread the lie that she had died at birth.
They gave her to a servant who loved and cared for her, but the servant slipped up once and almost let guests at her parents’ castle catch a glimpse of Margaret. To ensure that never happened again, her father, filled with the arrogance that marks the culture of death, had a single-room cell built next to a church in the forest and walled her into it. An interior window allowed Margaret to hear Mass; another window on an exterior wall let servants pass food into the girl.
The priest there discovered Margaret had a fine mind and loved God, so he spent time teaching her the faith. When her family fled from their home when she was a teenager, they took Margaret with them, only to lock her away in an underground vault near their new home.
A year later, her parents brought her to a tomb in Castello where people were said to be receiving miraculous cures of various ailments. When Margaret was not healed, her parents just abandoned her there. Two beggars befriended her and ultimately Margaret’s life began to improve, although with many setbacks along the way.
She died at the age of 33 on April 13, 1320, after having served for years in the habit of the Third Order of St. Dominic. It has been reported that the whole city attended her funeral – that was how well-known and beloved she had become – and that a crippled girl was healed during the Mass.
St. Margaret’s life offers many profound lessons for those of us in pro-life. She disappointed her parents twice at her birth, by being female and for failing to be perfect. Today, both of those things can prompt parents to choose abortion. The world is missing millions of girls because of this preference for sons in so many cultures.
Also, she was unwanted by the very people who were supposed to love and care for her, in much the same way the unborn are unwanted by those who have envisioned a different timeline for their lives.
St. Margaret’s profound physical ailments teach a powerful lesson about how every life – no matter how compromised, no matter how “imperfect” – has value and every person has a contribution to make.
And the question that challenges us most deeply is: If we were there, and knew Margaret was locked up in that cell, would we have spoken up?
St. Margaret’s canonization comes at an interesting time in the U.S., as more states are passing laws to protect babies from abortion based on their sex, race, or disability. Prenatal testing now allows parents to know long before their baby is born if he or she will be everything they have dreamed of and planned for. Babies falling short of that ideal – like those with Down syndrome or dwarfism – are frequently aborted.
I invite everyone who believes in the sanctity of every human life to join me in praying this prayer I wrote some years ago for Margaret of Castello, the newest saint for the pro-life movement.
Father,
Your care extends to every human person,
No matter what afflictions they suffer,
And you uphold the dignity of every human life,
Regardless of the false ways that the world may calculate its value.
You gave us St. Margaret of Castello as a sign and a challenge.
You permitted your glory to shine through her human weakness,
And called those around her to love her
Despite her physical limitations.
Forgive us when we fail to defend the least among us.
Through the intercession of St. Margaret,
Give us grace to speak up for the outcast
and to welcome those who are rejected.
When this brief life is over,
Grant that we who have welcomed all our brothers and sisters,
May be welcomed by you into the life that never ends.
We pray through Christ our Lord. Amen.
Father Frank Pavone is the National Director of Priests for Life.
Researchers are calling for clinical trials to track and document menstrual changes in vaccinated women after some women reported changes to their menstrual cycles after receiving a COVID vaccine.
Women have reported hemorrhagic bleeding with clots, delayed or absent periods, sudden pre-menopausal symptoms, month-long periods and heavy irregular bleeding after being vaccinated with one or both doses of a COVID vaccine.
“In terms of why women would have a heavier cycle, I think clearly we don’t know the answer to that,” Dr. Heather Huddleston, a reproductive endocrinologist at University of California, San Francisco, told ABC7News.
“However, we do know in addition to hormones being really important in a menstrual cycle, that there is a role for the immune system in the uterus,” she said. Huddleston suggested “if there are changes, perhaps due to a vaccine, maybe that would subtly affect the behavior of the immune system in the uterus.”
A researcher at the University of Illinois described her own experience on Twitter and asked if others experienced menstrual changes after vaccination. The response was robust, so she and her colleague at Washington University in St. Louis turned it into a formal survey.
So far, there’s no data linking COVID vaccines to changes in menstruation. But two Yale University experts wrote in The New York Times last week there could be a connection.
“There are many reasons vaccination could alter menstruation,” wrote Alice Lu-Culligan, an M.D. and Ph.D. student at Yale School of Medicine, and Dr. Randi Epstein, writer in residence at Yale School of Medicine.
“Every month the lining of the uterus thickens, driven by a steady increase in estrogen, so that a fertilized egg can implant. If there is no conception, levels of progesterone plummet, causing most of the uterine layer to slough off, causing the bleeding,” Lu-Culligan and Epstein explained.
But periods also involve the immune system, as “the thickening and thinning of the uterine lining are facilitated by different teams of immune cells and signals moving in and out of the reproductive tract.”
Vaccines are designed to ignite an immune response, and the female cycle is supported by the immune system, so it’s possible vaccines could temporarily change the normal course of events, Lu-Culligan and Epstein said.
“For example, an activated immune system might interfere with the usual balance of immune cells and molecules in the uterus,” they explained in the op-ed. “These types of disturbances have been found in studies to contribute to changes in periods, including heavy menstrual flows.”
Forbes health contributor Alice G. Walton agrees. She said a connection between the vaccine and menstrual irregularities is plausible given the interplay between the menstrual cycle and the immune system — the building up and shedding of the uterine lining are processes that each rely on immune function.
When the body mounts an immune response, either to an illness or to a vaccine, it can extend to the uterus and affect immune cells that help control menstruation. A number of doctors have explained how this might work, including fertility specialist Dr. Natalie Crawford.
“We know that the COVID vaccine causes an immune response to make antibodies very similarly to how a COVID infection would in your body, and there is actually a study talking about COVID infection and what it does to your period,” Crawford said.
A study in the Reproductive BioMedicine Journal, “Analysis of Sex Hormones and Menstruation in COVID-19 Women of Child-bearing Age,” retrospectively looked at women in China who had acquired COVID naturally and the affect of the infection on sex hormones, ovarian reserve and period.
The study found that 28% (or 1 in 4) women had a change in their menstrual cycle length, 25% had a change in their menstrual cycle volume and hormone concentrations were altered.
“If a quarter of women who get COVID are experiencing menstrual cycle changes, it is most likely from a cellular immunity response,” said Crawford. She said it would not be surprising if women experienced this from the vaccine as well, as it causes a similar immune response.
To find out whether the COVID vaccine truly disrupts the menstrual cycle, experts say there would need to be a controlled study with a placebo group. Currently, clinical trials omit tracking menstrual cycles, so there’s no evidence to put the women’s reports in context.
“Menstruation is something we don’t know enough about,” said Dr. Hugh Taylor, chair of the department of obstetrics, gynecology and reproductive sciences at Yale School of Medicine. “It’s an important indicator of a person’s health, like any other bodily function.”
If so many factors can affect periods, and periods are such an important indicator of health, why don’t we know more about how vaccines affect menstruation?
It’s part of a long history of medicine not taking women’s bodies seriously, Lu-Culligan and Epstein said. They explained that it wasn’t until 1993 that a federal law mandated the inclusion of women in government-funded research, which may account for why so little is known about how new drugs and treatments affect women’s health.
Rather than treat menstrual cycles as unimportant or too complicated, researchers should view tracking periods in future studies as a potential opportunity, they said. Clinical trials should track and document menstrual changes as they do other possible side effects.
For now, scientists are still in the dark about so much of female health, Lu-Culligan and Epstein said. But a conversation has begun, thanks to women speaking out.
We didn’t plan to have many kids. It just sort of happened. After our fifth child was born, a friend asked my wife how many children she planned to have. She said, “Two.” Yet each of our six kids has been both a joy and an endless source of parenting lessons. Whether you’re considering producing your own mini-platoon, or are merely curious as to how it’s possible for apparently sane adults to cope, I offer here a few insights and one piece of advice: don’t take yourself too seriously, hang on, and enjoy the ride.
How do you handle sickness?
Commercials where the kid has a cold and the parents give him cough syrup and lovingly tuck him into bed are a joke. Nursing numerous children is like playing whack-a-mole. One kid gets over his cold just in time for another to get it. No, they can’t all be sick at once. They must do it sequentially.
What to a normal family would be a three-day cold, to a large family is a month-long affair. When you have a lot of kids, you don’t quarantine the sick ones. You want them to infect each other as quickly as possible, because you need to process all of them before you come down with the bug yourself. You start to thank God for the blessing of acquired immunity that guarantees each kid will only get the disease once.
Then you discover pink eye.
If dealing with a cold is like playing whack-a-mole, dealing with pink eye is like playing a macabre game of telephone. Kid #1 gives it to Kid #2, who gives it to Kid #3. By this time Kid #1 is cured, but Kid #3 has given it to Kid #4. Now Kid #1 has forgotten your repeated warnings about washing his hands and keeping his fingers out of his brother’s eye, and sure enough, Kid #1 has it again. He gives it to Kid #2, and the whole cycle continues. You find yourself praying for a harsh winter so the freezing temperatures can kill off the germs these house creatures have painted on to every surface.
What do you call them?
We spent months selecting a name for our first child, Erika. We thought about how it sounded, what it meant, whether it had a long enough shelf life so it wouldn’t make her sound like an old lady just as she was hitting her college years. Ladies named Mavis, Opal, Inez, and Violet weren’t born 80 years old. They just lost the shelf life lottery.
We were quicker at naming our second child, largely because I am a science fiction freak and my hero, Isaac Asimov, had died just before our son was born. So Isaac it was. Our church friends thought it touching that we named him after the one of the biblical patriarchs. We didn’t have the heart to admit that we named him after a lecherous chemistry professor who wrote wicked sci-fi.
With names come nicknames. At first, you’re proud to tell people your baby’s name. “She’s Ivanka, after my wife’s mother. There’s been one Ivanka in each generation in my wife’s family going back five generations. Our little Ivanka is the sixth of that name.” But that doesn’t last. Where names are concerned, poetry eventually takes a backseat to practicality.
Nature has given toddlers the triple advantage of being quick, quiet, and small enough to fit into tiny spaces. When you want to sleep, they’re louder than a frat house on homecoming night. But when they’re getting into things they shouldn’t, they’re like incontinent ninjas. Sometimes the only way to find them is to follow the smell.
So, with locomotion comes the need to summon the little tykes. And this is where practicality comes in. When you finally put that name to work, you’ll regret not having picked an industrial-strength name like “Bob.” You can keep saying “Bob” until the cows come home. “Bob, where are you?” “Bob, come here!” “Bob, don’t bite the cat!”
But if you picked a poetic name, now is when you’ll regret it. Try repeating “Beatrix” or “Jacinda” ad infinitum. This is why God invented nicknames. The nickname is the name you should have given your kid but were too embarrassed to pick. It takes a while to whittle a flowery name down to something practical. And you can tell how much trouble a kid gets into by how quickly the parents adopt an industrial-strength nickname.
Over the course of three days, our lovely Ivanka became “Vonky,” then “Schpanky,” then “Schpank,” then “Spank,” then “Hank.” Now, Hank is an industrial-strength name. You can shout it all the livelong day, and the last use will be as potent as the first. You can put some serious air pressure behind that opening consonant, and the hard “k” at the end cuts off the sound to an immediate and ominous silence. “Hank” is the air horn of the naming world. “Beatrix” is the kazoo.
But nicknames quickly add up to a lot of words to remember. Our last two kids, Alexander and Benjamin, were born just a year apart. Since we both abhor the nickname Alex, we announced his nickname before we left the hospital. “He shall be known as Xander.” We didn’t like the nickname “Ben.” But since “Jamin” sounded like a reggae stoner, #6 stayed straight-up “Benjamin.”
As they tend to be inseparable, my wife has taken to calling Xander and Benjamin (as a conglomerate), “Xanjamin.” Kind of like Brangelina meets the Brady Bunch. “Xanjamin” exhibits a bit of creative flair, but at three syllables it’s not industrial-strength. Plus, if you want to summon just one of them, you have to go back to either “Xander” or “Benjamin,” which means that you now have three names to deal with instead of merely two. The efficient solution we evolved is to give each of them the same nickname: “Kid.” If we need to refer to one of them, we say, “the kid.” As in, “Tell the kid to take out the trash.” If the wrong one shows up, the other one is, automatically, “the other kid.” As in, “Kid, come here. No, the other kid.”
Last in the telling, though not the lineup, is Simon. Simon is the middle child. You hear about middle-child syndrome, where the poor middle child is ignored because he’s not needy like the teenagers or cute like the babies. Middle children, the story goes, grow up to be meek and unsure of themselves. Middle children stay in the shadows of their more outgoing siblings.
Simon does not have middle-child syndrome. If there is an opposite of middle-child syndrome, that’s what Simon has. Picture George S. Patton as a teenager. On a battlefield. In a tank. That’s Simon. When told that their older brother would be staying at college over the summer, the other children cried. Simon’s response was, “Excellent. That means we all move up in rank.”
What do you learn from having many children?
Humans are, hands down, the single most fascinating set of creatures on the planet. If you want to understand how humans work, just make a few, sit back, and watch them do their thing. But one or two won’t do. To understand humans, you need to observe enough of them so the individual quirks average out and you get to see the commonality in their behaviours. How many are enough? Probably several hundred thousand. As that was outside our budget, we settled for six.
What sorts of insights have we gained into Homo sapiens?
1. Children believe they are inventing the world as they experience it.
The child who, standing in front of you with chocolate all over his hands and face, insists that he most certainly did not eat the cake you left on the counter, believes he has invented lying. Had it occurred to the child that lying was invented about twenty minutes after language itself, he’d suspect that the parent would not only (a) know that lying was possible, but (b) be better at it than the kid, and (c) be able to spot it a mile away.
This belief — that just because they haven’t experienced something before, no one else has either — continues into the teenage years and can even be seen persisting into adulthood. Our teenager who thinks she’s getting away with sneaking out of the house doesn’t consider that her parents are not merely parents. They are also former teenagers who did the same things she is doing. No, she’s not getting away with anything. We’re allowing her to believe she’s getting away with something so she doesn’t up her stealth game and actually succeed in getting away with something.
2. Children believe they are smarter than their parents.
When I was a kid, I was embarrassed that my father couldn’t manage to programme the simplest electronic device. And I don’t mean “programme” in the sense of writing code that instructs the device to perform certain functions. I mean “programme” in the sense of any interaction more complicated than “turn it on.” Here he was, a senior executive at a multinational corporation, and he needed me — teenager — to set the time on his clock radio. If this, I thought, were typical of the caliber of mind populating corporate America, I would be running the country by my eighteenth birthday.
Now that I have teenagers on whom I rely to navigate Netflix, I realise the stark truth. I wasn’t a teenaged mental giant. My father simply had more important things to occupy his mind — things I had no idea even existed, like retirement contributions, mortgage payments, and tire rotations — such that he saw no point in wasting his time with a problem he could much more easily solve by telling his son, “Go fix that flashing thing in my room.”
Children believe they are smarter than their parents because children command nearly 100 percent of the knowledge they perceive to exist. The irony, of course, is that they are so aware of the things they know because the number of things they know is embarrassingly small.
3. Children have a keen but myopic sense of justice.
When you confront a child with the accusation that he has wronged someone, the child becomes a firehose of excuses as to why he is, in fact, not in the wrong. The young child will rely on his weak lying skills. The teenager, who has by this age has learned that he isn’t good at overt lying, turns to lying by omission and burying his accuser in a flood of irrelevance.
But when the child is the one who has been wronged, suddenly the kid becomes the world’s shrewdest prosecutor. The arguments that were so reliable in his defence — packed with misunderstandings, questions of interpretation, and mitigating circumstances — disappear. In their place are ice-cold facts and impeccable logic. In a way, this is heartening. It suggests that the child has no problem comprehending justice. It’s the equality of application that’s lacking.
Why have a bunch of kids?
Children are expensive. They are messy. They are frustrating. They can be selfish and argumentative. They are also immense fun. They are creativity unencumbered by talent. They are slow to judge and quick to forgive. They love not out of reciprocity or personal gain, but because that’s what they do. They are joyful packets of energy that upend your life and wreck your plans in every way possible. They are the most wonderful creatures you will ever have the pleasure to know.
When you reach the end of your life, you will look back on accomplishments that the world has long forgotten and at hard-won money, power, and prestige that have faded into the mists of time. And you will know that the single greatest accomplishment any person can achieve in this life is to populate the world with children who love each other, care for those less fortunate, and walk humbly with their God.
Antony Davies’ research interests include econometrics, public policy, and consumer behavior. Davies has authored over 150 op-eds for, among others, the Wall Street Journal, Los Angeles Times, Forbes,… More by Antony Davies
In recent years, pro-lifers have exposed the gruesome, ongoing practice of harvesting and buying and selling the body parts of aborted children for medical research.
A series of undercover videos released by pro-life researcher David Daleiden showed abortionists and executives of biomedical companies callously describing how they obtain the bodies and haggling over the prices for different body parts.
In one of the most disturbing videos that I have ever seen, Daleiden and his co-investigators captured footage of the dismembered body of a child aborted at 20 weeks in a dish. At one point the camera operator uses tweezers to lift up the fully intact hand and arm of the baby, who, we are informed, was a twin.
Unfortunately, Planned Parenthood, the abortion industry in general, and pro-abortion politicians and the media did everything they could to ensure that as few people as possible viewed the actual videos. When the media did report on the videos (which was very rarely), they slavishly called the videos “deceptively edited” – as if “editing” could possibly explain the gruesome images of the violated bodies of these children.
To this day, far too few people are aware of the macabre experimentation going on involving the bodies of children killed during legal abortions. Even fewer are aware that, in many cases, the federal government has funded this experimentation, using taxpayer dollars.
Biden Administration Renews Fetal Research
In two recent reports, Judicial Watch exposed that between 2012 and 2018, the federal government spent tens of thousands of dollars to buy human fetal tissue from California-based Advanced Bioscience Resources (ABR).
In 2018, however, the Trump administration cancelled the contract with ABR. They also clamped down on the funding of fetal tissue research in other ways.
According to the Susan B. Anthony List, the Trump administration committed $20 million to ethical alternatives to fetal tissue; “banned intramural (National Institutes of Health-based) research using tissue from elective abortions”; and convened an Ethics Advisory Board (EAB) to “review all new and renewable requests for research using tissue from elective abortions.” According to the SBA List, that EAB rejected many funding requests from researchers “due to major deficiencies with their consent process for women being solicited for tissue and organ donations.”
In the latest assault on the sanctity of human life, however, the Biden administration has announced that they are reversing some of the key restrictions on fetal tissue research. According to a statement from the Department for Health and Human Services (HHS) released Friday, April 16th, “HHS is reversing its 2019 decision that all research applications for NIH grants and contracts proposing the use of human fetal tissue from elective abortions will be reviewed by an Ethics Advisory Board.”
The move is hardly surprising, given the extreme pro-abortion views of newly confirmed HHS Secretary Xavier Becerra. However, religious leaders and pro-life groups vociferously condemned the decision, which uses our money to fund experiments that are almost too disturbing to fathom.
“The bodies of children killed by abortion deserve the same respect as that of any other person,” said Archbishop Joseph F. Naumann of Kansas City, Kansas, chairman of the U.S. Conference of Catholic Bishops’ Committee on Pro-Life Activities, in a statement. “Our government has no right to treat innocent abortion victims as a commodity that can be scavenged for body parts to be used in research.”
SBA List President Marjorie Dannenfelser noted that the Biden and Harris administration is “working hand-in-glove with radical appointees like Xavier Becerra…to pay back their abortion industry allies and wipe out pro-life progress made under the Trump-Pence administration.”
“Now,” she added, “they would force Americans to be complicit in barbaric experiments using body parts harvested from innocent children killed in abortions, with no limits of any kind. Pro-abortion Democrats push this deeply unpopular agenda at their own political peril.”
Real Children, Real Exploitation
As I have mentioned in the past, I am convinced that one of the reasons that abortion is still legal and widely accepted is that for most people it is basically an abstract issue. We may read about abortion in the news or on social media. But usually, the language used is so clinical, or so familiar, that we fail to grasp the physical reality of what is going on.
For decades now, some pro-life activists have attempted to awaken consciences by confronting people with the concrete, documentary evidence of the brutality of abortion. David Daleiden’s videos remain some of the most powerful recent instances of this strategy.
I have already mentioned perhaps the most heart-wrenching video – the one involving the 20-week-twin, whose mutilated body is captured on camera, while an abortion staff member boasts that sometimes “the organs come out really, really well.”
Another heart-stopping video is not so graphic, visually speaking, but is equally (if not more) damning and horrifying.
In the video, Cate Dyer, the CEO of StemExpress, one of the companies that trades in the bodies of aborted children, describes how her company sometimes ships the “intact” bodies of unborn children to academics at research institutes. Dyer explained that they have to warn the lab technicians on the other end that the shipment is coming, “so they don’t open the box and” scream. Sometimes, she admitted, “their lab techs freak out and have meltdowns.”
Dyer sounds positively contemptuous of the delicate feelings of these lab techs. “Academic labs cannot fly like that, they are just not capable,” Dyer says. “It’s almost like they don’t want to know where it comes from. I can see that.”
In some cases, Dyer says, they receive requests for the “limbs” of aborted children, but with the request that “no hands and feet need to be attached.” At one point Dyer agrees with the “joke” of one of the pro-life investigators that if you’re shipping the bodies of aborted children, they should make sure the “eyes are closed.”
Fighting for the Dignity of Unborn Victims of Abortion
It is important to emphasize that everything that Daleiden exposed in those horrific videos is still happening today. Just a few days ago, Fox News reported that StemExpress had provided the fingers of aborted children to researchers at Stanford University, who injected the human tissue into mice, in an effort to regenerate cartilage.
The papers of one of the studies bluntly explains the origin of the tissue. “Fourteen human fetal samples were obtained from Stemexpress (Folsom, CA) and shipped overnight,” it says. “Samples ranged in age from 10 to 20 weeks of gestation with no restrictions on race or gender.”
“Samples”! In other words: the bodies of children, some of them nearly old enough to live outside the womb had they had a chance to be born!
Although Daleiden’s videos had a huge impact in raising awareness, the powerful pro-abortion legal, media, and political apparatus went into overdrive attempting to crush and discredit him and his videos. Current U.S. Vice President Kamala Harris herself played a key role in persecuting Daleiden, during her time as California Attorney General. Harris colluded with Planned Parenthood executives to launch heavy-handed investigations, which included a raid on Daleiden’s home. Now, unsurprisingly, Harris is once again taking care of her good friends in the abortion industry, making them eligible for our money to support their gruesome and inhuman activities.
It angers me deeply to see Biden, Harris, the FDA, researchers, and biomedical institutes endorse and secure the atrocious actions of this macabre industry. Through words and actions, they blatantly deny human dignity and the personhood of unborn children, determining that they are not only unworthy of life but that these human beings can be treated as commodities – dehumanized and exploited for financial gain and for the benefit of others.
This dangerous mentality – denying the equal dignity of every person, born and unborn – has resulted in atrocious crimes and acts against human life, staining the landscape of human history. Its acceptance, justification, and perpetuation only further degrade our culture and society.
There is a dual injustice inflicted upon the unborn – murder and usury. The unborn has not relinquished its life, nor has the child given permission for its body to be scavenged and trafficked. It is time to end all experimentation on the bodies of unborn children killed by abortion; it has no place in a civilized society. Even if the outcomes of the research are medically helpful, the means are barbaric and evil, and evil means can never be used for a good end.
Human life is always good and from conception has dignity proper to a person that we are obliged to respect and defend, without exception. If a single life is determined to have no value, then no life has value, placing each of us in grave danger, not just the unborn.
Call and write your representatives, senators, and President Biden demanding that the bodies of unborn children killed by abortion be given the same respect as that of any other person. And at the same time let us add, stop the violence of abortion, and end the industry of death and exploitation it has created.
Did you know that Planned Parenthood, the country’s largest abortion provider, has infiltrated the public school system? In their own sneaky and conniving way, the abortion giant has convinced school administrations through veiled language that they can provide important assistance to their students.
For years, we’ve been telling you how Planned Parenthood is targeting children in an attempt to normalize abortion and perhaps, it hopes, create future customers to feed its unholy empire. We told you how a Planned Parenthood representative suggested the need for a “Disney princess who’s had an abortion” to plant the rotten seeds of abortion. Now the abortion giant has its sights set directly on your schools.
This year in New York, The Clarence Central School District’s Director of Health invited Planned Parenthood to give a presentation on their “services offered” to impressionable students in high school health class.
A parent contacted us after receiving a permission slip to allow her child to attend Planned Parenthood’s presentation because she was concerned that it would cover the topic of abortion. In its description of the presentation, the permission slip stated that the presentation covers “[s]ervices offered (Information about STI’s, getting STI tests, and birth control and many other services are mentioned).” It conveniently left off that abortion would in fact be addressed, leaving the parent to question the school’s apparent deception tactic.
The parent immediately reached out to the school district’s health director requesting permission to view the presentation before she signed the permission slip, which was her right as a parent. However, she was groundlessly denied any access to the presentation by the director, the superintendent, and the principal. According to the school, they had been giving this presentation for years, and it was never deemed a problem.
Being equipped with our letter and knowledge that the school was violating federal law, the parent again insisted that the health director allow her to review the presentation. She also requested that the school add the verbiage “many other services are mentioned, including abortion” onto future permission slips so that parents are no longer being deceived as to the true intentions of this vile presentation.
Not backing down, the parent made a compelling argument that there should be alternative resources for students, like a crisis-pregnancy center presentation, that explain how other options are available for young pregnant mothers.
We are proud to say that this parent was finally granted access to the materials, and the health director even agreed to include abortion as a topic on the permission slip for future classes. This is what advocating for your child can do. The parent has informed us that her work is still not done—she is planning on bringing this issue before the school board and insisting on alternative curriculums.
Normalizing abortion at a young age seems to be the name of the game for Planned Parenthood’s agenda, and it’s up to informed parents like you to advocate on behalf of your children. Don’t forget that these are YOUR tax dollars at work funding these reprehensible presentations and indoctrinating unsuspecting school children. This is why the ACLJ has redoubled our efforts to defund Planned Parenthood.
You can join the fight and be vigilant for your child and your community:
Start with understanding your right to inspect all curricula using the ACLJ’s parental rights memo. Ask to view all guest presentations, and know what your child is learning.
Once your information is compiled, use a grassroots strategy and inform other parents—start a petition, hold a parents conference, and bring your concerns before the school board!
Call on your local pro-life community to get more involved—find a local crisis pregnancy center willing to present at a school. Help them build a curriculum that could be presented as an alternative to Planned Parenthood’s presentation and provide it to the school board. Let them know that there are other options!
It’s time for the pro-life community to come alive and protect our innocent children. You can effect change in your cities’ and counties’ public schools, and the ACLJ is here to support you.
LifeNews Note: Christina Stierhoff writes for ACLJ.
April 19, 2021 (LifeSiteNews) – Thousands of women around the world are reporting disrupted menstrual cycles after receiving injections of COVID-19 vaccines.
The U.K.’s government vaccine adverse event system has collected more than 2,200 reports of reproductive disorders after coronavirus injections, including excessive or absent menstrual bleeding, delayed menstruation, vaginal hemorrhaging, miscarriages, and stillbirths.
In the U.K., the Yellow Card adverse event reporting system includes 2,233 reports of “reproductive and breast disorders” after reception of AstraZeneca and Pfizer vaccines.
The U.K. Yellow Card program reports 1,465 reactions involving reproductive systems as well as 19 “spontaneous abortions” (miscarriages), five premature labors, and two stillbirths in association with the AstraZeneca vaccine as of April 5.
The reports include:
255 cases of abnormal uterine bleeding
242 reports of unusual breast pain and swelling
182 women who experienced absent or delayed menstruation
175 cases of heavy menstrual bleeding
165 cases of vaginal hemorrhaging
55 reports of genital swelling, lesions, rashes or ulcerations
19 cases of postmenopausal hemorrhaging
12 cases of premature or “artificial” menopause
Another 768 reports of “reproductive and breast disorders” have been reported for Pfizer’s coronavirus vaccine in the U.K., as well as 42 “spontaneous abortions,” five premature labor onsets, and two stillbirths. These include:
265 reports of breast changes, including 22 reports of breast cancer and 177 reports of breast pain
134 cases of irregular menstrual bleeding
127 reports of absent or light menstruation
92 cases of heavy bleeding
73 cases of vaginal hemorrhaging
5 reports of postmenopausal hemorrhaging
5 cases of premature or ‘artificial’ menopause
Male reproductive disorders are fewer, but 75 Yellow Card reports on AstraZeneca’s vaccine include 63 erectile dysfunction reactions, 50 cases of testicular pain, 11 cases of scrotal pain and swelling, and three reports of haematospermia, or blood in sperm.
Pfizer’s Yellow Card includes 22 reports of testicular and scrotal pain and 21 counts of sexual dysfunction.
None of the Yellow Card reports reveal details about the individuals who experienced the side effects. However, 32-year-old Lorri Emmily Lowe of the U.K. said she felt cramping three days after receiving AstraZeneca’s vaccine in February.
“I also had a completely unusable arm for 24 hours,” she told LifeSiteNews. “It was excruciating and I was pretty much bed-bound just because of the arm. I had to laugh like a mad person for strange pain.”
Lowe said she felt “out of sorts” for about three days but what worried her most was that her menstrual cycle that had been predictably “perfect” for 10 years (not including pregnancies) suddenly vanished.
She had a strange “spotting” episode that she has never had in her life before and her period was five days late. “I’m never late. I’ve been consistent for many, many years,” she said, and when it did come on it was “super heavy and lasted eight days.”
Lowe’s cycle has returned to normal now but is quite heavy. “I do not see how out of the six years since I’ve birthed a baby, that was the one month my cycle decided to go haywire.”
The U.S. Vaccine Adverse Event Reporting System (VAERS) documents similar reproductive complications.
“My period has always been regular. Expected period was to begin on 02/22/2021 (after second vaccine dose) and bleeding did not occur,” a 25-year-old woman from Pennsylvania, who received both doses of Moderna’s vaccine, reported to the system, which is run by the U.S. Centers for Disease Control and Prevention.
One VAERS report describes a 51-year-old woman from Georgia who received a first dose of Pfizer’s vaccine in January and within three days developed a blood rash (petechiae) on her ankles that gradually spread to her knees. She was admitted to the hospital five days after her vaccine with vaginal bleeding and anemia. She was diagnosed with Disseminated Intravascular Coagulation, a blood clotting disorder, which led to her worsening liver function, painful leg swelling, and purple discoloration. She died February 11. [VAERS ID 1032163-1]
Write-up: Patient received dose #1 of COVID-19 vaccine on 1/16/21. Within 3 days, she developed petechiae up to ankles, later rising up to her knees. Pt admitted to hospital on 2/6/21 for symptomatic anemia 2/2 vaginal bleeding. Patient received 4 units FFP, 4 units PRBC, 1 unit cryoprecipitate, and vitamin K 5 mg IV. Also started on medroxyprogesterone 20 mg PO TID. Alectinib d/ced due to worsening liver function. Evalauted by OB/GYN and Hematology. Diagnosed with DIC. Patient with worsening bilateral lower extremity edema and purpura with pain and weakness. Palliative care consulted. Patient passed away on 2/11.
A 48-year-old woman from Texas received a first dose of Moderna’s COVID-19 vaccine in January and 13 days later was hospitalized with heavy vaginal bleeding and a critically low platelet count. [VAERS ID 0958885-1]
Write-up: The patient was seen in my office on 1/19/21 with complaint of heavy vaginal bleeding. A CBC was obtained which revealed an H/H of 12.2/36.1 and a platelet count of 1 (not 1K, but 1 platelet!) and this was confirmed on smear review. She was immediately sent to the Hospital ED and repeat CBC confirmed the critically low platelet count. She is currently hospitalized and she has received platelet transfusions but her platelet count is still critically low. She is also receiving steroids and immunoglobulin and is under the care of MD (Heme/Onc)
VAERS also includes 26 reports of miscarriage or other “fetal demise” events after COVID vaccinations.
A 40-year-old pregnant physician from California described a patient’s first dose of Pfizer’s vaccine as a “lethal event for the fetus” that led to her delivering the baby stillborn six days later. [VAERS ID 958755]
Write-up: Pt was 18 weeks pregnant at the time of the vaccine. Second pregnancy. Pt is a physician. Pregnancy was entirely normal up to that time. On 1/18/2021, she began to have heavy vaginal bleeding probably due to a placental abruption and subsequently delivered at 18 weeks. Baby was stillborn. Ultrasound done 1/15/2021 normal. Lethal event for the fetus. The patient did well.
“Something insulted this placenta to lead to fetal demise,” read another VAERS report on a 24-year-old woman who began bleeding two weeks after receiving a first dose of Pfizer’s COVID vaccine in February. [VAERS ID 1074788 ]
Write-up: At 8 weeks pregnancy (2 weeks after first shot) started bleeding and had a subchorionic hematoma. By 10 week subchorionic hematoma resolved. Received second shot and of Feb. 1 week later, at 12 weeks pregnancy , fetus had no heart beat! It measured normal size (as expected) and limited normal first trimester anatomy by ultrasound. But NO heart beat. Something insulted this placenta to lead to fetal demise.
In most cases, deaths of unborn babies were recorded only as “life-threatening” or as “hospitalizations” for the mother, as in the case of a 35-year-old Ohio woman. The woman lost her baby after she was vaccinated with a first dose of Moderna’s COVID vaccine on the same day that an ultrasound and genetic screening showed the 20-week-old baby to be in good health. [VAERS ID 1033412]
Write-up: 20 weeks gestation at time of vaccine administration. Saw OB that morning (1/12/21), normal exam and fetal heart rate. Normal anatomy scan 1/8/21, normal genetic screening. Fetal demise noted at 24 week OB visit on 2/9/21, stillborn baby delivered 2/12/21.
Moderna and Pfizer did not immediately reply to questions about their vaccine and fertility. “It has been incorrectly suggested that COVID-19 vaccines will cause infertility because of a shared amino acid sequence in the spike protein of SARS-CoV-2 and a placental protein,” Jerica Pitts, a Pfizer representative, claimed in an email to the Associated Press in December, however. “The sequence, however, is too short to plausibly give rise to autoimmunity.”
Animal studies to investigate the cross reaction of spike protein targeting COVID vaccines with Syncytin-1 have not been conducted to determine if autoimmunity can arise or not.
Fertility-disrupting ingredient in AstraZeneca coronavirus vaccine also present in HPV, flu shots
No mechanism to explain disrupted menstrual cycles or reproductive organ pain in males and females has been offered and public discussion of the reproductive reports has been minimal. However, polysorbate 80, a chemical that has exhibited delayed ovarian toxicity to rat ovaries at all injected doses tested over a tenfold range is an ingredient in AstraZeneca’s COVID vaccine, along with other vaccines including for influenza and HPV.
Concerns have been raised in the past about these vaccines’ impact on reproductive abilities. An Australian case study in the British Medical Journal described a 16-year-old girl whose regular menstruation ceased after receiving HPV vaccines and she was diagnosed with premature ovarian failure.
In 2014, Australian doctors published a case series of more teens who had entered premature menopause — a phenomenon they described as ordinarily “so rare as to be also unknown.” They raised troubling questions about some HPV vaccine ingredients’ documented risks to fertility including Polysorbate-80, cited serious deficiencies in preliminary vaccine trials and concluded that further research was “urgently required.”
Between 2006 and 2014, VAERS cited 48 cases of ovarian damage associated with autoimmune reactions in HPV vaccine recipients. Between 2006 and May 2018, VAERS catalogued reports of spontaneous abortion (256 cases), amenorrhea (172 cases), and irregular menstruation (172 cases).
A 2020 study of adverse event reports in VAERS reported a statistically significant association between the quadrivalent HPV vaccine (Gardasil) and premature ovarian insufficiency, including amenorrhea, irregular menstruation, and premature menopause.
Like the U.S. Vaccine Adverse Event Reporting System (VAERS), the U.K. Yellow Card program collects voluntary reports and does not prove causal connection between the vaccination and the reported symptom. As a voluntary system, however, it tends to capture only a fraction of adverse events. A Harvard Pilgrim Healthcare study found that fewer than 1 percent of vaccine adverse events are reported to VAERS, which means that the actual numbers of adverse reactions to vaccines are one to two orders of magnitude higher.
Former Pfizer VP’s warning of potential impact on fertility
In December, former Pfizer allergist and immunologist Michael Yeadon and German lung specialist Wolfgang Wodarg wrote a petition to the European Medicines Agency (EMA) in which they suggested that any vaccine against coronavirus spike protein, if it were to cross react with a similar human protein called Syncitin-1 in placental tissue, could result in loss of pregnancy and continued sterility in women who developed an autoimmune response to Syncytin-1 as a result of vaccination.
“There is no indication whether antibodies against spike proteins of SARS viruses would also act like anti-Syncytin-1 antibodies. However, if this were to be the case this would then also prevent the formation of a placenta which would result in vaccinated women essentially becoming infertile,” the doctors wrote in their urgent letter to the EMA.
Since pregnant and breastfeeding women were excluded from vaccine trials and women of childbearing age were included only if they were using pharmaceutical contraception, the letter added: “This means that it could take a relatively long time before a noticeable number of cases of postvaccination infertility could be observed.”
UK Government: ‘Insufficient evidence to recommend routine use of COVID-19 vaccines during pregnancy’
The menstrual side effects are getting traction on social media where hundreds of women have reported odd symptoms or gone looking for answers about their menstrual irregularities in the wake of receiving coronavirus vaccines. Sharon McGlinchey Seymour posted publicly on a COVID-19 vaccine side effects Facebook page that her obstetrician told her that she was seeing “lots” of women with complaints of uncommon hemorrhaging.
Dr. Kate Clancy, an associate professor at the University of Illinois, tweeted in February that she had been hearing of women who were having heavy periods after their shots. “I’m a week and a half out from dose 1 of Moderna, got my period maybe a day or so early, and am gushing like I’m in my 20s again,” she said.
Another woman who said she will be 65 in July replied that she started menstruating after the shot “fairly heavy.”
In Israel, the Health Ministry reported that it had received 13 reports of women with heavy and irregular menstrual bleeding by mid-February, though women under age 45 had not been eligible to receive the vaccine until the end of January.
The Health Ministry said that Pfizer, whose vaccine was in circulation in Israel, had not reported any menstrual irregularities in its vaccine’s clinical trials.
Media relations officer Fiona Cookson of AstraZeneca in the U.K. said the company does not have a formal response about the reproductive complaints and that the U.K. Government Medicines and Healthcare products Regulatory Agency (MHRA) would be responsible for monitoring and oversight of such side effects, rather than the vaccine manufacturer.
The Yellow Card reporting website states that 20.6 million first doses and one million second doses of AstraZeneca’s vaccine were distributed in the U.K. by April 5.
Moderna and Pfizer did not immediately reply to questions about reproductive side effects of their vaccines.
The U.K. Green Book, described as a “vital guide for public health professionals administering vaccines in the UK,” does not mention menstruation except for to say that “routine questioning about last menstrual period and/or pregnancy testing is not required before offering the vaccine.”
“As with most pharmaceutical products, specific clinical trials of COVID-19 vaccine in pregnancy have not been carried out,” according to the vaccine Green Book. As with other vaccines, no investigation of long-term effects on fertility or cancer is required for licensing or emergency use authorization of vaccinations.
The U.K. Green Book states that “developmental and reproductivity testing of the Pfizer BioNTech, Moderna and AstraZeneca vaccines in animals have not raised any concerns” and vaccines that use adenovirus vectors, similar to those used in the AstraZeneca COVID-19 vaccine, have been widely used to vaccinate women against Ebola” and “form trials of these vaccines in pregnancy are due to proceed.”
“Although the available data do not indicate any harm to pregnancy, there is insufficient evidence to recommend routine use of COVID-19 vaccines during pregnancy,” according to the government booklet. Yet the standard of practice has been to recommend the vaccine if it is thought that its benefits would outweigh its risks.
It’s ‘lunacy to get this experimental vaccine if you’re a young female’
Dr. Simone Gold of America’s Frontline Doctors has stressed the experimental nature of the vaccines, which have been granted Emergency Use Authorization only by the U.S. Food and Drug Administration, and are still undergoing phase III clinical trials.
“We know that the survivability rate [from COVID-19] for women of child-bearing age, as well as children, is exceedingly high at over 99.98% per the CDC even without treatment, and certainly without a new and unproven biological agent that is still only available under an Emergency Use Authorization (EUA) as an investigational treatment.,” Gold said in an emailed statement to LifeSiteNews. Using simple logic for a risk assessment would make the decision to give any of the COVID experimental vaccines to a pregnant woman extraordinarily reckless.”
While a year ago, women who were pregnant or planned on conceiving were hesitant to eat tuna because of its mercury content or to take a Tylenol, now they are being badgered into taking experimental injections.
“The desire to get pregnant is overwhelming. It’s not something that can be replaced by something else. It’s not something you can mess around with,” Gold told Michelle Malkin in an interview in February. “The cascade of events that has to go on in the human body to get pregnant and to maintain a pregnancy throughout is incredibly complicated and that’s why historically doctors and scientists have always excluded pregnant women from clinical trials because we don’t know all the details of what we don’t know.”
“It’s lunacy to get this experimental vaccine if you’re a young female,” Gold said. “I would flat-out forbid any young female from getting this vaccine and it’s very unethical for any physician to offer this to any young female.”
LifeSiteNews has produced an extensive COVID-19 vaccines resources page. View it here.
It was 1942 and a chemistry professor from Pennsylvania was looking for a cheap source of progesterone. The hormone had many uses at the time, including preventing miscarriages and treating women going through menopause.
In fact, Russell Marker already had invented a way to make progesterone from a chemical in certain plants. One option was the tubers of wild Japanese yams. But these were thin and weedy – they just didn’t contain enough of the hormone.
Marker scoured the land for alternatives, examining more than 400 species, but to no avail. Then he stumbled upon a drawing in an obscure botany book. This yam had fat, knobbly roots that reportedly weighed up to 100 kg (220lbs). He travelled to its native Mexico and smuggled one out of the country.
With an affordable source of progesterone found, researchers turned to its uses as a contraceptive. The birth control pill hit the market less than a decade later. Marker, on the other hand, mysteriously disappeared from public life and became obsessed with collecting silver.
The economic and social side effects of the pill were as profound as they are well-documented. Sex could be enjoyed without fear of pregnancy. Suddenly women could devote their 20s and 30s to furthering their education and careers, rather than housework and nappies.
But right from the beginning, the pill has had a secret.
In recent years, scientists have started to realise that the brains of women on the pill look fundamentally different. Compared to women who aren’t taking hormones, some regions of their brains seem to be more typically ‘male’.
There are behavioral changes, too. Women on certain types of pill aren’t as good at coming up with words – something our gender are usually highly skilled at. On the other hand, they’re better at mentally rotating objects, as is often the case in men. Finally, women on a different type of pill are better at recognising faces – something women are usually good at.
Confused? So are scientists. What’s going on?
We’re often told that the pill contains oestrogen and progesterone. But no pill contains either hormone
We’re often told that the pill contains oestrogen and progesterone. But no pill contains either hormone.
That is because, when taken orally, oestrogen and progesterone break down too quickly to be practical. Instead, the pill contains synthetic versions, which are built from more stable hormones that have been altered to mimic the hormones.
Every brand of combined pill on the market contains the same type of synthetic oestrogen, ethinyl estradiol, and one of eight synthetic progesterones, called progestins. Ethinyl estradiol prevents the body from releasing an egg every month, while progestins thicken the mucus at the entrance to the cervix and conspire to make the womb inhospitable. Even if an egg slips out and becomes fertilised, it won’t be able to settle down and start growing.
So far, so good. But though the hormones are effective at preventing pregnancy, they aren’t perfect matches for our natural hormones. The end result is that these synthetic versions also have effects that you would never get from raw progesterone.
The internet is awash with anecdotal reports of acne, sweating and unwanted hair growth after going on the pill. One women described sprouting hairs all over her cheeks, while another came down with “pizza face” after starting a new brand. These ‘masculine’ effects have been well-studied by scientists, and they are real: certain kinds of pill really do make them worse, especially in susceptible women.
But the reason is surprising. According to a study from 2012, 83% of US women who are on the pill are taking a version that contains progestins made from male hormones. This includes the popular brands Ortho Tri-Cyclen, Loestrin FE 1/20 and Tri-Sprintec®, among many others.
The male hormone that these pills use is a close relative of testosterone called nandrolone. A potent androgen (a hormone that influences the development of the male reproductive system), it can lead to the development of typically male characteristics.
It’s actually used for doping in men sometimes — Belinda Pletzer
“It’s actually used for doping in men sometimes,” says Belinda Pletzer, a cognitive neuroscientist at the University of Salzburg, Austria. It helps build muscle, so it’s popular with powerlifters and boxers: the former heavyweight world champion Tyson Fury recently served a two-year suspension after testing positive for the steroid in 2015 (he claimed it entered his system after eating the meat of an uncastrated wild boar.)
We’ve known about these side effects for decades: the first progestin ever made, norethindrone, was androgenic.
Back in the 1940s, 50s and 60s, pregnant women sometimes took norethindrone in large doses to help prevent miscarriage. But the hormone also caused some unsettling changes to their bodies.
The women were sweatier, hairier and spottier. Some noticed that their voices had deepened. Nearly one in five baby girls born to mothers taking it had masculinised genitals. Some of these unlucky children required surgery.
Today androgenic progestins are much less androgenic. The doses in contraceptive pills are much smaller, and the hormones are usually combined with synthetic oestrogen, which cancels out many of the masculine effects on our bodies.
But there are some side effects.
“These progestins, which were decreased in dose over the years, are still related to the chemical structure of testosterone. All the derivatives came out to levonorgestrel, which is the most used or known of the progestins,” says Regine Sitruk-Ware, a reproductive endocrinologist at the Population Council, New York. “It is still androgenic by itself, by the fact that it can bind to the androgen receptors.”
Over the years, there have been several generations of progestins. Though the earlier ones are nearly all androgenic, more recently scientists have developed versions made from synthetic progesterone, instead. These have the opposite effects – they are often prescribed to treat acne or excessive hair growth because they are ‘feminising’ (though they, too, can have undesireable side effects resulting from a hormonal imbalance). Some examples include Yasmin® and Ocella™.
Generally speaking, the older, cheaper brands of pill tend to contain androgenic hormones, while newer, more expensive ones tend to contain anti-androgens. This may be one reason that just 17% of women on the combined pill in the US take the anti-androgenic versions.
There are androgen receptors all over the body, particularly in the sweat glands and hair follicles, which explains why androgenic progestins can make some women sweatier, hairier and spottier. But these powerful, gender-bending steroids also affect the brain.
In men, the androgens released at puberty are known to remodel the brain. This is also true in women, where relatively small quantities of testosterone can cause certain areas to shrink and others to grow.
Given what we know about the power of these hormones, it’s perhaps surprising that until recently, no one had checked if progestins made from male hormones might have an impact.
“There has been a lot of research on their physical side effects,” says Pletzer. “There’s also been research on the emotional side effects, because that’s something that women keep complaining about. But very few studies have looked at the brain and cognition.”
But when she realised she was excluding those on the pill, she asked herself why. “We know that the steroids our own body produces, such as progesterone and testosterone, affect the brain. So of course I would expect any synthetic hormones to have an effect as well,” she says.
Pletzer abandoned her original idea and set out to test the effects of the pill instead. She recruited a mixture of men and women on and off hormonal contraception, then scanned their brains.
What she found was striking. The scans revealed that several brain areas were larger in the women on the pill, compared to those of women who weren’t. These areas just so happened to be larger in men than women, too.
The study involved a relatively small sample and didn’t separate androgenic and anti-androgenic contraception, so Pletzer cautions against reading too much into the results. But other research has hinted that both types of hormones actually may be changing our behavior.
Other studies have found that women on oral contraception remember emotional stories more like men
Other studies have found that women on oral contraception remember emotional stories more like men – recalling the gist more than the details. They’re also not as good at recognising emotions in others, such as anger, sadness, or disgust – just like men. It looks suspiciously like certain types of pill are “masculinising” women’s brains.
Crucially, these changes seemed to be affecting their behaviour.
Two brain areas were particularly engorged: the fusiform face area, a region about the size of a pea that processes facial information (from photographs of friends to cartoons), and the parahippocampal place area, which important for recognising places (such as cityscapes). These women were also better at recognising faces.
Facial recognition is something women are usually highly skilled at – even as babies – so this fits with the picture of oral contraceptives subtly influencing our brains. In this case, the anti-androgenic pills may be having a “feminising” effect.
Just as before, several brain areas were also larger in women on androgenic pills, including many which are typically so in men. The longer the women had been on the pill, the larger these areas were.
To complicate matters further, all combined pills contain synthetic oestrogen, which is feminising. This means that the same women may be experiencing both ‘feminising’ and ‘masculinising’ effects on their brains at the same time.
No one could have predicted that an ugly yam would give rise to a feminist revolution. The pill has repeatedly been called the greatest invention of the 20th Century and is said to be responsible for a third of the increase in women’s wages since the 1960s.
But contraceptive pills may have a darker side. As Pletzer wrote in 2014, when athletes take steroids we call it ‘doping’ – it’s considered abuse and strongly condemned by society. But we’re happy for millions of women to take these hormones every day, sometimes right through from puberty to menopause.
Scientists don’t yet know if any of the pill’s effects on the brain have much of an impact on our behaviour. But perhaps it is time we put it to the test.
Correction: An earlier version of this story implied that the ‘feminising’ effects of pills like Yasmin could lead to hair loss; while some women do experience hair loss while taking birth control pills, this tends to be for broader reasons such as a resulting hormonal balance. This has been changed.
One of the great achievements of Christian civilization has been the development of a thorough and robust account of the dignity of the human person – a dignity that outstrips that of any other being in physical creation, to the extent that the human person is viewed as an image of God Himself.
“The divine image is present in every man,” states the Catechism of the Catholic Church. “It shines forth in the communion of persons, in the likeness of the unity of the divine persons among themselves.” (no. 1702)
Those of us living in a historical time and part of the world so thoroughly indebted to the Judeo-Christian worldview often simply take for granted this view of the human person, failing to appreciate how unique and monumental it is in the history of the human race. Nowadays, even many (although not all) of the most hard-boiled atheists will profess to believe in the “dignity of the human person,” not pausing to appreciate that it is, in large measure, thanks to Christianity that this truth is so widely acknowledged.
It is true that in an increasing number of cases, certain ideologues are openly promoting a utilitarian or eugenic philosophy that measures the worth of human beings based upon various criteria (i.e., health, intelligence, productivity, degree of personal happiness, etc.). However, for the most part people still begin with the basic assumption of the Judeo-Christian worldview – that even those people who seem “useless,” or who have done great harm to others, are owed a basic respect, and certain rights, that they can never lose. We see this instinct manifested, for instance, in the movement against the use of the death penalty, even in the cases of the worst criminals – murderers.
Unfortunately, however, human beings are often inconsistent, and are blinded by their prejudices and selfish desires. In the past century, most of the world, including much of the Christian West, has carved out certain systemic “exceptions” to the dignity of the human person – escaping the duty of respect owed to other persons, often by simply denying that the other is a person to begin with. The primary victim of this movement has been the unborn child, although it is increasingly extending to the disabled, sick, and elderly.
Never before has there been more evidence in support of the humanity (and, therefore, the personhood) of the unborn child. And yet, never since ancient pagan times has the unborn child been so unprotected. This “de-personing” of the unborn child is simply the latest manifestation of the same tendency that led swathes of the world to deny the personhood and worth of black people and other enslaved races. It is the old, pagan view of the human being, escaping from the protective umbrella of Judeo-Christian civilization.
As Pope St. John Paul II wrote in Evangelium Vitae, “If such great care must be taken to respect every life, even that of criminals and unjust aggressors, the commandment ‘You shall not kill’ has absolute value when it refers to the innocent person. And all the more so in the case of weak and defenseless human beings, who find their ultimate defense against the arrogance and caprice of others only in the absolute binding force of God’s commandment.” (no. 57)
More Gaslighting: Abortion as a ‘Human Right’
Last week I wrote about the “gaslighting” of the gender ideologues, who deny the most self-evident truths – e.g., that a man cannot become a woman simply by wanting to – and then accuse those who disagree with them of being delusional or evil.
The same tendency toward gaslighting is present within the pro-abortion movement. Pro-abortion activists will call the baby in the womb – which we can now see on the ultrasound screen with our own eyes – a “blob of tissue,” and then turn around and accuse pro-lifers, who protest that this simply isn’t true, of being “anti-science” or not supporting “women’s rights.”
The pro-abortion position is filled with such flagrant absurdities and contradictions. Consider this recent document from Antony Blinken, President Biden’s new Secretary of State, which suggests that access to abortion and contraception is a “human right.”
As Live Action reports, during the Trump administration the human rights report prepared by the State Department did not mention women not having access to abortion or contraception as being a human rights violation. Blinken, however, indicated that a Biden administration will be reversing course.
“For many years, our human rights reports contained a section on reproductive health, including information about…discrimination against women in accessing sexual and reproductive health care, and government policies about access to contraception,” Blinken said in a statement. “And we are restoring the practice of documenting these rights in 2021 and future years.”
It is important to note that the phrase “sexual and reproductive health” is widely recognized as being a euphemism that includes access to abortion and contraception. In a statement to reporters, Blinken affirmed, “women’s rights – including sexual and reproductive rights – are human rights.”
Unpack the euphemism, and what Blinken is saying is: “The right to kill other innocent human beings is a ‘human right.’” Absurd. Especially when viewed from the perspective of the unborn child, who is stripped of that most fundamental of all human rights – the right to life – in the name of “human rights.”
Unfortunately, this is only one of several extremist attacks on the dignity of the unborn from the Biden administration in recent days. In a move that comes as no surprise, Biden has instructed the Department of Health and Human Services (HHS) to review President Trump’s Protect Life rule. That rule had forbidden Title X funding from going to health care providers who provide or refer for abortion. Because of the rule, Planned Parenthood had been withdrawn from Title X, losing tens of millions in taxpayer funding. That will now be reversed.
Recently, the Senate confirmed President Biden’s pick for the secretary of the HHS. Xavier Becerra has been described as a pro-abortion “extremist.” A letter signed by 60 pro-life leaders (HLI being one) called Becerra “an enemy to every pro-life policy and law” who has “demonstrated complete disregard for the religious and moral convictions of those opposed to the brutal act of abortion.”
Becerra previously served for 24 years in Congress. He infamously voted against the Hyde Amendment, which bans government funding for abortion. He also voted against the Partial-Birth Abortion Ban Act in 2003 and the Born-Alive Abortion Survivors Protection Act. He also twice voted against a law that would ban abortions at five months in pregnancy. In other words, he’s never met an abortion he didn’t support.
And yet, this is the man that Biden has chosen to promote “health”! Certainly not the health of hundreds of thousands of unborn children who are murdered every year in our country.
Unfortunately, Becerra, like Biden, is a lifelong “Catholic.”
In an astonishing statement, Sister Carol Keehan, the well-known Catholic religious sister who headed up the Catholic Health Association for a decade and a half, said she was “relieved and thrilled” at Becerra’s nomination. Sister Keehan called Becerra “a leader whose character is rooted in his Catholic upbringing and values.”
With Catholic leaders like this, who needs enemies!
The simple fact is that abortion is certainly the gravest, and most pervasive violation of human rights and the dignity of the human person being perpetrated in our world today. No one who actively promotes this enormous evil, conducted on an industrial scale, can possibly lay claim to being a “devout” Catholic.
“The deliberate decision to deprive an innocent human being of his life is always morally evil and can never be licit either as an end in itself or as a means to a good end,” said Pope St. John Paul II in Evangelium Vitae. “It is in fact a grave act of disobedience to the moral law, and indeed to God himself, the author and guarantor of that law; it contradicts the fundamental virtues of justice and charity.” (no. 57)
Fortunately, there are some Church leaders left who are willing to call a spade a spade. In a recent statement, Cardinal Raymond Burke once again reiterated the long-established teaching that Catholics who publicly support and promote abortion and other grave intrinsic evils automatically excommunicate themselves.
Cardinal Burke also clarified that “those who have been excommunicated or interdicted after the imposition or declaration of the penalty and others obstinately persevering in grave sin are not to be admitted to Holy Communion.”
To those who argue that the Church is using the Eucharist as a “political weapon” when it denies Communion to pro-abortion Catholic politicians, Cardinal Burke countered: “It is rather the Catholic politician, who publicly and obstinately promotes what is contrary to the moral law and yet dares to receive sacrilegiously Holy Communion, who uses the Holy Eucharist for political purposes. In other words, the politician presents himself or herself as a devout Catholic, while the truth is completely otherwise.”
Bishop Thomas J. Olmsted of the Diocese of Phoenix added his voice to this debate in his Apostolic Exhortation, Veneremur Cernui, published on April 1. “Holy Communion is reserved,” says Bishop Olmsted, “for those, who with God’s grace make a sincere effort to live this union with Christ and His Church by adhering to all that the Catholic Church believes and proclaims to be revealed by God.” This is, he emphasizes, why the “Church requires Catholic leaders who have publicly supported gravely immoral laws such as abortion and euthanasia to refrain from receiving Holy Communion until they publicly repent and receive the Sacrament of Penance.”
Moreover, states the bishop, “not all moral issues have the same weight as abortion and euthanasia. The Church teaches that abortion or euthanasia is an intrinsically grave sin and that there is a grave and clear obligation for all Catholics to oppose them by conscientious objection.” Quoting Evangelium Vitae, he adds that, “in the case of an intrinsically unjust law, such as a law permitting abortion or euthanasia, it is therefore never licit to obey it, or to ‘take part in a propaganda campaign in favour of such a law or vote for it.’”
If the Judeo-Christian teaching on the dignity of the human person is one of the most precious gifts of Christ and His Church to the human race, it must also be protected by Christians with enormous fervor, lest it be lost and forgotten. In these troubled times amongst rampant confusion and the torrential assault against truth, bereft of sound doctrinal teaching, the leadership of Cardinal Burke and Bishop Olmsted is a welcomed breath of fresh air. Their statements are simply an acknowledgement that no Catholic can support the systematic assault on the dignity of a whole category of persons, and still claim to be a faithful Catholic. The contradiction is simply too extreme, too deep.
In the face of the Biden administration’s assault on human dignity, we must, all of us, respond to Pope St. John Paul II’s “pressing appeal” in Evangelium Vitae: to “respect, protect, love and serve life, every human life! Only in this direction will you find justice, development, true freedom, peace and happiness!” (no.5)
A letter sent by the U.S. Food and Drug Administration (FDA) to the pro-abortion American College of Obstetrics and Gynecology (ACOG) indicates that the agency plans to “exercise enforcement discretion” in the dispensing of the abortion pill by mail during the COVID-19 pandemic. In other words, the FDA intends to continue to allow the distribution of these dangerous abortion drugs by mail for the duration of the pandemic.
The decision follows ongoing litigation filed by ACOG against the FDA asserting that requiring mifepristone (the abortion pill) to be dispensed to abortion clients in person during the COVID-19 pandemic is an undue burden. Under FDA’s REMS (Risk Evaluation and Mitigation Strategy), the abortion pill mifepristone (used in a regimen with misoprostol) must be dispensed by a certified prescriber at an approved hospital or clinic and is prohibited from being sold online or in a pharmacy.
Live Action News has previously documented how the abortion industry used the COVID-19 pandemic to lift the REMS and expand access to the abortion pill. In fact, well before the pandemic, the industry expanded its abortion pill clinical trials and then rolled out a “no test” abortion pill protocol, which some medical professionals have said endangers women. Around the same time frame, the ACOG also changed its recommendations to line up exactly with the abortion industry’s attempts to expand access to the abortion pill.
The ACOG is not an impartial medical organization; it is radically pro-abortion. It has been funded by organizations that directly received funds from U.S. abortion pill manufacturer Danco Laboratories. ACOG is also funded by the David and Lucile Packard Foundation, a Danco investor. In 2018, the ACOG received $1.4 million from the Buffett Foundation — a known abortion philanthropist —and has received hundreds of thousands from the foundation every year for the past several years. Buffett was also one of the first investors in Danco.
The letter was sent by Janet Woodcock, Acting Commissioner of the FDA under the Biden administration who previously served as Director of the FDA’s Center for Drug Evaluation and Research (CDER) when the Agency approved the abortion pill.
FDA letter to ACOG allows dispensing of abortion pill by mail outside Rems during COVID-19 Image Twitter
In the letter, Woodcock claims that CDER reviewed “postmarketing adverse events that reportedly occurred from January 27, 2020 – January 12, 2021” and found the “small number of adverse events reported to FDA during the COVID-19 public health emergency (PHE) provided no indication that any program deviation or noncompliance with the Mifepristone REMS contributed to the reported adverse events.”
What Woodcock failed to note is that changes made to the REMS by the FDA in 2016 no longer required the manufacturer of the abortion pill, Danco Laboratories or its generic GenBioPro to report non-fatal adverse effects.
The letter also indicates that CDER reviewed at least four studies published around the dispensing of the abortion pill via telemedicine. One of those “studies” was based on a TelAbortion Project sponsored by Gynuity Health Projects. Live Action News has previously documented the funding streams and conflicts of interest surrounding multiple abortion pill studies like this one.
The letter made clear that the FDA planned to “exercise enforcement discretion” with respect to in-person requirements as well as the dispensing of the abortion pill through the mail.
Provided the other requirements of the Mifepristone REMS are met and given that the in-person dispensing of mifepristone… may present additional COVID-related risks to patients and healthcare personnel… CDER intends to exercise enforcement discretion during the COVID-19 PHE with respect to the in-person dispensing requirement… [and] with respect to the dispensing of mifepristone through the mail either by or under the supervision of a certified prescriber or through a mail order pharmacy when such dispensing is done under the supervision of a certified prescriber.
SBA List president Marjorie Dannenfelser called the FDA’s decision “pure politics,” adding, “The Biden-Harris FDA is acting in the financial interest of the big abortion lobby. This is flagrant and dangerous disregard for the health and safety of American women and girls.”
In a press release, Live Action founder and president Lila Rose said:
Because of today’s decision, women will be home alone delivering a dead child, unsure whether the volume of blood loss they see is ‘normal’ for the abortion procedure or them hemorrhaging and bleeding out. Unsure if the pain they feel is the ‘normal’ pain of the abortion procedure or pain from their ectopic pregnancy going undiagnosed and now threatening their life. Now, due to the utter carelessness of the FDA, the door has been opened for sexual predators to have the abortion pill delivered by mail so they can administer it to their victims and destroy the evidence of their sexual crimes.
The FDA is out of line and the American people should respond en masse calling for them to pull the pill. In a move showing blatant disdain for the intellect of the American people, today’s letter from the FDA claims that the ‘small number of adverse events reported to the FDA during the COVID-19 public health emergency’ led to their decision.
In reality, there is no requirement for the manufacturer of the pill, Danco Laboratories, or its generic, GenBioPro, to report any adverse reactions except death under REMS since 2016. In addition, there are no federal laws in place to require or track abortion complications across all states.
In October of 2020, the first U.S. online pharmacy announced plans to ship abortion pills to patients across the country during COVID-19. Shortly thereafter, virtual abortion pill dispensaries began to flood the internet.
While the latest changes to FDA’s REMS are only in effect during the pandemic, the Biden-Harris administration is expected to pressure the FDA to permanently remove the REMS from the abortion pill. If this occurs, it will likely result in a surge of abortion pill sales far beyond the previously estimated $200 million annually.
Editor’s Note: Visit AbortionPillReversal.com for information on how to potentially stop the abortion pill process after it has begun.
By the end of March, 79 cases of rare blood clots had been reported in those who’d received the AstraZeneca vaccine the UK, with cases occurring more frequently in younger women. Because of this, comparisons have been drawn with the contraceptive pill, which carries a greater relative risk of clots. In the UK, blood clots have occurred in people taking the AstraZeneca vaccine at a rate of roughly one in every 250,000, whereas blood clots caused by the pill are estimated to affect one in every 1,000 women each year.
But this isn’t the only difference between the two. Although evidence is still emerging, the mechanisms behind the type of clotting linked to the vaccine and that linked to the pill appear to be quite different. It’s a reminder of how complex the blood and clotting is, with multiple parts of the process that can be disrupted.
The cause of vaccine-induced clots
With the AstraZeneca vaccine, a small number of clots have been reported, with individuals presenting with low levels of platelets in their blood, likely resulting from these clots forming.
Platelets are the smallest of our blood cells. Produced in our bone marrow, they travel to anywhere there is damage to blood vessels to help clotting (to prevent blood from escaping) and start the repair process. A normal number of platelets is anywhere between 150,000 and 450,000 platelets per microlitre of blood (there are 1,000 microlitres in one millilitre). If you have too few platelets, less than 150,000 per microlitre, then you have a deficiency – known as thrombocytopenia.
Thrombocytopenia can be inherited, acquired through lifestyle factors over time (such as poor diet combined with alcohol) or brought on by medicines or infections. And although yet to be confirmed, it seems the AstraZeneca vaccine, by causing blood clots, may be leading to low platelet levels in an extremely small number of people too. This potential new condition has been called vaccine-induced prothrombotic immune thrombocytopenia (VIPIT).
If blood clots occur when they shouldn’t, this can be fatal. In some people who have had the first dose of the AstraZeneca vaccine, unwanted clotting is being reported in the brain, known as cerebral venous sinus thromboembolism (CVST).
As blood leaves the brain, it drains into a dedicated space that exists around it – the cerebral venous sinuses – prior to it being channelled into the major veins that drain out of the head and into the neck, back to the heart.
Blood leaves the brain by moving into the venous sinuses (blue) and draining into the jugular vein.OpenStax/Wikimedia Commons, CC BY
But for some who’ve taken the vaccine, platelets appear to stick together in the venous sinuses of the brain, which causes a blockage that prevents blood draining out of the brain tissues. This creates back pressure in the small vessels of the brain and blood leaks into the brain itself, causing damage in the same way a haemorrhagic stroke would.
Accompanying symptoms include headache, tiny red spots under the skin, blurred vision, fainting or loss of consciousness, loss of movement in parts of the body, or coma. These typically appear between four and 20 days after vaccination.
These symptoms, as well as the mechanism underlying the formation of these clots, are similar to those from a different type of thrombosis, heparin induced thrombocytopenia (HIT), where specific antibodies bind to a molecule in the blood called heparin, causing platelets to become super sticky and clot. It’s been suggested some form of immune activation, similar to that seen in HIT, might be the cause of what is happening in some vaccinated people.
Clotting and contraception
Despite the combined oral contraceptive pill also increasing the risk of blood clots in those who take it, these clots are likely formed by a different mechanism to those seen in CVSTs.
Clotting is a complex system. It involves more than just platelets. There are also many proteins dissolved in the plasma of blood, which when damage to tissues or blood vessels occurs, launch a series of steps to produce fibrin, an insoluble protein that then combines with platelets and red blood cells to form a clot. These dissolved proteins are called clotting factors, and some of the ingredients in contraceptives increase the levels of certain clotting factors in the blood, which raises the odds of clots forming in veins.
Genetic factors can also work to increase the likelihood of abnormal clots forming in women taking the pill. For instance, having a genetic mutation that affects a specific clotting factor called factor V Leiden is associated with a three-fold increase in risk. About 5% of people categorised as white have this mutation, though it is much less common in other ethnic groups.
It’s plausible that there may be genetic factors that increase the risk of the AstraZeneca vaccine in some people in a similar way, but at this stage, we don’t know. And due to not knowing what the risk factors are for CVST, it is also not possible to say what the risk of taking the combined oral contraceptive pill and having the AstraZeneca vaccine might be. There are a lot of things that still need to be explored.
Oral contraceptives increase the risk of blood clots by raising the amounts of clotting factors in the blood.PATCHARIN SIMALHEK/Shutterstock
Finally, it’s important to note that COVID-19 itself has been reported to lead to thrombocytopenia in up to 41% of positive patients, with the figure rising to up to 95% in those with severe disease. There are many reports of small blood clots in multiple organs in COVID-19 patients causing organ damage, failure and death.
The mechanism behind this is also unclear, but the COVID-19 infection likely causes these clots either by destroying the bone marrow and preventing platelets from being made, by causing the immune system to destroy platelets, or by increasing the use of platelets to repair damage to lungs and other tissues as a result of the infection (or a combination of all these things).
With this in mind, it’s worth remembering that while there is a small risk of clotting in some individuals who take the AstraZeneca vaccine, this clotting risk is much less than with many other things, including contraceptive pills – and significantly less than the risk of clotting after a COVID-19 infection.
This article was amended on April 12 to correct the suggestion that thromobocytopenia causes blood clots. The likely mechanism is the other way round, with abnormal clotting leading to low platelet levels.
“Contraceptive cost of COVID: a million unplanned pregnancies” read headlines across many major media outlets on March 11. The viral headline was in response to a March 11 United Nations (UN) announcement that the COVID-19 pandemic was responsible for 1.4 million unplanned pregnancies, due to the estimated 12 million women in poorer countries who lost access to contraception because of various pandemic-related disruptions.
In its report, UNFPA lists the various pandemic-induced disruptions to contraceptive access, including hits to global manufacturing and supply chains, emptied out shelves, lockdowns and social distancing measures, fears of visiting health clinics, or the inability to visit clinics because of the overwhelm caused by the pandemic. Together, UNFPA believes that these disruptive factors, which they estimate lasted for an average of about 3.6 months in 2020, are responsible for at least 500,000 and as many as 2.7 million unplanned pregnancies (with 1.4 million being their medium estimate) across 115 low- and middle-income countries.
The UNFPA report actually highlights the reasons why pharmaceutical birth control is unsustainable in the face of a disaster (as many of these factors are not unique to a pandemic). Yet, the organization insists that further dependence on these methods of family planning is necessary, stating that contraceptive access must be prioritized for women and girls across the globe. In fact, the UN goes so far as to place contraceptives on a list of items which they consider “life-saving commodities.” But in essence, the UN is just placing more emphasis on the same unsustainable strategy, encouraging women and couples to rely on the same methods of pharmaceutical birth control that left them in a lurch this pandemic.
A new strategy for sustainable family planning
What the UN misunderstands is that the COVID-19 pandemic actually highlighted a dire need for family planning that is sustainable, independent of supply chains, and accessible beyond the clinic.
Thanks to scientifically-backed fertility awareness methods (FAM) (also known as Fertility Awareness-Based Methods, FABMs, or methods of Natural Family Planning, NFP), there are alternatives to pharmaceutical contraceptives that can better serve women and couples in meeting their family planning needs. FAMs are non-pharmaceutical, most require no or little equipment, and they provide sorely needed education and knowledge for women about their bodies and reproductive abilities—knowledge that won’t simply vanish as soon as disaster strikes.
The CDC has acknowledged that some fertility awareness methods have as low as a 2% typical use failure rate; while the CDC currently cites a range of 2-23% failure rate for FAMs, this reflects the range of fertility awareness methods with different efficacy rates. For example, FAMs that measure biological signs of fertility such as cervical fluid, basal body temperature, or hormone levels provide higher efficacy rates, while methods that use calendar estimates instead of biomarkers, are far less effective. Still, the efficacy of modern FAMs is often misrepresented, which leaves women with less quality information to make informed choices about the full scope of their family planning options.
The global applicability of FAMs
In truth, women all over the world have been successfully taught to use fertility awareness methods—and to use them with a relatively high degree of effectiveness. The Billings Ovulation Method (a cervical fluid-only method of natural family planning), in particular, has been taught to people in countries all over the world, in populations with every level of literacy (including no literacy).
For example, a 1996 field trial in India followed over 2,000 women who had been taught to use the Billings Ovulation Method; despite many of the women being illiterate, after 21 months, the method failure rate (for perfect use) was less than 2% per 100 users, and the user failure rate (typical use) was less than 17% per 100 users [2]. In a 1996 12-month multi-center study in China, the results were even more impressive, with a perfect use failure rate of 0, and a typical use failure rate of 0.5% [3]. Particularly noteworthy is the following conclusion from a World Health Organization-conducted, multi-continent study, published in 1981 in the journal Fertility and Sterility:
“The most striking finding was the demonstration that 94% of women representing a wide range of cultural, educational, and socioeconomic characteristics were able to recognize and record the cervical mucus symptom which allows self recognition of the fertile period” [4].
These studies indicate that the Billings method, a widespread and evidence-based method of fertility awareness, can be used by women across cultures and education levels to effectively prevent pregnancy. Even factoring in the initial instruction that women need to use these methods, they are still less expensive than any other form of birth control. Further, using a FAM does not require a prescription or a visit to a clinic or pharmacy to obtain, which makes them a form of uniquely sustainable family planning, especially in the face of a disaster (like a pandemic).
Diminished access to care for birth control side effects
While the UN report emphasizes increasing access to contraceptives, it does not address the increased access to healthcare women may need for side effects they could experience while on contraception (especially in the event of more serious side effects like blood clots, heart attacks, and strokes). Unmentioned in the UN report is how women in developing countries (or even women in developed countries during a disaster) may lack access to the care needed to change their birth control method, if health risks or serious side effects arise. Even more troubling in this regard are the long-acting reversible contraceptives (LARCs) such as intrauterine devices (IUDs) or the Nexplanon implant, which can produce uncomfortable and adverse effects for users, but which require a clinic visit for removal. Likewise, the Depo Provera shot, which despite its link to increased HIV transmission is one of the preferred methods of contraception in poorer countries, is not reversible at all. Biomedical scientist and author of Target Africa, Obianuju Ekeocha wrote in her 2012 Open Letter to Melinda Gates: “Where Europe and America have their well-oiled health care system, a woman in Africa with a contraception-induced blood clot does not have access to 911 or an ambulance or a paramedic. No, she dies.”
Environmentally friendly methods of family planning
In addition to being effective, sustainable methods of natural family planning, FAMs are the most environmentally friendly form of effective family planning. Most fertility awareness methods are zero waste, require no manufacturing, no shipping, and cause no endocrine-disrupting hormones to end up in our waterways.
With the UN’s continued focus on combating climate change, there is a large oversight when it comes to its dependence on pharmaceutical contraceptive drugs and devices, and its ignorance of more sustainable, “green,” and zero-waste forms of family planning. In 2019 alone, UNFPA boasts that it provided 1.3 billion male condoms, 16 million female condoms, 66.6 million oral contraceptives (28-day packs), 2.2 million IUDs, 47 million injectables, 9.9 million implants, and 2.9 million emergency contraceptives, with no mention of any provision of fertility awareness method education.
The UN is not alone in its near single-minded push of contraceptives. The World Health Organization also continues to push contraceptives, especially in poor countries, even though the organization recently acknowledged that breast cancer is now the world’s most-diagnosed form of cancer; the organization appears unconcerned about hormonal birth control’s established link to higher risk of breast cancer.
Accessible natural family planning
At the outset of the pandemic, Natural Womanhood realized that couples would need sustainable family planning more than ever. That is why we immediately published numerous articles to encourage women and couples to learn FAM when they might not have access to other forms of family planning. We have also been offering scholarships for women and couples to learn a FAM of their choice—for free. To date, we have awarded ten couples with a FAM scholarship. Some of these couples have admitted to us that without the scholarship, they might have resorted to hormonal contraception against their health preference or moral values, as their economic situation was too tenuous to allow for another child.
Although UNFPA stated in its report that “the situation could have been far worse,” and that “quick action,” “ingenuity,” and “creative efforts” “helped many health systems maintain or restore access to essential health services, including contraceptives,” those efforts were clearly not enough to help the estimated 1.4 million women avoid unplanned pregnancies [5].
Ms. magazine is the unabashed holy grail of feminism. Right on the masthead it says “More than a Magazine, a Movement.” But just what is feminism? Like many buzz words in our pestilential popular culture, the term is used like a sledgehammer to set the parameters of permissible public discourse. It is a set piece of the PC lexicon that you will fail to understand at your peril.
The Oxford English Dictionary, “the definitive record of the English Language”, defines feminism as “The advocacy of women’s rights on the basis of the equality of the sexes.”
Over here in the New World, Merriam-Webster defines feminism as “belief in and advocacy of the political, economic, and social equality of the sexes expressed especially through organized activity on behalf of women’s rights and interests.” (Interestingly, the American definition holds the prospective feminist to a higher more specific standard, requiring “belief in” as well as “advocacy” and even encouraging activism to boot.) Gloria Steinem, the doyenne of modern feminism, describes a feminist as “anyone who recognizes the equality and full humanity of women and men.”
Though I may be woefully unwoke otherwise, I have no problem with any of these basic ideas about feminism. It is when feminism spills over into misandrist grousings about “toxic masculinity” and hoked-up narratives of “oppression” that I part company. That is where feminism morphs into something else and is weaponized for political purposes.
But back to Ms. An interesting article just appeared in its pages, headlined: “Stop Panicking—There Are a Lot of Positives to the Baby Bust.” The article was subtitled: “We should celebrate that increased empowerment and equality are leading this trend of slowing growth and reducing pressure on the climate and environment.”
As an avid reader of headlines, I was struck by that one. Its message seemed to be “Relax, the baby bust is a good thing. Having empowerment and equality and not having children are things to be celebrated.”
Shocker: Is Ms. Magazine actually encouraging its readership of young women not to have children? To put it bluntly, oh yes.
Reading the piece, I hear Ms. saying, “The inability of people, particularly people of color, to access basic health care is a crisis. The climate emergency is a crisis. A million wildlife species going extinct in the coming decades is a crisis. People choosing to delay pregnancy or have fewer children is not.”
While a million species of wildlife going extinct soon would certainly be a crisis, the extinction of our own non-wildlife species, Homo sapiens, certainly is a crisis – and it is already underway. This is not mere alarmist rhetoric – it’s a fact. Believe the science! The global total fertility rate has declined a stunning 50% in the last 60 years. In pre-Covid 2020, the rapidly declining total global fertility rate was slightly above 2.4 and falling (2.1 being replacement level). And that was before the Covid baby bust. While I don’t mean to spoil the empowerment party, I’ll just say that today’s fast-falling fertility rate is nothing to celebrate.
The 2020 Lancet world fertility study projects global population peaking at approximately 9.73 billion in 2064 and declining to 8.79 billion by 2100 – a decline of more than 9% decline in just 31 years. And the rate of decline beyond that is projected to accelerate. While most demographic groups (with the exception of White American males) are living longer and thus slowing population decline, as fertility declines, each succeeding generation will shrink and will bear fewer children and have more elderly to support. The crisis is like a snowball rolling downhill, growing larger and picking up speed as it goes. Already China, Hungary, Russia and other countries are desperately promoting social and financial incentives to halt the decline. Their results thus far are mixed.
Demographers tell us that fertility tends to dip in times of war or pandemic, but the sustained decline in fertility we are now experiencing – over the past six decades – is unprecedented. Yet Ms. says, “Even as our population growth slows, our outsized consumption patterns and reckless industrial growth in the Global North continue to destroy the planet.”
I’ve been hearing a lot about the “Global North” of late. Those who toss the term about are usually talking about exploitative Whites and workaholic East Asians. These are said to be the populations that “continue to destroy the planet.” (Isn’t that racist?) At the risk of being sent to the Unwoke Gulag, I would say that it is folks in the Global North that drive the world economy, and in so doing, much improve the lives of folks in the Global South. The birth dearth is the worst in the Global North, where every major country has been saddled with below-replacement-level fertility for decades.
Ms. wraps the discussion, saying: “By focusing on the positive outcomes like sustainable fertility rates and empowering women, we can shift our perspective to embrace slowing population growth as a good thing and a way to create lasting change. The baby bust is not a signal of societal collapse but a positive indicator that we are getting closer to a sustainable, equitable world.”
This is so shortsighted.
To credibly assess any trend, considering the long-term consequences is essential. First, we do not have sustainable fertility rates, and we won’t see them anytime soon, if ever. The decades-long, unprecedented decline in fertility means unstoppable population decline. Our future could consist of a quasi-dystopia where there are fewer empowered women (and compliant men), so the burden of doing the jobs society needs will fall on fewer people. Elder care will be a big one. Artificial intelligence cannot fill the gap. And if countries resort to mass immigration to do the work, they risk the rise of a diversity dictatorship, and social cohesion will become a thing of the past, as in the United States today.
Personal finances, lack of religious faith and no confidence in the future are often cited as reasons for not having children. But not reproducing for purposes of individual comfort or convenience or ideological commitment pits personal preference against the survival of the species. It is that simple, and a choice must be made.
But what young magazine reader thinks of that, especially when she’s told she has a shot at Empowerment?
The battle over “my body, my choice” is not new; it has been raging over a century. A cartoon in the May 1919 issue of Margaret Sanger’s Birth Control Review shows a woman being crushed by a giant roll of paper labeled “Laws Controlling Women’s Bodies.” Another offensive but equally common slogans pro-abortionists use are variations are the indignant demand “What makes you religious fanatics think you can tell me what to do with my uterus?,” and the tiresome chant “Keep your rosaries off my ovaries!”
Interestingly, the first person to make the “woman’s body, woman’s choice” argument for abortion was the libertine and reprobate Marquis de Sade. His sexual writings actually inspired the word “sadism,” and he was, not surprisingly, guilty of blasphemy against the Catholic Church. In 1797, he wrote:
The penalty against child-murdering mothers is an unexampled atrocity. Who then has a greater right to dispose of the fruit than she who carries it in her womb? … To interfere with the usage a woman chooses to make of it is stupidity carried beyond any conceivable extreme.1
Let’s examine the science that disproves these claims.
What Should Be Our Pro-Life Response?
To begin with, it is impossible to reply directly to this slogan unless we have the user clarify what he or she means by it. We need to do is ask, “Why do you consider the unborn child to be a part of the woman’s body?”
The usual response is momentary hesitation, followed by one of three possible answers;
The fetus (unborn child) relies on the mother completely for its existence;
The fetus is inside her body, therefore it is part of her body; or
The fetus is a parasite.
You can give concise and effective answers to each of these.
(1) The unborn child relies on the mother
When asked to clarify, most pro-abortionists will argue that the unborn baby is totally dependent upon the mother. They are implying that this allows the mother the “right” to dispose of her baby.
These are separate arguments and should be treated as such. Certainly a newborn baby is just as dependent upon its parents for all of its needs as one not yet born, and will quickly die if not cared for. Does this mean that the newborn baby can be neglected or killed outright? As we see today in the infanticide debate regarding failed abortions where the child is born alive, the inevitable conclusion to draw if one is pro-abortion is affirmative. Some “intellectuals” have been arguing for decades that it is perfectly permissible to allow handicapped children to die, calling this “fourth-trimester abortion” or “post-natal abortion.” Moving the goal post means more and more killing is inevitable.
For example, Nobel Prize winner Dr. Francis Crick, one of the co-discoverers of DNA, actually claimed that “no newborn infant should be declared human until it has passed certain tests regarding its genetic endowment, and that if it fails these tests, it forfeits the right to live.”2 Hastings Center ethicist Joseph Fletcher has said, “It is ridiculous to give ethical approval to the positive ending of sub‑human life in utero, as we do in therapeutic abortions, but refuse to approve of positively ending a sub‑human life in extremis [after birth].”3
The pro-life answer is simple rebuttal. Every child who is born healthy is already entitled to care under the pain of prosecution for murder. And that baby, too, is completely dependent, so the argument is a non sequitur.
(2) The unborn child is inside the mother
The second assertion is that the unborn child is inside his or her mother, and is therefore part of her body.
Sometimes a pro-abortionist will also claim that the unborn child is inside the mother, depends on her completely, and is therefore part of her body. We can reply by describing an analogous situation involving astronauts in space. They are totally dependent upon their vessel for everything — their air, water, food, and all other needs. If they should exit the vehicle unprotected, they would be nonviable, and would die in minutes. This also holds true for a nonviable unborn baby. Yet no thinking person would argue that the astronauts are part of a space station!
Even the staff of Barack Obama, the most pro-abortion President in our nation’s history, recognized the unborn child as a separate human being. Pregnant women entering the White House must formally register their unborn children as separate visitors, with “Baby” as the first name, expected birth date, sex if known, and even “000-00-0000” as a Social Security number!
This silly policy demonstrates the totally illogical and schizophrenic nature of pro-abortion “thinking.”
(3) The unborn child as parasite
Pro-abortionists have a pressing need to dehumanize the unborn child in order to salve the guilt they feel when they support the practice of abortion or actually have one. Sometimes they will resort to the “fetus as parasite” argument, going beyond dehumanization to paint the unborn child as some sort of disgusting wormlike abomination draining the blood and life force from its “host.”
Third-trimester abortionist Warren Hern insists in his book Abortion Practice, “The relationship between the gravid female and the feto-placental unit can be understood best as one of host and parasite.”4
When pro-abortionists insist that the unborn child is a parasite, they are acknowledging its separate nature, because parasites are never part of their host’s body. They are biologically separate and distinct organisms. Anyone denying this fact is simply being anti-scientific.
One way to clarify your point is to ask the pro-abortionist a question. If they went to some underdeveloped part of the world and picked up a tapeworm because they ate some insufficiently cooked food, would they consider that parasite to be a part of their body?
In order to highlight the fact that the baby is a separate being, consider these facts, which not even the most ignorant pro-abortionist can deny:
All mothers are obviously female. About half of their children are male. How can a human being be both male and female?
The mother and baby frequently have different blood types.
The baby can be a different race from the mother.
Every cell in the mother’s body has a set of chromosomal characteristics that is entirely distinct from every cell in the baby’s body.
When the unborn child anchors to the uterine wall, there is a concerted attack by white blood cells to defeat him, and he must defend himself. The mother’s immune system recognizes it as “non-self.” Therefore, it is not part of her body.
The baby can die without the mother dying. The mother can die without the baby dying (the baby can be rescued if he is viable).
The unborn baby initiates a process that culminates in its leaving the mother’s body. Challenge a pro-abortionist to name any other body organ that does this.
Conclusion
Pro-lifers agree that a woman does indeed have the right to manage her own health. However, maintaining that right does not allow the mother to destroy her child’s body. When she conceived, she had already passed the right to life on to that new life.
Endnotes
The Marquis de Sade, quoted in “Yet another Effort, Frenchmen.” Juliette [New York City: Grove Paperbacks, Inc., 1968], pages 336, 782 and 783. It is interesting to note that de Sade’s novels were replete with several recurring themes, one of the strongest of which was the pleasure which certain disturbed individuals derive from killing both pregnant women and unborn children. In one of his grisly and deranged novels, he describes with great relish the skewering of a pregnant woman with a red hot iron rod driven through both her and her unborn baby, as described in Dr. Kenneth M. Mitzner. “The Abortion Culture.” Triumph, March 1973, pages 20 to 24.
Nobel Prize winner Dr. Francis Crick. Pacific News Service, January 1978.
Hastings Center ethicist Joseph Fletcher. “Four Indicators of Humanhood?: The Enquiry Matures.” Hastings Center Report, December 1974.
Abortionist Warren Hern. Abortion Practice. B. Lippincott Company, 1984.
(WASHINGTON, D.C., C-Fam) The state of New York quietly adopted a measure to make commercial surrogacy legal, raising objections by women’s rights and anti-trafficking groups. Meanwhile, Russia’s parliament is moving to restrict its own booming surrogacy industry. In a recent webinar hosted by C-Fam, experts in international surrogacy raised concerns about its harms to women and children and positioned the ongoing debate in the context of international human rights standards.
Surrogacy is a global, multi-billion-dollar industry, and while only a handful of countries explicitly allow commercial surrogacy, its legal status in other countries is ambiguous or exists in a legal vacuum.
According to scholar and Marie Curie Fellow Daniela Bandelli, surrogacy couples and individuals who want children, and are willing to pay a considerable cost to have them, and women who need money. “It is quite a risky activity,” said Bandelli, both for the mother, who is at higher risks of pregnancy and birth complications than those who conceive naturally, and for the child, who is deprived of physical contact, including breastfeeding, “with this person we usually call the mother.” The key question, says Bandelli, is “are women aware of all the risks they face in participating in the surrogacy industry?”
Jennifer Lahl, president of the Center for Bioethics and Culture, is an advocate for surrogacy abolition and creator of several documentary films highlighting the abuses that occur in the fertility industry. She contrasted the positions of those who, like her, believe there is no way that surrogacy can be practiced safely and ethically, and those who believe that it is better that surrogacy be legalized and regulated.
Lahl spoke about the harms experienced by surrogate mothers in the United States, including three who died from complications of the process. “We never want to forget that there are real human beings behind what can seem like a philosophical conversation about helping people build families.”
If such tragedies are occurring in the comparatively wealthy U.S. the plight of surrogates in the developing world is even more troubling. Emmanuele di Leo, president of the Steadfast Foundation, has documented the growing “reproduction-for-hire” industry in Nigeria, where young women and girls are recruited—by the same methods used to recruit women into prostitution—in poor villages and housed in “baby-factories.”
In all of these cases, the demand for surrogates often originates abroad, and arrangements are conducted through private surrogacy agencies. While few international organizations have taken a stand against the practice, including the European Parliament, most have either remained silent or, in the case of a growing number of UN experts, appeared to favor taking a more liberal approach.
A joint paper presented by C-Fam, Steadfast, and Bandelli’s project WoMoGeS points out that any defense of surrogacy would require watering down the right of the child to know and be cared for by his or own parents, as enshrined in the Convention on the Rights of the Child. C-Fam’s Director of Legal Studies, Stefano Gennarini, argued that this violates established standards for interpreting human rights obligations.
“As any human rights lawyer knows, human rights must be read as broadly as possible, and they must be restricted as little as possible.”
Editor’s Note: Rebecca Oas, Ph.D. writes for C-Fam. This article first appeared in the Friday Fax, an internet report published weekly by C-Fam (Center for Family & Human Rights), a New York and Washington DC-based research institute (https://c-fam.org/). This article appears with permission.
A recent Reuters article told the story of an anonymous 29-year-old Polish woman impacted by Poland’s recent ban on abortions for cases of fetal abnormality. The woman, referred to as Paulina, learned at an unspecified point in her pregnancy that her preborn child did not have kidneys and would be unlikely to survive after birth. The distraught mother was quoted as saying, “Everyone says that the reward after the pain of birth is holding your child in your hands. I would have nothing. I would give birth to a dead child, and that pain would be a thousand times worse.”
Eventually, Paulina found several healthcare professionals who, instead of equipping her with counseling and resources and support, were willing to assert that the fetal diagnosis was causing such a deterioration in her mental health as to qualify her for the “life of the mother” exception to Poland’s abortion ban. Sadly, she went through with the abortion.
Abortion is not a ‘treatment’
While abortion might seem to “stop the bleeding” by ending a pregnancy and seemingly also ending the emotional pain associated with the loss of a child before or shortly after birth, abortion is not a “treatment” for fetal abnormality.
Research suggests that women who choose to abort in such cases have worse mental health outcomes than those who carry their pregnancies to term. This makes sense, as abortions for cases of fetal diagnosis are inherently discriminatory and eugenicist, penalizing the weak and the sick. These discriminatory abortions strike at the heart of the natural bond of love and protection that grows between a mother and her preborn child, severing that connection.
The false dichotomy
The Reuters article mistakenly posited that Paulina had only two options after receiving a poor prenatal diagnosis: either choose to carry the pregnancy, soldiering on alone and emotionally broken, or have an abortion and presumably stop the emotional pain.
But this dichotomy is false, because abortion does not magically resolve the emotional pain of receiving an adverse fetal diagnosis, and in fact compounds that pain with the memory of permitting an act of violence against the defenseless preborn person. From a physical health and safety perspective, women often do not learn of fetal abnormalities until their second-trimester, when morbidity and mortality rates from abortion increase dramatically.
Furthermore, women like Paulina need not soldier on alone through a challenging pregnancy.
As Live Action News has previously reported, many life-affirming options such as perinatal hospices exist in Poland to help women bond with their preborn children, walking alongside them every step of the way, ensuring that they feel supported, not alone. Women who bear the heavy emotional burden of receiving such challenging news deserve to have full information about their baby’s diagnosis, treatment options, and resources for emotional, material, and financial support. Often, they are given little or incomplete information and instead are encouraged or even pressured to abort their sick children.
A few days ago the Vatican’s Congregation for the Doctrine of the Faith (CDF) somehow captured global headlines for doing something that is not particularly noteworthy, and certainly not surprising.
In a brief statement – called a Responsum – the CDF responded to a question about whether or not the Church can offer “blessings” to same-sex unions. The carefully-worded answer was, in brief, “no.” “[T]he Church does not have, and cannot have, the power to bless unions of persons of the same sex,” concludes the statement.
In other words, the CDF reiterated, once again, what the Catholic Church teaches and has always taught for the past 2,000-plus years: Marriage is the union between one man and one woman, and any sexual activity outside of marriage is sinful. Since the Church cannot bless sin, neither can it bless unions that are predicated upon sinful behavior.
None of this should come as a surprise to anyone. The Church’s teaching on marriage and the sexual act has been consistent throughout its history and is well-known to most people. As the Catechism of the Catholic Church states, quite unambiguously: “The sexual act must take place exclusively within marriage. Outside of marriage it always constitutes a grave sin and excludes one from sacramental communion.” (CCC 2390)
However, to read the many media reports on the Vatican’s statement, you would think that the CDF had done something very shocking indeed. Many spoke of a “ban” on blessing same-sex unions, as if the Church had come up with some harsh new rule specifically targeting individuals with homosexual inclinations.
To read the statement, however, is to wonder what the fuss is about. The CDF merely notes, with gentle wording, that the only moral use of the sexual act is within a marriage between a man and a woman open to life, and that blessings, as sacramentals, cannot be conferred on sinful sexual relationships. It reminds pastors that “men and women with homosexual tendencies must be accepted with respect, compassion, and sensitivity. Every sign of unjust discrimination in their regard should be avoided.” Because of the Church’s great care and respect for human dignity and each individual person, the CDF adds that it “does not preclude the blessings given to individual persons with homosexual inclinations who manifest the will to live in fidelity to the revealed plans of God as proposed by Church teaching.”
Furthermore, this “ban” does not exclusively target homosexual couples. The same approach would also apply to heterosexual couples in adulterous, fornicating, or polygamous relationships. Regardless of how much the people in such relationships love one another, their misuse of the gift of the sexual act means that the Church cannot endorse their relationship with a blessing.
As the CDF statement explains:
[W]hen a blessing is invoked on particular human relationships, in addition to the right intention of those who participate, it is necessary that what is blessed be objectively and positively ordered to receive and express grace, according to the designs of God inscribed in creation, and fully revealed by Christ the Lord. Therefore, only those realities which are in themselves ordered to serve those ends are congruent with the essence of the blessing imparted by the Church.
For this reason, it is not licit to impart a blessing on relationships, or partnerships, even stable, that involve sexual activity outside of marriage (i.e., outside the indissoluble union of a man and a woman open in itself to the transmission of life), as is the case of the unions between persons of the same sex. The presence in such relationships of positive elements, which are in themselves to be valued and appreciated, cannot justify these relationships and render them legitimate objects of an ecclesial blessing, since the positive elements exist within the context of a union not ordered to the Creator’s plan.
Rebellion Within the Church
On the one hand, I am quite encouraged by the CDF statement, which, while pastorally sensitive, is also unambiguous in its teaching.
In recent years powerful lobby groups, both within and without the Church, have been pushing for the Church to change its teachings on sexuality and marriage. At times, Pope Francis has seemed to indicate sympathy towards some of these efforts, something that I have found quite troubling. In a documentary released last year, for instance, the Holy Father appeared to endorse the idea of legalized “civil unions” for homosexual couples – something that the CDF under Cardinal Ratzinger had clearly said could not be supported (“In those situations where homosexual unions have been legally recognized or have been given the legal status and rights belonging to marriage, clear and emphatic opposition is a duty,” the CDF said in that 2003 statement). Whether justified or not, many people expected the Pope, or the Vatican, to soon go one step further, offering a formal endorsement of same-sex unions.
The fact that the CDF published such a clear statement, and that it was approved for publication by Pope Francis, is proof that whatever the forces pressuring the Church, the Holy Spirit is still guarding Her, and ensuring the preservation of true doctrine.
On the other hand, the reaction to the statement is deeply concerning, portending troubling times ahead. Unfortunately, it is not only the usual suspects outside the Church who are openly criticizing the statement – i.e., the secularist media and left-wing pressure groups. Many within the Church, including priests and bishops, are also openly criticizing the statement.
In Germany, 60 priests signed a statement saying they will defy the CDF, and bless same-sex couples. Another 350 priests in Austria signed a similar statement. Both of those statements used similar wording, saying that the priests will “continue” to bless such unions – highlighting the fact that many priests in Europe are already openly defying Church teaching. Another statement condemning the CDF responsum was signed by 230 theologians in Germany and elsewhere.
And it isn’t only priests that are signaling their dissent. Several bishops have also indicated their intent to pursue a different path, regardless of what the CDF says. “I feel ashamed for my Church. I mainly feel intellectual and moral incomprehension,” said Belgian bishop Johan Bonny in a statement. In the U.S. Cardinal Blase Cupich, while noting that the responsum said “nothing new” about marriage, also added that it is “understandable” that many people feel “disappointment”. Experienced Vatican watchers are also pointing to the fact that, while Pope Francis apparently approved publication of the statement, he himself did not affix his name to it – possibly suggesting that he has mixed feelings about it.
The boldness of some of these expressions of defiance suggests the existence of an undeclared schism within the church, with a considerable number of priests, bishops, and theologians holding and promoting a position that is wholly out-of-step with the Church’s teaching on a crucial matter.
Reclaiming Church Teaching
The widespread shock and anger found in much of the media reporting, and even from many Catholics, highlights the discouraging fact that many people are deeply confused about what the Church teaches about marriage and the sexual act, and why it teaches what it does. Many people simply view the Church’s teachings as being harsh and judgmental, condemning people who “love” one another for no good reason.
Clearly, our culture is deeply confused about human dignity and the sacredness of marriage and the sexual act, and this confusion has infiltrated the walls of the Church Herself. Where the Church, her ministers, and her faithful should be beacons of light, showing another way forward, a more loving way, all too often we are finding the exact same confusion as in the broader culture.
I am very grateful that at a time when confusion is reaching such a peak, the CDF’s new statement has provided us with a great opportunity to dispel the many misunderstandings about Church teaching!
Fundamentally, the CDF is upholding the truth about the human person. After all, written into the nature of the human person is a call to union and communion with and between one man and one woman. This union is indissoluble and by its nature procreative, participating in the generation of a new human life. Nature has a plan for human sexuality, and it doesn’t involve homosexual acts.
To “bless” any act contrary to the nature of the human person and the nature of marriage is contradictory. A same-sex couple cannot generate children because the nature of their sexual activity is not capable of procreation. There is no sexual complementarity. Moreover, there are two different kinds of sexual activity that should not be spoken of or treated as if they were the same – the conjugal act between one man and one woman, and a homosexual act.
Sexual intimacy is a mystery that symbolizes marriage and only belongs in marriage. Outside of marriage, conjugal relations are essentially untruthful. In upholding the good of the human person and of marriage, we are opposed to what threatens the context of sexual intimacy – i.e., premarital sex, extramarital sex, homosexual activity, etc.
Whereas the culture tends to view the modern approach to human sexuality and the sexual act as “broad–minded” and “liberating,” and the Church’s teaching on the same as being excessively “narrow” and “restrictive”, the reality is the exact opposite. The Church’s teaching on these subjects are so broad that they take into account the way the sexual act affects the whole person and impacts not only the people engaged in sexual behavior, but also others around them (especially their children), and society.
The modern approach, on the other hand, reduces the sexual act to a biological transaction that has no intrinsic meaning or purpose, and which is utterly private. This understanding of human sexuality is not only horribly reductionist, stripping the sexual act of much of its beauty and richness, but has also unleashed much suffering – through widespread divorce; the creation of an exploitative dating culture, characterized by mutual use rather than the pursuit of love; the consequent, ubiquitous disenchantment about romance and the possibility of finding true love; an explosion in STDs and out-of-wedlock births; the near-ubiquity of hardcore and degrading pornography, which exploits the actors and actresses, and enslaves many people in addiction, and so on.
The wisdom of the Church’s teaching is in how it captures the totality of what the sexual act is about: not just a source of physical pleasure, or even an expression of love between a couple, but also the means by which humans establish families, and contribute to the health and continuity of society. The Church’s view of sexuality is that the sexual act that is exclusively reserved to married couples is so noble and so powerful, that it must be carefully protected and nourished, integrated within the person, and within society.
The Church, in teaching that the sexual act is reserved for life-long unions of a man and a woman, is not against sex or against love. Instead, the Church is for sex and for love, including love for children, who have a right to be born into a stable union, and to be raised by a mother and a father. The problem with same-sex unions, or other sinful sexual relationships, is not that two people love one another, but that their love is expressed in a way that misuses and reduces the gift of sexuality, and thereby harms themselves and others.
For understandable reasons, this message is not nearly as popular as the message that people should pursue as much sexual pleasure as possible, in whatever ways they want. The good and the true are often not nearly as immediately alluring as the sinful and the untrue. To sin is easy; to be virtuous is hard. Nevertheless, the great saints and sages have always taught the same message: that the hard work involved in living in accordance with the good and the true is worth it. Wisdom is, in large part, the capacity to see through the superficial glitter of sin, and to recognize the subtle, but deep beauty of goodness and virtue.
The Church’s message about human sexuality, marriage and the sexual act, and the call to chastity, is a harder message to sell than the message of the Sexual Revolution. Nevertheless, it is our duty to do our best to find new ways to explain the truth about them, and to set the example ourselves by joyfully living according to this truth. I am grateful to the CDF for holding the line, and giving us some encouragement in this fight.
A February 2021 TIME magazine piece about the Natural Cycles birth control app mimicked the skeptical, gloom-and-doom tone of most mainstream commentaries on fertility awareness-based methods of family planning (FABMs). The article trotted out the same concerns about their potential “inconvenience” and difficulty of use, as well as the claim that “it takes a very specific patient to be a good candidate to use FAMs as contraception.” Fortunately for girls and women seeking a hormone-free alternative to conventional birth control, the facts about modern, evidence-based FABMs of family planning are far different from what potential users are often led to believe.
Myth: FABMs are “inconvenient” and “difficult” to use.
The TIME article quoted a Seattle-based OB/GYN taking issue with Natural Cycles’ utilization of the woman’s waking temperature each day. She stated, “Taking your basal body temperature should be done before you move out of bed in the morning. And depending on how well you wake up, getting that accurate reading is really difficult and usually takes months of practice, because you literally have to do it before you get up to pee or move your body. So you have to reach over and take your temperature and then have the wherewithal to record it as well. It’s difficult for most people to do.”
Portraying the taking and recording of one’s own temperature as “difficult for most people” is arguably an exaggeration, not a statement of medical fact — especially given the simplicity of typing it straight into an app. Why should a woman who is considered capable and motivated enough to take a birth control pill each day be incapable of checking her own temperature?
In a world where women in particular often pay extraordinary detail to the food they consume and the chemicals in the products they use, the “inconvenience” and “difficulty” arguments don’t hold water. Certainly, women have other fertility awareness options that do not require a daily recording of one’s temperature, but automatically assuming that many or most women are incapable of this basic task is patronizing.
Myth: Very few women can use FABMs to successfully prevent pregnancy.
One provider states that “If you’re someone who has irregular menses, or sometimes skips periods every other month, or has longer or shorter cycles, then this can make tracking your periods very difficult.” She adds, “An app (like Natural Cycles) does not take into account travel that you might be doing, stress from working night shifts, stress from childcare, stress from being in a COVID-19 pandemic, stress from an argument that you had at work, and all of those things can significantly affect your cycle.” She concludes, “These aren’t things that would necessarily be tracked in a fertility awareness method application, and a particular stress could make the fertility awareness method unsuccessful.”
The article fails to mention that Natural Cycles’ app takes into account the possibility of irregular periods, sickness, and more, and still boasts the effectiveness rate mentioned above. Other evidence-based FABMs also have similar pregnancy prevention rates even given the factors listed above. The single most important factor for pregnancy prevention when using an evidence-based FABM is learning the particular method from a trained instructor, who can answer follow-up questions and help the woman understand her own body as she begins to put what she learned into practice. Certainly there is a learning curve when a woman begins for the first time to get in touch with the natural patterns of her own fertility and infertility, and a trained instructor can help her interpret the signs and identify what she sees.
Here’s the truth: FABMs teach women to get in touch with their own bodies.
At one point, the TIME article accurately captures the beauty of FABMs, quoting a healthcare provider who says, “[FAMs] really allow the patient to become more aware of her own menstrual cycle and have a much greater awareness of her own body and her own fertility in a way that does not necessarily happen if she’s on some type of prescribed contraception.” This is exactly the message that truly pro-life, pro-woman health care communicates.
Women’s bodies are inherently beautiful, not broken, and fertility is actually an indicator of overall health, not a liability or a burden. Learning the natural patterns of fertility and infertility in their own bodies and utilizing that knowledge to plan their families empowers women at their core, in a way that suppressing, altering, or destroying a functioning reproductive system never can
The Abortion Pill Rescue Network, a subsidiary of Heartbeat International, is claiming it was targeted last week by a leftist independent global media organization in an effort to discredit their work.
Andrea Trudden, Sr. Director of Communications and Marketing at APRN, notified ifamnews.com via email of openDemocracy’s “deceptive work (which) stole hours of hotline consultants’ time… (preventing) women truly in need from receiving the timely help they deserved.”
APRN had noticed an irregular increase in international calls to their organization, and to Option Line – their 24/7 contact center. Hotline nurses, despite the red flag and the overwhelming number of calls, did not waver in their response and continued to provide the usual compassionate service and care intended for women in genuine need.
APRN’s suspicions were confirmed Monday when openDemocracy contacted Heartbeat International for response to their “findings” of its “investigative report” on the Abortion Pill Rescue Network.
The email sent to ifamnews.com also states that Heartbeat International President Jor-El Godsey had anticipated the ruse the week before. “We know that our team only supplied evidence that we love and care for women as they seek to make the choice to rescue their baby from a chemical abortion,” said Godsey. “The good news? Our team performed excellently.”
“We hear from women every single day who regret taking mifepristone to end a pregnancy and desire a way to continue their pregnancies and rescue their babies,” said Christa Brown, director of Medical Impact at Heartbeat International. “Abortion Pill Rescue Network listens to their requests and offers women real choices even after starting a chemical abortion.”
In a phone call with ifamnews.com’s Robert Siedlecki, Trudden stated the abortion pill reversal process uses doses of progesterone, “a time-tested FDA-approved treatment used for decades to prevent miscarriage and preterm birth.” Regarding openDemocracy’s wave of calls, Trudden also relayed that the callers wanted everything done via email – likely for the purpose of a “paper trail” – as opposed to using normal vehicles like various online chat platforms. What heightened the suspicion was that “a disproportionate number of callers went through the whole process and then suddenly said they didn’t want any help”.
For the online helpers at APRN and Option Line, time is of the essence in helping women in need. From the moment a woman takes the abortion pill, she has about 72 hours to change her mind and save her baby. The Abortion Pill Rescue Network answers more than 150 mission-critical calls a month from women who regret their abortion decision. Statistics show that more than 2,000 lives have been saved (and counting) through the abortion pill reversal protocol.
“The Big Abortion allies at openDemocracy may have grist for their hit piece, but what they really did was distract our good people from the life-saving work APR actually is,” Godsey said. “It will certainly be lost on openDemocracy that their efforts fail women.”
March 18, 2021 (L’Espresso) — Sandro Magister note: Published as received. The author of the commentary, Thibaud Collin, is a professor of philosophy at the Collège Stanislas in Paris and has written important essays on “gender” theory, same-sex marriage, and political secularism. His latest book, from 2018, is entitled: “Le mariage chrétien at-il encore un avenir?”
The starting point for his reflection is the appointment of Philippe Bordeyne, 61, moral theologian, rector of the Institut Catholique of Paris, as president of the Pontifical John Paul II Institute for Studies on Marriage and Family, replacing PierAngelo Sequeri.
The rotation will take place in September. And it will mark a definitive course reversal for the institute that bears the name of John Paul II, but is increasingly distant from the teaching of the pope who founded it and of his predecessor Paul VI.
The earthquake that rocked the Institute in 2018 was unleashed by its Grand Chancellor, Archbishop Vincenzo Paglia, on a mandate from Pope Francis and with the visible disagreement of pope emeritus Benedict XVI.
But still there as dean was Sequeri – a theologian of recognized talent and not suspected of conservatism – to courageously keep alive an interpretation of Paul VI’s encyclical “Humanae vitae” faithful to its original meaning: > Surprise. Among the Francis Men Is One Who Is Defending “Humanae Vitae”
But now this last levee has fallen as well. For years Bordeyne has backed the supplanting of that encyclical and the rethinking of the theology of the family, which for him – and in his judgment also for Pope Francis – “by no means ends with the little bourgeois triangle of a father, a mother and children,” but “is the place where each individual grows as a person in relationship,” so that “to despise different families would also be to despise this work of socialization” (interview with “La Croix,” April 8 2016).
Professor Collin’s turn.
But then let’s call it the “Amoris Laetitia” Institute
by Thibaud Collin
The announced appointment of Msgr. Philippe Bordeyne, current rector of the Institut Catholique of Paris, as dean of the Pontifical John Paul II Institute is the last stage of the refoundation carried out by Archbishop Vincenzo Paglia and Pope Francis of this institution explicitly desired by St. John Paul II and founded by Carlo Caffarra, the future cardinal. That confirms this refoundation is a real and true revolution.
The rich reflection of the Polish pope on the sexual body, marriage, and the family can be understood as a response to the failure of the reception of St. Paul VI’s encyclical “Humanae vitae.” Of course, this document does not touch upon the entirety of those themes, far from it, but it can be considered as the touchstone of the whole doctrine of the Church on sexuality and marriage. The contraceptive mentality that the encyclical opposes is in fact objectively the condition of possibility of the social legitimation of abortion, of the technologies of procreation, and of all LGBTQ demands.
The encyclical ‘Humanae vitae’ teaches that natural methods of controlling fertility are the only legitimate ones. However, it must be recognized that the distance between the practice of the faithful and the teaching of the magisterium has grown even wider. Is it simple deafness to the calls of the Spirit or is it the fruit of a work of discernment and responsibility in Christian couples subjected to the pressure of new ways of life? The human sciences and the experience of couples teach us that the relationships between desire and pleasure are complex, eminently personal, and therefore variable according to the couples, and evolve over time and within the couple. Faced with the imperative moral duty to fight against the temptations of abortion, divorce, and the lack of generosity in the face of procreation, it would be reasonable to leave the discernment on birth control methods to the wisdom of couples, placing the emphasis on a moral and spiritual education that would make it possible to fight more effectively against temptations in a context that is often hostile to Christian anthropology.
In this perspective, the Church could admit a plurality of paths for responding to the general call to maintain the openness of sexuality to transcendence and to the gift of life. […] The way of natural methods that involves continence and chastity could be recommended as an evangelical counsel, practiced by Christian couples or not, that requires self-control in periodic abstinence. The other way whose moral legitimacy could be admitted, with the choice entrusted to the wisdom of the spouses, would consist in using non-abortive methods of contraception. If the spouses decide to introduce this medicine into the intimacy of their sex life, they would be encouraged to double their mutual love. Only this latter is capable of humanizing the use of technology, at the service of a human ecology of procreation” (“Synode sur la vocation et la mission de la famille dans l’Eglise et monde contemporain. 26 théologiens répondent,” Bayard, 2015, pp. 197-198).
This quotation is a summary of what a large number of theologians and episcopates have said about the ethical norm recalled by St. Paul VI and founded by St. John Paul II anthropologically in the catecheses on the “theology of the body” and morally in the encyclical “Veritatis splendor.”
But now the circle is closed: the ecclesial spirit of the seventies has ended up conquering Rome! But why has the “distance” been so “widened” if not because most pastors, not having wanted to embrace this good news on birth control, identified as an unbearable burden, never really passed it on to those who had been entrusted to them? At that point why even speak of “deafness” to the calls of the Spirit as if His voice had actually reached the ears of the faithful?
The reality is that most of these have had no inkling of the Church’s doctrine on this issue except from the dominant media. Since the transmission work has not been done, it is not surprising that there has not been assimilation.
It is therefore quite a stretch to say that this document, not having been accepted, needs to be sifted through the human sciences and the “wisdom” of couples. Circular reasoning that allows it to be discreetly cashiered. Making natural birth control the object of a choice reveals that the sacrament of marriage is no longer perceived as oriented towards the holiness to which all the baptized are called.
How can we fail to see that these statements gravely relativize the teaching of the magisterium and mislead couples of good will, who consequently see this ethical norm not as a way to happiness but as an almost inhuman ideal? The doctrine of “Humanae vitae” certainly needs to be embodied in pastoral practice and in a “moral and spiritual education,” but this need not be measured by the human sciences, unable by their nature to grasp the truth of the language of bodies. The purpose of education is adequate subjectivation, meaning the free realization of the true human good.
Pastors and lay people engaged in the pastoral care of marriage must therefore work to make lovable the good to be realized in the free acts through which the spouses signify in the language of the body the truth of their conjugal love. Affirming that the choice of birth control methods should be left to the conscience of couples reveals that the ethical norm is applied externally, without engaging the person as a whole; in short, in a manner that is already technical, a bit as if I were asking myself: “I have to go to that place: do I take the bike or the car?” Hence that very revealing expression which is the “humanization of technology through love,” when instead the very introduction of technology ends up obscuring the gift of self, making the union of bodies a sort of lie, which no longer objectively signifies the communion of spouses. The height of confusion is reached when it is indicated that this humanization of technology must be placed at the service of human ecology!
Only the virtue of chastity, intrinsically linked to the good of conjugal communion and the source of temporary continence while however not being reduced to this, can safeguard, in the unity of the person in body and soul, the truth of love. Only chastity raises the sexual life of the spouses to the height of the value of the person and avoids reducing this to its sexual values alone. In the field of love, technology cannot and will never be able to replace virtue.
Finally, it is amazing to think of contraception as a kind of bulwark against abortion, when all the studies show on the contrary that the advancement of the contraceptive mentality actually encourages abortion, not to mention that today many pills are also abortifacient.
In short, the appointment as manager of a figure like Philippe Bordeyne confirms that the John Paul II Institute, in full hemorrhage of students, should for the sake of intellectual honesty change its name. It could be called, for example, the “Amoris Laetitia” Institute.
WASHINGTON (SBG) — Millions of women use implanted IUDs for contraception. The Food and Drug Administration has approved several brands as a safe and effective form of birth control. But one device, the Paragard IUD, is drawing thousands of complaints and dozens of lawsuits over concerns it can break, leaving women facing surgery and other complications. Now, some health advocates are calling for the FDA to step in and investigate so women can have more information about the device.
Anna Speaks lives in a rural area where she’s surrounded by forest, gardens and scenery. Her connection to nature has always made her careful about what she puts in her body. After her son was born in 2013, Speaks wanted a birth control method that didn’t involve hormones, so she decided to try Paragard. The popular and effective T-shaped IUD gets implanted in the uterus and is approved to stay there as long as 10 years. It is considered the only non-hormonal form of birth control, instead using copper to prevent pregnancy. Approved by the FDA in 1984, Paragard has been on the market since 1988.
Anna Speaks told Spotlight on America that Paragard seemed like a low maintenance, low fuss method. But she says she was never warned by her health care provider that the device could potentially break.
Anna Speaks says her Paragard IUD broke upon removal from her body (Photo: Alex Brauer)
After about five years with the device, Speaks decided to remove the IUD. While Paragard says the removal of its product should be done by a health care professional, there’s debate among experts, with some saying self-removal is safe and often the choice women make who don’t have access to care or insurance — just like Anna.
When Speaks removed the device, she immediately noticed a problem. The T-shaped device was broken and she knew a piece was still inside of her.
“When I realized one of the Ts had broken off, I just kind of started to freak out,” said Anna Speaks, a former Paragard user. “I was panicked. It was devastating, actually.”
Anna Speaks says when she removed her IUD, she immediately realized that a piece was missing (Photo: Anna Speaks)
Panicked, she realized the problem would now require an expensive and traumatic visit to a doctor to try to retrieve the broken piece. Eventually, surgery was required in an attempt to locate the missing fragment, which turned up on an X-ray supplied to Spotlight on America.
Our team discovered breakage like what Speaks experienced is a well-documented, yet little-publicized problem with the Paragard IUD. Spotlight on America dug through thousands of “adverse events” listed in a database known as FAERS – The FDA Adverse Events Reporting System, which tracks problems reported by individuals and health care providers.
According to the voluntary reports filed with the FDA since 2013 regarding Paragard, there have been:
3,186 reports of “device breakage”
1,910 of those events deemed “serious”
102 related reports of hospitalization or life-threatening complications
An exclusive Spotlight on America investigation found 3,000+ reports of Paragard breakage in an FDA database (Photo: Alex Brauer)
Those figures uncovered in our Spotlight on America investigation are attracting new attention from national leaders in women’s health. Cindy Pearson is Executive Director of the National Women’s Health Network, an organization that strives to empower women and promote equity in health care.
We shared what we found about the Paragard IUD with Pearson, who told us the complaints are just the tip of the iceberg, since they represent only those that took the time to file a report in a government system that is cumbersome and not well known to the public. The problem with voluntary reporting, Pearson says, is it’s hard to tell how often these issues happen, which specific lot numbers they may be tied to and whether the complication is related to the device or something specific about the individuals using it.
Getting the answers about the source of complications or adverse events after products hit the market can be difficult. Generally, companies are not obligated to look at the long-term effects or complications following FDA approval unless the agency instructs them to act or they voluntarily choose to conduct a study. But Pearson says with more than 3,000 Paragard breakage reports, it’s time for the FDA to take a closer look. “It’s a warning sign that deserves to be investigated,” said Pearson. “The FDA should now step in, investigate and use its authority.” Pearson says the agency could potentially require a study so that women can make an informed choice.
“That’s something that shouldn’t kill the method, it should just inform us,” said Cindy Pearson with the National Women’s Health Network. “If there’s no way to figure out what makes it more likely to break but we’re able to determine it breaks 1 in 25,000 times, then that’s a risk many women would still be willing to take, but we need to know.”
Cindy Pearson, Executive Director of the National Women’s Health Network, says IUDs are a safe & effective birth control method but women should be informed about potential complications
The FDA told Spotlight on America it is not currently requiring any new studies of the Paragard IUD. You can read their complete response to our questions at the bottom of this article.
For now, many impacted women are banding together on social media pages to discuss their experience with Paragard. One community on Facebook has more than 8,000 members, supporting one another by sharing personal stories. Some on the site have shared experiences discussing breakage of Paragard. Pearson says those collective experiences can prove powerful, with the FDA previously taking action on another birth control device, Essure, after a grassroots campaign on social media compelled the agency to look closer at complications. Essure is no longer on the market after advocates spent years highlighting problems with the device.
Health advocates say social media can be a powerful tool to compel the FDA to action, as was the case with the birth control device, Essure (Video: WJLA)
As women wait to see if the FDA will take a closer look, some are taking action in court. Spotlight on America discovered at least 55 recent lawsuits filed in more than 20 states by women who claim Paragard “has a propensity to break upon removal, causing complications and injuries, including surgeries to remove the broken piece of the device, infertility and pain.” The lawsuits were consolidated into multidistrict litigation in Georgia in December 2020 and are awaiting the next step.
Spotlight on America repeatedly tried to contact the maker of Paragard, reaching out by phone, email and even sending direct messages on social media platforms. Our requests to speak with the company were not returned.
Paragard has argued in the past that its warnings about the device are adequate, though you won’t hear any mention of breakage in the listing of potential side effects we found in commercials posted online.
When our team went through the prescribing packet for Paragard, we did find a mention of breakage in the fine print, “Breakage of an embedded Paragard during nonsurgical removal has been reported.” In a later section the company says, “Because these reactions are reported voluntarily from a population of an uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.”
The prescribing information for Paragard notes that because reactions like breakage are reported voluntarily, it is not always possible to determine how often they happen (Photo: SBG)
Anna Speaks says she was unaware of the potential for breakage and never saw a product label. She is sharing her experience, hoping it will help other women make informed choices. She filed a report with the FDA and says she is working with an attorney. Speaks encourages anyone who’s experienced a complication to share their story. “I do think there’s power in that,” Speaks said. “That’s how we create better regulations and how we create more transparency with these companies and help protect women and their bodies.”
If you’ve had experience with Paragard IUD breakage, contact us on Twitter or email us spotlight@sbgtv.com.
An X-Ray image shows a broken piece of the Paragard IUD in Anna Speaks’ uterus (Photo: Anna Speaks)
Spotlight on America reached out to the FDA to see if they are taking any action on Paragard and to get their reaction to criticism of the voluntary reporting system. The full Q&A is below:
1) Is the FDA currently doing any studies or follow-up research when it comes to adverse events involving the Paragard IUD?
Response: The FDA has been monitoring the safety of Paragard, as we do with all approved drug products, and remains committed to informing the public in a timely manner if and when the Agency identifies new safety issues that warrant FDA action. FDA is not currently requiring or requesting any studies on the Paragard intrauterine system. Also see our response to questions 3 and 4 regarding our use of the FAERS database and the strengths and limitations of FAERS.
2) Does the FDA perform any oversight of the manufacturing of the Paragard IUD – including inspections of materials, factory process, etc.?
Response: At the FDA, protecting patient and consumer health is our highest priority. For Paragard and other FDA-approved products, the FDA inspects manufacturing facilities and, when needed, takes action to enforce current good manufacturing quality standards and applicable regulations. When objectionable conditions are identified with manufacturing processes or controls, creating a risk of potentially producing an unsafe product, it’s important that the problems are quickly remedied. When needed, we exercise our regulatory authority commensurate with the assessed risk, including issuing import alerts, warning letters, and in the most serious cases, working with firms as they recall drugs, seizing drugs in commerce or enjoining manufacturers to prevent further violations. We continue to remain vigilant in our compliance and enforcement work, and we’ve taken a number of actions already this year. These actions are key parts of our commitment to ensure high-quality manufacturing, and to make sure Americans have confidence in the quality of products sold in the U.S.
3) Is there a threshold for the number of complaints to the FAERS database before the FDA will re-examine a drug?
Response: There is no specific threshold for the number of reports required before FDA will reexamine a drug. The FDA is monitoring the safety of Paragard, as we do with all approved drug products, and remains committed to informing the public in a timely manner if and when the agency identifies new safety issues that warrant FDA action. The reports in the FDA Adverse Event Reporting System (FAERS) database are routinely evaluated by FDA staff to monitor the safety of products after approval. On a weekly basis, FDA reviewers monitor individual spontaneous adverse event reports from the FAERS database. These staff also routinely monitor other sources of data, such as published literature and mandatory periodic safety reports from manufacturers. This information is collectively reviewed to inform whether regulatory action, such as labeling changes or other FDA communications, are needed. Additional information on postmarketing safety is available here.
Healthcare professionals, consumers, and manufacturers submit reports to FAERS. FDA receives voluntary reports directly from healthcare professionals (such as physicians, pharmacists, nurses, and others) and consumers (such as patients, family members, lawyers, and others). Healthcare professionals and consumers may also report to the products’ manufacturers. If a manufacturer receives a report from a healthcare professional or consumer, they are required to send the report to FDA as specified by regulations.
While FDA relies on the FAERS database as a drug safety surveillance tool after a product is approved and marketed, there remain limitations to the data that you should consider.
FAERS data by themselves are not an indicator of the complete safety profile of a drug.
Duplicate and incomplete reports are in the system: There are many instances of duplicative reports and some reports do not contain all the necessary information.
Existence of a report does not establish causation: For any given report, there is no certainty that a suspected drug caused the reaction.
Information in reports has not been verified: Submission of a report does not mean that the information included in it has been medically confirmed.
Rates of occurrence cannot be established with reports: The information in these reports cannot be used to estimate the incidence (occurrence rates) of the reactions reported or be used to make comparisons between products.
Differential reporting for one product over another may occur: Reasons for this include the time the product has been on the market, publication of literature reports related to an adverse event, and publicity surrounding the product or adverse event.
4) Because the FAERS database is voluntary, critics have asserted that it does not provide a complete picture of potential adverse reactions (i.e., It does not compel medical providers to report adverse events, which would help glean specific information about the frequency of specific issues, etc.) How does the FDA respond to that criticism?
Response: While there are limitations to FAERS (see response to Question #3), there are also notable strengths. FAERS data are particularly useful for identifying new (i.e., unexpected), rare, serious adverse events that are temporally associated with a product for which the background rate of events is low. Such adverse events are often not observed in the premarketing trials because these trials are limited in the number of patients, the types of patients included, and the duration of treatment. In addition, the spontaneous adverse event reports in FAERS can further refine or characterize a known adverse event.
As also noted in our response to Question #3, in addition to FAERS, other sources of postmarketing data are utilized to monitor and assess adverse events in the post-market setting.
During the Great Stem Cell debate, “the scientists” said they “only” wanted to be able to create and experiment on embryos up to 14 days of development, when cells begin to differentiate. Of course, at the time they couldn’t maintain them for longer than 14 days, so nothing was actually limited.
Now that they can, they plan to ditch the “14 day rule” as it is called — actually, it is a guideline since it isn’t legally binding — promulgated by the International Society for Stem Cell Research.
For the last 40 years, this voluntary guideline has served as an important stop sign for embryonic research. It has provided a clear signal to the public that scientists wouldn’t grow babies in labs. To researchers, it gave clarity about what research they could pursue.
Now, however, a key scientific body is ready to do away with the 14-day limit. The action would come at a time when scientists are making remarkable progress in growing embryonic cells and watching them develop. Researchers, for example, can now create embryo-like structures starting even from stem cells, and some hope to follow these synthetic embryo models well past the old two-week line.
And after that? Once embryos can be gestated in artificial uteruses, why not go to one month, three months, or six months? Hell, why not up to the point of birth? These are developing human beings, but there will always be a utilitarian excuse! Vermont has already passed a law that states no embryo or fetus has any rights of their own that have to be respected.
Much of this is learning how to engage eugenic manipulations:
Scientists are motivated to grow embryos longer in order to study — and potentially manipulate — the development process. But such techniques raise the possibility of someday gestating animals outside the womb until birth, a concept called ectogenesis.
According to [bioethicist Tetsuya] Ishii, new experiments “might ignite abortion debates,” especially if the researchers develop human embryos to the point where they take on recognizable characteristics like a head, beating heart cells, or the beginning of limbs.
Just know this: All of these talks of “limits” and “ethical boundaries” are a big con. Guidelines will not protect against abuse because those in charge will keep changing the guidelines.
And people wonder why there is so much distrust of our institutions.
LifeNews.com Note: Wesley J. Smith, J.D., is a special consultant to the Center for Bioethics and Culture and a bioethics attorney who blogs at Human Exeptionalism.
Earlier this year, we started a “Reasons Women Need Periods” series putting a spotlight on how women’s periods play a crucial role in other elements of women’s health. We talked about the importance of endogenous (i.e., naturally occurring) hormones and healthy cycles for immune system maturation, bone health, and heart and blood pressure regulation. Today we’re turning to the biggest and baddest organ of all—the brain.
Our noggin uses over 20% of our energy, making it the most “expensive” organ we have. And, you guessed it, our reproductive hormones (especially estrogen and progesterone) have really important effects on the brain. Brain health is another reason why you need a period—and therefore ovulation, and the healthy hormone production that makes your cycle possible.
Your brain and your hormones need each other
The first important thing to note is that steroid hormones (primarily estrogen and progesterone) are synthesized in the central and peripheral nervous system. This means they cross the blood-brain barrier and have organizational effects on the brain. Estrogen generates plasticity in the brain and improves cognitive function while progesterone regulates glial cells and promotes mood stabilization [1]. Before you think about these two hormones as independent players, they are anything but. If the effects of these hormones are not experienced in a balanced and cyclical way, the neuroprotective factors they are supposed to provide vanish.
In the first portion of our cycle (the follicular phase), estrogen is king. Or should I say—queen. As the dominant follicle in your ovary gears up for ovulation and grows, it produces increasing amounts of estrogen. This estrogen increases serotonin receptor levels as well as dopamine synthesis. This boils down to an increase in neuron excitability. These stimulated neurons increase structural plasticity of dendritic spines in the hippocampus, amygdala, and prefrontal cortex. Neuron excitability often translates to general feelings of an upbeat mood, increased energy levels, and improved verbal and lingual skills.
In the second portion of our cycle (the luteal phase), progesterone sweeps in and takes the stage. Progesterone is estrogen’s foil character. Instead of stimulating brain cells, it heals and maintains them by inhibiting dopamine-induced glutamate release. In this therapeutic phase, women often report mellowness in mood, decreased anxiety, and even more maternal tendencies. This is all thanks to GABA, the most inhibitory neurotransmitter in the brain. Progesterone (and allopregnanolone, which comes from progesterone) potentiates GABAergic synapses [2]. If there’s no progesterone, there’s no GABA. And interestingly, GABA has been shown in early studies to be an effective treatment for premenstrual dysphoric disorder (PMDD) [3].
Teens need their cycles for proper brain development
Have you ever wondered why teenagers and young adults seem to make more brash decisions and seem less grounded with risk assessment? It’s because quite literally, their brains—or more accurately, their prefrontal cortices—can’t process risk until they have fully matured. This full maturation usually occurs in the mid-twenties. Exposure to endogenous and balanced hormones (which occurs through regular ovulation and menstruation) throughout the teenage and young adult years helps develop and protect the brain. Without ovulation, the brain doesn’t have the same chance to mature. And even better, maturation under healthy endogenous hormones can help retain brain plasticity better for women after menopause.
Brain fog and depression: Birth control’s effects on the brain
You may think that the hormones in hormonal contraception have the same effect on brain health as endogenous hormones do. Unfortunately, the synthetic alternatives of estrogens and progesterone found in birth control have been shown to decrease serotonin concentrations and increase hepatic sex hormone binding globulin (SHBG). In effect, this makes your naturally occurring sex hormones harder for your body to utilize.
It’s well documented that the pill (and any of its relations, including the patch, the vaginal ring, the implant, the shot, and the hormonal IUD) comes with an increased risk of depression and mood disorders. Additionally, many women report “foggy brain” as a side effect of hormonal birth control. Some women don’t realize the symptom of brain fog until they get off birth control, and many women report feelings of “seeing in color for the first time” after returning to their cycles post-birth control. This is all related to the way the endocrine system acts on the brain. When you look at the bigger picture of how these synthetic hormones not only alter brain organization, but also rob the brain of exposure to endogenous hormones, these risks start to make sense.
You’re not crazy—your thoughts and feelings are very much tied to your hormones!
The Pill and your stress response—or lack thereof
Another glaring contrast in pill-taking brains as opposed to non-Pill-taking brains is the stress response, or rather the lack thereof.
“We should all be alarmed by the fact that the stress hormone profiles of women who are on the birth control pill look more like those belonging to trauma victims than they do like those belonging to otherwise healthy young women [6],” Hill exhorts.
When women’s bodies naturally ovulate and menstruate, women’s brains are enabled to mature, improve, and maintain cognitive function, and even protect their future neuroplasticity. When they take synthetic hormones that disrupt these natural reproductive processes, these brain developments are inhibited.
So, do you need a period? The answer lies in how much we care about women’s overall health as the interconnected ecosystem that it is—where hormone health affects heart health, immune system health, bone health, and now we can add brain health to the list. Since ovulation and menstruation have lifelong effects on cognitive function—which can affect how you interact with yourself and others in the world—there is a compelling case that these are vital aspects of women’s health.
References:
[1] Del Río J, Alliende M, Molina N, Serrano F, Molina S, Vigil P. Steroid Hormones and Their Action in Women’s Brains: The Importance of Hormonal Balance. Front Public Health. 2018;6. doi:10.3389/fpubh.2018.00141
[2] Boero G, Porcu P, Morrow A. Pleiotropic actions of allopregnanolone underlie therapeutic benefits in stress-related disease. Neurobiol Stress. 2020;12:100203. doi:10.1016/j.ynstr.2019.100203
[3] Hantsoo L, Epperson C. Allopregnanolone in premenstrual dysphoric disorder (PMDD): Evidence for dysregulated sensitivity to GABA-A receptor modulating neuroactive steroids across the menstrual cycle. Neurobiol Stress. 2020;12:100213. doi:10.1016/j.ynstr.2020.100213
[4] Study finds key brain region smaller in birth control pill users. ScienceDaily. https://www.sciencedaily.com/releases/2019/12/191204090819.htm. Published 2020. Accessed November 11, 2020.
[5] Petersen N, Touroutoglou A, Andreano J, Cahill L. Oral contraceptive pill use is associated with localized decreases in cortical thickness. Hum Brain Mapp. 2015;36(7):2644-2654. doi:10.1002/hbm.22797
[6]Hill S. This Is Your Brain On Birth Control. New York, NY: Avery; 2019.
Restrictions on abortion do not lead to an increase in women dying due to a lack of “safe” abortions, according to a new study highlighted by the American Association of Pro-Life Obstetricians and Gynecologists (AAPLOG).
In a recent tweet, AAPLOG cited a study published in the peer-reviewed medical journal BMJ Open, which examined maternal mortality in 32 Mexican states over a 10-year period, between 2002 and 2011. The study began by acknowledging the pro-abortion argument that “the legal status of abortion … is a factor that influences maternal health.” They also acknowledged the common argument that restrictions on abortion are thought to lead to “clandestine, or illegal, or unsafe abortions” leading to an increase in maternal deaths.
But instead of discovering data in support of that argument, the study instead found that “states with less permissive abortion legislation exhibited lower MMR [maternal mortality rates]” (emphasis added) than those where abortion laws are more permissive. In other words, pro-life restrictions on abortion did not result in higher maternal mortality rates.
Even in Mexican states that enacted constitutional amendments outlawing abortion, women’s health did not suffer: “No evidence of deleterious or beneficial effect [on maternal mortality] was found for the presence of constitutional amendments protecting the unborn over a 4-year study period.”
To be clear, the Mexico study’s authors did not find evidence that abortion restrictions were the cause of better maternal outcomes. Independent variables between the states explained most of the differences in outcomes. As AAPLOG’s tweet pointed out, “non-legislative factors (female literacy, birth weight, skilled attendance at birth, clean water, etc.) were leading causes” in the lower maternal mortality rates in the states with more abortion restrictions.
An attempted rebuttal published in the noted pro-abortion journal Contraception sought to undermine the Mexico study’s conclusions by attacking the authors’ use of the underlying data, while also engaging in ad hominem attacks. The paper claimed the Mexico study’s authors “have failed to respond to anti-abortion ‘junk science,’ which influences policy in the region,” claims an excerpt in Retraction Watch.
Yet the critique did not hold up to scrutiny. “Sincerely, I don’t know how our study is ‘influencing’ policies in the region, and of course I don’t consider our work as ‘junk science’,” said Elard Koch, the main author of the Mexico study. After an examination of the data and counter-argument in the paper, Koch pointed out a major statistical error in key calculations of the rebuttal that undermined the published conclusions. The flaws in the Contraception article were serious enough that the editors were forced to issue a public retraction.
The finding that abortion restrictions do not cause higher mortality rates deals a blow to a common line of argument for abortion activists. The notion that maternal health suffers when abortion restrictions are enacted is a narrative that abortion activists often trot out in response to the enactment of new pro-life laws. In 2019, in response to Georgia’s heartbeat bill, Hillary Clinton tweeted, “When anti-choice politicians limit access to reproductive care, women die.” She argued that “we must continue to fight the new wave of six-week abortion bans that make women collateral damage for extremist views.”
The misperception about abortion and maternal mortality has its origins in a big lie told by early abortion activists. In the years leading up to the legalization of abortion, abortion activists like Dr. Bernard Nathanson (one of the founders of NARAL) disseminated false statistics about the number of women dying each year from illegal abortions, as Live Action News has reported. The widely cited figure — that 5,000 to 10,000 women were dying each year from back-alley abortions — was a deliberate fabrication designed to advance the pro-abortion agenda. Dr. Nathanson, who later became pro-life, admitted to fabricating this number because it was a “nice, round, shocking figure.”
The Mexico study correlates with historical analyses of maternal mortality in the 20th century. As a Live Action Pro-Life Replies video notes, maternal mortality in the United States dropped precipitously in the decades prior to the legalization of abortion, and not as a result of legalized abortion. It was the advent of antibiotics like sulfa and penicillin in the mid-20th century, not abortion legalization, that resulted in the dramatic reduction of maternal mortality rates.
Current maternal mortality rate comparisons between countries further refute abortion activists’ arguments. Countries like Poland and Malta — which have tight abortion restrictions — have lower mortality rates, at three and nine deaths per 100,000 live births respectively, while the U.S. rate stands at 17 deaths per 100,000 according to the latest data, as Vox reported.
If the Mexico study is right, then the remedy for maternal mortality is not permissive abortion legislation, and abortion activists need to stop using a deceptive narrative to further their cause. By doing so, they prevent us from getting at the real solutions to maternal mortality, as identified by the Mexico study: the “non-legislative factors,” or medical, social, and educational variables, that were shown to have a causal effect on maternal mortality rates.
March 12, 2021 (LifeSiteNews) — The first vaccine in the United States to use an aborted fetal cell line in its production was the MMR vaccine in 1979. Currently in the United States there are many vaccines that contain aborted fetal DNA in the end product of the vaccine, while others use aborted fetal cells in their research and development.
There are four cell lines that are being used in vaccines currently available, including those expected to be available in the next month or two. These four cell lines are MRC-5, WI-38, PER C6, HEK293.
In addition to these cell lines, abortions were also done to obtain RA27/3 for use in the rubella vaccine. The rubella vaccine alone is the result of at least 99 abortions (32 for WI-38 and 67 for RA27/3). Yes, they came from abortions, not babies who died naturally in the womb.
The baby has to be alive when the tissues are taken. Otherwise, they are unusable.
MRC-6 and Wi-38 are both from the 1960s. PER C6 is from 1985, while HEK293 is from 1972. There are other aborted fetal cell lines that exist, but are not currently being used for vaccines.
The most recent aborted fetal cell line is from 2015 (Walvax2). This particular cell line is the result of 9 abortions.
Of those vaccines that are currently FDA-approved, all of the MMR (measles, mumps, rubella), hepatitis a, and chickenpox vaccines, including any combination vaccines for these illnesses, use aborted fetal cell lines. One of the shingles vaccine brands and one of the rabies vaccines also use aborted fetal cells.
As for experimental COVID injections, Johnson & Johnson and AstraZeneca both use aborted fetal cell lines on which to grow the virus for their vaccines. Pfizer and Moderna, for their COVID-19 injections, used the aborted fetal cell line HEK293 for the research and development of their vaccines.
With the exception of the Pfizer and Moderna vaccines, the others do contain aborted fetal DNA in the end product. It is next to impossible to remove all of the DNA from the virus grown in the aborted fetal cell lines. In fact, independent research has found levels as high as 142 to 2000 ng per dose, despite the FDA and WHO recommending limits of 10ng per dose.
The aborted fetal DNA contamination present in vaccines that use aborted fetal cell lines in their production come with risks. Specifically a risk of triggering autoimmune disease, as well as the risk of DNA insertion into the vaccine recipient’s DNA.
In addition to these risks, it is particularly interesting — given the current autism spectrum disorder (ASD) epidemic — that research shows that strong change-point correlations exist between rising ASD rates and when the first MMR vaccine with aborted fetal DNA was introduced, when the second dose was introduced, and when the chickenpox vaccine, which also contains aborted fetal DNA, was introduced in the United States.
The use of aborted fetal cell lines in vaccine research and production carries the serious moral concerns of abortion, trafficking of these babies, and denial of a proper burial, as well as serious health concerns.
As long as we as a society keep rolling up our sleeves for vaccines and other pharmaceuticals that use aborted fetal cells in their research, development or production, the situation is not going to get better, as there is no motivation for these companies to change their ways.
LifeSiteNews has produced an extensive COVID-19 vaccines resources page. View it here.
Dr. Marissa Brand is a board-certified Doctor of Natural Medicine and Doctor of Humanitarian Services, with a PhD in Natural Medicine.
Birth rates in the U.S. started their decline in 2006 — the same year the CDC recommended every American girl between the ages of 9 and 26 get Merck’s Gardasil HPV vaccine.
A CBS News story earlier this week sounded a recurring alarm about the record decline of birth rates in the U.S.
The news agency obtained records from health departments in more than two dozen states showing a 7% drop in births in December 2020 — nine months after the first lockdowns began.
As the Pew graph below illustrates, the overall drop in birth rates actually began in 2006.
Baffled “experts” blame everything from social media to the economy. But they overlooked one obvious possible explanation: the Gardasil HPV vaccine, which the Centers for Disease Control (CDC) and Prevention’ Advisory Committee on Immunization Practices recommended for every American girl between the ages of 9 and 26 — beginning in 2006.
Clinical trial researchers for Merck, Gardasil’s manufacturer, reported an explosion of reproductive injuries among the 20,000 trial volunteers. An astronomical 15% – 17% of trial participants experienced a range of reproductive harms, including premature ovarian failure.
CDC’s own graph shows that the steepest drops in births have occurred among teens — the age group most likely to have received the vaccine. Among this group, birth rates dropped a breathtaking 46% between 2007 and 2015. There were no changes in birth control or abortion rates that would explain this drop.
Gardasil contains three ingredients, L-histidine, polysorbate 80 and sodium borate that are all associated with reproductive disorders. The U.S. Food and Drug Administration has banned sodium borate in foods in the U.S., partially because of its strong association with premature ovarian failure. Merck nevertheless includes it in Gardasil.
During our Gardasil litigation, we have spoken to hundreds of girls suffering premature ovarian failure and a range of other reproductive problems. Gardasil victims and their mothers frequently tell us of girls who cease menstruating after receiving the Gardasil vaccine.
Merck knew that it was orchestrating a population-wide fertility experiment when it persuaded the CDC to effectively mandate Gardasil for every American teenager. Merck’s pre-licensing studies predicted the current national drops in fertility.
If Gardasil injured you, and you want to know your rights, call me at 844-RFK-HPV1.
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children’s Health Defense.
What are we doing to ourselves, and to our children? This is a question I am pondering a lot as of late, as I watch our nation, and so many parts of the world, racing to embrace ever more extreme and ever more destructive forms of anti-life and anti-family ideology.
With a kind of reckless abandon, we are casting aside common sense principles that have guided individuals and societies towards health and well-being for countless generations, replacing them with untested, unproven, and often flagrantly absurd ideas about sex, gender, marriage, family, life, and death.
In a way, I suppose I am “used” to the radicality and irrationality of the anti-life and anti-family revolutionaries. I expect bad and absurd ideas. After all, what could be more absurd than the claim that the unborn child is merely a “blob of tissue,” with no moral weight? And this in the 21st century, when we can watch detailed, 3D videos of the unborn child moving about in his mother’s womb!
And yet there is something that is somehow uniquely horrifying about the speed with which so-called “gender theory,” with its ever more implausible claims, has flooded the airspace in the past decade, going from something that most people had never given a moment’s thought to, to the dominant “social justice” cause of the day, with acquiescence demanded and enforced by the cultural and political elite.
Growing Intolerance
You would think that the burden of proof for the radical ideas of gender theory would rest on the revolutionaries who propose to turn our world topsy-turvy. Instead, however, in the historical equivalent of the amount of time it takes us to blink an eye, a new orthodoxy has swept our culture, quashing all dissent. Any amount of questioning or criticism is shouted down and shunned as a “dangerous” and “violent” assault on a vulnerable minority population.
Even merely to wonder, for instance, whether it is good for children and young teens to take puberty-blocking hormones, or to undergo irreversible surgical interventions, is proof-positive that one is “transphobic.” The only acceptable attitude to gender theory is unqualified enthusiasm. Anything less is a form of intolerance and bigotry that will – we are assured – drive transgender people to self-harm and suicide, and is therefore tantamount to “violence.”
At the moment, most of the enforcement mechanisms are social, rather than legal, taking the form of public shaming, and a growing censorship by private corporations. Any public figures who dare to publicly question any tenet of gender theory can expect an online mob to descend upon them, and for their employers to be pressured to cast them out into the darkness of unemployment. Often, the mob gets what they demand.
Meanwhile, the tech giants are increasingly ensuring that there is little space in the online world for expressing dissent. For years now, Twitter has banned so-called “dead-naming” – that is, referring to a transgender person by his or her birth name and/or biological sex. When President Biden recently appointed a transgender “woman” – i.e. a biological man who claims to be a woman – as the Assistant Secretary for Health, a conservative publication was suspended from Twitter for correctly noting that, biologically, he is a man. In other words, Twitter has formally banned stating a scientific truth as hateful and intolerant.
Recently, Amazon also stepped into the ring. Without notifying anyone, Amazon quietly pulled Ryan T. Anderson’s best-selling book When Harry Became Sally from their online store. Given that Amazon accounts for an overwhelming majority of online book sales, the disappearance of the book essentially makes it invisible to most online consumers. That, of course, is the whole point.
In the book Anderson had carefully scrutinized, and criticized, gender theory. It is worth noting that Anderson is no polemicist. He is a highly competent and highly respected conservative academic. In the book he presents his findings backed up by the best scientific data and takes enormous care to make his case in a way that is respectful towards individuals with gender dysphoria. And yet, none of that is enough for the progressive overlords at Amazon. As many commentators have rightly pointed out, you can buy Hitler’s Mein Kampf on Amazon, but you cannot find what is arguably the best book addressing one of the most hotly debated contemporary social issues.
Amazon eventually issued a terse statement saying that the book violated their “content policy.” That content policy states that Amazon reserves the right not to sell content “we deem inappropriate or offensive” – language that is so broad and subjective that it could be applied to just about anything. As Anderson noted in an article in First Things in response to Amazon’s move, “It’s not about how you say it, or how rigorously you argue it, or how charitably you present it. It’s about whether you affirm or dissent from the new orthodoxy of gender ideology.”
The Equality Act
Given the march towards censorship, it’s hardly surprising that a movement is afoot to take the next logical step – that is, to move beyond shaming and censorship, and to enforce this new ideology using the full apparatus of the State.
It is typical of the progressive left that they should disguise something so pernicious in language that sounds so harmless, indeed quite positive and uplifting. Who, after all, could possibly be against “equality”?
The Equality Act, which was passed just a few days ago in the U.S. House of Representatives, would ostensibly ban “discrimination” based upon “gender identity” and “sexual orientation.” In other words, it introduces the ill-defined, scientifically unsupported, and revolutionary notion of “gender identity” all throughout federal law.
The effect of the law would be widespread. Conservative commentators, including the U.S. Catholic bishops, have warned that the law would be used as a bludgeon against conscience rights, freedom of speech, and freedom of religion.
In a list of the effects of the Equality Act, the U.S. bishops note that it would require “women to compete against men and boys in sports, and to share locker rooms and shower facilities with men and boys.” The bill, they said, also “forces faith-based charities…to violate their religious beliefs,” “forces religiously operated spaces and establishments…to either host functions that violate their beliefs or close their doors to their communities,” and “jeopardizes existing prohibitions on the use of federal taxpayer funds for abortion.”
In a recent letter to Congress, the five committee chairmen of the U.S. Conference of Catholic Bishops warned: “The [Equality Act] represents the imposition by Congress of novel and divisive viewpoints regarding ‘gender’ on individuals and organizations. This includes dismissing sexual difference and falsely presenting ‘gender’ as only a social construct.”
They continued, “It is one thing to be understanding of human weakness and the complexities of life, and another to accept ideologies that attempt to sunder what are inseparable aspects of reality.”
Push Back
On the question of gender theory, there is no doubt about Pope Francis’ position. He has been vociferous, repeatedly and often condemning gender theory as a diabolical innovation.
During a speech in Poland in 2017, he warned that, “[T]oday children – children! – are taught in school that everyone can choose his or her sex. Why are they teaching this?” On one occasion, he even compared the imposition of gender theory to the propaganda of the Hitler youth.
More recently in a book prepared by Father Luigi Maria Epicoco commemorating the 100th anniversary of Pope St. John Paul II’s birth, Pope Francis, who offered commentary, was asked where he sees evil most at work today. “One place is ‘gender theory,’” said the pope. The Holy Father continued to say that gender theory is “dangerous” because it aims to erase “all distinctions between men and women, male and female.” It seeks to “destroy at its roots” the creative project that God wanted for each of us: “diversity, distinction. It would make everything homogenous, neutral. It is an attack on difference, on the creativity of God and on men and women.”
Indeed, I fear that we have barely begun to grapple with the impact that the ubiquity of gender propaganda in our schools and universities is having upon the younger generations, and what it portends for the future of our nation.
One shocking recent poll found that record numbers of youth are self-identifying as LGBT. Whereas in 2017, only 4.5 percent of the population identified as LGBT, that has since risen to 5.6 percent. A huge proportion of the increase can be traced to so-called Generation Z – that is, people born between 1997 and 2002. Nearly one in six members of Generation Z self-identify as LGBT, compared to 9.1% of millennials, and 3.8% of Generation X.
Pro-LGBT activists are interpreting this data as proof that more LGBT people feel comfortable “coming out,” due to more tolerant attitudes towards diverse sexualities. While it is possible that this is one contributing factor, I think it is naïve in the extreme to discount the ways that constant bombardment with pro-LGBT messages is recruiting more and more young people into experimenting with sexual identities and practices that would never have occurred to them otherwise.
Indeed, there are a growing number of stories of schools and communities where transgender identification has rapidly spread through the ranks of young teens. In many cases, these young people are immediately being shuffled towards “treatments” that are either completely irreversible, or have significant long-term impacts.
Courageous thinkers like Ryan Anderson are precisely what we need, to stand in the gap and question the dominant narrative using the best evidence available. Unfortunately, many people are being cowed into silence by the ideologues, afraid for their livelihoods and their reputations. The problem, however, is that every person who chooses silence and safety over truth, is one more person who gives the revolutionaries the space they need to steamroll others, and more of our culture, into acquiescence.
As always, hope in the face of lies and evil is found in adherence to truth and the willingness to fight to uphold it.
It is time for all Christians and people of good-will to rise up. One thing that every American can do today is to contact their senator, urging them to vote “no” to the deceptively-titled “Equality Act.” Do it today. The future of our country, and our youth, depends on it.
Abortion pill clients experiencing a complication are more likely to receive care from an emergency center than the abortion facility where they obtained the pills, according to an analysis of adverse events reports (AERs) submitted to the Food and Drug Administration (FDA) by abortion pill manufacturer Danco.
A team of over 30 board certified physicians spent three years reviewing thousands of pages of AERs and discovered glaring deficiencies in reporting on abortion pill complications and deaths. They also found that more than 60% of the surgeries due to abortion pill complications were not handled by the abortion facility, increasing the potential for large amounts of underreported complications.
Published by Issues in Law & Medicine, “Deaths and Severe Adverse Events after the use of Mifepristone as an Abortifacient from September 2000 to February 2019,” sheds doubt on whether deaths and adverse events are being properly tracked. The authors of the study included researchers from the American Association of Pro-Life Obstetricians and Gynecologists (AAPLOG). “[T]he analysis of the AERs revealed glaring deficiencies… Throughout the reports, there was also a lack of detail and many patients who were simply ‘lost to follow-up,’” the authors wrote.
Due to the dangers posed by the abortion pill, the FDA put in place a safety system called REMS. While anyone can submit an AER, the FDA currently requires AERs on the abortion pill (Mifeprex or mifepristone) to be submitted by Danco Laboratories, Inc. or by the abortion pill’s generic manufacturer, GenBioPro.
More ERs are treating complications than abortionists, which means complications may go unreported
The study found a greater percentage of emergency rooms were treating abortion pill complications than abortion facilities. And, since abortion pill complications are only reported to FDA once the prescriber (abortion facility) or Danco becomes aware, it is likely many complications are falling through the cracks unreported. Interestingly, Live Action News has documented how the abortion industry has advised women to present to ERs claiming miscarriage if they experience abortion pill complications.
Equally as troubling is that there is no federal mandate to report abortion-related complications across all 50 states.
AAPLOG’s executive director Dr. Donna Harrison and her team found that less than half of the women who experienced a complication received follow-up care from their abortion providers. Dr. Harrison said the AER reports indicated that “[m]ost of the time the women had to resort to the ER to get their care. And often it was after multiple visits to the abortion clinic.”
Reports suggested abortionists were often unaware of complications unless women returned to the abortion facility. As such, they would be unlikely to file reports in those instances.
“The information in the AERs is almost exclusively obtained from abortion providers, rather than the physician treating the complication, yet in this analysis, abortion providers managed only 39.75% of surgical complications (a number which is likely much lower since these are only the cases which are known to the abortion provider). Throughout the reports, there was also a lack of detail and many patients who were simply ‘lost to follow-up,” the authors wrote.
According to Dr. Harrison, “surgical complications” included a failed abortion requiring a complete D&C, an incomplete abortion (tissue left inside), a missed ectopic pregnancy and in a small number of cases, overwhelming infection leading to hysterectomies.
“Many of the AEs [adverse events] experienced by women were unknown to the abortion provider until the follow-up examination, which is troubling considering the poor follow-up rate and elimination of the requirement for an in-office follow up visit. Some of the patient deaths were not known to the abortion provider until they saw the death in an obituary or were contacted by an outside source,” the authors stated (emphasis added).
“Because of this, in addition to abortion providers, hospitals, emergency departments, and private practitioners should be required to report AEs,” the authors suggested.
How many women present to ERs for abortion complications?
“We know from other studies that about five percent of women end up in the emergency room,” Dr. Harrison stated.
Pro-abortion ER doctor Dara Kass confirmed this fact when she stated that eight percent of abortion pill patients end up in the ER. In 2019, Kass told Vice News, “[…] when patients are scared, or have pain or bleeding, they come to me.” She then pointed out, “Recently published results of the Gynuity pilot project showed that 8 percent of their patients who received abortion medication sought follow-up care at a local urgent care clinic or emergency department.”
Five to eight percent is no small number and may represent anywhere from 17,000 to 27,000 possible emergency or urgent care visits in one year, based off the most recent data (2017) showing 339,640 medication abortions were committed nationally out of 862,320 total abortions reported.
Dr. Harrison said her team of researchers found the information they reviewed to have scant details, and she described many of the AER reports as “uncodable.” Some indicated emergencies that did not specify whether the woman lived or died.
“No tests, no examination, no vital signs, no follow-up,” she described them. “Most of these reports we called ‘uncodable,’ and they were likely life threatening. We called these uncodable because there was no way to find out how sick she was or how much she hemorrhaged or how much blood was needed to save her life,” Harrison added. “And there’s no way that the FDA could tell that, either.”
Deaths and Complications
Live Action News has previously documented that, as of December 31, 2018, there were 24 women reported to have died from the abortion pill since its approval in 2000, “including two cases of ectopic pregnancy resulting in death; and several cases of severe systemic infection (also called sepsis), including some that were fatal,” the FDA’s website states.
The FDA also found nearly 4,200 adverse events including 1,042 hospitalizations and nearly 600 serious cases of blood loss along with over 400 cases of infection.
Despite thousands of adverse events and deaths, changes made by the FDA in 2016 no longer required Danco to report non-fatal adverse effects, so the true complication numbers are not known. In addition, despite numerous requests to the FDA and a requirement that Danco and GenBioPro report all known deaths, Live Action News has been unable to obtain more recent data.
Compromised and inadequate complication reports
The most important findings the researchers discovered, according to Dr. Harrison, was that the current FDA system to determine the safety of drugs like the abortion pill is inadequate.
The information given to the FDA was “compromised” and significantly underestimated the adverse events from mifepristone, Dr. Harrison said. In many cases, the researchers who reviewed reports found there was minimal to nonexistent clinical information for which to judge the severity of the events. Dr. Harrison suggested the reports may be filtered by the abortion pill manufacturer from an industry which has no motivation for accuracy.
“We found that almost one of six of the… reports didn’t even have enough information to tell the FDA or anyone else what actually happened to the woman. The FDA could not have used these reports to reassure anyone that Mifeprex is safe,” Dr. Harrison emphasized. “We are left with the sobering conclusion that the FDA now has no real-world idea of the number of women who are dead or injured from Mifeprex abortions.”
Dr. Harrison predicted the push to demedicalize abortion and lift REMS so women can obtain the abortion pill online, at a pharmacy, or over the counter would only serve to worsen the problem of faulty reporting. “More women will suffer complications invisible to oversight,” she said.
As such, AAPLOG is calling for the FDA to strengthen not weaken or eliminate the REMS on the abortion pill. In addition, they are also calling for mandatory abortion complication reporting to be implemented at the federal level for the safety of women.
Editor’s Note: For information on abortion pill reversal, visit AbortionPillRescue.
“No matter how thin you slice it, ladies and gentlemen, family planning is a euphemism. We don’t intend or desire to prevent conception for conception’s sake; we want to prevent conception because of what follows conception. Family planning is the prevention of births, and as birth is the end of a sequence which begins with the sexual urge, then family planning is anti‑conception, anti‑nidation, and the termination of the conceptus if implanted. This is the societal role of abortion in the future.”
― Professor Irvin Cushner of the Johns Hopkins School of Medicine in 1971.[1]
In 1986, Father Paul Marx, the founder of Human Life International, gave an excellent talk on contraception in my home town of Portland, Oregon. I met him afterwards and explained that I still didn’t understand the connections between contraception and abortion. After all, I asked, “Isn’t contraception designed to reduce the incidence of abortion?” For a moment, he stared at me as if I had suddenly sprouted a third eye in the middle of my forehead. Then he said, “Ve haff to talk.”
Half an hour later, I understood.
The Pro-Life Movement and Contraception
The pro‑life movement is currently divided into two schools of thought on the link between contraception and abortion.
The first group either sees no connection between the two practices, or takes a “no official position” stance on contraception in order to avoid controversy or to focus attention solely on abortion. But more and more pro‑life groups and individuals have seen their many connections and realize that, as long as contraception is widely available and the underlying anti‑life mentality reigns, the practice of abortion will never end.
Regardless of what a person thinks about the links between abortion and contraception, he should consider the following, and perhaps reflect on the relevance of contraception to his own life.
Even committed Christians rarely discuss the moral aspects of contraception any more. Mortal sin has become just another brightly-packaged consumer item on the grocery store shelf. Despite this profound silence, it remains one of the major life issues of our time because it serves as the foundation of the practice of abortion. Wherever contraception leads, abortion always follows, whether for a married couple, for a church denomination, or for an entire country.
At one time, the Protestant churches were united in opposing both contraception and abortion. After the Anglicans accepted contraception in limited cases during their 1930 Lambeth Conference, resistance to all of the anti‑life practices unraveled with amazing speed. All but a few of the many Protestant denominations now accept or at least tolerate contraception, abortion, divorce, homosexuality, euthanasia, and pornography. Today, most of the churches that actively oppose abortion are those that have steadfastly defended the Christian tradition against birth control.
The Sequential Connection
In Western nations, pro‑abortion groups work for school‑based birth control clinics and comprehensive sex education programs that include training children in the use of contraceptives. Alan Guttmacher revealed one of the primary purposes of value‑free sex education when he admitted, “The only avenue the International Planned Parenthood Federation and its allies could travel to win the battle for abortion on demand is through sex education.”[2]
The pro-abortion/population control strategy in the Southern Hemisphere is different. Population control groups spend billions of dollars annually in order to saturate developing nations with birth control. They know very well that contraception fails frequently, leading to an increasing demand for illegal abortion. Women begin to die from these illegal abortions, so the population controllers hugely exaggerate these numbers and then demand the legalization of abortion. This is a tried and tested formula that has worked successfully in more than one hundred nations.
The ultimate objective of the population controllers is to legalize abortion worldwide. NSSM-200, written in 1974, has not been amended and thus continues to represent official United States population control policy. It says, “No country has reduced its population growth without resorting to abortion.”[3]
Pro‑abortionists, population controllers, “family planners” and sex educators all over the world falsely claim as part of their propaganda campaigns that as contraceptive and abortifacient use increases, “unwanted pregnancies” and both illegal and legal abortions will decrease. At first glance, this allegation seems logical. After all, authentic (non-abortifacient) contraception is designed to stop conceptions and, if more conceptions are prevented, fewer abortions will occur.
As Father Marx explained to me long ago, however, this theory does not work in the real world, because the large‑scale use of contraceptives and abortifacients leads to a tremendously increased rate of sexual activity, which, combined with method and user failures, leads to a huge increase in the number of “unplanned pregnancies.”
But science and history do not deter the “family planners,” who continue to claim that increased contraceptive use reduces the number of abortions. They know that this message will appeal to the large segment of the public that uncritically accepts their assertions.
It would seem to be counterintuitive that a wider use of artificial contraception would lead to a great increase in the number of abortions, since the stated purpose of contraception is to prevent “unwanted” conceptions that lead to abortion.
However, there are two methods by which a greater general public use of contraceptives will lead to more, not less abortions.
Both of the co-inventors of the birth control pill have confessed that a greater use of contraceptives has led to greater promiscuity and carelessness, which inevitably leads to more abortions. Dr. Robert Kirstner said, “For years I thought the pill would not lead to promiscuity, but I’ve changed my mind. I think it probably has.”[4] And Dr. Min-Chueh Chang said, “[Young people] indulge in too much sexual activity … I personally feel the pill has rather spoiled young people. It’s made them more permissive.”[5]
Secondly, contraception is failure-prone, but people put so much confidence in it because it is advertised as being reliable. There are more than two million contraceptive failures in the United States annually, half of which end in abortion.[6] In fact, more than half of all women currently obtaining abortions were using contraception when they got pregnant.[7]
Up until the early 1980s, the most famous pro‑abortion leaders admitted that an increase in contraceptive availability inevitably leads to an increase in promiscuity and therefore abortions. None other than America’s most famous “sexologist,” Alfred Kinsey, admitted, “At the risk of being repetitious, I would remind the group that we have found the highest frequency of induced abortion in the group which, in general, most frequently uses contraceptives.”[8] And the world’s most experienced abortion statistician, Christopher Tietze, said:
A high correlation between abortion experience and contraceptive experience can be expected in populations to which both contraception and abortion are available. … Women who have practiced contraception are more likely to have had abortions than those who have not practiced contraception, and women who have had abortions are more likely to have been contraceptors than women without a history of abortion.[9]
Malcolm Potts, former Medical Director of the International Planned Parenthood Federation (IPPF), acknowledged the contraception-abortion link in 1981 when he said, “As people turn to contraception, there will be a rise, not a fall, in the abortion rate.”[10] Dr. Judith Bury of Canada’s Brook Advisory Centre confirmed Potts’ view when she said, “There is overwhelming evidence that, contrary to what you might expect, the provision of contraception leads to an increase in the abortion rate.”[11]
People’s laziness about using contraception has naturally morphed into laziness regarding abortion. Canadian sex educator David Robinson stated, “Today abortion is the most widely used birth control method in the world.”[12]
Indeed, some gender feminists see no distinction whatever between artificial contraception and abortion, seeing both as part of an unbroken continuum. Kristin Luker, in her revealingly‑entitled book Taking Chances: Abortion and the Decision Not to Contracept, says, “We would argue that since abortion has become a primary method of fertility control, it should be offered and subsidized in exactly the same way that other contraceptive services are.”[13]
The thinking behind the use of contraception is quite straightforward. Once a couple starts using contraception, they make lifestyle changes and commitments that do not allow room for children. When contraception fails and they become pregnant, their “life plan” wins out over their preborn children. Additionally, they have been conditioned to see their preborn child not as a gift from God, but as a “contraceptive failure” or a “mistake.” Since their contraceptive method has failed them, they feel cheated and therefore “entitled” to an abortion — using one method of medical technology to cover up for the failure of another.
View of the “Family Planners”
The primary mission of the research arm of the vast “family planning” industry is to develop more and more effective abortifacients. Every year, fewer women use true contraceptives and more are using abortifacient chemicals.
There are several reasons why abortifacients are preferable to contraceptives from a “family planning” point of view. To begin with, abortifacients are much more effective at ending pregnancies than contraceptives are at preventing them. The best user (‘real world’) effectiveness rates of the birth control pills, the IUDs, the injectables and the insertables average about 96-98%, and the best user effectiveness rates for the male and female condoms, cervical cap, diaphragm and sponge average only about 80%.[14]
There is another reason that “family planners” prefer that women use abortifacients. Despite all of the propaganda promoting “woman-controlled” birth control, the population controllers are actually more interested in increasing their own control of women’s fertility, primarily in developing nations. Abortifacients put more control into the hands of the medical profession and mean more money for the international pharmaceutical cartel than true contraceptives do. Abortifacients must be prescribed by health professionals. By contrast, contraceptives are controlled by the user.
Greater abortifacient use will ensure that physicians ― and, in some cases, the State ― will be able to strictly monitor and even control the fertility of the people. This is now happening in the People’s Republic of China and has happened on a smaller scale in more than thirty other nations.
The Legal Connection
The sequential link between contraception and abortion is not the only connection, however, between the two.
More than 25 years ago, pro-abortion lawyer Frank Susman recognized that the “rights” of abortion and contraception now actually merge:
For better or for worse, there no longer exists any bright line between the fundamental right that was established in Griswold and the fundamental right of abortion that was established in Roe. These two rights, because of advances in medicine and science, now overlap. They coalesce and merge and they are not distinct. The most common forms of contraception today ― IUDs, low‑dose oral contraceptive pills, which are the safest type of oral contraceptive pills available ― act as abortifacients.[15]
The principle used to justify all anti‑life practices in the United States is the “right to privacy,” which is not actually mentioned in the Constitution of the Unites States. The United States Supreme Court first used this term in its 1965 Griswold v. Connecticut decision, which legalized contraception for married couples nationwide. Three years later, the Court extended this “right” to unmarried people. And, of course, five years after that, it quickly applied the “right to privacy” to abortion in its Roe v. Wade decision.
Every American values personal privacy. Everyone wants the government to interfere with their private lives as infrequently as possible. So the “right to privacy” is used as a cover to justify practices that the public will not accept until it has been exposed to them for years. We can see this principle at work in the seamless progression from contraception to abortion to euthanasia. And the “right to privacy” is also used to justify homosexual acts, adultery, infanticide and all kinds of pornography.
The public has “evolved” to accept acts that were once universally believed to be immoral and loathsome. Anti‑lifers now label any opposition to abortion, euthanasia, pornography and other evils “anti‑choice,” “anti‑freedom,” and “anti‑American.”
The Psychological Connection
So there are legal, medical and practical connections between contraception and abortion. But they all pale in comparison to the most important connection of all: the fact that the belief system which accepts contraception will inevitably require abortion.
Most people — including most Christians — use contraception because they can’t afford a baby, they have problems with their relationships, they want to avoid single parenthood, they aren’t ready for the responsibility, they have all the children they want, or they are concerned about how a child (or another child) would change their lives.
These are exactly the same reasons women give for having abortions.[16] Underlying them all is the fundamental denial of God’s design of man and woman as sexual beings, and His plan for children in our lives. People today want to “plan” their families.
Why does a couple contracept? Because they don’t want a child. Why don’t they want a child? Because they have made Important Plans for Their Lives. And when contraception fails, the resulting “unplanned” child is often seen as an intruder, one who will spoil the couple’s carefully laid plans.
And when a couple has denied God’s plan for their lives once through contraception, it is so much easier to do it again through abortion. As St. Teresa of Calcutta observed:
In destroying the power of giving life, through contraception, a husband or wife is doing something to self. This turns the attention to self and so it destroys the gifts of love in him or her. In loving, the husband and wife must turn the attention to each other as happens in natural family planning, and not to self, as happens in contraception. Once that living love is destroyed by contraception, abortion follows very easily.[17]
For decades, pro‑abortionists have worked to blur the distinction between abortion and contraception in people’s minds. For example, a writer for “Catholics” for Choice said:
If RU‑486 is also used monthly, pro-lifers would have a hard time convincing the public that the drug isn’t just another contraceptive. Indeed, a 1982 New York Times story on [Etienne‑Emile] Baulieu and RU‑486 described the drug as “a new birth control pill.” Planned Parenthood released a “Fact Sheet” in October that refers to RU‑486 as a type of “interceptor (luteal contraception).” If most people hear a new drug described as “birth control,” they’ll think of the Pill and IUD, not abortion.[18]
And the National Abortion Federation has said, “If RU‑486 is referred to as an ‘abortion pill,’ it has significantly less support than if it is called a new form of birth control. In many polls, the description can change support by as much as 15‑20 points and determine if a majority of those polled are in favor of the Pill.”[19]
Conclusion: Pro‑Lifers and Birth Control
Some pro‑life activists will certainly be offended by the classification of artificial contraception as “anti‑life,” because they have completely separated contraception from abortion in their minds. As far as they are concerned, abortion and artificial contraception are two entirely separate issues.
I used to think that way until HLI founder Father Paul Marx set me straight.
Many pro‑life activists use artificial contraception. In fact, it is safe to say that many pro‑life women use “birth control” methods that are actually abortifacients. These men and women may not want to hear that they may be committing one or more “silent” abortions themselves every year, but it would not be intellectually or ethically honest to deny the truth in this matter. It is extremely ironic that a “pro‑life” woman who uses an intrauterine device or the Pill for a decade will suffer ten to twenty “silent” abortions, while a pro‑abortion woman using the same methods may only commit only one or two additional abortions through surgical means.
Alfonso Cardinal Lopez Trujillo, former Prefect of the Pontifical Council on the Family, said:
Getting human sexuality “right” is one of the great challenges of our time. Meeting this challenge is very much part of the work of the pro‑life movement. The mysterious links between sexuality, life, and death are part of our psychology and our experience of life. The anti‑life mentality began, not with abortion, but by separating sexuality from the transmission of life in contraception and sterilization. As the Holy Father points out in Evangelium Vitae [¶13], “Despite their differences of nature and moral gravity, contraception and abortion are often closely connected.”
I invite everyone here to think seriously about the roots of the anti‑life mentality. I urge you never to fall for the shallow argument that providing widespread contraception will reduce the number of abortions.[20]
Evangelium Vitae [¶13] points out, “Contraception and abortion are often closely connected, as fruits of the same tree.”
As such, all of this tree’s fruits ― whether they be contraception, abortion, euthanasia, homosexual activity, masturbation, or pornography ― are poisonous to the soul. Everyone who genuinely seeks God’s will for his or her life must avoid them like the spiritual plagues they truly are.
Endnotes
[1] Professor Irvin Cushner, Johns Hopkins School of Medicine, at the Symposium on Implementation of Therapeutic Abortion, International Hotel, Los Angeles, January 22 to 24, 1971. Quoted in the Marriage and Family Newsletter, July 1971, page 3.
[2] Alan Guttmacher quote of May 3, 1973, Humanity Magazine, August/September 1979, page 11.
[3]National Security Study Memorandum 200, “Implications of Worldwide Population Growth For U.S. Security and Overseas Interests,” December 10, 1974. Special footnote, “Worldwide Abortion Practices.”
[4] Dr. Robert Kirstner of Harvard Medical School, co-inventor of the oral contraceptive pill, quoted in “In Brief: Harvard, Mass.” ALL About Issues, June 1981, page 5.
[5] Dr. Min-Chueh Chang, co-inventor of the oral contraceptive pill, quoted in Charles E. Rice. “Nature’s Intolerance of Abuse.” ALL About Issues, August 1981, page 6.
[6] See Excel Spreadsheet F-21-03.XLS, “Statistics on Birth Control Methods Used by Women of Childbearing Age in the United States, and Total Annual Contraceptive Failures.” For a copy of this spreadsheet, e-mail Brian Clowes at bclowes@hli.org.
[7] Rachel K. Jones, Jacqueline E. Darroch and Stanley K. Henshaw. “Contraceptive Use Among U.S. Women Having Abortions in 2000-2001.” Perspectives on Sexual and Reproductive Health [formerly Family Planning Perspectives] [Guttmacher Institute], November/December 2002 [Volume 34, Number 6], pages 294 to 303. Table 1, “Percentage Distribution of Women Obtaining Abortions in 2002, by Contraceptive Method Used in the Month of Conception, and of Women at Risk of Unintended Pregnancy in 1995, by Contraceptive Method Used.”
[8] Alfred Kinsey, America’s most famous “sexologist,” quoted in Mary Calderone, M.D. [Editor]. Abortion in the United States [New York: Paul B. Hoeber, Inc., 1956], page 157.
[9] Christopher Tietze. “Abortion and Contraception.” In Abortion: Readings and Research [Toronto: Butterworth & Co.], 1981, pages 54 to 60.
[10] Malcolm Potts. “Fertility Rights.” The Guardian, April 25, 1979.
[11] Judith Bury, M.D., Brook Advisory Centre. “Sex Education for Bureaucrats.” The Scotsman, June 29, 1981. Also quoted in Rudolf Ehmann, M.D., “Consequences of Contraception and Abortifacient Birth Control,” Human Life International pamphlet.
[12] David Robertson, et al. Sex Education: A Teacher’s Guide. The Canadian Ministry of National Health and Welfare, Volume 4, pages 24 and 25.
[13] Kristin Luker. Taking Chances: Abortion and the Decision Not to Contracept, 1975, page 144.
[14] Robert A. Hatcher, et. al.Contraceptive Technology (18th Revised Edition) [New York: Ardent Media, Inc.], 2004. Table 31-1, “Percentage of Women Experiencing an Unintended Pregnancy During the First Year of Typical Use and the First Year of Perfect Use of Contraception and the Percentage Continuing Use at the End of the First Year. United States,” page 792.
Spermicides include foams, creams, gels, vaginal suppositories, and vaginal films. The female condom “Reality” is known as “Femy” in Spain and “Femidom” in the rest of the world.
Annual rates are not applicable since RU-486 effectiveness is measured on a per-use basis. For further information on the RU-486 abortion pill, see Chapter 2 of The Facts of Life, “Abortifacients.”
Eight major studies on the effectiveness of typical methods of natural family planning in the 1990s show an average user failure rate of 2.8%. These studies were carried out in a wide variety of cultures in Moslem, Hindu, Chinese and Christian cultures. The user failure rates by country were: United Kingdom 2.7%, Indonesia 2.5%, India 2.0%, Germany 2.3%, Liberia 4.3%, Europe 2.4%, China 4.4%, and Belgium 1.7% [Bob Ryder and Hubert Campbell. “Natural Family Planning in the 1990s.” The Lancet, July 22, 1995, page 233. Also see R.E.J. Ryder. “”Natural Family Planning:” Effective Birth Control Supported by the Catholic Church.” British Medical Journal, 1993;307:723-726].
[15] “Excerpts of Arguments before Supreme Court on Missouri Abortion Law.” Washington Post, April 27, 1989, page A16.
[16] Aida Torres and Jacqueline Darroch Forrest. “Why Do Women Have Abortions?” Family Planning Perspectives, July/August 1988, pages 169 to 176.
[17] Mother Teresa of Calcutta. “Whatever You Did Unto One of the Least, You Did Unto Me.” Address given at the National Prayer Breakfast in Washington, D.C., Thursday, February 3, 1994.
[18] Tony Kaye. “Are You for RU‑486?: A New Pill and the Abortion Debate.” Conscience [newsletter of ‘Catholics’ for a Free Choice (CFFC}], July/August 1986 [Volume VII, Number 4], pages 15 to 17.
[19] National Abortion Federation. Abortion: Moral Choice and Medical Imperative. “Abortion Practice Advancement, Sixteenth Annual Meeting Workbook, April 13‑14, 1992, San Diego, California,” page 133, “Successful Strategies: Managing the Media.”
[20] From the address by Cardinal Alfonso Lopez Trujillo, President of the Pontifical Council for the Family, given March 23, 1996 in Westminster Central Hall, London. “Evangelium Vitae and the Pro‑Life Movement.”
Scientists are witnessing an alarming trend: Men’s sperm counts are down, testosterone levels have plunged and erectile dysfunction is increasing. Male infertility is on the rise — and exposure to synthetic chemicals known as phthalates could be to blame, according to fertility scientist Shanna Swan, Ph.D., author of the new book, “Count Down: How Our Modern World Is Threatening Sperm Counts, Altering Male and Female Reproductive Development and Imperiling the Future of the Human Race.”
Citing Swan’s book, the New York Post reported that the global fertility rate has dropped 50% between 1960 and 2016, with the U.S. birth rate 16% below where it needs to be to sustain the population.
Although girls are experiencing early puberty, and women are experiencing declining egg quality and more miscarriages, emerging science is shifting the focus toward men as more couples suffer from infertility.
In 2017, Swan, one of the world’s leading environmental and reproductive epidemiologists, co-authored a meta-analysis that came to a staggering conclusion: The sperm count of average Western countries had fallen by 59% between 1973 and 2011.
Normal sperm counts range from 15 million sperm per milliliter to 200 million per milliliter. A rate below 15 million is considered “low” by the World Health Organization (WHO), but Swan argues that anything below 40 million creates challenges for reproduction. The average male is nearing that number at 47.1 million sperm per milliliter compared to his father who had an average of 99 million sperm per milliliter at the same age.
“If you look at the curve on sperm count and project it forward — which is always risky — it reaches zero in 2045, meaning the median man would have essentially no viable sperm,” Swan writes in her book.
Men are also experiencing lower testosterone levels. A 2006 study showed that a 65-year-old man in 2002 had testosterone levels 15% lower than a 65-year-old man in 1987. A 2020 study in the Urology Times Journal showed a similar drop with young adults and adolescents.
As a result, more men are getting prescriptions for testosterone replacement therapy, which increases testosterone levels but causes an even greater reduction in sperm count. “Ninety percent of men can have their sperm counts drop to zero while they’re on it,” according to Swan.
Sexual desire among men is also declining. Swan, who has studied infertility for more than 30 years, says men are seeking help for erectile dysfunction on average seven years earlier than they did in 2005, with 26% of men falling under the age of 40.
According to the New York Post, research shows an overall increase in genital abnormalities, including a higher rate of undescended testicles and unusually small penises. Growing numbers of sperm appear defective with some having two heads or wandering aimlessly instead of pursuing an egg.
Exposure to phthalates is a particular problem during pregnancy when fetuses are sexually differentiating in the first trimester, says Swan, and infants with greater exposure to phthalates during pregnancy are shown to have smaller penises.
Similar abnormalities have been observed in animals. Small penises are being reported in alligators, otters and minks. Polar bears have lower-than-normal testosterone levels, panthers are showing an increase in genital abnormalities, and fish, frogs and turtles are being born with both male and female organs.
Research points to endocrine-disrupting phthalates as likely cause
Phthalates are synthetic chemicals used to make plastics more flexible and harder to break. The chemicals are everywhere: plastics, shampoos, cosmetics, furniture, flame retardants, personal care products, pesticides, canned foods and even receipts.
In several studies over the last two decades, phthalates have been shown to disrupt male hormones like testosterone and to cause genital birth defects in male infants.
A 2018 systematic review published in Environmental International showed phthalates decreased testosterone and caused negative reproductive outcomes in men.
Flame retardants found in mattresses and foam furniture were linked to male infertility in a 2016 study published in the Reproductive Toxicology Journal, and chemicals in stain, water, fast-food packaging, paper plates, stain-resistant carpeting and other household items have been linked to a reduction in semen quality, testicular volume and penis length.
A 2017 U.S. study showed that 45 potentially harmful chemicals, including phthalates and flame retardants, were present in dust buildup in 90% of homes sampled, reported the New York Post.
Pesticides and herbicides have also been found to negatively affect male infertility. Atrazine, an herbicide used to prevent certain weeds from growing in corn, has been linked to lower sperm quality.
In her latest book, Swan writes:
“The problem isn’t that something is inherently wrong with the human body as it has evolved over time; it’s that chemicals in our environment and unhealthy lifestyle practices in our modern world are disrupting our hormonal balance, causing varying degrees of reproductive havoc that can foil fertility and lead to long-term health problems even after one has left the reproductive years.”
The cumulative effect of endocrine disruptors affect multiple generations. Patrician Hunt, a reproductive geneticist at Washington State University, conducted experiments on mice. When infant mice were exposed to disruptive chemicals for a few days their testes as adults produced fewer sperm. The mice passed on this propensity to their offspring, and after three generations of exposure, one-fifth of male mice were infertile.
“I find this particularly troubling,” Professor Hunt told The New York Times. “From the standpoint of human exposures, you could argue we are hitting the third generation just about now.”
Although more research, government regulation and corporate responsibility are needed, Swan offers practical suggestions to help men tip the scale:
Store food in glass containers and never microwave food in plastic.
Stop smoking and cut back on drinking. Cigarette smoke is associated with a lower sperm count and increased sperm defects, while more than seven drinks per week is harmful to sperm.
Buy organic to avoid pesticides and herbicides that interfere with male hormones, especially strawberries, spinach, kale, apples and grapes. Swan also recommends reducing full-fat dairy foods, which have been linked to greater sperm abnormalities and avoiding processed meats, which can harm the DNA of sperm.
Avoid saunas, binge watching TV and cut out stress, says Swan. A Danish study, “Psychological stress and testicular function: a cross-sectional study of 1,215 Danish men,” published in Fertility and Sterility Journal, showed that high levels of work stress resulted in a 38 percent lower sperm concentration.“Men who’ve experienced two or more recent stressful life events — such as the death or serious illness of a close relative, divorce or serious relationship problems, moving, or a job change — were more likely to have below-normal sperm concentration,” writes Swan.
Buy products labeled “paraben-free” and “phthalate free” and avoid skin-care products that are “antibacterial,” vinyl shower curtains, air fresheners, toxic household cleaners, and dust often to remove the build-up of chemicals, urges Swan.
“We can no longer afford to behave as though it’s business as usual,” Swan writes in her book. “The time has come for us to stop playing Russian roulette with our reproductive capacities.”
February 24, 2021 (LifeSiteNews) – Following the announcement that the radical pro-abortion and pro-LGBT Equality Act will be brought before the U.S. House of Representatives this week, pro-life and pro-family leaders have described the proposed legislation as “the most comprehensive assault on Christianity ever written into law.”
Dr. Bill Donohue, Ph.D., president of the Catholic advocacy group Catholic League, said that, contrary to U.S. House Speaker Nancy Pelosi’s claim that the Equality Act is “about ending discrimination,” that in fact the opposite is true, with Christians set to experience severe discrimination should the act be passed into law.
Donohue explained that, as well as amending the 1964 Civil Rights Act “to include sexual orientation and gender identity to the definition of sex,” a thing never intended or envisioned by the authors of that legislation, the Equality Act would “undermine the Religious Freedom Restoration Act by allowing gay rights to trump religious rights.”
Donohue said that the act’s broad scope would force healthcare providers to supply hormone therapies and even surgeries in accordance with “sex change” procedures.
Women’s sports, too, will become unfairly altered by the inclusion of boys and men who purport to be female. “These biological males can use the locker rooms, restrooms and shower facilities that have always been reserved for females,” he added.
But for Catholics and members of other religious groups who hold to a traditional understanding of human nature, they “could not raise religious liberty objections to any of the aforementioned rights of transgender women. In effect, religious entities would be secularized,” Donohue warned.
As an example, Donohue explained that “if the Equality Act were to become law, Catholic foster care programs would be shut down. They would either have to agree to allow two men to adopt children—a clear violation of Church teachings—or lose federal funding.”
Additionally, Catholic hospitals would lose any federal funding they receive under the proposed Equality Act if they refuse to perform abortions, “or be forced to get into the abortion business.”
“This is the kind of ‘gotcha’ type element that makes this bill so pernicious,” Donohue said.
Family Research Council (FRC) President Tony Perkins described the Equality Act as “a catastrophic loss of religious freedom in America.”
“The Equality Act is a grave and treasonous threat to our nation’s core values contained in our First Amendment. The fact that no Republicans have co-sponsored it, even those who co-sponsored in the previous Congress, underscores the Democrats’ lurch to the Left. This is a radical bill that uses the government to control, through coercion, how every American thinks, speaks, and acts on issues of human sexuality. It may be named the Equality Act, but as the details make quite clear, the only equal thing about it is how much damage it does to many facets of American life,” Perkins said.
“The bill erodes parental rights and positions the government as lord over churches and other faith-based institutions, potentially dictating how their facilities are used, who they hire, and even punishing them for not falling in step with a view of human sexuality that directly contradicts orthodox biblical teaching,” he continued.
“No person of faith or religious institution, whether school, church, synagogue, mosque, business, or non-profit, will escape the Orwellian reach of the Equality Act,” Perkins warned.
Mary Beth Waddell, FRC’s Director of Federal Affairs for Family and Religious Liberty, commented that the bill “politicizes the medical profession and denies biological reality, harming those it claims to protect.”
“In addition to obliterating the rights, privacy, and safety of women and girls, this extreme bill would politicize the medical profession, forcing doctors who provide legitimate hormone treatments and surgical procedures to offer those treatments against their conscience. It would put the threat of litigation over every medical professional who would dare to stand up for the science that indicates the harms of these treatments and surgeries, likely causing many to stay silent. The misnamed ‘Equality Act’ has no place in any just, fair, and tolerant society.”
Lila Rose, Founder & President of Live Action, described the Equality Act as “deceptively named and corrupt in its vision.”
“There is nothing empowering or ‘equalizing’ about killing innocent preborn children nor confusing what it means to be male and female. This deceptively named piece of legislation hides within it policies that override conscience rights, require employers to cover abortions in their healthcare plans, and nullifies pro-life laws and protections on a massive scale,” Rose said.
Experts from the Ethics and Public Policy Center (EPPC) agree. President Ryan T. Anderson, Ph.D., a specialist in bioethics, religious liberty, and political philosophy, said: “The so-called Equality Act is legislative malpractice that turns equality on its head.”
“It isn’t drafted as a shield to protect vulnerable minorities from unjust discrimination, but as a sword to persecute those who do not embrace new sexual and gender ideologies.”
Anderson cautioned as to the effect the act would have on religious agencies, like schools and adoption firms, warning that, if the act passes, they “would face federal sanction for operating according to basic biology and mainstream biblical teaching on sex and marriage.”
Anderson’s colleague and EPPC Fellow Erika Bachiochi, J.D., a legal scholar specializing in Equal Protection jurisprudence, criticized the bill as an attempt to “transform the great Civil Rights Act of 1964 into a mechanism for public funding of abortion.”
“But taxpayer funding of abortion — deeply unpopular among Americans — would only further incentivize employers to prefer abortion for their pregnant employees over far more costly accommodations for parenting,” Bachiochi said.
Andrew T. Walker, Ph.D., a scholar in EPPC’s Evangelicals in Civic Life criticized Biden in particular, whose “appeal to unity and moderation” he described as merely “a shallow political ploy.”
“This bill targets goodwill people of faith by making historic and reasonable claims about gender and sexuality suspect and ripe for exclusion from the public square,” he said.
The American Principles Project (APP), a national organization for pro-family advocacy in public policy, have released a scathing review of the impact of the Equality Act, recommending that Congress oppose the legislation on multiple grounds.
Terry Schilling, APP’s executive director, expressed dismay at the continued efforts of Democratic legislators to limit religious freedom, “now trying to make these changes permanent in federal law.”
“Of course, this has been their goal for a long time, and we know by now the very terrible consequences which will occur if the ‘Equality’ Act passes: female athletes will be forced to compete against biological males; women will be forced to share private spaces like bathrooms, locker rooms, and shelters with men; and religious charities will be coerced into violating their beliefs or else be shut down.”
A Connecticut anti-pregnancy center bill is moving forward after passing the Public Health Committee in a 19-12 vote on February 22, despite dozens of people testifying against the bill in a public hearing earlier this month. This is the fourth year in a row such a bill has been introduced in the Connecticut State Senate.
Senate Bill 835, aims to “prohibit deceptive advertising practices by limited services pregnancy centers.” After a pregnancy center moved into the same building as an abortion business and NARAL Pro-Choice Connecticut in Hartford, NARAL became the driving force behind the bill in an effort to dictate how pregnancy centers advertise their services (while simultaneously downplaying what those services are). The bill claims that pregnancy centers are dishonest and trick women into choosing life. Proponents of the bill also claim that pregnancy centers stall women, preventing them from getting abortions right away.
When women don’t know about their other options or the help available to them, they frequently feel abortion is their only choice. Many choose it out of desperation, without informed consent — and sometimes even against their wills. Pregnancy centers exist to be a safe place for women to learn about all their options without being pressured by a business which will make money from the sale of an abortion.
Pregnancy centers provide women with free pregnancy tests, free ultrasounds, free baby gear, free clothing, and assistance with other needs such as housing, medical care, education, parenting classes, job placement, and more. Some pregnancy centers also offer limited medical services and many have medical professionals serving on staff or as volunteers. Services vary from center to center and women have often shared their joy at having been given a way out of abortion.
Meanwhile, abortion businesses offer one option for women facing unplanned pregnancies: abortion. Women have stated that they were purposefully deceived by abortion businesses regarding the development of their babies as well as abortion procedures as well. Women deserve to know the full truth before they undergo an abortion and the time to make the decision rather than be rushed into an abortion. Pregnancy help centers give them just that.
“Breast cancer has now overtaken lung cancer as the world’s most commonly-diagnosed cancer,” reads a February 3 press release from the World Health Organization (WHO). The occasion for the press release was to mark World Cancer Day 2021 on February 4. Overall, the news was not good:
“In the past two decades, the overall number of people diagnosed with cancer nearly doubled, from an estimated 10 million in 2000 to 19.3 million in 2020. Today, one in 5 people worldwide will develop cancer during their lifetime. Projections suggest that the number of people being diagnosed with cancer will increase still further in the coming years, and will be nearly 50% higher in 2040 than in 2020.”
Breast cancer risk and birth control: The unmentioned connection
The WHO press release also highlights how the COVID-19 pandemic has exacerbated the global cancer burden, leading to later-stage diagnoses and decreased access to timely treatments. The WHO is urging their partners and stakeholders to take immediate action to combat rising cancer rates, and particularly rates of breast cancer, by “promoting breast health, improving timely cancer detection and ensuring access to quality care.” While these goals are admirable and necessary, the goal of promoting breast health is greatly undermined by another campaign of the World Health Organization—encouraging widespread use of hormonal contraceptives. Not only does the press release fail to mention the increased risk of breast cancer with frequently prescribed drugs such as the birth control pill, shot, patch, and vaginal rings, the WHO avoids mentioning the increased risk on pages that recommend birth control use. On the WHO’s dedicated webpage for contraception, there is no mention of cancer risk; instead the WHO doubles down on their perceived need to promote greater access to contraceptives across the globe:
“The Sustainable Development Goals set for 2030 will need to ensure that sexual and reproductive health services are widely available and used. This includes supporting contraceptive services through effective government policies and the provision of high-quality services for individuals.”
To make matters worse, the WHO often promotes hormonal contraception in countries that may not have the sophisticated medical systems needed to detect and treat cancer.
Breast cancer risk and hormone exposure go hand-in-hand
As we’ve written about before here and here, the theory that hormonal contraceptives may lead to increased risk for breast cancer is not new, and it has been borne out in multiple studies. One theory behind the increased risk is the increased exposure to (synthetic) sex hormones caused by hormonal contraceptive use. A 2017 study from the journal Evolution, Medicine, & Public Health found that “four widely prescribed formulations [of hormonal contraception] more than quadruple progestin exposure relative to endogenous progesterone exposure.” [1] This makes the findings from a 2018 meta-analysis from the American Journal of Lifestyle Medicine unsurprising, in that, “there appears to be an increased risk of breast cancer in women using combined oral contraceptives, regardless of progestin component or monophasic versus extended cycle administration. An increased risk was also identified in levonorgestrel-only oral and nonoral products” [2].
Birth control is an endocrine disruptor
As we learn more about the role of endocrine-disrupting chemicals (EDCs) in our environment, it has become increasingly clear that one’s risk of developing cancer is not merely a matter of genetics. This is especially true of hormone-sensitive cancers like breast cancer. As a 2013 paper from the Journal of Mammary Gland Biology and Neoplasia states: “In both humans and rodent models, environmental factors that act as endocrine disrupting compounds (EDCs) have been shown to disrupt normal mammary development and lead to adverse lifelong consequences, especially when exposures occur during early life” [3]. Given the connection between hormone exposure and breast cancer risk, there has been a push in recent years to limit exposure to potential endocrine-disrupting chemicals such as bisphenol A (BPA). Yet despite that the very purpose of hormonal birth control is to alter the actions of the endocrine system—making it quite literally a doctor-prescribed endocrine disruptor—there has not been the same push to limit exposure to the synthetic hormones found in birth control. Instead we see quite the opposite.
Promoting the science of fertility awareness helps combat breast cancer
Health organizations that are truly serious about combating all of the factors that may be contributing to increased rates of breast cancer across the globe should encourage alternate forms of family planning that do not involve the use of carcinogenic synthetic hormones. Fertility Awareness Methods (FAM) are safe, evidence-based, highly effective methods of family planning that do not require exposure to harmful synthetic hormones.
The CDC cites research showing that certain fertility awareness methods have as low as a 2% failure rate, revealing an effectiveness rate in pregnancy prevention that rivals (and even outperforms) the rates of some of the most highly prescribed contraceptives, like the Pill. Of fertility awareness methods as a whole, the CDC says “Failure rates vary across these methods. Range of typical use failure rates: 2-23%.” The wide range in that figure reflects the variety of methods included in the research analysis, as the study included less effective calendar-based methods alongside more effective symptom-based methods of fertility awareness in its analysis. Most of the most established modern fertility awareness methods—such as the Billings method, the Sympto-Thermal Method, the Creighton Method, and the Marquette Method—boast failure rates at 1% or lower for perfect use, and 10% or lower for typical use (read more on the exact rates for each particular fertility awareness method here).
FAMs have also been effectively taught to women and couples of all literacy levels across the world, including the visually impaired, and have the potential to meaningfully advance true gender equality and better, more comprehensive women’s health. The beauty of promoting fertility awareness is that it serves a dual purpose of promoting better health, and providing effective family planning options—all at the same time. FAMs prove that truly furthering women’s health does not require the tradeoff between increasing their breast cancer risk and providing them with effective family planning.
References:
[1] Lovett J, Chima M, Wexler J et al. Oral contraceptives cause evolutionarily novel increases in hormone exposure. Evol Med Public Health. 2017;2017(1):97-108. doi:10.1093/emph/eox009, https://pubmed.ncbi.nlm.nih.gov/28685096/
[2] White N. Hormonal Contraception and Breast Cancer Risk. Am J Lifestyle Med. 2018;12(3):224-226. doi:10.1177/1559827618754833, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6124967/
[3] Macon M, Fenton S. Endocrine Disruptors and the Breast: Early Life Effects and Later Life Disease. J Mammary Gland Biol Neoplasia. 2013;18(1):43-61. doi:10.1007/s10911-013-9275-7, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3682794/
New research has found that women who are pregnant or take estrogen either through birth control or hormone replacement therapy (HRT) may have a higher risk of developing blood clots if they contract COVID-19.
Though estrogen does not cause blood clots, if used in birth control or HRT it can increase a person’s risk by three- or fourfold. COVID-19 may exacerbate that risk.
Many COVID-19 patients in the intensive care unit (ICU) are developing blood clots that may contribute to respiratory failure.
Clotting with COVID-19 has been more common in patients who are older, male or have diabetes or obesity.
Some women who contract COVID-19 may need to discontinue their estrogen medications or begin anticoagulation therapy, according to the study, which published in the journal Endocrinology on Wednesday (December 2020).
According to the study, there have been no reports of increased incidence of venous thromboembolic events (VTEs) in pregnant women or people taking estrogen with COVID-19. Doctors have observed vascular abnormalities in the placenta of pregnant women with COVID-19.
Health experts say we need more research to fully understand how gender influences a person’s risk for severe COVID-19. Interestingly, women are generally less likely to die from COVID-19 compared to men, though it’s unclear as to why.
“My sense is, as with everything related to COVID, we are just beginning to understand gender as a risk for poor outcome in COVID and multiple factors are important, not just estrogen and clotting,” says Dr. Don L. Goldenberg, a rheumatologist and emeritus professor of medicine at Tufts University School of Medicine.
COVID-19 causes abnormal clotting
Several people who have been hospitalized with severe COVID-19 have developed blood clots.
VTEs are commonly reported in ICU patients — one found that 31 percent of ICU patients with COVID-19 experienced thrombotic complications.
Dr. Hamid Mojibian, a Yale Medicine interventional radiologist specializing in image-guided cardiac procedures, says there are a number of reasons COVID-19 may lead to clotting in some people.
Research has found that COVID-19 causes widespread inflammation in the body which may affect how well our platelets which are tiny blood cells that help regulate clotting — work and make them more prone to forming dangerous blood clots.
“Factors like overwhelming inflammation, vascular injury, platelet (blood cell) dysfunction, and pure immobility (stasis) contribute to blood clot formation,” Mojibian said.
Larger blood clots can prevent blood from flowing throughout our body and getting where it needs to be.
“During this pandemic, vein experts have found clots in the aorta, renal arteries, legs, and the brain,” says Mojibian.
Anytime blood supply is interrupted, there can be severe consequences, such as a stroke.
What is it about estrogen?
According to Goldenberg, estrogen is known to increase a person’s risk of VTEs.
With HRT and oral contraceptives containing estrogen, the risk of clots is highest in the first year of use amongst women with coagulation abnormalities.
Women without these abnormalities are also at higher risk for blood clots while taking these medications.
Estimates suggest 1 in 3,000 women who take birth control pills will get a blood clot each year.
Pregnancy, which causes the body to naturally produce more estrogen, is also linked to blood clots.
In fact, research shows the risk of venous thrombosis is six- to tenfold greater among pregnant women compared to nonpregnant women of the same age.
“Estrogen increases the gene expression of certain clotting factors and lowers factors which prevent blood clots. Overall, this leads to a ‘pro’ clotting state,” says Dr. Minisha Sood, an endocrinologist at Lenox Hill Hospital in New York City.
Evidence also suggests that estrogen impacts the immune system.
“Estrogen affects immune response and T cells as well as ACE-2 receptors, each important in COVID infection and severity,” says Goldenberg.
How can you cut your risk?
It may take some lifestyle changes, but health experts say it is possible to cut your risk of experiencing a clot.
Per the researchers findings, women who take birth control pills or HRT and get sick with COVID-19 may want to ask their doctor about alternative options that do not contain estrogen.
Sood doesn’t recommend discontinuing birth control or HRT as a preventative measure. If women taking these medications were to become severely ill with COVID-19, then it’s time to consider other options.
“There are still no firm guidelines but women not infected who are on HRT or oral contraceptives should consult with their physician regarding potential risk during the pandemic,” says Goldenberg.
Mojibian also recommends getting physical exercise as staying home and not moving increases your risk of venous thrombosis.
New research has found that women who are pregnant or take estrogen either through birth control or hormone replacement therapy may have a higher risk of developing blood clots if they contract COVID-19. Blood clots are a common complication reported in severe cases of COVID-19.
Some women who contract COVID-19 may want to discontinue any estrogen medications to cut their risk of clots, but it’s crucial to first consult a doctor.
C-Fam) Melinda Gates’ Family Planning 2020 (FP2020) coalition celebrated the progress they say they’ve made since its debut in 2012 and announced a new, updated partnership for the next ten years they are calling FP2030. Beneath the festive veneer, the awkward fact remains that FP2020 has fallen well short of its goals. What’s more, despite the partnership’s attempts to maintain neutrality, several participants used the event to promote abortion.
FP2020 was launched at a summit in London, sponsored by Melinda Gates, the United Nations Population Fund (UNFPA) and the government of the UK. Earlier that year, Gates announced that she wanted to make family planning her signature area of philanthropy, while stressing she wanted “no controversy” related to abortion or population control. “There’s a global movement waiting to happen,” she said.
However, there was already a global family planning movement, and its leaders were not interested in setting abortion to the side. Gates’ #nocontroversy hashtag quickly fell into disuse, and where FP2020 stayed relatively quiet on abortion, its partners and members of its steering groups filled the silence.
Speaking on a panel at the FP2020 event, Alvaro Bermejo, director of the International Planned Parenthood Federation (IPPF), said “the partnership has really made SRHR [sexual and reproductive health and rights] advocacy issues more effective” by bringing donors and implementing organizations together and creating accountability for governments. FP2020 executive director Beth Schlachter agreed, echoing his support for “family planning and SRHR more broadly.”
SRHR remains a highly controversial concept which has been rejected by the UN General Assembly for decades due to its associations with abortion, comprehensive sexuality education, and sexual orientation and gender identity.
Another frequent theme of the event was the Mexico City Policy, reinstated and expanded by former President Donald Trump, which blocked U.S. funds from going to foreign-based groups that promote or provide abortions, such as IPPF affiliates. “We made a specific decision to ensure that MSI [Marie Stopes International] and IPPF remained on the reference group to demonstrate that people could have different opinions […] but we as a community were going to try to find a way to work together,” said Schlachter.
“FP2020 managed to remain as the one convener where the U.S. government and staff and technical people and implementers like ourselves and other donors came around the table,” said Bermejo.
Numerous participants denounced Trump and his policies, including Simon Cooke, CEO of MSI, who also spoke stridently about abortion. “We have pathways for trans men to access abortion services” at MSI clinics, he said, acknowledging that “these are infinitesimally small numbers.”
Between providing opportunities for IPPF and MSI to promote their broader agendas, the event showcased FP2020’s crowning achievement: 60 million additional users of modern contraception since 2012. This fell significantly short of the partnership’s goal of adding 120 million new users in that time. FP2020’s progress had been off target for years, long before the COVID-19 pandemic created global disruption.
While FP2020 framed its work in terms of creating access to contraceptives, its metrics continue to rely on “unmet need,” which does not measure access and masks the fact that only a tiny percentage of women described as having such a “need” cite lack of access as the reason.
Editor’s Note:Rebecca Oas, Ph. D. writes for C-Fam. This article first appeared in the Friday Fax, an internet report published weekly by C-Fam (Center for Family & Human Rights), a New York and Washington DC-based research institute (https://c-fam.org/). This article appears with permission.”
On February 3, the Institute for Family Studies (IFS) reported research regarding American birth rates in the decade 2009-19. The results are not good. Even if we take 2008 as a baseline, the ensuing decade showed an implosion in birth rates. If birth rates had only stayed where they were in 2008 (remember, birth rates had been trending downward before that), there should be 5,800,000 more children in the United States than there are.
Drilling deeper into the data, the decline cut across all major demographic lines (white, black, Native American, Asian, and Hispanic). While some groups occasionally plateaued and others just plummeted, everybody ended the decade with birth rates markedly below where they had been ten years earlier. The biggest surprise, perhaps, was the collapse in Hispanic birth rates: almost half (47%) of that 5.8 million baby birth dearth are Hispanics. If Hispanic women had children at the rate they did in 2008, they would have reduced white mothers to a minority of population births in 2019. That they didn’t appears correlated with Hispanic women’s child bearing rates in 2008 (2.8) versus 2019 (2.0, i.e., below replacement).
Consider, also, that the 2009-19 birth dearth will probably be exacerbated by the annus horribilis of 2020 and COVID-19. As of this writing, the CDC attributes approximately 450,000 American deaths to the pandemic. And contrary to some initial hopes, there doesn’t appear to be a COVID-19 baby boom, but instead a baby bust.
A baby bust leaves its mark on society in a direct way for about 70-80 years (a typical lifespan) and an indirect one permanently. Our current lack of one-to-ten-year-olds will translate in a decade into a paucity of grade, high, and college students as well as first-job work entrants. The snowball multiplies across the decades, with fewer workers paying fewer dollars to subsidize entitlement programs, fewer people to marry, the not unreasonable possibility of their having fewer children…in short, a shrinking and aging society. It leaves its mark permanently by erasing from the picture all the activities (and children) those missing never do or have. Think George Bailey.
What caused the depressed birth rates of the past decade? A review of the history of those ten years suggests some obvious answers.
The 2008-11 recession obviously had an effect on marriage and parenthood. On the plus side, it reduced divorce, because two cannot live as cheaply as one flesh, especially in a society whose economic structure has geared itself to two-income households. On the minus side, it probably also drove down childbearing.
But while the economy appeared to recover (at least by the benchmarks economists employ) and, indeed, Americans arguably experienced a bull stock market in the Trump Administration, the question remains: Did Americans recover from their economic uncertainties? The 2016 election suggested that, at least for working/middle class Americans, the answer was “no.”
Further attention should be directed to the kinds of jobs created post 2008-11. While a “job” might mask unemployment, was the quality of those jobs (full v. part time, pay scales, benefits, permanence) more tenuous? For young people finishing schooling (high school or college) and seeking to enter the workforce in a first full-time job, were opportunities there? If there were, what were they and did they correlate with the economic situation of those first full-time workers? Were the jobs a high school graduate could obtain only slightly better than welfare? Were the jobs a college graduate could get allowing him to start paying down (student) debt?
Financial instability has been blamed as one of the reasons for why Americans are marrying later than ever or not at all. I’m not inclined to lay all the blame on finances—birth rates plummet even in economically secure European social welfare states—but neither would I minimize their impact. While materialism can always offer an excuse that “we’re not ready yet,” there is something to be said for the desire to enter marriage with some measure of financial security to enable a couple to do “married” things, like have children and buy their own house.
But financial factors alone do not affect marrying and childbearing. Cultural factors also devalue having children. Indeed, the lack of children is a perverse feedback loop: One of the factors the National Marriage Project (NMP) annually examines is what it called the “loss of child centeredness.” The time Americans spend with kids has progressively decreased. Fewer kids means less time with kids. A personal illustration: There is an 11 year span between my eldest and youngest child. Assuming (dato non concesso) that children start to go off on their own when they finish college, my wife and I will spend 33 years with a child in our lives before they theoretically make their ways in the world. Absent our youngest, that range would shrink to 24 years.
The time American adults spend with kids shrinks with fewer kids. Divorce tests one’s mastery of division: How does one parcel who “gets the kids?” Life expectancy reduces the ratio of a child’s life presence in an adult’s life. Growing childlessness cancels it altogether.
Our understanding of marriage affects childbearing. The states which sought to protect sexual differentiation as an essential element of marriage often argued that marriage and procreation had a natural nexus. The Supreme Court in Obergefell formally severed it, but its practical severance had occurred long before 2015 as contraception gained acceptance, even among nominal Catholics.
But the NMP also identified a seismic but generally insufficiently considered shifting in American thinking about marriage. Even as Catholic thought concedes that marriage and parenthood are distinct if related institutions, the rise of the “soulmate” model of companionate marriage fostered the view that those institutions are distinct but unrelated. While most people don’t bother themselves to think about the theoretical implications of what they believe, the practical effect has been that marriage has shifted from being about us-cum-future-family to simply us. As NMP research showed, children are, in fact, seen as an enemy to soulmate marriage because they necessarily shift the couple’s focus from us to them, rendering void all the assumptions about the nature of marriage that the “soulmate” model entailed.
There will clearly be little consensus to forge a public view of marriage as related to parenthood, at least from most present political forces; but it does accentuate the yeoman work for churches (and especially the Church) to reconstruct that marriage-and-parenthood vision. For the Protestant “mainline/old line” (to borrow Neuhaus’s term) that’s going to be hard, given their approval of contraception. But Catholic marital and sexual ethics are still congruent with a vision of marriage and parenthood as intrinsically and not just accidentally or functionally related. Its task is simply to teach what it says it believes. That just doesn’t mean a few doctrinal citations or a reading from Humanae vitae, but a whole vision of marriage as it fits into the life of the average believer, and that is as much practical as theoretical.
Let me give a simple illustration. Something that struck me when I first studied at the Catholic University of Lublin, Poland, was a discussion we had in a language instruction course on the topic: What kind of spouse would you want? The Polish teachers made it the topic of conversation because they considered it a topic college and older students would have ordinarily given some thought to and could expatiate upon. The Western students, especially the Americans, seemed surprised that the whole idea might be the subject of a public social conversation and repartee.
How do we expect to foster a vision of marriage if we don’t talk about it?
Because the Church’s role would be formative of a vision it would, as noted, be unlikely to find “common ground” with political discussions. Indeed, in the current climate of gender debates, the Church’s best hope would be to be left alone. But promote its vision it must. Two poles—the cultural vision and the economic conditions—are essential if we are to staunch the death spiral our growing rates of childlessness augur.
Two writers in the South China Morning Post reported research in January that, at least in East Asia, social and governmental efforts to promote marriage bolstered the birth rate. Chen and Yip note that every one percent increase in marriage rates among 25-29-year-old females was marked by an increase in fertility rates. While our two scholars “discovered” what most people knew about “the birds and the bees,” the Western fetish for numbers documenting claims helps make the case that promoting marriage promotes childbearing which promotes social stability.
The writing—or rather, the numbers—are on the wall.
Casual talk of birth control as a solution to women’s problems is abhorrent — and for a school that appreciates a proper, well-rounded education, I expected better.
The Curate women’s panel on Saturday covered many topics relevant to young ladies: careers, relationships, time management, and yes, menstrual cycles. One of the breakout sessions, led by a local pediatrician, was an “interactive talk on women’s menstrual health.” While I appreciated the open nature of the talk , the doctor mentioned birth control many times as the solution to women’s health problems.
For reasons beyond religious ones, contraceptives are problematic. Too often, young women are told that birth control can be a solution to their problems without knowing the side effects. Birth control has long-lasting detrimental effects on our bodies — ones that women should at least be informed about. Speaking of birth control as though it’s an easy fix to all of life’s problems is misleading, ill-informed, and wrong.
Birth control doesn’t actually “regulate” your body — it just creates an artificial cycle that takes longer for your body to adjust to. When women stop taking the pill, they have a high chance of what’s called post-pill amenorrhea, or when the body is forced to return normal hormone production, so the menstrual cycle is halted all together for up to six months.
The shot Depo-Provera (or DMPA), a popular form of birth control which is most frequently used by teenagers, can halt fertility for two years after the last injection. Say, for example, you took the shot in high school on the recommendation of your doctor. You enter college and by springtime in year four, you have that ring on your finger! When you and your financially stable partner are ready to consider conceiving, you go to your doctor. But wait — you might have to wait two years (or longer) until you welcome a new member into your family. Why wouldn’t your doctor tell you that contraceptive use can have long-term effects?
This is a phenomenon we see among quite a few young adults: doctors are quick to prescribe, slow to treat. The American Academy of Pediatrics even recommends over-the-counter purchase of contraceptives for teens.
A recent study found that many women are misdiagnosed with Polycystic Ovarian Syndrome (PCOS), a condition that makes it harder to conceive, makes cycles more painful, and causes depression. Women are told they may have difficulty conceiving and that the pill is the best solution for the disease. Twenty-one percent of young women are diagnosed with PCOS, and a shocking number of them are misdiagnosed. Further, many symptoms of PCOS go away after the age of 25.
But instead of waiting until young women have gone through puberty to see if symptoms go away, doctors prescribe them a hormone cocktail to fix problems they might not even have.
As young women, it’s easy to listen to the doctors who know more, the women with experience, or the friends whom we trust. It’s easy to look to a pill that might lessen cramp pains, relieve acne, or “regulate” your body.
It’s equally as easy to do your research about what birth control could mean for your body, long-term. Research what it means outside of pain relief or a “regular” cycle before you introduce an ocean of chemicals into your body.
So, what are the negatives? Hormonal birth control can trigger depression. Women are 23% more likely to become depressed while taking contraceptives, and teenage girls are 80% more likely to suffer from depression while on the pill. Not to mention the other emotional and physical side effects — anger, stress, weight gain, acne, and moodiness.
Birth control also causes increased cardiovascular morbidity and mortality, and increased breast and cervical cancer rates. In 2001, the World Health Organization classified contraceptives as Group 1 Carcinogens, or a substance known to cause cancer. Other Group 1 Carcinogens include cigarettes, mustard gas, and arsenic.
It’s not as if there’s no hope for women — natural alternatives are just as effective as hormonal birth control. In April 2007, professional nurses at Marquette University began a study to evaluate the effectiveness of a Natural Family Planning service. NFP works with a woman’s natural biology to determine fertility schedules, allowing women to get in tune with their body’s natural cycle. According to the study’s ongoing results, the Marquette method results in as little as a 2 – 6.8% failure rate, as opposed to the 9% failure rate of the pill.
It doesn’t matter if there’s a 1% chance, a 5% chance, or a 10% chance of harm from contraceptives; what matters is that you know the risk and act accordingly. Don’t fall victim to the slough of people who are more willing to prescribe than educate.
Haley Strack is a sophomore studying political economy. She is an assistant editor for the Collegian.
This week (Feb. 7-14) is “National Marriage Week” and Feb. 14 “National Marriage Day” (which coincides with St. Valentine’s Day). The USCCB Secretariat on Laity, Marriage, Family Life, and Youth even has a web page with some resources.
“National Marriage Week” happens to follow the release Feb. 3 of a short research piece by the Institute for Family Studies, “5.8 Million Fewer Babies: America’s Lost Decade in Fertility.” Its author, Lyman Stone, reports some disturbing numbers. He took the birth rate as it existed in 2008 (which had already been going down for some decades) and extrapolated it over the following 10 years. Next, he looked at the actual birth tallies for the period 2009-19. The result: there were almost 6 million fewer babies born in that period than actually should have been had the 2008 rate persisted.
Let me underscore several critical facts. First, Stone took 2008 as his baseline. That, in itself, was no high bar: it represented already declining trends. Second, the 2009-19 baby bust was not confined to one or a few demographic cohorts. All groups studied — whites, Blacks, Hispanics, Asian Americans, and Native Americans — went down. Hispanics were among the groups most in decline: just under 50% of that 5.8 million birth dearth was attributable to Hispanics.
Stone does not spend much time studying possible explanations for the decline, although he notes its future real and potential consequences. They range from a reduced workforce and military recruitment to increasingly polarized politics in an aging society competing for pieces of a non-expanding pie. I leave my readers to examine this disturbing report for themselves.
I raise it in the context of “National Marriage Week,” however, because of the correlation between marriage and parenthood. Yes, marriage and parenthood are theoretically distinct institutions and there are childless marriages. In reality, however, the first normally leads to the second and, as the Church itself teaches, “children are really the supreme gift of marriage” (Gaudium et spes, no. 50), not accessories or optional extras.
The National Marriage Project (NMP) has repeatedly tracked a phenomenon it calls the “loss of child-centeredness” in American life, including American marriage.
From a purely sociological viewpoint, the presence of children in American adults’ lives is in decline. Stone’s research cited above is one example: people are having fewer or no children.
Divorce is another: with the social acceptance and high incidence of divorce, those fewer children at best divide time between separate parents, with all the impacts such discontinuities entail.
Greater life expectancies is a third: an aging population increases the ratio of life lived apart from children, especially when one’s own children have fewer, if any children — no time with the grandkids. Our society economically squeezes kids by practically requiring and at least valuing higher both parents’ being in the workplace rather than with children.
Finally, we send all sorts of social messages. High tech IT firms offer ova freezing as a “benefit” for women to defer motherhood. I live in an apartment building in which the availability of a three-bedroom apartment is scarcer than hen’s teeth. And our elites convey their own anti-child messages: when my 13-year old was born in my late 40s, I received numerous unsolicited messages of sympathy for our “courage” in having a child, with the implicit assumption our precious and beloved Karol was some “mistake.”
All this is relevant as we mark “National Marriage Week” because there are two very strong trends in American culture that promote an idea of marriage which, in the end, is incompatible with Catholic marriage. The first is “soul mate” marriage, the second is the stripping away of characteristics Catholicism deems essential elements of marriage.
“Young adults today are searching for a deep emotional and spiritual connection with one person for life. At the same time, the bases for marriage as a religious, economic or parental partnership are receding in importance for many men and women in their twenties. Taken together, the survey findings present a portrait of marriage as emotionally deep and socially shallow.”
“Soul mate” marriage puts the focus on the spouse as fulfilling one’s emotional needs and goals, finding a kind of alter ego.
While some might think “soul mate” marriage tends to foster a noble and deep interpersonal relationship, its track record is far less impressive. Rather than drawing a person out of himself, “soul mate” marriage tends to foster an expectation that the other will be a reflection of the self. It also tends to focus on the emotive (feelings) rather than the volitional (commitments) side of relationships.
It tends to foster unrealistic expectations of Prince or Princess Charmings who can address the whole of one’s needs, a quite unrealistic burden to impose on another person. Because those expectations are so high, they in fact place a heavy burden on the relationship itself which, in a divorce-tolerant society, tends to lower the threshold at which the parties walk away from the marriage.
Finally, “soul mate” marriage tends to face critical stress in the face of childbearing because children, by their nature and dependence, are greedy, unavoidably shifting focus away from the “us” of the couple to the “them” of the children and the “us” of the family, something the very trajectory of such a marital paradigm does not prepare its “soul mates” for.
Spouses (especially fathers) have often felt “second fiddles” when a child is born, but the traditional model of marriage at least enforced an expectation that some shift of the “us” from each other to an “us” vis-à-vis “them” was natural, normal, and mature. The “soul mate” model, at least given the way people have been living them and the expectations they attribute to them, has not been doing that.
“Soul mate” marriage does not really account for children (certainly not as the “supreme gift of marriage”). To the degree, therefore, that we do not challenge this increasingly ascendant model of marriage (or try better to connect the idea of “soul mates” with the idea of becoming parents as part of that “soul mate” vocation), to that degree we acquiesce in a cultural model of marriage that depreciates the connection of marriage and parenthood, undermines a Catholic vision of marriage, and contributes to our ongoing birth dearth with its concomitant baneful implications for society. If this model is to remain, we have got to both deepen radically the understanding of “soul mate” as well as temper it with reality.
In practice, “soul mate” marriage dilutes the nexus between marriage and parenthood, shifting it from a Catholic view of “distinct but related” to one of “distinct but unrelated (unless we want it to be).” That attitude, in turn, bolsters a “contraceptive mentality” that sees one’s capacity to be a parent not as an intrinsically good part of my personhood but as a merely physically neutral biological phenomenon whose value is fixed by its convenience to my wishes. The result is that it undermines, even in Catholic minds, the idea that fruitfulness – openness to life – is an essential part of marriage as seen from a Catholic perspective.
There are, of course, other essential characteristics of marriage as understood from a Catholic perspective that are increasingly incomprehensible to the larger society. One of them is sexual differentiation. Another is permanence.
Exclusivity still gets lip service, in the sense that concurrent bigamy is both still illegal as well as frowned upon, but consecutive bigamy (divorce and remarriage) is broadly approved. Exclusivity also still receives lip service in that, even in the case of remarriage, we still expect just one “spouse A” and one “spouse B.” But if we really “believe” that “love is love” (as the woke lawn signs in my neighborhood proclaim), how can we logically limit “love” numerically?
My point in noting the question of how compatible what many people (including nominal Catholics) think about marriage with what the Church teaches about it is to recall a neglected teaching from Pope Pius XI’s encyclical Casti connubii. Early on in that document, the Pope affirms a principle whose mention we have unduly neglected: the scope of human freedom.
“This freedom, however, regards only the question whether the contracting parties really wish to enter upon matrimony or to marry this particular person; but the nature of matrimony is entirely independent of the free will of man, so that if one has once contracted matrimony he is thereby subject to its divinely made laws and its essential properties.”
Put simply, human freedom extends to whether or not John wants to marry and, if he does, whether he wants to marry Mary or Ann. Human freedom does not extend to what marriage is, e.g., whether he wants to “marry” Betty “till death do us part” or “for five years, subject to mutual agreement on extension of the contract,” or whether he wants to “marry” Sandy but positively exclude parenthood with her.
This distinction between freedom to marry versus freedom to redefine marriage — fundamental and uncontroversial to what Catholics have always understood in relation to marriage — is increasingly incomprehensible even to many Catholics today, with concomitant consequences for marital nullity. Restoring awareness and understanding would go a long way to addressing the crises even Catholic marriages today encounter.
I also strongly suggest that this educational-catechetical-formative focus deserves at least as much attention in our “National Marriage Week” observances as the celebratory/counseling/psychological element. Individual marriages are supported by the latter, but Christian marriages at large are made and nurtured by the former where, I venture to say, our public effort has been anemic.
Unless we also get that right, there aren’t going to be as many Christian marriages to celebrate during “National Marriage Week” … and likely even fewer offspring as marriage’s “supreme gift.” On the latter, the numbers are already in.
by Mary Cooney Our youngest child has Down Syndrome. We found out the day after he was born, when the pediatrician noticed several markers for T21. That day the nurses tried to draw blood so they could run a test to confirm the diagnosis. But the particular vein they needed to draw blood from was too tiny, and after seeing my son’s wrist full of needle holes, I asked them not to try again until he was older and his veins were bigger. My husband and I didn’t need immediate test results — T21 or not, he was our son and we loved him dearly.
Unbeknownst to my husband and I, the nurses drew blood for the test a week later. I didn’t know this until they told me that the test came back positive. I could have been upset that they drew blood without our permission, but I wasn’t. I could have been upset that the test came back positive, but I wasn’t. I was, however, tired and stressed because Junior wasn’t gaining weight, I wasn’t producing enough milk, and progress with his oxygen levels was painstakingly slow.
Later that afternoon, Junior’s nurse noticed that I was visibly upset. She thought it was because the test results had come back positive. “I’m sorry about the test results,” she said, sympathetically. Then she said something that shocked me: “Do you want to put him up for adoption?”
I was too exhausted to be indignant. Instead, I smiled at her sadly and just shook my head. But in my mind I thought, “How could you even think that I would put him up for adoption? Don’t you see me here ’round the clock pumping, nursing, and caring for him? Don’t you see how much I love him?”
It hadn’t occurred to me that perhaps her question was neither callused nor far-fetched.
For surely several mothers had come to that hospital and given birth to children that, for whatever reason, they were not able to raise. And after seeing their babies’ heartbeats, feeling their babies’ kicks in utero, and carrying their little ones for nine months, they had forged a bond of love for their babies, the way nature intended. Loving their babies as much as I loved mine, but without the support and resources they needed, these mothers had made a most heroic sacrifice: put their precious babies up for adoption. It was the most loving thing they could do.
I have always admired the heroism and selflessness of women in difficult circumstances who carry their unborn babies for nine long months and then give them up for adoption. But I never imagined the extent of their love and pain until I read The Lucky Few, by Heather Avis. In this autobiography, Avis details her struggles with infertility and how God led her to adopt three children, two with Down Syndrome. I think I read it in two days — it was that compelling.
But the chapter where she describes the day she met her youngest in the hospital had me in tears. Because the birth mother’s sorrow at leaving her baby was utterly heart-wrenching:
Sami’s bags were packed and waiting by the door. At the appointed time, Sami (the birth mother) went over to her sweet baby boy, clicked off the blue light, and gently picked him up.
She removed the mask and cradled him in her arms as she softly ran the back of her hand across his fresh cheeks. With tears streaming from her eyes, she whispered, “I love you” into his ear. Time stood still, and everyone in the room wept with her and poured out our love on this perfect baby boy. Lucy (Sami’s sister) handed her a fresh bottle, and we all watched as she sat on the bed to feed him one last time.
By the time he finished his bottle, it was almost time for him to go back under the blue light. Sami handed him to Lucy, and for the next few minutes he was passed around the room as aunties, grandma, and sister said good-bye. Then Sami held him close one more time, closing her eyes and pressing her face against his head. After one more “I love you,” he has back under the obnoxious blue light.
Everyone gave Josh (the adoptive father) a quick and teary hug, and he stayed with August (the baby) as I walked with them.
No one said a word. We did what had to be done and put one foot in front of the other as we headed to the elevator. One foot in front of the other into the elevator, tear-filled eyes glued to the floor. The door opened, and we put one foot in front of the other out of the hospital and into the cool evening air and all the way to their car.
Saying good-bye to Sami and her family was brutal. The loss they were experiencing weighed on me in a way I didn’t expect. I embraced her sisters and mom.
“Thank you for everything! For the gifts and the love. Thank you!” I said through tears.
“Take good care of him. We know you will,” Lucy said as she wept on my shoulder.
“I will. I promise I will.”
I gave Joy (Sami’s daughter) a long, tight hug, “You can see your brother any time you want. You just have your mommy call me, okay?”
She smiled and hugged me back, her youth offering her some protection from the gravity of the moment.
Then I made my way to Sami. We wrapped our arms around each other and sobbed. As I drenched her shoulder with my tears, I thought about how less than forty-eight hours ago, she had August in her womb, where she loved him and cared for him with all that she was. Now her womb and her arms were empty.
“I’m so sorry this is so hard,” I whispered. “I am so proud of you, Sami. I have never seen someone do such a selfless thing,”
“I love him so much, Heather.”
“I know you do.”
“Promise me you’ll take good care of him.” Her words came out broken and slurred between the sobs.
“I promise, Sami. The best care possible.”
Women like Sami are the unsung heroines of the pro-life movement. Difficult, messy, and painful as their own lives may be, they still choose life for their unborn babies. While the world tells them to make choices in their own best interests, they still choose what’s best for the babies in their wombs: life over death, adoption over abortion, hope over despair. These moms ought to be thanked and recognized for their heart-rending but life-giving sacrifices.
So today, when we usually would be Marching for Life in Washington D.C., I’ve been praying for all the moms who have given up a baby for adoption. Praying for the moms who are agonizing over what to do with an unplanned pregnancy or a baby with special needs. Praying that they will have all the love and support they need to make the loving choice and be honored for it.
May God bless these unsung heroines! May He heal their hearts and reward them for their selflessness. By their sacrifices and examples, we are one step closer to building a culture of life.
Republished with permission from Mary Cooney’s blog, Mercy for Marthas
Another dispatch from the Reproductive Revolution. BioEdge, MercatorNet’s associate site about bioethics, has been tracking the generosity of sperm donor dads for several years. Some men have fathered dozens of children, a few may have fathered hundreds. But in the case of Detroit gynaecologist and obstetrician Dr Philip Peven the word “thousands” is being used. It will be impossible to know, but since he delivered some 9,000 babies in his 40-year career, it seems possible. Some proportion of those children carry his genes.
Dr Peven is now 105 years old but is still in reasonably good health. Online DNA tests from sites like 23andMe and ancestry.com have united several of his offspring when they did some sleuthing into their genealogy.
Two of them confronted him early last year before the Covid-19 pandemic cut off personal contact. In the late 40s, he explained to them, medical students and young doctors often donated or sold sperm.
When he set up his own practice, he continued to use his own sperm to help women whose husbands had infertility problems – without informing them of the donor. At least once he was given a vial of sperm from a patient’s friend, but discarded it and used his own. He has no idea how many offspring he has, although he told his visitors that “My daughter thinks I could have fathered thousands of children.’”
Some of the offspring have noted that Dr Peven is an Ashkenazi Jew and people with that genetic heritage are prone to Gaucher disease, Tay-Sachs disease and cystic fibrosis. Many of his patients belonged to Detroit’s Jewish community, complicating matters still further. Their children could easily have married a half-sibling.
The Jewish News newspaper has covered this story extensively and found that other doctors were involved. One of the offspring of these other doctors made comments which apply to Dr Peven as well.
“I now realize that it was a different time, a time when doctors were not questioned, but I still consider the doctor’s behaviour unprincipled, unethical and possibly dangerous,” the person said. “The possibility was certainly there that half-siblings could meet, marry and have children. I do realize the doctor was trying to be helpful in enabling couples to have a child, but he should have told the mother he was using his own sperm. I doubt most women would have said yes to that scenario.”
As The Jewish News sought more information about Dr Peven, it unearthed deceptive donor sperm practices by other fertility doctors in Detroit. Dr Sylvester Trythall, who died in 1970, told one patient in the late 50s that he was going to mix her husband’s sperm with a medical student’s. But when a woman named Lynne Weiner Spencer investigated her genetic heritage, she found that she was really the daughter of Dr Trythall’s handyman, Hank Heemsoth, who died in 2006. Now it appears that Mr Heemsoth may have been the biological father of about 60 children – not many compared to Dr Peven, of course — but still noteworthy.
Secrecy is bad, of course, but the fundamental ethical problem with sperm donation is not secrecy; it is sperm donation. Every child deserves to be born as the beloved gift of a mother and father in a marriage. Sperm donation turns children into products and cuts them off from a father’s love, his own family connections, and a genetic heritage. However loving the child’s mother may be, erasing the father is a kind of child abuse. It should be banned.
But IVF clinics and sperm banks continue to promote it; the law continues to permit it. And as long as they do, some twisted men will take advantage of its legality for their own perverse reasons.
A horrifying feature in the New York Times this week shows a very dark side of sperm donation today. It examines the case of Jonathan Jacob Meijer, a Dutch musician in his 30s, who may have fathered 200 children – so far. Through donations to IVF clinics in the Netherlands, he has about 100; through private arrangements, another 80.
Even the New York Times suggests that at least more regulation is needed:
As an industry, however, it is poorly regulated. A patchwork of laws ostensibly addresses who can donate, where and how often, in part to avoid introducing or amplifying genetic disabilities in a population. In Germany, a sperm-clinic donor may not produce more than 15 children; in the United Kingdom the cap is 10 families of unlimited children. In the Netherlands, Dutch law prohibits donating anonymously, and nonbinding guidelines limit clinic donors to 25 children and from donating at more than one clinic in the country. In the United States there are no legal limits, only guidelines from the American Society for Reproductive Medicine: 25 children per donor in a population of 800,000.
The dismal truth is that some males get a kick out of spreading their genes far and wide. A member of Donor Offspring Europe, told the Times that some men travel around Europe trying to have as many children as possible.
“It’s kind of disgusting in a narcissistic way,” she said. “No sane person would want 100 children or more. The big question is why? These men want confirmation that they’re a great guy and everybody wants them.”
Mr Meijer, for instance, has been donating to a number of sperm banks outside the Netherlands as well. Ties van der Meer, the director of the Dutch Donor Child Foundation, told the Times that his offspring could number several hundred or even 1,000.
Mr Meijer says that this is “ridiculous” and appeals to an ersatz, mystical, flower-power version of love. “I am disappointed by the obsession of the numbers,” he says. “I became a donor not for any numbers but out of love to help parents with realizing their dream. I cannot understand how anyone can only focus on numbers and see my donor children as a number.”
Ultimately the problem is not more regulation. The Reproductive Revolution has to be unwound. We have to return to the notion that a new life is sacred and should only begin within marriage. That is where it is best protected.
Otherwise we end up with Genghis Khan wannabees like Philip Peven and Jonathan Jacob Meijer.
January 28, 2021 (Children’s Health Defense) — Pregnant women (unless they are at high risk of exposure to the COVID virus) and people under age 18 should not get Moderna’s COVID-19 vaccine until further studies are completed, according to new guidance issued today by the World Health Organization (WHO).
“While pregnancy puts women at a higher risk of severe COVID-19, the use of this vaccine in pregnant women is currently not recommended, unless they are at risk of high exposure (e.g. health workers).”
In an online briefing, as Reuters reported, WHO director of immunisation Kate O’Brien said, “There is no reason to think there could be a problem in pregnancy, we are just acknowledging the data is not there at the moment.”
WHO continues to recommend that “health workers at high risk of exposure and older people should be prioritized for vaccination.”
However, today’s recommendations also included this list of people who should not get the Moderna vaccine:
“Individuals with a history of severe allergic reaction to any component of the vaccine should not take this or any other mRNA vaccine.
“While vaccination is recommended for older persons due to the high risk of severe COVID-19 and death, very frail older persons with an anticipated life expectancy of less than 3 months should be individually assessed.
“The vaccine should not be administered to persons younger than 18 years of age pending the results of further studies.”
Last week, The Defender reported that allergic reactions had caused California health officials to hit pause on a large batch of Moderna vaccines. A few days later, Moderna said it was okay to resume using that batch.
Also last week, China health experts called for the suspension of Moderna’s and Pfizer’s COVID vaccines after reports that Norway and Germany were investigating the deaths of at least 43 elderly people (33 in Norway, 10 in Germany) who had received the COVID vaccine.
In the U.S., as of Jan. 15, 181 deaths had been reported to the U.S. government’s Vaccine Adverse Events Reporting System as possibly being related to COVID vaccines. A 2010 study by the U.S. Department of Health and Human Services concluded that “fewer than 1% of vaccine injuries” are reported to VAERS and experts say the government’s reporting system is “broken.” Both the Pfizer and Moderna vaccines use mRNA technology, never before used in vaccines. In the U.S., both are approved for emergency use only, which by the U.S. Food and Drug Administration’s definition, means that they are experimental.
(Right to Life UK) Filmmaker, author, and social activist Obianuju Ekeocha has called out the United States for repealing the Mexico City Policy which ensured that federal funding was not spent on abortions outside the United States.
President Joe Biden will revoke the policy put in place by the former US administration, likely resulting in a large increase in funds being made available to global abortion providers that target developing countries including MSI Reproductive Choices and International Planned Parenthood Foundation.
In a speech to the World Health Organization on Thursday 22nd January, Dr Anthony Fauci, Chief Medical Advisor to the President, said:
“To that end, President Biden will be revoking the Mexico City Policy in the coming days, as part of his broader commitment to protect women’s health and advance gender equality at home and around the world”.
The Mexico City Policy
The Mexico City Policy was originally announced by President Ronald Reagan in 1984. It required non-governmental organisations to agree, as a condition of receiving federal funding, that they “would neither perform nor actively promote abortion as a method of family planning in other nations”.
The policy, which essentially forbids federal funding from being used to perform and promote abortion outside of the US, has been a significant point of contention since its beginning, with successive Republican and Democrat Presidents instituting and then rescinding the policy.
The former administration had reinstituted it after the Obama era and expanded it into a policy called Protecting Life in Global Health Assistance.
Under the new President, federal funding for abortions outside of the US will once again be available for global abortion giants such as MSI Reproductive Choices and International Planned Parenthood Federation.
US funding of abortion in Africa
Social activist Obianuju Ekeocha has slammed the President for this move in a Tweet, saying:
“So Pres Biden intends to repeal the Mexico City Policy so that the United States can resume funding abortion organizations in Africa and other parts of the developing world…to kill our innocent unborn children. We will object”.
With the repeal of the Mexico City Policy, US federal funding, which ultimately comes from the US taxpayer, will now be available to fund abortions and the promotion of abortion in Africa.
In a report for Culture of Life Africa released last year, Ekeocha accused the UN and a number of Western nations, including Canada, the US and the UK, of “humanitarian blackmail” as they sought to capitalise on the global COVID-19 crisis by imposing abortion on the continent.
Illegal abortions, fake doctors and abortion bonuses
The move to repeal Mexico City Policy will likely mean that federal funding will once again be given to contraversial global abortion provider MSI Reproductive Choices.
MSI Reproductive Choices has recently rebranded from its previous name, Marie Stopes International, to hide their association with eugenicist and Nazi-sympathiser, Marie Stopes.
The organisation perform millions of abortions across the globe each year and received over £340 million from the British taxpayer over the last ten years, and continues to be surrounded by scandal.
In October 2020, the bodies of ten illegally aborted babies were found discarded and decomposing in a bin at a Marie Stopes International franchise ‘Medical Centre’ in Kenya, resulting in the closure of the clinic.
In 2017, a damning report from the UK’s Care Quality Commission (CQC) accused Marie Stopes International (now MSI Reproductive Choices) of paying staff bonuses for persuading women to have abortions.
In addition, the CQC found the abortion group was not following proper sterilisation and infection control protocols and was improperly disposing of the bodies of the babies they aborted.
In 2016, Marie Stopes International was forced to suspend abortion services for a month after an unannounced inspection by the CQC found “dead foetuses lying in an open bin and staff trying to give a vulnerable, visibly distressed woman an abortion without her consent”.
Right To Life UK spokesperson, Catherine Robinson, said:
“Thank you Obianuju Ekeocha for courageously speaking out against the US’s return to targeting developing nations with abortion funding”.
“The fact that President Biden has rescinded the Mexico City Policy should come as no great surprise. This is exactly what Barack Obama did when he came into office in 2009 with Joe Biden as his Vice-President. That it was one of his first acts as new President is an ominous sign of the priorities of this administration. They appear to have completely aligned themselves with an ideology concerned with expanding abortion access at all costs”.
“In the UK, this same ideology is on clear display in the case of those promoting ‘DIY’ abortions, regardless of the many serious safety concerns posed to vulnerable women. There are inadequate safeguards to prevent women being coerced into having an abortion, there are also inadequate safeguards to ensure the woman is taking the abortion pills at the ‘appropriate’ gestational age, and there is evidence of systemic underreporting of complications related to the use of ‘DIY’ abortions. None of these major concerns appears to matter to abortion providers who, like the Biden administration, have shown that they care as little for women as they do for their unborn children”.
Editor’s Note: This article was published at Right to Life UK and is reprinted here with permission.
In the fertility awareness world, it is no secret that we advocate for the medical community to consider the menstrual cycle a vital sign of health. Often sequestered to that aisle in the drug store or murmurs in the bathroom, periods have long gotten a bad rap. We’re learning now that not only do periods open a previously hidden door of new understanding into women’s well being and health, but healthy and balanced cycles have recently been linked with living longer. Finally, the PR for periods may be getting a long-overdue overhaul.
A landmark prospective cohort study out of Boston, published in the British Medical Journal this past August, found an association between irregular and long menstrual cycles* in adolescence and adulthood with a greater risk of premature mortality (described as death before the age of 70 years old) [1].
This association between menstrual cycles and premature death was independent of body mass index (BMI) and was present with or without signs of PCOS, endometriosis, or uterine fibroids. This indicates that hormonal disorders alone are not the culprit behind early death, but rather an indication that the lack of regular ovulation and menstruation could be the root of this association.
This is huge. It means if hormonal disorders are effectively treated, and regular ovulation is supported for women of reproductive age, then women with hormonal disorders can reap long-lasting health benefits just as well as women without such disorders.
The connections between irregular cycles, teenage birth control use, and early death
In an even more striking finding, the same study discovered an increased risk of early death among women who used oral contraceptives during their teen years, specifically between the ages 14-17.
This indicates two really important things that fertility awareness advocates have been positively shouting about for years: First, that having a regular, balanced period matters for a woman’s current and future health. Second, how the pattern of fertility cycles unfolds in a young woman’s early years matters.
It’s a sad irony that teens younger than 17 are more likely to be put on the Pill—or any other form of hormonal contraception—due to long or irregular periods, rather than for the express purpose of contraception. But irregular periods are more than merely annoying, and are thought to be a sign of something far more serious: a disrupted hypothalamic-pituitary-ovarian (HPO) axis. A disturbed HPO axis is associated with “non-communicable diseases, including ovarian cancer, coronary heart disease, type 2 diabetes, and mental health problems, through mechanisms probably related to a disrupted hormonal environment, chronic inflammation, and metabolic disturbances.”
While irregular periods can be normal in the beginning years of puberty, there should be a progression over time to more regularity. In the case that a young girl experiences irregular periods that don’t progress toward maturation, this is often a sign of some type of hormonal imbalance.
But what does this have to do with birth control? As we’ve discussed at length before, hormonal contraception doesn’t regulate anything about a woman’s cycle, but rather, it shuts down the all-important HPO axis. So instead of having a true menstrual period each month, a girl or woman on birth control has a false hormonal withdrawal bleed every month.
The missing link in irregular periods: Metabolic syndrome and hyperinsulinemia
It isn’t entirely clear why irregular periods are linked with premature death, but researchers are beginning to hypothesize that irregular and long menstrual cycles are strong predictors of a condition known as hyperinsulinemia [2]. That’s a fancy word for too much insulin—the hormone that regulates sugar—in your blood. Now it’s a question of what came first, the chicken or the egg: Did increased insulin cause irregular cycles or did irregular cycles cause increased insulin?
It’s no secret that modern diets are high in sugar, and that modern living is abundant in stress. Either one of these two things can wreak havoc on the endocrine system; together, they can cause a veritable firestorm in our bodies. Insulin resistance, when women have a much higher threshold of how much insulin is needed before their body recognizes it, is becoming the norm. And it has even been hypothesized that this condition could be cross generational [3]. This means that your great grandmother’s diet could have had an effect on your DNA, and insulin levels, even today. Wild. High insulin levels have been long thought to play a critical role in cancer, diabetes, and cardiovascular disease. And, in case you were wondering, cardiovascular disease is the top cause for premature death in women, and cancer and diabetes are a close second and third.
What can be done?
Before you get too down about this, consider that we do have a chance to rewrite our future generation’s DNA. It starts with the menstrual cycle. Women young and old can chart their menstrual cycles with a fertility awareness method (FAM), which can reveal cycle irregularities or hormonal imbalances that a FAM-aware doctor can help treat with restorative reproductive medicine.
Rather than putting a hold button on these issues, as hormonal contraception does, we have the option to teach teens how to chart their cycles which gives them an empowering relationship with their body as well as a family planning tool for when they need it. But more importantly, their cycle charts serve as an invaluable diagnostic tool helping them to know and manage their health risks, and alerting them to get the help they need when it matters most.
This is another reason medical professionals should learn more about fertility science and include information on cycle charting in their practice. If medical practitioners have enough knowledge about cycle charting and include menstrual characteristics as a vital sign of health, young teens can navigate cycles (regular or irregular) and utilize both complementary and conventional medicine to reduce future risk of adverse health outcomes.
*Irregular and long cycles can be considered normal in transitional seasons such as early puberty, post birth, during breastfeeding, and perimenopause.
When this article refers to fertility awareness methods (FAM), or natural family planning (NFP), we are referring to Fertility Awareness-Based Methods, evidence-based methods of cycle charting which can be used as effective forms of natural birth control when learned by a certified instructor.
References
[1] Wang Y, Arvizu M, Rich-Edwards J et al. Menstrual cycle regularity and length across the reproductive lifespan and risk of premature mortality: prospective cohort study. BMJ. 2020:m3464. doi:10.1136/bmj.m3464
[2] Wei S, Schmidt M, Dwyer T, Norman R, Venn A. Obesity and Menstrual Irregularity: Associations With SHBG, Testosterone, and Insulin. Obesity. 2009;17(5):1070-1076. doi:10.1038/oby.2008.641
[3] Fusco S, Spinelli M, Cocco S et al. Maternal insulin resistance multigenerationally impairs synaptic plasticity and memory via gametic mechanisms. Nat Commun. 2019;10(1). doi:10.1038/s41467-019-12793-3
CNA Staff, Jan 22, 2021 / 05:40 pm MT (CNA).- President Joe Biden’s statement backing legal abortion on the anniversary of Roe v. Wade drew swift reaction from the U.S. Conference of Catholic Bishops, whose pro-life chairman said the no president of the United States should ever defend denying the right to life of unborn children.
“We strongly urge the president to reject abortion and promote life-affirming aid to women and communities in need,” the U.S. bishops’ Committee on Pro-Life Activities head Archbishop Joseph Naumann of Kansas City in Kansas said Jan. 22.
“It is deeply disturbing and tragic that any president would praise and commit to codifying a Supreme Court ruling that denies unborn children their most basic human and civil right, the right to life under the euphemistic disguise of a health service,” he said.
The U.S. bishops’ conference responded to the statement from President Joe Biden and Vice President Kamala Harris on the anniversary of Roe v. Wade, the 1973 Supreme Court decision which mandated permissive abortion laws nationwide.
The president and vice president stressed their commitment to legal abortion, saying “The Biden-Harris Administration is committed to codifying Roe v. Wade and appointing judges that respect foundational precedents like Roe.”
Although Roe v. Wade was a critical pro-abortion rights decision, the statement did not mention abortion by name, preferring to use euphemisms such as “reproductive health” and “health care.”
“In the past four years, reproductive health, including the right to choose, has been under relentless and extreme attack,” they said. “As the Biden-Harris Administration begins in this critical moment, now is the time to rededicate ourselves to ensuring that all individuals have access to the health care they need.”
The U.S. bishops’ conference said the statement wrongly characterized the Roe v. Wade decision as “an advancement of women’s rights and health.” While the Biden-Harris statement did not mention religion, the bishops said Catholics cannot support abortion.
Biden has repeatedly emphasized his Catholicism, attending Mass the morning of his inauguration and citing St. Augustine of Hippo in his inaugural address. He has put a Pope Francis picture in the Oval Office.
Even on Biden’s first day in office, White House Press Secretary Jen Psaki cited Biden’s Catholicism when asked questions about abortion.
At a Jan. 20 press briefing, Owen Jensen of EWTN News asked Psaki what Biden plans to do regarding the Hyde Amendment and the Mexico City Policy, which Biden has opposed because they limit abortion funding.
“Well, I think we’ll have more to say on the Mexico City Policy in the coming days,” Psaki said.
“But I will just take the opportunity to remind all of you that he (Biden) is a devout Catholic, and somebody who attends church regularly,” she told reporters. “He started his day with attending his church this morning.”
In the bishops’ conference statement, however, Archbishop Naumann emphasized Church teaching on abortion.
“I take this opportunity to remind all Catholics that the Catechism states, ‘Since the first century the Church has affirmed the moral evil of every procured abortion. This teaching has not changed and remains unchangeable’,” he said.
The statement also emphasized politicians’ responsibilities to reject a right to abortion.
“Public officials are responsible for not only their personal beliefs, but also the effects of their public actions. Roe’s elevation of abortion to the status of a protected right and its elimination of state restrictions paved the way for the violent deaths of more than 62 million innocent unborn children and for countless women who experience the heartache of loss, abandonment, and violence,” said Naumann.
The president of the Franciscan University of Steubenville, Fr. Dave Pivonka, also reacted to the Biden-Harris declaration, saying their “aggressive pro-abortion statement … is saddening to Catholics worldwide. The policies they have promised to put forward are harmful to the dignity of the human person and are contrary to the teachings of the Church.”
Pope Francis has often rejected abortion as part of a “throwaway culture,” but some American pro-abortion rights advocates and politicians, and their supporters, have tried to claim the Pope has taken a non-confrontational approach at variance with most U.S. bishops.
On the day of Biden’s inauguration, Archbishop Jose Gomez of Los Angeles, in his role as president of the U.S. bishops’ conference, said he was praying for Biden. He noted areas of agreement and disagreement between the bishops and Biden.
“Catholic bishops are not partisan players in our nation’s politics,” Gomez said in a statement. “We are pastors responsible for the souls of millions of Americans and we are advocates for the needs of all our neighbors.”
“For the nation’s bishops, the continued injustice of abortion remains the ‘preeminent priority’,” he said, adding that “preeminent does not mean ‘only’,” and there are a wide variety of challenges and threats to human dignity facing the country today,” he said.
The U.S. bishops will engage with Biden with the aim of starting “a dialogue to address the complicated cultural and economic factors that are driving abortion and discouraging families,” Archbishop Gomez said.
Abortion has violently ended the lives of over 48 million Millennial (24.5 million) and Generation Z (24 million) babies combined, according to data published by Planned Parenthood’s former “special affiliate” and research arm, the Guttmacher Institute. Tragically, since the 1973 Supreme Court’s Roe v. Wade decision forced abortion upon the nation, a staggering 60 to 62 million preborn babies have been killed.
Guttmacher data from 2017 revealed that the lives of 2,363 preborn babies are violently ended every day by abortion in the United States.
Abortion at 8 weeks (Image credit: AbortionNo.org)
Using age definitions for the various generation groups published by Pew Research, along with reported abortion data published over the years by Guttmacher (note: the data has varied year to year due to estimations), Live Action News documented the following losses among the generations since Roe v. Wade:
Generation X = 8.7 million preborn lives lost to abortion
Between 1973 and 1980, there were an estimated 8,736,000 preborn lives lost to abortion among Generation X, identified by Pew as those born between 1965-1980. This is more than the entire population of the state of Virginia, and exceeds populations in all but 11 states in the US, according to 2019 population data estimates.
Millennials = 24.5 million preborn lives lost to abortion
Millennials are identified by Pew as those born between 1981 and 1996. In that generation, there were an estimated 24,514,400 Millennial preborn lives lost to abortion. Data by state published at infoplease.com for 2019 indicates that this would amount to more than the population of the state of Florida, and would exceed populations in all but two US states.
Generation Z = 24 million preborn lives lost to abortion
Pew Research defines Generation Z as those born after 1996. Between 1997 and 2017 (the last published report from Guttmacher), there have so far been an estimated 24,028,920 preborn babies from Generation Z lost to abortion. This, like those in the Millennial generation, also amounts to more people than the entire population of Florida in 2019, and would exceed populations in all but two US states.
The preborn lives lost to abortion among Millennials (24.5 million) and Generation Z (24 million) each outnumber the populations of a multitude of countries, according to a 2021 estimate published by WorldMeters.info. These include Niger, Taiwan, Sri Lanka, Burkina Faso, Romania, Chile, Guatemala, Syria and Cuba, among others. Collectively (48 million) they outnumber the populations of Spain, Uganda, Argentina, Algeria, Sudan, Ukraine and Iraq among many others.
Abortions by decade
Using data published by Guttmacher, we can also see the impact abortion has had in America by decade:
1973 to 1979: nearly 7.2 million
1980 to 1989: nearly 16 million
1990 to 1999: 14.3 million
2000 to 2009: 12.4 million
2010 to 2017 (last published year): nearly 7.7 million
Between 1973 and 2017 (the latest data published by Guttmacher), there were approximately 60 million abortions reported. Tragically, by end of 2020, the number of lives lost by abortion are now estimated to be as high as 62.5 million, according to National Right to Life.
As we enter the 48th year since Roe v. Wade, let us recommit to ending this horrific genocide of innocent children, so no more American generations will suffer loss from abortion.
Pro-life leader Joe Scheidler spent eight years as a Benedictine monk in Indiana, and though he discerned he wasn’t called to the priesthood, the founder of the Pro-Life Action League never stopped living the order’s motto of oraetlabora (prayer and work) during his many years in the pro-life movement, said his oldest son, Eric.
Joe Scheidler, who inspired many pro-life leaders and was chief defendant in a decades-long lawsuit filed by the National Organization for Women against pro-life efforts, died of pneumonia on Monday at his Chicago home surrounded by his family. He was 93. Scheidler is survived by his wife, Ann, seven children, 26 grandchildren and one great-granddaughter.
“He saw prayer as a foundation that you build work upon, the labora part, the work part,” said Eric Scheidler, who serves as executive director of the Pro-Life Action League, which recruits and equips pro-life Americans to help save unborn children through nonviolent direct action.
“He wanted to encourage people to do the work and to join him on the front lines. And the No. 1 work for him was going outside of abortion facilities because that’s where our witness is the most powerful.”
Recognized as an expert on the abortion culture, sidewalk counseling, battling the courts, fetal experimentation, the spiritual dimension of pro-life activism and the Church’s responsibility to fight abortion, Scheidler, easy to recognize in his trademark black fedora, also was a devout Catholic and daily Mass attendee, according to son Eric, who added that his father “very much saw what we were doing as a religious work, even though it has a public character, and it has a political character and we’re out in the public square. It was always rooted in faith. And he was passionate about sharing that faith, especially with his family.”
Scheidler was born in 1927, in Hartford City, Indiana. After serving in the U.S. Navy as a military police officer at the end of World War II, he earned a bachelor’s degree in communications at the University of Notre Dame and a master’s degree at Marquette University.
He spent eight years studying for the priesthood at St. Meinrad Seminary in St. Meinrad, Indiana. After discerning he was called to married life, Scheidler taught at Mundelein College in Chicago. During that time, he chaperoned a group of students on a pilgrimage to march with Dr. Martin Luther King Jr. from Selma to Montgomery, Alabama, in 1965.
Scheidler first got involved in the pro-life movement in 1972; and shortly after the 1973 Roe v. Wade decision legalizing abortion, he became a full-time pro-life activist. He founded the Pro-Life Action League (PLAL) in 1980 and wrote several books. For much of his life in the pro-life movement, he also could be found sharing the truth about abortion on street corners.
Targeted by the Abortion Lobby
In 1986, the National Organization for Women and a network of abortion facilities sued Scheidler and the Pro-Life Action League on racketeering charges for conspiring to deprive women of the right to abortion, according to the organization’s website. The case went to the U.S. Supreme Court three times before Scheidler won the case there in 2006, via a unanimous decision. The case didn’t completely end until 2014, however, when the U.S. Court of Appeals upheld a lower-court order instructing the National Organization for Women to pay the defendants more than $63,000 to compensate them for their legal costs.
Attorney Thomas Brejcha began working with Scheidler in 1986, when he took on the case. Brejcha, who went on to co-found the national public interest law firm the Thomas More Society with Scheidler, described him as a “towering figure” and compared him to the abolitionist William Lloyd Garrison.
Scheidler persevered as the court case dragged on and will be remembered for his advocacy in the face of persecution and oppression by litigation, Brejcha said of his longtime client and friend.
“He stood up and stood firm,” he said. “I can’t tell you how many times people told him to settle the case, give in, make peace with the opposition, and he refused steadfastly to do so.”
The nonprofit Chicago-based Thomas More Society, which seeks to restore respect in law for life, family and religious liberty, was founded during Scheidler’s case and from it, Brejcha said, adding that he learned how to fight major pro-life cases, including those against investigative journalist, David Daleiden, who exposed illegal activities of the abortion industry and for whom the society is currently providing legal services, due to Scheidler’s court battle.
Scheidler’s fight in the court case was a fight for the whole movement, and he can be considered a white martyr, said Peter Wolfgang, executive director of the Family Institute of Connecticut in Hartford, Connecticut.
“Something happens in a man when you give your whole life to something good and suffer for it,” Wolfgang said. “You just have this sort of presence about you, and people recognize that. That’s what everyone responded to whenever they were in a room with Joe Scheidler. You could feel his love for the unborn child. You could feel the purity of the man’s intention.”
‘A True Hero’
Scheidler also recognized the danger of new threats to religious liberty from the Obama administration’s contraception mandate introduced in 2012. He and the Pro-Life Action League organized simultaneous religious-liberty rallies across the country, Wolfgang said.
“I think they had an effect that, in some ways, continues to this day,” said Wolfgang, who added that Scheidler impacted his decision to work for the pro-life movement.
“It was Scheidler who rose manfully to the challenge of the 2010s, just as he did to the abortion challenge in the ’80s.”
Abby Johnson, founder and director of the pro-life apostolate And Then There Were None, remembered Scheidler on Facebook:
“Joe Scheidler was a true hero, someone whose opinion mattered in this fight for the unborn,” she wrote. “He was a giant in my own life, and I’m so grateful to have spent time with him and to have listened to his wisdom.”
Father Frank Pavone, national director of Priests for Life, and Janet Morana, Priests for Life’s executive director, honored Scheidler in a statement on Monday:
“I have countless memories of Joe, whether we were together fishing on Lake Michigan, praying to the Lord inside the Supreme Court as they were hearing his case, or saving babies in front of abortion mills,” Father Pavone said. “Every conversation with him was an inspiration to double my pro-life efforts.”
Morana called Scheidler the “godfather” of the pro-life movement. “In our early years, he was one of the people who taught us how to be pro-life activists,” she said. “He was an inspiration to us and gave us practical advice drawn from his many years as a passionate and fearless champion of the unborn.”
Scheidler’s passing on Jan. 18, the day when Martin Luther King Jr.’s legacy was remembered, is fitting because King’s work helped inspire the pro-life leader to activism, just as he went on to inspire others, Eric Scheidler said. “Seeing the impact that regular Americans could have by taking action against racial injustice inspired my father to mobilize Americans in the same way in the fight against the injustice of abortion.”
The following information was taken from America’s Frontline Doctors White Paper On Experimental Vaccines For COVID-19. More research is needed to determine the effects of experimental vaccines on fertility.
Experimental Vaccines & Other Unknown or New Problems
Frontline physicians have a very healthy respect for what is unknown. With these new experimental vaccines more is unknown than known, so this section is by definition, incomplete. But we already have suggestions of where serious problems will arise, based upon early data and mechanism of action. There is evidence to support that the vaccine could cause permanent auto-immune rejection of the placenta.
Placental inflammation resulting in stillbirths mid-pregnancy (second trimester) is seen with COVID-19 and with other similar coronaviruses. The way the experimental vaccines work, it is concerning that deleterious effect on the placenta, which in the wild only lasts as long as the acute illness, would instead be lifelong.
There is a case report of a woman with a normally developing pregnancy who lost the otherwise healthy baby at five months during acute COVID-19. The mother’s side of the placenta was very inflamed. This “infection of the maternal side of the placenta inducing acute or chronic placental insufficiency resulting in miscarriage or fetal growth restriction was observed in 40% of pregnant women with similar coronaviruses”54 Thus far SARS-CoV-2 appears to be similar.55 This issue has not been studied despite saying that “Additional studies of pregnant women with COVID-19 is warranted to determine if SARS-CoV-2 can cause similar adverse outcomes.” (Emphasis added)
The purported mRNA vaccines may instigate a similar reaction as the virus. There is a component in the vaccine that could cause this same auto-immune rejection of the placenta but indefinitely. In layman’s terms: getting COVID-19 has been associated with a high risk of mid-pregnancy miscarriage because the placenta fails – but the vaccine may do the exact same thing – but not for just a few weeks of being sick – but forever. Meaning repeated pregnancies would keep failing ~ mid-pregnancy. It is completely reckless to give this vaccine to millions of people who would otherwise all be expected to recover until we know the answer to that question!
i. Here is the scientific theory/explanation for the effect on the placenta (and possibly on sperm): the spike protein of Sars-Cov-2, against which teams are competing to develop a vaccine, is highly homologous with a human HERV protein, syncytin1. Syncytin-1, which is a HERV derived protein, causes fusion of cells in the trophoblast and has a role in placentation.56 The vaccinations are expected to produce antibodies against spike proteins of SARS-CoV-2. However, spike proteins also contain syncytin-homologous proteins, which are essential for the formation of the placenta in mammals such as humans. It must be absolutely ruled out that a vaccine against SARS-CoV-2 could trigger an immune reaction against syncytin-1, as otherwise infertility of indefinite duration could result in vaccinated women.57 58 (Emphasis added)
54 https://jamanetwork.com/journals/jama/fullarticle/2765616
55 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30311-1/fulltext
56 https://bjgplife.com/2020/05/21/of-hervs-and-COVID-19-questions-for-the-future/
57 https://2020news.de/en/dr-wodarg-and-dr-yeadon-request-a-stop-of-all-corona-vaccination-studiesand-call-for-co-signing-the-petition/?fbclid=IwAR3yoj0SCIK8WaaS0-w1vIoig4qNYydTxT3aK01NJDwHut3jWpygtnnbNY
Alignment of the endogenous elements Syn1 found on human chromosome 7, or Syn2 found on chromosome 6, or HERV-K expressed from chromosome 6, all show a number of sequence motifs with significant similarity to nCoV2019 spikeprotein.59
ii. As reported by Public Broadcasting Service, regarding placenta science: “The syncytiotrophoblast is the outermost layer of the placenta, the part that is pressed against the uterus. It’s literally a layer of cells that have fused together, forming a wall….This wall of cells keeps mom and baby working in harmony and not killing each other. There’s no other structure like this anywhere else in the body.”
60
Many scientists already agree the risk is much too high to release these experimental vaccines to the public at large. On December 1, 2020, the ex-Pfizer head of respiratory research Dr. Michael Yeadon and the lung specialist and former head of the public health department Dr. Wolfgang Wodarg filed an application with the European Medicine Agency responsible for European approval, for the immediate suspension of all SARS CoV-2 vaccine studies, in particular the BioNtech/Pfizer study on BNT162b. 61 62 One of the biggest reasons they cited was the possibility of lifelong infertility as described above and copied here.
America’s Frontline Doctors White Paper On
Experimental Vaccines For COVID-1958 https://2020news.de/wpcontent/uploads/2020/12/Wodarg_Yeadon_EMA_Petition_Pfizer_Trial_FINAL_01DEC2020_EN_unsi
gned_with_Exhibits.pdf
The Supreme Court has ruled that women must receive the abortion pill regimen in person, at an abortion facility, putting an end to dangerous mail-order abortions of mifepristone (brand name Mifeprex), also known as RU-486. The ruling affirms that the Food and Drug Administration’s (FDA) in-person abortion pill distribution requirements will remain in place, though as recently as October 2020, the Supreme Court “refused to rule on a request from the Food and Drug Administration to reinstate a rule banning the distribution of abortion pills by mail,” according to a previous report by Live Action News.
In the ruling, Chief Justice Roberts said the issue at hand was not whether or not the current requirements pose an undue burden upon women seeking abortion, but whether or not the District Court properly ordered the FDA to lift those requirements. “My view is that courts owe significant deference to the politically accountable entities with the ‘background, competence, and expertise to assess public health,’ ” Roberts wrote, adding, “In light of those considerations, I do not see a sufficient basis here for the district court to compel the FDA to alter the regimen for medical abortion.
The court’s three liberal justices — Stephen Breyer, Sonia Sotomayor, and Elena Kagan — dissented.
Previously, the pro-abortion American College of Obstetrician-Gynecologists (ACOG) had sued for the requirements to be suspended for the duration of the pandemic, and U.S. District Judge Theodore Chuang ruled in the group’s favor. “Particularly in light of the limited timeframe during which a medication abortion or any abortion must occur, such infringement on the right to an abortion would constitute irreparable harm,” he wrote in his ruling. “By causing certain patients to decide between forgoing or substantially delaying abortion care, or risking exposure to COVID-19 for themselves, their children, and family members, the In-Person Requirements present a serious burden to many abortion patients.”
Yet overturning the FDA requirements also put women at serious risk of harm, as the FDA itself argued in its appeal.
“Defendants will also suffer irreparable harm in the absence of a stay because they will be unable to enforce requirements that FDA has determined, based on its experience and scientific expertise, are necessary to ensure safe use of Mifeprex,” the appeal read. “Requiring patients to obtain Mifeprex at a clinic — as has been required for years — does not deprive women of the ‘ability to make a decision to have an abortion.’”
Though the abortion industry has repeatedly tried to claim the abortion pill regimen is completely safe, this is far from true. Potentially serious side effects have been well-documented, including uterine hemorrhaging, viral infections, sepsis, and death. At least 24 women have died, with thousands more adverse events, though the true number is likely to be even higher, as not every state requires abortion complications to be reported. The abortion pill has been shown to carry a four-times greater risk of complications than a first trimester surgical abortion. Women are put at greater risk when gestational age is not first properly assessed, when a life-threatening ectopic pregnancy is not ruled out, and when Rh factor is not tested (which can affect future pregnancies). Without an in-person visit, it’s also much easier for a woman to be coerced into an abortion against her will.
The simple reality is that the abortion pill is dangerous, and the FDA should remove it from the market altogether. But for now, at least, the Supreme Court has brought an end to mail-order abortions, a move that is likely to save some women’s lives.
XINJIANG, China (ChurchMilitant.com) – Decreases in the birthrate in the Xinjiang Uyghur Autonomous Region (XUAR) of China are stemming from the “eradication of religious extremism,” according to a new Chinese Communist Party (CCP) report.
The report, published on Thursday by the Xinjiang Development Research Center, said the elimination of what it calls “religious extremism” has allowed Uyghur Muslim women to become more autonomous and confident, according to the China Daily. They are less likely to resist family planning measures and now see themselves as more than mere “baby-making machines,” the report states.
Reportedly, the birthrate in Xinjiang decreased from 1.6% in 2017 to 1% in 2018.
Many critics see the CCP’s use of terms like “religious extremism” and “family planning” as euphemisms that imitate the radical feminist language and hide a sinister agenda.
China expert Steven Mosher, who witnessed the horrors of China’s one-child policy in the 1980s, told Church Militant recently: “Chinese communist propaganda mimics the language of Western feminists to disguise their ongoing genocide of the Uyghur people.”
“What is really taking Uyghur women out of the baby-making business,” Mosher added, “is the massive number of forced sterilizations and forced abortions that are being performed on Uyghur women who have two children.”
Chinese communist propaganda mimics the language of Western feminists to disguise their ongoing genocide of the Uyghur people.Tweet
The report claims “safe, effective and appropriate contraceptive measures are now available to couples of childbearing age in Xinjiang, and their personal decisions on whether to use those measures — which include tubal ligation and the insertion of intrauterine devices — are fully respected,” according to the China Daily.
“An increasing number of people in southern Xinjiang were deciding to marry and have children later in life, seeing the benefits of fewer but better births, and the change was due more to personal choice than government policy,” it added.
Evidence: Birth-Prevention Tactics
Mosher is not the only expert to criticize the CCP “family planning” policies and describe what’s happening as genocide.
Another China expert, Adrian Zenz, has put forth evidence of mass birth prevention and mass female sterilization of Uyghur Muslims in China. In an interview with NPR last summer, Zenz shared information he gathered from Xinjiang National Health Commission, local prefecture government and county websites. He stated:
I was able to uncover dedicated policies by Beijing in the [XUAR] region to systematically suppress birth rates and depress population growth. I uncovered evidence that the Uyghurs are subject to internment in camps if they violate birth control policies — have too many children. I also uncovered that there’s tools to implement intrauterine contraceptive devices and other intrusive surgical birth prevention mechanisms in at least 80% of the targeted women.
Zenz related the “harrowing” stories of Uyghur women who are:
caught up by the police and, as they’re being brought to the internment camp, the first thing is that they’re told “you’re going to go on the surgery table, and we’re going to put an intrauterine contraceptive device into your body because that’s standard policy for women who are put into a camp.” Other women report of forced sterilization, of abuse, even accounts of rape.
Pro-China Global Times reported that Chinese scholars from a Xinjiang think tank dismissed Zenz as “a far-right Christian” and accused him of “fabricating unfounded reports to slander China’s policies in Xinjiang” and “to cater to the U.S. and some Western countries’ aim of attacking China.”
But many anti-American mainstream sources have likewise reported on the annihilation of traditional Uyghur people. NBC News, for example, reported in late 2019 on how “[f]or at least the last three years, Chinese authorities in the far western region of Xinjiang have been rounding up men and women … and detaining them in camps designed to rid them of terrorist or extremist leanings.”
As to ridding Uyghur people of “extremist leanings,” Mosher added wryly: “I suppose we could call that ‘gender equality,’ CCP style. Neither sex can have children.”
Ohio Governor Mike DeWine has signed a new pro-life bill into law that will help save babies from abortions. The Ohio legislature approved a pro-life bill to ban a dangerous form of abortions that kill unborn babies but also put women’s health at risk.
Senate Bill 260, the Telemedicine Abortion Ban, passed out of the Ohio House of Representatives by a vote of 54 to 30. This legislation, spearheaded by Ohio Right to Life and Senator Steve Huffman, a physician, would prohibit the use of telemedicine for the purpose of selling abortion-inducing drugs and ensure that these killer drugs could only be provided in-person by the prescribing physician.
The Telemedicine Abortion Ban was introduced in January of 2020. During opponent testimony on SB 260, it came to light that Planned Parenthood had been committing abortions in Ohio using a form of telemedicine for several years. The total number of telemedicine abortions committed in Ohio by Planned Parenthood remains unknown, as they have yet to make the current statistics public.
“Ohio Right to Life is immensely grateful to our governor and our pro-life legislature for their work in ensuring that this much-needed protection became a part of Ohio law,” said Ohio Right to Life president Mike Gonidakis. “Although every chemical abortion is a tragedy than ends a baby’s life, this law helps prevent further loss of life by protecting women from an abortion industry which puts profits before safety. Planned Parenthood’s use of telemedicine to dispense abortion-inducing drugs cuts their own costs at the expense of basic health and safety standards. Patient safety shouldn’t have a price tag. Women deserve better.”
“The signing of the Telemedicine Abortion Ban into law is a victory for life and for women’s safety,” said Gonidakis. “No woman should be subjected to a dangerous telemedicine abortion in order to pad Planned Parenthood’s pockets. Pro-Life Ohio will not let the abortion industry continue to treat vulnerable women and children as money-making opportunities. Women and children deserve to be put first. This law is a crucial step towards that end.”
The abortion pills are dangerous to women.
The first pill in the chemical abortion pill regimen, mifepristone, is highly regulated by the FDA due to safety concerns. The FDA recorded nearly 4,200 adverse events from mifepristone between 2012 and 2018 and over 1,000 of those cases required hospitalization. Since the abortion pill regimen was first introduced in the U.S. in 2000, 24 women have died from chemical abortion complications.
Historically, Mifeprex, which comprises the first pill in the abortion pill regimen, has been highly regulated by the FDA, to the extent that they have imposed special safety requirements called Risk Evaluation and Mitigation Strategies (REMS) on the drug to reduce patient risk. Between 2012 to 2018 alone, the FDA recorded 4,195 cases of women being injured by the abortion pill. Twenty-four women have died from Mifeprex since the abortion pill was first introduced in the U.S. in 2000.
“Although every successful abortion is a tragedy which results in the ending of a human life,” says Senator Steve Huffman, “abortions committed through telemedicine have the potential to add one tragedy to another by subjecting women to dangerous abortions-inducing drugs without providing basic health and safety standards. Planned Parenthood may consider the financial boost of telemedicine abortion worth the very real risk to women’s lives, but as a physician, I certainly do not.”
Non-surgical abortions continue to make up a greater proportion of abortions performed in Ohio each year. In 2018, the [two-drug] Mifeprex regimen was used to perform 6,103 abortions, or approximately 30% of all abortions that year, and is the most commonly reported method of abortion before 10 weeks gestation.
Bishops in Argentina are urging faithful Catholics to be strong and are vowing to protect life despite the passage of a law legalizing abortion up to 14 weeks in the majority-Catholic country.
According to a statement published on December 30th, the bishops declared that, “together with brothers and sisters from different creeds and also many non-believers,” the Church’s leaders will “continue to work with firmness and passion for the care and service of life.” The bishops also decried the political leadership’s indifference to popular pro-life sentiment, “which has been expressed in various ways in favor of life throughout our country.”
In a separate statement, the bishops’ pro-life commission also expressed its solidarity with pro-lifers in Argentina: “With true conviction, we want to convey to you today that, despite what happened, life always triumphs over death. It is what Christ taught us, who overcame the death on the cross. All is not lost.” The commission urged Argentinians to “show the face of the God of Life and human love” in the new chapter of the Argentina’s pro-life struggle.
The statement, released the same day the country’s senate voted to become only the third in South American to legalize abortion, expressed the bishops’ sorrow and closeness with their flock. “We make their pain, their discomfort, their sadness our own, at the news of the sanction of a law that authorizes a mother to kill her child. We want each Argentine, each father, each mother, grandfather, son, to feel our closeness and understanding. We want to gratefully embrace all those who, from different convictions, from all creeds, without being discouraged, put their efforts, their hope and faith so that life triumph over death.”
The bishops invited pro-lifers in Argentina to redouble their efforts. “We feel called to work with more commitment than ever” in the face of this setback, and promised to work to strengthen the family. “That is why we want to invite you all, from different sectors, to join forces and work for a family that educates, contains, feeds, consoles, corrects, accepts and loves unconditionally,” the statement read.
Prior to the law’s late December passage, Argentina only allowed abortion in the case of rape or if a mother’s life were in danger. A similar pro-abortion effort in Argentina failed to pass in 2018. The bishops previously condemned the Argentinian government’s “feverish obsession” with abortion after President Fernandez vowed to legalize shortly after his election.
“The family has a special role to play throughout the life of its members, from birth to death. It is truly ‘the sanctuary of life: the place in which life – the gift of God – can be properly welcomed and protected against the many attacks to which it is exposed, and can develop in accordance with what constitutes authentic human growth.’ Consequently, the role of the family in building a culture of life is decisive and irreplaceable.”
─ Pope St. John Paul II, Evangelium Vitae, no. 92
“Is marriage becoming irrelevant?” That’s the jarring headline on Gallup’s website, reporting the results of a new survey. The answer to the question, unfortunately, appears to be a resounding “yes.” In key ways, marriage is becoming irrelevant for large numbers of people.
The results of the survey show a distressingly swift reversal in public attitudes towards the importance of marriage in relation to the marital act and the transmission of human life. According to Gallup, only 29% of people now believe it is “very important” for a couple to get married before begetting children. That’s a drop from 49% in 2006.
Meanwhile, 72% of respondents said that it is morally acceptable to engage in a sexual act outside of marriage. That’s up from 53% in 2001.
This poll tells a sad tale about how people in general view human sexuality, marriage, procreation, children, and the family. However, one especially discouraging finding is how dramatic the shift in opinion has been among church-going people.
In 2006, 65% of poll respondents who went to church weekly said it was “very important” for couples begetting children to be married. In 2020, however, it was just 45%, a drop of 20 percentage points! Among those who go to church monthly, the number has dropped from 58% to 32%, a difference of 26 percentage points!
The good news is that church-going people are still more likely than people who never go to church to think marriage is important (only 19% of non-church-going people said being married is “very important”, down from 32% in 2006); the bad news is that the opinions of church-going people have changed far more swiftly for the worse than those of non-church-going people.
The Gallup poll also found that only 38% of people believe that it is “very important” for couples who want to spend the rest of their lives together to get married. Unsurprisingly, perhaps, the number of respondents who say they are currently married has slid significantly in recent decades. Whereas in the early 80s, 64% of people said they were currently married, that number has since fallen to just 49%.
The Negative Effects of Family Breakdown
Unfortunately, none of these findings come as a great surprise. Ever since the introduction of contraception-on-demand and no-fault divorce, we have been witnessing the steady collapse of marriage and family life. This has been reinforced by the proliferation of a hedonistic attitude towards human sexuality that places greater emphasis upon personal pleasure, romance, and gratification. This attitude, in conjunction with the mentality and behavior it promotes, falsifies human sexuality, and divorces the marital act (an act meant to be exclusive to spouses) from its two-fold and inseparable ends, unitive and procreative. This kind of act is vastly different and contrary from the one God has made to be unique and complementary between spouses. The falsification of the inherent goods of marriage and the conjugal act has dire consequences, which impacts one’s view of self, others, marriage, and the family.
As Pope St. John Paul II wrote in Evangelium Vitae:
Thus the original import of human sexuality is distorted and falsified, and the two meanings, unitive and procreative, inherent in the very nature of the conjugal act, are artificially separated: in this way the marriage union is betrayed and its fruitfulness is subjected to the caprice of the couple. Procreation then becomes the “enemy” to be avoided in sexual activity: if it is welcomed, this is only because it expresses a desire, or indeed the intention, to have a child “at all costs”, and not because it signifies the complete acceptance of the other and therefore an openness to the richness of life which the child represents. (no. 23)
What we don’t seem to have yet realized, or at least not on any wide scale, is just how devastating the collapse of marriage and family life has been upon the health of our society. I am amazed, for instance, at how much conversation there is about poverty, violence, poor education, and homelessness, but how little is ever said of the systemic reasons behind these things, and where the remedy is to be found.
Study after study has found that children who do not grow up with both of their parents in the home suffer all sorts of negative consequences. As The National Review noted in response to a New York Times article minimizing the impact of single parenthood on poverty rates, the data is unequivocal: single parenthood is strongly associated with severe poverty.
“The social science tells us that children raised by single parents are significantly more likely to have children young, to drop out of high school, and to work less as young adults,” wrote W. Bradford Wilcox. “Not surprisingly, the children of single-parent families are more likely to end up poor as young adults.”
One Irish study found that the impact of divorce on children can even be worse than if one of the parents has died. According to that study, children of divorced parents are “more likely to develop depression, do worse in school, and have poor social skills compared to other children,” reported LifeSiteNews.
One of the researchers behind that Irish study said that she hoped their research would counteract the common narrative that paints divorce as inconsequential. “Nobody should delude themselves that divorce is easy,” she said. “Keeping a bad marriage together is difficult, but protecting children after a divorce can be even more difficult. Couples need to realise this.”
A Threat to the Common Good
The simple fact is that the redefinition and breakdown of marriage, exacerbated by the falsification of human sexuality and the acceptance of divorce and cohabitation, pose genuine and serious threats to the common good, the well-being of society. Marriage between a man and a woman, something that can be understood simply from the natural law, has been for millennia the foundation stone for civil society.
As the Catechism of the Catholic Church says:
The family is the original cell of social life. It is the natural society in which husband and wife are called to give themselves in love and in the gift of life. Authority, stability, and a life of relationships within the family constitute the foundations for freedom, security, and fraternity within society. The family is the community in which, from childhood, one can learn moral values, begin to honor God, and make good use of freedom. Family life is an initiation into life in society. (no. 2207, emphasis added)
Children, always welcomed as a blessing under any circumstance, have a right to be raised by their biological parents and nurtured within the family, this God-instituted school of learning. Today, however, children suffer widely from rejection, abandonment, divorce, and multi-relationship and single-parent households. Because of the falsification of human sexuality and wide acceptance of contraception, children are no longer seen as the fruit of conjugal love; they are, instead, labeled as a burden, an unwanted consequence of the sexual act. Moreover, children are being treated as objects to be exploited – engendered outside of the conjugal act, in petri dishes and laboratories, turning procreation into a “production” which dehumanizes children.
Unfortunately, the vices that are nourished in the privacy of family life have a tendency to perpetuate themselves across generations, and thence to spread out into society at large. One of the consequences of divorce is that children of broken families are in turn more likely to get divorced themselves. Divorce begets divorce, spreading like a virus, and bringing with it all the various negative personal and social consequences.
Building a Culture of Life by Defending Marriage
My question, then, is this: How can we build a virtue-based society, one that loves, respects, defends, and serves the sanctity of life and the dignity of the individual, if the original cell of social life (marriage and the family) upon which society is built is rejected, compromised, or re-created in the image of modern-day constructs and language?
After all, a building built on sand will collapse.
Unfortunately, with the legalization of same-sex “marriage” and the near-total triumph of the contraceptive mentality and the sexual revolution, even many conservatives and pro-life and family activists have lost sight of the importance of the battle over marriage, which is widely viewed as being “lost.”
Well, the battle may well be “lost”…for now. Or seem to be lost. But the fact that we must face is that the battle for a Culture of Life will never be won unless we turn the ship around, and begin to make some progress on the battle for marriage as well.
The data clearly show that the abortion rate among single and cohabiting women is way higher than among married women. This is hardly surprising. Biologically, women bear the brunt of the burden of having a child. Being in a stable marriage provides women with the security they need to feel safe bringing a child into the world. However, if the father of the child is either gone, or is likely to be gone sometime in the future, then it is far more likely that the mother will feel tempted to take drastic measures when she becomes pregnant.
However, the problem is even more basic than this. If most men and women don’t see any connection between sex and marriage, then they are more likely to engage in extra-marital sexual relations. The more people do this, the more unintended pregnancies there will be, and the more abortions there will be. The lives of countless unborn children depend on us defending marriage and pushing back against the lies of the sexual revolution.
In the fight against the culture of death, the church needs to get back to the basics. Christians have always taught that fornication and adultery are grave sins. However, as the Gallup poll findings suggest, churches are failing to educate their congregations in Biblical truths about human sexuality and marriage. As Pope St. John Paul II proclaimed, the “future of humanity passes by way of the family” (Familiaris Consortio, no. 75). Without strong marriages and families as its foundation, society will continue to disintegrate. If we restore, however, the centrality of marriage and the family, as designed by our Creator, they will serve as a catalyst for rejuvenating social life. Only by defending marriage and strengthening the family can society be revitalized.
Sarah Quale, president of Personhood Alliance Education, notes: “By promoting so-called ‘scientific benefits’ gained from children who were intentionally killed, regardless of when their deaths occurred, we continue to align ourselves with the evil of abortion. This includes harvesting aborted fetal cell lines in the past and in the present, which we know is currently happening for future vaccine production. By ignoring this, we help perpetuate and further legitimize the connection between abortion, biomedical science, and human trafficking.”
The Personhood Alliance warns that any effort to commodify aborted human beings in the design, production, and testing of vaccines will continue indefinitely unless and until Christians demand biomedical science be separated from the killing and trafficking of innocent human beings. “There remains an ethical dilemma here,” says Quale, “whether we want to ignore it for the sake of COVID-19 or not. Currently, there are ethical alternatives available for producing and testing COVID-19 vaccines. Why wouldn’t we use the time we have right now to demand a fully ethical vaccine be brought to market instead?”
Les Riley, interim president of the Personhood Alliance, adds: “Personhood formed a committee that spent months wrestling with these ethical issues—Doctors, bioethicists, researchers, pastors, and apologists. Based on direct evidence, they reported that 6 of the 8 COVID-19 candidates were unethically produced and/or tested, including the Pfizer vaccine. The two remaining ones will likely also be tested unethically.”
“This fact is not disputed by others who are arguing in support of these vaccines,” says Riley. “We are all citing the same research and using the same data. However, they are coming to a completely different moral conclusion, based on a Utilitarian ethic. What we are sure of is this: Producing and testing vaccines using the broken little bodies of aborted children should never be considered a ‘scientific benefit.’ We are continuing to dehumanize these babies, and it is repugnant.”
“This is why the pro-life movement as a whole is having such a difficult time ending abortion,” urges Riley. “Because we compromise. Because we allow exceptions; whether that be in abortion law or in trafficking the body parts of abortion’s victims. We pull the rug out from under our own feet, undermine our own principles, and dismiss the value God places on each and every life He creates. Talk about harming our own ability to effectively witness and share the Gospel!”
President of Personhood Alliance affiliate Personhood South Carolina, Dr. Matthew Clark—who is also a pastor and holds a Masters in Public Health from Harvard, with a specific focus on pediatrics, allergy, and immunology—lends his expertise: “Let’s not allow sophistry to cloud the obvious issue. Baby-murder was the source of cells used to test most of the currently available COVID vaccines. Every Biblically-minded Christian should reflect deeply on this fact. To ignore or minimize this fact is to be pro-death, not pro-life.”
~~~
The Personhood Alliance is a confederation of 28 independent pro-life organizations who pursue personhood as the essential strategy for restoring legal protections to every human being—from biological beginning to natural death, without exception—and who endeavor to uphold the Biblical worldview in 21st-century politics and culture by honoring God’s design for life, marriage, family, sexuality, and gender.
I was nine years old, and I was carrying a coffin.
Not just any coffin. This one held the tiny bodies of hundreds of aborted infants rescued from a dumpster, and I was among several children who were participating in their burial service at Holy Cross Catholic Cemetery in Milwaukee in 1984. Pro-life mourners and local media crowded around the gravesite, and I stepped carefully, conscious of how precious a load we bore. I remember the small box being lowered into the ground as we watched solemnly.
The grave marker read, “Holy Innocents” and in time, over a thousand victims of legalized abortion were laid to rest there, given a dignity in death they were denied in their brief lives.
It’s not the kind of thing one ever forgets, but this time of year our liturgical calendar resurrects the memory in a very poignant way.
On the fourth day of Christmas, the Church gives to us a somber memorial which concretizes what could very possibly become, thanks to elves and snowmen, an overly sentimental feast of Christ’s birth. Each year, December 28 marks the memorial of the Holy Innocents.
Then Herod, when he saw that he had been tricked by the wise men, was in a furious rage, and he sent and killed all the male children in Bethlehem and in all that region who were two years old or under, according to the time which he had ascertained from the wise men. Then was fulfilled what was spoken by the prophet Jeremiah:
“A voice was heard in Ramah, wailing and loud lamentation, Rachel weeping for her children; she refused to be consoled, because they were no more.” (Matthew 2:16-18)
This day we are asked to remember and honor the lives of the little boys of Bethlehem, cruelly slaughtered by the command of the jealous and grasping Herod. We are reminded that Christ came not only in poverty and humility but in grave danger – our little Savior was a hunted refugee. We recall that Christmas, far from just lights, gifts, and feelings of goodwill, was a real historical moment – when heaven plunged into earth, taking on time and space and shaking the foundations of the world. And evil, sensing the rumblings of its defeat, lashes out at the littlest ones. On this day, we weep with Rachel.
Even then, because we have a God who uses all for good, on this day, the Church gains her first martyrs. It may seem strange: children, not yet of the age of reason, and years before Christ would die for them, to wear a crown meant for saints who died confessing him. But martyrs they are. As the Collect for the day reads: “O God, whose praise the Innocent Martyrs on this day confessed, not by speaking, but by dying, mortify in us all the evils of the vices; that our life also may proclaim in its manners Thy faith, which our tongues profess.”
They confessed him not by speaking, but by dying. They died because of hatred of Christ, and they died in his place. St. Augustine speaks of this “pure host of infants,” saying of these children that they are “justly hailed as ‘infant martyr flowers’; they were the Church’s first blossoms, matured by the frost of persecution during the cold winter of unbelief.”
And so they are the first white-robed souls under the altar in the heavenly temple of Revelation, crying out to God (Rev 6:9-10). May their cries hasten not only his judgments but his healing mercy upon us and our land, and help us to remember, even in the midst of our joyful celebrations, that his coming exacted a steep price then and does so even now. Each of us, should we follow this tiny King, must be ready to lay down our lives – even if it be in the daily death to self that faithfulness demands.
Saints continue their missions even from heaven, and so the Holy Innocents have been given a fitting one: they have been appropriately named as patron saints of babies.
Therefore, we should entrust our own little children, grandchildren, and godchildren to their prayers.
We should beg the Innocents to intercede for the suffering children of the world. I thought immediately of the vacant stares in the faces of dusty, tear-stained orphans in Syria: “There is hope for your future, says the Lord, and your children shall come back to their own country” (Jer 31:17).
And as the gravestone in the Milwaukee cemetery reminds us, we must ask also that their cries in heaven be also those of supplication for this current massacre of innocents, the genocide of abortion, to end. That evil laws, like evil kings, will be no more. But most of all, that his laws – always good and perfect and true – be engraved within us.
“…I will put my law within them, and I will write it upon their hearts; and I will be their God, and they shall be my people…they shall all know me, from the least of them to the greatest, says the Lord; for I will forgive their iniquity, and I will remember their sin no more” (Jer 31:33-34).
Holy Innocents, first small martyrs, pray for us.
This post was originally published December 28, 2018.
(LifeSiteNews) – Each year, abortion groups celebrate the season by requesting donations and wishing everyone happy holidays. It is always ironic to see the spiritual descendants of Herod twist themselves into knots to acknowledge Christmas without being too religious, but I suppose it is also understandable. Nobody likes being left out, even those who spend the rest of the year dispatching God’s tiny gifts to the next world with scalpels and suction aspirators. This year, one abortion worker attempted to get particularly festive by topping a Christmas tree not with an angel or a star, but with a set of serrated forceps used to clamp on baby limbs and destroy baby bodies.
But there are other reasons abortion groups have such a complicated relationship with Christmas. Mary’s welcoming of an unexpected Child as a gift (indeed, to the whole world) is not the sort of story abortion activists wish to tell. Indeed, every year around this time some of the angrier feticide fans post memes fantasizing about the Virgin Mary having an abortion, revealing that abortion advocacy and hatred of Christianity are nearly always inextricably intertwined. Abortion ideology is predicated on the idea that we must not sacrifice for others, and the Christmas story is the ultimate rebuke to that idea.
Even the language abortion activists use reflects the fact that their worldview is antithetical to the Christmas message. This is my body, broken for you, said the Savior. My body, my choice—and we will sacrifice any who interfere with our lives, say the abortion activists. The abortion worldview is merely a perverse inversion of the Gospel message, the triumph of selfishness and bloodshed over innocence and beauty. They will deny it. They try to dress up their message in the language of rights. But the truth is incontrovertible. The result of an abortion is a dead baby. That is the point of abortion. That is why people get them.
When abortion activists, who traffic in death, misery, and regret, wish everyone a happy holidays, I suspect they know that it rings hollow. The abortion industry is responsible for millions of empty places at millions of tables. Their forceps and needles have stopped hearts and broken hearts, and the holiday season often reminds those who made this awful choice of those who are not with them. Planned Parenthood and their abortion allies have it all wrong. Success, to an abortion activist, is an empty cradle and a full grave. The essence of the Christmas story is a full cradle and an empty grave.
If you are pregnant, there is a great chance that your OB/GYN or a nurse will ask you what form of contraceptives you’re going to use after you deliver. If you’re planning on nursing your baby, you can tell them with confidence that breastfeeding is your method of “birth control,” along with a fertility awareness method (FAM).
Common questions about using breastfeeding for birth control
Fertility awareness while breastfeeding may sound counterintuitive to some women, because when you’re breastfeeding, your cycles usually change and the observable signs of fertility are affected. That’s why women considering using breastfeeding as birth control have questions like:
Is breastfeeding alone an effective method of natural birth control?
Can I still be fertile and get pregnant while I’m breastfeeding?
Can I chart my cycles accurately enough to know if I’m fertile or not while I’m breastfeeding?
Does my current method of fertility awareness or natural family planning (NFP) still work while I’m breastfeeding or will I need to change what I’m doing?
Where can I go for reliable information on breastfeeding, fertility, and family planning?
This article is not a scientific white paper on the extensive topic of using breastfeeding for family planning, but an effort to answer the above questions in a succinct way and to guide you to additional useful, evidence-based information on the subject.
1. Is breastfeeding an effective natural birth control?
Yes, breastfeeding does affect your fertility, and therefore under some specific conditions, breastfeeding alone can be an effective form of birth control/pregnancy spacing. Lactational Amenorrhea is a complicated-sounding term used to describe the connection between breastfeeding and the continued absence of periods (and fertility). Ecological Breastfeeding (EBF) and Lactational Amenorrhea Method (LAM) are two evidence-based methods of family planning that involve specific conditions for breastfeeding. Both methods have been proven to be highly effective when their respective required conditions are met, and both are widely used to postpone a pregnancy.
Here are a few encouraging statistics about LAM and EBF:
A 1997 study of LAM involving 519 sexually active women in 11 sites throughout the world showed a 98% success rate at preventing pregnancy [1].
Ecological Breastfeeding reports a 0% chance of pregnancy for first 3 months, 1% chance for the next 3 months, and 6% chance after six months (assuming no abstinence, no fertility charting at all, and that the mother’s cycles haven’t yet returned) [2].
Keep in mind, too, that these family planning methods are accomplished without contraceptives. That means they do not require putting any chemicals or devices into (or on) your body to be effective! However, if you’re not following the LAM or EBF criteria, or if you simply prefer additional insurance against pregnancy, you should be on the lookout for the signs of your body’s cycle returning, which formal training in a FAM or method of NFP can equip you to do.
2. Can I still be fertile and get pregnant while I’m breastfeeding?
Yes! You absolutely can still get pregnant while breastfeeding if you are not following the conditions set for by LAM, EBF, or your chosen FAM or method of NFP. For instance, if you’re not feeding at the breast exclusively (or nearly exclusively) and use supplemental bottles of formula or pumped milk, and/or start early feedings of solids to your baby, there is a much higher chance that your fertility will come back within six months. And this is important: Every woman, regardless of how she feeds her baby, will be fertile before her period returns, because a period is always preceded by ovulation. So it is highly beneficial to begin charting again as soon as you can after your baby is born, so that you can catch that first postpartum ovulation (and know when to expect your first postpartum period). You can begin charting your signs of fertility with your chosen method of NFP or FAM from the beginning after delivery of your baby, once bleeding stops and lochia lessens.
3. Can I chart accurately enough to know if I’m fertile or not while I’m breastfeeding?
Definitely. We surveyed a few natural family planning (NFP) teachers and this is what they had to say about fertility and charting while breastfeeding:
“I’ve taught many breastfeeding women and they have quickly and confidently learned their days of fertility and infertility,” said Tina Luther, teacher of the Creighton FertilityCare method. “While breastfeeding, there is (typically) not a menstrual period, so it’s a continuous chart. Women chart what they see—their most fertile sign at the end of the day. So we teach them how to discern their days of fertility.”
“The best way to answer the breastfeeding ladies is to tell them that fertility signs can always be charted, but you need to know what you are looking for,” says Cathy Nix, teacher of the Sympto-Thermal Method with Couple to Couple League. “The return to fertility is signaled by the presence of [cervical] mucus and the [basal body] temperature sign. At the first sign of mucus, it is recommended that a woman start to chart again and take her temp.”
The Billings method, another widely used fertility awareness method, offers a similar recommendation on their website: “When a woman is breastfeeding she remains infertile for a variable time. During this time she experiences, at the vulva, either a continuing sensation of dryness, or an unchanging discharge. The appearance of blood, or any change in the mucus or sensation alerts her to the possibility of her returning fertility.”
4. Does my current method of fertility awareness or natural family planning still work while I’m breastfeeding or will I need to change what I’m doing?
As mentioned above, FAM and NFP methods have individual processes to help you observe and interpret the signs of your fertility with a high degree of accuracy, and many have specific protocols to follow while postpartum and/or breastfeeding. If you haven’t learned a method yet, now is a great time to start—and to benefit from the pregnancy prevention efficacy rates, you must learn from a certified instructor in your chosen method. Some methods even have extensive classes specifically geared towards the postpartum period, which will teach you more about LAM and EBF. And if you choose not to follow LAM or EBF criteria, most methods will teach you specific protocols to follow in order to manage and chart the return of your fertility. Most of the major methods of NFP and FAM will help you with the specifics of charting, especially how to identify true cervical mucus after childbirth (the notable exception of which is the ClearBlue Fertility Monitor-based Marquette Method, which encourages mucus monitoring, but does not require it).
Another good reason to consider methods of NFP or FAM for postpartum family planning, compared with conventional forms of birth control, is that hormonal contraceptives can have a negative impact on breast milk production, supply, and duration. This problem seems more common with estrogen-containing combination pills (which is why the “mini-Pill,” i.e., the pill that only contains progestin, is recommended for new mothers who desire to breastfeed), but some women have reported similar issues with progestin-only pills as well. It is also likely that some small amount of the synthetic hormones contained within birth control pills passes through breast milk to the baby (although it is unknown what—if any—effect this may have on the baby).
5. Where should I go for reliable information on breastfeeding, fertility, and family planning?
If you have a FAM or NFP teacher already, you should talk to them while you are pregnant, so that you will be prepared to chart postpartum. If you don’t already have a method or an instructor, or want to learn more about breastfeeding and fertility, here are a few good sources of information:
Empowering yourself against the postpartum contraception push
We’ve heard stories from mothers who describe how hospital staff would push the Pill or the IUD on them a little before or after they had delivered. Women have even shared with us how they’ve been pressured to have their tubes tied after delivery! This push toward contraception or sterilization so close to the emotionally fraught time of delivery can be quite insensitive, distasteful, and even unethical. Fortunately, women can empower themselves with the knowledge of fertility awareness before they deliver, so that they can better advocate for their own individual needs and family planning desires postpartum. And if your doctor or nurse starts arguing with you and tries to discourage you from using a FAM postpartum, you can refer them to this article! Even if they don’t trust you, know that you can trust yourself, when you have all the information needed to effectively practice fertility awareness postpartum. Don’t let promoters of chemical methods of birth control intimidate you. You and your baby deserve better.
References:
[1] Labbok M, Hight-Laukaran V, Peterson A, Fletcher V, von Hertzen H, Van Look P. Multicenter study of the Lactational Amenorrhea Method (LAM): I. Efficacy, duration, and implications for clinical application. Contraception. 1997;55(6):327-336. doi:10.1016/s0010-7824(97)00040-1
[2] Bonyata K. Breastfeeding and Fertility • KellyMom.com. KellyMom.com. https://kellymom.com/ages/older-infant/fertility/#LAM. Published 2020. Accessed December 17, 2020.
When this article refers to fertility awareness methods (FAM), or natural family planning (NFP), we are referring to Fertility Awareness-Based Methods, evidence-based methods of cycle charting which can be used as effective forms of natural birth control when learned by a certified instructor.
This article was originally published on December 21, 2014 as written by Natural Womanhood CEO and Co-founder Gerard Migeon. It has since been updated by Natural Womanhood to offer more resources. Last updated December 17, 2020.
December 17, 2020 (LifeSiteNews) – Today marks the 250th birthday of one of the most famous and admired classical music composers, Ludwig van Beethoven.
On this occasion, it is worth watching the 2011 short film Crescendo, directed by the pro-life activists and filmmakers Jason Jones and Eduardo Verastegui. The film also had as executive producer Pattie Mallette, the mother of pop singer Justin Bieber, who said in 2012 that she herself rejected abortion.
Crescendo raised nearly $6 million for crisis pregnancy centers and won 15 international film festival awards. It also drew the praise of several pro-life leaders including Father Frank Pavone and Dr. Alveda King.
The pro-life film is set during “18th century Holy Roman Empire, [as] a series of events will turn an ordinary day into an extraordinary experience for a woman whose life will never be the same.” The story also displays the unimaginable potential of each human being, and how the murder of the unborn child takes away from the entire world.
This powerful 15-minute film is recommended for everyone ages 13 and older, but it makes for a great family movie night.
Many pregnant and postpartum women know what it’s like to field questions as they’re about to give birth and just after: “are we having an IUD inserted today?” or “what birth control will you be taking after birth?” Most recently, we’ve heard, “are we having our tubes tied today?” in reference to the sterilization procedure otherwise known as a bilateral tubal ligation.
While medical professionals may think they’re just helping women get the services they want after birth, there is a nature of the timing and the wording of these questions that produce an effect of asking “leading questions”—that is, questions that inherently direct patients toward a certain course of action regarding their reproductive health.
We have children and all three were born by C-section; our first was an emergency and the other two were planned. Little do people know when you go in for a planned C-section they ask you not just once but repeatedly: “honey, are we tying your tubes here today?”
And I’m like, “no, no we are not!
Why would I want to break something that is working exactly as it is intended to function?
Then they wheel you into the operating room; literally you’re about to have your beautiful little baby and they ask you again: “Are we tying your tubes here today?” And I’m like, “no! No, we’re not!”
Don’t feel pressured to decide on a tubal ligation—or any form of family planning—during such an emotionally fraught time
To time questions about a procedure as serious as a tubal ligation right before, during, or after the stressful experience of labor or surgery is to take advantage of a vulnerable moment, when no matter a woman’s long-term family planning goals, she may be ready to swear off children forever. It’d be like having a lawyer ask you to sign your will, determining which of your children will get what assets after you die, in the moment right after your teenage son slams the door in your face. Your judgment might be a little skewed at that moment, so most would recommend you make important decisions like this when you’ve had some space from stressful events and can think more clearly about the long view.
There are numerous reasons a woman may feel pressured in the moment to make a choice to sterilize herself via a tubal ligation that she wouldn’t have otherwise. Some women may feel judged in the moment for having hopes for a larger family, as if that is somehow selfish or bad for the planet, instead of acting according to her personal hopes and goals. Or perhaps her partner doesn’t want more children and she does, and instead of talking about it on their own time, the partner may take the medical professional’s prompting for a woman to “get her tubes tied” and pressure her to do “what the doctor suggests,” even though it’s not medically necessary. Never mind, also, how tubal ligation brings its own risks and complications to women’s health.
Moreover, there is no reason why such a decision needs to be timed at the “game time” of labor. Women have had numerous OB/GYN visits preparing for birth, and such a post-birth decision could and should be discussed long ahead of time. If a woman and her doctor have discussed the options ahead of time and she has refused birth control pills, the IUD, or tubal ligation ahead of time, that decision should be respected during labor, delivery, and recovery from birth.
There are better postpartum birth control options than getting your tubes tied
Offering patients birth control after birth has been happening for years, as I have experienced, most recently being offered an intrauterine device (IUD) immediately after birth. For me, it sounds like a horrible idea to insert an artificial device into the delicate area that is recovering from just giving birth. (If I can’t have relations with my husband for six weeks, how is having a metal device harmless?) But I also don’t want to postpone children for very long, because I’m in my late thirties, and what if I want to give my little new newborn a sibling that’s close in age (like I’m thankful my parents gave me)? If I was impressionable at that moment as opposed to geared to advocate for myself, I could have acted in a way that opposed my true wishes.
I am thankful for natural family planning and fertility awareness methods (FAM) because I feel well equipped to space children after birth without ruling them out completely, and without making any drastic changes to my hormonal makeup or physiology. Having learned the Creighton Method ten years ago, and having refreshed myself with an instructor before birth, I felt prepared on how to space children safely and effectively.
It’s one thing for providers to recommend a long-acting reversible contraceptive (LARC) such as an IUD after birth, as I was repeatedly offered after giving birth to my last child. But to suggest to women a sterilization procedure—tubal ligation—near that highly emotional moment of labor is ethically problematic. The risk is that the power of suggestion could guide a woman to make a choice she might otherwise have not made—and one she might regret when it is too late.
I never thought I’d see the day when I would have to praise the New York Times for waging a battle against a huge force within the culture of death that just about nobody else had the courage or conviction to take head on. But that’s what seems to have happened in the past week.
Nicholas Kristof, an opinion columnist at the Times, has in recent days set his sights on Pornhub, the largest porn website in the world. Pornhub reportedly welcomes some 10.5 billion visitors a month – surpassing even Netflix in viewership.
Pornhub, incidentally, is owned by a company called MindGeek, which is located in Montreal, Canada. MindGeek owns a huge consortium of over 100 porn websites, which together constitute by far the largest porn empire in the world.
There are many, many problems with Pornhub and Mindgeek, beginning with the fact that they traffic in porn, which is a dehumanizing industry that reduces vulnerable men, women, and children to objects to be consumed.
However, one of the most disturbing problems with Pornhub, is its complete and utter heedlessness about the massive amounts of outright illegal, violent, misogynistic, and morally heinous content that users upload and view on the site on a daily basis.
In the past year, Pornhub has come under increasing scrutiny. However, as a shadowy multi-billion dollar corporation, whose tendrils reach into almost every household on the planet, thus far it has arrogantly withstood every attack, brushing off the pro-woman and anti-porn activists who have tried to raise the alarm.
Even a petition signed by over two million people, demanding that Pornhub be shut down, has had almost no tangible effect to date.
The Children of Pornhub
But all that changed in the past couple weeks when Kristof decided to investigate and expose just how evil much of the content available on Pornhub is.
Pornhub’s site is infested with rape videos. It monetizes child rapes, revenge pornography, spy cam videos of women showering, racist and misogynist content, and footage of women being asphyxiated in plastic bags. A search for “girls under18” (no space) or “14yo” leads in each case to more than 100,000 videos. Most aren’t of children being assaulted, but too many are.
Some of the stories that Kristof has uncovered are so disturbing that it is difficult even to summarize them. There is, of course, the now-infamous case of the 15-year-old girl who went missing, and who was only found after her mother found 58 different pornographic videos of her on Pornhub.
Another 14-year-old girl, Serena Fleites, was convinced by her boyfriend to record sexually explicit videos for him. Pornhub allows users to upload their own pornographic videos to the site, as well as to download videos from the site to their computer. Soon enough, Serena’s videos ended up on Pornhub. Even though her mother convinced the site to remove the videos, within short order they were back. Every time they’re deleted, they promptly reappear, making it impossible for Serena to put this chapter of her life behind her.
Serena was so traumatized by the looks and remarks she was getting at school that she started skipping classes. Kristoff tells the rest of her story:
Fleites quarreled with her mother and began cutting herself. Then one day she went to the medicine cabinet and took every antidepressant pill she could find.
Three days later, she woke up in the hospital, frustrated to be still alive. Next she hanged herself in the bathroom; her little sister found her, and medics revived her.
As Fleites spiraled downward, a friend introduced her to meth and opioids, and she became addicted to both. She dropped out of school and became homeless.
Eventually, just to make ends meet, at the age of 16 Serena started shooting and selling more photos and videos, which also inevitably ended up on Pornhub. She is now off drugs, but living in her car. “A whole life can be changed because of one little mistake,” she says.
Kristoff interviewed other victims as well, many of whom eventually attempted suicide, and all of whom pointed out the brutal psychological fact that, while the physical assault they endured eventually ended, Pornhub prolonged the suffering by preserving it and displaying it to the world for the pleasure of others.
‘Epstein on an Industrial Scale’
Kristoff naturally, as a New York Times liberal, protests that he is not against pornography. He is only disturbed by the fact that MindGeek and Pornhub are profiting off of illegal and violent content, in which the participants have not, or legally cannot, consent.
He is wrong, of course, in so cavalierly dismissing the problems with porn in general. But we have to take what we can get. And when the Grey Lady (i.e. the New York Times) goes on the attack, people sit up and listen.
Kristoff notes,
Pornhub appears to be increasingly alarmed about civil or criminal liability. Lawyers are circling, and nine women sued the company in federal court after spy cam videos surfaced on Pornhub. The videos were shot in a locker room at Limestone College in South Carolina and showed women showering and changing clothes.
The good news is that following Kristoff’s column, a few relatively big things happened quite quickly. In the first place, Pornhub instituted (or claimed to institute) much stricter policies, including only allowing verified users to upload videos, and preventing users from being able to download videos from the site. Clearly, it would be better if Pornhub didn’t exist. But if these measures protect children and other victims of trafficking and rape, then it is something.
However, perhaps the biggest news is that Visa and Mastercard both announced that they have cut financial ties with Pornhub. PayPal had already previously cut ties. This change will put a huge dent in Pornhub’s bottom line. We can hope that it spells the beginning of the end, although given the size of MindGeek, it will likely take more than this.
Four U.S. senators have also introduced legislation that would make it easier for victims to sue porn companies. Canadian Prime Minister Justin Trudeau announced that Canada was looking into regulations to regulate companies like MindGeek. And, says Kristoff, various lawyers are contemplating civil and criminal suits against the company.
However, Kristoff rightly notes that this is barely scratching the surface. Other huge porn websites, not owned by MindGeek, also feature enormous numbers of videos tagged under disturbing key words suggesting that the girls featured are underage, and even preteen.
“Most of the results probably don’t involve children,” he writes, “but too many do, and the site is luring pedophiles who can then upload their own videos. This is Jeffrey Epstein on an industrial scale.”
Shut Down the Porn Industry
Though Kristoff is unwilling to address the elephant in the living room, I will. The problem with porn is not simply that unscrupulous criminals will take advantage of children or vulnerable women who have not consented. It is that pornography is inherently violent and dehumanizing.
The advent of the Internet unleashed a monster on the world. In the space of a few years, pornography went from something that was relatively fringe, difficult to obtain, and often low quality, to something that was streaming, in high definition video, in limitless quantities, on demand, into our bedrooms, and now, via the smartphone, into our pockets.
The old “free speech” arguments that allowed pornographic magazines and video companies to operate with impunity are simply not up to the task of responding to this brave new world. The world of high-definition porn on demand is simply way more addictive, way more destructive, and way more culturally damaging than anything that has ever gone before.
The statistics are clear: a significant majority of men, and a growing quantity of women, regularly view pornography. However, if you realize how much of the content they are viewing is unspeakably degrading, it will begin to dawn on you just how profoundly damaging this phenomenon is to the health of society, not to mention the profound spiritual harm to people’s immortal souls.
The Catechism of the Catholic Church is pretty succinct, but direct, about what governments should do about porn. Pornography, it says, “is a grave offense. Civil authorities should prevent the production and distribution of pornographic materials.”
Free speech does not protect grotesque obscenity. Sites like Pornhub are making their livings off the exploitation and degradation of men, women, and children. In many cases, even women who have allegedly “consented” turn out to have been strong-armed, or pressured by circumstances, to do something in a moment of desperation that they soon regret, and will regret for the rest of their lives.
Pornography is a true plague with disastrous effects. Kristoff’s column has started a conversation. But it is up to us to finish it, and bring it to its logical conclusion. It is time to denounce and shut down the porn industry.
Talk of COVID vaccines has taken center stage. As with all vaccines, pro-lifers want to know whether they are produced with a cell line from an aborted baby.
An analysis from Charlotte Lozier Institute (CLI), part of the Susan B Anthony List family, is on top of the issue and has produced an easy to understand summary of information to help you make an informed choice.
Funded by President Trump’s Operation Warp Speed, eight COVID vaccines are advancing toward distribution. Each was scientifically analyzed by CLI experts to determine whether production and testing involved abortion-derived cells.
Pfizer and Moderna, the two most mentioned vaccines, joined other companies and did not use aborted cells in the production of their vaccines. On the other hand, AstraZeneca and Johnson and Johnson used exclusively cells of aborted babies in their development. When utilized for production, the controversial cells are directly involved in making the final product, the vaccine that is injected in our arms.
When it comes to laboratory testing, at least six of the drug companies needlessly created a hurdle for American families wanting to avoid an abortion connection. They either used abortion-derived cells or utilized both abortion-derived cells and those not linked to abortion; two of the companies have not yet reported their testing process and the analysis was unable to determine either way.
According to Dr. David Prentice, VP and Research Director at Charlotte Lozier Institute, the testing process is another step removed from production of the vaccine for a recipient. “When an abortion-derived cell line is used in laboratory testing, that is not done within the production line.” He added, “It’s a confirmatory test done on the final vaccine, to validate what the scientists believe they’ve produced. The product is used to vaccinate mice or cells in culture, to verify a response.”
A new chart tracking each companies’ activities was produced by CLI for easy reference.
Four pro-life doctor groups have reported that two lead COVID vaccines—Pfizer and Moderna—did not use cells from aborted babies to develop their products. Still, false or misleading accusations have circulated, casting aspersions regarding Pfizer’s vaccine.
One is that their two-dose treatment isn’t safe for pregnant or nursing women because they were excluded them from clinical trials. But in reality,all vaccine trials exclude pregnant women and infants out of an abundance of caution, not because of any known risk.
Dr. Prentice explains the other. “A couple of doctors in Europe filed a claim with the European Medical Agency to stop the Pfizer trial because of potential fertility concerns.
“It started with a statement by Oxford Prof John Bell, who said: “These vaccines are unlikely to completely sterilize a population. They are very likely to have an effect which works in a %, say 60 or 70%.” By “sterilize” he means to rid the population of the virus and make the people immune, but the phrase was seized on by scaremongers who went looking for any connection to sterilization in terms of fertility, and thought they had found a protein similarity.
“They claimed a supposed similarity between the virus spike protein (the virus protein against which most of the COVID-19 vaccines are raised, not just Pfizer’s) and a protein that is expressed in the developing placenta called syncytin-1. They theorized that if the vaccine caused antibodies against spike, those might cross-react with the placental protein and inhibit placenta formation, causing infertility. But their evidence is faulty and claims unfounded.
“We did our own protein database check on similarity of the two proteins and found that it was minimal. And the region of the proteins where the supposed similarity was found is actually buried in the protein structure, covered up so that it can’t cause an antibody reaction. The region of the spike protein against which antibodies are formed has no similarity to the placental protein.”
CLI will continue to follow the science and keep you abreast of new developments. As you make decisions concerning vaccines, be informed about making the best choice possible.
LifeNews.com Note: Bradley Mattes is the President of Life Issues Institute, a national pro-life educational group.
To address the coronavirus (COVID-19) pandemic, Congress directed $10 billion to project Operation Warp Speed to develop vaccines, therapeutics, and diagnostics—so-called countermeasures.1 While the public health community and media laud the ambitious goal of producing enough vaccine for every person in the US by January 2021, other people have expressed concern that rapid development of a coronavirus vaccine might take shortcuts with proper safety testing. Indeed, 50 percent of Americans would not receive a coronavirus vaccine when one becomes available, and another 25 percent aren’t sure.2
Historically, vaccine development can take 10 years or longer,3 which may explain why many Americans, parents especially, lack trust in a coronavirus vaccine developed under such a hasty timeline.
Perhaps more people have experienced or learned of adverse safety issues with other vaccines and are suspicious of claims by government and vaccine manufacturers that vaccines are “safe and effective.”
Considering that coronavirus has a 99.8 percent recovery rate—similar to annual influenza—one could even question the need for a vaccine. Additionally, new coronavirus vaccines may be only 50 percent effective, similar to a yearly flu shot.4
Are “ethical” vaccines really ethical?
Another concern for people of faith is news that experimental coronavirus vaccines could be produced using tissue derived from aborted babies.5 In addition to future coronavirus vaccines, several vaccines used for other diseases can be designated as “unethical” because their production methods use tissues derived from aborted human fetuses to cultivate vaccine viruses.6 Children of God for Life has meticulously documented such vaccine origins.7 Its founder, Debra Vinnedge, was prominently featured in Meredith Wadman’s 2017 book The Vaccine Race, which offers a detailed history of vaccines developed using aborted human fetal tissue.8
If a vaccine is not derived from aborted fetal tissue, can it then be termed “ethical” and thus appropriate for administration to entire populations? Unfortunately, vaccines may be considered unethical for reasons beyond the use of fetus-derived tissue. After many years of vaccine research, I have found abundant evidence of corruption and unethical practices within drug companies and the government public health community.
Use of the term “ethical” to describe vaccines ignores the mandatory nature of vaccines and the potential for severe vaccine adverse effects, regardless of how the vaccines were made.
For example, within minutes of birth, babies are injected with the vaccine for hepatitis B—a disease of promiscuous homosexuals, heterosexuals, and intravenous drug abusers.9 This is a so-called “ethical” vaccine because it’s not derived from aborted human fetuses. But is it ethical to inject all babies with a lifestyle-disease vaccine?
In addition, pre-teens are injected with an HPV (human papillomavirus) vaccine with the unproven goal of preventing cervical cancer.10 Infection with certain high-risk types of HPV—a sexually transmitted disease—can cause cancer of the cervix, genital areas, or throat. Cervical cancer is commonly related to early sex with multiple partners or to having a male sexual partner who has had multiple sexual partners.11 The HPV vaccine is another so-called “ethical” vaccine because it’s not derived from aborted human fetuses. But is it ethical to inject pre-teen girls and boys with a lifestyle-disease vaccine?
Furthermore, mandating vaccines is a blatant violation of medical informed consent—a basic tenet of ethical medical practice. With numerous vaccines currently mandated for work, school, college, and daycare—and soon a coronavirus vaccine likely added to the list when marketed—the potential for harm increases.
Are vaccines totally safe?
If an adult or child is killed or injured by a vaccine, federal law—the National Childhood Vaccine Injury Act of 1986—prohibits the person from suing the drug company that made the vaccine. Despite the government’s narrowing criteria for injured parties to collect on vaccine death or injury, the taxpayer fund has paid out more than $4 billion to vaccine victims and their families. If vaccines are safe, why must drug companies be protected from lawsuits?
When recipients of a new coronavirus vaccine are killed or injured, they or their families will be prohibited from suing the vaccine makers.12 Since new COVID-19 vaccines are termed “countermeasures,” they are covered under the federal Countermeasures Injury Compensation Program.13 Described as a government “black hole” process with no transparency or accountability, the CICP appears to lack sufficient funding, reflected in its less than 10 percent payout rate for mostly H1N1 swine flu vaccine injury claims and limited one-year statute of limitations. Since the program began reviewing claims in 2010, it has received 485 claims, yet only 39 people have received compensation, prompting one critic to portray this as “the right to file and lose.”14
In congressional hearings leading to passage of the NCVIA, which gave lawsuit immunity to drug companies for vaccine injuries and death, Dr. Martin Smith, then president-elect of the American Academy of Pediatrics, compared children harmed by vaccines to military soldiers in combat. Dr. Smith stated: “This country does, and it should, provide compensation and continuing care for its soldiers who are injured in the defense of their country. It has been and is the contention of the [AAP] that the children of this nation are also soldiers in the defense of this country against disease.”15
This means the government is telling you to risk sacrificing your children instead of giving drug companies incentive to develop safer vaccines. In his testimony to Congress, polio vaccine pioneer Dr. Jonas Salk expressed concerns that the NCVIA would remove “the incentive for manufacturers and the scientific community to improve existing vaccines.”16 In recent years, adults have also been encouraged to receive an ever-increasing number of vaccines.17
When vaccines are mandated and the federal government (through taxes) pays the vaccine liability costs for drug companies, these companies have no incentive to make safer products or improve existing products.18
Moreover, the Department of Health and Human Services has ignored directives under the 1986 NCVIA to report every two years to Congress how the agency has improved vaccine safety. In a Freedom of Information lawsuit in 2018, the HHS revealed that it had never submitted a single biennial safety report in 30 years. In the meantime, HHS promotes and funds a growing vaccine schedule with little apparent concern for the safety of currently licensed vaccines.19
In their goal to achieve 100 percent vaccination rates, drug companies and government public health authorities withhold and distort an unconscionable amount of information. Common practices include inflating disease incidence data to mislead the public into thinking a disease is more common than it really is and minimizing reports on a vaccine’s adverse reactions.
Financial conflict of interest is another major area of concern. Individuals and organizations that determine national vaccination policies often receive grants from or own stock in the very companies they regulate.20
Do your own research
Just as we research different brands when choosing a refrigerator, a washing machine, or a car, we should spend at least similar effort in researching the pros, cons, and safety of vaccines. Vaccine consumer organizations can assist with such research.21 With social media censorship of vaccine consumer websites, we cannot rely solely on Google searches, which link to biased government and drug-company-sponsored sources.22
Simple justice dictates that Americans exercise their right to medical informed consent for vaccines (i.e., the right to opt out of vaccines for themselves or their children). Why should vaccines be any different from other medical procedures, all of which require informed consent?
Meredith Wadman, The Vaccine Race: Science, Politics, and the Human Costs of Defeating Disease, (Viking, 2017), Chapter 26.
“Hepatitis B Virus: A Comprehensive Strategy for Eliminating Transmission in the United States Through Universal Childhood Vaccination: Recommendations of the Immunization Practices Advisory Committee (ACIP),” MMWR, November 22, 1991, 40 (RR-13); 1-19, cdc.gov/mmwr/preview/mmwrhtml/00033405.htm.
Tom Hals, “COVID-19 Era Highlights U.S. ‘Black Hole’ Compensation Fund for Pandemic Vaccine Injuries,” Reuters, August 21, 2020, reut.rs/2ZBcELJ.
“Vaccine Injury Compensation: Hearings Before the Subcommittee on Health and the Environment of the Committee on Energy and Commerce, House of Representatives, 98th Cong., 2d Sess., on H.R. 5810, A Bill to Amend the Public Health Services Act to Provide for the Compensation of Children and Others Who Have Sustained Vaccine-Related Injury, and for Other Purposes,” September 10, 1984, p. 121, babel.hathitrust.org/cgi/pt?id=mdp.39015042797467&view=1up&seq=129&q1=smith.
National Childhood Vaccine-Injury Compensation Act: Hearing on S. 2117 Before the Senate Committee on Labor and Human Resources, 98th Cong., 2d Sess., S. Hrg. 98-1060 (May 3, 1984), at 166.
FACA: Conflicts of Interest and Vaccine Development—Preserving the Integrity of the Process, Hearing Before the Committee on Government Reform, House of Representatives, 106th Congress, Second Session, June 15, 2000, Serial No. 106-239, govinfo.gov/content/pkg/CHRG-106hhrg73042/html/CHRG-106hhrg73042.htm.
Rep. Adam Schiff Sued by Physicians for Censoring Vaccine Debate, Association of American Physicians and Surgeons, January 15, 2020, aapsonline.org/rep-adam-schiff-sued-by-physicians-for-censoring-vaccine-debate;“#MalkinLive: Interview with Del Bigtree after YouTube Bans The Highwire,” YouTube, July 30, 2020, youtube.com/watch?v=bPfTz3d0Zls; “Controversial Vaccine Movie Banned by Netflix & Apple,” YouTube, July 9, 2020, youtube.com/watch?v=FX95m5kXMBU; “CHD Holds Press Conference with Legal Team and Plaintiff in Lawsuit Against Facebook, Mark Zuckerberg, and Three of Facebook’s So-Called ‘Fact-Checkers,’” Children’s Health Defense, August 20, 2020, bit.ly/3bFVXU2.
A month and half ago, this writer predicted that China would end its two-child policy at the October meeting of Communist bigshots in Beijing. It was there that they hammered out their economic and social policies for the next five years, formally known as the “14th Five-Year Plan”.
I was hoping for a repudiation of a policy which had probably murdered more unborn babies than any other time in history and a formal announcement of the end of birth restrictions. I was correct — but in an underwhelming way.
The meeting did indeed announce further relaxations of the policy. But it did it ever so discreetly, buried deep in the pages of the CCP’s resolutions. The hated phrase “计划生育”, or family planning (an euphemism for the one-child policy in China), was finally dropped from the Five-Year Plan.
According to the English version of the semi-official Global Times, the plan also mentioned a much more “inclusive” policy, signaling that the era of child limits is coming to an end. Even Zhai Zhenwu, a population expert formerly employed by the National Family Planning Commission, a man who misled both the Chinese public and the tyrants in Beijing on China’s population prospects with both Malthusian theories and fudged statistics, admitted that: “Birth restrictions will definitely be phased out. We are moving in the right direction.”
Whilst this writer believes that we will only be on the right direction if and when people like Zhai and the officials who carried out mass sterilisations, forced abortions and cold-blooded murders of both pregnant women and babies are arrested, prosecuted and jailed for crimes against humanity, this is still a small victory.
But today I don’t want to talk about villains. I want to talk about the heroes. These are people who worked in a country with asphyxiatingly low levels of free speech and collective myopia on population policy, challenges the official population policy and changed hearts and minds. They helped to push China slowly towards demographic sanity.
Let’s celebrate the good guys for a change.
Big Country with an Empty Nest
The first is Yi Fuxian. He was trained at one of China’s top medical schools, Xiangya in his native southern Hunan Province (which as I profiled in one of my previous articles, was founded by missionaries from Yale University). By 1999 he was working in the University of Wisconsin-Madison’s Department of Obstetrics and Gynecology. He was one of the most skilled researchers and physicians in his field.
Yi had an unconventional hobby — researching China’s demographics. When he started in the early 2000s, the rhetoric and the research was monopolized by the advocates of the one-child policy. They were making absurd claims that China’s population would reach 4 billion people in 2050 without a one-child policy. Western critics criticized its human rights abuses. But everyone missed the elephant in the room: the policy was useless; it was all based on lies; and the guys in charge were demographic illiterates.
Yi exposed this. Spurned by the officials in Beijing, he posted his research on the Chinese internet, which was considerably freer back in the early 2000s. He went viral on popular forums such as Tianya, and gained millions of followers. He was the first to point out that China would never have 4 billion people and that all of Beijing’s population projections since the 1970s had been wrong. The National Family Planning Commission had deliberately amended statistics in consecutive censuses to artificially increase the birth rate and continue the population panic. There might even be 100 million fewer Chinese people than appeared in the official figures. Yes, fewer, not more. The draconian policy was unnecessary.
Yi has been vindicated repeatedly, humiliating the apparatchiks in Beijing. Even more worrying for the officials, he democratized opposition to the birth policy. Before Yi Fuxian, opposition to the one-child policy was taboo. But after his trailblazing research, it became much easier to oppose the policy and voices for reform grew ever louder.
Yi became subject to intense censorship. For years, he was not allowed to step foot in China. His influential book, Big Country with An Empty Nest, had to be published in Hong Kong in 2007 when the former British colony was still a haven for free speech in the Chinese world, because no publisher on the Mainland would touch it. For a decade he was not allowed to return to China, but his fanbase only grew bigger and bigger online.
When China loosened its one-child policy, first allowing couples to apply for a second-child quota if one of them were an only child, and then abolishing the one-child policy altogether. Yi was invited back to China, gave seminars in many universities and academic forums, and was even allowed to speak at the prestigious Bo’Ao Asia Forum (the Chinese version of Davos).
His book was published by a publisher with links to the government, and his Weibo account had hundreds of thousands of followers. Yi became a popular figure among both the Maoist hard-left and the pro-reform right. His book was endorsed by figures as diverse as Mao Yushi, a pro-democracy economist who won the Milton Friedman Liberty Prize, and Kong Qingdong, a Maoist Peking University professor who claims to be a descendant of Confucius. Hatred for the population policy may be the only thing left and right can agree on in China.
But then the Family Planning Commission decided to strike back even as it was on its way out. When Yi called for a full abolishment of all birth restrictions and declared that China’s population might have been exaggerated by the Chinese government in the tens of millions, making India more populated than China, his Weibo account was deleted and his articles and research were erased from the Chinese internet.
Yi retreated to Twitter and continues to post about his research online. He also maintains WeChat groups for thousands of his fans. Many of them were inspired to have more children by his writings and research. He provides advice for them on having children as well as how to evade punishment for violating birth restrictions.
Wang, a devout Christian, interviewed mothers who had abortions or were pressured to have them, to speak about their experiences. She regularly updated on her personal WeChat media account with the contents of her book and regularly wrote articles in Yicai critical of the one-child policy, focusing on the harsh fines handed down by officials to impoverished parents for having an “illegal” child.
As a journalist, she embarrassed Family Planning Commission officials at news conferences. At its peak before the end of the one-child policy in 2015, tens of thousands of anxious Chinese parents were following her, as she told them that the reform of the birth policy was near and that they did not need to give up on a second or third child.
Ms Wang and mother-activists against the one-child policy spoke at seminars organized by the pro-natalist Chinese website cnpop.org. She was also vocal about how her Christian faith influenced her beliefs against the birth policy. She has since receded from her spotlight and no longer writes for Yicai, since her articles and writings are probably too provocative under Xi Jinping.
But she saved many babies and started a grassroots movement against the one-child policy, contributions which should never be forgotten.
Too many people in China?
James Liang Jianzhang is not your average crusader. He is very much part of China’s elite, one of the many who benefited from China’s economic boom. He is the founder of ctrip.com, one of China’s largest travel websites.
When Liang did a PhD at Stanford University, he noticed the differences in attitude towards child rearing and fertility between China and the United States. He began his own research on population control and came up with a radical slogan — people are wealth, and not a burden.
He used his position as Chairman of Ctrip to implement pro-natalist policies within his own company. He backed start-ups which help relieve the immense pressure on child rearing in China. He opened company-funded childcare facilities in the company headquarters of Shanghai, allowing Ctrip employees with children to have a peace of mind.
Nowadays he uses his position of influence to promote his “people are a wealth not a burden” theme. He has even created comedy sketches which debunk Malthusianism. He has appeared on one of China’s most popular variety shows on iQiyi ( China’s Netflix) called U can U Bibi (奇葩说 ), to debate population reform.
Liang went viral when he declared that the Chinese people will go extinct in the next few hundred years as a result of the current population policy if things are not turned around quickly. Liang’s partner in demographic research, demographer Huang Wenzheng, is also very active.
His provocatively titled book, Are there too many people in China?, was followed by another book, the Demographics of Innovation. Liang is permitted far more space for his opinions than Yi Fuxia because he is not nearly as anti-establishment. It also helps that he is a wealthy businessman and chairman of one of China’s best-known companies.
Future Nobel laureates?
Change would not have been possible had these people and many others who woke up from population brainwashing not spoken out for reform. China continues to be reluctant to acknowledge human rights abuses and the huge mistake it made through its inhumane population policy. But at least it is becoming more pro-natalist in its thinking, a step in the right direction.
Someday the world will recognize that China’s one-child policy should be as infamous as Apartheid. When that happens I will nominate these three heroes for the Nobel Peace Prize.
Today the national pro-life group Susan B. Anthony List (SBA List) celebrated the continued momentum for pro-life women in Congress as Young Kim claimed victory in California’s 39th congressional district. Kim is the 17th new pro-life woman elected in the 2020 cycle. Out of these 17 women, nine have flipped seats formerly held by pro-abortion Democrats. This brings the total number of pro-life women in Congress to 27, more than double the previous record, with more races still to be called.
“This historic surge of pro-life women in Congress is continued proof that life is winning in America,” said SBA List President Marjorie Dannenfelser. “Nancy Pelosi and pro-abortion Democrats are now up against a stronghold of pro-life women who will stand up to their radical agenda and fight to protect longstanding pro-life policies including the Hyde Amendment and others like it, along with our gains under President Trump.
“These victories are a testament to the power of the life issue to motivate voters and unify Republicans to build a broad, winning coalition. Contrary to years past, today there is universal recognition in the Republican Party that protecting unborn children and their mothers is both morally right and politically smart. Following President Trump’s lead, pro-life candidates are going on offense to expose the extremism of their Democrat opponents and are finding tremendous success.”
A full breakdown of pro-life women victories and races yet to be called follows:
U.S. Senate:
Rep. Cynthia Lummis (R-WY) won election
Sens. Joni Ernst (R-IA), Shelley Moore Capito (R-WV), and Cindy Hyde-Smith (R-MS) won re-election
Sen. Kelly Loeffler (R-GA) advances to a runoff to take place January 5, 2021
Six pro-life women will serve in the U.S. Senate next Congress, seven if Sen. Loeffler wins the runoff
U.S. House:
All 11 pro-life women incumbents have won re-election
17 new pro-life women elected to the House with two races still to be called:
Maria Salazar (FL-27) – flipped Democrat-held seat
2 races featuring pro-life women yet to be called:
Claudia Tenney (NY-22)
Mariannette Miller-Meeks (IA-02)
SBA List and its partner Women Speak Out PAC recently announced a $4 million independent expenditure campaign to elect Georgia Senators Kelly Loeffler and David Perdue, and expose their opponents’ radical pro-abortion agenda to preserve the pro-life majority in the Senate. The multi-channel effort will reach one million voters and includes voter mail, digital ads, voter calls and texts, and door-to-door canvassing.
The groups’ Georgia efforts are an expansion of their overall $52 million campaign for the 2020 cycle. The biggest election effort in the organizations’ history reached more than eight million voters across 10 key battleground states: Arizona, Florida, Michigan, Montana, North Carolina, South Carolina, Iowa, Pennsylvania, Texas, and Wisconsin. Details of the campaign in each can be found in SBA List’s 2020 Election HQ.
Since the Supreme Court ruled on the legalization of birth control, millions of women—often oblivious to its dangers—have used one of its many forms. Manufacturers make billions off a woman’s desire to have sex with little to no consequences. While the pill is the most popular type, other methods continually entice women. Birth control implants are one such method.
A birth control implant is a device, about the size of a matchstick, used to prevent or impede pregnancy. A doctor inserts this device just under the skin of a woman’s inner upper arm. Usually containing levonogestrel, the implant releases this chemical into the woman’s body daily for years at a time.
Birth control implants are marketed as an easy solution to the “problem” of fertility. Women can have them inserted and then forget about them. This eliminates forgetfulness or user error. And it increases efficacy. But these implants have had a far-from-smooth introduction into the market. In addition, they do not prevent against STDs.
It all began with a device called Norplant. Norplant was first developed and approved abroad in the 1980s. But it wasn’t until 1990 that the FDA approved its use in America. Norplant was made of silicone and contained six capsules containing levonorgestrel. It was effective for up to five years.
Soon after Norplant was introduced, women found themselves facing health crises.
Side Effects of Norplant
Almost immediately, women began experiencing terrible side effects. These included:
severe headaches
anxiety and panic attacks
depression
acne
weight gain of 60 to 100 pounds
excess growth or loss of hair
ovarian cysts
breast pain
skin discoloration
infection at the implant site or numbness in the arm
a variety of menstrual disorders
These side effects were so harmful that over 36,000 women joined a class action lawsuit against American Home Products Corporation, the parent company of the maker of Norplant. The plaintiffs claimed that the company “misled customers about the severity of Norplant’s side effects.” In 1999, American Home settled without admitting any wrongdoing. The company agreed to pay more than $50 million total. The settlement gave each woman slightly under $1,500.
According to a lawyer for the women who sued the manufacturer, the most severe side effects that he knew of were “enlarged ovaries and fallopian tubes that burst, causing the need for hysterectomies and/or the removal of the tubes and ovaries.”
Following the class action lawsuit and public outcry, the distributor withdrew Norplant from the US market in 2002. Its production was discontinued worldwide in 2008.
But like a phoenix rising after its death, birth control implants would not stay dead long.
In came Jadelle—an FDA-approved implant that is only marketed overseas.
Jadelle
While Norplant had 6 matchstick-sized implants, Jadelle is a set of two. Each contains 75 mg of levonorgestrel.
Like Norplant, a doctor must insert the rods—one at a time—into the woman’s arm. The doctor uses a local anesthetic and makes the incision. Often, swelling, bruising, or discoloration result at the site. Some women report pain or itching. In addition, some women have had skin reactions such as blistering, tingling, numbness, or scarring.
According to RX List: “Immediately after insertion of Jadelle® . . . implants, a low continuous dose of the hormone is released into your body. Pregnancy is prevented by stopping ovulation (so eggs will not be produced regularly), and thickening the cervical mucus (making it more difficult for the sperm to reach the egg). There may also be other effects that contribute to pregnancy prevention.”
Abortifacient effects:
It doesn’t mention these “other effects.” But we know what they are. Jadelle—and other similar hormonal contraceptives—alters the lining of the endometrium to prevent implantation of a fertilized egg. That means that a baby has already been created. However, that baby is unable to attach to the wall of the endometrium to continue to grow. Because he cannot attach, he dies.
These three methods combine to give Jadelle a less than 1% failure rate.
Jadelle is effective for up to five years. If the woman weighs over 132 lbs, her doctor may recommend that she have the implant removed after the 4th year. This is done to maintain its efficacy.
Side effects:
No hormonal contraceptive comes without side effects. And Jadelle has many. About 10% of women suffer from:
Between 1 and 10% of women suffer more serious side effects. Some of these include:
Chest pain
Depression
Asthma
Fatigue
Palpitations
Bronchitis
Ovarian cysts
In addition, according to the Jadelle pamphlet, a woman may experience an allergic reaction to the device. Some of these reactions include:
shortness of breath
wheezing or difficulty breathing
swelling of the face, lips, tongue, or other parts of the body
rash, itching, or hives
The pamphlet also warns: “You may have a higher risk of an ectopic pregnancy if you get pregnant while your implants are in place. An ectopic pregnancy can be a serious and life-threatening condition. It can also cause problems that may make it harder for you to become pregnant in the future.”
Not only is the implant potentially deadly for a woman’s baby, but it’s potentially deadly for her as well.
Hormonal contraceptives can cause fatal blood clotting.
How are birth control implants removed?
Just as a woman must have a doctor insert the device, so must she return to the doctor to have it removed. While this is supposed to be an easy procedure, it is not always.
The overall incidence of removal difficulties in the clinical trials, including damage to the implants, was 7.5%. If removal of the implant(s) proves difficult, close the incision and bandage the wound, and have the patient return for another visit. The remaining implant(s) will be easier to remove after the area is healed. It may be appropriate to seek consultation or provide referral for patients in whom initial attempts at implant removal prove difficult.
So while many women have an easy time with the removal of the implant, a significant number of women experience difficulty. That difficulty has not gone unnoticed by the manufacturer.
Enter a new kind of device. This one is detectable on an x-ray.
Implanon and Nexplanon
Jadelle is not available in the US. So, in 2006, the FDA approved Implanon. Implanon was a single thin rod produced by a division of Merck that released etonogestrel. Its improved design made it easier to insert and remove.
However, just four years later, Merck replaced Implanon with Nexplanon. Nexplanon was designed to be visible through an x-ray, which makes it easier to find and remove. It also comes with an improved insertion device.
Nexplanon is currently the only available birth control implant in the US. The FDA has approved it for up to three years. Unlike Jadelle, which may not be as effective in women over 132 lbs, Nexplanon isn’t contraindicated in overweight women. Yet the information pamphlet also states that the device may lose its effectiveness in women with a BMI greater than 30.
Just like the other birth control implants, Nexplanon has a fewer than 1% failure rate. And its side effects are similar to those of its predecessors.
Cysts may develop on the ovaries and usually go away without treatment, but sometimes surgery is needed to remove them.
Besides changes in menstrual bleeding patterns, other common side effects reported in women using Nexplanon include: headaches; vaginitis (inflammation of the vagina); weight gain; acne; breast pain; viral infection such as sore throats or flu-like symptoms; stomach pain; painful periods; mood swings, nervousness, or depressed mood; back pain; nausea; dizziness; pain and pain at the site of insertion. Implants have been reported to be found in a blood vessel, including a blood vessel in the lung.
Again, we see significant dangers to women. Sadly, many women feel that the gains outweigh the pains.
Who uses birth control implants, and where do they get them?
According to the Kaiser Family Foundation: “In 2015-2017, the most recent years for which there are national data, about 4% of women ages 15-44 who currently use contraception used the implant.”
Those who use birth control implants tend to be younger women and women from low-income households. Many have Medicaid or are uninsured.
Researchers believe that women from these backgrounds prefer the implant because of its ease and because they want to prevent pregnancy for a longer period of time.
The Kaiser Family Foundation also reported the results of a 2016-2017 survey of obstetricians. This survey found that almost three out of four OBGYNs who provide obstetrical care offer the implant. Those who don’t offer it were asked why. They cited reasons such as lack of interest and the fact that their staff were not trained to insert it.
That brings us to another issue with birth control implants. Staff need special training to insert it. The FDA requires a two-hour, in-person training from the manufacturer. While the cost of the training is free, travel to the site and any other expenses incurred are the responsibility of the trainee. Some doctors don’t feel that it’s worth the effort.
Many low-income women use federally qualified health centers. However, because of the cost of the birth control implants, oftentimes these facilities do not stock them. Furthermore, their staff do not have the training. A 2017 study found that just over two-thirds of these facilities carry implants, Meanwhile, about 98% of Planned Parenthood clinics carry them. In addition, Planned Parenthood clinics allow a woman to come in for just one visit to have the birth control implants inserted. Some health centers require the woman to have an initial appointment and then return for the insertion.
Punitive Use?
When Norplant was still available in the US, it caused controversy for another reason. Judges in several cases made its use a requirement or part of a plea deal for women who had been accused of child abuse or endangerment.
According to Hastings Constitutional Law Quarterly: “Within months of its approval, several judges around the country had already succumbed to Norplant’s allure. In California, Nebraska, and Texas, judges imposed use of Norplant as a mandatory condition of probation for mothers convicted of child abuse….Elected officials, judges, and other interested parties began advocating and implementing widespread and sometimes mandatory use of Norplant, often as a means to fight poverty.”
Initially, officials targeted women using drugs. Their hope was that Norplant would prevent them from creating babies who suffered from addiction at birth. Sometimes Norplant was used as an incentive. If the woman agreed to using it, she would get something in return. And finally, it was used as a condition of probation for mothers who were convicted of child abuse.
But was this ethical? Is it morally right to coerce a woman to have chemicals inserted into her body?
Right to Privacy?
According to Hastings Constitutional Law Quarterly, “The United States and California Constitutions provide a right to privacy that protects decisions regarding procreation, parenting, and medical treatment from government intrusion.”
This right to privacy has been extended to include a person’s right to refuse “unwanted medical treatment and other invasions of bodily integrity.” Further, the Court allows a person to refuse medical treatment in a criminal setting as well.
The courts quickly realized that women could not be forced to undergo any kind of medical procedure. And that included birth control implants.
The Catholic Church is adamant about maintaining bodily integrity because the body is a temple of the Holy Spirit. As HLI’s Brian Clowes states: “Any mutilation of the body—including extreme ‘body modifications’…and attempts to cripple it for social reasons (including sterilization)—is to be condemned. Such mutilations ‘violate the integrity of the human person.’ Direct sterilization destroys the normal and proper functioning of a body system and is thus illicit in all cases.”
While birth control implants aren’t sterilization, they do destroy the normal and proper functioning of the human body for years at a time. In addition, forcing a woman to undergo this treatment is an offense against her dignity as a human being.
Final thoughts
Advertisements, organizations, and social media all paint a joyous picture of the freedom that women can experience while using birth control implants. Rarely will they acknowledge that this “freedom” comes at a cost.
Isn’t it time that women exercise true freedom? Isn’t it time they listen to the facts? The facts paint a very different picture. Yet the facts tell the truth. Hormonal birth control, including implants, is detrimental to a woman’s health. And sometimes they kill a baby.
Women, you only get one body. Treat it with respect.
Brittany died in December of 2012 of a deep venous thrombosis (DVT), a blood clot in a major blood vessel, caused by the contraceptive NuvaRing. She collapsed after an evening out with her sisters and was declared brain dead three days later. According to her father, “Her death diagnosis was acute respiratory failure, diffuse pulmonary hemorrhage, diffuse venous thromboembolism with deep venous thrombosis, [and] severe anoxic brain damage.”
Alex collapsed in 2013 on the landing in her apartment building after grocery shopping. Six hours later, she was dead. She suffered a massive pulmonary embolism — a blood clot in the lungs. Pulmonary embolisms are a known side effect of the birth control pill, which Alex was using for contraception. Both young women had minimal or no symptoms in the days leading up to their deaths.
In order to “educate other women and families about the very real risks associated with hormonal contraceptives and the incredible lack of data and information available to women to make an informed choice,” Malone developed BirthControlSafety.org, to which Rowan is a contributor. According to research cited on the website, 1,500 women will die of a pulmonary embolism due to the birth control pill, patch, or NuvaRing in the United States each year. “A woman is 4-10 times more likely to develop a potentially fatal blood clot if she uses [the] pill, patch, or ring than if she uses an IUD or an implant,” according to the site. Stories of dozens of women who experienced a serious injury or even death due to complications of hormonal birth control are can be found on the site.
Rowan also launched the Alexandra L. Rowan Memorial Foundation in his daughter’s honor. The foundation funds research into pulmonary embolisms because research has revealed newer generations of birth control pills actually increase the risk of pulmonary embolism. The foundation also seeks to establish a protocol for utilizing a screening test or vetting program that could help to identify the women most at risk for embolism so they can make an educated decision about whether to use hormonal birth control. The Foundation has also partnered with the National Blood Clot Alliance to raise awareness about the connection between contraception and blood clots.
“By the drug company’s own data, if you’re taking hormonal birth control, you have a 1 in 12,000 chance of dropping dead,” Rowan said in a Period Party podcast interview in 2019. Furthermore, he noted that most women are not screened for a known blood clotting disorder that significantly raises their risk of developing a pulmonary embolism prior to being prescribed hormonal birth control. “If you have something called the Factor V Leiden mutation, you’re eight times more likely to develop a blood clot on birth control than not… So, your 1 in 12,000 rate goes down significantly, then it becomes a very real risk,” he said.
On October 30th, Alex Rowan’s family honored the 7th anniversary of her untimely death by sharing her college graduation picture.
Brittany and Alex were not the first young women to die of complications from hormonal birth control, and unfortunately, they were also not the last. Women deserve to know the root causes of their various reproductive system issues, plan their families, and monitor their fertility and overall health in ways that respect and even restore the natural rhythms of their bodies. Evidence-based fertility awareness methods of family planning offer all of this, without hormonal birth control’s potentially devastating side effects.
WASHINGTON — U.S. Supreme Court should hear appeals backing HHS rules that block recipients of Title X family planning funds from performing or making referrals for abortions, a group of pro-life obstetricians and gynecologists and a Christian medical association have said.
The Supreme Court is considering whether to hear appeals seeking to overturn an appellate court’s ruling against the Protect Life Rule, created by the Trump administration’s Department of Health and Human Services. The rule prohibits recipients of Title X family planning funds from referring for or performing abortions. It requires Title X fund recipients to be both physically and financially separate from facilities that perform abortions.
“The Supreme Court has already recognized that the federal government has authority to prevent Title X funds from being used for abortion. The 4th Circuit chose instead to rely on the preferences of pro-abortion medical associations,” John Bursch, Alliance Defending Freedom senior counsel and vice president of appellate advocacy, said Nov. 9. “The Supreme Court should take this case and affirm that HHS has the authority to issue a rule that the high court already deemed constitutional.”
The Alliance Defending Freedom legal group filed the Nov. 9 amicus brief on behalf of the American Association of Pro-Life Obstetricians & Gynecologists, which claims 4,000 OB-GYN members and associates, and the Christian Medical and Dental Associations, which claims 20,000 members and 329 chapters in the United States.
The case, Azar v. Mayor and City Council of Baltimore, went before the 4th Circuit Court of Appeals. The Sept. 3 decision split 8-6, with the majority opposing the rule. The majority decision said the Department of Health and Human Services “failed to recognize and address the ethical concerns of literally every major medical organization in the country” and “arbitrarily estimated the cost” of implementing a section of the rules.
The amicus brief, however, argued that the final HHS rule essentially revives regulations previously approved by the Supreme Court in its 1991 case Rust v. Sullivan, which barred abortion counseling as a method of family planning in federally-funded facilities.
The brief further argued that the Fourth Circuit wrongly assumed that these prominent medical associations “promote objective truths, rather than abortion advocacy.”
One such organization, the American Medical Association, has a litigation center that promotes abortion. It has advocated unencumbered access to abortion.
“But this Court has never acquiesced to the AMA’s policy views simply because it is a significant medical association,” the amicus brief continued. “Quite the opposite, the AMA’s pro-abortion policy positions have not fared well in this Court, which rejected the AMA’s call to force a pro-life pregnancy clinic in California to advertise for the abortion industry based (in part) on its dubious view of medical ethics.”
The court has previously rejected the American Medical Association’s denial of pro-life sidewalk counselors’ First Amendment right to speak in public byways outside abortion clinics.
The Protect Life Rule has withstood other challenges.
On Feb. 24, the 9th Circuit Court of Appeals ruled 7-4 to uphold the rule. The majority opinion, written by Judge Sandra Ikuta, cited the 1991 Rust v. Sullivan case and said the Trump Administration rule was “less restrictive in at least one important respect” than the previous rule which had been upheld.
The Protect Life Rule does not reduce the amount of available Title X funding, but clarifies eligibility to receiving the funding. Title X is a federal program created in 1965 that subsidizes family-planning and preventative health services for low-income families, including contraception, breast and cervical screenings, and HIV testing. It has been frequently updated and subject to new regulations. Title X does not pay for abortions, but recipients have in the past been able to refer patients for abortion.
“Non-directive counseling” about abortion is still permissible under the new rules, which pro-life advocates have praised as a commonsense way to ensure enforcement of already-existing rules against taxpayer money being used for abortions.
Abortion advocates have characterized the restrictions as a “gag rule.” They said the rule for physical separation would have required many providers to change locations, conduct expensive remodels, or shut down.
After the new rules were announced, Planned Parenthood said it was exiting the Title X program in order to continue performing abortions. It is the largest abortion provider in the U.S., with some 300,000 performed every year. Its political arm is deeply influential.
Planned Parenthood had been receiving about one-fifth of the total amount of Title X funds distributed, and withdrawing from the program means a $60 million cut in federal funding for the organization each year.
Planned Parenthood still receives roughly $500 million annually in Medicaid reimbursement.
I’m a former Marine. These days, I work full time in manufacturing. I’m not one to go out and seek to be known or throw myself into the public arena. Yet, my wife and I are pro life speakers. I’m not the natural she is. That’s obvious within the first few minutes of me opening my mouth. But like my wife Jennifer says, “As God opens doors, we’ll walk through them.”
In 2014, Jen was a victim of a sexual assault so brutal it doesn’t bear thinking about. As painful as that was for both of us, separately and as a couple, what followed changed everything. What followed was a little boy. We named him Joshua.
We, as pro life men, have been cowed when it comes to the abortion debate. Especially when we’re talking abortion and exceptions. We have opinions. I have a very strong opinion. I hear the other side throw out the “but what about in cases of rape?” when debating, thinking that they’ve got a trump card. I know from my personal experience that things aren’t usually the way they say they are. I know from Jen’s experience and that of hundreds like her, that the child that came from rape has been nothing but happiness for them.
I’ve seen what our son has done for our family.
It irritates me that so many in the pro-choice world think they can talk for women who have conceived after assault.
I see the damage women have been dealt by being told that abortion erases trauma and NOT being told of the further damage abortion will cause. They’re never told that the baby can be a huge healing factor like Joshua has been for us. I know that’s not always going to be the case. That sometimes it would be best to consider adoption: A brave and beautiful decision.
Babies [are] created by God and human beings at conception. They are alive, they need to be spoken for, they should have rights like any other person.
Men need to be men… I get nervous about saying this because it might sound old fashioned or chauvinistic… but our job is to protect those weaker than us. Protect those who can’t protect themselves. An unborn baby is the most perfect example of one so vulnerable. Stand beside the mother. She has been fed lies for decades. She’s been taught that abortion is simple. Quick. Easy.
Stand for the baby.
They are 100% at the mercy of other people.
Love them both. Abortion cannot be seen as a solution. It doesn’t make you forget.
Some people call me a hero. Kind of weird. It’s a larger scale problem that we view keeping your vows, honoring your God, and loving your wife as heroic. Jen didn’t have any say in what happened to her. The baby didn’t have a say in it. Why would I lower my thinking to the level of putting the onus for some stranger’s actions on either one of them? I don’t know how to say this any better but it seems like such an immature, selfish way to look at the situation. That if your wife became pregnant after rape that you would want her to abort…
More often I’m called a cuck. A simp. Once I was called ball-less (which irked Jen mostly because it was written without a hyphen). Common attempts at digs from people who just don’t know what they’re talking about. They’re coming from a place where they believe “rapist’s spawn” is a thing. It’s not. I don’t even think the people saying these things believe them.
It doesn’t bother me. These are ridiculous arguments that have no weight to them. It’s this mindset that believes someone who marries a woman after she’s been raped is getting damaged goods. That staying with her makes him less of a man. If you ask me[, a]ny guy who so much as entertains that thought is already less of a man.
People talk about our son without even knowing him. They use phrases like demon seed and evil genes and talk about me being weak because I’m raising “somebody else’s” baby.
But he’s not somebody else’s baby. He’s my wife’s baby. He’s OUR baby who we loved from the very beginning. Childish, bogus arguments.
And while I’m at it[, s]top with the sins of the father being visited on the children stuff in reference to our story? That doesn’t fit. It should be the sins “of the donor.” Because I’M Joshua’s father. I’m his dad in EVERY sense of the word except for how he came about.
Life never turns out the way you expect. But character is revealed in the valley.
Be consistent, pro life men.
Be strong for the weak.
Defend the defenseless.
Protect EVERY life.
Leave a name your children will be proud to speak.
Carry on.
Editor’s Note: This article was originally published at Love Louder on Facebook and is reprinted here with permission.
In July of 2012, Ward Miles Miller was born three and a half months early weighing just 1.5 pounds. His father Ben chronicled the first year of Ward’s life in a heartwarming video that went viral and has now amassed more than 35 million views on YouTube. Viewers loved watching Ward grow from a tiny preemie with his mother holding him for the first time into a laughing and thriving one-year-old. Now, eight years old and in the second grade, Ward continues to thrive.
Born at 25 weeks, Ward required the use of numerous machines to support him as he fought to survive. He spent 107 days in the neonatal intensive care unit and his parents were unsure at times if he would survive, but Ward overcame obstacle after obstacle. Today, he’s a big brother to Jude, age four, and loves to play hockey, enjoys math class best at school, and wants to be a paleontologist when he grows up. Though he struggled with vomiting as a toddler, he now has no issues at all from being born so young.
In April 2020, Ben Miller created a follow-up video of Ward to show the world how well he is doing. “We are surrounded by coronavirus, people are on lockdown in their homes and have bad news streaming in all the time,” said Ben in the video. “And I thought this would be a great time to share an update about Ward and let you guys see how far he’s come from such a tiny baby.”
Ward’s progress truly is amazing. He’s not that fragile little baby with seemingly endless wires attached to him. He’s now just like any other little boy with sports heroes he admires, a little brother with whom he loves to play (and fight), and a love of dinosaurs.
Instagram.
Babies born at 25 weeks have about a 50% chance of survival, according to VeryWell. Though babies as young as 21 weeks have survived, the closer a baby is born to 34 weeks, the much better his chances of survival. By 27 weeks, the chances rise to 90% and by week 32, babies have a 95% chance of survival. Sadly, abortion is still legal at these ages in the United States.
In eight states, abortion is legal through the third trimester, when babies are capable of surviving outside the womb. One of those states, Colorado, rejected Proposition 115 during the 2020 election, which would have banned abortion in the state after 22 weeks. Alaska, New Hampshire, New Jersey, New Mexico, Oregon, Vermont, and New York also allow abortion up until birth. Most Americans have been misled into believing these late-term abortions are committed for health reasons, but this is untrue. If the baby is capable of surviving, there would be no need to commit a three-day abortion rather than carry out an emergency C-section if the mother’s health was truly on the line.
The Miller family has said that the first year of Ward’s life was difficult — spiritually, emotionally, and physically. But it was all worth it. In 2017, they allowed Live Action to alter and share the video of baby Ward in order to help educate Americans on the truth of life inside the womb and the fact that preborn children are human beings, not mere “tissue.” Ben Miller shared Live Action’s version of the video and said, “I hope people’s hearts are changed!”
Ward has definitely opened millions of hearts and minds with his story.
Even among young women, the risk of blood clot should be a serious consideration if they are on hormonal birth control. Very recently, a friend of mine had a big scare. Her daughter Anne was complaining about unexplained lower back pain, and my friend found out that she was on birth control. She was especially concerned that Anne was on a version of birth control that had a similar formulation as Yaz (which contains ethinyl estradiol), the infamous pill that caused many cardio-vascular accidents among women, resulting in a class-action suit settlement of over 19,000 claims including 100 deaths. Putting the two together, my friend quickly ascertained that Anne may have a blood clot, and urged her to get tested for clots.
This mom, a faithful reader of our website, knew about the tragic stories of other young women like Alexandra Williamsor Alex Rowan, whose early signs of blood clots, including lower back pain,were misread by medical professionalsuntil it was too late.
Anne, a 28-year–old educated and active professional, was using this particular birth control pill in part because of its relieving effecton her acne. She had been to urgent care to check on her back pain, and the doctor had ruled out a blood clot. But upon learning the type of pill she was on, Anne’s mom insisted that she get it checked more thoroughly. Her daughter also complained about being short of breath, another serious sign of blood clots. Besides, members of the family had a history of blood clots and vascular disease. Now, where should she go to find out for sure?
The three levels of thorough testing for blood clots
Beyond an external checkup commonly performed by an outpatient physician(such as swollen and/or warm areas in the leg), the actual detection of a clot requires thorough testing, which is usually performed in an ER setting. Hospitals rely on three main tests to really find out if someone like Anne has a blood clot:
The D-Dimer blood test
The Doppler Ultrasound
CAT Scan
D-Dimer blood test
The D-Dimer test is the first step of a thorough check for blood clots. It will effectively signal a blood clot risk, though it may not mean that you have a blood clot. D-dimers areprotein fragments produced as the result of the dissolving of blood clots. Elevated D-dimer levels in your blood is a possible sign of blood clots, or a sign of elevated risk for clotting, but doesn’t show where the clot is.
Note that this test can be done by regular labs and is not expensive. The advantage of going to the ER is that the analysis is done on-site and results are produced within the hour. This can make the difference that saves a life and if you’re very concerned, it is worth doing.
Anne went to the ER to get checked. Her D-dimer test results were higher than normal. The ER physician immediately ordered the next two exams, which were performed one after the other within the next hour.
Doppler ultrasound
The next exam Anne underwent to rule out blood clots was a Doppler ultrasound. This examis designed to check the blood circulation speed in the legs or the arms. It sends an ultrasound signal that bounces back off red blood cells. A Doppler ultrasound is non-invasive and painless. It can identify if there is a blockage or a clot.
CT Scan
The second exam, the CT Scan, is high precision imaging technology that will produce images of the veins and arteries and detect clots. Megan Henry, anOlympic athlete, was a young woman whose CT scan revealed a large number of clots around her lungs, an exam that saved her life. Note that the CT scan uses higher level radiation, which can have other side-effects.
Other tests for blood clots
Other possible tests include the ventilation/perfusion lung scan (“VQ scan”), which is a low-level radiation test reading a tracer injected in the patient’s veins, and a pulmonary angiogram, which is the most accurate but also the most risky. A MRI is also an option, and is usually administered to pregnant women for the safety of their baby.
Happily for Anne, both the Doppler ultrasound and CT scan were negative. She was able to go home safely, more aware of the signs of blood clots—and that her contraception method was a risk factor for her. What was next for her?
Preventing blood clots
As young women consider birth control options, they need to be thoroughly informed about the risk of vascular problems and the signs of blood clots. An estimated 300 to 400 young women die each year from blood clots caused by contraceptives, and 13,000 are hospitalized in the United States alone. Here are a few considerations for them.
Get tested for Factor V Leiden
At minimum, if a woman feels she must use contraceptive drugs, she should get tested for Factor V Leiden. Factor V Leiden is a genetic condition that greatly increases the risk of blood clots at any age. This condition can increase risk of VTE by 3 to 20 times. The blood test for Factor V Leiden is done by labs for patients who have a family history of blood clotting or show other risk factors. It is an expensive test ($180 to $280, but can be as high as $2,000) and not always covered by insurance (be sure to check). This doctor suggests thatclinicians should “first order a test to measure the activated protein C (APC) resistance in the blood before the blood test.”However, this CDC article about the merits of conducting this test states that “women with Factor V Leiden (FVL) who take oral contraceptives are at higher risk for developing VTE and, if tested and found to have FVL, can be prescribed a more appropriate non-hormonal contraceptive.”
Learn fertility awareness methods (FAM) for safe family planning
The safest option, as even women without the Factor V Leiden condition are at an elevated risk for blood clots while on birth control, is to avoid hormonal contraception altogether. While non-hormonal,non-chemical options exist, such as condoms, diaphragms, and so on, the most effective family planning approach will be a well-understood and managedfertility awareness method (FAM) or natural family planning (NFP). The effectiveness rates of fertility awareness methods vary depending on the method, but they are very similar to the pill and free of side-effects.
Sometimes the challenge for potential users of fertility awareness is that it takes more learning and planning than just popping a pill. But the sad irony is that busy young women areoften keen on carefully managing their diet and exercise, while at the same time daily ingesting a very powerful and dangerous drug out of ignorance of its side-effects and risks.
Two other factors may deter these young women from using a fertility awareness method: the possible lack of support from their partner, and the sense of uncertainty when using the method. We do recommend that a woman has a serious talk with her partner, which could actually be a test of commitment (“does he love me enough that he can take the change of birth control approach for the sake of my health?”). We also recommend that women and couples work with a professional teacher who can guide them through choosing the method that is best for their lifestyle and body, and help them gain confidence in reading the signs of their body for effective family planning.
Young women live busy lives. Regardless of their education level, managing partner relationships, work, career goals, and family plans is a lot to manage for anyone. In this context, it would seem that the birth control pill is a no-brainer, until they really understand the risks and side-effects to which they are subjecting themselves. A serious detection of any blood clot risk is critical if one has any doubt, followed by a pro-active search for good support and training in FAM.
If you’re a family member (especially a parent), this situation may trigger a range of feelings depending on your thoughts about birth control, from doubt and resistance if you believe that contraception is generally OK, to possible resentment if you’re strongly opposed to it. In any case, know that youcan make a big difference and play an active role as you engage with yourloved ones in a pro-active,non-judgmental and supportive way. A life may be at stake.
When this article refers to fertility awareness methods (FAM), or natural family planning (NFP), we are referring to Fertility Awareness-Based Methods, evidence-based methods of cycle charting which can be used as effective forms of natural birth control when learned by a certified instructor.
October 29, 2020 (Inside the Vatican) — At a prayer vigil in November 2009, I discerned the Lord asking me to interview Dr. Bernard Nathanson, the last surviving co-founder of NARAL — the National Association for the Repeal of Abortion Laws (later renamed NARAL Pro-Choice America). In the late 1960’s, Bernard Nathanson and Lawrence Lader crafted what they called the “Catholic Strategy,” later called “the most brilliant political strategy of all time.” It was a stealthy and effective scheme to destroy America’s historical protection of unborn life by undermining the spiritual authority of Divine Law and marginalizing the moral authority of the Catholic Church. As co-founders of NARAL, these two atheists deployed their Catholic Strategy with tactical precision and great efficacy. They were the pioneers of the sinister industry of abortion, which depended on political victory to deceive and destroy. And then a miracle of sorts happened, and Bernard Nathanson became immovably pro-life.
I was daunted by the prospect of interviewing Dr. Nathanson, and even doubted its possibility, but I felt I was supposed to try. Tracking down his phone number via a pro-life attorney, I dialed with trepidation. His wife answered and explained that her 83-year-old husband was very frail from terminal cancer and had not granted an interview in over a year. But she instructed me to fax my letter of request, and promised to present it to her husband.
A few days later she called to inform me that, much to her surprise, Dr. Nathanson had agreed to my request. On December 1, 2009, I flew to New York City to interview the man who trained Planned Parenthood how to kill children in the womb and who worked as Medical Director for the largest abortion center in the world, the Center for Reproductive and Sexual Health (CRASH). These credentials earned him the title “The Abortion King.” Yet, he was the same man who spent his final 35 years working tirelessly to undo what he had regrettably unleashed upon America: deceiving the courts, maligning clergy, manipulating the media, training doctors and crushing the souls of millions of mothers and fathers by stopping the beating hearts of their unborn children.
What Changed?In 1973, just a few months after celebrating the Roe v Wade decision, Dr. Nathanson witnessed for the first time a new technology: real-time ultrasound. He observed an unborn child in the womb — smiling, stretching, and wiggling her toes. He told me, “Real-time ultrasound was the bomb. It made everything come alive.” Science revealed the beauty, goodness and truth of life in this sacred space, demanding intellectual honesty from Dr. Nathanson; he had to acknowledge that abortion kills an existing human life, and admit that what he had been doing was morally wrong. In that moment, he realized he had two patients: the mother and her child. His job was to protect and save them both. In that moment, Dr. Nathanson’s pro-life journey began.
He spent two years persuading NARAL that real-time ultrasound exposed a major ethical and moral dilemma, but the organization cared little and would not alter its position.
Dr. Nathanson resigned from NARAL on the second anniversary of Roe v Wade. In his resignation letter, addressed to Lawrence Lader, he wrote: “The judgments of the Supreme Court were never meant to be infallible or eternal. And what if we’ve been wrong — if the Court should soon reverse itself on the abortion issue in the light of changing times and/or new scientific evidence? What an incalculable injustice will have been perpetrated. What an immeasurable, irretrievable loss will have been suffered. The annual dues to NARAL are ten dollars a year and the hubris of certainty. I can no longer afford those dues.”
By 1979, the father of America’s abortion industry had become 100% pro-life — without exceptions. The industry, in his words, grew “fecklessly out of control.” And fueling it was NARAL’s Catholic Strategy.
Following his defection from the abortion industry, Dr. Nathanson suffered nearly a decade of depression, frequently contemplating suicide, until he crossed paths with a priest who introduced him to the love and mercy of Jesus Christ. On December 8, 1996, America’s “Abortion King” was baptized at St. Patrick’s Cathedral in New York City, and was made new in Christ as a Child of Light.
Background: My Promise
As I sat beside Dr. Bernard Nathanson in the interview he had granted me, listening to his great remorse for orchestrating and leading the war on America’s unborn children, I felt a deep sense of empathy. He was too ill to get his message out anymore, which compelled me to make him an offer: if he had a message for America, I would deliver it across the country until it became common knowledge — or until Roe v Wade was overturned.
In a thin, raspy voice weakened by his illness, but coupled with a slight twinkle of hope in his eyes, he responded, “Yes, yes…Continue teaching about the strategy I used to deceive America, but also deliver this special message. Tell America that the co-founder of NARAL says to ‘Love one another. Abortion is not love. Stop the killing. The world needs more love. I’m all about love now.’” I reached over and shook his feeble hand, promising that one day America would hear his story — and his important message.
The non-profit pro-life organization I founded, named Hosea Initiative, is committed to revealing this vital piece of American history to the public. Our informal polling shows that more than 90% of our predominantly pro-life, Catholic audience lacks awareness of Bernard N. Nathanson’s “Saul-to-Paul” conversion or NARAL’s Catholic Strategy. This is essential information for Catholics walking into the voting booth this November 3.
The “Opposition Element”
NARAL successfully united a fractured pro-abortion movement and aggressively lobbied for the overturn of a 140-year-old New York law which protected infants from abortion. When Governor Nelson Rockefeller signed liberal pro-abortion legislation into law in April 1970, New York City became the nation’s abortion epicenter. Only nine months later, NARAL’s Executive Committee assembled for an emergency meeting to discuss a grave risk to their blossoming abortion crusade. An increasing number of infants were born alive following second-trimester saline abortions.
Executive Director Lawrence Lader showed no empathy for these salt-burned infants. He expressed just the opposite. Dr. Nathanson described Lader’s response in his post-conversion book, The Abortion Papers: Inside the Abortion Mentality (1983): “[He] saw these abortion survivors as an embarrassment to NARAL and was concerned that the press had made much of them and that the opposition elements were seizing upon them as a tactic in the abortion wars.”(p. 177)
Who Was the Most Feared “Opposition Element”? The Roman Catholic Church
The Catholic Church was NARAL’s primary opposition due to its long-standing, uncompromising doctrine regarding the sanctity of human life. While the Anglican Church reversed its position on contraception at the 1930 Lambeth Conference and other Protestant denominations followed, Rome held its position against contraception and abortion as destructive moral evils against God’s gift of life.
For a deeper understanding of the genesis of NARAL’s response to Catholic opposition, look to Lawrence Lader’s 1966 book Abortion, where he identifies the Catholic hierarchy as “a force inimical” to what he called “legalized abortion — the final freedom.”
Nathanson says Lader shows his true colors and the level of his vitriol against the Catholic Church in the sequel, Abortion II: Making the Revolution. In it, Lader names individuals with their religious affiliation (most Catholic) only if they did not support his agenda. (Interestingly, the current “cancel culture” phenomenon mirrors tactics from NARAL’s playbook.)
Naral’s Religious War
Together, Lader and Nathanson executed an all-out, anti-Catholic religious war: Anti-Catholic warp was a central strategy, a keystone of the abortion movement. It was, in a sense, the self-fulfilling prophecy: knowing that the Catholic Church would vigorously oppose abortion, we laced the campaign with generous dollops of anti-Catholicism, and once the monster was lured out of the cave in response to the abortion challenge and the nakedly biased line, we could make the Catholic Church the point man of the opposition. The more vigorously the church opposed, the stronger the appeal of the anti-Catholic line became to the liberal media, to the northeastern political establishment, to the leftist elements of the Protestant Church, and to the Catholic intellectuals themselves. (The Abortion Papers, p.196)
A copy of the magazine of Margaret Sanger, the founder of the Birth Control Federation of America
Lader also modeled his anti-Catholic bigotry after the queen of racism and eugenics, Margaret Sanger, the founder of the Birth Control Federation of America (later renamed Planned Parenthood).
She started her dirty deeds in 1916 as a fallen-away Catholic whose socialist father taught her to despise the Church. In the early 1920s, she strategically pitted Protestants against Catholics over the issue of contraception.
By 1939, she launched the “Negro Project,” an aggressive plan to reduce the black race by pushing birth control and sterilization onto minority communities under the guise of women’s healthcare. In the late 1950s, she led the charge for a little white pill which fueled an era of unfettered promiscuity and out-of-wedlock births. Then, she passed the baton of abhorrence of the Catholic Church to Lader, her biographer and admirer, who soon thereafter partnered with Nathanson to form NARAL.
Dr. Nathanson explained that NARAL braced itself for a response, especially from the Catholic hierarchy. But none came. And it only fueled NARAL’s confidence and purpose. “What continually surprised us in the planning sessions and strategy meetings at NARAL was not only the comparatively mild quality of the organized Catholic opposition, but also the virtual absence of response to what was blatantly an anti-Catholic campaign.” (Ibid., p.190)
Later, writing with a heavy heart, Nathanson described the tactics as morally detestable, with no modern parallel. He was convinced that “there has been, then, no social change in American history as sweeping, as potent in American family life, or as heavily dependent upon an anti-religious bias for its success as the abortion movement.” (Ibid., p. 197)
The efficacy of NARAL’s Catholic Strategy helps explain why the vast majority of current U.S. Senators who identify as Roman Catholics consider themselves “pro-choice” and voted against the “Twenty-week Fetal Pain Bill,” which would have banned abortions from 20 weeks gestation onward, as well as the “Abortion Survivor Infant Protection Act,” which would have guaranteed, by law, healthcare to babies who survive attempted abortion.
The Catholic Strategy
Like wartime strategists, NARAL’s Executive Committee stealthily devised four primary points of attack against their leading opposition, the Catholic Church.
First: Blame and Accuse the Hierarchy
Cardinals, bishops and clergymen were targeted relentlessly by the NARAL team. Every time a woman was maimed or died from complications of illegal abortion, NARAL never accused the physician of malpractice, but blamed the hierarchy and Church opposition to legal abortion. Every press conference, editorial, or published article linked the name of a clergyman with social ills or women’s woes.
The blame game included an endless indictment of Church leaders for starting a religious war, abusing tax-exempt status and even attempting to overturn the Bill of Rights!
Nathanson explained: “The anti-Catholic tactic was… central to the maintenance of unity within the High Command of the movement. In providing a palpable, visible opposition it allowed those of us setting policy and devising a strategy to occupy ourselves with the enemy. We were kept too busy to contemplate in any critical way the quintessential brutality of permissive abortion. There was always another bishop to denounce, another pastoral letter to be rebutted, another cardinal to excoriate.” (Ibid., p. 197)
Second: Support and Campaign for Catholic Pro-abortion Candidates
NARAL recognized and praised Catholic politicians who publicly expressed a softened stance on abortion. It assisted legislators with election campaigns, grassroots efforts, and financial support, regardless of party affiliation. As long as the candidate embraced legalized abortion, s/he was a candidate for NARAL’s backing. Using the complicit media, NARAL made it appear times were changing, and “pro-choice” politicians were the new majority. NARAL understood the power of perception.
Third: Split and Set Catholics Against Each Other
The Time magazine cover devoted to Pope Paul VI on the publication of his 1968 encyclical Humanae Vitae
NARAL recognized that John and Jacqueline Kennedy were models of the modern, enlightened twentieth-century Catholic, thinking for themselves “without obeisance to church dogma.” NARAL’s strategists recognized two categories of Catholic faithful: the well-educated, fashionable “Kennedy Catholics,” and blue-collar, conservative Catholics, only one generation removed from immigration. NARAL fueled divisiveness within the Catholic Church, pitting liberal against conservative Catholics. As Dr. Nathanson recounted it, everything was in place “for the portrayal of the Catholic Church as a political force, for the use of anti-Catholicism as a political instrument, and for the manipulation of Catholics themselves by splitting them and setting them against each other.” (Ibid., p. 181)
Let it be said: The Church helped us in NARAL. The papal encyclical of 1968 [Humane Vitae] denying both abortion and contraception to Catholics was a bonanza for us at NARAL at precisely the correct moment in history. By linking abortion and contraception in the encyclical, the Vatican made it impossible for those Catholics who were using birth control to split off the abortion issue, therefore leaving them to pick their own way through the confusing ethical and theological landscape.” (Ibid., p. 189)
The leap from practicing contraception to supporting legalized abortion proved an easy one.
Fourth: Execute the Straddle
Perhaps the most common and effective tool in the NARAL strategy toolbox was ‘the Straddle’: a separation of religious conviction from legislative judgment. Nathanson wrote that it was first proposed to the Board by “such notables as Robert Drinan, SJ, and Richard Cardinal Cushing.” (Ibid., p. 177)
“To maintain their appearance as enlightened and progressive while still retaining their bona fides as Catholics, we provided [Kennedy Catholics] with the now classic ‘straddle’ for Catholics in public positions: abortion is personally abhorrent, but everyone must be free to make their own choice. Now we were ready to use them to call over the more traditional, less trendy Catholics to our cause.” (Ibid., p.181)
Of course, substitute “slavery” for “abortion” and few would agree that one person can find slavery personally abhorrent while others are free to choose whether or not to own slaves. Yet, it’s a refrain we’ve heard for decades in politics. Dr. Nathanson prophetically warned that, as long as abortion is legal, there would be increased violence, increased public turmoil and the disintegration of the American family. These bitter fruits are everywhere apparent.
I believe the abortion ethic is fatally and forever flawed by the immorality of the means of its victory. A political victory achieved by such odious tactics is at best an unstable tyranny spawned by an unscrupulous and unprincipled minority. At the very least this disclosure of those odious tactics should compel those who are uneasy with permissive abortion to re-examine the issue. I believe that an America which permits a junta of moral thugs to foist an evil of incalculable dimensions upon it, and continues to permit that evil to flower, creates for itself a deadly legacy: a millennium of shame. (Ibid., p. 209)
This powerful quote of Dr. Nathanson’s is one of my favorites. It reveals how intimately he understood the diabolic industry. Abortion does not simply “happen” as civilizations evolve; it is created with evil intent. Dr. Nathanson wanted every bishop, priest and Catholic layperson to know how they were deliberately exploited, and be motivated to act in defense of their Faith and the sanctity of every human life. It’s time to challenge the anti-Catholic bias which marginalizes the prophetic voice of the Church. Pivotal in this effort is the courage to elect pro-life leaders with the power to reverse the ebbing tide of pro-life legislation. It’s time to abort our “millennium of shame.”
Researchers behind a study published Thursday in the journal Cell found that using the Crispr gene-editing technology in human embryos caused unintended and unwanted chromosomal changes, showing that the ethically problematic research may cause more harm than good.
The study focused on attempts to use Crispr to repair a gene that causes hereditary blindness. Forty human embryos were created for the study, using the sperm of a man who has hereditary blindness caused by a mutation on the EYS gene. Crispr-Cas9 was used to cut the father’s DNA at the site of the gene mutation that scientists wanted to correct. A Crispr-Cas9 enzyme was then injected into 37 of the embryos, with three embryos used as controls. However, the use of Crispr caused the elimination of large sections of chromosomes or entire chromosomes altogether in half of the embryos.
Dieter Egli, assistant professor of developmental cell biology at Columbia University and the study’s senior author, called it “a very adverse outcome,” but also said, “This study is not going to stop the field.”
Crispr allows researchers to cut, edit, and insert DNA, and has been highly controversial since first used in 2012. While scientists see it as a way to treat severe illnesses like cystic fibrosis, cancer, and sickle-cell anemia, the technology is also viewed as highly unethical, with opponents seeing it as a first step in creating “designer” human beings, and with embryonic studies using humans with disabilities as disposable guinea pigs.
According to The Wall Street Journal, in September 2020, an international commission sponsored by the U.S. National Academy of Medicine, U.S. National Academy of Sciences, and the U.K.’s Royal Society issued a report that said Crispr gene-editing technology is not ready to be used because scientists do not have a grasp on how to make the changes they want to make without causing dangerous health concerns. Twin girls, created using Crispr, were born in 2018, but virtually nothing is known about their health. Another baby created using Crispr is also believed to have been born, but again, nearly nothing is known about that baby’s health. The Chinese researcher who led the experiments that created those lives was sentenced to three years in prison for illegal medical practices.
Crispr can be used in experiments using adult cells, as was done in a study using intestinal stem cells from adults with cystic fibrosis. That study found that while cystic fibrosis might not be the “prime candidate for clinical application of adult stem cell gene therapy, this approach may present a safe complement to induced-pluripotent-stem-cell-based approaches, and in the future it could be applied to different single-gene hereditary defects.”
According to The Wall Street Journal, a paper that looked at the ethical issues surrounding the creation of genetically modified children was published in the Crispr Journal, and surveyed the policies regarding such technology in 106 countries. Ninety-six of the countries already had legislation, regulations, or international treaties regarding the gene-editing of embryos, with 75 of them prohibiting the creation of genetically modified embryos with the aim of implanting those embryos for continued development and birth. This was indicative, researchers said, of the possibility of creating an international consensus on the ethics surround gene editing and embryos.
“We’re all on Nexplanon,” says a recent ad for “the birth control that goes in your arm,” featuring actress Vanessa Hudgens.Seconds later, the ad warns that “if at any time you can’t feel the implant, contact your doctor right away… removal of the implant may be very difficult or impossible if the implant is not where it should be.”
Perhaps you remember the old slogan for Nexplanon,which used to be the clever “Armor Up.” Remember the ads, with the stylishly dressed young women in the workplace, flexing their biceps and telling us that they‘ve “armored up” against an unplanned pregnancy? Now, Nexplanon wants to show us that everyone—from moms to gamers to students to actresses (and not just women striving for the corner office)—are “all on Nexplanon.”
It’s true that more and more women are turning to long-acting reversible contraceptives (LARCs)such as Nexplanon. Like the IUD, theNexplanon implant is increasingly favored by patients and healthcare providers for its ease of use and compliance. The idea behind Nexplanon and other LARCs is to function as a “set it and forget it” method of birth control, promising women up to three years of protection against unplanned pregnancy without having to worry about taking a daily pill.
The trouble is, ever since women have been getting birth control implants in their arms, there have been reports that the matchstick-sized devices havethe rare but serious chance of moving from the arm to other places in a woman’s body.In 2016, the FDA updated the Nexplanon label to include warnings about the device’s ability to migrate, noting that a “deep” insertion is more likely to lead to issues with locating or removing the implant.
Nexplanon also shareshormonal birth control’s more common side effects such as headache, depression, weight gain, mood swings, breast pain, acne, nausea, loss of libido, and painful periods (among others)—as well as the less common but far more seriousside effects of blood clots, strokes, and heart attacks.
How does Nexplanon work?
Similar tohormonal IUDs, Nexplanon prevents pregnancy by continuouslyreleasing a steady, low dose of a synthetic form of the hormoneprogesterone, known as a progestin. Nexplanon’s particular progestin is known as etonogestrel, which prevents pregnancy through various functions, including preventing ovulation, thickening cervical mucus, and changing the lining of the uterus (etonogestrel can also be found in combination with ethinylestradiol, a synethetic estrogen, in vaginal rings such as the NuvaRing).
Nexplanon should be removed after three years, but if it is lost and/or cannot be retrieved, it may continueaffecting the body even after the three-year mark.During the COVID-19 pandemic, some women have had difficulty finding providers to remove their expired Nexplanon implants. However, providers are assuring women that the device is probably still pumping out enough synthetic hormone one to two years after its expirationdate to continue preventing pregnancy (although many providers advise condom use after an implant expires). The continued effects of the implant past its expiration may seem like a boon to some, but for those whose device has moved, making it difficult or impossible to retrieve (or if it has become lost, and impossible to retrieve, as has happened in some rare cases) the extended effects can be troubling.
Nexplanon’s risk of moving and informed consent
As it turns out, Nexplanon‘s issues with migrating are nothing new. Nexplanon is actually an updated version of a device called Implanon (which gained FDA approval in 2006), which was also a matchstick-sized hormonal LARC placed in the arm to prevent pregnancy for up to three years. With the FDA’s approval of Nexplanon in 2011, Implanon has gradually been phased out, but for many years was the subject of class action lawsuits from women “who allege they were not properly warned about the risks associated with using Implanon,” and from some for whom the device is irretrievable.
One of the issues with Implanon was not only that it had the potential to migrate to areas outside the arm—including the pulmonary artery, a vital blood vessel found in the lungs—but it was also impossible to find via x-ray. To fix this problem, Nexplanon was developed tocontain barium, which makes it radio-opaque. This means that if Nexplanon does move (as it still has the potential to do, despite the updates made to the original version), it can be located via x-ray. So, in a way, the updates to Nexplanon were developed with a specific awareness in mind of the implant’s potential to get lost inside a woman’s body.
When Nexplanon moves and can’t easily be found
Nexplanon migration is an uncommon occurrence, and an updated applicator is meant to keep healthcare providers from inserting Nexplanon too deeply (again, a deep insertion is believed to make migration more likely). However, migration to other areas of the body is still possible (including within blood vessels, and even blood vessels within the lungs), and it can be extremely serious. In fact, the FDA-approved label for Nexplanon notes that if the device cannot be located, chest x-rays may be required to ensure that the device is not located within the pulmonary artery.
Some women report they were not aware of Nexplanon’s ability to migrate when they had it inserted. One woman shared with the New York Post her ordeal having to undergo mandatory surgery to go “fishing” and “digging” for the implant after her Nexplanon merely moved to a different part of her arm. “I was angry,” says Tenayah Dawson, who was told she needed an MRI to locate her implant because it had moved. “I was like, what do you mean it moved? I was really concerned. It moved? How can it move?” Dawson says it took over an hour of surgery for her doctor to find and remove the device.
A way to prevent pregnancy that doesn’t require being “on” anything
The good news is there are family planning methods that don’t involve inserting foreign objects into your body.Fertility Awareness-Based Methods, more informally called fertility awareness methods (FAM) or natural family planning (NFP) have gained in popularity since the FDA approved the digital health app Natural Cycles as an effective form of birth control.
Fertility awareness methods aremodern, scientifically-based methods of family planning. They are 100% natural (they work with your body’s natural processes of fertility, not against them), have zero side effects, and can be just as effective as the Pill, the implant, and the IUD. As a proud, longtime user of the Sympto-Thermal Method of NFP, I’ll take a thermometer in my mouth any day over a matchstick in my arm—especially one that could end up in my lungs. If you feel the same, it’s time to start learning about your fertility awareness options today. Because, as it turns out, for women to reach the goal of scientifically proven and effective family planning, we don’t have to sacrifice our health—or be “on” anything.
The United States was joined by several countries on Thursday for a virtual ceremony to celebrate the signing of the Geneva Consensus Declaration on Promoting Women’s Health and Strengthening the Family. Co-sponsors of the declaration are the United States, Brazil, Egypt, Hungary, Indonesia, and Uganda. The Declaration currently has 32 signers and remains open, should more countries choose to sign on. Some countries who have already signed in agreement include Belarus, Burkina Faso, Cameroon, Democratic Republic of the Congo, Haiti, Iraq, Kenya, Poland, Sudan, and Saudi Arabia.
The Declaration intends to affirm and strengthen four major goals in international women’s health, including: “better health for women, the preservation of human life, strengthening of family as the foundational unit of society, and protecting every nation’s national sovereignty in global politics.” As part of attaining these pillars, the Declaration holds that “it is the sovereign right of every nation to make their own laws in regard to abortion, absent external pressure,” according to the Department of Health and Human Services. This comes as a significant step given the many external pro-abortion pressures often put upon historically and predominantly pro-life nations.
The Declaration also reaffirms “the inherent ‘dignity and worth of the human person,’ that ‘every human being has the inherent right to life,’ and the commitment ‘to enable women to go safely through pregnancy and childbirth and provide couples with the best chance of having a healthy infant.’” Additionally, the Declaration emphasizes that “in no case should abortion be promoted as a method of family planning” and that “the child… needs special safeguards and care… before as well as after birth.”
At the Declaration’s virtual signing ceremony, U.S. Secretary of State Mike Pompeo stated, “At its very core, the Declaration protects women’s health, defends the unborn, and reiterates the vital importance of the family as the foundation of society. The Declaration restates that there is no international right to an abortion. It goes even further, affirming that every country has its own sovereign right to determine its own laws with respect to abortion….”
The statements of the Declaration reflect the United States’ Protecting Life in Global Health Policy, which guides U.S. dealings with the World Health Organization and the United Nations and abides by the same pillars as the four goals of the Declaration (listed above).
As part of attaining these international improvements for women and children, the nations on the Declaration commit to working together to “ensure the full enjoyment of all human rights and equal opportunity for women.” Significantly, the Declaration also vows to “reaffirm that there is no international right to abortion, nor any international obligation on the part of States to finance or facilitate abortion,” a tenet “ consistent with the long-standing international consensus that each nation has the sovereign right to implement programs and activities consistent with their laws and policies.”
The Department of Health and Human Services states the Declaration “charts a positive way forward for accelerating progress on achieving this end.”
“I thought I knew everything about Karol Wojtyla, St. John Paul II. I did my doctoral work on his theology,” said Msgr. Start Swetland, host of Go Ask Your FatherTM on Relevant Radio®. But even Msgr. Swetland was surprised to learn a new fact about the early life of St. John Paul II and the heroic virtue of his parents.
Karol Wojtyla was born on May 18, 1920, in Poland to Karol and Emilia Wojtyla. It’s commonly-known that Emilia died when her one-day saint son was just a young boy, but did you know that her ailing health prompted doctors to recommend that she put her life ahead of her unborn son’s?
Emilia and her son, Karol Wojtyla (St. John Paul II)
“I knew that her health was delicate, but I did not know that it was so delicate and there were some complications in the pregnancy … that doctors had recommended to her that she terminate the pregnancy,” explained Msgr. Swetland.
This shocking fact was revealed in a book published recently in Poland about the saint’s early life. Several witnesses have testified to the fact that this is true.
“Of course, being a devout Catholic, knowing the right and holy thing to do, she did not and the rest, as we say, is history,” said Msgr. Swetland. “You can see how Satan works—Satan would have loved to kill the future saint in the womb, if he could have gotten away with it and inspire people to do those kind of things.”
It gives you goosebumps, doesn’t it… knowing that 100 years ago, parents were counseled by their doctors to kill such a holy and influential man before he was even born? Thanks be to God, Emilia and Karol Wojtyla Sr. made the good and holy decision to give their son the gift of life, setting aside their own health and fears to bring a future saint into the world.
Their prolife witness is a stunning example of how trust and faith are rewarded by God. The cause for canonization of St. John Paul II’s parents has recently been opened. Servants of God Emilia and Karol Wojtyla, pray for us!
“Laws which authorize and promote abortion and euthanasia are…radically opposed not only to the good of the individual but also to the common good; as such they are completely lacking in authentic juridical validity. Disregard for the right to life, precisely because it leads to the killing of the person whom society exists to serve, is what most directly conflicts with the possibility of achieving the common good. Consequently, a civil law authorizing abortion or euthanasia ceases by that very fact to be a true, morally binding civil law.” ─ Pope St. John Paul II, Evangelium Vitae, no. 72
It is a true but underappreciated fact that animals in the wild almost never die of old age. Long before old age finishes them off, weakened animals succumb to disease, predators, or starvation. I say this fact is underappreciated, because it points to one of the most remarkable things about human beings: i.e. that we look out for one another, including – or rather, especially – the weakest among us. Rather than abandoning our grandmother when she can no longer work, we sacrifice our time and resources to ensure she is cared for and lives and ends her life surrounded by love.
Two Visions of Human Society
Some early modern philosophers claimed that civilization only came to exist because of our fear of one another, and our desire to look out for our own selfish interests. We band together into cooperative tribes, they say, only so as to counteract the threat of violence, and so that we can ultimately get the things we want. Civilization, in other words, is just a bunch of people who have agreed to some version of this promise: “If you don’t take my stuff, I won’t take your stuff.”
This is an incredibly narrow vision of human nature, and a dangerously reductionist understanding of the nature of society. The Christian vision of society is radically different. It is perhaps best expressed in the phrase used so often by Pope St. John Paul II: i.e. “the civilization of life and love.” As the phrase suggests, in a truly healthy society, people are bound together not by fear or self-interest, but rather by bonds of love for one another.
This vision is the natural outflowing of a radically different anthropology. Instead of viewing humans simply as highly developed animals striving like other animals for nothing more than food, sex, pleasure, and social status, the Christian vision understands human beings as made in the image and likeness of God, with the capacity for self-transcendence, and destined for eternal bliss in the contemplation of the Divine Essence. As the United States Conference of Catholic Bishops (USCCB) writes in their document entitled Catholic Social Teaching:
“Catholic social teaching is based on and inseparable from our understanding of human life and human dignity. Every human being is created in the image of God and redeemed by Jesus Christ and therefore is invaluable and worthy of respect as a member of the human family. Every person, from the moment of conception to natural death, has inherent dignity and a right to life consistent with that dignity. Human dignity comes from God, not from any human quality or accomplishment.”
The Catechism of the Catholic Church makes the same point, when it notes that an authentic understanding of the “common good” presupposes “respect for the person as such.” In the name of the common good, public authorities are bound to respect the fundamental and inalienable rights of the human person.”
Within the civilization of love, one person does not protect the rights and welfare of another in a calculating tit-for-tat arrangement in the hope that the other person will do the same for him. Instead, a person looks out for another because it’s the right thing to do: because the other person, by virtue of being a person, merits and even demands our protection and love.
In Evangelium Vitae, Pope St. John Paul II pointed to “those daily gestures of openness, sacrifice and unselfish care which countless people lovingly make in families, hospitals, orphanages, homes for the elderly and other centers or communities which defend life.” For two thousand years the Church has spearheaded countless such charitable efforts, building up the common good in imitation of our Divine Master, who commanded His disciples, “Love one another. As I have loved you, so you also must love one another.”
Human beings are capable of self-transcendence, of looking out for the other with no other ulterior motive than to value the other person for the person they are, and to treat them with the dignity they deserve. It is this incredible capacity that the cynical modern philosophers completely overlooked. And yet, without this capacity, human society is not just built on a foundation of sand, but of quicksand. Any society that is founded purely on principles of self-interest will, at the first sign of instability, tear itself apart. Inevitably, it is the weakest members who will suffer most.
The Culture of Death
The vision of “society” described by some cynical modern philosophers looks a great deal like that formed by Satan and his minions, as depicted by John Milton in Paradise Lost. Though consumed by envy and loathing for one another, the demons are united by their common hatred of God and a desire to pervert the human race. Satan is the overlord of a true society in which the members cooperate to achieve a common aim; but what sort of a society, with what sort of a culture!
A culture of sin. A culture of death.
In our world the civilization of love has never existed in its pure form – not, at least, since that short-lived civilization of two in the Garden of Eden. Instead, the civilization of love and the culture of death are intermingled. In various times and in various places, one or another civilization is ascendant, while the other is ailing.
My fear, however, is that not only is the culture of death now dominant, but that in many cases we have even lost sight of the fact that any other form of culture is desirable, or even possible. Indeed, I fear that what we are experiencing now is a diabolic inversion, in which the anti-civilization embodied by Satan and his minions, in which the only bond uniting us together is selfishness and shared hatreds, is viewed as the ideal.
Less than Beasts
A few weeks ago, I quoted St. Augustine in On the Trinity, where he notes the paradox that in striving to become like God, human beings inevitably debase themselves, coming instead to resemble the beasts. In reality, however, the case is worse than this. In striving to become like God, humans often sink beneath the level of the beasts, becoming, as it were, more bestial than beasts.
A mother cat knows enough to treasure and care for her kittens. In our worship of radical “autonomy” and a diseased notion of “freedom” (that is, in our efforts to become like God), however, we now celebrate the “right” of mothers and fathers to choose to have their own children murdered. And while an adult cat may not do much to protect its mother or grandmother in their old age, we are now championing the “right” of our grandmother to kill herself or to have our grandmother killed. The thing that most distinguishes human society from that of the animals – our valuing of other humans not for anything they can do, but for what they are – is vanishing.
At root, this total inversion of values stems from our loss of the sense of the dignity of the human person, which in turn stems from our loss of the sense of God, in whose image the human person is made. To quote Pope St. John Paul II in Evangelium Vitae again: “when the sense of God is lost, there is also a tendency to lose the sense of man, of his dignity and his life; in turn, the systematic violation of the moral law, especially in the serious matter of respect for human life and its dignity, produces a kind of progressive darkening of the capacity to discern God’s living and saving presence.”
Building a Civilization of Love
Contrary to the claims of cynical pragmatists, the most useful thing in the world is an unattainable ideal. Even though this ideal be unattainable, the person with such an ideal at least knows in what direction he should be moving. The modern “pragmatic” conception of society, which views it merely as a means to protect “freedom,” without any notion of what freedom is for, at best leaves people lost and confused, and at worst sends them marching in precisely the wrong direction.
As Christians we need to constantly remind ourselves of the ideal – Pope St. John Paul II’s “civilization of love” – and to resist the allure of the deceptions of the evil one. Even in conservative circles one often encounters the idea that the only reason society exists is to protect our “freedom” – understood in the narrow sense of the ability to do whatever we want. In reality, society exists to protect and promote the common good, understood in the rich sense of human flourishing. The common good, says the Catechism, is “the sum total of social conditions which allow people, either as groups or as individuals, to reach their fulfillment more fully and more easily.”
Human beings, however, only achieve their true fulfillment in relationships of love, firstly with one another, and ultimately with God. This Christian understanding of the “common good” as the creation of a civilization of love is an unattainable ideal. Such a civilization will never exist in a perfect form this side of Heaven. Nevertheless, to the extent that we transform this world into a foretaste of Heaven, it will only be because we have pursued such an ideal.
With such a beautiful ideal in mind, we in the pro-life and pro-family movement will gain new strength to labor against the great threats to that ideal in our own culture of death: abortion, euthanasia, embryonic stem cell research, and other such attacks on human life and dignity. Let us pray, then, with Pope St. John Paul II, as he prayed in Evangelium Vitae, “May God strengthen us in our effort to bring about a culture of life and solidarity for the true good of the whole of human society.”
In May 2019, Sen. Amy Klobuchar criticized the Trump administration for attempting to cut Planned Parenthood’s federal funding. Klobuchar stated: “In their lifetime, one in five women go [to Planned Parenthood]. . . . And most of them are going there for contraception, birth control [and] . . . for mammograms.”
Her comments about mammograms caused confusion. Why? Because Planned Parenthood does not provide them.
“Mammograms” are an emotional tinderbox.
Breast cancer: Two words that rightly terrify women. It doesn’t matter what race, age, or color. According to MD Anderson, one of the nation’s leading cancer hospitals, breast cancer takes the lives of about 40,000 women per year. In addition, there are about 265,000 new diagnoses each year. Fortunately, the five-year survival rate is almost 90%. The earlier the cancer is caught, the better a woman’s chances.
So it’s natural that women are scared. It’s natural that they want to be screened and tested. It’s natural that they don’t want to lose a part of themselves. And it’s natural that they don’t want to die. Couple these fears with a lack of money, and you have a recipe for anxiety. Many women struggle financially. They often wonder how they’ll pay for a doctor, and they fear needing extra tests.
So where do low-income women turn when they need testing?
If you ask the average person, you may find that he/she recommends Planned Parenthood. After all, politicians have falsely claimed for years that the organization offers mammograms.
Who repeats the mammogram myth?
The reality is that Planned Parenthood gives only referrals for mammograms. Still the myth persists that it does them.
The way people phrase their speech often hides its real meaning. The media is particularly skillful at doing this. We see this specifically when it comes to Planned Parenthood’s funding.
The media wants people to believe that poor women cannot live without the services of Planned Parenthood. Yet, there are over 13,000 federally funded health clinics across the country. Planned Parenthood has just 587. Women do have choices. They can function without the nation’s number one abortion provider.
Let’s examine some of the instances in which noted personalities mentioned mammograms and Planned Parenthood in an attempt to mislead.
Cecile Richards, Planned Parenthood President
In 2011, Cecile Richards was president of Planned Parenthood. She sat for an interview with TV personality Joy Behar and discussed current issues. During the interview, they talked about a proposal in Congress that would take federal monies from Planned Parenthood. Richards said: “If this bill ever becomes law, millions of women in this country are going to lose their health care access—not to abortion services, but basic family planning. You know, mammograms, cancer screenings, cervical cancer.”
She didn’t specifically say that Planned Parenthood offers mammograms. However, those listening—including the media—jumped on the notion that women might lose access to necessary healthcare. And since Richards mentioned mammograms, the media and others ran with it. They began to say that women wouldn’t get the mammograms that they need. Thus, they either ignored or wrongly interpreted the meaning of the word “access.”
Barack Obama
Politicians and media personalities seem to enjoy creating fear in low-income women. They claim that women will lose access to healthcare if the government does not fund Planned Parenthood.
For example, during the 2012 presidential campaign, President Obama talked about Governor Romney’s desire to take funding from Planned Parenthood. He stated: “There are millions of women all across the country who rely on Planned Parenthood for not just contraceptive care. They rely on it for mammograms, for cervical cancer screenings.”
Several weeks later, Obama made that same claim again. He told a New Hampshire crowd: “Governor Romney said he’d end funding for Planned Parenthood, despite all the work it does to provide women with mammograms and breast cancer screenings.”
People want to trust the president. When he says something, people believe him. Many don’t even question his words.
And everyone else…
Fast-forward to September 2015. Representative Carolyn Maloney, a Democrat from New York, spoke to a government reform committee. Regarding Planned Parenthood funding, she said: “All of the [people signing the letter to support defunding Planned Parenthood] are men. None of whom will get pregnant, or need a cervical screening for cancer, or a mammogram, or a pap smear, or other life-saving services that are provided by Planned Parenthood.”
The Washington Post later addressed the inaccuracies that high-profile supporters repeat about mammograms. One example was comedian Margaret Cho “who tweeted about this repeatedly during the hearing.” Another was Whoopi Goldberg “who referred to it on The View the day after the hearing.” The Post also mentioned that Miss Tennessee made a statement about it during the Miss America contest. She stated that Planned Parenthood’s federal funding “goes for mammograms.”
That same year, Martin O’Malley, the former governor of Maryland, was asked if he had seen any Center for Medical Progress videos. These videos showed Planned Parenthood staff members talking about selling baby body parts. O’Malley stated that he hadn’t. He then followed that up with: “I do know that 97 percent of the work that Planned Parenthood does is about mammograms and preventative health.”
Unravelling the deception
O’Malley was wrong on two counts. He was wrong about the mammograms. And he was wrong about 97% of PP’s services going to healthcare. Planned Parenthood likes people to believe the myth that abortion is only 3% of its services. But it calculates this 3% number to purposely mislead. Planned Parenthood counts each service it provides as a “unique interaction.”
Instead of recording multiple services for one person, Planned Parenthood records each service included in the abortion process individually. It then divides the number of abortions by the total number of services it provides. This number comes out to a little over 3%.
It’s easy to see how that number is skewed. And it’s easy to see how the untruths about mammograms get continually passed along. When people hear a lie over and over, they begin to believe it.
What type of cancer screenings does Planned Parenthood offer?
In its 2018-2019 annual report, Planned Parenthood listed the services it currently provides. This list included 566,186 cancer screening and prevention services. Under this umbrella are things like pap tests and HPV vaccinations. Also included in that number are 265,028 services for “breast care.” This refers to the same kind of breast exam that a woman can do on her own at home. The doctor will feel for lumps. He also checks for any other problems. If he finds something of concern, he will provide a referral for a mammogram at an outside facility.
Some Planned Parenthood facilities have allowed a mobile unit to park outside. This mobile unit offers free mammograms to PP’s clients. A few affiliates, such as Planned Parenthood of Western Pennsylvania, have created a healthcare fund. This fund helps needy patients obtain services they cannot afford. In addition, the Center for Disease Control and Prevention runs the National Breast and Cervical Cancer Early Detection Program—a program for low-income women to get access to services. Some PP facilities will help women apply for this program.
Why does the myth persist?
We know that Planned Parenthood does not provide mammograms. A simple google search proves this. Yet politicians and TV personalities often state otherwise. Why?
We live in a culture where people have not learned to think for themselves. Nor do they search for facts. They are willing to believe whatever suits their belief system. They do so even if that belief system is based more on emotion than on facts. Oftentimes people put more stock in what they see on social media or on memes than in the truth.
The myth that Planned Parenthood provides mammograms exposes a larger and more widespread problem in our society. People believe everything they see or hear. They then pass this misinformation along to others. They don’t take time to check whether something is true or not.
Many politicians back Planned Parenthood. The media backs Planned Parenthood. Knowing this, we must all be cautious. We must fact-check what we read and what we see on social media. We must do our best to pass along only what is true.
The media does have an agenda. If we are not careful, we will fall prey to it, and then we will never see the truth. Now more than ever, we need the truth. Does Planned Parenthood do mammograms? Absolutely not.
Supreme Court nominee Amy Coney Barrett, currently in confirmation hearings before the Senate, has faced scrutiny for her pro-life stance. A Catholic mother of seven, a law professor at the University of Notre Dame, and a judge on the Seventh Circuit Court of Appeals, Barrett has never hidden her knowledge and understanding that life begins at fertilization (often referred to as “conception”).
In 2006, as a private citizen, Barrett publicly supported St. Joseph County Right to Life, also known as Right to Life Michiana, which has been called “extreme” for taking the scientific position that life begins at fertilization. The organization ran a full-page newspaper ad in the South Bend Tribune noting the need to “defend the right to life from fertilization to natural death,” and Barrett and her husband Jesse signed their names to it. That advertisement also referred to abortion as “barbaric.”
During her January 18, 2013, presentation titled “Roe at 40: The Supreme Court, Abortion and the Culture War that Followed,” Barrett spoke “to her own conviction that life begins at conception,” reported Notre Dame Magazine. Abortion advocates are attacking her for this, but science shows that Barrett’s convictions align with scientific fact.
In Human Life and Health Care Ethics, Vol. 2, James Bopp discussed this first moment of a new life:
The first cell of a new and unique human life begins existence at the moment of conception (fertilization) when one living sperm from the father joins with one living ovum from the mother. It is in this manner that human life passes from one generation to another.
In The Developing Human: Clinically Oriented Embryology, professors Keith Moore, TVN Persaud, and Mark Torchia also note that life begins at the moment of fertilization, writing, “Human development begins at fertilization when a sperm fuses with an oocyte to form a single cell, the zygote.”
Along with National Geographic, The Endowment for Human Development, a scientific non-profit group, released a documentary about the development of human beings inside the womb. Of fertilization, EHD stated:
The two cells gradually and gracefully become one. This is the moment of conception, when an individual’s unique set of DNA is created, a human signature that never existed before and will never be repeated.
Medical experts and medical textbooks concur that a new human life exists at that first moment of fertilization “in a bright flash of light as a sperm meets an egg….” That moment has been captured on film in “[a]n explosion of tiny sparks” that “erupts from the egg at the exact moment of conception.”
Thanks to ultrasound technology and other advances in science, gone are the days when people believed life began at the “quickening” or the first moment a woman felt her preborn child kick. Now, life inside the womb is better understood than ever before in history, including the fact that the human heart begins to beat between 16 and 22 days post-fertilization. Barrett’s so-called “extreme belief” that life begins at fertilization isn’t merely a belief — it is knowledge built from scientific data.
Abortion advocates call abortion “reproductive freedom” but instead of finding freedom, women who experience abortion can find themselves weighed down by mental health disorders, including depression. Research consistently points to the negative effects of abortion on women’s mental health — and personal stories from women corroborate these studies.
The Scientific Proof
A study published in July of 2016 — using data was collected from 8,005 women in the United States who were followed over a period of 13 years — associated abortion with an increased risk of mental health disorders and substance abuse in late adolescence and early adulthood. Dr. Donald Sullins analyzed the data and found that “abortion was consistently associated with increased risk of mental health disorders. Overall risk was elevated 45%.” This research confirmed 2005 study findings from Norway which showed that compared to women who have suffered miscarriages, women who have had abortions have “significantly higher” Hospital Anxiety and Depression Scale anxiety scores even five years later. In addition, a 2008 New Zealand survey of over 500 women found that women who had an abortion had a 30% increased risk of developing mental health disorders such as anxiety and depression.
A 2019 study on abortion and mental health examined at women who aborted “wanted” babies compared to women who aborted “unwanted” babies. The results of the study showed that both groups of women suffered increased risks to their mental health after abortion. Women who aborted “wanted” babies suffered from mental disorders 1.43 times more often than women who aborted “unwanted” babies. But women who said their pregnancies were “unwanted” had a 94% higher risk of subsequent suicidal thoughts than women who did not abort. They were also 270% more likely to abuse alcohol.
The Personal Stories
Women who have suffered the effects of abortion trauma often suffer in silence, shamed by the abortion industry into believing abortion is a “right” they should applaud. However, there are women who have come forward with their heartbreaking stories showing that abortion did not empower them.
On the Netflix dating show “Love is Blind,” contestant Amber Pike revealed the trauma she suffered from abortion. “After the fact, [my boyfriend and I] were just talking. I’m telling him, like, I’m trying to explain what I’m going through, like, I”m having a really hard time getting out of bed in the morning. I don’t eat. I’m not really sleeping. […] I can’t survive that again. It would destroy me.”
In a post-show interview with ET, Pike discussed her financial debt. “I had not been paying on my student loans, as previously mentioned. After my abortion, I had fallen into depression and dropped out of school. My mental health was more of a priority for me and I was slowly building my life together when I got the opportunity to be on this show.”
Still, Pike received criticism for speaking about abortion in a negative light.
TLC band member Chilli revealed in 2010 that her past abortion still weighs on her. “It messed me up,” she said during an interview. “I don’t know; It just, it broke my spirit. […] I feel like I became kind of like not my strong self anymore. […] And I would break down and I would just cry because I wasn’t a mommy. I cried almost every day for almost nine years and then I was caught up, I had to have a baby.”
Allison Duhon shared her abortion experience, saying it was both physically and emotionally painful. “I remember going numb for months after my abortion,” she wrote. “I remember the trust issues I had with everyone. I remember feeling extremely overprotective of my daughter because I thought I didn’t deserve a healthy child. I remember the pain when I found out my son had autism and thoughts of it being a punishment.” She said she felt “unforgivable.”
“I still cry for my baby,” she explained. “[…] I have to live forever with the excruciating reality that I ended my baby’s life. All my ‘right’ did was cause me a lifetime of pain. There was no empowerment in that.”
Another woman shared her experience with abortion after becoming pregnant from rape. On the website AbortionChangesYou.com, she wrote, “There are no words that can explain this depressing, and anxiety feeling I feel. Deep inside it kills me everyday knowing what I did was very stupid. I don’t think I could ever forgive myself. Not only does it haunt me but it’s very traumatizing knowing I did it. Having this happen not only did it affect my feelings, but it affected my life in so many ways…. I do regret what I did. If I could only go back to the day I would have never done it.”
In a horrific story out of Belgium, Julie Lambotte aborted her daughter because of a Down syndrome diagnosis and afterward suffered such grief that she killed two of her three born children. She drowned her 22-month-old daughter and stabbed her nine-year-old and seven-year-old children. The nine-year-old survived. Lambotte told authorities she did it because she “missed her little girl.”
The denial of the abortion industry
Abortion advocates deny that abortion trauma exists, but the abortion industry has a lot to lose financially if women choose life. Rosemary Candelario, who served as director of the Massachusetts Religious Coalition for Reproductive Choice, explained the abortion industry’s reasoning behind denying that abortion trauma is real. “I think the fear in the [abortion rights] movement is if we admit abortion is hard for some women, then we’re admitting that it’s wrong [….]” She then denied, of course, that abortion is wrong.
Abortion is a traumatic experience for many women, and also for many men, who have said that abortion “left deep scars” and that they felt “an extra weight pulling [them] down.” Another man admitted that after his girlfriend’s abortion, “I didn’t know how I was going to survive; I wasn’t going to jump off a bridge, but I probably would have drank myself to death. I’ve thought about what happened every day for the last 32 years.”
October 8, 2020 (LifeSiteNews) — The Susan B. Anthony List knows a thing or two about censorship. Three years ago, Twitter banned of their ads for including a quote from Mother Teresa, the world-famous nun who is now considered a saint in the Catholic Church.
Prudence Robertson works in the communication department for the Susan B. Anthony List, which is based in Washington, D.C. and works to elect pro-life politicians. She recently sat down with LifeSiteNews as part of our ongoing series Uncensored: Big Tech vs. Free Speech to explain how social media giants have unfairly targeted them for their pro-life messaging in recent years..
“It’s very frustrating that the majority of Big Tech groups continue to ignore us and continue to censor us. It’s been difficult to to fight this censorship,” Robertson explains. “It’s frustrating to see that they don’t value our pro-life speech and that they’re not willing to just give us a platform for conversation.”
Robertson pointed to several particular instances of censorship to support her claim that “Big Tech is becoming complicit with Big Abortion.”
“In 2018, when the election was coming around,” she began, “Facebook banned our ads, stopped them so that we could not reach pro-life voters and key persuadable voters, just weeks and days before the election…that’s critical for us to be able to reach those important voters.”
“And platforms like Twitter and TikTok and Pinterest have completely banned our friends at Live Action for their powerful, inspiring videos that expose the truth about abortion.”
Robertson said that despite the clear bias of Big Tech, she and her colleagues at the Susan B. Antony List are determined to fight back, and that they are using other platforms like Parler to get their message out.
“It hasn’t stopped us from standing up for the truth…we are as motivated as ever to reach voters and explain to them the extremism of the Democrat Party.”
“This election is a matter of life or death and President Trump will continue to fight for us in the White House as long as each and every pro-life voter gets out and votes.”
“I think the number one thing is to vote for President Trump, because in November it’s the Party of Death versus the Party of Life. President Trump will fight for life and Biden and Harris is the most radical pro-abortion ticket. It is crucial that each and every pro-life voter go out and vote.”
To watch more of LifeSite’s Uncensored: Big Tech vs. Free Speech series, click here for more info.
In 1937, Pope Pius XI wrote that the Rosary is “a powerful weapon to put the demons to flight, to preserve the integrity of life, to acquire virtue more easily, and . . . to attain real peace among men.”
October is not only the month of the Rosary, but it’s Respect Life Month as well. So it’s only fitting that we combine the two and begin the habit of saying a pro-life Rosary, not just in October, but throughout the year, for this powerful weapon is vital in rebuilding a Culture of Life
Our Spiritual Weapon
Tradition teaches that Our Lady gave the Rosary to St. Dominic, though this is possibly legend. We do, however, know that St. Dominic greatly advocated the use of the Rosary. Not only does Church history witness to the spiritual power of the Rosary, so does history, as well.
We see an example of this at the Battle of Lepanto. During the 1400 and 1500s, the Muslims and Christians were locked in battle, as Christians attempted to block increasing expansion of the Ottoman Empire. The decisive turning point came in 1571, when Pope Pius V sent a fleet comprised of Catholic European states to fight off the Muslims and protect the Mediterranean. He requested all the faithful say the Rosary, asking all to invoke our Blessed Mother’s intercession.
Despite being grossly outnumbered, the Holy League, as it was termed, won decisively. Pope Pius declared the Feast of Our Lady of Victory in honor of the Holy Virgin, which was later inserted in the universal Church calendar marking the date of the battle, October 7th. Today it is known as the Feast of the Holy Rosary. According to reports, the Muslims who later wrote of the battle recorded “seeing in the sky a lady dressed in armor holding a child.” While accounts vary, it is widely maintained that in battle the Ottoman side possibly lost as many as four times the number of ships as its enemies and Christendom was preserved from the would-be Muslim conquerors.
There are numerous testimonies to triumphs credited to the Rosary over the centuries, but here’s one other example. In 1628 King Louis XIII, the Catholic king of France, was attempting to put down rebellions by Protestant Huguenots. Fearing the possibility that his kingdom would be torn apart, he ordered “public rosaries and processions [to be] held nightly in Catholic churches all over France during the eight-month duration of the siege. Dominican friars accompanied the king to the battlefield and preached to the armies of the French the necessity of praying the Rosary daily for victory. The priests distributed more than 15,000 rosaries among the troops, with the soldiers praying together at set times during the day.” On October 28, the Huguenots surrendered, and the French were victorious.
Our Blessed Mother has often implored us to say the Rosary daily, and we know that she can and will hear our prayers if we persist. Starting now, in Respect Life Month, let us say a pro-life Rosary of the Joyful Mysteries and reflect upon the fact that every human being is sacred and valuable. With each decade, let us also pray that Mary will soften those hearts hardened by the Culture of Death.
Artist: Jean Bourdichon (1457?-1521?). Credit: Collection of New York Public Library.
When the Angel Gabriel appeared to Mary, he greeted her saying “The Lord is with you.” He told her that she had found favor with God, that she should not feel afraid, and that she would soon have a son.
As we reflect upon Gabriel’s words and how Mary must have felt, let us remember that there are many women suffering from anxiety and fear because of a surprise pregnancy. Maybe they’re scared because they don’t have enough money. Or perhaps they’re afraid because they’re young or unmarried. Maybe they’re in an abusive relationship. Maybe they’re vulnerable because they have no family to help them. Let us pray for Mary’s intercession so that these women know that God is with them, telling them in the words of Pope Saint John Paul II, be not afraid to open the doors to trust Christ! He will help provide all that they need. And let us pray that, even if these women think that no one else is with them, they will somehow know that they can always turn to God.
2. The Visitation
Mary, pregnant with Christ, went to visit her cousin Elizabeth, who was also expecting: “When Elizabeth heard Mary’s greeting, the infant leaped in her womb, and Elizabeth, filled with the Holy Spirit, cried out in a loud voice and said, ‘Most blessed are you among women, and blessed is the fruit of your womb.’” Even John the Baptist, still a baby in the womb himself, understood that he was in the presence of Christ. This realization made him jump with joy.
As we reflect upon the fact that John, as a preborn baby, was able to sense and feel, let us pray that those with hardened hearts toward the humanity of the preborn come to understand that babies in the womb are indeed human beings. They can feel both pain and joy and deserve to leap with joy outside the womb as well.
3. The Nativity
In Luke 2:12, we read, “You will find an infant wrapped in swaddling clothes and lying in a manger.” As we think about this holy night—this beautiful gift of love—let us reflect upon the fact that Christ came to us as a baby. He could have come in any way he wanted—as a fully grown man or as the son of a rich king. But he did not. He came as a tiny, helpless infant to a young mother who trusted in God, for Mary had said “Yes!” to life, and her “fiat” (Latin for “let it be done”) made our redemption possible. She named Him Emmanuel – meaning “God is with us.” We must remember that, if God humbled himself to come to a poor family and to be born among the animals, there is room for all of us. Money and status mean nothing compared to life.
Let us pray for all those women who feel that they are too poor, too young, too uneducated, or too unskilled to care for a baby. Let us pray that they feel the strength of God and that, like Mary, they will trust in Him to guide them and that they will find joy in the birth of their babies. Let us also invoke St. Joseph, as patron of the family, to help care for these women as he cared for Jesus and Mary with all his might.
4. The Presentation in the Temple
Luke 2:22 says, “According to the law of Moses, they took him up to Jerusalem to present him to the Lord.” As was tradition, Mary and Joseph took Jesus to the temple to present Him to God. While there, Simeon approached the Holy Family. God had promised him that he would live to see the Christ child. After seeing the baby, Simeon said: “My eyes have seen your salvation, which you prepared in sight of all the peoples, a light for revelation to the Gentiles, and glory for your people Israel.”
Let us pray that those who do not see the humanity of the baby in the womb also experience a light of revelation and come to understand that a baby is not just “a blob of tissue” or a “choice.” Let us pray that the callouses are removed from their eyes and that they work to protect even the smallest among us.
Artist: Stefan Lochner
5. The Finding of Jesus in the Temple
Joseph thought Jesus was with Mary. Mary thought that Jesus was with Joseph. When they realized He was not with the group as they traveled, they frantically searched for him. According to Luke 2:48, “When his parents saw him, they were astonished, and his mother said to him, ‘Son, why have you done this to us? Your father and I have been looking for you with great anxiety.’”
Jesus was lost, and both Mary and Joseph must have been beside themselves. If you have ever momentarily lost sight of a child—or if you have lost a child—you know that fear and despair. Let us pray for all those mothers and fathers who have lost a child—whether through miscarriage, through abortion, through an accident, or through spiritual loss—so that they find healing, understanding, and peace in Christ.
Final Thoughts
At Fatima, the Blessed Mother told the children, “Pray the Rosary every day, in order to obtain peace for the world, and the end of the war.”
We face a war every day. We are at war with the Culture of Death—a culture that devalues even the smallest among us. If we truly want to make the demons take flight and preserve the integrity of life, we will use the most powerful weapon given to us, not just by saying a pro-life Rosary in October, but throughout the year.
When Mary and Joseph found Christ teaching in the temple, Christ said to them: “I must be about my Father’s business.” Let us imitate His example and attempt to build a kingdom of our loving God on earth.
Some women who have struggled with getting pregnant wonder if their past use of birth control might have caused their infertility. While there are assurances all over the internet that the birth control pill does not cause infertility, the answer is a bit more nuanced than that.
Let’s say you are 33 years old and got married a year ago. In the past ten years, you have been using a variety of hormonal birth control methods. Now you and your partner are looking forward to starting a family. You get off the pill, hopeful and a bit anxious as you know time is working against you—“biological clock,” and all. You try for eight months to get pregnant, but nothing happens.
You start getting concerned, and worry that your long-term use of birth control might have something to do with your fertility struggles. So you talk your doctor into putting you on Clomid, a drug known to stimulate ovulation, in the hopes that it might “jumpstart” your cycles once more. Unfortunately, this drug could actually lower your chances of conceiving, unbeknownst to you (more on this later). A few more unsuccessful months pass, before you get your first appointment at a fertility clinic. There you discuss your options: namely, Intrauterine Insemination (IUI) and In-Vitro Fertilization (IVF). You brace yourself for several months of treatment and thousands of dollars in medical bills, being assured all the while that this is likely your best hope for achieving pregnancy.
But could all the anxiety, doctor visits, and interventions be completely unnecessary?
When your cycles have returned after birth control, but you still can’t seem to get pregnant
Most women see their cycles return fairly quickly (i.e., the return of ovulation and menstruation) once a contraceptive device like the IUD, ring, patch, or implant is removed. And while most women see a return of their cycles fairly quickly after discontinuing birth control pill use, in some cases, it can take up to a year for your fertility to return as you begin to cycle regularly once again. A woman who has used the birth control shot Depo-Provera may not see a return to fertility for up to 18 months or longer.
Although birth control pills or devices may not cause long-term cycle-suppression after discontinuation, they can still delay your return to fertility, i.e., your ability to get pregnant. One theory for the delay in fertility post-birth control is the pill’s impact on the production of cervical fluid, an essential component of conception. Another theory is the possible association with long term (i.e., 5+ years or more of) contraceptive use and a significantly thinner endometrial lining. Because a thickened endometrial lining is essential for proper embryo implantation, a thinner lining can make it difficult to achieve pregnancy, even if ovulation and conception can still occur. No matter the cause, the delay in a return to fertility after being on birth control can be critical as women tend to start their families much later in life now than in earlier decades.
The importance of cervical mucus in fertility
We are all taught in high school biology or sex-ed that it takes a sperm and an egg to make pregnancy happen. What is often left out of this equation is the cervical fluid, also known as cervical mucus.
In order for sperm to survive more than a few hours in the vagina, and then have the energy reserves to travel through the uterus all the way to the fallopian tubes and wait for the egg to arrive, it needs good quality, fertile cervical mucus. Cervical mucus also does the important job of filtering out “bad” sperm, i.e., sperm with poor morphology or motility, to maximize your chances of having a healthy pregnancy and baby.
Cervical mucus is secreted by pockets in the cervix known as “crypts.” The mucus changes in consistency and appearance as ovulation approaches, in order to better nourish sperm and help it to reach the egg. Before and after ovulation, cervical mucus is much thicker, and blocks access to the uterus (a mechanism that also protects the womb from infection). At the time of ovulation, the cervical mucus becomes thinner and stretchier, almost like raw egg whites, allowing the “good” sperm to swim easily through the vagina and the cervix, into the uterus and fallopian tubes. Once there, the sperm await an egg for fertilization, and can actually survive for up to 5 days in the female reproductive tract in the presence of fertile-type mucus.
Without sufficient, good quality mucus, there can be no baby.
How birth control works to prevent pregnancy
Hormonal contraceptives, as generally documented in scientific literature, don’t work to prevent pregnancy just by suppressing ovulation (although this is generally the primary mechanism of action for the most popular forms of birth control, such as combination pills). Another mechanism by which contraception prevents pregnancy is its effect on the production of cervical mucus. Hormonal birth control actually continuously thickens cervical mucus, which provides an additional barrier against pregnancy in case ovulation still takes place (which can happen, although exactly how often is unknown).
If a woman is not taking hormonal birth control, the cervix follows the marching orders of your body’s naturally occurring hormones. But when a woman is on hormonal birth control , the synthetic hormones in the pill (or patch, ring, implant, or IUD) override the natural ones, and run the cervix in a way so that it constantly produces this non-fertile mucus. But how do the synthetic hormones in birth control accomplish this feat?
What does birth control do to your cervix—and your cervical mucus?
One theory of how of birth control effects cervical mucus comes from the research of a man named Erik Odeblad. Dr. Odeblad was a Swedish professor and researcher born in 1922, who spent most of his life studying and explaining the secretion of cervical mucus: specifically, the various types of mucus produced at different stages in a woman’s cycle and in her life, and their role and composition.
Dr. Odeblad was one of the first scientists to use MRI technology for a medical purpose, and through his research, Dr. Odeblad discovered that there are at least three different types of cervical mucus. Dr. Odeblad called the different types of cervical mucus G, L, and S, and found that each has a different role, and is secreted by a different kind of cervical crypt at different times in a woman’s cycle and during different times in her life.
Dr. Odeblad found that right after puberty, a young woman has an abundance of S crypts, and as she ages, the number of S crypts decreases; the S crypts are then replaced by L crypts. Dr. Odeblad discovered that S mucus (which is secreted by S crypts) in particular is the type of mucus that is essential to fertilization: it provides passage, transport, and nourishment of sperm.
Dr. Odeblad appeared to find that hormonal birth control actually diminishes the amount of S crypts a woman has. From his findings, Dr. Odeblad concluded that “for each year the Pill is taken, the cervix ages by an extra year.” He posited that long-term use of hormonal contraception may impair a woman’s chances of conceiving, because of the degradation of S crypts in her cervix.
Although Dr. Odeblad’s data has not been evaluated with a peer-reviewed study, his findings are not without precedent, as there is other evidence suggesting that hormonal birth control can have some effect on the tissues of the cervix. Further, long term use of oral contraceptives is also associated with increased cervical cancer risk, as well as accelerated maturation and increased cell proliferation of cervical epithelial tissue.
Why a delayed return to fertility after birth control matters
For a variety of reasons, women are waiting longer than ever to start their families than in the past. Case in point: in 1970, the average age at first child birth was 22. Today, it has risen to 26.4 years old. In addition, more women are delaying their first pregnancy past age 30. The percentage of first birth to women over 30 went from just one in ten in 1970, to almost one in three in 2014. This late start to childbearing is significant, because on average, a woman’s ability to get pregnant takes a sharp decline after age 35, and is practically nil by the time she reaches her mid-forties.
If a woman waits until her fertility is already in a natural state of age-related decline to try to get pregnant—and especially if she has been on birth control for several years prior, possibly depleting her S crypts and chronically thinning her endometrial lining—she may face even more obstacles to conceiving. If a woman’s issues with fertility lie in a problem with proper cervical mucus production, and she is placed on Clomid, it could further thwart her chances of conception: a known side effect of this drug is to reduce the production of cervical fluid.
Further complicating matters, many women begin hormonal contraception as a means to “regulate” irregular or painful periods. Often, an irregular period is a sign of an underlying health condition such as endometriosis, polycystic ovary syndrome (PCOS), or some other hormonal imbalance—all of which are associated with infertility. If a woman began taking birth control to reduce symptoms for one of these conditions, she is likely to still be faced with painful and irregular periods once she discontinues birth control—and may also have trouble conceiving as a result of them not being treated.
How truly restorative reproductive medicine is the solution for infertility—even before you experience it
That is why it is so important that teenagers and young women have access to information about what’s known in the medical community as Fertility Awareness-Based Methods, more informally called fertility awareness methods (FAM) or natural family planning (NFP). Doctors who are trained in restorative reproductive medicine such as Natural Procreative Technology (NaProTechnology), can address the root causes of painful or irregular periods. With the treatment provided by fertility awareness doctors, a woman can get true relief from her symptoms, while healing her fertility for whenever she is ready for pregnancy. When a woman is faced with infertility, a thorough evaluation of both her ovulations and of her mucus production is needed, which is something restorative reproductive medicine and NaPro can provide.
We find here yet another great reason why young women who are hoping to get pregnant one day should avoid hormonal birth control all together and opt for evidence-based methods of natural birth control, by learning to chart their cycles with a fertility awareness method. Not only will these methods preserve their fertility, but when the couple is ready to achieve a pregnancy, the knowledge gained through training in a FAM will help them reach that goal more quickly and easily.
To find a restorative reproductive health practitioner who can meet via telehealth, check out this resource.
When this article refers to fertility awareness methods (FAM), or natural family planning (NFP), we are referring to Fertility Awareness-Based Methods, evidence-based methods of cycle charting which can be used as effective forms of natural birth control when learned by a certified instructor.
This article was originally published on March 11, 2017 as written by Gerard Migeon. It has since been updated by Natural Womanhood to offer more resources. Last updated October 3, 2020.
The month of October will be an incredibly important one for the pro-life movement across the world. Tensions are already growing in the United States on “filling that seat” on the Supreme Court, which may decisively turn the tide for pro-life conservatives for a generation in the highest court of the most powerful nation on Earth. Indeed, the next month may offer one of the greatest victories in a generation for the movement.
But on the other side of the world, another “October Surprise” may be on the cards. Speculation is growing that China may finally abolish a policy — 40 years too late — by removing all birth restrictions. This would end the two-child policy (at least for the ethnic Han majority, who suffered most under China’s birth restrictions). The move would come only five years after the one-child policy came to an end.
Although most mainstream media outlets have failed to pick up on this development yet, this writer will venture a prophecy — October 2020 is likely to be the month when the birth restrictions, which should never have been implemented, are finally abolished.
The monumental change, should it transpire, will take place at the 5th Plenary Session of the 19th Central Committee of the Chinese Communist Party (CCP). A mouthful of a meeting, it can be summarized this way: the entire core leadership of the Party will meet in Beijing to decide on a theme and make major resolutions on the issues related to that theme.
Themes may vary, with the Second Plenary Session of the 19th Central Committee in January 2018, dropping the bombshell that the CCP was amending its Constitution so that it could crown Xi Jinping as President for Life by abolishing term limits. However, most 5th Plenary Sessions have a constant theme — the drafting of the next Five-Year Plan.
Five-Year Plans, for those who are not fanboys of Soviet and Communist history, are relics from the Soviet Union, exported to Communist China after 1949. Basically a centrally planned platform for the socioeconomic directives and initiatives for the entire country over the following five years, China’s five-year plans have been in place since 1953. The present one is the “13th Five-Year Plan”.
The plans are drafted and then approved almost every single time at the 5th Plenary Session of a Central Committee, because their five-year term ends after every 5th plenary session, heralding the need for a new one. Next year will usher in the “14th Five-Year Plan”, which is exactly what Xi and his mandarins will be discussing this coming October in Beijing.
OK, so plenty of political jargon, but what signals show that the two-child policy may finally be abolished once and for all at this boring-sounding meeting of Communist tyrants? Well, there is precedent — every single time the birth policy was reformed, it occurred during a plenary session. It was the Fifth Plenary Session of the 18th Central Committee in October 2015 that ended the one-child policy. It wrote the two-child policy into the official draft document of the 13th Five-Year Plan, which China is in the process of implementing until the end of 2020.
And the reform before that? It came in 2013, during the 3rd session of the 18th Central Committee in November 2013, which saw Xi Jinping timidly begin to dismantle the one-child policy by allowing couples with one member who is an only child to apply for the quota to have a second child. Incredibly underwhelming, I know, but at that time it was unthinkable because the National Family Planning Commission of China vehemently denied any possibility of both reforms before the two Plenary Sessions.
So here’s the bottom line: if these birth policy reforms, including the eventual abolition of the entire birth restriction system, are ever going to happen, it can only take place at one of these plenary sessions. And this time around, Xi looks to plan at this meeting his entire blueprint all the way to the year 2035. This means that if no birth-policy reforms occur at this vital point in time, the two-child policy will probably be around for a very long time.
Just as the battle for the seat of the Supreme Court in America will decide the pro-life fight for the next few decades, this Plenary Session and any decisions the Central Committee makes will decide if millions of babies can be born, or not, at least for the next decade-and-a-half in China.
Right now, as the seat in DC is in the hands of Trump and Mitch McConnell, the decision which will make or break the lives of countless unborn Chinese lies with Xi Jinping. Now that does not deliver any confidence, for Xi Jinping and his regime has been ruthless in Xinjiang, sterilizing Uyghurs en masse (covered in depth in one of my earlier articles), but Xi may well be considering the nuclear option of ending birth restrictions at least for the Han majority due to a myriad of factors.
To understand why this might be happening, we need to take a closer look at Xi and his father Xi Zhongxun, who was also one of the most powerful men in China. It is important to be aware of their personal legacies in relation to China’s birth policies, to understand why Xi Jinping may well be the man to end the inhumane policy (due to completely self-serving and dehumanizing calculations of his own).
Xi Junior and his obedience to the one-child policy
In the 1980s, Xi Jinping was a 30-year-old deputy Party Chief at Zhengding County in rural Hebei Province near Beijing. His father had only been politically resurrected a few years before from political persecution following the end of the Cultural Revolution. (More on Xi Senior later). Xi Jinping had managed to land the job in Zhengding thanks to his father’s maneuvers, and actually gave up a military position in Beijing for the role of a local county governor.
He was largely ignored at first because everyone thought he was going to come and go, as most “red princelings” do these days — using the county position as a mere stepping stone to return to the nerve centre, Beijing. But Xi had a different plan. He wanted to make a name for himself in Zhengding and climb his way up. Therefore, as Deputy Party Chief and then Party Chief, Xi began to leave his mark on Zhengding aggressively.
Some of his policies were benign — getting a bus route to come to Zhengding from the provincial capital, Shijiazhuang, making use of Zhengding’s ancient Buddhist temple treasures to promote tourism, and building a “Dream of the Red Chamber” theme-park set to attract the shooting and production of films.
But the 1980s did not merely herald the beginning of the market economy in China — it also ushered in a period of full-on assault on the reproductive rights of the Chinese people. Xi, as a local mandarin eager to make an impression, launched an all-out assault on the women of Zhengding in 1983, which is also the year when National Family Planning Commissioner Qian Xinzhong rolled out his aggressive warlike national forced sterilization operations.
Xi had 31,000 women sterilized in Zhengding and had IUDs inserted into another 30,000 in late 1983 alone. When covering this for The New York Times in a profile of Xi Jinping as he was about to take over power in China, Times reporter Ian Johnson stated that there was “no evidence that Xi was more zealous than others” in the implementation. But it was still incredibly zealous — Zhengding only had around 400,000-450,000 people back in 1983, and Xi oversaw the sterilization of 61,000 women in that whirlwind campaign, which was more than a third of all women in Zhengding and probably nearly half of all women of reproductive age.
Xi Senior and his “rebellion”
Before Xi junior’s climb up the ladder, atop the wombs and fetuses of the Zhengding people, Xi Zhongxun was already trailblazing reforms in the coastal province of Guangdong as party secretary in the province with his partner Ren Zhongyi, who continued the reforms in Guangdong after Xi Senior returned to Beijing. Xi Zhongxun is remembered today for proposing to create the special economic zones in Guangdong and creating the first market-based economy in Communist China. But Xi Senior’s legacy in Guangdong has another interesting aspect — the aspect of human life.
Xi Zhongxun and Ren Zhongyi both understood something the Beijing leadership did not — that human resources and manpower are something to be cherished, not feared. They knew that China’s best resource in the 1980s was none other than its hard-working people eager to lift themselves out of poverty.
In order for the factories to flourish, cheap labour needed to come into the party and attract investment. Xi and Ren managed to get policies specifically catered to Guangdong — Paramount Leader Deng Xiaoping basically granted them the power of policy autonomy, or as he put it in guerilla warfare terms: “fight a bloody path out”. And when it came to population policy, Guangdong was far more radical than anywhere else in Han-majority China, just like its economic radicalism.
In 1980, just as the nationwide one-child policy was being rolled out, Xi Zhongxun’s Guangdong had a different approach. Xi Zhongxun allowed Guangdong women to have two children, something unheard of outside of ethnic-minority areas as the one-child frenzy began to take over pretty much every province.
In 1986 the policy changed to allow rural couples to have two children, but that was still considerably more humane than what was happening in the rest of China. Most other Han-majority provinces applied one-child quotas to every urban couple and only loosened the rules slightly to allow rural couples with a firstborn daughter to have a second child.
Xi and Ren’s two-child policy was universal in Guangdong at first and remained universal in rural Guangdong, and according to independent Chinese demographer Yi Fuxian, Xi Senior’s policy, which was only abolished in 1998 following immense pressure from the National Family Commission long after his retirement, may have allowed 5 million more births to occur in the province, which would not have occurred had he implemented the one-child policy like his son in Zhengding.
Xi Zhongxun was also resistant to the proclamation of any formal nationwide Family Planning Bill and repeatedly resisted the efforts to pass any such bill. It was only after his retirement that the National Family Planning Commission’s bid for such a bill succeeded in 2001, long after China had already reached sub-replacement fertility.
Fast forward a few decades, and now Xi Jinping is at the crossroads of a major choice. He no longer needs to impress any seniors with his implementation of baby slaughter. He actually has already dismantled a lot of the birth-control machine in China. But he is doing so because he has realized to some extent that China is falling off a demographic cliff. Xi mentioned in detail in his rationale for abolishing the one-child policy in 2015 that China faces a rapidly ageing population and the adverse effects this may have on the socioeconomic health of China — which is now his China. But he still did not have the courage to abolish all birth restrictions.
Since then, China’s birth rates have continued to plummet. Rumours had already begun to swirl suggesting that all birth restrictions would be lifted as early as 2018, with 2020 deemed “the latest” for the birth restriction to end. Initial feasibility studies had already been submitted to Premier Li Keqiang in 2018 about ending all birth restrictions. Every year, people in China thought the announcement would come through.
And now, in 2020, Xi is as vulnerable as ever due to his strategic blunders as well as his arrogance. If there is one policy announcement that could relieve him of some pressure, it would be an announcement to formally grant birth freedoms back to the Chinese people. It would not cause any controversy, and is unlikely to cause any baby booms, given how deeply entrenched the one-child and two-child norm is in Chinese society. It would be a purely symbolic gesture, but a hugely symbolic one.
Of course there are possible snags that could derail this prophecy about the October announcement. Ethnic minorities like the Uyghurs are now subject to 1980s-style mass sterilizations. Leftovers from the now defunct Family Planning Commission apparatus continue to spread Malthusian lies and demographic paranoia. But if there is one thing Xi can learn from his reformist father, it may be dismantling and opposing the family-planning apparatus, which has not only destroyed the lives of Chinese people (especially women), but could also derail Xi’s so-called “China Dream”. This is because an ageing, overburdened nation falling off a demographic cliff may be the one thing that could decisively cripple Xi’s ambitions.
So, we look to the October Surprise with bated breath. Both DC and Beijing may yet pleasantly surprise everybody.
Advertisements promoting one-child or child-free families are appearing around Vancouver, British Columbia, with the intention of convincing young people not to have children in order to save the environment. One advertisement features a smiling baby and states, “The most loving gift you can give your first child is to not have another.” Other ads state, “We Chose One!” and “We Chose Childfree!”
The ads were placed by the group “One Planet, One Child,” which aims to move society towards a “small family norm.” The group’s goal is to drop the world population from today’s 7.8 billion to below 3 billion 100 years from now. The group states on its website that it has placed similar ads in Minnesota and Colorado, with similar advertisements soon to come in other U.S. and Canadian cities.
A healthy replacement fertility rate is 2.1, and the global fertility rate currently sits at 2.4. However, researchers have found that the world fertility rate is falling, and will drop below 1.7 by the year 2100. Twenty-three countries are predicted to see more than a 50% decline in their populations. This drastic decline in the population will lead to an economic crisis, with countries unable to support health care programs or welfare systems. With not enough people in the workforce compared to those of retirement age, the retirement age will rise — predictably by 8.4 years by 2050. Economic disaster is so imminent in some nations, like Hungary, Denmark, Italy, and Singapore, that these countries have put incentives in place to encourage couples to have more, not fewer, children.
“To be successful we need a fundamental rethink of global politics,” Professor Ibrahim Abubakar of the University College London told the BBC. “The distribution of working-age populations will be crucial to whether humanity prospers or withers.”
It seems that groups like “One Planet, One Child” are more concerned with the future of the environment than the future of humanity. However, new innovations and ideas from future people — some who have yet to be born — have the potential to help the environment… but not if those people aren’t born. Not if humanity “withers.”
“One Planet, One Child” says it is “not dictating anyone’s family size” but simply “helping young couples make informed decisions.” It says, “The choice is theirs.” But the group’s advertisements are reminiscent of Chinese ads promoting the government’s one-child policy, which state, “Less births will be better for your child,” and “Fewer and better births, happiness throughout your whole life.” Eventually, the constant presence of those advertisements convinced Chinese young people that having one child was the right thing to do, not something they were being forced to do.
Some Canadians responded to the ads in Vancouver, telling City News, “If you want to be child-free, be child-free. If you want to have like 10 children, it’s maybe not so convenient but, go ahead,” and “If you want to have a big family you can go ahead.”
On Thursday, September 24, Natural Womanhood hosted Emily Sederstrand in a virtual conversation about empowering teenage girls to know and understand their bodies.
“I love foreign languages,” said Emily, “and so it was a great revelation to me to learn that fertility is like a language. But if you haven’t been taught, you don’t know how to interpret it. It’s not that it’s very complicated, but a woman does need to be taught.”
Emily talked with Natural Womanhood board member Jackie Aguilar and Natural Womanhood CEO Gerard Migeon about her mission to empower young women to understand the language of their fertility, and to appreciate the beauty of their bodies.
“Our girls today are being bombarded with images” remarked Emily, such as those found in popular music videos displaying graphic images of sexual abuse. She sees the language of fertility as a powerful tool for combating harmful messages our culture broadcasts to girls and young women via every media platform. Emily also offered resources and practical tips to parents of young daughters for protecting their innocence, physical health, and emotional wellbeing, and how fertility awareness goes hand-in-hand with these goals.
ByCassy Fiano-Chesser A new research study is looking to provide birth control over-the-counter, without a doctor’s supervision — and children are being recruited for it.
According to CNS News, Advocates for Youth, which works with Planned Parenthood, sent out a mass e-mail with the subject line, “Know anyone ages 11-15 to join this study?” The e-mail was promoting The Pill Study, through which researchers are looking to make birth control available from a pharmacy, but without a prescription — essentially, over-the-counter. The study’s website also confirmed that girls as young as 11 are eligible to participate.
Participants who qualify will make an appointment at a participating pharmacy, where they will receive the birth control. The study also will remain fully confidential, so a child’s parents will have no clue that their daughter is receiving dangerous contraception and potentially having sex at such a young age. On top of that, the study will pay participants $75, further incentivizing children to sign up.
There is not a single state in the entire country in which an 11-year-old can legally consent to sex.
Equally disturbing is the idea that a child would be able to get birth control without their parents’ knowledge and without a doctor’s supervision. Under those circumstances, it seems unlikely, if not impossible, that the child in question would be adequately counseled about the potential risks associated with hormonal birth control.
Studies have found that birth control can negatively impact women’s mental health, with high depression rates found specifically in teen girls. One study even found that women using hormonal birth control have triple the risk of suicide than women not using hormonal birth control. Other known risks include pulmonary embolism, heart attack or stroke, numerous cancers, potential infertility, and more. That doesn’t even include any potential contraindications.
A child as young as 11 or 12 could not be relied upon to give a pharmacist a thorough medical history. Just last year, a college student’s family was awarded $9 million after she died. The student, Hope Johnson, was prescribed contraception even though she was at high risk of developing blood clots. A month later, Johnson tragically died.
It’s beyond inappropriate, not to mention dangerous, for children to be encouraged to join a research study, where they will be paid to receive birth control, without being seen by a doctor, and without their parents’ knowledge or consent.
(Pregnancy Help News) — If you are providing life-saving services to families in need and are not getting taxpayer funding, why not?
Real Alternatives recently celebrated 25 years of serving 322,813 clients through 1,888,825 client visits in Pennsylvania. As the statewide administrator for Pennsylvania’s Pregnancy and Parenting Support Program, Real Alternatives assisted those 300-thousand-plus Pennsylvania residents via public funding.
Real Alternatives uses a network of 29 service providers with 86 pregnancy support centers, maternity homes and other pregnancy help sites in 33 counties, Heartbeat International affiliates among them, with 234 caring and compassionate trained counselors to provide free pregnancy support and parenting education services to women and families in Pennsylvania.
Kevin Bagatta is president and CEO of Real Alternatives, which has extended their operations into Indiana and Michigan. Thirteen other states have started taxpayer-funded operations with Real Alternatives’ assistance.
“When explaining the program to government officials from other states,” Bagatta said, “I’ll often ask them, ‘Do you know what they call a positive approach to the most controversial issue of our time? They call it a solution!’”
Vice President Mike Pence has supported Real Alternatives starting in 2014 as governor of Indiana, directing the state’s Department of Health to contract with them to start and operate a $1-million program modeled after Pennsylvania’s.
“For more than two decades, Real Alternatives has empowered women for life by providing positive, life-affirming pregnancy and parenting support services to women and families in need. I am grateful to all the men and women who have dedicated their time and talent through the Real Alternatives network,” Pence wrote in 2018 congratulating the organization.
In the Real Alternatives model (which could be duplicated in all 50 states) the state hires the organization to administer a statewide program that promotes childbirth rather than abortion. The PA group was the first Alternatives to Abortion Program to receive state and then federal funding. The Temporary Assistance for Needy Families (TANF) is the federally funded portion.
“After the pregnancy, especially with young people, that unplanned pregnancy, or unexpected pregnancy can become a crisis parenting situation,” Bagatta said. “We’ll be there with them for that time to make sure they are ready and are providing good parenting and good nurturing and are being taken care of during that first year of life.”
Real Alternatives is the only statewide faith-based program funded in Pennsylvania. At $7.263 million per year ($6.263 million state and $1 million TANF) taxpayers are empowering women to choose life and have the resources to thrive.
Real Alternatives’ goal is to provide life-affirming alternatives to abortion services throughout the nation. Therefore, Bagatta seeks to share the information with any pro-life organizations serving women and families in need.
Measurable outcomes of the program include the increase of women who choose life rather than abortion — among those served by Real Alternatives, 60% of abortion-minded clients and 89% abortion-pressured clients choose life.
As Real Alternatives’ network of programs thrive, there are increases in measured outcomes of physical and emotional support, knowledge of adoption, parenting skills, reproductive health due to STD education, and the modification of risky lifestyle behavior through abstinence education.
The Pregnancy and Parenting Support Program gets results for taxpayers’ investment, as health and Medicaid costs are lowered due to high rates of pre-natal and pediatric care, and immunization.
As Real Alternatives recently celebrated 25 years, national growth of their programs was highlighted at the organization’s banquet.
For six years Real Alternatives partnered with Texas Pregnancy Care Network (TPCN). In 2012, TPCN assumed sole administration of their program.
Among the award winners at the 25th Anniversary celebration was Mike Turzai, the former speaker of the Pennsylvania House of Representatives. He has been an avid supporter of Real Alternatives.
“Every single human being is beautiful. Everybody is capable and will contribute to this world,” Turzai stated, addressing the Real Alternatives banquet. “And everybody wants to feel the love of their family, friends and another human being. You are not only providing that love, protection and care during the pregnancy, but you are doing it after the pregnancy.”
Another award winner was former Governor of Pennsylvania, Mark Schweiker, who had increased funding of Real Alternatives with $1 million of TANF funds. These funds from the U.S. Department of Health and Human Services for alternative to abortion services programs were the result of U.S. Senator Rick Santorum pushing for the approval of TANF for such services.
Schweiker stated, “Real Alternatives steers women into the reassuring hand of service providers and away from fear and uncertainty.”
The Real Alternatives model demonstrates real potential for other states. Bagatta is eager to talk with any organization interested in knowing more.
“With the financial resources provided by taxpayers,” stated Bagatta, “the pregnancy support centers, Catholic Charities, maternity homes, and adoption agencies can hire more counselors and open more centers thereby compassionately serving more women in unexpected pregnancies and lower abortions!”
As studies have demonstrated, abortion-minded and abortion-vulnerable women need at least one person in their lives to empower them to choose life with confidence.
Bagatta points out this is the driving force of the Real Alternatives program.
“The real alternative to abortion is another person,” said Bagatta. “Connecting a woman with that one voice (counselor, pregnancy help center or other resource) is a dual empowering force for life. First for her own and for her baby.”
Accountability in billing for actual, specific services performed for women in need and the extensive tracking of funds is part of Real Alternatives’ history and is a vital aspect of working with government funded programing.
All billed services occur as a one-on-one service to women in need.
Any savings in administrative costs, which Bagatta’s team keeps as low as possible, are redirected toward advertising. This increases traffic to Real Alternatives’ website where women utilize the zip code specific referral system to locate local services.
Bagatta eagerly looks forward to the overturn of Roe vs Wade decision, but noted, “Even when that happens, we will still need to continue this work to support women who need help.”
For now he looks forward to hearing from more states eager to utilize this opportunity for taxpayer funded pro-life programs, stating, “The vision is for the citizens of every state to see their taxpayer dollars to be used to help at risk women, empowering them so they do not need to choose abortion.”
Note from the editor of Pregnancy Help News: Heartbeat International manages Pregnancy Help News.
Recent accusations of forced sterilizations have brought the United States’ dark history of eugenic, compulsory sterilization programs — which once targeted those deemed by elites as “unfit” — back into the spotlight.
The 1934 film, “Tomorrow’s Children,” portrayed a state’s coercive power to eugenically sterilize a young pregnant woman. While the woman portrayed in the film succeeded in stopping the state’s court order, actual eugenics programs within the United States resulted in the sterilization of an estimated 60,000 people — many minorities, who were eugenically sterilized against their wills. Many more have been subjected to these atrocities worldwide.
California’s eugenics: Coercive sterilization of over 20,000 people
In 1909, California passed the third sterilization bill in the U.S., which sanctioned the coercive sterilization of over 20,000 patients, noted an American Journal of Public Health report. According to author Edwin Black, “[T]he code permitted castration or sterilization of state convicts and the residents of California Home for the Care and Training of Feeble Minded Children in Sonoma County. Two institutional bureaucrats could recommend the procedure if they deemed it beneficial to a subject’s ‘physical, mental, or moral condition.’”
Eugene S. Gosney, founder and President of the Human Betterment Foundation (HBF), published a study with his his associate Paul Popenoe entitled “Sterilization for Human Betterment,” focusing on sterilizations ordered under California’s law. In July 1931, Margaret Sanger published Gosney’s views on sterilization in her Birth Control Review. He wrote, “Eugenic sterilization is, under usual state laws, ordered or permitted by the state, for the benefit of the state…. Eugenic sterilization starts where contraception stops. It is applied primarily to people or families without the intelligence, emotional stability, or self-control to handle contraceptives successfully. It succeeds where contraception would fail.”
In 1932, according to the New York Times, Gosney’s group published a paper warning America of “race degeneration” unless it adopted “eugenic sterilization of the large numbers of the mentally defective.”
Iowa’s eugenics: Planned Parenthood desired ‘wider application’ of coercive sterilization
Iowa’s first sterilization law passed in 1911. According to researcher Amy Vogel, “In 1929 the Iowa General Assembly created a Board of Eugenics to investigate persons who were a ‘menace to society,’ so that such ‘degenerates’ could be sterilized. Between then and 1977, when the legislature voted unanimously to abolish the board, it authorized the sterilization of more than two thousand individuals, three-fourths of them women.”
“Although the Iowa law was intended to be voluntary, there were undoubtedly instances when patients felt they had little choice,” she wrote. “… In Iowa, as in other states, many sterilizations were probably conducted without the knowledge or approval of the Board of Eugenics, but the extent to which physicians acted independently is unknown.”
Planned Parenthood was a referral agency for Iowa’s sterilization board, according to a 1969 report published in the DesMoines Register. Iowa State’s Eugenics Board Chairman Dr. S.M. Korson admitted a percent of their referrals came from the welfare office or Planned Parenthood.
When Korson noted a decrease in sterilizations due to a “more humane and enlightened attitude,” Rev. Robert L. Webber — the executive director of Planned Parenthood of Iowa — attacked board members, saying they “should reinterpret the law and give it wider application than they do now or they should quit.”
Minnesota’s eugenics: Wishing Hitler success
In 1925, Minnesota passed legislation allowing the sterilization of “feeble-minded” and “insane” residents of state institutions, according to the Minnesota History Center. Charles E. Dight, who was “largely responsible” for Minnesota’s Sterilization Law, also reportedly “fought unsuccessfully for expansion of the law to include sterilization of the ‘unfit’ who lived outside of institutions.”
In the 1930s, Dight joined the Minnesota Birth Control League, the forerunner of Planned Parenthood of Minnesota. In 1933, as president of the Minnesota Eugenics Society, Dight wrote a letter to Adolf Hitler wishing him success in “stamping out mental inferiority among the German people,”noting the Nazi leader’s efforts would “advance the eugenics movement in other nations as well as in Germany.”
According to Minnesota Magazine, the state’s eugenics program authorized the sterilization of 2,350 people.
Charles F Dight letter to Hitler ( Image from document provided by the Minnesota Historical Society)
North Carolina’s eugenics: Black men, women, and “feeble-minded” targeted
The state of North Carolina sterilized about 7,600 people before it ended in 1974, according to the Winston-Salem Journal which exposed the program in an award-winning series, “Against Their Will.” That program targeted many Black men and women for forced sterilization. One of those women was Elaine Riddick, who became pregnant after rape at age 13.
Watch Riddick’s emotional story from the documentary film Maafa21 below:
“Gamble helped found the Human Betterment League of North Carolina in 1947 to promote eugenic sterilization,” reported the Winston-Salem Journal.
According to the documentary Maafa21, “In 1947, Gamble called for the expansion of North Carolina State’s sterilization program, saying that for every feeble minded person sterilized, 40 more were polluting and degrading the bloodlines of future generation with their defective genes.”
Excerpt: Margaret Sanger Letter to Clarence Gamble, Negro Project
Another coercive eugenic sterilization program in the state was headed by Wallace Kuralt, who served as Mecklenburg County’s welfare director from 1945 to 1972. A 2014 Slate article in Slate noted that Kuralt believed sterilization would save taxpayer funding by reducing poverty among the “low mentality-low income families, which tend to produce the largest number of children.”
North Carolina later became the first state to offer any kind of restitution to sterilization victims.
Virginia’s eugenics: Over 8,000 sterilized
On March 20, 1924, the Virginia General Assembly passed “The Racial Integrity Act” overseen by eugenicist Walter Ashby Plecker. The Assembly also passed the state’s 1924 Sterilization Act, which became a model for other states, after the 1927 U.S. Supreme Court decision Buck v. Bell upheld it. The act was based on Model Law written by American Eugenics Society founder Harry Laughlin.
In 1933, Laughlin’s ideas were published by Margaret Sanger’s Birth Control Review, and in 1938 he became part of the Citizen’s Committee on Planned Parenthood. Laughlin was an unabashed Nazi sympathizer who, in 1936, “received an honorary degree from the Nazi-controlled University of Heidelberg as ‘a pioneer in the science of race cleansing,’” according to researcher Paul A. Lombardo.
Harry Laughlin author of Immigration Act signed Committee for Planned Parenthood
It is estimated that the State of Virginia sterilized more than 8,300 people.
Not all instances of eugenics were in America, but Americans were connected to efforts in Germany as well as Sweden:
Germany’s eugenics: Sanger’s cohorts praised Hitler, who sterilized hundreds of thousands
Fischer was in charge of the Kaiser Wilhelm Institute, where racist Nazi programs were developed. According to the DNA Learning Center at Cold Spring Harbor, the Rockefeller Foundation — which has long funded eugenics and abortion organizations including the Population Council — provided funds to construct the Kaiser Wilhelm Institute.
Fischer praised Hitler in a 1935 New York Times article, asking the World Population Congress to “Hail Fuehrer and Reich Chancellor Adolf Hitler.” According to the DNA Learning Center, “Hitler read Fischer’s textbook Principles of Human Heredity and Race Hygiene while in prison at Landsberg and used eugenical notions to support the ideal of a pure Aryan society in his manifesto, Mein Kampf… By the outbreak of the Second World War in 1939, an estimated 400,000 people had been sterilized.”
Eugen Fischer (Image: DNA Learning Center)
Another Sanger cohort, Lothrop Stoddard, traveled to Germany to observe a Nazi eugenics court.
Stoddard described this Nazi meeting in his book, “Into the Darkness: A Sympathetic Report from Hitler’s Wartime Reich.”
“The first case I saw looked like an excellent candidate for sterilization. A man in his mid-thirties, he was rather ape-like in appearance–receding forehead, flat nose with flaring nostrils, thick lips, and heavy prognathous jaw. Not vicious-looking, but gross and rather dull,” Stoddard wrote in part.
Sweden’s eugenics: Sterilization in the name of a ‘progressive, enlightened welfare state’
“From 1934 to 1974, 62,000 Swedes were sterilized as part of a national program grounded in the science of racial biology and carried out by officials who believed they were helping to build a progressive, enlightened welfare state,” wrote the Washington Post in 1997.
“No one can document with certainty how many of these sterilizations were involuntary, but those who have looked at the program believe that, at its peak, a sizable majority were forced… In some cases, couples judged to be inferior parents were sterilized, as were their children when they became teenagers,” they added.
The program was strongly supported by Gunnar and Alva Myrdal, the paper noted. Gunnar authored the 1500-page book, “An American Dilemma: the Negro Problem and Modern Democracy,” paid for by the eugenics-founded Carnegie Corporation. His wife Alva was published in Margaret Sanger’s Birth Control Review and was later honored by Planned Parenthood.
We now know that hormonal birth control, even progesterone-only forms like the IUD, traditionally considered to have only localized effects in the body, are associated with an increased risk of depression and that the risk is highest among new users in their teens. We also know that the pill in particular changes women’s brains.
This is because, says author Sarah E. Hill, far from acting only on the ovaries, “[s]ex hormones impact the activities of billions of cells in the body at once, many of which are in the brain. There, they play a role in influencing attraction, sexual motivation, stress, hunger, eating patterns, emotion regulation, friendships, aggression, mood, learning, and more.” This is particularly concerning because, notes Hill, “By changing what women’s brains do, the pill also has the ability to have cascading effects on everything and everyone that a woman encounters. This means that the reach of the pill extends far beyond women’s own bodies, having a major impact on society and the world.”
Many recently published articles about the harmful effects of hormonal birth control cite a landmark 2016 Denmark study, which was groundbreaking both because of its results and because of the sheer number of women studied (over one million women’s health records kept over 16 years). The results? “Women taking the combined oral contraceptive pill were 23% more likely to be diagnosed with depression, while those using progestin-only pills were 34% more likely.”
Many studies skewed and of poor quality
Regrettably, according to the lead author of the study, Dr. Ojvind Lidegaard, much of the research previously done on the connection between hormonal birth control use and poor mental health outcomes has been poor quality. “There has been a lot of research in hormonal contraception,” Lidegaard said. “On mental health, the quality of the studies have been poor and the results consequently unreliable. Those studies, for example, had not followed women from their first use of hormonal contraception in the way we did here has been a lot of research in hormonal contraception.”
A 2016 Harvard Health article concurred with Dr. Lidegaard’s assessment of the previous research literature, stating, “While many of these did not show a definitive association, a critical review of this literature revealed that all of it has been of poor quality, relying on iffy methods like self-reporting, recall, and insufficient numbers of subjects. The authors concluded that it was impossible to draw any firm conclusions from the research on this birth control and depression.”
Dr. Lidegaard offered another disappointing piece of information about research into hormonal contraceptives and mental health, saying that many research studies are “sponsored by the marketing holders” — in other words, the drug companies themselves. “I think it’s true that the companies who produce these pills are very willing to support proving that there are benefits to taking hormonal contraception. It is much more difficult to get support to study the negative reactions and demonstrate the adverse effects. Many more studies have been conducted to prove that [the pill] protects against ovarian cancer than that it can increase the risk of depression.”
The alternatives
While the status of research into contraceptive-caused adverse mental health outcomes leaves plenty to be desired, on the other hand fertility awareness-based methods of natural family planning are gradually losing their status as the “best-kept secret” for addressing women’s health holistically. Furthermore, NaProTECHNOLOGY and other similar approaches to women’s reproductive health can utilize women’s own “data” as the basis for diagnosis and treatment of common reproductive problems, even including treatment of issues like PCOS that historically have been assumed to require treatment with the birth control pill.
All across the country last weekend, pro-life advocates gathered to pray and remember the unborn babies who have been victims of abortion.
In Kansas City, Kansas, Catholic Archbishop Joseph Naumann led pro-lifers in mourning for the unborn at the Gate of Heaven Cemetery, one of 54 memorial sites for aborted babies in the U.S., according to The Leaven, the newspaper of the Archdiocese of Kansas City.
Local pro-life organizations sponsored the event, and Naumann spoke about the value and dignity of every human life, the report states.
In Pennsylvania, another group of pro-lifers placed flowers on a memorial for aborted babies at St. Jerome’s Cemetery in Tamaqua. The Republican Herald reports, during the special ceremony, pro-life advocate Cheryl Kiefer shared her testimony about aborting three of her unborn babies.
After her abortions, she said she turned to alcohol to drown out her pain and regret. Kiefer said God eventually changed her life, and now she looks forward to seeing her babies in heaven someday.
“He is here to forgive us and heal us,” she said. “I believe my babies are with God.”
Pro-lifers welcome Kiefer and others who have had abortions to mourn with them during the annual event.
Scheidler said they welcome mothers of aborted children and fathers who have participated in, coerced or tried to stop the abortion of their child. He said the day is for everyone to “mourn for those children, to take stock of our involvement, and to seek God’s healing and mercy.”
The pro-life groups that lead the nation-wide effort are Citizens for a Pro-Life Society, Priests for Life and the Pro-Life Action League.
The U.S. Supreme Court forced states to legalize abortion on demand in 1973 through Roe v. Wade. Since then, nearly 62 million unborn babies have been killed in abortions.
IRWIN COUNTY, Georgia, September 15, 2020 (LifeSiteNews) – A nurse has come forward to accuse a privately-run Immigration & Customs Enforcement (ICE) detention facility in Georgia of performing hysterectomies on female illegal immigrants en masse, without medical necessity. Whether the women consented or understood the procedure they were undergoing is unclear.
The activist groups Project South, Georgia Detention Watch, Georgia Latino Alliance for Human Rights, and South Georgia Immigrant Support Network have filed a complaint with the Department of Homeland Security (DHS) Office of the Inspector General (OIG) against Irwin County Detention Center (ICDC) on behalf of a nurse who used to work there, Dawn Wooten.
Law & Crimereports that Wooten and others allege witnessing several examples of “jarring medical neglect” at ICDC (which is run by the private prison company LaSalle Corrections), the most alarming of which is the claim that an outside physician was brought in to examine women, most of whom he performed hysterectomies on.
“Everybody he sees has a hysterectomy—just about everybody. Everybody’s uterus cannot be that bad,” Wooten says. “We’ve questioned among ourselves, like, goodness he’s taking everybody’s stuff out…That’s his specialty, he’s the uterus collector.”
“Recently, a detained immigrant told Project South that she talked to five different women detained at ICDC between October and December 2019 who had a hysterectomy done,” the complaint says. “When she talked to them about the surgery, the women ‘reacted confused when explaining why they had one done.’”
Among the complaint’s examples is a detainee who says she was improperly anthesized beforehand and subsequently heard the doctor had mistakenly removed the wrong ovary, destroying her ability to have children in the future:
Everybody he sees has a hysterectomy—just about everybody. He’s even taken out the wrong ovary on a young lady [detained immigrant woman]. She was supposed to get her left ovary removed because it had a cyst on the left ovary; he took out the right one. She was upset. She had to go back to take out the left and she wound up with a total hysterectomy. She still wanted children—so she has to go back home now and tell her husband that she can’t bear kids… she said she was not all the way out under anesthesia and heard him [doctor] tell the nurse that he took the wrong ovary.
LaSalle Corrections has so far refused to comment on the allegations. ICE has issued a statement claiming that it “does not comment on matters presented to” OIG, and while it “takes all allegations seriously,” it also maintains that “anonymous, unproven allegations, made without any fact-checkable specifics, should be treated with the appropriate skepticism they deserve.” ICE added that ICDC “has been inspected multiple times, with and without warning, and that the facility has been found to be in compliance with Performance Based National Detention Standards.”
In 2014, the California State Auditor released a report which of the 144 prison inmates “who underwent tubal ligations from fiscal years 2005-06 to 2012-13, auditors found nearly one-third were performed without lawful consent.”
“In some cases, physicians falsified the consent forms,” USA Today reported. The audit found “that all women receiving tubal ligations had been incarcerated at least once before, indicating that they were repeat offenders,” seeming to suggest they were targeted.
Beginning in 1932, what is now known as the infamous Tuskegee Study or Tuskegee Experiment was a “40-year experiment run by Public Health Service officials followed 600 rural black men in Alabama with syphilis over the course of their lives, refusing to tell patients their diagnosis, refusing to treat them for the debilitating disease, and actively denying some of them treatment,” The Atlanticsummarized.
Responsible men can become more deeply convinced of the truth of the doctrine laid down by the Church on this issue if they reflect on the consequences of methods and plans for artificial birth control. Let them first consider how easily this course of action could open wide the way for marital infidelity and a general lowering of moral standards. Not much experience is needed to be fully aware of human weakness and to understand that human beings – and especially the young, who are so exposed to temptation – need incentives to keep the moral law, and it is an evil thing to make it easy for them to break that law. (Paul VI, Pope, 1897-1978, Humanae Vitae, 17).
This quote from St. Pope Paul VI’s famous encyclical on artificial birth control, Humanae Vitae, has proven prophetic, even 50 years later. He affirmed Church teaching that marital love is about giving oneself completely to the other, using the words “total,” “faithful” and “fecund” (fruitful). He went on to discuss the damage that a relationship incurs when those principles are disregarded, and how it would damage society as a whole as well.
I spoke with Dr. Diann Ecret of the National Catholic Bioethics Center (NCBC) about artificial birth control. In addition to Church teaching, Dr. Ecret also spoke about the medical problems with artificial birth control. There are physical health risks such as heart disease, loss of bone density and even infertility after ceasing their use. She also discussed emotional side effects such as depression and lowered libido. The modern world downplays these risks, declaring them the tolerable side effects of a drug designed to cure an illness – as if pregnancy is comparable to death. Advocates of birth control also seem to presume that there are only two options for people: artificial birth control or pregnancy. They ignore the very real and positive choices of abstinence for single people and Natural Family Planning for married couples, a family-planning method that promotes respect, mutual love and other virtues essential for a fulfilling marriage.
On the other end of the fertility spectrum is help for those who are battle infertility. I spoke with Dr. Paul Day, a local family physician, about solutions for infertility. One of the more commonly-known methods today is in vitro fertilization (IVF), which is contrary to Church teaching for several reasons. First, it uses technology to replace the marital act, treating children as products. Secondly, IVF can lead to abortion if more embryos are successfully implanted than are desired. Finally, IVF produces multiple embryos, the majority of which are either discarded or frozen in storage. There are hundreds of thousands of human beings stored in fertility clinics around the world and possibly millions already discarded.
Is there hope for Catholics who suffer from infertility? The answer is, yes, and it is called NaPro Technology. This is treatment that works cooperatively with a woman’s body to restore fertility naturally. It begins with charting and hormone tests. Treatments can include hormone supplementation and/or corrective surgery, among others. To learn more, visit naprotechnology.com. Of course adoption and foster care are beautiful ways to make a family, as well.
This is neither the end of the story nor the end of bioethics topics. Tune in to the full interviews of Drs. Ecret and Day, as well as my interview with Dr. Ted Furton on common vaccines developed from aborted fetal tissue lines. I also interviewed Bobby Schindler on end-of-life issues in light of his experience with the 2005 court-ordered cessation of life support for his sister, Terri Schiavo. Watch the video interviews and listen to the podcasts from our website at www.catholicaoc.org/being-pro-life. Let us strive to educate ourselves so we can all take a stand for life on these important medical issues.
BEING PRO-LIFE PODCASTS Click on name to direct you to the podcast!
SEPT 1 Dr. Ted Furton, vaccines & aborted fetal cell lines
SEPT 8 Dr. DiAnn Ecret, artificial birth control
SEPT 15 Dr. Paul Day, ethical and unethical treatment for infertility
SEPT 22 Terri Schaivo’s death and Catholic teaching on end-of- life issues
Nineteen years ago on September 11, 2001, America was left shaken after a series of unexpected terrorist attacks served as a reminder of the inherent preciousness of human life. Three thousand Americans were killed after two hijacked planes were flown into the World Trade Center in New York, a third struck the Pentagon in Washington, D.C., and another crashed in a field in Shanksville, Pennsylvania. Buried deeply in the minds of many in the aftermath of the attacks was the heartbreaking impact of so many lives being lost in one devastatingly cruel and deliberate stroke.
To commemorate the 9/11 victims, the state of New York holds an annual Tribute of Light Ceremony. Two beams of light reaching into the sky are meant to evoke the fallen Twin Towers, and the event gives people the opportunity to come together and mourn. The iconic sight honors those who were killed, but it also represents a need for healing in the city where many deaths occurred on that awful day.
Which is why it was strange for Governor Andrew Cuomo to light up New York’s landmarks in pink after signing the Reproductive Health Act into law in January 2019, a radical bill that expanded the ‘right to abortion’ in the state up to birth. New York’s 9/11 lighting ceremony pays tribute to the lives that were lost, but Cuomo’s twisted version of it celebrated the ‘right’ of women to kill their own preborn children. In America alone, over 2,300 preborn children are killed every day by abortion.
9/11 did more than take the lives of thousands of innocent people – it wiped out future generations. This is why the names of pregnant women and their preborn children are inscribed on the 9/11 memorial. These women were mothers when they died, and their babies are mourned alongside them.
Dianne T. Signer was six months away from giving birth when she and her baby died in the World Trade Center. Signer’s mother, Patricia Signer, is pleased the 9/11 memorial honored the legacy of both her daughter and her grandchild.
“I’m so happy the baby is mentioned,” she said. “Because that baby will always be in my heart.”
On the morning of 9/11, Louis Massari and his wife Patricia were ecstatic when they learned Patricia was pregnant. The couple wept tears of joy together before Patricia left for work at the World Trade Center. Sadly, Patricia never returned home.
“Two things were taken from me on that day,” Massari said. “I was looking forward to being a father.”
The tragedy of 9/11 is not limited to the many individual deaths that occurred, but the families that were destroyed because of it. This is why 9/11 memorial president Joe Daniels expressed his belief that acknowledging the deaths of the preborn children killed that day in the tragedy was so crucial.
“It’s a special part of the memorial,” he said. “It reinforces that message about the whole project that the folks were just like us, that they were about to start these lives… It reminds us that they were who we are.”
Public Health England says that gonorrhoea cases have risen “to their highest level in more than 100 years”, with 70,936 cases diagnosed last year — a 26 percent increase on 2018. In the same year, all cases of sexually-transmitted diseases rose by five percent — from 447,522 in 2018 to 468,342 — with gonorrhoea “the second-most commonly diagnosed STI after Chlamydia, accounting for 15 per cent and 49 percent of all cases respectively”.
Their 2018 report found that among over-65s, gonorrhoea was rising at nearly double the national average. It blamed divorce and dating apps for the increase in promiscuity. Dr Hamish Mohammed of Public Health England said they “expect to see further cases of antibiotic-resistant gonorrhoea in the future, which will be challenging for healthcare professionals to manage”. He added: “The consistent and correct use of condoms with new and casual sexual partners is the best defence against all STIs.”
Official records of sexually-transmitted diseases began in 1918, but the only war we seem to be fighting at the moment is the war against disease. And yet, while the public is subjected to strict rules to protect us against the coronavirus, no one suggests that the “best defence” against Covid-19 is “the consistent and correct use” of a face mask.
And while the Government declares war on obesity, the official approach to promiscuity is that it “can’t be helped” like drug abuse, crime and even terrorism — but unlike smoking, eating and drinking alcohol. Indeed, for decades now, school children have been taught that having sex is inevitable. No wonder abortion is also at sky-high levels.
But the West’s other war is against population, which paradoxically requires promiscuity to function. Instead of forming families, individuals are encouraged to remain as individuals because of the alleged cost of new life. And judging by our precipitously declining birth rate, that is one war that we seem to be “winning”.
However, for those really interested in public health, the answer to promiscuity is not to make abortion easier and look for new antibiotics, but to encourage behaviour change. That presupposes the existence of free will, with its inescapable associations with outdated religion; but if we can choose to restrict our diet, then presumably we can also exercise control in other areas that impact on our health and welfare.
The alternative is to hire even more healthcare professionals to restrict our freedom, rather than being allowed to manage our own lives.
It turns out that religious teaching was right after all — free love does come with a price tag.
September 8, 2020 (LifeSiteNews) — How did we get modern sex education — and why? These are questions I frequently get from parents. A few years ago, I decided to pose them to Peter Hitchens, a well known journalist, author, and cultural commentator hailing from Oxford, England. He has had much to say about the idea of modern sex education in his various writings and media interviews. For more insight into how modern sex education in the West came about, I decided to interview him. According to his analysis, the suspicions of many parents are absolutely correct. In his view, the entire concept of sex education fails on its own terms.
“The problem with sex education,” he told me by phone, “is that the ostensible purpose for which it is advocated turns out not to be true. I did a study a few years ago of the development of sex education in my own country, and what I found is that it’s been justified really since the middle part of the Second World War, when of course there were a lot of venereal diseases, on the basis that if people were better educated about it, then it would reduce the amount of sexually transmitted disease and the amount of unwanted pregnancy. And yet if you watch the figures for both sexually transmitted disease and for unwanted pregnancy, and increasingly now for abortion, we find that despite the greater and greater extent of sex education in our society, more and more frankness about sex, and more and more pornography (which is also supposed to end repression), the number of people becoming pregnant when they didn’t want to continues to rise and the number of people contracting sexually transmitted diseases continues to rise.”
This is partially because, as the late National Post columnist George Jonas wrote during one sex education controversy, educating young people in an activity will increase that activity. Thus, the risk of abortion, sexually transmitted disease, and teenage pregnancy will only go up. If sex education’s intent, however, is not simply to prevent these things, but rather to re-educate, then it still can suit the purposes of the State quite nicely.
“It is said,” Hitchens noted, “that Gyorgy Lukas, who was commissar for education in the short-lived Bela Kun Soviet Government in Hungary in 1918, openly said that the purpose of sex education when he introduced it then — I think he was probably the first person to do so — was to debauch the minds and morals of religiously brought up young women particularly. It seems to me to make a certain amount of sense … because the kinds of things that people are taught in sex education are disinhibiting things. When I was in school no one ever mentioned masturbation. It would have been extremely bad manners to mention it anywhere, let alone for an adult teacher to talk to quite young children about it and about other sexual practices in class. The moment these things start being discussed, it disinhibits people, it takes restraints off them that previously were there. Now, you may believe, and a lot of people do believe and have believed for many years, that these inhibitions are bad for us. That’s a point of view. I don’t happen to share it, and if you follow that belief as a parent, I suppose you’re entitled to introduce your child to this sort of thing as early an age as you wish in a free country, but what bothers us in many cases [is that] parents don’t realize what is being done in classrooms until after it’s happened.”
“Discussing these things in the way that they’re discussed [makes these] things sound normal,” Hitchens pointed out. “So it’s assumed that children will have underage sex or unmarried sex or promiscuous sex, and it’s assumed that they will do so, and all the precautions they’re supposed to take is based on this idea that this will happen. ‘If you can’t be good, be careful.’”
That is why our public schools are so involved in handing out condoms and ensuring ready access to birth control pills — because they assume that people, even children, are entirely incapable of abstaining from sex outside marriage. Sex education, in essence, proceeds directly out of that assumption. And that assumption is very much promoted by our current political class.
“There [are] politics in sex,” says Peter Hitchens. “Much of those politics are about the family and the State. The state is increasingly hostile to the strong family, and the strong family is sustained by lifelong marriage and by a pretty stern and puritan attitude towards sexual relations — whereas the strong state benefits in many ways, as does modern commerce and the modern employer, from weak marriages and relaxed sexual relations. There’s also the point that Aldous Huxley makes, which is that we are increasingly going to embrace our own enslavement in the pursuit of pleasure, which [is a point] I believe actually the Marxist historian Eric Hobsbawm made … that there is absolutely no congruence in human history between sexual freedom and political freedom. Slaves have always been allowed to copulate. What they haven’t been allowed to do is marry.”
“And this,” Hitchens continued, “is an extremely important point. There is no necessary connection between a society which is sexually free and sexually uninhibited, and a society that is politically free and has free speech and freedom of assembly. It doesn’t necessarily follow at all. So [this is] a very, very profound philosophical battle about the nature of society, and it needs to be conducted in a very serious fashion. The difficulty is in finding anyone to give you a hearing.”
It’s a fascinating perspective, especially coming from someone who was once a radical Trotskyist as Hitchens was. When I pointed this out to him, Hitchens responded by noting that this is precisely the reason he is so well versed in the way the left thinks and does business.
“I decided to stop believing it because it seemed to me to be morally wrong and highly dangerous,” Hitchens told me. “But the great advantage which it gives me is that I know what left-wing people say and think in private when they’re not trying to please people on television shows. I know just how dogged and devastating this project is, which they want, and I know that the fundamental engine of left-wing activity, really since the 1960s, has not been to seize the post office and the barracks and the railway station; it’s been to seize the television station and the newspaper and the university, and to obtain victory through capturing the minds of people, and also to alter society not through the nationalizing of railways, but through the nationalizing of childhood.”
The nationalizing of childhood — a chilling idea that makes much sense. Give to the State and its education system the task of teaching children what to believe and which values to hold, and you’ve essentially co-opted the family structure.
“When they say children should speak for themselves,” Hitchens pointed out, “what they actually mean is that the parents should be removed from the discussion. They don’t actually want them to speak for themselves; they want the children to do what they want them to do, and they know the parental home is the biggest obstacle to this thing.”
This is why many states seek to ban practices that threaten this goal, like homeschooling: “There’s a certain amount of it in Britain, it’s actually illegal in Germany to this day because of the National Socialist law passed under Hitler, which has never been repealed, and attempts are being made to restrict it in Britain. They’re in their infancy, but they’re on their way, and I think parental resistance to it on that scale is probably the only effective answer. You say, ‘All right, well, if you feel that this is how you want to drive your power into my home and into my life, then I thank you very much, but I’m not going to let you. We’ll educate our children at home.’ And quite honestly, I don’t know what your public school system is like, but if it’s anything remotely like ours, it’ll probably come up with a much better general education on top.”
Parental resistance is, at the end of the day, the answer to the State’s attempt to educate and re-educate children, and that is already increasingly difficult. In many places in Canada and the United States, governments are stepping in and demanding that acceptance of certain sexual behaviors be taught. Officials are objecting to parents who want to opt their children out of sex education. Christian schools are being told that the day is soon coming when they will no longer be allowed to teach sexuality from the Christian point of view. Many people, after all, consider that point of view hateful and harmful.
First and foremost, it is essential that parents take the responsibility of educating their children on sexuality seriously. This is something Christians have often done quite badly, but it is the most effective way of inoculating the youth against many of the damaging ideas promoted everywhere in our society. If we teach our children nothing about biblical sexuality and send them out into a hedonistic and exhibitionist culture, we are practically guaranteeing that they will not be able to withstand the poisonous intellectual onslaught and torrent of temptation. Our children are the future, and if we do not educate them, the culture — and the state — will be more than happy to do it for us.
Happy birthday, BlessedMother! We love you dearly! This article was written by Fr John A Hardon S.J encouraging us to model our faith in the faith of Mary.
There is no human person in the annals of history whose faith was deeper or more precious in the eyes of God than that of His Mother, Mary. As we read the Gospels, we see something of what this means.
At the Annunciation, Mary believed that she was being invited to become the Mother of the Most High. When the angel explained to her how she would conceive the Redeemer, without losing her virginity, she made an act of faith, “Be it done to me according to your word.” She believed what the angel had told her, “Nothing is impossible with God.” When she conceived her Son, she believed that she was carrying her Creator in her womb. No mother’s faith before or since has ever been greater. In fact no woman’s faith can be Mary’s equal. When we say in the Hail Mary, “Blessed art thou among women,” we are affirming the fact that Mary was so blessed by God because she so deeply believed in the God whom she carried for nine months before His birth. This, we may say, is what the women of the world today most need to be blessed with by their Lord: something of the faith of the Blessed Virgin Mary, the Mother of our Creator.
At the Visitation, she believed what Elizabeth told her when she addressed Mary as “the Mother of my Lord.” She believed what Elizabeth told her when the unborn John the Baptist stirred with joy in his mother’s womb. Why did he stir with joy? Because Mary began to exercise her mediation of grace from Jesus whom she was carrying in her womb. Mary’s words in Elizabeth’s ears, as the Church believes, sanctified John and enabled him to be born without sin.
Mary believed every word that she said in the Magnificat:
that all generations would call her blessed,
that God’s mercy is on all who fear Him,
that God casts down the mighty from their thrones, and lifts up the lowly
At Bethlehem, Mary believed what the shepherds told her about the angels announcing the birth of the Savior. She believed that God does give His peace to those who do His will.
At the Presentation Mary believed that her Son would be contradicted, opposed, and finally crucified. She believed that her own soul would be pierced by a sword. She expected suffering. She knew that to accept Christ means to embrace the cross.
At Cana Mary believed that Jesus could work the miracle of changing water into wine. That is why, after apparently being rebuffed by Him, she told the servants to “do whatever He tells you.” Jesus worked the miracle that His Mother asked Him to perform.
During Christ’s public life, Mary believed that some, at least, would also believe in her Son’s divinity; that some, at least, would obey His teaching and would follow His example.
On Calvary Mary believed that the dying Man on the cross was God. She believed that Jesus would rise from the dead. Her faith never wavered. That is why over the centuries Saturday remains Mary’s Day or, as it is also called, Faith Day.
Our Faith Modeled on the Faith of Mary
There is nothing more needed in the Pro-life Movement than a deep faith in the providence of God. There is nothing which pro-life apostles need more than a share in the faith that Maryhad when she saw the Author of Life murdered by His own creatures.
What does it mean to model our faith on that of Our Lady? We must believe without comprehending. We must believe against all human odds. We must believe that God has an all-wise purpose in permitting the anti-life crimes in the world today. We must trust that He will bring good, even greater good, out of greater evil. We must trust in God’s providence, that where crime is so abundant there God’s loving mercy will be even more abundant.
Let us be clear, however. Christ is giving us this grace to believe the incomprehensible and to accept the humanly unbearable. But we must cooperate with this grace, even as Mary did. The heart of this cooperation is knowing what Christ wants and then doing it. That was Mary’s message to the servants at Cana. They did what Christ told them to do. Then, as the poet tells us, the water looked at its Maker and blushed.
Like Our Lady we should expect miracles. The highest miracle is not moving mountains. It is moving human wills from self-idolatry to submission to the will of God. This is the moral miracle that we should expect if we hope to convert a society in which innocent people are murdered, and the murderers become leaders in the modern world.
Prayer through Mary to her Divine Son
We commonly speak of praying to Mary. This is correct provided we understand what this means. What do we mean? We mean that because Mary is the Mother of Jesus, and Jesus is God; therefore whatever she asks of her divine Son, He will grant her. But we must ask. We must keep asking. We must keep asking confidently, trusting that our prayers will be heard.
That is why the Memorare is such an important prayer in Catholic Church and, I would say, indispensable in the Pro-life Movement. We tell Our Lady that “never was it known that anyone who fled to thy protection, implored thy help, or sought thy intercession was left unaided.” That is why we continue, “Inspired by this confidence, we fly unto thee, O Virgin of Virgins, our Mother, to thee we come, before thee we stand, sinful and sorrowful. O Mother of the Word incarnate, despise not our petitions, but in thy mercy hear and answer us. Amen.”
Mary’s power of intercession with her divine Son is beyond human calculation. It is no wonder, then, that most of world-famous shrines are dedicated to Our Lady. Centuries of Christian experience have taught the people that Mary is the wonder-worker used by her divine Son to do what only God can perform. Only God can change a culture that destroys human life into a culture that respects even the life of an unborn child. But Mary must be invoked by us so that she, in turn, may intercede with her Son to change hearts of stone into hearts of selfless love.
Recommendations
I wish to make two recommendations to those engaged in the Pro-life Movement. Following the example of Mary, they must grow in their faith; and they must cultivate a deep loving devotion to the Mother of God.
Growth in the Faith.
Thank God there are people from various faith traditions in the Pro-life Movement. There are Orthodox Jews and Evangelicals; there are Mormons and Southern Baptists; there are Anglicans and Eastern Orthodox Christians. But the leadership in the pro-life cause must come from believing, practicing, and instructed Catholics. Why do we say this? We must say this because the Catholic Church has the fullness of God’s revealed truth. Let us be honest. One reason for the rise of the anti-life forces throughout the world is that Catholics have not been as humbly believing, faithfully practicing, and well instructed in their faith as they should be. Concretely, this means that we must grow in our faith by becoming more Marylike in our belief.
By accepting, as Mary did, everything which God tells us,
By loyally living out what we believe, up to and including standing, like Mary, near Mary under the Cross of Jesus; as she stood in her Calvary, and we standing in our Calvary,
By striving to understand what we believe, especially following Mary’s example of “pondering the things we believe in our heart,” through daily meditation, mental prayer, and reflection on our faith in God’s presence, and in Mary’s company.
All of the foregoing are indispensable for lasting programs in the Pro-life Movement.
Devotion to Mary.
The Pro-life Movement will grow in the measure that we Catholics practice devotion to the Blessed Virgin Mary, Mother of God. Why? Because in the Pro-life Movement we are not struggling with mere flesh and blood but with the powers of darkness–in high places, which means with the devil and his human legions on earth.
In every major crisis over the centuries, the Church has appealed to Mary to overcome the forces of evil. That is why we absolutely must develop an extraordinary devotion to the Blessed Virgin Mary. The daily Rosary must become an essential part of our daily life. The daily Angelus, morning, noon, and night, should also become part of our daily living. A picture or statue of Our Lady should be an integral part of every Catholic household. Enrollment in a confraternity of the Blessed Virgin Mary and wearing a medal of the Blessed Virgin should become normal for every professed Catholic. Spiritual reading about Our Lady should become part of the mental diet of those, like us, who believe that Mary is the Mother of our God. Saturdays are not just ordinary days. For almost two thousand years, Saturday has been called Mary Day and Faith Day. Why? Because she alone of all the followers of Christ never wavered in her faith in His Resurrection from the dead. From childhood, my widowed mother and I never ate meat on Saturday. It was the least, I was told, that we can do to show our love for the Mother of Jesus.
It is surely not coincidental that the five hundred million Moslems throughout the world have a great love for Mary, the Mother of Jesus. In our day, the Moslems are almost unique in the non-christian world for their opposition to the pro-death movement which has reached a peak in the Beijing Conference which is now meeting, ironically, under the auspices of the United Nations.
May I suggest the following prayer to our Blessed Mother. You compose your own prayer, but this is what I recommend:
“Mary, Mother of God and our Mother, obtain for us from your divine Son something of His great love for human life, which He received from you and began in your womb. Help us to exert ourselves to the limit to safeguard the sanctity of all human life, whether born or unborn, whether helpless or strong. Ask Jesus, the Light of Life, to enlighten the leaders of nations that human life is to be loved, because that is why we are conceived–to serve God by loving others here on earth and be happy with Him and with our families, for all eternity. Amen.”
(ONE MORE SOUL NOTE: Although this is an interesting article about the pill and nutrition we do not agree with the author’s opinion that the birth control pill is essential and “life-saving”. The author mentions some serious life-threatening conditions associated with the use of the pill. A better way to keep optimal nutrition will be to eat a healthy diet, get supplementation when needed, and avoid harmful hormonal steroids such as birth control pills.)
You can eat your fruits and veggies, exercise regularly, and take the occasional gummy vitamin—but that may not be enough to reach optimal health if you’re currently on a hormonal birth control pill. One of the lesser-known side effects of the Pill is it’s ability to cause deficiencies in essential vitamins and minerals like vitamin B6, magnesium, vitamin b12, folic acid, vitamin C, and zinc, among others. With immune health being of critical importance these days, why aren’t more women aware of this side effect?
“The science is there, but it’s certainly not new,” says Dr. Charis Chambers, a Board-certified OBGYN who is known as The Period Doctor. “I mean, this has been written about and discussed since the ’70s.” She notes that B vitamins are “particularly important for women of reproductive years,” and in addition to preventing anemia, they also play a key role in the “normal development of a fetus.” Some of the key vitamins and minerals birth control pills deplete—like vitamin c, for example— can lead to an increase in oxidative stress, triggering a potential cascade of negative effects. Especially since birth control is something women take for years, sometimes decades.
So why does birth control impact your bioavailability of these nutrients? The science points to a variety of causes, all of which Dr. Jolene Brighten, a nutritional biochemist and naturopathic physician, covers in her book Beyond The Pill. Hormonal contraception impacts so many processes, Brighten explains, from how your liver functions to your gut permeability (and even who you’re attracted to). But both Brighten and Chambers agree that it’s largely the Pill’s impact on your liver function that’s to blame. “The human body is so complex,” says Chambers. “It’s mostly because these hormones are affecting your liver, which affects how everything is metabolized to your body.”
All this isn’t to say that birth control is bad—for many women, it’s essential and life-saving. It’s just worth noting that in addition to preventing pregnancy and quelling symptoms of PCOS, hormonal pills can also impact your nutritional health.
Chambers stresses that just because a vitamin or mineral shows up as low on a blood test doesn’t mean it automatically correlates to any serious health issues. “How am I helping you by letting you know, hey, that’s a little low? It doesn’t equal that you would have depression, it doesn’t equal that you would be anemic. It doesn’t even equal greater birth defects,” says Chambers. To understand your health is to look at the big picture.
So why isn’t this decades-old side effect more commonly discussed? Chambers explains that the reason doctors don’t usually tell their patients about this risk is because their time with you is quick, and they’d rather let you know about more serious complications like strokes and blood clots. “We have limited time and I want I don’t want to get so lost in the weeds that I miss an opportunity to help you reach your life goals, which is planning your life and your family,” she says. If you want to optimize your nutritional health, don’t be afraid to discuss any concerns with your doctor.
This begs the question: while you’re still on the Pill, how can you optimize your nutrition outside of a balanced diet? Some supplement brands are currently selling capsules designed specifically for women on the Pill to fill in the gaps, though critics say they’re not well-rounded enough. Brighten and Chambers both agree that all women of child-bearing age, whether they’re on birth control pills or not, should be taking a prenatal or women’s multivitamin, which will cover all of your nutritional bases.
“If you’re concerned about the nutrient depletions happening, get on a multivitamin or prenatal, but it’s not urgent right now for you to get b12 tested,” adds Brighten. Chambers also cautions against taking extreme measures to course-correct your nutrition at-home. “It doesn’t mean you should be like loading up on just B complex vitamins or chugging magnesium, or anything extreme,” she says.
In the age of COVID-19, it’s tempting to think more is better when it comes to immune-boosting and anti-inflammatory vitamins and minerals like vitamin C and zinc. That’s not the case. Other than taking a daily vitamin supplement, Brighten advises to only rush to a doctor if you’re exhibiting serious, life-threatening symptoms like difficulty breathing or chest pain that could indicate either a COVID infection or blood clot. “Will taking a multivitamin or prenatal prevent you from getting COVID? Absolutely not. Can you out-eat your way from contracting COVID? No,” says Brighten, who publicly battled the disease earlier this year. “So [supplements are] not a treatment and not a cure, and it’s not going to prevent it. But it is something that my doctors have said to me multiple times: if I had not had the diet and lifestyle that I did, I probably would have died from COVID.”
The goal to be a father, to be a mother, is a human right. An absolute human right.~Italian infertility specialist Severino Antinori.1
God bestowed men and women with an innate desire to procreate and to nurture their children. This is one of the most fundamental instincts of all, shared by all of God’s creatures. But sometimes God’s plan for our lives differs from our own, and couples find that they cannot have their own natural children.
In this most complex of issues―infertility and its possible resolutions―there is a great amount of confusion and misunderstanding regarding the teachings of the Catholic Church. After all, we have a virtual universe of surgical and medical procedures to evaluate, with new ones being announced on nearly a monthly basis. We must consider the impregnation of single women and lesbian couples with sperm; various forms of surgery to repair damaged reproductive systems; early human embryos grown in cow or other animal uteri (“xenotransplantation”); numerous variants of in-vitro fertilization (IVF); designer babies conceived solely to avoid (or even inherit) certain genetic diseases; reproductive cloning; and surrogate motherhood, to name just a few.
We must judge each specific procedure on its own merits, but underlying all of them is the fundamental question: “Is having children a right?”
IVF specialist Randy S. Morris, M.D., says, “A different [religious] view states that in order to determine God’s will, fertility treatments must first be tried. If God truly does not want a couple to have children, he will simply prevent the treatments from working.”
Unfortunately, Dr. Morris’ misunderstanding of Church teachings is shared by many. Under the same reasoning, I could point a gun at someone and pull the trigger. If God desires my intended victim to live, He will make certain that the gun jams or misfires. Whether it is reproductive technologies or outright murder, God permits us to bypass His will for our lives because He has given us the most precious gift of free will. He allows us to choose evil.
If a couple has no right to a child, then it can be argued that a doctor lacks the moral justification to help produce one for them. While it may be moral to treat a disease which hinders the body from producing a child, such as surgery to open blocked fallopian tubes, it would be morally unacceptable to use those treatments which aim to produce a child but still leaves a couple infertile. IVF would fall into this latter category.
In practice, impermissible assisted reproductive technologies do not seek to heal an illness or injury. They instead cater to a desire by bypassing or replacing the marital act. By contrast, licit ARTs actually treat an injury or a defect, with the intent of allowing the married couple to conceive naturally.
Is Having Children a, Right?
As the quotation at the beginning of this article demonstrates, many scientists equate urges and wants with “basic human rights.” Large multinational organizations are taking up this cause; the United Nations World Health Organization (WHO) recently published a document claiming that the inability to have children (including a lack of success in finding a sexual “partner”) constitutes a disability that governments are obligated to ameliorate, giving every person a “right to reproduce.”2 In other words, single men and women are by definition “infertile.” Fertility specialist David Adamson, one of the authors of the new and expanded classification of “infertility,” claims that the new definition
…puts a stake in the ground and says an individual’s got a right to reproduce whether or not they have a partner. It’s a big change. It fundamentally alters who should be included in this group and who should have access to healthcare. It sets an international legal standard. Countries are bound by it.
Apparently, the ivory tower medical bureaucrats at the WHO are blissfully unaware that every new “right” they invent necessitates a corresponding obligation on the part of others—in this case, the use of a woman’s body, a fact noted and rightly criticized by leading feminists.
Simply proclaiming something to be “an absolute human right” does not magically make it so. Even a happily married couple with ample resources does not have a right to a child, because a child is a person, and nobody has a “right” to another person.
We are all created in the image and likeness of God, and therefore share in His dignity. Unfortunately, our world is rife with violations of this dignity, especially at life’s beginning and at its end. In addition, married couples share an additional unique and precious dignity due to the fact that they have been united in one flesh. When other parties are introduced into their co-creation of a child, many problems―both spiritual and physical―will result.
Of all people, pro‑life activists can empathize with the yearning for a child that an infertile couple experiences. Crisis pregnancy center workers and sidewalk counselors, especially, are struck by the irony of abortionists killing thousands of perfectly healthy children every day―while thousands of couples undergo the stress and pain of a complicated and expensive series of tests and procedures so they can have what others are contemptuously disposing of as “biological waste.”
People who know infertile couples often wish that they could somehow miraculously present them with the infant they long for.
This kind response is commendable, but unfortunately it defines children as a “right” and intrinsically and unconsciously reduces their status from a supreme “gift of the Lord” (Psalm 127:3) to an acquisition or a possession. Worse, it seems that those who promote the most popular assisted reproductive technologies do not even begin to consider the impacts the procedures may have on resulting children.
Donum Vitae explains:
A true and proper right to a child would be contrary to the child’s dignity and nature. The child is not an object to which one has a right, nor can he be considered as an object of ownership: rather, a child is a gift, “the supreme gift” and the most gratuitous gift of marriage, and is a living testimony of the mutual giving of his parents. For this reason, the child has the right, as already mentioned, to be the fruit of the specific act of the conjugal love of his parents; and he also has the right to be respected as a person from the moment of his conception. [II,8]
Our Lord gives every one of us crosses to bear. Some of these involve losses close to us and are much more difficult to carry than others―such as the death of a child, the inability to conceive or lack of success in finding a spouse.
The thinking that there is a “right” to a child is a derivation of the mentality that is confused about the nature of true freedom. True freedom is doing what you should do, not what you want to do. Those who pursue their desires without regard for the moral law are enslaved to those wants and tend to trample any person or law that gets in their way.
Final Thoughts
We can respond to the severe trial of childlessness or an inability to find a spouse in one of two ways. We can struggle against them with all of our energy and strength, and, whether we conquer them or not, find ourselves afflicted with a strange emptiness of soul. Or we can use licit technology in an attempt to bypass our infertility, while acknowledging God’s mastery over our lives, knowing that our ultimate happiness is His concern.
Donum Vitae offers hope and solace to infertile couples:
Spouses who find themselves in this sad situation are called to find in it an opportunity for sharing in a particular way in the Lord’s Cross, the source of spiritual fruitfulness. Sterile couples must not forget that even when procreation is not possible, conjugal life does not for this reason lose its value. Physical sterility in fact can be for spouses the occasion for other important services to the life of the human person, for example, adoption, various forms of educational work, and assistance to other families and to poor or handicapped children. [II,8]
Endnotes
[1] Italian infertility specialist Severino Antinori, quoted in the Lexington Herald‑Leader, January 26, 2001 and the SPUC News Digest for 30 January 2001.
[2] Julian Vigo. “The World Health Organization And The ‘Right’ To Reproduce.” The Huffington Post Blog, October 31, 2016. Males could even be classified as “infertile” in the sense that “the inability to find a suitable sexual partner—or the lack of sexual relationships which could achieve conception—could be considered an equal disability.”
The abortion industry is highly skilled at marketing its “services,” changing tactics to suit various situations. From “safe, legal, and rare” to simply “legal,” pro-abortion businesses and organizations frequently change their terminology. In one recent example, the abortion pill has been compared at least twice to Tylenol, but in very different ways.
Some claim the abortion pill is “safer than Tylenol”
Former Planned Parenthood CEO Cecile Richards wrote an op-ed in the Los Angeles Times in 2018 in which she erroneously claimed, “There is no medical or health reason for [a] ban on medication abortion. Approved by the Food and Drug Administration in 2000, non-invasive medication abortion is safe by all measures — safer than Tylenol and Viagra, even.”
What Richards neglected to mention is that the abortion pill carries risks of abdominal pain, nausea, vomiting, diarrhea, headache, heavy bleeding, and maternal death — all of which can happen when taking the prescribed dosage on just one occasion. Additionally, the abortion pill can fail and lead to follow-up surgical abortions. Some women have died from infection or undiagnosed ectopic pregnancies after taking the abortion pill.
For these reasons, the U.S. Food and Drug Administration has specific safety regulations in place (REMS) which require one of the two drugs in the abortion pill regimen (mifepristone) to be dispensed by a certified prescriber at an approved hospital or clinic. (Some of these requirements have been suspended during COVID-19, a decision which the FDA is actively opposing.)
Tylenol is an over-the-counter medication which is not subject to REMS.
The abortion pill is clearly not safer than Tylenol.
Others claim the abortion pill is really “not the same as taking a Tylenol”
Yet this week in response to Florida House Bill 265, which requires that minors have written consent from their legal guardian for an abortion, pro-choice Generation Action board member Emma Moses said that the abortion pill is actually “not the same as taking a Tylenol” so that she could argue that a minor taking the abortion pill should not be forced to tell her parents, despite any safety risks.
She’s right, but perhaps not in the way she thinks. There are consequences to taking the abortion pill that are dangerous, yet Moses argues that telling parents that their child is taking the abortion pill is what puts girls in a “really dangerous” situation. That argument is misguided.
In reality, withholding that information from a minor’s parents could be dangerous because girls taking it could suffer major complications, including death. If a girl’s parents are unaware that she has taken the abortion pill, they cannot properly communicate with emergency responders. Additionally, a teen could potentially be a victim of sexual abuse by a teacher, an uncle, or a coach. Informing her parents about the abortion could be the one window of opportunity to save her from the abuse.
The abortion pill is not safer than Tylenol, as was claimed by Planned Parenthood’s former president.
Yet, despite the difference in safety, the major difference between Tylenol and the abortion pill is that only one exists solely to end the life of a human being.
Most women know that pharmaceutical birth control does not protect against STDs. But did you know that certain forms of birth control can actually increase your risk for contracting human immunodeficiency virus (HIV), which if left untreated, may progress to the deadly disease known as acquired immunodeficiency syndrome (AIDS)?
Depo-Provera (also referred to as DMPA, or DMPA-IM), a brand of birth control that is often referred to as “the birth control shot,” is one such form of birth control that introduces so much risk for users, that a group of doctors and researchers have petitioned the FDA for its complete removal from the market. While all forms of pharmaceutical birth control come with side effects, the FDA petitioners claim the health complications of the Depo-Provera birth control shot are too high to justify the benefits of pregnancy prevention.
The doctors and researchers who petitioned the FDA presented evidence that conclusively shows that Depo-Provera is responsible for increased transmission of HIV from men to women. Again, if left untreated, HIV will progress to the extremely deadly disease known as AIDS.
According to UNAIDS, between 31.6 million and 44.5 million people globally were living with HIV in 2019. An estimated 500,000 to 970,000 people globally died from AIDS-related illnesses in 2019. Sub-Saharan Africa alone contains more than two-thirds of all people living with HIV globally. Notably, according to data from the United Nations, Depo-Provera is the most popular method of contraception in Sub-Saharan Africa.
A 2016 meta-analysis of global survival rates from HIV diagnosis to AIDS onset, and from AIDS onset to death, found that “the majority of HIV-positive patients progress to AIDS within the first decade of diagnosis. Most patients who receive highly active antiretroviral therapy (HAART) will survive for >10 years after the onset of AIDS, whereas the majority of the patients who do not receive HAART die within 2 years of the onset of AIDS.”
Despite the established side effects of Depo-Provera, including increased risk to HIV—which is clearly still an extremely serious and deadly disease despite significant advances in HAART—this side effect is currently not reported by mainstream sources of contraceptive information, such as Planned Parenthood. Notably, when discussing the side effects and disadvantages of Depo-Provera, Planned Parenthood also neglects to mention another serious, well-established risk of the birth control shot: bone mineral density loss, which leads to an increased risk of bone fractures and osteoporosis later in life for women.
“four meta-analyses (3 reports, one of which is known as the 2015 Morrison SRMA trial) were published in 2015. Each used different inclusion criteria and compiled the data on different numbers of studies, yet all 4 came up with essentially the same result of significantly increased risk of male-to-female HIV transmission in women using DMPA. . . . Importantly, no consistent association has emerged with regard to oral contraceptives or other injectable or implantable contraceptives and the facilitation of HIV transmission.”
In contrast, organizations that downplay the risk of HIV for Depo-Provera users cite a study known as the ECHO Trial study which was conducted between Dec 2015 and Sept 2017 to examine the risk of HIV acquisition by women using the Depo-Provera birth control shot. Published in The Lancet in June 2019, the study concluded that the ECHO Trial Consortium of researchers “did not find a substantial difference in HIV risk among the methods evaluated [including Depo-Provera, the copper IUD, and the levonorgestrel implant], and all methods were safe and highly effective.”
According to the authors of the Citizen’s Petition to the FDA, ECHO’s conclusion is erroneous and also potentially disingenuous:
“a careful analysis of the design and results of the ECHO Trial reveals that in fact, the ECHO Trial results of 2019 provide a near perfect confirmation of the results of the 2015 Morrison SRMA trial, and that the authors misrepresent them as the opposite; as the exculpation of DMPA as ‘safe.’”
Closer inspection of their analysis reveals that the ECHO researchers decided that they would only consider a 50% increase in HIV risk as “meaningful” on the basis of “formative work with stakeholders to determine a meaningful difference that would inform policy change.” Thus, they instead advocate for “continued and increased access to these contraceptive methods.”
Understanding the ECHO study on HIV risk for Depo-Provera users
As it happens, the ECHO study did find that compared to the use of the levonorgestrel implant, Depo-Provera use was associated with an increased risk of HIV infection (with a hazard ratio of 1.29, as seen in their “continuous use” dataset in Table 2, almost identical to the Morrison SRMA trial, which concluded an increased HIV risk with Depo-Provera use). However, the study wasn’t statistically powered to measure the percent increased risk of hazard ratios below 1.3 (which would indicate a 30% increased risk). So while we can’t conclude with certainty from these data what exactly the increased HIV infection risk of Depo-Provera is, it does seem that there is at least some increased level of risk (especially when considered with other robust studies which have indicated similar levels of increased risk), despite the ECHO Consortium’s insistence to the contrary.
In the ECHO study, the exact level of risk has been obscured for unknown reasons, making it difficult for women to get accurate information about HIV risks and Depo-Provera use.
Since other robust studies have indicated an increased risk of contracting HIV for Depo-Provera users—even if it’s less than a 50% increase—women should be informed of it so that they may consent to taking the risk. Greater transparency about birth control risks is in fact what motivated the Citizen’s Petition writers to urge the FDA that, of all the birth control methods available, Depo-Provera should be removed from the market.
Given how many highly effective methods of birth control are available to women today, there is little justification for downplaying the risks women face by receiving the Depo-Provera birth control shot. If you have had a negative experience with the birth control shot, we encourage you to submit your experience as a comment on the FDA petition.
WASHINGTON, DC, August 27, 2020 (LifeSiteNews) — A religious sister who was formerly a colonel in the U.S. Army Medical Corps gave a knock-out speech at the Republican National Convention last night, moving from a description of her recent work with refugees to her concern for the unborn.
“Those refugees all share a common experience,” said Sister Deirdre “Dede” Byrne, POSC.
“They have all been marginalized, viewed as insignificant, powerless and voiceless. And while we tend to think of the marginalized as living beyond our borders, the truth is the largest marginalized group in the world can be found here in the United States,” she continued.
“They are the unborn.”
Sister Dede held up the Lord Jesus Christ both as an example of someone once an embryo and as a model of defending justice against political correctness.
“It is no coincidence that Jesus stood up for what was just and was ultimately crucified because what He said wasn’t politically correct or fashionable,” she said.
“As followers of Christ, we are called to stand up for life against the politically correct or fashionable of today. We must fight against a legislative agenda that supports and even celebrates destroying life in the womb.”
Sister Dede combined her roles as a spiritual leader and a doctor to get across her deeply pro-life, humanitarian, and unabashedly Christian message.
“Keep in mind, the laws we create define how we see our humanity,” she said.
“And we must ask ourselves, ‘What are we saying when we go into a womb and snuff out an innocent, powerless, voiceless life?’” she continued.
“As a physician, I can say without hesitation, ‘Life begins at conception.’ While what I have to say may be difficult for some to hear, I am saying it because I am not just pro-life; I’m pro-eternal life. I want all of us to end up in heaven together someday.”
Sister Dede told her audience of millions of American viewers that she had been praying to be allowed to be a voice for human life. She saw the invitation to speak at the Republican National Convention as an answer to that prayer and was firm in her support of the re-election of Donald Trump.
“Donald Trump is the most pro-life president this nation has ever had, defending life at all stages,” Sister Dede said.
“His belief in the sanctity of life transcends politics.”
In contrast, she described Biden-Harris as “the most anti-life presidential ticket ever” because together they support even late-term abortion and infanticide.
Therefore, Sister Dede declared, the president has two solid groups of allies.
“Because of his courage and conviction, President Trump has earned the support of America’s pro-life community,” she said.
“Moreover, he has a nation-wide of religious standing behind him. You’ll find us here with our weapon of choice, the rosary.”
“So thank you, Mr. President. We are all praying for you.”
One of seven children, Deidre Byrne studied medicine at Georgetown University, where she joined the U.S. Army. Her service, which included roles as both doctor and surgeon, lasted 29 years. According to the Catholic News Agency (CNA), she was asked to be on “standby” as personal physician to Mother Teresa when the saint visited Washington, D.C. in 1997. Byrne was also a first responder during the 9/11 attack on the Pentagon.
Convinced that she was being called to religious life, Byrne pronounced her first vows with the Little Workers of the Sacred Hearts of Jesus and Mary, which has a medical apostolate, in 2004. She continued to serve with the military, including in Afghanistan, until she retired in 2009 at her order’s request.
In the wake of Sister Dede’s speech, there has been a robust conversation on social media about how extreme the pro-abortion views of Joe Biden and Kamala Harris are.
Their opinions have certainly diverged in the past. Biden previously had only a 36% rating as a pro-abortion politician from NARAL, thanks to his previous support for the Hyde Amendment. However, Biden has subsequently rejected the amendment, and the anti-life organization now says it is “proud to endorse” him.
The Hyde Amendment bans federal funding for most abortions, anathema to radically pro-abortion politicians like Planned Parenthood ally Kamala Harris. Susan B. Anthony List president Marjorie Dannenfelser described Harris earlier this month as “an extremist.”
“Kamala Harris is an extremist who supports abortion on demand through birth, paid for by taxpayers, and even infanticide — an agenda rejected by the overwhelming majority of Americans, including millions of Independents and rank-and-file Democrats,” Dannenfelser said.
“As attorney general of California, Harris conspired with the abortion industry to launch a politically-motivated shakedown of brave citizen journalists who exposed Planned Parenthood’s role in the harvest and sale of aborted baby parts for profit.”
“The stakes are life and death and the choice is clear. Pro-life Americans must unite to defeat Biden-Harris.”
Pro-life activist Abby Johnson discussed her experience working at Planned Parenthood at the Republican National Convention Tuesday night, saying that her experiences with the nation’s largest abortion provider are why she advocates “so passionately for life.”
Johnson said Planned Parenthood approached her at a volunteer fair and convinced her to volunteer for the organization by talking about “helping women in crisis and their commitment to keep abortion safe, legal, and rare.” She began working for the organization, she said, and received Planned Parenthood’s employee of the year award.
“My supervisor assigned me a new quota to meet… an abortion quota,” she said. “I was expected to sell double the abortions performed the previous year. When I pushed back, underscoring Planned Parenthood’s public facing goal of decreasing abortions, I was reprimanded and told abortion is how we make our money.”
“But the tipping point came a month later when a physician asked me to assist with an ultrasound-guided abortion,” she continued. “Nothing prepared me for what I saw on the screen. An unborn baby fighting back, desperate to move away from the suction.”
Johnson said that she will “never forget” the doctor joking, “Beam me up, Scotty.”
“The last thing I saw was a spine twirling around in the mother’s womb before succumbing to the force of the suction,” Johnson said. The incident happened in August, she noted, and she left the clinic in October. Johnson says that she only looks back on her experiences there “to remember why I now advocate so passionately for life.”
“For me, abortion is real,” she continued. “I know what it sounds like. I know what abortion smells like.”
“Did you know abortion even had a smell?” Johnson asked the audience.
The pro-life activist said that she now supports President Donald Trump because “he has done more for the unborn than any other president.”
“During his first month in office, he banned federal funds for global health groups that promote abortion,” Johnson said. “That same year, he overturned an Obama-Biden rule that allowed government subsidy of abortion. He appointed a record number of pro-life judges, including two Supreme Court justices. And importantly, he announced a new rule protecting the rights of healthcare workers objecting to abortion, many of whom I work with every day.”
“This election is a choice between two radical, anti-life activists, and the most pro-life President we’ve ever had,” she concluded, urging viewers to take action and vote to re-elect Trump.
“And do it with our very most vulnerable Americans in mind – the ones who haven’t been born yet,” she added.
WATCH:
LifeNews Note: Mary Margaret Olohan writes for Daily Caller. Content created by The Daily Caller News Foundation is available without charge to any eligible news publisher that can provide a large audience.
It has been so long since America lived through Griswold v. Connecticut, followed by Roe v. WadeandDoe v. Bolton, that our citizenry may not realize that our current national plague of systemic violence has roots. But really, it is not at all surprising.
If you are wondering how Supreme Court decisions dealing with human sexuality could lead to mayhem, murder, and a general disregard for human dignity, let us explain.
French archbishop Michel Aupetit explains that a lack of appreciation for the gift of fertility is the beginning. He argues that rejection of Pope Paul VI’s Humanae Vitae by Catholics—including many members of the hierarchy—led to an acceptance of contraception and abortion. In the midst of this calamitous shift away from “genuine loving interpersonal relations” there came a “corrosive shift in the way people think about parenthood and childbearing.”
At this point, the human family began to disintegrate, and systemic violence took root, first by the slow disappearance of men as the head of the family, and at the same time, the emergence of women’s liberation as a way of life.
Rejection of fertility as the norm was the first fatality. That was followed by chemical and mechanical interventions to avoid pregnancy and the elimination of the preborn baby by an act of direct killing. In this milieu, systemic violence took root, and from there things both sexual and cultural have only gotten worse.
Contraception conditions men and women, and therefore the cultures which they form, to deny the obvious and intrinsic relationship between sex and the conception of new life. Contraception pits couples into a kind of unknowing war with themselves. . . . It is as if they are saying to one another, “yes, I’m yours, but not all of me.” This subtle and unknowing war with the partner and with the self inevitably leads to alienation, to atomization, and, eventually, to a kind of loneliness.
Alienation, manipulation, distrust, and disregard for the uniqueness of the human person are just some of the repercussions. If that is not a path to hostility, I do not know what is.
READ >>Let the Supreme Court Decide
Americans in general do not want to get to the root cause of systemic violence because a desire to dig deeper would create discomfort, so why bother? Blame it on some radical group, a political party, or a respectable entity like a local police department and move on.
While such trivial excuses summarize the prevailing attitude today, we know that babies are still dying, women and men are still suffering, and families are in shambles. The deadly carnage resulting from the sexual revolution obliges us to bring it to the attention of anyone with ears to hear.
Believe me, politicians will never do it. Judges will not acknowledge their roles in it, and far too many religious leaders prefer to turn a blind eye than confront the evil in our midst.
At this moment in time, we need a restoration of moral sanity.
And while the Democrats and the Republicans are jockeying for their version of political moral high ground, the real answer is here before us, and it has no partisan label. It is simply common sense—a recognition of truth. All we need to do is take our cue from St. John Paul II, who wrote that the Gospel of Life was “meant to be a precise and vigorous reaffirmation of the value of human life and its inviolability, and at the same time a pressing appeal addressed to each and every person, in the name of God: respect, protect, love and serve life, every human life! Only in this direction will you find justice, development, true freedom, peace and happiness!”
READ >>A Supreme Court Folly: The Same-Sex Union Decision
In the service of life, each of us can help stem and eradicate the systemic violence that begets hatred. Where there is disdain, we are called to sow the seeds of hope as we teach the meaning of true freedom, peace, and happiness in Jesus Christ.
I have received your kind email, in which you inform me of the initiative you have scheduled for this coming September 5 for the protection of the physical, moral, and spiritual health of your children. In responding to you, I address all the mothers of Italy.
The demonstration you are promoting intends to express the dissent of citizens and in particular of parents against the norms that the government, abusing its power, is preparing to issue in view of the new school year; norms that will have very grave repercussions on the health and psychosomatic equilibrium of students, as authoritative experts have rightly demonstrated.
First of all, the systematic effort to demolish the family, the foundation of society, must be denounced, with the multiplication of ferocious attacks not only against conjugal life, which Christ has elevated to a Sacrament, but also against its very natural essence, against the fact that marriage is by nature constituted between a man and a woman in an indissoluble bond of fidelity and reciprocal assistance. The presence of a father and a mother is fundamental in the upbringing of children, who need a male and female figure as a reference for their integral and harmonious development; nor can it be permitted that children, during the most delicate phase of their infancy and adolescence, be used to advance partisan ideological claims, with serious damage for their psychosomatic equilibrium, by those who with their own rebellious behavior reject the very idea of nature. You can easily understand the impact of the destruction of the family on the civil consortium: today we have right before our eyes the results of decades of unfortunate policies that inevitably lead to the dissolution of society.
These policies, inspired by principles that are repugnant both to the Law of nature inscribed in man by the Creator as well as to the positive Law of God given in the Commandments, combine to permit children to be placed at the mercy of the whims of individuals, and that the sacredness of life and conception become objects of commerce, humiliating motherhood and the dignity of woman. Sons cannot be bred by mares for a fee, because they are the fruit of a love that Providence has ordained must always be an enduring love, even in the natural order.
Parents have the responsibility, as a primary and inalienable right, to educate their children: the State cannot arrogate this right, much less corrupt children and indoctrinate them in the perverse principles that are so widespread today. Do not forget, dear mothers, that this is the distinctive sign of totalitarian regimes, not of a civil and Christian nation. It is your duty to raise your voice so that these attempts to steal the education of your children may be denounced and rejected with force, because you will be able to do very little for them if your faith, ideas, and culture are judged incompatible with those of an impious and materialistic state. And it is not just a matter of imposing a vaccine on your children and teenagers, but also of corrupting their souls with perverse doctrines, with gender ideology, with the acceptance of vice and the practice of sinful behaviors. No law can ever legitimately make the affirmation of the truth a crime, because the authority of the law ultimately comes from God, who is himself the highest Truth. The heroic testimony of the martyrs and saints responded to the oppression of tyrants: may you too today be courageous witnesses of Christ against a world that would like to subject us to the unleashed forces of hell!
Another crucial aspect in this battle for the family is the defense of life from conception to natural death. The crime of abortion, which has claimed millions of innocent victims and that cries out for vengeance from heaven, is today considered as a normal health service, and just in recent days the Italian government has authorized the more widespread use of the abortion pill, encouraging an abominable crime and keeping silent about the terrible consequences on the psychological and physical health of the mother. If you think about how during the lockdown all care of the sick was suspended and yet abortions continued, you can understand what the priorities of those who govern us are: the culture of death! What progress can be invoked when society kills its own children, when motherhood is horribly violated in the name of a choice that cannot be free, since it involves the ending of an innocent life and violates one of God’s Commandments? What prosperity can our country expect, what blessings from God can it hope for, if human sacrifices are being made in our clinics just as in the times of the most bloody barbarism?
The idea that children are the property of the state repulses every human person. In the Christian social order, the civil authority exercises its power to guarantee its citizens that the natural well-being is ordered towards the spiritual good. The common good pursued by the state in temporal things therefore has a well-defined object that cannot and must not be in conflict with the Law of God, the Supreme Legislator. Every time that the State infringes on this eternal and immutable Law, its authority is diminished, and its citizens ought to refuse to obey it. This certainly applies to the hateful law on abortion, but it should also be applied to other cases, in which the abuse of authority regards the imposition of vaccines whose danger is unknown or that, by their very composition, are ethically problematic. I am referring to the case in which a vaccine would contain fetal material coming from the bodies of aborted children.
But there are other disturbing aspects now envisaged, which regard not only the content of instruction but also the method of participation in the lessons: social distancing, the use of masks and other forms of presumed prevention of contagion in classrooms and school environments cause serious damage to the mental and physical equilibrium of children and young people, compromising their ability to learn, the interpersonal relations between pupils and teachers, and reducing them to automatons that are not only ordered what to think but also how to move and even how to breathe. It seems that the very notion of common sense that ought to govern choices fraught with consequences in social life has been lost, and it seems that an inhumane world is being heralded in which parents have their children taken away from them if they test positive for an influenza virus, with mandatory health treatment protocols applied as in the most ferocious dictatorships.
It is also very perplexing to learn that the WHO has chosen Mario Monti as the President of the European Commission for Health and Development, who has distinguished himself by draconian measures imposed on Italy, among which, it must not be forgotten, is the drastic reduction of public appropriations for hospitals. These perplexities are confirmed by Monti’s membership in supranational organisms like the Trilateral Commission and the Bilderberg Club, whose aims are in clear contrast to the inalienable values protected by the Italian Constitution itself, which are binding on the Government. This mixing of private interests in public affairs, inspired by the dictates of Masonic and globalist thought, should be vigorously denounced by those who are representatives of the citizens, and by those who see their legitimate powers usurped by an elite that has never made a mystery of its true intentions.
We should not lose sight of a fundamental element: the pursuit of ideologically perverse goals is invariably accompanied by an interest of an economic nature, like a parallel track. It is easy to agree on the fact that there is no profit in the voluntary donation of umbilical cords, just as there is no profit in the donation of hyper-immune plasma for the treatment of Covid. Conversely, it is extremely profitable for abortion clinics to provide fetal tissue and for pharmaceutical companies to produce monoclonal antibodies or artificial plasma. Thus it is not surprising that, following a logic of mere profit, the most reasonable and ethically sustainable solutions are the object of a deliberate campaign to discredit them: we have heard self-styled experts make themselves promoters of cures offered by companies in which they themselves – in a clear conflict of interest – hold shares or are well paid consultants.
Having said this, it is necessary to understand whether the solution of a vaccine is always and everywhere the best health response to a virus. In the case of Covid, for example, many exponents of the scientific community agree in affirming that it is more useful to develop a natural immunity rather than inoculate the depowered virus. But also in this case, as we know, herd immunity is attained without any costs, while vaccination campaigns involve enormous investments and guarantee equally large profits for those who patent and produce them. And it should also be verified – but in this the experts will certainly be able to speak with greater confidence – whether it is possible to produce a vaccine for a virus that does not yet seem to have been isolated according to the protocols of science-based medicine, and what potential consequences may come from using newly generated genetically modified vaccines.
The world health industry, led by the WHO, has become a true multinational corporation that has as its primary end the profit of shareholders (pharmaceutical companies and so-called philanthropic foundations), and its means of pursuing it is the transformation of citizens into chronically ill people. And it is obvious: the pharmaceutical companies want to make money by selling drugs and vaccines; if eliminating diseases and producing effective drugs leads to a reduction in the number of sick people and thus of profits, it will only be logical to expect that the drugs they make will be ineffective and that the vaccines they promote will be the instrument of spreading diseases rather than eradicating them. And this is precisely what is happening. How can we think that the search for cures and therapies is being promoted in a disinterested way if those who finance the search profit disproportionately from the persistence of pathologies?
It may seem difficult to persuade ourselves that those who ought to be protecting health instead wish to ensure the continuation of illnesses: such cynicism repulses – and rightly so – those who are strangers to the mentality that has been established in healthcare. And yet this is what is happening right before our eyes, and it involves not only the emergence of Covid and vaccines – in particular anti-influenza vaccines, which were widely distributed in 2019 right in those areas where Covid has had the highest number of victims [in 2020] – but all treatments and therapies, as well as childbirth and care for the sick. Such cynicism, which is repugnant to the ethical code, sees in each of us a potential source of profit, while instead what should be seen in every patient is the face of the suffering Christ. We therefore appeal to the many, many Catholic doctors and all doctors of good will, asking you not to betray the Hippocratic oath and the very heart of your profession, which is mercy and compassion, love for those who suffer, and selfless service to the weakest among us, recalling the words of Our Lord: “As often as you did these things for the least of my brothers, you did it for me” (Mt 25:40).
The Catholic Church, especially in recent decades, has intervened authoritatively in this debate, thanks also to the Pontifical Academy for Life founded by John Paul II. Its members, up until a few years ago, gave medical-scientific directives that did not conflict with the inviolable moral principles of any Catholic person.
But just as in civil society we have witnessed a progressive loss of responsibility of individuals as well as those who govern in the various spheres of public life, including health care, so also in the “Church of Mercy” that was born in 2013 it is preferred to adapt the commitment of the Pontifical Dicasteries and the Academy for Life to a liquid vision – and I dare say a perverse vision because it denies the truth – which embraces the demands of environmentalism with connotations of Malthusianism. The fight against abortion, which opposes the reduction of births desired by the New World Order, is no longer the priority of many pastors. During the various pro-life demonstrations – such as those held in Rome in recent years – the silence and absence of the Holy See and the hierarchy has been shameful!
Obviously the moral principles which form the basis for norms to be adopted in the medical field remain perennially valid, nor could it be otherwise. The Church is the guardian of the teaching of Christ and she has no authority to modify or adapt it to her own liking. We remain bewildered, however, as we witness the silence of Rome, which appears to be more concerned with promoting recycling – to the point of writing an encyclical about it – rather than the lives of the unborn, the health of the weakest, and the assistance of the terminally ill. This is only one aspect of a much wider problem, a much greater crisis, which as I have said many times stems from the moment in which the deviant part of the Church, led by what was once the Society of Jesus, seized power and made her a slave to the mentality of the world.
When we consider the new orientation of the Pontifical Academy for Life (whose presidency has been entrusted to a person who is well-known for having shown the best of himself when he was bishop of Terni), we cannot expect any condemnation of those who use fetal tissue from voluntarily aborted children. Its present members hope for mass vaccination and the universal brotherhood of the New World Order, contradicting previous pronouncements of the same Pontifical Academy.[1] In recent days the Bishops’ Conference of England and Wales[2] has entered this anomalous wave. On the one hand it recognizes that “The Church is opposed to the production of vaccines using tissue derived from aborted fetuses, and we acknowledge the distress many Catholics experience when faced with a choice of not vaccinating their child or seeming to be complicit in abortion,” but it then affirms, in very grave contradiction with the stated unchanging principles of Catholic morality,[3] that “the Church teaches that the paramount importance of the health of a child and other vulnerable persons could permit parents to use a vaccine which was in the past developed using these diploid cell lines.” This statement lacks any doctrinal authority and instead aligns itself with the dominant ideology promoted by the WHO, its principal sponsor Bill Gates, and pharmaceutical companies.
From a moral point of view, for every Catholic who intends to remain faithful to his or her Baptism, it is absolutely inadmissible to accept a vaccination that utilizes material coming from human fetuses in its process of production. This has also been restated authoritatively recently by the American Bishop Joseph E. Strickland in his April 27 Pastoral Letter[4] and in his August 1 tweet.[5]
We must therefore pray to the Lord, asking him to give Pastors a voice, in such a way as to create a united front that opposes the excessive power of the globalist elite which would like to subjugate us all. It should be recalled that while the pharmaceutical companies are proceeding on the plane of economic interests only, there are people operating on the ideological plane who, using the opportunity of the vaccine, would also like to implant devices for identifying people, and that these nanotechnologies – I am referring to project ID2020, “quantum dots” and other similar initiatives – are being patented by the same individuals who patented the virus as well as its vaccine. Furthermore, a cryptocurrency project has been patented to allow not only health identification but also personal and banking information to be monitored, in a delirium of omnipotence that up until yesterday could have been dismissed as the ranting of conspiracy theorists, but that today has already been initiated in several countries, including for example Sweden and Germany. We see the words of Saint John taking shape right before our eyes: “It forced all the people, small and great, rich and poor, free and slave, to be given a mark on the right hand and the forehead; so that no one could buy or sell without having the mark” (Rev 13:16-17).
Given the gravity of the situation, we must also speak out with regard to these aspects: we cannot remain silent if the public authority would make vaccines obligatory that pose serious ethical and moral problems, or that more prosaically do not give any guarantee of obtaining the promised effects and that are limited to promising benefits that from a scientific point of view are absolutely questionable. May the pastors of the Church finally raise their voice to defend the flock entrusted to their care in this systematic attack against God and man!
Do not forget, dear Mothers, that this is a spiritual battle – even a war – in which powers that no one has ever elected and that do not have any authority other than that of force and the violent imposition of their own will seek to demolish all that evokes, even only remotely, the divine Paternity of God over His children, the Kingship of Christ over society and the Virginal Motherhood of Mary Most Holy. This is why they hate to mention the words father and mother; this is why they want an irreligious society that is rebellious against the Law of God; this is why they promote vice and detest virtue. This is also why they want to corrupt children and young people, securing hosts of obedient servants for the foreseeable future in which the name of God is being cancelled and the Redemptive Sacrifice of his Son on the Cross is blasphemed; a Cross that they want to banish because it reminds man that the purpose of his life is the glory of God, obedience to His Commandments and the exercise of Christian charity: not pleasure, self-exaltation, or the arrogant overpowering of the weak.
The innocence of children and their trusting recourse to Mary Most Holy, our Heavenly Mother, can truly save the world: for this reason the Enemy aims to corrupt them in order to distance them from the Lord and to sow the seed of evil and sin in them.
Dear mothers, never fail in your duty to protect your children not only in the material order but also, even more importantly, in the spiritual order. Cultivate in them the life of grace, with constant prayer, especially through the recitation of the Holy Rosary, with penance and fasting, with the practice of the corporal and spiritual works of mercy, assiduously and devotedly frequenting the Sacraments and Holy Mass. Nourish them with the Bread of Angels, the true food of eternal life and our defense from the assaults of the Evil One. Tomorrow, they will be honest citizens, responsible parents, and protagonists of the restoration of the Christian society that the world would like to cancel. And please also pray, dear mothers, because prayer is a truly fearful weapon and an infallible vaccine against the perverse dictatorship that is about to be imposed on us.
I take this occasion to assure you of my prayer and to impart my Blessing to all of you: to you, dear mothers, and to your children, and to all those who are fighting to save our children and each one of us from this ferocious global tyranny that is striking our beloved Italy.
+ Carlo Maria Viganò, Archbishop
15 August 2020 Assumption of the Blessed Virgin Mary
[5]Tweet of August 1, 2020: “I renew my call that we reject any vaccine that is developed using aborted children. Even if it originated decades ago it still means a child’s life was ended before it was born & then their body was used as spare parts. We will never end abortion if we do not END THIS EVIL!”
Pharmaceutical giant Bayer announced Thursday it had agreed to pay $1.6 billion to settle nearly all claims filed in the United States over controversial birth control implant Essure.
“The company will pay approximately $1.6 billion to resolve these claims, including an allowance for outstanding claims, and is in resolution discussions with counsel for the remaining plaintiffs,” the German company said in a statement.
“There is no admission of wrongdoing or liability by Bayer in the settlement agreements,” the statement said, and the settlement does not apply to claims filed in other countries.
Essure, a non-hormonal coil implant used to prevent pregnancy, has in some cases caused chronic pain, perforation of the uterus and fallopian tubes and led to hysterectomies, news reports say. It was discontinued in 2018. Nearly 39,000 women had sued Bayer or hired lawyers over their use of Essure.
Approved in the United States in 2002, the device’s perceived advantage is that it is a less invasive alternative to tubal litigation, in which a small hole is cut into the abdomen and the surgeon blocks or cuts the fallopian tube.
Bayer’s pharmaceutical division said in the second quarter it took a charge of 1.25 billion euros for litigation, primarily for claims around Essure.
All told, Bayer reported a loss of 9.55 billion euros in that quarter, which was mostly reflective of a US settlement of thousands of claims that its glyphosate weed killer may have caused cancer.
Previously, Live Action News has discussed how emergency contraception (EC) can act as a potential abortifacient. Emergency contraception is typically taken by a woman to prevent pregnancy if her preferred method of birth control has failed or was not used. In order to understand how things like the Morning After Pill (Plan B) or Ella (a different type of EC) might cause early abortions, it’s important to know how emergency contraception differs from the abortion pill (RU-486). It is easy to confuse Ella or Plan B with the abortion pill (mifepristone), but they are not the same.
Women deserve to know if a contraceptive method has the potential to harm them physically or emotionally, or if it terminates a pregnancy. Let’s see how the abortion pill, Plan B, and Ella compare.
What Happens After a Woman Takes the Abortion Pill?
A chemical abortion (abortion pill regimen) involves two different drugs: mifepristone and misoprostol. Mifepristone blocks the progesterone hormone needed to sustain the pregnancy. It breaks down the lining of the mother’s uterus to deprive the baby of the nutrients needed to survive.
About 24-48 hours later, misoprostol is taken to cause contractions that will expel her dead baby from her body.
The FDA has only approved mifepristone (the abortion pill) to be taken up through 10 weeks of pregnancy. Taking the abortion pill is said to be four times more dangerous than a surgical abortion. So far, we know at least 24 women have died after taking the pill.
Because approximately half of U.S. states are not required to report abortion complications, it is difficult to know the full impact of the abortion pill and surgical abortions on women. Abortion groups have admitted that they coach women who suffer side effects from the pill to lie to emergency room staff and say they are experiencing a natural miscarriage.
Not only is the abortion pill dangerous, it is clearly designed to end the life of a preborn child.
When it comes to emergency contraception, do Ella and Plan B operate the same way?
Plan B
Plan B is composed of 0.75 mg of levonorgestrel, and its primary function is to prevent ovulation (the release of an egg from a woman’s ovary). However, the manufacturer’s insert for Plan B admits the product may prevent the implantation of an already fertilized human embryo. Since life begins at fertilization, this means it is possible for Plan B to stop a human being that has already come into existence from implanting inside his mother’s womb, even though that is not Plan B’s primary, intended function.
Distributors of Plan B claim it does not end a pregnancy because in 1959, the American College of Obstetricians and Gynecologists (ACOG) voted to redefine pregnancy — changing its definition from the moment of fertilization to the moment of implantation into the wall of the uterus. This is incredibly misleading, and women deserve to know Plan B can act to prevent an already developing human being from continuing its development.
Even Barr Pharmaceuticals, the manufacturer of Plan B, has acknowledged it has potential abortion-inducing effects. The Food and Drug Administration (FDA) concurred, stating, “Plan B One-Step is believed to act as an emergency contraceptive principally by preventing ovulation or fertilization. . . . In addition, it may inhibit implantation (by altering the endometrium). It is not effective once the process of implantation has begun.”
Ella
Ella (or ella) works differently from Plan B, as it is made of a different chemical compound. This type of EC actually has properties similar to the abortion pill. Ella is composed of 30 milligrams of ulipristal acetate, and like the abortion pill (mifepristone), acts as a “selective progesterone receptor modulator” (SPRM). Because it blocks progesterone receptors, Ella can cause the death of an already-implanted embryo, unlike Plan B.
The European Medicines Agency (EMEA) discovered that Ella “is embryotoxic at low doses, when given to rats and rabbits” and“[was] approximately equipotent at the dose levels of 10 and 30 mg/day in terminating pregnancies in guinea-pigs.” The similarities between Ella and mifepristone, combined with studies conducted through animal testing, has led researchers to conclude that a 30 milligram dose of Ella can abort a preborn child.
The pro-life American Association of Pro-Life Obstetricians and Gynecologists (AAPLOG) has found similar evidence to support the conclusion that Ella acts as an abortifacient. The ability of ulipristal, according to the AAPLOG, “to destroy established pregnancies, as well as prevent implantation, makes it an embryocidal drug.”
Conclusion
While the abortion pill is not the same drug as either kind of emergency contraception, it seems that of these three drugs, Plan B alone does not have the ability to abort an already implanted embryo (though it has the potential to end the life of one that has not yet implanted). Women deserve to know the differences and similarities of these three drugs. They also deserve to know that there are better methods of preventing pregnancy (see more here on fertility awareness methods) that do not deprive a preborn child of his or her life.
Americans have recently become much more aware of the prevalence of child sex trafficking amid the unraveling of the secrets of Jeffrey Epstein and Ghislaine Maxwell. But sex trafficking has been a profitable industry for decades, having a symbiotic relationship with the porn and abortion industries.
DKT International was founded by Philip Harvey, who has made millions of dollars selling pornographic films and sex toys through his company, Adam & Eve. Those films, according to a report by National Review, likely contain footage of sex trafficking victims forced to participate in pornography. DKT International receives 25% of the profits from Adam & Eve ($75 million in sales in 2019) and then in turn funds the overseas birth control and abortion industry. Harvey sits on the board of the UK-based Marie Stopes International, one of the largest abortion chains in the world.
Meanwhile, sex trafficking victims are frequently forced to undergo multiple abortions to be able to continue ‘working.’ Abortionists are, therefore, making money off of sex trafficking.
“The prevalence of forced abortions is an especially disturbing trend in sex trafficking,” wrote study authors Laura J. Lederer and Christopher A. Wetzel. “One victim noted that ‘in most of [my six abortions,] I was under serious pressure from my pimps to abort the babies.’ Another survivor, whose abuse at the hands of her traffickers was particularly brutal, reported 17 abortions and indicated that at least some of them were forced on her.”
Despite clear signs of abuse, abortion businesses frequently fail to report these instances to authorities, though they are mandated to do so. Instead, they collect money for abortions and return victims to their traffickers and abusers.
“The abortion industry is profiting tremendously [from sex trafficking] …financially,” explained Nita Belles, regional director for Oregonians Against Trafficking Humans.
It’s a cruel, inhumane, brutal circle in which Planned Parenthood can often be found at the center.
Planned Parenthood’s role in sex trafficking
“Survivors [of human trafficking] also had significant contact with clinical treatment facilities, most commonly Planned Parenthood clinics, which more than a quarter of survivors (29.6%) visited,” reported Lederer, former senior advisor for trafficking in person for the U.S. Department of State. “… Since pimps and traffickers generally exercise nearly complete control of their victims, these points of contact with healthcare represent rare opportunities for victim identification and intervention.”
One victim who took part in the study explained that no one at any clinic she ever visited, including Planned Parenthood, ever asked her questions about her situation. “No one ever asked me anything anytime I ever went to a clinic. … I was on birth control during the 10 years I was on the streets – mostly Depo-Provera shots [which increase women’s risk of contracting HIV by 40%] which I got at the Planned Parenthood and other neighborhood clinics. I also got the morning-after pill from them. I was young and so I had to have a waiver signed in order to get these.”
That waiver, it turns out, could be signed by the victims’ abusers — as was revealed during Live Action’s Aiding Abusers investigation into Planned Parenthood’s willingness aid abusers and traffickers, and cover up sexual abuse.
In 2011, Live Action investigators posed as a pimp and one of his prostitutes seeking a place that would handle STI treatments for his sex trafficking victims — some as young as 14. Planned Parenthood employees at seven facilities across the nation actually worked to help the “sex traffickers” by telling them how to get victims tested, the best way to skirt the laws to get abortions for them, and how to lie on paperwork about the ages of the girls so Planned Parenthood could avoid mandated reporting laws. One Planned Parenthood staffer even encouraged the “pimp” to sign the paperwork as the girls’ guardian.
Planned Parenthood manager Amy Woodruff worked at the facility in Perth Amboy, New Jersey, and was videotaped coaching the “sex traffickers” on where to get abortions for underage girls:
WOODRUFF: You never got this from me, just to make all of our lives easier.
PIMP: Ok.
WOODRUFF: If they’re 14 and under…
PIMP: Yeah, yeah.
WOODRUFF: [circles clinic paper] … just send ‘em right there if they need an abortion. OK? [Laughter].
WOODRUFF: … Here’s the thing too. If they’re minors, just tell them to put down that they’re students.
PIMP: Students?
WOODRUFF: Yeah, just kind of play along that they’re students. We want to make it look as legit as possible…
While these “sex traffickers” were actually undercover investigators, their experience supports what trafficking victims are saying. One trafficking victim said in an interview that she was “trusted” by her pimp and was given the task of scheduling abortions for the other girls. “The pimps and the traffickers would get fake I.D.’s for the girls and we would take them to have abortions,” she explained.
She added that abortion businesses like Planned Parenthood would commit the abortions without question. “[H]onestly they had to know that these were teenagers,” she said, “they were not adult women.”
After Live Action’s Aiding Abusers investigation was released, Planned Parenthood quickly fired the staffers caught aiding the “sex traffickers” and even announced they would be retraining their staff to spot abuse. This was false.
According to former Planned Parenthood manager Ramona Trevino, who was present for one of these retraining sessions, she and her fellow staffers were taught how to spot undercover investigators and determine whether or not they were being recorded — not how to identify trafficking victims.
As more information comes to light about sex trafficking in the U.S., those who have covered it up for decades, like Planned Parenthood, must be held responsible for aiding the abuse of thousands of children and women.
Many of us have been there: we’re eating right, we’re exercising, but still the scale won’t budge, and our clothes are still fitting the same. What gives? For some women, their birth control might be to blame for thwarting their fitness goals, possibly causing them to gain weight, changing where their body stores fat, altering their eating patterns, or even keeping them from gaining muscle.
Which kind of birth control can make you gain weight?
Weight gain has long been a contested side effect of birth control, and not all women gain weight when they go on the Pill–so why do some women gain weight on birth control, and is it really the birth control’s fault?
According to new research, women with certain genetics may be more prone to weight gain when using a certain type of birth control–namely, the etonogestrel contraceptive implant, otherwise known as Nexplanon. The study, which followed the weight of women implanted with Nexplanon, found that women with two copies of a certain estrogen receptor 1 variant in their DNA gained an average of 30 more pounds than the women in the study without that ESR1 genetic variant. While the study only included women implanted with Nexplanon, etonogestrel (a synthetic form of progesterone, known as a progestin) can also be found in the vaginal ring (such as the NuvaRing) in combination with the synthetic estrogen ethinylestradiol; the study authors therefore remark that other forms of birth control could conceivably have similar effects on women with a particular genetic makeup.
Birth control and weight gain: Genetics or behavior?
Whether or not birth control actually causes weight gain is a pretty hotly contested subject. Like many birth control side effects, weight gain is often disregarded as “just in her head,” or the fault of the woman herself. Sometimes, when the potential for weight gain on birth control is admitted, it is simply chalked up to temporary “fluid retention” or bloating (which is a commonly reported side effect of birth control).
But what about the women who gain more weight than can simply be attributed to retained fluid?
As seen with the Nexplanon study, your DNA could be at play. It’s also possible that the question “Does birth control cause weight gain?” might be something of a red herring altogether. Because it might not be the birth control itself causing weight gain for some women—it might be the changes in eating patterns that birth control could be causing.
In her book, This is Your Brain on Birth Control, author and evolutionary psychologist Sarah E. Hill describes what birth control may be doing to your eating habits to cause you to eat more, and therefore gain weight.
Hormonal birth control tricks your body into believing it’s perpetually in the luteal phase of your cycle (the time after you ovulate, and prior to when your period begins), so that your body never releases another egg (and no egg = no chance of getting pregnant).
Dr. Hill describes how humans (and other animals) tend to eat less when gearing up for ovulation (when it is possible to get pregnant), and eat more in the aftermath of ovulation (when a woman’s body is preparing itself for the potential months of pregnancy to come). The theory behind this decreased intake during the first half of the cycle, Hill says, is that it “reflects an unconscious motivational trade-off in which women’s increased sexual motivation comes at the expense of decreased motivation to do other things, like eat and digest.” So, if your body constantly thinks it’s in “we need to eat ALL THE THINGS” mode because that’s what the Pill is making it believe, it would make sense to see some weight gain while on the Pill.
The possible birth control-stress-weight gain connection
Yet another theory Dr. Hill posits in her book for why some women may gain weight on birth control is the way it affects how women process stress. We’ve discussed before how birth control causes a woman’s HPA-axis to go into overdrive, sending her cortisol levels through the roof. This results in women’s bodies on hormonal contraception actually mimicking bodies under chronic stress (after the body simply cannot take the elevated stress response anymore, and the HPA-axis basically shuts itself down). Cortisol actually sends fat and sugar out into the bloodstream, so that a healthy body can react as needed in a tense, fight-or-flight situation.
“In the long term, though (as in the context of chronic cortisol signaling), this isn’t great for the body” writes Hill. “Higher-than-normal levels of fat and sugar in the bloodstream can increase the risk of glucose intolerance (pre-diabetes), weight gain (especially abdominal fat), and coronary heart disease.”
How birth control can change your body shape—even if you’re not gaining weight
Maybe your birth control has never made you gain weight, but that doesn’t mean that it can’t affect your shape in other ways. Hill cautions in her book that for the time being, the reasons for possible weight gain on the Pill are just theories—but other research has found that women on the Pill tend to have more of a “pear-shaped” figure, and have more subcutaneous fat than women who aren’t on the Pill (even if it doesn’t necessarily make women on the Pill weigh more).
In another example of the Pill affecting body shape, a 2009 study by an exercise physiologist from Texas A&M University found that women on the Pill gained 40% less lean muscle mass than women who weren’t of the Pill, after the women completed a ten-week exercise regimen designed to build muscle mass. The researchers found that women on the Pill had much less DHEA—a naturally occurring steroid precursor that signals the body to grow muscle, among other functions—circulating in their bloodstream. They deduced that birth control pills containing a certain progestin (synthetic progesterone) may compete with DHEA for the same binding sites, prohibiting the DHEA from doing its job to signal muscle growth.
Weight gain on the Pill might be a complicated discussion, but what’s clear is this: birth control has far more effects on a woman’s body than simply preventing her from getting pregnant. By altering a woman’s hormones, birth control has the potential for downstream effects that many are unaware of until doing their own research. If you’re tired of playing a game of roulette when it comes to the various forms of birth control and their myriad side effects, but you still want effective family planning, it might be time to learn more about fertility awareness methods (FAM) or natural family planning (NFP).
“There are any number of reasons why women switch from hormonal contraception to a fertility awareness method, but the whole ‘not putting synthetic hormones in my body’ bit is often the most popular. By regularly ovulating, women protect their future bone and heart health, often find better intimacy, improve their gut health, lower their risk of depression, and gain important insight into their hormonal health.”
Women shouldn’t have to suffer side effects while planning their families. As women are learning more about evidence-based and effective fertility awareness methods, many are finding freedom from the unwanted weight gain and mental health effects of birth control.
When this article refers to fertilityawarenessmethods (FAM), or natural family planning (NFP), we are referring to FertilityAwareness–BasedMethods, evidence-basedmethods of cycle charting which can be used as effective forms of natural birth control when learned by a certified instructor.
August 13, 2020 (Live Action News) — Given the multiple side effects and risks of hormonal birth control, there has never been a better time for women to learn about evidence-based methods of fertility awareness. A growing number of medical professionals are utilizing fertility awareness–based methods (FABMs) of natural family planning as they seek to address root causes of infertility, and others are seeking to offer their female patients additional treatment options beyond a prescription for hormonal birth control to manage painful periods, irregular cycles, and more.
Dr. Summer Holmes Mason of Ohio is one such provider. In a 2019 interview with Natural Womanhood, she said that initially in her practice she considered hormonal birth control “bread and butter gynecology for me. It was probably one of the largest tools I had in my arsenal as an OBGYN to treat medical issues.” Yet, she found that birth control was not a good fit for some of her patients.
“After a couple of years, I realized people were coming back to me with more side effects than I thought was acceptable,” she said, recalling one patient who experienced a blood clot, a potentially life-threatening complication of hormonal birth control. Additionally, Dr. Holmes Mason saw other patients “cycle through birth control. They’d be on, sometimes, five or six or seven different kinds of birth-control pills . . . and they couldn’t find one that worked well for them.” Just as troubling, she found that hormonal birth control was masking symptoms rather than resolving underlying problems.
“Often times I see women in my office who have been on the Pill for 5 or 10 years, and they’ve had menstrual dysfunction since they were 12 or 13 years old. . . . I’m seeing them for the first time, and we don’t really know why their menses were dysfunctional,” Dr. Holmes Mason said. “The Pill has been masking whatever pathology was going on. Maybe they want to come off the Pill, for whatever reason — a medical issue, or they want to get pregnant. But the original issue still remains.”
She wanted to offer her patients more options, but her only exposure to FABMs during medical school and residency was learning about the rhythm method, a 1930s precursor to today’s evidence-based methods. She was surprised to find a podcast that featured an interview with Dr. Marguerite Duane, co-founder of the Fertility Awareness Collaborative to Teach the Science (FACTS), a group of medical professionals and others which works to “provide information about natural or fertility awareness based methods of family planning with the medical community.” When Dr. Duane specifically addressed the use of FABMs for medical management of common reproductive issues, Dr. Holmes Mason thought, “Aha! This does exist!”
Fast forward several years, and Dr. Holmes Mason is now certified in FEMM Medical Management, which along with Neo Fertility and NaProTechnology has treatment protocols for various reproductive problems that work to restore health by identifying and treating underlying root causes. For her part, Dr. Holmes Mason now says she has “so much more to offer” patients besides hormonal birth control.
Public perception about FABMs is slowly shifting, amongst medical professionals and users alike. Growing numbers of providers have incorporated FABMs, leading to significant increases in patient load. Georgetown University is now offering an elective on FABMs to med students. In 2019, the CDC finally updated its effectiveness statistics for FABMs. What’s more, a 2018 survey found that more than 4 in 10 women were open to hearing about FABMs from their OB/GYN.
Evidence-based FABMs offer women holistic options to restore reproductive health without side effects, and can be used to either achieve or avoid pregnancy. Their growing popularity is worth celebrating.
Do healthy hormone levels and ovulation help women battle COVID-19? According to a recent study, the answer seems to be yes.
One of the most important principles of FEMM education and medical management is that ovulation is a sign of health. As explained in the FEMM White Paper, “a woman’s biomarkers indicate the vital signs of her entire health. Since ovulation is a sign of both health and fertility, understanding these changing hormonal fluctuations through biomarker observation allows a woman to understand and manage her long-term health.” Learning to chart her cycle using FEMM or a similar method can help a woman to identify potential underlying health problems and collaborate with her doctor to find solutions that improve, rather than suppress, the functioning of her ovulatory cycle.
With this in mind, it should come as no surprise that new research is still revealing important connections between ovulation and improved health outcomes. As the world continues to reel from the COVID-19 pandemic, however, one new study is particularly noteworthy. The study, titled “Potential Influence of Menstrual Status and Sex Hormones on Female SARS-CoV-2 Infection,” explicitly links healthy hormone levels and ovulation to improved outcomes in women suffering from COVID-19.
The researchers behind the study were motivated by a puzzling phenomenon: studies have shown that women are generally less vulnerable to COVID-19 than men, demonstrating lower morbidity and mortality, as well as a lower severe case rate. As early as February, data had begun to emerge suggesting that men were disproportionately affected by COVID-19. In fact, one study in China showed that the death rate for men with COVID was 2.8 percent, while it was only 1.7 percent for women. Theories abounded about the reasons for this, and as early as April, some doctors in the US were testing their hypothesis that female sex hormones could be the key. No one was sure what caused the disparity in outcomes, though. The researchers behind this most recent study readily admit that there is still a need for further research, but their work is a significant step toward answering the “why.”
Through their studies involving COVID-19 patients in China, the researchers discovered that the key factor in the disparity between male and female outcomes may not be just be sex, but hormone levels and ovulation. While non-menopausal women with COVID-19 fared better than men of the same age, menopausal women (i.e. women who no longer ovulate) had outcomes similar to men of their age. In particular, the non-menopausal women were less likely than their menopausal counterparts to be hospitalized, and when they were, they were generally discharged more quickly. This implies that “female hormones of pre-menopausal women may provide protection.” In other words, women who ovulate seem to have an advantage when it comes to fighting COVID-19.
The researchers concluded that this may be due to the high levels of E2, or estradiol, that are present in women who ovulate. Estradiol is a type of estrogen, which in turn plays a crucial role in the ovulatory cycle; if estrogen doesn’t reach a high enough level in a given cycle, ovulation fails to occur. While the researchers stopped short of drawing a definitive causal connection between E2 and improved COVID-19 outcomes, they did note a strong correlation and suggested that E2 likely offers protection through its regulation of cytokines (cell proteins that play an important part in the immune system’s functioning).
While this is good news for ovulating women, it might seem discouraging to women who have reached menopause or who struggle with anovulatory cycles (i.e. cycles in which no ovulation occurs). In reality, however, this study is good news for everyone. As doctors learn about COVID-19, they can make treatment decisions tailored to the specific needs of their patients. Identifying ovulation and hormone levels as important factors in managing COVID-19 opens up new possibilities for treatment, even for women who don’t ovulate regularly and have low levels of estrogen. The researchers behind this study suggested that hormone therapy might benefit COVID-19 patients. In particular, it seems likely that estrogen replacement could improve outcomes for menopausal women, as well as women with anovulatory cycles and low levels of estrogen.
Today, many women are taught that female hormones and ovulation are inconveniences that ought to be suppressed. In some societies, menstruation is considered to be shameful. Too often, complaints of severe symptoms that could indicate underlying conditions fall on deaf ears. Fortunately, many women have been able to break free of this mentality through hormonal health education programs like FEMM. As women learn to chart and understand their cycles, they are able to work with their doctors to significantly improve their health. The need for education on the importance of ovulation existed before COVID-19, and it will still exist once the pandemic ends. In the meantime, however, this study is a reminder that women’s reproductive health can never be separated from overall health and wellbeing. Let’s hope that this study inspires more women to learn about their bodies and gives doctors much-needed insight into the best treatments for COVID-19.
Child playing on outdoor playground. Kids play on school or kindergarten yard. Active kid on colorful swing. Healthy summer activity for children. Little boy swinging in tropical garden.
An expert New Zealand researcher is warning women to “please have children” as, mirroring other Western nations, New Zealand’s fertility rate reaches an all-time low. The country’s total fertility rate is now 1.71 children per woman, well below the population replacement level of 2.1.
Increasingly, greater numbers of researchers are acknowledging the grave problems associated with a society that delays having children and seemingly celebrates career milestones over marriage and parenthood.
It is likely that, for many couples, the increased cost of housing and food in New Zealand also plays a part in their decision about family size. The current global uncertainty surrounding the Covid-19 pandemic could well now contribute too.
Dr Pushpa Wood, who is the director of Massey University’s financial education and research centre, says that if the downwards trend continues New Zealand will be left with an ageing population, more retired people needing care, and fewer people to care for them, with devastating impacts on the country.
“Without population replacement or growth, economies decline. A nation’s strength lies in its young: their energy, innovation, risk-taking and entrepreneurship. The new blood drives the exchange of ideas and experimentation. If these attributes aren’t home-grown, they have to be imported. At an individual level, single person households are the fastest growing household type in New Zealand. Increasingly people face old-age with few or no family supports.”
As the working-age population reduces globally in the coming years, it will likely become untenable for New Zealand to simply rely on immigration. Wood suggests that the Government needs to take action by incentivizing people to have children. Measures could include increased parental leave, financial support for childcare, and initiatives such as the “baby box” which the Finnish Government provides to new mothers, and includes items such as clothes, sheets, and toys.
(National Review) While COVID-19 dominates the news cycle, a battle is being fought over a deadly drug that has killed over 3.7 million children and at least 24 women. The drug is Mifeprex — commonly known as the abortion pill. On July 13, an Obama-appointed federal judge enjoined the Food and Drug Administration requirements governing the prescription of Mifeprex. He ruled that requiring pregnant women to complete an in-clinic appointment to procure the drugs was a “substantial obstacle” to abortion and was to be suspended during the COVID-19 pandemic. This ruling suspends, for the abortion pill, the Risk Evaluation and Mitigation Strategy (REMS), the FDA’s rules for “certain medications with serious safety concerns to help ensure the benefits of the medication outweigh its risks.”
Women procuring abortion drugs without proper education or evaluation are at greater risk of complications and death due to undiagnosed ectopic pregnancy, hemorrhaging, infection, and more. This dangerous judicial activism should compel elected officials, entrusted with the care of their constituents, to take a stand when federal agencies jeopardize public health and safety.
The first drug in the abortion-pill regimen, Mifeprex was approved by the FDA in 2000 after a highly politicized scramble within the Clinton administration. Beverly Winikoff is the founder of one of the abortion pill’s loudest proponents, Gynuity Health Projects. Winikoff claimed that the September 11 terrorist attacks “saved” Mifeprex because the nearly 3,000 Americans killed that day overshadowed news of a woman killed by the abortion pill a day prior. Mifeprex was designed specifically to kill the developing child and is approved for use up to ten weeks, at which point a child has arms, eyelids, toes, fingers, and organs.
Since the drug’s approval, over 4,000 adverse maternal reactions have been reported to the FDA. The FDA acknowledges that adverse reactions are notoriously underreported, and most women experiencing hemorrhaging and severe infections will seek follow-up care at emergency rooms instead of returning to the abortion clinic. Yet emergency rooms are not required to report adverse reactions. And as of 2016, the Obama administration changed the requirement so that abortion-pill manufacturers must report only maternal deaths to the FDA. The number of women seeking blood transfusions and emergency intervention is likely much greater than 4,000.
The Mifeprex regimen has unleashed horrors on America’s women and children while providing no medical benefit. Killing innocent children, endangering mothers, and abusing the health-care system to do harm is tragic. And as long as this deadly drug remains on the U.S. market, it will pose a serious health risk.
Pregnancy is not a disease and abortion is not health care. The abortion pill is not medicine. No child deserves to be killed by a drug, and pregnant women deserve better. FDA commissioner Stephen Hahn should acknowledge the subversion of the abortion industry and its allies, which are using a national pandemic to instigate abortion expansions that could remain long after the pandemic is over. The FDA should protect the public health of Americans and pull this lethal drug, Mifeprex and its approved generics, from the market immediately.
Ted Cruz is a U.S. senator from Texas and a member of the Senate Committee on the Judiciary. Lila Rose is the president and founder of Live Action, a nonprofit human-rights organization educating on abortion and the abortion industry.
Editor’s Note: This article was published at National Review and is reprinted here with permission.
August 10, 2020 (LifeSiteNews) — The city of Cleveland, Ohio is putting the lives of its children at risk. And it is receiving federal taxpayer funds to do so.
No, it’s not COVID. For that low-risk disease, children are sheltered, masked, kept away from many schools, and scared to death by the hovering helicopter government bureaucracy.
But what about advice to teens that leads to lifelong complications from underage sexual promiscuity, along with the high likelihood of emotional disaster? And may cause the death of a child through abortion?
Who will be held accountable for this?
Cleveland is not alone, but let’s look specifically at what Cuyahoga County, Ohio communicates to teens on a website the health department operates, www.216Teens.org (216 is the Cleveland area code).
It’s funded by the U.S. Department of Health and Human Services and claims to tell the truth about sexuality for adolescents. But very quickly the extreme bias is evident. The site includes zero pro-life or abstinence-focused resources. There is a nominal page on abstinence, which dismisses it quickly as almost impossible. Adolescents who visit the site will read biased, X-rated, high-risk, pro-abortion, and pro-homosexual advice encouraging early experimental sex.
216Teens is not “medically accurate” and “evidence-based” as it claims to be. All the best medicine and evidence points to providing youths with an unequivocal message that delaying sex until marriage is positively correlated with life success and healthy outcomes. Premature sexuality leads to the opposite result.
A YouTube video produced by Protect Ohio Children lays out the irresponsible, dangerous messages of 216Teens and its pro-abortion, pro-“LGBTQ,” condom-obsessed, anti-abstinence advice.
For instance, the 216Teens Facebook page included a recent post from NARAL (National Abortion Rights Action League) that trashes authentic abstinence. “Say it with us. Abstinence only programs don’t work. No matter how many times the anti-choice movement pushes its lies about sex ed, science isn’t on their side. EVERY young person deserves inclusive, evidence-based sex ed at school. ”
Ohio parents need to recognize that this is open defiance of an Ohio law mandating that sexuality education shall emphasize abstinence until marriage. Where are Ohio lawmakers and the Ohio State Board of Education to hold the Cuyahoga County Board of Health accountable for this illegal, child-endangering action?
On March 17, 216Teens posted on Facebook this pandemic advice for teens: “While you are out purchasing all the toilet paper and water consider adding these items to your emergency preparedness list: filled birth control prescriptions, emergency contraception, menstruation products, condoms.” What happened to social distancing?
Along with rioting, looting, and Democrat politicians’ funerals, does the virus cease being a threat during progressive activities like underage teen sex?
How stupid does this health department think Cleveland’s people are?
Another post on June 5 told kids, “Guess what? There isn’t an age requirement for buying condoms.” Take that, parents! And another post gave the phone number and website for Preterm, a Cleveland area abortion clinic, while another on July 24 offered this helpful information: “Did you know there are 64 terms that describe gender identity and expression?”
No, this is a lie. There are two sexes, male and female. Facts, not mythology, is what a health department should be offering to teens.
The good news is that the Protect Ohio Children video gives the phone number for Ohio governor Mike DeWine (614-644-4357) and Ohio attorney general Dave Yost (614-466-4986).
But Bedsider is way beyond birth control, providing sex advice for “Frisky Fridays” and asking, “Is the pandemic wrecking your libido?” It provides teen readers a list of topics from aphrodisiacs to sex toys.
Just what every Ohio teen needs from a health department. Ohio has an abstinence education law. Right? Right.
Meanwhile, through 216Teens, “Bedsider” is being promoted to teens as young as 13 in northeast Ohio.
Power to Decide (Bedsider’s parent group) raises a whole nest of new questions. Power to Decide/Bedsider has a Pop Culture Partners section on its site and serves as an “expert adviser” to Cosmopolitan, Bustle, Glamour, and Teen Vogue magazines; the sex-drenched “progressive” programs Grownish, Good Trouble, The Fosters, The Bold Type, Blackish, Unexpected, and East Los High; the program Sex Education on Netflix; Disney’s Andi Mack; MTV’s 16 and Pregnant and Teen Mom; and Hulu’s Shrill.
Power to Decide launched a social campaign, “Thanks Birth Control!,” picked up by many of these pop culture partners. Ever wonder why the “early sex is normal and cool” message seems to be everywhere? This explains some of it.
Power to Decide joined SIECUS, Planned Parenthood, Advocates for Youth, and others to start the campaign “Sex Ed for All” in May 2019. In announcing this effort, they’ll “no longer observe National Teen Pregnancy Prevention Month.” Why? With the new focus on “LGBTQ” behaviors, the sex ed cartel is way beyond concerns about pregnancy alone.
This coalition is committed to selling underage teens on their sexual “rights” with a new emphasis on “justice” for “LGBTQ” identifiers and non-white teens.
And 216Teens picked up this “justice” emphasis with a recent Facebook post inviting teens “13 to 19” to an online summit to learn about the intersection of “racial and reproductive justice.”
Pro-abortion groups are beginning to capitalize on trending concerns about racial inequality to conflate it with access to abortion and contraception. These are “justice” issues, teens will be taught. “You have ‘rights’ that are being denied!”
So will abstinence messages become “racist”? That’s where many fear this is going.
What can Ohioans do? Call the governor and the attorney general. Ohio children are being corrupted and exploited by 216Teens.org and comprehensive sexuality education in general. It’s promiscuity promotion, plain and simple. And our kids deserve the “right” to hear the truth.
Ohio has an abstinence education law, and we need to follow it!
“NO JUDGMENT, JUST CARE.” These words cover the walls of a bus stop near my house. It is an ad for Planned Parenthood—the organization that, depending on one’s perspective, is known as America’s largest, best-funded abortion provider, and/or as a champion of women’s health. For Planned Parenthood, the term “women’s health” is synonymous with access to abortion and contraception. Yet their sole focus of “women’s health” on methods that seek to prevent motherhood has played a part in the United States’s comparatively dismal state of maternal health among the developed countries of the world.
An incomplete picture of “women’s health”
Last year, Planned Parenthood ousted president Dr. Leana Wen after just eight months at the organization’s helm. The exact circumstances that led to Wen’s departure (or removal) from Planned Parenthood are murky, but rumors swirled that Wen’s desire to focus more intensely on non-abortion care—such as maternal health—produced “philosophical differences” with the organization’s board chairs.
When women’s health groups focus on abortion and contraception access first, it suggests that preventing or postponing motherhood are the top goals for women regarding their health today. But the majority of women in the United States say they desire to be (and will eventually become) mothers. Of course, there are some women who will not become mothers, some by circumstance and others by choice. But given the fact that most women will eventually bear children at some point, it seems that a conception of “women’s health” predominantly focused on preventing motherhood misses an extremely significant aspect of the life and health of the average woman. It is one of many potential reasons why the United States has the highest maternal mortality rate (MMR) among the developed nations of the world.
Pregnancy and childbirth in the United States
Around 4 million babies are born in the United States each year, and the CDC estimates that about 700 women die each year from pregnancy or childbirth-related complications. While these numbers indicate that death from childbirth is still a blessedly rare occurrence in the United States, the maternal mortality rate appears to be rising. But the MMR alone presents an incomplete picture with regards to maternal health: investigative reporting in 2017 by NPR and ProPublica found that for each American woman who dies in childbirth, an additional 70 come close to dying (suffering from what is known as severe maternal morbidity). Therefore, while death in pregnancy or childbirth might be rare, nearly dying during those times is much less so.
The reasons why our MMR is on the rise are likely multifactorial. On the whole, Americans are increasingly unhealthy, suffering from obesity and associated risks like diabetes and hypertension, and American women are increasingly delaying childbirth until an older age than prior generations. All of these conditions increase the likelihood of complications in pregnancy, delivery, and during the postpartum period.
When mothers’ concerns go ignored
In interviews with NPR and ProPublica, many of the mothers who almost died from pregnancy, childbirth, or related complications expressed that they felt like their health concerns were not taken seriously, or were completely dismissed until things became blatantly dire. For women who did die, their family members reported feeling the same way.
In the course of writing this article, I put out a call for personal stories on social media about pregnancy, childbirth, or postpartum complications that could have been avoided if doctors took their patients’ concerns more seriously, and the responses came flooding in. There are too many to include them all here, and of course, all of the women who answered my call are fortunately still alive, but for some, death came too close for comfort. One woman shared with me how she almost lost her life from an ectopic pregnancy that could have been caught earlier if her “extreme pain and bleeding” had been taken more seriously. Another shared how after a miscarriage led to complications, she had to “beg and plead for appointments, antibiotics, and attention,” and ultimately was hospitalized for an infection that had worsened due to lack of care.
Many women have experienced the incredibly frustrating experience of being turned away at the hospital while in labor; this can be even more frustrating for women who have had babies before and know when they are in labor. This happened to Haley Stewart, who was sent away from the hospital with assurances of, “No, you’re not in labor,” as she moaned through painful contractions during the end of her fourth pregnancy at age 32. This led to an incredibly fast birth (with almost no time to get into a hospital bed) a mere three hours later. Recounting the birth story on her blog, Haley says, “I do feel angry that my instincts were dismissed and that I was told not to listen to my body.”
Amy Garlick was 27 at the time of her first pregnancy, and also felt her health concerns were disregarded to the point of serious risk. Incredibly sick during the first trimester of her pregnancy and plagued by severe panic attacks, Garlick’s doctor told her more than once to stop “being a baby” when she shared her symptoms. It took until her 12-week appointment when she weighed in at under 100 pounds, for her doctor to start taking her concerns seriously. It turned out that Garlick had Hyperemesis Gravidarum (HG), a serious condition that can require hospitalization if it causes severe enough dehydration and weight loss.
Melissa Kobialka, 32, experienced postpartum depression (PPD) and postpartum anxiety (PPA) after the birth of her first child at age 27 that resulted in “suicidal ideation and full blown panic attacks if I heard a crying baby (any baby, even someone else’s child or a doll that made crying sounds).” Shockingly, Kobialka was not even screened for PPD at her six-week postpartum visit. Instead, she was screened at her daughter’s two-month pediatric appointment, but the pediatrician “blew off” the positive results of Kobialka’s PPD survey. It wasn’t until seven months postpartum, when Kobialka says she “started to wish I was dead,” that she finally received help for her PPD.
The MMR for black mothers in the United States is a shocking three to four times higher than what it is for white mothers. The C-section rate is also higher for black mothers.
A study from the American Journal of Public Health concluded that black mothers are more likely to die from conditions such as “preeclampsia, eclampsia, abruptio placentae, placenta previa, and postpartum hemorrhage” than white mothers who have the same conditions. This terrible disparity holds true even across income and education levels: the MMR for black women with at least a college degree is 5 times as high as it is for white women with a similar education. Status and experience in public health won’t save a black woman from pregnancy morbidity or mortality, either: whether she is a famous athlete (Serena Williams, who very nearly died in childbirth), an epidemiologist (Shalon Irving, who died three weeks after giving birth via planned C-section), or a former American Hospital Association staffer (Arika Trim, who recently died one week after giving birth via emergency C-section). According to the NPR/ProPublica MMR investigation, the disparity in maternal health outcomes between white and black women is “the main reason the U.S. maternal mortality rate is so much higher than that of other affluent countries.”
The reasons for the disparity in maternal health outcomes between white and black women are complex and multi-faceted. Obesity and hypertension are more prevalent in black women, and both can adversely affect pregnancy outcomes. On the whole, black women are also less likely to have access to early prenatal care, the lack of which is associated with worse maternal and fetal outcomes. Again, however, having a higher income and/or higher education level is not protective for black women or their babies against the increased risk of maternal or fetal death. This has led many in public health to theorize that an insidious form of racism may be at play in black women’s interactions with the medical system, putting them at higher risk of death when their concerns are dismissed as “not a priority.” Bias in medicine (and a vile legacy of historical mistreatment of Black Americans in health care and medical research) has perhaps fostered a culture of mistrust between black patients and their health-care providers, especially in situations where women cannot be treated by a provider with whom they have had an opportunity to establish a trusting relationship.
Babies vs. mothers: a false choice
Whether the mother is white or black, some say that the United States’ focus on saving babies during and after childbirth is largely to blame for the state of maternal health. There may be some truth to this claim (as long as the babies are wanted and viable, of course). The NPR/ProPublica investigation found that “federal and state funding show only 6 percent of block grants for ‘maternal and child health’ actually go to the health of mothers.”
Consider also the current disparity in follow-up care after childbirth for moms versus their babies. The prenatal period is full of dozens of checkups, but after childbirth, most mothers are afforded only one quick check-up at four to six weeks postpartum which will be covered by insurance. For women who have had any sort of complications in pregnancy or childbirth, this can literally be too little, too late; the CDC estimates that one-third of pregnancy-related deaths occur one week to one year after delivery. This is also prime time for postpartum mental health issues to appear, from postpartum depression, to postpartum anxiety, to postpartum psychosis, which if gone undiagnosed and untreated, can lead to devastating outcomes for mothers and their babies. New babies, meanwhile, will have several thorough checkups within their first six months of life. The contrast in care sends a clear message: “Mom’s health doesn’t matter.”
How can we decrease the maternal mortality rate?
What are we to do about the increasing MMR in the United States? First, it is clear that we must shift our focus to recognize the truth that a healthy mother makes for a healthy baby, and that both are worthy of the same level of dignity and care. Too often, mothers’ health concerns go ignored, and they need to be taken seriously by healthcare providers before it is too late. No child should have to lose his mother on his birthday, and no mother should have to lose her life on what should be a most joyful and meaningful day.
Practically speaking, it is clear from the NPR/ProPublica reporting that doctors and nurses need better training in recognizing and treating the leading, treatable causes of maternal mortality and morbidity, such as hemorrhage and preeclampsia. States like California have made significant strides in this direction. The recent standardization of maternal mortality reporting data across all 50 states, Washington D.C., and U.S. territories will also, one hopes, prove to be a useful tool in better identifying the leading causes of maternal mortality and in developing data-driven protocols for how to better recognize, prevent, mitigate, or treat these causes. The United States also needs to make a concerted effort in improving postpartum care. A single appointment at four- to six-weeks postpartum is insufficient to safeguard the physical or mental health of new mothers. Especially for women who have experienced any complications in pregnancy or delivery, additional care (preferably in the form of home visits) is needed, as is education of the mother and her partner/caregiver for warning signs of any serious complications that require immediate attention.
It is also clear that the disparity in MMR across racial differences deserves far more attention than it has received. Health-care providers need a better awareness of the conditions that disproportionately plague black mothers, and how to recognize and treat them earlier. More initiatives like the Black Child Legacy Campaign, which pairs black women with doulas to assist and advocate for them during labor (based on research that shows better outcomes for mothers and their babies when the mother has continuous support during labor), are needed on a wider scale, especially in areas where racial disparities are highest. Increased focus on identifying and mitigating possible implicit biases in health-care providers is also of vital importance, as is a commitment on the part of providers to forming trusting doctor-patient relationships.
Better care for women who aren’t seeking pregnancy termination
There is some good being done to increase awareness of both the maternal mortality rate and the racial disparities in MMR in the United States, but there is a long way to go. Further, the focus on abortion access has somewhat stunted women’s health conversations when it comes to pregnancy. The sad irony is that maternal health is suffering as abortion and pregnancy prevention takes up all the oxygen in the women’s health conversation.
Recall how the World Health Organization listed “unsafe abortion” as one of the leading causes of maternal deaths worldwide. Yet the WHO also doubles down on abortion as a way to prevent maternal deaths: “To avoid maternal deaths, it is also vital to prevent unwanted pregnancies. All women, including adolescents, need access to contraception, safe abortion services to the full extent of the law, and quality post-abortion care.” Abortion providers constantly assure us that legal abortion is an extremely safe procedure—in fact, Planned Parenthood says it “is one of the safest medical procedures you can get.” Abortion advocates stress that unsafe abortions will kill women, but in the same breath, many fight against legislation that would hold abortion clinics to medical standards prioritizing patient care. When the Supreme Court recently struck down a Louisiana law requiring that abortionists have admitting privileges at a local hospital in the event of abortion complications, the ruling was heralded as a victory for women’s health. Ensuring widespread access to abortion was prioritized over ensuring that women could get immediate, emergency care in the event of a complication.
Of course, some states have instituted their own abortion restrictions in recent years, while others have become even more liberal. Take New York and its recently signed Reproductive Health Act, which notably allows for late-term abortions up until birth. New York consistently tops the list of states with the most abortions performed per thousand women, and that number is disproportionately made up of black women; in fact almost half of black pregnancies in New York City are ended through abortion rather than through delivery (notably, NYC also happens to be the location of Planned Parenthood’s headquarters). And yet despite the access to (and utilization of) abortion services by black women in NYC, they are still twelve times more likely to die in pregnancy or childbirth than white women.
The New York City example showcases that the WHO’s recommendation that “to avoid maternal deaths, it is also vital to prevent unwanted pregnancies” is like placing a dirty Band-Aid over the open wound of our maternal mortality crisis. Is abortion truly the best we have to offer women so that they don’t die in childbirth? It is sad if this is the implication—but it is also untrue.
Pregnancy prevention at all cost
From a young age, American girls are put on hormonal contraceptives and conditioned to treat their fertility as something to be controlled, covered up, and little understood. Pharmaceutical birth control has been used as a symptom cover-up for common reproductive issues (like endometriosis and PCOS) for so long, that it has disincentivized doctors and researchers from investigating root causes for these disorders and developing effective treatments for them.
In America, instead of seeking answers as to why a young woman is having intensely painful, irregular periods, cystic acne, and debilitating PMS, we place her on a birth control method that will simply mask her symptoms—at least, for as long as she stays on it. When she gets off it, her symptoms may be worse. If later in life she’s trying to get pregnant, she may face infertility due to an underlying condition that could have potentially been treated years earlier.
If we are to expand to a more comprehensive view of women’s health, beyond pregnancy prevention and toward greater reproductive health, we should equip girls from a young age to understand their fertility. Widespread contraceptive access has not convincingly reduced the numbers of women seeking abortion for unplanned pregnancies, since about half of all abortions are obtained by women who were using contraceptives at the time they conceived.
Hope for comprehensive women’s health
These days, some of the most substantive advances in women’s health toward solutions for reproductive disorders have come from the corners of medicine specializing in what’s called “fertility awareness.” There is a growing field of restorative reproductive medicine that uses health information collected by women charting their cycles with fertility awareness methods, such as the Creighton Model, Fertility Education & Medical Management (FEMM), Marquette Method, and Sympto-Thermal Method. Doctors specializing in restorative reproductive medicine are able to use information from a woman’s monthly charts and any accompanying symptoms to pinpoint and treat reproductive health disorders like PMS, PCOS, and endometriosis, including disorders that can cause infertility. In addition, since fertility awareness methods teach a woman how to identify the signs of her fertility, a woman using fertility awareness can work with her body to plan for or avoid pregnancy without side effects (and, depending on the method, with rates as effective as the leading methods of contraception).
Advances in fertility awareness and restorative medicine offer hope that the field of women’s health can incorporate a more holistic view of women’s health and doesn’t have to pit pregnancy avoidance against maternal health. This vision of women’s health puts each woman back in the driver’s seat of understanding her unique body and fertility, equipping her with greater self-knowledge and agency to be a more active participant in her reproductive and overall health care.
Given the sad fact that too many pregnant and postpartum women cannot trust the medical field with their lives in the moments that count the most, we need a paradigm shift away from one-size-fits-all prescriptions and toward more personalized care to treat the unique woman in the doctor’s office. The best path toward greater transparency and accountability for poor care is a more informed patient base. Toward that end, the greater self-knowledge and agency that comes with fertility awareness may be exactly what the field of women’s health needs most.
A doctor in a white robe and blue gloves holds a syringe with a coronavirus vaccine. Injection of the vaccine from covid-2019. Pandemic coronavirus 2020. vaccine test. Covid-2019. Pandemic 2020.
The race is on to develop a vaccine for Covid-19. More than 140 vaccines are being tested around the world, according to the World Health Organisation. In Australia alone at least half a dozen vaccines are being trialled.
At the same time, the WHO and various experts keep warning us that, even with a vaccine, the coronavirus will remain a threat and that we must adapt our habits accordingly. Among other things, they are worried about community take-up of anti-Covid vaccines as they become available – whenever that is.
Mistrust of vaccination has grown in recent years. In his bizarre announcement of a bid for the US presidency, rapper Kanye West appealed to anti-vaccine sentiment, saying vaccines are “a mark of the beast” and are among the things that “make God mad”.
A recent YouGov survey found that one in six UK respondents indicated they “definitely” or “probably would not” get vaccinated if a coronavirus vaccine became available. A further sixth of respondents to the survey were unsure what they would do. “Worryingly, this means up to a third of UK people could turn down a coronavirus vaccine,” writes an Australian academic.
One reason she does not mention is that some essential vaccines have been developed from the cells of aborted foetuses. This is not the only or even the main reason for the “anti-vaxxer” movement, although it may be the reason for Kanye West’s attack.
The link between abortion and some vaccines is real
For years, opponents of abortion were dismissed as crazy scaremongers for advancing this objection to vaccines. But in 2013 their concerns were acknowledged by the editors of the leading science journal, Nature, following a scandal over another cell line, HeLa, derived from the cancerous cervical cells of a woman named Henrietta Lacks in 1951.
From this article we learn that in 1962 a Swedish woman had a legal abortion at four months because she did not want another child. The lungs of the fetus were removed and sent to the Wistar Institute for Anatomy and Biology in Philadelphia where they were processed and cultured by Leonard Hayflick. WI-38 was distributed to drug companies and researchers around the world and used to create vaccines for rubella, rabies, adenovirus, polio, measles, chickenpox and shingles.
The leading issue with both HeLa and WI-38, as far as Nature’s editors were concerned, was the absence of the women’s consent, which was certainly unethical. However, pro-life objections concern primarily the injustice of abortion and the question of moral complicity in a particular abortion through acquiring foetal tissue, using it to make a product, and administering or receiving vaccines derived from it.
Are some of vaccines now in development on that list of morally questionable therapies?
And just what does that mean for people with a conscientious objection to abortion?
Covid-19 vaccine research does not need foetal cells
According to a briefing paper put out by the Anscombe Bioethics Centre (Oxford) in April, the answer to the first question is, yes. The author, Helen Watt, says:
“One such cell-line used in COVID-19 vaccine research (including a project of the University of Oxford5) is the HEK 293 cell-line modified from tissue taken from the kidney of an unborn child aborted probably in 1972, while another is the PER C6 cell-line from the retinal tissue of an 18-week baby aborted in 1985.”
Even people who do not object to abortion in general, Watt points out, may object to a late-term abortion like that used for the PER C6 cell line. In any case drug companies and researchers are aware by now of such objections and should take them into account.
In the US, new research using fetal tissue is effectively banned. In June last year the Health and Human Services Department (HHS) issued a statement which includes the following principle: “Promoting the dignity of human life from conception to natural death is one of the very top priorities of President Trump’s administration.”
However, this is keeping a leading researcher, Kim Hasenkrug, from using “humanised” mice to test potential therapies. These mice have human-like lungs with tissue derived from aborted human fetuses.
Democrats in the House of Representatives have attacked the ban. In a letter to Health and Human Services Secretary Alex Azar in April, they wrote: “Because of your restrictions, NIH is unable to utilize human fetal tissue to develop animal models of COVID-19 that can test potential vaccines and treatments to decelerate or even end this global health crisis. This inaction may ultimately put Americans further at risk of disease or death from COVID-19. “
Republicans in the House and Senate rubbished these claims, pointing to the dozens of Covid-19 treatments already being investigated without the use of fetal cells. In the Anscombe briefing Helen Watt mentions such ethically uncontentious sources as insects, tobacco plants, and hamster ovaries. One Australian trial is adapting the BCG vaccine, which was designed to protect against tuberculosis and has been around for 100 years – well before permissive attitudes to abortion made fetal tissue possible as a medium.
Complicity and conscientious objection
Chances are, then, that vaccines will be available which are not tainted by abortion. But what if you are a conscientious objector and your government decides to buy the one that is? This a question particularly in welfare states like New Zealand where governments fund the bulk of healthcare; and particularly, should a government try to make vaccination compulsory.
The Anscombe briefing is very helpful here, providing an ethical framework for those involved in any way with the provision or reception of such vaccines and aware of their origin.
It begins by pointing out: “There is a chain of actions from the original abortion and harvesting of fetal tissue, to the creation of a fetal cell-line, to its use in the creation of a vaccine, to the vaccine’s marketing and purchase, and offer to and use by members of the public. Is complicity involved at every stage, and if so, to what extent?”
The original act is ‘deeply immoral’
The original collection, involving arrangements between the scientist and the abortionist (with possibly an agent in between) for the cells of a particular baby, is deeply immoral. The scientist’s needs will dictate the precise way in which the abortion is done (as described, for example, in the 2015 undercover videos of an interview with a Planned Parenthood medical director) and using a go-between cannot sanitise his actions.
Such arrangements could encourage more abortions. They could make a woman who is ambivalent feel better about going ahead, because something good might come of it, and yet create subsequent conflicts for her.
“After the event, the knowledge that tissue was taken from her child with her consent will complicate her thoughts and feelings about the abortion: any grief, pain and guilt she experiences may be even harder to process and resolve.”
What if the cells were created long ago?
More morally complex is the use of cell lines already created, perhaps long ago.
“The more pairs of hands that separate us from the original wrongdoers, and the less we are part of an organised system, the less scandalous the messages we send out and the more likely it is that our actions are defensible. However, these actions are, conversely, less likely to be defensible if the wrongs in question, as with abortion and foetal tissue harvesting, not only continue to the present day, but continue with some degree of social sanction.”
It may be possible that a scientist does not know the provenance of a particular cell line. However, it is difficult to plead ignorance once a controversy about it has developed (and the pro-life movement can be counted on to create that controversy). Using the cells under these circumstances is a serious moral issue and can convey approval and encourage continuing fetal tissue experiment.
Conversely, there is an opportunity (and a moral obligation) to discontinue use and promote alternative research: “One scientist who formerly used an embryonic stem cell-line obtained from another institution led his laboratory colleagues to conclude that the end (scientific discoveries from embryonic stem cell research) must justify the means (destruction of IVF embryos).”
Catholic responses
Though objections to fetal tissue research are not limited to religious people, religious people tend to be more sensitive to the morality. A 1995 Vatican document, Dignitatis Personae (The Dignity of Persons), is the most authoritative statement of the Catholic Church’s position. It says that scientists have a duty to refuse the use of illicitly-produced material “even when there is no close connection between the researcher and the actions of those who performed the artificial fertilization or the abortion”.
This duty, it claims, “springs from the necessity to remove oneself, within the area of one’s own research, from a gravely unjust legal situation and to affirm with clarity the value of human life.”
However, the document states that “within this general picture there exist differing degrees of responsibility. Grave reasons may be morally proportionate to justify the use of such “biological material”, reasons relating to the health of children, for example.
“Thus, … danger to the health of children could permit parents to use a vaccine which was developed using cell lines of illicit origin, while keeping in mind that everyone has the duty to make known their disagreement and to ask that their healthcare system make other types of vaccines available. Moreover, in organizations where cell lines of illicit origin are being utilized, the responsibility of those who make the decision to use them is not the same as that of those who have no voice in such a decision.”
What about boycotts?
Watt discusses protesting a morally fraught vaccine by refusing to use it:
“Boycotting a COVID-19 vaccine in the absence of an alternative is a serious action that should be carefully considered, because of its potentially grave risks both for the person and for others. These risks will in turn depend on such factors as the person’s state of health and family and work circumstances and the presence of the virus (or immunity to the virus) in the community in which he or she lives.
“To give just two examples, for health care professionals and those with vulnerable family members living with them, a boycott may be incompatible with retaining a role in health care, or living with/caring for the family member.”
This is especially applicable to Covid-19. But, if truly ethical alternatives for vaccination against this virus are available, those who can access them “without excessive difficulty” have a moral duty to do so, “as a witness to the value of human life and life-respecting research.”
“If an alternative is not reasonably available, some will decide, under protest, that they have grave reasons (in the words of Dignitas Personae) to accept a vaccine out of concern for their own health and the health of others they may infect. Such individuals should make their views on use of foetal cell-lines known to the health authorities, as Dignitas Personae urges, in the hope of raising awareness and helping to change the brutal culture in which abortion products are so widely used.”
In other words, boycotting unethical vaccines is a matter for the individual conscience, and “some will feel, whether rightly or wrongly, called to a boycott even if no alternative vaccine is available to them.”
However, governments should seek to fund research on vaccines that do not depend on the killing of human beings, and to purchase them.
That is something for pro-life people everywhere to add to discussions about Covid-19 research, in the hope that, in the words of Helen Watt, “morally uncontentious vaccines will be made widely available to all peoples of the world, both to fight the COVID-19 pandemic and to combat other threats to life and health.”
As experts have known for years, unborn children begin to feel pain as early as eight weeks after fertilization, and definitely no later than 14 weeks. In fact, University of Arkansas Professor Kanwaljeet Anand, the world’s leading authority on fetal pain, says that preborn children probably feel pain much more acutely than adults. Their nervous systems develop early in gestation, but their pain modulation pathways do not begin to function until about six weeks after birth.1
Science proves that an unborn child, when being aborted in the second or third trimester, feels hideous pain as he or she is cut apart by the razor-sharp instruments of the abortionist. As more and more testimonies from pro-abortionists show, many of them do indeed acknowledge that a baby aborted late in pregnancy feels pain but say that this factor should not carry any weight when a woman decides whether or not to have an abortion. (Strangely, many of these same people are champions of animal rights, in particular efforts to ban any treatment of animals that might lead to their unnecessary pain or suffering.)
Pro-abortionists often dismiss pro-life concerns by saying that there are only a few third-trimester abortions performed in the United States each year, and only for the most extreme cases, as if the rarity of an evil makes it any less evil. For example, the National Abortion Federation claimed, without evidence, “This particular procedure [partial-birth abortion] is used only in about 500 cases per year, generally after 20 weeks of pregnancy, and most often when there is a severe fetal anomaly or maternal health problem detected late in pregnancy.”2 Planned Parenthood stated in a November 1, 1995 press release: “The procedure, dilation and extraction (D&X), is extremely rare and done only in cases when the woman’s life is in danger or in cases of extreme fetal abnormality.”
The question we must ask is whether these unsubstantiated claims are true.
Why Do Women Have Late-Term Abortions?
What Abortionists Say
But the partial-birth abortionists themselves have repeatedly contradicted the National Abortion Federation and Planned Parenthood. Martin Haskell, the inventor of the partial-birth abortion procedure, said that 80% of the procedures he performs are “purely elective.”3 Partial-birth abortionist James McMahon says that the primary reason given by those requesting the procedure is “depression.”4
The National Abortion Federation even contradicted its own 1993 statement that most partial‑birth abortions are performed for such reasons as “lack of money or health insurance, social‑psychological crises, lack of knowledge about human reproduction, etc.”5
Third-trimester abortionist George Tiller said at the 1995 National Abortion Federation conference in New Orleans, “We have some experience with late terminations; about 10,000 patients between 24 and 36 weeks and something like 800 fetal anomalies between 26 and 36 weeks in the past 5 years.” This means that Tiller alone did 2,000 partial-birth abortions every single year, and only eight percent of them were for birth defects.
The Statistics
In addition to the testimony of the partial-birth abortionists themselves, there is a large body of evidence showing that the procedures are much more common than most people believe.6
The number of abortions that have been done since legalization is so huge that even the small percentage of late abortions done results in a very large number. For example, in 2019 alone over 860,000 abortions were performed in the United States, according to the Guttmacher Institute.
The Guttmacher Institute also surveyed a large number of women obtaining late abortions and asked them their reasons for doing so. It found:
Only about one percent of second- and third-trimester abortions are performed for fetal anomalies, or eugenics
One-third (31%) of the women surveyed said that they misjudged how far along they were
One-fourth (27%) said that they found it hard to arrange an earlier abortion
14% said that they were afraid to tell their parents or their “partner”
The rest gave reasons such as taking their time to decide or waiting for a change in their relationship.8
Remember that Planned Parenthood claims that all partial-birth abortions are done for fatal birth defects or to save the life of the mother. It turns out that the actual number done for these reasons is about one percent.
The Quick Slide to Infanticide
The fundamental nature of evil is that it always expands unless it is relentlessly opposed. Certainly this is true of abortion. Typically, its supporters first demand an exception just to save the mother’s life, then more exceptions for rape and incest, then for the mother’s mental and physical health, and finally abortion for any reason whatsoever throughout all nine months of pregnancy.
Now we see them agitating for so-called “after-birth abortion,” as more and more “ethicists” baldly advocate infanticide in prestigious medical journals. As one example, it is only necessary to read the beginning and end of one article published in 2012 in the British Medical Journal to see where this train of thought is transporting us:
By showing that (1) both fetuses and newborns do not have the same moral status as actual persons, (2) the fact that both are potential persons is morally irrelevant and (3) adoption is not always in the best interest of actual people, the authors argue that what we call ‘after-birth abortion’ (killing a newborn) should be permissible in all the cases where abortion is, including cases where the newborn is not disabled.…If economical, social or psychological circumstances change such that taking care of the offspring becomes an unbearable burden on someone, then people should be given the chance of not being forced to do something they cannot afford.9
This is how far we have fallen down the slippery slope. The two professors who wrote this article callously approve of the murder of a newborn if the mother “cannot afford” to raise him or her. We have arrived at the point where many say that we do not even have to justify the killing of a newborn; now the little ones have to somehow wordlessly prove that they are worthy of life, as the above article’s title reflects: “After-Birth Abortion: Why Should the Baby Live?”
In reality, American abortionists have been practicing “after-birth abortion” for a long time.
Alisa LaPolt Snow, a lobbyist for the Florida Alliance of Planned Parenthood Affiliates, gave startling testimony during the Florida House debate over a state Infants Born Alive Act in 2013. She said that helping a healthy newborn who has survived a botched abortion “inserts politics where it doesn’t belong.” She suggested that such infanticide is part of “a woman’s ability to make her own personal medical decisions.” Representative Jim Boyd asked her “So, um, it is just really hard for me to even ask you this question because I’m almost in disbelief. If a baby is born on a table as a result of a botched abortion, what would Planned Parenthood want to have happen to that child who is struggling for life?” Snow replied without hesitation “We believe that any decision that’s made should be left up to the woman, her family, and the physician.”
And then, of course, we have the example of abortionist Kermit Gosnell, who routinely delivered full-term babies in his Philadelphia abortion mill and then severed their spinal columns with scissors. This was done with the full knowledge of the National Abortion Federation, which had inspected his clinic, and other Pennsylvania pro-abortionists. Not one major so-called “pro-choice” group has condemned Gosnell. They are willing to say that he is the exception, not the rule, but that is as far as they are willing to go.
Gosnell is certainly not the first abortionist who has engaged in infanticide of born-alive babies. There have been many cases of abortionists being brought to trial for either murdering these babies outright or setting them aside and allowing them to die of starvation and thirst.
Conclusion
Statistics show that that late-term abortions are rarely done for the “hard cases” of the health of the mother or fetal deformities—and the excruciating pain experienced by the baby during a late-term abortion should remind us that even in the hard cases, abortion cannot be permissible.
After all, if it is legal to kill a preborn child just hours before birth, what is to stop people from killing them after they are born?
Endnotes
[1] Annie Murphy Paul. “The First Ache.” The New York Times Magazine, February 10, 2008.
[2] “Fact Sheet” on the National Abortion Federation (NAF) web page, downloaded on February 18, 1997.
[3] Partial-birth abortionist Martin Haskell, of Dayton, Ohio, quoted in Gene Peterson. “Senator, Former Official Equate Late Term Abortion to Infanticide.” Ludington Daily News, October 21, 1996, page 4 (original quote in American Medical News, November 20, 1995).
[4] Partial-birth abortionist James McMahon, quoted in a Sixty Minutes episode of June 2, 1996 entitled “Partial Birth Abortion Ban.”
[5] 1993 National Abortion Federation internal memorandum, quoted in United States Senator Bill Frist. Bill Frist: A Senator Speaks Out on Ethics, Respect, And Compassion (Washington, D.C.: Monument Press), 2005, page 247.
[6] There is abundant evidence that there are many more third-trimester abortions performed than there are reported, and that most of them are done for relatively trivial social reasons:
A former employee of third-trimester abortionist George Tiller, Luhra Tivis, wrote:
I witnessed evidence of the brutal, cold blooded murder of over 600 viable, healthy babies at seven, eight and nine months gestation. A very, very few of these babies, less than 2%, were handicapped.…I thought I was pro-choice and I was glad to be working in an abortion clinic. I thought I was helping provide a noble service to women in crisis.…I was instructed to falsify the age of the babies in medical records. I was required to lie to the mothers over the phone, as they scheduled their appointments, and to tell them that they were not “too far along.” Then I had to note, in the records that Dr. Tiller’s needle had successfully pierced the walls of the baby’s heart, injecting the poison that brought death.
Luhra Tivis. “Where is the Real Violence?” Celebrate Life (American Life League), September/October 1994.
I have been protesting at Carhart’s on Mondays since December 6 [2010]. During this time, I have had the opportunity to speak with over twenty-five mothers who were there seeking late-term abortions. There has only been ONE case of a mother seeking a late-term abortion because of a poor prenatal diagnosis. The other mothers were reportedly there because, even at this advanced stage in their pregnancy, they decided that the baby was an inconvenience. One mother, Kiesha, who came to Carhart’s for a late-term abortion decided to save her baby. She just gave birth to a beautiful, healthy baby girl.
Midtown Hospital was Georgia’s largest abortion mill, a member of the National Abortion Federation and heartily endorsed by Planned Parenthood. Eventually, it was closed by officials due to its filthy conditions and endangerment of patients. One former employee testified in an affidavit:
On April 18, 1998, at approximately 7:00 a.m., I witnessed a patient deliver an intact fetus in the toilet of a bathroom in the waiting room area. After expelling the baby and the afterbirth, the patient walked to the operating room because there were no wheelchairs. I opened the fetal sac so that the fetus could be weighed. The weight was approximately 3029 grams [over 6 pounds, 10 ounces]. It was a very big fetus. My impression is that at Midtown Hospital a procedure will be done at any gestational age as long as the patient has the money.
“Men Behaving Really Badly.” Life Insight (National Conference of Catholic Bishops Secretariat for Pro-Life Activities), Volume 9, Number 8, October 1998.
An article in the September 17, 1996 Washington Post said:
It is possible, and maybe even likely, that the majority of these abortions are performed on normal fetuses, not on fetuses suffering from genetic or developmental abnormalities. Furthermore, in most cases where the procedure is used, the physical health of the woman is not in jeopardy.
In After Tiller, a 2013 pro-abortion propaganda film that lionizes four partial-birth abortionists, Susan Robinson, who performs third-trimester abortions at her clinic in Albuquerque said:
Women whose fetuses have terrible abnormalities…are a lot easier for people to understand. The husband and wife want to spare their baby whatever suffering that baby would have. Then there’s the group of women who didn’t know they were pregnant. They were told they were not pregnant for one reason or another and they are just as desperate. “I already have three children, my husband just lost his job and I can barely put food on the table. If I add a new baby to this family, we’ll all go under.”
Sarah Terzo. “Third-Trimester Abortions in America: ‘Healthy Babies at Seven, Eight and Nine Months Gestation.’” LifeSite Daily News, February 8, 2013.
[7] Aida Torres and Jacqueline Darroch Forrest. “Why Do Women Have Abortions?“ Family Planning Perspectives, July/August 1988 (Volume 20, Number 4), pages 169 to 176, Table 4, “Percentages of Women Who Reported that Various Reasons Contributed to Their Having a Late Abortion and Who Cited Specific Reasons as Accounting for the Longest Delay.”
[8] Alberto Giubilini and Francesca Minerva. “After-Birth Abortion: Why Should the Baby Live?” British Medical Journal Online, March 2, 2012.
PORTLAND, Maine, August 5, 2020 (LifeSiteNews) ― A recent paper has suggested that women who use the birth control pill may be particularly susceptible to blood clots if they contract COVID-19.
Doctors Daniel I. Spratt, an endocrinologist, and Rachel J. Buchsbaum, a hematologist, published “COVID-19 and Hypercoagulability: Potential Impact on Management with Oral Contraceptives, Estrogen Therapy and Pregnancy” in the Endocrinology journal on July 29.
The physicians wrote that one of the consequences of contracting the coronavirus seems to be an increased risk of blood clots.
“The novel coronavirus, SARS-CoV-2, has proven unusual with respect to the spectrum of its pathological effects,” they wrote.
“In addition to damage inflicted on the lungs, kidneys, heart and other organ systems, reports have emerged of hypercoagulable states in patients hospitalized with COVID-19.”
These clots and their travels from one part of the body to another “occur with a troublesome frequency” in coronavirus patients, they added.
Given this situation and other emerging COVID-19 research, the authors suggest there may be a chance that risk of blood clots and strokes for pregnant women and those using the pill or hormone replacement therapy is heightened by the virus.
“As more information emerges regarding the effects of SARS-CoV-2 on coagulation, questions arise as to whether infection with this virus aggravates the risk of [venous thromboembolic events (VTEs)] and strokes associated with combined oral contraceptives (COC’s) and other estrogen therapies as well as pregnancy-associated risks,” they wrote.
High doses of estrogen already have their dangers, and not just for older women and, for that matter, not just for women.
The doctors noted that contraceptive pills are linked to a “2- to 6-fold increase in risk for VTEs.”
“The risk for stroke is increased in young women from about 4 to 8 in 100,000 women per year,” they wrote.
“Similar data exist for oral hormone replacement therapy (HRT) in menopausal women and oral estrogen therapy in male-to-female transgender patients [sic].”
Pregnancy also carries a heightened risk for VTEs, they wrote, increasing 4-5 fold.
The doctors added that, although there is no “clear data” to support this advice, it is commonly recommended that people stop taking estrogen two weeks before they do something that could also increase their risk of blood clots, like surgery or long flights.
Spratt and Buchsbaum also noted there have so far been no reports of increased incidents of VTEs among women with coronavirus who are pregnant or using estrogen products. However, one “preliminary report” has suggested that “vascular abnormalities in the placenta” can accompany a COVID-19 infection. Also, given the relationships between the virus and blood clots, the doctors believe that more research must be done for women already at a higher risk for the latter.
Their questions include concerns for the effect of the coronavirus’s tendency to cause hyperinflammation on the health of unborn babies, as well as the measures that should be taken to reduce the risk of blood clots to pregnant women, women who use estrogen products, and women with the virus.
The doctors stressed the importance of these questions by predicting that the novel coronavirus will be around for years to come.
“We do not know how long the current pandemic will endure and can be reasonably certain that, like the H1N1 virus causing the 1918-1919 influenza pandemic, SARS-Co-V-2 will return cyclically for years if not decades,” they wrote.
“Thus, the importance of undertaking research to answer these questions will continue with findings likely to be applicable in a wide range of clinical situations.”
As yet doctors do not know why or how the virus has an impact on blood coagulation. Spratt and Buchsbaum called for researchers and clinicians, and for endocrinologists and hematologists to work together to find the answers.
Rachel J. Buchsbaum, MD, is the Director of the Cancer Center and Chief of the Division of Hematology/Oncology at Tufts Medical Center in Boston. Daniel Spratt, MD, works in the Division of Reproductive Endocrinology and Infertility at the Maine Medical Center in Portland, Maine.
LifeSiteNews reached out to Dr. Spratt for further comment today and is awaiting a reply.
In the 1960’s the pill was revolutionary, giving women the ability to control their fertility and advancing their equality in the workplace and in society. But when the pill came onto the market, women were not fully informed of the side effects and risks. Sixty years later, any conversation around the drawbacks of hormonal birth control remains politicized and suppressed.
Today, over half the women prescribed hormonal birth control are on it for non-contraceptive reasons like acne, irregular or painful periods, PCOS and endometriosis. Hormonal birth control has been linked to depression, autoimmune disease, cervical cancer, fatal blood clots and other chronic conditions; yet it is still prescribed to healthy women as a panacea for every hormonal and reproductive issue.
With pharmaceutical companies making billions on blockbuster products and reproductive rights under attack, exposing the downside of hormonal birth control is controversial. Yet, as the scientific research grows, there is a rising consciousness around the mental and physical impacts of these medications and the landscape is shifting: A Danish study found an 80% increase in the risk of depression for teenagers on hormonal contraception. Younger generations want to avoid endocrine-disrupting chemicals and are scrutinizing everything they put in their bodies. Femme-tech and fertility awareness methods are becoming mainstream and hormonal health coaches are reframing natural menstrual cycles as more empowering than suppressing ovulation.
Looking at the complex relationship of hormonal contraception to women’s health and liberation, The Business of Birth Control features the stories of activists, doctors and scientists who are blowing the whistle on how hormonal birth control affects the mind and body. The film revisits the 1970’s Nelson Pill Hearings, where feminists disrupted the proceedings to demand informed consent and follows a courageous group of bereaved parents who are fighting to get warning labels on Yaz and NuvaRing fifty years later.
The filmmakers trace the shocking history of how hormonal birth control has been weaponized against communities of color, while capturing a revived feminist health movement that is embracing body literacy and redefining reproductive justice. The Business of Birth Control is primed to ignite the next women’s health revolution. It is sure to be required viewing for anyone with a uterus.
Will Covid-19 lockdowns allow some babies to be born this year who would otherwise be aborted? Yes – and that’s not, it seems, a good thing, according to a report on “compromised abortion” from the Indian abortion provider Ipas.
It says that redeploying abortion facilities and staff to prioritise care for Covid-19 patients has had deleterious effects on India’s abortions, including the fact that some may not take place at all.
It urges that all stops be pulled out to provide abortions for Indian women, including second-trimester abortions. “Unwanted” pregnancies, as they are baldly described, must not be allowed to go to term. Missing in the report is any reference to “unwanted” fetal sex, a frequent motivation for abortion in India; female children who succeed in being born may well have escaped an abortion precisely on this ground.
There is great social pressure on women in India to abort female babies for a host of cultural reasons. The huge sex imbalance in the country is troubling even to those who support abortion. In-laws and husbands push for sex-selective abortion, and pregnant women, willingly or otherwise, comply. Indeed, this also applies in the immigrant population in the US where, unlike in India, there are no legal restrictions on antenatal sex screening.
Despite the law in India concerning screening, abortions based on sex continue in large numbers. It is clear from other reports where Ipas’s priorities lie: efforts to stop sex selection must not, they admonish us, get in the way of abortion provision. So if more baby girls die this year simply for being girls – including those who die because of the zealous efforts of Ipas – Ipas will not be, it seems, to blame.
Ipas are not alone in seeming to regret the births of unaborted babies. Regretting lost opportunities to abort, whether due to Covid-19 or to other factors, is a regular feature of British abortion advocacy. Recently, we saw the abortion provider BPAS shaking its head over the fact that women presenting for late-term abortions are being “compelled to continue pregnancies they do not want”. This is, it seems, an intolerable means to the surely good end of birth when the pregnancy is completed.
It is doubtful whether the mothers who requested these late-term abortions now regret their baby’s birth. After all, even the famous and flawed Turnaway study of women refused an abortion found that the great majority did not regret having the baby.
Even for those who did, the value of children is not conferred by parents: no child should have to prove, by “wantedness”, her right to remain in the land of the living. The answer to reluctant or simply challenged parenthood is serious support for parents – or in extreme cases, but only then, transfer of care.
Abortion is something many women mourn, particularly those who were conflicted or coerced, who wanted the baby, or who believed that abortion was morally wrong. Surprising as this may seem, even if the baby is terminally ill, abortion seems to produce for women significantly more despair, depression and avoidance than going through with the pregnancy. The hospice/palliative care approach, here as later in life, carries huge emotional benefits for those left behind.
Of course, most women are aborting not for fetal disability or sex selection, but simply due to personal circumstances. Women in poverty, and those who have been abandoned or abused, need real and positive help with their pregnancies. Such help is available from various sources in Britain, though not often publicized by abortion clinic personnel. The organization Be Here for Me gives a voice to women, often migrants lacking access to public resources, who accepted such positive help at the very last minute – help of which the clinic certainly did not make them aware. Again, far from regretting their born children, these women cannot speak too warmly of their children and of the support they received to keep them in some extremely fraught situations.
Redeploying abortion resources to Covid-19 care, as in India, is the medical equivalent of beating swords into ploughshares. Contemplating peace and its challenges, the union leader Walter P Reuter remarked in 1953 that it was “fantastic and inhuman” that those in Wall Street and elsewhere should be afraid that “peace will break out”, and depression then follow.
For some of us, it is no less “fantastic and inhuman” that activists across the world should be so afraid of the escape of – hopefully – many babies in 2020, whose mothers will have not a mere painful memory, but a child in their arms.
In a newly-released eight-minute video, “The Billionaires Behind Abortion,” Live Action exposes the “who’s who” behind the push for population control—by means of contraception and abortion—from its beginnings to today. “Without the financial support of these billionaires,” says the video, “abortion would not be nearly as prevalent as it is.” The video is part of a new exposé by Live Action, “Abortion Pill Kills,” which reveals the largely unknown details surrounding a dangerous drug that has killed millions of preborn children and which has also injured and even killed women.
So who are these influential billionaires? Their names are probably very familiar. Watch:
The top funders of contraception and birth control worldwide are, according to the video, the foundations of Bill Gates (founder of Microsoft and the second richest man in the world), Warren Buffett (successful investor and the fourth richest man in the world), and William Hewlett and David Packard (the founders of the Hewlett-Packard corporation). Other funders include George Soros, The Ford Foundation (Henry Ford), and the Rockefeller Foundation (John D. Rockefeller, the world’s first billionaire).
The video notes that population control is the motive behind these philanthropists, stating that the Rockefeller family “was influential in the development of the American eugenics movement of the 1920s” which “later served as the basis for the eugenics movement in Nazi Germany.” John D. Rockefeller founded an organization called the Population Council after the atrocities of World War II.
Frederick Osborn, Rockefeller’s successor at the Population Council, was also the founding member of the American Eugenics Society. He believed strongly in birth control and abortion as “the great eugenic advances of our time.” A later Population Council president, Bernard Berelson, suggested that if voluntary birth control efforts were unsuccessful among the population, birth control agents should be put into the water supplies of urban areas.
Today, the Population Council is still operating full force, and is funded by many of the previously mentioned billionaires.
Microsoft founder Bill Gates has long funded population control efforts through the Bill and Melinda Gates Foundation and, as seen in the video, has stated that funding “reproductive health” efforts has always been “the main thing” on the Gates Foundation’s list of priorities, especially “in the very poorest places.”
Billionaire Warren Buffett reportedly had a “Malthusian dread of overpopulation’s potential negative effects.” Billionaire David Packard, likewise, was concerned that overpopulation would cause other societal problems to “become unmanageable.”
Today, as the video states, these same billionaire philanthropists are funding efforts to expand access to the abortion pill. French pharmaceutical company Roussel-Uclaf donated the abortion pill’s patent rights to The Population Council in 1994. The Council formed Danco Laboratories to manufacture and market the pill in the U.S.
Screenshot
Danco has been “shrouded in secrecy,” notes the video, has “refus[ed] to release the names of its investors and executives,” and “has been shielded by the FDA, who in an unprecedented maneuver concealed the name and location of the manufacturer… as well as the names of the experts who reviewed the pill.” Buffett, Packard, and Soros have all invested financially in Danco. Gynuity Health Projects, a sponsor of U.S. clinical abortion pill trials, is also funded by many of these billionaire foundations, as is DKT International, which sells the abortion pill internationally.
As the video sums up, “The abortion movement has always been fueled by ultra-wealthy individuals as a means to control global populations, promoting the killing of children and exploitation of women under the guise of reproductive health and women’s rights.”
In 2018, the BBC published several articles noting that British women were beginning to trend away from the birth control pill and were instead opting for long-acting, reversible contraceptives (LARC) like IUDs and the implant. Reasons for this transition vary, including a desire for a “set it and forget it” method that doesn’t require taking medication at the same time every day. For other women, the side effects of the birth control pill led them to seek an alternative. In a brief video, the BBC shared a snapshot of these women’s experiences. Though a switch to LARCs is unsettling, what should not be overlooked is these women’s shared negative experiences taking birth control pills.
Each of the women interviewed for the BBC had a different reason for taking the Pill; some started taking it for health reasons, others were looking for reliable birth control. One woman had grown up believing that “if you were going to be having sex, like with a partner or anything, you would have to be taking the Pill. You know, you could use condoms, but if you were going to be in a relationship, you needed to go on the Pill.” Another woman started the Pill as a teen due to heavy periods that were causing her to miss high school.
And all of the women experienced side effects severe enough to outweigh any possible benefits to them.
Some of the side effects were physical. Two of the women developed blood clots, which are six times more likely to occur in women who are on the Pill versus non-users. While blood clots anywhere in the body are dangerous, one of the women developed a pulmonary embolism, a blood clot in the lungs which can cause death even without prior symptoms. Other physical side effects of the Pill included significant weight gain “right off the bat,” whole-body muscle aches and heart palpitations, and migraines, which one woman said “would shock my body into so much pain that I would have seizures.”
Several of the women additionally experienced new onset mental illness. One woman recalled, “I would be awake for three days straight, because I had such insane anxiety attacks that I couldn’t sleep” and also would “have depressive attacks so bad that I couldn’t get out of bed, couldn’t go to school.” Even antidepressants and anti-anxiety medications did not resolve her struggles. Another woman reported developing depression and decreased sex drive. Unfortunately, new-onset depression, especially amongst teenage girls who go on the Pill, is far from uncommon. In fact, according to the BBC video, which cited CDC statistics, about 30% of American women who stopped taking the Pill did so due to “dissatisfaction,” with side effects being the most common reason for their dissatisfaction.
Despite all of these issues, when these women went to their doctors reporting new health concerns, few were told that the Pill might be causing their problems. The woman who experienced seizures due to Pill-induced migraines saw nine different neurologists in the United States and the UK over the course of two years, and tried out over 30 different medications for her migraines. The woman with the pulmonary embolism was misdiagnosed with “exercise-induced asthma” when she first went to her doctor with breathing difficulties. The woman on antidepressants and anti-anxiety medications said she asked her doctor multiple times about a possible link between the Pill and anxiety and depression, but said, “No one once said anything about it, not the psychologists, or therapists, or gynecologists.”
Each of the eight women in the video eventually stopped taking the Pill, with unanimously positive results. The woman who went on antianxiety and antidepressant medications experienced significant improvements in her mental health after stopping the birth control. She asserted, “We should be telling young girls that they have options and that there are other ways to take care of your body and other ways to take charge of your reproductive health.”
That woman was right. Women and girls do have options for pregnancy avoidance and reproductive health issues that respect and work cooperatively with the natural rhythms of their bodies. Fertility awareness methods of family planning enable women to become experts about their own bodies and to use that information to achieve their personal and health goals, without any nasty side effects.
Denver Newsroom, Jul 24, 2020 / 04:51 pm MT (CNA).- As someone who teaches couples about Natural Family Planning (NFP), Jeanice Vinduska most often fields questions of doubt from couples who are used to artificial means of contraception, such as birth control pills and IUDs.
It can be difficult to convince some people that a natural means of planning and spacing children is effective and worthwhile, especially in a culture where artificial contraception is widely accepted and used, Vinduska told CNA.
But Vinduska also fields questions from Catholics and Christians who are dubious of NFP because they are concerned it could be contraceptive too.
“I had a woman in my parish who said…’Well, this is just natural contraception,’” Vinduska recalled. Vinduska works as the co-director of the FertilityCare Center of Omaha, with the St. Paul VI Institute, which specializes in teaching women and couples the Creighton method of NFP.
The Creighton method is a method of NFP that tracks cervical mucus as a symptom of fertility in women. It can be used by couples to achieve or avoid pregnancy, and it can also help diagnose conditions like endometriosis.
But methods of NFP differ from artificial means of contraception in that they do not do anything to disrupt the sexual act, Vinduska said. “Contraception basically prevents fertilization. It prevents human life,” she said. “Oral contraception can even act as an abortifacient.”
NFP, on the other hand, allows married couples to track their fertile and infertile days and to decide when to be sexually intimate and when to abstain from sex, based on what is best for their family at that time, Vinduska said.
And unlike contraception, NFP is approved by the Catholic Church as a means of planning and spacing children in accordance with God’s plan.
The ‘quiverfull’ movement
Some Christians are part of the “quiverfull” movement, which gets its name from Psalm 127: 3-5: “Certainly sons are a gift from the LORD, the fruit of the womb, a reward. Like arrows in the hand of a warrior are the sons born in one’s youth. Blessed is the man who has filled his quiver with them.”
Christians with a “quiverfull” mentality towards family planning believe that they should have as many children as God will give them, and refuse the use of contraception or Natural Family Planning. They also do not attempt to resolve any physical defects that cause infertility, which they also see as God’s will.
But the “quiverfull” mentality has never been a part of the teaching of the Catholic Church, Vinduska said.
“That’s never been a teaching. It’s more about being open to life and finding a responsible way of family planning, of fertility regulation.”
Dr. Janet Smith is a Catholic theologian and author of “Humanae Vitae: A Generation Later” and “Self-Gift: Essays on Humanae Vitae and the Thought of John Paul II.” She has frequently written and spoken about Humanae Vitae, including in her signature talk, entitled “Contraception: Why Not”.
Smith said the Catholic Church instead teaches that God has given humans reason and freedom to choose to have children freely, or to abstain when they are fertile.
“God gives us the possibility of pursuing many goods; he forbids us from doing evil, but permits us to choose freely between goods,” Smith told CNA.
“Some couples are blessed with many resources both material and spiritual that enables them to have many children, but others need to limit their family size because of various difficulties in their lives. Certainly couples should be generous in their child-bearing, but the Church teaches that for serious or just reasons spouses may limit their family size,” she said.
NFP differs from contraception by allowing the couples to fully participate in the marital embrace without removing the possibility of conceiving, Smith noted. The Church supports NFP because it does nothing to change the meaning of the marital act.
“Contraception undercuts that meaning since it removes the commitment-making power of procreation.”
Church teaching also differs from the quiverfull mentality in that couples experiencing fertility are also free to attempt to remedy physical defects so that they may have children, Smith said.
“[I]f couples have correctable physical defects that prevent them from conceiving, it is fully in accord with God’s will that they attempt to have those defects repaired,” she said.
Humanae Vitae
Pope Paul VI, for which the institute in Omaha is named, wrote one of the most oft-referenced encyclicals on the subject of marriage, sexuality and family planning in his encyclical letter, Humanae Vitae.
In it, Pope Paul VI first states that “the transmission of human life is a most serious role in which married people collaborate freely and responsibly with God the Creator. It has always been a source of great joy to them, even though it sometimes entails many difficulties and hardships.”
In section 10 of the letter, the pope states: “Married love, therefore, requires of husband and wife the full awareness of their obligations in the matter of responsible parenthood, which today, rightly enough, is much insisted upon, but which at the same time should be rightly understood.”
Rightly understood, responsible parenthood is exercised “[w]ith regard to physical, economic, psychological and social conditions…by those who prudently and generously decide to have more children, and by those who, for serious reasons and with due respect to moral precepts, decide not to have additional children for either a certain or an indefinite period of time.”
What serious reasons are serious enough?
Pope Paul VI wrote that while Catholic couples are free to exercise their reason and freedom in planning their families, they also must involve God in their decisions.
“[T]hey are not free to act as they choose in the service of transmitting life, as if it were wholly up to them to decide what is the right course to follow,” he wrote. “On the contrary, they are bound to ensure that what they do corresponds to the will of God the Creator. The very nature of marriage and its use makes His will clear, while the constant teaching of the Church spells it out.”
Smith said that there are a variety of serious reasons for which couples may decide to avoid having children for a time or an indefinite period, depending on the circumstances.
“For example, if a family is financially strapped and can’t pay the bills, it would make sense to postpone having a child; if the wife has serious health conditions that a pregnancy would exacerbate or if she has duties that are so consuming (such as caring for an elderly parent or challenging child) another child may be an excessive burden,” Smith said.
Vinduska said she has worked with couples to avoid pregnancies for certain periods of time for such reasons. For example, she said, one woman was on a strong medication for a disease that made her bones brittle that would have caused serious defects if she were to become pregnant; other women with cancer have needed to avoid pregnancy while going through treatment.
The woman was successfully able to avoid a pregnancy while on the medication using the Creighton method, Vinduska said.
“We want to make sure that they are using a natural system and following their moral beliefs,” she said. “And they don’t have to be Catholic to do this. We teach NFP for everybody.”
Smith said that NFP could even be used for lesser reasons. During a 2018 talk at for a symposium at Benedictine College, Smith noted that couples can morally abstain from having sex for all kinds of non-fertility related reasons: someone has a headache, the couple wants to catch a sports game, or finish a movie, or they are staying somewhere with thin walls, and so on.
In those instances, Smith said, it is perfectly moral to abstain from sex.
“So I have a simple question for you. Why would it be wrong not to have sex because it’s not a good idea to have a child at that time?” she said.
The Church does not mandate any particular amount that couples must be sexually intimate, she said.
However, she told CNA, couples should “keep praying that God will let them know if they are being selfish,” although she added, “that selfishness is usually incompatible with long term use of NFP since only the virtuous and unselfish can use NFP over a long period of time.”
The benefits of NFP for marriage
Both Vinduska and Smith said that using a method of Natural Family Planning can be very beneficial for couples.
Vinduska said one of the biggest benefits of using NFP in a marriage is that it improves “communication, especially communicating where they’re at with their fertility and infertility. If the couple is charting together, it’s not such a surprise for either one of them where they’re at in their cycle.”
Something else that benefits couples using NFP is using the periods of abstinence to reconnect in ways other than sexuality, Vinduska said. She said she encourages couples she works with to use these times to develop common hobbies and interests, which serve to strengthen their relationship in other ways.
“Once you’re married, you kind of slip a little bit in doing the things like you did when you were dating,” she said. “But you shouldn’t have to always spend a lot of money. If you both like the outdoors, find a time to set aside to go hiking, go to a park. Maybe they can garden together, take up a new activity that gives them that sense of doing something together.”
The low divorce rates among NFP using couples speak for themselves, Smith added.
“The fact that couples using NFP almost never divorce…is a very revealing fact. NFP is a lot more than abstaining during the time a woman is fertile; it is a method that requires a lot of communication and shared values,” she said.
“It fosters the virtues of patience and ability to sacrifice. Women in couples who use NFP believe their husbands are exceptional (and husbands love that) and know their husbands love them for more than their sexual availability – a feeling that delightfully leads to them wanting to be more available (and their husbands love that).”
BELLEVUE, Nebraska, July 22, 2020, (LifeSiteNews) – Pro-life advocates in Nebraska joined together for a prayer rally across the parking lot of an abortion center that included adoration of the Blessed Sacrament. The prayer rally included a priest making the sign of the cross over the killing center with the Blessed Sacrament.
Pro-lifers on the ground told LifeSiteNews that after the prayer rally, there were no abortion appointments at the center on the usual killing days (Friday and Saturday), something that has not happened since they’ve been doing sidewalk advocacy there. It remains unclear if abortions will resume tomorrow (Thursday).
On July 16, the pro-life group Life Runners sponsored an Ablaze prayer vigil at Carhart abortion facility in Bellevue, known as “Bellevue Health Clinic.” LIFE Runners, a pro-life organization, teamed up with Ablaze, a Catholic ministry program, to organise an evening of prayer, singing, and adoration across from the abortion center. About 75 people gathered for the event.
At one point during the prayer event, Fr. Michael Voithofer, the founder and leader of Ablaze, made the sign of the cross over the abortion center with the Blessed Sacrament. He also prayed the St. Michael prayer written by Pope Leo XIII and recited the litany of the saints.
Dr. Patrick Castle, the founder of Life Runners, told LifeSiteNews that their goal is to “end abortion now.” He pointed out how “one in three women in America have had an abortion; one in five conceptions in America end in abortion.”
Pro-lifers pray and sing in front of abortion center in Bellevue, Nebraska, July 16, 2020.
Castle said that abortion takes more lives than all “combat casualties in the history of our country.” He explained that the fight to end abortion is a “spiritual war.”
“We did a holy battle there,” he continued, “to push back the demonic, to claim that space in the Lord’s name.” Castle hopes to “memorialize the unborn that have been slaughtered there (at the abortion center).”
“Abortion is the greatest WMD, weapon of mass destruction,” Castle said. “It is the leading cause of death on the planet.” He said that the Holy Eucharist, “the most powerful spiritual weapon,” was used to fight abortion during the July 16 rally.
“The ground is blessed now so the mothers that go into the clinic will be walking on blessed ground in their moment of crisis,” he continued.
This was the first known time that the sign of the cross was made over the center with the Blessed Sacrament. Just last month, a Mass was celebrated across from the abortion center.
Pro-lifers lift their hands in prayer in front of abortion center in Bellevue, Nebraska, July 16, 2020.
In an interview with LifeSiteNews, Fr. Michael said the fight to end abortion is a “spiritual battle.” He explained that, “praise is really a weapon we can use to ward off evil.”
“Our battle is not against people; it’s against demons,” he continued. “The devil wants to sacrifice these children.”
Offering prayer to God through singing is like a “blast of light that demons can’t stand,” said the priest.
By making the sign of the Cross with the Blessed Sacrament over the abortion center, Fr. Michael said he fought against “the demons and spirits that are behind this evil of abortion.”
“What perpetuates the abortion industry,” he explained, “is a demonic stronghold” that seeks to “destroy human life.”
“Every pregnant woman is a reminder to Satan that he’s done — he lost — because every pregnant mother reminds Satan of the Blessed Mother.”
The Carhart center is open for abortion usually on Thursday, Friday, and Saturday each week. However, after the prayer rally on Thursday evening, the center did not perform abortions Friday and Saturday, according to pro-life eyewitnesses on the ground. It remains to be seen if the center will resume abortions later this week.
“They didn’t have any abortion appointments on Fri and Sat. We were there. Fri and Sat without abortion appointments hasn’t happened since I’ve been doing sidewalk advocacy there, 3 years. Praise God!,” Castle told LifeSiteNews.
Castle encouraged pro-lifers to go to abortion centers to fight with the weapon of prayer.
“We know that that is often enough for a mom to not turn in to that abortion facility,” he said.
The prayer vigil occurred during the pro-life Across America Relay, sponsored by LIFE Runners. The relay began on July 4 from the north, south, east, and west coasts of the United States. Four groups will walk or run 5359 miles in 5-kilometer legs, meeting in Kansas City on August 9 for a mass celebrated by Archbishop Naumann.
The only requirement to be a LIFE Runners is to wear a “REMEMBER The Unborn” jersey as “a public witness to impact hearts and minds for saving lives.” LIFE Runners has 14,657 members in 2,553 cities across 39 nations.
Castle explained the importance of wearing these jerseys, “78% of post abortion mothers say that if just one person had encouraged them to choose life of if they saw an encouraging sign to choose life, they would not have aborted their child.”
Castle explained that pro-lifers can sign up to remotely participate by walking or running 5 KM legs while wearing LIFE Runners jerseys anywhere in the world.
The curriculum suggested by the United Nations health organization promotes aberrant sexuality for children, claiming their guidelines supersede those of the parents. This takes on chilling implications when considering the history of rape and pedophilia within the organization.
In the wake of the organization mishandling the ongoing COVID-19 pandemic, President Trump removed US funding from the World Health Organization (WHO). Many people criticized the decision but a closer look shows that not only is the WHO incompetent at performing the function for which it was created but it has side agendas that are shocking indeed. One such program that began more than ten years ago is focused on indoctrinating children under the age of four in the “enjoyment and pleasure of masturbation” and that even for children, sexuality is a “normal part of everyone’s life.”
The WHO Collaborating Centre for Sexual and Reproductive Health, established in 2003 at the German Federal Centre for Health Education (BZgA) focused on establishing standards for sexuality education, providing guidance for implementation and support the implementation of training programs for educators. The program has been translated into several languages and used internationally. The program was produced in a framework document for the development of sexuality education. It has been used in at least 14 countries to develop or adapt curricula for sexuality education and/or for advocacy towards decision-makers.
The WHO curriculum suggests that children ages four to six, the be given information “about friendship and love towards people of the same sex” and “same-sex relationships,” and be guided to develop “an open, non-judgmental attitude.”
As per this program, children under the age of four are introduced to masturbation including “playing doctor” (i.e. sexual activity with another person of unspecified age). Children from 4-6 are introduced to “same-sex relationships” (i.e. homosexuality).
The WHO also removes the authority of the parents in such matters, establishing its standards as superseding those.
“As argued,” reads the document, “parents, other family members, and other informal sources are important for learning about human relationships and sexuality, especially for younger age groups.
“However, in modern society, this is often insufficient, because these informal sources themselves often lack the necessary knowledge, particularly when complex and technical information is needed (such as that pertaining to contraception or transmission modes of STI).”
In 2018, Andrew MacLeod, the former chief of operations at the UN’s Emergency Co-ordination Center claimed that an estimated 60,000 cases of sexual exploitation had been committed over the last decade by 3,300 pedophiles working in the organization.
“Child rape crimes are being inadvertently funded, in part, by United Kingdom tax-payers,” he said in an interview with British tabloid The Sun. At the same time, UN Secretary-General António Guterres admitted that the UN had “wrestled for many years with the issue of sexual exploitation and abuse,” as reported by the British newspaper The Times. In early 2017 the United Nations Secretary-General admitted to 145 incidents involving 311 victims in 2016 alone, mainly in peace operations.
In one case that is disturbingly relevant to the WHO education program, Canadian humanitarian worker Peter Dalglish, who helped found the charity Street Kids International, was taken in by police in Nepal over claims he was involved in pedophile activities in Kavre district, around 50 kilometers north of the capital, Kathmandu.
“Under the guise of community worker, claiming to educate poor kids and provide the necessary support, he had been sexually exploiting these children. We have developed a sound network to track down and arrest pedophiles entering Nepal. We had been following Dalglish’s activities for the last two weeks after we were tipped about his activities,” CIB chief and Deputy Inspector General of Police, Pushkar Karki said, according to the Kathmandu Post.
Prior to his stint in Nepal, he had worked for a number of United Nations agencies and was the U.N.-Habitat country representative for Afghanistan.
He was also part of the U.N. Mission for Ebola Emergency Response in Liberia until January 2016 and has been an advisor to the World Health Organization to help tackle the spread of the disease.
Multiple possible coronavirus vaccines that are on a fast track for development as the world awaits a vaccine to deal with the international pandemic. But one of the COVID-19 vaccines that is receiving the most attention is also the most controversial because it relies on cells from the body part of an aborted baby.
Despite a strong outcry from pro-life and Catholic leaders and despite ethical alternatives being available, a number of research teams still are using the cells from aborted babies in their work. These include Janssen Research & Development USA, a Johnson & Johnson subsidiary, and the University of Oxford and AstraZeneca, which could be the first to make a coronavirus vaccine available in the United States.
The Oxford/AstraZeneca team appears to be in first place in the vaccine race and doses of the vaccine were given to 1,077 healthy adults aged between 18 and 55 in five UK hospitals in April and May as part of phase one of the clinical trial. A new paper published in The Lancet medical journal revealed the vaccine appears safe and induces a strong immune response following the first phase of human trials. It also appears to be helping the human body make antibodies by the body’s B cells, which is very helpful in staving off the virus in the future.
But the vaccine is not without ethical concerns.
The team at Oxford University is developing the vaccine using the HEK 293 cell-line. This cell-line was originally created from tissue taken from the kidney of an unborn child probably aborted in 1972.
Dr Anthony McCarty, a pro-life physician in the UK, spoke out about the moral concerns.
“For those of us who see the original abortion as the unjustified taking of the life of the unborn child, such use of the products of abortion, even a cell line derived from the original tissue, risks sending out a harmful social message concerning the value of early human life,” he said.
Dr McCarthy added: “Even those not opposed to all abortion may well have serious and substantial moral concerns over practices which seem to treat opportunistically the remains of an aborted unborn child. Society needs to respect the consciences of its members who uphold the inviolability of human life from conception and who do not wish to be involved in anything they may see as complicit with the unjust taking of such life.”
In April 2020 the British pro-life group SPUC wrote a letter to Jo Churchill the Parliamentary Under-Secretary at the Department of Health and Social Care), requesting that the Government make available vaccines which are not made using cell lines originally derived from the tissue of aborted unborn children.
Some vaccines are being developed without the use of foetal cell lines. These vaccines may involve plant or animal cells. For example: cells from insects, tobacco plants and hamster ovaries. A team at Imperial College London is working on a ‘synthetic’ vaccine i.e. a ‘cell-free’ method. There are no pro-life concerns with these vaccines.
Other researchers also using cell lines from aborted babies include CanSino Biologics, Inc. and the Beijing Institute of Biotechnology and the University of Pittsburgh, Science reports. Some are using a cell line from a baby who was aborted sometime around 1972, while others are using one from a baby who was aborted in 1985.
University of Pittsburgh researcher Andrea Gambotto said the cell lines from aborted babies are more useful than ethically-derived sources.
“Cultured [nonhuman] animal cells can produce the same proteins, but they would be decorated with different sugar molecules, which—in the case of vaccines—runs the risk of failing to evoke a robust and specific immune response,” Gambotto said.
But other scientists disagree. Earlier this year, the Charlotte Lozier Institute identified 60 potential treatments for the virus that are being investigated using materials that do not come from aborted babies.
Respected researchers Drs. James L. Sherley, MD, PhD and David A. Prentice, PhD recently reviewed the vaccines in development for the coronavirus and published a list identifying which are being made ethically and unethically. They found at least 10 companies that are not using cell lines from aborted babies in their vaccines.
Pro-life leaders also have highlighted how ethical alternatives to cell lines from aborted babies are available, including pluripotent stem cells and tissue from placentas, umbilical cords and amniotic fluid. In 2018, the Trump administration created a $20 million grant to invest in these ethical research alternatives.
Catholic and pro-life organizations have been advocating against research using aborted baby body parts for years. During the coronavirus crisis, they have renewed calls to scientists to abide by basic ethical standards in their efforts to save lives.
According to the Catholic News Agency, a Canadian Catholic archbishop recently took his pro-life advocacy a step further by donating thousands of dollars to an ethical vaccine research project at the University of British Columbia.
Earlier this spring, the U.S. Conference of Catholic Bishops sent a letter urging the Food and Drug Administration (FDA) to ensure vaccines are being produced ethically.
“… we think it’s very important at this moment to let the voice not only of the Church but other concerned citizens to voice that we want to—we all want a vaccine, we realize that’s important for our public health, but we also want a vaccine that has no ethical problems in the way it’s developed,” said Archbishop Joseph Naumann, chairman of the U.S. bishops’ Committee on Pro-Life Activities, earlier this spring.
Natural Family Planning (NFP) Awareness Week is slated for 19 to 25 July this year, and has for its theme: “Live the truth and beauty of God’s plan for married love!”
This annual week-long event is a national educational campaign of the Natural Family Planning Program of the U.S. Bishops’ Conference that promotes Catholic beliefs about human sexuality, conjugal love and responsible parenthood.
According to the U.S. Bishops, Natural Family Planning is the general title for “the scientific, natural and moral methods of family planning that can help couples either achieve or postpone pregnancies.”
The week highlights the anniversary of the papal encyclical Humanae Vitae (25 July 1968) on human life, and the feast of Saints Joachim and Anne (26 July), the parents of the Blessed Virgin Mary.
Natural Family Planning
The Church teaches that the “Sacrament of matrimony symbolizes Christ’s relationship with His Church…a relationship of total, faithful, permanent and fruitful love,” the Bishops explained in their Prayer and Liturgy guide for the event.
Therefore, when couples live out their vocation according to the Church’s teachings, especially with regard to the transmission of life, they grow in “holiness and consequent deepening of their respect and awe of God’s gift of human sexuality, marriage and family.”
NFP methods are based on the “observation of the naturally occurring signs of symptoms of the fertile and infertile phases of a woman’s menstrual cycle, ” the Bishops said. It requires “no drugs, no devices or surgical procedures” to avoid pregnancy
2020 NFP Awareness Week
Every year, the USCCB’s Natural Family Planning Program issues a poster, alongside basic supportive materials for the campaign. However, it is individual dioceses that offer a variety of educational formats best suited for the local church to focus on NFP methods and their use in marriage.
The USSCB materials for this year’s event include among others, homily aids for priests and deacons, documents and articles on the Church’s teachings on NFP, and stories from real-life couples who have put the method to use.
In one of the stories, the writer recounts that after taking an NFP class, she understood “the relationship that God designed between the marital act and procreation” and it made her “open to life.”
“Today, I am confident that had I not been open to life in the practice of NFP,” she said. “I would not have needed to depend on God, and not have grown as a person. This growth benefits my family and the people I meet in everyday life. Jesus calls us to serve others. Marriage and parenthood are ways we can immediately apply this call in our lives.”
(National Review) Yesterday, a federal judge ruled that, during the COVID-19 pandemic, women do not need to abide by a policy requiring that they go to a medical facility in order to obtain chemical-abortion drugs. The ruling by a U.S. district judge in Maryland, Theodore D. Chuang, stated that the “in-person requirements” were a “substantial obstacle” to women seeking abortions. As a result, the ruling allows health-care providers to mail or otherwise deliver abortion pills directly to women.
During the recent pandemic, supporters of legal abortion have been aggressive in their efforts to expand access to chemical abortions. In March, a coalition of 21 state attorneys general wrote to the commissioner of the FDA requesting that it loosen its safety regulations for chemical abortions. In June, more than 100 members of Congress made a similar request of the FDA.
Unfortunately, this decision by Judge Chuang likely will have adverse effects on women’s health. There is a body of research suggesting that chemical abortions pose significantly greater health risks to women than surgical abortions do. One of the best studies on this subject was published in 2015 after obtaining comprehensive and reliable data from Medicaid billing records in California. It found that chemical abortions result in a complication rate four times higher than the complication rate for first-trimester surgical abortions. The risk of a major complication with a chemical abortion was nearly twice as high as the risk of a major complication with a first-trimester surgical abortion. It seems likely that, if a higher number of chemical abortions are conducted without medical supervision, the risks of a complication will only increase.
Some supporters of loosening restrictions on chemical abortion cite a study published in Obstetrics and Gynecology surveying chemical abortions provided via tele-medicine im Iowa and purporting to show that those procedures were safe. However, that study had a number of shortcomings.
For instance, it used data from a survey of Iowa hospitals, with only a 35 percent response rate. It also failed to hold constant the gestational age of the unborn child and other factors that could increase the health risks involved with obtaining an abortion. Finally, the authors of the study admitted that some respondents might not have reviewed medical records and instead relied on their recall of events, making it possible that some adverse events were excluded. As a result of those shortcomings, this study should not be taken as a definitive data point regarding the safety of tele-med abortions.
There is evidence that the incidence of abortion has increased during the pandemic. According to a CBS News article from April, some abortion facilities have reported an increase in the number of women seeking abortions.
Meanwhile, ABC News reported that many “abortion funds,” which use private donations to subsidize abortions, had seen an increase in requests for help funding abortions. Data from Florida this spring show that the number of abortions in the state has increased by nearly 7 percent since a similar point in time last year. It is unfortunate that judges and policymakers are prioritizing access to medically risky chemical abortions instead of finding creative ways to support pregnant women in need.
Editor’s Note: This article was published at National Review and is reprinted here with permission.
The coronavirus pandemic has served for many as a forceful reminder of our mortality as humans. A recent Wall Street Journal article noted that the transhumanism movement capitalizes on such fears, touting the promise of “eternal life through advanced technology” to bolster support for what otherwise might be considered extremist or unethical goals.
Currently, nanorobots (and other artificial intelligence), prosthetics and implants, and genetic engineering are the most favored technologies of the transhumanist movement, whose 1998 Transhumanist Declaration sought “the possibility of broadening human potential by overcoming aging, cognitive shortcomings, involuntary suffering, and our confinement to planet Earth.” According to a 2019 Areo magazine article, these ideas are being adopted and used by companies like Google, Apple, Tesla, and Space X and financially backed by Silicon Valley executives like Jeff Bezos of Amazon, Elon Musk of Tesla, and Peter Thiel of PayPal and Palantir, and more.
In some ways, transhumanism’s pursuit of a future without suffering is already being aggressively pursued through artificial reproductive technologies (ART). Preimplantation genetic testing and genetic testing during pregnancy offer a false hope for a future without suffering—and surrogacy, womb transplants, and three-parent babies promise a baby at all costs.
All of these technologies lead to the commodification of human beings, dehumanizing the weakest and most vulnerable among us.
Preimplantation genetic testing, preimplantation genetic screening, and “designer babies”
On the surface, preimplantation genetic testing done on embryos conceived through IVF seems like a positive means of preventing disease. When performed on embryos who have one parent with a known genetic abnormality, it is known as preimplantation genetic diagnosis (PGD). When performed on embryos as a generic screen for a plethora of potential problems, it’s called preimplantation genetic screening (PGS). Families in which one parent has cystic fibrosis are just one example of potential candidates for PGD. Yet some would go so far as to say that even if families don’t have trouble getting pregnant, they have a “duty” to themselves and/or their potential children to use IVF to avoid having children with the same genetic condition. Families who have sought IVF after years of unexplained infertility are also potential candidates for PGS.
In plain language, the thinking goes that if getting pregnant is this costly and time-intensive, you had better be getting your money’s worth. While screening embryos with the goal of avoiding future suffering is understandable (yet misguided), that’s not the only reason for preimplantation genetic testing. “Designer babies” can also be chosen based on arbitrary characteristics like height, weight, eye color, and more. No matter what the reason, PGD and PGS lend themselves to the commodification of human beings, treating preborn people as “manufactured goods,” with the natural end results of genetically inferior embryos being discarded like so much excess waste.
Prenatal genetic testing for eugenic purposes
Once children have been conceived, via whatever means, they face another existential threat in the form of prenatal genetic testing. While genetic testing falsely promises to alleviate future suffering, it has been used repeatedly for eugenic purposes. Initially developed for “high-risk” mothers only, genetic testing is now offered to all expectant mothers in the United States as part of routine prenatal care. These screening tests are not 100% accurate, and positive results are meant to be confirmed with other diagnostic tests like amniocentesis or chorionic villus sampling, but there have been known cases of abortion based on the results of screening tests alone.
Surrogacy, womb transplants, and three-parent babies viewed as “progress”
The Areo article noted, “Some transhumanists view a wish to obtain satisfaction from natural bodily functions, such as carrying a baby to term and experiencing the various associated biological and emotional sensations, as anti-progress.” Since part of transhumanism has a goal of pushing the limits of what is physically possible, it is no wonder that surrogacy, womb transplants, and three-parent babies are all promoted in the name of progress.
Surrogacy has been criticized internationally as reproductive human trafficking by essentially turning women—especially poor women—into “wombs for hire.” Even in situations of “altruistic surrogacy” in which the mother is not paid, the potential for abuse still exists, as surrogate mothers are vulnerable to pressure to abort the babies they carry if the genetic parents change their minds.
Womb transplants are also fraught with ethical concerns, like potential risks to both mother and baby, and the exploitation of vulnerable women as with surrogacy. Three-parent babies are already being born in Europe. Speaking of this process, which involves manipulation of two women’s eggs before fertilization by a man’s sperm in a laboratory, bioethicist Fr. Tad Pacholczyk noted, “The final egg produced really belongs to neither woman, so that the technological manipulations introduce a fissure between any child conceived from the engineered egg and both ‘mothers.’ The child becomes ‘distanced’ and to a significant degree ‘orphaned’ from both women involved in the process.”
Transhumanism’s tenets are already being promoted within the artificial reproductive technology (ART) industry, and these current practices are already leading to devastating situations. This shouldn’t surprise us. After all, as Areo states, “If we see bodies as little more than parts, to be artificially generated, assembled and disassembled, we need not associate them with human rights, nor should any biological process be viewed as exclusive to any particular group.”
July 14, 2020 (LifeSiteNews) – On Thursday, July 16, some of the most well-known pro-life heroes from all over the world will proclaim that out of love and reverence due to Our Lord they would never receive Holy Communion in the hand.
That message will be apart of the, “Love and reverence to Our Lord: Let’s always receive Holy Communion on the tongue” online conference, which is set to begin at 12:00 p.m. noon EST and run until 2:30 p.m. EST on Thursday, July 16, 2020. You can watch the conference on LifeSite’s YouTube channel and on the LifeSiteNews Catholic Facebook page for free. To visit the LifeSite YouTube channel, click here. For more information about the conference, click here.
Some of the world’s most famous converts to Catholicism will explain why they will never receive Communion in the hand. Those voices who you will hear from include Abby Johnson, the head of the March for Life in Italy, the founder of the March for Life in New Zealand, the President of the largest pro-life group in Canada, the President of the organization best known for pro-life lobbying at the United Nations, the CEO of the oldest pro-life group in all the world based in the UK and the daughter of a proclaimed saint in the Catholic Church who’s mother was proclaimed a saint for giving up her life so that her unborn child could live.
Have you ever wondered why pro-life advocates are making such a big deal about receiving Holy Communion on the tongue kneeling and not receiving Holy Communion on the hand? Doesn’t that seem strange? Why would they be doing that? Why would they risk the credibility they have to push for something so seemingly obscure? I’m going to tell you why so many of them are ready to sacrifice themselves, and their reputations for this.
Pro-life activists all over the world spend their lives defending the reality of hidden life, of the child hidden in the womb of his or her mother. That life is not recognized, not valued, by most of society. Many fail to recognize the inestimable value of the child in the womb precisely because these children are not seen, the truth of their lives, even though they are there and very much-alive is concealed in the wombs of their mothers.
In very much the same way Jesus, truly present in the Blessed Sacrament, is not seen and thus not recognized for Who He truly is in the Sacred Host. Our Lord and God conceals Himself under the appearance of a wafer of bread, and yet it is He, the Creator of the Universe, the King of Kings and Lord of Lords-in-the-flesh Whom we are called to receive in Holy Communion.
The same Savior Who sacrificed Himself in the terrible passion and crucifixion to save you and me from eternal damnation is right there before us in Holy Communion. If we truly recognized Him how could we fail to show Him the reverence He is due? If we bow before Princes and Kings of this world, if we salute the powerful and make acts of self-effacing love towards those on earth to whom we are most devoted, how can we not be on our knees before Almighty God and Our Greatest Love compared to Whom we are to disdain all earthly loves?
Now what I’m about to say may be very controversial but it’s a thought that came to me while praying and meditating about this subject. It was that kind of inspiration that makes you feel you have to share it even though it seems very socially awkward and you worry about it being offensive to some.
It is relates the pro-life struggle directly to Communion in the Hand. Of course the primary reason for not receiving Holy Communion in the hand is the awe and reverence due Our Lord and the need to have the consecrated hands of the priests and ordinary ministers of Holy Communion handle Our Lord in the Eucharist with consecrated hands. However, from the most ancient times of the Church, the Fathers spoke of the need to guard the fragments of the Eucharist from being lost.
The most well known quote used to promote Communion in the hand is attributed to St. Cryril of Alexandria in the 300s. However the quote of his used is most often taken out of context. While he did speak of receiving Communion in the hand, his main emphasis was to warn against losing the fragments.
Here is what he said in full:
Approaching therefore, do not come forward with the palms of the hands outstretched nor with the fingers apart, but making the left [hand] a throne for the right since this hand is about to receive the King. Making the palm hollow, receive the Body of Christ, adding “Amen”. Then, carefully sanctifying the eyes by touching them with the holy Body, partake of it, ensuring that you do not mislay any of it.
Be careful that you do not lose anything of the Body of the Lord. If you let fall anything, you must think of it as though you cut off one of the members of your own body. Tell me, I beg you, if someone gave you kernels of gold, would you not guard them with the greatest care and diligence, intent on not losing anything? Should you not exercise even greater care and vigilance, so that not even a crumb of the Lord’s Body could fall to the ground, for It is far more precious than gold or jewels?
So where does this tie in to the pro-life movement?
One of the things that has been most distressing over the last 50 years has been the deception that has gone on in the medical field concealing the grim realities of abortion. One of the biggest deceptions was over the abortifacient nature of the birth control pill. For decades women were unaware that the birth control pill could cause abortions, for decades women were inadvertently aborting their children and had no clue about it.
They were told by doctors that the pill was healthy, even good for their ability to have children when they wanted them. And yet the grim reality was that the pill caused the lining of the uterus to be inhospitable to life such that with breakthrough ovulations resulting in conception of a new life, that newly conceived child could not implant in the uterine wall.
It struck me that this is very very similar to what we’ve experienced in the Church for the last 50 years, where with Communion in the Hand our bishops and priests for the most part never told us of the danger of the fragments falling to the floor. Never explained the reality of Jesus being present in those small fragments as He is in the full Sacred Host.
We have for 50 years been counselled to receive Our Lord in such a way that had us participate inadvertently in the trampling of Our Lord with our feet at Mass. We were told communion in the hand was a better way to receive, a more dignified way, a superior way for mature Christians. And now we have some bishops and priests suggesting, despite contrary opinion from some physicians, that communion in the hand is a healthier way to receive due to Coronavirus. And never in all that time did they explain about guarding the fragments.
These thoughts were germinated with the statement of Bishop Athanasius Schneider written in his most recent book-length interview with former LifeSite correspondent Diane Montagna, Christus Vincit.
“There is the grievous fact of the loss of Eucharistic fragments because of Communion in the hand. No one can deny this,” he wrote. “Fragments of the consecrated host fall to the floor and are subsequently crushed by feet. This is horrible! Our God is trampled on in our churches! No one can deny it.”
That part about the Our Lord’s Body in Holy Communion being ‘crushed’ via the practice of reception of Holy Communion in the hand
Pro-lifers seek to stop abortionists from laying their hands on the child in the womb and violating them, literally stop them from crushing the precious child in the womb.
And that is exactly the same with the Holy Eucharist which when received in the hand has fragments and particles scattered on the floor and trampled and crushed by the feet of parishioners. Even though each particle is Jesus Himself. The awe and reverence due our Lord and this desecration of the Holy Eucharist are exactly why Communion in unconsecrated hands was banned for over 1000 years in the Church until it was reintroduced in 1969, right around the same time abortion came to most of the world.
WASHINGTON, July 15, 2020 (LifeSiteNews) — A new study on global population trends by researchers at the University of Washington’s Institute for Health Metrics and Evaluation has concluded that falling fertility rates will lead to a dramatic decline in global population by the end of this century.
Professor Christopher Murray, one of the authors of the study published in The Lancet, told the BBC that the findings are “jaw-dropping.”
The BBC report says that in 1950 an average of 4.7 children were being born for every woman, but that by 2017 that number had fallen to 2.4 and is expected to continue to fall significantly in the coming years.
In many countries the fertility rate is already beneath 2.1, the minimum average number needed for a population to replace itself.
This means that while global population numbers continue to reach all-time highs, the numbers are expected to peak before rapidly declining later this century.
Japan, Italy, Spain, Portugal, Thailand, and South Korea are among 23 countries “expected to see their population more than halve” by 2100.
“It makes me worried because I have an eight-year-old daughter and I wonder what the world will be like,” he said, “we need a soft landing.”
The BBC report says that the fall in fertility rates is “being driven by more women in education and work, as well as greater access to contraception, leading to women choosing to have fewer children” and says that “[in] many ways” this is a “success story.”
“Responding to population decline is likely to become an overriding policy concern in many nations, but must not compromise efforts to enhance women’s reproductive health or progress on women’s rights,” Professor Stein Emil Vollset, another of the study’s authors, said.
“I find people laugh it off; they can’t imagine it could be true, they think women will just decide to have more kids,” Murray said.
“If you can’t [find a solution] then eventually the species disappears, but that’s a few centuries away,” he added.
The study also predicts that the population of sub-Saharan Africa will treble in size to more than three billion people by 2100, with Nigeria becoming the world’s second biggest country.
“We will have many more people of African descent in many more countries as we go through this,” Murray said.
Noting the role played by migration in sustaining population numbers where the fertility rate is below replacement level, such as the U.S., Canada, and the majority of Western European nations, Murray says that “[w]e will go from the period where it’s a choice to open borders, or not, to frank competition for migrants, as there won’t be enough.”
Population analysts have long argued that policies around the world promoting contraception and abortion are leading to an inevitable “demographic winter.” In 2007 a U.N. report described the global demographic trends of decreased fertility and ageing populations as “a process without parallel in the history of humanity.”
Many social commentators have noted that while birth rates continue to decline among post-Christian secularists in European nations, the birth rate among Islamic communities in those countries is generally considerably higher.
Do you remember your first “very special” health class? Mine was taught by a middle-aged lady whose first priority was eliminating dirty fingernails. She stalked around our fifth-grade public school classroom, examining each girl’s hands, prepared to name and shame any offenders.
Besides the hygiene review, we also received a blurry diagram of the female reproductive system. The teacher unconvincingly strove to impress upon us that we each had inside ourselves a duplicate of this diagram, and that soon these organs would power on, like a self-aware computer. As far as I was concerned it may as well have been a map of the battle of Gettysburg, labeled entirely in French.
She explained that an egg would one day travel down one of our tubes like a marble, and if that egg wasn’t fertilized by sperm, “it” would happen. “It,” the teacher made clear, was an unstoppable part of life. The train was bearing down upon us and there was no way to unstrap ourselves from the track. Carnage—ahem, menstruation—was inevitable.
We also watched a sappy video produced under the mistaken assumption that all tween girls long with their whole hearts to get their periods, grow breasts, and most of all, be noticed by boys. I was in no hurry to grow up, and I experienced the same feeling of loneliness I got from reading Judy Blume novels. The girls in the video, like the characters in the Judy books, seemed anxious and very unhappy, so I was glad their problem was not my problem. Still, was there something wrong with me? Should I be worried that I wasn’t worried about eggs and tubes and bras?
Unless you were very lucky, you can probably tell a similar story about your first sex-ed experience. It was probably strange, awkward, and not what you needed. Can you imagine another way? What if the way kids learned the “facts of life” was positive, useful, and even feminist?
Fertility awareness has been grabbing headlines recently as women discover one of medicine’s best kept secrets—that they can plan their families without being chained to a pill bottle. But fertility awareness is not, at its core, about avoiding pregnancy. It proposes the radical notion that women are people with bodies that deserve to be studied, understood, and appreciated. I spoke with three women helping lead the fertility awareness charge to find out what that looks like with teenagers.
Sex ed that teen girls actually want to learn
Cassie Moriarty is a women’s health dynamo based in New York City—she’s a certified breastfeeding counselor, a trained DONA postpartum doula, and knows multiple methods of natural family planning. She’s also a certified teacher for FEMM, a comprehensive women’s program that helps women understand how their cycle intersects with their health.
“I got involved with TeenFEMM when I was training with FEMM,” Moriarty says. “I saw it as such an opportunity. I view sex ed as something that happens periodically throughout one’s life rather than a conversation that happens once; sex ed should happen even throughout your twenties. The idea of teaching teens about fertility awareness sets a great foundation for young girls with their bodies.”
Moriarty works with clients of all ages, usually in small groups or in one-on-one sessions, sometimes even with OB/GYNs alongside teens who are dealing with hormonal disorders. Regardless of the setting, the material hits home.
“Honestly teens are some of my best students!” says Moriarty. “For one, they are in the swing of learning. They are used to having homework and pop quizzes. Almost everyone I have taught has been bright, mature, curious, and excited . . . they are usually more intrigued than embarrassed. I joke that the couples I work with who are getting married sometimes act more squeamish than a 13-year-old girl.”
I asked Moriarty what young women can learn from fertility awareness that they may never discover otherwise.
“The biggest most obvious piece is cervical fluid. That is something virtually every teen girl experiences, and just about all of them aren’t taught about it in their public school sex ed. A lot of young girls, like myself at that age, experience shame about a totally normal bodily function,” she told me. She also says that students benefit from hearing “a different angle” than simply “Don’t get pregnant!”
I remember as a 13-year-old feeling like pregnancy wasn’t even close on my radar . . . but I did want to know more about that strange bleeding I was experiencing. And headaches and cramps.
“Sex ed is usually built upon the message of ‘here’s how pregnancy happens, here’s how to avoid it’ rather than ‘here are these amazing (and sometimes annoying, strange, and intrusive) things your body is doing.’ I hardly even talk about pregnancy in the first few classes. I talk more about mental health, hormonal health, and cycle health.”
Your body is feminist
Leah Jacobson had been working with young people and moms for more than a decade by the time she founded the Guiding Star Project in 2011. She saw a deep, unmet need for an initiative to bring together whole-woman feminism and women’s health. Guiding Star Centers around the country offer a variety of location-specific health-related services like childbirth education, breastfeeding support, postpartum care, and family planning to help women achieve or avoid pregnancy. It also includes fertility awareness outreach to young girls.
“The core of these programs and our philosophy on fertility, is that there’s nothing wrong with our fertility. It’s a really beautiful part of who we are,” Jacobson says. “It’s our belief that by giving [young people] the tools and the education to understand their bodies, they’re going to make better decisions that are in line with avoiding risky behaviors. They’re going to care for their dignity and the dignity of their partner.”
In our culture, which regards a woman’s fertility as an obstacle or a potential threat to her success and happiness, Jacobson has seen first hand how women have lost touch with their bodies.
“It’s sad; we have had women come in for the first time to learn how to chart their cycle, and you explain to them more than once that they have to come off the Pill to chart,” Jacobson told me. “They don’t understand, because they somehow think that they have a natural cycle, when what they actually have is withdrawal bleeding [when they take the ‘inactive’ drugs in their pill pack]. That’s an incredibly shocking and alarming situation for women to be in. They feel empowered, they feel like they’re ‘doing something’ because they’re taking the Pill. But for them to not even know that they’re not ovulating and that they don’t have a cycle . . . that’s disturbing, because it means they don’t at all understand the function of these drugs that they are [taking].”
For so many of us, that confusion starts at the very beginning, with that first period. Almost as a rite of passage, many moms take their daughters to the doctor, who may perform a pap smear but who almost certainly will want to discuss medication to “treat” and control her new, risky state of natural fertility.
The result is that thousands of children are prescribed synthetic hormones. It’s clear many kids are never told how the Pill works, nor are they routinely screened and warned about the Pill’s links to depression and breast cancer. Some girls stay on the drug for decades, until they decide to have children—only to confront the reality that they know virtually nothing about what to expect from their bodies once the medication leaves their system.
This is even more so the case if girls complain of symptoms like cripplingly painful periods or irregularity. Few OB/GYNs make the effort to find out what is wrong when hearing of period symptoms.Take for example endometriosis, a painful condition that affects one in every ten women and can destroy a woman’s quality of life and fertility. Even though it is one of the most common diseases affecting women’s health, it takes a woman an average of seven years of suffering, begging, and doctor-shopping before she can get a diagnosis. Because hormonal contraception covers up the symptoms of diseases like endo, doctors often employ birth control as an easy fix for any potential reproductive problem—as if passing the buck to the next doctor to figure out whatever it may actually be. One study from the Guttmacher Institute found that more than 80 percent of teens on the Pill had been prescribed contraceptive meds for non-contraceptive reasons.
“What is our health-care system doing? This is a complete act of paternalism,” Jacobson says. “It’s dignifying to tell girls the truth about themselves. It should be the core of feminism. Feminism that fails to acknowledge the female body does not have women’s best interests at heart. All it is, is a facade for a male normative culture. Fertility is a liability to how success is currently defined in [that culture].”
Authentic feminism, according to Jacobson, will “redefine the worldview—not just accept the male normative world and say we have a right to fit ourselves into it. It’s confusing to tell our daughters, your breastfeeding is good, you should breastfeed, but your fertility is dangerous, you should suppress that. We have to have a consistent narrative. It’s all good.”
Each Guiding Star center has different programs, ranging from the Guiding Star Cycle Show—a five-hour, interactive, hands-on experience for young girls—to offerings that can be accessed online, particularly useful in the era of coronavirus. Jacobson specifically points out that the programs are science-based and secular. “Our presentations don’t have a religious aspect. . . . We want every girl regardless of any religious affiliation to understand this applies to her,” she says. They’re already used in public schools in Germany, China, and the United Kingdom.
The Chinese government is allegedly taking forceful measures to slash birth rates among Uighurs and other minorities as part of a sweeping campaign to curb its Muslim population, according to an alarming new report on aggressive birth control policies in China’s Xinjiang province.
The report by China scholar Adrian Zenz, released on Monday, has prompted a coalition of leading international politicians to call for an independent United Nations investigation into human rights abuses in Xinjiang, to prevent the further suffering of the Uighur people.
A statement by the interparliamentary alliance on China (IPAC) cites “a body of mounting evidence” of alleged “mass incarceration, indoctrination, extrajudicial detention, invasive surveillance, forced labour, and the destruction of Uighur cultural sites,” as the basis for action by the UN General Assembly.
Professor Zenz’s new research suggests that the sudden fall in Uighur birthrates coincides with reports of a Chinese state policy of intrusive birth prevention, including female sterilization.
“This may indicate that the Chinese government is pursuing and enforcing a coordinated policy to reduce the population of minority groups. The world cannot remain silent in the face of unfolding atrocities,” said the statement by IPAC, a cross-party international group of politicians, including Conservative MP Iain Duncan Smith and Baroness Helena Kennedy QC.
The findings by Professor Zenz, an independent contractor with the nonprofit Victims of Communism Memorial Foundation in Washington, shows that population growth rates fell by 84% in the two largest Uighur prefectures between 2015 and 2018, declining further in 2019.
The report links the drop to state-driven efforts to forcibly suppress Uighur birthrates relative to the numbers of ethnic Han Chinese, using measures that include mandatory birth control, family separations and sterilisations.
“Since a sweeping crackdown starting in late 2016 transformed Xinjiang into a draconian police state, witness accounts of intrusive state interference into reproductive autonomy have become ubiquitous,” it claims, adding that anecdotal accounts have been confirmed for the first time through “a systematic analysis of government documents.”
According to the research, “documents bluntly mandate that birth control violations are punishable by extrajudicial internment in “training” camps” and “reveal plans for a campaign of mass female sterilisation in rural Uighur regions, targeting married women of childbearing age.
Among the conclusions, it claims the project targeted southern Xinjiang and continued in 2020, likely aiming to sterilise women with three or more children.
“Budget figures indicate that this project had sufficient funding for performing hundreds of thousands of tubal ligation sterilisation procedures in 2019 and 2020, with least one region receiving additional central government funding,” it reports.
It adds that by 2019, Xinjiang planned to subject at least 80% of women of childbearing age in the rural southern four minority prefectures to intrusive birth prevention surgeries -IUDs or sterilisations – and reveals that in 2018, 80% of all new IUD placements in China were performed in Xinjiang.
“This is part of a wider control campaign to subjugate the Uighurs,” Mr Zenz told the Associated Press.
The practice of forced birth control is far more widespread and systematic than previously known, according to the AP’s own investigation based on government statistics, state documents and interviews with 30 ex-detainees, family members and a former detention camp instructor.
They include women like Gulnar Omirzakh, a Chinese-born Kazakh, who was ordered by the government to get an IUD inserted after she had her third child.
Four officials in military camouflage also came knocking at her door to threaten Ms Omirzakh, the penniless wife of a detained vegetable trader, with a $2,685 fine for having more than two children. Failure to pay, they warned would result in her incarceration in an internment camp.
“To prevent people from having children is wrong,” Ms Omirzakh told the newswire. She fell deep in debt to scrape together the money and later fled to Kazakhstan. “They want to destroy us as a people.”
Having too many children is a major reason people are sent to detention camps, the AP found, with the parents of three or more ripped away from their families unless they can pay huge fines.
The campaign over the past four years in the far west region of Xinjiang has prompted some experts to call it a form a form of “demographic genocide.”
The interviews and data reportedly show that women are even subjected to forced abortions, and that the hundreds of millions of dollars the government pours into birth control have transformed Xinjiang from one of China’s fastest-growing regions into one of its slowest in just a few years.
One former camp detainee, Tursunay Ziyawudun, said she was injected until she stopped having her period and kicked repeatedly in the lower stomach during interrogations. She now can’t have children and often doubles over in pain, bleeding from her womb, she said.
Ms Ziyawudun said women at her camp were made to undergo gynecology exams and get IUDs, and their “teacher” told them they would face abortions if found pregnant.
Zumret Dawut, a Uighur mother of three, said after her release from an internment camp in 2018, authorities forced her to get sterilised. If she didn’t, they told her she’d be sent back to the camp. “I was so angry,” she said. “I wanted another son.”
The Chinese Foreign Ministry and the Xinjiang government have not responded to the reports. However, Beijing has said in the past that the new measures are merely meant to be fair, allowing both Han Chinese and ethnic minorities the same number of children.
ODESSA, Texas — The inhaled steroid Budesonide is being hailed by one West Texas doctor, Richard Bartlett, as the ‘silver bullet’ for COVID-19.
Midland Memorial Hospital seems to disagree with him, telling us Tuesday that there is no such thing a ‘silver bullet’ for the virus.
But Bartlett’s patients credit the treatment for saving their life. He has treated well over a dozen patients and has had a 100% success rate.
Even with patients who have preexisting conditions.
“I’m in my 60s, I’m living with two different types of non-hodgkin’s lymphoma,” Kathy Lollar, Dr. Bartlett’s patient and COVID-19 survivor, said. “In fact I’m on daily chemo.”
Lollar is one of many at-risk patients Bartlett has treated.
“I’m 48-years-old, I’m diabetic and I’m a bit overweight,” Eric Rodriguez, another one of Dr Bartlett’s patients and also a COVID-19 survivor, said.
When they were diagnosed with the virus, they both thought the worst-case scenario.
“I was scared, fearful, desperate,” Rodriguez said. “I starting thinking about my children without a father.”
Rodriguez lost his 31-year-old brother, who had no preexisting conditions, to the virus in June. For that reason, Rodriguez sought a different treatment and reached out to Dr. Bartlett for help.
He started taking Budesonide twice a day.
The inhaled steroid Budesonide is being hailed by one West Texas doctor, Richard Bartlett, as the ‘silver bullet’ for COVID-19. Midland Memorial Hospital seems to disagree with him, telling us Tuesday that there is no such thing a ‘silver bullet’ for the virus. But Bartlett’s patients credit the treatment for saving their life. He has treated well over a dozen patients and has had a 100% success rate. Even with patients, like the ones I talked to, who have preexisting conditions.
“The difference? It’s life and death right now,” Rodriguez said.
As for Lollar, she believes it would have been a different outcome if it were not for Dr. Bartlett.
“I would have been at the hospital on a ventilator,” she said. “Trying the Budesonide I could tell improvement. It wasn’t a miracle but I was improving.”
Dr. Bartlett tells us budesonide works well if COVID is diagnosed early like it was for Lollar and Rodriguez.
He also tells us he is not taking any more patients. He suggests people ask their own physician to see if Budesonide can work for them.
WASHINGTON, D.C., July 8, 2020 (LifeSiteNews) – The US Supreme Court ruled 7-2 Wednesday in a decision siding with the Little Sisters of the Poor and their bid to stop being forced to distribute abortifacient and contraceptive drugs to their employees.
The Obama administration had first mandated that employers subsidize the provision of contraceptives, including abortifacient drugs, to their employees under the auspices of the Affordable Care Act (ACA), better known as Obamacare. The Little Sisters of the Poor, a Catholic institution that provides support for the elderly poor, refused to comply, as did other religious employers, sparking years of litigation.
In November 2018, the Trump administration announced two final rules to protect Americans from being forced to subsidize abortion in government-mandated health insurance plan, one to cover conscience objections on the basis of “sincerely held religious beliefs,” and another for small businesses and nonprofits with non-religious moral objections.
In January 2019, multiple federal judges granted injunctions to several liberal states that had challenged the Trump rule, preventing it from taking effect.
According to the religious-liberty firm Becket Fund, the federal government admitted that it broke the law by trying to force the Little Sisters and others to provide contraception in their health plans that violated their religious beliefs. The government issued a new rule in October 2017 that protected the religious exemptions of the Little Sisters and others.
Despite the announcement, the state of California sued the federal government to eliminate the religious exemption. California has numerous contraceptive programs of its own, and it never filed suit over the much larger secular exemptions created by the Obama administration for corporations such as Pepsi and Chevron, according to Becket, that applied to tens of millions more people than the religious exemption. Also, the state has not identified a single person who had contraceptive coverage but will lose it because of the new rule.
The Supreme Court heard oral arguments to this effect in May of this year, which ultimately won the day. Justices Elena Kagan and Stephen Breyer joined the majority, while Justices Ruth Bader Ginsburg and Sonia Sotomayor dissented.
The Third Circuit Court of Appeals’ judgement that federal agencies had no authority to exempt the Little Sisters in the first place “was erroneous,” Justice Clarence Thomas wrote in his majority opinion. ‘We hold that the Departments had the authority to provide exemptions from the regulatory contraceptive requirements for employers with religious and conscientious objections.”
In a concurring opinion, Justices Samuel Alito and Neil Gorsuch went a step further and argued that not only were the Departments allowed to exempt the Little Sisters, but the federal Religious Freedom Restoration Act (RFRA) actually “compels an exemption for the Little Sisters and any other employer with a similar objection to what has been called the accommodation to the contraceptive mandate.”
While ultimately voting with the majority, Kagan explained in a concurring opinion that while she believed the relevant departments did have “statutory authority to exempt certain employers from the mandate,” she also believes the accommodation made for the Little Sisters was broad enough that it could still be invalidated under the federal Administrative Procedure Act. So while the ruling is a major victory the Little Sisters and other opponents of compulsory birth control coverage, Kagan’s opinion also provides ammo to a potential future challenge.
“The Supreme Court was right to, in the face of outrageous legal challenges from Pennsylvania and New Jersey, allow the Trump administration to protect the freedom of these religious nuns and so many other religiously affiliated groups,” Heritage Foundation senior research fellow Ryan Anderson said. “This case stemmed from mandates that the Obama administration promulgated that put unreasonable demands on employers to cover potentially life-ending drugs, contraception, and sterilization. Hopefully, this brings an eight-year ordeal for the Little Sisters of the Poor to a close and they can focus entirely on ministering to the poor in our communities.”
This ruling, and the Supreme Court’s 7-2 ruling in favor of religious schools’ right to judge their own educators’ understanding of the faith, represent significant victories for religious liberty, and may help reassure conservatives stung by the court’s recent pro-abortion ruling in Louisiana that there remain significant differences between the judicial nominees of President Donald Trump and the type who would be appointed by former Vice President Joe Biden.
As a defender for the Orlando Pride women’s soccer team, 26-year-old Carson Pickett is no stranger to the spotlight. But last year, a photo of her went viral not for her athletic achievements, but for her meeting with a very special fan.
Pickett was born missing her left hand and part of her forearm, and after one of her games in April she met a young fan with the exact same disability. The Orlando Pride shared a video from their meeting on social media, and it generated so much positive support that some called it the 2019 Picture of the Year.
Even though Joseph Tidd was not yet two years old at the time, Carson told USA Today that “Literally within five minutes of me meeting him, we had an instant bond. It’s interesting, though, because for a kid that young, I didn’t expect him to connect the way he did. Even though we both have the same [birth defect], it was amazing to me that it felt like he realized why we were bonded.” She added, “I know I might be seen as his role model, but he’s also mine. It’s just a gift to feel so much emotion from a little boy who understands you in a way other people can’t.”
In an interview with CBS Evening News, she shared, “”Seeing him gives him and me just as much joy as seeing my best friends.”
The two met as part of Carson’s partnership with the Lucky Fin Project, which raises awareness about the 2,500 children born with limb differences in the United States each year. Groups like the Lucky Fin Project ensure that children who are born missing limbs grow up in a different world than Carson, who didn’t know anyone who looked like her as a child. Joseph Tidd’s parents are part of that effort, maintaining his Instagram account to continue supporting children like him.
A year later, Joseph Tidd is still raising awareness for children with limb differences.
Commenting on her ongoing friendship with little Joseph back in 2019, Pickett said, “When I was younger and I didn’t know how the world works, it was hard. My parents always tell me that God put me here for a reason. The biggest thing I’d want Joseph (and others) to know is that even if people see you as different, it’s what’s in your heart that counts.”
In late May of this year, Pickett told Just Women’s Sports, “I want [people] to ask me what happened because then I can educate more people about limb difference. It’s not that I want to stand out, but I want to help people who are like me. And I know I’m also reaching people who have both of their hands, but who may be struggling with other problems. Everyone has their own story, everyone is different, everyone has gone through struggles and has weaknesses. It’s how you use that story and those weaknesses and the struggle to best help people in the world. Now that I’m able to reach so many diverse groups, it’s really become more of a blessing.”
A recent investigation from the Associated Press (AP) is finally opening the world’s eyes to the genocide against Uighur Muslims in China. In addition to the concentration camps holding an estimated one million Uighurs, the AP investigation revealed that the Chinese government is taking “draconian measures” to prevent Uighurs from having children – including forced birth control and abortion, sterilization, and even ripping infants away from their mothers while they breastfeed.
The AP’s sources for what it has labeled a “demographic genocide” include government statistics and documents, as well as interviews with 30 ex-detainees, family members, and a former detention camp instructor. Uighur women, along with other Chinese minorities, are regularly subjected to pregnancy checks by government officials. They are also being forcibly sterilized, are forced into intra-uterine device (IUDs) insertion, and are even forced into abortions. The AP estimates that this affects hundreds of thousands of people. Women who do not comply with government demands are sent to a concentration camp.
Gulnar Omirzakh spoke to the AP about her experience as a victim of China’s communist regime. After having a third child, she was ordered to have an IUD inserted and to pay a $2,685 fine, though her husband was already detained and she was struggling financially. She was threatened with imprisonment if she did not comply. “God bequeaths children on you. To prevent people from having children is wrong,” Omirzakh told the AP tearfully. “They want to destroy us as a people.”
Uighur birth rates are drastically falling in comparison to nationwide Chinese birth rates, making Xinjiang —a Uighur majority area—one of China’s slowest-growing areas. Just a few years ago, it was one of the fastest-growing. “This kind of drop is unprecedented… there’s a ruthlessness to it,” explained Adrian Zenz, a China scholar and expert in the country’s minority regions. “This is part of a wider control campaign to subjugate the Uighurs.”
The Chinese government denies these claims, as it has denied the existence of concentration camps and torture. Yet experts refuse to accept their explanations. “It’s genocide, full stop. It’s not immediate, shocking, mass-killing on the spot type genocide, but it’s slow, painful, creeping genocide,” Joanne Smith Finley, who works at Newcastle University in the U.K., told the AP. “These are direct means of genetically reducing the Uighur population.”
It is estimated that the targeting of Uighurs began in 2017, with people thrown into camps simply for praying or traveling abroad. Government officials went door-to-door, looking for pregnant women and children. All minorities were required to attend flag-raising ceremonies each week, and women were forced to take pregnancy tests afterward. Abdushukur Umar was one of the people who fell victim to this terror; the father of seven children, he was put into a camp in 2017, sentenced to a year in prison for each of his children.
“How can you get seven years in prison for having too many children?” Zuhra Sultan, Umar’s cousin, said to the AP. “We’re living in the 21st century — this is unimaginable.”
Leaked data obtained by the AP revealed that one of the most common reasons for detainment was having “too many” children.
In the camps, women have been forced to get IUDs and “pregnancy prevention shots,” although they have never been explicitly told what the shots are. After being released, many have later discovered only they could no longer have children. Dina Nurdybay, one of the women forced into a camp, said married women were separated from the unmarried women. Those who were married were forced to get IUDs. An official who stopped by her cell one day insulted the women, saying, “Do you think it’s fair that Han people are only allowed to have one child? You ethnic minorities are shameless, wild and uncivilized.”
Nurdybay was eventually transferred to a facility which also had an orphanage, with hundreds of children separated from their parents. “They told me they wanted to hug their parents, but they were not allowed,” she said. “They always looked very sad.”
Tursunay Ziyawudun, another detainee, told the AP she is now sterile. While in the camp, she was repeatedly kicked in the stomach and was given numerous injections. One of the pregnant women who was detained with her disappeared. Gulbahar Jelilova, another detainee, said pregnant women were forced into abortions there. Jelilova also told the AP that one woman’s infant was cruelly taken from her, and she was still leaking breastmilk. The mother did not know where her baby had gone or what had happened to her.
Gulzia Mogdin, another victim, was forced into an abortion at two months pregnant. “That baby was going to be the only baby we had together,” Mogdin told the AP. “I cannot sleep. It’s terribly unfair.”
Zumret Dawut was put into a camp simply because she had an American visa. Later, she was forcibly sterilized. “I was so angry,” she said. “I wanted another son.”
Congress and the Trump administration recently worked together to pass legislation to hold the Chinese Community Party responsible for the genocide against the Uighurs, and Secretary of State Mike Pompeo wasted no time responding to this latest revelation, calling it “horrifying” and “an utter disregard for the sanctity of human life and basic human dignity.” In a statement to Reuters, he said, “We call on the Chinese Communist Party to immediately end these horrific practices and ask all nations to join the United States in demanding an end to these dehumanizing abuses.”
Five thousand, two hundred years ago, long before Stonehenge, long before the Pyramids, farming communities in the Boyne Valley of Ireland built a gigantic passage tomb, called Newgrange. It covers 4,500 square metres, or more than one acre, of ground. The builders heaped alternating layers of stone and earth until it was 12 metres high.
Every year, on the winter solstice, a shaft of sunlight pierces a passage formed by gigantic stone slabs which illuminates a chamber 19 metres within. Archaeologists have found human remains, some cremated, in the passage.
Newgrange, in County Meath — older than Stonehenge and the Pyramids
Newgrange is just the best preserved of a number of Neolithic tombs scattered across the Irish landscape. Another is the Poulnabrone portal tomb, in County Clare, on the other side of the island, which was probably built before Newgrange, between 4200 and 2900 BC. The remains of 22 people – 16 adults and six children — were discovered beneath it by archaeologists in the 1980s.
Who constructed these monuments? Why?
Whoever they were, they left no written records, just elaborate art motifs scribed into sandstone or limestone slabs. But genetic detective work just published in the journal Nature opens a window onto the human drama of these ancient peoples.
First of all, the skull of a male interred at Newgrange’s inner chamber points to first-degree incest: he was the offspring of brother and sister or perhaps parent and child. For the archaeologists this was an amazing find.
Inbreeding is a near universal taboo across continents and centuries. It only happens among ruling elites – typically within a deified royal family. It was customary in Hawaii, the Inca Empire and ancient Egypt. By breaking the rules, archeologists hypothesise, an elite separates itself from the general population, intensifying hierarchy and thereby legitimizing its power. Extravagant monumental architecture often co-occurs with dynastic incest. A faint echo of this is found in the mediaeval Irish name for one of the passage tombs, Fertae Chuile, or “Hill of Sin”.
Second, and more relevant to our own times, is the genetic analysis of the people buried in Poulnabrone. Previous investigations suggested that they, too, were members of an elite. Judging from the manpower and organisation required to build a portal tomb, they must have ruled over a numerous and fairly sophisticated society. Even so, their lives were tough. Only one adult had lived past the age of 40. They suffered bouts of infection and malnutrition. They lived with violence. One individual may have died after being struck by an arrow; another had a crushed skull; still another a rib broken by an aggressive blow.
Don’t believe that old cliché. These Neolithic people could teach us a thing or two about human dignity – as the archaeologists discovered when they examined the genome of PN07.
PN07 – we’ll never know what name his mother gave him – was a male infant with Down syndrome. He is, the archaeologist proudly report, “the earliest definitive discovery of a case of Down syndrome”. Up until now, the earliest remains of an individual with Down syndrome dated from the 5th or 6th Century in France. Furthermore, genetic analysis reveals that PN07 had been fed from his mother’s breast.
What does this suggest?
The lives of these Neolithic people were harsh beyond our comprehension. Every day was a struggle to survive. They battled wild animals, disease, injuries, rival tribes, the weather, hunger. A Down syndrome boy must have been a heavy burden on their scarce resources. His tribe or clan must have known that he would never be a warrior and that he would not live long. Yet they nurtured him as best they could. They made him feel loved. And when he died they treated his body with the dignity due to the child of an elite household.
If the true measure of a society is to be found in how it treats its most vulnerable members, the Poulnabrone people were civilised.
Indeed, they compare favourably, very favourably, with us. We abort at least 90 percent of all of our Down syndrome babies – even though research shows that 99 percent of parents with Down syndrome children love them and 97 percent are proud of them.
Perhaps we can learn something from the 5,000-year-old tenderness of PN07’s mum.
Today, by a vote of 5 to 4, the U.S. Supreme Court struck down a Louisiana law requiring abortionists to have admitting privileges at hospitals within 30 miles of their practice. The opinion in June Medical Services v. Russo is quite fractured and legally technical. It does not bring the pro-life movement any closer to overthrowing Roe v. Wade and Planned Parenthood v. Casey; but it does not likely move us further away from that end either. More litigation to that end is still required.
In June, a plurality of Justices (Breyer, Ginsburg, Sotomayor and Kagan) voted to strike down the Louisiana law on the grounds that the burdens it imposed upon women were greater than its claimed health benefits, just like the Texas admitting-privileges law struck down in the 2016 case of Whole Woman’s Health v. Hellerstedt. Chief Justice John Roberts provided the fifth vote for the Court’s holding in a concurrence in which he disagreed with the plurality’s standard for striking the law down, but agreed that the law was unconstitutional under the standard established by the Court in the 1992 Planned Parenthood v. Casey decision.
Justices Clarence Thomas, Neil Gorsuch, Samuel Alito and Brett Kavanaugh dissented, with only Thomas using his opinion as an occasion to also declare Roe v. Wade an unprincipled decision that should be overturned.
June Medical raised several legal questions with important implications for the future of abortion law: first, whether or not abortionists have what is called “standing” to challenge laws that were enacted in order to better vet abortionists to ensure that they provide safe medical services to women. “Standing” requires that the party challenging a law has or will suffer an actual injury to a legally cognizable interest. This question is important because the vast majority of cases seeking to overturn abortion restrictions are filed by abortion doctors and clinics, not by individual women. It is also important because of the obvious conflicts of interest in cases like this one, where abortionists are seeking to quash a law that could make abortion safer for their patients.
The five justices in the majority concluded that the abortionists and abortion clinics had standing, even though abortionists do not have any sort of “right” to practice abortion that the Louisiana law burdens.
The plurality claimed that the state of Louisiana had “waived” the problem of third-party standing in the two lower federal courts that had heard the case. But they also noted that abortionists had previously generally been permitted to sue to defeat abortion restrictions, and that they should be permitted to challenge a law that might “indirectly” harm women’s interests in obtaining a convenient abortion.
Three of the dissenters (not including Kavanaugh) agreed that abortionists and clinics lacked standing to challenge the Louisiana law. In lengthy treatments of Supreme Court precedents about the importance of standing in order for the Court even to have the authority to hear a case under its Article III powers, Justices Thomas and Alito forcefully pushed back on the majority. Alito and Gorsuch spoke particularly fervently about the dangerous conflict of interest in allowing doctors to overthrow laws designed to safeguard the patients in their care. Gorsuch penned a detailed portrait of the dangers that abortionists in Louisiana pose to their patients. He noted the extraordinarily lax reviews the clinics conduct prior to hiring abortionists, reporting that abortion clinics had previously allowed ophthalmologists and radiologists to perform abortions! He also pointed to the “dozens” of ethical and safety violations that Louisiana abortion clinics had committed in the past.
The next important question the Court considered is the appropriate standard for reviewing abortion laws. The plurality justices stood by the standard that the Court (then including Justice Anthony Kennedy) adopted in Whole Woman’s Health. It allows the Court to conduct the kind of test that legislators use when they evaluate whether or not to pass a law: whether the benefits of the law outweigh the burdens the law imposes, considering the law’s object. This test differs from the one announced in the Casey decision. There, the Court did not claim a right to balance benefits and burdens; rather, it analyzed whether the effects of an abortion restriction constituted a “substantial obstacle” or “undue burden” upon a woman’s access to legal abortion.
Which test the Court adopts matters a great deal. The Whole Woman’s Health test allows the Court to perform a legislative task forbidden to it under Article III of the Constitution. It allows the Court to pick and choose what evidence it wants to highlight on benefits and burdens and give almost no deference at all to state legislatures’ findings. This is equivalent to (in a famous legal phrase about cherry picking) “looking over the crowd and picking your friends.” It means more state abortion restrictions become subject to the whims of the Court’s reigning majority.
Five justices, including Chief Justice Roberts and the four dissenters, rejected the Whole Woman’s Health test. But because Roberts believed that the Louisiana law would constitute a substantial obstacle to abortion for a large fraction of Louisiana women, he voted to strike down the law, even as he disagreed with the test the majority employed to do it!
The third important question June Medical considered concerns whether or not the law makes abortion too difficult to obtain for a large number of Louisiana abortion clients. The majority held that it did. Employing detailed geographic and doctor-specific details (and even maps, printed in the opinion), the Court concluded that the vast majority of doctors and clinics would go out of business were the admitting-privileges law to stand, leaving many women without a sufficiently-close-by abortionist.
This part of the plurality opinion extended tremendous deference to the claims of the abortionists and the clinics, regarding how hard they had tried to obtain admitting privileges, and what would happen if they failed. On this matter, Justices Alito and Gorsuch were particularly appalled. Justice Alito — continuing his theme of abortionists’ conflicts of interest — pointed to the doctors’ lackluster efforts. He highlighted emails from one of the abortionists revealing that during his alleged “good faith” search for admitting privileges, he took into consideration that a denial of privileges would best support a victory for his side of the case. Justice Gorsuch noted that one Louisiana doctor already had such privileges, that one hospital was already changing its admitting-privileges rules in order to make it easier for abortionists to succeed, and that privileges requirements applied to other types of ambulatory surgical centers (for, e.g., colonoscopies, Lasik eye treatments) had not diminished the number of those centers able to continue operating.
Furthermore, even while objecting to the majority’s “balancing test,” Justice Gorsuch wrote a detailed summary of all the health benefits of the law attested by experts testifying before the Louisiana Legislature. In addition to those described above (ameliorating lax clinic rules for licensing doctors, improving clinics’ ethics and safety records), Gorsuch highlighted the testimony of women abandoned by their abortionists to seek follow-up care, after the doctors had botched their abortion procedures.
Finally, only Justice Thomas took direct aim at Roe and Casey. In memorable language, he referred to the reading of the Constitution on which it is based as “legal fiction” and the “putative right to abortion [as] a creation that should be undone.” He wrote that it is “farcical” to imagine that the legislators who created the 14th Amendment’s “due process” language intended it to protect a procedure nearly completely banned in every state and territory in the U.S. at the time it was passed. He called Roe a “demonstrably erroneous” decision.
On this subject, Gorsuch, Alito and Roberts only noted that no one had asked for a reconsideration of the constitutional right of abortion. Roberts, instead, opined that the work before the Court involved only the application of existing precedent — in this case Whole Woman’s Health and Casey — to the question of the constitutionality of the Louisiana law before it.
Helen Alvaré is a professor of law at the Antonin Scalia Law School, George Mason University
An eye-opening article from the November/December 1979 issue of Mother Jones suggests that for decades, the United States has had a “double standard” when it comes to “dumping” unsafe contraceptives in developing countries.
IUDs
Throughout the 1970s, hundreds of thousands of dangerous Dalkon Shield IUDs were distributed in 42 developing nations, despite the growing list of documented serious or life-threatening side effects experienced by U.S. women, including pelvic inflammatory disease, sepsis, miscarriages, ectopic pregnancies, uterine perforations, and hemorrhage. Even after the Shields were taken off the U.S. market in 1975 (after at least 17 deaths were attributable to their use), the IUDs continued to be “dumped” overseas by the United States International Agency for Development (USAID) as well as NGOs like the International Planned Parenthood Federation (IPPF) that it funded.
Just as disturbing, many of the IUDs were unsterilized, provided in boxes of 1,000 with only a few applicators and instructions that were not in the language of the people administering or receiving them. This lack of standards was considered acceptable in developing nations because the IUDs were cheaper and aided the goal of population control in order to maintain U.S. economic interests, so USAID officials turned a blind eye. Women seeking care at family planning clinics in Paraguay, Israel, Tunisia, Pakistan, India, and 37 other countries were left to deal with the disastrous consequences.
High dose birth control pills
But Dalkon Shields were only the beginning of unsafe contraceptive “donations” by USAID to developing countries, writes Mother Jones. After that came the “contraceptive inundation program” in the 1970s, which ” disseminat[ed] contraceptives through any outlets, to any and all takers.” USAID and its NGO partners distributed birth control pills to countries like Bangladesh where it was available without a prescription or any medical oversight. Additionally, after U.S. health officials recommended that birth control pill dosage be decreased from 80 mcg to 50 mcg because of health risks, the 80 mcg pills became much cheaper to obtain and were distributed en masse overseas instead of their safer but more expensive counterparts.
Depo-Provera shots
The next phase of the contraceptive inundation program was a population control advocate’s dream. Depo-Provera, an injectable medication that provided contraception for three to six months at a time, did not require any effort or maintenance by users. As an added bonus, many users associated injections with “safe, effective, modern medicine.” But as Mother Jones noted, “The overseas consumer of Depo [didn’t] know that the ‘latest research’ is what prevented the contraceptive from being approved for use in the United States, and that [was] why it [was] being dumped.”
Risks
In research on animals, the shot caused breast nodules and reproductive system cancers. In humans, the shot caused severe bleeding, increased susceptibility to infection, long-term or permanent sterility, and birth defects when given accidentally to pregnant women. In breastfeeding women, it appeared to decrease their breastfed children’s susceptibility to diarrheal illness, a leading cause of infant mortality in impoverished nations.
FDA rejects for U.S., but shot distributed among poor women in other countries
On March 7, 1978, the drug maker’s manufacturer Upjohn received a letter from the FDA stating their decision not to approve the drug for use in the U.S. Despite this, Depo-Provera was distributed for “research” purposes to 8,000 poor women in San Pablo Autopan, Mexico, as well as 120,000 women in Sri Lanka, some 250,000 women in Bangladesh, and hundreds of thousands more in Thailand. One report noted that at an International Planned Parenthood-sponsored clinic in Thailand, each woman was given only 60-90 seconds for “the time to make her ‘free choice’ and have the injection….”
Though the U.S. was not the only Western nation pouring contraceptives into developing Countries, the Swedish International Development Agency (SIDA), to its credit, decided in 1980 to stop distributing Depo-Provera overseas. SIDA found that “[t]he use of Depo-Provera needs continuous medical follow-up by health staff in a well-functioning health system. We know this is lacking in many of SIDA’s programme countries. Without a good health infrastructure, there are risks that the clients are not given enough information to make an informed choice of contraceptive method.”
Safety of shot has not improved
Given that Depo-Provera is now widely used in the United States, one might expect that its safety has drastically improved since the 1970s. This is not the case. Since 2004, the shot has had a black-box warning (used by the FDA to highlight special concerns about a drug) about the shot’s potential to decrease bone density when used long-term in young women. Decreased bone density can lead to bone fractures, and to osteoporosis later in life. This risk is logically compounded in already malnourished women living in less developed nations. These effects may not be reversible after the drug wears off.
Depo-Provera use has also been associated with an up to 40% increased risk of HIV infection, as well as increased risk of contracting gonorrhea and chlamydia, just as it was associated with increased susceptibility to infection almost 50 years ago. As a previous Live Action News article noted, “More than half of the 36.7 million people living with HIV reside in eastern or southern Africa, and DMPA [Depo-Provera] is the primary birth control used in sub-Saharan Africa. It is used by over 50 million women around the world.”
Whereas American women have ready access to treatment options if they experience significant side effects from the Depo-Provera injection or other forms of birth control, women in developing countries continue to suffer to this day from the “beneficence” of Western nations.
In an effort to increase the birth rate and repair the stalled economy, Italy’s parliament passed a bill last week to encourage couples to have more children.
“The Family Act” will provide a universal monthly allowance for children to be paid to families beginning in the seventh month of pregnancy until the child turns 18, which may be in the form of a direct payment or a tax credit. These payments will be on a sliding scale based on the income of the parents. Fathers will be given ten days of mandatory paternity leave and there will be salary supplements for mothers returning to work. Each parent has the choice of taking an additional two months of leave. The government will also triple the amount of money spent to help parents pay for daycare from €1,000 to €3,000 a year depending on the parents’ income, and there will be additional allowances for children with disabilities. These changes will take effect in the next two years.
“We have approved the Family Act to support parenting, combat the falling birth rate, encourage the growth of children and young people, and … help parents reconcile … family life with work, especially for women,” said Premier Giuseppe Conte after the law’s passage.
In 2018, Italy had its lowest birth rate on record with just 464,000 births, the lowest in all of the European Union. “If Italians don’t start having more babies, you have to wonder what Italy will look like in the next few decades,” said Francesco Scalone, a demographer at the University of Bologna. Last year, the Italian government said it would begin building a plan on how to combat this issue.
While Germany and Scandinavian countries offer new fathers weeks to months of paternity leave, 10 days is double what Italian fathers had been given previously and meets the 10-day minimum paternity leave requirement of the EU. Other countries, including Singapore and Hungary, have taken similar steps to encourage couples to have more children to reverse their declining birth rates and aging populations as well. Despite the common societal belief that overpopulation is a serious threat, it is actually a decline in population that is causing problems for the economies of many nations, including the United States.
Concern for our environment is the most altruistic of the several primary motivations which drive the activities of the population control movement. Unfortunately, the leaders of many population control groups think that the best way to preserve our natural surroundings is to decrease the number of people in the world by whatever means are available.
Environmentalism and Population Control
Environmentalism has led to many drastic measures in the name of population control.
For example, we have witnessed forced abortion and sterilization programs in China, Vietnam, Peru and many other countries, partly in support of programs to preserve the environment. There have been vast numbers of women sterilized or fitted with IUDs without their knowledge or consent for the same reason.1 Animal rights activists and environmentalists have caused tens of millions of dollars of damage with arson and sabotage, and have tried to murder researchers and loggers with nail bombs and tree spikes. They have also published many “how-to” guides with titles such as:
Ecodefense: A Field Guide to Monkeywrenching
Setting Fires with Electrical Timers
How to Sink Whalers, Driftnetters and other Environmentally Destructive Ships
Killing People to Save the Animals and the Environment.2
Rachel Carson’s 1962 book Silent Spring is widely credited with launching the modern environmentalist movement. Carson’s book focused on documenting the detrimental effects of pesticides on the environment, with a particular emphasis on birds. One of the deadliest impacts of this book was the banning of DDT, which was effectively used to hold down mosquito populations all over the world. This led to a dramatic increase in the incidence of malaria, typhus and dysentery, resulting in tens of millions of additional deaths and unspeakable suffering, mostly among Africans.3 Despite this terrible tragedy and scant evidence that DDT causes harm to birds, most radical environmentalists today continue to lobby for the continued ban on the pesticide, essentially meaning that they hold bird eggs in higher esteem than the lives of poor Africans.
Six years later, in 1968, Zero Population Growth founder Paul Ehrlich kicked off the modern population control movement with his atrociously-researched book The Population Bomb. He predicted that more than 90% of the population of the United States would die of starvation and radiation sickness by 1999 in an event he called the “Great Die-Off.”4 Every one of the other major predictions he made in his book did not even come close to being fulfilled.
Despite the glaring failings of Carson’s and Ehrlich’s books, population controllers found “cover” for their activities by claiming that they were acting in the best interests of the environment, and therefore humanity at large. Many influential people began to advocate measures that completely disregarded the most basic of human rights. For example:
In 1969, Bernard Berelson, President of the Population Council, recommended punishment for large families and a widespread program of “involuntary fertility controls.”5
Also in 1969, Frederick S. Jaffe, Vice-President of Planned Parenthood-World Population, recommended that the United States government “encourage increased homosexuality;” place “fertility control agents in water suppl[ies],” and “require women to work and provide few child care facilities.” He also recommended “compulsory abortion of out-of-wedlock pregnancies;” “compulsory sterilization of all who have two children,” and “stock certificate type permits for children.”6
In his 1971 book The Case for Compulsory Birth Control, Professor Edgar Chasteen proposed a stringently-enforced two-child law for the United States, with every child being immunized against fertility at the age of ten.7
Even the United States Postal Service jumped on the bandwagon, releasing an eight-cent stamp in 1972 showing a perfectly-groomed, white, “gender‑balanced” family joyously embarking on the wide and smooth road to the Brave New World. The USPS proudly declared, “The new stamp will serve as a reminder for all members of our society of the current world environmental situation and the need for planning to have a better America and a better world.”8
Thanks in large part to Carson and Ehrlick, a misguided concern for the environment has led to the suggestion of drastic population control measures.
Government Response
It did not take long for these views to insinuate themselves into government agencies and documents. The 1972 Report of the Commission on Population Growth and the American Future (“The Rockefeller Report”) is larded with scores of statements and recommendations for holding down the population of the United States for the sake of the environment. The foundational document of the United States international population control program, the 1974 National Security Study Memorandum 200, echoes much of what the Commission said.
Many influential people still hold these views. John P. Holdren, Obama’s “Science Czar,” has never repudiated the views he expressed in his book Ecoscience:Population, Resources, Environment, which he co-authored with Paul and Anne Ehrlich in 1977. He called for seizure of all illegitimate children from their mothers, forced abortions and sterilizations for unmarried women, mandatory implantation of a reversible infertility drug in all adolescent children, a national two-child policy, and the addition of sterilizing agents to the water supplies of our nation (so long as they did not affect livestock or pets). Most appalling of all, Holdren and the Ehrlichs recommended a United Nations-run “Planetary Regime” that would control population by whatever means necessary.
Others recommended even more extreme measures. In 2006, Professor Eric R. Pianka of the University of Texas said that we should manufacture and then release the Ebola virus, thereby killing 90% of the world’s population in order to preserve the environment. Pianka does not seem to care that Ebola sufferers die an agonizing death over several days as their internal organs slowly liquefy. He said:
We’ve got airborne 90 percent mortality in humans. Killing humans. Think about that….We’re no better than bacteria!…And the fossil fuels are running out, so I think we may have to cut back to two billion, which would be about one-third as many people….You know, the bird flu’s good, too. We need to sterilize everybody on the Earth.”9
As always, we cannot eliminate a class of people until we dehumanize them. Hitler called the Jews “vermin,” racists called blacks “animals,” and pro-abortionists call preborn children “blobs.”
In order to eliminate people in general, we now have to dehumanize ― ourselves.
In 1966, the United States Department of State declared, “Mankind is the cancer of the planet.”10 Since that time, hundreds of influential leaders have repeated this view until it has become a virtual mantra of the environmentalist movement.11 Some have suggested that we excise this “cancer” by whatever means are available. For example, Jacques Cousteau, said, “Our society…is a vicious circle that I compare to cancer….In order to stabilize world population we must eliminate 350,000 people a day.”12
Final Thoughts
We must not make the mistake of dismissing these people as mere cranks. The first step towards implementing any idea, no matter how ridiculous it may seem at the time, is to talk about it. And talk about it. And talk about it. This leads first to outrage among the people, then irritation, and finally indifference as they become desensitized to the message. Twenty years ago, people laughed when radicals talked about homosexual “marriage,” but now it is being rammed down our throats while its opponents are being silenced, punished and persecuted.
You can find bumper stickers online that say “Humans are a Pestilence,” or which show the outlines of two people and say “Worst Species Ever.” This depressing worldview is in total opposition to the Christian view of Man, who is made in the image and likeness of God.
St. Paul wrote, “What is man that you are mindful of him, or the son of man, that you care for him? You did make him for a little while lower than the angels, you have crowned him with glory and honor, putting everything in subjection under his feet” (Hebrews 2:6-8).
We must care for our natural surroundings without violating the rights of humanity. Evangelium Vitae says:
As one called to till and look after the garden of the world, man has a specific responsibility towards the environment in which he lives, towards the creation which God has put at the service of his personal dignity, of his life, not only for the present but also for future generations.
Losing sight of this balance means the inevitable proliferation of horrible human rights abuses all over the world.
Endnotes
[1] Just one of these programs sterilized thousands of women in the area around Cebu City in the Philippines. A “Safe Motherhood” program funded by the West promised to give all women in the area free pelvic examinations. While doing so, the doctors placed IUDs in all of the women without their knowledge. Years later, the Dominican sisters in the area, who are also qualified as medical doctors, ran clinics to remove these IUDs, many of which were impacted or had migrated into the abdominal cavity (witnessed by Brian Clowes in November 1996 in Cebu City).
[2] These books are definitely not “for entertainment purposes only.” For electronic copies of these books, e-mail Brian Clowes at bclowes@hli.org. The liberal establishment has defended the publication of all of these manuals under the banner of free speech; but try to imagine how they would react if somebody published a guide on how to blow up an abortion mill (oh, wait, they already screamed in outrage when someone published the anti-abortion “Army of God Manual”).
[3] Dr. Henry Miller, Senior Fellow at the Hoover Institution, and Gregory Conko Senior Fellow at the Competitive Enterprise Institute. “Rachel Carson’s Deadly Fantasies.” Forbes Magazine, September 5, 2012. A 1970 study by a committee of the National Academy of Sciences found that “to only a few chemicals does man owe as great a debt as to DDT. In a little more than two decades, DDT has prevented 500 million human deaths, due to malaria, that otherwise would have been inevitable.”
[4] Zero Population Growth (ZPG) founder Paul R. Ehrlich. The Population Bomb (New York City: Ballantine Publishers), 1968; Paul R. Ehrlich. “Looking Backward from 2000 A.D.” The Progressive, April 1970, pages 23 to 28.
[5] Bernard Berelson. “Beyond Family Planning.” Studies in Family Planning (Publication of the Population Council), February 1969, pages 1-16. For a PDF copy of this article, e-mail Brian Clowes at bclowes@hli.org.
[6] February 11, 1969 memorandum from Frederick S. Jaffe (Vice-President of Planned Parenthood-World Population) to Bernard Berelson (President of the Population Council) found in “Activities Relevant to the Study of Population Policy for the U.S.” Table 1, “Examples of Proposed Measures to Reduce U.S. Fertility, by Universality or Selectivity of Impact.” For a PDF copy of this Table, e-mail Brian Clowes at bclowes@hli.org.
[7] Edgar R. Chasteen. The Case for Compulsory Birth Control (Englewood Cliffs, New Jersey: Prentice‑Hall), 1971, back cover.
[8] United States Postal Service (USPS) comments on its 1972 eight‑cent stamp. Shown in “Family Planning Gets ‘Stamp of Approval’ from U.S. Postal Service.” Pittsburgh Planned Parenthood newsletter, February‑March 1972, page 4. The USPS unveiled its new “Family Planning” stamp at the winter meeting of the Planned Parenthood‑World Population Board of Directors in New York City on March 17, 1972.
[9] Professor Eric R. Pianka, University of Texas lizard expert and evolutionary ecologist, during a speech before the Texas Academy of Science. He received an enthusiastic and prolonged standing ovation for his remarks, and five hours later, the President of the Texas Academy of Science awarded him the title of 2006 Distinguished Texas Scientist. Reported by Forrest S. Mims III. “Meeting Doctor Doom.” The Citizen Scientist, March 31, 2006.
[10] “U.S. Presents Views on Population Growth and Economic Development.” Department of State Bulletin, January 31, 1966, page 176.
[11] Some examples of famous people referring to mankind as a “cancer:”
Third-trimester abortionist Warren Hern (“Anthropologist Symposium Calls Human Beings a Cancer Infecting Planet Earth.” Catholic Family & Human Rights Institute (CAFHRI) Friday FAX, January 1, 1999).
Oceanographer Jacques Cousteau, in a November 1991 UNESCO Courier interview.
Environmentalist and broadcaster David Suzuki (Victoria Branden. “The Abortion Merry‑Go‑Round.” Humanist in Canada, Autumn 1989, pages 14 to 15).
National Park Service Research biologist David Graber (“Mother Nature as a Hothouse Flower.” Los Angeles Times Book Review, October 22, 1989, page 10).
Dr. Lynn Margulis of the University of Massachusetts, coauthor of the “Gaia Hypothesis” (“Anthropologist Symposium Calls Human Beings a Cancer Infecting Planet Earth.” Catholic Family & Human Rights Institute (CAFHRI) Friday FAX, January 1, 1999).
Ingrid Newkirk, Director of People for the Ethical Treatment of Animals (PETA), who famously said, “We [humans] have grown like a cancer. We’re the biggest blight on the face of the earth” (Charles Oliver. “Liberation Zoology.” Reason Magazine, June 1990, pages 22 to 27).
[12] Oceanographer Jacques Cousteau in a November 1991 UNESCO Courier interview.
A recent Instagram discussion between documentary producer Ricki Lake (“The Business of Being Born” and the forthcoming “The Business of Birth Control” slated for release later in 2020), and Chelsea VonChaz, co-founder of #HappyPeriod, centered on “The Anti-Black History of Birth Control.”
During the discussion, VonChaz admitted that ‘birth control has this kind of dark connection with eugenics, population control, and just the feeling of superiority, or feeling as if this specific intelligence or this specific trait—physical trait—is superior over the other….” She added that “because of racism… so many individuals… in the past used fake news, fake science, fake research to uplift the narrative that whites are better and Black is not.”
And this philosophy—that Black women were ‘less than’—led to human atrocities. “… [A] lot of individuals who [were] men, specifically, white men… spent a lot of time experimenting on Black bodies and Black female bodies, and using their research findings as a means to push the narrative [of racism] in the healthcare system,” added VonChaz.
Lake responded, “So when was this happening? Because I know that Margaret Sanger has a complicated history.” But here, Lake is being much too generous with Sanger, a staunch eugenicist who believed the “unfit” should not reproduce and who stacked her American Birth Control League (which later became Planned Parenthood) with white supremacists and fellow eugenicists.
While VonChaz had not referenced Sanger, she immediately referenced Sanger’s work in the 1920s and 30s—and in particular, the Negro Project, which she said gave Sanger “a lot more success within the Black community, claiming that “when [Sanger] and her group went to the South… they saw that in the 30s pretty much everyone was suffering.” She continued, “So they just felt like ‘ok, well, since they are famished, since a lot of their babies are dying because they don’t have good diets, maybe it’s solely because they are the lesser race, the weaker race, and maybe they really don’t want to have kids, maybe we should figure out how we can “empower” them in a way.’”
But the Negro Project had nothing to do with empowering Black women, and everything to do with finding a way to halt their reproduction. And VonChaz seemed to have a sense of this, because she added an immediate caveat:
I actually—to be honest with you—I’m really iffy with Sanger because there’s really no proof to what her intention was when it came to [the Negro Project]…. Is she for the “advancement” of whiteness or was she really for women in general? Especially when they started the Negro Project. That was when they went into Black communities, they told Black mothers, “Hey, take this pill, take this powder [birth control was originally developed as a powder]…. This will help you….”
This was a way of them connecting with women and connecting with communities and they would also even use organizations like churches to get the word out, but there was nothing as far as going back into the community and building the community, so of course all of the funding would go back into Sanger or into the Negro Project. Nothing would go towards aiding the women at the time.
Rather than addressing malnutrition and other causes of high infant mortality in the Black community at the time, Sanger’s “solution” was birth control and more birth control – and later, Planned Parenthood pushed for the legalization of abortion. Little has changed; today, Planned Parenthood still offers only abortion as a “solution.” As a result, Black women have 38% of all abortions in the U.S. even as Black Americans make up just 12% of the population.
VonChaz added that this “project” bled over into other projects through the decades where the “Black body was the subject, the Black body was the guinea pig” for medical research, and “unfortunately, some women were sterilized without even knowing it.”
She was referring to the trials of the early birth control pill on “women of color across the diaspora, from the U.S. to Puerto Rico, the majority of the studies being in Puerto Rico, where women used this product and they ended up being sterilized. A lot of them also ended up being very, very sick and actually did not know why they were sick.” As Lake noted, informed consent for these women was virtually nonexistent, and they were left alone in an impoverished U.S. territory with no resources to deal with the consequences.
As she made clear near the end of the Instagram video, VonChaz does not consider herself pro-life, specifically stating, “I don’t want people to think, ‘Oh, she’s anti-birth control. She’s anti-choice.’” But as she also made clear during the video, with a little research, anyone can come to understand the racist origins of birth control.
WASHINGTON, D.C., June 23, 2020 (LifeSiteNews) — The National Institutes of Health (NIH) has approved 70 new embryonic stem cell lines for use in projects eligible for federally funded research.
The new cell lines, which come from human embryos created and destroyed in a laboratory, were approved by the NIH last month. The new cell lines come from the Shaare Zedek Medical Center in Israel.
Despite President Donald Trump’s many pro-life accomplishments, pro-lifers have expressed concern about NIH director Francis Collins, an Obama appointee who has defended research using tissue from aborted babies. In 2018, the March for Life and Live Action called for Collins to be ousted.
Collins’ replacement should be “someone who recognizes that children who are killed by abortion should be mourned, not experimented on,” Live Action President Lila Rose said at the time.
President George W. Bush’s administration banned public funding of research involving the creation of new stem cell lines through the destruction of new human embryos. In other words, he stopped taxpayer funding of the creation of new human beings in laboratories whose sole purpose for being created was so they could then be destroyed for research.
During Bush’s presidency, private funding of such research was not prohibited, and research using existing stem cell lines was permitted to continue.
But in 2009, shortly after he first assumed office, via executive order, President Barack Obama reversed Bush’s ban on public funding for research involving new stem cell lines created through the destruction of new human embryos.
Last year the Trump administration removed funding from some projects using human fetal tissue from aborted babies. The administration also instituted a policy which had the effect of making it more difficult for projects which use fetal tissue from aborted babies to receive federal funding. However, federal funding applications for projects using embryonic stem cells or embryonic cell lines were not impacted and the policy specifically excluded them in its definition of research involving human fetal tissue.
The year 2020 marks the 25th anniversary of an incredible document defending the sanctity of human life.
Evangelium Vitae [“The Gospel of Life”] by Pope John Paul II has definitely stood the test of time. Its powerful arguments are as relevant today as they were two-and-a-half decades ago.
The Pontiff issued this warning about attacks on human life:
…not only is the fact of the destruction of so many human lives still to be born or in their final stage extremely grave and disturbing, but no less grave and disturbing is the fact that conscience itself, darkened as it were by such widespread conditioning, is finding it increasingly difficult to distinguish between good and evil in what concerns the basic value of human life.
In contrast, Pope John Paul II offered his “Gospel of Life”:
…the splendour of truth which enlightens consciences, the clear light which corrects the darkened gaze, and the unfailing source of faithfulness and steadfastness in facing the ever new challenges which we meet along our path.
The Pope also presented a powerful Biblical rationale for preserving and protecting life from the very moment of conception.
The New Testament revelation confirms the indisputable recognition of the value of life from its very beginning. The exaltation of fruitfulness and the eager expectation of life resound in the words with which Elizabeth rejoices in her pregnancy: “The Lord has looked on me … to take away my reproach among men” (Lk 1:25). And even more so, the value of the person from the moment of conception is celebrated in the meeting between the Virgin Mary and Elizabeth, and between the two children whom they are carrying in the womb. It is precisely the children who reveal the advent of the Messianic age: in their meeting, the redemptive power of the presence of the Son of God among men first becomes operative.
The Gospel of Life is available online here. In these difficult days, reading or re-reading this classic work can help give you the strength you need to speak out boldly and convincingly for the sacredness of life.
LifeNews.com Note: Maria Gallagher is the Legislative Director and Political Action Committee Director for the Pennsylvania Pro-Life Federation and she has written and reported for various broadcast and print media outlets, including National Public Radio, CBS Radio, and AP Radio.
June is the month devoted to the feast of the Sacred Heart of Jesus. It reminds us of the mystery of the Holy Trinity and of God’s revelation of Himself to us. Not too long ago the Holy Father Pope Francis declared: “Mercy is the Lord’s most powerful message.” Where does this mercy come from? You guessed right- from the loving Heart of Jesus. He truly has a Pro-life heart.
With the Indian summer just coming to an end everyone braving the monsoon with the wind and rain which is welcoming and soothing. It is like welcoming the sight of an oasis in a desert. The heat of the sun and the humidity can be exhausting and life ebbing. A person exposed to this bears a tired body which languishes for nourishment and the sagging spirit deeply desires to be uplifted; that is exactly when a person longs for the sight of an oasis. Truly then the month of June is welcome as it becomes joyful, life giving and exhilarating. It is also exciting after a long vacation to look forward to a new season and routine for children and family.
We have all been babies once upon a time. Babies have hearts that radiate love like the sun in the tropics. But as we grow up, the bumps and bruises, and hardships of life gradually force us to layer our heart with toughness and defensiveness locking the love inside and disallowing the love of people from entering. The common factors that close the heart are Fear, Resentment, Unsolved grief, Jealousy, Pain, Attachments, and Ego. This leaves us with a closed or cluttered heart. Only selfless people can keep their hearts always open like Jesus, Mother Mary and extraordinary human beings like Mother Teresa. The radiance of their open merciful, compassionate hearts is likened to a ‘pro-life mystery.’ They are fully life-giving.
If anyone wants to have a pro-life heart then kindness is the key to unlock the Love, Compassion and Forgiveness present in this mysterious heart. When your heart is filled with love, you feel happy and peaceful for no external reason. The basic energy is the loving, life-giving energy of the heart. Compassion is the response to the suffering of others that motivates a desire to reach out, help another and soothe his pain. It literally means “to suffer together”. In order to cultivate compassion in others, we should start modelling kindness and show love first in the family, where each person can experience very deeply and intimately the love of Jesus. It can be quite contagious and spreads to friends, neighbours and others around.
Resentment which is past anger is normally built over months and years; it is the junk that clogs the free flow of love in and out of your heart. It also forms a crust over the heart like plaque making it hard and perhaps diseased. In that situation forgiveness is the only universal solvent that washes the crust away. When you open your heart and allow yourself to fill it with love, you will feel the clouds around your heart wafting and dispersing. When you ask for forgiveness you are saying, “Please take me back into your heart.” Imagine how you would feel when slowly the layers of resentment and pain peel off with forgiveness. Many gifts and blessings will follow and be bestowed upon you. When we make this our motto in life it will help create a unique society. We need to reach out to others as channels of mercy and compassion.
The life of Jesus is rooted in love; all the miracles he worked were the result of his Pro-life heart. His love is total and unconditional; His heart is sensitive and responsive to the needs of all his people. His love is universal, embracing all, the rich, the poor, the dregs of society, the prostitute the sinner et al. He does not refuse anyone. Jesus’ love is persevering and enduring to the end. His love unites and binds together in community. Truly His Sacred heart is patient, forgiving, active, practical and efficacious to the end.
As we rejoice in His glory we remember the gifts of His Heart and feel drawn us closer to His love. May the Prolife heart of Jesus bring all humankind into His kingdom of justice, peace and love.
Dr Jeanette Pinto, an educator for the past 5 decades, headed the Department of History was Vice Principal of St. Xavier’s College Mumbai, and retired as Principal of Sophia College, Mumbai. She is a counsellor and conductor of Personal Enrichment Programmes for students and teachers.
She set up the Human Life Committee in the Archdiocese of Bombay. As a sex educator she has given talks on Human Sexuality in India and abroad. In 2014 she received the Rachana Outstanding Woman of the Year for her Pro-life work presented by the Diocese of Mangalore. She has attended many National and International Pro-life conferences and given talks at other fora on various women’s issues.
She is author of a couple of books, her most recent ones are titled: I’m Pro-Life Are you? & Sex Talk: Parent to Child. She has also written a number of articles on a variety of themes and subjects, which have been published in research journals, The Examiner and other Catholic publications.
An experiment that involved editing the DNA of unborn babies at their earliest stage of life and then destroying them ended in disaster, scientists in London reported this month.
Medium reports the research by biologist Kathy Niakan and her team at the Francis Crick Institute is being widely regarded as a warning sign about the dangers of trying to create a genetically modified human being.
Niakan used the CRISPR gene-editing technology to experiment on 25 human embryos, all less than 14 days old, according to the report. Although the embryos were in their earliest stage of life, they already were individual human beings with their own unique DNA.
According to the report, the London scientists used CRISPR to remove a gene known as POU5F1 in 18 of the embryos. Afterward, when they examined the 18 embryos and compared them to the seven that had not had their DNA edited, the scientists said about half had major DNA abnormalities that they did not intend.
Though the full impact of DNA editing is unknown, the scientists predicted that the abnormalities could cause birth defects, cancer and other problems, the report states. It also is unknown how DNA edits could affect any future children of those children.
Here’s more from the report:
The researchers then used sophisticated computational methods to analyze all of the embryos. What they found was that of the edited embryos, 10 looked normal but eight had abnormalities across a particular chromosome. Of those, four contained inadvertent deletions or additions of DNA directly adjacent to the edited gene.
A major safety concern with using CRISPR to fix faulty DNA in people has been the possibility for “off-target” effects, which can happen if the CRISPR machinery doesn’t edit the intended gene and mistakenly edits someplace else in the genome. But Niakan’s paper sounds the alarm for so-called “on-target” edits, which result from edits to the right place in the genome but have unintended consequences.
After the experiment, the scientists said they destroyed all the embryos.
Genetic experts at the University of California Berkeley and the University of Pennsylvania reacted strongly to the research and warned other scientists about moving forward with similar experiments.
Professor Fyodor Urnov at UC Berkeley said the disastrous results should be regarded as a “restraining order for all genome editors to stay the living daylights away from embryo editing.”
Kiran Musunuru, a cardiologist at the University of Pennsylvania, said the experiment suggests DNA editing is much more complicated and dangerous than initially thought.
“What that means is that you’re not just changing the gene you want to change, but you’re affecting so much of the DNA around the gene you’re trying to edit that you could be inadvertently affecting other genes and causing problems,” Musunuru said.
For pro-life advocates, the experiment is troubling on multiple levels. The destruction of human life, no matter how early, is always wrong. From the moment of conception, unborn babies are unique, living human beings. Yet, their bodies are destroyed and used for experiments in laboratories across the world.
Genetic editing also has many concerned about the possibility of “designer babies,” or children whose genes have been edited to produce desired traits, such as height, hair color and sex.
In late 2018, a Chinese scientist caused international outrage after he announced that he had successfully changed the DNA of twin girls Lulu and Nana when they were embryos. The experiment involved editing a gene associated with HIV infections to make the twins resistant. One of the problems with the experiment, however, is that no one knows the effects of genetically altered DNA on human beings or their offspring.
In December, the Chinese news agency Xinhua reported the scientist, He Jiankui, was sentenced to three years in prison for illegally practicing medicine and fined 3 million yuan (about $430,000).
Meanwhile, international health agencies are considering international guidelines for genetic editing.
This randomized controlled trial done in Sweden assessed whether the fertility awareness counseling tool known as Reproductive Life Plan (RLP) could increase men’s fertility awareness. The authors sought to address the limited awareness many people have about the factors that affect their fertility. They noted this lack of fertility awareness was especially problematic for men, at least partly due to the general paucity of attention directed at men’s reproductive health both in terms of education and research.
Background
The Reproductive Life Plan provides a structured format for people to consider whether or not they are interested in having children in the future. It is intended to motivate individuals to reflect on their reproductive goals and create a plan to achieve them. Additionally, it creates the setting for a conversation with a health care professional, during which patients can discuss factors that affect their fertility. RLP-based counseling has been shown to have positive results with women. However, prior to this research, it had not yet been studied in men.
Methodology
This trial included 201 men ages 18-50 who visited one of two sexual health clinics in Sweden for sexually transmitted infection (STI) testing. All 201 men received the care and STI testing for which they presented to the clinic. Additionally, 101 of them (the intervention group) received oral and written RLP-based information about fertility and lifestyle factors that can affect fertility. The RLP-based counseling was carried out by nurse midwives who, in Sweden, are responsible for much of the sexual and reproductive health care for healthy young adults.
During the RLP-counseling session, the nurse midwives consulted a list of fertility facts as a guideline and checked off any topics that were discussed. Furthermore, they emphasized relevant fertility information and lifestyle recommendations based on a predetermined checklist. After the counseling session, participants were sent home with a brochure about male fertility and lifestyle.
Assessment
The authors assessed any change in the men’s fertility awareness by administering a questionnaire before the intervention, and comparing the results via a telephone survey administered three months later. The initial questionnaire included general background questions, six open-ended questions about reproduction, and two open-ended questions about lifestyle factors relevant to fertility. The questions sought to assess the participants’ general knowledge about male fertility and reproduction. As an example, one question stated, “How long does sperm usually survive in the uterus/fallopian tubes after intercourse?”
The follow-up phone survey occurred three months after the RLP-counseling session, and the participants were asked the same knowledge questions as they had during the initial assessment. All the answers were given a score of 0-2 points based on a correction template, with the maximum possible total score being 12 points.
Results
In terms of participant characteristics, many had STI’s (75% had Chlamydia), one out of three (33%) had been involved in at least one pregnancy, and most of those resulted in induced abortions. 71% of participants wanted children in the future and, for the intervention group, the number of men who stated they wanted children increased from 58% before the intervention to 76% at follow-up.
Regarding the six general fertility questions, men in the intervention group increased their average score from 4.6 to 5.5, whereas there was no improvement in the control group. Regarding the two questions about lifestyle factors, men in the intervention group increased their average number of accurate lifestyle factors listed from 3.6 to 4.4, while the control group had no improvement.
As for feedback received about the RLP-counseling, some participants suggested a mobile application would be helpful. Three out of four participants (75%) noted they would likely make a pre-conception lifestyle adjustment if planning for a pregnancy.
Discussion
This research suggests RLP-based counseling targeted toward men can increase fertility awareness and ultimately help men adjust lifestyle factors that may impact their fertility. Given the fact that the recruited participants were all seeking STI testing, an important next step will be to determine if this research is reproducible with a larger, more diverse patient population.
Editor’s Note: It is encouraging to see this type of research taking place during a time when many couples are seeking healthier, safer, and more natural alternatives for family planning. The research by Bodin et al uncovered limited knowledge in the population studied concerning potential impact of age, weight, STI’s, and chemicals known to affect the endocrine system. It also identified and attempted to rectify misinformation about factors the men thought impact fertility, yet studies have shown they do not. We hope future research will incorporate more strategies to provide pre-conception counseling to educate men about modifiable lifestyle factors impacting their fertility.
Resources [i]Bodin M, Tydén T, Käll L, Larsson M. Can Reproductive Life Plan-based counselling increase men’s fertility awareness? Ups J Med Sci. 2018;123(4):255‐263. doi:10.1080/03009734.2018.1541948.
Forty years have passed since the U.S. Food and Drug Administration first authorized physicians to prescribe a drug that would subvert the institution of motherhood. May 9, 1960, was the day on which the authorization was granted; it was, by ironic coincidence, the day after Mothers’ Day. The drug, of course, was Enovid, a/k/a “the pill.”
Developed by Dr. Gregory Pincus and Dr. John Rock and manufactured by the Searle Pharmaceutical company, “the pill” was hailed by feminists at the time as a great liberator, providing women for the first time in history with a level playing field, allowing women as equals to compete with men in the work force and in the pursuit of sexual pleasure. For women who preferred a more formal and lasting commitment rather than the one-night stand, marriage itself, so went the prevailing wisdom, would be transformed by the new freedom from the encumbrance of unwanted children.
Every child would henceforth be a welcomed child and the fear — or the reality — of unwanted children would no longer put marriages under stress.
There were, to be sure, certain naysayers who did not line up promptly to salute the pill as an unmixed ‘benefaction. The Catholic Church, after careful study, found oral contraceptives to be nothing more than a more sophisticated method of frustrating God’s plan for the upbuilding of mankind.
Even certain secular thinkers were expressing concern at the likelihood of the collapse of sexual guidelines that had proved to be beneficial over time. Some political economists were fretting in public about the pill’s potential for catastrophic reduction in population levels, though such were gainsaid by the larger throngs of alarmist “experts” who feared that the Earth had already far too many people for the planet’s limited resources to sustain. And some physicians could be heard muttering in the corner about the pill’s potentially deleterious effects on women’s health.
But these demurrers were in the minority. The crowd was shouting: “Three cheers for the pill!”
Looking back from our vantage point today, we can see that there was reason indeed for second thoughts about the pill. In its original form, the pill had a dangerously high concentration of synthetic variants of progesterone and estrogen. That such was the case is attested by the fact that current forms in use today have less than a hundredth of the estrogen dosage found in the original form of the pill. Even at the time of the pill’s introduction, astute observers took note of the fact that while many physicians were assuring the public that the pill was perfectly safe, not a few of those physicians were loath to recommend the use of this medication to their own wives.
In a commemorative article in The New York Times (May 9 issue), Health reporter Jane Brody writes, “For the first time millions of young, healthy women were taking a potent drug every day, raising legitimate concerns about the drug-induced health risk. . . . And, as predicted, serious, even fatal, complications did occur among users of oral contraceptives, especially among women who smoked or were over 35 and those who used the early high-dose pills. These problems prompted a host of warnings and stimulated research that resulted in safer products containing far smaller hormone doses.”
Brody goes on to comment, however, that even the mini-doses available today are by no means utterly risk-free. “The pill today is sold with an insert mandated by the FDA (the Food and Drug Administration) and filled with . . . facts, figures, and warnings that . . . women . . . should know if they wish to avoid becoming a statistic. Blood clots, which can result in heart attacks, strokes, thrombophlebitis, pulmonary embolism, or vision-impairing eye damage, are the most common serious side effects and are most likely to occur in women who smoke and in older women. A smoker in her middle to late 20s is seven times as likely to die as a non-smoker from the pill-related clots, and the older the woman, the more smoking increases her risk if she also takes the pill.
“Women who have already had a clot-related disorder are advised not to take the pill. Women who have had cancers of the breast, lining of the uterus (endometrium), cervix, or vagina are advised not to take the pill, since it is possible that the hormones it contains could stimulate the growth of such cancers. . . . While there is at present no clear evidence that the pill increases a woman’s risk of developing breast cancer, women taking the pill who have strong family histories of breast cancer or those who have had breast nodules or abnormal mammograms should be monitored closely by a doctor.”
Thus the risk to a woman’s physical health present in the use of oral contraceptives is by no means negligible even today. But the moral and social and even economic damage wrought by the pill is equally disturbing. Today every nation in Europe is rapidly aging as the number of children drops well below — in the case of Russia, drops far below — the number needed just to preserve the numerical status quo, let alone to maintain a vigorous growth in the economy.
What masks the situation in the United States is massive immigration. On the moral front, the pill has vastly popularized the “playboy philosophy” among men. So many men in the age of the pill now look upon women as little more than casual accomplices in sensual satisfaction, accomplices to be nonchalantly discarded as fresh accomplices come upon the scene. A woman’s dignity as potentially a mother, to be revered by her children and by her faithful husband, is swept away.
And if, against expectation, a child is conceived from such casual liaisons, this turn of events is now thought to be the woman’s “fault”; it is accordingly her responsibility to provide a “solution” for the “problem,” either by aborting the child or by rearing it on her own.
The liberated male admits no obligation: “If you had taken the pill we wouldn’t have this problem” is his likely retort as he heads out the door.
The moral harm wrought by the pill within marriage has been similarly calamitous. Our national divorce rate of 50 percent is the predictable outcome of the prevailing mindset in which, thanks to the pill, the humble and complete gift of oneself to one’s spouse is replaced by exploitation of the other in self-centered satisfaction in the impeded marriage act. Living side by side with another person soon becomes intolerable in the absence of mutual respect. And when one regards one’s partner as mainly a means to one’s own selfish ends, mutual respect will wither and die.
To regard another person as a means to an end is to reduce that person to the status of a thing, an instrument to be manipulated for one’s own advantage. One can offer another person no greater insult. That is precisely what contraception does. Accordingly contraception erodes the foundations of a stable and happy marriage.
The most destructive impact of contraception, however, is what it does to one’s relationship with God. The pill frustrates the natural order by telling a biochemical lie. The hormonal content of the pill sends a woman’s body a false signal to the effect that she has already conceived. Nature being thus deceived, ovulation is suppressed and actual conception becomes impossible as long as the false signal is maintained. Thus the basis of the pill’s effectiveness in frustrating the natural order is cleverly orchestrated mendacity. As such, it carries the family features of the “Father of Lies.”
To reject in any fashion the natural order governing human relations is to reject the order’s author, Almighty God. To reject that order in a serious matter is to separate oneself from God. Since human life is preeminently sacred, to misuse the sources of human life is to sin in a serious matter, i.e., to commit a mortal sin. Contraceptive misuse of sexual power is accordingly seriously sinful. In thus separating the soul from God, contraception empties the soul of grace and of that fullness of peace that is the companion of grace, the peace that God wishes each soul to possess, to possess already in this life.
Far worse, contraception, in separating the soul from God, places the soul in danger of losing God for eternity.
Taken all in all, and in each point severally, the Age of the Pill has been a disaster.
Most American women use some type of contraception in their lifetimes, according to the Centers for Disease Control and Prevention. Nearly 13% of women aged 15 to 49 are currently on the pill, while about 10% use an intrauterine device or contraceptive implant.
Those birth control options are often touted as safe and effective methods for preventing pregnancy or addressing hormonal imbalances.
But Dr. Jolene Brighten suggests that isn’t the whole story. Dr. Brighten, a naturopathic physician and women’s health specialist by training, explores the effects hormones can have on women’s health.
That’s why she wrote the book “Beyond the Pill: A 30-Day Program to Balance Your Hormones, Reclaim Your Body, and Reverse the Dangerous Side Effects of the Birth Control Pill,” to delve deep into the issues that can arise with the use of the pill.
“I wanted to provide women with a user’s manual for their bodies and give them the information I wish I’d been given early in life,” Dr. Brighten said.
If women are diagnosed with a hormonal issue, they’re often offered the pill as the first — or sometimes only — solution. But Dr. Brighten seeks to educate women about the effects hormone imbalances can have on their well-being. The book also offers advice to remedy these imbalances through lifestyle changes, supplements, and nutritional modifications.
Some women experience side effects when they start birth control, including hair loss, lagging libido, extreme fatigue, and chronic infection. And those issues aren’t always taken seriously by their doctors. But women may not realize that they don’t have to live with those problems. Dr. Brighten discusses in her book how to locate the root cause of hormonal issues, attain a pain-free, manageable period free of cramps, acne, stress or PMS, and how to support liver detox, among other helpful topics.
“The book also provides them with tools to have a more productive conversation with their doctors and monitor and support their health if they do choose hormonal birth control,” Dr. Brighten said.
In addition to books, her website, www.drbrighten.com, has articles and resources to help women identify their symptoms and have more informed interactions with their doctors.
Birth Control May Not Be Right for Every Woman
Dr. Brighten said she doesn’t think women always have the right tools to understand their own bodies. Instead, she believes that women are often recommended birth control without clearly understanding its risks.
Birth control can lead to a variety of issues in women, including thyroid dysfunction, adrenal problems, loss of libido, menstrual irregularities, PMS, and anxiety.
Women don’t always link these problems to birth control or hormones, however. Until they read Dr. Brighten’s writings or consult with her, many believe they have to live with these symptoms.
“We serve women all over the world who are struggling and feeling dismissed by doctors about their concerns,” Dr. Brighten said.
But Dr. Brighten said she doesn’t think that birth control is inherently bad. Instead, she said she believes that women should have all the information about it when making choices about what to put in their bodies.
Nutritional Advice and Supplement Guidance Promote Hormonal Health
In addition to reaching a global audience with her writing, Dr. Brighten is also a clinician who works with clients.
In her clinical practice, she focuses on teaching women to make better choices that support their wellness. Often, that focus turns to diet and supplement changes to promote hormonal balance.
Dr. Brighten’s expertise on the connection between women’s hormones and nutrition informs those recommendations. She also shares that nutritional healing advice on her website.
“As both my family and myself leverage supplements, I wanted to have a line of the highest quality products I could trust to give to my family and take myself. One of our core values is to think about our customers like our family,” Dr. Brighten said.
In April of this year, President Trump temporarily halted funding from the World Health Organization over concerns that it had grossly mishandled the COVID-19 crisis. Since then, he has threatened to make the decision to withhold funding permanent.
For the WHO, the loss of U.S. funding is no small thing: The U.S.’s contributions of some $400-$500 million per year to the WHO amount to approximately 14 percent of the organization’s operating budget.
However, for pro-life Americans—and indeed pro-life individuals globally—the Trump administration’s decision was welcome for a reason completely separate from the organization’s missteps on the pandemic. The WHO has long been one of the most pro-abortion organizations on the planet, using the ostensibly humanitarian nature of its mission as cover to promote the killing of preborn babies throughout the world.
The same is true of a number of departments and organizations associated with the United Nations. The UN was founded as a political body intended to protect peace and uphold human rights around the world, yet large segments have been hijacked by radical pro-abortion activists. Disturbingly, the UN’s pro-abortion agenda has been on prominent display throughout the coronavirus pandemic, as various agencies—including the WHO—have attempted to promote abortion access as somehow being a crucial part of the response to the pandemic.
Trump Admin Opposes Hijacking COVID-19 for Abortion Advocacy
Thankfully, the Trump administration has been at the forefront of the efforts to get out ahead of this anti-life agenda.
In a letter dated May 18, John Barsa, the acting USAID administrator, blasted the United Nations’ drafted “Global Humanitarian Response Plan.” The Global HRP is supposed to be the UN’s formal reaction to the coronavirus pandemic, laying out a united global plan for how to respond. However, instead of putting a laser focus on the pandemic, the statement included troubling and divisive language promoting abortion.
In his letter, Barsa urged the UN not to use the pandemic “as an opportunity to advance access to abortion as an ‘essential service.’” “Unfortunately,” Barsa continued, “the Global HRP does just this, by cynically placing the provision of ‘sexual and reproductive health services’ on the same level of importance as food-insecurity, essential health care, malnutrition, shelter, and sanitation. Most egregious is that the Global HRP calls for the widespread distribution of abortion-inducing drugs and abortion supplies, and for the promotion of abortion in local country settings.”
Barsa made it clear to UN Secretary General António Guterres that the U.S. will—quoting President Trump’s address to the UN—“never tire of defending innocent life.” “Indeed, the UN should not intimidate or coerce Member States that are committed to the right to life,” he continued. “To use the COVID-19 pandemic as a justification to pressure governments to change their laws is an affront to the autonomy of each society to determine its own national policies on health care. The United States stands with nations that have pledged to protect the unborn.”
Amen. I will never tire of seeing the leadership of our country stepping forward and boldly defending the dignity and right to life of the preborn on the global stage.
Just last week, the Trump administration also rejected another attempt to insert pro-abortion language into a UN document. In a statement entitled the “U.S. Mission to the United Nations,” the administration said that it would not sign on to the proposed resolution for the 2020 ECOSOC Humanitarian Affairs Segment at the UN, specifically due to the inclusion of the terms “sexual and reproductive health care services” and “sexual and reproductive health.” These terms are understood by many UN bureaucrats to include not only contraception, but legalized abortion.
“The United States rejects any interpretation of international human rights to require any State Party to provide access to abortion,” the U.S. statement said bluntly.
Austin Ruse, the head of the pro-life organization C-FAM, which lobbies at the UN, said in response: “This is a great victory for pro-lifers around the world who are justifiably concerned that COVID funding would be used to promote abortion in humanitarian assistance. We thank the Trump administration for taking this strong stance in favor of true humanitarian assistance and in favor of the unborn child.”
The WHO’s Extensive Abortion Advocacy
In his encyclical Caritas in Veritate, Pope Benedict XVI expressed his dismay that international organizations were using their clout to promote abortion, particularly in third world nations. He wrote:
Some non-governmental organizations work actively to spread abortion, at times promoting the practice of sterilization in poor countries, in some cases not even informing the women concerned. Moreover, there is reason to suspect that development aid is sometimes linked to specific healthcare policies which de facto involve the imposition of strong birth control measures. Further grounds for concern are laws permitting euthanasia as well as pressure from lobby groups, nationally and internationally, in favor of its juridical recognition.
The Holy Father wrote movingly of the ills that NGOs are guilty of when they promote abortion instead of authentic development. “Openness to life is at the center of true development,” he said. He continued:
When a society moves towards the denial or suppression of life, it ends up no longer finding the necessary motivation and energy to strive for man’s true good. If personal and social sensitivity towards the acceptance of a new life is lost, then other forms of acceptance that are valuable for society also wither away. The acceptance of life strengthens moral fiber and makes people capable of mutual help. By cultivating openness to life, wealthy peoples can better understand the needs of poor ones, they can avoid employing huge economic and intellectual resources to satisfy the selfish desires of their own citizens, and instead, they can promote virtuous action within the perspective of production that is morally sound and marked by solidarity, respecting the fundamental right to life of every people and every individual.
Unfortunately, as one recent in-depth study makes clear, the WHO—which should, by virtue of its name, be promoting health—is one of the leading organizations promoting the “suppression of life” rather than an “openness to life.” In a white paper entitled The World Health Organization’s Abortion Overreach, Dr. Rebecca Oas exposes how the WHO is lobbying to legalize abortion throughout the world and strives to make abortion more prevalent by promoting the use of dangerous abortion drugs, including those taken without medical supervision. She also exposes how, in some cases, the WHO has trained doctors in pro-life countries to perform abortions and promotes “comprehensive sexuality education” that includes pro-abortion propaganda aimed at children. In addition, her white paper explains how the WHO’s abortion advocacy has distracted the organization from addressing the actual healthcare needs of women and infants.
Dr. Oas traces many of these shady activities to the WHO’s Department of Sexual and Reproductive Health and Research (SRH). Behind the SRH is a group of wealthy, pro-abortion Western nations and nonprofits—including the Ford, MacArthur, and Packard Foundations—as well as (unsurprisingly) International Planned Parenthood. Unfortunately, in the latest records available (2016-17), the United States was also listed as a donor to the SRH.
Another outsized influence, observes Dr. Oas, is the Bill and Melinda Gates Foundation, which is the second largest donor to the WHO, second only to the United States. Dr. Oas notes that the influence of this foundation is troubling, since it “derives its influence from the wealth of a single family, and is not subject to the norms that govern the UN and its agencies, such as the need for global consensus.” While the Gates Foundation carefully massages its messaging to focus on contraception rather than abortion, it also donates huge sums of money to leading abortion organizations, like Marie Stopes International and International Planned Parenthood. With the Gates Foundations’ deep pockets and enormous influence at the WHO, it’s unsurprising that the WHO has increasingly openly promoted abortion, despite the opposition to abortion held by many UN Member States.
In the end, the clear picture that emerges from the evidence presented by Dr. Oas is that the WHO is diligently working to give a veneer of credibility to abortion by calling it “essential health care” and then using its considerable wealth and power to impose abortion—in flagrant violation of the law if necessary—in developing nations. The same is true of other UN agencies, including the UN Population Fund, UN Women, and the UN Children’s Fund (UNICEF). With a $50-billion-a-year budget, the UN is arguably the biggest engine of the Culture of Death today. That is why pro-lifers everywhere can celebrate the Trump administration’s decision to halt funding to the WHO as well as to the United Nations Population Fund (UNFPA), with its horrific history of supporting coercive abortion and sterilization.
However, as Dr. Oas argues, it is time to go further. Until the UN and WHO stop meddling in the affairs of pro-life nations and pushing the killing of innocent human beings under the guise of “health care,” they should never again receive another dime of U.S. taxpayer money.
The two primary female reproductive hormones are estrogen and progesterone. When estrogen zigs, progesterone zags. They are like foil characters that have important balancing characteristics. We see the impact of this balancing act on our bone health, mood stabilization, and even our libido. We also see it in our heart health: recent research has found a connection between cardiac functioning and our natural monthly cycles of endogenous estrogen and progesterone, and it has also indicated a relationship between our cycles and heart disease risk. As heart disease is one of the leading causes of death for post-menopausal women, it is crucial to understand why and how Fertility Awareness-Based Methods (FABMs) can help.
The estrogen-dominant phase of the menstrual cycle is often referred to as spring and summer: Libido is high, the endometrium proliferates and grows, brain cells are stimulated, and bone mass is built. Following this is the progesterone-dominant phase, which is often compared to fall and winter: Libido drops, moods are stabilized, the endometrium maintains, and brain cells restore and repair, as does bone mass.
As these hormones have an effect on our brain, bones, libido, and moods, it should come as no surprise that even our heart is affected by them, too.
Your heart loves your hormones (especially estrogen and progesterone)
Recent findings show that resting heart rates follow distinct patterns across the menstrual cycle. Resting heart rate is slower in the menstrual and follicular phase (the first half of the cycle, when estrogen dominates), while it is significantly faster in the ovulatory and luteal phase (the second half of the cycle, when progesterone dominates).
We also know that estrogen has a preventative effect on coronary artery calcification (CAC). CAC can cause blood vessels to narrow and lead to the development of heart disease, but estrogen helps prevent the buildup of calcium in the arteries. Estrogen also positively influences myocardial contractile reserve, which gives the heart the ability to pump harder when it needs to, and to rest easier when it doesn’t.
Progesterone plays an important role in cardiovascular health, too: it decreases blood pressure through vasodilation and decreases angiotensin-II vaso-responsiveness. Vaso what? Angiotensin-II is a blood vessel constrictor that increases blood pressure, and progesterone helps moderate that response. See? Zig and zag.
When you pair these effects of estrogen and progesterone on cardiovascular functioning with other research that connects reproductive factors and incidence of heart failure, the importance of the cyclical effects of these hormones for optimal heart health becomes even more striking. In a 2017 paper, researchers found that a “shorter total reproductive duration [defined as the time from menarche to menopause] was associated with a higher risk of incident total heart failure hospitalization in post menopausal women.”
More research is needed to determine the exact relationship between endogenous (that is, naturally occurring) progesterone and estrogen exposure, but these results seem to indicate that a longer reproductive lifespan seems to reduce one’s chances of developing cardiovascular disease and/or having a cardiovascular event later in life: according to the study, “a total of 1494 women (5.2%) were hospitalized for adjudicated incident heart failure, with women who had fewer total menstrual cycles having a greater risk for incident heart failure at 1 year.”
Your heart on birth control
But reproductive duration isn’t necessarily measured in time alone. It’s what is actually happening during those cycles throughout those prime years of reproductive potential that matters the most.
So what should be happening during those prime reproductive years? Well, ideally, you’d be ovulating and menstruating in a predictable, healthy manner. But if you are on hormonal contraception of any kind, you are not ovulating or cycling at all. This, by definition, means shorter time of potential fertility. Even though the same amount of time is passing than would be off the Pill, your reproductive duration is shortened because there is no exposure to biological cycles—the zig-and-zag of your naturally occurring estrogen and progesterone.
When a woman takes hormonal birth control, instead of ovulating and experiencing the cyclical effects of her naturally occurring sex hormones, the menstrual cycle is suppressed, and the heart is no longer experiencing this beneficial balancing act. And, in case you’re wondering whether the synthetic forms of estrogen or progesterone found in hormonal contraception have this same beneficial effect, the answer, unfortunately, is “no.”
It is commonly known that smokers and women over 35 are not good candidates for hormonal contraception, but women with high blood pressure, diabetes, and high blood cholesterol are also at higher risk for developing coronary heart disease, which makes hormonal contraception a riskier family planning choice for them, too. Hormonal contraceptive use itself has been linked with increased risk of blood clots, and their associated cardiovascular events like stroke and heart attack. High blood pressure, diabetes, and high cholesterol are all associated with hormonal contraceptive use, too.
Healthy cycles for a healthy heart
Of course, even if you aren’t on birth control, cycling alone is not enough to reap the benefits of your hormones’ balancing act for optimal heart health. Similar to our discussion with Dr. Prior on bone health and ovulation, we know that healthy, ovulatory, and functional cycles are needed for our bodies to reap the benefits of our cycles. Hormonal disorders—which usually correspond with irregular, anovulatory, progesterone deficient, and/or estrogen dominant cycles—can mess with this delicate balance, even if a woman is not on birth control.
Good nutrition and regular, moderate exercise can go a long way in balancing hormones, but they are not the *only* variables—sometimes more interventions may be needed to find balance. This is where charting cycles with a Fertility Awareness-Based Method (FABM) can be a vital tool in assessing a woman’s overall health. Healthcare providers who understand how to use the biological information gleaned from a woman’s menstrual cycle can diagnose and treat the hormonal disorders that may be affecting a woman’s health—from her fertility, to her immune functioning, to her bone and heart health, and everything in between.
What’s happening to my heart if I’m pregnant or breastfeeding?
Obviously, pregnancy is a time of anovulation (that is, when ovulation does not occur). Women who are breastfeeding also may not see a return to fertility for weeks, months, or even years. But whether you are breastfeeding, pregnant, or both, those are the only times (except for puberty and pre/post menopause) when it is considered biologically normal to go without the zig-and-zag of progesterone and estrogen that cause the regular cycle of ovulation and menstruation. And your body—savvy as it is—has a fix for that! The incredible amounts of endogenous progesterone and estrogen that a woman is exposed to throughout her pregnancy more than recoup for the effects of anovulation due to pregnancy or breastfeeding. Further, prolactin (better known as the lactation hormone) has indirect, beneficial effects on the new mom’s heart. Prolactin actually modulates neural pathways in the brain to decrease stress, which decreases cortisol. And as we all know, cortisol is that greedy stress hormone that (when left unchecked due to chronic or long term stress), can rob your body of estrogen and progesterone, and raise your risk for heart disease.
It is true that pregnancy is a time of complicated risk factors for heart disease—and pregnancies before age 20 especially seem to increase one’s risk for heart disease. But this is where it comes in handy to have had those years of protective exposure to endogenous hormones prior to pregnancy. Just another reason why teens and young women need a (regular, functional) period! It’s also another big point in favor of FABMs, which allow women to cycle naturally whether they are trying to achieve pregnancy or not.
Women need periods
If we haven’t already convinced you how important menstruating (and ovulating) is for your heart health, consider that heart disease is one of the leading causes of death for post-menopausal women. While more research is needed to determine the exact effects of progesterone and estrogen on the heart, the decades of natural, cyclical, endogenous hormone exposure throughout a woman’s reproductive life could have an important impact on her heart disease risk. It’s certainly something to take into account when considering your family planning options.
The more we learn about feminine health, the more reasons we encounter why #womenneedperiods. Regular and functional ovulation benefits the development and maintenance of your immune system, the building and protecting of your bone mass, and the functioning and preservation of your heart. As hard as it may feel to appreciate at times, your period actually does a lot of good for you.
June 8, 2020 (LifeSiteNews) – Many of the greatest defenders and proponents of stay-at-home orders and Black Lives Matter protests are rabidly pro-abortion, yet their responses to COVID-19 and the death of George Floyd reveal staunchly pro-life principles.
The entire narrative built by politicians and the mainstream media following the government’s stay-at-home orders was that we had to temporarily sacrifice our lifestyle and freedoms in order to protect the vulnerable. We were told every day that we didn’t have the right to endanger the health and lives of others.
Similarly, if every other form of bodily rights can or should be temporarily restricted in a pandemic to save lives, why shouldn’t abortion, which always ends a life? Many politicians and pundits argued that social distancing and stay-at-home orders illustrated that your right to bodily autonomy should be regulated if your actions risk harming others. Regardless of whether those orders were justified, this is the exact case pro-lifers make for protecting the unborn: A pregnant woman’s bodily autonomy ends the moment that exercising that autonomy harms or kills others.
Obviously, pro-lifers maintain there is a difference between unintentionally infecting a vulnerable person at Disneyland and having an abortion, which always involves the direct and intentional killing of a human being. But this only strengthens the case for regulating bodily autonomy when it comes to abortion.
It is not unreasonable for the government to temporarily restrict a pregnant woman’s bodily autonomy to protect the health and life of her vulnerable child.
Then, after two months of stay-at-home orders, a police officer in Minneapolis brutally mistreated and killed a black man named George Floyd, whom he held down on the street with his knee placed directly on Floyd’s neck for a full eight minutes.
This incident incited protests and riots all around the country. While there is a clear distinction between peaceful protestors truly angered by Floyd’s murder and the criminals using his death to “justify” their looting and burning, the protests were nearly all called Black Lives Matter, which quickly became the trending hashtag on social media platforms.
Putting the question of systemic racism in the police force aside, it is obvious that Americans are united in calling racism evil. We all believe that Black Lives Matter, not because they’re black but because they’re human beings with intrinsic dignity. Everyone agrees that intentionally harming or killing innocent human beings without proper justification is wrong.
But if Black Lives Matter because they’re human beings, then they matter from the moment they ARE human beings. If systemic racism is true and Gayle King at CBS This Morning is right that there is an “open season on black people,” such that we need to initiate systemic change to correct injustice, then how can we continue to tolerate the injustice of abortion, which quite literally is “open season” on black people?
While the claim that there is systemic racism in America’s police force targeting black lives is not verifiable, it is proven that the abortion industry targets black lives because of their race. Fully aware of the disproportionate amount of abortions that black America obtains, Planned Parenthood strategically places their death camps in black neighborhoods. A study by Protecting Black Life found that “79 percent of Planned Parenthood’s surgical abortion facilities are strategically located within walking distance of African and/or Hispanic communities.”
If Black Lives Matter, then ALL Black Lives Matter, both born and pre-born. There is no greater assault on black lives than the one the abortion industry wages, as they specifically target black babies to increase profits.
Both the COVID-19 and Black Lives Matter responses reveal the self-evident nature of the pro-life position: Human beings have intrinsic dignity and value that should be respected and protected.
Unfortunately, after decades of pro-abortion propaganda, that self-evident truth is not as self-evident as it used to be. While recognizing this truth as it applies to born people, too many of our countrymen still don’t believe it applies at the beginning of a human being’s existence!
Those who really care about women’s health and safety should be deeply concerned about the latest push to expand chemical abortion via telemedicine and look for ways to communicate the serious risks involved.
The use of chemical abortion was already on the rise in the United States, but calls to expand access have become even louder during the coronavirus pandemic. In October, the Guttmacher Institute (originally the research branch of Planned Parenthood) reported that the use of chemical abortion over the past two decades has ballooned. “Medication abortions increased from 5% of all abortions in 2001 to 39% in 2017, even while the overall number of abortions declined,” reads the report. In 2001, there were approximately 71,000 chemical abortions; in 2017, this number climbed to 340,000. It will very likely increase during the pandemic.
Billed as safe and effective by the abortion industry, chemical abortion is arguably much harder on women’s health than surgical abortion — and there’s certainly less medical oversight. A study out of Finland showed that women are four times more likely to suffer severe complications as a result of chemical abortion than they are as a result of surgical abortion.
Chemical abortion is grueling and takes a nasty toll on a woman’s body, in addition to ending the life of her unborn child. It is a two-step regimen. The first step requires a woman to take a drug called mifepristone, which blocks progesterone and prevents an unborn baby from receiving vital nutrients, effectively starving the baby to death. The second drug, misoprostol, causes strong uterine contractions that expel the unborn baby from the uterus. With both drugs come vaginal and abdominal bleeding and cramping, according to the Mayo Clinic, and the clinic advises that anyone who has an at-home chemical abortion to get access to a doctor and emergency services.
The use of telemedicine only to prescribe a chemical abortion eliminates critical medical oversight afforded by an ultrasound. Ultrasounds should always be performed to determine the gestational age and location of the baby; if not, chemical abortions can pose potentially fatal risks to women. Perhaps the most dangerous possibility of all is if a woman uses chemical abortion when she has an ectopic pregnancy — that is, when the baby has attached to her fallopian tubes rather than the uterine wall. It’s a life-threatening situation that ultrasound can either rule out or accurately diagnose.
The gestational age is also important because, for safety reasons, the Food and Drug Administration has approved chemical abortion only up until 10 weeks into pregnancy. And an ultrasound is generally needed to date a pregnancy accurately because many pregnant women aren’t certain about the date of their last menstrual period.
A peer-reviewed study from 2015 on the safety, efficacy, and acceptability of self-administered abortion pills through 70 days showed that almost 30% of the 40 women taking chemical abortion did so after the FDA-approved time frame of 63 days. Very sadly, 62% of these women had incomplete abortions. Surgical evacuation was required for 68% of these patients, and 23% of these women had a failed abortion. For 12.5% of them, they received surgical evacuation with blood transfusion. The authors concluded that “unsupervised medical abortion can lead to increased maternal morbidity and mortality.”
When chemical abortion was approved by the FDA in 2000, the drugs required a “black box warning” because of mifepristone’s known ability to suppress the immune system and issues with bleeding. In the years since chemical abortion was approved, the FDA has reported adverse events, the latest information shows that at least 24 women have died as a direct result of chemical abortion in the U.S. between 2000 and 2018, and there have been thousands of serious adverse event reports submitted to the FDA including hospitalizations and blood transfusions. With increasing numbers of women using telemedicine to obtain a chemical abortion, the number of complications and deaths caused by chemical abortion will very likely increase.
In light of the many risks associated with chemical abortion, it is profoundly troubling that anyone would advocate for telemedicine abortion — or demand that the FDA relax the policies designed to mitigate those risks. No one claiming to champion women should prioritize “access” above their health and safety.
When I was in college was when I first heard about Fertility Awareness-Based Methods (FABM) and about six months before I was to be married, I learned how to chart a specific method.
A few months after we were married, we went on a trip to Guatemala, and while we were there I was charting out my cycles and noticed that something was bizarre. I was trying to figure out the days that I was fertile and infertile, and wasn’t able to do so. At that point, though, I had no other symptoms and so I ended up calling my instructor to see if she could guide me.
My instructor told me, after taking a look at my charts and my cycles, that she agreed that something odd was occurring and she referred me to my fertility awareness doctor who was trained in the specific method that I had learned.
When I saw my doctor, she took a look at my chart; she agreed with me that it was definitely strange that I couldn’t tell when I was fertile or infertile.
And so she decided to do an exploratory ultrasound just to figure out if there was something we could be missing.
So we did the ultrasound, and she told me she found a six-centimeter tumor on my left ovary.When I heard that information from my doctor, it was very shocking, and I remember entering into her office and just feeling like the world around me was going in fast motion–but I was still stuck in slow motion, almost as if I was in a movie.
After the surgery, they did a biopsy of the tumor and found that it was a borderline tumor. A borderline tumor is one that is a slow-growing nonmalignant cancer. And I remember that as the surgeon was explaining to me about this that my husband had asked her, “what would have happened if we had waited two months to find out?” And the surgeon replied back to him, “honestly I wouldn’t have wanted you to wait another two weeks to have this removed.’
Many women are put on birth control for irregular menstrual cycles– but if I had been using an artificial means of birth control, I may not have found out that I was sick.
That was four years ago, and I am happy to report that I’m healthy—that all is well. Originally I was fearful that I wouldn’t be able to conceive with one ovary, but we were able to have a child two years ago; and so we have our little Gigi, and our life is very blessed.
Ultimately it was charting that saved my life. I have no other symptoms, and it was only by charting the natural signs of my cycle that I was clued into there being anything wrong. If I had been using an artificial means of birth control, I may not have found out that I was sick.
Since then I have spoken to many people who have found out about health problems solely through charting, and I am very passionate about getting the information out there about these methods, so much so that I now teach a Fertility Awareness-Based Method myself.
Fertility awareness is learning the signs of your body and charting them out to be able to achieve or avoid pregnancy, and ultimately to know your reproductive health.
My hope in sharing my story is to really empower women to not be afraid to learn the natural signs of their bodies, and to learn these methods that can truly be beneficial to their lives and their health.
Many millennials and gen-z-ers never had the experience of “going out to play” in generally safe neighborhoods without constant parental supervision. High divorce rates and the rising influence of the Internet deprived them of this particularly formative part of their childhoods. Their schools reinforced the idea of constant supervision by an education philosophy that is long on ideology and short on truth.
Not only do the newer generations have difficulty going out to play but they have fewer playmates. Fewer couples are having children. Statista relates that 49.5 million families in the U.S have no children under the age of eighteen, 14 million have a single child, 12.8 million have two children, and only 7 million have three or more. While these figures do not reflect homes where children are grown, the trend is undeniable. Children are vanishing in America.
The Long Term Trends
The fertility rate in the United States has been on a steady decline since 2007. It is now at an all-time low. According to a report from the Centers for Disease Control’s National Vital Statistics System, “The general fertility rate was 59.0 births per 1,000 women aged 15–44, down 2% from 2017 and another record low for the United States.”
The Hill presented the overall picture as it rolled out over time. “[T]he TFR (Total Fertility Rate) hovered above 3.0 in the early twentieth century; declined to replacement levels of about 2.1 in the 1940s; reached a peak of 3.7 in the post-World War II baby boom; and then declined rapidly to relatively stable low levels in the seventies. Declines in fertility have accelerated since 2010 — raising questions about the economic and public policy implications if this latest trend continues.” The Washington Post pegs the current fertility rate at 1.73.
Reasons for the Decline
The reasons for this decline are well-known. Contraception is more common and available everywhere. Couples wait longer to get married, and then delay childbearing until they consider themselves more financially secure. The costs of raising children – especially daycare and education – continue to rise faster than the general cost of living. Many couples simply decide never to have children.
The influence of culture and government also contributes to this trend. Many schools and other public agencies promote contraception and abortion among the young. Such efforts are often done in tandem with Planned Parenthood. Under Obamacare, contraception drugs are mandated for all health insurance packages. The United Nation’s World Health Organization actively promotes abortion and contraception worldwide. Much of the environmental movement favors fewer people since the mere existence of humanity is the source of the coming global collapse.
This depopulation trend has massive social and economic consequences.
Children and the Family
Neighborhoods that once crawled with children are now relatively quiet. Rather than neighborhood games of tag, baseball, or other games, which could go on for hours, the now-common “playdate” is more likely to be indoors and have a set end time. The playdate is tailored to the dwindling number of children that now must play by appointment only.
The playdate is a poor substitute for the neighborhood. The limits on the parents’ time make these occasions relatively rare, which makes forming lasting friendships more difficult. The pool of children is limited and thus makes it more difficult to develop social skills with groups that should develop naturally.
When the playdate has to be called off or postponed, the most available alternative is “screen time.” That screen might be attached to a television, a computer or a video game, which is a poor replacement for human interaction.
Can A Shrinking Society Support Itself?
Most couples who delay or limit childbirth cite economic reasons. They may not realize that a shrinking society carries severe economic costs.
Euromonitor International reported on the global impact of an aging consumer base. Its study is ominously titled Developed Cities with Lower Birth Rates Forecast to Register Slower Real GDP Growth by 2030. The report finds that “While new opportunities will certainly arise in light of a growing elderly demographic,… continuously low birth rates will inevitably lead to a drop in total consumption in the future as overall population will begin to decrease.”
Euromonitor also reported on the negative impact of a decreased number of workers. “The shrinkage of the working-age (15-64) population is the single biggest danger for the economic health of cities. This age category is the main supplier of productive labour for businesses, which means the working-aged are also the taxpayers and the care providers for the age-dependent.”
Boston College’s Center for Retirement Research also described this impact in March 2019. “[L]ower fertility has serious consequences: a smaller future workforce will result in slower overall economic growth and higher tax burdens to support pay-as-you-go programs such as Social Security. According to the 2018 Social Security Trustees Report, a total fertility rate of 1.8 children per woman instead of 2.0 would increase the program’s 75-year deficit by 0.41 percent of taxable payrolls or a present value of almost $2 trillion.”
Eventually, the Social Security System may collapse or be restructured as a taxpayer-subsidized welfare program. Of course, there will be fewer taxpayers.
European and Asian Situations Are Even Worse
While American population trends are troubling, the situation is far worse in Western Europe and parts of Asia. Figures compiled by The World Bank find that no European Union nation hits the population replacing 2.0 fertility rates. Malta’s rate is lowest at 1.2. Cypress, Italy and Spain are at 1.3. France is the highest at 1.9.
Japan has not replenished its population since 1975 and currently sits at slightly under 1.4, according to the website Macrotrends. Even the liberal New York Times acknowledges that China’s low birth rate has “undesirable side effects” stemming from its tyrannical thirty-five year “One Child Policy” that was slightly changed in 2015. “It upended traditional structures for supporting older adults and led to a widening imbalance in the number of men and women, one that could sow social unrest.”
Indeed, the present generations are too selfish to reproduce. Like most selfish behavior, it is short-sighted. Individuals and families think they are short-term advantages to having small families. However, these “advantages” will come to haunt them as they age and the smaller generations that follow struggle to keep society running.
During the recent virtual meeting of the World Health Assembly-the decision-making body of the World Health Organization (WHO)-the US submitted its written Explanation of Position (EOP) on the COVID-19 Response Resolution, disassociating itself from a number of paragraphs, including two related to “sexual and reproductive health”.
The US statement expressed regret at the failure to achieve consensus language in all areas of the resolution and explained:
“The United States dissociates from operative paragraphs 7.5 and 9.4. The United States strongly supports women reaching the highest attainable outcomes for health, life, dignity, and well-being throughout their lives. We champion access to high-quality health care for women and girls across the lifespan. However, we do not accept references to “sexual and reproductive health,” or other language that suggests or explicitly states that access to abortion is included in the provision of population and individual level health services. The United States believes in legal protections for the unborn, and rejects any interpretation of international human rights (such as General Comment 36 on the International Covenant on Civil and Political Rights) to require any State Party to provide access to abortion. As President Trump has stated, ‘Americans will never tire of defending innocent life.’
Each nation has the sovereign right to implement related programs and activities consistent with their laws and policies, free from external pressure. There is no international right to abortion, nor is there any duty on the part of States to finance or facilitate abortion. Further, consistent with the 1994 International Conference on Population and Development Programme of Action and the 1995 Beijing Declaration and Platform for Action, we do not recognize abortion as a method of family planning, nor do we support abortion in our global health assistance.”
UN “Experts” Object to US States’ Right to Decide Abortion Policy
According to Elizabeth Broderick, Vice-Chair of the Working Group, “We regret that the above-mentioned states, with a long history of restrictive practices against abortion, appear to be manipulating the crisis to severely restrict women’s reproductive rights.
“This situation is also the latest example illustrating a pattern of restrictions and retrogressions in access to legal abortion care across the country. We fear that, without clear political will to reverse such restrictive and regressive trends, states will continue pursuing this pattern.”
The Working Group also expressed its opposition to USAID’s letter to the UN Secretary General which requested the removal of references to “sexual and reproductive health and its derivatives” from the Global Humanitarian Response Plan (HRP) on COVID-19.
Broderick said, “We reiterate that sexual and reproductive health services, including access to safe and legal abortion, are essential and must remain a key component of the UN’s priorities in its responses to the COVID-19 pandemic.”
PNCI notes that the Working Group disregards UN consensus agreed to in the 1994 International Conference on Population and Development Programme of Action which states in 8.25 “Any measures or changes related to abortion within the health system can only be determined at the national or local level according to the national legislative process”. State legislators are the ones to determine state policy on abortion, not abortion activists who are appointed by the Human Rights Council to serve on Special Procedures.
Over at National Review, Michael Brendan Dougherty recently discussed the latest fertility figures from the United States. Once again, they were in decline: in 2019 the total fertility rate (the number of children each woman on average is expected to have over her life) dropped to 1.7. This is well below the replacement rate of 2.1 and means that, absent large scale immigration, the USA’s population will start to naturally decline.
This fertility rate is the lowest on record and marks about the twelfth year in a row in which it has declined (from just before the GFC). This is now a trend which has reduced the USA’s position as the outlier among western nations – for many years America had a fertility rate closer to replacement than its East Asian and West European competitors and allies.
Dougherty worries about the atomisation that this trend will bring. Family trees will collapse inwards: there will be fewer siblings, aunts, cousins and uncles. As he puts it “more people in the future will grow up with shrivelled kin networks, fewer relations with people who are obliged to socialise and network with each other”.
This reduces our sense of comfort and confidence in the world: the school and support which the family provides to us all will be weakened, especially in its role as the first of the independent civic associations that undergird society.
Without a strong family network, society loses a bulwark against the forces of social conformism. (I’m not sure about the States, but this is something desperately obvious in New Zealand – the last few weeks have shown us comprehensively that we are a nation of conformists.)
More generally, low fertility societies are low confidence societies: too few are investing in the future by investing in the next generation. They also tend towards suspicion and paranoia: immigrants aren’t seen as reinforcements to the nation’s mix, but replacements of the nation’s natives.
A large part of the decision to delay having children, or forgo doing so at all, is due to concern that we have material prosperity sorted before bringing children into the world. We need to have finished our education, have a secure job lined up, and preferably be on the property-owning ladder before we feel settled enough to have children. Even if all of these material goals are met, having children is pushed back into the late 20s or early 30s. Making child rearing dependent on material security also means that fertility rates are depressed by economic downturns and recessions.
But even when the economy is growing, the lack of extended family trees and social networks in which more than two children are the norm means that it is hard for a society to increase its fertility rate. There are fewer social support networks available: older parents means older grandparents who can contribute less to the raising of grandchildren.
What can be done? Is this a problem which merely requires policy tinkering like maternity leave or increased day care? Are we instead witnessing something greater: the beginning of the end of our current economic/social/culture milieu as we fail to replace ourselves? And if so, what will replace us?
If a society is not even guaranteeing its future through replacement generations of children, then it is a failing society. We need to start acknowledging this.
You can tell something about a person by the company she keeps, and the same applies to organisations. Marie Stopes International, a high profile British birth control non-profit, was outed in The Mail on Sunday recently for receiving cash and goods worth 7.5 million pounds from American porn tycoon Phil Harvey over the past 15 years.
Harvey himself has been a direct player in the international “reproductive health” game since the 1970s, funding his own and other charities through Adam & Eve, a business that sold 60 million pounds worth of sex toys and pornographic film in 2019.
What does this say about Marie Stopes?
At best that it suffers from poor taste. It also has a strange attitude to women. MSI touts its contraceptive and abortion services as empowering “women and girls all over the world to choose when or whether to have children.” Yet it works hand in glove with an industry that disempowers women by making them sexual playthings, if not facilitating sexual assault and human trafficking.
Harvey’s sex business offers an array of pornographic material including female sex robots which promote the fact “her inflatable body is also practical if you need to store her or take her on journeys.” An huge list of pornographic films is also flaunted on his sex website.
But by peddling contraception and abortion to vulnerable women in developing countries, MSI, like Planned Parenthood and the rest of them, is handmaiden to every man who would sexually exploit a woman. Yet it is blasé about the connection.
Its response to the Mail on Sunday was: “Phil Harvey has spent his life defending sexual and reproductive health rights, and played a significant role in expanding access for women across the world. We are proud that he continues to contribute to the organisation.”
Harvey, 82, is not the only unsavoury mogul to cosy up to the birth control industry. Hugh Hefner, the founder of Playboy, used his magazine to campaign for legalised abortion. Harvey Weinstein apparently posed as a cheerleader of Planned Parenthood. It makes sense: the women they used or encouraged other men to use might need the odd abortion, and it goes down well with the liberal crowd.
However, Phil Harvey’s US$9 million equivalent over a decade or two looks paltry compared to what Marie Stopes gets from other sources every year. The UK government alone gave them £48million last year which helped them deliver around five million abortions and pay its CEO £434,000 – among other things. Harvey’s position as a board member of MSI signals that he is much more important to the organisation than his cash grants.
A profile of him in Mother Jones magazine back in 2002 reveals that the relationship between Harvey and Marie Stopes goes back more than 50 years, to when he was a graduate student at the University of North Carolina’s School of Public Health, on a Ford Foundation fellowship (Ford being one of the main powerhouses of the population control movement). There he worked with a young British doctor, Tim Black, who went on to rescue the bankrupt Marie Stopes Foundation in 1975 and turn it into a “social business” with its current name.
Both Harvey and Black had spent time in developing countries and were convinced that what the poor of the world needed more than food was fewer babies. As part of their thesis work they came up with a plan to test social marketing of contraceptives in the American marketplace. With a university grant they began a mail order business, running clever ads in college newspapers and selling condoms to students. Next they added other merchandise and eventually struck gold when they threw in sex magazines. This was the genesis of Adam & Eve, which under Harvey surfed the wave of the home video boom in the 1980s and survived efforts to shut it down under the Reagan administration.
But Harvey and Black hadn’t forgotten the poor: perhaps social marketing of condoms would work in the developing world as well. To this end they set up a dual venture: a profit-making arm called Population Planning Associates, and a separate nonprofit, Population Services International (PSI), which by 1975 was running condom-marketing programmes in Kenya and Bangladesh. PSI remains one of the big guns of population control alongside International Planned Parenthood.
Harvey left PSI in the late 1970s and focussed on his porn business, but a few years later he founded another non-profit, DKT International, to take up marketing and supplying cheap condoms to the poor again.
In 2017 DKT launched a “WomanCare” platform “to dramatically increase the use of high-quality contraceptive, safe abortion, and reproductive health products.” In 2019, DKT WomanCare sold 222,123 manual vacuum aspiration abortion kits, 1.8 million cannulae and 1.4 million implants (linked with high rates of HIV in some African countries) in 90 countries. The organisation’s homepage currently features an example of its social marketing in the form of an article headed, “5 People Share Why Their Abortion Was Beautiful”.
This seems to be the real value of Phil Harvey to MSI and the whole international birth control industrial complex. As an entrepreneur he will use some of his own profits from porn to boost the supply of something like manual vacuum aspiration kits where, say, the British foreign aid agency or the Bill and Melinda Gates Foundation or the UN Population Fund might hold back until the product is more acceptable to recipient governments.
Perhaps in somewhere like Kenya, where, although Marie Stopes says it only does abortions where they are legal, it more or less openly flouts the country’s highly restrictive law, and cloaks its activity with the saintly garb of “after abortion care” – that is, cleaning up after illegal abortions, which MSI dramatises (and inflates?) in order to push its abortion rights barrow.
On its home turf in Britain, MSI has had to clean up its own operations after unannounced official inspections. A highly critical Care Quality Commission report found major safety flaws at MSI clinics, with more than 2,600 serious incidents reported in 2015. A follow-up report in 2017 found there were 373 botched abortions in just the first two months of that year. MSI had issues with infection control and staff at one clinic complained of a “cattle market” approach with incentives for putting through as many abortions as possible.
No doubt there was some kind of idealism driving the founders of MSI and PSI/DKT, as there may be among those working for the organisations today – an actual belief that preventing births is a real favour to women and to the world in general. After all, the rich and respected of the world, the Fords, the Hewletts, the Gates and others have thought and continue to think so.
But the pornography connection that has helped so many of their projects along shows the true character of the birth control enterprise. Harvey told Mother Jones in 2002 that in the early days he was “terrified that, because of Adam & Eve, we were going to lose support for some of our programs.” Then he added: “But it never happened. I think part of the reason was that the key people in charge of family planning overseas, even in conservative governments, are not the types who are likely to be upset by sex products. After all, they’re in the sex business themselves.”
Yes, sex boils down to business for the so-called family planning establishment. A business requiring certain products to make it “safe” if not enjoyable for all concerned. And porn is one of those products, nearly as important as the condom itself, and often more effective since it removes the need for any human contact whatsoever. In that way, however, the pornographers could drive MSI and company out of business, ending a beautiful friendship, as beautiful as abortion.
When you think about cycling and menstruation, you don’t typically think about your bone health. But important research has emerged in the last few decades linking the natural cycle of women’s reproductive hormones to their bone health and development. That’s right, yet another thing your cycles are good for, is protecting your current and future bone health–which is especially important for women. Just another reason why, yes, you do “need” a period!
How bones work
We often think of our skeleton as a fixed structure, just there to hold our bodies upright. But the truth is that our bones are anything but static; they have a life cycle that involves building up, tearing down, and rebuilding tissue constantly. Kind of like construction at the LaGuardia airport.
Kimberly Reda-Wilson is a four-year apprentice in the program Bones For Life, which offers classes that “explore movement intelligence of bone strength and weight-bearing posture,” as a preventative measure against osteoporosis. Reda-Wilson explains, “Bones are living tissue. They have blood vessels and are made of living cells, which help them to grow and repair themselves. They are just as alive as your heart or brain or lungs.”
There are two main types of cells that comprise bone tissue: Bone forming cells and bone resorbing cells. The types of cells that form bone are called osteoblasts and osteocytes. The type of cells that resorb bone are called osteoclasts. Bone also contains nonmineral matrices of collagen and noncollagenous proteins called osteoids, as well as mineral salts. The higher your bone mineral content, the denser your bones are—which, as you might guess, is a good thing. The denser your bones, the less likely you are to experience fractures. Low bone density can lead to osteoporosis, a condition where bones become dangerously porous and fragile, increasing their risk of fracturing.
Hormones, cycles, and their roles in bone health & development
It is well established that estrogen plays a role in bone formation. The major physiological effects of estrogen are to inhibit bone resorption and to promote bone growth. For years, researchers have surmised that post-menopausal bone loss is attributed to the lack of estrogen that occurs after menopause. But estrogen isn’t the only thing post-menopausal women lack. After cycles cease, progesterone is low as well. Mounting research indicates that bones need progesterone just as much estrogen.
In this 2010 research paper co-written by two of the leading researchers on reproductive hormones and bone health, Dr. Jerilynn Prior and Dr. Vanadin Seifert-Klauss, it was confirmed that “In vitro studies of human osteoblasts in culture, prospective studies in adolescent, premenopausal, perimenopausal, and post-menopausal women all indicate that progesterone—likely working through bone formation pathways—plays an active role in maintaining women’s bone and in osteoporosis prevention.”
Dr. Jerilynn Prior is the director of the Centre for Menstrual Cycle and Ovulation Research (CeMCOR) and her life’s work has been researching and educating about progesterone’s relationship to bone health.
“You need ovulation, as well as normal cycles, for healthy bones,” Dr. Prior told me in a virtual meeting. “Women spend the first 25 years of their lives building bone mass. If they are ovulating normally, they should be able to keep that bone mass throughout their reproductive life and beyond.”
That means post-menopausal bone health is decided by hormone processes that occurred decades earlier. “The story that everyone hears is that it’s estrogen deficiency that causes post-menopausal bone loss. But in reality, it’s the long time of pre-menopausal bone loss that’s silent if you’re not cycling regularly over the course of your reproductive years,” Dr. Prior explains.
In other words, if you’re not ovulating during your prime reproductive years, your bone density will be negatively impacted, and those effects will manifest in your post-menopausal years.
So, how we can support bone health for post-menopausal women? Dr. Prior says plainly, “You need to put bone mass in your bank in those [prior] critical years—and the only way to do that is by ovulating [regularly and functionally].”
Progesterone: the “heal and repair” hormone
Considering what we know about the effects of estrogen and progesterone in the body, Dr. Prior’s message makes intuitive sense.
We know that estrogen and progesterone have complementary effects on our reproductive and general health. Estrogen proliferates the endometrium and breast tissue, elevates blood sugar, dilates blood vessels, stimulates brain cells, and gives women a general boost of energy and feeling of well-being. Progesterone, estrogen’s alter ego, maintains endometrium tissue, relaxes blood vessels, normalizes blood sugar, maintains and heals brain cells, and promotes mood stabilization. We need both. Can you imagine being stimulated all of the time without the heal-and-repair mode?
So it should come as no surprise that the same is true of our bones. In this paper by Dr. Prior, she explains that, “when menstrual cycles are normal length and normally ovulatory, estrogen and progesterone are balanced and bone mineral density is stable. However, clinically normal cycles commonly have ovulatory disturbances (anovulation, short luteal phases) and low progesterone levels; these are more frequent in teen and perimenopausal women and increased by everyday stressors: energy insufficiency, emotional/social/economic threats and illness.”
Dr. Prior claims that the main contributor to ovulatory disturbances these days is … drum-roll … stress. “Women are expected to perform in the workplace the same as men. Yet, they’re also doing all the traditional things at home with little to no help. Women have an incredible burden today.” It’s true, women are under great demands emotionally, socially, culturally, financially, and physically in a fast-paced world. You could argue that women don’t get a “heal and repair” mode both hormonally and literally in their daily lives.
Synthetic hormones are not created equal
“Great,” you may be thinking. “I’m on hormonal contraception, and doesn’t that contain a form of progesterone? That should be good for my bones.” Unfortunately, you’d be wrong.
Hormonal contraception contains an artificial form of progesterone known as progestin. There are six different compounds of progestins used in hormonal contraception. But Dr. Prior warns that progestins do not have the same positive effect on our bone health (nor on our general health, either) as natural or bio-identical progesterone does. “Progestins do not have a class effect except for two things that are signified in their name,” Dr. Prior says. The first effect is “to preserve an existing pregnancy, and the other is to transform the proliferative effect of estrogen on the endometrium to a secretory one. Those are the only two things all progestins do.”
So, progestin in birth control may send a negative feedback signal to the part of the brain that wants to start a new cycle (the same thing that preserves an existing pregnancy), but it does not do anything to preserve your bones. In fact, it could actually be robbing them of a crucial opportunity to build bone mineral density.
Does hormonal contraception use negatively affect bone health?
Remember the ovulatory disturbances Dr. Prior talked about? As it happens, another huge correlation to ovulatory dysfunction is hormonal contraceptive use. One third of women who go on the Pill do so for solely gynecologic reasons, such as irregular or painful periods. These are usually glaring symptoms of an ovulatory dysfunction, which then goes untreated as a woman is prescribed birth control that masks the underlying dysfunction without actually doing anything to resolve it.
When I asked Dr. Prior if hormonal contraceptive use affects bone health, she gave a resounding “Yes!” After all, hormonal contraception creates an “ovulatory dysfunction” itself, in that it prevents pregnancy by preventing ovulation. Ovulation is the only thing that can produce progesterone, so if there is no ovulation, then—you guessed it—there is no progesterone. And we’ve already talked about how vital progesterone—the real stuff, not synthetic progestin—is for bone health and development!
It’s especially problematic for their future bone health when teenagers and young women start birth control. Since the teenage years are so critical for building bone, it is that much more important for adolescent girls to have normal menstrual maturation undisturbed by artificial hormones. “Birth control use in adolescent girls has been shown to be significantly negative for spinal bone gain,” says Dr. Prior. “That’s something everyone needs to know.” The detrimental effects of progestin on bone health for adolescent girls was confirmed in a 2001 study that focused on Depo-Provera use. The Depo shot, which comprises one high dose shot of medroxyprogesterone acetate (a progestin) every 3 months, also happens to be the highest progestin dose of all hormonal contraceptives. And, as shown by the study, it also happens to significantly decrease bone mass density (BMD). This is just one more reason why women, and teenagers especially, need a (regular, post-ovulatory) period.
Cycles and stress-management: Keys to good bone health & preventing osteoporosis
So what does this mean for women hoping to maximize their bone health and maybe even evade osteoporosis?
Dr. Prior makes the point that perimenopause and menopause—and the bone density loss they come with—are very normal parts of life. If a woman has had the opportunity to cycle normally through puberty and onward, she should be well-equipped to withstand the natural loss of bone density that occurs in those years. And Dr. Prior makes it clear that while estrogen is important, progesterone deserves its 15 minutes of fame, too. “Although the dominant osteoporosis paradigm for women is, and should remain, centered on estrogen, progesterone is emerging as an important partner hormone that collaborates with estrogen,” she says.
Kimberly Reda-Wilson’s work with Bones for Life focuses on women in the post-menopausal years, and the things women can do to combat osteoporosis as they age. “While there are common denominators (diet, exercise, and stress management) among bone loss prevention programs, each one seems to emphasize a different component,” Reda-Wilson explains. “Originally the Women to Women’s program (now Women’s Health Network) emphasized an alkaline-based diet, exercise, supplements, and stress management. The Save Our Bones program also emphasizes an alkaline-based diet, exercise, supplements and stress management,” she says.
There it is again . . . the word stress! Both Reda-Wilson and Dr. Prior agree that stress management is a huge component in osteoporosis prevention. Of course, not all stressors are within each individual woman’s control—in fact, many stressors could be systemic, cultural, and political. But healthy stress management is certainly something healthcare providers should prioritize discussing with their patients. If women can bring down the stressors in their life, cycle naturally, and minimize ovulatory dysfunctions, it is quite reasonable to expect their bone health to benefit.
So there you have it. Having a period improves your immune system (as we discussed last week, here), and it also improves your bone health. These are two pretty darn good reasons women need their cycles–that is, they need to ovulate and have periods–for optimal health, and why Fertility Awareness-Based Methods (FABM), which allow women to cycle naturally while planning their families with high effectiveness rates, are far superior to contraception when it comes to safeguarding women’s health while preventing pregnancy.
Stay tuned for more in our “Reasons Women Need Periods” series in the coming weeks.
When she was a teenager, Angela Retchless was told she should never become pregnant. But thanks to an incredible gift from her dad, she was able to have the family she had always dreamed of.
Diagnosed with kidney disease at the age of nine, a doctor gave her devastating news as a teenager: it would be too dangerous for her to ever have a child. “I was only 16, but I’d always imagined that one day I’d be a mother,” she wrote for That’s Life!, an Australian magazine. “Glancing over at my mum, Julie, I could tell she was heartbroken for me too.” With her diagnosis, Retchless was told that her kidney function would continue to worsen until she would need to go on dialysis, and eventually, need a transplant. Her father, Leon, promised that he would give her one of his.
At 23, Retchless said she met her future husband Luke and had to break the news to him that she couldn’t have children; though she said he took it well, she knew deep down he wanted a family as she did. And after getting married, she had to deal with the pain of constant questions from people wanting to know when they would have kids. At first, Retchless thought her only option was IVF.
“[I]t was distressing to be asked when I knew the odds were stacked against us,” she said. “About a year after we were married, my doctors gave us the green light to try IVF. Then, my kidney function dropped to 40 per cent. Cross that off the list, I thought, devastated.” A friend offered to be a surrogate for her, but her kidney function was so dangerously low, that even egg retrieval was too dangerous. Meanwhile, she began to feel worse and worse.
“My head throbbed constantly and I woke up exhausted. To make sure I had enough energy to go to work on a Monday, I’d have to spend all Sunday resting,” she wrote. “‘If you don’t get a transplant, you’ll be on dialysis by the end of the year,’ my specialist said.”
But then, her dad stuck to his promise to give her a kidney — and even better, he was a perfect match.
“The 12-month recovery was tough. But almost instantly, with Dad’s kidney inside me, I felt better,” she said. “Before, I didn’t have the energy to go to the gym at all – now I was working out four times a week! And Luke and I were able to go on lovely weekends away.”
After she began feeling better, she and her husband decided to try IVF. But she needed to take a pregnancy test before they could get started. “What?! I thought, shocked, as two pink lines appeared,” she wrote. “That can’t be right, I decided, going outside to hang up some washing. Walking back inside, I half expected the lines to have disappeared. But they hadn’t.”
When she broke the news to her husband, it was an understandably emotional moment. “I was bawling,” she recalled. “‘Are you okay?’ he asked, worried. ‘I’ve got a baby in my belly!’ I sobbed even harder. Doing two more tests, together, both came up positive too! After eight years of trying, we’d fallen pregnant naturally.”
But that wasn’t the only surprise for the happy couple. At 13 weeks, she had an ultrasound and found out even more exciting news.
“As the sonographer slid the wand over my belly, I could see two little moon-like shapes on the screen,” she said. “‘There’s two, isn’t there?’ I asked. ‘Yes, you’re having twins,’ she said.” Doctors made sure to monitor her carefully, and Retchless said she had a “dream pregnancy.”
At 31 weeks, she successfully gave birth to her twin boys, Wyatt and Morgan. Each weighing less than four pounds, they were premature but still healthy. “[T]hey were tiny but perfect,” Retchless said. The twins are now three years old, and “best of mates.” And she said she will always be thankful for the gift her dad gave her.
“Each year on our transplant anniversary, Dad and I have a special outing for coffee and cake to celebrate,” she said. “I’ll never stop thanking Dad for the gift he gave me. Without his kidney, my body wouldn’t have been able to sustain a pregnancy. He gave Luke and me our beautiful twins!”
Your doctor rattled off those words like he was calling roll in a classroom. But each one made you cringe a little more than the last. You could feel your eyes widening as the list grew. Side effects—for a drug you don’t even need, for a drug not designed to alleviate a sickness. You look at him dubiously, as if maybe he’s joking. These can’t all be side effects from one drug, you think. But the look on his face tells you that he is not joking. In fact, he is very serious. And luckily for you, he cares enough about you to tell you what could happen if he prescribes the drug you’re asking for. You start to think to yourself: I don’t want to do that to my body. I value my health too much. I respect my body more than that.
You wonder why you never heard any of this before, and you realize you’re going to have to rethink your desire for hormonal birth control.
The Petition
In June 2019, 10 doctors and researchers who had formed a Contraceptive Study Group published a document entitled Petition on Hormonal Contraceptives. This document evaluated existing literature and synthesized studies on hormonal birth control in order to present information on their side effects in one comprehensive document. The Contraceptive Study Group’s goal was to not only warn potential users, but also to petition the government to add black box—or warning—labels onto the boxes of contraception and to include warnings on patient-related information so that women know and understand the risks of the chemicals they put into their bodies. This article serves as an overview of just some of the major findings and of the information this group desperately wants to put forward for all to know.
The members of the Contraceptive Study Group understand the damage hormonal contraceptives do to women, to the babies they may carry, and to the families who love them. That is why they undertook the daunting task of reading, interpreting, compiling, and then disseminating the information they found. In all, this petition cites 230 outside sources—not counting those related to the environmental impact. This petition was not only a labor of love and compassion for their fellow human beings but also serves as a wake-up call to people who unknowingly—or knowingly—ingest these harmful chemicals.
Millions of women take hormonal birth control or receive contraceptive injections without any idea about the poison they’re putting into their bodies. According to the petition, “Based on data from the Guttmacher Institute, a conservative estimate of 11 million women aged 15-44 in the US take some form of hormonal contraceptive each day. A 2015 study reports that about 21 percent of women of reproductive years are using some form of hormonal contraceptive, which equates to about 13 million women (Daniels 2015).”
In addition, millions of babies die when these contraceptives thin the lining of the uterine wall, thus preventing the baby from implanting.
Hormonal contraceptives have been on the market for over 50 years, yet the scope of the devastation and health ramifications they have caused can never be known. Some women don’t even realize that the causes of the health problems they face may be contraception. If this petition succeeds in its intent, pharmaceutical companies will have to disclose these side effects.
The petition begins by listing the side effects of combined estrogen-progestogen contraceptives (COCs). Many are mentioned in the first paragraph above. COCs include oral, intravaginal, and transdermal formulations. The petition lists the brand names of all of these—in six pages.
According to the team, progestogen-only contraceptives (POCs) “have not been extensively studied, but one large registry study did show a significantly increased risk of breast cancer with use of POCs.”
Furthermore, the International Agency for Research on Cancer (IARC) classifies COCs as Group I carcinogens, meaning they can cause cancer in humans.
Recommendations
The petition recommends that the government “remove from the market the injectable contraceptive Depot Medroxyprogesterone Acetate (DMPA; Depo-Provera) based on conclusive evidence that it facilitates the transmission of HIV from men to women.” It then recommends that black box warnings should be added for the following diseases and conditions: breast cancer, cervical cancer, inflammatory bowel disease, systemic lupus erythematosus, depression and suicide, venous thrombosis, and cardiovascular events. In addition, safety information should be added to advertisements and patient-related materials about multiple sclerosis, bone fractures, body mass effects, and urogenital problems.
Countless women suffer the side effects of hormonal contraception. Countless women feel duped by healthcare providers, by pharmaceutical companies, and by organizations that tout the benefits of COCs. Rarely do they hear of these side effects—side effects that can appear after long-term use, after a few months, or even after just a few short weeks.
In conjunction with the petition, the public is asked to post comments or stories to this site in order to encourage the government to add warnings to contraceptive labels. Many of these comments reference tragic and heartbreaking stories of loss—loss of life, loss of health, and loss of autonomy.
You might wonder why many physicians don’t warn their patients about these side effects. Dr. Ken Stone offers some insight:
It is common practice that physicians do not discuss any significant adverse effects of oral contraceptives or require an informed consent. Some colleagues have said to me that they do not want to say anything that would deter them from using the pill. Standard adverse effects in formularies for prescribed contraceptive medicines usually do not mention the most severe ones like pulmonary embolus, stroke, breast cancer, liver disease, etc.
This petition for removing certain contraceptives from the market, listing those adverse effects that should have black box warnings in prescribed contraceptives, and those that need additional safety warnings in prescribed contraceptives provide[s] more than adequate research data to require the actions requested. As a family practice physician for the past 41 years, I believe the scandal of not informing women of the known side effects of contraceptives is an egregious injustice and needs immediate correction.
The members of the Contraceptive Study Group believe that the public should know the truth. Throughout the next several pages, we will discuss some of the findings and data they presented regarding many of the major side effects of hormonal contraception. To read the petition in its entirety, and to see the comprehensive list of side effects, visit the petition’s site.
HIV Transmission
Depo-Provera, or DMPA, is an injectable contraceptive that is administered quarterly. However, according to the study group: “Evidence began emerging in the 1990s, which has become compelling in recent years, that DMPA is unique among contraceptives in its property of facilitating the transmission of HIV.”
How is this so?
According to research, DMPA has an immunosuppressant quality. It binds to the glucocorticoid receptor of human leukocytes, which, in layman’s terms, means that it represses the woman’s innate immune responses and allows for an increase in HIV replication. Thus, when an infected man has intercourse with a woman taking DMPA, her compromised immune system cannot fight off the disease.
Because of this, the authors want DMPA taken off the market.
Breast Cancer
According to the petition, there are 1.7 million cases of breast cancer diagnosed every year. It is the most common form of cancer among women in developed countries and accounts for 20% of cancers in females.
The International Agency for Research on Cancer classifies COCs as Group 1 carcinogens. That means they can cause cancer in human beings. Studies have long shown the link between breast cancer and COCs. The New England Journal of Medicine published an article in 2006 that found that COCs increase the risk of breast cancer. That same year, the Mayo Clinic Proceedings (a medical journal sponsored by the Mayo Clinic) published a meta-analysis that confirmed the findings that COCs increase the risk of premenopausal breast cancer.
According to the Contraceptive Study Group, “Studies that looked at recent use (within 1–5 years) or current use of COCs in premenopausal women showed the most dramatic increased risk for breast cancer.” The most significant study found that women between the ages of 20-49 who had used COCs “within a year had an increased risk of breast cancer.”
Other studies corroborate these findings as well. Most found that women who used COCs for a year or more had a higher risk of breast cancer. A Danish study found that a woman’s risks increased even after she discontinued use if she had used COCs for five or more years.
The comments site offers many stories from women who have suffered from breast cancer and from the doctors who have treated them. Included among them are these:
As a general surgeon, me and my partners ask our breast cancer patients about OCP [oral contraceptive pills] use since our best cancer textbooks describe an increased risk of breast cancer with OCP use. It is ethically imperative that women are made aware of the risks of ingesting hormones into their bodies.
At age 31, I found a small breast lump. I went to more than one doctor, but the last one I saw was the head of the UCSD Cancer Institute, a Dr. Barone, in San Diego, where I lived at the time. He told me that it was small, movable and I didn’t have any pain but that I should GET OFF THE PILL. 19 years later that very same lump grew and became malignant, and I ended up having a mastectomy.
An anonymous writer says: “Recently diagnosed with breast cancer; I was on the pill for 10 years.”
The authors recommend that a black box warning be included with COCs, along with warnings on patient-related materials, so that women understand the risks they face.
Cervical Cancer
According to the petition, approximately 260,000 women in the United States have cervical cancer. The American Cancer Society claims that there will be about 14,000 new cases this year alone. Research has shown that there is an increased risk of cervical cancer associated with COCs and that the risk increases for women currently taking hormonal birth control. In addition, the risk increases with the length of time the woman has taken the COCs.
The risk also increases if the woman has tested positive for HPV—the human papilloma virus.
The authors recommend both a black box warning and a warning on patient-related materials.
Depression, Mood Disorders, Suicide
According to the study group, “The largest study of incident depression and use of anti-depressant medication (Skovlund 2016) indicates significantly increased risks for both COCs and POCs for both outcomes. The same group studied for suicide attempts and suicides (Skovlund 2018). Elevated risks were seen, and this was the case for both COCs and POCs. The recent NCHA study (Gregory 2018) showed a similar trend.”
The authors claim that their research has shown an “increased risk for depression, suicide risk, and suicide within 3 months of beginning to use the drugs and tapering off after 6 months, partly due to attenuation of symptoms, partly due to discontinuation due to adverse effects.”
The comments section of the website paints a dismal picture and offers evidence that these hormones cause new mental health problems and exacerbate existing or latent ones.
Julie Baltz, a family practice clinician who has practiced medicine for over 20 years, states that she has seen the psychological harm caused by hormonal contraceptives. She wrote:
Even more subtle and more underreported are the psychological effects. These patients simply state “I didn’t feel right” and often think that there something wrong with them that they don’t tolerate this type of medication. I’ve seen insomnia, anxiety, depression, anhedonia, anorexia, and poor libido directly improved within my clinical office by discontinuing a combined OCP.
In 2011 I was prescribed hormonal birth control to “fix” a very irregular cycle. Three months later I started to struggle with crippling fatigue, loss of appetite and disinterest in everything except sleeping. I was shortly after that diagnosed with Major Depressive Disorder, and still to this day have to be on medication to remain functional. I still struggle with my energy levels, unfortunately medication can’t cure depression and make it disappear. My doctor and I both believe that the hormonal birth control was likely a trigger to a predisposition for Major Depressive Disorder.
In my early twenties I was prescribed birth control pills. The first cycle I took the pills as prescribed. I began to feel depressed, anxious, crying daily, with mood swings. Prior to beginning the oral contraceptive pills, I had none of these symptoms. After completing the first 2 weeks of the medication packet, I called the nurse practitioner at the OB/GYN clinic that I originally got the prescription. She told me that the changes in my mood, depression, and anxiety among others, could not be due to the new medication, that it must have just been life. She changed me to a lower dose contraceptive pill. After three weeks of taking the second prescription pack as directed I decided to discontinue use of oral contraceptives due to the side effects. I had gained 15 pounds and felt terrible.
The site is filled with story after story of people who have suffered—mentally and physically—because of these drugs. The authors want a black box warning about this side effect and warnings on patient-related materials.
Body Mass
While studies have varied regarding weight increase in women who use COCs, the strongest data found that levonorgestrel-releasing IUDs do, in fact, affect body mass. The authors stated that “a significant increase in % fat mass with a corresponding decrease in % lean body mass was observed in both studies where these were measured.”
Women have found this side effect all too real. For example, a woman who wishes to be anonymous said:
When I was taking hormonal birth control (HBC) I underwent a massive weight gain. From 120 lbs. to 155 lbs. That’s almost adding 30% to my body weight! I also suffered with severe stomach cramping, constant discomfort, constipation and diarrhea. My doctor diagnosed it at IBS. I was only on HBC for 8 months and got pregnant while taking it. I stopped taking it upon pregnancy and have never touched the stuff again!
The authors believe that all patient-related materials and advertising (print, radio, etc.) should convey information about this risk to the consumer.
Urogenital (Urinary and Genital) Effects
The authors found evidence of several different kinds of urogenital problems in women. These include interstitial cystitis (a condition that causes bladder pain and pressure), bacterial infections, urinary tract infections, vulvovaginal candidiasis, vaginal dryness, female sexual dysfunction, and more. They state that the risk increases for adolescents and if the woman uses COCs for at least two years.
A woman who wishes to remain anonymous experienced a whole host of problems, including urogenital. She said:
I was put on birth control by my parents when I was only 15 years old after a sexual assault incident. I then continued it for another 5 years before I began to question it. In that time frame I experienced extreme weight gain and loss from one pill to another, was diagnosed with bipolar disorder because of my manic depression and severe mood swings (I am not bipolar), experienced a miscarriage, developed cysts in my breasts, had continuous pregnancy symptoms (including morning sickness every day), and had frequent UTIs and yeast infections. No one ever associated any of my problems, other than the breast cysts, to my birth control pills. It wasn’t until I discontinued the use once learning of the cysts that I began to feel normal and realized the association between my symptoms and the pill.
The authors believe that all patient-related materials and advertising (print, radio, etc.) should convey information about this risk to the consumer.
Venous Thromboembolism, Atherosclerosis, and Cardiovascular Events
Venous Thromboembolism
A venous thromboembolism (or VTE) is a condition in which a blood clot forms in a vein, most often in the leg, arm, or groin, and then lodges itself in the lung. This is an extremely dangerous health problem that can cause death. Even the American Heart Association website agrees that COCs can cause a VTE: “In women, pregnancy and the use of hormones like oral contraceptives or estrogen for menopause symptoms can also play a role.”
The comments regarding this side effect address the tragedies that have befallen women and families as a result of hormonal birth control. For example, Carol Pepin wrote about the loss of her daughter:
My 19-year-old daughter Shelby Pepin . . . died. Shelby was very athletic, did not smoke, and had no history of a blood disorder. The coroner’s report confirmed that Shelby had died from a pulmonary embolism. She had a DVT [deep vein thrombosis] behind her left knee that traveled to her lungs causing her bilateral embolism. The coroner also confirmed that her DVT was caused by her birth control the NuvaRing. Shelby had been on the NuvaRing for 18 months.
Our daughter died at age 29 in the Intensive Care Unit of her local hospital where she had been transferred after presenting herself at her local walk-in clinic. Her death was five weeks to the day after getting married and one day before [her] scheduled departure on a delayed honeymoon cruise. The autopsy report stated that she had “bilateral pulmonary thromboemboli” with a thrombus present in the left popliteal fossa. She had been using NuvaRing at the time of her death [which] had been removed at the walk-in clinic prior to transport to the hospital. . . . The [ICU] doctor stated that she believes that hormonal birth control was a significant contributor to the death of our daughter.
Kimberly Phipps-Nichol shared her personal story of survival:
Last year, at the age of 46, I was hospitalized with a cerebral thrombosis that was literally caught right before causing a stroke. The ER docs told me that if it had not been for the fact that the people I was with at the time of the event were trained to recognize the signs of stroke and called 911 for a stroke paramedic unit that arrived quickly, I would have been somewhere between a vegetative state and severely disabled. After countless CT scans and MRIs, along with a thorough study of my family history, the neurologist and hematologist teams determined it was the oral contraceptives that I was taking that had caused the thrombosis.
Diagram of thrombosis
An anonymous family physician claims to have seen the negative side effects of contraceptives firsthand and tells of several cases, including her treatment of a young woman in her late 20s who went into a coma brought on by a pulmonary embolism. The only known risk factor was that this woman was taking hormonal birth control. In addition, a medical colleague of this doctor suffered a pulmonary embolism that was attributed to OCP.
Nancy Brockoff wrote to say that she had four friends, who were all young mothers, who died of blood clots related to hormonal birth control.
Atherosclerosis and Heart Disease
Atherosclerosis is a disease of the arteries caused by plaque. Arteries clogged with plaque lead to heart problems. Even as long ago as 1982, researchers understood and took interest in the fact that vascular disease and COCs were linked. According to the petition, these researchers “found that combination oral contraceptives (COCs) caused ‘greater cell proliferation and incorporation . . . in both human arterial smooth muscle cells and dermal fibroblasts.’ Smooth muscle cell proliferation is an integral feature of all atherosclerotic lesions (Bagdade 1982). In 2007, a presentation at the American Heart Association meeting described a study of 1,301 Belgian women, which showed that women had a 20 to 30 percent increase of plaque for every decade on COCs (Rietzschel 2007).”
Furthermore, the Danish Heart Association “released the results of a 15-year historic cohort study looking at thrombotic stroke and myocardial infarction, which observed over 1.6 million women. The results demonstrated that women taking COCs with ethinyl estradiol at a dose of 20 [micrograms] had a risk of arterial thrombosis that was 0.9 to 1.7 times higher than non-users, while those taking a dose of 30 to 40 [micrograms] had a 1.3 to 2.3 higher risk” (Lidegaard 2012).
The current black box warning about thrombotic events mentions smoking and age, which the authors believe misleads the consumer into thinking she’s safe if she doesn’t smoke or if she’s younger than 35. They want the warning amended to read: “Warning: Increased risk of serious cardiovascular events including blood clots.” Additionally, they request warnings on all advertising and patient-related materials.
Environment
The synthetic hormones that women take are continually released from their bodies through their waste products. When researchers noticed changes in the aquatic environment—especially in fish—they began conducting studies to determine the cause of these changes. What they found astounded them.
The Contraceptive Study Group explained:
EE2 [the synthetic estrogen ethinylestradiol] is metabolized in the liver undergoing first pass metabolism, but ~6% of the administered dose appears as untransformed EE2 in the urine and ~9% in the feces (Stanczyk 2013)….Even at low concentrations, these compounds can act as potent endocrine disruptors, affecting the growth, development, and reproduction of exposed aquatic organisms (Tyler 1998, Larsson 1999).
While wastewater treatment plants have the ability to filter out many chemicals and pollutants, they cannot filter out EE2.
Studies have found that these synthetic chemicals cause changes in male fish. A 1995 paper found that male fish in nearly 30 rivers throughout Britain had become “feminized” by these pollutants.
The Contraceptive Study Group also referenced a seven-year long study of the effects of EE2 on Canadian lakes. In that study, researchers approximated the amount of EE2 that would reach the waterways from a town of 200,000 people. They immediately saw the feminization and transgendering of male fish and a “near extinction” of the population of the fathead minnow there. Once the researchers stopped adding EE2 to the water, the population of minnows returned to normal.
We find further evidence in a study that looked at the fish populations near three Colorado sewage treatment plants. There, researchers found a significant difference between the fish upstream of the plant and those downstream. They stated:
The fish in the upstream locations enjoyed a balanced 1:1 female-to-male sex ratio. Downstream there were five female fish for every one male, and twenty percent of the reduced male population demonstrated intersex characteristics, such as eggs in their testes and the presence of vitellogenin, an egg yolk protein normally found only in fertile females. The consequences also appeared to ascend up the food chain in a measurable way, specifically with the feminization of trout, mink frogs and green frogs (Parke 2009). Both the predicted and the measured concentrations of EE2 in the US, including effluent of waste water treatment plants, surface water, or ground water, exceeds the predicted no-effect concentrations on fish populations (Kostich 2013).
Conclusion
In addition to these diseases and the pollution in the environment, the economic costs from these side effects and their resultant diseases/health problems to the patient and to the community are in the billions.
This article touched upon some of the most egregious side effects. To read the full list of side effects and the studies referenced, to read all of the comments, or to add your own comment, visit regulations.gov/document?D=FDA-2019-P-2289-0001.
This health crisis affects us all. Whether you are male or female, elderly, middle aged, young, a mother, or a father, hormonal birth control does affect your life in some way because these hormones affect your wives, your mothers, your sisters, your cousins, your best friends, the environment, and even your dinner table. It’s time to speak up and tell the government that women must know the truth. It’s time to help women understand that their health is more important than a drug that can alter their body and mind. Synthetic hormones and their deleterious effects leave a lasting impact and crush our society.
In a recent podcast, 40 Days for Life president and CEO Shawn Carney and two other 40 Days for Life directors — Steve Karlen, and Robert Colquhoun — tackled the topic of contraception and how it relates to abortion in society.
Historically, children were viewed as a gift
Steve Karlen, director of North American Outreach for 40 DFL, noted that our current cultural mindset represents a major shift from centuries past, saying, “Throughout all of human history, children have been viewed as a blessing,” adding, “We all know this to be true, and at the same time we have this schizophrenia where we have mass use of contraception that says ‘no, we don’t really want children around here.’”
Karlen further characterized contraception as “contrary to human nature” because he believes human beings “have this innate longing to bring children into the world and to love them and to make the world a better place for them.”
A contraceptive mentality increases abortions
40 DFL CEO Shawn Carney defined a contraceptive mentality as one that divorces the idea of babies from sex, primarily via hormonal birth control that acts against (“contra”) conception.
Because we expect contracepted sex to be sterile and for the purpose of pleasure only, when a child does result, as Karlen pointed out, we tend to view him or her as “an intruder, an invader, an uninvited guest. And that makes abortion so much easier to justify at that point.”
Robert Colquhoun, director of International Campaigns for 40 DFL, said many people believe “if we just use birth control, we can reduce abortions.” In actuality, he said, increased use of contraceptives correlates with increased rates of sexual activity. When the contraceptives fail, as some inevitably do, there’s an increase in unintended pregnancies accompanied by an increase in abortions to “deal” with them. He added, “Planned Parenthood wouldn’t be handing out contraceptives if they knew that they led to a decreased abortion rate.”
Some contraception may cause abortions
As Karlen, Carney, and Colquhoun noted, the science behind contraceptives acting as abortifacients is not complicated. Contraceptives act in several ways to prevent ovulation, but they also thin the lining of the uterus, making implantation of an embryo much more difficult. Once fertilization occurs, a genetically unique human being is created. Preventing implantation, then, would mean that a child dies.
Contraception’s negative impacts on society
Karlen said, “Contraception is not good for our relationship with children in the womb” because it leads to a classification of children as “wanted” or “unwanted” depending on whether their parents intended to get pregnant or not.
As Shawn Carney recalled, decades ago, the Catholic Church was considering whether to change its longstanding prohibition on contraception, and Pope Paul VI released a 1968 document called Humanae Vitae. In that document, he made three predictions about what would happen if contraceptive use became widespread: 1) a rise in divorce, 2) a decreased respect for the wellbeing of women, and 3) governmental coercion of human reproduction (i.e. China’s One Child Policy and the forced sterilization of thousands of U.S. women between the 1920s and 1970s). These predictions have sadly come true.
Life of chastity brings ‘great peace, great hope’
Carney noted that while 40-50% of couples who contracept reportedly divorce, the divorce rate among couples who use fertility awareness-based methods is only 3-5%. Carney believes this is due to a fundamental difference in mindset among those using NFP — one that values the woman as a whole person and doesn’t pathologize her fertility, and which views children as a blessing and a joy rather than a burden.
When Amanda Nichols and her husband Charlie were trying to become pregnant, Natural Family Planning (NFP) led them to the discovery of the causes of their infertility. And when Tara Horesowsky and her husband Bryan were ready to start having children, they were able to use NFP to know on which days they were most likely to conceive. NFP has been belittled by the fertility industry and birth control industry for years, with doctors telling women that it simply doesn’t work — but this couldn’t be further from the truth, and recent studies have shown how incredibly effective it is. NFP isn’t the rhythm method our grandmothers used, but rather a way of understanding one’s own personal fertility and making decisions based on each body’s unique rhythm.
After using their chosen method of NFP, the Horesowskys learned when they had reached peak fertility, and within a couple of months, they were expecting their first child.
“It was the most incredible news and it was so clear to us that NFP helped us prevent pregnancy when it wasn’t the right time, and helped us achieve pregnancy when we felt that calling,” Horesowsky told the Catholic Messenger.
There are a variety of ways to practice NFP, and every couple can choose for themselves which works best for them.
Types of NFP
The Billings Method/Cervical Fluid. By observing changes in cervical (cervix) fluid, a woman can notice when she is infertile and when she is near peak fertility as well as when she reaches peak fertility. Used in combination with basal body temperature reading, understanding cervical fluid can help a couple achieve pregnancy. The Billings Method uses cervical fluid to help women chart their cycles.
The Couple to Couple League/Sympto-Pro Method. Examples of the Sympto-Thermal Method are the Sympto-Pro Fertility Education and the Couple to Couple League methods. Through these, couples can combine the cervical fluid and basal body temperature methods in order to achieve pregnancy. By using a thermometer that measures her basal body temperature, a woman can take her temperature each morning before getting out of bed. Before ovulation, her temperature will be at her lowest and after ovulation, her temperature will rise about half a degree and remain elevated. By observing and charting these changes together, a woman can better track fertility and interpret her unique chart to find her most fertile days. Women who have irregular cycles can do well with this method as it is based on their own unique fertility.
The Marquette Model. With the Marquette Method of NFP, couples can use modern technology to monitor fertility. By using urine fertility biomarkers, along with the observation of cervical mucus or basal body temperature, couples use a fertility monitor that shows them when certain hormones have been detected in the woman’s urine which indicate ovulation is about to occur. It is easy to use and understand and when using the ClearBlue Fertility Monitor, women can look back on their cycles for the last six months to determine their personal fertility patterns or issues with their cycle.
The Creighton or FertilityCare Method. This method not only helps women understand their cycle, but is the basis for NaProTECHNOLOGY, a revolutionary method of achieving pregnancy for couples struggling with infertility. The Creighton Model FertilityCare System (CrMS) is built off of the Billings Method and requires the participation of both spouses. NaProTECHNOLOGY has helped couples who have been struggling with frequent miscarriages, premature births, abnormal bleeding, and ovarian cysts, as well as other fertility problems.
Couples who use NFP aren’t sitting on the sidelines of their fertility. They have taken control and are therefore able to know when is not only the best time to conceive but when to refrain from sex if seriously trying to avoid pregnancy. Over 6 million women in the United States struggle with infertility. In Vitro Fertilization is expensive, highly controversial, and has a success rate only as high as 30 percent per cycle. NaProTECHNOLOGY, however, has up to an 80 percent success rate for couples struggling with infertility through the use of charting along with medical or surgical restorative treatments that address the cause of infertility.
Nichols and her husband were struggling to become pregnant when they reached out to Dr. Monica Minjeur, who is trained in CrMS. Minjeur used NFP to help identify why the couple was having trouble conceiving because Nichols had been charting her cycles. Minjeur noticed that Nichols’ temperatures were lower than normal which was a sign of a thyroid condition. She was able to diagnosis Nichols with Polycystic Ovarian Syndrome as well, which explained infrequent ovulation. In addition, low progesterone was determined to have been the reason that they weren’t able to conceive even when she did ovulate. With changes in her diet and the addition of progesterone supplements, the couple was able to become pregnant and gave birth to a baby girl.
NFP has been disparaged by industries built on making money off of women’s bodies and fertility. But in reality, a woman’s ability to gain understanding and knowledge of her body and her unique cycle is empowering, allowing her to be freed from the constraints and health risks associated with hormonal birth control.
At 27 years old, recovering drug addict Laura Amoretti discovered that against all odds, she was pregnant. She had only been sober for 90 days and her sister pressured her to have an abortion, kicking Amoretti out of her home when she refused.
“I began having problems with drugs and alcohol at 19 after an abusive relationship and serious depression left me broken, lost, with an overwhelming sadness and dislike for myself,” she wrote in an essay for Love What Matters. “As my addiction progressed, I found myself 27 years old with a crippling heroin addiction and I hadn’t gone a day in 8 years without drinking. I was a master at hiding my addiction from family and friends but when I was alone, I was an absolute mess. I cried myself to sleep every night and woke up in full blown withdrawal almost every day. When I wasn’t falling asleep smoking cigarettes I was escorting or partying.”
After finally telling her family the truth, they helped her quit drugs and get through “the most painful and debilitating withdrawal.” Amoretti also found support in a fellow-recovering addict, until one day he was tragically robbed and killed. His death nearly sent her back to drugs, but instead, she found herself at a meeting for recovering addicts. “… I spoke and told everyone what happened and told them I was so distraught I couldn’t think of what to do but to go back to addiction,” she said.
A week later, after her friend’s funeral, Amoretti texted her dealer and set up a time to meet him. “[I]n that exact instant I received a different text that I believe saved my life. A guy from that meeting texted me asking if I was ok, how was I doing. I stopped and made a decision right there not to use drugs that day. It was GOD was showing me there was something else waiting for me if I just stayed sober,” she explained.
The two soon began dating, and two months later – only 90 days sober – Amoretti learned she was pregnant. She was shocked. At 13 years old she had been told it would be nearly impossible for her to become pregnant because of Polycystic Ovarian Syndrome. But there they were — two recovering addicts expecting a baby. Her sister, with whom she was living, insisted that she abort, but Amoretti refused. “I was soon forced to leave her house because she didn’t agree with my decision and in a scramble and with almost nothing to work with, me and him found the tiniest guesthouse to live in. We both found jobs and slowly but surely created a modest life to bring our baby into.”
Abortion isn’t the solution
Unfortunately, this sort of treatment is common toward women dealing with unplanned pregnancies, and it’s even worse for pregnant women battling addiction. Rather than helping women, abortion has been tied to an increased risk of drug and alcohol use. One study found that women who aborted unwanted pregnancies were “270% more likely to report subsequent alcohol abuse or dependence.” And post-abortive women are more likely to become addicted to drugs than women who choose life (15.8 percent vs. 5.3 percent). Based on this, abortion could certainly send a recovering addict into a downward spiral.
As for babies conceived while their mothers are addicted to drugs, they do not deserve death. When we help the mother, we help the child in the womb as well; the focus should be on assisting women in overcoming their addictions. The effects on the child depend on the type of drug abused during pregnancy, and killing a child through abortion is not a morally acceptable response to the fear of a substance’s effect on that child’s body.
While society’s “solution” of aborting a child is often cloaked in a misguided sense of compassion and a desire to avoid suffering, eliminating the sufferer is surely not a proper way to avoid life of potential suffering. After all, “suffering is not evil,” noted the Daily Wire’s Michael Knowles in a recent video. “Actually, suffering is morally neutral…. What is good or evil is how you react to suffering. You can react in a way that is ennobling, dignified, and good. Or you can react in a way that is selfish, wicked, evil, and wrong.” Reacting with killing — abortion — is wrong.
Coercion isn’t the solution
Other individuals, such as Barbara Harris, believe that the best way to help women who are addicted to drugs is to coerce them into sterilization. Harris travels the country in an RV, offering cash to women struggling with addiction in exchange for being permanently sterilized. “Nothing positive comes to a drug addict who gives birth to eight children that are taken away from her. This is a win-win for everybody,” she said. Harris has reportedly paid more than 7,000 women to be sterilized.
While on the surface, this might seem reasonable, it isn’t. Lynn Paltrow, executive director of National Advocates for Pregnant Women, says Harris’ method of assistance isn’t morally acceptable. “[Harris] perpetuates really destructive and cruel myths about pregnant women and their children,” she said. She sees Harris as operating under the false narrative that the children of drug addicts have no hope and that drug addicts themselves have no chance at recovery. This is far from the truth.
For many addicts, becoming pregnant actually saves them from their addiction, as they feel a new sense of responsibility and purpose in life.
Leilani is one woman who discovered she was pregnant while she was homeless, addicted to drugs, and had already been in jail for stealing. She chose life for her baby and for herself with the help of Ventura County Pregnancy Center. She was able to continue her education, find a job, and be the mother she wanted to be, all because she said yes to life and had the support to do so. Another drug addict, Kailee, was dating and living with her dealer when she learned she was pregnant. He and her stepfather both wanted her to abort, but she knew she wanted her baby. Still, they told her she “would be doing [her] baby a favor” with abortion, and that taking her child’s life “would be the best thing for me.” They told her she would be a terrible mother. But a pregnancy center helped her choose life and Kailee was able to go to rehab. Her baby’s father also quit drugs and got a job. The two married and have since had two more children.
As for Amoretti, she and her boyfriend also overcame addiction and welcomed a baby boy. They work hard to stay sober for his sake. Amoretti says that together they are “sober, stronger, and happy as can be.”
“The odds were fully stacked against us,” she said, “but we both stayed sober and in a mountain of grief and chaos we brought light into the world.”
Babies are a light in the world and a miracle in the darkness of addiction.
Author’s Note: If you are pregnant and living with addiction, contact OptionLine for help in your local area.
WASHINGTON, D.C., May 6, 2020 (LifeSiteNews) – Today, the Little Sisters of the Poor, pro-life nuns who care for the elderly, are once again part of a case before the U.S. Supreme Court. Their goal is to stop the government from forcing the Catholic community to participate in the provision of contraceptives and life-ending drugs to their employees.
The Supreme Court began hearing oral arguments at 10:00 a.m. EST. Given the coronavirus restrictions on public gatherings, everything is set to take place remotely by phone.
“The Court will provide a live audio feed of the arguments to FOX News (the network pool chair), the Associated Press, and C-SPAN, and they will in turn provide a simultaneous feed for the oral arguments to livestream on various media platforms,” the Supreme Court announced.
Preceding the oral arguments, there was a “virtual” rally to support the Little Sisters of the Poor. “Leaders from around the country will offer messages of support for the Little Sisters of the Poor as they head (virtually) to the Supreme Court,” the organizers stated.
The rally closed with a rosary prayed by different religious communities.
The Obama administration had first mandated employers to participate in or help facilitate the provision of contraceptives, as well as abortifacient drugs, to their employees. The Little Sisters of the Poor refused to go along with the new policy, as did Hobby Lobby and other religious entities.
If the Little Sisters of the Poor – pro-life Catholic nuns – were forced to provide contraceptive and life-ending drugs and devices, they would explicitly contradict their mission of respecting the dignity of every human life.
On October 6, 2017, the Department of Health and Human Services came out with an updated, broad religious exemption protecting communities like the Little Sisters of the Poor from having to provide goods and services that would violate their conscience.
Thus, the Trump administration admitted that the federal government broke the law by trying to force the Little Sisters and others to provide services like the week-after-pill in their health plans that violated their religious beliefs.
Nevertheless, the state of Pennsylvania went on to sue the federal government, arguing the religious exemption should be removed.
“Pennsylvania admits that it already has and already uses many government programs to provide contraceptives to women who need them,” wrote Becket Law, the religious liberty law firm representing the Little Sisters of the Poor.
“Pennsylvania never challenged the Obama Administration for creating much larger exceptions for secular corporations – exceptions that covered tens of millions more people than the religious exemption,” Becket pointed out. “Pennsylvania does not even have its own contraceptive mandate at all. And Pennsylvania’s lawsuit does not identify a single real person who previously had contraceptive coverage but will lose it because of the new Rule.”
If Pennsylvania Attorney General Josh Shapiro, a Democrat, prevails before the Supreme Court, and the sisters refuse to comply, they would be forced to pay millions of dollars in fines.
Beginning in November 2017, Becket intervened on behalf of the Little Sisters of the Poor in California and Pennsylvania, working its way through the court system.
Countless groups, including the United States Conference of Catholic Bishops and the Knights of Columbus, as well as many legislators, have filed amicus curiae briefs, supporting the Catholic nuns in their fight.
Justice Ruth Bader Ginsburg phoned into oral arguments from Johns Hopkins Hospital in Baltimore, Maryland, where the 87-year-old underwent “non-surgical treatment for acute cholecystitis, a benign gallbladder condition” on May 5, according to the Court.
BALTIMORE, Maryland, May 4, 2020 (Lepanto Institute) — A sixth investigative report on Catholic Relief Services projects, published by the Lepanto Institute, shows that CRS both implemented and promoted comprehensive sexual education curriculums that include pornographic images and the promotion of contraception.
The first curriculum profiled by the Lepanto Institute, called Go Girls!, was linked to directly by a CRS copyrighted document about its DREAMS/4Children project in Lesotho titled, “TWO PLUS TWO EQUALS TEN.” The CRS-produced document says that the Go Girls! curriculum was adapted for use by CRS Lesotho, and a footnote referencing the curriculum provided a link directly to it.
“The Go Girls! curriculum not only pushes contraception and promotes masturbation, but has a pornographic illustration that actually demonstrates the genital use of a condom,” said Michael Hichborn, president of the Lepanto Institute. “Why on Earth would someone at CRS ever think this curriculum would be acceptable on any level? The leadership at CRS needs to ask why a morally acceptable curriculum wasn’t used, because CRS paid for this immoral curriculum and provided it to a vulnerable community.”
The Lepanto Institute’s report also showed that CRS had implemented a curriculum called Aflateen, and maintains a close relationship with Aflateen’s parent company, Aflatoun. Not only does the Aflateen curriculum clearly promotes the use of contraception, but Aflatoun publicly signed a statement announcing its support for the abortion-funding initiative called “She Decides.” But despite this, CRS has been found to be promoting the curriculum to other agencies.
“Curriculums like this have to be paid for when they are implemented, which means that even if CRS claims to have implemented a sanitized version of them, they still paid for them,” said Hichborn. “These curriculums might as well have been created by Planned Parenthood; would CRS purchase curriculums from Planned Parenthood with the intention of using only the morally acceptable portions? If the answer is no, then CRS is guilty by purchasing and distributing these curriculums.”
“For the last two months, we have been issuing heavily documented proof that there are serious problems with Catholic Relief Services projects, and despite an initial promise to investigate and respond, CRS has yet to address a single concern,” Hichborn added. “It is for this reason that we continue to call upon the bishops of the United States to conduct an independent, third-party investigation of CRS, and to withhold their support for the agency until such an investigation is convened.”
A woman living with a disability in the United Kingdom will be forced to receive a long-term contraceptive implant against her will, thanks to a court ruling from a judge.
According to Metro, the woman, who was not named, is in her late twenties and has had children before, all of whom were taken away from her and placed into child protective services. She is currently pregnant and did not want to receive an implanted birth control device.
The woman arrived to testify on her own behalf for the Court of Protection and explained that she was willing to use birth control — specifically, the birth control shot, which lasts for three months at a time. “It’s my body and it’s my life,” she said. “I should have the choice on what I want.” Yet Justice Gwynneth Knowles disagreed, and ruled that when the woman undergoes a c-section, the implant should be put in anyway. Knowles said that she lacks the mental capacity to make the decision for herself.
In addition to ignoring the woman’s willingness to use birth control, Knowles’ justification for her decision highlights an inherent problem in her logic. If the woman in question is not capable of making the decision for herself on what kind of birth control to use, then she does not have the ability to consent to sex, meaning that every sexual encounter she has had has been rape. Yet it doesn’t seem that there is much concern for finding the men assaulting her — as long as she isn’t getting pregnant, it doesn’t seem to matter. On top of that, the issue also seems to be that she’s having children, raising the question of how Knowles would have responded if the woman was having multiple abortions, rather than giving birth to living children. Would she be considered capable if that were the case? There are also alternatives to forcing her to be on a method of birth control she does not want, like providing her with liaisons or aides to ensure her safety.
People with disabilities are routinely mistreated in the United Kingdom. It’s far from the first time that someone with a disability has been forced onto birth control there, and around the world, forced sterilization, abortions, and birth control for people with disabilities are common, both throughout recent history and in the present day. Even a Paralympian felt compelled to speak out after she was pressured to have an abortion because of her disability. The country’s Equality and Human Rights Commission has found “deeply concerning” evidence that people with disabilities there routinely face abuse, mistreatment, bullying, and exclusion. And yet, when these people come forward to report the abuse they face, authorities don’t believe them. Doctors in the United Kingdom have also been known to issue DNRs for people with intellectual disabilities — without their or their families’ knowledge or consent. Other families report receiving substandard health care for their loved ones with a disability.
This kind of decision should be troubling for all people because ultimately, it sets a disturbing precedent: that at any time, a judge can decide that someone isn’t capable of making decisions for themselves, and thereby be forced into birth control, abortion, or sterilization. Yet what makes this worst of all is that because cases like these involve people with disabilities, next to no one will step forward and say that this is wrong.
The World Health Organization (WHO) proved itself to be an advocate for abortion and sexual liberation after it declared abortion to be an essential service during the coronavirus (COVID-19) pandemic. Health officials with the organization said the possibility of a woman being infected with the virus should not impede her ability to access abortion, and if she lives in a state with restricted access to abortion, the woman should seek an at-home, do-it-yourself abortion. This is not only dangerous, but it exposes the radical agenda behind a group that is supposed to prioritize the health and well-being of individuals.
WHO has partnered with the International Planned Parenthood Federation (IPPF) in the past to promote abortion and various sexual practices. This collaboration has included promoting the idea that programs geared towards encouraging sexual abstinence are harmful to “young people’s sexual and reproductive health and rights.” WHO and IPPF’s programs encourage impressionable youth from 9-12 years of age to masturbate in private, discourage teenagers from 15-18 years of age from holding their parents’ views on sex, and teach kids from ages 12-15 how to derive pleasure from sexual acts without risking pregnancy.
But these combined efforts to enforce comprehensive sex education also include educating adolescent girls about ‘abortion rights’, as well as information about using emergency contraception. While advocates for Plan B, Ella, and the Morning After Pill insist these pills merely prevent pregnancy without acting as abortifacients, this is misleading. In an effort to capitalize on the normalization of hormonal birth control, the American College of Obstetricians and Gynecologists (ACOG) altered the definition of conception.
Instead of life being recognized as beginning at fertilization, in 1965, the ACOG contended that it began at implantation, which enabled the marketers of emergency contraception to claim that it did not cause abortions. But in altering the lining of a woman’s uterus, emergency contraceptives like Ella or Plan B can create a hostile environment for a developing embryo, preventing as a secondary action the implantation of the new life that has already begun. While the Morning After Pill may not always induce an abortion, it can function in this way if ovulation is not prevented.
Another reason to be concerned about WHO’s agenda is that hormonal birth control and emergency contraception can dramatically alter women’s bodies. It’s especially concerning when hormonal contraceptives like this are promoted to young girls, as they can not only change their reproductive systems in unhealthy ways, but in the case of emergency contraception, a woman may find herself at an increased risk for an ectopic pregnancy.
Recently, President Donald Trump’s administration announced that funds originally directed towards WHO would instead be directed to the Red Cross and Samaritan’s Purse in order to combat COVID-19. This comes at a time when, based on WHO recommendations, the United Nations has attempted to push a $2 billion spending plan for the virus that includes funding for abortions.
The documentary “Pro-Life Feminist,” originally released in 2018, was recently made viewable for free online via YouTube.
Aimee Murphy, founder of Rehumanize International, a nonprofit best known for its “consistent life ethic” approach, opens the film commenting on an unfortunate contradiction in the modern-day feminist movement. “There are some who say that equality for the preborn is contrary to the liberation of women. You know, that perspective is really pitting women against their children.” She also notes in the film, “Feminism is about human equality. You can’t just leave some humans out.”
Viewers also meet Christina Marie Bennett, a writer for Live Action News who worked for years at a Connecticut pregnancy center and now works for Family Institute of Connecticut. She too understands the abortion issue as part of a larger framework – the struggle for human rights for all humans. “I’m not ok with injustice in any way, shape, or form…and so I came to this realization that I am a feminist. And it’s okay. It’s okay, because I am going to redefine [feminism]. To think that, because we value the littlest women of all, just as much as any other woman at any other stage in her life, means that we are against womanhood, or that we are disconnected to the reality of the pains and struggle and trauma associated with being a woman…are not we women? Do we not hurt and ache in the same way?”
Destiny Herndon-De La Rosa is also featured in Pro-Life Feminist. She founded New Wave Feminists because of her son, whom she had at 16. The organization received significant media attention due to its inclusion in and then subsequent exclusion from the Women’s March on Washington in 2017 because of its pro-life position. From her perspective, “The pro-life side, a lot of times, they see one person, they see the unborn child. And the feminist person, they see one person. The woman. But pro-life feminists see two people. We want to protect two people.”
Aimee, Christina, and Destiny’s pro-life feminist stories make clear that the old stereotype of pro-lifers as a bunch of old white men imposing their religious beliefs on women’s uteruses is just as much a relic of the past as the chilling accusation from the Roe v. Wade audio recordings that opponents of abortion want to “force” women to continue pregnancies. On the contrary, far from “forcing” anything on anyone, these three women seek justice, freedom, and equality for all. And they’re shaking up both the pro-life and feminist movements in the process.
April 23, 2020 (Pregnancy Help News) — Rita and her fiancé were in the midst of a three-hour car drive home when she began hemorrhaging. She was eight weeks pregnant and had just left an abortion facility where she had begun a chemical abortion.
As Rita would later recall, she was bleeding “so severely it was dripping like a faucet that wouldn’t turn off.”
Rita’s fiancé rushed her to the hospital where she was given a blood transfusion and monitored for the next three days.
“I was in so much pain it felt like I was being ripped apart internally!” she said.
Despite the terror of those few days at the hospital, Rita discovered something that would bring her immense happiness: She was still pregnant and her baby still had a heartbeat.
With that news, Rita was able to find a life-saving treatment known as abortion pill reversal. To Rita’s joy, it worked.
Now, nearly two years after that fateful day on the road, Rita is the mother to a happy one-year-old boy.
“He’s 15 months old now and is the sweetest, happiest and most beautiful little boy I have ever laid my eyes on!” she wrote on a Facebook post made by pro-life advocate Laura Klassen. “God was truly with me, and now I see why, my son’s my biggest blessing.”
So impactful was the experience on Rita’s life that today she is outspokenly pro-life.
According to a message she sent to Klassen, that wasn’t always the case.
Rita explained that she grew up believing that abortion was a “choice” and that an unborn child in the womb wasn’t a human life. Her own mother had two abortions.
But because of the transformative experience of saving her baby, Rita was able to help her mother become pro-life, as well.
“I should have never been able to take my son’s life,” Rita wrote to Klassen. “And seeing him here today is such a blessing! He’s a radiant soul with a happy, laughing, and smiley energy that radiates a room! He, like all other babies, deserves life!”
That’s exactly what the team at Abortion Pill Rescue is hoping to ensure. The group — a network of more than 800 medical providers run by Heartbeat International — has helped save more than 1,100 from in-progress chemical abortions since it launched more than a decade ago.
“Many women regret their abortions and often that regret sets in right away,” said Christa Brown, director of Medical Impact for Heartbeat International. “Many women contact the APR hotline as soon as they get to their cars in the abortion clinic parking lot. Or, like Rita, regret already begins on their way home from the clinic. The realization sets in that they are ending the life of a child and they want to know if they have options.”
A chemical abortion — often referred to as the “abortion pill” or RU-486 — actually involves two drugs. The first, which Rita took, is mifepristone, a drug that destabilizes the pregnancy by blocking progesterone receptors. The second, typically misoprostol, triggers contractions, forcing the woman’s body to expel her baby in very premature labor, often at home.
If a woman changes her mind after taking the first drug, she may be able to save her baby with help from the Abortion Pill Rescue Network. By calling the 24/7 helpline (877-558-0333), she is connected with a local medical provider who offers the treatment.
Brown says that even in seemingly dire cases — like Rita’s — babies have been rescued.
“Many assume that some bleeding after taking mifepristone means it’s too late to save the baby,” Brown said. “But that isn’t necessarily true.”
She said that mifepristone is known to cause fever, heavy bleeding, abdominal pain and nausea.
“The FDA states that cramping and vaginal bleeding are expected with mifepristone and warns that one in one hundred women who have taken just the mifepristone will have bleeding so heavy they will require a surgical procedure to stop it,” she said.
When combined with the second drug, misoprostol, the effects of a chemical abortion are more alarming still.
“I’m very concerned about the abortion pill because aside from the fact that it’s killing babies, it’s being marketed heavily to young women as ‘easy’, and ‘safe’, and that you can ‘do it in the comfort of your own home,’” Laura Klassen told Pregnancy Help News in an email. “But I am hearing the horror stories regularly.”
“What I have come to find is that the RU-486 pill is much more bloody and painful than the abortion industry portrays it,” Klassen said. “What I am hearing is that women are often sent to the hospital during the process because of hemorrhaging, or else they’re having to go weeks later to have surgery because parts were left inside.”
Brown says the Abortion Pill Rescue Network hears similar accounts.
“The medical staff of APR hear from women who are scared, alone and bleeding heavily,” she said. “Because chemical abortion is often advertised as ‘inducing a period,’ and because abortion providers often describe the bleeding as spotting, many women are shocked by the amount of pain and bleeding the abortion pill causes.”
Yet if a woman contacts the Abortion Pill Rescue hotline soon enough after taking the first drug, she may not suffer the same experience.
In cases where an ultrasound can still detect a baby’s heartbeat — even a faint one — the abortion pill reversal treatment can begin. To initiate that process, a medical provider prescribes bioidentical progesterone, such as Prometrium, to the pregnant woman. The hope is that by flooding her body with progesterone, they can restabilize the pregnancy.
“It works to outnumber and outcompete the mifepristone for those receptor sites in the uterus and placenta and is successful about 68 percent of the time,” Brown said, referring to a study by physician George Delgado, one of the founders of the Abortion Pill Rescue Network.
With more and more babies being rescued by the treatment, Brown says the protocol is an important form of empowerment for women.
“APR empowers women with real choice,” Brown said. “No woman should ever feel pressure to complete a medical procedure she no longer desires.”
Your doctor rattled off those words like he was calling roll in a classroom. But each one made you cringe a little more than the last. You could feel your eyes widening as the list grew. Side effects—for a drug you don’t even need, for a drug not designed to alleviate a sickness. You look at him dubiously, as if maybe he’s joking. These can’t all be side effects from one drug, you think. But the look on his face tells you that he is not joking. In fact, he is very serious. And luckily for you, he cares enough about you to tell you what could happen if he prescribes the drug you’re asking for. You start to think to yourself: I don’t want to do that to my body. I value my health too much. I respect my body more than that.
You wonder why you never heard any of this before, and you realize you’re going to have to rethink your desire for hormonal birth control.
The Petition
In June 2019, 10 doctors and researchers who had formed a Contraceptive Study Group published a document entitled Petition on Hormonal Contraceptives. This document evaluated existing literature and synthesized studies on hormonal birth control in order to present information on their side effects in one comprehensive document. The Contraceptive Study Group’s goal was to not only warn potential users, but also to petition the government to add black box—or warning—labels onto the boxes of contraception and to include warnings on patient-related information so that women know and understand the risks of the chemicals they put into their bodies. This article serves as an overview of just some of the major findings and of the information this group desperately wants to put forward for all to know.
The members of the Contraceptive Study Group understand the damage hormonal contraceptives do to women, to the babies they may carry, and to the families who love them. That is why they undertook the daunting task of reading, interpreting, compiling, and then disseminating the information they found. In all, this petition cites 230 outside sources—not counting those related to the environmental impact. This petition was not only a labor of love and compassion for their fellow human beings but also serves as a wake-up call to people who unknowingly—or knowingly—ingest these harmful chemicals.
Millions of women take hormonal birth control or receive contraceptive injections without any idea about the poison they’re putting into their bodies. According to the petition, “Based on data from the Guttmacher Institute, a conservative estimate of 11 million women aged 15-44 in the US take some form of hormonal contraceptive each day. A 2015 study reports that about 21 percent of women of reproductive years are using some form of hormonal contraceptive, which equates to about 13 million women (Daniels 2015).”
In addition, millions of babies die when these contraceptives thin the lining of the uterine wall, thus preventing the baby from implanting.
Hormonal contraceptives have been on the market for over 50 years, yet the scope of the devastation and health ramifications they have caused can never be known. Some women don’t even realize that the causes of the health problems they face may be contraception. If this petition succeeds in its intent, pharmaceutical companies will have to disclose these side effects.
The petition begins by listing the side effects of combined estrogen-progestogen contraceptives (COCs). Many are mentioned in the first paragraph above. COCs include oral, intravaginal, and transdermal formulations. The petition lists the brand names of all of these—in six pages.
According to the team, progestogen-only contraceptives (POCs) “have not been extensively studied, but one large registry study did show a significantly increased risk of breast cancer with use of POCs.”
Furthermore, the International Agency for Research on Cancer (IARC) classifies COCs as Group I carcinogens, meaning they can cause cancer in humans.
Recommendations
The petition recommends that the government “remove from the market the injectable contraceptive Depot Medroxyprogesterone Acetate (DMPA; Depo-Provera) based on conclusive evidence that it facilitates the transmission of HIV from men to women.” It then recommends that black box warnings should be added for the following diseases and conditions: breast cancer, cervical cancer, inflammatory bowel disease, systemic lupus erythematosus, depression and suicide, venous thrombosis, and cardiovascular events. In addition, safety information should be added to advertisements and patient-related materials about multiple sclerosis, bone fractures, body mass effects, and urogenital problems.
Countless women suffer the side effects of hormonal contraception. Countless women feel duped by healthcare providers, by pharmaceutical companies, and by organizations that tout the benefits of COCs. Rarely do they hear of these side effects—side effects that can appear after long-term use, after a few months, or even after just a few short weeks.
In conjunction with the petition, the public is asked to post comments or stories to this site in order to encourage the government to add warnings to contraceptive labels. Many of these comments reference tragic and heartbreaking stories of loss—loss of life, loss of health, and loss of autonomy.
You might wonder why many physicians don’t warn their patients about these side effects. Dr. Ken Stone offers some insight:
It is common practice that physicians do not discuss any significant adverse effects of oral contraceptives or require an informed consent. Some colleagues have said to me that they do not want to say anything that would deter them from using the pill. Standard adverse effects in formularies for prescribed contraceptive medicines usually do not mention the most severe ones like pulmonary embolus, stroke, breast cancer, liver disease, etc.
This petition for removing certain contraceptives from the market, listing those adverse effects that should have black box warnings in prescribed contraceptives, and those that need additional safety warnings in prescribed contraceptives provide[s] more than adequate research data to require the actions requested. As a family practice physician for the past 41 years, I believe the scandal of not informing women of the known side effects of contraceptives is an egregious injustice and needs immediate correction.
The members of the Contraceptive Study Group believe that the public should know the truth. Throughout the next several pages, we will discuss some of the findings and data they presented regarding many of the major side effects of hormonal contraception. To read the petition in its entirety, and to see the comprehensive list of side effects, visit the petition’s site.
HIV Transmission
Depo-Provera, or DMPA, is an injectable contraceptive that is administered quarterly. However, according to the study group: “Evidence began emerging in the 1990s, which has become compelling in recent years, that DMPA is unique among contraceptives in its property of facilitating the transmission of HIV.”
How is this so?
According to research, DMPA has an immunosuppressant quality. It binds to the glucocorticoid receptor of human leukocytes, which, in layman’s terms, means that it represses the woman’s innate immune responses and allows for an increase in HIV replication. Thus, when an infected man has intercourse with a woman taking DMPA, her compromised immune system cannot fight off the disease.
Because of this, the authors want DMPA taken off the market.
Breast Cancer
According to the petition, there are 1.7 million cases of breast cancer diagnosed every year. It is the most common form of cancer among women in developed countries and accounts for 20% of cancers in females.
The International Agency for Research on Cancer classifies COCs as Group 1 carcinogens. That means they can cause cancer in human beings. Studies have long shown the link between breast cancer and COCs. The New England Journal of Medicine published an article in 2006 that found that COCs increase the risk of breast cancer. That same year, the Mayo Clinic Proceedings (a medical journal sponsored by the Mayo Clinic) published a meta-analysis that confirmed the findings that COCs increase the risk of premenopausal breast cancer.
According to the Contraceptive Study Group, “Studies that looked at recent use (within 1–5 years) or current use of COCs in premenopausal women showed the most dramatic increased risk for breast cancer.” The most significant study found that women between the ages of 20-49 who had used COCs “within a year had an increased risk of breast cancer.”
Other studies corroborate these findings as well. Most found that women who used COCs for a year or more had a higher risk of breast cancer. A Danish study found that a woman’s risks increased even after she discontinued use if she had used COCs for five or more years.
The comments site offers many stories from women who have suffered from breast cancer and from the doctors who have treated them. Included among them are these:
As a general surgeon, me and my partners ask our breast cancer patients about OCP [oral contraceptive pills] use since our best cancer textbooks describe an increased risk of breast cancer with OCP use. It is ethically imperative that women are made aware of the risks of ingesting hormones into their bodies.
At age 31, I found a small breast lump. I went to more than one doctor, but the last one I saw was the head of the UCSD Cancer Institute, a Dr. Barone, in San Diego, where I lived at the time. He told me that it was small, movable and I didn’t have any pain but that I should GET OFF THE PILL. 19 years later that very same lump grew and became malignant, and I ended up having a mastectomy.
An anonymous writer says: “Recently diagnosed with breast cancer; I was on the pill for 10 years.”
The authors recommend that a black box warning be included with COCs, along with warnings on patient-related materials, so that women understand the risks they face.
Cervical Cancer
According to the petition, approximately 260,000 women in the United States have cervical cancer. The American Cancer Society claims that there will be about 14,000 new cases this year alone. Research has shown that there is an increased risk of cervical cancer associated with COCs and that the risk increases for women currently taking hormonal birth control. In addition, the risk increases with the length of time the woman has taken the COCs.
The risk also increases if the woman has tested positive for HPV—the human papilloma virus.
The authors recommend both a black box warning and a warning on patient-related materials.
Depression, Mood Disorders, Suicide
According to the study group, “The largest study of incident depression and use of anti-depressant medication (Skovlund 2016) indicates significantly increased risks for both COCs and POCs for both outcomes. The same group studied for suicide attempts and suicides (Skovlund 2018). Elevated risks were seen, and this was the case for both COCs and POCs. The recent NCHA study (Gregory 2018) showed a similar trend.”
The authors claim that their research has shown an “increased risk for depression, suicide risk, and suicide within 3 months of beginning to use the drugs and tapering off after 6 months, partly due to attenuation of symptoms, partly due to discontinuation due to adverse effects.”
The comments section of the website paints a dismal picture and offers evidence that these hormones cause new mental health problems and exacerbate existing or latent ones.
Julie Baltz, a family practice clinician who has practiced medicine for over 20 years, states that she has seen the psychological harm caused by hormonal contraceptives. She wrote:
Even more subtle and more underreported are the psychological effects. These patients simply state “I didn’t feel right” and often think that there something wrong with them that they don’t tolerate this type of medication. I’ve seen insomnia, anxiety, depression, anhedonia, anorexia, and poor libido directly improved within my clinical office by discontinuing a combined OCP.
In 2011 I was prescribed hormonal birth control to “fix” a very irregular cycle. Three months later I started to struggle with crippling fatigue, loss of appetite and disinterest in everything except sleeping. I was shortly after that diagnosed with Major Depressive Disorder, and still to this day have to be on medication to remain functional. I still struggle with my energy levels, unfortunately medication can’t cure depression and make it disappear. My doctor and I both believe that the hormonal birth control was likely a trigger to a predisposition for Major Depressive Disorder.
In my early twenties I was prescribed birth control pills. The first cycle I took the pills as prescribed. I began to feel depressed, anxious, crying daily, with mood swings. Prior to beginning the oral contraceptive pills, I had none of these symptoms. After completing the first 2 weeks of the medication packet, I called the nurse practitioner at the OB/GYN clinic that I originally got the prescription. She told me that the changes in my mood, depression, and anxiety among others, could not be due to the new medication, that it must have just been life. She changed me to a lower dose contraceptive pill. After three weeks of taking the second prescription pack as directed I decided to discontinue use of oral contraceptives due to the side effects. I had gained 15 pounds and felt terrible.
The site is filled with story after story of people who have suffered—mentally and physically—because of these drugs. The authors want a black box warning about this side effect and warnings on patient-related materials.
Body Mass
While studies have varied regarding weight increase in women who use COCs, the strongest data found that levonorgestrel-releasing IUDs do, in fact, affect body mass. The authors stated that “a significant increase in % fat mass with a corresponding decrease in % lean body mass was observed in both studies where these were measured.”
Women have found this side effect all too real. For example, a woman who wishes to be anonymous said:
When I was taking hormonal birth control (HBC) I underwent a massive weight gain. From 120 lbs. to 155 lbs. That’s almost adding 30% to my body weight! I also suffered with severe stomach cramping, constant discomfort, constipation and diarrhea. My doctor diagnosed it at IBS. I was only on HBC for 8 months and got pregnant while taking it. I stopped taking it upon pregnancy and have never touched the stuff again!
The authors believe that all patient-related materials and advertising (print, radio, etc.) should convey information about this risk to the consumer.
Urogenital (Urinary and Genital) Effects
The authors found evidence of several different kinds of urogenital problems in women. These include interstitial cystitis (a condition that causes bladder pain and pressure), bacterial infections, urinary tract infections, vulvovaginal candidiasis, vaginal dryness, female sexual dysfunction, and more. They state that the risk increases for adolescents and if the woman uses COCs for at least two years.
A woman who wishes to remain anonymous experienced a whole host of problems, including urogenital. She said:
I was put on birth control by my parents when I was only 15 years old after a sexual assault incident. I then continued it for another 5 years before I began to question it. In that time frame I experienced extreme weight gain and loss from one pill to another, was diagnosed with bipolar disorder because of my manic depression and severe mood swings (I am not bipolar), experienced a miscarriage, developed cysts in my breasts, had continuous pregnancy symptoms (including morning sickness every day), and had frequent UTIs and yeast infections. No one ever associated any of my problems, other than the breast cysts, to my birth control pills. It wasn’t until I discontinued the use once learning of the cysts that I began to feel normal and realized the association between my symptoms and the pill.
The authors believe that all patient-related materials and advertising (print, radio, etc.) should convey information about this risk to the consumer.
Venous Thromboembolism, Atherosclerosis, and Cardiovascular Events
Venous Thromboembolism
A venous thromboembolism (or VTE) is a condition in which a blood clot forms in a vein, most often in the leg, arm, or groin, and then lodges itself in the lung. This is an extremely dangerous health problem that can cause death. Even the American Heart Association website agrees that COCs can cause a VTE: “In women, pregnancy and the use of hormones like oral contraceptives or estrogen for menopause symptoms can also play a role.”
The comments regarding this side effect address the tragedies that have befallen women and families as a result of hormonal birth control. For example, Carol Pepin wrote about the loss of her daughter:
My 19-year-old daughter Shelby Pepin . . . died. Shelby was very athletic, did not smoke, and had no history of a blood disorder. The coroner’s report confirmed that Shelby had died from a pulmonary embolism. She had a DVT [deep vein thrombosis] behind her left knee that traveled to her lungs causing her bilateral embolism. The coroner also confirmed that her DVT was caused by her birth control the NuvaRing. Shelby had been on the NuvaRing for 18 months.
Our daughter died at age 29 in the Intensive Care Unit of her local hospital where she had been transferred after presenting herself at her local walk-in clinic. Her death was five weeks to the day after getting married and one day before [her] scheduled departure on a delayed honeymoon cruise. The autopsy report stated that she had “bilateral pulmonary thromboemboli” with a thrombus present in the left popliteal fossa. She had been using NuvaRing at the time of her death [which] had been removed at the walk-in clinic prior to transport to the hospital. . . . The [ICU] doctor stated that she believes that hormonal birth control was a significant contributor to the death of our daughter.
Kimberly Phipps-Nichol shared her personal story of survival:
Last year, at the age of 46, I was hospitalized with a cerebral thrombosis that was literally caught right before causing a stroke. The ER docs told me that if it had not been for the fact that the people I was with at the time of the event were trained to recognize the signs of stroke and called 911 for a stroke paramedic unit that arrived quickly, I would have been somewhere between a vegetative state and severely disabled. After countless CT scans and MRIs, along with a thorough study of my family history, the neurologist and hematologist teams determined it was the oral contraceptives that I was taking that had caused the thrombosis.
Diagram of thrombosis
An anonymous family physician claims to have seen the negative side effects of contraceptives firsthand and tells of several cases, including her treatment of a young woman in her late 20s who went into a coma brought on by a pulmonary embolism. The only known risk factor was that this woman was taking hormonal birth control. In addition, a medical colleague of this doctor suffered a pulmonary embolism that was attributed to OCP.
Nancy Brockoff wrote to say that she had four friends, who were all young mothers, who died of blood clots related to hormonal birth control.
Atherosclerosis and Heart Disease
Atherosclerosis is a disease of the arteries caused by plaque. Arteries clogged with plaque lead to heart problems. Even as long ago as 1982, researchers understood and took interest in the fact that vascular disease and COCs were linked. According to the petition, these researchers “found that combination oral contraceptives (COCs) caused ‘greater cell proliferation and incorporation . . . in both human arterial smooth muscle cells and dermal fibroblasts.’ Smooth muscle cell proliferation is an integral feature of all atherosclerotic lesions (Bagdade 1982). In 2007, a presentation at the American Heart Association meeting described a study of 1,301 Belgian women, which showed that women had a 20 to 30 percent increase of plaque for every decade on COCs (Rietzschel 2007).”
Furthermore, the Danish Heart Association “released the results of a 15-year historic cohort study looking at thrombotic stroke and myocardial infarction, which observed over 1.6 million women. The results demonstrated that women taking COCs with ethinyl estradiol at a dose of 20 [micrograms] had a risk of arterial thrombosis that was 0.9 to 1.7 times higher than non-users, while those taking a dose of 30 to 40 [micrograms] had a 1.3 to 2.3 higher risk” (Lidegaard 2012).
The current black box warning about thrombotic events mentions smoking and age, which the authors believe misleads the consumer into thinking she’s safe if she doesn’t smoke or if she’s younger than 35. They want the warning amended to read: “Warning: Increased risk of serious cardiovascular events including blood clots.” Additionally, they request warnings on all advertising and patient-related materials.
Environment
The synthetic hormones that women take are continually released from their bodies through their waste products. When researchers noticed changes in the aquatic environment—especially in fish—they began conducting studies to determine the cause of these changes. What they found astounded them.
The Contraceptive Study Group explained:
EE2 [the synthetic estrogen ethinylestradiol] is metabolized in the liver undergoing first pass metabolism, but ~6% of the administered dose appears as untransformed EE2 in the urine and ~9% in the feces (Stanczyk 2013)….Even at low concentrations, these compounds can act as potent endocrine disruptors, affecting the growth, development, and reproduction of exposed aquatic organisms (Tyler 1998, Larsson 1999).
While wastewater treatment plants have the ability to filter out many chemicals and pollutants, they cannot filter out EE2.
Studies have found that these synthetic chemicals cause changes in male fish. A 1995 paper found that male fish in nearly 30 rivers throughout Britain had become “feminized” by these pollutants.
The Contraceptive Study Group also referenced a seven-year long study of the effects of EE2 on Canadian lakes. In that study, researchers approximated the amount of EE2 that would reach the waterways from a town of 200,000 people. They immediately saw the feminization and transgendering of male fish and a “near extinction” of the population of the fathead minnow there. Once the researchers stopped adding EE2 to the water, the population of minnows returned to normal.
We find further evidence in a study that looked at the fish populations near three Colorado sewage treatment plants. There, researchers found a significant difference between the fish upstream of the plant and those downstream. They stated:
The fish in the upstream locations enjoyed a balanced 1:1 female-to-male sex ratio. Downstream there were five female fish for every one male, and twenty percent of the reduced male population demonstrated intersex characteristics, such as eggs in their testes and the presence of vitellogenin, an egg yolk protein normally found only in fertile females. The consequences also appeared to ascend up the food chain in a measurable way, specifically with the feminization of trout, mink frogs and green frogs (Parke 2009). Both the predicted and the measured concentrations of EE2 in the US, including effluent of waste water treatment plants, surface water, or ground water, exceeds the predicted no-effect concentrations on fish populations (Kostich 2013).
Conclusion
In addition to these diseases and the pollution in the environment, the economic costs from these side effects and their resultant diseases/health problems to the patient and to the community are in the billions.
This article touched upon some of the most egregious side effects. To read the full list of side effects and the studies referenced, to read all of the comments, or to add your own comment, visit regulations.gov/document?D=FDA-2019-P-2289-0001.
This health crisis affects us all. Whether you are male or female, elderly, middle aged, young, a mother, or a father, hormonal birth control does affect your life in some way because these hormones affect your wives, your mothers, your sisters, your cousins, your best friends, the environment, and even your dinner table. It’s time to speak up and tell the government that women must know the truth. It’s time to help women understand that their health is more important than a drug that can alter their body and mind. Synthetic hormones and their deleterious effects leave a lasting impact and crush our society.
The BBC recently reported that African countries do not have enough ventilators to treat people affected by the coronavirus (COVID-19). The World Health Organization’s Director for Africa, Dr. Matshidiso Moeti, stated that “the issue of ventilators is one of the biggest challenges that the countries are facing.” Other concerns include limited personal protective equipment (PPE) and a lack of access to soap and clean water. Unfortunately, there aren’t enough supplies for every country in the continent, as the Associated Press detailed how one major shipment included “more than 400 ventilators… for sharing among all 54 countries.”
So how did the Swedish International Development Cooperation Agency (Sida) respond to the crisis African people are facing? While they created a $2 million aid plan, the money is not going towards these urgent medical needs. Instead, Sida plans to use the $2 million to fund abortion kits for the continent.
“Our program is especially important for vulnerable women and girls in the region. We need to address the effects of COVID-19 quickly to have their human rights safeguarded, so they are able to decide for themselves when and with whom they will have children,” Sida Director General Carin Jämti.
Sida will send funding to DKT International, an organization funded by the Bill and Melinda Gates Foundation that provides products such as manual vacuum aspiration kits and abortion drug kits. On its webpage, DKT boasts that about 8 million pregnancies have been “averted” because of its services. The kits Sida obtains from DKT International are to be sent to the Democratic Republic of Congo, Ethiopia, Kenya, Mozambique, Tanzania, and Uganda.
The agency will also allocate funds towards the education of local health care workers, community leaders, and individuals. Instead of providing African countries with the equipment necessary for saving lives, Sida is focused on promoting a radical abortion agenda.
Pro-life activist Obianuju Ekeocha has spoken extensively about this attempt by Western societies to force abortion and contraception into African culture. According to Ekeocha, the beliefs of most African women do not align with the radical views pro-abortion groups are trying to push on them.
“I don’t know many African women who would choose contraception over everything else,” Ekeocha said in a statement printed at Catholic Digest. “Africans cherish babies and celebrate motherhood even in the midst of poverty.”
Ekeocha has detailed how pro-choice organizations sneak their agenda into Africa under the guise of philanthropic work. While their intention is to push young girls to have abortions and take contraceptives, Ekeocha says these groups disguise their goal by claiming their actions are part of a “maternal mortality reduction” program.
Now, as Africa is suffering in the midst of COVID-19 due to a lack of medical equipment, Sida — through DKT International — is attempting to do the same thing. Despite claims that abortion is necessary healthcare, more than 30,000 American doctors have refuted this point, calling it “medically irresponsible” to allow such procedures to continue during a global pandemic.
Instead of saving lives, groups like Sida are dedicating funds towards ending them.
WASHINGTON, D.C. — Development of an effective, safe and widely available vaccine for the novel coronavirus is deeply important, but its development should avoid unethical links to abortion, said pro-life leaders in a letter to the Trump administration.
“It is critically important that Americans have access to a vaccine that is produced ethically: no American should be forced to choose between being vaccinated against this potentially deadly virus and violating his or her conscience,” said the April 17 letter to Dr. Stephen M. Hahn, commissioner of the U.S. Food and Drug Administration.
“Fortunately, there is no need to use ethically problematic cell lines to produce a COVID vaccine, or any vaccine, as other cell lines or processes that do not involve cells from abortions are available and are regularly being used to produce other vaccines,” it continued.
The letter’s signers include Archbishop Joseph Naumann of Kansas City in Kansas, chair of the U.S. Conference of Catholic Bishops’ Committee on Pro-Life Activities; the heads of three other bishops’ conference committees; and leaders of many other Catholic and non-Catholic groups.
The letter comes after the release of the Trump administration’s gradual three-phase plan to remove restrictions on economic and social life while seeking to contain the coronavirus spread, especially spread to vulnerable populations. A coronavirus vaccine, if effective, could help prevent infection and speed economic recovery.
The letter’s signers “strongly support” vaccine development “as quickly as possible.” At the same time, they urged the federal government to “ensure that fundamental moral principles are followed in the development of such vaccines, most importantly, the principle that human life is sacred and should never be exploited.”
“We are aware that, among the dozens of vaccines currently in development, some are being produced using old cell lines that were created from the cells of aborted babies,” signatories said.
They cited the case of Janssen Pharmaceuticals, Inc, which has a “substantial contract” from the U.S. Department of Health and Human Services and is working on a vaccine produced using “ethically problematic cell lines.”
The letter encouraged other vaccine development that uses cell lines not linked to these “unethical procedures and methods.” These are in development by companies like Sanofi, Pasteur, and Inovio, they added, while also noting the work of the Iowa-based John Paul II Medical Research Institute.
The letter was copied to President Donald Trump, Vice President Mike Pence, and Secretary of Health and Human Services Alex M. Azar, II.
Besides Archbishop Naumann, other bishops signing the letter are Archbishop Paul Coakley of Oklahoma City, chair of the Committee on Domestic Justice and Human Development; Bishop Kevin Rhoades of Fort Wayne-South Bend, chair of the Committee on Doctrine; and Bishop John Doerfler of Marquette, chair of the Subcommittee on Healthcare Issues.
Signers include Russell Moore, president of the Southern Baptist Ethics and Religious Liberty Commission; Michael Parker, president of the Catholic Medical Association; Joseph Meaney, president of the National Catholic Bioethics Center; Ellen Gianoli, president of the National Association of Catholic Nurses, U.S.A.; Marianne Linane, director of the National Association of Pro-Life Nurses; Donna J. Harrison, executive director of the American Association of Pro-Life Obstetricians and Gynecologists; Michael P. Farris, president, CEO and general counsel at Alliance Defending Freedom; Travis S. Weber, vice president for policy and government affairs at the Family Research Council; Kristan Hawkins, president of Students for Life America; and Lila Rose, president and founder of LiveAction.
Catholic teaching acknowledges the right to well-formed conscientious objection to many legal mandates and medical procedures, while also emphasizing vaccination as a matter of public responsibility.
A 2005 document from the Pontifical Academy for Life considered the moral issues surrounding vaccines prepared in cell lines descended from aborted fetuses. The Vatican group concluded that it is both morally permissible and morally responsible for Catholics to use these vaccines.
The pontifical academy also noted that Catholics have an obligation to use ethically-sourced vaccines when available, and have an obligation to speak up and request the development of new cell lines that are not derived from aborted fetuses.
The 2008 Vatican document Dignitatis Personae strongly criticized aborted fetal tissue research. However, as regards common vaccines, such as those for chicken pox and measles, mumps, and rubella (MMR), that may be derived from cell lines of aborted babies, the Vatican said they could be used by parents for “grave reasons” such as danger to their children’s health.
In a 2017 document on vaccines, the Pontifical Academy for Life noted a “moral obligation to guarantee the vaccination coverage necessary for the safety of others… especially the safety of more vulnerable subjects such as pregnant women and those affected by immunodeficiency who cannot be vaccinated against these diseases.”
Editor’s note: L.J. and Joan Helferty believed they had every good reason to use contraception in their Catholic marriage. But then everything started falling apart. Their story, published exclusively on LifeSiteNews, is one of the best testimonies about the spiritual blindness that follows the sin of contraception and about the mercy of God that follows true repentance.
April 17, 2020 (LifeSiteNews) – Sunday Dec 10, 2000. About 7:00 a.m. A cold crisp cloudy Sunday morning. I was the first one awake and out of bed. That was normal. I usually stoked the furnace and got our farmhouse warmed up before calling everyone. Mass was at 9:00. There would be just enough time to get ready. We had eleven children, nine at home and two older ones away at post-secondary institutions.
I had slept in this morning. We had installed a new furnace that weekend and I was exhausted by the time we were finished on Saturday evening. When I went downstairs into the kitchen on my way outside to the furnace, I noticed a hand-written note on the table, at the place where our 15-year old son Matthew usually sat for family meals.
Curious, I glanced at the first line.
“By the time you are reading this, I’ll already be dead. Hey, it’s Matthew. You’ll find my body in the front field…”
I froze. “Not possible,” I thought. This boy had everything going for him – brilliant, thoughtful, lots of friends,… “Okay, this has to be some sort of terrible joke or experiment, because it just isn’t possible.”
I ran upstairs to his bedroom. The bed was neatly made up. It hadn’t been slept in. I awoke my wife and told her to call 911 and ran outside, shouting his name, hoping that he would be sitting somewhere, not able to go through with his plan. I was too late – only by minutes – he had used a hunting rifle in one decisive act.
When I returned to the house with the heart-breaking news, my wife Joan made the necessary phone calls while I sat on the kitchen steps in disbelief.
When she got off the phone, she came over to me and said, “It’s because of the tubal.”
I couldn’t believe she was saying that.
After our eleventh child was born, we had secretly arranged for Joan to have a tubal ligation. We hadn’t told anyone because we had always professed to be in union with the Catholic Church’s teaching regarding the use of the natural cycles to limit the size of your family, if there was a serious reason to do so.
We seemed to lack the discipline to make that work for us, and we thought that we were at the point where we needed to stop having children, so we opted for tubal ligation. Both of us went to confession afterwards, but the sacrament can’t help you much if you don’t have contrition and don’t plan to make satisfaction for the damage you have done.
The thoughtfulness and generosity of our parish priest, the police, our parish members, friends, and our funeral director became manifest as soon as the terrible news spread, and helped to sustain us through the coming days, weeks and months. It is impossible to describe the impact suicide has on each family member, especially the parents and the closest siblings. Thankfully, in His generosity, God gave us several consolations, allowing us to be confident that Matthew’s eternal salvation was assured.
In Loving Memory of Matthew Helferty SOURCE: Pete Baklinski / LifeSiteNews
After the wake and funeral, I became driven, attempting to understand how we had lost our son in such a terrible manner.
Eventually, it became evident that Matthew had descended into deep depression and that he was listening to music on his personal CD player that would further contribute to his depression and offer the ultimate solution. He had also been playing violent video games and a card game called ‘Magic: The Gathering’ with some of his friends. But… this explanation was incomplete. Lots of kids listen to this terrible music and play those games and have depressing lives, but they don’t commit suicide. Matthew was part of a loving family, and we hadn’t even noticed that he was depressed, until we looked back and saw some of the obvious signs.
As the months went by, Joan continued to insist that the tubal ligation was the explanation for our loss of Matthew.
I was not convinced.
To settle the matter, we decided to visit our former spiritual director and family friend, Father Jim Duffy of Madonna House. He had called us on the day of Matthew’s death, to offer prayers and condolences. He was perplexed that this had happened. I agreed that I would accept that the tubal was the explanation, if Father Jim said so. It was Divine Mercy Sunday, 2001. When we arrived at Madonna House in Toronto – it’s a 4-hour drive from our home – Father Jim offered mass for our intentions in their chapel, then we went to a nearby restaurant & park for lunch.
When Joan told him that she had undergone a tubal ligation, he stopped eating and his countenance dropped.
He gravely explained that our experience was simply the re-telling of the stories of the Old Testament. When the Jewish people strayed from the ways of God, when they rejected His teachings, they experienced suffering and loss. When they realized their faults and turned back to God, their lives were restored.
I was devastated.
But, I knew that Father Duffy, a devout and holy priest, with many decades of experience, would not mislead us. During the drive home, we decided to arrange for a reversal of the tubal ligation and to confess this sin again, this time with true contrition.
Divine Mercy Image
We realize now that when we had the tubal ligation, we cut our family off from many of God’s graces and guidance and protection. We were blind. Matthew was the one that suffered the most, and we didn’t even notice. We are convinced that if we had been living within God’s order, either the perfect storm of circumstances and events that plunged Matthew so quickly into such deep depression would not have occurred or we would have noticed the seriousness of his condition and been able to save him.
Since the reversal and confession of that sin, our family has been blessed tremendously. There are still lots of challenges, but sincerely attempting to live within God’s order provides spiritual protection and peace of mind that we treasure dearly.
After the reversal of the tubal ligation, we were hoping for more children, but each pregnancy ended in miscarriage. We have accepted that when you tamper with the natural law, there are natural consequences. Nineteen years later, several of our children are married and we currently have close to 20 grandchildren. One of our sons is a priest and one of our daughters is a Sister. All of these things bring great joy to Joan and me.
The consequences of our sin were severe, but God has restored our lives miraculously. Deo Gratias!
We hope that by sharing our experience, we will help others to avoid the sins related to artificial contraception and sterilization. We have learned that God’s way is the best way, regardless of how difficult it may seem at the time. Please observe the Catholic Church’s teachings regarding family planning in Humanae Vitae. Our son’s death on December 10, 2000 was the worst day of our lives. Divine Mercy Sunday in 2001 was indeed the day our lives were restored.
(NRL News Today) When Angela Primachenko told Sheinelle Jones on the TODAY show this morning,” I feel like I’m a miracle walking,” she was not exaggerating. Consider…. The 27-year-old respirator therapist from Vancouver, Washington, who was 33 weeks pregnant, had among other symptoms a fever, and was tested for COVID-19 on March 24, Scott Stump of NBC/Today reported.
Eight days later she… was fighting for her life on a ventilator while in a medically induced coma.
At the same time, she gave birth to her daughter after doctors at Legacy Salmon Creek Medical Center induced labor to give Primachenko more of a fighting chance while also protecting her child. …
Primachenko was taken off the ventilator on April 6, and one look down at her body told her that her baby must have been born.
“Obviously nobody expected that I was going to get that sick, so no, absolutely not, I did not expect to deliver my child,” she said. “After all the medication and everything I just woke up and all of a sudden I didn’t have my belly any more. It was just extremely mind-blowing.”
Stump explained that Primachenko, who was released from the hospital Saturday, has not been able to hold daughter Ava who is in neonatal intensive care. Fortunately, neither her husband David nor their 11-month-old daughter, Emily, have tested positive for COVID-19, so they are able to hold the newest member of the family. Primachenko has had to content herself with FaceTime.
Another blessing: Ava has tested negative for COVID-19.
NBC/Today detailed the loving contributions of Primachenko’s supportive family and friends.
Her twin sister, Oksana Luiten, had been keeping family and friends updated through Primachenko’s frightening ordeal, asking for prayers on Instagram for a “miraculous healing.”
Primachenko also had a moment she’ll never forget when she was wheeled out of the intensive care unit in her bed.
“Everyone did a standing ovation and just clapped me out of the ICU, which is so amazing and such a huge thing to be able to leave the ICU and go to the floor — it’s just the grace of God,” she said.
Washington state has been hit hard by COVID-19. Primachenko said she “is hoping her story can send a positive message during a difficult time.”
“That there’s hope,” she said. “That even in the hardest days and the hardest times that there’s hope and you can rely on God and people and community. The amount of community and people that were praying for me is just unbelievable. I was blown away, and I’m so incredibly thankful.”
Giving her daughter the name Ava also has a special meaning, particularly after everything that mother and daughter have endured.
“It means ‘breath of life,”’ Primachenko said. “So she’s our new little breath of life.”
Editor’s Note: This article was published at NRL News Today and is reprinted here with permission.
Birth control is touted as one of the greatest medical advancements ever made for women, allowing them to take charge of their sexuality without worrying about unplanned pregnancies — or so the narrative goes, anyway. But birth control has risks that go along with it, and those who use it should weigh those risks before taking it. Unfortunately, many women aren’t properly informed of the risks beforehand. For certain kinds of birth control, those risks include an increased susceptibility to getting a sexually transmitted disease (STD).
DEPO PROVERA
Depo Provera is a birth control injection given four times a year, and is intended for women who don’t want to take a pill every day. It works by suppressing ovulation — preventing ovaries from releasing an egg — and thickening cervical mucus, so that sperm are less likely to reach an egg, should one be released.
However, Depo Provera has been found to possibly increase the chances of contracting chlamydia, gonorrhea, and HIV. It’s not clear why this happens, but it should serve as a warning to women who choose Depo Provera. “These findings underscore the need to counsel all sexually active women who use DMPA and who are not in a mutually monogamous relationship to use condoms consistently and correctly,” Dr. Charles Morrison, the first author of one of the studies that found this increased risk, said in a press release. “For sexually active women not in a mutually monogamous relationship, limiting the number of partners may also help to reduce the risk.”
It should be noted that limiting one’s number of sexual partners always reduces one’s risk of getting an STD.
COPPER INTRAUTERINE DEVICE (IUD)
IUDs have become popular in recent years, as they’ve allegedly become safer (although there are still plenty of horror stories) than in past decades. The copper IUD is considered a non-hormonal contraceptive device, and works by triggering an inflammatory reaction from the copper wire coiled around the device. The copper is toxic to both sperm and eggs. It can be left in place for up to 10 years, and can be removed at any time, making it seem like a very attractive option for women.
Yet there are questions being raised about whether it may make women more susceptible to contracting STDs. KQED noted that along with the rise of IUDs in California, STDs — including chlamydia, gonorrhea and syphilis — also drastically skyrocketed, and the “why” behind this is still unclear. “These are things that are happening at the same time and in tandem, but we can’t necessarily say there’s causality between them,” Stephanie Arnold Pang, director of policy and government relations at the National Coalition of STD Directors, told KQED.
Meanwhile, a medical paper posited that a potential risk might exist between using copper IUDs and HIV, specifically in women who have copper sensitivity. It’s because in these women, the copper IUD causes severe dermatitis; this, along with the excessive menstrual bleeding women sometimes experience, could put them at higher risk. Other studies, however, found no difference in HIV risk between copper IUDs and hormonal IUDs.
ORAL CONTRACEPTIVES
The birth control pill, or oral contraceptives, was the first modern birth control method created. It works by preventing a woman’s egg from fully developing each month, and therefore, unable to accept sperm and become fertilized. The pill also thickens cervical mucus, making it more difficult for sperm to reach any egg that might be released. However, birth control pills are notorious for their side effects. One of the lesser known side effects is an increased chance of STDs.
The Guttmacher Institute, the former research arm of Planned Parenthood, published a study showing that women who used oral contraceptives were more likely to get chlamydia and vaginal candidiasis, compared to women who don’t use them.
Women should be aware that there are effective, risk-free natural methods available for them, should they choose to forgo artificial birth control methods. Women deserve to know what they’re risking before they take birth control, whether it’s an increase risk of pulmonary embolism or STDs. True empowerment comes when women are given all the information they need beforehand so they can make informed decisions.
The Wuhan virus pandemic has begun to attack the very foundation of the Culture of Death.
Media reports show the pandemic is causing the shuttering of some abortuaries as well as the canceling of “gay pride” events.
But the effect on contraception has been largely ignored.
The Wuhan pandemic is causing supply shortages for pharmaceutical companies around the world, creating shortages of chemical contraceptives.
Likewise, restrictions on doctor visits is also diminishing access to contraception.
The normal protocol of getting an exam, blood test and consultation before obtaining a prescription has been curtailed. And without a prescription, one cannot purchase or refill contraceptive pills, which act as abortifacients.
Further, Malaysia-based Karex Industries, responsible for 20% of the world’s condoms, has shut down factories in China and India due to government lockdowns, slowing the distribution of condoms worldwide.
The United Nations is warning of “devastating” consequences.
Even Planned Parenthood of Pennsylvania has announced it has dropped all birth control services during this time.
Faithful Catholics are hoping diminished access to contraception and abortion will force young people to reflect on the importance of chastity, the sanctity of marriage and the dignity of human life; and that God will use this to lead many souls back to Him — and, perhaps, save Western civilization in the process.
Heartbreaking stories have emerged from the coronavirus pandemic in Italy. Hospitals are too full. Doctors are overworked. People die alone. Coffins pile up. The Pope walks through empty Roman streets, praying alone.
The coronavirus has created these scenes. Yet, behind the scenes of the crisis is another one. Slow-moving, largely hidden, yet destructive both physically and socially, a problem people prefer to ignore. I am speaking of demographic winter: the worldwide fertility decline. This problem aggravates the coronavirus crisis.
The coronavirus is especially lethal for the elderly. The death rate (deaths per number of cases) is 15% for people over 80, 8% for people in their 70s, 3% for people in their 60s and less than 1% for people under 50. The countries with the highest number of cases and fatalities per capita are countries with a large percentage of elderly people. For instance, Italy’s fertility rate is now 1.33 children per woman, far below the replacement level of 2.1. As a result, Italy has a rapidly aging population. Almost a quarter (23%) of Italy’s population is now over 65 years of age. In 2019, the median age was 46.3, projected to rise to 51.4 by 2050. An aging population is creating and will continue to create rising costs for both pensions and health care.
But beyond the dollars and cents are the human costs. Low fertility rate means fewer young people to take care of the increasing number of older people. Even if the fear of contagion had not prevented family visits, more and more people have no young relatives to come visit them. Even without coronavirus, for example, Japan has so many childless elderly people who die alone that the culture has developed a special term: “lonely death.” People die in their apartments, alone, sometimes undiscovered for days or more, sometimes much more. The first person to whom the term was applied, evidently, was a man who was discovered three years after his death.
We are so accustomed to hearing about “overpopulation” and “The Population Bomb” that we scarcely consider the opposite problem of underpopulation. Yet the fact is that birth rates in most of the world are well below replacement rates. And the problems are becoming harder to ignore and harder to solve.
Political scientist Nicolas Eberstadt of the American Enterprise Institute stated in a depressing article entitled, Growing Old the Hard Way:
“Left unaddressed, the mounting pressures that population aging would pose on pension outlays, health care expenditures, fiscal discipline, savings levels, manpower availability, and workforce attainment could only have adverse domestic implications for productivity and economic growth in today’s affluent societies.”
These pressures have been pretty much “left unaddressed” during the 15 years since Eberstadt penned those words. Public policy around the globe still emphasizes the need to slow population growth. The problems created by population decline never seem to get the same attention.
You may reply that lower fertility is one of the costs of women’s greater participation in higher education and the professions. Women are choosing delayed and reduced fertility, because they believe they will benefit from it. That is only true up to a point. What kind of “choice” is it, when we women hear all about the benefits of delayed fertility and never hear about the costs?
Did you know that most college educated women end up with fewer children than they originally wanted?* Most people don’t know this. Yet this is the case in pretty much every rich country. The “fertility gap” is highest in Southern European countries, such as Italy and Spain, where the coronavirus just happens to be the most virulent.
There is no world overpopulation crisis. The bigger problem is that we don’t have enough people. We cannot solve this problem overnight. There is nothing we can do today to increase the number of 40 year-olds we have tomorrow. Sure, we could increase immigration. But that is neither a global, nor a long-term solution.
In fact, we know today with absolute certainty the maximum number of 40-year-olds there could possibly be in the world in April 2060. (Demography is predictable that way.) We can’t do anything about that. But we can do something about how many 40 year-olds there will be in January 2061 because we can do something about how many babies we have in January 2021.
The COVID-created enforced “social isolation” could well result in a baby boom. Some “experts” offer you a free abortion as a “solution” to your “unwanted” pregnancy. I offer a different suggestion: Have the baby. Pull yourself together to take care of that baby, even if you didn’t “plan” it. Lots and lots of people who didn’t “plan” their babies will tell you later they don’t regret having them.
We baby boomers were, frankly, idiots on this point. We thought we were so smart, putting off our pregnancies and “planning” our families. We planned ourselves right into the personal heartbreak of infertility and the social crisis of demographic winter.
Of course, we as good Christian citizens must do our best to limit the spread of the coronavirus. But we must also understand the role of demographics in making us more vulnerable to this pandemic. A nation without children has no future, no matter what diseases may emerge.
For the love of God and all mankind, be not afraid! Have the baby! With any luck, and by the grace of God, Italy and all of us, will experience a post-COVID baby boom.
She is the founder and president of The Ruth Institute, an international interfaith coalition to defend the family and build a civilization of love.
*See figures 1-3 of the linked article, which states on page 527, “Highly educated women generally show the largest gap between intended and realized fertility.”
Our Lady of Fatima cautioned us and gave remedies. So did Our Lady of Akita. So did Our Lady of America.
But instead, the heedless world has been in the hot pursuit of what Cardinal Arinze pointed out as the three major “P’s” — Pleasure, Power, Possessions. A lot of that has come to a halt in the last few weeks.
Most aren’t familiar with Our Lady of America and what she said. Beginning in late 1956, Our Lady came and identified herself as Our Lady of America to bring warnings and solutions. I desire that my children honor me, especially by the purity of their lives, she told Sister Mary Ephrem (Mildred Neuzil), a cloistered nun in Ohio. I desire to make the whole of America my shrine by making every heart accessible to the love of my Son.
Our Lady wished America to be the country dedicated to my purity. The wonders I will work will be the wonders of the Soul. They must have faith and believe firmly in my love for them. I desire that they be the children of my Pure Heart.
I desire, through my children of America, to further the cause of faith and purity among peoples and nations. Let them come to me with confidence and simplicity, and I, their Mother, will teach them to become pure like to my Heart that their own hearts may be more pleasing to the Heart of my Son.
Our Lady said she was coming to us children of America, as a last resort. I plead with you to listen to my voice. Cleanse your souls in the Precious Blood of My Son. Live in His Heart, and take me in that I may teach you to live in great purity of heart which is so pleasing to God.
Here’s a mother pleading with her wayward children to please listen and then do what she’s telling them. If they don’t? In January 1957, Our Lady did not mince words.
The hour grows late. My Son’s patience will not last forever. Help me hold back His anger, which is about to descend on sinful and ungrateful men. Suffering and anguish, such as never before experienced, is about to overtake mankind. It is the darkest hour.
We know Jesus is merciful, more than we could imagine. Earlier he told St. Faustina “before I come as a just Judge, I first open wide the door of My mercy.” Again, “I never reject a contrite heart. Sooner would heaven and earth turn into nothingness than would My mercy not embrace a trusting soul.”
Our Lady told Faustina, “I am Mother to you all, thanks to the unfathomable mercy of God.” One of her titles proclaims her Mother of Mercy. She is that also — and refers back to Fatima too — as she appeared as Our Lady of America and continued: But if men will come to me, my Immaculate Heart will make it bright again with the mercy which my Son will rain down through my hands. Help me save those who will not save themselves. Help me bring once again the sunshine of God’s peace upon the world.
There’s great hope because Our Lady said mercy is ready and waiting. Remember, this was back 63 years ago. When life was simpler, and on Sundays, churches were filled. Look at society’s downhill race since.
Next, Our Lady of America requested, Reform of life is what I ask as the sign and proof of my children’s love for me. God looks at the heart, and if it resembles the Heart of His Divine Son, it is with the greatest pleasure He regards it…But to make your hearts grow more and more like to the Heart of the Son, you must go to the Mother, whose heart is most like His. From this Pure and Immaculate Heart you will learn all that will make you more pleasing to the Divine Heart of the Son of God.
Again, the message is similar to Fatima’s. Now 40 years later people still hadn’t listened enough. Our Mother was again trying to get our attention. Come to me, my children, come to me and learn. There is much I would teach you. It is for your own happiness and eternal salvation. Do not disregard the voice of your Mother. It is the voice of love trying to save you from eternal ruin.
She said her Immaculate Heart desires to see the kingdom of Jesus established in everyone’s heart. Now I have pleaded with my children to open their hearts to Him, but most are cold and indifferent.
Three months later Our Lady again warned: Unless my children reform their lives, they will suffer great persecution. If man himself will not take upon himself the penance necessary to atone for his sins and those of others, God in His justice will have to send upon him the punishment necessary to atone for his transgressions.
But her children were stopping their ears and hearts.
On Aug. 22 (the feast of the Queenship of Mary), she said, What am I to do…when my children turn from me? The false peace of this world lures them and in the end will destroy them. They think they have done enough in consecrating themselves to my Immaculate Heart. It is not enough. That which I ask for and is most important many have not given me. What I ask, have asked, and will continue to ask is reformation of life…I will work my miracles of grace only in those who ask for them and empty their souls of the love and attachment to sin and all that is displeasing to my Son.
Oh, what grief my children have caused me!
Another Message for America
Then on the feast of the Most Holy Rosary, Oct. 7, Our Lady, holding a rosary, gave a warning, and still another avenue of hope. [W]hat I am about to tell you concerns in a particular way my children in America. Unless they do penance by mortification and self-denial and thus reform their lives, God will visit them with punishments hitherto unknown to them.
My child, there will be peace, as has been promised, but not until my children are purified and cleansed from defilement, and clothed thus with the white garment of grace, are made ready to receive this peace, so long promised and so long held back because of the sins of men.
My dear children, either you will do as I desire and reform your lives, or God Himself will need to cleanse you in the fires of untold punishment. You must be prepared to receive His great gift of peace. If you will not prepare yourselves, God will Himself be forced to do so in His justice and mercy.
Let’s be honest. Look how in the last few decades the world has speeded up turning Genesis upside down — declaring as good something that was unheard of and would shock the people during that 1950’s message.
Oh, if you knew the punishments I am holding back from you by my pleading and intercession on your behalf! Will you do as I wish at last, my children? she continued.
Repent. Stop sinning. Live according to God’s commandments, not man’s. She taught,
Making the Rosary a family prayer is very pleasing to me. I ask that all families strive to do so. But be careful to say it with great devotion, meditating on each mystery and striving to imitate in your daily lives the virtues depicted therein. Live the mysteries of the Rosary as I lived them, and it will become a chain binding you to me forever. They who are found in the circle of my Rosary will never be lost. I myself will lead them at death to the throne of my Son, to be eternally united to Him.
Earlier the next year, Our Lady assured, My Immaculate Heart will win in the end, and the Spirit of Christ will dwell in the hearts of men. Those in whom this Spirit is not found will be condemned to eternal hell-fire.
She then reminded that because nothing is accomplished without pain there needed to be preparation to suffer much. She showed the sword she suffered in her own heart. It is also the sword of grief plunged therein by my children who refuse to let me teach them the true way. There is only one true way to the Father, my child, only one way to eternal union. That, she affirmed, is through her Son Jesus.
But my children will not heed; they will not listen. Every other way they will take, but not this one.
Did people finally listen and change? A year later, in 1959 Our Lady said, I come again to warn and to plead. Oh, penance, penance! How little my children understand it! They give me many words, but sacrifice themselves they will not. It is not me they love but themselves. Oh, what blindness, sweet child, what blindness! How it pierces my heart!
See, I weep, but my children show me no compassion. They behold the sword in my heart but will make no move to withdraw it. I give them love; they give me only ingratitude.
Weep, then, dear child, weep with your Mother over the sins of men. Intercede with me before the throne of mercy, for sin is overwhelming the world and punishment is not far away.”
At the time she also said she had a great interest in America’s young people, for them to become the next leaders of renewal.
Plans for the United States
Obviously, things didn’t get better. On the day after the feast of St. John the Baptist, June 25, 1967, Our Lady of America came once again because people didn’t change. Their sins cry to heaven for punishment. I hold out help, but they will not receive it…they only spurn the efforts of my love.
Then on Nov. 22, 1980, a Saturday, Our Lady came with a message specifically for the United States:
It is the United States that is to lead the world to peace, the peace of Christ, the peace that he brought with Him from heaven in His birth as a man in the little town of Bethlehem…
Unless the United States accepts and carries out faithfully the mandate given to it by heaven to lead the world to peace, there will come upon it and all nations a great havoc of war and incredible suffering. If, however, the United States is faithful to this mandate from heaven, and yet fails tin the pursuit of peace because the rest of the world will not accept or co-operate then the United States will not be burdened with the punishment about to fall.
The warning ramped up on Jan 23 (the old feast of the Espousal of Joseph and Mary).
The world was paying no attention to what Malachi (2:17) said — “You have wearied the Lord with your words. Yet you say, ‘How have we wearied him?’ By saying, ‘Everyone who does evil is good in the sight of the Lord, and he delights in them.’” — and what Isaiah (5:20) made clear — “Woe to those who call evil good and good evil, who put darkness for light and light for darkness.”
Our Lady of America reminded us of this on Holy Saturday in 1981, saying, Evil is so insidious it often passes for good. The simple and pure of heart alone can detect the difference. Many good works and many a good person or persons are thwarted or destroyed by apparently good people who are manipulated by the powers of evil because they do not possess that finer sense of being able to detect a false spirit form a true one.
In the next two years she again repeated, O my children, you still aren’t listening. I see the destruction coming but you do not believe me…The Divine Spirit is there but you are continuing in your blindness and so blotting out the Divine Light and closing your ears to eternal truth. I beg of you to heed my voice or there will be no more time for you to turn back the Divine Wrath. I weep for you because I love you and wish, my dear children, to spare you this terrible suffering.
Hope Remains — A Chance Too
In 1984, on Jan. 3 (the Feast of the Holy Name of Jesus), Our Lady of America gave a Final Message:
If my warnings are taken seriously and enough of my children strive constantly and faithfully to renew and reform themselves in their inward and their outward lives, then there will be no nuclear war.
There must be much more good then evil prevailing in order to prevent the holocaust that is so near approaching.
Yet I tell you, my daughter, even should such destruction happen because there were not enough souls who took my warning seriously, there will remain a remnant — untouched by the chaos who, having been faithful in following me and spreading my warnings, will gradually inhabit the earth again with their dedicated and holy lives.
These will renew the earth win the power and light of the Holy Spirit. These faithful ones of my children will be under my protection and that of the Holy Angels, and they will partake of the life of the Divine Trinity in a most remarkable way.
The choice is clear. Listen to Our Lady. Do what she says. Never lose hope. Pray.
April 2, 2020 (LifeSiteNews) ― Planned Parenthood is begging supporters for protective equipment and other supplies while other doctors and nurses go without as they try to save the lives of coronavirus patients.
Sue Dunlap, the president and CEO of Planned Parenthood Los Angeles, wrote a message to the abortion giant’s mailing list asking for “all of the same supplies you are hearing about on the news.”
“In order to keep our patients, staff, and sites moving through this emergency, we need all of the same supplies you are hearing about on the news,” she wrote.
“As gloves, masks, and medications run low, we are doing all that we can to procure supplies for the essential care our community is depending on us to provide.”
Like the World Health Organization, Planned Parenthood considers the killing of unborn human life “an essential service,” and abortion businesses remain open in most American states while other elective services, like dental care, are suspended. Nevertheless, Planned Parenthood is asking not only for scarce medical resources, but also for extra funds for its “almost-500 coworkers in order to help them cover groceries, child care, or any other expenses they are incurring while working and supporting Planned Parenthood patients through this difficult time.”
Much of California, including Los Angeles, is under lockdown, and social distancing between households is being encouraged. Hundreds of daycares have been shut, so it is unclear whom Planned Parenthood employees are paying to care for their children.
Planned Parenthood Keystone, which operates in Central and Eastern Pennsylvania, is also asking for supplies to continue aborting children during the pandemic. In late March, it asked for donations of “hand sanitizers, home sewn masks, shoe covers, and surgical hats.” According to National Right to Life News, Planned Parenthood Keystone is providing only abortions, and no other services, during the national health emergency. Meanwhile, the government of Pennsylvania has suspended all elective surgery in the state.
Catholic writer John Zmirak said Planned Parenthood’s determination to keep harvesting human beings even during the pandemic shows the organization for what it is.
“Planned Parenthood wants masks and gloves? Fine. Send them Halloween masks, since they’re a pack of ghouls,” Zmirak told LifeSiteNews via social media.
“Send them baseball gloves, since they only play at providing health care. What they are is a murderous cult, little better than the Manson Gang,” he continued.
“The fact that they want us to divert life-saving surgical masks and gloves away from real health care providers, so they can go on stealing organs from tiny Americans and selling them, tells us all we need to know. These people belong in prison cells.”
Selene Cerankosky of Students for Life of America told LifeSiteNews that Planned Parenthood’s days of insisting that abortion is only part of what they do are over.
“I think they can never again be defended as an organization who ‘does more than abortion,’ considering they are defaulting to this ‘service’ over any other during this time,” she said via social media.
“They are so dead set on profiting over caring for women that they’ll attempt to rob women suffering from the coronavirus of essential supplies,” Cerankosky added.
“Why not ask for supplies to perform pap smears,” Cerankosky wondered, “or STD tests? It’s because they’re well aware abortion is their most profitable engagement, and they’ll leave everything else they do unaddressed in order to cash in on ending lives.”
March 27, 2020 (LifeSiteNews) — I’ve always been close to my family, but the coronavirus pandemic and the requisite social distancing have reminded me not to take them for granted. Never again will I “just drop by” my parents’ place without being reminded that it is a blessing to be able to do so. My toddler daughter is so fed up with not seeing her extended family that she frequently demands that we video-call her grandparents, aunts, and uncles. Like everyone else, I worry about my elderly grandparents. In the midst of the panic, many of us are feeling profoundly grateful for the families we have been blessed with.
But if you are a certain type of progressive, this global upheaval presents an opportunity. Open Democracy, for example, published an essay this week with this headline: “The coronavirus crisis shows it’s time to abolish the family.”
Open Democracy’s motto is “free thinking for the world,” and I certainly hope nobody is paying for that garbage. But the group’s essay is a good reminder that many progressives see this crisis as an opportunity to further their political agenda, especially as large swathes of the population are at this point willing to accept massive government oversight of their lives in order to flatten the curve and protect the elderly and the vulnerable. This crisis has taught us that our families are essential and that our elderly are valuable, and I hope we remember these lessons when this is all over.
But if you’re one of the clowns over at Open Democracy, the crisis is leading you to entirely different conclusions — conclusions such as the fact that we must get over “the mystification of the couple-form; the romanticisation of kinship; and the sanitization of the fundamentally unsafe space that is private property.” And why do we have to “get over” the idea of marriage and cease “romanticizing kinship,” whatever that means? Because of “the power asymmetries of housework (reproductive labor being so gendered) … of patriarchal parenting and (often) the institution of marriage.” One genuinely wonders what the author of this gibberish had to suffer in order to produce such twisted nonsense.
Homes, Open Democracy informs us, are fundamentally unsafe: “[q]ueer and feminized people, especially very old and very young ones, are definitionally not safe there: their flourishing in the capitalist home is the exception, not the rule. It follows that, upon closer inspection, both terms — ‘social distancing’ and ‘sheltering in place’ — appear remarkable as much for what they don’t say (that is, what they presume and naturalize) as what they do. Sheltering in what place…and in whose? Distance from whom…or everyone but whom?”
Obviously, domestic abuse is an enormous issue, and the sad fact is that some people will feel trapped in their homes. But I would argue that family breakdown has contributed to abuse rather than lessened it, and that the idea of getting rid of the family to eliminate domestic abuse would exacerbate the problem rather than mitigate it. But according to Open Democracy, “the pandemic is no time to forget about family abolition.” In fact, even when homes are safe, the author theorizes, they are still awful and should still be abolished:
[E]ven when the private nuclear household poses no direct physical or mental threat to one’s person — no spouse-battering, no child rape, and no queer-bashing — the private family qua mode of social reproduction still, frankly, sucks. It genders, nationalizes and races us. It norms us for productive work. It makes us believe we are ‘individuals.’ It minimizes costs for capital while maximizing human beings’ life-making labor (across billions of tiny boxes, each kitted out — absurdly — with its own kitchen, micro-crèche and laundry). It blackmails us into mistaking the only sources of love and care we have for the extent of what is possible. We deserve better than the family. And the time of corona is an excellent time to practice abolishing it.
I suspect that there is as much of Freud as Marx in all of that, as the logic of attempting to contain a pandemic by collectivizing and moving us into large group homes escapes me. Perhaps it escapes the author, as well, as I see that this essay is long on abolishing things and short on what, exactly, those things will be replaced with. (Smart Marxists always remain fuzzy on the details.) But I think this crisis, whatever else it brings, will be doing precisely the opposite of what the progressives over at Open Democracy hope. Yes, there are genuinely tragic situations occurring. But for most of us, our families are the silver lining in all of this. Trying to figure out where all of this is headed and to plan for the future is stressful, but all of that can vanish the minute your two-year-old tugs on your sleeve and says: “Hey, Daddy. Wanna snuggle for a minute?”
Providers have challenged being included in the suspension of elective procedures, arguing that their work is ‘essential’ and ‘vital.’
COLUMBUS, Ohio, March 30, 2020 (LifeSiteNews) – As states order suspensions of non-essential medical procedures in order to conserve resources and contain the spread of the coronavirus, abortion facilities in Ohio are calling on the courts to step in and allow abortions to proceed as usual.
U.S. Surgeon General Jerome Adams and the federal Centers for Disease Control (CDC) have advised healthcare facilities to reschedule non-urgent appointments and elective procedures, both to limit the spread of the coronavirus and to free up time and resources to focus on patients afflicted by COVID-19 (the illness caused by the coronavirus).
Compliance with this guidance has been mixed, leading numerous states to mandate that facilities temporarily halt “non-essential” procedures, with Ohio among them. On Monday, state abortion centers, including Planned Parenthood of Southwest Ohio, filed a motion demanding that the Ohio Department of Health be blocked from applying the order to them, The Cincinnati Enquirerreported.
The abortion centers argue that abortion should be deemed “essential” because it’s time-sensitive in nature, even when sought for economic or lifestyle reasons rather than medical ones.
“As leading medical groups have recognized, abortion is essential and time-sensitive health care,” said attorney Elizabeth Watson of the left-wing American Civil Liberties Union (ACLU). “We hope the court will recognize the urgency of this matter and grant relief for our clients so that they can continue the vital work of providing care to their communities.”
“The idea that all abortion care is essential is overblown,” responded Ohio Right to Life executive director Stephanie Krider. “If a woman needs an abortion for some sort of life-saving situation, she’s not going to Planned Parenthood for that abortion. She is going to a hospital.”
Planned Parenthood and other pro-abortion groups are also suing Texas over a similar suspension in that state.
Pro-life medical professionals have assailed the notion that the abortion industry should get a pass from the same standards currently being applied to every legitimate field of medicine.
The American Association of Pro-Life Obstetricians and Gynecologists (AAPLOG) says that while “elective abortion is neither ‘essential’ nor ‘urgent,’” it “does consume critical resources such as masks, gloves, and other personal protective equipment, and unnecessarily exposes patients and physicians to pathogens.”
“Elective abortion, both surgical and drug induced, also generates more patients to be seen in already overburdened emergency rooms,” AAPLOG continued. “Most abortion providers instruct women to go to an emergency room if they have any concerning symptoms after the abortion. Approximately five percent of women who undergo medication abortions will require evaluation in an emergency room, most commonly for hemorrhage. Surgical abortions can also result in hemorrhage. Emergency room personnel – who are already struggling to meet the demands of the COVID-19 pandemic – will be further strained to provide care to these women.”
How many times have we thought – or heard someone say: “I don’t want to be kept alive by a machine.”
As COVID-19 spreads around the globe, the public is learning about the importance of mechanical ventilators in providing temporary breathing support for many of those infected. Ventilators are saving lives!
A false understanding of respirators and ventilators has become commonplace in recent years. Many people think that these and similar machines’ only role is prolonging the dying process. The widely publicized treatment of COVID-19 patients is helping to dispel that myth. Many patients rely on machines temporarily every day for any number of reasons and go on to make full recoveries.
Unfortunately, many individuals have completed advance health care directives stating or suggesting that they do not wish to receive breathing assistance through mechanical ventilation.
Please take the time to review any advanced medical directives (including POLST forms) signed by you or your loved ones to make sure they are clear that mechanical ventilation is not among the forms of care that are refused. If there is any ambiguity, you may want to consider writing, signing, and dating an addendum specifying that mechanical ventilation is authorized.
If you have not already done so, we also encourage you to think about preparing an advance health care directive—especially if you are in a high-risk group. It is important to be sure your documents indicate that you want mechanical ventilation in the event you are unable to express your health care wishes. Click here for Life Legal’s guidance on advance health care directives, which includes a link to state-specific advance directive templates.
If you or someone you know is having trouble receiving life-sustaining medical care, please contact us at info@lldf.org or 707.224.6675.
The new book From the Depths of Our Hearts by Cardinal Sarah and Pope Benedict XVI continues the Church’s ongoing discussion about clerical celibacy, but it seems to me that the whole topic has been kicked into a new category by the invention of artificial contraception.
What has contraception to do with celibacy? The quick-witted might observe that celibacy is the most effective “contraception.” It’s also a sure fire way to prevent sexually transmitted diseases.
However, that’s not the point of the headline. Instead I’ve been thinking about the way artificial contraception has radically changed the whole idea not only of sexuality, but of celibacy, and especially of the celibate priesthood.
Artificial contraception has changed celibacy because it has separated sexual activity from procreation, and once it separated sexual activity from procreation it follows that sexual activity might just as well also be separated from marriage, for marriage is not only for the support and love of the spouses, but also for the security and well-being of children.
The secularist might argue that if sex is not about procreation it is not necessarily about marriage either.
Artificial contraception has made sex into recreation rather than procreation, and therefore the meaning of marriage has also changed. Marriage is intended to be a sacrament of self-sacrifice. Now for the majority of Americans it is a sacrament of self-gratification.
Consequently, celibacy has also lost its meaning. Celibacy only has meaning within the context of marriage. Marriage is a lifelong commitment within which two people grow into the maturity of love and (ideally) do so within the natural dynamic of a large and loving family. Celibacy reflects that love, because when the celibate person sacrifices marital love and family love to make their own lifelong commitment to the greater love of God and others.
The husband and wife love one another and their children completely and fully win a lifelong commitment. The celibate loves God and the human family of his parish and church as fully and completely as he can in a lifelong commitment. Contraception, however, reduces the fullness of marriage and family life to unlimited sexual gratification and thus pulls the meaning out from under marriage and not only pulls the meaning and purpose out of marriage but also pulls the meaning and purpose out of celibacy.
Because artificial contraception turns marriage into little more than sex it therefore turns celibacy into little more than “not having sex.”
Both celibacy and marriage, however, are far richer and deeper and more beautiful than “just sex” or “not having sex.”
Artificial contraception has not only degraded marriage, but it has completely altered the popular conception of marriage. This, as a result, has changed totally the conception of the celibate priesthood.
Let me explain with a practical example. Before artificial contraception, marriage was a sacrament of self-sacrifice. For the vast majority of men and women, marriage meant a large family, long hours of hard work to support that family and a difficult, but rewarding life of sacrifice, work, trials, tribulations, joys and sorrows. To be a celibate priest was also a rewarding life of self-sacrifice but by a different path.
Think for a moment of the choice a young man would have had in a Catholic community in a place like Philadelphia in the 1940s.
He would have seen his uncles and father and older brothers who had chosen marriage. Perhaps they lived in a little row house with a wife and half a dozen kids. The man would work long hours to support his large family. He and his wife had a joyful but hard life of self-sacrifice.
The young man might be considering the priesthood, and for him the celibate life was not so bad. He got an education. Maybe he had the chance to travel. He lived in a big rectory with three or four other priests with a nice Italian grandma to cook for them and look after them. In the extended family in his part of the city he had mom and pop and brothers and sister and uncles and aunts and nieces and nephews. He served them as “father” in the way his brothers served their own kids. It was also a way of self-sacrifice, and compared to his brother’s big family it has equal joys and sorrows of its own.
The choice between celibacy and fatherhood was between one way of total sacrifice and another way of total self-sacrifice. Self-sacrifice as a father and husband or self-sacrifice as a father-priest.
Now think of the choices facing a young Catholic man today: the models he has for fatherhood are mostly men who have used contraception to have two or maybe three children. The wife works. Double income. Trophy house. A good retirement plan. Kids in private school. Not much suffering or difficulty at all. It seems to him like the modern American Dad has it all because contraception has provided the way for him to “have it all.”
The young man who is considering the priesthood is likely to face a life living alone in a big rectory, being suspected of being a pedophile and working long hours for little reward or recognition. His celibacy seems like a curse not only of loneliness, but a reminder that he has given up everything the suburban man takes for granted. Contraception has not only given the suburban man endless child-free sex. It has given him access to a previously unimagined level of wealth.
Marriage has therefore become not a sacrament of self-sacrifice, but a sacrament of self-gratification. Whereas, for our grandfathers marriage was a way to give all, for us marriage is a way to get all.
No wonder the celibate may think from time to time that it is all very unfair. Not only does he give all, but the very meaning of what he is giving is pulled out from under him because the meaning of marriage (in which the meaning of celibacy is rooted) has been destroyed. Conversely, while marriage gives celibacy meaning, it may be now that celibacy may begin to give meaning back to marriage.
This could be reversed, however. The self-giving service of the celibate priest may start to remind people of the true meaning of marriage. The true meaning of marriage is that it is a sacrament of self-sacrifice and service. Married people may observe the self-sacrificial sacrifice of the priest and be reminded that as the priest is “married to the church” in loving service, so too, they are to be married to their spouses in a lifelong commitment of loving service.
This is why the Catholic Church will soon become the sole defender of marriage: because it has continued to be the sole defender of celibacy.
By Anne Marie Williams “Every single person is made by God for love. Every single person is made for a great and beautiful purpose.” Since their founding in 1991, the Sisters of Life, a vibrant order of Catholic religious sisters, have been sharing this message with women experiencing unplanned pregnancies or suffering in the aftermath of an abortion.
What started out as a local ministry to women near their New York City convent spread over time to missions in Washington D.C., Philadelphia, and Toronto. Then, five years ago, they began bringing this good news to college campuses in Colorado. Live Action News spoke to Sr. Maris Stella, one of the sisters living at the Denver convent, about why they are called the Sisters of Life, what brought them to minister on college campuses, what a day in their life looks like, and how their work is building up a culture of life.
While all religious sisters take vows of poverty, chastity, and obedience, the Sisters of Life take a fourth vow “to protect and enhance the sacredness of human life.” Sr. Maris Stella said that this vow flows from their understanding that “every person is good and valuable, and their life has meaning.” While the sisters have been inviting pregnant and post-abortive women to accept this radical love for years, Sr. Maris Stella told Live Action News that she and her fellow sisters in Denver undertook “a mission of evangelization on college campuses because this population is most vulnerable to abortion. Oftentimes, a pregnant woman in college feels that the only way to preserve her dreams is to end the life of her child.”
The sisters in Denver aim to meet women in this place of overwhelming uncertainty and fear with another option: “You can make choices that will help your life flourish.” The Sisters have found that “when people experience being loved for who they are, they thrive, live in joy, and dream about their futures.”
Five school years ago, the sisters launched their ministry on three college campuses. Now, the Sisters minister monthly to six campuses, five in Colorado and one in North Dakota. They typically travel in teams of several sisters, and occasionally all six together, for three days at a time to each place. Their schedules usually include hosting a women’s night, composed of a dinner, a talk on some aspect of God’s plan for life and love (often as part of a semester-long series), and a holy hour of Adoration.
The sisters also engage in “tabling,” setting up a table and engaging students in high-traffic areas of each campus. Sr. Maris Stella shared a story from a recent project where the sisters passed out stickers with messages like, “Created by God: Irreplaceable.” One young woman walked by the group, head down, and a sister called out to her, offering her a sticker. The woman looked up with a hostile expression and refused. The sister said, “it just says ‘you’re irreplaceable.’” The woman stopped in her tracks and received the sticker.
In a completely different tone of voice, the young woman said, “Thank you. I needed to hear that because I have been feeling very replaceable lately.”
The sister said, “She left believing something different about herself and her identity.”
The sisters also spiritually mentor 150-180 young women each month. The goal listed on their website is “to accompany students in discovering their beauty, value, and uniqueness. We want you to know, deep down, that your life is a gift, full of meaning and purpose. We are here to walk with you as you come to discover your inner greatness and the gifts that you are destined to share with the world.” Sr. Maris Stella commented that this can serve “as a point of integration for all aspects of their lives.”
While the Sisters may not always speak directly to abortion-vulnerable women, through their evangelistic efforts they can reach the people these women are likely to turn to in times of crisis: their roommates and friends.
Overall, the Sisters’ most important “task” is to pray for four hours each day. All of their work flows from this primary relationship with Jesus Christ. Having first been loved by Him, they can then “bring a maternal presence” to the college campuses, a presence that includes a listening ear and a warm, open heart that accepts and welcomes the other person in. This unconditional love builds up a culture of life.
March 20, 2020 (LifeSiteNews) –– Scientists who are now claiming that the Trump ban on fetal tissue usage is blocking coronavirus treatment research are using the current pandemic opportunistically to reinstate the usage of tissue derived from aborted babies at government research facilities.
“A senior scientist at a government biomedical research laboratory has been thwarted in his efforts to conduct experiments on possible treatments for the new coronavirus because of the Trump administration’s restrictions on research with human fetal tissue,” blared the lede in a Washington Post article.
Kim Hasenkrug, an immunologist at the National Institutes of Health’s (NIH) Rocky Mountain Laboratories in Montana, told the Post that he has been arguing for a month that the pandemic “warrants an exemption to a ban imposed last year prohibiting government researchers from using tissue from abortions in their work.”
‘Humanized mice’
U.S. scientists had found last year that “mice could be transplanted with human fetal tissue that develops into lungs — the part of the body the new coronavirus invades,” according to the Post report. These “humanized mice” are seen as important by some because they “could then be infected with coronaviruses — to which ordinary mice are not susceptible — closely related to the one that causes the new disease, covid-19.”
The fetal tissue to create the “humanized mice” that researchers like Hasenkrug would like to access would have to be provided by women undergoing elective abortions.
Hasenkrug, who works at an NIH research lab, has been prohibited from using aborted baby body parts since Health and Human Services (HHS) announced last year that it had changed its policies concerning the use of fetal tissue.
“Promoting the dignity of human life from conception to natural death is one of the very top priorities of President Trump’s administration,” an HHS statement explained.
Playing on people’s fears
“Those who advocate experimentation using body parts harvested from aborted children are shamelessly exploiting the coronavirus pandemic, playing on people’s fears at a vulnerable time so that a select few can continue to use aborted fetal tissue in their research,” declared a statement released by the Charlotte Lozier Institute (CLI) in Washington, D.C.
“The fact is that there are modern, successful alternatives available,” continued the CLI statement. “Already, over 60 potential treatments are under investigation — none of which need aborted fetal tissue to fight coronavirus.”
“Instead of wasting precious time listening to these dishonest claims, we should continue to focus our attention on successful, ethical alternatives that don’t require the exploitation of baby body parts, taxpayer dollars, and public sentiment that just wants a swift and compassionate end to this crisis,” said CLI.
Last month, CLI criticized claims made in a USA Todayopinion piece by San Francisco–based professors Irving Weissman and Joseph McCune. The pair made an appeal similar to Hasenkrug’s, asserting, “People will suffer and die for lack of adequate treatments,” because aborted fetal tissue could not be used for research.
In December 2018, CLI’s vice president and research director, Dr. David Prentice, and senior fellow in life sciences Dr. Tara Sander Lee testified before Congress regarding the array of ethical alternatives to experiments using aborted baby parts and that fetal tissue research is medically unnecessary.
Sander Lee explained that less than 0.4 percent of the NIH’s budget is currently going toward research involving fetal tissue; that “after over 100 years of research, no therapies have been discovered or developed that require aborted fetal tissue”; and that researchers have access to a wealth of ethical sources for human tissue, including cells that can be given the coveted quality of pluripotency, or the ability to become other types of tissue.
The CLI scholar went on to detail how the original polio vaccine was first developed with monkey kidney cells; how vaccines for measles, mumps, and rubella can be produced with cell lines from chicken eggs, human placentas, human kidney cultures, monkey cells, and chick embryo fibroblasts; how the vast majority of the research currently being done on the Zika and Ebola viruses does not use fetal tissue; and how even the vaccines currently being produced in the United States with fetal tissue are using cell lines from the 1960s rather than newly obtained tissue from abortions.
Ethical alternatives currently available to researchers “include, but are not limited to, fresh human tissues from adult and pediatric populations, donated and discarded biopsies and surgical specimens, from both living and post-mortem individuals,” she continued. “There are numerous examples of investigators successfully using these ethical alternatives for research and clinical trials for studying the most complex processes, such as brain development and neurodevelopmental disorders, immune response to pathogens, and stroke.”
Sander Lee is an associate scholar with the pro-life Charlotte Lozier Institute. She holds a Ph.D. in biochemistry, studied molecular and cell biology at Boston Children’s Hospital and Harvard Medical School, and has 20 years of experience with both academic and clinical medicine.
Trisomy 18, also known as Edwards syndrome, has been labeled as “incompatible with life” by some doctors. Those doctors will often advise expectant parents to terminate their pregnancies when babies are determined to have the condition. But, as difficult as it might be, there are people living their lives every single day with the condition, and proving that Trisomy 18 and life are not incompatible when they are given a chance.
Faith Smith
Faith. Photo courtesy of Smith family.
When Faith Smith’s parents Brad and Jesi were told by doctors that there was no hope for her survival and that they should undergo amniocentesis to confirm the diagnosis so they could abort, they refused. Doctors said Faith would destroy their finances and ruin their marriage, but the couple insisted that they would not end their daughter’s life.
After Faith was born, she was officially diagnosed with Trisomy 18, and her parents did everything in their power to get her the care she needed. They often had to fight doctors — and even an ethics committee — to ensure Faith was cared for. It paid off. Faith is now 11 years old and just underwent spinal surgery for scoliosis and kyphoscoliosis in February.
“She is now several inches taller, back to walking in her gait trainer, and playing her keyboard with such great posture that our family is encouraged to sit straighter too,” Jesi Smith told Live Action News. “She has somehow gained extra sympathy from her siblings due to the surgery and has us all trained to give her back rubs. Really, with as much attention and love she gets from all of us her life is enviable.”
Melody Thenhaus
Melody practicing walking with her monkey bars built by her dad. Photo courtesy of Thenhaus family.
Melody Thenhaus wasn’t diagnosed with Trisomy 18 until after birth. She had just one marker for the condition during pregnancy, and doctors weren’t concerned. Her parents, Jennifer and Andrew, named her Melody partly because of how she loved music even while in the womb. But at birth, she did not open her eyes, cry, or move.
“That evening my husband decided to play music from the Eden String Quartet on his phone. All of a sudden we saw movement in Melody’s little isolette,” her mom Jennifer Thenhaus recalled. “Little toes wiggled, hands moved, and then eyes popped open. […] This incident was a significant gift from the Lord that gave us a glimmer of hope.”
Melody is now seven years old! “She is healthy, happy, and full of personality,” her mom told Live Action News. “She is extraordinarily charming. It is not uncommon for someone who works with her on a regular basis to exclaim that she is the sweetest child on the planet. She is exceptionally lovable. Melody currently has no health issues. Although Melody has delays in her development, she has been making remarkable advances lately. She loves to read books, play, cuddle, and drive her pink Porsche.”
Kayden McClanahan
Photo: Marta McClanahan Facebook
Now almost 19 years old, Kayden has been defying the odds for nearly two decades. His parents were told he wouldn’t survive to see his first birthday, but last year, he graduated from high school, pushed across the stage by his big brother. On his 18th birthday, his mother Marta Johnson McClanahan shared photos of him throughout his life, saying he had lived “an amazing 18 years full of LOVE, happiness and lots of fun!”
“Drs talked about no quality of life does this look like no quality???” she wrote.
McClanahan told Live Action News that Kayden underwent open-heart surgery this year and is doing well. He is looking forward to receiving a new adaptive bike. Kayden lives a happy life and is adored by his family.
Bella Santorum
Photo: Bella Santorum via Karen Santorum Facebook.
Bella Santorum is the 11-year-old daughter of former Senator Rick Santorum and his wife Karen. Doctors predicted she wouldn’t survive long enough to be discharged from the hospital, but she has proven them all wrong.
“When I think of being pro life, an image comes to my mind,” Bella’s sister Elizabeth Santorum Marcolini wrote on Facebook. “It’s not a baby in a womb or a mother in distress, it is my 11 year old sister. Bella was born with a rare genetic birth defect called Trisomy 18. According to medical textbooks, she is ‘incompatible with life,’ but from where I’m sitting, that’s the biggest lie we were ever told. Bella is full of life.”
Marcolini describes Bella’s “beautiful giggle, her joy, her sweetness” and considers how many children like Bella are missing from the world because of abortion. Her mother calls her “the happiest little girl in the world.”
While Trisomy 18 is a very serious health condition and not everyone who has it will survive as long as these individuals, what’s important to realize is that each of these lives is precious and deserves to be lived to the fullest. Even if a baby with Trisomy 18 lives for only hours after birth, his or her life is a gift and should be honored with love rather than tossed away through abortion.
In 1940, an Italian Catholic priest known as Padre Pio announced his plans to found a “Home for the Relief of Suffering” (Casa Sollievo Della Sofferenza), a hospital that would serve as “a haven of relief from suffering for all of God’s children in pain in body or soul.” The Casa’s doors opened in 1956, with 300 beds. At the same time, Padre Pio developed a worldwide prayer ministry to support the work of the Casa. Today, the Casa is a thriving 1,000+ bed hospital facility, considered “a model of community of Catholic Christian health delivery.” All this is despite its location in “one of the most remote, desolate and poorest parts of Italy,” some four hours from Rome.
Fifty-three years later, Padre Pio is a canonized saint in the Roman Catholic Church, and in October of 2009, the administration of the Italian Casa entered into formal agreements with the administration of Catholic Healthcare International to bring the Casa model to the United States.
In early 2020, Catholic Healthcare International announced that it is actively moving forward with plans to break ground in the Diocese of Lansing, Michigan. According to the CHI website, the Casa USA has a three pillar vision: 1) a medical school faithful to the teachings of the Catholic faith, to be called the School for the Relief of Suffering; 2) a Casa USA hospital; and 3) a Catholic physician practice network.
A recently released bulletin also listed a worldwide prayer ministry, an on-site perpetual adoration chapel, and planned collaboration with the Terri Schiavo Life & Hope Network to “establish a safe-haven center” for “patients with traumatic brain injuries” like Schiavo’s. There will also be a partnership with the Christ Medicus Foundation to include a National Center for Public Policy on-site. According to the CHI flyer about the project, the Casa USA will serve as a “‘Beacon
of Light’ of faithful Catholic health care delivery for all Catholic providers of care and medical education in the US.”
Far from having implications for Catholic health care professionals alone, the Casa USA endeavor bears watching for all pro-lifers in health care. In a culture increasingly desensitized to the innate dignity and value of human life, the Casa model represents hope for ethical health care for all of us.
The results of a small study in China that followed four pregnant women infected with COVID-19 during pregnancy, suggest that the viral infection doesn’t pass from mother to infant at birth. All four mothers in the study, which focused on the health of their newborns, gave birth at Wuhan’s Union Hospital. The report, published in the journal Frontiers in Pediatrics, is the second to come out of China within a month to find that mothers infected with the SARS-CoV-2 virus did not infect their babies.
“Importantly, we found neither SARS-CoV-2 diagnostic positivity nor immediate evidence of symptomatic COVID-19 among these infants born to symptomatic, test-positive mothers,” commented Yalan Liu, PhD, at Huazhong University of Science and Technology, and colleagues in their Frontiers in Pediatrics report, which is titled, “Infants born to Mothers with a New Coronavirus (COVID-19).” Liu also works in the Department of Pediatrics at Union Hospital.
The study by Liu and colleagues follows on from a report by researchers in China, and published in The Lancet in February on the results of a study in nine pregnant women with laboratory-confirmed COVID-19 pneumonia. This report had also concluded that there was “… currently no evidence for intrauterine infection caused by vertical transmission in women who develop COVID-19 pneumonia in late pregnancy.”
Liu et al. followed four pregnant women who presented with symptomatic COVID-19 infections during the 3rd trimester of pregnancy. Four full-term infants were born. Cesarean sections were performed for 3 patients in the acute phase of the disease, and the fourth patient underwent a vaginal delivery because of the onset of labor. The nine mothers followed in the prior study in The Lancet had all undergone Caesarian sections.
“To avoid infections caused by perinatal and postnatal transmission, our obstetricians think that C-section may be safer,” Liu said. “Only one pregnant mother adopted vaginal delivery because of the onset of the labor process. The baby was normal. Maybe vaginal delivery is OK. It needs further study.”
None of the four infants in the latest study developed any serious symptoms, such as fever or cough, which are associated with COVID-19, although all four were initially isolated in neonatal intensive care units and fed formula. Three of the four tested negative for the respiratory infection following a throat swab, while the fourth child’s mother declined permission for the test. “ … we found neither SARS-CoV-2 diagnostic positivity nor immediate evidence of symptomatic COVID-19 among these infants born to symptomatic, test-positive mothers,” the investigators noted.
One newborn did experience a minor breathing issue for three days, and this was treated using non-invasive mechanical ventilation. Two babies, including the one with the respiratory problem, exhibited body rashes that eventually disappeared on their own. The team acknowledged it’s not possible to conclude whether there’s a connection between these other medical issues and COVID-19. “We are not sure the rash was due to the mother’s COVID-19 infection,” said Liu. All four infants remained healthy, and their mothers also fully recovered.
In previous coronavirus outbreaks, scientists found no evidence of viral transmission from mother to child, but SARS and MERS were both associated with “critical maternal illness, spontaneous abortion, or even maternal death,” according to Liu.
The authors said further investigations into other aspects of potential COVID-19 infection in newborns and children are needed. For example, the sensitivity of the current diagnostic test for detecting the virus is about 71%, they noted, and its reliability should be evaluated in children. “Further study for viral infection in placenta, amniotic fluid, neonatal blood, gastric fluid and anal swab, and the viral depending receptor on children will be detected in future,” they further commented.
(MRC-TV) Amid mass panic over the seemingly inevitable coronavirus outbreak sweeping the country, some in the abortion industry are using the widespread alarm to tout the importance of…abortion.
Why? Well, that’s unclear, given that abortion has nothing at all to do with the coronavirus. Even still, several abortionists and abortion advocates have taken to Twitter to stump for the public’s “right” to access abortion pills via telemedicine (i.e., an online consultation without having to physically see a doctor).
Dr. Dustin Costescu, an OBGYN, associate professor and “sexual medicine specialist” at McMaster University, tweeted that “self-managed abortion is safe” and “avoids in person appointments,” inexplicably predicting that telemedicine abortion “will be necessary to address the increased incidence of unintended pregnancies that will result from self-quarantine.”
Dr. Dustin Costescu@BirthControlDoc
#COVID2019 is a good time to remind you that Self-Managed abortion is safe, avoids in person appointments, and will be necessary to address the increased incidence of unintended pregnancies that will result from self-quarantine.
After claiming that at-home abortions via the abortion pill are “safe,” Costescu seemingly contradicted himself by adding that “Systems need to be prepared to respond to possible complications from failed self-management, including ectopic pregnancy and bleeding.”
Pregnant patients with low risk of ectopic pregnancy and with reasonable certainty of their last period being within 8 weeks can safely use mifepristone followed by misoprostol with over 95% probability of successful completion without medical intervention.
Dr. Dustin Costescu@BirthControlDoc
Systems need to be prepared to respond to possible complications from failed self-management, including ectopic pregnancy and bleeding.
But abortion by telemedicine or self management are safe and effective strategies to reduce visits during the outbreak.
“But,” he simultaneously said, “abortion by telemedicine or self management are safe and effective strategies to reduce visits during the outbreak.”
Dr. Daniel Grossman, another vocal abortionist with a large Twitter following, retweeted Costescu’s statements, adding that the coronavirus is “a reminder of why we must expand telemedicine to patients, including for medication abortion.”
“Patients should have access to healthcare, whether they are able to make it to the clinic or not,” he wrote. “Self-managed abortion and telemedicine can ensure they receive care.”
This is also a reminder of why we must expand telemedicine to patients, including for medication abortion. Patients should have access to healthcare, whether they are able to make it to the clinic or not. Self-managed abortion and telemedicine can ensure they receive care. https://twitter.com/BirthControlDoc/status/1237177485336416258 …
Dr. Dustin Costescu@BirthControlDoc
#COVID2019 is a good time to remind you that Self-Managed abortion is safe, avoids in person appointments, and will be necessary to address the increased incidence of unintended pregnancies that will result from self-quarantine.
The big push for online abortion pills prescribed via telemedicine comes just after the Ohio state Senate passed a bill that would outlaw telemedicine abortions within the state, requiring instead that physicians be certified to distribute the drugs, as well as mandating that an in-person evaluation be conducted before a patient is prescribed the abortion medication.
The drug centers on two drugs. Mifepristone, or “Mifeprex,” is a synthetic steroid. When taken in conjunction with misoprostol, the combination carries a 95 percent success rate of forcing a woman’s body to miscarry. Because of its function, it’s recommended that the drug only be taken up until the 10th week of pregnancy. The roughly five percent of children who survive the process are at much greater risk of birth defects.
While abortion supporters say the medication carries a low risk of complications, the FDA warns against women with certain conditions taking these drugs, as side effects can include uncontrolled bleeding that requires surgery, sepsis, flu-like symptoms and even death. The FDA added it has “received reports of serious adverse events in women who took Mifeprex, including “one case of ectopic pregnancy resulting in death; several cases of severe systemic infection (also called sepsis), including some that were fatal; and a single case of non-fatal heart attack.”
Editor’s Note: This article was published at MRC-TV and is reprinted here with permission.
A pro-life ministry in Omaha, Nebraska, has found an innovating new way to reach the next generation. Heart of a Child Ministries has been using ultrasounds to show people the humanity of preborn children within the womb. Founded by Bernie and Nikki Schaefer in 2012, the ministry offers ultrasound presentations, along with pro-life prayer pillows, to help build a culture of life.
One of their recent presentations at a Catholic high school was highlighted in a story in the Omaha World-Herald. Haley Lubeck, who is 24 weeks pregnant, sat for an ultrasound conducted by Angela Himmelburg, a professional sonographer who graduated from the University of Jamestown and University of Nebraska Medical Center. Himmelburg narrated throughout. “Can you see the eyes?” she asked, then pointing out, “Here’s an arm right here… there’s a foot digging into the placenta.”
Focus on the Family has also used ultrasounds to try to change hearts and minds, and even hosted a live ultrasound presentation in Times Square last year. Approximately 20,000 people watched what Paul Batura, vice president of communications for Focus on the Family, described to the Omaha World-Herald as a “game-changer,” explaining that the ultrasounds serve as “a window on the womb.”
Along its ultrasound presentations, Heart of a Child Ministries also gives scientific information about fetal development. The group’s goal is to fully illustrate the indisputable humanity of children in the womb.
Each presentation is tailored to the specific age of the students attending. “My kids loved it. I felt like they did a great job explaining things at their level,” a first grade teacher said in a testimonial on the ministry’s website. A third grade teacher added, “The students were totally entranced with the presentation and the live ultrasound. The ‘props’ (seeds) made it so much easier for the kids to understand. The small groups were phenomenal and explained everything so well. And who doesn’t like gifts?… rosary, baby, brochures. Wow! So awesome! GREAT presentation!!”
The subject of abortion is not brought up until seventh or eighth grade, in specific middle school presentations.
“Seeing the live ultrasound made me want to cry,” said Liv, a seventh-grader, in a testimonial on the website. “It is so undoubtedly amazing how something only 17 weeks old is circulating its own blood, has working organs, and continuously moves around. Hearing the baby’s heartbeat is the most amazing thing. It shows that it is more than just a lump of tissues and cells. It is a baby and it is fully alive.”
In addition to school presentations, the group offers presentations for adults as well, often hosted by Nikki Schaefer, who has a master’s degree in social work. Schaefer has also worked for pregnancy resource centers, as well as in art therapy and parenting groups with pregnant and parenting teens. During adult presentations, she focuses on seeing the heart of each child, and what the ministry calls “the three pro-life calls of prayer, action and truth.”
Showing young people the truth of humanity of the preborn is a unique, powerful, and positive way to help create a new generation of pro-life activists.
Hormonal contraceptives such as the Pill could be sabotaging women’s success, a study suggests.
Women were found to give up quicker than those who were not on contraceptives when presented with both simple and difficult problem solving tasks.
This in turn caused them to score worse, and it could have implications for their performance at school, college and work, the researchers at Texas Christian University said.
Previous research has shown a link between hormonal contraception and altered brain function in areas responsible for motivation, emotion and attention.
PhD candidate Hannah Bradshaw and colleagues set out to explore how hormonal contraceptives affect perseverance on tasks using the brain.
Studies show the ability to persevere, even if a task is challenging, can predict a person’s success in many areas of life.
However, evidence is emerging the hormonal contraceptives may negatively affect this trait.
Ms Bradshaw said: ‘A growing body of research suggests that HC use may be associated with important structural and functional differences in brains areas important for executive function and the cognitive control of behaviour.
‘Research suggests that HC use may also have effects on women’s brain structure and function.’
The team recruited college students from a university in southern US. It compared women who had either been using a HC for two months, or off them for at least three months.
The first study asked 149 women, of which 73 were on HCs, to do a simple ‘spot the difference’ task using an image from the film Frozen.
Naturally cycling women who were not on HCs spent significantly more time on the task than women on HCs, 81 seconds compared with 67 seconds.
Analysis showed that women on HCs performed worse because they gave up quicker, the researchers said.
The second study, consisting of 175 female undergraduates, 89 of whom were on HCs, involved more challenging tasks.
First, women had to solve eight mathematical tasks with the help of a calculator.
Results show naturally-cycling women spent 97 seconds on the task compared with women on HCs who spent 78 seconds on it, who also performed worse.
Next, women unscrambled jumbled letters – an anagram – to make words. Some were ‘fake’ because they were unsolvable.
In both the real and fake anograms, women who did not take HCs spent more time trying to figure them out.
The researchers said timing how long participants took on each task relative to how well they scored was a measure of their perseverance.
Concluding their findings, the authors wrote: ‘These results suggest that HC use may affect women’s perseverance on simple and challenging tasks.’
The study did not attempt to uncover why HCs may alter cognitive performance, but Ms Bradshaw and colleagues suggested some reasons based on previous research.
HC users have been shown to have decreased connectivity in the brain’s executive control network, responsible for paying attention, organising and planning, initiating tasks, regulating emotions and keeping self-control.
Additionally, oestrogen levels, which are generally lower for HC users, are found to play a key role in hippocampal function, also involved in emotion control as well as motivation.
The authors said: ‘While additional research in humans is needed to evaluate these possible mechanisms, the current results provide compelling evidence that differences in perseverance during cognitive tasks exist between women who take HCs and those that are naturally-cycling, which can lead to decrements in performance.
‘It is, however, important to note that HC use can also aid in women’s educational attainment by allowing them to prevent unintended pregnancies, which can be an insurmountable barrier for those who wish to further their education.’
Approximately three million women in the UK take the contraceptive pill, and a further 11million women in the US use hormonal contraceptives.
In July 2019, 20-year-old Ally Givens got out of bed to use the bathroom, collapsed, and died. She was just two days shy of her 21st birthday. Her boyfriend said she fell to the floor and he quickly called 911, but Givens was unable to be revived, and died from a pulmonary embolism caused by blood clots that formed when she began using the NuvaRing for birth control. Sadly, Givens isn’t alone. Many women have suffered the consequences of hormonal birth control — including death — after believing it was safe.
1. Pulmonary Embolism
Though pulmonary embolism is rare, it is deadly for one-third of the people who are not immediately diagnosed with blood clots that can move from the other parts of the body to the lungs. Combination birth control pills including Yasmin and Yaz carry a risk of pulmonary embolism, especially for women who have pre-existing factors, which they may not even realize. Even when women are told of the risk of blood clots, they may not know their complete family history or what the signs of blood clots are until it is too late. Before taking birth control, it is vital that a woman knows any family history of blood clots and it is important that she understands the symptoms so that she can get help if and when she needs it.
2. Heart Attack or Stroke
Just as with pulmonary embolism, heart attacks and strokes can occur when blood clots form. A review of different studies found that compared to women who don’t use oral contraceptive pills, there is a 1.6-fold increased risk of a blood clot in an artery that obstructs blood flow to major organs — including the heart and brain — in women who do use contraceptive pills. The risk is twice as high for women taking pills with higher doses of estrogen.
3. Breast Cancer
The risk of developing breast cancer is greater for women who use hormonal birth control compared to women who have never used it. Higher estrogen levels are linked to birth control, and The New York Times stated that for every 100,000 women, hormonal contraception use causes an additional 13 cases of breast cancer each year. According to Cancer.gov, women who are currently using oral contraception have a 24 percent increased risk of developing breast cancer. That risk declines when oral contraception use is suspended.
4. Cervical Cancer
According to Cancer.gov, women who have used oral contraception for five or more years are at a higher risk of developing cervical cancer than women who have never used oral contraception. And the longer women use oral contraception, the higher the risk. One study found a 10 percent increased risk when oral contraception was used for less than five years. A 60 percent increased risk existed for women who used oral contraception for five to nine years. And the risk doubled for women using oral contraception for 10 or more years. The risk dropped after women stopped using oral contraceptives.
5. Depression
Another major side effect of hormonal birth control is depression, especially in teens. A study from Denmark found that “women taking the combined oral contraceptive were 23% more likely to be diagnosed with depression and those using progestin-only pills (also known as the ‘mini-pill’) were 24 percent more likely.” Teens had an 80 percent increased risk of depression when taking the combined pill and double the risk with the progestin-only pill.
6. Alterations in the Brain
Research released in 2019 found that women using birth control pills had “significantly smaller hypothalamus volume” compared to women who do not take the pill. The hypothalamus is at the base of the brain and is responsible for producing hormones, and helps to regulate things like body temperature, mood, appetite, sex drive, sleep cycles, and heart rate. The study also found greater anger and symptoms of depression among women using hormonal birth control.
7. Implant Migration
Implanted birth control is a long-acting device put into a woman’s body; however, in some cases, these devices can migrate in the body, even breaking into pieces that move in separate directions. A study from July 2019 shared the story of a 31-year-old woman whose birth control implant migrated from her arm to her lung. Another woman suffered major health issues when her IUD migrated from her uterus to her stomach, then to her liver, and then broke into as many as five pieces. She developed sepsis after surgery, eventually had to have her ovaries and uterus removed, and lost her toes.
8. Increased Risk of HIV
Hormonal contraception, most notably the injectable birth control Depo-Provera, has been linked to an increased risk of HIV transmission. This is said to be due to biological changes caused by hormonal birth control, including changes to the cells that line the vagina and cervix.
9. Infertility
The use of hormonal birth control carries an increased risk of short-term infertility among women who take birth control for two years or longer. Fifty-four percent of women who try to become pregnant after using condoms as birth control delivered a baby within a year, compared to just 32 percent of women who used hormonal birth control. Women who used an IUD for more than six years had the highest rate of infertility.
10. Rare Brain Tumors
A Danish study found that the use of hormonal birth control can increase a woman’s risk of developing a rare type of brain cancer called a glioma. Women under age 50 who were diagnosed with glioma “were 90 percent more likely to have been using hormonal contraceptives for five years or more, compared with women from the general population with no history of brain tumor,” according to the study leader Dr. David Gaist. The risk appeared to rise according to the length of time women were on birth control.
Unfortunately, these are just some of the risk factors that are associated with the use of hormonal contraception. For decades, women have been told that hormonal birth control is safe and has remained ill-informed of the risks to their health as well as the risk of unintended abortion that can be caused by birth control.
In the last post, we explored how the hormones in birth control interfere with the normal process of maturation of the reproductive system in a teen girl. Doctors may have good intentions when they prescribe these medications, but most do not realize the potential harmful effects that may develop as a result of taking this medication, such as significantly increasing the risk of breast cancer later in life. For this and many other reasons, we must be cautious when considering prescribing birth control to teens.
There is no disputing the fact that the hormones found in the birth control pill are classified as carcinogens. Not just mild carcinogens but the most dangerous type – Group 1 carcinogens[1]. This is the same category where you would find nicotine and asbestos. The hormones in birth control increase the risk of breast, cervical, and liver cancers. The link between hormonal contraceptives and breast cancer is significant. I was skeptical when I first heard this until I studied the mechanisms by which this can occur.
Breast cancer is an epidemic in the United States. One in every 8 women are diagnosed with breast cancer. The incidence of breast cancer has significantly increased in the last 50 years since the birth control pill was introduced. Although there are many factors that have likely contributed to this increased incidence, we must consider birth control as to be a major contributor given its effect on breast tissue. Many newly diagnosed breast cancer patients have told me on the first visit after their diagnosis, quite defensively, that they could no longer take any hormonal contraceptives due to the breast cancer diagnosis. They frequently lamented that they took birth control pills in the first place.
Whether a woman’s breast cancer risk is increased by hormonal birth control or not depends on when in her life she is exposed to the hormones in birth control.
Let’s look at the natural process of breast maturation. Prior to a woman’s first full-term pregnancy, her breast tissue remains in a very immature, fragile stage of development. At this stage, her breast tissue is much more susceptible to the carcinogenic effects of birth control. For example, the estrogen-like component in hormonal birth control (ethinyl estradiol) mimics natural estradiol but is not the same hormone; therefore, its effects on the breast, and other organs, are different, and in many cases, toxic. All hormones are not created equal, remember.
credit: Breast Cancer Prevention Institute
Breast tissue becomes fully mature during pregnancy/breastfeeding, and only then becomes much less vulnerable to carcinogens compared to the breasts of adolescent girls. Breast tissue is made of lobules, where milk is made, and ducts, the passageways through which milk flows to the nipple. Consider the analogy of an oak tree. When an oak tree is young, its leaves and branches are tiny and vulnerable to damage from storms. However, when that tree is decades older, it is much more likely to withstand the weather. Breasts are similar in that over time, maturation occurs so that breast tissue is much more resilient and less likely to be harmed by carcinogens. For a woman, this maturation occurs when she becomes a mother during pregnancy due to the continued high levels of estradiol, progesterone, and hCG (human chorionic gonadotropin) hormones. The further the woman’s first pregnancy continues, the more mature (cancer resistant) the breast tissue becomes.
Interestingly, if a pregnancy is terminated (by abortion or pre-term delivery) before the breast tissue has become significantly mature (at about 32 weeks gestation), her risk of developing breast cancer increases. If a pregnancy is interrupted by abortion or pre-term delivery, the natural process of tissue maturation is suspended and the developing cells are then more vulnerable to carcinogens. [2]
You may have heard that women who have never been pregnant are at higher risk of breast cancer. This makes since if you understand the process of breast tissue maturation. These women have breast tissue that has remained in an immature state that is more susceptible to carcinogens.
Bottom line: Having babies is good for breasts, birth control is not.
If you would like to read more about this topic, here are some resources:
Book – Breast Cancer: Its Link to Abortion and the Birth Control Pill by Chris Kahlenborn, MD
In recent years, the birth control pill has become a very common medication prescribed to adolescent girls for a number of apparently good reasons. It appears to help with irregular periods, acne, ovarian cysts, premenstrual syndrome, menstrual cramps, and (of course) pregnancy prevention. I took birth control as a teen and I prescribed birth control to teens – until I stepped back to consider what this medication is actually doing to these girls. In medical school and residency, I was taught that this was a rather innocuous medication that may have some side effects but I was told that the side effects were rare and that the benefits of birth control outweighed the risks. This is simply not true. Let’s take a look at why.
In this post, we will consider the physiology of a teen girl’s developing reproductive system and how the hormones in birth control disrupt this development. This is the case whether we are using birth control to “treat” a symptom or to prevent pregnancy.
Mothers of teens should be well informed before making the decision to allow their daughters to take birth control.
My hope is that this information would be used to help make better decisions.
In the years after a woman’s first period, her body is working hard to establish healthy communication between the brain and the ovaries that is critical to healthy ovulation. There are two glands in the brain – the hypothalamus and pituitary – that are trying to connect to the ovaries via hormone messengers in order to direct the ovaries to make estrogen and progesterone each cycle through the process of ovulation. Think of this as a sort of symphony. Just like an actual symphony, it takes time and practice in order to get it right. This practice can take up to ten years in adolescents in order to establish a healthy system of brain-ovary communication that results in regular periods and healthy hormone production. The idea is that by the time the system is perfected, the woman might have gotten married and then, if everything works well, a baby might be welcomed sooner or later.
As a result of normal process of maturation, it is normal for girls to have irregular periods during their teen years. They may bleed too frequently or too infrequently. Either way, moms get worried and bring their girls to the doctor. Doctors might be too busy to explain the information above so they quickly offer a prescription of birth control to “regulate” the periods. The problem is that the pill does not fix the problem. Instead, it suppresses the “symphony” that simply needs time and practice to perfect itself. In most cases, irregular periods in teens are simply due to an immature hypothalamic-pituitary-ovarian (HPO) axis. In some cases, irregular periods are caused by a disease process such as an eating disorder, thyroid disease, a benign pituitary enlargement, polycystic ovarian syndrome (PCOS) and/or other problems. Either way, the answer IS NOT to shut down the ovaries. We should look for a solution and support the HPO axis in the meantime.
This is my approach to irregular periods in teens:
1. Listen to the teen and her mother. I ask about her diet, sleep habits, stressors and family history of period/fertility problems.
2. If there are any worrisome symptoms – very heavy periods, severe cramps, etc., then I may order tests or I may prescribe natural progesterone to aid the HPO axis as it struggles to get healthy (this really works). We talk about possible causes for her symptoms such as endometriosis or PCOS. Sometimes I recommend supplements or pain relievers that have been researched to be effective for certain symptoms.
3. I ask the teen to start tracking her periods using an app on her phone or paper calendar.
4. I explain to her how her reproductive system works and how she can help it to function well so that she will feel her best.
5. Together with mom, we come up with a personalized strategy to help ease this most beautiful (but challenging) transition from girl to woman.
If you would like to learn more about restoring cycles (and treating other problems) without birth control, I highly recommend the book Period Repair Manual by Lara Briden, ND.
What about using birth control in teens for, well, birth control? I can’t wait to share my thoughts on that in future posts but for now consider this fact:
Hormonal birth control is the only medication in the history of medicine that is given to a healthy person with the intention of making them unhealthy.
Sounds crazy, right? A woman who is ovulating normal is healthy (remember the symphony analogy?). The hormones in birth control are designed to deliberately disrupt this state of health. This disruption causes dysfunction in the woman – physically, emotionally and relationally. Stay tuned for more…
Editor’s Note: The opinions expressed in this guest submission are those of the author and do not necessarily represent the views of Live Action or Live Action News.
As a pro-life activist, I have watched young women walk into abortion facility doors, and I weep, knowing when they walk out, they will no longer be the same. It might not happen immediately, but a change occurs. As the hole in the heart left by the lost baby grows larger, the soul darkens, and hope begins to evaporate.
How do I know? I’ve been there. Twice. It was not long after Roe v. Wade became law that I had my first abortion. I was career-oriented and a die-hard, left-wing feminist. I believed the rhetoric about abortion being a source of empowerment – the power to choose what happens to my own body.
During what I now call my “dark days” (post-abortion), I made very bad choices… many of them encouraged by my best friend, alcohol. Booze was a convenient way to mask all my emotions, especially the guilt and shame of my abortions.
Those choices caused many losses back then — relationships (including two marriages), respect of my family and friends, and a successful career in the government. But the most grievous loss was my fertility. Of all, this was the one that had the most impact.
You see, at the age of 30, I convinced a doctor to give me a tubal ligation. I lied to myself, saying I didn’t want to have any children, but the truth was I felt I didn’t deserve to have any. The guilt and shame of killing my two precious babies resulted in my never being able to conceive again.
I ended up a broken, drunk, and barren woman – because I believed abortion would empower me.
I eventually hit a suicidal bottom and ended up in a mental hospital. When I entered the facility, the psychiatrist asked me why I wanted to die, and for some reason, the first time in decades, I told the truth. I was already dead inside and wanted to finish the job. Through therapy and subsequent alcohol rehab, my head began to clear, but for some reason, I still felt empty, and it remained that way for many years … even with sobriety and continued therapy.
It wasn’t until I began going to church and heard a woman speak about how her abortion affected her life that I was able to connect the dots. I was still carrying regret and shame of my abortions and mourning the deaths of my babies and fertility.
I attended a healing retreat not long after and was able to come to terms with what I had done and finally understand why I sabotaged so much in my life and why my heart was still in pieces. After the retreat, I felt almost whole again. The pieces of my heart were put together by acknowledging my babies’ existence and welcoming them into my life, but the abortions still haunt me and probably always will. I also chose to see my tubal ligation as a blessing that brought me a son through foster care adoption, but the thought of never experiencing carrying a baby to term and giving birth still stings.
I can’t turn back the hands of time. All I can do is speak out and make it abundantly clear: abortion is far from empowering. It’s “unpowering.” It strips power from within and replaces it with years of guilt, shame, and self-loathing, and I want to prevent others from experiencing it all.
BALTIMORE, Maryland, March 3, 2020 (Lepanto Institute) — Following a year-long investigation into Catholic Relief Services (CRS) programs and documents, the Lepanto Institute has published the first of a series of reports showing that CRS was both, directly and indirectly, involved in the promotion of contraception and condoms teens and children as young as 10. CRS is the official overseas relief and development agency of the United States Conference of Catholic Bishops.
In the first report, the Lepanto Institute provided links and screen-captured images of CRS documents that encourage young people to use condoms whenever they have intercourse, while indicating that condoms are effective in preventing the transmission of HIV and pregnancy.
“Catholic Relief Services has long-maintained that it never promotes condom use in its programs, but these documents prove otherwise,” said Michael Hichborn, President of the Lepanto Institute. “Sadly, this isn’t even the worst of what we discovered in our year-long investigation.”
One document produced and copyrighted by CRS in 2017 says (in French), “Condom use should be correct and consistent for any occasional sexual intercourse or with a non-regular partner.” Another CRS-produced document from 2017 (also in French) says, “You can do a number of things to stay as healthy as possible … [such as] use a condom during sex to reduce the risk of sexually transmitted diseases, including HIV, and pregnancies” and then later adds, “For adolescents who need access to HIV prevention methods, such as condoms, it is important for them to know where to access them.”
“In March of 2019, we provided our initial findings regarding these documents to CRS officials and were promised answers,” said Hichborn. “Not only were we never provided answers, but several of the documents disappeared from the CRS.org website, while other condom-promoting documents appeared later in the year.”
A CRS-produced document that was published in December of 2019 indicates to a counselor that a core idea being taught to adolescents in a CRS-run program is, “Delaying sex, limiting the number of sexual partners, and always using a condom are good practices.”
“We’ll be revealing a lot more in subsequent reports, but this is one of the primary reasons we’re asking bishops of the United States to withdraw their support for CRS until there is an independent, third-party investigation of CRS, and CRS is forbidden from receiving federal money,” said Hichborn.
The petition asking bishops to withdraw their support from CRS can be found at the link here.
“The fetal tissue that we’re talking about—if we don’t use it for research, it will be discarded,” said University of California San Diego scientist Lawrence Goldstein, who sometimes uses aborted baby parts in his research. “That’s the choice. Discard the fetal tissue in the trash, or use it for valuable research.”
But that “tissue” comes from human beings, unborn babies whose lives were destroyed in abortions. Some states, prohibited from banning abortions under Roe v. Wade, are trying to at least provide dignity to aborted babies in death by requiring a proper burial or cremation.
The Trump administration also has been working to restore dignity to the unborn child by ending the unethical practice of using aborted baby body parts in taxpayer-funded research. Earlier this month, it announced the formation of a new ethics board to oversee the matter within the National Institutes of Health. Last summer, the NIH introduced new requirements for taxpayer-funded research grants, including detailed explanations from scientists about why they want to use tissue from aborted babies rather than ethically-obtained materials.
The rules apply to tissue and cell lines taken from baby parts from elective abortions only; human tissue donated from miscarried babies and other ethical sources are not subject to the rules.
Microbiologist Carolyn Coyne at the University of Pittsburgh expressed frustration about the future. She told The Scientist that she uses cells from aborted babies to study how viruses penetrate the placenta, but she is concerned about future funding for her research.
“It’s impacted almost all of the facets of the lab,” Coyne said.
Some scientists, like Thomas Reh, a biologist at the University of Washington, have found private donors to fund their research, according to the report. But other scientists noted that not all private foundations will fund research using aborted baby body parts either.
In California, politicians are trying to counteract the Trump policies with their own funding. According to the report: “In California, the state’s stem cell agency, the California Institute for Regenerative Medicine (CIRM) has provided funding for stem cell studies using fetal tissue since it was founded in 2004. That fund is about to run out, but a bill that would provide $5.5 billion in funding to CIRM will come before voters in November.”
Scientists have ethical alternatives, including cells from miscarried babies and pluripotent stem cells, which do not involve destroying human lives. The Trump administration also has been investing in alternative materials. In 2018, it announced a new $20 million grant for exactly that purpose.
But Anita Bhattacharyya, a stem cell scientist at the University of Wisconsin-Madison’s Waisman Center, complained that tissue from miscarried babies is harder to get and often is not intact, according to the report. Bhattacharyya has used brain tissue from aborted babies in her research on Down syndrome and fragile X syndrome, the report states.
Mana Parast, a stem cell and placental biologist at the University of California San Diego, argued that pluripotent stem cells “are fairly new and not yet broadly accepted, it is still necessary to validate them with cells from human placentas,” the report continues.
Goldstein expressed concerns about the new NIH ethics board refusing grants for research using aborted baby body parts.
“[We’ll] see whether the administration is going to act in good faith and appoint a decent ethics review committee, or if they’re going to ignore the value of the scientific and medical research that needs to be done in this area and let ideology weigh out over logic,” he said.
But ethics in research is important, and other scientists contend that aborted baby parts are not necessary in scientific studies.
“We do not need fetal body parts from aborted babies to achieve future scientific and medical advancements. Very little research is actually being done that currently relies on abortion – derived fetal tissue,” said Tara Sander Lee, Ph.D., an associate scholar with the Charlotte Lozier Institute.
In 2018, Sander Lee told Congress that cells from aborted babies never have been the exclusive means necessary for breakthroughs in vaccines and other medical advancements. She said parts from aborted babies have been used in research for more than a century, but “no therapies have been discovered or developed that require aborted fetal tissue.”
Over the past several years, the Trump administration has been listening to pro-life leaders’ pleas to stop using taxpayer funding for research using aborted baby body parts.
The U.S. Department of Health and Human Services also is conducting an audit of all acquisitions involving human fetal tissue to “ensure conformity with procurement and human fetal tissue research laws and regulations.”
In the past, the federal government has given hundreds of millions of dollars to fund research using aborted baby parts. Pro-life groups and conservative news outlets have been uncovering new details about government spending on this unethical research. Some of the government contracts have used tax dollars to pay for body parts of healthy, late-term aborted babies – including potentially viable unborn babies up to 24 weeks.
In 2018, a CNS News report shed light on how taxpayers’ money is being spent on these ethically troubling experiments. It exposed the NIH contract with University of California San Francisco for aborted body parts to conduct experiments involving “humanized mice.”
Aborted baby body parts used in the experiments were taken from healthy, later-term unborn babies. According to the report, the aborted babies were 18 to 24 weeks gestation from “women with normal pregnancies before elective termination for non-medical reasons.” Another article indicated aborted babies’ livers and thymuses also were used. They were between 20 weeks and 24 weeks gestation.
A 2017 journal article indicates researchers also used aborted babies’ intestines in their experiments.
Dr. Imre Teglasy’s life dispels the myth of “my body, my choice.”
Born in 1952 in communist Hungary, Teglasy survived multiple abortion attempts on his life. Today, he is a dedicated pro-life advocate who has helped to save tens of thousands of unborn babies from abortion.
His parents’ circumstances were extremely difficult in 1951 when he was conceived. Teglasy said his father had been a major in the Hungarian army during World War II, but when the communists took over, he was declared an enemy.
Teglasy said his father, mother and older brothers were removed from Budapest and forced to resettle in a poor, rural area in northern Hungary. His father struggled to find work, and the family nearly starved.
“While in this sad plight, my mother realized she was pregnant. My father did not favor the abortion, but my mother did not want to carry me to term,” he said.
Desperate, his mother tried to find a doctor willing to abort him, but abortions would not become legal until five years later. Teglasy said she tried to throw herself against a desk, took hot baths and eventually took quinine pills to attempt to induce labor. Nothing worked, and, in 1952, he was born.
The relationship between mother and son was strained, though Teglasy did not know why for many years.
“When I was a little boy of 3 years old, I kept looking for my ‘real’ mother since I could not accept … that she was my mother,” he said.
He remembered how his godmother treated him with more love and care than his birth mother did.
“As a child, I could not ask her about the strange relationship we had because I simply did not know about her abortion attempts,” he said.
Then, one day when he was about 12 years old, he accidentally overheard his father talking to a relative about the abortion attempts, Teglasy said. It was not until his mother was on her death bed, decades later, that the two finally reconciled.
“Only then at the end, I felt I could draw close to her,” he told LifeNews. “The experience of reconciliation was so bittersweet … I hope she experienced forgiveness in the sense of knowing herself guilty of serious offenses but throwing herself on God’s mercy.”
In those final moments together, Teglasy said he also realized that he had been wrong to resent his mother. At her bedside, he said he cried and asked God to forgive both of them.
Teglasy believes his life is a “miracle,” and he has dedicated it to helping others in need. He envisions a future where pregnant mothers view their pregnancies “not as burdens or curses but rather as an expecting, joyful and glorious stage of their motherhood.”
Since 1956, more than 6 million unborn babies have been legally aborted in Hungary, but were it not for Teglasy, there could have been many more.
He began working with Human Life International after meeting Father Paul Marx, the founding president of the pro-life organization, in 1992. Four years later, Teglasy formed his own pro-life organization, Alpha Alliance, which has provided support for approximately 43,000 mothers and babies to date.
“I am truly thankful to her since she, by her brilliant talent, made me and many thousands of good, willing people to understand the deeper dimensions and meaning of our own tragedies,” he said.
Faces of Choice has been helping to shed light on the reality of abortion through the stories of abortion survivors. Despite ultrasounds and other modern medical advances, Teglasy said people are still deceived by the myth of “choice.”
“We live in a time when, in spite of all the highly developed technical advances, abortionists usually turn away the screens of their ultrasound machines to conceal the reality of children before birth from the eyes of their parents,” he said.
“This means that they have fear of admitting that children before birth are real persons and faces of mankind,” he continued.
“We have the mission of encouraging all the modern followers of Doubting Thomas by saying this to them: Open your ears and hearts to the heartbeat of ours,” Teglasy said. “Put your finger on our face. Take our hands and not our lives. Touch the wounds of our bodies and souls. Stop doubting and believe.”
What drives your commitment to promoting the sanctity of innocent human life? Was there an eye-opening moment when a life-changing incident forced you to come to grips with the tragedy of abortion?
For Tracy, a candidate for the Pennsylvania state legislature, the defining moment occurred when she was pregnant.
As Tracy wrote to me, the life issue came up front and center—and she could not avert her eyes.
“This issue is very close to my heart,” Tracy noted.
“I was offered a ‘selective reduction’ when carrying my twins, based on a non-confirmed diagnosis.”
“Selective reduction.” Code words for aborting a living preborn baby, while allowing her twin to live.
Tracy would have none of it. She was determined to give birth to both her girls.
“My daughters were born at 28 weeks,” Tracy said. “Emily passed (away) shortly after birth, but we were given time to hold her and say goodbye.”
As for the other twin?
“Alyssa graduates from college in May,” Tracy stated.
This incident is just one more example of the beauty of respecting life—even when circumstances look bleak. Imagine what Tracy’s emotional pain would have been if she had agreed to the abortion? She never would have had that profound peace that came with holding her baby in her arms.
Tracy is one of the many women who courageously resist a doctor’s call to abort their offspring. They choose the path of life—and they are grateful for it. Tracy is eternally thankful that she had the opportunity to spend time with Emily…to embrace her…and to love her before the twin passed into eternity. She received a sense of closure that an abortion would not have given her.
How about you? Was there one particular incident that propelled you to defend human life? Sharing that personal story may be just what is needed to save an innocent, unrepeatable human being!
LifeNews.com Note: Maria Gallagher is the Legislative Director and Political Action Committee Director for the Pennsylvania Pro-Life Federation and she has written and reported for various broadcast and print media outlets, including National Public Radio, CBS Radio, and AP Radio.
The review found “little evidence that [comprehensive sex education] programs are effective at producing positive impact on their participants.” Of 103 total sex education studies, only six had evidence of “real effectiveness” without negative effects after 12 months. Yet even in these six studies, there was no evidence that these six successful studies led to increased consistent condom usage, teen abstinence, fewer instances of sexually transmitted diseases, or fewer teen pregnancies. Meanwhile, 16 studies actually showed negative effects on teen sexual behavior and sexual health, including increases in teen sexual activity and other risky behaviors.
The negative behaviors found included increased pregnancies, STDs, and sexual activity including oral sex, more sex partners, increases in forced sex/rape, and increases in paid sex. Meanwhile, there were decreases in condom use. Part of the problem, according to the review, is that certain factors dealing with sexual behavior aren’t addressed in the classroom.
“[M]any factors outside the classroom influence adolescent sexual behavior — factors related to the home, peer, social media, and cultural environments,” the review noted. “Significant and lasting increases in sexual risk avoidance may be amplified by a multi-pronged prevention strategy that addresses these various factors directly.”
Comprehensive sex education, as defined by Planned Parenthood, takes place in grades K-12, and is “high quality teaching and learning about a broad variety of topics related to sex and sexuality, exploring values and beliefs about those topics and gaining the skills that are needed to navigate relationships and manage one’s own sexual health.” Organizations like the American Medical Association, the American Academy of Pediatrics, and the American College of Obstetricians and Gynecologists all support comprehensive sex education in schools.
And despite the growing trend of comprehensive sex education in schools, it’s not just this one analysis that has found problems. Even the Centers for Disease Control (CDC) has found that the number of sexually transmitted diseases are growing, with cases of syphilis, gonorrhea, and chlamydia reaching an all-time high. Newborn deaths related to congenital syphilis are also increasing, which the CDC says is a direct result of the STD “epidemic.”
Proper sex education is vital for young people. But comprehensive sex education may not be the answer that society has been led to believe.
WASHINGTON, D.C. — While the Catholic Church teaches that procuring an abortion is always immoral, a majority of U.S. Catholics do not believe abortion is intrinsically evil and say it should be legal in all or most cases.
According to a RealClear Opinion Research poll sponsored by EWTN and published on Monday, 47% of Catholics in the U.S. believe abortion is “intrinsically evil,” while a 53% hold otherwise.
A majority — 51% — say that abortion should be legal in all or most cases, with 31% saying it should be legal except for late-term cases and 20% saying it should always be legal.
The poll of 1,512 Catholic registered voters was conducted between Jan. 28 – Feb. 4, 2020, and surveyed U.S. Catholic opinion on a range of subjects, including political affiliation, preferred presidential candidate, the morality of abortion, and religious practices.
U.S. Catholics were slightly less likely to support legal abortion than Americans overall. According to 2019 Gallup polling, 25% of Americans think abortion should be “legal under any circumstances,” while 20% of Catholics take that position, according to Monday’s poll.
But while 21% of Americans believe abortion should be “illegal in all” circumstances according to the Gallup poll, only 11% of Catholics think so.
Michael New, a visiting professor of social research and political science at the Catholic University of America, told CNA that religious practice, not self-identification, is the strongest predictor of opinions on abortion.
“What is a much stronger predictor” for Catholics, he said, is “attendance at Mass.”
Among Catholics attending Mass at least weekly, the majority, 55%, answered that abortion should be illegal in all or most cases.
More than one-third of weekly Mass-goers, 35%, said abortion should be illegal except in cases of rape, incest, or “to save the mother’s life.” Twenty percent said that abortion should always be illegal. Meanwhile, 20% of weekly Mass-goers said abortion should be legal in all cases, and 22% said it should be legal except for late-term cases.
Among Catholics who say they accept everything the Catholic Church teaches, and that their lives reflect Church teaching, a substantial number 27% said that abortion should be legal in all cases, and 15% said it should be legal except in cases of late-term abortion. A majority said that abortion should be illegal in all or most cases.
While they remain divided on the question of the legality of abortion, a far greater number of Catholics in who attend Mass weekly or say they accept everything the Catholic Church teaches also believe abortion to be “intrinsically evil,”
More than seven-in-ten Catholics, 71%, who say they accept all the Church’s teachings believe abortion is intrinsically evil. 66% of “weekly-plus” Mass attendees answered the same way—far more than the 47% of Catholics overall who answered this way.
“The term ‘intrinsically evil’ isn’t used all that much” in society, New told CNA, and thus this term might seem “unnecessarily harsh” to describe abortion if Catholics are not well-versed in the language of moral theology.
Catholics of other demographics did not vary with great significance in their answers on the morality of abortion. Catholics of generations X, Y, and Z were only slightly less likely than Catholics of the Boomer and Silent generations to believe abortion is intrinsically evil.
Hispanic Catholics offered perspectives on abortion similar to Catholics overall; 21% said abortion should be legal in all cases, and 32% said it should be legal except in late-term cases. Only 48% said abortion is intrinsically evil.
Beliefs about abortion vary significantly among political party affiliations. Catholics identifying as Republicans were more likely to say abortion is intrinsically evil, with 63% answering thus. In this subset, only 37% said it should be legal all or most of the time while 61% said it should be illegal all or most of the time.
Two-thirds of Catholics identifying as Democrats said abortion should be legal in all or most cases, compared to just 37% of Republicans. Meanwhile, just 36% of Democratic Catholics said that abortion is intrinsically evil, compared to 63% of Republican Catholics who said it is.
February 19, 2020 (LifeSiteNews) – People who had more sexual partners throughout their life have a higher chance of being diagnosed with cancer, according to a study published in the journal BMJ Sexual & Reproductive Health.
“Compared to women who reported one partner or none, those who reported 10 or more were 91% more likely to have been diagnosed with cancer. Similarly, men with 10 or more partners were 64% more likely to have been diagnosed with cancer compared to men with one partner or none,” Reuters reported on the findings of the study.
Dr. Jennifer Roback Morse, founder and president of the Ruth Institute, an international organization that defends the family, was not surprised by the results of the study.
“Goodness! A big expensive study to tell us that having multiple sexual partners is unhealthy! Who knew? I’ll tell you who knew: Your grandma, the Church and what used to be called ‘common sense,’” she remarked to LifeSiteNews.
Lee Smith, one of the co-authors of the study, speculated on the reason for the higher risk in women. “This may be because the link between certain [sexually transmitted infections] and cancer is stronger in women, such as HPV and cervical cancer, compared to HPV and penile cancer,” she told WebMD.
The study was based on data provided by 2,537 men and 3,185 women over 50 who had participated in the English Longitudinal Study of Ageing. This study tracks a certain number of people for a longer time, creating a better opportunity to observe changes in the participants.
As the study published by BMJ Sexual & Reproductive Health explains, the participants stated the number of sexual partners during their lifetime. They also provided “self-rated health and self-reported limiting long-standing illness, cancer, coronary heart disease, and stroke.”
Reuters broke down the numbers: “Among men, 29% reported one or zero sexual partners, 29% had two to four, 20% had five to nine and 22% reported having 10 or more. Among women, just under 41% had one or zero sexual partners, 36% reported two to four partners, 16% reported five to nine partners and 8% said they had 10 or more.”
“Indeed, a higher number of sexual partners means greater potential exposure” to sexually transmitted infections, the director of research at the Cambridge Centre for Sport and Exercise Sciences at Anglia Ruskin University in England summarized.
While the study shows an association, it cannot prove that having more sexual partners throughout life directly causes a greater likelihood of having cancer. However, a more promiscuous lifestyle often goes hand in hand with other behaviors known to increase the risk of cancer.
“Those who reported a higher tally of sexual partners were more likely to smoke, drink frequently, and do more vigorous physical activity on a weekly basis,” inews wrote.
Pro-abstinence organization Love Facts offers a chart that allows people to calculate the extent of their sexually transmitted disease (STD) exposure based on their number of sexual partners. According to the chart, a person who had 10 sexual partners, each of whom also only had 10 partners, will have been potentially exposed to the STDs of 1,023 others.
Robert Edwards, a professor of obstetrics, gynecology and reproductive sciences at the University of Pittsburgh School of Medicine, told Reuters that “smoking and alcohol consumption amplify the risk for cancer with certain sexually transmitted diseases.”
Lee Smith emphasized the need for using “appropriate protection,” reducing “the risk of related cancers going forward.”
However, STDcheck.com, a service that facilitates STD testing, explains that many STDs can be transmitted even if a condom is used during intercourse. The website lists, among others, HPV, genital herpes, syphilis, and pubic lice.
The Centers for Disease Control and Prevention, a federal agency and the leading national public health institute of the United States, is equally cautious.
“However, condom use cannot provide absolute protection against any STD. The most reliable ways to avoid transmission of STDs are to abstain from sexual activity, or to be in a long-term mutually monogamous relationship with an uninfected partner.”
Morse provided different advice. “As a happily married woman, I have an ‘active sex life,’ but absolutely zero ‘risky encounters.’ These researchers should be telling people to get married, stay married and only have sex with the person you are married to. That would solve a lot of problems, including health problems.”
LifeNews Note: Priests for Life recently hosted a meeting with pro-life leaders and activists. They released the following statement to encourage pro-life Americans to continue fighting and praying to end abortion:
A Statement of Encouragement for the Pro-life Movement
Having gathered in Titusville, Florida for a national strategic summit meeting, we, as leaders in the pro-life movement, want to issue a word of encouragement and a call to action.
The year 2020 brings us to a momentous and pivotal point in the effort to end abortion and to restore protection to children in the first nine months of their lives, as well as to protect vulnerable people from euthanasia and assisted suicide.
The Supreme Court is currently hearing another case regarding abortion. The outcome of this case could make it easier for the states to protect mothers from the devastating actions of an unregulated and unscrupulous abortion industry.
We call on our brothers and sisters in this movement to inform themselves about this case, discuss it with others, and pray for a favorable outcome. Many members of Congress have expressed to the Court their support for the pro-life side of this case, and we should thank those who have done so. Numerous mothers who suffer from a past abortion have also let their voices be heard in this case; we should listen to and spread their testimonies to all our fellow citizens.
This year 2020 also brings us to national, state and local elections which will shape our courts for decades to come, decide the fate of tens of millions of children, determine whether we will continue to fund the abortion industry, and impact how much longer it will take to end the violence of abortion in our land.
We urge our fellow citizens to be active and informed voters, to see the right to life as the most fundamental electoral issue, and to educate and mobilize other voters to do the same. Likewise, we urge everyone to pray for our nation as we elect our leaders.
Thanks to the perseverance, faith, and tireless efforts of a very large and diverse pro-life movement for five decades, we have saved countless lives, changed countless minds and healed countless hearts. We have passed numerous laws, prevented the abortion industry from doing even more damage than it has done, and brought our nation closer to the fulfillment of its creed of equal justice under law.
Grateful for all these efforts, we look forward to our continued progress and encourage all in our movement to redouble their efforts on behalf of our youngest brothers and sisters and their mothers, and to redouble their confidence that those efforts will succeed.
Fr. Frank Pavone
National Director
Priests for Life
Janet Morana
Executive Director
Priests for Life
Evangelist Alveda King
Civil Rights for the Unborn
Priests for Life
Jor-El Godsey
President
Heartbeat International
Bradley Mattes
President
Life Issues Institute
Kristan Hawkins
President
Students for Life of America
Students for Life Action
Allan E. Parker, Jr.
President
The Justice Foundation
Thomas Glessner
President
National Institute of Family and Life Advocates
Joe Langfeld
Human Life Alliance
Shari Richard,RDMS
Unborn.com
Connie Eller, Founder
Missouri Blacks For Life
Joel Brind, PhD
Member, Medical Advisory Council
Heartbeat International
Rev. Arnold M. Culbreath
Director of Ministry Engagement
Douglass Leadership Institute
Larry Cirignano
Children First Foundation
Chris Slattery
Founder and President
Expectant Mother Care-EMC FrontLine Pregnancy Centers
John J Jakubczyk
Southwest Life & Law Center
Bryan Kemper
President – Stand True Youth Pro-life Outreach
Ann Lauren Rooney Morris
Florida Director
National Life Chain
Matthew and Cathy Connolly
Red Rose Rescue
Jeff White
Survivors of the Abortion Holocaust
Cheryl Conrad
Survivors of the Abortion Holocaust
JoAnn Gerling
Coalition on Abortion and Breast Cancer
Rev. Patrick Mahoney
Christian Defense Coalition
Dr. Michael New
Pro-life Researcher
Brendan H. O’Connell
Life Matters TV and Media, Inc.
My name is Szilvia. I am a 40-year-old quality manager and mother of two little children, living in Germany.
Not long ago, I found the Natural Womanhood site when searching birth control side effects while on the copper IUD. I found so much important information on the copper IUD and copper toxicity in an article by Kathleen Taylor, who cited the podcast of Julie Casper on the topic.
I can say from lived experience that what was published in that article is 100 percent true.
After having two children, my partner and I decided to use a non-hormonal form of birth control, and my gynecologist told me about the copper IUD. Regarding side effects, the only thing she said was that the copper IUD can cause heavier bleeding; that was the only side effect I heard. I had to undersign it that I was aware of the possibility for heavier bleeding; I received no information about other possible side effects.
A Dark Period
After the insertion of my IUD, my monthly bleeding did become heavier, but I experienced other changes as well. My period cycle became much shorter and my hair became thinner—about one-third the volume it was before. But this was not the worst of it; I experienced immense depression. I had all the symptoms: depressed mood, anger, mood swings, anxiety, insomnia, rage, racing thoughts, palpitations, and suicidal thoughts.
I was prescribed pills for depression and sleep at night, but they didn’t help my depressed days.
I started to take notes about when exactly I had the worst days. A trend emerged: the days when I experienced the worst moods were precisely the days during the bleeding. It was not a dip in mood before the bleeding, as in premenstrual syndrome (PMS); instead, my worst depressive symptoms persisted for the whole length of my bleeding phase.
Once I realized the timing of my mood changes, I decided to search online to see if other women noticed this. I found reports of women all over the world who claimed the same connections between having the copper IUD and depression. It finally clicked: my depressive symptoms were a result of the IUD. Only after hearing the experiences of other women in testimonials did I see clearly enough to make the decision: I had the IUD removed, and this was the first step in my recovery.
A New Day
Now that my IUD is removed, my symptoms have completely changed: I have no mood swings, no depression at all. I wish I had never had these experiences, which almost destroyed my life and that of my family.
Thanks to articles that shed more light on this, and testimonials of women revealing their bad experiences, I can say today that I am healed.
Women need to speak up about their IUD side effects. It makes a big difference! Only by listening to women’s experiences—by spreading information, by standing up—do others have the chance for healing. Before starting my own investigation, I was never informed of any correlation between all the mentioned symptoms and the copper IUD. Here in Germany, there is not much information about the IUD and possible side effects.
I am one of the lucky ones because I got the information. Without it, I might have taken antidepressants my whole life, and I would not understand why this dark cloud became a persistent part of my life.
My experience has led me to view the pharmaceutical industry with skepticism. I no longer believe it is in the interest of the pharmaceutical industry to make us healthy—quite the contrary; it is their interest to keep us in a state that requires medication. They can sell their products, not only the IUD, but also the antidepressants and other pills we get prescribed after developing adverse symptoms.
With my copper IUD removed, I am feeling 100 percent myself again. Most importantly, my little family has their mum back, as I was before: a shining woman with a lot of energy, funny, and optimistic.
I do not wish to bring attention to myself in writing this. My aim in writing this is to warn others. We women have to stick together.
As of January 1st 2020, A Personal Choice Tubal Reversal Center is offering free tubal reversal surgery by sponsoring the first ever Free Tubal Reversal Surgery Contest. This opportunity to have free tubal ligation reversal surgery is the first of its kind.
Dr. Charles Monteith is a sterilization reversal surgeon who is responsible for sponsoring the contest. He is the Medical Director of A Personal Choice Tubal Reversal Center, which is a specialty surgical center located in Raleigh, North Carolina. The center exclusively offers patients affordable, outpatient sterilization reversal for both women and men. Those who enter the Free Tubal Reversal Surgery Contest will have a chance to win a sterilization reversal surgery valued at up to $8,000. Each year, Dr. Monteith will select up to four (4) lucky winners who will be eligible to win either tubal ligation reversal surgery or vasectomy reversal surgery at no cost to them. This is the first time free sterilization reversal surgery has been offered in the United States.
Tubal ligation and vasectomy are very popular forms of permanent birth control. Each year approximately 700,000 tubal ligation surgeries (female sterilizations) and up to 500,000 vasectomy surgeries (male sterilization) are performed each year in the United States. Medical research has demonstrated up to 30% of women who have tubal ligation and 10% of men who have vasectomy will regret their sterilization procedures and desire to have more children. Their options for having another child are limited to adoption, in-vitro fertilization (IVF), and sterilization reversal. All of these options are expensive and none of them are guaranteed.
Adoption can cost up to $50,000 and up to 15% of adoptions will not be successful. A single cycle of IVF can cost up to $15,000 and a single IVF treatment cycle is approximately 30% successful. Sterilization reversal surgery is not guarantee but can be more successful than IVF. Sterilization reversal surgery can be up to 95% successful for men and up to 80% successful for women. Costs of sterilization reversal surgery range from $7,000 to $30,000 depending on where the surgeries are performed. Unfortunately, most health insurance plans consider surgeries to reverse self-imposed sterilization as non-essential, elective medical treatments and most plans will not cover the cost of either reversal surgery or IVF. This leaves many couples having to pay out of pocket for the treatment of their regret.
Many couples will quickly realize sterilization reversal surgery can be the most affordable option providing the best chance of pregnancy success. Despite sterilization reversal being more affordable, many who choose sterilization reversal will have to spend their life’s savings, borrow from their retirement plans, or endure high surgery financing interest rates in an effort to afford reversal surgery. Dr. Monteith continually receives requests from couples in despair because they can not afford the high cost of reversal surgery. These couples asking if he would consider performing free or probono reversal surgery on their behalf. Many will tell him they are not able to afford the surgery and inquire if there are research trials offering free infertility treatment. After years of continually receiving these request, Dr. Monteith decided he could help a few of these couples each year by sponsoring a reversal surgery contest.
Applications are already rolling in! Within the first two weeks, Dr. Monteith has already received over 800 contest entries. Some of the statements made by those entering the contest are truly heartbreaking and revealing of the many different reasons people regret their sterilization surgery.
One contestant wrote on her application, “Thank you so much for offering this contest. I lost my children in a house fire and have been emotionally devastated. I looked into IVF and was not able to afford IVF. My local fertility doctor quoted me over $20,000 for reversal surgery. Your contest is giving me hope that I can one day be a mom again.”
Another contestant wrote, “I was in an abusive relationship and the victim of domestic violence. I had my tubes tied so I would not be further trapped with my abuser by having more children with him. I have since divorced and now I am with a man who is the love of my life. He supports me, is not abusive to me, and is a real father to my children from my previous relationship. Tubal reversal surgery would allow me the chance to give him a child.”
Another entry read, “I was advised to have a tubal ligation after being diagnosed with a potentially deadly heart condition. I have never had children. My health has dramatically improved over the last 10 years. I have spent over $30,000 on three IVF treatments and have not become pregnant. Although tubal reversal may not work…at least it will give me hope and a chance…”
Although it can be easy to blame those who chose sterilization and easy to have a “that is what you get” attitude, one can easily see by reading the above comments submitted by contestants that the decision to have sterilization and the decision to reverse sterilization are influenced by many different life circumstances. Dr. Monteith has extensive experience in the field of reproduction and understands the complexity of his patient’s lives. This is why he chose to offer the first contest giving away free tubal reversal surgery and offering couples hope and a chance of becoming new parents again.
For more information about A Personal Choice Tubal Reversal Center, call (919) 977-5050 or visit https://www.tubal-reversal.net:
CONTACT INFORMATION:
A Personal Choice Tubal Reversal
Dr. Charles W. Monteith, Jr., M.D.
(919) 977-5050
ContactUs@tubal-reversal.net
3613 Haworth Drive, Raleigh NC 27609
I received the most wonderful gift on St. Valentine’s Day a few years back. It made me so happy, I wept tears of joy. My friend Kathy and I were fulfilling our commitment to pray every Thursday outside the Planned Parenthood Center in St. Paul, Minn. We had been there about three hours.
We prayed for Kim, the pro-life sidewalk counselor with the warm smile and outstretched hand as she offered literature to a young woman, listing alternatives to abortion. We heard her say, “Hi, I’m Kim. Here’s some information for you.”
The Planned Parenthood escorts tried to distract the woman from Kim by placing themselves between her and Kim. They talked continuously to the young woman.
Nonetheless, Kim persisted: “You do have other choices. There is a Life Care Center right over there,” she said, pointing to a nearby building. The escorts brought the woman inside the clinic, and the door slammed shut.
All we could do was wait and hope that something Kim said would sink in, and that God’s grace would touch someone’s heart inside the center. Kathy and I continued to silently pray. Shortly after, three people from the Legion of Mary came by and prayed a Rosary and The Divine Mercy Chaplet.
We saw the escorts leave. This meant all the women were inside for their abortions. Soon, two women came out carrying little brown bags of medications and other things needed after an abortion.
How my heart aches when I see them come out. Many of them are alone, clutching the brown bag with one hand and holding their stomach with the other. They look sad and bewildered. There are no escorts with them when they come out.
Often, we give them a list of post-abortion counseling centers or at least shout the 1-800-WECARE number. At that number, they can talk to someone who’s had an abortion and who knows what they are going through.
On this Valentine’s Day, I dreaded the “brown paper bag” scenario. Each brown bag means a little life lost. It means a wounded mother who will grieve her lost baby and never be able to bring the child back. It means death chosen over life. It means a feeling of failure for me.
I had difficulty focusing on my prayers, feeling grief-stricken. I decided to say the Divine Mercy Chaplet again after having prayed it several times. In the middle of the prayer, the clinic door burst open. Out hurried two young women in tears. Neither carried a brown paper bag!
One got on her cell phone, sobbing as she talked: “I didn’t do it. I couldn’t go through with it.”
My heart leaped for joy, and tears fell freely as I hollered across the parking lot to her: “There is a Life Care Center right on the corner just beyond that flag. There are lots of people who want to help you.”
I stood there crying and thanking God for the women’s courage, for His grace, and for all the people I knew who were praying and fasting for the protection of the unborn. What they would give to see the miracle I saw on St. Valentine’s Day at Planned Parenthood.
Pat Wittkop is a mother of seven and a freelance writer. She volunteers as a sidewalk counselor for Pro-Life Action Ministries, St. Paul, Minn.
Committed pro-life activists are often accused of being too focused on abortion: “If you really cared about babies, you would also care about Issue X!”
True, children need many things to survive and thrive, and pro-lifers should work on those issues as well as the abortion issue. But the “Seamless Garment,” as a rhetorical strategy, is often perceived by pro-lifers as a subtle or not-so-subtle attempt to undermine them. All too often, these suspicions are well-founded. So my next statement may surprise you: The pro-life movement needs a Seamless Garment of its own. Let me explain.
The Ruth Institute conducted a survey of pro-life student opinion at the Students for Life Pro-Life Summit on Jan. 25 in Washington, D.C. More than 3,000 people attended this summit the day after the 47th-annual national March for Life. Nearly 10% of the attendees stopped by the Ruth Institute booth and took our survey. Their ages ranged from 12 through 76, with an average of 28. The respondents were 71% women and 77% Catholic.
We asked them: “What other related issues concern you? Check all that apply.” Of the 305 people who answered, the following percentages flagged these issues:
83% said they were concerned about euthanasia.
83% said they were concerned about the decline of marriage.
66% said they were concerned about contraception.
59% said they were concerned about comprehensive sexuality education.
50% said they were concerned about surrogacy, egg donation and sperm donation.
47% said they were concerned about the worldwide decline of fertility.
True enough, these are not the issues that advocates of the Seamless Garment generally mention. Back when Cardinal Joseph Bernardin of Chicago popularized the Seamless Garment, the issues included government programs supporting the material needs of children.
Today, the issues are more apt to be climate change or immigration, but the subtle accusation is clear enough: “If pro-lifers really cared about children, they would care about them after birth.” So let us look at our survey of the Students for Life participants through this lens of children’s needs after they are born.
Of course, everyone knows that children need food and shelter and clothing. But children also need love. The “failure to thrive” syndrome shows that, in some way, the non-material needs of children are more important than their physical needs. Children who “fail to thrive” have their material needs met. They have food, shelter, clothing and medical care. But they do not grow. They may even die. The commonly accepted explanation for failure to thrive is that kids need more than food. They also need to be fed and nurtured, by a person who holds them, rocks them, looks into their eyes and loves them.
In other words, kids need their parents. Mom rocks the baby. Dad supports Mom while she rocks the baby. She can’t get it done alone.
I conclude that authentic care for children must include care for their need to be loved by both their parents. We should provide systematic social structures to ensure that as many kids as possible get to grow up with their own parents who love them and each other. Children have a birthright to their own parents. That means a stable relationship with their biological parents wherever possible and stable, child-centered provision for adoption where the biological parents are permanently unavailable.
What might those structures look like? Adult society affirms that people should be having sex only with the person we are married to. We get married before having sex. We stay together unless someone does something really awful. We cut out petty criticism of our spouses. We have a social norm of patiently bearing with our spouse’s faults.
In other words, the most reliable systematic plan for ensuring that kids get to have the love and attention of both their parents is lifelong married love, supported by traditional Christian sexual ethics. The respondents to our survey at the Students for Life Summit seem to be quite well aware of this. “The decline of marriage” option comes in at the top of the list of their concerns, with more than 80% support.
Two-thirds of the activists mentioned contraception as an area of concern. Only an idiot can overlook the connection between the constant promotion of the contraceptive ideology and people’s casual choices of sex partners. If you care about kids, you should make it easier, not harder, for people to make good decisions about the identity of their child’s other parent.
Nearly 60% of the respondents were concerned about comprehensive sexuality education. This, too, shows that these activists are sensitive to the needs of children. Much of what passes for sex education amounts to propaganda for the sexual revolution, inflicted on small children, too young and impressionable to defend themselves.
Schools, public and private alike, convey to children that sex is a recreational activity: They safely can partake of it, as long as they use a condom every time. This message has no place in a Seamless Garment that treasures the rights of children to their parents, and therefore demands self-control from adults.
Half the survey participants were concerned about third-party reproduction issues. Is this because children of donated sperm or eggs are cut off from one of their biological parents? Or are these respondents mainly concerned about all of the death-dealing that goes on in the infertility industry, by discarding or freezing unwanted embryos? Either way, these pro-lifers’ care for babies extends well beyond the abortion issue.
When we conceived the idea for this survey, we just wanted to get an idea of where these participants at the Students for Life Summit stood on the Ruth Institute’s issues. Viewing the results reveals something more.
The pro-life movement really has matured from a single-issue battle, fought in a single way, to a multi-issue movement. The most committed participants in the movement understand that we need to defend the rights of children and parents to be in stable relationships with each other. Children have a birthright to their parents, as well as a birthright to be born in the first place.
And this survey also shows us that we are closer than we realized to having a pro-life Seamless Garment of our own.
ROME, February 11, 2020 (LifeSiteNews) ― The seventh annual Rome Life Forum will bring together pro-life, pro-family Catholics from all over the world to discuss “authentic purity” as the way to counter “attacks on human life, the family, and our faith.”
Rome Life Forum 2020 will take place on May 20-21, introducing two more days of pro-life activities leading up to the 10th annual Rome March for Life on May 23. The Forum will be held in the world-famous Pontifical University of St. Thomas Aquinas, also known as the Angelicum.
The theme this year is “Opening the door to purity and closing the door to vice.”
Cardinal Raymond Burke, Cardinal Willem Eijk, and prior emeritus of the Monks of Norcia, Fr. Cassian Folsom, OSB, will be among the speakers.
Another of this year’s speakers, John Smeaton of the Society for the Protection of Unborn Children (SPUC), told LifeSiteNews that this international gathering is a “unique opportunity” for Catholic pro-life leaders to gain strength from one another.
“The Rome Life Forum provides leaders within the pro-life and pro-family movement, united in their love for the Church, with a unique opportunity to strengthen one another in fidelity to the truth, and in working to restore a truly Christian civilization worldwide,” Smeaton told LifeSiteNews.
SPUC’s chief executive noted that Forum participants have come from the United States, United Kingdom, Ireland, Canada, New Zealand, Australia, Italy, Austria, Belgium, the Netherlands, Germany, France, Spain, Poland, the Philippines, Romania, Brazil, Venezuela, Nicaragua, Albania, Malta, Chile, Argentina, South Africa, India, Portugal, Switzerland, Czech Republic, Sweden, and Hungary as well as other countries.
“One thing which unites us all is a clear understanding that the pro-life movement cannot win the pro-life and pro-family battle on their own,” Smeaton said.
“The Church must recover her teaching authority to save her children. And at this time of trial, the faithful at all levels of the Church Militant must mobilise to fight for her.”
Rome Life Forum a ‘foretaste’ of heaven
Past speaker Michael Hichborn, president of the Lepanto Institute, told LifeSiteNews that going to the Rome Life Forum is like a “foretaste” of heaven.
“I’ve been to the Rome Life Forum every year since 2014, and each one is better than the last,” he said enthusiastically.
“It’s like a mini-retreat for me, and the reunion of so many good friends is like a foretaste of the reunion we’ll enjoy for eternity in heaven.”
Hichborn said “the wonderful thing” about the Roman Forum is that anyone can attend ― and all faithful Catholic should.
“Those Catholics who wish to have a solid understanding of the current rebellion in the Church should attend,” he said.
“Over the course of three days, faithful Catholics will not only be able to hear brilliant presentations, but have one-on-one access to various Catholic leaders from around the world.”
‘A wonderful sense of fellowship’
Canadian Catholic journalist Deborah Gyapong told LifeSiteNews that the Forum is an excellent networking opportunity.
“Nowhere else have I experienced such an international gathering of pro-life and pro-family leaders and experts from as far away as New Zealand, from all over Europe and the UK, and from North and South America,” Gyapong said.
“There is a wonderful sense of fellowship and joy at the Forum, a gathering of happy warriors. For me as a journalist, it was a forge for ideas and source of contacts.”
Gyapong told LifeSiteNews that she believes the Rome Life Forum is a “huge encouragement and chance to share victories and strategies” for pro-life leaders and activists.
“For young people who attend, it’s a great chance to find mentors.”
Margaret Akers of SPUC Scotland is one of the younger pro-life leaders participating in the Rome Life Forum 2020. She told LifeSiteNews that she very much enjoyed talks given last year by Fr. Linus Clovus and Cardinal Raymond Burke, both of whom will be speaking again at the Forum this May.
“I was particularly struck by the talk given by Fr. Linus Clovis, who spoke beautifully about the role of Our Lady in the Church and our lives; it was incredibly moving,” Akers said.
“I am always pleased to hear Cardinal Burke and last year’s conference was no exception,” she added.
“He framed patriotism and commitment to one’s ‘fatherland’ in a way one doesn’t often hear in an age of globalism, and it was inspiring.”
Akers said she believes this year’s theme, “Opening the door to the virtue of purity,” is particularly necessary today.
“I look forward to hearing how each of the speakers chooses to expand on this topic,” she said.
Dr. Joseph Shaw, chairman of the UK’s Latin Mass Society, will be speaking at the Roman Life Forum for the first time this year. While pondering the theme of purity, Shaw told LifeSiteNews that intellectual honesty is key.
“It is very evident today that much thinking about theology and morality is conditioned by the need to justify certain conclusions — conclusions justifying or permitting lifestyle choices which one does not wish to confront or reconsider honestly,” Shaw said.
“Whether the problem arises from one’s own past decisions, or those of people one loves, or those accorded value by one’s circle, true intellectual honesty is a real risk, an adventure in which one faces the possibility of losing friends, status, and career.”
Shaw said intellectual work that is constrained by these worldly considerations is “worthless.”
“We must rediscover our love of the truth, and a true commitment to it, because it is in the truth that we find God, who is Truth, and not in some sordid intellectual compromise,” he concluded.
‘The food is always great at the Forum’
A five-day trip to Rome uses up one’s vacation time, but Gyapong argued that the location and the price of the Rome Life Forum have been right.
“The food is always great at the Forum,” the journalist said.
“The price is really modest, and you can’t beat the location ― Rome,” she added.
“Participants find opportunities to worship together at daily Mass, the city is wonderful, and the weather is just right in May. Participants in the Forum also join the Italian March for Life, another joyous occasion that has grown substantially over recent years.”
The Rome Life Forum is also a chance to make a spiritual pilgrimage. Hichborn told LifeSiteNews that his fondest memory of the Rome Life Forum is from his first trip there.
“My wife and I attended with our (then) four-month-old daughter, Maria Faustina,” he recalled.
“We landed in Rome on the very day St. Faustina was being canonized, and we happened to walk into the church where St. Catherine of Siena is buried. We were able to actually touch her tomb and pray there. While we were at the Forum, Cardinal Raymond Burke gave a blessing to all three of us. For me, this memory will always signify what the Rome Life Forum is.”
The full price of the Roman Life Forum registration is £110/€130 (approx. $143 US). A one-day ticket is £65/€75 (approx. $84 US). To register and see the complete schedule, please visit voiceofthefamily.com.
The science of pregnancy gets more and more fascinating. To think of the mother simply ‘hosting’ her baby is so, well, 1973. What’s going on in the womb is really a marvelous co-operative venture that may last a lifetime, as Dr Kristin Collier, an Assistant Professor of Internal Medicine at the University of Michigan Medical School, explains in the following interview with MercatorNet.
* * * * * *
MercatorNet: For most of us, Pregnancy 101 means there’s a baby developing inside the mother, attached to the placenta by the umbilical cord. And, thanks to ultrasound and the photographs of Lennart Nilsson, we know what that looks like. But there’s a lot more to this inside story, isn’t there – could we start with the placenta?
Dr Kristin Collier Yes! There is so much more to the “inside story.” Since you asked about the placenta, let’s spend some time exploring this organ, as part of the “inside story.” The placenta is amazing. Why you might ask? Well, for one, it is the only organ made in cooperation by two people. It is made from the growing baby’s tissue and the mother’s tissue together. Therefore, the placenta is known as a ‘feto-maternal’ organ. It is the first time that mother and baby come together to do something in cooperation.
The placenta, as many of your readers know, is the organ through which the baby and mother interface. This name ‘placenta’ is derived from the Latin word for a type of cake, as it is a flat organ and averages about a pound in weight. It is attached to the wall of the mother’s uterus and is connected to the growing baby by his or her umbilical cord. The placenta is the only purposely transient organ in human beings.
It also is amazing because it functions as many organs in one. The placenta helps the prenatal child get rid of waste, helps provide nutrition and also produces hormones and protects the baby against infection. The placenta is acting like a lung, kidney, gastrointestinal tract and the endocrine and immune system. Pretty amazing for this one organ to have so many important functions.
In New Zealand, the indigenous Maori people have treated the placenta with reverence, traditionally burying it in ancestral land, which reinforces a link between people and land. Their intuitions seem to prefigure the importance of “the afterbirth” that science has discovered…
This information is beautiful to hear. It sounds like these indigenous people recognized the importance of the placenta even before modern science started to take a deeper interest. As you mentioned, the placenta has long been called the ‘afterbirth’ as it is delivered after the baby. This ‘afterbirth’ often got short-shrifted in attention as an ‘afterthought’. But no longer.
In fact, the placenta is so important, that the National Institutes of Health (NIH) in the United States has a research arm dedicated to the placenta called the Human Placenta Project (HPP), and on its website says ‘The placenta is arguably one of the most important organs in the body.’ A healthy placenta is not only crucial for healthy development of the prenatal child, but also affects the health of the child and mother for years to come.
On a side note, it sounds like the Maori people were into the field of human ecology even before the field had its formal name. This is unsurprising as these fields of study are often just a way to give a formal name to something that has been there the entire time, often practiced authentically by indigenous peoples and only recently fractured by modern life and technology.
Is there more to discover about this ‘transient organ’?
Yes, there is always more to discover. One goal of the human placenta project is to better understand the placenta with the ultimate goal of improving maternal and child health. One interesting thing we know now about the placenta, although the full extent of this knowledge is not fully understood, is that along with functioning as many organs as one, there is a unique transfer of cellular material that happens across the placenta.
In science, microchimerism refers to the presence of a small population of genetically distinct and separately derived cells within an individual. In pregnancy, small amounts of cells travel across the placenta. Some of these cells are the prenatal child’s cells that travel from the baby into her mother, and some cells also pass from the mother into her child. The cells from the prenatal child into her mother are pluripotent, which means they haven’t yet differentiated into the type of cell specific for one organ or tissue in particular. These cells find their way into mother’s tissue and start acting like the tissue in which they find themselves. This process is known as feto-maternal microchimerism.
That is fascinating! In what ways can these fetal cells protect the mother in later life – or put her at risk?
Their full impact is still being understood, but some of these cells have been hypothesized to help mom in the time after birth and also for years to come. For example, these cells have been found in Caesarean sections incisions helping to make collagen to help mom heal after a surgical delivery. These cells have also been found in the maternal breast and have been hypothesized to help reduce mom’s risk of breast cancer in her later years.
The ’gift’ of these cells from the baby, entering into mom’s body and helping her heal and protecting her from cancer, is amazing to think of and really challenges our ideas of people as autonomous beings. In reality, many human beings carry remnants of other human beings in their body. These cells may even play a part in how future siblings are spaced.
What is also interesting, these cells that enter the mother are allowed to survive and are not attacked by the mother’s immune system, even though they are somewhat ‘foreign’. This again speaks to a cooperation, at the cellular level, between mother and child. And it would be one thing if these cells were inert and existed as a gift of sorts, from the child in the mother, but to think of these cells in some ways benefiting the health of the mother really speaks to a radical mutuality at the cellular level between two people that only serves to enhance our understanding of the maternal-child bond.
And what are the implications for involuntary pregnancy loss?
Miscarriage can be a devastating event in the life of both the expectant mother and father. I’ve heard from many women that they felt, even after they lost their baby, that their baby was somehow always still with them in a way. And now, through the knowledge of the science of microchimerism, we know that this is true. Many women do have the presence, in their bodies, of a biological piece of their child and this cellular material may be aiding and assisting her not only now but in the future in ways we are only beginning to understand.
Obviously this science throws new light on the abortion debate, in particular on a woman’s autonomy when it comes to ending a pregnancy. She would be ending an irreducibly cooperative venture rather than a ‘kidnap’ (as Judith Jarvis styled it) and harming herself as well, would she not?
Every dehumanizing ideology succumbs to the same temptation – to see the undesirable other as a non-person. In the abortion debate, as in similar debates around marginalized vulnerable populations, language is used when describing the undesirable other that is dehumanizing. In the abortion debate, the prenatal child is referred to as a ‘clump of cells’ or even as a ‘parasite’.
As my friend Charlie Camosy writes in his book Resisting Throwaway Culture: How a Consistent Life Ethic Can Unite a Fractured People, we must resist appeals to individual autonomy that detach us from our duty to aid others, and resist language, practices and social structures that detach us from the full reality and dignity of the marginalized. A radical view of autonomy that leads to the end of another human life is one that is anti-life and oppresses the rights of another in the name of ‘freedom’.
So yes, the language that should be used to highlight the beautiful cooperation that exists in the dyad of the mother-prenatal child relationship instead has been perverted to one that brings to mind a cancer, an infection or a crime (like a kidnapping or hostage situation). Those of us who feel called to stand up for the vulnerable and marginalized among us, should call out such language not only in the abortion discourse but also in the discourse involving other marginalized vulnerable populations.
In a world focused on avoiding pregnancy it’s not surprising that we have heard little or nothing about these amazing pregnancy facts. Are there other reasons?
That is an interesting question. I don’t know why this information isn’t more widely known. One reason is that there are so many other ‘practical’ things to know when you are pregnant that these other details of awe and wonder get marginalized.
Having had four pregnancies myself, I remember getting inundated with information around things to expect in pregnancy regarding my body – physical changes, symptoms etc. I remember reading in a book about what my baby was doing and looking like at each week of gestation, but I don’t remember getting information that exceeded the ‘practical’ domain.
Pregnancy and childbirth are wondrous, miraculous events! In my opinion, using language that reflects awe and wonder doesn’t discredit us in medicine, but only legitimizes the emotions and feelings the pregnant mother is likely already feeling.
What are the theological implications of these scientific insights, in your view?
I am not a theologian, however in talking with those who are, I’ve come to think of biology now, more generally, in a relational sense that mirrors the nature of God. The scriptures speak of a God who is in relationship with his people. We then would only expect that God, being the author of biology, would create our bodily nature in a way that was also relational – even down to the level of the cell.
And in particular, when I think of the science of fetomaternal microchimerism, I think of the theological implications of cells from the incarnate word of God, Jesus Christ, in his mother, the Virgin Mary. We can say that Mary not only carried the Son of God in her body when he was in her womb, but that she likely carried his cells in her body throughout her life in a way that further magnifies her position as the glorious Theotokos. This highlights Mary’s glorious position as the Mother of God in a way I had never thought of before.
Kristin Marguerite Collier is an Assistant Professor of Internal Medicine at the University of Michigan Medical School where she practices general Internal Medicine. She serves as an Associate Program Director of the Internal Medicine Residency Program and is the Director of the Program’s Primary Care Track. In addition, she is the Director of the University of Michigan Medical School Program on Health, Spirituality and Religion. She was interviewed by Carolyn Moynihan, Deputy Editor of MercatorNet.
**CORERCTED**February 10, 2020 (LifeSiteNews) – One Child Nation won the Grand Jury Award at Sundance in 2019. **It did not win Academy Award. **The film is a harrowing expose of the devastation caused by the womb police who enforced China’s One Child Policy. But the film goes beyond that. It is a scorching indictment of Communism itself.
First, a caveat. The film begins with the statement that China ended the One Child Policy in 2015, making it seem as though the film serves as a memorial to a tragic era gone by. The film does not mention, however, that forced abortion continues under the Two Child Policy. The new rule is that every couple is allowed to have two children. Single women and third children are still forcibly aborted. In its recent report, released January 8, 2020, the Congressional Executive Commission on China stated: “Local-level officials reportedly continued to enforce compliance with family planning policies using methods including heavy fines, job termination, and coerced abortion.”
The atrocities described in the film continue to this day, and the battle to stop them must continue until all coercive population control in China has ended. We cannot explore China’s dark past and ignore China’s dark present.
Nevertheless, the film is remarkable in the intimacy of the portraits it paints, while at the same time giving rise to agonizing conclusions regarding the world’s most massive social engineering experiment gone shockingly awry.
The Chinese Communist Party has boasted that it “prevented” 400 million births through its One Child Policy. This statistic is mind-numbing, inconceivable. The filmmakers, Nanfu Wang and Jialing Zhang, shows us how this was accomplished in Wang’s village.
Wang returned to China after having given birth to her son, to learn what her family and community experienced under the One Child Policy. The interviews Wang records are heartbreaking in their candor. Here we meet the uncle who left his infant daughter in a marketplace, hoping that someone would take her in. No one did. Over several days, he watched as she slowly starved to death.
We meet the family planning official who said that women with illegal pregnancies were tied up and dragged “like pigs” for forced abortions. We see one of the local “womb police” – a midwife personally responsible for more than 50,000 forced abortions and sterilizations – who now seeks to atone for her “sins” by helping infertile couples conceive. We meet the artist who, devastated at finding full-term babies in trash heaps, lovingly preserved and photographed them as a testimonial to the lives that could have been. Wang was courageous in keeping the disturbing images in the film, though doing so caused the film to be rated “R.”
Wang asks those she interviews if they think the One Child Policy was a good thing, worth the sacrifice. Astonishingly, the answer is an overwhelming yes – it was necessary to fight the “population war.” This view is consistent with the collectivist attitude of Communism and its powerful propaganda machine: sacrifice the one for the good of the many.
Do those interviewed really believe that the policy was a good thing, despite the excruciating pain it has caused them personally? Or did they merely say so, because they were being filmed and knew that their statements could get back to the Chinese government, resulting in persecution if they defied the Chinese Communist Party on one of its central policies?
When asked why they did not take measures to save their babies, the overwhelming answer is, “We had no choice.” This is the hallmark of Communism: the peacetime killing of its own citizens. The true face of Communism is never more clearly seen than in the faces of the Family Planning Police, dragging women out of their homes, strapping them to tables, and forcing them to abort babies they want. Anyone who thinks that Communism is a good thing must see this film.
I asked a pro-life friend if he had seen One Child Nation. He replied, “No, I would never see a film that advocates for abortion.” He was referring to the filmmaker’s statement at the end of the film that she thinks it ironic that she has left a nation where women are forced to have abortions only to come to a nation that restricts abortion, evincing an ill-conceived moral equivalency between China and the United States.
It is unfortunate that the filmmaker, having made a film of unparalleled power regarding the brutality of forced abortion in China, chose to take a wholly unnecessary stand on the America abortion debate. The filmmaker’s comment is a non sequitur. Ignore it, and see the film.
You can watch the trailer here and rent the film on Amazon Prime here.
Reggie Littlejohn is the President of Women’s Rights Without Frontiers. A video on her work to stop forced abortion in China can be viewed here.
The 50-minute documentary “Strings Attached,” produced by Culture of Life Africa founder and president Obianuju Ekeocha exposes the funding pipeline from Western countries to African nations, specifically for abortion and contraceptive “services,” and shares first-hand accounts of the harm countless women have experienced at the hands of global abortion giant Marie Stopes International.
In the fall 2019 issue of American Life League’s Celebrate Life magazine, Ekeocha said that the documentary’s title “Strings Attached” is meant to “capture[] the nature of the ‘gifts’ of some of Africa’s wealthiest donors.” In the documentary, Ekeocha explains how she came to become a vocal pro-life advocate after the Bill and Melinda Gates Foundation announced in 2012 that it would dramatically increase its “family planning investment” around the world, including across the African continent.
The documentary reveals how, following President Trump’s reversal of the Mexico City Policy — a move that abortion advocates call the ‘Global Gag Rule’ — European nations came together to pledge hundreds of millions of dollars to “make up for ” the funds diverted from abortion providers. The Organization for Economic Aid and Development reported in 2014 that “Africa received more funding for population programs than for education, healthcare, water and sanitation.”
Screenshot from Strings Attached documentary
Marie Stopes International Provides Sub-Standard Care
The documentary chronicles Marie Stopes International’s (MSI) troubling history of providing substandard medical care, as documented in European countries. In December 2016, the UK’s healthcare regulator Care Quality Commission issued what one UK physician called “a very critical, some might say, a damning report of Marie Stopes” due to 2,634 incidents of “serious breaches of practice” between 2015 and 2016. A year later in 2017, the doctor reported, “nearly 400 botched abortions were carried out in just two months.” He asked the next logical questions: “What about in developing countries where the health service is not as good, where there’s not a regulator, where people aren’t carrying out inspections? If [Marie Stopes International] is not following instructions here, what are they going to do in an unregulated situation [like in African countries]?”
“They Ruined My Life”
“Strings Attached” exposes the harm African women have experienced from illegal abortions and dangerous contraceptives provided by Marie Stopes International. Multiple women went on record describing horrific experiences of illegal abortions thanks to abortion pills dispensed and surgical abortions performed by staff of Marie Stopes International (MSI), which has clinics in 37 countries globally.
Jacqueline Gandhi was an MSI employee in Kenya who staffed a hotline for women trying to obtain abortions, even though abortion is illegal in Kenya. She personally had four abortions during her eight years working for MSI. She said that in its reporting, MSI reports abortions as “post-abortion care.” She also said, “Clinics got bonuses if they surpassed their targets [for number of abortions].” She personally knew of multiple “cases where we heard that ladies died because of abortions done by Marie Stopes.”
Another woman Ekeocha interviewed, Akeech Aimba, experienced an unplanned teenage pregnancy, and a trusted friend referred her to MSI for a second-trimester surgical abortion. She said, “I was not put under any anesthesia. The doctor went on and on, and I remember screaming and crying and trying to crawl out of that bed…. And after the procedure, he showed me the pieces of my baby.”
A third Kenyan woman shared her medication abortion experience anonymously, reporting tremendous pain during the procedure, and saying that afterwards she suffered from “post abortion stress syndrome. I’m still trying to recover from it. They [MSI] ruined my life.”
A fourth woman reported “there was no counseling or anything. They just did it.”
Ekeocha also secretly recorded a call placed to the Eastleigh, Kenya, MSI clinic by a woman purportedly seeking an abortion. The MSI employee she spoke to over the phone offered her her choice of an in-clinic abortion or “we deliver the pills at your place.” A second call placed to a different Kenyan MSI clinic several months later yielded the same offer for an illegal abortion.
Dr Seyoum Antonio, an Ethiopian surgeon, told the story of a 16-year-old girl “who has gone to Marie Stopes International to get abortion, where she sustained uterine perforation, and then she had a serious infection. She was brought to the hospital and a hysterectomy was done, at the age of 16.”
“Even if You Refuse, This is the Best”
Ekeocha told American Life League that “nothing prepared me for the deep wounds inflicted on African people and communities by Western donors. Some of the women I interviewed had such painful stories about their experiences. I believe that they’re victims of human rights abuses by Western pharmaceutical companies in collaboration with organizations like Marie Stopes International.”
Anna-Theresa Amo was one of 12 women from her village who visited a MSI facility and was pressured to have IUDs implanted. Through a translator, Anna-Theresa said that when the women objected, requesting some other form of contraception, staff told them, “even if you refuse, this is the best” and then locked the women inside the room and inserted the IUDs. The women experienced terrible abdominal pain and infections — side effects they were never warned about.
Other women Ekeocha interviewed received the Norplant contraceptive implant years after it had been taken off the market in the United States due to disturbing side effects. One woman she interviewed described “abdominal pain, paralysis in hands and legs, vaginal discharge, and severe headache on one side” caused by the implant. Another woman said that when she requested removal of the Norplant, she was told that it would cost her the equivalent of a week’s worth of food for her family to do so.
Dr. Anthony, a physician in a small, rural Ugandan clinic reported seeing “as many as one hundred women every week” due to serious side effects from Norplant, including “heavy vaginal bleeding, some of them come complaining of headache, severe headache. Some of them have a lot of pain. Some patients come here and they are saying the husbands beat them up because there is a loss of libido. So the man thinks the woman’s going out hitching around.”
He reported one case where a woman had had an IUD in place for 12 years, a not uncommon experience in rural parts of Africa where followup to contraceptive insertion or implantation is nonexistent. He said the woman was “rotting up there,” and that “some patients do die, by the way.” While American women received financial settlements from the makers of Norplant, Ekeocha did not know of a single African woman who had been compensated for damage caused by a contraceptive from a Western country.
“These organizations say that they’re empowering women, but they are abusing the Africans, especially the ones in the most rural areas who don’t have access to a doctor,” Ekeocha said. “The African people are treated as sub-humans.”
What Africans Really Want
Speaking of her travels to 10 African countries and 20 African cities, Ekeocha said “none of the women are telling me how much they want contraception. None of them are telling me how much they want abortion. Every time I’m speaking with, especially, young African girls, they tell me that some of them want to be doctors. They want to go to med school, they want to go to law school, they want to go to engineering school. These are the dreams that I hear the African girls speaking about.”
“Strings Attached” is available for rental or purchase on Vimeo and Amazon. Ekeocha’s book, “Target Africa: Ideological Neo-colonialism of the Twenty-First Century,” is available on Amazon.
(Pregnancy Help News) On a spring day in 2018, Sarah walked into a Planned Parenthood under immense pressure. Already a single mother of three children, she was pregnant with her fourth, and the baby’s father had one thing in mind: an abortion.
Against her better judgment, Sarah took the first drug in the chemical abortion regimen, returned home, and began to cry.
“I couldn’t look at my other three children in the face without breaking down and telling myself this baby deserves love just as much as these three in front of me,” she said.
With that thought in mind, she decided to act, turning to the internet to see if there was any way she could save her unborn baby.
In that moment, Sarah, like hundreds of other women, discovered a fast-growing treatment known as Abortion Pill Reversal. She quickly dialed the 24/7 Abortion Pill Rescue helpline (877-558-0333) and was put in touch with one of the network’s 800-plus medical providers.
Once she was at the doctor’s office, the baby’s heartbeat was detected and Sarah was able to begin the Abortion Pill Reversal treatment.
Used as an antidote to the abortion drug mifepristone (otherwise known as the “abortion pill” or RU-486), the reversal protocol works by flooding a woman’s body with progesterone, the natural hormone that is needed to sustain a healthy pregnancy. If administered within 72 hours of taking the abortion drug, progesterone has a 68 percent success rate in saving unborn babies.
“I prayed for God to help me through,” Sarah said. “I wanted to try whatever I could to reverse the worst decision I had made.”
Today, Sarah’s life looks vastly different from the heartache she faced earlier that spring day. That’s because the little baby she thought was aborted is alive and well, having recently celebrated his first birthday.
To Sarah’s immense joy, the Abortion Pill Reversal protocol worked. Her baby boy Isaiah has become an integral member of her family and has stolen the hearts of his aunts, grandparents, cousins, and siblings.
“Isaiah is starting to walk,” Sarah wrote in a message to Heartbeat International, the group that manages the Abortion Pill Rescue Network. “He’s starting to babble more and is always hungry. He is a ham and knows it. He loves jumping in on the action when his siblings are playing.”
The miracle of her child’s life is not lost on Sarah. Since the experience of rescuing Isaiah from abortion, she has been overcome with unshakable gratitude and the desire to share her story with others.
“All my children bless me daily,” she wrote. “Each one taught me lessons, but Isaiah began my new life. This morning when he woke up and smiled at me it touched my soul. I will forever be grateful that there are people out there who hold life in the highest regard.”
“I am ashamed I went for an abortion for my son,” said Sarah, “but I will forever be humble that God broke through my life and saved his life and mine with the aid of selfless, caring individuals.”
“One day, we will end abortion,” she continued. “And no woman will ever have to feel that regret and shame again and will either get to look with love at their child, or gift a couple with the blessing they have been praying for. I want everyone who works for APR to know just how much we appreciate their work!!”
Christa Brown, who oversees the Abortion Pill Rescue Network for Heartbeat International, says the feeling is mutual. She is encouraged by Sarah’s willingness to share her experience in the hopes of helping other moms who regret their abortions. She is also struck by Sarah’s perseverance and grace as a mother of four.
“As a single mom, we know this last year has been difficult at times for her, but we are so proud of Sarah,” she said. “She is so beautiful inside and out. As a loving mom, she accepts every challenge willingly in order to provide the best life for her little family.”
Brown says that Sarah has become an ardent champion of pregnancy help centers and other pro-life organizations and that her faith in God has been renewed. Later this spring, Sarah will return to school to pursue further education.
As Sarah prepares for that new chapter, Brown can’t help but reflect on the rippling effects of Sarah’s decision to change her mind and rescue her baby from abortion. Not only has Sarah been restored as a mother and Christian, but her family has also experienced profound renewal.
“They all love Isaiah dearly and couldn’t imagine life without him,” she said. “Abortion impacts so many and seeing the joy Isaiah has brought to this entire family makes the saving of his life even more miraculous.”
Editor’s Note: This article was first published at Pregnancy Help News and is reprinted here with permission.
Politicians and medical professionals alike are calling for Australia to make conscientious objection to things like abortion and contraception illegal — and one doctor in particular seems to be at the middle of the controversy. Dr. Hong Nguyen, who works at Torquay Medical Health and Wellness Clinic near Melbourne, recently posted an announcement saying she would no longer prescribe contraception or consult for abortion or IVF. When a local politician noticed, he set off a firestorm after posting the photo.
Andy Meddick posted a photo of the announcement on Twitter. “Shocked to see this in my town. Yes, legal. But likely emboldened by Religious Discrimination Bill,” Meddick wrote. “Federal MPs must vote it down – or lives and safety will be at risk. This is reproductive healthcare and nobody should ever be denied it.”
Photo shared on Twitter
The image was retweeted over 500 times, and hundreds of people chimed in to express their outrage. And Meddick has further spoken out about it, arguing that people with a religious objection to things like abortion shouldn’t be involved in health care.
“I think it’s absolutely appalling. It’s disgraceful and incredibly concerning,” he said in an interview with Yahoo News Australia. “If this particular doctor is making this decision based upon religious beliefs it should be reversed because religious decisions don’t have a place in reproductive healthcare. Nobody should ever feel ashamed to see a doctor and it’s a vulnerable time.”
Currently, the Australian government is considering a religious discrimination law which would allow conscientious objection in health care to be protected. But Meddick isn’t the only one who opposes it; Chris Moy, president of the Australian Medical Association, opposes the legislation too, according to The Sun:
When you sign up to be a doctor, we have a code of ethics and professional standards – and one of the key things is having responsibility for our patients. Now the problem is this legislation is a crude tool. We have this law that says you have this consent but the legislation now says “I can walk away” if you have an objection to something like a deeply religious belief. [But] it confuses and creates a lower bar when compared to professional standards and ethics, and the flow and affects in terms of how the fabric of the current health system where there is a balance between doctors’ rights to conscientiously object, and their requirement to always be there for the patient.
We have an obligation to the patient and not abandon them. We actually have to be able to make sure that we don’t impede their care, and to facilitate them. We’re pretty unhappy about [legislation]. What AMA is concerned about is how the conscientious objection is undermining the professional standards. Patients trust me as a doctor so I’m not going to let them down.
However, what is ignored by people like Meddick and Moy is that patients are not actually being deprived of any care.
Torquay Medical Health and Wellness Clinic released a statement addressing the controversy, and pointed out that other doctors within that very clinic offer the services Nguyen doesn’t want to. “We do support women’s health and the rights of women to make their own health decisions,” the statement read, adding, “Our practice sits in the middle, a group of people who are medical practitioners, nurses and reception staff that together between all of us provides care to EVERYONE who needs it, regardless others beliefs, religion or political views or cultures. We are a diverse team that between us cares for everyone who uses our clinic.
The clinic said it has received so many abusive comments that it had to shut down its social media page.
It is disturbing that people are arguing that medical professionals should be forced to violate their own beliefs and principles or be banned from practicing medicine altogether. The idea that a child in the womb of a human mother is also a human is a scientific fact, not a “religious belief.” As the clinic itself pointed out, other doctors there were still willing to provide contraceptions or abortions. However, to those who seek to promote abortion, it isn’t enough. Instead, they demand that all doctors in Australia support abortion, or be forced out of the profession.
That’s a chilling mindset, and if the legislation doesn’t protect doctors like Nguyen, it’s a worrying sign of what the future may hold for pro-life health care providers in Australia.
An advocacy group for the rights of disabled persons in Spain has introduced a measure that would end the current practice of forced sterilization of the disabled. Shockingly, under the current law, even those with what are considered “high-functioning” disabilities such as Asperger’s or other mild forms of autism, can be forcibly sterilized without their knowledge or consent, or with diminished consent under severe pressure from family or other authorities.
The regressive policy has come under fire from international human rights organizations in recent years. According to article 156 of the Spanish criminal code, all that is necessary to carry out this act is a judge’s authorization and acknowledgement of the “incapacity” of the individual in question. A 2018 report from the European Disability Forum showed that, from 2010-2013, 400 women — whom doctors deemed as having some form of disability regardless of mental capacity — were forcibly sterilized in Spain. The report highlights the story of a deaf woman who was sterilized without her consent.
“And these are just the cases we know about,” a report in Equal Times points out. “Far more often, forced sterilization procedures don’t leave traces in official records because doctors typically go it alone, performing sterilizations on women with no due process.”
When Ciudadanos party MP Sara Gimenez brought the issue to public consciousness in a tweet in January, Euronews illustrated the problem with the story of Cristina, who was diagnosed with autism at the age of 18. Her parents immediately pressured her to undergo tubal ligation.
“They kept telling me that it would be irresponsible to have sex because I could get pregnant; that I was not going to be able to take on the responsibility of being a mother,” she told EuroNews. “That, as I was Asperger, my children would also be born Asperger; and this insistence fixed in my mind the idea that I was not capable of having children.”
The pervasive societal belief at the heart of the policy is that persons with disabilities cannot be good mothers, or that the disability would be passed on and the resulting child would be a “burden,” both on the family and on the state which sometimes lacks appropriate resources. In some cases, the forced sterilization is also portrayed as being for the good of women, “protecting” them from potential future pregnancies due to possible abuse.
Grave moral problems are tearing the country apart. For many, this is apparent in the form of broken homes, procured abortion, shattered communities and lost Faith.
Many people get it right when pointing out the problems. However, they get it wrong when looking for solutions.
Some get it wrong because they look for solutions that address symptoms, not causes. Others search for a way out that involves the least possible effort. In these politically correct times, people are told not to offend anyone by their proposals. Thus, they automatically exclude the only real solution, which is a return to Christendom. They are willing to consider any other solution, no matter how absurd or improbable—anything but Christendom.
Christendom! It may seem shocking since its days seem long past. We are supposed to be in a post-Christian era. However, the urgency of our times call for it. We need a Christian civilization if we are going to overcome the present crisis. It needs to be at least considered.
A Rejected Proposal
Because our problems are moral, our solutions must also be moral. The rich treasury of Western thought and traditional Church teaching prove that the natural law and Christian morality are the norms that are best suited to our human and social nature. We find our greatest happiness inside institutions and social structures that take us to the end for which we are created—God.
Thus, we should naturally tend to favor Christendom. Everyone, Christian and non-Christian alike, finds the best conditions for prospering inside a family of nations that facilitates virtue and promotes social harmony in this vale of tears.
But everyone avoids this conclusion. We have long been conditioned to reject this line of thought. This Anything But Christendom (ABC) Syndrome curiously applies alike to the political left, right and center. It embraces both secular and religious America. The most rigid tyranny bars anyone from thinking outside the materialistic box.
The ABC Syndrome and the Political Spectrum
Each political sector has its reasons for denying Christendom.
For radical liberals, the ABC Syndrome makes sense. They resent any moral limits to their acts and do not care if there are harmful consequences. Individual pleasure reigns supreme regardless of self-destruction or the death of babies. Thus, a Christian moral code represents an unbearable restriction on their desires to do, think and be whatever they want. Their variant of the ABC Syndrome is to allow Everything But Christendom. Use any letter of the LGBTQ+ alphabet, but never use C for Christendom.
Those on the right have a different approach. We find Christians who truly desire a Ten-Commandment-based moral code, for example. However, they dare not propose Christian morality because the people and media who oppose it appear to be numerous. For them, it has no chance of winning. Thus, they subscribe to the Anything But Christendom approach on how society should be run. Every concession must be made to accommodate others who refuse to accommodate them. Christians dance around all the issues touching on Christendom, but no one dares say the word.
And then there are the radical moderates who want to appear non-radical. In their radicalism, these extremists purge all moral references from the debate. They prefer to tweak the status quo, hoping to avoid the Christendom issue altogether. As society falls apart, this effort proves elusive and ineffective.
Imposing the Christian Will Upon Others
Three main fallacies are used to justify the ABC Syndrome. The first is the mistaken belief that proposing Christendom imposes the Faith on non-believers.
Liberals think that establishing any moral limits means imposing Christianity on others. And yet they have no qualms whatsoever with imposing their anti-Christian will on Christians, on Christian feast days such as Christmas, and the Little Sisters of the Poor. They have no scruples about stuffing a Drag Queen Story Hour world of perversion down the throats of society, despite protests from concerned parents.
Christians cannot impose their Faith on those who do not believe because Faith is a gift from God. It cannot, by its nature, be imposed. However, Christians can and should enact reasonable laws based on the natural law that call for moral restraint to form a just and harmonious society.
Since Aristotle, moralists taught that this natural law is valid for all times, places and peoples. By advocating such moral limits in the law, Christians merely obey the nature of all law, which restricts what individuals might do for the sake of the higher common good.
In proposing Christendom, we are not imposing but returning to an order that conforms to our human nature and which favors our development and sanctification. In submitting their Everything But Christianity agenda, the left imposes on society a destructive system that brings it to ruin.
Hopelessly Outdated
The second fallacy is that Christendom is so far removed from society’s current state that it is impractical to propose it. The Christian agenda is hopelessly outdated for postmodern times, it is falsely claimed.
There is nothing more outdated than today’s anti-Christian agenda. As Catholic thinker Plinio Corrêa de Oliveira notes, there is nothing new about divorce, procured abortion, nudity, and moral depravity. Most “modern” proposals are merely recycled pagan vices from antiquity. Moreover, what could be more foreign to our American Christian heritage than the sudden appearance of transgenderism or the current mainstreaming of Satanic movements?
Indeed, most Americans identify with a return to our Christian roots. They have problems adjusting to the latest barbarisms proposed by a neo-pagan culture. The debate should not be centered on the age of the ideas proposed but their merits. The automatic exclusion of ideas because some claim they are outdated is foolish and wrong. The only thing that matters is if they are true or false.
A Long Time Frame
Finally, there is the fallacy that it is impossible to change society quickly, especially when most people seem to subscribe to the opposite of a Christian civilization. At best, a Christian restoration is a futile effort, they erroneously claim.
Again this argument sidesteps the merits of ideas. It focuses on the practicality of implementing them. However, this fallacy is as flawed as the other two.
Captivating ideas like homeschooling, for example, have drastically changed individuals and families in a short time. As the last elections have proven, voters will change their positions when convinced of the need to change.
Societies, too, can quickly and radically change. Consider the Sexual Revolution. Within the space of a decade, the sixties radically changed the mores, fashions and manners of that generation and all those that followed. Most people in the fifties were not hippies, but many adopted hippie ways in the seventies as these became mainstream.
The history of the Church is full of fervent missionary efforts in which whole peoples, burdened by their paganism, were quickly converted to the Faith by the efforts of men and the action of grace. These peoples changed their lives wholesale, adopting Christian ways in a short time.
People change their ways when times are empty, and ideas are exhausted. Indeed, it is in times like ours that grand ideas like Christendom have their greatest appeal.
Where Christ Is King
Thus, the time is ripe to debate Christendom. It should be done openly, unapologetically and enthusiastically. Many do not know what Christendom is. Indeed, the ABC Syndrome represents old liberal prejudices that distort the true nature of a Christian society. For too long, our shallow, materialistic society has suppressed the notions of wonder, sublime, and the sacred that correspond to the deepest desires of the human soul.
By engaging in the debate over Christendom, we address the emptiness of our nihilistic society that finds no meaning or purpose in life.
Above all, the failure to debate Christendom is fatal since it means the continued descent into an anti-Christendom of anarchy and unrestraint. This anti-regime is already seen in the dark yearnings of Antifa, anarchists and Satanic movements that call for a world without morality. They advocate the destruction of our nation and the persecution of those who keep the Faith.
These topics need to be discussed. We should not be afraid to proclaim our desire to see Christ as King. Numerous popes have described this Christian society as one that affirms the social Kingship of Christ. In his encyclical Quas Primas, Pius XI says that “Once men recognize, both in private and in public life, that Christ is King, society will, at last, receive the great blessings of real liberty, well-ordered discipline, peace and harmony.”
Only Christendom can be a truly just society for all.
Even many people in the pro-life and pro-family movements do not fully appreciate the deep threads that tie together many seemingly disparate social issues. Contraception, abortion, euthanasia, divorce, pornography, same-sex “marriage”, and gender ideology (to name some of the big ones) are not isolated social or spiritual problems. Rather, they are deeply interrelated, and, more importantly, they feed off one another.
There is an interior logic to the Culture of Death, if not short-circuited by a return to perennial truths, that causes it to eat its own tail, so to speak, with death leading to more death, and loneliness and isolation to further loneliness and isolation. This dynamic is something that Human Life International’s founder Fr. Paul Marx, OSB, was keenly aware of. As he wrote in From Contraception to Abortion, “In every country, bar none, contraception has led to abortion, and once abortion, to infanticide, the prelude to full-blown euthanasia. Once the purposes of sex are torn loose from procreation and the family, the homosexual thrust rears its ugly head.”
The Demographic Alarm
One of the most underappreciated areas where we see this perverse logic at work is in the relationship – alluded to by Fr. Marx – between the contraceptive/anti-natal mentality, and the growing demand for legalized euthanasia and assisted suicide.
Many anti-life campaigners believe that they are advocating for legalized euthanasia because they believe in the principles of “freedom” and “autonomy”. What they don’t realize is that in fact they are responding to pressure to find a “solution” to a growing problem that exists in large part only because their ideology created it in the first place – by demolishing the supporting structure of the family and by promoting an anti-natal mentality that has robbed families and society of the children they so desperately need.
Even many mainstream publications and liberal politicians are beginning to wake up to the slew of problems caused by the demographic winter that was conjured by the dual forces of overpopulation alarmism and the sexual revolution. Consider this recent article in Canada’s Globe and Mail, a far-left, but widely-read newspaper. In it, author John Ibbison warns about the financial and social tsunami that is looming on the horizon, thanks to that country’s rock-bottom fertility rate.
As the teaser below the headline handily summarizes: “Every generation is having fewer children than the one before it, leaving fewer and fewer people to care for us in our increasingly long lives. It is a crisis we ignore at our own peril”. This crisis is a simple matter of mathematics: many of our social and financial structures have been built upon the presupposition that there will exist a large and healthy population of young people to enter the work force, pay their taxes, and support their aging parents and relatives. But, as it turns out, those young people are no longer there.
Fertility rates in Canada (and throughout the Western world) began to plummet in the early 1960s. From a peak of nearly four children born per woman during her lifetime in the late 1950s, the rate rapidly fell in Canada to the current 1.5 or so. According to Statistics Canada, the last year during which Canada’s fertility rate was at replacement level was in 1971. For nearly five decades, then, the country has had below-replacement-level birth rates. The only thing keeping the country’s population stable is immigration. As Michael Nicin, executive director of Ryerson University’s National Institute on Ageing, told the Globe, “This is a fundamental, paradigmatic shift in society, and for too long we’ve buried our heads.”
As Ibbitson notes, the decrease in fertility has coincided with an increase in longevity, with a result that we now have an aging population of retirees that is also living longer than ever before. Already there are a growing number of couples hitting retirement age and beyond, many of whom (as Ibbitson notes) have not saved nearly enough money to pay for their living expenses and health care until their deaths. Furthermore, they don’t have any children that they can rely on for financial assistance or (much more importantly) the kind of personal care and companionship that are so vital for their happiness and overall well-being. And finally, since everybody else has also stopped having children, neither will there exist the workers and associated tax revenues that will make it possible for the government to pick up the tab for their long-term care.
Enter Euthanasia
Is it any surprise, then, that Canada legalized euthanasia a few years ago?
The pro-euthanasia advocates will deny this link, of course. As mentioned above, they think they’re advocating for what’s right based upon a dispassionate principle. They think the “right to die” or “death with dignity” is a human right, and they are the selfless crusaders willing to go the distance to pressure government to protecting that right. In reality, they are merely putting the nails in the coffin of the Culture or Death.
A healthy society does not seek to find ways to ensure that its most venerable and elderly citizens have the easiest path possible towards offing themselves. In a healthy society, there wouldn’t even exist any such demand for euthanasia or assisted suicide, as there now does. In a healthy society, the elderly live out their final days in dignity, surrounded by families and loved ones, embedded within a loving community of relationships that has supported them through life, and is there to support them as they pass on to the next life. Few people in such humane circumstances give much thought to whether and how they should kill themselves.
However, within a society that has built itself on the principle of radical autonomy, explicitly repudiating the centrality of relationships of dependence and love, above all those that exist within the family, the inevitable result is a growing number of isolated, lonely, embittered, and suffering elderly. If that society has also enthusiastically embraced utilitarian and consumerist values, in which the worth of a life is judged by its levels of pleasure or social utility, then the result is that those same elderly become viewed as – and even more pernicious, view themselves as – dead weight, costing others money, time, and mental energy that they don’t have to spare. In other words, if there is now a demand for euthanasia and assisted suicide, it is only because the Culture of Death first created that demand, by embracing contraception, anti-natalism, abortion, and divorce.
Nobody that I know of is explicitly pushing for euthanasia and assisted suicide as a cost-saving device. However, in those nations where euthanasia has been legalized, there are a myriad of macabre tales of elderly individuals being pressured into opting for euthanasia, often by overwhelmed and underpaid long-term care staff who are fighting for limited pools of government funding. It’s the logic of the thing. A single elderly patient could end up costing the government hundreds of thousands of dollars if they happen to pull through this current health crisis and go on to live for another five or ten years; why not just encourage them to put an end to their suffering once and for all right now, and sign on the dotted line?
As I wrote in this same column last year:
During a papal audience with Pope St. John Paul II in 1979, Fr. Marx offered his insights with the saintly pope saying that “once contraception is widespread, the rest is predictable. In every country contraception always leads to massive abortion.” He further emphasized that “once you have contraception and legalized or widespread abortion, birthrates fall; nations collapse; young people follow their parents in the abuse of sex, and increasing numbers live together without the benefit of marriage.” As if capable of looking into the future, Fr. Marx also discussed the intimate link between contraception, abortion, and euthanasia. For “if you can kill before birth, why can’t you kill after birth? So, euthanasia is inevitable.”
The Slippery Slope
Not only is euthanasia in some sense “inevitable”, or at least the logical consequence of embracing contraception and anti-natalism, so too is the gradual expansion of euthanasia once accepted. The “slippery slope” phenomenon has been well attested to in the Netherlands, where euthanasia has been extended even to people suffering from mental illnesses. In the Netherlands it would be illegal for a severely depressed person to shoot themselves, but perfectly legal for him to give himself a lethal injection if the poison is provided by a licensed doctor at taxpayer expense. This is the double-think we are increasingly called upon to blithely accept.
Pro-euthanasia activists always claim that they only wish euthanasia to be legal in a select few, “extreme” circumstances; but if recent experience is any indication, those “extreme” circumstances turn out to be very many indeed. Already, a court in the Canadian province of British Columbia has ruled that a requirement in the recently-passed Canadian euthanasia/assisted suicide law that patients requesting euthanasia be facing a “reasonably foreseeable” death is unconstitutional. It was only in 2016 that the Canadian Supreme Court suddenly “discovered” the right to assisted suicide and euthanasia in the constitution. And now, just three years later, another court has somehow discovered a “right” for people who aren’t dying to ask doctors to help kill them! Unless pro-life and family Canadians and disability advocates mount a strenuous opposition, this will undoubtedly only be the beginning: it will only be a matter of time before those suffering from depression, dementia, and other non-terminal illnesses will be deemed “eligible” for, and (subtly or not-so-subtly) pressured into euthanasia or assisted suicide.
Speaking of the macabre interior “logic” of the Culture of Death: it turns out that in Canada there has been a big boom in the number of organ “donations”. And who are these organs coming from? From people who have legally killed themselves or been killed by doctors. The mainstream media thinks this is a wonderful thing. In reality, however, this the monstrous outcome of the Culture of Death: elderly or ill patients who, according to utilitarian standards, have outlived their “usefulness”, being told they can do something “positive” by helping another person with their organs if they would just put a premature end to their miserable existences. And, of course, it is a great benefit that the organs in these cases are so wonderfully “fresh”. This is the Culture of Death in action. Death leads to death.
A former NFL star who shunned an invitation to the White House in 2013 to protest President Barack Obama’s embrace of Planned Parenthood says he’s pro-life in part because of the mothers of his two adopted children.
In remarks to the National Pro-Life Summit in Washington, D.C., on Jan. 25, Matt Birk, who played that year for the Super Bowl-winning Baltimore Ravens, urged his audience of mostly high school and college-aged pro-life activists to combat the celebration of abortion and to rejoice in life.
Birk, the father of eight, made headlines in June 2013 after the Ravens’ victory in his 14th and final season in the NFL. Because of his pro-life beliefs, he declined to take part in the team’s invitation to the White House, saying Obama had said “God bless Planned Parenthood” about six weeks earlier.
According to a CBS Sports report at the time, Obama had concluded a speech to the organization’s national conference in April 2013 with “Thank you, Planned Parenthood. God bless you. God bless America.”
“I wasn’t ready for what happened next,” Birk told his audience of more than 3,000 at the Marriott Marquis hotel. “All of a sudden, I got introduced to the 24-hour news cycle.”
Birk explained why he held pro-life convictions strongly enough to say no to an invitation from the president, noting that his Catholic faith and his own family played into those beliefs.
“I am pro-life because God is the originator of all life, and my life has dignity, not because my mother said so, but because I am a child of God,” said Birk, who played 10 seasons for the Minnesota Vikings and four with the Ravens and was a six-time Pro Bowl selection.
Birk, 43, said his family owes its existence in part to two women who chose life.
“Two of my eight children are adopted, and I cannot tell you the gratitude that I have to their birth mothers,” he said. “They committed the greatest act of love I have ever witnessed in my life—to give a child up for adoption.”
He says that fact informs his belief that abortion is wrong.
“You’ll never see a woman walking out of an abortion clinic with a smile on her face, because there’s nothing to celebrate,” Birk said. “You’ll never hear someone say, ‘Here’s my daughter. She’s two years old, and I wish I had aborted her. This means only one thing—that abortion must be evil.”
Birk said that while he was always pro-life intellectually, he started “doing pro-life” after he got a call from the Catholic archbishop of Baltimore in 2012, asking him to speak at the Maryland March for Life, where his eyes were opened to the harsh reality of abortion.
“I was so shocked by the hundreds of women who had an abortion who regret it, and are still hurting from it. And they don’t want other women to make the same mistake,” he said.
Birk concluded by urging the audience to pray and to show up for pro-life events, but not to be discouraged.
“It’s not our job to win this fight, but it is our job to try,” he said. “We are a movement rooted in truth. We don’t have to defend the truth, because the truth is like a lion that you just have to let out of its cage.”
Abortion proponents not surprisingly object to sex education that doesn’t promote artificial contraception.
By Martin M. Barillas
BRASILIA, Brazil, January 29, 2020 (LifeSiteNews) — Damares Alves, Brazil’s Minister for Women, Family and Human Rights, recently asked parents to consider telling their teenage children to wait until adulthood to have sex, thus unleashing a rash of negative comments from leftists in the South American republic.
Minister Alves responded to the growing rate of sexually-transmitted disease and teenage pregnancies by promoting sexual abstinence among adolescents. She is collaborating with a campaign sponsored by evangelical Christians, dubbed “I Choose to Wait,” that fosters traditional Christian teachings about sexuality, chastity, and marriage. Alves is a leader in the evangelical Christian community in Brazil and one of the most visible cabinet members in the current government.
Pro-abortion and LGBTQ advocates denounced the campaign, citing fears that it is effectively a merger of Church and state. According to The New York Times, Brazilian law professor and abortion activist Debora Diniz said that program will have “terrible consequences” and lead to further cases of teenage pregnancy and sexually transmitted infections (STI).
Diniz claimed that abstinence doesn’t work. Abortion providers such as Planned Parenthood and advocates such as Guttmacher Institute also regularly discredit delaying sex as a method of avoiding pregnancy and sexually-transmitted diseases among adolescents.
The I Choose to Wait campaign states that it is “centered on the importance of living a life in holiness and purity based on the Holy Scriptures.” According to Daily Wire, Alves said of underage sex, “Our young people, by and large, are having sex as a result of social pressure. You can go to a party and have lots of fun without having sex.”
Brazilian President Jair Bolsonaro has accused his leftist rivals of encouraging teenage sex. He stopped a campaign to address homophobia in schools that leftist predecessor Dilma Roussief had begun before her sudden departure from government. He said it amounted to a “homosexual kit” that intended to “pervert” children.
Bolsonaro’s campaign and subsequent actions in government have won him friends among conservative Catholics and evangelical Christians, the latter of which is a growing sector in political importance.
In an essay published in the daily Folha de São Paulo, Alves insisted that she was not diminishing the use of contraceptives and condoms to minimize teenage pregnancy and STI.
“We are cooperating with all of the ministries to offer additional material at each step when people make decisions,” she wrote, adding that this does not mean her government is imposing anything, but is “informing, through which autonomy is reinforced.”
Alves said her critics use the term “abstinence” in order to discredit the program. Recently, she said previous programs have not worked, given the fact that teens are having sex at an earlier age than in previous years. She also pointed out that teens are further endangered by a bill now before Brazil’s congress that would lower the age of consent to 12, which she said would thus legalize pedophilia.
After being named to Bolsonaro’s presidential cabinet, Alves said she wants to rescue women and children from abortion. “The greatest human right is the right to life … I am against abortion,” she said. “We want a Brazil without abortion. How? A Brazil that prioritizes public policies of family planning, where abortion is never seen as a contraceptive method.”
She went on to say that women don’t want abortion, but they exercise this option when they believe there is no other alternative, adding that while “pregnancy is a ‘problem’ that lasts only nine months, abortion is a burden you carry your whole life. We will always fight to save two lives: the woman and the child.”
The abstinence program is slated to kick off next month. Alves wrote that abstinence programs in the United States have been successful in limiting teenage pregnancy.
In an email response to LifeSiteNews, Dr. Michelle Cretella, president of the pro-life American College of Pediatricians, applauded the Brazilian government’s move. According to Dr. Cretella, a board-certified pediatrician specializing in adolescent health, the “so-called comprehensive sex education (CSE) programs” in U.S. schools have not shown long-term effectiveness at increasing sexual abstinence among adolescents, nor have they been shown to increase long-term condom and contraceptive use among sexually active youth.
“This should come as no surprise since CSE programs send a double message to teens,” Dr. Cretella said in the email. “In contrast, school-based sexual risk avoidance (SRA) curricula, traditionally known as abstinence education, focus on the primary public health principle of risk avoidance’ and thereby uphold the highest attainable standard of health for all students.”
She said SRA programs have significantly delayed sexual activity among teens. “The American College of Pediatricians,” Dr. Cretella said, “recommends the adoption of sexual risk avoidance (SRA) programs by all school districts in lieu of curricula described as comprehensive sex education (CSE).”
January 29, 2020 (LifeSiteNews) – The basic outlines of the Church’s teaching on family life, in terms of what we must on no account do, are clear, but we need to beware of the more subtle ways our thinking has been warped by our contraceptive culture. This is a hugely complex topic and I want to look at just one aspect of it: the attitude to large families.
It has become a joke, albeit a boring one, that many people can’t see a family of more than three children without having a dig at the parents. My lifestyle does not expose me to much of this but I did get a “You should get a TV” from a stranger recently, which was intended as light-hearted. (Actually, I’d rather have the children.) Such comments can be particularly upsetting when they come from fellow Catholics. No less annoying is the counter-pressure occasionally found in those pockets of Catholic society where larger families are more common. It is such a stupid thing to ask mothers if they are going to have another baby. Who knows what has been going on? Just don’t do it.
These opposing remarks have something in common, which is the odd way they hold parents to account for having or not having children, and see a certain family size as the right one for everyone: whether is it two children, six, or none. This is obviously absurd in ignoring the particular circumstances of different families, above all biological factors which are of no concern to complete strangers. But it also puts an artificial limit to family size, whether the limit small or large.
One motive for this is a concern about the environment, or the supply of food. Without going into too much detail, the Netherlands, one of the richest countries in the world, has a population density of 521 people per square kilometer, and enormous national parks; China has a density of 153. There is no shortage of space, nor, now vertical farming technology has rendered calculations about arable land irrelevant, need there be any shortage of food. It is impossible to escape the impression that some environmentalists just don’t like people very much, and see the coming demographic winter in developed countries, and the projected decline of the world’s population, as a cause for rejoicing.
(Here’s a fun fact. When will or did the world population growth rate begin to slow? 1968.)
A more pervasive motive, however, is the question of “what I (or you) can cope with”. Not, you understand, a concern about health problems for the mother or actual malnutrition among the children: I mean, in relation to what we might call lifestyle expectations.
People who have never experienced a large family often assume that they must be proportionately more chaotic than a smaller family. ‘It is must be mayhem at your house at Christmas!’, my butcher cheerily informed me, no doubt based on an experience of two or three children extrapolated to six or eight. Obviously, things don’t work like that. Large families have their challenges, but the biggest challenge is keeping the mayhem under some kind of control with just one child.
The same goes for estimates of the cost of “raising a child”. This page, based on US government figures, talks about the enormous cost of one child, and makes no reference to the marginal cost of additional children. The implication is that readers should double the cost of one child if they are considering two, and to quadruple it for four, which would be an obvious mathematical fallacy. Indeed, it is silly to invite people to consider if they can afford the average cost of a child. This average is composed of super-wealthy parents going to all sorts of non-essential expenses with their children, and the rest of us not doing so. What has the average cost got to do with what it will cost you, if you are relatively poor? No-one is going to force you to buy every child an iPad.
I would like to invite young people starting or considering a family to set aside not only this kind of demonstrable nonsense, but also the more realistic worry about maintaining the expectations associated with small families, such as children not having to share a bedroom. Similarly, in large families there tends to be more wearing of cast-off clothes, and flying with the whole brood can become very expensive (no sibling discount there). There are many things which need to be adjusted, gradually, as the head-count increases. There may be typical middle-class things you could do if you have only two children and can’t do if you have six. There’s no denying it, and having a large family in this sense is a real sacrifice. You know, however, exactly what you are getting instead. Children.
St Augustine wrote that Christian mothers, as well as consecrated virgins, should be praised, because they bear children for the Church (De Virginitate). This is the end, the goal, of the vocation of marriage. Don’t place too many limits on God’s generosity.
Thank you for the kind invitation to address the 2019 National Youth Conference here in the Diocese of Kasana- Luweero. I am delighted to be able to learn more about Uganda, as I only know a few things about your country. I am aware of the Ugandan Martyrs. In union with the worldwide Catholic Church, I observe the liturgical feast of St. Charles Lwanga and his companions every year on June 3.
I also know that Uganda had a successful strategy for combating the spread of HIV-AIDS in the 1980s and 1990s. Your country did not blindly follow the lead of the international agencies that were promoting condoms as the one and only solution to the spread of the HIV virus. You developed your own program, encouraging people to reduce the number of sexual partners they had. And you continue to take a wholistic approach, seeing the person in his social and spiritual context.
My topic today is the sexual revolution. The sexual revolution is not native to Africa. Wealthy and powerful people have spent vast sums of their own money to promote the sexual revolution. These same people have captured the use of governments and international agencies to impose this ideology around the world. This is a new form of colonialism. We could call it sexual colonialism or ideological imperialism, to distinguish it from economic colonialism or imperialism.
I want you to know that many, many Americans share your pro-life and pro-family values. Many Americans have come to realize that the sexual revolution is a totalitarian ideology. Those same Americans are deeply ashamed when they realize how our government has historically thrust the values of the sexual revolution on people around the world, including you here in Uganda. I am not talking only about American Catholics. Eastern Orthodox Christians, evangelical Protestants, Latter-day Saints and observant Jews in America also share your family values. On behalf of those Americans, I apologize for our country’s role in spreading the sexual revolution to your country.
I sometimes hear confused reports that Uganda has the death penalty for homosexuality or is considering the death penalty for homosexuality and that American Christians are somehow to blame. So I wish to say something to this all-Catholic gathering.
As Catholics, we stand by the Catechism of the Catholic Church, on the death penalty, as on all other serious matters. Pope St. John Paul II revised the Catechism to say:
“The traditional teaching of the Church does not exclude … recourse to the death penalty. … Today, given the means at the state’s disposal to effectively repress crime by rendering inoffensive the one who has committed it, without depriving him definitively of the possibility of redeeming himself, cases of absolute necessity for [the death penalty]… ‘are very rare, if not practically nonexistent’” (2267).
We cannot support the death penalty for homosexuality. We don’t need to belabor the point.
My purpose here today is to convince you that you should exercise all morally acceptable means for keeping the toxic ideology of the sexual revolution out of your country. One step in protecting your country is to refuse to use the terminology of the sexual revolutionaries. They have invested millions, by now, perhaps billions, of dollars to create certain associations of ideas and words. If you use their terminology, you will place yourself at a disadvantage.
For instance, the term “feminist” carries many positive associations for many people. “Feminism” means “freedom” and “equality” and “education for girls” and “women get to have good jobs.”
But “feminism” has other ideas associated with it. “Feminism” means “women don’t really need men,” and “women are too good to waste by staying home and caring for children,” and “children hold women back.” With these associations, “feminism” comes to mean abortion and contraception.
This word “feminism” has ideological assumptions built into it. The interest of men and the interests of women are necessarily distinct from and in conflict with each other. The word “feminism” also assumes that “feminists” and only “feminists” have the right to speak for all women.
That is why I avoid using the word “feminism.” I urge you to avoid it, as well.
Another important term to avoid is the word “gay.” I strongly recommend that you not use the word “gay,” or even “homosexual.” I especially urge you to avoid these words as free-standing nouns, as in “He is a homosexual,” or “I’m gay.”
Speaking in this way has ideology baked into it. It suggests that the person is defined by his sexual desires and behaviors. The term suggests that those desires and behaviors are permanent and can never change.
These associations with the word “gay” come from the United States. Let me tell you the backstory.
As you know, the United States has the terrible history of importing people from Africa to be used as slaves. The trans-Atlantic slave trade persisted for 200 years. We have spent the past 150 years trying to deal with its aftermath. All of this troubled history has left us with many problems of racial discrimination and prejudice. We have tried to solve these problems with laws forbidding discrimination.
The basic idea of anti-discrimination law is simple enough. People who are the same should be treated the same. People who behave differently, can, of course, be treated differently. For instance, employers must treat people who are equally qualified for a job in the same way, regardless of their race.
By now, America has a well-developed body of law defining permissible and impermissible differences in how people are treated in employment, housing, education and so on. Unlawful discrimination is treating people differently on the basis of inborn characteristics over which the individual has no control. People cannot be treated differently on the basis of what the law calls “immutable traits.”
The sexual revolutionaries seized upon this distinction between “immutable traits” and “chosen behavior” in American law. Their strategy was to create the impression that “being gay” is comparable to “being black.” If they could succeed in making this comparison, then the whole body of anti-discrimination law could be used to protect homosexual acts.
Let me pause to assure you that American blacks deeply resent the way that the sexual revolutionaries have used this comparison between race and homosexual acts. Many American blacks are serious Christians who oppose homosexual acts. They are deeply offended by what they consider the hi-jacking of the civil-rights movement for defending a set of behaviors and political commitments.
Despite the protests of American blacks, sexual radicals have made a strong effort to create the belief that people are “born gay.” They say, no one chooses to be gay. Being gay is something a person cannot change, they say. It is an “immutable trait.” The sexual revolutionary elites have spent an enormous amount of money and effort to create the impression that these points are true. But none of them actually are true.
We now know that there is no “gay gene.” People may experience same-sex attraction as a deep part of their personality. They may not remember ever feeling differently. But no one is “born gay.” The scientific and psychological professions must now admit (somewhat reluctantly):
There is no scientific consensus on how and why some people develop same-sex attraction and others do not.
Sexual orientation is fluid in many people, meaning that it can change.
In short, “being gay” is nothing like “being black.”
My advice that you avoid the term “gay” is more than just a rhetorical strategy. It is also part of Church teaching. Homosexual desires do not define a person’s identity. This is why the Church uses the phrase “men with deep-seated homosexual attractions.”
So, instead of saying “gay,” use a phrase that more accurately describes what you are actually talking about.
Instead of “gay” say, perhaps, “same-sex attracted” if you mean someone who experiences these feelings. Instead of “gay,” say, perhaps, “men who have sex with men.” This is what medical researchers say, for instance, when they are studying the spread of disease. Instead of “gay” say, perhaps, “self-identified homosexual” if you mean someone who does in fact identify himself with his patterns of attraction.
And if any of you, dear young people, find yourself feeling same-sex attraction, do not label yourself as “gay.” Seek help and counseling. But do not let anyone call you “gay,” or draw you into what they call the “LGBT community.” Be assured that, with prayer and counseling, those feelings can diminish, and you can live a normal life as a husband and father or as a wife and mother. These feelings do not define who you are.
That is conclusion my young friend Hudson Byblow came to. He was not very athletic. He was slightly built. The other boys teased him. He was confused about himself. He doubted his manhood. Then an older man molested him. So Hudson thought to himself, “I must be gay.” It took him a long time to overcome the problems he created for himself by adopting that label and the behaviors that went along with it. But now, as he says, he is doing “something more beautiful.” He has moved from “LGBT to Jesus Christ.”
Conclusion: New Colonialism, New Slavery
As I said at the beginning, the sexual revolutionary ideology is not native to Uganda. It is actually a new form of colonialism. The old economic colonialism attempted to dominate the physical resources of the African continent. The new ideological imperialism attempts to dominate the soul of Africa.
But I will tell you a secret: The sexual revolution is an intellectual house of cards. It is fragile because it is untrue. It opposes the law of nature and nature’s God. Therefore, the sexual revolution needs to be propped up, coddled, protected. The sexual revolution needs conformity. Evidence that contradicts it is a direct threat. People who dissent are a direct threat. Every chaste teenager is a threat. Every person and institution of faith is a threat.
And you are a threat. The ideologues fear your vitality and your fertility and your faith. The new Western colonialists do not want to extract resources or material wealth from you. They want your conformity. They want your hearts and minds.
Chattel slavery and the trans-Atlantic slave trade was the old form of Western exploitation of Africa. Today, Western influence has the potential to create an even more serious form of slavery. Jesus told us to have no fear of those who could kill the body. Rather, we should fear those who can kill the soul. And St. Paul warned us long ago about the enslaving power of sin. In Galatians 5, St. Paul told us, “For freedom Christ set us free; so stand firm and do not submit again to the yoke of slavery” (1).
That is why we must continue to be inspired by the Ugandan Martyrs. These martyrs died for their faith at the hands of the king. Sometimes when the story of the Ugandan Martyrs is recounted, the homosexual element is omitted from the story. But we should not omit the fact that the king was a sexual predator who preyed upon young men. The king believed he was entitled to do whatever he wanted and that everyone was required to submit to his desires. Charles Lwanga and his companions refused the king’s sexual advances. The king was enraged and ordered their execution.
When Western aid agencies come around here pestering you to adopt their ways, tell them you reject sexual colonialism. Do not accept the lies of ideological imperialism. Remember the Ugandan Martyrs! The truth really will set you free.
New research provides more evidence that hormonal birth control pills can negatively impact women’s cognitive performance. The study, published in the journal Hormones and Behavior, found that women taking contraceptive pills tend to have reduced perseverance when completing both simple and complex cognitive tasks.
“My colleagues and I first became interested in this topic after learning that women taking hormonal contraceptives don’t experience a spike in cortisol that is typically found after one encounters a stressor. While people usually talk about cortisol as a bad thing, this cortisol spike allows people to adequately meet challenges in their environment,” explained Hannah K. Bradshaw (@HKBradshaw), a PhD candidate in Experimental Psychology at Texas Christian University and corresponding author of the study.
“After we started looking through the literature, we also found that, compared to non-users, women taking hormonal contraceptives exhibit decrements in brain areas that play an important role in learning, attention, and memory.”
“For instance, compared to non-users, women taking hormonal contraceptives have decreased hippocampal volume. This led us to wonder whether hormonal contraceptive use is associated with differences in perseverance and performance on simple and challenging cognitive tasks that one might encounter in their day-to-day lives.”
In two studies, 324 female undergraduates completed various cognitive tests as the researchers timed them. Roughly half of the participants had been on hormonal birth control for at least two months, while the remainder had not used hormonal birth control for at least three months.
In the first study, participants completed a simple spot-the-difference task in which they were shown two similar images and asked to find 10 subtle differences. In the second study, participants completed more complex mathematical problems and word scramble problems from the Graduate Record Examinations (GRE) test.
The researchers found that women on hormonal birth control tended to spend less time on the problems, which in turn was associated with their relatively worse performance on all of the cognitive tasks.
“Our data suggest that hormonal contraceptive use is associated with decreased perseverance on both simple and challenging cognitive tasks. These differences in perseverance drove decrements in performance. That is, women taking hormonal contraceptives performed worse on these tasks than non-users because they spent less time on the tasks,” Bradshaw told PsyPost.
“The major takeaway here is that hormonal contraceptive use carries a myriad of consequences beyond mere pregnancy prevention; additional research is desperately needed to more fully understand what these consequences may be.”
The study — like all research — includes some limitations.
Randomized experiments are the gold standard in scientific research, but there are obvious problems with trying to randomly assign women to receive hormonal birth control. “We didn’t randomly assign women to the hormonal contraceptives (vs. non-user) group, so it’s possible that our effects may, in part, be due to previously existing differences between women,” Bradshaw explained.
“Secondly, hormonal contraceptives can include different hormones and various ratios of these hormones. We didn’t collect information about this, so it’s impossible to know what specific hormones or hormonal ratios are responsible for our results. Future research is needed to address these limitations.”
The findings may have important implications for women, but the real-world impact of decreased perseverance is unclear. Future research is needed to help “understand how hormonal contraceptive use might influence women’s perseverance in their education, careers, and relationships,” Bradshaw said.
“My colleagues and I don’t have an anti-birth control agenda. By enabling women to take control of their fertility, hormonal contraceptives have helped women meet their educational and career goals,” she added.
“However, it’s important that we understand the unintended consequences associated with hormonal contraceptive use. Millions of women worldwide take hormonal contraceptives. While several women complain about negative emotional and mental side effects, their concerns are largely written off. We need to be less cavalier with women’s health and women’s hormones.”
Researchers have conducted a controversial study that involved paying dozens of young women at a hospital near Puerto Vallarta, Mexico, to get artificially inseminated so their embryos could be flushed out of their bodies and analyzed for research purposes.
The study showed that embryos created that way appear to be as healthy genetically as embryos created through standard in vitro fertilization. Physically, the embryos appear to, possibly, even be healthier, the study found.
The research, published online in the journal Human Reproduction, suggests the approach could offer couples a simpler, less expensive way for some couples to have healthy children than is currently available via IVF, the scientists and others say.
“We have now a method that can produce embryos that are of good quality or better than in vitro fertilization,” says Santiago Munne, a reproductive geneticist who led the study when he worked at CooperGenomics in Livingston, N.J. Munne now works at Overture Life, a Madrid-based company that makes infertility treatment equipment.
But others denounce the research as unethical.
“What this essentially does is use a woman’s body as a petri dish,” says Laurie Zoloth, a bioethicist at the University of Chicago. “And there’s something about that that seems so profoundly disturbing.”
The women received hormone injections to stimulate their ovaries to produce eggs, which is a standard way to obtain donor eggs that are to be used for women experiencing infertility problems.
But instead of having eggs extracted via a needle from their ovaries and fertilized in the lab — a standard procedure during IVF — the women in the study were inseminated by sperm. Four to six days later, the women underwent a procedure known as “lavage,” which involved using a specialized device to flush out any resulting embryos from the womb.
The researchers then analyzed the embryos, comparing them to embryos produced by 20 of the women who also underwent standard IVF.
Embryos produced by both methods looked similar genetically, while those created using the lavage method looked slightly healthier physically, the researchers reported.
The women were paid about $1,400, the equivalent of more than two month’s average wages in the area, raising questions about what motivated them to volunteer, Zoloth says.
The women also had to get injections of powerful hormones to stimulate their ovaries, which can pose some risk. In addition, some women underwent surgical or chemical abortions afterward, when tests indicated some of the embryos might not have been successfully removed.
“I think this research was unethical,” Zoloth says.
Munne defends the research, noting that it was reviewed extensively and approved by the Ministry of Health of the State of Nayarit, in Mexico, and the Western Institutional Review Board in the United States. The women were fully informed of any potential risks, Munne says.
“We passed all the ethical committees and all the ethical checks and balances,” he says.
The primary purpose of the study was to try to find a way to help couples who carry the gene for certain inherited diseases, such as beta thalassemia or cystic fibrosis, have healthy babies, Munne says. Currently, the reason such couples create embryos through standard IVF is so the embryos can be tested in the lab, and only those found to be healthy need be implanted, Munne says.
“For couples that have genetic abnormalities and are at risk of transmitting them …. by selecting the embryos that are not affected, they can have a normal baby,” he says.
So Munne and his colleagues decided to see if he could do the same thing without IVF, which requires a painful extraction of eggs, and expensive laboratory procedures. The study involved 81 women who were recruited at Punta Mita Hospital in Punta de Mita, Mexico.
“This is the first time that human embryos conceived naturally have been analyzed genetically to see if they are normal or not,” Munne says.
“The advantage is that these embryos are conceived naturally — so you don’t need in vitro fertilization to do the genetic testing of the embryos. In theory, it should be much cheaper.”
In addition to helping couples avoid transmitting a genetic disease to their children, he says, the approach could offer an alternative way for lesbian couples to share the experience of having a baby.
“You could use this for lesbian couples [when] one wants to conceive the embryos and the other wants to carry the embryos,” Munne says. “So one could have the embryos fertilized and then the embryos are transferred to the other woman to carry them. So they can share the pregnancy.”
Several researchers told NPR the research could be valuable.
“We may actually have here a technology that in the future may be very helpful for couples trying to complete their families at a lower cost, which is important,” Racowsky says.
But others agree with Zoloth that the study raises serious ethical issues.
“Yes, it is quite a series of things that do raise your eyebrows,” says C.B. Lambalk, the editor-in-chief of Human Reproduction.
Lambalk says the journal decided to publish the study only after verifying that the research had been thoroughly reviewed, and published it along with an editorial and a commentary exploring the ethical concerns.
“We could have made ourselves a very easy out — by just saying: ‘No, no, we don’t want this,’ ” Lambalk says. “But we decided to go the hard way and publish it.” The findings could be useful, he believes, and the journal wanted to draw attention to the ethical issues the study raises.
Galia Oron, an infertility expert at the Rabin Medical Center in Israel, who wrote the accompanying commentary as an associate editor at the journal, believes the study was ethically questionable.
“Everything was technically kosher,” Oron says. “But, I’m afraid to say, maybe kosher but smelly.”
For his part, Munne says the process the women in the study went through is essentially the same as what women routinely go through in the United States when they donate eggs to help infertile women. Eggs donors in the U.S. are also routinely paid.
“There is no difference between an egg donation cycle and what we did here,” Munne says.
Embryos produced in the study already have been used to create at least five pregnancies and three healthy babies.
The remaining embryos have been frozen for use by other couples experiencing infertility problems, according to John Buster, another member of the research team.
In a proclamation signed on Monday, President Donald Trump declared January 22 to be National Sanctity of Human Life Day, signifying the importance of valuing human life from the moment of fertilization until natural death.
“Every person – the born and unborn, the poor, the downcast, the disabled, the infirm, and the elderly – has inherent value,” he wrote. “Although each journey is different, no life is without worth or is inconsequential; the rights of all people must be defended.”
Today, January 22, is a date of great significance in the pro-life movement as it was on January 22, 1973, that the Supreme Court legalized abortion in the Roe v. Wade ruling. Trump, following the lead of other presidents, has declared January 22 to be National Sanctity of Human Life Day in 2018 and 2019. Presidents Ronald Reagan, George Bush, and George W. Bush each did the same.
As noted in the proclamation, there has been a decline in the national number of abortions since 2007, however, abortions at Planned Parenthood, the nation’s largest abortion provider, rose from 332,757 in 2017 to 345,672 in 2018. Planned Parenthood now commits 40 percent of all U.S. abortions.
“All Americans should celebrate this [national] decline in the number and rate of abortions, which represents lives saved,” wrote President Trump. “Still, there is more to be done, and, as President, I will continue to fight to protect the lives of the unborn.”
Trump wrote that he has asked Congress to work to end abortions on preborn children who can feel pain. Though Trump mentioned that these would be “later-term babies,” new information from a pro-abortion researcher shows that preborn children are likely capable of feeling some form of pain starting around 13 weeks gestation – including when they are dismembered during an abortion. The researcher believes the current “consensus” that preborn children don’t experience pain until 24 weeks is inconsistent with the scientific evidence. Other research has indicated preborn children as young as eight weeks are capable of feeling pain to an even greater extent than adults.
Approximately 60 million preborn human beings have been killed in the years since Roe v. Wade was decided.
“On National Sanctity of Human Life Day, we celebrate the wonderful gift of life,” wrote President Trump, “and renew our resolve to build a culture where life is always revered.”
I winced at reading Rob Port’s Jan. 2 column scolding social conservatives for not supporting North Dakota State University’s new “Junk Mail” initiative, which aims to curb unplanned pregnancy through mailing students free “safe-sex” education and prophylactics.
My unrest isn’t so much that Port called out pro-lifers for not backing this program, despite fervently disagreeing with it and him. I’m more troubled that so many can’t see the forest through the trees. As a mother and wife, woman of faith and child of God, I feel wholly discouraged, because this scenario has “we’ve completely failed our youth” all over it.
What grieves me most is Port’s assumption that unmarried couples “need” sexual intimacy. He begins by minimizing the effects of abortion-restriction laws, likening them to certain laws on drugs and alcohol. Illegalization of these substances only leads to black markets, he says, since people “want and need” these drugs and will find a way to obtain them somehow.
The “Junk Mail” program bets on “education” and “safe sex” as the solutions to lowering unplanned pregnancy. Again, going with their and Port’s logic, we must accept as fact that people “want or need” abortion, and, preceding that, to be sexually active outside of marriage.
The initiative will fail, firstly because it sends the wrong message. “People are going to drive fast so let’s increase the speed limit” is an apt parallel. (I can see the accidents already.) And like the drug-abuse crisis, it doesn’t even begin to address the “whys.” Why do people “need” drugs? Why do unmarried couples “need” to be sexually active? We’re starting with the wrong premise.
In truth, we’re dealing with an epidemic of broken relationships, porn addiction and a devastating mindset of use versus love. It is a crisis of men and women engaged in sexual intimacy before making themselves irreplaceable to one another through the bonds of marriage, along with any children who might result.
What if, instead of throwing condoms and pills at young people, we reaffirmed the primary reason for sexual intimacy – to bear children? What if we returned to teaching our youth that the purpose of dating is to find a spouse? What if we didn’t scoff at couples marrying before obtaining their graduate degrees?
Remember this? “Bobby and Janie sitting in a tree, K-I-S-S-I-N-G. First comes love, then comes marriage, then comes Billy in a baby carriage.” The childhood song might seem elementary, but it contains prudent wisdom. Cultivating a culture with an appreciation for this proper order of love would offer an enduring solution, exponentially more effective and satisfying than a pack of condoms.
Rightly ordered relationships bring comfort and safety to couples, along with children who know they’ve been loved and wanted from the beginning and feel assured their parents are committed to each other and them.
Despite how far away we’ve gotten from this beautiful vision, our youth deserve to know this reality. They’re worth our true, considerate caring, not just careless condoms.
ENGLAND – A 33-year-old British woman says she nearly died after birth control pills led her to develop two “massive” blood clots in her lungs.
Lauren Dyer, of Tamworth, England, told Birmingham Live that she suddenly fainted while home in February 2019. Her brother, who was with her at the time, called an ambulance for Dyer, who was later unable to talk or move “without gasping for air,” the outlet reported.
Tests at Good Hope Hospital in Birmingham revealed Dyer was suffering from two pulmonary embolisms in each of her lungs. The clots started in her pelvis but eventually moved to her lungs, doctors told her.
“I’m very lucky to be alive today,” she told Birmingham Live, adding she didn’t have any warning signs before she passed out. “Usually with blood clots, they start in the legs and your legs will swell and give you pain. Treatment can be given before the travel closer to your heart or brain, but mine developed in the pelvic area and when I passed out [the clots were] passing through my heart.”
Dyer was hospitalized for a number of days, during which time she received a drug that would break up the clots.
“It was a really scary time for me, but mostly my family and close friends,” she said, noting she was worried the health care would force her to cancel a May 2019 trip to southeast Asia.
“I was concerned I wasn’t going to be able to go traveling or it is delayed massively, but the treatment worked within 10 minutes of the drugs being administered. My heart rate started to go down, I gradually needed less oxygen and, before I knew it, over the next 24 hours I was in the clear,” she recalled, adding she spent a few more days in the hospital before she was released.
“I was a bit battered and bruised from all the tubes and drips, had to go on medication for the next six months but I was alive, my heart was OK and everything was all good.”
Birth control pills do not cause blood clots, but they do increase a woman’s risk of developing them. That said, the risk is relatively low. “The rate for getting clots is about 0.3 [percent] to 1 [percent] over 10 years for a woman on the pill,” states one report on the increased risk.
Women who take combination oral contraceptives — birth control pills that contain both estrogen and progestin — are the most at risk. Increased estrogen levels can cause blood clots to develop more easily, according to the Cleveland Clinic.
Does the termination of an unwanted pregnancy harm women’s mental health? No more than giving birth in such circumstances, according to mainstream social scientists and medical associations. Perhaps. But what about women who terminate a wanted pregnancy?
A new study by sociologist Donald Paul Sullins focuses on this neglected minority – about 1 in 7 of reported abortions in the United States – and finds there is no room for complacency about the effects of abortion among them. In the following interview he talks to MercatorNet about this study, the first of its kind, published in November in the Swiss medical journal Medicina.
* * * * *
Golden Globes award winner Michelle Williams more or less shouted her abortion as a good career move that she does not regret. She has a daughter of 14 and is happily pregnant again at age 39. Isn’t Williams living proof of the therapeutic value of abortion?
Ms. Williams’ declaration is very consistent with the results of my study. The child she aborted clearly was not a wanted pregnancy, and the study found that women who only aborted one or more unwanted pregnancies experienced much lower affective distress (depression, anxiety, suicidality). This is why ignoring wanted pregnancy abortions, acting as if only unwanted pregnancies were ever aborted, tends to understate how much hurt is out there for women after abortion.
There is no question that the chances for advancement in a highly demanding, competitive career often improve by removing inconvenient persons and commitments, whether through divorce, not crediting someone else’s work, character assassination, or– in Michelle Williams’ case — killing an inconveniently conceived child before birth. Civilized people generally do not boast about exercising such brutal career realpolitik, but Ms. Williams probably (let us hope for her sake) does not comprehend the humanity of the unborn life she took.
She has no way of knowing what the acceptance and love of that terminated life, a close reflection of her own being, may have contributed to her own growth in dignity and humanity. For all she knows, her career may have been improved, or maybe her career would have suffered but her life and happiness improved. We have no way of knowing what pain and struggle may lie (lay?) behind her defiant public mask. Why did she feel the need, after announcing her abortion, to reassure her living child of her love for her? Did she sense that her daughter (and we) may wonder?
In the #MeToo era, it is also appropriate to ask who was the father of the child she felt she needed to abort. Would presenting this man with a child after having sexual relations with him have impeded her career? Male sexual exploitation does not end just with hurt feelings or degradation for the woman. Perhaps this was not the case for Ms. Williams, but for every actress who found a pregnancy inconvenient to her career there are probably several men in the film industry who have urged or insisted that she obtain an abortion.
The career obstacle for both men and women of having a child at the wrong time is a mirror image of the career and personal obstructions met by women who refuse to have sex with the right men. Whatever her personal circumstances, Ms. Williams’ statement reflects the typical Hollywood product, in which women’s sexuality exists primarily to service male desire, and women consequently have little agency. As one Hollywood actress (don’t remember who) said of her new boyfriend, voicing a common feeling of young women today, ” I have to give him what he wants, or he will get it somewhere else.”
Even if some women experience mental health problems after an abortion, research seems to show that these are no greater on the whole than those of women who give birth, and that they soon pass away. Have researchers been missing something?
Yes. Both the idea that mental health problems are not increased by abortion and that they are not reduced by childbearing are myths perpetrated by poor research, in this case studies that follow women for only a very short time, some only a few days and often only a few months. So far, every study that has followed women 10 years or longer post-abortion have reported significant mental health problems, compared to women who give birth.
It is important to note that most of this difference is not due to psychological deficits from an abortion but to psychological benefits from having a child. In the Add Health data I studied, childbirth reduced mental health risk by 29% following wanted pregnancies and by 12% even with unwanted pregnancies.
The reasons for this defect in the research, I believe, is that most abortion researchers tend to think of an abortion as a detached clinical event, and do not take into account the way that having an abortion, including making the choice and defending it, alters the life course, relationships and outlook of the woman involved. As I put it in the paper:
“The experience of deciding upon, experiencing, and recovering from the termination of a pregnancy brings many life factors to bear for women, all of which may influence subsequent mental health. For these reasons, it may be more accurate to conceive of an abortion, not as a discrete cause of mental health outcomes (a clinical event), but as one factor in a complex of influences (a life event) that together affect a woman’s level of psychological well-being or distress.”
It seems amazing that yours is the “first study ever” of wanted pregnancy abortions. Surely there is plenty of evidence of them, especially with the increase in terminations for fetal abnormality, and all we hear about #MeToo and domestic violence?
The most influential researchers have simply assumed that only unwanted pregnancies are aborted. Many studies simply define aborted pregnancies as unwanted, even when not preceded by contraception. In 2008 the American Psychological Association (APA) dismissed all wanted pregnancy abortions as due only to fetal abnormality, but (as I show in the study) such abnormalities, even if we could detect them perfectly (we detect only about 60%) and even if all of them were aborted (many are not), could account for only a small proportion of reported wanted pregnancy abortions. When not forced to check a box on a survey, very few women spontaneously describe their aborted child as “unwanted”. There is almost always a level of ambivalence, regret and resignation, that is expressed in complex feelings about the abortion.
It is difficult for OB/GYNs in other countries to understand the sales-like pressure to have an abortion faced by women in American abortion clinics. The movie “Unplanned” does a good job of illustrating this. The abortion rate in the United States has been much higher than in countries where abortions are performed in public hospitals with no profit incentive. A recent study of Utah clinics found that just a three-day waiting period resulted in 8% of women reversing their initial decision to have an abortion.
There have been one or two studies of fetal abnormality abortions, and studies that have looked at all abortions regardless of pregnancy intention have thereby included wanted pregnancy abortions mixed in with all the others, but mine is the first study of all wanted pregnancy abortions as a distinct category.
In your study, what data and measures did you use and what did they reveal about wanted pregnancy abortions? How serious were the effects compared to giving birth or unwanted pregnancy abortions?
The study examined the National Longitudinal Study of Adolescent to Adult Health (Add Health), which followed a representative cohort of 3,935 ever-pregnant U.S. women from age 15 to age 28, gathering data from three successive interviews. I looked at seven psychological disorders which Add Health measured using criteria from the APA’s Diagnostic and Statistical Manual (DSM): depression, suicide ideation, anxiety, and abuse of or addiction to hard drugs, alcohol, opioids or marijuana. Mental health was compared both before and after pregnancy, abortion and birth, and was adjusted for 20 covariates that, my previous research had suggested, account for higher mental health problems, apart from an abortion. These were 1 = childhood physical abuse, 2 = childhood sexual abuse, 3 = childhood verbal abuse, 4 = depression, 5 = anxiety, 6 = suicidal ideation, 7 = alcohol abuse, 8 = drug abuse, 9 = nicotine dependence, 10 = cannabis abuse, 11 = conduct problems in school, 12 = neuroticism, 13 = neighborhood integration, 14 = grade point average (gpa), 15 = ever raped, 16 = relationship satisfaction, 17 = educational attainment, 18 = respondent poverty income, 19 = marital status, and 20 = intimate partner violence.
I found that by age 28, U.S. women who had ever had an abortion of a wanted pregnancy were 84% more likely to experience higher numbers of the seven psychological disorders than were women who had carried all wanted pregnancies to term. Women who had ever aborted any pregnancy were 74% more likely to experience higher psychological disorders compared to those who had given birth.
Experiencing wanted pregnancy abortion led to higher affective distress (depression, anxiety and suicidality) than abortions of unwanted pregnancies, relative to the corresponding births. Risk of these psychological difficulties was only 18% higher following abortion of only unwanted pregnancies, but 69% higher following abortion of one or more wanted pregnancies.
What is the significance of your finding about substance abuse?
I was surprised to find that whether an aborted pregnancy had been wanted or unwanted had no effect on post-abortion rates of substance abuse. Overall, risk of substance abuse (of alcohol, opioids, marijuana, or illegal drugs) was twice as high (elevated 100%) for women following any abortion, but was unaffected by pregnancy intention. Only a few studies have examined the association of abortion and substance abuse; more study is needed to understand what is going on in this area.
My hunch is that pregnancies that may be subject to abortion and substance abuse reflect risk-taking, self-destructive behavior, and their co-occurrence reflects a system of mutually reinforcing moral hazard. I hope to explore this idea in a future study.
What is it about the design of your study that gives you confidence in its findings?
By comparison to cross-sectional studies that only take a snapshot of women at a single point in time, my study is more like a series of pictures that can show changes over time. The exact same women were interviewed at three points in time to determine the effect of their prior pregnancy history on their current mental health. Only a handful of abortion studies have used such rigorous longitudinal designs.
In addition, the Add Health data, funded by a consortium of U.S. federal agencies, are widely acknowledged to be among the most comprehensive and accurate in the world. Response rates and follow-up rates are high (over 80%) and the measures are well-designed and independently validated.
Having said that, it is important to acknowledge that no empirical study can offer definitive proof, and this one is subject to several limitations. Most importantly, every study of abortion using population data is limited by the fact that many abortions are not reported, so we can only talk about the abortions we know of. Since a woman who is more troubled by her abortion is less likely to report it, I think my study probably understates the true level of post-abortion distress for U.S. women. Other limitations are discussed in the study.
No doubt the fact that you are a Catholic priest working in a Catholic university will provoke some prejudice against your research, so it is interesting that studies by secular researchers in Scandinavia and by David Fergusson in New Zealand support your findings. What do their studies show?
Pedersen (studying women in Sweden) and Fergusson found similar problems for women following abortions because they used a similar longitudinal design that followed women for a decade or more after their abortion. Fergusson found that ever-aborting women had 1.4 times higher overall risk (not relative to births) of mental health problems; my study found 1.2 times higher risk.
The similarity has nothing to do with their personal religious or moral convictions about abortion as public policy. Several recent studies from Finland, by scholars who reflect that culture’s uncontroversial acceptance of abortion as reproductive health care, have found similar persistent problems for post-abortion women, such as a doubled risk of suicide, 25% higher overall mortality, and higher emotional distress among women who wanted to give birth. This doesn’t reflect an anti-abortion bias, but just the fact that Finland has excellent health registry population data and is able to follow women’s health for a long time to see the outcomes.
Accusing me of anti-abortion bias because I am Catholic reflects a shallow ignorance of the Catholic enterprise. Many scientists today do not even believe in objective truth, and so cannot imagine someone who does not approach scientific topics with anything more than a narrow ideology to propagate. It is very true that my faith strongly affects my research, but not in the manner critics think. The principles of the Catholic faith, out of which modern science developed, call for faithful scientists to be rigorously objective in their research. Only by looking as hard as I can to find empirical evidence that contradicts the claims of my faith can I then have confidence that any resulting findings which may be consistent with faith-claims have any validity. This process — the logic of the null hypothesis — is not external to the scientific method, but is central to what every scientist should be doing.
There is a great deal of bias in abortion research, but it’s not from the religiously oriented scholars for the most part. The main difference between myself and most scholars who research U.S. abortions is that I am not employed or funded by an abortion provider. Over 90% of U.S. abortion studies have as one or more co-authors a researcher who works for an abortion provider or a research center funded by an abortion provider. Their assertively benign findings about the experience and effects of abortion are highly self-serving and rarely withstand careful scrutiny.
What, so far, has been the response to your latest study from other researchers?
It is too soon to tell much. Friendly researchers I know (most, but not all, opposed to abortion) have written words of appreciation and praise, and invited a couple of lectures to explain the findings further. Pro-life attorneys have been ecstatic. With the study I published a “crosswalk” that addresses some critical responses to a similar earlier study from pro-abortion researchers. I will be interested to see what their eventual responses will be to the measures I took in this study to address those concerns.
Rev. Donald Paul Sullins, MDiv., PhD, is a Research Associate Professor of Sociology at The Catholic University of America and Senior Research Associate at The Ruth Institute. He is also Director of the Leo Institute for Catholic Social Research.
Reference: Sullins DP. Affective and Substance Abuse Disorders Following Abortion by Pregnancy Intention in the United States: A Longitudinal Cohort Study. Medicina. 2019 Nov;55(11):741. Available at: https://www.mdpi.com/1010-660X/55/11/741 The article can be freely accessed and reproduced.
On the night of January 4, a baby box in the Czech Republic received the 200th child safely surrendered through baby boxes in the country. According to BRNO Daily, the newborn baby boy was safely deposited in a baby box in Blansko.
Ludvík Hess, who spearheaded the effort to bring baby boxes to the Czech Republic in 2005, released a statement that the boy was healthy. After being received in the baby box, the baby was transferred by ambulance to a hospital in Boskovice. Hess revealed that the baby had been named Jan in honor of Jan Juchelka, one of the donors to the baby box project. According to BRNO, “A babybox basically works as a newborn incubator; when a baby is placed in the device, the heating and ventilation systems switch on and, with a slight delay, an alarm alerts medical staff that the baby is there.”
The first baby box in the Czech Republic was installed in 2005, and there are now 76 in the nation. The Blansko baby box which received baby Jan was installed in 2018.
For parents in crisis, the baby box can provide a means of surrendering a newborn without question and without revealing their identity. Baby boxes are becoming more common in many parts of the world. One baby box in the United States received its first newborn less than 30 days after going into operation last fall. Raising public awareness about baby boxes and the life-saving alternative they can provide for families in crisis helps to combat potentially fatal newborn abandonment and ensures people have a place to turn.
Because of baby boxes, in less than 15 years, 200 Czech babies were safely transferred to resources and potentially life-saving care. Hess, who launched the baby box system in the Czech Republic, joked after the 200th baby, “So if there are now 111 girls, how many boys are there?” Each of those 111 girls and 89 boys have had a chance at life because a safe alternative was provided to their birth parents who may not have been able to provide for them in a difficult time.
OFFICE FOR THE LITURGICAL CELEBRATIONS OF THE SUPREME PONTIFF
The most ancient practice of distributing Holy Communion was, with all probability, to give Communion to the faithful in the palm of the hand. The history of the liturgy, however, makes clear that rather early on a process took place to change this practice.
From the time of the Fathers of the Church, a tendency was born and consolidated whereby distribution of Holy Communion in the hand became more and more restricted in favor of distributing Holy Communion on the tongue. The motivation for this practice is two-fold: a) first, to avoid, as much as possible, the dropping of Eucharistic particles; b) second, to increase among the faithful devotion to the Real Presence of Christ in the Sacrament of the Eucharist.
Saint Thomas Aquinas also refers to the practice of receiving Holy Communion only on the tongue. He affirms that touching the Body of the Lord is proper only to the ordained priest.
Therefore, for various reasons, among which the Angelic Doctor cites respect for the Sacrament, he writes: “. . . out of reverence towards this Sacrament, nothing touches it, but what is consecrated; hence the corporal and the chalice are consecrated, and likewise the priest’s hands, for touching this Sacrament. Hence, it is not lawful for anyone else to touch it except from necessity, for instance, if it were to fall upon the ground, or else in some other case of urgency” (Summa Theologiae, III, 82, 3).
Over the centuries the Church has always characterized the moment of Holy Communion with sacredness and the greatest respect, forcing herself constantly to develop to the best of her ability external signs that would promote understanding of this great sacramental mystery. In her loving and pastoral solicitude the Church has made sure that the faithful receive Holy Communion having the right interior dispositions, among which dispositions stands out the need for the Faithful to comprehend and consider interiorly the Real Presence of Him Whom they are to receive. (See The Catechism of Pope Pius X, nn. 628 & 636). The Western Church has established kneeling as one of the signs of devotion appropriate to communicants. A celebrated saying of Saint Augustine, cited by Pope Benedict XVI in n. 66 of his Encyclical Sacramentum Caritatis, (“Sacrament of Love”), teaches: “No one eats that flesh without first adoring it; we should sin were we not to adore it” (Enarrationes in Psalmos 98, 9). Kneeling indicates and promotes the adoration necessary before receiving the Eucharistic Christ.
From this perspective, the then-Cardinal Ratzinger assured that: “Communion only reaches its true depth when it is supported and surrounded by adoration” [The Spirit of the Liturgy (Ignatius Press, 2000), p. 90]. For this reason, Cardinal Ratzinger maintained that “the practice of kneeling for Holy Communion has in its favor a centuries-old tradition, and it is a particularly expressive sign of adoration, completely appropriate in light of the true, real and substantial presence of Our Lord Jesus Christ under the consecrated species” [cited in the Letter “This Congregation” of the Congregation for Divine Worship and the Discipline of the Sacraments, 1 July 1, 2002].
John Paul II, in his last Encyclical, Ecclesia de Eucharistia (“The Church comes from the Eucharist”), wrote in n. 61: “By giving the Eucharist the prominence it deserves, and by being careful not to diminish any of its dimensions or demands, we show that we are truly conscious of the greatness of this gift. We are urged to do so by an uninterrupted tradition, which from the first centuries on has found the Christian community ever vigilant in guarding this ‘treasure.’ Inspired by love, the Church is anxious to hand on to future generations of Christians, without loss, her faith and teaching with regard to the mystery of the Eucharist. There can be no danger of excess in our care for this mystery, for ‘in this sacrament is recapitulated the whole mystery of our salvation.’”
In continuity with the teaching of his Predecessor, starting with the Solemnity of Corpus Christi in the year 2008, the Holy Father, Benedict XVI, began to distribute to the faithful the Body of the Lord, by placing it directly on the tongue of the faithful as they remain kneeling.
In a webinar sponsored by And Then There Were None, former Planned Parenthood worker Jayne explained how Planned Parenthood endangered their patients’ future pregnancies. Rh-negative women were not given RhoGAM shots.
If a woman has Rh-negative blood type and aborts a baby who has a positive blood type, a condition called Rh incompatibility can develop in future pregnancies. When fetal red blood cells mix with maternal cells, which can happen during an abortion, miscarriage, or delivery, the woman’s body will develop antibodies. If a future baby also has a positive blood type, these antibodies can attack the child’s red blood cells. This can cause a miscarriage or cause the baby to be born with severe complications leading to jaundice, swelling, brain damage, or death.
To keep the mother from developing these antibodies, she should be given a shot of the drug RhoGAM. The website Medline Plus says that a shot of RhoGAM should be given to every woman with Rh-negative blood type “after a miscarriage or abortion.”
With the way many abortion facilities rush women through theirabortions, one can only wonder how many abortion facilities neglect to give these shots.
Jayne describes how women at the Planned Parenthood where she worked weren’t given RhoGAM shots:
[A]t Planned Parenthood, because of the high volume and high-speed, patients were not – you only have 45 minutes to see a patient, and that’s when they come in, as soon as they come off the table it’s one blood pressure. You only take three blood pressures and they’re out the door, even if they’re groggy. [It] doesn’t matter because they have to keep moving. So, if you’re in charge and you have your 10 patients, there’s no way that you’re going to – things are going to get missed. And in this case, many cases, many times these patients were leaving, and not being given that shot – the RhoGAM.
Jayne is now a fertility care nurse practitioner. She sees women come in with frequent miscarriages and infertility and wonders how many of them might have previously had abortions at Planned Parenthood.
The problem in Jayne’s abortion facility was exacerbated by the fact that if women went out the door without the shot, Jayne was not allowed to call them and tell them to come back:
As soon as I saw those couple women going out without that shot, I was like, well we need to call them. They need to come back. They have to have that shot. And it was like, we can’t, because everything is kept kind of on the down low so to speak, and so you can’t just call them back…. We can’t call them because, you know, it was a secret kind of thing. So, you don’t call them, and these patients go out.
Because Planned Parenthood wanted to keep the women’s abortions secret, their policy was not to contact any of the women after they left. Their fear was that a family member might discover the abortion and make trouble for the woman or the facility. Because of this, Jayne says, many women never knew they needed a RhoGAM shot. They were set up to have future miscarriages and seriously ill or dying babies, without ever knowing they’d been put at risk.
Jayne gives an example of a patient who nearly left without her RhoGAM shot. In this case, it was because untrained staff made a mistake with her bloodwork:
I had a patient that was [Rh] negative and she had come in, and she was again, you know, zip zip, three blood pressures and you’re out the door.… I said, okay, you’re good, this is your medicine, blah blah blah you’re out the door, and she’s like, well, you know, when I had my son they said that I was supposed to always get a shot, and I was like immediately, oh my gosh, I looked back to make sure, because of course, you’re rushing – am I making a mistake? I went back and I flipped it and and I’m like no – you know what – hold on though, hold on a second, because if you’re saying that you were at the hospital and they said you had a blood type and needed a shot, you’re going to need a shot here. So, let me just get them to redo your bloodwork…. You’re not even getting bloodwork that’s reliable.
If this woman hadn’t spoken up, she would have left without the shot.
This one Planned Parenthood facility put many women at risk for future miscarriages and child loss, just because they had untrained staff who rushed women through the facility. Planned Parenthood wanted to make a profit and didn’t care about women’s future babies, even if those babies were wanted. There is no way to know how common this problem is at Planned Parenthood.
I am a doctor and a caregiver, but above all else, I am a woman of faith. It is my faith that drew me to become an OB-GYN, called me to open my own practice to treat women with dignity and compassion, and that helps me navigate the daily challenges of my profession. But two months ago, Planned Parenthood and the state of New York convinced a court to strike down federal regulations that protect medical professionals like me from being forced to perform procedures—like abortions and physician-assisted suicide—that violate our consciences.
Supported by my colleagues at the Christian Medical and Dental Associations and by the federal government, I have asked a federal appellate court to intervene and allow me to continue to provide compassionate medical care without being forced to violate my conscience.
As an OB-GYN, I am present during the most intimate moments in the life of a mother, father, and child. I have the privilege of placing children into the arms of their mothers for the very first time. I also have to deliver the life-altering news of infertility and guide mothers and fathers through the tragedy of a lost pregnancy.
This work cannot be done impersonally. I cannot leave my humanity at the door. I give all my patients the degree of care that I would a close friend or loved one. I provide them the advice that I would want to receive, bringing my best judgment to their situations.
While walking with women through some of their greatest joys and sorrows, I am called to offer more than just my medical expertise. I am called to provide the compassionate guidance of a friend, to be Christ’s outstretched arms for the women who enter my practice. But if Planned Parenthood and New York succeed in blocking conscience protections for medical professionals, I may be forced to either perform procedures that violate my conscience or leave my practice and the profession entirely.
These federal conscience protections, known as the Conscience Rule, merely allow the government to enforce laws that have been on the books with bipartisan support for decades. These laws, like the Weldon Amendment and the Coates-Snow Amendment, simply prevent tax dollars from being used to force pro-life doctors like me from performing abortions.
But Planned Parenthood and New York don’t like that, so they sued to render those long-established and bipartisan laws toothless. Without the Conscience Rule in place, religious doctors and nurses across the country are at greater risk of being forced to perform procedures that violate our core beliefs.
I cannot take the life of a child in one room and guide another child into this world in the next. Nor can I care for one elderly woman while helping another end her life. That would not only undermine my most deeply held religious beliefs and my medical judgment, but also the oath I took as a medical professional.
Medical professionals have the privilege and the honor of serving those in need. For doctors like me, our job is our calling. And we do not take this calling lightly. Each and every day, we make decisions in reliance on our medical judgment and the best interest of our patients. Government bureaucrats should not insert their politics into these critical and deeply personal medical decisions.
My faith is at the heart of who I am. It is what drives me to put the needs of women and their children first every day. It makes me a better doctor. For decades, our country has recognized that a big, diverse nation like ours can deliver high-quality medical care without making taxpayers force people of faith to violate their core beliefs. If we forget that insight, we’ll hurt both doctors and patients.
Dr. Regina Frost is an OB-GYN and a member of the Christian Medical and Dental Associations.
(Save The 1) “Is Kristi pregnant?” That was never a question I expected my pastor and friend to ever ask me over the phone on a Sunday afternoon after we arrived home from church the morning of April 22nd, 2018. I thought, if my 18 year old daughter was pregnant, he would have heard it from me, or from us, right?
I answered with a slow, “No… Ah… I don’t know… Let me call you back.” It seemed my words sounded as if they were purposely edited as special sound effects for a film. I felt as if my head for the first time completely emptied itself. The only thought or sound left was like a very far off siren that rang “Kristi’s pregnant, Kristi’s pregnant, Kristi’s pregnant.” How could that be? And suddenly, I knew she was.
It was one more crisis to deal with. My mother had just died of cancer a month earlier. A few months before that, my father fell down some icy steps walking outside a restaurant in Munich, breaking up the right side of his body: shoulder, arm, hip, knee and leg. After he got out of the hospital, I went to Munich to help take care of him for a few months.
Prior to that, we’d had a busy year, having just premiered our first full-length feature film in our local town. We produced, wrote, directed and acted in it — a true story about our personal testimonies surrendering our lives to the Lord. It was 15 years ago that I learned I had a 3-year-old daughter named Kristi and was struck with awesome joy, even though I knew nothing about her, her mother, or even if she really was my daughter until DNA testing was complete. We spent a year non-stop making that film and had a crew of about 40 people using our house as a full-time production office.
The day following our premiere, we were given notice we would have to move from our rented rural Montana house where I’d lived for 19 years. I loved that house — a 4-acre property by the edge of the woods and near the river, 6 miles out of town. As a single parent, I raised Kristi there most of her life. The property was old and going to be torn down to be commercially redeveloped.
Within 12 hours of completing the move into our new house, I lit a fire in the fireplace, and after I fell asleep, the rafters in the attic caught on fire. Everything was ruined and uninhabitable, but thank God Kristi was away at a dance that evening. The Fire Captain told me the smoke detector saved my life.
Whatever we had left was moved into storage and during the next few months, we moved in and out of several motels, various friends’ houses and eventually a small camp trailer with a door which wouldn’t completely shut.
With all of that going on, it’s no wonder I didn’t know Kristi was pregnant. She was very small and didn’t show for the first 6 ½ months, especially through her winter clothes.
After the call from my pastor, I hung up the phone, waited a moment, took a deep breath, looked up at God saying in my heart, “I need you again please” and walked into Kristi’s room. Immediately, I was emotionally struck and began hugging her telling her how much I love her and how proud I am of her. Even though I didn’t mention anything else, nor did I know any of the details, she instantly realized I knew she was pregnant and we both started crying together. For me, it became tears of joy.
We cried and talked for a long while as I learned she was almost 7 months into her pregnancy. I spoke to my grandchild in the womb, introducing myself as Papa. Kristi hadn’t filled me in yet about having been raped, and was vague in talking much about the father. I do remember having felt something wasn’t right about it, but didn’t want to spoil the moment. I happily knew Kristi would keep her baby, no matter what.
I learned later that she wanted to tell me all along about the pregnancy, but with so much tumult going on in our lives, she didn’t want to just blurt it out. Kristi still had high school graduation ahead and couldn’t seem to find the right time to tell me. She was one of the top students in her school, but the only known girl in that small Christian school ever to graduate pregnant. Still, they supported and loved her through it all.
But most significantly, she was pregnant by rape — a young man who was someone we knew, whose family attended our small church. Of course, no one else knew Kristi had been raped or that she was pregnant. Kristi was afraid to share the details out of fear I would do something bad to this young man and get myself in trouble, and perhaps she was right. As you can imagine, there were in fact bad thoughts going on in my head once I learned what he’d done to my daughter.
In time, my daughter explained how at 17, she had been forced to have sex while locked in this 19-year-old’s car. Kristi had been afraid to go to the police due to being young and under peer pressure, which I understood. This young man supposedly was well-liked and popular, and we were living in a very small mountain town community.
I brought the matter up with the pastors of our church. The rapist, both of his parents, two of the pastors, Kristi and myself had a meeting at the church office one evening where the young man willingly admitted what he had done. While I appreciated his truth-telling and hoped I could find it within me to extend forgiveness, there was no true sign of any remorse on his part.
What really surprised me was that one of the pastors (not the one who had called me) recommended that Kristi and her rapist try marriage counseling “just to see if they could become compatible to raise a baby together!” Of course, Kristi said no, and I wholeheartedly agreed, but then we were told that if she wouldn’t follow the recommendations of the church leaders, she was being selfish and would no longer be welcomed in their church.
At first, we were devastated. We had been attending, serving and being served in that church for over 12 years. It was my first church ever. It had been our extended family. We loved everybody and were loved, until that time. We were there every time the doors were open and involved with several of its ministries. I even headed a couple of ministries and had started a prison ministry there.
But now they wanted us to conceal a crime which had been committed — a crime against my daughter which would change her life forever! So, we left.
On July 27th, 2018, I got to witness Adeline Marie Kollar being born early in the morning at 6:31a.m.. I was the first person she opened her eyes to and smiled at having recognized my voice. I fell in love in one second! It was my gift from God having not known about and missed the first three years of Kristi’s life.
The rapist refused to sign Adeline’s birth certificate, so she was thankfully given our last name; however, his parents tried to start a custody case, while I finally convinced Kristi to file for child support. After our attorney listened to Kristi’s story, he strongly recommended she meet with Victim’s Services. The nice young counselor there convinced Kristi that she really should report the crime to the police — even though it had been 10 months — just so the police would have the young man on their radar, against other possible assaults.
At the police station, I too was interviewed by a young female detective who seemed like she wanted to charge the young man after learning about the story, but that would now depend upon the State. Meanwhile, the detective went to interview the pastors of our former church, the young man, and his parents. She later contacted us and said everyone denied that the young man had made that confession back at the church office meeting….
BIO: Robert Kollar is a single father, grandfather, post-abortive, and pro-life speaker / blogger for Save The 1. He is also a filmmaker, writer, prison minister, and fatherhood speaker. For more info on his film projects, go to mwmcornerstone.com
Editor’s Note: This article was published at Save The 1 and is reprinted in part here with permission.
RICHMOND, Virginia, January 8, 2020 (LifeSiteNews) — A Democrat-sponsored bill in Virginia would treat minors as adults for the purpose of consenting to birth control, vaccines, and “medical or health services required in case of … pregnancy or family planning except for the purposes of sexual sterilization.”
The bill, Senate Bill 104, includes the stipulation that the commonwealth’s law requiring parental consent for abortion would remain in effect. It would also allow minors to receive “[m]edical or health services needed to determine the presence of or to treat venereal disease or any infectious or contagious disease that the State Board of Health requires to be reported.”
The bill is sponsored by Sen. Barbara Favola, a Planned Parenthood–endorsed leftist whose website touts her work as a “lifelong pro-choice advocate” and her “LGBTQ Rights” activism. Favola represents parts of Arlington, Fairfax, and Loudoun counties.
For the first time in 26 years, during November’s elections, Democrats seized control of both chambers of the Virginia legislature and the governorship. They have promised to implement a progressive agenda focusing on a variety of liberal issues, including abortion on demand.
Efforts to give minors birth control, HPV shot, PrEP sex drug without parental involvement
One of the most serious side effects of hormonal birth control is blood clots, which can be fatal. In 2016, a 17-year-old Romanian ballerina living in England died from a blood clot caused by hormonal contraception. She is not the only young woman to have died from taking the pill.
“We strongly support the right of loving parents to make informed medical decisions with and for their children,” Michael Ramey, executive director of parentalrights.org, told LifeSiteNews in a previous interview. “Natural bonds of affection lead parents to act in the best interest of their children.”
“Now lawmakers want to steal that role from the parents at the behest of the pharmaceutical companies,” he said. “Unlike lawmakers, parents aren’t getting campaign contributions; their only motivation is the health and well-being of their child.”
For more than a decade, there have been efforts underway in New York to allow teens to receive the Human Papilloma Virus (HPV) vaccine without parental consent. The New York Department of Health ultimately simply changed regulations after legislative efforts failed.
A May 2019 New Jersey bill would have allowed minors as young as 14 to receive various shots without parental consent. California; Delaware; and Washington, D.C., allow minors to be vaccinated for HPV and hepatitis B without parental involvement.
Meanwhile, “no jurisdiction explicitly prohibits minors’ access to PrEP” — a daily sex drug meant to lower risk of HIV contraction — “without parental/guardian consent,” according to the Centers for Disease Control (CDC).
“Sixteen jurisdictions have statutes/regulations that explicitly allow minors of a particular age to independently access PrEP; the age for access varies by jurisdiction,” the CDC says. “However, minors might still be legally allowed to access PrEP without parental/guardian consent in some jurisdictions without explicit statutes/regulations.”
PrEP is intended for people who engage in risky sexual activity with partners of unknown or positive HIV status and those who share needles when injecting drugs. It does not guarantee protection from HIV.
Whether kid is competent to ‘consent’ totally up to ‘health care practitioners’
S.B. 104 comes amid an aggressive push to force more children to receive optional medical interventions — i.e., vaccines — regardless of parental concerns about aborted fetal tissue in most vaccines and the shots’ manufacturer-acknowledged risks, such as seizures, diabetes, and death. There has been widespread panicked media coverage about vaccine “foes” and diseases like measles, with social media giants censoring or putting warnings above content that questions the safety of vaccines.
If S.B. 104 becomes law, there will be no guarantee parents will know if their children had received vaccines at daycare, at school, or at another location. It seems that under the proposed law, after having been deemed “to the satisfaction of a health care practitioner” to possess “the ability to understand at the same comprehension level as an adult the risks and benefits associated with vaccinations and immunizations,” there is no mechanism in place to notify parents after their children “consented” to a vaccine.
“A minor shall also be deemed an adult for the purpose of accessing or authorizing the disclosure of medical records related to” the subdivisions of the bill that allow minors to consent to vaccines and birth control, the bill says. That language originally did not cover vaccinations — only medical records about birth control, STDs, and some mental health or substance abuse-related matters.
If a child experienced serious side effects from a vaccine or birth control, parents’ lack of knowledge of the shot or drug having been administered could prevent them and emergency room doctors from effectively treating the child. It’s unclear if parents would ever be able to access the medical records indicating that their child had received birth control or a vaccination.
The bill also opens the door for children to, unbeknownst to parents, receive double doses of government-recommended shots. This could happen if at daycare or school a child was deemed by a “health care practitioner” to be mature enough to consent to a vaccine, received that vaccine, did not tell his parents, and then was subsequently administered by a family pediatrician the same vaccine with parental permission.
In Virginia, minors need parental permission to be given Advil in school or have their ears pierced.
Concerned citizens can find contact information for legislators HERE and HERE.
Rebekah Hagan is grateful for the life of her six-year-old son, and she wants to give back by helping other moms facing adversity in pregnancy.
After making a courageous decision in the spring of 2013 to try and save her son’s life through Abortion Pill Reversal, the California mom of three speaks to audiences about her experiences, works to raise awareness about APR (see Editor’s note below), and she helps other young women make their own brave choices.
Nearly seven years ago, Hagan began the Abortion Pill Reversal protocol after she had taken mifepristone, the first pill of the two-pill chemical abortion process, at a Planned Parenthood facility in Sacramento.
“I thought of all the reasons to abort,” she said. “I already had a child and was newly single. I was afraid of losing my home with my parents. I had a fear mind-set, and I didn’t plan to tell anyone.”
She’d had her first son, Eli, when she was 18 and still in high school. The father of this child was also Eli’s father. However, “it was a toxic relationship,” she recalled. She had left the man and returned to her parents’ home.
“I knew Eli and I were not safe (with him),” Hagan said.
Because of these circumstances, she thought abortion was her only option.
“Sometimes abortion looks like hope,” she said.
After taking that first abortion pill, however, she immediately experienced regret.
“I thought to myself, ‘Oh, my gosh, what did I just do?’” she recalled. “You don’t know how to advocate for yourself. I didn’t think to ask questions. You are sent on your way with a little brown bag and are told, ‘There’s no going back.’”
This was March 13, 2013, and Eli had been born on March 14. The coincidence with the dates hit her hard.
“I prayed for forgiveness and then began searching online for how the abortion might be stopped,” she said.
She discovered information about Abortion Pill Reversal, originally spearheaded by Dr. George Delgado. With the help of a doctor in her area, she began the progesterone regimen.
Somehow, the Planned Parenthood facility found out; the staff contacted her and told her the baby would have birth defects if it survived the treatment, Hagan said.
They were proven wrong.
“I have a healthy and active six-year-old boy,” she said.
She named him Zechariah. “I liked the meaning of the name,” Hagan said.
The Hebrew meaning is ‘The Lord has remembered.’
“I see God’s hand in it all,” she said.
Hagan recently had her third child, a girl whom she and husband Kramer named Lydia.
Serving and raising awareness
Hagan was raised in a Christian home, however, like some young people raised in a faith-based family, she made choices that went against her family’s beliefs. After finding hope and redemption with the assistance of Abortion Pill Reversal, she began sharing her experience with others. Public speaking opportunities came, and she responded with enthusiasm.
“I wanted to give back,” she said. “The public speaking has grown. It was a natural progression because of the relationship with people involved.”
Hagan speaks between 15 and 20 times a year, in churches, pregnancy centers and schools. She has also testified before state legislators regarding informed consent bills.
She is also able to personally connect with women who find her on Facebook, and she’s able to provide them encouragement.
For example, 25-year-old “Samantha”* was in an emotionally abusive relationship and though she started a medical abortion, she changed her mind.
“Although she wasn’t with the guy anymore, he still controlled her,” Hagan said. “I’d recite truth to her. She delivered a baby boy at the end of November. Even when you choose life, things don’t just go away. (But) she is grateful she didn’t go through with the abortion.”
Additionally, 17-year-old “Jessica”* who had gotten involved with the “hook-up culture” on the East Coast, according to Hagan, was put in contact with her.
“Her main concern was disabilities,” Hagan said. “There is so little information, truthful information, out there online. Women wonder if they will be okay and if the baby will be okay. I want to help them.”
Hagan said she is grateful to help women like Samantha and Jessica.
“These moms have been spared the trauma of abortion,” she said.
Hagan also serves at a California pregnancy center.
For the past three years, she has worked as the community outreach coordinator for Sierra Pregnancy & Health in Roseville, near Sacramento. This year, the center plans to add Abortion Pill Reversal to their services offered to women.
As a decade dawns, more than 900 babies’ lives have been saved thanks to APR and courageous women like Hagan.
The Abortion Pill Rescue Network is now coordinated by Heartbeat International, with support from Dr. Delgado and many other medical professionals.
Hagan continues to advocate for APR, saving women and babies from the horror of abortion, giving women another choice and a second chance for themselves and their unborn children.
“The reality is the majority of women are conflicted … in this decision. APR gives women another choice and a second chance,” Hagan said. “It’s life-changing and life-saving.”
January 7, 2020 (LifeSiteNews) – After Michelle Williams used her award acceptance speech to promote abortion at the Golden Globes on Sunday, a Catholic model in labor took the time to record an Instagram video challenging Williams’ statement that abortion was integral to her success as an actress.
“I’m here getting ready to deliver my fifth baby,” said Leah Darrow, a former contestant on America’s Next Top Model, from her hospital bed. “And I want to let all you women know, all you young ladies who haven’t had babies or are maybe listening to what the culture says about birth, and women, and babies, and choice.”
“Babies don’t keep us from our dreams,” she declared.
“I’m getting ready to deliver a baby that will not keep me from my professional growth, but will make me better because of it,” she continued. “And I’m so honored and excited, and I can’t wait to have this baby.”
Darrow wasn’t the only one who took to social media to push back against Williams’ Golden Globe speech in which she hinted that having an abortion enabled her to succeed professionally.
Eric Sammons@EricRSammons
A little reminder to last night’s Golden Globe winners, especially Michelle Williams.
“How sad it must be to trade an innocent human life for a tiny golden statue. Praying for Michelle Williams,” tweeted Abby Johnson, the former Planned Parenthood director whose conversion to pro-life activism is depicted in the film Unplanned, drawing a comparison that many others did as well.
Abby Johnson@AbbyJohnson
How sad it must be to trade an innocent human life for a tiny golden statue. Praying for Michelle Williams.
“Only in Hollywood are you able to announce that you murdered a baby in exchange for a hunk of metal with your name on it and have the crowd cheer for you,” said Elizabeth Fortmeyer in a video she posted on Twitter.
“Abortion is not birth control. Abortion is premeditated murder of an innocent child, depriving them of their right to life,” she continued.
“As a woman, I am sick of this belief that all women should be okay with murdering their children for personal gain,” said Fortmeyer. “Real women are pro-life.”
Elizabeth Fortmeyer @eafortmeyer
Yesterday, Michelle Williams accredited ABORTION for her Golden Globe, and suggested that all women should be in favor of it.
As a woman, I am sick of this belief that all women should be okay with murdering their children for personal gain.
Real women are pro-life.
Sara Gonzales asked those in the audience who applauded Michelle Williams’ pro-abortion speech, “Why are they clapping? You’re clapping for dead babies. Stop!”
“Only in Hollywood can you get [cheers] for telling the crowd that you traded a baby for an award,” said Gonzales. “That a piece of metal is infinitely better than the tiny human life that you created inside you. That the fancy gown and the jewelry that you’re wearing is way more important than your own flesh and blood.”
“Hollywood, you all are messed up,” she added.
Sara Gonzales
✔@SaraGonzalesTX
Michelle Williams proudly thanked her abortion for her Golden Globe…WHAT is WRONG with these people?!
“Michelle Williams, while visibly pregnant, claims she wouldn’t have won her Golden Globe Award if she didn’t kill her previous child,” tweeted Live Action Founder and President Lila Rose, who gave birth to her first child days ago.
“No trophy is worth more than a child’s life,” said Rose. “Sacrificing our children to pursue our dreams is the total antithesis of women’s empowerment.”
Lila Rose
✔@LilaGraceRose
Michelle Williams, while visibly pregnant, claims she wouldn’t have won her #GoldenGlobes Award if she didn’t kill her previous child.
No trophy is worth more than a child’s life.
Sacrificing our children to pursue our dreams is the total antithesis of women’s empowerment.
Princeton Professor Robert George, former Chairman of the U.S. Commission on International Religious Freedom, described the Hollywood crowd’s response to Williams as “Pavlovian” and “drearily predictable.”
Robert P. George@McCormickProf
Michelle Williams’ little speech and the crowd’s drearily predictable–nearly Pavlovian–response crystallized the self-focus, shallowness, narrowness of vision, insularity, parochialism, and groupthink of the celebrity culture. There it was, on full display, for all to see. https://twitter.com/xan_desanctis/status/1214208667370823680 …
Alexandra DeSanctis
✔@xan_desanctis
Last night at the Golden Globes, Michelle Williams said she couldn’t have been successful without “employing the right to choose,” telling women everywhere that they need abortion in order to succeed. My latest: https://www.nationalreview.com/corner/the-right-to-choose-what-michelle-williams/ …
“Dear Michelle Williams,” wrote Kristan Mercer Hawkins, President of Students for Life, on Facebook: “Your remarks at the Golden Globes were heartbreaking. Like many post-abortive mothers, you disguised your hurt with a political speech to seek absolution from the world for your past abortion decision(s). It’s so sad that you credit an act of violence, abortion, for your career success. The second wave of Feminism has clearly failed as millions of women like you have been deceived into believing that you must kill another in order to succeed in your career.”
“Abortion is the opposite of female empowerment,” said Hawkins. “An abortion says you thought you weren’t strong enough to achieve your goals and care for the new human you created. It’s the pro-life movement that seeks the full empowerment of women, showing women they are superheroes and can do both.”
Chiefly, it’s the underlying idea that human lives are a worthy trade-off for career achievement. If someone put a gun to a child’s head on the Golden Globes stage and said to Williams, “You can have your award, but the price is this child’s life,” hopefully she would have said “F— that award, save the child.” But here she is on a global stage, not only admitting that she has already done essentially the same thing to an even smaller human, but also encouraging other girls and women to do likewise — to repeated Hollywood applause.
I can think of few stronger expressions of moral corruption than “This child must die so I can live as I please.” Yet this is the tradeoff we are constantly told epitomizes women’s empowerment. Bunk. What does it profit a woman to gain a major industry award if the price is the life of an innocent child? What kind of “success” is it to rise at the cost of other people’s existence? What kind of society encourages people to think and live this way? A sick, self-cannibalizing one.
National Review’s Alexandra DeSanctis took Williams to task for couching her message in terms of “a woman’s right to choose” rather than speaking straightforwardly about abortion.
No one disagrees that women have the right to make their own choices. The abortion debate exists not because a large faction believes women should be deprived of the “right to choose” but rather because of the choice in question: to end the life of a distinct human being. Abortion-rights supporters such as Williams aren’t part of the debate at all because they are intentionally deceptive about the heart of the argument. And who can blame them? It’s far easier to issue euphemistic speeches about women’s empowerment to thunderous applause than it is to defend the taking of an innocent human life.”
A man who wishes to remain anonymous remarked to LifeSiteNews:
I wonder if a day will come when Williams will look at this worthless Golden Globe trophy she’s holding and wish she were cradling her missing child instead.
As we enter the 2020s, the world has become increasingly cognisant of the need for more babies after a decade of worryingly low growth.
In the United States the population grew by only 0.48% between 2018 and 2019, according to newly released Census Bureau estimates. That is the lowest annual growth rate since 1918.
In fact, according to analysis from the Brookings Institute, it “caps off a decade that should show the slowest 10-year population growth since the first census was taken in 1790.”
The United States birth rate fell to a 32-year low in 2018, and 30 states experienced decade-wide declines in youth population, with California losing as many as 400,000 young people. The nation as a whole sustained an absolute decline of 1.14 million youth between 2010 and 2019.
The dramatic decline in the youth population comes at a time when there is a large ageing population which will increasingly rely on young people for support, through their friendship, employment and their taxes.
As a result, the Census Bureau projects that from 2030 immigration will account for more than half of the nation’s population growth. Thus, racial proportions will shift significantly. By 2030, whites will have dropped to 55.8% of the population, and Hispanics will have grown to 21.1%. The percentage of black and Asian Americans will also grow significantly.
What are the root causes of such an unprecedented situation? Family life is changing dramatically the world over. According to Steve Mosher, president of the Virginia-based Population Research Institute, we need to offer more positive encouragement to young couples to get married and have children. He considers there are three fundamental root causes of low fertility:
Abortion: “The first thing that we as a people must address is abortion on demand, which has led to sex without responsibility, and the wanton destruction of the unborn.”.
The porn epidemic: “The second thing we must address is the porn epidemic, which is devastating young men. It has undermined healthy relationships between the sexes, and led to virtual sex replacing procreative sex.” This trend haunts many countries and is an increasingly scary factor as porn usage surges. In an era of celebrated female liberation it is ironic that women have never been more objectified.
Student loans: “The third thing we must deal with are student loans. These ‘debt traps’ have left millions of young people saddled with tens of thousands of dollars in debt that will take years, or even decades, to pay back, depressing marriage and birth rates.” According to the College Board, the total amount borrowed by grad students in particular has been climbing. Mosher suggests the forgiveness of student debt in proportion to how many children a couple have; a type of family subsidy tied to student loan debt. Other countries also provide examples of less crippling systems than the United States, such as systems where paying off student loan debt is tied to future income, and effectively paid as an additional payment (collected along with tax payments) on all future income until it is paid off.
Many places continue to fail to address the underlying issues facing young people and families, but as Mosher warns: “Children are the only future a family has. Indeed, they are the only future a nation has.” The 2020s may mark a turning point as we continue to see people wake up to this.
LOS ANGELES — When officials from the County of Los Angeles announced a new program to staff “Well-Being Centers” on 50 high-school campuses with Planned Parenthood employees, they noted that the “full range of sexual services” provided to students at these centers will be completely confidential.
Thanks to Title X, students as young as 12 years old can already legally access Planned Parenthood’s services without their parents’ knowledge. But inserting Planned Parenthood in public-school campuses, and allowing students to leave class to visit these centers, is a dangerous further step toward cutting parents out of their children’s lives, concerned observers warn.
“One of the things that Planned Parenthood always said when I was training them is that parents are a barrier to service,” Monica Leal Cline, the executive director of It Takes a Family, told the Register. “They recognize that a parent will naturally want to protect their child and keep them from an environment that would put them into danger.
“They are aware that when a parent knows that a child is accessing services at a Planned Parenthood, they are going to stop that and then start to educate the child themselves, which means Planned Parenthood loses a customer. So they don’t want the parent to be involved.”
Cline spent 10 years working with Planned Parenthood as a sex educator. She started doing street outreach as an HIV prevention educator after being trained by Planned Parenthood on how to reach teenagers and eventually went on to be a Title X training manager for all of Texas and New Mexico. She worked for a company that provided government-mandated trainings for clinics receiving Title X funding, including Planned Parenthood, and spent a lot of time training Planned Parenthood employees.
Cline had a religious conversion 10 years ago and founded It Takes a Family to “equip and strengthen parents to reclaim parenthood and become their children’s greatest advocates and educators.”
In the Los Angeles Health Department’s press release about the new centers last month, Sue Dunlap, CEO of Planned Parenthood Los Angeles, highlighted the secrecy possible when students can get to Planned Parenthood at school and don’t have to explain to anyone, even their parents, where they went. She said that when students leave campus, it “means time away from class, money for transportation, and explaining your whereabouts to others, all hurdles that loom large for teens.”
In contrast, when Planned Parenthood is installed on a campus, parents never need to be informed that their child is accessing sexual services.
‘Cycle of Hopelessness’
Another boon for Planned Parenthood, and blow to parents’ rights, is California’s Healthy Youth Act (HYA), which came into effect in 2016 and mandates comprehensive sex education for public middle- and high-schoolers and encourages sex education beginning in kindergarten. In accord with the HYA, the California Department of Education K-12 curriculum guidelines include, for example, suggestions that first-grade students write reports on a book that describes the sexual act and that teachers of fourth- to sixth-grade students use another book that encourages masturbation in order to “initiate dialogue for the group chats.”
“If a child believes and follows everything that they are being taught through graphic sex education in California, then they will naturally have a need for condoms, lubrication, hormonal contraception, STI testing and treatment and abortion,” Cline said about how the HYA benefits Planned Parenthood. “It is the perfect sales tools to have a lifelong customer. That’s the hopelessness that they are selling.”
“The only hope of comprehensive sex education is this: become sexually active,” Cline said. “That is the expectation. Get comfortable with the fact that you will get a disease, but you can lessen the chance of it by using condoms and lubrication. And when that doesn’t work, you can get tested. And then you get treated. And when you have an unplanned pregnancy, you get an abortion. Then you just continue on that cycle your whole life. It’s a cycle of hopelessness for our children that is destroying them emotionally and physically.”
Astrid Bennett Gutierrez, the executive director of Los Angeles Pregnancy Services and a speaker for the VIDA Initiative, has, like Cline, seen how Planned Parenthood encourages sexual activity among students.
“I was a Planned Parenthood volunteer in college when they recruited me for an AIDS-prevention program,” Gutierrez said. “I got to see how they work to break down modesty and the values most parents want to transmit to their children. The topic of sex is treated in an utterly disrespectful way. The message of chastity as an alternative would have no place in the atmosphere they create.”
“It has never been the intention to stop school-age children from having sex,” Cline agreed. “It has always been the intention to just teach them how to do it ‘safer.’ Comprehensive sex education and Planned Parenthood are all about meeting school-age children where they’re at and leaving them there. They believe our children are sexual from birth, which is why we see Planned Parenthood — and anyone who supports comprehensive sex education — hypersexualizing children even in elementary school.”
Cline also noted the health department’s announcement that Planned Parenthood will train students to reach their peers.
“Not only will the children be exposed to graphic sex education that only sets up the expectation for becoming sexually active and normalizing STIs and all of that,” she said, “but they’re also going to train those school-age children to teach graphic sex education to each other.”
Planned Parenthood Los Angeles and the County of Los Angeles Public Health Department did not respond to requests for comment about the health-centers initiative.
Student and Parent Concerns
Frida Plata, who attends Gahr High School in southeast Los Angeles, is committed to fighting back against Planned Parenthood’s promotion of contraception and abortion.
“At school I’ve had debates with teachers and students on the topic of abortion,” she said. “The fact that Planned Parenthood is trying to go into high schools is really devastating.”
Plata said she knows multiple girls from her high school who have had abortions. Four years ago, Plata gave information about Rachel’s Vineyard post-abortion healing retreats to a middle-school classmate who had had an abortion and regretted it.
What if Planned Parenthood comes into Plata’s school?
“I’m definitely going to take action and go around handing out flyers and informing students about the truth of what happens behind the doors of Planned Parenthood and what their true evil plans are. I would organize marches. I would do anything that is possible for Planned Parenthood not to be in my school.”
Although parents have a legal right to have their children excused from instruction that “conflicts with the[ir] religious training and beliefs,” the onus is on parents to obtain the instructional materials from their children’s schools, review them and submit a written request to have their children excused from the objectionable classes.
Gutierrez, a Los Angeles native, has worked for almost 20 years with the families being targeted by the new Los Angeles County program and speaks to thousands of parents every year in Los Angeles-area churches.
“Few parents are aware of Planned Parenthood’s agenda to indoctrinate their children into embracing abortion and contraception as a good, and as inevitable, and to break down their innocence at an early age,” Gutierrez said. “They are also unaware of the many ways Planned Parenthood attempts to usurp their role as parents.
“Through the ‘well-being centers,’ Planned Parenthood is attempting to be the primary confidante when it comes to questions about sexuality. In my presentations, I seek to equip parents to assume their God-given role as the primary educators of their children. Parents must send a clear message to Planned Parenthood that they are not welcome in their schools and communities.”
“I’m scared,” said Lucy Koes, whose son will start Alhambra High School in the fall. “My job is to protect my child at any cost, and they are taking that from me. That’s my concern with my son going off to public high school. I’m already trying to talk to him, trying to get the message across: Just be careful what they’re presenting to you.”
“The unfortunate thing is they’re only presenting one side,” Koes said about the HYA curriculum. “I just remember in high school the same thing when they had sex education. It was: You’re going to do it. They never once brought up abstinence and self-control. I remember feeling so disrespected and thinking, ‘Give me all the information so I can make a proper decision.’ But they’re controlling what information you’re given, so they control what you do.”
“I’m sure there are other parents in the same situation who don’t have a choice but to send them to public school,” Koes said. “We’re basically going to lose our children. I have sleepless nights over that and just a lot of prayer: Lord, help me here.”
“It’s pretty scary,” Cline said, regarding Planned Parenthood’s sexualization of children. “And the only way they can make it happen is to keep parents ignorant and to ensure that they have like-minded legislators and decision-makers that will help pass it, regardless of how parents feel about it.”
Saving Lives and Souls
Gutierrez believes parents’ influence can save lives.
“Just last night, I saw a young woman who I had counseled some years ago when she found out she was pregnant at the age of 18,” Gutierrez said. “At first she thought about abortion, and she understood how easy it was to get one, due to the pro-choice sex education at her school, but she thought about her parents and the values they had taught her, and she decided instead to speak to her priest about her excruciating dilemma. He referred her and her mom to Los Angeles Pregnancy Services. Last night she was radiant with joy and gratitude, and I got to shake the hand of a beautiful 5-year-old boy who she says is the light of her life.”
“It is more important than ever for parents to pray and fast for their children and to take seriously and actively their role as primary educators — especially in the area of chastity,” Gutierrez said. “And they must remain vigilant regarding Planned Parenthood and their insidious, taxpayer-funded programs to ensnare the lives and souls of their children.”
Register correspondent Mary Rose Short writes from Southern California.
January 2, 2020 (LifeSiteNews) – Like all public figures, I get my share of crank letters in the mail. Most of these go right where they belong—spiraling downward into the circular file that sits on the floor by my desk.
But every so often one comes in that catches my attention, like the “Certificate of Recognition” I recently received from a former Stanford colleague of mine.
In it, he hammers me for my “Pro-Natal Conduct” and my “reprehensible ignorance” of “Climate Change Science.” Don’t I know, he says, that more people means “an Unraveling Social, Economic and Environment, Extreme Weather Events, Massive Midwest Flooding, Rising Oceans, Never-Before-Seen tornado and Hurricane Seasons.”
Running out of room on the “Certificate”–but not out of words–he ranted on for three more pages about how I was “betraying my grandchildren.” Among other things, he claimed that “the world is adding 87 million people a year,” “a billion people have no access to fresh clean water,” “energy resources are finite,” and “minerals will definitely run out.”
Such is the value of a Stanford education these days that he is completely, absolutely, and fundamentally wrong on every single point.
“Climate Change”
My hysterical colleague (along with every single Democratic candidate for president) apparently believes that global temperatures are reaching the boiling point. But the best evidence, published recently in the Asia-Pacific Journal of Atmospheric Sciences, shows a warming rate of just 0.095C per decade over the last 38 years. One-tenth of a degree every ten years is about half the rate predicted by the computer models on which the UN’s Intergovernmental Panel on Climate Change and various government agencies rely for their predictions of climate doom.
Why is that significant? Because it suggests that someone is tinkering with the models–the only basis for predictions of future temperature—to suggest that the warming will be much more dramatic than it actually is. This is what happens when scientific questions are heavily politicized–as questions concerning the cause, extent, and threat of global warming have been.
“ … An Unraveling Social, Economic and Environment.”
My colleague echoes AOC in suggesting that “The end is near.” But by every available metric, from life spans to caloric consumption, human beings are better off than they have ever been in human history. Over the past 250 years or so, living standards have improved so dramatically that the average person on the planet now lives longer, eats better and enjoys better housing than European nobility in the Middle Ages. What would King Henry VIII of England have given for a refrigerator, much less for a smartphone or penicillin?
We live in the best of times, not the worst of times.
To listen to my hysterical colleague, we are experiencing the last days of the Planet Krypton. But the evidence simply does not bear this out. Take the issue of hurricanes, for example. Even the UN’s Intergovernmental Panel on Climate Change (IPCC) was forced to admit in 2012: “There is low confidence in any observed long-term (i.e., 40 years or more) increases in tropical cyclone activity (i.e., intensity, frequency, duration), after accounting for past changes in observing capabilities.”
“Low confidence” is science-speak for “there is no evidence.”
“ … The world is adding 87 million people a year,”
Typical exaggeration on the part of the gloom and doom types. The world actually added 81 million people in 2019. Global population numbers may be somewhat inflated as well. There is some evidence that China, for example, has overcounted its population by some 100 million people.
The more important fact is that fertility rates are falling worldwide, including in the United States, which long had the highest birth rates in the developed world.
Many countries are currently literally dying — filling more coffins than cradles — and many more will soon follow. Even populous China has one foot in the grave, demographically speaking, as its aging population begins dying off. The population of the entire world will start shrinking shortly after mid-century.
“… A billion people have no access to fresh clean water,”
Another gross exaggeration. According to the World Health Organization, since 1990 some 2.6 billion people have gained access to an “improved” drinking water source, that is to say, one that is designed to protect against contamination. By 2015 the number of people who still drank water from unprotected sources had been reduced to 663 million, and that number has been reduced in the years since as global poverty is reduced.
At the same time, we are becoming far more efficient where the use of water is concerned, especially in agriculture. This in turn leaves more water available for basic human needs.
Notice what my Stanford colleague isn’t saying. He’s not talking about famine, because hardly anyone starves to death any more. He’s not talking about child mortality, because fewer and fewer children die in infancy. And he’s not talking about disease, because such scourges as malaria, polio, and heart disease are all on the decline.
“… Energy resources are finite,”
Fossil fuels are theoretically finite, although we keep discovering new reserves, and more ways to extract existing ones, with each passing year.
Other sources of energy, however, are clearly not finite. Environmentalists constantly hector us on the need to use wind and solar. Leaving aside the difficulties of capturing such diffuse forms of energy, do they think that the wind will stop blowing, or the sun will stop shining? And what about the virtually infinite amount of energy that can be generated by clean nuclear energy from fission or, one day soon, fusion?
My colleague can’t have it both ways. Either energy resources are finite or they are not. And they are not.
“… Minerals will definitely run out.”
This claim has definitely passed its “sell by” date. It owes its origins to a book called The Limits to Growth published almost 50 years ago which asserted that the world would run out of silver, zinc, copper, mercury and–well, just about everything–by the year 2000. Stanford ecologist Paul Ehrlich and others argued from this that radical population control programs were the only answer.
My friend Julian Simon disagreed, arguing that if any metal grew scarce human ingenuity would enable us to find substitutes. After all, he noted, the Stone Age did not end for lack of stone. He bet Ehrlich that any five metals that he (Ehrlich) picked would cost less—not more–in 1990 than they did in 1980. Prices fell over the decade, as Simon had expected, and he won the bet hands down. Ehrlich paid up, but not without taking a parting shot at Simon, saying “The one thing we’ll never run out of is imbeciles.”
I’ll let you judge for yourselves who the imbecile is in this equation, given that, thirty years further down the road, none of the metals Ehrlich picked has run out or even significantly risen in price.
Another happy but unheralded fact comes from MIT scientist Andrew McAfee, whose book More from Less documents how we are using less water, less land, and less metal to produce more food and more goods. In other words, the future promises to be greener and more abundant without denying people the right to drive their own cars, own and heat their own homes–or have as many children as they want.
In fact, the anti-people crank who wrote me got things exactly backwards. Our long-term problem is not going to be too many people, but too few people.
That’s the real “Progeny Calamity” and it is occurring right before our very eyes. Steven W.
Steven W. Mosher is the President of the Population Research Institute and the author of Bully of Asia: Why China’s Dream is the New Threat to World Order
More human beings died in abortions than any other cause of death in 2019, a new report indicates.
A heartbreaking reminder about the prevalence of abortion, statistics compiled by Worldometers indicate that there were over 42.3 million abortions world-wide in 2019. The independent site collects data from governments and other reputable organizations and then reports the data, along with estimates and projections, based on those numbers.
When contrasting the abortion numbers to other causes of death, including cancer, HIV/AIDS, traffic accidents and suicide, abortions far outnumbered every other cause.
By contrast, 8.2 million people died from cancer in 2019, 5 million from smoking, 13 million from disease, and 1.7 million died of HIV/AIDS. Deaths by malaria and alcohol are also recorded.
Worldometers estimates about 58.6 million deaths world-wide in 2019, but that number does not include unborn babies’ abortion deaths. Unborn babies are not recognized as human beings even though biology indicates that they are unique, living human beings from the moment of conception and they die brutal, violent deaths in abortions.
The abortion number is incomprehensible, but each of those 42 million abortions represents a living human being whose life was violently destroyed in their mother’s womb. Each unborn baby already had their own unique DNA, making them distinct from their mother. That DNA indicated if the child was a boy or girl, their eye and hair color, their height, possible genetic disorders and other disabilities, and much more. In most cases, the unborn babies’ hearts are beating when they are aborted, too.
An estimated 61 million unborn babies have been killed in abortions in the U.S. since Roe v. Wade in 1973. In January, pro-life advocates will gather for the annual March for Life in Washington, D.C. to remember the anniversary of that infamous decision and call for restored protections for the unborn.
“To evangelize means: to show this path – to teach the art of living … This is why we are in need of a new evangelization – if the art of living remains an unknown, nothing else works. But this art is not the object of a science – this art can only be communicated by [one] who has life – he who is the Gospel personified.”
— Cardinal Joseph Ratzinger, Address to Catechists and Religion
Teachers, Jubilee of Catechists 2000
“Bewilderment” is perhaps the word that best sums up my feelings as I survey the events of the past year. If there is anything that is a constant in this world, it is change. And yet, it seems to me that 2019 was a year characterized by unusually rapid, seismic, and often-confusing change: political, social, and spiritual.
If there is any one issue that I would say sums up this reality of rapid change and pervasive confusion it would be transgenderism and gender ideology. Even though I have paid close attention to the progress of the Culture of Death for many years, I would never have guessed, even as little as two or three years ago, that the most radical forms of gender ideology would sink their teeth into our culture so deeply and as quickly as they have done.
Indeed, one could well argue that 2019 was the year of gender ideology. Every single day, it seemed, we were being asked to accept ever more bizarre and improbable claims: that biological men can become pregnant, for instance, or get a period; or that the right for biological males to compete in women’s sports is a fundamental “human right”; or that we should celebrate when allegedly “transgender” toddlers are trotted out in front the world’s media to show how tolerant and progressive their parents are.
Equally dismaying was the sight of so many ordinary people bowing their heads and accepting every new outrageous demand, regardless of the very real cost on our freedoms, our culture, and the happiness, health, and even lives of our youth.
The confusion of 2019 was hardly confined to the world of social progressivism, however. The world of politics seemed to many to be increasingly characterized by division, chaos, and extremism. It often seemed, for instance, that each of the Democratic presidential candidates was consciously striving to outdo one another in the extremism of their pro-abortion and anti-family positions. And I hardly need mention how the year ended with a vote to impeach our president, and the exposure of deep political divisions even within the Christian community.
Christ, Our Rock
Meanwhile, for many Catholics, 2019 was the year they realized that the confusion and corruption in Holy Mother Church goes deeper, and higher, than they had previously realized. For faithful Catholics this is, without doubt, the most discouraging source of confusion of all. As the culture has descended into moral chaos, we have relied upon the stability of Holy Mother Church as the one and only reliable refuge against the madness of our age. We counted on the Barque of Peter to carry us calmly across the heaving ocean of the Culture of Death, and the moral madness of our age. Now, however, it sometimes feels as if that Barque is taking on a dangerous amount of water.
At the end of 2019, then, this year characterized by such disorienting change, it is a good time to remind ourselves of certain fundamental truths, truths that can provide a stay against the confusion. The first of these is that Christ is and must be our rock, and that – whatever the temporary appearances – it is only in Christ, and in the Church that He founded that we can find the stability, peace and the salvation for which our hearts so yearn.
Recall the despair of the Apostles in the boat, as they crossed the Sea of Galilee in the storm. Christ was right there, in their midst. They could see His peacefully sleeping form. Their Lord, their Christ, the Son of God, the Word made flesh, their Savior, lay but an arm’s length away from them. What more could they have wanted? And yet their courage failed when they saw the storm and the waves. Despairing, they woke Christ, daring even to rebuke Him: “Teacher, do you not care if we perish?”
The evangelist recounts: “And He awoke and rebuked the wind, and said to the sea, ‘Peace! Be still!’ And the wind ceased, and there was a great calm.” Then Christ turned toward his apostles sadly, asking, “Why are you afraid? Have you no faith?’” (Mark 4:39-40)
“Why are you afraid?” Many of us right now might feel like the Apostles in that boat. Like the Apostles, the Church is carrying us amidst the waves and winds of a world gone mad. And yet, like the Apostles, we lose faith, we lose courage. The waves seem so large, the winds blow so fiercely, and the boat itself heaves and spins in the waves. And yet, all the while, Christ Himself is among us, His resting form quietly awaiting us within the tabernacle, ready to impart His peace and grace to our troubled souls, if only we would turn to Him and trust in His promises.
As I have said so often in this column, the answer to the Culture of Death and the confusions of our age does not lie in political or social activism, no matter how brilliant. Yes, we need brilliant and committed activists and political leaders. However, even more than this we need men and women of deep prayer, in whose hearts has been kindled the fire of Divine love. We need men and women who have drunk deeply of Christ’s loving presence, and who yearn to bring His love to all the world, beginning with their family, friends, and neighbors.
My New Year’s Wish
My dearest New Year’s wish is this: to see people, especially within the Christian fold, adopt this motto and to live by it: “Whatever happens to my brother or sister happens to me. Whatever affects my brother or sister affects me.” For, as Jesus says, “Whatever you did for one of these least brothers of mine, you did for me.” (Matthew 25:40)
The greatest act of love that we can do for our neighbors is to bring to them the truth of Christ’s life, death, and resurrection, and His gift of salvation – to evangelize. If more people lived by this reality, our cultures would be radically different. Our problem is that most have been desensitized to the inalienable dignity of the human person. Therefore, we must first re-teach the inherent and immutable dignity of the human person, a dignity that was revealed to us in its fullness by Christ’s incarnation. If we do not understand our nature and dignity, we will make little to no progress.
The Culture of Death has been very successful in dehumanizing the human person and our concern for each other. By assaulting the family, it has unlinked us from each other and our obligations to each other. The Culture of Death has peddled its wares well in convincing people to reject long-held Judeo-Christian beliefs and moral doctrines. Moral relativism reigns. For most, their conscience is either numb or dead. And, “The supernatural,” says Cardinal Robert Sarah, “is swallowed up in the desert of the natural” (The Day is Now Far Spent).
We need to re-evangelize, starting within the Church. Ultimately, the solution to the current cultural and moral crisis is the pursuit of greater holiness. As our Enemy is sin itself, the easiest sins to do battle against are those festering in our own souls. As St. Francis of Assisi put it, “The soldier of Christ must begin with victory over himself.”
Christ in the House of His Parents – John Everett Millais
Victory over our sins is possible only once we have united our hearts with Christ, the “stone which the builder’s rejected” which “has become the cornerstone” of our whole lives. As Pope Benedict stated in 2010, “[A]t the root of all evangelization lies not a human plan of expansion, but rather the desire to share the inestimable gift that God has wished to give us, making us sharers in His own life” (Ubicumque et Semper, 2010). To build our lives on this rock is to protect ourselves against the winds of confusion and the storms of discouragement: “And the rain descended, the floods came, and the winds blew and beat on that house; and it did not fall, for it was founded on the rock.” (Matthew 7:25)
While many make New Year’s resolutions for superficial things, we should pledge, using all our abilities, to be more active in the pro-life and family movement. We need to stand in unity against the radical assault upon life, marriage, the family, and our children. We need to educate ourselves on the issues, get more involved in the political life of our country, support people in leadership who actively support our causes, and expose and confront those who are in opposition to our values. We need to be more sensitive to what is happening around us – i.e. anti-life and anti-traditional marriage legislation and policies, the indoctrination of perverse sex education programs and gender ideology, legalization and normalization of euthanasia, etc.
I say to you: Make perfect your will.
I say: take no thought of the harvest,
But only of proper sowing.
— T.S. Eliot – Choruses from the Rock
Even more importantly, since we are in a spiritual battle, we need to recommit to deeper spiritual lives. In this time of confusion and change, we need men and women who, as T.S. Eliot put it in the poem above, have made perfect their wills; who never give into the temptation of discouragement, but paying no need to the harvest – which is Christ’s business – put their hands to the plow in the sowing – which is our business. “For here the saying holds true, ‘One sows and another reaps.’” (John 4:37)
We must lay all our trust in Christ, our rock. We must recommit ourselves to deep prayer, to frequent confession and reception of the Eucharist, to Eucharistic Adoration, to the family rosary, and to mortification of our passions. These are the weapons that the Church recommends to us, and that have served so many saints so well over the centuries.
As we begin this new year then, let us make concrete, achievable spiritual resolutions, which we can begin to put into practice immediately, and that will – if we adhere to them – carry us through the year ahead with the deep peace that only Christ can impart in our hearts.
A recent article by Washington Post columnist Alexandra Petri ridicules pro-life advocates’ contention that unborn humans should not be treated like medical waste.
Referring to legislation that requires dignified treatment of the remains of human embryos and fetuses (whom Petri inaccurately calls “fertilized ova”), Petri writes: “Why such concern for these fertilizing spermatozoa, more than others? Those spermatozoa have passed into the beyond after making connections that elude millions of their brethren. Why honor them?”
She goes on to sarcastically suggest that if we have funerals for embryos and fetuses, then we should have funerals for sperm too:
State legislators, if you have such concern for the select few, remember the unfortunate millions! We must, of course, give honor above all to those who went to the halls of glory without glimpsing even a hint of an ovum. This is the least we owe those who lived in hope—and died—in states of single blessedness.
Satire can be powerful, but not when it’s founded on scientific illiteracy. Petri’s mistake is that she confuses human beings with human gametes. They are two very different things.
Pro-life people have no concern for “these fertilizing spermatozoa.” We do not wish to “honor them.” Pro-lifers have concern, rather, for the individuals who come to be upon fertilization. These individuals, as middle- and high-school biology students (hopefully) learn, are neither spermatozoa nor ova (both of which cease to exist when fertilization is successful). They are human organisms—members of the species Homo sapiens.
They are called zygotes at the one-cell stage, and then embryos (through eight weeks), fetuses (eight weeks until birth), infants, toddlers, adolescents, and adults as they develop themselves throughout life.
“Human development begins at fertilization when a sperm fuses with an oocyte to form a single cell, a zygote,” explain Keith L. Moore and T.V.N. Persaud in their embryology textbook The Developing Human. “This highly specialized, totipotent cell marks the beginning of each of us as a unique individual.”
Human zygotes, embryos, and fetuses are human organisms. And since pro-life people think all human beings are important—they oppose discrimination on the basis of age, appearance, or ability—they care about the treatment of these unborn children.
Spermatozoa, by contrast, are not human organisms. They are gametes (reproductive cells with only 23 chromosomes), which are parts of the parent. They don’t develop as human beings—because that’s not what they are. Their purpose is to unite with an egg and thereby cease to be. That’s why we would never think to have funerals for them. A sperm isn’t one of us. It’s just a sperm.
Petri is far from alone in conflating living individuals with mere parts of living individuals (either gametes or somatic cells). But sound ethics requires sound science. Before we can know how to treat unborn children, we must know what they really are.
What are human embryos and fetuses? They are human beings. Science tells us so.
CHICAGO — Researchers studying the brain found that women taking oral contraceptives, commonly known as birth control pills, had significantly smaller hypothalamus volume, compared to women not taking the pill, according to a new study presented today at the annual meeting of the Radiological Society of North America (RSNA).
Michael L. Lipton, M.D., Ph.D., FACR
Located at the base of the brain above the pituitary gland, the hypothalamus produces hormones and helps regulate essential bodily functions including body temperature, mood, appetite, sex drive, sleep cycles and heart rate.
Structural effects of sex hormones, including oral contraceptive pills, on the human hypothalamus have never been reported, according to the researchers. This may be in part because validated methods to quantitatively analyze MRI exams of the hypothalamus have not been available.
“There is a lack of research on the effects of oral contraceptives on this small but essential part of the living human brain,” said Michael L. Lipton, M.D., Ph.D., FACR, professor of radiology at the Gruss Magnetic Resonance Research Center at Albert Einstein College of Medicine and medical director of MRI Services at Montefiore Medical Center in New York City. “We validated methods for assessing the volume of the hypothalamus and confirm, for the first time, that current oral contraceptive pill usage is associated with smaller hypothalamic volume.”
Oral contraceptives are among the most popular forms of birth control and are also used to treat a host of conditions, including irregular menstruation, cramps, acne, endometriosis and polycystic ovary syndrome. According to a 2018 report from the Centers for Disease Control and Prevention’s National Center for Health Statistics, from 2015 to 2017 approximately 47 million women aged 15–49 in the U.S. reported current use of contraceptives. Of those, 12.6% used the pill.
In his study, Dr. Lipton and colleagues recruited a group of 50 healthy women, including 21 women who were taking oral contraceptives. All 50 women underwent brain MRI, and a validated approach was used to measure hypothalamic volume.
“We found a dramatic difference in the size of the brain structures between women who were taking oral contraceptives and those who were not,” Dr. Lipton said. “This initial study shows a strong association and should motivate further investigation into the effects of oral contraceptives on brain structure and their potential impact on brain function.”
Other findings from the study, which Dr. Lipton described as “preliminary,” were that smaller hypothalamic volume was also associated with greater anger and showed a strong correlation with depressive symptoms. However, the study found no significant correlation between hypothalamic volume and cognitive performance.
Co-authors are Ke Xun Chen, M.D., Sandie Worley, B.S., Henry J. Foster, B.S., David Edasery, M.D., Shima Roknsharifi, M.D., and Chloe Ifrah, B.A. The study was funded by the National Institutes of Health/National Institute of Neurological Disorders and Stroke and by The Dana Foundation.
Note: Copies of RSNA 2019 news releases and electronic images will be available online at RSNA.org/press19 beginning Monday, Nov. 25.
RSNA is an association of over 53,400 radiologists, radiation oncologists, medical physicists and related scientists, promoting excellence in patient care and health care delivery through education, research and technologic innovation. The Society is based in Oak Brook, Ill. (RSNA.org)
Editor’s note: The data in these releases may differ from those in the published abstract and those actually presented at the meeting, as researchers continue to update their data right up until the meeting. To ensure you are using the most up-to-date information, please call the RSNA Newsroom at 1-312-791-6610.
For patient-friendly information on brain MRI, visit RadiologyInfo.org.
December 24, 2019 (LifeSiteNews) – Twenty-six Christmases ago – our ninth together as man and wife – my wife, Valerie, and I experienced an unexpected miracle.
After discovering we were infertile early in our marriage, we had employed the help of doctors to the extent our consciences would allow, and when that proved unfruitful we quickly and happily went to work with an adoption agency. A few years and thousands of dollars later, amid soul-crushing disappointment, we reluctantly gave up our hope of ever having children.
We resigned ourselves to childlessness and tried to find comfort in the possibility of a lifetime of increased disposable income, of travel and other little luxuries. Over the next few years we put the thought of raising a family out of our minds. Or at least, we tried to.
Then something extraordinary happened.
Four days before Christmas, shortly after I had arrived home from work, the phone rang. On the other end of the line was a neighbor who explained that her sister was a foster parent for newborns, and that she was caring for a two-day-old baby boy who might be a difficult placement because he was biracial.
“I understand this might be a door you don’t want to re-open,” she said, “but I thought I should let you know. Are you interested?”
A bit dazed by the call, I thanked her and hung up the phone. My mind raced. Did I really want to risk tearing the scab off this deep wound, knowing that this could be another heartbreaking dead end?
I said a quick prayer, and when my wife walked in the door I suggested we go out for dinner at our favorite restaurant.
Halfway through our second glasses of wine – amid the Christmas decorations and carols softly playing in the background – I told her about the phone call and popped the question.
Over the next few days it was wonderful to witness the pure joy, peace, and hope return to my wife’s soul after having steeled herself against the pain of childlessness. Our celebration of the birth of the Christ Child that year took on new meaning as we at last could enter into the joy and anticipation of Mary and Joseph in a way we that we hadn’t been privy to previously.
Although it took a while to undergo another home study, Michael came to us just before Easter and, in a sense, resurrected our lives. For us, Michael was and always will be a miracle.
Then nearly two years later, another equally extraordinary event occurred.
A few days after submitting the paperwork to the same agency seeking to adopt a second child, the phone again rang. It was the head of the agency. I naturally assumed she was simply calling to acknowledge receipt of our application. I was wrong.
“Mr. Mainwaring, you’re not going to believe this but Michael’s birth mom just contacted us. She is eight months pregnant by the same man and they both want you and Valerie to have the child.”
Goosebumps popped up all over my arms and legs. At that moment I knew I was witnessing – and in the middle of – another miracle, a perfect answer to prayer that went beyond our wildest dreams, something that would never even have occurred to us to ask for.
Just a few weeks later, we brought home Christopher. He, too, is and always will be a miracle.
I’ll never forget that Christmas week a quarter of a century ago, when out of the blue God showed His love toward us after we had given up hope.
When we were completely unable to give each other a child, and every path had been blocked, God displayed his munificence toward us. Not once, but twice.
Among G.K. Chesterton’s many brilliant aphorisms is the following: “There is a law written in the darkest of the Books of Life, and it is this: If you look at a thing nine hundred and ninety-nine times, you are perfectly safe; if you look at it the thousandth time, you are in frightful danger of seeing it for the first time.”
Chesterton was a great lover of Christmas and wrote numerous poems and essays celebrating this most mystical and poetical of Christian feasts. I have no doubt that he would have agreed with me when I say that Christmas tops the list of those things that many of us have seen countless times, and yet have never truly seen.
Let us consider the barest, historical facts of the matter: God, Whose name is “I AM,” Who created all things, Whom heaven and earth cannot contain, lowered Himself by assuming a human body and sharing in the nature of one of His creatures. He was born as a helpless baby to an unknown and uncelebrated peasant woman, amidst the humblest beasts of burden in a stable in a backwater town belonging to a little-known people, who at the time lay crushed under the thumb of foreign conquerors.
And for what? To live 30 years in near-complete anonymity, engaged in the humblest manual labor, after which He spent a mere three years as a poor, itinerant preacher, a career that was brought to an ignoble and abrupt end through the betrayal of one His closest associates, who handed Him over to a brutal death by one of the most painful and humiliating forms of execution ever devised by man.
These are the barebone historical facts. And if we profess the Christian faith, but are not eternally astonished that such things could ever have happened, it is most likely because we have seen these facts 999 times, and yet have not seen them.
But now, let us go beyond the barebone historical facts. Let us turn our attention towards the meaning of these historical facts. We can do no better than to quote John 3:16: “For God so loved the world that he gave his one and only Son, that whoever believes in him shall not perish but have eternal life.”
God loved the world. He loved the human race! He loved us so much, that He saw fit to become one of us, and, by subjecting Himself to scorn, humiliation, and suffering, to offer us the opportunity to partake of His own life in a state of perfect, loving communion with Him for all eternity. He came, that is, to offer us the gift of salvation.
In his Christmas message in 1959, Pope St. John XXIII marveled at what this fact of Divine condescension says about the dignity of the human race, and every individual human being. “He ‘loved me and gave himself up for me.’ Thus spoke St. Paul to the Galatians (Gal. 2:20). And if God has loved man to such a degree, that indicates that man is of interest to Him and that the human person has an absolute right to be respected.”
Artist: Gerard van Honthorst – The Childhood of Christ
God’s coming to earth in human flesh was and is the greatest affirmation that, whatever the mysteries, messiness, sufferings, and sins that mar human existence in our fallen state, every single human life is endowed with infinite value and dignity, a dignity beyond telling. There is not one among us who is not infinitely precious in God’s sight.
The Rise of Anti-Human Pessimism
It may seem a very curious thing to reference a rather bleak scene from the movie The Matrix in a column about Christmas. But bear with me, and I think you will understand. The scene comes towards the end of the movie, when the villain – Agent Smith – is interrogating the character Morpheus. Morpheus is a leading figure in the last, desperate resistance against the reign of super-intelligent machines, who are ruthlessly exploiting humans to fuel their dystopian society.
Agent Smith, who is himself a super-intelligent computer program, muses on what he has learned about the human race. Contrary to every other mammal on the planet, he says, human beings seem incapable of developing an “equilibrium” with the environment. “You move to an area and you multiply and multiply until every natural resource is consumed and the only way you can survive is to spread to another area,” he says. “There is another organism on this planet that follows the same pattern. Do you know what it is? A virus. Human beings are a disease, a cancer of this planet. You’re a plague and we are the cure.”
Humans are a “plague,” a “virus,” a “disease” and a “cancer”. Where have we heard these sentiments of late? The brilliance of this scene is that it speaks directly to a deep-seated self-loathing that has plagued the human race for as long as humans have pondered the meaning of their existence. It is also a form of radical self-doubt and pessimism that is making a resurgence right now in the form of militant atheism, hedonism, nihilism, and anti-humanism.
Several weeks ago, I wrote about the philosophy of a South African philosopher named David Benetar. Benetar preaches “anti-natalism.” He argues that not only is human life intrinsically meaningless, but that it is essentially harmful, since to live is to suffer, and to suffer is to undergo pain for no reason. For this reason, Benetar thinks it is a moral evil to bring other human beings into the world.
In one way it is remarkable that Benetar’s philosophy should have gained such an audience and such a foothold in a time of unprecedented wealth and comfort, where the sufferings that have long beset human existence have been so dramatically reduced by near-miraculous scientific advancements and growth in wealth. On the other hand, it is not remarkable at all: for we live in an age that has turned our backs on the Gospel message, with the inevitable consequence that we have lost sight of the dignity of the human person.
Child rescued from “baby dumping” in Kenya
And, as Chesterton predicted, the moment we lost sight of the dignity of human existence, we lost sight of the need to respect human rights. How else can we explain the bloody revolutions and genocides in the atheistic regimes of the 20th century, and the growing comfort with eugenics, abortion, and euthanasia in the increasingly secular and apathetic West? As Pope St. John XXIII said in the same Christmas message quoted above: “The disturbances which unsettle the internal peace of nations trace their origins chiefly to this source: that man has been treated almost exclusively as a machine, a piece of merchandise, a worthless cog in some great machine or a mere productive unit.”
The Need for Christmas
Compare the anti-natalist philosophy of Benetar, to the gorgeous ruminations of St. Peter Chrysologus, who spoke so eloquently about Christ’s incarnation and human dignity, and whose writings make an appearance in the Roman breviary around this time of year. I strongly encourage you to read this beautiful quotation in full:
…Why then, man, are you so worthless in your own eyes and yet so precious to God? Why render yourself such dishonor when you are honored by him? Why do you ask how you were created and do not seek to know why you were made? Was not this entire visible universe made for your dwelling? It was for you that the light dispelled the overshadowing gloom; for your sake was the night regulated and the day measured, and for you were the heavens embellished with the varying brilliance of the sun, the moon, and the stars.
The earth was adorned with flowers, groves, and fruit; and the constant marvelous variety of lovely living things was created in the air, the fields, and the seas for you, lest sad solitude destroy the joy of God’s new creation. And the Creator still works to devise things that can add to your glory. He has made you in his image that you might in your person make the invisible Creator present on earth; he has made you his legate, so that the vast empire of the world might have the Lord’s representative. Then in his mercy God assumed what he made in you; he wanted now to be truly manifest in man, just as he had wished to be revealed in man as in an image. Now he would be in reality what he had submitted to be in symbol.
And so Christ is born that by his birth he might restore our nature. He became a child, was fed, and grew that he might inaugurate the one perfect age to remain for ever as he had created it. He supports man that man might no longer fall. And the creature he had formed of earth he now makes heavenly; and what he had endowed with a human soul he now vivifies to become a heavenly spirit. In this way he fully raised man to God, and left in him neither sin, nor death, nor travail, nor pain, nor anything earthly, with the grace of our Lord Christ Jesus, who lives and reigns with the Father in the unity of the Holy Spirit, now and forever, for all the ages of eternity.
Christ, by taking on human flesh and a human nature, has permanently elevated human existence. As St. Pope John Paul II did not tire of repeating: “Christ reveals man to himself.” Christ was God, but also man. And as the perfect, sinless man, He has revealed the heights of dignity for which every human being was intended, and to which he is called. As the Second Vatican Council puts it:
Human nature, by the very fact that it was assumed, not absorbed, in [Christ], has been raised in us also to a dignity beyond compare. For, by his Incarnation, he, the son of God, in a certain way united himself with each man. He worked with human hands, he thought with a human mind. He acted with a human will, and with a human heart he loved. Born of the Virgin Mary, he has truly been made one of us, like to us in all things except sin…
This is marvelous truth contained in the familiar story of Christmas. It may well be we have seen it nine-hundred and ninety-nine times. But let us pray for the grace, this Christmas, to see it for the thousandth time. To really see it. And then let us put our hands to the plow and respond to Christ’s call to preach this Good News to the four corners of the globe.
December 20, 2019 (LifeSiteNews) – At pro-life presentations across North America, audience members often ask me how to bring the subject of abortion up with children. After all, when parents are participating in pro-life activism or attending pro-life events, it is perfectly natural for a child to wonder what, exactly, it means to be “pro-life” in the first place. And considering that pro-life is anti-abortion and abortion is an act of violence perpetrated against a child, parents can understandably be unsure of how to approach the subject.
Enter Bethany Bomberger, a mom of four with a Bachelor’s Degree in Education and Family Studies and a Master’s Degree in Education from Regent University who has taught in both public and private schools. Bomberger is also a pro-life activist, working alongside her husband Ryan (who shared his story on my podcast earlier this year) at The Radiance Foundation, a “life-affirming organization that is rooted in the belief that we are all created in God’s image and have undeniable purpose.”
Drawing from these three wells of experience: Mom, educator, and pro-life activist, Bomberger has written an extraordinary book titled Pro-Life Kids! Paired with engaging and adorable illustrations by Ed Koehler, Bomberger’s book walks gently through the pro-life worldview, introducing a difficult subject in an age-appropriate way reminiscent of a Dr. Seuss book: “Pro-life means for life, We’re cheering for you. Your life is important. There’s only one you.”
Page of ‘Pro-Life Kids!’
From the facts of life before birth to the reality that many deny these facts (“Sadly, there are those who don’t understand…that life has purpose, whether planned or unplanned”), Bomberger manages to cover virtually everything, from the denial of personhood to what abortion actually is. Her description is simple, sad, and age-appropriate: “Abortion is when, some say it’s okay, to take that baby’s, precious life away.” Pro-life people, on the other hand, fight for all life, no matter what age or size.
To emphasize that the pro-life movement follows in the footsteps of other great social reform movements, Bomberger explains that people have always stood up for those who were denied their rights, comparing the civil rights marchers (there is a very clever illustration of the march across Edmund Pettus Bridge) to the March for Life in Washington, D.C.
The book ends with a call to action, emphasizing that even if you are young, you can be empowered to do something:
We are Pro-Life Kids
so dreams come alive.
We are Pro-Life Kids
so our future survives.
Bomberger ends with a personal note and a list of “Ten Ways You Can Show You’re a Pro-Life Kid,” including options like praying that abortion will end, attending a pro-life event, and going to the March for Life. Following this are stories of “real pro-life kids” to inspire and empower kids who may think they are too young to do something for the pro-life cause.
Page of ‘Pro-Life Kids!’
The book has been so popular that its first run is already sold out.
“The response to our book has been overwhelming!!! We actually sold out of our first run of books! Thousands more arrive on Monday, Dec 16th!,” Bomberger wrote on the book’s website.
I was thrilled to see this book published because it fills a much-needed void. In today’s culture, parents are searching for age-appropriate ways of educating their children on difficult social issues, and Bomberger has written the book that many of us have wanted for a long time. I’ve already read it to my little daughter, and she loved the story (Ed Koehler’s illustrations certainly helped with that.)
Pro-lifers must also keep in mind that according to data sets from across North America, many young people lose their pro-life convictions once they enter university. In some places, the numbers are staggeringly high. One of the reasons for this is that we are not doing an effective enough job of teaching our children our beliefs and passing on our convictions. One reason for this is that parents do not know how to broach these difficult issues, and thus often hope that their views will be passed on by osmosis. This is wishful thinking, and more often than not, their children embrace a different worldview.
Page of ‘Pro-Life Kids!’
Bethany Bomberger’s book removes parental excuses, and I heartily recommendPro-Life Kids! to each and every one of you. It makes the perfect Christmas present.
Jonathon’s new podcast, The Van Maren Show, is dedicated to telling the stories of the pro-life and pro-family movement. In his latest episode, he interviews Gianna Jessen, a well known abortion survivor and pro-life advocate. Ms. Jessen has been mentioned in speeches by President George W Bush. The Archbishop of Canterbury and the Archbishop of Westminster have said that her story could impact the abortion debate. Jessen survived a saline abortion and now uses her story to show people what an abortion. “I am alive. Just by the miraculous power of Christ.”
In chapter one of the first book of the Bible, we find a remarkable, even revolutionary statement – indeed, a series of such statements.
At the end of each day, after God has put the finishing touches on one more part of His creation, He pauses to survey His handiwork. And, the Bible says each time, “He saw that it was good.” The water and dry land are “good.” The stars and the sun and the moon are “good.” The birds of the air, and all the animals and fish are “good.”
On the sixth day, God creates human beings. “In the image of God, He created them,” says Genesis. And after God has blessed them, He commands them to “be fruitful and multiply.” And then, with this crown jewel of His creation completed, He steps back and takes in the whole of His cosmos. The first chapter of Genesis concludes: “God saw all that He had made, and it was very good.”
The Creation of Adam by Michelangelo
You may be wondering, “What is so remarkable or revolutionary about this? Surely, there is nothing so very groundbreaking in the idea that God is good, and that everything He has made is good. This is Theology 101!”
In reality, however, the idea that everything we see around us – above our fellow human beings – is in some deep, metaphysical, unshakeable sense “good,” is simply not self-evident. Quite the contrary. There have existed and do exist many human beings, and many philosophical and religious systems, that insist that material things are evil through and through, that human beings are a blight upon the earth, and that life itself, far from being “good,” is a curse, and that the one truly “good” thing would be the extinction of our consciousness, or the melting of that consciousness into a state of oblivion.
St. Augustine, for instance, before his conversion to Catholicism, famously believed in Manicheism. Manicheism is but one of countless “dualistic” philosophical systems, a form of Gnosticism, that proclaimed that matter was created by an evil deity whose power rivaled that of God. God Himself, the creator of a “spiritual” world, had no part whatsoever in material creation. The whole point of life was to escape matter and the body.
The Return of Pagan Despair
Certain pagan creeds advocated a worldview far more bleak even than Manicheism. The idea that life itself is evil is captured most famously and pungently in a line in the play Oedipus at Colonus by the Greek tragedian Sophocles. In that line, the chorus declares: “Never to have been born is best. Everyone knows that, and a close second, once you have appeared in this life, is a quick return, as soon as you can, to where you came from.”
This is dark stuff.
But, is also a sentiment that is making a comeback. Indeed, South African philosopher David Benetar turned to Sophocles when searching for the title of his book outlining the case for his philosophy, called “antinatalism.” The subtitle of the book is, “The Harm of Coming into Existence.”
Antinatalism is not a subtle theory. It is precisely what it proclaims itself to be: a philosophical theory that argues that human existence is essentially and irredeemably an evil thing. Benetar does not hesitate to draw out the logical consequences of this theory. If life is evil, then it is immoral to give life to another human being – that is, to have children.
The basic tenet of antinatalism is simple but, for most of us, profoundly counterintuitive: that life, even under the best of circumstances, is not a gift or a miracle, but rather a harm and an imposition. According to this logic, the question of whether to have a child is not just a personal choice but an ethical one – and the correct answer is always no.
Though we might be inclined to dismiss Benetar as a fringe lunatic, the first thing to note is that he is currently the head of the Department of Philosophy at the University of Cape Town. More importantly, his ideas are gaining traction.
A sub-forum on the social media site Reddit dedicated to antinatalism currently has some 45,000 followers. Earlier this year, antinatalism got a big publicity boost after Raphael Samuel, an Indian man, sued his parents for giving him life. Though the lawsuit was in some respects merely symbolic – he was asking for a tiny sum of money – Samuel was deadly serious. “It was not our decision to be born,” he told the BBC. “Human existence is totally pointless.”
Forms of antinatalism have also embedded themselves deeply in contemporary environmentalism. More and more we are hearing A-list celebrities declare that there is a moral duty not to bring any more human beings into the world. Their views may not be as bleak as Benetar’s. They may not, for instance, believe that human life is intrinsically evil, as such, but only evil insofar as it harms the planet. But clearly, the ideas are closely related. And many philosophical antinatalists are also (unsurprisingly) environmental extremists.
Christian Hope and the Meaning of Life
It’s quite natural for many of us to recoil in horror from Benetar’s theories. And yet, the first thing I want to point out is that there is a perverse logic to his worldview. Benetar is quite right to point to the fact that human life, even in the best of cases, is suffused with suffering. Further, in the end, all of us will have to face the dark and terrifying mystery of death. In the face of these hard facts, there is cause for our courage to fail.
Even in the Judeo-Christian worldview, we find this bleak strain of thought. Psalm 84 refers to this world as a “vale of tears,” and that phrase has been picked up by countless saints and spiritual writers. At the end of every rosary we pray the Salve Regina, which describes Christians as crying out to the Blessed Mother, “mourning and weeping in this valley of tears.” Christianity and Benetar see eye to eye in acknowledging this: life can be difficult and full of suffering.
But where the antinatalists and Benetar radically depart from Christians is on the place and the meaning they give to suffering.
For Benetar and the antinatalists, suffering is the final word. Life is suffering and death. Full stop. For Christians, suffering and death are but one part of life, and by far the least important part. For Christians, human beings are not destined for death. Quite the contrary: God intended for every human being to spend all of eternity with Him, enjoying the greatest happiness conceivable. Perfect happiness. Happiness without even the hint of suffering. And though suffering and death entered the world through sin, human beings still have the option to attain to the high dignity for which God intended them. Death, therefore, far from being the final word, is merely a footnote. It is but one step on the path to the fullness of life.
The noble purpose of human existence is summarized by Pope St. John Paul II at the very beginning of his encyclical Evangelium Vitae. There he writes:
Man is called to a fullness of life which far exceeds the dimensions of his earthly existence, because it consists in sharing the very life of God. The loftiness of this supernatural vocation reveals the greatness and the inestimable value of human life even in its temporal phase. Life in time, in fact, is the fundamental condition, the initial stage and an integral part of the entire unified process of human existence. It is a process which, unexpectedly and undeservedly, is enlightened by the promise and renewed by the gift of divine life, which will reach its full realization in eternity (cf. 1 Jn 3:1-2).
It is this supernatural calling, says the saintly pope, “which highlights the relative character of each individual’s earthly life. After all, life on earth is not an ‘ultimate’ but a ‘penultimate’ reality.”
“The Redeemer suffered in place of man and for man. Every man has his own share in the Redemption. Each one is also called to share in that suffering…” ~JP II
Remove a human being’s supernatural destiny from the picture, and “antinatalism” may well be the most logical conclusion. But place all of the suffering and pain of our earthly existence against the background of our eternal supernatural destiny, and suffering and death fade from view. Indeed, not only are suffering and death no longer the final word, but they become integrated into our great destiny. Seen with the supernatural eyes of Christian revelation, suffering and death take on a whole new meaning, and can be seen as one of the means by which we attain eternal life. Suffering embraced can be the means by which we are purged of our selfishness and sinfulness and rendered fit for eternal life with God.
Antinatalism feeds upon the despair that comes when human life is flattened. If this life is all there is, then the prevalence of suffering leads inevitably to despair. And this despair is what the Culture of Death is built upon. Viewed at with the eyes of faith, however, it is the deep joys present even in this life that are seen to be the only truly real things. Viewed this way, life is indeed seen as the great and wonderful gift that it is, and the bringing of new life into this world as an astonishing miracle.
Over two decades ago, journalist Andrew Coyne, responding to the case of Robert Latimer, who murdered his daughter Traci because she had cerebral palsy, wrote the following prophetic words: “A society that believes in nothing can offer no argument even against death. A culture that has lost its faith in life cannot comprehend why it should be endured.”
Prophetic, I say, because since Coyne wrote these words, the perverse mentality that he described has only grown in prevalence. More and more jurisdictions have legalized so-called “mercy killing.” Increasingly, even those suffering from mental illnesses are being deemed candidates for euthanasia and assisted suicide. No longer are we to find the meaning in suffering, or to peer through the façade of suffering to discover the inherent dignity of human life.
The Culture of Death feeds upon the despair that gives rise to the philosophy of antinatalism. Without God, antinatalism is the logical outcome. This is why I continuously hammer home the reality that it is not sufficient to fight the Culture of Death through political or social activism. The Culture of Death has a spiritual origin. And if we are to fight back and win, then we must fight with spiritual weapons.
We must return to the first chapter of Genesis. God created all things and all things are good. The antinatalists are fatally wrong. Life, indeed, is a great gift and a miracle. This is the good news of the Gospel of Life. In our efforts to fight abortion, euthanasia, and all the self-destructive tendencies of our Culture of Death, we must continuously strive to preach this Good News.
“Physicians who seek to advocate for their female patients’ best interests should become aware that medical abortion results in complications far more often than its proponents acknowledge,” wrote Dr. Ingrid Skop, M.D., a San Antonio obstetrician.
Skop said abortion providers are encouraging women to choose drug-induced abortions, which involve a combination of the drugs mifepristone (Mifeprex or RU486) and misoprostol (Cytotec). They are used to abort unborn babies up to 10 weeks of pregnancy in America.
Currently, about 39 percent of abortions in the U.S. are drug-induced, according to Skop’s research.
Though safety regulations require that a doctor prescribe the drugs, the abortion industry sometimes skirts the requirement by using webcams to remotely dispense them. The method is cheaper for the abortion industry, but women never actually see a doctor in person before taking the drugs.
According to the research, risks include ruptured ectopic pregnancies, hemorrhage, infection and retained pregnancy tissue, which require surgery in as many as one in 20 women. The FDA reports at least 24 women have died along with their unborn babies from the drugs, and thousands more have been injured. In total, the number of adverse events from 2000 to 2018 is now 24 deaths, 97 ectopic pregnancies, 1,042 hospitalizations, 599 blood transfusions, and 412 infections (including 69 severe infections), with a total of 4,195 adverse events reported, according to the FDA.
Abortion activists claim the drugs are very safe, but Skop said the little research on their safety is “heavily biased.” She said only 28 states require abortion facilities to report complications.
“Vocal abortion advocates are aggressively using the court systems and pro-choice media sources to advocate for removal of safety restrictions on abortions,” Skop wrote. “They have also begun to advocate for illegal use of mifepristone and misoprostol when restrictions are in place, despite the demonstrated increase in adverse events that occur when these medications are used without close medical supervision.”
This includes lobbying for mail-order abortion drugs, telemedicine and abortions performed by non-physicians. California recently mandated that the abortion drugs be provided on all public college campuses, and the New York legislature is considering a similar proposal.
De-regulating abortion drugs also would make women and their unborn babies more vulnerable to abuse. Already, LifeNews has reported on several cases of forced abortions or abortion attempts by men who did not want their partners to have the baby.
Skop concluded her report by urging doctors to be aware of the biased information coming out of the abortion industry and to consider their patients’ safety.
As a child, I never knew exactly what my dad did, but I knew that his office was the first place where I had ever seen anatomical pink and magenta models of the uterus and the embryo. I remember sitting with my mother in our family station wagon and looking up into the exotic jungle of scarlet bougainvillea that pressed against the glass of his beautiful corner office, displaying its deeply ridged flowers, just like the pink plastic model.
My father and I used to race each other up the stairs of the Population Center, and I remember the feeling of my heart pounding in my chest as I reached the last step before he did. I would triumphantly turn around and wait for his brown shoes and white cotton socks to appear on the top step before jumping out so that he could pretend to be surprised.
Beating my father up the stairs confirmed my feeling that someone wanted me. I was strong and fast, and thus worthy of my father’s love. (Later, this would develop into a mania for long-distance running and endurance training.)
“Wantedness” was originally a term coined to describe a mother’s attitude toward the birth of a child. Sociologists decided that the degree to which a birth was wanted could be measured by accounting for less than perfect timing, less than perfect finances, or simply emotional hesitancy on the part of the mother.
Yet its wider applications had more to do with phenomenology than with science. It could describe a person’s value in the social economy and the environmental factors limiting that value.
As I grew older, moved out, went to college, and began a career, my father would return periodically to the question of wantedness. He would ask me if I was content with my life’s circumstances, my partner or boyfriend, and so forth. It was his way of measuring my happiness.
He taught me that there was nothing more important than arranging your life in such a way as to create a balance between your “wantedness” and the events of your life. It was essential to make careful choices in order to achieve the outcomes you wanted. Yet, to me, it seemed even more important to make the right choices to ensure that I would continue to be wanted by others. At any of life’s crossroads, I might slip into a state of “unwantedness” simply by making the wrong decision.
Where family planning stated that educated reproductive choices resulted in better families, the unspoken assumption was that educated sexual choices would help separate sex from reproduction. As a child, I concluded that the “right” behaviors were those that resulted in being continually wanted by my parents, and then by friends and peers. Surprisingly enough, the result of being exposed to wantedness was not conformism, but a rigid perfectionism based on achievement.
My conclusions were shared by a whole generation of women and men who could only prove self-worth through professional achievement. As adults, we switched academic institutions and professional specializations frequently, and did not let ourselves be taken in by marriage or even by long-term professional commitments. Being depressed or heartbroken was just the price of having a career.
The unspoken promise that was embedded in perfectionism was that the political system would eventually reward high-achieving people by having our sexuality set free from the conditions of biology through advances in contraceptive technology—a promise especially aimed at women academics: do everything right, and the political system will make sure that sex stayed far away from sexual reproduction.
The Gospel of public health
I grew up within the emerging culture of population studies and maternal and child health. My father, J. Richard Udry, and his colleagues sought to bring the new science of fertility measurement to third-world countries, thereby preventing an imagined population explosion of unwanted births. Behind the new science of population studies, however, lay the old science of eugenics.
North Carolina, like many other southern states, still had sterilization programs in place until the mid-nineteen-seventies. Politically and culturally liberal social scientists reframed eugenics in updated language, emphasizing the need to give women control over their fertility and then rewarding them if they made decisions to have fewer children.
In the fairy tale world of public health, no mother would ever again have a baby and then suffer with feelings of guilt or regret, and no child or teenager would ever again feel pressured into gender roles that didn’t suit his or her deepest inclinations. Potential fathers would voluntarily register for sterilization rather than produce children in less than ideal environments or prevent their wives from pursuing educational and financial opportunities. All this would come about by discipling communities in the new science of family planning.
The gospel of public health said that women’s desire to have children and nurture the young could be modified through education. Educating the mother of the household about contraceptives would result automatically in smaller families, because that’s what “everyone wanted.” Public health continuously projected the image of reproductive progress: a perfectible male and a perfectible female to go along with a perfectible human family, shorn of excesses to fit into a modern world.
One of the target geographical areas for the new science of fertility control was southeast Asia, and Thailand in particular. As the Population Center’s funding grew, it began to attract large numbers of students from Thailand and India. On Friday nights, graduate students from Thailand would gather at our house to play table tennis and talk shop in the basement. Part of the idea of these get-togethers was to introduce the graduate students to American academic culture and to model the benefits of family planning and fertility control.
The family was presented not just as a procreative and biological unit, but as an aesthetic and social one. The symmetrical ideal was a family of four, and this “family planning pyramid” began to appear everywhere on posters and flyers related to family health. As one part of a two-child family, my sister and I were supposed to model this ideal—the lower the number of children, the more likely it is that the individual child will be intelligent, gifted, and nurtured. I felt this pressure keenly. To be loved and wanted, and to do my part to spread the gospel, I knew that I had to play my part perfectly.
A dangerous dance
In his work, my dad made numerous trips to Bangkok. Once, he brought me a little dancing golden prince from Thailand, with crescent shoes and a hat shaped like a little, upside-down golden cup. He danced with one arm up and one arm down, standing on the end of one of his long, pointed shoes.
In spite of his placid expression, the prince’s dance looked very difficult. If he moved too quickly to one side or the other, the pagoda hat might slide off. If he did not stand correctly, his shoes would surely bend, and he would stumble to the ground. To me, negotiating friendships felt like the dance of the Thai prince: my ankles ached and my arms throbbed, but I didn’t dare stop proving that I was worthy of being wanted.
One day, in the fourth grade, we learned a polka in which we had to change partners. I was so upset at the thought of my best friend dancing with someone else that I walked up to the new girl and kicked her sharply in the shins. Any time I was rejected in a friendship, I interpreted it as a final judgment on my worth as a human being. Any time I attempted a new undertaking, it had to be perfect. I already knew that I had to continually win my parents’ approval and attention to continue to be “wanted.” It was only natural that the same should apply to my other relationships.
When I was ten years old, my father’s sister died after an overdose of sleeping pills. My parents told me it was because “she could not control her own fertility.” I did not know if they meant that she had suffered through an unplanned pregnancy and abortion, or if my four cousins were just too much for her. In any case, I concluded that motherhood had gotten in the way of what my aunt really wanted: fewer children.
Clearly, “being in control” was very important. I must learn to do it very well, for if I failed, I might pay with my life. The prospect that losing control over fertility could so quickly lead to lethal “unwantedness” made the idea of having a family very dangerous. Since I was female and soon to enter puberty, it seemed to make me dangerous, too.
The gospel of family planning was not only preached in Southeast Asia. It was also taught to us at school. “Health class” now meant “sex” class, and sexual experimentation seemed to be the only acceptable way to become a healthy person. I was taught to apply the new philosophy of sexual freedom to constructing myself.
Any conclusions based on biological clues as to my sex were to be ignored on the grounds that they were too conservative and would constrain me to follow traditional gender roles. All conclusions based on my individual gifts, inclinations, and predispositions were to be evaluated according to the social standard of progress, and I was rewarded for making decisions that went counter to my own biological sex.
Well into college and graduate school, my perfectionistic quest to be wanted corroded my soul, mind, and body. There were now so many conditions being placed on what could make me desirable—as a student, as a potential mate, or as an employee—that I couldn’t win. I could no longer reliably know how to make myself desirable in the eyes of the world. It was better, I decided, to work on fulfilling my own wants and desires.
The fear I had developed about friendships in grade school turned into a tendency to verbally tear down other women who dared to challenge my fragile ego. Sarcasm had been the daily catechism in our house—a form of verbal warfare in which science always won. Contempt was heaped on those of differing political, cultural, or intellectual views. Even as an adult, these lessons lingered. I had a pathological need to prove that I was smart by putting others down—a practice that has sadly become a standard feature of social science.
The language of “wantedness” hurts children—and adults
Today, we are living in a society where the ideals of family planning that were envisioned in the seventies have largely been realized. The way couples talk about family size and fertility in casual settings has been so touched by “the magic wand of family planning” that we imagine there is one-hundred-percent correspondence between an imagined number of births and the shape of the families we have.
Not only family size, but the sex and genetic makeup of a birth are subject to the rubric of “wantedness.”
Even when people talk about their personal fertility, no one questions the logic of “wanted vs. unwanted births.” Yet when this kind of rhetoric permeates a society, the first thing to go is the capacity to form and sustain long-term relationships of the kind that hold the family together, like marriage. The decision to have children ceases to be something that people plan for by becoming married. Instead, it is viewed as extraneous to marriage as an institution.
The effects of the family planning rhetoric of the 1970s changed a generation. One can hear the echoes in the way we talk about the family today. Classifying human beings as “wanted” and “unwanted” has insidious and enduring effects. Instead of family bonds, it creates groups of human beings who have to prove they are worthy of life before receiving it.
For my generation of late baby-boomers, we were not so much career-driven as driven to achieve in any area. We delayed child-rearing, and opted for long-distance relationships that lasted only until the next academic opportunity arose. Instead of being resilient, we were unable to endure conflict and were crushed under criticism, a disease that ruined collegial cooperation and stifled academic discourse. Our assumptions could not be criticized, and any challenge had to be met with total resistance.
The ideology behind the perfect family was not nearly as pretty as the sterile plastic models of the womb looked. The beautiful pink and magenta models of the womb in the big, sunny office never became what they should have become: life. The ideology said that families would be improved when sex was kept far from birth, and that when a relationship or a person was no longer wanted, one simply did away with it, setting it aside to die like one of my father’s potted plants.
Over time, anatomical models became frightening to me, because they never changed—the embryos were always suspended, never complete. The plants in the office window continued to fascinate me though, especially the “Crown of Thorns,” a tangled tree that forced scarlet flowers up through wooden thorns. Messy, tangled, and uncontrolled, it was a survivor, a desert tree, that continued to produce life even in old age.
Susan Martin writes about gender, fertility and memory from the perspective of a non-Jewish person walking on the soil where the killing of millions of Jewish people took place. She studies the boundaries between historical record and the recording of memory in the body as it influences current cultural issues of gender identity. This article has been republished, with permission, from Public Discourse.
A British mother decided to speak out publicly after watching the medical community discriminate against her unborn son because he has Down syndrome.
Speaking with The Sun, Cheryl Bilsborrow, of Lancashire, England, said prenatal testing is fueling increased discrimination against unborn babies with disabilities.
Parents often feel pressured to consider abortion after a Down syndrome diagnosis. In Bilsborrow’s case, she said she repeatedly was asked if she wanted an abortion, including when she was 38 weeks pregnant.
“Never!” she replied, but they kept asking.
Today, her son Hector is a happy, affectionate 2-year-old. His mother said he loves to sing, and he is beginning to talk.
“He’s got beautiful white hair and blue eyes, and he is always smiling and laughing, blowing kisses and coming for hugs,” Bilsborrow said. “But when I was pregnant I was made to feel like his life would have no value and that I should abort him. Why? Because he has Down’s Syndrome.”
New research from 26 hospitals in England found a 30 percent drop in the number of babies born with Down syndrome since the NIPT prenatal test became widely available. All NHS hospitals are supposed to begin offering the test soon, according to the report.
Bilsborrow described the situation as a “national travesty.”
She said she agreed to have the screening test done “without much thought.” When the results came back, however, they were a huge shock, and the so-called options counseling did not help.
“Each time I went back for my midwife appointments over the pregnancy, they spoke to me about the possibility of abortion,” Bilsborrow said. “There was no offer of counselling, no discussion about how my life might be enhanced by this baby.”
Though she was extremely worried and anxious about her child, she repeatedly refused to abort him.
Yet, “abort and get rid seemed to be the only answer” that she was given.
“What if the midwife had phoned me and said: ‘Please don’t be alarmed. You’re having a baby with Down’s syndrome. We can offer you some counseling and help you meet a family with a child with Down’s syndrome so you can learn more,’” she said. “Instead, they made out it was the worst news in the world.”
Bilsborrow said families deserve better.
“Now, having had Hector, I know there was nothing to be frightened of,” she said. “But the joys of having a baby with Down’s Syndrome aren’t spoken about when the NIPT test results first come back.
“It spoke volumes to me about the perception of children with Down’s syndrome,” she continued.
In England, abortions are legal up to birth for babies with Down syndrome and other prenatal diagnoses. Bilsborrow believes the expansion of prenatal testing would be “disastrous” for babies like her son because there is so much stigma about people with the disability.
“So given babies like my son can live perfectly happy, normal lives, why are millions of pounds are being spent on Down’s Syndrome screening each year – which in turn encourages mothers to abort their unborn children?” she asked.
Down syndrome discrimination is a problem across the world. Several years ago, CBS News report shocked the nation with its exposure of the discriminatory trend. According to the report, nearly 100 percent of unborn babies who test positive for Down syndrome are aborted in Iceland. The rate in France was 77 percent in 2015, 90 percent in the United Kingdom and 67 percent in the United States between 1995 and 2011, according to CBS.
Did you know that the Pill affects how we process stress? Sometimes this is viewed as a positive since research shows women on hormonal contraception do not exhibit the body’s classic response to stress (i.e., elevated levels of the stress hormone, cortisol, courtesy of HPA-axis signaling) in stressful situations. But this aspect of the Pill isn’t all positive; unfortunately, it can lead women to feel out of touch with healthy stressors, and it can also lead to chronic stress.
Hormonal birth control disrupts healthy stress processing
While at first glance it may seem that the Pill’s disruption of stress responses would lead to less stress—which sounds good—the problem is that hormonal contraceptives disrupt our bodies’ normal way of processing stress, even good stress. As a matter of fact, there is such a thing as healthy stress. The stress response is our body’s way of letting us know that something significant is happening and helping us react accordingly. Some stress is normal (in fact, needed) to help us live meaningful, interesting, lives—and to make a quick getaway in dicey situations. That’s why a healthy person will exhibit increased cortisol in dangerous or exciting situations, but will also experience a drop in cortisol once the precipitating event has passed.
But what happens if your body doesn’t experience that drop—if the stress response is always on? This is what is known as chronic stress, and it’s when stress becomes chronic that it causes all sorts of negative effects, such as depression and anxiety, memory and concentration impairment, weight gain, and headaches. Unfortunately, the bulk of the research on stress and hormonal contraception indicates that the bodies of women on hormonal contraception seem to react to stress similarly to bodies under chronic stress.
Women’s bodies on hormonal contraception mimic bodies under chronic stress
In her new book, This is Your Brain on Birth Control, Dr. Sarah E. Hill discusses the effects of hormonal contraception on women’s stress response, describing how current research indicates that the HPA-axes of women on the Pill appear to be in “shutdown mode”:
“The Pill-taking women’s pattern of HPA-axis function looks suspiciously similar to that of someone who has experienced chronic stress, suggesting that the Pill might actually cause the HPA axis to go into overdrive, requiring it to take coordinated action to blunt itself.”
It is perhaps this self-shutdown of the HPA-axis that negatively affects a woman’s body on birth control from being able to effectively cope with stress, paving the way for all sorts of other issues associated with hormonal contraception, like depression and anxiety.
Further, Hill points out, “despite the fact that too-much cortisol signaling can increase women’s risk of brain-volume loss, serious depression, and certain health problems, no one really knows why this happens, how it unfolds, or whether it is reversible.”
No one knows the full effects of birth control on the brain
I think Hill’s finding above is so disturbing I had to put it in bold. Certainly, more research and awareness in this area is needed. But, for now, we can keep sharing articles like these, so women can grow in the knowledge of how their birth control may be affecting their health.
So, what does this mean for you if you’re on the Pill, or thinking about going on it? It’s hard to say, as the research into the relationship between hormonal contraception and its effects on the stress response is fairly preliminary, and because the Pill (and different formulations of hormonal contraception) seem to affect different women in different ways. But if potentially throwing your body’s response to stress way out of whack sounds like a gamble you’d rather not take, then rest assured that there are other options available that will keep your brain and body intact while still allowing you to effectively postpone pregnancy. Fertility Awareness-Based Methods (FABM) are science-backed, effective, natural forms of family planning that rival and sometimes exceed the effectiveness of the Pill.
To benefit from the high, research-backed effectiveness rates of Fertility Awareness-Based Methods, begin by connecting with a trained FABM instructor. You can expect to find life-changing knowledge in a judgment-free zone, and begin a journey toward greater wellness and better-informed health decisions. And best of all, you can say goodbye to days of chronic stress.
If you are involved in the pro-life movement for any length of time, you will encounter the image of Our Lady of Guadalupe. There are many connections between this particular image of Our Lady and the pro-life cause.
On December 12, 1531, the Blessed Virgin Mary appeared to an Indian named Juan Diego and requested that a shrine be built and dedicated to her on the Hill of Tepeyac. Juan Diego, upon reporting this event to the bishop, was disappointed because the bishop didn’t seem to believe him. Juan returned to the place of the apparition where Our Lady again appeared. She told him to return the next morning when she would give him a sign that would convince the bishop of the truth of her appearance and her request.
The following morning Our Lady told Juan to go to the top of the hill and gather Castilian roses that he would find there. Although he knew that only cactus grew there, he obeyed, and his simple faith was rewarded by the sight of beautiful roses growing where she had told him they would be. He gathered them and showed them to Our Lady who rearranged them for him. Juan returned to the bishop. As he opened his tilma (a type of pancho), the roses fell to the floor. All who were present were startled to see an image of Our Lady on the tilma. Today this image is still preserved on Juan Diego’s tilma, which hangs over the main altar in the basilica at the foot of Tepeyac Hill just outside of Mexico City. In the image, Our Lady is pregnant, carrying the Son of God in her womb. Her head is bowed in homage, indicating that she is not the Goddess, but rather the one who bears and at the same time worships the one true God. Many articles have been written on dozens of other theological lessons drawn from the details of the image.
When asked who the lady was, Juan replied in his Aztec dialect, “Te Coatlaxopeuh,” which means “she who crush the stone serpent.” His answer recalls Gen. 3:15 and the depictions of Mary as the Immaculate Conception, her heel on the serpent’s head. The devil exalts himself above God and above God’s law (see Isaiah 14:12-15), whereas Mary submits to God (see Luke 1:38). Some promote abortion as a “choice.” Self-will is exalted. We reject abortion because we, like Mary, submit all our choices to God. That spirit of obedience crushes evil and sin. Our Lady’s image reminds us to live in that obedience each day.
Human Sacrifice Then and Now
Some nine million Aztecs were converted to Christ by the power of the image of Our Lady of Guadalupe. At that time, the Aztec peoples were practicing human sacrifice. As a result of the image’s presence among the people, their hearts were converted to the true God and the practice of human sacrifice was abolished. A key theological dynamic operating here is that Our Lady turned the Aztecs from a worldview of despair to one of hope, from a conviction that the gods were against them to a conviction that God was so much for them that He became one of them.
We can listen to stories of Aztecs cutting out their victims’ hearts or placing their heads on poles and say, “Oh, how terrible that was!” But America is not doing any better, as the hearts and heads of innocent babies are destroyed by abortion! The image is therefore being used again to change the hearts of our people.
A Theology of Despair
The Aztects had a complicated mythology-theology. The universe for them was essentially unstable, and in that universe humans played a very small role. This view led to pessimism, and a fear that they needed to always appease the deities. Their view was that the present world was the “Fifth world,” made by the “Feathered Serpent.” The previous four worlds had been destroyed by gods who turned people into monkeys or dogs. The present world, they thought, would be destroyed by an earthquake, as a result of which skeleton creatures would come out of the ground to destroy the surviving inhabitants of earth.
This is a theology of despair. Whatever moral aversion they may have had to human sacrifice, their despair made them feel they had no choice but to practice it.
The dynamics behind abortion are essentially the same. While there may not be a mythology of feathered serpents and skeletons, there is real despair. People do not get abortions because of “freedom of choice”; they get them because they feel they have no freedom and no choice. They feel trapped, abandoned, desperate, and afraid. The thousands of case-studies that Priests for Life has collected from post-abortive women are permeated by the theme expressed by the woman who said, “My friends told me I had no other option. The clinic did not offer me any alternative, and I was almost crying out for one.” As author Frederica Mathewes-Green has said, a woman does not choose an abortion like she chooses a Porsche or an ice-cream — rather, she chooses it like an animal caught in a trap chooses to gnaw off its own leg. Her experience is that she either chooses to end the life of this baby, or her own life will end. “I cannot handle it, I can’t do it, nobody will support me, it’s impossible.”
The rationalizations offered for abortion are also full of despair for the child. “Why bring a child into this world, into these circumstances, where he/she will have to suffer so much?”
From Despair to Hope
How does the image of Our Lady of Guadalupe answer the theology of despair, both for the Aztecs and for the Americas?
Our Lady is carrying God within her womb. The God of the Universe has now become a human being. No longer is there any question as to whether God is on our side. He is not a God who will destroy us; He is a God who has become our brother. He is not a God far away who waits to be appeased by blood. He is a God who shares our own flesh and blood, and is as close to the human family as an unborn child to his mother.
In this framework, human beings no longer play a small part in the universe. On the contrary, as the Second Vatican Council proclaimed, “By his incarnation the Son of God has united himself in some fashion with every human being” (Pastoral Constitution on the Church in the Modern World Gaudium et Spes, 22). The result of that is the promise of Revelation 3:21, “I will give the victor the right to sit with me on my throne.”
The universe into which Our Lady of Guadalupe invites us is no longer an unstable universe. God clearly reveals Himself as the only God, who is and shares both love and life. This truth brings hope. There is no longer need for human sacrifice, whether on pagan altars or in abortion clinics, because both the present and the future are in the hands of a God who is “God with us.”
The Image and the Pro-life Movement
The image of Our Lady of Guadalupe which converted the Aztecs has been replicated and travels the United States on an explicit mission to end abortion. It is carried into Churches and it is brought in front of abortion clinics nationwide. I have been with the image many times in these settings. In one instance in Florida, a Catholic girl who was already in the clinic’s waiting room looked outside and saw us praying, and decided to cancel her abortion. She came out to talk to us. We arranged for all the assistance she needed, and later that year I had the joy of baptizing her baby, whom she named “Guadalupe.”
The image speaks to these girls a message of hope. It also speaks to the pro-life people a message about the task before us. We who fight abortion do not see abortion walking down the street. Instead, we see a girl, frightened and in the grip of despair. We, the Church, are to reach out to her in what is the most critical pastoral mission of our day.
That mission is illustrated by the Annunciation and the Visitation. When Mary is told she will be the Mother of Christ, she does not get wrapped up in herself, thinking about what has just been said and isolating herself from others in order to absorb some unique spiritual experience. Rather, she seems to pay more attention to what Gabriel said about Elisabeth, Mary’s cousin, that about Mary! She runs in haste into the hill country and tends to Elisabeth’s needs during her pregnancy. The message for us is that authentic religious experience and true worship never turn us in on ourselves. Rather, the more real our encounter is with God, the more attentive and responsive we are to the needs of our brothers and sisters.
Our Lady of Guadalupe has been declared the “Patroness of the Unborn.” They will be saved by the message of hope she brings, and by the message of concrete charity with which she challenges the Church. Among the many and varied groups that carry out this pro-life mission, one of special note in this context is “Indians for Life.” The outreach department of the National Right to Life Committee, as well as Priests for Life, have fostered and encouraged the growth of this yet small organization, coordinated by Clementine “Little Hawk” Hernandez. Archbishop Charles Chaput, OFM Cap., has been among the strong supporters of this effort, which gives concrete expression to the reverence of Native Americans for the gift of life.
Conclusion: For the little ones, for us
When Our Lady appeared to Juan Diego, she addressed him as “Juanito” (signifying the weakest or smallest member of the family), and as “Son”, and spoke of herself as both his “Mother” and the “Mother of the One, True living God.” All of this indicates another reason why Our Lady of Guadalupe should be entrusted with the unborn.
Today she addresses to us who defend life the same words she addressed to Juan Diego:
“Hear and let it penetrate your hearts, my dear little ones. Let nothing discourage you, nothing depress you; let nothing alter your heart or your countenance. Do not fear vexation, anxiety or pain. Am I not here, your Mother? Are you not in the folds of my mantle, in the crossing of my arms? Is there anything else that you need?”
After falling into despair following the start of a chemical abortion last year, Jessica pursued abortion pill reversal, and she is now the mother to five-month-old-baby Arya, who brings joy to her life.
“I’m really happy that I was able to reverse the abortion and that she is part of my life,” she said of her baby girl. “I couldn’t imagine it any other way.”
Mindful of those who didn’t have this same chance, she is speaking up about her experience in hopes that others can learn about Abortion Pill Reversal.
“There are other women who didn’t have that option,” Jessica told Pregnancy Help News.
She had just begun her first year of nursing school when found out she was pregnant with her second child. Jessica’s three-year-old son had just been diagnosed with autism, and she’d also left her spouse, citing problems with drug and alcohol, and his mental and emotional abuse.
Jessica recalled discovering that she was pregnant, finding herself out of breath walking up the hill to her car after class, which was strange.
After running to the store, purchasing and taking three pregnancy tests, which all turned positive, she was then on her bathroom floor sobbing.
“I didn’t know what to think,” Jessica said. “I went back and forth from wanting to keep my baby, to trying to focus on the life I already struggled with at times.”
She thought about being a single mother, now with two children, her son’s diagnosis and her trying to finish school, all without support from her children’s father.
“It was really hard on me,” Jessica recalled.
After an ultrasound in October of last year confirmed she was six weeks pregnant, she continued to mull over her situation while discussing options with her doctor.
“I really was unsure of my decision; part of me wanted to focus on my new goals in life and another part of me wanted to keep this precious baby,” she said. “It was later on that day that I decided I would take the first abortion pill.”
Jessica said she immediately began to cry after she took the abortion pill.
“I remember sitting in my car in the parking lot staring, not knowing what I had just done,” she said.
It was Thanksgiving weekend in Ontario, and she was driving to her mother’s house the following day, crying through the entire drive.
“I felt horrible,” Jessica stated. “How could I want to abort my beautiful baby? … The life that was growing inside of me…”
“I was so upset with my decision that I didn’t want to live anymore,” she told Pregnancy Help News. “Then I thought about my three-year-old son, and that I can’t not want to live because I have another child.”
Jessica continued to sob with regret after arriving at her mother’s home and talking with mom.
Her mother suggested that there might be some way to reverse the chemical abortion process, and Jessica began searching on the internet, coming across the website abortionpillreversal.com.
She spoke with a helpline consultant, who told her that a nurse would call her back.
The consultant was very supportive, Jessica said, reassuring her that she would do everything she could to help her.
The few minutes waiting for word on the next steps were the longest of her life, said Jessica, “I just kept thinking, “Please, I hope someone can help me, can help my beautiful baby.”
When the Abortion Pill Rescue Network nurse called her back, Jessica said she was so polite and helped reassure her that she was not alone in this situation.
“She gave me all the information that I needed and called local hospitals,” said Jessica, to determine whether they knew the APR protocol.
She estimates that it was about 30 hours after taking the abortion pill that she started her progesterone treatment.
The chemical abortion process consists of two pills; the first, mifepristone blocks the effects of progesterone, the natural hormone in a pregnant mother’s body necessary for her pregnancy to thrive. The abortion drug causes the uterine lining to break down and the placenta to begin to fail, thus starving the baby of oxygen and nutrients.
The second chemical, misoprostol, taken one to two days later, completes the chemical abortion, by causing the mother to deliver her deceased baby.
The Abortion Pill Reversal protocol works by giving the mother extra progesterone up to 72 hours after she takes the first chemical abortion drug. The treatment has the best chance for success when begun within 24 hours.
Jessica was followed closely by doctors throughout her pregnancy and had numerous ultrasounds. She continued to worry about her daughter even after completing the progesterone treatment at 18 weeks, but carried her baby to full term, delivering her one day after her due date.
“My daughter Arya Alexandria is the most amazing gift,” Jessica beamed. “I call her my miracle baby.”
Arya was born perfectly healthy, she said, and is very happy, sleeping a lot, and getting along well with her son.
“I’m just really happy that this worked out,” Jessica told Pregnancy Help News. “She brings a lot of joy to my life and also to my son’s life.”
She said she’ll be forever grateful to have found the APR website and receive treatment as soon as she could.
Jessica hopes for more women to find help and support in these situations. And she believes everyone should be educated on the Abortion Pill Reversal process “because it truly is an amazing thing.”
“So many babies have been saved by this process, and by saving babies you could also be saving a mom,” she said.
“There are other options if you do take the abortion pill,” said Jessica. “That one option (APR) really changed my outlook on things. It gave me hope.”
Pregnancy Help News is a project of Heartbeat International, which manages the Abortion Pill Rescue Network, a 24/7-365 provider network of more than 800 clinicians that provide the APR protocol.
LifeNews Note: Lisa Bourne is Managing Editor of Pregnancy Help News and Content Writer for Heartbeat International. This originally appeared at Pregnancy Help News.
Another young woman has died as a result of hormonal birth control.
Alexzandria “Ally” Givens died in July, two days before her 21st birthday, after collapsing when she got out of bed to use the bathroom, according to Fox 17. Her boyfriend, Eli Richards, called 911. Then he called Ally’s parents.
Carla Givens, Ally’s mother, told Fox 17 that Ally hadn’t been feeling well the night before. While she was unable to describe exactly what was wrong, Ally had complained of pain in her neck and shoulder as well as her leg during her time using the NuvaRing. No one realized it was connected to the birth control. When her parents received the call that she had collapsed, they rushed to her side.
“It was a worst nightmare phone call you’d ever get in your life,” Carla Givens explained. “We got it and we rushed out of bed and went to his house and when we got there, the door was open and she was laying there and they were trying to revive her and they couldn’t.”
The medical examiner determined that Ally had died of pulmonary embolisms caused by blood clots that had formed as a result of the NuvaRing, listing “History of Exogenous Hormone Use” in the official report.
Carla Givens told Fox 17 that while she believes Ally’s doctor told her what risks are involved in taking hormonal birth control like the NuvaRing, she doesn’t think the doctor explained how those side effects present themselves. So while Ally may have been made aware that blood clots could develop when using NuvaRing, she wasn’t told what the actual signs and symptoms would be.
Many women aren’t made aware of the full list of side effects that accompany hormonal birth control and even if they are warned about them, these serious side effects are often played down by medical professionals as being rare and unimportant. However, when a woman dies, it shines a light on just how vital it is for women to know exactly what they’re getting into when they choose to use hormonal birth control.
The Givens family won’t be suing Merck, the manufacturer of the NuvaRing, for Ally’s death, but they are asking that they stop selling the product altogether.
“I just want it off the shelf,” said Carla Givens. “I don’t want another girl to die from it and have those parents feel like I do.”
But it isn’t just the NuvaRing that can kill women. All hormonal birth control comes with major concerns for women’s health including an increased risk of depression and suicide, heart attack and stroke, breast cancer and cervical cancer, infertility, blood clots, and death. In fact, research shows that up to 400 women a year die as a result of taking hormonal birth control. Pulmonary embolisms and strokes have always been rare in young adults; however, as reported by The Federalist, once birth control hit the market, the number of young people experiencing cardiovascular problems such as these increased.
College student Hope Johnson died in 2014 from a pulmonary embolism linked to birth control, and her family was recently awarded $9 million in a wrongful death medical malpractice lawsuit against Auburn Urgent Care in Alabama. After a blood test found that Hope was at a high risk of developing blood clots, the results weren’t properly filed and she was given birth control known to cause blood clots anyway. Despite a few trips to the ER for help, her condition was not properly diagnosed, and she died about a month after she began taking birth control.
Twenty-year-old Alexandra Williams died in 2018 after collapsing in her parents’ driveway. She had been suffering from back pain that doctors failed to recognize as a sign of blood clots in her lungs. She had been on hormonal birth control pills for nine months, which Planned Parenthood had prescribed. According to The Federalist, Alex was not made completely aware of the side effects and health risks that come with hormonal birth control, and her doctors failed to properly diagnose her once symptoms began.
Women are suffering from the effects of birth control, yet major media outlets and doctors are ignoring the facts. Birth control is failing women and girls, yet the school systems bring Planned Parenthood into their buildings to dole it out to children. How many women are going to be sacrificed at the altar of the sexual revolution?
Top scientists found that women taking the contraceptive pill have a significantly smaller hypothalamus – a brain region responsible for regulating hormones.
Damage to the hypothalamus can wreak havoc with a women’s sex drive, mood, appetite, heart rate and sleep cycles.
The shocking revelation comes following a study, presented at the annual meeting of Radiological Society of North America, that examined 50 women – 21 of whom were using the Pill.
All 50 women underwent a brain scan, and doctors measured the size of the hypothalamus of each participant.
And doctors were stunned to discover the difference in brain structures in women taking the Pill compared to those who weren’t.
Impact on brain function
Dr Michael Lipton, professor of radiology at Albert Einstein College of Medicine in New York, said: “We found a dramatic difference in the size of the brain structures between women who were taking oral contraceptives and those who were not.
“This initial study shows a strong association and should motivate further investigation into the effects of oral contraceptives on brain structure and their potential impact on brain function.”
Dr Lipton also found a strong correlation between smaller hypothalamic volume and greater anger and depressive symptoms.
Despite this, he said that this finding was currently “preliminary”.
Pill plays Cupid
This is the first time structural effects of sex hormones, including oral contraceptive pills, on the human hypothalamus have been reported, according to the researchers.
It comes after it was revealed the Pill can dictate who you fall in love with and significantly lower your sex drive.
Top psychologist Dr Sarah Hill revealed that it affects “sex, attraction, stress, hunger, eating patterns, emotion regulation, friendships, aggression, mood, learning, and so many other things”.
She said women on the Pill are attracted to less masculine men and are less interested in sex.
That’s because the hormone progesterone, which sends a message to the body that ovulation is not required, is dominant throughout your cycle.
She said: “Rather than experiencing an increased preference for sexy men at high fertility like naturally cycling women do, Pill-taking women exhibit an unwavering preference for men with less masculine faces and voices.
“This is the sort preferred by naturally cycling women during the second half of their cycles, when progesterone is high.”
TULSA, Oklahoma, December 5, 2019 (LifeSiteNews) — A pro-life mother accomplished a world record for fastest half-marathon while pushing her baby daughter in a stroller. This happened despite race officials’ objections to the pro-life messaging she and her teammates put forth during the race.
Julia Webb (36) won the Route 66 women’s half marathon in Tulsa on Sunday, setting a world record while she pushed her 10-month-old daughter, Gabriella, in a stroller. Wearing a t-shirt that proclaimed, “Remember the unborn,” she came in at 1:21:24, according to race organizers. The official results are pending ratification from the Guinness Book of Records.
Fox News reported that Julia said, “I have just felt called to run my whole life.” She added, “This is what I was made for. Especially as a mom of three kids, I need some me-time…everything that it entails, I just absolutely love it.” Saying that she enjoys competition, Julia said that decided to combine running and motherhood by running with her children in a stroller.”
In an interview with LifeSiteNews, she said that in 2016, she clocked a similar time, pushing her daughter Jonni is stroller, but did not have video evidence to prove it as required by Guinness.
Both Julia and her husband Alan Webb are active with LIFE Runners, the largest pro-life running group in the world. LIFE Runners has over 13,000 Christian runners in 39 countries all over the world who raise money and draw attention to the pro-life cause. During the summer, Julia trained with fellow LIFE Runners for the race on Sunday. “They were a big reason I was able to break the record this season,” she said. LIFE Runners founder Dr. Patrick Castle said in an interview with LifeSiteNews that running for the pro-life cause gave Julia the extra push she needed to accomplish her record run.
A pro-life advocate, Julia wore her blue LIFE Runners t-shirt bearing the words “Remember the unborn” as she ran to victory. She is currently preparing to run marathon trials this February in Atlanta in order to qualify for the next Olympic Games. LIFE Runner and husband Alan is an athlete,too, and famed for having set the unbeaten American record in the mile (3:46.91). Both Julia and Alan are devout Catholics.
The decision to join Life Runners was not easy. For most of my life I never wanted to stand up for anything. I wanted to be agreeable with everyone and everything, offending as little people as possible … 2016 my husband had a conversion and has challenged me on every level ever since.
I realized I was most of the time ashamed of Christ and His Church. I was embarrassed to be ‘out there’. Also I have always been Pro Life but I was terrified to take a public stand against abortion. I just wanted to be accepted and having approval feels good.
Respect to all beliefs but I feel called to be a witness to Christ. There are days I am dragging and want to hide behind a Nike logo but it’s time for me to be uncomfortable. Standing up for the littlest in society matters. Anyone else brave enough to join?
In a telephone interview with LifeSiteNews, Julia credited LIFE Runners at the Tulsa race for helping her achieve her record. “There was so much charity and love and support for families,” she said, on the part of LIFE Runners at the race. She said she arrived fatigued and somewhat dispirited to the race. But the enthusiasm and warmth of her teammates buoyed her energy level. Before the race, she felt that the Holy Spirit was at work in her, lending the confidence she needed to make the win.
Credit: LIFE RunnersLIFE Runners
Having joined LIFE Runners earlier this year has not been without a cost, she said in the interview. Pro-abortion acquaintances and fellow runners have criticized her for wearing the LIFE Runner t-shirt and have questioned her motivations.
Julia told Fox News that she wants to see LIFE Runners movement continue to grow, adding, “… if it can save one woman from getting an abortion it will be worth it.” In a separate statement, she wrote: “When I am competing for LIFE Runners it is for a cause much greater than myself and this is the extra I need to achieve big goals.”
In a statement, LIFE Runners founder Dr. Castle, a nano-analytical chemist and pro-life advocate, declared, “Julia set that world record in a LIFE Runners jersey supported by her 13,857 teammates in 39 nations.” He added that more than 100 fellow Christian LIFE Runners were on hand to cheer her on at Route 66 Marathon events.
In an email, Castle wrote that 35% of LIFE Runners in 50 chapters are age 22 and younger. For example, Baby Gabriella Webb wore a LIFE Runner onesie under her parka during the race.
Race officials squelch free speech
In an extensive interview with LifeSiteNews, Dr. Castle said some race officials objected to LIFE Runners’ use of pro-life messaging on t-shirts, their team booth, and banners. He said Route 66 Marathon executive director Destiny Green told him on the sidelines of the race, “Stay in the confines of your booth.” Dr. Castle said Green gestured to a line in front of the team’s table as the boundary that should not be crossed. When he pointed out that the booths of other teams exceeded their assigned space, Green responded: “But you have an agenda.” He pointed out to her that other teams also had an agenda, which included pushing handicapped people in jogging carts to make them feel part of the race.
In another instance of apparent prejudice, Dr. Castle said a race official called on the LIFE Runners, “Lose the jackets!” in reference to the blue jackets that bear the team logo and messaging.
Other race officials also expressed objections to the LIFE Runners’ pro-life messaging. For example, a race director told Bishop Thomas Paprocki of Springfield, Illinois to remove the LIFE Runners’ “political banner from the start area.” Paprocki refused, telling the official: “We have a First Amendment right to be here with this message.” The race official retorted, “I don’t care if you are a bishop!” Dr. Castle, who was also on hand, responded that they would move only if asked by the local police. No police subsequently asked for the removal of the messaging.
Credit: LIFE RunnersLIFE Runners
Bishop Paprocki ran a half-marathon on Sunday. Forthrightly pro-life, Paprocki issued a statement earlier this year telling Catholic politicians who have affirmed pro-abortion legislation that they should not present themselves for Holy Communion.
There’s a general assumption in public policy discourse that economic policy and social policy are separate universes.
When economic policy is the topic, we think about taxes, government spending, business, jobs, etc. When social policy is the topic, we think about marriage, family, children, abortion, etc.
But, in reality, the line between economic policy and social policy is ambiguous, if it exists at all.
In recent years, for instance, family structure has gotten increasing attention as an important factor to consider in policy discussions about poverty.
Now we have a new academic paper by economists—Maxim Massenkoff and Evan Rose, both doctoral candidates in economics at the University of California, Berkeley—that makes it even clearer that what we generally think of as social policy can fall into the realm of economic analysis.
The paper—”Family Formation and Crime”—examines the connection between the incidence of pregnancy, childbirth, and marriage, and the incidence of crime.
The conclusion, in the words of the authors: “Our event-study analysis indicates that pregnancy triggers sharp declines in crime rivaling any known intervention. For mothers, criminal offending drops precipitously in the first few months of pregnancy, stabilizing at half of pre-pregnancy levels three years after the birth. Men show a smaller, but still important 25 percent decline beginning at the onset of pregnancy, although domestic violence arrests spike for fathers immediately after birth.”
Marriage, according to the authors, “is a stopping point, marking the completion of a roughly 50 percent decline in offending for both men and women.”
The analysis, again per the authors, is “by far the largest such study ever conducted in the United States.” They tapped information on over a million births and, using data in the state of Washington, matched records on “criminal offenses, births, marriages, and divorces.”
George Mason University economist Alex Tabarrok discusses the work on his enormously popular blog Marginal Revolution.
Tabarrok notes his own research on crime deterrence, which shows that in the case of three-strikes laws, the prospect of an additional 20 years to life imprisonment reduced criminal recidivism by 17%. Compared with this, notes Tabarrok, “the effect of pregnancy is astoundingly large.”
Of course, demonstrating statistical correlation and explaining why the occurrences correlate are different things. Why is incidence of pregnancy followed by significant drops in criminal activity in both women and men?
What is it about birth and marriage that contributes significantly to reducing crime?
Tabarrok conjectures it’s about “socializing and civilizing both men and women.”
I would speculate that it is similar to why, when a pregnant woman sees an ultrasound image of the child developing within her, she is less likely to abort that child.
It’s a wake-up call to the awe and mystery of life, which produces a sense of meaning and personal responsibility.
It follows that we ought to be concerned about the decline in Americans’ sense of importance of marriage and children.
In a newly published survey from Pew Research Center, 57% of men and 46% of women said “having a job or career they enjoy” is “essential for a … fulfilling life.”
Compared with this, only 16% of men and 17% of women said marriage is “essential for a … fulfilling life.”
And only 16% of men and 22% of women said children are “essential for a … fulfilling life.”
I love my work and agree that satisfying and meaningful work is rewarding. But I think something is wrong when Americans are saying work is three times more important for a fulfilling life than marriage and children.
The public policy implications of this research showing a drop in crime after pregnancy are not clear. But what is clear is we should be thinking more about how our culture can do a better job conveying the importance of marriage and children.
LifeNews.com Note: Star Parker is the founder and president of the Coalition on Urban Renewal and Education (CURE) and is a leading pro-life advocate within the African-American community.
This is Your Brain on Birth Control, a new book by Dr. Sara E. Hill takes a remarkably deep dive into the myriad ways that hormonal contraception alters women’s bodies, demonstrating that our sex hormones have an enormous impact on how our brains and bodies function. As we learn more about the consequences of altering women’s hormonal balance with contraception, we’ve come to find that those consequences can be very serious, indeed—in some cases, even fatal. Although the book is about the consequences of meddling with the hormones of women of reproductive age, it should also serve as a cautionary tale against male contraception and the risks of fiddling with men’s hormones.
While women’s sex hormones (estrogen and progesterone) tend to get more attention because of their relationship to the monthly cycle and to pregnancy, men’s sex hormones (primarily testosterone), are often something of an afterthought (unless a man is experiencing some form of sexual dysfunction or infertility), mostly because they don’t cycle on a monthly basis as women’s do. But interesting research about men’s changing testosterone levels in response to fatherhood shows that men’s hormones drive their brains and bodies as much as women’s. Testosterone appears to have an impact on who men are the same way that estrogen and progesterone do on women.
For instance, a 2011 study came to the following conclusions:
You read that right: becoming a father is associated with a large drop in a man’s testosterone levels, which from an evolutionary perspective, is thought to promote more caregiving behavior in men, and better long-term family stability.
One has to wonder if continued research will uncover the further impact testosterone has on other behaviors and functions. Testosterone has physical and emotional effects beyond a man’s fertility, much like female sex hormones do in women. The preliminary signs seem to point in that direction, and furthermore, while the results are mixed, some studies have found a correlation between testosterone replacement therapy and increased risk of cardiovascular events like stroke and heart attack, and possibly heightened the risk of prostate cancer, too, as for women using hormonal contraceptives.
If one thing is clear from all of our experimentation with sex hormone tinkering thus far, it’s that it’s difficult—if not impossible—to use them for a single, precise, desired outcome (like pregnancy prevention) and that unintended consequences and side effects will typically abound. That’s why calls for a “male birth control pill” as an answer to women’s woes with the Pill (and other forms of hormonal contraception) thoroughly miss the mark. There should be no doubt that anything that would pump men full of synthetic hormones—as female hormonal contraception does—would just be shifting the same burden over to men, affecting them in ways that we can’t even know about yet. And frankly, in an era with highly effective, side-effect-free Fertility awareness-based Methods (FABMs), it’s simply a burden that’s unnecessary for anyone to bear.
So let’s not make the mistake of believing that men’s sex hormones—and tinkering with them—are any less complicated than are women’s. There’s still so much we don’t know about how our sex hormones work within our bodies, but the preliminary research indicates that they do quite a bit and that messing around with synthetic versions can lead to some pretty serious effects in our brain and bodies. That’s precisely why FABMs have so much to offer men and women: safe, effective family planning, the natural way.
(National Review) The Centers for Disease Control (CDC) has released abortion data for 2016, indicating that the U.S. abortion rate has continued to decline, a trend that began in 1980. Between 2015 and 2016, both the number of abortions and the abortion rate (the number of abortions per 1,000 U.S. women of childbearing age) decreased by about 2 percent. The decline was fairly consistent, as 33 of the 46 states that reported abortion data saw their numbers decline. This is good news for pro-lifers, and for anyone who wants to see the incidence of abortion decrease.
While much of the analysis of new abortion data typically focus on short-term trends, the long-term decline in the U.S. abortion rate is even more impressive. According to the CDC, the abortion rate has fallen by more than 25 percent between 2007 and 2016 among the 47 states that reported abortion data consistently during that timespan (excluding California, Maryland, and New Hampshire, which did not report abortion numbers). The data also indicate that the abortion rate has fallen by approximately 50 percent since 1980. The abortion trends reported by the CDC are similar to those shown by estimates from the Guttmacher Institute, which in September released its estimates for U.S. abortion data for 2017.
Most of the media coverage of declining abortion numbers typically credits increased contraception use. But commentators often overlook a key factor in the long-term abortion-rate decline: the fact that a higher percentage of women with unintended pregnancies carry them to term. Data from Guttmacher show that between 1981 and 2011, the percentage of unintended pregnancies that resulted in abortion fell from approximately 54 percent to 42 percent.
Since the early 1990s, pro-lifers have made gains in public opinion, enacted a higher number of pro-life laws, and established more pregnancy-help centers. The declining abortion numbers and the fact that more unintended pregnancies are being carried to term is nice evidence that these pro-life efforts have been effective. Hopefully, the new CDC data will encourage pro-lifers and inspire them to continue their lifesaving efforts.
Editor’s Note: This article was published at National Review and is reprinted here with permission.
November 29, 2019 (LifeSiteNews) – A couple of years ago, some of you might remember, California state Senator Scott Wiener of San Francisco sparked outrage by putting forward legislation that would reduce knowingly exposing others to HIV from a felony to a misdemeanor. In other words, withholding the information that you are HIV-positive from the partner you are sleeping with has become no longer a felony in California. The same legislation also applied to those who give blood to a blood bank without disclosing that they are HIV-positive. Wiener himself, unsurprisingly, is HIV-positive, and trumpeted the legislation as a way of “reducing stigma” around those who have this condition.
I’m not precisely sure how hiding this very important information from a sexual partner who might contract that condition as a result of this omission does anything to “reduce stigma”—it seems to me that it might do precisely the opposite. But Wiener’s crude little crusade is nothing compared to how ludicrous New Zealand’s attempt to reduce the stigma round HIV is. According to The Telegraph, the Kiwis have “launched the world’s first HIV positive sperm bank in an effort to reduce the stigma round the virus.”
The description of this bizarre new endeavour is — irony alert — sure to have ladies lining up for blocks to take this totally unnecessary risk that does absolutely no good to anybody whatsoever: “Online sperm bank ‘Sperm Positive’ has begun with three HIV positive male donors, who all have an undetectable viral load, meaning the virus cannot be passed on even through unprotected sex. While the amount of the virus in their blood is so low it cannot be detected by standard methods, it does not mean the HIV has been completely cured by the treatment.”
I’m sure you’ll agree — irony alert — that the above description sounds very reassuring.
The cold and brutal reproductive technology industry has already spawned the strange scenario of women poring over profiles as they attempt to select which sperm donor they want to use to conceive their (generally) fatherless children, determined to pick the perfect genetic specimen as their stud. But some activists apparently feel that those same women would be perfectly willing to select sperm from HIV-positive donors just to help “reduce the stigma” of—what, exactly? A condition that can, potentially, lead to the dreaded and fatal AIDS?
Unsurprisingly, Sperm Positive donor Damien Rule-Neal told The Telegraph that he was pleased to participate as “there is a lack of education and understanding in New Zealand about what an undetectable status meant, and that he had experienced stigma about living with HIV in his personal life and his professional life.” In fact, he says, he knows many people with HIV who went on to have children, and The Telegraph noted that “HIV-positive men can father children with minimal risk of transmission to their partner or their baby as long as they have up-to-date advice, support, and HIV medications, even if their virus is detectable.”
And so now there are apparently some people who genuinely thought it was a good idea to start a sperm bank where women who are on the hunt for the seed of HIV-positive men can finally have all their dreams come true.
Most people, I suspect, will read the news of this new endeavour and roll their eyes or shake their heads. Willingly placing other people at risk of becoming HIV-positive in order to “reduce stigma,” even where there is “minimal risk,” is immoral and unconscionable.
But if you listen to Wiener and Rule-Neal, other people—be it partners or in this case, children—must be willing to run a potentially deadly risk in order to “reduce stigma” for others.
The very suggestion of it will probably do precisely the opposite.
November 27, 2019 (LifeSiteNews) – Fertility rates in the United States have been declining for years, and reached a record low in 2018, according to government statistics released Wednesday.
The National Center for Health Statistics announced that 2018 saw 59.1 births for every 1,000 American women of childbearing age, the New York Timesreports, a drop of approximately 15% since 2007.
Birth rates are tied to a number of economic factors, including a country’s ability to replace retiring or dying workers and the size of a future tax base to fund government programs. Rates tend to drop with economic downturns and rise with growth, but the latter hasn’t been the case for the latest U.S. numbers.
“It’s clear that the traditional age-fertility pattern that held for Baby Boomers and Gen X women is shifting,” Brookings Institution senior demographer William Frey told the Times, pointing to evidence that millennial women are waiting until later in life to marry and have children, particularly after obtaining college degrees and finding career success.
“Is it a permanent shift? We just don’t know yet,” said Johns Hopkins University demographer Professor Alison Gemmill. If so, there “might be implications for society at large, say for funding Social Security — but I don’t think we are there yet.”
Others argue the evidence already shows America is in a precarious situation.
The annual rate of births per woman, which for 2018 was 59.1/1000, is known as the general fertility rate. A different metric, the total fertility rate, measures the likely number of children the average woman will have during her lifetime, if current fertility patterns hold.
“For 2018 the [total fertility rate, the number of children an average woman will have] stood at 1.73, according to a Pew study released in May,” Zachary Evans writes at National Review. “This means that women are having fewer than two children on average, below replacement level for the general population.”
“If birth rates continue to decline, and immigration drops off, the impact on the U.S. economy could be significant,” the Population Research Institute warns. “Economists estimate that as much as one third of economic growth is attributable to workers being added to the labor force every year. Low birth rates correspond to aging population. The U.S. is facing a substantial increase in its dependency ratio as the Baby Boomers retire, and working-age adults must replace the productivity thus lost and pay for entitlement programs like Social Security and Medicare.”
While countries like Iceland have grossly celebrated the eradication of individuals with Down syndrome from their society (eugenics as its worst) – we are teaming up to send a new message to our country’s leaders, employers, educators, healthcare providers, future parents and most importantly, individuals with Down syndrome – life for people with Down syndrome matters.
Our life’s passion and work, in different corners of our great country, brought us together with this common moral – “pro-life for all of life.” For the two of us, a future that doesn’t include people with Down syndrome is very personal (Chloe is a self-advocate from Pennsylvania who is one of the fiercest advocates on the planet and Weir is the former President & C.E.O. of the National Down Syndrome Society and a candidate for U.S. Congress).
Today, we are calling on all Members of Congress, regardless of party, to put your differences aside and help us ensure that our society embraces diversity, embraces differing abilities and, most importantly, stands for life, from the very beginning to natural death, by supporting a new bill, the Down Syndrome Discrimination by Abortion Prohibition Act, which places a federal ban on the performance of an abortion because an unborn child has been diagnosed with Down syndrome.
There continues to be a widespread increase in the Down syndrome prenatal screening tests in the United States (and across the world) which is leading to a decrease in the number of babies with Down syndrome. And while these screening tests (called noninvasive prenatal screening tests (NIPT)) are intended to only screen for Down syndrome (not diagnose), the pressure to not seek further testing, and terminate a pregnancy is real. For instance, the most recent stats available to the public estimate that 67% of babies with Down syndrome are terminated in the Unites States, 77% in France, 98% in Denmark and 100% in Iceland.
Chloe Kondrich, who happens to have Down syndrome, is from Pennsylvania and has fought to pass her own bill “Chloe’s Law” which requires support and educational materials to be provided for families after a diagnosis of Down syndrome – a model law that is working itself through state legislatures around the country. Chloe has met the President and Vice President and appeared twice at the United Nations in NYC.
Chloe and her father Kurt speak at events and venues across the country to end this prenatal eugenic movement against Down syndrome, and Weir is setting her sights, with Chloe’s support, on taking their collective message to the United States Congress by representing her home district in Kansas to continue to give a voice to the voiceless. Kansas also happens to be a battle ground state for the pro-life movement, as we seek to advance an amendment next year to reverse the State of Kansas’ recent court decision that found the right to an abortion in the Kansas Constitution. Weir and the Constitutional amendment will find themselves on the same ballot in 2020.
For the two of us, as women, this possibility that our society won’t include people with Down syndrome is unacceptable. We are speaking up and speaking out to help influence generations of women and families that people with Down syndrome matter – and will continue to advocate at the federal and state levels to “Embrace, and not erase” our community. We hope you join us!
LifeNews Note: Sara Hart Weir, (38) a pro-life Republican US Congressional Candidate in Kansas’ Third District, most recently served as the President & C.E.O. of the National Down Syndrome Society (NDSS), the leading human rights organization for all individuals with Down syndrome, inspired by her best friend, Kasey, of over 20 years who happens to have Down syndrome, is hoping to continue her life’s work by giving a voice to the voiceless in Congress.
CHICAGO, Illinois, November 20, 2019 (Operation Rescue) — According to documents and a 911 recording obtained by the Pro-Life Action League, a previously unknown medical emergency at the Near North Planned Parenthood in Chicago, Illinois, has resulted in a medical malpractice case filed by a woman who fell and broke her neck after a medical procedure.
On May 2, 2019, Morgan Castro sued Planned Parenthood Federation of America, Planned Parenthood of Illinois, abortionist Amy Whitaker, and other clinic employees for damages in excess of $50,000 due to serious injuries she suffered during an appointment for insertion of intrauterine contraception (IUC).
Castro reported to the Near North Planned Parenthood on May 24, 2018, for the IUC procedure. Castro’s complaint stated that she was informed by Planned Parenthood workers that after the procedure, she might become dizzy or experience cramping. Castro did in fact become dizzy and informed a Planned Parenthood worker.
Castro was alone and unmonitored when she lost consciousness and fell off a table. A Planned Parenthood employee later discovered her on the floor and called for an ambulance.
Once at Presence St. Joseph’s Hospital, an MRI revealed fractures to two vertebrae in Castro’s neck. Due to her severe injuries, she was transferred to Presence Resurrection Hospital where she was fitted with a Halo brace to stabilize her neck.
Planned Parenthood has been accused of negligence for failing to monitor Castro, failing to recognize and treat her dizziness, and failing to prevent her from falling off the table.
Operation Rescue has documented 19 medical emergencies at the Near North Planned Parenthood, with the help of the Pro-Life Action League.
“Planned Parenthood loves to tell everyone what great healthcare they provide and how caring they are — ‘no matter what.’ But that is just public relations spin. In truth, they should change their motto to ‘Negligence — no matter what,'” said Operation Rescue President Troy Newman. “If the general public knew all we have learned about Planned Parenthood through our research monitoring life-threatening abortion facility medical emergencies, failed inspection reports, and heartbreaking malpractice/wrongful death suits, Planned Parenthood would have no customers left!”
Editor’s note: More than once at Natural Womanhood, we have received emails from parents whose daughters have tragically died as a result of her birth control. A few months ago, we received a different kind of note—one from a woman who had a close call and was able to share her story with us. Cheyenne, whose name has been changed, found Natural Womanhood in a search for help when experiencing birth control side effects; it’s that Google search that led to a Natural Womanhood article on copper IUDs, which she credits with saving her life.“Thank you so much for your article. I had a close encounter with death just this afternoon.” Cheyenne then shared her story. She ended her note with these words: “Thank you for your website, which saved my life. I’m forever grateful.”
Here is Cheyenne’s story.
All I can say in a nutshell about life: You do not know what life is until death comes knocking at your door.
Back in my home country of Malaysia, I used to work in the TV and advertising industry. But now living in South Africa I cannot work because of my Visa, even though I am married to a South African. I travel to Malaysia every two years to renew my Visa.
I have been married for three years. Because of our financial situation, it’s not the right time for us to have kids. So I am a full-time homemaker. I manage my vegetable garden and I am a mommy to my fur-baby, my dog.
When it comes to family planning, I cannot use the Pill; I can’t use the implant; nothing works. The Pill gives me spotting every day, and that’s terrible. I’ve tried everything. Once a doctor recommended a hysterectomy to me due to my endometriosis. Everything here is “Can’t deal with it? Remove it.”
I decided to get the IUD on my next trip to Malaysia because it is more affordable there.
I thought this would be like any other procedure because I had used the IUD before. Due to my endometriosis, my threshold of pain is extremely high so the initial pain is nothing to me. It was about 4:30 p.m. and I was walking to a mall 20-30 minutes away. While walking I noticed that I was experiencing something that was not quite right—light-headed, nauseous, and imbalanced. Of course, I had cramps, and that could be from the procedure, but other symptoms were not quite right.
I thought I probably was just tired and needed to rest, so I went into town and dinner with a friend. I left the restaurant with a huge migraine, which I have never had in my life. It was mostly on the right side of my face, around my eyes, but my whole face was painful. I didn’t know what was going on. The cramping pain was elevated. Back home after dinner, I vomited. Then I came down with a fever.
Still, I thought I could sleep it off. I told my husband by phone, took two panadol (Acetaminophen), and dozed off.
Dizziness and the IUD
When I woke up in the morning, within a half-hour all the symptoms had come back in double force. I was extremely imbalanced, and now dizzy, light-headed, and breathless.
I went to eat breakfast with my friend, and I told her I wasn’t feeling well. I needed to run an errand in town but was really, really feeling off. The symptoms started to escalate. I started having palpitations, shortness of breath, brain fogginess, extreme hunger, nauseousness, and slight weakness in my legs.
While waiting for my friend in the car, I did a quick research on copper toxicity and it was only Natural Womanhood’s website that described my symptoms.
My friend took me straight to the gynecologist. She was busy with patients, so the nurses said the doctor would call me back.
My friend took me back home, and that’s when things got scarier. When I was going up the stairs, I almost blacked out; I grabbed hold of the railing and my body felt intoxicated. I had to use all my strength to hold onto the railing and get up the stairs to my water bottle.
That’s when I knew something wasn’t right, and it was the IUD. The doctor called me back, and my friend rushed me there. I struggled to walk because my legs were extremely weak. I noted that I had lost my balance. And while I was explaining the symptoms to the doctor, I noted that I started slurring and was leaning to one side.
My doctor agreed with my assessment that we should remove the IUD. By the time she removed it and I went back home, my symptoms were reduced by 80 percent. By the next morning, I was 100 percent better.
Dangerous but hidden birth control symptoms
If I had never made it—if I collapsed in the house, no one would have known the cause, what had happened, even if an ambulance came. Who would ever figure out it would be an IUD?
When I Googled “copper toxicity,” I found a generalized article that did not actually state my symptoms. It suggested that what I was experiencing can’t happen, or that it always differs for individuals. But after I did more research on it, I came across the same symptoms I was experiencing, in a Natural Womanhood article.
I believe it was God who sent me to the Natural Womanhood article. When I Googled copper toxicity, it came up on the first page, in the third spot. In the article, I read further and it made a lot of sense on how the biochemistry, and the IUD, and your body all work together. I really respect the author for writing it because I really want to know the details of why I’m experiencing what I’m experiencing. It was written with a lot of heart and patience and understanding and time.
I want to pass my thanks to the author for writing it and to Natural Womanhood for publishing it. I am happy to share my story in hopes it will save someone else’s life.
Over the last two years, I noticed my Facebook and Instagram feeds filling with ads urging me to donate my eggs or to become a surrogate. At first I laughed it off. But the more ads I saw, the more concerned and uncomfortable I felt. So, I started a small experiment. Every time I saw an ad from a fertility company, I took a screenshot.
Here are just some of the results, from over thirty unique ads replayed numerous times:
It troubled me that women were portrayed as Easter Bunnies; that their ovaries were compared to egg cartons; and that the donors, especially Asian women, were fetishized as exotic, smart, sexy finds, ideal for making a baby. These fertility companies ask young women like me to make a choice―somehow simultaneously altruistic and lucrative―either to sell their eggs for up to $10,000 per ovulatory cycle, or to serve as a surrogate for a couple who just wants a child of their own (for upwards of $75,000). For a college student on a tight budget, or a low-income mother trying to make ends meet, that’s a tempting offer. And I fear that the monetary compensation obfuscates the fact that this system inherently exploits women’s and children’s bodies.
It troubled me that women were portrayed as Easter Bunnies; that their ovaries were compared to egg cartons; and that the donors, especially Asian women, were fetishized as exotic, smart, sexy finds, ideal for making a baby.
A Dangerous Industry
The fertility industry targets and exploits low-income populations: wealthy companies and the powerful elite offer to pay for eggs and wombs from poor women. India, Nepal, and Thailand have recently banned commercial surrogacy because of its predatory nature. Prior to the bans, many women signed contracts with foreigners without knowing the consequences―like facing dangerous Caesarean sections—and with no guarantee of receiving postpartum care.
The fertility industry targets and exploits low-income populations: wealthy companies and the powerful elite offer to pay for eggs and wombs from poor women.
In Jennifer Lahl’s documentary Eggsploitation, women recount the devastating medical problems that they experienced as a result of donating their eggs, including Ovarian Hyper Stimulation Syndrome; puncture, torsion, or loss of their ovaries; infertility; strokes; and reproductive cancers.
Surrogacy can have even worse consequences. Some surrogateshave died in childbirth or sufferedseverecomplications from pregnancy. Women that participated in both egg donation and surrogacy told Jennifer how no one informed them of the risks. When many women faced catastrophic health issues, their doctors ignored them, and fertility agencies did nothing to cover the costs of their massive medical bills. Because of their desire to help others, many of these women lost the ability to have their own children, and paid far more than they had bargained.
The European Union has also banned commercial surrogacy, declaring the practice “reproductive exploitation,” which “undermines the human dignity of the woman, since her body and its reproductive functions are used as a commodity.” However, in the United States, the practice continues, because there the desires of wealthy and privileged adults currently trump the rights of poor women and vulnerable children.
The truth is that no one has the right to a child, and that the bodies of women and children should never be treated as commodities.
Who’s the Parent?
In even the most routine of surrogate pregnancies or donor conceptions, a child can have as many as six parents: the genetic father, the genetic mother, the surrogate mother, her spouse, and the intended parents.
Unfortunately, the state views parents as legally interchangeable. In California, a new law went into effect last year that requires birth certificates to list only the intended parents as the “natural parents.” Biological and surrogate parents will no longer be listed. The stamp of parentage is now arbitrarily decided by a contract that names each individual as parent, partner, surrogate, or donor.
Consider the case of Melissa Cook, a surrogate mother of triplets from Orange County. The intended father, Shannon Moore, a deaf single man living in his parents’ basement, urged Melissa to abort one of the triplets since he couldn’t pay the extra cost of another baby. Melissa refused and did not charge Shannon any money after the births of the children. She only wanted these babies to have a good, loving home.
Months after the triplets’ placement with Shannon, Melissa was horrified to learn that the intended father had a history of killing pets, lives with unstable family members, left the infants alone for hours, forced them to eat off the dirty floor of the basement, and changed their diapers so infrequently that the baby boys suffered severe rashes and had to be taken to the hospital. Shannon’s sister even contacted social workers begging them to take the triplets, saying that her brother was “unable to care for the children.” Heartbroken, Melissa sued for custody to protect the boys from abuse and neglect. Because surrogates are considered legal strangers to the children they carry, her request was denied. To this day, Shannon retains exclusive custody of the triplets as both their legal and “natural” parent.
The Rights of the Child
According to the UN Convention on the Rights of the Child, a child has the right “to know and be cared for by his or her parents,” to “preserve his or her identity,” including “family relations,” and not to be separated from parents against his will. In case a separation becomes necessary, the child has the right to “maintain personal relations and direct contact with both parents on a regular basis.”
Americans are generally very aware that adopted children suffer from being separated from their natural parents. For proper psychosocial development, children need to form attachments with their biological parents, siblings, and extended family. They need to know their heritage and identity. Adoptive families and agencies show immense sensitivity to adopted children’s needs and work hard to remedy the trauma of adoption. Many of them practice open adoption, preserve records, identify the child’s cultural roots, and incorporate traditions from the child’s birth culture into family life. And yet, at the same time, our society sanctions the creation of children for the express purpose of separating them from their biological family. The desire to create a family and to love a child is good and noble. But it is neither noble nor loving to create a child so that it can suffer separation and loss.
Gestational surrogates also bond with the children whom they carry throughout the nine months of pregnancy, as they feed, shelter, nurture, love, and protect them. But the attachment is severed at birth. Research shows that children who are carried by gestational surrogates are more likely than the general population to experience depression. The surrogate mothers also face severe emotional experiences. This correlation suggests that, even though the child and mother lack biological ties to each other, they still feel a loss when they are separated. Thus society creates these children in order to make them suffer twice over: from being separated not only from their genetic parents but also from the women who carry them.
Lost Identity
The first generations of children who were conceived by donors and borne by surrogates are now adults, and many are searching for themselves. Message boards like the Donor Sibling Registry allow young people to find half-siblings and relatives whom they never knew to exist. The community that these platforms help to create is growing, but not all the members’ stories end happily. One young woman, Kathleen LaBounty from Texas, discovered that she had been conceived by a sperm donor who was a Texas A&M medical student. She contacted every man who had attended the school during the years prior to her conception. Although she heard from hundreds of men, she still did not discover her father. In an open letter, Kathleen describes feeling “empty and extremely cheated out of important aspects of life.” She desperately wants to find out if her “interests, appearance, life views, and personality” match those of her biological father.
Scores more children have written on the site Them Before Us to share their stories of longing and loss. One daughter reflected soberly about her traditional surrogate mother (that is, who conceived the child by her own ovum and artificial insemination): “When you know that a huge part of the reason that you came into the world is due solely to a paycheck, and that after [the payment is received] you are disposable, given away and never thought of again, it impacts how you view yourself.” Just as surrogates are treated as wombs for rent, surrogacy turns children into a commodity to be bought and sold.
Women and Children Should Not Be for Sale
Surrogacy and donor-conception are frequently in the news as more and more celebrities pay for these services. Missing from the Instagram posts and tabloids are the stories of the other family members that are affected by these actions. What do donor-conceived and surrogate-born children think of their conception and family history? What about the surrogate mothers and donor parents? Lost in the legal and financial drama are the rights of children to know their biological parents and the rights of women to receive full information about the risks of these procedures.
The truth is that no one has the right to a child and that the bodies of women and children should never be treated as commodities. Just because we can do something does not make it right. And in the case of reproductive technology, the least society can do is to protect the right of children to know who they are and to protect the right of women not to be exploited.
Natural family planning (NFP) needs a slogan, because as a “product” — if I might adopt business-speak — it’s not selling too well. According to some surveys, about 90 percent of professed Catholics reject the Church’s teaching on birth control. Even among priests, fewer than one in three considers artificial contraception to be “always” sinful.
So let me propose a new rallying cry: “Use NFP: It Doesn’t Work!”
You think I jest.
The case for NFP should, by rights, be the case for more babies. To have them is good. Not to have them is to be deprived. Every wife deserves to be a mother, and every mother’s son deserves a brother and a sister. And since a cat-o’-nine-tails has nine tails, surely having nine children is the proper way to scourge selfishness right out of one’s family.
As a slogan, “Use NFP: It Doesn’t Work!” has many strong arguments in its favor. First, it is true. NFP proponents tout its 99 percent effectiveness rate, but they neglect to mention that this is true only if the husband is in the Navy and assigned to extended, uninterrupted sea duty of three-year tours or longer. Otherwise, for most Catholics I know, NFP means a baby every two years or so, though the rate can slow with age, as the couples learn a proper respect — that is, fear — for each other and are too tired in any event for what Catholics call “the conjugal act.”
Now I know there will be inevitable protests and testimonials by those who swear by NFP. And who am I to say that my own experience is not colored by the fact that I am excessively virile? Indeed, there is plenty of evidence that this is the case.
But another reason for NFP’s allegedly high success rate is that couples who use it are prepared to welcome children and so don’t blame NFP for unexpected pregnancies. Four of my own five children came the NFP way — that is, totally unexpectedly — and that’s a good thing, because without them bouncing in as surprises, excuses to delay (the sort of excuses one might hear from a recruit in parachute training) might have gone on for a very long time. As it is, in a mere matter of ten years, my wife and I assembled a complete basketball team. And if menopause doesn’t strike my wife soon, who knows what sort of team we might assemble.
Rather than bite one’s nails to the quick at the prospect of baby number ten — which, if one marries in one’s early 20s and practices NFP, is a definite possibility — we should encourage the attitude of the more the merrier, which is a far more attractive case to make than all the goo-goo language about how NFP helps couples “communicate” and about the joy of charting temperatures and discharges and plotting one’s conjugal acts as a captain might chart a course for his ship.
Frankly, as far as I’m concerned, the charts can be thrown away (what’s so “natural” about them?). And to hell with improving “communication” as a dogmatic defense of NFP. For men, the whole point of marriage is to avoid communicating; all that dating conversation stuff can finally be foregone. Married communication, as successful husbands know, is best limited to grunts and hand signals — one upraised finger meaning, “I need a beer”; two upraised fingers meaning, “You need to change the brat’s diapers”; three upraised fingers meaning, “Honey, why don’t you mow the lawn while I watch football?,” and so on. No words are more doom-laden than a wife’s sitting down and saying, “Let’s talk.” Communication is, of course, the first step toward divorce.
Tom Hoopes pointed out in the November 2004 issue of crisis that there are no apparent data to support the widely touted statistic that only 2 percent of NFP couples divorce. If there is any validity to this number, I suspect it lies in the fact that NFP couples have no time to communicate. The husband has to hold down several jobs to pay the family’s bills, and a wife with little ones barely has time to shower, let alone talk to her husband, save to pass a pregnancy test result across the breakfast table through splodges of spilled porridge as she sighs, & 2000 #8220;Here’s another fine mess you’ve gotten me into.”
I grant you, there is one form of communication that NFP certainly does advance — it makes a public statement. Not so very long ago, I was invited to speak at a Confederate Memorial Service. There I was with my Robert E. Lee tie, my wife (a blond California beach babe) wearing a Confederate battle flag scarf, and the five little members of our own Critter Company lined up in a row. A friendly chap meandered over and told us, apropos of nothing, “My daughter’s a Catholic, too. Three kids.”
No need for a secret handshake. Kids tell the story.
As a slogan, “Use NFP: It Doesn’t Work!” puts the focus where it belongs — on babies — and away from a technique, a technique that wrongly strikes most lay Catholics as medieval. If only it were medieval, then it would be effective: a sturdy, padlocked, handsomely designed, pewter chastity belt.
Instead, NFP is shiny, modern, and scientific, as its advocates are always quick to emphasize. In his book The Truth of Catholicism, George Weigel approvingly quotes several paragraphs from a woman in love with NFP. She reminds us that:
Natural Family Planning is not the justly ridiculed rhythm method, which involves vaguely guessing when the woman expects to ovulate and abstaining for a few days around day fourteen of her cycle. The full method involves charting a woman’s waking temperatures, changes in cervical fluid, and the position of the cervix.
Nothing unnatural or artificial about that, is there? Her raptures climax with NFP apparently transformed into “Narcissism For Pleasure”:
But the turning point came for me as I watched, month after month, as my temperature rose and fell and my hormones marched in perfect harmony. I had no idea I was so beautiful. I found myself near tears one day looking at my chart and thinking, “Truly, I am fearfully and wonderfully made.” My fertility is not a disease to be treated. It is a wonderful gift. I am a wonderful gift.
Er, if you say so, missy. If my wife talked like this, I’d have her committed. Happily, my wife, bless her heart, takes a more robust line: “Barefoot and pregnant is better than high-heeled and professional!” That’s the spirit!
There is no shortage of people wandering around these days thinking they are wonderful gifts. In fact, there are rather too many of them — and they shouldn’t be encouraged. What’s lacking are married couples who think that having a family big enough to fill up a minivan (or for the younger, stronger, and more ambitious, a small bus or modified hearse) is a wonderful gift.
A neighboring priest has noted how many young married women these days are without children but doting over dogs. One suspects that such women are less in need of NFP training than they are of a push into motherhood (and thereby full-fledged adulthood) with a reminder that children are what marriage and life are all about.
So rather than focusing on NFP, premarital preparation should go like this:
Father O’Counselor: “Now I want you two to understand that the primary and fundamental purpose of marriage is not companionship, not romantic love, not moonlit strolls on the beach, or any other balderdash but the begetting and raising of children — lots of ’em, and starting soon. The optimum number is enough so that you can lose a few at the grocery store and not notice. That’s giving without counting the cost, and at that point, you won’t care anyway. As a priest, my sacrifice for the good of the Church is celibacy. As a married couple, yours is to propagate children — who will incidentally annually propagate fierce storms of influenza in your house. If you haven’t already studied up on communicable diseases and basic first aid for children jumping off sofas, I’d do it now. But you will find children and their challenges to be the great tutor of not only the medical but the moral virtues.”
Potential Husband: “You mean, I’m screwed?”
Father O’Counselor: “In a manner of speaking, yes.”
Potential Husband: “Is it too late to enroll in the seminary?”
We can thus improve Catholic marriages and alleviate the priest shortage at the same time.
In fact, we forget how inspiring parents’ confessions are to priests:
Penitent: “Forgive me, Father, but I lost patience when my children used my wedding china as Frisbees, took my necklace and used it as a line and fishhook in the toilet, and took my toothpaste to give the cat a bath.”
Priest (sotto voce): “Thank God I’m celibate.”
Penitent: “What did you say, Father?”
Priest: “I mean to say, why not just laugh about it? These years will pass all too quickly. And when they’re over, you’ll know why you have gray hair and high blood pressure. Now, a Hail Mary and an Act of Contrition, if you please.”
So, let us step out boldly and fly the banner high. Say it proudly — “Use NFP: It Doesn’t Work!” But babies sure as heck do.
In the book, Women, Sex, & the Church, contributing writer Angela Franks observed that “the contraceptive mindset cannot avoid scapegoating women’s bodies as the cause of both personal and societal problems.” Franks cited birth control crusader and Planned Parenthood founder Margaret Sanger’s firm belief that tyranny, war, and famine were ultimately caused by women because of their failure to use birth control.
Franks notes that modern society tells modern women and girls that they “need to turn against their bodies in order to be liberated,” disavowing their fertility with pills, patches, shots, and so on. Anticipating that these cultural attitudes may not seem to impact the average individual woman, Franks queries,” how many women do you know who seem at home in their bodies?”
In contrast to the women’s-bodies-are-the-problem attitude, the “natural” in fertility awareness-based methods of natural family planning refers to what mirrors the dignity of the human person. Rather than reducing women to sex objects, FABMs view women’s fertility as an integral part of their whole persons. Furthermore, a woman’s fertility is a physical reflection of her innate and unique ability to nurture others, whether by physically bearing children or by emotionally nurturing others.
Children Aren’t the Problem
In the contraceptive mindset, an unplanned pregnancy is the ultimate “method failure.” Society seems to have forgotten that conceiving a baby from sex during the fertile part of the cycle is actually a sign of health. But because contraception promises baby-free sex without regard to the woman’s cycle, the logical implication is that babies are a problem to be avoided at all costs.
This mindset leads to an implicit “need” for abortion when contraception fails, as noted in the 1992 Planned Parenthood vs. Casey Supreme Court case ruling that the “Roe rule’s limitation on state power could not be repudiated without serious inequity to people who, for two decades of economic and social developments, have organized intimate relationships and made choices that define their views of themselves and their places in society, in reliance on the availability of abortion in the event that contraception should fail.”
On the other hand, FABMs understand children to be human persons with worth and dignity. In fact, children invite their parents in a unique way to a new level of personal growth in selflessness. Women, Sex, and the Church contributor Jennifer Roback Morse wrote about the birth of her first child, “I experienced for the first time the genuine neediness of another person. I had to bend my schedule and my life to her, as did my husband. This newfound ability to give of ourselves, while often painfully won (colic and all), was the most important growth that we experienced in our lives. It was also the single best thing that ever happened to our marriage. We experienced what is true for every human being: self-gift, while difficult, makes us flourish.”
Rather than forcing the woman to bear the responsibility of pregnancy achievement or avoidance alone, FABMs involves a woman and her partner having a monthly conversation about their intention to avoid or achieve pregnancy and then working cooperatively with the woman’s cycle in light of their goal. When couples using FABMs do get pregnant, the understanding that parenthood is a shared responsibility is already in place. In this way, FABMs promote a positive environment for children to enter into.
A twist on the old joke, “a ___ walks into a bar” might be “a girl walks into an OB office” followed by the predictable punchline “and walks out with a prescription for birth control.” Hormonal birth control, whether via the Pill, the Patch, or other hormonal medications, is routinely prescribed to teenage girls for everything from acne to heavy bleeding to irregular periods to pregnancy prevention. No matter what’s wrong, birth control seems to be the answer. But is it? What’s the cost of putting young women still going through adolescence on hormones for potentially years on end?
Hormonal birth control is a Band-Aid
Everyone seems to know someone who went on the Pill for heavy bleeding as a teen, typically without much investigation into the cause. A 2015 bulletin by the American College of Obstetricians and Gynecologists called “Menstruation in Girls and Adolescents: Using the Menstrual Cycle as a Vital Sign” showed a graphic of no less than 14 different issues, some very serious, that abnormally heavy bleeding could indicate. Birth control represents a band-aid for a symptom without addressing, let alone fixing, what’s wrong. In fact, hormonal birth control represents a band-aid approach in many cases, as it only takes away the symptoms of irregular periods or painful periods, etc.
Source: ACOG.org
Lizzy, a 31 year old from Illinois, told Live Action News that she was placed on prescription pain medication as a teen for extremely painful periods, and then the Pill at age 21. Even though her pain persisted despite the medicine and the Pill, she was always told that “everything’s fine.” Only after she was married and unable to conceive did she learn that her infertility was due to Stage III endometriosis, a growth of uterine tissue outside the uterine cavity on other abdominal organs that can cause excruciating pain.
Hormonal Birth Control Creates New Problems
Just last month, CNN.com reported on a new study in the medical journal JAMA Psychiatry that found an increase in crying, sleeping, feeling worthless, suicidal thoughts, and other symptoms of depression amongst teens who went on birth control compared with non users. The connection between birth control use and depression is nothing new, and in fact a 2016 study from Denmark found that teen girls placed on hormonal patches, coils, and rings were at even higher risk for depression than those placed on the Pill. This latest research confirms that teenage girls are hardest hit by depressive symptoms amongst new birth control users, even when researchers controlled for other potentially confounding factors like ethnicity and socioeconomic status.
Depression isn’t the only problem that the Pill and other methods of hormonal birth control can create. Both birth control pills and the Depo-Provera synthetic progesterone shot have been found to decrease bone density in teen girls and young women, a particularly concerning finding given that bone density growth should be most significant amongst this population. This can translate into higher osteoporosis risk later on in life.
Another major side effect of birth control use in teenagers is the increased risk of blood clots, which can be life-threatening and even fatal. Live Action News recently reported that an Alabama teen’s family was awarded $9 million after their daughter died due to a blood clot caused by her birth control. In that case, taking a thorough family medical history before giving the girl birth control could likely have saved her life, as her own mother had a history of blood clots. Live Action News also recently reported on a Tennessee girl who nearly died due to a blood clot in her lungs caused by her birth control. Yet another story from 2019 is of an Irish girl whose birth control caused a blood clot in her legs that broke off and traveled to her lung. She, too, almost died.
Live Action News has previously reported on the benefits of teaching teen girls to track their menstrual cycles. The 2015 ACOG bulletin mentioned above specifically addressed how the menstrual cycle can be a fifth vital sign in girls and adolescents. According to the bulletin, “Just as abnormal blood pressure, heart rate, or respiratory rate may be key to diagnosing potentially serious health conditions, identification of abnormal menstrual patterns in adolescence may improve early identification of potential health concerns for adulthood.” This is because the menstrual cycle is an indicator of overall health in the young woman’s body. Certain patterns in menstrual cycle charting can prompt trained clinicians to suspect hormonal abnormalities, which can have a whole host of effects on various body systems.
What’s more, as Leslie Carol Botha found out in the late 1980s, teaching girls to chart their cycle can truly be life-changing. Botha worked with young women in restorative care homes, whose typical profile included a history of sexual assault, running away from home while still a minor, drug and/or alcohol use, and jail time. She found, according to the Natural Womanhood article on her work, that “these young women hadn’t been equipped with an understanding of the hormonal shifts in their cycles and how these changes were driving their moods and behaviors.” Astonishingly, she found that of the girls who had gone to jail, some 90% of them had been in the premenstrual phase of their cycle at the time of their criminal behavior. Within just three months of learning to chart their cycles, she found that they began to take control over their own lives, understanding when to expect the “rabbit hole” of premenstrual symptoms to begin… and when it would end.
In fact, research done on the TeenStar program that incorporates menstrual cycle charting in teaching teens self-awareness and responsible decision making found that “this program is effective in reducing the rate of pregnancy, delaying the onset of sexual activity, decreasing sexual activity in sexually-active youth, and improving attitudes towards abstinence, compared with students in the no-treatment groups.”
With benefits like these, and the risks of hormonal birth control on the other hand, what’s not to love?
A Texas court has stepped in to stop a Fort Worth hospital from pulling the plug on a 9-month-old baby without her mother’s consent.
Cook Children’s Fort Worth was slated to pull the plug on 9-month-old Tinslee Lewis against her mother’s will on Sunday. But pro-life advocates helped Tinslee’s mother fight for her in court.
Baby Tinslee is a 9-month-old girl with congenital heart disease and is breathing with the assistance of a ventilator. She is sedated but conscious. Cook Children’s Fort Worth Hospital informed Tinslee’s mother, Trinity, on October 31 that they would pull the plug on her daughter against her directive in 10 days, scheduling her to die on Sunday.
According to Texas Right to Life, the hospital committee cited no physical health reason for their decision to seize Tinslee’s ventilator against her mother’s will but instead cited their own “quality of life” judgments.
Baby Tinslee’s mother was in a race against the clock this weekend to save her daughter. Texas Right to Life provided a lawyer to defend the patient after the family contacted us for help, but the Texas 10-Day Rule legally allows this form of euthanasia.
The 10-Day Rule is a provision in the Texas Advance Directives Act (Chapter 166.046 of the Texas Health & Safety Code) that allows a hospital ethics committee to withdraw basic life-sustaining care, like a ventilator or dialysis, from a patient against his expressed will, his advance directive, or the instruction of his surrogate decision-maker. Ten days after informing the patient or surrogate of the committee’s decision, the hospital can remove basic life-sustaining care from a patient.
Committees can withdraw care for any reason and the patient cannot appeal the decision. Even if the patient is conscious, coherent, and actively requests to stay alive, the 10-Day-Rule allows the hospital to overrule the patient’s will.
Thankfully, a court has stepped in to grant Tinslee and her mother more time.
The controversial 10-day rule essentially allows hospitals to euthanize patients after a 10-day notification. Attorney Wesley Smith, a noted writer and author on end of life issues, testified in favor of the legislation. During his testimony he broke down the problems with the 10-day rule:
In Texas, patient autonomy is essentially a one-way street. Here, if a doctor disagrees with the patient’s decision to maintain life—and the patient or family refuses to permit the life-extending treatment to be withdrawn—the doctor can take the controversy to the hospital bioethics committee for a quasi-judicial hearing and binding ultimate ruling.
If the committee agrees with the doctor, the patient or family has only 10-days within which to find an alternative source of treatment and arrange a transfer. If they can’t, the life-extending treatment can be terminated over the patient or surrogate’s objection—meaning the patient will be forced into a death at a time when life could have been maintained.
To fully comprehend the unjust nature of Texas law in this regard, realize that these “futile care” or “inappropriate care” decisions do not terminate treatment because it won’t work, but because it does. It is keeping the patient alive when the doctor/bioethics committee thinks the patient should die.
This isn’t an objective medical determination, but a subjective value judgment. And given the subjective nature of such decision making—which involves the question of whether the among of suffering the intervention may cause outweighs the desire to maintain life—the law should give the ultimate power to decide such questions to patients, families, and duly appointed surrogates who know the patient most intimately, not to bioethics committee members who are strangers to the patient.
MADRID, November 12, 2019 (LifeSiteNews) – Guinean Cardinal Robert Sarah strongly criticized LGBT ideology that he said is overrunning governments and education centers while tracing the ideology to the root of the widespread acceptance of contraception about seven decades ago.
“The destructuring of sexual identity, which is often called ‘gender theory,’ against which Pope Francis has harsh words and an attitude of absolute intolerance, can be understood as the anthropological consequence of a practical mutation,” said Cardinal Sarah, the Vatican’s Prefect of the Congregation for Divine Worship and Discipline, at a Nov. 7 conference at Madrid’s San Pablo University in advance of the 21st Congress of Catholics and Public Life of Spain. His talk was titled “The importance of education in the Church’s mission today.”
Gender theory holds that male or female sexual organs do not determine an individual’s “sexual identity” but a person’s inner sense of being a man, a woman, or whatever it is that a person wants to identify as (dozens of ‘gender options’ have been invented to help people identify how they feel about themselves). The theory holds, for instance, that a person born with a male organ of reproduction can choose to identify as “female” and that it’s discriminatory not to support the individual’s choice, including the male’s choice to use female pronouns. The theory also holds that a person’s “gender identity” is fluid and can change over time.
“The first link in the process involved women,” Cardinal Sarah continued: “In fact, the contraceptive mentality that has extended strongly after 1950 has made possible a profound disconnection between the woman and her body, a disconnection that has radically changed the way of understanding human sexuality, marriage, filiation and of course education.”
The Catholic Church reaffirmed its condemnation of contraception in the 1968 Encyclical Humanae Vitae. Pope Paul VI prophetically warned that widespread acceptance of contraception would lead to the “general lowering of moral standards” among other things.
The Cardinal credited French writer Simone de Beauvoir’s phrase “You are not born a woman, you become a woman” as summarizing the essence of gender theory.
“Let’s add that for de Beauvoir, the family, Marriage and motherhood are the source of female ‘oppression’ and dependence. The pill would have ‘freed’ women by giving them ‘control of their body’ and the possibility of ‘freely disposing’ of it. Under the feminist motto ‘my body belongs to me’ a deep alienation of the incarnated subject is actually hidden. In fact, behind this ‘freedom’ statement lies an instrumentalization of the body itself as a material available to the most indeterminate desires,” he said.
The Cardinal then showed the link between contraception and the distancing of a person from his or her male or female body.
“The contraceptive mentality has engendered a dualism between individual freedom seen as unlimited and almighty, on the one hand, and the body as an instrument of enjoyment, on the other. In that perspective, the sexed body can no longer be lived as a sign and instrument of the gift of self, whose purpose is the communion of the spouses. The intrinsic link between the two meanings of the conjugal act, the procreative dimension and the unitive dimension, is broken. This link becomes optional, and logically, sexuality ends up being considered only in its relational and pleasure-producing dimension. The destabilizing effects of such a mentality have not been long in coming,” he added.
The Cardinal noted that one of the major destabilizing effects of the contraceptive mentality was the “social legitimization of homosexuality.”
“In fact, if sexuality is no longer perceived in the light of the gift of life, how can homosexuality be considered a perversion, an objective and serious disorder?” he said.
Cardinal Sarah said logically accompanying these changes regarding sexuality was a “redefinition of sexual identity, considering it as purely constructed.”
“If the intrinsic link between the two meanings of the conjugal act is denied, the difference between the sexes loses the first foundation of their intelligibility.” From then on, he said, the “sexed body” can more and more be considered as a “material that individual consciousness can model to its liking.”
The Cardinal then explained the mechanism at work as “sexual minorities” publicly demand equality and freedom to live according to their perceived identities.
“In the name of the fight against the ‘discrimination’ of which the ‘sexual minorities’ would be victims, the agents of the anthropological subversion take the public authorities and the legislator hostage in their revindications. In the name of ‘equality’ and ‘freedom’, they demand that all social discourse, especially in schools and the media, be ‘respectful’ with the sexual indeterminacy of individuals and the free choice of their identity,” he said.
“Then, each one can affirm that it is by self-designation and proclaim: ‘I make my own choice. I am proud of it and I affirm myself in that choice. I do not admit that another or society tell me what I am. I do not receive my being and my existence from anyone but myself. I decide for myself who I am. Society must assume my choice and adapt to my orientation changes.’”
For the LGBT movement, the Cardinal pointed out, the battle is no longer about “claiming tolerance” but about “imposing a new conception of the human being” and creating a “new” human being.
“Under the guise of freedom, this deconstruction at the service of a radical constructivism can be compared with the totalitarian attempts to produce a ‘new man,’” he said.
“Its innocent victims are mainly children, whose parents, permeable to libertarian slogans and bewitched by contemporary sirens, do not support [authentic] human growth and the formation of their [genuine] sexual affectivity. All this presupposes an erroneous conception of freedom, understood as the fact of not being prevented from following your immediate desires. How far we are from true freedom, which is the realization of the person when he uses his free will to seek the truth and choose his true good,” he continued.
“The anthropological revolution violently disrupts intellectual and moral education, because it creates mental and social dispositions that separate people from themselves,” he added.
The Cardinal said that Catholics should be aware of the gravity of the crisis, “given the atheist atmosphere or of indifference to religious or moral issues which permeate education and school structures.” What should be understood is that the goal of education is for students to “acquire the virtues that permit them to unfold and structure their humanity and personality in accord with the truth that is intrinsic to them.”
He called for the Church to become more active in defending the truth about man in sectors of civil society where that truth has been abandoned, especially in education.
“As has been the case several times in history, the Church has a duty to assume a substitute role to compensate for the collapse of entire sectors of civil society and public authorities,” he said.
“The Church assumes this function of substitution through all its children who are present in this magnificent educational task,” he added.
‘Dirty and unhealthy’ environment destroys children
Following his presentation, Cardinal Sarah answered questions from participants who are concerned about secular influences upon their children.
Likening schools to aquariums where fish are regularly fed fresh food, he said, “But the water in the aquarium is dirty and unhealthy.” Despite the good food, he said, the fish are slowly poisoned and eventually perish. In the learning environment, “even while there are well-disposed students and dedicated teachers, there are substances in the environment that are toxic to the students mental health,” said the Cardinal.
When he was asked how the water in the aquarium could be made clean, he said, “What poisons the environment are dangerous ideologies,” citing “marxism” and “transhumanism.”
He continued, “If we cannot explain who is man, who it is that God wants him to be, logically the aquarium is contaminated.” The water can be cleansed by rediscovering, he said, “the identity of human beings created in the image and likeness of God.”
“Identity is not something we give,” he said, “God gives it to us.” The West, he said, arrogantly “refuses to accept” that identity.” “The great issue are the economic and media leaders who contaminate the environment concerning the identity of the human person.” This is, he said, “the rejection of God.”
Asked what the Church should do in an environment where God is excluded, the Cardinal said, “The Church should be the first to combat toxic ideologies.”
The Church, he said, should focus on “the unprecedented anthropological and moral crisis of our time which demands that the Church should assume a greater responsibility and commitment to propose its doctrinal and moral teachings in a clear, precise and firm manner.”
Javaid Perwaiz, an OB/GYN in Virginia, has been arrested and charged with health care fraud after being accused of sterilizing women without their consent. The FBI had been investigating Perwaiz for over a year after a hospital employee gave them a tip about his unethical actions.
According to the Virginian Pilot, women were sent to the hospital by Perwaiz for what they thought were “annual cleanouts,” without actually knowing what kind of procedure they would be undergoing. He would then be performing hysterectomies, D&Cs, or tubal ligations without their knowledge or consent.
One patient was given a D&C each year by Perwaiz because she believed she had endometriosis; at least once, the procedure was done without Perwaiz seeing her for an office visit beforehand. Another patient, a breast cancer survivor, was told that she had pre-cancerous ovarian cells present; she agreed to have her ovaries removed. But when she woke up, she found out that Perwaiz had done a complete hysterectomy, and perforated her bladder. She ended up with sepsis, and her medical records later showed that no pre-cancerous cells were present. Still another patient had tried unsuccessfully to conceive a child, only for a fertility specialist to eventually tell her that her fallopian tubes had been completely removed, burned down to nubs.
Many of the women Perwaiz victimized were Medicaid patients. Doctors often need to use hysteroscopes to be reimbursed by insurance for a hysterectomy, and a Medicaid analysis showed that Perwaiz claimed to have used his hysteroscope over 80 times in both 2016 and 2017. Yet in 2010, an inspection found that his hysteroscope was broken; it was repaired but hadn’t been serviced since then. He also didn’t use anesthesia when using the instrument on his patients, though it can cause pain, and he only used the scope for around 10 seconds at a time — not long enough to properly view the uterus.
Perwaiz’ medical license had previously been revoked in 1996, after he pled guilty to tax evasion, but was reinstated in 1998. He also has faced numerous malpractice lawsuits.
Many women have been sterilized without their consent; this is often due to ethnicity, disability, or income status. Medicaid patients are likely to be either minorities or low-income. While it’s not known why Pervaiz did this, this kind of behavior is one of the worst injustices that can be visited on someone. And it has, understandably, left many of his patients scared and speaking out.
Every patient he sees he orders surgery on them,” one woman wrote on Facebook, the Virginian Pilot reported. Another woman said she wanted to get an ultrasound to make sure nothing had been removed. “I’ve been a patient of his since 2008 and to read about this today is very disturbing,” a third patient said on Facebook. “I’ve had several procedures performed by him to include major surgeries in which I was scheduled to have an appt at the end of this month. My concerns are what he’s done to me thus far. There is no amount of money to compensate many of us for the things and procedures that he’s performed as some aren’t reversible.”
LIMA, Peru, November 7, 2019 (LifeSiteNews) – After more than 20 years, women who were forcibly sterilized will have their day in court as prosecutors in Peru intend to charge a former president and government officials with serious human rights abuses.
Former President Alberto Fujimori of Peru (1990-2000) and other former high-ranking government officials will face a court in December for their involvement in forced sterilizations of women, which caused the death of at least one woman in the Andean republic. Fujimori, 81, promoted his Voluntary Chemical Contraception Program in the 1990s to supposedly level the playing field and provide to poor women contraception that they would not be able to afford without government assistance. Contraception services in Peru were subsidized by U.S. taxpayers through the U.S. Agency for International Development (USAID).
This was despite a 1978 amendment to the Foreign Assistance Act of 1961 that prohibits the use of U.S. dollars “to pay for the performance of involuntary sterilizations as a method of family planning or to coerce or provide any financial incentive to any person to undergo sterilizations.”
The Congressional Research Service reports that as a result of the forced sterilizations in Peru, “In October 1998, Congress enacted an amendment introduced by Representative Todd Tiahrt as part of the FY1999 Foreign Operations, Export Financing, and Related Programs Appropriations Act that directs voluntary family planning projects supported by the United States to comply with five specific requirements.”
Those requirements lay out stricter guidelines that are supposed to prevent funding from going to coerced sterilizations.
This amendment, “which became known as the Tiahrt amendment, has been included in foreign operations appropriations in each subsequent fiscal year,” the Congressional Research Service reports.
‘They cut me up like a hog’
According to Spanish website LaRazon, Gloria Basilio, 46, recalled that government nurses came to her home in the 1990s, telling her that because she already had three children, she should not bear any more.
“They explained to me ‘in the future, we will privatize schools and hospitals and there won’t be any money.’ My children wouldn’t have an education, so it was obligatory to tie my [Fallopian] tubes. They didn’t pay me anything, so I told them, ‘I’ll think about it.’” Two days later, she said, the nurses returned and told her that she should take advantage of the government program because sterilization would soon become expensive.
She says they told her, “Women in the countryside multiply like guinea pigs, like rabbits.”
When the nurses returned for a third visit while Basilio’s husband was travelling, Basilio agreed to the procedure.
“They came for us at five in the afternoon, then they tied down our arms, blindfolded us, and without any machines. Through the blindfold, I could see the surgical saws and how the blood sprayed on the doctors from my abdomen. But I couldn’t move because I was anesthetized. They cut me up like a hog.”
Basilio and thousands of other poverty-stricken Peruvian women are demanding justice and a hearing of their concerns.
Another of the victims of the contraceptive program was María Mamérita Mestanza Chávez, a woman from an indigenous community in the mountainous Cajamarca region of Peru. According to various media reports, she agreed to demands for sterilization after 10 threatening visits from government medical personnel. On March 27, 1998, personnel of the Peruvian Ministry of Health operated on and sterilized her without a doctor present. The officials did not offer any information about the risks and consequences of the operation or any further medical assistance. In less than two weeks, on April 4 of that year, Mestanza Chávez died as a result of an infection.
Besides Mestanza Chávez, Peruvian prosecutors have identified four other women who died as a result of forced or involuntary sterilizations: Alejandra Aguirre Auccapina, Reynalda Betallaluz Aguilar, Marían Espinola Otiniano, and Celia Ramos Durand. The number of victims of Fujimori’s sterilization campaign range as high as 300,000. Of these, 272,000 were female and 22,000 were male. Of these, 2,166 have presented complaints before prosecutors. Approximately 1,316 victims of sterilization have been added to the case so far. There are 5,758 women whose names appear on the National Victims Registry that is maintained by the Ministry of Justice.
Some women were sterilized unknowingly when government medical personnel performed caesarean deliveries for them. Many of the victims are illiterate and are non-native speakers of Spanish. The indigenous people of Peru speak the pre-Columbian Aymara or Quechua languages. According to Adolfo Castañeda of Human Life International, many of these women agreed to be sterilized only after being offered food for themselves and their hungry children.
Peruvian feminist Giulia Tamayo told the Peruvian website LaMadre that she observed in the poorest districts of her country that government agencies had quotas to fulfill for sterilizations among women. Many of these districts are heavily populated by indigenous people. Some of these districts were targeted, she said, because the government judged them to be under the control of narcotraffickers and armed leftist insurgents.
USAID was funding Peru’s health system during the period that sterilizations were widespread. Other organizations involved in the campaign were the United Nations Population Fund (UNFPA) and the nonprofit Japanese NIPPON Foundation.
Concerning the Peruvian victims, in an email to LifeSiteNews, PRI President Steven Mosher wrote: “These women not only deserve compensation, the government needs to apologize to them for violating their human rights.”
“President Alberto Fujimori, elected to a second term in mid-1995, had wasted no time in legalizing sterilization as a method of birth control. He ordered the country’s Ministry ofHealth, headed by Dr. Eduardo Yong Motta, to focus its efforts on family planning, specifically, on tubal ligations. To train Peruvian doctors and officials in how to structure and run a sterilization campaign, Dr. Motta brought in Chinese, Indian and Colombian doctors who had carried out such campaigns in their own countries. To monitor the success of the campaign, Fujimori himself set national targets for the numbers of sterilizations to be performed—100,000 in 1997 alone—and demanded weekly progress reports.
Mobile sterilization teams, a fixture of such campaigns, were soon being assembled in the capital city of Lima. These teams of doctors and nurses, who often had no prior training in obstetrics or gynecology, were hurriedly taught how to do tubal ligations, and then sent to the countryside to conduct a series of one- or two-week ‘ligation festivals.’ Prior to a team’s arrival in an area local Ministry of Health employees would hang banners announcing the forthcoming ‘Ligation Festival,’ and fan out across the countryside to captar [ ‘bring in’ or ‘capture’ in English] women for tubal ligations. The effort was focused on the poorer provinces, home to a high percentage of Peruvians of Indian descent.”
In 1974, during the Nixon administration, bearing the title “Implications of Worldwide Population Growth For U.S. Security and Overseas Interests, National Security Study Memorandum (NSSM-200 or so-called Kissinger Memorandum, which bore the name of erstwhile Secretary of State Henry Kissinger) set out the American foreign policy goals for demographic collapse of Latin America and other regions of the world. The secret document was declassified in 1989.
Dr. Brian Clowes of Human Life International analyzed the document, noting, “In order to protect U.S. commercial interests, NSSM-200 cited a number of factors that could interrupt the smooth flow of materials from lesser-developed countries…to the United States, including a large population of anti-imperialist youth, who must…be limited by population control.”
As for former Peruvian President Alberto Fujimori, he remains in prison after the country’s supreme court overturned a presidential pardon in 2018. He was sentenced in 2005 to a 25-year sentence for human rights violations involved in using death squads to fight leftist insurgents in his country.
The early morning hours of March 15 were filled with terror for the Labuschagne family. 14-week-old baby Michael unexpectedly suffered cardiac arrest. His mother, Emma Labuschagne, described the moment in a video shared on Facebook, writing, “We watched our baby breathless, gasping for air while his heart stopped and paramedics worked to save his life. In that moment I did not think Michael would make it through.”
Remarkably, Michael did survive and was rushed to the hospital, where he was placed in a medically induced coma. In her video, Michael’s mother writes that the family was told their son was not likely to survive the ordeal, and if he did, he “would not be the same baby.” Michael had been without oxygen for 9 minutes during the medical emergency, leading his medical team to believe that he would be severely brain-injured. Families of patients in such situations are often not given any reason to hope.
Five days later, when doctors removed some of the sedatives and Michael began to wake up, he gave his family an unmistakable sign of hope. His mother wrote, “The first thing he did when he opened his beautiful brown eyes was smile at his daddy.”
“It’s a moment I will cherish with every inch of my heart,” Labuschagne told CNN. “To be really honest, it’s got to be the happiest moment of my life. He is a living miracle, and we have never felt prouder of him.”
Michael’s medical problems, however, were far from over. Doctors discovered that the infant had a 5 cm cardiac fibroma, a tumor in the left chamber of his heart. The condition is so rare that doctors in the United Kingdom, where the Labuschagnes live, have no experience operating to remove the tumor. They placed a pacemaker and defibrillator but are unable to offer any hope of improvement beyond waiting for a heart transplant.
Through research, the Labuschagnes found an alternative: traveling to the United States for potentially life-saving surgery. Boston Children’s Hospital, the premiere hospital in the world for these types of conditions, has experience with the surgery Michael needs. His mother told CNN, “We researched the hospital and specifically the cardiac surgeons, Dr. (Pedro) del Nido and Dr. (Tal) Geva.” The surgeons have a 100% success rate, so the family had no doubt that they would do whatever is necessary to make the journey.
Michael’s mother said, “When we received a response from Boston confirming that he would be a good candidate for surgery, it did not matter what the cost was. We would pay any amount of money to save our child’s life.”
Since the family began fundraising for the trip and cost of the surgery, they have received tremendous support. Emma Labuschagne said, “We have had well-wishers and donations from all over the world! We are unbelievably thankful!”
For now, Michael, who is now 10-months-old, lives a surprisingly ordinary life, despite his significant medical challenges. His mother says, “Looking at him, he is like any other baby.”
She told CNN, “He is always smiling and grinning widely. His older brothers dote on him and he is a strong little character in our family. We are just so grateful for him, even with his medical troubles.”
Michael’s story, which seems likely to have a happy ending, recalls other stories from the United Kingdom of families seeking medical care in other countries. The world watched in horror as first Charlie Gard and then Alfie Evans were held captive in UK hospitals with the courts ruling in favor of anti-Life bureaucracy. In those cases, the medically vulnerable boys were not able to leave the hospital and that meant their families were unable to move their sons for potentially life-saving treatment.
Every family has the right to advocate for the care of their loved ones. Anti-Life laws that give hospitals power over life-and-death decisions must be repealed. Every child, like Michael, deserves the care his family thinks is best.
The chemical abortion pill, marketed as Mifeprex and referred to as a medication abortion, is the future of the abortion industry. The number of chemical abortions in America has increased dramatically while the overall tally of abortions has declined.
Those who advocate for and provide this abortion drug almost always downplay the excruciating process that awaits unsuspecting women, doing a grave disservice to them.
Tammi Morris was no stranger to abortion. She had previously had seven of them, so when an abortion provider told her the chemical abortion process would be “safe, near painless, and private,” she agreed to use it. Shortly after taking the second dose of pills, however, Tammi realized it wouldn’t be anything like what the abortion center staff had described.
“They didn’t prepare me for this,” Tammi said. Instead, what she endured was an experience she described as “savage” and “horrific.” She found herself alone, “feeling like I was going to give birth to death.” Profuse bleeding forced Tammi to seek medical intervention.
Elizabeth Gillette’s experience with the abortion drug was similarly traumatizing. In her case, the falsehoods exceeded the abortion staff’s mischaracterization of the drug’s effects. Elizabeth told them she was undecided about the abortion and wanted to view the ultrasound. At first, she was rebuffed, but Elizabeth persisted.
A staff member finally showed her a still shot of the monitor, saying, “Do you see? There’s no heartbeat. There’s no movement. Your pregnancy’s not viable.” Elizabeth said the facility had lied to her in an attempt to tip the scale of her uncertainty about the abortion.
“No one counseled me. No one told me what the options were.” As for the abortion process, Elizabeth says she was told, “You’ll experience some light cramping. It’ll be like a heavy period. Shouldn’t hurt.”
Elizabeth confessed, “I had no idea what was coming. No idea.” The cramping was “deep and very painful. I’ve had three children since then, and it felt like labor.”
The physical ordeals of these women were just the beginning of more horrors to come. Common to Tammi and Elizabeth’s experience during their chemical abortions, facilities send women home to abort alone, with no one to shield them from what they will see and feel.
Numerous medical experts understand the added physical and emotional trauma inflicted by chemical abortion. OB-GYN Donna Harrison likened the process, which is four times more likely to require medical intervention afterward than a surgical abortion, to “almost patient abandonment.” She sees the irony in feminists demanding safe, legal abortion while “pushing a chemical coat hanger on women.”
During her chemical abortion — really an induced miscarriage — Tammi felt the urge to push and then looked down. What she saw left her devastated. “There was my baby, in a toilet. This wasn’t fetal tissue. This was a formed, recognizable, undeniable baby. My baby.”
Through tears, Elizabeth also described coming face to face with her unborn son. “I held him. The doctor promised me that I would feel relieved.” But what Elizabeth described wasn’t relief. Instead she felt an “overwhelming guilt, a sickness inside that I couldn’t put away. Nightmares started shortly after. I stopped eating. I became anorexic. I was later diagnosed with acute post-traumatic stress disorder.”
Tammi and Elizabeth then faced the struggle of daily emotional turmoil enveloping their lives as a result of what they had done and seen.
“How does a mother who killed her own child in the womb intentionally, how does she grieve outwardly?” Tammi questioned.
Elizabeth felt a burning passion to warn other women. When facing a second unexpected pregnancy, she made a video that quickly became popular, encouraging other women to persevere. “Hiding in the silence is just your own personal death sentence. But when you stand up and say enough is enough. This hurt me and it’s hurting women everywhere, it set me free.”
“Our society is breeding fear,” Elizabeth said. “We tell our women to go out and get a job and be everything you can be, except being a mom. And that’s a lie.” To her, abortion is “a regret you can’t reconcile. It’s forever.”
Grassroots organizations and people who have seen or experienced these devastating effects are making an effort to give a voice to women who have been physically or emotionally harmed by chemical abortion. They’ve created a safe, confidential place women can go to tell their stories about their experience. Sharing can often be therapeutic.
The landscape of the abortion debate was altered during the 1980s when women who had experienced abortion and its aftermath came forward to tell their stories. By speaking out, the victims of chemical abortion can spare countless other women and their babies from enduring a similar tragedy.
Hear Tammi and Elizabeth’s stories and learn more about chemical abortion below, or watch the full documentary here.
LifeNews.com Note: Bradley Mattes is the President of Life Issues Institute, a national pro-life educational group.
Victimization is a prominent leitmotif in contemporary culture, and our morally relativistic, “non-judgmental” times tend to take self-claims of injury at face value. But, as contemporary Polish philosopher Zbigniew Stawrowski has observed, today’s “sleek barbarians”—those who, employing traditional terms like “rights” and “justice” empty them of their received meanings, pressing them into service of what had once been deemed wrongs and injustice—often employ the victim card to parry what once would have been called “chutzpah.” Case-in-point: Bryce Cleary.
Bryce Cleary is a physician who, as a student at Oregon Health and Science University (OHSU) 30 years ago, apparently liberally donated his sperm. He claimed his motivation was to help the infertile and to foster research. He caveated his gifts: the sperm should be used by five couples on the U.S. East Coast, while the rest should go for research. He’s now suing OHSU for $5.25 million, claiming fraud.
See, thanks to modern technology, the internet and Ancestry.com, Cleary discovered that he had fathered at least 17 children (in addition to the four he publicly acknowledged as a father within marriage), most of whom lived nearby in Oregon. And that’s what’s got him peeved: his acknowledged and unacknowledged offspring can intermix (and apparently have) without their even knowing it.
A narrow, autonomy-centered paradigm might say, “Well, that’s what he was concerned about, and that’s what OHSU failed to prevent. He’s been lied to.”
Perhaps, however, we ought to expand the concept of “lie.”
“Oh, what a tangled web we weave//when first we practice to deceive,” goes the old axiom. Cleary thinks he was deceived. But so were his children.
Bryce Cleary is responsible for 17 lives with which he clearly never intended to have any contact. Sperm donation has long been shrouded in secrecy, and Cleary had no problem with being at least partially a liar. After all, “’I can’t emotionally be invested in all these people’” he says.
Well, then, you shouldn’t have become their father.
This case is tragic, but not the way Bryce Cleary sees it. It is tragic because real people—real kids—do not know whom their real father is, have probably been lied to all their lives, and do not know whom their brothers and sisters are (or even how many they have).
Letting Cleary define the parameters of this case would be wrong. The situation shows that parenthood is not just a matter of “personal autonomy” but has social implications in which society as a whole has vital rights and interests, in no small part “in the best interests of the children.” Yes, we’ve forgotten that test of social policy.
A person’s right to know his true parentage and relations and the prevention of incest are not just Cleary’s private concerns. They are all our concerns. Cleary’s lawsuit suggests that, because he donated his sperm, he is the policymaker for whether and how to achieve these ends.
So does that mean he could decide a child has no right to know his true genetic parentage? Even as we recognize that orphans have a right eventually to know who there is true parents are, we would give genetic fathers a veto over another person’s rights to their very identity? This would guarantee making that person an orphan, not just physically but spiritually and intellectually? Afflicting the orphan, like maltreating the widow, is among the Bible’s worst crimes.
The artificial insemination industry has, of course, long been shrouded in secrecy. Artificial insemination by donor (AID) has been cloaked by its own “don’t ask, don’t tell” policy, where one’s real father excludes himself from his child’s life, while an often infertile man pretends to be the “father” of this child – until the ugly truth comes out (usually not voluntarily). (For the perspective of lied-to children, see “Anonymous Father’s Day,” a great documentary film, here).
When this “gentlemen’s agreement” of secrecy was confined to AID, its impact was circumscribed: the number of people resorting to artificial insemination, especially using the gametes of a third party, was in the past limited.
But the fertility industry today is an enormous (and enormously profitable) business, which depends on AID, ovum donation and surrogacy. It is also a largely unregulated business: America at large is, as Jennifer Lahl puts it, “the Wild West” of surrogacy, and some states (e.g., California) are wilder than others.
Trends in delayed marriage, subordination of parenthood to career milestones, and growing infertility fuel that fertility industry. So, too, does “same-sex marriage.”
The fallacy behind Obergefell’s establishment of “same-sex marriage” was the Supreme Court’s claim that sexual differentiation was irrelevant to marriage because marriage had no inherent nexus to procreation. But the Court is inconsistent in its own logic, because homosexual activists increasingly argue that, unless they have a “right to parenthood” (notwithstanding their own natural sterility), then Obergefell’s promise of “same-sex marriage” is empty.
Lest this proposition end on some maudlin slogan about “the right to choose whom you love,” understand what it implies. If there is a “right to parenthood” notwithstanding the natural incapacity of two people of the same sex to conceive children, it means that parenthood as it has been understood in every culture throughout history (and as it biologically exists) has no right to be privileged or given priority in law. Parenthood as the natural outcome of the union of a man and woman is just “one alternative” parenthood, and the state must support any method of conceiving children so long as it fulfills the problem of overcoming the “discrimination” apparently established by “nature and nature’s God.” Natural law itself would become practically unconstitutional.
If one has any doubt that legal preference of parenthood as it has existed as long as there have been men and women would be undermined, consider already what has been going on with birth certificates. A number of states have been complicit in the “gentlemen’s agreement” of AID by establishing presumptions about paternity when it comes to issuing birth certificates: if a child is conceived in wedlock, the law presumed that the husband of the wife is the child’s father. If a couple agreed to use AID, neither spouse had an interest in disclosing true paternity, and the birth certificate simply covered up that fact.
With the advent of “marriage” without sexual differentiation, however, there also arose the question of whom to list as “parent one” and “parent two” on the birth certificate. (Note the disappearance of “father” and “mother,” presumably as “discriminatory” sexual residue. A child may now be entitled to two parents, but he is not entitled to a father and a mother). Several states balked at applying the “paternal presumption” in the case of two lesbians, since clearly (a) there was no male “married” to these two persons and (b) the female “spouse” clearly could not have exercised the genetic paternal role. But the federal courts, applying Obergefell, have insisted that—biology notwithstanding—the “parental presumption” requires listing the same-sex “spouses” as “parents” on the birth certificate, regardless of their natural incapacity to give life.
What this clearly means is that birth certificates need not have any necessary relationship to truth, i.e., need not necessarily tell us about who is father and mother of this child. What it means is that the law increasingly ratifies and countenances the parcelization of parenthood, sliced and diced into genetic, gestational and social components, with the implicit presumption that the social component – those who chose to raise the child –is the “parenthood” that matters.
The poor kid: who gets the Father’s and Mother’s Day cards? The anonymous gamete donor? The gestational “womb for rent?” The woman or man that signed the check for the braces?
Sperm is not just “another bodily fluid,” whose “donation” is as anonymous as blood or plasma or bone marrow. It’s time we stopped pretending it is. Newsweek featured a story in 2011 about the new “paternity,” of a man hired by two women for his semen, who went into a Starbucks bathroom, ejaculated into a cup, handed his free will donation to the woman, who then employed it, after which they all shared a Venti Dolce Latte.
Is society to affirm “fatherhood” as an ejaculate handed over in a coffee shop? Cahal Daly once observed that the way one treats sperm is the way one would treat a human being. I didn’t grasp his existential meaning when I read that line 45 years ago, but I get it now.
It’s also time to stop pretending that a child born from his real mother’s womb is no different from one from another’s womb or commissioned as a product from a hatchery. All methods of “family production” are not created equal.
These are profound and radical changes with enormous social implications, but they are advancing with little, if any, social debate. And the real victims, because they are deceived about their origins, are the children. Instead, pseudo-“victims” sue in the name of their violated autonomy.
We need to refocus on those who are the real victims: the kids.
All views contained herein are exclusively those of the author.
BOSTON – A new study found that the use of birth control pills was associated with more depressive symptoms in teenage girls, including crying, excessive sleeping and eating issues, compared to their peers who don’t take oral contraceptives.
The study, published recently in JAMA Psychiatry, included more than 1,000 participants in the Netherlands between the ages of 16 to 25 over a period of nine years. On average, researchers found that the 16-year-old participants who were using oral contraceptives reported more crying, sleeping and eating problems than those who weren’t on the pill.
Previous studies have found an association between adolescents who take oral contraceptives and the risk of depression into adulthood. This study, led by investigators at Brigham and Women’s Hospital, University Medical Center Groningen and Leiden University Medical Center, aimed to examine the more subtle depressive symptoms.
“Depressive symptoms are more prevalent than clinical depression and can have a profound impact on quality of life,” said co-author Hadine Joffe with Brigham’s Department of Psychiatry. “Ours is the first study of this scale to dive deep into the more subtle mood symptoms that occur much more commonly than a depression episode but impact quality of life and are worrying to girls, women and their families.”
Researchers analyzed data from a cohort study, called Tracking Adolescents’ Individual Lives Survey, and assessed the participants’ birth control usage at ages 16, 19, 22 and 25.
Each participant filled out a survey with questions about depressive symptoms, such as crying, eating, sleeping, suicidal ideation, self-harm, feelings of worthlessness and guilt, energy, sadness and lack of pleasure. Their responses were used to generate a depressive symptom severity score.
Among the 1,010 participants between ages 16 and 25, the team found no association between oral contraceptive use and depressive symptoms overall. But they did find that the 16-year-old participants who were using oral contraceptives had depressive symptom severity scores that were 21 percent higher on average than those who were not taking the pill.
The study authors noted the findings don’t prove that birth control pills cause depressive symptoms. While birth control pills might contribute to these symptoms in girls — it also could be that more severe symptoms may prompt teen girls to start taking them, researchers said.
“Because of the study design, we can’t say that the pills cause mood changes, but we do have evidence suggesting that sometimes the mood changes preceded the use of the pill and sometimes the pill was started before the mood changes occurred,” said author Anouk de Wit, a trainee in the Department of Psychiatry at University Medical Center Groningen.
The authors also pointed out that the study only included females in the Netherlands, a relatively homogenous population, and a more diverse group may have produced different results.
“One of the most common concerns women have when starting the pill, and teens and their parents have when an adolescent is considering taking the pill, is about immediate depressive risks,” said de Wit. “Most women first take an oral contraceptive pill as a teen. Teens have lots of challenging emotional issues to deal with so it’s especially important to monitor how they are doing.”
Kanye West recently came out against abortion during an interview for his new album Jesus is King. During that bold statement, he mentioned Plan B, the “emergency contraception” product that claims to prevent pregnancy in the event of contraception failure. Many people, including the manufacturers of Plan B, concluded that West was likening Plan B to abortion, and it caused a stir.
“Democrats had us voting Democrat for food stamps for years, bro,” said West, speaking about the Black community. “What you talking about? Guns in the 80s, taking the fathers out of the home, Plan B, lowering our votes, making us abort our children. Thou shall not kill… I can’t tell y’all how to feel. But what I can tell you honestly is how I feel.”
Foundation Consumer Healthcare, the pharmaceutical company that makes the Plan B One-Step pill, seems to believe that West was labeling their product as an abortion. They were so concerned about what West had to say that they told TMZ, “Plan B helps prevent pregnancy before it starts by delaying ovulation. Plan B is not an abortion pill – it will not harm an existing pregnancy and it will not be effective if a woman is already pregnant.” But that’s not the whole truth.
A Planned Parenthood rep also spoke to TMZ saying, “As Black women, we make our own decisions about our bodies and pregnancies, and want and deserve to have access to the best medical care available. Misinformation like this is meant to shame us and keep us from making our own health care decisions. Black women want and deserve support and access to the full range of reproductive health care, but this persistent lie is threatening our ability to obtain it.” But if West was calling Plan B an abortion-causing product (though it isn’t clear that he was; after all, Plan B and “abort our children” were not mentioned contiguously), he wasn’t lying.
Close-up of the back of a Plan B box.
While Plan B states on the box that it “will not harm an existing pregnancy” it also states that it will “prevent […] attachment of a fertilized egg to the uterus.” And thatis the unnatural ending of the life of a new human being, and therefore, Plan B can function as an abortifacient.
Science is clear – life begins at fertilization. Ending that life on purpose is an act of abortion and, therefore, by potentially preventing implantation, Plan B can cause an abortion. Plan B sticks to the term “fertilized egg” instead of zygote to try and distract people from the reality of the fact that a new human being is present the moment an egg is fertilized.
As President of Students for Life of America Kristan Hawkins pointed out during an event at Villanova University, The American College of OBGYNs altered the definition of pregnancy in 1965 after birth control was introduced. They decided to start considering pregnancy to begin at implantation rather than fertilization, despite the scientific proof that says a human being is present days prior to implantation.
“So that allows the makers of Plan B to say, ‘Woah, woah, woah, we’re not killing anybody. We’re just not letting anything implant,” said Hawkins. “What aren’t you letting implant? ‘Oh, it’s just a fertilized egg.’ Why do we use the word fertilized egg? Because fertilized egg doesn’t sound like human being. […] So what the Plan B manufacturers said today was disingenuous and they’ve been lying all along.”
But don’t take Kanye West’s word for it. All anyone has to do to realize that Plan B actually can cause an abortion is read the Plan B box.
Washington D.C., Oct 31, 2019 / 04:58 pm (CNA).- Cardinal Timothy Dolan of the Archdiocese of New York has responded to questions about the denial of Holy Communion to former Vice President Joe Biden last Sunday.
On an Oct. 31 interview with Fox News, Dolan said that he thought the incident was a good teaching moment about the Eucharist and the seriousness of denying Church teaching, but that he would not himself deny anyone reception of the Eucharist.
“So whether that prudential judgment was wise, I don’t want to judge him either,” Dolan said of Fr. Robert Morey, who denied Holy Communion to Biden. “I wouldn’t do it.”
“Sometimes a public figure will come and talk to me about it. And I would advise them, and I think that priest (Morey) had a good point, you are publicly at odds with an issue of substance, critical substance, we’re talking about life and death and the Church,” Dolan said.
Receiving the Eucharist “implies that you’re in union with all the Church believes and stands for. If you know you’re not, well, integrity would say, ‘uh oh, I better not approach Holy Communion.’ That’s always preferable than to make a split-second decision and denying somebody,” Dolan added.
“Sadly, this past Sunday, I had to refuse Holy Communion to former Vice President Joe Biden,” Morey, who is the pastor of St. Anthony’s, explained in a statement sent to CNA.
“Holy Communion signifies we are one with God, each other and the Church. Our actions should reflect that,” Morey added. “Any public figure who advocates for abortion places himself or herself outside of Church teaching.”
In denying Biden communion, Morey was following a diocesan policy set forth in a 2004 decree signed jointly by the bishops of Atlanta, Charleston, and Charlotte. The decree states that supporting pro-abortion legislation is “gravely sinful” and that public figures who do so must be denied communion until they repent.
Joseph Zwilling, director of communications in the Archdiocese of New York, told CNA that the archdiocese does not have such a policy.
Dolan told Fox & Friends he agreed with what Morey said, though he would not personally deny a public figure the Eucharist.
“I think what he said was very to the point, I thought that was a good teaching moment,” Dolan said.
The cardinal said the issue has never come up for him personally – he has never seen a public figure in his Communion line who he knew was publicly advocating for policies that violate Church teaching.
“I’ve never had what you might call the opportunity, or I’ve never said ‘Uh oh, should I give him or her Holy Communion’, it’s never come up. Sure could,” Dolan said.
Dolan faced heavy criticism in January from Catholics who felt that he should have explicitly barred from communion New York’s Governor Andrew Cuomo, who had signed into law an expansive abortion bill.
“Especially if you have a governor who enjoys this and wants to represent himself as a kind of martyr to the cause, doing what is right. He is proud to dissent from the essentials of the faith. He’s proud with these positions.”
“For me to punish him for it? He would just say, ‘Look at the suffering this prophet has to undergo,’ the cardinal added.
Dolan said Oct. 31 that he frequently sees public figures at St. Patrick’s Cathedral in New York, and that he “admires” them when they do not approach the Eucharist out of their own awareness of their sin and separation from the Church.
“They seem to know – ‘I shouldn’t do that. That could be hypocritical at this moment,’” Dolan said.
“On the other hand, we also remember Pope Francis. We…I personally can never judge the state of a person’s soul. So it’s difficult, that’s what I’m saying. I’m not up there as a tribunal, as a judge, distributing Holy Communion, I’m there as a pastor, as a doctor of souls,” Dolan said.
“So it’s difficult to make a judgment on the state of a person’s soul. My job is to help people make, with clear Church teaching, make a decision on the state of their soul and the repercussions of that.”
When asked if priests could refusing other people communion because of their sins, Dolan said that communion is intended for sinners.
“If only saints could receive Holy Communion, we wouldn’t have anybody at Mass, including myself, alright?” Dolan said.
“So sinners are who Holy Communion is for, it’s medicine for the soul, it’s an act of mercy, so it’s intended for sinners…but sinners who want to, who are sorry and want to repent. Then anybody’s welcome, come on up,” he added.
Canon 915 of the Code of Canon Law states that “Those who have been excommunicated or interdicted after the imposition or declaration of the penalty and others obstinately persevering in manifest grave sin are not to be admitted to holy communion.”
Edward Peters, who teaches canon law at Sacred Heart Seminary in Detroit wrote in The Hill this week that “however the decision to withhold holy communion from Biden made headlines, it was unquestionably the pastor’s decision to make and he made it, in my view, correctly.”
“While there are relatively few examples of pastors withholding holy communion from Catholic politicians who support abortion, the refusal that Biden experienced should not have come as a surprise. He had been warned about approaching for holy communion in 2008 by Bishop Joseph Martino of Scranton, who told Biden that, because of his support for abortion, he would be refused holy communion if he approached that prelate, and by Archbishop Charles J. Chaput (then of Denver, now of Philadelphia), who implied likewise,” Peters wrote.
While not addressing Dolan’s remarks Peters addressed a point Dolan made during his interview, which Peters called the “reddest herring” in defense of Biden.
Specifically, he criticized the argument “which implies that withholding holy communion requires a minister to peer into the soul of a would-be recipient and judge it unworthy. Nonsense. To confuse the private examination of one’s conscience as envisioned by Canon 916 with the recognition that some public acts warrant public consequences under Canon 915 is to show either ignorance of or indifference to well-established Catholic pastoral and sacramental practice.”
In a memorandum to the U.S. Catholic bishops in 2004, explaining the application of Canon Law 915, then-Cardinal Joseph Ratzinger said “the minister of Holy Communion may find himself in the situation where he must refuse to distribute Holy Communion to someone, such as in cases of a declared excommunication, a declared interdict, or an obstinate persistence in manifest grave sin.”
The case of a “Catholic politician” who is “consistently campaigning and voting for permissive abortion and euthanasia laws” would constitute “formal cooperation” in grave sin that is “manifest,” the letter added.
Biden has declined to comment on the communion incident telling reporters that it was “just my personal life.”
“I’m a practicing Catholic. I practice my faith, but I’ve never let my religious beliefs…to impose that view on other people,” Biden said this week.
While Biden served in the Senate, he largely supported the Supreme Court’s 1973 decision that found a legal right to abortion, Roe v. Wade. He called his position “middle-of-the-road,” in that he supported Roe but opposed late-term abortions and federal funding of abortions.
Since then, he has supported taxpayer funding of abortions via the repeal of the Hyde Amendment and Mexico City Policy in his 2020 platform and has called for the codification of Roe v. Wade as federal law. Biden also favors reinstating taxpayer funding for Planned Parenthood, the nation’s largest abortion provider.
A Personal Choice Tubal Reversal Center is a center where couples can regain their natural fertility through tubal ligation reversal surgery and vasectomy reversal surgery. Dr. Charles W. Monteith, MD is the Medical Director of this unique specialty center a surgical center located in Raleigh, North Carolina. Dr. Monteith exclusively specializes in fertility surgery and using his unique surgical skills he is able to offer couples affordable outpatient reversal surgery to couples who travel from across the world to have surgery at his specialty center.
Tubal ligation, more commonly known as ‘getting one’s tubes tied’, is one of the most common surgical procedures performed in the United States. Unfortunately, research has shown that up to 30% of women will regret their tubal ligation procedure. Most women regret tubal ligation because they would like to have more children. Some regret their tubal ligation because they have developed troublesome symptoms after tubal ligation.
Tubal ligation regret is a common problem that can cause immeasurable guilt and anxiety in women. If you suffer from tubal ligation regret and would like to have more children then you only have three choices; tubal reversal surgery, in-vitro fertilization (IVF) or adoption. Most people are unaware that tubal reversal surgery can be more successful and far more affordable than in-vitro fertilization. Tubal reversal provides a woman a chance to become pregnant every month and more than one time. In-vitro fertilization is an expensive and lengthy medical process that may not be as successful as tubal reversal. On average about 2 out of every 3 women who have tubal reversal will become pregnant. In comparison, 1 out of every 3 women who have IVF will become pregnant.
The cost of tubal reversal surgery with Dr. Monteith is approximately $6,900. The cost of IVF is approximately $14,000 for each cycle attempted. You can easily see how Dr. Monteith offers patients a better option for having more children with outpatient tubal reversal surgery at A Personal Choice.
Some women will develop abnormal tubal ligation symptoms after having their tubes tied. These women will often complain of irregular periods, heavier periods, pelvic pain, hair loss, joint pain, and memory issues. Although tubal ligation side effects are rare, Dr. Monteith specializes in helping these women. Tubal reversal allows these women a surgical evaluation of their tubes and the chance at improving their symptoms. Often during these surgeries Dr. Monteith will discover undiagnosed endometriosis or pelvic scar tissue. Many times these women will have completely normal findings. Dr. Monteith has observed over 80% of his patients who have reversal for abnormal symptoms report improvement after reversal surgery.
Patients travel from across the United States and around the world to have reversal surgery with Dr. Monteith. Many patients will find it easier and more affordable to travel to Raleigh NC to have surgery with Dr. Monteith than with a less experienced surgeon in their hometown. Scheduling surgery at A Personal Choice is easy. Patients can determine if they are a candidate for surgery by faxing or emailing Dr. Monteith a copy of their tubal ligation records for a free review. Scheduling surgery occurs over the phone and by email. Patients then travel to Raleigh for surgery and spend two nights and three days. The consultation is on the first day, the surgery is on the second day, and the postoperative visit is on the third day. After the postoperative visit, patients are free to return home. Surgery at A Personal Choice is extremely safe with a very low surgical complication rate. Patients are encouraged to start trying to become pregnant as soon s they feel comfortable. Most will report pregnancy within the first 12 months. Those who have abnormal symptoms often report improvement within the first week!
Dr. Monteith’s success is illustrated by the many testimonials shared on his website and Facebook page. A new mom who traveled to Dr. Monteith from North Haledon, New Jersey to have reversal of burned tubal ligation submitted a testimonial saying, “Our second tubal reversal son was born August 8th 2019. His older brother is 4 years old. These are true miracles from God through the guided hands of Dr. Monteith and his staff. We are so blessed and thankful for these two boys! We can’t thank you enough!”
In another testimonial, a happy mother, writes, “Fifteen years of suffering from tubal ligation symptoms brought my husband and me to Dr. Monteith. He did a great job and I felt the symptoms vanish soon after my reversal. Our baby (born on the one year anniversary of my reversal) is an amazing blessing!”
Those looking to learn more about A Personal Choice to have more children after their tubes have been tied or to evaluate abnormal symptoms after tubal ligation can find extensive information and statistics on the website of A Personal Choice. In addition, A Personal Choice also maintains an active company Tubal Reversal Facebook page and Facebook Tubal Reversal Group, where they share updates with those desiring more information about tubal ligation reversal and vasectomy reversal surgery.
For more information about A Personal Choice Tubal Reversal Center, call (919) 977-5050 or visit https://www.tubal-reversal.net:
CONTACT INFORMATION:
A Personal Choice Tubal Reversal
Dr. Charles W. Monteith, Jr., M.D.
(919) 977-5050
ContactUs@tubal-reversal.net
3613 Haworth Drive, Raleigh NC 27609
Servando Carrasco and Alex Morgan are a match made in soccer heaven. The couple, who married in 2014, are both major soccer stars; Carrasco plays professionally with the L.A. Galaxy, while Morgan is co-captain of the United States national team, which just dominated in the 2019 World Cup, where she won the Silver Boot award for second-most goals scored. But now, they’re celebrating a new achievement: a new baby girl, due next April.
Carrasco and Morgan announced their pregnancy on Morgan’s Instagram account, posing on a beach with a onesie, and a sign that read “Baby Girl April 2020.” In the caption, Morgan wrote, “We are already in love and we haven’t even met her yet.”
Carrasco likewise celebrated the news on Instagram, with a picture of them posing with their two dogs. “Can’t wait to meet my baby girl,” he wrote. They also spoke to PEOPLE about their exciting news. “We are so overjoyed to grow our family,” Morgan said. “She’s the best World Cup gift I could have asked for.”
Their soccer family likewise took the occasion to celebrate with them. “Bringing another powerful woman into the world. Love to see it,” the US Women’s National Team account posted on Instagram. “Congrats [Alex] & Servando! Your #USWNT fam is ecstatic!”
Morgan is the latest elite female athlete to show that motherhood does not get in the way of achieving goals, or that having an amazing career does not keep one from being a mother. Serena Williams, considered to be one of the greatest tennis players of all time, won a Grand Slam tournament while two months pregnant. Kerri Walsh Jennings, a star volleyball player who has won numerous Olympic gold medals, likewise won Olympic gold while pregnant with her daughter Scout, and she credits her children for giving her the drive to succeed.
“She knows she’s golden,” she said of Scout in an interview. “I don’t know if she knows how big of a part she played in that [Olympic win]. My boys certainly do.” Another Olympian, Alysia Montano, is a seven-time United States champion, a two-time American record holder, and she’s won three Olympic medals. She competed in the 2017 USATF Outdoor Championships at almost six months pregnant, her baby bump proudly on display; she had previously competed in the USATF’s USA Outdoor Track and Field Championships in 2014 while eight months pregnant.
Allyson Felix is another Olympic runner, and is the most decorated Track and Field Olympian of all time. She became pregnant, and was almost immediately threatened the loss of her sponsorship by Nike. Felix, however, fought back, successfully pressuring Nike to change their policy towards pregnant athletes, and ensuring that women who play sports will not be punished for having children. Her fight marked a huge victory over pregnancy discrimination for athletes everywhere.
U.S. women’s soccer coach Vlatko Andonovski and general manager Kate Markgraf have shown support for Morgan and her goal of returning to the Olympic team in late July.
“[…] we’re going to do everything in our power, use the resources that the federation is providing, whether it’s high-performance director, staff, anything that we can do on our side to help her get back for the Olympics,” said Andonovski.
These women, together, are making a huge difference for women everywhere. They’re proving that women can do anything — from being Olympic stars to doting mothers — and they don’t have to choose between their children and their dreams.
Data collected by Prof. Abigail Aiken and the team at Project SANA (Self-managed Abortion Needs Assessment) do give us some valuable insight into exactly who is seeking chemical self abortion and why.
Distribution by age of those inquiring about abortifacients online tended to be about what they were for the general population of abortion patients. About 72% were under thirty, 24%-25% were women in their 30s, and between 3% and 4% were women over forty.
Just over half (about 53%) already had given birth to at least one child ; past national figures from the CDC put the number for aborting women who have already given birth at closer to 60%.
More than 7 in 10 (72.3%) reported the age of their unborn baby at less than seven weeks (the FDA’s original cut off for chemical abortions with mifepristone). The remainder said they were between seven and ten weeks pregnant (the FDA’s current cut off).
Though we know from reports that clinics across the U.S. have often attempted to chemically abort women with gestations greater than ten weeks, the Women on Waves (WoW) website currently tells women these pregnancies are too far advanced and will end the consult.
Because this data is based on self reporting, factual confirmation of these details are lacking. Moreover, there are still questions about the representativeness of this sample. Nonetheless, there are interesting claims made by women in the study about the circumstances under which they became pregnant and why they wanted abortions.
Nearly half (48.9%) said that they were not using birth control at the time they became pregnant. Another 45.4% said their contraception “failed.” About one in twenty (4.9%) said that they were pregnant as a result of rape.
Reasons given for seeking to chemically self-abort were largely consistent with those we have heard for all abortions.
More than six in ten (60.7%) reported “lack of money.”
About four in ten (38.7%) said they “want to finish school.”
Three in ten (30.4%) said they were “too young”; one in twenty (4.8%) said they were too old.
More than two-thirds (68.8%) simply said, ”I just cannot have a child at this point in my life.” (What this meant was not further specified in the form; women were able to pick out multiple reasons, so percentages do not add up to 100.)
Less than one in fifty (1.9%) cited unspecified “illness” as the reason for their abortion, while one in five (20%) simply stated that their “family is complete.”
Aiken and her team tried to generate separate statistics for those women contacting WoW from “hostile states” and those from “supportive states.” (The categories depended on how many laws had passed with regard to parental involvement, informed consent, abortion funding, clinic regulation, etc.)
Differences were slight with regards to gestational age, contraceptive use, and reasons for seeking abortion. Women from “hostile states”–those with more pro-life laws–tended to be more likely to have previously given birth (55.7%) than those from “supportive states” (44.6%).
Reasons for online abortion pills not as expected
Abortion advocates have tried to argue that limits on abortion in those “hostile” pro-life states are driving women to seek out abortion pills online. Despite their best spin and efforts, the data here in this study generally doesn’t seem to support that view.
For example, when asked why they were seeking abortion pills online from WoW, less than a fifth cited “state laws.” Just 18.1% cited this as a reason for trying to get the pills in the so-called “hostile” states, and almost as many (14.1%) gave this as a reason in states that the research team deemed “supportive.”
Beyond the low percentage, the minimal difference between perceptions in “hostile” versus “supportive” states shows that the actual presence or absence of such laws in a given state isn’t that big a factor in pushing women into the arms of the online abortion merchants.
What about the distance involved in having to travel to an abortion clinic, often cited by abortion advocates? This was slightly more of an issue for women in “hostile” states (29%) than it was for those in “supportive” states (21%). However this may be a function of geography (e.g., being in a state with a spread out population) or of their generally being a higher concentration of abortion clinics in those abortion sympathetic states.
The other reasons given for seeking abortion pills online are pretty much what might be expected of women looking for an alternative to an abortion at a clinic. About half said being able to abort in the “privacy” (49.3% for “hostile” states, 48.5% for “supportive” states ) or “comfort”(47% for hostile” states ,44.5% for “supportive” states) of their own home environment was factor.
This is something that was a huge early selling point for these abortions, attractive to those unaware of the physical dangers and psychological trauma associated with the chemical abortion process.
The quarter of potential WoW customers that said they sought the pills online because of the “ability to have others present” (25.3% for “hostile” states, 25.8% for “supportive” states) may have included some with a better understanding of the risk involved.
A sizeable number of women appear to have bought into the myth (or at least thought that it sounded like an attractive feature) that at home abortions with pills bought over the internet give them “a feeling of autonomy” (41.9% in “hostile” states, 43.7% in “supportive” states) or a “feeling of empowerment” (10.8% for “hostile” states,12.8% for “supportive” states).
About four in ten (39.6% in “hostile” states, 43.2% in “supportive” states) cited the “need to keep abortion secret” as their reason for turning to online abortifacients. Just over a third (34.4% in “supportive states,” 32.5% in “hostile” states) said that getting the pills online helped them avoid problems involved in getting time off from work or school.
Less than 20% from either “hostile” or “supportive” states mentioned “perceived abortion stigma,” “protester harassment” or “difficulty finding childcare” as reasons they might prefer a method that would enable them to avoid going to the clinic.
By far, the biggest reason women gave for seeking out online abortion pills was the “cost of clinic abortion.” This was cited by 71.1% of women in “hostile” states and 62.9% in “supportive” states, tops in both categories. [1]
This clearly means that interest in online abortifacients is driven, not by those seeking a way around pro-life laws, but by women unhappy with clinic abortion prices looking for a bargain on the internet.
Either way, that’s an industry issue, a marketing issue, not a legal one.
These results presents the industry with a dilemma. Clinics are struggling to get enough clients to stay open, to pay the bills, cover the rent, pay the staff, and give the abortionists their cut. Cut prices and the margin is even lower.
Online abortion pill peddlers don’t have all the overhead of a physical clinic, all the extra employees, thus enabling them to charge lower prices. The more women go online for their abortions, the less business there is for the “brick and mortar” clinics.
This may explain why you see other people and other groups out there promoting these online pills but not abortion giants such as Planned Parenthood.
More a marketing report than a study
Ostensibly a study to show how pro-life laws are driving pregnant women to seek the means to self-abort online, Aiken et al.’s study instead exposes how well the abortion industry’s widely touted and heavily promoted effort to come up with a new and improved abortion method to address problems with clinic abortions like cost, time, travel, etc., is faring.
The answer appears to be “not well.”
There are some women, accustomed in this day and age to shop for bargains on line, who are looking for something cheaper, something better that they can get at home rather than the expensive, inconvenient abortions for which they’d normally have to take the day off work and drive to the abortion clinic.
The pitch of a cheap, easy, safe abortion a woman can do in the privacy of her own home is clearly attractive to some women, even if the reality is something far different. What should be surprising to the Aiken team is how relatively few women seem to have sought the option.
Advocates of “self-managed abortion” are anxious to portray this as an “access issue,” where state laws and FDA drug policies interfere with a woman’s ability to exercise what they think is her “right to abortion.” Creating “evidence” of this supposed interference and demand is a critical part of making their case to the FDA to loosen controls on prescription and distribution of these abortion drugs to overcome these barriers.
Although that was clearly the intention of this study’s authors, their data tell us it really wasn’t the reason most of the women sought the abortion pills online. They simply weren’t satisfied with the product and the prices currently being offered at America’s abortion clinics.
Eventually, in spite of the latest marketing pitch, women will figure out that it is the same product, just with new packaging being delivered in a new and riskier setting. And no matter the price, they will discover that the cost in lost lives and wounded souls is just too high
[1] That about 8% fewer in the “supportive” states mentioned cost in some cases may be because many of those states cover abortions with state funds.
WASHINGTON, D.C., October 25, 2019 (C-Fam) — Several major family planning groups recently revealed how they are working to integrate abortion into their humanitarian work. The groups were quite open about this at an event hosted by the Wilson Center in Washington, D.C.
Millions of people around the world are affected by war and natural disasters, with many displaced from their homes. Humanitarian crises can last for years, during which families must continue to raise their children; access health care and education; and protect themselves from violence, often exacerbated in fragile situations.
But such crises are also opportunities to change gender norms, promote contraception and abortion, and campaign for changes to abortion laws, according to speakers at panel. The event was co-sponsored by Save the Children, CARE, the International Rescue Committee (IRC), and Family Planning 2020. Although the theme was providing family planning in humanitarian settings, the panelists frequently discussed their work in providing abortion.
“Norms have a way of changing in acute settings,” said Seema Manohar of CARE, an organization working to undermine the current U.S. administration’s pro-life policies abroad. CARE opposes the Protecting Life in Global Health Assistance (PLGHA) policy blocking U.S. funding to foreign groups that promote or provide abortions.
As an example, Manohar said that in one area of the Democratic Republic of the Congo, only short-acting contraceptives had been available. After conflict in the region necessitated a humanitarian response, longer-acting methods were being provided.
Manohar said that her organization’s work includes the provision of “safe abortion” and she cited a guidance called the Minimum Initial Services Package, or MISP, which calls for “safe abortion to the full extent of the law” in humanitarian settings. The MISP was created by the Interagency Working Group for Reproductive Health in Emergencies, of which CARE is a steering committee member.
On multiple occasions, the presence of abortion in the MISP has led to its exclusion from negotiated UN documents.
Erin Wheeler, IRC’s Contraception and Abortion Care Advisor, also discussed her organization’s work to promote abortion, focusing on Venezuelan refugees in Colombia. She noted that IRC “strives to be a feminist organization” and provides abortions in eight countries. In Colombia, IRC works with local affiliates of the International Planned Parenthood Federation, where they refer patients for abortions after 13 weeks’ gestation. For earlier pregnancies, Wheeler said her organization provides them with abortion pills.
Comparing different sites in Colombia, Wheeler said providing abortions was more difficult in Medellín, both because of local regulations and health workers’ attitudes. “We’re actually finding some providers a bit reluctant to offer this service, we’re seeing conscientious objections, but also they’re requiring hospitalization for even first-trimester abortion, which actually has been dramatically increasing our costs.”
Wheeler said IRC was working with local leaders to find ways to “improve staff attitudes” and document “delays” to accessing abortions.
All panelists stressed the importance of advocacy in addition to providing humanitarian services. Wheeler said that in order to change norms nationally, one key was finding groups already working on those issues and helping them with partnerships and financing. She pointed to the example of a “nexus-wide” effort to liberalize the abortion laws in the Democratic Republic of the Congo.
In response to an audience question about the impact of PLGHA, Wheeler noted that IRC is U.S.-based, and therefore exempt from the policy, which she referred to as a “benefit” of their structure.
Wheeler echoed the sentiments of the panel regarding the administration’s pro-life policy: “Hopefully we don’t see it in the future.”
A dialogue of discomfort in the face of an epidemic:
A. What could be more important to a developing country than highly effective contraception for its women?
B. Preventing HIV-AIDS, perhaps?
A. That is equally important, but not more important.
B. We agree. But what if the most effective method in such a country seems to be increasing the risk of HIV?
A. Well, none of the evidence for that so far is very strong. We must do some research that will give us a definitive answer to this question.
That, very simplistically, is the conversation that has been going on for at least a decade between the international population control establishment (A) and the HIV-AIDS prevention establishment (B) – a conversation that resulted in a World Health Organisation press release in June headlined, “New study finds no link between HIV infection and contraceptive methods”.
The definitive research has been done and the main finding is greatly reassuring to the WHO and the sexual and reproductive health NGOs providing contraceptive services in southern and south-eastern Africa. This is the region of the world where the HIV epidemic is now concentrated, especially among young women – the population which is also deemed to be most in need of highly effective contraception.
For 30 years, as the AIDS epidemic took hold in many countries, evidence has been accumulating that women on hormonal contraceptives, in particular the injection best known as Depo-Provera, were more likely to become infected with HIV than those not using modern contraception. Targeted studies over the last decade showed increased risk levels of 50 and 100 percent.
This was disappointing to the WHO and others because Depo-Provera – a synthetic progesterone shot lasting three months and usually injected into muscle tissue in the upper arm (also named DMPA-IM) — and a similar injectable were regarded as the most effective method for women living far from family planning clinics (or any regular health service) and in traditional communities where birth control was suspect.
Did this highly effective method of preventing too many births in fact pose a special risk? And if so, how much of a risk?
The ECHO trial
To answer these questions a clinical randomised trial was designed with the title, Evidence for Contraceptive Options and HIV Outcomes (ECHO). Its main purpose was to compare HIV infection rates among women using DMPA-IM and two other methods: the Levonorgestrel implant (also known as Jadelle), and a (non-hormonal) copper-bearing IUD.
Sexually active young women (ages 16 to 35) who wanted effective contraception were recruited in 12 community settings (nine sites in South Africa, and one each in Eswatini, Kenya and Zambia) with high HIV prevalence, they had to be HIV negative and not have used any of the methods during the previous six months. After screening, 7829 women were enrolled in the trial and randomly assigned to one of the three methods.
The women were followed for 12 to 18 months and received ongoing health services, including counselling on HIV prevention and care, screening and treatment for sexually transmitted infections. To remain in the trial they had to contribute at least one HIV test. Retention rates were over 90 percent.
When the results were reported in The Lancet Online in June there was good news and bad news.
The good news: “We did not find a substantial difference in HIV risk among the methods evaluated, and all methods were safe and highly effective.”
The bad news: “HIV incidence was high in this population of women seeking pregnancy prevention, emphasising the need for integration of HIV prevention within contraceptive services for African women.”
The take-home message: “These results support continued and increased access to these three contraceptive methods.”
In other words: Shame about all the HIV – we need to do something about that – but it’s nothing, or nothing much to do with the contraceptives we like so much.
‘Reassuring’ – and ‘sobering’ results
In the WHO press release, a member of the ECHO Management Committee said that the results were both “reassuring” and “sobering”:
“After decades of uncertainty, we finally have robust scientific evidence about the potential relationship between hormonal contraception and the risk of HIV from a rigorous, randomised clinical trial,” said Professor Helen Rees, Executive Director of the Wits Reproductive Health and HIV Institute at the University of Witwatersrand in Johannesburg. “The results on this question are reassuring, but our findings are also sobering, because they confirm unacceptably high HIV incidence among young African women.”
At the end of August, WHO issued an updated guidance on the contraceptives in question that means they can be used without restriction.
So, all methods safe? Full steam ahead?
Not everyone in the conversation about contraception and HIV is equally reassured. Those involved in HIV prevention and advocacy, in fact, find it very sobering.
Responding to the WHO’s reclassification of DMPA-IM, the New York based Global Advocacy for HIV Prevention (AVAC) said it was “gravely concerned that this guidance will be used to justify a ‘business as usual’ approach.” The Civil Society Advocacy Working Group on contraception and HIV went further, saying that, “The ECHO results are not ‘good news’.”
Listening carefully to ECHO
To understand why requires listening carefully to ECHO, to three notes in particular.
1. The number of women who became infected with HIV during the trial – despite counselling and treatment – was 397, an annual rate of 3.8 percent (4 percent in South Africa) that the authors of the Lancet report describe as “alarmingly high”. The WHO requires a preventive drug regime known as PReP for rates above 3 percent.
Under these circumstances, as the advocacy groups cited above said, any increased risk associated with method use is unacceptable. However, the trial was geared to detect a 50 percent increased risk (or hazard ratio) and could not reliably detect ratios below 30 percent.
2. ECHO only compared three methods to one another, not the absolute risk of using a method compared to using no hormonal or other “highly effective” form of contraception, as most previous studies have done.
Dr Jokin de Irala, who holds the Chair of Preventive Medicine and Public Health at the University of Navarre in Spain, told MercatorNet that he agrees with the ECHO authors that, given the design of the trial, having a placebo group would have been unethical, but a comparison with HIV rates in the areas from which the women came would have been useful. As it is, “the only valid conclusion from the trial is that the three groups compared have similar rates of HIV.” Given the high rate of infection inthe trial, he adds, the ECHO finding that “all methods are safe misses some criteria of safety.”
3. ECHO did find increased risks in its comparisons; these were (per annum) as follows: 4 percent for DMPA-IM compared with the copper IUD; 23 percent for DMPA-IM compared with the implant LNG; and 18 percent for the copper IUD compared with LNG. (In a secondary analysis the first two figures were 10 percent and 29 percent.) What was “reassuring” was that these figures were “similar” and all below 30 percent – that is, not statistically significant in terms of the study design.
STIs – the other epidemic
In truth, it is hard to see how anyone can feel reassured by these results from a region with what AVAC calls a “soaring epidemic [of HIV] among young women,” (who can also, by the way, infect new partners.) Among those in the ECHO trial there were high rates of other infections as well: at enrolment 18 percent had chlamydia and by the end of the trial, despite treatment, gonorrhoea stood at 5 percent. Some had herpes. It is well known that these other STIs increase the risk of HIV in the long run.
WHO officials quoted by the Kenyan paper, The Nation, said the infection figures in ECHO were “a wake-up call”, that “STIs have been forgotten” and that family planning clinics should be offering testing. Ironically, it’s long-acting contraceptives like DMPA, and even more, the implant and the IUD, that keep women away from clinics and their other services.
At the same time, as Dr de Irala points out, these “very effective” methods might lead young women to take more risks with their sexual behaviour – what is known as risk compensation. The ECHO study authors themselves noted “post-randomisation differences in self-reported HIV risktaking behaviours between groups.”
Biological reasons are also in play for young women. It is thought that hormonal contraception reduces the immunology of the vagina and cervix, which in younger adolescents is immature. A scientific report in Nature in January suggested the mechanisms by which this happens with DMPA-IM.
Anything but behaviour change
Both the population control and HIV-AIDS prevention establishments agree that there is an urgent need for “integration” of their respective services and training of providers. AVAC and others insist that injectables are not suitable for all women and that there must be a greater choice of contraceptives for them, as well as PReP for those most at risk of HIV. How they will achieve all this, and who will continue to fork out the funds required is not clear. Some are pinning their hopes on a magic pill that will prevent babies and HIV at the same time.
The last thing they will consider, apparently, is behaviour change. In the 1990s the Ugandan population living with AIDS fell from 15 percent to 5-6 percent through the presidential-led ABC campaign: abstain, be faithful to one partner, or if you can’t, use condoms. This strategy has been used in other African countries also with some success, where it is more consistent with traditional values.
But Western elites underestimate the peoples of the developing world, and in their continued hurry to bring down birthrates that are already falling – and are just where they should be in Africa – they undermine local cultures and make whatever is faulty in them worse. Much of this is done in the name of “empowering” women, who, in southern Africa at least, are now the population most vulnerable to HIV, and from an early age.
The trouble with rich elites is that when they intervene in other cultures, they only look for echoes of themselves. This is why they cannot really help African women, as the plight of those in the ECHO study demonstrates.
By now most readers are aware that U.S. birth rates have fallen to all-time lows. Early data for 2019 suggest that this slide is likely to continue. Those interested in demography more generally may also be aware that birth rates are falling in other countries. Most recently, reports of Finland’s baby bust have made headlines. Why are birth rates plummeting across so many countries?
Before the “why” question can be answered, it’s important to get a handle on the scope and scale of the decline. Where is fertility falling? Is the decline more severe in some places than in others?
To answer that question, I’ve put together the most up-to-date database of fertility statistics available anywhere, covering 61 countries for recent years. Major sources like the World Bank and the United Nations are only updated through 2017; I have updated through 2018 where data is available, and where year-to-date 2019 data is available, I’ve estimated what 2019 fertility rates are likely to be.
The data shows that very low fertility rates are becoming increasingly normal across the globe. Current declines are probably not just cyclical, but likely reflect a “new normal” with most countries having birth rates between 1.4 and 1.9 children per woman.
Presenting 61 countries’ fertility rates in a single graph is not feasible. Instead, below I show the average annual change in each country’s birth rate from 2007 to the latest data (2017, 2018, or 2019) for a variety of countries, grouped by various regional or historic ties. The groups are arranged from left to right, with the highest fertility region as of 2007 (the Middle East and North Africa) at the left, and the lowest-fertility region as of 2007 (East Asia) at the right.
As the figure shows, fertility fell the most in the highest-fertility regions, and it rose somewhat in lower-fertility regions. Put in statistical terms, the amount of variation among these 61 countries declined by half between 2007 and 2019. This was not only because of fertility declines among very-high-fertility countries, what demographers call “demographic transition,” but also because of modest fertility increases in low-fertility countries, and declines in medium-fertility countries.
The graph below illustrates this even more clearly, with the change in fertility rates since 2007 compared to actual fertility in 2007.
Basically, countries with birth rates above 1.6 or 1.7 children per woman experienced fertility declines. Countries with birth rates below that saw more stability or even increases. What we appear to be seeing is a global convergence around fertility rates of 1.6 or 1.7 children.
This is not just a rich-world phenomenon. Birth rates in Mexico are around 1.9 to 2 kids per woman, so below the rate needed to sustain Mexico’s current population levels. Brazil’s birth rate is even lower, at 1.75, similar to Colombia’s at 1.77. Costa Rica is even lower, at 1.66. El Salvador, Argentina, and Venezuela are all just barely “breaking even” demographically. Other countries like Guatemala are higher but falling fast.
Across the Pacific, Sri Lanka, Bangladesh, and India are all around 2 or 2.2 kids per woman, while Malaysia has fallen to about 1.8. Thailand is even lower, at 1.5 kids per woman. Even Muslim countries like Turkey (2), Iran (1.8), and Tunisia (2.1) have near-replacement fertility, with speedy declines still ongoing.
Data for Africa is not sufficiently recent or high-quality to speak to very recent declines, but the trend there is also one of extremely rapid fertility decline, as I’ve written previously for IFS.
Thus, while recent fertility declines are not globally shared, they nonetheless point to an emerging norm of below-replacement fertility. We should not expect that the future will be one of growing populations, but rather one where most countries face serious demographic challenges.
Why is this happening? A few specific country examples may help point the way to an explanation.
Asian Tigers? Asian Pandas.
Many commentators use “Japan” as a by-word for demographic decline. But while Japan does face demographic challenges, it appears to be rising to meet them. Today, Japan actually has the highest fertility rate in East Asia, once we exclude the hermit kingdom of North Korea and the post-Soviet nomads of Mongolia.
Japan’s birth rates have been rising for some time. But beyond this rise, Japan has been getting creative to encourage births at all levels of society and is also successfully opening its doors to immigration. The perception of Japan as an ultra-low fertility, unfriendly-to-families, closed-to-immigration country is increasingly outdated.
On the other hand, Korea’s birth rate has plummeted to astonishingly low levels. If current trends hold, 2019 will report birth rates of around 0.92 expected children per woman, one of the lowest numbers ever reported by any country. Korea is trying to boost fertility rates, but their efforts are misguided and failing. Without serious labor reforms aimed at de-prioritizing “workist” career-competitiveness, Korea’s birth rate will continue to fall.
Korea’s case is unique, but the forces driving it, especially the unchecked power of the labor market over peoples’ lives, are shared with many countries.
The Mongol Horde
The universality of the forces reducing fertility is sometimes obscured by impressive-looking short-term fluctuations. And indeed, elsewhere in Asia, there’s a baby boom.
Mongolians averaged 7.3 kids per woman in 1974: a figure that fell to 2.5 by 1993, and below 2 by 2005. But then, something happened. Since 2005, Mongolian birth rates have rocketed upwards and now stand at around three children per woman. The consequences of this baby boom on school crowding, the challenges it poses for children’s health in Mongolia’s highly polluted capital, and the role played by improving rural maternal health services, have all been featured in international media. More generally, Mongolia’s economic boom driven by growing global, and especially Chinese, investment almost certainly had a role to play. Meanwhile, this fertility gain has not come at the expense of gender equality, as Mongolian women remain better educated than Mongolian men, and are making more and more inroads into traditionally male-dominated fields.
But while Mongolia’s case appears unique for Asia, offering some cause for hope, that optimism would be misplaced. Mongolia’s true peers are not other Asian countries, but other post-Soviet countries.
Many former Soviet countries had a “baby bust” just like Mongolia did during the 1990s due to the chaos and disruption of the fall of communism. And many of those countries are now enjoying a recovery to fertility rates nearer their 1980s levels, just as Mongolia is. These recoveries probably will not last forever, and indeed may already be fizzling out. In time, despite its currently-impressive fertility trends, it is most likely that Mongolia’s “Soviet recovery boom” will fade, and the gradual forces of economic modernization will push its birth rates down to similar levels seen in other countries.
Modern Greenland
Economic modernization is a funny thing. Sometimes it comes naturally, sometimes, it’s forced. One of the most striking cases of “engineered modernity” comes not from the Soviet Union, but from Greenland, a constituent part of the Kingdom of Denmark.
Denmark had owned and colonized Greenland for a long time when, starting in 1950, the government embarked on an ambitious project to modernize the people of Greenland: economically of course, but also, perhaps especially, culturally. Notably, this was despite a 1946 decision by Greenland’s native leaders to reject modernization.
The first step of modernity was to introduce the sale of alcohol into Greenland, with predictably deleterious effects. Then, from 1952 to 1968, the Danish government embarked on a massive campaign of housing and infrastructure expansion designed to encourage Greenlanders to move out of small, traditional villages, into a few urban centers, where public services could be more easily delivered. The most infamous of these new housing developments was Blok P, an enormous and notorious public housing project that eventually housed nearly 1% of the total population of Greenland, but few of them happily. During the modernization period, education was also switched to Danish. Political modernity arrived as well, with the usual democratic, socialist, liberal, and rightist parties forming during the 1970s.
Overall, Denmark’s aggressive modernization campaign provoked anti-colonial resistance and helped lead to the movement for Greenlandic home rule in 1979, self-government in 2009, and perhaps someday independence.
But that wasn’t all. Fatefully, in 1967, the Danish government began a major campaign to promote IUDs. The results of aggressive modernization, intentional cultural disruption, and aggressive contraceptive campaigns were as might be expected.
In the span of just eight years from 1966 to 1974, fertility rates fell abruptly from 7 children per woman to 2.3. This is the fastest fertility transition in human history.
Of course, Greenland’s fertility did not fall to extremely low levels and remains near replacement rate today, although it is gradually declining. But the country is an example of the striking influence that can be exerted by a determined government. A full-court-press of political reform, urbanization, healthcare, education, and industrial transformation radically altered Greenlandic fertility. Not even China’s one-child policy was so dramatically successful at reaching its goals and, certainly, no pro-natal initiative has ever been so successful.
People of the Promise
So, if a government can engineer a cultural change to reduce fertility, can it do the opposite?
In any discussion of fertility, one country comes up a lot: Israel. Virtually alone among rich countries, Israel has a fertility rate of around 3 children per woman. And this is not just thanks to a minority group within Israel, like Muslims. The majority-population of Israeli Jews have birth rates around 3 kids per woman. While the ultra-Orthodox Jews have the most children, even secular Jews have above-replacement-rate fertility in Israel.
This also cannot be solely attributed to the general policy environment. While Israel does encourage births, many previously very-high-fertility groups in Israel, like the Druze, now have near-replacement-rate fertility. Rather, Israel’s high birth rates appear to be in some sense a product of cultural norms within the Israeli Jewish community.
However, if early data for 2019 is to be believed, Israeli Jewish fertility is now falling as well. If even Israel’s pro-family culture and aggressively pro-natal policies can’t stave off fertility declines, what can?
Looking Forward
Birth rates are falling. Around the world, it seems like fertility rates are likely to reach stability between 1.4 and 1.9 kids per woman, and most plausibly around 1.6 to 1.7. This is considerably below the assumptions of most population forecasting bodies like the United Nations, which typically assumes stable fertility rates of between 1.8 and 2.1. In other words, the ongoing global fertility slump suggests that the future human population will be smaller than expected.
Lyman Stone is a Research Fellow at the Institute for Family Studies, and an Adjunct Fellow at the American Enterprise Institute. Republished from the Institute for Family Studies blog, with permission.
PAMPLONA, Spain, October 22, 2019 (LifeSiteNews) — The use of oral contraceptives among women increases the risk of obesity, according to new research.
Researchers at Spain’s University of Navarre analyzed the results of a longitudinal study of nearly 5,000 women over the course of eight years. Lead researcher Alfredo Gea and colleagues at the university’s Center for Research on Obesity and Nutrition (Ciberobn) published their findings in the International Journal of Obesity. The study is titled “Oral contraceptives use and development of obesity in a Mediterranean cohort: the SUN (Seguimiento Universidad de Navarra) Project” and was published in August.
According to the study, the use of oral contraceptives by women over the course of two or more years is related to an increase of 78% in the probability of obesity in the following eight years. The abstract of the study stated, “The use of oral contraceptives (OC) has been suggested to represent a potential risk factor for the development of obesity.”
Regarding methodology, the authors noted that the study population consisted of 4,920 female university graduates who were identified as “initially nonobese” with a mean age of 28.2 years. The use of oral contraceptives was self-reported, while the body mass index of the subjects was assessed at the onset and every two years thereafter. For the purposes of the study, the female subjects were divided into two groups. The women of one group were regular users of oral contraceptives, while those of the other group were not.
The results of the study showed that obesity becomes especially prevalent among women who consistently use oral contraceptives over time. Researcher Álvaro San Juan Rodríguez of the University of Pittsburgh told Spanish newspaper ABC that the study proved that “the risk of developing obesity in the following years practically doubles among the women who regularly used oral contraceptives and almost tripled among those who used it continuously for more than two years.”
Gea urged caution in the use of oral contraceptives, which are more and more commonly used.
The study noted that obesity has become a global public health issue that has reached “epidemic proportions” and presents a major challenge to human health. According to the authors, “obesity increases the risk of diabetes, hypertension, coronary heart disease, stroke, obstructive sleep apnea, and certain types of cancer, among other diseases.”
The authors wrote that available evidence is highly inconsistent as to how oral hormonal contraceptive may cause weight gain. “Weight gain may be a result of fluid retention, fat deposition, muscle mass gain, or any combination of the aforementioned elements,” the study said.
No previous large prospective studies have assessed the long-term risk of oral contraceptive use, wrote the authors.
Previous studies have indicated links between oral contraceptive use and debilitating or deadly blood clots. Oral contraceptive pills can cause elevated levels of cholesterol, migraine headaches, high blood pressure, various forms of cardiovascular disease, and cancer. According to the National Cancer Institute, women who have used oral contraceptives are at a slightly higher risk for breast cancer. The government agency noted that women who have used oral contraceptives are also at a higher risk of endometrial and cervical cancer.
The family of a college student who died in 2014 from a pulmonary embolism linked to birth control has been awarded $9 million in a wrongful death medical malpractice lawsuit against Auburn Urgent Care in Alabama.
Hope Johnson was prescribed hormonal birth control by her gynecologist even after a blood test determined that she was at a high risk of developing blood clots. The doctor’s office, however, failed to properly file the lab results and Johnson was prescribed birth control that was a risk to her health and life. According to AL.com, her mother had a history of blood clots and had a pulmonary embolism while pregnant.
About a month after being prescribed the hormonal birth control, Johnson was struggling with shortness of breath, chest pain, headache, and a sore throat. On December 2, 2014, she went to Auburn Urgent Care for help. She was diagnosed with bronchitis and was prescribed an antibiotic. She was directed to come back if her condition worsened.
The next day, she had “severe shortness of breath” and her chest pain had gotten worse. However, the doctor at Auburn Urgent Care did not give her a physical exam, according to AL.com, but diagnosed her with a high white blood cell count and shortness of breath. She was given an inhaler. It was the first day on the job for a new doctor at the clinic and he had been directed by the medical director to treat patients without having any access to their current or past medical records. The lawsuit stated that Johnson’s condition was critical and she should have been taken by ambulance to East Alabama Medical Center.
The following day, on December 4, Johnson died of a “massive pulmonary emboli” according to the lawsuit, which was filed against Auburn Urgent Care, Dr. Zenon Bednarski – the clinic’s senior partner, owner, and supervising physician – and Dr. David Willis, the doctor who saw her at the urgent care. The lawsuit states that Bednarski did not give Willis login credentials that would have enabled him to view patient histories. It was Willis’s first day on the job. The verdict is the largest ever in a Lee County medical-malpractice suit.
“We are very pleased with the jury decision in the wrongful death case of our precious daughter Hope,” the Johnson family said in a statement. “We continue to feel her absence every day and pray this decision brings about much-needed change. Our chief desire is that this case will set a precedent that will prevent this from happening to another family or college student, not just in Lee County, but in Alabama as a whole.”
Hormonal birth control carries numerous risks to women’s health, which are frequently downplayed by doctors and the media. Women are often not fully informed about the potential risks to their health when they are prescribed birth control. These dangers include an increased risk of depression and suicide, heart attack and stroke, breast cancer and cervical cancer, infertility, and blood clots — as was the case with Johnson.
“Hope’s death is tragic because it was entirely preventable,” said Brett Turnbull of Turnbull Law Firm, representing the Johnson family. “We don’t know the exact number of patients seen that day, but it was too many. Patient well-being, not profits, should be the primary goal of healthcare.”
The pro-life movement is marked by many prayers. For people of faith, prayer unites us to the Lord of Life, and calls Him to make present the Victory of Life. We pray for our own conversion and for the conversion of the mothers, the fathers, the abortionists, and the general public.
Among Catholics, few are more popular than the Rosary and the Chaplet of Divine Mercy.
The Rosary has been constantly recommended by Popes and saints. In its prayers can be found all of salvation history. It immerses us in Scripture. It has gained great victories for Christianity through the ages.
And it is particularly well suited to our movement to end abortion. There are a number of reasons.
The Rosary honors a Mother, and calls “blessed” the fruit of her womb. This counteracts the abortion mentality, which sees motherhood as more of a burden than a blessing and sees the fruit of the womb as disposable.
In the Rosary, we proclaim that we are sinners. “Pray for us sinners.” “Forgive us our trespasses.” It proves false the accusation of abortion supporters who tell us we are “self-righteous.” Rather, we are the ones who need to repent of our negligence and inactivity regarding abortion.
Often the Rosary is used at the prayer vigils at abortion facilities, where we confront the killing, lies, and exploitation that go on inside.
The Rosary has a calming effect as our fingers handle the beads, our lips repeat the Hail Marys, and our mind calmly reviews the Mysteries. An abortion mill can be a place of great tension, especially if there are counter-demonstrators. The Rosary helps diffuse the tension.
The format of the Rosary allows everyone to participate, whether at an abortion mill or during a march. It can be prayed while walking and can be adjusted to any time frame. A practical suggestion is to have half the group say the first part of the Hail Mary and the other half respond. If there is only one person leading the prayer, most people cannot hear it, especially with the noise of traffic.
Because of the popularity of the Rosary among pro-life activists, various forms of “pro-life Rosaries” have been developed. Some of these have different colored beads associated with each decade, each representing a specific intention (the babies, the mothers, the abortionists, etc.). Some rosaries bear the image of the unborn child on each bead.
The Divine Mercy Chaplet grew out of a series of visions experienced by St. Faustina, who was a religious sister in Poland in 1935.
In the revelations of Divine Mercy to St. Faustina, abortion was the primary sin for which God asked us to cry out for his mercy. Moreover, God allowed St. Faustina to experience severe abdominal pains, to signify the pain of mothers aborting their children. The devotion to Divine Mercy deserves particular emphasis for those who have had abortions and for abortionists and clinic workers.
Because of all this, we at Priests for Life have just begun a daily broadcast of the Rosary at 3 p.m. ET on EndAbortion.TV and about twenty social media video platforms simultaneously.
The Joyful Mysteries will be recited on Mondays and Saturdays; the Sorrowful Mysteries, on Tuesdays and Fridays; the Glorious Mysteries, on Wednesdays and Sundays, and the Luminous Mysteries, on Thursdays.
Following the rosary each day, I will also pray the Divine Mercy Chaplet of St. Faustina. Each broadcast lasts about 28 minutes.
Please join us, and let’s continue to bring the power of prayer to the most important, urgent and fundamental human rights struggle of our day: restoring protection to the children in the womb!
A measure to force public universities to offer dangerous abortion pills on college campus, recently signed into law by California Governor Gavin Newsom, will initially be set up using funds from pro-abortion groups. However, pro-life student group Students for Life of America (SFLA) notes that student fees will also be used to fund on-campus abortions, since those fees underwrite the costs of campus healthcare centers. SFLA also pointed out how the conscience rights of students and healthcare workers will be violated if forced to participate with abortions. “This law includes funds that can go to Planned Parenthood for ‘consulting’ and new funds for ‘security’, allowing the nation’s number one abortion vendor to sit back and cash checks, enjoying the chaos of abortions taking place at schools without any of the risk,” said SFLA president Kristin Hawkins.
The bill requires student health care services centers at the state’s 34 University of California (UC) and California State University (CSU) campuses to offer medication abortion on and after January 1, 2023. According to a Department of Financial Bill Analysis, SB 24 “establishes the College Student Health Center Sexual and Reproductive Health Preparation Fund under the administration of the Commission on the Status of Women and Girls.” It requires the Commission, whose current chair Alisha Wilkins previously worked for Planned Parenthood of the Pacific Southwest in Riverside, “to provide grants of $200,000 to each student health center, and a grant of $200,000 to both the UC and CSU system to become prepared to offer abortion by medication techniques and develop associated back-up medical supports.”
The Buffett Foundation, identified by the Washington Post in 2000, writing, “The Buffett Foundation… made at least $2 million in interest-free loans to the Population Council… according to tax documents filed in 1995. That money was in turn used to conduct clinical trials of RU-486 [the abortion pill].”
A number of other abortion pill investors chose to remain unnamed, according to internal documents reviewed by the Wall Street Journal
Packard Timeline shows it invested in abortion pill distributor
To update campus student health center procedures, provide training, and purchase equipment at UC, the Department’s analysis estimated:
One-time system wide readiness General Fund costs between $4.6 million to $7.8 million…
Ongoing General Fund costs of $2.2 million to $3.3 million commencing in 2023 to provide abortion by medication services in each campus student health center and provide access to 24-hour telehealth services.
At CSU, the initial costs were “unknown” but raised concerns it could likely range in the millions to low tens of millions of dollars.
CSU on costs of law mandating abortion pills on California campuses (Image: CBS Sacramento)
“While this bill and its sponsors indicate that private financing would cover all the costs associated with this bill, Finance notes this bill could create future General Fund cost pressures to the extent sufficient private funding cannot be raised to support readiness grants, the costs to comply with this bill’s requirements exceed the proposed grant funding, or to the extent the UC and CSU incur ongoing costs after January 1, 2023,” the analysis said.
Lila Rose on law mandating abortion pills on California campus (Image: Twitter)
According to a statement by the ACLU, a “[C]onsortium of funders, including the Women’s Foundation of California and Tara Health Foundation,” has raised the initial funds.
Tara Health Foundation (THF):
A pro-abortion philanthropic organization which funds abortion projects and abortion facilities.
According to the Guttmacher Institute there were 132,680 abortions committed in California in 2017. A previous analysis by Live Action News revealed that taxpayers in the state paid over half a billion dollars (nearly $700 million) for abortions from 1989 to 2014. In 2017, the pro-abortion Advancing New Standards in Reproductive Health (ANSIRH) — a research group at the University of California, San Francisco (UCSF)’s Bixby Center for Global Reproductive Health, which trains abortion providers — estimated, “Approximately 23% of CSU students and 12% of UC students are enrolled in Medi-Cal.”
Medi-Cal FFS abortion expenditures in California 1989 to 2014
“Students across UC and CSU campuses obtain 1,038 abortions each month,” ANSIRH wrote adding, “[W]e estimate there would be between 322-519 medication abortions occurring across UC and CSU campuses every month.”
SFLA claims there was no need for the law because abortion facilities are less than 6 miles from every California public university and college campus. The group also claims there are no safeguards are in place to protect women who may be dosed with the drugs without their consent. Live Action News previously documented how many of those behind the push for these dangerous pills to be readily available on campus are also pushing for FDA safety requirements to be lifted. To date, at least 24 women have died from the abortion pill and literally thousands have been hospitalized with serious complications.
Are you feeling tired? You’re not alone. Roughly 25% of women have trouble sleeping at any given time. As our female bodies go through seemingly endless hormonal changes, it can be hard to fall asleep and stay asleep. But researchers have found there may be an unexpected factor contributing to the modern epidemic of exhaustion: the birth control pill.
To understand how hormonal contraception can affect a woman’s sleep, it’s important to first know how human sleep is structured. Shut-eye actually happens in phases. In stage 1, which only lasts a few minutes, we experience brain waves called alpha and theta waves. This is very light sleep where we can still be easily awoken. In stage 2, the brain causes a sudden increase in wave activity. Stages 3 and 4 are where the deep, restorative rest we all long for happens. This is slow wave sleep, in which the brain is producing delta waves. We get our energy for the next morning, consolidate what we learned during the day for our long-term memory bank, and repair our bodies during this time. Finally, there’s Rapid Eye Movement or REM sleep. This stage is when most of our dreaming occurs.
Ladies actually have a special sleep advantage: We are naturally capable of getting more of that deep, stage 3 sleep, compared to men. But researchers have discovered that women taking the artificial hormones found in the Pill don’t get the same benefit. Their body temperatures were elevated, and they experienced less stage 3 sleep compared to women who were experiencing their natural menstrual cycles without the synthetic hormones found in contraceptives. I asked Dr. Lynn Keenan about this phenomenon. She is Program Director of the Sleep Medicine Fellowship, and a NaProTECHNOLOGY expert, at the University of California, San Francisco – Fresno.
What natural hormones have to do with good sleep
“This was also found in women after menopause taking the synthetic progestin,” Dr. Keenan told me. “They have worse sleep quality than those taking bio-identical progesterone.” Bio-identical hormones are the same, at a molecular level, as those naturally produced in the human body.
Women who are paying close attention to their bodies through Fertility Awareness-Based Methods (FABM), or modern methods of natural family planning (NFP), may find their fertility charting to be a helpful tool for understanding the intersection of their reproductive cycle and their sleep.
“Charts can give you hints that there may be a coexisting sleep disorder that is impacting the woman’s quality of life,” Dr. Keenan said. “I have had women who only had sleep walking or sleep talking in their luteal phase, and when taught to chart, we found lower than normal progesterone, and the timed administration of bio-identical progesterone controlled their [sleep walking].
“Some women with Polycystic Ovary Syndrome, or PCOS, have very heavy menses, and I find that group in particular have a high chance of sleep apnea,” she noted. “The oxygen drops associated with sleep apnea can really affect the ovaries and endometrium, and when the sleep apnea is controlled, I have seen significant improvements in menstrual flow. Both PCOS and sleep apnea have lower than normal progesterone,” she said.
Dr. Keenan has even observed a connection between women’s health and sleep conditions like narcolepsy and Restless Legs Syndrome, also known as RLS.
Given all the multi-tasking, care-giving and problem-juggling women have to cope with, it’s fair to say we have enough to keep us up at night, without disrupting the most restful stage of the sleep we do get. It’s just one more reason it’s wise for women to make the switch from birth control to Fertility Awareness-Based Methods; they work with our bodies—and our sleep goals—instead of against them.
Melissa Villalobos woke up on May 15, 2013, to find herself in a pool of blood.
That morning she was alone with her four children. Her husband, David, had left the family home in Chicago earlier that morning and was just then boarding a flight to Atlanta for a business meeting.
Bleeding had been noticed some weeks earlier during the first trimester of this, her sixth pregnancy. An ultrasound had shown that the placenta had become partially detached from the uterine wall, “so there was a hole in the placenta and that hole was allowing blood to escape,” Melissa explained to the Register July 22. To make matters worse, she had developed a subchorionic hematoma, a blood clot two and a half times the size of her unborn baby. This had lodged in the fetal membrane.
Her doctor ordered immediate bed rest for Villalobos.
But this was easier said than done. Melissa had four small children, aged 6, 5, 3 and 1. Although the 36-year-old mother had formerly practiced as a lawyer, her husband was the family breadwinner now. He had a high-pressure job that regularly took him away from home. No family members were close at hand to help: Melissa had been brought up in St. Louis, and David was raised in Texas. Apart from a few neighbors and friends, they were alone: Six months’ bed rest until the birth of their new child was nearly impossible.
In any event, the bleeding continued, and was getting worse since Melissa was admitted to a hospital emergency room on May 10, 2013. At that time, the medics warned the couple about a possible miscarriage. If the baby survived the pregnancy, they said, she would probably be born prematurely with attendant complications. The medical prognosis was heartbreaking, and now, less than five days later, the worst seemed to be happening.
Seeking Heavenly Aid
Sadly, David and Melissa had been here before. In February 2013, Melissa’s fifth pregnancy had ended in miscarriage, and Blessed John Henry Newman had been a part of that story, too. In that earlier pregnancy, the doctors, after detecting no heartbeat for weeks, had offered the mother a procedure to remove the unborn baby. Melissa refused. She was determined to carry the child to delivery, even if she knew the child could not live.
Perhaps no one, other than David, understood the grief that Melissa carried in her heart during those weeks before that first miscarriage. As she put it, at that time, she feared “the grief of that miscarriage would kill me of a broken heart.” So she prayed. The person to whom she prayed was a 19th-century English Catholic convert whom she had seen discussed on an EWTN television show and then whose prayer card had been brought home unexpectedly by her husband and now stood on a mantelpiece in the family home: “Please, Cardinal Newman, help me with this.”
Melissa Villalobos prayed as never before. She prayed for the child she carried; she prayed that, if her baby died, she could still believe, still trust, still love the God who had sent her this cross. But, most of all, she prayed that God’s will be done.
Her prayer was heard. As the dead child was buried, Melissa Villalobos remained faithful to the God of love. She knew that her prayer had been heard: that her faith, hope and love were intact, and that Newman’s intercession had been instrumental in this. Today, of that time, she simply says: “I lost the baby. But I had kept my faith — thanks to Cardinal Newman, my rock.”
Desperate Prayer
With the experience of her miscarriage still fresh in her heart and mind and concern for who would tend for her four young children, this young mother lay in bed, helpless, in a pool of her own blood on the morning of May 15, 2013.
Terrified thoughts ran through her consciousness: “I was afraid … of losing the baby and what would become of the four children downstairs if I were to bleed to death. How would they be raised? These things were crashing through my mind.”
Although she continued to bleed, she delayed calling 911, worried about her children should she be admitted to the hospital. Finally, she knew she had to call an ambulance, but she then realized she didn’t have her cellphone near her. She also knew that in trying to find it and make a call she would cause even more damage to her body.
Eventually she struggled to her feet. She began to make her way downstairs. Somehow she managed to get the children all in the kitchen and watched as they helped fix breakfast. Then, firmly, mustering all the strength she had, she ordered them: “Don’t get out of your seats no matter what!” They fell silent as their mother left the room. Melissa ascended the stairs.
At last she reached the bathroom. She locked the door behind her, fearing the children would see the blood on the floor. The next thing she remembers was opening her eyes after having collapsed. Now a feeling even more debilitating overtook her physical weakness: desperation.
Was it on this bathroom floor that she was to die, Melissa asked herself, while downstairs her four children sat silently waiting for her?
She prayed: “Please, Cardinal Newman, make the bleeding stop!”
It did.
Immediately.
“‘Please, Cardinal Newman, make the bleeding stop.’ Those were my exact words. Just then, as soon as I finished the sentence, the bleeding stopped.”
She knew instantly that something physical had changed. As she checked, something else occurred. “Just then the scent of roses filled the bathroom,” Melissa recalls, “the strongest scent of roses I’ve ever smelled.” In hindsight, she says: “The injury was unseen so the roses gave me the confidence to go downstairs to see the children.”
She made her way downstairs again. This time she was praying a different prayer than that uttered only minutes previously: “Thank you, Cardinal Newman. Thank you.” During all this time she heard no sound in the house. This had unnerved her. She felt panicked, thinking that the children had gone outside. She rushed to the kitchen only to find four silent faces looking at her. As they told her later, she had asked them to remain there, and that is exactly what they had done, simply and quietly waiting for their mother to come back to them.
The children may not have registered the fact that their mother’s mood had changed from one of utter anguish and dereliction to euphoric elation. “I thought to myself in that moment, ‘Oh my goodness! My baby is okay. I’m okay. My four children are okay. We’re all okay.’ And I said, ‘Thank you, Cardinal Newman.’”
Then her cellphone rang. It was David. He had arrived in Atlanta. There was a problem with his hotel. But all he wanted to know was how his wife was doing. His wife’s reaction was as unexpected as it was welcome: “Everything is going to be fine. … Everything is going to be great! … I’ll explain later. …Take care of your hotel and call me back.”
As it happened, that afternoon Melissa had a scan prearranged at the hospital, as the doctors were understandably still worried about the health of their patient. So, later that day, her complete recovery was confirmed. The doctors told her everything was now “perfect.” There was no longer a hole in the placenta.
Seven months later, on Dec. 27, 2013, a baby girl, Gemma, was born. She weighed 8 pounds, 8 ounces. The child has had no medical problems then or since, nor has her mother.
Canonization Cause
Villalobos waited until after Gemma was born to report the healing to the promoters of Cardinal Newman’s canonization. Officials from the Archdiocese of Chicago conducted the initial inquiry. A report was then forwarded to the Vatican for another series of investigations. This process officially concluded on Feb. 13, when Pope Francis announced the miracle was accepted: Cardinal Newman would be canonized. At no stage in this process was Melissa in any doubt: “I knew it was a miracle.”
Saintly Expression of Love
Melissa loves the family life she shares with David and her now seven children. When she was ill, it was the disruption to the family’s ordinary life that she found hardest to bear. She could not cook and clean and was unable to lift anything; she could not play with her children, for fear that if they bumped her it would set off more bleeding. She feared she would never return to normal family life. That changed instantaneously — and for good: “I was able to resume my full, active life as a mom,” she said. “I was cured through Newman’s intercession so that I could continue an ordinary life, but at the same time be completely devoted to him and to God and his Church.”
That devotion will open a new chapter this October when Melissa makes her first trip to Europe. She will travel with her family to Rome to witness the Pope proclaim a saint that same 19th-century English Catholic convert priest whom she feels now she knows well.
Melissa’s devotion to Newman started with an EWTN television discussion and a prayer card dedicated to him. It was his face upon the card that drew her interest. Newman’s eyes and expression seemed to understand her mood, her preoccupations when, from time to time, she passed by the card on the mantle. The more she read about Newman’s life and witness, the more she felt he understood her. Above all, she says, she learned of how Newman was a true shepherd to all. She wondered if, spiritually, she, too, could become part of his flock, “one of his spiritual children.”
That prayer is now answered — definitively. Now, John Henry Newman is linked to Melissa Villalobos. “To be in the same sentence as Cardinal Newman is a blessing beyond words,” she said, “a display of God’s mercy and Newman’s humility.”
Melissa says that Gemma, now age 5, is not aware of what took place, not yet, although the other day she asked her mother: “What does ‘cured’ mean?”
Today, as Melissa watches her children play and as she plays with them, Newman’s spiritual child reflects: “Several times a day I think of what has happened and try to show my gratitude, just to be as loving as I can be.”
October 14, 2019 (LifeSiteNews) – In 2018, cases of syphilis, gonorrhea, and chlamydia were at an all-time high in America, according to a report released last week by the U.S. Centers for Disease Control and Prevention (CDC).
The three most common sexually-transmitted diseases (STDs) rose to more than 115,000 cases of syphilis, more than 580,000 cases of gonorrhea, and more than 1.7 million cases of chlamydia, the CDC said in a press release. While all three are treatable by antibiotics, without treatment they can be spread to other people and lead to heightened risks of HIV, infertility and ectopic pregnancies.
The most alarming detail in the new report is a 40 percent spike in the number of infants born with syphilis to 1,300.
“There are tools available to prevent every case of congenital syphilis,” Gail Bolan of the CDC’s Division of STD Prevention said. “Testing is simple and can help women to protect their babies from syphilis – a preventable disease that can have irreversible consequences.”
The CDC report attributes the increases partly to drug use and decreased condom usage, as well as “poverty, stigma, and unstable housing” reducing “access to STD prevention and care,” as well as “cuts to STD programs at the state and local level.”
Social conservatives argue that something more fundamental is at work.
On Thursday, Family Research Council (FRC) president Tony Perkins interviewed Dr. Michelle Cretella of the American College of Pediatricians and FRC’s own David Closson, who attributed the numbers to “liv(ing) in such a sexually saturated culture” and to venturing “outside of God’s design and the boundaries that he’s given us,” respectively.
Cretella faulted the CDC’s statement for emphasizing secondary prevention (treatment after the fact) over primary prevention (discouraging risky behavior). She noted that government and society have no hesitation about telling young people to abstain from smoking (often employing frightening and judgmental language and imagery in the process), but tends to treat sexual promiscuity differently.
Pro-lifers have long argued that so-called “comprehensive” sex education, particularly as operated by Planned Parenthood, actually encourages underage sexual activity, partly out of far-left ideology and partly in order to generate more demand for Planned Parenthood’s services.
A 2016 report from the Obama-era U.S. Office of Adolescent Health found that, across six different Planned Parenthood affiliate partners, more than 3,500 students, and 87 schools, a Planned Parenthood-backed sex-ed program left students “significantly more likely than controls to have ever been pregnant or to have caused a pregnancy.”
Activists with green handkerchiefs, which symbolizes the abortion rights movement, demonstrate to mark the revival of their campaign to legalize abortion, in front of the National Congress in Buenos Aires, on May 28, 2019. – Activists and lawmakers in Argentina relaunched a bid to legalize abortion on Tuesday with a new bill before Congress and a major demonstration, resuming a battle that has divided the homeland of Pope Francis ahead of October’s general election. (Photo by Emiliano Lasalvia / AFP) (Photo credit should read EMILIANO LASALVIA/AFP/Getty Images)
Obianuju Ekeocha, pro-life founder of Culture of Life Africa, has coined the phrase “ideological colonization” to describe how well-funded abortion activists in the West push for the killing of preborn babies in developing countries, many of which have strong pro-life cultures. Although abortion activists are most overt in their ideological colonization in Africa, Latin America is also an important, if oft-overlooked, battleground in the struggle for life. A recent AP overview of the current hotspots in Latin America reminds us that abortion activists’ ideological colonization efforts are alive and well in the region.
Argentina
Argentina has long been a strong protector of the rights of the preborn, with abortion illegal with limited exceptions since the 1880s, making it a prime target of ideological colonization in Latin America by abortion activists.
Last year, Argentina came close to legalizing abortion after abortion activists’ well-organized and internationally backed campaign. As Live Action News reported, influential abortion colonizers like the International Planned Parenthood Federation (IPPF) and Amnesty International were directly involved with pressuring the Argentine government into taking up the bill. Many other groups supported the effort, including Human Rights Watch, which in 2018 called Argentina’s pending pro-abortion legislation a “landmark opportunity to end [the] harmful policy.”
Green scarves worn by protesters are well-recognized symbols of the pro-abortion movement in Argentina green scarves. The origin of these scarves is deeply, painfully ironic; the inspiration was drawn from the legacy of Argentine mothers of the desaparecidos, or disappeared, who wore white scarves in remembrance of their children who went missing under the military dictatorship. But instead of speaking up for their missing children, the green scarf-clad abortion supporters are wearing those symbols instead to advocate for their right to disappear their own children, through the violence of abortion.
Last year the effort to legalize abortion failed by a 38 to 31 margin in the Senate after widespread civic action by pro-lifers. However, this has not deterred the pro-abortion groups. As PRI reported, abortion activists reintroduced an abortion legalization bill on the symbolic date of May 28th, which abortion activists have termed the International Day of Action for Women’s Health. The day is an initiative of the Women’s Global Network for Reproductive Rights, whose members include leading ‘abortion colonizers’ like Amnesty International, the Center for Reproductive Rights, the International Centre for Reproductive Health, the International Planned Parenthood Federation, and Pathfinder International.
Mexico
Like most of Latin America, Mexico has long afforded preborn babies legal protections, but those seeking to expand abortion have been chipping away at its protections for decades. Planned Parenthood Global claims that its work in Mexico is “growing” and has as its primary goal to “reduce abortion stigma.” The predominantly Catholic country has traditionally been opposed to abortion with the exception of Mexico City, which legalized abortion in 2007. Last month, the state of Oaxaca became the first state outside the capital to legalize abortion when the state’s lawmakers approved a bill allowing abortion up to 12 weeks of pregnancy.
Although Mexico’s President Andres Manuel Lopez Obrador has not publicly taken a position on abortion, the fact that his party dominates Oaxaca’s legislature does not bode well. In another ominous sign, according to The Guardian, the federal government tweeted a note of support for Oaxaca’s abortion legalization: “Our democracy is strengthened with the extension of rights and the recognition of the autonomy of women to make decisions over their own bodies.”
Planned Parenthood Global celebrated with a tweet rife with undertones of ideological colonization; the abortion giant claimed that Mexico is finally emerging from its so-called backwardness and now “takes a crucial step in the protection of women’s rights.”
El Salvador
The small Central American republic of El Salvador has one of the most staunchly pro-life laws in the world. The country has come to the forefront in the news recently for controversies surrounding its abortion law and the case of a woman who was charged with inducing an abortion. International groups have been using this woman’s case, as well as the country’s controversial practice of prosecuting women who procure abortions in general, as a wedge and an opening to advance their ideological colonization.
Despite the flurry of recent press coverage, abortion supporters have targeted the country for years. In 2013, they tried to use the case of a 22-year-old named Beatriz (who requested an abortion because she had lupus and her baby had anencephaly) as their rallying cry, and they falsely claimed she needed a “life-saving abortion” when she was offered an emergency c-section (not the same as an abortion). The Supreme Court denied her request and upheld the abortion ban in 2013. In 2016, Amnesty International railed against El Salvador’s abortion restrictions as “tantamount to torture,” as Live Action News reported. Abortion groups like IPPF have even been caught covertly funding abortion advocacy organizations in El Salvador, as the Population Research Institute has reported. And in 2017, 21 pro-abortion Congressmen from the U.S. threw their weight behind the abortion colonizers by formally calling for El Salvador to decriminalize abortion, as reported in a Center for Reproductive Rights press release.
Despite losing U.S. federal funding, the abortion colonizers have retained significant influence around the world pushing their agenda, including Latin America. As Senior Counsel for Alliance Defending Freedom International Neydy Casillas said in an interview last year with Live Action News, Central and South America “have been targets for the abortion movement” for a long time. Some Latin America watchers are even trying to paint recent pro-abortion developments in Latin America as part of a “green tide,” an allusion to the green scarves of Argentina’s abortion activists.
Yet pro-life laws in many Latin American countries remain deeply rooted in pro-life cultural values that draw from the traditional influence of the Catholic Church and, more recently, the growing presence of evangelical Protestant groups. As Casillas has pointed out, despite the efforts of wealthy international abortion colonizers, “In Latin America, it has not been easy for them because most of the constitutions throughout the region protect life, but furthermore the value of life lives in people’s hearts.”
Issues In Law & Medicine published a new meta-analysis done by the Breast Cancer Prevention Institute 20 retrospective case-control studies from January 1, 2000 through June 30,2017 were analyzed. Overall, the 20 studies resulted in a 151% increase in breast cancer with induced abortion. These results were statistically significant. There was a 291% increase in the 5 studies that differentiated induced from spontaneous abortions as well as a dose response i.e. there was greater risk with more abortions. You can see a copy of this study here
Children, including infants, are being sexually abused, and then suffering the further degradation of having their abuse filmed and shared amongst an army of online perverts, on a scale that beggars belief.
“The Internet Is Overrun With Images of Child Sexual Abuse,” states the title of a New York Times investigative article, published last week, exposing the epidemic of child porn. According to the Times, in 1998 there were some 3000 reports of images depicting child sex abuse. A decade later, that number grew to over 100,000. By 2014, the number of reports broke one million, before ballooning to over 18.4 million by last year. Those reports, says the Times, “included over 45 million images and videos flagged as child sexual abuse.”
The scale of the problem is so vast that it is beyond the capacity of law enforcement agencies to respond. Officials interviewed for the article lamented that they are continually being forced to make impossible decisions about how to prioritize their resources – focusing, for instance, on identifying and rescuing the youngest and most vulnerable victims, knowing that by doing so they are abandoning countless other children to ongoing abuse. Furthermore, once the images are in circulation, they are almost impossible to delete: their existence haunting the lives of their victims indefinitely.
According to one law official, less than two percent of cases in which a computer in the U.S. has shared child porn will be investigated. “We are overwhelmed, we are underfunded, and we are drowning in the tidal wave of tragedy,” said Special Agent Flint Waters.
Some of the increase in the number of reports over the years can, no doubt, be explained by the implementation of better technology, such as artificial intelligence, to detect child porn. However, the experts interviewed by the Times leave no room for doubt – the underlying problem is an exponential increase in the number of individuals producing and sharing child porn.
It is tempting to envision the perpetrators of this horrific crime as being a tiny sliver of sub-human scum lurking somewhere “out there.” But the numbers defy this interpretation. One online forum on the “Dark Web” dedicated to sharing child porn reportedly had some one million members. Another such forum had over 30,000 members. The creator of that site – an Ohio man – had over three million images of child sex abuse on his computer when authorities caught up with him.
The members of these forums not only share child abuse images, but they also encourage one another to produce new images (i.e. to find children to abuse, and to film it), and exchange tips on how to evade the authorities. One of the creators of one such site, a daycare worker, admitting to abusing over a dozen children, as young as three months old. I cannot bear to type even the briefest description of what he did to the children.
Equally Deviant, “Legal” Porn Must End
As grateful as I am that the Times has drawn attention this epidemic, I was also troubled by a bizarre companion piece that they ran alongside their investigative article. This article strongly endorsed the hypothesis that the origin of pedophilic sexual attraction is “largely biological.” As James Cantor, director of the Toronto Sexuality Center, says in the article: “The biological clues attached to pedophilia demonstrate that its roots are prenatal.” In other words, people who are sexually attracted to children are “born that way.”
Now, I will not dismiss the possibility that early biological development may play a role in predisposing some people to experiencing unwanted sexual attraction to children. And if that is the case, such people bear a heavy cross. However, if – as the article itself acknowledges – scientific research on the topic is in its infancy, then why do other possible causes of pedophilic attraction receive scarcely a passing mention? In fact, the article avoids any mention at all of the elephant in the living room: the explosion in so-called “legal” porn use, and its connection to the growth of deviant forms of porn, including child porn.
Indeed, many people who work fighting child porn have argued that there is a clear link between legal porn use, and the rise in child porn. As Margaret Healey, a former adjunct professor at Fordham School of Law, put it in a report prepared for the 1996 World Congress against Commercial Sexual Exploitation of Children:
[W]ith the emergence of the use of computers to traffic in child pornography, a new and growing segment of producers and consumers is being identified. They are individuals who may not have a sexual preference for children, but who have seen the gamut of adult pornography and who are searching for more bizarre material.
Muireann O’Brian, who leads the Bangkok office of the organization “End Child Prostitution in Asian Tourism,” made the same point. “[A]rrests have shown men with perfectly normal sexual proclivities become seduced, then involved and finally addicted to child pornography,” she said. “Their addiction may manifest itself by them just keeping and looking at the images … But it has been found that the addiction leads many men into seeking out children to abuse.”
Certainly, there is no doubt about the existence of the phenomenon of “escalation” among regular porn users. Many users of legal porn will admit that the kinds of material that once excited them no longer excite them. In order to achieve the same sexual “high” they used to experience, they have instead found themselves searching out more and more deviant forms of pornography. A habit that at first seemed innocent and “normal” gradually led them down a rabbit hole into a cesspool of the grotesque and the violent.
The world-renowned psychiatrist Norman Doidge, author of the best-selling book The Brain That Changes Itself, has argued that routine porn use can alter the brain itself, creating new reward pathways that can only be stimulated by more and more extreme material. Doidge objects to the simplistic claim that the only problem with porn use is that some people may use too much of it. The problem with porn addictions is even more sinister, he says. Porn addictions have the power to “change sexual taste.”
It’s a simple matter of science, he notes: “One key driver of plastic change [in the brain] is the reward centre, which normally fires as we accomplish a goal.” He further explains:
A brain chemical, dopamine, is released, giving us the thrill that goes with accomplishment. It also consolidates the connections between neurons in the brain that helped us accomplish that goal. As well, dopamine is secreted at moments of sexual excitement and novelty. Porn scenes, filled with novel sexual ‘partners’, fire the reward centre. The images get reinforced, altering the user’s sexual tastes.
Not all regular porn users will become child porn users. However, many porn users will find themselves becoming gradually desensitized – or even attracted – to forms of porn that once disgusted them. Studies have found that people who view such material are also far more likely to want – and attempt – to act out what they have seen. Some will end up in the very darkest corners of the Internet. Indeed, it is madness to discount the possibility that some child porn users began as “regular” porn users, and that the normalization of pornography has not in some way contributed to some of the worst crimes imaginable.
What to Do: The Porn Stops Now
In the face of such horrific evil, it is easy to feel powerless. However, there are several concrete steps we can do to respond to this epidemic:
Pressure lawmakers to put more resources into fighting child porn – The New York Times article gets this part right. Law enforcement agencies need more resources to fight this filth. Demand that your local, state or federal legislator prioritize this issue.
Pressure lawmakers to prosecute “normal” porn – As Patrick Trueman has pointed out, hardcore pornography breaks obscenity laws already on the books. Despite this, lawmakers and law enforcement agencies have allowed our society to be immersed in a sea of filth. We should be prosecuting the big porn platforms and porn creators, and passing tighter restrictions on porn sites, so that children can never “accidentally” encounter pornography. This may not end child porn, but it will do yeoman’s labor in making it harder for people who are disposed to addiction to obscene materials from going down that dark road. Stop the problem at the source.
Quit porn – If you’re a regular porn user, you’re part of the problem. No, you may not be viewing illegal material involving children. But chances are you’ve already become comfortable with seeing forms of porn that once caused you discomfort. Furthermore, the porn industry in general is predicated on exploitation. The big porn sites are full of hardcore material involving young women who, in a moment of vulnerability, agreed to do something that they will regret for the rest of their lives. You are training your brain to be ok with violence and exploitation. Don’t feed the porn industry. Quit.
Talk to your children – In this day and age, parents simply cannot afford to be complacent about the harsh realities of our pornified society. Child sex abusers will often show their victims legal pornography in order to lower their inhibitions. The average age of exposure to pornography is now around 11 years old. When children are exposed to porn, they are more likely to become addicted, to be potential victims of abuse, and in some cases, to abuse others themselves. Talking about sex and porn with your kids is hard. But it’s your job. There are lots of helpful materials out there. One book lots of people I trust recommend is called “Good Pictures, Bad Pictures.” Buy a copy, or look for other books, and then approach the topic with your children in a frank, non-threatening and prayerful fashion. Arm them with the tools they need to protect themselves from abusers, and to protect their souls and their minds from the scourge of porn addiction.
Earlier this year, Rep. Sean Duffy resigned from his position in the United States House of Representatives to focus on his family. He and his wife, Rachel Campos-Duffy — both alums of the MTV reality show “The Real World” — were expecting their ninth child together, and had discovered the baby had a heart defect. This week, their baby girl was born, and that baby has a little something extra to love: an extra chromosome! Daughter Valentina StellaMaris has Down syndrome.
In August, Duffy took to Facebook to announce his resignation and explain why he was stepping down. “Recently, we’ve learned that our baby, due in late October, will need even more love, time, and attention due to complications, including a heart condition,” he wrote. “With much prayer, I have decided that this is the right time for me to take a break from public service in order to be the support my wife, baby and family need right now.”
The baby ended up being born a month early, and Duffy explained that their daughter would not only need open heart surgery within a few months, but also would have developmental delays, leading some to speculate that the little girl has Down syndrome. Yesterday, that news was confirmed, when Campos-Duffy made the announcement on her Facebook page.
Campos-Duffy said that Valentina remains in the NICU, and is the “sweetest, most perfect angel we’ve ever seen.” She also said that she does, in fact, have Down syndrome. “Valentina was born with a heart defect (2 holes in the heart and valves that need to be fixed). She will need surgery in 3-4 months,” Campos-Duffy wrote. “As we suspected, Valentina was also born with an extra chromosome, which means she also has Downs Syndrome. That extra chromosome certainly made her EXTRA cute. Life is wonderful!!” Both parents report that the family is already very much in love with their beautiful little girl.
Duffy is an outspoken pro-life advocate, including fighting for minority children to be protected while in the womb.
In 1985, I was asked to show the new film “The Silent Scream” (still online) at a local community college for the students. I was anxious to show this amazing 30 minute film showing an actual abortion on ultrasound and narrated by the late Dr. Bernard Nathanson, a former abortionist who was the co-founder of the National Association for the Repeal of Abortion Laws (NARAL) in 1969.
Dr. Nathanson later deeply regretted his actions, and earned the enmity of the abortion movement by exposing the “deceptions, dirty tricks, and other tactics that helped make abortion legal and socially acceptable in the United States”.
His “The Silent Scream” film was his effort to get the truth about abortion to the nation and it caused a lot of controversies.
When I showed the film at the community college, I was seven months pregnant and had a bumper sticker that said: “Every child deserves a birthday”. My mother supported my pro-life work but was worried about my speaking publicly. “Someone may try to shoot you!” she warned.
I just laughed at the time but when I got to the college I saw an armed guard also attending. He said he was there because there were death threats about showing this film. Although nothing happened and the students were very receptive to the film’s message, I was a bit shaken but hopeful that this film would help end the abortion nightmare.
34 years later, the battle to end abortion continues.
I thought of Dr. Nathanson’s film when I was finally able to see the 2019 movie “Unplanned” that, like “The Silent Scream”, also caused tremendous controversy. Some theaters refused to show it and many film critics panned it but the movie was a surprising success at the box office.
“Unplanned” is a great sequel to “The Silent Scream” because it depicts the true story of Abby Johnson, an ambitious young woman who became the director of an abortion clinic and thought she was helping women.
Abby slowly and painfully finally learns the truth about both medical and surgical abortions and the real effects on women-including herself. The effect is both eye-opening and heartbreaking. Abby Johnson now helps other abortion clinic workers like herself as well as the public to see the truth about the enormous damage abortion causes.
It’s been ten years since the Great Recession ended. Yet, despite robust economic growth and low employment over the past two years, births in the United States have continued to plummet.
Before the Great Recession, the fertility rate—the number of children women have on average during their lifetimes—had been on the rise. But once the recession hit and unemployment rose to 10%, many couples put off having children and birth rates declined.
Demographers and economists had long anticipated the birth rate would rebound when the economy recovered. After all, birth rates in the U.S. have historically fallen during economic downturns and risen during times of economic recovery. But despite a fifty-year low in the unemployment rate, rising earnings and wages, and a robust 2-3% growth in GDP almost every quarter since the start of 2017, birth rates are still falling
Earlier this year, the National Center for Health Statistics reported that the birth rate in 2018 had fallen to 59 births per 1,000 women 15-44 years of age—the lowest birth rate ever recorded in U.S. history. But before 2018, the 2017 birth rate had been the lowest birth rate ever recorded. And the year before that, the 2016 birth rate had been the lowest. In fact, of the 10 lowest birth rates on record, 9 of them have occurred in the past 9 years.
America’s total fertility rate is also at an all-time low with women on average giving birth to 1.73 children over their lifetimes. This is far below the replacement fertility rate, which is about 2.1 and is the minimum fertility rate needed for the current generation to replace itself without having to be propped up by immigration.
Despite low birth rates, however, preferences for childbearing in the U.S. have not declined.
According to Gallup, Americans on average think 2.7 children is the ideal number of children to have. This is virtually unchanged from the number of children Americans considered ideal back in the 1970s. In fact, Americans’ ideal family size today is larger than it was before the recession started in 2007—and in 2007, the fertility rate had peaked to the highest level on record since 1971.
So if childbearing preferences are not declining, why have birth rates continued to decline in spite of robust economic growth and low unemployment rates? As it turns out, there is no single driving reason why birth rates have fallen. The decline in the birth rate is the result of a variety of factors—including economic factors, postponement of marriage, demographic changes in the marriage market, and changing ideas on marriage—all of which happen to be converging right about now.
This week’s article will discuss the economic reasons behind the falling birth rate while next week’s article will discuss the cultural and demographic reasons behind this trend.
Lost Millennial Wealth
Perhaps the most potent reason driving the falling birth rate is that many adults, particularly young adults in their prime marrying-age years, are finding it difficult to afford having children or are finding it difficult to get their finances in order so that they can have a family. Nowhere has this effect had more impact than on Millennials who now make up the bulk of women in their childbearing years.
Financial concerns have weighed particularly heavily on Millennials as they were the generation hardest hit by the Great Recession. According to the Federal Reserve Bank of St. Louis, Millennials born in the 1980s accumulated 34% less wealth than they would have had the recession not occurred. By comparison, adults born in the 1970s lost 17% of their wealth and those born during the 1960s lost only 11%.
Many Millennials, who faced high employment and underemployment early in their careers, were not able to accumulate as much income or savings as prior generations had when they were entering the workforce. For some young adults, this has made it more difficult for them to achieve enough financial stability to start a family. As adults aged 20-34 years of age make up the bulk of childbearing in the U.S., lower birth rates among the Millennial generation has directly translated into falling birth rates overall.
For one, wages and earnings for young adults in their prime marrying years are less than they were a generation ago. Inflation-adjusted median weekly earnings for adults 25-34 years old today are lower than what they were in 1979 and during the early 2000s. Meanwhile, wages for the workforce overall has increased—an indication that while older adults are still seeing their real wages rise, adults in their prime marrying years are being left behind.
Today’s young adults are not only making less than they used to, they are also making less compared to the workforce overall. During the early 1980s, adults aged 25-34 years on average made more than the overall workforce and made close to what most adults over the age of 25 made. But during the late 1980s, median earnings for adults 25-34 years of age dropped below the workforce average. And since 2002, the wage gap has been steadily widening. Today, median usual weekly earnings for adults 25-34 years of age are almost 9% lower than the workforce average.
Due to high unemployment and slow wealth accumulation early on in their careers, Millennials are at risk for becoming a “lost generation” in terms of wealth, according to the Federal Reserve Bank of St. Louis. This has likely forced Millennials to put off milestones like getting married, buying a house, and having children.
The loss of wealth accumulation has affected low-income, lower socioeconomic, and minority young adults in particular. The little savings men and women in these demographic groups were able to accumulate were often spent on supporting aging parents or paying for basic living expenses rather than on things like education, transportation, and job training which could have helped to advance their careers.
Additionally, when it comes to getting a college education, young adults today (and their parents) have faced skyrocketing tuition costs. According to tuition statistics tracked by College Board, the inflation-adjusted cost of tuition at four-year private colleges has risen by 134% since the 1986-1987 academic year. At public colleges, the rise in tuition has been even steeper, increasing by 215% since the 1986-1987 academic year.
Meanwhile, wages have not kept pace. Since 1986, real median household income has only increased by 15.7%, according to the Federal Reserve Bank of St. Louis.
The steep and rising cost of college education has forced young adults to take on unprecedented amounts of student debt. The amount of outstanding student debt nationwide is now $1.48 trillion, according to the Federal Reserve Bank of New York, which is now greater than the amount of debt Americans owe through either credit card debt or auto loan debt. And since 2011, student debt has been rising at a faster rate than either credit card debt or auto loan debt.
The rapidly rising cost of student debt is likely part of the reason why birth rates have been declining in the U.S. According to a study from Ohio State University, every $1,000 in student debt a college graduate is historically linked to a 1.2% drop in the birth rate.
Due to mounting student debt and slow wealth accumulation, young adults have put off owning a home more than previous generations. While 43.3% of adults under the age of 35 owned their own home in 2005, in 2015, only 34.6% of young adults did.
Birth rates for women in their late 20s have plummeted since the recession (before the recession, they had been rising). A slight rise in birth rates among women in their early 30s (30-34 years) has not made up for the difference either. And while birth rates among women in their early 30s had been on the rise since 2011, in 2017, the birth rate for this age group also fell for the first time since the end of the recession.
The Rising Cost of Child Care
But there are many other reasons for the declining birth rate in the U.S. and it would be incorrect to fully attribute falling fertility to lost Millennial wealth due to the Great Recession.
A recent New York Times/Morning Consult survey found that the number one reason men and women today cite for having fewer children than their ideal number is that child care is too expensive.
Indeed, the cost of child care is quite steep. According to Child Care Aware of America, the cost of daycare for infants averages between $5,000 – $23,000 per year, depending on the state of residence. For most low-income parents, these costs can be prohibitive.
After child care, concerns related to finances, the economy, and the cost of raising a child were among the foremost reasons adults in the New York Times/Morning Consult survey cited for expecting to have fewer children than they wanted. Nearly 40% also cited not having paid leave through their employer or not having enough paid leave as reasons for not having as many children as they wanted. Presumably, if these couples had the financial security to take time off from work to have another child, they would. A full 36% of adults also said they struggled with striking a work-life balance, in part perhaps due to the fact that many adults do not feel secure enough in their careers or savings to devote sufficient time to family.
Some adults have even chosen to forgo childbearing altogether due to financial reasons. Those who say they do not want to have children most often say they want more leisure time or say that they haven’t found a suitable partner yet. But 31% say they do not want children because they cannot afford child care.
The cost of raising a child has skyrocketed in recent years. Since 2000, the cost of raising a child has risen by 41%. According to the United States Department of Agriculture (USDA), middle-income married households with two children making up to 107K per year spent on average $233,610 per child through age 17. And that does not even include costs associated with putting a child through college. A middle-income couple today with two children can expect to spend about $12,680 per year on a child until the child turns 3.
Even for married couples making less than $59K per year, the cost of raising a child is not much different. Parents making less than $59K shell out on average $174,690 per child in a two-child family.
According to the USDA, the biggest expenditure associated with the cost of raising a child is the cost of housing. In recent years, home prices have soared. In the past five years alone, the cost of housing has jumped by 33% nationally, according to the Federal Housing Finance Agency.
After the cost of housing, the cost of food is the second largest expenditure for parents when raising children, according to the USDA. The cost of child care and education is a close third and the cost of transportation a close fourth. But for parents with children under the age of five, the cost of child care is often a larger expense than either food or transportation.
Lack of access to paid leave in the U.S. is also a significant hurdle for many couples. According to a report prepared for the U.S. Department of Labor, 46% of Americans in 2012 who qualified under federal law to take unpaid leave for medical reasons, military deployment, or for the birth of a new child did not take it because they could not afford to do so.
Very few Americans have access to paid leave. According to the Bureau of Labor Statistics, only 17% of Americans as of 2018 had access to paid leave through their employer.
Other Economic Reasons
Studies have also hinted at other possible economic reasons for why the birth rate in the U.S. continues to tank.
High unemployment during the Great Recession, for instance, may have a significantly negative hindering effect on how many children Millennials have in the long term. According to a study published in the Proceedings of the National Academy of Sciences, women who live through high unemployment rates while in their early 20s may have significantly fewer births over their lifetimes. The study found that every 1% point increase in the unemployment rate experienced by women in the early 20s correlates with a 14-point drop in the birth rate by age 40.
But perhaps even more impactful on the birth rate than high employment has been the permanent loss of manufacturing jobs that were wiped out during the recession. According to one study, the loss of manufacturing jobs since the recession accounts for anywhere from 25%-50% of the drop in the birth rate, depending on race. The study found that the loss of manufacturing jobs during the recession had a stronger effect on the declining birth rate than even the unemployment rate. The loss of manufacturing jobs has driven down the birth rate for all major racial and ethnic groups, but the effect has fallen particularly hard on Hispanic women.
In a society obsessed with chemical-free everything, interest is growing in fertility awareness methods, which respect a woman’s physical “ecosystem” rather than disabling her fertility with chemical toxins. On September 30th, Fertility Care practitioner Melissa Buchan hosted a webinar titled, “How to Manage your Menstrual Cycle without the Pill.” Buchan was a co-host of the first ever Cycle Power Summit held in May of this year. During the webinar, she shared 3 Secrets to Tapping into Body Literacy for Self-Awareness and Health Advocacy.
Understanding your unique cycle is the foundation to confidently using natural birth control
Buchan spoke about how knowledge is power when it comes to fertility awareness. Each woman’s body speaks a “language” through the signs and symptoms of her fertility. Charting observable signs like cervical mucus and/or basal body temperature allows a woman to learn that language over time by identifying her unique body’s predictable patterns. Buchan stressed that confidence in using fertility awareness methods comes most importantly from learning an evidence-based method of natural family planning from a certified teacher. “Drive-by” self-teaching of natural family planning from a mishmash of online articles is insufficient and could potentially put a woman at risk of an unintended pregnancy. Furthermore, ongoing contact with a certified teacher is necessary, both for accountability and to answer questions that the woman may have as she navigates various situations like illness, the postpartum period, etc.
Charting your cycle is the first step to identifying reasons behind unexplained infertility
Buchan emphasized that infertility is a symptom of an underlying issue, not the primary problem, as a prominent infertility expert concurs. Infertility is a sign that something is wrong in the woman’s body that needs to be explored, and hopefully managed successfully or even cured.
In September, Live Action News shared several stories of women who conceived after infertility related to polycystic ovarian syndrome (PCOS) through Natural Procreative (NaPro) Technology. NaProTechnology is a reproductive health science that utilizes charting from the standardized CREIGHTON Model FertilityCare System. This charting serves as a starting point for exploring the root causes of abnormal bleeding, irregular periods, unexplained infertility, and more by helping guide fertility care clinicians in their choice of diagnostic tools. Multiple days of brown bleeding at the end of a woman’s period, for example, would generally indicate that a clinician should run a blood test to check for low progesterone levels. Low progesterone is one of a number of causes of infertility, as well as recurrent miscarriage.
Living a charting lifestyle is a powerful tool for self-advocacy
Buchan referenced a 2015 bulletin from the American College of Obstetricians and Gynecologists called “Menstruation in Girls and Adolescents: Using the Menstrual Cycle as a Vital Sign.” So often, a teenage girl with abnormally heavy periods is simply counseled to go on the Pill, which can have a whole host of dangerous and even life-threatening side effects. However, the graphic below shows a list of conditions that abnormal bleeding patterns in a teenage girl can indicate, which could be masked by the “band-aid” approach of going on the Pill to stop the bleeding.
Imagine the possibilities if a girl starts charting her cycle in her teens, learning her body’s unique patterns long before she needs to use them to navigate family planning. By the time she gets married and is ready to have babies, she is confident of how her body works (does she experience double-peaks? does she have little to no mucus on one hand, or continuous mucus on the other?) and if needed, has proactively sought medical help if she saw deviation from her norm, or if her charting instructor noticed abnormalities in her charting. She has already addressed any personal risk factors she has for miscarriage or preterm labor. This woman truly embodies every feminist catchphrase — she is empowered by knowledge, and free to make choices about her body that will benefit her and her whole family.
Medical leaders representing more than 30,000 doctors said intentionally killing a baby in an abortion is never necessary to save a mother’s life.
The American Association of Pro-life Obstetricians and Gynecologists (AAPLOG), the American College of Pediatricians (ACPeds) and the Christian Medical and Dental Associations (CMDA), representing over 30,000 medical professionals, issued a correction of the recently released joint statement on abortion from the American College of Obstetricians and Gynecologists (ACOG) and Society for Family Planning (SFP).
Today, Dr. Donna Harrison, executive director of AAPLOG, emphatically stated that “there is a difference between elective abortion – a procedure done to ensure that a baby is born dead – and the separation of the mother and the baby in order to save the life of the mother. ACOG leadership is deceptively hiding behind the confusion about the definition of ‘abortion’ to imply that such treatments to save the life of the mother are the same as elective abortions.”
Dr. Cretella, executive director of ACPeds explained, “a separation procedure to treat maternal pathology INTENDS to save the lives of both the mother and her baby if possible. In contrast, an abortion, which the general public understands to mean ‘elective abortion’, INTENDS to deliver a dead baby every single time. That is why a baby born ALIVE after an elective abortion is called a ‘Failed Abortion’. The separation of the baby from the mother did not fail. What failed to occur is that her baby ‘failed’ to be killed.”
Finally, Dr. Michael Chupp, chief executive officer of CMDA pointed out that “ACOG leadership’s advocacy of elective abortion is out of step with the 85% of OB/GYN’s who do not perform abortions. Their extreme advocacy for elective abortion through birth does not represent the majority opinion of either ACOG membership or the majority opinion of all the rest of the obstetricians and gynecologists in this country.”
The full statement follows:
As organizations representing over 25,000 medical professionals, we would like to correct the errors and assumptions of the recently released joint statement from the American College of Obstetricians and Gynecologists (ACOG) and Physicians for Reproductive Health (PRH).
We state unequivocally that there is a difference between elective abortion – a procedure done to ensure that a baby is born dead -and the separation of the mother and the baby in order to save the life of the mother. ACOG leadership is deceptively hiding behind the confusion about the meaning of the word “abortion” to imply that such treatments to save the life of the mother are the same as elective abortions.
A separation procedure to treat maternal pathology INTENDS to save the lives of both the mother and her baby if possible. In contrast, an abortion, which the general public understands to mean “elective abortion”, INTENDS to deliver a dead baby. That is why a baby born ALIVE after an elective abortion is called a “Failed Abortion”. The separation of the baby from the mother did not fail. What failed to occur is that her baby “failed” to be killed.
We are glad that ACOG and PRH leadership recognize what all pro-life obstetricians know – that sometimes treatments which result in the separation of the mother and the baby are necessary to save the mother’s life. However, ACOG and PRH leadership disingenuously imply in their statement that these life saving procedures are the same as elective abortions.
The ACOG leaders’ advocacy of elective abortion is out of step with the 85% of OB/GYN’s who do not perform abortions. Their extreme advocacy for elective abortion through birth does not represent the majority opinion of either ACOG membership, or the majority opinion of all the rest of the obstetricians and gynecologists in this country.
Respectfully,
Donna J. Harrison M.D. dip. ABOG
Executive Director
American Association of Pro-Life Obstetricians and Gynecologists
Mike Chupp MD, FACS, FCS(ECSA) CEO
Christian Medical Dental Association
Michelle Cretella, M.D.
Executive Director
American College of Pediatricians
BALTIMORE, Maryland, October 3, 2019 (LifeSiteNews) — A mother is furious after discovering that her 16-year-old daughter’s headaches and soreness were caused by a birth control implant inserted by a school nurse without her consent.
Nicole Lambert was shocked to learn from her daughter’s pediatrician that the pain her daughter was experiencing had been caused by a tiny tube containing the contraceptive “Nexplanon,” which had been improperly inserted in her daughter’s upper arm.
Not only did the doctor recommend that the tube be removed to alleviate the child’s discomfort, but he further warned that the contraceptive could cause far worse side-effects, such as blood clots.
“I actually started crying because just to hear that your child, anything could happen to your child and you don’t even know what’s going on,” Lambert told WMAR-2 News. “It’s a scary feeling.”
“I actually went to the school. I was furious. I was mad, so I went to the school and the nurse told me, ‘I don’t have to talk to you about absolutely nothing,’” said Lambert. “I’m like that is my child, I take care of this child, you can talk to me about my child.”
“And they put me out of the school,” said Lambert.
“They call me for Tylenol, but they don’t call me about birth control,” continued the concerned mom. “You gave my daughter this insertion so she might be suffering from that, but do they even look at that?”
“Other kids out here could be going through the same thing and their parents don’t know about it. And I just think these kids, if they have it incorrectly or whatever it is, they should be checked because anything could happen to these kids,” she added.
Disturbed that her daughter — and others — could, without parental notification, undergo such an invasive medical treatment that comes with potentially serious side-effects, Lambert has hired attorney David Ledyard to investigate.
“Ms. Lambert wasn’t given the choice to pick the medical provider where her daughter would feel comfortable going and receiving these services, who she knew did a comprehensive medical exam, who she knew her medical history,” Ledyard explained.
“There’s no transparency in the training or certification of the school health centers,” Ledyard told PJ Media.
“Are they looking at the medical history of the students and doing a full workup before implanting these devices?” asked Ledyard. “What is the certification process and training of the nurses?”
Lambert’s daughter attends Digital Harbor High School, which is home to one of Baltimore City’s 17 School-Based Health Centers (SBHC), several of which offer birth control to students.
According to the Baltimore City Health Department, 164 students were using birth control provided at school during the 2017–2018 school year, including oral contraceptive pills, Plan B, Depo-Provera, NuvaRing, and Nexplanon.
Maryland’s health code states, “A minor has the same capacity as an adult to consent to treatment for or advice about contraception other than sterilization.” Minors are also able to consent to treatment for or advice about drug abuse, alcoholism, venereal disease, and pregnancy, as well as to consent to physical examination and treatment of injuries from — or to obtain evidence from — an alleged rape or sexual offense.
According to PJ Media’s report, the surgery to remove the Nexplanon implant from Lambert’s daughter also entailed removing skin and tissue damaged by the device.
Although the Nexplanon implant was inserted into her daughter’s body without Lambert’s knowledge, a doctor could not remove it without Lambert’s consent.
Lucy Jones, A top psychologist found that the contraceptive pill can significantly affect a woman’s brain and change their personality, she claims. Dr Sarah Hill revealed that it affects “sex, attraction, stress, hunger, eating patterns, emotion regulation, friendships, aggression, mood, learning, and so many other things”.
In particular, she said women on the Pill are attracted to less masculine men and are less interested in sex.
That’s because the hormone progesterone, which sends a message to the body that ovulation is not required, is dominant throughout your cycle.
Dr Hill told the Daily Mail: “When you’re on the Pill, progesterone dominates the entire cycle.
“And rather than experiencing an increased preference for sexy men at high fertility like naturally cycling women do, Pill-taking women exhibit an unwavering preference for men with less masculine faces and voices.
“This is the sort preferred by naturally cycling women during the second half of their cycles, when progesterone is high.”
Less interested in sex
Several studies have supported this – with one led by Craig Roberts at the University of Stirling revealing that those not taking the Pill when they met their partners generally found their other halves sexier.
On the other hand, those who had met their partner while they were on the Pill didn’t have as good sex lives.
Despite this, women who chose their partners when they were on the Pill were more satisfied with their partners’ financial providing and intelligence than the women who chose their partners when they were off it.
And women who chose partners when they were on the Pill were significantly less likely to divorce than women who chose their partners when off it.
Dr Hill added: “It seems a natural cycle makes a woman more attuned to sexiness thanks to oestrogen levels, but progesterone dominance in Pill-taking women emphasises qualities that would have helped to keep them safe and secure when preparing for pregnancy.”
More desirable to men
On top of this, the Pill makes your brain “less interested in sex” and can “dial down your sexual motivation”.
This may have an impact on how attractive a woman may look.
Dr Hill revealed that women not on the Pill are more open to “new experiences” and put more effort into their appearance as they’re at a high fertility.
She said: “When women are coming into their fertile period, hormones do their utmost to make them attractive to a mate.
“Women at high fertility also wear more make-up, wear sexier clothes, and wear more red, a colour known to make women appear particularly attractive and desirable to men.”
One unconventional study, taken out by the University of New Mexico, even revealed that dancers at a strip club earned more money when they were not on the Pill in comparison to those that were.
Dancers not on the Pill earned an average of £56 per hour, whereas those on the Pill averaged around £30 per hour.
It revealed that while women on the Pill can tell if someone else is happy or scared, they’re 10 per cent less likely to pick up on pride or contempt.
Dr Alexander Lischke, from the University of Greifswald in Germany, said: “More than 100 million women worldwide use oral contraceptives but remarkably little is known about their effects on emotion, cognition and behaviour.
“Findings suggest oral contraceptives impair the ability to recognise emotional expressions of others, which could affect the way users initiate and maintain intimate relationships.”
Earlier this year, parents in North Carolina faced heartbreaking news in the second trimester of pregnancy—their twin girls had developed a disease called twin-to-twin transfusion syndrome, a life-threatening condition for both babies, caused by connections in the blood flow between identical twins who share one placenta.
That leads the smaller (donor) twin to pump blood to the other, larger (recipient) twin. If left untreated, advanced forms of the disease are fatal between 80% and 100% of the time.
The news was devastating, and the potential outcome for both babies was grim. But the medical team at the Charlotte Fetal Care Center offered a glimmer of hope.
They could perform laser surgery on the placenta to correct the defect, while the twins remained in their mother’s womb. If performed promptly (the next day), the surgery could significantly increase the odds that one or both of the baby girls would survive.
The North Carolina couple decided courageously to embrace this lifesaving treatment. Dr. Courtney Stephenson performed the in-utero surgery on the babies at 21 weeks, and even with some unexpected turns during the procedure, both girls survived with no lingering health issues. A news account can be found here.
Fetal surgery, in which babies receive lifesaving treatment while in the womb, is one of the next frontiers of medicine.
The first procedure used to treat twin-to-twin transfusion syndrome was pioneered and performed in 1988 by Dr. Julian E. De Lia in the United States. Opportunities for intervention have markedly improved since then, but the underlying goal has remained the same; namely, stop progression of the disease and optimize outcomes for both babies.
Fast-forward 30 years, and this minimally invasive surgery—formally called fetoscopic laser ablation—is now the preferred treatment, particularly when the disease is identified in its early stages, for patients between 16 and 26 weeks’ gestation.
High-volume fetal therapy centers, such as the Children’s Hospital of Philadelphia’s Center for Fetal Diagnosis and Treatment, report a higher than 90% survival rate of at least one baby and a higher than 80% survival rate of both babies after laser ablation. The Cincinnati Children’s Fetal Center reports similar data of higher than 80% overall survival of at least one or both twins.
The advanced technology uses endoscopes (small fiber-optic guided instruments) and one small incision to seal off the blood connection between the twins. Mom and both babies are under anesthesia, and the entire operation lasts less than two hours and requires only a one- to three-day hospital stay.
It is routine that women with twin pregnancies at increased risk of developing twin-to-twin transfusion syndrome receive increased surveillance to catch the disease in its early stages, should it develop. Women should be referred to a maternal-fetal medicine specialist for this close monitoring and for review of the options for treatment, including fetoscopic laser ablation.
Yet women still report instances where this procedure was not offered to them. In a recent study, one woman reports, “My [maternal-fetal medicine specialist] told me to abort babies and that laser was not an option for me … . I had surgery after I found a clinic … on my own, and both babies survived and are healthy.”
A 2017 Vice article describes a pregnancy with twin-to-twin transfusion syndrome to argue in favor of abortion beyond 20 weeks, with no mention of the latest treatment modalities in fetoscopic laser surgery.
Termination of one baby, called selective fetal reduction (or selective feticide), regrettably remains an option for babies with twin-to-twin transfusion syndrome, despite the fact that laser surgery has a proven record of saving both babies at all stages of the disease.
Selective reduction is rare and typically offered as a last resort in the presence of severe problems affecting one of the babies. In this procedure, cord blood flow to one twin is surgically blocked, causing death to that twin with the purpose of trying to improve the outcome for the other twin.
Studies have shown that selective fetal reduction offers no better outcome, with maximum survival of 50% for one twin, a rate much lower than laser surgery with a higher than 80% survival of one or both babies. And this termination procedure will guarantee 0% survival for at least one twin.
Furthermore, it can be hard to define which fetus has the worse prognosis.
A study in the Netherlands reported intentional fetal and neonatal demise in almost 10% of all twin-to-twin transfusion syndrome pregnancy cases, due to abortion, fetal reduction, and withdrawal of neonatal intensive care. A study in India reported performing fetal reduction up to 27 weeks of pregnancy, with survival rates still no greater than laser ablation procedures.
A 2019 U.S. study reported that the majority of twin-to-twin transfusion syndrome patients referred to a single surgery center in California for fetal therapy underwent fetoscopic laser ablation (96.4%), but a small percentage still opted for selective feticide (0.8%). Of those patients that did not undergo any form of fetal therapy, 42.6% terminated both twins.
Twin-to-twin transfusion syndrome is a particularly challenging and dynamic disease, with progression that is often unpredictable. Some cases remain stable throughout pregnancy, or even regress, while others develop quickly with rapid deterioration of twins within days.
The aforementioned U.S. study also highlights the critical role of time and suggests that the rapid progression of twin-to-twin syndrome, along with delays between diagnosis and treatment, contributed to a subset of women becoming ineligible for fetal surgery and resulted in fetal demise.
Clearly, there is a real need for immediate consultation in these women to determine eligibility for laser ablation surgery to give them the greatest chance of survival for their babies.
Resources such as the TTTS Foundation and Be Not Afraid can offer help to women in crisis who need immediate attention.
The story out of North Carolina is a beautiful reminder that amid the pain and despair in receiving a diagnosis of twin-to-twin transfusion syndrome, there is real hope of survival with fetal surgery.
It just takes a courageous medical team to do everything it can to give both babies the chance at life they so desperately deserve.
Physicians who remain diligent in following advances in this and other types of lifesaving fetoscopic surgery to treat a previously incurable disease can drastically improve outcomes for families and contribute to the advancement of medical science in the 21st century.
LifeNews Note: Tara Sander Lee, Ph.D., is an associate scholar for the Charlotte Lozier Institute. She is a scientist with almost 20 years’ experience in academic and clinical medicine. Kathryn Nix Carnahan, M.D. is an obstetrics and gynecology resident in Wisconsin and an associate scholar at the Charlotte Lozier Institute. Prior to attending medical school, Dr. Carnahan was a health policy analyst at the Heritage Foundation.
On September 27, 2018, a 20-year-old woman named Alexandra Williams died at Duke University Medical Center in Durham, North Carolina. The days prior had been normal for Alexandra, until she spontaneously collapsed in her driveway on September 26. In the months prior, she had experienced some back pains, which doctors did not understand were the setup of what ultimately became fatal blood clots in her lungs.
What no major media covered in the year since her death is that Alexandra Williams lost her life due to her birth control.
Alex, as her family calls her, was a college junior at North Carolina Central University. She loved to travel, had career ambitions, and showed a dedication to women’s empowerment.
Just nine months before her death, Alex received a birth-control prescription from a local Planned Parenthood clinic. The generic combination pill, Levora, is marketed as one of the “safer” birth control pills available. Like many women, Alex was not fully aware of the health risks associated with her birth control, as she and doctors struggled to identify health complications that resulted just months later.
Alex’s father Anthony Williams shared with Natural Womanhood that Alex’s visit to an Urgent Care center resulted in a muscle-strain diagnosis, and an ER visit later resulted in a diagnosis of a lung infection and prescribed antibiotics. “However, at various times up until her death,” Williams said, “Alex still mentioned occasional discomfort in her back and her overall energy level fluctuated more than normal.”
No medical professional identified the real problem—not even the Duke Medical Center doctors who tried to revive her on September 26. Then, on September 27, 2018, a brain scan revealed no brain activity, and Anthony and Lisa Williams let their daughter go.
The Least-Discussed Killer of Women Today
Not until the autopsy of their daughter did the Williamses learn it was blood clots in Alex’s lungs—a pulmonary embolism—that led to Alex’s sudden death.
Pulmonary embolisms, strokes, and such cardiovascular events used to be rare in people Alex’s age. But those numbers have increased since birth control has become the most mass-prescribed drug on the market. A systematic review published this year found 300 to 400 U.S. women die yearly of birth-control related health complications like those Alex faced.
Researcher Lynn Keenan, MD, and Natural Womanhood CEO Gerard Migeon cowrote an article expounding that, “comparing users of HC [hormonal contraception] to nonusers, and including more than seventeen million woman-years of observation, we found that using HC increases a woman’s risk of being diagnosed with VTE by three to nine times. For women under thirty, the risk is increased thirteen-fold during the first year of use, when the risk for clot formation is highest.”
While we might not hear much about this in news headlines, pharmaceutical companies are highly aware. After a major lawsuit, Bayer settled more than 10,000 claims between 2009 and 2016 from patients who took the drug Yaz and suffered venous thromboembolism. The Yaz label suggested a risk of “cardiovascular events” with “cigarette smoking,” misleading many women into believing they were safe if they weren’t smokers.
Poor labeling and inadequate informed consent for highly prescribed birth control drugs have recently led a group of researchers to launch an FDA Citizen’s Petition on birth control to seek more accurate black box warnings on these drugs, as well as other safety information. In addition to sharing more than 100 pages of research on the health risks caused by birth control, the Citizen’s Petition has gathered more than 130 comments, including stories of women who say they suffered blood clots and strokes due to birth control. Many comments also come from doctors, loved ones, and parents whose daughters died of blood clots and didn’t live to tell about it.
In one such comment, Laura Bonnet shares, “2 years ago, my daughter died from a blood clot in her brain caused by the birth control, Yasmin. It was prescribed to her for acne and she believed it was safe. She had no risk factors, no clotting disorders. In the hospital, the doctors told us they see 3-5 patients EVERY WEEK with blood clots from birth control. That’s one hospital in a small metropolitan area in Wisconsin. I can’t imagine what other hospitals are experiencing…”
In another comment, Carol Pepin explains, “My 19 year old daughter Shelby Pepin had died. Shelby was very athletic, did not smoke and had no history of a blood disorder. The coroner’s report confirmed that Shelby had died from a pulmonary embolism. She had a DVT behind her left knee that traveled to her lungs causing her bilateral embolism. The coroner also confirmed that her DVT was caused by her birth control the NuvaRing…”
Deaths Like Alex’s Can Be Prevented
One other comment in the recent FDA Citizen’s Petition on birth control health risks is from a woman whose symptoms sounded remarkably like those of Alex Williams.
Amanda Jean Beaulieu shared in a comment that she nearly died five days before her 27th birthday due to a “massive pulmonary embolism” that caused her to collapse in the arms of a security guard while literally running toward the hospital. “When I came to I was told a heart attack was ruled out and the doctor explained it could be an infection in my lungs. As he left the room and paused and asked me are you on birth control?” When Amanda said she was on the Nuvaring, “he explained that he was going to run a d-dimer test to rule out blood clots.”
Scans revealed “a clot the size of a ten cent gum ball was stuck in the valve between my left lung and heart. If it moved to my heart I would die… I had a stroke right in the ER and my life was forever changed. When I arrived to the ER my O2 level was below 40% and I should have been dead. . . . I was the one out of five who got to walk away…”
What bothers Amanda the most is knowing that the health risks she experienced were “100% preventable.” She says, “If I had never used the Nuvaring none of this would have happened to me. My pulmonary embolism with infarction and stroke were a direct result of my Nuvaring usage.”
Just like Amanda, Alex’s doctors at one point thought her symptoms indicated a lung infection. Tragically, no one made the connection between her birth control and blood clot possibility until it was too late.
It’s time that birth control side effects and health risks receive greater attention both in the medical community and the media at large. It’s time birth control receives the same treatment as every other drug with adverse health effects—with accurate black-box warnings, product recalls, and even the discontinuation of particularly dangerous drugs from the market.
Today, Alex would have just celebrated her 21st birthday. We owe it to her to do better.
Mary Rose Somarriba, who completed a 2012 Robert Novak Journalism Fellowship on the connections between pornography and sex trafficking, is editor of Natural Womanhood and associate editor of Verily Magazine. Follow her at maryrosesomarriba.com.
We recently shared the results of our months-long investigation into the Hidden Harms of various drugs and medical devices. In doing so, we hoped to shed light on the many ways in which patients can be misled by confusing or incomplete drug and medical device labels. Today, we continue those efforts by kicking off our Hidden Harms blog series. Each post in the series will focus on one drug or device from our investigation, exposing the contrast between marketing messages and reality—as experienced by actual patients.
We begin our series with Essure, the non-surgical implant once touted as an ideal alternative to tubal ligation. The silicone and metal Essure inserts were supposed to provide a convenient, safe form of permanent sterilization, but many implant recipients experienced life-altering side effects. More than 30,000 of the women harmed by Essure have filed lawsuits claiming Bayer and Conceptus—the original manufacturer—failed to warn them of risks associated with the device.
Keep reading to understand how Essure marketing and labeling materials failed to communicate possible risks, leading many women to unexpected and serious consequences.
Keisha Carney and her husband had eight children between them. “God has blessed us abundantly,” she told the Washington Post, “We knew we were done.” After speaking with her OB-GYN, Keisha underwent permanent sterilization through Essure implantation.
At first blush, the procedure seemed to be a success. But then strange symptoms appeared. Keisha suddenly developed recurrent, serious tooth infections, eventually losing five teeth. Her hair started falling out. She lived with constant brain fog and fatigue, whether she slept or not, and she gained weight.
Then she missed a period. She wanted to believe she couldn’t be pregnant, because her doctor had assured her that Essure was “the most effective method of permanent birth control available.” But Keisha wanted reassurance, so she bought a drugstore pregnancy test.
She was pregnant.
Keisha went online where she learned that other Essure recipients were experiencing symptoms similar to her own, including unplanned pregnancy. She wanted the implants out but couldn’t do anything about it until she delivered the child she was carrying.
Keisha’s pregnancy was plagued with problems: widespread pain, lower back pain that sometimes paralyzed her, and depression. Doctors attempted to remove her Essure devices during Cesarean section delivery, but they couldn’t retrieve a fragment that had migrated near her colon.
A hysterectomy finally removed the last known Essure fragment from Keisha’s abdomen, a hysterectomy she never intended to have. She says her symptoms changed immediately. The stabbing pains in her back stopped, her hair started to grow back, and the recurrent tooth infections disappeared. Keisha says she still struggles with brain fog and a few aches and pains, but overall, things have improved since ridding her body of the Essure devices.
Nothing about Keisha Carney’s Essure experience conformed to the information she received from her doctor. Similarly, Keisha’s Essure saga contrasts sharply with expectations set by the patient brochure and label information.
Essure Patient Brochure and Label Messaging
Though patients should have access to the official device label and instructions for use, many only ever examine the patient information booklets for implants. In the case of Essure, patients were given a 19-page document replete with smiling, middle-aged women extolling the virtues of the Essure implants.
The first page of the 2007 brochure proclaimed Essure a “Simple Option for Permanent Birth Control” in large, bold, blue lettering. Turning the page, potential users learned the benefits of Essure:
Effective
Covered by Most Insurance Plans
No Cutting Into the Body
Rapid Recovery
Can Be Done in An Office Setting
Confirmation of Placement
High Patient Satisfaction
Hormone-free
No General Anesthesia Required
Readers learned of Essure’s 99.8% success rate in preventing pregnancy in addition to the user comfort ratings ranging from good to excellent within 1 week of implantation.
The brochure informed women that a simple test could confirm proper placement of the inserts and give them peace of mind about their sterilization status. Buried deep in the later portions of the brochure, women who continued reading learned that they would have to use alternative birth control for 3 months prior to confirming placement and function of the inserts.
The brochure did not inform women that they absolutely could not rely on the Essure inserts until and unless they underwent the confirmation test with positive results. Keisha Carney never had the test done, because her insurance would not cover it.
Nickel Allergies
The original patient brochure instructed women with confirmed nickel allergies not to go forward with Essure, but the FDA later approved a label change downgrading this contraindication to a warning. “The data did not meet the threshold of a known hazard,” according to an FDA spokesperson. Some women asked their doctors about potential nickel allergies only to have their concerns dismissed, possibly as a result of this labeling change.
Essure’s Hidden Harms
During our Hidden Harms investigation, we analyzed over 40,000 Essure adverse event reports hoping to distill the true incidence of adverse events mentioned and unmentioned in the Essure patient and physician materials. Ultimately, such reports could not provide reliable estimates of side effect incidence, but scientific studies could.
Chronic Pelvic Pain
A clinical study in Canada found that 4.2% of Essure users developed chronic pelvic pain after device implantation. Neither the term “chronic pelvic pain” nor any of its derivatives appear anywhere in the Essure Instructions for Use or the Patient Information Brochure.
Unintended Pregnancy
Many studies have attempted to estimate the rate of unintended pregnancy after Essure sterilization, but few have succeeded. A 2014 study used a mathematical model combined with published Essure placement success rates and short-term unintended pregnancy rates to predict the expected long-term unintended pregnancy rate. The model indicated that 1 in 10 Essure recipients would have an unintended pregnancy over a ten year period.
According to Essure materials, almost every other form of birth control has a lower failure rate than the one found for Essure. Keisha Carney said she felt betrayed by the contrast between the rosy message presented in Essure materials and the stark reality of the device’s relatively frequent failure to prevent pregnancy.
Informed Women Stopped Choosing Essure
After years of public outcry from Essure users, the FDA finally took additional steps to ensure transparent risk communication with potential patients. Once the FDA began requiring physicians to complete a mandatory communication checklist prior to Essure implantation, sales plummeted. Bayer announced Essure’s removal from the market just months later.
The original Essure marketing materials did not communicate risks transparently. Some were buried in text-heavy pages, and others were entirely absent. Women did not fully understand the implications of Essure implantation, and many were then surprised by the health consequences of the device.
When patients truly understood the risks, they did not choose Essure. Based upon the success of the Essure patient communication checklist, we hope to see similar communication requirements for drugs and medical devices of the future. You can find additional examples of transparent risk communication in our Hidden Harms Risk Explorer.
September 25, 2019 (LifeSiteNews) – The United Kingdom announced Monday that it will spend £600 million on “family planning supplies” for third-world nations, including abortion and contraception.
UK International Development Secretary Alok Sharma made the announcement at the United Nations, claiming that “universal sexual and reproductive health and rights” were essential to achieving “universal health coverage.”
The plan is to spend £600 million over the next five years for various “family planning supplies” in the world’s poorest countries, such as Bangladesh, Syria, and Yemen. That sum will cover some legitimate health services such as medicines to prevent death in childbirth, and the UK government’s press release speaks only in euphemisms such as “reproductive health care,” but the supplies will include “condoms, the contraceptive pill[,] and safe abortions,” according to the Telegraph.
“The UK has been at the forefront of global efforts to promote sexual and reproductive health and rights for women and girls living in the world’s poorest countries,” Sharma declared. “This UK aid will help give millions of women and girls control over their bodies, so they can choose if, when[,] and how many children they want. That is a basic right that every woman and girl deserves.”
Hailing the announcement, the International Women’s Health Coalition claimed access to abortion and contraception was “at the core of your freedom as a human being,” and called the UK’s move a “stark contrast to the policies of the United States,” which under President Donald Trump has blocked foreign aid to entities that commit or promote abortions, leading the UK-based abortion organization Marie Stopes International to close hundreds of locations across Africa.
Pro-lifers had the opposite reaction. “There is no internationally recognised right to abortion, and the British Government, along with the UN, should not be acting as if there is,” Right To Life UK spokeswoman Catherine Robinson responded. “The British public does not want its taxes being used in this way. 65 [percent] have stated they are opposed to their taxes being used to fund overseas abortions.”
“This is nothing short of neo-colonialism, where the British Government is using its resources to fund abortions in foreign nations,” she declared.
U.S. officials took the opposite approach to abortion at the UN this week, from the president rebuking the international body for pressuring pro-life countries to accept abortion, to Health and Human Services Secretary Alex Azar declaring there is no so-called right to abortion and condemning the use of euphemistic language such as “reproductive health” that can be used to assert one.
Concerned parents in Austin, Texas rallied Monday against a new sex education curriculum that they say would “sexualize” young children in the city public schools.
Texas Scorecard reports the abortion chain Planned Parenthood is involved in the developing the curriculum that the Austin Independent School District is considering.
The program would teach children in third through eighth grades about gender identity, sexual orientation and other controversial issues, according to the Austin Statesman.
On Monday, local parents held a rally before the school board meeting to discuss the issue. Several parents also spoke during the crowded meeting, urging the school board not to adopt the curriculum.
“These types of lessons are sexualizing our children,” Lorie Meynig said. “Please focus on reading, writing, and arithmetic.”
Caryl Ayala, co-founder of the local group Concerned Parents of Texas, said she is concerned that the curriculum will pit students against each other and violate “students’ rights to hold a different opinion regarding boundaries of sexual behavior according to their family’s values.”
She said Hispanics like her and her family also feel that the teachings violate their cultural values, according to the Scorecard.
“I am offended that this school district is grooming 46,000 Hispanic children to accept these behaviors,” Ayala said. “I consider this a direct assault on Hispanic family culture.”
Here’s more from the report:
“Many of us are concerned that the national sexuality education standards that have been adopted by the AISD board are not in compliance with the laws of the state of Texas,” said grandparent and district taxpayer Don Dores, who brought up the age of consent laws in the Texas Education Code. One example of questionable age-appropriateness is an incident in 2017 where AISD Covington Middle School sent children home with a Planned Parenthood information sheet that included YouTube links to the abortion business’ consent video series, videos that feature gay and lesbian couples undressing each other and preparing for sex.
“It’s time for us to stand up to the board, tell them to go back to the drawing board, and give parents another opportunity to give their input in what their children should be taught,” said Mary Elizabeth Castle with Texas Values, who spoke at the pre-meeting rally.
The school board is slated to vote on the issue later this fall.
Among some of its worst teaching points, the abortion chain tells children that promiscuity is not unhealthy. “There’s nothing bad or unhealthy about having a big number of sexual partners,” Planned Parenthood tells students on its Tumbler page. Planned Parenthood’s booklet for HIV-positive youth, “Healthy, Happy and Hot,” also tells young people that it is their “human right” to not tell their partner that they have HIV.
Numerous communities across the United States have rejected Planned Parenthood as a sex education teacher. The whole Massachusetts legislature recently rejected a bill that recommended Planned Parenthood’s middle school sex education curriculum. The program teaches children as young as 12 “how to perform oral and anal sex.”
Planned Parenthood teaches sex education to at least 221,000 students in 31 states, according to CBS News. It also aborts about 330,000 unborn babies every year.
If she hadn’t become pregnant, Courtney Greer wouldn’t have learned so quickly that she had ovarian cancer. It was during her first pregnancy ultrasound, usually performed around eight to ten weeks, that the doctor noticed the tumor on her ovary. When that doctor said she suspected it wasn’t cancerous, but they wouldn’t be able to biopsy it until after the baby was born in nine months, Greer decided to get a second opinion.
“My mind was racing, I had a million questions,” she wrote in an essay for Love What Matters. “[…] after talking to a few friends and family members, they suggested a second opinion. I noticed one doctor’s name kept coming up. I did not find this to be by chance, (it’s a God thing) so I called and made an appointment. I wanted a second opinion and I wanted it to be from a well-respected physician who knew what he was talking about.”
After meeting with this doctor, Greer knew he was the one who would take the best care of her and her growing baby. They came up with a plan that made her comfortable and moved forward taking measurements of the tumor to monitor its growth. Unfortunately, it kept growing. But Greer, though originally upset at the prospect of having surgery to remove the tumor while she was 15 weeks pregnant, soon found it to be a blessing.
“I was a big ball of nerves with ‘what ifs’ and ‘is my baby going to be okay?’ A million things go through your mind as a Mom. However, I trusted my doctor and believed in him,” she wrote.
The surgery went well but just days later, the doctor told Greer and her husband Micah that unfortunately, it was cancer.
“I’m so excited to see this doctor and tell him how I’m recovering, thank him for everything, and find out is this baby a boy or a girl?!” she wrote. “When he walks in, I can see his demeanor isn’t quite what it usually is. He tells us we need to talk. What we removed wasn’t a fibroma. It’s cancer…”
Greer barely reacted to the news. She didn’t cry. She didn’t worry. But she was in shock. She was healthy. She wasn’t experiencing any symptoms. How was it possible that she had cancer? And then she came to a realization.
“Finally, I look at Micah and say, ‘How blessed are we that I got pregnant?! I would’ve never even know I had a tumor if it weren’t for the baby,” she explained. “I had no symptoms. I felt fine. I couldn’t see or feel it.”
“My doctor tears up and says, ‘Wow. I didn’t even think of that.’ Then he tells me that divine intervention brought me to him. He grabs a tissue and points at a photograph on the wall. He can’t get the words out. I just knew, through the tears I ask him, ‘Is that your daughter?’ … after a few moments he speaks. ‘Yes. In all my years practicing, she is the only case of this cancer that I’ve seen.’ We all break into tears,” she said.
After meeting with an OB oncologist, Greer learned that it appears they got all of the tumor during surgery. There is a 25 percent chance of the cancer coming back, so she will wait to do chemo until after her baby is born. In the meantime, she will be closely monitored and may end up not needing chemo at all.
“This little miracle inside me saved me from letting cancer go further,” said Greer. “I would’ve never known I had it if I didn’t go in for my first ultrasound. Who knows how long this would’ve gone on for? I thank you God for listening to me and making me listen to You. I feel beyond blessed for every single thing in my life and I felt compelled to share this message.”
According to the American Pregnancy Association, only up to 5.7 percent of pregnant women will have a mass on their ovary. Only about 5 percent of those cases turn out to be cancerous. Each case is different and will require a different course of action based on the doctor’s recommendations.
While ovarian cancer itself will not pose risks to the preborn child, treatments for ovarian cancer can. Depending on the severity of the cancer, the risks to the baby will be weighed against the risks to the mother with doctors focused on carrying for both of them.
CARDIFF, U.K., September 23, 2019 (LifeSiteNews) – A restoration of true femininity is essential to restoring Christian civilization, said Maria Madise, International Director of Society for the Protection of Unborn Children, at a U.K. Catholic conference earlier this month.
Madise made the case that the revolutions behind today’s culture of death have specifically targeted women to play an essential role in a worldwide corruption of morality.
“She [women] is a strategic target of the revolution, because of her influence on the family and society,” Madise said.
Madise’s talk (read full talk below), titled “Women and the rebuilding of Christian civilisation,” was given at a conference organized by Voice of the Family, an initiative of LifeSiteNews and the Society for the Protection of Unborn Children. The Sept. 6-8 conference, titled “Handing on the Deposit of the Faith,” was held at Newman Hall, University Catholic Chaplaincy, in Cardiff, UK.
The corruption of morality has been necessary for evil to thrive both in general society and within the ranks of Christian communities, Madise noted.
“The Reformation and the French Revolution tempted the woman to rebel against her position in society. The Communist revolution turned the rebellion against her position in the family. The sexual revolution incited rebellion against her very womanhood. In the current phase of the revolution we see an attempt to introduce these errors into the Church,” she said.
The remedy, Madise puts forward, is a “counter-revolution” of women who discover what it means to be a woman by imitating the example of the person of Mary, Mother of God, who was crucial in overturning the great supernatural revolution against God and His order.
“Mary’s ‘Fiat!’ reconciles the human race with God and forms the troops of the counter-revolution,” she said.
“To fulfil her destiny, to be truly happy, every woman must take Mary as her example. Regardless of her particular role or state in life, if she is to be a joyful counter-revolutionary, she must submit herself wholly to God in everything she does,” she added later.
Drawing throughout her talk on the writings of Alice von Hildebrand and Edith Stein, Madise addresses several key issues Christian women face, including modesty in dress and behavior.
“Vigilance is required to maintain purity of mind and body. By the way we look, speak and act we can give witness that God exists. A fact so well hidden today! We should look and sound Catholic. Our appearance, therefore, should not contradict what we believe. We are in the battle. Soldiers in slippers cannot be taken seriously at wartime. Their uniform, on the other hand, shows their readiness and competence to fight. We should look like Catholic women ‘on duty’ at all times,” she wrote.
“Christian mothers must have special regard to the holiness of their children. ‘All children have an instinct for the sense of dignity and decorum of their mother,’ observed Cardinal Siri. This is why modesty in dress, comportment and speech is necessary not only in public, but also at home. By guarding the innocence of their children, Christian mothers foster wilful purity in their children in later life,” she added.
Madise concluded by challenging women to embrace their true calling.
“Since Eve, only one woman has had the right attitude of complete surrender, the attitude of Fiat. Let us seek to imitate that woman. Let us adopt her attitude to the Truth – protect it as a mother would protect her child and submit to it as she submitted to her Child who was the Truth. Let us be part of her army under the command of Her Immaculate Heart, turned always to God, while crushing the devil with her heel. We are her little children called to the battle.”
This talk is printed in full in the current edition of Voice of the Family’s quarterly magazine ‘Calx Mariae’. Copies of the magazine can be ordered here.
***
Women and the rebuilding of Christian civilisation
By Maria Madise
Introduction
“To a great extent the level of any civilization is the level of its womanhood,” noted Archbishop Fulton Sheen. We can only fathom the full dignity and beauty of Christian civilisation when we consider that its level is none other than the Blessed Virgin.
Today’s world looks even more fallen than after the Fall and wholly unworthy of her. However, we should not forget the perseverance of those who lived between Eve and Mary, ceaselessly imploring God to send a saviour to reopen the gates of Heaven. Their prayer was successful. So we should also pray – and work – for the speedy triumph of the Immaculate Heart.
Mary is our surest and shortest way to Christ. The closer we are to her, the closer we are to Christ. They are so intimately united that St Louis de Montfort claimed: “it were easier to separate the light from the sun, the heat from the fire”. “Nay,” he said “it were easier to separate from Thee all the angels and the saints than the divine Mary, because she loves Thee more ardently and glorifies Thee more perfectly than all the other creatures put together.”1
If she is our true help and comfort, our chief commander and sovereign, we need to know where to find her. With her marvellous assistance, she could be present anywhere, but we can surely find her at the foot of the Cross. The Cross is at the heart of Christian civilisation, of which Mary is the mother and crown.
Alice von Hildebrand points to the privileged position that has been granted to women in the economy of redemption from the Annunciation to bringing news of the Resurrection. The holy women, in the company of Our Lady, followed and served Christ as He taught, made their way to Pilate’s courtroom, accompanied Him to Calvary and assembled at the foot of the Cross.2 Amid complete despair, when God Himself was dying, woman received her new mission. The Apostles had fled. St John did come back and it was he that the dying Saviour entrusted to His Mother: “Woman, behold thy son.” Her task was not finished, but extended. And with her, each woman, who wants to fulfil her role, must share in her motherhood wrought at the foot of the Cross.
This article will consider how the revolution against Christian civilisation has sought to instrumentalise women and womanhood – so tightly connected to the Cross – and how, consequently, the counter-revolution is dependent on women.
Order and revolution
The revolution is a perpetual attack on God’s order. Recalling the success of the serpent, revolutionaries often seek to achieve their goals through the woman. She is a strategic target of the revolution, because of her influence on the family and society.
By “revolution” we mean a movement that aims to destroy a legitimate order and replace it with an illegitimate power or state of things (not order). It is the subversion of the moral order and denial of God. This, in fact, is how “revolution” is defined by Dr Plinio Corrêa de Oliveira (1908-1995),3 the Brazilian thinker and author of the book Revolution and Counter-Revolution, essential reading for all counter-revolutionaries.
Dr Plinio explains that all big revolutions in history, whether the Reformation or French or Communist revolution, as well as any of the more localised and limited forms of revolution, are fruits of the same tree – the denial of God and His order. Thus, revolution has a universal character.4 He also argues, that each “episode” of the revolution contains within it all previous stages.5 So the key elements of the Reformation can be seen in the French Revolution, and the key elements of both, the Reformation and French Revolution, in the Communist Revolution and so on. It is no surprise then, that we may identify many Marxist and socialist ideas in the revolution we are witnessing in the Church today.
Given that the aim of revolution is to destroy the Christian order mothered by Mary, logically, the aim of the counter-revolution is to stop the revolution and to restore the authentic Christian civilisation in its beauty, goodness and truth.
In principle, the temptation inciting the woman to co-operate with the revolution derives from God’s command for her. Through the sin of our first parents, the original or natural order, created by God, became fallen. The relationships between man and God, as well as between man and woman, changed dramatically. Man and woman were punished each according to their main domain and privilege in the natural order, which for the woman was giving birth to new life. God said to her: “I will multiply thy sorrows, and thy conceptions: in sorrow shalt thou bring forth children, and thou shalt be under thy husband’s power, and he shall have dominion over thee.”6 In each of the following episodes of the revolution, therefore, the woman is especially tempted to protest against the sentence she received for her first sin: against being subject to the man and making sacrifices for her family.
However, tempting her has become more challenging after Mary’s “Fiat!”. For her pride, Eve was humbled, but through the perfect humility of the Blessed Virgin, the authentic dignity of women is restored. Eve’s disobedience echoed the rebelling angels’ “non serviam!”. But Mary’s “Fiat!” reconciles the human race with God and forms the troops of the counter-revolution. The gate of Heaven closed behind Eve, while Mary became the gate of Heaven herself. The Fall and Incarnation frame the loss and restoration of order that kaleidoscopically form countless new patterns in Christian history.
Given what happened in the Garden of Eden, we may consider that it follows that love of sacrifice and perseverance are inherent in the female nature. It was through atoning sacrifice that her disobedience was to be redeemed. Until then she was to be completely powerless in healing the wound that she had inflicted on her relationship with God. All she could do was to persevere in hope for the sacrifice to be offered for her and all her children born in exile. This love of sacrifice, so deep-rooted in women’s nature, is reflected in the words of Edith Stein: “After every encounter in which I realise my inability to influence others directly, I become more intensely conscious of the urgent need for a personal holocaustum.”7
Yet, Mary raised this to a completely new level. Her love of sacrifice was not the love of a sinner hoping for reconciliation, but the love of the mother, completely united with her Son who was the Sacrifice. Eve was sentenced to bring forth her children in sorrow. In her tremendous sorrow under the Cross, Mary became the mother of all and was ordered to love all. Since then every woman is called to take part in the sacrificial motherhood of Mary, be it naturally or spiritually, and raise citizens for Heaven.
Love of sacrifice and perseverance is what the revolution wants to destroy in every single woman and also in a culture. For the revolution, these are intrinsically related, because the woman who can nurture souls, can also nurture the culture.
Woman and revolutions
How has each episode of the revolution sought to appeal to women and deform their mission? The Reformation and the French Revolution tempted the woman to rebel against her position in society. The Communist revolution turned the rebellion against her position in the family. The sexual revolution incited rebellion against her very womanhood. In the current phase of the revolution we see an attempt to introduce these errors into the Church.
We cannot study these attempts fully in the scope of this article. However, we can consider some of the key elements in the main episodes of the revolution in connection with women, while seeking to strengthen our commitment to Our Lady’s counter-revolutionary army today.
Early progress of the revolution against Christian civilisation
Dr Plinio Corrêa de Oliveira identifies some of the essential factors in the Protestant revolution as: loss of the love of sacrifice, loss of true devotion to the Cross; the rise of sensuality and the importance of man’s own merits; the rise of natural above the supernatural.8 These were all changes that deeply affected the woman’s mission. Dr Plinio goes on to explain: “Pride begot the spirit of doubt, free examination and naturalistic interpretation of Scripture, and revolt against superiority which wrought ecclesiastical egalitarianism… On the moral plane, the triumph of sensuality was affirmed by the suppression of priestly celibacy and by the introduction of divorce.”9 This first episode of the revolution in the Christian world laid out the plan for destroying the protective walls of Christian morality – enshrined in the commandments and sanctified by the sacraments.
We could make two observations here in connection to the woman. Firstly, the long term consequence of the growth of pride and sensuality became evident in the later stages of the revolution, especially in the Communist and sexual revolution, when divorce, combined with its allies, contraception and abortion, ensnared women in moral chaos. It took time to reach that point. However, we should not miss the first blow to the sacramental order of marriage, which made all further blows possible.
Secondly, we must consider the inevitable and immediate conflict between these developments and the Blessed Virgin who is a constant reminder of God’s order. From the early episodes of the revolution in the Christian world, statues of Our Lady, her images and devotions had to be violently removed in pursuit of the design that so wholly contradicted her.
Like the Reformation, the French Revolution entered into a direct conflict with the blessed Virgin. A“Goddess of Reason” was enthroned in the Cathedral of Notre Dame. A temple of Philosophy was erected in the nave and decorated with busts of philosophers. At its base was an altar dedicated to Reason, and before it a torch of truth. The true Seat of Wisdom, however, was driven from her own cathedral.
According to Dr Plinio, the French Revolution was “the heir of Renaissance neopaganism and Protestantism, with which it had a profound affinity.”10
“The political work of the French Revolution was but the transposition to the sphere of the State of the ‘reform’ the more radical Protestant sects had adopted in the matter of ecclesiastical organization: the revolt against the King corresponding to the revolt against the Pope; the revolt of the common people against the nobles, to the revolt of the ecclesiastical “common people”; the faithful, against the “aristocracy” of the Church, the clergy.”11
Central to the French Revolution was the emergence of the Freemasonic lodges and the role they played in spreading revolutionary ideas. When the permanent instruction of Alta Vendita (Italian high lodge) came to light, it revealed a strategic plan to subvert the Catholic Church. Both Pope Pius IX and Pope Leo XIII ordered this revolutionary document to be made public. Also, the letters, which have survived from the members of the lodge, leave no room for doubt of their plan:
“Catholicism does not fear a very sharp sword any more than the monarchies feared it. But, these two foundations of Social Order can collapse under corruption; let us never tire to corrupt them… from the blood of martyrs Christians are born; let us not make martyrs; but, let us popularise vice among the multitudes; may they breathe it through their five senses; may they drink it and be saturated. Make vicious hearts and there will be no more Catholics.
“It is corruption on a big scale that we have undertaken… a corruption that should one day enable us to lead the Church to its grave. Lately, I heard one of our friends laughing philosophically at our projects saying: ‘To destroy Catholicism, we should do away with women.’ The idea is good in a certain way, but since we cannot get rid of women, let us corrupt them with the Church. ‘Corruptio optimi, pessima.’ The best dagger to strike the Church is corruption.”12
Notably, in this correspondence, in the universal corruption of Catholicism, women were considered to have an important role. This programme of corruption was determinedly pursued and in association with the feminist movement in the 1960s, these efforts bore ample fruit. Showing remarkable continuity with the Masonic letters of the previous century, the magazine L’Humanisme wrote at that time:
“The first conquest to be done is the conquest of women. Woman must be freed from the chains of the Church and from the law. […] To break down Catholicism, we must begin by suppressing the dignity of women, we must corrupt them together with the Church. We spread the practice of nudity: first the arms, then the legs, then all the rest. In the end, people will go around naked, or almost, without batting an eyelid. And, once modesty has been removed, the sense of the sacred will be extinguished, the morality will be weakened and faith will die of asphyxiation.”13
Until recently, the Church zealously protected the purity of her daughters. In his address to a group of Catholic girls, Pope Pius XII lamented:
“Many women… give in to the tyranny of fashion, be it even immodest, in such a way as to appear not even to suspect what is unbecoming. They have lost the very concept of danger: they have lost the instinct of modesty.”14
Later, he commented on the inherent connection between the morals of an individual and the morals of the culture and the nation, so well-known to the enemies of the Church:
“It is often said almost with passive resignation that fashions reflect the customs of a people. But it would be more exact and much more useful to say that they express the decision and moral direction that a nation intends to take: either to be shipwrecked in licentiousness or maintain itself at the level to which it has been raised by religion and civilization.”15
Our Lady herself issued warnings against the corruption of her daughters. “Certain fashions are to be introduced which will offend Our Lord very much,” she said in Fatima. “Those who serve God should not follow these fashions. The Church has no fashions. Our Lord is always the same.”
Already much earlier, 1594-1634, in Quito, Ecuador, Our Lady of Good Success had said:
“Unbridled passions will give way to a total corruption of customs because Satan will reign through the Masonic sects, targeting the children in particular to ensure general corruption.
“In those times the atmosphere will be saturated with the spirit of impurity which, like a filthy sea, will engulf the streets and public places with incredible license… Innocence will scarcely be found in children, or modesty in women.”16
Communist Revolution
The Communist Revolution instrumentalised women with enormous profit. In his article “A Great Beginning” (1919), Vladimir Lenin asserted that “we have far more organising talent among the working and peasant women than we are aware of.”17 And the party vowed that it is principally important to employ these talents in state business and social work. With that manoeuvre, the family was left to be mothered by the state.
The influential Communist women Inessa Armand (1874-1920), a member of the executive committee of the Bolshevik party, also Lenin’s lover, and Aleksandra Kollontai (1872-1952), the first Soviet People’s Commissar for Social Welfare, argued that sexual liberation was a necessary premise for the realisation of a socialist society. Kollontai wrote, in 1920, in the journal Kommunistka:
“In place of the individual and egoistic family, a great universal family of workers will develop, in which … men and women, will above all be comrades… These new relations will ensure for humanity all the joys of a love unknown in the commercial society, of a love that is free and based on the true social equality of the partners…The red flag of the social revolution which flies above Russia and is now being hoisted aloft in other countries of the world proclaims the approach of the heaven on earth.”18
In 1921 she explained:
“The economic subjugation of women in marriage and the family is done away with, and responsibility for the care of the children and their physical and spiritual education is assumed by the social collective. The family teaches and instils egoism thus weakening the ties of the collective and hindering the construction of communism.”19
Nothing like the powerful alliance of Communism and feminism has employed women more ferociously in the destruction of the family. To assume their responsibilities as “talented organisers” they were either to abort their children or hand them over to the Communist educational model that in the words of Kollontai, would “take upon itself all the duties involved in the education of a child.”20 Once the family was out of the way, immorality and liberalism would pave the way to “free love”. Incidentally, sex education in our schools today is the fruit of the seeds sown at this stage of the revolution.
Lenin congratulated himself on the progress made with regard to the position of women. He claimed:
“In this field, not a single democratic party in the world, not even in the most advanced bourgeois republic, has done in decades so much as a hundredth part of what we did in our very first year in power. We really razed to the ground the infamous laws placing women in a position of inequality.”21
The speed of the Bolshevik attack on the true mission of women and the family was remarkable indeed. On 17 December 1917, a few weeks after Bolsheviks seized power, divorce was introduced; in 1920 abortion was legalised without restriction (Soviet Russia was the first country in the world to allow this); in 1922 prostitution and homosexuality were decriminalised.22 In 1923 Leon Trotsky wrote: “The first period of family destruction is still far from being achieved. The disintegration process is in full swing.”23
Communist movements grew out of the French Revolution, which was the heir to the Protestant revolution – and nothing could be more logical, as Dr Plinio explains:
“The normal fruit of deism is atheism. Sensuality, revolting against the fragile obstacles of divorce, tends of itself toward free love. Pride, enemy of all superiority, finally had to attack the last inequality, that of wealth. Drunk with dreams of a one-world republic, of the suppression of all ecclesiastical or civil authority, of the abolition of any Church, and of the abolition of the State itself after a transitional dictatorship of the workers, the revolutionary process now brings us the twentieth-century neobarbarian, its most recent and extreme product.”24
On the eve of the Communists’ seizure of power, the Blessed Virgin appeared in Fatima. Her Immaculate Heart desired the Consecration of Russia, to prevent it from spreading its errors throughout the world. But the world had rejected the humble Virgin and enthroned a common woman worker instead.
Sexual revolution
In the realm of the family, the sexual revolution was the refinement and globalisation of the Communist revolution. When considering the territories and populations conquered by Communist regimes, we see that at this stage, the revolution had truly built an empire. Dr Plinio also points out that through its networks and infiltration of every social and professional sphere “the Third Revolution applies with devastating efficacy the tactics of psychological conquest.”25
What the sexual revolution added to the refinement and spread of the revolution was contraception.
In her book Adam and Eve after the Pill, Mary Eberstadt notes, “it may be possible to imagine the Pill being invented without the sexual revolution that followed, but imagining the sexual revolution without the Pill and other modern contraceptives simply cannot be done.”26 The pill redefined the most elemental human relationships. It is perhaps the single greatest change in the relationship between men and women after the Fall. The individual and social consequences of contraception predicted by Humanae Vitae (1968) – including 1) lower moral standards; 2) greater infidelity, 3) less respect for women by men, and 4) coercive use of reproductive technology by governments – are all fully vindicated today.
Nothing has ever done more for woman than Christianity. But nothing has enslaved and harmed women more than “sexual liberation”. There is ample empirical evidence – which Eberstadt presents in her book – that people in faithful married relationships “score better on all kinds of measures of well-being”. Other data “testifies to the propositionthat families headed by a married couple are better off than those headed by a cohabiting couple.”27 Children who grow up with both of their biological parents do better emotionally, financially, educationally, mentally than children who grow up with a single parent.28 Secular research tells us that lifelong, faithful marriage is better for children, better for adults and better for society.
The ideological position that women need to be freed from marriage and their fertility in order to enjoy unrestricted sexual relations, along with its permanent back-up plan, abortion, is a lie that subjects them to a grave injustice. It robs them of their right to be honoured and protected as women.
The sexual revolution suggests that, as a result of continued offences against God, woman “was severely punished in the very domain of her glory – to give life.”29 Only she is no longer suffering in the pain of childbirth, but rather in the fruitless pain of the sacrifice of her children on the altars of the revolution. The moral blindness of our society has grown to the extent that the killing of fifty million unborn children worldwide each year is no longer considered a crime that cries out to heaven. Consequently, millions of women walk the earth wounded to the core – in their femininity, motherhood and ability to love, to say nothing of those who share in these wounds, even if they also share responsibility for inflicting them.
After being tempted to rebel against God, against man, against her family and children, the woman is incited to rebel against her own nature and against womanhood. G.K. Chesterton wrote that the feminist is someone who “dislikes the chief feminine characteristics” and that “feminists want to destroy womanhood”.30 Alice von Hildebrand added, “the new age philosophy of feminism, in waging war on femininity, is in fact waging war on Christianity. For in the divine plan both are intimately linked.”31 Feminism leaves the culture without femininity, without the mother and without the queen.
Revolution in the Church
All phases of the revolution share one main target – the Church. At the heart of the revolution is the subversion of God’s order and a desire to institute disorder without God. The revolution will never be satisfied as long as the Holy Catholic Church, the earthly shrine of God-given order, stands strong. It desires to corrupt the Church, as it has corrupted the world. Let us recall the correspondence of the Alta Vendita:
“…let us popularise vice among the multitudes… make vicious hearts and there will be no more Catholics… it is corruption on a big scale that we have undertaken…a corruption that should one day enable us to lead the Church to its grave.”
Instead of attacking her directly, the revolution allures her children to take everything it has achieved in the world today – secularisation, divorce, contraception, abortion, homosexuality, gender ideology, and bring these things into the Church. And once morality is corrupted, doctrine is corrupted. If she were to accept any of these sins of her children without calling them to repent, all her teachings would wither.
Yet, at this stage of the revolution, even more seems to be under attack than her moral and doctrinal health – namely, the very relationship with her Son which is at the foundation of the salvation of mankind. This brings us to the upcoming Amazon synod.
Concerns about the synod are dominated by proposals to adopt pagan, syncretistic, egalitarian, tribal ideas and practices incompatible with Catholic teaching and the admission of married men to the priesthood. It is the discussion of an official ministry that could be conferred on women that is relevant for us.32
Tradition opposes female ordinations, Sacred Scriptures reject it, canon law forbids it, popes throughout history have ruled against it. Christ came to earth as the Son of Man. He established his priesthood in persona Christi, in the person of Christ. Therefore, all ministers ordained to His ministry must be men.
This is not ordered so as to exclude women. On the contrary, Christ bound Himself on earth intimately to one woman, the Blessed Virgin, who would have been most qualified of all women to share in His ordained ministry, if that were part of the divine plan. But the plan for the woman is different. Edith Stein writes:
“He formed her so closely after His own image as no other human being before or after; He gave her a place in the Church for all eternity such as has been given to no other human being. And just so, He has called women in all times to the most intimate union with Him: they are to be emissaries of His love, proclaimers of His will to kings and popes, and forerunners of His Kingdom in the hearts of men. To be the Spouse of Christ is the most sublime vocation which has been given, and whoever sees this way open before her will yearn for no other way.”33
Marriage is between two parties. One cannot be married to oneself. Women can never carry out a ministry in the person of Christ. Women cannot be ordained deacons either, because all other ranks of ordained ministry are ordered after the ministry of the High Priest. Women’s role is fashioned after that of the Spouse of Christ, the Church, who is the fruitful mother of souls that are borne to Him.
The institution of marriage in this world is under continual attack. Today it is fiercely assaulted by the homosexual and transgender agenda. Proposals to ordain women, however, direct these attacks on the supernatural marriage of Christ and His Church. Words fail to convey the gravity of such a desecration. However, this shows why churchmen who do not recognise this desecration are incapable of resisting the evil of homosexuality and gender ideology.
Once again, a revolutionary proposal seeking the input of women, is founded on the same premise as the ancient Fall. The serpent suggests we will gain something we are denied, while retaining everything we have now. What was the reality? Eve got the apple, but Paradise was lost. There was no gain to speak of.
Thanks to the merits of the Blessed Virgin, instead of human equality, women are offered a dignity and honour in the Catholic Church unparalleled to what they have received in any other institution. This is rooted in humble service of the handmaid of the Lord. Her “Fiat!” is the greatest word ever said after Logos. Her word brought forth the Incarnation of the Word.
Conclusion
A similar examination of the key episodes of the revolution could be taken through the perspective of men, formation of children and youth, religious life or in a number of other ways. However, women have their own particular, and irreplaceable, role in countering the revolution.
The pure image of feminine nature stands before our eyes in the Immaculata, the Virgin, writes Edith Stein.
“The most pure virgin is the only one safeguarded from every stain of sin. Except for her, no one embodies feminine nature in its original purity. Every other woman has something in herself inherited from Eve, and she must search her way from Eve to Mary. There is a bit of defiance in each woman which does not want to humble itself under any sovereignty. In each, there is something of that desire which reaches for forbidden fruit. And she is hindered by both these tendencies in what we clearly recognise as woman’s work.”34
To fulfil her destiny, to be truly happy, every woman must take Mary as her example. Regardless of her particular role or state in life, if she is to be a joyful counter-revolutionary, she must submit herself wholly to God in everything she does. Edith Stein continues:
“Whether she is a mother in the home, or occupies a place in the limelight of public life, or lives behind quiet cloister walls, she must be a handmaid of the Lord everywhere. So had the Mother of God been in all circumstances of her life, as the Temple virgin enclosed in that hallowed precinct, by her quiet work in Bethlehem and Nazareth, as guide to the apostles and the Christian community after the death of her Son. Were each woman an image of the Mother of God, a Spouse of Christ, an apostle of the divine Heart, then would each fulfil her feminine vocation, no matter what conditions she lived in and what worldly activity absorbed her life.”35
What practical conclusions could we draw?
We should of course share in all the tasks that come with our time to defend and spread the faith, but women today seem to be required specifically to exercise discipline of the senses and focus on the divine. To lead, so to say, a “Eucharistic life” – to love and adore the Lord in the Holy Eucharist as a bride loves her husband. Bridal love of Christ makes His business one’s own, says Edith Stein. And His business is none other than saving souls.
Vigilance is required to maintain purity of mind and body. By the way we look, speak and act we can give witness that God exists. A fact so well hidden today! We should look and sound Catholic. Our appearance, therefore, should not contradict what we believe. We are in the battle. Soldiers in slippers cannot be taken seriously at wartime. Their uniform, on the other hand, shows their readiness and competence to fight. We should look like Catholic women “on duty” at all times. The Catechism of Perseverance speaking of the first century Rome recalls: “The admirable purity of our ancestors appeared in their exterior. Nothing was more striking than the contrast between Christian and pagan women in this respect.”36
Christian mothers must have special regard to the holiness of their children. “All children have an instinct for the sense of dignity and decorum of their mother,” observed Cardinal Siri. This is why modesty in dress, comportment and speech is necessary not only in public, but also at home. By guarding the innocence of their children, Christian mothers foster wilful purity in their children in later life.
Religious are called to manifest the fidelity of true brides in every detail. These traditions nurture the hidden life in this special and most privileged union. A bride has more perfect opportunities to offer signs of affection and service to her husband compared to any other.
In all of these roles, interiorly, we must unite ourselves with Our Lady – through the Sacraments, through the Rosary, and through consecrating our entire lives to her.
Since Eve, only one woman has had the right attitude of complete surrender, the attitude of Fiat. Let us seek to imitate that woman.
Let us adopt her attitude to the Truth – protect it as a mother would protect her child and submit to it as she submitted to her Child who was the Truth.
Let us be part of her army under the command of Her Immaculate Heart, turned always to God, while crushing the devil with her heel. We are her little children called to the battle in the way described by St Louis de Montfort:
“… the power of Mary over all the devils will especially break out in the latter times, when Satan will lay his snares against her heel; that is to say, her humble slaves and her poor children, whom she will raise up to make war against him. They shall be little and poor in the world’s esteem, and abased before all, like the heel, trodden under-foot and persecuted as the heel is by the other members of the body. But in return for this, they shall be rich in the grace of God, which Mary shall distribute to them abundantly. They shall be great and exalted before God in sanctity, superior to all other creatures by their animated zeal, and leaning so strongly on the divine succour, that, with the humility of their heel, in union with Mary, they shall crush the head of the devil, and cause Jesus Christ to triumph.”37
Endnotes:
[1] St Louis de Montfort, True Devotion to Mary, Saint Benedict Press, Charlotte 2010, p. 30.
[2] Alice von Hildebrand, The Privilege of Being a Woman, Sapientia Press, Ave Maria 2002, p. 18.
[3] Dr Plinio Corrêa de Oliveira, Revolution and Counter-Revolution, The American Society for the Defense of Tradition, Family and Property (TFP), Spring Grove 2008, p. 40.
[4] Ibid., p. 11.
[5] Ibid., p. 4.
[6] Genesis 3:16.
[7] Sister Teresia de Spiritu Sancto, O.C.D., Edith Stein, Sheed and Ward 1952, London and New York, p. 77.
[8] Dr Plinio Corrêa de Oliveira, Revolution and Counter-Revolution, TFP, Spring Grove 2008, pp. 14-16.
[9] Ibid., p. 16.
[10] Ibid., p. 17.
[11] Ibid.
[12] Letter of Vindice to Nubius [pen-names of two leaders of the Italian ‘Alta Vendita’], dated 9August 1838, International Review of Freemasonry, 1928; quoted by Robert T. Hart in Those Who Serve God Should Not Follow the Fashions, Little Flowers Family Press 2017, p. 6.
[13] Quoted by Virginia Coda Nunziante in Countering the Challenges of Today’s Society as Catholic Women, Voice of the Family 2018; http://voiceofthefamily.com/countering-the-challenges-of-todays-society-as-catholic-women/
[14] Pius XII, Address to a group of Catholic Action girls on 6 Oct. 1940, quoted by Robert T. Hart inThose Who Serve God Should Not Follow the Fashions, Little Flowers Family Press 2017, p. 5.
[15] Pope Pius XII, Address to a Congress of the “Latin Union of High Fashion”, 8 Nov. 1957; quoted by Robert T. Hart in Those Who Serve God Should Not Follow the Fashions, Little Flowers Family Press 2017, p. 26.
[16] Prophecies of Our Lady of Good Success About Our Times, TFP 2000.
[17] Vladimir Lenin, A Great Beginning, Marxists Internet Archive, https://www.marxists.org/archive/lenin/works/1919/jun/19.htm
[18] Alexandra Kollontai, Communism and the Family, first published in Komunistka, No. 2, 1920, https://www.marxists.org/archive/kollonta/1920/communism-family.htm
[19] Alexandra Kollontai, Theses on Communist Morality in the Sphere of Marital Relations, first published in Kommunistka, No. 12, 1921, https://www.marxists.org/archive/kollonta/1920/communism-family.htm
[20] Ibid.
[21] Vladimir Lenin, A Great Beginning, Marxists Internet Archive, https://www.marxists.org/archive/lenin/works/1919/jun/19.htm
[22] Cf. Givanni Cadevilla, Dalla Rivoluzione bolscevica alla Federazione Russa, Froanco Angeli, Rome 1996; quoted by Prof. Roberto de Mattei, A History of Revolutions and their Consequences for the Family, Voice of the Family 2017, http://voiceofthefamily.com/roberto-de-mattei-a-history-of-revolutions-and-their-effects-on-the-family/
[23] Leon Trotskij, Problems of everyday life, Monad Press, New York 1986, p. 37, quoted by Prof. Roberto de Mattei, A History of Revolutions and their Consequences for the Family, Voice of the Family 2017, http://voiceofthefamily.com/roberto-de-mattei-a-history-of-revolutions-and-their-effects-on-the-family/
[24] Dr Plinio Corrêa de Oliveira, Revolution and Counter-Revolution, TFP, Spring Grove 2008, p. 18.
[25] Ibid., p. 130.
[26] Mary Eberstadt, Adam and Eve before the Pill. Paradoxes of the Sexual Revolution, Ignatius Press, San Francisco 2012, p. 12.
[27] Ibid., p. 25.
[28] Ibid., p. 27-30.
[29] Alice von Hildebrand, The Privilege of Being a Woman, Sapientia Press, Ave Maria 2002, p. x.
[30] Quoted in ibid., p. 2 and p. 8.
[31] Ibid.p. 32.
[32] Instrumentum Laboris, No. 129, a), 3., http://www.sinodoamazonico.va/content/sinodoamazonico/en/documents/pan-amazon-synod–the-working-document-for-the-synod-of-bishops.html
[33] Edith Stein, Essays on Women, ICS Publications, Washington 2010, p. 84.
[34] Ibid., p. 119.
[35] Ibid., p. 54.
[36] Abbé Gaume, The Catechism of Perseverance, Vol. III, p. 78. Dublin; quoted by Robert T. Hart in Those Who Serve God Should Not Follow the Fashions, Little Flowers Family Press 2017, p. 33.
[37] St Louis de Montfort, True Devotion to Mary, Saint Benedict Press, Charlotte 2010, p. 24.
TORONTO, September 19, 2019 (LifeSiteNews) — A growing number of students from around the world are pledging not to bear children until their governments do something to combat so-called climate change.
Launched by 18-year-old Canadian Emma Lim, the initiative asks students to refrain from having children until their government takes action.
“I pledge not to have children until I am sure my government will ensure a safe future for them,” the initiative’s website states.
“I am not the only young person giving up lifelong dreams because they are unsure of what the future will hold. We’ve read the science, and now we’re pleading with our government. Please, keep us safe. Please act while there is still time,” she writes on her website.
Carleton University professor Michael Hart argued in his 2016 book Hubris, however, that climate change advocacy is based on “poor science” and is being used as a Trojan horse for ramming through a social agenda on an unsuspecting population.
“I learned that both domestic and international actors had succeeded in using the poorly understood science of climate change to advance an ambitious environmental agenda focused on increasing centralized control over people’s daily lives,” he told LifeSiteNews in an August 2016 interview.
“Left-wing politicians discovered in climate change renewed ways to press their agenda of social and economic justice through coercive government programs. As John Sununu, the former governor of New Hampshire, sees it, ‘The alarmists have learned well from the past. They saw what motivates policymakers is not necessarily just hard science, but a well-orchestrated symphony of effort … announce a disaster; cherry pick some results; back it up with computer modeling; proclaim a consensus; stifle the opposition; take over the process and control the funding; and roll the policymakers,’” he said.
On Tuesday, Lim told CBC Montreal’s Daybreak program, “Our government isn’t doing enough.” She said her country’s legislators are “nowhere near the action needed.” On Twitter, supporters can use the “No Future, No Children” hashtag to register their position. Lim has launched a website where they can announce their decision.
As of Thursday, more than 1,000 people had registered at Lim’s website. While Lim herself claims she wants children, she says she wants them only if they can be “safe.”
Lim believes that global climate change will cause mass migration. Comparing it to the Holocaust, she said she fears that her children will have to “again face the very worst of humanity.” On CBC, Lim said, “It’s clear that our leaders aren’t taking this seriously, and this is a serious issue,” referring to the approval of the Trans Mountain oil pipeline by the Canadian government.
Lim’s website is linked to the Climate Strike Canada website, which is calling on students to leave their classrooms on Friday to demonstrate their support for climate change doctrine. Among student testimonies collected by the website, “Emma” is quoted: “Just 100 companies are responsible for 70% for GHG [greenhouse gas] emissions, [yet] convenient rhetoric keeps the blame and responsibility off their shoulders. I strike because I believe change is possible and because there is so much in this world worth protecting.”
According to its website, Climate Strike Canada endorses a Canadian Green New Deal and supports the Global People’s Platform for a Livable Future. Among its proposals is the reduction of greenhouse gas emissions of 75% over 2005 levels by 2030.
Students of all ages are expected to walk out of school, starting on Friday, as part of a global climate strike. In Canada, some school boards are allowing or even encouraging students to skip class. Among the institutions in support are the Toronto District School Board, Dawson College of Montreal, and the University of British Columbia. The Toronto board has asked schools to avoid scheduling tests on September 27 so as to ensure that students are not penalized academically for taking part in the rally outside the Ontario legislature. Students under 18, said the authorities, must obtain parental permission to skip class.
The University of British Columbia told student participants that they should talk to their instructors first, while faculty members were told to inform students in advance should they participate in the strike.
New York City schools declared recently that students participating in the strike will receive excused absences. Students around the world are set to participate.
Media attention has been focused on Greta Thunberg, a 16-year-old climate activist from Sweden who has been largely credited with starting the student movement in her country. She testified before the U.S. House of Representatives this week, appearing at a hearing on Wednesday. She offered a copy of the United Nations’ report from the Intergovernmental Panel on Climate Change, which offered findings of scientists to be used by government leaders.
“I am submitting this report as my testimony because I don’t want you to listen to me,” Thunberg said, adding, “I want you to listen to the scientists. And I want you to unite behind the science. And then I want you to take action.”
Less than 30 days after installing a Safe Haven Baby Box, Franciscan Health Hospital in Hammond, Indiana, received a healthy newborn baby girl. ABC7 Chicago reported the baby was retrieved by first responders in less than 90 seconds. An alarm sounded when the baby was placed in the box, and the emergency department of the hospital responded.
ABC7 Chicago interviewed Monica Kelsey, founder and CEO of Safe Haven Baby Boxes. Kelsey was adopted, and later learned that she was abandoned as a newborn. After seeing a baby box at a church in Cape Town, South Africa, where parents could surrender a newborn without face-to-face interaction, Kelsey started Safe Haven Baby Boxes to create a way for mothers to ensure their child’s care, and educate people about Safe Haven Laws, gwhich allow parents of newborns to surrender a newborn without facing legal consequences.
In regards to the newborn recently placed in the hospital baby box, Kelsey said, “That is my hope and my goal for this little girl, is to grow up knowing she was loved from the beginning. Her mom just felt that this was best for her, and hopefully one day she changes the world and does something amazing.”
The story of this newborn safely delivered to authorities is a contrast to many recent stories that could have ended tragically. Over the summer, one newborn baby girl was found abandoned in the woods in a plastic bag in Georgia. Another baby girl, likely just hours old, was found naked in the woods of Silver Spring, Maryland. In both cases, the babies were rescued when passersby heard crying and investigated. Tragically, many cases of abandoned newborns do not end with the child safely rescued.
Indiana Safe Haven Laws allows parents to place a newborn in care at any hospital emergency room, police or fire station without any questions or legal consequences. As the recent story shows, laws like this save lives. For information about Safe Haven Laws in your state, you can visit Baby Safe Haven or call 1-888-510-BABY.
Kiera Meldrum, aged 20, was offered an abortion every single week following her 21-week scan, which discovered that her unborn baby had severe ascites to the bowel.
The young mum from York, bravely defied the doctors’ orders to abort her baby, every week, and describes how constantly being offered an abortion made her feel “horrific.” At 34 weeks, Kiera delivered her baby girl, Lillee-Rose, who had to undergo life saving surgery and spend eight intensive weeks in hospital.
However, Lillee-Rose is now happy and home with her family. Despite having a delicate bowel, doctors are satisfied that she should live a healthy and normal life.
According to The Scotsman, Lillee-Rose’s mum (Kiera) said: “Doctors told me every week to terminate my pregnancy, and hearing that advice over and over again was horrific, but something told me Lillee-Rose would make it through.
“I refused to terminate Lillee-Rose every time they told me to, and I’m so happy I listened to my heart instead of the doctors. There was no way I was terminating my pregnancy – I’d waited so long to become a mum and I was determined to do all I could to protect my baby
“My baby girl never stopped fighting and finally having her home with me is a blessing. I always had a feeling that she’d be ok, and seeing her grow up healthy and strong just goes to show that a mother always knows best. She is my little miracle.”
“Always go with your gut instinct”
Earlier this year, SPUC reported on the case of Scottish mother, Lauren Webster, who was also repeatedly offered an abortion during the course of her pregnancy, as her unborn child was suspected of having a low chance of survival. Ms Webster resisted the medical pressure to abort, and later gave birth to a healthy baby boy as she had a “gut feeling he would survive.”
PRO-LIFE COLLEGE STUDENT? LifeNews is looking for interns interested in writing, social media, or video creation. Contact us today.
Similarly, mother Natalie Halson was advised to abort her baby, Mirabelle, ten times after she was diagnosed with spina bifida, and was told by doctors that the baby would have a ‘poor quality of life.’ Ms Halson resisted the pressure from medical staff to abort and later gave birth to a healthy baby, who after a spinal operation is likely to live a happy and normal life.
Ms Halson said: “I would recommend to any parents who are advised to abort that it isn’t the only option, no matter what the hospitals try to tell them. Always go with your gut instinct; something inside told me that my baby was going to be ok- and look at her now, she’s perfect.”
“Mothers should not be facing such pressure”
SPUC Scotland, Director of Communications and Campaigns, Michael Robinson said: “Whilst these stories of survival are heart-warming, they also highlight the immense and unacceptable pressure on mothers from medical staff.”
“These brave mothers chose life for their child and now cannot imagine life without them. It is saddening to reflect on the pressure brought upon them during their pregnancy- what should have been a hopeful and happy time.”
LifeNews Note: Courtesy of SPUC. The Society for the Protection of Unborn Children is a leading pro-life organization in the United Kingdom.
Imagine for a moment that a courageous undercover journalist embedded herself among a group of powerful and wealthy businessmen involved in some horrific crime – sex-trafficking, for instance. Imagine the journalist had surreptitiously recorded conversations in which these powerful men openly haggled over the prices of their victims and spilled the details about how they circumvent the law.
Now, imagine that this journalist publicly released these damning recordings. And then imagine that, instead of investigating the businessmen, congressmen and law enforcement officials instead investigated the journalist – for the “crime” of secretly recording the businessmen!
The scenario is absurd, you might say. The public outrage in the face of such a gross miscarriage of justice would be swift and ferocious. After all, even if the secret recordings were technically illegal, clearly this kind of hard-hitting undercover journalism is an important exception.
However, we don’t really need to “imagine” such a supposed absurd scenario. Right now, two heroic pro-life investigators are fighting for their freedom in a Californian courtroom. Their crime? Exposing the horrific illegal practices of abortion clinics and biomedical companies who traffic in the bodies of aborted babies.
David Daleiden and Sandra Merritt are the two journalists, working for the Center for Medical Progress (CMP), who secretly recorded abortionists and other officials in the abortion industry describing how they harvest the body parts of unborn victims of abortion, and then sell them for a profit to various buyers. The pair publicly released the shocking videos in 2015.
They are now facing 15 felony counts for allegedly “illegally” taping the conversations with the abortion officials. If convicted, they face up to 10 years in prison!
The horrifying truth
I’ve watched the videos. To say they are nauseating is an understatement. One of the most haunting of them shows a medical worker digging through a petri dish filled with the crushed remains of aborted 20-week twins. At one point, the tweezers seize upon an object, and then proceed to lift the dismembered arm of a baby for the camera to see. Each of the fingers is vividly, searingly visible. This is the arm of a human being…a human being that was fully alive but minutes before, but whose mangled body is now being sorted through for intact parts that can be sold to pad the bottom line of the abortion clinic.
Then there’s the video in which the CEO of Stem Express, a tissue procurement company, described how in order to harvest “insanely fragile” brain tissue, it’s best just to ship the whole head of the fetus to researchers. “Just make sure the eyes are closed,” Daleiden (one of the pro-life investigators) remarks at this point. “Yeah,” the CEO laughs in response, “Tell the lab techs it’s coming…it’s almost like they don’t want to know what it is.”
Just about anybody with an intact conscience who saw these videos knew they were looking at something morally repugnant. In our bizarre legal system, however, the mere fact of harvesting the bodies of unborn babies who have been deliberately murdered is not, in itself, illegal. However, some of the practices that abortionists and other officials in the video explicitly admit to engaging clearly violate the law.
For instance, though it is technically legal to harvest human body parts from abortion and to provide them to biomedical companies or universities for macabre “research,” there are regulations against profiting from the sale of these body parts. Furthermore, there are regulations that forbid abortionists from altering the abortion procedure in order to obtain better or more intact “specimens.” The reason why is obvious: the abortionist could put the baby’s mother at risk if he decides to change his normal practices because he wants “better” body parts to sell.
In the videos released by Daleiden and Merritt, however, it’s clear that the abortionists and biomedical companies are very, very interested in money. In one of the most notorious of these videos, Dr. Mary Gatter, president of Planned Parenthood Federation of America’s for-profit Medical Directors’ Council, haggles over the price of baby body parts. At one point she even jokes, bizarrely, that she “wants a Lamborghini.” In the same conversation, Gatter says she would be willing to ask their abortionist if he would be willing to alter “the protocol” they follow during abortion to procure the body parts. In other words, Gatter appeared to violate the law on both counts in a single conversation.
A politically motivated prosecution…that might backfire
Unsurprisingly, the abortion industry responded to CMP’s videos by doing everything in their power to browbeat the pro-life investigators into silence. Unfortunately for Daleiden and Merrit, the abortion industry has powerful friends in high places.
One of these is former California Attorney General Kamala Harris – now a stridently pro-abortion presidential candidate for the Democratic party – who first initiated the investigation into CMP, partially in response to the urging of four Democratic congressmen (frankly, I’m not sure she needed much urging). And another is Harris’ successor, current California Attorney General Xavier Becerra, who is known as a staunch pro-abortion advocate with ties to Planned Parenthood.
According to Peter Breen, one of the lawyers defending Daleiden and Merritt, the case against CMP is the “first time in California history” that an attorney general has prosecuted anyone under California’s law banning illegal taping. As Breen observed, this is bizarre. “We as a society made a value judgement, we as a society value undercover journalism,” he said. And (it should come as no surprise), “Undercover journalism requires surreptitious taping.” But in the quest to protect legal child-killing, it appears just about any stick is good enough to beat pro-lifers with.
Daleiden was also previously hit with a nearly $200,000 fine after a California judge concluded that Daleiden and his lawyers had violated a gag order he had placed on CMP’s videos.
It’s possible, however, that the abortion industry’s strategy of suing and investigating CMP into oblivion will backfire. As Daleiden pointed out late last month, before the current hearing began, if Planned Parenthood’s lawsuit against CMP proceeded, many of the abortionists and abortion officials featured in their videos would have to take the stand and testify under oath about their nefarious activities. Which is precisely what CMP wanted in the first place.
That, in fact, is currently happening. The first week of the preliminary hearing into Planned Parenthood’s lawsuit wrapped up last week, and the case will be ongoing this week. Several key witnesses have already taken the stand and described some the macabre business of harvesting fetal body parts. And while the pro-abortion attorney general requested a gag order that would seriously impede media reporting on the case, the judge overseeing the preliminary hearing last week rejected that request.
Perhaps the most chilling testimony of all, so far, came from Daleiden himself, who last described on the stand how he was motivated to investigate fetal tissue procurement after seeing a 2012 documentary in which a whistleblower who worked in Planned Parenthood clinics described receiving the intact bodies of aborted babies, and “cutting open the chest and seeing the heart was still beating.” Daleiden then explained that Stem Express itself provided researchers at Stanford University with fetal hearts. According to Daleiden, the methods used by those researchers would have required that they receive living human hearts.
The CEO of Stem Express herself admitted in court last week that her company provided fetal hearts and heads, and that in some cases the heads would be attached to the bodies of the baby, or could “be torn away.” As Daleiden’s lawyers pointed out, this raises questions about how Stem Express is obtaining intact bodies of babies, and whether the babies may well have been alive at the time they were born or were victims of illegal partial-birth abortions.
Pray for Daleiden, Merritt and their lawyers
At this point in the preliminary hearing, Daleiden and Merritt’s lawyers feel confident that they are winning. They are arguing that the laws against illegal taping do not cover cases when the conversations being taped can reasonably be expected to be overheard. This would include many of the conversations in CMP’s videos, which were recorded in public restaurants and at trade shows with numerous people milling about in the vicinity. The lawyers are also arguing that the law doesn’t apply to instances when those doing the recording reasonably believe that they are investigating a violent crime – which, clearly, Daleiden and Merritt were doing.
However, as anyone who has worked in the pro-life movement knows, legal proceedings involving the issue of abortion often go in unexpected directions. Lawyers who defend pro-life advocates often must prepare themselves for things that they have never experienced in their entire legal career: e.g.seemingly slam-dunk, routine preliminary motions arbitrarily denied, or judges tortuously interpreting the law in novel ways to arrive at decisions that go against the pro-lifers.
Daleiden and Merritt are courageous pro-life witnesses, who have done immeasurable good for our unborn brothers and sisters. Thanks to their efforts, the sheer, horrific barbarity of abortion has been exposed for countless millions of people to see. Right now, they are fighting for their freedom. They need our support in any way we can give it to them. And they and their lawyers need our prayers – for wisdom, and spiritual protection. I hope you will join me in praying for them throughout this court case.
A study published in the Journal of Child Psychology and Psychiatry found that teenagers who use birth control are “1.7 times to 3 times more likely to be clinically depressed in adulthood, compared to women who started taking birth control pills as adults, and to women who had never taken birth control pills.”
According to UBC News, the researchers collected data on over a thousand women in the United States, which led them to see that use of hormonal birth control during adolescence increases vulnerability to depression in adulthood even if the woman has been off of birth control for years. “Adolescence is an important period for brain development. Previous animal studies have found that manipulating sex hormones, especially during important phases of brain development, can influence later behavior in a way that is irreversible,” said the study’s first author, Christine Anderl, a psychology postdoctoral fellow at the University of British Columbia.
While the study’s authors say that this doesn’t prove that birth control causes depression, they hope that dialogue will continue on the topic. Meanwhile, the researchers behind this study are working on a new study to “investigate how hormonal changes during adolescence can affect teenagers’ emotions, social interactions, and mental health.”
Given what we know both about the side effects of hormonal birth control and the ever-fluctuating hormones of teenagers, this correlation comes as no surprise. Depression and anxiety are cited as some of the most common side effects of hormonal birth control, and this is not the first study to make this connection. Another study from 2017 published in The American Journal of Psychiatry looking at nearly a million Danish women and girls found that those on “hormonal contraception were 97% more likely to attempt suicide than those not taking the drugs, and were 200% more likely to succeed in their suicide attempt.”
All this being said, it is important to note that many women will experience anxiety and depression whether or not they have been prescribed hormonal birth control. However, one of the beauties of FABMs is that it can help women regulate stress and mood swings and help with self-care and emotional health.
One hopes that these recent findings—echoing concerns we’ve had for a while now—will be taken seriously and be considered by healthcare providers when they are caring for teen girls. Women and girls should not have to suffer mental-health side effects in order to prevent anything from pregnancy to acne to polycystic ovary syndrome (PCOS). Thank goodness for fertility awareness and the freedom and clarity that it can bring!
September 12, 2019 (LifeSiteNews) — A group of scientists revealed the opening of another Pandora’s box this week with a new paper detailing a method for quickly producing large quantities of organic structures similar to human embryos, for the purpose of studying human life in its earliest stages.
The paper, published Wednesday in Nature, details the development of “microfluidic devices” capable of mass-producing embryoid bodies, which are “cystic teratoma-like structures consisting of semi-organized tissues representing all three embryonic germ layers.”
These devices, the researchers say, offer a “powerful experimental system to advance knowledge of human embryology and reproduction,” which “could assist in the rational design of differentiation protocols of hPSCs for disease modelling and cell therapy, and in high-throughput drug and toxicity screens to prevent pregnancy failure and birth defects.”
Describing these embryoids as “synthetic embryos,” NPR reports that the research has sparked a conversation about the ethics of creating organic entities so similar to newly conceived human beings.
Rockefeller University embryologist Ali Brivanlou said the development opens “windows to aspects of development that we have never seen before,” the “Holy Grail of human embryology.” But Harvard and Case Western bioethicist Insoo Hyun called on researchers to be “very careful not to model all aspects of the developing human embryo, so that they can avoid the concern that this embryo model could one day become a baby if you put it in the womb.”
Jianping Fu, the lead researcher on the paper, acknowledged he was “pushing the boundary” but insists he made sure these embryoids only “resemble a portion of the human embryo — the core of the early human embryo,” and that his team had “zero intention” of creating a “complete human embryo.”
That approach satisfied some of the researchers who spoke to NPR, but Georgetown bioethicist Daniel Sulmasy sounded concerned.
“That would be sort of a very early sort of Frankenstein model, right? Taking different parts and stitching them together in order to try to create an organism,” he said. “If somebody tried to do it and it were even at the earliest stages of embryonic development, and they tried to then let it develop further, that would be a problem.”
Tackling the question of whether embryoids are, in fact, living human beings, Heather Zeiger of the Center for Bioethics & Human Dignity writes that they “seem to have many of the features that define a biological organism. They respond to environmental stimuli, exhibit self-organization, undergo growth and development, and consume energy. The cells within embryoids can be said to reproduce in the same sense that embryonic cells grow and divide. However, the embryoid itself lacks the necessary cells to grow into a human that, in turn, can reproduce. Furthermore, its self-organization is local in contrast to the global and directional organization of embryos.”
Ethical guidelines currently accepted by the scientific establishment dictate that scientists can experiment on an embryo only for up to fourteen days after its creation, a restriction that Fu touts embryoids as circumventing. In 2017, scientists from Harvard argued that the advent of embryoids necessitated replacing the 14-day rule with a more rigorous framework based on the precise nature of the entities being created.
“These and related experiments raise more foundational issues that cannot be fixed by adjusting the 14-day rule, because the framework underlying the rule cannot adequately describe the ways by which synthetic human entities with embryo-like features (SHEEFs) might develop morally concerning features through altered forms of development,” they wrote at the time. “We propose that limits on research with SHEEFs be based as directly as possible on the generation of such features, and recommend that the research and bioethics communities lead a wide-ranging inquiry aimed at mapping out solutions to the ethical problems raised by them.”
Abortion pills on state college campuses may soon become a reality, depending on how the California legislature votes tomorrow on SB 24, a bill that would allow California campus health centers to dispense the abortion pill regimen to students.
Live Action News previously detailed how at least 24 women have already died and how literally thousands have been hospitalized with serious complications from the abortion pill, all while the pill regime was monitored under a safety system (REMS) put in place by the FDA. But many of those now pushing for these dangerous pills to be readily available on campus are also pushing for these same safety requirements to be lifted.
What does this mean?
According to the pro-abortion Rewire news website:
The California state legislature has until Friday to vote on the College Student Right to Access Act, sponsored by state Sen. Connie Leyva (D-Chino). If it does not move forward this week, the bill will be “carried over” to 2020…. A previous version of the bill was vetoed by Gov. Jerry Brown (D) last year, but California’s new governor, Democrat Gavin Newsom, has signaled he would sign the bill into law.
Should SB24 be approved, Rewire says, “Starting in 2023, each campus of California State University and the University of California would receive $200,000 to cover the startup costs of offering medication abortion services at their health centers.”
Rewire fails to point out that, as Live Action News previously documented, the funds for campus abortion pill distribution were promised by Tara Health Foundation (THF) — a radically pro-abortion organization pushing to expand abortion.
TARA Health foundation funds abortion pill on college campus
Packard Timeline shows it invested in abortion pill distributor
THF recently funded a study on TelAbortion (telemedicine), claiming abortion pill expansion is safe. This study was published by the Journal Contraception, which has failed to list previous financial conflicts tied to the abortion pill’s manufacturer, DANCO, in past reports. The Journal’s editorial board has been stacked with abortion industry insiders, including a National Abortion Federation board member and members of the Population Council (responsible for bringing the abortion pill into the US and forming DANCO, the manufacturer of the pill).
Who are the people behind the studies claiming that distributing the abortion pill this way is safe?
Abortionist Daniel Grossman, director of Advancing New Standards in Reproductive Health (ANSIRH) at the University of California, San Francisco (UCSF), told Rewire that Tara Health’s funding of the abortion pill on California college campuses “should be ‘more than enough’ to train staff and get student health centers ready to provide abortion care.”
Grossman was also recently recruited to issue “fact checks” for Facebook, targeting Live Action. (Live Action News has been exposing Grossman’s ties to big abortion.)
Daniel Grossman ( Image credit: University of Texas at Austin)
Rewire also quoted Ushma Upadhyay,associate professor at ANSIRH. “In one study,” Rewire writes, “[Upadhyay] and her colleagues found that the average student at a California state school had to wait about a week for an off-campus appointment and pay an average of $600 for medication abortion services.” That study, published by the Journal of Adolescent Health, deliberately hid its funding source, noting it was a “private anonymous donor.”
Ushma Upadhyay abortion study anonymous funding
Hiding funding sources isn’t new among abortion insiders. Live Action News uncovered that the Buffett Foundation — another DANCO abortion pill manufacturer investor — has been an anonymous funding source for at least one abortion pill study. And we have documented several times that Buffett and Packard were original investors in DANCO, as was billionaire George Soros (Open Society Foundations).
In past years, Buffett gave $78 million to the University of California — and according to New York Times, Buffett is the primary financier of the Bixby Center’s Ryan Residency Program at UCSF, where Daniel Grossman works. In 2016, ProPublica revealed that “Buffett’s main academic partner (receiving at least $88 million from 2001 to 2014) has been the University of California, San Francisco…” where Grossman is on staff.
Buffett funds UCSF Bixby Ryan program where Grossman is staff and Family Planning Fellowship
Additional connections:
ANSIRH:Founded by abortionist Felicia H. Stewart, previously awarded by Population Council which brought the abortion pill to the US and set up Danco Laboratories.
ANSIRH has for years pushed for abortion expansion in California with funding from DANCO investor, the Packard Foundation.
Bixby trains abortionists, as Live Action News previously documented, and receives funding from a number of organizations collaborating to expand abortion, including DANCO’s original investor the Packard Foundation.
University of California is heavily funded by DANCO’s investors (Packard and Buffett), and sponsoring clinical trials to expand abortion in U.S.
Upadhyay studies have been funded by Danco investor, Packard.
ANSIRH recently collaborated with Danco-funded Ibis to publish a report entitled, “A roadmap for research on self-managed abortion in the United States.”
Daniel Grossman works with Ibis funded by abortion pill mfg Danco
September 11, 2019 (LifeSiteNews) – This week on The Van Maren Show, Jonathon Van Maren speaks with Mary Eberstadt about the sexual revolution. Eberstadt provides an intellectual and precise commentary on current culture, philosophy, and the fate of the post-modern man. She is the author of the new book Primal Screams: How the Sexual Revolution Created Identity Politics, and also wrote How the West Really Lost God and Adam and Eve after the Pill.
The sexual revolution is a topic that Van Maren has covered extensively on his LifeSiteNews blog and on The Van Maren Show. The sexual revolution has impacted every corner of society, from the so-called LGBT movement to pornography and sex-education to attacks on freedoms of speech and religion.
Eberstadt dives into the concept of “the loneliness epidemic” and how it relates to the sexual revolution. According to Eberstadt, to say there has been an explosion of loneliness in every single advanced country is not at all an overstatement. It is traceable to the fact that a lot of people simply aren’t having children. She states that children and marriage are nature’s solution to loneliness. However, more and more people are not getting married and are deciding against having children.
“This is, to me, one of the most poignant manifestations of the revolution’s fallout. And it’s something that we’re going to be dealing with for a long time to come,” she explains.
Van Maren and Eberstadt spend some time discussing the #MeToo Movement and third-wave feminism, which are consequences of the sexual revolution. Eberstadt summarizes the rage that we see all the time in the third-wave feminism movement by stating that “the problem is the sexual revolution has unleashed predation and made it harder to find what most women, even now, will say they want most, which is marriage and family.”
Despite the far reaches of the sexual revolution and the massive impact it has had on today’s culture, Eberstadt wraps up this episode with a good bit of hope: “I think there are all kinds of reasons for hope, including that we are rational animals.”
She cites several examples of positive social transformation in history, and argues that young people today being more likely than their Baby Boomer parents to be pro-life is evidence of a rollback of sexual revolution ideology.
Eberstadt’s commentary is simply amazing. This episode of The Van Maren Show is a must-listen. Additionally, be sure to read Eberstadt’s books, available at Amazon or her website.
The ability to delay and space childbearing is crucial to women’s social and economic advancement. Women’s ability to obtain and effectively use contraceptives has a positive impact on their education and workforce participation, as well as on subsequent outcomes related to income, family stability, mental health and happiness, and children’s well-being. However, the evidence suggests that the most disadvantaged U.S. women do not fully share in these benefits, which is why unintended pregnancy prevention efforts need to be grounded in broader antipoverty and social justice efforts.
With rave reviews like this, what’s not to love? Plenty, as it turns out.
In the Beginning
Contraception, beginning with the development of the only medication to be so widely known that it’s simply called “the Pill,” marked a major shift in men and women’s understanding of the purpose of sex. Classically understood, sex was for babies and bonding between the partners. Not every act of intercourse led to babies, certainly, but couples understood that the possibility of conceiving existed.
Contraception was originally marketed using a kind of salvation messaging. Promiscuous sex — including with married men — and a career would give a single girl’s life meaning, according to Helen Gurley Brown’s best-selling book “Sex and the Single Girl.” And sex without the possibility of more mouths to feed would make married women happy and free as described in the pages of Cosmopolitan magazine. In this narrative, birth control was the ticket to making both single and married women’s wildest dreams come true. Unfortunately, the Pill hasn’t made good on all of its glitzy promises.
Reality Check
Separating fact from fiction in the Guttmacher Institute’s claims above, it’s true that 33% of modern-day women will graduate college, versus just 7% in the 1960s, and some 60% of recent college graduates are female. It’s also true that at the time contraception was introduced, women were often fired for becoming pregnant, as described by Sue Ellen Browder in her book, “Subverted: How I Helped the Sexual Revolution Hijack the Women’s Movement.” Legal policy changes, ultimately, not contraception, were the driver in ending pregnancy discrimination. In fact, contraception plays right along with the misogynistic idea that women have to be just like men (unable to bear children) in order to succeed professionally.
While the Guttmacher Institute also insists that contraception makes women economically better off, data from the United States Census Bureau show that more children, not less, are living with single mothers than in decades past. And, those single mothers, 27% of whom are living in poverty, are significantly more likely to be poor than the far fewer numbers of single fathers raising children. In fact, economist Timothy Reichert found that “the contraceptive revolution has resulted in a massive redistribution of wealth and power from women and children to men” by setting up “what economists call a ‘prisoner’s-dilemma game, in which each woman is induced to make decisions rationally that ultimately make her, and all women, worse off.”
The Guttmacher Institute also claims that contraception contributes to family stability, yet we know that divorce has skyrocketed since the 1960s. Speakers in the 2018 documentary Unprotected pointed out the logical connection between contraception and divorce, given the basic premise that human beings need deterrents to do the right thing and that contraception removes a historical deterrent to infidelity by dramatically reducing the risk of an unexpected pregnancy. Infidelity is commonly cited as a reason for divorce. Timothy Reichert’s analysis of research from the social sciences bore out this connection as well.
Improved “mental health and happiness” is also credited to contraception in the quote above, and yet directly contradicts a major study finding that women’s happiness “has declined both absolutely and relative to men” when compared to women in the 1970s. This makes sense given that the Unprotected documentary mentioned above noted how young girls face pressure to “sext” nude pictures of themselves to teenage boys. In college, rates of sexual assault on young women are staggering. The trend of disrespect for women continues in the workplace and beyond, as catalogued by the #metoo movement.
According to the Unprotected documentary, this decline in women’s well-being due to a loss of respect for women was directly predicted by Pope Paul VI in his 1968 papal document “Humanae Vitae,” which reaffirmed the Catholic Church’s traditional prohibition on contraception. Specifically, Pope Paul VI anticipated that if contraception became widespread, “the man” would lose respect for “the woman” and “no longer (care) for her physical and psychological equilibrium,” and would go so far as “considering her as a mere instrument of selfish enjoyment and no longer as his respected and beloved companion.”
In fact, Pope Paul VI also predicted an increase in “infidelity and moral decline,” described above, as well as governments using coercive measures to control population size and poverty. China’s regressive One-Child Policy comes to mind, as well as the United Kingdom’s new “Two-Child Limit” on welfare benefits for poor couples.
While contraception has proved far from an unqualified good for women, modern, evidence-based methods of natural family planning (NFP) enable women to work with their bodies to plan family size and monitor their reproductive health. Natural family planning maintains the integral unity of sex, rather than separating babies from bonding. Couples utilize the woman’s fertile window if they are trying to become pregnant, and to abstain from sex during that time (growing their relationship in other ways) if their goal is to avoid pregnancy.
With apps like Daysy and FEMM, and at-home fertility monitors like the Clear Blue Monitor, technology is assisting more and more women in understanding their own bodies and achieving their reproductive goals in ways that respect their fertility rather than viewing it as an obstacle. At the end of Unprotected, presenter Christopher West emphasized that working cooperatively with the woman’s body via NFP is a game-changer for couples. In fact, research suggests that rates of divorce amongst couples using NFP are less than 5%. Respecting the woman’s body, rather than treating her fertility as the enemy, can bring benefits that contraception can’t ever achieve.
September 9, 2019 (LifeSiteNews) – The European physician behind an organization that circumvents medical regulations by sending abortion pills through the mail has filed a federal lawsuit against the U.S. Food & Drug Administration (FDA) over actions it has taken to block their activities.
Created by Dutch abortion activist Rebecca Gomperts, “Aid Access” sends women the abortion-inducing drugs mifepristone and misoprostol after just an online consultation with a “doctor,” for the express purpose of getting around the costs and unavailability of abortions in their area, as well as regulations such as waiting periods or parental involvement requirements. The group claims it’s safe to take the pills at home, without medical supervision.
The FDA opened an investigation into Aid Access last October, and in March warned the organization that it was “facilitating the sale of…unapproved and misbranded” products, and to “promptly cease” doing so or face regulatory action potentially “including seizure or injunction, without further notice.”
On Friday, Gomperts filed a suit in U.S. District Court for the District of Idaho against the FDA and Health and Human Services (HHS) Secretary Alex Azar for seizing up to ten doses of abortion drugs Aid Access had “prescribed” since that letter, NPR reports, as well as allegedly blocking some payments to the group. The suit seeks to stop what Gomperts calls “bullying” and “intimidation” by the FDA.
Gomperts’ attorney Richard Hearn claims that Aid Access merely helps women carry out the so-called “right” to abortion. “Some women in the United States can exercise that right just by going down the street if those women happen to live in New York or San Francisco or other major metropolitan areas on either one of the coasts,” he told NPR. “But women in Idaho and other rural states, especially conservative states…cannot exercise that right.”
“FDA remains very concerned about the sale of unapproved mifepristone for medical termination of early pregnancy on the Internet or via other channels for illegal importation, because this bypasses important safeguards designed to protect women’s health,” the agency responded in a statement to NPR. It didn’t comment on potential future actions against Aid Access, but said it “generally does not take enforcement action against individuals” who receive such unapproved drugs.
Part of the FDA’s March warning to Aid Access was that its business circumvents federal requirements that the approved prescription version of mifepristone, Mifeprex, be only made available via a Risk Evaluation and Mitigation Strategy (REMS) program and obtainable only from REMS-certified healthcare providers. This, it said, ensures that providers can “assess the duration of the pregnancy accurately, diagnose ectopic pregnancies, and provide surgical intervention in cases of incomplete abortion or severe bleeding, or to have made arrangements for others to provide such care”; give women “access to medical facilities for emergency care”; and more.
Pro-lifers also warn that even when “properly” taken, abortion pills are not only lethal to preborn children but more dangerous to women than advertised.
“As of December 31, 2018, there were reports of 24 deaths of women associated with Mifeprex since the product was approved in September 2000, including two cases of ectopic pregnancy resulting in death; and several cases of severe systemic infection (also called sepsis), including some that were fatal,” the FDA warns, on top of 2,740 cases of severe complications from 2000 to 2012.
“Protecting women from the known dangers of abortion-inducing drugs is good and safe policy,” Students for Life of America spokesperson Kristi Hamrick said in a statement about the lawsuit. “Risking women’s lives so that an international sales team for abortion pills can more easily operate is not in the interests of American women. It’s easy to understand why a profit driven industry for chemical abortion pills wants fewer health and safety standards but protecting women from the known dangers of the pills is the right public policy.”
Sarah was 26 years old when she got the shock of a poorly-timed, positive pregnancy test. Already a mother of three, she was concerned about the course of her life. Her boyfriend insisted she have an abortion, so she scheduled the appointment, fearing being a single mother of four and feeling she needed to “save face,” succumbing to the father’s pressure to “take care of this.”
Sarah was given two pills to complete the abortion. But after she took the first pill, she dissolved into tears. “It was awful,” she told The Catholic Telegraph. When she looked at her other children she thought, “I love you and we’re making it. Why does this baby not deserve that same chance to love and be loved and be a sibling?”
Soon after, she began combing the internet for a way to undo the effects of the abortion pill, which is when she discovered Abortion Pill Rescue, which offered the process of the abortion pill reversal. She discovered there was a doctor in her area who could see her in just a few hours to begin the process.
Abortion pill reversalworks by countering the effects of the first phase of the two-step abortion pill process. In the first step, a woman takes mifepristone in order to block the effects of progesterone, essential cutting off nutrients the baby needs to survive. Mifepristone will eventually lead to the death of the baby. The second pill, misoprostol, causes contractions that expel that baby’s body.
Reversing the process involves administering high dosages of progesterone to counteract the first abortion pill, mifepristone, and its harmful effects. As the American Association of Pro-Life Obstetricians and Gynecologists (AAPLOG) explains, “[U]sing progesterone to counteract the effect of mifepristone is the logical extension of simple principles of toxicology and poison control.” And while some abortion activists baselessly claim that administering high doses of progesterone is dangerous to women and can cause birth defects, Live Action News has shown that these are lies. On the contrary, administering progesterone has been a standard part of OBGYN care for decades.
As Live Action News has reported, Dr. Bill Lile, an obstetrician and gynecologist licensed in Alabama and Florida, has explained that abortion pill reversal is analogous to a patient who has overdosed on narcotics and is given the reversal agent Narcan. “[J]ust like we give Narcan to reverse a bad decision, we can give Prometrium [micronized progesterone] to reverse a bad decision. And we’ve been very successful around the country with reversal protocols.”
After Sarah began the treatment, her baby showed a strong heartbeat, and the doctor who gave her the regimen continued to treat her and Isaiah, who was born healthy. Isaiah’s father left after Sarah told him the “abortion didn’t work.” But despite the roadblocks in her life, she is doing better now than she could have imagined.
“I have a job now that I couldn’t even see myself having when I found out I was pregnant, wondering how I was going to make it work,” she said. “But God sets things in motion, and I’m benefiting from believing in His plan.”
Sarah’s story is being told in an upcoming episode of the Being Pro-Life podcast, airing September 12th.
Editor’s Note: If you have taken the first of the two-dose abortion pill and regret it, visit abortionpillreversal.com or call their 24-hour helpline at 877-558-0333.
Mother Teresa is best known for her work among the poorest of the poor, caring for “all those people who feel unwanted, unloved, uncared for throughout society” in the slums of Calcutta. By her death in 1997 the order she founded, the Missionaries of Charity, had grown from a 13-member Calcutta congregation to more than 4,000 sisters who managed orphanages, AIDS hospices and charity centres worldwide, caring for refugees, the blind, disabled, aged, alcoholics, the poor and homeless and victims of floods, epidemics and famine.
However, she was also praised (and fiercely criticised) for her staunch opposition to abortion. She spoke up for the unborn on the biggest stages imaginable, including when she accepted her Nobel Peace Prize. She didn’t let famous people off the hook either, keeping up correspondence over many years with Hilary Clinton to try and change her mind on abortion.
So, on this twentieth anniversary of her death, what lessons does Mother Teresa have for pro-lifers today?
1) Dare to speak out
Speaking out about abortion can be hard. It is such a controversial topic, and people’s reactions can be so extreme, that we can all feel the temptation to be quiet about our beliefs, or perhaps stick to more socially acceptable causes. Mother Teresa’s main work was with the poor and hungry, and I’m sure it would have been easier for her to stick to that work and enjoy the praise she received for it. But she didn’t. She used the platform her fame had won her to speak out for the most marginalised, the unborn. When accepting her Nobel Peace Prize in 1979, she said:
“And I feel one thing I want to share with you all, the greatest destroyer of peace today is the cry of the innocent unborn child. For if a mother can murder her own child in her womb, what is left for you and for me to kill each other?”
She reiterated the sentiment at the National Prayer Breakfast in Washington, D.C, on February 5, 1994, where guests included the then President Bill Clinton, and his wife Hilary.
“But I feel that the greatest destroyer of peace today is abortion, because it is a war against the child, a direct killing of the innocent child, murder by the mother herself.”
Here, she stood in front of the most powerful people in America, if not the world, and dared to call out abortion for what is it – the killing of a child.
2) Reach out in love
However, Mother Teresa also reminds us that we must spread this truth with love. This quote is also taken from the prayer breakfast address:
“How do we persuade a woman not to have an abortion? As always, we must persuade her with love and we remind ourselves that love means to be willing to give until it hurts.”
While I’ve yet to encounter the pro-lifer of common stereotypes, who shouts “murderer!” at women seeking abortion, we can never be reminded too often that the only way to reach out to an abortion-minded woman is with love, and by offering support.
3) Recognise the real difficulties
This also means recognising the very real situations that people find themselves in. Mother Teresa knew that keeping a baby often isn’t easy – love means to be willing to give until it hurts. Working with people in the most unimaginable circumstances, she knew better than anyone how difficult it can be, and that a baby changes the parents’ lives beyond recognition.”So, the mother who is thinking of abortion, should be helped to love, that is, to give until it hurts her plans, or her free time, to respect the life of her child. The father of that child, whoever he is, must also give until it hurts.”
4) Do your part
This recognition requires those of us fighting for the cause to give of ourselves. Mother Teresa told the assembled VIPs in Washington what she and her sisters did to put her pro-life rhetoric into action. “We are fighting abortion by adoption — by care of the mother and adoption for her baby. We have saved thousands of lives. We have sent word to the clinics, to the hospitals and police stations: ‘Please don’t destroy the child; we will take the child.’ So we always have someone tell the mothers in trouble: ‘Come, we will take care of you, we will get a home for your child.’”
We may not be able to personally care for mothers and babies to this extent, but we should all be willing to translate our beliefs into real action – we too must give until it hurts. This could be by volunteering, or by making it known to those around you that you would help them in any difficulty, or by lobbying your MP, or simply by speaking up for your beliefs. To use another famous quote from Mother Teresa, “I alone cannot change the world, but I can cast a stone across the waters to create many ripples.”
5) The greatest destroyer of peace
Perhaps the greatest lesson Mother Teresa can give us is an understanding of just what it is we are fighting. Abortion doesn’t just kill babies and damage mothers, it affects the whole of society. It isn’t just those women and those babies that are affected, but all of us. Abortion certainly affects the fathers: “…that father is told that he does not have to take any responsibility at all for the child he has brought into the world. The father is likely to put other women into the same trouble. So abortion just leads to more abortion.” It also affects the entire country where abortion is permitted: “Any country that accepts abortion is not teaching its people to love, but to use any violence to get what they want. This is why the greatest destroyer of love and peace is abortion.”
There are many other causes worth fighting for, but we must never let ourselves be convinced that the pro-life fight is a side-issue, or one that affects only a small number of people. It’s not just that we care about babies, and also their mothers – we care about everyone. A final quote from the Washington address:
“Many people are very, very concerned with the children of India, with the children of Africa where quite a few die of hunger, and so on. Many people are also concerned about all the violence in this great country of the United States. These concerns are very good. But often these same people are not concerned with the millions who are being killed by the deliberate decision of their own mothers. And this is what is the greatest destroyer of peace today — abortion which brings people to such blindness.”
Recent numbers released by the American Academy of Dermatology revealed a dramatic spike in the incidence of melanoma cases among young women. Melanoma is the most dangerous type of skin cancer, and for women aged 18-39, its rates have increased by 800% from 1970 to 2009. In Caucasian women under 44, the number of cases has increased by just over 6% annually. (1)
Now, in addition to being the most dangerous, melanoma is one of the most common cancers in young adults (especially young women). More than 7,000 people in the United States are expected to die of melanoma in 2019—about 4,740 men and 2,490 women, (2) and the American Cancer Society estimates that about 96,480 new melanoma cases will be diagnosed in 2019. (3)
The introduction of indoor tanning is likely to have played a major role in this spike. However, we should take a hard look at exactly what role highly prescribed drugs like birth control play in the epidemic of skin cancer cases among pre-menopausal women.
Connections between skin cells and estrogen receptors
Anyone who has encountered breast cancer in their family history is probably familiar with a receptor known as HER2. I was, but I really didn’t know much about it beyond its name until I began researching for an article I was writing on breast cancer.
According to the NIH, a cancer that is HER2 positive, “describes cancer cells that have too much of a protein called HER2 on their surface. In normal cells, HER2 helps to control cell growth. When it is made in larger than normal amounts by cancer cells, the cells may grow more quickly and be more likely to spread to other parts of the body.”
HER2 stands for human epidermal growth factor receptor 2. Each cell in our body can contain many types of receptors. These receptors are proteins, usually on the surface of the cell, seeking to bond with another very specific molecule. Together, these partners fulfill many different types of functions in the body, especially the immune system. As a receptor, HER2’s primary partner is Epidermal Growth Factor (EGF), a protein believed to play a role in how cells normally grow.
For me, the first clue that birth control could play a role in skin ailments came when I read that scientists at the University of Colorado recently discovered that the presence of estrogens can stimulate astrocytes in the brain to produce EGF. (3)
With all this “epidermal” terminology and the estrogen connection, I couldn’t help but wonder what effect hormonal birth control might have on the skin. It didn’t take much digging to learn that hormonal contraceptives are commonly linked to things like acne, hyperpigmentation, and melasma (5), but I was surprised to learn that they have also been linked to skin cancer. Honestly, given that estrogen receptors can be found in nearly every cell of the body, I’m not sure why it surprised me; but this is one birth-control side effect that definitely flew below my radar.
Connections between hormonal contraceptives and skin health
In 1978, the New York Times reported on a ten-year study of nearly 18,000 patients, which found that women who took birth control for more than four years faced almost twice the risk of developing malignant melanoma.
A follow-up study out of the University of Oxford in 1981 showed that the risks weren’t significant in the short term. However, after five years of use, the increased relative risk climbed to nearly 60% (6).
A 1999 study demonstrated that premenopausal women who took hormonal birth control were nearly three-and-a-half times more likely to develop melanoma (7), while a 2018 French study showed that the increased risk for ten-year users was only 33%. (8)
While studies show mixed numbers, they all show a risk increase
Clearly, the results are mixed, and there’s a lot of debate in the scientific community about how significant birth control’s impact is on skin cancer. But, whether the increased risk is 33% or 350%, the studies seemed unified in signifying that a woman’s risk increases the longer she takes birth control.
Another recent health scare that made headlines may offer insight into how birth control could contribute to this increased risk. When scientists recently questioned whether some ingredients in sunscreen could actually be causing cancer, one of their concerns was that most brands contain parabens and phthalates, which, like hormonal birth control, are known endocrine disruptors. Endocrine disruptors are estrogenic chemicals that mimic natural hormones (in this case, estrogen) by binding to receptors within cells and thereby blocking the body’s natural estrogens from binding to these same cells.
In his enlightening book, Estrogeneration, Anthony G. Jay, Ph.D. explains how the UV light from the sun can fuse the disruptors to the estrogen receptors. Jay says, “If or when this chemical reaction occurs, the estrogen receptor would be stuck in the ‘on’ position. Biochemists call this a ‘constitutively active receptor.’”
Having this “light switch” stuck in the “on” position leads to longer-term damage, because the receptor switch is turned on for far longer than nature ever intended for our bodies. (9)
A Two-Pronged Attack
Given all this research, I’ve come to view the relationship between hormonal birth control and skin health much like a messy tenant in an apartment building—leaving the lights on for UV damage and piling up its dirty laundry in the form of overproduced Epidermal Growth Factor. This disorderly behavior disturbs two very important receptors in skin cells. Considering the spike in melanoma rates since the introduction of the Pill, it may be time to clean house.
From 1960 to 2016, the number of U.S. children living with two married parents dropped 19 percent — and the number of children living with just their mother tripled from nine percent to 23 percent of all children under the age of 18. This represents about 17 million children. Numbers from the Pew Research Center report that 27 percent of single mothers live in poverty. Even though there are five times more single mothers raising children than single fathers, single mothers are significantly more likely to be poor than single fathers are.
In 2010, economist Timothy Reichert argued that contraception actually has devastating economic consequences for women and children. He suggested that “the contraceptive revolution has resulted in a massive redistribution of wealth and power from women and children to men,” because it “sets up what economists call a ‘prisoner’s-dilemma’ game, in which each woman is induced to make decisions rationally that ultimately make her, and all women, worse off.” Despite being a lose-lose situation for women, and the children that rely on them, he wrote that because of the “prisoner’s dilemma,” contraception would continue to be the law of the land “unless legal restrictions or social mores ‘tax’ men and ‘subsidize’ women and children.”
Contraception creates a Marriage Market and a Sex Market
Reichert argued that birth control separated what has historically been a mating market, inhabited by roughly equal numbers of men and women, into two separate markets. One market, called the sex market, includes men and women seeking sexual relationships without any plan for marriage or a permanent future together. The other market, called the marriage market, is inhabited by people seeking what its name suggests. This split of one mating market into sex and marriage markets becomes a problem when “imbalances exist in these markets (so) that the ‘price’ of either marriage or sex tilts in favor of one or the other gender.”
Reichert explained how at any given time, more men are likely to be in the sex market because they don’t have a “biological clock” necessitating that they move into the marriage market by any certain age. Women in the sex market tend to “have more bargaining power than men” for two reasons: relative scarcity and age. Firstly, they are typically in shorter supply in the sex market. Secondly, women in the sex market tend to be younger, as a typical woman will decide by her early 30s that she is interested in marriage and a family, and thus leave the sex market. Younger women tend to be interested in older men, and vice versa, whereas younger men are not equally likely to be interested in older women.
Using charts, graphs, and research from the social sciences to illustrate his point, Reichert contrasted the sex market with the marriage market. In the marriage market, women face significant challenges in finding marriageable men because there are fewer men in the market than women. Reichert isn’t the only one to have made this observation. Riffs on the topics “Why can’t I find a good man?” and “Why are good men hard to find?” abound online, backing up Reichert’s economic analysis with personal anecdotes. He went on to argue that women become more likely to settle for less in order to get married, and then end up getting divorced later on. A 2017 study by Stanford University found that in 2,500 divorce cases studied, women initiated 69% of them.
Reichert further argued that the creation of separate sex and marriage markets caused by contraception correlated with a higher “cost” of infidelity to women than men, higher rates of divorce (and women heading up single-parent households), a “need” for abortion, and even — surprisingly — a driving up of the cost of real estate.
The “Prisoner’s Dilemma”
Reichert considered contraception a “prisoner’s dilemma,” or a situation in which “all parties have a choice between cooperation and noncooperation, and where all parties would be better off if they choose cooperation. But because people in a prisoner’s dilemma setting cannot effectively coordinate and enforce cooperation, all parties choose the best individual choice, which is noncooperation. The social result is disastrous, and everyone is made poorer.” He wrote that “women (and, by implication, children) would be better off had there been no separation of the mating market into separate sex and marriage markets,” because of the long-term negative consequences of the imbalance between the two markets on women, children, and society at large. But, they are nonetheless highly motivated to continue using contraception because of the short-term benefits to themselves.
There are people in every generation who believe the generation following theirs is either going to the dogs or will ruin the country.
A new Wall Street Journal/NBC News poll lends credence to that way of thinking, especially where Generation Z/millennials (those born in the mid-1990s to mid-2000s) and Generation X (those born in the early-to-mid 1960s to the early 1980s) are concerned.
The poll of 1,000 adults earlier this month found that “younger generations rate patriotism, religion and having children as less important to them than did young people two decades ago.”
The poll contrasts with a similar survey conducted by the Journal 21 years ago. When asked then which values were most important, respondents sounded like their parents and grandparents, saying “hard work, patriotism, commitment to religion and the goal of having children.”
Not only will these current findings likely impact next year’s election (most of those running for president with more than single-digit polling numbers are much older men and women and thus represent a generation gap), they could also have serious implications for the future of the country.
The Founders and subsequent generations — perhaps excepting the Gilded Age and the horrors of slavery — mostly believed in the virtues younger people either now reject or approach with indifference.
How can this be? What has happened between the World War II generation, which gave so much so their children and grandchildren might enjoy the blessings of liberty, and the current generation, which seems cool to what once seemed to matter most?
Generalizations are always problematic, but I have lived long enough and witnessed the general decline to make some.
Prosperity is one explanation. People who make more money than previous generations and possess a lot of stuff seem less inclined to participate in community (how many of us know our neighbors, who are here today and move tomorrow?). Stuff and the personal satisfaction of achievement lead to a decline in one’s need for God — too much money, too little purpose.
Politicians become a god-substitute and politics their religion. Creeping secularism has affected theological truth to the point where people can believe whatever they want — or nothing at all — and escape correction. Heresy, even apostasy, has infiltrated many churches.
Then there is culture. Younger people are exposed to what we collectively call “media” more than any previous generation. Most of what constitutes culture proceeds from a singular worldview that denigrates, or does not promote, patriotism, belief in God and values previous generations not only took for granted, but instilled in their children.
Unrestricted abortion has cheapened how many young people view the value of human life. For growing numbers of the young, marriage has become passe as children witness the pain of their parents’ divorce and decide that living together without a formal, legal, or spiritual commitment is better than risking the cost and pain of ending a marriage. For some, children are viewed as a financial burden and an intrusion on adult lifestyles.
Sociologists and historians will tell us these things are cyclical, like weather. That has been true in the past when spiritual revivals often followed a fallow period of faithlessness and a focus on self. I’m not sure that cycle will repeat with younger people, given what they are taught at public schools and in liberal universities.
The values that shaped and sustained America through economic downturns and wars had to be taught and instilled in the next generation. Today’s younger people, as reflected in the poll, seem intent on making their own rules (if they can be called rules) and creating their own gods.
They will eventually learn the impossibility of it all as their substitutions will fail them. The question is can America survive when our moral, spiritual, and patriotic foundations are destroyed? If you don’t love your country, what’s the point of having one?
LifeNews.com Note: With a twice-weekly column appearing in over 600 newspapers nationwide, Cal Thomas is the most widely read and one of the most highly regarded voices on the American political scene.
(Pregnancy Help News) Despite their public statements to the contrary, Planned Parenthood did not turn down $60M in Title X federal funds because a new “gag rule” is against their freedom of speech (the new federal “Protect Life Rule” prohibits Title X recipients from referring for abortion).
Nor did Planned Parenthood turn down Title X because they are so committed to “women’s reproductive health” — however skewed it is to think that an abortion referral could ever be construed as “health care.”
Nor did Planned Parenthood turn down the money because it would be too onerous to separate their abortion services from their Title X funded services in geographical location and financial recordkeeping as the new federal rule requires (much smaller faith-based groups that receive federal dollars comply willingly with similar requirements that separate their tax-funded services from their faith-based ones).
Planned Parenthood’s refusal to accept the conditions of the Title X grant proves, without a doubt, how closely tied contraception is to abortion in their strategy.
A required service for Title X recipients is comprehensive family planning (not including abortion). Planned Parenthood’s “cash cow” is abortion. How are the two connected?
The first time I became aware of the connection was years ago when I first heard Carol Everett’s story. She was the owner of several Texas abortion clinics before she became pro-life and authored Blood Money. The sooner she and her staff could get girls and women on the pill (they aimed for middle school), the sooner they would get pregnant (because of contraceptive failure rates), and the sooner Carol’s abortion clinics would provide abortion as the “back up.”
Carol’s business plan was based on their family planning clients having multiple abortions before graduating from high school.
Abby Johnson, former Planned Parenthood clinic director, now a pro-life advocate and author of Unplanned, tells a similar story.
As the clinic director, she thought she was helping women by providing contraceptives. But her Planned Parenthood bosses were really motivated by the “bottom line” — increasing income from abortions.
Bring them in for birth control, develop a relationship, sell them an abortion. That was Abby’s assignment.
After all, once a woman commits to the idea that the worst possible outcome of her sexual activity is a pregnancy, she is a prime candidate for abortion when her contraceptive fails.
Planned Parenthood’s “family planning” clinics (funded primarily by Title X) are the pipeline for their abortion clinics. If these family planning clinics don’t refer for abortions, might women whose contraception fails find another abortion provider?
Planned Parenthood has the nation’s largest chain of abortion clinics, their annual abortion numbers continue to increase so that they now perform slightly more than half of all reported abortions in the USA [Live Action News Editor’s Note: According to Planned Parenthood’s annual reported abortions compared to the Guttmacher Institute’s latest abortion statistics, Planned Parenthood currently holds approximately 35-36% of the U.S. abortion market share.] But the overall number of abortions is decreasing, the “market” is getting smaller. All a woman needs to do is google the word “abortion” to find lots of competition for Planned Parenthood.
Planned Parenthood is no doubt hoping that a scheduled Court hearing on September 23 will go in their favor, the new federal rule will be overturned, and things will be “back to normal.” If not, they are counting on a different President in 2021 so things will go “back to normal.”
Meanwhile, I can’t see Planned Parenthood ever cutting back their “family planning” services (even though they now whine that “women will have to travel further . . .”). Birth control accompanied by abortion referral is too crucial to Planned Parenthood’s overall strategy.
Plus, Planned Parenthood can afford to provide low cost or “free” contraceptive services even if they never again receive Title X funds.
After all, $60M (the amount of Title X money they are refusing) is only about 12% of the $500M they receive each year in federal and state tax dollars for their services (not including abortions), much of it from Medicaid. For abortions, in addition to private pay, Planned Parenthood receives millions of state tax dollars in NY, CA, and some other states. (See GAO data in Heritage Foundation report, 2018.) Planned Parenthood’s balance sheet also shows millions of dollars in assets.
No matter what happens with Title X, Planned Parenthood won’t abandon the contraceptive pipeline to their abortion engine.
Editor’s Note: This article was published at Pregnancy Help News and is reprinted here with permission.
Planned Parenthood is having a terrible few weeks.
It began with the news that on the same day that the movie Unplanned was released on DVD, it shot up to become the #1 selling DVD on Amazon. Apparently, sales haven’t slowed down much since. Over a week later, Unplanned is still sitting right next to Avengers: Endgame on Amazon’s “Best Sellers” list. In case you don’t know (and you should!), Unplanned tells the true story of Abby Johnson, the former Planned Parenthood clinic manager who became pro-life. The movie exposes both the truth about abortion (that it kills a living human being) and Planned Parenthood (that it never met an abortion it didn’t like). How inspiring to see this comparatively low budget pro-life film holding its own against blockbuster films that cost hundreds of millions of dollars to make. As it turns out, the public doesn’t just want glitzy popcorn entertainment: they are hungry for films that tackle serious topics and promote the pro-life and pro-family worldview. Hollywood, take note.
Then, Planned Parenthood announced that due to new rules promulgated by the Trump administration, they would be foregoing $60 million in taxpayer funding. Under the new rules, clinics receiving Title X funding cannot refer for abortions. However, rather than abiding by this rule, Planned Parenthood announced they would withdraw from Title X altogether. ABC News reports that abortion clinics around the country, including Planned Parenthood clinics, are worried about being able to keep their doors open in the wake of the loss of funding. Good! Killing babies and authentic reproductive health have nothing to do with one another. Planned Parenthood’s PR machine went into overdrive in the wake of the decision, bombarding people with the notion that somehow this new rule will harm poor women, who won’t be able to get the care they need. Nonsense. In reality, there are myriad community health clinics all across the country that perform all the other services that Planned Parenthood does, except for killing babies. Many of them are woefully underfunded, in large part because Planned Parenthood’s well-oiled lobbying and marketing machine sucks up most of the money.
Then came perhaps the biggest blow of all, at least to Planned Parenthood’s public image: a jury in Arizona ordered Planned Parenthood to pay $3 million to a former clinic manager who had exposed all manner of malfeasance going on at Planned Parenthood clinics. Mayra Rodriguez had worked for the organization for 17 years and had run three different clinics. In other words, she knew what was going on behind the walls of Planned Parenthood. She was fired from her job after she raised concerns about the fact that an unusual number of women were experiencing complications after having abortions at the hands of one particular abortionist. She also complained that the doctor was falsifying medical records, that the clinic failed to report a case of statutory rape, and about poor procedures for handling narcotics, among other things. Rodriguez is now working with And Then There Were None, the pro-life organization founded by Abby Johnson to help abortion clinic workers to leave their jobs and to embrace the pro-life position.
Power to Change the Culture
In case it need be said, developments like these don’t just “happen.” Each one of them came about as the result of weeks, or even years of hard work and savvy strategizing on the part of various pro-life groups and individuals. Each one of them is a testament to the growing sophistication, commitment, investment and influence of the pro-life movement.
Planned Parenthood is not alone in having a rough time these days. The whole pro-abortion movement in the United States is on the defensive. I’ve noticed a significant change in tone in a lot of the pro-abortion rhetoric in the past couple of years. The pro-abortion movement has always claimed that reproductive rights are “under attack,” and that people need to donate to them in order to stop the “anti-choice” fanatics from undermining “women’s rights.” Lately, however, I’ve started to notice that this urgency, and even fear, no longer sounds like a fundraising strategy. Pro-abortion activists are legitimately worried that they’re losing.
Pro-life Generation, Walk for Life 2019, San Francisco
As well as they might. As one liberal publication put it recently: “For America, it seems, this is a year of reckoning on the issue of abortion.” The article continues, “In the past few months, a slew of states have passed restrictive abortion laws, with the explicit intent to have them challenged in front of the Supreme Court.” It also does the heart good to read the recent headline in the New York Times, “‘This Is a Wave’: Inside the Network of Anti-Abortion Activists Winning Across the Country.” The article itself begins, “State after state is passing sweeping abortion restrictions this year…”
But it’s not just the growing number of pro-life laws that are changing the landscape on this issue. These laws are coming about as the result of the experience and hard work of a growing body of shrewd pro-life lawyers, legislatively-focused organizations, and pro-life lawmakers. But even as these types of pro-life individuals and groups are grinding away at the often thankless and unseen work of paving the way for pro-life state and federal laws, a huge army of pro-life individuals are chipping away at the Culture of Death in their own ways, both big and little.
Looking at the modern pro-life movement makes me think of St. Paul’s words to the Corinthians: “Now there are varieties of gifts, but the same Spirit; and there are varieties of service, but the same Lord; and there are varieties of working, but it is the same God who inspires them all in every one.” The glut of pro-life laws being put forward is inspiring. But there’s no way we’d be able to pass pro-life laws if it weren’t for the crack troops of the Culture of Life: the volunteers at the thousands of pregnancy help centers across the country providing love and concrete help to women in trouble; the thousands of prayerful protesters outside abortion clinics; the groups working on college campuses to change the minds of the next generation; the pro-life media organizations; the Knights of Columbus councils that fund pro-life initiatives; organizations committed to helping post-abortive women heal; organizations committed to helping abortion workers leave their jobs and repent; parish-level pro-life groups…and on and on.
Walk for Life 2019, San Francisco
Each one of these groups is necessary. And every one of these groups is constituted of individuals who felt God’s call to do something about the massacre of the innocents and responded. There is a need for some form of concrete pro-life witness or activism in every single one of our lives. For the busy stay-at-home mom, it might just be a matter of witnessing to her own children about the sanctity of life by the love she shows them, and the gratitude with which she welcomes new life. For the working father, it might just be a matter of budgeting a portion of his pay to go to the local pregnancy help center, or offering up a weekly holy hour for the end of abortion.
Or it might be more than that. It might be opening your heart to adopt an unwanted child, or to fostering some of the many children who our culture tells us are “unwanted” and probably better off aborted. It might be putting a roof over the head of a pregnant woman desperate for a place to stay while she figures out the next steps in her life. Or it might be starting that pro-life council at your parish, or taking a shot at launching that big pro-life idea that’s been on your heart for years.
What there’s no excuse for, is doing nothing. If you’re grateful about the visible pro-life progress that’s being made these days, don’t give in to the temptation to relax. This progress would never have been possible had it not been for the handful of dedicated pro-life pioneers in the early 1970s who courageously forged the way for us and without the small and unseen sacrifices of pro-life citizens like you. Rather than relaxing, renew your resolution to do more, providing further energy to this great push in favor of the sanctity of life.
When it comes to chemical abortions (“medication” abortions, in pro-abortion parlance), rhetoric and reality have increasingly been on a collision course.
Advocates have diligently argued that chemical abortions are so simple and safe that women can do them on their own (the rhetoric). But simultaneously many have also insisted that women “denied” access to abortion would be in danger if they tried to self-abort (the reality).
What do abortionists who have encountered such women in their clinics—as opposed to activists and academicians–say?
Safety concerns about chemical self-abortion stand out in a study published April 16, 2019 in the journal Contraception. It is titled “Abortion Providers’ experiences and views on self-managed medication abortion, an exploratory study” (abstract at www.contraceptionjournal.org/article/S0010-7824(19)30143-X/pdf)
Between July and September of 2017, researchers from the University of Iowa did an online survey of the memberships of the Society of Family Planning, the Association of Reproductive Health Care Providers and the Abortion Care Network. They inquired about their experiences with and opinions of “self-managed abortion.”
Of the 650 respondents, just over half (359, or 55.1%) were abortionists. Results?
More than two thirds (230) of the abortionists reported having experience with women trying to abort on their own. More than three quarters (153) of those with such experience indicated those women were using mifepristone (RU-486) and/or misoprostol, the abortion drugs currently sold in the U.S., but legally available only through an abortionist who meets certain conditions laid down by the Food and Drug Administration (FDA). *
Women have been known to pick up misoprostol – which can be used alone to abort, though not as successfully – on the black market at places like border town flea markets [1] and have been able to order packets of foreign manufactured mifepristone and misoprostol from the internet [2].
Certain abortion researchers and advocacy groups (e.g., Aid Access, Women on Web [3] have been promoting the idea of self-managed abortion with pills bought over the internet. One, Gynuity, has been conducting trials in several states where abortion drugs can be mailed to women after an online consult [4]
In the University of Iowa survey, though, barely half (53.3%, or 171 of 321 abortionists**) said they thought the use of misoprostol/mifepristone for the self management of abortion was safe. That means that nearly half of those who did abortions were not satisfied that it was safe for women to use drugs to perform their own abortions.
More than a third (34.9% or 117 of 335 abortionists**) said they had witnessed complications from self-abortion. The most common complication was an incomplete abortion, but also reported were hemorrhage, sepsis (infection), and uterine rupture.
What the study tells us
Several results are very much worth noting.
One obvious thing is that “incomplete abortion” was mentioned so frequently as a complication in the study that failure is clearly a far bigger issue than advocates would have us believe. These results fly in the face of assurances by promoters that these drugs have proven to be “highly effective” (Aid Access at http://aidaccess.org/en/page/427/what-is-a-medical-abortion, accessed 4/25/19).
If official statistics from Danco, the U.S. distributor of mifepristone are accurate (claiming 93-98% effectiveness), this still means that perhaps one of every 20 patients may require surgery to either stop the bleeding or to complete the abortion. This would actually be a lot of cases for a drug we are told is used by hundreds of thousands of American women a year.
Promoters of the abortion pill have tried to soft-pedal complications
The University of California-San Francisco’s ANSIRH (Advancing New Standards in Reproductive Health) compiled an August 2016 Issue Brief on the “Safety and effectiveness of first-trimester medication abortion in the United States.” The Issue Brief claimed that there are serious complications with mifepristone and misoprostol in less than 0.5% [one half of one percent] of patients.
These admissions seem at odds with the experiences of abortionists who participated in the University of Iowa survey.
From the figures given, we don’t know the percentage of self- aborting patients that had problems. But we do know that they were frequent enough that at least a third of the abortionists in the survey encountered them–and that some were quite serious, serious enough that almost half the abortionists were unwilling to tell researchers they considered it safe.
The FDA reported that 24 patients are known to have died in the U.S. during that time, at least a third from rare bacterial infections. (Some of the 11 mifepristone patients who died in other countries also died of these infections.)
The over 4,000 figure includes over a thousand hospitalizations, more than 500 patients requiring transfusions, and more than 400 “severe infections.”
No matter how many thousands managed to endure the drugs’ grueling, painful process without any obvious immediate or enduring damage, if such a number of women have died or faced serious complications, it is a clear indication that the drugs are potentially quite dangerous.
And note this: most of these deaths and complications are associated with standard clinical use of the drugs, before studies of mail order abortions were launched and before webcam abortions became available in very many states. And there is nothing about the webcam or mail order abortions that would make complications like incomplete abortion, ruptured ectopic pregnancies, or deadly infections any less likely. It just might make medically qualified, timely help less likely–something that would concern any good doctor.
Abortionists at odd with Activists and Academicians
Perhaps the most significant finding in the University of Iowa study is that many of the rank-and-file abortionists do not appear to be on the same page as the academics and advocates who are pushing hard for at-home chemical abortions.
Those advocates are doing their own studies. They then tell the public that women can order these abortifacient drugs on line or pick them up at their local pharmacy and “manage” their abortions themselves with little or no supervision.
Daniel Grossman, popular abortion researcher, chemical abortion “expert,” and advocate, raved about self-abortion in an interview with National Public Radio [3/11/15]: “It would really be quite easy for women to actually use this [mifepristone/misoprostol] on their own…. It could almost be eligible for the kind of medication that could be available over the counter.”
In February of 2013, Grossman told Contraception that “Women can use misoprostol on their own and with accurate information; they do not necessarily need a health care provider to use it safely and effectively.”
He told CNN on November 5, 2018 that “When it comes to self-managing abortion, research shows that when people have accurate information and high-quality medication, they can use the abortion pill safely and effectively on their own.” (Emphasis added.)
Beverly Winikoff, of Gynuity, is currently in the middle of the “TelAbortion Study” using telemedicine (webcams) to counsel and screen patients and then mailing them the mifepristone and misoprostol to use at home. Winikoff claims that there had been no problems with the 200 women who had enrolled in the study as of November of 2018. (CNN, 11/18/18.)
Women, she said, were satisfied. “The results are equivalent to what’s happening in the clinics.”
The World Health Organization said “There is no evidence that home-based medical abortion is less effective, safe or acceptable than clinic-based medical abortion” (Vox 10/22/18).
Yet nearly half of the abortionists who answered the University of Iowa survey seem to think otherwise. Many of those who deal with aborting women at their clinics on a regular basis, who have practical, clinical experience versus the detachment of a university researcher or an activist, won’t call it safe. They don’t seem willing to consider self-managed abortion a good idea.
Winikoff and her Gynuity pals are likely to come out soon with a study of their own, claiming to have proven that mail order abortion drugs taken at home after an online consult are “safe” and “effective,” along with an assurance that women found them “satisfactory.” When they do, remember this University of Iowa study and the abortionists with the real life experience that led them to a far different conclusion.
*The FDA approved mifepristone, used in conjunction with misoprostol, for abortion in September of 2000. However it has limited its distribution to “certified healthcare providers” who 1) have the ability to date pregnancy accurately & diagnose ectopic pregnancy; who 2) provide (or have made arrangements for) surgical intervention in cases of incomplete abortion or severe bleeding ; and who 3) indicate they have read and understood the prescribing information (which contains warnings about possible “serious and sometimes fatal infections or bleeding”).
** We did not have full numerical tables when it came time to post. But apparently different numbers of abortionists responded to different survey questions.
A remarkable, cutting age medical intervention has given joy to a family and life to their baby boy who was threatened by a rare illness in the womb.
Baby Edward, also known as Teddy, developed anaemia whilst inside the womb. In response, Doctor Amarnath Bhide, used an ultrasound sensor to insert a needle through the uterus and into the umbilical cord which injected Teddy with donated blood.
Teddy received five blood transfusions before he was born, these were some of the earliest in-utero interventions to ever be performed.
SPUC Scotland, Director of Communications, Michael Robinson, described the interventions as “extraordinary.”
Saving life through in-utero surgery
Whilst the life-saving intervention performed on unborn baby, Teddy, is indeed ‘extraordinary,’ the option of in utero surgery, which can save and improve the life expectancy of unborn children, is becoming a far more positive prospect.
Currently, in utero surgery, can treat a number of foetal health conditions including Spina Bifida, foetal tumours, Cerebral Palsy, foetal cardiac conditions and Hyperthyroidism.
In May of this year, the UK witnessed the astonishing account of doctors who performed key-hole surgery on an unborn baby with Spina Bifida, which was the first operation of its kind in the United Kingdom. Unborn baby, Jaxon, received the operation at just 27 weeks gestation, and as a result had the ability to move his legs after being born six weeks later.
Similarly, unborn child, Ethan Leibbrandt, underwent in utero surgery to remove the benign tumour which consumed 50% of his lung space. The in utero surgery was successful and life saving as without it, Ethan would have died of cardiac failure.
Human beings worth protecting
SPUC Scotland, Director of Communications, Michael Robinson, said: “The early interventions that can now be used to treat and save unborn children are truly astonishing. The story of Edward once again proves that science is on the side of the pro-life movement. Indeed, scientific developments and new technology is now instilling a sense of awe that society never really had before, about the beauty and dignity of every unborn child.”
Mr Robinson continued: “This case illustrates the terrible irony that medical teams spend enormous effort, time, and money to deliver babies safely and nurse premature infants back to health. Yet, in the UK we routinely and deliberately end the lives of 600 babies a day. Whilst pro-abortion campaigners insistently refer to unborn children as ‘blobs of cells’ or ‘parasites’, the use of in utero surgery, highlights that unborn children are human and worth saving and protecting.”
LifeNews Note: Courtesy of SPUC. The Society for the Protection of Unborn Children is a leading pro-life organization in the United Kingdom. File photo.
There is a very funny scene in the 1980 film Airplane! that speaks to the current assumptions about what the West thinks is best for developing nations.
The movie features a young couple, Ted and Ellen, who visit the fictitious “Malombo” tribe in Africa as Peace Corps volunteers.
Instead of focusing on practical solutions that might best help the tribe to which they are assigned, the couple spends time introducing Western solutions that, while well-meaning, completely overlook the real needs of the people. For example, Ellen hosts a Tupperware party for the women of the village to help them “stretch” their food dollars and to “keep hot dog buns fresh for up to a month.”
The cognitive dissonance in the scene is, of course, part of the humor, but it also draws a bead on the mixture of ignorance and arrogance that has defined much of what passes as Western “aid” to developing countries.
Like this idealistic young couple in Airplane! Melinda Gates, the wife of Microsoft founder Bill Gates, seems to have her heart in the right place. She has a love for the poor and a genuine desire to relieve the suffering of others. She understands the influence that her position in society brings.
Unfortunately, Gates’ primary solution to the problems plaguing African and other developing countries is no better (and often a great deal worse) than Tupperware: Gates is strident in promoting widespread use of artificial contraceptives, as she argues in her new book, The Moment of Lift: How Empowering Women Changes the World.
Gates’ argument for contraception is experienced-based. She holds that contraception is the primary path for women to freedom and equality and cites her own success as a career woman “to work and have the time to take care of each” of her and Bill Gates’ three children, who are precisely spaced three years apart.
Moreover, she says that when it comes to contraception, “no woman I knew went without it.” If Western women are healthy, educated and powerful — a packet of adjectives she comes back to frequently — Gates reasons that such benefits are a result of unlimited access to contraception.
But Gates is a puzzle. She is passionate about contraception and yet she also professes to have a great love for her Catholic faith.
As she relates, she received a Catholic education through high school, attending the prestigious Ursuline Academy — a Catholic boarding school in Dallas — before attending Duke University. She also takes pride in noting that her parents attended a Marriage Encounter retreat (at her father’s insistence) and her mother not only “believes in the Church” but also “goes to Mass five times a week … reads, goes to silent retreats and explores spiritual ideas with passion.” Nevertheless, despite the great influence that she says the Church has had in her life, Gates has apparently never encountered a woman who in her married life has followed Church teaching on contraception.
It is telling that The Moment of Lift includes no references to the tremendous advances in non-contraceptive (and Church-approved) methods of achieving and avoiding pregnancy.
For instance, one wonders what Gates would make of technology like the natural fertility app developed by a Swedish nuclear physicist, or how she might consider the potential benefits to the poor provided by “CycleBeads,” a reproductive physiology-based method promoted by the Institute for Reproductive Health at Georgetown University. CycleBeads is well-known as a simple, low-cost, easy-to-teach and natural family planning method that has greatly benefited women in developing nations. The method — which relies on the woman’s natural fertility cycle — does not require women to walk miles and miles every few months to receive contraceptive “shots” or have their IUDs adjusted.
It is equally telling that, in a later chapter, Gates describes natural family planning in general as “the rhythm method,” even though neither teachers nor practitioners in the fertility-awareness-based field have used that term for more than 40 years.
Such misnomers, though, may not indicate Gates’ animus toward fertility-based-awareness methods, so much as her ignorance of such methods — either in how they work or how they can benefit women. Indeed, this can only be the case if she has surrounded herself, intentionally or otherwise, with peers who have only known and used artificial contraception.
Indeed, we might assume that Gates’ ignorance regarding fertility awareness extends even to the Church’s teaching on such matters. But her own words indicate rather a truculence to such teaching.
In her book, Gates points out that it is “hugely reassuring” to her “that a huge majority of Catholic women use contraceptives.” She also claims to have met with “high-ranking officials of the Church” to discuss her disagreements with the Church’s teaching on family-planning methods — although she doesn’t name the officials nor the topics covered. Instead, she simply notes that the Church officials shared “similar concerns” about the plight of the poor.
Gates does provide some horrifying stories about the ravages of poverty and its particular impact on women and girls. These stories include personal anecdotes and experiences shared with her by those who serve the poor in countries in Africa and Asia.
For example, she relates how young girls can be married off as early as age 11. She also points out the prevalence of female genital mutilation and sexual trafficking. In one poignant passage, Gates reports on children as young as 5 “baby-sitting” for tiny infants so that their mothers could go out and scrape together enough food for the day. She also tells about children looking through garbage dumps for food, children dying from diarrhea, mothers dying in childbirth and newborns dying because they don’t receive even basic postpartum care.
Likewise, Gates’ book is valuable for expressing concern — and outrage — at the substandard hospitals the poor must rely on and at the lack of educational opportunities for women. In her book, she also helps raise awareness about the need in these countries for neonatal care, preschool programs, healthy food initiatives and microloans to small family businesses.
However, as Nigerian-born pro-life activist Obianuju Ekeocha points out in her “Open Letter to Melinda Gates,” none of these problems are solved by contraception, and the millions of dollars spent on contraceptive pills, implants and devices imported to African nations and other developing countries by wealthy Western aid organizations would be better used to address the conditions that necessitate such aid in the first place.
Why is the bulk of Western financial aid, as Ekeocha notes, focused on ensuring “that the African woman is less fertile” — especially when most African cultures welcome and celebrate new life as a gift from God?
Ekeocha rightly notes that there are multiple risk factors associated with the use of hormonal contraceptives, as American women have long complained, while no similar side effects exist with the use of fertility-awareness methods.
As Ekeocha asks, does “a woman in Africa with a contraception-induced blood clot … call 911 or an ambulance or a paramedic? No, she dies.” Moreover, Gates does not even touch the issue of the failure rate of hormonal and injectable contraceptives, which Great Britain’s leading abortion service, BPAS, has admitted. Nor does Gates acknowledge the increased risk for HIV infection among African woman who use hormonal injections (which The New York Times admitted poses “an alarming quandary”).
In a news clip that went viral, Ekeocha instructed a BBC talk-show host on the real needs of African women, of the side effects of hormonal contraceptives that are not fully disclosed to them when promoted, and of the “ideological colonization” that contraceptive programs sponsored by the West represent.
Even if the poor do achieve a momentary “lift” from the widespread use of artificial contraceptives, as Melinda Gates contends, it is a lift that will likely have no lasting impact. You don’t eliminate poverty by eliminating the poor.
After using contraceptives, women may have fewer children, but they won’t necessarily have a new maternity hospital, or a new preschool, or successful crops, or educated daughters.
The Catholic Church has much wisdom and lived experience to share with Melinda Gates. Perhaps, with the help of testimony from Ekeocha and other women outside her peer group, she may still inquire into how the Church can help women around the world achieve a true moment of lift.
Mary FioRito is the Cardinal Francis George fellow at the Ethics and Public Policy Center in Washington.
(Ivanhoe Newswire) – When people get new prescriptions, they very often don’t look at the list of side effects. One woman in Seattle started taking the birth control shot, Depo-Provera not knowing all the side effects. She became one of the less-than-one-percent who developed life-changing, life-threatening blood clots in her lungs.
Marilyn Wightman thought losing weight would ease her sudden mysterious shortness of breath in 2009. It didn’t. Then, she fainted on the stairs.
“The first question my doctor asked was, ‘Are you taking Depo-Provera?’ I’m like, ‘Yeah.’ And he’s like, ‘Oh, that’s it,’” said Wightman.
He put her on blood thinners, but she was in and out of the hospital until last year when her doctors told her that without surgery, she had a ten percent chance of living five years.
Michael Mulligan, MD, Cardiothoracic Surgery, UW Medicine shared, “In a very small fraction, however, patients develop a response to the clot, where the clot breaks down, but then you start to develop scar-like plugs that obstruct the vessels and make it harder and harder for the blood to be pumped through the lungs.”
In a six-hour procedure that left a scar, Dr. Mulligan removed 15 clots mixed with scar tissue from Marilyn’s lungs. First, he had to raise her oxygen level, lower her temperature and metabolism, stop her heart and drain her blood.
“You work very quickly to expediently tease out these clots that are multi-branched without puncturing the vessel, which is wafer thin,” continued Dr. Mulligan.
Marilyn says she wouldn’t have taken Depo-Provera if her doctor had told her about the blood clot risk.
“So, I’m telling my story because I want at least one woman to ask the question. When your doctor is trying to give you a new drug, ask the question. What are the side effects?” stated Wightman.
Dr. Mulligan says as long as Marilyn stays on her blood thinners, her clots should not return. It shouldn’t be long until she has her normal life back again.
The UK’s biggest abortion provider, British Pregnancy Advisory Service (BPAS), has attacked pharmacists who do not sell the ‘morning after pill’ for conscience reasons.
After one incident where a pharmacist would not dispense emergency contraception to a woman for ‘personal’ reasons, BPAS condemned both the pharmacist and the conscience protections provided to pharmacists. A petition was also set up to prevent pharmacists from claiming freedom of conscience rights.
Under the current law, covered by guidance from the General Pharmaceutical Council (GPhC), pharmacists with a genuine conscientious objection to selling the pill can refer the customer to another pharmacist.
However, BPAS complained that it is ‘impossible to overstate the significance of even one pharmacist conscientiously objecting to selling the morning-after pill’.
Fortunately, the General Pharmaceutical Council, in this case, upheld their guidelines and the consequent media coverage has now died down, temporarily at least.
This may seem like a one-off minor incident, but it is an illustration of increasing pressures on freedom of conscience protections. It is often assumed that the role of the conscience in medicine is relevant only to a few specialised and limited areas such as contraception or abortion, but in fact, the concept of the conscience goes right to the heart of what it means to act in a moral way, to act with integrity.
If we do not stand by those who are under pressure, the problems will only get worse and will spread. A well-known quote often attributed to Burke, which may have actually come originally from JS Mill warns: “He should not be lulled to repose by the delusion that he does no harm who takes no part in public affairs. He should know that bad men need no better opportunity than when good men look on and do nothing.”
CMF has therefore written to the GPhC to ensure they are aware of our concerns and to thank them for holding to their guidance. The text of our letter is as follows, with their response after it:
‘I am writing to you following the recent news coverage of a Lloyds pharmacy worker who, according to news reports, conscientiously objected to selling the morning after pill and directed a customer to another pharmacy instead.
I note that a petition has since been set up to prevent pharmacists from claiming conscientious objection rights.
The Christian Medical Fellowship is the UK’s largest faith-based group of health professionals and we contributed with both written and oral evidence to your review of your Guidance on Religion, Personal Values and Beliefs. We publicly welcomed the new Guidance and the statement accompanying it, in which the Chief Executive of the General Pharmaceutical Council highlighted the positive contribution that pharmacists’ faith can make in their provision of care. We also welcomed the clear statement that: ‘Pharmacy professionals have the right to practise in line with their religion, personal values or beliefs’.
We all aspire to person-centred care. In any care scenario, there are (at least) two parties – the carer and the one receiving care – each of whom has rights. The General Pharmaceutical Council guidance helpfully achieves a balance between the patient’s right to service access and the pharmacist’s right to freedom of conscience.
Respect for the sincerely held religious and moral beliefs of employees is essential and we are concerned that some of the demands being made, based on this one recent case, would marginalise the beliefs, values and religion of pharmacists disproportionately and unnecessarily, and trivialise their right to freedom of conscience under the law. Despite widespread coverage of this case, we have yet to see evidence of recurring complaints under the present provisions.
While we strongly support the right to freedom of conscience for pharmacists, we do also emphasise the importance of openness and sensitive communication with colleagues and employers; any refusal to supply should be made courteously and sensitively.
On behalf of CMF, I want to thank the Council for protecting the right of pharmacists to refuse to engage in certain procedures that violate their most profound moral convictions.
I also encourage the Council to continue to make it clear, publicly, that all pharmacy professionals have the right to practise in line with their religion, personal values or beliefs.
Yours faithfully
Dr Mark Pickering
Chief Executive, CMF
In response, the GPhC replied with the following two sentences:
‘Our existing guidance ‘In practice: Guidance on religion, personal values and beliefs’ (to which you refer) remains in place. We have no current plans to review it.
As you are aware, the guidance sits under our standards for pharmacy professionals and relates to standard 1, Pharmacy professionals must provide person-centred care.
The point here is simple but vital; if we care about liberty and personal integrity, we must make a reasoned defence of it in the public square, from the smallest incident to the biggest.
Philippa Taylor is Head of Public Policy at CMF. She has an MA in Bioethics from St Mary’s University College and a background in policy work on bioethics and family issues. Republished from the CMF blog with permission.
When parents are told that their preborn child has Trisomy 18, the diagnosis is often followed up with the words: “incompatible with life.” But as a team of doctors at Children’s Hospital and Medical Center in Omaha is proving, children with the condition can live and thrive when doctors treat them as equal human beings.
“If you look at the old textbooks, and a lot of them are still being used, the outcome is death,” explained Dr. Meaghann Shaw Weaver, division chief of Palliative Care in an interview with Children’s. “It was one of the few diagnoses that was named lethal.”
Because it was considered “lethal” for so long and still is by many, most doctors automatically write-off preborn children with Trisomy 18 and consider them as good as dead, often advising parents to abort. For Meredith Willard, mom of one-year-old Rose, even meeting with the comfort care team to discuss her baby’s birth wasn’t allowed by the doctors in their home state of California.
Rose was diagnosed with Trisomy 18 at 12 weeks gestation. Trisomy 18 can cause congenital heart defects, physical and mental developmental delays, and feeding and breathing problems. Doctors said Rose wouldn’t survive. For choosing life for their daughter, Willard says they were called “cruel” and told they had to “let this child go.”
“I said, ‘There’s a heartbeat and she’s here, let’s let her be,’” explained Willard. “When I said I wasn’t going to terminate, there really was no more help for me there. I went weeks with no one.”
Finally, a doctor advised them that they should speak to a heart surgeon because he felt that their baby would live through pregnancy and birth, but would need heart surgery. 50 percent of children with the condition have a ventricular septal defect (VSD or hole in the heart) while the rest have defects that can be fixed with the right surgery. None of the heart surgeons in California would operate — strictly because Rose has Trisomy 18.
“You’re angry, but it fuels you,” said Willard. “You know that kids are treated. We just wanted that for our kid.”
That’s when they learned of Children’s Hospital in Omaha, 1,500 miles away, from a support group called SOFT – Support Organization for Trisomy 18, 13 and Related Disorders. Doctors there agreed to operate on Rose. And while it was a big deal to the family, for Dr. James Hammel, division chief of Cardiothoracic Surgery, it was just another day at work.
“If a family didn’t want surgery for an infant with VSD or tetralogy or even pulmonary atresia, we would take them to court, take the child out of the family and take care of them,” explained Dr. Hammel. Yet for children with Trisomy 18, it’s considered “cruel” to perform surgery despite the fact that without care they die, and with care they can live for much longer than originally thought. Seventy to 80 percent of babies with Trisomy 18 survive heart surgery, and 50 percent will still be alive 16 years later, according to Dr. Hammel. Others say the rate of survival is as high as 90 percent.
In the video below, Dr. Hammel gives a fascinating and instructive web lecture on heart surgeries for children with Trisomies 13 and 18:
“Most physicians view this as a hopeless diagnosis – but there is always hope,” he said. “Yes, these kids have functional limitations, but there is plenty of room to make their life better…. I’ve always said if I can improve a child’s chance of survival from five percent to 10 percent, I’m perfectly happy to take that on if that’s what the parents want to do.”
Thanks to the dedication of Dr. Hammel and his colleagues, families from across the country are self-referring to Children’s Hospital. The team at Children’s aims to treat the whole child and the whole family. They say that the medical treatments they provide for these children would be “absolutely obligatory for a child without trisomy” but other hospitals refuse to do them simply because of the trisomy diagnosis.
“Going to Omaha, we were treated the most normal you could be treated with such a medically fragile child,” said Williard. “It was like nothing fazed them, nothing scared them. They’re like, ‘No worries – we’ve got this, Mom. Go get a coffee.”
Rose was born with multiple heart defects and suffered from apnea, which is the cessation of breathing. After surgery, the apnea stopped.
“At the hospital we were at, they kept telling me, ‘She has Tri-18; her body is not meant to survive.’ I said, ‘It’s because of her heart.’ When Dr. Hammel repaired her heart, she never had one more episode of apnea. We flew home commerical with her on no oxygen… and I was told this child could never live outside the hospital.”
Doctors said Rick Santorum’s daughter Bella, who has Trisomy 18, was incompatible with life. She is proving them wrong.
Rose still has health concerns. She uses a feeding tube to get proper nutrition, she takes two heart medications as well as medication to help stop seizures, and she sees multiple specialists. But her life with her parents and four older brothers is a happy one.
“I’m super excited to see what she can do and explore and experience,” said Willard. “I was told this kid wasn’t a survivor. I knew she was.”
Terra Spiehs-Garst, Nebraska’s state chairwoman for SOFT, has a now seven-year-old son named Emerson who has Trisomy 18. Spiehs-Garst and her husband Tyson Garst learned Emerson had Trisomy 18 when Terra was 17 weeks pregnant. Doctors advised abortion. The couple told Live Well Nebraska that they wanted Emerson to be in control. He had heart problems that were able to be controlled with medication; now, he no longer needs them. He had surgery on his jaw, which helped his breathing improve. He underwent treatment for kidney cancer at 15 months old and is still tumor-free. He uses a communication device to talk to his family, and he loves dancing and hugs from his three brothers.
Dr. Hammel notes that there are other hospitals in the United States that do provide care for children with Trisomy 18, but they aren’t the established multidisciplinary team that exists at Children’s. Thanks to social media, more and more families are learning about the program at Children’s and are able to properly care for their children with Trisomy 18. Dr. Hammel is happy to provide this crucial care to families.
“In the end,” he said, “we will be judged by how we treat the most vulnerable people in our society.”
Thanks to the doctors at Childen’s, vulnerable children with Trisomy 18 are being treated as equal and whole human beings worthy of life.
As a physician assistant specializing in OB/GYN, I have prescribed birth control to everyone for everything . . . irregular cycles, painful periods, unusual bleeding, PMS, acne, Polycystic Ovarian Syndrome (PCOS), endometriosis, perimenopause and, of course, to avoid pregnancy.
It wasn’t until my own struggles with infertility that I began to research more about the consequences of using artificial hormones. Although I was taught in school that the birth control pill was a treatment for these disorders, I learned that artificial hormones are only FDA-approved to treat two things: to avoid pregnancy, and for hormonal acne. Other than that, the Pill only masks the symptoms of underlying disorders. Actually, for estrogen-dominant disorders like PCOS and endometriosis, the excess estrogens in the Pill can make these disorders worse!
After many years of my own struggle with infertility, I was diagnosed with atypical PCOS and realized that I had symptoms starting at 15 years old. Now, I know that if I had been treated for PCOS instead of being placed on the Pill to “regulate my periods,” I would not have had to struggle with infertility.
The Search
Fast-forward 8 years and 4 precious children later, I was diagnosed with a dangerous heart condition and was told it would be medically unwise to become pregnant again. I was given the choice of different forms of birth control, as well as permanent sterilization options. As a Physician Assistant, my medical knowledge instilled the fear of risks of surgery, as well as the risks and side effects of artificial hormones. I had just been through a very difficult 8 years of struggles with infertility and related health problems, and did not need to deal with any more problems. So began my search for a natural method of avoiding pregnancy.
The method I chose had to be very reliable in avoiding pregnancy and had to be fairly easy to learn as I now had four children under the age of 6 to take care of. I investigated the Sympto-Thermal methods, Marquette (using ovulation predictor kits), and the Creighton Model System. I chose the Creighton System due to the medical studies and statistics backing its accuracy, as well as the benefit of NaproTechnology, the branch of medicine which seeks to naturally cure underlying disorders causing the symptom of infertility. I learned that the Creighton Model System came with a 99.5% efficacy rate for perfect use and 98.6% typical-use effectiveness rate in avoiding pregnancy in one year. This is amazing, since other forms of birth control come with only a 97% use effectiveness, and they have the added risks and side effects that I was seeking to avoid.
After only 3 months of using this system, and working with my FertilityCare Practitioner (Creighton teacher), the specifics of my PCOS were revealed: I had estrogen dominance combined with low progesterone. Although all my previous bloodwork with fertility doctors appeared normal, my Creighton chart revealed a different story. I began seeing a NaproTechnology doctor and learned that I was also insulin resistant (my previous doctors had only tested my glucose for diabetes, and missed this very important diagnosis). After taking bio-identical progesterone, adding a few supplements, and drastically changing my diet, I started ovulating regularly, felt much better, and I developed a confidence in recognizing my fertile and infertile days shown within my Creighton chart.
“I felt normal for the first time in my life”
As it happens, the very simple methods of diagnosis provided by my Creighton cycle charting revealed not only the causes of my infertility, but also my life-long struggle with my weight and the causes of my mid-cycle anxiety and premenstrual depression (“mood swings”). With NaproTechnology, I was able to feel healthy and normal for the first time in my life!
Although I physically felt better, emotionally, I became angry . . . very angry! Why was I not taught this in medical school? Why didn’t my supervising physician and mentor have any options for women besides artificial hormones? Why did my “fertility doctors” not investigate further the causes of my infertility? Why, now that I am in my forties and unable to have more children, have I not heard about NaproTechnology sooner? This anger spurred me on to do something about it. I became trained both as a Creighton Model Practitioner (FCP) and a NaproTechnology Medical Consultant (NFPMC).
In my new role educating and assisting women with their cycle and hormonal health, I have seen numerous women who had painful periods and/ or ovulation, painful sex, heavy or long periods, were diagnosed with endometriosis and then put on the Pill to lessen their symptoms. Years later, in order to conceive a baby, they got off the Pill. Not only were their symptoms worse, but now they had infertility to deal with, too. They suffered from regret: if they had only used a Fertility Awareness-Based Method for avoiding pregnancy, and treated the endometriosis with supplements, diet changes, and/ or surgery early on, then they would not only be pain-free, but would have been able to start their families by now!
I have seen teenagers with symptoms of PCOS: irregular, long cycles, facial hair, acne, difficulty losing weight. The traditional approach of putting them on the Pill would add to their estrogen-dominance and, later in life, they may have insulin resistance or diabetes, obesity, depression, and/or infertility. However, when these girls start early-on charting their menstrual cycles with a Fertility Awareness-Based Method, learn about their bodies, diagnose underlying problems, and start with natural treatments and diet changes, their futures can be symptom-free!
A missed diagnosis
When women are given artificial hormones to treat PMS, a key underlying disorder is missed: low progesterone. We know that the vast majority of PMS is caused by low progesterone. When charting one’s menstrual cycle Fertility Awareness-Based Method, women see this diagnosis within their charting in the form of brown spotting prior to their periods starting, or brown spotting at the end of their periods. A short luteal phase may also be recognized. With NaproTechnology, the progesterone can be replaced, instantly eliminating the symptom of PMS. This has long-range benefits, as low progesterone is also linked to infertility and recurrent miscarriages. So, instead of masking the symptoms of low progesterone, women using natural methods of family planning can diagnose themselves, seek treatment, and prevent future miscarriages!
These are the most common disorders diagnosed and treated with Fertility Awareness-Based Methods and NaproTechnology, but there are many more. Using artificial hormones, whether to avoid pregnancy or to reduce unwanted symptoms, can not only delay diagnosis and treatment, but also add unnecessary risks. Artificial hormones have side effects such as headaches, weight gain, nausea, bloating, irregular spotting, decrease in libido, and are linked to blood clots, strokes, and even breast cancer.
Fertility Awareness-Based Methods have side effects, too: increased relationship bonding due to an increase in communication, a 50% decrease in divorce rate, as well as early detection of medical disorders. Some forms of FABMs are up to 99.5% accurate in avoiding pregnancy, equivalent or better than any form of artificial hormones and even sterilization—all without the side effects.
I truly wish I had known about natural family planning and NaproTechnology sooner, even before I was trying to achieve pregnancy. However, now that I am having to avoid further pregnancies for health reasons, I am so grateful to be able to reap the many benefits of using a Fertility Awareness-Based Method.
Posted by Allison Jung, PA
Allison Jung is a Physician Assistant with more than 18 years of experience in OB/GYN and fertility. She is also a health educator, teaching the Creighton Models System and NaproTechnology for almost 4 years. Through her own story of PCOS and infertility, Allison found the validity in a holistic approach to healthcare—searching for the causes of symptoms, instead of the routine treatment of covering up symptoms with artificial hormones, painkillers, or anti-depressants. Allison loves working with women with symptoms of irregular cycles, painful periods or PMS who have been told that birth control is their only answer, and showing them not only the reasons behind their symptoms, but curing them often with natural means. Allison’s approach to women’s healthcare is one of hope and freedom.
A study published in the July 2019 edition of BMJ Case Reports details the case of a 31-year-old woman in Portugal whose birth control implant migrated from her arm to her lung. The implant’s migration was only discovered because the woman experienced abnormal vaginal bleeding for three months and was referred to a gynecologist.
Upon examination, the implant, originally placed in her upper arm, could not be found. Subsequent ultrasound revealed the implant had migrated to her chest. An X-ray and CT scan showed the implant was in the lower lobe of the left lung.
This alarming complication (which is not unique) resulted in surgery to extract the implant from the woman’s lung. After four days in the hospital, she was released, apparently without further complication.
The woman had been using the Implanon NXT implant for eight years and had two implants before the most recent one, one in 2010, another in 2013. The most recent, placed in 2017, is the one that migrated to her lung.
The Implanon NXT — and other contraceptive implants like it — is a small rod inserted under the skin of the upper arm. Once inserted, the implant gradually releases the hormone progestin to alter a woman’s cervical mucus to prevent conception.
The article in the BJM Case Reports notes that risk factors for migration include having the implant placed too deeply or participating in vigorous physical exercise… even when an implant is properly placed. Many women are never told of this rare but severe complication of implanted devices. For an implant in the arm, the device can migrate to the chest cavity where is can be difficult to locate. In fact, this happens often enough that the implant’s material was updated to be easier to locate on a diagnostic scan “if it ever moves from its original location.”
The risk of migration is alarming enough on its own, but hormonal contraception like this comes with a slew of other side effects and complications that are often not discussed. Physical and mental side effects can be devastating for women using hormonal contraceptives.
In the video below, one woman documents her “horror story” with getting the Nexplanon contraceptive implant in her arm, which actually ended up migrating and causing nerve damage. She says in the video that she will never get an implant again, and instead intends to use natural family planning. Below the video on YouTube are several comments from women who also had scary experiences with their implanted birth control:
There are alternatives to hormonal contraceptives, including modern natural family planning methods. Natural family planning (fertility awareness-based methods) is slowly gaining recognition as a viable and effective form of child-spacing that respects a woman’s body and does not undermine her physical and mental health.
According to a horrifying report, not a single girl has been born in the last three months in the Uttarkashi district of India.
The discovery has launched an investigation into whether sex-selective abortion or female feticide is being practiced in the region, which has a population of over 300,000. The district magistrate Ashish Chauhan spoke to ANI saying: “We are monitoring these areas to find out what is affecting the ratio. A detailed survey and study will be conducted to identify the reason behind it.” Officials are also holding emergency meetings with local health care workers.
According to official data, 216 children were born in the district’s 132 villages in the last three months. None were female. The area has been marked as a “red zone,” meaning it will be scrutinized more closely and the government has asked health care workers to be on alert. In recent days, the government has attempted to prevent sex-selective abortions through its BBBP program, which among other things helps to educate on the importance of the Child Sex Ratio (CSR) and promises girls in India a good education.
In a 2011 census report by the United Nation Population Fund, India’s CSR had declined from 927 to 914 girls for every 1,000 boys. Although abortion on the basis of sex is illegal in India, the practice is widespread based on cultural views of girls as potential liabilities, and boys as breadwinners and parental caretakers in old age.
Live Action News recently reported that 550,000 preborn baby girls are killed each year due to sex-selective abortion in India, with a total of 15.8 million girls lost to sex-selective abortion since 1990. India has also been found to be the “most dangerous country in the world for women” on account of its astronomical numbers of rape and sexual assault. Parents are also frequently pressured to pay dowries when daughters marry, even though the custom was abolished in 1961. Kalpana Thakur, a social worker from the region, pointed out that these alarming numbers show that the government isn’t doing enough.
“No girl child was born for three months in these villages,” said Thakur. “It cannot be just a coincidence. This clearly indicates female foeticide is taking place in the district. The government and the administration are not doing anything.”
While sex-selective abortion is more prominent in countries such as India and China, it is accepted here in the United States. Planned Parenthood has spoken out against proposed laws to ban sex-selective abortions and Live Action’s undercover investigation revealed that the abortion corporation has no problem aborting simply because the preborn child is a girl.
New research provides some preliminary evidence that hormonal contraceptives could influence how things are remembered. The study in Psychological Reports found that women taking birth control pills tended to recall less negative emotional information compared to women who were not taking them.
“I have previously conducted a number of studies on the effects of oral contraceptives on mood and have always been interested in this area of research,” said Kirsten Oinonen, an associate professor of psychology at Lakehead University and the corresponding author of the new study.
“I know many women who have reported experiencing emotional side effects from oral contraceptives and I think it is imperative that researchers continue to examine the effects of hormonal contraceptives on mood, cognition, and perception. It is critical that women are fully informed about these potential effects so that they can make informed decisions about birth control options.”
“I have a graduate student, Brandi Person, who was also extremely interested in exploring how oral contraceptives affect emotion and cognition. Given previous research suggesting that hormones can affect both mood and cognitive ability, we felt that looking at the effects of ‘the pill’ on emotional memory would be an important area to study,” Oinonen explained.
For their study, the researchers recruited 58 women who were using oral contraceptives, 40 women who were not using oral contraceptives, and 37 men.
The participants completed an Emotional Spatial Memory test, in which they viewed a variety of emotionally-charged and emotionally-neutral items that had been set up on a tray. Shortly after viewing the tray of items, the participants were asked to list as many items as they could remember and also to indicate where each item had been placed.
One week later, the participants completed the same tests of memory recall again.
The researchers found that oral contraceptives users tended to recall more positive items and fewer negative items than nonusers in the short-term recall test. In the long-term recall test, there was no significant difference between users and non-users.
“Hormones have the potential to influence emotions and cognitive ability. Thus, women should be alert to any such changes they notice in themselves when taking hormonal contraceptives,” Oinonen told PsyPost.
“The findings of our particular study suggest that women taking ‘the pill’ may experience a change in their memory for emotional information. In particular, the findings suggest that women taking the pill may show a memory bias in terms of being less likely to remember negative information than nonusers.”
“This could result in women taking the pill viewing situations, people, or objects as more positive than they might have if they were not taking the pill (i.e., because they are relatively more likely to remember the positive versus the negative information),” Oinonen said.
The researchers controlled for a number of variables that could impact mood and memory, including menstrual cycle phase. But like all research, the study includes some limitations.
“Any new research finding needs to be replicated before it can be accepted with confidence. That applies here as well. Thus, future studies need to replicate the findings with larger and more diverse populations,” Oinonen said.
“As we looked at memory for visual stimuli, future studies should examine if women also show a tendency to recall less negative verbal, olfactory, auditory, and kinesthetic stimuli. Brandi Person and I are examining some of these questions in her PhD dissertation. Of course, a future placebo-controlled trial to look at the effects of oral contraceptives on emotional memory would provide the strongest evidence to support these findings.”
WASHINGTON, D.C., July 26, 2019 (LifeSiteNews) — According to the Centers for Disease Control, the fertility rate in the United States reached an historic low in 2018.
In a report issued Wednesday, the CDC confirmed provisional figures that were released in May that “the 2018 general fertility rate fell to another all-time low for the United States.”
The Atlanta-based government institution found that the fertility rate among women ages 15 to 44 dropped by two percent between 2017 and 2018. This represented a drop from 60.3 births per 1,000 for women ages 15-44 to 59.1 percent. In addition, the percentage of preterm and early-term births increased: For babies delivered at less than 39 weeks, the percentage increased from 9.93 percent in 2017 to 10.02 percent in 2018. Full-, late-, and post-term deliveries declined.
The general fertility rate for the United States declined two percent in 2018 to 59.1 per 1,000 women ages 15-44 from 60.3 in 2017.
Fertility rates declined for the three largest race and Hispanic-origin groups from 2017 to 2018, down two percent for non-Hispanic white and non-Hispanic black women and three percent for Hispanic women.
In 2018, the fertility rate was highest for Hispanic women (65.9), followed by non-Hispanic black (62.0) and non-Hispanic white (56.3) women.
In May, provisional figures released by the National Center for Health Statistics of the CDC showed the total fertility rate, or average number of children born per mother, was 1.7, which is far below the demographic replacement rate of 2.1.
Also, statistics showed that in 2018 fewer than 3.8 million children were born in the United States. Despite a peak year in 2007, birth rates have fallen in all but one of the last 11 years.
The U.S. showed a continuing trend of diminished fertility among younger women during that period.
The average age of first-time mothers has risen by more than five years: in 1968, the average age was 21.4; today, it was registered as 26.8. In 2018, childbirth rates in the 20-24 age cohort dropped by four percent, and three percent among women ages 25-29. However, women in the 30-35 age cohort had a higher rate of births than those ages 25-29. Thus, this is the first time that women in their early 30s were leaders in birthing babies.
In February, Hungarian Prime Minister Viktor Orban announced that women with four children or more will be exempt from paying income tax for life in an effort to encourage births. The Hungarian fertility rate is currently 1.45 children per woman.
The Lancet medical journal published a report in November 2018 that showed that almost half of the countries on earth do not exhibit sufficient birth rates to outdistance deaths. In South Korea, for example, there were seven births per 1,000 people in 2017, a number that has since fallen. In Spain, a report issued in Marchshowed evidence that the abortion rate is contributing to the nation’s birth dearth and its overall aging.
Experts have long warned about the economic and social costs of a declining birth rate. This has long been documented in Japan, which has a current birth rate of 1.43. Small families, contraception and abortion have led to an aging population. Fewer births means fewer workers to support the growing number of pensioners, for example. Experts contends that a birth dearth may curtail any country’s plans to sustain and increase social welfare programs that currently depend on population growth.
In Japan, official encouragement for mothers to be more open to childbirth has largely failed. Immigration has not met with much acceptance in Japan, either.
July 24, 2019 (LifeSiteNews) — It’s already been dubbed “The Best Soccer Image of the Year,” and it has gone viral.
A toddler from Florida expressed sheer joy encountering his new friend who is just like him. The faces of 21-month-old Joseph Tidd and professional soccer player Carson Pickett — both born without a left forearm — register delight as they “fist bump” after Carson’s game.
Joseph’s mom, Colleen Tidd, snapped the photo, which quickly went viral on Instagram and has exploded all over all social media.
Young Joseph and 25-year-old Orlando Pride defender Carson Pickett first met last spring, according to a Today.com report. Pickett exclaimed to Joseph, “We have the same arm!”
The “instant bond we can’t begin to understand”
“Carson knelt down next to Joseph and showed him her arm,” Joseph’s dad, Miles Tidd, told TODAY Parents. “It was this instant bond we can’t begin to understand.”
The now viral picture of the two clearly displays their special bond.
Pickett, for her part, said the feeling was mutual.
“I know I might be seen as his role model, but he’s also mine,” Pickett told USA Today Sports. “It’s just a gift to feel so much emotion from a little boy who understands you in a way other people can’t.”
“Literally within five minutes of me meeting him, we had an instant bond,” said Pickett. “It’s interesting, though, because for a kid that young, I didn’t expect him to connect the way he did. Even though we both have the same arm (birth defect), it was amazing to me that it felt like he realized why we were bonded.”
“Honestly the best part of the photo is that it was so real and wasn’t planned,” said Pickett. “It was the true pure reaction we both had.”
“Pictures mean a lot so hopefully when he gets older he can see that and feel even more of what it means,” continued Pickett. “When I was younger and I didn’t know how the world works, it was hard. My parents always tell me that God put me here for a reason. The biggest thing I’d want Joseph (and others) to know is that even if people see you as different, it’s what’s in your heart that counts.”
Joseph, still three months shy of his second birthday, may well end up following in Pickett’s footsteps.
“Carson believes she can do anything,” said his dad, Miles, “and that is the mindset we want Joseph to have as well.”
“Football, basketball, baseball, soccer, he does it all,” mom Colleen told TODAY Parents. “He maneuvers his arm a little bit differently, but he makes it work.”
According to new research from the University of Pittsburgh and the U.S. Department of Veterans Affairs, and published in USA Today, distributing 12-months of birth control pills at a time will reduce unintended pregnancies.
The study’s lead author has stated that the distribution of more birth control at one time will reduce the healthcare costs associated with pregnancy, making it economically beneficial.
However, there are serious concerns surrounding this potential plan. At this time, there are 17 states plus Washington D.C. that have laws that require insurers to provide 12-months worth of birth control pills at a time, however, most people have difficulty getting more than a 90 day supply at a time.
According to Cathryn Donaldson, communications director for American Health Insurance Plans, some insurance companies are reluctant to provide this 12-month supply because, as with any medication taken in the long term, birth control comes with risks.
“Side effects and improper use of prescription drugs can have a serious and potentially life-threatening impact on a patient, which is why it is recommended patients regularly consult their physician, pharmacist or other care provider,” wrote Donaldson. She also states that this 12-month supply could cause “waste, fraud, abuse and increased costs.”
There serious reasons to be concerned about how a 12-month prescription system could affect women. While this system may sound convenient, it doesn’t account for the long-term side effects of birth control that may go unaddressed in a woman who is only required to consult with her physician about her medication once a year.
Safer, More Effective Options
Fertility Awareness-Based Methods (FABM), also known as “natural birth control” or natural family planning, allow women to manage their health without putting loosely regulated drugs (that come with many health risks and side effects) into their bodies. When taught by a certified FABM instructor, these methods of family planning are more effective than the birth control pill in preventing pregnancy. In addition, Fertility Awareness-Based Methods are economically feasible. It’s reassuring to know that methods like FABMs exist, which allow women to take their health into their own hands in an empowered and safe way.
A 12-month prescription of birth control may seem convenient, but it eliminates the need for frequent visits with a physician, which are necessary in order to reassess a woman’s health and address medical side effects. Considering how many women suffer painful and even life-threatening side effects of birth control, from depression to blood clots, women being prescribed birth control today deserve more medical care and attention, not less.
Now streaming on Amazon Prime, Eggsploitation (2010, updated and expanded version released in 2013) is a documentary short about some of the unheard victims of the $6.5 billion per year infertility industry. It follows the stories of several women from a variety of demographic backgrounds who chose to become egg donors for the promised financial and altruistic benefits, yet suffered terrible consequences. Stroke, ovarian torsion, unexpected cancer, and ultimately damage to or loss of their own fertility are some of the painful prices these women paid, despite not being adequately counseled on serious risks ahead of the procedure.
Produced on a $25,000 budget, the award-winning 45-minute independent film Eggsploitation is the first in a series of Jennifer Lahl’s exposés on the shady business of breeding in the laboratory. These include Anonymous Father’s Day (2011), Breeders: A Subclass of Women? (2014), and Eggsploitation: Maggie’s Story (2015, also streaming on Amazon Prime).
As the stories in Eggsploitation reveal, the venture can be eerily reminiscent of human trafficking, with women treated as commodities rather than respected as autonomous beings in a reasonable economic exchange.
With offers as high as $100,000 floating in advertisements, young women (usually targeted for their physical beauty and academic success — one woman in Eggsploitation had to take an IQ test) are easily baited into signing up for the initial procedure. When their ovaries don’t release as many eggs as preferred in the first cycle, they feel pressured to continue the risky operation or settle for less money and possibly disappoint their recipients.
Lahl, R.N. and founder and president of the Center for Bioethics and Culture Network (CBC), decided to create the documentary when she encountered many women hurt by the egg donating process. She takes a sympathetic approach to the subject, understanding the charitable intentions many young women have towards those who struggle to conceive. The ethics of egg donation, in vitro fertilization, and other infertility treatments are left to the viewers’ discernment. But when it comes to the ethics of treating patients, Eggsploitation makes it quite clear that there is a problem.
“If you are an organ donor and you donate your kidney, you will forever live in a database that will monitor you long term to find out how you do five, ten, twenty years later after you donate a kidney,” Lahl says in an interview with Women Now. “That’s not the case with egg donors,” whom she says are not even treated as patients because their importance becomes secondary to the woman pursuing a fertility remedy. “Because they’re not sick, we don’t even keep medical records on egg donors,” says Lahl.
“This whole industry of fertility medicine is relatively new,” Lahl, says in the aforementioned interview. “It’s only been around for about three decades, so we’re only now starting to see some of the negative longer term risks, and those are predominantly cancers.” These risks apply not only to women donating eggs, but to women who collect their own eggs for in vitro fertilization, and possibly to children conceived through these alternative methods.
The risks are due to tampering with the hormones that control a woman’s reproductive cycle. While a man normally produces millions of easily released sperm every day, a woman normally produces a single egg every month that is matured and released on a delicate hormonal schedule. Since this is commercially impractical, the egg donation procedure must hijack the menstrual cycle with hormonal injections that cause the woman to produce an abnormal amount of eggs (a range from 20 to 70) at once, which are then surgically removed.
A British study published last year notes, “[a]ssisted reproduction cycles usually involve exposure to supraphysiological levels of oestradiol, exogenous gonadotropins, and multiple ovarian punctures, all potentially carcinogenic. Most concern surrounds the risks of breast, endometrial, and ovarian cancers after such exposures.”
Eggsploitation reports that the procedure begins by inducing temporary menopause in order to synch the egg donor’s cycle with that of the egg recipient. This is done by the woman self-injecting Lupron, a drug the FDA has not approved for fertility use. Next, the ovaries are prompted to super ovulate, which can lead to the dangerous ovarian hyperstimulation syndrome (OHSS). A final injection is given to release the mature eggs, which are afterward sucked out via a vaginal catheter under anesthesia.
Even though the featured women began experiencing extreme discomfort (the ovarian swelling alone is miserable) and some severe side effects, their symptoms were dismissed as “normal,” and their commitment to the donation kept them in denial.
But it’s not just the women who came forward in Eggsploitation who can testify to this. A quick Google search highlights a sisterhood of suffering egg donors. One Canadian blogger who documented her experience is disappointed in how the risks were downplayed at the outset, and cautions other women to do more thorough research.
“Are we fulfilling one woman’s dream at the expense of another woman’s health?” This is the question at the heart of Eggsploitation. While society may have grown past the ancient days of women using slaves as their surrogates, humanity’s baser instincts in the face of desperation to conceive have not necessarily become less barbaric.
Natural family planning, or NFP, is increasingly becoming an attractive option for women and couples alike as they rethink conventional contraceptives. Unlike birth control, NFP can be used to track a woman’s monthly cycle, not only avoid pregnancy, but to help couples get pregnant, and to help women better understand their own bodies. And one app that helps with this sort of tracking has been credited with helping the US Women’s National Team with the FIFA World Cup.
The women’s soccer team thrilled fans across the country as they not only became world champions, but also scored the most goals ever in a Women’s World Cup. According to the coaches, using NFP was crucial. “I feel like it’s one of many strategies that we deployed that helped us win,” Dawn Scott said in an interview with Good Morning America. “I feel like [the U.S. is] leading the way on this.” Scott, the high performance coach for both the USWNT and the National Women’s Soccer League (NWSL), had been tracking her players’ cycles for years, but as the World Cup approached, she realized she needed a more advanced and individual approach.
“For a few players, I always noticed that just before they started their cycle, their recovery fatigue was increased and their sleep was less,” she said. “I was noticing it for three or four players and thought, ‘We’re six months out from the World Cup, how we can help that?’” So with the help of Dr. Georgie Bruinvels, a research scientist, the problem was solved, thanks to Fitr Woman, an app Bruinvels created that tailors workout schedules and nutrition advice based on their unique monthly cycle. Each player filled out an individual survey, explaining the timing of their cycles, the symptoms they felt, and how those symptoms impacted their playing. That information was used to keep the athletes in peak condition as they competed for almost two months for the World Cup.
FitrWoman app
“We could see what [menstrual cycle] phase a player was in and what some of their symptoms were,” Scott explained. “I would just text or say to a player, ‘Hey you’re in phase three and we know you get disrupted sleep, so make sure you do x, y and z.’”
This outlook was lauded by several medical professionals, who said it is long overdue for women who compete in sports. “We do know that there are parts of the cycle where women may have less ability to sleep and may have different eating habits,” Dr. Richard Beckerman, chairman of the Department of Obstetrics and Gynecology at Sibley Memorial Hospital in Washington, D.C., explained to ABC News. “But just as we find people are affected differently by different things, it can be very variable.”
ABC News chief medical correspondent and OB/GYN Dr. Jennifer Ashton agreed. “For anyone who understands the complexities of women’s health, the fact there can be fluctuations in physical or mental stamina, or changes in sleep or dietary behaviors corresponding to changes in a woman’s menstrual cycle come as no surprise,” she said. “The ability to individualize behaviors that have the potential to optimize athletic performance exists and absolutely should be considered when dealing with any athlete, male or female.”
She added, “The fact is, female athletes are biologically, hormonally and physically different, and the sooner that reality is embraced instead of resisted, the more potential exists for that athlete to optimize her training behaviors. An app that tracks the menstrual cycle absolutely has the potential to improve a female athlete’s behaviors.”
In Scott’s case, she wanted to go public to break the taboo surrounding menstruation. “For the 15-year-old girl who doesn’t have the support of a national team, I want to make it so she can talk about it with a female coach and a male coach,” Scott said. “We need to make people aware of it and not embarrassed by it. This is physiologically what female athletes deal with.”
While NFP has long been maligned, especially by the abortion industry, pro-lifers have been its strongest advocates over the past several decades, and it has only grown in popularity. The reality is, NFP is more effective than women are often led to believe. And though traditional birth control comes with serious side effects, which roughly half of women have “serious trouble” with, NFP has no side effects — and, as the USWNT shows, it can be used for more than just avoiding pregnancy.
Stars from the “Bachelor” franchise, as well as other celebrities, have likewise been increasingly open about using NFP apps that help them understand their own bodies, how they are affected by their cycle, and how it has helped them to both avoid and achieve pregnancy. It is this kind of information that empowers women, giving them the ability to see how their hormones and cycle affect them, as well as to take charge of their fertility without potentially using an abortifacient or feeling like they must subject themselves to unpleasant and potentially dangerous side effects.
Empowering a woman begins with educating her about the amazing way her body and her fertility works.
ROME — The anthropological vision of John Paul II on love, life and human sexuality, developed in his “theology of the body” (TOB) catechesis, has become a polestar for a whole generation. Gathering a series of 129 catechetical addresses pronounced during his Wednesday audiences in St. Peter Square from Sept. 5, 1979, to Nov. 28, 1984, the theology of the body remains a key element of John Paul’s thought and a major papal contribution to the Church’s teaching on human sexuality..
Although the Pope’s addresses remained relatively unknown until the 1990s, this crucial work is now widespread — and continues to spread — thanks to the commitment of individuals around the world who have dedicated their lives to teaching John Paul’s vision, notably through the organization of large conferences and the creation of institutes and associations.
One of these associations is the Dallas-based Theology of the Body Evangelization Team, known as TOBET, founded in 2001 by a group of educators and parents. TOBET’s aim is to “‘translate’ this philosophically dense, theological reflection so that families and people of all ages can access this life-affirming teaching.”
Its executive director, Monica Ashour, a national speaker and author, wrote a number of books designed to help people live according to the anthropology espoused by the theology of the body in a more concrete and authentic way, including through books for children entitled The Body Matters.
In May 2015, Ashour was a participant in an ad hoc committee for the Pontifical Council for the Family led by the council’s president at the time, Archbishop Vincenzo Paglia. Three years earlier, in November 2011, she attended the Theology of the Body International Symposium in Rome and presented a talk about how to teach teens the TOB.
The Register met her during her recent pilgrimage to the tomb of St. John Paul II in Rome.
For many years, you’ve been dedicating a significant part of your life to spreading St. John Paul’s TOB, through TOBET. Why are these teachings so important nowadays?
I think John Paul II saw the problem in our current culture. In the mid-fourth and early fifth century, St. Augustine sought to address the problem of what it means to be human; 800 years later, St. Thomas Aquinas addressed this question, as well; and 800 after Thomas, St. John Paul, in turn, sought to answer a similar question. St. John Paul saw that the body was not being seen properly in modern society. He describes our understanding of our bodies as “detachment.” We [as a modern society] are, John Paul II claims, detached from the truth of our own bodies. We don’t see them as a sacrament, as revealing something about God, about ourselves, about love. So John Paul II focuses on the body and its meaning, and I think this focus is perfectly fitting for this culture.
How did John Paul II develop these teachings from his own experiences?
Karol Wojtyla lived during World War II, during which, in [Nazi] concentration camps in Poland and neighboring countries, there would be experiments on people, especially on Jews, whose bodies were seen as objects of scientific study. And then with the sexual revolution — John Paul was a young priest back then — he saw people abusing the body as mere tools for pleasure. This is how he came to understand that the body matters.
In John Paul II’s TOB addresses, the importance of the body is underscored by the fact that the word “soul” appears 55 times, “spirit” 99 times and “body” 1,319 times.
But today, things are not much better than they were during John Paul II’s time. When we look around, we see so many tattoos on people, and there is rampant sexual promiscuity — all because we see the body in the wrong way. The sacred dimension of our body is so often lost.
This is what I think St. John Paul saw at the time. And he anticipated even transgenderism. In TOB, he says that, in today’s society, a person has difficulty in identifying with his or her own body. When he wrote that in the 1980s, he may have seen transgenderism as it was going to become many years later. Many at the time did not understand the meaning of being a “body-person,” a term coined by him. In this way, John Paul II doesn’t give us only a theology of love, of marriage, and of matrimony, but he also gives us the theology of the body.
You see a continuity of thought linking St. Augustine, St. Thomas Aquinas and St. John Paul II. What are their distinctive features?
Regarding the theology of the body, St. Augustine says that procreation and education of children is the purpose of conjugal and marital intercourse. Then, 800 years later, St. Thomas Aquinas further developed St. Augustine’s idea of the union of spouses as a secondary and subordinate end to procreation. And 800 years after Thomas, St. John Paul, agreeing with both Augustine and Thomas, further develops our understanding of the body’s nature by pointing out that the body speaks a natural language, a language of a free, full, faithful, fruitful person-to-person encounter.
In the theology of the body, John Paul II says to the husband and wife that their bodies speaks through the language of gift. He draws inspiration from Vatican II, Gaudium et Spes, 24, which says men and women “cannot fully find [themselves] except through a sincere gift of [themselves].” That is the meaning of life. In a similar way, Pope John Paul sees the meaning of life in Genesis 2:25 (“Adam and Eve were naked and did not feel ashamed”). Why? Because before the Fall, the human body revealed who we were as humans, and we knew our bodies were meant to be a gift. After the Fall, we lost sight of this sense of gift. So the gift — and recovering that sense of gift — itself is the meaning of life.
Even if I am single, I can give the gift of my body to others, although in a way quite different from how a married couple give their bodies to one another, of course. It is important to know that we all, married and single, speak the language of gift through our bodies — because we are gifts to each other. Right now, for example, my vocal cords are directed towards your eardrums. I am giving something to you, and you’re giving something back by receiving, by smiling at me, and together as we interact we are more than the sum of our parts.
God is love, so whenever all of us love together, we reveal God. And how can we express that love to one another? A primary and fundamental way of expressing this love is through our bodies. We are a composite body and soul. But I think John Paul moves away from the expression “body and soul” and just says that the body shows you that you have a soul, that you’re made for love and that finding that sense of love in our bodies and souls is the meaning of life.
A significant part of your work focuses on young people, to whom you dedicated a series of books. Why do you think it is important to reach young people with these teachings?
A few years ago, I received a phone call from Toronto, in Canada. I’ve been urged to teach TOB to children because, in a school there, the small children were told that their sexuality was fluid. “Close your eyes,” the teachers instructed the children. “Think about whether you’re a boy or a girl, and don’t let anybody tell you. You decide your own sexuality.” Naturally, parents were outraged at this sort of activity, and the school’s sex-education curriculum provoked great controversy among the parents.
After I heard that story about students being encouraged to decide their own sexuality, and many others like it, I consulted the bishops on our TOBET advisory board and they advised that I write books for children that would counter these false secular teachings on human sexuality. This is how my series of books called The Body Matters started. We hope we can spread them in Catholic schools as well as in parish catechetical programs. And we want parents to read these books as well because many may not know the theology of the body. These books are a good way to establish a dialogue between parents and children.
Some commentators lamented the fact that the synod on young people, in October 2018, didn’t give enough space to sexuality. Do you agree with them?
I believe there wasn’t much discussion about TOB during the synod on young people, which I think is a problem. There needs to be some focus on sexuality, and that focus should not be at the exclusion of anthropology — that is, at the exclusion of what it means to be human. I wish the synod would have integrated Pope John Paul’s understanding of the human person as a gift made in God’s image because I think he knew what we need now — that is a TOB based on Scripture.
How would you have integrated TOB into the synod on young people?
I would have advised participants to take seriously what Pope John Paul was trying to do. He warned against seeing the body in “detachment” or that the body doesn’t have meaning. If I was an adviser in this kind of event, I would start by asking, “How does the body teach you many lessons?” Then I’d point out that the body teaches us that we’re human, first and foremost. This basic teaching — the humanity of our bodies — will become more important in the future because another thing that is coming is transhumanism, which is very scary.
Next, I would point out that the body teaches us that we are male or female (“boy body” or “girl body” is how I put it for children in the TOBET books), not neutral. This, too, is vital for children to know, as I’ve heard that people are even building sex robots to replicate — and replace — authentic human sexual experience. So, if we don’t talk to young people about the truth of their existence as male and female sexual beings, then they’re going to be brainwashed by erroneous views of sexuality as a neutral thing. My advice is that young people should take seriously the people who have studied and understood the truth of the child, the truth about the human person, and the truth about sexuality and about the body mattering in all these truths.
Your first book was on marriage preparation. What would be your first piece of advice to a young couple getting married?
Engaged couples need to understand that the body is a revelation of the person. So often, we wrongly think that the body is separated from the person. It is seen as a tool for pleasure, not a sacrament. Engaged couples must see the body as a gift and the other as a gift. Only then will they be able to see how the teachings about sexuality come into play — even though, of course, marriage is about much more than sexuality.
All of TOB is about ultimately getting to heaven, where we will be in union with God and others, with our “spiritualized” bodies. So, through TOB, engaged couples will truly come to now that “I am meant to be for you and you for me.”
When I give talks before engaged couples, one of the last things I explain to them is how, for instance, two fiancées, Katy and Joe, will enter into a mutual self-giving in marriage. “When you get married, Joe,” I say, “you become Joe for Katy, and, Katy, you become Katy for Joe.” In other words, Pope John Paul says a person is a “being-for-another.” So they become gifts for each other, and they get to journey this life together. And, ultimately, they get to see each other face-to-face, with their bodies, in heaven. Marriage gives you a taste of heaven.
In the priesthood and religious life, too, individuals are self-giving and likewise live for all. In either case, married or religious life, this self-giving is a taste of what heaven is about. Both of those vocations give a taste of heaven. It is all about the Father, the Son and the Holy Spirit — and the Church — all being at the center of one’s life.
You’re in Rome for a pilgrimage to the tomb of St. John Paul II. What does this trip mean to you?
I am here is to show my gratitude. I am grateful to God, to my parents for raising me in the Catholic faith, and to Pope John Paul who gave us TOB. I am going to be in front of his tomb, praying and thanking him for his gift, a gift which is going to transform the culture, one person at a time, for Jesus and his Church.
Solène Tadié is the Register’s Rome-based Europe correspondent
There is no more unifying experience among women around the globe than menstruation. All women understand what it feels like to have their period—even if they don’t exactly understand what it is.
And yet, the topic of menstruation continues to hold significant stigmas, and embarrassment or hesitation to discuss this vital function of the female body has created gaps in our knowledge of how the menstrual cycle affects a women’s overall health.
Therefore, it was a welcome shock to discover that the May 2019 issue of Scientific American magazine is primarily dedicated to the science of women’s reproductive health—or rather, the lack thereof. In one particularly revealing article, “What is the Point of a Period?” by Virginia Sole-Smith, the author investigates the long-standing menstrual taboo and the devastating effect it has had on women’s reproductive health, including the unique problem concerning menstrual suppression through hormonal birth control.
Coming from a nationally esteemed scientific magazine as Scientific American(the longest continuously published magazine in the United States), this article is truly a breakthrough for women’s reproductive health, for several reasons.
The medical and scientific repercussions of the global menstruation taboo
All women of child-bearing years experience menstruation. There is nothing strange or unhealthy about it, even if global taboos are still very much alive. In fact, the female menstrual cycle is necessary for reproduction—necessary for human survival. But still, most people are too scared or embarrassed to talk about or even acknowledge it. As Sole-Smith explains, “That aversion has influenced women’s relationships to their own bodies as well as how the medical establishment manages women when things go wrong with their reproductive health.”
Somehow, many doctors still do not understand the intricacies of the menstrual cycle (especially how charting one’s cycle using a Fertility Awareness-Based Method can help diagnose and treat common health problems). Too many doctors don’t realize that periods offer clues that often reveal underlying issues concerning a woman’s reproductive and overall health.
The scientific community has offered very limited help. As Sole-Smith explains, “It is hard to measure how much money is spent on period research, but experts agree the subject is underfunded.”
At the heart of this menstruation taboo is a lack of knowledge and understanding. Many women may know that their period signals the shedding of their uterus’s lining. But what exactly does that mean? Sole-Smith answers this question thoroughly and concisely: “The endometrial lining of the uterus thickens over the course of a woman’s cycle as her estrogen level rises. If none of the eggs she releases at ovulation joins with a sperm and implants in that lining as a fertilized zygote, then levels of estrogen and another hormone called progesterone drop, triggering the uterus to shed the thickened endometrium so it can start fresh in the next cycle.”
Essentially, a woman’s uterus lining thickens every month to prepare for the possibility of a fertilized egg and pregnancy. If the egg does not get fertilized, then the uterus sheds this lining and it leaves the body as menstrual blood.
While scientists are still struggling to understand exactly what menstrual blood is, Sole-Smith writes that “Even less is known about why so many women—up to 80 percent by some estimates—experience cramps, bloating, fatigue, anger, or other symptoms just before the onset of menstruation.” She quotes Tomi-Ann Roberts, president of the Society for Menstrual Cycle Research, who reveals that “We know so little about menstruation. . . . Because of this, our attitudes toward menstruation are overwhelmingly negative. This has real consequences for how we can begin to understand healthy menstruation, as well as menstruation-related disorders and the treatment options available.”
“Having periods is not a disease. But when they go wrong, they offer clues into disorders that require intervention. The medical field has largely done a poor job of identifying and treating them with precision. Clinicians tend to wield synthetic hormones like a hammer, liberally prescribing the birth-control pill for all kinds of pain—which is partly why serious diseases of the female organs such as endometriosis take an average of eight years to be diagnosed. That women’s symptoms are often dismissed does not help.”
Which brings us to the question of why doctors started covering up the female menstrual cycle via hormonal birth control in the first place, and why they are just now—decades later—starting to adequately research the effects of menstrual suppression.
The problem of birth control’s long-term suppression of menstruation
In her article, Sole-Smith explains how research on menstruation evolved from ludicrous conclusions “that menstrual blood contained a kind of poison” in 1920 to research on how to prevent pregnancies in the 1950s in large part to the work of Margaret Sanger (future founder of Planned Parenthood). In the first large-scale, FDA-approved trial of hormonal birth control, 265 low-income Puerto Rican women were recruited (as Sole-Smith notes, “without the level of ‘informed consent’ required today”), and 22% of the women dropped out of the experiment after experiencing adverse side effects. “The study’s medical director argued that the pill ‘caused too many side reactions to be generally acceptable.’ Nevertheless, it went to market.”
This is how birth control came to be—tested on poor women in another country without proper consent, with their blatant side effects brushed aside. While the Pill is celebrated as a liberating breakthrough for women, Sole-Smith goes on to explain: “But liberation came with a price. By the late 1960s patients across the U.S. were reporting the same symptoms documented during the Puerto Rican trial. Despite many reformulations over the ensuing decades, side effects remain a problem for many women on the pill; risks for breast cancer, blood clots and stroke may also be higher.”
Elizabeth Kissling, a professor of women and gender studies at Eastern Washington University, explains how this new “reproductive freedom” did not seem to take into consideration the consequences of “shutting down a woman’s natural cycle.” Sole-Smith sums it up well: “scientists figured out how to supplant periods long before they began trying to understand why they work the way they do.”
The article explains how scientists did not truly investigate “the larger question of why menstruation happens at all” until the late 1980s. She explains the research of evolutionary biologist, Beverly I. Strassmann, including her investigation into why humans do not reabsorb their menstrual blood like other animals do, stating: “Our physiology doesn’t permit reabsorption, so much of the blood gets discharged as menstruation.” This led her to conclude that bleeding during one’s menstrual cycle is “an insignificant by-product of evolution rather than an advantage.”
Does that mean a woman’s cycle is insignificant, and should be suppressed by artificial birth control? After all, Sole-Smith notes that “Skipping that monthly ordeal can mean avoiding debilitating pain . . . and other symptoms that can dramatically impair a woman’s quality of life.” But as Kissling notes, “The pill isn’t a treatment for these conditions. It’s a way of refusing to treat them.” Endocrinologist Jerilynn Prior explains how “it can take up to a decade or longer from disease onset for a woman to be diagnosed with endometriosis, for example, in part because doctors are so quick to prescribe the drug to teenagers reporting bad cramps without investigating to see if there is an underlying cause.” The Pill masks often serious underlying problems and manipulates natural hormone functions.
Reason for concern
Strassmann, for one, is rightly skeptical about the long-term effects of “medically induced menstrual suppression”—namely, the higher hormone levels with which women become exposed. She says, “It’s true a monthly menstrual period is not necessary. But taking more progestin to skip your period is not living like our ancestors did 500 or 1,000 years ago.”
As the article “What is the Point of a Period” reveals, “analyzing data from 12 studies, as well as the information on birth-control package inserts, Strassmann’s team concluded that some types of the Pill exposed women to a quadruple dose of progestin (a synthetic form of progesterone contained in the Pill), relative to the progesterone their naturally cycling body would produce.”
Ultimately, this crucial article reveals that what we know about menstruation and the long-term effects of birth control on menstruation is that we still don’t know enough. Sole-Smith explains, “Nobody knows for sure what that exposure to synthetic hormones will mean long term for women using the Pill to suppress their cycles indefinitely. This knowledge gap speaks to broader concerns about our ignorance around menstruation.” And if this is not concerning, then I do not know what is.
What I do know is that I do not want to be part of this experiment. I find myself asking the same questions that Moskowitz poses, “What might be different if researchers had investigated the evolutionary purpose of periods before they developed a Pill to shut down a woman’s cycle? Why are women expected to shoulder health trade-offs in exchange for avoiding pregnancy?”
I find it tragic that more women do not see their menstrual cycle and fertility as a vital sign of health and that they are not given adequate information by their doctors about their cycle and natural options for family planning and treatment of common health issues, other than birth control. Too many women are not given the option of—or even information on—safe, natural, side-effect-free, Fertility Awareness-Based Methods, modern methods based in science.
In a closing sentence that left me with chills, Kissing suggests that “Long-term menstrual suppression via birth control is the largest uncontrolled medical experiment on women in history.” Here’s to stopping experiments when it comes to women’s health.
Book Review:American Restoration: How Faith, Family, and Personal Sacrifice Can Heal Our Nation. By Timothy S. Goeglein and Craig Osten (Regnery Gateway, 216 pages, $28.99).
Liberty can no more exist without virtue than the body can live and move without a soul. — John Adams
Bowling alone, coming apart, two nations, alienated America, sexual suicide — these phrases, all taken from titles of books both recent and dated, describe in painful detail the collapse of a cohesive society in which stable families, social mobility, and a common moral vision, however imperfectly lived, enabled a rising middle class to prosper. The familial collapse first identified by the late Daniel Patrick Moynihan in his prescient 1965 report on the decline of the African-American family has now become a generalized, systemic condition for a large segment of white and Hispanic America, too.
“As of 2014, more than seventy percent of all African American children are now born out of wedlock — triple the percentage Moynihan reported in the mid-1960s when the Great Society was launched to solve the problem (hopefully) of fatherless children in African American homes,” Goeglein and Osten write.
“In 2014, more than half of Hispanic children were born out of wedlock, as well as one-third of all American babies born to Caucasian mothers,” they continue. “As recently as 1970, only 15 percent of all American babies were born outside of marriage. The combined rate of all racial groups is now a whopping 40 percent.” And this despite $22 trillion spent over fifty years on Great Society programs.
As a mountain of social science data shows, single-parent families, usually without a father and husband, are an economic and social calamity for children, especially boys. A University of Pennsylvania study found that young men who grow up fatherless are twice as likely to end up in jail as those who come from traditional two-parent families.
For these authors, the cause of our problem is fundamentally cultural and religious, inextricably tied to a “propulsive postmodernism” and a demiurge for “self-fulfillment” without tether to Judeo-Christian morality or even the cardinal virtues discerned by ancient writers such as Plato, Aristotle, Cicero, Augustine, or Aquinas. In truth, these sources of the Western tradition are denigrated by the bien pensant, the current elites, the Brahmins presiding over our universities, the media, and much of corporate America today.
As the Catholic writer and social critic Mary Eberstadt opined:
“Politics did not create these problems. The sexual revolution did. That’s why politics will not solve them, either.”
Goeglein and Osten proceed to outline the origin and extent of the rot in American culture in several tight, well-developed chapters treating culture, family, the judiciary, religious liberty, education, medical ethics, and a variety of moral virtues required of a free and democratic people.
Their philosophy is grounded in the Christian idea that men and women are made in the image of God — imago Dei. This informs their view of the need for civility and the recovery of the concept of the gentleman regarding whom John Henry Newman said, “It is almost a definition of a gentleman to say he is one who never inflicts pain.” Unfortunately, the authors do not discuss the concept of a lady, probably too fraught a topic in this day and age for males to address.
Nevertheless, their hero is another great gentleman, George Washington, who, in his first inaugural address, stated that “religion and morality” are the “finest props of the duties of men and citizens,” adding that they are the pillars supporting “the dispositions and habits which lead to political prosperity.”
“Reason and experience both forbid us to expect the national morality can prevail in exclusion of religious principle,” the first president proclaimed.
While realistic regarding the forces arrayed against a moral restoration in America, they do not subscribe to the more extreme forms of the “Benedict Option,” which seem to counsel a complete withdrawal from the public square into an exclusively private zone disengaged from politics, culture, and social matters not exclusively en famille, so to speak. The authors do concur with the proponents of this idea that one must deepen oneself spiritually and morally in faith and humility. But that should not lead one to flee the slings and arrows of a hostile culture. Engagement grounded in a religious worldview is the correct posture.
Goeglein and Osten write, “We must not despair.”
Citing the work of David Brooks and James and Deborah Fallows on the vibrancy of positive, local restorative action in communities across America, these authors state boldly that “we must continue to be faithful. The key to America’s restoration is to be found in remaining engaged in our neighborhoods, in our communities, and in our nation — doing so faithfully and knowing God is in control.” They urge Americans to take up the charge offered by the great English philosopher and statesman Edmund Burke:
To be attached to the subdivision, to love the little platoon we belong to in society, is the first principle (the germ as it were) of public affections.
These writers are nothing if not hopeful — sometimes maddeningly so. But hope is a theological virtue grounded not in reason but in faith. They urge us to live that virtue and become “salt and light” in a country well worth the effort.
G. Tracy Mehan III is an adjunct professor at Antonin Scalia Law School, George Mason University. This article was first published in The American Spectator and is republished here with permission.
“In its most profound reality, love is essentially a gift; and conjugal love, while leading the spouses to the reciprocal “knowledge” which makes them “one flesh,” does not end with the couple, because it makes them capable of the greatest possible gift, the gift by which they become cooperators with God for giving life to a new human person. Thus the couple, while giving themselves to one another, give not just themselves but also the reality of children, who are a living reflection of their love, a permanent sign of conjugal unity and a living and inseparable synthesis of their being a father and a mother.”
— Pope St. John Paul II (Familiaris Consortio, 14)
The English writer G.K. Chesterton loved pointing out that we are surrounded by seemingly “ordinary” things that are in fact so suffused with beauty and mystery, that we ought by all rights to be walking about in a perpetual state of stunned wonder. As he famously put it: “There is a law written in the darkest of the Books of Life, and it is this: If you look at a thing nine hundred and ninety-nine times, you are perfectly safe; if you look at it the thousandth time, you are in frightful danger of seeing it for the first time.” What he meant is, that thousandth time, you might slough off your old pereptual habits that took the thing for granted and see the thing for what it is: a pure, mysterious gift.
G. K. Chesterton, aged 31
One of the ordinary things that Chesterton sought to show us in a new light was the family. A quote often attributed to him goes like this: “The most extraordinary thing in the world is an ordinary man and an ordinary woman and their ordinary children.” Now, I can’t seem to find a source for this quote. But the sentiment is unquestionably Chestertonian in nature. The fact of a man and a woman falling in love, their desire to unite their lives together with an unbreakable vow, and the children that – God willing – naturally follow: on the one hand these are utterly straightforward things, and on the other, filled with an unspeakable beauty and mystery. These ordinary things are really the most extraordinary things.
However, as Most Reverend José Gomez, archbishop of the diocese of Los Angeles, recently pointed out in a profoundly challenging speech hosted by the University of Notre Dame McGrath Institute for Church Life, marriage and children seem to be becoming “extraordinary” in a totally new way. That is to say, for the first time in the history of our civilization, it seems that a vast, and growing number of people, are consciously rejecting these things, refusing marriage, and consciously avoiding having any children at all.
Most Reverend José H. Gomez
Archbishop of Los Angeles, photo courtesy of the Archdiocese
For thousands of years, just about everyone intuitively understood that it was a good thing to commit one’s life to another in marriage, and then to bring children into the world. But for unusual cases, such as those entering the priesthood, or monasteries and convents, this is what the overwhelming majority of people would aspire to, and expect to do. Now, however, for a variety of reasons, “many young people are debating whether it is ‘ethical’ to have kids,” the archbishop noted. “There is an even larger conversation going on among millennials about the ‘value’ of starting a family.”
The ostensible rationale given for much of the anti-natalist attitude is concern for the natural environment – the fear that more children simply means more resource-hogging humans damaging the earth. We saw this attitude expressed memorably earlier this year by Democrat congresswoman, Alexandria Ocasio-Cortez. In a Q&A session live-streamed on Instagram to her 2.5 million followers in February, Ocasio-Cortez mused about environmental questions: “It is basically a scientific consensus that the lives of our children are going to be very difficult, and it does lead young people to have a legitimate question: is it OK to still have children?”
In his speech, Archbishop Gomez didn’t discount the need for serious concern for the environment; however, he suggested that this growing ambivalent – and even hostile – attitude towards children “tells us far more about the state of the family today” than many of the other problems that we usually associate with the crisis in marriage and the family: “contraception and abortion; divorce rates, out-of-wedlock births, people living together rather than getting married…the growth of same-sex unions and the confusion about sex that we see in our society.”
In rejecting marriage and children outright, he said, “Our society has rejected what 20 centuries of Christian civilization considered a basic fact of nature.” He stated: “Now marriage, family, and children have all become an open question, a ‘choice’ that individuals must decide for themselves.”
Recovering the Radical Christian Message
In response to this peculiarly sinister modern crisis, Archbishop Gomez firstly urged the need “to rediscover the radical ‘newness’ of the Christian message about the family.” We have heard the basic Christian teaching about marriage so often that we have lost sight of how radical, and how radically beautiful it is, both in itself, and in the context of historical attitudes towards marriage.
“When St. Paul said: ‘Husbands, love your wives, as Christ loved the Church and gave himself up for her’ — he was announcing a revolution in human thought and human society,” the archbishop said. “Before Christianity, no one had ever spoken about marriage in terms of a love that lasts a lifetime, or as a calling from God, or as a path that can lead to holiness and salvation.”
“It was a new and thrilling idea to speak of man and woman becoming ‘one flesh’ and participating in God’s own act of creating new life.” Indeed, it was through the profundity of their love for one another, and the way they lived that love in concrete ways, that the first Christians spread the Gospel. Not only did they approach marriage as a “life-long relationship of friendship and mutual devotion,” but they rejected the anti-life practices of their pagan neighbors: “They rejected birth control and abortion and welcomed children in joy as a gift from God and treated them as precious persons to be loved and nurtured and brought up in the ways of the Lord.”
The Marriage at Cana – 14th century fresco at the Visoki Decani Monastery
Archbishop Gomez went on to quote the early Church Father Tertullian. The quotation is so beautiful, that I feel compelled to include it here in full:
How beautiful … the marriage of two Christians, sharing one hope, one desire, one way of life. They are truly two in one flesh; and where the flesh is one, the spirit is one, also. They pray together, worship together, fast together; instructing one another, encouraging one another, strengthening one another. Side by side they visit God’s church and partake of God’s Banquet; side by side they face difficulties and persecution, share their consolations. They have no secrets from one another… they never bring sorrow to each other’s hearts. They visit the sick and assist the needy. … Hearing and seeing this, Christ rejoices.
I can’t help but think how different society would be if all Christian couples lived up to this beautiful vision!
Life is a Gift
However, continued Archbishop Gomez, not only must we recover the radicalness of the Christian message about marriage, but “we need to recover the Christian narrative, the Christian vision for life and human happiness.” This section of the archbishop’s speech is so theologically profound, and beautiful, that I urge you to read the whole thing if you can.
The archbishop lamented that many Christians are taking their cue about the meaning of life from our technologically obsessed and consumeristic society, rather than Christ and the Scriptures. The Scriptures reveal to us the great mystery that even God Himself is a family – a Trinity of persons united in love. “We need to tell this good news to our neighbors — that this God of love, who created the galaxies and oceans and mountains in the beginning, is still at work today, still creating,” said the archbishop. “And God intends his plan for creation, for history, to unfold through the human family.”
Jesus Christ, God Incarnate, entered into history in the womb of His mother, and raised within the beauty and hiddenness of the family. It is this great mystery that reveals to us how we humans are called to participate in God’s loving act of creation. “We are called to help every married couple realize this vocation — to live their love forever in a mutual and complete gift of self; to renew the face of the earth with children, who are the fruits of their love and the precious love of our Creator.”
Within this rich Christian view, children can never be viewed merely as “takers” and parasites, to be viewed with suspicion, and prevented through invasive, immoral means. On the contrary, “Every child who is born is also a sign of God’s love — a mystery, a gift, a miracle. In every child, even those in the womb, we glimpse the mystery of the Christ Child, in whom we come to know God.”
The archbishop warned that a society that does not welcome children is a society that has forgotten the meaning of life and has abandoned hope. “It is not about just giving birth to children. It is about hope,” he said. “It is about living with confidence in God’s Providence, knowing that he loves us and will never abandon us — no matter what this world may bring.”
The archbishop concluded this remarkable speech with this moving expression of his hope for those listening. “If you are married,” he said, “love your spouse with a great affection and raise your children well. Work for them, sacrifice for them; teach them to talk to God and listen for his calling in their lives. We cannot be afraid to call our young people to greatness, to be saints.”
“Life is not ours to sanction or command. Life is a beautiful gift — the child received by a husband and wife is as beautiful and precious as anything we find in nature.”
“By the love in our homes — by the sacrifices we make and the love that we hold in our hearts and pass on to our children — we are called to testify to this God who is our Creator and Father. This God, who holds all of this world — and every one of us — in his loving hands.”
I have nothing more to add to this beautiful and inspiring message. God bless Archbishop Gomez for his courage and fatherly concern in calling his flock (indeed all of us) to holiness in this way.
For the pro-life community, prenatal screening can be a source of contention, but for parents faced with the diagnosis of their preborn child, prenatal screening can be the technological gift that allows them to properly and effectively care for their child. The problem is, prenatal screening has been hijacked by the abortion industry.
Though the more routine use of tests such as ultrasounds and amniocentesis didn’t begin in the United States until the 1970s, the development of these tools was already in the works two decades prior. Well before Roe v. Wade legalized abortion through all nine months of pregnancy in 1973, researchers were developing ways to learn more about not only the development of the preborn child but also whether or not a child would be born with any health conditions. The controversy is, of course, what happens with the information that is gathered from prenatal testing. In a pro-life society, that information would simply be used to give the mother and child the best possible care for the best possible outcome at birth and throughout the child’s life. But in a pro-abortion society, that information is used to instead discriminate against the child in the womb and kill that child through an act of eugenics.
When used appropriately and ethically, prenatal testing is a pro-life tool.
For example, prior to prenatal testing, a woman who was carrying a child with anencephaly – a condition in which the child’s skull doesn’t properly form and he isn’t likely to survive more than a few hours after birth – would have absolutely no idea that the precious child she was so thrilled to give birth to was dying. There was no way to prepare her or the child’s father or grandparents or siblings for this tremendous loss. Now, however, parents can learn this information ahead of time, allowing them time to grieve and prepare so that when they meet their child at birth they are able to focus on him, not his diagnosis, and even have family photos taken. They can spend their time loving him instead of having him whisked away for tests. They will have had time to get a plan in place for the baby’s funeral or for family members to have traveled from long distances to arrive in time to meet him.
Likewise, for the parents of a child with Trisomy 21, better known as Down syndrome, receiving the diagnosis ahead of time allows them to not only emotionally prepare, but it helps them to plan for their child’s needs. Knowing that their child may need extra care because of a heart condition or anticipated developmental delays would give parents the opportunity to meet with specialists prior to the child’s birth in order to give the child the best care possible. Knowing of a diagnosis such as Down syndrome ahead of time may also alter the family’s financial plan so they are better prepared for the future.
Similar arguments could be made for prenatal testing that allows treatment plans to be set in place for conditions such as cystic fibrosis and spina bifida. About 10 percent of children with cystic fibrosis will need bowel surgery immediately after birth, making it important to keep an eye on their bowels via ultrasound. Early animal testing has even shown that treating CF while the child is still in the womb can treat male infertility, which affects 98 percent of men with CF. As for spina bifida, fetal surgeons are now performing surgery on babies while they are still in the womb with amazing success rates, including the increased likelihood of independently walking. The results of prenatal surgery for spina bifida are proving to be better than surgery after birth.
Photo: EBU Photography
Parents who learn their child has Trisomy 18 (Edward’s syndrome) prior to the child’s birth will likely be told that their baby is “incompatible with life” and told to abort. But the truth is that these children aren’t necessarily going to die at birth as in decades past. New information and the right doctors are helping children with the condition to live longer and healthier. One man with the condition just celebrated his 18th birthday.
While some conditions will need an amniocentesis in order to confirm a diagnosis, many parents may not wish to go through with this test because it carries a small risk of miscarriage. That is completely understandable. But going through with any prenatal testing, especially non-invasive testing that doesn’t carry a risk of harming the baby, in no way should lead to the assumption that those parents don’t love their child. In the pro-life community, many parents will say that they skipped all testing because it didn’t matter to them if their child had certain health conditions or not. And it is their right to do so. But if a parent is determined to choose life no matter what, and if a blood test or ultrasound could help a child live better and even survive, then taking that test is not unloving. It is preparing.
Betsy Leaf insisted that she was keeping her little boy, Jacen, even after he was diagnosed with anencephaly and she was offered abortion.
Prenatal testing can help certain children live longer and healthier lives, so why do the doctors who diagnose them push abortion on the grieving and scared parents? One very sinister reason is that they are actually trying to eliminate people who may cost more money to care for, especially if the child is going to be using government healthcare programs. Or they may want to eliminate people with disabilities because they think that these lives aren’t worth living. It’s discrimination. It’s eugenics. And it must stop.
Another reason doctors may push invasive testing and abortion is that they fear facing lawsuits. And that fear isn’t unfounded. There have been numerous cases of parents suing doctors for the “wrongful births” of their children because they went undiagnosed during pregnancy and the parents didn’t have the chance to kill them before birth. Doctors could lose their entire livelihood over it.
The reality is that prenatal testing is a game changer, but it makes a big difference which team parents and doctors are playing for. When we approach a prenatal diagnosis with a pro-life vision, amazing things happen. When we approach a prenatal diagnosis with a pro-abortion vision, death happens.
Earlier this month a heartbreaking story about an IVF “mix up” was reported. It seems the fertility clinic responsible for handling embryos during the IVF process accidentally implanted the wrong embryos into a woman. Instead of giving birth to twin daughters, the woman gave birth to two boys who were not genetically hers. Not only did this woman have to relinquish the children she just gave birth to, but the clinic has yet to locate her unborn daughters.[i] These cases may not be the norm but they’re not unheard of either, and as more infertile couples turn to IVF and more profit is to be made by the fertility industry,[ii] the frequency of these tragedies will increase.
Most people are rightly horrified by this story. Unfortunately, the conversations elicited by this story rarely extend to the broader debate surrounding artificial reproductive technologies (ART). In vitro fertilization (IVF) is a type of ART, which involves,
[C]ombining extracted eggs and sperm in a lab. The process involves producing multiple embryos and transferring them. . . into the woman’s womb, in hopes one would implant and cause a pregnancy. Today, many embryos are usually frozen, as couples opt to transfer the most viable one at a time to avoid multiple births. Unused embryos may be stored indefinitely, donated to science or destroyed….[iii]
Surrogacy also requires the creation of embryos through IVF, but in the case of surrogacy a third party is hired to carry the child created through IVF for another intended “mother”; with just IVF, the woman who gives birth to the child created though IVF is also the intended mother (unless the wrong babies were put inside of her, of course).
Sadly, not only are people not morally outraged by IVF, but they see it as a social good – the ends justifies the means. Some even think IVF as something they are owed by the US taxpayer.
Of course, infertility is a heavy cross to carry, and infertility caused by a combat injury even more so. No one is disputing the untold sacrifices that disabled veterans have made for this country, but even a disabled veteran is not above the moral law.
In 2016, with some qualifications, Congress authorized benefits for disabled veterans that covered IVF treatments, a benefit already available to active duty. Currently, the benefits for the disabled veterans must be reauthorized every year. It is the annual re-authorization of this program which, creates thousands of disposable embryos, that is in contention.[iv]
Putting aside the emotional aspect of disabled veterans, the arguments used to justify entitlement to this benefit are just as morally hollow as any other defense of IVF. According to one military wife, who’s already had three failed IVF attempts, and is now on her fourth try using donor embryos, “IVF gives . . . couples trying to conceive the ability to bond with their babies as soon as physically possible, unlike alternatives such as adoption and surrogacy. . . . By using donor embryos, you have all those memories, you have all those firsts. . . .You’re not having to make yet more sacrifices, more compromises.”[v]
It is absolutely frightening that the argument presented here isn’t even about a “right” to a child or “right” to be a parent. Rather, IVF and the destruction of offspring is justified based on a preferred way of bonding, making memories, and not comprising; all paid for by the taxpayer.
Proponents of IVF rarely, if ever, discuss the ethical and moral dilemmas associated with the child that they desire. “[C]ouples usually freeze many embryos, test for health problems and transfer the most viable one at a time to avoid multiple births. That often means leftovers once the desired family is complete.” One study estimates that 1.4 million embryos are currently in frozen storage.[vi]
One reason so many embryos are left in storage is due to the hesitancy of couples who suffered from infertility, who went through so much to create a family, now must destroy their leftover offspring. Offspring who, if given the chance, could have been additions to the family they fought so hard to create.[vii]
It is evident that the issue of IVF is rife with moral questions and concerns: creation of embryos in the first place, the exploitation of vulnerable infertile couples at the hands of the fertility industry instead of focusing research on medical treatments that actually treat infertility, putting embryos in the wrong woman, the psychological trauma inflicted on couples, and of course the pressing issue of the destruction on leftover embryos.
I say “pressing issue” because these embryos are being created and destroyed right now. These embryos are being denied their humanity, treated like nothing more than a commodity. This is not some abstract debate; this is the very real situation we are faced with in this moment. If we believe life begins at conception, we need to start acting like it. IVF is a pro-life issue. No one else is going to defend the humanity of these children. Pushing policies that recognize the humanity of and protect frozen embryos should be just as important as pushing policies that protect children in the womb.
Until the pro-life movement addresses the moral dilemmas inherent with IVF, we will continue to live in a country where children are “misplaced” or put into the wrong mother; where the destruction of embryos is completely justified so long as people get what they want. It’s time for pro-lifers to step up.
LifeNews Note: Ana Brennan, J.D., is the Vice President of the Society of St. Sebastian. She also serves as the Senior Editor for the Society’s publication, Bioethics in Law & Culture. Ms. Brennan began her pro-life activism in college, continued through law school, and ultimately worked at the national level in Washington, D.C. As a State Legislative Associate for the National Right to Life Committee, working closely with grassroots lobbyists, state attorney generals, and governors she helped state affiliates pass pro-life legislation.
Lauren Webster, a Scottish woman, has gone public about being repeatedly pressured to undergo an abortion after being told her preborn baby had a fatal birth defect. In an interview with the Scotsman, Webster said that after refusing an abortion, her son was born healthy.
Webster, 21, had previously suffered two miscarriages, but was hopeful about her latest pregnancy. “When I found out I was pregnant, I was very scared because of what had happened before,” she told the Scotsman. “But I just had a gut feeling that this was my time.” But then, at 13 weeks, she had an ultrasound at the Princess Royal Maternity Hospital in Glasgow and was told there was a problem with her baby.
“I was scared when I found out I was pregnant with Ollie,” she said. “I just thought, this is going to happen again. Because I had had two miscarriages previously, I got two early scans but there was a heartbeat so they weren’t concerned. But when I went for my 13-week scan, the doctor told me he had a bladder obstruction. She asked me if I wanted to terminate, saying there was a low chance he would survive.”
After Webster refused to have an abortion, she was told to come in for weekly ultrasounds to monitor the baby — but her wish to save her baby’s life wasn’t honored. “Every week she was asking me if I wanted to terminate,” Webster recalled. “She said she had to ask me. It was around Christmas time and I was feeling very down. I said to her ‘don’t ask me that again because I’m keeping it.’ By 18 weeks she had noticed that the bladder had repaired itself.”
But her problems were far from over — doctors then told Webster that her baby might have Edwards syndrome, and the pressure to have an abortion resumed again. Doctors told her that her baby wouldn’t survive past the age of four, but then doctors found out that he didn’t actually have the condition.
“After that, the doctor was shocked about how perfect he turned out in the scans,” Webster said. “I went into labour early and had to get an emergency caesarean because his heart rate was going up and down. Ollie was in the special care unit for a week but he came out absolutely fine. He was a good weight, he was 5lb 14oz. He’s a big boy. He’s got a condition called talipes which means his feet are a bit turned and he had to undergo a minor hernia op but apart from that is healthy. He sleeps good and is feeding well, he’s great. If someone else was to go through that experience, I wouldn’t want them to terminate because you don’t know what’s going to happen.”
This kind of pressure to have an abortion isn’t unusual at all; many parents report being pushedtowardendingthe livesof theirpreborn babies. Some parents, like Webster, have found that there ended up being no medical problems with their children, but others steadfastly chose life regardless of a diagnosis, knowing that the value of someone’s life is not dependent on the lack of a disability, or on how long they will live. As for Webster, she had a simple reason for telling her story in the end, saying, “I just think everyone should read my story and never give up hope.”
Nexplanon, an artificial birth control arm implant, launched a recent ad campaign using the slogan “Armor Up.” It shows pictures of attractive young women with battle ready faces, flexing one bicep while pointing to the implant. The ad reads: “Pregnancy protection for up to 3 years. Over 99% effective. Your life. Your way.” This ad campaign merely takes the common phrasing of birth control as “protection” to its logical extreme. Against whom are women to “armor up?” Well, babies, it would seem. According to Nexplanon, a baby would be an invader, an enemy even.
This marketing technique promotes and plays into women’s fears that children mean the end of life. It perpetuates the idea that becoming pregnant is something to fear, unless it is meticulously planned. But protection, of course, comes at a cost. The risks and side effects include the possibility of blood clots, stroke, and death. More common, the website reports that 10 percent of women stopped using Nexplanon because it caused “an unfavorable change in their bleeding pattern.” The implant is only one of many varieties of hormonal birth control medications that pose similar risks.
There is an irony in the contraceptive mentality, as it purports to give women ultimate control over their bodies and reproduction. In reality though, women become dependent on pharmaceutical drugs that can cause a range of side effects, some of which are a nuisance, to those that threaten lives. In the end, the sense of “control” is an illusion. A pharmaceutical company recently recalled packets of birth control pills because of a packaging error that placed placebos where active pills should have been. This is not a lone incident. In 2015, 100 women filed a lawsuit against multiple pharmaceutical companies they held responsible for their pregnancies after another placebo pill mix up.
It is not uncommon to find women who become pregnant while using
contraceptives. Yet the prevailing message is that if you “protect yourself,” you have nothing to fear. “99% effective,” proclaims the Nexplanon ad. That means some women will become pregnant while using the implant. How shocked will they be? Will they embrace this baby they were protecting themselves against, or seek an abortion?
Despite the messaging, artificial contraception takes control away from women in at least two ways. First, most forms suppress a woman’s natural hormones and cycle which give her important information about her reproductive and overall health. Second, they make women dependent on the pharmaceutical companies that make them, and government programs or insurance companies to pay for them.
Fortunately, there is a better way to avoid pregnancy when it’s not the right time for a baby. The dramatic language of the Nexplanon marketing campaign highlights the stark differences between Natural Family Planning (NFP) and artificial birth control. Birth control promotes the idea that babies are something to fear. They will derail your life so you don’t want to take any chances. “Armor up,” suppress your natural hormones, and accept side effects as the cost of this security. NFP recognizes that there are times when conceiving would not be wise. But instead of telling women that their bodies’ natural cycles are a threat and something to thwart, NFP gives women more information about what is going on with their bodies to allow for informed choices each cycle. NFP offers women an arsenal of information about fertility, hormonal health, and more. It educates women about their own bodies, which makes women stronger, independent, and more empowered than an implant or pill ever could.
The miraculous recovery of a stillborn baby, whose parents turned to Venerable Archbishop Fulton Sheen for help, has been officially approved by Pope Francis, thus paving the way for the beatification of the popular televangelist.
According to the National Catholic Register, the Vatican approved the miracle on May 14 and authorized the Congregation for the Causes of Saints to promulgate a decree regarding this decision. Plans can now get underway to set a date for the Archbishop’s beatification.
The popular television star and host of Life is Worth Living, a show that ran from 1951 to 1957, was declared Venerable in 2012 by Pope Benedict XVI after being recognized for his heroic virtue.
However, the cause was suspended by Bishop Daniel Jenky of Peoria in 2014 on the grounds that the Holy See expected the Archbishop’s remains to be in the Peoria diocese rather than in the archdiocese of New York.
Apparently, Archbishop Sheen indicated that he wished to be buried in New York, but his niece and closest living relative, Joan Sheen Cunningham, later said that he would have wanted to be interred in his home diocese of Peoria, Illinois if he knew he was going to be considered for sainthood.
A years-long legal struggle ensued between the family and the Archdiocese of New York that ended in May of 2019 when the New York Court of Appeals dismissed the archdiocese’s appeal and granted the family’s wishes of having the Archbishop’s remains transferred from St. Patrick’s Cathedral in New York City to Peoria. Once this was accomplished, the cause was permitted to continue.
During this time, a miracle was already under consideration. It occurred on September 16, 2010, when Bonnie Engstrom gave birth to a stillborn baby boy. During delivery, the baby’s umbilical cord became knotted and cut him off from essential oxygen and nutrients, resulting in his death.
The child’s parents, who live in the Peoria-area town of Goodfield, watched their little boy receive CPR and immediately turned to Archbishop Sheen for his intercession. Even though the baby showed no signs of life while the doctors worked on him, and was without vital signs for 61 minutes, the child miraculously returned to life.
“Moments before the doctor was going to declare the infant to be dead, suddenly and without any medical explanation, the infant’s heart began to beat normally and the baby breathed normally,” Peoria Bishop Daniel Jenky said in a statement. “After a few weeks in the hospital, the infant was sent home and has now grown into a healthy young child.”
Eventually, seven medical experts agreed that the sudden recovery of the child, named James Fulton Engstrom, was miraculous.
A date for the beatification of Archbishop Sheen has not yet been set.
Five states in 2019 have passed pro-life measures requiring abortionists to inform women using the abortion pill about the possibility of abortion pill reversal. But the simple act of providing potentially life-saving information to women has been viciously opposed by pro-abortion activists — for instance, in North Dakota, where the pro-abortion American Medical Association (AMA) joined with the Center for Reproductive Rights to launch a legal challenge against the new mandate in court.
To justify their opposition, abortion activists are engaging in fear-mongering and the spreading of misinformation about abortion pill reversal. A recent article published in the Huffington Post is a good case study in these types of deceptive scare tactics, which abortion activists are using with greater frequency.
False Claim #1: Abortion pill reversal is junk science
The HuffPost article cites attorney Molly Duane with the pro-abortion Center for Reproductive Rights, who claims, “The notion of ‘abortion reversal’ is based on junk science.” But as the American Association of Pro-Life Obstetricians and Gynecologists (AAPLOG) explains in a 2019 position statement that “using progesterone to counteract the effect of mifepristone is the logical extension of simple principles of toxicology and poison control.” AAPLOG adds, “There is a very long and solid history of safety of the use of natural progesterone in pregnancy.” A 2018 study observed 754 women who attempted the Abortion Pill Reversal procedure and concluded that “reversal of the effects of mifepristone using progesterone is safe and effective.” In addition, AAPLOG executive director Donna Harrison recently told Live Action News that there are “multiple studies” — not just the 2018 Delgado study — which suggest the legitimacy of abortion pill reversal, including Davenport 2017, Yamabe 1989, and Baulieu 1989.
Many abortion activists with ulterior motives are pinning their hopes on a new study that, as Live Action News’s Carole Novielli has shown, should be viewed with great suspicion. It is being funded by organizations with deep ties to the abortion industry, including investments in abortion pill manufacturer DANCO. The study clearly lacks independence, as its backers all stand to gain financially from an outcome that would support the unfettered and widespread adoption of the abortion pill and the discrediting of abortion reversal. The study itself, which is being conducted by California abortionist Mitchell Creinin, involves a disturbing methodology that will involve the death of 40 preborn babies. Watch the video below to see how the abortion pill actually works:
False Claim #2: Abortion pill reversal is not effective anyway
According to the HuffPost article, abortion reversal is an “experimental practice” that is based on “false and nonscientific information.” Actual research and experience, however, paint a different picture. As AAPLOG points out, “By giving a woman progesterone, the Mifeprex abortion can be stopped and the chances of the baby surviving increase from 25% (the survival rate without natural progesterone) to 68% (the average survival rate after giving natural progesterone).” While the efficacy of progesterone supplementation can depend on the method of progesterone delivery and how far along the pregnancy is, abortion pill reversal has been demonstrably effective at increasing the likelihood of survival. A growing number of physicians, like Dr. Robert Snyder and Dr. George Delgado, are advocating and using abortion pill reversal with great success. And countless stories from real-life women seeking abortion reversal continue to testify to the efficacy of the treatment.
False Claim #3: Abortion pill reversal is dangerous to women
The HuffPost article cites abortionist and pro-abortion researcher at UC Davis, Dr. Daniel Grossman (who is involved with Planned Parenthood). He claims that “there is no evidence” that abortion reversal is safe for women, and that “patients deserve to know if there are any safety risks.” This is another scare tactic. The reality of abortion reversal involves nothing more than administering high doses of progesterone — a natural hormone treatment — to women to counteract the effects of mifepristone, a progesterone blocker. And decades of medical practice have shown overwhelmingly that progesterone is safe for women. As the 2018 Delgadostudy explains in a section titled “Progesterone Safety,” progesterone “has been used safely in pregnancy for over 50 years.”
As a result, according to the study, “The American Society of Reproductive Medicine states that no long-term risks have been identified when progesterone is used in pregnancy. The FDA has given progesterone a category B rating in pregnancy, in contrast to synthetic progestins.” In fact, progesterone can be used safely and effectively more or less continuously for some women, such as peri- and post-menopausal women. And while there has been some question about whether progesterone support in early pregnancy is effective at preventing miscarriages, there is no evidence that it is unsafe for women.
False Claim #4: Abortion pill reversal could cause birth defects
The HuffPost article cites abortionist Kathryn Eggleston, who raises questions about the drug’s safety as it relates to preborn children (yes, you read that correctly). “Scientists thus do not know what impact, including potential birth defects, the administration of these drugs could have on the children,” said Eggleston. Aside from the dark irony of an abortionist feigning concern about preborn babies’ health, this again is fear-mongering without evidence. The 2018 Delgado study found that, among 257 women who had successful reversals, the percentage of children born with birth defects — at just under 3% — was the same as the general population.
The Society for Assisted Reproductive Technology (SART) agrees, saying “there is no convincing evidence that progesterone causes birth defects. This seems to make sense, since progesterone is a natural hormone and is identical in structure to the progesterone which is produced during the menstrual cycle and during pregnancy,” adding that “long-term adverse consequences of progesterone therapy have not been identified in humans and appear unlikely.”
Although abortion activists seem desperate to discredit abortion reversal, their claims cannot withstand objective analysis. Still, these false claims will be repeated widely, since the notion of abortion reversal strikes at the heart of abortion advocates’ core narrative: that abortion is a positive good to be celebrated, and therefore women can’t and don’t regret it. Meanwhile, abortion pill reversal will hopefully continue to be a blessing for vulnerable women and their children.
The rat is a valuable animal model of human disease. Humans and rats share many common genetic features and by examining the physiology, neurology, neurophysiology and the resulting behaviours such as the response to stress, of a rat, scientists can gain valuable insights into how humans function. The rat is one of the primary models for studies of human reproduction.
Which is why the findings of a new peer reviewed study on the effects of a drug induced medical abortion on rats is so fascinating. And since 71% of women having an abortion in England and Wales have a medical rather than surgical abortion (over 140,000 women per year), research on the effects is needed.
In a medical abortion, two drugs are administered, mifepristone then misoprostol, up to 48 hours apart. The effects of medical abortions are debated, especially the mental health consequences, but some of the known physical complications are detailed in this briefing.
In the rat experiment the same drug protocols were followed as with humans, but with the major advantage in that rats, unlike humans, can be randomly assigned to different groups. So out of 81 rats there was a control (non-pregnant) group, a pregnant group and a group that was administered mifepristone and misoprostol at the equivalent of 28–40 days gestation for humans.
The researchers measured rat body weight, food intake, vaginal impedance, sucrose consumption and home-cage activity.
The results were striking.
The rats with a full-term pregnancy increased their weight throughout as expected. The rats that experienced a natural miscarriage stopped increasing weight but did not lose weight, their weight stabilised. But the rats given the medical abortion lost significant weight. They simply stopped eating as much and their sucrose consumption dropped dramatically. The ‘miscarriage rats’ and pregnant rats ate normally throughout. Weight is a useful indication of health, well-being and stress in rats and a drop in sucrose consumption and weight suggests depression-like behaviour. In this research, the ‘abortion rats’ demonstrated moderate to severe stress.
Activity levels also measure depression-like behaviour. This showed that the average distance, speed and time moved per week was far less for the ‘abortion rats’, even compared to the ‘miscarriage rats’, which moved as much as the full pregnancy ones. When measuring ‘rearings’ (standing on hind legs – an indication of normal interest in their environment), the medical abortion group displayed a significant decrease relative to all the other groups.
The time spent in cage corners was also measured and showed that the ‘abortion rats’ separated themselves from the others and spent far more time than the other rats in the far back corner of the cage, indicating increased anxiety.
Additionally the ‘abortion rats’ did not show healthy rat behaviour. They did not groom themselves , they had unkempt coats, their posture was more hunched, and they showed a reduction in exploratory behaviour (sniffing and rearing).
The researchers concluded that the rats who had had a medically induced abortion showed moderate to severe stress, as indicated by their physiological effects measured. The observed effects of stress were specific to the induced abortion not the loss of a pregnancy through miscarriage.
The authors also note that the effects of the drug induced termination were not short-term. The effects on food intake lasted for seven days which is the equivalent of 244 human days. The biochemical observations were still visible at the end of the experiment which equates to around six and a half human years.
‘Our findings strongly suggestthat pregnancy termination at mid-term (first-trimester human equivalent) induces significant negative biological and behavioural changes in the rat. Additionally, such a procedure appears to be associated with a potential absence of beneficial effects of carrying a pregnancy to full-term. Moreover, our findings also appear to indicate a significant difference between induced pregnancy termination (medical abortion) and natural miscarriage.’
The researchers say that this is the first research that investigates the biological and behavioural effects of drug-induced abortion in an animal model. It seems that the focus of other research has been primarily directed at the success (effectiveness and speed) of terminating a pregnancy. Which leaves me questioning what rigorous pre-clinical therapeutic investigation has taken place with the administration of these powerful drugs on women.
Obviously, as this research was done on rats and not women, the results cannot be directly extrapolated across. But as I state at the outset, knowledge from rat models has benefitted many disorders and contributed significantly to the progress of medicine, so it cannot be easily dismissed. It was also a controlled, objective and ethical assessment – no one can argue that rats suffered these consequences because they were reflecting on what they had done, or were being made to feel guilty by society for having an abortion.
These findings at the very least emphasise the need for further objective research into the physical and behavioural effects of drug induced abortion. Particularly since 86.1% of abortions in Scotland and 71% of abortions in England and Wales are performed using these drugs – over 150,000 women per year. I wonder how many of these women have any idea of the potential physical and emotional consequences to their long-term health?
Philippa Taylor is Head of Public Policy at Christian Medical Fellowship. She has an MA in Bioethics from St Mary’s University College and a background in policy work on bioethics and family issues. Republished with permission from the CMF blog.
You may already know that a Citizen’s Petition was recently filed to the FDA (Food and Drug Administration) requesting more transparency and patient warnings regarding potential side effects for different forms of hormonal contraceptives. We have been talking about it for a few weeks now, and, as Natural Womanhood CEO Gerard Migeon invited readers weeks ago, we encourage anyone who has suffered from birth control side effects to share their story by making a comment on the petition, to which dozens of people have already commented.
But what exactly does this petition contain? At almost 100 pages, this hefty document can appear a little intimidating at first glance. So we’re happy to break down the content into a digestible FAQ format.
What is the goal of the petition?
In brief, the Citizen’s Petition aims to make all healthcare providers and consumers of hormonal contraceptives aware of their possible, proven side effects. To do so, it is urging the FDA to add black box warnings to certain prescribing information, as well as other safety information, and to remove one of the worst culprits from the market completely.
A black box warning is a label on a prescription medication that warns both providers and consumers about serious safety concerns of that drug, usually adverse (and potentially life-threatening) side effects. The FDA can decide to require the manufacturer to add a black box warning to a medication’s packaging at any time after that drug is approved to be on the market.
What exactly would these potential changes be?
If accepted, this petition would, first of all, remove one drug from the market altogether—the injectable contraceptive Depo Provera, known medically as Depot Medroxyprogesterone Acetate (DMPA). Evidence definitively shows that it is responsible for increased transmission of HIV from men to women (a side effect that is currently not even reported in online sources of contraceptive information, like Planned Parenthood). As the FDA petition documents:
“four meta-analyses (3 reports) were published in 2015. Each used different inclusion criteria and compiled the data on different numbers of studies, yet all 4 came up with essentially the same result of significantly increased risk of male-to-female HIV transmission in women using DMPA. . . . Importantly, no consistent association has emerged with regard to oral contraceptives or other injectable or implantable contraceptives and the facilitation of HIV transmission.”
Besides the request that Depo Provera be removed from the market, the majority of this petition’s impact would be to affect the advertising of many contraceptives, which would then affect those being advertised to—that is, everyday consumers. The petition requests that the FDA add black box warnings concerning the proven, reported, adverse side effects of breast cancer, cervical cancer, inflammatory bowel disease, Systemic Lupus Erythematosus (SLE), depression and suicide, venous thrombosis (blood clots), and cardiovascular events.
Additional safety information that the petition requests should be added to contraceptive labels include: the increased risk of developing Multiple Sclerosis (MS), a higher risk of bone fractures, a significantly increased percentage of fat body mass (which can lead to other serious conditions such as diabetes and cardiovascular problems), and an increased risk of urogenital problems. Potential urogenital problems include a significantly higher risk for the development interstitial cystitis, an increased risk of urinary tract infections, vaginal dryness, Female Sexual Dysfunction (FSD) caused by OC-induced dyspareunia, reduced sexual desire and libido, and other problems. (Visit the FDA document for all cited research).
Currently, these potential risks and side effects are either not added to black box warnings on most hormonal contraceptives, or they are downplayed or misleading at best. Just as it took years for cigarettes to add appropriate health warnings onto their packages, it seems that it is taking an unacceptably long time for the FDA to add sufficient warnings to the packages of hormonal contraceptives.
Even with some current warnings on birth control pill packaging, the implication is that certain risks—like blood clots (which claimed the life of 20-year-old Alexandra Williams)—only occur when combined with cigarette smoking, and increase with “heavy smoking” and an increase in age. This misleads users to think their risk is null if they don’t engage in cigarette smoking and/or are not over 35 years of age. It also suggests it is not the contraceptive that causes the blood clot but the cigarette smoking. If the FDA heeds this petition, it will follow the request that such labels be changed to state: “WARNING: INCREASED RISK OF SERIOUS CARDIOVASCULAR EVENTS INCLUDING BLOOD CLOTS.”
What forms of contraception does the petition cover?
As the Preliminary Statement explains, hormonal contraceptives have been around for 50 years. When most people think about birth control, they think of “the Pill,” but it is not always realized that there have been numerous different formulations of it over the years. Further, other methods of hormonal contraceptives besides oral pills have been increasingly gaining in popularity, such as intravaginal rings, transdermal patches, implants, and the IUS/IUD.
The Citizen’s Petition differentiates between combined estrogen-progestogen contraceptive formulations (COCs) and progestin-only contraceptive formulations (POCs), in listing the many different contraceptive “agents,” or pharmaceutical names of different kinds of hormonal contraceptive. The overwhelming majority of these fall under the “COC” banner as Combined Estrogen-Progestin (EE-P) Pills—from Natazia to Ortho-Novum to Yasmin. There are two types of COC patches and one vaginal ring (the popular Nuvaring). The number of “POC” Progestin-Only Pills is much smaller, although there are several POC injectables, implants (Nexplanon has been on the hot seat this year), and IUS/IUDs (the Mirena IUD has also had its share of unfortunate connections).
What is the research behind this petition?
A lot of work went into the creation of this petition, which was spearheaded by Dr. William V. Williams, Editor in Chief Emeritus of the Linacre Quarterly. An official “Contraceptive Study Group” of medical professional and experts (including Natural Womanhood’s CEO, Gerard Migeon), compiled all of the information and extensive research necessary for the FDA to make their decision regarding the proposed changes.
The petition goes into depth about each adverse side effect for which it requests a black box, citing research from various studies over past decades, as well as a series of comprehensive, well-documented literature studies. In the case of Depo Provera (DMPA), the one contraceptive drug that the petition advises should be immediately removed from the consumer market, the petition provides both epidemiological evidence from various studies and reports, as well as mechanistic and experimental evidence—including in vitro evidence of increased HIV replication at the cellular level. As the petition concludes: “In the United States, where the availability of a wide range of contraceptive drugs and devices is virtually universal, and where, among these contraceptive choices, one and only one particular method—DMPA—is now known to increase the transmission of an often-fatal viral infection (HIV/AIDS), there can be no justification for such a drug’s continued availability in the marketplace.”
Extensive research and statistics are provided concerning the causal relationship of hormonal contraceptives and cancer—both breast and cervical—including tables of case control studies. PubMed literature reviews back up claims of causal links to Crohn’s Disease, Ulcerative Colitis, Multiple Sclerosis, and Systemic Lupus Erythematosus. Various studies of contraceptives and depression, mood disorders, and suicide are provided, as well as studies about every other proven side effect of hormonal agents. (Again, all of this research is cited in the supporting documentation of the FDA petition.)
The economic impact of contraception
The conclusion explains how all of the data reviewed above reflects many of the known side effects that are not properly represented in current prescribing information (indeed, as it explains, warning information is often presented in a misleading manner). The conclusion also begs the FDA to consider the many environmental and economic impacts of hormonal birth control, stating:
“Many millions of women are currently receiving COCs and POCs. Many millions more have been exposed to these agents at some point in their lives. They should receive updated information regarding risks which have not been conveyed, or not adequately conveyed, in the past. All women who have been exposed to COCs or POCs should be informed so that they can take this information into account as they may encounter some of these adverse effects in some cases many years after cessation of use.”
This statement is immediately followed with numerous studies documenting the various environmental impacts of hormonal agents; for example, highlighting the effects of synthetic hormones on fish populations and other species. It calculates the estimated economic impact by taking into account both those women who are currently using COCs and those who have ever used them. It cites reports and studies that show an estimate of just how much money hormonal contraceptives are costing our society, by considering different cases of cancers, diseases, and mood disorders.
In short, the conclusion reveals that there are even more reasons to be opposed to hormonal contraceptives than the many obvious (and serious) health concerns.
So what can I do to help?
The FDA is seeking comments from both medical providers who have witnessed adverse birth control side effects firsthand, or from patients who have experienced them. If you or someone you know has, indeed, suffered at the hands of hormonal contraception, now is the time to make your voice heard.
Please comment directly on the petition (by clicking the “Comment Now!” button on the right-hand corner), or share with someone you think would like to know about it. With your help, we can make an enormous impact and greatly increase awareness of the many proven risks involved with various forms of birth control. Lives could be saved! Your assistance is very much appreciated.
Too many women are given a prescription without an explanation. Too many women are wholly uninformed and misled about the dangerous (and even potentially fatal) effects of hormonal birth control. The overall goal of this petition is to amend this cycle of misinformation. In turn, the hope is that doctors might also start thinking twice before prescribing some of these contraceptives to their patients and offer effective natural alternatives in their practices (as some doctors have already told us they are doing). We currently live in a world where a woman has much more information on possible side effects of her ibuprofen than her birth control—and that needs to change.
When couples, by means of recourse to contraception, separate these two meanings that God the Creator has inscribed in the being of man and woman and in the dynamism of their sexual communion, they act as ‘arbiters’ of the Divine plan and they ‘manipulate’ and degrade human sexuality – and with it themselves and their married partner – by altering its value of ‘total’ self-giving. Thus, the innate language that expresses the total reciprocal self-giving of husband and wife is overlaid, through contraception, by an objectively contradictory language, namely, that of not giving oneself totally to the other. This leads not only to a positive refusal to be open to life but also to a falsification of the inner truth of conjugal love, which is called upon to give itself in personal totality.
— Pope St. John Paul II (Familiaris consortio, n.32)
Late last month The Washington Post ran a lengthy obituary upon the death of George Rosenkranz, a Hungarian-born chemist. You might be thinking that chemists aren’t usually the subject of lengthy articles in publications as prestigious as The Washington Post, and you’d be right. Rosenkranz, however, was world-famous due to his instrumental role in devising one of the most revolutionary drugs in all of human history – the birth control pill.
George Rosenkranz
Though responsibility for the invention of the pill can be attributed to a host of scientists, Rosenkranz was one of the first to create a synthetic version of the female hormone progesterone. Ironically, norethindrone – as the synthetic hormone was called – was initially intended to help prevent miscarriage. However, the pharmaceutical company that Rosenkranz worked for soon realized its potential as a contraceptive, and released their version of the pill in 1964, making the company (and Rosenkranz) immensely wealthy.
As The Washington Post summarizes, the release of the pill on the market was “a watershed moment in the feminist movement as well as the culture wars — allowing women to enjoy sex without fear of becoming pregnant, permitting couples to decide when and whether to begin families, and setting off an enduring debate about sexual values.”
It truly is hard to overstate the impact of the pill on our world. As Evangelical Pastor Albert Mohler observes in writing about the death of Rosenkranz, the invention of the pill is truly one of those rare events in history, the consequences of which are so seismic that it constitutes a dividing line – before the pill, and after the pill. Only in the 1960s, for the first time in human history, did humans widely have access to a relatively reliable method of separating sex from procreation. And, as Mohler observes, “once that separation took place, you basically redefined human sexuality.”
The Church was Right
The question that hangs over us to this day is whether this redefinition has been for good or for ill. Dr. Rosenkranz himself seemed ambivalent about the question, focusing instead on the purely practical question of technical achievement. “I leave to others any debate about the ultimate worth of the pill,” he said, while receiving an honor from the University of Mexico in 2001 for his work.
It’s no secret that the Catholic Church, and a small number of other Christian denominations and thinkers, have consistently opposed artificial contraception. This opposition is often based on, or at least supported by the observation that separating sex from marriage and procreation has helped unleash a sexual revolution that has devastated traditional sexual ethics.
As Mohler notes, the pill not only enabled couples (more or less reliably) to control their fertility, “it also gave technological authorization to adultery and premarital sex and extramarital sex and just about everything you can imagine.”
The “everything you can imagine” includes a whole lot. Indeed, it is difficult to imagine, for example, the grotesque excesses of the LGBT movement – which were so prominently on display during last month’s “Pride” celebrations – and the widespread public support for them, without the redefinition of sexuality that the pill precipitated. Once sex became viewed as just another pleasurable pastime, rather than the immensely sacred, powerful, and private act by which a married couple express their love for one another and create new life, there was nothing stopping all manner of sexual excess – from the explosion of pornography, to the celebration of various deviant and violent sexual practices, to the systematic grooming of children through so-called “comprehensive sex education.”
However, the Church’s critique of contraception has always gone beyond concerns about sexual morality, to the far-reaching practical consequences. Many people scoffed at the Church’s claim that more contraception would lead to more abortion. It seemed self-evident to the early birth control pioneers that if women had the means to prevent unwanted pregnancy, then abortion rates would drop. What they didn’t account for was the way contraception would drastically alter sexual behavior. With routine casual sex becoming the norm, contraception’s “small” failure rate of several percent suddenly translated into millions of “unwanted pregnancies.” The result was that the abortion rate exploded even as the rate of contraceptive use increased.
The early birth control pioneers also failed to anticipate other dire consequences of the illusion of unfettered “sexual freedom,” both for the individual and society. Monsignor Pope recently summarized some of the these in an insightful article, writing:
Since contraception’s widespread use began, abortion has skyrocketed, as has divorce. Other consequences included an increase in sexually transmitted diseases (such as AIDS), teenage pregnancy and single motherhood, absent and irresponsible fathers, the breakdown of the families, and the poverty and dysfunction that goes with all of this. There is also a pornification of our culture that assists in spreading sexual confusion to include the celebration of homosexual acts and so-called transgenderism.
Growing Secular Opposition to Contraception?
Lately, however, I have noticed a fascinating trend. More and more non-religious people are starting to take note of the downsides to artificial contraception. In a surprising number of cases, they are instead turning their attention to natural methods of family planning. Case in point: the explosion of secular-developed mobile apps to assist women in fertility tracking. While in many cases the moral outlook of these developers doesn’t match Catholic teaching (for instance, they happily promote using barrier methods of contraception during fertile periods), it’s astonishing how many secular people seem to be coming to the same conclusions about the harms of contraception as the Catholic Church reached long ago.
Many women, for instance, are realizing that they disproportionately (indeed, almost entirely) bear the burdens and responsibilities that come with artificial contraception. Even worse, they are increasingly realizing that they are doing so in order that men can use them for meaningless sexual encounters that they are far less likely to desire in the first place.
Among the burdens born by women are the myriad side effects of pumping their bodies full of artificial hormones. One recent article in a widely-read secular German publication is titled “Depression and Suicide: The Dark Side of the Birth Control Pill.” The article focuses on the story of one woman who developed suicidal tendencies after going on the pill. But as the article observed, she’s far from alone. Indeed, it’s not hard to find forums online where thousands of women share terrifying and sometimes heart-breaking stories of emotional side effects they suffered once they went on birth control – severe depression, anxiety, mood swings, personality changes, loss of libido, and on and on.
Other side effects are less obvious, but possibly far more pervasive, and equally troubling. One study released earlier this year suggested that using hormonal contraceptives can interfere with women’s ability to detect emotional cues from others. While this is a relatively small study, it adds to the growing body of evidence that hormonal contraception interferes with women’s cognition and psychology in subtle ways that, multiplied hundreds of millions of times, may in fact be altering society in far more substantial ways than anyone realizes.
Some studies, for example, have suggested that the pill significantly affects how women perceive men as potential mates. This might not sound like a big deal. But as the authors of one study observed, “[T]he use of hormonal contraceptives may not only affect initial partner choice but also have unintended consequences for women’s relationship satisfaction if contraceptive pill use subsequently changes.” That is, women who were attracted to their partner while on the pill may suddenly find that the attraction changes or goes away when they cease using contraception. Again, multiply this effect potentially several hundred million times, and you see how the pill may be affecting lives and society in ways that the pill’s inventors never anticipated.
Other well-documented physical side effects from hormonal contraception include increased risks of certain types of cancer, pulmonary embolism, heart attack, stroke, weight gain, headaches, nausea, and decreased libido.
Many women are now waking up to the fact that they have been the subjects of a vast, largely untested scientific and social experiment, often for the sake of the pleasure of others. And they are beginning (rightly) to ask themselves whether this is true female “empowerment.”
The Wisdom of the Church’s Teachings
Pope St. Paul VI, author of Humanae Vitae
In a way, it is easy to understand why contraception became as popular and widespread as it did, or why so many even within the Church urged Pope St. Paul VI to change Church teaching on contraception. All the pleasures of sex without any of the consequences? Who wouldn’t want that?
The problem, of course, is that the promises of contraception are a lie. The really Big Lie is that contraception eliminates the risk of pregnancy. It didn’t, and still doesn’t. Even the most effective methods of contraception have a failure rate. Even if only a few percent risk per year, that translates into an enormous number of unwanted pregnancies. The contraceptive mentality, and its false promise of total control, primes men and women to view these unwanted pregnancies as unjust encroachments on their freedom, instead of the natural consequences of their sexual behavior. Inevitably, many of them turn to abortion to fix the “problem.” Indeed, data suggests that a solid majority of abortions may involve women who were using contraception at the time they became pregnant.
However, the other Big Lie is that pregnancy is the only “consequence” of sex, and that once we get rid of that, sex can be rendered simply “fun.” As we are learning, the “contraceptive mentality” can change society. It fundamentally changes the way men and women relate to one another, the kinds of sexual behavior society deems acceptable, the way we pursue romance, the meaning of marriage, the values that people treasure, the education our children receive, the entertainment we watch, the structure of the family, the physical and psychological health of our populace. And on and on, into every aspect of society.
The Catholic Church saw all this from its very beginning. Pope St. Paul VI saw this when he resisted the immense pressure put on him to lift the Catholic prohibition on contraception, and instead upheld that teaching in Humanae vitae. Pope St. John Paul II saw this when he repeatedly and emphatically reemphasized the Church’s teaching, despite the reality of widespread dissent from Church teaching.
Herein we find one more proof of God’s providence operating through His Church – that despite the confusion in the world, the Church could chart a clear path through that fog of confusion, upholding a beacon of truth, showing Christian couples (indeed all couples) the way to contribute to a true “Civilization of Love.”
July 1, 2019 (LifeSiteNews) — Twin babies were saved when their mother changed her mind after beginning the process of a chemical abortion.
“Alexis” was around six weeks pregnant when she sought an abortion at Charlotte, North Carolina’s busiest abortion provider, A Preferred Women’s Health Center.
During an ultrasound, the technician casually remarked, “Oh, twins,” giving her pause, because she had always wanted twins.
While she processed the fact she was carrying twin babies, Alexis, a pseudonym, was given the first of two drugs in the chemical abortion process, along with the second dose to be taken in the next 48 hours.
As she left the abortion center, a sidewalk counselor was able to reach Alexis through her state of bewilderment and initiate the process of saving her twins.
“It might not be too late for you,” the counselor told her, “AbortionPillReversal.com, they can still help you save your baby.”
After Alexis left the abortion facility, she pulled into the nearest parking lot and searched on her phone for the website mentioned by the counselor and called the helpline, which coordinated assistance for her at a local pregnancy center.
“We got her started on the abortion pill reversal treatment extremely fast,” said Courtney Parks, abortion pill reversal coordinator for HELP Pregnancy Center. “It was a matter of hours.”
The “abortion pill,” or RU-486, refers to a chemical abortion that uses two pills: mifepristone and misoprostol. Mifepristone is taken first, destabilizing the pregnancy by blocking progesterone receptors and reducing progesterone levels in the mother’s blood. The abortion is then finished when misoprostol induces labor, forcing the mother’s body to expel the baby.
Abortion pill reversal treatment works by giving the mother extra progesterone up to 72 hours after she takes the first chemical abortion pill.
HELP medical director Matt Harrison and California physician George Delgado developed the reversal treatment over a decade ago.
The Abortion Pill Rescue Network (APRN) includes 450 professional health care providers in the U.S. and 11 other countries that assist women who call the helpline that Alexis had called. The helpline is staffed 24 hours a day, seven days a week, and is a project of Heartbeat International, a global network of 2,600 pregnancy help organizations.
Acting within that 72-hour window is crucial, and Alexis was fortunate to make contact with the helpline early enough in that timeframe. Her twins are two of the 750 babies who have been saved by abortion pill reversal.
Once at her appointment with HELP Pregnancy Center, Parks and HELP sonographer Kelly Byrum gave Alexis what the abortion facility did not: the opportunity to see her babies on an ultrasound.
“They were tiny, little babies and they had beautiful, little heartbeats,” Parks said. “I just remember sitting with her in that ultrasound room and her crying, and just hoping that this would work for her so that she could save her babies.”
Parks saw to it that Alexis had follow-up ultrasound scans in the following several weeks, to be certain the babies were still healthy and thriving.
The abortion pill reversal protocol worked, and roughly a month later, the center connected her with a doctor who provided her with prenatal care for the remainder of her pregnancy.
Parks and his HELP team kept in touch with Alexis, throwing her a baby shower along with another ministry.
“She has had everything that these babies need for several years provided for her,” Parks said. “She told me, ‘If I had known what I know now and I had seen how the Lord has provided for these babies, I would have never even walked into that clinic.’ So she’s just been overwhelmed with just how good God has provided for her throughout this.”
HELP Pregnancy Center has seen four babies saved by the abortion reversal protocol.
The rest of Alexis’s pregnancy was otherwise uneventful, and she delivered her babies early this year.
Parks said Alexis is thriving as a single mother, and she has the support of her own mother, who moved in with her to assist with the twins.
Alexis “is just head over heels in love with these babies,” Parks said.
Byrum is glad for the awareness created for abortion pill reversal by Alexis’s story.
“It’s really neat that it’s getting some press now and people are becoming aware of it,” she said. “We have heard women come out of this [abortion] clinic that have told us that they told them inside that once you take this pill, there’s nothing you can do to reverse it, that it’s just not
I once heard a very young boy call out for his daddy in a beautiful, clear, and diminutive voice while he was playing. The father, moved by it, responded lovingly,“Yes, my heart?” And something about that interaction touched me. If that boy is his father’s heart, then he is the most important thing to him. The heart is the core or center of a person in a figurative way. And, in the most literal and physical sense, the
heart is the engine or the motor of the body. It pumps our entire lives, never sleeping. It keeps us alive. If a father can love his son to the core of his being so that he calls him his heart, then we can understand more how Jesus must love us.
In the image of the Sacred Heart, Christ extends to us His flaming heart that has been lanced and pierced with thorns. It is a suffering heart. Christ loves us by saving our lives in exchange for His life. We, as the Body of Christ, are called to do the same.
One way this love is embodied is in prolife work. It is, at its essence, a work of self giving love for children in the womb who don’t even know we are loving them. And it is a lifesaving work that comes with a cost. The crown of thorns on the heart and the piercing with the lance symbolize the suffering that all those who defend the unborn will undergo; defend the unborn and you will be treated like them. Despite suffering, Christ’s heart keeps on beating inside His body. So must we persevere within the Body of Christ.
And we worship the Sacred Heart of Jesus. His heart is part of His body, and it is the body of God.The Feast of the Sacred Heart, and our devotion to that heart throughout the year, bring to the forefront the reality of the Incarnation. And so does pro-life work. Just as the heart is a physical organ, pro-lifework is a physical concern, not just a spiritual one. We must pray for the children in the womb, but we must also encounter them physically and defend them physically. We pray at the places where they are being killed, we counsel the moms in whose wombs they are nourished, we bury the bodies of those we could not save. We act, in the body, because we are moved by His love, which He shows us in His Body.
Moreover, the passion of love in the Sacred Heart is also the passion of love by which we defend the baby in the womb; His heart of mercy is the mercy we extend to all who have been involved in abortion. Pro-lifers are often stereotyped as being single-mindedly concerned with saving babies and nothing more. This claim couldn’t be further from the truth. Our ministry at Priests for Life ministers to everybody. Rachel’s Vineyard offers healing retreats for families broken by abortion. Silent No More gives them a voice and a vote. This is the work of mercy.
Jesus said He is meek and humble of heart, and this also brings us to the heart of the pro-life movement. The attitude of humility is the opposite of pro choice, which asserts itself. Humility humbles itself and accepts the choices of God. It accepts that God’s will and plans are better than our own, even if they come unexpectedly. A story recently broke about an Olympic athlete who discovered she was pregnant weeks before the Olympics. Blindsided and panicked by the pregnancy, she hastily aborted so she couldparticipate in the Olympics. But the decision was met with instant regret. She and the father realized that what they decided demonstrated a desire to control their circumstances. She wishes she had had a more open heart.
The Sacred Heart is a welcoming and open heart.It welcomes the unexpected. When we have Jesus’ heart, we see Him in the stranger. We must not treat our children as strangers in the womb, but we must welcome them as if we were welcoming Christ. We make room for the woman in crisis as if we were welcoming Christ. We open our hearts to the brokenhearted who regret their abortions. And we even open our hearts to those who have yet to see the error of their ways. We see Christ in each of these and we choose love.
The Sacred Heart of Jesus, and our worship of that heart,represent the heart of the pro-life movement, and enable us to be transformed according to that heart. Every aspect of the pro-life movement is motivated by love, and that’s why we can be confident of victory, for“Love is stronger than death, more powerful even than hell” (Song of Songs 8:6). Sacred Heart of Jesus, lead us to the victory of life and of love!
We’ve already talked a bit here at Natural Womanhood about how the Pill can negatively affect your gut health. So for our regular readers, it should come as no surprise that the development of Crohn’s Disease, an inflammatory bowel disease, has been linked to the use of oral contraceptives since researchers and physicians first began observing the connection in the 1970s.
Crohn’s disease can be a painful, debilitating, and even life-threatening disease for those affected by it. According to the Mayo Clinic, the chronic inflammation of the bowel in Crohn’s disease can “lead to abdominal pain, severe diarrhea, fatigue, weight loss and malnutrition.” The exact cause of the disease is unknown—researchers are divided on whether the chronic inflammation of Crohn’s is due to the immune system attacking itself or something else within the gut—but heredity and risk factors like smoking and obesity seem to play a role in the development of Crohn’s.
Although the incidence of Crohn’s among young women spiked disproportionately to the incidence in young men after the widespread introduction of the birth-control pill in the 1970s, today the disease affects men and women at mostly equal rates. However, a recent study out of Australia found evidence that for reasons as yet unknown, women with Crohn’s tend to fare worse than do men with Crohn’s, facing more complications, more hospitalizations, and less chance of remission. The chief investigator of the study, Professor Rupert Leong, posited that “hormonal differences may also account for the accelerated disease progression seen in women,” citing the “weak association” found between the use of oral contraceptive pill and the onset of inflammatory bowel diseases like Crohn’s.
Weak association or not, research both old and new continues to reveal some link between the development of Crohn’s and contraception use. A recent, large-scale study from Harvard researchers found that American women who had used the birth-control pill (or morning after pill/Plan B) for five or more years were three times more likely to develop Crohn’s disease. The same researchers found an association between long-term contraception use and increased risk for surgery among Swedish women with established Crohn’s disease. Lead researcher Dr. Hamed Khalili stresses that a combination of genetic factors and contraception use is likely at play in the development of Crohn’s, and recommends that physicians take into account family and personal history of Crohn’s when considering prescribing hormonal contraception to patients.
The Bigger Picture
As I mentioned in my piece detailing the connection between birth control and Lupus, research continues to uncover the effects of hormones on the immune system. The colon is chock-full of estrogen receptors, and synthetic hormones are known to affect both the gut’s permeability and microbiome. The Pill’s deleterious effects on the gut may be the culprit behind an entire cadre of digestive issues in women, ranging from the annoying (like bloating and irregularity), to the downright dangerous (like Crohn’s and Small Intestinal Bacterial Overgrowth, or SIBO)—some of which may be reversed, and some of which could be permanent.
As more evidence comes to light about the Pill’s effects on the gut (and in turn, the immune system) more women (and especially women with a family history of immune diseases) should seriously consider non-hormonal family planning options like Natural Family Planning and Fertility-Awareness Based Methods.
Told that her son would never survive after he was diagnosed with Trisomy 18, Marta Johnson McClanahan couldn’t hold back her joy at the fact that her baby boy just turned 18. She turned to Facebook to share her excitement in an emotional post.
“Screaming from the top of my lungs HAPPY 18th BIRTHDAY to my amazing, STRONG and happy boy Kayden! To think we were told he wouldn’t live,” she wrote. “He sure has proved them all wrong!”
McClanahan explains that Kayden has had the odds stacked against him his entire life, but that the doctors were wrong about both his quantity and quality of life. She says he has truly lived “an amazing 18 years full of LOVE, happiness and lots of fun!”
“Drs talked about no quality of life does this look like no quality???” she wrote, sharing photos of Kayden throughout this life. She also thanks God for Kayden and for allowing her to care for him.
“We are all so very blessed and pray we have many more years with him,” she said.
Many doctors consider children with Trisomy 18 to be “incompatible with life” and tell parents that their children will die at birth or shortly after. However, it has come to light in recent years that not only are children with Trisomy 18 compatible with life but that when they receive proper health care, they can and do thrive.
Rick Santorum’s daughter Bella has Trisomy 18 and recently turned 11 years old. Her mother calls her “the happiest little girl in the world.” Little Evelyn received a similar prognosis when doctors diagnosed her with Trisomy 18 in the womb. Doctors told her parents that “everything is wrong” with her and that they couldn’t keep their daughter. Now Evelyn is a big sister who is proving the doctors wrong.
Despite how well these children are doing, parents of children with Trisomy 18 have discovered, to their horror, that doctors will initiate what’s known as “slow code” when they have a child with the condition under their care. Put simply, in this situation, medical personnel avoid taking measures to save the child’s life or treat underlying health conditions, yet act as if they are taking steps to help. Parents of children with Trisomy 18 must find a doctor they can trust.
Kayden is proving that not only can doctors be wrong, but that every human being has value regardless of any health condition they may have. Each person has his or her own gifts to bring to the world — even those who may live shorter than average lives.
Is a ‘TelAbortion’ (telemedicine abortion pill) FDA clinical trial actually a Trojan horse intended to skirt important abortion pill safety requirements put in place under the FDA? Live Action News has been analyzing the effort to expand abortion, and has documented the various abortion pill collaboratorsworking behind the scenes on various clinical trials, studies (read more here) and funding streams, which all happen to be closely connected. In addition, Live Action News has documented the push for illegal dispensing of the dangerous pills and the effort to discreditabortion pill reversal. Now, we’ve analyzed changes reported under the Direct-To-Consumer protocol (pills sent via mail after a TelAbortion or telemedicine interview) and are seeing that FDA regulations are being skirted in the name of continually broadening “clinical trials.”
BACKGROUND:
The abortion pill regimen is made up of two drugs: Mifeprex and Misoprostol.
The Packard Foundation and other pro-abortion philanthropy groups seeded DANCO.
Packard is now funding groups and studies that claim abortion pill expansion is safe.
Packard Foundation invested in abortion pill manufacturer DANCO (Image: David and Lucile Packard Foundation )
FDA’s SAFETY REQUIREMENTS KNOWN AS REMS:
The FDA currently requires Mifeprex to be placed under a safety system called REMS (Risk Evaluation and Mitigation Strategy), which is a “safety strategy to manage a known or potential serious risk associated with a medicine and to enable patients to have continued access to such medicines by managing their safe use.”
Under the REMS Program, the FDA states, “Mifeprex and the approved generic version of Mifeprex”…
… [may] only be supplied directly to healthcare providers who are certified to prescribe the drug product and who meet certain qualifications.
… are only available to be dispensed in certain healthcare settings, specifically, clinics, medical offices and hospitals, by or under the supervision of a certified prescriber.
… are not available in retail pharmacies and are not legally available over the Internet.
Without REMS, abortion pills could be ordered online, picked up at any pharmacy, and prescribed by any health care provider.
TelAbortion a workaround abortion laws
TELABORTION CLINICAL TRIAL:
In theory, clinical trials are used to test a specific drug and hopefully alleviate safety issues that arise. But with expansion of this abortion pill clinical trial there is a growing concern it is less of a clinical trial and more of a permanent way to skirt the FDA’s REMS system. In fact, a recent interview with the co-leader of this Gynuity sponsored trial, Erica Chong, by the online media group Fast Company, noted, “The hope is to get enough providers on board so TelAbortion can eventually go from research study to full-blown service.”
The TelAbortion clinical trial was announced in 2015. When the (then cohort) clinical trial began recruiting in 2016, they anticipated an enrollment of 50 participants with eligibility ages between (believe it or not) 11 to 50 years old and an estimated completion that same year.
In 2016, there were only two locations for the trial listed, as seen in the screen below.
TelAbortion screen from 2016 two locations
However, as of the date of this article (June 2019) the now defined “case-only” (instead of “cohort”) clinical trial currently intends to enroll 1,000 participants with age eligibility as young as 10 years old. Why Gynuity Health Projects moved the recruitment age even lower is not stated, but this is concerning, given past abuses by abortion facilities and Planned Parenthood centers’ failure to report child sexual abuse, along with potential violations of parental consent and notification laws in certain states.
Feasibility TelAbortion clinical trial ages 10 to 50 accessed June 20 2019
In addition to those changes, the completion date continues to be pushed out, and is currently set for June of 2020. There is also a growing list of locations (see below), enabling the abortion pill to be dispensed even more widely, without existing REMS safety requirements.
In other words, the study just keeps getting bigger and broader, with no FDA safety requirements in place.
Locations:
Planned Parenthood of the Rocky Mountains (Denver, CO, and New Mexico)
Planned Parenthood Columbia Willamette (Portland, OR, and Washington)
Oregon Health and Sciences University Women’s Health Research Unit (Portland, OR, and Washington)
Carafem (Atlanta, GA)
Maine Family Planning (Augusta, ME)
The University of Hawaii Women’s Options Centers (Honolulu, HI)
Choices Women’s Medical Center (Jamaica, New York)
The aforementioned media group, Fast Company, noted another “workaround” to existing laws, writing:
In some cases, TelAbortion providers are physically located in one state but licensed in another, which allows them to reach clients there as well…. TelAbortion obviously cannot expand into states where telemedicine abortion is illegal, but one workaround Chong is exploring is to introduce the program in neighboring states. “If we can get into a neighboring state, it’s possible for a woman in Texas, for example, to maybe cross the border into New Mexico,” Chong says. “She can have her consult there, and then pick up her package at a Fedex office that’s holding the package for her, or something like that.”
These kind of “workarounds” to intentionally bypass existing laws and safety regulations are clearly not the intention of any FDA clinical trial.
TelAbortion locations screen accessed of June 20 2019
Abortion generally is not without complication or risks. Recently, the FDA updated its adverse effects reports through 2018, revealing 24 deaths of women associated with the abortion pill since it’s September 2000 approval. To date, the report documents nearly 4,200 reported adverse effects, including hospitalization and other serious complications. But under 2016 changes, the drug’s manufacturer, DANCO, no longer has to report non-fatal adverse effects, so we can only imagine what the number really is.
Population growth can have an impact on controversial bioethical issues like abortion, contraception, aged care and euthanasia. That’s why a projection of world population trends from United Nations, released this week, should be of great interest.
There are no big surprises, but the UN has revised its projections downward. Two years ago, it predicted that global population in 2100 would be 11.2 billion. The 2019 projection is only 10.9 billion.
The UN’s figures are not definitive. In fact, there are dissidents who believe that the UN is seriously overstating population growth. While the UN projects that world population will peak and begin to stablilize or decline in 2100, others think that decline will begin as early as 2050. Even the UN acknowledges that there is “roughly a 27 per cent chance that the world’s population could stabilize or even begin to decrease sometime before 2100.” For more on this, read Wired’s review of the book Empty Planet – which is headlined, chillingly, “The world might actually run out of people”.
* * * * * * *
1. The world’s population continues to increase, but growth rates vary greatly across regions. The world’s population is projected to grow from 7.7 billion in 2019 to 8.5 billion in 2030 (10% increase), and further to 9.7 billion in 2050 (26%) and to 10.9 billion in 2100 (42%). The population of sub-Saharan Africa is projected to double by 2050 (99%). Other regions will see varying rates. These include Australia and New Zealand (28%) and Europe and Northern America (both 2%).
2. Nine countries will make up more than half the projected population growth between now and 2050. The largest increases in population between 2019 and 2050 will take place in: India, Nigeria, Pakistan, the Democratic Republic of the Congo, Ethiopia, the Tanzania, Indonesia, Egypt and the US (in descending order of the expected increase). Around 2027, India is projected to overtake China as the world’s most populous country.
3. Rapid population growth presents challenges for sustainable development. Many of the fastest growing populations are in the poorest countries, where population growth brings additional challenges in the effort to eradicate poverty, achieve greater equality, combat hunger and malnutrition, and strengthen the coverage and quality of health and education systems.
4. In some countries, growth of the working-age population is creating opportunities for economic growth. In most of sub-Saharan Africa, and in parts of Asia, Latin America and the Caribbean, recent reductions in fertility have caused the population at working ages (25-64 years) to grow faster than at other ages, creating an opportunity for accelerated economic growth.
5. Globally, women are having fewer babies, but fertility rates remain high in some parts of the world. Today, close to half of all people globally live in a country or area where fertility is below 2.1 births per woman over a lifetime. The global fertility rate, which fell from 3.2 births per woman in 1990 to 2.5 in 2019, is projected to decline further to 2.2 in 2050.
6. People are living longer, but those in the poorest countries still live 7 years less than the global average. Life expectancy at birth for the world, which increased from 64.2 years in 1990 to 72.6 years in 2019, is expected to increase further to 77.1 years in 2050.
7. The world’s population is growing older, with persons over age 65 being the fastest-growing age group. By 2050, one in six people in the world will be over age 65 (16%), up from one in 11 in 2019 (9%). Regions where the share of the population aged 65 years or over is projected to double between 2019 and 2050 include Northern Africa and Western Asia, Central and Southern Asia, Eastern and South-Eastern Asia, and Latin America and the Caribbean. By 2050, one in four persons living in Europe and Northern America could be aged 65 or over. In 2018, for the first time in history, persons aged 65 or above outnumbered children under five years of age. The number of persons aged 80 years or over is projected to triple, from 143 million in 2019 to 426 million in 2050.
8. Falling proportions of working-age people are putting pressure on social protection systems. The potential support ratio, which compares numbers of working-age people aged 25-64 to those over age 65, is falling around the world. In Japan, this ratio is 1.8, the lowest in the world. An additional 29 countries, mostly in Europe and the Caribbean, already have potential support ratios below three. By 2050, 48 countries, mostly in Europe, Northern America, and Eastern and South-Eastern Asia, are expected to have potential support ratios below two.
9. A growing number of countries are experiencing a reduction in population size. Since 2010, 27 countries or areas have experienced a reduction in the size of their populations of 1% or more. This is caused by low levels of fertility and, in some places, high rates of emigration. Between 2019 and 2050, populations are projected to decrease by 1% or more in 55 countries or areas, of which 26 may see a reduction of at least 10%. In China, for example, the population is projected to decrease by 31.4 million, or 2.2%, between 2019 and 2050.
10. Migration has become a major component of population change. Between 2010 and 2020, Europe and Northern America, Northern Africa and Western Asia, and Australia and New Zealand will be net receivers of international migrants, while other regions will be net senders.
The National Embryo Donation Center (NEDC) of Knoxville Tennessee recently gathered families from around the country to celebrate the 800th birth of a child conceived by a donated embryo through the clinic. WATE 6 reports that the group has been collecting leftover embryos for 16 years.
NEDC president Dr. Jeffrey Keenan told the news station, “It’s been exciting, it’s been awesome. It’s in some respects put Knoxville on the map, as far as a fertility destination because many of these families, to be honest are out of options and don’t have really any other good option for conceiving except to come here and receive donated embryos.”
Many people view in-vitro fertilization (IVF) as a positive scientific development that has allowed many couples struggling with infertility to conceive children. But this rosy view ignores the serious ethical problems with IVF, which include treating children as manufactured goods.
Reporting on NEDC’s celebration, the reporter said, “Many people attending the event are alive because of the donated embryos.” Meanwhile, the remaining embryos, also created outside the womb and kept frozen, are also alive. They are in suspended animation, frozen indefinitely and treated as products to be discarded, made into jewelry, or traded for a more desirable offering. The NEDC estimates there are at least 700,000, and possibly more than 1 million, “surplus” embryos currently frozen in the United States.
The NEDC states, “Many biological parents store their frozen embryos for future use. But when those parents have completed their families, they must decide what to do with their remaining embryos. Donating them to another infertile couple is an increasingly popular option. It benefits both the genetic family and the recipient family.”
These types of donations are sometimes called “snowflake adoptions,” referring to the unique and unrepeatable attributes of each individual child frozen at the embryonic stage. Embryo adoption can be a way to recognize the human dignity of children through IVF, but there are still myriad ethical concerns with the process.
The NEDC’s celebration of 800 births demonstrates the massive scale of the unintended consequences of IVF: the hundreds of thousands of children kept frozen indefinitely. Couples struggling with the heartbreak of infertility deserve to know the full consequences of undergoing IVF before they make a decision, and they deserve to know that there are ethical alternatives.
SALT LAKE CITY, UT – APRIL 26: In this photo illustration a one dose bottle of measles, mumps and rubella virus vaccine, made by MERCK, is held up at the Salt Lake County Health Department on April 26, 2019 in Salt Lake City, Utah. (Photo Illustration by George Frey/Getty Images)
WASHINGTON — As part of its push to eliminate or greatly restrict federal funds involved with fetal-tissue research, the Trump administration canceled a medical research contract with the University of California, where fetal cells were infused with mouse immune systems.
The June 5 decision from the Department of Health and Human Services is the latest example of the administration pledging to find “adequate alternatives” to research that has depended on fetal tissue and to make sure “efforts to develop such alternatives are funded and accelerated.”
“Promoting the dignity of human life from conception to natural death is one of the very top priorities of President Trump’s administration,” the decision stated.
The announcement may give hope for Catholics that the time has come to push for the development or distribution of ethical vaccines whose source cells did not involve the taking of a human life by abortion.
Most vaccines are derived from ethically derived sources, such as animal or insect cell lines, and not from unborn children whose tissues were harvested following elective abortions. But a number of vaccines Americans rely on today, such as the Mumps, Measles, Rubella (MMR) vaccine, are derived from cell lines whose origins go back to the tissues of unborn children aborted decades ago.
In Kentucky, Jerome Kunkel, a Catholic high-school senior at Our Lady of the Sacred Heart/Assumption Academy in Walton, refused a chicken pox vaccine for this reason, citing his objections to abortion.
He sued the Northern Kentucky Health Department after it barred him from going to school for several months due to concerns over possible contagion from his lack of a chicken pox vaccination. Kunkel came down with chicken pox in May and since returned to class.
The Catholic Church opposes using fetal tissue derived from abortion for medical research and vaccine development. However, the Church also recognizes that in the absence of ethically sourced alternatives, parents and individuals may use those vaccines until an alternative is available, explained Jozef Zalot, staff ethicist at the Philadelphia-based National Catholic Bioethics Center.
A 2005 instruction from the Pontifical Academy for Life stated that people who have no access to ethically sourced vaccines would be “right to abstain from using these vaccines if it can be done without causing children, and indirectly the population as a whole, to undergo significant risks to their health.”
The Vatican’s Pontifical Academy for Life explained that there is “proportional reason” to use such vaccines “on a temporary basis” to avoid considerable dangers to public health, particularly in the case of diseases such as rubella (German measles), which is fatal to unborn children. It said “the burden of this important battle cannot and must not fall on innocent children and on the health situation of the population — especially with regard to pregnant women,” but this unjust situation of forcing parents or individuals to violate their consciences through passive material cooperation to avoid worse evils “must be eliminated as soon as possible” by production of ethically derived alternatives.
Zalot explained that while Catholics have a moral responsibility to communicate their demand for ethical alternatives to vaccines derived from fetal tissue, the burden of responsibility increases for those in positions of power and authority. He pointed to leaders of Catholic health care systems that have contracts for hundreds of millions of dollars with pharmaceutical companies that provide such vaccines as one example.
Catholic health care systems, Zalot said, “have some clout, and because of that, I would say their moral responsibility to call for ethically sourced vaccines is greater than [that of] your typical John Q. Public.”
Generating Grassroots Pressure
Dr. Barbara Golder, the editor in chief of TheLinacre Quarterly and a member of the Catholic Medical Association, said that because the vaccine issue is one of moral law and not spiritual matters, Catholics need to make sure the discussion on ethical alternatives to vaccines derived from fetal tissue does not get confined to the Catholic or religious world, but is part of the general conversation.
However, she said Catholics should arm their advocacy with awareness about the alternatives in existence and make sure their allies in the pro-life movement are informed about them. Golder said there is also more at stake than the ethical source of the vaccine.
“It is unreasonable to put a patient in the position of choosing to violate his conscience for an essential medical procedure, in this case, vaccination,” Golder said.
Golder, however, cautioned that refusing to take vaccines at all is “counterproductive.”
“The rising incidence of vaccine refusal is leading in some places to an elimination of exemptions altogether, which undermines the argument for religious conscience in general,” she said.
Conversations about ethical alternatives could build to grassroots-level engagement that could “involve medical societies, large practices or other community groups.”
She said Catholics — and other people of goodwill — should be informed about ethical vaccines and “ask for them by name when the time comes” to one’s physician, pharmacist or health department. She recommended rewarding practices that provide ethical vaccines and protesting when “alternative vaccines are not available because the hospital, practice or insurance company has elected not to cover them.”
Golder suggested that Catholic physicians, organizations and institutions should become intentional about getting behind this effort. Universities might also have the heft to raise funds to support ethical vaccine development.
But she said it is important for Catholics to speak up and organize to generate “a growing sense of demand that can’t be ignored” so lawmakers and policymakers can act on the development of ethical alternatives.
“We have a responsive administration just now — it makes sense to take advantage of it,” she said.
Some in Congress have echoed similar sentiments in welcoming the Trump administration’s HHS decision.
“Ethical scientific practices are paramount to discovery, but they should never include the harvesting of developing baby hearts, eyes, livers and brains following elective abortions,” U.S. Rep. Vicky Hartzler, R-Mo., said in a statement.
Toward Newer, Ethical Vaccines
The Trump administration’s decision to close the federal spigots on fetal-tissue research could help vaccine development stay focused on vaccines that are not only ethically sourced, but far more effective in the long run.
Tara Sander Lee, a senior fellow and director of life sciences at the Washington-based Charlotte Lozier Institute, told the Register that the new Ebola and shingles vaccines, engineered with Vero monkey cell line and engineered hamster cells respectively, have proven more effective than their fetal-tissue based alternatives. Lee said the new Ebola vaccine proved to be 97% effective, and Shingrex (the new vaccine for shingles) showed “greater than 90% effectiveness.”
Lee said scientific research is demonstrating that the new vaccines from animal cells are just as effective, if not more so, than the ones derived from fetal cells. She noted that none of the vaccines currently in use today by Americans are affected by the decision to close off fetal-tissue research.
“The vast majority of vaccines are already being produced with ethical alternatives [to fetal tissue],” she said, such as monkey kidneys, insect cells or Chinese hamster cells.
Scientists in the past have used fetal cell lines because fetal cells replicate much faster than adult tissues when it comes to cultivating vaccines. But Lee said they were not the exclusive source — vaccines such as for polio now use animal cells.
Lee also pointed out that there are more ethical alternatives that have been developed, but they are not available in the U.S.
“There is an ethical version for MMR [Measles, Mumps and Rubella], but it is only available in Japan,” she said. Japan’s rubella vaccine is derived from quail egg and rabbit cell lines.
However, she said companies like Merck are reluctant to reformulate vaccines or get the Food and Drug Administration to approve distribution of ethical vaccines when they see no financial incentive to do so.
Stopping this practice of fetal tissue-based research now, with renewed pressure from the administration, Lee said, would encourage scientists to focus their research on non-fetal-tissue-based alternatives that make more effective vaccines in the long run.
“There’s no need for them to continue to use these fetal cell lines from abortions that took place back in the ’60s. There’s just no need,” she said.
“The newer, most advanced way is using ethical vaccines.”
A Wisconsin high schooler is speaking up for stroke awareness after she suffered a stroke of her own during gym class, WAOW reported—an event her doctors said was brought on by her birth control pills.
Like two-thirds of women her age and up, Hannah Drummond, 18, was prescribed birth control with low expectations of any serious side effects. Loyola University Medical Center researchers previously found women who don’t have any other medical problems are safe to take the pill, but in those with comorbidities, it can be a riskier call.
Drummond was taken to the hospital after experiencing numbness and tingling during her gym class, quickly learning she’d suffered a stroke. Her care team said the culprit was her birth control, and that the estrogen in her pills had caused a blood clot that then slipped through a previously undiscovered hole in her heart and up to her brain.
“It was actually scary knowing I was so young, I’m 18, this is happening to me,” she told WAOW. “If you don’t feel something is right, say something, tell someone.”
Drummond is still suffering from impaired vision but is expected to make a full recovery.
The promotion of promiscuity through comprehensive sex education and condom-distribution campaigns is continuing to fuel an STD epidemic that is now seeing more than one million new cases of sexually transmitted infections (STIs) and diseases (STDs) every year.
According to the AFP, the World Health Organization (WHO) is expressing alarm over the lack of progress in curbing the rampant spread of sexually transmitted diseases worldwide since 2012.
“WHO found that there were more than 376 million new cases of chlamydia, gonorrhoea, trichomoniasis and syphilis registered around the world in 2016 — the latest year for which data is available,” the AFP reports. “That is basically the same number as WHO reported in its previous study, based on data from 2012.”
The WHO, which promotes comprehensive sex education and condom distribution rather than abstinence as a way to fight this epidemic, now blames the continued spread of these infections on dating apps and a more complacent attitude about the spread of HIV because of new antiviral drugs that have proven to be very effective.
People are “more complacent about protection,” said Teodora Wi, a WHO expert on STIs, which she believes is dangerous because this attitude is coming at a time when “sex is becoming more accessible (through things like) dating apps”.
Peter Salama, WHO’s executive director of Universal Health Coverage, expressed concern over the “lack of progress” in stemming the tide of these diseases and infections, and called the latest numbers to be a “wake-up call” for authorities.
The numbers are indeed grave. In 2016, the most recent year for which data is available, an estimated 127 million people between the ages of 15 and 49 were infected with chlamydia. Another 87 million contracted gonorrheoea, and 6.3 million contracted syphilis. In addition, 156 million were infected with trichomoniasis, a parasital disease commonly called “trich.”
This amounts to one in 25 people globally that have at least one of these STIs.
What makes these diseases so difficult to prevent through mere comprehensive sex education and condom distribution campaigns is because some have no early symptoms. This means people who are engaging in casual sex unwittingly spread the diseases which, if left untreated, can lead to serious conditions. These include infertility, stillbirth, neurological and cardiovascular disease, as well as increased risk of contracting HIV.
The only real way to stop the spread of STIs and STDs is to promote abstinence until marriage, but the WHO is once again choosing to follow the same failed path by recommending regular screening and the proper use of condoms. They tend to promote comprehensive sexual education, which supposedly contains abstinence-only material, but analyses of these programs finds that only a small percentage of the content is actually devoted to authentic abstinence education.
How many more young lives will be ruined before officials at the World Health Organization hear this “wake-up call” for what it is – a call to admit that their strategies are failing and the time has come to challenge youth to live chastely until marriage?
Multiple Sclerosis (MS) is an autoimmune disease (AI) that attacks the central nervous system, often to the point of causing severe disability. It is also a disease that has always loomed large in my life. My paternal grandmother had MS, and it caused her to be bed-ridden from the time my dad was a small boy, until her death when he was in his early 20s. Various aunts and uncles have also been diagnosed with MS, and I know I am not the only one among my cousins who lives with the fear of receiving that diagnosis someday, too.
So you can imagine that I try to do what I can to avoid triggering the monster that might very well be lying dormant in my genes. After all, the prevailing theory is that for an autoimmune disease to occur, one must have the right (or rather, wrong) genetics, and that some “triggering event” must occur to spring the disease into action. Different theories abound about what the different triggers may be, but one theory has not been given nearly enough light: the possibility of hormonal contraception as an autoimmune trigger.
As guest author Mike Gaskins wrote for Natural Womanhood:
“When our body’s natural estrogens attach to receptors on T cells (the “soldiers” of the immune system), it arms the soldiers and gives them their marching orders. Natural estrogen basically points out the invader and triggers the command to attack. But when disruptive agents that mimic natural estrogen enter our body, they attach to the receptors. Suddenly, the soldier is armed but doesn’t know what to attack because the synthetic estrogens don’t carry the code our natural estrogen would have provided. This can cause the armed immune system to battle our body’s healthy tissue, which will result in an AI for those who are genetically predisposed.”
In the case of MS, the immune system attacks myelin within the central nervous system, which includes the brain, spinal cord, and optic nerves. Myelin is “the fatty substance that surrounds and insulates the nerve fibers—as well as the nerve fibers themselves, and the specialized cells that make myelin.” So who—or rather, what—is giving the orders for the body’s attack on the central nervous system when it comes to MS? The cause is still unknown, but perhaps clues can be found in the way the disease disproportionately affects women, especially keeping in mind the role estrogen plays in the immune response.
Multiple Sclerosis Disproportionately Affects Women
In general, most AIs affect women more greatly in severity and/or number of cases, and MS is no different. Researchers have found that while MS has always disproportionately affected women, the gap in incidence (number of new cases) between women and men has widened considerably in the last five decades. This suggests that a possible environmental factor is at play, and it just so happens that the increased incidence of MS in women (especially as compared to men) coincides with the widespread use of hormonal contraceptives.
While this might seem like a leap in logic to some, others have noted that as we learn more about the role of estrogen on the gut—and particularly, the huge number of immune receptors located in the gut—we’ve also learned a bit more about autoimmunity’s “female” preference.
Researchers identified 305 women who had been diagnosed with MS or its precursor, clinically isolated syndrome, during a three-year period from the membership of Kaiser Permanente Southern California and who had been members for at least three years before the MS symptoms began. Then they compared them to 3,050 women who did not have MS . . .
Women who had used hormonal contraceptives were 35 percent more likely to develop MS than those who did not use them. Those who had used the contraceptives but had stopped at least one month before symptoms started were 50 percent more likely to develop MS.
So while autoimmune diseases presents a unique mix of genetic, epidemiological, and environmental factors, perhaps there is something to the theory that the synthetic estrogens from hormonal birth control—which our bodies and environment have been awash in for more than fifty years, now—could be the culprit behind skyrocketing rates of autoimmune diseases (and especially so in women).
Whether or not the birth control-MS link is substantiated further, I’m thankful that, with 50 million Americans currently suffering from an autoimmune disease, and a known genetic link to the disease in my own recent family history, I have ways to plan my family that are both effective and hormone-free. Of course, Ican’t do much about the synthetic estrogens polluting our environment—and, in particular, our water—but at least I know that in foregoing hormonal contraception in favor of a Fertility Awareness-Based Method (FABM) of family planning or Natural Family Planning (NFP), I’m not taking a Pill, receiving an injection, or carrying an implant that is exposing me daily to a substance that could seriously affect my health.
Organizers of “Gay Pride” events have successfully conditioned the media and the public totalk about these parades as if they were simply celebrations of “equality.” However, even some people who are fully on board with the LGBT agenda have pointed out the obvious: these parades are often less about celebrating equality than they are about celebrating promiscuous sex – the more debauched the better.
A few years ago an openly homosexual columnist in a major Canadian newspaper defended themuch-derided declaration by Toronto’s former mayor that the world-famous Toronto Pride parade is just an event where “middle-aged men with pot bellies” run down the street “buck naked.” “I’d say that was just an accurate description of what goes on,” admitted Josh Dehaas. “Disturbingly, more and more parents are bringing young children to watch the parade, exposing them to provocative displays of sexuality that no child should witness. If a politician believes in family values, why would he or she want to be associated with such debauchery?”
Truth be told, I still have a hard time wrapping my head around the fact that any parent, no matter how liberal, would bring their kids to these parades. A lot of things happen at so-called “gay pride” parades that aren’t fit for polite adult conversation, let alone for the eyes of children. It seems to me that keeping Pride parades child-free should be something that liberals and conservatives couldeasily agree on. After all, what benefit could there possibly be to exposing children to public nudity, simulated sex acts, highly sexualized displays of affection and dancing, etc.?
Alas, there is no such common ground to be found. After all, we now live in a world where parents openly and proudly encourage their threeand four-year-old children to explore “diverse” sexualities, helping them cross-dress in sexually provocative clothing, or bringtheir pre-pubescent children to gay bars to dance for money, or to appear on national TV shows, where they are lauded and feted by sycophantic hosts and cheering audiences. Furthermore, we have now reached a point where even the mildest expression of dissent from even the most extreme instantiations of the LGBT agenda is greeted with rage
Bishop Tobin’s Tweet
Recently, one of the United States’ Catholic bishops learnedthe hard way just how bad things have gotten. One June 1, the first day of a month that has been co–opted as “Pride month” by LGBT activist, Bishop Thomas Tobin sent out a tweet reminding Catholics that they should not be supporting or attending “Pride” events, which, he said, “promote a culture and encourage activities that are contrary to Catholic faith and morals.” Such events “are especially harmful for children,” noted the bishop.
Courtesy of Twitter
The response to this rather mild tweet was extraordinary. As of this writing, there are over 95,000 responses to the tweet – the vast majority of which are deeply, even violently critical. For simply doing the bare minimum of what his job entails – i.e., stating and defendingwhat the Catholic Church believes and has always taught – the bishop found himselfin the international spotlight, portrayed as an odious purveyor of hatred and bigotry.
Articles about his tweet appeared on CNN, The Daily Mail, the Irish Post, and countless other news publications. Famous actors and actresses took to Twitter to vent their outrage. The mayor of Providence Rhode Island, and the governor of the state, both issued statements condemning the bishop’s remark. One of the priests in Bishop Tobin’s own diocese was featured in numerous news articles, after he pleaded with homosexual parishioners not to leave the Church over the bishop’s tweet.
The next day, Bishop Tobin issued a statement expressing “regret,” not so much for the tweetitself, as the way it was received. “The Catholic Church has respect and love for members of the gay community, as do I,” the bishop stated. “Individuals with same-sex attraction are beloved children of God and our brothers and sisters.” However, he added, “As a Catholic Bishop…my obligation before God is to lead the faithful entrusted to my care and to teach the faith, clearly and compassionately, even on very difficult and sensitive issues.”
The Lessons We Can Learn
This disturbing episode is illuminating in more ways than one. Unfortunately, some of the lessons to be learned are far from encouraging.
In the first place,it seems that we are now at a point in which a completely straight-forward, non-emotional, impersonal, and non-confrontational expression of Catholic teaching – and, for that matter, moral common sense – is widely viewed as de facto intolerance, bigotry and hatred. The organized venom aimed at Bishop Tobin is – and, one suspects, was meant to be – a message sent to every faithful Christian in the country: the mere fact that you believe what Christians have always believed about sexuality makes you an enemy and a persona non grata. Either change your views and conform or be prepared to be hounded into silence.
Bishop Tobin of the Diocese of Providence (courtesy of LifeSite News)
Indeed, the thing that stands out most strongly to me is how mild Bishop Tobin’s tweet was. To anyone with an ounce of common sense, it is clear that Gay Pride parades are harmful to the innocence of children. And to anyone who understands an iota of Catholic moral teaching, it is clear that Gay Pride parades are completely incompatible with life as a faithful Catholic. Bishop Tobin stated both of these facts in a calm, straightforward manner, without a hint of animosity. He was, in other words, doing what any priest or bishop charged with leading a flock should be expected to be doing on a regular basis – instructing the faithful in how to be better Catholics. Given the filth that young children are routinely exposed to at these parades, the bishop could easily have been justified in using stronger language.
As Catholic journalist Phil Lawler recently observed, “what is remarkable about Bishop Tobin’s tweet is that it was so unusual—that other bishops and pastors have not routinely issued similar cautions.” Indeed, one discouraging effect of Bishop Tobin’s tweet has been to highlight how rare it has become for Catholic shepherds to speak unpopular moral truths, particularly on sexual matters. If our priests and bishops were routinely catechizing the faithful on the totality of Catholic moral teaching,then the media would have had a very difficult time making Bishop Tobin’s tweet into a national story. Instead, the good bishop would have been just one among countless other bishops and priests saying exactly the same thing.
We are awash in extremist LGBT propaganda. This is especially true now, in this month of June, when nearly all the large corporations use LGBT-themed marketing, which fills our streets and airwaves. Understandably, many Catholics in the pews simply don’t know what to think, or how to respond. They do not realize how Catholic teaching is grounded in an authentic compassion for homosexual individuals, or how Catholic teaching promotes the happiness and flourishing of individuals and societies by showing how God’s gift of sexuality is best put to use: in a loving union of a man and a woman oriented towards the begetting and raising of children. In the absence of clear voices from the pulpit presenting Catholic teaching in a compelling and unapologetic way, many Catholics are simply being swept away by the prevailing message in the culture. They feel overwhelmed, confused, and brow beaten.
“[W]e wish to make it clear that departure from the Church’s teaching, or silence about it, in an effort to provide pastoral care is neither caring nor pastoral. Only what is true can ultimately be pastoral. The neglect of the Church’s position prevents homosexual men and women from receiving the care they need and deserve.”
The Church’s teachings on sexuality provide the road map for human fulfillment. For a pastorto remain silent out of a fear of losing social esteem or of “offending” Catholics in the pews is to abandon the sheep to the wolves.
Indeed, a natural response to the controversy over Bishop Tobin’s tweet would have been for every other priest and bishop in the country to re-tweet the exact same message, or, at the very least, to issue a public statement supporting the bishop, and explaining Catholic teaching in a loving, compassionate way. What a great opportunity for evangelization that would have been! What a powerful message that would have sent! Instead, as the wolves circled for the kill, Bishop Tobin had more the look of a lone sheep than a shepherd among shepherds.
Even worse, the day after Bishop Tobin posted his Tweet, one extremely prominent Catholic cleric, who even enjoys an advisory role at the Vatican, tweeted out a message saying, “Catholics need not be wary of June’s #PrideMonth.” The previous day this same cleric posted a message wishing a “Happy #PrideMonth”. This is a breathtaking form of moral blindness.The Catholic Church’s vision of sexuality, which has remained consistent since the earliest days of the Church, is one characterized by wholesomeness, fruitfulness, modesty, self-giving and joy. “Pride” celebrations proclaim a diametrically opposed message. It is quite true that we require creative thinkers to pursue pastoral approaches to reach out to homosexual persons in compassion and love in an effort to help them arrive at the fullness of Christian truth. However, there are simply no compelling arguments that supporting participating in wholly worldly public celebrations of sin does anything except spread confusion, at the enormous cost of souls. The hyper-sexualization of children – including the expectation that parents should bring their children to “Pride” events that is increasingly a feature of the LGBT movement is especially dismaying.
As Catholics we have to support our pastors when they speak difficult truths, as well as challenge them to speak up when they remain silent.A petition supporting Bishop Tobin has received over 25,000 signatures. That’s a good start. I hope you will join me in praying for Bishop Tobin, and all of the Church’s pastors, including myself, that we will be filled with the courage that comes from the Holy Spirit, and that we will imitate the early Apostles by fearlessly proclaiming the totality of the Gospel, regardless of the personal cost.
This essay is adapted from remarks delivered at the Heritage Foundation.
The media and Hollywood celebrities, like Kim Kardashian and Jimmy Fallon, present surrogacy as a wonderful and beautiful thing. Even Ben Shapiro said “surrogacy can be useful and wonderful in some cases” when he spoke at this year’s March for Life. But I’m happy to discuss what you won’t hear about in the media: the health risks to women, and to the children to whom they give birth, of commercial contracted pregnancies.
On October 8, 2015, an American surrogate mother named Brooke Brown died from complications related to pregnancy. Brooke was a commercial gestational surrogate, not the biological mother. She was being paid to carry twins for a couple from Spain, where surrogacy is illegal. This had been an otherwise uncomplicated pregnancy; Brooke was just a day away from a scheduled caesarian section. But then she suffered a complication, called placental abruption (the premature separation of the placenta from the uterus), that proved fatal. The twins died, too.
Almost immediately after the loss of these three lives, women calling themselves Brooke’s “Surro Sisters” set up a GoFundMe page in order to raise $10,000 for Brooke’s family; although in the end they weren’t even able to raise $7,000.
A healthy society would not create a multi-billion-dollar fertility industry at the risk of the health and well-being of women and children. The spirit of proper medicine, expressed in the principle “First, do no harm,” requires us not to allow healthy women to engage in entirely elective, medically risky procedures that do not benefit them in any way and might harm them or lead to their death.
In the process of making documentary filmson surrogacy, I have met and interviewed several surrogate mothers whose experiences harmed them, physically and emotionally, and nearly took their lives. Several academic studies have reached the same conclusion. In December 2017, a study in the prestigious journal Fertility and Sterility compared “spontaneous” (that is, “regular”) pregnancy with surrogate pregnancy. It reported that,
Neonates born from commissioned embryos and carried by gestational surrogates have increased adverse perinatal outcomes, including preterm birth, low birth weight, maternal gestational diabetes, hypertension, and placenta previa, compared with the live births conceived spontaneously and carried by the same woman.
The report also found that these pregnancies are more likely to end in cesarean section rather than vaginal birth, which carries more risks both for the surrogate birthmother and for the baby.
Need more evidence of the medical risks to women who serve as surrogates, or to the babies they carry? Dr. Allen Merritt, a perinatologist at Loma Linda Medical Center, in my state, California, published a snapshot of the medical outcomes of the surrogate deliveries that took place at his Medical Center in 2012 and 2013:
RESULTS: Analysis of sixty-nine infants delivered from both gestational and traditional surrogate women found an increase in multiple births, NICU admission, and length of stay, with hospital charges several multiples beyond that of a term infant conceived naturally. Among singletons and twins, hospital charges were increased 26 times . . . and in triplets charges were increased 173 times . . . when compared to a term infant provided care in a normal nursery at our center.
CONCLUSION: Maternity costs for surrogates exceed those of women who conceive naturally, and these costs are especially magnified in women with triplets and multiple births.
Why are these costs so high, and why are the hospital stays so long? Because these are high-risk pregnancies. A woman’s body is not designed to carry another woman’s baby, even just one baby.
Still not convinced? Just a few months ago, in February 2019, the American Journal of Obstetrics and Gynecology published findings titled “Risk of Severe Maternal Morbidity by Maternal Fertility Status: a U.S. Study in Eight States.” The study compared the pregnancies of six groups of women: one group that had no fertility issues (called simply “fertile”); one that underwent treatments for infertility; and four that bore children conceived by in vitro fertilization (IVF).
This study is significant for several reasons. First, its sample size was huge: it examined 1,477,522 pregnancies and births. Second, the results are quite disturbing (although, as my research assistant said, “it doesn’t seem like fertility doctors even paused to consider their own findings”). I highlight some of the findings below. Keep in mind that gestational surrogate mothers are those who become pregnant by means of IVF and a donor’s eggs.
All four groups of women with IVF pregnancies were more likely to require a blood transfusion at delivery.
Women with IVF pregnancies who gave birth vaginally were more likely to suffer third- or fourth-degree lacerations to the vagina at delivery.
Women with IVF pregnancies that used donors’ eggs, whether fresh or thawed, were more likely to require an unplanned hysterectomy.
All groups of women with IVF pregnancies had higher rates of diabetes during pregnancy (“gestational diabetes”) than the group of “fertile” women.
The groups of women with IVF pregnancies that used donors’ eggs had the highest rates of hypertension (high blood pressure) for the whole duration of the pregnancy (that is, both pre-gestational and gestational hypertension).
The children conceived by IVF were more likely to be admitted to a neonatal (newborn) intensive care unit (NICU).
Children conceived by IVF from donors’ eggs had the highest rates of admission to the NICU, and their birth mothers had the highest rates of admission to the ICU (the general intensive care unit).
When Brooke Brown died, I immediately sent a letter to the Attorney General’s office in Idaho (the state where she had lived) asking for an investigation. I received no response. I contacted the press in the hope of getting her story out to the media; but again, no response. My office reached out to the local Baptist church that held Brooke’s memorial service, inquiring about services for the twins who had died. We were told no one knew what had become of the infants.
Brooke’s doctors, and the fertility industry, surely knew that this woman’s body, which had carried her own three children to term and then five surrogate babies, was at high risk of grave injury. We have no business, by any principle—ethical or otherwise—building a multi-billion-dollar industry at the risk of the health and well-being of women and children. In the end, the public deemed Brooke’s life, and those of the infants she carried, to be worthy of no news coverage and of barely $7,000. There’s nothing wonderful, beautiful, or useful about that.
Jennifer Lahl is the Founder and President of the Center for Bioethics and Culture and producer of the documentary films, Eggsploitation, Anonymous Father’s Day, Breeders: A Subclass of Women?, and Maggie’s Story. In 2018 she released #BigFertility which is an official selection in the Silicon Valley International Film Festival. Republished with permission from The Public Discourse.
ROME, June 5, 2019 (LifeSiteNews) — A respected Brazilian neurologist is seeking to blow the lid off the “brain death” myth, saying it is being perpetuated to supply an international multi-billion-dollar transplant industry.
Doctor Cicero G. Coimbra, MD PhD, a neurologist and professor of neuroscience at the Federal University of São Paulo, Brazil, has also said recovery for comatose patients is often possible, but a tightly controlled medical establishment is not giving doctors and medical students the facts they need to “do the best they can” for their patients.
In this interview (read full text below), Dr. Coimbra explains that the term “brain death” was coined in the 1960s, after the first successful human heart transplant “triggered a demand for transplantable vital organs to be harvested from patients” who were considered to be “hopelessly comatose” according to medical knowledge at that time.
There was “no preliminary scientific research” on the brain-death concept before the name was used, he said. But calling these patients “dead” enabled the medical community to overcome all of the legal hurdles associated with removing vital organs from these comatose patients.
Their main mistake, Dr. Coimbra argues, was to consider these patients “irreversibly” brain damaged.
By the 1980s, when organ transplants were performed around the world, medical researchers experimenting on animals discovered that when blood flow to the brain is reduced from the normal range to just 20-50 percent, the brain would “fall silent” — but was neither “dead” nor “irreversibly damaged.” By the end of the 1990s, this phenomenon — called “ischemic penumbra” — was demonstrated in humans, shattering the “brain death” myth.
The brain is silent but not dead, he said.
“Why is the ‘brain death’ theory still so prevalent, and what are students in medical school being taught about this?” LifeSite asked Dr. Coimbra.
The Brazilian neurologist explained that while medical students might hear about this if “information is provided to the general public,” they will not learn it in medical school.
“In medical schools, these concepts that I am telling you about — although they are published — are not available in medical textbooks. They are not available in medical meetings. In medical conferences you cannot find them,” he said, adding that information is being withheld to supply the organ donation industry.
If you speak to doctors one-on-one, they will often tell you they agree, Dr. Coimbra said, but “they don’t want to mess with the transplant system,” which has one of the most “well controlled systems” of information sharing in the world.
“The transplant system is a wealthy system; it is a powerful system,” Dr. Coimbra said. “They are everywhere in the medical community. They are in medical councils and medical academies; they are everywhere … Politically, they are very powerful.”
“In the United States alone, in 2016 the transplant system involved business to the tune of approximately 25 billion dollars,” he noted. “By 2025, it is expected to reach 51 billion dollars per year.”
It is “big business,” he said.
Dr. Coimbra continued:
The brilliant idea of the transplant system was to call what they thought to be irreversible brain damage “brain death.” Because whenever you say someone is against “brain death,” you think: “How can someone possibly be…against death? They don’t believe in death?” But “death” is just a word that was given to a “hopelessly comatose” patient — but they were “hopelessly comatose” at the end of the 60s, not now.
“In a very large number of those patients, they have no damage at all — no brain damage at all — they just have a silent brain,” he added.
To compound the problem, Dr. Coimbra said the standard test used for screening “brain death” — called the “apnea test” — can actually induce irreversible brain damage to an already comatose patient, by reducing the blood and oxygen to the brain for 10 minutes.
Dr. Coimbra said he has seen firsthand that there is hope for patients who have been labeled “brain dead.” If doctors would simply replace three essential (thyroid and adrenal) hormones, “the normal circulation to the brain would be restored,” he explained. But when these hormones are not replaced, the patient progresses “into a disaster.”
The Brazilian neurologist again noted that doctors and medical students are not taught this:
They know what is in the neurology textbook of medicine … They know what’s there, and this is not there. The importance of replacing thyroid hormone is not discussed in meetings related to brain injuries, and how to treat brain injuries. Not one single intensive care unit in the world replaces thyroid hormones — not a single one that I know of.
To illustrate how much the “brain death” myth has gripped the minds of the medical community, Dr. Coimbra tells the story of a 15-year old girl who began to show signs of brain activity once he administered the necessary hormones. Seeing notes of progress Dr. Coimbra had made in the girl’s medical chart, a doctor on call in the ICU that night wrote: “Once a patient is declared ‘brain dead,’ the patient is dead. It doesn’t matter if later on the patient no longer fulfills the criteria for ‘brain death.’ The patient is legally dead, because it was once diagnosed as ‘brain dead.’”
In the end, Dr. Coimbra said it all comes down to the duty of doctors to honor their sacred oath to “do no harm” and to “do the best they can” for the health and wellbeing of their patient.
By the end of the 1960s, the first human heart transplant performed by the surgeon Christiaan Barnard in South Africa triggered a demand for transplantable single vital organs to be harvested from those patients considered to be “hopelessly comatose.” It was the common understanding that, by using all possible techniques and knowledge available at that time, those patients could not be restored to a normal life and would rather eventually evolve to cardiac arrest within a matter of days; they would not recover consciousness. An ad hoc committee at Harvard Medical School decided to call their clinical condition “brain death,” so that they could remove vital organs maintained viable due to sustained heart beating (maintained supply of oxygenated blood) and use those organs to improve the health [of] other people — patients, for instance, who had liver failure, kidney failure, or end-stage heart failure. These people would benefit from having the organs from patients who were “hopelessly comatose.”
Calling these patients “dead” enabled the ad hoc committee to overcome all legal problems related to removing vital organs from comatose patients that could not recover according to the concepts and medical scientific knowledge that we had available by that time, i.e. by the end of the 1960s.
In order to transplant organs, they had to be removed from someone while they are still alive, while the heart is still beating?
Yes, they removed them from a comatose patient. But they thought it would not be possible to recover those patients, because they did not have the technology and knowledge to recover them.
The main mistake was to consider those patients “irreversibly” brain damaged, but their brain damage was considered irreversible due to the limited knowledge that they had at that time. Later on, as time went by, new knowledge and neurological scientific achievements offered other ideas about what was really going on in these patients. For instance, by the end of the 1960s — when the concept of “brain death” was introduced into medicine — doctors believed that, when there were no signs of brain activity that could be detected by neurological examination, the only possible reason would be the absence of blood circulation in the brain. And because the absence of brain circulation would destroy the brain within minutes, they decided to call it “brain death.”
The problem is that in the 1980s everything started changing. The practice of transplanting vital organs had already spread across the world, but already by 1984 or 1985 experiments carried out in animals — in rodents — demonstrated that when you decrease blood flow to the brain to only 50 percent of the normal range, the brain falls silent. This is because there is not enough energy to sustain what we call “synaptic activity.” Synapsis is the site where one neuron communicates with another neuron. Synaptic activity, which is the release of neurotransmission at the synaptic site, was no longer possible in these brains, because the brain blood flow was 50 percent of the normal range, and that would not provide enough energy for synaptic activity, for neurons to communicate with one another. So, the brain was silent, but the neurons would not die just because the blood flow was reduced to 50 percent.
So, the brain was silent but not dead…
Yes, silent but no neuronal death — no “brain death.” Necrosis, i.e. the process of neuronal death, is a process that takes several hours and is triggered when the blood flow is lower than 20 percent of the normal range.
This interval (approximately between 20 percent and 50 percent of the normal level of circulation) is now known as the “penumbra zone.” It was initially described in situations where there is an obstructed artery that supplies part of the brain. In the peripheral area of this so-called “ischemic” part of the brain, there was a collateral flow of blood supply between 20 and 50 percent of the normal flow, as demonstrated in animals. If you could recirculate that artery, you would save the peripheral area because it was only silent. It was not necrotic; it was not destroyed.
It is quite clear that when you have a patient with head trauma, and the brain is swelling, at some point the arteries that supply blood to the brain start being compressed, because the brain size is increasing within the intracranial space. The intracranial space is protected by bones, and bones cannot expand to accommodate the increase in brain volume. So, if the size of the brain increases as a result of what we know as “brain edema” or “brain swelling,” then the vessels are progressively compressed, and the blood flow to the whole brain decreases proportionally to increases in intracranial pressure. At some point, you will reach the level of a 50 percent decrease as compared to normal range. At this point the whole brain is silent — not a part of it but all of it is silent — but it is still recoverable. It is not dead; it is alive. And that situation was unknown at the end of the 1960s, when the concept of “brain death” was introduced into medicine.
So, it is clear that some of those patients are actually alive. What do I mean by alive? The brain was not destroyed; it was only silent. And the transplantation system has been taking organs from patients who had brain tissue that theoretically could be recovered. That brain tissue is not destroyed.
To me, it was quite clear by the end of the 1990s when the phenomenon of “ischemic penumbra” — a silent brain but no brain destruction — was demonstrated in humans, not only in rodents, that this situation could be called “global ischemic penumbra.”
The problem is that one of the tests used to diagnose “brain death” — called the “apnea test” — involves switching off the respirator. You disconnect the respirator for 10 minutes. When you do that, the high level of carbon dioxide increases sharply. This in turn further increases intracranial pressure and may decrease arterial pressure. So, you increase the compression on the brain vessels and you decrease the pressure within the brain vessels during the apnea test.
What was the purpose of the apnea test?
The aim of the apnea test is to demonstrate that the patient cannot breathe on his own.
In any culture in the world, it would be unacceptable to say that someone who is breathing is dead. Spontaneous breathing in any culture means life. So, for instance, when a baby is born, and it never breathes, you say that it was born dead. But if the lungs expanded at least once, for legal purposes, even if the baby immediately dies, you say that the baby is alive. The question of whether the baby is alive or dead when the baby is born has considerable legal consequences. No one in any culture of the world — Indian culture or Western culture, etc. — would accept anyone to be dead if that person is capable of breathing on his own. So, the purpose of the apnea test is to demonstrate that the patient cannot breathe on his own and can be regarded as dead.
But imagine for a moment: the respirator is disconnected from the lungs for 10 minutes. In order to breathe on your own, you need your respiratory centers in your brain to be working. They control the diaphragm and the respiratory muscles in general. If you switch off the respirator, and there is no breathing for 10 minutes, they say: “Ok, you see, this is one more piece of evidence that the patient is dead, because he cannot breathe on his own.” The apnea test is considered the fundamental test to diagnose “brain death.” No medical doctor anywhere in the world would diagnose “brain death” without doing this test. So, whenever you hear that a certain patient has been diagnosed as “brain dead,” you know that the apnea test has been performed.
Why isn’t the apnea test legitimate?
It’s not legitimate. Actually, it disrupts the most basic concepts of medicine. For instance, imagine if I prevent you from breathing for 10 minutes, what will happen? You will die.
But in this case, a respirator is helping the person to breathe.
Yes, right. The respirator is helping the person to breathe. You’re correct, no problem about that. The issue is: you are testing the vitality of the respiratory centers. But what will happen to the respiratory centers in a silent brain if you induce a test that decreases the blood flow to the respiratory centers? The respiratory centers were already silent, because they need synaptic function to work. If the blood flow is within the penumbra zone — between 20 and 50 percent — the respiratory centers cannot work, not because they are irreversibly damaged but because they are silent. You would not diagnose this as “brain death.” You will not differentiate the condition of global ischemic penumbra from irreversible brain damage by testing the respiratory function.
You can actually destroy the respiratory centers — as you can damage all parts of the brain — by further reducing the blood flow during the apnea test. Forty percent of the patients who are submitted to the apnea test have a major drop in their blood flow, in their blood pressure. Blood pressure is the pressure that is within the arteries; it’s the pressure that provides the driving force to maintain circulation in the brain. So, when you perform the apnea test, you may actually induce irreversible damage to the brain when you were only supposed to diagnose irreversible brain damage.
That would seem to go against the Hippocratic oath? You are harming the patient in order to apparently test whether a silent brain is dead.
The silent brain is not dead. You induce irreversible damage to the respiratory centers and to the whole brain just by performing the apnea test. So, as you said, they are not respecting the Hippocratic oath, because the most basic concept of medical practice is what you just said: First, “do no harm.” And the second is, “do the best you can.” So, neither of these basic concepts of the Hippocratic oath are being respected in this situation.
If this research has been done in humans as well as in rodents, why is the “brain death” theory still prevalent? And what are students in medical school being taught about this? Would they hear about this latest research?
Well they may hear about it, if you provide information to the general public as you were trying to do. But in medical schools these concepts that I am telling you about — although they are published — are not available in medical textbooks. They are not available in medical meetings. In medical conferences you cannot find them.
Nowadays the transmission of information within the medical community in general — not only in this country or that, but worldwide — is probably, or certainly, the most well controlled system of transmitting information, because it is worth billions of dollars per year. If you put information in a textbook, it can redirect the flow of money from one sector to another. It’s the most well controlled type of transmitting information in our society that I know of.
Are you saying that, for the sake of the organ donation and organ transplant industry, the general public and medical students are not being given this information?
Yes, I have been trying to talk to the neurological community in my country and in other countries, and the reaction that we see is that some [doctors] will tell you — “Okay, I understand what you are saying, but never tell anyone that I agree with you” — because they don’t want to mess with the transplant system. The transplant system is a wealthy system; it is a powerful system. They are everywhere in the medical community. They are in medical councils and medical academies; they are everywhere. They are very powerful. Politically, they are very powerful.
What could happen to a doctor if he tried to go against the system?
Well, maybe what happened to me. I had to fight in court to hold on to my license to work as a doctor for 19 years in Brazil. And that was a long time. So, you understand why some doctors that are aware of what is happening do not want to talk freely about that. They simply do not want to mess with powerful people.
They even control and have an influence in the press. Sometimes it is said, “Oh that doctor is against ‘brain death.’” The brilliant idea of the transplant system was to call what they thought to be irreversible brain damage “brain death.” Because whenever you say someone is against “brain death,” you think: “How can someone possibly be against death? They don’t believe in death?” But “death” is just a word that was given to a “hopelessly comatose” patient — but they were “hopelessly comatose” at the end of the 60s, not now.
Now you can understand that, in a very large number of those patients, they have no damage at all — no brain damage at all — they just have a silent brain. And that was confirmed in the middle of the 70s. In the mid 70s, some people from histopathology or pathologist[s] started wondering how a doctor since 1968 (when “brain death” was introduced into medicine) can say that there is necrosis of the whole brain — that there is irreversible damage of the cells in the whole brain, just by doing a neurological examination? Pathologists started wondering what is happening here. They wondered: “How can they possibly use a term like ‘necrosis,’ which is the terminology that only pathologists use when they look at the tissue under the microscope.”
So, they started checking into this. They did histological examinations in patients who were diagnosed as “brain dead” for 48 hours — so time enough for full necrosis to occur. No signs of brain activity, no evidence of blood flow for 48 hours. The whole brain should be necrotic; it’s time enough for full necrosis. When they examined those brains — I think the article was published by 1976 — they saw that about 60 percent of those brains had no signs of necrosis at all.
People who were in favor of “brain death” had to defend themselves when these papers were published. They said, “Okay, necrosis in those cases is indicated by such tiny signs that you cannot see it in the microscope. That’s why you cannot see it, but we know it’s there. We know, because there is no possible explanation for absence of blood flow for 48 hours.” Again, when more and more evidence was available to demonstrate that what they had thought in 1968 — which was complete absence of blood flow — was not true, they tried to say something else or invent something else in order to explain it — even as a hypothesis.
You saw that in this conference [on “Brain Death”: A Medicolegal Construct: Scientific & Philosophical Evidence] — it was said several times — that when the practice of “brain death” was introduced into medicine, there were no scientific papers to support it, no scientific research. It was simply a concept: “Ok, we believe that those patients have no blood flow, because they have such a severe edema that the blood vessels are completely compressed. There’s no blood flow. There is no way that the brain could survive after a few hours under no blood flow. So, we will call it ‘brain death’ because that’s what we believe is going on.”
But as I told you, and as you heard from several speakers, there was no preliminary scientific research on the concept of “brain death” to support the concept of “brain death.”
While they claimed that the brain was “dead,” what was going on in the body? The heart is still beating…
Yes, because if it’s not beating you cannot use vital organs. If there is an arrest in circulation, you have damaged organs that you’re trying to transplant to other people.
Dr. Coimbra, when people hear “brain death,” they think the brain is dead. But as you have explained, the brain is actually silent. When the brain is silent, what is the state of the other organs and systems in the body?
This is a very important question, because one of the parts of the brain that is possibly within the range of ischemic penumbra, between 20 percent and 50 percent of the normal levels of circulation, is the hypothalamus.
The hypothalamus produces several hormones that control other glands in our body. And there are at least three hormones that are very important to our discussion. Because the hypothalamus is also under low levels of circulation, the production of those hormones is decreased.
For instance, one of these hormones is the hormone that releases TSH from the pituitary gland. TSH is “thyroid stimulating hormone.” So, you have the hypothalamus producing TSH-releasing hormone. TSH-releasing hormone induces the production of TSH by the hypophysis [pituitary gland]. The hypophysis releases TSH into the circulation, and then the thyroid gland located in our neck keeps producing thyroid hormone.
Thyroid hormones have an action in the brain. They have actions in all of our organs. One of the most important actions is to prevent fluid from leaking into the tissues. So, when you have a patient who has had a brain trauma, for instance, and that trauma has increased the volume of the brain, and now the blood vessels are compressed, the blood vessels that supply blood to the hypothalamus are also compressed. And then you get into a state that is called “Central hypothyroidism.” In this state, the thyroid gland decreases the production of thyroid hormones, because the thyroid gland is not receiving enough stimulation from the brain.
So, the lack of thyroid hormones increases brain damage and brain edema, i.e. brain swelling. This is a critical situation, which I could put this way: if you don’t replace thyroid hormone the brain tissue will die, because the brain swelling will progress, progress, and progress up to the point that the blood vessels are fully compressed, and you have no blood flow at all. Then you have irreversible damage to the brain. But when the blood supply to the brain is within the range of “ischemic penumbra” (a silent but not irreversibly damaged brain) or progressing to that situation (progressing into deeper levels of coma – with reduced, but not absent neurological signs of brain activity) you can rescue the brain, just by giving three hormones.
One of the most important ones is the thyroid hormones. If you give the comatose patient thyroid hormones, you will prevent further leakage of liquids from the intravascular space (the space within blood vessels) into the brain tissue. The progress of brain swelling will stop and reverse, the brain vessels will no longer be compressed, you will increase the blood supply to the brain and the patient will start recovering brain functions.
But this situation starts long before the beginning of [the] screening test for “brain death.” We have a scale to measure the level of coma. It’s called the “Glasgow Coma Scale.” A normal person who is fully awake is at level 15 on the Glasgow Coma Scale. When there are no signs of brain activity, you are at level 3. When you reach level 3, you start screening the patient for the diagnosis of “brain death.”
But when the Glasgow Coma Scale is far away from 3 — when it is around 8 or 7 — most if not all patients have low circulating levels of thyroid hormone. By that point the brain edema is now turned into the so-called “brain myxedema,” because the edema is now caused by a lack of enough amounts of thyroid hormones. Therefore, if you start replacing thyroid hormones when a patient of a traumatic brain injury is at the Glasgow levels of 8 or 7 — the patient’s neurological state can improve and even all neurological functions can be normalized. And this is an obligation, this is not something that you say, “Okay, I will leave it like that.” No, you see that something is wrong, and you can save the life of a patient. Hypothyroidism is a lethal disorder; if you don’t treat it patients will die.
It goes back to what you said about the Hippocratic oath. The most basic part is “do not harm” to your patients. But the second part is “do the best you can” to save the life of your patients, to improve their health, to improve the wellbeing of your patient.
So “do your best” and now you’re not following the second aspect of the Hippocratic oath. You should replace thyroid hormones in order to prevent so-called “brain death.”
And is this generally done? Are these three hormones generally given?
No, it’s not done anywhere.
Why not?
This is a question that the medical community should answer. Why are they not following the second principle of the Hippocratic oath in this situation? It’s been published since the 80s.
So they know … it’s not as though the doctors who are dealing with these patients don’t understand what happens to the thyroid …
When you say they “know,” I have to say that it’s published, but I would not say that the doctors “know” because they don’t know everything that is published. They know what is in the neurology textbook of medicine, like the neurology textbook. They know what’s there, and this is not there. The importance of replacing thyroid hormone is not discussed in meetings related to brain injuries, and how to treat brain injuries. Not one single intensive care unit in the world replaces thyroid hormones — not a single one that I know of. Because, you know, if you would replace thyroid hormones when the Glasgow Coma Scale is at 7 or 8, probably almost no patient would progress into so-called “brain death.” So, it’s not done — it’s simply not done.
What happens to the brain when these thyroid hormones are not given to the patient?
As the brain swells because thyroid hormones are not replaced, the hypothalamus stops or decreases the production of other hormones that are very important for the survival of the comatose patient.
One of the most important ones is the so-called ACTH. ACTH is a hormone that is produced under the stimulation of the hypothalamus. It is produced by the hypophysis [pituitary gland], and it stimulates the adrenal glands to produce hormones that keep your blood pressure within the normal range.
If you can compose the whole situation in your mind: you have a decreased level of thyroid hormones — that’s why the brain is swelling, that’s why the blood flow is decreased: because blood vessels are being compressed in the intracranial space. The patient is evolving to the so-called…“brain death.” And now, the pressure within the vessels that is necessary to supply blood flow to the brain is also decreasing, because the adrenal glands are not providing enough amounts of what we call “mineralocorticoids” to stabilize the blood pressure. So, the blood pressure within the vessel is going down — the pressure which is necessary to supply blood flow to the brain.
So, you have these two circumstances that co-operate to damage the brain: you have increased intracranial pressure because of lack of thyroid hormones, and you have decreased blood pressure because of low levels of adrenal hormones. And again, because those adrenal hormones are not replaced, the patient – the whole organism — is progressing into a disaster.
You said that three hormones should be given. What is the third?
There is a third hormone that should be given to those patients and it’s also produced by the hypothalamus and the hypophysis. It is called ADH, which stands for “antidiuretic hormone.” It prevents your kidneys from releasing large amounts of fluid that would further decrease the volume within your vessels. The further decrease in pressure within the blood vessels comes from the fact that you don’t have enough volume within your circulatory system to sustain circulation.
This third hormone is the only one that is sometimes given to those patients, because it’s impossible not to identify this situation. If you want to identify the situation when thyroid hormones are low, you have to measure them. If you want to identify a situation where adrenal gland hormones are low, you have to measure them. But you know whether the patient is producing low levels of ADH, you know it because he (she) is eliminating a lot of urine — 6 liters, 8 liters, or even 10 liters of urine every day.
The lack of these three hormones will lead the organism into a disaster. And they are not replaced. Because what should be done is not being done, this patient will die within a few days. Nearly these patients will die within a few days due to cardiac arrest. But that’s because you are not considering part of the second Hippocratic oath, which is: you should do the best you can to save the life of your patient. You’re not replacing thyroid hormones; you’re not replacing adrenal hormones; you’re sometimes not replacing ADH, so those patients will die in a few days.
How do those who support “brain death” defend this?
Believe it or not, people who are in favor of “brain death” say it doesn’t matter what you do. The say that, even with the most aggressive intensive care treatment, these patients will die within a few days, so it’s a good idea to take their organs to save the lives of other people. But, actually, those patients have not been treated as they should. The most basic treatment, that is, replacing of all these three hormones, is not done, so the patient will die.
Hypothyroidism is known by the medical community to be a lethal disorder if it’s left untreated. Adrenal failure, which I just described, is also known to be a lethal disorder if it’s left untreated. And the same is true for diabetes insipidus, which is due to the lack of ADH. So, you have three lethal disorders in the same patient, and you don’t treat them. Instead, you say: “Those patients will die even if you give them the most aggressive intensive care treatment.” It’s not true. You don’t know what’s happening. You don’t know the pathophysiology of what is happening with this patient.
Medical doctors are not taught to give thyroid hormones or adrenal hormones; sometimes they are not even taught to give ADH. Doctors sometimes say this is happening “because the brain is dying.” But, actually, the brain is dying because they not replacing those thyroid hormones. If doctors would replace these three types of hormones, the normal circulation to the brain would be restored and the hypothalamus will restart producing normal amounts of all those hormones.
Have you treated patients who have recovered from severe brain trauma through the use of these hormones?
Yes, I treated a 39-year-old woman who was declared “brain dead”… It was a surgical accident that caused the damage to the brain, and I started the replacement of these hormones four days after the event. I have to tell you that it should have started beforehand, not four days later. But she was already diagnosed as “brain dead” and the family had been told. So, we started replacing the thyroid hormones at day four. Eight days after the beginning of the replacement of thyroid hormones and the other hormones, the patient started to breathe on her own. Therefore, the patient could no longer be recognized as someone who is dead, because she was breathing. As I said before, the ability to breathe on one’s own is a sign of life in any culture of the world, so that patient was alive.
One month later, she was able to communicate with her parents. Because she had a tracheostomy she had to communicate by lip reading. She would only move her lips, because there wasn’t sufficient air to vibrate the vocal cords. There was no sound, but she could communicate by lip reading and that continued for two or three months.
Unfortunately, she died because she was in bed too long and she had clot formations within the veins of her legs and the clots moved to her lungs. She died because of pulmonary embolism.
But she was able to communicate with her parents before she died.
Yes, for two or three months she could communicate with them…
Which is all the difference for the family…the fact that the parents were able to communicate with their daughter.
Her brain was functional. Of course, she had some severe neurological problems related to movement. Her movements were severely restricted. But we did not know what would have happened in the next few months, if she would start moving her arms and legs or not. Unfortunately, she had this clinical complication and died because of that.
Since you asked, it is important to say that, before this lady, I treated a 15-year-old girl. I started the treatment one month after the accident. She had already been submitted to three apnea tests. She breathed in the first and the second, but not in the third. They were done on consecutive days, so each of the tests were an additional aggression to the patient, to the brain circulation, and finally she could not resist the third. She was in a deep coma with no respiratory reflexes.
That patient was not in the same city where I worked, and the family moved from another state in Brazil to the state of São Paulo. I started the replacement of the thyroid hormones too late, but at some point, about two weeks later, under thyroid hormone replacement and the replacement of other hormones, that patient was having seizures, convulsions, on the right side.
But a person who is “brain dead” doesn’t have brain seizures, do they?
No, a dead brain cannot have a seizure. That’s what I wrote on the patient’s chart.
The doctor on call that night in the ICU was someone involved in a transplant system. And he wrote something [in the chart] like: “once a patient is declared ‘brain dead,’ the patient is dead. It doesn’t matter if later on the patient no longer fulfills the criteria for ‘brain death.’ The patient is legally dead, because it was once diagnosed as ‘brain dead.’”
I can prove this. I have a copy of the patient’s chart. So, you see the conflict of interest here. In the United States alone, in 2016 the transplant system involved business to the tune of approximately 25 billion dollars. By 2025, it is expected to reach 51 billion dollars per year.
On the internet, you can find announcements suggesting that you should buy shares from those pharmaceutical companies, because they will be increasing profits and you can earn a lot of money by buying their shares. So, this is big, big business. You can see how powerful these people are.
Imagine that you knew a very well-known, prestigious transplant surgeon, who has been performing vital organ transplants for 30 years. He is very skillful surgeon, possibly world-renowned. And then you come to him and say that “brain death” is not death anymore, because now we know much more than we knew in 1968, when brain that was introduced into medicine.
Imagine that you tell him he should stop doing vital organ transplants. He has been doing them for 30 years, and he is very skillful, perhaps a world-renowned doctor. Do suppose that he will accept that peacefully? It’s difficult. After 30 years, all the prestige that has accumulated and then you tell him he should look for another way of making money — another specialty because transplants are no longer possible.
It seems it goes back to the Hippocratic oath. A doctor makes a vow when he becomes doctor. It is a sacred vow.
Yes, definitely.
***
See below the complete 41-minute talk by Dr. Coimbra given May 20, 2019 at the John Paul II Academy for Human Life and the Family Conference in Rome.
A preborn baby is beautiful and fascinating, and technology is revealing the development of this tiny human person growing in his mother’s womb. The amazing moment that a mother can hear the heartbeat of her preborn child has been captured thousands of times on video, and shared on YouTube and other social media.
Below are some of these precious moments which prove, yet again, that the baby in the womb is very much alive and deserves our full protection:
5 weeks:
6 weeks:
7 weeks:
8 weeks:
9 weeks:
10 weeks:
“When a heartbeat can be detected, a life should be protected” — this is the impetus behind “heartbeat bills” which ban abortion after a preborn child’s heartbeat can be detected, usually by six weeks.
On November 1, 2017, a federal Heartbeat Protection Act received a hearing before a Congressional Subcommittee on the Constitution and Civil Justice. The bill, H.R. 490, was sponsored by Representative Steve King (R – Iowa), who is also the Chairman of the Subcommittee. The bill did not succeed.
By just 22 days after conception, a baby’s heart is confirmed to be beating in utero. But more recent studies show it might actually start beating as early as 16 days after conception.
Do some products contain fetal parts? The short gruesome answer: Yes.
Today’s consumer products are not the soap and lampshades of recycled Nazi concentration camp victims. The new utilitarian use of people is a sophisticated enterprise, not visible to the human eye.
Fetal Parts in Daily Life
Perhaps you are a diligent supporter and promoter of pro-life legislation, only vote for pro-life candidates, avoid entertainment from musicians and actors who openly support Planned Parenthood. Regardless, you may unwittingly be cooperating in aborted fetal cell research by purchasing products that use aborted fetuses, either in the product itself or in its development.
One might take Enbrel (Amgen) to relieve Rheumatoid Arthritis. Your husband was given Zoastavax (Merck), a Shingles vaccine, at his annual physical. Your mother with diabetes and renal failure is prescribed Arensep (Amgen). Your grandfather is given the blood product Repro (Eli Lilly) during an angioplasty. The local school district requires that your grandchildren receive the MMRII (the Merck Measles-Mumps-Rubella vaccine). Your daughter and son use coffee creamers and eat soup with artificial flavor enhancers (Senomyx/Firmenich) tested on artificial taste buds engineered from aborted fetal cells.
Because of the vagary of FDA labeling, unless you are proficient at reading patents and pharmaceutical inserts you wouldn’t know aborted fetal parts were there without someone to tell you.
Luckily, that someone is the watchdog group Children of God for Life (COG), a pro-life public citizen group which tracks the use of aborted fetal parts. Under the leadership of Executive Director Debi Vinnedge, COG publishes a downloadable list of products that use aborted fetuses currently available in the U.S.
Products That Use Aborted Fetuses
Products related to fetal material can be broken down into roughly 3 categories: artificial flavors, cosmetics, and medicines/vaccines.
1. Food and Drink
To be clear, food and beverages do not contain any aborted fetal material; however, they may be tastier because of it. How is that?
The American biotech company Senomyx has developed chemical additives that can enhance flavor and smell. To do this, they had to produce an army of never-tiring taste testers–that is, flavor receptors engineered from human embryonic kidney cells (HEK 293, fetal cell line popular in pharmaceutical research).[1] These artificial taste buds can tell product developers which products the public will crave. The goal is to do a taste bud “sleight of hand,” creating low-sugar and low-sodium products that taste sweet or salty while actually using less sugar or sodium in the product.
Does your Nestle Coffee-mate Pumpkin Spice refrigerated creamer taste more like autumn? Does your Maggi bouillon taste just like chicken? Thank Senomyx.
The laboratory-created artificial enhancers do not have to be tested at length by the FDA because the Senomyx chemical “flavor compounds are used in proportions less than one part per million” and can be classified as artificial flavors.[2]
In 2005, Senomyx had contracts to develop products for Kraft Foods, Nestle, Campbell Soup and Coca-Cola.[3] However, when it was discovered in 2011 that PepsiCo was using Senomyx to develop a reduced sugar beverage, a boycott ensued that caused Kraft-Cadbury Adams LLC and Campbell Soup cancelled their contracts with Senomyx. In a 2012 letter to Children of God for Life, PepsiCo stated, “Senomyx does not use HEK cells or any other tissues or cell lines derived from human embryos or fetuses for research performed on behalf of PepsiCo.”[4] To that effect, PepsiCo is working with Senomyx on two products developed with Sweetmyx 617, a new Senomyx sweet taste modifier.[5]
In November 2018, the Swiss company Firmenich acquired Senomyx, Inc. Firmenich describes itself as “a global leader in taste innovation and expert in sweet, cooling and bitter solutions.”
2. Cosmetics
The fountain of youth…is babies.
Commercially, it’s known as Processed Skin Proteins (PSP), developed at the University of Lausanne to heal burns and wounds by regenerating traumatized skin. The fetal skin cell line was taken from an electively aborted baby whose body was donated to the University.[6]
Neocutis, a San Francisco-based firm, uses PSP in some of their anti-aging skin products. Their website claims the trademarked PSP “harnesses the power of Human Growth Factors, Interleukins and other Cytokines, to help deliver state-of-the-art skin revitalization.”
3. Vaccines and Medicine
The Vaccine Card at the Sound Choice Pharmaceutical Institute (SCPI) website lists over 21 vaccines and medical products that contain aborted fetal cell lines. The Card is updated yearly, and also lists ethical vaccine alternatives when there are any.
SCPI is a biomedical research organization headed by Theresa Deisher, who has a PhD in Molecular and Cellular Physiology from Stanford and 23 patents in the field to her name. Dr. Deisher, the first person to identify and patent stem cells from the adult heart, has an insiders understanding of genetic engineering having worked in the industry leaders such as Amgen, Genetech, and Repligen.[7]
Among other things SCPI “promotes awareness about the widespread use of fetal human material in drug discovery, development and commercialization.”
No vaccine product is completely pure: “You will find contaminating DNA and cellular debris from the production cell in your final product. When we switch from using animal cells to using human cells we now have human DNA in our vaccines and our drugs.”[8]
The problem is three-fold. Aborted fetal parts are used for experiments, aborted fetal cell lines are used, and fetal cellular DNA debris are in vaccines and medicines.
But it is not just human DNA that is left over, so are some of the chemical stabilizers that keep the product from degrading, as well as, stimulants to rev up the immune system.
“Vaccines are a virus that have been put into a vial, in a liquid, which is the buffer, which we call excipients, and companies have put in stabilizers so that the virus won’t degrade and other things that kind of rev up your immune system so that they can use lower amounts of the virus and have a greater profit margin. And immune stimulants are things like aluminum and thimerosal, they are stabilizers but they rev up the immunes system, so all of these things are in the final product, including contaminates from the cell lines that are used to manufacture the vaccines.”[9]
Why aren’t the contaminates removed? Because nobody wants a pediatric vaccine that costs a few thousand dollars.[10]
In finance, the yield is inversely related to the price. In chemistry, the yield is inversely related to purity. The price of inexpensive mass-produced vaccines is that the medical establishment accepts that the vaccines contain a high amount of fetal contaminates.
“[I]f they have purified out the containments from the cell lines, the yield would be so low that they wouldn’t make any money, or no one would pay a thousand dollars or ten thousand dollars for a vaccine. And so because of that case remnants from the cell lines, in that case, fetal cell lines are in the final product. And they are at actually very high levels. And in the chicken pox, the fetal DNA contaminates are present at twice the levels of the active ingredient which is Varicella DNA.”[11]
The Fetal Tissue Marketplace
Much research is currently being done with fetal cells.
We know this because, for one, there’s a market for fetal parts. In a series of undercover videos, David Daleiden of The Center for Medical Progress exposed Planned Parenthood abortion clinics selling fetal parts to investigators posing as and medical researchers. And for his efforts his office was raided in 2016 by then California Attorney General Kamala Harris, now a Senator and 2020 Presidential Candidate Harris.[12] Daleiden is currently being pursued in court by current California Attorney General, and former Democrat California Congressman, Xavier Becerra.
We already knew this was happening from the testimony of scientists themselves. On January 11, 2018, professor emeritus Dr. Stanley Plotkin, the lead developer of the Rubella vaccine for the Wistar Institute (Philadelphia) in the 1960s, was deposed as an expert witness on Vaccinology in a Michigan child custody case.[13] Dr. Plotkin was asked how many aborted fetuses he has used in his experiments:
QUESTION: So in your, in all of your work related to vaccines throughout your whole career, you’ve only ever worked with two fetuses?
PLOTKIN: In terms of making vaccines, yes.
But after being presented with Exhibit 41 (Proceedings of the Society of Experimental Biology and Medicine), the two fetuses involved in his experiment grows exponentially to 76 aborted fetuses.
QUESTION: So this study involved 74 fetuses, correct?
PLOTKIN: Seventy-six.
QUESTION: And these fetuses were all three months or older when aborted, correct? PLOTKIN: Yes.
A true enough response. Fetal cells, for that matter all normal cells, have a finite capacity to replicate following the principle of cellular aging. The vaccine trail needed many cell lines in order to achieve its end.
An interesting aside, during questioning Dr. Plotkin answered affirmatively that some of his subjects for experimental vaccine trials had been children of “mothers in prison,” the mentally ill, and “individuals under colonial rule” [Belgian Congo].
Dr. Theresa Deisher first became aware of the introduction of fresh aborted fetal material in drug discovery in 1996.[14] Fresh fetal parts are a time-saver compared to the days spent washing and prepping animal tissue, like monkey hearts, for laboratory experiments. While it is not legal to sell aborted fetal tissue, it is still available in catalogues and comes with high prices for shipping and handling.
A Better Option
According to Dr. David A. Prentice Vice, President of the Charlotte Lozier Institute and Adjunct Professor of Molecular Genetics at the John Paul II Institute, adult stem cells are the benchmark for research that has led to actual cures for patients.
“The superiority of adult stem cells in the clinic and the mounting evidence supporting their effectiveness in regeneration and repair make adult stem cells the gold standard of stem cells for patients.”[15]
Then why are we still using embryonic cell lines when adult stem cells have become the Gold Standard? There seems to be little excuse for products that use aborted fetuses.
U.S. Policy on Products That Use Aborted Fetuses
President Bill Clinton
On the 20th Anniversary of Roe v. Wade in 1993, President Clinton signed five abortion-related memorandums which included the reversal of the George H. W. Bush era moratorium on creating new fetal tissue for research, claiming at the time that, “This moratorium has significantly hampered the development of possible treatments for individuals afflicted with serious diseases and disorders, such as Parkinson’s disease, Alzheimer’s disease, diabetes and leukemia.”[16]
While a bio-ethics debate transfixed the country in 2006 as to whether the United States would allow the use of new aborted fetal stem cells in research, [see White House Fact Sheet on Stem Cell Research Policy], the medical research community had already decided that the future lay with human-animal hybrids and new aborted fetal cell lines. According to a statement submitted to the President’s Bioethics Council:
“Aborted human DNA in our vaccines is not the end, it is only the beginning, as the creation of human-animal hybrids demonstrates. A new aborted fetal cell line has been developed, called PerC6, and licenses have been taken by over 50 partners, including the NIH and the Walter Reed Army Institute, to use this cell line for new vaccine and biologics production. The goal of the company that created the PerC6 is to become the production cell line for ALL vaccines, therapeutics antibodies, biologic drugs and gene therapy.”[17]
And this has largely come to pass.
In 2019, the Department of Health and Human Services granted a second 90-day extension to a contract it has with the University of California at San Francisco that requires UCSF to make “humanized mice” for on-going AIDS research. The human fetal tissue comes from late-term abortions.
CNSNews reported that “according to an estimate it has published on its website, the National Institutes of Health (which is a division of HHS) will spend $95 million this fiscal year alone on research that–like UCSF’s “humanized mouse” contract–uses human fetal tissue.”[18]
See here for news on how the Trump administration limited the sale of fetal parts.
Stop Ebola? Prevent Zika Virus? Cure AIDS? Look for more, not fewer, aborted fetal products in the future.
Writer Andrea Byrnes was the first producer of U.S. March for Life coverage at EWTN Global Catholic Network, which she continued to supervise for seven years. She attended her first HLI conference in 1989, where she first met Servant of God Dr. Jerome Lejeune. She and her husband would later pray for Lejeune’s intercession for her son’s health difficulties discovered before birth, and thanks be to God, he is thriving.
Notes
[1] Melanie Warner, “Pepsi’s Bizarro World: Boycotted Over Embryonic Cells Linked to Lo-Cal Soda.” CBS News Moneywatch. June 3, 2011.
[7] Theresa A. Deisher, Phd. “Testimony on Conscience Rights related to biologic drug disclosure and alternative drugs.” President’s Council on Bioethics Archive. Georgetown University. September 8, 2008.
[8] Theresa A. Deisher, Phd. “Testimony on Conscience Rights related to biologic drug disclosure and alternative drugs.” President’s Council on Bioethics Archive. Georgetown University. September 8, 2008.
[9] “Dr. Theresa Deisher Guelph, Ontario Canada June 23, 2018.” Vaccine Choice Canada published on YouTube. August 2, 2018.
[16] Robin Toner. “Settling In: Easing Abortion Policy; Clinton Orders Reversal of Abortion Restrictions Left By Reagan and Bush.” New York Times. January 23, 1993.
[17] Theresa A. Deisher, Phd. “Testimony on Conscience Rights related to biologic drug disclosure and alternative drugs.” President’s Council on Bioethics Archive. Georgetown University. September 8, 2008.
[18] Terence P. Jeffrey. “HHS Extends Contract to Make ‘Humanized Mice’ With Aborted Baby Parts for Another 90 Days.” CNSNews. March 1, 2019. 5:16 PM.
According to an article published by Wisconsin Public Radio, Republican lawmakers in Wisconsin are introducing a new bill that would allow pharmacists to prescribe birth control pills and patches. As of now, only doctors can prescribe birth control under Wisconsin state law.
Under this proposed law, all that would be required of patients would be to fill out a questionnaire and undergo a blood pressure test in order to receive a prescription. The two lawmakers pushing for this bill, Reps. Mary Felzkowski and Joel Kitchens, “wrote in a memo seeking co-sponsors that they want to give women more choices for reproductive care and reduce unplanned pregnancies.”
Unfortunately, despite these representatives’ intentions, data shows that increased access to birth control does not always decrease unplanned pregnancies but sometimes increases them, by providing couples with a false sense of security that they cannot have a pregnancy when using it. All forms of birth control have a failure rate and when we consider the high number of people are using birth control, the number of those who get pregnant using it is not insignificant.
As former Planned Parenthood director Abby Johnson describes it to Natural Womanhood, “according to Guttmacher themselves, Planned Parenthood’s own research arm, is that 54% of women who are having abortions are using contraception at the time when they get pregnant. So the idea that contraception is working for women and that it’s preventing [unplanned pregnancies and] abortion is not true. If it were, that number would not be 54%.”
TURNING PATIENTS INTO CUSTOMERS
At present, pharmacists can prescribe birth control in California, Colorado, Hawaii, Maryland, New Mexico, Tennessee, Utah, Washington D.C., and Washington state. Each state has different requirements and restrictions, and pharmacists in these states can opt out of providing this service.
This push towards eliminating the step of visiting the doctor’s office to get prescription medication rings familiar, as Natural Womanhood contributor, Lindsay Schlegel recently wrote about the rise of direct-to-consumer medicine providing websites. In this model, the patient—who is now better described as a customer—fills out an online questionnaire through the website. Their questionnaire is then used to prescribe the customer with the proper medication, which is then mailed directly to their doorstep.
Although this model is certainly convenient, Schlegel addressed the overwhelming concern of where this system might lead us:
“Skipping a visit to the doctor’s office and pharmacy is certainly more convenient than dealing with uncertain wait times. Still, we have to consider that in this model, ‘doctors can’t address secondary issues that surface during a consultation and can’t add information to a patient’s home medical record,’ notes Vishal Khetpal, third-year medical student at the Warren Alpert Medical School of Brown University, in his essay ‘The Worrisome Rise of Direct-to-Consumer Medicine’ published at Undark, an editorially independent magazine.”
While we recognize that by having pharmacists prescribe birth control we are not eliminating face-to-face interaction, this does dispose of the aspects of personal care for the whole health of a patient that only a doctor can provide. In general, pharmacists are not permitted to prescribe drugs, only handle and administer them. Whereas a doctor has the opportunity to treat a patient more holistically, the interaction with a pharmacist is brief and puts them in the position to be more of a drug gatekeeper.
As the access to hormonal birth control is made more easily available without doctors’ involvement, we should be concerned with her women will become collateral damage in a system that treats them like customers buying harmless products rather than as patients with individual health needs, considering taking a very powerful hormone-altering drug.
Fertility Awareness-Based Methods (FABM), also known as “natural birth control” or natural family planning, allow women to manage their health without putting loosely regulated drugs (that come with many health risks and side effects) into their bodies. While our medical system seems to be becoming less and less patient-oriented, it’s reassuring to know that methods like FABMs exist, which allow women to take their health into their own hands in an empowered and safe way.
Posted by Gabriella Patti
Gabriella Patti is a journalist currently located in Michigan.
Americans are having fewer children than ever before. According to new data released by the Center for Disease Control (CDC), for the fourth year in a row the number of children born in the United States has fallen. Last year, 3,788,235 babies were born in the U.S. – a drop of 2% from the previous year, and the lowest number in 32 years.
Behind the drop in total births, however, is an even more dramatic and troubling statistic. The overall fertility rate (i.e. the number of children born per woman) has fallen to its lowest level ever, at just 1.72. As a general rule, for a population to replace itself, the average birth rate needs to be 2.1 children born per woman.
Up to a point, birth rates tend to reflect the health of the economy. The healthier an economy, the more confident parents are that they can provide for their children, and the more likely they are to have children. At least, that’s the theory. Demographers had previously linkedthe downturn in the birthrate over the past decade to the effects of the 2008 recession. However, even though the economy has since recovered, birth rates continue to fall – something that has taken population experts by surprise.
“I keep expecting to see the birthrates go up, and then they don’t,” demographer Kenneth Johnson of the University of New Hampshire’s Carsey School of Public Policy told the Associated Press. Johnson noted that if the fertility rate had remained at the same level as it was before the recession, some additional 5.7 million babies would have been born. “That’s a lot of empty kindergarten rooms,” he noted.
Many mainstream media outlets seemed puzzled about how to frame the latest numbers. On the one hand, many clearly felt compelled to try to put a bright face on the data, suggesting that the reduction in birth rate is a consequence of the greater “reproductive freedom” (i.e. access to contraception and abortion) enjoyed by women. However, underneath the façade of celebration, many news reports also contained a pervasive note of concern. As well they might.
One doesn’t need to be pro-life to recognize that a nation without children is a nation without a future. With an aging population, increasing pressure will be placed on an ever-dwindling work force to keep the economy going, to pay the taxes that support social security, health care for the needy and other social programs, and to provide care for aging parents and grandparents. Furthermore, the smaller number of young people carrying this heavier social and economic burden will be the same people we need to produce children for the next generation.
Where There is God, There is Fruitfulness
However, as one demographer pointed out, America’s increasingly bleak demographic statistics are, in fact, nothing unusual. Quite the contrary. “This is an important change,” Dr. Johnson-Hanks told the New York Times about the latest CDC numbers, “but it is not one that is making us extraordinary. It is making us more like other rich countries. It is making us more normal, in a sense. This is what Canada looks like; this is what Western Europe looks like.”
I suppose Dr. Johnson-Hanks meant this observation to be comforting. But the fact is, on the data he’s absolutely right: this is the new “normal” all across the developed world. In many European countries, the number of deaths has long exceeded the number of births, and many countries have birth rates far, far below that of the U.S.
While some politicians and economists are starting to wake up to the dire economic outlook created by shrinking populations, my own concern is the spiritual crisis that precipitated the demographic one. Indeed, this is where I think the demographers go wrong. The reason the U.S. birth rate isn’t rebounding goes far deeper than the lingering effects of a brief recession: at root it’s not an economic problem, it’s a heart problem…and a theological problem.
In a 2017 homily, Pope Francis addressed this issue head on. “Fill the earth, be fruitful! It is God’s first commandment,” the Holy Father noted, adding that where “there is God, there is fruitfulness.” “[S]ome countries come to mind,” he said, “that have chosen the path of infertility and suffer from that bad disease that is ‘demographic winter’. We know them…. They don’t make children.”
To have such countries “empty of children” is “not a blessing” he lamented. Because “fruitfulness is always a blessing of God.” In concluding his homily, the pope asked: “How is my heart? Is it empty? Always empty, or is it open to continuously receive life and give life? To receive and be fruitful? Or will it be a heart preserved as a museum object that has never been open to life and to give life?”
Pope Francis is right. Children are a blessing from God. The fact that couples are no longer interested in having children, and deliberately prevent them from coming into being, is a sign that – as the Holy Father warned – the hearts of many in the developed world have become museum objects. Our hearts are hearts of stone, and not of flesh.
Nowadays, rather than opening their hearts to new life, many couples prefer to jealously guard their love, viewing children as threat to their relationship, personal wellbeing and autonomy. What these couples fail to understand, is that, as St. Thomas Aquinas said, love, by nature, is diffusive. Love is a fire, and like a fire it yearns to spread, and must spread in order to live and be healthy. Many couples soon learn, the hard way, that by stifling the natural creative fecundity of romantic love, they have also stifled the love itself: the result is disillusion and divorce. This is why I say the demographic crisis is a heart problem.
It is also a theological problem, because the ultimate source of love is God, who is Love itself. However, in the developed world we have thrust God out of public and private life. The three theological virtues of faith, hope, and love are the surest sign of God’s presence in our hearts. They are also interrelated. Without faith in the living God, hope dies, and love withers. Without theological hope – the steadfast assurance that, in the end, all things work to the good, and that our destiny is perfect happiness – our fears overwhelm us. Many couples now are so crippled by fear, that all they can see are the “risks” involved in having children – the financial burdens, the possible illnesses and suffering, the limits of their own characters. And without the burning fire of a generous love for God – and the inevitable experience of God’s infinite love in return – many couples can only put their trust in human love, only to find human love, apart from Love itself, is petty and fallible. Without the experience of God’s infinite love, many couples simply do not see the point or the attraction of fruitfulness.
The Contraceptive Mentality
This is the great evil of the “contraceptive mentality” that I wrote about a few weeks ago. Contraception is sold as a means of enabling greater expression of erotic love: but even as it frustrates the natural consequences of sexual behavior, so too does it frustrate the love it is supposed to feed. It does this by quietly replacing the self-sacrificial, outward-looking, self-transcendent nature of authentic love, with a cheap and lifeless verisimilitude.
As I pointed out the other week, in an audience with Pope John Paul II in 1979, Father Marx foretold the collapse in the birthrate with the triumph of the contraceptive mentality. “[O]nce contraception is widespread, the rest is predictable,” he said. “[O]nce you have contraception and legalized or widespread abortion, birthrates fall; nations collapse; young people follow their parents in the abuse of sex; and increasing numbers live together without the benefit of marriage.”
This is the logic of the Culture of Death. If where there is God, there is fruitfulness, then we should not be surprised that inverse is also true: that where God is ignored and banished, there is barrenness and sterility. Further, just as love is self-diffusive, so, in a sense, is sterility. And so we now see the great scandal of developed Western countries that long ago embraced the hopelessness of the contraceptive mentality and the Culture of Death feverishly working to spread their self-destructive ideology elsewhere.
Pope St. John Paul II warned about this in his encyclical Evangelium Vitae. “In the rich and developed countries there is a disturbing decline or collapse of the birthrate,” he wrote. The opposite is true in poorer countries, where couples have many children. However, he said, the powerful and rich nations of the world now behave in the same way as Pharaoh did towards the Israelites, killing their children out of fear of their ascendency.
The powerful elite, said the late Holy Father, “are haunted by the current demographic growth, and fear that the most prolific and poorest peoples represent a threat for the well-being and peace of their own countries. Consequently, rather than wishing to face and solve these serious problems with respect for the dignity of individuals and families and for every person’s inviolable right to life, they prefer to promote and impose by whatever means a massive program of birth control. Even the economic help which they would be ready to give is unjustly made conditional on the acceptance of an anti-birth policy.”
As I have suggested, many people who look at the demographic collapse see only the impending financial repercussions. I see the personal and spiritual repercussions: couples who were called to a great love, but who turned their back on their vocation, to their own personal and spiritual impoverishment; children murdered in abortions and their mothers physically, emotionally, and spiritually scarred; a whole generation of elderly people yearning for the love of children and grandchildren, and living out their final years in loneliness and regret.
In his 1994 Letter to Families, Pope St. John Paul II spoke of the need for families to contribute towards building a “civilization of love.” As Pope Francis observed in his homily, love is inherently fruitful. At this time in history, when so many people are deliberately preaching an anti-Gospel of sterility, we need courageous couples to open their hearts to new life, to recognize the truth that “fruitfulness is always a blessing of God.” In my travels I have met many such families, which evidence an infectious joy that comes of living in God’s love. It is from families such as these that the civilization of love will emerge.
As Pope St. John Paul II explained in the Letter to Families: “The civilization of love evokes joy: joy, among other things, for the fact that a man has come into the world (cf. Jn 16:21), and consequently because spouses have become parents. The civilization of love means ‘rejoicing in the right’ (cf. 1 Cor 13:6). But a civilization inspired by a consumerist, anti-birth mentality is not and cannot ever be a civilization of love.”
Ohio House Bill 182, introduced in April, aims to limit insurance coverage for abortion procedures in which the life of the mother is not at risk. In addition, it would ban birth control drugs or devices such as IUDs that do not prevent fertilization but rather the implantation of the human blastocyst — meaning they technically cause an abortion. But, oddly, the bill also calls for health insurance to cover the re-implantation of an ectopic pregnancy — a procedure that is currently not possible.
An ectopic pregnancy is one that occurs outside of the uterus. Most are located in a fallopian tube, but some are found in the mother’s abdomen. One to two percent of all pregnancies are ectopic, and risk factors include pelvic inflammatory disease due to chlamydial infection, smoking, tubal surgery, history of infertility, and in vitro fertilization — which actually increases the chances of experiencing a tubal pregnancy. While the future of medicine is wide and hopefully someday babies involved in ectopic pregnancies can be saved along with their mothers, the technology simply doesn’t exist today.
The odds of successfully carrying an ectopic pregnancy to term are non-existent if the baby is growing in a fallopian tube, and just one in three million for babies developing in their mother’s abdomen. An ectopic pregnancy is one of the most common causes of death among women during the first trimester. The danger exists in the ectopic pregnancy going undiagnosed and the fallopian tube rupturing. If a procedure existed to save both mother and child, doctors would be performing it. Unfortunately, such a procedure doesn’t exist.
The bill also removes a section of the current law that states women can be reimbursed for the “termination of an ectopic pregnancy.” It’s important to note that surgically removing an ectopic pregnancy is not an abortion.
Abortion is a violent act intentionally committed with the purpose of ending the life of the preborn child. In an ectopic pregnancy, the preborn child is removed in order to save the life of the mother. It is not the intentional killing of a preborn child. If the child was left in the fallopian tube, the mother and baby would both die; therefore, by removing the baby, the mother has a chance of surviving. The baby’s death is an unintended and tragic side effect of the surgery performed to save the mother.
Ectopic pregnancy is a tragedy, but abortion isn’t needed in order to save the mother’s health or life; in fact, abortion is never needed to save a woman’s life. And as medical science advances, we hope that someday both mothers and babies involved in ectopic pregnancies can be saved.
For some, the name Marie Stopes speaks of an organisation, one of the biggest abortion providers in the world. For others, it speaks of a person, a feminist icon and pioneer of birth control and family planning.
Both are true, but few people know the full story about Marie Stopes the woman, the author, palaeobotanist, family planning pioneer, and eugenicist. It is Marie Stopes the woman that I focus on here because she is key to understanding the organisation that bears her name today.
Marie Stopes is widely lauded today as a feminist hero and women’s rights campaigner.
The BBC history page dedicated to Marie Stopes introduces her as a “campaigner for women’s rights and a pioneer in the field of family planning” and says nothing negative about her. A biography on the Manchester University website describes her as “truly an extraordinary woman. Despite the hardships she had faced from her opponents, she continued to pursue the causes she believed in, and remains to this day as a much loved and respected figure. In honour of her name the charity Marie Stopes International [was] established in the 1970s.” Readers of The Guardian voted Stopes Woman of the Millennium in 1999. In 2008 she was chosen by an all-female, all-feminist committee to be one of six women pioneers in the Royal Mail’s Women of Distinction collection.
The organisation named after her, Marie Stopes International (MSI) is clearly proud of its link to her, their website making clear that their present work is built on her legacy:
“The way we provide contraception and safe abortion services has been shaped, to a large extent, by our history. And by the lives of two pioneers of the family planning movement, Dr Marie Stopes and Dr Tim Black. Both built reputations for their client-centred approach and their willingness to push boundaries – qualities that are central to how we work today.”
Stopes the eugenicist
However, both the MSI website, the BBC historical figures page dedicated to Stopes, and many other biographies leave out a great deal of interesting information. In particular, her openly racist and eugenic beliefs and practices have been largely overlooked and ignored or, at best, framed as an embarrassing footnote to her achievements.
Here are some less well-known facts about Marie Stopes and her beliefs:
1. From 1918 to the early 1930s she published several books on marriage and birth control. One of these was Radiant Motherhood (1920) and in a chapter headed ‘A new and irradiated race’ Stopes reveals her underlying (and repulsive) agenda behind her push for widespread birth control: ‘it is the urgent duty of the community to make parenthood impossible for those whose mental and physical conditions are such that there is a certainty that their offspring must be physically and mentally tainted…’ She wants their sterilisation made immediate and made compulsory otherwise there will be an: ‘…ever increasing stock of degenerate, feeble-minded and unbalanced who will devastate social customs…like the parasite upon a healthy tree.’
2. She did not just write, but actively lobbied the Prime Minister and Parliament to pass Acts to enforce compulsory sterilisation in order to: ‘…ensure the sterility of the hopelessly rotten and racially diseased…by the elimination of wasteful lives.’
3. Stopes also urged the National Birth Rate Commission to support the compulsory sterilisation of parents who were diseased, prone to drunkenness or of ‘bad character’. To use a selection of her words, the: ‘hopelessly bad cases, bad through inherent disease, or drunkenness or character’, ’wastrels, the diseased…the miserable [and] the criminal’, ’degenerate, feeble minded and unbalanced’, ’parasites’, and the ‘insane’. In Wise Parenthood she explains: ‘Our race is weakened by an appallingly high percentage of unfit weaklings and diseased individuals.’
4. Marie Stopes’ first family planning clinic was in North London in 1921 and was run by an organisation she founded: The Society for Constructive Birth Control and Racial Progress. It was no coincidence that her birth control clinics were clustered in deprived areas, to focus on reducing the birth rate of the poor lower classes and prevent the birth of those whom she considered to be ‘the inferior, the depraved, and the feeble-minded’.
5. Her views were not a passing fad. In 1934 she publicly stated that ‘the half-caste’ should be sterilised at birth. In 1956, two years before she died, Marie Stopes asserted that one-third of British men should be forcibly sterilised, ‘starting with the ugly and unfit’.
6. Stopes cut her own son out of her will simply because he married a girl who wore glasses. Instead, the bulk of her estate went to the Eugenics Society.
7. Stopes was a Nazi supporter. In 1935, she attended a Nazi Congress for Population Science in Berlin. Four years later she sent Hitlera gushing personal letter along with a volume of her love poems: ‘Dear Herr Hitler, love is the greatest thing in the world: so will you accept from me these that you may allow the young people of your nation to have them?‘ A poem of hers from 1942, at the height of the Jewish Holocaust, has this to say: ‘Catholics and Prussians, The Jews and the Russians, All are a curse, Or something worse…’ The irony of people today praising Stopes is captured by Anthony Ozimic of SPUC: ‘Praising Marie Stopes as a woman of distinction should be as unacceptable as praising Adolf Hitler as a great leader. Both promoted compulsory sterilisation and the elimination of society’s most vulnerable members to achieve what they called racial progress.’
8.The BBC website states that the Catholic Church was Stope’s fiercest critic. They fail to clarify it was actually the Catholic Church that most opposed her appalling eugenic beliefs. In the 1920s, a legal victory against the rising eugenic tide was won by Dr Sutherland, with the support of the Catholic church, over Marie Stopes. Sutherland actually opposed eugenics long before he became a Catholic. Yet Stopes is lauded today as a feminist hero, while the story of the eugenics libel trial, and the Catholic role in trying to stop eugenics, has been either overlooked or dismissed as simplistic Catholic opposition to contraception.
9. Moreover, Dr Sutherland and others were actively trying to prevent and cure tuberculosis, (the disease of poverty) while at the same time influential eugenicists decried their efforts as a waste of time. Eugenicists considered tuberculosis was a ‘friend of the race’ because it was a natural check on the ‘unfit’ and poor, killing them before they could reproduce.
How ironic that Stopes, who describes poor children as ‘puny-faced, gaunt, blotchy, ill-balanced, feeble, ungainly, withered’ is the one now feted as a feminist heroine, and Sutherland who tried to treat and heal them is forgotten.
10. The deliberate excision of Stopes’ eugenic legacy has made her a secular saint. The abortion industry in particular, and liberalism in general, have effectively erased Stopes’ racism and hatred of the poor (such inconvenient historical facts) from their collective memory. Yet the truth is, Marie Stopes was not motivated by a kind of early feminism but rather ‘by the urge to reduce the numbers of the ‘burgeoning Lumpenproletariat.’
Stopes and other eugenicists endorsed legalised birth control because the working class was too ‘drunken and ignorant’ to be trusted to keep its own numbers down.
This all helps to explain why today, Marie Stopes International, arguably the biggest abortion and birth control provider in the world, focuses on providing cheap abortions in developing countries directly to the poorest women in the world.
Recall, as I quoted above, the MSI website: ‘The way we provide contraception and safe abortion services has been shaped, to a large extent, by our history. And by the lives of two pioneers of the family planning movement, Dr Marie Stopes and Dr Tim Black.’
I agree with them: Marie Stopes’ eugenic and racist goals in family planning shape MSI even today:
The truth is, liberal abortion legislation and ‘safe abortion’ provision in developing countries has no effect on maternal mortality rates ie. women’s health. (An attempt to discredit these findings had to be retracted!). Liberalising abortion laws increases numbers of abortions but what genuinely improves maternal mortality rates and health and thus truly helps women (and their unborn children) is education, nutrition, clean water, sanitation and maternal health care for women.
It seems that a neo-colonial and eugenic agenda carries on, with a different cloak and mantle and exported to a different part of the world, but with the same underlying agenda that Marie Stopes had. ‘History repeats itself, but in such cunning disguise that we never detect the resemblance until the damage is done.’
Philippa Taylor is Head of Public Policy at Christian Medical Fellowship. She has an MA in Bioethics from St Mary’s University College and a background in policy work on bioethics and family issues. Republished with permission from the CMF blog.
When it comes to gun violence in schools, people get outraged about children in danger of losing their lives. It’s a worthy concern. According to Education Week, in 2018 28 students were killed in school shootings, while so far in 2019, 2 children have been killed.
That is tragic. But it’s not about the math; it’s about the loss of life … and 30 lives forever gone are 30 too many. But have you noticed that when it comes to babies born during abortions — or viable babies aborted after 20 weeks — all you hear is that it’s not that many? But how many are there?
Consider this, according to the Centers for Disease Control and the abortion-industry think tank the Guttmacher Institute, “only” about 1.3 percent of abortions are late-term (after 21 weeks). With an abortion rate of 879,000 in 2017, that’s more than 11,400 increasingly viable babies at risk.
Those increasingly viable babies face pain, suffering and loss of life.
And what of those who may be exposed to infanticide, allowed to die only because they were born during an abortion, how many might there be?
USA Today notes: “The Centers for Disease Control and Prevention recorded 143 deaths between 2003 and 2014 involving infants born alive during attempted abortions,” with CDC also reporting “it is possible that this number (143) underestimates the total number of deaths involving induced termination.” In another report, the CDC also notes, “Although unlikely, the induced abortion procedure may result in a live birth.”
May? Many abortion survivors are alive and available to tell their own stories. Articulate people like Melissa Ohden, the founder of the Abortion Survivors Network, Josiah Presley or Claire Culwell, speak eloquently about life after almost death at the hands of an abortionist.
In fact, Ohden’s Abortion Survivors Network reports that 279 people have come forward saying that their birthday began in an abortion vendor’s office, in a life and death struggle from their first breath of life.
And how many infants lose their lives because of what happened on the night of their conception?
The New York Times proudly has proclaimed an often-reported number, that babies conceived in rape or incest are “only” 1 percent of those targeted with abortion. With an abortion figure of 879,000, that’s at least 8,790 people who were discriminated against based on the night of their conception.
Children conceived in rape are still children, unique and valuable, deserving of their own chance to make a mark on the world. A civil society does not execute children for the crimes of their fathers, yet when it comes to abortion the knee-jerk assumption is that they should pay the ultimate price rather than putting the focus on the criminal guilty of violence.
Consider that if my father commits a sexual assault today society would not allow his victim to legally kill me tomorrow. The sins of the fathers are not passed on to the children under our system of justice, and my ability to be seen and heard makes that kind of death unthinkable. As it should be. Yet children conceived in rape must endure the constant messaging that the world would be better off if they were dead, and many do end tragically through abortion.
Alabama legislators made a courageous and counter-cultural choice when they said that they cared most about mother and preborn child by focusing their law on the abortionist preying on women, by putting in protections for mothers whose lives were at risk and by telling the world that they loved the children whose stories began in a moment like rape or incest. That moment did nothing to detract from their worth or right to enjoy a chance at life.
In the United States, birth certificates are not issued with points awarded based on your parents’ race, income, marital status or the events on the night of your conception. Birth certificates note one thing: a unique human being has entered the world.
And as we look at the math, it’s clear that the victims of abortion for even the most “rare” cases still number in the thousands. How many need to die before the math just doesn’t add up for a civil society?
When it comes to gun violence in schools, people get outraged about children in danger of losing their lives. It’s a worthy concern. According to Education Week, in 2018 28 students were killed in school shootings, while so far in 2019, 2 children have been killed.
That is tragic. But it’s not about the math; it’s about the loss of life … and 30 lives forever gone are 30 too many. But have you noticed that when it comes to babies born during abortions — or viable babies aborted after 20 weeks — all you hear is that it’s not that many? But how many are there?
Consider this, according to the Centers for Disease Control and the abortion-industry think tank the Guttmacher Institute, “only” about 1.3 percent of abortions are late-term (after 21 weeks). With an abortion rate of 879,000 in 2017, that’s more than 11,400 increasingly viable babies at risk.
Those increasingly viable babies face pain, suffering and loss of life.
And what of those who may be exposed to infanticide, allowed to die only because they were born during an abortion, how many might there be?
USA Today notes: “The Centers for Disease Control and Prevention recorded 143 deaths between 2003 and 2014 involving infants born alive during attempted abortions,” with CDC also reporting “it is possible that this number (143) underestimates the total number of deaths involving induced termination.” In another report, the CDC also notes, “Although unlikely, the induced abortion procedure may result in a live birth.”
May? Many abortion survivors are alive and available to tell their own stories. Articulate people like Melissa Ohden, the founder of the Abortion Survivors Network, Josiah Presley or Claire Culwell, speak eloquently about life after almost death at the hands of an abortionist.
In fact, Ohden’s Abortion Survivors Network reports that 279 people have come forward saying that their birthday began in an abortion vendor’s office, in a life and death struggle from their first breath of life.
And how many infants lose their lives because of what happened on the night of their conception?
The New York Times proudly has proclaimed an often-reported number, that babies conceived in rape or incest are “only” 1 percent of those targeted with abortion. With an abortion figure of 879,000, that’s at least 8,790 people who were discriminated against based on the night of their conception.
Children conceived in rape are still children, unique and valuable, deserving of their own chance to make a mark on the world. A civil society does not execute children for the crimes of their fathers, yet when it comes to abortion the knee-jerk assumption is that they should pay the ultimate price rather than putting the focus on the criminal guilty of violence.
Consider that if my father commits a sexual assault today society would not allow his victim to legally kill me tomorrow. The sins of the fathers are not passed on to the children under our system of justice, and my ability to be seen and heard makes that kind of death unthinkable. As it should be. Yet children conceived in rape must endure the constant messaging that the world would be better off if they were dead, and many do end tragically through abortion.
Alabama legislators made a courageous and counter-cultural choice when they said that they cared most about mother and preborn child by focusing their law on the abortionist preying on women, by putting in protections for mothers whose lives were at risk and by telling the world that they loved the children whose stories began in a moment like rape or incest. That moment did nothing to detract from their worth or right to enjoy a chance at life.
In the United States, birth certificates are not issued with points awarded based on your parents’ race, income, marital status or the events on the night of your conception. Birth certificates note one thing: a unique human being has entered the world.
And as we look at the math, it’s clear that the victims of abortion for even the most “rare” cases still number in the thousands. How many need to die before the math just doesn’t add up for a civil society?
I am troubled by what appears to be a growing trend of violent attacks on peaceful pro-life activists.
Perhaps the most famous recent instance was caught in a dramatic video last fall. The video shows a twenty-something-year-old man wearing a purple sweater, with a pentagram (a pagan symbol) on a necklace around his neck. He asks the pro-life woman behind the camera what should happen if a 16-year-old gets pregnant by rape. From his tone, it is clear that he doesn’t really want an answer. Still, the woman begins to explain that the child is still a child, and should not be murdered, regardless of how the baby is conceived. Before she can finish, however, the young man sticks out his tongue, winds up, and kicks her. The camera falls and clatters on the ground. A female voice is heard crying, “Someone call the cops!”
The woman who was assaulted, Marie-Claire Bissonnette, described in a written account the astonishing indifference of the Toronto police who arrived on the scene. Eventually, however, the attacker was identified, and charges were filed. As it turns out, the same man was responsible for another violent assault on a pro-life activist some months before.
Courtesy of Lifesite – Marie-Claire Bissonnette, Youth Coordinator for Campaign Life Coalition
As Bissonnette points out, the attack on her is far from an isolated incident. And while the video of the assault against her was viewed millions of times, most of these assaults receive little to no public attention. On the very same day that Bissonnette was attacked, for instance, a woman walked up to a pro-life man who was silently praying at a location just West of Toronto and poured paint down his back. This was mild in comparison to what happened just days before, also in Toronto, when Gabby Skwarko, a member of the Ryerson Reproductive Justice Collective, walked up to pro-life activist Blaise Alleyne and proceeded to repeatedly punch her, attempted to grab her bag, and threw a metal dolly at her.
One elderly woman recently had her leg broken when she was assaulted outside Kentucky’s only abortion facility, in Louisville. Another elderly man, participating in the recent Lenten 40 Days for Life campaign, was thrown to the ground and viciously and repeatedly kicked. Then there’s the woman who was left bruised after being punched outside a clinic in Alabama. Or the young man who was repeatedly punched by a pro-abortion woman during a pro-life demonstration at the University of North Carolina.
As a life-long pro-lifer, Bissonnette has participated in pro-life demonstrations for years. She says she has repeatedly suffered physical and verbal assault. “Rocks have been thrown at me,” she writes. “I’ve been spat upon multiple times and pushed. Men have aggressively asked how I would like it if they raped me and forced me to have an abortion.”
Brian Sims’ Contemptible Attack
Thankfully the issue of aggression and violence against peaceful pro-life activists is receiving some (but still shockingly limited) media attention right now, thanks to the contemptible antics of Pennsylvania Democratic Representative Brian Sims. Earlier this month Sims posted a video of himself harassing a pro-life woman who was praying the rosary outside an abortion facility, calling her “shameful,” “disgusting,” “racist,” as well as “old white lady.”
Even worse, he also filmed himself approaching two young girls (aged 13 and 15), calling them “a bunch of pseudo-Christian protesters who’ve been out here shaming young girls for being here.” Sims then offers $100 to anybody who can identify the girls. This is called “doxing” – that is, publicly identifying ordinary citizens in order to subject them to systematic shame and harassment. It’s a terrible practice. Coming from an elected politician, aimed at young, minor girls, it’s downright evil.
Ironically, in posting the footage of his harassment of the girls, Sims accused the pro-life activists of “prey[ing] on young women.” People who protest Planned Parenthood” use white privilege, & shame,” he claimed. “They’re racist, classist, bigots who NEED & DESERVE our righteous opposition.”
Got that? According to Sims, young pro-life girls “need” to be harassed by grown men such as himself. Astonishingly, at the time of this writing, Sims has neither resigned, nor been dismissed from office, though he did record and release a video apology. If instead of a pro-abortion Democrat, it had been a pro-life Republican who berated and doxed young teen girls I think this story would have ended quite differently.
Democratic State Representative Brian Sims has harassed pro-lifers on more than one occasion.
Both Discouraging and Hopeful
Obtaining reliable statistics on assaults against pro-life activists is difficult, and so I can’t say with certitude that there are more of these types of attacks than in the past. What is certain, however, is that reports of these attacks have been coming out with surprising frequency these past few months, and that many of them have been unusually brutal. I’m far from the only one to notice this.
What does this trend mean? On the one hand, it is clearly a discouraging sign of the spiritual sickness of our culture, the growth of a violent underbelly in our national discourse, a testament to the woundedness of so many men and women, and evidence in many cases that pro-abortion activists are held to a completely different standard than pro-lifers by the media, politicians, and the public.
Sims, for instance, clearly believed that pro-life activists were “fair game” for his vicious anger. Why else would he have proudly broadcast his harassment to the world? From his perspective, pro-life women had forfeited their rights to be treated with even a modicum of decency and respect.
This kind of dismissive attitude towards just about anyone who holds traditional moral values is becoming alarmingly common. Consider, for instance, the fact that, as far as I can find, no prominent liberal politicians, media figures or activists have publicly condemned Sim’s misbehavior. Truth be told, many so-called “progressives” now see almost no difference between ordinary social conservatives who believe such things as that marriage is between a man and a woman, and neo-Nazi skinheads.
On the other hand, one senses that the desperation that motivates these attacks stems in part from anger in the face of the fact that the pro-life movement is succeeding as never before. And this is cause for hope. One of the recent attacks, for instance, was in Alabama, which just last week passed the single-most restrictive abortion bill in the country, a bill that would ban almost all abortions in the state, and that was designed directly to challenge Roe v. Wade. This was only the latest of several strongly pro-life bills explicitly crafted as a test to overturn Roe v. Wade.
There are further reasons to think that the growing instances of assault on pro-lifers are a cause for hope. Consider, for example, the obvious fact that in order for pro-life activists to be assaulted in the first place, they need to be in a public space, proclaiming their pro-life beliefs, and trying to prevent abortions from taking place. As it turns out, on any day of the week, all across the country, in rain, shine, snow or hail, thousands of peaceful pro-life activists are gathering outside abortion clinics to pray. Others are holding signs on public streets, or demonstrating on college campuses. That so many are willing to sacrifice their time, and to take the risk of boldly defending human life, is a great sign of hope.
2019 Walk for Life, San Francisco
Another reason for hope is the response of the pro-life activists who are the victims of these assaults. Consider Donna Durning, the pro-life woman whose leg was broken after she was shoved to the ground. “I believe that the lady who caused this injury needs prayers,” Durning said after the attack, “and I’m forgiving her and I would hope that people would also pray for her.” Abby Johnson, who recently spoke at a public rally protesting Brian Sims’ harassment, had much the same message. “I don’t know that I’ve ever seen anybody that needs Jesus more than that man right there,” she said about Sims.
Indeed, it is very likely that many of those perpetrating these assaults are themselves deeply wounded by abortion. Perhaps they themselves had an abortion, or paid for an abortion; or perhaps some close loved one, perhaps even their own mothers, had abortions. Their anger and their violence against pro-lifers is evil, but I strongly suspect that in many cases they are the products of deep pain, pain that only love – above all the love of Christ – can heal. Clearly the pro-life message is Gospel-motivated. However, it is deeply encouraging to see how thoroughly the Gospel has penetrated into the pro-life movement, so that even those pro-lifers who have been violently assaulted by our ideological opponents can say, along with Christ, that most Christian of all prayers: “Father forgive them, for they know not what they do.”
Walk for Life 2019, San Francisco
I hope that you will join me today in praying both for the victims of these attacks, and for the perpetrators. Furthermore, I hope that these incidents, far from discouraging our efforts, will cause us to redouble them. Though more common than I should like, such violent attacks are still relatively rare in comparison to the number of pro-lifers participating in peaceful prayer vigils and the like. Certainly, these attacks should not frighten us away. We need more and more pro-lifers to listen to the call of Christ, and to physically place themselves where the killing of innocents is taking place, so that they can serve as a voice for the violence against pro-lifers///. Thanks to the many silent prayer warriors who participate in 40 Days for Life vigils, or other peaceful protests, untold numbers of babies have been saved, and mothers and fathers spared life-long regret. Will you respond to Christ’s call, and join their life-saving efforts?
As a busy woman with a lot on her plate, I am all for streamlining where possible and making time to focus on the things that are important to me: my family, my work, and my health. I’m often for it when technology makes daily tasks quicker, easier, and cheaper. Grocery shopping from home? Yes, please. Buying a gift online when my child is invited to a birthday party? Absolutely. Working out to a video in my living room rather than driving to the gym? Let’s do this.
And yet I can’t help but see a forest of red flags raised at the prospect of women buying hormonal birth control online or via an app, without having an in-person consultation with a doctor.
The Virtues of the Middleman
“Direct-to-consumer medicine” is a new and rapidly growing e-commerce market that seeks to improve our existing healthcare model in terms of efficiency and convenience by offering prescriptions to reverse hair loss, treat erectile dysfunction, treat skin conditions, and prevent pregnancy by mail. According to an article via Yahoo! (sponsored by Nurx, one of the sites offering the service for birth control), “Gone are the days of being blindsided by unexpected costs, judgy doctors or pharmacists, long waits for appointments and other health care woes.”
A more objective article at the New York Times puts it this way: “The sites invert the usual practice of medicine by turning the act of prescribing drugs into a service. Instead of doctors making diagnoses and then suggesting treatments, patients request drugs and physicians serve largely as gatekeepers.”
In one of the testimonials in that Nurx-sponsored article, Ilena writes, “The customer support team is incredibly helpful. Every time I have a question, like if I’m getting weird symptoms, I always hear back right away.”
We should be concerned about replacing patient-doctor conversations with those of customer support teams—because the priorities of each are inherently different. At my doctor’s office, there are doctors and nurses, but no “customer support team”—because in my doctor’s care, I’m a patient whose health is the first priority, not a customer to whom my provider is looking to sell a product. And because my doctor knows more about me than a survey can communicate, she can help make recommendations for my care as a whole, not with only one concern in mind.
Until recently, advertising for pharmaceuticals—whether online, on TV, or in magazines—concluded with, “Talk to your doctor about…” Now, the doctor is virtually cut out of the equation. Sites like Hims, Hers, Nurx, The Pill Club, and PRJKT RUBY are more like online retail shopping than a trip to the doctor.
Skipping a visit to the doctor’s office and pharmacy is certainly more convenient than dealing with uncertain wait times. Still, we have to consider that in this model, “doctors can’t address secondary issues that surface during a consultation and can’t add information to a patient’s home medical record,” notes Vishal Khetpal, third-year medical student at the Warren Alpert Medical School of Brown University, in his essay “The Worrisome Rise of Direct-to-Consumer Medicine” published at Undark, an editorially independent magazine.
Khetpal says that his conversations with patients usually begin with what brought them in, but typically broaden to include previous diagnoses, new concerns, end-of-life care, and evidence-based preventative measures such as improving diet and scheduling screenings. “We [act] on the concerns of the present,” he says, “but also anticipate the needs of the future.”
Is This the Path We Want to Be On?
The future, indeed. We know that we skim more than read on our screens, so reading that a writer at Slate who used the Pill Club got a list of side effects via text message to which a reply was not required, is less than ideal. We should be concerned that changing access to birth control in this way means there will likely be less informed consent in receiving medications that have a proven history of serious side effects and other possible abuses that are yet to be seen.
Hormonal birth control is often touted as being a safe, healthy choice for women to take control of their sexual lives. That claim has been proven false, by reports of deaths caused by blood clots and the increase in depression in women on hormonal birth control. Too often, hormonal birth control is prescribed to mitigate symptoms of other conditions, rather than seeking out and treating the root cause. This is one of the reasons I use and encourage my family and friends to consider the natural birth control alternatives known as fertility awareness-based methods (FABMs), whether they are sexually active or not. Making access to hormonal birth control even easier and even less concerned with the person popping the pills (or inserting the shot, or giving herself the injections—seriously) seems to me a dangerous road to travel down, particularly when there are other options available.
Personal Decisions Made in an Impersonal Way
For those who have current prescriptions, direct-to-consumer sites offer discreet, unmarked packaging; free shipping (sometimes with treats like chocolate and stickers thrown in); and recurrent deliveries to keep users in supply. In the 38 states where it’s legal, sites also generate new prescriptions. In the latter case, customers fill out an online questionnaire, which the organization says will be reviewed by a licensed medical professional. The customer will be contacted if there are any questions, but the implication seems to be that ideally, most cases will receive the stamp of approval without any direct interaction between the provider and the customer. What’s more alarming is that on these sites, I found it difficult or impossible to find background on the doctors and nurse practitionerswriting the scripts.
I get that waiting in line at the doctor’s office is a pain, and that it can feel like we have better things to do. But as Khetpal makes clear, there’s a difference between filling out a questionnaire and discussing the responses with a human being.
Furthermore, a common theme on the sites I researched was that they were not intended to replace primary care physicians. Maybe not intended, but I can see it happening pretty easily. Half the customers at one site said they used the service to get their first hormonal birth control prescription. And if it’s that much easier and costs the same or less, many people would say, why not?
We can’t forget that there’s good reason prescription medications typically allow only a certain number of refills before the patient needs to check in with her healthcare provider. Again, note my use of “patient” here, rather than “customer.” If we get used to healthcare being this expedited, yearly screenings and simply establishing care with a doctor could fall by the wayside without much of a second thought, creating more damage to public health than good.
Supervision TBD
Because this technology is new and developing, the legal system hasn’t quite caught up yet. Customers should be aware that “there is no single federal or state agency in charge of overseeing online prescription drug services.” These services claim not to be “health providers,” which means they quite literally don’t have to play by the same rules as physicians.
What does that look like? Well, for one thing, researchers who have tried out the services to gauge the quality of the sites found, more than once, that important usage information was delivered inconsistently. For another, we’ve been taught since we were children never to take another person’s medication. Yet one site, Kick, sells a blood pressure medication to customers who are interested in its potential side effect of calming performance anxiety. These issues, I fear, are only the beginning. Without instituting ethical and consistent practices, this industry could cause a lot of harm in a field whose focus is supposed to be healing.
At the end of the day, when it comes to something as important as our health, convenient isn’t always better.
ROME, Italy, May 17, 2019 (LifeSiteNews) — The Church of England’s endorsement of contraception at its 1930 Lambeth Conference has led to the “diabolical monstrosity” of “procreative medicine,” German Cardinal Walter Brandmüller told the Rome Life Forum on Friday (read full talk below or here).
It also led to the American Protestant Federation of Churches collectively endorsing contraception in 1961 as “morally justified if the motives are just,” and essentially obliged the Catholic Church to “tackle the matter of contraception” at the Second Vatican Council, Cardinal Brandmüller said in an address delivered in Italian on “The Prehistory of Humanae Vitae.” His talk was given in Rome at the Pontifical University of St. Thomas Aquinas (Angelicum).
By that time, a “number of Catholic theologians, to a greater or lesser extent” had also endorsed contraception, and the “concept of situational ethics” on which that position is based had “penetrated Catholic moral theology,” said Brandmüller, a dubia cardinal and president emeritus of the Pontifical Committee for Historical Sciences.
Thus Pope Paul’s 1968 encyclical Humanae vitae reaffirming Catholic teaching, which had been affirmed by Pius XI in Casti Connubii and by Pius XII and John XXIII, that contraception is intrinsically evil, “triggered a fierce storm of protest within the Church.”
The acceptance of contraception — which separates the sexual act from procreation — has now resulted in practice of “procreative medicine” — in-vitro fertilization, genetic engineering, eugenic prenatal screening, abortion — in which “man has seated himself on the throne of the Creator,” Cardinal Brandmüller said.
Practitioners of reproductive medicine carry out experiments that “sacrilegiously violate the sanctity of human life” and interventions “of an almost diabolical monstrosity, today heralded as spectacular breakthroughs,” he observed.
“We hope for a renewed reception, adoption and more profound transmission of the truly prophetic teaching of Paul VI in our days,” the cardinal concluded.
Talk by Cardinal Walter Brandmüller
Give at Rome Life Forum, Rome, May 17, 2019
Pontificia Università di San Tommaso d’Aquino (Angelicum)
An insight into the pre-history of Humanae vitae
Last year we commemorated Pope Paul VI’s Encyclical Humanae vitae, published in July 1968, in the midst of the cultural revolution in that year.
Among other things in this encyclical, Paul VI put an end, in doctrinal terms, to disputations pursued with great fervor even within the Catholic Church on the lawfulness and moral reprehensibility of artificial contraception. The encyclical therefore triggered a fierce storm of protest within the Church.
The matter became a subject of controversy in the Catholic world when, at the 1930 Lambeth Conference, the Church of England reached a decision, based on a vote of 193 in favor and 67 votes against, entirely in keeping with the secular spirit of the time, in favor of contraception. The first person to be open to neo-Malthusian propaganda after the First World War was probably the Anglican Bishop of Birmingham, Russell Wakefield. Conversely, in 1920 the Lambeth Conference — the Church of England’s assembly of Bishops — decisively opposed any attempt to put forward medical, financial or social justification for birth control.
Nevertheless, a poll of priests showed that half of the lay people interviewed did not use contraceptives, while the other half used prophylactics or coitus interruptus. However, the personal physician to the head of the Church of England, Lord Dawson di Penn declared, in contradiction of the decision of the 1921 Lambeth conference, that birth control should not be refused from either a medical or an ecclesiastical standpoint. Hence a barrier had been broken down and the Anglican Church assumed a leading role in influencing opinion in the non-Catholic world.
At the beginning however, this was not the case. Eminent representatives of Lutheranism and the Methodist Episcopal Church South saw in contraception one of the “most repugnant modern travesties”, a return to morally ruinous paganism. On 2 April 1931 The Presbyterian wrote as follows on the adoption of the Lambeth Resolution by the USA Federal Council of Churches: “Its recent pronouncement on birth control should be sufficient cause, even if there were no others, for the withdrawal of its support from that body, which declares that it speaks for the Presbyterian and other Protestant Churches in ex cathedra pronouncements.”
Surprisingly, on 22 March 1931 the Washington Post joined with the protests against the adoption of the Lambeth decision: “Carried to its logical conclusion, the [Lambeth] Committee’s report, if carried into effect, would sound the death-knell of marriage as a holy institution by establishing degrading practices which would encourage indiscriminate immorality. The suggestion that the use of legalized contraceptives would be ‘careful and restrained’ is preposterous.”
The Encyclical of Pius XI, Casti connubii, published on 31 December 1930, which presented the Catholic position with great clarity, met with an impressive ecumenical consensus.
However, this fortuitous period came to an abrupt end. In spite of the Encyclical, disputations multiplied, in the Catholic world also, to be interrupted only by the Second World War. A number of Catholic theologians, to a greater or lesser extent, endorsed the position of the USA Federal Council of Churches and its resolution of 23 February 1961:
The majority of Protestant Churches regard contraception and periodic abstinence as morally justified if the motives are just. It is generally believed by Protestants that the motives, rather than the methods, constitute the principal moral problem, providing that the methods are limited to the prevention of conception. Protestant Christians are in agreement in condemning abortion and any method which destroys human life, unless the health or life of the mother is at risk.
The fact that behind this statement was the concept of situational ethics cannot be ignored: illustrious names such as J. Paul Sartre, Albert Schweitzer, Martin Buber and finally A. T. Robinson denied the existence of permanently binding moral standards. This idea then penetrated Catholic moral theology.
These, in broad terms, were therefore the circumstances under which the Second Vatican Council was obliged to tackle the matter of contraception. During the debates, Catholic voices were raised in the Council chamber calling for endorsement of the American Protestant position described above.
The ingenuity with which Cardinal [Leo] Suenens [of Belgium] believed he could compare the development of modern contraceptives to the discoveries of Galileo Galilei is to be noted.
We also recall in this regard the warning from Cardinal Suenens — in fact the spokesperson of Döpfner, Alfruk and Hélder Câmara, The Rhine flows into the Tiber — issued with terrible pathos to the Council fathers, that the Church should not, for the love of God, create a new Galileo case, by once again opposing the discoveries of modern science through its refusal of contraception, an utterance which certainly failed to demonstrate any great knowledge of the Galileo affair.
Today however, we are confronted with the results of a process of erosion initiated at the 1930 Lambeth Conference which, from the approval of artificial contraception, has led us to the monstrosity of what is today known as procreative medicine, by which man has seated himself on the throne of the Creator.
Goethe’s Prometheus said: “I am here and I create men in my image …”.
These words, written more than two hundred years ago, in fact mirror this notion of self which, today, is driving the protagonists of so-called reproductive medicine to carry out these experiments, through which they sacrilegiously violate the sanctity of human life. These are interventions — and there are almost no words to describe them — of an almost diabolical monstrosity, today heralded as spectacular breakthroughs … It only remains for us to wait until these Prometheic persons arrive at the same destiny as their mythical hero.
It is therefore, and in the context of these circumstances, that tribute should be paid to the Encyclical Humanae Vitae published in 1968, a doctrinal document whose prophetic nature has, over time, also been acknowledged by leading non-Catholic thinkers. One of the most illustrious of these was Max Horkheimer, first among the leaders and then among the critics of the Frankfurt School, who allied himself with Paul VI. The journalist Malcolm Muggeridge, at that date still a Communist, gave a favourable welcome to the Pope’s Encyclical.
In this encyclical, Paul VI brought temporary closure to a series of doctrinal affirmations on the matter of contraception, instigated by Pius XI in Casti Connubii and continued by Pius XII and John XXIII. These were ultimately taken up, developed and deepened by John Paul II.
Humanae Vitae provides an extraordinary example of the workings of the process of parodosis, which means transmission of the doctrine of the Church. When the truth of faith is received, adopted and transmitted, what happens is that what is received, when adopted and transmitted, responds with deeper understanding and more precise expression to the needs of the respective present, while continuing to be identical to itself. In all of this, contradiction between yesterday and today is impossible: it is the Holy Spirit who acts in the Church of Jesus Christ to guide this process of paradosis. It is the Holy Spirit who ensures that the faith of the Church develops in the course of time, just as an adult person continues to be identical to the infant it was in the past, an intuition formulated by Vincent of Lérins as early as 430 and elaborated upon by Blessed John Henry Newman.
*
Today, we hope for a renewed reception, adoption and more profound transmission of the truly prophetic teaching of Paul VI in our days.
IRVINE, May 15, 2019 (Center for Medical Progress) – The Center for Medical Progress (CMP), the citizen journalism organization responsible for the undercover video series exposing Planned Parenthood’s sale of aborted baby body parts, revealed today that over the past month, government-funded researchers at University of California San Diego (UCSD) have sought to purchase hearts and pancreases from aborted fetuses from CMP.
CMP is a well-known citizen journalism organization that advocates against the commercial exploitation of aborted fetal body parts. The Frazer Laboratory at UC San Diego runs in part with NIH grants—but the NIH spending database does not classify the Frazer grant money as related to human fetal tissue experimentation.
In April, UCSD’s Frazer Laboratory emailed CMP “searching for human fetal pancreas from 4-5 donors.” CMP investigative journalists then engaged in an email dialogue with the Frazer Laboratory to learn more about the Lab’s demand for fetal body parts from abortions. While never promising to provide fetal tissue, CMP asked the Frazer Lab for more details about the project and probed the Lab’s engagement with the market in aborted fetal organs and tissues.
Startlingly, while asking for body parts from first trimester aborted fetuses, the Lab also wrote that fetuses up to six months “should be compatible with our experimental design.” When informed that the “market price” for fresh fetal organs was $500 to $750 per specimen, the Frazer Lab was not fazed, replying “please let me consult the pricing with Prof. Frazer. We are indeed in contact with a few other organizations in California however it is critical for us to find a reputable and reliable source which could provide the samples.” The Lab continued, “we will most certainly choose the option of the fastest possible delivery of fresh (not frozen) samples.”
Later in April, the Lab left multiple voicemails for CMP seeking to discuss options for ordering aborted fetal body parts. By then the Frazer Lab had increased its request, writing, “Also, would like to ask for heart specimens from 3 donors (ideally pancreas and heart specimens from the same donors).”
CMP Project Lead David Daleiden notes, “Government-funded laboratories are so greedy for fresh aborted baby body parts that they will try to buy them from anybody—without even bothering to check who they are emailing.”
Daleiden continues, “Even as the Department of Health and Human Services continues an agency-wide audit of fetal experimentation and the U.S. Department of Justice investigates the sale of aborted fetal tissue at Planned Parenthood and their business partners, government-funded researchers do not seem to have curtailed their appetite for aborted baby body parts one bit. It is far past time for HHS to end the barbaric practice of taxpayer-funded fetal experimentation, and for the Department of Justice to do their job and hold Planned Parenthood and other baby body parts traffickers accountable to the law.”
Amina Khamis Juma is 22 years old and lives in Mbande-Kisewe, near Dar es Salaam, Tanzania. After delivering her first child in 2016, she was persuaded by her sisters to begin using contraception since the couple did not wish to have another child. Her sisters suggested using condoms, but they caused pain and discomfort, so Amina and her husband soon stopped. When Amina became pregnant, the couple was unwilling to have a child at that time and tragically opted to abort.
Amina Khamis Juma, a Tanzanian wife and mother.
When sexual partners rely upon technology to prevent conception and the technology fails, they often expect they will not have to deal with the “unwanted” consequence – a baby. This way of thinking is called the “contraceptive mentality.” When sexual partners with this mentality engage in a sexual act while inhibiting the procreative element, they are unwilling to consider pregnancy. It is expected that the contraceptive method employed will do what it claims, prevent conception. However, when the contraceptive fails and they become pregnant, the couple often succumbs, like Amina and her husband, to fear and opts for abortion as the “backup choice” – the method of correction.
Father Paul Marx, who held a doctorate in sociology, spent his life affirming Church teaching on life, marriage, and family, testifying to the toxic mindset created by the “contraceptive mentality.” “The foolproof contraceptive does not exist,” said Father Marx, “and sociological studies have shown, almost without exception, that intensive contraceptive programs, by emphasizing the prevention of unwanted pregnancies, also reinforce an intention not to bear an unwanted child under any circumstances; that is, there is a greater likelihood that women experiencing contraceptive failures will resort to abortion.”
During a papal audience with Pope St. John Paul II in 1979, Father Marx offered his insights with the saintly pope saying that “once contraception is widespread, the rest is predictable. In every country contraception always leads to massive abortion.” He further emphasized that “once you have contraception and legalized or widespread abortion, birthrates fall; nations collapse; young people follow their parents in the abuse of sex; and increasing numbers live together without the benefit of marriage.” As if capable of looking into the future, Father Marx also discussed the intimate link between contraception, abortion, and euthanasia. For “if you can kill before birth, why can’t you kill after birth? So, euthanasia is inevitable.”
Fr. Paul Marx, the Founder of Human Life International.
Colonization of the Mind
Hamidou Kane, a Senegalese novelist, coined the expression “colonization of the mind.” He said there are two ways to control a people: through brute force by waging war with bombs and guns; or through a more permanent and less costly method, to get the people to accept new attitudes through propaganda directed at breaking down the two most important custodians of a nation’s and culture’s values – Faith and the family.
The Church of England, at its 1930 Lambeth Conference, was the first Christian denomination to suggest that the use of artificial contraception by married couples might be morally licit in certain difficult circumstances. It is important to note that leaders at the Conference assumed that the non-use of contraception would be the norm for believing Christians and that its use would only be resorted to in “extreme” cases. But as we know, the “hard case” mentality always leads to greater perversion. It makes for bad law – gradually the lines become blurred. Contraception became respectable, even touted as “good” for married life and society. What was once considered shameful and unmentionable to a great majority of Christians (and even within the general population) became acceptable and even “necessary.”
This growing acceptance of contraception rapidly transformed the culture with the seductive idea of uninhibited “free sex,” made palatable – even virtuous – by an ever-expanding list of seemingly lofty rationales: If reliable contraceptives could not be used, how could married couples express their love for one another without the possibility – threat – of a baby? How could parents (especially the poor) raise a large family with today’s social and economic conditions? What about the threat of an ever-expanding population? How could any woman find fulfillment while she is enslaved to her “biology?”
The minds and hearts of the nation and its people had been corrupted. Whatever reasons Christians might formerly have had for condemning contraception became irrelevant!
Formation of a Contraceptive Mentality
Contraception is the direct intention of preventing by mechanical or chemical means the possible natural and procreative consequence of sexual intercourse – the conception of another human being. The purpose, therefore, is to separate intercourse from procreation so that contracepting partners can enjoy the pleasures of sex without the fear that their sexual activity could lead to pregnancy.
A “mentality” is an attitude of mind, a way of thinking. It is established when a person (group or society) reacts automatically to a situation without thinking of the consequences. A “mentality” is very difficult to correct since it is shielded by unconscious assumptions and preserved by consistent behavior and habit.
The “contraceptive mentality” exists when: (1) sexual intercourse is separated from procreation, (2) the rational is assumed to be normative, and (3) in employing contraception, the couple sever themselves from all responsibility for a conception that might take place as a result of contraceptive failure. This is a pervasive “mentality” that is aware of the immediate benefit but fails to consider the future repercussions. The “contraceptive mentality” implies that a couple has not only the means to separate intercourse from procreation, but also the right or responsibility to do so. It is also important to remember that at the very core of the “contraceptive mentality” is a fear or rejection of something perfectly natural as a result of sexual intercourse – a baby.
Many wrongly believe contraception prevents abortion. This belief is not borne out by studies and statistics. Research clearly shows that contraception leads to riskier behavior, more unplanned pregnancies, and consequently, more abortions. Dr. Malcolm Potts, former Medical Director of the International Planned Parenthood Federation (IPPF) openly stated, “As has been pointed out, those who use contraceptives are more likely than those who do not to resort to induced abortion … the epidemiological evidence points to the fact that induced abortion services are most needed by those adopting any form of fertility regulation.” When contraception fails – as it inevitably does – couples, and especially single mothers, are tempted and even pressured to eliminate the “unwanted” life.
Scandalously, national studies reveal that around 72 percent of all married Catholic couples of childbearing age in the United States use some form of artificial contraception or sterilization to limit childbearing. Studies also reveal that nearly 41% of high school students are sexually active, supported by contraception and its deceptive offer of so-called sexual freedom. How many Planned Parenthood facilities and private abortion clinics now exist to “serve” these young people with the consequences of failed contraception? An entire industry has developed in response to an ever-expanding market – i.e. more sex, more contraception, greater need for abortion.
Pope St. Paul VI, in his landmark encyclical Humanae Vitae, prophetically spoke of some of the consequences of the “contraceptive mentality,” warning that “responsible men… [should] reflect on the consequences of methods and plans for artificial birth control. Let them first consider how easily this course of action could open wide the way for marital infidelity and a general lowering of moral standards… [men] —and especially the young, who are so exposed to temptation—need incentives to keep the moral law, and it is an evil thing to make it easy for them to break that law. Another effect that gives cause for alarm is that a man who grows accustomed to the use of contraceptive methods may forget the reverence due to a woman, and, disregarding her physical and emotional equilibrium, reduce her to being a mere instrument for the satisfaction of his own desires, no longer considering her as his partner whom he should surround with care and affection.”
“Finally, careful consideration should be given to the danger of this power passing into the hands of those public authorities who care little for the precepts of the moral law. Who will blame a government which in its attempt to resolve the problems affecting an entire country resorts to the same measures as are regarded as lawful by married people in the solution of a particular family difficulty? Who will prevent public authorities from favoring those contraceptive methods which they consider more effective? Should they regard this as necessary, they may even impose their use on everyone. It could well happen, therefore, that when people, either individually or in family or social life, experience the inherent difficulties of the divine law and are determined to avoid them, they may give into the hands of public authorities the power to intervene in the most personal and intimate responsibility of husband and wife.”
Because of successful propaganda and the rejection of Judeo-Christian values concerning marriage, human sexuality, and family life, many people in our society have the attitude that human life is sometimes inconvenient and an unnecessary burden. Pope St. John Paul II saw this “mentality” as a root cause of abortion. When we see any human life as a troublesome burden that we must manage, rather than a sacred gift entrusted to our care, there is a dangerous temptation to get rid of the burden by any means necessary. As Father Marx predicted, we see this same attitude and behavior today with the euthanasia movement.
Indoctrination
Proponents of the “sexual revolution,” supported by legalized contraception and abortion, have successfully inflicted upon this generation the burdensome and insidious manifestations of their revolution. Faith and the family are no longer the custodians of our nation’s (our world’s) and culture’s values. Sadly, many of today’s youth have embraced a secular, laissez-faireattitude toward religion, life, sex, marriage, and family life.
Sex is now seen primarily as a matter of “self-expression” or “self-fulfillment.” Responsibility, morality, self-mastery, self-giving, and sacredness which belong to any Christian view of the human person or human sexuality are absent and outwardly rejected. The inevitable consequence of such a point of view is the “contraceptive mentality.” One can’t, after all, have sex without being “free” from the burden of conception and “free sex” is clearly incompatible with any sound idea of marriage and family life. Sexuality is thus divorced not only from possible procreation but also from marriage itself. This explains why many young people delay marriage or opt not to marry at all.
Contraception laid the groundwork for this evolution of thought.
Radical sex ed is being forced on children as young as 5 around the world, often without parental consent.
The indoctrination has been successful in creating a sex-saturated culture – I would dare say a sex-addicted culture – fixated upon satisfying any and all urges, supported by the “contraceptive mentality.” This indoctrination is now being systematically introduced into school classrooms, mostly through courses in so-called “sex education or family life education,” in social science courses, and in “population education.” I have personally witnessed these programs in action. I have seen children as young as five being introduced to sexual experimentation and modern contraceptive devices. Our young are being indoctrinated, propagandized, and convinced that contraception, like abortion, is a positive good. They are taught that it is good for themselves and for society in general, and that they have a “moral” obligation to embrace these so-called “truths.” The moral judgments of religion and their parents are passé; “anything goes” is now in vogue.
Lest We Forget
In this great battle for life and family, we can no longer ignore the proverbial skunk in the room – the “contraceptive mentality.” Our effort to end the violence and plague of abortion requires that we address this fundamental, underlying issue. The “contraceptive mentality” is the root from which abortion flows, and failure to address it enables juggernauts like Planned Parenthood Federation of America and IPPF to flourish. As Father Marx said, “while we need a variety of pro-life groups hacking away at the anti-life monster, it is enormously futile and indeed grossly short-sighted to overlook the chief source of baby-killing, which is contraception.” To come full circle to Amina Khamis Juma at the beginning of this article, she outright rejected contraception after her abortion, a failed marriage, terrible effects on her health and even forcibly implanted birth control. After hearing HLI Tanzania on the radio, she reached out and our staff got her immediate help at a Catholic hospital; she is now recovering and learning safe, natural natural family planning (NFP), which is fully open to life.
Sadly, there is much confusion and dissent within the Church regarding contraception, but as faithful Catholics (Christians), we must reclaim an authentic understanding of the human person, life, marriage, and human sexuality, along with the language to articulate these truths to an errant culture. If we truly want to put a permanent end to the violence of abortion, heal the deep wound it causes, and protect the sacredness of human life, marriage, and the family, then we must continue to confront contraception head-on, along with its “mentality” feeding the entire abortion industry.
Sader Issa, a third-year dentistry student living in Syria, credits the love and support of his parents for his success and happiness in life. In fact, he is so proud of his parents, especially his father, that he wants everyone to know that he grew up happy and well-cared for by a father who has Down syndrome. He says it might not have been easy, but his father made it seem like it was.
“A child who grows up in the lap of a person with Down syndrome will have all the love and tenderness that anyone can offer,” said Issa in the video below, shared by Symphony homeland. “This will lead up to a person who has an emotional and social well balance and is able to achieve anything he wants.”
Unfortunately, the majority of men with Down syndrome cannot have children or have a lower fertility rate than the average male. Only about half of women with Down syndrome are able to have children.
Issa said that his father, Jad Issa, is like any other father and worked hard to provide for him at the wheat factory. But his father is also a vulnerable person and that has inspired Issa to be the “best person for the sake of this person who worked hard.”
When his father introduces him to someone new, Issa said he is full of pride. “It’s like he’s saying: ‘I have Down syndrome, but I raised my son and did everything to help him become a doctor who treats people. I’m proud of him.’”
Issa says his parents’ relationship is just like any other couple who has been together for decades. Married for 23 years, they may disagree at times, but they enjoy “a life full of love, simplicity and humility in all respects.”
Issa and his parents when he was young. Photo via Facebook.
Because of his upbringing, Issa has a unique perspective on life with Down syndrome. He said his father is loved and respected by everyone in their community, and he is using his life experience to ask the government to respect people who live with the condition, even those who are still in the womb.
“For many people, the idea of a woman pregnant with a baby with Down syndrome may be the worst scenario,” he said. “You can expect a number of people can resort to abortion. If my grandmother was convinced of this idea, I wouldn’t be here with you.”
Through the video above as well as social media and at least one radio interview, Issa has dedicated himself to sharing the truth about Down syndrome and fighting for the right to life for those diagnosed with the condition before birth.
With countries such as Iceland bragging about having a 100 percent abortion rate of babies with Down syndrome and the United States aborting 67 percent (or higher) of preborn children with the condition, it is vital that people like Issa speak up. The truth is that abortion kills people with Down syndrome through a violent act of discrimination. When we see that people with Down syndrome are capable of living what society deems to be “normal” lives, it becomes apparent just how inhumane abortion is and that we need to rethink how society views persons with disabilities.
Lawmakers in Washington, D.C., are calling on the Food and Drug Administration (FDA) to crack down on illegal online sales of the abortion pill. According to information from Rep. Michael C. Burgess, M.D. (R-TX) and Rep. Martha Roby (R-AL), the Congressional letter, sent to Dr. Norman Sharpless, Acting Commissioner of the FDA, was signed by 117 members of Congress. It comes on the heels of information showing that Aid Access and Rablon, two foreign companies, have been distributing the chemical abortion drug Mifeprex by mail-order to U.S. customers in violation of the FDA’s safety protocols. Live Action News previously documented a larger push by pro-abortion organizations to lift the FDA’s safety requirements, known as REMS, to expand abortion pill dispension to mail order and online sales, via self-managed abortions.
FDA warns consumers to not buy abortion pills over the internet (Image: FDA)
The Congressional letter urges the FDA to “continue to conduct oversight” of the entities following FDA warning letters to Aid Access and Rablon ordering them to halt dispensing the pills. Lawmakers point out that the pills are prescribed by an abortionist in the Netherlands and filled by a pharmacy in India. A fact sheet published by Charlotte Lozier Institute research organization found that “72 unique websites” were selling the pills online.
An email from the FDA to Live Action News clarified that “Mifeprex may only be supplied directly to healthcare providers who are certified to prescribe Mifeprex….”
The FDA stated the drug is “only available to be dispensed in certain healthcare settings, specifically, clinics, medical offices and hospitals, by or under the supervision of a certified prescriber. It is not available in retail pharmacies, and it is not legally available over the Internet.” They added:
FDA has warnedconsumers not to buy Mifeprex over the Internet because doing so bypasses the distribution restrictions that are in place to ensure the safe use of the drug. Drugs purchased from foreign Internet sources are not the FDA-approved versions of the drugs, and they are not subject to FDA-regulated manufacturing controls or FDA inspection of manufacturing facilities.
Congressman Burgess expressed his concern, “As an OB/GYN who practiced medicine for nearly three decades, I am concerned about the consequences of unapproved mail-order abortion drugs. The dangerous business that Aid Access is conducting is harmful to the health of American women, who deserve quality health care throughout the course of a pregnancy.”
Rep. Martha Roby stated, “By violating the FDA’s safety protocols, Aid Access and other European mail-order abortion companies endanger the health of American women and their children. The FDA must take decisive action against these illegal activities immediately…. Aid Access circumvents the Food and Drug Administration’s safety requirements, placing the lives of women and their children at risk. We would like to… voice our support for ongoing oversight of this and any other rogue mail-order abortion operation.”
Watch as SBA List president Marjorie Dannenfelser discusses the illegal sale of the abortion pill online:
Weeks ago, the FDA updated its adverse events report through 2018, documenting “24 deaths of women associated with Mifeprex since the product was approved in September 2000….” The FDA also noted additional adverse effects in the thousands. Under 2016 changes, the drug’s manufacturer, Danco, no longer has to report non-fatal adverse effects, so we can only imagine what the number really is.
Live Action News previously documented that Danco itself is incredibly secretive about its stakeholders and controlling parties, who (from the limited information we can glean) appear to stand to gain financially from a broad abortion pill expansion. And a previous Live Action News report revealed that the FDA recently approved a generic version of the abortion pill Mifeprex known as GenBioPro.
FDA reported deaths for abortion pill December 2018
In an e-mail exchange with Live Action News, FDA officials assured us that, “FDA monitors sponsors’ compliance with REMS, including assessment evaluations and on-site inspections. In addition… Mifeprex is not legally available over the Internet. The agency is aware of media reports regarding the sale of unapproved mifepristone in the U.S. through online distribution channels and is actively evaluating the reports in order to assess potential violations of U.S. law.”
An FDA representative told Live Action News, “The agency is aware of media reports regarding the sale of unapproved mifepristone in the U.S. through online distribution channels. We assure you that the agency is extremely concerned about the activities described in these reports and is actively evaluating the reports in order to assess potential violations of U.S. law. As I’m sure you understand, however, the agency is unable to discuss potential or pending investigations, if any such exist.”
Full text of the Congressional letter can be found here.
Editor’s Note: Learn more about Abortion Pill Reversal here.
Jonathan Abbamonte and Steven W. Mosher MAY 7, 2019
Bureau du siège de l’ONU à Genève
The U.N. Human Rights Committee has taken broad aim at pro-life laws and policies in the United States.
Meeting last month, the Committee called on the Trump administration to “review” a number of its pro-life policies, suggesting that these were incompatible with international law. The Committee singled out for criticism President Trump’s Mexico City Policy,[1] his executive order “Protecting Free Speech and Religious Liberty,” and his executive order which protects religious employers like the Little Sisters of the Poor from being forced against their religious beliefs to pay for contraceptives in their employer-sponsored health plans.
Specifically, the Committee called for the Trump administration to explain the “compatibility” of these pro-life policies with the International Covenant on Civil and Political Rights (ICCPR), suggesting that the U.S. is bound by its own Constitution and by international law to observe the Committee’s interpretation of this international human rights treaty as legitimating abortion.
What is driving this new assault on American efforts to protect the unborn is the Committee’s General Comment no. 36—a document adopted late last year by the Human Rights Committee that claims that every country that has ratified the treaty “must provide…legal and effective access to abortion” in cases of rape, incest, health of the mother, and when the pregnancy “is not viable.”
The Committee has ordered the Trump administration to respond to its inquiry “in the light of the Committee’s General Comment No. 36.” What the Committee did not say was that General Comment No. 36 is the very first document ever adopted by a U.N. treaty body to suggest that the ICCPR treaty, or any other U.N. treaty, requires countries to legalize abortion. Nor did it mention that its radical interpretation of the treaty has been rejected by a number of countries.
The Committee also took sweeping aim at the hundreds of pro-life laws that have been passed in the U.S. on the state level over the past few years. Explain how these pro-life state laws are in compliance with U.S. obligations under the ICCPR Treaty, the Committee told the Trump administration.
The U.N. Committee did not specify which state-level abortion restrictions it wanted the U.S. Government to review in particular, but broadly requested that the administration include any pro-life laws which “restrict women’s access to reproductive health and abortion services and create new barriers to them in practice.”
One can understand why international abortion advocates are in panic mode over state-level initiatives to protect life. Literally hundreds of pro-life laws have already been enacted by various states over the past few years. Just since January 1 of this year, more than 250 new pro-life laws have been introduced in state legislatures. And these laws restricting abortions have been saving many lives, as Michael New has recently documented.
While the U.S. Supreme Court’s decisions in Roe v. Wade and Planned Parenthood v. Casey prevent states from banning abortion outright, states have successfully banned abortion after 20 weeks when a child can feel pain, required basic health standards for abortion facilities, prohibited taxpayer funding for abortion, provided women seeking abortion with informed consent. States have also banned certain kinds of abortions, such as sex-selective abortion and or the abortion of unborn children diagnosed with Down Syndrome or other congenital defects.
While the U.N. Committee rejected in General Comment No. 36 the imposition of criminal sanctions on abortionists, many of the state-level pro-life laws in the U.S. do just this to ensure compliance.
Another area where the U.N. Committee’s positions are at odds with current U.S. practice is in the area of conscience rights. In 2016, the Committee called on Poland and Colombia to require that doctors who conscientiously object to performing an abortion provide abortion referrals, even if it violates their conscience to do so. General Comment No. 36 returns to this issue, instructing countries to remove “barriers” to abortion, “including barriers caused as a result of the exercise of conscientious objection.”
The Trump administration has just done the opposite. The U.S. now has in place a broad-based policy of protecting the conscience rights of healthcare entities and individuals.
The U.N. Committee justified its request to the Trump administration by pointing to Article 40 of the ICCPR, which authorizes it to periodically request reports from countries on their progress in implementing the treaty. The Committee has long used such reviews as occasions to harass countries into loosening restrictions on abortion.
The Committee’s request last month to the Trump administration is unprecedented, however. It represents the first time the Committee has officially criticized U.S. laws protecting the
unborn — under the guise of “requesting” the Trump administration to comment how such laws comport with the Committee’s radical interpretation of the ICCPR treaty.
It will be interesting to see how the Trump administration will respond.
We recommend that it simply reject General Comment No. 36 altogether, along with any other interpretation of the ICCPR treaty that undermines American sovereignty and democracy.
[1] The Mexico City Policy is a policy that prohibits U.S. foreign aid in global health programs from being used to financially support foreign non-governmental organizations (NGOs) that perform or promote abortion. The Mexico City Policy was reinstated in 2017 as one of President Trump’s first acts in office and has since cut millions of dollars in U.S. funding to international abortion groups such as the International Planned Parenthood Federation (IPPF) and Marie Stopes International (MSI).
As parents of three children (currently 6, 4 and 13 months), how many children my husband and I should have – and what would be best for our children themselves – is a question we have thought about.
We have contemplated whether or how a range of factors should affect our decision about each pregnancy. These include the temperaments and health of our current children, how far away our extended family lives, how our children might benefit from another sibling, how much money we have, how much stress or anxiety we currently feel, how much community support we have, work, the cost of school or necessary expenses (and what are necessary expenses?), how strong our marriage feels, how sick I get in pregnancy, and how many adult children we would like to have in the future.
And then there is the absolute amazingness of having the power to create a whole new human being and another beautiful little newborn baby to cuddle, and the expansion of love, sacrifice, growth and community that comes with each new family member.
Joe Pinsker ofThe Atlantic interviewed economist Bryan Caplan to see what he considers the optimum number of children. Over and above being an economist, he is described as “a dad who has thought a lot about the joys and stresses of being a parent”, and is author of the 2011 book, Selfish Reasons to Have More Kids. He said,
“If you have a typical level of American enjoyment of children and you’re willing to actually adjust your parenting to the evidence on what matters, then I’ll say the right answer is four.
Though Caplan himself does currently have four children, apparently he even suspects that more than four would be optimal for him.
He suggests that parents should revisit their child-rearing approach and then, if they can afford to, consider having more kids, because kids can be fun and fulfilling. He also considers that many of the time- and money-intensive things that parents do in the hope of helping their children succeed, such as multiple extracurricular activities and sending them to private schools, don’t actually contribute much to their future earnings or happiness.
Since having a child at school, it is interesting to me how much the emphasis on extracurricular activities really does affect parents. One parent told me that having a third baby was “an excellent advertisement for a fourth,” were it not for the fact that she then hit extracurricular activities, ‘taxi driving’, and a very busy household. (By the way, in my experience parents seem to really enjoy third babies, and I am one of those parents! At this point, we are often not worrying as much about the intensity of the baby years as we might have been the first and second time around.)
According to Ashley Larsen Gibby, a Ph.D. student in sociology and demography at Penn State, the societal norm also affects how many children will make you happiest. So, if the norm changes, the number of children that will likely make parents happiest changes as well.
It is much harder to have a big family in a society where the norm is small (currently two children in most places). This makes sense because a lot of community and business services won’t be aimed at meeting your family’s needs in the way they would be if bigger families were the norm. You will also likely feel different to many of the parents around you (and maybe even endure regular amazed comments about your family size), something which is harder for some temperaments than others.
Pinsker writes:
In general, the experts I consulted agreed that the optimal number of children is specific to each family’s desires and constraints.
“When a couple feels like they have more interest in kids; more energy for kids; maybe more support, like grandparents in the area; and a decent income, then having a large family can be the best option for them,” says Brad Wilcox, the director of the University of Virginia’s National Marriage Project.
“And when a couple has fewer resources, either emotional, social, or financial, then having a smaller family would be best for them.”
However, one thing is certain from the research. Women are measureably less happy when they are unable to have as many children as they would like to; something to bear in mind for the many women who now put off having children until their thirties, or those contemplating an additional child.
Per the General Social Survey, in 2018, 40 percent of American women ages 43 to 52 had had fewer children than what they considered ideal.
“Part of the story here is that women are having children later in life, compared to much of human history, and they’re getting married later in life as well,” Wilcox says.
“So those two things mean that at the end of the day, a fair number of women end up having fewer kids than they would like to, or they end up having no kids when they hoped to have children.”
Though the root causes can differ, this mismatch between hope and actuality is seen worldwide, and appears to make women measurably less happy. So, while people’s ideal family size may vary—and is highly individualized—they’ll probably be happiest if they hit their target, whatever it may be.
Two children is currently the preferred option for most, but it seems from the research that many families may actually be happier with more — especially if they rethink some of their unproven intensive parenting practices. And the more people who do have one more (thereby contributing to a change in the norm), the more happy those with a slightly larger family will be.
Shannon Roberts is co-editor of Demography is Destiny, MercatorNet’s blog on population issues.
A recent paper published in the peer-reviewed journal Issues in Law and Medicine details lifesaving treatment and prenatal surgery being given to babies in the womb. The study, titled “Perinatal Revolution” affirms that the preborn child is a unique and separate patient from the mother. When doctors treat both the mother and the “patient within the patient,” successful treatment of conditions that might otherwise be severely life-limiting are possible, increasingly so as technology continues to advance.
The paper’s authors are Drs. Colleen Malloy, Monique Chireau Wubbenhourst, and Tara Sander Lee. Two of the study’s authors are associate scholars with The Charlotte Lozier Institute. The research is being publicized so that doctors and other health care professionals are made aware of these lifesaving procedures, so that they are less likely to recommend or coerce patients into aborting their children rather than carrying to term. The study notes that a doctor’s personal views about abortion and the availability of prenatal treatment can directly affect whether a mother decides to end her child’s life in an abortion or carry to term. The authors write, “In several studies of families receiving diagnoses of Trisomy 13 or 18, a majority of parents (61%) felt pressured to terminate the pregnancy.”
Doctors and other medical professionals are not the only ones who can benefit from this information about the emerging treatment for babies before birth. If parents are unaware of life-affirming treatment options, they are more likely to fall prey to coercion to terminate a child with a potential disability. However, knowing about the rapidly developing field of prenatal treatment and the dramatic increase in the successful treatment of premature babies empowers families to make life-affirming decisions for their children.
The paper details how advances in genetics and medical technology have made it possible for doctors to treat babies more effectively while still in the womb. Prenatal surgery has been available for decades, but with technological advances, treatment can be better and less invasive, and may be done at even performed at earlier gestational ages. Some of the conditions discussed in the paper that can now be treated or mitigated in the womb include cerebral palsy, fetal hypothyroidism and hyperthyroidism, spina bifida, and cystic fibrosis.
The authors write about these technological developments:
“With the ability to see the fetus in real time came the ability to diagnose problems and to consider how best to help the affected fetus, to follow affected fetuses and to monitor treated fetuses, over the course of pregnancy. This shifted the focus from the newborn, with a severe disorder that could not be corrected after birth, to the possibility of prenatal medical or surgical intervention that could help ameliorate the clinical manifestations of disease…These diagnostic capabilities led to further research and clinical trials and the realization that the fetus was, and is, a patient.”
Successes with these prenatal surgeries have far surpassed conventional treatments given to newborns with these conditions. Study author Tara Sander Lee wrote in another paper about a peer-reviewed study of prenatal surgery for spina bifida published in the New England Journal of Medicine. The babies who received prenatal surgery fared so much better than babies who received the conventional surgery at birth that the study was halted before completion so that all babies would receive the superior prenatal surgery.
The most recent paper notes that the types of surgery and interventions available continue to evolve. The authors write that cellular therapy for babies before birth, tissue engineering, gene therapy, and the artificial womb may be available to treat babies soon, as these methods are rapidly developing. They note that these therapies are uniquely suited to treating preborn babies, writing, “Many of these cell-based techniques take advantage of the fact that the fetal environment is constantly remodeling and ideal for accepting stem cell therapies that facilitate regeneration.”
Despite these dramatic advances in lifesaving treatments for mothers and their preborn babies, many people, including doctors, are not aware of the potential. The more people know about these technologies, the more families may have the courage to give each child a chance at life. Not every child with a medical condition diagnosed prenatally will be cured through these emerging techniques, but the study notes that even in these cases abortion is not the only option. The rapid expansion of perinatal hospice, and the much better mental health outcomes for families, demonstrates that abortion is not a solution.
Finally, the study authors note that these emerging technologies have ethical implications that require oversight and ongoing engagement in public discourse. In this area, pro-lifers have contributions to make, as these emerging technologies reveal what pro-lifers have already recognized: the preborn child in a human being worthy of life, protection, and care.
CNN interviewed discredited environmental catastrophist Paul Ehrlich in its coverage of the United Nations’ latest warning of ecological collapse due to human activities and climate change.
Humanity will need to start “consuming less, polluting less and having fewer children” if it’s going to stop mass extinction in the coming decades, CNN correspondent Nick Watt said summarizing the U.N. report, which was released Monday.
Ehrlich, a Stanford University professor, told CNN he was “pessimistic” that countries could solve predicted ecological disaster in part because of President Donald Trump pledging to leave the Paris climate accord.
Tom Elliott@tomselliott
CNN: If we don’t start “having fewer children” a million species will die.
Note that the “expert” they interview is Paul Ehlrich, the discredited “Population Bomb” prof who’s been predicting imminent mass starvation since the 1960s.
The U.N. called for “lowering total consumption and waste, including by addressing both population growth and per capita consumption differently in different contexts” to limit ecological damage.
The U.N. report blamed “rapid population growth” and the development and pollution that entails for putting 1 million plant and animal species at risk of extinction.
“The other organisms of the planet are our life support system,” Ehrlich, a Stanford University professor, told CNN. “You don’t have to worry about them if you don’t care about eating, if you don’t care about breathing, if you don’t care about having fresh water and so on. Then you can just forget about it and die.”
Ehrlich’s writings came out as environmental concerns were beginning to become top priorities for western countries, including the U.S. and Europe. In general, Ehrlich is a leading predictor of mass starvation and collapse of nature because of rapid population growth.
Ehrlich’s 1968 book “The Population Bomb” called on the U.S. government to take “whatever steps are necessary to establish a reasonable population size.” His ideas included taxing children, mass sterilization and abortions to limit population growth.
John Holdren, President Barack Obama’s science czar, co-authored pieces with Ehrlich, warning the human population was growing too quickly for the planet to sustain. Lawmakers criticized Holdren during his confirmation for his past writings.
But the mass starvation and ecological collapse predicted by Ehrlich and others never came to pass. However, Ehrlich maintains his dire predictions are certain to happen in the coming decades.
LifeNews Note: Michael Bastasch writes for Daily Caller. Content created by The Daily Caller News Foundation is available without charge to any eligible news publisher that can provide a large audience.
Alex Schadenberg, Executive Director – Euthanasia Prevention Coalition, May 2, 2019
Wesley Ely, who, among his other professional accolades, holds The Grant W. Liddle Chair in Medicine at Vanderbilt University Medical Center, wrote an insightful article that was published in the USA Today titled: Death by organ donation: Euthanizing patients for their organs gains frightening traction.
Dr Ely has written his article from the point of view of a former co-director of Vanderbilt University’s lung transplant program and a practicing intensive care unit physician. His article is a response to presentations made at International medical conferences concerning organ donation and euthanasia and the ethical debate concerning euthanasia by organ donation. Ely writes:
At international medical conferences in 2018 and 2019, I listened as hundreds of transplant and critical care physicians discussed “donation after death.” This refers to the rapidly expanding scenario in Canada and some Western European countries whereby a person dies by euthanasia, with a legalized lethal injection that she or he requested, and the body is then operated on to retrieve organs for donation.
At each meeting, the conversation unexpectedly shifted to an emerging question of “death by donation” — in other words, ending a people’s lives with their informed consent by taking them to the operating room and, under general anesthesia, opening their chest and abdomen surgically while they are still alive to remove vital organs for transplantation into other people.
The big deal here is that death by donation would bypass the long-honored dead donor rule, which forbids removal of vital organs until the donor is declared dead. Death by donation would, at present, be considered homicide to end a life by taking organs.
Ely, who opposes euthanasia by organ donation, explains how euthanasia by organ donation would work.
The mechanics of obtaining organs after death from either euthanasia or natural cardiac death (both already legalized in Canada, Belgium and Netherlands) can be suboptimal for the person receiving the transplant, because damage occurs to organs by absence of blood flow during the 5 to 10 minutes-long dying process. This interval is called ischemia time. Death by donation purports to offer a novel solution. Instead of retrieving organs after death, organ removal would be done while organs are still being receiving blood. There would be no ischemia time and organ removal would be the direct and proximate cause of death.
If you think that euthanasia by organ donation is not a threat, Dr Ely explains:
Recently, the New England Journal of Medicine (NEJM) published an article by two Canadian physicians and an ethicist from Harvard Medical School, who contended it might be ethically preferable to ignore the dead donor rule if patients declare they want to die in order to donate their organs.
Dr Ely then argues that society should oppose euthanasia. According to a 2015 article in the NEJM, of the 3,882 deaths due to physician-assisted suicide or euthanasia in Flanders, Belgium, in the year 2013 alone, 1,047 (27%) were due to medication dosages to hasten death without patients’ consent. Such patients are generally unconscious and may or may not have family members around. In 2014, a statement on end-of-life decisions by the Belgian Society of Intensive Care Medicine asserts that “shortening the dying process” should be permissible “with use of medication … even in absence of discomfort.” When discussing these facts, two prominent physicians, one from the Netherlands and another from Harvard, told me that where they come from, they call that murder.
When physicians are participating in a procedure designed to take a person’s life, will patients feel 100% certain that their physician is firmly on the side of healing? What message does it send about the value of every human life when physicians endorse the exchange of one life for another? What effect has it already had on physicians complicit in such death-causing procedures?
Finally Dr Ely compares the discussion about euthanasia to the 1973 movie Soylent Green. In the 1973 science fiction classic “Soylent Green,” detective Frank Thorn searches for answers to dying oceans and a deteriorating human race on overcrowded Earth. He discovers the high-protein green food produced by the Soylent Corporation is recycled, euthanized humans. “Soylent Green is people!” he screams.
“Soylent Green” was set in 2022. We are three years away.
Dr E. Wesley Ely is building awareness with the discussion and concerns with euthanasia by organ donation. Belgian doctor supports euthanasia by organ donation.
Sadly, once society accepts that killing can be an acceptable solution to certain human problems, then the only question is which human problems can killing be a solution for?
Once society accepts euthanasia, then it naturally follows that euthanasia by organ donation will be considered. If the issue is debated based on its efficacy, then euthanasia by organ donation will be become a reality because it is a very effective way to obtain healthy organs for transplanting.
The central focus of the Baho Neza Campaign is the promotion, distribution, and provision of “family planning” and “family planning services” for the sake of increasing the contraceptive prevalence rate of the country. According to an article about the campaign by Hope Magazine, the Baho Neza campaign:
… is an innovative approach that includes additional components of Family Planning and Early Childhood Development (ECD) to address various health related issues, including the availability and accessibility of family planning services, as well as closing the existing gaps.
The article also explains that the campaign:
… will focus on raising awareness countrywide on available information and services related to Family Planning, Early Childhood Development, Antenatal Care and Postnatal Care, the importance of Parents-Adolescents Communication and Teenage Pregnancy prevention.”
At the launch of the campaign, Dr Diane Gashumba (left) urged Rwandans to embrace family planning, saying, “the goal is the best possible services, this year will be dedicated to the promotion of cleanliness as a means of disease control and the practice of family planning.”
On 21 December 2018, Applied Monitoring Services Ltd, posted a job announcement looking for a consultant to conduct a base-line assessment for the Baho Neza project. In the background information on the project, the announcement stated that the overall goal is
… increasing access to long-acting reversible contraceptives and strengthening health care providers capacity to offer post-partum family planning and post-abortion care services countrywide.
Right: Contraception on display for the Baho Neza launch ceremony.
Another Rwandan news site boldly claimed that the primary message parents should be receiving in this campaign is:
… test for pregnancy; in pregnancy, take care of the health of the baby in the first 1000 days of her life; the role of men in following up development, caring for children, protecting children through all the needs; family planning, rehabilitation, to avoid and to prevent pregnancy.
The campaign will combat malnutrition, early pregnancies, seek to increase the number of people practicing long-term family planning methods, and take other measures to improve social well-being.
‘Baho Neza’ is aimed at sensitizing all Rwandans to avoid and fight disease, to care for child and mother health, to attend and use child care services for children, to prevent pregnancy, and to adopt and use family planning services.
Already, it is clear that the purpose of the Baho Neza project is completely incompatible with Catholic moral teaching. Its overall focus and goal include the spread of contraception to vulnerable women and adolescents. But we can expect that CRS will respond by providing us with the same old tired excuses it always gives regarding other projects such as these in which it has been found to be participating.
In the event that CRS actually bothers to respond to questions as to why it is participating in this project, we can anticipate that the answers will include any combination or all of the following:
The real goal of the project is to save lives, and so CRS is saving lives by helping to bring health care to the people of Rwanda.
CRS never participates in the promotion or distribution of contraception or condoms, and is exempt from such things regarding the Baho Neza project as well.
CRS’s role in family planning with the Baho Neza project is to promote Natural Family Planning, thereby giving an alternative to the contraception being promoted by the other implementing partners.
CRS is providing nutrition and medicine through the project and is not participating in the contraception-promoting aspect.
Regardless of the reason CRS is participating in this campaign, the fact of the matter is that CRS is lending the name of the Catholic Church to a campaign whose overall goal is the spread of the Culture of Death. In fact, the Campaign itself makes clear that it is using the religious community to spread its contraceptive messaging. The article in Hope Magazine says, “Religious Leaders will also play a leading role in the campaign to ensure a wide reach and meaningful impact.” Bizimungu François, Health Advisor at Rukomo Health Center in Rwanda, said that some of the barriers to family planning include the churches and churches that are inadequate and the lowest sensitivity of the population. The danger of Catholic Relief Services being associated with a campaign intent upon the spread of contraception is the grave possibility of scandal. The mere attachment of the name “Catholic Relief Services” to the Baho Neza campaign will carry a lot of weight.
But the problem of scandal is not just limited to lending the name Catholic to the campaign. By partnering with groups intending to spread contraception as an end-goal of the campaign, whatever role CRS plays assists in the success of the project. Supposing that CRS has no direct involvement in the contraception-promoting and spreading element of the project, CRS’s work in other areas lightens the burden of those working to spread the contraception. In other words, whatever work CRS does in the campaign, other organizations won’t have to do it, freeing them up to focus on contraception.
We’ve said it before, but it bears repeating … if we exchange the word “contraception” with “sex-trafficking 8-year-old children,” it should hopefully go without saying that CRS would never participate in such an effort. So, either CRS doesn’t view the spread of contraception as a mortal sin whose spiritual effect is just as deadly as sex-trafficking children, or it does but enjoys the funding too much to care.
Contact Catholic Relief Services and tell it what you think about its participation in this project.
Even if the idea of using Fertility Awareness-Based Methods (FABM) for family planning and overall health is starting to gain traction with more women, there is still a conspicuous lag when it comes to the medical community.
The overwhelming majority of medical professionals are not fully (if at all) informed about modern FABMs, or Natural Family Planning (NFP), and do not understand how the biological information recorded on women’s charts can help diagnose and treat common women’s health issues.
Because of this disparity, many women feel they must become advocates for their own health or look for support outside of their primary physician and OBGYN when seeking Fertility Awareness-Based Methods. But with a little education on the benefits of charting for patients, doctors can easily expand their options available to patients, while learning more about how to best treat any symptoms that come up.
Here are just some of the reasons why doctors would benefit from adding Fertility Awareness-Based Methods to their practice.
1. Today’s patients want side-effect free options for family planning.
The truth is, more women than ever are dissatisfied with hormonal birth control methods, in great part due to the disagreeable (and even life-threatening) birth control side effects they are experiencing. Women report they have not felt heardin their desire for safer, natural, effective methods of family planning and solutions for helping with their reproductive health issues. When doctors give women the impression they are not capable of learning and observing their bodies’ natural signs of their menstrual cycle, the medical community is underappreciating not only their patients’ abilities but also the benefits.
In a recent Natural Womanhood interview, Dr. Summer Holmes Mason, a board-certified OBGYN, shared how she came to start offering fertility awareness options in her practice. Since she had limited education about FABMs in medical school, she had to educate herself, but she found it was worth it. While prescribing hormonal contraceptives was her primary method of treating women with various medical issues, Dr. Holmes Mason explains, she eventually started noticing that these contraceptives were not always producing desirable effects. She recalls, “After a couple of years, I realized people were coming back to me with more side effects than I thought was acceptable.”
She knew that there had to be more options for her patients, which led her to discover FABMs, a safer, side-effect-free option for preventing pregnancy and managing women’s health issues. Now, Dr. Holmes Mason offers both hormonal birth control and natural FABM options to her patients, as she explains: “I really try to utilize the informed consent process. I feel like my patients will know what they are getting into if they are getting hormonal contraceptives, and let them make that choice for themselves . . . for those people who don’t want to, after having that discussion, I have so much more to offer.”
Women today are seeking doctors with more to offer them for their family planning and health issues than hormonal methods of birth control. Even the supposedly natural, hormone-free copper IUD affects patients’ natural hormonal balance since copper affects the thyroid. Too many women are tired of experiencing adverse effects of their contraception methods and are searching for truly natural and safe methods.
2. Offering fertility awareness methods will help doctors retain patients.
Because women are not typically offered natural options for family planning by their doctors, women who want such options are starting to look harder for doctors who are knowledgeable on Fertility Awareness-Based Methods. Many women are taking their reproductive health concerns into their own hands by seeking doctors who offer more than pharmaceutical birth control as a one-size-fits-all solution for all range of health issues.
As one woman named Andrea recently shared with us:
“I was most worried about my doctor being knowledgeable enough to help me use FABMs. I asked my gynecologist (part of a world class healthcare system) for information about fertility awareness-based methods of contraception, but she stared at me blankly. When I clarified and called it [Natural Family Planning], she referred me to the Institute for Reproductive Health, which was fine, but it’s geared toward women in third-world countries. Therefore, I didn’t stay with that practice. I found a more informed gynecologist who not only can read charts, but can also understand me perfectly when I say something like, ‘I’m getting a lot of tacky fluid during phase 2.’ While it is sad that I knew more than my first doctor, it was well worth changing doctors to someone who could better assist me in using FABMs.”
Dr. Marguerite Duane, a board-certified family physician, explained in a Fertility Friday podcast why medical professionals are typically not educated about FABMs in their medical training (herself included). First, FABMs are not profit-generating like birth control, so they have difficulty competing against highly marketed pharmaceutical products. Second, medical professionals are given less than accurate accounts of FABM effectiveness rates. Third, with the way our healthcare system is currently set up, most physicians do not have time to explain fertility awareness to their patients and review their cycle and charts (sadly, it’s much easier and quicker to simply prescribe a pill). And fourth, many doctors are misinformed in their medical training, wrongly associating modern Fertility Awareness-Based Methods with the outdated rhythm method.
With these obstacles standing in the way, it’s no surprise that more doctors are not aware of fertility awareness methods. As Dr. Duane stated in the podcast, “I firmly believe as a physician and as a woman, this information should be available to every woman, and every medical professional that provides women’s health services should be trained in these methods.”
3. Charting will give more information about a patient’s health to assist in a treatment plan.
The primary reason doctors should consider adding fertility awareness-based methods in their practice is because doing so serves the health of their patients. At the recent Fertility Appreciation Collaborative to Teach the Science (FACTS) Conference in Cleveland, Ohio, I observed a presentation by two doctors called “The Female Cycle as the Fifth Vital Sign” that confirmed the medical value of charting. Dr. Kim Vacca, a pediatrician, explained how charting using FABMs is for more than just family planning, since it can contribute to a woman’s overall health, starting from adolescence.
Mothers are desperately searching for birth control alternatives for their teenage daughters, who are being prescribed the Pill for things like irregular periods, PMS, or acne, only to find that it is only covering up their symptoms, not treating their problems, and often providing even worse side effects.
At the FACTS Cleveland conference, family physician Dr. Kathleen Heimann explained that if doctors were to properly treat women in their entirety, they would look at five vital signs, rather than just the usual four signs observed by most doctors.
Dr. Heimann and Dr. Vacca are not the only ones who believe that doctors need to start paying more attention to a woman’s cycle. The Committee on Adolescent Health Care in the American College of Obstetricians and Gynecologists statesthat “by including an evaluation of the menstrual cycle as an additional vital sign, clinicians reinforce its importance in assessing overall health status for patients and caretakers.”
In short, doctors need to become more informed as to the importance of empowering their female patients to managing their health with access to and information on Fertility Awareness-Based Methods. Not only will natural family planning options provide doctors with side-effect-free pregnancy prevention options patients today are seeking, and retain more patients in the process, but FABMs will give today’s doctors a new tool in their kit equipping them to truly help women—and to help women help themselves.
April 29, 2019 (Renew America) — The “dead donor rule” — a person must be dead before his vital organs are extracted for transplantation — is the basic principle guiding organ donation. A dead body is a corpse. Excising vital organs from a corpse does no harm. But, if we are not certain the individual is dead, removing vital organs is a grave matter.
The Catechism of the Catholic Church (2296) states: “… it is not morally admissible directly to bring about the disabling mutilation or death of a human being, even in order to delay the death of other persons.” Furthermore, even though Pope John Paul II stated that organ donation is an act of charity, in Evangelium Vitae (n. 15) he cautioned: “Nor can we remain silent in the face of other more furtive, but no less serious and real forms of euthanasia. These could occur for example when, in order to increase the availability of organs for transplants, organs are removed without respecting objective and adequate criteria which verify the death of the donor.”
We have been asked, “How and why does HALO differ from the National Catholic Bioethics Center’s position on ‘brain death’ and the use of ‘brain dead’ individuals as organ donors?” This paper is HALO’s answer.
HALO’s position is that a diagnosis of brain death does not mean that it is morally (or scientifically) certain the person is dead. Therefore, the practice of removing vital organs from “brain dead” individuals should be suspended and alternative means for extending the lives of individuals with failing organs should be pursued.
The National Catholic Bioethics Center’s Position
The NCBC’s most well-known authority on brain death, Father Tad Pacholczyk, makes four assertions:
1. “The [brain dead] individual has undergone a traumatic event resulting in the complete and irreversible cessation of all brain functions.”
2. “Brain dead individuals cannot be kept going on machines forever. In fact, there is usually a period of only a few days that it may be possible to extend the functioning of their organs by keeping them on a ventilator.” He suggests that “somebody is likely to have cut some corners in carrying out the testing and diagnosis” in cases where individuals have survived for months or years after a brain death diagnosis.
3. “Genuinely brain-dead individuals never ‘wake up.'”
4. “Defining brain death as the irreversible cessation of all functions of the entire brain, including the brainstem, is compatible with a Christian understanding of the true nature of man.” [1]
We do not disagree with Father Pacholczyk’s fourth assertion. However, after diligently searching for the answer to our question (this paper’s title), we have reached an uncomfortable conclusion: If physicians wait long enough to be certain that all functions of the entire brain have irreversibly ceased — that is, that the person is truly dead — the deceased person’s organs will have begun to deteriorate and therefore will not be transplantable. If the goal is to salvage healthy organs, haste is of the essence in determining brain death. Haste can lead to cutting corners and to errors. Also, as Pope John Paul II suggested, furtive euthanasia may occur as a means of increasing the supply of transplantable organs. (This is a reasonable concern since organ transplantation is a very lucrative business and “the love of money is the root of all kinds of evil…” — 1 Timothy 6:10).
To address Father’s first assertion, it is necessary to ask a question. How is it possible to establish “the complete and irreversible cessation of all brain functions” when the person is exhibiting signs that some parts of the brain are functioning — signs which we can see with our own eyes?
Should We Believe Our Senses?
When our senses tell us someone is alive, but doctors tell us he is dead, what are we to believe? Two things which contradict each other cannot both be true. A human being is either alive or dead.
Before organ transplantation was possible, physicians made every effort to judge the moment of death in the direction of protecting life from a death-dealing mistake. Circulation and respiration had irreversibly ceased — the body was cold, blue and stiff. Our senses told us that the person was dead.
Brain death is declared while the patient has a beating heart because removal of vital organs must be done before they begin to deteriorate due to loss of circulation. We bury dead people, but we would never bury a person with a beating heart because we know that a beating heart is a sign of life. Also, consider these facts:
• A person can be pronounced “brain dead” while he or she has a normal pulse, blood pressure, color and temperature. All signs of life.
• “Brain dead” people
• “Brain dead” children grow.
• “Brain dead” pregnant women have gestated and delivered healthy babies and produced milk.
• “Brain dead” patients’
• During the excision of organs, the donor is sometimes given paralyzing drugs to control muscle spasms; the heart rate increases, and blood pressure shoots up. Dead people don’t move or react to pain in these ways.
The legal definition of brain death is “the irreversible cessation of all functions of the entire brain, including the brain stem.” Yet “brain dead” patients display signs that their brains retain many essential functions. [2]
If a person who has been determined to be brain dead is truly dead, then our senses are deceiving us.
Pursuing the Truth Wherever It Leads
There are good people who support vital organ donation after a determination of brain death and good people who oppose it. It is not HALO’s purpose to judge anyone who has decided to donate organs or to undergo transplant surgery. We do, however, strongly suggest that people consider all the evidence before making these decisions and prior to taking a position on this crucial moral issue.
Renowned theologian Christian Brugger believes there is reasonable doubt that “brain dead” bodies are dead and concludes, “Since we should not treat as corpses what for all we know might be living human beings, it follows that we have an obligation to treat BD individuals as if they were living human beings.” [3] Dr. Paul Byrne and other experts in the fields of medicine, philosophy, and theology explain why they maintain that “‘Brain Death’ is Not Death” in an illuminating essay by that name. [4] HALO highly recommends reading this brief, yet thorough set of arguments against using neurological criteria alone to determine death.
John Haas, President of the NCBC, says that those who express doubt or deny that brain death is true death “create confusion in the minds of a number of the faithful” and “run the risk of unsettling the consciences of the faithful on a life-and-death ethical matter for which the authentic magisterium of the Church has provided clear guidance.” [5] However, we find Church guidance on this matter to be anything but clear and interpretations of Church guidance vary widely. Brugger, Byrne, Pacholczyk, and Haas are just a few of the many Catholic experts who express differing positions on “brain death.” (Perhaps this is a topic for another paper.)
The evidence HALO has thus far examined leads us to agree with the experts who say we cannot be morally certain that a person who has been declared “brain dead” is truly dead before organs are removed. But we will never cease our search for the truth. At the very least, those who believe brain death is death should concede that this is one diagnosis where doctors need to be correct 100% of the time — and, for the sake of all who trust them, admit that there is a growing body of evidence that this diagnosis is not accurate in at least some cases, and perhaps in many cases.
Father Pacholczyk asserts, “Genuinely brain-dead individuals never ‘wake up.'” Every time a recovery occurs after a determination of brain death we are told the diagnosis was wrong; that perhaps corners were cut in testing, or mistakes were made, or the person doing the testing was not qualified, etc. Thus, how can anyone know for certain that a person is “genuinely brain dead?” The only way is to wait and see.
People who have been determined to be “brain dead” using the most rigorous neurological criteria have awakened and recovered. It is safe to say that they would not have recovered had they been stripped of their vital organs before their injured brains could begin to heal. Here are two cases in point.
Trenton McKinley, a 13-year old Alabama boy, was declared brain dead after suffering skull fractures and a traumatic brain injury in March 2018. He reportedly passed all the tests for determining brain death. His mother signed papers to donate his organs. Fortunately, he regained consciousness before his vital organs were removed. Trenton was taken off the ventilator and eventually went home. He is now conscious, walking and talking. [6]
In 2007, Zach Dunlap, a 21-year-old Oklahoman, flipped over on his 4-wheeler and suffered catastrophic brain injuries. Thirty-six hours after his accident, doctors at United Regional Healthcare System in Wichita Falls, Texas determined he was “brain dead.” They had subjected Zach to a battery of tests including a scan that showed a complete absence of blood flow to the brain. Preparations to harvest his organs were underway when a relative scraped the bottom of his foot with a pocket knife and he jerked his foot away. Just months later, Zack was walking and talking. He recalled hearing a doctor say he was dead and being “mad inside” but unable to move. [7]
Father Pacholczyk also maintains that “there is usually a period of only a few days that it may be possible to extend the functioning of [brain dead individuals’] organs by keeping them on a ventilator.” We point out that some people who have been diagnosed as brain dead have lived for years even though they have not made remarkable recoveries. For example:
On December 9, 2013, 13-year old Jahi McMath underwent surgery to remove her tonsils and adenoids at a children’s hospital in Oakland, California. Shortly thereafter, she started to bleed and suffered cardiac arrest. She was declared “brain dead” three days later. Her family disagreed with the diagnosis and fought for Jahi’s life when the hospital sought to remove her life-support. Keeping her alive required moving her to New Jersey. Bobby Schindler, President of the Terri Schiavo Life & Hope Network (https://www.lifeandhope.com/), explains: “After Jahi was ruled to be brain dead, she and her family found themselves in an incredible situation wherein Jahi was considered legally dead in California, but legally alive in New Jersey due to that state’s religious accommodations.” Jahi’s mother took excellent care of her at home. Jahi breathed with the aid of a ventilator. She responded appropriately to commands and underwent pubertal development. Her true death occurred on June 22, 2018. Her death certificate, completed by the NJ physician treating Jahi, listed her cause of death as bleeding as a result of liver failure. Various news outlets subsequently reported that Jahi McMath had died, underscoring the fact that Jahi was a living human being for four and a half years after being issued a death certificate in California. [8] To learn more about Jahi’s condition read “The Case of Jahi McMath: A Neurologists’ View” by D. Alan Shewmon, The Hastings Center Report, December 25, 2018 (https://onlinelibrary.wiley.com/doi/10.1002/hast.962).
Father Pacholczyk contends that such cases “indicate a failure to apply the tests and criteria for determination of brain death with proper attentiveness and rigor.” This explanation is not reassuring for people who have signed up to be organ donors, trusting that doctors don’t make erroneous declarations of death.
One final point. There are many different sets of diagnostic criteria that may be used to determine brain death. A person who would be declared brain dead in one hospital could be considered alive and receive potentially life-saving treatment in another hospital.
Even if you believe that brain death is true death, consider that you do not know where you might be hospitalized in the event you suffer a severe brain injury. What criteria will be used to determine brain death? Will the doctors who do the testing be qualified, careful, and honest? Will your organs be more important to them than your life?
“Should I Refuse to Be an Organ Donor?” Is a Prudent Question
Let us be clear. HALO does not reject vital organ donation by itself. We question the validity of brain death, particularly when “brain dead” individuals are slated to be organ donors or when a brain death determination is made not in order to be certain a patient is truly dead, but to justify stopping all life-sustaining treatment. Our position is compatible with the Church’s position. The Catholic Church is not opposed to organ transplantation but insists that persons must not be killed in order to procure their organs or for any other reason.
HALO cautions people: When in doubt, err on the side of life. We advise that you sign a wallet card refusing to be an organ donor [9] and carry it with you at all times, but the decision is up to you.
NOTES:
[1] Father Tad Pacholczyk, Director of Education, The National Catholic Bioethics Center, “Making Sense of Bioethics: Brain Dead Means Dead,” November 2005, www.ncbcenter.org.
[5] John M. Haas, “Catholic Teaching regarding the Legitimacy of Neurological Criteria for the Determination of Death,” The National Catholic Bioethics Quarterly, Summer 2011.
In the 1930s or 1950s, how often did the parish priest talk about contraception in homilies? Only occasionally. It might be proposed once a year by the diocese, but generally they didn’t preach much on it. Instead, they would bring mission preachers in regularly and get them to take on hard topics like this.
We have lost these parish mission preachers for the most part. Leslie Woodcock Tentler, author of Catholics and Contraception: An American History, thinks that a large part of the collapse of the missions was how they treated contraception. However, I wonder if we should bring them back precisely for contraception but maybe with some slight changes to adapt to the modern situation. Let me point out why parishes relied on mission preachers to talk about contraception, canon law, and how I might adapt this to the future.
Why Mission Preachers?
Giving preaching on contraception to itinerant preachers served a few purposes. First, it avoiding scandalizing children. It is always challenging to bring up adult sins while not giving inappropriate ideas to the children present at Sunday Mass. When I worked more in youth ministry, we would simply say, “Did you look at anything on the internet you shouldn’t have?” if younger teens were present to avoid giving them ideas about pornography. In a related vein, missions were generally preached only to adults, and often preached to single-sex audiences.
Second, it is hard for a pastor who is close to his flock and “smells like the sheep” to bring up a sin that is common, serious and secret. Bringing in a priest to preach on it lets the pastor just say, “Yes, Fr. Jack was right,” when anyone asks, which might avoid some parish conflicts.
Third, it is a difficult topic to preach on well. Even for a priest with the courage to bring it up, it is hard to make a homily that is engaging, at the level of the everyman and actually explains the reasons behind Catholic teaching.
Canon Law on Parish Missions
Even though parish missions have fallen out of favor in many places, Canon Law still asks for frequent parish missions.
The law in force from 1917-1983 set a rather long time between missions: “Canon 1349.1: The ordinary [bishop] should be vigilant that at least every 10 years that sacred parish missions be held. Parishes priests are to ensure this happens.” In the U.S., most parishes used to have them far more frequently than every 10 years.
The 1983 code dropped the 10-year requirement, and offered other formats, but kept the requirement for extra preaching in parishes: “Canon 770: At certain times according to the prescripts of the diocesan bishop, pastors are to arrange for those types of preaching which are called spiritual exercises and sacred missions or for other forms of preaching adapted to needs.”
Thus, every parish is still called to have regular preaching by outside priests. I know many parishes do this regularly, but my experience makes me think some forget about this.
Parish Missions Going Forward
Although I disagree slightly with Tentler’s analysis of the collapse of parish missions, she seems like a serious historian to rely on for facts about how these missions preached on contraception.
Today, I don’t know if we could excite the people who need to hear the Church teaching on contraception to a weeknight preaching. I’d hedge my bets. Often a priest will need to get coverage for one or two Sundays a year while he’s out. Why not get a priest specifically trained in contraception to celebrate the Masses and preach one weekend?
I think this would fully resolve two of the three reasons above that mission preachers were relied on before, and it could manage the third. It would solve the issues of being tough to preach well and a pastor looking to avoid parish conflicts. Obviously kids would be present at a Sunday Mass, but I’ve seen a few priests preach in ways that explain Church teaching without giving kids inappropriate ideas.
I think in doing so, we can do something better than the missions 75 years ago. Often these missions just told people to obey the Church on the issue or gave secondary problems that might result from contraception. Instead, modern homilies I’ve seen on this do a far better job of describing the natural law and theological reasons than any of the varied mission homilies Tentler quotes in her book.
I am not the first to suggest this idea. I have heard similar suggestions of training a few priests to give amazing homilies on these tough topics and send them out to cover different parishes each weekend. However, I have yet to seen it done much.
Such missions would need to be timed with classes on NFP/Fertility Awareness of the parish starting right after. Helping couples see how to live without contraception helps change their mind about whether they use it.
If we keep on our current trajectory, we will keep having an official Church teaching that many Catholics ignore. We need a way to teach Catholics this in a way that they are open to accepting the teaching. I think priests who regularly preach on this in different parishes is one way. Let’s bring back parish missions.
Have you ever heart of the “sweaty T-shirt test?” No, not the quick pit-check you do after a morning at the gym to see if it’s still socially acceptable to run into the coffee shop or grocery store on your way home. I’m talking about the study performed by Swiss scientists in the nineties in which women literally sniffed a whole bunch of men’s sweaty T-shirts. Why did these women subject themselves to such an experiment (and unique form of torture)? For science, of course!
What the Swiss researchers found was that when it comes to the immune system, opposites attract. The women in the study were more attracted to the scents of the men whose major histocompatibility locus (MHC) genes (“one of the immune system’s key markers of identity”) were more dissimilar to their own.
As it turns out, there is an evolutionary advantage to such an adaptation: the offspring of mice with genetically dissimilar immune systems tend to have stronger immune systems—and are therefore healthier—than the offspring of two individuals with genetically similar immune systems. Thus, it made good evolutionary sense that the rule of opposite attraction was observed in the Swiss sweaty T-shirt study: the scent of a man who had MHC genes that were too similar to the woman who sniffed his T-shirt was perceived as less appealing.
What stood out to researchers is that this was the case for all women, except for women who were on birth control.
For women on the Pill, the medication actually altered how they perceived the smell of a potential romantic partner, making them more likely to be attracted to men with genetically similar immune systems, rather than to those with immune systems that differed from their own. This has to do with the way that hormonal birth control “tricks” a woman’s body into believing she’s in a perpetual state of pregnancy, which (evolutionarily speaking) makes her more attracted to men with genetically similar immune systems—i.e., men who are more likely to be related to her—because of the “protection” such relationships can provide in her more vulnerable state.
Future effects on children
Recently, a Danish study made headlines by declaring that there was no evidence for birth defects in the children of mothers who had been on hormonal contraceptives immediately prior to, or during the first few months of, pregnancy. But another recent study went even farther back, before those children were in the picture, to determine whether women who were on birth control when they met their romantic partner produced less healthy offspring than women who met their partners while they were not on any form of hormonal contraception. The findings, reported in the journal Evolutionary Psychological Science, were astounding:
“Our findings show that children of women who were on the Pill during relationship onset are more often reported by their mothers to be infection-prone and require medical care, suffer from a higher frequency of common sicknesses, and are perceived as generally less healthy than their peers as compared with children of women who were not on contraceptive pills during relationship onset.”
Put simply, what researchers found was that, not only can being on the Pill alter your preferences for a romantic partner, but it might actually have downstream effects on the health of your offspring, too—even if they don’t come in the form of obvious birth defects.
Similarly, there is also some recent evidence that being on the Pill within six months of conceiving a child may also raise that child’s chances for developing leukemia. And the more we find out about the effect of hormones on the gut, the more we may also learn about the impact the Pill’s gut-wrecking effects may have on our future children.
It turns out that a little pill contains quite a lot of power over a woman’s future, her children’s futures, and the future of human evolution.
Safe and effective alternatives
Thankfully, there are ways for women and couples to plan their families that won’t mess with their (very helpful!) evolutionary adaptations—and which can be just as effective at pregnancy prevention as the Pill. Fertility Awareness-Based Methods, also known as modern methods of Natural Family Planning, have effectiveness rates comparable to those of hormonal birth control, especially when women and couples take the time and effort to learn a method from a certified instructor.
Women are increasingly turning to natural methods of family planning and cycle charting apps, not only to avoid birth control side effects, but to have greater confidence in theirhealthcare management. With this latest research in mind, they might also make the switch to protect their relationships and children as well.
BUDAPEST, Hungary — The Hungarian Parliament passed sweeping pro-family legislation April 1, guaranteeing various married couples and families interest-free loans, mortgage assistance and even childcare allowances for grandparents.
The seven-point package is an “important milestone” in the history of Hungarian family policy, says Katalin Novak, Hungary’s minister for the family, in a Europe that is renouncing its Christian culture and “slowly committing suicide.”
Novak also explains in this April 12 interview with the Register why Hungary has pursued such an overt pro-family approach since 2010, one that statistics show has led Hungary’s abortion rate dropping by 33.5% from 2010 to 2018, marriage increasing by 43%, and divorce decreasing by 22.5% between 2010 and 2017.
She also explains how the Hungarian government has persisted with its pro-family policies despite being demonized as “far-right.” The radicals are those who “believe that immigration should be the only path to choose,” Novak argues. “It’s not normal, for example, to compare family support to Nazism.” Mrs. Novak, how important was the recent World Congress of Families in Verona — which brought together pro-family leaders from all over the world — to your work in support of the family, and how might it influence your policy formulation in the future?
As a pro-family politician, I appreciated the opportunity to promote the priority and importance of families and present the Hungarian family-friendly model. The event in Verona was a very good opportunity to spread the word to my colleagues about best practices that actually work in Hungary.
We are building a family-friendly country, and we’ve achieved quite a lot in this field. Last year, the birth rate was at its highest for 20 years, as was the number of marriages. I was more than happy to share our experiences with other countries’ representatives and decision-makers.
What were the main points of your talk?
In my speech, I talked about a Europe that is slowly committing suicide. If we renounce our Christian culture and at the same time stop promoting the importance of the family and children and just accept anything that might happen to our continent, we are in practice sacrificing ourselves and committing suicide.
I presented the Hungarian model’s family-policy measures. The Hungarian government has been pursuing a strong family policy and the goal of being a family-friendly country since 2010. This seeks to achieve a turnaround in demographic trends by supporting legislation, financial incentives, assistance, services and a family-friendly mentality. We are also helping those who are already raising children as much as possible. Traditional strong families represent an asset which we intend to defend — not only in Hungary, but internationally, as well.
Were you surprised by the extent of opposition to the congress, and why do you think it drew so many attacks?
I wasn’t surprised, as we’re used to the habits of the left-liberal media, NGOs and politicians that label everything not in line with their views as wrong, radical and far-right extremism. We’re not radicals — we simply want to strengthen families as much as we can, instead of prioritizing immigration.
In Central Europe, we not only understand the demographic crisis we face, but we also want to find our own solutions that address our young people who would like to have children. This is the difference between Central and Western Europe. Western political elites don’t want to dig deeper into the problems, and they choose the simplest path: mass immigration.
We believe that the demographic crisis can only be solved in the long run by relying on our own internal resources. We’ve asked Hungarians many times about how they imagine their future, who they want to live with, and how many children they want.
The answers were crystal-clear: Hungarians are family-oriented; and they love their families, their culture and their traditions. We’ve been given this direction by the Hungarian people. We want to strengthen families, women and young people. We want to provide security, and we want to protect our Christian culture.
In relation to your government’s support for the family, how have you managed to introduce such policies in the face of opposition, and what can other countries learn from your example?
After we won the election in 2010 with a two-thirds majority, we decided to build a family-friendly country and to strengthen families raising children. We thought the opposition would be a partner in this, but since then there have been very few decisions in the field of family policy that they’ve supported. So if we had always taken the opposition’s opinion into account, Hungary would now be on the brink of collapse. There wouldn’t be such a comprehensive family-support system, a family-friendly tax system, a housing program, 800,000 new jobs, and many opportunities to create a balance between life and work. The socialists have driven our country into deep crisis before, and they would do it again. They’re only interested in grabbing power again; to achieve this goal, they’ve even joined forces with the Hungarian far right.
We now spend twice as much on families as in 2010: almost 5% of total GDP, exceeding the OECD average by almost 100%. We have a very complex, comprehensive support system, and we help families in many different fields, including nursery developments, the tax system, housing and pension policy. We are open to sharing our experiences and best practices worldwide.
How can policies supporting the family be separated from the demonizing label of “far right”?
In many cases, everything is considered “far right” that is to the right of a given position. Is it far right and extremist to support families, just because of this? The question itself is misleading.
In our eyes, the radicals are those who believe that immigration should be the only path to choose. It’s not normal, for example, to compare family support to Nazism — as one Swedish minister has done. Our main aim is to provide opportunities and to make it possible for young Hungarians to freely decide about their lives. Is this far right?
How do you see the future? Do you see the tide turning and governments adopting more pro-family policies in the coming months and years?
The starting point is that in Europe there is a battle between anti-migration and pro-migration countries. We want to solve the demographic challenges by strengthening families, while they prefer migration over empowering young Europeans to have more children.
Meanwhile, there are more and more people that are deeply worried about the unchecked influx of illegal immigrants and the rise of terrorist attacks. Europewide I see that there is an increasing demand for good policies that enable people to live better, to have more choice and to receive help when needed.
The European Parliament election in May will be an important milestone. The question is very much about whether the EU is able to renew and strengthen itself by putting families at the core, instead of surrendering.
One thing is clear: We shall continue to support families in the future, and in this we hope to have more and more allies — like Poland or Italy, among others.
What measures does this new legislation, the Family Protection Action Plan, include?
This seven-point package is an important milestone in the history of Hungarian family policy and also in our attempts since 2010 to build a family-friendly country. The law has just been approved by Parliament and will be effective from July 1:
· Married couples in which the wife is under 40 will be eligible for an interest-free, general-purpose loan of 31,000 euro. Repayment can be suspended, significantly reduced or written off entirely if the couple go on to have children.
· Families raising at least three children will be eligible for a grant of 7,800 euro to buy a new car seating at least seven people.
· There will be universal crèche [baby crib] provision by 2022. Therefore, we will be creating 21,000 additional crèche places over the next three years.
· We are providing the opportunity for families to reduce their mortgage loans by 3,100 euro upon the birth of a second child. Upon the birth of a third child, this amount increases to 12,500 euro.
· The preferential home-loan scheme will be extended: Families will be able to use it for purchasing existing properties as well as new ones. The amounts on which repayment relief is available are up to 31,000 euro or 48,000 euro, depending on the number of children.
· And from Jan. 1, 2020: We are providing lifetime exemption from personal income tax for Hungarian women who have given birth to at least four children or who will give birth to a fourth child.
· Grandparents will be eligible for childcare allowance.
This is not the end of our work. There is more to come! Hungarian families can count on us.
Edward Pentin is the Register’s Rome correspondent.
Where are you headed? This is not just a question the cabbie asks when you get into his car in a big city somewhere in America. It is also a question we ask ourselves as Catholics. With Lent in progress, we know the answer: We are headed to Easter and we get there by following the apostles Peter and John in their run to the empty tomb. We do not, however, run through Lent. Lent is a time to slow down and think seriously about serious matters.
By thinking seriously about serious matters, I do not have in mind the intricacies of Trinitarian theology or the subtleties in atonement theology—although it is never unwise to think about these matters. What I have in mind are the realities of ecclesial life in large swaths of the United States at the present time.
Decades ago, I had the good fortune to meet a dedicated religious priest at a wedding. At the reception following the nuptial Mass, we were seated next to each other, and from that time forward we were friends. In the discussions that good friends have over the years, good priest friends, that is, the topic of the Church was ever present. Often, my priest friend would remark, “The Church means less and less to more and more Catholics.”
Never mind that this priest had me by more than a few years, but he had also travelled widely in the United States because of responsibilities related to his ministry. Having age and experience on his side, I was inclined to trust my friend’s observation. In fact, I did not have to extend the benefit of the doubt to him in the matter of what the Church means to Catholics today. I could see with my own eyes and hear with my own ears what was occurring in the lives of Catholics whom I met in pastoral setting after pastoral setting. My own ministry was already showing me what had been manifested to my friend over a much longer span of time.
What you may ask at this point is: what are you referring to, Monsignor? What examples can you give in support of your thesis? Well, let me offer a few illustrations.
Every year at the Easter Vigil, in most parishes, men and women are baptized and received into the Church. In some places, the numbers are small but that is not always the case. In a diocese, when you add up all the parishes, the numbers of baptisms and receptions into full communion run into the hundreds or perhaps exceed one, two, or three thousand in large archdioceses. What happens when the Church marks the Second Sunday of Easter or the Solemnity of Pentecost? The newly initiated and the newly received—most of them, anyway—vanish and are not seen again in our parishes by priest or congregant.
Regular churchgoers have known for a while now that Mass attendance is not what it used to be. Reliable surveys indicate that weekly attendance is somewhere in the range of 18 to 25 percent, with higher and lower median averages depending on specific locale and other factors across the nation. Not so well known to Catholics are the steep falloffs in infant baptisms, weddings, and funerals. In just one of the categories mentioned, weddings, estimates are that church weddings are off by two-thirds in heavily Catholic areas compared with only thirty years ago. If you are doubtful about the downward shifts in weddings, infant baptisms, and funerals, you would do well to check out the statistics for these indices of Catholic life through the publication of the annual The Official Catholic Directory, which was known for the longest time as the Kenedy Directory. Go back fifty years, forty years, thirty years, twenty years, or even just a decade and you will be amazed at the enormous differences in reported sacramental celebration.
One thing The Official Catholic Directory will not be able to tell you is the massive decline in sacramental confessions. For that, you will have to show up in your parish church at the regularly scheduled period for celebrating the Sacrament of Penance. Thirty years ago, it was not unusual for a priest to sit in a confessional for ninety minutes and hear confessions without any “downtime.” Not today though. It is mostly “downtime” with very few penitents going to have their sins absolved.
Much can be adduced to explain the phenomena cited above from a sociological perspective. Surely that would be helpful but only to a point. What is needed is a more fundamental explanation, one which must concern itself with the Church’s nature and how this is, unfortunately, lost on many Catholics today.
Since sociology helps but only up to a point, let us start there. Sociology, as an academic discipline, studies institutions and the services they provide to those within the social matrix. According to the applicable taxonomy, the Church is a mediating institution. She mediates between persons and the society to which they belong. She is a “go-between,” putting persons in a more salutary relationship with each other and over against other, more “depersonalizing” institutions. However, this kind of mediating is basically along a functionalist axis, and thus has nothing to do with what Catholics believe as Catholics.
The Church, by her nature, is mediating. But the mediation she exercises does not start with what we do. It begins with Christ, the Mediator (cf. 1 Tim. 2:5). He is the One who puts us in a relationship, an ontological relationship, with the Blessed Trinity, and this new reality commences for us with baptism. It is important to note however, that baptism inaugurates but does not complete our sacramental incorporation into Christ. In the sacramental ministry—from baptism through the Anointing of the Sick—the Church has a concrete means by which Jesus the Mediator reaches people who were not on earth when he was. Through the sacramental ministry—again, from baptism through the Anointing of the Sick—the mediation accomplished once and for all in Christ reaches people today through his Body, the Church.
All of this is put forward succinctly and directly for us in Lumen Gentium where the Fathers of the Second Vatican Council say that “the Church, in Christ, is in the nature of sacrament.” (1) She is the sacrament par excellence because “[t]he one mediator, Christ, established and ever sustains [her as] the community of faith.” (8)
Just a few years after the close of Vatican II, then-Father Joseph Ratzinger delivered lectures that he would later publish as Introduction to Christianity (1968). In this volume, the future Pope Benedict XVI writes: “[T]he sacramental idea … forms the heart of the concept of the Church: Church and sacrament stand or fall together; a Church without sacraments would be an empty organization, and sacraments without a Church would be rites without meaning or inner connection.”
The problem we need to face up to, pastorally, is why so many Catholics choose to forsake sacramental celebration as a regular feature of Catholic life. Could it be that so many of our brothers and sisters in Christ view the Church as “an empty organization?” Or do they see the sacraments as “rites without meaning or inner connection?” As then-Father Joseph Ratzinger says above, “Church and sacrament stand or fall together.” Right now, these two pillars of faith are not standing all that well.
Some concerns in the pro-life community today are with supporters who are personally pro-life but believe they cannot impose on others their opinion that abortion is wrong, and pro-lifers who believe in “certain circumstances” abortion should be an option. These pro-life supporters may have well intentions but are misinformed or do not hold pro-life values as a high priority. They may vote for legislators whether or not their “personal” stance on abortion is shared. This attitude occurs in communities everyday. This “pro-lifer” could be your best friend, your relative, or a fellow parishioner at your church.
The Catholic church, for example, has always considered abortion a mortal sin. Their doctrine forbids all abortions, but church members are sometimes divided on the issue; some Catholics are pro-abortion, and some are pro-life. Additionally, there are other Catholics who are apathetic, or care personally, but are politically indifferent. With the increasingly radical abortion laws being passed across the country, many Catholics and pro-life supporters have voiced their outrage at their government and these morbid, inhumane laws, even permitting infanticide. But were they passionately advocating for their position on election day when it mattered?
It is easy to blame pro-abortion politicians, even pro-abortion Catholic politicians like Governor Andrew Cuomo in New York, but it is time for pro-life supporters and pro-life Catholics to look in the mirror.
Archbishop Jerome Listecki of Milwaukee Wisconsin argued, “The real problem lies with our Catholic community that justifies the voting for candidates who would support anti-life actions.”
Why are we compromising our morals and beliefs by voting for these politicians? We deserve better. These politicians need our votes. We are letting these so-called leaders pass these laws. To make a difference, Catholic pro-life supporters need to stand up.
Listecki also urged, “Therefore, it begins with us making our voices heard as politicians vie for our votes, and refusing to accept the rationalization that we can make these heinous acts rare and limited. Human life demands our respect, protection, and nothing less.”
Indirectly, when pro-life supporters and pro-life Catholics do not vote for pro-life politicians, they are condoning abortion or even supporting infanticide. In historical times of human atrocities, it was similarly vital for people to take a moral stand.
During World War II, millionsof people were being slaughtered, yet there were Nazi soldiers and others who knew it was wrong, but did nothing. Some were intimidated by fear.
Similarly today, some pro-life supporters may not be vocal for fear of a controversial issue. Pro-life supporters voting for pro-abortion politicians, however, are no different than those passively complicit in other injustices.
Thus, pro-life Catholics who vote for extremist pro-abortion politicians arguably share the blame, which is why it is important for Catholics and other Christians to advocate for the preborn and educate others.
Together, the Church can take positive steps to end abortion if we are willing to start the difficult dialogue and vote our values.
I recently learned that this week is National Infertility Awareness Week. While those who’ve experienced infertility are surely painfully aware of its difficulties, for the rest of us, it presents a great opportunity to learn more about this struggle that affects 1 in 8 couples. If we listen, we can better understand how to come alongside these men and women to encourage and support them.
A message of faith, hope, and life from Washington, D.C.
Many news outlets ran stories this week highlighting some of the famous women and couples who’ve experienced infertility and its heartbreak. First up was Second Lady Karen Pence, who shared a rare interview with The Federalist’s Melissa Langsam Braunstein. The article is poignant in its rawness relating how painful, consuming, and exhausting the infertility journey can be.
“It took us six years before we were able to get pregnant with our first child…We were ready to start our family, and it just didn’t happen. And when you experience that, all of your friends are getting pregnant, all of your relatives are getting pregnant, I remember my little niece looked up at me one day and said, “Auntie Karen, why don’t you have any babies?” It can be a very heartbreaking experience, and so for us, we thought, maybe we’re just not going to be a couple that has children.”
For the Pences, adoption proved to be a great alternative, but just as an opportunity came up, Mrs. Pence learned she was pregnant. Still, it took a lot to get to that point, including questioning and ultimately trusting God to bring children into their lives in His perfect timing.
“For us, it was really a matter of just letting God bring us kids when He was ready to bring us kids, and that’s where they come from, and so we just had to wait until He was ready. And now it’s so clear to us that that was the perfect timing, these kids are the perfect kids for us, and we couldn’t be more grateful every day that He gave us that privilege.”
The message of faith is not surprising coming from the Second Lady, and it sure is a welcome addition to the mainstream conversation about infertility. It’s a message I’ve seen echoed by many Christian women who have been bold in sharing their struggles in the midst of such a deep desire to become mothers. For these women, the pro-life message is simply understood. They know that a baby in the womb is a gift—and his or her life is just as precious at the moment of conception as it is at the moment of birth.
The Hollywood pro-life, pro-woman message
For me, I was more amazed to hear such a strong pro-life, pro-woman message coming from Hollywood celebrities who have experienced infertility. The Huffington Post ran an article titled, “13 Celebrities Who’ve Shared Their Struggles With Infertility,” and the comments in that article struck me as so staunchly pro-life and pro-women, that I couldn’t help but wonder how those celebrities reconcile some of their policy positions with their own statements.
For example, actress Jaime King, a strong supporter of Planned Parenthood who even donated to the abortion giant in Mike Pence’s name, struggled for seven years with infertility. And yet, her heartbreaking story is a testament to human life in the womb and the beauty of womanhood.
“Nobody knew how long it took me to get pregnant, that for seven years I had so many losses, I’d been trying for so long and I was in so much pain… Somewhere in our subconscious when someone tells you, ‘Oh, you might not be able to do that,’ you feel like it’s the one thing that you have … I feel like it’s detrimental for me as a woman to not be honest about that and that it’s detrimental that women don’t talk about these things because when you go through it you feel like you’re suffering in silence by yourself.”
Singer Beyoncé, who is currently pregnant with twins and has surprised many with her pro-life tributes to her unborn children in recent months, echoed King’s story of hope and tragic loss.
“About two years ago, I was pregnant for the first time. And I heard the heartbeat, which was the most beautiful music I ever heard in my life. I picked out names. I envisioned what my child would look like … I was feeling very maternal. I flew back to New York to get my check up—and no heartbeat. Literally the week before I went to the doctor, everything was fine, but there was no heartbeat… it was the saddest thing I’ve ever been through.”
While these are just a couple of examples from the article, it’s encouraging to see these women speak so openly, not only about their experiences, but about their understanding of life in the womb and the unique capacity that women have to bring new life into this world.
Infertility is a deeply personal journey
If you’re anything like me, you desire ways to better understand infertility and be there for the friends and family in your life who are experiencing it. But if there’s anything I’ve learned from reading these stories and hearing others, it’s that infertility is personal. Some may want to share; others may not. The only thing we can do is be more aware, be sensitive to the realities (1 in 8 couples!), and pray that those who experience infertility will find peace, joy, and fulfillment in whatever God brings their way.
My heart hurts for these women and men who so desperately want to become mothers and fathers. And while I don’t know their experience, their emotions, or their pain, I am thankful for their message and for their strength in sharing it.
Almost 11 years ago, Sarah Wickline Hull received some of the worst possible news that a pregnant mother could hear: She had aggressive cancer, and both she and her unborn baby could die.
Wickline Hull said her doctors encouraged her to have an abortion, but she refused.
Today, she is cancer free and her daughter is a happy, healthy 10-year-old.
In a Facebook post in January, Wickline Hull shared her story as the debate about legalized late-term abortions erupted again in the United States.
“People are talking about the medical necessity of abortion to save the mother’s life. I was one of those mothers,” she wrote.
She struggled with infertility for years before becoming pregnant with her daughter. Then, at 20 weeks, Wickline Hull was diagnosed with an aggressive form of cancer that was cutting off her airway.
“I will never forget when the first doctor, an oncologist, mentioned abortion,” she said.
Immediately, she rejected the idea of aborting her unborn daughter, saying, “I knew I would rather die and give birth.”
A second doctor also urged her to consider abortion after listing a number of problems that her baby may have.
“I stood my ground and refused,” she remembered. “He said, ‘That is ok. The baby will probably spontaneously abort anyway.’”
Eventually, Wickline Hull said she found doctors who supported her decision to choose life for her baby. At 34 weeks of pregnancy, she gave birth to a healthy baby girl.
“I will be celebrating 10 years cancer free in May,” she said. “I have a healthy, beautiful, bright, precious 10 year old daughter who is a living reminder that doctors do not know everything.”
Of all the holidays and events on our calendars, I believe none are more important than Easter Sunday.
The pro-life movement’s entire reason for existing is to promote and protect the value of human life because it is created in the image of God. If it were not – if human life were simply highly-evolved amoeba fighting to survive in a dog-eat-dog world – then the best we could hope for is to appeal to a supposed charitable nature for the good of society.
Instead, we can point to Psalm 139 and speak of how God knits each of us together in the womb. Critics will say it is merely Jewish poetry or laugh at it as an ancient attempt to explain the mystery of fetal development.
We can appeal to the common concern man has for man as a sign of God-given compassion when tragedy strikes at places like Sandy Hook Elementary School. Critics will point to Auschwitz or Dachau and say that man is an animal.
We can talk about teachings in the Christian church on the sanctity of life. Critics will call it superstitious, biased against other faiths, or lies.
But when we talk about the Creator of Life, we can point to an empty tomb as validation that the God of the universe is who He says He is.
Easter must not be a three-day weekend that places our programs and efforts on hold. It must be the central event in human history that we must hold on to as proof that we each bear the fingerprints of God.
How can we not protect so precious a gift?
May you and your family enjoy a blessed Easter.
LifeNews Note: Mike Fichter is the president of Indiana Right to Life.
(Life Site News) 40 Days for Life’s current initiative has only been going on for a little over a month, yet the pro-life effort has already saved hundreds of unborn lives from abortion.
Timed to coincide with Lent, the latest 40 Days campaign began on March 6 in 377 cities across the United States, United Kingdom, and 29 other countries around the world. Volunteers have been stationed outside abortion facilities for 12 hours a day to conduct prayer vigils and offer sidewalk counseling to women considering abortion.
“The whole point of this is to take a positive and upbeat pro-life message to the whole community,” Robert Colquhoun, 40 Days’ Director of International Campaigns, told LifeSiteNews last month. “It is simple, and effective because it works. Lives are saved, hearts and minds and changed and eternal souls are impacted. Abortion workers leave [their employment] and abortion centers close.”
Since then, 40 Days has received 446 confirmed reports of mothers choosing life for their babies, the group revealed Monday. The post shared several examples of the fruits of their efforts.
In Memphis, Tennessee, a man named Marcus who reluctantly accompanied his girlfriend to Planned Parenthood spoke with the sidewalk counselor, who promised help and convinced him to text her to leave the building before going through with the abortion. The couple left “smiling” and eager to go to a pregnancy center instead, and Marcus even participated in the prayer vigil.
In Cincinnati, Ohio, a traffic delay kept a woman from leaving Planned Parenthood’s parking lot long enough for a 40 Days volunteer to offer help, to which she revealed, “I changed my mind. I didn’t do it. It’s a baby!”
Not every interaction has been positive. Late last month, an 85-year-old pro-life volunteer was shoved to the ground and repeatedly kicked outside a San Francisco Planned Parenthood location. But the overall fruits of 40 Days’ efforts have been encouraging, and 40 Days says it plans a live webcast on April 30 to recap volunteers’ impact.
“Father, we have done battle with the power of evil, and therefore we can have compassion on those still within its grip,” 40 Days for Life president Shawn Carney wrote. “We have been freed from the kingdom of darkness, and therefore we can bear witness to your Kingdom of Light. May the witness of all your people through these 40 Days for Life bear abundant fruit.”
Last year, 40 Days for Life reported that it has saved 14,000 since its campaigns first started in 2007.
Editor’s Note: This article was published at Life Site News and is reprinted here with permission.
The FDA has approved a generic version of the abortion pill Mifeprex, at a time when more deaths are being reported and the abortion industry is pushing for the dangerous abortion inducing chemicals to be dispensed online or by mail. According to a notice from the FDA, the generic version is approved for use as an abortifacient. This news comes just a day before the FDA updated its adverse effects reports through 2018, stating, “As of December 31, 2018, there were reports of 24 deaths of women associated with Mifeprex since the product was approved in September 2000, including two cases of ectopic pregnancy resulting in death; and several cases of severe systemic infection (also called sepsis), including some that were fatal…” The FDA’s 2017 report put the number of deaths at 22.
This means that in 2018 alone, two more women died from taking the abortion pill. And yet, now a generic version is going to be made available.
To date, the report documents nearly 4,200 reported adverse effects, including hospitalization and other serious complications.
On April 11, 2019, the FDA approved GenBioPro, Inc.’s abbreviated new drug application for a generic Mifeprex, which, when used with Misoprostol is approved as an abortion pill regimen. The FDA states (emphasis added), “This approval reflects FDA’s determination that GenBioPro’s product, Mifepristone Tablets, 200 mg, is therapeutically equivalent to Mifeprex and can be safely substituted for Mifeprex. Like Mifeprex, the approved generic product is indicated for the medical termination of intrauterine pregnancy through 70 days gestation….”
Generic abortion pill by GenBioPro approved by FDA
The FDA also states clearly that although they modified the Mifeprex application to include “mifepristone products,” this change in no way removes the FDA’s REMS (Risk Evaluation and Mitigation Strategy), “a safety strategy to manage a known or potential serious risk associated with a medicine and to enable patients to have continued access to such medicines by managing their safe use.”
Of note, on April 11, 2019, FDA approved a supplemental application for Mifeprex, approving modifications to the existing approved REMS for Mifeprex to establish a single, shared system REMS for mifepristone products (including Mifeprex as well as the approved generic version of Mifeprex) for the medical termination of intrauterine pregnancy through 70 days gestation. In establishing the single, shared system REMS, no changes were made to the substantive elements of the REMS. This single, shared system REMS is known as the Mifepristone REMS Program.
Find approval information for this 2019 supplement here.
The approved generic version of Mifeprex generally has the same labeling as Mifeprex…Under the law, the approved generic version of Mifeprex is required to use a single, shared system REMS with the brand product, Mifeprex. This single, shared system REMS, known as the Mifepristone REMS Program, sets forth the distribution requirements that must be followed for both Mifeprex and the approved generic version of Mifeprex.
Requiring that the generic be subject to FDA’s REMS is good news for now, because, as Live Action News has previously reported, the abortion lobby is attempting to expand access to the abortion pills via mail order or pharmacy by pushing “self-managed abortion,” described by Guttmacher as ending a pregnancy “without direct supervision by a health care provider.” To accomplish this, REMS, must be eliminated.
Dr. Donna Harrison, Executive Director American Association of Pro-Life Obstetricians and Gynecologists(AAPLOG), agreed, telling Live Action News (emphasis added):
Allowing a generic equivalent of Mifeprex basically means that the patent restrictions have run out. So, new drugs have a patent which is time limited… and in the case of Mifeprex, the patent was held by the Population Council. So, now that the patent has run out, generics are allowed. But this does not change the restrictions. REMS are still in place until FDA changes the restrictions. So, just to clarify, this does not mean that Mifeprex is OTC [over-the-counter]. It just changes how much quality control goes in to the pill manufacturing process and how much Danco can charge for the drug.
The move towards a generic drug is being hailed a victory by abortion advocates, specifically Dr. Daniel Grossman, who has deep ties to the “self-managed” abortion pill push.
FDA Approves generic abortion drug (Image Twitter Dr. Daniel Grossman)
FDA Approves generic abortion drug NWHC (Image: Twitter)
Under the Mifepristone REMS Program, the FDA states, “Mifeprex and the approved generic version of Mifeprex” may:
[O]nly be supplied directly to healthcare providers who are certified to prescribe the drug product and who meet certain qualifications.
[T]he products are only available to be dispensed in certain healthcare settings, specifically, clinics, medical offices and hospitals, by or under the supervision of a certified prescriber.
They are not available in retail pharmacies and are not legally available over the Internet.
The original drug (Mifeprex) was approved in 2000 after being brought to the U.S. by the eugenics-founded Population Council, and was seeded by the Packard Foundation among other pro-abortion philanthropy groups. They then set up a highly secretive company named Danco to manufacturer the drug.
The generic version is produced by GenBioPro, Inc., which also appears to have the financial supportof abortion collaborators. In fact, Packard gave GenBioPro, Inc. $185,000 in 2016 and 100,000 in 2017. According to the Nevada Secretary of State, a 2007 filing for the company was permanently revoked. A new filing in 2011 is active and shows a registered agent of CSC Services of Nevada, Inc.and the only officer listed is E. Masingill.
The FDA warns consumers they should not buy Mifeprex or GenBioPro, Inc.’s approved generic version of Mifeprex, Mifepristone Tablets, 200 mg., over the Internet because they will bypass important safeguards designed to protect patient health.
Artist Caitlin Solan calls herself “passionately pro-life” and expresses that love for life through colorful paintings which capture the lives of her littlest clients during their time living inside their mothers’ wombs.
“I started creating sonogram art about 3 1/2 years ago,” she told Live Action News. “I wanted to use my art talent to glorify God and make a positive difference. I have always felt strongly about fighting for life and being a part of the pro-life movement.”
Solan explained that she uses bright, bold colors and “expressive” brushstrokes along with splatter art to portray the beauty of life inside the womb. She enjoys turning what is normally a black and white image into a colorful work of art.
“My goal is to show that these babies are alive and their lives are beautiful,” she said. “My sonogram paintings are one way that I fight for life in a positive way, without bringing attention to any negative aspects of the debate, but just focusing on the beauty of life.”
Solan is thankful that she is able to create art that is meaningful and personal to her clients. Sonograms are parents’ first pictures of their child, and sometimes, sadly, it’s the only one they get. Solan has created paintings of babies who have been miscarried, as well as rainbow babies, and even one baby who was aborted. The mother had been pressured to abort and deeply regretted it, so a friend gifted her with the painting.
“I hope my paintings of lost babies bring comfort to the families and that the artwork will be a positive remembrance of their child,” Solan explained.
Sonogram artwork has become a popular way to display the first image of a child, rather than the usual placement of the black and white image in a simple frame. Some new parents coordinate the artwork to the nursery they lovingly decorate for their new arrival or use it as a way of announcing their pregnancy. Friends and family can even gift the artwork as a baby shower present. Some moms have even taken to having their children’s sonogram images painted on their fingernails.
April 15, 2019 (Calx Mariae) — Sacred Scripture has a great deal to say about education, which starts within the relationship between parent and child, and, in order to be purposeful and true, must also begin with knowledge and fear of the Lord (Prov. 1:7–8, Deut. 11:19, 32:46, Eph. 6:4). This principle of the parent as “primary educator”, who has both the God-given role and responsibility to teach a child “in the way he should go” (Prov. 22.6), has consequently been an established and consistent tenet of authentic Catholic teaching. It is the father and mother, through their participation in God’s work of creation, who have conferred life on their children and have the closest natural relationship with them.
The Church affirms that this God-given parental right and duty is, in the words of Pope John Paul II, “irreplaceable and inalienable, and therefore incapable of being entirely delegated to others or usurped by others”.1 They have the “right to educate their children in conformity with their religious and moral convictions” and “should also receive from society the necessary aid and assistance to perform their educational role properly”.2 This is even more so the case with “Relationships and Sex Education” (RSE), as the government now refers to this most intimate area of our children’s learning and development, especially given the potential influence of such learning not only on children’s health, well-being, purpose, and fulfilment in this life, but their vocation in the Spirit and eternal salvation in the next life.3 Consequently, Pope John Paul II insisted that “sex education, which is a basic right and duty of parents, must always be carried out under their attentive guidance, whether at home or in educational centres chosen and controlled by them. In this regard, the Church reaffirms the law of subsidiarity, which the school is bound to observe.”4 In The truth and meaning of human sexuality, the Pontifical Council for the Family explained: “Other educators can assist in this task [of education for chastity] but they can only take the place of parents for serious reasons of physical or moral incapacity.” (Section 23)
A SHIFT IN THE CHURCH’S POSITION?
Catholic parents worldwide therefore have been severely challenged by the march of the comprehensive sex education agenda, and, in many countries, the growing imposition, if not virtual takeover, by the state in this sacred area of parental responsibility. Equally disconcerting has been the more than just apparent shift of the Holy See in this important area during the pontificate of Pope Francis. His controversial post-synodal apostolic exhortation Amoris laetitia (2016) overlooks the Church’s previously clear teaching on the matter in its section entitled “Yes to Sex Education” (translated in the English version as “The Need for Sex Education”) (Ch.7). This section does not make any reference to the role of parents in educating their children in the area of sexuality, but only refers instead to the role of “educational institutions”. Pope Francis reaffirmed his position in a recent interview on the plane returning from World Youth Day in Panama (28 January 2019). He stated:
I believe that we must provide sex education in schools. […] But we need to offer an objective sexual education, as it is, without ideological colonization. […] Sex as a gift from God must be taught, not with rigidity. […] I don’t say this without putting myself in the political problem of Panama. But they need to have sex education. The ideal is to start from home, with the parents. It is not always possible because there are so many different situations in families, and because they do not know how to do it. And so the school makes up for this, because otherwise it will remain a void that will then be filled by any ideology.5
The Pontifical Council for the Family also no longer abides by the Church’s perennial teaching. After the promulgation of Amoris laetitia, it published its own sex education programme, titled “The Meeting Point,” in 2016. This programme, which is intended to be taught in schools, in mixed classrooms, and not by parents, has been widely criticised by Catholic and pro-life commentators for its failure to adequately convey Catholic moral teachings, for its secularising approach, and use of inappropriate images. Psychiatrist Rick Fitzgibbons MD, who has worked extensively with Catholic youth harmed psychologically by family breakdown, sexual abuse, pornography, and other consequences of the permissive society, has described the programme as being, “in my professional opinion, the most dangerous threat to Catholic youth that I have seen over the past 40 years”; it “reveals an ignorance of the enormous sexual pressure upon youth today and will result in their subsequent confusion in accepting the Church’s teaching”.6
THE BISHOPS OF ENGLAND AND WALES, AND THE CES
The Bishops of England and Wales, via the Catholic Education Service (CES), have been even more advanced in this agenda. From 1999 until 2008 the Chairman of the CES was Archbishop Vincent Nichols of Birmingham (now Cardinal Archbishop of Westminster). Under the chairmanship of Archbishop Nichols the CES developed a policy that resulted in providing children in Catholic schools, including adolescents under the legal age of consent, with access to abortion and contraception services without parental knowledge or consent, through a state-run confidential advice agency, named “Connexions”.
Also under his chairmanship the CES joined the Sex Education Forum and agreed to policies directly contrary to Catholic teaching and the natural law. Membership of the forum required agreement with the Sex and Relationships Education Framework (2003, reissued 2005), which, for instance, “welcomes” the “diversity of society” in the area of “sexuality”, regards sex education as “an entitlement for all boys as well as girls; those who are heterosexual, lesbian, gay or bisexual”, and requires that children should be given “relevant information” which “is accurate and non-judgmental” about “the potential consequences of unprotected sex” including “abortion”.
In April 2010 the CES, now under the chairmanship of Malcolm McMahon (then Bishop of Nottingham, now Archbishop of Liverpool), appointed as deputy director, Greg Pope, a former Labour member of Parliament, who had an extensive anti-life, anti-family voting record. Pope remained in that post until his promotion, in 2017, to be the Assistant General Secretary of the Bishops’ Conference of England and Wales.
BETRAYAL OF CATHOLIC PARENTS IN ENGLAND
For Catholic parents in England recent developments are bringing the threatened state takeover of their God-given role to a critical new reality, and the conduct of the Catholic Education Service, which should be at the vanguard of protecting their rights, as well as the God-given rights of all parents, has instead been, in certain specific ways, complicit in their betrayal.
In March 2017, Parliament passed the government’s Children and Social Work Act (2017) which made the new subjects of Relationships Education compulsory in all primary schools in England, and Relationships and Sex Education (RSE) compulsory in all secondary schools in England, including faith and independent schools. It was announced that the required content of these new subjects would be subject to public consultation, although from the outset government spokespersons, including the Prime Minister, stated that Relationships Education would be “LGBT” inclusive.7The government stated that parents would be able to withdraw their children only from the “sex education” parts of RSE at secondary school.
Archbishop Malcolm McMahon, chair of the Catholic Education Service for England and Wales, issued a statement welcoming the government’s announcement that it was acting to change the law:
Relationship and Sex Education (RSE) forms part of the mission of Catholic schools to educate the whole person. Our schools have a long track record of educating young people who are prepared for adult life as informed and engaged members of society, and high quality RSE plays an important part of this.
We welcome the government’s commitment to improving Relationship and Sex Education in all schools. Catholic schools already teach age-appropriate Relationship and Sex Education in both primary and secondary schools. This is supported by a Catholic model RSE curriculum which covers the RSE curriculum from nursery all the way through to sixth form.
We additionally welcome the government’s commitment to protect parental right of withdrawal and involve parents in all stages of the development and delivery of RSE in all schools. It is essential that parents fully support the school’s approach to these sensitive matters. The experience of Catholic schools is that parental involvement is the basis for providing consistent and high quality RSE at home and at school.
We look forward to working closely with the government to shape any new guidance to enable Catholic schools to continue to deliver outstanding RSE, in accordance with parents’ wishes and Church teaching.
Despite the apparently strong statements with regard to parental involvement, it is telling how much the statement conforms, not to established Catholic teaching on the matter, but to the new secular “orthodoxy” and government policy regarding this area of a child’s learning. It is now the “mission” of the school to “educate the whole person” — rather than this principally being the parents’ mission and responsibility. The parent is simply granted an “involvement” in the process, because “it is essential that parents fully support the school’s approach”. There is no reference to the fact that the “right of withdrawal” at this time was only for the “Sex Education” parts of RSE, and, in any case, the government’s actual distinction between “sex” and “relationships” education is still very much unclear. There are echoes of all the key buzzwords of the sex education lobby in the statement — the changes are all about “improvement” and providing “high quality RSE” (by whose criteria?), which is essential to prepare them “for adult life as informed and engaged members of society”, or as the Department for Education puts it, “to support all young people to stay safe and prepare for life in modern Britain”.8 After all, who wouldn’t want our children to be “safe” and “prepared for life in “modern Britain”? Except do we serve them best by preparing them to either counter or conform to those aspects of “life in modern Britain” which are opposed to the Gospel? What will keep them the safest: following the true teachings of the Church in the area of sex and relationships, or following instead the new secular moral code of the LGBT and sex education lobbies?
Leaving aside for a moment the assumption that all Catholic schools in England and Wales offer genuine “Catholic teaching” in every respect, what about the 90 per cent of children, including many Catholic children, who do not attend a Catholic school? Should we be concerned at all for their temporal and eternal welfare? Does the Church not have any kind of mission to evangelise the nation, to shine the light of God’s truth into every corner of public policy?
There is a submissive ghetto mentality here reminiscent of the bishops’ role in the issue over adoption by homosexual couples. The bishops of England and Wales appeared to take the line that, of course we accept that same-sex couples should be allowed to adopt because that was in the Labour government’s manifesto, but we are just requesting a “bit of diversity in the system”, and requesting an opt-out for Catholic adoption agencies when it comes to same sex adoption — even though Archbishop Nichols admitted that Catholic adoption agencies had been giving up children for adoption by single (but active?) homosexuals and also by unmarried but cohabiting heterosexual couples. Moreover, the bishops had no objections to allowing Catholic adoption agencies to refer homosexual applicants to agencies that would place children with homosexual couples.9
Naturally in both practising and freely admitting this highly compromised position there was no witness whatsoever as to why deliberately denying an adopted child the natural situation of having a father and mother was wrong, or why the homosexual lifestyle was wrong. The government regarded such a weak, compromised, and contradictory stance with absolute contempt, brushing it aside and insisting it would be done regardless. All but one of the twelve diocesan adoption agencies either voluntarily closed themselves down or cut their ties with the Church — exactly what the enemies of the Church wanted in the first place.10 This should also perhaps serve as a forewarning to us of what will happen to Catholic schools when the government wants to drive the LGBT juggernaut over a red line that is too far even for the Bishops of England and Wales.
MISSED OPPORTUNITY FOR CHURCH ACTION
The government announced a public “Call for Evidence” in December 2017, which closed in February 2018, concerning what should be the content of the new compulsory subjects. Seeing as this was a public consultation, where numbers clearly matter, one would have thought it might have been a good idea to encourage Catholics, especially Catholic parents, to participate and make submissions? The message from the CES, however, seemed to be that we can just trust and leave everything to them, that everything is and will be fine with Catholic schools, and that everything the government is doing with regard to RSE is positive and can be perfectly compatible with the Church’s teaching. A number of pro-life and pro-family organisations, including SPUC, did, however, campaign hard to rally parents and their supporters to respond to the “Call for Evidence”. This helped contribute to an impressive 23,000 submissions. The government’s reporting on the results of that consultation, however, has been highly inadequate, and what it had produced showed no evidence whatsoever for any claims of consensus, especially from parents, for the agenda it is pursuing.
In July 2018 the government issued its Draft Guidance and Regulations regarding the proposed content and delivery of the new subjects, and simultaneously launched a second public consultation on their acceptability. There was some evidence of the positive impact of campaigning by the pro-life and pro-family lobby. There was an acknowledgement that parents are the primary educators in certain of the matters covered by the new subjects, and that it would be mandatory for schools to consult with parents on RSE policies and programmes. However, where do the parents stand when, following the consultation, they are still unhappy about what the school proposes to teach? Overall the Draft Regulations and Guidance seriously undermine parental rights, and also present a completely one-sided view of human sexuality, marriage, and the family which is contrary to what the Catholic faith teaches.
The children’s programme of study is required to be “LGBT inclusive” throughout and present homosexual relationships and family structures in a positive manner. In primary school, children must be made to understand and accept that families “sometimes” look different from their family, but that they should respect those differences and know that other children’s families are characterised by “love and care for them”; also that marriage, including same-sex “marriage” and civil partnerships, represents “a formal and legally recognised commitment of two people to each other which is intended to be lifelong”.11 In other words, primary school children will have to demonstrate “respect” for the idea and practice of homosexual relationships and not just for the people involved in them, and will be expected to agree that such relationships, including when they have children, are just as valid, positive and beneficial as those based on real marriage.
In RSE at secondary school teenagers will be further encouraged to “explore” their developing “sexual orientation” and “gender identity”. It presents dangerous and immoral lifestyle choices as equally valid as marriage. Abortion is presented simply as one of the available options during pregnancy and pupils will be signposted to contraceptive and abortion services, without any parental knowledge or consent.
The right of parents to withdraw their children from the “sex education” parts of RSE, which the government had promised to retain, has now been removed and replaced only by a “right to request” withdrawal, with the final decision going to the headteacher. Even this much compromised parental right is withdrawn altogether when the children reaches 15, when they will be allowed to overrule their parents’, as well as their headteachers’, wishes if they choose, as they are being given the right to have sex education provided to them by the school. Moreover, it is a statutory requirement for schools “to have regard” to the final published Guidance when delivering the new subjects, which means they have to deliver the required content unless they have a “good reason” not to. The experience of a number of independent faith schools, particularly independent and Orthodox Jewish schools, who have been failed or severely penalised by OFSTED (England’s schools inspection agency)12 for not teaching LGBT issues in a satisfactory way, shows that the fact that LGBT ideology is against the tenets of the Christian, Jewish, or Islamic faith is not considered a good enough reason.
CES CONTINUES TO BACK THE GOVERNMENT OVER RSE
The CES were one of the favoured selected groups listed who had been involved in the deep consultation process with the Department for Education, though that is not to say that they necessarily agreed with all of the resultant Draft Guidance. However, their public statements so far have expressed only support for the government’s plans.
Following the publication of the Draft Regulations and Guidance in July 2018 the CES issued another press release again stating that the Catholic Church “welcomes” the government’s moves to “improve” Relationships and Sex Education, as well as how “the government had used the Catholic model curriculum as examples of best practice”. It also “welcomes” how “the recommendations are clear that the right for parents right of withdrawal [sic] will be maintained”, even though the Draft Regulations only allow parents the right to request withdrawal, with a right to refuse being given to the headteacher. It also welcomed that “schools with a religious character” will be able to deliver RSE “within the tenants [sic] of their own faith”.13However, the Children and Social Work Act (section 34:3(b)), as well as the Draft Regulations, only stipulate that “the education is appropriate having regard to the age and the religious background of the pupils”, which is open to interpretation and a much weaker requirement than such teaching needing to be in line with the “tenets” of a particular faith. A school may “have regard” for the fact that a pupil comes from a Catholic family, but still deem it necessary to teach the pupil things that do not conform to the tenets of the Catholic faith. The Draft Guidance uses similarly vague language and also adds that “schools must ensure they comply with the relevant provisions of the Equality Act (2010)”. OFSTED inspections have interpreted that to mean a school must clearly teach about active homosexuality and transgenderism in a positive light, so that children who may identify themselves by one of the “protected characteristics” do not feel marginalised or discriminated against, and that children are adequately prepared for “life in modern Britain”. For instance, in May 2017 Vishnitz Girls School, an Orthodox Jewish primary school, failed its third OFSTED inspection in a year specifically because the school acknowledged that it did not teach its young children (aged 3–11) about homosexuality and transgenderism. The original report stated that “the school’s approach means that pupils are shielded from learning about certain differences between people, such as sexual orientation. […] They acknowledge that they do not teach pupils about all the protected characteristics [of the Equality Act 2010], particularly those relating to gender re-assignment and sexual orientation. This means that pupils have a limited understanding of the different lifestyles and partnerships that individuals may choose in present-day society.”14
Christian schools have also been targeted by OFSTED. Pupils at Grindon Hall Christian School and Durham Free School faced intrusive questioning on transsexualism, homosexuality and same-sex “marriage” by OFSTED inspectors, who then claimed that they found evidence of “homophobic behaviour” in both schools — a claim rejected by staff, pupils, and parents. Despite the outcry, The Durham Free School was closed down in April 2015 and Grindon Hall — one of the best performing schools in the North East — was rated “inadequate”, and was forced by the Department for Education to be taken over by a secular trust.15
A further public consultation (July–Nov 2018) was announced regarding the Draft Regulations and Guidance for the new subjects. However, rather than initiating a campaign to encourage Catholics, and others who attend Catholic schools, to participate in this consultation, so that protections for parents could be genuinely safeguarded, the CES had already embarked on a mini-PR campaign in support of government policy, with an article which appeared on the CES website and the Catholic press informing us that the government’s proposals were only to be welcomed, that there was nothing to worry about, that Catholic schools already do a fantastic job teaching RSE (in line with the Church’s teaching), and, falsely, that the government is committed both to allowing faith schools flexibility to teach according to the tenets of their faith, and protecting the parents’ right of withdrawal.16
Given the content of the government’s Draft RSE Guidance it is very hard to conceive of how a Catholic school can deliver the subjects in a way which “has regard to the Statutory Guidance” whilst still in conformity with the tenets of the Catholic faith. The CES’s current “model policy for RSE”, which the CES boasts has been praised by the Department for Education, features an uncomfortable mix of Catholic teaching with elements of the statutory SRE Guidance (2000) and contemporary secular sex education programmes shoehorned into it. So at Key Stage 1 (ages 5–7) children are to be taught to “identify and correctly name their ‘private parts’”; and at KS 2 (ages 7–11) they are taught “that similarities and differences between people arise from several different factors (see protected characteristics of the Equality Act 2010, part 2, ch. 1, sections 4-12)”. In other words, they are taught about “sexual orientation” and “gender reassignment” (LGBT issues).17
The ambiguity of elements of the policy at the very least allow scope for teaching which is not in accordance with the faith. For example, the RSE secondary school policy stipulates teaching children about “recognising and valuing their own sexual identity and that of others”, or to “ensure RSE is sensitive to the different needs of individual pupils in respect to […] their own sexual orientation”.18 This is especially the case when we have had the scandal of homosexual lobby-group Stonewall being invited into Catholic schools and colleges to train teachers on how to deal with “homophobic bullying”.19
Although the model RSE policy stresses that “teachers will be expected to teach RSE in accordance with the Catholic Ethos of the school”,20 and the CES proclaims its confidence that authentic Catholic RSE is and will continue to be taught in Catholic schools, even after 2020; it is not clear, judging by some of the recent publications of the CES, that the CES has the same idea as many Catholic parents, or the perennial teachings of the Catholic Church, about what exactly the “tenets” of the Catholic faith are when it comes to human sexuality and the teaching of RSE.
BISHOPS AND CES PROMOTE LGBT IDEOLOGY IN SCHOOLS
An RSE guide for Catholic educators published by the Catholic Bishops of England and Wales in 2017, entitled Learning to Love, declares its admiration for Pope Francis’ Amoris laetitia, as “an inspirational document, rich with insights and fresh descriptions of the Church’s teaching on this vital subject”.21 On the subject of homosexuality, the Bishops’ Learning to Love offers its own “fresh description” of the Church’s teaching:
Here we would like to emphasise that this exalted form of love exists just as powerfully in relationships between people of the same sex as it does in heterosexual relationships. We applaud the great progress that has been made in countering all forms of discrimination against homosexuality in recent times, and wish to collaborate with efforts to make such discrimination obsolete. (p.17)
Note that we are now talking about “discrimination against homosexuality” as something that should be countered, as opposed to “unjust discrimination” against homosexual persons as the Catechism states (2358). “Homosexuality” itself has now been transformed from an “inclination, which is objectively disordered” to what can be an “exalted form of love”; and what does it mean “to collaborate with efforts to make such discrimination obsolete”? To actively promote the LGBT and Pride agenda? To shut down freedom of speech on the issue and persecute Christians and others who try to speak the truth about homosexuality?
An even more pernicious document is Made in God’s Image: Challenging homophobic and biphobic bullying in Catholic schools, a joint publication by the CES and St Mary’s University, Twickenham — first published in 2017 and which has even been given a second edition, without any major alterations, despite its deep and scandalous conflicts with the Church’s teaching being widely pointed out by commentators.22
Under the guise of “guidance” for the “pastoral care of pupils”, Made in God’s Image is designed to intimidate Catholic schools into introducing a concerted LGBT indoctrination programme for children, in the form of an eight-lesson scheme of work. The sum of the message that children will take away from this is that being “lesbian, gay, bisexual or transgender” is part of their God-given purpose and identity, an integral part of being Made in God’s image, something that must be celebrated, and that any true Catholic should act to report and help robustly stamp out any sign or attitudes of disapproval. An example from the introduction illustrates the strategy being taken:
The Church teaches that homosexual persons ‘must be accepted with respect, compassion and sensitivity’ (Catechism of the Catholic Church 2358). The School should be mindful that the Church teaches that homosexual inclinations are not sinful. For older pupils who may publicly identify themselves as such, Church schools should be havens of respect and custodians of the true dignity of each human being. They should be as attentive to the possibility of homosexual pupils being marginalized and bullied as they are to discrimination based on religion, gender, race or disability.23
Although the Church does indeed teach that involuntarily experiencing same-sex attraction is not itself a sin, the Catechism also adds that the inclination itself is “objectively disordered” (2358), and that authoritative Catholic teaching has also always declared that “homosexual acts are intrinsically disordered”, “basing itself on Sacred Scripture, which presents homosexual acts as acts of grave depravity” (2357). The Congregation for the Doctrine of the Faith has instructed bishops that “although the particular inclination of the homosexual person is not a sin, it is a more or less strong tendency ordered toward an intrinsic moral evil; and thus the inclination itself must be seen as an objective disorder.”24 There is no mention of this in the document, or indeed any mention whatsoever of Catholic doctrine on marriage, or any attempt to present the true meaning and purpose of human sexuality between man and woman. Indeed the only thing presented as sinful (although it does not directly employ the term “sin”) is the new sin of “homophobia” which “should have no place among Catholics. Catholic teaching on homosexuality is not founded on, and can never be used to justify homophobic attitudes”. In one of the word games that children are encouraged to play “homophobia” is defined as:
A range of negative attitudes and feelings toward homosexuality or people who are identified or perceived as being lesbian, gay, bisexual or transgender (LGBT). It can be expressed as antipathy, contempt, prejudice, aversion, or hatred, may be based on irrational fear, and is sometimes related to religious beliefs. (p.16)
Notice again how, as with Learning to Love, it is negative attitudes towards “homosexuality”, and not just “homosexual persons”, that is condemned here. And “homosexuality”, according to the Catechism at least, refers to “relations” between same-sex attracted men or women, including “homosexual acts”. Conveniently, if not outrageously, the actual word of God on the subject of homosexuality is never quoted or referred to.
It is undeniable that a deliberately misleading sleight of hand is in play throughout, with the document’s omissions and selective quotations from both Catholic documents and the Bible. That such a secular and distorted presentation of human sexuality, saturated with LGBT ideology, is being presented to children is hardly surprising when, as has been widely pointed out on Catholic blogs and by at least one English bishop, much of the material has been lifted directly from pre-existing propaganda programmes from Stonewall and LGBT Youth Scotland.25
Chillingly, Made in God’s Image even offers lesson material which encourages children to judge and challenge their own parents’ and families’ attitudes, based on provided examples of expressions of “homophobia”, including typical comments made whilst watching television programmes. It is ironic that a document purported to be concerned with “anti-bullying” engages in a highly pernicious form of bullying against faithful Catholic children and their parents by labelling them “homophobes” and “bigots”.
The pro-LGBT Made in God’s Image programme is said to have been prompted by a survey conducted by the CES on “homophobic” bullying in Catholic schools. However, the small print reveals that only 12 per cent of Catholic schools responded to this survey — the whole justification of this programme therefore being based on completely unrepresentative data (p. 31). Catholic headteachers would have been rightly reluctant to respond as the survey itself was ideologically loaded and intimidating (employing the un-qualified terms “homophobic” and “transphobic” throughout), with questions posed in a way that would make it very difficult for a faithful Catholic to respond, without compromising Christian truths on issues of sexuality.
WHERE ARE WE HEADING?
So where does this all leave us for the future if this agenda remains unchallenged? Scotland and Wales already show where the direction of travel is going in the immediate future. As a statutory part of Wales’s new curriculum which will be in place from 2022, the Welsh government announced that it is introducing “LGBTQI+ -inclusive Relationships and Sexuality Education” for all learners aged 5–16. Kirsty Williams, Welsh Education Secretary, has stated: “The days of traditional sex education are long gone; the world has moved on and our curriculum must move with it. […] Of course, thirty years on from the introduction of Section 28, we will also ensure that RSE is fully inclusive of all genders and sexualities and meets the needs of LGBTQI+ learners.”26
The Welsh government is adopting the recommendations of a specially commissioned report on the future of SRE in Wales produced by an “SRE Expert Panel”, headed by Prof. Emma Renold of Cardiff University, a sociologist whose research on child sexuality, as her university profile informs us, is characterised by “feminist, queer and post-humanist approaches”. Neither the Catholic Church, nor any other faith groups, were represented in the “expert panel” — no doubt they were not invited to be. The Catholic Bishops of England and Wales have issued no response to what is an all out assault on the childhoods of all Welsh children, including those of Catholic families.
“Post-humanism”, by the way, is one of the latest pseudo-intellectual fads of western academia. In the same way that “gender” and “sexuality” are regarded as mere social constructs, and therefore open to deconstruction, so now too is the very notion of what it is to be a “human being”. The “natural” distinctions between human, animal and machine are also regarded as arbitrary boundaries to be explored, redefined and transgressed. It should not be too hard to envisage the even more disturbing future of “sexuality” once such last remaining taboos have also been removed.
The Scottish government has so far gone the furthest in Britain along this trajectory, having proudly announced recently that Scotland will become “the first country in the world to have lesbian, gay, bisexual, transgender and intersex (LGBTI) inclusive education embedded in the [whole] curriculum” — not just in relationships and sex education.27 Naturally if ideological indoctrination is to be truly effective then thought must be controlled at all times, and not just within the confines of certain lessons. Unbelievably this development was also “welcomed” by Scottish Bishops, who added that they hope the “impact of these recommendations will be positive for all.”
So how should parents respond in the face of this situation? For times like this God tells us to “rejoice in hope, be patient in tribulation, be constant in prayer” (Rm. 12:12). We should hold on more strongly than ever to the fact that God Himself has still ordained us to be the primary educators of our children, a right which as Pope John Paul II reminds us “is irreplaceable and inalienable”; that the right of parents to bring up their children to know, love and serve Him is His holy will. Scripture tells us to “be strong and courageous”, to “not be afraid or terrified because of them, for the Lord your God goes with you; He will never leave you nor forsake you” (Deut. 31:6). “Where sin abounds, grace abounds all the more” (Rm. 5:20), and we are now seeing encouraging signs of a strong and powerful parents’ rights movement rapidly rising up to confront what Church officials have been unwilling to confront.
This is an issue which unites many people of different faiths and none. For instance, a Parliamentary petition concerning the parental right of withdrawal from RSE recently gained in excess of 100,000 signatories, which resulted in a Parliamentary debate on the petition in February 2019. Many Muslim parents, in particular, have provided an example of peaceful, but vocal and resilient parent power, with hundreds of parents witnessing weekly outside Parkfields Primary School, Birmingham, where their children were being subjected to an LGBT propaganda programme called “No Outsiders”.
This is a time for faith, not fear or compromise. In that spirit SPUC Safe at School has recently launched a major campaign in defence of the parental right to withdraw their children from Relationships and Sex Education and it has already gained tremendous support from parents from different backgrounds and communities. To find out how you can become involved visit: www.spuc.org.uk/rsebriefing
Dr Tom Rogers is the SPUC Education Manager. He has been working full-time for the pro-life cause since 2016. An academic and educationalist, he previously lectured in English literature at University, and has also taught in the secondary and further education sectors. He is the author of God of Rescue: John Berryman & Christianity (2011). He is married with two children.
This article was originally published in Calx Mariae, Voice of the Family’s quarterly magazine. To order copies or subscribe, please visit this website.
ENDNOTES:
John Paul II, Apostolic exhortation Familiaris consortio, 22 Nov 1981, 36.
Charter of the Rights of the Family, presented by the Holy See, 22 Oct 1983, Article 5.
Familiaris consortio, 37.
Familiaris consortio, 37; Charter of the Rights of the Family, Article 5, c.
Diane Montagna, “Pope Francis: ‘We must provide sex education in schools’”, LifeSiteNews, January 28 2019; https://www.lifesitenews.com/news/pope-francis-we-must-provide-sex-education-in-schools
Rick Fitzgibbons MD, “Psychiatrist: The Vatican’s sex ed is the most dangerous threat to youth I’ve seen in 40 years”, LifeSiteNews, 2 September 2016; https://www. lifesitenews.com/opinion/exclusive-the-new-threat-to-catholic-youth-the-meeting-point
For instance, Nick Gibb MP, stated in response to a Parliamentary question (3 July 2017) that “we expect schools to ensure that all pupils, whatever their developing sexuality or gender identity, feel that relationships and sex education is relevant to them and sensitive to their needs. As part of our engagement programme, we will consider ways to ensure that our guidance and regulations are inclusive of LGBT issues. We plan to work closely with organisations such as Stonewall and the Terrence Higgins Trust, amongst others.” Prime Minister Teresa May affirmed her support for ‘LGBT inclusive’ RSE in English schools in her speech at the Pink News LGBT Awards 2017.
Department for Education, “Policy Statement: Relationships Education, Relationships and Sex Education, and Personal, Social, Health and Economic Education”, March 2017, (p.1).
The then Archbishop of Birmingham, Vincent Nichols, made these comments and admissions over two interviews with Jon Snow (Channel 4 News) and Jeremy Paxman (BBC 2 Newsnight) on the evening of 23 January 2007. See also “Birmingham Archbishop: ‘Oh by the way,’ Britain’s Catholic Adoption Agencies Already Adopt to Gay Singles”, LifeSiteNews, 29 Jan 2007; https://www. lifesitenews.com/news/birmingham-archbishop-oh-by-the-way-britains-catholic-adoption-agencies-alr; “UK Catholic Bishops Compromise on Gay Adoption Leads to Charges of Hypocrisy”, LifesiteNews, 23 March 2007; https://www.lifesitenews.com/news/uk-catholic-bishops-compromise-on-gay-adoption-leads-to-charges-of-hypocris
Only Leeds-based Catholic Care in the diocese of Lancaster continued until forced to shut down. See Hilary White, “UK Catholic Church Agency to Cease Adoption Work As government Forces Homosexual Adoption”, LifeSiteNews,July27,2007; https://www.lifesitenews. com/news/uk-catholic-church-agency-to-cease-adoption-work-as-government-forces-homos
See learning outcomes on pp.16-17 in Department for Education, “Draft Statutory Guidance on Relationships Education, Relationships and Sex Education and Health Education”, July 2018; https://consult.education.gov.uk/pshe/relationships-education-rse-health-education/
The Office for Standards in Education, Children’s Services and Skills is a non-ministerial department of the UK government, reporting to Parliament.
Catholic Education Service, “Catholic Church welcomes move to improve Relationship and Sex Education in all schools”, Press release, 19 July 2018: http://catholiceducation.org.uk/component/k2/item/1003657-catholic-church-welcomes-move-to-improve-relationship-and-sex-education-in-all-schools
OFSTED, “Vishnitz Girls School: School Progress Monitoring Inspection Report”, 10 May 2017 (ref. 138516). Note, following the justifiably negative publicity on publication of this report, OFSTED subsequently replaced the original report with a redacted version (ref. 138515_5) on its website — one which had removed any direct references to ‘sexual orientation’ and ‘gender reassignment’, hence attempting to conceal the real reason why the school was failed.
For a summary and further details of these and similar cases, see The Christian Institute, “OFSTED and ‘British Values’”, June 2017; available online at: https://www. christian.org.uk/resource/ofsted-british-values/
Catherine Bryan, “Why Relationship and Sex Education is a must for all Catholic schools” [online article], Catholic Education Service, 20 June 2018; http://www.catholiceducation.org.uk/component/k2/item/1003652-why-relationship-and-sex-education-is-a-must-for-all-catholic-schools. The same article also appeared in “The Catholic Times”, 15 June 2018, (p.28).
See learning outcomes 1.2.4.4 (p.7) and 2.1.3.4 (p.4) in Catholic Education Service, “A model Catholic Primary RSE curriculum”, Autumn 2016; http:/catholiceducation. org.uk/schools/relationship-sex-education
For instance, it was reported that St Mary’s Catholic Primary in Wimbledon invited Stonewall to train staff on homophobic bullying “in order to comply with OFSTED requirements”, and subsequently became a Stonewall “Primary School Champion”. “Gay rights group called in to advise primary teachers”, Evening Standard, 15 May 2013; https:/www.standard.co.uk/news/education/gay-rights-group-called-in-to-advise-primary-teachers-8616681. html. It has also been reported that students training to be teachers were subjected to a Stonewall-run session on ‘homophobic bullying’ at the Catholic St Mary University, Twickenham; https://spuc-director.blogspot. com/2013/06/stonewall-scandal-at-catholic.html
“Learning to Love: An Introduction to Catholic Relationship and Sex Education (RSE) for Catholic Educators” (2017), Department of Catholic Education and Formation and Catholic Bishops’ Conference of England and Wales; https://www.catholiceducation.org.uk/images/ Learning2love.pdf.pdf
Catholic Education Service, “Made in God’s Image: Challenging homophobic and biphobic bullying in Catholic schools”, 2018 edn; http://catholiceducation.org.uk/ images/CES-Project_Homophobic-Bullying-Booklet_ JUN18_PROOF-9.pdf. For comment see, for instance, Deacon Nick Donnelly, “UK bishops’ group pushing radical LGBT propaganda in Catholic schools”, LifeSiteNews, 18 May 2017; https://www.lifesitenews.com/opinion/ uk-bishops-group-pushes-radical-lgbt-materials-in-catholic-schools. Also, Bishop Egan of Portsmouth has commented on the ‘ideological colonisation’ at work in our schools, including the influence of Stonewall and LGBT Youth on the CES’s “Made in God’s Image” document. Deacon Nick Donnelly, “Interview: UK bishop questions LGBT involvement in Catholic schools’ sexed program”, LifesiteNews, 22 May 2017; https://www.lifesitenews. com/news/interview-english-bishop-questions-lgbt-involvement-in-catholic-schools-sex
CES, “Made in God’s Image” (2018), section 2, (p.5).
Congregation for the Doctrine of the Faith (signed by Cardinal Ratzinger), “Letter to the Bishops of the Catholic Church on the Pastoral Care of the Homosexual Persons”, 1 October 1986; http://www.vatican.va/roman_curia/congregations/cfaith/documents/rc_con_ cfaith_doc_19861001_homosexual-persons_en.html
As pointed out, for instance, in three 2017 blog posts by the “Counter Cultural Father”: https://ccfather.blogspot. com/search?q=Made+in+God%27s+Image; See also Bishop Egan’s comments in an interview in LifesiteNews, 22 May 2017; https://www.lifesitenews.com/news/interview-english-bishop-questions-lgbt-involvement-in-catholic-schools-sex
Welsh government, “Kirsty Williams announces focus on healthy relationships in major reforms to ‘Relationships and Sexuality’ education”, Press release, 22 May 2018; https://gov.wales/newsroom/educationandskills/2018/ kirsty-williams-announces-focus-on-healthy-relationships-in-major-reforms-to-relationships-and-sexuality-education/?lang=en
Scottish government, “LGBTI education: Scotland will lead the way in inclusive education”, Press release 8 Nov 2018; https://www.gov.scot/news/lgbti-education/
All of these terms mean the same thing, and each one can lead to the same thing for anyone afflicted with it: progressive, and potentially permanent, blindness.
And according to multiple class action lawsuits, and backed up by research, intracranial hypertension (ICH) is also a rare, albeit extremely serious potential risk from intrauterine levonorgestrel, a synthetic progestogen widely distributed in the Mirena IUD (although other contraceptive formulations containing levonorgestrel, including Plan B—may also carry the same risk to varying degrees).
Pseudotumor cerebri (PTC) literally translates to “false brain tumor,” and the term is used to describe increased cerebrospinal fluid (CSF) pressure within the skull precisely because the symptoms it produces are highly similar to those caused by brain tumors—although, in cases of PTC, there is no actual tumor present. Just as someone with a brain tumor might experience changes or loss in vision, headaches, nausea and vomiting, and tinnitus among other symptoms, so too will someone with PTC be affected by these debilitating symptoms. In particular, the increased CSF pressure within the skull causes swelling of the optic nerve, which can cause changes and/or loss in vision, which may be permanent.
For many, the exact cause of PTC is unknown. Women, and particularly obese women, seem to have a higher risk of developing the condition, and pregnancy, thyroid conditions, and chronic kidney failure may all further exacerbate one’s risk. If the cause of PTC cannot be determined, it will be termed “idiopathic.” But for far too many women, the cause may be linked to their choice in contraceptive.
And although researchers have known for more than two decades that other levonorgestrel-releasing contraceptives (like the Norplant) have been linked with PTC, it is a complication that many women have suffered from—and a risk many claim was downplayed or unmentioned by their doctors and the drugs’ pharmaceutical companies alike.
This is sadly unsurprising news, given the conclusion of a recent study reviewing the number of Mirena-associated intracranial hypertension cases reported to the FDA’s Adverse Events Reporting System (FAERS). Although researchers discovered “a higher than expected number of reports of ICH with Mirena in the FAERS database,” they nevertheless concluded that “the small risk of ICH may outweigh the risk of unintended pregnancies.”
Safer Family-Planning Options for Women
What I wish these researchers would acknowledge—and even more so, what I wish the women whose vision may be permanently damaged because of their choice in contraceptives knew—is that there is a better way for women to plan their families that involves absolutely no risk of PTC or its associated symptoms.
While long-acting reversible contraceptives (LARCs) like IUDs and implants may be among some of the most effective methods on the market at preventing pregnancy, modern methods of Fertility Awareness-Based Methods (FABM) and Natural Family Planning (NFP) can be just as effective at preventing pregnancy (depending on the method), and carry none of the debilitating, dangerous, or permanent risks of LARCs. And, although most women with an IUD will never experience PTC, wouldn’t it be better if doctors and pharmaceutical companies were open and honest about the very real risks presented by the various types of birth control, and knowledgeable about the many risk-free alternatives?
Unfortunately, there is very little money to be made by the medical establishment from FABM and NFP, especially when compared to all of the pharmaceutical options. So until more in the medical community embrace the science and research on fertility charting, women will have to be their own healthcare advocates and learn more about natural options of family planning. We always recommend that, if women are seeking FABM for pregnancy prevention, she should reach out to a certified FABM instructor to benefit from the highest effectiveness rates.
Many women who have made the switch from pharmaceutical birth control to natural family planning report that they couldn’t feel more empowered to know they have more awareness of what is going on in their bodies. They can also have the confidence of knowing they aren’t exposing themselves to drugs that could hurt them.
April 12, 2019 (LifeSiteNews) – Marriage and family provide the foundation for Christian society, Bishop Joseph Strickland said in an interview. And there’s so much broken about that foundation, he said, as well as in the Church and the world today, that it’s imperative to help young couples who are seeking marriage with a strong formation in the Catholic faith – including teaching them about why contraception is morally wrong.
The Tyler, Texas bishop spoke with LifeSiteNews (read full interview below or click here) about his call as a bishop to teach the Catholic faith and a bold initiative to do so in his diocese wrapping up its second year. Strickland released the Constitution on Teaching in May 2017 and also established the Saint Philip Institute of Catechesis and Evangelization, tasked with teaching the Catholic faith in his diocese.
The comprehensive plan to evangelize his flock includes a year of marriage formation that incorporates natural family planning and the Church’s teaching that Catholics are called to be open to life in marriage, embracing Pope St. Paul VI’s document Humanae Vitae. The truth of Church teaching is so profound, he said, that even though it’s not had acceptance in the last 50 years by many Catholics, it’s begun to resonate in and outside the Church.
“And with the 50th anniversary of Humanae Vitae, we’ve focused on in the diocese that this is a truth that the Church has been teaching for those 50 years.”
The Church teaches in the 1968 encyclical that using contraception is always and in every case wrong. “Each and every marital act must of necessity retain its intrinsic relationship to the procreation of human life,” states the document. According to this teaching, contraception blocks the marital act from its God-given procreative purpose, contradicting the husband and wife’s promise to give themselves to each other, totally and unreservedly — where nothing must be held back, including one’s own fertility.
The document has been largely ignored by the faithful, said Strickland, by priests and even by bishops. Strickland told LifeSiteNews he had to admit, while he’s always believed what the Church said, that as a parish priest for many years, he also didn’t focus on it that much, because it really wasn’t very popular to focus on.
In Humanae Vitae Paul VI foretold various social ills that would befall the culture, such as marital infidelity, a general lowering of morality, growing disrespect for women and population control.
“If you read Humanae Vitae,” Strickland said, “Pope St. Pope Paul VI, in #14 of Humanae Vitae, he basically is prophetic and he lays out – This is where we’re headed if we ignore God’s plan for a married couple, open to life and not using contraception.”
“And I think we’ve ended up exactly where his prophetic prediction said we would end up,” continued Strickland. “So with all of that being realized, I felt that we need to start at the very foundation of the Christian community, which is marriage, and then the families that are formed on a solid marriage. “
Natural family planning, which respects the natural rhythms inherent in the human body, is part of this, he said.
Strickland, who has become noted for verbalizing the Church’s teaching on subjects such as sexual morality and abortion, discussed a number of things in the interview, speaking candidly about contraception.
He emphasizes that in speaking out about Church teaching he is doing his job as a bishop, and in most cases he is addressing his local flock in northeast Texas. But because it is relatively uncommon for a bishop to speak out, he’s come to stand out.
He tells LifeSiteNews that the Church’s teaching isn’t his truth; it’s Christ’s truth. And he’ll vocalize it as long as he’s a bishop. The fact it seems remarkable, he said, shows how secular society has become.
“Sadly, after 50 years of Humanae Vitae, it’s somewhat revolutionary to do what we’re doing,” Strickland told LifeSiteNews, “but it’s in line with what the Church has continued to teach for these 50 years. It’s been the official teaching. It’s been not emphasized that much.”
While it may be possible to overemphasize it, he says, he thinks it is very significant, because society’s problems today stem from disobedience to God, and contraception has become entrenched in the culture, including with Catholics.
“I guess the way I would put it is, everything traces back to ills of our society,” said Strickland, “which has been the case since Adam and Eve, it traces back to disobedience to God’s plan and to God’s will.”
“And so the contraceptive mentality that is very much in the Catholic community, and certainly in the non-Catholic, or even just humanity, contraception is accepted as something that is smart to use,” he said. “And it’s like you’re strange or you’re delusional if you’re not using contraception.”
“So it’s kind of a revolutionary idea,” he added, “but it is the teaching of the Church and I think there’s tremendous wisdom there.”
Strickland said there’s a real desire there on the part of many couples to learn NFP, especially after it’s really explained to them what God’s plan is and how natural family planning can be used properly.
This is true even in his area of Texas, he said, where less than 10 percent of the population in the geographical area of the diocese is Catholic.
“We’re finding more and more non-Catholics who are saying, ‘Hey, I think the Catholic Church has something here that we need to pay attention to,’” said Strickland.
“Because really, the Catholic Church — even as eroded as it is as far as Catholic practice — continues to teach that contraception is not morally acceptable,” Strickland said. “And we’re the only church that even attempts to teach that, and many of the non-Catholics individually are saying, we want to learn more about this because we think the Catholic Church is on to the truth of God’s plan.”
Strickland’s Constitution on Teaching can be accessed here.
Writing nearly half a century ago (1970), the Italian Catholic philosopher Augusto Del Noce noted that
I often find myself envying unbelievers: Does not contemporary history provide abundant evidence that Catholics are a mentally inferior species? Their rush to conform to the opinion about Catholicism held by rationalist secularists is stunning.
Those words from his essay “The Ascendance of Eroticism” open Del Noce’s brilliant reflections—part analysis, part prophecy—on Europe’s then-current sexual revolution. At a time when a young priest named Joseph Ratzinger was predicting a smaller, more hard-pressed, but purer Church of the future in his 1969–70 German and Vatican radio interviews, Del Noce was explaining how it would happen. He foresaw that “the decisive battle against Christianity [can] be fought only at the level of the sexual revolution. And therefore the problem of sexuality and eroticism is today the fundamental problem from the moral point of view.”
History has proven him right, and for obvious reasons. Sex is both a powerful bond and a fierce corrosive, which is why, historically, nearly all human cultures have surrounded it with taboos that order its harmonious integration into daily life. The naive eagerness—“stupidity” would not be too strong a word for Del Noce’s purposes—of many mid-century Church progressives in accepting, or at least accommodating, sexual license as a form of human liberation, spearheaded the intellectual collapse of an entire generation of Catholic moral theology. Since the 1960s, license has morphed into widespread sexual and social dysfunction, conflict, and suffering—also foreseen by Del Noce.
Unfortunately, the lessons of the ’60s are steadfastly ignored today by much of the Church’s own intellectual class: Simply put, sex is tied intimately to anthropology, to human self-understanding and the purpose of the body. Thus, for the Church to remain the Church, there can be no concordat with behaviors fundamentally at odds with the Word of God and the Christian understanding of the human person as imago Dei. All such attempts lead inevitably to what Ratzinger (now Benedict XVI, pope emeritus) once called silent apostasy. The current situation with Germany’s bishops’ conference comes to mind; but the problem is wider than a single local Church.
In his April 10 essay “The Church and the Scandal of Sexual Abuse,” a much older Joseph Ratzinger looks at the abuse phenomenon through the lens of his own life experience, dividing his text into three parts: origins of the crisis, initial Church responses, and what now needs to be done to heal Catholic life. The essay lacks some of the rigor of his earlier formal writings, and it will not satisfy those critics who see John Paul II and Benedict as slow in addressing the scale and gravity of the problem, but his words are nonetheless as clear and penetrating as ever.
Like the laypeople they serve and lead, priests are shaped by the culture from which they emerge. They should be held, rightly, to a higher standard because of their calling. But priests and bishops have no miraculous immunity to the abnormality bubbling around them. Ratzinger locates the seed of the current crisis in the deliberate turn toward sexual anarchy that marked much of Europe in the 1960s, and the complete failure of Catholic moral theologians to counter it—a failure that more often resembled fellow-traveling. He also notes, as did Del Noce, the dirty little secret of the sexual revolution: Relaxing sexual norms does not reduce an appetite for violence, including sexual violence. It does exactly the opposite.
Ratzinger acknowledges that “In various seminaries homosexual cliques were established which acted more or less openly and significantly changed the climate in the seminaries.” He also notes a problem that infected leadership: “Above all, a criterion for the appointment of new bishops [became] now their ‘conciliarity,’ which of course could be understood to mean rather different things.”
Ratzinger seeks to explain the initially slow and inadequate Church response to the abuse problem. He correctly saw the abuse issue as a crisis impacting the integrity of the faith and not merely as a legal matter grounded in the rights of accused clergy. Thus he successfully forced the transfer of abuse cases from Congregation of the Clergy jurisdiction to the Congregation for the Doctrine of the Faith where dealing with cases could be expedited. But even there, the scope of the problem proved larger than anyone anticipated. He remains silent on what many see as the continuing resistance of Rome to candidly name the core issue of the clergy abuse problem, which is not primarily a matter of clerical privilege but rather a pattern of predatory homosexuality.
Throughout his brief text, Ratzinger has moments of insight and genius that fall like rain in a desert, especially today. As in: “There are values which must never be abandoned for a greater value and even surpass the preservation of physical life. There is martyrdom. God is [about] more than physical survival. A life that would be bought by the denial of God, a life that is based on a final lie, is a non-life.” And: “A world without God can only be a world without meaning.” And: “A paramount task, which must result from the upheavals of our time, is that we ourselves once again begin to live by God and unto him.”
The words of the pope emeritus are especially piercing when he speaks of the many contemporary Catholics who treat the Eucharist—the Real Presence of God in our midst; the source and summit of Christian life—as “a mere ceremonial gesture . . . that destroys the greatness of the Mystery.” Or when he notes that the Church today “is widely regarded as just some kind of political apparatus,” and even many bishops “formulate their conception of the Church of tomorrow almost exclusively in political terms.” And finally this:
Today the accusation against God is, above all, about characterizing his Church as entirely bad, and thus dissuading us from it. The idea of a better Church, created by ourselves, is in fact a proposal of the devil, with which he wants to lead us away from the living God through a deceitful logic by which we are too easily duped. No, even today, the Church is not just made up of bad fish and weeds. The Church of God also exists today, and today it is the very instrument through which God saves us . . .
Today’s Church is more than ever a Church of the Martyrs, and thus a witness to the living God. If we look around and listen with an attentive heart, we can find witnesses everywhere today, especially among ordinary people, but also in the high ranks of the Church, who stand up for God with their life and suffering. It is an inertia of the heart that leads us to not wish to recognize them. One of the great and essential tasks of our evangelization is, as far as we can, to establish habitats of faith and, above all, to find and recognize them.
Amen. Not much more need be said.
Toward the end of his own 1970 essay, Augusto Del Noce noted that “an enormous cultural revision will be necessary in order to really leave behind the philosophical processes that have found expression in today’s sexual revolution.” The bad news is that too many of today’s Catholics seem to lack the will and ability to pursue that task. The good news is that some of our leaders still have the courage to speak the truth.
Charles J. Chaput, O.F.M. Cap., is the archbishop of Philadelphia.
COLUMBUS, April 11, 2019 (LifeSiteNews) – Ohio legislation to ban abortion once a fetal heartbeat can be detected is finally becoming law Thursday, after a lengthy battle last year came up one vote short of overcoming a veto by the state’s previous governor.
Senate Bill 23 would ban aborting any baby once a heartbeat can be detected (around 6-8 weeks), except in cases of a physical threat to the mother. Violating physicians would face up to a year in prison and suspension or revocation of their medical licenses (with medical board fines going to finance foster and adoption services). Women would also be able to sue abortionists for wrongful death.
The legislation passed the state Senate in March, and passed the state House Tuesday on a 56-40 vote, Cleveland.com reports.
“Today is a historic day. The legislature and Governor DeWine have declared that no longer should the beating hearts of humans too young to be born be violently torn apart by abortion,” Mark Harrington, president of the pro-life group Created Equal, said in a statement. “If pro-abortion lobbies present a legal challenge to this Act, we will defend these babies all the way up to the Supreme Court. Changes on the bench signify an even better day for preborn babies may be on the horizon.”
Democrat state Rep. Beth Liston, who is a physician and a professor at Ohio State University, denied that preborn babies are alive by week 12. “Simply put, you need lungs and a brain in order to live,” she claimed. “And there’s no science or technology that we have that can replace that need.” In fact, settled biological criteria and numerous medical textbooks establish (and various abortionists admit) that a living human being is created upon fertilization and is present throughout the entirety of pregnancy.
As protesters loudly gathered outside the chamber, Democrats tried and failed to add multiple amendments to the bill, including rape and incest exceptions and a proposalby state Rep. Janine Boyd to specifically exempt black women from the ban, ensuring black babies would still be legally killable.
The legislature passed a nearly-identical heartbeat ban last year, but came one vote short of overriding a veto by former moderate Republican Gov. John Kasich, who claimed it was “contrary to the Supreme Court of the United States’ current rulings on abortion” and therefore wouldn’t be worth the cost of a drawn-out legal battle. This time around, Republican Gov. Mike DeWine has vowed to “absolutely” sign it into law.
Numerous states have introduced or enacted heartbeat bills over the past several months. They ban abortion much earlier than the “viability” standard set by Roe v. Wade, which some cite to claim the bills would waste time and money on a doomed legal battle. But supporters argue that most state pro-life measures get sued anyway, and that the heartbeat ban will force a Supreme Court review that could finally overturn the 1973 ruling.
“Will there be a lawsuit? Yeah, we’re counting on it,” Republican state Rep. Ron Hood said. “We’re excited about it. Because this will be the law that ultimately reverses Roe v. Wade. Or there is several things they could do. They could hand it down to the states.”
Students for Life reports that due to the proposal of a school-based health center, public high school and middle school students at Sedro-Woolley High School and nearby middle school in Washington state may have IUDs inserted without their parent’s knowledge.
Initially, the proposal included referring students to Planned Parenthood for abortions. After strong objections from the community, PeaceHealth, a Catholic hospital that would conduct the proposed health center, decided not to refer minors to Planned Parenthood for abortion.
As Students for Life recently reported, a spokesperson for PeaceHealth said, “Our providers are empowered to discuss options with patients, including abortion; however, they can not give referrals.” However, girls as young as 13 could receive a referral for an IUD at PeaceHealth or another medical clinic without their parents finding out. The spokesperson clarified that IUDs would not be inserted in the school health center, but added, “if, within the context of the confidential patient/provider relationship, it is decided that an IUD is medically necessary, a PeaceHealth provider can insert an IUD.”
IUDs can have severe, sometimes life-threatening, complications if they migrate. Women are sharing their stories of complications they experienced with IUDs that are not often discussed. Many women who experienced complications said they were not informed about the severity of the potential issues. Minors receiving an IUD without their parent’s knowledge are taking on risks without guidance from an adult, and if complications do occur, those minors and their parents could face significant costs.
According to local news, Christina Jepperson, Sedro-Wooley High School Board President, insisted, “This isn’t going to be a condom clinic.” Trying to assuage parent’s fears, she said, “This really is primary care services. This isn’t any different than if you would go see your primary care or family doctor for.” However, Washington state law allows minor over the age of 13 to request confidential medical services, including getting IUDs and undergoing abortions. By placing a health center in the school that can give minors access to dangerous and abortifacient contraceptive devices, many parents still have valid concerns about the proposal.
Katie Lodjic, Washington Regional Coordinator for Students for Life of America and a Sedro-Woolley High School alumna said, “Healthcare corporations like PeaceHealth should not be allowed to circumvent parents by inserting IUDs into minor girls without their parents’ knowledge. Parents deserve to be involved in the medical decisions of their minor children but the school board plan would undermine parental rights.”
In the Guardian, Yvonne Roberts writes about how grim the sexual revolution was. She was there, and describes the sexual permissiveness not as something liberating but something monstrous dressed up as “peace and love.” It was a dystopia that gave rise to a rape culture. But today she notes the marked decrease in sexual activity among young people. Porn is ubiquitous, and addictive, and exemplifies the Final End of the sexual revolution. Loveless, abusive, soul-destroying. We reached peak sex, and it wasn’t even good. She asks:
“Are we satiated? As a commodity, is junk sex now on the wane, just like shopping on the high street? Are the young beginning to recalibrate sex and also understand its invaluable connection with intimacy, social skills, self-awareness and mutual self-respect?”
Oddly, in a progressive culture which despises priestly celibacy, which is voluntary, some progressive writers are now willing to admit that the sexual revolution was a dystopic failure and that the rise of involuntary celibacy is “a sign of progress.”
That’s quite the admission. I wonder if they might actually arrive at a better view altogether. Sex is sacred. It is an earthly union which cooperates in the divine act of creating immortal beings. It belongs in the the temple of marriage alone, and nowhere else. Sex isn’t for selling, it’s for creating.
Men and women who give up this great good, this urge of our nature, should only do so for a much greater good: the salvation of souls. But most of us should not give up on sex. We should start trying to understand what it really is, and where it belongs.
The Vatican cardinal discusses his hard-hitting new book in this exclusive interview with La Nef
Cardinal Robert Sarah is publishing the third of his book-length interviews with Nicolas Diat: The Day is Far Spent. An unflinching diagnosis, but one full of hope in the midst of the spiritual and moral crisis of the West.
1) In the first part of your book, you describe “a spiritual and religious collapse.” How does this collapse manifest itself? Does it only affect the West or are other regions of the world, such as Africa, also affected by it?
The spiritual crisis involves the entire world. But its source is in Europe. People in the West are guilty of rejecting God. They have not only rejected God. Friedrich Nietzsche, who may be considered the spokesman of the West, has claimed: “God is dead! God remains dead! And we have killed him…” We have murdered God. In view of God’s death among men, Nietzsche would replace him with a prophetic “Superman.”
The spiritual collapse thus has a very Western character. In particular, I would like to emphasize the rejection of fatherhood. Our contemporaries are convinced that, in order to be free, one must not depend on anybody. There is a tragic error in this. Western people are convinced that receiving is contrary to the dignity of human persons. But civilized man is fundamentally an heir, he receives a history, a culture, a language, a name, a family. This is what distinguishes him from the barbarian. To refuse to be inscribed within a network of dependence, heritage, and filiation condemns us to go back naked into the jungle of a competitive economy left to its own devices. Because he refuses to acknowledge himself as an heir, man is condemned to the hell of liberal globalization in which individual interests confront one another without any law to govern them besides profit at any price.
In this book, however, I want to suggest to Western people that the real cause of this refusal to claim their inheritance and this refusal of fatherhood is the rejection of God. From Him we receive our nature as man and woman. This is intolerable to modern minds. Gender ideology is a Luciferian refusal to receive a sexual nature from God. Thus some rebel against God and pointlessly mutilate themselves in order to change their sex. But in reality they do not fundamentally change anything of their structure as man or woman. The West refuses to receive, and will accept only what it constructs for itself. Transhumanism is the ultimate avatar of this movement. Because it is a gift from God, human nature itself becomes unbearable for western man.
This revolt is spiritual at root. It is the revolt of Satan against the gift of grace. Fundamentally, I believe that Western man refuses to be saved by God’s mercy. He refuses to receive salvation, wanting to build it for himself. The “fundamental values” promoted by the UN are based on a rejection of God that I compare with the rich young man in the Gospel. God has looked upon the West and has loved it because it has done wonderful things. He invited it to go further, but the West turned back. It preferred the kind of riches that it owed only to itself.
Africa and Asia are not yet entirely contaminated by gender ideology, transhumanism, or the hatred of fatherhood. But the Western powers’ neo-colonialist spirit and will to dominate pressures countries to adopt these deadly ideologies.
2) You write that “Christ never promised his faithful that they would be in the majority” (pg. 34), and you go on: “Despite the missionaries’ greatest efforts, the Church has never dominated the world. The Church’s mission is a mission of love, and love does not dominate” (pg. 35). Earlier, you wrote that “it is the ‘small remnant’ that has saved the faith.” If you will pardon a bold question: What is the problem exactly, seeing that this “small remnant” does in fact exist currently and manages to survive even in a world hostile to the faith?
Christians must be missionaries. They cannot keep the treasure of the Faith for themselves. Mission and evangelization remain an urgent spiritual task. And as St. Paul says, every Christian should be able to say “If I proclaim the gospel, this gives me no ground for boasting, for an obligation is laid on me, and woe to me if I do not proclaim the gospel!” (1 Cor 9:16). Further, “God desires everyone to be saved and to come to the knowledge of the truth” (1 Tim 2:4). How can we do nothing when so many souls do not know the only truth that sets us free: Jesus Christ? The prevailing relativism considers religious pluralism to be a good in itself. No! The plenitude of revealed truth that the Catholic Church has received must be transmitted, proclaimed, and preached.
The goal of evangelization is not world domination, but the service of God. Don’t forget that Christ’s victory over the world is…the Cross! It is not our intention to take over the power of the world. Evangelization is done through the Cross.
The martyrs are the first missionaries. Before the eyes of men, their life is a failure. The goal of evangelization is not to “keep count” like social media networks that want to “make a buzz.” Our goal is not to be popular in the media. We want that each and every soul be saved by Christ. Evangelization is not a question of success. It is a profoundly interior and supernatural reality.
3) I’d like to go back to one of your points in the previous question. Do you mean to say that European Christendom, where Christianity was able to establish itself throughout the whole of society, was only a sort of interlude in history; that it should not be taken as a model in the sense that in Europe Christianity “dominated” and imposed itself through a kind of social coercion?
A society permeated by the Faith, the Gospel, and natural law is something desirable. It is the job of the lay faithful to construct it. That is in fact their proper vocation. They work for the good of all when they build a city in conformity with human nature and open to Revelation. But the more profound goal of the Church is not to construct a particular model society. The Church has received the mandate to proclaim salvation, which is a supernatural reality. A just society disposes souls to receive the gift of God, but it cannot give salvation. On the other hand, can there be a society that is just and in conformity with the natural law without the gift of grace working in souls? There is great need to proclaim the heart of our Faith: only Jesus saves us from sin. It must be emphasized, however, that evangelization is not complete when it takes hold of social structures. A society inspired by the Gospel protects the weak against the consequences of sin. Conversely, a society cut off from God quickly turns into a dictatorship and becomes a structure of sin, encouraging people toward evil. That is why we can say that there can be no just society without a place for God in the public sphere. A state that officially espouses atheism is an unjust state. A state that relegates God to the private sphere cuts itself off from the true source of rights and justice. A state that pretends to found rights on good will alone, and does not seek to found the law on an objective order received from the Creator, risks falling into totalitarianism.
4) Over the course of European history, we have moved from a society in which the group outweighed the person (the holism of the Middle Ages) – a type of society that still exists in Africa and continues to characterize Islam – to a society in which the person is emancipated from the group (individualism). We might also say, broadly speaking, that we have passed from a society dominated by the quest for truth to a society dominated by the quest for freedom. The Church herself has developed her doctrine in the face of this evolution, proclaiming the right to religious liberty at Vatican II. How do you see the position of the Church toward this evolution? Is there a balance to be struck between the two poles of “truth” and “freedom,” whereas so far we have merely gone from one excess to the other?
It is not correct to speak of a “balance” between two poles: truth and freedom. In fact, this manner of speaking presupposes that these realities are external to and in opposition to one another. Freedom is essentially a tending toward what is good and true. The truth is meant to be known and freely embraced. A freedom that is not itself oriented and guided by truth is nonsensical. Error has no rights. Vatican II recalled the fact that truth can only be established by the force of truth itself, and not by coercion. It also recalled that respect for persons and their freedom should not in any way make us indifferent in relation to the true and the good.
Revelation is the breaking in of divine truth into our lives. It does not constrain us. In giving and revealing Himself, God respects the freedom that He Himself created. I believe that the opposition between truth and freedom is the fruit of a false conception of human dignity.
Modern man hypostatizes his freedom, making it an absolute to the point of believing that it is threatened when he accepts the truth. However, to accept the truth is the most beautiful act of freedom that man can perform. I believe that your question reveals how deeply the crisis of the Western conscience is really in the end a crisis of faith. Western man is afraid of losing his freedom by accepting the gift of true faith. He prefers to close himself up inside a freedom that is devoid of content. The act of faith is an encounter between freedom and truth. That is why in the first chapter of my book I have insisted on the crisis of faith. Our freedom comes to fulfillment when it says “yes” to revealed truth. If freedom says “no” to God, it denies itself. It asphyxiates.
5) You dwell at length on the crisis of the priesthood and argue for priestly celibacy. What do you see as the primary cause in the cases of sexual abuse of minors by priests, and what do you think of the summit that just took place in Rome on this question?
I think that the crisis of the priesthood is one of the main factors in the crisis of the Church. We have taken away priests’ identity. We have made priests believe that they need to be efficient men. But a priest is fundamentally the continuation of Christ’s presence among us. He should not be defined by what he does, but by what he is: ipse Christus, Christ Himself. The discovery of many cases of sexual abuse against minors reveals a profound spiritual crisis, a grave, deep, and tragic rupture between the priest and Christ.
Of course, there are social factors: the crisis of the ‘60s and the sexualization of society, which rebound on the Church. But we must have the courage to go further. The roots of this crisis are spiritual. A priest who does not pray or makes a theatre out of the sacraments, especially the Eucharist, a priest who only confesses rarely and who does not live concretely like another Christ, is cut off from the source of his own being. The result is death. I have dedicated this book to the priests of the whole world because I know that they are suffering. Many of them feel abandoned.
We, the bishops, bear a large share of responsibility for the crisis of the priesthood. Have we been fathers to them? Have we listened to them, understood and guided them? Have we given them an example? Too often dioceses are transformed into administrative structures. There are so many meetings. The bishop should be the model for the priesthood. But we ourselves are far from being the ones most ready to pray in silence, or to chant the Office in our cathedrals. I fear that we lose ourselves in secondary, profane responsibilities.
The place of a priest is on the Cross. When he celebrates Mass, he is at the source of his whole life, namely the Cross. Celibacy is a concrete means that permits us to live this mystery of the Cross in our lives. Celibacy inscribes the Cross in our very flesh. That is why celibacy is intolerable for the modern world. Celibacy is a scandal for modern people, because the Cross is a scandal.
In this book, I want to encourage priests. I want to tell them: love your priesthood! Be proud to be crucified with Christ! Do not fear the world’s hate! I want to express my affection as a father and brother for the priests of the whole world.
6) In a book that has caused quite a stir [In the Closet of the Vatican, by Frédéric Martel], the author explains that there are many homosexual prelates in the Vatican. He lends credibility to Mgr Viganò’s denunciation of the influence of a powerful gay network in the heart of the Curia. What do you think of this? Is there a homosexual problem in the heart of the Church and if so, why is it a taboo?
Today the Church is living with Christ through the outrages of the Passion. The sins of her members come back to her like strikes on the face. Some have tried to instrumentalize these sins in order to put pressure on the bishops. Some want them to adopt the judgments and language of the world. Some bishops have caved in to the pressure. We see them calling for the abandonment of priestly celibacy or making unsound statements about homosexual acts. Should we be surprised? The Apostles themselves turned tail in the Garden of Olives. They abandoned Christ in His most difficult hour.
We must be realistic and concrete. Yes, there are sinners. Yes, there are unfaithful priests, bishops, and even cardinals who fail to observe chastity. But also, and this is also very grave, they fail to hold fast to doctrinal truth! They disorient the Christian faithful by their confusing and ambiguous language. They adulterate and falsify the Word of God, willing to twist and bend it to gain the world’s approval. They are the Judas Iscariots of our time.
Sin should not surprise us. On the other hand, we must have the courage to call it by name. We must not be afraid to rediscover the methods of spiritual combat: prayer, penance, and fasting. We must have the clear-sightedness to punish unfaithfulness. We must find the concrete means to prevent it. I believe that without a common prayer life, without a minimum of common fraternal life between priests, fidelity is an illusion. We must look to the model of the Acts of the Apostles.
With regard to homosexual behaviors, let us not fall into the trap of the manipulators. There is no “homosexual problem” in the Church. There is a problem of sins and infidelity. Let us not perpetuate the vocabulary of LGBT ideology. Homosexuality does not define the identity of persons. It describes certain deviant, sinful, and perverse acts. For these acts, as for other sins, the remedies are known. We must return to Christ, and allow him to convert us. When the fault is public, the penalties provided for by Church law must be applied. Punishment is merciful, an act of charity and fraternal love. Punishment restores the damage done to the common good and permits the guilty party to redeem himself. Punishment is part of the paternal role of bishops. Finally, we must have the courage to clearly apply the norms regarding the acceptance of seminarians. Men whose psychology is deeply and permanently anchored in homosexuality, or who practice duplicity and lying, cannot be accepted as candidates for the priesthood.
7) One chapter is dedicated to the “crisis of the Church.” When precisely do you place the beginning of this crisis and what does it consist in? In particular, how do you relate the “crisis of faith” to the crisis of “moral theology.” Does one precede the other?
The crisis of the Church is above all a crisis of the faith. Some want the Church to be a human and horizontal society; they want it to speak the language of the media. They want to make it popular. They urge it not to speak about God, but to throw itself body and soul into social problems: migration, ecology, dialogue, the culture of encounter, the struggle against poverty, for justice and peace. These are of course important and vital questions before which the Church cannot shut her eyes. But a Church such as this is of interest to no one. The Church is only of interest because she allows us to encounter Jesus. She is only legitimate because she passes on Revelation to us. When the Church becomes overburdened with human structures, it obstructs the light of God shining out in her and through her. We are tempted to think that our action and our ideas will save the Church. It would be better to begin by letting her save herself.
I think we are at a turning point in the history of the Church. The Church needs a profound, radical reform that must begin by a reform of the life of her priests. Priests must be possessed by the desire for holiness, for perfection in God and fidelity to the doctrine of Him who has chosen and sent them. Their whole being and all their activities must be put to the service of sanctity. The Church is holy in herself. Our sins and our worldly concerns prevent her holiness from diffusing itself. It is time to put aside all these burdens and allow the Church finally appear as God made Her. Some believe that the history of the Church is marked by structural reforms. I am sure that it is the saints who change history. The structures follow afterwards, and do nothing other than perpetuate the what the saints brought about.
We need saints who dare to see all things through the eyes of faith, who dare to be enlightened by the light of God. The crisis of moral theology is the consequence of a voluntary blindness. We have refused to look at life through the light of the Faith.
In the conclusion of my book, I speak about a poison from which are all suffering: a virulent atheism. It permeates everything, even our ecclesiastical discourse. It consists in allowing radically pagan and worldly modes of thinking or living to coexist side by side with faith. And we are quite content with this unnatural cohabitation! This shows that our faith has become diluted and inconsistent! The first reform we need is in our hearts. We must no longer compromise with lies. The Faith is both the treasure we have to defend and the power that will permit us to defend it.
8) The second and third parts of your book are about crisis in western societies. The subject is so vast, and you touch on so many important points–from the expansion of the “culture of death” to the problems of consumerism tied to global liberalism, passing through questions of identity, transmission, Islamism, etc.–that it is impossible to address them all. Among these problems, which seem to you to be the most important and what are the principal causes for the decline of the West?
First I would like to explain why I, a son of Africa, allow myself to address the West. The Church is the guardian of civilization. I am convinced that western civilization is passing at present through a mortal crisis. It has reached the extreme of self-destructive hate. As during the fall of Rome, elites are only concerned to increase the luxury of their daily life and the peoples are being anesthetized by ever more vulgar entertainment. As a bishop, it is my duty to warn the West! The barbarians are already inside the city. The barbarians are all those who hate human nature, all those who trample upon the sense of the sacred, all those who do not value life, all those who rebel against God the Creator of man and nature. The West is blinded by science, technology, and the thirst for riches. The lure of riches, which liberalism spreads in hearts, has sedated the peoples. At the same time, the silent tragedy of abortion and euthanasia continue and pornography and gender ideology destroy children and adolescents. We are accustomed to barbarism. It doesn’t even surprise us anymore! I want to raise a cry of alarm, which is also a cry of love. I do so with a heart full of filial gratitude for the Western missionaries who died in my land of Africa and who communicated to me the precious gift of faith in Jesus Christ. I want to follow their lead and receive their inheritance!
How could I not emphasize the threat posed by Islamism? Muslims despise the atheistic West. They take refuge in Islamism as a rejection of the consumer society that is offered to them as a religion. Can the West present them the Faith in a clear way? For that it will have to rediscover its Christian roots and identity. To the countries of the third world, the West is held out as a paradise because it is ruled by commercial liberalism. This encourages the flow of migrants, so tragic for the identity of peoples. A West that denies its faith, its history, its roots, and its identity is destined for contempt, for death, and disappearance.
But I would like to point out that everything is prepared for a renewal. I see families, monasteries, and parishes that are like oases in the middle of a desert. It is from these oases of faith, liturgy, beauty, and silence that the West will be reborn.
9) You end this beautiful book with a section entitled “Rediscovering Hope: The Practice of the Christian Virtues.” What do you mean by this? In what way can practicing these virtues be a remedy for the multifarious crisis we have spoken about in this interview?
We should not imagine a special program that could provide a remedy for the current multi-faceted crisis. We have simply to live our Faith, completely and radically. The Christian virtues are the Faith blossoming in all the human faculties. They mark the way for a happy life in harmony with God. We must create places where they can flourish. I call upon Christians to open oases of freedom in the midst the desert created by rampant profiteering. We must create places where the air is breathable, or simply where the Christian life is possible. Our communities must put God in the center. Amidst the avalanche of lies, we must be able to find places where truth is not only explained but experienced. In a word, we must live the Gospel: not merely thinking about it as a utopia, but living it in a concrete way. The Faith is like a fire, but it has to be burning in order to be transmitted to others. Watch over this sacred fire! Let it be your warmth in the heart of this winter of the West. “If God is for us, who is against us?” (Rom 8:31). In the disaster, confusion, and darkness of our world, we find “the light that shines in the darkness” (cf. Jn 1:5): He who said “I am the Way, the Truth, and the Life” (Jn 14:6).
Translated from the French by Zachary Thomas (Original)
Note: the French text published by La Nef edited the text of the interview given by the Cardinal. This is a translation of the integral text supplied by the Cardinal.
Ignatius Press has announced the 2019 publication of an English translation entitled The Day is Far Spent, available for pre-order on their website.
To anyone who’s been paying attention, it’s clear that the pro-life movement is gaining enormous momentum. However, if you still have any doubts about pro-life progress, you need only glance at Planned Parenthood’s latest press release, responding to data just published by the Guttmacher Institute, Planned Parenthood’s former research arm.
According to the Guttmacher Institute, since the beginning of this year over 250 pro-life bills have been introduced in over 41 states. Almost 50% of those bills would ban abortion in “some or all circumstances,” says the organization. In fact, according to Planned Parenthood’s analysis, legislators in seven states have proposed bills that would completely ban abortion, while six states are considering or have passed “trigger bans” that would ban abortion if or when Roe v. Wade is repealed.
Elizabeth Nash, the Senior State Issues Manager at the Guttmacher Institute, linked the glut of pro-life bills to both the conservative shift on the Supreme Court, and the increasingly open efforts of the pro-life movement to enact total abortion bans. “Energized by a new Supreme Court, anti-abortion activists and politicians have kicked into high gear their decades-long agenda to ban abortion through a series of increasingly radical and dangerous abortion bans,” she stated.
Nash claimed, disingenuously, that the pro-life bills being introduced “are about exerting control and power over pregnant people.” But, for the growing number of Americans who call themselves pro-life, this claim is simply absurd. The goals of the pro-life movement have nothing to do with controlling pregnant women; they have to do with protecting the lives of the unborn children that science and ultrasound technology have revealed beyond any shadow of a doubt to be just as fully alive and human as you or I.
Extremist leftist organizations like Planned Parenthood, which have built their ideology on denying or conscientiously burying basic scientific truths, are struggling to remain relevant now that those scientific truths are so undeniable and publicly accessible, thanks both to technology and the tireless efforts of the pro-life movement.
Indeed, the absurdity of the Guttmacher Institute’s ideological extremism is on display in Nash’s remark about pro-lifers wanting to control “pregnant people.” One of the pro-abortion movement’s latest dogmas is that men can get pregnant – i.e. so-called “transgender men,” which is to say, biological women who now claim that they are men. This claim is at least as absurd as the claim that the unborn child is just a “blob of tissue” that magically becomes a living human person either the moment the “pregnant person” (i.e. mother) decides that she wants the baby, or that the baby emerges from the birth canal.
Planned Parenthood Panicking
Another immensely encouraging piece of news from the Guttmacher Institute’s report is that six states have only a single abortion facility left. In other words, these states are on the verge of eliminating surgical abortions from their borders even without passing legislation banning abortions. In fact, statistics show that the number of abortion clinics across the country has plummeted over the last two decades. According to Operation Rescue, in 2018 the total number of abortion clinics in the U.S. fell to 697. That’s a decrease of 79% since 1991. The Washington Postblames many of these closures on the successful passage of pro-life progress in legislation.
The massive growth in such pro-life legislation, and closure of abortion clinics, coincides with a dramatic decrease in the U.S. abortion rate. According to the CDC, the U.S. abortion rate reached a historical low in 2015. That translates into millions of lives saved.
Planned Parenthood President Dr. Leana Wen sounds panicked, as well she might. “Today, the reality we live in is a terrifying one for women around the country,” she claimed. As is typical of Planned Parenthood, Wen deceptively attempted to link the reduction in abortion clinics to disruptions in access to services like cancer screenings and STD and HIV testing. In reality, pro-lifers have thoroughly debunked Planned Parenthood’s past claims to offer mammograms (Even the pro-abortion Washington Posthad to admit that pro-lifers were right). Meanwhile, Planned Parenthood’s own public numbers show that most of their non-abortion-related services have been declining for years, while abortions keep climbing.
Click to read more about the real Planned Parenthood and its genesis.
However, Wen is quite right when she bemoans the fact that “access to abortion care is disappearing in states.” But far from a “terrifying” reality for women, this means that many more young girls will have a chance to be born, rather than being flushed down the drains at Planned Parenthood’s abortion facilities before they ever even have the opportunity to pursue their dreams. So, too, many more young women will have the opportunity to pursue a happy, meaningful life without carrying the burden of shame and regret that so often follows after accepting Planned Parenthood’s bleak, self-centered, and murderously-maintained worldview.
Crucially, many of the bills introduced around the country are so-called “heartbeat bills,” which would ban abortion after the point when the baby’s heartbeat can be detected. Such bills would not only prevent the overwhelming majority of abortions from taking place but present a direct challenge to Roe v. Wade. If passed into law, such bills would inevitably be challenged in court, ultimately ending up at the Supreme Court, which would have the opportunity to revisit the notorious case that ushered abortion-on-demand into the United States. Pro-abortion activists clearly believe that they may very well see Roe v. Wade overturned within months or a few years. It’s up to us, with God’s grace, to ensure that their fears are well-founded.
Interestingly, even many of the massive liberal corporations which, in the past, have not hesitated to use their influence to threaten individual states if they should pass legislation that goes against the leftist agenda have declined to publicly oppose the heartbeat bills being introduced in states like Georgia. I think the reason why is obvious: public opinion is trending pro-life. Corporations that threatened Georgia for passing religious liberty legislation a few years ago know that they can’t risk associating their brand with the killing of unborn babies.
The Pro-Abortion Movement’s Worst Year Ever?
Amidst the hundreds of pro-life bills that have been introduced, a more conservative Supreme Court, a president who seems determined to fulfill his pro-life promises in the face of any amount of backlash, and the release of what may well be the most successful pro-life movie ever made – Unplanned, telling the story of former Planned Parenthood director Abby Johnson – the abortion industry in the United States seems set to have what may well turn out to be its worst year since the Supreme Court first passed Roe v. Wade.
Click for more on “Unplanned” and the truth about Planned Parenthood. Footage courtesy EWTN
That said, pro-lifers should be wary of growing even a little bit complacent. Pro-abortion forces are terrified, and in response they are rallying their supporters and legislative allies to push back…hard. As Planned Parenthood noted in its release, the pro-life bills “have triggered a counter response from constituents and reproductive health care champions”. This, in part, explains the glut of attempts (some of which have been successful) to pass laws enshrining the most extreme versions of legal abortion in states like New York and Virginia.
We live in chaotic times, and there is much to be worried about in terms of the state and future of our culture. However, if respect for the sanctity of human life is, as Pope St. John Paul II so often proclaimed, the necessary foundation for a healthy society, then it would seem we have great reason for both hope and gratitude: gratitude that so many lives are already being saved thanks to our country’s pro-life direction, and hope that within our lifetimes we may yet see the end of the reign of terror that is legalized abortion-on-demand.
ST. LOUIS, Missouri, April 4, 2019 (LifeSiteNews) — A new scientific study has found that pre-born babies’ brains show significant differences between sexes and thus before any parental or societal conditioning.
In the April 2019 edition of Developmental Cognitive Neuroscience, an article titled “Sex differences in functional connectivity during fetal brain development” details the authors’ study of 118 unborn babies (70 male, 48 female) between 25.9 and 39.6 weeks gestational age. By looking at 16 distinct networks of the brains, they found differences between male and female fetuses in functional connectivity across gestational age. They concluded, “These observations confirm that sexual dimorphism in functional brain systems emerges during human gestation.”
“Specifically, female fetuses demonstrated long range gestational-age related changes in functional connectivity between subcortical and cortical regions,” the authors reported. “The present study demonstrates for the first time that development of fetal brain FC [functional connectivity] varies with sex,” the researchers wrote. The networks they found in the unborn babies’ brains reveal, they wrote, “building blocks” for brain development later in life. Using MRI scans of unborn babies, the researchers examined the neural connections or F.C. in the various areas of the fetal brain. Connections they found in unborn girls were nearly absent among the boys.
The study concluded, “The differential development of FC over gestation in male and female fetuses likely acts as a precursor to sex-related brain connectivity differences observed across the lifespan. Further, the fetal brain networks observed in the present study likely serve as the building blocks for nascent neonatal, toddler, and adult networks.”
Dr. Leonard Sax, a physician and psychologist, wrote in Psychology Today that the new study is in line with previous studiesshowing that female infants “have significantly greater brain volume in the prefrontal cortex compared with males.” He wrote that some of the sex differences the researchers found are “truly amazing.” Girls showed differences in the connections in the left cerebellum, for example, as well as other areas of the brain, when compared to boys. The cerebellum lies near the base of the skull and has an important role in motor control. It may also be involved in functions such as attention, language, and the regulation of fear and pleasure responses.
In an interview with CNA, Sax said the importance of the study is that it shows that sexual differences in brain development come before birth. “Exactly what those differences signify is controversial,” he added.
Sax recalled in the Psychology Today article that Professor Judith Butler, a non-scientist, has been celebrated for her idea that “male” and “female” categories are social constructs. He quotes Butler, who says that “because gender is not a fact, the various acts of gender creates [sic] the idea of gender, and without those acts, there would be no gender at all.” Butler’s book, Gender Trouble, has been influential for decades among transgenderism advocates, who have argued that sexual differences are conditioned by parents and societal norms. The new study throws the resultant gender theory into doubt, Sax writes, because it focuses on babies before birth and thus before any influence from parents or society.
While transgender advocates attribute gender differences to societal prejudices and norms, for Sax, “girls and boys are different,” according to CNA. Sax believes that “girl” and “boy” are “meaningful categories” that are not a performance or social construct.
KETTERING, April 2, 2019 (LifeSiteNews) — An embattled abortion facility in Ohio has lost the latest round of its legal battle to stay open despite lacking the required hospital transfer agreement, with the next step potentially being the state Supreme Court.
In 2016, state health officials revoked Women’s Med Center of Dayton (WMCD)’s ambulatory surgical facility license, citing alleged rule violations. County court judge Mary Wiseman let WMCD remain open while challenging the decision but went on to rule that the “court lacks the jurisdiction” to intervene in the case.
Women’s Med, which is roughly four miles away from two hospitals, has been unable to secure a written agreement with area hospitals to admit patients in cases of complications. But Jennifer Branch, an attorney representing WMCD, claims the requirement is “medically unnecessary and politically motivated” because hospitals would be required to take emergency patients anyway.
Operation Rescue notes, however, that WMCD has a history of medical emergencies, including a 26-year-old woman hemorrhaging after a surgical abortion last month and an unconscious woman rushed to the hospital the month before after the abortion center’s staff were unable to treat her seizures. WMCD is owned by the infamous late-term abortionist Martin Haskell, who has been credited with inventing the partial-birth abortion procedure.
Ohio’s Second District Court of Appeals took up Women’s Med’s appeal on March 12, and on Friday a three-judge panel sided with the state, the Dayton Daily Newsreports.
The panel ruled that the Ohio Department of Health (ODH) “had the authority to revoke [WMCD’s] license based on the failure to comply with the administrative rule requiring a written transfer agreement with a nearby hospital”; that ODH’s finding of noncompliance “was supported by reliable, probative and substantial evidence”; and that WMCD failed to demonstrate that ODH commited an “abuse of discretion.”
“It is ridiculous for an abortion facility that cannot comply with licensing standards to stay open for four, five, or six years until the appeals can be exhausted and the clinic finally closed,” Operation Rescue president Troy Newman said. “In the meantime, women are suffering abortion complications and are being transported away by ambulance. These all could have been avoided had the appeals process allowed for the closure of this dangerous abortion clinic within a reasonable time frame.”
“The state’s law is intended to protect the health of the mother and the unborn child, and clearly the court agreed,” said Republican state Rep. Niraj Antani. “If the clinic decides to appeal to the Supreme Court, I’m confident the state law will continue to be upheld. Otherwise, the clinic should be immediately closed, and countless lives in the Dayton region will be saved.”
Branch confirmed that WMCD intends to appeal the case to the Ohio Supreme Court.
“We are one step away from one ending the child-killing career of one of the most notorious full-term abortionists in America,” Newman said. “It’s just unfortunate that it will likely take another year of appeals before we can finally see Haskell’s late-term clinic closed.”
Today I recommend to you some interesting demographic insights from Lyman Stone, speaking on The Federalist Radio Hour. You can listen here. Some of the points I found interesting are:
– Are demographers considering what individual people actually want for their lives? Lyman Stone argues that this is the meaningful question demographers should ask, particularly in relation to developing countries, and it is often a blind spot.
– The United States is at the lowest fertility rate in its history, as are many other countries around the world, so we are in an anomalous period in the world’s history.
– People often think the fewer people there are in the world, the more of the ‘pie’ will be left for them. This is wrong because, in fact, the ‘pie’ gets a lot smaller when there are fewer people, and there is less for everyone. The economy will get smaller, and who will be left to buy your assets such as your house and stocks? How will businesses you invest in stay afloat with no new innovative people?
So, while it might make financial sense at an individual level to have fewer children and have more money left for you, at a societal level there will be less for everyone when you do this.The perspective of individuals does not match what society as a whole needs in this case.
– Climate change is a challenge of creativity and reducing emissions intensity. The good news is we’re good at this. In fact, the only meaningful thing we can do about emissions based on the current generally agreed scientific projections (if you take these as fact), is to come up with new innovations and technology at this point – which helps every country in the world lower their emissions too. Reducing population is too delayed based on the arguments and projections driving climate change.
There is a law that the time required to complete a task matches the time available. The feast of the Annunciation fits conveniently in the Lenten cycle this year, as the season comes unusually late. Our Lady conceived when she said “Yes” to the Creator. Many today are saying “No.” In some parts of our country there is growth in the number of seminarians, but in most places the harvest is sparse, and that is directly related to the dearth of children. The birth rate is the lowest in history: 60.2 births for every 1,000 women. We may be contracting a contagion of barrenness from Europe, which is dying because of a birth rate of 10 per 1,000 women and is desperately trying to survive by radically transforming its culture through massive immigration. It is projected that within ten years, the European Union will experience a 14% decrease in its workforce and a 7% decrease in its consumer populations.
A birth dearth reflects moral sterility. There is one condition shared by the heads of state or government in France, Germany, Britain, Italy, Sweden, Holland, Scotland, Romania, Lithuania, Latvia and Luxembourg: none of them have any children. Why should they care about future generations? There actually are voices calling for a complete elimination of births, on the claim that anthropogenic “climate change” will destroy the world in twenty years anyway. Many of them, whose mothers were of a different school of thought, may not remember that fifty years ago, a book titled The Population Bomb predicted that within ten years, hundreds of millions would have died of starvation and that most of its readers would have starved to death by now. Practicing what he preached, the author had a vasectomy and now—at the age of 85—still has an adequate food supply. Confident that theory takes precedent over fact, he maintains that his core thesis was correct.
State legislation and cultural pressures are increasingly hostile to families, which in various ways are looked on as threats to government. Governmental and societal forces promote contraception, abortion, easy divorce, and welfare structures that encourage fatherless households. If the Church is true to herself in her teaching and example, she will be the solace of civilization in this new demographic dark age.
Giving thanks in these Lenten days for Our Lady’s “Yes,” we look to the words of Saint John Paul II: “I wish to invoke the protection of the Holy Family of Nazareth. … It is therefore the prototype and example for all Christian families. … St. Joseph was a ‘just man’… May he always guard, protect and enlighten families. May the Virgin Mary, who is the Mother of the Church, also be the Mother of ‘the Church of the home.’ . . . May Christ the Lord, the Universal King, the King of Families, be present in every Christian home as He was at Cana, bestowing light, joy, serenity, and strength” (Familiaris Consortio #86).
Thirty-five years ago I admired the neo-Gothic buildings of a Catholic college in Westchester County. But I was surprised to find that the confessional in the beautiful chapel was being used as a broom closet. There had been some misunderstanding about aggiornamento, or bringing the practice of the Faith up to date. That was the College of New Rochelle, begun in 1904 by the Ursuline sisters whose Religious institute was founded by Saint Angela Merici and who have graced the Church since 1535 with hospitals and schools and missionary work. They have not been unique in their numerical decline. In the United States since 1965, when the Second Vatican Council ended with sentiments of a “New Springtime” of the Church, Religious sisters have declined from 181,421 to 47,160, and most of those left are aged. This year the College of New Rochelle will close.
While various factors for all this may be cited, many Religious orders, trained in obedience, accepted bad advice from misguided and misguiding theologians and leaders. Bishops often have been at fault, timorous about correcting error, cheerily giving out diplomas while the spiritual foundations of the schools sank. It took courage usually lacking to point out that serious mistakes were being made, and many Religious dug into their errors, abandoning community life and even Religious habits, and replacing doctrine with secular dogmas about “Peace and Justice” and “climate change”—all witness to the dictum, attributed to various sources, that ”Insanity is repeating the same mistakes and expecting different results.”
Such need not be the case, given a dose of humility and sanity. Those who stubbornly will not admit mistakes are easily annoyed when shown new Religious orders, faithful to classical doctrine and religious practice, that are rapidly growing. Something similar is happening in education. Take just two examples: Thomas Aquinas College has emphasized quality over size since its founding in 1971 and has become one of the best regarded colleges in California. This year, it is opening a beautiful additional campus on an historic site in Massachusetts. Its California chapel, built in the Spanish Mission style, is a magnificent witness to Catholic heritage, as is the new chapel planned for Christendom College in Virginia, which was founded just a few years after Thomas Aquinas College. In the few years of their existence, although primarily lay institutions, Thomas Aquinas has produced 60 priests, 44 consecrated Religious women and men, and 26 seminarians; Christendom boasts so far 80 priests, 55 Religious, and 22 seminarians. Those colleges have not turned their confessionals into broom closets.
Any individual or institution that seeks happiness on its own terms will not find it. Chesterton asks, “Do you have joy without a cause…?” On Laetare Sunday, the Church rejoices in the true cause of joy, which is God Himself. The failings evident in practical experience testify to what happens when vanity tries to usurp Him.
March 29, 2019 (LifeSiteNews) — Each year, over 250,000 women get sexually assaulted in the United States, while the actual number of victims is likely far higher, considering that less than 40% of victims report their assaults. Of the women who do go to an emergency room, almost all will get a pregnancy test, and if the test is negative, almost all will receive emergency contraception, usually Plan B, which consists of a hormone called levonorgestrel, given with the hope that it will prevent pregnancy. The main ethical debate concerns the question of whether this medication works via preventing pregnancy or via ending pregnancy (i.e., an early abortion).
So what is the policy of Catholic hospitals in the United States with regard to the dispensation of emergency contraception? A few Catholic hospitals forbid its use; however, many Catholic hospitals dispense emergency contraception under certain conditions and follow the Peoria Protocol, which was invented in Peoria, Illinois, under then-bishop Myers.
Simply put, this protocol states that it is ethical to dispense emergency contraception such as Plan B to a woman who is sexually assaulted if she is not pregnant and has not yet ovulated. The premise behind the protocol is that Plan B will stop a woman from ovulating if she is about to ovulate and therefore prevent any potential pregnancy.
However, recent research has shown that giving Plan B to women who are about to ovulate does little to stop the upcoming ovulation, as noted by researchers Noe and Croxatto (2011, Contraception), who found that one could easily measure when a woman ovulates by high-tech ultrasound and noted that about 80% of the women ovulated if Plan B was given 2–5 days prior to ovulation.
So if Plan B does not effectively prevent ovulation, then how does it stop pregnancy? The answer is that these women are likely getting pregnant, but the embryo dies prior to ever implanting in the uterus — that is, an early abortion.
In light of the newest data, the Catholic Medical Association, the largest group of Catholic physicians in the United States, has published its official position on its website, concluding that the Peoria Protocol is flawed and that the dispensation of emergency contraception such as Plan B in Catholic emergency rooms is immoral.
The obvious question is, why is Plan B still being given out in Catholic hospitals’ emergency rooms?
One of the problems regarding Plan B and its mechanism of action is that it is a very technical area, so those who favor the dispensation of Plan B often make old claims that are not supported by the most current medical literature. In response, the Polycarp Research Institute has produced a video that goes into more detail and refutes these older arguments while presenting the most current evidence.
It is everyone’s hope that rape victims, whether pregnant or not, receive the most compassionate and effective care available. Unfortunately, using Plan B and continuing to cite the faulty Peoria Protocol, based upon what we now know, is simply an immoral compromise — with the unintended consequence of the loss of human life and the abandonment of truly loving and courageous Christian health care.
March 27, 2019 (Society for the Protection of Unborn Children) — Scientists have created unprecedented 3D images of a baby’s heart while still inside the womb — a development which could help the treatment of babies with congenital heart disease.
Standard 2D images were taken using an MRI machine, and the images were then put through a powerful computer program developed by experts at King’s College London and Guy’s and St Thomas’ NHS Trust. The technology pieces the images together and adjusts for the speed of the baby’s heartbeat and its movements in the womb to create an unprecedented 3D image of the heart.
This then gives doctors a clear view of any abnormality.
To help babies with heart disease or screen them out?
Congenital heart diseases affect up to eight in every 1,000 babies born in the UK. According to a Danish study, the rate of abortion for babies with major congenital heart disease (CHD) increased from 0.6% in 1996 to 39.1% in 2013 — a 65 fold increase.
However, Prof Reza Razavi, a consultant paediatric cardiologist, told the BBC that he wanted to improve the diagnosis of the birth defects after his daughter was born with one. “We thought we were going to lose her, that was a strong motivator… we should be able to pick up the problem in the womb,” he said.
He describes the 3D images as “beautiful” and says they let doctors clearly see the problem and improve care. He said: “We can have complete certainty and plan ahead what treatment is needed, what’s the operation we need to do.
“It really helps the parents to have the right support to know what’s going to happen. But it also really helps the babies because they get the right operation at the right time and have the best outcomes.”
The research is part of the iFind project, which also produced this incredible video of a twenty-week-old baby in the womb.
Let’s hope that this incredible technology is used to provide care for babies with heart disease, and is not used as another tool to screen them out.
March 27, 2019 (Lepanto Institute) — Catholic Relief Services is currently in the middle of a national fund-raising campaign, and Catholics all around the country have been contacting the Lepanto Institute, asking if CRS is still involved in the promotion of contraception. Sadly, the answer is a resounding “yes.” Last year, we reported that CRS is a dues-paying member ($56,000 per year) of an organization called InterAction, which actively lobbies Congress for the expansion of contraception and the end of the Mexico City Policy. Last week, we reported how CRS Executive Vice-President William O’Keefe testified before Congress to request nearly $9 billion for USAID, PEPFAR, and the Global Fund, which comprise the largest distributors of contraception and condoms throughout the world.
Our latest report on a CRS project (which can be read in full by clicking here) shows that from 2013 to 2018, Catholic Relief Services participated in a project which had the stated objective of spreading contraception to vulnerable women living in poverty in rural areas of Madagascar. CRS’s role in this project was to create a self-sustaining financial mechanism that would provide funding to Community Health Volunteers, whose job (among other things) it was to teach women all about contraception and to sell them various pills and devices.
Background
The USAID Mikolo Project, which ran from August 2013 to July 2018, was a continuation of another project in Madagascar called SanteNet2. At the close of SanteNet2 in March of 2013, USAID noticed that its efforts to spread contraception through Community Health Volunteers was not achieving the level of independent sustainability it had hoped. In January of 2013, USAID conducted an “Assessment of Community Health Volunteer Program Functionality in Madagascar” wherein it sought “how to finance the CHV program to make it sustainable.” The report said:
Recommendations included determining how to finance the CHV program to make it sustainable. One representative called for a line item in the Government budget at decentralized levels to cover CHV services. Another said that some FP services were free at health centers but that CHVs had to ask for a fee to recoup the costs of medicines and supplies, though the service was free. This particularly applied with medications that were purchased through the community. Poverty in remote areas precluded asking for contributions from the communities.
Analamanga’s community representatives were concerned about stimulating and sustaining CHVs’ motivation. They acknowledged the efforts CHV had to make and cited a need for financial incentives. One representative explained that the work interfered with a CHV’s personal (especially marital) life, since many were approached at night, especially for MNCH emergencies. In one case, a CHV’s husband opposed his wife’s CHV activity due to the frequent disruptions. Financial incentives, e.g., compensation for travel expenses, could help retain CHVs. Providing resources to communities to organize incentives was suggested.
The answer to this problem of providing incentives for CHVs to continue their work in the community (and away from their homes and farm work) while making sure the project was self-sustaining (as in, not reliant upon outside funding) came in the form of Savings and Internal Lending Communities (SILC).
The most common financial incentives across all interviewed CHWs included per diem for attending trainings and meetings, user fees from the sale of medicines and commodities, performance-based financing (PBF) incentives, and referral payments for FP [family planning] services. Some CHWs were also involved in program-supported savings and internal lending communities (SILCs) and income generating activities, while others received free enrollement [sic] in community health insurance schemes.
The Problem
There are two basic elements to the project which must be understood in order to grasp the problem: Community Health Volunteers (CHV) and their role in promoting contraception; Savings and Internal Lending Communities (SILC) and their role in financing CHVs.
Community Health Volunteers and Contraception
The role of the Community Health Volunteers (CHVs) is very clear. They are to provide service delivery for various health-related issues in rural communities, including contraception. The Final Performance Evaluation of the Mikolo Project, which was published in Dec. of 2017, gives a concise explanation for the use of CHVs in the project:
Working in eight of Madagascar’s 22 regions, in 43 Districts, 506 communes and 3,557 fokontany (communities) over the past three years, the Project has re-established a strong community based service delivery mechanism through the strengthening of the quality of service delivery by more than 6,500 community health volunteers (CHV). By focusing on communities which are greater than five kilometers from a nearest health facility, the Mikolo Project is ensuring that the most underserved of Madagascar’s population are receiving quality integrated health services for women and children under five years old. CHVs are the community linchpin in ensuring a strong continuum of care by:
offering family planning services to women of reproductive age, including youth …
In the very first report for the Mikolo Project (1 August–30 September 2013) it was established that the promotion and distribution of contraception was a priority. The report identifies on page 7 what it referred to as sub-purpose 2 of the project, namely, “increase the number of CHVs, fortify linkages with providers of long-acting and permanent methods (LAPMs) of FP, and improve commodity security.” In other words, CHVs were to be used as mules for contraception throughout the community.
Further explaining sub-purpose 2, the report goes on to state that the project will be ensuring that the curricula for training CHVs includes instructions on how to inject hormonal contraception, Depo Provera.
What is clear from this information is that Catholic Relief Services would have known from the very beginning of this project that the spread of contraception was integral to its success. In fact, in the portion of this report which delineates CRS’s responsibilities regarding the establishment of microfinance institutions is a statement that CRS will not be asked to provide service delivery related to family planning and reproductive health:
CRS will not be asked to provide service delivery related to family planning and reproductive health. Specifically, it is expected that CRS will lead all activities related to microfinance. Drawing from international and Madagascar specific experiences, CRS will facilitate the establishment of commune-level COSAN Savings and Loans Funds (CSLF)/Village Saving and Loans Associations (VSLAs). CRS will establish partnerships with Microfinance Institutions and determine the demand for client centered loan products available through COSANs.
Volunteers also provide community-based family planning services. These services include counseling, pregnancy screening, method eligibility screening, and provision of short-acting contraceptive methods. CHVs inform and refer clients for long-acting and permanent methods available through mobile outreach and private and public service providers. CHVs socially market many of the products that they distribute; this modest income serves as a motivation for CHVs and sets Madagascar apart from other countries that pay direct stipends. CHVs also provide a link to youth peer educators in the community to reproductive and other health services.
Savings and Internal Lending Communities
As explained earlier, Catholic Relief Services’ role in the Mikolo Project was to “lead all activities related to microfinance.” In June of 2018, MSH (the lead on the Mikolo Project) published an article explaining how the SILCs work and the relationship between the SILCs established by CRS and the Community Health Volunteers. It is important to note that this is the first time that SILCs would be used to finance a health-related project.
In rural Madagascar, people have limited access to savings programs or credit. This impacts community health when people cannot afford to pay for health care. In partnership with Catholic Relief Services (CRS), the USAID Mikolo Project promoted the creation of savings and internal lending communities (SILCs) at the Fokontany (village) level to encourage individuals and families to regularly save income and to provide them with access to credit on favorable terms.
CRS first developed the SILC approach for general community development, and USAID Mikolo implemented it for the first time in the field of public health. SILC groups offer easy access to financial services for households and health care providers, especially women, as well as social capital. The main objective of SILCs is to provide funding, borrowing, and savings opportunities for community members.
SILCs are groups of 15-25 community members that meet on a weekly basis. Each member contributes money into the SILC fund. Members can borrow money at a fixed interest rate, e.g. to start up a small business. After a full cycle (9-12 months), the total savings accrued throughout the period are distributed to members based on how much each has saved, as a percentage of the overall savings.
This idea of SILC groups is not new to Madagascar; however, what makes the USAID Mikolo model unique is that the underlying premise is that rural development is inherently connected with health. USAID Mikolo-supported SILC groups enable members to both improve their livelihoods and lead healthy lives.
In fact, community health volunteers (CHVs) participate in the SILC groups not only as members, but also as health educators to improve quality of life by considering personal and family health. Life in a rural village is very difficult, and without financial stability simple healthy behaviors may seem out of reach for many families, such as purchasing needed medicines, soap, family planning methods, or healthy food. CHVs encourage these behaviors, and with the SILC program these and other health-promoting activities can become regular habits rather than unattainable conventions.
In short, CRS is responsible for creating local microfinance groups called SILCS, which in turn provide funding to CHVs, whose mission is to spread contraception to women in the village.
To put into perspective the effectiveness of CHVs in promoting and spreading contraception, this chart, which is on page 95 of the final evaluation we cited earlier, illustrates how “new users of family planning” was by far the most popular service provided.
Further Evidence in Video
Catholic Relief Services knew fully well that it was being used by USAID in order to create a financial engine for the spread of contraception through Community Health Volunteers. The project itself identified CRS as being responsible for all matters pertaining to microfinance, it showed how CHVs were being funded by these microfinance groups, and it showed how one of the primary missions of the CHV was to introduce and spread contraception. The very fact that CRS had a disclaimer indicating that it would not be directly responsible for the delivery of family planning is further indication that CRS knew exactly what this project was about.
But another and more direct piece of evidence comes from CRS itself.
On YouTube, USAID had uploaded a series of videos on the Mikolo Project intended to explain various aspects of the project itself. Several of these videos had closing credits showing that they were written, produced, and owned (copyrighted) by Catholic Relief Services itself.
The primary goal of the project is to increase the use of primary healthcare services to local community and the adoption of health enhancing behavior. The project relies on human capital to achieve this goal. The establishment of CSLF or Cosen Savings and Loans funds, which are savings groups of community health volunteers is one way to achieve this. The CSLF presents an opportunity for community health volunteers to have access to financial opportunities such as credit and savings. This practice also enables them to develop their social capital into the community health volunteer’s professional network.
While the narrator for the video is saying this, the B-roll footage shows a CHV entering a woman’s hut, where he pulls out a box of something from his backpack (image above). Blowing the picture up (left) reveals that the box being taken from the backpack is a box carrying the label “Confiance.”
A few seconds later, the contents of the box are set out on the table while the CHV examines the instructions on the back of the box. The contents included a small vial and a syringe (see the image below). According to a document produced by Family Planning Watch, a project of Population Services International, Confiance is an injectable contraceptive equivalent to Depo-Provera, produced by the Pfizer corporation.
This video, along with this report, was sent to Catholic Relief Services in September of 2018. After several months, Catholic Relief Services claimed that the video, which bears its closing credits and its copyright, was not its video and that a local production company mistakenly attached CRS’s credits and copyright to the end of the video. Not only is this explanation the same kind of thing CRS said about the government documents indicating that CRS was involved in the promotion of contraception in the SAIDIA Project, and the inventory reports showing that CRS had received and distributed 2.25 million units of contraception in Project AXxess, but since CRS was specifically identified as having been responsible for all of the matters pertaining to microfinances, there simply isn’t any other entity for whom this video would have been made.
After receiving CRS’s explanation that the video isn’t actually theirs, we have discovered that the original now has the ending credits and copyright attributed to CRS blurred out. However, the Lepanto Institute saved the video in case something like this should happen. You can see the original version with the closing credits at the link here.
Conclusion
There is absolutely no way of denying that Catholic Relief Services played a willing role in a project designed to spread contraception to poor people in rural Madagascar. The project identified the spread of contraception by Community Health Volunteers as a priority from the very beginning. The Community Health Volunteers were being funded by the microfinance communities called SILCs, and those communities were being established by Catholic Relief Services.
Another way of looking at this is that the CHVs are legalized drug-dealers (contraception instead of heroin), and CRS created the self-sustaining mechanism that would keep them funded.
CRS may claim that its role in the project was very small, but what it overlooks is that its small part was also one that was vital to the overall “success” of the project. The battery on a car is a very “small part,” but without one, a car won’t go anywhere.
But one more thing CRS has to atone for is the grave scandal it caused to the Malagasy people. On June 26, MSH and USAID Mikolo announced the role of the Mikolo Project in helping to draft Madagascar’s new law that allows universal access to contraception and enables CHVs to provide short-term contraception. While CRS may not have played a direct role in the drafting of this new law, because of its participation in a gravely and intrinsically immoral project, the name of the Church is now attached to this result.
Big families are not unusual in the Ukrainian village of Glynne. While the country’s population is falling, this highly religious community has more than 100 families with seven or more children. But one couple has gone further than most, recently welcoming their 19th child. Can they even remember all of those names? BBC Video by Roman Lebed
MICAIAH BILGER MAR 26, 2019 | 5:04PM WASHINGTON, DC
Popular Christian recording artist Matthew West released a new song Friday that focuses on the value of the “unplanned” baby in the womb.
His song, “Unplanned,” comes out in coordination with the release of the film by the same name, which follows the story of Planned Parenthood director-turned pro-life advocate Abby Johnson.
CBN News reports West wrote the song as the title track for the movie. His inspiration came from memories of hearing his own daughter’s heartbeat for the first time.
“I wrote this from the perspective of someone seeing their baby for the first time,” West said. “I tried to capture the feelings I had when I first heard my own daughter’s heartbeat; the overwhelming sense of life that is precious, a life that is a miracle, and a life that is a gift.”
West, whose music video is interspersed with clips from the film, said he hopes the song will move people.
“Oh I don’t believe in accidents/Miracles, they don’t just happen by chance,” West sings. “As long as my God holds the world in his hands/I know that there’s no such thing as unplanned.”
March 25, which is nine months before the celebration of the Birth of Christ, is the Annunciation, when Jesus was conceived within the body of the Virgin Mary as she accepted her call to be the Mother of God.
Priests for Life, along with many other pro-life groups, urges believers to celebrate this day as a Day of the Unborn Child, with special observances that highlight the Church’s pro-life teachings.
In 2019 take a journey through pregnancy from March 25th (Day of the Unborn Child) to Christmas Day, 2019 A coalition of national pro-life groups are urging people to observe March 25th as the “Day of the Unborn Child” (already celebrated in various countries), and then to journey through the nine months of pregnancy, until Christmas Day, with prayer, outreach, and education, so that people may learn about the development of the unborn child. For project details see www.BabyChris.org.
Fr. Frank
The Magisterium’s most comprehensive statement on the sanctity of life, the encyclical Evangelium Vitae, was issued on March 25, 1995, the Solemnity of the Annunciation. This feast marks the moment at which the Incarnation took place. At Mary’s “Fiat,” God began existing in a human nature – a human nature at the earliest stages of its development within Mary’s body.
“Mary’s consent at the Annunciation and her motherhood stand at the very beginning of the mystery of life which Christ came to bestow on humanity” (Evangelium Vitae, 102).
At a time when our society is beset with the evil of abortion, and when the human embryo is treated as a mere object for scientific research, Priests for Life believes that the celebration of the Feast of the Annunciation is more important than ever. By celebrating this Feast with special solemnity, and by spending more time meditating on its doctrinal and spiritual lessons, the faithful can be even more solidly rooted in their pro-life convictions, and spurred on to effective action in defense of life.
We pray that the pastors of the Church will lead their congregations in special pro-life observances on this Solemnity each year.
A special prayer that can be used as you observe this Feast:
Redeemer in the Womb
Lord Jesus Christ, we thank you that when Mary, your Mother, said “Yes” at the Annunciation, You took our human nature upon Yourself. You shared our life and death, our childhood and adulthood.
You also shared our time in the womb. While still God, while worshiped and adored by the angels, while Almighty and filling every part of the universe, You dwelt for nine months in the womb of Mary. You were our Redeemer in the womb, our God who was a preborn child.
Lord Jesus, we ask You to bless and protect the children who today are in their mothers’ womb. Save them from the danger of abortion.
Give their mothers the strength, like Mary, to say “Yes” to you. Give them grace to sacrifice themselves, in body and soul, for their children.
Help all people to recognize in the preborn child a brother, a sister, saved by You, our Redeemer in the womb, who live and reign forever and ever. Amen.
By Leticia Velasquez, Co-founder of KIDS (Keep Infants with Down Syndrome)
When abortion was unthinkable in the fifties, abortion activists had to find a chink in the armor of society’s love for the unborn child to justify abortion. They had to find the original hard case.
They looked to the children who were less loved than others, the children we abandoned at birth and sent to institutions, those with Down syndrome. After all, a mere 10 years earlier such people had been designated “life unworthy of life.” They were forced into institutions which, under the Nazi’s infamous T4 Program, operated as death camps where they were systematically chosen for death and killed by their doctors and nurses.
No longer executed yet considered ineducable in the sixties, mothers allowed doctors to convince them that it was “for the best” to institutionalize newborns with Down syndrome. Oftentimes a death certificate was issued so that the parents could cut ties with their child. See the film. ‘The Memory Keeper’s Daughter” for an idea of the mentality of that era.
It wasn’t until Geraldo Rivera’s expose documentary of the horrible conditions at Willowbrook that the public began to reconsider inviting individuals with Down syndrome into society. But tragically it was too late: a combination of scientific advances sealed the fate of generations of unborn babies with Down syndrome.
French physician Dr Jerome Lejeune discovered in 1958 that the cause of Down syndrome was an extra copy of the 21st chromosome. As his daughter Clara Lejeune Gaymard wrote in her memoir, Life is a Blessing,
“He might have called it Lejeune’s syndrome, like so many other diseases that bear the name of the one who discovered them. But what was important to him was restoring the dignity of those who are ill and their families. Trisomy 21 is a genetic accident, it is not contagious, and syphilis is not the cause of it. From now on people would not cross the street any more to avoid contaminations their future offspring when the afflicted child passed with its mother. From not on families would know if their child was ill, they were not at fault. The term mongolism called too much attention to the physical imperfection. Trisomy 21 would be from now on the name. . .” p16
Dr. Lejeune made it possible to identify a child with Down syndrome by their genetic karyotype, or unique genetic footprint. Around the same time, Dr. William Alfred Liley perfected the technique for prenatal diagnosis in New Zealand, hoping as Dr Lejeune did, to treat babies in utero. He had become famous for developing a treatment of inter-uterine blood transfusion for Rh-negative babies.
But these Catholic family men found their discoveries led to a reversal of their noble intentions. “Thanks to amniocentesis and karyotyping the technology was in place for eliminating “undesirable specimens” before birth. Their discoveries were diverted from their original objective.” (Life is a Blessing, p. 40)
In a desperate attempt to stop the militant march of abortion legalization, both Drs. Lejeune and Liley became leaders in the burgeoning pro-life movement in the 1960’s but the die had already been cast. Prenatal testing and abortion were possible. Elimination of the “unwanted” baby was possible. The abortion activists had the hard case they would use to pry open the door to unlimited abortion.
For years since the discovery that as women age, the likelihood of bearing a child with Down syndrome increases, doctors had been scaring women with that statistic. Some doctors considered age of the mother as a reason to abort in case they might be carrying a child with Down syndrome. Now, the certainty that a child with Down syndrome could be diagnosed in utero, prenatal testing was hailed as ‘life-saving.’
Its cost to the lives of unborn babies with Down syndrome was disregarded, the only babies worth saving were those deemed perfect. The doors to legal abortion were pried open for such tragic cases.
In the ensuing years the language has changed little. Abortion is touted as lifesaving even though thousands of babies are aborted every year and those with Down syndrome are aborted at a rate close to 90% after prenatal screening and diagnosis. New prenatal screening tests, such as Materni T21. boast of a 99% accuracy rate using only the mother’s blood in the 10th week of pregnancy increasing the “opportunity” to abort babies with Down syndrome.
Drs. Lejeune and Liley collaborated in trying to save babies who were being killed because of the tragic misuse of the discoveries they meant to save lives. Dr. Lejeune dedicated the rest of his career until his death in 1994, to finding a cure for Down syndrome.
He said, “I see only one way left to save them, and that is to cure them. The task is immense—but so is Hope.”
Editor’s note. Leticia Velasquez is the author of “A Special Mother is Born.”
BISMARCK, N.D. — There’s a scene in the middle of The Lord of the Rings, a fantasy series written by Catholic author J.R.R. Tolkien, where the quest to destroy an evil, all-powerful ring seems to be utterly hopeless. Darkness and danger have surrounded and hounded Frodo, the little hobbit ultimately given the mission to destroy the ring, ever since he set foot out of the Shire, the idyllic and safe home he left behind for this quest.
(The Daily Signal) The Cut recently ran a piece by Jen Gann, an outspoken, pro-choice mother who details her journey through in vitro fertilization (IVF) and genetic testing as she aims to conceive a healthy child. Her first pregnancy resulted in a son with cystic fibrosis, a life-threatening disease, and what she considers a missed opportunity to abort him.
In 2017, Gann filed a wrongful [birth] lawsuit against her doctors for inadequate genetic testing that she claims would have likely determined her son had cystic fibrosis and would have then provided her the option to abort him.
I responded to her lawsuit two years ago, because this story is very personal to me. Not only because I believe life is the most valuable gift generously bestowed upon mankind, but because I also have a child living with cystic fibrosis.
It pained me, again, to see Gann reiterate in print her desire to end her sick child’s life.
Sadly, we see this far too often. The left pushes a false narrative when it comes to human dignity. Masked in the so-called desire to prevent a sick child from suffering, pro-choice activists actually devalue the sickest among us. Their drive to abort unhealthy babies sends the message that those who live with a medical condition are somehow less than or an unwanted burden.
All human beings, regardless of disease, illness, ailments, and deformities, have the right to life. They too are fearfully and wonderfully made. Their value is in no way decreased because of their disease or any subsequent pain and suffering that disease brings.
Inaccurately, Gann’s piece focuses heavily on women’s empowerment and the amount of influence a woman holds in her ability to make a choice to end or continue a pregnancy.
The reality is that women don’t give life—God does. Yes, we have the biological ability to carry a child in the womb, provide it the nutrients needed to grow and the environment to thrive, as well as give birth. But we do not form a child in the womb, knit together its genetic makeup, or will it to live.
Furthermore, despite the feminist movement’s desire to vilify men, male DNA is also needed to produce a child. The fact that women carry a child does not make way for absolute female control.
I fully agree that women should be empowered, just like all humans should be encouraged and free to reach their upmost potential. But ending the life of another human is not empowerment—it is the highest form of oppression.
Terminating a child is devaluing its existence and saying it doesn’t share equal status with others who are currently living. No matter what reason is given for the abortion (choice, convenience, compassion, etc.), the act erases a human life and the lasting mark it would most certainly leave on others.
The abortion industry also claims to promote empowerment for women, but such “empowerment” is extremely exclusive, limited only to those women living outside the womb. The women growing in utero, on the other hand, are completely voiceless, powerless, and subjected only to the will of others, unable to defend themselves.
To no surprise, not once in the piece does Gann focus on the actual horrors of abortion, the pain it brings women and families, and the emotional toll it can take on a person. Instead, she glorifies it as a normal health care procedure and a thankful option she has if the “perfect” child isn’t conceived:
I had a child at home; if, when, this didn’t work, I would be fine. Besides, pre-implantation genetic testing isn’t perfect. If this embryo’s results were discovered to be inaccurate later on, I knew I’d terminate.
This rhetoric normalizes murder in an attempt to make others feel as though it’s natural and easy, when in reality that is not the case.
Our society has a major problem if we continue to sit by silently while abortion is used as a tool to erase the sickest and weakest among us. We must not follow the dark path of countries like Iceland and Demark, which have publically bragged about “eradicating” the Down syndrome gene through abortion.
Every single child, regardless of illness or disability, deserves access to the most basic and fundamental right of mankind, the right to life. And we should tirelessly fight to see that they do.
Editor’s Note: This article was originally published at The Daily Signal and is reprinted here with permission.
ROME, March 20, 2019 (LifeSiteNews) – Is it morally permissible to harvest the organs of a person in a coma declared “brain dead” by doctors? Why and when did organ transplantation first come about? And what is the Church’s teaching on using organs from a person deemed to be “brain dead”?
These questions and more are answered by Doyen Nguyen during an in-depth interview with the Italian magazine Radici Cristiane (read full interview below), where she blames a “consumerist culture” for causing many to accept the idea of “brain death,” a term she refers to as an incoherent, “medical fiction.”
Nguyen is a lay Dominican and professor at the Pontifical University of St. Thomas Aquinas (Angelicum) in Rome. She will be presenting on the topic of “brain death” at the A Medicolegal Construct: Scientific & Philosophical Evidence conference hosted by the John Paul II Academy for Human Life and the Family in Rome May 20-21.
Professor Josef Seifert, Bishop Athanasius Schneider, and Fr. Edmund Waldstein, among others, will present to the gathering as well, which will be held at the Hotel Massimo D’Azeglio. Click here to register.
In the far-reaching interview, Nguyen says that an Ad Hoc Harvard Committee in 1968 redefined the term “brain death” to mean someone in an irreversible coma. Nguyen says this was done in order to serve the interests of the organ transplantation industry and to avoid public outcry that would have viewed transplant surgeons as organ-stealing killers.
Nguyen refutes the invention of the term “brain death” to describe someone in an “irreversible coma” by arguing that the term “irreversible coma” itself “indicates that the patient is alive, for the simple reason that only a living person can become comatose or remain comatose. In other words, it would be an oxymoron to say that a corpse is in coma!”
When a doctor declares a comatose patient to be dead, that patient does not thereby become dead, she said.
Nguyen criticized John Paul II’s 2000 Address to the 18th International Congress of the Transplantation Society for its shortsightedness. Nguyen says John Paul’s remarks, which suggest “brain death” in certain cases “does not seem to conflict with the essential elements of a sound anthropology,” did not take into consideration all the literature available on the topic at the time. Nguyen says that the address should be “amended, or better yet, retracted.” Nguyen proceeds to explain how the Church should understand “brain death.”
***
Radici Cristiane’s full interview with Doyen Nguyen
Radici Cristiane (RC): There are people who think that “brain death” is a great deception. Do you agree?
Doyen Nguyen (Nguyen): Yes. “Brain death” has been a medical fiction from its very inception. The evidence for this can be found in the manuscript-drafts of the Ad Hoc Harvard Committee report which introduced “brain death” on August 5, 1968. The Committee, headed by its chairman, Dr. Beecher, worked swiftly on this report from March through June 25, 1968. In the first manuscript-draft, Beecher wrote:
The question before this committee cannot be simply to define brain death. This would not advance the cause of organ transplantation since it would not cope with the essential issue of when the surgical team is authorized—legally, morally, and medically—in removing a vital organ.
In the penultimate manuscript-draft on June 3, 1968, Beecher wrote:
With increased experience and knowledge and development in the field of transplantation, there is great need for the tissues and organs of the hopelessly comatose in order to restore to health those who are still salvageable. (1)
The language in the manuscript-drafts of the Harvard report is thus overtly explicit with regard to the connection between organ donation and the “birth” of “brain death.” In other words, the real reason why the Harvard Committee redefined irreversible coma as death (and gave it a new name, “brain death”) is for a two-fold purpose: (i) to have fresh, viable organs more readily available for the transplantation enterprise, and (ii) at the same time, to avoid any public outcry that transplant surgeons were organ-stealing killers.
In the final draft which became the Harvard report, the explicitly utilitarian language in the earlier drafts was toned down by Ebert (then the dean of the Harvard Medical School), in order to make it seem that transplantation was not the primary cause of the “birth” of “brain death.”
So, in a nutshell, “brain death” is a construct to serve the interest of organ transplantation.
RC: What is the scientific/medical evidence showing that “brain death” is not true human death?
Nguyen: Here I will answer you with a long quote taken from a peer-reviewed article written by Kompanje and De Groot. They are supporters of organ transplantation and therefore, of “brain death.” Yet, because of academic honesty, they have to admit that “brain death” is a construct for the purpose of organ transplantation. They wrote:
Suppose one of your loved ones is admitted to an ICU with a subarachnoid hemorrhage and you are sitting next to her bed, overwhelmed by emotions and holding her hand. She is deeply comatose, connected to a ventilator; intravenous vasopressors are needed to keep her blood pressure stable. You are hoping for the best, but fear the worst. And the worst comes. The intensivist tells you her brain is dead. Then he asks you for permission to take out her organs. You, and your loved one, had never thought about this scenario of dying. You had heard about brain death, but you don’t have a picture of it in your head. You ask the doctor: “when will she die”? He answers: “she is already dead.” You don’t believe him because there are so many signs of life. Her skin is warm, her heart is beating. […] Taking out her organs while her heart is still beating seems like a scene from a cheap horror film. […] We are, as most intensivists, greatly in favor of organ donation for transplantation. The whole concept of organ donation is founded on the concept that the potential organ donor is really dead at the moment that brain death is declared. This is pivotal in order to gain even remote public acceptance of organ donation. They have to be ensured that their loved one is dead before the organs are taken out. But, the bare fact that many brain-dead patients can continue to perform a variety of integrative functions over indefinite time periods, including maintaining body temperature, persistent and adequate hypothalamic hormonal function, regulating salt and water homoeostasis, digesting administered food, healing wounds, increase of infection markers and healing infections, stress responses to bodily interventions such as surgery and gestating fetuses in pregnant brain-dead women, makes some wonder whether a brain-dead patient is as ‘dead’ as the doctors say. Or they mistrust the statement that the patient has been pronounced ‘dead.’ For example, it is very difficult to see a ‘brain-dead’ pregnant woman, in whose womb a fetus grows over a time period for 2–3 months after the determination of brain death, as ‘a cadaver.’ There are just too many signs of life. Declaring these patients ‘dead’ solely on the basis of ‘a definition’ seems to contradict our common sense of what it is to be alive. Brain death is, since the first definitions in the scientific literature in 1968, closely related to organ donation. This is why, some scholars considers equating brain death to death as a moral and legal fiction. […] Without the needs of transplantation medicine, ‘brain death as death’ would not exist at all, but would be seen as […] irreversible […] coma (le coma dépassé). (2)
In fact, the above quote should remind us of the opening statement in the Harvard report which states: “Our primary purpose is to define irreversible coma as a new criterion for death.” Note however, the term “irreversible coma” itself indicates that the patient is alive, for the simple reason that only a living person can become comatose or remain comatose. In other words, it would be an oxymoron to say that a corpse is in coma!
Moreover, both life and death are realities the nature of which is mind-independent. The world is what it is regardless of what anyone says or thinks about it, and that world includes phenomena such as life, death, diseases, and all natural things from inorganic matter to human persons. Such natural entities are not open to revision or stipulation. In other words, death (understood as a biological phenomenon) is not the kind of thing that occurs by fiat like in the case of marriage. When a doctor declares a comatose patient (whose heart is beating, and whose skin is warm and pink) to be dead, that patient does not thereby become dead.
RC: A threefold question regarding John Paul II’s 2000 Address to the 18th International Congress of the Transplantation Society, the problem which this Address has caused, and what should the Catholic faithful do?
Nguyen: For a detailed answer to this question please read my article: Doyen Nguyen, “Pope John Paul II and the Neurological Standard for the Determination of Death: A Critical Analysis of His Address to the Transplantation Society,” Linacre Quarterly 84, no. 2 (2017): 155–186. A more expanded treatment of the topic can be found in my book: Doyen Nguyen, The New Definitions of Death for Organ Donation: A Multidisciplinary Analysis from the Perspective of Christian Ethics (Bern: Peter Lang, 2018) on pages 457-483.
In this interview, I can only give you a brief synoptic answer to this very complex question. The bulk of my answer is found in sections 3.2 and 3.3.
3.1 First point: About the hierarchy of the different types of Magisterial teaching
The ordinary teaching of the Church’s Magisterium includes several gradations, from the higher end (e.g., the teaching of an encyclical such as Veritatis Splendor) to the lower end which consist of interventions in the prudential order, in which some Magisterial documents might not be free from all deficiencies since they might not have taken into immediate consideration every aspect or the entire complexity of a particular issue (see Donum Veritatis, no. 24). In addition, the importance of a particular Church’s teaching can also be inferred from the insistence with which it has been repeated.
In this regard, John Paul II’s address to the Transplantation Society in 2000 belongs to the category of interventions of the prudential order. Moreover, the Pope’s statement (contained in that address) with regard to “brain death” has occurred once and only once in the whole of the teaching of the Magisterium. In particular, John Paul II did not even make a reference to that statement in his 2005 address to the participants of the conference “the Signs of Death” (February 2005) sponsored by the Pontifical Academy of Sciences.
3.2 Second point: John Paul II’s statement in his 2000 address
John Paul II’s statement in his 2000 address is as follows:
Vital organs which occur singly in the body can be removed only after death, that is from the body of someone who is certainly dead. […] The death of the person is a single event, consisting in the total disintegration of that unitary and integrated whole that is the personal self. It results from the separation of the life-principle (or soul) from the corporal reality of the person. […] For some time certain scientific approaches to ascertaining death have shifted the emphasis from the traditional cardio-respiratory signs to the so-called ‘neurological’ criterion. Specifically, this consists in establishing, according to clearly determined parameters commonly held by the international scientific community, the complete and irreversible cessation of all brain activity. […] It can be said that the criterion adopted in more recent times for ascertaining the fact of death, namely the complete and irreversible cessation of all brain activity, if rigorously applied, does not seem to conflict with the essential elements of a sound anthropology.
There are several key points in the Pope’s statement:
(a) Death is the separation of the soul from the body. In other words, the Pope’s teaching on death is grounded in Christian anthropology, according to which: (a) man is the substantial unity of body and soul and, (b) the soul is the life principle of the body. In medical/scientific terms, the separation of the soul from the body manifests itself as the loss of somatic integration, i.e., the process of corruption of the material constituents which once composed the living body.
(b) Vital organs can only be removed after death. In this regard, it is necessary to understand that because human beings belong to the same genus of warm blood mammals, the biological manifestations of the death phenomenon in a human being are no different from that observed in other mammals such as a pet dog or a pet cat – no heartbeat, no respiration, no movements, no responses to any stimulation. The temperature of the dead body quickly drops to the same level as the ambient temperature; and livor mortis and rigor mortis set in within a few hours.
(c) The Pope’s endorsement of the neurological criterion for the determination of death (i.e., “brain death”) is a conditional endorsement, clearly indicated by the conjunction “if” and the verb “does not seem.” According to the Pope’s statement, in order to be acceptable, the “brain death” criterion must fulfill three requirements:
(i) the loss of somatic integration, i.e., the physical evidence that the soul has left the body;
(ii) a consensus of the parameters that constitute the “brain death” criterion (i.e., in the Pope’s words: “clearly determined parameters commonly held by the international scientific community”). The parameters here refer to the clinical tests used for determining “brain death;” and
(iii) the rigorous application of these parameters.
3.3 Confronting John Paul II’s 2000 statement and the reality of “brain death”
3.3.1 Without going into details, suffice it to mention that even brain-death advocates have to acknowledge that there is no global consensus on the parameters of the “brain death” paradigm, but rather a confusion of practice. For instance, in a well-known study by Greer and colleagues, within the United States alone, there is wide variability in the practice and determination of “brain death” among the top 50 institutions for neurology and neurosurgery. The most worrisome aspect of this wide variability is the variability in apnea testing, recognized by Greer and colleagues as “an area with the greatest possibility for inaccuracies.” (3)
Moreover, the parameters can only be clearly determined if they have undergone rigorous validation prior to being introduced into clinical practice. Such a validation process was never done prior to the introduction of “brain death” by the Harvard Committee. No validation study has been performed since that time either.
3.3.2 Perhaps the most grievous aspect regarding John Paul II’s 2000 Address is the fact that it did not take into account the wealth of peer-reviewed literature, published prior to 2000, which clearly provided the evidence that “brain death” is not death. Examples of such literature include:
(i) Shewmon’s 1998 report of a series of chronic “brain death” survivors;
(ii) many reports since the 1980s on brain-dead pregnant mothers who, with aggressive life support, were able to carry their pregnancy until the time when their babies could be safely delivered by Cesarean section;
(iii) many critiques of “brain death” authored by scholars who supported organ transplantation, but who, in conformity to academic honesty and scientific realism, publicly acknowledged that “brain death is a social construct created for utilitarian purposes, primarily to permit organ transplantation.” (4)
(iv) The most important publication which the Pope’s 2000 Address should have known about and should have taken into account is the document of the Quality Standards Subcommittee of the American Academy of Neurology published in 1995 to provide the guidelines for determining “brain death.” According to the guidelines, the presence of – “spontaneous movements of the limbs and reflexes of the limbs (e.g., rapid flexion in arms, raising of all limbs off the bed, grasping movements, spontaneous jerking of one leg, etc.) as well as responses such as profuse sweating, blushing, tachycardia, and sudden increases in blood pressure” – is compatible with the diagnosis of brain death.” (5)
A review done by Saposnik in 2009 shows that up to 80% of brain-dead patients can manifest such movements. Although movements in any particular brain-dead patient may be very infrequent, they nevertheless occur.
Put simply, according to the guidelines for the determination of “brain death,” the brain-dead patient can be declared dead even though he or she may have movements from the arms and legs. The obvious question that any average person should ask is: how is it that a corpse can move? And the obvious question which every Christian should ask is: if the soul has left the body, then what is the principle which accounts for the spontaneous movements and reflexes of the arms and legs in the brain-dead patient? According to the sound tenets of the Church’s anthropology, the soul is the principle by which the body lives, and the principle of our nourishment, sensation, and local movement; and likewise of our understanding. (6)
There, without the soul, there can be no movements, no sweating, no blood flow, no heartbeat, etc.
In a nutshell, given that the brain death criterion admits the presence of spontaneous movements and reflexes, then in what way can it be claimed that “the complete and irreversible cessation of all brain activity, if rigorously applied, does not seem to conflict with the essential elements of a sound anthropology”? (7)
Such a statement can only reflect a gross oversight of the medical, scientific, and bioethical literature publicly available before 2000. For this very reason, such a statement needs to be seriously amended, or better yet, retracted – for the good of the Church and her children, the faithful.
Truth is the conformity of the mind to reality (veritas est adaequatio rei et intellectus). Given that (i) John Paul II’s 2000 address ranks at the lower end of ordinary Magisterial teaching (the kind which may contain inaccuracies), (ii) the teaching was mentioned once and only once in the entire Magisterial teaching of the Church, (iii) John Paul II himself did not even allude to it in his subsequent address in 2005, and (iv) the statement itself contradicts the medical reality of brain-dead patients, then indeed it cannot be said that the teaching in the 2000 address has any binding force on Catholic believers.
RC: About the interests and pressures on the Church and society in general, such “brain death” is universally accepted?
Nguyen: It should be evident to readers by now that “brain death” is a medico-legal fiction, a social construct for utilitarian purposes. It does not take much imagination to figure out that the transplantation enterprise is a multi-billion dollar (or Euro) business. Even the most staunched defender of “brain death,” Bernat, had to admit (albeit very reluctantly) that the concept of “brain death” is incoherent; but, according to him, in the real world of public law and policy, we must compromise so that death can be declared and organs procured. (8)
It is not correct to say that “brain death” is universally accepted. As Brugger points out, doubt about “brain death” has become an international consensus, in the sense that quite a number scholars in medicine, philosophy, and bioethics from countries worldwide have recognized that the “brain death” paradigm is unsound. (9)
It would be more correct to say that “brain death” has been universally imposed by legislation in different countries. The materialistic, utilitarian mindset of a consumerist culture has led to the so-called worldwide acceptance of “brain death.” It is part and parcel with the culture of death. Surprisingly, somehow this mentality has also penetrated into the Church, probably under the guise of charity and solidarity, especially since in the writings of John Paul II, organ donation has been exalted as a new way for man to make a sincere gift of himself and fulfill his constitutive calling to love and communion and, moreover, the gift of vital organs donated after death gives the donors the possibility to project beyond death their vocation to love. (10)
Certainly, as taught in the Catechism no. 2296, the Church encourages organ donation, because it is a noble act of charity and solidarity. But, it is not morally admissible to bring about the death of a human being, not even in order to delay the death of other persons. In a nutshell, it is not morally permissible to do evil to achieve a good. “Brain death” does exactly that: the deeply comatose patient (usually a young patient who has suffered a traumatic brain injury) is declared dead, so that his or her organs can be removed for transplantation purposes.
Notes:
(1) the drafts of the Harvard report are part of what is known as the “Beecher manuscripts,” preserved at the Francis Countway Library of Medicine at Harvard. They are not accessible to the public, they are made available only to some selected scholars.
(2) the quote is taken from: Erwin J.O. Kompanje and Yorik J. de Groot, Sounding board: is mandatory recovery of organs for transplantation acceptable? Intensive Care Medicine (2015) 41:1836–1837.
(3) data taken from David M. Greer, Panayiotis N. Varelas, Shamael Haque, Eelco F.M. Wijdicks, Variability of brain death determination guidelines in leading US neurologic institutions. Neurology 70, no. 4 (2008): 284–89]. Ironically, the apnea test is a cornerstone bedside clinical test for making the declaration of “brain death.”
(4) quoted from Robert Taylor, “Reexamining the Definition and Criteria of Death,” Seminars in Neurology 17, no. 3 (1997): 265.
(5) this quote is derived from Eelco F. M. Wijdicks, “Determining Brain Death in Adults,” Neurology 45, no. 5 (1995): 1007.
(6) see Thomas Aquinas, Summa Theologiae, I, q.76, a.1.
(7) this is the statement taken from the 2000 Address.
(8) see James L. Bernat, “The Whole-Brain Concept of Death Remains Optimum Public Policy,” Journal of Law, Medicine & Ethics 34, no. 1 (2006): 41
(9) see E. Christian Brugger, “Are Brain Dead Individuals Dead? Grounds for Reasonable Doubt,” Journal of Medicine and Philosophy 41, no. 3 (2016): 355
(10) see John Paul II, “To Participants of the First International Congress of the Society for Organ Sharing (20 June 1991)
March 18, 2019 (LifeSiteNews) – Did you know that having an abortion carries serious health risks? I found over the years of following the news on abortion that the health risks of getting an abortion are cast aside. Research shows that getting an abortion carries serious health complications.
You may wonder why the media and many health experts neglect to give this warning. Abortion clinics, which include Planned Parenthood, are in business to make a profit. Therefore, it is not in their best interest to provide information that may make the patient think about alternatives to abortion, such as adoption.
Putting the moral argument aside for now, there is growing evidence that shows that women who have abortions are at much higher risk to develop serious physical and emotional problems in the future.
Abortion breast cancer link
A meta-analysis was conducted of Chinese females between induced abortion (IA) and breast cancer risk. The conclusion?
“IA is significantly associated with an increased risk of breast cancer among Chinese females, and the risk of breast cancer increases as the number of IA increases. If IA were to be confirmed as a risk factor for breast cancer, high rates of IA in China may contribute to increasing breast cancer rates.”
In other words, the more abortions the women had, the higher their risk of breast cancer. This could possibly explain the US rates of breast cancer. 1 in 8 women will develop breast cancer in her lifetime. An estimated 1 in 4 women will have an abortion by age 45.
Emotional/spiritual toll
Many women who have had abortions resort to drugs and alcohol and even try to take their own lives. In one study, 49% of post-abortive women abused drugs and 39% started using or increasing their alcohol intake. About 14% admit that they have been addicted to drugs or alcohol. 60% suffered from suicidal tendencies and 28% in the study attempted suicide. Of those that attempted suicide, half continued attempted suicide two or more times.
Isolation is a side effect that occurs for a number of women who have had abortions. They keep their struggles and demons internal, pretending their life is normal and happy. They also could be completely out of touch with their feelings and only feel numb. The research shows that many women go through a 5 to 10 year period of denial where they will repress their emotions.
Studies have found within weeks following an abortion, 40 to 60% of women report negative outcomes. 2 months after, 55% felt guilty, 44% had nervous disorder reactions, 36% had sleep problems, 31% experienced regret, and 11% had been prescribed psychotropic drugs.
Women who have had abortions have a harder time connecting to their already born children or their future children. There is evidence that women can be violent against their own children as a result of having an abortion. One woman beat her 3-year-old to death after her abortion. Another woman jumped off a bridge with her two children, aged 2 and 5, a week after her second abortion, apparently in order to punish herself (the mother and 5-year-old survived). In both cases, experts concluded their behavior was in response to their abortions.
Possible side effects 2-4 weeks after an abortion according to American Pregnancyare abdominal pain and cramping, nausea, vomiting, diarrhea, and spotting and bleeding. More serious complications from an abortion include heavy or persistent bleeding, infection or sepsis, damage to the cervix, scarring of the uterine lining, perforation of the uterus, damage to other organs, and death – yes even death.
Approximately 3-5% of women who have had abortions suffer from sterility. If a woman has an STI at the time of the abortion, her risk is even greater. If a woman contracts an infection from an abortion, her risk of an ectopic pregnancy is 4 times greater. Cervical damage is another complication of abortion. Due to forced dilation of the cervix, the cervical muscles become microscopically torn nearly every time. Sometimes the dilation results in the uterine wall being severely ripped. Because of the weakening of the cervix, a woman who has had an abortion is more likely to suffer from a miscarriage or premature birth in future pregnancies.
Placenta previa risk
There is an increased chance of having placenta previa in future pregnancies if a woman is post-abortive. Placenta previa is a serious problem during pregnancy where the placenta covers some or all of the opening to the cervix.
Death
Tonya Reaves, Cree Erwin, Jennifer Morbelli, and Lakisha Wilson all died from complications of abortion. Here is a partial list of women who have also died from abortion. These women’s lives mattered and so did the lives of their babies. To say that abortion is a “safe” procedure because it is legal is not only incorrect but dangerous. The mainstream media makes women think that abortion is no more serious than going in to get their teeth cleaned at the dentist. Women have died. Some have had irreparable damage to their bodies. Lives have been changed forever.
Childhood leukemia risk
Having abortions could also harm your future children. According to a meta-analysis in 2014, there may be an increased risk for childhood leukemia if the mother had an abortion. The risks for childhood acute myeloid leukemia and acute lymphoblastic leukemia were strongly associated with maternal abortions.
Think twice
There are many grave health risks involved in having an abortion. It is not simply just a medical procedure. It is surgery in many cases with very serious health risks and complications. The mainstream media and abortion organizations are not upfront about this. They try to cover any health risks abortion poses because it would discourage women from seeking abortions if they told the truth.
Abortion also ends the life of the new human person developing inside your body. Abortion has health risks for the woman and is certainly never healthy, but deadly, for the fetus. It is my hope in writing this article that anyone considering an abortion will think twice and reflect on the potential health consequences.
If you have had an abortion or been affected by one, you should also know that there is healing through programs such as Rachel’s Vineyard and Silent No More. Countless people have attended retreats by these organizations and participated in their programs and have found true peace.
If you or someone you know are pregnant and need help, I have listed crisis pregnancy resources below.
There is also hope for abortion workers. Abby Johnson, former Planned Parenthood director, runs the organization And Then There Were None to provide financial and emotional support for abortion workers who are feeling trapped and wanting to leave.
Sarah Ruiz is a certified Integrative Nutrition Health Coach, Weston A. Price chapter leader for High Point, NC and is an active blogger through her website Health By Sarah.
A federal appeals court Tuesday upheld an Ohio law that strips Planned Parenthood of state funding, handing pro-lifers in the state a major victory three years after the law was passed.
Former Republican Gov. John Kasich signed the law, which prohibits money from the Department of Health going to organizations that perform or promote abortions. Planned Parenthood, the nation’s largest abortion provider, gets roughly $1.5 million from the department each year.
Judge Jeffrey Sutton, writing for the 11-6 majority, ruled that the law does not violate the U.S. Constitution because it does not prohibit women from obtaining abortions. The ruling overturned a lower court decision.
“Planned Parenthood must show that the Ohio law, if implemented, would impose an undue burden on a woman’s right to an abortion,” wrote Sutton, who was nominated by President George W. Bush. “Its vow to keep performing abortions sinks any pre-enforcement action, and any speculation about what would happen if it changed its mind is just that.”
Further, Sutton wrote, Ohio “may choose to subsidize what it wishes – whether abortion services or adoption services, whether stores that sell guns or stores that don’t,” as long as “the subsidy program does not otherwise violate a constitutional right of the regulated entity.”
“The Supreme Court has never identified a freestanding right to perform abortions,” Sutton wrote. “To the contrary, it has indicated that there is no such thing.”
Four of the 11 judges in the majority were nominated by President Trump, according to Politico.
Pro-life and religious liberty groups applauded the decision.
“Ohio Right to Life is absolutely thrilled that Planned Parenthood will not get any more of our state tax dollars,” said Michael Gonidakis, president of Ohio Right to Life. “Thanks to this very encouraging decision, Ohioans of conscience won’t have to worry about whether their tax dollars are going towards abortions.”
Mat Staver, founder and chairman of Liberty Counsel, agreed.
“We celebrate that the Sixth U.S. Circuit Court of Appeals has upheld the Ohio law that blocks nearly $1.5 million in taxpayer funding for Planned Parenthood,” Staver said. “Planned Parenthood does not have a constitutional right to receive taxpayer funds for abortions and the state of Ohio should withhold all public funding. Not one penny of taxpayer dollars should ever go to fund the killing of innocent children.
ROME, March 14, 2019 (LifeSiteNews) – The “sordid history” of vaccine production using aborted babies began with eugenicists like Planned Parenthood foundress Margaret Sanger and has become a billion-dollar industry that threatens parents’ rights and fills the pockets of pharmaceutical companies and abortion providers, a leading advocate for ethical vaccines has said.
Speaking to a packed hall in Rome on Wednesday, March 13, Debi Vinnedge of “Children of God for Life” revealed the “horrific history” of vaccine production using aborted fetuses, sought to separate myth from fact using documentation from scientists directly involved in vaccine research, and explained why aborted babies are still being used in vaccine production today.
LifeSite spoke with Debi Vinnedge ahead of her talk at the Rome conference. In our interview, Vinnedge briefly sketches out the “horrific history” of vaccine research using aborted fetuses, including the “barbaric” practice of ensuring babies were aborted alive so that their organs might be harvested without anesthetic.
Speaking to the legality of aborted fetal research, Vinnedge explains that it has been federally funded in the US since 1993, when President Clinton signed it into law after intense lobbying by the pharmaceutical industry.”
“There is a huge market worth billions of dollars due to the creation of patents, sale of the cell lines by companies that actually store and resell aborted fetal material,” Vinnedge said.
The founder of Children of Life for God pointed out that such research and vaccine production is filling the pockets of “universities, biotech companies, the pharmaceutical industry and of course, Planned Parenthood who was caught in an undercover sting discussing how they ensure obtaining intact organs for sale.”
“Even the medical profession and our Catholic Church” is unaware of the “horrific history of forced abortions involved in vaccine research and thousands more that led to the ultimate final production,” Vinnedge said.
“The truth needs to be made known about this sordid history and it is my goal to see that is done, and ultimately to put an end to this barbaric practice.”
Vinnedge explained further that a “major roadblock” to “making progress to stop this injustice” is “the tacit approval of using the aborted fetal vaccines when there is no alternative.”
In fact, as recently as 2017 the Pontifical Academy for Life — under the leadership of Archbishop Vincenzo Paglia — made a disturbing shift in support of aborted fetal vaccines, on the grounds that “in the past vaccines may have been prepared from cells from aborted human fetuses,” but today “the cell lines used are very distant from the original abortions.”
“Until our physicians and clergy leaders unite worldwide demanding the moral alternatives, the pharmaceutical industry is not going to change,” Vinnedge insists. “In fact, as history and the current trends are proving, it’s only going to get worse.”
Here below is LifeSite’s interview with Debi Vinnedge and a video of her presentation at the March 13 conference sponsored by Renovatio 21, under the theme: “Faith, Science and Conscience: using aborted fetuses for pharmaceutical production.”
LifeSiteNews (LSN): Debi, what personally led you to found ‘Children of God for Life’?
Debi Vinnedge (DB): I have always been pro-life but in 1999 when I read about proposed federal funding for embryonic stem cell research I was deeply disturbed. And I was even more upset to learn that none of my prolife friends had ever heard of this, nor did they even know what a stem cell was. Back then, there just wasn’t much information available and so, with the help of Richard Doerflinger who was then at the USCCB prolife office, and members of the Catholic Medical Association, I began to educate the public and massive protest campaigns began. When the Clinton administration tabled the idea a couple of months later, I was happy and thought my work was over. But within weeks I learned about the use of aborted fetal cells in vaccines and medicines and I knew God had a plan and my work was cut out for me. Children of God for Life was founded with the sole purpose of educating the public and putting an end to this gross exploitation of our unborn.
LSN: There is considerable debate surrounding vaccines. Some people are completely against vaccines, others are completely for them, while still others are somewhere in the middle. What is your general position on vaccines?
DB: I believe the decision about whether to vaccinate or not lies solely with the parents. Children are a gift from God to the parents. They are not owned by the State, nor should the State try to make their medical decisions. One thing I have learned over the past 20 years is that children are not like cattle. All children develop differently and have different needs. Without question, vaccines can and have caused serious adverse reactions and deaths as evidenced by our own government payout of nearly $4 billion to the families of vaccine damaged children. Certainly not all children have these reactions, but one cannot deny the fact that they exist. I find it utterly disgusting when parents are ridiculed and persecuted simply because they do not want to risk the vaccines — either for medical or moral reasons.
LSN: In your presentation, you discuss some of the history of experimentation with aborted fetuses, and how this led to using aborted fetal cell lines in vaccines. Can you share with our readers the main points of this history?
DB: This is probably one of the most shameful eras in the history of our country dating back over 100 years to a time when the eugenics movement became widespread under people like Harry Laughlin and Margaret Sanger. People with any type of handicap and unfortunately, women who were unwed mothers were deemed “feeble-minded” and “unfit to breed.” They force-sterilized these women and in many of these women, they also force-aborted their babies. At the same time, there was a worldwide polio epidemic and scientists began working on producing a polio vaccine. In the 1930s they openly admit to using these aborted fetuses in their polio vaccine research.
In one such science publication the researcher noted that “In many cases the (fetuses’) hearts were still beating at time of receipt in the polio research labs.” This is absolutely unconscionable! What they were trying to do is create what is known as a “cell line” for culturing the polio virus. To explain, viruses grow well on various types of tissues — both human and animal as well as other culture mediums. So in order to produce thousands of doses, scientists established cell lines taken from various tissues in several organs such as heart, thymus, retinal and lung. They culture the cells from the tissue in the labs and once there is a healthy stable growth, this is now a cell line that can be frozen and then reconstituted and used over and over in the future. But, just as all humans have finite lifespans, so do the normal human cells used in vaccines. Most of the vaccines today that use aborted fetal cell lines were derived from the aborted babies’ lung tissue.
LSN: How widespread is research on aborted fetuses today? And how are aborted fetal cell lines being used today? Are there particular vaccines that contain them? How can parents inform themselves about which vaccines are safe and ethical and which are not?
DB: Because of the finite lifespan of these cell lines which Leonard Hayflick discovered in his research on cell senescence, scientists have developed more and more aborted fetal cell lines to replace the current WI-38 (Wistar Institute, specimen number 38) and MRC-5 (Medical Research Council, specimen number 5) which were created over 50 years ago. The newest to be introduced by China is WALVAX 2 – from a 3 month gestation female baby lung tissue, the 9th abortion that was part of their research. It is intended to replace these two cell lines. In addition, there are several vaccines and medicines using other aborted fetal cell lines such as PER C6, HEK-293, IMR-90, IMR-91, WI-26 and lambda hE.1. But unless one reads the package insert or in some cases, the actual patents, they would have no way of knowing and doctors do not give that information prior to vaccination. Children of God for Life keeps an updated list on our website that can be viewed here— or from the home page click on the “Vaccine” tab, then “Vaccine Chart.”
LSN: Is the US government supporting it? And does US law require that parents be informed of what vaccines contain?
DB: Aborted fetal research has been federally funded in the US since 1993 when President Clinton signed it into law after intense lobbying by the pharmaceutical industry. And while right now, there is no legal obligation for physicians to advise parents, many prolife doctors do! In addition, there is legislation pending in at least one state – Illinois, HB0342 that would require vaccine recipients to be fully informed. See the proposed bill here.
LSN: Who is profiting from the use of aborted fetal cell lines in vaccines and more broadly by aborted fetal research?
DB: Universities, biotech companies, the pharmaceutical industry and of course, Planned Parenthood who was caught in an undercover sting discussing how they ensure obtaining intact organs for sale. And one university in Washington reported fulfilling over 4,400 fetal material requests in just one year! There is a huge market worth billions of dollars due to the creation of patents and sale of the cell lines by companies that actually store and resell aborted fetal material. A quick browse through companies such as Coriell Cell Repository and American Type Cell Culture provides the cell lines, the source, the gestation of the baby and more.
LSN: In your presentation, you talk about the need to separate myth from fact in the discussion on vaccines? What are the main myths out there? And what are the facts?
DB: Unfortunately, misinformation is widespread but here are the most common misconceptions and the actual facts:
MYTH: “The abortions were not done with intention of vaccines…”
FACT: Documentation from the researchers themselves clearly show their direct involvement and intent for over 100 years.
MYTH: “Descendant cells are not part of the original aborted fetus…”
FACT: The DNA is intact and identical to first cells harvested. If not, FDA and WHO would require a test each time cells were used. By its very definition, these are human diploid cells that contain the DNA from both parents – they do not morph into anything else over time.
MYTH: “It was only a couple of abortions from the past …”
FACT: Hundreds of abortions were performed before perfecting cell lines.
MYTH: “No further abortions are needed now or in the future…”
FACT: New aborted fetal cell lines — thousands of new abortions
LSN: What is the message you want people to take away from your presentation?
DB: There is a great deal of information in my presentation that even the medical profession and our Catholic Church is not aware of, especially regarding the horrific history of forced abortions involved in vaccine research and thousands more that led to the ultimate final production. It never ceases to amaze me when some of the myths I mentioned before have been taken as fact, especially the number of abortions and direct participation by the pharmaceutical industry in the research. To give you an example, years ago when we wrote to Merck to ask them to produce moral alternatives to the aborted fetal vaccines, they stated they had nothing to do with the original aborted fetal research. Yet in one of Leonard Hayflick’s published science papers in which he was describing his work with the aborted fetuses to produce a cell line, at the end he gives grateful acknowledgment to Dr. Anthony Girardi, Merck Research Institute for his help. The truth needs to be made known about this sordid history and it is my goal to see that is done, and ultimately to put an end to this barbaric practice.
LSN: What advice would you give new parents to help them navigate the issue of vaccines?
DB: Talk to their doctor about their concerns with the vaccines and the possible use of moral alternatives for at least some of the vaccines. For example, one of the first vaccines a baby will get is Pentacel which combines DTaP with Polio and HiB. That vaccine uses aborted fetal cells in the polio portion and there are moral options. Parents should ask their doctor for those alternatives and if he/she refuses to listen, find another doctor! Sometimes parents ask me if they should or should not use the vaccines if there is no moral option, but that is a question they need to take to God in prayer and then do whatever He puts in their heart.
LSN: Is there anything you wish to add?
DB: The tacit approval of using the aborted fetal vaccines when there is no alternative is a major roadblock to making any progress to stop this injustice. Until our physicians and clergy leaders unite worldwide demanding the moral alternatives, the pharmaceutical industry is not going to change. In fact, as history and the current trends are proving, it’s only going to get worse.
March 13, 2019 (American Thinker) — Back in college, I participated in one of those summer-long, Koch-funded libertarian internship programs. During the final week of the program, clusters of us interns, fresh off working in the “real world” for two total months, were tasked with arguing an esoteric philosophical point of our choosing.
One group of impish participants decided to argue against having children. The argument was fiendishly simple: the very act of existing invites pain, so it’s morally questionable to bring young ones into a world guaranteed to harm them. With toothy grins, wrinkled slacks, and tousled hair, these students made their nihilistic argument, finely exercising their ability to, as F. Scott Fitzgerald said, “hold two opposed ideas in the mind at the same time, and still retain the ability to function.”
At the time, the arguers didn’t believe their own position. The no-harm logic, while sound on the surface, meant human extinction when taken to its logical conclusion.
A mélange of college students hopped up on Leonard Read essays and overpriced beer understood the implications of eschewing childbirth. But what’s Democrats’ excuse?
It turns out my puckish colleagues may have been prophets for the most visible newcomer in America’s liberal party. Alexandria Ocasio-Cortez, the socialist and de facto Democratic leader, questions the wisdom of having kids. During an Instagram livestream, the 29-year-old congresswoman explains, in her termagant, ditzo manner, that Millennials like her don’t want to bring children into a world where China and India are pushing the global temperature a jot or tittle higher.
“There’s scientific consensus that the lives of children are going to be very difficult. And it does lead young people to have a legitimate question: Is it OK to still have children?” she asked her legions of followers from her kitchen, wearing a beige turtleneck sweater to warm her body against one of the coldest winters in years.
Rep. Ocasio-Cortez posits the same ethical challenge my fellow interns did years ago: is it morally kosher to have children if they will, someday, possibly suffer harm?
If you apply Ocasio-Cortez’s thinking to any time in human history absent the short time period of post-World War II to the present, it doesn’t stand up. Until the mid-twentieth century, many children had to contend with high infant mortality rates, slavery, sexual exploitation, hard labor, and a myriad of untreatable diseases like polio and hemophilia. What we think of as the relatively harmless lifestyle fit for children today — mandatory schooling through 18 years of age, widespread immunizations, Sesame Street — is so new to human existence that some grandparents alive today never experienced it.
You wouldn’t be reading this column in the year 2019 had earlier generations become conditioned to Ocasio-Cortez’s paralyzing fear. Yet the longue durée of human survival is increasingly forgotten by liberals who share a skeptical view of the future. A duo of fretting Cassandras recently appeared on a BBC program touting something called “Birthstrike,” a movement to withhold the gift of life in service to apocalyptic prediction.
“The natural world is collapsing around us, and that’s actually happening right now. And I’m so disappointed by the response by authorities to this crisis, and so freaked out by everything I’ve read that I’ve — I’ve basically last year I came to the decision that I couldn’t bring a child into that,” Blythe Pepino, founder of Birthstrike, explained to an audience currently experiencing a record-low birth rate. Her partner in petrification, Alice Brown, concurs, ratcheting up the fear a notch: “We are destroying biodiversity so quickly that it threatens our food … the U.N. have said that can lead to the risk of our own extinction.” Brown explains that her decision not to have children “has come from not wanting to pass that fear on to someone else.”
Petrifying everyone else with world-ending divinations is perfectly fine, apparently.
There’s a name for this swearing off procreation: anti-natalism. The philosophy — if self-imposed genocide can be called a philosophy — is, at its core, a deadening of everything it means to be human. It is both anti-life and misanthropic. “Homo sapiens is the most destructive species, and vast amounts of this destruction are wreaked on other humans,” writes anti-natalist philosopher David Benatar.
How Benatar maintains the will to live with such a bleak view of himself isn’t addressed. Like climate alarmists who pay thousands of dollars to travel around in carbon-emitting machines, Benatar doesn’t seem to take his own philosophy seriously.
The divide between anti-natalist liberals and conservatives is, as Russell Kirk said of all political problems, spiritual at heart. Conservatives view life as intrinsically valuable — that all children are formed in the image of a loving God. Even if a baby will one day grow to harm someone else, he is still not denied his inner worth.
Along with neoliberal types concerned that Africa’s high birth rate puts too much of a strain on economic resources, anti-natalists commit the dangerous fallacy of putting sublunary concerns above higher values. The road to despotism is paved with such intentions.
Editor’s note: The letter below was written by a Catholic father to his three children. He writes: “The letter is a sort of final testament of my witness to the Truth, that there will never exist any confusion among my own children about my actual beliefs and firm steadfastness in our shared Catholic Faith, and the mortal dangers that lurk everywhere in the current secular culture.” It is reprinted by permission of the author.
Well into the final third of this earthly life, I am focused on the ultimate goal, the saving of my soul and the souls of my children and grandchildren. Eyes on the Prize. When I asked Mom if this email was too much, she replied: “If their house was on fire, would we tell them? . . . and the spiritual threat to them is so much greater.” So here goes. Please forgive the length.
With the combination of aging, life experiences, the love of Mom, the Catholic Faith, and the grace of God, during the past two decades, I have gained wisdom and knowledge. As a parent who prays that you and your children reach heaven, I am compelled to share these insights with you.
Mom and I often reflect on the unbelievable changes in the culture that have occurred in our lifetime and the amazing speed in which these changes have occurred. Unlike the scientific and technological fields, where breakthroughs occur on a frequent basis and at a dizzying pace, during the past fifty years there have been no significant advances in understanding the Truth of the word of God. No Thomas Aquinas or Augustine has emerged to enlighten and elucidate our knowledge of moral law. Neither the Holy Bible nor Natural Law has changed. The Catholic catechism essentially remains the same. Yet the culture has truly undergone a revolution, a revolution fueled by many evil influences. If still alive, Grandma & Grandad and Grandpa & Grandma would have been abhorred by the radical changes in mores.
Compared to the generation in which I was raised, and even the one in which you were raised, these cultural changes have made the task of being a responsible parent an extremely difficult, nearly impossible, undertaking. Surrounded on all sides by this secular and permissive culture and with easy access to the internet, your children face imminent and immense spiritual dangers, literally unimaginable to our generations. Mortal danger lurks as close as their cellphone, or that of their friends’ cellphone or laptop.
In our midst evil hides in plain sight. Everywhere. Pornography, for example, is one of the most immediate and pressing threats to the souls of your children. Eleven is the average age children are exposed to the degrading, visually vivid, lurid, and addictive images of pornography. You must maintain constant vigilance to protect your children. Be proactive. Talk with them about good and evil. Pray daily. Dedicate time to pray the Rosary with your children. Ask the Blessed Mother for her intercession and assistance. Pray to cousin Gloria to beseech God and St. Michael the Archangel to guide and safeguard your family.
My dear children, please slowly read and thoughtfully ponder this letter. It describes changes in the culture, none positive, lies of the culture, and specific consequences of those lies. It includes comments on the orchestrated attack on free speech by the left via fear, shaming, and intimidation, both in the public arena and on the internet/social media, where your children will seek information and learn much about the world. Finally, it concludes with personal reflections on an appropriate response to such changes. Here are the unvarnished truths of our culture.
The Past 50 years: A Frontal Assault on our 4,000-year-old Judeo-Christian Culture
During the past 50 years, there has been a direct frontal assault on our 4,000-year-old Judeo-Christian Culture. The Church, the family, and marriage, cherished institutions foundational to our culture, have been viciously attacked by the progressive left, including much of the media and Hollywood. Contraception, abortion, casual sex, divorce, and most recently, gender fluidity, have been actively promoted as cultural advancements that should be heralded.
However, the product of these forces has been a cesspool of moral corruption with striking increases in adultery; homosexuality; premarital sex; out of wedlock pregnancy; abortion; confused, unwanted and unloved children; drug abuse; euthanasia; assisted suicide; and pornography. These cultural myths have been based on lies and deception, repeated so often that, sadly, many now accept them as true. Here are some of the more damaging lies.
The Big Lies of the Modern Secular Culture & Direct Consequences: Is Any of this Good?
The Biggest Lie: A baby in the womb is not a real person
Murder of 60 million infants by abortion in the United States alone
Legalization of the murder of infants born alive after an “unsuccessful” abortion & public celebration of passage of that law
The lie that some human beings lack God-given dignity and are no longer worthy of life
Promotion of Physician-Assisted Suicide & Euthanasia
Murder of 5,000 black Americans each year, 90-95% by other black males (of that total, less than 100 unarmed blacks killed by police)
The lies that human beings must act on their sexual urges and that the previously esteemed virtue of chastity, as well as many other virtues, are no longer relevant to modern man
The lie that sexual intercourse is merely a casual recreational behavior between consenting individuals for selfish pleasure, rather than a sacred and beautiful procreational and unifying act of unselfish, unconditional love between a married man and woman
The lie that marriage is not exclusively the union between one man and one woman
The lies that marriage is not a permanent moral contract, that no-fault divorce is painless, and that children, irrespective of age, are not significantly and permanently harmed by divorce
The lie that children do not need both a mother and a father
Rampant STD’s in teenagers and young adults (“steep sustained increases”)
“A record 918 neonates in the US infected by their mothers with syphilis in 2017”
Increased number of divorces
Explosion in single-parent families & the directly related increase in poverty
Increased sexual abuse of women
Increased sexual abuse of children
Increased number of children/teenagers both exposed to and addicted to pornography
650,000 deaths from AIDS in the US alone; about 40,000 new infections of HIV annually
The incredibly personally destructive lie that gender is not biologically determined
The promotion of transgenderism and resulting confusion in many children & parents
The increase in both attempted and completed suicide by teenagers
The lie that diversity, rather than greatness or excellence, is an important stand-alone goal
Classification of individuals by skin color and/or sexual orientation, rather than by content of character, is a nightmarish version of Martin Luther King’s “I Have a Dream” speech
The lie that socialism, rather than capitalism, is the better system to create wealth, raise the standard of living for everyone, decrease poverty, and protect and promote individual & religious freedom
The lie that past injustices against one’s ancestors, the resulting victimhood, and systemic racism are the major determining factors in one’s individual success or failure, rather than the love and encouragement of parents, personal responsibility, God-given talent, and hard work
The lie that work is demeaning and it is merciful and charitable for the government to subsidize individuals unwilling but physically and mentally able to work
Legacy of welfare & victimhood passed from one generation to the next
Promotion of envy and jealousy between lower and higher economic classes and of racial animosity among minorities directed toward successful white individuals
The lie that homosexual activity and the tolerance of that sexual behavior by the hierarchy is not a fundamental factor in the sexual abuse crisis in the Catholic Church
Failure of the hierarchy to effectively confront the sexual abuse crisis among the clergy
Childhood innocence destroyed and lives irreparably damaged and lost
Hate Speech. The Progressive Left’s Orwellian Definition
Differing opinions, previously considered a normal and essential part of civil discourse, now are framed as hate speech. To avoid hurting someone’s feelings, free speech is scorned in favor of the “correct” opinion, increasingly dictated by the progressive left. Opposition is silenced by fear, intimidation, and even violence. Virtue signaling abounds. Noise, rather than logical reasoning, fills the void. Only one side is heard. Knowledge and truth are the casualties.
“Hate Speech” is defined by the progressive left as any opinion that differs from their own. If you disagree and have the courage to voice another opinion, you are targeted by social media and labeled a racist, bigot, homophobe, misogynist, prejudiced, hateful and/or just simply stupid or ignorant. Even wearing the wrong hat makes one a target. No one is immune from this type of irrational, personal attack. You or your children could be the next target. The left is unsparing and relentless as it advances a progressive, often non-Christian agenda.
The Frontal Assault on the First Amendment to our Constitution
Examples in which the progressive left, in an attempt to intimidate, responds with name calling and insults rather than engages in an honest and respectful dialogue include:
Marriage is the union of one man & one woman = Homophobe
Life begins at conception = Misogynist; Sexist
Sexual Behavior & Natural Law = Homophobe
Immigration & Respect for the Law = Racist; Fearful of Latinos / Hispanics / People of color
Man Made Climate Change = Science Denier
Right to own guns = Pro Violence
Pro Police = Racist; Fascist
Pro Capitalism = Hater of the poor / minorities
Pro Trump / MAGA Cap = Racist; Misogynist; Homophobe: Hater; Bigot; Fascist; Nazi; Stalinist
What can you do in a “World Gone Wrong”?
Jesus asks each of us: “But who do you say I am?” What is your answer? Study the tenets of your Catholic religion in the catechism, read the Holy Bible, and pray. Fully embrace and practice your Catholic Faith, a precious gift God has bestowed upon you. Pass that precious gift unto your children. But it will not be easy. Pray daily to God for wisdom and courage.
Do not be distracted or discouraged by the moral failures and abominations of far too many priests and leaders in the Church’s hierarchy. They represent human and institutional weaknesses and failures. Their individual sins, no matter how inexcusable and horrific, neither diminish nor alter the Truths of our Catholic Faith. Remain steadfast in that Faith.
You have a unique opportunity to swim against this rising tide of moral corruption and cultural decline and lead a singular life of heroic virtue. One person can and does make a difference. Be that one person. Ignite a counterrevolution in your own family and social circles. Forsake the false idols and myths of our modern secular culture. Be an authentic warrior for Christ.
Speak fearlessly and with moral clarity, in a loving and merciful voice, to your children. Teach your children to love the sinner but hate the sin. Reconsider the values of our traditional cultural and moral norms as you educate and guide your children to heaven in a secular culture that threatens their very salvation. Lies and deceit are everywhere. Confusion reigns. Satan is active. Your children desperately need your active guidance. You are their sole moral compass.
As you already do in your personal and professional lives, strive for greatness in your spiritual lives. Pray the Rosary. Live like a Saint. It is what God is calling you to do. For your own sake, and that of your loving spouse and beautiful children, answer that call with a resounding yes!
You are always in our prayers. I believe in you. I love you, Dad
When I first became a registered nurse in 1969, ICUs (intensive care units) were still new. The first one I worked was set up in the former visitors’ lounge and we learned how to read EKGs (heart tracings) by using a book.
By the early 1970s, I worked in a surgical/trauma ICU where we used sophisticated ventilators like the MA-1. We were able to get almost all our patients off ventilators by weaning, the process of gradually lowering ventilator support until the patient can breathe on his or her own.
But in 1976, I was shocked by the Karen Quinlan case that changed everything.
Karen was a 21 year old woman who suffered brain damage after apparently taking drugs at a party. She was hospitalized and placed on a ventilator. When she was thought to be in a “persistent vegetative state”, her adoptive parents asked that her ventilator be removed. The doctors disagreed and they case eventually went to the New Jersey Supreme court that allowed the removal of the ventilator on the grounds of an individual’s right to privacy. Shortly afterward, California passed the first “living will” to refuse “life support” if or when the signer is incapacitated.
Ironically, Karen lived 10 more years because, as some ethicists criticized, she was weaned off the ventilator instead of just abruptly stopping the ventilator.
My experience with ventilators became personal in 1983 when my baby daughter Karen died on a ventilator before she could get open-heart surgery. Unfortunately, one young doctor earlier offered to take her off the ventilator to “get this over with”. I reported him to the chief of cardiology who was furious with the young doctor.
In the 1990s, I returned to working in an ICU and was shocked by the development of the “terminal wean” for some patients on ventilators. Often the families were told that there was no hope of a “meaningful” life. The terminal wean involved abruptly disconnecting the ventilator and “allowing” the patient to die. I brought up at least trying regular, gradual weaning and oxygen as we did for the other patients on ventilators but I was ignored.
After I retired from bedside nursing, I was asked to be with an elderly man on a ventilator who had had a massive stroke and the family was told that he would never have any quality of life and would die soon anyway. I tried to bring up weaning but some members of the family were adamant.
When the ventilator was stopped. I held the man’s hand and prayed while he gasped for air and turned blue. I asked the nurse to at least giving him oxygen for comfort but she ignored me. Instead, she gave frequent doses of morphine intravenously until the man’s heart finally stopped after 20 minutes.
I am still haunted by this man’s death.
INFORMED CONSENT?
The medical definition of informed consentrequires understanding “the purpose, benefits, and potential risks of a medical or surgical intervention…”.
But most people seem to have a vague understanding of ventilators when they sign a “living will” or other advance directives and thus have very little information about this often life-saving medical intervention.
As a nurse, I found that most people-especially the elderly-tend to automatically check off ventilators without understanding that a sudden problem with breathing can come from a number of treatable conditions that don’t require long-term use of a ventilator such as asthma, drug overdoses, pneumonia and some brain injuries.
In some circumstances such as certain spinal cord injuries and late-stage neurodegenerative diseases like amyotrophic lateral sclerosis, the ventilator is necessary long-term to live. But even then, people like Christopher Reeve and Stephen Hawking have used portable ventilators to continue with their lives. Some people with disabilities use small ventilators only at night.
It is important to know that ventilators move air in and out of the lungs but do not cause respiration-the exchange of oxygen and carbon dioxide that occurs in lungs and body tissues. Respiration can occur only when the body’s respiratory and circulatory systems are otherwise intact. A ventilator cannot keep a corpse alive.
It’s also important to know that not all machines that assist breathing require the insertion of a tube into the windpipe. Non-invasive positive-pressure ventilation like the BiPap successfully used for my elderly friend Melissa allowed her to use a face mask to assist her breathing until antibiotics cured her pneumonia.
WEANING FROM A VENTILATOR
Many patients are easy to wean from a ventilator but some patients are more difficult.
Years ago, I cared for an elderly woman with Alzheimer’s who needed a ventilator when she developed pneumonia. She had made her son and daughter her medical decision makers in her advance directive.
However, the doctors found it very difficult to try to wean the ventilator after the woman improved. They spoke to the family about removing the ventilator and letting her die. The daughter agreed but the son was adamantly against this.
The woman was totally awake after the sedation to keep her comfortable on the ventilator was stopped. She was cooperative and made no effort to pull out the tube in her windpipe. She just smiled when asked if she wanted the ventilator stopped.
Having known of some great respiratory therapists in the past who were able to successfully wean difficult patients from ventilators, I suggested that she be transferred. She was transferred and a week later we were told that she was successfully weaned from her ventilator.
About a year later, I encountered the woman again when she was recuperating after a routine surgery. Although her Alzheimer’s disease was unchanged, she was doing well in an assisted living residence.
CONCLUSION
As a student nurse, I was as initially intimidated by ventilators as anyone else. But as I learned how to use them and saw the constant improvements not only in the technology but also in our care of patients on ventilators, I came to see ventilators as a great blessing when needed.
And while we are never required to accept treatment that is medically futile or excessively burdensome to us, sometimes this can be hard to determine-especially in a crisis situation. Most of my patients on ventilators recovered but some could not be saved. We were surprised and humbled when some patients with a poor prognosis recovered while others who seemed to have a better chance died unexpectedly. There are no guarantees in life or death.
That is why my husband and I wrote our advance directives that designate each other as our decision maker with the right to have all current options, risk and benefits of treatment fully explained.
We don’t want an advance directive that could be hazardous to our health!
I’m Michael Voris coming to you from the annual Bringing America Back to Life Symposium in Cleveland, Ohio.
Each year in the second weekend of March, organizers bring in speakers from all over the country and the world to talk about the growing threat to human life and dignity in areas of culture, science, politics and governments.
We at Church Militant pay special attention, as you know, to the threat to not just temporal human life, but also — most importantly — spiritual life.
It’s why we have and continue to concentrate so many of our resources toward unearthing the rot in the Church, and doing this every day, we can tell you the rot and betrayal of the truth goes a lot deeper than almost anyone realizes and happens in a million different ways.
We often talk about things on a macro level — the big picture — but we sometimes talk about things on a micro level, specific examples, and show how each of them relates, or feeds back into the big picture.
Today, a micro example, from the diocese of Lansing, Michigan and the bishop there Earl Boyea. Back in 2014, a sexual assault victim informed Boyea of an assault perpetrated against him by a priest who had gained some notoriety on Ave Maria Radio out of Ann Arbor.
The priest is Fr. Pat Egan and his show on Ave Maria was entitled Fully Alive. Egan is a priest of the archdiocese of Westminster, London, England. He has been in the U.S. for a number of years now. When the victim reported the assault to Boyea in 2014, Boyea did nothing of relevance.
He told the victim, an adult male, who had also been an adult at the time of the assault, that since Egan was not a Lansing priest, he couldn’t do anything, like remove his faculties. However, four years later in 2018, once word got out about Egan, Boyea did then remove his faculties.
In a very untransparent press release, Boyea kept most of what he knew close to his vest, revealing only the barest minimum he could get away with. The relevant part read that Egan “has had his priestly faculties removed due to a credible allegation of inappropriate sexual behavior with an adult male.”
What it does not say, which is what the point is:
One, the assault happened four years earlier.
Two, Boyea knew about it back then.
And three, it was not just “sexual behavior” — it was an assault, a homopredator clerical assault. Those missing details are important because of the implication attached.
Why would Boyea conceal that it was an actual assault — he kept that hidden. Why? Why did Boyea keep hidden that the assault happened four years earlier? Why would Boyea not acknowledge that he had personal knowledge of this four years earlier?
Reading the press statement, it could be easily interpreted to mean that Boyea just became aware of a consensual homosexual relationship involving a priest, and the moment he discovered it, being the strong bishop he is, he immediately stepped in and fixed the matter.
Nothing could be further from the truth. Boyea concealed — deliberately — the most relevant facts to cover for his own inaction.
Egan had an earlier charge against him that Boyea knew about as well. In that case, the diocesan review board, Boyea says, determined that the earlier accusation was not credible.
Again, in a case of covering up and making misleading statements, Boyea failed to acknowledge that on the diocesan review board was none other than Fr. Egan’s religious superior who went to bat for him and got the charge deemed not credible. But Boyea never revealed that little piece of info, either.
This is a small example of why growing numbers of Catholics — increasing every day — are looking at their bishops and saying they simply cannot be trusted — period.
If they aren’t out-and-out lying — like Cardinals Wuerl and Cupich and Tobin and Farrell — then they are parsing their words and publishing deliberately ambiguous statements with the intent to mislead. All the bowing at the altar of transparency and offering incense to the gods of accountability is pure bunk.
It is no longer a case of the credibility of these men being destroyed, but the truth of the Faith. The Church Herself is being damaged by these scoundrels who treat the Church as their own private company, pretending to care about the faithful all the while holding them in contempt.
Church Militant was given an audio recording made at a public gathering where Boyea was confronted about his wrongdoing, and the sarcasm and contempt in his answers is palpable — no remorse, nothing, just sarcasm and lashing out in almost accusatory tones.
These men live in a surreal world where no one is allowed to question them, and they rarely if ever suffer the consequences of their actions — only in the most heinous of cases.
Brother bishops defend them in a kind of suicide pact mentality, ensuring that if one goes down, many others would follow, so they enjoy a kind of mutually assured destruction, careful to keep as much under wraps as possible.
Well, here’s a thought for the bishop and others to chew on. The original assault happened in 2014 — a sexual assault — that’s a crime. The statute of limitations has not run out on that crime.
Boyea knew about the crime and did not report it, quite possibly making him an accessory after the fact, because he knowingly protected a criminal or someone he should have had reason to believe was a criminal.
Likewise, because the 2014 crime was related to the earlier crime, and Boyea knew that the decision of that diocesan board may have been rigged, his knowledge could very well open that case up again.
This is all stuff, of course, for lawyers to look at, and Church Militant has information that the Michigan state attorney general is indeed looking at this case. A few years ago, a bishop in Kansas City, Bp. Finn, was removed for failing to report a case of sexual assault involving a minor male.
In 2014, Bp. Boyea failed to report a case of sexual assault involving an adult male. The statute of limitations had run out on the Kansas case. It has not run out on the Lansing case.
So the obvious question is: Why is Boyea still bishop of Lansing? And, are criminal charges possibly awaiting him?
Is it not OK to sexually assault a child; but it is apparently acceptable for a priest to sexually assault a male adult. The entire mindset of the U.S. bishops has to change, and it has to change now — no more secrets, no more deflections, no more arrogance.
There has been a paradigm shift that has occurred and is occurring in the battle to end abortion. I would summarize the focus of this shift to be about three primary aspect. First, we have begun speaking the blunt and hard truths of what abortion is. Instead of speaking of it as a healthcare issue or with euphemisms, we have begun to expose this murder for what it is in all its graphic and barbaric forms. We have used graphic images and videos of abortion. We have called it murder. We have refused to talk about it as healthcare.
Two, we have refused to compromise with the slaughter of children. There can be no compromise in any way with the intentional murder of children. There are no exceptions. This means that groups that pass bills compromising on the issue are being exposed as compromisers and are called to do what is right. We do not support exceptions for rape, incest, or health issues. Abortion is murder, period. We don’t support measures that regulate abortion or say its ok to murder your baby if the abortion doctor can’t find a heartbeat that they really won’t be looking to find.
Thirdly, we are acknowledge that there is no such thing as neutrality. You will either submit to and obey God or you will rebel against him. The Supreme Court is not neutral nor are they God. The paradigm shift is pushing the “prolife” movement to acknowledge that either Christ is our God or the Supreme Court is our God. These three things, no neutrality, no compromise, and no flinching from the truth, are enabling those who battle this evil to do so with the power of God through faithfulness to him. This is having no small effect. There are and have been many haters and many difficult battles to make this shift but God is working and will be glorified. We are seeing because of this shift a change in the conversation nationwide even among those who are still operating under the old paradigm shift. Even those who are pro-abortion are having to acknowledge that this shift is happening.
This same paradigm shift must occur in the church’s battle with sexual immorality and the protection of the family. We must realize that there is no such thing as neutrality. The LGTB alphabet soup mafia does not believe in neutrality on this issue. They want to eradicate any and all opposition to their views. They readily acknowledge that they want to indoctrinate children and are doing so in the public library, public schools, and entertainment media. We in the church must recognize that there is no neutral ground on this issue. You will either celebrate this evil or you will hate it. You will either bow to the Supreme Court on this issue or you will obey God. We cannot give pretense to neutrality. We must call men to repentance and faith in Christ on this issue.
Secondly, we must recognize that compromise is unfaithfulness to our Lord. Where we compromise on sexual immorality in our personal lives, families, or churches, we are being unfaithful to God and will find ourselves losing this battle. Compromise on this issue starts with compromising on the distinction between male and female. It starts with women usurping authority and men shirking authority. It starts with failing to raise our boys to be boys and our girls to be girls. We teach our daughters to find their identities in their careers instead of preparing them to be the kind of young women Titus 2 says they should be. We are compromising by ordaining women in the church or having them be the primary leaders of worship.
Compromise happens when we fail to see how seriously the bible takes sexuality. In the very first chapter of the Bible we learn that God made male and female. All throughout scripture, we find that God takes sexual immorality very seriously. Things like adultery, incest, sodomy, and bestiality are considered crimes in the bible and God destroys nations for tolerating them. But we compromise by failing to take things like modesty, chaste speech, and what we entertain ourselves with seriously. We compromise by our pretense to neutrality. We do this by adopting a live and let live mentality. We say “what you do in your own bedroom is none of my business. Who am I to judge?” But this filth is not staying in the bedroom and those who practice it are all too ready to judge. We will either judge rightly or be judged.
Thirdly, and perhaps the hardest for us to to today, is that we are going to have to speak about this with the same blunt and forcefulness as we speak about abortion as murder. Those supporting sexual immorality have spent years working to change the paradigm on the issue. They have couched it all in terms of relationships and love. In turn, many in the church have been put on the back foot. We have started speaking about sodomy as something that just isn’t best for human flourishing. I guess you could say that when God reigned down fire from the sky on Sodom that humans were not flourishing too well that day. But we have began to soften the biblical and historical Christian witness against the sins. We have seen this in terms of relationship instead of abomination.
We have also embraced the terminology of sexual orientation. Many talk about same-sex attraction as if it is some neutral thing. This terminology of sexual orientation is a useful tool for those pushing this sexual immorality. To give one example, it has been used to try and distinguish between men who sleep with men and men who sleep with boys. That is they have tried to argue that no gay man abuses boys. The truth is that every time a man sexually abuses a boy, he is committing a same-sex sex act. That is homosexuality at work. But we have been taught that we can never make this connection.
The use of orientation language is often used to position those who commit sexual immorality as victims. They are victims of something they never chose. It is all God’s fault they are “gay”. The hard truth is that these men and women who give into to sexual temptation are morally culpable. They are not perpetual victims. Even if some of these people have been victims of sexual abuse, they are responsible for how they respond to that abuse. The “LGBT” movement has been good at painting themselves as victims in order to garner sympathy and support for their position.
The sexually immoral have managed to pull the wool over the eyes of the culture and of the church. Our work is going to be the hard and difficult task of pulling that wool off and exposing this evil for what it truly is. The bible commands us to expose the unfruitful deeds of darkness. We are going to have to get over our addiction to being liked and being nice and speak the blunt truths of sexual immorality. We are going to have to work to restore the shame to this evil. We need to speak the hard truths of scripture and call these sins what they are, abomination, perversions, attacks on nature and nature’s God, filthy and disgusting sin worthy of death. We are going to have to expose the truth about the connection between sodomy and child abuse. We are going to have expose how sodomy destroys men’s bodies, minds, and souls.
Why must we do this?
1. We love God. And we want to be faithful to his word and his created order.
2. We love the church. We don’t want to see the church compromise and be stained with impurity. We don’t want it to lose its saltiness. Nor do we want to see future generations of the church facing the consequences of our inaction.
3. We love our children. We do not want to see them assaulted with lies and sexual perversion. We don’t want to see them fall into the destructive patterns of these sins. Nor do we want them to be a part of a nation that experiences the full wrath of God.
4. We love our country. God has placed us here and we are to be salt and light to it. We want to see it fall on its knees before Christ and honor him in the culture and the laws it enacts. We also don’t want to see it continued to be destroyed. We don’t want to see God wipe it from the earth as he has done with other nations that have followed this path.
5. We love those who are caught in these sins. We love those who practice these sins that destroy their minds, bodies, and souls and therefore we warn them truthfully, without compromise, and without neutrality. For their sake we cannot pretend there is some neutral ground where God is not to be obeyed, where Christ is not king. We cannot pretend as if the gospel cannot save them if they will humble themselves. For their sake we don’t compromise letting them continue in their pride. For their sake we speak the hard blunt truths that put the shame on what they are doing so that they may be humbled by the demands of God’s law and look to the only hope of forgiveness, Jesus Christ.
It is love that demands we refuse neutrality, refuse compromise, and refuse to speak soft words of peace when there is no peace. Love demands that we have nothing to do with the unfruitful works of darkness, but instead expose them. Church its time for a paradigm shift.
A preborn baby in the womb is no different from a baby on the outside; one is just as precious and worthy of love and protection as the other. This is the message conveyed by the by the #MeStillMe hashtag that has recently gained traction on social media.
It all started when Nichole Rowley and her husband Tyler gave birth to their baby, Fulton, in August. They received a congratulatory note from the governor of their home state of Rhode Island, but the well-wishes made Nichole feel uneasy. That’s because Rhode Island is poised to pass an extreme abortion bill on par with, and in fact more extreme than, New York’s. Despite the fact that 74% of Rhode Islanders oppose unrestricted abortion up until birth, Governor Raimondo has promised to sign it into law. “The card expressed the joy of having children, but the sentiment didn’t make sense coming from Governor Raimondo,” said Rowley to NBC 10 News. “If children are such a special gift, as the card claims, why does she offer those children no rights before they are born?”
To combat the dehumanization that helps many like Raimondo feel comfortable with taking away the lives of preborn babies, Nichole combined the powerful tools of social media and ultrasound imaging: “We combat the lie of dehumanization by showing a side-by-side photo of the child in the womb (Me) and outside the womb (…Still Me), clearly presenting the continuum of human life from the womb to the crib.”
We’re voters, and we’re watching! @CharleneLimaRI 74% of Rhode Islanders oppose abortion right until the moment of birth. VOTE NO ON H5125 Sub A. #MeStillMe#SaveTheBabies
Nichole sent the card back to the governor, along with her #MeStillMe images of her oldest son and newest baby. She later created a Facebook page and a Twitter account to spread the hashtag. Pro-lifers from about half a dozen other states have shared the hashtag, and two pro-life Catholic media outlets, EWTN and Relevant Radio, have shared with millions of followers. Many have taken up the hashtag to share photos of their own babies, both born and preborn.
Nichole said she has been overwhelmed by the outpouring of support after creating the hashtag. She told the National Catholic Register, “I have been so moved by the people who have reached out to me personally. Women have told me incredible stories. They tell me I encourage them but it’s really their incredible stories of choosing life in this culture of death that is encouraging. Their kindness and thankfulness gives me the confidence to keep fighting.”
Growing numbers of Americans are looking with horror at what has become of our Church and country. Moral confusion and indifference to human life is common. Legal boundaries continue to be stretched to favor abortion, same-sex marriage and pornography without limits. Finally, the Church seems to be rotting from within from a massive problem of homosexuality among the clergy, including bishops and cardinals, as reports surface of a number of homosexual bishops preying on seminarians.
But we must take heart. Societies have broken down before and caused great human misery — but help did come. In times past, Our Lord sent His Blessed Mother to rescue His people in the midst of similar evil and suffering.
In fact, our times bear similarities to the Mexico of 500 years ago, a time when human life was also vulnerable to the powers of the state. In that case, it was the Aztec rulers who were brutally sacrificing hundreds of thousands of human beings on pagan altars. Then, in 1531, God sent Mary to a humble peasant, Juan Diego, and through this now canonized saint offered to an entire country the Christian message of peace and hope. In just 20 short years, nine million Aztec pagans were converted to Christianity by people’s obedience to the message of Our Lady of Guadalupe.
In that famous and beloved apparition, Mary appeared as Our Lady of Guadalupe, also known as Our Lady of the Americas, to signify her motherly care over all the countries of the western hemisphere.
Five centuries later, many people believe that Our Lady appeared again under a similar title, Our Lady of America, to signify her care over our specific country, the United States of America.
This series of apparitions began in 1956 in Indiana and continued over three decades into the 1980s. They earned the approval of the local bishops. However, today, few Americans are aware of these appearances of Mary, who identified herself under a new title Our Lady of America. Perhaps people believe that they can solve today’s problems without extraordinary help from God.
In any case, when Mary began appearing to a quiet nun in Indiana, religious devotion was common in the U.S., and the legal system largely respected faith institutions and their constitutionally protected role under the First Amendment. But a troubled future was rapidly approaching — if we only knew. Today, we appreciate the prophetic quality of her message, as Mary reached out like a good mother with warnings for our country’s future, warnings which clearly fit our confused and troubled 21st century.
Our Lady’s appearances were made to Sister Mildred (Mary Ephrem) Neuzil (1916-2000) while she was living in Rome City, Indiana and later, in Fostoria, Ohio. Our Lady told Sister Mildred that troubling times were ahead, specifically for the United States of America. Yet Mary also held out encouragement and hope — that, yes, America can be reformed and many lives will be saved if people will turn to God and turn away from sin, especially sins of sexual impurity.
You may well be asking: since there have been so many bogus and unconfirmed apparitions — why believe in this one?
Most important of all, this apparition earned the support and approval of Paul F. Leibold auxiliary bishop of Cincinnati, who gave the imprimatur to the messages of Our Lady of America first in 1960 and later in 1971 when he was Archbishop of Cincinnati. As Archbishop of Cincinnati he also commissioned a statue and a devotional medal. In 2007 Archbishop Leibold’s action received the support and encouragement of Cardinal Raymond Burke, at the time Archbishop of St. Louis. In a letter to the National Conference of Catholic Bishops dated May 31, 2007 he wrote this about devotion to Our Lady of America:
What can be concluded canonically is that the devotion was both approved by Archbishop Leibold and, what is more, actively promoted by him. In addition, over the years, other bishops have approved the devotion and have participated in public devotion to the Mother of God under the title of Our Lady of America (italics added).
At the United States Bishop’s Conference on Nov.15, 2006 Archbishop Burke publicly displayed and blessed a new statue of Our Lady of America.
Today, there are those who point out that the apparition of Our Lady of America had not reached the final stages of official Church approval before the death of Archbishop Leibold in 1972. This caution certainly cannot be criticized. No Catholic is forced to believe in apparitions (even those with full approval) and it is fully understandable that many Catholics will not listen to any Marian message until the Pope has given full “canonical approval.”
Still, if one weighs the credibility of these purported apparitions to Sr. Mildred, a number of things stand out. First, Sr. Mildred never sought publicity (hunger for the limelight is a discrediting sign). Second, she submitted Our Lady’s messages to her Episcopal superiors and was obedient to their direction. Third, the message itself was granted an imprimatur of a bishop of the Church and was accepted by other bishops. Finally, there is the fact that the message is so clearly in accordance with Holy Scripture, and that it carries a prophetic warning for our times. For all these reasons, isn’t it more prudent to believe the message, especially when these predictions have already begun to come true?
Why should the messages of Our Lady of America be taken seriously?
Overall, Our Lady of America’s message was twofold. It contained an encouragement of faith but also a warning of terrible times ahead if there was not widespread repentance.
First, Mary revealed to Sister Mildred that this country could be a great source for spreading the true faith across the world. Our Lady said: “I desire, through my children of America, to further the cause of faith and purity among peoples and nations.”
At the time, her directive seemed most appropriate, because the United States was experiencing a time of both world tension combined with a deep spiritual devotion to Mary. Yes, the threat of nuclear war with the Soviet Union was intense, but faith was intense also, as Catholics were inspired and directed to bombard Heaven with prayer from their homes and parishes. Every Mass concluded with prayers “for the conversion of Russia.” In 1950 the pope had declared the doctrine of the Assumption, and the acknowledgment of Our Lady’s special role in salvation unleashed a huge wave of devotion in the United States, both among Catholics and secular society. Archbishop Fulton Sheen became one of the country’s first “network TV stars,” and he dedicated much of his ministry to Mary and wrote many books about her. Father Patrick Peyton launched the Family Rosary Crusade and filled stadiums across the U.S. for his Rosary rallies. He was flanked in many of his public appearances by Hollywood stars that were proud to be identified as Catholics. Pastors nationwide encouraged their parishioners to pray the Rosary every night.
Also, during this time, the American bishops reinforced their proclamation of the Blessed Virgin Mary, conceived without sin, as Patroness of the United States. This was first proclaimed at the Council of Baltimore in 1846. The bishops capped this directive by completing and opening the National Shrine of the Immaculate Conception in Washington D.C.
On September 25, 1956, Sr. Mildred recorded this message from Our Lady: “I am pleased, my child, with the love and honor my children in America give me.” Then Our Lady promised to reward their love by working “miracles of grace among them.”
But she immediately added: “I do not promise miracles of the body but of the soul.”
In other words, Mary’s mission was not to work physical healings and to make people happy in this life. By promising miracles of the soul —instead of the body — it’s clear that Our Lady’s primary goal is to help people change morally so they will be saved.
As at Guadalupe, she showed herself as a most tender mother and invited each of us to turn to her for help.
And, as at Lourdes, Our Lady of America proclaimed one of the great mysteries of our faith, that she is the Immaculate Conception. In fact, Mary, under the title of Our Lady of America, gave her specific approval of the Cathedral of the Immaculate Conception, telling Sr. Mildred, “This is my shrine, my daughter. Tell my children I thank them.” Our Lady encouraged the shrine as a pilgrimage site and promised, “It will be a place of wonders.”
And, as at Fatima in 1917, she asked Americans to reform their lives, especially in matters of purity and chastity, before it was too late and our nation succumbed to terrible sufferings.
Priests were called to a special role. Mary said American priests should submit to penance and self denial and in this way lead the renewal of the Church in America.
The second part of her message was just as crucial, but more ominous. In subsequent apparitions, Mary’s messages became more somber and urgent. “I come to you, children of America, as a last resort . . . Be my army of chaste soldiers ready to fight to death to preserve the purity of your souls.”
Our Lady added: “Make the Rosary a family prayer …. Those found in the circle of my Rosary will never be lost.”
Our Lady also spoke sternly about the future of the United States and the world. She spoke specifically about “my children in America.” “Unless they do penance by mortification and self-denial and reform their lives, God will visit them with ‘punishments as yet unknown.’”
But what could she be talking about?
What Should We Make of the “Punishments”?
Any Christian would be unsettled to hear of “punishments as yet unknown.” But what punishments did Mary come to save America from?
If we stop to think about it, the answer clearly involves major trends we know too well: We live in a time of homes without fathers, and sexual relationships without marriages. Deep moral confusion which has destroyed the peace of families and the justice of many of our nation’s laws. Every day we hear of new acts of violence. Sexual depravity has become “mainstream.” Women and children are the special targets of predators. And though the “Cold War” has ended, we have entered a new era of war waged by terrorists.
So, it isn’t as if we aren’t already experienced the punishments warned of by the Blessed Mother. Besides the historic changes of legal abortion and same sex marriage (two groundbreaking legal precedents which people in the 1950s couldn’t have imagined), we also have the rise of religious persecution in our own country (Remember the government’s legal threat against the Little Sisters of The Poor.)
Today, in both Mexico and the U.S., murder routinely begins in the womb and ends in the street. Are we really surprised? After all, just as love and life are mysteriously related, so is hatred and death. When the U.S. Supreme Court opened the door to legal abortions in 1973, in effect, it swung open the door to a world of hatred and death. Recall that, when Mother Teresa of Calcutta received the Nobel Peace Prize on Dec. 11, 1979 in Oslo, Norway, she declared: “if a mother can kill her own child, what is left for me to kill you and you to kill me? There is nothing between.”
But there is one more type of “punishments as yet unknown” which Our Lady of America says will happen if Americans do not reform their lives: War. Yes, we already experience war in distant countries, but now the reality has come to our own cities. We used to worry about terrorism from the Mideast, and nuclear threats from rogue nations like North Korea. Now we have to worry about bloodbaths in our own hometowns, like San Bernardino, California!
By comparison, the memory of the Cold War arms race between the U.S. and the Soviet Union almost looks like peacetime. Clearly, our civilization is sinking into depths that, to anyone granted a glimpse of the future in the 1950s, would have seemed like a nightmare.
How Mary’s heart must be breaking for us.
A final plea to the United States
Take these troubling examples all together and it’s no great stretch to realize we face a world that is growing just as dangerous, brutal and unforgiving as the ancient Aztec culture of 500 years ago. But again, Our Lady has stepped forward to help. Like a good mother, she comes not just to warn us, but to show us the way out of our difficulties.
First, however, Mary issued an apparent “final” warning and correction for her children and this country. She told Sr. Mildred: “Unless the United States accepts and carries out faithfully the mandate given to it by Heaven to lead the world to peace, there will come upon it and all nations a great havoc of war and incredible suffering.”
She also added a consoling message: If Americans make a concerted and prayerful effort to reject the secular and evil trends consuming the country, the U.S. can escape the worst of the “incredible suffering” about to fall on the world. Mary also told Sr. Mildred that even if America “fails in the pursuit of peace because the rest of the world will not accept or cooperate, then the United States will not be burdened with the punishment about to fall.”
This stern, but absolutely crucial, part of Our Lady of America’s message occurred in the 1980s, which has caused some skeptics to discount it (or even shrug off the entire series of apparitions.) By then, Archbishop Leibold had died and so the later messages were not afforded the same Episcopal scrutiny as those 20 years earlier. Let me repeat: The Church never compels anyone to believe in an apparition. But in the case of these credible apparitions of Mary, as Our Lady of America, to Sr. Mildred, and the fact that so many of Mary’s warnings have come true, isn’t it more prudent to believe, than not to believe?
Our Lady, ever the good mother, didn’t conclude her visits on a note of despair. She announced through Sr. Mildred that God was giving America a special gift — one which she herself relied on in this world — the protection of St. Joseph.
Mary said: “My holy spouse has an important part to play in bringing peace to the world.”
That’s right — the apparition of Our Lady of America has a special role for St Joseph. This great saint, mostly silent throughout history, but so powerful, also appeared to Sr. Mildred. On March 18, 1958, St. Joseph told her that “Fatherhood is from God and it must take once again its rightful place among men.” For this to be done fathers must have the moral strength and courage to enter into only holy marriages and accept the responsibility of remaining with their families and training their children especially in Christian doctrine.
If fathers turn to St. Joseph by praying to him and imitating his virtues, like honesty and chastity, they will receive the moral strength and courage to be good fathers. St. Joseph told Sr. Mildred that “Through me the Heavenly Father has blessed all fatherhood, and through me He continues and will continue to do so till the end of time.”
All in all, there are many reasons to have hope. In the years since Our Lady of America’s stern but supportive apparitions, John Paul II issued his prophetic words that a “springtime in the Church” is underway. Today, we have proof that spring is upon us. The number of young practicing Christians in the United States is growing, if still numerically small. But their faith is pure and very courageous — in other words, they are fit for battle. As it says in 1 Maccabees 3:19: “victory in war does not depend on the size of the army but on the strength that comes from Heaven.”
The role of young people in renewing the Church and society is part of the message given to Sr. Mildred. She stated: “Our Lady made it known to me that she is particularly interested in the youth of our nation. It is they who are to be the leaders of this movement of renewal on the face of the earth. Their ranks will be swelled by youths of other nations whom Our Lady also calls to help in the accomplishment of this great renewal.”
So, while the message of Our Lady of America is pointed and troubling, it is also worthy of a mother who greatly loves her wayward children: To save ourselves from disaster here and in eternity, all we have to do is All we have to do is try.
How do you get your tubes untied with Medicaid? How do you get your private insurance plan or company to pay for tubal ligation reversal surgery?
Surprisingly, the answer to both of these questions is the same – it will be very hard.
Here is the bottom line. Both Medicaid and private insurance plans may pay when there is a covered medical reason for each possible step: upfront testing, the procedure itself, and any post-operative issues.
In addition, supplemental policies and state-based infertility mandates open the door for alternative approaches. These avenues could be a more affordable way to restore your fertility and have another baby – or two.
Get Your Tubes Untied With Medicaid
How do you get your tubes untied with Medicaid? Medicaid is a public health insurance plan for low-income families, women, and children. The federal government provides much of the funding, and each state administers the programs and set rules for eligibility and coverage.
In general, Medicaid will not pay for tubal reversal surgery in any state unless you can cite a medically necessary reason. Therefore, getting your tubes untied with Medicaid may mean finding alternatives.
Covered Medical Reasons
Medicaid and other private insurance plans may pay for three types of covered medical reasons relating to your pending tubal reversal procedure. Each phase or category must be medically necessary. Medically necessary means that procedure prevents, diagnoses, or treats an injury, disease, or symptoms.
Pre-Surgery Testing
You may be able to get your Medicaid or private insurance plan to cover certain tubal reversal pre-surgery testing steps. Ask your clinic to code the test for a medically necessary reason.
Pre-operative bloodwork to spot infections (STD, HIV, or Hepatitis)
Ultrasound and exam to visualize the health of reproductive organs
Surgical Procedure
It is unlikely that your Medicaid or private insurance plan will cover the tubal reversal surgery itself as it corrects earlier voluntary sterilization. The purpose is rarely a covered medical reason – unless the procedure corrects an underlying disease or symptom.
Post Tubal Ligation Syndrome (PTLS) is the rapid decline of estrogen/progesterone hormone levels caused by damaged blood supplies to the ovaries
Dysmenorrhea is pain and cramping during your menstrual cycle
Also, related services rendered while under the knife might be covered. For example, removal of uterine fibroids and polyps could be medically necessary and needed to restore fertility.
Post-Operative
It is more likely that your Medical or private insurance policy will cover any complications arising from your tubal reversal operation. The surgery is very safe. However, things can go wrong and these complications are often covered medical reasons.
Bleeding
Infection
Damage to nearby organs
Reactions to anesthesia
Get Private Insurance To Pay for Tubal Reversal
How do you get your health insurance plan to pay for tubal ligation reversal surgery? Follow the same logic as for Medicaid plans – specify the medically necessary portions of the procedure (upfront testing, PTLS or Dysmenorrhea, post-operative complications).
However, health insurance plans issued in the private marketplace offer two possible opportunities to make having a baby again more affordable.
Supplemental policies cover the expected outcome
Infertility mandates may cover other treatment options
Supplemental Insurance
Supplemental health insurance covers tubal reversal outcomes – not the surgical procedure itself. Remember, the purpose of this procedure is to restore your fertility and have another baby.
Therefore, you may need to take unpaid maternity leave and find yourself with leftover hospital bills after your labor and delivery.
A baby girl in England is doing well inside her mother’s womb after doctors performed an innovative new procedure to fix a hole in her spine.
The baby’s mother, Bethan Simpson, of Burnham, Essex, chose to undergo the surgery in December instead of aborting her unborn baby, as doctors suggested, Yahoo News reports.
“We were offered continuing pregnancy, ending pregnancy or a new option called fetal surgery – fixing her before she is born. We had to do it. Our lives were such a rollercoaster for the next few weeks,” Simpson wrote on Facebook.
She and her husband, Kieron, learned that there was something wrong with their unborn daughter during a 20-week pregnancy scan. Doctors later diagnosed her with spina bifida, according to the report.
Simpson told the BBC that she refused to consider an abortion because she “couldn’t justify terminating a child I could feel kicking.”
In December, they became the fourth mother-child pair to undergo fetal surgery to repair spina bifida in the UK, the report states. Doctors from University College Hospital and Great Ormond Street Hospital in London removed the baby girl from her mother’s womb at 24 weeks of pregnancy and repaired a hole in her spinal cord, according to the report. Then, they placed her back in the womb.
“I came out of surgery at one o’clock and could feel her moving that evening,” Simpson said. “It was reassuring to feel that first kick after the anaesthetic wore off.”
Simpson said the lesion on her daughter’s spine was small, and doctors deemed the surgery a success. While she is sore and fragile, she said the risks were worth it to give her daughter a better life.
Other babies are not so fortunate. About 80 percent of unborn babies diagnosed with spina bifida are aborted, according to the BBC. Even though fetal surgery is becoming more widely available and more successful, many mothers still choose abortion.
Medical professionals warn parents that the surgery is risky and it does not cure spina bifida. However, fetal surgery can greatly lessen the severity of the disease. In 2003, the National Institute of Health’s Management of Myelomeningocele Study (MOMS) found that closing the spinal defect in utero reduced the need for shunts after birth and boosted the child’s chances of walking independently. Doctors think fetal surgery also may reduce the odds of learning disabilities.
With a growing number of success stories to point to, Simpson urged parents to choose life for babies with spina bifida.
“There are unknowns – it’s major surgery, and the biggest decision you’ll make in your life,” she said. “But remember most children born with spina bifida today are walking and reaching normal milestones.
“Yes, there are risks of things going wrong but please think more about spina bifida, it’s not what it used to be,” she continued. “I feel our baby kick me day in and day out, that’s never changed. She’s extra special, she’s part of history and our daughter has shown just how much she deserves this life.”
An abortion pill study which seeks to provide the deadly drugs to women who are not even pregnant yet has begun in California. The “experimental” study, published at the FDA’s Clinical Trials website for participants who are “not currently pregnant and not desiring to be pregnant in the next year,” appears to be in its beginning stages. It will be conducted under the direction of abortionist Daniel Grossman by the University of California, San Francisco (UCSF) and is expected to be completed in April of 2020. Study participants will receive:
Currently, under the FDA’s REMS system, the pill (Mifeprex) is only permitted to be “dispensed in clinics, medical offices, and hospitals by or under the supervision of a certified healthcare provider,” which have the ability to (1) date pregnancies accurately and to diagnose ectopic pregnancies, and (2) provide any necessary surgical intervention, or have made arrangements for others to provide for such care.
However, this abortion study’s participants will not be examined for pregnancy, but will receive a mere “over the phone” consultation, with pregnancy to be estimated based on the date of the last recalled menstrual period.
What could possibly go wrong? Well, a lot, actually.
Abortion drug study for non pregnant women Daniel Grossman
In this model, patients at risk of unintended pregnancy and with a desire to avoid pregnancy will be assessed by a clinician and provided counseling on pregnancy recognition and testing, as well as how to administer MAB at home. For this pilot study, only patients who have previously had a MAB will be included, since this population has reported the highest interest in the model, and they are also already familiar with how to use the medications.
But in this trial, abortion inducing pills will be given to women before becoming pregnant:
The clinician will provide Mifeprex® and misoprostol to the patient at the time of counseling in case the patient becomes pregnant and wants to terminate the pregnancy using the medications up to 10 weeks gestation. Patients will contact a study clinician for an over-the-phone assessment of eligibility for MAB, including assessment of gestational age, before self-administration of Mifeprex® and misoprostol, and then attend a follow-up visit with the clinician.
Despite the potentially risky possibility of miscalculating the pregnancy and then taking the pills past the gestational limit of 10 weeks — or an ectopic pregnancy, which often requires ultrasound to determine — the posted “secondary outcome” states, “Gestational age will be calculated by last menstrual period during the over-the-phone clinical evaluation with a study clinician. Ultrasound data will be analyzed if obtained.”
“Participants will be given clear instructions on study participation and returning unused medicationsin an appropriate time frame,” the study claims.
Daniel Grossman ( Image credit: University of Texas at Austin)
If the name ‘Daniel Grossman’ sounds familiar, it might be because he has been leading the push for so-called “self-managed” abortion. He has sponsored another study which involves pharmacy dispensing of the abortion pills.
Grossman has a previous association with manufacturer of the abortion pill, DANCO, and is deeply entrenched in the abortion industry. Grossman:
served as a liaison member of the PPFA National Medical Committee.
served as consultant in 2016 to Planned Parenthood Federation of America to provide input on medical abortion using telemedicine.
In addition to Grossman, study contacts include Katherine Ehrenreich, Project Manager at UCSFs’ Bixby Center for Global Reproductive Health – ANSIRH (Bixby trains abortion providers), and Rana Barar, Senior Project Director for the Alternative Provision of Medication Abortion Program at ANSIRH.
Barar has written casually about her own abortion, one that she claims she does not regret. “I was 40 years old, my family was complete, and my husband and I made the decision easily and without angst,” she said.
I told my son, who was 13 at the time, that I was having an abortion a few days before the procedure. I explained to him that contraception can fail and even someone who knows a lot about reproduction can get pregnant unexpectedly. I told him that while I was sure I would grow to love a new baby just as much as I loved him and his sister, I also feared I would resent the havoc it would wreak on all our lives, and the attention it would take away from them. He wanted to know if I would be OK, if it would hurt.
I waited to tell my daughter, who was 9 at the time, until my story was going to be on the local radio. Neither of my kids ask about it now, but if they did, I would tell them that the decision I made was the right one for me and our family. I would tell them that mostly, I don’t think about that pregnancy as a baby, but sometimes I do. I would tell them that mostly when I do think of the baby that could have been, I do so with dread. But sometimes I think of the joy it could have brought.
If these abortion extremists have their way, ending the life of a living human baby in the womb will become even more casual and common than it already is. This study to provide abortion pills to women who are not even pregnant yet is another clear indication of how fanatical true abortion supporters have become.
Last September, at a Gates Foundation event held during a General Assembly meeting of the United Nations in New York, French President Emmanuel Macron opined that high fertillty in parts of Africa were “not chosen” but the result of girls not being well educated and marrying too young. Quoting himself he said: “Present me the woman who decided, being perfectly educated, to have seven, eight or nine children. Please present me with the young girl who decided to leave school at 10 in order to be married at 12.’”
Macron is not the only politician or expert to spout such views, but this effort brought a spirited response from North of the Equator in the form of #PostcardsToMacron from highly educated mothers of large families in the US and elsewhere. This month, seven couples from Ivory Coast added their voice, the (well educated) wives signing the following superb testimony. published in the newspaper Fraternité Matin on February 15.
* * * * *
A persistent opinion from the North claims that large families are a problem for Africa. And, what is perhaps more serious, some go so far as to say that if African women have seven or more children it is out of ignorance: an educated woman, claim these scholars, doesn’t allow herself to be trapped but knows how to avoid having many children.
Well, we, African women with an advanced degree and practicing a profession, would like to say that we are very happy with our large families, our children around the table, their cries when they welcome us, the joy of sharing a loving union of dad-mother-children — which is priceless. Even if needs that come with the lifestyle make themselves felt, happiness does not depend on it.
Mutual love, devotion to one another, the concern of everyone to make everyone else happy, these are the sources of true happiness. We feel rich as individuals and as couples in acquiring and developing personal and marital skills in the education of our children. That can neither be quantified nor bought and sold.
By the way, in our opinion, it is children who have grasped this aspect of happiness who will eventually become responsible citizens, in solidarity with others.
It is very likely that we have a vision of family and happiness that some of those trying to teach us neither share nor know. This is a shame, and we can only feel a certain compassion for those who confuse purchasing power with happiness.
We know that many of our African sisters have few children, either because they could not have more children, or because they preferred to limit their number, for sometimes serious reasons. We understand them and will not pretend to tell them what to do. We will simply say that we, our husbands and our children are very happy.
In addition, we want to transmit to our children our vision of life, happiness and the beauty of conjugal love. They need to be educated so that they know how to build a happy home in the future, and are able to appreciate and live married fidelity and dedication to the children, who are the source of a truly successful life. And if they (our children) are led to limit the number of children, let them know that the means and methods are not neutral.
We would like to ask the international bodies that seem so concerned about our happiness that they let us educate our children according to our convictions and that they do not come to impose their ideas about contraception or sexual health. And we would also like to ask our authorities to protect us and our children from these foreign ideological currents.
Finally, we kindly ask you to believe us: we are very happy! And, if you do not want to believe it, at least leave us alone and leave our children alone.
Mrs. Tra Lou Gohi Clémence, Senior Administrator of Financial Services, 7 children
Ms. Aminata Toure, Masters in Business Management and Finance, 5 children
Dr. Achi Flavie, medical doctor, pediatric specialist, 8 children
Ms. Soro Fonondia Ella, Master Financial Engineering, 6 children
Ms. Arlette Yao, law degree, certified in Business Administration
Ms. Sandra Essoh, licensed in English and Communication
Mrs Ahekpa N’Guessan Laetitia, Graduate INTEC (National Institute of Economic Techniques and Accountants) of Paris, 7 children
(Translated from the French. Email addresses were supplied with the original article)
An infant born weighing less than 10 ounces is home from the hospital and doing well after his record-breaking survival.
Doctors at Keio University Hospital in Japan believe the boy is the smallest premature baby ever to survive, CBS News reports. His weight, 268 grams, is about the same as an average onion.
“There is a possibility that babies will be able to leave the hospital in good health even though they are born small,” said Dr. Takeshi Arimitsu, who helped care for the baby boy.
The infant spent five months in the hospital after his emergency delivery in August. Around 24 weeks of pregnancy, doctors realized that the unborn boy had stopped growing, and his life was in danger, The Japan Times reports. They performed a cesarean section in an attempt to save his life.
Initially, neither doctors nor his parents knew if he would survive.
“I can only say I’m happy that he has grown this big because honestly, I wasn’t sure he could survive,” the baby’s mother said.
Last week, the baby boy was deemed well enough to go home. He now weighs about 7 pounds, according to the hospital.
The Tiniest Babies Registry, run by the University of Iowa, puts the baby boy as the smallest ever to survive, the Times reports. It lists 23 babies born weighing less than 300 grams who survived.
A Duke University study published in 2017 reported that babies born at just 23 weeks gestation are surviving outside the womb at a greater rate than ever before. Researchers examined 4,500 babies between 2000 and 2011 and found a “small but significant drop in fatalities for babies born between 23 and 37 weeks gestation,” as well as a decrease in premature babies manifesting neurophysiological problems, the Daily Mail reported.
While more micro-premature babies are surviving, some hospitals will not treat them. Research published in 2015 in the New England Journal of Medicinefound that 23 percent of premature infants survive as early as 22 weeks of pregnancy, but some hospitals have policies against treating babies at such an early age.
These troubling policies also came to light with the story of Maddalena Douse in 2012. The British infant was born weighing just 13 ounces at birth. Many British hospitals have policies against trying to save premature infants who weigh less than 1 pound. However, when one of the medical staff weighed the baby girl, they accidentally left a pair of scissors on the scale, bumping her weight up to the minimum. Doctors, who did not realize the mistake until later, treated Maddalena and saved her life.
Women who have been hurt by a copper IUD known as ParaGard are calling a silly commercial full of dancing girls “condescending, deceitful garbage.”
The commercial is hard to miss. It features a girl in a bright yellow dress who dances and sings about the virtues of the “hormone free” IUD that has been on the market since 1988. In the most embarrassing moment in the commercial, the woman playfully pinches the IUD between her fingers. As usual, the goofy presentation lays on a thick layer of hype while giving not even a hint about why being “hormone free” doesn’t necessarily mean safer.
ParaGard is a small IUD made of flexible plastic that has been wrapped in a thin layer of copper. Manufactured by Duramed Pharmaceuticals, its only active ingredient is copper which has been clinically proven safe and effective for pregnancy prevention and has been FDA-approved since 1988. It is implanted in the uterus by a healthcare provider during a routine office visit and can be kept in place for up to 10 years.
The method of action in ParaGard comes from the copper which repels sperm. The other way it prevents pregnancy is by irritating the uterine lining which inhibits implantation.
This last action is why ParaGard is often inserted within a few days after unprotected sex because it can prevent a fertilized egg from implanting in the womb.
As the Henry J. Kaiser Family Foundation explains, “The copper IUD begins working immediately after insertion and consequently does not require a woman to use a backup method of contraception after insertion. Because of this, the copper-IUD can also be used as emergency contraception within five days of unprotected intercourse or method failure and is more effective at preventing pregnancy than emergency contraceptive pills. Unlike Plan B emergency contraceptive pills, the effectiveness of IUDs does not vary based on a woman’s weight.”
Judging by the looks of the commercial, which features a group of girls playfully dancing around, women might be inclined to think that having a hormone-free birth control device is something to celebrate. However, the women weighing in on a Facebook page entitled “Paragard Don’t Get One: Women Helping Women To Be Informed” tell a much different story.
One of the more common complaints on the page, which has more than 11,000 followers, is from women who had a toxic response to the copper in the device.
For example, this woman described a host of symptoms such as fatigue, brain fog, PMS, bloating, dry skin, and mood swings, and said, “I’ve lost so much hair, it just fell out in globs. Also developed pulmonary hypertension, which is rare and can be caused by excess copper in the blood, while having the IUD.” She was forced to have it removed.
Another issue is the dislodging of parts of the device. As this woman explains: “I’m at home recovering from surgery. I just had the broken arm of the Paragard removed from my womb and the muscle layer. Like other women on this site. The IUD broke when it was being removed 3 hard tugs and it came out missing one arm. Scans showed it had embedded into the womb lining and migrated into the muscle layer beyond. I’ve been struggling with sharp stabbing pain and unbearable back aches. They were able to remove the entire 15 mm piece yesterday and the abdominal pain is gone!”
She added: “I wish I could sue these buggers but no one seems to be interested anymore. I am so happy to have this bit of shrapnel gone!”
Although there were many good reviews on Drug.com, there were even more negative ones.
One woman only had the device in for a few days which she described as “the worst time for my health.” From the moment the device was implanted, she had tingling in her left arm. The tingling remains even though it was removed and doctors say it may be with her for the rest of her life. She was in perfect health before ParaGard but experienced “vomiting ,bleeding, dizziness, cramps ,losing weight in a short time, sweating at nights” after it was inserted. To those women who are considering the use of ParaGard she warns, “Please think!”
Another woman was equally blunt. “You are putting your future fertility, and possibly your life, at risk with this version of a Copper T. Ask any older woman about the horror stories from when this device was first introduced. Just think about the shape of your uterus and what the plastic arms of the “T” could do to it! To be clear, I mean it can poke a hole into the uterus when it is implanted or in place for any length of time. I am shocked that the FDA allows this dangerous device to stay on the market.”
She adds: “Further, I am completely disgusted by the current TV commercials with young women dancing in floral dresses. What condescending, deceitful garbage.”
The contraception industry uses the same tactic over and over again to promote potentially dangerous drugs and devices to women. For example, they promoted NuvaRing with a group of women in bathing suits who sit in a circle in a pool. What it didn’t tell women is that hormone delivery from the device causes spikes that make women more susceptible to blood clots. In some cases, the clots were fatal. In 2014, the manufacturer, Merck, settled more than 1,700 lawsuits for a combined $100 million to litigants who claimed the active ingredient in the drug, etonogestrel, was inadequately tested before NuvaRing’s 2002 release.
Then there’s Yaz and Yasmine, birth control pills that were introduced to the public with the same kind of deceptive advertising which made the use of these drugs look hip. There are scores of lawsuits pending against Bayer HealthCare Pharmaceuticals for the the drug’s “fourth generation” progestin known as drospirenone which has been linked to blood clots, gall bladder disease, stroke, heart attack and death in young women. As of 2013, Bayer paid out more than $750 million to settle 3,000 cases from women harmed by the drug; however, Bayer has not admitted liability in settling any of these cases.
The reason these deceptive marketing tactics work so often, to the detriment of women’s health, is because too many health care providers are not giving women the information they need to make informed choices. Instead, they are handed packages containing lengthy small-print inserts that no one with a life has time to read.
Thankfully, women are banding together to give one another the kind of full disclosure they deserve. For example, the women who formed the Facebook community known as Essure Problems raised such a ruckus that this deadly “permanent sterilization” product was eventually withdrawn from the market!
The only way we can help each other is to stay informed. Click here for a downloadable pamphlet detailing the many injuries and lawsuits pending against these dangerous drugs and devices.
Whenever people ask me what I think the biggest challenge we face today in regards to abortion it can be tempting to think in terms that are far too narrow. For example, I could respond by saying that the seemingly continual attempts by our politicians to introduce more extreme abortion laws are a major issue.
I could talk about the fact that the pro-life movement has extremely limited funding, resources, and personal with which to try and carry out one of the most monumentally important works of justice in human history.
Or perhaps I could highlight the unrelenting push to reduce medical professionals to subservient technicians incapable of exercising true clinical judgement by denying them their vitally important right to freedom of conscience.
All of these things are very real and very serious, but at the same time they need to be properly understood as the symptoms of a much bigger crisis. The fact that we are now living in a culture where authentic community has all but been usurped by rampant individualism.
There are many causes of this crisis. One could even say that it is a perfect storm of factors that are coalescing with catastrophic results.
Unparalleled development and widespread embrace of technologies increase our connectivity at the cost of human community. The rise of nihilistic relativism results in the loss of a unifying vision of reality in the West. A culture of self-gratification, with no desire for self-regulation through virtue mstems from the false belief that individual choice is the same thing as freedom Rampant consumerism reduces profoundly important goods and even human persons to mere objects.
And there is an almost obsessive fixation on global “community,” even though forming community on such a scale is beyond any possibility. Just witness the ideologies which reduce and separate us based on individualistic identifying characteristics rather than our shared common humanity.
In a nutshell, we have made the technologically enhanced, individualistic, self-gratifying consumer the most important good in our society.
Sadly, not even Christianity has been immune to this. How often do we come to church now as individual consumers seeking out products (‘I’ll take one satisfying sermon and four rousing worship anthems thanks’) for our personal happiness?
How many people in our church do we know as more than a face at Sunday service? Are we genuinely invested in each other’s lives and wellbeing beyond a mere handshake? Or is community just a buzzword that looks great when it appears in front of our church name in the Sunday notices or on the billboard out front?
Aristotle once declared that the greatest and most important relationship we can form with another person is one where we seek their good and not our own personal happiness or material gain. Through such a relationship of self-giving love, not only does the recipient flourish and become more fully human, but so do we, the giver.
Tragically, in a misguided quest for human fulfilment, much of modern culture has inverted this important truth, and as a result a destructive and deadly anti culture has arisen.
Which brings me back to my original question about abortion.
It is my contention that the biggest challenge we face is about recognising that abortion isn’t simply a political or social issue. It is a symptom of this culture of death that has made the gratification of individuals more important than community, and the wants of the strong more important than the needs of the vulnerable.
In doing so, this culture is not only dehumanising us, but it is also making abortion increasingly more appealing. The more people find themselves living isolated from community, the more they find themselves without the most essential and empowering element to be able to choose life for their unborn children – the concern and care of others.
Worst of all, this culture of death is now actively trying to sell us the lie that abortion, and its inseparable culture of lonely consumerism, is the path to human fulfilment and flourishing that we should be demanding as a human right.
Yes, we must continue to be unflinching and courageous in telling the hard truths about abortion, but it is now more vitally important than ever before that we become people living a culture of life — the culture of intentional community and self-giving love for the other.
Brendan Malone is the founder and Director of LifeNET. He has been working in pro-life, marriage and family ministry in New Zealand and Australia for the last 14 years. He lives in Rangiora with his wife Katie and their 5 rambunctious kids. He can be found online at www.lifenet.org.nzRepublished with permission from The Catholic Weekly, Sydney
Editor’s note: An international group of lay Catholics held a public demonstration in Rome yesterday just outside the Vatican, demanding that Pope Francis and the world’s bishops address homosexuality during the upcoming abuse summit as the major cause of the sexual abuse crisis in the Catholic Church. The following statement was given by Arkadiusz Stelmach during a press conference at the event. Read all statements here.
February 20, 2019 (LifeSiteNews) – I come from Poland, the country that owes its existence to the Catholic Church. I come from a country which, by virtue of the royal act, declared the Blessed Virgin Mary the Queen of Poland.
Like the entire Catholic world, we Poles are sad about the condition of the Church and Christian Civilization. Yes, the Church and Christian Civilization are being destroyed for over five centuries by the gnostic and egalitarian Revolution.
Today we see a dramatic struggle between the Revolution and the Counter-Revolution within the Church.
We see how the red dragon in a new form of neo-Communism or neo-Marxism got insidiously into the Church, making in Her previously unknown devastation.
Unfortunately, also my beloved Poland is not free from this scourge. We are living part of the Catholic Church. We are struggling with the crisis of Faith – manifested in the fall of vocations to the priesthood, the decline of religious practices especially among young people, the scourge of immorality, the promotion of homosexuality and gender ideology. Unfortunately, our seminaries and universities are not free from the terrible ideology of progressivism, which effectively undermines doctrine, discipline, and pastoral work of the Church.
A year ago, the Fr. Piotr Skarga Institute, who I represent, conducted a completely unique campaign of Polonia Semper Fidelis in defense of the indissolubility of Catholic marriage and in defense of the Blessed Sacrament. This action was an expression of the concern of Polish Catholics with an unclear and thus dangerous doctrine on the indissolubility of Sacrament of Marriage contained in the papal document Amoris Laetitia. The Polish episcopate received, in effect, over 145,000 letters, the vast majority of them by traditional post. In the letters, the Polish faithful appealed to the Polish Bishops’ Conference to confirm the Church’s teaching on the indissolubility of marriage, as well as to prevent of receiving Holy Communion by divorced Catholics that are living in the non-sacramental unions.
It’s sad that until now we didn’t receive any answer from the Polish episcopate for the campaign.
Unfortunately, the past months have brought further information about the extent of the crisis and confusion in the Church.
Letters from Archbishop Viganò, unmasking scandals of sexual abuse against children and clerics; attempts to democratize and destroy the hierarchical structure of the Church arouse our greatest concern.
Unfortunately, it also coincides with the increasingly furious attacks on the Church in Poland by external enemies. A sad example of this is the movie “Clergy” that presents a deformed and one-sided picture of the Church as a corrupt organization.
This very tragic situation of the Church calls us to be faithful to the clear traditional Catholic teaching and doctrine. In Poland — my country — the Mother of God, Blessed Virgin Mary, was always venerated and was our hope in most dark hours of our history. That’s why we need to stand with Her and pronounce: “Credo in Unam, Sanctam Catholicam Ecclesiam” (I believe in one, holy, Catholic Church) and that gates of hell will not destroy the Church.
While still in his mother’s womb, the British boy was diagnosed with a long list of life-threatening ailments, including hydrocephalus and chromosomal abnormalities.
His mother, Shelly Wall, of Abbeytown, England, recently told Good Morning Britain that doctors suggested they abort their son five separate times. The couple refused.
“We wanted to give Noah the chance of life,” her husband, Rob Wall, said.
Today, Noah is 6 years old and defying doctors’ expectations. His parents said Noah can talk, and he is learning to walk, surf and ski.
His brain, which at birth was just 2 percent of the size it should have been, has grown to 80 percent of its full size – stunning doctors, according to the report.
“It’s a very emotive subject. Some people say you can’t grow a brain,” Rob Wall said. “Other people say it must have always been there. But if it was and squashed up it would have been so severely damaged he would have been very mentally and physically disabled.”
His wife added: “Before he was born they gave me the option of a termination five times. We got taken into a room and they drew a circle saying ‘this brain will only be half a brain.’”
Noah was diagnosed with hydrocephalus, chromosomal abnormalities, spina bifida and other problems just three months into the pregnancy, his mother said.
Even after they chose life, she said they did not know if Noah would be born alive. The parents remembered the hope that they felt when Noah came into the world screaming,
The Walls said Noah still has medical problems and will need more surgeries, but he is doing so much better than everyone predicted.
“Every time we see the doctors they just shake their head. They’re just amazed at what he can do,” his mother said.
His story also is one of many reasons why abortions are wrong. There always is a chance that a child may survive, heal, grow and live a happy, fulfilling life.
It’s true that not every child with a serious or fatal disability will have the same miraculous recovery as Noah. But these children are just as valuable, whether they live for a few minutes or days or years outside the womb. Children with disabilities deserve the utmost care and compassion. But that compassion never should include the violent ending of a child’s life in an abortion.
February 18, 2019 (LifeSiteNews) — Ask anyone if the world is overpopulated, and you know what he will say.
The idea that we humans are breeding ourselves to death — and taking the planet with us — is in the air that we breathe.
It was drummed into us in high school biology, where we were told that the world is like a tiny “lifeboat.” We have to lighten the load, our teachers told us, or the “lifeboat” will sink, and we will all die.
And who can forget Al Gore’s doomsday scenario, in which he warned us that a “black hole” will engulf us if we do not stop having babies? Armageddon, anyone?
But It’s worth thinking about what would happen if everyone actually abandoned childbearing. Because it turns out that a lot of young people are already doing exactly that.
While on the fantasy island of overpopulation, human numbers are always exploding, a close look at the real world reveals an increasingly barren reality. Many nations, especially in Europe, are already in a death spiral, filling more coffins than cradles each year. Listen closely, and you will hear the muffled sound of populations crashing.
The birth dearth that began in post-war Europe has now spread to every corner of the globe. China is dying, and India and Latin America are rapidly growing old, while the Middle East is barely holding its own. Even in once prolific Africa, birth rates are in free fall.
You may be forgiven for not knowing this, because the United Nations continues to beat the overpopulation drum. Human numbers will balloon to 9.5 billion people by 2050, it chants, and reach 11 or even 12 billion by 2100.
This will happen, the U.N. says, because a secret fertility rebound is brewing. Women in largely barren places like Germany, France, and Japan will soon start having more children — in fact, many, many more children. Never mind that there is zeroevidence to back up such a claim, which itself seems like nothing more than a desperate attempt to breathe new life into a dying theory.
From the U.N. Population Division’s latest projections, “World Population Graph.”United Nations
Buried in the U.N. data is another, far more accurate, projection called the “low variant.” But because it doesn’t fit the “overpopulation” narrative, neither the U.N. nor the media gives it much airtime.
The “low variant” assumes that once birth rates go low, they stay low. It accepts that educated, urbanized young women in Paris, London, or Tokyo who today want only one child — or none — are not suddenly going to want a second tomorrow. Women in the rest of the world will follow, and global fertility will fall to European levels, or about 1.3 children per woman.
The bottom line: global numbers will peak at something less than 9 billion around 2050. After that, the human die-off will begin, slowly at first, but faster and faster as the years go by. By the end of the century, we will be back to our present numbers — about 7.5 billion — but we will be, collectively, far older and grayer.
What this means is that our present problem is not too many babies; it’s too few babies.
Many of today’s young adults are too enamored of sex, the city, and the single life to think about marriage, much less about replacing themselves. Education delays marriage and provides other opportunities for women besides marriage and family. A single Swedish woman may eventually bear one child as her biological clock approaches midnight, but she is unlikely to bear a second.
For materially minded couples in countries where the state provides old age benefits and charges high tax rates in consequence, the way to get ahead is to remain perpetually childless. The cradle-to-grave welfare programs that have now spread throughout the world have not merely made children superfluous to wealth; they have made children themselves the enemy of wealth. They are now, as the Chinese say, “goods on which one loses.”
Why give up a second income to bring a child into the world who will never, at least in material terms, repay your investment? Why provide for the future by having children to care for you in your dotage, if the government has pledged to keep you out of the poorhouse anyway?
A young Florida woman, who was commuting 100 miles a day to her well paying job, once complained to me about how little time she had to spend with her only child, a four-year-old son. Perhaps she could get a job locally so she could be home more, I suggested helpfully, even though it would mean selling her expensive SUV. “You don’t understand,” she said, aghast. “My husband and I love this SUV.”
These are the calculations driving the old age tsunami that is about to hit the world, not just in places like New York, but in Rio and Nairobi as well.
For a long time, population growth has been seen as the enemy, particularly by those who did not realize that it was a key driver of economic growth. Now, with young people becoming a scarce resource, the linkage is clear. Absent a nuclear war, global plague, or a collision with a comet, business from now on is primarily going to be a numbers game.
The rapid aging of the population, by reducing the amount of human capital available, will dramatically darken humanity’s prospects in countless ways.
Population growth has been an important escalator of consumer demand. Try selling cars, houses, refrigerators — or anything else, for that matter — in a depopulating country. Try seeking profitable investments in the stock market when millions of elders start slowly liquidating their IRAs and 401(k)s to survive.
Some sectors, such as pharmaceuticals and health care, will still do well, but shrinking demand elsewhere will more than offset these gains.
The ranks of workers will thin with each passing year, while the number of elderly will grow. Countries will be forced to slash pensions or raise the retirement age. Living standards may fall, and economies may well shrink.
Within the next couples of decades, the world will enter a “low-birthrate recession.” Unlike other recessions, this one may never end.
Shrinking birthrates also threaten social isolation as family circles collapse. Those seniors who lack close family ties will be socially isolated and painfully lonely.
As Ben Wattenberg once remarked, “Young DINKs (double income, no kids) may be cute. Old LINKs (low income, no kids) may be tragic.”
So stop telling us that we are having too many children already. Our long-term problem, which is now upon us, is too few children.
This is the real “black hole.” And it threatens to devour us all.
Steven W. Mosher is the president of the Population Research Institute and the author of Population Control: Real Costs and Illusory Benefits.
Planned Parenthood of Illinois has announced that affiliates across the state will offer free birth control for a year to women who cannot afford the cost. The Chicago Tribune reports that the initiative, Access Birth Control (ABC), is being funded by “private philanthropy” and will offer a wide range of contraceptives to low-income and uninsured women.
The program seems altruistic until you take a closer look at the contraceptives on offer to women in the program. The options include IUDs, vaginal rings, injectable birth control, and the pill. These forms of contraceptives carry significant health risks for women, both physical and mental, as hormonal contraception has been strongly linked to depression.
It’s also important to note that Planned Parenthood is the organization administering the birth control. Planned Parenthood is not a comprehensive health provider — in fact, they have, for example, never provided mammograms. Planned Parenthood is an abortion corporation. Over the past several years, legitimate health services have declined. Meanwhile, as the national abortion rate has continued to decline, Planned Parenthood’s market share of abortions has increased.
While the “free” contraception program is presented as philanthropy by Planned Parenthood and their friends in the media, a more accurate description might be “marketing campaign.” By offering ‘free’ contraceptives to vulnerable women, Planned Parenthood builds brand loyalty, so that women will continue to come to them for other “services” — for instance, when those contraceptives occasionally fail, which is not at all unusual, those women are likely to turn to Planned Parenthood for abortion. With the many health risks of these contraceptives and the increased chance of paying Planned Parenthood for an abortion, the program is not really “free.”
While this may seem alarmist, we should keep in mind that Planned Parenthood is a business that ends the lives of more than 330,000 preborn babies each year. They are unlikely to tell women about ethical and effective alternatives that carry none of the health risks.
VANCOUVER, February 15, 2019 (LifeSiteNews) – Teen girls who use hormonal contraception like ‘the pill’ showed significant bone loss, increasing their risk of “later life fractures,” a new scientific study has found. The authors of the study say that their findings are “of concern” and present a “potential public health problem.”
According to Dr. Jerilynn C. Prior of the department of medicine at the University of British Columbia (UBC), a meta-analysis of controlled, observational studies found that healthy teenage girls who used combined hormonal contraception (including estrogen and progestin via several delivery methods) showed significant spinal bone loss over two years.
Dr. Prior is a professor of endocrinology and metabolism at UBC, and founder and scientific director at the Centre for Menstrual Cycle and Ovulation Research in Vancouver. She told Endocrine Today, “Instead of using combined hormonal contraception as the go-to, routine therapy in adolescent girls, we need to use evidence-based and physiological ways to treat cramps, heavy flow, irregular cycles and acne, and nonhormonal methods for contraception.” The study, titled “Adolescent use of combined hormonal contraception and peak bone mineral density accrual: A meta‐analysis of international prospective controlled studies” was published Jan. 7, 2019.
The study indicates “adolescence is a key time in women’s life cycle for bone accrual, for decreasing later life osteoporosis and lifetime fragility fracture risk,” and peak bone mass density (BMD) is “gained in women ages 16 and 19 years and lumbar spine peak BMD is achieved between ages 33 and 40…” Citing the risk of loss of BMD, the study states: “Those who achieve a lower peak BMD are widely believed to be at increased risk of later life fractures, although prospective BMD and incident fragility fracture data are scarce.”
The study was conducted in Brazil, Canada, China, and the United States and showed bone mass density loss over one to two years. Prior and her colleagues analyzed data from nine clinical trials and observational, longitudinal studies that included teen girls who were using hormonal contraception (including estrogen and progestin in oral, patch or ring preparation). Those monitored for 12 months showed bone loss, while bone loss continued to be evident for the girls in the 24-month study.
In summary, the study showed that teen girls on contraception showed significantly less bone growth than those not using contraception, even when they are prescribed lower estrogen doses than in previous years. Because hormonal contraception is increasingly used even for “treatment of mild symptomatic, non‐contraceptive reasons such as acne and cramps,” the authors of the study fear that a “negative public health impact” may result.
The American College of Obstetricians and Gynecologists (ACOG) — a notoriously pro-abortion organization — has released a so-called “fact sheet” on “later” abortions, titled, “Facts Are Important: Abortion Care Later in Pregnancy is Important to Women’s Health.” In it, they take issue with the use of the phrase “late-term abortion,” claiming it “has no medical definition and is not used in a clinical setting or to describe the delivery of abortion care later in pregnancy.” While the ACOG may make this claim, abortionists who commit abortions late in pregnancy have used the term for years and still do. And before pro-abortion organizations like the ACOG gave the abortion-friendly media their marching orders in the past few weeks, the phrase “late-term abortion” was used frequently by news outlets as well.
The ACOG typically makes claims in lockstep with the abortion industry’s public relations personnel, and the American Association of Pro-Life Obstetricians and Gynecologists (AAPLOG) stands firmly in opposition to the death-promoting speech of the ACOG. AAPLOG released a fact sheet of its own about abortions late in pregnancy. Its document, titled, “Facts ARE Important: Abortion, including later in pregnancy, is NOT healthcare,” directly takes on the ACOG’s “fact sheet” claims.
Claim #1: Late abortions are “rare.”
Truth: That’s at least 11,000 human beings every year.
First, the ACOG does what every abortion supporter does when speaking about late-term (or “later”) abortions: it points out the “rarity” of such procedures. “Abortion after 21 weeks accounts for slightly more than 1 percent of all abortions that occur in the United States. Abortion later in the second trimester is very rare, and abortion in the third trimester is rarer still, accounting for less than one percent of abortions.” It’s “rare” only in comparison to the hundreds of thousands of abortions happening earlier in pregnancy… as if that makes the brutality of killing fully developed children so late in pregnancy somehow acceptable.
AAPLOG counters (emphasis added):
A recent release from the American College of Obstetricians and Gynecologists (ACOG) stated that policy related to abortion care “must be based on medical science and facts”. We could not agree more….
Although abortions in the second half of pregnancy only account for 1.3% of all abortions, this still amounts to over 11,000 fetal pain-capable human beings that are being killed each year.
It is undisputed scientific fact that at the moment of fertilization, a new distinct living human being comes into existence. This human being came from two human parents and therefore can be nothing but human. Even very early in pregnancy, this human being meets all of the scientific criteria for a living organism and is completely distinct from her mother, not a part of her mother’s body. This is scientific fact.
Claim #2: Abortion is medically necessary.
Truth: It’s never necessary to deliberately kill an innocent human being in the womb.
ACOG writes, “The need for an abortion later in pregnancy could arise for a number of reasons, including fetal anomalies or complications that threaten a woman’s health.” (Notice the term “need.”) ACOG goes on (emphasis added): “Women, in consultation with theirphysicians, must be able to evaluate all appropriate treatments and make informed choices about what’s best for their health and their pregnancies. Depending on the circumstance, this might include abortion care….”
AAPLOG points out that abortion is never actually medically necessary, and that it’s not healthcare. Oh, and about those “physicians”….
Abortion is NOT healthcare, much less an essential part of women’s health care. If it were, more OB/GYN’s would do them.
Currently, greater than 90% of abortions are done by dedicated abortion providers, not by awoman’s personal physician.
In other words, the woman has likely never seen that doctor before she walked through the doors of that facility (unless she’s had a previous abortion there) — a facility often dedicated solely to the practice of aborting human beings.
Claim #3: There could be complications with the baby or mother, making abortion necessary.
Truth: Killing an ill child helps no one, and abortion also puts women at risk — both now and in future pregnancies.
The ACOG’s “fact” sheet goes on to say that sometimes severe fetal anomalies occur. “In these cases, where death is likely before or shortly after birth, patients may decide whether to continue the pregnancy and deliver a nonviable fetus or have an abortion” for “what she feels is best for her health and her family.” The ACOG goes on to say, “Abortion later in pregnancy may also be necessary when complications severely compromise a woman’s health or life, conditions which may also reduce the possibility of fetal survival.”
However, abortion reduces the possibility of fetal survival every time it’s done as intended.
AAPLOG makes this point:
… [T]he intentional killing of a fetal human being (often through barbaric means such as dismemberment), does not treat disease and does not improve a woman’s health. It is 100% lethal for one of our two patients, and has significant health ramifications for our adult patient. For example, there is now substantial evidence for the link between surgical abortions and very preterm birth (prior to 32 weeks) in subsequent pregnancies, and this risk increases exponentially with each abortion a woman has.
And having an abortion at such a late stage typically involves two to three days of dilation. If a woman’s health truly is “severely compromise[d],” dilating the cervix over three days seems unwise. AAPLOG adds that the risk of death from abortion so late in pregnancy is higher than the risk of dying during birth, adding:
There are rare circumstances during pregnancy in which a mother’s life is in jeopardy…. It is extremely rare for this to occur prior to the point of viability (currently 22-23 weeks). In this circumstance, delivery is indicated. Intentional killing of the fetal human being, however, is not necessary. We can save the life of the mother through delivery of an intact infant and then give both the care that they need….
In cases where the mother’s life is in danger in the latter half of pregnancy, there is not time for an abortion, which is typically a two to three day process. Immediate delivery is needed in these situations, and can be done in a medically appropriate way….
AAPLOG also recommends perinatal hospice for parents facing a diagnosis of a terminal condition for their child, writing that not only does this “improve outcomes for the family” and mother, “but also honors the life of their child and allows them to have an intact child to hold and grieve.”
ACOG claims in its “fact sheet” that “The best health care is provided free from political interference in the patient-physician relationship.” But AAPLOG gives a slam dunk response to this platitude, writing, “when the issue at hand is the killing of innocent human beings as well as the harming of women through deceptive practices, it is the responsibility of the government in any civilized society to protect its innocent citizens from harm.”
In the face of growing confusion about the doctrine of the Faith, many bishops, priests, religious and lay people of the Catholic Church have requested that I make a public testimony about the truth of revelation. It is the shepherds’ very own task to guide those entrusted to them on the path of salvation. This can only succeed if they know this way and follow it themselves. The words of the Apostle here apply: “For above all I have delivered unto you what I have received” (1 Cor. 15:3). Today, many Christians are no longer even aware of the basic teachings of the Faith, so there is a growing danger of missing the path to eternal life. However, it remains the very purpose of the Church to lead humanity to Jesus Christ, the light of the nations (see LG 1). In this situation, the question of orientation arises. According to John Paul II, the Catechism of the Catholic Church is a “safe standard for the doctrine of the faith” (Fidei Depositum IV). It was written with the aim of strengthening the Faith of the brothers and sisters whose belief has been massively questioned by the “dictatorship of relativism.”
1. The one and triune God revealed in Jesus Christ
The epitome of the Faith of all Christians is found in the confession of the Most Holy Trinity. We have become disciples of Jesus, children and friends of God by being baptized in the name of the Father and of the Son and of the Holy Spirit. The distinction of the three persons in the divine unity (CCC 254) marks a fundamental difference in the belief in God and the image of man from that of other religions. Religions disagree precisely over this belief in Jesus the Christ. He is true God and true Man, conceived by the Holy Spirit and born of the Virgin Mary. The Word made flesh, the Son of God, is the only Savior of the world (CCC 679) and the only Mediator between God and men (CCC 846). Therefore, the first letter of John refers to one who denies His divinity as an antichrist (1 John 2:22), since Jesus Christ, the Son of God, is from eternity one in being with God, His Father (CCC 663). We are to resist the relapse into ancient heresies with clear resolve, which saw in Jesus Christ only a good person, brother and friend, prophet and moralist. He is first and foremost the Word that was with God and is God, the Son of the Father, Who assumed our human nature to redeem us and Who will come to judge the living and the dead. Him alone, we worship in unity with the Father and the Holy Spirit as the Only and True God (CCC 691).
2. The Church
Jesus Christ founded the Church as a visible sign and instrument of salvation realized in the Catholic Church (816). He gave His Church, which “emerged from the side of the Christ who died on the Cross” (766), a sacramental constitution that will remain until the Kingdom is fully achieved (CCC 765). Christ, the Head, and the faithful as members of the body, are a mystical person (CCC 795), which is why the Church is sacred, for the one Mediator has designed and sustained its visible structure (CCC 771). Through it the redemptive work of Christ becomes present in time and space via the celebration of the Holy Sacraments, especially in the Eucharistic Sacrifice, the Holy Mass (CCC 1330). The Church conveys with the authority of Christ the divine revelation, which extends to all the elements of doctrine, “including the moral teaching, without which the saving truths of the faith cannot be preserved, explained, and observed” (CCC 2035).
3. Sacramental Order
The Church is the universal sacrament of salvation in Jesus Christ (CCC 776). She does not reflect herself, but the light of Christ, which shines on her face. But this happens only when the truth revealed in Jesus Christ becomes the point of reference, rather than the views of a majority or the spirit of the times; for Christ Himself has entrusted the fullness of grace and truth to the Catholic Church (CCC 819), and He Himself is present in the sacraments of the Church.
The Church is not a man-made association whose structure its members voted into being at their will. It is of divine origin. “Christ himself is the author of ministry in the Church. He set her up, gave her authority and mission, orientation and goal (CCC 874). The admonition of the Apostle is still valid today, that cursed is anyone who proclaims another gospel, “even if we ourselves were to give it or an angel from heaven” (Gal 1:8). The mediation of faith is inextricably bound up with the human credibility of its messengers, who in some cases have abandoned the people entrusted to them, unsettling them and severely damaging their faith. Here the Word of Scripture describes those who do not listen to the truth and who follow their own wishes, who flatter their ears because they cannot endure sound doctrine (cf. 2 Tim 4:3-4).
The task of the Magisterium of the Church is to “preserve God’s people from deviations and defections” in order to “guarantee them the objective possibility of professing the true faith without error” (890). This is especially true with regard to all seven sacraments. The Holy Eucharist is “source and summit of the Christian life” (CCC 1324). The Eucharistic Sacrifice, in which Christ includes us in His Sacrifice of the Cross, is aimed at the most intimate union with Him (CCC 1382). Therefore, the Holy Scripture admonishes with regard to the reception of the Holy Communion: “Whoever eats unworthily of the bread and drinks from the Lord’s cup makes himself guilty of profaning the body and of the blood of the Lord” (1 Cor 11:27). “Anyone conscious of a grave sin must receive the sacrament of Reconciliation before coming to communion” (CCC 1385). From the internal logic of the sacrament, it is understood that divorced and civilly remarried persons, whose sacramental marriage exists before God, as well as those Christians who are not in full communion with the Catholic Faith and the Church, just as all those who are not disposed to receive the Holy Eucharist fruitfully (CCC 1457), because it does not bring them to salvation. To point this out corresponds to the spiritual works of mercy.
The confession of sins in Holy Confession at least once a year is one of the Church’s commandments (CCC 2042). When the believers no longer confess their sins and no longer experience the absolution of their sins, salvation becomes impossible; after all, Jesus Christ became Man to redeem us from our sins. The power of forgiveness that the Risen Lord has given to the Apostles and their successors in the ministry of bishops and priests applies also for mortal and venial sins which we commit after Baptism. The current popular practice of confession makes it clear that the conscience of the faithful is not sufficiently formed. God’s mercy is given to us, that we might fulfil His Commandments to become one with His Holy Will, and not so as to avoid the call to repentance (CCC 1458).
“The priest continues the work of redemption on earth” (CCC 1589). The ordination of the priest “gives him a sacred power” (CCC 1592), which is irreplaceable, because through it Jesus becomes sacramentally present in His saving action. Therefore, priests voluntarily opt for celibacy as “a sign of new life” (CCC 1579). It is about the self-giving in the service of Christ and His coming kingdom.
4. Moral Law
Faith and life are inseparable, for Faith apart from works is dead (CCC 1815). The moral law is the work of divine wisdom and leads man to the promised blessedness (CCC 1950). Consequently, the “knowledge of the divine and natural law is necessary” to do good and reach this goal (CCC 1955). Accepting this truth is essential for all people of good will. For he who dies in mortal sin without repentance will be forever separated from God (CCC 1033). This leads to practical consequences in the lives of Christians, which are often ignored today (cf 2270-2283; 2350-2381). The moral law is not a burden, but part of that liberating truth (cf Jn 8:32) through which the Christian walks on the path of salvation and which may not be relativized.
5. Eternal Life
Many wonder today what purpose the Church still has in its existence, when even bishops prefer to be politicians rather than to proclaim the Gospel as teachers of the Faith. The role of the Church must not be watered down by trivialities, but its proper place must be addressed. Every human being has an immortal soul, which in death is separated from the body, hoping for the resurrection of the dead (CCC 366). Death makes man’s decision for or against God definite. Everyone has to face the particular judgement immediately after death (CCC 1021). Either a purification is necessary, or man goes directly into heavenly bliss and is allowed to see God face to face. There is also the dreadful possibility that a person will remain opposed to God to the very end, and by definitely refusing His Love, “condemns himself immediately and forever” (CCC 1022). “God created us without us, but He did not want to save us without us” (CCC 1847). The eternity of the punishment of hell is a terrible reality, which – according to the testimony of Holy Scripture – attracts all who “die in the state of mortal sin” (CCC 1035). The Christian goes through the narrow gate, for “the gate is wide, and the way that leads to ruin is wide, and many are upon it” (Mt 7:13).
To keep silent about these and the other truths of the Faith and to teach people accordingly is the greatest deception against which the Catechism vigorously warns. It represents the last trial of the Church and leads man to a religious delusion, “the price of their apostasy” (CCC 675); it is the fraud of Antichrist. “He will deceive those who are lost by all means of injustice; for they have closed themselves to the love of the truth by which they should be saved” (2 Thess 2:10).
Call
As workers in the vineyard of the Lord, we all have a responsibility to recall these fundamental truths by clinging to what we ourselves have received. We want to give courage to go the way of Jesus Christ with determination, in order to obtain eternal life by following His commandments (CCC 2075).
Let us ask the Lord to let us know how great the gift of the Catholic Faith is, through which opens the door to eternal life. “For he that shall be ashamed of me, and of my words, in this adulterous and sinful generation: The Son of Man also will be ashamed of him, when He shall come in the glory of his Father with the holy angels.” (Mark 8:38). Therefore, we are committed to strengthening the Faith by confessing the truth which is Jesus Christ Himself.
We too, and especially we bishops and priests, are addressed when Paul, the Apostle of Jesus Christ, gives this admonition to his companion and successor, Timothy: “I charge thee, before God and Jesus Christ, Who shall judge the living and the dead, by His coming, and His kingdom: Preach the word: be instant in season, out of season: reprove, entreat, rebuke in all patience and doctrine. For there shall be a time, when they will not endure sound doctrine; but, according to their own desires, they will heap to themselves teachers, having itching ears: And will indeed turn away their hearing from the truth, but will be turned unto fables. But be thou vigilant, labour in all things, do the work of an evangelist, fulfil thy ministry. Be sober.” (2 Tim 4:1-5).
May Mary, the Mother of God, implore for us the grace to remain faithful without wavering to the confession of the truth about Jesus Christ.
United in faith and prayer,
Gerhard Cardinal Müller, Prefect of the Congregation for the Doctrine of the Faith 2012-2017
Editor’s note: After this text was published, the cardinal’s office submitted to CNA three amendments to the text originally submitted to CNA. Two were minor syntactical corrections. The third change replaced the word “to” with “cannot” in the following phrase: “just as all who are not properly disposed, to cannotreceive the Holy Eucharist fruitfully (CCC 1457) because it does not bring them to salvation.”
The bishop also said that a pope’s words are not necessarily ‘authentic doctrine’
Bishop James Conley of Lincoln, Nebraska has said there is “uncertainty and confusion” within the Church over moral teaching, including “at a very high level” of the hierarchy.
While praising Pope Francis, the bishop also discussed the role of the papacy, saying that even popes “cannot overturn what has been infallibly taught”.
Bishop Conley’s remarks came in an interview with Professor Robert George of Princeton University, which appears as a chapter in a new book, Mind, Heart, and Soul: Intellectuals and the Path to Rome.
The bishop was asked about the divisions within the Church. He replied that “there seem to be some voices within the Church, some at a very high level, that are calling into question some fundamental truths about the human person”. Bishop Conley, who chairs the US bishops’ Subcommittee for the Promotion and Defense of Marriage, said he was especially referring to truths about marriage and sexuality.
“These truths have long been taught by the Church,” Bishop Conley told Professor George, “and were strongly reaffirmed by Pope John Paul and Pope Benedict. Questions concerning the nature and function of conscience, sin and the moral act, intrinsic evil, and the natural law.”
Bishop Conley said that “some voices” were “very disturbing. And some of them are very important voices – theologians and even bishops, archbishops, and cardinals”. But despite these “deepening divisions”, the bishop said he was not “shaken”. “I have confidence that the Holy Spirit will eventually sort it all out and not let the Church go off the rails.”
Bishop Conley said he thought Pope Francis upheld the Church’s teachings. The bishop also considered “what the faithful Catholic would be bound by conscience to do if, God forbid, his or her properly formed conscience were to come into conflict with something a pope says. It could be Pope Francis or any pope.”
Under such circumstances, the bishop argued, it would be necessary to “go with the sensus fidelium” – “the belief of the Church through the ages, yesterday, today, and forever”. Bishop Conley distinguished between the sensus fidelium – “the Church’s firm, constant, and true teaching” – and modern dissent about, for instance, contraception.
Bishop Conley said that there were “rare” times in history when a pope has said “something that contradicts or is logically inconsistent with the firm and constant teaching of the Church on a matter of faith or morals”. If this happens, he said, it is important to remember that “the pope cannot overturn what has been infallibly taught, whether by the papal magisterium itself or by an ecumenical council or by the ordinary universal magisterium.” Popes are “not dictators”, he said, and “the faith of the Church does not lie in a pope”.
Bishop Conley said that Blessed John Henry Newman could help Catholics to “understand the office of Peter, especially in the present pontificate”. While Newman “had a very healthy respect, obedience, and admiration for the papacy”, he also “knew that not every utterance that came out of a pope’s mouth is necessarily authentic Christian doctrine.” Bishop Conley said this awareness made Newman unpopular with powerful figures, and may have prevented Newman from being made a bishop.
NFL tight end Ben Watson had some powerful pro-life words for men in an interviewwith Fox News anchor Martha MacCallum.
As a husband and father of seven children (two currently in the womb), the NFL star explained that men should “step up and lead,” which could “eradicate” many of the abortions occurring today.
He added that abortion is “the ultimate form of sexism against women.”
“I look in the mirror and encourage myself as a husband and father…If men stood up…a lot of this would be eradicated.”
Watson explained that “men are in a role of leadership in many areas. Men are protectors—we are providers. Many women would not be seeking abortions if the men involved in their lives were doing what they’re supposed to be doing.
“And that’s a challenge to myself, that’s a challenge to all men who are listening, that’s a challenge to men everywhere to step up and be men.
“A lot of the issues that we face in our country, whether it’s the abortion issue, or education, or whatever it may be, sometimes incarceration, whatever it may be, if men were doing their job, these things would be eradicated.
“My message to men is a lot of times, me looking in the mirror and encouraging myself as a father, as a husband, to do what it takes to stand in the gap, to step out, and to lead, because manhood is really falling by the wayside.
“The crazy thing is that abortion itself is really the ultimate form of sexism against women. And if men were standing up doing what they were supposed to do, much of this would be eradicated.”
Watson also presented a similar message at the 2017 March for Life:
Doctor and Kansas Rep. Roger W. Marshall wrote an op-ed saying there aren’t any reasons why a late-term abortion is necessary to protect a woman’s health.
“To this day, I can’t think of a single scenario where I thought a late-term abortion would help to improve a woman’s mental health,” Marshall wrote in a Monday op-ed published by Fox News. “Contrary to the pro-abortion movement, regardless of the mother’s underlying medical health, I never saw the scenario where we had to choose between a mom’s life and a baby,” Marshall wrote.
Marshall is an obstetrician who has delivered more than 5,000 babies in Western Kansas over 25 years. He also served as an OB-GYN at a state mental health hospital and prison.
Pregnant women face much higher risks for uterine perforation and life-threatening hemorrhaging during late-term abortions, according to Marshall. The procedures also pose a high risk of infection, permanent scarring and infertility, according to the doctor.
“Point blank, late-term abortions are unsafe and are more dangerous than naturally occurring childbirth in almost any situation,” Marshall wrote.
A number of states, including Rhode Island, Vermont, Virginia, Maine, New Mexico and Maryland, are considering proposals to expand abortion access allowing women to abort in the late stages of pregnancy.
New York passed the Reproductive Health Act on Jan. 22, codifying a woman’s ability to abort under state law and allowing women to have abortions after 24 weeks in cases where “there is an absence of fetal viability, or at any time when necessary to protect a patient’s life or health,” according to the legislation.
Marshall called New York’s law “inhumane” for both mothers and children.
“I urge you to tell all of your elected federal officials to support the Born Alive Abortion Survivors Protection Act, which is the first step to immediately protect those babies who have survived botched abortions and mandate that they receive proper medical care,” the doctor and state representative also urged.
Seventy-five percent of Americans support significant abortion restrictions and say abortion should be limited to the first three months of pregnancy, according to a January Marist survey.
LifeNews Note: Grace Carr writes for Daily Caller. Content created by The Daily Caller News Foundation is available without charge to any eligible news publisher that can provide a large audience.
The most effective prison has no guards with guns, nor cells with bars. The enslavement of the mind in the prison of false narrative is so deceptive we submit to it willingly.@prayingmedic
Thirty-three years after America ended the horrific practice of enslaving Blacks, the Supreme Court restored the habit of treating people differently based on the color of their skin. Eugenicists and segregationists cheered the Plessy v. Ferguson decision as they continued terrorizing former slaves, using skin color to keep them divided from the community they once were forced to embrace.
The segregationist culture began to shift in the mid-1950s, when the Civil Rights movement exposed the horror and terror embedded in the Jim Crow laws. Most of America grew to reject discrimination based on skin color. Realizing the passage of the Civil Rights Acts would impede their agenda of controlling the Black birth rate, eugenicists like Planned Parenthood founder Margaret Sanger and Alan Guttmacher turned to the federal government to continue their population control maneuvers. With racist allies like President Richard Nixon, a devout population control enthusiast, Sanger and Guttmacher set the stage for abortion on demand. By 1973, their dogma won out when Roe v. Wade established the so-called right to abortion.
Abortion on demand also aided the government’s establishment of an office to administer family planning programs, specifically for the poor. On Christmas Eve 1970, the Democrat-controlled Congress rejoiced that Public Law 91-572, 84 Stat. was passed, ushering in the age of population control in America to be administered through the Office of Population Affairs (OPA). This office exists under the U.S. Department of Health and Human Services (HHS). Despite the law prohibiting organizations that “use abortion as a family planning method” from receiving Title X funds, the Office of Population Affairs has provided Title X funds to Planned Parenthood, the nation’s leading abortion provider, almost from the passage of Roe v. Wade.
Today, Planned Parenthood commits more than 30 percent of all abortions carried out in this country and receives more than a half-billion taxpayer dollars while doing so. Camouflaging their eugenic intent in the rhetoric of providing “access to health care,” they have long targeted the Black population while collecting taxpayer dollars through Title X and Medicaid.
Every administration since 1970, whether Democrat or Republican, has ignored the violation of Title X and other federal laws that ban using federal dollars for abortion. Planned Parenthood has committed Medicaid fraud, has ignored laws regarding child sexual abuse, has enabled sex traffickers to maintain their “trade,” and has sold the body parts of babies they aborted, among other crimes. Despite all these egregious acts, they continue to freely dip into the taxpayer coffers because the United States Department of Health and Human Services refuses to enforce the laws related to family planning.
More than 60 million babies later, 20 million of whom are Black, it may be time to shift America’s culture yet again. President Trump’s HHS has not fulfilled its self-proclaimed mission of protecting the weakest among us. Instead it is choosing to follow the business as usual model that has allowed a genocide on America’s most vulnerable.
The time has come to end the genocide and to hold those committing the genocide accountable. It is time to strip away the false narrative that abortion is akin to a civil right. It is time to open the prison bars and liberate those who are enslaved to the false narrative that abortion is safe and rare. The time has come to “Speak up for those who cannot speak for themselves; ensure justice for those being crushed” (Proverbs 31:8) by dismantling the Office of Population affairs and pursue all avenues of prosecution against Planned Parenthood for its decades of atrocities.
WASHINGTON, D.C., February 7, 2019 (LifeSiteNews) – The United States Supreme Court is being asked to weigh in on whether embryonic children are persons or property. Thomas More Society Special Counsel Rebecca Messall, J.D. has filed a petition with the high court for a writ of certiorari to the Colorado Supreme Court in Rooks v. Rooks, a controversial Colorado embryo custody case.
Messall, acting on behalf of Colorado mother Mandy Rooks, is requesting that the United States Supreme Court reverse an earlier ruling by the Colorado Supreme Court and affirm the fact that embryos are human persons, as “recognized in law hundreds of years ago.”
Mandy Rooks is the mother of six cryopreserved babies. The embryos are those remaining in cryogenic storage after in-vitro fertilization procedures. Those procedures allowed Ms. Rooks to deliver a son, and later twins, while married to Drake Rooks, the children’s father. Despite the couple’s divorce, Ms. Rooks wants to keep the babies for future implantation. Her now ex-husband has asked the court to deliver the six embryos to him for destruction.
Both a district court and the Colorado Court of Appeals awarded custody to Mr. Rooks, but the Colorado Supreme Court ordered a stay of execution for the embryos because the lower courts considered what it labeled “inappropriate factors” in attempting to balance the divorced couples’ interests. The case was remanded to the trial court.
The Petition for review by the United States Supreme Court enumerates multiple reasons for the highest court in the land to rule on the most basic question: Is a human embryo a person or property?
Classifying human life as property conflicts with a plethora of federal and state laws, as well as high court precedent.
The express language of the United States Constitution’s preamble conflicts with a “property” designation.
Human embryos are entitled to substantive due process as persons under the Fourteenth Amendment.
Science is firm on when a person comes into being.
Family rights are more precious than property rights.
The Colorado Supreme Court has violated Ms. Rooks’ sincerely held religious beliefs.
The lower courts are in conflict.
Messall states in the appeal to the high court, “Granting human embryos the status of persons cannot be left up to fifty states, any more than the Kansas-Nebraska Act could leave the status of slaves to each state. The test of who is a ‘person’ must be decided for the entire nation in order to uphold the principles of ‘Equal Justice Under Law.’”
She holds that the arguments for the personhood of Dred Scott and his family, which the courts got wrong, denying the enslaved citizens their personhood, remain as true today as they were in the infamous 1857 trial.
The petition also points out that scientific reality confirms the terms “reproduction” and “procreation” as referring to a new human person, not property, and not to an in-between classification.
Attorney Rita Gitchell, Thomas More Society Special Counsel, explained some of the issues at stake in Rooks v. Rooks: “These cryogenically preserved children are already developing human beings, before implantation. Colorado courts are relying on their state law that does not protect unborn children from third party liability for harm done to the unborn and case law extracted from old, out-of-date science that had not yet understood that embryo body cells, along with the placental and other cells, are present before implantation of the embryo in the womb.”
Parental constitutional rights to bear and raise offspring were not considered even though the trial court found the embryos to be human life.
“While it is a simple fact that those who provide an egg and a sperm which unite to become an embryo become genetic parents,” continued Gitchell, “It is not fact that while the embryos are developing, that the parents are ‘becoming genetic parents.’ That is comparable to suggesting that a woman who is seven months pregnant is ‘becoming pregnant.’ Until the courts or legislatures grasp the facts of created life, the Constitutional rights of parents to protect their created offspring are not being considered, nor are the human rights of the embryo considered. This results in human embryos being treated like chattel or property, not unlike the treatment of African slaves in the pre-abolition era.”
She added, “Mr. and Ms. Rooks are forever genetic parents of these created embryos. A court can terminate his or her legal parental rights, but can never terminate the genetic fact that these tiny embryos are their biological children.”
A response from the United States Supreme Court on whether they will consider the issue is expected by February 25, 2019.
Read the Petition for A Writ of Certiorari to the Colorado Supreme Court, submitted to the United States Supreme Court in Rooks v. Rooks by Thomas More Society Special Counsel Rebecca Messall, on behalf of Mandy Rooks, on January 22, 2019 here.
Read the amicus curiae submitted to the Colorado Supreme Court in Rooks v. Rooksby Thomas More Society attorneys on behalf of the American Association of Pro-Life Obstetricians and Gynecologists here.
GEORGE WEST, Texas, February 5, 2019 (LifeSiteNews) ― A mother who refused to abort her unborn son despite being told he had a fatal abnormality prayed for a miracle — and got one.
Last summer, Kate Bledsoe McKinney, the mother of three daughters, was told that her unborn son had a cystic hygroma, a malformation of the lymphatic system, and that it was so big he could not survive.
“I was encouraged to go ahead and terminate,” McKinney recounted Sunday on her Facebook page.
“In fact, they could even do it that same day,” she continued. “It was nothing to them.”
When she began to cry, the doctor left the room and McKinney recalled that she had been advised 10 years before to abort her twin daughters.
“We were told they only had a 32.8 percent chance for both to be born alive,” she said. “I was encouraged to terminate them, also. I couldn’t believe I was here again.”
McKinney told the doctor that she wouldn’t abort her child and stuck to her guns despite his advice.
“He then told me about the risks of continuing the pregnancy and what would happen during a stillbirth,” she reported. “He was still trying to persuade me to abort.”
Fortunately, McKinney then met someone with a different philosophy of medical care. When a nurse came in to draw blood from the tear-stained mother, she shyly asked her how her appointment was. When McKinney said it could have gone better, the nurse took a risk.
“She gently placed her hand on my arm and looked me in the eyes and said, ‘Just have faith. Nothing is too big for God,’” McKinney recalled.
“In a doctor’s office, where it seemed like they were handing out lollipops with abortions, this woman was an angel,” she continued.
“I know God put her there to tell me that. I needed to hear it.”
After weeks of being offered — and refusing — an abortion multiple times at each medical appointment, McKinney prayed for a miracle. The next day, she noticed that the sonogram technician didn’t measure the cystic hygroma as usual, and asked what was going on. The sonogram technician said the doctor would explain.
Here’s what happened next:
“The doctor walked in. A new one. I had never seen her before during my visits. She was sweet and soft spoken. She had bedside manner. If anyone was going to give me bad news, I wanted it to be her. Immediately, I asked about the cystic hygroma not being measured. She gave me this sweet smile and told me that there was nothing there to measure. It was gone. I’m not sure who seemed more shocked. I had her repeat the news several times because I could not believe what was coming out of her mouth. There are cases out there (believe me, I read them day and night) where these things have resolved on their own. I knew there was a possibility. It was a very small chance, but it was there.”
McKinney’s baby boy was born November 4. The proud mother describes him as “perfect.” Although the doctors were shocked and ran test after test to find something seriously wrong with him, all they found was a small heart murmur that would resolve itself.
McKinney shared her testimony of grief, faith and hope over social media on February 5. She had always meant to share the story but indicated she was doing so now because of the radically pro-abortion, pro-infanticide law that passed in New York state.
Reflecting on the reality that she could have aborted her baby up to the day he was born, the happy mother said she could not believe it.
“I cannot fathom the idea that I could have changed my mind on November 4th. Just said, ‘To heck with it,’ because I changed my mind about having this baby,” she wrote.
“I firmly believe my faith was tested during this pregnancy. God wanted to see if I would do the unthinkable and terminate His plan. He wanted to see if I would believe in Him to heal our baby. Boy, am I glad I did,” she continued.
“I choose life. Yesterday, today and tomorrow. I will pray for New York and the leaders that made that decision. As I know all too well, nothing is too big for God.”
McKinney concluded by saying she made her story public so it could be shared.
“I hope it helps someone that may be going through something of their own,” she wrote.
One of the most prominent features of the Culture of Death is its short-sightedness. It puts grand plans into action and makes sweeping promises about how many lives will be saved or improved by its initiatives. And then its architects are invariably shocked and surprised when a galaxy of negative unintended consequences quickly emerge, usually making the situation much worse than it was before. To put it simply, the Culture of Death is entirely ignorant of sinful human nature.
The classic example of this absolute lack of foresight is the birth control pill.
From the very first day it was introduced, “family planning” experts hailed the Pill as the conclusive solution to “unwanted pregnancies.” But continued promises of high efficiency, combined with the easy availability of abortion as a “backup,” inevitably led to widespread careless use and abuse of the Pill. When the Pill failed to prevent pregnancy, many women felt entitled to an abortion because they believed that medical technology had failed them and that another type of medical technology was the “answer” to their problem.
Use of the Pill requires care and consistent attention. Each cycle of pills must be taken in the proper order every day at about the same time. So women often forget to take pills, take them at the wrong time, or lose them. This is the major contributor to an incredible number of unintended pregnancies, especially among younger women. U.S. women who are on the Pill experience nearly a million unintended pregnancies annually, and more than 40 percent of these occur among girls and women 15 to 24 years old.[i]
The method effectiveness of the Pill is 99.7 percent per year. This percentage is extremely high, but it refers to the efficiency of the Pill when a woman is in excellent health and uses the Pill without error. When user error and illness are factored in, the result is the actual, or “real world” user effectiveness rate. In the case of the Pill, this is only 91 percent per year.[ii] This means that nine percent of women on the Pill will become pregnant in any given year of use. In other words, the Pill itself is responsible for only about three percent of all failures, and the users are responsible for the remainder.
The 91 percent “real world” effectiveness rate for the Pill still sounds high until we calculate the probability of a woman becoming pregnant over an extended period of time when using it.
She has a nine percent probability of becoming pregnant in the first year, a one in four (25%) probability in three years; 38% in five years; and 61% in ten years.[iii]
In summary, if a sexually active girl of 15 starts using the Pill continuously, there is a nearly 50 percent chance that she will become pregnant by the time she is 22!
This statistic is verified by pro‑abortionists, including Dr. Christopher Tietze, who said that “within 10 years, 20 to 50 percent of Pill users and a substantial majority of users of other methods may be expected to experience at least one repeat abortion.”[iv] Note that Tietze is speaking about repeat (second or more) abortions here. These statistics are significant when one considers that one of the primary goals of school‑based clinics (SBCs) is to distribute contraceptives and abortifacients to teenagers without parental consent or knowledge.
These rates are in line with Alan Guttmacher Institute figures that show that half of all abortion patients thirty years ago were practicing contraception during the month in which they conceived. Additionally, the majority of abortion patients who had stopped using a method prior to becoming pregnant said they had most recently used the Pill.[v]
The situation has not improved, despite decades of saturation propaganda campaigns by everyone from big pharma to Neofeminist groups. A 2007 Marie Stopes International study found that 43 percent of aborting women were using the Pill when they got pregnant, and another 27 percent were using condoms.[vi] And in 2014, the British Pregnancy Advisory Service, the largest chain of abortion mills in the United Kingdom, found that 27 percent of women obtaining abortions were on the Pill when they got pregnant, while 35 percent were using condoms.[vii] BPAS Executive Director Ann Furedi confirmed what pro-lifers have always claimed when she acknowledged that “Ultimately women cannot control their fertility through contraception alone, and need accessible abortion services as a back-up for when their contraception lets them down.” [viii]
The Pill: Unsafe At Any Speed
Even after the shift from high-dose to low-dose pills, United States Federal courts classified the birth control as “unavoidably unsafe.”[ix] This means that, implicit in a woman’s consent to use the Pill is an acknowledgement of physical risk ― even if she is not entirely informed of all (or any) of its dangers.
This legal classification means that women injured by the Pill have a much harder time recovering damages. Dr. John Hildebrand, an expert in the field of human reproduction, estimated that more than 500 women die every year because of pill‑induced effects. This startling number is confirmed by figures provided by the Alan Guttmacher Institute (the world’s foremost abortions statistics analyzer) and one of the foremost abortionists in the United States, Warren Hern. His textbook Abortion Practice contains figures that lead to the conclusion that more than 30,000 American women have died due to direct side effects of the Pill since it was adopted in the United States ― with a current average of 600 to 700 deaths per year.[x]
It is ironic indeed that the same pill that the radical feminists pushed so hard as part of their solution to illegal abortion deaths now kills five to seven times as many women per year as illegal abortions themselves did before Roe v. Wade. And, with a few minor exceptions, these feminists do not breathe a word about it.
In 2010, major magazines, newspapers and pro‑abortion organizations celebrated fifty years of “The Pill,” and trumpeted how it has freed women from “unwanted childbearing” and drudgery. Perhaps they should tell that to the loved ones of the more than thirty thousand women who have died from the fatal side effects of the Pill.
The manufacturers of each of the more than 125 brands of birth control pill issue patient information pamphlets (PIPs) which give detailed information on each one. These standardized forms each have sections entitled “Warnings and Precautions” and “Adverse Reactions,” which list anywhere from 50 to 67 side effects of the Pill. The most serious of these include cardiovascular and breast problems.
The most dangerous and well‑documented side effects commonly associated with the Pill are heart attacks and strokes. The eight‑year Nurse’s Health Study at Harvard Medical School found that Pill users are 250 percent as likely to have heart attacks and strokes than those who don’t use the Pill, probably because the Pill greatly increases blood clotting ability. One of the major findings of the study was that women who get off the Pill have rates of cardiovascular disease equal to that of the general population after a period of one year.[xi] All of the patient information pamphlets produced by the manufacturers of the Pill confirm that the drug increases these risks.
Soon after the high-dose pills were phased out in favor of the low-dose regimen, the Pill came under intense scrutiny by researchers. In 1988, scientists at the Boston University School of Medicine, the University of Pennsylvania, and New York’s Memorial Sloan‑Kettering Cancer Center showed that the longer women took the Pill, the greater were their chances of contracting breast cancer. The risk of developing breast cancer was found to be twice as great by age 45 for women who had used the Pill for less than ten years and four times as great for women who had used the Pill for greater than ten years.
After a decade of accumulating evidence, the International Agency for Research on Cancer (IARC) classified combined oral contraceptives as “carcinogenic to humans” (Group 1). In 2005, the IARC confirmed this classification and has not changed it since.[xii]
Researchers at the Mayo Clinic followed up this classification with the most comprehensive review of studies on the Pill-breast cancer link ever performed. They found that 21 of 23 large well-conducted studies found that there was an average of a 44 percent increased risk of breast cancer in women who were taking the Pill prior to their first pregnancy.[xiii]
Indirect Impacts of the Pill
We have seen that the birth control pill is so ineffective that it fails hundreds of thousands of times annually in the United States, leading to hundreds of thousands of surgical abortions. We have also covered some of the more serious physical side effects inflicted upon women by the Pill, including more than 30,000 deaths and tens of thousands seriously injured since its introduction.
The indirect impacts of the Pill are much more diffuse, but are terribly damaging to society in general. The Pill impacts not only women, but men and children.
Since its introduction, the Pill has contributed heavily towards sexual promiscuity, the increase of illegitimate births, the explosion of venereal diseases, and the degradation of marriage and the family.
Increased Promiscuity
Immediately after the Pill was introduced in the mid‑1960s, pre‑marital sex and cohabitation both almost doubled in only five years. Currently, 48 percent of all couples living together are not married.[xiv] People of all ages (but especially teenagers) are having premarital sex more than ever before. Wife‑swapping clubs, organized orgies, membership in sex addiction treatment organizations like Sexaholics Anonymous, hard‑core pornography, and ‘fantasy [sex] tours’ to Far East nations have increased tremendously.
After witnessing two decades of this social carnage, the developers of the Pill admitted that its wide availability appeals strongly to those persons with little regard for sexual ethics. Dr. Robert Kirstner of Harvard Medical School said, “About ten years ago, I declared that the Pill would not lead to promiscuity. Well, I was wrong. The birth control pill has been a major causal factor in the rapid increase in both V.D. and cervical cancer among adolescents by stimulating higher levels of promiscuity.”[xv] And Dr. Min‑Chueh Chang acknowledged, “[Young people] indulge in too much sexual activity … I personally feel the Pill has rather spoiled young people. It’s made them more permissive.”[xvi]
Dr. Alan Guttmacher, former Medical Director of the International Planned Parenthood Federation, also drew a clear picture of the link between abortion and contraception within the context of increased promiscuity nearly fifty years ago; “When an abortion is easily obtainable, contraception is neither actively nor diligently used. If we had abortion on demand, there would be no reward for the woman who practiced effective contraception. Abortion on demand relieves the husband of all possible responsibility; he simply becomes a coital animal.”[xvii]
Finally, psychologists Eugene Sandburg and Ralph Jacobs noted the obvious connection between contraception and abortion as birth control; “As legal abortion has become increasingly available, it has become evident that some women are now intentionally using abortion as a substitute for contraception.”[xviii]
Drs. Kirstner and Min‑Chueh were certainly correct in their assessment of the situation. In 1970, only 4.6 percent of all 15‑year‑old girls had experienced premarital sex. By 2000, this rate had increased more than eightfold to 40 percent. Of all unmarried girls in the 15 to 19 age bracket, 28.6 percent had had premarital sex in 1970. This rate had more than doubled to 61.4 percent by 1990[xix] and about 80 percent by 2000.[xx]
Illegitimate Births
The inevitable result of the combination of increases in premarital sex and of ‘unwanted pregnancy’ is an increase in illegitimate births and abortion. This principle is so obvious that leading “family planners” recognized it in the early 1970s.
Professor Kingsley Davis of the United States Commission on Population Growth and the American Future stated that
The current belief that illegitimacy will be reduced if teenage girls are given an effective contraceptive is an extension of the same reasoning that created the problem in the first place. It reflects an unwillingness to face problems of social control and social discipline, while trusting some technological device to extricate society from its difficulties. The irony is that the illegitimacy rise occurred precisely while contraceptive use was becoming more, rather than less, widespread and respectable.[xxi]
The illegitimacy rate for births among teenaged girls hovered around five to seven percent for decades until about 1960. Between 1960 and 1970, it doubled as the birth control pill ushered in the “Sexual Revolution.” After 1970, the teenage illegitimacy rate exploded with the introduction of comprehensive sex education programs and school‑based clinics.
The overall illegitimacy rate for all children born in the United States was 5 percent in 1960. This rate had increased 700 percent to 40.7% by 2008.[xxii]
This phenomenon is not just an ethical or religious concern, it is a profoundly practical one. Social workers know that children born into one‑parent families are much more likely to be abused and abusive, to be undereducated, to be under‑ or unemployed, to have illegitimate children themselves, and to be far more likely to become involved in criminal activity.
Degradation of Marriage and Family
In 1965, before the Pill became widely available, about 15 percent of all couples lived together before marriage. The major reason for the relatively low incidence of this arrangement was simple: Living together meant more sex, and more sex meant a greater chance of a pregnancy in a nation where abortion was still illegal.
Today, many young unmarried women are on the Pill and abortion is readily available as a backup. They feel that they have no reason not to be sexually active and “shack up” before marriage.
As a result, nearly half of all couples in the United States now live together before marriage.[xxiii] This in turn causes great problems because more than 75 percent of all couples who lived together before marriage eventually divorce.[xxiv] The Pill has also contributed greatly to our country’s exploding divorce rate, which was about 18 percent in 1965 and now stands at about 50 percent.[xxv]
Predictably, the innocent children of divorced couples are always those who suffer the most. But the gender feminists and sexologists simply write them off as a sort of necessary “collateral damage,” inevitable victims of the Sexual Revolution and the war against one’s own sexuality.
Implications for Pro‑Lifers
Millions of women in the USA and all over the world use the Pill. Many women who would never consider a surgical abortion now use low‑dose pills that cause them to abort a new life an average of once or twice every year. A large number of women who claim to be pro‑life use these pills, many at the urging of their husbands. These are usually women who are ignorant of the Pill’s abortifacient mode of action, those who think that their way of life requires that they use the Pill, or those who cannot mentally make the connection between contraception and abortion.
Pro-abortionists play upon this theme constantly. For example, `Catholic’ House Minority Leader Nancy Pelosi claimed that “98 percent of Catholic women use birth control to determine the size and timing of their families.”[xxvi] The reality is that 83 percent of Catholic women use artificial birth control (32% have been sterilized), and only 31 percent of Catholic women use the Pill.[xxvii]
Researchers have calculated that the birth control pill directly causes between 1.53 and 4.15 million chemical abortions per year in the United States ― up to four times the total number of surgical and medical abortions committed every year! We can calculate that about 750 million “silent abortions” have occurred in the United States since the birth control pill began to come into wide use in 1965.[xxviii]
To put this into perspective, for every surgical and RU-486 abortion that has been performed in this country, a dozen “silent abortions” have taken place.
This means that otherwise pro‑life women who are using the Pill or some other means of abortifacient birth control are committing abortions themselves on a frequent basis. These abortions are “silent” and unseen, but they are no less abortions than are gruesome third‑trimester D&X abortions. There are many pro‑lifers who are using these pills and who are involved in their promotion and distribution. These people must consider whether they can, in good conscience, criticize women whose action differs from their own only in that they have to drive to an abortion mill to commit it.
Conclusion
When Pope Paul VI overrode the recommendations of his Birth Control Commission and wrote Humanae Vitae in 1968, he was exposed to widespread criticism, dissent and ridicule. But the four predictions he made in his great encyclical have undeniably come true. These are; (1) infidelity and moral decline; (2) loss of respect for women; (3) abuse of power by public authorities; and (4) a false sense of unlimited dominion over one’s body.[xxix] Today, most women (and men) see contraception as essential to their lives, and what was once mortal sin has “evolved” in the minds of most Catholics into an absolute necessity of life, something they simply cannot do without.
The great irony in all of this is that those who follow Church teachings regarding sexual morality are not only happier, they find their lives less difficult and complicated in the long run.
This is how Our Lord planned it, and this is the way we should live.
Endnotes
[i] See Chapter 21 of The Facts of Life, “Contraception,” for calculations and documentation.
[ii] Robert A. Hatcher, et. al.Contraceptive Technology (20th Revised Edition) [New York: Ardent Media, Inc.], 2011. Table 26‑1, “Percentage of Women Experiencing an Unintended Pregnancy During the First Year of Typical Use and the First Year of Perfect Use of Contraception and the Percentage Continuing Use at the End of the First Year. United States,” page 791.
[iii] For references and calculations, e-mail Brian Clowes at bclowes@hli.org and ask for Excel spreadsheet F-02-05.XLS, “Probability of Pregnancy over Time for Fertile Women Who Use Various Methods of Birth Regulation, Ranked by User Effectiveness Rates.”
[iv] Christopher Tietze, quoted in the National Abortion Rights Action League’s A Speaker’s and Debater’s Guidebook. June 1978, page 24.
[v] Christopher Tietze, quoted in the National Abortion Rights Action League’s A Speaker’s and Debater’s Guidebook. June 1978, page 24.
[vi] Steven Ertelt. “British Abortion Business Admits Birth Control Doesn’t Prevent Pregnancy.” LifeNews.com, January 29, 2008.
[vii] Peter Baklinski. “Two-Thirds of Women Seeking Abortions were Using Contraception: Britain’s Largest Abortion Provider.” LifeSite Daily News, February 5, 2014.
[viii] Peter Baklinski. “Two-Thirds of Women Seeking Abortions were Using Contraception: Britain’s Largest Abortion Provider.” LifeSite Daily News, February 5, 2014.
[ix] Thomas P. Monaghan, Co‑Chairman, Free Speech Advocates. “Unavoidably Unsafe.” Fidelity Magazine, October 1987, pages 14 and 15.
[x] For references and calculations, e-mail Brian Clowes at bclowes@hli.org and ask for Excel spreadsheet F-02-06.XLS, “Estimate of Annual Deaths Attributable to Use of the Birth Control Pill in the USA, 1960-2014.”
[xi] Dr. Meir J. Stampfer. New England Journal of Medicine, November 24, 1988. This study was based on an eight‑year follow-up of 119,061 female nurses, ranging in age from 30 to 55 in 1980. 7,074 were current pill users and 49,269 were previous users. Overall, there were 380 heart attacks, 205 strokes, and 230 cardiovascular deaths among pill users.
[xii] UNDP/UNFPA/WHO/World Bank Special Program of Research, Development and Research Training in Human Reproduction (HRP). “Carcinogenicity of Combined Hormonal Contraceptives and Combined Menopausal Treatment,” September 2005, page 1.
[xiii] Chris Kahlenborn, M.D., Francesmary Modugno, Ph.D., MPH, Douglas M. Potter, Ph.D., and Walter B. Severs, Ph.D. “Oral Contraceptive Use as a Risk Factor for Pre-Menopausal Breast Cancer: A Meta-Analysis.” Journal of the Mayo Clinic, October 2006, http://www.mayoclinicproceedings.org/article/S0025-6196(11)61152-X/fulltext and http://www.polycarp.org/statement_mayo_clinic_article.htm, November 5, 2014.
[xiv] Centers for Disease Control and Prevention (CDCs), Division of Vital Statistics. Casey E. Copen, Ph.D., Kimberly Daniels, Ph.D. and William D. Mosher, Ph.D.. “First Premarital Cohabitation in the United States: 2006–2010 National Survey of Family Growth.” National Health Statistics Reports, Number 64 [April 4, 2013], http://www.cdc.gov/ nchs/data/nhsr/nhsr064.pdf.
[xv] Dr. Robert Kirstner, Harvard Medical School, one of the original developers of the birth control pill. Quoted in Barret L. Mosbacker. Special Report: Teenage Pregnancy and School‑Based Clinics [Washington, D.C.: Family Research Council], 1986, and in ALL About Issues, June 1981, page 5 [emphasis in the original].
[xvi] Dr. Min‑Chueh Chang, one of the inventors of the birth control pill. Quoted by Charles E. Rice. “Nature’s Intolerance of Abuse.” ALL About Issues, August 1981, page 6.
[xvii] Dr. Alan Guttmacher in a discussion at the Law, Morality and Abortion Symposium, held at Rutgers University Law School, March 27, 1968. Rutgers Law Review, 1968(22):415‑443.
[xviii] Eugene C. Sandburg, M.D. and Ralph I. Jacobs, M.D. “Psychology of the Misuse and Rejection of Contraception.” American Journal of Obstetrics and Gynecology, May 15, 1971, pages 227 to 237.
[xix] “The US Family Staggers into the Sexy Secular Future.” Family Research Newsletter, January‑March 1991, page 1, Table 1, “Percentage of Women Aged 15‑19 Who Reported Having Had Premarital Sexual Intercourse, By Race and Age ― United States, 1970‑1988.” Numbers from 1988 to 1992 are linearly extrapolated using 1985‑1988 rates.
[xx] United Nations Children’s Fund (UNICEF). “A League Table of Teenage Births in Rich Nations.” July 2001, page 2.
[xxi] Professor Kingsley Davis. “The American Family, Relation to Demographic Change.” Research Reports, United States Commission on Population Growth and the American Future. Volume I, Demographic and Social Aspects of Population Growth, edited by Robert Parke, Jr., and Charles F. Westoff [Washington, D.C.: United States Government Printing Office], 1972, page 253.
[xxii] United States Department of Commerce, Bureau of the Census. Reference Data Book and Guide to Sources, Statistical Abstract of the United States [Washington, DC: United States Government Printing Office], 2012 (132nd Edition). Table 78, “Live Births, Deaths, Marriages and Divorces: 1960 to 2008,” shows 4,248,000 total births for the year 2008, and Table 85, “Births to Unmarried Women by Race, Hispanic Origin, and Age of Mother: 1990 to 2008” shows 1,727,000 births to unmarried mothers in 2008, for a percentage rate of 40.7%. The entire Statistical Abstract for the current year in PDF format is available on the Census Bureau Web site.
[xxiii] Centers for Disease Control and Prevention (CDCs), Division of Vital Statistics. Casey E. Copen, Ph.D., Kimberly Daniels, Ph.D. and William D. Mosher, Ph.D.. “First Premarital Cohabitation in the United States: 2006–2010 National Survey of Family Growth.” National Health Statistics Reports, Number 64 [April 4, 2013], http://www.cdc.gov/ nchs/data/nhsr/nhsr064.pdf.
[xxiv] In 1989, James Bumpass, James Sweet, and Andrew Cherlin of the University of Wisconsin completed a long‑term study to determine the effect of prenuptial cohabitation on marriage. Described in Dale Vree. “Hey, it Sounds Plausible.” National Catholic Register, May 7, 1989, page 5.
[xxv] United States Department of Commerce, Bureau of the Census. Reference Data Book and Guide to Sources, Statistical Abstract of the United States [Washington, DC: United States Government Printing Office], 2010 (130th Edition). Table 78, “Live Births, Deaths, Marriages and Divorces: 1960 to 2007.” The entire Statistical Abstract for the current year in PDF format is available on the Census Bureau Web site.
[xxvi] House Minority Leader Nancy Pelosi (D-Calif.), February 16, 2012. Glenn Kessler. “The Claim that 98 Percent of Catholic Women Use Contraception: A Media Foul.” The Washington Post, February 17, 2012, http://www.washingtonpost.com/blogs/fact-checker/post/the-claim-that-98-percent-of-catholic-women-use-contraception-a-media-foul/2012/02/16/gIQAkPeqIR_blog.html.
[xxvii] Rachel K. Jones and J. Dreweke. “Countering Conventional Wisdom: New Evidence on Religion and Contraceptive Use.” Guttmacher Institute, 2011, and unpublished tabulations of the 2006–2008 National Survey of Family Growth. http://www.guttmacher.org/media/resources/Religion-FP-tables.html.
[xxviii] For references and calculations, e-mail Brian Clowes at bclowes@hli.org and ask for Excel spreadsheet F-02-A.XLS, “Birth Control Methods Used by United States Women, and Overall Estimated Number of “Silent Abortions,” 1965-2013.”
[xxix] For a short but excellent summary and exposition on the four prophecies of Pope Paul VI in Humanae Vitae, see Janet Smith. “Pope Paul VI as Prophet: Have Humanae Vitae’s Bold Predictions Come True?” at http://www3.nd.edu/~afreddos/courses/264/ popepaul.htm.
February 4, 2019 (C-Fam) – If a woman visits a doctor in Delaware for a sore throat or a sprained ankle, she may be asked a surprising question: “Do you want to become pregnant in the next year?” If she says no, she could leave the clinic that same day with a long-acting contraceptive implant or intrauterine device.
Promoting contraception as a way to reduce poverty is the result of a partnership between the state of Delaware and an organization called Upstream. The approach has received national attention and is being considered for a national expansion. Although this approach may seem innovative in the United States, it looks very familiar in an international context.
For decades, women in developing countries have surveyed about whether they would like to become pregnant in the near future. Those who answer no are described as having a “demand” for family planning, even if they say they have no intention of using a method.
The global contraceptive market has become increasingly saturated, and knowledge of methods is near universal. Meanwhile, family planning organizations have redoubled their efforts to increase demand among women on the ground through mass marketing campaigns, including radio and TV dramas. To donors and governments, they offer contraceptives as a solution to poverty, conflict, and environmental degradation.
Like all marketing experts, family planning organizations have done extensive research on how to increase “sales.” Recent years have seen a broad international push to integrate family planning into all areas of health care. In practice this means any woman of reproductive age may be offered contraceptives when she visits a health clinic, regardless of the reason for her visit.
As retailers know, most impulse buying occurs when people are already in stores, and may be followed by buyer’s remorse. But unlike food or an item of clothing, the insertion of a long-acting reversible contraceptive (or LARC) is a major medical decision that carries risks and side effects. Researchers found that four in ten women who stopped using long-acting contraceptives did so because of health concerns. Nevertheless, Upstream focuses on promoting such contraception over other methods due to their low failure rates. A spokeswoman for the pro-abortion National Institute for Reproductive Health expressed concern to the New York Times that the Upstream approach may be “tipping the scale” in favor of these methods.
Some women currently seeking to avoid pregnancy may want to return to fertility in the near future. As Lyman Stone notes in The Federalist, women accepting long-acting contraception may not realize that the effects can last up to a year after removal.
Whether in Delaware or sub-Saharan Africa, decisions around procreation are best made within the context of the family. The campaign for same-visit delivery of long-acting contraceptives eliminates the opportunity for women to consult their partners – or parents, in the case of adolescents – before making a decision.
Delaware’s former governor Jack Markell started the partnership with Upstream in 2014. He now sits on the organization’s board of directors, alongside an Upstream co-founder who worked as a lobbyist for Planned Parenthood and other pro-abortion organizations.
As for the hope of reducing poverty, the data is mixed. Brookings Institution fellow Isabel Sawhill told the New York Times, “It’s very expensive and very hard to reduce poverty. Reducing unplanned births is easy by comparison.”
SPOKANE, Washington, February 4, 2019 (LifeSiteNews) – A Catholic bishop has warned pro-abortion politicians who call themselves “Catholic” and who reside in his diocese that they “should not” present themselves to receive Holy Communion.
“Politicians who reside in the Catholic Diocese of Spokane, and who obstinately persevere in their public support for abortion, should not receive Communion without first being reconciled to Christ and the Church,” wrote Bishop Thomas Daly of Spokane, citing Canon 915 of church law (read full letter below).
In a tweet, the bishop said that “willful murder of unborn children is a grave evil,” and called on Catholics to read his Feb. 1 letter.
Bishop Thomas Daly@Bishop_Daly
Friends, please read my letter on the abortion legislation that has been passed in New York and considered in other states. The willful murder of unborn children is a grave evil. Let us pray for life to be protected from conception until natural death. http://ow.ly/VNxa30ny1mw
A spokesperson for the Spokane diocese said that Bishop Daly’s letter is not commenting directly on any politician in his diocese, but seeks to clarify that the “Catholic faith and public abortion advocacy are incompatible.” Those who publicly support access to abortion, the spokesperson said, “should refrain from receiving Holy Communion,” according to CNA.
The issue of pro-abortion politicians receiving Communion has been stirred of late ever since New York Gov. Andrew Cuomo (D), a Catholic, signed one of the most liberal pro-abortion laws in the country on Jan. 21. Various bishops have shown support for excommunication of Cuomo, but Cardinal Timothy Dolan of New York has called such a move “not an appropriate response.”
Bishop Daly mentioned Cuomo in his letter, stating that it is “unacceptable” to call oneself Catholic and champion abortion.
“The champion of this abortion legislation is Andrew Cuomo, a Catholic and governor of New York. Governor Cuomo frequently cites his Catholic faith in support of legislation he favors. His public witness as a Catholic politician, coupled with his stalwart support of abortion, is unacceptable,” the bishop wrote.
“Efforts to expand access to abortion, allowing murder of children up to the moment of birth is evil. Children are a gift from God, no matter the circumstances of their conception. They not only have a right to life, but we as a society have a moral obligation to protect them from harm,” he stated.
Bishop Daly concluded his letter by calling on Christians “to turn to Our Lord in prayer for our political leaders, entrusting them especially to the intercession of St. Thomas More, a public servant who preferred to die at the hands of civil authorities rather than abandon Christ and the Church.” Finally, he wrote: “Let us also keep the unborn, as well as all pregnant mothers, in our prayers.”
The future pope wrote that pro-abortion politicians must be admonished not to present themselves for Holy Communion. When “precautionary measures” have been to no avail, and the person continues to present himself to receive the Holy Eucharist, Ratzinger wrote, “the minister of Holy Communion must refuse to distribute it.”
***
Bishop Daly’s Feb 1, 2019 letter:
February 1, 2019
Dear Friends,
Each January as the nation commemorates the sad anniversary of the Roe v. Wade decision, marches are held, and vigils are prayed. Those committed to the cause of human rights of the unborn make their voices heard. This year, pro-abortion politicians fearing increased restrictions on abortion have advocated for and passed laws expanding access to abortion in the state of New York. Similar attempts have been made in Virginia.
Efforts to expand access to abortion, allowing murder of children up to the moment of birth is evil. Children are a gift from God, no matter the circumstances of their conception. They not only have a right to life, but we as a society have a moral obligation to protect them from harm.
The champion of this abortion legislation is Andrew Cuomo, a Catholic and governor of New York. Governor Cuomo frequently cites his Catholic faith in support of legislation he favors. His public witness as a Catholic politician, coupled with his stalwart support of abortion, is unacceptable.
Politicians who reside in the Catholic Diocese of Spokane, and who obstinately persevere in their public support for abortion, should not receive Communion without first being reconciled to Christ and the Church (cf. Canon 915; “Worthiness to Receive Holy Communion. General Principles.” Congregation for the Doctrine of the Faith, 2004).
The Church’s commitment to the life of every human person from conception until death is firm. God alone is the author of life and for the civil government to sanction the willful murder of children is unacceptable. For a Catholic political leader to do so is scandalous.
I encourage the faithful to turn to our Lord in prayer for our political leaders, entrusting them especially to the intercession of St. Thomas More, a public servant who preferred to die at the hands of civil authorities rather than abandon Christ and thI encourage the faithful to turn to our Lord in prayer for our political leaders, entrusting them especially to the intercession of St. Thomas More, a public servant who preferred to die at the hands of civil authorities rather than abandon Christ and the Church. Let us also keep the unborn, as well as all pregnant mothers, in our prayers.
George Mason University, starting in late October of 2018, rolled out a new initiative that was approved by university officials which was being lobbied for by the pro-abortion student group, Patriots for Choice. The newly approved initiative gave the green light to a third party to supply the Plan B pill, to be sold in one of the on-campus vending machines to students. The vending machine is located in the building on campus referred to as “SUB 1,” which is the equivalent to a common hub or union on a college campus where students eat and study. And the university stands to make a commission from the sales.
According to an October 15th article in The Fourth Estate, the Patriots for Choice organization’s leadership claimed on a flyer that the pill being sold “helps prevent pregnancy when taken within 72 hours of unprotected sex or birth control failure.” The pro-abortion student group also made the claim that the contraceptive “is not an abortion pill,” and “will not work if [the user] is already pregnant.” The Wall Street Journal also previously reported on the growing trend across the country for higher education institutions to offer Plan B in vending machines.
In light of George Mason University approving the Plan B pill and placing it into the vending machines, Live Action News launched an investigation into determining why this occurrence happened at the public institution by means of filing a FOIA (Freedom of Information Act) request. The findings suggested that there was not only little push back against the student organizations request, but also that “the Pill will be sold in the Vengo Vending Machines for $30 and the University will receive its previously negotiated commission of 9%.”
Additionally, emails between the Executive Director of GMU Student Health Services, Dr. Lisa L. Park, and GMU’s Administrative Director of Student Health Services, Dr. Carol J. Filak, responded to the request by offering times to meet in person, and later approving the ladder steps for the permanent placement of the pill on campus.
According to other FOIA documents requested by Live Action News, Patriots for Choice requested and was approved to spend $749 on November 15th, 2018 for an event billed as “Feminist Open Mic Night.” Students fees and outside tax dollars go to funding these activities through the office of the GMU Student Government. Live Action News has reached out to GMU’s pro-abortion student group, Patriots for Choice, for comment on the story multiple times but the group has not responded. University spokesman Michael Sandler did comment to Live Action News with a statement that the “9 percent commission is the standard flat rate that applies to all products sold from the Vengo Vending Machines.”
Further, a representative for Canteen, the Vending Machine company, wrote in an email to a GMU administrator, David Atkins, that “in the event we receive any negative feedback that we believe impacts our ability to continue to offer the product, we will remove them from the campus.”
Rose Pascarell, Vice President for University Life, told Live Action News, “The product was requested by students, and the university was able to accommodate. The product is sold over the counter at most local drug stores with no restrictions. Our students now have access and are able to purchase the same product on campus.”
HC George Mason@HCGeorgeMason
*Chris Traeger voice* This is LITERALLY one of the best things to ever happen!
Patriots for Choice@gmu4choice
We are so excited to announce that SUB 1 now has emergency contraception in a vending machine! Students can now access emergency contraception every day from 7:30am-10pm.
“Although the product is medically safe for people to self-administer and does not require a prescription, we would always prefer that students talk with medical or counseling practitioners about preventing unwanted pregnancy before using,” Pascarell continued. “However, some students who may not want to or don’t feel comfortable entering a health care agency are also able to access and our goal is to be responsive to student needs.”
The Patriots for Choice student page states that their purpose on campus is to “support and protect, as a fundamental right and value, a woman’s freedom to make personal decisions regarding the full range of reproductive choices…”
Currently, the student group is seeking positive feedback to report back to university officials. “We need your experience to help demonstrate the need for EC on campus and how it helps student well being,” the pro-abortion organization wrote in a November 14th Facebook post.
The group is currently seeking to expand the placement of the pills to be placed in more Vengo vending machines on the Fairfax campus along with a push to drown out opposition to their agenda.
Zachary Petrizzo is a sophomore at George Mason University. His previous work has appeared in The Daily Caller, Townhall, Campus Reform, and The College Fix, among others.
January 31, 2019 (LifeSiteNews) – The movie about Abby Johnson’s pro-life conversion has found a distributor and will be coming to 800 screens in March. The film’s backers released a two-and-a-half-minute trailer of the much-anticipated film today.
Pure Flix, the distributor for God’s Not Dead, is releasing “Unplanned” on 800 movie screens March 29, the Hollywood Reporter (THR)reports.
Unplanned is a dramatic film adaption of Johnson’s best-selling 2010 autobiographical book of the same name. It tells the story of Johnson’s journey from Planned Parenthood facility manager to pro-life activist.
“I thought I was helping women,” said Abby Johnson, founder and director of And Then There Were None, an organization that helps abortion workers exit the industry and find new jobs.
“But I was doing more harm than good. It wasn’t until I saw a child fight for its life that my world came crashing down and I understood the enormity of my actions. I had to leave. No one will be able to walk away after seeing this movie and say ‘I didn’t know,’” she added.
In the trailer, Johnson’s character is warned by Planned Parenthood that by crossing to the pro-life side she’s made an enemy of “one of the most powerful organizations on the planet.”
Unplanned was written and directed by Cary Soloman and Chuck Konzelman, the writers and co-producers for God’s Not Dead, God’s Not Dead 2 and Do You Believe. Daryl Lefever (I Can Only Imagine) is also a producer.
Pure Flix distributed the two God’s Not Dead films and Do You Believe theatrically as well.
“We had other offers but felt they would be our strongest partner because of the great success we’ve had together in the past,” Konzelman said of Unplanned.
Unplanned was filmed in secret and under a different name due to its content, and the filmmakers had to pull back from using some mainstream pop songs in the movie, because major record labels refused to license the music to them for the film.
Blake Kanicka, music supervisor for Unplanned, told THR that nine out of the 10 initial requests he’d made for licensing were denied. Among those turning the request down were Disney, Sony/ATV and Universal Music.
Some faith-based bands also denied the filmmakers use of their songs, telling Kanicka that they could not risk the possible controversy.
Actress Ashley Bratcher (War Room, 90 Minutes in Heaven) who plays Johnson, told the Fox & Friends program in December that she had been warned that she would probably be blacklisted for acting in the movie.
The $6 million cost for making Unplanned was financed in part by Mike Lindell, the multimillionaire founder of My Pillow, who invested $1 million in the film. Lindell, a pro-life Christian, told THR he plans to continue supporting films that represent his values.
The film has the endorsement of Kansas City Kansas Archbishop Joseph Naumann.
Naumann, also chairman of the United States Conference of Catholic Bishops’ Committee on Pro-life Activities, said during his homily for the March for Life Vigil Mass at the Basilica of the Immaculate Conception in Washington D.C., “If you see one film this year, see Unplanned… I warn you, Unplanned is graphic, it’s painful, but at the same time, inspiring…”
In addition to Bratcher, the movie stars Brooks Ryan as Johnson’s husband, Doug; Robia Scott (CSI, Buffy the Vampire Slayer) as Johnson’s superior at Planned Parenthood; Emma Elle Roberts (Hunger Games: Mocking Jay, I Am Not Ashamed, ) as Marilisa Carney, Kaiser Johnson (Little Boy, Vampire Diaries, Sleepy Hollow); and Jared Lotz (Of Little Convenience, Thanksgiving) as 40 Days for Life President Shawn Carney.
Pope John Paul II was born Karol Wojtyla, a man from a small town in Poland who lost all of his immediate family — mother, older brother, an infant sister and father — by the time he was 20 years old. Shortly thereafter, he vowed a life of celibacy as a Catholic priest. And yet Wojtyla would go on to be remembered as the “Pope of the Family.”
Twenty-five years ago next week, on Feb. 2, 1994, Pope John Paul II penned his “Letter to Families,” the subject of which was spurred by the United Nations’ declaration that 1994 would be the “Year of the Family.”
At the time, U.S. divorce rates were higher — about 4.6 per 1,000 people, compared with 2.9 in 2017. But marriage rates were also higher: 9.1 compared with 6.9 for those same years. Legalized same-sex “marriage” was still considered a taboo political idea and would remain so for more than a decade. And Bruce Jenner still went by Bruce Jenner.
But even though it was written 25 years ago, many Catholics in family-life ministries believe that the Church is only beginning to see the fruits of John Paul II’s message to families.
Although he was a celibate priest, Father Wojtyla became very close to a circle of young people whom he pastored while serving as chaplain to university students in Krakow. As they married and had children, Father Wojtyla offered spiritual and pastoral guidance to their families that would inform his work well into his years as Pope John Paul II.
“He was able to support these young families, to help them live the faith at a time when communist society was really trying to undermine the family,” said Jared Staudt, who is the director of formation for the Archdiocese of Denver, where he also leads “Building Family Culture” retreats for families.
When the Communist Party ruled Poland, family work and school schedules were arranged in such a way that they spent as little time together as possible. The state, and not the family, was, according to the government, the ultimate good and end of society.
“So he was in this battle for family life very directly in Communist Poland,” he said of Father Wojtyla.
Much of what Father Wojtyla came to know about the sanctity and importance of marriage and family life can be found in his 1994 “Letter to Families.”
Man, Woman and Child: The Family as Vocation
John Paul II wrote prolifically on the family, but this letter is one of his more personal and concise works, detailing much of his thought on marriage and family.
He was known for elevating the idea of the vocation of marriage and family life to a level that had not yet been articulated in the Catholic Church.
“John Paul literally started a revolution when it comes to the Catholic Church and family,” said Steve Bollman, founder of family ministry Paradisus Dei.
“What John Paul did is he truly identified the family as the pathway to holiness,” Bollman said. “In this letter, it’s the family that’s placed at the heart of the great struggle between good and evil, between life and death, between love and all that’s opposed to love.”
In his letter, John Paul II wrote that men and women, particularly in their roles as fathers and mothers in the family, are key to building up a “civilization of love,” in which families are able to give and receive love at individual and societal levels.
“If the first ‘way of the Church’ is the family, it should also be said that the civilization of love is also the ‘way of the Church,’ which journeys through the world and summons families to this way; it summons also other social, national and international institutions, because of families and through families. The family, in fact, depends for several reasons on the civilization of love, and finds therein the reasons for its existence as family. And at the same time the family is the center and the heart of the civilization of love,” John Paul II wrote (13).
Bollman said that by telling families that they were at the heart of the Church, it called them to holiness in a way that hadn’t yet been articulated.
“The vast majority of people become holy as a husband and father and wife and mother, not in spite of that,” Bollman said. John Paul II’s teachings on the family are at the foundation of Bollman’s work at Paradisus Dei, which includes a couple’s ministry and “That Man Is You,” a ministry for men that particularly focuses on their roles as husbands and fathers.
“Our tagline is ‘Helping families discover the superabundance of God.’ That’s what we are: We’re all about family and finding God within the family,” he said.
Cultural Attacks on the Family
Staudt called John Paul II’s letter “prophetic” because it addresses not only the crucial importance of the family’s place in society, but some of the key ways it is under attack.
And if attacks on the family were urgent in 1994, they are all the more so today, Staudt said.
“John Paul’s famous line from the letter — ‘The history of mankind, the history of salvation, passes by way of the family’ — is actually chilling, at this point,” Staudt noted, “because what we’re seeing is that we don’t have hope for the future [as a society]; we’re not investing for the future of society or for the Church. We’re just living for the present moment for our own selfish desires. So I think John Paul was already recognizing that the foundation of society itself is already in jeopardy, if people are not getting married, if they’re not having kids, they’re saying No to the future.”
According to Pew Research Center, the marriage rate in the United States is currently hovering at around 50%, meaning half of U.S. adults aged 18 and older are married, a steep decline compared to the peak rate of 72% in 1960. The fertility rate is also at a 30-year low in the United States and sits below replacement levels. As of 2014, less than half of children were living in a traditional nuclear home with their married mother and father.
By many measures, marriage and family life today are in crisis, in ways that are perhaps even more pronounced than when John Paul II wrote this letter.
“I think the ‘crisis of concepts’ that John Paul II speaks of is an enormous challenge for the family today,” Sister John Mary, of the Sisters of Life, told CNA.
“Who can deny that our age is one marked by a great crisis, which appears above all as a profound ‘crisis of truth?’” John Paul II wrote. “A crisis of truth means, in the first place, a crisis of concepts. Do the words ‘love,’ ‘freedom,’ ‘sincere gift’ and even ‘person’ and ‘rights of the person’ really convey their essential meaning?” This crisis now seems to be even more profound than when the Pope first wrote these words, Sister John Mary said.
“Even more so today than when the ‘Letter to Families’ was written, modern culture does not recognize the truth of who the human person is, what we are made for, what constitutes a family, what freedom and human rights are,” she said. “So to truly live Christian family life becomes more and more radically countercultural. John Paul II addresses this in the letter by proposing the anthropology that corrects this crisis of concepts and allows for a civilization of love to grow by way of marriage and family,” she noted.
Another major challenge faced by families is the “radical individualism” present in current culture, Sister John Mary said, which is something else John Paul II addressed in the letter.
According to John Paul II, radical individualism is “based on a faulty notion of freedom and proposes personalism as the antidote,” Sister John Mary said. “The family is the first place where love is given and received. But if parents do not model authentic, self-giving love to their children, families become groups of persons pursuing their own selfish ends.”
Papal Cure for a Sick Society
Though John Paul II’s descriptions of these crises and the current state of affairs of marriage and family in the world paint a dark picture, John Paul also provides families and the Church a way out.
Bill Donaghy is a senior lecturer and content specialist with the Theology of the Body Institute. The mission of the institute is to educate and train men and women to understand, live and promote John Paul II’s teachings in his theology of the body catechesis.
Donaghy told CNA that not only does he consider John Paul II’s “Letter to Families” the blueprint on how to live a holy life personally as a husband and father, he also considers it the “antidote” to everything that goes against a “civilization of love.”
“Without a doubt in my mind, in the providence of God, who could foresee today’s crisis in marriage and the family, the attempt to redefine marriage and the explosion of gender ideologies that detach our identity from our humanity, St. John Paul II’s thought is the antidote, the cure, the clear truth of who we are and how we are to live as human persons made by Love,” he said.
“I think the vision presented in this letter is actually more relevant now than it was 25 years ago,” he said. “It contains the secret for our joy, the mystical meaning of marriage, the way home for the prodigal sons and daughters who’ve tried everything else to bring joy and failed to find it.”
For himself, Donaghy said building the “civilization of love” starts in his own home — by treating his wife with love and respect, by spending time with and listening to his children and by modeling sacrificial love. At the parish level, he said the Church must help families by creating space for “real human interaction, conversation and formation.”
“Again, the ‘Letter to Families’ is a goldmine of a teaching, a school of love for humanity. But we’ve got to make time and space for it to enter into the everyday dynamics of our own family,” he said.
Staudt also told CNA that the words and teachings of Pope John Paul II on the family have deeply inspired his work in family ministry.
“It really is through John Paul’s teachings, the letter and his other teachings … that I’ve discerned that the way to build Christian culture is through family life,” Staudt, the father of six children, told CNA.
For the “Building Family Culture” retreats that he leads, Staudt said that he focuses on teaching families how to pray, the importance of which is heavily emphasized by John Paul II in his letter.
“Prayer must become the dominant element of the ‘Year of the Family’ in the Church: prayer by the family, prayer for the family and prayer with the family,” John Paul II wrote. “Prayer increases the strength and spiritual unity of the family, helping the family to partake of God’s own ‘strength.’”
“I think we take that for granted, that families know how to pray, and I don’t think they do. So I think that’s the foundation, that’s the core, and John Paul does talk a lot about that,” Staudt said. After prayer, he also focuses on how to build a family culture, which includes doing things that form children’s imagination in positive and beautiful ways.
Staudt said he hopes that more in family ministry “wake up” to the urgency of helping families become what John Paul II has called them to be.
“I don’t think enough people have woken up to the urgency in supporting family life and really making that a priority in their parishes, their dioceses, in catechesis, in evangelization,” he said.
“John Paul, I think, is truly prophetic in pointing us to the fundamental realities of man, woman, human love, family life as crucial for the Church and society at this time — that these are the key issues that we need to face.”
Sister John Mary and her fellow Sisters of Life say they help build a “civilization of love” through the women they help in crisis pregnancies, the women they counsel after abortions, or the young people who are early on in their journeys of faith.
Sister John May said that because John Paul II was speaking about universal truths of the human person, his words will continue to be relevant for families and the Church throughout time. “John Paul’s ‘Letter to Families’ explores universal truths: the goodness of the human person, the dignity of marriage and the very real challenges facing families today,” she said. “Marriage and family are God’s plan to satisfy the universal longings of the human heart, so speaking of them is always timely.”
“We are all called to do something great with our life and our love,” she added. “We are made for love and communion with God and others. John Paul II reminds us of this lofty call and encourages us that true love is possible.”
January 28, 2019 (LifeSiteNews) – America’s top abortion chain is rolling out a new product meant to cut out any middleman between themselves and children searching for information and guidance about sex, contraception, and abortion: a new automated chat program to directly answer whatever questions they may have.
Roo is a “chatbot” operated by artificial intelligence and accessible via smartphones. Intended for kids between the ages of 13 and 17, it is meant to compensate for children who “don’t have access to sex education or only have access to programs that teach abstinence,” the Wall Street Journalparaphrases Planned Parenthood CEO Leana Wen as explaining.
“Roo answers all your awkward questions about sexual health, relationships, growing up, and more. Chatting with Roo is free and private, so go ahead and ask the things you don’t want to ask out loud,” Planned Parenthood says on its “Ask Roo” web page. Its “answers are backed by professional health educators from Planned Parenthood,” and the chatbot “gets a little bit smarter every time you ask a question.”
Young people will flock to the service because “they’re concerned about privacy, and skeptical about anything that seems to lecture or talk down to them or sounds like parents,” added Gene Liebel, a founding partner at the tech company Work & Co. that helped develop Roo.
Users can type in their own questions or choose from a selection of frequently-asked questions. Asking “What is an abortion” results in “Abortion is a legal and safe way to end a pregnancy […] there’s many reasons why someone may decide to have an abortion and only you can decide what is best for you.”
“What’s the right age to have sex for the first time” yields “it’s all about picking the right age for you, which might be totally different than the right age for other people. It may seem like everybody you know is having sex, but that’s definitely not true. The average age when people have sex for the first time is around 17.” It then displays an animated graphic of the phrase “you do you.”
Roo answers “When are you no longer a virgin” by claiming that while most people consider it “after the first time they have sex,” sex also “means different things to different people, so it’s up to you to decide what virginity means to you.”
Readiness to have sex is simply defined as a “big decision” that should be discussed “with a non-robot person you trust.” In response to “How do you have sex without getting pregnant,” Roo suggests various forms of birth control, but leaves out the fact that none are 100% effective.
In response to “how do I get birth control without my parents knowing,” Roo says parental permission is usually unnecessary except in certain states, and that Planned Parenthood can help teens “get started on birth control.” It accepts as a given that kids should bypass their parents, and makes no effort to suggest that teens at least consider discussing the matter with them.
Notably, when LifeSiteNews manually typed the following queries – “when does life begin,” “does human life begin at conception,” “are fetuses alive,” and “I heard abortion kills babies” – Roo was unable to process any of them and suggested either rephrasing the question or speaking to a live Planned Parenthood worker.
The Daily Callernotes that the last collaboration between Planned Parenthood and Work & Co. was TrackingTrump.org, a timeline documenting decisions by the Trump administration related to contraception, sex education, and “anti-LGBT” appointees.
Will the world’s population really reach 11.2 billion in 2100? This week The Guardian provides a good summary of alternate world population projections which challenge this United Nations figure, and casts doubt on whether the world’s population will really continue to grow until the end of this century.
The United Nations bases its population projections on a range of uncertain assumptions about fertility and mortality. Its most likely current estimate is that world population will reach 11.2 billion by 2100, and then stabilise and slightly decline.
The UN is not the only international body to project world population, and the various demographers are certainly not in agreement. A key question is whether Africa’s fertility will remain at current rates, or will drop to follow Western low fertility trends. The Guardian discusses some of the alternate projections:
Jørgen Randers, a Norwegian academic who decades ago warned of a potential global catastrophe caused by overpopulation, has changed his mind. “The world population will never reach nine billion people,” he now believes. “It will peak at 8 billion in 2040, and then decline.”
Similarly, Prof Wolfgang Lutz and his fellow demographers at Vienna’s International Institute for Applied Systems Analysis predict the human population will stabilise by mid-century and then start to go down. [Marcus discussed these predictions here, back in 2014.]
A Deutsche Bank report has the planetary population peaking at 8.7 billion in 2055 and then declining to 8 billion by century’s end.
Since 1970, a sharp global decline in fertility has occurred. In the United States, all of Europe, and much of the rest of the West, fertility is now actually below the replacement level of 2.1 children and will eventually lead to population decline, unless those countries can attract enough immigrants to sustain current population levels. In fact, many European countries may almost cease to exist by 2300 if low fertility persists and migration does not intervene, according to the most recent United Nations long-term population projections.
According to The Guardian:
Already, almost two dozen countries are getting smaller every year, from Poland to Cuba to Japan, which lost almost 450,000 people in 2018. In these countries, women have fewer than the 2.1 babies that they must produce, on average, for a population to remain stable. The population decline would be even steeper were it not for steadily increasing life expectancy.
The fertility rate in the UK is 1.7. Most population growth in the UK today is the result of international immigration, according to the Office of National Statistics. Without immigrants, Great Britain would eventually enter an era of population decline.
More old people and fewer young people place an increased strain on society’s ability to generate the wealth and taxes needed to fund, among other things, healthcare for the old.
The really big news, however, is found in the large countries of the developing world, where the great majority of people live. There, declines in birth rates have been simply astonishing. China, the world’s largest country, has a fertility rate of 1.5, lower than Britain’s. India, soon to overtake China as the world’s most populous nation, is at the replacement rate of 2.1 and falling. Brazil, the fifth most populous country, has a fertility rate of 1.8.
One cause of the accelerating decline in fertility is urbanisation. In 2007, for the first time in human history, the majority of people in the world lived in cities. Today it is 55% and, in three decades, it is expected to reach 66%.
Currently, Africa has the highest fertility rates in the world and the majority of the world’s population growth is coming from that continent. Yet, sub-Saharan Africa is also the fastest urbanising part of the world, with annual urban population increases of 4%, twice the global average. This is a factor in the expectation by many demographers that African fertility rates will continue to decline.
According to The Guardian, “Population decline is not a good thing or a bad thing. But it is a big thing. It’s time to look it in the eye.”
Over the past few decades world leaders have compelled people to have fewer children, often in the euphemistic name of reproductive and sexual health. The United Nations itself gave its first population award to both the Chinese minister for population and the Prime Minister of India for their work initiating family planning and sterilisation programmes, forced abortions and sterilisations and all. Vincenzina Santoro points out that the Guttmacher Institute jointly accepted the most recent annual Population Prize of the United Nations last June.
As more people seemingly begin to realise that the world does not have a population spiralling out of control, but instead a soon to be declining one, let’s look the forced taking of life, the abuse of women, and the thousands of dollars of aid and public “health” money spent in the name of population control in the eye too.
While 700,000 marchers flocked to Washington, D.C. to stand up for the rights of the preborn, a record number were also marching for in Paris. The March for Life in Paris, a non-denominational and non-partisan event, is the largest annual pro-life gathering in Europe, and the number of attendees continues to grow. In 2009, a reported 20,000 people came to march. This year’s 13th annual event saw an estimated 50,000 people, a massive increase, attend the January 20th protest, many of whom were between 18 and 35 years old.
François, 20 ans, porteur de #trisomie21, devant 50 000 manifestants de la Marche Pour La Vie: “J’ai un cœur comme vous, je suis comme vous, j’aime la Vie. Ma vie est belle même avec la #trisomie21. Je vous demande de toujours protéger les plus faibles.”
Vive la Vie !#MPLV2019pic.twitter.com/xjEZtEEJUj
One powerful witness came from one of these young people. Francois, a 20-year-old man with Down Syndrome, addressed the crowd. “I have a heart like you,” he said. “I am like you. I love life! My life is beautiful, even with Trisomy 21. I ask you always to protect the weakest.”
People with Down syndrome are routinely targeted for eugenic abortion, especially in Europe. In France in 2015, the abortion rate after a diagnosis of Down Syndrome was reported as 77%. In many parts of the European Union, it’s much closer to 90%. In Iceland, it is almost 100%, with just one or two children born with the condition each year.
The March for Life in Paris began in 2005, as French pro-life organizations came together to protest 30 years of legalized abortion. It is held on or around the January 18th anniversary of the legalization of abortion in France. This year’s Paris March for Life had as a theme the issues of conscience protections for health care workers, among others.
Life offers no guarantee, but abortion gives no chance.
Also forefront among the issues in this year’s march was the recommendation of France’s highest bioethics body that IVF should be available to all, and an “expansion of eugenic policies.” Nicolas Sévillia of the Jérôme Lejeune Foundation, which helps organize the Paris march, has put this march in the context of the “yellow vest protests.” The protests are a populist movement, whose social and political influence points to the possibility for popular manifestation to change the national discourseon various issues. Hitherto, bioethical and social issues have been excluded from what has been called “the great national debate.” The March hopes to change that, as yellow vest protesters joined the pro-life march.
lf a native of Argentina, addressed the March through the Papal Nuncio, saying, “All the evil done in the world can be summed up in contempt for life.” He encouraged the participants to “bear witness to the inalienable values of human dignity and human life.”
France has around 220,000 abortions per year. It is estimated that one in three French women have abortions in their lifetimes.
When we Catholics defend our Church’s teaching about contraception, we almost always use philosophical arguments that appeal to the natural law without relying on God or revelation. These kinds of arguments are great, as they can appeal to people of any faith (or even no faith), but there is another approach we can take as well, one that is particularly helpful when discussing the issue with other Christians: we can look to the teaching of Scripture on the subject. The Bible does not explicitly address the morality of contraception, but there is a passage that very strongly implies that it’s wrong.
The Story of Onan
In the book of Genesis, we find the story of a man named Onan, the most famous and (to my knowledge) only user of a contraceptive method in all of Scripture. Granted, modern contraceptive methods were not around in biblical times, but the ancients did have ways of making their sex non-procreative, and Scripture tells us that Onan used one such method:
“Then Judah said to Onan, ‘Go in to your brother’s wife, and perform the duty of a brother-in-law to her, and raise up offspring for your brother.’ But Onan knew that the offspring would not be his; so when he went in to his brother’s wife he spilled the semen on the ground, lest he should give offspring to his brother. And what he did was displeasing in the sight of the Lord, and he slew him also.” (Genesis 38:8-10)
This passage can be a bit confusing for us 21st century Americans, so let me give a bit of background. In ancient Israel, when a married man died childless, it was his brother’s duty to marry his widowed sister-in-law and have a child with her, and that child would legally be considered the dead man’s heir.
Once we understand the cultural context, the story becomes easy to follow. Onan’s brother died without any kids, so it was Onan’s responsibility to have a child with his sister-in-law. However, he knew the child would not be his, so when they had sex, he used an ancient method of birth control (pulling out before ejaculating) to render their sex non-procreative. This angered God, so he punished Onan by killing him.
The Big Question
The story raises an obvious question for us: what exactly was wrong with Onan’s action? Unfortunately, the text doesn’t give us an answer, so we have to figure it out for ourselves. Essentially, there are three possible reasons for God’s anger with Onan:
1) Onan’s sin was refusing to perform “the duty of a brother-in-law.”
2) Onan’s sin was failing to continue the line of the patriarch Judah (his father), the line from which Jesus would eventually come.
3) Onan’s sin was using an ancient method of contraception.
So which is it? Which of these three is the reason God killed Onan? To figure that out, we need to read the story in the larger context of Scripture as a whole, and when we do that, we’ll find that the answer becomes pretty clear.
The Wrong Answers
Let’s begin by considering the first possible answer. Did God kill Onan simply because he failed in his duty to his sister-in-law? Probably not. If we look at the rest of the Old Testament, the punishment in ancient Israel for this kind of sin was not death (Deuteronomy 25:7-11). Granted, Onan lived before the Jewish Law was given, but if God did not think that failing to raise up children for one’s dead brother was a sin worthy of death for the Israelites after the Law was given, he probably did not think that way before it was given either. As a result, it’s unlikely that this was the reason why he killed Onan.
Next, let’s look at the second possibility. Did God punish Onan because he failed to continue the line of Judah? Again, not likely. While we know from the rest of Scripture how important that family tree would become, at this point in the story, there is not even a hint of it. The first indication in the Bible of Judah’s future importance comes later on, towards the end of Genesis (Genesis 49:8-12), so it would not be fair for God to expect Onan to understand that at this point. As a result, it is unlikely that this was the reason why Onan was put to death.
The Right Answer
At this point, we might be tempted to say that the third answer (that Onan’s sin was using an ancient method of contraception) has to be right simply by process of elimination, but let’s dig a bit deeper. Let’s see if there is any evidence supporting this option other than the failure of the other two alternatives. Specifically, take a look at these passages from the book of Leviticus:
“If a man has sexual relations with a man as one does with a woman, both of them have done what is detestable. They are to be put to death; their blood will be on their own heads.” (Leviticus 20:13)
“If a man has sexual relations with an animal, he is to be put to death, and you must kill the animal. If a woman approaches an animal to have sexual relations with it, kill both the woman and the animal. They are to be put to death; their blood will be on their own heads.” (Leviticus 20:15-16)
At first, it might be tough to see just what these passages have to do with the story of Onan, but let’s ponder them a bit. In these texts, God is prescribing death as the penalty for homosexual activity and bestiality, two acts that share something in common with contraception: all three of them are non-procreative forms of sexual activity. Sex with an animal or with someone of the same gender is intrinsically incapable of producing a child, and contraception artificially removes the procreative potential of the act.
Once we recognize that similarity, we can see that the third possible explanation for Onan’s punishment is most likely the right one. God didn’t think that failing to raise up children for one’s dead brother merited death for his ancient people, but he apparently thought that non-procreative forms of sex did, so Onan’s fate makes perfect sense. God killed him because he spilled his seed on the ground, thereby removing the procreative potential of his sex with his sister-in-law and making it similar in that key respect (but, we should note, not necessarily in any others) to homosexuality and bestiality, two sins that merited death in the Old Testament era.
Scriptural Support
Like I said before, this approach to the issue of contraception is particularly helpful when talking to other Christians. The story of Onan complements the philosophical arguments we normally use by confirming that our philosophy is in fact correct. It shows us that the Church’s teaching on the matter is supported by both reason and revelation, so if a fellow Christian is having a tough time understanding or accepting the philosophy behind it, the fact that Onan was punished for rendering his sex non-procreative can help them see that the teaching is true even if they cannot fully see why it is true.
January 23, 2019 (LifeSiteNews) – As a people of life, we pro-lifers are naturally pro-natal. We not only abhor abortion, we offer positive encouragement to young couples to get married and have little blessings—lots of them.
Yet we live in a wider culture that teaches young people that babies are burdens and not blessings. Add to this government policies that discourage marriage and childbearing, and it is not surprising that U.S. birthrates continue to fall. In fact, our birth rate, which first dropped below replacement way back in 1971, is now the lowest it has ever been in American history.
Indeed, they are the only future a nation has. And we are simply not having enough.
Consider that the total fertility rate needed for a population to sustain itself over time is 2,100 births per 1,000. But America is not even close to that. We are currently averaging, according to the U.S. National Center for health Statistics, an anemic 1,765.5 births per 1,000 women. This is a recipe for demographic decline.
So, what can we as a country do about these dismal numbers?
The first thing we ought to do is overturn Roe v. Wade, the infamous Supreme Court ruling that has led to the deaths of 60 million unborn children over the past 45 years. In 2016 alone, the lives of 884,524 Americans were snuffed out before they saw the light of day.
This number is roughly equal to the shortfall in births. In other words, absent abortion, the American fertility rate would be just about at replacement.
At the same time, we also have to address the “push factors” that propel young women into abortion clinics. Often it is not a matter of “her choice” at all, but rather pressure from a husband, a boyfriend, or a parent or grandparent that forces her hand.
How many of these women would have chosen life if just one friend or family member had stood by her side? Most of them, reported one study. So it is incumbent upon pro-lifers to be there for young women in need.
The second thing we have to do is help young people avoid the “debt trap” of student loans. Far too many millennials find themselves graduating from college with tens of thousands of dollars in debt that will take years, or even decades, to pay back. Others don’t graduate at all, which makes their student loans even more difficult to pay back.
Over the last two years, the rapidly improving economy should have sent birth rates higher. After all, factories are now moving back to the U.S., and unemployment rates are at historic lows. But a trillion-and-a-half dollars in outstanding student loans stand in the way of a fertility rebound. In a sense, student loans may be the most effective contraceptive ever invented.
Who would risk marriage with someone who is heavily in debt, or undertake the decades-long project of raising a family together? Instead they simply live together, an arrangement that is far less likely to produce children than tying the marriage knot.
Encouraging millennials to marry and have children requires giving them a way out of the debt trap they find themselves in. One way would be to forgive the student loans of those who are willing to marry and have children. The first child would result in one-third of your debt being forgiven, the second two-thirds, and with the third your entire debt might be forgiven.
The slogan of the new policy might be “With three you study free.”
We at Population Research Institute (PRI) have long argued that couples who are willing to raise three or more children should be sheltered from all federal taxes. After all, such couples are providing for the future of their country in the most fundamental way, by providing the future generation, often at great personal sacrifice.
Such a policy would obviously encourage couples to be more generous in having children, since each additional child would, in a sense, pay for itself.
There are many benefits to a higher birthrate, including a natural and gradual easing of the entitlement crisis. More younger taxpayers improves America’s worker/dependency ratio, making it easier for us to honor our social security promises to the elderly. For every one-tenth of an increase in the total fertility rate, for example, Social Security will remain solvent for an additional three years.
Raising the birthrate and strengthening families is a good in itself, of course. But the American people have been a great force for good in the world as well, and ensuring their survival is a worthy goal in itself.
Editor’s note: Steven W. Mosher is the President of the Population Research Institute and the author of “Bully of Asia: Why China’s Dream is the New Threat to World Order.”
In a recent piece for The Wall Street Journal called “When Your Daughter Defies Biology,”author Abigail Shrier described the plight of mothers whose daughters have come home from college with newly-grown mustaches and recently removed breasts.
Shrier had been contacted by a mother whose daughter had some anxiety issues during her first semester at college. Along with some friends, her daughter “decided their angst had a fashionable cause: ‘gender dysphoria.’” Over the course of a year, she began a course of testosterone, shaved her head, and began to wear boys’ clothes.
Shrier went on to interview 18 parents in the same situation, desperate to save their daughters, but unable to find allies. “Nearly every force in society is aligned against these parents: Churches scramble to rewrite their liturgies for greater ‘inclusiveness.’ Therapists and psychiatrists undermine parental authority with immediate affirmation of teens’ self-diagnoses,” Shrier writes. “Campus counselors happily refer students to clinics that dispense hormones on the first visit.”
In fact, health plans at 86 colleges around the country, including most of the Ivy League schools, cover cross-sex hormones and surgery.
Gender dysphoria is believing yourself to be the opposite gender from your biological sex. What these young women suffer from is rapid onset gender dysphoria, i.e., when such feelings manifest themselves suddenly — within days or weeks — without having been present in early youth. Shrier refers to sudden onset gender dysphoria as a social contagion — one that, like anorexia and bulimia, overwhelmingly affects girls.
Yes. Regarding transgender identification, social contagion is unleashed on teens via the internet, mainstream and social media, messaging in schools, peer pressure, and sadly, from the medical elites who propagandize gender ideology as science.
For example, the American Academy of Pediatrics policy statement on the issue declares that all children, regardless of age, should be immediately affirmed in accordance with their self-proclaimed gender identity.
As I write in my forthcoming book, Don’t Let the Culture Raise Your Kids, the influence of social media on young people — when it comes to gender ideology and so many other issues — can’t be underestimated. Shrier lists Reddit, Tumbler, Instagram, and YouTube as places where young women can find affirmation that “transitioning” is the answer to all their problems.
At The American Conservative, Rod Dreher writes about a mother who went to speak to her seventh grade daughter’s guidance counselor when she started claiming to be a boy. The counselor advised her to “accept your son as he is.”
The College Fix website wrote about this issue and received several emails from moms who described their ordeals.
Here’s one mother’s tragic story:
Our daughter went off to the college of her dreams. She seemed to do well her first year away. During her second year at college, she experienced a mental health breakdown. We received sketchy details of her struggles from her and a couple of her friends. There was no outreach from her college – due to privacy concerns. Following much pleading on our part, she came home for a visit. We were met with a very different visage upon picking her up at the airport. Her face was covered in acne, she sprouted an obvious mustache, her entire appearance was disheveled…Her voice was somewhat deeper, I might note here. She seemed very disturbed – not at all her old self. What was she like before this? No, not a tomboy as a child. She was an ambitious student, an animal lover, she loved to spend time in the kitchen baking. As for gender, she was typical (whatever that means). For her high school prom, she had her hair and makeup professionally styled…When our daughter was visiting, we asked her what was wrong. I inquired about the acne and mustache – that is not natural, I said. She insisted that she had always had a mustache. Not true. Before we knew what had hit us, she returned to her college. We discovered that she had obtained testosterone in the student clinic. And, she refused all contact with her family. Her college was complicit in all of this.
Another mother tells her daughter’s story:
She left for college in the fall of 2016 as a National Merit Scholar, all AP classes, involved in countless activities including bands, orchestra, theater, dance, literary magazine editor, starting women’s studies club, part time job… She honestly was on top of the world with so much potential. She also happened to be gender conforming. She had a significant merit scholarship at a well-respected east coast university in a large city. Sometime the second semester sophomore year things went horribly wrong… She called us in a deep voice stating she was transgender and had changed her name. She was unable to even think clearly around this issue and was obviously horribly confused. Within a week she completely severed ties in an email to us. No one in her immediate or extended family can believe what has happened. Within a year she had a double mastectomy. Our family is absolutely devastated by all of this.
Another mother, responding to Dreher’s piece, asks for our prayers:
You can’t imagine what it’s like to have the entire educational/med/psych/media world fighting against your parental values and common sense… If you’re not having to deal with such a thing, thank your God for that blessing. Be aware of what’s being taught in your schools. And say a prayer for the rest of us.
The New York Senate and Assembly each passed an expansive pro-abortion bill on Tuesday, within 90 minutes of each other. Governor Andrew Cuomo immediately signed the Reproductive Health Act into law and then celebrated by lighting the state up pink. Sitting with Cuomo as he signed the bill was Sarah Ragle Weddington, the lawyer who represented Jane Roe in Roe v. Wade and the woman whom Roe would later say manipulated her and lied about her in order to convince the Supreme Court to legalize abortion. Roe, whose real name was Norma McCorvey, said Weddington lied about McCorvey having been raped. McCorvey said that Weddington simply needed a vulnerable pregnant woman to help open a court case. McCorvey, who was homeless, fit that bill. Still, Cuomo thanked Weddington for her work in ensuring legalized abortion.
Third-trimester abortion will be allowed under the new law when a preborn child is diagnosed with a condition that will cause him or her to die at or shortly after birth. In addition, the new law removes protections for babies born alive after an abortion — meaning they could be left to die after birth — by rescinding a portion of NY’s public health law, seen below.
NY public health law nixed by Reproductive Health Act
The law also allows for abortion through all nine months of pregnancy when the mother’s life or health is at risk – which is completely unnecessary, as delivering a live baby via C-section is faster and safer than killing the baby in a two-day late-term abortion. Former abortionist Dr. Anthony Levatino explains in the video below:
The new law also allows non-physicians to commit non-surgical abortions and moves the abortion law from the state’s penal code to its health code – which removes any threat of the prosecution of abortionists. Senate Republicans, however, said that change could make it impossible for a woman who loses her preborn child because of an assault to have her assailant prosecuted. In addition, according to the New York Law Journal, “Lawmakers also codified into state law on Tuesday regulations promulgated by the state Department of Financial Services that require health insurance companies to provide coverage for contraceptives in New York. Both bills take effect immediately.”
Live Action
✔@LiveAction
This is the sound from the NY Senate chamber after the 38-24 vote to:
New York has an abortion rate of 23.1 per 1,000 women, twice the national average of 11.8 per 1,000 women. 25 to 27 percent of pregnancies in New York State end in abortion. In New York City, 78 percent of abortions are on African American babies. More black babies being killed through abortion than being born in the city. Cuomo’s new abortion law will likely increase those numbers.
The Senate passed the bill first by a vote of 33-24. The Assembly then voted 92-47 in favor of the bill. It is the first change to New York’s abortion laws since 1970, and while the federal law set by Roe v. Wade in 1973 trumps New York’s law, Cuomo pushed the abortion expansion out of fear that Roe v. Wade could be overturned by the U.S. Supreme Court.
Live Action president Lila Rose issued a statement on the bill, saying, “Convicted criminals aren’t subjected to the death penalty in New York state, but now children up until the ninth month of pregnancy can be given lethal injections and poisoned to death. This is no different than infanticide…. New York’s law is barbaric and inhumane and rejects modern science and medical advancements that reveal the development and humanity of life in the womb…. A recent Marist poll showed 75 percent of Americans believe abortion should be limited to – at most – the first three months of pregnancy.”
Editor’s Note, 1/23/19: Added graphic of NY public health law protecting abortion survivors, which was eliminated by the Reproductive Health Act and statement on contraceptive coverage (HT: Carole Novielli). Also added statement by LA president Lila Rose.
Every day in our country, thousands of pregnant women enter so-called medical “clinics.” When they emerge hours later, they are no longer pregnant. Their babies, so recently living and growing within the warmth and safety of their mothers’ wombs, have been suctioned out with a vacuum, or injected with poison or scalded to death with saline fluid and then pulled apart limb by limb with forceps.
The gruesome reality of what happens to those babies is disguised by a veneer of medical respectability, by the white gowns worn by profiteers who play at being “doctors” and “nurses.” And it is hidden by the plethora of carefully crafted euphemisms designed to cast a pall of confusion over the abortion debate: “products of conception,” “blob of tissue,” “reproductive rights,” “freedom of choice,” etc.
But no number of white gowns, and no number of euphemisms coined by clever propagandists can ever change the cold reality of what happens in every abortion mill every day of the week – the deliberate, calculated killing of living human beings.
The first part of the mission of the pro-life movement, then, is to peel back these layers of obfuscation and deception and to show to the world what – or rather who – is at the center of the abortion debate: the unborn child. And the second part of our mission is to speak for that unborn child, who has no voice of his own.
The March for Life: A Voice for the Voiceless
In my books, the annual March for Life in Washington D.C. is one of the most effective tools devised by the pro-life movement to accomplish both of these goals.
Though the mainstream media works mightily to ignore the March for Life – actually, any pro-life and family march – the growing phenomenon of social media and independent conservative media has ensured that the witness of the hundreds of thousands of pro-life Americans willing to stand in frigid and often inclement weather in D.C. to support the right to life of all human beings is broadcast around the world.
Furthermore, even the mainstream media can’t entirely ignore the March, especially these past few years when both the President and Vice-President have addressed those participating. As a consequence, millions of people have been exposed to pro-life information, arguments and witness.
They have seen, first-hand, how much the actual pro-life movement differs from the media caricatures. Far from being a fringe minority, pro-lifers have created the largest annual human rights march in U.S. history. And far from being hateful zealots, pro-lifers are decent, ordinary people motivated by an extraordinary love.
“This is a movement founded on love and grounded in the nobility and dignity of every human life,” said President Trump in his address to the March this year. “When we look into the eyes of a newborn child, we see the beauty and the human soul and the majesty of God’s creation. We know that every life has meaning and that every life is worth protecting.”
As one popular pro-life blogger noted on Twitter on the day of the March, what makes the March for Life so unique, is that “nobody in attendance is marching for themselves. Nobody is demanding rights or privileges for themselves. Everyone is marching on behalf of those who cannot march.”
What a witness!
Pro-Life = Pro-Science
Pro-abortion advocates want everyone to believe that abortion is a highly “complex” matter rife with shades of grey. But it’s not. Ultimately it comes down to one, simple, scientifically-answerable question: is the unborn child human or not?
At this year’s March for Life, Ben Shapiro, a wildly popular young, Jewish conservative media star, answered that question with his trademark clarity during an hour-long broadcast from the main stage – a broadcast likely watched by hundreds of thousands of people.
Shapiro systematically dismantled ten of the most popular pro-abortion arguments, noting that the core pro-life arguments, far from being politically partisan or faith-based, are politically agnostic and purely empirical. As he put it, the pro-life cause is based upon the “sheer, unadulterated science of human life.”
Furthermore, he noted, victory is inevitable since the “science is moving in the direction of our movement.”
St. Teresa of Calcutta (Mother Teresa) once succinctly summarized this unassailable and scientifically-backed pro-life argument. “If the right [to] life is an inherent and inalienable right, it must surely obtain wherever human life exists,” she said. “No one can deny that the unborn child is a distinct human being, that it is human, and that it is alive. It is unjust, therefore, to deprive the unborn child of its fundamental right to life on the basis of its age, size, or condition of dependency.”
Even more succinct still is this statement by Dr. Jerome Lejeune, the world-famous scientist who discovered the cause of Down Syndrome: “Life has a very long history, but each of us has a very neat beginning, the moment of conception.”
A couple of years ago, Bill Nye and a bunch of other pro-abortion and liberal activists organized a so-called “March for Science.” As it turns out, however, the March for Life is the original March for Science – a march supporting the unassailable “scientific consensus” on when human life begins, against the hopelessly outdated, faith-based arguments of pro-abortion “human-life deniers.”
The Sacred Value of Human Life
But though the pro-life position is entirely defensible using science and reason alone, faith has a way of cutting through the rhetoric and personal prejudices and opening hearts to receive the arguments from reason.
Pro-abortion activists like to point out that a huge number of the participants at the March for Life are religious. Every year, for instance, hundreds of priests, seminarians, bishops and cardinals participate in the Vigil Mass for Life at the National Shrine of the Immaculate Conception, while tens of thousands of Catholic youth attend various youth masses on the morning of the March.
Abortion activists seem to think that this somehow amounts to “proof” that the pro-life cause is simply fueled by religious “bigotry.” I wonder, however, if they would say the same thing about the historical fact that huge numbers of those involved in the effort to abolish the slave trade were also religious, and explicitly motivated by religious arguments? Were their efforts, too, just religious bigotry?
In Scripture, children are always viewed as gifts from God, and divine image-bearers. Thus Psalm 127 depicts the man whose quiver is filled with children as being blessed. Psalm 128 depicts that same man as doubly-blessed if he exercises great care and faith in the raising of his children to walk in the fear of the Lord.
And then there is Psalm 139, which reads: “You formed my inmost being; you knit me in my mother’s womb. I praise you, because I am wonderfully made; wonderful are your works! My very self you know. My bones are not hidden from you, when I was being made in secret, fashioned in the depths of the earth.” (Psalm 139: 13-16).
The mass participation of Christians at the March for Life, and the central place given to prayer, is not a cause for shame, but rather a badge of honour. It shows that the profound respect for human life found in the Scriptures has seeped into our bones and imbued us with the spiritual energy needed to take risks and make sacrifices to defend the right to life of all human beings. It also emphasizes the truth that the flourishing of a Culture of Life can only come about as a consequence of widespread conversion of heart.
The only shame about the presence of Christians at the March for Life is that there are not so many hundreds of thousands more – that every Christian pastor in the country is not there and has not exhorted his flock to attend.
We Must Act
Our culture desperately needs to be reminded that all humans are made in the image of God – Imago Dei – and that human life has inherent and inalienable dignity and value.
As Pope St. John Paul II lamented at World Youth Day in Denver: “In our own century, as at no other time in history, the ‘Culture of Death’ has assumed a social and institutional form of legality to justify the most horrible crimes against humanity: genocide, ‘final solutions’, ‘ethnic cleansings’, and the massive ‘taking of lives of human beings even before they are born, or before they reach the natural point of death’.”
The “father of lies,” said the pope, “relentlessly tries to eradicate from human hearts the sense of gratitude and respect for the original, extraordinary and fundamental gift of God: human life itself.”
Given the stakes at play, there is not one of us who is not responsible in some way for stemming the tide of this Culture of Death. “Woe to you if you do not succeed in defending life,” the pope warned the youth in Denver. “The Church needs your energies, your enthusiasm, your youthful ideals, in order to make the Gospel of Life penetrate the fabric of society, transforming people’s hearts and the structures of society in order to create a civilization of true justice and love.”
One of the simplest, most effective ways to declare your support for the Gospel of Life is to attend a March for Life. As Pope St. John Paul II stated, “Do not be afraid to go out on the streets and into public places, like the first Apostles who preached Christ and the Good News of salvation in the squares of cities, towns and villages.”
Though the March for Life in Washington D.C. is the largest march in the U.S., it has fostered hundreds of imitation marches around the world. Even if you cannot attend the Washington March, I urge you to look up the march closest to you, and to attend – to join the “Great Campaign in support of Life” (Evangelium Vitae, ¶95).
Our country, and the world, are thirsting for Christians who eschew the lure of comfort, and proactively swim against the tide of the Culture of Death. Stand-up, therefore, and make your voice be heard, for your voice is the only voice that the unborn have. Silence is not an option.
Most people volunteer for the pro-life movement. I consider myself a draftee.
I was a young intensive care unit nurse when the Roe v. Wade decision came down in 1973. Like most people I knew, I was shocked when abortion was legalized. As a medical professional, I couldn’t imagine good doctors and nurses condoning — much less participating in — such a brutal act. However, my medical colleagues were split on the issue with those supporting what was then said to be “only” early abortions the most vocal and insistent. Our formerly cohesive unit began to fray.
However, I was professionally offended by the pro-life argument that legalizing abortion would lead to the legalization of infanticide and euthanasia. It was one thing to deny the truth with an early and unobserved unborn baby but it was quite another to imagine any doctor or nurse looking a born human being in the eye and killing him or her.
How wrong I was!
INFANTICIDE AND MEDICAL DISCRIMINATION AGAINST PEOPLE WITH DISABILITIES
My eyes were opened with the 1982 Baby Doe case in Indiana. Baby Doe was a newborn baby boy with an easily correctable hole between his esophagus (food pipe) and trachea (windpipe) who was denied this lifesaving surgery by his parents and a judge because he also had Down Syndrome. Six days later, Baby Doe starved and dehydrated to death while his case was being appealed to the Supreme Court.
My husband and I wanted to adopt Baby Doe when we read the story but all offers of adoption were refused. I did not know at the time that my expected third child also had Down Syndrome and a life-threatening problem.
When Karen was born a few months after Baby Doe, we were stunned that she had both Down Syndrome and a severe heart defect but I was determined that she would not become another Baby Doe.
But even when the cardiologist told us that Karen had an 80-90% chance of survival with one open-heart surgery by age 6 months, he also gave us the “choice” to let Karen die. I was outraged that he could even consider not treating my daughter like any other baby with the same heart defect.
Even worse, when my daughter was hospitalized with pneumonia at 4 months, I was tipped off that my trusted pediatrician had made her a “do not resuscitate” without my knowledge or consent because “Nancy is too emotionally involved with that retarded baby”. I then realized that “choice” was just an empty slogan that had infected medical ethics.
Although Karen survived that incident, she unfortunately died at age 51/2 months just before her scheduled surgery. I finally joined the disability rights and the pro-life movements.
THE “RIGHT TO DIE” MOVEMENT
A few years after Karen, I was shocked by the so-called “right to die” movement that pushed “living wills” to refuse even food and water by tube if or when a person became incapacitated. I became involved in both the Nancy Cruzan and Terri Schiavo cases involving seriously brain-injured, non-dying young women declared “vegetative”, a term invented in 1972. I wrote an op-ed for my local paper predicting that the potential pool of victims would expand if death by starvation and dehydration was allowed. I was thinking about my own mother who had Alzheimer’s and cancer and indeed I was asked at one point if our family was going to feed her. I replied that my mother would die naturally from her condition, not starvation and dehydration.
The “right to die” movement ultimately did expand into the Compassion and Choices organization, the well-funded former Hemlock Society that promotes physician-assisted suicide by lethal overdose. In the late 1990s, Oregon became the first state to legalize assisted suicide. Now a handful of states and the District of Columbia have followed Oregon but the relentless effort to legalize physician-assisted suicide continues in the other US states.
Over the years, I had cared for many suicidal people and I saw the seductive effect of people like Jack Kevorkian, the infamous “Dr. Death”on them. As a nurse, I knew how dangerous it was to portray suicide as a “solution” to many at-risk people.
But it became personal when my 30-year-old daughter Marie killed herself using an assisted suicide technique that she learned reading the pro-assisted suicide book “Final Exit”. My Marie had struggled with drug addiction for 16 years and despite our best efforts and those of her therapists, she finally succumbed to despair. She was the only suicidal person I ever lost.
I was not surprised when two people close to Marie became suicidal after her death. Fortunately, they were saved.
I also discovered that it’s only a short step from “I wouldn’t want to live like that” for assisted suicide to “No one should have to live like that” for euthanasia.
Ironically and around the same time, I was threatened with termination after I refused to increase a morphine drip “until he stops breathing” on an older man who did not stop breathing as expected after his ventilator was removed. The patient was presumed to have had a stroke when he did not wake up from sedation after 24 hours. I reported the situation up the chain of command at my hospital but no one supported me. I escaped termination that time but I refused to back down.
An autopsy later showed that the man had no lethal condition or brain injury.
But until and unless we are ready to recognize what we unlock when we legalize “just a little bit” of medical killing, we may find that the slippery slope has no bottom and that no one is safe.
And I saw it all start with the Roe v Wade decision legalizing abortion.
The year is 1980. The town is Cuapa, near the middle of Nicaragua — 59 straight miles northeast of the capital of Managua and 96 miles via highways and roads.
The date is April 15. While carrying out his work as a simple church sacristan in what was called the “old chapel,” Bernardo Martinez sees a statue of the Blessed Virgin Mary producing a supernatural light — heaven’s way to announce he would soon see the Blessed Mother.
He would later recount for his bishop this beginning and everything to follow. There was no natural explanation because “the light came from her,” he would write. “That was a great mystery for me, with the light that came from her one could walk without tripping. And it was nighttime.”
Our Lady Appears
In May — the same month as Our Lady first appeared at Fatima — she appeared to Bernardo. Like at Fatima, she would appear other times, the last visit being in October.
Bernardo described how after a lightening flash, there appeared a pure white cloud on which stood Our Lady. “The dress was long and white. She had a celestial cord around the waist. Long sleeves. Covering her was a veil of a pale cream color with gold embroidery along the edge. Her hands were held together over her breast. It looked like the statue of the Virgin of Fatima. I was immobile. I had no inclination to run to yell. I felt no fear. I was surprised.”
He described how “she extended her arms — like the Miraculous Medal which I never had seen, but which later was shown to me. She extended her arms and from her hands emanated rays of light stronger than the sun.”
Similarly, in Our Lady’s first apparition in May at Fatima, Lucia described how Our Lady opened her hands and the children “were bathed in a heavenly light that appeared to come directly from her hands. The light’s reality cut into our hearts and our souls, and we knew somehow that this light was God, and we could see ourselves embraced in it.”
At Cuapa, it seemed Our Lady was echoing Fatima in the same way. Bernardo asked her name. “She answered me with the sweetest voice I have ever heard in any woman, not even in persons who speak softly. She answered me and said that her name is Mary…She told me with the same sweetness:
I come from heaven. I am the Mother of Jesus.
He asked what she wanted and, like at Fatima, she told him:
I want the Rosary to be prayed every day…I want it to be prayed permanently, within the family…including the children old enough to understand…to be prayed at a set hour when there are no problems with the work in the home.
Bernardo later explained: “She told me that the Lord does not like prayers we make in a rush or mechanically. Because of that she recommended praying of the Rosary with the reading of biblical citations and that we put into practice the Word of God.” He asked where are biblical citations? “She told me to look for them in the Bible.”
Our Lady continued:
Love each other. Comply with your obligations. Make peace. Don’t ask Our Lord for peace because if you do not make it there will be no peace.
Remember, during her first visit at Fatima on May 13 she told the children, Say the Rosary every day, to bring peace to the world and an end to the war. In July, Our Lady told the Fatima children, Continue to say the Rosary every day in honor of Our Lady of the Rosary, to obtain the peace of the world and the end of the war, because only she can obtain it. She also said in July, If you do what I tell you, many souls will be saved, and there will be peace.
And the obligations? Might they be daily duties (more later)?
In Cuapa there then came another Fatima connection. Our Blessed Mother told Bernardo:
Renew the five first Saturdays. You received many graces when all of you did this.
Bernardo admitted people had previously gone to Confession and Communion every first Saturday but no longer did so.
Our Lady then said:
Nicaragua has suffered much since the earthquake. She is threatened with even more suffering. She will continue to suffer if you don’t change.
Pray, pray, my son, the Rosary for all the world. Tell believers and non-believers that the world is threatened by grave dangers. I ask the Lord to appease His justice, but, it you don’t change, you will hasten the arrival of the Third World War.
Remember at Fatima during her July apparition Our Lady warned, This war [World War I] will end, but if men do not refrain from offending God, another and more terrible war will begin during the pontificate of Pius XI. When you see a night that is lit by a strange and unknown light, you will know it is the sign God gives you that He is about to punish the world with war [World War II] and with hunger, and by the persecution of the Church and the Holy Father.
Next Visits
On June 8, the Blessed Mother gave Bernardo “the same message as she had done the first time,” he wrote, then he gave her many requests from the people. “She answered me by saying: Some will be fulfilled, others will not.The petitions and answer echoed those of Lucia and Our Lady at Fatima.
As the Fatima seers saw in the sky the October vision of Our Lady and the Holy Family, here Our Lady directed Bernardo, Look at the sky.
He did, and Our Lady “presented something like a movie” during which he felt “transported” and saw different groups of people including those from the early Christian communities now in celestial joy, to the first to receive the Rosary from her, to a present day countless multitude carrying rosaries.
She said:
I have shown you the Glory of Our Lord, and you people will acquire this if you are obedient to Our Lord, to the Lord’s Word; if you persevere in praying the Holy Rosary and put into practice the Lord’s Word.
On July 8 Our Lady appeared in a dream. Bernardo wrote she told him to “pray for Nicaragua and for the whole world because serious dangers threaten it.” Again, echoes of Fatima because of the lack of peace when her directives are ignored.
On Sept. 8, at the place of the apparitions, Our Lady directed Bernardo,
Restore the sacred temple of the Lord [meaning ourselves].In you is the gratification for the Lord. She added:Love each other. Love one another. Forgive each other. Make peace. Don’t first ask for it. Make peace!
“Peace” was mentioned more than once at Fatima, too.
Before leaving, Our Lady told Bernardo she was going to return. On Oct. 13. Again, the Fatima connection. Oct. 13 would be the date of her last appearance in Cuapa as it was at Fatima.
October 13 Apparition
As Bernardo joined by others was praying at the site of the apparitions, Our Lady appeared and “extended her hands and rays of light reached all of us.”
He continued, “She raised her hands to her breast in a similar position to the statue of Our Lady of Sorrows…her face turned pale, her mantle changed to a gray color, her face became sad, and she cried. I cried too. I trembled to see her like that.”
Recall on Oct. 13 at Fatima, Our Lady appeared as Our Lady of the Rosary, Our Lady of Mount Carmel, and also Our Lady of Sorrows.
When Bernardo asked why she was crying, she answered,
It saddens me to see the hardness of those persons’ hearts. But you will have to pray for them so that they will change.
At Fatima on Oct. 13, Our Lady told the children, People must amend their lives and ask pardon for their sins. They must not offend our Lord any more, for He is already too much offended!
Earlier at Fatima, on July 13, Our Lady similarly directed, Make sacrifices for sinners, and say often, especially while making a sacrifice: O Jesus, this is for love of Thee, for the conversion of sinners, and in reparation for offences committed against the Immaculate Heart of Mary. In August she told the children, Pray, pray very much. Make sacrifices for sinners. Many souls go to hell, because no one is willing to help them with sacrifice.
Returning to Cuapa, in that Oct. 13 visit Our Lady continued, repeating in a different way what she had said before and also echoed Fatima:
Pray the Rosary, meditate on the mysteries.
Listen to the Word of God spoken in them.
Love one another. Love each other.
Forgive each other. Make peace. Don’t ask for peace without making peace; because if you don’t make it, it does no good to ask for it.
Fulfill your obligations. (Fatima’s Lucia revealed this meant doing your daily duties as the sacrifice required.)
Put into practice the Word of God.
Seek ways to please God.
Serve your neighbor as that way you will please Him.”
After Our Lady said this, to answer Bernardo’s petitions for people’s requests, she said, in part,
Ask for faith in order to have the strength so that each can carry his own cross. The sufferings of this world cannot be removed. Sufferings are the cross which you must carry. That is the way life is. There are problems with the husband, with the wife, with the children, with the brothers. Talk, converse so that problems will be resolved in peace. Do not turn to violence. Never turn to violence. Pray for faith in order that you will have patience.
Before leaving she repeated, again in ways echoing her message at Fatima:
Do not be grieved. I am with all of you even though you do not see me.
I am the Mother of all of you, sinners. Love one another. Forgive each other.
Make peace, because if you don’t make it there will be no peace.
Do not turn to violence. Never turn to violence.
Nicaragua has suffered a great deal since the earthquake and will continue to suffer if all of you don’t change.
If you don’t change you will hasten the coming of the Third World War. Pray, pray, my son, for all the world.
A mother never forgets her children. And I have not forgotten what you suffer. I am the Mother of all of you, sinners.
Related to that, Our Lady requested that she be beseeched this way: Holy Virgin, you are my Mother, the Mother to all of us sinners…
Our Lady also gave Bernardo this prayer: St. Mary of Victory,Favorite Daughter of God the Father, give me your faith; Mother of God the Son, give me your hope; Sacred Spouse of God the Holy Spirit, give me your charity and cover us with your mantle.
That title was originally the name of the feast St. Pius V declared after the victory at Lepanto and which was soon changed to the feast of Our Lady of the Rosary — the title with which Mary identified herself at Fatima.
Approval of the Apparitions
In 1982, Auxiliary Bishop Bosco M. Vivas Robelo of the Archdiocese of Managua, authorized the publication of the narration of the apparitions of the Blessed Virgin Mary in Cuapa. Bishop Pablo Antonio Vega Mantilla, of Juigalpa, (the diocese of the apparitions) was studying the authenticity of the events “in order to be able to assist in discerning the true value of the alluded to message.” In 1994 Bishop Robelo who then led the Diocese of Leon stated, “I hereby authorize the publication of the story of the Apparitions of the Blessed Virgin Mary in Cuapa and the messages given to Bernardo Martinez…May this publication help those who read it to have an encounter with Jesus Christ in the Church through the mediation of the Mother of Our Lord.” Bernardo Martinez was ordained a priest.
At the 2019 March for Life on Friday, conservative author, speaker, and attorney Ben Shapiro reminded pro-lifers that what’s right is not always popular and what’s popular is not always right. As he took on U.S. and Canadian political leaders’ criticisms of pro-lifers, Shapiro aimed to motivate pro-lifers to keep going against adversity.
“So perhaps we are out of line with the rest of society – to which I say good,” he said. “So were the abolitionists. So were the civil rights marchers. So were the martyrs in Rome and the Jews in Egypt. Righteousness doesn’t have to be popular. It just has to be righteous.”
Shapiro’s comments are in reference to Canadian Prime Minister Justin Trudeau’s remarks that pro-lifers are “not in line with where we are as a government and quite frankly as a society.” Shapiro also pointed to New York’s Governor Andrew Cuomo as an example of someone who has “excised those who stood for life.” In 2014, Cuomo said during a radio interview that pro-lifers “have no place in the state of New York.”
These examples of prejudice from government leaders show how frightening it can be to proclaim one’s pro-life position. It opens a person up to criticism and even discrimination. Shapiro points out that pro-choicers have reversed good and evil when it comes to abortion, and preborn children and pro-lifers bear the brunt of that confusion. Abortion is based on lies, he said, and pro-choicers have blinded themselves to the truth. It’s up to pro-lifers to expose the truth despite the tribulations that may arise.
Shapiro reminded the crowd at the March for Life that “America was founded on the promise of God-given rights, chief among them the rights to life and liberty.” Some people, however, were “unjustly omitted” from receiving those rights. As America grew, hard-fought battles were won for people to receive their God-given rights, but one group was left behind, he explained.
“That group had once been the most prized possession of a great and moral people,” said Shapiro. “Its children. The souls entrusted to us by the Creator – given to us with care and love. We built this country for our children. We built our lives for our children. And then something happened. We, as a country, decided to erase them.”
This is why pro-lifers march, said Shapiro. Not for any attention or recognition, because major media outlets will continue to ignore the tens of thousands who march in favor of life and speak out against abortion. Pro-lifers march for the children who have been aborted and to hopefully save the lives of children at risk of abortion.
“Our children, slaughtered over the decades, remember. They look at us from above and they know that they meant something,” said Shapiro. “That they do mean something so long as we keep them in our minds and in our hearts.”
As the “guardians” of God’s precious children, Shapiro believes the children of pro-lifers will take up that job as they grow into adults and that all pro-lifers will “stand between America and the darkness, and we will march until that darkness is banished forever, and all of our children can stand together in the sunlight.”
Shapiro delivered a one-hour long podcast earlier in the day from the March for Life stage during which he addressed pro-choice arguments, interviewed Vice President Mike Pence, and said that the pro-life movement will prevail.
For years, the Little Sisters of the Poor, a group of Catholic nuns, have been fighting an Obamacare mandate that would require them to fund birth control that could potentially cause an abortion, like the morning-after pill. As this is a direct contradiction of the teachings of the Roman Catholic Church, the Little Sisters are opposed and have been fighting the mandate on the basis of religious liberty. In 2017, it appeared that they finally had found a reprieve when the Trump administration expanded religious exemptions for the mandate… only for pro-abortion attorneys in 13 states to file lawsuits to overturn the new religious exemption. And today, a federal judge ruled against the Trump administration and the Little Sisters in another ruling that is sure to be a disappointment to pro-lifers and defenders of religious liberty alike.
U.S. District Judge Haywood Gilliam, Jr. ruled that the administration’s expanded religious exemptions would harm the 13 states that sued, which were mostly Democratic states (California, Connecticut, Delaware, Hawaii, Illinois, Maryland, Minnesota, New York, North Carolina, Rhode Island, Vermont, Virginia and Washington). Washington, D.C. also joined in the lawsuit, and Gilliam’s ruling blocks the religious exemption from affecting the 13 states and Washington, D.C., which now means that the Little Sisters of the Poor, along with other religious employers, will be forced to fund birth control methods that could potentially cause abortions. Another court in Pennsylvania is also considering a request, and if the court rules against the administration there, it could potentially have national implications.
The Department of Health and Human Services responded by slamming Gilliam’s decision in a statement. “No American should be forced to violate his or her own conscience in order to abide by the laws and regulations governing our health care system,” Caitlin Oakley, spokeswoman for Health and Human Services, said. “The final rules affirm the Trump Administration’s commitment to upholding the freedoms afforded all Americans under our Constitution.”
Mark Rienzi is the president of the Becket Fund for Religious Liberty, which has been representing the Little Sisters of the Poor. In a statement provided to Live Action News, he promised to keep fighting. “Yesterday’s decision will allow politicians to threaten the rights of religious women like the Little Sisters of the Poor,” Rienzi said. “Now the Little Sisters have no choice but to keep fighting this unnecessary fight so they can protect their right to focus on caring for the poor. We are confident this decision will be overturned.”
In a previous statement, Mother Loraine Marie Maguire of the Little Sisters said they simply want to focus on their mission, and cannot because of this legal battle. “We just want to be able to continue our religious mission of caring for the elderly poor as we have over 175 years,” she said. “We pray that these state governments will leave us alone and let us do our work in peace.”
HYATTSVILLE, Maryland, January 11, 2019 (LifeSiteNews) – The U.S. National Center for Health Statistics has announced that the national fertility rate is the lowest it has been in 30 years.
The American birth rate has been insufficient to sustain the population since 1971, but the 2017 numbers indicate a 30-year low. According to CNN, the federal agency reported that the total fertility rate for the U.S. overall that year was 1,765.5 per 1,000 women, 16 percent below the level needed for a population to replace itself: 2,100 births per 1,000 women.
The total number of births in the U.S. in 2017 was 3,853,472, a drop of two percent from 2016.
“The general fertility rate was 60.2 births per 1,000 women aged 15–44, down 3% from 2016 and another record low for the United States. Birth rates declined for nearly all age groups of women under 40, but rose for women in their early 40s. The birth rate for teenagers aged 15–19 was down 7% in 2017 to 18.8 births per 1,000 women; rates declined for both younger (aged 15–17) and older (aged 18–19) teenagers.”
There were some interesting differences between birth rates for states.
South Dakota and Utah were the only states to reach “replacement rate.” South Dakota was the biggest winner overall, with a rate of 2,227.5 live births per 1,000 women, and Utah came in second with 2,120.5. North Dakota nearly made it with a rate of 2,065 live births per 1,000 women. The same can be said for Nebraska, which had a rate of 2,062. In contrast, the birth rate in Washington, D.C. was 1,421 per 1000 women.
CNN published remarks by Dr. Georges Benjamin, executive director of the American Public Health Association, who said that fertility rates have been dropping consistently.
“We’ve been seeing fertility rates go down, and I think it has a lot to do with women and men, couples in particular, having much more control over their reproductive lives,” he said.
Benjamin did acknowledge that a low fertility rate isn’t necessary good for society.
“I think the concern is – and there is a concern – having a fertility rate that doesn’t allow us in effect to perpetuate our society,” he said. “But we may very well over time start seeing this reversed or flattened out, but that remains to be seen.”
CNN noted that “between 2007 and 2017, total fertility rates in the United States fell 12% in rural counties, 16% in suburban counties and 18% in large metro counties, according to a separate CDC data brief released in October.”
The shocking abuse against a disabled woman has outraged the nation. The woman, a patient at Hacienda HealthCare in Phoenix, Arizona, is described by CNN as having been in a vegetative state for more than a decade, gave birth to a baby boy on December 29. The media are not releasing her name, because she is a victim of sexual abuse.
Many people are surprised that a patient who appears to be unconscious could give birth. Dr. Deborah Feldman, Hartford HealthCare Medical Group director of maternal fetal medicine, told CNN that it is very rare but does happen. Dr. Feldman stated that the case “speaks to the fact that the patient actually had largely normally functioning organs.” Recent research has shown that patients in a vegetative state can also have awareness and mental functioning far beyond what most people realize. A neuroscientist found that at least 20 percent of people in a vegetative state are completely aware of their surroundings and experience but unable to move or respond.
John Micheaels, an attorney for the victim’s family, told CNN, “The family would like me to convey that the baby boy has been born into a loving family and will be well cared for,” adding, “The family obviously is outraged, traumatized and in shock by the abuse and neglect of their daughter at Hacienda HealthCare.” Detectives are gathering DNA samples from men at the facility as part of an ongoing investigation of the crime.
Terry Rambler, chairman of the San Carlos Apache Tribe of which the victim is a member, called for justice. He told CNN, “When you have a loved one committed to palliative care, when they are most vulnerable and dependent upon others, you trust their caretakers.” He added, “Sadly, one of her caretakers was not to be trusted and took advantage of her.”
This abuse, committed against a vulnerable disabled woman, is dehumanizing and horrific. Her family’s loving care for her baby boy born last month shows that the crime in no way diminished the humanity of her child, conceived in such difficult circumstances. All vulnerable lives — including disabled persons and the preborn conceived in rape — deserve to be treated with dignity and respect.
The 163 Catholics in the new Congress are split on abortion: almost all Republicans are pro-life and almost all Democrats are abortion-rights advocates.
For incumbents, we checked their voting record as scored by NARAL and National Right to Life. Typically, those who received a 100% NARAL score garnered a 0% rating from National Right to Life (which would be most Democrats), and vice versa (which would be most Republicans).
For Freshmen, we checked their stated positions on abortion, and the endorsements they received from pro-life and abortion-rights groups.
There were a few notable exceptions. Among them are Rep. Daniel Lipinski, a Democrat from Illinois: he received a 51% rating from NARAL and a 75% score from National Right to Life.
More Republicans than Democrats differed with the majority in their own party.
For example, Sen. Lisa Murkowski of Alaska agreed with NARAL 42% of the time, and with National Right to Life 28% of the time. Sen. Susan Collins of Maine received a 45% score from NARAL and a 42% score from National Right to Life. Rep. Walter B. Jones of North Carolina garnered a score of 51% from NARAL and a rating of 85% from National Right to Life.
It is obvious that religion is not a reliable predictor of the way a Catholic member of the Congress will vote on abortion. Party matters—not religion.
Tim was not supposed to be born, and certainly not to live. Now the man who survived a failed late-term abortion in 1997 has died aged 21.
Tim – known in the media as the “Oldenburg baby” – was diagnosed with Down syndrome in the 20th week of gestation. German abortion rules limit terminations to the first 13 weeks, except in cases when the mother feels – for health or psychological reasons – unable to carry the baby to term.
As the mother in this case threatened to take her own life, the late-term abortion – legal up to 22 weeks – was scheduled. But things didn’t go according to plan.
In Tim’s case the doctor did not use potassium chloride to stop the heart, assuming he would not survive labour.
Born weighing just 690g (1½lbs), nurses wrapped him in a towel, where he spent the first nine hours of his life alone. After that, realising he was still alive, doctors and nurses began to provide him with medical care.
Doctors gave him one, maximum two, years to live because of various health difficulties, including underdeveloped lungs, which made him susceptible to infections.
After his mother and father declined to keep him he was raised by Bernhard and Simone Guido. They had applied to be foster parents but were offered a very different baby than they expected.
“It was supposed to be a healthy girl,” wrote Simone Guido later in a book about her life with Tim.
But seeing him in the hospital in 1997, she said, was like love at first sight: “We immediately thought: he belongs with us.”
As a result of adopting Tim, their life took on a very different direction. Through a book and website, the Guidos became campaigners against late-term abortions in Germany – and the use of pre-natal tests to allow abortions. In Germany an estimated nine out of 10 Down syndrome diagnoses lead to an abortion.
Later, a German MP sued the doctor who performed the failed abortion, but the case was dismissed.
As a result of his condition, as well as lack of after-birth care, Tim suffered from other medical conditions. He was autistic, could barely speak and underwent many operations during his life.
As well as Tim and their two own children, the Guidos fostered two further children with Down syndrome
In a statement on their website, they said Tim had died without warning after a “wonderful Christmas” at home with his family, days after contracting a lung infection.
They said: “We are very sad and don’t yet know how we should come to terms with the loss of our son who was unique, full of life and spread joy.”
ATASCADERO, California, January 9, 2019 (LifeSiteNews) – A California woman is taking her doctor and pharmacy to court for allegedly writing and filling an accidental prescription for the abortion pill, which she unwittingly took without knowing it would kill her preborn baby.
According to a lawsuit filed Monday in San Luis Obispo County Superior Court, Lorena Anderson went to see Dr. Maria Rasul at Bishop’s Peak Women’s Health on March 20, 2018, to confirm she was pregnant. Rasul then allegedly “carelessly and negligently” ordered a prescription for misoprostol – one half of a chemical abortion – without informing her of its “nature and effects.”
The suit says Rasul realized her mistake and contacted the pharmacy to cancel the prescription, but did not contact Anderson to warn her not to take the prescription if she picked it up – which she did the same day at Rite Aid Pharmacy’s Atascadero location. Rite Aid staff “carelessly and negligently” filled it anyway, according to the suit, and subsequently failed to inquire whether Anderson was pregnant or explain what it would do.
Anderson took the pill on March 20 and suffered a miscarriage, she says. Her suit, which names Rasul, Bishop’s Peak, Rite Aid, and Bishop’s Peak parent Dignity Health, is seeking damages for “fright, horror, anger, disappointment, emotional distress, mental suffering,” and “physical injury.”
“As a direct and proximate result” of the defendants’ actions, the suit continues, Anderson “was compelled to and did fall and sustain serious injuries,” including “shock and injury to her nervous system” that has incurred ongoing medical expenses and loss of earnings, and may result in “some permanent disability.”
“She was very excited to learn she was pregnant, and she was looking forward to being a mother,” Anderson’s attorney, Garrett May, told the San Luis Obispo Tribune. The first hearing in the case is slated for May 13; Anderson’s legal team is seeking a jury trial. Dignity Health has yet to comment on the lawsuit.
For chemical abortions, abortionists give women mifepristone, or RU-486, in an office and then have them take misoprostol at home. Pro-lifers have long argued that even when “properly” taken, abortion pills are not only lethal to children but more dangerous to women than advertised.
The U.S. Food and Drug Administration lists 2,207 adverse health events in women who used mifepristone between 2000 and 2011, including 14 deaths, 612 hospitalizations, 339 hemorrhages requiring transfusion, and 256 infections.
Mifepristone can be reversed by the practice of abortion pill reversal, if extra progesterone (the natural hormone mifepristone functions by blocking) is taken quickly enough. Its pioneers credit it with saving more than 400 babies since 2007, yet “pro-choice” advocates fiercely oppose promoting the option.
December 19, 2018 (LifeSiteNews) – The Catholic Church continues to be rocked by highly credible allegations, most powerfully voiced by Archbishop Carlo Maria Viganò, of homosexual corruption in the highest echelons of the hierarchy. The rot appears to run from the top down to the level of dioceses and seminaries, where countless adolescents and seminarians have suffered sexual predation at the hands of men who should have been their spiritual fathers. The problem appears to be virtually universal in Europe, Latin America, and the Anglophone world. The Church now finds itself in what may be the most wretched state of moral decadence that it has ever suffered in its long history.
It might seem that the Catholic Church is simply suffering from a particularly virulent infiltration of the clergy by a powerful and extensive fifth column, one that only must be detected and rooted out to eliminate the problem. Indeed such exposure is crucial to winning this battle of Catholic restoration, and that is a work to which LifeSite and many other Catholic journalists and activists are dedicated. However, I would argue that it isn’t remotely enough. The reality is that the crisis is a far more general one, and largely stems from a perverse pact made between a degenerate clergy and a deeply corrupt laity. Until both the laity and the clergy are reformed, we will never extricate ourselves from this terrible crisis.
Most of the Catholic laity are addicted to their own version of sodomy
Any casual observer of the ecclesiastical scene can find countless examples of parishes that are served by a weak and effeminate “Fr. Feelgood” (perhaps accompanied by his assistant, the ever-dissenting “Sister Angrynun”), whom we can easily blame for the compromised moral and spiritual state of the parish. “Fr. Feelgood” tends to create in his parish a watered-down version of the Catholic faith in which notions of sin, sacrifice, and salvation are deemphasized or eliminated in favor of a low-content sentimentalism that tends to affirm the carnal mentality and worldly tendencies of the congregation. “Fr. Feelgood” may be an outright homosexual or merely a “tame” beta male who exhibits a similar mentality, but the effects of his leadership (or lack thereof) will tend to be the same.
However, what is often overlooked is the more silent and passive but equally essential element in this perverse partnership, and that is the laity of the parish who seem untroubled and even grateful for Fr. Feelgood’s weak character and pandering ministry. Underlying this attitude is a troubling fact that is passed over in silence, and that is that virtually all of the sexually-active members of the parish are themselves involved in the sin of sodomy.
Yes, that’s right: sodomy. That’s the term used historically in the Church for a sin that is currently rampant among sexually-active Catholics, even those who attend Mass every Sunday. It’s the use of contraception, which poll after poll since the 1970s have indicated is used by the majority of sexually-active Catholics, even those who attend mass regularly.
Contraception has always been understood in the Catholic Church as a grave sin against nature, a perversion that is similar to other abuses of the sexual act that deny its natural unitive and procreative purposes. Couples that use artificial birth control are seeking the pleasure of sexual intercourse in a way that denies its ultimate end, which is to bring forth life and simultaneously to reinforce their marriage union for the purpose of cooperating in the education of their children. Instead, they are seeking the pleasure of the act as an end in itself, and treating the body of their companion as an object of lust.
A recent Pew Research poll (p. 26) reinforced what previous research has demonstrated repeatedly about the attitudes of Catholic laity regarding contraception. It found that of those Catholics who attend mass weekly only 13% regard contraception as “morally wrong.” Of the rest, 45% say it is morally acceptable, and 42% say it’s “not a moral issue,” in the words of the poll. This is reflective of so many other studies that have found a similar acceptance of contraception. There can be no doubt that the vast majority of sexually-active Catholic couples are engaging in this destructive vice.
The contraceptive mentality, which separates the sexual act from reproduction and reflects a hedonistic and narcissistic ethos, leads easily to other sins. If the ultimate purpose of the sexual act isn’t reproduction, but just selfish pleasure, then why should couples marry at all? Extra-marital sexual activity and cohabitation easily follow from this conclusion, as well as abortion when the “unwanted” unborn child inconveniently enters into the picture – after all, if people have a right to their selfish pleasure without consequences, an unborn baby is seen easily as an intruder in their relationships.
Divorce is also closely associated with the sin of contraception. Various studies comparing married couples who don’t use birth control with those who do have found that the divorce rates of the latter are much higher. A study of users of Natural Family Planning (which is used often by those who reject contraception) found that those who have used NFP have a divorce rate half of that of those who have never used NFP.
At the end of this continuum of perversion are the worst abuses of the sexual act, which themselves follow from the logic of contraception. Among them is the vice of homosexual sodomy, which differs from heterosexual contraception not so much in kind, as in degree.
That’s why St. Peter Damian, the Catholic Church’s greatest defender of sexual morality among all of its canonized saints, regarded the contraceptive sin of Onan in the Old Testament as a type of sodomy. Onan engaged in the most simple and easiest form of contraception, withdrawing from his brother’s wife and “spill[ing] his seed upon the ground” (Gen. 38:6-10). God struck Onan dead for this evil act – even though the penalty for not bringing up offspring for one’s dead brother was not death, but public humiliation – because Onan had perverted the sexual act.
“Certainly, this disgrace (sodomy) is not unworthily believed to be the worst of all offenses,” writes Damian in his Book of Gomorrah, which he wrote to denounce a crisis of sodomy among the clergy and monks of his day. He soon adds: “[God] struck Onan, the son of Jude, with an untimely death because of this nefarious offense, according to the Scripture, which says, ‘Onan … knowing that the children should not be his, when he went in to his brother’s wife, he spilled his seed upon the ground, lest children should be born in his brother’s name. And therefore the Lord slew him, because he did a detestable thing.”
The resulting situation is a Catholic laity that has a mentality similar to that of practicing homosexuals. In their own relationships, the vast majority of lay Catholics are using artificial birth control. In general, they do this because they have a hedonistic and consumeristic notion of marriage, and indeed of life itself, one that is characteristic of modern neoliberal secularist democracies, where happiness is absurdly sought in the transient pleasures and perishable goods of this world.
Those involved in this heterosexual form of sodomy, will naturally tend to have a deep and implicit sympathy for homosexual sodomites, whose only major difference is the preference of a same-sex partner in their unnatural sin of lust. This is why the vast majority of Catholics seem to be unperturbed by the effeminate and worldly attitudes of their pastors – they resonate with the contraceptive mentality of the laity. If Fr. Feelgood rarely mentions the doctrines of hell, or sin, or repentance and amendment of life, and seems uninterested in prayer or sacrifice, he is little more than a reflection of his own hedonist and consumerist congregation, which would rather not hear about such unpleasantries. Of course, such priests never trouble their parishioners with the Church’s doctrine condemning contraception, despite their obviously small family sizes.
As a result, less than a third of Catholics told the Pew Research Center that homosexual behavior is “morally wrong,” and even among those who attend Mass every Sunday, only 50% held that view (again, p. 26). The Catholic Church’s clear doctrine condemning sodomy, expressed repeatedly in Sacred Scripture, the writings of the Church Fathers, in the Catechism of the Catholic Church and in the official pronouncements of the popes, is either ignored or rejected outright in most parishes. This attitude is a natural consequence of the embrace of contraception by the laity; although their version of sodomy and hedonism is more bourgeois and conventional than that of homosexuals, their own addiction to sexual lust and perversion entails the same essential reality.
Contraceptive parishes, contraceptive liturgies
The contraceptive mentality that runs through most Catholic parishes is not only facilitated by the false doctrines of wayward priests, but also by the generally degraded state of the Roman Rite liturgy. It should be unsurprising that the decline of the liturgy occurred at the same time as explosion of contraceptive practice among Catholics.
Although the formal intention of the liturgical reform was to encourage participation by the faithful, the effect has been to facilitate a style of worship that dovetails with the self-centered, narcissistic mentality that underlies contraceptive unions. The priest who faces the people from behind the altar encourages the notion of the “community celebrating itself” in the words of Cardinal Josef Ratzinger, later Pope Benedict XVI. The childish liturgical translations, which were somewhat corrected by Pope Benedict but now appear on their way to being restored by Pope Francis, the trite and breezy hymns, the reception of communion in the hand by the laity, the worldly architecture, all are alien to the traditions of the Church, and all tend to undermine the sense of reverence in the liturgy.
In light of the results of liturgical reform, which the same Cardinal Ratzinger regarded as gravely botched, it hardly seems coincidental that the massive liturgical changes that came about in 1969-1970 followed on the heels of the equally massive rejection of Pope Paul VI’s encyclical letter Humanae vitae in 1968. After years of speculation that the Church might reverse its condemnation of artificial birth control, Paul VI in Humanae vitae reaffirmed the ancient doctrine that contraception is “intrinsically evil” and a mortal sin. However, the vast majority of Catholics rejected the doctrine, and their pastors appeased them by ignoring it and ignoring their own parishioners’ immersion in this sin. Soon after, the liturgy was altered in ways that facilitated the new mentality, and numerous priests departed from the priesthood, which appeared to many to have been deprived of its sacramental meaning. They left behind a largely weak and effeminate clergy that sought to pander to modern sensibilities rather than to exercise manly leadership on behalf of Christ.
It shouldn’t be surprising that the absolute condemnation of contraception reaffirmed by Humanae Vitae is a major focus of the current attack carried out by homosexualist theologians against Catholic sexual morality. The acceptance of contraception is the foundation of the entire sexual revolution, including the acceptance of cohabitation, abortion, and same-sex sodomy. The lavender mafia that currently holds power in the Church depends deeply on this evil pact with contracepting laity, who support them morally and financially.
Catholic pastors are called to a particular sort of courage in the face of pressure from their confused congregations, who are accustomed to regarding the priest as a facilitator of their lifestyles rather than as a prophet who calls upon them to repent. The duty of the priest is to speak the truth to the laity, even at the risk of persecution, as St. Paul notes in his second letter to Timothy, whom he had personally ordained to the priesthood:
I charge thee, before God and Jesus Christ, who shall judge the living and the dead, by his coming, and his kingdom: Preach the word: be instant in season, out of season: reprove, entreat, rebuke in all patience and doctrine. For there shall be a time, when they will not endure sound doctrine; but, according to their own desires, they will heap to themselves teachers, having itching ears: And will indeed turn away their hearing from the truth, but will be turned unto fables. But be thou vigilant, labour in all things, do the work of an evangelist, fulfil thy ministry.
Amanda Schuster and husband Robert wanted to give their son Baron a sibling, but months went by and they weren’t conceiving. They underwent testing and discussed measures that might help, but before they could take any steps, they got a “beautiful positive test.” Then, after weeks of pregnancy bliss, the couple was devastated after a 20-week scan revealed a condition that would cause doctors to advise them to abort their baby girl immediately.
“At 20 weeks, we went in for the routine anatomy scan with no concerns whatsoever,” Schuster wrote in an essay for Love What Matters. “We held hands and laughed when we saw her on the screen. We couldn’t wait for pictures to show her grandparents.”
That joy quickly turned to fear as the ultrasound technician became quiet and continually scanned the baby’s head. Then she excused herself to speak to the radiologist. Schuster knew that something was wrong.
The doctor informed the couple that there was an “anomaly” with the baby’s skull and they needed to go to maternal fetal medicine the next day for a better scan with more advanced machines. It was there that the doctor diagnosed their baby girl, named Emmy, with a type of dwarfism that she said would be fatal. She advised them to abort — and fast.
“This was taken after they had rushed her to the other OR to evaluate her breathing and we had been just waiting to hear ANYTHING. Seeing her and knowing that she’s breathing and doing okay was just so overwhelming.” – Amanda Schuster, Facebook
“She told us we had to hurry because our time for legal abortion was coming to an end and I would have to fly out of state if I waited too long,” said Schuster.
Despite the pressure to make a decision, Schuster refused to make a decision so abruptly. She wanted a second opinion. The doctor referred them to another doctor in the craniofacial department who determined the original diagnosis to be wrong.
“He took one look at her scans and said that the initial diagnosis was completely incorrect and that he was 98% sure she’d have Pfeiffer Syndrome,” wrote Schuster. “He told us the good and the bad but assured us that she could live and have a very good life. She would need surgeries – probably many – but she could be a happy child with a fairly normal life.”
“She’s a very happy girl. She smiles all the time. She loves being held and cuddled and talked to and sung to.” – Amanda Schuster,Facebook
People with Pfeiffer Syndrome have premature fusion of the skull during development. Because of this, the head and face don’t grow normally, eye sockets will be shallow and the face will be small, leaving the airway too narrow.
“Even though we had prepared ourselves the best as we could, it was still a shock to see Emmy in the flesh,” wrote her mother. “Her eyes were huge, her skull was misshapen, and they intubated her immediately before I even got to look at her. She also has the most beautiful blue eyes and dark hair.”
Schuster recalls that the delivery room was silent which carried an eerie feeling. Emmy was immediately whisked away to get checked out by the doctors. She had surgery to place shunt to drain the fluid, and would spend four months in the Neonatal Intensive Care Unit undergoing more surgeries and surprising everyone with her continued progress.
Now 18 months old, Emmy is doing well. She has had no less than 20 surgeries, including repairing intestinal malrotation, receiving a g-tube to help nourish her, a tracheostomy, and three skull surgeries to help her brain develop. She struggles with sleep apnea and will need more surgeries in the future, but she is a happy, well-loved girl who adores her big brother.
“[Her brother is] really going to be such a champion for her. He loves her just so unconditionally and it takes my breath away to just see how much love and adoration flow between them. They needed each other and they both lucked out in the sibling lottery.” – Amanda Schuster, Facebook
“She’s doing remarkably well these days… probably more so than anyone ever expected,” said Schuster. “We’ve had hospital stays and emergencies, we’ve had PICC lines and long nights of worry, but she smiles through it all. She continues to grow and develop, albeit at a slower pace than other kids her age, but she shows a determination that is unbelievable. She’s got parents that love her, a brother that thinks she hangs the moon, grandparents that encourage her, and a team of doctors, nurses, and therapists that give her every tool possible to thrive.”
Her family knows that life won’t always be easy for Emmy and they worry about bullies in her future, but they hope that by sharing her story, other families will see that she’s a fun-loving child like any other and would love to play.
Doctors are often quick to advise abortion, especially if the state they work in has abortion restrictions. That pressure to abort can cause families to choose abortion without having the time to think it over. Families who are faced with this can learn something from the Schusters: always seek a second opinion. An obstetrician is a specialist in pregnancy and delivery, not in every health condition on earth. The Schusters followed their instincts, got a second opinion, and chose life for their beautiful girl who has become the light of their lives.
I was greatly moved by a December 21, 2018 op-ed in the Wall Street Journal by Gayle Somers titled “Life Is Worth Living, Even if It Is Painful and Short” with the subtitle “My son’s addiction caused great suffering and ended with a fatal overdose. I’ve never regretted his birth”
In this op-ed, Ms. Somers told the story of her son’s birth and eventual death 33 years later from an accidental overdose after a 14 year battle with drug addiction. That resonated with me since I lost my 30 year old daughter Marie to suicide using an assisted suicide technique after a 16 year battle with addiction.
But it was Ms. Somers’ wonderful statement “I’ve never regretted his birth” that caused me to write a letter to the editorthat was published today:
“As someone who has lost a daughter to suicide and has also lost another daughter and a grandson to medical conditions, I really appreciate and agree with Gayle Somers’ op-ed “Life is Worth Living, Even if it is Painful and Short” (Dec. 22). My first daughter died at 30 after struggling with substance abuse for 16 years.
As a nurse and friend of bereaved parents, I also have never met a parent or grandparent who regretted the birth of his or her lost child.
I once was asked for advice by a bereaved mother after her 2-year-old son with Down Syndrome died unexpectedly. She wanted to know what might help her accept her son’s death with a hopeful outlook. From my own personal experience, I told her that solace comes when a lost child’s life rather than his death becomes the most important fact about him. The love itself never dies.
Nancy Valko
St. Louis
CELEBRATING LIFE
Ms. Somers also wrote in her op-ed that:
“These days pregnant women can take prenatal tests to learn about genetic defects their babies may have. Sometimes I’m grateful that no test allows you to see how a child’s life will unfold. All parents instinctively shrink from the excruciating expectation of a child’s suffering and, inevitably, their own suffering.
Some parents are so frightened at the prospect of raising a child with a genetic abnormality that they end the child’s life in the womb. While I understand this temptation—to spare the child the struggle, to spare yourself the pain—reflecting on the time I spent with my son convinced me that life is worth it despite the suffering.”
This also resonated with me since I lost my 5 1/2 month old daughter Karen who had Down Syndrome and a severe heart defect just before her scheduled surgery in 1983.
Two years later, I was pregnant again and the doctor strongly urged me to have an amniocentesis to test for Down Syndrome. I refused not only because of the unnecessary risk to the baby but also because I knew I would love this baby regardless of any condition or lifespan. Because of Karen, I was not afraid to welcome this baby.
Happily, my daughter Joy was born healthy and now has a baby daughter of her own to share with us.
CONCLUSION
Over the years, I’ve been inspired by many parents who have lost children of all ages. Some of these children died of natural causes and some from medical malpractice, tragic accidents, suicide and even murder.
The pain of losing a child is naturally devastating, especially at first. However, I have seen those same parents also rise up and honor those children’s lives by helping others or fighting injustices.
I consider Ms. Somers one of those inspiring parents, especially how she ended her op-ed by writing:
“Even knowing what we know now about how our children’s lives would end, all of us would choose life, no matter how short, no matter how painful. We welcomed our children into our families. We gave them names, and then, one day, we began to learn how to do what all parents must do—love without limits, comfort during the pain, not shrink from the suffering, give thanks for the gifts our children are to us.”
As a non-Catholic teenager, I didn’t know this — in fact, I was told the opposite was true. It wasn’t.
When I was 19, in the summer after my freshman year of college, I was prescribed birth control after experiencing two cycles of more painful than usual menstrual cycles.
At the time, I wasn’t Catholic. I had no awareness of the negative effects of the pill, and was in fact assured that there were no negative effects, only positive ones. It would stop my cramps, reduce my acne, and, the doctor assured me, “control mood swings.”
Mood swings were not something I was prone to at the time. I loved college, loved my friends, loved my classes, and was in fact deliriously happy with life. But that changed after I started taking birth control. It wasn’t dramatic — it was more of a slow decline, a gradual loss of interest in classes that led to sleeping in, skipping class, and my grades dropping ever so slightly. As promised, my cramping subsided and my acne got marginally better, but I began gaining weight. It was the weight gain more than anything that prompted to me to stop taking the pill six months after I started. At the time, I didn’t connect the boost in my mood and improvement in my grades during the second semester of my sophomore year, but looking back, it’s clear that the pill had altered my mental state during the brief period of time when I took it.
A survey conducted by the team behind the documentary, titled The Contraceptive Pill: How Safe Is It?, found that one in four women taking the pill said it had negatively affected their mental health.
Danielle, 31, is one of these women. Speaking in the Horizon episode, she recalls how her side effects were “completely debilitating and terrifying,” adding that she’d never experienced poor mental health prior to taking the pill. “I went from being fine to having suicidal thoughts within six months,” she adds …
Dr. Zoe Williams, who presents the documentary, explains that all medicines have potential side effects, but the pill is different to most because it is taken by women who are well, rather than to prevent or treat illness or disease. “Therefore side effects that significantly impact on quality of life, in a negative way, are not acceptable,” she tells The Independent.
One of the biggest problems with the pill is that depression and anxiety, well-known side effects of progesterone, are not named in the literature distributed with it. Instead, the first potential side effect listed is “mood changes,” which could mean anything. It’s almost as if the manufacturers of the pill are attempting to hide the pill’s serious side effects.
This is a real problem, particularly with something as widely and cavalierly prescribed as birth control. Growing up, I knew girls taking birth control for everything from acne to endometriosis. Like me, they were assured by their doctors that the medication was virtually risk-free, and in fact came with a host of positive benefits.
But altering a woman’s natural hormonal balance is not a panacea, particularly when it’s being done for frivolous reasons. I’m glad to see this research making its way to the public, because countless young women deserve to know that birth control is not harmless, nor is it consistently beneficial. Regardless of their beliefs on ethics and morality, young women deserve to know that the pills they’re being given could cause more harm than good.
January 4, 2019 (LifeSiteNews) — Unable to sleep the other night, I began to think back over my life. I reflected on my turbulent youth as a child of the 60s: the men, the drugs and drinking. I came of age in a tumultuous time; everything was in a state of change and upheaval.
I got to thinking about an old college friend and his family. I decided to Google my friend’s father who had an unusual name and was sadly influential in my life. I found an obituary for the father, Garrett Hardin.
As I read it, I was in shock.
At 18, I was a freshman at the University of California, Santa Cruz, facing an unplanned pregnancy. I could have shared the pregnancy with my parents, who were against abortion and would have helped me parent my child. I turned instead to this college friend and his family.
As I struggled to accept the reality that I was pregnant, the Hardins persuaded me that I could get rid of the pregnancy and then after the procedure I could return to my pre-pregnancy life. That’s exactly what I wanted.
But in 1968 abortion was still illegal. Not to worry. Garrett Hardin had another option that would make my problem go away.
One particular paragraph of Hardin’s obituary hit me especially hard. I was not the only woman he helped get rid of the problem:
“Mr. Hardin and his wife were longtime supporters of Planned Parenthood, and … helped operate an ‘underground railroad’ in which 200 local women went to Mexico seeking abortions.”
I am one of those 200 local women who went to Mexico on that Hardin Underground Railroad of Abortion.
Garrett Hardin was tragically wrong. That abortion did not magically return me to my pre-pregnancy life. Pregnancy and childbirth are life-changing events. But abortion is also a life-changing event.
At 18, I really had no idea what I was doing on that journey to Mexico. One of the Hardin family women went with me. We drank the whole two days. I’m surprised they were able to do anything medical given my blood-alcohol level. I’m sure it was through the roof.
For a short time after that trip, life seemed sort of OK. The only problem was that my drinking, drugging and promiscuity all got worse. After two more unplanned pregnancies and two more abortions, I was a mess.
I finally had a child and then got sober. After a number of years floundering around, I returned to my childhood Catholicism. I then found an abortion healing program called Rachel’s Vineyard that began my journey back to peace and serenity.
In Garrett Hardin’s obituary, a friend of his shared:
“Mr. Hardin’s research and writing on reproductive rights ‘were fundamental in getting the state Legislature (California) to pass therapeutic abortion bills in the 1960s.’”
I also learned something else about Hardin. His aggressive advocacy for abortion rights led him inexorably to the promotion of euthanasia.
The first parents of our human family faced the temptation to “become like gods,” and rebel against the providence of their Creator. In their anguish and shame, they learned the painful lesson that some choices do not lead to liberation and freedom but to spiritual and physical death.
This temptation to rebel against God’s absolute providence over our lives, and the lives of the unborn, remains a powerful and deadly temptation that still rages in the hearts of women and men.
The obituary revealed the final chapter in the life of Garrett Hardin. He was a member of the pro-euthanasia Hemlock Society. Faced with illness and disability, Hardin and his wife died in a double suicide.
Susan Swander lives in Oregon and is a member of the Silent No More Awareness Campaign
KRISTAN HAWKINS JAN 3, 2019 | 10:21AM WASHINGTON, DC
The anniversary of Roe v. Wade and Doe V. Bolton approaches, marking the beginning of the debate over whether abortion is truly a Constitutional right and what that looks like in daily life.
Abortion advocates argue for access to their product along with federal funding and accommodation, justifying their demands because they say they have a legal product found in the Constitution. And since 1973, they have the court documents to prove it despite the uneasy legal foundation even in the eyes of six Supreme Court justices.
Though a right to abortion is never mentioned by the authors of our nation’s birth certificate, abortion has been hung on the concept of privacy (also not mentioned in the Constitution) and defended for more than 45 years.
But given the blanket assertion that constitutionality equals governmental facilitation, let’s consider how that might apply to something actually found in the constitution at our founding … the right to bear arms … actual guns that are sold with considerable scrutiny.
Planned Parenthood has taken numerous states to court and won when legislators decided that healthcare dollars would go to full service healthcare providers and not simply abortion vendors. Through numerous federal and state programs, Planned Parenthood has brought in more than half-a-billion in taxpayer funds annually, and they argue for more.
Ending preborn life should be an absolute right especially for the poor, according to Planned Parenthood’s new President, Dr. Leana Wen, who is direct that ending preborn life is necessary to avoid class struggle.
“Our narrative on choice is incomplete without recognizing choice is predicated on privilege and it’s all of our responsibilities to fight against systemic injustices that have gotten us to where we are,” she told ThinkProgress.
But why stop at abortion when it comes to issues of life, death and justice for the poor?
Those in poverty also endure an increased crime rate. In fact a recent study found that “the poorest Americans are 12 times as likely to be sexually assaulted as the wealthiest.” Does that mean government subsidized guns should be made available for their protection, to save their lives or their bodies from harm? Wouldn’t that also be a pro-woman policy — federally funded guns and gun safety classes in the name of access to a constitutional right that should not be unavailable because of financial resources?
Access is an important word for the abortion lobby today that could be defined as a commute. A 2017 story at CNN noted a study showing that women traveled 11 miles to get an abortion for the most part. The abortion lobby finds this a bridge too far, and in fact any travel for abortion is a problem.
Recently, the former governor of California, Jerry Brown vetoed a bill that would have forced California publicly-funded colleges and universities to dispense chemical abortion drugs on campus, pointing out that studies showed abortion facilities were 4-6 miles from every campus, and therefore reconfiguring school health centers into abortion vendors was “not necessary.”
Abortion advocates were outraged. “There are so many campuses where the pill is not close by and even within a mile or two or three, women don’t always have transportation,” Sen. Connie Leyva (D-Chino) told reporters.
Writing in the LA Times, columnist Robin Abcarian observed: “It takes a particularly privileged, out-of-touch person to tell California college students that it’s no big inconvenience for them to travel up to seven miles to obtain an abortion pill.”
Imagine the outrage when people find out that the average commute to a job is 16 mileseach way or that gun stores are not easily accessible by all Americans and require background checks and other time consuming screens.
But in the name of access, abortion vendors have also fought against health and safety standards like an emergency plan if a woman was dying or requiring that an abortionist operating an abortion facility follow the safety laws that govern other types of outpatient medical centers. Case in point, Whole Woman’s Health v. Hellerstadt in which Texas officials had to fight for such protections.
Sadly abortion “access” won the day as Justice Stephen Breyer wrote for a five-justice majority finding, “We conclude that neither of these provisions offers medical benefits sufficient to justify the burdens upon access that each imposes.”
Abortion advocates are practically libertarians in their free market view of their product as any regulation that slows down an abortion from taking place is too horrifying to imagine. Imagine burdening abortion vendors with women’s safety.
With the logic of the abortion lobby, a short commute, a federal subsidy, and an unregulated process are hallmarks of a constitutional right. It’s a less-is-more philosophy until it comes time for taxpayer support.
Some may call this an apples and oranges comparison, between abortion and gun ownership, as guns can carry a risk to others, can end life and therefore need some scrutiny. But the same can be said of abortion, which always ends one life and leaves another harmed by the experience.
Most of the time, that fact that something is constitutional opens the door for a discussion on how to proceed, rather than ends the argument. It’s hypocritical to push regulations of one constitutional right while arguing that something not even mentioned in the Constitution must be singled out as deserving of governmental facilitation and billions of tax payer dollars. Even if one believes abortion is a constitutional right (and I don’t), that still does not mean it should be forced on Americans nationwide and paid for with precious taxpayer resources.
More human beings died in abortions than any other cause of death in 2018, a new report indicates.
A heartbreaking reminder about the prevalence of abortion, statistics compiled by Worldometers indicate that there were nearly 42 million abortions world-wide in 2018. The independent site collects data from governments and other reputable organizations and then reports the data, along with estimates and projections, based on those numbers.
Breitbart contrasted the abortion numbers to other causes of death, including cancer, HIV/AIDS, traffic accidents and suicide, and found that abortions far outnumbered every other cause.
Here’s more from the report:
As of December 31, 2018, there have been some 41.9 million abortions performed in the course of the year, Worldometers revealed. By contrast, 8.2 million people died from cancer in 2018, 5 million from smoking, and 1.7 million died of HIV/AIDS. …
It also records the total number of abortions in the world, based on the latest statistics on abortions published by the World Health Organization (WHO).
Globally, just under a quarter of all pregnancies (23 percent) were ended by abortion in 2018, and for every 33 live births, ten infants were aborted.
Worldometers estimates about 59 million deaths world-wide in 2018, but that number does not include unborn babies’ abortion deaths. Unborn babies are not recognized as human beings even though biology indicates that they are unique, living human beings from the moment of conception and they die brutal, violent deaths in abortions.
The abortion number is incomprehensible, but each of those 42 million abortions represents a living human being whose life was violently destroyed in their mother’s womb. Each unborn baby already had their own unique DNA, making them distinct from their mother. That DNA indicated if the child was a boy or girl, their eye and hair color, their height, possible genetic disorders and other disabilities, and much more. In most cases, the unborn babies’ hearts are beating when they are aborted, too.
An estimated 60 million unborn babies have been killed in abortions in the U.S. since Roe v. Wade in 1973. In January, pro-life advocates will gather for the annual March for Life in Washington, D.C. to remember the anniversary of that infamous decision and call for restored protections for the unborn.
Duc in altum! These words ring out for us today, and they invite us to remember the past with gratitude, to live the present with enthusiasm and to look forward to the future with confidence: ‘Jesus Christ is the same yesterday and today and forever’ (Heb 13:8).
These are the words of Christ to Simon Peter, commanding him to lower his nets into the sea. Peter did as the Lord told him, but not before expressing doubts, for he and his companions had been fishing all that night, without success. But, when Peter and his companions hauled up their nets, the nets began to break, so great was the catch of fish. Astonished at the miracle, St. Peter cast himself at the feet of the Lord: “Go away from me, Lord; I am a sinful man!”
These are also the words that Pope St. John Paul II chose to begin and end his apostolic letter Novo Millenio Ineunte, in which he celebrated the dawn of the third millennium by urging Christians to renew their commitment to the Gospel and Christ’s evangelical mandate: “Go into the whole world and proclaim the gospel to every creature” (Mark 16:15).
The Great Catch of Fish mosaic in the St. Peter’s Basilica
Though the pope wrote this letter to greet a new millennium, its message is perennial. Indeed, the whole of the pope’s letter is intended to emphasize that no matter the year or the century or the millennium, no matter the time or the season, every Christian is called to commit him or herself to the self-same mission: to live in Christ (“It is no longer I who live, but Christ lives in me” – Gal. 2:20), and to preach Christ to all the world.
Many of you reading this column are formulating your New Year’s resolutions. But the pope’s letter reminds us that there is only one New Year’s resolution that truly matters: to become saints.
The Perennial Christian Program
You have made us for yourself, O Lord, and our heart is restless until it rests in you.
In June of 1979, Pope St. John Paul II visited Poland. During one speech in Warsaw, the Holy Father spoke of the urgent need for spiritual and cultural renewal. Within the vast throng of some one-million people gathered there, a great cry spontaneously rose up: “We want God! We want God!”
In a Poland oppressed by the atheistic and totalitarian communists, the worship of God had been made difficult by the oppressive crackdown on the Catholic Church, and the pervasive propaganda in the schools and media. But the Polish people knew that the materialistic utopianism of the communists could not give them that for which they yearned.
The same desire for God is just as operative (if not more so!) in our own increasingly materialistic and atheistic culture, so weighed down by the burden of sin: That neighbor crushed by a recent painful divorce is crying out, “I want God!” That friend at school who has threatened to commit suicide is crying it, “I want God!” The nephew who has fallen into a life of drug use and sexual immorality is crying out: “I want God!” The niece whose life fell apart after she aborted her child is crying out: “I want God!” And if we would only cease our frenetic activity long enough to listen, we would find that our own hearts, too, are crying out: “I want God!”
We have all encountered misguided pastors who are obsessed with “change,” with devising or implementing clever new programs to help the Church “get with the times” and to “speak to the current generation.” Unsurprisingly these programs rarely work, for the world is not thirsting for the trendy and up-to-date. Indeed, our world is drowning in the trendy and up-to-date, which can be found in super-abundance at the nearest mall or movie theater.
The world is thirsting for the transcendent; and the transcendent is not a thing that changes with the times or that needs to be updated for one generation over the next. The desire – and the remedy – will be the same in 2019 as it was in 2018, as 1018 for that matter.
“It is not therefore a matter of inventing a ‘new programme,’” said Pope St. John Paul II in Novo Millenio Ineunte.
The programme already exists: it is the plan found in the Gospel and in the living Tradition, it is the same as ever. Ultimately, it has its center in Christ himself, who is to be known, loved and imitated, so that in him we may live the life of the Trinity, and with him transform history until its fulfilment in the heavenly Jerusalem. This is a programme which does not change with shifts of times and cultures, even though it takes account of time and culture for the sake of true dialogue and effective communication. This program for all times is our program for the Third Millennium.
‘What Must We Do?’: A Christian’s New Year’s Resolution
In this time of bewilderingly rapid and misguided social change, we may feel a sense of helplessness, anxiety and even fear: How do we respond when our efforts seem so small in the face of the Culture of Death? What is our path to achieving the radical transformation of culture and people? At a time when the media, politics, and popular culture are so virulently hostile to religious belief, and Christianity in particular, how are we possibly to catch the great catch that our world and Church so desperately need?
As Pope St. John Paul II emphasized and re-emphasized, the answer is always and everywhere the same: Christ.
Jesus calls the Apostles St. Andrew and St. John by Francesco Gessi (1588 – 1649).
Conscious of the Risen Lord’s presence among us, we ask ourselves today the same question put to Peter in Jerusalem immediately after his Pentecost speech: “What must we do?” (Acts 2:37). We put the question with trusting optimism, but without underestimating the problems we face. We are certainly not seduced by the naive expectation that, faced with the great challenges of our time, we shall find some magic formula. No, we shall not be saved by a formula but by a Person, and the assurance which he gives us: I am with you! It is not therefore a matter of inventing a “new program”. The program already exists: it is the plan found in the Gospel and in the living Tradition, it is the same as ever. — Novo Millennio Ineunte, ¶29
However, our hearts are fatally fickle and our resolutions in continual need of renewal. In this New Year, let us resolve to pay heed to the universal cry for God, beginning with the cry of our own hearts. Let us resolve to reflect the life Jesus calls us to live, to open our hearts to God’s transforming activity, to submit our lives to His will, to follow the Gospel, to put on Christ (Rom. 13:14).
In this New Year let us resolve to become saints!
To the extent that Christians are living as Christians, they are also heralds of the Gospel – for they will continuously preach Christ in their every word and deed: in their peaceful demeanor, in their charitable speech even about those who hate them, in their generosity to the poor and the downtrodden, in their rejection of shallow consumerism and the depraved dominant morality, etc. This will in turn become the hinge upon which a Culture of Life will be constructed – defending life from conception to its natural end and upholding the dignity and the inalienable rights of every man, woman and child.
We must remember the miracle of the great catch of fish. Before and after Christ arrived, Peter and his companions were doing the exact same thing: working hard to catch fish using the best methods and equipment at their disposal. Their efforts did not change; only the results changed. Without Christ, there was no catch; with Christ, the catch surpassed their wildest hopes.
We will only succeed in building a Culture of Life and Civilization of Love when we live authentic, transparent lives in Christ: holiness is the universal call which will infuse our ability to transform cultures and peoples. It is not enough that truth and grace are offered through the proclamation of the Gospel of Life. It needs to be accepted and experienced in every practical situation, in the way Christians lead their lives.
I will conclude with one more quotation, filled with hope, from Pope St. John Paul II’s letter Novo Millennio Ineunte, adapted for the beginning of a new year:
A new [year] is opening before the Church like a vast ocean upon which we shall venture, relying on the help of Christ. The Son of God, who became incarnate two thousand years ago out of love for humanity, is at work even today: we need discerning eyes to see this and, above all, a generous heart to become the instruments of his work. … Now, the Christ whom we have contemplated and loved bids us to set out once more on our journey: “Go therefore and make disciples of all nations, baptizing them in the name of the Father, and of the Son and of the Holy Spirit” (Mt 28:19). The missionary mandate accompanies us into the [new year] and urges us to share the enthusiasm of the very first Christians: we can count on the power of the same Spirit who was poured out at Pentecost and who impels us still today to start out anew, sustained by the hope “which does not disappoint” (Rom 5:5).
Patrice (not her real name) is a woman living with HIV. In a consultation with her doctor, she explained that she and her partner were planning to have a child. The doctor is said to have told her that she was wicked to want to get pregnant and pass the virus on to her child.
While our allies in the healthcare system are far greater than in previous years, Patrice’s story is one example of the discrimination that people living with HIV face from some healthcare workers.
With the widespread availability of antiretroviral treatments, people living with HIV have been living long and productive lives for years now. This includes healthy sexual and reproductive lives. Proper adherence to treatment and medical supervision significantly reduce the chances of transmitting the virus to one’s partner and virtually eliminates the chance that a woman will transmit HIV to a foetus. Despite these advances, there is significant evidence to suggest that some healthcare workers in Jamaica regularly coerce HIV-positive women to undergo tubal ligation (tie-off).
Women must never be denied the opportunity to give full and informed consent for sterilisation or other long-term contraceptive procedures because they are HIV-positive. Coerced sterilisation is a grave violation of the human rights of HIV-positive women, even classified by the OHCHR as an act of torture and cruel, inhuman, and degrading treatment. It manifests itself in ways that include offering financial incentives, deliberately providing misinformation, or using intimidation practices such as denying healthcare serves in an attempt to compel positive women to undergo the procedure.
This discriminatory practice is linked to the false belief that HIV-positive women are somehow not fit to be mothers or that HIV-positive women who become pregnant are irresponsible and incapable of managing their own healthcare needs and those of their families.
This practice also prevails because of weak or non-existent informed consent policies and procedures to protect patients’ rights or where medical personnel who violate such policies are generally not held accountable.
FORCED CONTRACEPTIVES
Additionally, there is evidence to suggest that HIV-positive women are also unwittingly placed on long-term contraceptives without consent or consultation. In a recent PLHIV training workshop, three different women shared their experiences of being told to go to ‘X’ clinic on ‘Y’ date to get a contraceptive method. The requisite consultation regarding their preferences and the details (side effects, etc) of type of method being issued were not provided in these cases.
In support of our members across the island and also the approximately 30,000 Jamaicans living with HIV, we encourage a joint approach from the Ministry of Health and Ministry of Justice to bring the practice of coerced tubal ligation to an end and make amends to the affected persons. Our first line of defence must be to provide continuous and comprehensive education and sensitivity training for our healthcare workers. This is a must if we are to make healthcare in Jamaica more effective, improve the lives of people living with HIV, and eradicate HIV altogether in Jamaica.
We must also be prepared to take action against violators of human rights and establish accountability, a process that includes introducing mechanisms so that violations are not permitted in the future.
In offering redress to persons affected by coerced sterilisation, JN+ advocates that we offer free sterilisation-reversal procedures. Law enforcement, including the judiciary, must also be trained to appropriately investigate, prosecute, and adjudicate allegations of violations of reproductive rights, especially as they relate to HIV-positive women.
In discussing female contraception, the general assumption is that you’re talking about the Pill. But new findings released by the Centers for Disease Control and Prevention (CDC) show that another method has surpassed oral contraceptives in popularity: female sterilization.
According to the data, which was released Wednesday and gathered between 2015 and 2017, nearly 65 percent of the 5,500 women aged 15 to 49 who participated in the survey said they had used some form of contraception in the month before they were interviewed. The most common methods used were female sterilization (18.6 percent), oral contraceptives (12.6 percent), long-acting reversible contraceptives (LARCs), such as intrauterine contraceptives (10.3 percent), and male condoms (8.7 percent).
The last time the survey was conducted (between 2011 and 2015), only 14 percent of women reported they were relying on female sterilization, i.e. tubal ligation, a surgical procedure in which the fallopian tubes are closed to prevent future pregnancies. Today, more women are opting for this method, the older they get. About 4 percent of women between the ages of 20 and 29 choose this method, compared to nearly 22 percent of 30- to 39-year-olds, and 39 percent of 40- to 49-year-olds. The researchers also found that rates of female sterilization declined and the use of the Pill increased with higher education.
Tubal ligation is a big choice. It’s a permanent form of birth control and requires surgery, the American College of Obstetrician and Gynecologists points out. During a tubal ligation, a woman’s fallopian tubes are cut, tied or blocked to prevent future pregnancy, by keeping an egg from traveling from the ovaries through the fallopian tubes or a partner’s sperm from traveling up the fallopian tubes to the egg, the Mayo Clinic says. It generally doesn’t affect a woman’s natural menstrual cycle.
“Tubal ligation permanently prevents pregnancy, so women no longer need to use birth control,” women’s health expert Jennifer Wider, MD, tells Yahoo Lifestyle. “It’s convenient and a popular option among women who are done having family or know they don’t want children.”
Jessica Shepherd, M.D., a minimally invasive gynecologist in Texas, tells Yahoo Lifestyle that the numbers are “shocking, given that this is a permanent procedure.”
The procedure comes with some risks. One is an increased risk of ectopic pregnancy (where the fetus develops outside the uterus), which can be life-threatening for a woman, Wider says. “Other side effects include cramping and bleeding,” she adds. Given that this also involves surgery, there are risks of complications, including chronic pain and even death, Christine Greves, MD, a board-certified ob-gyn at the Winnie Palmer Hospital for Women and Babies, tells Yahoo Lifestyle. “Some people also complain that their periods aren’t as nicely controlled after a tubal ligation, but they often were using a hormonal method of birth control beforehand, which makes your periods a lot better,” Greves says.
Clearly, this isn’t a hugely popular choice among younger women, but it’s an important one for some. Life coach and hypnotherapist Bri Seeley tells Yahoo Lifestyle that she’s “known pretty much my entire life that I don’t want to be a mom. I feel like it’s just part of who I am.” After being on birth control for years, Seeley asked her doctor about getting a tubal ligation when she was 24, and her request was denied. Even though she repeatedly asked, her doctor wouldn’t even give her a referral to have someone perform the procedure on her until she was 30, which Seeley says was hard to take.
“It was frustrating because I know myself. To have someone tell me that I don’t know myself well enough to make this decision was super-frustrating,” Seeley tells Yahoo Lifestyle. Seeley ended up finding a doctor herself and had the procedure done six years ago. “I went from being worried about getting pregnant all the time to now it’s something that hasn’t crossed my mind over the last six years other than ‘Thank God,’” she says. “I’ve seen female friends have to fight to get birth control, and I always think, ‘Thank God I don’t.’”
“I’ve seen this quite a bit for women in their 20s who have had children earlier in life — after their third or fourth child, they may ask for a tubal ligation,” Greves says. But Greves says she’s also seen women like Seeley who know they don’t want to have children and request a tubal ligation. Shepherd has too. “Some people will say, ‘I do not want kids ever,’ but we always go back to the LARC when they say that, because we want to give them the option to change their mind,” she says. Research has shown that there is a high percentage of women who regret having had the procedure done if they decided to do it before they were 30, she says, and doctors are well aware of that. “You’ll have people who say, ‘I’m so sure that I don’t want kids anymore,’ and later get into a relationship or get married and regret their decision,” Shepherd says.
Producing a film that argues for the moral and practical superiority of natural family planning over modern contraceptive technology when practically “everyone” takes the latter approach for granted must be either an act of madness or an act of faith. “Sexual Revolution: 50 Years Since Humanae Vitae”, is both.
But it is more: the documentary, inspired by the prophetic encyclical of Pope St Paul VI, is also a testament to reason and to truth; philosophical reason, scientific truth.
The film tilts towards a Catholic audience (funding issues alone made this necessary) and it’s Catholics who are in most need of hearing its message. As popular writer Peter Kreeft says at the beginning, there is no Catholic teaching more “despised, hated and disobeyed” – by Catholics themselves –than that contained in Humanae Vitae.
Yet the number of true believers is not small and their intellectual leaders are impressive. Witnesses assembled by the film’s director Daniel diSilva include some of the biggest Catholic names in American scholarship: Robert P. George, Janet Smith, Helen Alvare, Brad Wilcox, Mary Eberstadt… Theological writers and apologists such as Dr Kreeft and Chris West appear in a line-up that includes Archbishop Charles Chaput of Philadelphia and Archbishop Anthony Fisher O.P. of Sydney.
Not least in this gallery are the scientists dead or alive, who gave a large part of their lives to setting natural family planning on a sophisticated, scientific footing: Australian neuroscientist John Billings and his paediatrician wife Evelyn; New Zealand chemist, James Brown; Swedish physicist and gynaecologist Eric Oderblad…
Mother Theresa, whose nuns introduced NFP to India, makes an appearance.
And the narrator is a young woman who knows one of the downstream effects of the Pill from personal experience: Alana Newman, long-haired, strumming a guitar and singing of love, evokes the era of Woodstock and “free love” even as she speaks about of the wound of not knowing her father, not even who he is. The child of an anonymous donor, she created an organisation for such victims of the reproductive anarchy unleashed by the Pill: Anonymous Us.
For all the weight of authority in its cast, however, the project is up against a massive wall of prejudice.
The vast majority of people cannot see anything wrong with the Pill and other modern forms of contraception. Though some have practical problems with it, moral and philosophical objections don’t wash with the general run of humanity. How could you question the value of something that has shaped society as we know it, liberating women from constant childbearing, allowing them to use their brains and earn their own money, slowing population growth and thus protecting the planet we live on?
As the various experts in the film demonstrate, however, these grand claims wilfully ignore the damage that contraception, with its promise of “free” and “no consequences” sex, has done to individuals and society: the explosion of single motherhood and fatherless children; the decline of marriage, delayed parenthood, disease, infertility and the boost it has given to embryo experimentation, anonymous donor dads and poor women exploited as surrogate mothers; and, of course, countless millions of abortions of “unwanted pregnancies” – to name only the most obvious harms.
Women themselves have been kept in ignorance about the physical risks of hormonal contraception: its contribution to breast and cervical cancer, blood clots and strokes, and harm to the reproductive organs themselves, such as premature ageing of the cervix — a cause of infertility.
Indeed, there is a general unwillingness to teach women to understand their reproductive system and thus give them the choice to work with its natural symptoms and rhythms to achieve, with spouses or partners, their own family goals. Public and private interests alike would prefer to see healthy women medicating themselves daily for years on end rather than taking control of their own bodies, though the latter was always supposed to be the goal of “women’s liberation”.
The decades-long effort to make out that NFP is unscientific and very unreliable – even to persistence in referring to it as the “rhythm method”, which was based solely on charting the menstrual cycle – hides the truth of the painstaking research that has gone into identifying changes in cervical mucus as the key indicator of ovulation and the monthly fertility window.
(The focus in this film is squarely on Billings Ovulation Method of NFP, which relies on mucus symptoms only. Some NFP organisations insist on the necessity of charting temperature as well.)
The history of this research is probably the most important aspect of the film for younger adults, most of whom will have no idea that there were two paths to choose between back in the 1960s. No idea of the eugenic inspiration for mass contraception (ask Black America), of its unethical testing, and the way it prepared the ground for population control programmes in China, India and elsewhere, involving massive abuse of human rights.
And no idea, either, of how to read their own bodies and respond with appreciation and respect. This is particularly hard for a generation who have learned that the body is something you can change to suit your own idea of sex and sexuality. But the seeds of this idea were already present 60 years ago when the Pill told us that the body is just something to use, not something with its own laws, which we disregard at the risk of disease and unhappiness.
Commercially, it was a “very clever idea to get every woman on earth to take a pill [nearly]every day of her fertile life,” says Archbishop Fisher in the film. “Now we know how this technology messes up the body and relationships.” And again, “Are we any happier? Better at maintaining our marriages? Demonstrably not.”
At the close of the film he looks forward to a natural family planning counter-revolution that will sustain what John Paul II called “a civilisation of life” and love, and sees forces in Western culture at the moment that “point exactly in that direction.”
I think he is right. After all, everyone wants to be healthy and happy – two things that are eluding many of us today.
Since 2012, Jeanne Mancini has been president of the March for Life Education and Defense Fund, the organization behind the March for Life. During an interview with Catholic News Agency’s CNA Newsroom podcast (Episode 5), Mancini shared her thoughts on the state of the pro-life movement and hinted at plans to continue expanding the reach and impact of the annual March for Life in Washington, D.C., which is the annual capstone event of the pro-life movement. With echoes of the great Civil Rights marches of the 1960s, tens of thousands of citizens from across the United States brave the freezing weather in our nation’s capital each year to demand an end to legalized abortion.
Jeanne Mancini took the mantle of the March for Life from famous pro-life activist Nellie Gray. Gray organized the first March for Life in 1974, the year following Roe v. Wade, and continued to do so each year until her death in 2012. Mancini has brought fresh energy and dynamism to the March for Life. “The founder of the March for Life was 88 when she passed away, and so she wasn’t that engaged in social media,” Mancini explained.
During her tenure thus far, Mancini has been able to capitalize on the vigor and enthusiasm of a young pro-life movement including spreading the message using all forms of mass communication. “We’ve also worked to grow our social media presence quite a bit,” Mancini said. “And so it’s been fun to work with young people and to grow that presence.” In spite of the media continuously downplaying the event’s significance, the March for Life is thriving and growing through the organization’s dynamic outreach. In fact, some sources estimated the March for Life in 2018 drew a crowd of 100,000.
Theme of 2019 March for Life
Over the decades, attendance at the March for Life has become the way for pro-life leaders to take a public and powerful stand in defense of the preborn. In 2017, Vice President Mike Pence became the first sitting VP to address the March for Life. In 2018, President Trump became the first sitting president to address the march via live video. Previous pro-life presidents, including George W. Bushand Ronald Reagan, also regularly delivered remarks via telephone.
Despite the preponderance of Republican politicians at the event, Mancini reiterated her commitment to keeping the March for Life a nonpartisan event. “We always try to have both sides of the political aisle represented at the March for Life, and sadly that’s become harder and harder,” she acknowledged. The case of pro-life Democrat Dan Lipinski, who cancelled his appearance in 2018 after President Trump’s address to the march, made this increasing polarization all too palpable. “But we also seek to get legislators from around the country and state houses, for example, because there are many pro-life Democrats at the state level, so that is something that we’re hoping to see at this year’s March for Life.”
Mancini revealed that the March for Life Education and Defense Fund has been working for over a year to develop an action plan to expand the March for Life throughout the country. “We’re starting to embark upon state marches, and that’s something that I’m hoping to explain a little bit more to people in January,” she said.
Mancini hinted at broader initiatives to inspire year-round activism. “We also just want to make sure that marchers that get so excited the day of the march, and it’s almost a life-changing experience in terms of motivation and enthusiasm and all of that, that they take that energy home and make a difference in their local communities. And so we’re trying to do what we can to really tool up the grassroots,” Mancini explained.
With the 45th annual March for Life coming up in January, Mancini is shaping the march into a prominent expression of the pro-life movement in a rapidly changing social and political landscape. Around the world, inspired by the example of the annual U.S. March for Life, international Marches for Life have sprung up in a variety of countries. From Lisbon, to Ottawa, to Rome, to Lima and beyond, pro-life activists worldwide have taken to the streets to demand a recognition of the rights of the preborn.
Director Frank Capra‘s 1946 family classic It’s A Wonderful Life is a poignant tale which reminds us that even in turmoil, it is a mistake to presume we can choose what makes life worth living. It may not have been originally intended to be confined to the Christmas genre, but the hot-cocoa-and-popcorn comfort flick was destined to be a life-affirming masterpiece from its conception.
The story, which begins on a Christmas Eve night with a suicidal father, came to historian and author Philip Van Doren Stern in a dream in 1938. Originally titled The Greatest Gift, Van Doren Stern’s short story was rejected by publishers, so he sent the story as a Christmas letter to friends in 1943. It was eventually printed in several magazines, with the character names nearly identical to those in the film that was produced after Capra bought the story rights.
The movie wasn’t a hit when it was first released, but it earned five Oscar nominations and one win (Technical Achievement Award for its innovativefaux snow!). It became a popular holiday rerun on television during the 1980s, and is now ranked among the greatest films of all time.
What makes It’s A Wonderful Life such a compelling classic?
George Bailey (James Stewart) is somewhat a small town American embodiment of Job: a devoted, selfless member of his family and community who comes under misfortune due to no fault of his own, and then makes a fatal, even hubristic error – deciding that his sorrows make his life unfit and disposable. An angel named Clarence (Henry Travers) intervenes to show George that from his finite perspective he has no idea what he’s throwing away.
Screenshot from It’s a Wonderful Life
This life-affirming theme isn’t only at the crux of the story, however, but is manifested throughout the plot. From his youth, George wrestles with envisioning career success as the benchmark for making life meaningful, even while he repeatedly denies himself his dreams of leaving Bedford Falls to do the right thing instead. Mary Hatch (Donna Reed), who becomes his wife, challenges this dynamic by being a college-educated woman who isn’t ashamed to give up a glamorous honeymoon for a fixer-upper house and lifestyle as a homemaker and mother to four children. At a time when the word “pregnant” was still rather taboo for the screen, George and Mary’s first baby is featured in the story while pre-born (“George Bailey lassos stork” and “on the nest” were the charming euphemisms).
Together, the Baileys work to improve the lives of the threatened and impoverished in their town, from stumbling society girl Violet Bic (Gloria Grahame) to Italian immigrant family the Martinis. George’s little brother Harry (Todd Karns) becomes a Medal of Honor hero for saving lives in the war, ultimately grateful to George risking his own life to save him during a childhood accident. Everything the Baileys do seems to affirm the truth that every human being’s life matters.
Meanwhile, antagonist Mr. Potter (Lionel Barrymore) values life only according to a monetary and convenience basis. It is Mr. Potter who kicks George when he’s down, scolding him with the fateful words, you’re worth more dead than alive, which George internalizes and surrenders to against better judgment.
It is in that vulnerability, made so perfectly relatable by Jimmy Stewart’s performance, that George goes to the brink of defying the entire theme the story has constructed. But in the end, George realizes that life, with its unique miseries, is still better than death. Finally, for arguably the first time in the story, he is actually rewarded for making the right decision, when his family and town shower him with support in the tear-jerking final scene.
The film’s unspoken theme — that life, even though it may have terribly dark times, is worth living — seems to resonate year after year with viewers, making the film a celebrated holiday classic that’s definitely worth watching.
The darkening that comes with the year’s shortest hours of daylight is like the lowering of the lights in a theater as the play is about to begin. But in the “Drama of Salvation” by which the human race is offered the promise of restoration to its original glory, “all the world’s a stage,” and the acts and actors are real. The creation of the world was not a mere myth, otherwise we would not be here. Nor are good and evil abstractions, for they always have had real consequences.
One of the most dramatic events in the progress of man, to which Saint Jude would later allude (Jude 1:7), was the destruction of Sodom and Gomorrah about 1,700 years before the birth of Christ. He knew that the story of that destruction was not the sheer theatrics of fiction. Until recently, it was convenient for some scholars to pass it off as an instructive legend. Archeologists in a symposium this past month concluded that those cities north of the Dead Sea were utterly destroyed, and their land became uninhabitable for the next six hundred years. The substantial theory is that upwards of 60,000 inhabitants were wiped out by a meteor exploding at low altitude with the force of a ten-megaton bomb, dropping platinum and molten lava on the larger area called Middle Ghor, and unleashing a temperature the same as the sun.
Wise ones interpreted this as punishment for the corruption of that culture. There is a symbiosis between matter and morality. When souls are disordered, there are consequences in all creation. So it was, that at the climax of the Drama of Salvation, when Christ died on the cross, the sky grew black.
It has been quipped that if God does not punish our culture for its decadence and contempt for natural law, He owes Sodom and Gomorrah an apology. It was to save us from total destruction that the Word, whose utterance brought all things into being, became flesh and then appeared on a day now called Christmas.
Twice did our Lord speak of Sodom, saying that its fate was less severe than that of anyone who by an act of willful pride, rejects Him and all that He requires in the way of obedience to His truth (Matthew 10:15; 11:24). Such severity is the outcry of the Christ who wants that none be lost and that all be saved. This is a reminder never to infantilize the Babe of Bethlehem for, while He may whimper in the manger, this is the Voice that made all things and judges all at the end of time. And in His humility by making Himself frail and fragile in a stable, He reveals a mercy more powerful even than an exploding meteor.
“For their sake He remembered His covenant and showed compassion according to the abundance of His steadfast love” (Psalm 106:45).
In June, doctors told Roxli Doss she had an inoperable brain tumor called diffuse intrinsic pontine glioma, or DIPG, KVUE [Fox News] reports.
According to doctors, the disease is “very rare” and causes a “decreased ability to swallow, sometimes vision loss, decreased ability to talk, eventually difficulty with breathing,” said Dr. Virginia Harrod with Dell Children’s Medical Center.
The little girl went through weeks of radiation and all her parents, Gena and Scott Doss, could do is pray for a miracle.
“When I first saw Roxli’s MRI scan, it was actually unbelievable,” said Dr. Harrod. “The tumor is undetectable on the MRI scan, which is really unusual.”
“[Doctors] at Dell Children’s, Texas Children’s, at Dana-Farber, at John Hopkins, and MD Anderson, all agreed it was DIPG,” said Scott Doss.
And now with no trace of the tumor, the family is thanking God.
The family tells KVUE they will continue to watch her closely and continue to undergo treatments as a precaution.
Most people ask for assisted suicide because they have given up hope or they fear for their future.
December 20, 2018 (LifeSiteNews) – A few years ago I was helping a friend and her family re-organize their personal library and came across a book titled “A Child is Born.” I asked innocently if it belonged in the Christmas section. The answer was an emphatic no, as I was informed that the photograph-driven bestseller about a baby’s development in the womb was not, in fact, a retelling of Christ’s Nativity.
Even so, I realized that Christ’s development in Mary’s womb was something that could be better understood by our more detailed knowledge of the natural world. After all, if it is sensible to say with generations of logic students that, “All men are mortal; Socrates is a man; therefore, Socrates is mortal,” then it seems rational to apply newfound knowledge about embryology to the infant Jesus.
Beginning at the beginning, then, we can confidently say that Jesus became “incarnate,” literally “took on flesh,” about nine months before that distressing night outside the Bethlehem inn. (None of the gospels specifies that it was an exactly nine-month pregnancy, though there is no particular reason to believe that it deviated from that human norm.)
Dr. Keith L. Moore’s 2011 textbook Human Embryology states: “Human development is a continuous process that begins when an oocyte (ovum) from a female is fertilized by a sperm (spermatozoon) from a male.” The Encyclopedia Britannica’s article on pregnancy puts it this way: “A new individual is created when the elements of a potent sperm merge with those of a fertile ovum, or egg.” That fertilized oocyte, called at that earliest stage of development a zygote, is how Jesus began his life on earth, what Christians call the mystery of the “Incarnation,” when the “Word became flesh.”
Now, here are two ways of interpreting “The Holy Spirit will come over you, and the power of the Most High will overshadow you; therefore the child to be born will be called holy—the Son of God” (Luke 1:35 ESV). One possibility is that after Mary’s “Yes,” God the Father could have implanted a spermatozoon into her fertile ovum, having formed the spermatozoon literally out of nothing, so that the now fertilized ovum (zygote) could implant in her womb. Another possibility is that he could have placed in Mary’s womb a miraculously fashioned zygote to grow and develop in safety there. Either one would be at the same time a profound mystery as well as a short order for the one who began the world by creating everything from nothing, and for whom “all things are possible” (Matthew 19:26 ESV).
Jesus’ bodily development would have continued apace from then on. Eighteen days in and his heart would have been forming; around three weeks in and that heart would have begun pumping blood through his body—blood separate from Mary’s circulatory system and of whatever blood type he would have throughout his whole life on earth, a blood type that for all we know would have been different from his mother’s as son’s blood types often are.
More body parts’ formations are noted by Randy Alcorn in his Pro-Life Answer to Pro-Choice Arguments: “By thirty-five days, mouth, ears, and nose are taking shape. At forty days the preborn child’s brain waves can be recorded . . . By forty-two days the skeleton is formed . . . By eight weeks hands and feet are almost perfectly formed, and fingerprints are developing . . . By twelve weeks the child is kicking, turning his feet, curling and fanning his toes, making a fist, moving thumbs, bending wrists, and opening his mouth.”
Meanwhile, every component of the baby Jesus’ body is presently formed. “In the remaining six months in the womb nothing new develops or begins functioning. The child only grows and matures,” says Alcorn (emphasis original). And at the same time the baby is busy developing rationally.
An article in Newsweek (coincidentally titled “Do You Hear What I Hear?”) stated, “With no hype at all, the fetus can rightly be called a marvel of cognition, consciousness and sentience.” The same article goes on to note that, “After 32 weeks, the fetus spends half its time in REM sleep, the brain state associated with dreaming.” What the infant Jesus could have been dreaming about is anyone’s guess. But that he was dreaming seems relatively clear.
Similarly, even before birth, Jesus would have been listening and even responding to Mary’s speech (which was probably Aramaic). The above Newsweek column breaks down a study that tracked mothers reading stories to their children before birth and afterward and was, in the words of the researcher, “the first direct demonstration that human speech has a discernible effect on the fetus.”
The specifics of Jesus’ growth inside Mary’s virgin womb could be continued, of course, from the double helix structure of his twenty-three chromosomes’ DNA to the contours of his brain waves (which, consistent with our earliest measurements, would have appeared by six weeks).
These findings of modern science give us a more vivid window into what happened some two thousand years ago in Bethlehem and a greater appreciation for the miracle that is every pregnancy and every new human life.
When Culture of Life Africa founder Obianuju Ekeocha tweeted about dangerous birth control devices, like IUDs, on November 28, 2018, she asked her followers to share their stories of using natural fertility awareness methods. They not only responded to what she asked, but they also shared their birth control “gone wrong” stories.
Referring to birth control devices as “shackles & chains”, Ekeocha said she “can’t believe women are convinced to put these devices into their bodies.” The truth is that most women and their partners don’t know the true risks of these birth control methods, because no one tells them. In a lot of cases, they find out the hard way.
Obianuju Ekeocha
✔@obianuju
I can’t believe women are convinced to put these devices into their bodies (some of which could harm them)…shackles & chains.
I want to hear from friends here who use fertility awareness methods or those who would like to learn this healthier option
My best friend developed cancer at the spot her IUD perforated her uterus. She is ok now but how horrifying to get that diagnosis as a single working mother of four.
I would never put a foreign object into my body that could potentially harm me, no matter how it’s sold to me. My sister in law had to have her uterus removed due to a device that made her very sick. It was sold to her as a method that was safe.
Birth control, whether it’s the pill or a device such as an IUD, is touted as safe, despite the risks of blood clots, infertility, and even death. Like most people do when given a prescription or a medical device, women taking birth control listen to what their doctor tells them, and often don’t bother to read through the paperwork filled with fine print about the side effects and risks associated with it. So if their doctors aren’t telling them the full story, they don’t know.
Women also seem to be kept out of the loop when it comes to understanding their own bodies and menstrual cycles. Natural Family Planning is an accurate way to know when to skip sex if you are trying to avoid pregnancy and what days during the month are your most fertile when trying to get pregnant. It is not the rhythm method, as so many doctors still believe. There are multiple methods, including the Marquette method, which allows women to use the ClearBlue Fertility Monitor to track their cycles. When used properly, NFP is as effective as birth control. In the case of the Marquette Method, it is 98 percent effective in preventing pregnancy. But just like with birth control, you can’t skip a day if you want it to work. Ekeocha’s followers shared their stories about NFP:
Does hormonal birth control equate to “shackles & chains” as Ekeocha states? Here are the facts: it comes with a 70 percent increased risk of depression, an increased risk of blood clots, heart attack, and stroke, a 20 percent increased risk of breast cancer (after 10 years of use that jumps to 38 percent), and an increased risk of cervical cancer. Some hormonal birth controls can decrease bone density, which can lead to osteoporosis. Others can cause benign liver tumors. In addition, hormonal birth control can lead to infertility and unintended abortion.
NFP carries none of those risks, and all of the benefits of understanding your body and your cycle. That’s empowerment.
BETHLEHEM, December 17, 2018 (LifeSiteNews) — Thousands of babies are safely born in Bethlehem thanks to a Catholic hospital named for the Holy Family.
Holy Family Hospital is a Catholic teaching hospital with a state-of-the-art maternity and neonatal critical care center. It serves poor women, children, and babies throughout the West Bank of Palestine. It has been likened to a “modern day manger,” not only because it is located just 1,500 steps from where Jesus was born, but because it offers shelter to families and babies in need. Over 4,300 babies are born there annually.
The hospital is a work of the Order of Malta, the oldest Catholic charity. Every family who walks through the doors is immediately given a 50 percent subsidy, thanks to the hospital’s donors. No one is ever turned away. Meanwhile, the hospital provides work for 170 Palestinians in the impoverished region: it is Bethlehem’s second largest employer.
The president of the Holy Family Hospital Foundation is Michele Burke Bowe, who travels to the hospital often from her home in the United States. Bowe is also the Ambassador of the Sovereign Military Order of Malta to Palestine.
Ambassador Bowe told LifeSiteNews that the French order of the Daughters of Charity founded a general hospital in Bethlehem in the 1880s, but after 100 years they couldn’t run it any more.
“Not enough money, not enough Daughters,” Bowe explained.
Deeply distressed that the people of Bethlehem would no longer have a hospital, the Daughters of Charity called John Paul II for help. He told them that the Order of Malta would take over. When the pontiff consulted the Order of Malta they agreed, but on their terms.
“They said, ‘Let’s be orderly about it,’” said Bowe.
Looking at the needs of the area, the Order decided that the hospital would specialize in neonatal and infant care.
“It took a little time to do some reconfiguring to get it repurposed to be an infant and maternity hospital,” Bowe explained.
The first baby was born in the refurbished hospital in 1990.
Ambassador Bowe grew up in Amman, Jordan and returned often to the Middle East during her studies at Georgetown University. She worked in the field of development until her duties as a mother intervened. Eventually she became a member of the Knights of Malta and then a board member of the Holy Family Hospital Foundation. Now the foundation’s president, the ambassador speaks Arabic, French, Spanish, and Italian. She has five children, too.
“I love babies,” said Bowe. “I have a soft spot for babies.”
The ambassador told LifeSiteNews that one of her most powerful experiences of the Holy Family Hospital happened during the Gaza War, when Bethlehem was a “ghost town.” During her visit, Bowe became friendly with the father of twins born after just 26 weeks’ gestation. One was born weighing 1,500 grams; the other weighed only 700 grams.
Despite the war, the difficulties of travelling from his home in Hebron, and the privations of the Muslim fasting season of Ramadan, the twins’ father, a construction worker, came to visit them every day. Because of the dangers, their mother stayed at home.
“It was the most powerful witness of fatherhood,” Bowe recalls.
She remembers vividly when the father finally dared to touch his tiny daughters. A nurse put the larger girl, finally five pounds, on his lap.
Bowe told the quiet man that although the girls would not remember his daily visits, “their hearts are so touched.”
“Holy Family Hospital taught me to be a good father,” the man replied. Apparently he had been afraid of pain of the girls dying, but the care the hospital showed them inspired him to care for them too.
After three months in the neonatal intensive care unit, the babies were able to go home.
The man’s quiet fidelity reminded Bowe of St. Joseph.
“It made me think about what a wonderful father Joseph was and what a wonderful husband he was to Mary,” she said.
When asked what she would like readers to know about Holy Family Hospital, Bowe’s reply was swift: “That the doors are always open, no matter what the patient’s creed or need.”
She also stressed that the Catholic teaching hospital has raised the level of education and health awareness throughout the region. In addition to its services for mothers and babies, it now has a clinic for older women, who often have not received any medical advice or attention since they last gave birth.
In a region where Christians now comprise only two percent of the population, the hospital is also important because it provides a place where Muslims and Christians can work together, Bowe said.
Meanwhile, it is always Christmas in Bethlehem – and not just because of all the babies. Katie DeMoss of TAN Books told LifeSiteNews via email that it’s a “little known fact” that the Church of the Nativity in Bethlehem celebrates the Christmas Vigil Mass every day of the year.
According to a new study in the British Journal of Medicine, women who are victims of domestic violence are twice as likely as other women to use emergency contraception.
Researchers at the University of Bristol and Queen Mary University of London analyzed the medical records of over 200,000 women of reproductive age. “Our findings are in line with evidence from studies in other countries suggesting that women experiencing domestic violence and abuse (DVA) use more emergency contraception than other women,” said Joni Jackson, an author of the study.
Jackson said that community pharmacists and sexual health practitioners are “at the frontline responding to these requests” and have the opportunity to help women who are being abused. Fellow author of the study, Dr. Natalia Lewis, added that this “means that healthcare services are an important point of contact for DVA victims and survivors.”
Homicide is the second leading cause of death among pregnant women, behind car accidents. When men who are actively abusive (or have the potential to be abusive) learn that their partners are unexpectedly pregnant, the lives of women and their preborn children are in danger.
Women who are victims of domestic violence and fear becoming pregnant may be so afraid of their partners abusing a child that they feel that emergency contraception (which may either prevent pregnancy or, if that fails, make the uterus inhospitable to the newly-created human life) is the first way they have of preventing this. They also may desire to escape the abuse, and fear that having a baby would forever tie them to their abuser (which is not the case if they receive proper help to flee). Even if an abused woman doesn’t want an abortion, she may feel it is her only option. And despite what the media claims, emergency contraception is capable of causing an abortion.
According to Veronica Gillispie, an obstetrician and gynecologist in New Orleans, “reproductive coercion” occurs when an abusive partner gets a woman pregnant against her will through rape or by “birth control sabotage” as was reported by 25 percent of teen girls with abusive partners and 15 percent of women with abusive partners. Abusive men may use pregnancy or birth control and emergency contraception as means to exert power and control over their victims.
When a doctor or pharmacists comes into contact with a woman requesting emergency contraception, they can refer her to the National Domestic Violence Hotline at 1-800-799-SAFE. This latest study’s researchers are asking that their findings be included in the existing domestic violence awareness programs for doctors.
Editor’s Note, 12/16/18: The words “and become pregnant” in paragraph five have been changed to “and fear becoming pregnant” for clarity.
Miracle baby Royce Cannon was born premature at just 30 weeks gestation after his mother, Felice Renfroe, was diagnosed with preeclampsia. Royce was delivered via emergency c-section at Akron Children’s Hospital.
“I had protein in my urine and they were scheduling me to take steroid shots,” Renfroe told Fox 8. “The first day I was fine, then the second day I went to take another steroid shot and they ended up admitting me because of my high blood pressure.”
Baby Royce weighed just three pounds, two ounces at birth, and since his lungs weren’t fully developed, he required oxygen. “I thanked the nurse and I thanked the doctor,” said Renfroe. “And he was like, ‘Don’t thank me. It was only by the grace of God.”
Royce is now a month old, and excluding the first hour after his birth, his mother, who is a nurse’s aide, has never left his side in the Neonatal Intensive Care Unit.
“I think that makes such a huge difference in babies’ development and how well they do in the NICU when their parents are there all the time,” said Stephanie Sykes, a neonatal nurse practitioner.
Little Royce is gaining weight and doing well, but he must be able to eat by mouth eight times a day, continue to gain weight, and maintain a certain temperature before he is able to go home. It will likely be weeks. “He’s just soaring, he’s just doing what he’s supposed to do and I’m just blessed I got a chance and I do have a chance to be here every day,” said Renfroe. “… I think he’s my miracle baby because he, just like I said, he’s striving every day.”
Babies the same gestational age as Royce have an amazing chance of survival, thanks to advances in modern medicine. According to current research, after 28 weeks, babies have a 96 percent rate of survival. If they weigh less than three pounds, four ounces like Royce, they can face a tougher fight and are more at risk for disabilities than babies who weight more. Despite the fact that these babies are capable of surviving outside of the womb, it is still legal in the United States to kill a child this age through abortion.
NEW HAVEN, Connecticut, December 11, 2018 (LifeSiteNews) – Students at Yale University’s Silliman College will soon be able to obtain condoms, lubricant, and even abortifacient “emergency contraception” as easily as putting some money in a vending machine.
A so-called “wellness to-go” vending machine will be installed in the campus’s Good Life Center before winter break, the school newspaper Yale Daily Newsreported. Accessible 24 hours a day and seven days a week, the machine will offer the Plan B morning-after pill, condoms, lube, and other over-the-counter medications.
Plan B is already available for free to students with Yale’s Hospitalization/Specialty Care Coverage plan, and Yale spokeswoman Karen Peart says “emergency contraception” can be obtained for free at Yale Health Pharmacy or at Acute Care regardless of what insurance plan someone has.
But student Grace Cheung, who first proposed the machine, argued that Plan B isn’t covered by the school’s basic insurance plan, and that students seeking it shouldn’t have to go through the “humiliating process” of purchasing it.
“The point of this is to make Plan B more accessible and to make medications in general more accessible,” said student Ileana Valdez ’21, a Yale College Council (YCC) representative who pushed for the machine. “Hopefully, this will set a precedent for more machines to show up around campus that contain other things so Yale students don’t have to go out of their way to go to CVS, especially students from the new colleges.”
Melanie Boyd, the college’s Assistant Dean of Student Affairs, told the paper she was “glad that the YCC is working to publicize awareness of the easy availability of Plan B at Yale Health.”
The “wellness” machine will charge a price “comparable to or lower than” that of pharmacies for Plan B, according to the Daily News. CVS and Walgreens list $50 for a single pill; both companies offer a variety of other contraceptive products for significantly cheaper.
More significantly, however, Plan B doesn’t simply prevent fertilization; it can function by killing an already-conceived embryonic human depending on when it’s taken.
“If Plan B is taken five to two days before egg release is due to happen, the interference with the LH signal prevents a woman from releasing an egg, no fertilization happens, and no embryo is formed,” explains Dr. Donna Harrison of the American Association of Pro-Life Obstetricians and Gynecologists.
Many Plan B defenders point to this mechanism to paint it as an alternative to abortion, but Harrison notes that if Plan B is taken during the “two-day window in which embryos can form but positive pregnancy tests don’t occur,” studies indicate it “has a likely embryocidal effect in stopping pregnancy.”
The U.S. Food and Drug Administration’s online guide to birth control methods admits that Plan B “may also work (…) by preventing attachment (implantation) to the womb,” resulting in the death of an embryonic human being.
Other methods are similarly fraught with controversy. More and more women have begun speaking out over the past few years about negative physical and mental reactions to birth control pills. Oral contraceptives have been linked to an 80 percent increased likelihood of depression and as much as a sixfold rise in the risk of thrombosis, as well as heightened risks of blood clots, hair loss, Crohn’s disease, brain shrinkage, breast cancer, hardening of the arteries, glaucoma, and cervical cancer.
Responding to the news, the Family Institute of Connecticut faulted the college for framing the machine as offering “emergency contraception” without informing women the pills may cause abortions rather than prevent them.
“Do parents send their high-achieving children off to this top Ivy League school to read the classics, engage in challenging intellectual debate, rub elbows with some of the nation’s top academics and lay the path for a successful and bright career, or to be indoctrinated with godless SJW ideology and engage in casual sex?” asked Elizabeth Johnston of the Activist Mommy blog.
At Breitbart, Dr. Susan Berry observed that data indicate the “safe sex” trend is leaving America’s children far less safe. “As recently as August, CDC released data revealing the number of cases of STDs had skyrocketed for the fourth consecutive year,” she wrote. “Of the 20 million new STDs reported each year, about half occur among young people between the ages of 15 to 24.”
November 5, 2018 (40 Days for Life) – Men’s role in abortion often starts by not respecting women enough to practice abstinence before marriage.
Once a pregnancy occurs, many men are stunned to learn that a father has no legal right to protect his own child from abortion. But even if a dad can’t rely on the law, he can use his voice. Sometimes, all it takes is a loving word and a promise of support.
An abortion-bound father named Chuck told Cathy in Atlanta that he didn’t really want the abortion…but he and his fiancée, Jenny, have a seven-month-old baby. They worried that a second baby so soon would be a financial burden.
“He said it was bad timing, and they thought they would abort this baby and try again in a year,” Cathy reported.
Cathy described the devastating toll abortion takes on a woman – and on a couple’s relationship. She also encouraged Chuck to tell Jenny he doesn’t want the abortion, that he will stand by her, and that they can take care of a second child together.
Showing him a fetal model, she continued, “This is about the size of your baby now. Can you please go protect that baby? That baby is precious and needs protecting. Now go get her out of there and let me treat you to breakfast!”
When Chuck and Jenny left the abortion center a short time later, applause broke out on the sidewalk.
“Jenny put her hand over her mouth and was crying,” Cathy said. “They gave me a big hug! They were BEAMING!”
At breakfast, Jenny repeatedly said how happy she was to have walked out on her abortion appointment.
“Praise God that this man was a warrior for his child,” Cathy said. “Jenny was so relieved.”
New York
During her shift on the sidewalk, Colette spoke to a man whose girlfriend was in Planned Parenthood, about to have an abortion. She showed him a video on fetal development and a non-graphic video of the abortion procedure.
After more than 20 minutes of discussion, the man said he couldn’t stand by while his girlfriend had the abortion and texted her asking her to leave the abortion facility. She immediately wrote back saying she didn’t want the abortion either.
“I’m glad I’m not standing here crying,” the relieved dad said. “Now I’m happy!”
Fargo, North Dakota
The son of a 40 Days for Life volunteer in North Dakota found out an acquaintance was bringing his girlfriend to Fargo for an abortion. He took the opportunity to talk with the father about the way abortion hurts babies…and also their parents.
“This man-to-man discussion had a tremendous impact on the father,” said Fargo leader Colleen. “Consequently, the father decided against abortion, and their appointment was cancelled.”
This child is the 82nd saved baby since Fargo’s first 40 Days for Life campaign in 2007!
Boston, Massachusetts
“Will you pray with me?” the man asked Boston 40 Days for Life leader Rita.
He had previously ignored Rita’s attempts to engage him but now he admitted he had been involved in a previous abortion and “could not do that again.”
Rita sent him back into Planned Parenthood to tell the mother of his child that he loved her, that he would be there for her, and that he wanted both mom and baby.
“It worked!” he exclaimed when he re-emerged from the abortion facility. “She rescheduled her appointment, and I have more time to convince her.”
For one day, at least, the baby has been spared. “Please pray for this couple,” Rita said. “The woman seemed very much at risk for an abortion.”
He will wipe every tear from their eyes. There will be no more death or mourning or crying or pain, for the old order of things has passed away. He who was seated on the throne said, “I am making everything new!”
— Revelation 21:4-5
Father, you are the God of hope. Your word fills us with the vision of the world to come, when every tear will be wiped away, and death will be no more. Father, how we need that hope, how we are strengthened by that vision! Keep our hearts focused on heaven, and diligent in the labors of earth. As we struggle against the culture of death, root our souls in the assurance of victory.
61508340 – stop abortion sign with sunny background
The “safe and legal abortion” myth suffered yet another blow on Friday when the Florida Board of Medicine revoked the medical license of late-term abortionist James Scott Pendergraft, IV who was arrested for operating an illegal home abortion and drug distribution business out of the back of his van. As usual, the so-called “pro-woman” mainstream media utterly ignored the story.
According to Operation Rescue, the revocation occurred on December 7 when the Florida Board of Medicine voted to revoke Pendergraft’s license after discovering that he was practicing medicine out of the back of a van in South Carolina where he holds no license to practice medicine.
Cheryl Sullenger, Senior Vice President of Operation Rescue, the grass-roots pro-life organization that filed the initial complaint, attended the Board meeting when the disciplinary action was announced.
Sullenger reports: “Pendergraft was arrested on October 5, 2015, in Spartanburg County by Sheriff’s Deputies who were conducting a routine traffic stop. Deputies found illegal drugs, including Fentanyl, LSD, and marijuana in his vehicle along with bloody abortion instruments with tissue still attached used in illicit home abortions.”
This led to Pendergraft’s conviction of ten drug offenses. He is currently serving a five-year term of probation.
What should alarm all women, whether they are pro-life or pro-abortion, is that at the time of this arrest, Pendergraft was serving his fifth license suspension in Florida where he operated a chain of abortion facilities, some of which have permanently closed.
“Ownership his other clinics have been transferred to his former wife, while yet others have been converted into medicinal marijuana clinics,” Sullenger reports.
Despite the transfer of business ownership on paper, pro-life activists tell Operation Rescue that Pendergraft is still seen regularly entering his so-called “former” abortion facilities during business hours and holds an interest in the medicinal marijuana businesses.
“This license revocation was years in the making and was the result of the work and prayers of countless pro-life activists on the ground outside Pendergraft’s abortion facilities and in our office,” said Troy Newman, President of Operation Rescue. “This is a victory for all of us, especially women and babies who will no longer be placed at risk by James Pendergraft’s dangerous practices.”
Despite how relevant this information is to the overall picture of abortion in America, there was not a single report published by the mainstream media about this man who lost his license for operating an abortion business out of his van.
Looking out for the “reproductive health care” of women in America means reporting all the facts, not just those that support the pro-abortion view. All women, regardless of where they stand on the abortion issue, deserve to know that seedy abortionists like Pendergraff are very much a part of the “safe and legal” abortion establishment in the U.S.
BRAD WILMOUTH DEC 10, 2018 | 10:22AM WASHINGTON, DC
On Friday, the NBC Nightly News took the time to devote an entire story to the case of a Michigan woman who survived a near-death experience which illustrates that doctors can sometimes make the wrong diagnosis and give up on comatose patients too soon.
Anchor Lester Holt recalled description of the surprise recovery as a “miracle” as he set up the report: “We’re back now with what a family is calling a medical miracle — a woman considered almost brain dead who recovers after the gut-wrenching decision to remove her life support.”
In a pre-recorded piece, correspondent Kristen Dahlgren then recounted for viewers that Michele De Leeuw was hospitalized after having a heart attack and, at one point, was diagnosed as nearly brain dead with only five percent brain function.
Her husband, Karl, was seen explaining how difficult it was for him to decide to have her life support removed by doctors who advised that she would never recover, but then she woke up and began talking a few days after life support was disconnected, and has improved substantially since then.
LifeNews.com Note: Brad Wilmouth is a news analyst for the Media Research Center and a graduate of the University of Virginia. This column originally appeared on the NewsBusters web site and is reprinted with permission.
“The victory, if it comes, will come through Mary.” These were the dying words of Cardinal August Hlond, as recounted by Pope St. John Paul II in his book Crossing theThreshold of Hope. Reflecting on the Cardinal’s prophesy, the pope wrote:
During my pastoral ministry in Poland, I saw for myself how those words [of Cardinal Hlond] were coming true. After my election as Pope, as I became more involved in the problems of the universal Church, I came to have a similar conviction: On this universal level, if victory comes it will be brought by Mary. Christ will conquer through her, because He wants the Church’s victories now and, in the future, to be linked to her.
Human Life International founder, Father Paul Marx, shared the Holy Father’s conviction. That is why he chose Our Lady of Guadalupe – whose feast day we celebrate in just a few days – as HLI’s patroness.
Fr. Marx, who tirelessly devoted his life to the defense of Life and Family, personally understood the hardships of the great battle between the forces of Life and Death and encouraged all, in every age, to turn to Our Lady of Guadalupe as the solution against fear and hopelessness. “In contemplating her simplicity, we find the strength to emulate her faith,” he said, “and proceed with confidence in the knowledge that God will overcome the seemingly insurmountable barriers looming over the world today.”
“Be Not Afraid”Bless
Fear and hopelessness are a risk whenever we forthrightly confront the evils in our culture. In the past few decades, while there have been many victories, there have also been many – and catastrophic – losses. Despite the tireless efforts of so many committed pro-life and pro-family activists, abortion is still legal and untold millions of babies have been slaughtered; euthanasia activists are gradually gaining ground; same-sex ‘marriage’ is the law of the land; contraception, divorce, and immoral “reproductive technologies” have been normalized; pornography is epidemic; and gender ideology is sweeping our cultural institutions.
In the face of a lost culture wandering ever further from the truth about God, man, and morality, one risks becoming discouraged. But in moments of such discouragement, I often recall the booming voice of Pope St. John Paul II, thundering above the massive crowds who flocked to see him: “Be not afraid!”
Pope St. John Paul II first issued that memorable exhortation on October 22, 1978, after which he adopted it as a recurrent theme of his papacy. In Crossing the Threshold of Hope, the Holy Father explained the meaning behind this unofficial motto and linked the fearlessness that he was calling for to Mary’s example. “Be not afraid!’ Christ said to the apostles and to the women after the Resurrection,” he wrote. “According to the Gospels, these words were not addressed to Mary. Strong in her faith, she had no fear.” Mary’s fearlessness arose from her unshakeable conviction in the power of Christ’s redemption, and in the goodness of God.
We too should have no fear, said the saintly pope, because “man has been redeemed by God,” and because “the power of Christ’s Cross and Resurrection is greater than any evil which man could or should fear.” Our own fearlessness in the face of evil will arise in proportion to our dependence upon Mary, and the extent to which we emulate her example.
Our Lady of Guadalupe: Hope for a Culture of Life
Perhaps no Marian apparition provides such cause for hope as does Our Lady of Guadalupe. Before she appeared to the humble peasant Juan Diego, Aztec culture was still in throes of bloody-thirsty paganism. The conquistadors reported that, before they managed to partially curtail the practice of human sacrifice, the Aztecs had routinely sacrificed 10,000 human victims each year, tearing the still-beating hearts out of their victims’ chests. Many of those victims were children.
16th century image, showing Aztec sacrifice
Mere human calculations would have said that demonic paganism was so deep-seated in Aztec culture that it would take hundreds of years of missionary toil to succeed in ripping it up by the roots. That is the human way: the best we can hope is to change the world by changing one mind and one heart at a time through slow, toilsome work. Instead, within just a few years after Mary’s apparition, paganism had been swept aside, and millions of Aztecs had been converted and baptized as Catholics. Human sacrifice came to an abrupt end. Mary claimed Mexico as her own.
In 1910 Our Lady of Guadalupe was declared Patroness of Latin America by Pope St. Pius X, and in 1945 Pope Pius XII declared her to be the Empress of all the Americas. On January 22, 1999 Pope Saint John Paul II named Our Lady of Guadalupe patroness of the Americas and raised December 12 to the rank of Feast for all the countries of the Americas.
Our own culture’s bloodthirsty paganism is sanitized and hidden behind a veneer of clinical efficiency. But, as Fr. Marx never tired of observing, in substance it is no different from the horrors witnessed in the most degenerate pagan civilizations, such as the Aztecs. “In ever greater numbers, society sacrifices our young and aged at demonic altars, hurrying them to destruction through abortion, sex education, prostitution, pornography, infanticide and euthanasia,” said Fr. Marx, “foolishly believing that just a little more contraception, just one additional population control program, and we will be blessed with the happiness and peace that we so desire.”
In the face of the systemic, deep-seated, industrial-scale anti-life juggernaut that takes the lives of untold unborn children every year, we may feel a sense of helplessness and even powerless in the face of such evil.
But Mary is not powerless. There is no fear in her.
In the apparition at Guadalupe, Mary appeared as a young, pregnant native mother. She is carrying the Christ-child in her womb. What a potent symbol! God is present among us, but in a position of utmost dependence: an unborn child in his mother’s womb! Our Lady of Guadalupe is an icon of tender maternity and maternal strength, and of the utmost value and dignity of human life from its earliest stages. If Christ was with us from the first moment of His conception, then each unborn child, made in His image, shares in that dignity. And if Mary could change the course of human history by saying “yes” to God, and serving humbly as His mother, then we too can bring about the end of evil by our own daily “yes” to God, and through our daily work and sacrifices.
As the moral decline of the Americas [and the world] intensifies and spreads across the globe, we are in desperate need of renewal, conversion, and amendment of life. We need heavenly guidance and intervention. Sadly, most have accepted and embraced the “wide” path that leads to destruction of which our Lord warns. (Matt. 7:13-14) We are witnessing firsthand a “dramatic” confrontation between two diametrically opposing views, the “Culture of Death” and the “Culture of Life.”
Our Lady of Guadalupe brought the “Culture of Life” to pagan Aztec civilization with a speed that defied all human expectations. We need recourse to Mary to win the battle. We must pray the daily Rosary. By meditating on the life, death and resurrection of Jesus we obtain the graces to live for Christ alone! We must consecrate ourselves to Mary’s Immaculate Heart. We must pray novenas to Our Lady of Guadalupe, begging for the conversion of our culture.
Pope St. John Paul II promulgated the following prayer to Our Lady of Guadalupe, entrusting Life and Family to the Holy Virgin’s intercession. Please join me in praying this prayer, making it part of your daily devotion. The way to heal our country and the Americas, indeed all the world, is through Our Lady’s motherly guidance that leads us to her Son instructing us to “do whatever he tells you” (John 2:5).
Prayer of Pope St. John Paul II to Our Lady of Guadalupe
O Immaculate Virgin, Mother of the true God and Mother of the Church, who from this place reveal your clemency and your pity to all those who ask for your protection, hear the prayer that we address to you with filial trust, and present it to your Son Jesus, our sole Redeemer.
Mother of Mercy, Teacher of hidden and silent sacrifice, to you, who come to meet us sinners, we dedicate on this day all our being and all our love. We also dedicate to you our life, our work, our joys, our infirmities and our sorrows. Grant peace, justice and prosperity to our peoples; for we entrust to your care all that we have and all that we are, our Lady and Mother. We wish to be entirely yours and to walk with you along the way of complete faithfulness to Jesus Christ in His Church; hold us always with your loving hand.
Virgin of Guadalupe, Mother of the Americas, we pray to you for all the Bishops, that they may lead the faithful along paths of intense Christian life, of love and humble service of God and souls. Contemplate this immense harvest, and intercede with the Lord that He may instill a hunger for holiness in the whole people of God, and grant abundant vocations of priests and religious, strong in the faith and zealous dispensers of God’s mysteries.
Grant to our homes the grace of loving and respecting life in its beginnings, with the same love with which you conceived in your womb the life of the Son of God. Blessed Virgin Mary, protect our families, so that they may always be united, and bless the upbringing of our children.
Our hope, look upon us with compassion, teach us to go continually to Jesus and, if we fall, help us to rise again, to return to Him, by means of the confession of our faults and sins in the Sacrament of Penance, which gives peace to the soul.
We beg you to grant us a great love for all the holy Sacraments, which are, as it were, the signs that your Son left us on earth.
Thus, Most Holy Mother, with the peace of God in our conscience, with our hearts free from evil and hatred, we will be able to bring to all true joy and true peace, which come to us from your son, our Lord Jesus Christ, who with God the Father and the Holy Spirit, lives and reigns forever and ever.
Heather Crockett Oram was just 13 years old when she discovered she would never be able to have biological children. At a baby, her ovaries had been removed because they had not formed properly — and almost immediately, knew she would adopt children one day. “As I grew older my biggest fear was to have to someday tell a prospective spouse that I would never be able to birth our children,” she said in an article she wrote for Love What Matters. “Then I met Jason. He was a single dad to 2 wonderful little boys and we fell head over heels.”
She cried as she told him, but he told her it didn’t matter, and he would happily pursue adoption with her.
“Last June we were approved to adopt,” she said. “After a lot of research, we didn’t want to go through an agency. There were too many shady ones out there and they cost close to $55K when all is said and done. So we set out to do it on our own.” They instead used the internet and social media to find biological parents looking to give the gift of adoption, and at first, many of the responses they got were scams. “Then we got a message on Facebook,” she explained. “A young woman emailed us telling us that her friend was pregnant and looking for a family.”
They spoke with the mother over the phone for weeks, but she never sent them proof of her pregnancy. Then, another mother contacted them, and wanted to meet.
Two days later we met in a little diner 20 minutes from our house. Just when we thought she had stood us up, in walked a very pregnant girl and her mom. We hugged and she showed us the ultrasounds of a little baby boy. He then started kicking and she had me feel her belly. Towards the end of breakfast she asked us how we felt. She then asked us if we would adopt her baby and love him forever. Jason and I sobbed. In the middle of a diner. In complete shock. 3 weeks later we stood there and watched as our son Andy was born. I was the first to hold him and kiss his tiny hands. That was October 30th, 2017.
After taking Andy home, Oram continued to keep in contact with the first mother they had been matched with, who told them she had found another family for her baby. Still, they continued speaking, and in January, they got a shocking phone call. “She told me she had just told the other family she did not feel good about them adopting her baby,” Oram said. “She then told me that she knew this baby was supposed to be ours. I stood there holding my 3-month-old baby boy and she sent me pictures of an ultrasound of the baby boy growing in her stomach. I was speechless. But I also knew. Deep down I knew.”
After much prayer, the couple decided to welcome another newborn into their family, just months after adopting Andy. They flew to Missouri and met the birth mother and her three children, just before she was scheduled for an induction. “We all instantly connected,” she said. “The next day we stood at her bedside and watched as our son Ellis was born. Jason even got to cut the cord. I was first to hold him and again kiss his tiny hands.”
Since then, they have maintained open adoptions with both of their sons’ biological parents. “We talk and send pictures and recently met up with Andy’s birth parents at a nearby park,” she explained. And doing so led to another surprise.
Four months after Ellis was born we had a strong feeling to reach out to his birth mom and she had mentioned they were in a rough spot. Jason and I decided to then fly her oldest child out to visit us for 10 days so he could spend some time with Ellis. Sean had never been on a plane or been that far away from his home. We instantly fell in love with this sweet boy. 10 days eventually turned into all summer.
At the end of summer, he asked if he could to watch his new friends try out for football. Before we knew it, he was talking to the coaches and asked if he could try out. Sean made the top football team for 8th grade in his first year ever playing an organized sport. He called his mom and asked her if he could stay. She said whatever would make him happy. Sean has now been living with us for 6 months and his football team made it all the way to playoffs.
All together, the Orams accepted three children in less than nine months into their family, and she is thankful for the family she now has.
Much of the world is watching as the state funeral of former President George H.W. Bush unfolds. America does a good job of honoring our nation’s highest leaders when God calls them home.
George H.W. Bush supported abortion as a candidate for president, one of the reasons Reagan prevailed. When Ronald Reagan named Bush to run on the ticket with him during the Republican Convention, there was considerable disappointment from rank and file pro-lifers.
Dr. Jack Willke, my former colleague and founder of Life Issues Institute, was then president of the National Right to Life Committee. Upon hearing the news of a Reagan/Bush ticket, he went to the hotel that served as the Republican headquarters and asked to see Mr. Bush. Instead he was introduced to Bill Casey, Reagan’s campaign manager who went on to be Director of the CIA. Jack explained the need to see Mr. Bush and Casey agreed. He was ushered into a room where it was just the two of them.
Jack stressed to Bush the need to elect Ronald Reagan, he conveyed the complication of having a running mate who supported abortion and suggested to the candidate that he brief him on the abortion issue. Mr. Bush began to share his opinion on the issue, but Jack interrupted him saying that he’d rather hear Mr. Bush’s position on abortion after the briefing.
Then Jack added, “I need four hours to thoroughly brief you.” Bush reacted with mild shock, but he pressed on. “We represent a lot of pro-life Americans. If we can tell them that you thought this issue was so important, you dedicated a substantial amount of time to be briefed, it will make a favorable impression on our people.” Bush responded, “You make a valid point. Let’s do it.”
Jack pressed even further, asking to bring in a few pro-life leaders after lunch to discuss the campaign. Bush agreed.
A few weeks later Jack was seated on the couch in Bush’s Kennebunkport, Maine home with a slide projector between them.
Using effective imagery, Jack introduced the vice-presidential candidate to the beauty of life in the womb, as well as the shocking reality of what abortion does to babies and their mothers. They also discussed key arguments for and against abortion.
At the end of their time together Jack then asked Mr. Bush where he was on abortion. Mr. Bush smiled, realizing the strategy of their time together. “I wasn’t here before, but I am now. I will support an amendment to the Constitution to forbid abortion and overturn Roe v. Wade, as a state’s rights amendment.”
Mission accomplished!
That meeting changed the course of history and many babies are alive today because of the pro-life policies of President George H.W. Bush’s administration. You can watch Dr. Willke recount this story in a brief interview here.
President Bush was good to his word.
As President, he directed his attorney general to ask the Supreme Court to overrule its pro-abortion decisions in Roe v. Wade and a later case that reaffirmed Roe’s holdings, Webster v. Reproductive Health Services.
President Bush worked to limit Title X funds from going to organizations that promote abortion and maintained the Mexico City policy, which stops U.S. taxpayer funding of the abortion industry overseas.
President Bush also used his veto pen to protect unborn babies. He vetoed an entire spending bill when congressional Democrats sought to loosen the Hyde Amendment. Overall, he lodged 10 vetoes of bills that lacked protections for the unborn.
And he issued sanctity of life proclamations annually. President Bush’s 1991 proclamation told Americans his administration “championed compassionate alternatives to abortion, such as helping women in crisis through maternity group homes, encouraging adoption, promoting abstinence education, and passing laws requiring parental notification and waiting periods for minors.”
We join the nation in mourning this good and decent man. His pro-life conversion is a lasting testimony to the power of education, the foundation on which pro-life political and legislative victories are built.
Please keep the family of President George H.W. Bush in your prayers.
LifeNews.com Note: Bradley Mattes is the President of Life Issues Institute, a national pro-life educational group.
The speed with which gender ideology has grown from the radical fringe to a movement dominating our media, legislation, education and entertainment is nothing less than staggering. Unless you are a professional LGBT activist, keeping up with the bewildering lexicon of new terms and “gender-neutral” pronouns is an exercise in futility. Even more disorienting is how quickly their use has become mandatory by the gatekeepers of culture and political correctness.
Last week, news broke that Twitter had introduced a new “hateful conduct” policy. The policy bans, among other things, “misgendering” and “deadnaming.” To “misgender” someone is to refer to them by a gender other than the one they currently claim to have. That’s relatively self-explanatory.
But I had to look up “deadnaming.” Apparently, this is when you refer to someone by the name they were given or used before they “transitioned.” If you were to refer to the Olympic athlete who now calls himself Caitlyn Jenner as “Bruce,” you would be guilty of “deadnaming” him. And for this, you are a hater, and worthy of banishment by Twitter.
But as self-evidently totalitarian as the gender movement is becoming and has become, nothing disturbs me as much as what this movement is doing to children.
Celine Dion, and Prepubescent Drag Queens
Celine Dion is making news this week for all the wrong reasons. With a new video, Dion has launched a new line of ‘gender-neutral’ babies and children’s clothing. In the video, which can only be described as bizarre, Celine breaks into a hospital maternity ward, where she finds two rows of newborn babies, boys and girls. Celine unzips a black leather bag, from which she takes out a package of black glitter which she blows over the sleeping children. Immediately the pink and blue clothes vanish and are replaced with drab, gender-neutral clothes in shades of black, white and grey.
Drab, in fact, is a generous description. Some of the clothing in Celine’s new line –CELINUNUNU – look like something out of a dystopian nightmare. Many of the shirts are emblazoned with the words “New Order” – presumably referring to Celine’s mission to eliminate traditional gender-roles. Some of the other articles of clothing bear skulls…lots of skulls. There are lots of photos of children and babies on the website for Celine’s new clothing line. None of them are smiling. In one photo a young child, who appears unhappy (other product shots show children staring blankly ahead) is covered in a “onesie” of skulls.
Anyone who has been around children knows that, given they are well-loved, they are naturally happy. Children are energetic, rambunctious; they love to laugh, they love to play. They love a good story, a good joke, a good game. Any parent or educator worth their salt wants to protect this carefreeness, to carve out space for children to develop their personality and talents without being burdened by the complicated troubles of the adult world. Instead, LGBT activists seem hell-bent on inaugurating children into a bleak word of politicized ideology and hyper-sexualization.
Earlier this month Good Morning America, one of the most-watched television shows in America, featured 11-year-old “drag queen” Desmond Napoles. The co-hosts of the show tripped over each other in their efforts to praise Desmond for his “bravery.” The audience beamed and clapped and laughed. But watching this young boy, who should be outside playing tag and catch and riding his bike, slither up the aisle, strutting like a show-girl is enough to make one weep. Who is responsible for this? Who has stolen this boy’s innocence?
Desmond and the hosts of the show furiously pretended that he was simply “expressing himself” and being “true” to himself. But this is a lie. Eleven-year-old boys do not sprawl sensually on the floor and writhe and strut and put on wigs and makeup and elaborate costumes, unless someone has coached them on how to do so.
Boys love to be boys!
The Real Agenda: Grooming
Drag queens, once exclusively encountered in the kind of “adult” establishments where decent folk wouldn’t dare set foot, have emerged from the brothels and strip clubs and ended up – of all places – in our children’s schools and libraries. Across the country libraries are hosting children’s Storytime with drag queens. This week, one such drag queen openly admitted what he is doing. “This is going to be the grooming of the next generation. We are trying to groom the next generation,” said Dylan Pontiff.
And the next generation is indeed being groomed. One UK teacher recently stepped forwardanonymously, describing how at her school there are currently seventeen children transitioning their gender. Seventeen! This teacher explained that when one student approached her about her gender dysphoria, she supported the child and referred her to a transgender clinic. She now regrets that decision, since the girl – who is autistic – is now planning on going through a double mastectomy. Other children at the school, many of whom are also autistic, are taking hormone blockers, and planning on irreversible surgical mutilations of their bodies.
The teacher says she is convinced most of the children aren’t even suffering from gender dysphoria. They’re simply vulnerable to persuasion. “They are just young people with mental health problems who have found an identity and want to be part of a group of like-minded people,” she said. She says the first student began “educating” other students on transgenderism. She described this as a form of “grooming.” The media, celebrities like Celine Dion, and many politicians are enthusiastically cooperating with this grooming by presenting gender dysphoria as normal, admirable, and a cause for celebration.
And what kind of life is it that Mr. Pontiff and his ilk are “grooming” children into? One eye-opening essay published by the New York Times this month gives us some idea. In the essay, titled “My New Vagina Won’t Make Me Happy,” author Andrew Long Chu (a biological male who “identifies” as female) describes how he is planning on undergoing sex change surgery, even though he knows that it likely won’t make him happy. On the contrary. When Mr. Chu started taking female hormones to “transition” this made the psychological distress caused by his gender dysphoria “demonstrably worse.” The surgery will likely only do the same; after all, the fake “vagina” that the surgeons will construct, says Mr. Chu, will be treated by his body as a “wound” (which it is) until the day he dies. But Mr. Chu thinks he should be able to get the surgery anyway. Why? Because he wants it. This is the radical “freedom” that our culture now celebrates, and into which gender ideologues are co-opting our children: the “freedom” to be miserable.
Children are vulnerable to peer pressure and fads. Adults – above all parents – are supposed to be the voices of reason in the room, standing up against irrational trends and protecting children from manipulative ideologues who want to claim them as feathers in their cap. Instead, in many cases the children’s parents are encouraging the children’s confusion, actively pushing them into a sexual subculture that, statistically, is rife with depression, drug abuse, and suicide. In many cases, one can’t help but suspect that it is the parents who planted the first seeds of gender confusion in the first place. Why would any parent want to do that?
The Diabolical Attack on Children
This week many mainstream media sources are roundly mocking a Catholic exorcist who responded to Celine Dion’s gender-neutral clothing line by speculating that the spread of gender ideology is of demonic origin. “The devil is going after children by confusing gender,” said Msgr. John Esseff, an exorcist in the diocese of Scranton, Pennsylvania. “When a child is born, what is the first thing we say about that child? It’s a boy, or it’s a girl. That is the most natural thing in the world to say. But to say that there is no difference is satanic.”
Many media outlets are treating this as self-evidently preposterous. And yet, who with clear vision can acknowledge the deliberate effort to co-opt even the youngest and most innocent children into this extreme ideology, with all the physical and psychological dangers involved, and not conclude that this is diabolical?
This is not to say that any one person involved is evil. On the contrary, many gender-confused people are struggling with an enormous cross and urgently need our compassion and prayers. Many others promoting gender ideology at least seem to believe that they are motivated by compassion. But even if we must resist any impulse to demonize people, we must acknowledge gender ideology as a form of mass delusion that is threatening the innocence and lives of our children. Satan is real and he is the Father of Lies. As social pressure continues to mount to either support or stay silent in the face of gender ideology, we must resist the temptation to capitulate. We must keep our eyes open, and engage productively, calmly, compassionately and rationally in this crucial cultural debate.
As Canadian psychologist Jordan Peterson noted about this issue: “If you don’t stand your ground, then all that happens is people push you backwards… But if you don’t stand up and do something about it, especially when it affects your own family, then all that’s going to happen is that it’s going to continue to spread.”
St. Michael the Archangel
This has been a bleak column to write, and I’m sure it is a bleak one to read. But as Jeeves once told Wooster, it is better to know “what tune the devil is playing.” We can’t afford to close our eyes. But neither do we need to give in to hopelessness. On the contrary, we cling to hope. We must hold close to Christ and his mother. We must invoke their protection on our families and culture. And finally, as I always urge, we must pray. I agree with Msgr. Esseff that there is a diabolical origin to the cultural confusion we are witnessing right now. That is one reason why I believe that we must resurrect the prayer to St. Michael, which I hope you will join me in praying:
Holy Michael, the Archangel, defend us in battle. Be our safeguard against the wickedness and snares of the devil. May God rebuke him, we humbly pray; and do you, O Prince of the heavenly host, by the power of God cast into hell Satan and all the evil spirits who wander through the world seeking the ruin of souls.
SAN PEDRO, California, December 3, 2018 (LifeSiteNews) – A California mother of three facing leukemia while expecting twins received news last week that may save her life after tens of thousands stepped up to potentially donate bone marrow.
Susie Rabaca was praying for a perfect match so she could stay alive for her kids. She is due December 6 with her twins and needs a bone marrow transplant to save her life.
“I was devastated, emotionally devastated,” she told NBC News, regarding learning her diagnosis months ago.
Rabaca’s sister is a 50 percent match, but doctors said the match wasn’t sufficient to treat her cancer, an aggressive form of acute myeloid leukemia.
She needs a 100 percent match, but Rabaca’s mixed heritage – Latina and Caucasian – has made finding a match problematic. No one from some 30 million people registered worldwide was a complete match for her.
Rabaca, with the help of daughter Riley, made an online plea for more possible donors.
Her story went viral, and since then more than 50,000 people registered with the national marrow donor program Be The Match, a record-breaking number.
She received word of a 100 percent match Wednesday.
“Oh, my God, that to me is beyond amazing,” Rabaca said. “It’s an overwhelming feeling of just joy and happiness. It really is.”
More tests will be needed, but the hope is that she will be able to undergo the transplant after delivering some time in the next week.
“It’s so exciting,” Rabaca said. “It’s the best Christmas gift, it’s everything.”
In a Facebook post Thursday, the pregnant mom said:
“With tears running down my face and my heart full of hope I want to say THANK YOU LORD! And thank you from the bottom of my heart to every single person that has said even 1 prayer for me and my family! Thank you to my family, friends, people around the country that I don’t even know that have shown support and especially that have signed up for BE THE MATCH!!!!! Journey isn’t over but a huge step forward!!! Thankful for you all lots of love! Keep Praying thank you!!!!”
One would think that ten years is not a very long time to measure change in such timeless matters as family and sexuality. But these are not ordinary times.
The gap between 2008 and 2018 has been far more dynamic than most decades. As a sociologist, my specialty is behavior, so that will be my main focus. Here are five noteworthy narratives from the past decade. Each story constitutes a profound change, or reflects changes occurring within our most intimate relationships.
1. Same-sex marriage becomes law in all fifty states.
This is the easiest to identify, and arguably most significant, shift in the marital landscape. Around two out of every three Americans approve of same-sex marriage today.
How many Americans have entered into civil same-sex marriages? It’s hard to say, since same-sex households themselves have never been simple to count.
The Treasury Department, leaning on tax returns, identified about 250,000 same-sex marriages (filing jointly) in 2015, a figure that characterizes just under one-half of one percent of married tax filers in the United States. The Census Bureau estimates that the true figure is about 60 percent higher, and the Williams Institute thinks it’s higher still.
What are these couples like? Their tax returns suggest they’re generally younger and less likely to have dependent children—especially the men. They are also well-to-do. The average adjusted gross income of male couples was nearly $166,000, a number well above the $118,000 for female couples and the $115,000 for different-sex couples.
What is more striking is the income reported by male couples with dependent children, clocking in at an average of $264,000. This is more than double what opposite-sex married couples with children tend to report ($122,000). Such couples tend to congregate in major coastal metropolitan areas. But even there we tend to overestimate the presence of married same-sex couples.
In San Francisco, for instance, same-sex couples comprise only about 1.5 percent of all marriages, in a city not known for its embrace of matrimony. And that’s the highest rate among American cities.
Will same-sex marriage rates increase? As I wrote in Cheap Sex, I doubt it. Gallup data reveals a modest uptick in Americans reporting being married to someone of the same sex—six-tenths of one percentage point—between the first and second years after Obergefell.
That’s not exactly the outcome you’d expect from pent-up demand. Some hold that the Obergefell case is enabling yet further changes in American family and sexual behavior. Toward that end, there is evidence of rising same-sex sexual behavior at levels outpacing that of growth in the share of Americans who identify as gay or lesbian.
2. Transgender is trending.
If there was an immediate legacy of the Obergefell case—a cause célèbre birthed by the legal success of same-sex marriage—it is the transgender movement. Unlike marriage, which managed to unite gay and lesbian Americans, the support base for the transgender issue seems to have emerged from somewhat different corners.
Unlike homosexuality, which is often publicly undiscerned and privately unrevealed until late adolescence or early adulthood, the transgender moment seems to hinge more directly on children, teenagers, and supportive parents.
Moreover, transgender matters entail “transition” decisions to be made about the body—ones that can have irreversible effects. Hormonal treatments to delay or prevent puberty or menarche, for example, can prompt permanent infertility, while surgeries replace functional (but unwanted) organs with sculpted substitutes.
Adolescent and youth transgender claims are nevertheless surging, creating conflicts over pronouns, bathrooms, and sports teams, to name just three domains.
So just how many transgender minors are there? It’s a moving target. The Williams Institute thinks it’s 0.7 percent, but a new study in the journal Pediatrics reveals a statewide survey in Minnesota estimates it at just under 3 percent—a number that’s four times as large. Who’s right? Who knows. The terrain is unstable—and treacherous to map.
Brown University professor Lisa Littman, writing in the open-access, peer-reviewed journal PLoS One, documented the reality of the rapid onset of gender dysphoria (ROGD) in adolescents. By “rapid” she means that it happens suddenly either during or after puberty among teenagers who displayed no indications of such tendency in their childhood.
The teens’ parents tended to note that ROGD occurred in groups of friends and alongside a surge in the kids’ internet or social media use. In fact, only 13 percent of parents noted no evidence of a “social influence.” Critics, concerned that the transgender moment might unravel, pounced. Littman maintains she saw what she saw.
3. “Queer” has gone mainstream.
Most of the growth in non-heterosexual self-identification nevertheless has come in the form of bisexuality. This is also true of behavior. In the past twenty-five years, in fact, most of the growth in same-sex sexual activity has come from those who report both men and women as partners.
The share of the population that reports at least one partner of the same-sex has grown from 3.6 to 8.7 percent of women and from 4.5 to 8.2 percent of men.
Yet we shouldn’t read too much into long-term bisexuality. When such young adults marry, they still tend to do so with someone of the opposite sex. While that could be a matter of simple numbers—there are more heterosexual options—it’s also a reflection of what economists call observed preferences.
How do bisexuals differ from the other identifiers we are beginning to hear about, including pansexuals and omnisexuals? It’s a good question—and one for which an answer will have to wait.
But you’re not the only one who finds the explosion in sexual self-identifiers confusing. Sexual fluidity is in. Talk of immutability remains, and was helpful in securing legal victories in Windsor and Obergefell, but the concept has not been widely accepted among scholars of sexuality for years, especially as it concerns female sexuality.
Sexual plasticity among women is now conventional scholarly wisdom.
“Queer” has become mainstream, and “cisgender” and “heteronormative” are no longer terms understood by a tiny fraction of the population. The term “queer” has now become a catch-all for the panoply of non-heterosexual options available today—identities, behaviors, relationships, preferences, and speech.
4. Married and cohabiting Americans are having less sex.
If you suspect that all this sexual fluidity, combined with the surge in approval and use of pornography, would have led to a place where the sex act had become so normal and common, like drinking a glass of water, you would be in good company. And yet mistaken.
A November 2017 article in the Archives of Sexual Behavior reported that, on average, Americans have sex about nine fewer times a year than they did in the late 1990s. And that was without the 2016 data, which revealed an additional drop in sex—a statistically significant one—in just two years.
The trend, ironically, is most pronounced among younger adults. Controlling for age and time period, people born in the 1930s had the most sex, whereas those born in the 1990s are reporting the least.
Blame quickly turns to the ubiquity of smart phones, grabbing attention away from the relationship in front of us and toward the lives of those more distant. Other suspicions include the surge in antidepressant use—a drag on the libido—that now characterizes one in every eight adult Americans.
5. Divorce rates are dropping (because marriage rates are dropping).
One of the reasons for pessimism about the long-term uptake of same-sex marriage is because short-term interest in marriage continues to turn cold, with rates tracking downward for well over forty years. To suggest that same-sex marriage might invigorate a lagging institution, showing straight Americans how to get hitched again, is silly. People don’t work like that.
So why not try another positive angle: millennials are divorcing at rates notably lower than their parents’ generation. It’s true. While it is heartwarming to see the media get excited about one of the classic hallmarks of marriage—the idea that it should be permanent—there are better explanations for the phenomenon than millennials’ newfound commitment to something/anything.
Divorces are getting rarer precisely because marriage is getting rarer. Marriage is receding. By how much? The share of Americans in the “sweet spot” of getting married (twenty-five to thirty-four years old) who are actually married today has shrunk dramatically—dropping from 80 percent to 40 percent—since the downturn began around 1970. And the rate of decline has shown no evidence of diminishing.
What it all means is that Americans are getting pickier about marriage. It’s called selectivity, and it means that many marriages that may (or may not) have been less satisfying, or less desired, are not being entered into today. Predictably, some of those would have failed. Now they can’t, since they never happened.
Marriage is, as sociologist Andrew Cherlin has explained, in the throes of “deinstitutionalization.” It is no longer a shelter to be ducked into, a way for two to construct something together out of nothing but love. And it’s no longer expected. Instead, it’s a symbol, an unnecessary but nice luxury item, a capstone of a successful young adulthood.
Americans now hold out for picket fences, figuratively speaking. Why? Because they can, because they have been taught to, and—at least for men—because sex is cheap.
Unfortunately, not everyone can afford this new type of marriage. Although the benefits of marriage are still—in theory—available to all, marriage is increasingly a middle- and upper-middle-class thing. As a result, income inequality—a social phenomenon often aided by getting married—is getting worse.
A Liminal Spot
There are other patterns of less clear nature, including MGTOW, Red Pill, and the #MeToo movement. Each is consequential, but far more difficult to gauge in terms of popularity, shared meaning, and what we ought to expect as a result of them.
For example, the #MeToo movement has considerable name recognition, is influential in calling out (mostly) men who have capitalized on their power to coax or force sexual acts. But to identify with it on social media can mean quite different things.
It can yield much, in the case of Harvey Weinstein’s accusers—who have witnessed an indictment of the man—or it can yield very little, as is the case for most women who have experienced assault, garnered the courage to talk about it publicly, and yet have witnessed little or no change in the real world.
By comparison, the five patterns or social realities discussed above are not so heavily dependent on social media.
We find ourselves in a liminal spot, one between long-taken-for-granted traditional relationships anchored in marriage and the future relationship system characterized more consistently by “confluent love.” There will not be two dominant systems.
Meant to be a “haven in a heartless world,” as the late social critic Christopher Lasch described it, marriage has become another tenuous social arena in competition with the economic marketplace (for our limited time and energy) and the remarriage market (for second chances and sexual variety).
Marriage will not disappear, of course, but it may well become a minority practice.
Mark Regnerus is Contributing Editor of Public Discourse, Professor of Sociology at the University of Texas at Austin, and a senior fellow at the Austin Institute for the Study of Family and Culture. Republished with permission from The Public Discourse.
The birth control pill was approved for use in the United States in 1960, and then in the United Kingdom in 1961. Right away, it was controversial; the pill includes serious side effects like blood clotsand breast cancer, as well as more benign, yet still frustrating, side effects like weight gain, nausea, headaches, and bloating. However, a new documentary from BBC Two is bringing to light lesser-known risks of the birth control pill: depression, anxiety, and suicidal ideation.
The documentary, titled, “The Contraceptive Pill: How Safe Is It?”, notes that 1 in 4 women taking the birth control pill reported in a survey that it had a negative impact on their mental health. The hormone responsible for the increase in mental health problems is believed to be progesterone. Danielle, age 31, said her side effects were “completely debilitating and terrifying. I went from being fine to having suicidal thoughts within six months.” She explained that she had never had any problems with mental health before she began taking the pill.
Vicky Spratt, editor-in-large of Grazia, likewise had negative side effects. “I remember thinking ‘if this is what the rest of my life is going to be like, I don’t want to live it’,” she said in the documentary. The Independent notes that numerous studies, including one of 800,000 women in Sweden, have confirmed these findings, linking the birth control pills to poor mental health.
Part of the problem, according to Spratt, is that women are not being adequately warned about the risks they are taking when they take the birth control pill. The only side effect listed on NHS pamphlets, Spratt said, is ‘mood changes.’ “What does that even mean? It could refer to anything,” she said. “I think the NHS is sticking with ‘mood changes’ because they’re nervous about women being deterred from taking the pill and unwanted pregnancies rising as a result. It surprises me that despite known links between progesterone and depression, the NHS aren’t looking into it and, as a result, we don’t know how many women are affected by this in the UK.”
The goal of this documentary is not to dissuade women from taking birth control, but to bring attention to the issue and encourage more research, so women can be informed of the risks and trulygive informed consent. Dr. Zoe Williams, who presented the documentary, also pointed out that birth control is often not taken the way other medications are, out of necessity to prevent disease or treat an illness. “Therefore side effects that significantly impact on quality of life, in a negative way, are not acceptable.” she said.
November 27, 2018 (LifeSiteNews) – Offering Mass ad orientem “enhances beauty” and “enhances reverence,” Bishop Robert Morlino, who died Saturday, told LifeSiteNews two years ago. LifeSiteNews releases footage of those comments for the first time today.
In 2016, Morlino became the second U.S. bishop to officially adopt the ad orientemposture facing the altar with the people while offering Mass at his regular cathedral parish. He said his flock received this well because he made catechesis on the liturgy a focus of his episcopate.
“The particular community that worships with me have been made aware and catechized about the meaning of ad orientem for years now,” he said. “When I announced to them that I would begin to celebrate in the adorientem in the Ordinary Form, they smiled and nodded yes.”
Offering Mass this way “enhances beauty, it enhances reverence, and it enhances that feeling of comfort, that predictability that somehow the priest is much less likely to share off-the-cuff when he’s celebrating ad orientem,” said Morlino.
Before the promulgation of the Novus Ordo Mass by Pope Paul VI, Masses were offered with the priest facing the tabernacle along with his congregation. The rubrics of the post-Vatican II Mass suggest that liturgy should still be offered ad orientem, a fact often ignored by liturgical innovators and left-wing clerics.
Morlino, who the Catholic blogosphere fondly nicknamed the “Extraordinary Ordinary” because he offered Mass in the Extraordinary Form and allowed it to flourish in his diocese, explained to LifeSiteNews that “predictability” in the liturgy allows people to worship without worrying and wondering about what will happen next.
“St. Ignatius said repetition is the mother of studies, and we know from the Church fathers and many others that repetition is a key to prayer,” said Morlino. “So there must be a certain predictability in the liturgy so people can relax and not wonder, ‘what’s going to happen next and how exactly am I gonna respond to it?’ That approach is I think what’s harmed the Church so much — particularly maybe in the United States since the [Second Vatican] Council – that the participation in the Eucharist became unpredictable.”
Morlino’s diocese experienced a surge in vocations to the priesthood while many dioceses in the West have struggled to recruit men to become priests. Morlino said he thanks God every day for the seminarians of his diocese, who are “tremendous,” “wonderful,” and “terrific.”
“Seminarians in liturgy want really a couple things,” he said. “The most important thing is they want reverence… generally, the young men who are coming forth to be seminarians want reverence, they want beauty, and they want to relax so that they can participate. They want to know what’s going to happen next” rather than having to wonder what liturgical innovations will be introduced.
‘You have shepherded your flock well’
Bishop Morlino was well-known for his defense of orthodoxy and the pro-life and pro-family causes, in addition to his reverent Masses and focus on sacred liturgy.
On Monday, Dan Miller of Pro-Life Wisconsin wrote that Morlino made an enormous difference for the state’s pro-life movement and inspired his flock by joining them at prayer vigils outside abortion centers:
Pro-Life Wisconsin is so blessed to be a part of your community. Bishop Morlino, what you have done here is beyond a mere mortal’s words. Your leadership has inspired people to make great sacrifices to end abortion. You have shepherded your flock well. Look at the time your sheep have given! Thousands of cumulative hours spent out in front of Planned Parenthood making a difference. Your prayers. It wouldn’t surprise me if there were more than a million rosaries prayed throughout the years in front of Planned Parenthood to end abortion. Your finances. Millions of dollars you have sacrificed so that our brothers and sisters in Christ may have a better chance of making it out of the womb ALIVE! If the life of the pro-life movement is any indicator of a faithful Bishop, you are absolutely guilty of leading your flock well! Thank you! You are a sign that the hope of Christ is alive and well. Let us rejoice and be glad for your steadfast love for Christ, your vocation and for the people you serve and have served so well.
“The death of Bp. Morlino of Madison has had the effect of demonstrating that he truly deserved the nickname [the] Extraordinary Ordinary,” Father John Zuhlsdorf wrote on his well-trafficked blog. “I have received a flood of emails and text messages from all over the world expressing sorrow at his passing, admiration for his work and for his sheer goodness, and hope with prayers for him and for the continuation of what he set in motion.”
Zuhlsdorf shared a few of those messages, some of which were from priests telling him they would be offering Masses for the repose of the bishop’s soul.
“Bishop Morlino did more than encourage speaking truth to power[;] he modeled it,” Madison priest Father Richard Heilman wrote of his late ordinary. “His Sunday homilies were, classically, a refutation of what was on the news that previous week. He was not going to let them get away with manipulating his flock. He was shockingly to the point. But, while clear and unambiguous in his teachings, he remained charitable in his approach. He spoke these words whenever he could, ‘Truth with love.’”
“Bishop knew that a strong force of believers would not come from a soft Catholicism,” Heilman continued. “Moreover, Bishop understood that a strong
Bishop was an avid disciple of Pope Benedict XVI, and he agreed with the holy pope who wrote about what laid at the very heart of the crisis in our Church: ‘I am convinced that the crisis in the Church that we are experiencing today is, to a large extent, due to the disintegration of the liturgy.’”
Late Bishop Robert Morlino on Radio Maria May 2014 “The Quest for a Culture of Life in America”
On September 21, the well-known German magazine, Der Spiegel, featured a long article on the whole career of Pope Francis under the title “The Greatest Crisis in the History of the Church.” The immediate issues brought up concerned the pope’s handling of abuse issues while he was still in Argentina. Most people are by now also familiar with the issues in this same area brought up by Archbishop Carlo Maria Vaganò’s testimony concerning former Cardinal McCarrick’s unfortunate record. In a situation such as this, most people also want to be as fair as possible to the pope. And most people want to know the facts.
People are also puzzled by the pope’s refusal to answer what seem to be quite legitimate and straightforward questions about what he teaches. Common sense would normally suggest that, if someone is not guilty, he would be anxious to state why, to clear the record, as it were. The pope’s silence, fairly or unfairly, suggests to most people of good will that something was covered up, something is not quite right.
People at all levels and particularly Catholics strive to know what is at stake. They are not interested in gossip or innuendo. They rightly want to know the truth; they want to hear a fair assessment of the situation from the pope himself; but they do not want their concerns dismissed. Their spiritual wellbeing depends on a Church sound enough to proclaim the truth, including the truth about its own members who are sinners. Catholics are not afraid of sin unless they cease to believe in the Church’s major teaching about sins, namely, that Christ came not to deny them but to forgive them. Even if the Church is no longer credible, we still remain in sin. That is good Pauline teaching.
Admittedly, this on-going saga brought up by Der Spiegel need not be the greatest crisis in Church history. Whatever ranking we want to give it—the worst, the second worst, the tenth worst, or a minor glitch—in the public eye, it certainly is a crisis of major proportions that challenges the credibility of the Church on its own terms. We would all like to see it just go away. Indeed, we would all like to think it never happened. But we are realists. What happened, happened. We must deal with it, but not before knowing the truth of what went on.
Pope Bergoglio himself seems willing to talk about almost every subject but his own beliefs and record. They seem most at issue. The crisis at this stage, whether we like it or not, is precisely about the present pope, what he believes and which decisions he made. It is not directly about whether Catholicism is objectively true or not. Rather it is a question of whether the Catholic Church, in its own testimony about itself, is consistent with its own teachings.
As the reporting in Der Spiegel and the New York Times shows, people from outside the Church, not just Catholics, are now carefully watching this drama. They realize the long-term implications to our culture if Catholicism can no longer claim for itself a consistency with its past or with the integrity of its teaching. It is analogous to a question of whether, say, the Communist Party in its hay-day was consistent with its own tenets, and whether it was objectively consistent with its own premises or not.
The headlines in the September 7 issue of L’Osservatore Romano presented the pope’s Letter on the World’s Day of Prayer for Creation. The Letter is about access “to clean water.” The ancient Romans were famous for building aqueducts to bring water into cities. If anyone lacks water today, it is not because we do not know how to purify and distribute water resources. It is almost entirely due to economic and political choices. The technical means or know-how for providing water is not a major theological concern of Christianity as such. Christ walked on water, turned water into wine, helped a woman at a well draw it up, and was baptized with it in the Jordan. He never designed a dam to provide water for Nazareth or Jerusalem. He evidently assumed that men could eventually figure this task out without the need of revelation.
A pope can mention the problem of water availability or other such issues, but his is not the task to provide technical solutions even if he had a doctorate in water engineering. One can question whether the pope’s views of economics and politics that tend toward socialism encourage a system that easily provides water on a large-scale basis. Many people of good will wonder why, if the pope can talk of clean water, he cannot talk about his own record or the views he holds on issues that certainly do fall within his competency. These latter issues are what perplex people and give impetus to the reportage of Der Spiegel.
II.
We might reasonably ask ourselves: “What would the Church’s ‘greatest’ crisis be, if it were to have one?” It would have something to do with pride, as in placing a human opinion over a divinely revealed or rational teaching. It would have to be an embracing of “this world,” spoken of in John’s Gospel as a world that rejects Christ’s coming and his Cross.
Passages in 2 Timothy and in Matthew 25 do indicate that a serious crisis can erupt when unworthy priests and prelates are found within the Church itself. The pope speaks much of clericalism and Pharisees in the Church itself. People are fond of citing Paul VI’s “smoke of Satan” in the Church. Ezekiel and St. Augustine give us warnings that unworthy shepherds might prevail among us. On the other hand, at least the papacy was supposed to have been a place where “the gates of hell” did not prevail. Popes could be sinful in their personal lives but still would not teach false doctrine or approve immoral activities.
By implying that this crisis is the “greatest” in the Church’s history, Der Spiegel is taking the Church at its own word. It compares the Church’s own teachings with what is practiced or proposed by Pope Francis. Ross Douthat’s book, To Change the Church, is along these lines also. The implication is that the crisis is of the Church’s own making. It is not due to some barbarian invasion, a Masonic plot, or some other outside force imposing on it or threatening it. It is being threatened by its own ministers not only for not living according to Christian moral standards but also in not teaching what is good. The irony, to be specific, is that disordered man-man sexual relations have become a civil “right” in many countries but the same relationship is a natural law aberration according to Church teaching.
The world watches to see if the Church will join the world in approving these relations as “rights” in the public order and in the Church. Or will it reject them? In other words, the Church is being watched to see if it upholds the natural law in its own teachings and practices or whether it joins the world and thereby undermines its claim to consistency and truth of doctrine since its beginning.
The “greatest crisis” of the Church, then, would not be the discovery that clerics are themselves sinners. Christ was sent not for the just but the unjust. He was sent to grant forgiveness to whoever asked for it. But he also told us to stop sinning. Therefore, the fact that sinners populate the world and the Church, even after Christ established rules to live by, cannot surprise anyone. There are, of course, many kinds of sin. The current flair-up is over the sixth commandment in its many consequences. They all relate to the integrity of the family and its members.
Indeed, the current issue is largely the result of ingrown, acquired habits that are difficult, but not impossible, to break. Generally speaking, in seeking to make a fair judgment on priest and bishop sinners, their victims were neglected. This latter concern is now central, as it should be. The greatest “crisis” is not about the fact of sin or sinners. It is about the internal order of the Church itself, whether it believes and upholds its own doctrines, whether true or not.
Many do not think that the aberrations some priests and bishops are accused of committing are sins or disorders. But even these realize that the Church is the last bastion of moral integrity as seen in its classical philosophic and religious form. They also see that the serious troubles the Church itself is in are primarily due to its own actions.
We can say that the issue is not over whether the pope is a sinner, naïve, or weak, but whether he has approved teachings or moral behaviors that he is obliged to oppose. If he has taken this step in some obviously authoritative way, then Der Spiegel will be proved right. A reversal of fundamental teaching at the highest levels of the Church would constitute the “greatest crisis” in Catholic history. It is an act of faithfulness to respectfully hope Pope Francis clarifies his own teachings. It does not seem like too much to ask and many, including Der Spiegel, are asking it.
In a recent video linked on Facebook, Dr. William Lile, an OB/GYN in Florida, speaks about how children in the womb are distinct human beings from their mothers, and also how they should be viewed as persons because they can receive prenatal medical treatment.
In the video below, Lile says that “the mom is a patient, and the baby is a patient.” The mother’s body, he says, doesn’t see the baby’s body as just another one of her organs — which is so often the implication of pro-abortion slogans such as ‘my body, my choice’ — but as a “foreign entity.” Sometimes, he adds, the mother’s body even makes antibodies against the baby. In cases like this, antibodies cross the placenta and begin to attack the baby, and the child’s blood count may become low enough that a blood transfusion is necessary… in-utero. It can be done “as early as 19 weeks,” says Lile, and can be done every four weeks to continue to ensure the health of the baby, because the baby is viewed as a separate patient.
Lile notes that some hospitals are finding heart defects using ultrasound at around 13 weeks gestation and are performing prenatal surgery for things like left hypoplastic heart syndrome, in which the baby’s heart fails to pump enough blood from the left side of heart. Doctors can do this kind of surgery as early as 21 weeks gestation using ultrasound guidance, says Lile. A catheter is guided through the wall of the uterus and into the baby’s heart. For some conditions, stents can even be added, which will remain in place until after birth.
Lile mentions the fact that corrective spina bifida surgeries can be done as early as 21 weeks in the womb, and these babies usually have better outcomes than those who have surgery after birth. In other conditions affecting the placenta, laser surgery can even be done to save babies when placental blood vessels aren’t functioning properly.
Lile notes that the American College of Obstetricians and Gynecologists talks about “informed consent… the risks, benefits, alternatives…” and says we need to treat the patient as a person.”Well, when is a baby in the womb a patient? I would say that if we’re doing heart surgery… spinal surgery, placental surgery, blood transfusions… doing so many interventions… that I think clearly they’re a patient,” Lile says. “And if they’re clearly a patient, then they’re clearly a person.”
Lile notes that though the Supreme Court decided in Roe v. Wade that the preborn baby isn’t a person with rights, the very existence of prenatal surgery clearly shows that these babies are patients and, therefore, persons.
It has been a busy week or two for the powerful birth control lobby in the United States. Between the Midterm elections and Thanksgiving they have been rousing their faithful, sending messages to politicians and launching a new campaign that embraces all the gender-related issues beloved of progressives.
They have been encouraged by the blue ripple that brought a Democratic majority to the House, bearing a pink raft of new women members; but there are signs that their cause may have peaked and become irrelevant to the needs of millennial America. And the #MeToo experience gives the lie to the myth that their prize product has been a great liberation for women.
On Monday this week the new president of the Planned Parenthood Federation of America, Dr Leana Wen, started her first official day at work with a softball interview on CBS This Morning. Kindly hosts led her through a set of talking points about PPFA’s wonderful history of preventing unintended pregnancies and “saving lives”. The delicate subject of abortion – which accounts for by far the greatest part of the organisation’s “services” and has taken tens of millions of lives – was barely mentioned.
Abortion certainly contributes to controlling the number of births, but hiding it under the term “birth control” and selling it all as “basic health care” is deceptive. Former Planned Parenthood boss Cecile Richards alleges that Ivanka Trump and Jared Kushner told her that the Trump administration would increase funding for her organisation if it stopped doing abortions – a gesture she described as a “bribe.” Of course, it went down like a lead balloon. Since then the White House has adopted a rule that would require “physical as well as financial separation” between entities that receive federal funds for birth control and those that provide abortions.
So, when “Thanks, Birth Control Day” came around on Tuesday, it brought an appeal from PPFAs executive vice-president, Dawn Laguens, to sign a message to the Trump-Pence administration (copy to your Congressional Representative) calling for a stop to “attacks on accessing care at Planned Parenthood health centers” and to the roll-back of the Obamacare contraception mandate. The latter, because the White House last week confirmed its interim concessions to the conscience rights of some Christian institutions and a few other employers with sincerely held moral objections to covering abortifacient contraceptives in insurance plans.
“America just elected a pro-reproductive health care majority to the U.S. House and I urge you to join them in defending access to basic health care, like birth control,” the message asserts.
New names for old campaigns: Power to Decide, UNSTOPPABLE
It turns out that Thanks, Birth Control Day is “catalysed” annually by Power to Decide, “the campaign to prevent unplanned pregnancy,” once known as the National Campaign to Prevent Teen Pregnancy, but facing a shrinking market among teens. To support its political campaign the influential group commissioned a poll of 1000 Americans 18+ showing that 78 percent consider birth control (including abortion?) to be “a basic part of women’s health care.” Not men’s, note, even after 50 years.
Among the cute social media plugs, merchandise and celebrity testimonies (“Shay Mitchell loves being in total control over her reproductive health…”) on Power’s flash website there are some grateful messages from the team that runs it. Among them, three about freedom to travel, a couple about how expensive kids are, plus “My next baby will be a cat”, “Keeping me kid-free”, “Cause it’s my life and it’s my body,” and – my favourite — “Because all women should have control over their bodies” – as if she hasn’t handed the control over to technology so she doesn’t have to think about her body.
Planned Parenthood has also poured some of its ample profits into a creative campaign called “UNSTOPPABLE”, which sets birth control in the context of other progressive causes like paid family leave, equal pay, freedom from sexual violence and LGBT rights. In August the first of a series of videos was launched, the work of New York producer Tanya Selvaratnam, who told the UK Independent last month (in another puff piece for Planned Parenthood): “It’s a beautiful experience to bring together a vital organisation that’s more than a hundred years old with a lot of creative people who are honoured to support such work.”
And yet here the “thanks, birth control” story begins to unravel.
The victims include sex itself
Ms Selvaratnam is not a good advertisement for the boom years of birth control and Planned Parenthood. A Harvard graduate who moves in elite circles, she would not have lacked access to birth control. In fact, she was in her late thirties before she attempted motherhood, only to suffer repeated miscarriages. In 2014 she published a book, The Big Lie: Motherhood, Feminism, and the Reality of the Biological Clock, in which she complained about her generation being brought up in ignorance of their own fertility and its decline with age. She wrote:
“I didn’t think about that reality when I was growing up or even later during my college years when I was pondering my future. My generation was going to be different from that of our mothers. We were reaping the benefits of feminism. No one was going to tell us what to do, and we could control our bodies. But crucial information was missing, and we didn’t know to seek it out: We have a finite supply of eggs, and if we wait until we are in our late thirties to start having kids, many of us may be disappointed.”
The other thing Selvaratnam didn’t get was sexual relationships. She is divorced, though she could have been the innocent party in that. In 2016, in her mid-40s, she met the (now former) Attorney-General of New York, Eric Schneiderman, and began a sexual relationship with him. How that turned out became very public knowledge when The New Yorker published an exposeabout his abusive, violent behaviour with her and three other women earlier this year. Yet she stayed in the relationship for more than a year.
Although its details are unique, her story in its main features – marital failure, infertility, childlessness, abusive sexual relationships – has become a very common one in the era of mass birth control, as her own book and the #MeToo movement witness. To repeat: contraception and abortion may have liberated women for education, work – and, of course, travel – but it has played havoc with the things that matter most, to most women: marriage and motherhood.
Or did. There are signs that today’s young adults are losing interest not only in marriage but in sexual relationships, and even the sexual act itself. The Atlantic’s December issue was published online a couple of days ago with a cover story on a “sexual recession” that can be blamed partly on technology that is more magical than the pill: the internet — and porn.
Now, why would porn replace sex if it wasn’t more exciting than the real thing? Why would the Eric Schneidermans of the world want to act out throttling and slave-master routines with a beautiful woman who’s looking for love? Isn’t it because sex routinely divorced from the possibility of procreation is simply boring? Simply mechanical and pointless?
The idea that women should be thanking birth control for a culture marked by divorce, infertility, childlessness, involuntary celibacy, sexual aggression and violence is bizarre. Tanya Selvaratnam is smart enough to see through the birth control myth; she would be doing Millennials a real favour if she could turn her creative gifts towards exposing it, and leave Planned Parenthood to peddle its own dreary culture of meaningless sex.
MICAIAH BILGER NOV 19, 2018 | 8:00PM WASHINGTON, DC
A California mother displayed selfless courage earlier this month as a California wildfire approached the hospital where she had just given birth.
The San Francisco Chronicle profiled Rachelle Sanders and others who survived the horrible wildfire that has claimed dozens of lives and destroyed the homes of thousands more.
Sanders had just given birth to her third child Nov. 8 at the Feather River Hospital in Paradise when emergency response teams began evacuating the town, according to the report.
Her baby, Lincoln, was born via C-section because Sanders had a high-risk pregnancy, but he was healthy, she told the newspaper.
Not long afterward, Sanders said the evacuation order came.
According to the report:
They put Sanders in a wheelchair, the infant in her lap. A line of patients snaked from the emergency room to the ambulance bay. Orange glowed in the digger pines, needles aflame. Time was short, so the staff began loading patients into each other’s cars.
Sanders was hustled into a stranger’s white sedan. Her intravenous line hung from the rearview mirror. No seat belt, because of her incision. She slipped a mask over the baby’s mouth and nose and covered her own face with her pink hospital gown.
“Go with David,” they said.
The situation went from bad to worse as they got onto the roads. Traffic was jammed with people trying to escape, and the flames were getting close – so close that they melted the plastic taillights on the vehicle that David, an employee of the hospital, was driving, according to the report.
Some people jumped out of their cars and began to run away on foot, but that was not possible for Sanders.
The report continues:
As the flames roared closer, Sanders stroked Lincoln’s cheeks and made a pact with the stranger to her left.
“If it comes down to it, if you have to run, take the baby,” she said to David. “Leave me behind.”
Sanders would have sacrificed her life for her son in that terrifying blaze. Fortunately, she did not have to. Although her family lost their home in the fire, they all are alive and safe.
According to the report, David was re-routed back to the hospital, which narrowly escaped the fire. Eventually, Sanders said she and her son were transferred to another hospital and reunited with her husband and two older children.
She could have lost her life to give her son a chance at his, sacrificing everything for him. When others were panicking and fearing for their own lives, she thought only of her son. Sanders is a true heroine.
Issues in Law & Medicine, Volume 33, Number 2, 2018
A catholic hospital is decreasing the prevalence of disabilities in its Neonatal Intensive Care Unit (NICU) survivors. The hospital developed guidelines that encourage parents to allow their premature baby to die. Using extremely negative message framing, a physician guides the prospective parents to choose to forego an examination of their baby when it is born. Making this choice before birth ensures that no intervention or health care will be provided. The goal is to decrease the probability that the family will leave the hospital with a baby who will be disabled. The outcome is the death of a baby who may or may not have been disabled.
MICAIAH BILGER NOV 19, 2018 | 2:41PM WASHINGTON, DC
A nationally-recognized scientist who has testified in support of unborn babies is President Donald Trump’s new choice for the National Science Board.
Dr. Maureen Condic, an associate professor at the University of Utah who specializes in neurobiology, is widely known for her work on spinal cord repair, according to the Salt Lake Tribune. Earlier this month, Trump chose her to fill one of the 25 seats on the National Science Board.
“I’m just thrilled that it’s an opportunity to serve my country and the greater scientific community,” Condic said in response to the news.
She obtained her Ph.D. from University of California, Berkeley, and is a widely published scientist whose works have appeared in a variety of peer-reviewed journals.
Her work has been instrumental to the pro-life movement in its pursuit to protect unborn babies from painful abortions. In 2003, Condic testified before Congress that unborn babies have the capacity to feel pain as early as eight weeks.
“The neural circuitry responsible for the most primitive response to pain, the spinal reflex, is in place by 8 weeks of development,” she explained. “This is the earliest point at which the fetus experiences pain in any capacity.”
She asked lawmakers to pass the Pain-Capable Unborn Child Protection Act to protect unborn babies from the “cruel” and unnecessary pain of abortion.
“Imposing pain on any pain-capable living creature is cruelty,” Condic said. “And ignoring the pain experienced by another human individual for any reason is barbaric. We don’t need to know if a human fetus is self- reflective or even self- aware to afford it the same consideration we currently afford other pain-capable species. We simply have to decide whether we will choose to ignore the pain of the fetus or not.”
Abortion activists are attacking her nomination, as they have in the past with other pro-life individuals who Trump chose to help lead his administration.
Among the critics is Utah abortionist Leah Torres, who accused Condic of being “willfully ignorant or not up-to-date.”
“An adviser is not supposed to be using opinions,” Torres told the newspaper. “She does not heed the stance of the American College of Obstetricians and Gynecologists or that of maternal-fetal medicine and does not respect current scientific evidence.”
Condic defended herself against these accusations, telling the newspaper:
Condic responded Thursday, defending her position as being based on “undisputed, uncontested data” and a number of peer-reviewed scientific publications cited in her testimony. She said the consciousness argument isn’t the final conclusion because there are animals without the same brain structures as humans that can still detect pain. And a fetus at eight weeks, she added, shows “the most rudimentary form” of pain response.
“I’m not reporting bad science,” she said. “I’m reporting an interpretation of science that’s open to discussion.”
She also said the process for her appointment is confidential, but she doubts “seriously that any one position is driving this nomination.” Condic believes any researcher who says she supports “junk science” hasn’t read all of the literature on the topic.
“Pain is a really nuanced kind of thing,” she said. “The debate over fetal pain has very little to do with the evidence.”
“As the family goes, so goes the nation and so goes the whole world in which we live.” — Pope St. John Paul II
One of the most remarkable things about the Gospels is also one of the least remarked upon – perhaps, in part, because this most remarkable thing is more about what’s not in the Gospels than what is.
The biographers of the world’s “great men” love to trace the genealogy of their subjects’ greatness, relishing tales of their advanced aptitude as children and analysing the influence of their family and friends, the schools they attended, the books they read and the heroes they admired. Not so with the Gospel writers. Other than a handful of stories about Christ’s birth, and even fewer about his childhood, we are told almost nothing about his first 30 years. After one brief anecdote from when Christ was twelve, Luke says only that Jesus returned to His family home and “was subject unto” Mary and Joseph, and that Mary “kept all these things in her heart” (Luke 2:51). After this, the Gospel writers draw the veil.
I love to imagine what those 30 years in Nazareth must have been like. Jesus, Mary and Joseph must, on the outside, have resembled many other families. Mary must have gone to the market and haggled for a fair price for meat and produce, and labored long hours cooking and keeping the house tidy; as a carpenter, Joseph must have been a typical small businessman, taking orders from his customers, building and delivering the final product and receiving payment; Jesus, eventually, must have worked alongside Joseph in the workshop, probably attached to their home. On the Sabbath, they surely attended the Synagogue like every other Jewish family.
Ordinary…and yet the furthest thing from ordinary. For what warmth, what peace, what love, and what full, prayerful silence must have reigned in that little home in Nazareth! I have often been struck by the warmth and welcome I find when I enter the homes of close, loving families. In such homes, love is made tangible, and one catches a glimpse of how humans were made to live alongside one another. But, if this is so in the case of a family of ordinary sinners, how much more must it have been the case with the Holy Family!
If a family peacefully praying the rosary in the candlelight of the advent wreath is a little foretaste of heaven (and it is!), how much greater must have been the peace when Jesus, Mary and Joseph spent time together in prayer. How beautiful must have been their conversations as they gathered for refreshment around the dinner table. How welcome and fortunate their friends and family must have felt when they visited the Holy Family’s humble dwelling and were privileged to observe and participate in the harmony of that home.
“Through God’s mysterious design, it was in that [Holy] family that the Son of God spent long years of a hidden life,” writes Pope St. John Paul II in Familiaris Consortio. “It is therefore the prototype and example for all Christian families. It was unique in the world. Its life was passed in anonymity and silence in a little town in Palestine. It underwent trials of poverty, persecution and exile. It glorified God in an incomparably exalted and pure way” (¶86).
Love Begins in the Family
The point is this: Nothing that Christ did was by accident. Christ chose to spend the first three decades of his life, not in the kind of conspicuous preparations for greatness that we might expect from a world-changing political or religious leader, but rather quietly serving his earthly parents in their home. The only preparation that he received that we know of, was an outwardly ordinary life lived in an extraordinary way within a family. And it was there that “Jesus grew in wisdom and stature, and in favor with God and man” (Luke 2:52).
The conclusion is obvious: If the Holy Family glorified God “in an incomparably exalted and pure way,” then every family, insofar as it imitates the Holy Family, also exalts God in a similarly lofty way.
In the last century we were fortunate to have two larger-than-life saints – Pope John Paul II and Mother Teresa – who constantly drew our attention to the dignity and value of the family, and its fundamental importance for the common good. St. Mother Teresa’s favored approach to transforming the world was not ambitious political or social reform, but rather practicing daily self-sacrificial love towards those closest to us. And as she never tired of saying, this begins in the family. “The way you help heal the world is that you start with your own family,” she insisted. And again: “What can you do to promote world peace? Go home and love your family.”
If this seems simplistic, it is only because the past century and a half we have become enamored with the search for vast technological solutions to our problems, not realizing that the worst of our problems are not a consequence of bad technology, but the failure to love. Modern technology has alleviated much suffering, but bad technology was not responsible for the Holocaust or the Gulags or the killing fields of Cambodia. Perhaps you remember the idealistic doctor’s pithy saying in The Brothers Karamazov. “The more I love humanity in general,” he lamented, “the less I love man in particular.” To such men as this doctor, St. Mother Teresa replied: “It is easy to love the people far away. It is not always easy to love those close to us. Bring love into your home, for this is where our love for each other must start.”
The family is – or should be – the school of love. If the parents show one another love and create a culture of love that is imbibed by the children, then this interior love spreads outwards. For as St. Thomas Aquinas noted, “good is self-diffusive.” It spreads. Love begins in the family, but it does not stop there. “The problem with our world is that we draw the circle of family too small,” said St. Mother Teresa. The nuclear family is where we learn to be family, which is to say, we learn to love freely and unconditionally. With this knowledge in hand, we are then free to draw the circle of the family larger and ever larger. Children who have learned to love in a family, leave the home and go into their schools, universities, offices, clubs, and churches equipped with the knowledge of how to treat others as if they, too, are family – as indeed they are.
“The family is the first and fundamental school of social living,” wrote Pope St. John Paul II in Familiaris Consortio. “[A]s a community of love, it finds in self-giving the law that guides it and makes it grow. The self- giving that inspires the love of husband and wife for each other is the model and norm for the self-giving that must be practiced in the relationships between brothers and sisters and the different generations living together in the family. And the communion and sharing that are part of everyday life in the home at times of joy and at times of difficulty are the most concrete and effective pedagogy for the active, responsible and fruitful inclusion of the children in the wider horizon of society” (¶37).
Again, and even more succinctly, he said: “The fostering of authentic and mature communion between persons within the family is the first and irreplaceable school of social life, and example and stimulus for the broader community relationships marked by respect, justice, dialogue and love” (¶43).
The Family Under Attack
The Catholic Church has always affirmed the importance of health of the family, not just as an intrinsic value, but as the necessary precondition for the health of society at large. The family, says the Catechism, is “the original cell of social life” (CCC, ¶2207). Again: “Authority, stability, and a life of relationships within the family constitute the foundations for freedom, security, and fraternity within society” (CCC, ¶2207).
The framework, in today’s world, for public discourse is often focused on the rights and freedom of the individual. The Catechism of the Catholic Church, however, seeks to re-orient our view, looking at the individual as a member of a family, and at the family in relation to society. The Catechism speaks about the duties of children and of parents, of citizens and of civil authorities. It emphasizes the social dimension of human existence and provides the required antidote to an increasingly fragmented and fundamentally anti-social view of humanity.
One of the great challenges of our day, especially in secularized societies, is the attempt to change laws which, over centuries, even millennia, have recognized the plan of God for marriage and family as founded in the created order. “The vocation of marriage is written in the very nature of man and woman as they came from the hand of the Creator,” says the Catechism (CCC, ¶1603). Further: “In creating man and woman, God instituted the human family and endowed it with its fundamental constitution” (CCC, ¶2203).
Tragically, and disastrously, over the past century and a half we have witnessed a concerted attempt by ideologues to either entirely eradicate the institution of the family (an explicit goal of Communism), and, when that failed, to fatally undermine its stability (divorce and “free love”) or fundamentally transform its nature (contraception, same-sex “marriage” and “polyamory”). The results have been catastrophic: an unprecedented spike in divorce, children traumatized by being abandoned by one or the other of their parents, a huge increase in fatherless households and poverty among single-mother homes, huge increases in public spending on welfare, an increasingly hostile war of the sexes, an epidemic of STDs, and, of course, the deaths of millions of unborn children to the violence of abortion.
That’s why I was so delighted recently to hear Fox News Host Tucker Carlson using his highly visible platform to draw attention to the value of the family. “A country without strong families is a weak country,” he noted. “It is a volatile place, a chaotic place. It’s a place susceptible to political demagoguery.” Carlson expressed his fear that this is precisely “what America is becoming,” and exhorted: “If you want to stop that slide, support families. It’s that simple.”
While the ways in which the Democratic Party attacks families are obvious, Carlson also took Republicans to task. “If your supposedly conservative economic program doesn’t make it easier for young people to get and stay married and have kids, how is it really conservative?” he asked. “If couples are too poor to have children and you’re not helping, why should I as a conservative vote for you?” And: “Supporting marriage and children is the best, maybe the only way for Republicans or any of us to save the country.”
To this, I can only say, Amen! One of the great tasks of government is to protect the integrity and stability of the family and to preserve its freedom.
There isn’t space in this column to speak of all the ways that we can work to respond to the many and growing assaults on the family today. However, there is something that we can all do. It is reflected in Pope St. John Paul II’s famous cry in Familiaris Consortio: “Family, become what you are”! Let all families renew their resolve to be the school of love they are called to be. Let every family look for inspiration to the Holy Family, and model themselves on that great emblem of the union of human and divine love.
And, of course, we can all pray for the family. In concluding, I would like to ask you to join me in reciting this prayer of Pope St. John Paul II for the family:
Lord God, from You every family in Heaven and on earth takes its name.
Father, You are love and life. Through Your Son, Jesus Christ, born of woman, and through the Holy Spirit, the fountain of divine charity, grant that every family on earth may become for each successive generation a true shrine of life and love.
Grant that Your grace may guide the thoughts and actions of husbands and wives for the good of their families and of all the families in the world.
Grant that the young may find in the family solid support for their human dignity and for their growth in truth and love.
Grant that love, strengthened by the grace of the sacrament of marriage, may prove mightier than all the weaknesses and trials through which our families sometimes pass.
Through the intercession of the Holy Family of Nazareth, grant that the Church may fruitfully carry out her worldwide mission in the family and through the family.
We ask this of You, Who is life, truth and love with the Son and the Holy Spirit. Amen.
MICAIAH BILGER NOV 16, 2018 | 11:13AM LONDON, ENGLAND
The extent to which the medical community now pushes abortion for unborn babies with disabilities is alarming.
Jordan Squires, of Middlesborough, England, told the Daily Mail that she was infuriated when doctors pressured her to abort her unborn son because he might have Down syndrome.
Squires refused, and she is so glad that she did. Her son Jay, now a toddler, was born healthy.
The pressure to have an abortion began at Squires’ 12-week pregnancy scan. She said she realized something was wrong when the medical staff took her and her partner, Johnathan, into a room after the ultrasound.
“They told us that the baby was highly likely to have Downs Syndrome due to the large amount of fluid that was placed high on the back of his neck,” Squires said.
“Straight away I was told that they advised terminating the pregnancy without giving us any other options or support,” she continued. “We were so angry … There was no way I was going to do that, we had waited so long for this baby and we would love our child regardless of the disability.”
The couple refused an amniocentesis test, which would have given them a better idea if their son had Down syndrome, because it also would have put his life at greater risk, according to the report.
Squires continued with her pregnancy, thinking her son would be born with Down syndrome. But to her great surprise, Jay was born healthy, weighing 9 pounds, 2 ounces, the report states. He now is a toddler.
Thinking about mothers in similar situations, Squires said she understands why some choose abortion: Medical professionals often encourage it.
“I was furious that they were encouraging people to do that and if it had been someone different then they could of been persuaded by the doctors, then they would have ended a healthy pregnancy,” she said.
The young mother urged other families to get a second opinion if they feel pressured to have an abortion.
“There was so much pressure on us to have a termination with no offer of us having support or advice should we want to carry on,” Squires said. “When you’ve been told your baby has a disability you’re obviously in a vulnerable position and it can be easy to make quick rash decisions.
“We could have lost a healthy baby if we had decided otherwise,” she continued.
Many parents succumb to the pressure. In Iceland, nearly 100 percent of unborn babies with Down syndrome are aborted. CBS reports the rate in France was 77 percent in 2015, 90 percent in the United Kingdom and 67 percent in the United States between 1995 and 2011. Some put the rate as high as 90 percent in the United States, but it is difficult to determine the exact number because the U.S. government does not keep detailed statistics about abortion.
Research published in the Journal of the American Medical Association suggests that manywomen are not receiving adequate counseling about prenatal testing for Down syndrome and other disorders.
Stories like Squires’ help to expose the discrimination and provide hope to families, who are wrongly led to believe that killing their sick child is their best option.
COLUMBUS, Ohio, November 15, 2018 (LifeSiteNews) – The Ohio House of Representatives voted Wednesday to pass legislation that would ban the vast majority of abortions upon detection of a fetal heartbeat.
House Bill 258 would ban committing an abortion on any preborn baby with a detectable heartbeat, except in cases of a “substantial and irreversible” physical threat to the mother. Any physician that violates the statute would face up to a year in prison. Preborn babies’ hearts finish forming around 7-8 weeks into pregnancy.
Heart beat bill clears Ohio House 58-35. Not a veto-proof margin.
HB 258 now goes to the overwhelmingly-Republican state Senate, where Senate President Larry Obhof says he has the votes to pass it, the Cincinnati Enquirerreports. He hasn’t decided whether or not to hold a vote, however, because the bill is opposed by Ohio’s ostensibly “pro-life” Gov. John Kasich.
Kasich vetoed a heartbeat abortion ban in 2016, instead signing a late-term abortion ban and arguing the state would only lose an inevitable lawsuit defending the stronger law, gaining nothing but legal bills. He’s expected to do so again, and the bill’s 58-35 margin isn’t large enough to override a veto.
If the outgoing governor again vetoes the bill and lawmakers can’t muster enough votes to override it, pro-lifers will have another chance when Governor-elect Mike DeWine, previously the state’s attorney general, takes over in January. DeWine, who in his previous role defended the states’ efforts to defund Planned Parenthood, has already pledged to sign the bill.
“Right to Life of Greater Cincinnati has supported Ohio’s human heartbeat protection strategy since efforts began in 2011. In the years since, these efforts have educated many on the true nature of abortion’s toll on women, men, and their unborn children,” the group said Wednesday. “Establishing human heartbeat protections in Ohio is a historic opportunity for those committed to the cause of life.”
Currently, the strongest state-level protections for preborn babies are Iowa’s heartbeat abortion ban and Mississippi’s 15-week abortion ban, both of which are currently tied up in the courts. The Ohio measure is all-but-certain to face a similar legal challenge, but several pro-lifers, such as Rep. Steve King of Iowa, argue that now is the time to press such a legal battle.
The U.S. Supreme Court has repeatedly upheld Roe v. Wade since 1973 and has not yet upheld any pre-viability abortion bans, but heartbeat supporters argue that President Donald Trump’s nomination of Justice Brett Kavanaugh to replace the pro-abortion Justice Anthony Kennedy has shifted the court’s ideological balance to the point where the pro-life case has a fighting chance.
It’s not known how Kavanaugh or Trump’s first nominee, Justice Neil Gorsuch, will vote on Roe. Both alarmed some pro-lifers by expressing significant respect for Roe’s status as “precedent,” though other pro-lifers argued they were merely phrasing their answers diplomatically to navigate a narrowly-divided Senate confirmation process.
WASHINGTON, D.C., November 14, 2018 (LifeSiteNews) – Trump administration health officials are meeting with national pro-life leaders in hopes of resolving concerns over the pro-life administration’s continued funding of medical research using tissue obtained from aborted babies.
In August, a notice from the U.S. Food and Drug Administration (FDA) surfaceddetailing a contract to the fetal tissue procurement firm Advanced Bioscience Resources, Inc. (ABR) to acquire “Tissue for Humanized Mice.” The tissue was meant to give mice a “humanized” immune system for the purpose of drug testing.
Forty-eight pro-life leaders representing LifeSiteNews, the Center for Medical Progress, Susan B. Anthony List, Priests for Life, Operation Rescue, and other groups sent a letter to Health and Human Services (HHS) Secretary Alex Azar on September 11 demanding the contract’s cancellation. Eighty-five U.S. House members sent a letter to FDA commissioner Scott Gottlieb, as well.
The administration terminated the contract in September and promised to review all remaining research involving fetal tissue, but concerns remained over nearly $100 million in tax dollars that continued to pay for other research using tissue and organs from aborted babies.
Last week, the administration began to arrange meetings to discuss cancelling the remaining projects, Politicoreported Tuesday. Both sides of the issue will be represented, with scientists who use fetal tissue invited to defend their work and pro-life groups such as Susan B. Anthony List invited to critique it.
“HHS is holding multiple listening sessions with various stakeholders [like] scientists, pro-life groups, ethicists, on this topic,” an HHS spokesperson confirmed to to Politico. One such session has been scheduled for this Friday, and is slated to last an hour. Among the groups attending are the American Society for Cell Biology, Federation of American Societies for Experimental Biology, International Society for Stem Cell Research, and the Society for Neuroscience.
“HHS leadership is inviting a select group of experts from diverse backgrounds to obtain their individual views on the use of fetal tissue in biomedical research and development,” an invitation obtained by Politico states. It reportedly tells attendees to prepare not only a defense of fetal tissue, but suggestions for alternatives.
Assistant Secretary for Health Brett Giroir will be leading the review and has been tasked with issuing final recommendations afterward. He is reportedly “enthusiastic” about finding ethical alternatives to fetal tissue.
The FDA’s continued funding of aborted tissue research stands in stark contrast to the Trump administration’s robust pro-life record, which has included various pro-life appointees, defunding Planned Parenthood abroad and partially defunding it at home, and working to protect conscience rights and religious objections against participating in abortion or contraception.
Preliminary research provides evidence that the use of birth control pills is associated with an increased frequency of mind wandering in women. The study, published in the journal Psychoneuroendocrinology, could help explain why women face higher risks of depression and other mood disorders.
“Oral contraceptives (OC) are the most common type of contraceptive method used in industrialized countries. It is estimated that one woman out of four who are of reproductive age currently use OC and more than 80% of women report to have used it at some point in their lives,” said study author Catherine Raymond of the University of Montreal
“Still, around 10% of OC users report experiencing mood side effects (e.g., depressive symptoms, irritability, mood swings, etc.). Recent large studies also suggest that OC use is associated with the onset of major depression and antidepressant intake.”
“What we wanted to assess in the current study was whether OC use in healthy women was associated with cognitive processes associated with depression in women who do not (or not yet!) suffer from depression. Mind wandering is one of such cognitive process. It refers to all of the thoughts that one has that are not associated with the task at hand. Studies on the subject show that the more you mind wander, the less happy you are,” Raymond said.
“Furthermore, recent studies suggest that mind wandering might be a precursor for cognitive vulnerability among individuals who are at higher risk for mood disorders.”
The researchers compared 28 women currently using OC, 14 naturally cycling women in the luteal phase of their menstrual cycle and 29 men. All of the participants were between the ages of 18 and 35. The researchers also excluded women who had used antidepressants or previously received a psychiatric diagnosis.
Raymond and her colleagues found that women currently using OC reported significantly greater frequency of mind wandering than men. Naturally-cycling women, on the other hand, did not differ from men.
In particular, women currently using OC tended to report having less attentional control — meaning they had trouble concentrating. But they had similar levels of depressed and guilt oriented thoughts and positive constructive daydreaming as the other groups.
“What we found is that healthy women using OC present increased mind wandering frequency (which means that they mind wander more often on a daily basis) as opposed to naturally cycling women and men. Our findings are important in showing that utilization of OC in women could explain some of the sex/gender differences in vulnerability to various mental health disorders,” Raymond told PsyPost.
“Indeed, it was shown many times that women are twice as vulnerable as men to suffer from stress related psychopathologies such as depression. Given previous studies showing that mind wandering can confer increased cognitive vulnerability to mood disorders, our results suggest that an increase in the frequency of mind wandering in OC users could serve as a marker of risk for depressive disorder in women.”
The study — like all research — includes some limitations. Future research could benefit from longitudinal designs and larger sample sizes.
“As for every correlational study, the question of ‘the chicken or the egg’ remains. Therefore, we still wonder whether OC intake causes an increase in mind wandering, or whether women that mind wandering more frequently present an increased tendency to use OC,” Raymond explained.
“Causational studies (where we would ask women who have not used OC before to use it and measure mind wandering before and after cessation – for example) would be necessary to fill this gap in the literature.”
It is still unclear what effects OC use has on female brain development.
“Not only do adult women use OC, we know that adolescent girls use it more and more. Preliminary data in animal models show that the chronic secretion of some hormones (such as cortisol, for example) during brain development (which ends around 21 to 25 years old in humans) may be problematic for the development of some brain regions that are necessary to regulate the stress response in adulthood,” Raymond said.
“Since synthetic sex hormones that are contained in OC also access the brain, we think that more studies are needed to understand the effect of OC on the developing brain.”
November 5-11, marked the first ever Post-Birth Control Syndrome Awareness Week. Hosted by Dr. Jolene Brighten, the effort sought to help women “make informed decisions about birth control—whether you want to get on, get off or reverse/prevent side effects.”
Dr. Brighten was on the Pill for 10 years before she realized the damage she was doing to her system. Her moods were unreliable and she’d developed acne from her prescription. She was already trained in nutritional biochemistry and was on her way to a medical degree. Despite her doctor not taking her concerns about her side effects seriously, she knew there had to be another way.
This week, she hosted over 50 hours of online presentations that explore why the Pill does what it does to women’s bodies and how we can counteract those side effects. Brighten believes, “there’s a reason you’re feeling fatigued, frazzled, irritable and struggling with your hormones. There is a root cause to autoimmune disease, PMS, fertility issues, brain fog, chronic pain, and digestive disorders.” Treating the symptoms doesn’t remedy the issue, and chances are that an unresolved issue will continue to rear its head in other ways down the line, perhaps most painfully when a woman is trying to conceive.
The Pill—as well as the patch, implant, shot, and IUDs—work by manipulating a woman’s hormones. Especially when ingested for years at a time, the damage caused can be challenging to undo. The symptoms that triggered the prescription may still be present, and new issues like Pill-induced acne now need to be managed as well. Some women have an easy transition and their period resumes within three months. But for others, it can take time for the body to regulate. Still, conventional medicine doesn’t always recognize this as a real problem.
Post-birth control syndrome can present itself in a range of symptoms, experienced four to six months after going off of hormonal birth control: headaches, hair loss, libido loss, mood swings, insomnia, depression, chronic yeast infections and UTIs, acne and rashes, irregular periods, and difficulty conceiving. According to Dr. Brighten, “It is well documented that birth control leads to nutrient depletions, mood symptoms and scarier side effects like cancer, blood clots, strokes, and heart attacks. And women round the world have complained of post-birth control syndrome symptoms since the introduction of hormonal birth control.”
It’s unfortunate that the struggle of going off the Pill has been overlooked for as long as it has. Trading symptoms for side effects is not a winning solution.
Thankfully, as more and more women turn away from the Pill, their concerns are being taken more seriously, and more resources are becoming available in femtech and beyond. Post-birth control syndrome can be treated with a combination of good nutrition (restoring the key nutrients the body lost while taking the Pill), improved sleep patterns, supplementation, stress reduction, and a particular focus on the gut and liver. For those who have looked to the Pill for contraception, there are plenty of more natural, healthier, evidence-based options to track your fertility, as well as your overall health. Charting your cycle can take a variety of forms, but all of the modern charting methods have one thing in common: no harmful side effects, and a healthier, stronger you.
The road to a healthier, happier, hormone-balanced life is no longer one any woman needs to walk alone.
In a lyrical essay originally published in Crisis Magazine, Catholic philosopher and Senior Fellow of Human Life International, Donald DeMarco, Ph.D., poignantly paints the stark division between the pro-life worldview, and the worldview espoused by the Culture of Death. Invoking T.S. Eliot’s seminal poem The Waste Land, Dr. DeMarco suggests that Eliot captured the essential characteristics of the Culture of Death.
In such a culture, death is presumed to have the final say, and as such is the measure of all things: life leads to death, and then no more. Given this, life is suffused with a sense of bleak hopelessness, a “tale told by an idiot…etc.” Children – the most tangible sign of a society’s hope for and investment in the future – are a thing to be prevented through contraception, sexuality is reduced to the tawdry and transactional, suicide ever lurks on the peripheries, and beauty and fertility appear as things painful and threatening (“April is the cruellest month.”).
“Children – the most tangible sign of a society’s hope….”
Against this bleak pessimism, Dr. DeMarco sets up the testimony of an array of poets who saw beneath even the worst of life’s struggles and sorrows a rich ore of beauty and meaning, and who celebrated life. Often inspired by the Christian gospel, they presumed that resurrection, and not death, is reality’s final word, and that the apparent tragedy of death is but a preparation for resurrection. Death’s finality is only an apparent finality. “Life is real! Life is earnest! And the grave is not the goal,” exclaimed Longfellow.
“The label ‘pro-life’ hardly begins to do justice to the rich poetic expressions of life,” concluded Dr. DeMarco. “Yet ‘the fine art of Life,’ as the contemporary poet, Edwin Leibreed has said, ‘is to make another Soul vibrate with a song of joy.’ God is the author and paragon of life, which, in its pilgrim form, becomes a challenge, an adventure, a sublime and luminous possession, a great gift, an inexhaustible treasure, and the way to heaven. We should live out our lives with the full understanding of how infinitely valuable life is.”
The Richness of the Term “Pro-Life”
I admit that such speculations can seem somewhat far removed from the pragmatic political purpose that the label “pro-life” was designed to serve. I am sympathetic to the argument that we ought not excessively to broaden the meaning of the term “pro-life,” so that it no longer immediately testifies to our opposition to the deliberate slaughter of unborn children. There is a risk that by meaning everything, the term “pro-life” will come to mean nothing. And indeed, we have seen some in the “liberal” wing of the Church attempt to co-opt the term to serve their own questionable political purposes.
On the other hand, the pro-life movement and its founders and shapers selected the term “pro-life” in part precisely because they recognized that the battle against baby-killing is not just a battle against this one particular form of evil, but against a whole worldview – a worldview that, in some real way, favors and celebrates death. I am not one of those who necessarily gets offended if someone refers to me as an “anti-abortion activist.” I most certainly am someone who is against abortion, and there is nothing shameful about that. Indeed, it is a badge of honor. On the other hand, I do lay claim to the admittedly more imprecise “pro-life” label, precisely because my opposition to abortion is an expression of a more comprehensive worldview that not only precludes the killing of innocent unborn babies, but also rejects the spiritual and psychological root causes that would lead anyone to desire to kill innocent unborn babies in the first place!
More than anyone else, St. Pope John Paul II pointed towards the common thread uniting the abortion holocaust to other forms of evil in our modern world, including not just the direct attacks on life itself, but attacks against the moral truths and societal structures designed to protect life: above all the moral truths pertaining to sexuality, and the structure of the family. The abortion holocaust is only one manifestation of this Culture of Death. The Culture of Life, on the other hand, is one in which the absence of abortion is merely the natural outflowing of a radically life-affirming worldview.
If Dr. DeMarco’s description of the pro-life worldview seemed excessively poetic, consider this alternately gorgeous and chilling passage from St. Pope John Paul II’s homily on the Solemnity of the Assumption of the Blessed Virgin Mary in 1993:
This marvelous world – so loved by the Father that he sent his only Son for its salvation (Cfr. Io 3,17) – is the theater of a never-ending battle being waged for our dignity and identity as free, spiritual beings. This struggle parallels the apocalyptic combat described in the First Reading of this Mass. Death battles against Life: a “culture of death” seeks to impose itself on our desire to live, and live to the full. There are those who reject the light of life, preferring “the fruitless works of darkness” (Eph 5,11). Their harvest is injustice, discrimination, exploitation, deceit, violence. In every age, a measure of their apparent success is the death of the Innocents. In our own century, as at no other time in history, the “culture of death” has assumed a social and institutional form of legality to justify the most horrible crimes against humanity: genocide, “final solutions”, “ethnic cleansings”, and the massive “taking of lives of human beings even before they are born, or before they reach the natural point of death.”
Diabolical child sacrifice extends to ancient times. The Canaanites sacrificed thousands of 1-2 month old infants to the false god Moloch or Baal.
The sainted pope took the same approach in his deservedly famous pro-life encyclical Evangelium Vitae. That incisive exploration of the cultures of life and death is framed within an initial discussion of the profound value and dignity and destiny of human life. Compared with the subsequent ethical analyses of specific moral acts such as abortion, euthanasia, artificial reproductive techniques, etc., this discussion may seem excessively abstract. But St. Pope John Paul II knew that just as laws are downstream from culture, so is culture downstream from theology. A Culture of Life cannot and will not begin merely with the correct laws, as important as they are. It can only flow out from the correct theological and metaphysical principles: our concepts of God and man.
“Man is called to a fullness of life which far exceeds the dimensions of his earthly existence,” he writes at the beginning of Evangelium Vitae, “because it consists in sharing the very life of God.”
The loftiness of this supernatural vocation reveals the greatness and the inestimable value of human life even in its temporal phase. Life in time, in fact, is the fundamental condition, the initial stage and an integral part of the entire unified process of human existence. It is a process which, unexpectedly and undeservedly, is enlightened by the promise and renewed by the gift of divine life, which will reach its full realization in eternity (cf. 1 Jn 3:1-2). At the same time, it is precisely this supernatural calling which highlights the relative character of each individual’s earthly life. After all, life on earth is not an “ultimate” but a “penultimate” reality; even so, it remains a sacred reality entrusted to us, to be preserved with a sense of responsibility and brought to perfection in love and in the gift of ourselves to God and to our brothers and sisters.
The Bleak Culture of Death
How vastly different is this transcendent optimism from the bleak pessimism of various popular philosophies that have so enamoured and ensnared so many minds in the past century: the nihilism that proclaimed that God is dead and that life holds no meaning; the existentialism that proclaimed that meaning is something that humans futilely wrest from a fundamentally “absurd” universe; the communism that eschewed hope in a transcendental paradise and that murdered over a hundred million people in the name of creating an earthly one; the fascism that proclaimed the value of the master race and the worthlessness of all others; the eugenics that proclaimed the dominance of the “fit” and the worthlessness of the “unfit.” And on and on.
Our own age is still haunted by the spectres of each of these hopeless ideologies, and many others created since. Indeed, one is astonished, at times, at the extent to which simple, wholesome, fruitful, productive, happy normalcy is looked down upon and scorned as “old-fashioned” and unsophisticated, while all manner of hopelessness, sterility, deviancy, and bleakness are openly celebrated as the only “sophisticated” and praise-worthy things.
I think it safe to say that we saw this dynamic played out in the recent election. There are, no doubt, many things that one could criticize about the Republican Party as it exists today. And yet, it is difficult to wrap one’s head around the furious apostolic zeal with which the Democratic party systematically advocates things destructive, evil, and hopeless. Whatever one thinks of the national spectacle that was the nomination hearings of Supreme Court Justice Brett Kavanaugh, for instance, there is no doubt in my mind that a great deal of the irrational hysteria manifested in much of the media coverage and in public protests was directly traceable to one issue: abortion. The Democratic Party has openly and explicitly committed itself to defending the right to kill – murder – unborn babies in just about any imaginable circumstance and for just about any reason. With the nomination of Kavanaugh, Democrats were petrified that their fabricated Constitutional “right” to abortion would be taken from them, and no measures were too extreme to prevent that from happening.
Recently the Trump administration reported its intent to return to the scientific, text-book definition of “sex” – contrary to the Obama administration’s novel use of an entirely subjective definition – was greeted with outrageous claims that Trump was “erasing” the existence of transgender people. This was only the most recent indicating that the Democratic party has wholly allied itself with an extremist, tyrannical and tawdry conception of LGBT ideology and sexual ethics, in which objective scientific truth is subordinated to subjective feelings; in which no age is too young to introduce children to gross sexual immorality (i.e.drag queens reading to children at public libraries); in which the nuclear family is perceived as an oppressive and outmoded institution to be replaced with fluid “open” and “polyamorous” unions; in which vast public spectacles are devoted to celebrating anonymous, unnatural, sterile, promiscuous sex; in which the quiet pleasures of true romance and life-long commitment are subordinated to the unmitigated, hedonic search for pleasure; and in which even gentle expressions of conscientious opposition are to be subject to crushing retribution.
We are told that all these things are to be accepted in the name of “tolerance” and “love” and “freedom.” But in truth, one finds little of any of these among their advocates. On the other hand, when I attend pro-life events such as the “March for Life” in Washington, D.C., I always find a super-abundance of all three. Rather than the vulgar outrage that characterizes so many pro-abortion events, at the March for Life one finds a hopeful, joyful optimism. There are families. There are children. There is an abundance of common decency. And this is because most pro-life activists are not merely against abortion, but because their opposition to abortion is the natural outflowing of a wholly different worldview. Even if they do not realize it, they are giving voice to a fundamental metaphysical conviction that life is stronger than death, and not the other way around. Death is not the bleak conclusion of all things, but rather the prelude to resurrection.
March for Life, 2018
To be pro-life then, most certainly involves conscientious, explicit activism targeted at ending abortion, and all other systematic attacks on human life in our society. However, it also involves witnessing to what St. Pope John Paul II called the Gospel of Life, without which our pro-life efforts are doomed to long-term failure. In addition to pro-life activism, the lay faithful are called to deeply culturally transformative activities such as building a community of loving families, providing an authentic Christian presence in the world rooted in prayer and contemplation, charitable service and evangelization, artistic and liturgical renewal, etc.
The laity’s life is called to integrate all activities into one meaningful whole – to give witness in the ordinary of one’s day in an extraordinary manner. The Culture of Death feeds off an anti-Gospel. The only truly long-lasting antidote to this anti-Gospel is the true Gospel, and the instantiation of that Gospel as a lived reality in our daily lives, by which the culture is transformed from a Culture of Death to a Culture of Life from the very roots up.
Sharran Sutherland’s tenth pregnancy was going well. Early ultrasound images showed a healthy baby and placenta. At 11 weeks, Sutherland saw her baby’s heartbeat blinking on the screen. But a couple of weeks later, it was gone.
Sutherland’s doctor didn’t want her to miscarry the baby at home. She could hemorrhage. The doctor advised a dilation and curettage, or D&C. But she knew what that meant. “I was not okay with that,” she told The Stream in an interview.
“So, I said, ‘No, I want to deliver my baby.’”
Not Medical Waste
Her doctor became annoyed. Why wouldn’t she have a D&C? “I don’t want my baby to come out in pieces,” Sutherland told her. “I want to see him, I want to hold him.”
Although she felt that a funeral would be too extreme, she wasn’t going to let the doctor throw him away, either. The doctor referred to him as “medical waste.”
“I was angered by that,” she recalled. “I was like, there’s no way I’m letting them dispose of [him] as medical waste. [He’s] not medical waste.”
Help us champion truth, freedom, limited government and human dignity. Support The Stream »
She gave birth to the baby boy, whom she named Miran, and got to hold him. She thought he’d look like the images in books about pregnancy. “I was amazed at how he looked like a little baby. There were no words to describe how I felt.” She saw his gums, his tongue, every tiny part of him. “I was curious. I thought, ‘Holy cow, this is a full baby.’ I thought he was so beautiful and I was so in awe over how he was made. How he was formed.”
Sutherland took pictures and even captured his footprints and handprints. Because she also showed him to his siblings. She wanted her daughters to see that he was a baby. She wanted her sons to recognize life. If they were ever in a situation where they were thinking about an abortion, she wanted them to know the truth. “They were in awe. It was a valuable lesson.”
His Soul is in Heaven
The hard part was getting ready to bury him. “I knew he was gone — his soul is in heaven — but I felt like it gave me time that I was never going to get to spend with him again.” She is thankful for the memories the time with him gave her.
Not long after, a friend asked if she could share the pictures of Miran and Sutherland’s story on social media. Sutherland agreed. If someone was contemplating aborting her child and sees Miran’s image, perhaps they would choose life.
The images stirred up viewers. Most readers thanked Sutherland for sharing the pictures. Others were quite critical of her decision. But others shared their stories with her. Two others decided against abortion after seeing her son. Miran had made an impact.
In early October, Sutherland was praying for her children. When she got to Miran, she began thanking God for the time she had with him. She asked God, “How do I honor him and bring You glory?” She felt God prompt her to help young pregnant moms who face consequences of choosing life: those who don’t have anywhere to go or are otherwise estranged from their families. She’d call it “Miran’s House.”
She’s got a lot going on with her children and sports and other responsibilities. But she told her family about it. “We’ll just see what God does,” she said.
He Was Real
Sutherland thought she was past the grief. She thought she’d handled it well. Then came the day when, at her daughter’s sports game, she saw a woman holding a newborn. “I was crying. I thought, ‘I should be holding Miran.’”
When his due date came, she wanted some recognition for him as a baby. “He’s my son. He was my son, he was my baby and he was real.” So she shared the original post again. She asked people to share with someone who might be thinking about getting an abortion.
Within days, she couldn’t keep up with the social media notifications. There were kind words. There were harsh words. Then there were vile words. There were posts claiming Miran was a plastic doll. There was even a post of Miran’s face on an alien body. “I was drained physically and exhausted,” she said. Contrary to what some said, “I wasn’t trying to shame women who’ve had an abortion.” She just wanted to spread awareness about babies’ development in the womb.
She recognized the enemy, however. “[Evil] is freaking out that [I’m] shining a light on truth, and it’s trying to shut it off.”
Saving Lives
Between all of the posts about Miran, responses have been in the thousands. The posts and private messages from women surprised her. Many women shared their personal stories of abortion or miscarriage. Doctors told them it wasn’t a baby. It was just a clump of cells. It wasn’t a human.
Sutherland didn’t get angry at the women. She got angry for the women — for how the doctors treated them. “If a woman is going to have an abortion, she should be able to see what she’s doing, not be lied to and told it’s just tissue, it’s just a clump of cells, it’s not human. [The women] don’t understand what they’re doing.”
She began to realize that these women have been kept in the dark about early pregnancies and the development of their babies. “I’m willing to share my story if it’s going to save lives,” said Sutherland.
She’ll never believe that Miran’s death was in vain. “I know I’m going to see him again. … If Miran’s purpose was just to show the world in a different way of what a baby looks like, I’m glad. I’m thankful God chose me. … Miran’s life has touched so many people. How incredible it is that he’s already saved two lives?”
COLUMBUS, Ohio, May 23, 2018 (LifeSiteNews) – Twin premature newborn boys died at an Ohio hospital last year while staff stood by refusing to give them medical assistance, a pro-life group is reporting, and the hospital classified the boys’ deaths as stillbirth.
Both boys were born alive at 22 weeks and 5 days gestational age at Riverside Methodist Hospital in Columbus, according to the report.
The first born, Emery, survived for 45 minutes. His younger brother, Elliot, lived for two and a half hours, even crying, and his mother, Amanda, begged for help to no avail.
Alarming footage released today by Created Equal shows both boys just after their births.
Amanda is shown in the video beseeching in the case of Emery, “You guys are going to save him, right? Promise me they’re going to save him.”
Amanda then says, “Look at him, please save him.”
Amanda is shown holding and speaking to her newborn boys in the video.
Later in the video, she tells Elliot, “Mommy tried, Mommy tried.”
Amanda had been told by the hospital her boys would be stillborn or breathe only for a moment after birth, according to her statement included in the Created Equal report, but the video shows otherwise.
Additionally, an attending physician’s notes confirm the boys were born at 22 weeks, five days, the time at which many healthcare professionals say is the marker of viability.
Even though Emery and Elliot were born alive, Riverside Methodist Hospital released Amanda with stillbirth discharge papers.
“I was discharged with instructions for care after stillbirth,” Amanda said. “But Emery and Elliot were not stillborn. They were born alive and died as Riverside Methodist Hospital staff denied my pleas for help.”
The pro-life group released the video after attempts to have the incidents addressed internally were unsuccessful, the hospital calling the matter “closed.”
LifeSiteNews inquired with the hospital regarding its policy on determining when medical aid is provided to preterm babies. Media relations staff responded initially saying the inquiry was being submitted to leadership for women’s health at the hospital, but a response could not be guaranteed by press time.
Amanda begged repeatedly for help
While the video footage is heartbreaking, Created Equal Director Harrington said it represents just a portion of Amanda’s appeals to Riverside Methodist staff save her children.
“She pleaded with them many times before and after birth to aid the babies,” Harrington told LifeSiteNews.
Harrington said as well that some of Amanda’s paperwork had been changed, and the boys’ ages were scratched out.
“Which makes me think they needed to cover their tracks,” Harrington said.
“There is evidence that Amanda’s children were either right at the limit or below when it comes to receiving care,” he said. “Determining the age of a preborn baby is not an exact science. Still, the staff should have erred on the side of life, being that the children were apparently born at 22.5 weeks, even though the age put on the paperwork is disputed.”
‘We consider this matter closed’
Created Equal had assisted Amanda in filing a complaint with OhioHealth’s Ethics and Compliance office, but the group said those efforts were rebuffed.
“The ethics and compliance department has investigated and addressed the concern brought by the caller,” the hospital compliance office said in its response. “If further incidents occur, please notify compliance line or local management …. We consider this matter closed.”
“Hospital regulations and rules don’t take into the account the human factor,” said Harrington. “I understand that hospitals need to limit when to use their resources to save a premature baby, but the cold and calculated way the staff disregarded the pleas of Amanda is outrageous.”
“Rules should be guidelines,” he said, “but not black and white determiners of life and death.”
They can feel pain, they could live
Harrington noted that Ohio law penalizes abortionists who kill unborn children after 20 weeks because science considers that viability.
“We need to be consistent and save premature babies born alive below 22 weeks gestational age,” he added.
To date, there has been no real recognition from the hospital of the incident, according to the Created Equal report, nor condolences communicated to the grieving family.
“The family is very disturbed by what happened,” Harrington told LifeSiteNews.
Amanda, the boys’ father Shaun and others, continue to grieve the loss of Emery and Elliot, he said, and they are greatly concerned for others to whom similar incidents may occur. While they do want justice, the family’s last name is redacted for their privacy.
OhioHealth is a non-profit, charitable healthcare system of the United Methodist Church. Based in Columbus, it consists of 10 hospitals, more than 200 ambulatory sites, hospice and other assorted health services throughout a 47-county area.
Emery and Elliot
Amanda went to Riverside Methodist Hospital on June 24, 2017 with bleeding, concerned for her twins. She was at 22 weeks, 2 days in her pregnancy.
Hospital staff informed her that if she delivered prior to 22 weeks, 5 days gestation, there’d be no assessment of her boys and no attempt to resuscitate them.
Emery and Elliot were born three days later at 22 weeks, 5 days gestation.
Despite making it to that critical point in gestation set out by the hospital, Riverside Methodist staff still told Amanda as she labored the boys were coming too early and that its neonatal intensive care unit would not attempt to aid the boys.
“Emery was born first,” Amanda said. “No medical team member was present. He landed on the edge of the bed.”
“My mother demanded assistance from the nurse’s station,” she continued. “A neonatal doctor did come in, but just wrapped Emery in a blanket, put him under a heat lamp, and opened his mouth.”
“Emery did not merely “breathe for a moment,” said Amanda. “He survived for about 45 minutes before passing away without any assistance from hospital staff.”
A couple of hours later, she began to contract again. This time, a doctor delivered Elliot, cut the cord, and laid him on her chest.
“Elliot was bigger than Emery,” Amanda recalled. “Not only was he breathing, like Emery, but he was also crying. But no one assessed his needs. He lived for two and a half hours while they did nothing.”
“Though I repeatedly asked staff to help or assess my babies, I was told they were born too young,” she said. “But there is no documentation to prove they were born too young.”
“In fact, I had been told previously they would not help if the babies were born before 22 weeks and 5 days. Documentation shows I was admitted at 22 weeks 2 days and the babies born at 22 weeks 5 days,” Amanda said. “Nevertheless, when I begged for help, they refused.”
Viability
Harrington points to a 2015 study by the New England Journal of Medicine that says babies born at 22 weeks have a greater probability of survival than was previously thought – provided they are given assistance.
The study’s lead author, Dr. Edward Bell, a pediatrics professor at the University of Iowa, told The New York Times at the time that he considers 22 weeks the new standard of viability.
“That’s what we think, but this is a pretty controversial area,” Bell said. “I guess we would say that these babies deserve a chance.”
At the time of the 2015 New England Journal of Medicine study, a Newsweek reporton the study said there are about 5,000 babies born at 22 weeks in the U.S. each year.
Harrington told LifeSiteNews incidents like what happened with Amanda and her boys are occurring elsewhere, and he believes they are the result of the Obamacare healthcare law. While this is the first case he’s aware of with this hospital, Harrington said he’s certain the case is not unique.
He cautions people not to trust the medical profession will always have you or your family’s best interest in mind.
“The tragic story of Amanda and her twins Emery and Elliot is not an isolated incident and is taking place in hospitals across America,” he said. “Amanda just happened to capture this incident on film.”
Contact information for respectful communications:
This Saturday, November 10, 2018, representatives from 12 pro-life organizations will present an online summit on how pro-lifers can become more effective at helping pregnant college students. The Save Lives U seminar will be held from 1-4 p.m. EST, and is completely free of charge. Those who register will also have access to free, recorded replays of all the seminar sessions. Register and find out more on the event, speakers, and topics included in the seminar here.
College age students account for nearly half of those who choose abortion, and Planned Parenthood places 79 percent of its facilities within 5 miles of college campuses.
Through genuine friendships, empathetic listening, careful communication, loving care, and local resources, you can meet students where they are, and help in their time of need.
By the end of SaveLivesU, you’ll know exactly how God can use you to save lives, heal wounds, and impact eternal souls while building a culture of love and life on campus.
The seminar will offer “step-by-step training on how to identify a student facing an unexpected pregnancy, and learn what to say and do to provide compassionate help and connect her with life-saving resources.”
Join the 500+ other registrants and REGISTER TODAY to get training on how to be more effective at reaching and giving life-affirming support to college students experiencing unplanned pregnancies.
The Trump administration has just finalized a rule change that allows employers with “religious or moral objections” to opt out of paying for birth control for employees, including potentially abortifacient types of contraceptives. The Department of Health and Human Services noted in its press release about the conscience protections:
The first of today’s final rules provides an exemption from the contraceptive coverage mandate to entities that object to services covered by the mandate on the basis of sincerely held religious beliefs. The second final rule provides protections to nonprofit organizations and small businesses that have non-religious moral convictions opposing services covered by the mandate.
The religious and moral exemptions provided by these rules also apply to institutions of education, issuers, and individuals. The Departments are not extending the moral exemption to publicly traded businesses, or either exemption to government entities.
Fox News reports, “The rule, set to take effect after a 60-day comment period, does not bar any employer from providing contraceptive coverage.”
HHS’ press release also points out that the rule change is expected to affect “no more than approximately 200 employers with religious or moral objections.” It also makes clear that “government programs that provide free or subsidized contraceptive cover to low income women, such as through community health centers,” will be left in place, and the rule change does “not ban any drugs or devices or prohibit any employer from covering contraceptives.”
In other words, no contraceptive is being banned; this rule change simply ensures that employers who object to providing contraceptives on moral or religious grounds will not be forced to do so — a departure from the Obama administration. Fox notes, however, that “[l]arge companies whose stock is sold to investors won’t be eligible for the opt-out, and neither will governmental employers.”
In addition, HHS also issued a “proposed rule” that would, if finalized, “protect[] rights of conscience by… requir[ing] issuers to send a separate bill to consumers who selected a[n Affordable Care Act] plan with abortion coverage for the portion of premiums attributable to abortion services for which public funding is prohibited.”
There is already plenty of evidence to show that in vitro fertilization, or IVF, has led to the commodification of children. An article published in the New York Post is certain to fan those flames. A mother named Lisa explained that she is looking to trade her last remaining embryo with another mother — simply because the embryo is female instead of male.
The mother, “Lisa,” explained that her five-year-old son desperately wants a brother, not a sister, because a brother will be someone he can share a room with, go to soccer games with, and cheer on the Boston Red Sox with. “I’m doing this for my son,” she said. “My husband grew up with sisters and wants a boy too. This is the way we want to complete our family.”
Lisa said her daughter is the last embryo she has remaining after going through multiple rounds of IVF.
She reached out to IVF groups on Facebook, writing, “Hello, we have been trying to give my child a sibling for three years… we want to complete our family with a son. We have a great quality female embryo. Would you like to consider a trade?” While most people expressed outrage, and her plea was even removed from one group, one woman in California showed interest in the trade. “She already has a toddler, and she has two male embryos left over,” Lisa explained. “Her husband… has six sons from another marriage and then they have a boy together. Her husband said: ‘If we are going to go through this again, it’s going to be a girl!’”
Both women have their children frozen at IVF storage centers.
Lisa and her husband began their IVF process in 2012 when they spent $15,000 to create four embryos — four children. They implanted one, and had their son, who quickly began asking for a brother. “He’s our world and a beautiful child,” Lisa said. “But, as soon as he could talk, he was asking for a sibling. Every time he sees other kids — there’s a lot in our family and in our neighborhood — he is like: ‘He has a brother. Why don’t I have a brother?’ And I’m like: ‘Don’t make it any harder on me than it already is.’ He has no idea.”
After several unsuccessful IVF attempts with other male embryos, they tried again, and froze their daughter. Altogether, they have spent over $45,000 on IVF and pay $1,000 a year to to keep the embryo frozen. And they say that their financial situation also is a factor in their decision to trade their daughter for a son. “Economically, it makes sense for us to have a boy,” Lisa said. “We have a two-bedroom house with no space for a third bedroom. We bought it when Daniel was an infant, and now prices have risen so much in this neighborhood. There is no way we could afford [a separate bedroom for a girl]. We’d have to move to Nebraska.” They claim that adoption is too expensive.
Disturbingly, Lisa seems to understand completely that she sees her child as nothing more than a product to be bought… and sold. “I made up my mind as a reaction to losing the $12,000. Now I have a commodity — something I can leverage,” she admitted.
“Lisa’s” story shows just how far our twisted view of preborn children has become. No longer do we accept their humanity. Instead, they are just things we can create at will, and then throw away when they’re not wanted.
November 6, 2018 (LifeSiteNews) – In a new video published just in time for election day, young men and women explain why they are placing pro-life considerations ahead of all others when choosing which candidates they will support.
“I’m voting pro-life first because I support women and their pre-born infants,” says one young man, adding, “Love them both.” A young woman makes a startling, sober declaration, saying, “I’m voting pro-life first because too many people in my generation are missing because of abortion.”
In a rapid-fire litany, several college-age men and women profess they are voting “pro-life first” because:
“We have an opportunity this election to save pre-born lives and change our country for generations to come.”
“I’m voting pro-life first because we only need a few more votes to end fifth month late term abortion.”
“I am voting pro-life first because I don’t want Planned Parenthood receiving any of my tax dollars.”
“I’m voting pro-life first because we need to ensure pro-life judges and Supreme Court justices are confirmed.”
Watch them make their case in the short – just 1 minute, 22 seconds – video:
The video, titled “We Vote Pro-Life First,” was produced by Students for Life of America, which “exists to recruit, train, and mobilize the Pro-Life Generation to abolish abortion.”
November 2, 2018 (LifeSiteNews) – What’s your main motivation to vote? When you are choosing a party or particular candidate, what’s the most important issue on their platform?
Education? The local or national economy? Health care? Support of programs for families and children? Immigration? Foreign policy?
Many people would not list a candidate’s position on abortion as a primary voting factor. Those who support abortion have done a good job of framing the abortion issue as a private, personal health care decision by a woman (and hence, none of our business.)
Yet, when you look at the bigger picture of the longer-term impact of abortion, and the personal and social costs, you may decide to move up abortion on your list of concerns when casting your vote.
After over 25 years working with thousands of women and men after their abortion procedures, the reality is far more complex than the pro-abortion rhetoric of rights and choice. Abortion has emotional and physical consequences that can negatively impact women and men, their relationships and families.
The poor and minority communities thought to be most in need of abortion “services” have the highest rates of abortion [1]. Tragically, it turns out that they also have the greatest risk for post-abortion reactions that feed addictions, abuse, and the breakdown of family life. Why are they at higher risk?
While abortion may initially appear to solve the problem of an unplanned pregnancy, the unfolding consequences of the procedure can be devastating for women with a previous history of sexual, emotional, and physical abuse.
If we look at the rate of sexual abuse among African-Americans, we find a group of women that is especially vulnerable to post-abortion complications. Statistics reveal that 1 in 4 or 3.3 million African-American women have been sexually abused [2].
The intimately invasive and painful abortion procedure can be experienced as a traumatic re-enactment of the physical and emotional violation of previous abuse. After the abortion these women may experience a powerful resurgence of trauma-related symptoms: addictions; impulsive acting out in relationships; episodes of rage, anxiety, depression; self-injury; nightmares; and difficulty sleeping.
These symptoms can contribute to problems parenting their living children. Women are left more vulnerable to ongoing exploitation, dysfunction, and abuse in their relationships. We know that this instability and dysfunction in relationships leads to breakdown in family life, leaving women and their children vulnerable to predatory relatives, partners, and friends. Economic and social problems are closely connectedto family instability.
The cycle continues: more abuse, more trauma, more abortions, more death.
Breaking the cycle of death
Abortion prevention and abortion healing – if possible after the initial abortion – are essential to help break dysfunctional patterns in the lives of the poor. (Keep in mind repeat abortions make up close to half of all procedures – with higher repetition rates among minorities.)
The emotional and spiritual recovery process helps to significantly reduce destructive symptoms and behaviors and provide a foundation to build a healthier relationship with God, spouses/partners, and living children.
Even women and men with no previous history of trauma can suffer painful symptoms after their abortions:
An increase in depression and anxiety [3].
Even among those that feel a sense of relief after the procedure, unresolved feelings and memories of that loss lead to the abuse of substances and self-destructive behaviors that can lead to personal and relational dysfunction [4].
Subsequent abortions are common after the first procedure (half of all procedures are repeat abortions with the highest rates in minority communities.) Repeat abortion raises the risk of miscarriage and infertility.
When you go to the polls on November 6, make sure the candidate you’re voting for understands the impact of abortion on a woman’s emotional and physical health, her partners, and family.
[1] According to the Census Bureau, the rate of abortions in 2006 among black women was 50 per 1,000, compared with 14 for white women and 22 for “other” women. In New York City, 6 out of every 10 unborn African Americans are aborted.
[2] Robin D. Stone. No Secrets No Lies: How Black Families Can Heal from Sexual Abuse. Harmony (March 8, 2005)
[3] Carlo V. Bellieni MD. Abortion and subsequent mental health: Review of the literature. First published: 16 July 2013
[4] Priscilla Coleman, Ph.D. Abortion and mental health: quantitative synthesis and analysis of research published 1995–2009. 02 January 2018
November is a month set aside to recognize the love and support of adoptive parents and families who provide thousands of children with loving homes each year and to help all Americans realize that adoption is a powerful way to show women they are not alone in an unexpected pregnancy.
“We celebrate the life-changing act of adoption, bring attention to the millions of Americans who are eager to adopt, and express our gratitude to the families who have welcomed children into their lives and homes,” the president said in this year’s official proclamation.
“My Administration also acknowledges the courage of those mothers and fathers who place their child for adoption. Our Nation grows stronger because of the love and sacrifice of parents, both birth and adoptive.”
According to Heartbeat International, the first major effort to promote awareness of the need for adoptive families began in 1976 with Massachusetts governor Michael Dukakis who initiated the first “Adoption Week.” The idea quickly grew in popularity and spread throughout the country.
President Gerald Ford issue the first National Adoption Week which was expanded to the month due to the number of states participating and the number of events promoting adoption.
“During the month, states, communities, public and private organizations, businesses, families, and individuals celebrate adoption as a positive way to build families. Activities and observances across the nation, such as recognition dinners, public awareness and recruitment campaigns, and special events shed light on children who are in need of permanent families,” Heartbeat International reports.
“The month also includes National Adoption Day, traditionally a Saturday, which is observed in courthouses across the nation, where thousands of adoptions are finalized simultaneously.”
A particular focus of the month is on children who are currently in foster care and who are seeking permanent homes.
“Unfortunately, many youth leave foster care at the age of 18 without lasting family connections,” the president states. “These children deserve a permanent family, which can provide them with love, stability, support, and encouragement as they pursue personal, educational, and employment goals and confront life’s opportunities and challenges.”
Adoption affirms the inherent value of human life and signals that every child born or unborn is wanted and loved, he concludes.
“Children, regardless of race, sex, age, or disability, deserve a loving embrace into families they can call their own. This month, we honor the thousands of American families who have grown because of adoption. We also stand with those children in foster care, and we appeal to families, communities, and houses of worship across our great Nation to help these children find a permanent home.”
Adopthelp.com lists nine ways to celebrate this special month, ranging from retelling your family’s adoption story to thanking an adoptive family and spreading awareness through social media.
And, most importantly, let’s set aside this month as a time to intensify our prayers for those families who have adopted children, are considering adoption, or who are confronting an unexpected pregnancy. May God give us the grace to make this nation once again become a land where everyone is deserving of life and love!
The total population of North, Central, and South America is less than a billion. Europe’s population is much less. Africa’s population is about one billion. In the last 100 years the world has eliminated one billion children through abortion. In other words, whole continents. World War II was a walk in the park compared to this. The US alone has aborted 58 million infants (the total population of the US as it came into the twentieth century, and almost the same as the total populations killed in World War II, the bloodiest war in human history. The “body-count” in the Holocaust pales in comparison to this, US-only “body count”.
Clearly, we “do sex” wrong. Humankind has never, ever, done it so wrong.
In the US, for children who survive pregnancy and make it to birth, most of their parents cannot stand each other enough to live their lives together and raise their children to adulthood. Slavery has returned to the US—in the form of sex trafficking. Pornography addiction (to some degree or other) is almost universal among young men. Cohabitation is the majority’s choice despite the widespread knowledge of its bad effects. STDs are “through the roof” and are now mega epidemics — having been epidemic for decades. Motherhood is frowned upon in the academic world and most businesses put up with mothers only because they are forced to if they want female workers.
The list could go on and on— and that is without going near what is being taught and not taught in churches— of all denominations!
As a society we have really lost our way. Leaders in all institutions have lost their way or their courage. There are some who know how to get sex right but most don’t, or are afraid, and public schools and academia are not only totally lost, they lead down the wrong and debilitating path — even in the face of overwhelming data. Proof? Just look around you.
Where do we start to rebuild?
This rebuilding starts with men — with fathers in particular.
Fathers, take back your sons
The fundamental correction involves all fathers taking back from everyone else the sexual education of their sons. Mothers need to do the same for their daughters. However, the sine qua non is that fathers become the sexual tutors of their sons, because, given the nature of males, men have much greater and difficult task to achiever bringing their sexual impulses under total control.
The program is simple. Every father worthy of the title, wants his son to end up happily married to the girl of his dreams and wants to show him the way to pull that off. This is what fathers do: make men out of their boys.
Now that presents a difficulty, because most fathers today have not achieved that status or have lost it: they are single or married to some other woman. Thus, they are quite handicapped in giving what they do not have. However, let us leave that major difficulty to the side for the time being and focus instead on what has to be achieved: lifelong marriage of a boy to the girl of his dreams.
As a nation — as a culture — we either go for this or we break apart into factions, because sex, at every level of social organization from the couple to the polis, either powerfully binds us together or powerfully splits us apart. Those who do not go for the gold of lifelong marriage, ultimately allow our nation be split into pieces. Too strong a claim? What happens to families after divorce? Multiply that by millions and then by two or three generations and then you have a nation and culture falling apart. The choice is not just an individual one, it is political (in the pure sense of the polis).
Feminists cannot help you
How men deal with their sexuality is at the bedrock level of society. This is something the marxist feminists understood very well, though for nefarious purposes.
Feminists and lots of other women are clear on what they don’t want men to do sexually, and they are right! But they are NOT clear on what they want men to DO. And without a clear destination anyone is lost. So, feminists, though correct in their attacks on predation, are totally wrong on the nature of sex.
There is only one destination that makes sense of sex: marriage and procreation — procreation within marriage — both entwined. There are lots of secondary purposes and benefits but these two, procreation within marriage, are non-negotiables if we are to avoid social chaos, if justice is to be done to every child, and if we are to be a people who want justice for every child.
Maybe the biggest natural barrier to achieving this justice is a universal fact about being male: for every man a huge proportion of females are physically attractive — and will remain so throughout his life, no matter his marital status. Men see, and immediately register the beauty and attractiveness of a woman before they know anything else about her. And if a man permits himself to pursue that attraction to its logical end (intercourse) he can be in big trouble for the rest of his life. Worse still, he will have caused chaos in the life of the woman, in her extended family, his own extended family, and in particular, and most disastrously, will have severely damaged any children that result from that intercourse (either eliminating them through abortion or leaving them with split parents for the rest of their lives – and the grandchildren’s lives.)
The only way that sexual attraction can be properly handled is by channelling it towards one person only — the future bride. Finding her is a long and delicate process for which a good father is the best guide, by far.
Begin instructing your sons early
The journey to the bride starts in childhood. It used to start in adolescence for most of human history but now, with pornography being universally and aggressively obtrusive, it starts for boys around age seven or eight, because with his first exposure to it he is beginning to go down the right path or the wrong path.
(By the way – I am all for the death penalty for pornographers. The human suffering unleashed by pornography is so large it is beyond comprehension.)
Back to the task: fathers now have to begin tutoring early if they are not to be too late. By age 7 or 8 it is already urgent and assumes a good level of affection between father and son for this next phase to be successful.
The good father lets his boy know (despite his son not yet being interested in girls) that he wants him to end up as a great young man with a beautiful young wife who will be his companion and best friend for life. Even the father who has failed to achieve this for himself can lay this out for his son.
Gradually – and differently for each son – he leads him to understand the fundamental complementarity between male and female; that this complementarity between his mother and father brought him into existence and an even greater complementarity and unity between them is needed to raise him to be a great young man. The father reminds his son that he exists because he, his father, used his sexuality to bring him into existence. (This is a most powerful lesson each modern boy needs to hear from the lips of his father. Without this exchange a father is neglecting the growth of his son).
He lets his son know that his father, and he alone, is the one to guide him in learning about sexuality and that his son should take it from no one else unless his father says it is OK. He even goes so far as to teach his son how to demand this his right, in the classroom and any other place. He teaches his boy how to be a modern warrior — and gentleman — in these sexually hostile times.
The father holds up, repeatedly, the goal of the great woman to be won over – by his son being a great man. He teaches him that in this domain “like attracts like!” He cannot have a great woman without being a great man. It is impossible. (At the same time the boy’s mother is teaching a similar lesson to his sister).
The father teaches his son that along the way there are many traps and snares for every man; that there always has been and always will be. The first snare that modern boys confront is pornography — new, modern and powerful in its intrusiveness and alluringness (that is what makes it a snare). The father tells his son (at the appropriate time) how he combats his own temptations to look at pornography. He does it in a way that invites the son to lean on his father for help whenever that struggle is present – and it will be.
The father promises to protect him within the home and at school but tells him he has to learn how to protect himself when his father is not around. And he reminds him constantly that all this is for the sake of that wonderful girl he is going to win some day. The purer his heart the stronger it will be and the more easily she will sense it and be attracted by it. And he in turn will be able to recognize a woman with a similarly pure heart – ready to give it to the right man but only to the right man and only to one man!
Time for another revolution
Anybody with an ounce of sense will agree with the above. Anyone who does not is an enemy of children. Harsh? Yes — but true and fundamental to a just and peaceful society.
In all my years working with couples and families, with data and research, with evaluating programs and trying to figure out how best to help couples and families, I have concluded that nothing is more fundamental in the life cycle of individuals and nations than that the father be the one to induct a boy in sexuality. No one else. All else is fraud — dressed up no doubt, but fraud.
Given this, I think it is time for another Revolutionary War. This war is not fought with guns (though, if it is not won there will be a war with guns). It is the revolution by which fathers take back from everyone else, no matter who they are (teachers or clergy), the sexual education and formation of their boys.
We all love appropriate battle cries, such as New Hampshire’s “Live Free or Die”. The one every father needs close to his heart, and on his lips when need be, is, “Keep your hands off my son’s sex!”
If we get enough fathers taking “sex ed” (it really is sexual malformation) back out of the schools (public and private, denominational or secular) we can change America. If we don’t, we lose it.
Too simple? No, no matter the difficulty of doing it. I see nothing more foundational than this in the cycle of human existence, handed on from one generation to the next.
(By the way, this is the ultimate reform the Catholic Church needs to rectify its own sexual ethics for all vocations — for marriage, priesthood, religious celibacy or single lay life. It was the “program” proposed in plenty of time by Pope Pius XII back in the 1950’s. It is a pity of historical proportions that Catholic bishops and religious teaching orders did not take that to heart.)
May fathers take back the formation of their sons’ sexuality from everyone else! It belongs to no one else. If anyone wants to do any “sex ed” let them help fathers and mothers do it — and most of them will need help to do this well. But any other form of sex-ed is only adding to the problem. Proof? Just look around you.
It is already very late. It is time to start this New Revolution.
Pat Fagan is the director of the Marriage and Religion Research Initiative at The Catholic University of America. He is publisher and editor of Marripedia.org. Republished from the MARRI blog with permission.
In recent days, one teacher has been in the spotlight for not only allowing a college student to bring her baby to class, but for holding the student’s baby in a carrier while teaching the class. But this teacher isn’t the only example:
To be pro-life is to support and “make room” for pregnant women in our communities and for young mothers struggling to care for their little ones. We should reassure women that ALL their babies are welcome. That is why I love this video so much!
Earlier this year, married Savannah State University student Jarquita Arrington was caught off guardwhen her husband had to work late on her first day of class. Not knowing what to do, she told her professor — who told her to bring her son to class. The professor held Jarquita’s seven-month-old son so she could take notes.
In 2017, single mother and college student Morgan King didn’t know what to do when she couldn’t find childcare for her three-month-old daughter. Her professor wrote to her, saying that anytime she might find herself in that situation, to “feel free to BRING HER with you to class. I would be absolutely delighted to hold her while I teach, so that you can still pay attention to the class and take notes.”
While most college campuses aren’t equipped to deal with students who are also parents , in our changing world, it isn’t unusual for a high school or college-aged student to become parents. While pro-abortion groups are working toward the abortion pill being made readily available on certain campuses, on-campus options for students who want to choose life are scarce. Perhaps as colleges spend money to build larger sports facilities and other things to draw future students to campus, an investment could be made in the lives of pregnant and parenting students by offering childcare on campus, along with other support services for expectant parents and their children. Students and professors dedicated to helping pregnant and parenting students will be the ones to make the difference — in fact, it is evident from the video above that they already are.
As Culture of Life Africa’s Obianuju Ekeocha noted in her tweet above, “To be pro-life is to support and ‘make room’ for pregnant women in our communities and for young mothers struggling to care for their little ones. We should reassure women that ALL their babies are welcome.”
President Trump, in the stirring rallies he has been holding across the country to show voters the tremendous progress we have all made under Republican leadership and the dangers we face from the Democratic Party, has called this an election of common sense. And he names this as his reason for embracing the policies he has been advancing.
There appear to me five immediate ways that common sense would lead us to vote Republican in the midterms of 2018.
1. When you are making progress, you keep going! The president’s rallies provide a handy checklist of tremendous progress towards making America great again. In less than two years, 4.2 million new jobs have been created. Unemployment is at its lowest in 50 years; female unemployment is the lowest in 65 years, and unemployment in other demographics, including the African-American community, are at all-time lows. The GDP is over 4 percent, median income up more than 4 percent, and wages are on the upswing. Consumer confidence has reached an 18-year high. Our military is stronger, a new trade deal with Mexico and Canada has replaced NAFTA, North Korea is no longer shooting off rockets, veterans are receiving better care, taxes are lower, and religious freedom is more secure. And that’s not the half of it.
Common sense would dictate that if you’re getting good results, you have a good thing going. You don’t change course; you don’t, at a point like that, put leadership in the hands of the opposing political party.
2. If you don’t have borders, you don’t have a country. This is as self-evident as saying if you don’t have a front door, you don’t have a house. Even the Vatican has very high walls protecting its boundaries. Yet the Democratic Party is full of advocates of “open borders,” people who are either oblivious to the dangers of just letting anyone walk in to their country (or their house), or who think that the rest of us are oblivious. Strong borders, and a willingness to insist on laws that control who crosses them, have never constituted prejudice against anyone who wants to come in, or a lack of appreciation of the tremendous value and blessing that immigrants bring to our nation. Rather, it’s just, well, common sense.
3. Everyone is innocent until proven guilty. This bedrock principle of our legal system, and of civilized society, was thrown out the window by the Senate Democrats and their allies during the recent Kavanaugh hearings. The lesson here for the midterms is that this was not an aberration, but rather has now become the modus operandi of Democratic opposition to the progress the Republicans are making in transforming the courts. I looked and listened in vain to hear a simple, straightforward answer from the opponents of Kavanaugh to the question, “Isn’t he to be presumed innocent until proven guilty?” but, sadly, their answers lacked the requisite simplicity and common sense.
4. You don’t give matches to an arsonist, and you don’t give political power to an angry mob. This has been one of the president’s best quotes in his rallies, referring to the very disturbing behavior of Democrat-supported left wing groups who pounded and clawed at the doors of the Supreme Court recently, and, following the advice of Democratic members of Congress like Maxine Waters and Cory Booker, got in the face of Trump supporters and drove them out of restaurants. Neither should voters lose sight of the “logic” of Hillary Clinton. She recently declared that you cannot be civil with a political party that opposes what you stand for, and that civility will return only when the Democrats return to power. This means either that what Republicans stand for doesn’t matter, and therefore can be destroyed by Democrats without any reaction, or it is an unintended compliment that Republicans and their allies know how to disagree peacefully, and use the processes America provides for making peaceful change rather than resorting to mob rule. In any case, commonsense dictates not to give matches to arsonists.
5. You don’t kill babies. The arena of my own fulltime advocacy is that of calling for the protection of children in the first nine months of their existence. I never cease to be amazed at the blind spot that the Democratic Party has to the children in the womb. The fact that they are human is common sense. And the duty of any civilized society to protect its youngest children is self-evident. If you analyze the roll call of the all the abortion-related votes in the current 115th Congress as well as in the 114th Congress, you will see that every one of them broke down along party lines. Whether it was about direct protection of the babies in the womb, or the financing of abortion, the Republicans always voted in favor of protecting these children and the Democrats always voted in favor of abortion. The crossover votes in each case were either non-existent or could be counted on one hand. There was even a vote on whether to protect babies born alive after a failed abortion, and the Democrats opposed that too. To lack common sense on something as basic as the protection of children is the most disturbing point of all.
The president is right. The midterms of 2018 really don’t require complex analysis of political trends or a highly nuanced understanding of the many issues confronting our nation and its leaders. It really is an election of common sense. And it is a moment to pray that common sense prevails.
Fr. Frank Pavone is one of the most prominent pro-life leaders in the world. He became a Catholic priest in 1988 under Cardinal John O’Connor in New York. In 1993 he became National Director of Priests for Life. He is also the President of the National Pro-life Religious Council, and the National Pastoral Director of the Silent No More Campaign and of Rachel’s Vineyard, the world’s largest ministry of healing after abortion. He travels to about four states every week, preaching and teaching against abortion. He broadcasts regularly on television, radio, and internet. He was asked by Mother Teresa to speak in India on abortion, and was asked by then-candidate Donald Trump to serve on his Pro-life and Catholic advisory councils. He has served at the Vatican as an official of the Pontifical Council for the Family, which coordinates the pro-life activities of the Catholic Church. To read more of his reports — Click Here Now.
October 31, 2018 (LifeSiteNews) – Several years ago, my wife and I spent some time in Africa for our honeymoon. One night after she’d gone to sleep in the tent, our safari guide and I stayed up chatting. He was about my age, and was telling me what it was like growing up in Tanzania and about his wife and children. He asked what I did “for a job,” and I explained that I worked in the pro-life movement.
I still remember the stunned look on his face when I explained that in Canada, abortion was not only legal, but legal until birth.
“This would never happen here,” he told me, shaking his head sadly.
It was that conversation I thought back to as I watched Obianuju Ekeocha’s new documentary, Strings Attached.
Ekeocha is a Nigerian-born pro-life activist and founder of Culture of Life Africa, and her journey into the pro-life movement is an interesting one. While working as a biomedical scientist in the United Kingdom, she saw Melinda Gates on television, talking about the desperate need for birth control in Africa. Insulted, Ekocha wrote an open letter to Melinda Gates, explaining that contraception is not what African women are asking for. It went viral, and a pro-life champion was born.
Strings Attached is the documentary version of her 2018 bookTarget Africa: Ideological Neocolonialism in the Twenty-First Century, a damning look at Western meddling in Africa. She begins by pointing out that the Mexico City Policy—referred to by opponents as the Global Gag Rule, which ensures that American foreign aid cash cannot be used for abortion—is not only supported by 83% of American taxpayers, but is also supported by 70% of pro-choice and Democrat voters. The same is true in the UK, where 65% of British voters disagree with funding abortion overseas. Despite this, nations like Canada and the Netherlands are giving millions of dollars to a Global Abortion Fund to make up the shortfall caused by Trump’s withdrawal of cash.
Ekeocha’s documentary exposes a number of staggering facts. Despite Western pretensions of having Africa’s best interests in mind, for example, it very much appears as if limiting the number of Africans is high on the EU and UN priority list. The 2014 Report for the Organization for Economic Cooperation and Development, which tracks foreign aid, found that African countries received more money for so-called population programmes than they received for education, healthcare, and water sanitation.
Ekeocha’s outrage is justified: In what universe, she wants to know, do Africans need IUDs and abortion more than clean water and reliable medicine?
The international abortion-peddler Marie Stopes, meanwhile, is making a killing. Named for a notorious eugenicist (much like Planned Parenthood’s Margaret Sanger), Marie Stopes is operating in 37 developing countries despite a track record of botched butchery. One report found 2,600 instances of concern, and there were 373 botched abortions at clinics in the UK in only two months, with women being rushed to the hospital for surgery and blood transfusions. Ekeocha asks a cutting question: If Stopes has a record this terrible in countries where they are regulated, how bad are they in countries where they are unregulated?
She spends much of Strings Attached answering that question. A secret video recording reveals Paul Cornelissen, the regional director for South Africa of Marie Stopes International, stating in a meeting to chuckles from the audience that “We do illegal abortions all over the world.” Multiple calls made to various Marie Stopes clinics throughout Africa revealed that most were willing to refer women to abortionists, and some were willing to actually perform them. Marie Stopes is a prominent recipient of cash from countries like Canada, and when Canadian MP Garnett Genuis asked Canada’s Minister of Foreign Affairs Chrystia Freeland if she was confident that Marie Stopes was not breaking the law in the countries where it operates, she refused to answer and instead went on a tirade about Liberal support for abortion.
Obianuju Ekeocha
✔@obianuju
Dear friends, many of you contributed to the crowdfunding, many of you prayed so I’m glad & grateful to share this short teaser of “Strings Attached” our new documentary…
While African women are being provided with contraceptives, they are not being informed of the risks or the side effects—for example, the fact that many oral contraceptives are categorized as a Class 1 carcinogen by the World Health Organization. Ekeocha interviews women who tell horror stories about the side effects of the birth control they got at Marie Stopes clinics. Some women died as a result. While Planned Parenthood and other so-called “reproductive health” organizations like to claim that “women will die” if they do not have access to their services, Ekeocha points out that in many instances, the precise opposite is the case.
The most heartbreaking stories are those of African women who got abortions and suffered horribly as a result. One woman’s story was truncated and brutal: “In about twenty minutes, my baby was gone. I walked in there, and I walked out without my baby.” Another described screaming and crying in desperation—the abortionist showed her pieces of her baby when the procedure was over. Abortion is brutal, but it is also a cash cow for organizations like Marie Stopes, which performs 70,000 abortions per year in the UK—but 3.53 million internationally. Many of these abortions are illegal, which is why Stopes has been banned from countries like Zambia.
While politicians like Justin Trudeau pledge millions of taxpayer dollars to support organizations running illegal abortion rackets in the developing world, Ekeocha points out that this is simply another version of Western colonialism, this time powered by donor cash rather than armies. Across ten African countries, Ekeocha spoke to girls and women and asked them what they wanted. The answer was always about education, and never about abortion or birth control. In fact, interview after interview with women and girls—even the impoverished in a Ugandan slum—revealed that they thought abortion was evil. But as it turns out, nobody is asking them.
Strings Attached is a must-see documentary for politicians, pro-lifers, and those interested in how their tax dollars are funding an assault on African values, African women, and African children. High schools should screen it in their social studies classes. Pro-life organizations should organize screenings for the public. And university clubs should bring it to campuses. Obianuju Ekeocha has a message for the West, and we need to sit down and listen carefully.
In news that shows how prevalent discriminatory attitudes towards babies with Down’s syndrome still are within the medical profession, a mother has spoken out about her horror at being told the point of prenatal screening was to abort babies with the condition.
“It was horrible”
Leah, a mother of two who did not give the BBC her full name, recently went for a dating scan and asked for the screening so she could be prepared if her baby had the condition, which it did not. She has a sister with Down’s syndrome, and told the midwife that she would not terminate the pregnancy if the test came back positive.
The midwife told her “the purpose of the test is for terminations”, and kept repeating the word for the short amount of time they were in the consultation. Leah said that had she not had experience with Down’s syndrome she might have gone along with the midwife’s insistence that it was normal to abort babies with the condition, something she described as “scary”.
“We came out of the consultation, my husband and I, literally as if we’d been punched in the guts. We were sat there with tears in our eyes looking at each other and we couldn’t believe what we’d just heard,” she said. “It was just horrible. Really horrible.”
“Totally biased towards terminations”
The news comes as the Welsh Government has been forced to scrap a leaflet given to women who choose to have the screening, after it was criticised for overly focusing on medical problems their baby could face.
The information was produced to accompany a non-invasive prenatal test (NIPT) for chromosomal conditions which was rolled out by NHS Wales in April. Campaigners said pregnant women were being “pushed towards terminations”.
One mother said that the support offered is “totally biased towards termination” with counselling only offered to mothers who decide to terminate the pregnancy, and not to those who continue.
People, not a medical condition
In a letter to a campaigner Health Secretary Vaughan Gething admitted the initial booklets given to mothers having the test had to be replaced after the Nuffield Council on Bioethics said the information was “overly focused on the medical problems associated with the screened-for conditions”, “lacking in important information about NIPT” and “difficult to navigate”.
The new leaflet has altered some medical information, and states: “most children and adults who have Down’s syndrome lead healthy and fulfilled lives and are included in their community. Most say they enjoy their lives and relationships. Many adults are capable of work and live in their own accommodation, with support.”
ROME, October 19, 2018 (LifeSiteNews) – Archbishop Carlo Maria Viganò today has issued a third explosive testimony, in response to an open letter from Cardinal Marc Ouellet, Prefect of the Congregation for Bishops.
Here below we publish the official English text of Archbishop Viganò’s third testimony, dated October 19, the liturgical Feast of the North American Martyrs.
On the Feast of the North American Martyrs
To bear witness to corruption in the hierarchy of the Catholic Church was a painful decision for me, and remains so. But I am an old man, one who knows he must soon give an accounting to the Judge for his actions and omissions, one who fears Him who can cast body and soul into hell. A Judge who, even in his infinite mercy, will render to every person salvation or damnation according to what he has deserved. Anticipating the dreadful question from that Judge – “How could you, who had knowledge of the truth, keep silent in the midst of falsehood and depravity?” — what answer could I give?
I testified fully aware that my testimony would bring alarm and dismay to many eminent persons: churchmen, fellow bishops, colleagues with whom I had worked and prayed. I knew many would feel wounded and betrayed. I expected that some would in their turn assail me and my motives. Most painful of all, I knew that many of the innocent faithful would be confused and disconcerted by the spectacle of a bishop’s charging colleagues and superiors with malfeasance, sexual sin, and grave neglect of duty. Yet I believe that my continued silence would put many souls at risk, and would certainly damn my own. Having reported multiple times to my superiors, and even to the pope, the aberrant behavior of Theodore McCarrick, I could have publicly denounced the truths of which I was aware earlier. If I have some responsibility in this delay, I repent for that. This delay was due to the gravity of the decision I was going to take, and to the long travail of my conscience.
I have been accused of creating confusion and division in the Church through my testimony. To those who believe such confusion and division were negligible prior to August 2018, perhaps such a claim is plausible. Most impartial observers, however, will have been aware of a longstanding excess of both, as is inevitable when the successor of Peter is negligent in exercising his principal mission, which is to confirm the brothers in the faith and in sound moral doctrine. When he then exacerbates the crisis by contradictory or perplexing statements about these doctrines, the confusion is worsened.
Therefore I spoke. For it is the conspiracy of silence that has wrought and continues to wreak great harm in the Church — harm to so many innocent souls, to young priestly vocations, to the faithful at large. With regard to my decision, which I have taken in conscience before God, I willingly accept every fraternal correction, advice, recommendation, and invitation to progress in my life of faith and love for Christ, the Church and the Pope.
Let me restate the key points of my testimony.
In November 2000 the U.S. nuncio Archbishop Montalvo informed the Holy See of Cardinal McCarrick’s homosexual behavior with seminarians and priests.
In December 2006 the new U.S. nuncio, Archbishop Pietro Sambi, informed the Holy See of Cardinal McCarrick’s homosexual behavior with yet another priest.
In December of 2006 I myself wrote a memo to the Secretary of State Cardinal Bertone, and personally delivered it to the Substitute for General Affairs, Archbishop Leonardo Sandri, calling for the pope to bring extraordinary disciplinary measures against McCarrick to forestall future crimes and scandal. This memo received no response.
In April 2008 an open letter to Pope Benedict by Richard Sipe was relayed by the Prefect of the CDF, Cardinal Levada, to the Secretary of State, Cardinal Bertone, containing further accusations of McCarrick’s sleeping with seminarians and priests. I received this a month later, and in May 2008 I myself delivered a second memo to the then Substitute for General Affairs, Archbishop Fernando Filoni, reporting the claims against McCarrick and calling for sanctions against him. This second memo also received no response.
In 2009 or 2010 I learned from Cardinal Re, prefect of the Congregation of Bishops, that Pope Benedict had ordered McCarrick to cease public ministry and begin a life of prayer and penance. The nuncio Sambi communicated the Pope’s orders to McCarrick in a voice heard down the corridor of the nunciature.
In November 2011 Cardinal Ouellet, the new Prefect of Bishops, repeated to me, the new nuncio to the U.S., the Pope’s restrictions on McCarrick, and I myself communicated them to McCarrick face-to-face.
On June 21, 2013, toward the end of an official assembly of nuncios at the Vatican, Pope Francis spoke cryptic words to me criticizing the U.S. episcopacy.
On June 23, 2013, I met Pope Francis face-to-face in his apartment to ask for clarification, and the Pope asked me, “il cardinale McCarrick, com’è (Cardinal McCarrick — what do you make of him)?”– which I can only interpret as a feigning of curiosity in order to discover whether or not I was an ally of McCarrick. I told him that McCarrick had sexually corrupted generations of priests and seminarians, and had been ordered by Pope Benedict to confine himself to a life of prayer and penance.
Instead, McCarrick continued to enjoy the special regard of Pope Francis and was given new responsibilities and missions by him.
McCarrick was part of a network of bishops promoting homosexuality who, exploiting their favor with Pope Francis, manipulated episcopal appointments so as to protect themselves from justice and to strengthen the homosexual network in the hierarchy and in the Church at large.
Pope Francis himself has either colluded in this corruption, or, knowing what he does, is gravely negligent in failing to oppose it and uproot it.
I invoked God as my witness to the truth of my claims, and none has been shown false. Cardinal Ouellet has written to rebuke me for my temerity in breaking silence and leveling such grave accusations against my brothers and superiors, but in truth his remonstrance confirms me in my decision and, even more, serves to vindicate my claims, severally and as a whole.
Cardinal Ouellet concedes that he spoke with me about McCarrick’s situation prior to my leaving for Washington to begin my post as nuncio.
Cardinal Ouellet concedes that he communicated to me in writing the conditions and restrictions imposed on McCarrick by Pope Benedict.
Cardinal Ouellet concedes that these restrictions forbade McCarrick to travel or to make public appearances.
Cardinal Ouellet concedes that the Congregation of Bishops, in writing, first through the nuncio Sambi and then once again through me, required McCarrick to lead a life of prayer and penance.
What does Cardinal Ouellet dispute?
Cardinal Ouellet disputes the possibility that Pope Francis could have taken in important information about McCarrick on a day when he met scores of nuncios and gave each only a few moments of conversation. But this was not my testimony. My testimony is that at a second, private meeting, I informed the Pope, answering his own question about Theodore McCarrick, then Cardinal archbishop emeritus of Washington, prominent figure of the Church in the US, telling the Pope that McCarrick had sexually corrupted his own seminarians and priests. No pope could forget that.
Cardinal Ouellet disputes the existence in his archives of letters signed by Pope Benedict or Pope Francis regarding sanctions on McCarrick. But this was not my testimony. My testimony was that he has in his archives key documents – irrespective of provenance – incriminating McCarrick and documenting the measures taken in his regard, and other proofs on the cover-up regarding his situation. And I confirm this again.
Cardinal Ouellet disputes the existence in the files of his predecessor, Cardinal Re, of “audience memos” imposing on McCarrick the restrictions already mentioned. But this was not my testimony. My testimony is that there are other documents: for instance, a note from Card Re not ex-Audientia SS.mi, signed by either the Secretary of State or by the Substitute.
Cardinal Ouellet disputes that it is false to present the measures taken against McCarrick as “sanctions” decreed by Pope Benedict and canceled by Pope Francis. True. They were not technically “sanctions” but provisions, “conditions and restrictions.” To quibble whether they were sanctions or provisions or something else is pure legalism. From a pastoral point of view they are exactly the same thing.
In brief, Cardinal Ouellet concedes the important claims that I did and do make, and disputes claims I don’t make and never made.
There is one point on which I must absolutely refute what Cardinal Ouellet wrote. The Cardinal states that the Holy See was only aware of “rumors,” which were not enough to justify disciplinary measures against McCarrick. I affirm to the contrary that the Holy See was aware of a variety of concrete facts, and is in possession of documentary proof, and that the responsible persons nevertheless chose not to intervene or were prevented from doing so. Compensation by the Archdiocese of Newark and the Diocese of Metuchen to the victims of McCarrick’s sexual abuse, the letters of Fr. Ramsey, of the nuncios Montalvo in 2000 and Sambi in 2006, of Dr. Sipe in 2008, my two notes to the superiors of the Secretariat of State who described in detail the concrete allegations against McCarrick; are all these just rumors? They are official correspondence, not gossip from the sacristy. The crimes reported were very serious, including those of attempting to give sacramental absolution to accomplices in perverse acts, with subsequent sacrilegious celebration of Mass. These documents specify the identity of the perpetrators and their protectors, and the chronological sequence of the facts. They are kept in the appropriate archives; no extraordinary investigation is needed to recover them.
In the public remonstrances directed at me I have noted two omissions, two dramatic silences. The first silence regards the plight of the victims. The second regards the underlying reason why there are so many victims, namely, the corrupting influence of homosexuality in the priesthood and in the hierarchy. As to the first, it is dismaying that, amid all the scandals and indignation, so little thought should be given to those damaged by the sexual predations of those commissioned as ministers of the gospel. This is not a matter of settling scores or sulking over the vicissitudes of ecclesiastical careers. It is not a matter of politics. It is not a matter of how church historians may evaluate this or that papacy. This is about souls. Many souls have been and are even now imperiled of their eternal salvation.
As to the second silence, this very grave crisis cannot be properly addressed and resolved unless and until we call things by their true names. This is a crisis due to the scourge of homosexuality, in its agents, in its motives, in its resistance to reform. It is no exaggeration to say that homosexuality has become a plague in the clergy, and it can only be eradicated with spiritual weapons. It is an enormous hypocrisy to condemn the abuse, claim to weep for the victims, and yet refuse to denounce the root cause of so much sexual abuse: homosexuality. It is hypocrisy to refuse to acknowledge that this scourge is due to a serious crisis in the spiritual life of the clergy and to fail to take the steps necessary to remedy it.
Unquestionably there exist philandering clergy, and unquestionably they too damage their own souls, the souls of those whom they corrupt, and the Church at large. But these violations of priestly celibacy are usually confined to the individuals immediately involved. Philandering clergy usually do not recruit other philanderers, nor work to promote them, nor cover-up their misdeeds — whereas the evidence for homosexual collusion, with its deep roots that are so difficult to eradicate, is overwhelming.
It is well established that homosexual predators exploit clerical privilege to their advantage. But to claim the crisis itself to be clericalism is pure sophistry. It is to pretend that a means, an instrument, is in fact the main motive.
Denouncing homosexual corruption and the moral cowardice that allows it to flourish does not meet with congratulation in our times, not even in the highest spheres of the Church. I am not surprised that in calling attention to these plagues I am charged with disloyalty to the Holy Father and with fomenting an open and scandalous rebellion. Yet rebellion would entail urging others to topple the papacy. I am urging no such thing. I pray every day for Pope Francis — more than I have ever done for the other popes. I am asking, indeed earnestly begging, the Holy Father to face up to the commitments he himself made in assuming his office as successor of Peter. He took upon himself the mission of confirming his brothers and guiding all souls in following Christ, in the spiritual combat, along the way of the cross. Let him admit his errors, repent, show his willingness to follow the mandate given to Peter and, once converted let him confirm his brothers (Lk 22:32).
In closing, I wish to repeat my appeal to my brother bishops and priests who know that my statements are true and who can so testify, or who have access to documents that can put the matter beyond doubt. You too are faced with a choice. You can choose to withdraw from the battle, to prop up the conspiracy of silence and avert your eyes from the spreading of corruption. You can make excuses, compromises and justification that put off the day of reckoning. You can console yourselves with the falsehood and the delusion that it will be easier to tell the truth tomorrow, and then the following day, and so on.
On the other hand, you can choose to speak. You can trust Him who told us, “the truth will set you free.” I do not say it will be easy to decide between silence and speaking. I urge you to consider which choice– on your deathbed, and then before the just Judge — you will not regret having made.
+ Carlo Maria Viganò
Arcivescovo tit. di Ulpiana
Nunzio Apostolico
19 Ottobre 2018
Feast of the North American Martyrs
The great “IUD rush” of 2017 proved to be an unnecessary race to obtain an implanted, long-acting intrauterine birth control device before President Donald Trump — as some claimed — could end no-cost health insurance coverage for it. That fear was unfounded, and many women ended up regretting their decision to implant IUDs. While some women report no issues with the device, others are coming forward with stories of immense physical and emotional suffering brought on by IUDs — and it’s time their stories are heard.
WARNING: Images may be disturbing for some.
Cynthia’s IUD lodged in her uterine wall
She never wanted an IUD, but fear of becoming pregnant again so soon after having a baby led Cynthia to have an IUD implanted. She told Live Action News she immediately had horrible cramping and light bleeding, but it wasn’t until a year later that she learned something was terribly wrong.
A UTI that doctors failed to immediately diagnose led to a kidney infection and sepsis. A CT scan found the kidney infection… as well as the fact that the IUD had embedded itself in Cynthia’s uterine wall. Doctors were extremely concerned and after she had healed from the kidney infection, they scheduled surgery to remove the IUD.
While the doctors told her she shouldn’t have long-term physical damage despite having a hole in her uterus, Cynthia told Live Action News she suffers emotionally from what she went through.
Tanai lost her uterus, her ovaries, and toes because of an IUD
Live Action shared the story of Tanai Smith of Baltimore, who had an IUD placed six months after her daughter was born. But she wasn’t told of a possible risk of the IUD migrating in the body. Smith’s IUD wedged itself into the wall of her stomach, leaving her feeling as though she had been stabbed.
Her doctor said surgery was needed to remove the IUD, but scheduled it several weeks after — during which time the IUD migrated again, this time to her liver, where it broke into pieces. What was supposed to be a quick surgery with one incision ended up longer, with three incisions to locate the pieces. The next morning Smith woke up with severe pain and heavy bleeding.
Tanai Smith’s hand after her IUD migrated and surgery to remove it led to sepsis.
Doctors said her ovaries and uterus had blackened and needed to be removed with surgery. She spent weeks in and out of consciousness, developing sepsis and losing kidney function. Eventually, the toes on her left foot and the tips of the toes on her right foot were removed due to loss of blood flow. One day she noticed her middle toe had simply come off. While she is grateful she didn’t lose her limbs completely, she is heartbroken to not be able to give her daughter siblings.
Amanda told MamaMia that her IUD made her “crazy.” After she had it implanted, she bled for more than 10 days at a time and dealt with spotting as well, and she was “an emotional wreck.” She became depressed and angry, and her sex drive was uncomfortably high.
Amanda was diagnosed with Premenstrual Dysphoric Disorder, a depressive syndrome that includes feelings of anxiety, fatigue, sleep issues, and anger. She was put on antidepressants, which came with more side effects. She wanted the IUD removed, but her doctor refused. After a few more months went by, she saw a different doctor who agreed something was wrong. The IUD was finally removed. Six months later, Amanda was back to feeling like herself again.
Tanai Smith lost the toes on one foot and the tips of her toes on the other after surgery to remove an IUD that had migrated.
Melissa’s IUD broke and embedded into her uterus
Despite her initially positive experience with an IUD, Melissa Petro is now concerned for women who get them. In an article for The Week, she says her doctor never told her the IUD’s potential side effects — and for nine years all seemed well, until she lost her insurance.
Two years after this, she was experiencing bleeding during intercourse and went to Planned Parenthood for help. She says she paid out of pocket to have the IUD removed, but they refused. The IUD had migrated, but since she didn’t have backup birth control, Planned Parenthood’s doctor advised her to leave the IUD in.
“Bad advice: A displace(d) IUD can compromise its effectiveness and result in an ectopic pregnancy – but again, when you don’t have insurance, you don’t get a second opinion,” she wrote, “even when the advice you receive from the first physician doesn’t sound right.”
Four years later, Amanda was married with health insurance, and wanted to start a family. She went to have her IUD removed, but the doctor discovered that a piece of it had broken off and embedded into the uterine lining. A different doctor was able to remove it without surgery, but Amanda was told she may have trouble carrying a baby to term. In a happy ending, she was eventually able to get pregnant, but she is concerned that women are being pushed into getting IUDs without being properly warned of the risks.
Tanai Smith in the hospital after surgery to remove the IUD that had migrated.
Saskia suffered an ectopic pregnancy because of an IUD
Three years after Saskia Longaretti had an IUD implanted, she experienced abdominal pain, a five-week long period, and a hard lump at the base of her cervix. Her doctor diagnosed stress-induced irritable bowel syndrome and sent her on her way. But her conditioned worsened.
The pain escalated, and while on the toilet, Saskia felt something fall out of her. She went to the emergency room where doctors discovered she was miscarrying an ectopic pregnancy — her child had begun developing outside her uterus because of the IUD. She had to have her ruptured fallopian tube and preborn child removed.
Esther and Isobel experienced anxiety and hair loss from their IUDs
One month after Esther Colner got an IUD, she began losing her hair and having panic attacks. Her doctor had only great things to say about IUDs so Esther felt she had been scammed — another woman who wasn’t warned of the potential side effects of IUDs.
Isobel Larkin had a similar experience of anxiety and hair loss, along with acne and extreme abdominal pain. When she told her doctor, he said it wasn’t related to the IUD and ran multiple tests before finally deciding it was the IUD causing Isobel’s symptoms. It took a year for it to be removed.
Tanai Smith’s IUD was found in her stomach before it ultimately migrated to her liver and broke.
While some in the medical community downplay the IUD’s risks and cases like these, women are often not informed of the risks; when symptoms do arise, many doctors are quick to dismiss them. Some doctors blame small cervixes for IUD migration and recommend that only women who have already had a child should implant an IUD. However, many women affected had already given birth before they got IUDs.
Hormonal contraception — like the Pill and the IUD — has been linked to depression and a higher risk of suicide, as well as physical risks like the ones these women have suffered. Women have other options, and they deserve to know the risks before they do something that could negatively affect their reproductive systems.
October 22, 2018 (LifeSiteNews) – I was reading an interesting book recently by Antoine Arjakovsky on the historical development of the notion of Christian orthodoxy, and I came across a quotation from a French patrologist, Jerome Alexandre, that made me pause and think:
The flesh, like language, acts as a sign. It signifies a reality that only trust can attain. This is why the substantial difference between soul and flesh is so important: the soul knows that the flesh attached to it is other than itself, that it can neither take full possession of it nor separate itself from it. It must hence resolve to trust it, respect it, and love it.
My flesh is part of who I am—it is not an appendage or a machine or a piece of property, but myself in matter. At the same time, my consciousness of myself is not the same as the flesh; we know there is a distinction between my thoughts and my body. As a result, my flesh, like the language I speak with my lips, is itself a sign of me and of my intentions and my priorities. What I do in the flesh and to it and with it signifies what I think and desire. It is not only not irrelevant to my personhood, it is the primary language through which my person speaks, even before a particular word is uttered.
Therefore the flesh is also a reality that must be respected. I do not absolutely “own” it nor can I live without it (at least, in a natural way; how we live after death is mysterious and certainly no longer simply “natural”). I have to acknowledge the reality and goodness of the flesh, “trusting” it as I go through life, trusting that my embodiment is part of my perfection, and that the body’s limitations, as regards both pleasure and pain, are also for my benefit, if I have learned to respect and love it for what it is (and not for what it is not).
Then I began to ponder how contraception and abortion contradict Alexandre’s insight. What are you saying about your own flesh when you impede what is the most normal and natural functioning of your body—namely, to give rise to other human beings, and to nurture them into existence, to maturity? What are you saying about your self when you treat your flesh, which is part of yourself, as a locus of threat, danger, antagonism, competition? What this says is that a person is profoundly sick, divided from himself or herself, internally at war. Or it might say that the soul would treat the body as an industrialist treats raw materials, stripping them from nature, exploiting them and extracting every last benefit without regard to the health of the “body politic.”
Take one step further. What is the person who thus divides himself from himself (or herself from herself) saying to a partner, a spouse, about the other’s flesh? Your flesh is also the enemy of my soul, my desire, my self-conception; there is something in you that I do not trust, respect, or love. I will take your appetite, I will take the comfort of your matter, but I will not take you yourself in your wholeness. I will do violence to your materiality, as I do (or am willing to do) violence to mine, so that we can be disembodied and embodied together. Is there not in all this a hatred of the flesh mixed in with the love of it?
The language such a couple speaks to one another is a language of desperate half-truths and evasions, politely covered over with conventions, but reducible to self-interest—and as we have seen, not even the interest of one’s entire self.
It gets worse with abortion, for here, the hatred of one’s own flesh is magnified to include the flesh (and soul) of another. To seek to rid oneself of the flesh of a child is to hate the child himself or herself, since the body is the person in his or her material aspect. Thus the civil war that began in the person in whom disordered desire has created self-hatred extends to encompass the person with whom he or she lies (in both senses of the term) and all the persons implicit in this relationship, which is naturally fruitful and must be violently attacked to preclude or excise the fruit.
If the flesh, then, is a language, what are contracepting and aborting couples saying to themselves? What are they saying to each other? What are they saying to their potential or actual offspring? “I do not trust you. I do not respect you. I do not love you.”
Anti-euthanasia activists have been pointing out for years that wherever euthanasia is legalized, it is not long before the “strict safeguards” touted by pro-death politicians and activists as protection to ensure euthanasia is only used in extreme cases begin tumbling down or being wantonly ignored.
Such is the logic of the Culture of Death. Once we permit the killing of the innocent as an acceptable solution to a certain problem, then suddenly there is nothing stopping us from using death to solve an ever-widening set of problems. Indeed, the temptation to use death becomes quite acute. Killing, after all, is relatively easy and cheap; whereas, solving a problem like how to care for people suffering great pain is extremely difficult and expensive.
“Euthanasia is a false solution to the drama of suffering, a solution that is not worthy of man. The real answer cannot be, in fact, to give death, as ‘gentle’ as this may be, but to testify to the love that helps us to face pain and agony in a humane way.”
— Pope Benedict XVI, February 1, 2009
The pattern is clear in countries like Belgium and the Netherlands. Legalize euthanasia for extreme cases involving adults suffering incurable terminal illness, and before long we’re: euthanizing newborn babies born with non-lethal conditions like spina bifida; euthanizing patients without their consent (I’m pretty sure that’s still called “murder”); euthanizing people suffering from mental illnesses like depression; and completely ignoring regulations requiring doctors to report cases of euthanasia, making it impossible to know whether a patient was legally euthanized, or simply murdered.
In the Netherlands, some patients are being killed because they’re “tired of living.” They’re not sick. They’re not dying. They just want to die. And rather than helping them, doctors gladly administer the lethal injection. In one case, a 47-year-old woman in the Netherlands was killedat her request because she was suffering from tinnitus – that is, the condition where a person hears a persistent “ringing” in their ears. The clinic that euthanized the woman was subsequently “reprimanded” because the doctors hadn’t fully researched whether there might be treatments that would help this woman with her problem. There might have been a treatment that could have helped her. But she’ll never find out.
Horrifying New Development in Canada
Astonishingly, while most people would likely agree with me that all of the “abuses” above are horrifying, very few people know about them, and even less speak up against them. They receive very little media attention. And when they do, they’re often presented in news articles in the form of statistics. And, as Stalin is reported to have said: “One death is a tragedy. A million deaths is just a statistic.”
However, maybe one recent development in Canada is sufficiently disturbing that it will wake some people up to what lies in wait once euthanasia is legalized.
The situation is summed up chillingly in the first sentence of an article that appeared in several Catholic newspapers. It begins: “In a prestigious medical journal, doctors from Toronto’s Hospital for Sick Children have laid out policies and procedures for administering medically assisted death to children, including scenarios where the parents would not be informed until after the child dies.”
The article continues: “The Canadian Council of Academies is specifically looking at extending so-called assisted dying to patients under 18, psychiatric patients and patients who have expressed a preference for euthanasia before they were rendered incapable by Alzheimer’s or some other disease.”
Of course, by this point killing patients suffering from Alzheimer’s or psychiatric problems is old hat. But killing children without their parents’ consent? That’s something even I haven’t heard of before. And how do these prestigious doctors writing in this prestigious medical journal working at this prestigious children’s hospital justify this terrible, terrible idea?
Well, they explain with impeccable logic, euthanasia is now legal in Canada. That makes euthanasia just another form of healthcare. Canada already allows competent minors to make some decisions about healthcare without their parents’ knowledge or consent, including the decision to stop futile extraordinary care. If we’re going to be consistent, then we need to consider allowing them to make decisions about euthanasia too. As the doctors put it: “If we regard MAID [Medical Aid in Dying] as practically and ethically equivalent to other medical decisions that result in the end of life, then confidentiality regarding MAID should be managed in this same way.”
And there’s the logic of the Culture of Death in a nutshell. If (and what a big if this is!) we accept that actively killing people is “practically and ethically equivalent” to other forms of healthcare, then all manner of things that people historically considered self-evidently evil very quickly become justifiable – like having doctors kill minors without telling their parents.
The Abortion/Euthanasia Connection.
Often, even pro-life people fail to see the connection between abortion and euthanasia. But the connection runs deep.
Euthanasia is always presented to the public as an act of compassion, a way to alleviate unbearable suffering for people who are already in their final days. For people who haven’t thought about the issue in a lot of depth, this argument seems quite compelling. Especially to anyone who has been at the death bed of a loved one dying from a painful illness. Euthanasia in such extreme cases only seems humane.
The same is true of abortion. Pro-abortion activists always focus on extreme cases: e.g. cases of rape, incest or life-threatening pregnancies. In fact, the woman who was the famous “Roe” in the Roe v. Wade court case that legalized abortion in the United States, Norma McCorvey, later admitted that she had lied about being raped. But the rape made a compelling story for the Supreme Court. It made abortion seem humane.
In both cases – abortion and euthanasia – killing was only supposed to be a last resort. An extreme solution for an extreme case. But as we know, that is not what happened. As soon as abortion was legalized it opened a flood-gate. Now, abortions in cases of rape or incest are only a tiny minority of all abortions. The vast majority of abortions are for “social reasons” – in other words, a quick fix. McCorvey herself later became pro-life, and lamented that the lawyers who convinced her to join the abortion case never told her: “That what I was signing would allow women to come up to me 15, 20 years later and say, ‘Thank you for allowing me to have my five or six abortions. Without you, it wouldn’t have been possible.’ Sarah [one of the lawyers] never mentioned women using abortions as a form of birth control. We talked about truly desperate and needy women, not women already wearing maternity clothes.”
When euthanasia was legalized in Canada in 2016, Canadians were told that it would just be for “terminally ill” patients. Scarcely two years later, they’re now being told they might have to accept euthanasia for their own children, or for mentally ill patients who aren’t dying, or for people who have just been diagnosed with dementia and aren’t dying. In all likelihood, there will be very little outcry. Canadians have already been conditioned to accept death as a solution. What’s a little more death?
The Hôtel Dieu, Paris: interior showing patients being nursed by monks and nuns. France’s oldest hospital was founded by St. Landry in 651 AD.
Killing is Easy. Caring is Hard.
Euthanasia and abortion are two sides of the same coin. Once we accepted abortion as a solution to “problems” at the beginning of life, it was only a matter of time before we began to accept death as a solution to problems at the other end of life.
After all (and I’ll repeat it again): Killing is easy. Caring for people is hard.
It’s easy for a man to fork over a few hundred dollars and tell his mistress to go abort the baby that is the result of his search for selfish pleasure. It’s hard for him to man up and take responsibility for his actions. It’s easy for a national healthcare system or insurance company to save money by pressuring a patient diagnosed with dementia to opt for euthanasia. It’s hard for that healthcare system or insurance company to allocate resources to invest into research and palliative care that can alleviate suffering while respecting the dignity of every patient.
As it turns out, it’s something of a law of nature that the hard thing is often the right thing to do; and the easy thing is often also the wrong thing. One of the reasons we have criminal laws is to turn that formula on its head, to protect the common good by creating incentives to do the right thing and avoid the wrong thing. It’s easy to rob a bank and spend the rest of your life as a wealthy man. But the law makes robbing banks hard by introducing the threat of imprisonment. Bank robbery is such a serious crime that we would never consider legalizing bank robbery for “extreme cases.” The reason why is obvious. It sends the message that robbing banks is an acceptable solution to our problems. It tears down a crucial wall, and thereby creates social havoc.
If there’s anything that the past several decades have proved, it’s that when a society allows killing as a solution, it’s almost impossible to keep it to extreme cases. Legalize killing in some cases, and the incentives against killing have been removed. The finger has been pulled from the dike. The flood follows soon after. Eventually, society will not be able to defend the most vulnerable and abused.
There is an inner logic to the Culture of Death. Death leads to death. What is happening in Canada right now is not just a Canadian issue. It is a universal issue – a human issue. It will reverberate across the U.S. and beyond.
Agreeing with euthanasia and its mentality is an affirmation that, depending on the circumstances, some lives are not worth living and need to be terminated. This callous view should evoke disgust, urgency and a need for repudiation. Human life, at every stage, is sacred and no one may dispose of it at will. Every person, no matter the circumstance, has an inalienable and immutable dignity that must be defended, especially those who cannot defend themselves. If silence and indifference toward this grave threat remain, evil will grow, innocent lives will be destroyed, and the conscience of people will be further desensitized, unable to distinguish good from evil.
We Must Speak Out
I believe our response and action to these anti-life ideologies and philosophies is best summarized by St. Pope John Paul II in his letter to the bishops of world (May 19, 1991, Church Must Proclaim the Gospel of Life). Though the letter is specifically addressed to bishops, it equally applies to us, disciples of Jesus and people of good will, actively called to participate in the Great Campaign for Life:
A source of particular concern, however, is the fact that people’s moral conscience appears frighteningly confused and they find it increasingly difficult to perceive the clear and definite distinction between good and evil in matters concerning the fundamental value of human life.
However serious and disturbing the phenomenon of the widespread destruction of so many human lives, either in the womb or in old age, no less serious and disturbing is the blunting of the moral sensitivity of peoples’ consciences. Laws and civil ordinances not only reflect this confusion, but they also contribute to it. When legislative bodies enact laws that authorize putting innocent people to death and states allow their resources and structures to be used for these crimes, individual consciences, often poorly formed, are all the more easily led into error.
In order to break this vicious circle, it seems more urgent than ever that we should forcefully reaffirm our common teaching, based on sacred Scripture and tradition, with regard to the inviolability of innocent human life…. Moreover, we must encourage scientific reflection and legislative or political initiatives which would counter the prevalent “death mentality.” Through the coordinated action of all the bishops and the renewed pastoral commitment which will result, the Church intends to contribute, through the civilization of truth and love, to an ever fuller and more radical establishment of that “Culture of life,” which constitutes the essential prerequisite for the humanization of our society.
October 19, 2018 (LifeSiteNews) – Chesterton said: “It is the paradox of history that each generation is converted by the saint who contradicts it most.”
Thinking on this Chesterton quotation, it came as no surprise to learn that Chiara Corbella Petrillo is being considered for canonisation. To be more exact that her cause could be opened a mere six years after her untimely death on 13 June 2012.
Pause for a moment. Go check your email history for 13 June 2012. I did. There was little of note, a lot that was mundane – everyday communication dealing with the petty and the ordinary. And yet, on that day, a Christian witness of epic proportions had just ended.
*****
Enrico and Chiara were married in September 2008. Soon after Chiara became pregnant. The newlyweds were overjoyed. Their joy was to be short-lived, however. An ultrasound scan revealed the child was deformed. “Of course, you will abort?” the doctors asked. But as Chiara looked back at the image of the helpless child, she was determined to continue with the pregnancy. Even if the child were to live but a short time, she determined that child would live nonetheless.
Maria Grazia Letizia was born on 10 June 2009. She lived for 30 minutes, long enough to be baptised by a priest. Later Chiara was to write:
‘If I had aborted her, I do not think that I would have remembered the day of the abortion as a day of celebration …It would have been a moment that I would have tried to forget, a moment of great suffering. But the day of Maria’s birth I shall always recall as one of the most beautiful days of my life …The amount of time (as parents) does not matter: one month, two months, a few hours. What matters is that we have had this gift …and it is something that can never be forgotten.’
Maria Letizia’s funeral took place two days after her birth. On the small white coffin, her parents left a card with the following words:
We were content to hold you in our arms, for even half an hour, we were fine.
We were not able to stop looking at your nose, the same as mine, and those little hands, and those little feet.
We did not have much time to tell you… that we love you… It does not matter how much time we spend together…
What is necessary is to know the Father…
And you were born ready, I do not know how to tell you how proud we are of you.
We accompanied you as far as we were able.
Now you shall know the Father…
Another pregnancy soon followed. This time scans showed that the child in the womb was missing one leg and had a stump for another; further scans showed the child had no kidneys and so, as a consequence, the lungs would not develop; the baby would have trouble breathing. The prognosis for survival was poor. Once more there was discussion with medical staff about whether to proceed with the pregnancy. Medical staff discussed with Enrico and Chiara whether to end the life of their child while on the screen in front of them a child kicked and pushed for life.
A baby is not a lifestyle choice for any couple but a gift from God. And so, for this Catholic couple the pregnancy continued until eventually Davide Giovanni was born.
Immediately upon entering into this world, the child was embraced by his mother as she tenderly whispered: ‘My son, my love’. Like his sister, the child was baptised at once by a waiting priest. Then Enrico placed a small wooden cross around his newborn son’s neck. Thirty minutes later, just as with his sister before him, silent now, Davide was carried by his father to the hospital mortuary.
But the couple could no more block the wellsprings of life than stop loving each other. Another pregnancy soon followed. As this child grew in Chiara’s womb something else was growing in her body though. A tumour had been discovered on her tongue. Soon it would spread to the neck and to her eyes. Various treatments were proposed. Chiara refused any that could endanger the life of her unborn child, preferring to put them off until after the birth.
Eventually, another child, Francesco, came into the world. His parents were beside themselves with happiness. He was also a healthy child.
For a short time after the birth, the couple, with their newborn baby, enjoyed something close to a ‘normal’ family life, something they both craved. They relished every minute of having a child in their home, being with other mothers and fathers, having their first excursions as a family, even the sleepless nights. It was a precious time; it proved to be borrowed time. Chiara did not know then that just as she had ushered new life into the world, her own was slowly beginning to ebb away.
The tumour proved malignant. There was little that could be done. After some time in hospital, it became clear that no treatment was ever going to work. Finally, medical staff took Enrico aside to explain to him of how bad the situation really was. Now it was for Enrico to go and explain this to his 28-year-old wife, the woman with whom he had expected to grow old, the woman whom he hoped would rejoice alongside him with their children, and one day their grandchildren.
Finally Enrico was able to compose himself. Finding his wife, and then gently taking Chiara by the hand, he led her to the hospital’s chapel. It was there before the Blessed Sacrament that he explained matters to her.
After some time, they embraced each other. Then the young couple once more repeated their marriage vows. Chiara made her husband promise not to tell her how long she had left; she wanted to live in the present moment with her husband and beloved child.
It was the Wednesday of Holy Week.
*****
As in the best love stories, theirs was a chance meeting. It took place in the summer of 2002. Both were visiting a Marian shrine although they had travelled there separately, Enrico with his then girlfriend. The latter had quickly departed the scene, though, and so Enrico Petrillo found himself sitting alone in the dining room of his hotel when a young woman entered. When his eyes fell upon Chiara for the first time he thought she was the most beautiful woman he had ever seen. There was only one free seat in the whole dining room. And so their eyes met as she walked across the room.
*****
Just as the Angelus bell rang out at noon on 13 June 2012, Chiara’s eyes closed for the last time. She was 28.
In this world, she had so wanted to be a mother; yet, sooner than she could have imagined, she went to where two of her children already awaited her, and where now she waits to be reunited with all those she loved when finally their many tears shall be wiped away.
The story of Chiara Petrillo is of our time, but, also, for our times. To quote Chesterton again: “The saint is a medicine because he [or she] is an antidote. He will generally be found restoring the world to sanity by exaggerating whatever the world neglects.”
In this faithless age when the fraudulent mislead the faithful; when the most vulnerable are eliminated as a matter of course; when “choice” is more important than the life extinguished as a result of that choice; when the sick, seen as an inconvenience, are hurried to death; when lies about the human condition have become “facts”; in fact, when the stench of the whole rotten Culture of Death is experienced daily all around us – then it does seem we are being offered a “saint” for our times.
For Chiara was faithful to God’s plan for her; she was faithful to the vows she made when she married; she was faithful to the Church’s perennial and unchanging teaching; she was faithful to her vocation as mother, regardless of the condition of the children sent into her care; she was joyfully faithful until the end, even if that end became her very own Golgotha.
WASHINGTON, D.C., October 17, 2018 (LifeSiteNews) – Proud, smart moms with big families are fighting back on social media against France’s president for suggesting it was impossible to find a woman who was “perfectly educated” and who had “seven, eight, nine children.”
Women with big families are using the “#PostcardsForMacron” hashtag to send Emmanuel Macron pictures of their large and happy families. Hundreds of highly educated women have used the hashtag to send Macron beautiful photos of their large families.
Macron made the derogatory comment about African women having big families at a Goalkeepers event in the shadow of the United Nations in New York last month. Goalkeepers is an event hosted by tech giant Bill Gates and his wife Melinda’s pro-abortion and pro-contraception Gates Foundation.
“One of the critical issues we have regarding the African demography is the fact that this is not a chosen fertility,” said Macron. “I always say, ‘Please, present me the lady who decided, being perfectly educated, to have seven, eight, nine children.”
The French president’s insinuation that a lack of education is what is fueling big families has offended many mothers with big families, many of whom are very well-educated.
But, if Macron wanted examples of educated women with big families, he’s certainly getting that now.
On Twitter, women from throughout the world are setting the French president straight by posting photographs of themselves and their large families – and noting their educational achievements.
Meet Dr. Catherine R. Pakaluk.
She earned her doctorate in economics at Harvard University and is now an assistant professor at The Busch School of Business and Economics and a faculty fellow at the Institute for Human Ecology at The Catholic University of America.
On the Twitter thread she started, #postcardsforMacron, Pakaluk posted a photograph of herself and six of her children.
She followed up that tweet stating: “Eight children by choice.”
@CRPakaluk PhD Harvard (2010), AM Harvard (2002), BA UPenn (1998). Eight children by choice. Keep it going ladies, add your own. #postcardsforMacron
She’s also urged other women with big families to post pics of themselves with their kids on that thread.
And it’s catching on.
Already on Wednesday, more than 1,000 people had “liked” Pakaluk’s tweet and 304 people had re-tweeted it. Many women – and their husbands – are also answering the call with photographs of their big families and educational credentials.
Stanford graduate Beth Hockel is both a mother of 11 and an electrical engineer. Hector Mauricio Peña showed off his six children and their mother who, incidentally, has a doctoral degree.
“Robbbbbb” posted a photograph of his five young children and noted “My wife has a PhD in music and was once a college professor. This is her best work.”
Sue Anne Smith, who has both a degree in pharmacology and a master of business administration, is the proud “mom of seven.” University of Dallas grad Kristina Joyce Cyr, chairwoman of the Republican Central Committee for the City of St Louis, was also happy to tell the French president she has seven children.
Elizabeth Foss tweeted about her nine children: “Yes, they’re all mine. And so is my UVa degree. #postcardsforMacron.”
Despite the growing number of very well-educated women with fancy degrees stepping forth to proudly show off their families, though, Pakaluk wants to be clear that this is not just about either fancy degrees or large families.
“This is about … debunking the notion that high-fertility is a consequence of ignorance,” she tweeted.
It’s important to Pakaluk that people realize that high fertility is in no way an obstacle to economic growth.
They prayed for babies, and boy, did they get them: Five children in less than a year, providing a crash course in parenthood for a couple who couldn’t be happier.
Sarah and Andy Justice of Tulsa, Okla., wanted a family but had trouble conceiving, so they adopted triplets. But soon after, Sarah found out she was pregnant with twins.
“I was shocked and a bit overwhelmed because I got to thinking, added it up and I’m like, wow, if they go to term we’re about five babies in eight months. But we were really excited because it was something we’ve been dreaming of and longing for for years,” Sarah told the TODAY anchors, who had their hands full cradling the babies. Some were a little fussy during their national television debut.
The couple had been struggling with infertility for years when they turned to adoption. Just after they arranged to adopt the triplets last year, Sarah’s doctor discovered she was having twins.
The couple didn’t want to give up the triplets and officials told them they could still get all three if they didn’t back out, Tulsa World reported.
Now, their life revolves around their five kids, with lots of help from their family and their church. They get about three hours of sleep each night, though not necessarily in a row, Andy noted.
“My husband says all we do is babies, everything else in life has pretty much stopped,” Sarah said. “But it was something we’ve wanted so badly that we love it. It’s not to say it’s not a lot of work and we’re not tired a lot but it’s great. We just really love having these children.”
October 18, 2018 (LifeSiteNews) – It is rare that a new pro-life organization emerges that does something utterly unique, but that is precisely what Laura Klassen and Choice42 have done. In the past several months, they have released a series of viral videos that have taken the Internet by storm, with Klassen and her now signature pink wig playfully poking fun at popular pro-choice arguments—and racking up millions of views and copycat videos in a wide range of different languages.
Their now famous “Magical Birth Canal” video has over one million views on their Facebook page alone.
Klassen first became aware of what she calls “the horror of abortion” when she was quite young. “I saw a graphic abortion image on the street,” she told me by email.
“That image always stuck with me. I started volunteering at my local pregnancy resource centre when I was in university. It was there that I realized the huge potential for reaching out to abortion-minded women online and so I started Choice42.”
The result was a massive online hub containing every pregnancy resource centre in the country, a one-stop shop for whatever a woman might need in crisis.
And then came the videos.
“Our #JustSaying series was created to challenge the abortion status quo by addressing various pro-choice arguments,” Klassen explained. “Usually a certain pro-choice argument will be making the rounds on social media, and then a script starts brewing. We’ve had to build some pretty random props—you can’t buy a giant sparkly birth canal on Amazon, go figure—and those take some time. We’ve spent a lot of time gathering costumes for our next video, which we’ll be filming soon! We usually take a half-day to film a video with a small crew and then we do the editing ourselves.”
The videos have triggered massive reactions right across the spectrum—especially because Klassen has a knack for at poking the pro-choice activist arguments in a way that drives them crazy.
“The Magical Birth Canal” cleverly exposed a fundamental abortion apologetic as ridiculous—the idea that your physical location has anything to do with your humanity or your value. “No Uterus, No Opinion” (which features Klassen explaining to me why I can’t have an opinion on an issue of human rights because I am a man) highlighted how bizarre it is to say that you can’t have an opinion on an injustice unless you’ve directly experienced it yourself. And if there is one thing abortion activists cannot stand, it is being made fun of.
“Abortion supporters are quite offended by our work,” Klassen noted. “We receive a lot of hate mail and threats. The comments on our videos from people who don’t agree with them are usually just insults with no real argument. We have opened a lot of eyes though…especially with the ‘Magical Birth Canal’ as even many abortion supporters did not realize that you don’t gain your human rights until you are fully born.”
Success for women in the pro-life movement always comes with a backlash: Klassen puts up with some of the most repulsive and misogynist online hate that I’ve seen in a long time.
Klassen’s latest video tackles the lazy slander that pro-lifers only care about babies until they’re born, and features her and a masked colleague breaking into a “fake clinic”—the moniker given to crisis pregnancy centres by abortion activists—and filling it with thousands of dollars worth of free diapers.
“The idea for our latest video came because we wanted to do a big ‘pro-love’ gesture,” she explained. “The atmosphere here in Canada regarding the abortion issue is very tense right now with all of the violence against pro-lifers. We felt it would be a good time to do something really positive. We bought $2500 worth of diapers and did a reverse robbery at a Pregnancy Resource Centre. We ‘broke in’ to the centre and filled it with all of the diapers. We were addressing the myth that, ‘pro-lifers only care up until the point the baby is born’ which couldn’t be further from the truth. We also wanted to bring more awareness to the Pregnancy Resource Centres and all that they offer for women and their families for YEARS after the birth.”
Many more videos are being planned—and not just the hilarious parody videos Klassen has become famous for. Choice42 has put out riveting and heartbreaking stories of women who regret their abortions, and beautiful stories of women who chose life in spite of horrific circumstances. It is a powerful one-two punch of real-life stories and the clever popping of pro-choice myths—an online pro-life juggernaut that fills a unique role in the movement. Until now, there has been no group doing work quite like this—and it is tremendously effective.
“The response to our videos has been amazing,” Klassen told me. “We’ve gotten world-wide attention and have been accused of trying to sway other countries’ votes [in Ireland] regarding the pro-life issue. We’ve had women write in to say that they decided to choose life after watching our ‘Choose Life’ videos. Pregnancy Resource Centres across the globe are showing videos to their clients.”
In just a few short years, Klassen and Choice42 have managed to make an international impact. I’m sure we will be seeing much more of them in the future.
JOHN STONESTREET OCT 17, 2018 | 10:34AM WASHINGTON, DC
A recent story in the Washington Post described the story of Kianni Arroyo, who is on a three-year quest to meet all of her half-siblings. It’s not as idyllic as it sounds… So far she has found forty-four of them. They live in eight states and four different countries.
The “father” of these children was, of course, a sperm donor, known affectionately to Kianni as “Donor #2757.”
As the story’s title “44 Siblings and Counting” suggests, there may be even more. Apparently, “Donor #2757” was very popular with customers of the sperm bank. Some women “liked his looks and his artistic background.” Others liked his family pedigree. Still others thought — I’m not making this up — that he seemed like the kind of guy they’d like to date.
That’s how Kianni wound up with “forty-four siblings and counting.” And “Donor #2757” is nowhere near the record-holder. One Canadian donor has fathered at least 150 children.
As with abortion, the U.S. is one of the most permissive countries when it comes to sperm donations. According to the Post, “while Britain, Norway, China and other countries have passed laws limiting the number of children conceived per donor, the United States relies solely on voluntary guidelines.”
In fact, the FDA recently rejected an attempt to limit the number of children a donor could father because it claimed to lack jurisdiction. This was fine according to “a spokesman for the American Society for Reproductive Medicine,” who said that the proposal would have “infringed on the right to privacy and to procreate, giving government ‘control over who has children with whom.’”
This is nonsense. The government already controls “who has children with whom.” When my wife and I applied for a marriage license, one of the questions we were asked was if we were related to each other.
It’s a legitimate question of government concern due to the health risks for any offspring. In a world where one man can have dozens or hundreds of offspring, the same risk is real.
Ten years ago, a married British couple discovered to their horror that they were fraternal twins who had been adopted by different families as infants. When you have dozens, even hundreds, of half-siblings the chances of “accidental incest” are much higher.
Even if that challenge is avoided, children conceived through sperm donation face obstacles others don’t. A 2010 study found that “donor offspring are twice as likely as those raised by biological parents to report problems with the law before age 25.” They were twice as likely to report substance abuse and fifty percent more likely to report mental health problems.
The obvious, but rarely asked, question is “Why?” The authors’ conclusion was that “there’s really no such thing as a ‘donor.’ Every child has a biological father.” The absence of a connection to that father is felt keenly by these children.
Then there’s the elephant in the room: According to the Donor Sibling Registry, less than one-fifth of the parents of its members are married couples. Half are single women and a third are same-sex couples.
In other words, the vast majority of donor-conceived children are born to women who either can’t or won’t provide them with a father whom they can ever hope to know.
To put it bluntly, the needs of children have taken a back seat to adult self-fulfillment. It’s the most repeated lie of the sexual revolution: “The kids will be fine.” Little wonder that half of donor-conceived children expressed “concerns or serious objections to donor conception.”
Actually there’s no wonder. Our society repeatedly chooses to ignore the risks that our illusions of autonomy heap on the heads of our children. And so, we’ve sentenced a whole group of people to spend their lives searching for connections that should be theirs by birthright.
KANSAS CITY, Missouri, October 5, 2018 (LifeSiteNews) – Doctors told an expectant mom that her son had spina bifida and might never walk. But thanks to his parents’ love and prenatal surgery, adorable toddler Roman Dinkel has become an internet walking sensation.
A video of Roman taking some of his first steps, with the aid of tiny crutches, has gone viral, seen millions of times. Last month the toddler appeared on “Good Morning America” with his mom Whitney, dad Adam, and the family puppy, Maggie. Maggie appears in the eight-second clip, as Roman squeaks, “Look, Maggie! I’m walking!”
Thousands of people have posted messages to the Dinkel family’s Facebook page, “Defying Odds: Roman Dinkel’s Journey,” and Youtube to say how much joy and inspiration Roman has given them.
Roman was diagnosed with spina bifida, a congenital defect of the spine in which the spinal cord is left exposed through a gap in the backbone, when he was 20 weeks in the womb. His father Adam said on “Good Morning America” that the first option doctors give parents of unborn babies diagnosed with spina bifida is “termination.” But the Dinkels do not believe in it.
“I would never judge a person for making that decision,” mom Whitney told LifeSiteNews. “It is obviously not what we believe. But often times doctors paint a very grim picture of what the life of a child with spina bifida will look like. They say [he’ll have] severe brain damage, will be paralyzed, in pain their whole life, and they make you believe that you will bring them into this world suffering until they die. But those things just aren’t true. That’s outdated information.”
Adam and Whitney decided that the best thing they could do for their son was to have doctors operate on his spine before he was born.
“The theory is that the quicker you get the nerves back inside the body the less damage they will sustain. So getting his nerves back in at 25 weeks [versus] 40 weeks is huge,” Whitney said.
She told LifeSiteNews that she was frightened that the operation, performed in St. Mary’s Hospital, would cause Roman to be born prematurely.
“It was scary,” she said. “But at the same time I knew it was the best decision we could make for him so I had peace about it. But the fears that he could have been born that day, at 25 weeks, or that he could have been born anytime after, were real.”
With two small children, Layton and Gracie, already in the house, and her husband with his chiropractic practice to attend to, Whitney relied on the help of her mom, who moved in when the expectant mother was advised to rest. The family was also sustained by their faith.
“We had so many people praying for us and I definitely know that the peace I felt came from God,” Whitney said. “I knew He pointed us in this direction and I knew that He would take care of the rest, no matter how that turned out. We just had to trust in Him. And we did.”
Roman was born in Kansas City’s Children’s Mercy Hospital on May 5, 2016, healthy, happy, and adorable. Although his parents were warned that he might have cognitive delay and be paralysed from the knees down, Roman turned out to be a clever little boy determined to walk as soon as he could. Thanks to the operation, therapy, and the help of his parents, this became a reality.
“We do believe getting the fetal surgery gave him a higher chance [of being able] to walk,” Whitney told LifeSiteNews. “It’s been proven that fetal surgery allows you to function better.”
Now able to take steps without a walker, Roman is still on his journey to full mobility. He gets regular chiropractic adjustments and physical therapy. His parents work with him at home, and he wears braces, called SMOs, on his ankles to keep his feet properly aligned.
“He doing awesome with walking,” his proud mother reported.
Adam Dinkel told “Good Morning America” host Michael Strahan that he and Whitney want to show parents of babies diagnosed with spina bifida that “this is an amazing life.”
“This is what you get,” he said happily, as Roman clambered to his feet on the couch.
“A lot of kids do have many more issues than Roman, but they’re happy and their family is happy to have them,” Whitney Dinkel told LifeSiteNews. “So we want people who get this diagnosis to think of Roman and how amazing he is.”
There’s a young woman in my parish called Lupita. She’s Mexican, and about as pretty and charming a woman as you would ever hope to see. She carries a little copy of herself on her hip, most days — a little toddler called Mercedita whose hair is always perfectly slicked into a ponytail and whose hands are always sticky.
Lupita is certified in a natural family planning technique called NaPro, and she teaches it to married couples as a vocation. She is the perfect ambassador, because she radiates joy and confidence in God’s perfect plan.
In this you could say she is very much in the spirit of Blessed Pope Paul VI. But also you could say that she is very much in the spirit of Blessed Oscar Romero, even if this connection is not so obvious.
NaPro is short for Natural Procreative Technologies, a scientific approach to women’s reproductive health that works with nature, not against it. Lupita teaches married and engaged couples how to use NaPro to space their children, whom they rightly consider the highest gift of marriage.
Where the birth control pill does violence to the rhythmic dance of female hormones, NaPro uses biomarkers to monitor the delicate intricacy of the female cycle so that a man and his wife can plan their intimacy around them.
Instead of side effects from the pill (caused by suppression of natural hormonal functions) such as depression, stroke, and cancer, Lupita’s system has side effects like increasing a man’s respect for his wife’s complex femininity and enhancing mutual thoughtfulness and consideration.
Pope Paul VI understood how only a marriage in which the husband accepts and cherishes his wife’s totality, even her healthy, natural fertility, can truly be said to mirror divine love. Abstaining for part of the month can be hard, or tantalizing, depending on how you look at it.
Then, when the infertile period recurs, the couple “use their married intimacy to express their mutual love and safeguard their fidelity to one another. In doing this they certainly give proof of a true and authentic love.”
That quote is from “Humanae Vitae,” Pope Paul’s momentous encyclical that sang an elegy to marriage as representing the union of Christ and his Church.
It also explained just how artificial contraception would cause a “general lowering of moral standards” by teaching men to “forget the reverence due to a woman,” thus reducing women to an instrument for the satisfaction of desire.
He also wrote of the terrible temptation of governments, especially of those of developing nations, to address their understandable anxieties through antenatal programs that trample on the essential dignity of man.
What a strong temptation, when material goods are scarce or unevenly distributed due to selfishness or corruption, to encourage the poor to prevent their own joy by preventing their children — or worse — abort them.
This bring us to Blessed Romero. He was a man who drank deeply of the suffering of his brothers and sisters, the peasants who eke out a bare subsistence with all their drudgery, and too often go hungry.
He is the darling of many progressive liberals, who assume that he would have supported the legalization of abortion and the spread of artificial contraception from Yankee do-gooders as a liberation from the rigors of biology.
But they are wrong.
Romero spoke out forcefully against what Pope Francis would later call “ideological colonization,” the system by which affluent countries impose their decadent values on the vulnerable poor.
He railed against the “foreign specialists in the suppression of life” who came to El Salvador to teach the people that completely materialistic conception of family where a child is not a blessing but only a drain of scant resources.
He criticized secular societies like ours in the U.S., where pleasure and material well-being are the only yardsticks of fulfillment and cause a deep and wide hedonism that leads to all sorts of social injustice.
One of these is government policies that keep the poor immiserated, but another is what he called the “entire terrible campaign of contraceptives, of abortions … sins against the faith of Abraham; against the God who, as a gift, makes men and women fertile in their core.”
He was a firebrand, Romero, and it is no wonder he was martyred while celebrating Mass. Lupita is not a firebrand, but she lives a bit of martyrdom.
Pope Paul VI and Archbishop Oscar Romero in an undated photo (EQUIPO MAIZ, COURTESY CAFOD, JUST ONE WORLD)
It’s hard, even in Catholic circles, to be a spokeswoman, no matter how pretty and charming, for something so countercultural as living marriage in joyful cooperation with God’s love. It leads to children!
And her smile and that little Mercedita on her hip are sure signs that through them, it leads to joy.
Dr. Grazie Pozo Christie grew up in Guadalajara, Mexico, coming to the U.S. at the age of 11. She has written for USA Today, National Review, Washington Post and the New York Times, and has appeared on CNN, Telemundo, Fox News andEWTN. Her Angelus column, “With Grace,” earned a Catholic Press Association award for “Best Regular Column: Family Life” in 2018. She practices radiology in Miami, Florida, where she lives with her husband and five children.
One of the biggest claims made by advocates of emergency contraception — also known as the Morning After Pill, Ella, Plan B, and more — is that these pills do not cause an abortion. Supporters insist that the pills, no matter their brand, simply prevent a pregnancy from occurring in the first place. Planned Parenthood tells women there’s no way the Morning After Pill can cause an abortion, and the British Pregnancy Advisory Service (BPAS) insists the pills merely work “by preventing or delaying ovulation, not by terminating a pregnancy.”
Unfortunately, this is misleading to women, and many women know it. Bustle reports, “35 per cent of respondents to ellaOne’s survey thought the pill ’causes a mini abortion’, while 47 per cent of those surveyed by FPA ‘thought using emergency contraception was like an abortion, or weren’t sure.’” While the abortion industry dismisses these women’s suspicions as misinformation, they are actually rooted in fact.
In order to understand exactly how the Morning After Pill (and emergency contraception in general) can cause early abortions, one must understand the science behind pregnancy. Scientific textbooks from the disciplines of embryology, biology, and genetics all agree on when a new human life begins: at the moment of fertilization, when a woman’s egg cell and a man’s sperm cell fuse.
For years, science expressly taught that pregnancy began at fertilization, also known as conception. It was only when those who wanted to normalize hormonal birth control began to propose a more convenient definition that the lines were blurred. The year before the first oral birth control pill was approved by the FDA, the American College of Obstetricians and Gynecologists (ACOG) paved the way to argue that hormonal pills for women would not end their pregnancies.
In 1959, ACOG voted to change the definition of conception: instead of conception being equivalent with fertilization (the scientifically accurate view), the term “conception” was now altered to mean the same thing as implantation. With this change in definition, birth control manufacturers — and later, the makers of Plan B, the Morning After pill, and other emergency contraception — would be able to claim that these pills would not end a pregnancy.
A closer look at the manufacturers’ inserts reveals that they do still admit their products can prevent implantation. (Notably, hormonal birth control manufacturers and the makers of the copper IUD admit the same thing.) This means, of course, that fertilization can occur; a child can begin her life. But before she has been given the chance to implant in her mother’s womb — a process that generally occurs within six to 12 days — she is flushed out, her life ended.
Notice the parsing of words here — “pregnant” being used to describe when that new human life has fully implanted in the uterus. But that human life is already in existence prior to implantation and is making her way toward the uterus. When she arrives, it — according to Plan B itself — implantation may be “inhibited” or prevented, which means that human being will die.
Similar to the well-known types of hormonal birth control, emergency contraception floods a woman’s body with hormones her body would not normally be producing. The levels of the hormones are greater with the Morning After Pill and other forms of emergency contraception. This is not healthy or beneficial to a woman’s body, and can alter her reproductive system in dangerous ways.
Manufacturers and doctors alike admit that women who use emergency contraception are at a much higher risk of ectopic pregnancies, specifically if the pill fails to end the child’s life. If the child survives, but the womb has become an inhospitable environment due to the actions of the Morning After Pill, the child may attach herself elsewhere in the woman’s body, creating an ectopic pregnancy. Dr. Mary Maina studied the risk of ectopic pregnancies in women who had taken emergency contraceptives. She reported, “The risk of ectopic pregnancy increased 12 times in women who had used the pills.”
Women deserve the truth: the Morning After Pill and other emergency contraceptives can cause abortions, and they can create ectopic pregnancies where the child almost always dies (with rare exceptions) and the mother’s life is also at risk.
However, it is also a fact that the Morning After Pill does not always cause an abortion. The same is true with hormonal birth control in general and copper IUDs. They do not always cause early abortions. They can indeed prevent ovulation, thicken cervical mucous, and operate in preventive ways. However, the fact remains that the so-called “back-up” mechanism of these pills and devices is to stop a new human child from implanting, growing, and developing. No woman can know with an absolute certainty which mechanism is working in her body, and at what time.
Women are right to be concerned that emergency contraceptives may actually abort their newly-conceived children.
I did not think I would ever be a biological mother. This didn’t bother me; I was too busy anyway and much too afraid of the sheer pain of it all. I winced to hear the word “labor” in connection with childbirth. But love won me over.
It started with my need to be loved and cherished by someone. I know you have that need, too. A woman wants nothing quite as much as arms to hold her and a heart to lay her head on. Let’s be honest: this is at the root of some of our worst decisions, driven by passion, fueled by lust. We let ourselves be scorched by the heat of our hook-ups because we want someone to hold and harbor us and our fears. But it isn’t where we find love. My husband, however, knew how to love me unconditionally and it was in the comfort and security of his love that I found my true self.
But this letter isn’t about me, it’s about you. It’s about your desire for love. I want you to experience the strong, solid tethers of a true union, bound by marriage, within which love bears its most beautiful fruit — the birth of a child.
I gave birth to my first-born three months ago; a year ago she was conceived. And, yes, I labored, long and hard, to bring her into this world. But love once again won me over. Hers is like her father’s love, but even more so in its untainted innocence; she looks at me with a tender love that knows no limits. I am the first person she loved.
Every time she looks at me, she recognizes that I am unique – I am her mother – and she loves me uniquely. To be loved so fully and perfectly, to be embraced by her and know that to her, I am everything (for now), is a reward in itself.
Young woman, look no further for love than in the eyes of a child. They are like the eyes of God — in them you can see yourself anew and recognize that you are loved unconditionally. I can’t imagine now who I would be without my little daughter to teach me every day who I am. I can’t imagine how much love I would have lost without her.
Young woman, what is it worth to gain the world and not experience love? The love of a child is too beautiful to refuse. Choose life and you will find love.
Reprinted with permission from MercatorNet.
About the author Julia Dezelski is the assistant director for Marriage and Family Life, and Laity in the Secretariat of Laity, Marriage, Family, Life and Youth at the United States Conference of Catholic Bishops.
VATICAN CITY — In his general audience Wednesday, Pope Francis said that abortion “suppresses innocent and helpless life in its blossoming.”
“Is it right to take a human life to solve a problem? It’s like hiring a hitman,” Pope Francis said in St. Peter’s Square Oct. 10, in a departure from his prepared remarks.
“Violence and the rejection of life are born from fear,” the Pope added.
For this reason, parents who learn that their unborn child will have a disability need “real closeness, true solidarity to face reality, overcoming understandable fears,” he explained.
Pope Francis lamented that parents receiving a difficult prenatal diagnosis often “receive hasty advice to stop the pregnancy.”
It is contradictory to suppress “human life in the womb in the name of safeguarding other rights,” the Pope insisted.
“How can an act that suppresses innocent and helpless life in its blossoming be therapeutic, civil or simply human?”
The Pope’s remarks on abortion came during a reflection on the Fifth Commandment, “Thou shall not kill.” In recent weeks, the Pope has dedicated his weekly general audiences to a series of lessons and reflections on the Ten Commandments recorded in the scriptural books of Exodus and Deuteronomy.
“One could say that all the evil done in the world is summarized in this: contempt for life,” Pope Francis told the pilgrims gathered in St. Peter’s Square.
“What leads man to reject life? They are the idols of this world: money, power, success. These are incorrect parameters to evaluate life. The only authentic measure of life is love, the love with which God loves it!”
The positive meaning of the Fifth Commandment is that “God is a lover of life,” he continued.
“In every sick child, in every weak old man, in every desperate migrant, in every fragile and threatened life, Christ is looking for us; he is looking for our heart to disclose the joy of love. It is worthwhile to accept every life because every man is worth the blood of Christ. We cannot despise what God so loved!” Pope Francis said.
While a sick child or an elderly person who needs assistance can be viewed as a burden, this can actually be “a gift from God,” explained the Pope. This vulnerable life can “pull me out of self-centeredness and make me grow in love.”
Demographers have previously thought that low fertility among US women is a result of the 2008 Great Recession and will recover at some point, just as it has following historic recessions. It was thought that many women were simply delaying pregnancy and there would be a cyclical rebound. However, it seems increasingly likely that structural changes may mean that the US fertility rate never recovers.
A recent study undertaken by The Center for Retirement Research at Boston College backs this up. Among its key findings is that, while fertility typically rises in expansions, in the current expansion it has actually declined more than it did during the recession.
The following four structural changes suggest the decline in the birthrate between 2001 and 2016 may be more permanent than previously thought:
a falling birthrate among Hispanics – this group has historically had a higher birthrate than the general U.S. population and was previously propping it up but is no longer doing so;
a rising share of women with college degrees – this group tends to have fewer babies;
increasing numbers of people who do not identify as religious, another group which tends to have fewer babies; and
a rise in the female-to-male wage ratio, meaning women are more likely to be focusing on career over motherhood and are therefore likely to continue to have fewer babies.
This spells trouble for future retirees. As the reports states,
“The future of the fertility rate is important in that it determines the age structure of the population, the ratio of workers to retirees and, hence, the finances of the Social Security system (which operates largely on a pay-as-you-go basis).
According to the 2018 Social Security Trustees Report, a total fertility rate of 1.8 children per woman instead of 2.0 would increase the program’s 75-year deficit by 0.41% of taxable payrolls or a present value of almost $2 trillion.”
The total fertility rate in 2017 was just 1.76 births per woman, according to the paper. That was a slight increase from 2016 when it stood at just 1.7, the lowest birth rate in American history.
Not only do lower birth rates mean a struggle to pay benefits at existing rates, they also mean that there will be a decline in the number of family members and friends available in the future to freely care for the elderly, likely increasing demand on state care and decreasing quality of life for the dependent elderly.
So what should the US do? Increase immigration or create a culture and develop incentives which mean US women have more babies?
CHRISTINA VAZQUEZ OCT 8, 2018 | 3:04PM WASHINGTON, DC
A recent report from the Medical Journal of Australia found that many who had used some form of contraception ended up becoming pregnant anyway. The data published in the report comes from the results of a national, random survey of Australian women aged 18 to 45, according to AJP News.
The report continues:
Most women who had unintended pregnancies (205 of 362, 56.6%) reported not having used contraception at the time. Of the 150 women (41.4%) who had an unintended pregnancy while using contraception, 96 (64%) had used oral contraceptives and 40 (26.9%) had used condoms as their primary methods; nine (6%) were using long-acting reversible contraception.
The researchers warned that while nearly one in five women who had been pregnant reported an abortion, this number was likely lower than the actual figure due to “under-reporting on this sensitive topic”.
In other words, four in 10 women facing an unplanned pregnancy were using contraception at the time, according to the report.
Not only does contraception have a spotty track record for preventing pregnancy, but it has led to some other harmful side effects through the years.
Abby Johnson, a former Planned Parenthood employee turned pro-life advocate, discusses the risks of contraception on her website. Some hazardous risks of “the pill,” a known group-1 carcinogen, are breast, cervical and liver cancers, as well as heart attacks.
Meanwhile, reductions in contraception have connections to reductions in teen pregnancy and abortion. A 2017 study from the Journal of Health Economics found that recent budget cuts in Great Britain’s sex-education program were correlated with statistically significant reductions in both the teen pregnancy rate and the teen abortion rate.
Regardless of the pro-abortion movement’s insistence on contraception, it has shown time and time again that it is not the best way to prevent pregnancy. Thomas Peters of CatholicVote.org says the contraception-to-prevent-abortion argument is weak.
“When faced with the raw numbers that contraceptive use does not rule out ‘unplanned’ pregnancies, Planned Parenthood responds by saying we need more contraceptive use. That’s like a textbook definition of insanity: doing the same thing over and over again and expecting a different result,” Peters said.
By Felix Carroll (Oct 5, 2018) This is what tuberculosis can do to you: Attack the lungs, kill tissue, and spread to the brain and the bones. Coughing becomes a given — sometimes mucus, sometimes blood. Breathing can become difficult. You may wheeze and feel chest pains and sweat excessively. You may become fatigued and feverish and lose weight such that you become a mere fragment of your former physical self.
Eighty years ago, on Oct. 5, 1938, St. Maria Faustina Kowalska, the great apostle of Divine Mercy, died at the age of 33 from complications from tuberculosis and other ailments, which included internal hemorrhaging.
Firsthand accounts collected by biographers over the years attest to the fact Faustina suffered a physically agonizing death. Yet, just as Faustina shows us how to live — united to God’s will — in her death, Faustina shows us how to die. She was prepared and unafraid.
Here is how Sr. Stella Kozlowska described the once-attractive Faustina just days before her death, as explained in Ewa K. Czaczkowska’s Faustina: The Mystic & Her Message (Marian Press): “Her face was gaunt, and its shape had changed. Her skin was yellow, and her eyes were huge and sunken … .”
Other sisters later said they found it painful to even look at her. Yet they reported that, all the while, Faustina remained stoic, even cheerful and smiling.
“Sister dear, you are not afraid of death?” Sr. Crescentia asked her, according to Maria Tarnawska in her now-out-of-print Marian Press book, Sister Faustina Kowalska — Her Life and Mission.
“Why should I be?” Faustina responded from her deathbed. “All my sins and imperfections will be consumed like straw in the fire of the Divine Mercy.”
On the day of her death, Faustina, in agony, announced, “Today Jesus is going to take me with Him,” writes Czaczkowska. Faustina said so, not only with confidence, but with longing. The sisters gathered around her for one last time and prayed for her as her mind began to dim. The future saint took her last breath at 10:45 p.m. In her last moments, she lay quiet and peaceful.
The sisters who visited her in her last days reported feeling God’s presence in the room. Even those few sisters who showed ambivalence with regard to Faustina in her healthier days reported feeling they were in the presence of a saint.
Her pursuit of mystical union
Saint Faustina’s now-famous Diary gives us a fuller picture of her state of mind as she approached death. As her physical pain and exhaustion grew in intensity, so, too, did her mystical union with Christ.
She details a three-day retreat less than four months before her death (see Diary, 1753-1779).
During the retreat (led by Christ Himself), He assured her of the sanctification and salvation available through the Sacraments, particularly the Holy Eucharist and Confession. He taught her to totally abandon herself to His will; to put her “self-love in the last place”; shun gossip “like the plague”; act kindly to those who sought to cause her harm; hide in His Heart whenever confronted by temptation and discouragement; trust He is always with her; pray for the sick and dying; and to always be adorned by the virtues of humility, purity of intention, and love.
But He also minces no words with regards to the sufferings ahead. He says He will “not delude” her “with prospects of peace,” and tells her that her “body and soul will often be in the midst of fire.”
“Although you will not feel My presence on some occasions,” Christ says, “I will always be with you. Do not fear; My grace will be with You” (1767).
Jesus directs His words as much to Faustina as to us. Her recording of the retreat reads like a crash course geared to all who seek holiness.
An eternal ellipsis
Prepared thusly, Faustina’s happiness, spiritual strength, and glorification of Jesus became all the more pronounced.
By then, she could no longer live a normal community life. Still, strengthened through the Holy Eucharist, she taught herself to put her sufferings to divine use, to transform them into a daily oblation for the salvation of souls.
Though undated, Faustina’s final Diary entry is believed to have been in mid-June 1938. She no longer had the strength to continue. But by then, what else could she say? Save for a final Confession and Last Rites, she was fully prepared to die. In her final Diary entry, she writes:
Today, the Majesty of God is surrounding me. There is no way that I can help myself to prepare better. I am thoroughly enwrapped in God. My soul is being inflamed by His love. I only know that I love and am loved. That is enough for me. I am trying my best to be faithful throughout the day to the Holy Spirit and to fulfill His demands. I am trying my best for interior silence to be able to hear His voice … (1828).
That’s how the Diary ends — with an ellipsis. That’s how St. Faustina died, too, with an ellipsis, so to speak, a dot, dot, dot indicating that the story continues. Yes, life everlasting has only just begun.
As it was for a saint, so it is for ourselves: When we keep our eyes fixed on Jesus’ Merciful Heart, we should rest assured that someday, like Faustina, we will rest in peace.
Around 80 per cent of pregnant women report some kind of morning sickness and up to 2 per cent will be diagnosed with hyperemesis gravidarum, a severe form likened to the nausea caused by chemotherapy and from which the Duchess of Cambridge suffered.
In final clinical trials Xoneva was found to reduce the amount of nausea by two thirds and cut the number of episodes of sickness from four a day to just one.
Unbearable symptoms driving women to abortion
Some 15% of HG pregnancies in the US end in abortion, and abortion provider BPAS estimates that 1000 pregnancies a year are terminated in the UK because of debilitating symptoms. Last year, a charity warned that suffering women were being denied help by NHS staff, driving many into abortion.
SPUC researcher Fiorella Nash, who suffered from the condition in all four of her pregnancies, says that HG is “one of the most distressing and misunderstood complications of pregnancy”. In her book the Abolition of Woman, she writes that the overwhelming majority of abortions triggered by HG “are unwanted, causing high levels of grief, guilt and anger from women who are driven to abortion as a result of being unable to cope with their symptoms.”
“This is a very welcome breakthrough,” she said. “HG is an incredibly distressing condition, which as well as damaging the woman’s health and elevating the chance of miscarriage, drives a significant minority into abortions they do not want. If this new drug goes any way to alleviate women’s suffering, it’s very good news.”
Attitudes need to change
However, she said that a change in attitude from the medical profession was also needed. “Women have reported being patronised, dismissed, instructed to pull themselves together, or being told it was ‘all in the mind’. My own doctor lectured me for being so silly as to ‘purposefully’ dehydrate myself when I came to her vomiting blood. It’s disgraceful that in the 21st century women with pregnancy complications that can lead to high levels of miscarriage, and the sort of desperation that leads them to abort, are not being given the care they need.
“When women end up having abortions because of HG, it’s because they’re in such a state of despair that they literally can’t see any other way out,” she continued. “What kind of choice is that? Women who are that sick are incredibly vulnerable, and it’s ludicrous that they are left with no support. What’s really tragic is that these are often very much wanted babies, and inadequate care drives women to do something they never usually would. These women don’t need abortion, they need to be taken seriously and have their very serious medical condition treated.”
Let’s hope that this new drug and better medical care means that women feeling there is no way out of their sickness than abortion is a thing of the past.
October 1, 2018 (The Catholic Thing) – Like other professional men, if I want to attend weekday Mass, I have a choice between an early Mass in my parish and a mid-day Mass near my work. I love seeing colleagues at the later Mass, and the thrill of the sacrifice, which comes specifically from putting work aside for the moment and giving that time directly to God. But at the morning Mass I have the great blessing of being instructed in Christian wisdom by the moms there with little children.
My parish is St. Jerome’s in Hyattsville, celebrated as a strong community in a “Benedict option” sort of way. Many families live within walking distance of the church. On any weekday, there can be ten or fifteen moms at Mass. Most have one child with them, but some bring two or three – perhaps one in a sling, another in a stroller, and a third getting around on his own steam. If the family is homeschooling sometimes older children, too, get up early and lend a hand.
At most parishes there will be a couple of moms like this, not always the same ones at every Mass. In a city, where there are many parishes, and people improvise to catch the most convenient Mass, these moms with children will come to know one another, forming a kind of secret conspiracy of real Catholic devotion.
I mentioned being schooled in Christian wisdom, first of all – paradoxically – by the example of the husband and father, who is not there. These moms are mainly homemakers, although some, of course, will have jobs on the side. The point is that the husband has not insisted that they go out into the workforce full time, as many do. He is willing to accept the cares and occasionally large sacrifices that go along with raising a family on a single income. That is, he is a highly noble figure in our day. The mom and the father together testify to the priority of their children over wealth and security.
Secondly, I am instructed by the heroism of the mom. It’s important to emphasize that it is heroism, “above and beyond the call of duty” (more shortly on “duty”). How heroic? Morning Mass is a deeply ordered act, which the mom manages to set up at the start of the day, at a time of life that inherently resists order. Her presence at that service has all of the character of a beachhead on Iwo Jima; the consecration and her Communion, a raising of the flag.
To get there at all, she’s wrestled a child to change a diaper, and wrestled with a couple others too, or pleaded and cajoled, to get them dressed. In winter, there are layers of clothing, potentially depressing to put on, knowing that they have to come off and be put away in an hour. Always there is the principle of household entropy at work, the tendency to disorder.
Her path goes all uphill. The church will be cold in the winter and hot in the summer. Most likely the homily will be uninspiring: she’s grateful if it doesn’t knock her back (“women don’t have to breed like rabbits”) or promote a heresy, like the one she was arguing against with a Protestant friend at a book club last week. Don’t discount the small mortification of often appearing in public not “put together.” (In that sense she did give up the heels and lipstick, as in the abortion ad.)
But above all there is the repeated mortification involving the “main show,” the reason she is there at all, to pray and worship. Her children are fussy or asking her for things. They can’t sit still and run all over. She has to take them to the back, yet again. She sits on a chair in the vestibule, plays give-and-take with her toddler, and can barely hear anything in the sanctuary. It’s far from the romantic ideal of peaceful communion with God. What is the point of this? It’s not even clear she’s improving in anything, she thinks.
But her perseverance proves important truths, to which over time she becomes a “martyr” or witness. Others may read about them in books, but she at least learns them by concrete experience. Consolations in prayer do not matter. We give ourselves to God through the will, not the imagination. Grace will assuredly be imparted by the objective character of the sacrament and a believer’s subjective willingness to receive.
In simply getting to “the place of grace” in the morning, she is standing beside the Cross with Mary and becomes, like her, a “spiritual vessel, vessel of honor.” She cannot “feel” the grace that she gains at the Mass, and that flows out from her to her family, relatives, friends, and prayer intentions, but as an exercise of faith she trusts that it is so.
We live in a society where people are afraid to praise anyone (but in personal life only) for fear of seeming to criticize everyone else. I know that. Let’s be plain then: there are many moms who want to get to weekday Mass but can’t manage it, or who started and couldn’t continue. Likewise, there are couples where the mom would love to stay at home and can’t, or in conscience before God believes she can and should work full time. I am not criticizing these brethren in the slightest, not by a long shot.
I say, instead, for Christians the strange “logic” of a parable seems at play. Remember the workers who were hired at the last moment but got the same payment as those who bore the brunt of the day’s work? Yes, there are degrees of glory, but that parable would seem to hold for more than differences in time. Who knows how the Lord will repay in his generosity?
But that moms at Mass are heroes of the faith, among others not at Mass, that is a sure thing.
KATIE FRANKLIN OCT 1, 2018 | 4:37PM WASHINGTON, DC
For more than a decade, women have used Abortion Pill Reversal as a means to stop their in-progress chemical abortions and save their unborn babies’ lives.
“This new milestone represents not only 500 lives saved, but 500 women who were given a second chance to choose life and save themselves and their babies from a terrible fate,” said Jor-El Godsey, president of Heartbeat International, a global network of more than 2,600 pregnancy help locations. “Thanks to the prayers and commitment of all the medical providers, pregnancy help centers, and generous donors who make the Abortion Pill Rescue Network possible, 500 precious children are alive today.”
Abortion Pill Rescue—the network of more than 400 medical practitioners who administer the protocol—answers well over 100 calls per month from its 24-7 helpline (1-877-558-0333) run by Heartbeat International’s Option Line. That figure is up from 50 calls per month since the hotline changed hands this spring.
Abortion Pill Reversal’s Proven Success
With chemical abortions accounting for as many as 40 percent of abortions throughout the U.S., the need for Abortion Pill Reversal is great.
Otherwise known as the “abortion pill” or RU-486, chemical abortions actually involve a two-pill regimen.
The first pill, mifepristone, works by telling a woman’s body to stop producing progesterone—a natural hormone that is necessary to sustain a healthy pregnancy—thereby starving the baby of nutrients. The second pill, typically misoprostol, induces labor, forcing her body to expel the baby.
Pioneered by doctors George Delgado and Matt Harrison in 2007, the Abortion Pill Reversal treatment works by giving women extra progesterone up to 72 hours after a woman takes the first pill, mifepristone.
Research released by Delgado this year revealed the protocol’s success. According to his study, up to 68 percent of women who changed their mind about an abortion and started the Abortion Pill Reversal treatment were able to give birth to a perfectly healthy baby.
The findings, though reaffirming of Abortion Pill Reversal’s validity, were not altogether surprising since progesterone has been used as an FDA-approved protocol to prevent miscarriages since the 1950s.
Now, successful Abortion Pill Reversal has been reported in 46 states and 17 countries, including the U.S. There are 430 medical practices, in addition to 84 pregnancy help centers that prescribe Abortion Pill Reversal.
Although abortion advocates have dismissed the life-saving treatment as “junk science,” dozens of women are now publicly sharing their success stories, putting faces and names to the human beings who are alive today because of Abortion Pill Reversal.
Emily is one of them.
Emily’s Story
At 19, when Emily discovered she was pregnant, she was happy, surprised, and scared all at the same time. A freshman in college and living at home, she feared her parents’ reaction.
Although her sister and her best friend built her up with encouragement, her ex-boyfriend, the father of her baby, responded with anger.
“[He] told me I deserved it, it was my fault, and I was a horrible person who he wanted nothing to do with…I decided abortion was my only choice,” Emily writes in a reflection.
At four weeks pregnant, she made an appointment at Planned Parenthood. Her experience there was far from optimal.
“They rushed through my appointment and gave me the first half of the abortion pill,” she wrote. “I felt horrible being at Planned Parenthood. They treated me as if nobody cared about me.”
She left Planned Parenthood feeling terrible.
“When I went home from Planned Parenthood at 5:30 pm on a Friday in downtown California traffic, it was pouring rain and I felt like it was God crying tears for me,” she writes. “I cried the whole way home. I felt so sad that I took the pill in the little white cup at Planned Parenthood.”
Worse still, this was the second time she’d done it. At 17, she had her first abortion, what she says is her “worst memory, the worst thing I’ve ever done.”
“I regret it everyday of my life and it breaks my heart continually,” she says.
When she got home, things began to change as she prayed, asking God for help.
“As soon as I got home I took a shower to hide how much I was crying from my parents,” Emily writes. “I cried under the water for a few minutes before I decided an abortion is not what I wanted. I wanted my baby. I began to pray as hard as I could for forgiveness and help.”
Then, she had an idea: Maybe she could “reverse” the abortion.
“I know God put it in my mind because I had no idea what that was previously or if it was possible,” she writes.
With her sister at her side, she did a Google search and found a hotline number, which she dialed immediately. A woman answered her call and connected her to a local pregnancy help center where she made an appointment for early the next morning.
“They showed me models of the baby at various stages of pregnancy and I saw how tiny, vulnerable and beautiful a baby was,” she said.
As soon as I got home I pulled my mom into my bedroom and told her everything. She cried when I said I got an abortion but was happy but weary when I told her about the reversal. She came with me to my next appointment on Sunday and joined me once and for all. To this day she’s never left my side or support. She supported me my whole pregnancy and she does now as the best grandma (to) my child. I heard the heartbeat in November right before Thanksgiving and I was so happy to know the reversal worked! I thanked God so much as I continue to everyday for my blessing. At nineteen weeks I discovered I was having a boy. I named him Ezekiel, which means “God Strengthens.”
Today, Emily is married to a man who she says loves Ezekiel as much as she does. Zeke, as they call him, is in preschool and Emily works as a paraeducator for special needs third graders.
“God saved my life by saving my son’s life,” Emily says. “Zeke means everything to me and is the best thing that’s ever happened to me. Being a mom came so naturally to me and it gave me the strength to get to know God again, go back to college, get a good job and buy a house. Everything I do, I do for Zeke and because of Zeke. He is the absolute light of my life and I love him with my whole heart. There’s nothing I wouldn’t do for him.”
LifeNews Note: Katie Franklin is managing editor for Pregnancy Help News and content writer at Heartbeat International. She previously served as director of communications for Ohio Right to Life and is a graduate of Denison University where she earned a B.A. in history in 2013. Katie lives in Columbus, Ohio with her husband Miles and daughter Elizabeth.
September 26, 2018 (LifeSiteNews) – Several centuries before Christ, Aristotle had observed in his work Nicomachean Ethics: “Children seem to be a bond of union. Hence sterile couples separate more readily, for children are a common good of both parties; and what is common maintains friendship.” In the thirteenth century St. Thomas Aquinas commented as follows on this passage:
Next, he [Aristotle] indicates a means of making this friendship [of marriage] strong. He remarks that children seem to be a cause of a stable and lasting union. Hence, sterile couples who fail to have children are separated more readily. In fact, divorce was granted in former times because of sterility. And the reason for this is that children are a common good of both husband and wife whose union exists for the sake of children. But what is common continues and preserves friendship which also consists in sharing (communicatio), as has been pointed out.
A moral philosopher who was well acquainted with both Aristotle and Aquinas, Pope John Paul II seemed to have just this thought in mind when he wrote in his Letter to Families:
In the newborn child is realized the common good of the family. Just as the common good of spouses is fulfilled in conjugal love, ever ready to give and receive new life, so too the common good of the family is fulfilled through that same spousal love, as embodied in the newborn child.
Even the Enlightenment philosopher Baruch Spinoza (1632–1677)—a hard-core modern who asserted that things in nature do not act for an end and that final causes are the products of our fantasy—could not deny in his Ethics that marriage is inherently bound up with children. It was as if the facts themselves compelled his assent:
As concerning marriage, it is certain that this is in harmony with reason, if the desire for physical union be not engendered solely by bodily beauty, but also by the desire to beget children and to train them up wisely; and moreover, if the love of both, to wit, of the man and of the woman, is not caused by bodily beauty only, but also by freedom of soul.
We are thus not completely unprepared for the rather sharp observation of Blaise Pascal (1623–1662) in his Pensées that children are so much the good of marriage that married people who avoid them selfishly are worse than fornicators:
It is not the nuptial blessing [of the Church] which takes away the sin from procreation, but the desire to procreate children for God, which is only genuine in marriage . . . The daughters of Lot, for example, who only wanted to have children, were purer without marriage than married people who have no desire for children.
What is the problem with such a lack of desire? What does it tell us? We could begin with the probing remarks of Gabriel Marcel, who in his work Homo Viator descries the contradiction of contraception:
The advocates of birth control claim more or less sincerely that it is out of pity for their possible descendents that they refuse to give them the chance of existence; but we cannot help noticing, all the same, that this pity which is bestowed at small cost, not upon living beings but upon an absence of being or nothingness, is found in conjunction with a suspiciously good opportunity for indulging the most cynical egoism, and can scarcely be separated from an impoverished philosophy which measures the value of life by the pleasures and conveniences it provides.
What Marcel is pointing to is the inherent selfishness of wanting to “keep marriage just for the two of us.” This is contrary to its very nature as a good thing, since good things are meant to be shared, spread out, multiplied, and perpetuated. If we do not want to multiply the loaves and fishes that God has given us a natural power to multiply, we are starving ourselves and others. If we do not seek a living image of our love, by which it can transcend itself and demand still more love, we are purposefully throwing up a barrier to the maturation of friendship, the increase of virtues, the growth of our humanity. In short, it is self-crippling, self-enclosing, self-imploding. It is all about me, a little about you inasmuch as you serve my perceived needs, and nothing about anyone else. No wonder Aristotle and Aquinas think such a relationship unstable and ready to break apart.
Granted, this description would only apply in full to those who are in the grip of an extreme anti-family mentality, of which, sadly, there seem to be an increasing number in the contemporary Western world. But it is the nadir, the limit case, of a trend of thinking and feeling that fails to see or refuses to see how spousal love is literally “embodied in the newborn child.”
The wisdom of the Catholic Church is far different from the folly of the world. Her teaching inspires, challenges, and consoles. In his encyclical Casti Connubii, Pope Pius XI voices this wisdom:
God wishes men to be born not only that they should live and fill the earth, but much more that they may be worshippers of God, that they may know Him and love Him and finally enjoy Him for ever in heaven; and this end, since man is raised by God in a marvelous way to the supernatural order, surpasses all that eye hath seen, and ear heard, and all that hath entered into the heart of man. From which it is easily seen how great a gift of divine goodness and how remarkable a fruit of marriage are children born by the omnipotent power of God through the cooperation of those bound in wedlock.
What a privileged way of sharing the greatest of goods—to baptize sons and daughters, bring them up in the fear and love of the Lord, and set them on their way to eternal life with Him and the whole company of the blessed—and to do so as a couple, as a family!
In news that adds further evidence that home abortion is risky for women, a large Swedish study has suggested that the practice is the reason complications for medical abortion have doubled in six years.
The study, published in BMC Women’s Health, concludes: “The rate of complications associated with medical abortions [at less than 12 weeks gestation] has increased from 4.2% in 2008 to 8.2% in 2015. The cause of this is unknown but it may be associated with a shift from hospital to home medical abortions.”
The Westminster Government last month announced it plans to follow the Scottish and Welsh governments in approving the medical abortion pill for home use – a decision SPUC is fighting in the courts.
What does the study say?
The study analysed all the women who underwent abortions at Skaraborg Hospital in Sweden between 2008 and 2015 – a total of 4945 abortions.
For most of these women, medical abortion at home was the recommended procedure. Home abortion has increasingly become the norm in Sweden; by 2015, 85.2% of all medical abortions before the 9th gestational week were carried out at home – an increase of over 10% from 2008-9, when the number was 74.6%.
In the same time frame, the complication rate (bleeding, infections, and most commonly, incomplete abortions) for medical abortions before 12 weeks has increased from 4.2% to 8.2%.
Why is this?
The researchers suggest several times that the increase in abortions at home may be to blame. “There was a significant increase in the share of complications related to medical abortions…One potential reason is that the proportion of induced abortions performed at home has risen. It is likely that women who have medical abortions at home will visit our outpatient clinic in a greater extent since they do not have the direct help and support from a midwife.”
Important implications
SPUC is currently appealing a decision by a judge at the Edinburgh Court of Session to back the Scottish Government’s home abortion policy.
Deputy Chief Executive John Deighan said: “This study appears to back what we have been saying all along – that home abortions are risky for women. Sweden is known to have very good data on abortion, and the conclusions of a large scale study like this, where home abortion has been the norm for more than a decade, are not to be taken lightly.
“We call on the Government to urgently review their decision to allow home abortion in light of this new evidence.
“We are still of the view that abortion at home is not lawful and the evidence shows the threat it poses to women’s health,” he concluded. “This latest research suggests that women taking the abortion pill at home cannot be ruled out as a factor leading to a significant increase in complications in a country where it has been extensively tried.”
LifeNews Note: Courtesy of SPUC. The Society for the Protection of Unborn Children is a leading pro-life organziation in the United Kingdom.
It’s been a tough summer for Catholics this year, and I would not be surprised if by now you’re tired of hearing and reading about church scandals, church politics, and maybe even church in general. As we wait for our bishops, cardinals, and the Pope to shed light on how they will address these problems and “clean house”, we lay people can feel rather helpless. Especially as we watch our beloved Church get attacked from the outside and ripped apart from within.
But I have news for you… well not quite news, but an important reminder: as parents, we can reform the church by the way we raise our children.
This is so important. The scandalous and tragic events that are rocking the church should impel us to take ever more seriously our vocation as parents to raise holy men and women devoted to God. Families are the seedbed of vocations; from our homes come the future priests, nuns, and leaders of the church. Holy families make a holy church.
The other scandal: ignoring Humanae Vitae
I don’t think it’s a coincidence that the 50th anniversary (July 25, 2018) of Humanae Vitae came shortly before the revelations of McCarrick’s scandalous behavior and the Pennsylvania Grand Jury’s report. Fifty years of disregarding and watering down the Church’s teachings on human sexuality have, as Pope Paul VI predicted, eroded society’s moral sense, even among practicing Catholics.
Somehow, too many Catholics have bought into the secular lie that sexual sins are not really sins at all because they’re private and therefore don’t affect other people. But they do. All sins hurt the body of Christ, but especially sexual sins, because they are so damaging physically, emotionally, psychologically, and spiritually. Sexual sins not only debase and demoralize individuals, they also ruin couples and therefore families, which are the keystone of society.
Thus, pre-marital sex and the use of contraceptives, which the Catholic Church has always considered to be mortal sins, are today considered the norm. Pornography runs rampant along with sexual abuse, homosexuality, marital infidelity, and family breakdowns. Millions of babies have been aborted since Roe vs. Wade. And now we learn that leaders in the Church have been covering up sexual abuse of minors and seminarians for decades. If Catholics had only embraced Humanae Vitae instead of ignoring or dissenting from it, the church (and society at large) might not be in the deplorable mess it’s in right now.
Where do seminarians and priests come from? Not straight from heaven. They come from families, which today live in a conscience-deadened society. We often think of the church as having an effect on society, but society also has an effect on the church. For the church is both divine and human, and therefore subject to the weaknesses and imperfections of human nature. So when seminarians and priests come, by and large, from a sickened and licentious society, should it really be so shocking (albeit scandalous and disturbing) that a few or maybe more of them commit sexual sins?
The church needs families who are radically pursuing holiness, families who can “purify the air” around them by their witness to love and joy. Families can be the wellspring of a new evangelization. They can bring forth a new generation dedicated to Christ and His teachings who will, with the grace of God, transform society. But the radical holiness of a family begins with the love between husband and wife, a love that is unconditional and faithful, unitive and procreative. A love that embraces the tenets of Humanae Vitae.
Here are the main points of Humanae Vitae in a nutshell:
Married love is total, faithful, and fecund (life-giving). “Marriage and conjugal love are by their nature ordained toward the procreation and education of children. Children are really the supreme gift of marriage and contribute in the highest degree to their parents’ welfare.” (HV 9)
The exercise of responsible parenthood requires that husband and wife, keeping a right order of priorities, recognize their own duties toward God, themselves, their families and human society. Thus, they are bound to ensure that what they do corresponds to the will of God the Creator. (HV 10)
Each and every marital act must of necessity retain its intrinsic relationship to the procreation of human life. (HV 11)
An act of mutual love which impairs the capacity to transmit life which God the Creator, through specific laws, has built into it, frustrates His design which constitutes the norm of marriage, and contradicts the will of the Author of life. … But to experience the gift of married love while respecting the laws of conception is to acknowledge that one is not the master of the sources of life but rather the minister of the design established by the Creator. (HV 13)
The direct interruption of the generative process already begun and, above all, all direct abortion, even for therapeutic reasons, are to be absolutely excluded as lawful means of regulating the number of children. Equally to be condemned, as the magisterium of the Church has affirmed on many occasions, is direct sterilization, whether of the man or of the woman, whether permanent or temporary. Similarly excluded is any action which either before, at the moment of, or after sexual intercourse, is specifically intended to prevent procreation—whether as an end or as a means. (HV 14)
If … there are well-grounded reasons for spacing births, arising from the physical or psychological condition of husband or wife, or from external circumstances, the Church teaches that married people may then take advantage of the natural cycles immanent in the reproductive system and engage in marital intercourse only during those times that are infertile, thus controlling birth in a way which does not in the least offend the moral principles [described in Humanae Vitae]… (HV 16)
Being open to life is not easy. In fact, it can be so hard and scary that most people think that not contracepting is irresponsible and foolish. But when a couple allows the Lord to permeate every facet of their lives, including what happens in the bedroom, and trustingly welcomes every child God gives them, God blesses their marriage and family immensely. And He uses their families to sanctify the world around them.
Saints are the proof
Let’s look at some of the great saints who have had a substantial impact on the life of the Church: St. Ignatius of Loyola, founder of the Jesuits, was the youngest of 13 children. St. Catherine of Siena, third Order Dominican who convinced Pope Gregory IX to leave Avignon for Rome, was the youngest of 25 children. St. Charles Borromeo, who played a key role in the Counter Reformation, was the third of six children. St. Louis de Montfort, the great Marian saint, was one of 18; 11 of his siblings had died in infancy. St. Francis de Sales, Doctor of the Church, was the oldest of six. St. Bernadette of Lourdes was the eldest of nine. St. Faustina Kowalska was the third of ten children. St. Therese of Lisieux, Doctor of the Church, was the youngest of nine children. The list of saints born to parents who were open to life goes on and on. (And yes, even in the Middle Ages there were ways of contracepting.)
Of course, this is not to say that to produce a saint, one must have a large family. After all, it is God who makes saints, not parents or the saints themselves. But God so loves the generosity and steadfast faith of those parents who are open to life that He often blesses them with children who would change the world and bring them eternal joy. In any case, it is not the number of children that matters, but the openness to God’s will in our lives and the faithfulness with which we live out His commands as taught to us through the Church.
My favorite example is St. Pope John Paul II , who was one of four. It is interesting to see the spacing of the siblings in his family: John Paul II (born Karol Wojtyla) had an older sister who died before he was born. His brother Edmund was thirteen years older than he. And his mother died in childbirth at the age of 45, when he (Karol) was only eight. The wide spacing of the children in the devoutly Catholic Wojtyla family suggests that the parents were open to life even when his mother was at an advanced age, and it is an example that being open to life does not necessarily result in a large family.
Considering that John Paul II’s mother died in childbirth, one might think he would have condoned the use of artificial contraceptives, at least in cases of advanced maternal age or other extenuating circumstances. Yet during the drafting of Humanae Vitae, Cardinal Wojtyla strongly supported and assisted Paul VI in his writing. He fully understood that “the teaching of the church regarding the proper regulation of birth is a promulgation of the law of God Himself” (HV 20). Indeed, it is only with the eyes of faith that can we see God’s loving and provident hand in the untimely death of Karol’s mother. The example of the Wojtyla family shows us that being open to life does not spare us from suffering, but it does draw forth tremendous blessings, such as having holy children.
So, as bishops and cardinals look for new ways to reform the church, let us who are married do our part by being faithful to our vocations as spouses and parents. By our example, let us show our children the beauty of conjugal love and marriage as God planned it. Doing so will confer upon us “a deeper and more effective influence on the education of [our] children.” (HV 21) Co-operating with God in this way, we can raise strong, convicted men and women who are committed to living lives of holy purity while protecting and upholding the Church’s teachings on love and marriage.
The renewal of the Church can come from the heart of our homes.
Mary Cooney is a home-schooling mother of six who lives in Maryland. The above article is a slightly abridged and edited version of one published on her blog, Mercy for Marthas. Read the original article.
WASHINGTON, D.C., September 25, 2018 (LifeSiteNews) – The Trump administration has canceled a $15,900 contract for medical research using aborted babies’ remains, but pro-lifers warn that far more funding – nearly $100 million – for similar experiments remains in place.
Last month, a notice from the U.S. Food and Drug Administration (FDA) surfaceddetailing a contract to the fetal tissue procurement firm Advanced Bioscience Resources, Inc. (ABR) to acquire “Tissue for Humanized Mice.” The tissue was meant to give mice a “humanized” immune system for the purpose of drug testing.
Between the use of tissue from aborted babies and ABR’s past work with Planned Parenthood in the abortion giant’s 2015 scandal over selling aborted baby parts, 48 pro-life leaders representing LifeSiteNews, the Center for Medical Progress, Susan B. Anthony List, Priests for Life, Operation Rescue, and other groups sent a letter to Health and Human Services (HHS) Secretary Alex Azar on September 11 demanding the contract’s cancellation.
“We expect far better of our federal agencies – especially under the leadership of a courageous pro-life president – entrusted with the health of American citizens,” the pro-life letter reads. “It is completely unacceptable to discover that the FDA is using federal tax dollars and fomenting demand for human body parts taken from babies who are aborted.”
85 members of the House of Representatives also sent a letter about the contract to FDA commissioner Scott Gottlieb on September 17, declaring, “unborn children are not commodities to be bought and sold” and the “practice of conducting research using the body parts of children whose lives have been violently ended by abortion is abhorrent.”
On Monday evening, HHS released a statement announcing it has terminated ABR’s contract because the department “was not sufficiently assured that the contract included the appropriate protections applicable to fetal tissue research or met all other procurement requirements.”
The statement also announced an “audit of all acquisitions involving human fetal tissue to ensure conformity with procurement and human fetal tissue research laws and regulations” and a “comprehensive review of all research involving fetal tissue to ensure consistency with statutes and regulations governing such research, and to ensure the adequacy of procedures and oversight,” and that it will continue researching ethical alternatives to using fetal tissue.
But pro-life leaders say the move hasn’t resolved the controversy.
“Canceling a single contract and conducting a review is a small step forward, but overall is completely inadequate,” said Susan B. Anthony List president Marjorie Dannenfelser, noting that almost $100 million continues to fund other research using tissue and organs from aborted babies. She added that Congress is slated to increase funding for the National Institutes of Health (NIH) without restrictions on these kind of experiments.
“Pro-life Americans are horrified and outraged by revelations that the pro-life Trump Administration contracted with a notorious baby parts trafficker to purchase ‘fresh’ aborted baby body parts for research, at taxpayer expense,” Dannenfelser said. “Unfortunately, HHS’s response does very little to alleviate the outrage. Secretary Azar must show decisive leadership and fix this problem immediately.”
Last week, Center for Medical Progress (CMP) founder David Daleiden said it was “unconscionable that the United States government would be sending the message with taxpayer dollars that these children are worth more to the U.S. government dead than alive,” in a speech to the Values Voter Summit in Washington, D.C.
In 2015, CMP revealed Planned Parenthood’s fetal organ harvesting activities with a series of undercover videos that suggested the abortion giant was breaking multiple federal laws pertaining to human tissue sales and abortion procedures. Their work led to a congressional panel referring ABR, among other entities, for criminal investigation.
“When you commodify human beings, and you commodify the body parts of aborted children, [then] you create incentives for abortions to happen,” Daleiden warned. “When you commodify human beings, you create incentives for bad things to happen.”
Of Monday’s announcement from HHS, Daleiden said:
“So long as HHS trades taxpayer dollars for freshly-aborted baby body parts, the U.S. government is setting its own abortion quotas and sending the message that these children are worth more dead than alive. By terminating a grotesque contract for ‘fresh’aborted baby parts from Planned Parenthood’s business partners ABR that never should have been signed in the first place, HHS has taken a small first step to stop the epidemic of trafficking tiny baby hearts, lungs, livers, and brains from late-term abortion clinics into government-sponsored laboratories for taxpayer-funded experimentation. HHS’smission to ‘serve all Americans from conception to natural death’ cannot permit trafficking unborn children to stitch their body parts into lab rats.”
“HHS’s newly-announced review of fetal tissue procurement and experimentation must be exacting, and it must terminate all other agreements for baby body parts with ABR, StemExpress, and similar business partners with Planned Parenthood and the abortion industry,” insisted Daleiden. “HHS should provide 110% transparency about the extent of taxpayer-funded harvesting from and experimentation on unborn children, and to this end, CMP will file a federal Freedom of Information Act request in the coming days to surface all the relevant facts and details about the $100 million in taxpayer money spent on HHS’s most recent round of baby body parts contracts and projects.”
(Natural News) Kavanaugh accuser Christine Blasey Ford, who claims — without any evidence — that Kavanaugh inappropriately touched her at a drunken party while in high school, turns out to have ties to an abortion pill pharmaceutical company called Corcept Therapeutics. This discovery brings to light an obvious conflict of interest in Blasey’s story, revealing that she works for a pharmaceutical company that manufacturers an abortion pill drug, whose profits could be strongly impacted by future Supreme Court decisions on abortion rights.
Corcept Therapeutics (Corcept.com) manufacturers and markets an abortion pill drug called mifepristone, and Christine Blasey Ford is a co-author of at least eight published scientific papers produced by the pharmaceutical giant to promote its pills. You can see Blasey’s name listed on several publications at this Corcept.com web page detailing their research papers.
Corcept Therapeutics, Inc., a $166 billion market cap company (stock symbol CORT) reportedly has current annual sales of $216 million. The company offers just one drug, mifepristone, which is widely known as an “abortion pill” or RU-486. Many drugs have multiple uses, and mifepristone — brand name “Korlym” at Corcept — is currently marketed by the company for the treatment of Cushing’s syndrome. (h/t to The Gateway Pundit for initial work on this breaking story.)
Like all FDA-approved drugs, mifepristone is frequently prescribed off-label, meaning doctors prescribe it for conditions that it has never been approved to treat. It is well known throughout the medical industry that doctors routinely prescribe this drug to terminate unwanted pregnancies. It is a covert “abortion drug,” in other words.
If Kavanaugh were to be confirmed on the U.S. Supreme Court and be part of a decision that overturns Roe vs. Wade, it would make the prescribing of Corcept’s drug for abortion illegal, directly impacting the bottom line profits of the company for which Christine Blasey works.
See this Medscape explanation of how this abortion pill works, where it explains the drug is “Indicated for the medical termination of intrauterine pregnancy through 70 days gestation in combination with misoprostol.”
The Corcept company even issues a strong warning about its abortion potential on its marketing website, offering the “warning” as a wink, wink message to doctors that this is actually an abortion pill.
The “warning” explains:
Mifepristone is a potent antagonist of progesterone and cortisol via the progesterone and glucocorticoid (GR-II) receptors, respectively. The antiprogestational effects will result in the termination of pregnancy.
“Mifepristone, also known as RU-486, is a medication typically used in combination with misoprostol, to bring about an abortion. This combination is more than 95% effective during the first 50 days of pregnancy,” says the Wikipedia entry on mifepristone. The World Health Organization currently promotes the drug as an abortion pill, calling it “safe and effective.” (Safe for the mother, not the child, of course.)
Christine Blasey scrubs her internet history to eliminate evidence of hazy, drunken sex parties documented in her high school yearbook
Christine Blasey Ford, whose middle name is Margaret, is known as “Blasey CM” on the science papers she’s published with Corcept Therapeutics.
Before going public with her baseless accusations against Brett Kavanaugh, Christine Blasey scrubbed her internet history, removing her Linked In pages and even managing to have her entire high school year book completely removed from the internet. (Natural News has now posted the recovered yearbook files at this link – PDF.) As InfoWars reports, the high school yearbook of Christine Blasey is full of accounts of wild, drunken sex parties attended by Blasey and others:
“And there were always parties to celebrate any occasion,” reads one passage. “Although these parties are no doubt unforgettable, they are only a memory lapse for most, since loss of consciousness is often an integral part of the party scene.”
The reasons for Blasey working so hard to scrub her own history are obvious: Even while she claims that Kavanaugh’s history should be researched and brought to light, she didn’t want anyone looking into her own history, including her wild, alcohol-induced party days and her ties with Corcept Therapeutics and its abortion pill drug profits.
But the ties cannot elude internet researchers like Natural News. A Palo Alto University document from 2015 (see page 97) confirms that Christine Blasey, Ph.D. is a professor at Palo Alto University and a “Director of Biostatistics at Corcept Therapeutics.” See the screen shot from that document:
Blasey is the co-author of numerous published studies funded by Corcept
Blasey also appears on numerous published studies at PubMed, where her author ID is 19888560. These studies are all funded by Corcept Therapeutics of Menlo Park, CA. They all center around uses of mifepristone for uses beyond the typical “abortion pill” application. They include studies such as:
Some of Blasey’s colleagues in this pharmaceutical research include Coleman Gross, Dr. Henry Fein, Dr. T. Brooks Vaughan III and Dat Nguyen.
This P.R. announcement from Corcept, intended to entice investors, states that, “Corcept is exploring mifepristone (the active ingredient in Korlym) as a treatment for triple-negative breast cancer with a multi-center, Phase I clinical study currently underway in patients with metastatic or locally advanced unresectable breast cancer. It is also supporting investigator-led clinical studies of mifepristone in the treatment of ovarian cancer and castration-resistant prostate cancer.”
Furthermore, the company is also working to get FDA approval for mifepristone in the treatment of psychiatric disorders, saying, “[The company] owns or has licensed extensive intellectual property covering the use of GR antagonists, including mifepristone, in the treatment of a wide variety of metabolic and psychiatric disorders and triple-negative breast cancer.”
What’s clear is that Corcept is working to aggressively expand the approved uses of its drug, obviously in an effort to increase prescriptions and profits.
See the full details of this story in our REAL.video report
The full details of this article, by the way, are available in this REAL.video report, just filed today:
MILFORD, Connecticut, September 20, 2018 (LifeSiteNews) – The quarterback for the Los Angeles Chargers made an interviewer gasp with amazement when he confirmed that he has eight children – and wants more.
Dan Patrick of The Dan Patrick Show chatted with NFL player Philip Rivers, 36, over the phone on September 17 about the surprising mid-game retirement of Vontae Davis and other football gossip before getting down to family matters.
“We were trying to bet on how many kids you have now,” the interviewer said. “I went with eight.”
“You’re on it,” said Rivers happily.
“You got eight?” gasped the host.
“You nailed it. Six girls and two boys.”
The interviewer then asked the question so familiar to parents of large families everywhere.
“Are you done?”
“Heck no!” answered Rivers proudly. “I hope not.”
“I should talk to your wife,” joked Patrick. “Does your wife know that you want to have more?”
“Oh yeah, she’s all in,” Rivers assured him, but the interviewer interrupted to gasp, “Six GIRLS?”
“Yeah, six girls,” said the quarterback.
“But I’ll tell you what,” he added, as if to reassure the interviewer that being the father of six girls is a blessing, not a curse, “the three oldest are girls. Now they’re 16, 13, and 12, so we have a lotta little mamas in the house, helping out.”
Patrick stammered a little as the host continued to gasp “My Gawwwwd!”
“It’s awesome,” Rivers insisted.
“Do they think you’re stupid, though?” Patrick asked, as if girls invariably think their fathers are stupid. In fairness, though, Patrick has three daughters and a son, so he may have been reflecting on his own experience of family life.
“No,” said the quarterback. “Well, sometimes. Just in general, you know, like ‘Dad!’”
But Rivers insisted that his family life is awesome.
“There’s always a lot of action in the house as you can imagine,” he said.
“Any boys come over yet?” the host asked.
Rivers seemed puzzled but went along with jokes about which NFL players would be best to stand in the doorway to warn young men to behave with Rivers’ 16-year-old daughter.
The football player revealed that he was 19 and his wife was 18 when they married but that he doesn’t see his daughter Halle marrying that young: no sweetheart has turned up just yet, so her dad believes she’s on “a different path.”
The couple’s other children are named Caroline, Clare, Grace, Gunner, Peter, Rebecca, and Sarah Catherine.
Philip Rivers is a devout Catholic and his wife Tiffany, who was his junior high school sweetheart, is a convert to the faith. They grew up in Alabama and married in 2001 when Rivers was a sophomore at North Carolina State. He was the #4 overall pick in the 2004 NFL Draft.
WASHINGTON — The purchasing of aborted fetal tissue for use in research is “abhorrent” and must stop, said 85 members of the U.S. House of Representatives in a letter to the Food and Drug Administration.
The FDA in July gave a $15,900 contract to Advanced Bioscience Resources (ABR) for “fresh human fetal tissue,” which would be transplanted into mice in order to create human-like immune systems for research purposes. It is the eighth contract between the FDA and the company since 2012, and seven of the contracts appear to relate to the same or similar programs.
Federal law prohibits the sale of human fetal tissue for “valuable consideration.” Furthermore, the letter states, Congress investigated ABR in 2016 as a part of its investigation into the fetal-tissue procurement and late-term abortion industries, finding ABR’s practices to be unethical and possibly illegal.
The 2016 investigation was spurred after David Daleiden, a pro-life advocate and a journalist with the Center for Medical Progress, released a series of videos that called into question the fetal-tissue procurement and sales practices of Planned Parenthood.
“ABR plainly admitted to Congress that it obtained tissue by collecting human fetal remains from abortion clinics, paying $60 per ‘singe aborted fetus’ — and then upselling the child’s body parts separately to researchers at fees of $325 per ‘specimen’ — brain, eyes, liver, thymus and lungs,” the letter states.
Congress referred ABR to the Department of Justice, the Federal Bureau of Investigation and the District Attorney’s Office of Riverside County, California, for further investigation.
Rep. Chris Smith, R-N.J., said Sept. 17 that the FDA is using taxpayer dollars “to fund a barbaric research method that treats babies like research guinea pigs.”
More ethical methods of research exist, Smith said, such as developing human-like immune systems from human bone marrow or umbilical cord blood instead of obtaining tissue “through the destruction of unborn children.”
Rep. Vicky Hartzler, R-Mo., who was part of the House investigation into ABR in 2016, said that she was “alarmed” that the FDA would partner with ABR, which has a “checkered history of purchasing the remains of aborted children and reselling the babies.”
“While our letter calls on the FDA to cancel its contract with ABR, I would go the next step and call on all federal agencies, including the National Institute of Health (NIH), to cease and desist in furthering the abhorrent and highly unethical practice of using aborted babies as research specimens. This is a grisly, disturbing and unnecessary business,” she added.
Rep. Mark Walker, R-N.C., said that companies such as ABR “have suffered no consequences” despite the findings of Congress’ 2016 investigation.
“Considering President Trump’s pro-life promises, the FDA should immediately cease all government business with ABR and no longer use any aborted fetal cells for future research,” he added.
On Sept. 10, Daleiden said of the contract that it is “unconscionable that the United States government is still paying top-dollar in taxpayer money for the freshest, most high-quality dismembered baby hearts, lungs, livers and brains.”
September 19, 2018 (LifeSiteNews) – As if Canadians did not already have enough to be ashamed of with Prime Minister Justin Trudeau’s aggressive promotion of abortion around the world, Canada has now joined the Netherlands in lobbying the World Medical Association to change its longstanding position in opposition to assisted suicide. Nations that decide to fundamentally mangle the definition of medicine are never satisfied with simply changing their own laws – they must always bring their bloody practices to other places, as well.
Some Canadian doctors are advocating that Canada follow the Netherlands in other ways, as well. As I described in my 2016 bookThe Culture War, physicians in the Netherlands have begun to both advocate and implement the practice of harvesting organs from euthanized patients. The medical journal Applied Cardiopulmonary Pathophysiology published a description of how this is carried out in 2011:
Donors were admitted to the hospital a few hours before the planned euthanasia procedure. A central venous line was placed in a room adjacent to the operating room. Donors were heparinized [a drug to maintain organ viability] immediately before a cocktail of drugs was given by the treating physician who agreed to perform the euthanasia. The patient was announced dead on cardiorespiratory criteria by 3 independent physicians as required by Belgian legislation for every organ donor…The deceased was then rapidly transferred, installed on the operating table, and intubated [in preparation for organ removal] …
Ponder the enormity of what was done here. Four people—who were not otherwise dying—were killed and then swiftly wheeled into a surgery suite to have their organs removed. Three of the donors were struggling with neuromuscular disabilities—people who often face social isolation and discrimination—and one was mentally ill. In a particularly bitter irony, the latter patient was a chronic self-harmer, the “treatment” for which was a willing professional team ready to administer the ultimate harm.
That’s just the beginning. Prominent voices among the medical elite have called for the overturning of the “dead donor rule”—the ethical backbone of organ transplant medicine requiring that a patient die naturally from injury or illness before vital organs can be procured. These advocates argue that consent should be the primary ethical concern and criteria for organ harvesting—not that a donor is dead. Thus if living patients or their surrogates give the okay, doctors should be allowed to euthanize by means of live harvesting.
Two doctors from Ontario’s Western University along with a bioethicist from Harvard Medical School, Robert Truog, are already advocating that Canadian laws and medical protocols be changed so that organ donation can be paired with euthanasia in Canada, as well. Euthanasia, a report on their proposal notes, “offers significant advantages for transplant surgeons” – if the customary delay where the physicians wait for blood circulation to cease in order to ensure that any organ donation takes place after cardiac death takes place is done away with. In that short period of time, which may be only several minutes, the “quality of the organs declines,” and thus if “they were removed in a coordinated operation from a euthanasia patient, they would be as fresh as possible.”
Several very important changes would need to take place before these coordinated operations could begin to take place in Canadian hospitals. First, they noted, the “staff of intensive care wards are trained to keep people alive; in organ donation after euthanasia they would have to kill the patient. At the moment, too, a firewall exists between the staff handling withdrawal of life support and the staff handling organ donation so that patients are not killed for their organs. But with legalised euthanasia, there will be no need for the firewall.” Read those words again carefully, and let them sink in.
Other significant changes would include doing away with the “dead donor” rule that has so long been essential to medical institutions. Canadian law also stipulates that a death by euthanasia is, by definition, a death “caused by the administration of a ‘substance,’” which would need to be changed so that death could instead be caused by “organ retrieval.” Of course, some medical professionals would presumably object, and so the authors of this proposal recognize that something will have to be done about “conscientious objectors”:
Hospitals and organ-procurement organizations must therefore have protocols that allow clinicians who object to opt out. Organizations also need to consider where to draw the boundaries of legitimate conscientious objection. Does the right to opt out extend to laboratory and pharmaceutical staff? What about the disposition of these organs — should clinicians be permitted to opt out of participating in the transplantation of donated organs, and should potential recipients be informed about the source of the organs in case they may want to decline transplantation?
In other words, some medical professionals might not be able to object to cooperating with these medicalized killings, regardless of how appalled they might be at the idea of killing somebody by pillaging their body for “fresh organs.” Considering Canada’s track record on conscientious objection in the medical field, it seems very unlikely that physicians with functioning consciences would not be in danger of being forced into some level of cooperation with this horrifying new step into sanitized barbarism.
At this stage, euthanasia-by-organ-donation is only a proposal, and we can hope that Canada does not continue to follow in the footsteps of the Netherlands. These practices would make an awful situation even worse, with some sick patients perhaps being encouraged to consider organ donation for healthier people—and feeling obligated to do so—or using organ donation as a way of attempting to find meaning for their lives. The potential implications are endless. For the sake of vulnerable men and women everywhere, these practices must be emphatically rejected.
The attached 1991 Inaugural Address by Dr John J. Ring, M.D. as President of the American Medical Association, includes the following statement:
“We can accept nothing that threatens this relationship by trying to turn medicine into a mere trade, a dispassionate business venture, an impersonal public utility. We can accept nothing that threatens this relationship by maneuvering us to work for anyone other than our patients. We can accept nothing that threatens this relationship by trying to make us agents of any effort that would violate our duty “to do no harm” — by asking us to ration needed care, to assist in suicide, or to kill people — even in state-sanctioned executions.”
“Do no harm” medicine is fast becoming extinct. Contemporary health care is increasingly under the sway of a utilitarian bioethics that makes the elimination of suffering the prime directive—to the detriment of traditional standards of medical morality that deem all human life equally worthy of care and protection.
The prestigious New England Journal of Medicine has been among the instigators of this shift. As early as 2005, the journal published (without significant criticism) the so-called Groningen Protocol—a bureaucratic checklist from the Netherlands that instructs Dutch doctors which terminally ill or seriously disabled babies they can lethally inject. In 2010, NEJM published advocacy in favor of an invidious health-care rationing measure known as the QALY (“quality-adjusted life year”), adoption of which has the effect of limiting care to the disabled and disadvantaged whose lives are bureaucratically rated as lower in quality than the lives of others.
In its September 6, 2018, edition though, NEJM has outdone itself. With Belgium and the Netherlands already allowing the conjoining of organ donation and euthanasia, and with Canada debating whether to follow them off that moral cliff, the journal has published a radical proposal that would demolish the ethical foundation of transplant medicine—the “dead donor rule.”
The rule requires that donors be declared dead before vital organs are procured and that the surgical transplant procedure not be the cause of the donor’s death. In their NEJMpiece “Voluntary Euthanasia—Implications for Organ Donation,” Dr. Ian M. Ball and bioethicists Robert Sibbald and Robert D. Truog urge that those rules be loosened in countries where euthanasia is legal:
Although some patients may want to be sure that organ procurement won’t begin before they are declared dead, others may want not only a rapid, peaceful, and painless death, but also the option of donating as many organs as possible and in the best condition possible. Following the dead donor rule could interfere with the ability of these patients to achieve their goals. In such cases, it may be ethically preferable to procure the patient’s organs in the same way that organs are procured from brain-dead patients (with the use of general anesthesia to ensure the patient’s comfort).
In other words, rather than wait for the patient’s heart to stop after lethal injection—as currently is done in the Netherlands and Belgium—the patient could be anesthetized and his organs procured while he is still alive.
Bear in mind that legal euthanasia in Belgium and the Netherlands is not limited to the terminally ill. In Canada, the euthanasia patient’s death need only be “foreseeable,” whatever that means, and even that vague limitation is under court attack. And bear in mind, too, that patients requesting euthanasia usually do not receive any suicide counseling services before they are killed.
Conjoining euthanasia with organ donation would thus send the insidious message to vulnerable people that their deaths have greater social value than their lives. For the particularly vulnerable, that could be the point that tips their decisions. Moreover, following the path the authors urge would transform a life-saving medical sector into one that also ends lives, imposing on transplant specialists the dual role of both healer and killer.
The NEJM was once one of the most powerful institutional opponents of medical utilitarianism. In 1949, it published a famous and powerful argument against allowing such values into the practice of medicine. Writing after the revelation of the depraved practices of the Nazi regime’s doctors, who engaged in infanticide, the killing of disabled adults, and many other infamies in the name of science, Leo Alexander, a psychiatrist and medical adviser to the office of chief counsel at the Nuremberg war crimes trials, warned that the utilitarian infection that destroyed German medical ethics could spread:
Whatever proportions these crimes finally assumed, it became evident to all who investigated them that they had started from small beginnings. The beginnings at first were merely a subtle shift in emphasis in the basic attitude of the physicians. It started with the acceptance of the attitude, basic in the euthanasia movement, that there is such a thing as life not worthy to be lived.
All it took for doctors to be led astray, Alexander warned in “Medical Science Under Dictatorship,” was utilitarian calculation, “the infinitely small wedged-in lever from which this entire trend of mind received its impetus”:
Physicians have become dangerously close to being mere technicians of rehabilitation. . . . In an increasingly utilitarian society these patients [with chronic or terminal diseases] are being looked down upon with increasing definiteness as unwanted ballast. A certain amount of rather open contempt for the people who cannot be rehabilitated with present knowledge has developed. . . . At this point Americans should remember that the enormity of a euthanasia movement is present in their own midst.
Would today’s NEJM publish Alexander’s powerful anti-utilitarian advocacy? How could it? By running articles openly supportive of infanticide, health-care rationing by “quality” of life, and now of conjoining euthanasia and organ harvesting, the NEJM has become the very wedge against which Alexander so powerfully inveighed.
Perhaps it is time for a name change. I suggest that the New Euthanasia Journal of Medicine more accurately identifies the values it embraces.
LifeNews.com Note: Wesley J. Smith, J.D., is a special consultant to the Center for Bioethics and Culture and a bioethics attorney who blogs at Human Exeptionalism.
“It is essential, therefore, that the values chosen and pursued in one’s life be true, because only true values can lead people to realize themselves fully, allowing them to be true to their nature. The truth of these values is to be found not by turning in on oneself but by opening oneself to apprehend that truth even at levels which transcend the person. This is an essential condition for us to become ourselves and to grow as mature, adult persons.”
— Fides et Ratio, St. Pope John Paul II, ¶25
By this point, even the most wild-eyed apologist for the sexual revolution can scarcely deny that something has gone terribly wrong. For the fourth year in a row, STD rates in the U.S. are up. In fact, they’re at the highest level they’ve ever been. In 2017, gonorrhea rates soared 67%, chlamydia 21%, and syphilis 76%. The executive director of the National Coalition of STD Directors thinks President Trump should declare that STDs are a “public health crisis.”
For some reason, when the hippies preached their gospel of free love, they never mentioned venereal disease. Neither did they mention the routine visits to the abortion clinic down the street to “take care of the problem,” or the massive amounts of synthetic hormones women would have to pump into their bodies to prevent the children for which their hearts are yearning, or the trillions of dollars spent on the divorces produced by an epidemic of infidelity.
I could go on. But what I have said is already more than enough to show that the sexual revolution of the 60s and 70s has failed. Even a child can see that. Indeed, far too often it is precisely our children who do, when they are aborted en masse, or abandoned by their parents, too obsessed with their own fleeting “needs” to notice how the consequences of those needs redound upon the heads of their children.
What we desperately need now is a new sexual revolution; or rather, not a new revolution at all, but a reprisal of the original sexual revolution.
The Sexual Revolution: No Revolution at All
It is ironic that the sexual revolutionaries of the 60s ever convinced themselves they were doing something especially new. Viewed from the standpoint of the preceding centuries, yes, the sexual revolution appeared radical. Unheard of, however, it was not. Our historical memory is far too brief. Christians are often sneered at for wanting to “turn back the clock.” In reality, a great deal of what the sexual revolutionaries advocated turns out to be little more than a case of “turning back the clock” – with the same, predictable consequences.
The Romans enslaved the conquered but were likewise enslaved by their own sexual debauchery before the advent of Christianity.
As Dr. Benjamin Wiker observes in a recent article, radical sexual libertinism is scarcely an invention of liberated 20thcentury hippies: it was, in fact, the norm in many pre-Christian pagan societies. You can see it openly depicted in the pornographic wall paintings of the ancient Romans or read it in their literature. In some respects, in ancient Rome sexual liberation was even more complete: pedophilia, for instance, was not only not taboo, but encouraged, as were prostitution, pornography, homosexuality, and even public sex (e.g. the public bacchanalia).
If anything deserves the title of the first sexual revolution, it was the truly radical revolution that accompanied the arrival of Christianity.
In the first place, the early Christians were sexual ascetics. They knew what the depraved aesthete does not know: that there are goods that transcend physical goods, and pleasures that are more pleasurable than bodily pleasures, and that these are the only goods and pleasures ultimately worth pursuing. The early Christians subordinated everything to the pursuit of spiritual goods, including happiness in the life to come. They did not reject sex as such (St. Paul is quite clear on that point), but they knew that without asceticism even sex soon loses its power to please, and worse.
This truth is far from obvious to the members of a dying, decadent society that has lost all sense of the spiritual. As Dr. Peter Kreeft writes, the sexual revolution of the 60s could not have happened “without the loss of true religion, the loss of spiritual joy, the loss of religious passion, the passionate love of God.” The human heart is infinitely restless. Through bitter failure, St. Augustine learned that the heart is restless until it rests in God. Without God, all we have is our restlessness. To fill it we often cast about for the best substitute for God we can find. Sex is frequently the first alternative we hit upon. And no wonder: sex is that overwhelmingly pleasurable experience by which, in this life, we are most intimately united with another person, in which we most completely overcome our individuality and rest in another. That is, sex is ecstatic.
Or rather, sex can be ecstatic. However, as the ancient Romans learned, and as the sexual revolutionaries of modernity have learned, the moment we make an end of sex – that is, we make sex an idol – is the moment sex turns on us. Sex untamed by asceticism becomes a devouring beast. Rather than transcending ourselves, we debase ourselves, and others. Hence the endemic sexual slavery, prostitution, infanticide, and exploitation of ancient Rome. Hence the disease, loneliness, divorce, abortion, and pornography of modernity.
In the second place, and more importantly, the Christians recaptured the two-fold purpose that God inscribed within the sexual act between husband and wife – that of union and procreation. The Christians had Genesis, and the teaching of Christ, and the writings of St. Paul to guide them. Each make clear that sex is not simply the exchange – or, worse yet, the taking – of pleasure. As great as the pleasure of sex may be, the pleasure turns out to be the least good part of sex. Better yet is the capacity for the conjugal act to draw a man and a woman (husband and wife) closer together in a bond of self-giving love – a love that is permanent and mutually enriching and fruitful.
Love, I say, and not lust – a rich, meaningful love that peels back the layers of our selfishness and allows another person into the depths of our heart, and vice versa. “Husbands,” says St. Paul, “should love their wives as their own bodies.” How different is this from the violent lust of the Roman aristocrat, unscrupulously using his sex slaves to satiate his insatiable appetites! And how different is this from the contemporary millennial, cruising the bars or his “dating” apps looking for a one-night stand – for a partner to scratch the itch of his desire. The pleasures of this deeper love are less frenetic and vehement than the purely physical pleasures of sex, and they require much in the way of self-sacrifice, but they speak to and satisfy the quieter, deeper cravings of our heart: for meaning and union.
But even better yet is the creative power of sex, which power is practically God-like, so much so that Christian theology views parents as “co-creators” of their children. To the Christian, the creative power of sex is not some peripheral quality of sex, but self-evidently intrinsic to it. To put aside, or ignore, this creative power is tantamount to pretending that drinking is not for quenching thirst or eating for nourishing the body. Furthermore, to reject sex’s creative potential is not freeing, but is rather to reject sex’s greatest gift of all – a new human being who is the symbol and fruit of the self-giving love of husband and wife. In ancient Rome, as in modern day Western society, this rejection was and is not only symbolic, but horrifically, murderously literal: in the widespread practice of infanticide and abortion.
The Likeness of God
It is hard for human beings in our fallen state to see beneath the surface of things. The pleasures of sex are self-evident to any who has experienced sexual desire. The layers of the meaning of sex, though perfectly accessible to the non-Christian, are less self-evident. Concupiscence blinds us. Christ, however, is the light that dispels the shadows. Pagan society labored in the shadows of concupiscence and sin. Christ showed ancient society a better path forward – one based upon the truth about the human person, and the high dignity of our destiny.
Thus, the “new sexual revolution” that I am advocating will not be transformative by simply “turning back the clock,” but by capturing what has always been true – man is a spiritual being made in the image of God. We see what God intended for his sons and daughters in Mary, the mother of Jesus. She, who was destined to be the Mother of God by the grace of her Immaculate Conception, was conceived without sin; therefore, she did not have consequences of original sin. Being spotless, she did not suffer the rupture and effects of concupiscence. Her intellect and will were united with the will of God. “Do whatever He tells you to do,” Mary says.
The immediate consequence of original sin is shame, which is manifested by Adam and Eve’s denial of Love as the source of creation. The serpent tempts them to accept that God is withholding Himself from them: “For God knows that when you eat of [the tree of the knowledge of good and evil] …you will be like God knowing good and evil.” — Gen 3:5
What is the implication revealed by the tempter? – God doesn’t want you to be like Him – God is not Love. If you want to be like God, you must grasp this likeness to God to possess it for yourself. This is a story that has a tragic ending. What is forgotten is that man and woman have already been freely given this most precious gift – the likeness to God.
A Revolution of Tenderness
Our youth and young adults are overwhelmed by a torrential onslaught of moral filth in all forms of media. Even their schools and institutions are not immune from instruction in promiscuity and perversion. The widespread propaganda in support of immorality – impurity, contraception, abortion, homosexuality, and divorce – signify an assault on family and life and the Christian understanding of the human person and human sexuality that is unparalleled since the days of ancient paganism.
The new sexual revolution I am advocating will be revolutionary only in the sense that someone who is walking precisely the opposite direction needs to be spun around, face-forward. Our culture is walking straight towards a cliff; in the past six decades, the bodies (both literal and figurative) have been piling up.
Most revolutions are loud, violent affairs. The communists preached the brotherhood of man, and we got the gulags. The sexual revolutionaries preached universal love, and we got STDs, AIDS, and abortion. However, the first, Christian, sexual revolution was a different kind of revolution. It was, to use a term coined by Pope Francis, a “revolution of tenderness.” It built – to use St. Pope John Paul II’s phrase – a “civilization of love.”
The violent, lustful deities of pagan Rome were gradually exorcised. Laws against pedophilia and sexual slavery were passed. The truth about human nature was inscribed in the structures of law and culture, eradicating the worst abuses, protecting the vulnerable, and creating the conditions for stable societies. In jettisoning all of this, the sexual revolutionaries of the 60s have simply re-opened Pandora’s Box, unleashing anew upon the world the myriad evils that Christian civilization had, at the cost of great effort, restrained.
Ultimately, however, as Dr. Peter Kreeft rightly observes, this new sexual revolution cannot even be a sexual revolution as such. It must, as it was in the early Church, be first and foremost a spiritual revolution.
“What then do we need to defeat this [sexual] revolution, which has brought about such immense destruction, and eventual death, to families, and eventually to society?” he writes. “Reason, logic, argument, science, facts, common sense, compromise, return to tradition – none of these are strong enough. What is strong enough? Only one thing. Nothing less than Jesus Christ will do.
“Why? Because the heart of the error of the Sexual Revolution is the identifying of love with sex. Christ undoes this fundamental confusion by showing us – not just telling us, but showing us – what love is.”
During the canonization of Maria Goretti in 1950, Pius XII spoke about her fortitude in safeguarding her purity and virginity. Even as a young girl of twelve confronted by evil, Maria understood the demands of living the life won for her in Christ Jesus. She was aware of the dangers and consequences. She remained vigilant to defend her chastity, preserving in prayer and entrusting her purity to the motherly love of Our Lady.
Over 500,000 people gathered around the Holy Father on this momentous occasion to celebrate the heroic witness and virtue of this young, poor farm girl. Recognizing the moral crisis of his day, prompted by the Holy Spirit, Pius XII prophetically challenged the young people and families gathered:
“Dearly beloved youth, young men and women, who are the special object of the love of Jesus and of us, tell me, are you resolved to resist firmly, with the help of divine grace, every attempt made to violate your chastity?
“You fathers and mothers, tell me—in the presence of this vast multitude, and before the image of this young virgin who by her inviolate candor has stolen your hearts…in the presence of her mother who educated her to martyrdom and who, as much as she felt the bitterness of the outrage, is now moved with emotion as she invokes her, tell me, are you ready to assume the solemn duty laid upon you to watch, as far as in you lies, over your sons and daughters, to preserve and defend them against so many dangers that surround them, and to keep them always far away from places where they might learn the practices of impiety and of moral perversion?”
His challenge rang true then as it rings true today!
Dr. Wiker and Dr. Kreeft beautifully and rightly pinpoint the transforming power of the Gospel. It changed how our world viewed sex, marriage and the meaning of life. The Culture of Death seeks to rob man of his inherent dignity and recreate him as a secular atheistic being. It reshapes his view of self, including his understanding of human sexuality. The world is starving for love. Human beings were made for love. This latest sexual revolution has drained sex of love, and practically all its transcendent meaning. The time is ripe for a revolution against the revolution, a revolution that will be kindled in the hearts and homes of every Christian and in turn set the world alight with love.
September 13, 2018 (LifeSiteNews) – Brittany sat in the courtroom weeping, her face hidden in her hands. How had it come to this?
She looked up as the bailiff took her boyfriend, Harold, away to serve a life sentence in prison. For murder. She was only 17; he was 19.
“Please send me to jail, too!” she pleaded with the judge. After all, what they had done, they had done together.
The tragic story of Brittany and Harold (not their real names) shows how our culture has lost its sense of right and wrong, good and evil.
Like many teens, they had believed they were in love. As time passed, they grew closer, first emotionally and then physically. Eventually, they began having sex, believing that, since they were in love, everything was OK.
Then Brittany got pregnant, and she and Harold decided they didn’t want to have the baby. They didn’t want the responsibility or the embarrassment.
The best plan of action, they decided, was to have Harold apply pressure to Brittany’s stomach to induce premature labor. After several days, the inevitable happened. In the middle of the night, at 21 weeks pregnant, Brittany started having contractions and delivered not one baby, but two – into the toilet. Harold was charged with double homicide.
Brittany faced no charges; state law did not allow a pregnant woman to be prosecuted for causing the deaths of her own fetuses.
Brittany testified in Harold’s defense. But the law that protected Brittany did not protect Harold, and it treated the babies as what they were: human beings. Harold was convicted on two counts of homicide.
We have lost our sense of sin. The apostle Peter tells us that “the devil prowls around like a roaring lion looking for someone to devour” (1 Peter 5:8). He begins by influencing us in small choices, but he doesn’t stop there. Little mistakes lead to bigger ones, gradually enticing us to be more and more under his influence.
No one grows up wanting to get pregnant out of wedlock or have an abortion. If these things happen, they originate in the small steps we don’t realize are leading us in the wrong direction.
When this story hit the media, a Planned Parenthood official said the case was evidence of the government trying to give fetuses the same status as adult human beings, ignoring the tragedy of the two babies losing their lives. He also complained, “Abortion is getting less accessible.”
His comments reveal the cold and insensitive mindset required to justify abortion rights. A mentality that doesn’t want to recognize this “choice” for what it is or treat the root of the problem. A mentality that mentions “abortion getting less accessible” after twins have died at home. A mentality that doesn’t want to right the wrong – that just wants to call it by a different name. A mentality that wants to keep the wrong but make it sound better.
A Fox News reporter asked Harold’s attorney, “Why didn’t she just go for an abortion? Why do this grisly thing?” The reporter’s question implies that abortion is not grisly. The worst part of this tragedy is not that it was grisly, or even that it was illegal, but that two babies lost their lives. It’s as if we have learned to approve of evil as long as it seems clean or professional or is portrayed as a right.
Yet nothing escapes our deepest human nature. When Brittany saw what she had done, she was heartbroken. She was reminded, in a very difficult way, that those twins weren’t problems that needed a solution – they were her children.
She still visits their graves today. Abortion doesn’t go away, no matter how grisly or clean we are told it is. Brittany will carry the pain of this tragedy forever.
September 13, 2018 (LifeSiteNews) – They say that Pope Pius X’s favorite bedside reading was The Soul of the Apostolate by Dom Jean-Baptiste Chautard. I am beginning to wonder if Pope Francis’s favorite bedside reading is Niccolò Machiavelli’s The Prince.
Authors like Ross Douthat, Phil Lawler, and Henry Sire have provided copious documentation of the Pope’s Machiavellian modus operandi. It may help to recall, in the midst of Viganògate, a few egregious examples from the past that demonstrate how it works.
We remember when the pope deliberately washed the feet of women, against the universal liturgical law that limited the washing of feet to men. Then he changed the law to allow for the inclusion of any baptized member of the faithful—and proceeded to violate his new law by washing a Muslim’s feet. Even if one argues that the pope, as the highest legislator, is not bound by these laws in the same way as his subjects are, he should (as popes in the past have done) set the first and best example of observing Church discipline, since others will, in fact, take their cue or their justification from him. Thus, his public actions contrary to discipline are meant to transmit a spirit of contempt for law, with the message that subjective motives of “charity” or “mercy” can and should lead to the practical neutralization of Church discipline.
We have seen the same contempt, message of neutralization, and stirring up of confusion in regard to the German bishops’ disputes over whether communion should be given to Protestant spouses of Catholics. The pope first feinted to the left, favoring the liberal bishops, then feinted to the right, seeming to support backpedaling from the CDF, and finally let it be understood that the bishops could do whatever they pleased, even if the result will be a cuius regio eius religio checkerboard of dioceses with contradictory policies.
Then, in his manner of modifying the Catechism of the Catholic Church as well as in the new content that was ordered to be inserted, Pope Francis pushed through another victory for progressivism by effecting a change in doctrine, or initiating a motion towards that end, without having used a form of language that is unequivocally heretical. We saw that he did precisely the same thing in Amoris Laetitia (taken together with the Buenos Aires guidelines), in his revisions to the annulment process, and in many other cases, using techniques such as equivocation, studied ambiguity, internal contradiction, false quotation, and stalling tactics between phases to accomplish his purposes.
Again and again he displays this duplicity, playing off one side against the other, keeping people guessing—and keeping employed an army of anxious conservative Catholics who rabbinically reshape each act or statement. But a situation in which it is thought necessary to bend over backwards to defend the pope against undeniable appearances of doctrinal rupture and moral corruption is already a crisis of unprecedented scope. It means, at very least, that this pope has permanently lost the trust of many, and has therefore introduced a strong note of instability into the very office of the papacy, since future popes will be governing from a weak foundation. All of this coming from a Pope who told youths at a Mass in 2015 to “make a mess.”
There are still some Catholics who are digging in their heels. They refuse to believe that any pope can be as bad as this pope would have to be, if the most natural “reading” of things turns out to be true—so it must not be true! “Perhaps all of these doctrinal contradictions and moral meanderings and policy flip-flops are being misreported or misunderstood. Let’s circle around and defend the Pope at all costs from these naysayers, scandalmongers, and calumniators!” By doing this, they are effectively consigning their heads to a permanent vacation in the sand. This is one kind of coping mechanism: it effectively denies that there is a problem. It is like a child who puts his hands over his ears and says some loud nonsense in order to avoid having to hear what an adult is saying to him.
There is another group I have known, a smaller and more rarefied one, made up of intellectuals who have convinced themselves that whatever the pope is saying must either be true (since he is, after all, the vicar of Christ, and we want to be on his team, right?), or be able to be deftly rendered true by clever scholastic distinctions about the level of authority of a given statement, the location of a prepositional phrase, a faulty translation into French, etc. This is, I believe, a psychological coping mechanism for not dealing with the now notorious fact that we have a pope who is somewhat like a truck with failed brakes careening out of control down a steep mountain and heading for a mighty crash.
By this point, people who evade the truth about Francis are oddly like the Pharisees who, instead of surrendering to the divine reality of Our Lord, argued ceaselessly about their human traditions in the interpretation of the Law and whether or not He was violating this or that aspect of it. In other words, rather than face up to the big reality, they sought refuge in their Jewish scholasticism. In our present case, the big reality is not something good and holy like Our Lord in the midst of His disciples, but something sinister and repugnant, like Judas stealing from the common purse, betraying with a kiss, and hanging himself.
But, as many have pointed out, this situation is no cause for despair. It is, on the contrary, a dramatic and long-overdue end to an unsustainable exaltation of the papal office, where the pope is cast as a combination Delphic oracle, globetrotting superstar, dynamo of doctrinal development, and standard meter bar of orthodoxy. This is not only contrary to Catholicism, it is corrosive of it, because it replaces the primacy of inheriting the deposit of faith from divine revelation through apostolic transmission with the primacy of papal voluntarism. Such a distortion of the dogma of Pastor Aeternus could only end in flames.
Irish mom Grace Slattery is thrilled to have four beautiful children — but if doctors had their way, she would only have two children with her today. Slattery and her husband, James, had long struggled with infertility, and had suffered multiple miscarriages. Then, they were given a miracle: the couple had naturally conceived quadruplets, which is extremely rare. The odds of conceiving quadruplets naturally is 1 in 700,000, and the Slatterys were thrilled.
“When I fell pregnant naturally with quadruplets I couldn’t believe it as we had struggled for three years and I’d suffered four miscarriages,” Grace said. “We couldn’t afford IVF and when tests showed nothing was wrong I was baffled as to why we couldn’t have children.” But their happiness soon turned to sadness, when doctors told Grace to have an abortion. She was 17 weeks along, and they wanted her to undergo a “selective reduction” to kill two of her preborn children. But the parents refused. “[D]espite being offered to abort two of them before they were even born as they were classed as high risk, we decided to let fate decide,” she said.
The children selected for death would likely have been given a fatal shot of potassium chloride into their hearts, and then be left while their surviving siblings would continue to grow and develop. But at 17 weeks, preborn children targeted for abortion are typically subjected to a dilation and evacuation (D&E) abortion, a violent procedure in which the preborn child is literally ripped apart limb by limb.
Instead, Grace carried the four babies to 32 weeks, and all four — Lucas, Amelia, Lily-Grace, and Mollie — were born safely, weighing between two and four pounds each. Now, all four children are healthy and thriving, even Amelia, who was born with her organs in the wrong place. And they’re all starting preschool together, complete with matching uniforms.
“They are definitely little miracles and we still can’t believe we got four babies all at once,” Grace said. “All of them love school and as they wear a uniform now it makes it a lot easier as trying to think of four outfits for them every day takes a long time. They are going to be in the same classes at school and they are inseparable when together.”
There are also no regrets about keeping all four of her children, even though doctors recommended against it. “I couldn’t be more proud of the quadruplets and seeing them in their school uniforms is amazing,” she said. “Life is hectic with quadruplets but we wouldn’t change it for the world even though it had made us realise that our family is now complete.” And though she’s excited for them to start school, she admitted that it’s a bittersweet notion. “I will miss them when they go back to school but it will be nice to get some peace and quiet after the summer,” she said. “The school run will be fun as it’s almost impossible to keep my eye on all four but the quadruplets love making new friends so I know they’ll love it.”
The Slatterys are not the only family with quadruplets who were pressured to have an abortion. The Robbins family in Bristol, England, likewise were told to abort after becoming pregnant with quads. “Each time I went to the hospital it was all about the risks and asking me to consider aborting the twins to save the other two babies,” Mrs. Robbins said. “But I knew that each time I looked at my surviving babies I’d also be thinking about the ones I’d lost. The thought of it broke my heart.” Doctors told her over and over again to abort, but she steadfastly refused, and she gave birth to all four of her boys, now five years old.
Shontae Minor and Khristian Rohena were also pressured to abort after finding out they were carrying quadruplets after being told that Rohena would never be able to father children. But Minor refused, saying, “God gave me these kids for a reason, so I’m not going to abort.”
Pregnancies with multiples do come with increased risks, but advances in medicine prove that these babies are capable of being safely carried until birth, and of living healthy lives. Nevertheless, doctors continue to pressure mothers to undergo selective reduction. But the right to life is the most basic and important of all human rights, and every life is valuable, even if that life is inconvenient, fragile, or short.
September 11, 2018 (LifeSiteNews) – It is hard to believe that it was already seventeen years ago that our world changed forever, when airplanes turned into flying bombs by fundamentalist fanatics cleaved history in two with their fiery explosions of mass murder. When the morning of September 12, 2001 dawned with smoke still rising from the rubble of the Twin Towers, we had arrived in what would soon be called “the post-9/11 world.” Altogether, 2,977 people perished in the events of the day of fire that ended an age.
Looking back at that day, with all the fear and fury that followed, most remember an utterly rare sense of total unity. The heroes were clear: The first responders, firefighters, and cops; the men who had charged the hijackers on Flight 93; the countless acts of selflessness and sacrifice that played out in the stairwells of collapsing skyscrapers. The villains were clear, too: They were the men who had used jetliners filled with innocent people to incinerate and crush buildings filled with other innocent people, and the terrorists who had laid the plots and paid the bills.
Like many others, I have been back to the site of the Twin Towers since then. There are now nearly 3,000 names inscribed in bronze surrounding the footprints of where the Tower once stood—and eleven pre-born children are also recognized as the victims who were taken from us. Following the names of eleven expectant mothers is the phrase “and her unborn child.” Joe Daniels, the 9/11 Memorial president, explained why: “it’s a special part of the memorial. It reinforces that message about the whole project that the folks were just like us, that they were about to start these lives…It reminds us that they were who we are.”
One 9/11 widower, Louis Massari, discovered that his twenty-five-year-old wife Patricia was pregnant on the morning of September 11 that they were expecting a child. They wept tears of joy, he remembered, before she left for work at the World Trade Center. “Two things were taken from me on that day,” Massari told Newsdayin 2002. “I was looking forward to being a father.” Patricia never returned. Brian Howley, another 9/11 widower, has said that his pre-born child will be mentioned along with his wife Jennifer during the annual reading of the names of the victims of the September 11 attacks.
There are so many reasons to weep over the new revelations of sex abuse and other grave moral failings by some priests and bishops within the Catholic Church: the unimaginable suffering of the victims, the lost faith of the millions of Catholics scandalized by these latest revelations, and the missed vocations by the many good men who were turned away or left the seminary after witnessing scandalous behaviour among their peers and superiors.
For me, in my role as president of Human Life International, there is one additional cause for sorrow: the irreparable damage that this crisis has done to the pro-life and pro-family cause. In truth, these latest revelations have made my job, and the job of so many pro-life leaders, so much more difficult than it already was.
Throughout the past century, as our culture has abandoned the truths about Life and Family, the Catholic Church has remained conspicuously unmoved and unmoveable. Even non-Catholic pro-life activists often admit that they look to the Catholic Church for leadership, clear teaching and inspiration. In the face of the onslaught of secularism and the triumph of the sexual revolution, including within the vast majority of Christian denominations, the Catholic Church has not only strongly reaffirmed its teachings on Life and Family, but developed new and more sophisticated arguments and evangelical tools to proclaim what St. Pope John Paul II called the “Gospel of Life.”
And yet, all the while, it seems, the devil has been hard at work. Knowing that a frontal assault on the Church could not work, he has silently fomented corruption, weakness and treachery within Her very walls. Even as the Church has presented a strong public front, the corrosive force of evil has been eating away at Her inner structures. We know that the Church will never fall. Christ has promised that the gates of Hell shall not prevail. Her supporting pillars are no less than Christ, the Scriptures and Sacred Tradition: and against these all attacks come in vain. The Church, too, is the mother of the saints, and among our clergy and bishops there remain many who are faithful, sacrificing their lives for Christ and His Church.
And yet, it would be foolish to avert our eyes from the truth of our situation: for it is only in the knowledge of the truth that we may discover and apply the cure.
Church Historian: This Crisis is Way Worse Than You Think
There are two primary ways in which the sex abuse crisis feeds directly into the Culture of Death: 1) This crisis, involving as it does gross violations of morality, above all sexual morality, gravely undermines the credibility of the Church to speak on the most urgent moral issues of our age. If so many, even at the highest levels of the Catholic Church, are either guilty of sexual crimes, or have actively covered up the predatory sexual behavior of others, how can we expect members of an increasingly secular culture to listen when we urge them to embrace a high moral standard that demands the practice of continuous self-denial? 2) The complicity of far too many of our clergy and bishops, even those who are “conservative” or outwardly “faithful,” ensures that their voices are silenced or weakened precisely on those issues where they are most needed: such clerics inevitably lack the moral backbone to take risks for the sake of the truth, knowing how they themselves have failed and are even open to exposure and charges of hypocrisy should they speak in defense of truths they have violated. Thus, the spiritual strength of the Church is imperceptibly eviscerated by the hidden immorality and weakness of some of her ministers.
In (rightly) much-maligned remarks recently given during a TV interview, one leading cardinal claimed that revelations that Cardinal Theodore McCarrick sexually abused seminarians as well as at least one young boy is not “some massive, massive crisis.” In one of the best articles I have seen in response, a professor of political science at Franciscan University argues that – au contraire – this is one of the greatest crises the Church has ever faced.
Placing the sex abuse scandals in an historical context, Benjamin Wiker observes that in pagan cultures, prior to the arrival of Christianity, the practice of grown men pursuing and having sex with adolescent boys was widespread. The same was also true in the case of sexual slavery, abortion, infanticide and euthanasia – all of which were common, and actively defended. With the spread of Christianity, however, came the first sexual revolution, establishing sex within a lifelong marriage as the ideal and cultural norm, while pedophilia, ephebophilia and sexual slavery came to be viewed with revulsion, and made illegal. “They became moral issues, rather than accepted pagan social practices,” writes Wiker, “only because of Christian evangelization.”
In the past two decades, however, we have learned details about a disturbingly widespread, and sometimes organized network of homosexual priests and bishops in dioceses and seminaries, many of whom focused their predations primarily on young adolescent boys and men. This network, observes Wiker, is actively bringing the “de-Christianization of the world” by “literally recreating Greco-Roman sexual culture in our seminaries and dioceses.” [Editor’s note: such pictures are too graphic to include here.]
Indeed, says Wiker, those priests, bishops and cardinals complicit in sex abuse and active homosexuality are not merely one cause among many of the “devangelization, de-Christianization, repaganization” of culture, they are the “chief agents” of the aforesaid. For, as he rightly notes, “there is nothing, nothing, that undermines the moral and theological authority of the magisterium more quickly and thoroughly than the devilish marriage of scandal and hypocrisy. It destroys the ability to evangelize.”
“That’s a rather horrible irony, isn’t it?” queries Wiker. “The very men most authoritatively charged with the evangelization of all the nations are full-steam ahead bringing about the devangelization of the nations. In doing so, these priests, bishops and cardinals at the very heart of the Catholic Church are acting as willing agents of repaganization, undoing 2,000 years of Church History.”
Even this is putting it mildly. It is hard to imagine a worse and more cruel irony than watching shepherds tasked with the sacred duty of caring for their flock using their God-given authority to abuse and abandon the innocent and vulnerable in the most grotesque ways. Even furiously pro-abortion media, politicians and celebrities cannot do as much damage to the Church’s evangelical mission, then one highly placed prelate who abuses or abandons those under his authority.
Is it any wonder that so many have simply written off the Catholic Church, walking away in disgust, and dismissing every word from the mouths of its representatives as rank hypocrisy? How are we, who still believe the truths taught by Christ and His Church, despite the sins of her ministers, to tell those in the world that they must resist the sexual libertinism of our age, when our rectories, chanceries and seminaries have been infected with the same?
The Way Forward: Purgation and Conversion
What the McCarrick scandal in particular has exposed is that, even after the so-called “Long Lent” of 2002, when the secular press exposed many of the horrors of the Catholic sex abuse scandal, we have not yet fully understood or expunged the “filth” (as Pope Benedict called it) that has entered our Holy Mother Church. And yet, sunlight is a disinfectant. I mourn that we have learned the things we have learned these past few weeks. But I rejoice that they are no longer hidden.
What is needed now is a purgation and purification. Our first purgation began in 2002. Much has changed since then, and many efforts have been taken to protect the innocent and vulnerable. Thankfully, the numbers of abuse claims have fallen dramatically. I have heard from many priests and seminarians that many of the worst seminaries have been cleaned up. But still, more is needed.
In 2002 and afterwards many, including many of our bishops, were content to treat the scandal as involving illegal pedophilia by a small number of priests. Many of the policies that were adopted were aimed at curbing such predatory pedophilia. Unfortunately, however, the bishops put in place no measures to hold themselves accountable, nor did they broaden the scope of their concern to include not only obviously illegal abuse, but also other forms of sexual immorality that threaten the credibility and spiritual witness of the Church. In the short term, investigations, including those by secular authorities, should be launched and welcomed. In the long term, what is needed is the conversion and sanctification of the Church, above all her ministers and shepherds.
This quote from St. Paul to Titus strikes at the heart of the matter:
St. Paul
“For a bishop, as God’s steward, must be blameless; he must not be arrogant or quick-tempered or a drunkard or violent or greedy for gain, but hospitable, a lover of goodness, master of himself, upright, holy, and self-controlled; he must hold firm to the sure word as taught, so that he may be able to give instruction in sound doctrine and also to confute those who contradict it. For there are many insubordinate men, empty talkers and deceivers . . .; they must be silenced, since they are upsetting whole families by teaching for base gain what they have no right to teach.” (Titus 1:7-11)
The teacher should be an example to those whom he teaches. St. Paul often exhorted his audience to imitate him and to follow the example that he set (1 Cor 4:16; 11:1; Eph 5:1; Phil 3:17; 2 Thess 3:9) and urged both Timothy and Titus to be examples to the churches in which they ministered (1 Tim 4:12; Titus 2:7). We do not need priests and bishops who are administrators. We need shepherds who are holy, living righteous lives. Seminary rectors and vocation directors must actively recruit only young men who love Holy Mother Church and must ensure that their training challenges them to live by the highest possible moral standards, seeking holiness. Priests and bishops are primarily responsible to Christ and those entrusted to their pastoral care. They must hold each other accountable, must approach and cooperate with secular authorities when warranted, and must eschew any false notion of “fraternalism” that is infected with clericalism or groupthink.
The faithful have a right to demand higher standards from their shepherds. However, and in conclusion, we all have a responsibility to pursue holiness; the Mystical Body of Christ is one, and every member is valuable to is functioning. If ever there was a time for prayer and fasting, this is it. Our Church and our world need saints. Let us restore the purity and integrity of Holy Mother Church by becoming those saints and acting as examples to the world. Then, as in the early Church, the world may pause and pay attention to the Christians, inspired by their integrity, generosity and holiness, so different from the grasping selfishness of the Culture of Death.
On World Suicide Prevention Day, Sept. 10, we recognize suicide as the tragedy it is. Yet at this very moment, activists are agitating to expand—not to prevent—physician-assisted suicide.
This practice promotes the idea that some lives are more valuable than others, an idea that rips apart the social fabric of our nation.
No one should receive suicide assistance over suicide prevention.
Stories like Jeanette Hall’s remind us that the appropriate response to human suffering must always be loving care and solidarity, not destruction.
After losing her brother to suicide and receiving a cancer diagnosis in 2000, Hall approached her doctor, Dr. Kenneth Stevens, about a prescription for lethal barbiturates.
Instead of counseling her to die, Stevens reminded Hall of everything she had to live for, including her son’s upcoming graduation and—someday—his wedding.
“That’s what kept me back,” she said. “That one sentence.”
So, she decided to pursue chemotherapy instead. She was ultimately cured of cancer, and celebrated her 70th birthday in 2015.
“I was just going to say, ‘Give me the barbiturates; call it good,’ not even thinking that I would do [to] my own son the same thing that my brother did to me,” Hall said. “Suicide is awful. And here, knowing that, I was still going to do it.
“That would have been just heartbreaking for me,” said Hall’s son, Scott Walden.
Hall’s story reminds us that we all play a role in counseling and protecting the sick, the weak, and the elderly, whatever their background or circumstances.
Physician-assisted suicide is antithetical to a culture of life for a whole host of reasons.
For one, physician-assisted suicide sets up arbitrary guidelines about who receives suicide prevention and who receives suicide assistance.
Patients of a certain age or with a certain qualifying condition are told to end their lives with professional help, whereas others receive support in order to keep living. These circumstances are completely arbitrary and subject to change on a whim.
Ultimately, physician-assisted suicide guidelines communicate that some lives are simply more valuable than others. A mentality that privileges some lives over others infects culture on multiple levels.
Contrary to the prevalent myth that physician-assisted suicide is mainly an option for those in excruciating pain, studies suggest that the leading cause of physician-assisted suicide is not pain, but existential distress.
Ending one’s life does not solve loneliness, depression, or anxiety. It neglects the problem at the ultimate cost—that of the person.
Physician-assisted suicide also attacks the relationships that form the fabric of society.
When physician-assisted suicide is on the table, so too are less-than-pure motives to choose—or pressure someone to choose—death over life.
Family members may be increasingly tempted to think that suicide is what sick or elderly relatives “would have wanted” when facing down the emotional and financial toll of caring for others.
Patients might think themselves “better off dead” when accounting for the toll that additional medical care might take on their families.
Doctors might violate the Hippocratic Oath and their promise to never harm their patients when suicide is treated as a mercy.
Patients might withhold information from their doctors for fear they will be counseled to take their own lives.
Then there’s the uncomfortable fact that it is cheaper for health care systems and insurers to “do away with” patients who require additional, more expensive care.
So-called legal “safeguards” are gravely insufficient to protect against these negative social trends. Waiting periods, written requests, sign-offs from physicians—none of these requirements remove the pressure on patients to kill themselves or protect against other forms of abuse.
Physician-assisted suicide creates a culture where the weakest among us are the least able to protect themselves from pressure to end their lives.
Physician-assisted suicide devalues human life in circumstances that require the most protection and empathy. Life is treated as disposable, which helps explain why many European countries that have legalized physician-assisted suicide now have expanded into non-voluntary euthanasia.
The U.S. is hardly safe from these dangerous trends. Thus far, six states have legalized physician-assisted suicide.
But there is still time to change course. America can still choose life over death.
This World Suicide Prevention Day, we must recommit ourselves to a unilateral defense of human life.
LifeNews Note: Monica Burke is a research assistant in the DeVos Center for Religion and Civil Society at The Heritage Foundation. This first appeared at the Daily Signal and is reprinted with permission.
It was 1942 and a chemistry professor from Pennsylvania was looking for a cheap source of progesterone. The hormone had many uses at the time, including preventing miscarriages and treating women going through the menopause.
In fact, Russell Marker already had invented a way to make progesterone from a chemical in certain plants. One option was the tubers of wild Japanese yams. But these were thin and weedy – they just didn’t contain enough of the hormone.
Marker scoured the land for alternatives, examining more than 400 species, but to no avail. Then he stumbled upon a drawing in an obscure botany book. This yam had fat, knobbly roots that reportedly weighed up to 100 kg (220lbs). He travelled to its native Mexico and smuggled one out of the country.
With an affordable source of progesterone found, researchers turned to its uses as a contraceptive. The birth control pill hit the market less than a decade later. Marker, on the other hand, mysteriously disappeared from public life and became obsessed with collecting silver.
The economic and social side effects of the pill were as profound as they are well-documented. Sex could be enjoyed without fear of pregnancy. Suddenly women could devote their 20s and 30s to furthering their education and careers, rather than housework and nappies.
But right from the beginning, the pill has had a secret.
In recent years, scientists have started to realise that the brains of women on the pill look fundamentally different. Compared to women who aren’t taking hormones, some regions of their brains seem to be more typically ‘male’.
There are behavioural changes, too. Women on certain types of pill aren’t as good at coming up with words – something our gender are usually highly skilled at. On the other hand, they’re better at mentally rotating objects, as is often the case in men. Finally, women on a different type of pill are better at recognising faces – something women are usually good at.
Confused? So are scientists. What’s going on?
We’re often told that the pill contains oestrogen and progesterone. But no pill contains either hormone
We’re often told that the pill contains oestrogen and progesterone. But no pill contains either hormone.
That is because, when taken orally, oestrogen and progesterone break down too quickly to be practical. Instead, the pill contains synthetic versions, which are built from more stable hormones that have been altered to mimic the hormones.
Every brand of combined pill on the market contains the same type of synthetic oestrogen, ethinyl estradiol, and one of eight synthetic progesterones, called progestins. Ethinyl estradiol prevents the body from releasing an egg every month, while progestins thicken the mucus at the entrance to the cervix and conspire to make the womb inhospitable. Even if an egg slips out and becomes fertilised, it won’t be able to settle down and start growing.
So far, so good. But though the hormones are effective at preventing pregnancy, they aren’t perfect matches for our natural hormones. The end result is that these synthetic versions also have effects that you would never get from raw progesterone.
The internet is awash with anecdotal reports of acne, sweating and unwanted hair growth after going on the pill. One women described sprouting hairs all over her cheeks, while another came down with “pizza face” after starting a new brand. These ‘masculine’ effects have been well-studied by scientists, and they are real: certain kinds of pill really do make them worse, especially in susceptible women.
But the reason is surprising. According to a study from 2012, 83% of US women who are on the pill are taking a version that contains progestins made from male hormones. This includes the popular brands Ortho Tri-Cyclen, Loestrin FE 1/20 and Tri-Sprintec®, among many others.
The male hormone that these pills use is a close relative of testosterone called nandrolone. A potent androgen (a hormone that influences the development of the male reproductive system), it can lead to the development of typically male characteristics.
It’s actually used for doping in men sometimes — Belinda Pletzer
“It’s actually used for doping in men sometimes,” says Belinda Pletzer, a cognitive neuroscientist at the University of Salzburg, Austria. It helps build muscle, so it’s popular with powerlifters and boxers: the former heavyweight world champion Tyson Fury recently served a two-year suspension after testing positive for the steroid in 2015 (he claimed it entered his system after eating the meat of an uncastrated wild boar.)
We’ve known about these side effects for decades: the first progestin ever made, norethindrone, was androgenic.
Back in the 1940s, 50s and 60s, pregnant women sometimes took norethindrone in large doses to help prevent miscarriage. But the hormone also caused some unsettling changes to their bodies.
The women were sweatier, hairier and spottier. Some noticed that their voices had deepened. Nearly one in five baby girlsborn to mothers taking it had masculinised genitals. Some of these unlucky children required surgery.
Today androgenic progestins are much less androgenic. The doses in contraceptive pills are much smaller, and the hormones are usually combined with synthetic oestrogen, which cancels out many of the masculine effects on our bodies.
But there are some side effects.
“These progestins, which were decreased in dose over the years, are still related to the chemical structure of testosterone. All the derivatives came out to levonorgestrel, which is the most used or known of the progestins,” says Regine Sitruk-Ware, a reproductive endocrinologist at the Population Council, New York. “It is still androgenic by itself, by the fact that it can bind to the androgen receptors.”
Over the years, there have been several generations of progestins. Though the earlier ones are nearly all androgenic, more recently scientists have developed versions made from synthetic progesterone, instead. These have the opposite effects – they are often prescribed to treat acne or excessive hair growth because they are ‘feminising’ (though they, too, can have undesireable side effects resulting from a hormonal imbalance). Some examples include Yasmin® and Ocella™.
Generally speaking, the older, cheaper brands of pill tend to contain androgenic hormones, while newer, more expensive ones tend to contain anti-androgens. This may be one reason that just 17% of women on the combined pill in the US take the anti-androgenic versions.
There are androgen receptors all over the body, particularly in the sweat glands and hair follicles, which explains why androgenic progestins can make some women sweatier, hairier and spottier. But these powerful, gender-bending steroids also affect the brain.
In men, the androgens released at puberty are known to remodel the brain. This is also true in women, where relatively small quantities of testosterone can cause certain areas to shrink and others to grow.
Given what we know about the power of these hormones, it’s perhaps surprising that until recently, no one had checked if progestins made from male hormones might have an impact.
“There has been a lot of research on their physical side effects,” says Pletzer. “There’s also been research on the emotional side effects, because that’s something that women keep complaining about. But very few studies have looked at the brain and cognition.”
But when she realised she was excluding those on the pill, she asked herself why. “We know that the steroids our own body produces, such as progesterone and testosterone, affect the brain. So of course I would expect any synthetic hormones to have an effect as well,” she says.
Pletzer abandoned her original idea and set out to test the effects of the pill instead. She recruited a mixture of men and women on and off hormonal contraception, then scanned their brains.
What she found was striking. The scans revealed that several brain areas were larger in the women on the pill, compared to those of women who weren’t. These areas just so happened to be larger in men than women, too.
The study involved a relatively small sample and didn’t separate androgenic and anti-androgenic contraception, so Pletzer cautions against reading too much into the results. But other research has hinted that both types of hormones actually may be changing our behaviour.
Other studies have found that women on oral contraception remember emotional stories more like men
Other studies have found that women on oral contraceptionremember emotional stories more like men – recalling the gist more than the details. They’re also not as good at recognising emotions in others, such as anger, sadness, or disgust – just like men. It looks suspiciously like certain types of pill are “masculinising” women’s brains.
Crucially, these changes seemed to be affecting their behaviour.
Two brain areas were particularly engorged: the fusiform face area, a region about the size of a pea that processes facial information (from photographs of friends to cartoons), and the parahippocampal place area, which important for recognising places (such as cityscapes). These women were also better at recognising faces.
Facial recognition is something women are usually highly skilled at – even as babies – so this fits with the picture of oral contraceptives subtly influencing our brains. In this case, the anti-androgenic pills may be having a “feminising” effect.
Just as before, several brain areas were also larger in women on androgenic pills, including many which are typically so in men. The longer the women had been on the pill, the larger these areas were.
To complicate matters further, all combined pills contain synthetic oestrogen, which is feminising. This means that the same women may be experiencing both ‘feminising’ and ‘masculinising’ effects on their brains at the same time.
No one could have predicted that an ugly yam would give rise to a feminist revolution. The pill has repeatedly been called the greatest invention of the 20th Century and is said to be responsible for a third of the increase in women’s wages since the 1960s.
But contraceptive pills may have a darker side. As Pletzer wrote in 2014, when athletes take steroids we call it ‘doping’ – it’s considered abuse and strongly condemned by society. But we’re happy for millions of women to take these hormones every day, sometimes right through from puberty to menopause.
Scientists don’t yet know if any of the pill’s effects on the brain have much of an impact on our behaviour. But perhaps it is time we put it to the test.
Correction: An earlier version of this story implied that the ‘feminising’ effects of pills like Yasmin could lead to hair loss; while some women do experience hair loss while taking birth control pills, this tends to be for broader reasons such as a resulting hormonal balance. This has been changed.
SPUC SEP 5, 2018 | 2:02PM GUATEMALA CITY, GUATEMALA
Last month, pro-lifers celebrated as a bill to legalise abortion was rejected by the senate of Argentina. However, in Guatemala, it didn’t even come to a vote, as pressure from the pro-life majority forced women’s groups to drop a clause that would legalise abortion in some circumstances.
A bill sponsored by the leftist Convergencia opposition party had included a clause that would allow underage girls that have been the victims of sexual abuse to abort in the first 12 weeks.
Defending human life
Guatemala only allows abortion when the mother’s life is at risk, and has strongly opposed any moves to impose widespread abortion. Last year, the military blocked a Dutch ship distributing illegal abortion pills, saying it would defend “human life and the laws of our country”.
On Sunday 20,000 people, backed by the Catholic and Evangelical churches, took to the streets in protest of the bill and in support of life and family. This fierce opposition forced activists into a hasty retreat, leading to them deciding to remove the clause yesterday.
Without the abortion clause, the bill, which aims to provide social and educational support for girls who become pregnant, is likely to be adopted by Parliament. Also due to be debated is a bill which as well as toughening abortion laws, prohibits same-sex marriage and defines family as being limited to a father, mother and children.
The fight around the right to life for the unborn is continuing across Latin America, with ongoing proposals for liberalising abortion in Chile and Brazil, but the victory in Guatemala and the recent victory in Argentina shows that a united pro-life effort can be enough to uphold the rights of the unborn.
LifeNews Note: Courtesy of SPUC. The Society for the Protection of Unborn Children is a leading pro-life organization in the United Kingdom.
The release of a new report by the Centers for Disease Control and Prevention (CDC) which revealed another record high for STD infections in 2017 is being met with the usual response calling for more “safe sex” rather than getting to the root of the problem – rampant promiscuity.
According to the CDC, nearly 2.3 million cases of chlamydia, gonorrhea, and syphilis were diagnosed in the United States in 2017. This surpasses the previous record set in 2016 by more than 200,000 cases and marked the fourth consecutive year of sharp increases in these sexually transmitted diseases.
The CDC analysis of STD cases reported for 2013 and preliminary data for 2017 shows steep, sustained increases:
• Gonorrhea diagnoses increased 67 percent overall (from 333,004 to 555,608 cases according to preliminary 2017 data) and nearly doubled among men (from 169,130 to 322,169). Increases in diagnoses among women — and the speed with which they are increasing — are also concerning, with cases going up for the third year in a row (from 197,499 to 232,587).
• Primary and secondary syphilis diagnoses increased 76 percent (from 17,375 to 30,644 cases). Gay, bisexual and other men who have sex with men (MSM) made up almost 70 percent of primary and secondary syphilis cases where the gender of the sex partner is known in 2017. Primary and secondary syphilis are the most infectious stages of the disease.
• Chlamydia remained the most common condition reported to CDC. More than 1.7 million cases were diagnosed in 2017, with 45 percent among 15- to 24-year-old females.
“We are sliding backward,” said Jonathan Mermin, M.D., M.P.H, director of CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. “It is evident the systems that identify, treat, and ultimately prevent STDs are strained to near-breaking point.”
Chlamydia, gonorrhea, and syphilis are curable with antibiotics, yet most cases go undiagnosed and untreated — which can lead to severe adverse health effects that include infertility, ectopic pregnancy, stillbirth in infants, and increased HIV risk.
Prior studies suggest a range of factors may contribute to STD increases, including less frequent condom use, socioeconomic factors like poverty, stigma, and discrimination; and drug use. Others believe dating apps like Tinder may be contributing in some way to the spread of these diseases.
“We have seen steep and sustained increases over the last five years,” said Dr. Gail Bolan, director of the Division of STD Prevention at the CDC. “Usually there are ebbs and flows, but this sustained increase is very concerning. We haven’t seen anything like this for two decades.”
David Harvey, executive director of the National Coalition of STD Directors, told CBSthat the United States now has the highest STD rates in the industrialized world.
“We are in the midst of an absolute STD public health crisis in this country. It’s a crisis that has been in the making for years,” Harvey said.
As tragic as these numbers are, they are not surprising given the fact that the same failed strategies are being used over and over again. “Safe sex” education programs which promote the use of condoms have been used for decades to no avail while programs that encourage youth to embrace the only sure method of preventing STDs – abstinence – are widely disdained.
However, when practiced consistently, “abstinence provides the most effective protection against unplanned pregnancy and sexually transmitted diseases including HIV infection,” writes the Department of Health and Human Services (HHS).
Promoting abstinence is more important now than ever, especially with growing fears of antibiotic-resistance in certain STDs over the past few years that have experts fearing an uncontrollable disease outbreak.
For example, a new strain of gonorrhea known as “super gonorrhea” is already untreatable with standard antibiotics. In 2013, resistant strains accounted for just one percent of samples tested by the CDC. By 2017, that number jumped to four percent.
“We expect gonorrhea will eventually wear down our last highly effective antibiotic, and additional treatment options are urgently needed,” Dr. Bolan said. “We can’t let our defenses down — we must continue reinforcing efforts to rapidly detect and prevent resistance as long as possible.”
The CDC is also recommending that doctors make STD screening a part of all routine medical appointments.
Until our sexual health programs put more focus on helping youth to live chastely rather than encouraging them to practice “safer sex,” this epidemic will only continue to worsen.
by: Paul A. Byrne, M.D. and The Rev. George M. Rinkowski
Introduction
Physicians, clergy and everyone ought to uphold basic principles to do good and avoid evil, not to harm and not to kill. A physician and a Catholic priest offer the following statement to medical personnel and
clergy in an effort to inform others about the serious matters of sodomy and “homosexuality.”
The Declaration of Independence states that people “assume among the powers of the earth, the separate and equal station to which the Laws of Nature and Nature’s God entitles them.” The truths declared in this Declaration does not provide a basis for sodomy and “homosexuality.”
There is no “innate instinct,” rather there is a will that can be the cause of evil actions. After Original Sin God gave man the gift of mastery of desires. The first effect of this mastery of desires is the right of liberty, which is the ability to do good and avoid evil. Liberty includes the right to safeguard life and forecast happiness. “That to secure these rights, Governments are instituted among Men to guard Life, Liberty and the pursuit of Happiness.
The Science of Medicine is to guard the life of persons. Civil Government is to guard liberty and justice so that every citizen can pursue happiness here and hereafter. The Science of Medicine has goals to aid, to heal, not to harm and not to kill. This can be stated philosophically to protect, preserve, and prolong life and to postpone death. The province of medicine is not justice and rights, rather it is to treat and care for the life and health of persons.
DAVE ANDRUSKO AUG 31, 2018 | 4:21PM WASHINGTON, DC
Happily for me, earlier today I ran across a guest column written by the Rev. Charles Chaput, the archbishop of the Archdiocese of Philadelphia, for the Delaware County Daily Times, a Pennsylvania newspaper. Naturally, his column was exquisitely reasoned, brilliantly composed, and wonderfully persuasive.
Archbishop Chaput, as he often does, ponders the “meaning and dignity of the human person,” and begins with a conference he attended decades ago on the theme of “supercomputing and the human person.”
What leads him to a discussion of particular interest for us begins with his remembrance that “the nickname for the human body among the attendees was ‘wetware,’ or more crudely, ‘meat puppet.’” However, he reminds us, “Our flesh is not morally neutral. It’s not simply ‘wetware’ or raw meat or modeling clay for the will, but a revelation of God’s glory demanding reverence and stewardship.”
After I repost his next paragraph, I will offer three brief comments:
This makes us witnesses to a meaning and dignity of the human person that puts us at odds with the spirit of our age, an age perfectly captured by the 1973 Supreme Court Roe v. Wade decision and its license to kill the unborn. The cultural civil war triggered by Roe and its enshrinement of permissive abortion has never abated, and it continues full force (and rightly so) today. The stakes are high. Without a guaranteed right to life — a right that includes and recognizes the humanity of the unborn child — all other rights are legal fictions.
#1. “The stakes are high.” Why? For the same reason that the right to life is the first of “certain unalienable rights.” To put it in the negative, without the right not to be killed, all other rights, including “Liberty and the pursuit of Happiness,” are, in Archbishop Chaput’s perfect description, “legal fictions.”
#2.There truly is a “spirit of our age.” Whatever its origins—and they are legion—the underlining ethos is a refusal to see the uniqueness of each and every human being.
If we are nothing more than glorified (or not so glorified) “meat,” what follows? For starters, that we are essentially interchangeable. For another, to firmly avow that you, I, allof us are of transcendent value invites the listener who is a captive to the spirit of the age to roll his or her eyes in disbelief.
#3. I have often quoted the following passage from the late Rev. Richard John Neuhaus: “Thousands of medical ethicists and bioethicists, as they are called, professionally guide the unthinkable on its passage through the debatable on its way to becoming the justifiable until it is finally established as the unexceptionable.”
The unthinkable eventually becomes the unexceptional because the creed of contemporary bioethics begins with the rejection that any one of us, let alone all of us, is exceptional in any way that matters.
For us, the equality of life ethic means each man or woman, boy or girl, born or unborn is of equal/inestimable worth. Notice how the bioethicist, almost all of whom are secularists, twists the equality of life ethic to mean we all are equally unexceptional.
The idea (to quote Archbishop Chaput) that we are an embodied “revelation of God’s glory demanding reverence and stewardship” is not only unintelligible but an offense to them.
That is the Spirit of the Age which we combat every day. It is a battle for our culture that we cannot afford to lose.
Too many powerless people, born and unborn, are counting on you and me.
LifeNews.com Note: Dave Andrusko is the editor of National Right to Life News and an author and editor of several books on abortion topics. This post originally appeared in at National Right to Life News Today —- an online column on pro-life issues.
SACRAMENTO, California, August 30, 2018 (LifeSiteNews) – The California Assembly voted 52-25 this week to approve legislation that would require all public colleges and universities to provide chemical abortion pills in their campus health centers, despite the fact that these pills kill tiny human beings and pose health risks to women.
Effective starting in 2022, SB 320 requires that “each public university student health center shall offer abortion by medication techniques.” It provides for grants to cover the costs of any necessary equipment or training, “telehealth services” (also known as webcam abortions), and backup medical support.
“Abortion care is a constitutional right and an integral part of comprehensive sexual and reproductive health care,” the bill declares. “The state has an interest in ensuring that every pregnant person in California who wants to have an abortion can obtain access to that care as easily and as early in pregnancy as possible,” and “public university student health centers should treat abortion by medication techniques as a basic health service.”
The bill’s mention of “pregnant people” instead of “pregnant women” is likely a nod to transgender activists, who claim that “men” can be pregnant, too.
The measure previously passed the state Senate 25-13 in January, and now returnsto the Senate for final legislative approval. Pro-abortion Gov. Jerry Brown is expected to sign it into law.
The pro-abortion Rewire.News highlights state committee analysis stressing that the abortions would be financed through private grants rather than taxpayer funding. But between the bill’s odes to “basic health service” and “easily accessing” abortion, and its reminder that abortion “must be covered” by the state’s Medi-Cal program, pro-lifers remain wary.
Regardless of who pays for the abortion pills, pro-lifers argue that the bill offers bad medicine to young Californians.
“California politicians put the interests of the abortion industry ahead of the needs of both students and the colleges and universities with this shortsighted vote today,” Students for Life of America President Kristan Hawkins said Wednesday, vowing to fight for student health center workers unwilling to facilitate abortions and students who don’t want their fees going to them. “Schools should be focused on educating the next generation, not ensuring that it’s easy to end the lives of future generations.”
The bill does not specify the type of abortion drugs to be offered beyond “abortion by medication techniques,” but “medication abortion” typically refers to taking mifepristone in an abortuary office, then misoprostol at home.
Despite California Democrats and groups like Planned Parenthood insisting the pills are safe, the U.S. Food and Drug Administration lists 2,207 adverse health events in women who used mifepristone (also known as RU-486) between 2000 and 2011, including 14 deaths, 612 hospitalizations, 339 hemorrhages requiring transfusion, and 256 infections.
Mifepristone can also be reversed by the practice of abortion pill reversal, if extra progesterone to counteract mifepristone’s effects is taken quickly enough. Progesterone is the natural hormone developing babies require to survive, which mifepristone blocks. Its pioneers credit it with saving more than 400 babies since 2007, yet “pro-choice” advocates fiercely oppose making the option accessible to women.
California is one of the most aggressively left-wing states in the union. It was rebuked by the U.S. Supreme Court earlier this year for trying to force pro-life pregnancy centers to advertise tax-funded abortions, and is currently on the verge of enacting a far-reaching ban on treatment for both adults and minors who want to overcome unwanted same-sex attractions.
For the past four weeks, the Church has read from John 6, Jesus’ teaching about Communion, the Eucharist. She wraps that extended study today.
For the past four weeks, we explored the meaning of communion as it relates to giving of human life, illuminated by the teaching of Humanae vitae. We discussed the person of the spouse and of the child, and what love demands in order to create and sustain a communion of persons between myself and them.
Two closing thoughts on this catechesis of communion.
John F. Kippley, the great American pioneer of the natural family planning movement, has written about the relation of marriage, parenthood and the Eucharist. (If you have not read it, see his Sex and the Marriage Covenant). Some might be deterred by his frank association of the relationship of the Eucharist—communion between God and the Christian—and marriage—the communion between man and woman in sexual intercourse.
But there are two important points to draw from that association.
First, the question of openness. To benefit from the Eucharist, we have to be open to receiving Jesus as He is – Truth and Goodness incarnate – and making ourselves more worthy of the gift of the Person we are receiving. To benefit from marriage, we have to be open to receiving the spouse as he or she is – including them as potential parents – and making ourselves worthy of that gift of the person we are receiving.
Second, the question of sacrilege. To receive Communion but not want its graces, to receive Communion but refuse its transformative power, to receive Communion as a sign of wanting to be with God while clinging to mortal sin, is a sacrilege. I am not open to what I am receiving. Likewise, to mutilate sexual intercourse by receiving the person as he or she is while not wanting life, while clinging to my closed attitude toward parenthood, is a sacrilege.
The Church is not devaluing sex. The Church is demanding that we accept the nobility of what God has given us.
As Jesus wraps up His laying out the truths of the Eucharist, today’s Gospel treats us to the reaction. His audience announces, “This saying is hard; who can accept it?” And the result is that “many returned to their former way of life.”
Isn’t the same true of Humanae vitae? Yes, that “saying is hard; who can accept it?” Life is so complicated; children cost so much; times have changed; the world is different. And many “returned to their former way of life.”
The difference is that John does not say Jesus’ “disciples” who “returned to their former way of life” were just “dissenting” Christians. It doesn’t say that they recognized that Jesus’ Eucharistic Teaching was a matter of whether it was acceptable to their “conscience.” And John does not say that, even though Jesus laid down a clear marker of what His Teaching meant, the “Holy Spirit” was creating a new “sensus fidelium” among those other “disciples,” so that they were just “Christians” with a “different” take on the Eucharist. No—they “went away” to “a former way of life,” which is not the life of a follower of Jesus.
Note that their “consciences” too must have told them that Jesus was nuts in saying “this is my body, this is my blood.” And perhaps some, in good conscience, said He’s off His rocker and left. In that, they did right—they did not violate their conscience. But, at the same time, we know in faith the objective truth: their choice in conscience is objectively wrong, and so their conscience is in error.
So why do we equivocate when today’s “disciples” want to pretend that being Catholic but rejecting Humanae vitae is compatible? Yes, conscience is sacred, but not infallible. Conscience still must account to the Truth (not just “my” truth).
My guess is that some of those who turned away thought about what Jesus said and consciously rejected it. But my guess is also that most of those in that crowd simply did not understand Him and were not about to take the time to try. Life is, after all, so complicated, the world has changed, times are different, people are busy …. And, so, they went off, with nary a thought about returning to “their former way of life.”
How many of those who have heard cursorily that “the Church is against birth control” don’t even bother to inquire what Humanae vitae really teaches—and why—but simply go off, with nary a thought about returning to “their former way of life?” After all, times have changed, life is so complicated, people are busy, kids are costly ….
Likewise, Jesus did not adjust His Teaching. He did not dial back its demands. He did not propose a “gradualism” of the Real Presence. He’s pretty clear. Watching the masses depart, Jesus does not offer a watered down Eucharistic-lite teaching to His disciples. He puts the question to them: “Do you also want to leave?” Because, in the Father’s house, doors are not locked from the inside.
Jesus’ question here in John 6:67 is analogous to the question he poses in the Synoptics to the Apostles: “who do you say I am?” (Mark 8:29; Matthew 16:15; Luke 9:20). That profession of faith is the pivot in Mark’s Gospel: do you stay or do you go?
Like today, Jesus first reports “just the facts.” Today—that the crowd turned away. In the Synoptics—“who do people say I am?” to which Jesus gets the report, “John,” “Elijah,” “some prophet.”
But then the questions turn existential: now what about you? Because what you say (“who do you say I am?”) or what you do (“do you also want to leave?”) is an existential turning point: are we going to go on together or not? There’s no compulsion, but there’s also no compromise.
And, like in the Synoptic Gospels, Peter answers. “You are the Christ!” “Where else can we go?” And the Gospel is clear about the other 11: they follow Peter. They don’t say, “Well, this guy tends to be precipitous in his declarations, we’re kind of with you, we’ll see.”
And Peter—especially through Paul VI—also answered an existential dilemma for modern Catholics. Are we like the other 11? Or do we turn and go? Because, contrary to some modern theologians, there is no “fifth column” among the other Apostles.
That’s not to say they understood it all, even less that they wouldn’t fail. Peter himself is proof of that. But they did commit themselves to a “way of life” that others did not, because “you are the Christ, where else shall we go?”
What should that teach today’s Catholic, for whom the teaching about communion of persons in Humanae vitae is also, undoubtedly, “hard?”
ST. LOUIS, Missouri, August 28, 2018 (LifeSiteNews) – An article in the Journal of the American Medical Association (JAMA) bashes pro-life pregnancy centers, places that protect the tiniest of human beings, for allegedly presenting “false and misleading information” to women.
In the article, Dr. Rita Rubin mentions the findings about crisis pregnancy centers of an assistant professor of epidemiology and biostatistics at the University of Georgia College of Public Health, Dr. Andrea Swartzendruber.
“Georgia pregnancy resources centers’ websites contain false and misleading health information,” the article alleges.
“Virtually all of them advertised pregnancy testing and counseling about options,” it read. “However, 58 percent failed to mention that they did not provide or refer for abortion, while 53 percent included false or misleading statements, such as inflated statistics about the chance of a miscarriage and links between abortion and future health problems.”
There is a host of evidence supporting the link between abortion and future health problems such as breast cancer, preterm birth, and miscarriage.
Elsewhere, the article refers to Dr. Amy Bryant, who has claimed crisis pregnancy centers are unethical.
But Nancy Valko, a spokesperson for the National Association of Pro-Life Nurses, said the American Medical Association is simply playing politics with that article, which it has so far published in two of its publications.
“They’re extremely liberal and they go by the polls,” Valko said in an interview. “They see more people are for abortion than against it.”
Although the AMA was once against abortion, it changed its position in 1970 after a few American states legalized it, just before Roe v. Wade and Doe v. Bolton, which legalized abortion on demand in the U.S.
“I remember how upset many doctors were with the AMA after Roe v. Wade and many dropped out of the AMA,” wrote Valko on her blog. “Now, there are over one million MDs in the [U.S.] but less than 25 percent of practicing doctors are members of the AMA, down from 75 percent in the 1950s. (This is not just because of abortion but also the politics of the AMA.)”
“The AMA today now stands firmly for abortion rights and even against common sense conscience rights protection,” she explained.
According the career nurse, many of the criticisms levelled against crisis pregnancy centers in the JAMA article – including the allegation that these centers overplay the dangers of abortion – are simply untrue.
“They say we exaggerate it but I’ve seen the effects of abortion,” she said. “I’ve known women who have had abortions.”
Years ago, Valko cared for an 80-year-old woman suffering through the final stages of congestive heart failure. Fluid had built up in her stomach and it was distended and needed to be measured regularly. As Valko measured her patient one day, the elderly woman remarked she looked like she was pregnant. And then, she added she felt her suffering was a punishment for an abortion she’d had 60 years before.
Wracked with guilt and a sense of loss, she confided to Valko that even the legalization of abortion had not helped her forgive herself for that abortion.
“She said, ‘I know I’ve aborted the only little boy I ever had,’” recalled Valko.
Other women who have had abortions and later become pregnant were sometimes shocked when they learned about the prenatal stages of human development, said the nurse.
It’s a reaction she says pregnant women who visit crisis pregnancy centers share when they see ultrasounds of their preborn babies.
“Seventy-eight percent of women change their minds about abortion at the crisis pregnancy centers when they get the ultrasound,” she said. “They’re just looking at the truth.”
Despite the powerful impact ultrasounds can often have on pregnant women at crisis pregnancy centers, the JAMA article refers to these ultrasounds as medically unnecessary in the first trimester and “emotional manipulation.”
However, ultrasounds are a regular part of medical care during pregnancy, with OBGYNs typically performing them at around six or eight weeks to confirm the baby’s heartbeat and that the pregnancy is not ectopic, and again roughly once a month during a normal pregnancy.
The article in the medical journal also criticizes crisis pregnancy centers for not offering birth control, something Valko says is unnecessary.
“They’re called crisis pregnancy centers,” she said. “They’re already pregnant. They’re not going to need birth control.”
Nearly half of all women experiencing unintended pregnancies were taking hormonal contraception, according to the pro-abortion Guttmacher Institute.
The Pennsylvania grand-jury report was released on the very day that I had chosen (long beforehand) to begin a week-long vacation. I had vowed that it would be a real vacation—that I wouldn’t hop back to post news items on this site—and I held to that vow. Still I could not escape the news; everyone I met wanted to hear my take on the scandal.
So I told people what I have been telling people since 2002: that the Dallas Charter addressed only one part of a three-part scandal; that our bishops have still not recognized the depth of the problem; that the crisis will continue until Church leaders demand true reform.
This new outcropping of the scandal has roused much, much more anger than the earlier revelations of the “Long Lent” in 2002. And whereas sixteen years ago the public was shocked primarily by the loathsome activities of predatory priests, this year the focus is—quite rightly—on the bishops. Our shepherds failed us. They misled us. They told us that they had fixed the problem, and they hadn’t. They told us that there would be no more cover-ups, but there were. They told us that they now understood the problem, but they didn’t. And I’m afraid that, as a group, they still don’t. If the American bishops understood the depth and breadth of the rage that is mounting among the Catholic laity—and is most evident among the most loyal, the most active, the most prayerful Catholics—they would follow the example of their Chilean counterparts and resign en masse.
Against this background it was refreshing, on my first full day back on the job, to go to morning Mass and hear the reading from Ezekiel (34: 1-11):
The word of the LORD came to me:
“Son of man, prophesy against the shepherds of Israel, prophesy, and say to them, even to the shepherds, Thus says the Lord GOD: Ho, shepherds of Israel who have been feeding yourselves! Should not shepherds feed the sheep?
You eat the fat, you clothe yourselves with the wool, you slaughter the fatlings; but you do not feed the sheep.
The weak you have not strengthened, the sick you have not healed, the crippled you have not bound up, the strayed you have not brought back, the lost you have not sought, and with force and harshness you have ruled them.
So they were scattered, because there was no shepherd; and they became food for all the wild beasts.
My sheep were scattered, they wandered over all the mountains and on every high hill; my sheep were scattered over all the face of the earth, with none to search or seek for them.
“Therefore, you shepherds, hear the word of the LORD:
As I live, says the Lord GOD, because my sheep have become a prey, and my sheep have become food for all the wild beasts, since there was no shepherd; and because my shepherds have not searched for my sheep, but the shepherds have fed themselves, and have not fed my sheep;
therefore, you shepherds, hear the word of the LORD:
Thus says the Lord GOD, Behold, I am against the shepherds; and I will require my sheep at their hand, and put a stop to their feeding the sheep; no longer shall the shepherds feed themselves. I will rescue my sheep from their mouths, that they may not be food for them.
“For thus says the Lord GOD: Behold, I, I myself will search for my sheep, and will seek them out.
Dozens of bishops have released public statements about the scandal in the past few weeks. Some of these statements have been hard to credit: prelates claiming that they did not know what so many people around them knew, that they did not hear what they had been told. Others have been lawyerly and bureaucratic: mistakes were made, committees will be formed, procedures will be instituted. Most, to be fair, have been solid statements, full of apologies, recognizing a need for corrective action, promising reform.
Unfortunately we have heard the apologies and the promises before. The time for strongly worded statements has passed. It is time for action. Urgent action.
Last week a young Catholic woman asked me what our bishops are likely to do. “They’ll meet in November,” I began—and she interrupted with a shout: “In November??!!” She could not believe that, in the midst of this crisis, Church leaders would be content to wait several weeks before doing… anything. I share her frustration. I think Ezekiel shares it, too.
I said above that the time for statements has passed, but that was a slight exaggeration. There are two sorts of statements that a bishop could issue to catch my attention and earn my respect:
“I recognize that I have betrayed my people and irreparably damaged my credibility as a pastor of souls and a teacher of the faith. I resign.”
“I have done my best, despite my failings, to fulfill my episcopal duties. But my colleagues, [here supply names], have betrayed their people and irreparably damaged their credibility as pastors of souls and teachers of the faith. I call upon them to resign.
New statements, new policies, new committees, new procedures cannot resolve this problem. If our bishops cannot institute serious reform, then we need new bishops.
August 27, 2018 (Operation Rescue) – Judge Mary Wiseman issued a decision Wednesday upholding an Ohio Department of Health order to revoke the Ambulatory Surgical Facility license of the Women’s Med Center, a late-term abortion facility owned by Martin Haskell located in the Dayton suburb of Kettering.
Attempts to close the infamous abortion facility began in 2015, after the Health Department determined that the Women’s Med Center had failed to meet licensing requirements by not obtaining an approved hospital transfer agreement.
The abortion facility has 30 days to file an appeal.
Last year Christian musician Nichole Nordeman shared a humorous but tragic anecdote. She described overhearing a couple at the airport on a video chat with their “baby” and the baby’s “grandparents.” The parents, she said, were clearly suffering separation anxiety. “They are cooing and gushing and exclaiming “well look at YOU, big boy! So big! So handsome!” she wrote. Then followed a “million questions” for “Nana” about the baby’s eating and bathroom habits, and toys.
“I’m literally crying into my latte because it’s so precious,” recounts Nordeman, “and I turn around to try and get a sneak peek at the baby on their FaceTime video.”
It was a Labrador puppy!
According to The Washington Post, it’s not just our imaginations: younger couples really are consciously choosing to forego having children and instead to have pets, which, in many cases, they treat as if they actually were human children. Not only are millennials far more likely to own pets, but according to one study, 44% of millennials who have a pet view their pet as “practice” for having a child. In reality, as psychologist Jean Twenge observes, “pets are becoming a replacement for children.”
According to The Post, the pet industry has grown three-fold since 1996, becoming a $70 billion/year industry in the U.S. How absurd has it become? As journalist Matthew Walther wryly observes this week, we now have: “Dog strollers, dog birthday parties, dog hotels, dog therapy, dog aromatherapy, dog yoga, dog church, the Exquisite Dog Coloring Book: Mindfulness and Stress Relieving Patterns,” and “The 6 best dog swimming pools to buy in 2018.”
One Minnesota company recently hit the New York Times for deciding to offer employees the option to work from home for a week after they get a pet. They call it “fur-ternity” leave. Another company offers two weeks paid “paw-ternity” leave for any employee that adopts a dog or exotic pet. In the U.S. many working mothers of actual newborn babies won’t even get two weeks of paid leave!
The Selfishness of Voluntary Childlessness
Pope Francis has little patience for this sort of thing. In a 2014 homily, the Holy Father lambasted the “culture of well-being” that convinces couples that: “It’s better not to have children! It’s better! You can go explore the world, go on holiday, you can have a villa in the countryside, you can be care-free … It might be better — more comfortable — to have a dog, two cats and the love goes to the two cats and the dog.”
In the end, he warned, such a marriage “comes to old age in solitude, with the bitterness of loneliness. It is not fruitful, it does not do what Jesus does with his Church: He makes His Church fruitful.”
How different is this modern attitude from the traditional attitude, which is reflected in the language of The Catechism of the Catholic Church. The Catechism, quoting the Second Vatican Council, describes children as “the supreme gift of marriage.” Not just one gift among many. But the “supreme” gift! Indeed, as the Catholic Church has repeatedly insisted over the years, marriage is primarily oriented towards the procreation and education of children. And, as the Catechism also states, it is in children that marriage “finds its crowning glory.”
Sadly, whereas in past generations the truth of this statement would have been self-evident, it now strikes many young couples as preposterous. Indeed, an enormous amount of what we hear about children these days is profoundly pessimistic. I often hear from young couples, “We are not ready to have children.” “We cannot afford to have children, or more than two children.” “The world is overpopulated. It would be selfish for us to bring another child into it.”
Many young couples will agonize over every single detail of parenthood, worrying about the effects on their lifestyle, how they will pay for their child’s education, the stability of their careers, the size of their house, and myriad other such details. Sadly, the more they agonize the more they find compelling reasons not to have a child, because, truth be told, the ideal circumstances to have a child simply do not exist! Often, they will couch their hesitancy as a selfless concern for their non-existent child’s future, or the planet, when in reality they are merely worried about the threats to their comfort and sense of security.
In the meantime, they become older and more and more set in their ways, so that having a child appears ever more daunting and disruptive to their comfortable lifestyle. In the end, such couples will often find good reasons to delay starting a family until well past the woman’s peak fertile years. Indeed, they often find to their dismay that they have delayed too long and are forced to resort to expensive and immoral “reproductive technologies” to have the children they could easily have had in their mid-twenties.
Pope Francis powerfully put into words the consequences when a tired, decadent society eschews its very future by refusing children in this way. “A society with a greedy generation, that doesn’t want to surround itself with children, that considers them above all worrisome, a weight, a risk, is a depressed society,” he warned in 2015. “The choice to not have children is selfish. Life rejuvenates and acquires energy when it multiplies: It is enriched, not impoverished.”
“The joy of children makes their parents hearts throb and reopens the future,” he added. “Children are not a problem of reproductive biology, or one of many ways to realize oneself in life, let alone their parent’s possession. Children are a gift. Do you understand? Children are a gift.”
Children: The “Supreme Gift” of Marriage
I personally witness the truth of this statement everywhere I travel. Indeed, there is nothing in the world like the warmth that I find whenever I enter the home of a growing, rambunctious family whose parents have been generous in welcoming new life.
Children in church
In many of the poorer parts of the world that I visit, the parents may have had to sacrifice enormously in order to provide for their children. And yet, what joy reigns in such households! Often, I am mobbed at the door by children, eager to be the first to greet me. The pride that the parents take in each of their children is infectious, and they will gladly entertain me with stories about the adventures and gifts of each child. Mealtimes are riotous affairs, filled with lively conversation, laughter, stories, and – yes – numerous spills. The older children often keep a look-out for their younger siblings, playing games with them, reading to them, and making sure they get served at table, while the younger children clearly adore their older siblings. Sometimes the houses are a mess, but I truly wouldn’t trade that merry mess for all the spotless, silent, lifeless mansions of the voluntarily childless couples that populate our wealthy cities and suburbs.
Of course, family life comes with great challenges. Often at the end of the day, the parents fall into bed, bone tired. Yes, having a large family often means that the parents cannot go out as often as they would like, or afford expensive vacations, and all the other perks that our advertising industry constantly convinces us that we need. And yes, sometimes there is profound heartbreak, as when a child suffers a grave illness, or makes choices that harm the child’s physical or spiritual welfare.
But, as so many parents have told me, the rewards of family life are enormous. They may not be glamorous, but they are deep, and full of meaning. Working side by side in overcoming the challenges of raising a loving family is an ongoing education in love, and often brings the couple far closer than they might have been had they not had children. Their relationship has been forged into something resilient and beautiful by the habitual practice of sacrificing for the welfare of their children and for each other. Their love is not the immature puppy love of a young couple, highly vulnerable to the vicissitudes of life; theirs’s is a deep, rooted love, characterized by a depth of mutual understanding that is the hard-won fruit of years, or decades of shared labor, struggles, sacrifice, triumphs, joys and prayer.
Child having fun in the kitchen with Mom
As the Catechism states, children are not only the “supreme gift” of marriage, but they also “contribute very substantially to the welfare of their parents.” This becomes especially clear as the parents age. The many challenges of raising a large family give way to the irreplaceable joys of watching one’s children growing into mature adults who often count their siblings among their closest friends. Then there are the happy family reunions, the joyful family dinners and birthdays, the births of grandchildren. Even as they physically age, many parents of large families scarcely seem to get older: they are surrounded by so much life and love that they maintain an astonishing youthfulness of spirit into old age. Nor do they face the dark prospect of spending their declining years alone. They live in the happy confidence that their children will care for them, and that they will always have the lively presence of their grandchildren to lighten their twilight years.
It is true, as Pope Francis says, that, “it takes courage to start a family.” To bring a child into the world is a powerful act of defiance against the uncertainties and tragedies of life. Parenthood is the greatest act of hope, a resounding affirmation that life is worth living and full of meaning, that God’s creation is good, and that love is always fruitful and self-transcendent. To start a family is to open wide one’s arms to uncertainty and possible heartbreak; but to do so with a deep faith in the prevailing power of God’s providence, is to invite authentic joy into one’s life.
These young couples who are “practicing” parenthood by having pets will never know the joy of the first time when their child says, “I love you”! They will never know the subtle, rich and deeply rewarding pleasure of working side-by-side with one’s spouse in the most magnificent of all human tasks – that of cooperating with God in creating and nurturing new life! They will not learn that the glamour of this world leads only to boredom, disillusionment, and estrangement, and that the only path to the lasting love every heart craves is the sacrificial gift of self to another.
To all couples, and especially to young couples, I would urge that you do not allow yourselves to be overwhelmed by the anti-child pessimism of our age. Have courage! Have hope! Starting a family is daunting. But God’s grace is great! Learn to pray together as a couple, and then make that supreme act of hope and start a family. You will find great challenges; you will be stretched; you will experience moments of difficulty. But if you persevere in hope and love, nurturing the sacrament of your marriage through prayer, you will also experience greater rewards and joys you can now imagine
Bishops and priests attend Pope Francis’ celebration of Mass marking the feast of Sts. Peter and Paul in St. Peter’s Square at the Vatican June 29. In an Aug. 20 letter to all Catholics, the pope blamed clericalism for helping to support and perpetuate sexual abuse committed by clergy. (CNS photo/Paul Haring) See VATICAN-LETTER-ABUSE-CLERICALISM Aug. 22, 2018.
VATICAN CITY (CNS) — Pope Francis blamed “clericalism” in the Catholic Church for creating a culture where criminal abuse was widespread and extraordinary efforts were made to keep the crimes hidden.
Throughout his pontificate, Pope Francis has targeted clericalism as an illness in the church, an ailment that pretends “the church” means “priests and bishops,” that ignores or minimizes the God-given grace and talents of laypeople and that emphasizes the authority of clerics over their obligation of service.
“To say ‘no’ to abuse is to say an emphatic ‘no’ to all forms of clericalism,” the pope wrote in a letter Aug. 20 to all Catholics.
Clericalism, he said, involves trying “to replace or silence or ignore or reduce the people of God to small elites,” generally the clerics.
Kathleen Sprows Cummings, a professor of history at the University of Notre Dame and author of an Aug. 17 New York Times op-ed piece on the abuse scandal, told Catholic News Service, “I was blown away” by the pope’s focus on clericalism as the problem, “because that’s what I felt.”
What was different with the Pennsylvania grand jury report, she said, was not just the overwhelming scale and magnitude of abuse, “but that it really indicted the culture — the culture of clericalism — that allowed this abuse to continue and allowed it to be hidden.”
“It’s not just ‘a few bad apples,’ as we used to say, but it’s this entire culture that makes it possible,” Cummings said.
Natalia Imperatori-Lee, a professor of theology at Manhattan College, told CNS: “There is no doubt that clericalism is at the root of the abuse crisis. Clericalism is isolating and insular — it cuts off the ‘oxygen’ of genuine solidarity and sharing-of-life with laypeople by creating a separate class, even a separate caste, within the church.”
When people create “small elites” as Pope Francis called them, she said, “the temptation is to preserve ‘us’ and ‘our vision/lives/privilege’ at the expense of ‘them’ — the laity, ‘those who don’t understand,’ ‘those who aren’t burdened the way we are.'”
For more than two decades, Russell Shaw, an author and writer, has been warning of the disaster clericalism poses for the church. His book, “To Hunt, To Shoot, To Entertain: Clericalism and the Catholic Laity,” was published in 1993.
Writing Aug. 6 for Angelus News, the news site of the Archdiocese of Los Angeles, Shaw looked particularly at accusations of sexual abuse and misconduct leveled against now-Archbishop Theodore E. McCarrick.
“Clericalism doesn’t totally account for what happened,” he wrote in Angelus. “But it is an important part of the explanation, and it’s essential that we understand how that was so,” particularly in explaining how the archbishop was able to rise so high in the church’s hierarchy.
Giving any kind of integrity to a church investigation of the scandal will require the participation of laypeople, Shaw wrote, because “it would be a serious mistake to investigate the damage done by clericalism in a clericalist manner.”
Australia’s Royal Commission Into Institutional Responses to Child Sexual Abuse issued its report last December after five years of hearings and investigations, and it concluded that “clericalism is at the center of a tightly interconnected cluster of contributing factors” to abuse within the Catholic Church.
“Clericalism is linked to a sense of entitlement, superiority and exclusion, and abuse of power,” the report said.
In addition, it said, “clericalism caused some bishops and religious superiors to identify with perpetrators of child sexual abuse rather than victims and their families.”
The bishops of Australia plan to release a formal response to the report at the end of August. But in the meantime, Archbishop Mark Coleridge of Brisbane, conference president, told CNS that while the report is “essentially a secular eye upon church,” it “seems to me fairly accurate to claim that ‘clericalism is at the center of a tightly interconnected cluster of contributing factors.'”
“In seeking to combat clericalism,” he said, “we need to be careful not to throw the baby out with the bath water. Clearly, it requires a radical revision of how we recruit and prepare candidates for ordination. Much has changed in our seminaries, but one has to wonder whether seminaries are the place or way to train men for the priesthood now.
“There will also have to be a change in the culture associated with the Catholic priesthood, which of course is more easily said than done,” he continued in an email response to questions. “Part of that change will involve proper professional supervision for the sake of greater accountability, but also a greater sharing of responsibility with laypeople — which in turn requires a reconsideration of our structures of decision-making.”
“It will also involve a serious and practical consideration of the diagnosis of clericalism offered by Pope Francis over the years of his pontificate — a diagnosis which is both disruptive and consoling, just like the Holy Spirit,” Archbishop Coleridge wrote. “To accept and act upon that diagnosis won’t in any way diminish the priesthood — as some fear — but will show what the priesthood can be in the very different circumstances we now face.”
The Royal Commission report also tried to tackle some Catholic theology, claiming, “The theological notion that the priest undergoes an ‘ontological change’ at ordination, so that he is different to ordinary human beings and permanently a priest, is a dangerous component of the culture of clericalism. The notion that the priest is a sacred person contributed to exaggerated levels of unregulated power and trust which perpetrators of child sexual abuse were able to exploit.”
Archbishop Coleridge said his acceptance of the idea of clericalism as a contributing factor to the abuse crisis obviously does not mean he accepts the Royal Commission’s understanding of the theology of holy orders.
The phrase “ontological change” is what the church uses to describe what happens in ordination, he said; it affirms that “God actually does something in ordination, something which reaches into the depths of a man’s being” and that “once a man is ordained, his relationships with other people and with God are radically and permanently changed.”
So, while teaching that ordination brings a permanent change can contribute to clericalism, it does not have to, the archbishop said.
Imperatori-Lee also mentioned the teaching when commenting to CNS on how clericalism can infect the laity as well as priests and bishops.
“The laity, told repeatedly that the priest is special and uniquely holy — ‘ontological change,’ ‘indelible mark’ — is not inclined to believe the clergy capable of sin,” she said, “and then when these allegations arise, and are corroborated, the breakdown in trust is irreparable.”
“There are ways in which clericalism hurts everyone,” she said: “The laity is victimized and infantilized; the clergy is isolated and expected to be superhuman.”
Marie Collins, an abuse survivor and former member of the Pontifical Commission for the Protection of Minors, also welcomed the pope’s aim at clericalism.
Tweeting Aug. 20, she said, “The condemnation of clericalism in the letter is good to see, as it plays a big part in the ignoring of the laity, survivors and experts. It gives rise to the ease with which church leaders can feel comfortable protecting fellow clerics despite their crimes against children.”
ROME, August 25, 2018 (LifeSiteNews) — What you are about to read is an explosive testimony of the former apostolic nuncio to the United States, implicating Pope Francis and several senior prelates in covering up Archbishop Theodore McCarrick’s alleged sexual abuse of seminarians and priests.
In an extraordinary 11-page written statement (see official English text below), Archbishop Carlo Maria Viganò, 77, claims that Pope Francis knew about strict canonical sanctions imposed on McCarrick by Pope Benedict XVI but chose to repeal them.
Archbishop Carlo Maria Viganò at the Rome Life Forum on May 18, 2018.Steve Jalsevac / LifeSiteNews
In his testimony, dated August 22, Archbishop Viganò, who served as apostolic nuncio in Washington D.C. from 2011-2016, states that in the late 2000s, Benedict had “imposed on Cardinal McCarrick sanctions similar to those now imposed on him by Pope Francis,” and that Viganò personally spoke with Francis about the gravity of McCarrick’s abuse soon after his election in 2013.
But he says that Francis “continued to cover him” and not only did he “not take into account the sanctions that Pope Benedict had imposed on him” but also made McCarrick “his trusted counselor” who helped him to appoint a number of bishops in the United States, including Cardinals Blase Cupich of Chicago and Joseph Tobin of Newark.
Archbishop Viganò also implicates Cardinals Sodano, Bertone and Parolin in the cover-up and insists various other cardinals and bishops were well aware, including Cardinal Donald Wuerl, McCarrick’s successor as Archbishop of Washington D.C.
“I myself brought up the subject with Cardinal Wuerl on several occasions, and I certainly didn’t need to go into detail because it was immediately clear to me that he was fully aware of it,” he writes. The Cardinal’s “recent statements that he knew nothing about it … are absolutely laughable. He lies shamelessly.”
“Cardinal Wuerl, well aware of the continuous abuses committed by Cardinal McCarrick and the sanctions imposed on him by Pope Benedict, transgressing the Pope’s order, also allowed him to reside at a seminary in Washington D.C. In doing so, he put other seminarians at risk,” he attests.
A widely respected figure, Archbishop Vigano says his “conscience dictates” that the truth be known as “the corruption has reached the very top of the Church’s hierarchy.” He ends his testimony by calling on Pope Francis and all of those implicated in the cover up of McCarrick’s abuse to resign.
In comments to LifeSiteNews on August 25, Archbishop Viganò said: “The main reason why I am revealing this news now is because of the tragic situation of the Church, which can be repaired only by the full truth, just as she has been gravely injured by the abuses and coverups. I do this to stop the suffering of the victims and to prevent new victims, and to protect the Church: only the truth can make her free.”
Viganò said the second reason he chose to write his testimony is “to discharge my conscience before God of my responsibilities as bishop of the universal Church. I am an old man and I want to present myself to God with clean conscience.”
Asked if he is concerned about critics who might suggest he is breaking the pontifical secret — a code of confidentiality applying to matters that require greater than ordinary confidentiality — he said: “The secrets in the Church, also the pontifical ones, are not taboos. They are instruments for protecting her and her children from her enemies. The secrets are not to be used for conspiracies.”
“The people of God have the right to know the full truth, also regarding their shepherds,” he said. “They have the right to be guided by good shepherds. In order to be able to trust them and love them, they have to know them openly in transparency and truth as they really are. A priest should be a light on a candlestick always and everywhere and for all.”
This is a breaking story. Follow LifeSite for further updates.
Here below is the official English text of Archbishop Carlo Maria Viganò’s Testimony. (You can download a PDF of the English translation here, and a PDF of the original Italian here.) Emphasis not added.
TESTIMONY
by His Excellency Carlo Maria Viganò Titular Archbishop of Ulpiana Apostolic Nuncio
In this tragic moment for the Church in various parts of the world — the United States, Chile, Honduras, Australia, etc. — bishops have a very grave responsibility. I am thinking in particular of the United States of America, where I was sent as Apostolic Nuncio by Pope Benedict XVI on October 19, 2011, the memorial feast of the First North American Martyrs. The Bishops of the United States are called, and I with them, to follow the example of these first martyrs who brought the Gospel to the lands of America, to be credible witnesses of the immeasurable love of Christ, the Way, the Truth and the Life.
Bishops and priests, abusing their authority, have committed horrendous crimes to the detriment of their faithful, minors, innocent victims, and young men eager to offer their lives to the Church, or by their silence have not prevented that such crimes continue to be perpetrated.
To restore the beauty of holiness to the face of the Bride of Christ, which is terribly disfigured by so many abominable crimes, and if we truly want to free the Church from the fetid swamp into which she has fallen, we must have the courage to tear down the culture of secrecy and publicly confess the truths we have kept hidden. We must tear down the conspiracy of silence with which bishops and priests have protected themselves at the expense of their faithful, a conspiracy of silence that in the eyes of the world risks making the Church look like a sect, a conspiracy of silence not so dissimilar from the one that prevails in the mafia. “Whatever you have said in the dark … shall be proclaimed from the housetops” (Lk. 12:3).
I had always believed and hoped that the hierarchy of the Church could find within itself the spiritual resources and strength to tell the whole truth, to amend and to renew itself. That is why, even though I had repeatedly been asked to do so, I always avoided making statements to the media, even when it would have been my right to do so, in order to defend myself against the calumnies published about me, even by high-ranking prelates of the Roman Curia. But now that the corruption has reached the very top of the Church’s hierarchy, my conscience dictates that I reveal those truths regarding the heart-breaking case of the Archbishop Emeritus of Washington, D.C., Theodore McCarrick, which I came to know in the course of the duties entrusted to me by St. John Paul II, as Delegate for Pontifical Representations, from 1998 to 2009, and by Pope Benedict XVI, as Apostolic Nuncio to the United States of America, from October 19, 2011 until end of May 2016.
Niall McGrath stunned doctors when he came out of his coma in 2010 and has been steadily recovering ever since.
The Daniel O’Donnell fan has been helped by his mother, Mary, and sister Sandy Roper, as well as the Donegal singer who sang to him while he was on life-support and kept in touch with the family.
The Mullingar lad incurred massive brain damage when he allegedly fell down steps in a London pub on March 6, 1989.
However, cold-case detectives have launched an investigation after a doctor at St Bartholomew’s hospital, London said he believed Niall had received “a massive blow to the head with a block of wood”.
Six operations and ten days later, a week before his 21st birthday, doctors pronounced him “clinically dead”.
His sister said: “They actually withdrew him off life-support three times. He was a write-off.” But instead of rapidly wasting away, Niall began to breathe.
He was moved to the National Rehab centre in Dun Laoghaire and later St Joseph’s Care Home in Longford, where he has remained since.
Niall could not speak or move up to eight years ago and “now he’s able to stand up for 25 minutes and he can transfer himself from the wheelchair to the bed”.
He also uses an iPad, and attends speech therapy.
In between sessions, Sandy voice-coaches him. “In the beginning he struggled to say my name. All he could say was ‘Ssss’. Then one day he said to me: ‘I love you.’ He even sang a few bars of a Daniel O’Donnell song, Footsteps, after we played it at his bedside.
“Then another time he said ‘F***!’ He was cursing because he was frustrated. Now he’s got a lot of words. If you ask him ‘How are you?’ he says ‘Very well, thank you’.”
But while the now 50-year-old is making massive strides, Sandy, who works as a therapy attendant for disabled people, believes he would make even more progress if he didn’t have to live with older patients.
“All the other residents are elderly. It’s depressing for him. The staff do their best but there isn’t enough money put into therapy for people like Niall.”
She visits him every lunchtime and brings mother Mary, 73, to visit every evening.
The rest of the family also visit, including two nieces, a grandniece and grandnephew who weren’t even born when Niall went into the coma.
As has been obvious to many Catholics for many years, broad swathes of the American Church have been very cavalier and accepting of homosexual behavior, despite the fact that the Church is crystal clear that such behavior is gravely sinful.
So, I wanted to share a brief story.
My RCIA Experience
When I decided I had to become Catholic, I went to a local RCIA Program. RCIA stands for “Rite of Christian Initiation for Adults.” It is the program most converts go through in order to become Catholic.
So, I went to my first class. The instructor was a nice lady. But she had one major flaw: She took it upon herself to tell the students that she disagreed with the Church’s teaching. On what you may ask? You guessed it: homosexuality.
Up until she said that (and no student even brought it up) I had been very engaged in the discussion. But when she said it, I went dead silent. I didn’t know how to respond. I was so disappointed that an instructor in the Catholic faith wasn’t even standing by it that I determined the most prudent course of action, for a first class, would be to simply be silent — and if God intended me to speak, He would open the door.
An Open Door
Well, He did. The instructor noticed I went from lively and engaged to dead silent. “So Joshua, what do you think?”
“Oh, I’m happy to just listen,” I said, attempting to give her an out.
“No, I’d really love to hear what you think.”
I gave her another out, but then the other instructor, a middle-aged man who was subbing for the Deacon (who was sick) chimed in and said he’d love to hear my thoughts as well (he had not stood up to the lead instructor when she said she disagreed with the Church’s teaching on homosexuality).
Speaking Up
Taking this as my cue, and after giving 2-3 chances for them to opt out of getting a response from me, I looked the instructor in the eye, and firmly, but politely said:
“I am here precisely because I am no longer a Protestant; thus, I intend to obey and stand by the Church’s teachings.”
The room fell pin-drop silent. After about 5-10 seconds (which seemed like an eternity), I spoke up again:
“Also, you misquoted the Catechism.”
She had claimed that the Church taught that homosexual persons were intrinsically disordered, and that was discriminatory. I said, “That is absolutely false. That’s not what the Catechism says. It says that homosexual acts are intrinsically disordered.”
Sure enough, she looked it up, and I was correct. Paragraph 2357 said exactly what I said: “homosexual acts are intrinsically disordered.” Persons who have homosexual dispositions are to be loved and honored as persons. But homosexual acts are intrinsically disordered.
Again, silence.
“And by the way,” I said, “the Catechism states that many actions I would be prone to as a heterosexual man are also ‘intrinsically disordered.’ So if the Church discriminates against homosexuals, it is also discriminating against me, a straight man, I guess.” Sure enough, when the Catechism was opened, turns out I was correct. Many such actions are described as “intrinsically disordered.”
Suffice it to say I left that class horrified. How could the instructor in the Catholic faith (1) Openly declare rebellion against it; and (2) mangle the Catechism to make her point?
Baffled
To add insult to injury, the other instructor only stood up for the Church’s teaching against the dissenting instructor after I stood up for it! How on earth could this be happening? I wasn’t even in the Church yet, and yet I was standing up for her teachings more than the Catholics who were instructing me.
I was baffled.
I was even more baffled when I told the RCIA coordinator about it. The response was horrible. All I got was: “Thanks for letting us know.”
No changes were made, nothing. Someone was openly teaching error to potential converts, and they were allowed to continue doing so.
Not a Mystery
There were other troubling things that occurred during that RCIA class, but I trust the point is clear. There is a rot that has infested far too many Catholic parishes from parish leadership itself. That is why so many lay people are so furious right now. Nor was this a mystery to me prior to deciding to convert. I knew all about it, having had many discussions with Catholic friends.
But church leaders are attendants. They are not the Bridegroom. You don’t flee the altar, as many of the faithful are threatening to do.
You don’t leave. In fact, you can’t leave. You stick it out. People will always, always disappoint. But the Church remains the beneficiary of Christ’s promises.
So, you don’t leave, for this is to base faith on men. You stay, for that is to base faith on Christ.
MICAIAH BILGER AUG 21, 2018 | 5:36PM NEW DELHI, INDIA
A mother in India recently gave birth to a baby boy while in a coma and then surprised doctors by waking up when she heard her son’s cries.
The Indian news site Manorama Online reports Betina, of Kottayam, India, fell on Jan. 2 and sustained a severe head injury. The report described her as “half dead” when she arrived at the Caritas Hospital.
Doctors later determined that she had brain damage and, another complication, she also was about 9 weeks pregnant.
Tests determined that her unborn baby’s heartbeat was low and doctors feared the baby, a boy, would not survive to birth. They recommended an abortion.
Betina was transferred to the Kottayam Medical College Hospital where her unborn baby was supposed to be aborted, but doctors there gave a different opinion. According to the report, they said the abortion would put Betina’s health at even greater risk. Their decision proved to be life-saving.
Two weeks later, another scan showed the unborn baby was growing normally, and his heart rate had increased to a normal rate, according to the report.
At the same time, Betina was battling several life-threatening infections, but she also pulled through. Doctors said their hope for the mother and her unborn son began to grow steadily with each week.
Her husband, Anoop, said he sometimes put his hand on his wife’s stomach to feel the baby kicking.
At 37 weeks of pregnancy, a test revealed that the amniotic fluid in Betina’s womb was unusually low, and they decided to deliver her baby via cesarean section, the report states. Baby Elvin was born on June 14.
Doctors said his life was a miracle. But the miracles did not end there.
When Elvin began to cry, doctors said they noticed that Betina’s eyes began to move, slightly at first, according to the report. They laid Elvin beside her, and her eyes began to fill with tears. Doctors said she made an effort to move her arms to touch her son, the report states.
The doctors said they kept Elvin by his mother’s side as much as possible, and his laughter and cries seemed to help his mother more than anything else. They said she improved significantly over the next several weeks.
Though she remains in the hospital, Betina now can move her hands and fingers, and she often tries to hold her baby boy, according to doctors.
The report concluded:
The baby was christened Elvin, meaning “beloved friend” as he has been to his mother. On the day of Elvin’s baptism ceremony, Betina was made to sit in a wheelchair for the first time. When baby Elvin was placed on her lap, she smiled and touched him with all the love of a mother.
His tiny life almost was destroyed in an abortion, but because doctors allowed him to live instead, both he and his mother now have hope for the future.
God always knows what we need. God always gives us what we need. Sometimes we need comfort. Sometimes we need assistance. Sometimes we need correction. Often, we need all three.
In the midst of this dark time in the Church, where the people of God have been so rightly scandalized by the wickedness and cowardice of many of her priests and bishops, that axiom has proven itself true once again in the liturgies God’s providence has given us this week.
On Monday we celebrated the memorial of St. Bernard of Clairvaux. This great saint lived in the 12th century, a dark period when rival claimants to the papacy left the Church shattered by division and confusion. He devoted himself to the healing of this terrible schism and to the restoration of clarity, peace and concord within the Church. He was also an extraordinary reformer of religious life; his reforms of monasticism led to the foundation of the Cistercian Order.
He is a great reminder that fidelity, reform and holiness bring with them great fruitfulness: He himself founded more than 150 monasteries which, by the time of his death, had grown to well over 300 monasteries. The efforts of this one, dedicated man almost singlehandedly brought about an era of profound revival and flourishing — a true “new springtime” of religious life.
On Tuesday we were given the memorial of Pope St. Pius X. As we experience a crisis of Church hierarchy today, both domestic and worldwide, holy mother Church provides us with this example of a truly saintly bishop and pope, known above all for his personal piety and holiness. He too was a great reformer, instituting important changes in Church law and in the administration and oversight of seminaries. Additionally, his reform of the missal and breviary helped lead the clergy, and indeed the entire People of God, to a deeper understanding of the riches of Sacred Scripture and the liturgy.
And now today the Church gives us the great celebration of the Queenship of the Blessed Virgin Mary, the timing rendered even more perfect by the fact that the daily cycle of readings gives us as our first reading today the famous “wicked shepherds” passages from Ezekiel 34:
“Woe to the shepherds of Israel who have been pasturing themselves! Should not shepherds, rather, pasture the sheep? … You did not strengthen the weak nor heal the sick nor bind up the injured. You did not bring back the strayed nor seek the lost, but you lorded it over them harshly and brutally. So they were scattered for the lack of a shepherd, and became food for all the wild beasts.”
And in response to the situation, this is the promise God made to the wicked shepherds of Israel, and it is the promise He makes to the wicked shepherds today:
“I swear I am coming against these shepherds. I will claim my sheep from them and put a stop to their shepherding my sheep so that they may no longer pasture themselves. I will save my sheep. …”
Given what we are facing, it might behoove every priest and bishop in our Church to print out a copy of Ezekiel 34 and tape it to the wall next to his bed. And every morning, upon waking, read that passage and be reminded of the recompense that comes when shepherds abuse their authority.
In the midst of it all, we draw strength from God’s promise: “I will save my sheep…” Christ, the Good Shepherd, never will abandon his Church, nor abandon the sheep of his flock. We belong to him, and in that is our great comfort and our hope.
So, too, we draw hope from the Blessed Virgin Mary, “our tainted nature’s solitary boast,” to use the beautiful phrase of the poet Henry Wordsworth. She who is the Mother of the Church and the Queen of the Church is always with us, and her resplendence shines forth like a beacon into the darkness we are now facing.
On this memorial of her queenship, we recognize the need for a new generation of priests and bishops in our Church. Men devoted to Our Lady, who will be her servants and her knights, who will place themselves at her feet and allow her to guide them in serving her Divine Son and faithfully shepherding his people. We also need a new generation of faithful believers, sons and daughters of our heavenly mother, who will confidently place themselves under her mantle and form a great cohort of disciples, imitating in their own lives those virtues which shone forth so splendidly in the life of their queen. And by the power of the sacrifices, penances, and prayers lifted up by this vast army of saints-in-the-making, we pray for the hastening of that moment when all might see, piercing through the darkness of our time, the morning star rising, signaling that the darkness has been conquered and that Christ, the Sun of Justice, dawns anew in our Church and in our world.
O Mary, Mother of the Church, pray for us who have recourse to thee!
O Mary, Queen of Heaven and Earth, pray for us who have recourse to thee!
(This reflection is adapted from a homily delivered Aug. 22.)
Dominican Father John Paul Walker is the pastor of St. Mary’s Parish in New Haven, Connecticut.
Kevin B. McCarthy, J.D., S.T.L. For Our Lady of America
In The Name, The Heart, The Blood and The Divine Will of Our Lord Jesus Christ, through The Heart of The Blessed Virgin Mary, Our Lady of America, Greetings! This message communicates once again a prayer program (this one for 36 days in duration beginning on August 22nd) in support of the Catholic bishops of the United States of America doing the right thing and holding that solemn procession and permanent placement of the Our Lady of America statue into the National Shrine Church of The Immaculate Conception in Washington DC.
Today, many Christian faithful are already beginning a 54-day Novena of Holy Rosaries, and many are also confronting the news concerning the lack of purity in the clerical hierarchy of the Catholic Church for many years in the Commonwealth of Pennsylvania, and otherwise throughout Holy Mother Church. Many, many, Christians have expressed a conviction that this situation may be due, in part, to a failure to respond to the request of Our Lady of America for that procession and placement of Her statue. In any event, for many reasons, many Christians cry out for this event with a real hope that it will release or trigger a great flow of Divine graces of purity which they believe Our Lady of America offered to the United States and to the World. See the approved message of Our Lady: https://docs.wixstatic. com/ugd/34849b_ab8b398c01fb41b598b32a78d1990389.pdf
Nonetheless, some may question the reason for this. How is it that the bishops could hope for such a widespread infusion of purity in the populace of the United States of America? We find the answer both in understanding how vast indeed is the love and intercessory power of Our Heavenly Mother and in what She stated as Our Lady of America in Her messages. On September 27, 1956, the day after She appeared for the first time as Our Lady of America, She said: “I desire to make the whole of America my shrine by making every heart accessible to the love of my Son.” The virtue of purity, the habit of living a pure life in the state of grace, is essential for a Christian actually to enter into such a close union with The Indwelling Trinity that The Blessed Virgin Mary can make their hearts consistently accessible to Her Son, Our Lord Jesus Christ. This is why She later declared: “I am Our Lady of America. I desire that my children honor me, especially by the purity of their lives.” And, “I desire, through my children of America, to further the cause of faith and purity among peoples and nations.”
How do we know that this procession and placement of the statue is so critical, that honoring the Mother of God in this way is essential? The visionary gives us the answer: “On the morning of November 15, 1956, Our Lady taught me this little prayer: ‘By thy Holy and Immaculate Conception, O Mary, deliver us from evil.’ “Our Lady then asked me to draw a picture of her first appearance. She also requested a statue made according to this likeness and placed, after being solemnly carried in procession, in the Shrine of The Immaculate Conception in Washington, D.C. She wishes to be honored there in a special way as Our Lady of America, the Immaculate Virgin.”
“On February 23, 1959, Our Lady came to me and admonished me to work on the ‘message’ as soon as possible so that it might be placed in the hands of the Bishops who would be responsible for its fulfillment.” And, Our Lady had already told the visionary in January 1957: “Tell the Bishops of the United States, my loyal sons, of my desires and how I wish them to be carried out.” Because the Shrine of The Immaculate Conception at Washington, D.C. is the property only of the Catholic bishops of the United States of America, they alone can satisfy this singular request of Our Lady of America for that procession and placement of the statue. Let us pray that the United States bishops do this no later than this Fall, 2018.
Please pray a Rosary each day (whenever possible in a Holy Hour before The Most Blessed Sacrament) in a 36-day novena beginning on Wednesday, August 22nd the Feast of The Queenship of Mary, through the Anniversary of the original appearance of Our Lady of America, Wednesday, September 26th, 2018 for the intention that the bishops of the United States will manage to hold a beautiful solemn procession of the Our Lady of America statue into the National Shrine of The Immaculate Conception yet this year, even doing so without much advance notice or publicity, placing that statue (which displays Her Immaculate Heart and the Lily of Purity) permanently in our National Marian Shrine Church at Washington dedicated to The Immaculate Conception of Our Lady. Just as the immaculate and perfect purity of Our Lady was essential to Her becoming She Who actually physically carried God entirely within, so also is the virtue of purity essential to the rest of all Christians such that we can generally have The Most Holy Trinity spiritually dwelling within us. Let us overcome the widespread reports of evil by these prayers and by this advice from the Word of God:
“Have no anxiety about anything, but in everything by prayer and supplication with thanksgiving let your requests be made known to God. And the peace of God, which passes all understanding, will keep your hearts and your minds in Christ Jesus. Finally, brethren, whatever is true, whatever is honorable, whatever is just, whatever is pure, whatever is lovely, whatever is gracious, if there is any excellence, if there is anything worthy of praise, think about these things.”
—Philippians 4:6–8 (R.S.V.)
“By Thy Holy & Immaculate Conception, O Mary, deliver us from evil!”
People with severe brain injuries from accidents, strokes, illness, etc. are often in comas at first. If they don’t die or spontaneously wake up, they can progress to a “persistent vegetative state” (PVS) described as “awake but unaware” and/or a “minimally conscious state. ” MCS is described as “definite, but extremely limited, awareness of self or environment, and limited means of communication.”
People with both conditions have had court battles over removing their feeding tubes such as the 1988 Nancy Cruzan (PVS) and the 2001 Robert Wendland (MCS) “right to die” cases.
Now, an August 9, 2018, Medscape article, “New Guideline for Minimally Conscious, Vegetative States Released,” reveals that three specialty societies, including the American Academy of Neurology, have just published a new guideline with 15 recommendations for “accurate diagnosis, prognosis and treatment for these conditions.”
The reason for the new guidelines, according to Dr. Joseph Giacino, who was one of the authors of the study, is because
“Misdiagnosis of DoC (“disorders of consciousness”) is common because underlying impairments can mask awareness — in fact, there is a 40% rate of misdiagnosis, leading to inappropriate care decisions as well as poor health outcomes.”
“Clinicians should refer patients with DoC (disorders of consciousness) who have achieved medical stability to settings staffed by multidisciplinary rehabilitation teams with specialized training to optimize diagnostic evaluation, prognostication, and subsequent management, including effective medical monitoring and rehabilitative care.”
and
“When discussing prognosis with caregivers of patients with DoC (disorders of consciousness) during the first 28 days after injury, avoid statements suggesting that these patents “have a universally poor prognosis.”
According to Dr. Giacino, “Approximately 20% of individuals who have disturbance in consciousness from trauma regain functional independence between 2 and 5 years post-injury, even though they may not return to work or pretrauma functioning.”
The study also cites as potentially helpful the drug amantadine and brain imaging showing that the brain can still respond normally to stimulus even though the person seems unaware.
What about the “right to die” for these people? Ominously, the guideline does mention“1 study found that hospital mortality was 31.7%, with 70.2% of those deaths associated with the withdrawal of life-sustaining therapy.”
Is the “40% misdiagnosis” rate really news?
In the 1990s doctors such Dr. Keith Andrews of the UK and U.S. doctor Mihai Dimancescu published medical journal articles showing that around 40% of patients in a so-called “persistent vegetative state” were misdiagnosed. And in 1987, the Royal Hospital for Neuro-Disability in the UK opened a “vegetative state” unit and later developed the “Sensory Modality Assessment and Rehabilitation Technique (SMART)” as a clinical tool for the assessment and rehabilitation of people with disorders of consciousness following severe brain injury.
Despite this, most media stories about cases like Terri Schiavo’s and “right to die”/assisted suicide groups continued to insist that “PVS” is a hopeless condition for which everyone should sign a “living will” to ensure that food and water is withheld or withdrawn to “allow” death.
This happened despite articles like the New York Times’ 1982 article “Coming Out of Coma” about the unexpected return of consciousness of Sgt. David Mack over a year after the famous “right to die” neurologist Dr. Ron Cranford predicted ”He will never be aware of his condition nor resume any degree of meaningful voluntary conscious interaction with his family or friends.”
There have also been articles about people like Terry Wallis who in 2003 regained consciousness after 19 years in a “minimally conscious” state. Unfortunately, such cases were often explained away as just “misdiagnosis” or a “miracle.”
My Experience
Just before Drs. Jennet and Plum invented []the term “persistent vegetative state” in 1972, I started working with these many comatose patients as a young ICU nurse. Despite the skepticism of my colleagues, I talked to these patients as if they were awake because I believed it was worth doing it for the patient if hearing is truly the last sense to go.
Because of this, I unexpectedly saw some amazing recoveries. One patient later told me that he would only respond to me at first and refused to respond to the doctor because he was angry when heard the doctor call him a “vegetable” when the doctor assumed the patient was comatose.
Over the years, I’ve written about several other patients like “Jack”, “Katie,” and “Chris”in comas or “persistent vegetative states” who regained full or limited consciousness with verbal and physical stimulation. I also recommend Jane Hoyt’s wonderful pamphlet “A Gentle Approach-Interacting with a Person who is Semi-Conscious or Presumed in Coma” to help families and others stimulate healing of the brain. Personally, I have only seen one person who did not improve from the so-called “vegetative” state during the approximately two years I saw him.
Conclusion
It is good news that the American Academy of Neurology and other groups are finally rethinking their approach to people with severe brain injuries, especially the recommendation to start rehabilitation therapies as soon as the person is medically stable and the recommendation for periodic and thorough testing over time.
This is crucial because the often quick prognosis of “hopeless” attached to people with severe brain injuries can–and has–led to early withdrawal of feeding tubes and ventilators as well as DCD (donation after cardiac/circulatory death) for these non-brain dead people.
Dr. Joseph Fins, MD, and chief of Medical Ethics at Weill Cornell Medical College perhaps says it best when he praises the new guideline as “a real step forward for this population that has historically been marginalized and remains vulnerable” and “suggests that brain states are not static, but dynamic, and that people can improve over time.
After the recent fall of Catholic Ireland to the abortion regime, pro-abortion forces appeared confident that they could gain another victory for their ideology – this time Catholic Argentina.
Instead, after a bill was introduced to legalize abortion-on-demand up to 14 weeks of pregnancy, millions of ordinary pro-life Argentineans took to the streets in peaceful protests, demanding that their legislators stand for life. The Argentinean Bishops conference actively urged Catholics to get involved in the debate. Some 70 Argentinean bishops reportedly sharedimages of themselves on social media holding signs saying, “Every life counts,” and urging their flock to stand for life. A pro-life petition signed by over 400,000 people was presented to the Argentinean legislature.
Every life counts
Hundreds of pro-life medical doctors, the same people who would be expected to kill unborn babies, organized protests, making it clear that they would have nothing to do with abortion. “I’m a doctor, not a murderer,” read one of their signs. The country’s Academy of Medicine pointed out that life begins at conception, and that “to destroy a human embryo means impeding the birth of a human being.“ Hundreds of hospitals expressed their opposition to the bill. Ernesto Beruti, chief of obstetrics at the Austral University Hospital, summed up the resolve of medical professionals to stand for life. “How far are we willing to go to?” he asked. “Jail. Even if the law is passed, I’m not going to eliminate the life of a human being. The most important right is the right to live.“
And when Pope Francis, who is from Argentina,denounced abortion in June as being similar to the Nazi’s murderous eugenic programs, Argentineans took notice.“Last century, the whole world was scandalized by what the Nazis did to purify the race. Today, we do the same thing but with white gloves,“ the Pope had said, speaking of the practice of aborting unborn babies diagnosed with health conditions.
Everything came to a head in the early morning hours of August 9, after what has been described as a “marathon”16-hour debate in the Senate. Pro-life and pro-abortion protesters thronged outside the legislature. At around 3am, the Argentinian senate voted 38-31 to reject the abortion bill. Senator Silvia Elías de Pérez, one of those who stood firm for life, cut through all the rhetoric, observing that the bill would have established “new discrimination between those who are wanted and those who are not.““To legalize abortion is really to admit plainly and simply the failure of the State.“
Amen. In the end, the simplicity of this argument won.The unborn child is human. To kill an unborn child is an unaccountable act of murderous discrimination. The State exists to defend the right to life of all, no exceptions.
Abortion is a crime disguised as a solution
No Complacency
Unfortunately,Argentinean pro-abortion activists are not likely to give up their efforts.Pro-life Argentineans can’t afford to let their guard down for a moment. Much as it defied belief to see young Irish literally dancing in the streets after their country voted for abortion, it boggles the mind to see pro-abortion Argentinians literally rioting in the streets after the Senate’s vote for life. One of HLI’s own, Graciela Lopez Clair, says that this debate has riven the country. Pro-life activists have adopted the colour blue, pro-abortion activists the colour green. Huge protests featuring these two colours have taken place. “Even though the results were good, we live as if we were enemies,” she says sadly.
That wound will not soon heal. In a recent article on Amnesty’s website, Mariela Belski, the Executive Director at Amnesty International Argentina, proclaimed that the momentum enjoyed by the pro-abortion activists is “unstoppable.” Pro-abortion legislators are already talking about when they will introduce the next abortion bill.
Meanwhile, wealthy foreign abortion organizations will continue to fund pro-abortion efforts. Planned Parenthood has reportedly poured as much as $5 million into Argentina in recent years to legalize abortion.Father José María “Pepe“ Di Paola, one of Argentina’s renowned “slum priests,” who serves in the slums in Buenos Aires, blames the machinations of the powerful International Monetary Fund (IMF) for the recent abortion push.
It’s clear to me, however, that Argentina isn’t only facing the threat of worldly money and power. This is a fight involving principalities and powers.
In recent years, we have seen extremist pro-abortion feminists try to set fire to a cathedral in northern Argentina. In another incident that truly belies description, a horde of feminist protesters descended on the cathedral in the city of San Juan, where they violently and obscenely assaulted a group of Catholic men who had surrounded the church and were peacefully praying the rosary. In fact, vicious demonstrations by Argentinian pro-abortion feminists, aimed at Catholic churches, have become an annual tradition.
It is difficult to watch video footage of these demonstrations without concluding that there is something more than human at work. The diabolical rage in the faces of the pro-abortion protesters, the hatred with which they assault peacefully praying men, the gratuitous obscenity of their slogans and actions –all of these scarcely seem like the actions of rational human beings.These are the same activists who are behind the recent push for abortion.The devil is hard at work in Argentina – and around the world.
Argentina and Hope
On the other hand, I have long been hauntedby the footage of those faithful Argentinean menwith their arms around one another,praying the rosary stalwartly, peacefully defending their cathedral in the face of violent rage. It seems to me that this sums up so much of the war between the Culture of Life and the Culture of Death. The forces of darkness can sometimes seem to be the more dramatic, the more energetic, even the more powerful. Pro-life activists do not lob molotov cocktails, or set churches and government buildings on fire.
Indeed, I am often struck by the difference between pro-life and pro-abortion protests. Pro-abortion protests are often characterized by rage and the prevalence of obscenity. They are noisy, raucous affairs, and their participants rarely ever seem happy; children are few and far in between. Pro-life protests, on the other hand, are typically peaceful and even prayerful, with a huge percentage of children and families. They are not populated by professional agitators and protestors, but rather by ordinary people and stay-at-home moms and dads who are building the kingdom by raising children to love Christ and goodness.
Pro-abortion protesters in Argentina made a lot of noise. They had the support of the global media. They filled the airwaves with their slogans. But in the end, millions of ordinary pro-life Argentineans stood up en masse and said, “no.” Argentina shows us that the pro-life battle will be won by ordinary citizens, willing to sacrifice their time and money to stand up for what they believe.It will be won by the kind of men who are rooted in prayer, and who are willing to sacrifice themselves, including their own safety,to surround and defend their beloved local cathedral.It will be won by the kind of womenwho do not assert their femininity through violent and obscene protests, but who are convinced rather that their womanhood achieves its highest purpose and expression in the act of sacrificially nurturing new life. It will be won by bishops and priests and religious who do not allow themselves to be silenced by the mockery of the media, or by the moral failures of their fellow clergy, but speak the truth without fear of the consequences.
Argentina gives pro-lifers everywhere hope. Despite an extremely well-funded campaign, the efforts of ordinary Argentineans bore fruit. It is amazing to consider just how many lives will be saved by the Senate’s vote. Instead of another Ireland, we now have a country that has shown the rest of Latin America how they too can defend their traditional cultural and family values against the international abortion juggernaut. The pendulum is swinging back towards life. For that, we should all give thanks.
Father Tad Pacholczyk
Director of Education
The National Catholic Bioethics Center
Recent news articles exploring the post-#MeToo world of romance have noted the phenomenon of cell phone “consent apps,” allowing millennials to sign digital contracts before they have sex with their peers, sometimes strangers they have just met. Many of these apps are being refined to include a panic button that can be pressed at any time to withdraw any consent given. Lawyers reviewing the practice, as might be anticipated, have urged caution, noting that consent apps are not able to provide definitive proof of consent, because feelings may “change throughout an evening, and even in the moments before an act.”
When we look at modern views about sex, it’s not a stretch to sum them up this way: as long as two consenting adults are involved, the bases are covered.When it comes to “sex in the moment,” consent is touted as key, allowing for almost all mutually-agreed upon behaviors or practices.
Yet this approach to sex is fundamentally flawed, and it’s often the woman who is the first to notice. Even when consenting unmarried couples scrupulously use contraception, there remains an awareness, particularly on the part of the woman, that a pregnancy could follow, and a concern about who will be left holding the bag if that were to happen. Sex between men and women involves real asymmetries and vulnerabilities, with men oftentimes being, in the words of sociologist Mark Regnerus, “less discriminating” in their sex drives than women, eager to forge ahead as long as there appears to be some semblance of consent. Women often sense, rightly, that consent for a particular sexual act ought to be part of something bigger, a wider scope of commitment.
Consenting to sex, of course, signifies the surrendering of our self to another. Sex ultimately speaks of giving our self, and receiving another, in a total, rather than a fragmentary way. This is part of the reason why this unique human activity holds a perennial fascination for us; it goes far beyond other forms of communication, exchange, and bonding. To give our self fully to another, and to receive that person fully, forms a bond with them that extends beyond the morning dawn. Human sexual union is not a mere joining of bodies, but is preeminently a joining of human hearts. It is, at its core, consenting to share one of the deepest parts of our self with another. As Dr. Angela Franks has perceptively noted:
Sexuality is not simply a matter of something that I have, as though my body is another possession just like my wallet or my car. If, as Gabriel Marcel said, I am my body, then sexuality has to do with my very person, which has a deep value. To use the language of Pope John Paul II, when a person is reduced to being merely an object for another’s desire, then the experience violates the core of one’s sense of self.
In casual sexual encounters, the consent we give each other may seem sincere and genuine, expressing our desires within the moment, but this kind of consent is largely transactional and temporary. By consenting to pre-marital or extra-marital sex, we declare, in effect, that we are giving ourselves, our bodies and our hearts to each other, although in truth, our giving remains partial and conditional, and we may be out the door the next morning or the next month. Our consent, limited and qualified as it is, amounts to little more than an agreement to use each other as long as it’s convenient, and when the break up occurs, we are hurt, because we thought we had something special, even though we didn’t really want to commit to anything special.
In the final analysis, human sexual activity calls for something much deeper and more abiding than mere transactional consent, namely, the irrevocable and permanent consent of spouses. Professor William May describes it this way:
In and through his act of marital consent… the man, forswearing all others, has given himself irrevocably the identity of this particular woman’s husband, while the woman, in and through her self-determining act of marital consent, has given herself irrevocably the identity of this particular man’s wife, and together they have given themselves the identity of spouses. …Husbands and wives, precisely because they have given themselves irrevocably to each other in marriage, have established each other as irreplaceable, non-substitutable, non-disposable persons and by doing so have capacitated themselves to do things that non-married individuals simply cannot do, among them to ‘give’ themselves to one another in the act proper and exclusive to spouses—the marital act—and to receive the gift of life.
Through the enduring commitment of marital consent, a man and a woman establish the foundation for personal sexual consent. In the absence of that larger marital commitment, all other consents, even with legalized authorization or electronic notarization, ring hollow.
A downloadable, pdf version of this article is available here at: Making Sense of Bioethics, The National Catholic Bioethics Center Archives of Making Sense of Bioethics are available here.
Dear brothers and sisters in Christ of the Diocese of Madison,
The past weeks have brought a great deal of scandal, justified anger, and a call for answers and action by many faithful Catholics here in the U.S. and overseas, directed at the Church hierarchy regarding sexual sins by bishops, priests, and even cardinals. Still more anger is rightly directed at those who have been complicit in keeping some of these serious sins from coming to light.
For my part — and I know I am not alone — I am tired of this. I am tired of people being hurt, gravely hurt! I am tired of the obfuscation of truth. I am tired of sin. And, as one who has tried — despite my many imperfections — to lay down my life for Christ and His Church, I am tired of the regular violation of sacred duties by those entrusted with immense responsibility from the Lord for the care of His people.
The stories being brought into light and displayed in gruesome detail with regard to some priests, religious, and now even those in places of highest leadership, are sickening. Hearing even one of these stories is, quite literally, enough to make someone sick. But my own sickness at the stories is quickly put into perspective when I recall the fact that many individuals have lived through them for years. For them, these are not stories, they are indeed realities. To them I turn and say, again, I am sorry for what you have suffered and what you continue to suffer in your mind and in your heart.
If you have not already done so, I beg you to reach out, as hard as that may be, and seek help to begin to heal. Also, if you’ve been hurt by a priest of our diocese, I encourage you to come forward, to make a report to law enforcement and to our Victim’s Assistance Coordinator, so that we might begin, with you as an individual, to try and set things right to the greatest extent possible.
There is nothing about these stories that is okay. These actions, committed by more than a few, can only be classified as evil, evil that cries out for justice and sin that must be cast out from our Church.
Faced with stories of the depravity of sinners within the Church, I have been tempted to despair. And why? The reality of sin — even sin in the Church — is nothing new. We are a Church made of sinners, but we are sinners called to sanctity. So what is new? What is new is the seeming acceptance of sin by some in the Church, and the apparent efforts to cover over sin by them and others. Unless and until we take seriously our call to sanctity, we, as an institution and as individuals, will continue to suffer the “wages of sin.”
For too long we have diminished the reality of sin — we have refused to call a sin a sin — and we have excused sin in the name of a mistaken notion of mercy. In our efforts to be open to the world we have become all too willing to abandon the Way, the Truth, and the Life. In order to avoid causing offense we offer to ourselves and to others niceties and human consolation.
Why do we do this? Is it out of an earnest desire to display a misguided sense of being “pastoral?” Have we covered over the truth out of fear? Are we afraid of being disliked by people in this world? Or are we afraid of being called hypocrites because we are not striving tirelessly for holiness in our own lives?
Perhaps these are the reasons, but perhaps it is more or less complex than this. In the end, the excuses do not matter. We must be done with sin. It must be rooted out and again considered unacceptable. Love sinners? Yes. Accept true repentance? Yes. But do not say sin is okay. And do not pretend that grave violations of office and of trust come without grave, lasting consequences.
For the Church, the crisis we face is not limited to the McCarrick affair, or the Pennsylvania Grand Jury Report, or anything else that may come. The deeper crisis that must be addressed is the license for sin to have a home in individuals at every level of the Church. There is a certain comfort level with sin that has come to pervade our teaching, our preaching, our decision making, and our very way of living.
If you’ll permit me, what the Church needs now is more hatred! As I have said previously, St. Thomas Aquinas said that hatred of wickedness actually belongs to the virtue of charity. As the Book of Proverbs says “My mouth shall meditate truth, and my lips shall hate wickedness (Prov. 8:7).” It is an act of love to hate sin and to call others to turn away from sin.
There must be no room left, no refuge for sin — either within our own lives, or within the lives of our communities. To be a refuge for sinners (which we should be), the Church must be a place where sinners can turn to be reconciled. In this I speak of all sin. But to be clear, in the specific situations at hand, we are talking about deviant sexual — almost exclusively homosexual — acts by clerics. We’re also talking about homosexual propositions and abuses against seminarians and young priests by powerful priests, bishops, and cardinals. We are talking about acts and actions which are not only in violation of the sacred promises made by some, in short, sacrilege, but also are in violation of the natural moral law for all. To call it anything else would be deceitful and would only ignore the problem further.
There has been a great deal of effort to keep separate acts which fall under the category of now-culturally-acceptable acts of homosexuality from the publically-deplorable acts of pedophilia. That is to say, until recently the problems of the Church have been painted purely as problems of pedophilia — this despite clear evidence to the contrary. It is time to be honest that the problems are both and they are more. To fall into the trap of parsing problems according to what society might find acceptable or unacceptable is ignoring the fact that the Church has never held ANY of it to be acceptable — neither the abuse of children, nor any use of one’s sexuality outside of the marital relationship, nor the sin of sodomy, nor the entering of clerics into intimate sexual relationships at all, nor the abuse and coercion by those with authority.
In this last regard, special mention should be made of the most notorious and highest in ranking case, that being the allegations of former-Cardinal Theodore McCarrick’s (oft-rumored, now very public) sexual sins, predation, and abuse of power. The well-documented details of this case are disgraceful and seriously scandalous, as is any covering up of such appalling actions by other Church leaders who knew about it based on solid evidence.
While recent credible accusations of child sexual abuse by Archbishop McCarrick have brought a whole slew of issues to light, long-ignored was the issue of abuse of his power for the sake of homosexual gratification.
It is time to admit that there is a homosexual subculture within the hierarchy of the Catholic Church that is wreaking great devastation in the vineyard of the Lord. The Church’s teaching is clear that the homosexual inclination is not in itself sinful, but it is intrinsically disordered in a way that renders any man stably afflicted by it unfit to be a priest. And the decision to act upon this disordered inclination is a sin so grave that it cries out to heaven for vengeance, especially when it involves preying upon the young or the vulnerable. Such wickedness should be hated with a perfect hatred. Christian charity itself demands that we should hate wickedness just as we love goodness. But while hating the sin, we must never hate the sinner, who is called to conversion, penance, and renewed communion with Christ and His Church, through His inexhaustible mercy.
At the same time, however, the love and mercy which we are called to have even for the worst of sinners does not exclude holding them accountable for their actions through a punishment proportionate to the gravity of their offense. In fact, a just punishment is an important work of love and mercy, because, while it serves primarily as retribution for the offense committed, it also offers the guilty party an opportunity to make expiation for his sin in this life (if he willingly accepts his punishment), thus sparing him worse punishment in the life to come. Motivated, therefore, by love and concern for souls, I stand with those calling for justice to be done upon the guilty.
The sins and crimes of McCarrick, and of far too many others in the Church, bring suspicion and mistrust upon many good and virtuous priests, bishops, and cardinals, and suspicion and mistrust upon many great and respectable seminaries and so many holy and faithful seminarians. The result of the first instance of mistrust harms the Church and the very good work we do in Christ’s name. It causes others to sin in their thoughts, words, and deeds — which is the very definition of scandal. And the second mistrust harms the future of the Church, since our future priests are at stake.
I said that I was tempted to despair in light of all of this. However, that temptation quickly passed, thanks be to God. No matter how large the problem, we know that we are called to go forward in faith, to rely upon God’s promises to us, and to work hard to make every bit of difference we can, within our spheres of influence.
I have recently had the opportunity to talk directly with our seminarians about these very pressing matters, and I have begun to, and will continue to, talk with the priests of the diocese, as well as the faithful, in person and through my weekly column and homilies, making things as clear as I can, from my perspective. Here now, I offer a few thoughts to those of my diocese:
In the first place, we must continue to build upon the good work which we have accomplished in protecting the youth and vulnerable of our diocese. This is a work on which we can never rest in our vigilance, nor our efforts to improve. We must continue in our work of education for all and hold to the effective policies that have been implemented, requiring psychological exams for all candidates for ministry, as well as across-the-board background checks for anyone working with children or vulnerable individuals.
Here again, I state, as we have done consistently, if you have knowledge of any sort of criminal abuse of children by someone in the Church, contact law enforcement. If you need help in contacting law enforcement contact our Victim’s Assistance Coordinator and she will help connect you with the best resources. If you are an adult victim of sexual abuse from childhood, we still encourage you to reach out to law enforcement first, but even if you don’t want to, please still reach out to us.
To our seminarians: If you are unchastely propositioned, abused, or threatened (no matter by whom), or if you directly witness unchaste behavior, report it to me and to the seminary rector. I will address it swiftly and vigorously. I will not stand for this in my diocese or anywhere I send men for formation. I trust that the seminaries I choose, very discriminately, to help form our men will not ignore this type of scandalous behavior, and I will continue to verify that expectation.
To our priests: Most simply, live out the promises you made on your ordination day. You are called to serve Christ’s people, beginning with praying daily the Liturgy of the Hours. This is to keep you very close to God. In addition, you promised to obey and be loyal to your bishop. In obedience, strive to live out your priesthood as a holy priest, a hard working priest, and a pure and happy priest — as Christ Himself is calling you to do. And by extension, live a chaste and celibate life so that you can completely give your life to Christ, the Church, and the people whom he has called you to serve. God will give you the graces to do so. Ask Him for the help you need daily and throughout every day. And if you are unchastely propositioned, abused, or threatened (no matter by whom), or if you directly witness unchaste behavior, report it to me. I will not stand for this in my diocese any more than in our seminaries.
To the faithful of the diocese: If you are the victim of abuse of any kind by a priest, bishop, cardinal, or any employee of the Church, bring it forward. It will be addressed quickly and justly. If you have directly witnessed sexual advances or any type of abuse, bring it forward as well. Such actions are sinful and scandalous and we cannot allow anyone to use their position or power to abuse another person. Again, in addition to injuring individuals, these actions injure the very Body of Christ, His Church.
Furthermore, I add my name to those calling for real and sustained reform in the episcopate, priesthood, our parishes, schools, universities, and seminaries that would root out and hold accountable any would-be sexual predator or accomplice;
I will hold the priests of the diocese to their promise to live a chaste and celibate life of service to you and your parish, and evidence of failure in this regard will be justly addressed;
I will likewise hold every man studying for the priesthood for our diocese accountable to living a chaste and celibate life as part of his formation for the priesthood. Failure to do so will lead to dismissal from diocesan sponsorship;
I will continue to require (with our men and our funds) that all seminaries to which we send men to study be vigilant that seminarians are protected from sexual predators and provide an atmosphere conducive to their holistic formation as holy priests, in the image of Christ;
I ask all the faithful of the diocese to assist in keeping us accountable to civil authorities, the faithful in the pews, and to God Almighty, not only to protect children and the youth from sexual predators in the Church, but our seminarians, university students, and all the faithful as well. I promise to put any victim and their sufferings before that of the personal and professional reputation of a priest, or any Church employee, guilty of abuse;
I ask everyone reading this to pray. Pray earnestly for the Church and all her ministers. Pray for our seminarians. And pray for yourselves and your families. We must all work daily on our own personal holiness and hold ourselves accountable first and, in turn, hold our brothers and sisters accountable as well, and
Finally, I ask you all to join me and the entire clergy of the Diocese of Madison in making public and private acts of reparation to the Most Sacred Heart of Jesus and to the Immaculate Heart of Mary for all the sins of sexual depravity committed by members of the clergy and episcopacy. I will be offering a public Mass of reparation on Friday, September 14, the Feast of the Triumph of the Holy Cross, at Holy Name Heights and I ask all pastors to do the same in their own parishes. In addition, I ask that all priests, clergy, religious, and diocesan employees join me in observing the upcoming Autumn Ember Days (Sep. 19, 21, and 22) as days of fasting and abstinence in reparation for the sins and outrages committed by members of the clergy and episcopacy and I invite all the faithful to do the same. Some sins, like some demons, can only be driven out by prayer and fasting.
This letter and these statements and promises are not intended to be an exhaustive list of what we can and need to do in the Church to begin to heal from, and stave off, this deep illness in the Church, but rather the next steps I believe we can take locally.
More than anything else, we as a Church must cease our acceptance of sin and evil. We must cast out sin from our own lives and run toward holiness. We must refuse to be silent in the face of sin and evil in our families and communities and we must demand from our pastors — myself included — that they themselves are striving day in and day out for holiness. We must do this always with loving respect for individuals but with a clear understanding that true love can never exist without truth.
Again, right now there is a lot of justified anger and passion coming from many holy and faithful lay people and clerics across the country, calling for real reform and “house cleaning” of this type of depravity. I stand with them. I don’t know yet how this will play out nationally or internationally. But I do know this, and I make this my last point and last promise, for the Diocese of Madison: “As for me and my household, we will serve the Lord.”
Last month, the Catholic Church was rocked by a grotesque reminder that things are not all right for the institution that stands, singularly and without exception, against every form of “cheap sex”—masturbation, pornography, birth control, and divorce. Ironically, the allegations against Theodore McCarrick became public just days before the fiftieth anniversary of Humanae Vitae, the encyclical letter that condemned the use of the pill, reaffirming the ancient teaching of the Catholic Church against contraception. For many, the revelation of sexual abuse and cover-up at the highest levels in a Church that asks its members for seemingly unattainable purity is too much to bear.
But while journalists, commentators, and media outlets scramble to make sense of the rot in the Catholic hierarchy, most would do well to have another look at the latest and most ambitious monograph from University of Texas-Austin sociologist Mark Regnerus, called Cheap Sex: The Transformation of Men, Marriage, and Monogamy (Oxford, 2017). Despite being better known for the controversial New Family Structures Study, Regnerus previously authored Forbidden Fruit: Sex and Religion in the Lives of American Teenagers (Oxford, 2009) and Premarital Sex in America: How Young Americans Meet, Mate, and Think About Marrying (Oxford, 2011). Like those works, Cheap Sex mixes nationally representative survey data with qualitative interviews, presenting a vivid picture of the relationship behaviors of American adults. Regnerus’s conclusion is that cheap sex has left American men so chokingly awash in orgasmic experiences that the meaning of maleness itself is under threat. Where the biblical story of Jacob, who “served [Laban] seven years for Rachel . . . because of his love for her” (Gen. 29:18-20), once stood for male virtue par excellence, it is now merely incomprehensible.
Forget about seven years. Sex is standard on a first date—as thirty-two-year-old Sarah explains in the introduction—and men give up little to get it. Regnerus finds that American adults have a difficult time navigating a path to long-term, stable relationships, especially marriage, and he presents extensive data on the use of the pill, digital pornography, and online dating. In the penultimate chapter, Regnerus makes the case that American men have not become better human beings, and certainly not more marriageable ones, by giving up less in pursuit of a sexual partner.
But Regnerus isn’t interested in merely describing the state of affairs. At the heart of Cheap Sex is a sustained economic argument about the etiology of the crisis in men and marriage. His central claim is about technology: that the birth control pill and the rise of internet porn decreased the cost of sexual access so substantially as to affect a fundamental shift from a world in which sex servedhigher goods to a world in which sex is the higher good.
This is a world in which the term “sex life” has any kind of meaning (it shouldn’t), a world in which “sex is, like, a big, big, big, big part of everything now,” as one of the interviewees stated, a world in which “[s]exual expression—and how we experience it—is [understood to be] close to the heart of being human.” In this world, “quality sexual experiences are increasingly perceived to be just as pivotal to human flourishing as clean air, potable water, edible food, ample shelter, and antibiotics.” Regnerus supplies examples, but it is easy to supply more. Characteristic of his clinical tone, Regnerus groups these developments under the epiphenomenon of “The Genital Life,” discussed in his final, and perhaps most troubling, chapter.
And wherever they stand doctrinally, Regnerus tells us that churches from Jerusalem to Rome and Athens, Georgia, seem to have lost the battle against the shift toward The Genital Life. “What is happening in the wider mating market is affecting religious Americans, too, as well as their congregations and denominations,” he observes. Indeed, it has. He could have added that whatever is happening is affecting clerics, pastors, and religious leaders as brutally as it afflicts their congregations. Regnerus asks us to consider that the reason for this isn’t an insufficiency of belief, but an underestimation of the effects of sexual technologies that make what is forbidden too easy, too costless, and too secret.
In what follows, I aim first to explain why Regnerus’s book has not received the attention it deserves. Second, I present a simple thought experiment designed to illustrate what seems to be the central argument of Cheap Sex. Finally, I will return to the difficulty of a Church that rejects the pill while clinging to an ideal of purity that has been mocked from within as much as from without.
Economic Determinism and Free Will
Cheap Sex has not been read and heralded with due importance for a simple reason: its central argument is an economic argument, regardless of the narratives Regnerus brings to that case. By economic I mean that the analysis proceeds using a model of mating-market sexual exchange in which there are suppliers (women), demanders (men), and points of equilibria that “determine” the exchange price of sexual partnership. When there is an upward shock to supply—thanks to, say, decreased direct or indirect costs for suppliers (the pill)—exchange prices naturally float downward. The result is cheap sex.
And the problem with economic arguments is that they are, first of all, difficult. Rarely can an economic argument be sustained in one step. And this amounts to saying that complete economic arguments are always dynamic: first this, then this, and then this. By the third step, most readers—including academic economists—are bored, confused, or unconvinced. This also amounts to saying that economic arguments apply to movements over time. Even a “simple” supply and demand analysis requires a time horizon, since time is the currency of change.
A consequence is that isolating the effects of a single, causal variable, such as the pill, is exceedingly difficult. In the scholarly literature, in fact, economists are highly skeptical of papers aiming to show a causal claim. (For one of my own attempts, see joint work, in progress, with Andrew Beauchamp on the pill and non-marital fertility.)
And all of this difficulty, formidable indeed, comes before we get to the real problem with economic arguments, which is harder to describe than the first: Economic arguments rest on an odd sort of paradox about human behavior that is troubling to those who, in this case, might be most friendly to Regnerus’s conclusions—namely, Christians and conservatives. (See, for instance, this review at Crisis Magazine, where Regnerus ought to have been given a better read.) The paradox is that the voluntary choices of free men and women do tend to follow patterns that exhibit enough regularity as to be—not inaccurately—called “rules” or “laws.” But this feels like economic determinism, at odds with the notions of free will and personal responsibility that Christians and conservatives tend to celebrate.
Is Regnerus saying that men and women in mating “markets” are bound to act in ways that they do? Is he saying that we are determined by blind economic forces? Of course not. Yet it is difficult to ignore the similarity between what a model of sexual economics predicts and what seems to have unfolded in contemporary dating and mating markets.
Thus, men and women with free will appear, freely, to act in predictably similar ways when faced with similar pressures, incentives, costs, and expectations. And yet, for all of this, every free choice is still free. This tension threatens any good economic argument, including the one Regnerus makes.
Work: The Anti-Pill Technology
There’s no way around it: Cheap Sex is a difficult book. Though I was familiar with its central argument before it was released—indeed, a portion of my dissertation took up the implicit costs of sex within a Beckerian fertility model with contraceptive shocks—I have nevertheless struggled to find the best way to frame the findings that Regnerus presents. I’ve settled on the following dis-analogy.
Imagine that instead of the pill, a different sort of technology shock hit the sexual exchange market in 1960. Suppose that a fabulous machine was introduced into society, a machine that could make a man absurdly wealthy if he merely used it for a few hours a day; suppose further that it was originally invented in North Dakota, and was known in just a few villages. In this scenario, men in those villages would soon have to pay a higher exchange price—or marriage price—for sexual unions. This is not because women would simply demand a higher price. Rather, some men (those with the machine) could start to outbid other men for the “best” women; remaining women in the market would wish to have the same fine gifts and offers, and little by little average marriage prices would go up.
Soon, men without the machine would have little luck of a successful marriage offer without the wealth afforded by this device. Aware of this, men in North Dakota might even try to keep their machine hidden, but women outside the borders of North Dakota would greatly admire and envy their well-to-do neighbors over the border. The race to discover that machine would become quite intense. He who could discover it would have his pick of a marriage partner, and so on. Soon the price for marriage would be very high. In addition to marriage, monogamy, and financial support, some men might even offer gifts worth seven machine-years of work, and, like the biblical Jacob, they would count it as nothing.
Of course, the imaginary technology is already available in the form of hard work.
This thought experiment illuminates the particularly distorting character of the pill as Regnerus presents it, and other close substitutes. Because they make the supply of sex less costly, women—sexual gatekeepers—can and do undercut each other in a race to the bottom. These technologies slice through mating markets as a kind of “anti-work” technology. Men have no need to compete for sexual partners. Instead, women do the competing, lowering their prices. It is their side of the “market” that has been disrupted. Such a world cannot sustain many Jacobs: the costs and incentives just don’t add up.
The dis-analogy depends only on our willingness to accept the features of the so-called “market” for sexual exchange. Regnerus unpacks the evidence for this market in his first chapter. Though it will strike many readers as crude, hardly anyone will dispute that the model of a sexual market captures some important, timeless, and often comical aspects of the male-female dynamic—a state of affairs that has been something like “common knowledge” until recently—a world in which men pursue and women are pursued, men court and women are courted, men offer and women reject, and in which men sacrifice, labor, and attempt various noble deeds to win the heart (and hand) of a beloved. This is a world in which a Jacob is not an alien of a man, but rather one man among many generations of heroic suitors—a man to be admired not for doing what no one does, but for having done better what all others wish to do.
The Genital Life, Humanae Vitae, and the Way Forward
It is difficult to think about responding to a humanitarian crisis of the proportion that Regnerus describes. Doubtless, in the face of an obviously over-sexed culture, it falls on everyone to seek to understand what has happened—hence to read Regnerus’s work—to make an appraisal of those facts, and to work within their own spheres of influence to undo the damage.
The situation is not completely hopeless. At least one near-universal and destructive habit—cigarette smoking—was reversed in a generation or two following careful study and owning up to the facts. I am confident that online pornography, masturbation, and casual sex would eventually be appraised in that way—as destructive habits that serve no human good—if the facts were widely known and disseminated. (Incidentally, much of the careful study that is obviously warranted has simply not been done, thanks to the anti-religious biases of the academy.)
Whether intended or not, Regnerus’s chapter on The Genital Life has almost defined the worldview of those who do not accept the teaching articulated in Humanae Vitae. If “quality sexual experiences are increasingly perceived to be just as pivotal to human flourishing as clean air, potable water, edible food, ample shelter, and antibiotics,” then a teaching that limits sexual activity to the sole instance of married couples ready to accept a child is going to have to give way. Openness to life—as many have pointed out—is just as much an obstacle to the pursuit of “quality sexual experiences” as same-sex attraction, a commitment to celibacy, or the unfortunate condition of being in love with someone who isn’t one’s spouse.
These “difficulties” all line up together. Either sexual experiences are subordinated to some higher ordering principle, or they are not. And when sex is as cheap as it is now, there is little natural incentive to keep them so ordered. Thus, difficult as it may be, it remains for us to strive instead through force of conviction to make sex more costly again, restoring what was lost from the natural balance of things.
Difficult, but worth it. What we stand to gain by making sex expensive isn’t just the reclaiming of men, marriage, and monogamy—we stand to reclaim greatness. This is because The Genital Life simply can’t provide a ratio for the most important human goods. A ratio is something like the motivating force: the reason for which things are done. No man will do a great deed for an orgasm, which he could, after all, provide for himself in a moment of foolishness. But every great man has done what was great for love—of God, of country, or a beloved. Jacob counted seven years of work as nothing since he loved Rachel.
It’s high time for the Catholic Church and her vicars to recover a path to greatness—and not a bad time for the rest of us besides.
C.R. Pakaluk is Assistant Professor of Economics at The Catholic University of America, and head of the Social Research area at The Busch School of Business.
Medication abortion, also known as the abortion pill, has been marketed as a simple answer for women who want an abortion, offering them the convenience of taking their preborn baby’s lives in the privacy of their own homes. But in reality, medication abortion has had destructive effects — not just on preborn children, but on women and society.
Approved by the Food and Drug Administration (FDA) just 18 years ago, the “abortion pill” consists of two different medications. One medication, mifepristone, is “a synthetic steroid [that] interferes with a fertilized egg’s ability to adhere to the lining of the uterus.” Mifepristone works together with misoprostol, a medication which causes uterine contractions. At the time of approval, FDA Commissioner, Dr. Jane Henney, said the FDA approved mifepristone after a “careful evaluation of the scientific evidence related to the safe and effective use” of the drug.
But that “safe and effective” drug combination operates more like a human science experiment with deadly results.
The impact on women
1. Incomplete abortions.Focus on the Family reports that sometimes medications abortions are incomplete, and if so, “the woman has the option of taking another round of drugs or having a surgical abortion….”
Initially, the abortion pill was only available for 49 days past the woman’s last menstrual period; however, in 2016, the FDA upped that to 70 days, which, in turn, increased the risk for women, despite promises of safety. When it was approved in 2000, Gloria Feldt, then-president of Planned Parenthood, called it “as significant a technological advance for women’s health as the birth-control pill was 40 years ago. It will enable them, if they choose to terminate a pregnancy, to do that earlier (and) to do it without surgery.” For many women, Feldt claimed, this is “positive.”
2.Frightening side effects. Research on the abortion pill’s side effects and complications, however, is anything but positive… it’s disturbing. Side effects include pain, weakness, bleeding, nausea, vomiting, diarrhea, chills, and fever. Focus on the Family notes that bleeding “can potentially last for several weeks, and can be severe enough to require a transfusion.” Every woman “will experience” bleeding, which “is more common the earlier a woman is in her pregnancy.”
Beyond side effects, though, are serious complications that may occur. In a medical office, complications can be treated immediately and adequately, but a secret at-home abortion risks the mother’s life and takes the baby’s.
Still, Women on Web, an organization distributing abortion pills to women where abortion is illegal, insists that “[t]his risk [of using the abortion pill] is equal to that of requiring medical care for an allergic reaction after using penicillin.”
3. Misogynist attitudes persist. In California, public universities may soon be forced to offer the abortion pill to students. Instead of focusing on offering childcare and other help for pregnant and parenting students on campus, lawmakers prefer to push the idea that women can’t be students and mothers. Instead, they must sacrifice their children at the altar of their educational goals. This view is not pro-woman.
In the workplace, it’s no better. Working women who become pregnant are still punished, denied promotions, and even fired. Men who become fathers, however, experience the complete opposite. The availability of abortion (and now, the implied “ease” of taking a pill to end a pregnancy) has hindered, rather than helped, working women.
The impact on society
1. Profits take precedence over women’s safety. In 2006, several women died while using abortion pills prescribed by Planned Parenthood. Planned Parenthood responded by changing they way it administered the pills. It had cut corners by requiring fewer office visits, and the result appeared deadly, though the abortion corporation refused blame. And there have been other reports of death from the abortion pill.
Surprisingly, however, medical groups aren’t demanding that medication abortion be stopped; instead, it seems it nets some of them more money for less time — regardless of the effects on women. That’s certainly true at Planned Parenthood. In 2016, Fortune reported on the uptick in women opting for medication abortions, stating that in 2010, Planned Parenthood’s medication abortions accounted for 35% of its abortions; in 2014, that percentage increased to 43%. But Planned Parenthood and its friends in the abortion industry still make their money, charging approximately the same amount for medication abortions as for surgical procedures.
Medication abortions have been steadily increasing, even as overall abortion numbers are decreasing. According to the Guttmacher Institute, “Over the past 15 years, it has been used in more than 2.75 million abortions in the United States.” For population control enthusiasts, this may be welcome news — but for economies attempting to maintain a healthy population replacement ratio and sustain a workforce, it isn’t.
The Center for Disease Control’s last Abortion Surveillance Report, which reports trends from 2005-2014 (Table 22), notes that in 2014, nearly 23 percent of all abortions were “performed by early medical abortion” before 8 weeks gestation. “However,” the report states, “these numbers are not reliable on their own, as the counts are actually higher since 16 states either don’t report medication abortions, or don’t account for it in its own category or gestational age. Those states include some known for their high abortion numbers, such as California… and New York State” (NYC reports separately). The report notes that “it is only possible to speculate on what the real numbers are, but it’s clear they are growing.”
2. At-home abortions are a dangerous trend. The abortion pill puts women in the position of at-home physician, in effect, supervising their own ‘planned miscarriages’ (abortions). Medical abortion also leads to mail order and telemedicine abortions, two things the abortion industry is pushing for. In effect, these allow women to conduct alternate procedures on themselves, without ever physically encountering a physician.
Recent changes in FDA prescribing protocol have made medication abortion more affordable and accessible, as well as more dangerous, as it removes restrictions for in-person follow-ups, and it removes requirements for the abortion pill providers to be medical doctors, according to the Guttmacher Institute.
Besides women self-administering their abortions, sometimes their partners have done so — withoutthe women’s consent. In one recent case, a doctor didn’t want his girlfriend to have their child, but she refused to abort. He invited her for drinks and slipped the pills into her drink — at four times the effective dose. Another boyfriend gave his girlfriend the abortion pill by tricking her into thinking they were antibiotics. Worldwide, this kind of story has been repeated too many times.
The abortion pill has only promoted egregious medical ethics and health violations, all in the name of “choice.”
Editor’s Note: If you have taken only the first medication in the abortion pill regimen and are experiencing regret, there is a chance you may be able to reverse the abortion. Visit AbortionPillReversal.com.
Summer is, in a lot of ways, the “revelation of the body.” That’s true, even on the most natural level. People wear less. Just peruse the typical woman’s or, even more, teen magazines in April or May. There’s always an article about the agony and ecstasy of bathing-suit season. Summer reveals the body.
That’s especially true in the Church in the first half of August. No, I’m not talking about wearing clothes more typical for the beach to Mass: We have forgotten about the concept of one’s “Sunday best,” but that’s a subject for another day. What I’m talking about are two feasts that bookend early August and, in fact, form a nice, nine-day novena between them: the feast of the Transfiguration (Aug. 6) and the Solemnity of the Assumption (Aug. 15). They, too, are about the “revelation of the body.”
The Transfiguration permeates much of the liturgical year. The Gospel account of Jesus taking Peter, James and John up Mount Tabor shows up twice in the Lectionary: Aug. 6 and the Second Sunday of Lent.
Right up front in Lent we are reminded that we mortify the body (the Gospel of the First Sunday of Lent is always of the Temptation in the Desert) because it is destined for glory (Second Sunday’s Gospel of the Transfiguration). But, apart from these two references, the Transfiguration pervades the entire liturgical year. How so? Well, the Transfiguration is the foretaste and promise of the Resurrection (which is the central fact of Christianity; see I Corinthians 15:12-22), and Easter is the heart of the liturgical year and Christian life.
So, already on the Second Sunday of Lent, the Church is pointing us to the resurrection of the body at Easter. And, because Easter is the center of the liturgical year, every Sunday of the year is a “little Easter” because it is a remembrance of the resurrection of Christ: Every Sunday reminds us that we are Christians and saved because Jesus Christ “rose from the dead in his human body.”
The Transfiguration reminds us that, even beneath the seeming ordinariness of human flesh, lies great potential. The human body is not destined to be food for worms (at least not forever); nor is it simply compost material for recycling into the next generation of human beings or interstellar dust, as some nebulous “spiritualities” suggest today. Why?
Because the body is personal. The body is me. I am not just an “I” in a body. I just don’t “wear” my body like I wear my clothes or a summer swimsuit. It’s not just “body armor” like a turtle’s shell.
All those impersonal images hark back to an understanding of human beings — an “anthropology” — that is not Christian but gnostic. The ancient world was infected by Gnosticism. Greek dualism downplayed the significance of the body: The body was a prison, a covering like a snake’s, to be slithered out of in joyous escape at death. The old euphemistic phrase about death — “shedding our mortal coil” — embodied that.
But Catholic theology does not think of the body as a “prison” to be “escaped.” Yes, there have been times in Catholic spirituality that embodiment has been underappreciated, but that is certainly not the case in modern Catholic theology, especially after St. John Paul II’s masterful “theology of the body.” The body is an integral part of me.
Why so? Because what I do, I do in and with my body.
Let’s take it, step-by-step. An act is both the deed in itself and an intention. Both must be good. I may intend to stop somebody from suffering, but it’s wrong if I do it by giving the patient a fatal shot. I may give somebody a charitable donation, but it’s wrong if my motive is to bribe them into silence about something wrong. A good act has to be good both in deed and in intention.
But to do any act — good or bad — requires the whole person, body and soul. I may intend to give charity, but it is this hand that hands over the money or writes the check. I may want to steal, but it is this hand that takes what is not mine. I intend to commit adultery, but I do it with this body. I want to praise God, but I do it with this voice.
And, because God is just, both body and soul share the fate of the person. It would be manifestly unfair if the good person’s soul enjoyed heaven forever (or the evil person’s soul suffered hell forever) but the bodies of both faced the same fate: the grave. That is why “I believe in the resurrection of the body” — and not just the eternal life of the soul.
That is what the Resurrection was about: Jesus is risen, body and soul. He lives forever, in heaven; the Second Person of the Trinity, body and soul, is alive. The hands that mixed mud for the blind man’s eyes, the hands that touched lepers, and the “sacred and venerable hands” that took bread all live forever in heaven.
And that is what Jesus wanted to show Peter, James and John at the Transfiguration.
At the other end of the August novena is the Assumption. The Church infallibly and solemnly teaches that “at the end of her earthly life” Mary was taken body and soul into heaven. A Marian privilege? Yes. But more than that.
It would have been manifestly unjust for the “womb that bore thee and the breasts that suckled thee” (Luke 11:27) to have ended in corruption. It would have been unjust, for she was conceived without sin, to suffer the punishment of sin that is death as we know it. And God is not unjust.
So Mary’s Assumption is also a sign and confirmation of who she was. Like Jesus, the full person of Mary — body and soul — stands in heaven. But it doesn’t end there.
In 1 Corinthians 15:20, St. Paul speaks of Jesus’ resurrection as the “first fruits of those who have fallen asleep.” The ancient Israelites brought the first fruits gleaned in the harvest to offer in the Temple because they symbolically embodied the whole harvest. So, when St. Paul speaks of Jesus’ resurrection as “first fruits,” he means that Jesus’ resurrection is not an isolated event, but the first step in a chain that ends in the General Resurrection of all men.
And, in that light, Mary’s assumption is the “second fruits,” the first application of the power unleashed at Easter. The renewal of the earth that began with Jesus and to which “we look forward” in the Resurrection of the Dead has already paid its first installment in Mary. The Assumption is Mary’s privilege, but it is also our promise.
Her body, like her Son’s, has gone to where we hope one day also — body and soul — to go.
That’s the “revelation of the body” the Church reveals to us in early August. So, despite the occasional complaint that the holy-day obligation of the Assumption “ruins a perfectly good beach day,” realize that it, too, reveals more about the body than what one sees at the beach.
August 14, 2018 (LifeSiteNews) – Since its release in April 2016, Amoris Laetitia in its eighth chapter has shown itself to be the Trojan Horse by which progressive, liberal, and modernist clergy have been able to introduce old errors, new abuses, and more sins into the City of God. In this fiftieth anniversary year of Humanae Vitae, we will see the same clergy utilize two strategies to set aside the perennial teaching contained in that encyclical.
One strategy will make use of the “canonization” of Pope Paul VI. As with John XXIII and John Paul II, this politically motivated canonization is intended to remove Paul VI to a distant pedestal as an “example” of living the Christian life “in his particular circumstances”—i.e., not in our particular circumstances. It is paradoxically a way of excluding him from the current conversation by wrapping his life and work in a haze of hagiographical admiration that, in a sense, “discharges” all of our obligations towards his moral magisterium. Those who are manipulating his memory can create a smokescreen behind which they will be more free to do as they please. The same thing happened, of course, with John XXIII, whose canonization cemented in place a carefully contrived picture of him as the great revolutionary of Vatican II, and with John Paul II, whose canonization meant that Veritatis Splendor, Familiaris Consortio, and a host of other documents could be sealed up in the reverent tomb of his earthly remains.
The reasoning goes like this: Humanae Vitae was understandable in its context, that is, the confusion of the late 1960s, when the subject of birth control was still in its infancy (if you’ll pardon the expression), and we should applaud and admire a pope who had the courage to take a stand in defense, as he viewed it, of the goods of marriage. But in the twenty-first century, there is no longer any doubt that “times have changed.” The Church has a deeper and broader understanding of the goods of marriage, especially the union of spouses, such that the scholastic and natural-law categories relied on by theologians in the last century are now seen to be simplistic and outmoded. Moreover, the Church in her “motherly compassion” for weak human beings, and in her grave concern for the ecological health of the planet under the pressures of overpopulation, understands that there are competing goods that Paul VI may have overlooked—for he is a saint not due to how well he governed or how true his doctrine is, but because of the goodness of his heart.
So this is one strategy, and the whiff of sulphur is more than noticeable.
The other strategy will be a continuation of the divorced-and-remarried refrain, namely, that the Church’s traditional teaching is too difficult for some people in some circumstances to follow. They simply cannot do it; it is “morally impossible” and therefore not required of them.
But Pope Paul VI—well advised on this particular topic, if not always on others—anticipated that very line of argument and cut it off decisively:
The teaching of the Church regarding the proper regulation of birth is a promulgation of the law of God Himself. And yet there is no doubt that to many it will appear not merely difficult but even impossible to observe. Now it is true that like all good things which are outstanding for their nobility and for the benefits which they confer on men, so this law demands from individual men and women, from families and from human society, a resolute purpose and great endurance. Indeed it cannot be observed unless God comes to their help with the grace by which the goodwill of men is sustained and strengthened. (HV 20)
This, in a nutshell, is just what Pope John Paul II would later argue at length in Veritatis Splendor and other documents: while fallen man on his own is incapable of following God’s law, Christian man with the help of grace is certainly able to follow it, even if there will be faltering and failure, with the need for continual repentance and conversion. Put simply, a Christian is obliged to live as a Christian—and God will never deprive any of the baptized of the grace it takes to do that, if they sincerely ask Him for it. If they do not so live, then the Church’s motherly compassion consists not in a wink-wink, nudge-nudge toleration, but in reminding them, gently and firmly, of the truth by which we are saved, and of the need for God’s help to live according to it.
A different application of the archetypal error of Amoris Laetitia consists in maintaining that, even if contraceptive sex is wrong, it is a lesser moral evil than other evils such as infidelity, divorce, and abortion, and therefore can be condoned if only to prevent those greater evils. Pope Paul VI once again anticipates this devious dodge and refutes it utterly:
Neither is it valid to argue, as a justification for sexual intercourse which is deliberately contraceptive, that a lesser evil is to be preferred to a greater one, or that such intercourse would merge with procreative acts of past and future to form a single entity, and so be qualified by exactly the same moral goodness as these. Though it is true that sometimes it is lawful to tolerate a lesser moral evil in order to avoid a greater evil or in order to promote a greater good, it is never lawful, even for the gravest reasons, to do evil that good may come of it—in other words, to intend directly something which of its very nature contradicts the moral order, and which must therefore be judged unworthy of man, even though the intention is to protect or promote the welfare of an individual, of a family, or of society in general. Consequently, it is a serious error to think that a whole married life of otherwise normal relations can justify sexual intercourse which is deliberately contraceptive and so intrinsically wrong. (HV 14)
We must be prepared for the Machiavellian and, to speak truthfully, Luciferian strategies of the enemies of human nature, natural law, and holy matrimony. Pope Paul VI will be our ally, if, instead of elevating him to a lofty niche of irrelevance, we allow him to remain near us as the complicated and problematic figure he was, through whom nonetheless St. Peter spoke when he passed on the unbroken teaching of the Church about the intrinsic evil of contraception.
One of the most common combined oral contraceptive pills has a negative impact on women’s quality of life but does not increase depressive symptoms. This is shown by a major randomised, placebo-controlled study conducted by researchers at Karolinska Institutet in Sweden in collaboration with the Stockholm School of Economics. The results have been published in the scientific journal Fertility and Sterility.
“Despite the fact that an estimated 100 million women around the world use contraceptive pills we know surprisingly little today about the pill’s effect on women’s health. The scientific base is very limited as regards the contraceptive pill’s effect on quality of life and depression and there is a great need for randomised studies where it is compared with placebos,” says professor Angelica Lindén Hirschberg at the Department of Women’s and Children’s Health at Karolinska Institutet.
She has led just such a study together with Niklas Zethraeus, associate professor at the Department of Learning, Informatics, Management and Ethics, Anna Dreber Almenberg from the Stockholm School of Economics, and Eva Ranehill of the University of Zürich. 340 healthy women aged between 18 and 35 were treated randomly over the course of three months with either pills with no effect (placebos) or contraceptive pills containing ethinylestradiol and levonorgestrel, the most common form of combined contraceptive pill in Sweden and many other countries. Neither the leaders of the experiment nor the subjects knew which treatment was given to which women.
The women who were given contraceptive pills estimated their quality of life to be significantly lower than those who were given placebos. Both general quality of life and specific aspects like mood/well-being, self-control and energy level were affected negatively by the contraceptives. On the other hand, no significant increase in depressive symptoms was observed.
May be of clinical importance
Since the changes were relatively small, the results must be interpreted with a certain amount of caution, the researchers emphasise. In the case of individual women, however, the negative effect on quality of life may be of clinical importance.
“This might in some cases be a contributing cause of low compliance and irregular use of contraceptive pills. This possible degradation of quality of life should be paid attention to and taken into account in conjunction with prescribing of contraceptive pills and when choosing a method of contraception,” says Niklas Zethraeus.
The type of combined contraceptive pill that was used in the study (etinylestradiol + levonorgestrel) is recommended in many countries as the first choice since it is considered to entail the least risk of thrombosis among the combined contraceptive pills. The findings from the study cannot be generalised to other kinds of combined contraceptive pills because they may have a different risk profile and side-effects.
The study was supported by research grants from Jan Wallander and Tom Hedelius Foundation, Knut and Alice Wallenberg Foundation, Swedish Council for Working Life and Social Research, the Swiss National Science Foundation, the Swedish Research Council, Karolinska Institutet, and the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet.
Publication
Niklas Zethraeus, Anna Dreber, Eva Ranehill, Liselott Blomberg, Fernand Labrie, Bo von Schoultz, Magnus Johannesson, Angelica Lindén Hirschberg
A first choice combined oral contraceptive influences general well-being in healthy women – a double-blind, randomized, placebo-controlled trial Fertility and Sterility, online 18 April 2017, doi:10.1016/j.fertnstert.2017.02.120
August 8, 2018 (Society for the Protection of Unborn Children) – Abortion supporters appear determined to ignore the dangers of DIY abortion in their support to license abortion pills for home consumption. BPAS Chief Executive Ann Furedi recently branded abortion pills “safe and simple” in a Spiked Magazine article this week.
With an array of pro-abortion publications peddling the same message, they also appear to possess the same blind-spot. Whilst repeating snappy slogans such as ‘we trust women’ they refuse to acknowledge the 24 women who consumed abortion pills and are now dead. The cause of death? Abortion pills. The same pills branded ‘safe and simple’ by Furedi.
Fatal complications
Two women in the United Kingdom have been killed by abortion pills in the past five years according to the 2017 abortion statistics. The same statistics also exposed that medical abortions hold a higher complication rate compared to surgical abortions. Complications include sepsis and haemorrhaging.
It was only this year that the Food and Drug Administration updated their guidance to reveal the disturbing fact that 22 American women have been killed by abortion pills. The official website stated: “As of December 2017, there were reports of 22 deaths of women associated with Mifeprex since the product was approved in September 2000, including two cases of ectopic pregnancy resulting in death; and several cases of severe systemic infection (also called sepsis), including some that were fatal.”
It is reported that the deceased women perished from a range of complications associated with the abortion pills including; liver failure, sepsis, toxic shock syndrome and haemorrhaging.
Indifference to suffering
However, the FDA report further described the appalling side effects inflicted upon women taking the pills. Between 2000-2012, there were 2740 cases of severe complications. In the last five years, there have been 289 complications each year including, 273 hospitalisations,103 infections and 182 cases of blood loss resulting in urgent transfusions.
It appears that publications and providers such as Furedi simply refuse to acknowledge findings that do not match their agenda of liberalising abortion. The deaths of women are disregarded and the suffering of thousands ignored.
SPUC Director of Communications and Campaigns Michael Robinson said: “It is perplexing that women who claim to care for their fellow women refuse to acknowledge 24 of their sisters now dead and continue to reject the suffering of thousands.”
SPUC Scotland’s legal challenge on the Scottish Governments policy of providing abortion pills at home was heard in May and a judgement is expected around the end of August.
Okay, pretend you didn’t read the headline. It’s more fun that way.
Tatiana Guerra, 30, is from Brazil, and was 20 weeks pregnant when this video was taken. When she was 17, she’d lost her sight.
Courtesy of Huggies Brazil and the digital design firm, The Goodfellas, what you see on YouTube is the unfolding of a minor miracle– at least to we who are sighted and especially to those of us who grapple with understanding 3D printing.
The YouTube is less than 4 minutes long. We are immediately introduced to Tatiana and “Dr. David.” He seems to have a gentle touch and a reassuring voice, the perfect bedside manner.
After the opening “hellos,” the video cuts to Tatiana at home. She caresses her swollen abdomen and talks quietly and persistently to Murilo.
Clearly, Tatiana is passionately in love with her unborn son. “Mommy can’t wait to feel your little body, your little face, your little hands ….So come,” she says. “Mommy is counting the days. …You don’t need to be afraid.”
The video cuts back to Dr. David as he is performing the ultrasound. They chat back and forth.
“What does his face look like?”
“His nose looks like yours,” Dr. David says. “His two little eyes are closed.”
Tatiana smiles and giggles when she is told her son has a “small mouth” and a “chubby hand.”
All the while a 3D printer is transforming ultrasound images of Murilo’s face into something solid.
“And if…if you could touch him, would that let you know what he’s like?”
“Yes,” she responds.
At that juncture Dr. David hands Tatiana the 3-D sculpture of her unborn son’s face wrapped in a white cloth.
“That is your son.”
“What do you mean!?”
“That’s an image of your son. See if he feels the way you think he does.”
And then, the tear-jerking moment. She read a message, written in Braille…
“I am your son.”
She explores her son’s face–his nose, his eyes, his forehead and says (gulp)
“I am so happy to meet Murilo…Before he’s born.”
A moment’s pause.
“Thanks, Doctor.”
LifeNews.com Note: Dave Andrusko is the editor of National Right to Life News and an author and editor of several books on abortion topics. This post originally appeared in at National Right to Life News Today —- an online column on pro-life issues.
In 1803 Thomas Robert Malthus, an English clergyman who was concerned about the origins of poverty, published an Essay on the Principle of Population. This was a moment when the world’s population was increasing at a faster rate than it had in the past and some people were concerned about overpopulation.
Malthus had a novel idea: that the growth of the population would eventually outstrip the growth of resources needed to support the increasing number of people, especially food resources. He was convinced that population was growing exponentially and doubling every 25 years, while food resources could only increase arithmetically in the same time.
Malthus deplored the large families of the poor and held that the tendency of the working classes to reproduce was largely responsible for their poverty. The large numbers of dependent poor would eventually put a strain on the state and result in bankruptcy. He advised a decrease in population growth through abstinence and delayed marriage. He also advocated the use of artificial methods of contraception as he believed abstinence would not always be observed.
About 50 years later, in 1859, Charles Darwin published his masterpiece, The Origin of Species.Darwin is said to have been influenced by Malthus’ writing. Darwin’s theory of evolution reversed the Judeo-Christian doctrine of the fall of man from perfection as a consequence of man’s transgression, to a quest for perfection through natural selection. Natural selection would result in the survival of the strong and fit and the elimination of the weak and vulnerable, who would die out naturally. Their passing was essential for progress. Death became an essential element for making humanity better by improving the lineage.
The eugenics movement, an offspring of Darwinism, developed in Europe by the late 1800s. In Great Britain, Darwin’s cousin, Sir Francis Galton, introduced the concept of eugenics as a science. Eugenicists argued that many of the maladies of man were due to inferior inherited traits. They encouraged the fit middle and upper classes to have large families; the unfit, poor, especially minorities and immigrants, were to breed less.
By the late 19th century, supported by a utilitarian ideology and the doctrine of natural selection, the concept of a “right to death” surfaced in Europe. In Germany, in 1920, Karl Binding and Alfred Hoche published Allowing the Destruction of Life Unworthy of Life (Die Freigabe der Vernichtung lebensunwerten Lebens). Binding was a prominent jurist and Hoche a professor of psychiatry – members of the German intellectual elite. True to their utilitarian ethics, purportedly to benefit society, the authors advised killing those whose lives were devoid of value. This was justified as “compassion” and “release from suffering.” The slow, natural elimination of the unfit by natural selection had evolved into the notion of actively killing the unfit.
This ideology was adopted by German doctors. The victims would be those near death, those in a comatose state and the mentally impaired. Advocates of euthanasia, few at first, gradually increased. Many were professors at medical schools.
Systematic killing began in the 1930s. It started with infants and children with congenital defects and mental retardation and was followed by disabled and mentally ill adults and the terminally ill. The killing criteria expanded to include adults and children with “antisocial behavior” and those with minor handicaps. Children and adults in psychiatric hospitals were killed by lethal injection. When this method proved costly and awkward, gas chambers were built in some hospitals and patients were transferred for extermination. The impetus for the program was medical economics. (J.C. Willke, Assisted Suicide and Euthanasia). The Nazi government supported the program and decriminalized the killing. With the assistance of the state, the killing became impersonal and automatic.
It is important to note that this program was not established by the Nazi government; it was the initiative of members of the German medical community. Nazi ideology accepted eugenics and later on many German physicians accepted Nazi racial doctrines. Medical researchers conducted lethal experiments on inmates in concentration camps.
Binding and Hoche were respected scholars. They were convinced that their arguments for killing the sick and disabled were based on sound economics and were supported by the law. In the preface to the English translation of their book, Anthony Horvath observes that statements made by intellectuals in a scholarly dialogue were adopted by men of action who went on to slaughter the sick and disabled and eventually “inferior races”. The killing by physicians of those whose lives were considered unworthy occurred barely a decade after the publication of Allowing the Destruction of Life Unworthy of Life.
The eugenics movement in the United States
In the United States, the eugenics movement was also embraced by academics. Funding for eugenics research was provided by the Rockefeller, Carnegie, and Ford Foundations. Faculty from Stanford, Yale, Harvard and Princeton Universities were active promoters.
Compulsory sterilization of “defectives” was carried out. Forced sterilization laws were enacted in 27 states by 1909. Justice Oliver Wendell Holmes endorsed the practice of sterilization of “defectives” in a 1927 United States Supreme Court decision, Buck v. Bell. This decision encouraged supporters of coercive sterilization. In fact, American eugenic sterilization programs and genetic laws inspired the Nazi extermination plan (see Edwin Black, The Horrifying American Roots of Nazi Eugenics). Margaret Sanger, the founder of Planned Parenthood, was a leader in the US eugenics movement.
The death, or at least the sterilization, of an unfit, inferior person was considered a benefit to society. This was purportedly based on science and economics and ultimately the common good and justified ethically as a compassionate release from suffering.
The new eugenics
Over the past 20 years, scientists and philosophers have been proposing a more liberal kind of eugenics. Julian Savulescu, a prominent Australian ethicist, director of the Uehiro Centre for Practical Ethics at Oxford University, and John Harris, a British bioethicist, director of the Institute for Science, Ethics and Innovation at the University of Manchester, are leading figures in the new eugenics.
The supporters of the new eugenics affirm that technology rules and human beings must obediently follow. A basic tenet is human enhancement. Humanity must adapt to the new technologies. Those who do not will not survive or at least will not thrive. The new eugenics envisages that enhancement will be done genetically.
Harris and Savulescu argue that human enhancement is not only the result of a human being’s desire to improve himself but also that it is a moral obligation. If one is truly concerned about the well-being of future generations, parents must be obliged to produce the very best children possible. This is based on what Savulescu calls “procreative beneficence”.
The new eugenics claims that it will create better opportunities for children and that itis based on good science and individual consent. The old eugenics was unscientific, concerned with the improvement of the race, and coercive.
But is the new eugenics really free of coercion? Those who choose not to enhance might be considered unsatisfactory parents, who are not acting in the best interests of their children. Unenhanced children could place a larger financial burden on society. The social pressure on these parents could eventually lead them to consent to their child’s enhancement.
The old eugenics tried to improve the species by encouraging the reproduction of persons with desirable genetic traits and discouraging the reproduction of undesirables. The new eugenics views genetic selection as an improvement on Darwin’s natural selection. But don’t they have fundamentally the same aims: the development of a superior individual and the consequent elimination of those considered inferior?
The slippery slope
The concept of eliminating the unfit persists. In the Netherlands, voluntary euthanasia and physician assisted suicide have been legal since 2002. However, since 1984 the courts had failed to regulate these practices. This unofficial approval led to widespread use by the medical community and eventual acceptance by the public. Frequently it is a Dutch physician who decides who lives and who dies.
Surveys have showed that euthanasia of newborns and infants was a common practice in the Netherlands. In 2002, the Groningen Protocol for newborn euthanasia was developed to regulate the practice of actively ending the life of some newborns and to prevent uncontrolled and unjustifiable killing. It specified that the newborns to be killed were those with congenital defects who were facing “hopeless and unbearable suffering.” Belgium has followed the Netherland’s lead.
In 2012, two bioethicists, Alberto Giubilini and Francesca Minerva, published an article in the Journal of Medical Ethics, “After birth abortion: Why should the baby live?” The authors admit that the fetus and the newborn child are human beings, albeit non-persons or what they consider “potential” persons. They are non- persons because they are “unable to make aims [set goals] and appreciate their own life.” “Neither can be considered a person in a morally relevant sense, as a subject with a moral right to life.”
The authors conclude with this chilling logic: “If criteria such as the costs (social, psychological, economic) for the potential parents are good enough reasons for having an abortion even when the fetus is healthy, if the moral status of the newborn is the same as that of the infant [fetus] and if neither has any moral value by virtue of being a potential person, then the same reasons which justify abortion should also justify the killing of the potential person when it is at the stage of a newborn.” Note their words, “even when the fetus is healthy”. It is no longer just the unfit who are eligible for euthanasia.
A heated debate ensued in the media. The authors responded with an open letter in the Journal of Medical Ethics. They expressed their surprise at the uproar their article had sparked outside of their philosophical circle. They explained that they had been writing for like-minded ethicists and that the article was meant to be an academic exercise and an exercise in logic. “We are not policy makers, we are philosophers and we deal with concepts, not with legal policy,” they wrote.
Their rationale was reminiscent of the situation in the 1920s. After the publication of Binding and Hoche’s Allowing the Destruction of Life Unworthy of Life, academics and other intellectuals debated their proposals. Shortly thereafter, they were implemented by the Nazis.
The free exchange of ideas ought to be encouraged in a democratic society. But responsible citizens must be aware of the consequences their words will have on culture and society.
Felipe E Vizcarrondo MD, MAis the president of the Miami Guild of the Catholic Medical Association.
References
Binding, K., Hoche, A., Allowing the Destruction of Life Unworthy of Life, Suzeteo Enterprises, 1920, translated by Modak, C., 2012-2015, commissioned by the Policy Intersections Research Center, www.lifeunworthy of life.com
Black, E., The Horrifying American Roots of Nazi Eugenics, History News Network, The George Washington University, Washington D.C., 2003.
Buck v. Bell, http://en.wikipedia.org/wiki/Buck_v._Bell)
Darwin, C., The Origin of Species, 1859, Barnes and Noble Classics, New York, 2004.
Giubilini, A., Minerva, F., After-birth abortion: why should the baby live? Journal of Medical Ethics, (2012). doi:10.1136/medethics-2011-100411
Savulescu, J., (2001). “Procreative Beneficence: Why We Should Select the Best Children”. Bioethics. 15 (5–6): 413–26. doi:10.1111/1467-8519.00251. PMID12058767.
One of my favorite actors, Nick Searcy, a the lead role in “Gosnell: The Movie,” which finally opens this October reportedly in over 700 theatres. The film is one of the largest crowd-sourced movies of all time.
For that tiny handful of pro-lifers who might not know, Kermit Gosnell, who operated the notorious “House of Horrors,” was a West Philadelphia abortionist who was convicted of three counts of first-degree murder, one count of involuntary manslaughter, and a bevy of other lesser charges. Over the decades Gosnell delivered hundreds of very late-term babies alive and then murdered them by slicing their spinal cords.
Mr. Searcy appeared at NRLC’s 2018 annual convention, along with Executive Producer John Sullivan. The year before, Ann McElhinney, the producer of Gosnell the Movie and co-author of the New York Times Best Seller Gosnell: The Untold Story of America’s Most Prolific Serial Killer, was a featured speaker.
Ann told us an incredibly true-life story about the making of the film which I failed to pass along but which critic Christian Toto wrote about this week.
Tessya Whatley plays Viola Brown in the film. Viola considers an abortion but eventually chooses to give her baby life. “It’s a similar situation to what Whatley went through several years ago,” Toto writes. Whatley’s own son is now 6.
“I also was young and pregnant once,” she told the Daily Wire in an exclusive interview. “I went to actually abort my baby, and the nurse had let me hear my son’s heartbeat.”
As Whatley lay on the surgical table listening to her baby’s heartbeat while the nurse was out of the room, “I just started crying and decided it was something I couldn’t do, I couldn’t kill my baby,” she said.
“So I put my clothes on, I went out to my grandpa, I told him I couldn’t do it, he said, ‘let’s go,’” Whatley explained.
We will keep you updated as the movie locations are released.
LifeNews.com Note: Dave Andrusko is the editor of National Right to Life News and an author and editor of several books on abortion topics. This post originally appeared in at National Right to Life News Today —- an online column on pro-life issues.
August 1, 2018 (Human Life International) – In Evangelium Vitae, St. Pope John Paul II identified a sinister paradox in contemporary culture. “Precisely in an age when the inviolable rights of the person are solemnly proclaimed and the value of life is publicly affirmed,” he lamented, “the very right to life is being denied or trampled upon, especially at the more significant moments of existence: the moment of birth and the moment of death.”
This “strange contradiction,” he warned, means that in practice a great deal of the lofty talk about human rights spoken in legislatures, courts and conference rooms around the world amounts to little more than a “futile exercise of rhetoric.” In this blistering passage, the pope singles out one instance of the hypocrisy of many ostensibly liberal modern democratic states: i.e. their insistence that international “aid” sent to impoverished countries be contingent upon “arbitrary prohibitions against procreation” – in other words, “soft” coercive population control.
Marina and Norina in Tanzania, pressured to use Norplant implants. Celina’s implant “wandered” and a long scar in her arm is the result of cutting it back out, when she experienced bad side effects. They are relatives of Regional Anglophone Africa Director, Emil Hagamu.
“Should we not question the very economic models often adopted by States which, also as a result of international pressures and forms of conditioning, cause and aggravate situations of injustice and violence in which the life of whole peoples is degraded and trampled upon?” he queried.
Attack on Human Dignity – the Root of the Culture of Death
Over the past several weeks, we have been exploring Blessed Pope Paul VI’s prophetic encyclical Humanae Vitae, published just over 50 years ago. To a large number of people (including – alas – many Catholics) Humanae Vitae’s reaffirmation of age-old Christian teaching against artificial contraception is outdated, oppressive, and tangential to any of the “real” problems that our society is facing. Why, when we are facing grave issues like human trafficking, mass migration, political polarization, and gun violence is the Catholic Church still wasting its breath on questioning what consenting adults are doing in the privacy of their own bedrooms?
Liberal thinkers frequently make the same accusation against the Church’s condemnations of abortion. Why, when there are children starving and suffering other grave indignities does the Church continue to waste its time and energies on trying to prevent women from exercising their “right” to “control their own bodies”? Why is the Church so concerned with undeveloped fetuses when there are born children whose rights and dignity are being daily violated?
A clear and compelling answer is found in both Humanae Vitae and Evangelium Vitae. As we have seen, Blessed Pope Paul VI prophetically predicted that the moral effects of artificial contraception would not remain hermetically sealed in the bedrooms of the nation, but would seep out into the most public realms, including, in the most terrifying cases, in decisions by governments to coercively enforce population control using the new methods of contraception. He also saw the connection between contraception and abortion, warning in Humanae Vitae that abortion is “to be absolutely excluded as lawful means of regulating the number of children.” Thus, a practice that seemed to the sexual revolutionaries of the 60s to be transparently benign – artificial birth control – turned out to erode crucial structures and strictures that protected the dignity of the weakest among us.
In Japan, post-War many babies were aborted after women were raped or became pregnant by whites, to preserve the purity of Asian blood. Here Regional Director for Asia, Dr. Ligaya Acosta, visits a Shrine to the Unborn.
In Evangelium Vitae St. Pope John Paul II is even more explicit in explaining how direct attacks on human life, above all via abortion and euthanasia, undermine every effort to protect human dignity:
A society lacks solid foundations when, on the one hand, it asserts values such as the dignity of the person, justice and peace, but then, on the other hand, radically acts to the contrary by allowing or tolerating a variety of ways in which human life is devalued and violated, especially where it is weak or marginalized. Only respect for life can be the foundation and guarantee of the most precious and essential goods of society, such as democracy and peace. There can be no true democracy without a recognition of every person’s dignity and without respect for his or her rights. Nor can there be true peace unless life is defended and promoted.
Human Dignity in the Scriptures
To understand why radical respect for the dignity ofevery human being from the moment of conception is the precondition of all human rights, it is helpful to turn to the Scriptures. It is there that we find the theological and anthropological basis for St. Pope John Paul II’s assertion above. Indeed, much of the Scriptures amount to a protracted argument that human beings are vested with such a dignity that the value of a single human exceeds that of the entire physical universe.
That argument begins in the very first book of Genesis, where the Scriptural author asserts that God created man “in his own image” (Gen. 1:27). Due to overfamiliarity, I suspect we often lose sight of the seismic significance of this declaration. If humans are made in “God’s image” then we are, truly, in some meaningful sense “God-like.” What, precisely, does this mean? In brief: Unlike the rest of material creation, human beings are self-conscious, thinking beings invested with the capacity for free choice, and possessing immortal, spiritual souls capable of union with God through the direct contemplation of His essence in eternal beatitude in Heaven. Already created with a spark of the divine, human beings are truly capable of being “divinized” by receiving God’s life through grace.
As the psalmist puts it, “[Y]ou have made [man] a little lower than the heavenly beings and crowned him with glory and honor. You have given him dominion over the works of your hands; you have put all things under his feet, all sheep and oxen, and also the beasts of the field” (Psalm 8:5-7). In one of the most explicitly “pro-life” passages of Scripture, Jeremiah recounts God telling him, “Before I formed you in the womb I knew you, before you were born I set you apart.” The psalmist too echoes this message, speaking of the intimate, personal solicitude with which God created him: “For you formed my inward parts; you knitted me together in my mother’s womb” (Psalm 139:13). Job too marvels at God’s completely personal interest in his life and well-being: “You clothed me with skin and flesh and knit me together with bones and sinews. You have granted me life and steadfast love; and your care has preserved my spirit” (Job 10:8-12).
“Before I formed you in the womb I knew you, before you were born I set you apart” (Jeremiah 1:5).
After Christ, this message of the innate dignity shared by every human being is elevated even further by a new awareness of just how great God’s personal love for every human being is, and how lofty is the human destiny. “For God so loved the world, that he gave his only Son, that whoever believes in him should not perish but have eternal life,” marvels John the Evangelist. St. Paul exhorts his readers: “Do you not know that you are God’s temple and that God’s Spirit dwells in you” (1 Cor. 3:16). John echoes this same message in one of his letters: “See what kind of love the Father has given to us, that we should be called children of God; and so we are” (1 John 3:1-2).
Abortion and Human Dignity
What is so historically astonishing is these Scriptural passages do not admit of any exceptions. Every human being is created in “God’s image.” Every human being was “knit together” in his or her mother’s womb by a God intimately interested in their individual welfare. Every human being has the potential to become a “child of God.” Christ sacrificed himself for the salvation of every human being.
It is no accident that the very concept of universal “human rights” was hammered out and flourished in a culture deeply imbued with the principles of the Judeo-Christian Scriptures. For if there is anything history teaches us, it is that the equal dignity of all human beings is by no means self-evident to most peoples and cultures. Sadly, even in countries that have ostensibly had Christian roots, we have seen the horrific fruits of an abandonment of the Scriptural truth about universal human dignity: slavery and genocide.
Indeed, there seems to be an inexorable logic to the denial of universal human rights: once the pendulum starts swinging in that direction, the criteria for qualifying for human rights become progressively stricter and more arbitrary. In the long run, any country or civilization that deliberately and systematically undermines the fundamental rights of a particular class of human beings falls prey to the arbitrary whims of a powerful few. “To claim the right to abortion, infanticide and euthanasia, and to recognize that right in law, means to attribute to human freedom a perverse and evil significance: that of an absolute power over others and against others,” says St. Pope John Paul II. “This is the death of true freedom.”
This is why the Church insists upon the prioritization of the fight against direct, deliberate and grave attacks on the dignity – above all the right to life – of human beings. This does not mean that She does not consider other issues to be of importance: on the contrary, She consistently draws attention to all attacks on human dignity and praises every effort of whatever kind to raise the downtrodden to their rightful dignity.
Nevertheless, St. Pope John Paul II was crystal clear that direct attacks on human dignity are especially pernicious, to the point that he insisted that laws legitimizing such attacks are no laws at all, and that they even preclude a society’s capacity to achieve the common good in any meaningful sense.
Laws which authorize and promote abortion and euthanasia are radically opposed not only to the good of the individual but also to the common good; as such they are completely lacking in authentic juridical validity. Disregard for the right to life, precisely because it leads to the killing of the person whom society exists to serve, is what most directly conflicts with the possibility of achieving the common good. Consequently, a civil law authorizing abortion or euthanasia ceases by that very fact to be a true, morally binding civil law.
But, even this scathing passage does not fully capture the great pope’s scorn for laws that enshrine attacks on human life. Any time such laws are passed, he said, “the ‘right’ ceases to be such, because it is no longer firmly founded on the inviolable dignity of the person, but is made subject to the will of the stronger part.” In such cases, even so-called “democracies” are in fact declining into “a form of totalitarianism.” The State “is transformed into a tyrant State,” he said, “which arrogates to itself the right to dispose of the life of the weakest and most defenceless members, from the unborn child to the elderly, in the name of a public interest which is really nothing but the interest of one part.”
This applies even – or perhaps especially – in cases where abortion and euthanasia have been legalized by popular ballot. Such a vote may give the impression of being strictly legal and democratic. But, he said, “Really, what we have here is only the tragic caricature of legality; the democratic ideal, which is only truly such when it acknowledges and safeguards the dignity of every human person, is betrayed in its very foundations.”
The Weakness of the ‘Seamless Garment’
These are strong words.
They also help explain why pro-lifers have always rejected the common misuse of the so-called “seamless garment” theory. If the person using this term only means that all moral issues are connected – i.e. that all goodness is ultimately One and all individual goods are mutually reinforcing, and that all evils are equally interconnected and mutually reinforcing – then there is nothing necessarily wrong with it. Sin begets sin, and virtue begets virtue. True enough.
But in practice the theory is frequently used to level all moral evils to equal status, or, even worse, to raise certain lesser evils, or even prudential matters above those that involve grave, intrinsic evils, such as attacks on human life. The image itself facilitates this fallacy: for it seems that every thread of a seamless garment is just as important as any other. A much better image is the image used by St. Pope John Paul II in a passage quoted above: of a building and its foundation. Every brick of a building is crucial for the structural integrity of the building, but some are more important than others. Those that form the foundation are the most important of all. As grandiose as the structures built on such a foundation may be, they are all the more shaky for that.
Of course, nothing that I have said suggests that Catholics should only be involved in fighting for certain issues or causes. Every Christian is gifted with their calling, their own particular charism. We need Catholics to bring solid Christian principles based upon a true understanding of human dignity to every conceivable social and political issue: immigration, healthcare, housing, education, hunger, gun violence, penal justice, work conditions, legal reform, etc. However, what it does mean is that Christians must be wary of self-declared “human rights” campaigns or initiatives that are built on shifting sand: i.e. on a selective application of human dignity. We see this, for instance, in cases where ostensible “charities” attack the culture and dignity of peoples in impoverished countries by exploiting the offer of legitimate charity such as healthcare to introduce grave intrinsic evils like abortion. No matter how enticing the gift in one hand, the dagger held in the other undermines whatever good the gift might have done.
“The theory of human rights is based precisely on the affirmation that the human person, unlike animals and things, cannot be subjected to domination by others,” stated St. Pope John Paul II. As long as we live in a society that systematically and deliberately dominates the weakest among us, stripping them of their basic rights, we must always be aware that every attempt we make to protect human rights risks collapsing due to an infirm foundation. All true charity is at least implicitly built upon a commitment to defend the dignity of every human being: and any charity that lacks this commitment risks devolving – whether intentionally or not – into exploitation, all the more sinister for arriving in the guise of a “gift.”
Ever since 1928, Gerber Baby Foods has illustrated its products with a sketch of a beautiful child who was chosen after a nationwide contest. Beginning in 2012, Gerber supplemented its cherubic logo with an advertising campaign featuring an additional child, also chosen in an open competition.
This year, out of 140,000 submitted entries, Gerber chose a smiling two-year-old named Lucas. Last month, Gerber arranged for the two babies—the original 1928 Gerber baby and the 2018 Gerber baby—to meet.
This year’s baby, Lucas, has Down syndrome. Lucas is happy. Lucas is lucky to be alive.
Estimates vary, but in the United States, abortions of children whose Down syndrome is detected in the womb are in the range of about 67 percent. The lethal discrimination practiced against such persons has become a worldwide phenomenon. Iceland has trumpeted its success in eliminating people with Down syndrome from the island. Denmark, whose people heroically saved over 95 percent of the Jews living there during World War II, now boasts that 98 percent of unborn children with the condition are aborted. Italy, Germany, France, Switzerland, England, and Belgium all have rates exceeding 90 percent.
Hitler wanted Europe to be judenrein, scrubbed clean of Jews. It seems that today Europe aspires to be DownSyndromerein.
Despite the fact that a majority of children with Down syndrome are aborted in the United States, each year about 6,000 babies with Down syndrome survive pregnancy and are born here. In Europe, the situation is more dismal. In England, about 700 are born each year. In 2017, only four children whose Down syndrome was detected in the womb were permitted to be born in Denmark. There are virtually none in Iceland.
Protecting Babies with Down Syndrome
Down syndrome, or trisomy 21, occurs when there is an extra copy of chromosome 21. It most often occurs in pregnancy of women who are over thirty-five years of age. Common effects of Down syndrome include a smaller stature, a slight flattening of the rear of the skull, slightly upward slanting eyes, a degree of mental retardation, and heart and eyesight problems. Life expectancy is now around sixty years. Just forty years ago, life expectancy was only twenty-five years, and in 1929, it was a mere nine years. In the main, Down syndrome children are happy and outgoing.
On December 22, 2017 Governor John Kasich of Ohio signed the Down Syndrome Non-Discrimination Act, which prohibits abortions of unborn children who have been diagnosed with Down syndrome. In March 2018, federal district judge Timothy Black, responding to a suit by the ACLU, issued a preliminary injunction preventing the Act from going into effect. Similar laws in Indiana and Louisiana have also been stayed, but a North Dakota law protecting unborn children with Down syndrome has taken effect.
The Humanity of the Unborn Child
For the last twenty years, in the United States, states have passed myriad statutes attesting to the humanity of the unborn person. In addition to Down syndrome laws, they include such measures as fetal homicide acts, born alive acts, pain-capable restrictions, ultrasound requirements, sex-selection prohibitions, twenty-week bans, informed consent laws, heartbeat bills, and counseling and adoption opportunities. The next stage in abortion jurisprudence will be to grapple with the central fact of the humanity of the unborn person, to which all of these statutes attest.
In 1948, in reaction to the crimes against humanity perpetrated by the National Socialist regime in Germany, the Universal Declaration of Humans Rights was adopted. Drafted by men such as personalist philosopher Jacques Maritain, the Declaration had a basis in natural law. In the same year, the Genocide Convention was adopted. It seems that seventy years later, Europe and North America have circled back to the time when eugenics sought the sterilization or eradication of certain kinds of human beings. Because of the ideology of abortion, we have now traveled the road from termination of the pregnancy to the extermination of the kind of human being we no longer wish to abide in our midst.
The abortion decision is no longer just that baleful utilitarian calculus, “In order to enhance my life’s prospects, I must utterly destroy your life’s prospects.” It is now, “You may not live, because of who you are.” Recall that the first group Hitler sought to destroy was gay people—because of who they were. In China, girls are aborted—because of who they are. In Rwanda, the Tutsis were slaughtered—because of who they were. In America, we have something called pregnancy reduction—a euphemism—when one of twins or triplets is aborted, usually because he or she is smaller than the other. You’re short—you go.
With Down syndrome, as the columnist George Will has written, “it is simply the deliberate systematic attempt to erase a category of people.” In other words, it is a form of genocide. It goes beyond eugenics, for Down syndrome people rarely reproduce.
What Gives Someone the Right to Live?
When we tolerate the killing of people simply because of who they are, we lose our own moral standing to exist. Recall what Abraham Lincoln wrote about the justifications offered in defense of slavery.
You say A. is white, and B. is black. It is color, then; the lighter, having the right to enslave the darker? Take care. By this rule, you are to be slave to the first man you meet, with a fairer skin than your own.
You do not mean color exactly?—You mean the whites are intellectually the superiors of the blacks, and, therefore have the right to enslave them? Take care again. By this rule, you are to be slave to the first man you meet with an intellect superior to your own.
But, say you, it is a question of interest; and, if you can make it your interest, you have the right to enslave another. Very well. And if he can make it his interest, he has the right to enslave you.
Do you lose your right to life because of who you are? Because you are gay, or a girl, or a Tutsi, or black, or a Jew, or a Christian, or have an extra chromosome?
Does a person lose his right to live because of his geography? Did a person lose his right to live in Mao’s China because of where he was? Would he have retained that human right had he been in Taiwan? Does a person not have a right to live because he is a few centimeters inside the birth canal and then gain it when he is a few centimeters outside of it?
Is it time? Did a persecuted Jew during the anti-Jewish period in the Soviet Union have no right to live during the waiting period of his six-month exit visa? Did he then possess that right when he finally exited the country? Does a child six months away from delivery have any less a right to live than one who is just born?
Is it power? Does a citizen of North Korea have no right to live because Kim Jong-un can kill him at will, while a citizen of England has a right to live because Theresa May cannot? Does a child in the womb not have a right to live simply because someone else has the power to end her life?
During the mass starvation in Ukraine caused by the Soviet government, Joseph Stalin was quoted as having said, “If only one man dies of hunger, that is a tragedy. If millions die, that’s only statistics.” That glib comment is callously wrong. Ukraine’s millions of famine-induced deaths weren’t a statistic. They were a moral catastrophe. The mass extermination of unborn children today is likewise a moral catastrophe. Every year, we track the statistics on abortion. But behind each one of the twenty million or more deaths under Stalin, there was an individual person. Behind each one of the abortion statistics, there is an individual human person, unique, just like you and me, with a life, just like yours and mine, never to be replicated—for all time.
Just like Lucas.
David F. Forte is Professor of Law at Cleveland State University. He was formerly a Visiting Scholar at the Center for the Study of Religion and the Constitution at the Witherspoon Institute. This essay is derived from a presentation to a conference commemorating the Universal Declaration of Human Rightssponsored by the Forum of Rights and Freedoms, in Warsaw, Poland.
I have had many relatives and friends who lived in nursing homes and, especially as a nurse, I am always saddened by how few of the other residents had any visitors, even family members. I have even heard relatives say they would just prefer to remember their relative “the way they were”.
This is not only tragic for the family member’s or friend’s psychological well-being but also potentially for their safety. Nursing home residents without visitors are at greater risk of neglect or even abuse. With sometimes inadequate staffing and/or high nurse and aide turnover, it is important that people in a nursing home have someone who knows them to look out for them.
Here are 3 tips that can help safeguard a friend or relative:
Get to know the staff and tell them about your friend or relative, especially likes or dislikes. Visit at different times or days in order to know the staff and when it is most convenient to talk with them.
Notice “red flags” like poor personal hygiene, unexplained injuries, weight loss, emotional changes, environmental hazards etc. and know who to contact if you see a problem.
Especially if you are have health care power of attorney for your relative or friend, ask about care conferences so that you can attend them. Such conferences usually cover how the resident is doing in terms of activity, possible pain, eating, mobility, etc. It is also crucial to know what medications have been ordered and given, especially the PRN (as needed) ones. For example, you may notice a change such as sleepiness or fatigue that can be helped with a medication change.
According to the CDC, 1.4 million people are nursing home residents in the US and, as I wrote in last week’s blog “‘Rational’ Suicide and the ‘Elderly’”, those residents really benefit from visitors as do all of us who volunteer to help the elderly!
This week I have been swamped with messages from loyal Catholics who have been shaken and disgusted by the latest eruption of the continuing sex-abuse scandal in the Church. I wish I saw some sign that our bishops recognized the rising tide of anger—righteous anger—among the most active lay Catholics.
Unfortunately, Bob Royal is on target when, borrowing a line from Leo Strauss, he says that the American bishops are like Nero, except “they know neither that they are fiddling nor that Rome is burning.” Royal sums up the general level of dismay by saying that it is imperative for Church leaders to learn how the cancer metastasized:
Finding out how this was possible is going to call for some painful self-examination, both here and in Rome itself. But the alternative is business as usual. And that business is now in danger of bankruptcy.
In my view the most distressing development of the week was the craven public statement from Cardinal Sean O’Malley—who, as chairman of the special papal commission on sexual abuse, should be leading the charge against clerical misconduct. Instead he offered a bureaucratic response. He invoked the mossy old dodge that a crucial letter did not reach him. Notice that the cardinal did notsay that he was unaware of the letter’s contents. But if he wasn’t aware, he should have been; and if he was aware, he should have taken action.
In National Review, Michael Brendan Dougherty did a thorough job of deconstructing Cardinal O’Malley’s letter, along with the protestations of ignorance by Cardinal Kevin Farrell. He argues persuasively that the problem is not an absence of standards, policies, and procedures, but “a fear of confrontation, insufficient zeal, or—most likely of all—…moral compromise and passivity…”
In some cases, bishops showed themselves to be simply tone-deaf: unable to recognize that the patience of their people has been exhausted. Bishop Thomas Tobin of Providence, Rhode Island, who has often been a breath of fresh air because of his willingness to speak plainly, blundered badly with a Twitter comment, saying that despite the latest uproar he was proud of his brother bishops. That prompted a very lively rejoinder at Catholic World Report by Christopher Altieri, who had a simple, blunt message for the American bishops: “You have all failed us.”
(I am sorry that Bishop Tobin, shaken by the vitriolic reaction to his post, announced that he was deleting his Twitter account, convinced that the forum was an occasion of sin for himself and for others. He will be missed.)
If Altieri was rough on the US bishops, Ross Douthat of the New York Times was scathing in his analysis. Douthat made the trenchant observation that although the Catholic blogosphere is buzzing with news and analysis about the scandal, the secular media have taken a much less aggressive approach. Douthat believes that “because of secularization and polarization and the bonfire they have made of their own moral authority, the Catholic bishops are now somewhat protected from media scrutiny by virtue of their increasing unimportance.”
There is a great deal of truth in that argument. The scandal is an important matter for those of us who think that the Catholic Church is important. But for those who are indifferent or hostile to Catholicism, the devastation wreaked upon Church authority during the “Long Lent” of 2002 may be sufficient. On the other hand, Douthat does not deal with another obvious reason why the secular media have shown less interest in revisiting the story: The latest stories are very clearly stories about homosexual misconduct, and the secular media are, by and large, favorably disposed to the homosexual cause.
Nevertheless I think Douthat captures the importance of this moment for the Church:
The question that the church’s leaders need to ask themselves, in America but especially in Rome, is whether they are happy with this settlement—happy to be ignored so long as they can also evade accountability for what’s still rotten in the church, happy to serve out their time as stewards of a declining institution than demanding the heads of the men whose culpable ignorance made the decline much steeper than it should have been.
If anyone reading his column has somehow missed the uproar, J.D. Flynn provides a thorough briefing on the major elements of the story. Rod Dreher has written on the topic early and often, and his treatments— just one example among many here—have been exhaustive.
Of course I have been busy, too. My analyses are available here and here and here and here andhere on the Catholic Culture site, as well as for First Things.
When I was a child and preparing to receive my First Holy Communion, I remember being taught to do so the traditional way: on the tongue. In fact, if memory serves, we received Holy Communion via intinction that first time i.e. the priest carefully dipped the host in the Precious Blood before placing it on our tongues. (We were further instructed to allow the host to dissolve and not chew it; I believe this was very practical advice, for if we chewed it particles might have gotten caught in our teeth, which could then fly out if we coughed, sneezed, or just talked.)
Ever since that important day in my life – though there were many years when I did not go to church in-between – I have always preferred to receive Holy Communion on the tongue. It just seems right. And even now, as a priest, on the occasions when I simply attend Mass in choir, I still receive on the tongue.
In fact, once I was ordained and started reflecting at much closer range, so to speak, on these things – reflections often connected with practical matters, like how to distribute Communion well and efficiently, how to purify the sacred vessels properly, etc. – I went from having a personal preference against Communion in the hand to having serious misgivings about it for more objective reasons. I also started to be aware of the fact that many other priests shared these misgivings as well.
From the lack of reverence that many people show when receiving in the hand (oh, the stories!), to the dirty hands that they present… From the particles of the Sacred Host that most certainly end up on their hands and on the floor (Lord have mercy!), to the real possibility of theft for malicious purposes (which has happened in many places)… Communion in the hand has become something that greatly distresses me. I do not deny that the Church allows it – in the United States, at least – but I do not think that it is an advisable choice for us to make.
Fr. Bryan Jerabek
Regarding the very widespread practice of Communion in the hand, there are also particular problems with children receiving that way. Besides the fact that they frequently have dirty hands from playing before (or during!) Mass, they also often lack coordination and judgment: it has happened several times that children have dropped hosts that I placed squarely in their hands, due to their movements or a lack of attention.
I remember preaching about the proper way to receive Holy Communion in the hand on one occasion, in particular: about the need to form a “throne” with one’s hands, to consume the host right away, and then to check for particles on the hand, and so forth. And I noticed exactly zero change in how people approached and walked away from the Communion line at that very same Mass! It seemed to fall on deaf ears.
Why did it fall on deaf ears? I think it is because there has been a loss of faith in the Real Presence. Few Catholics would openly deny this dogma with their lips; but in practice, we see it denied all the time. I think this teaching has become something kind of “magical”, if I may put it that way: Christ is sort of mystically present in the host, but he’s not worried about crumbs. Even if such an erroneous belief is better than not believing in any sort of Real Presence, no matter: it is erroneous, not at all what the Church teaches.
Father Bryan W. Jerabek, J.C.L. is Rector of the Cathedral of St. Paul in Birmingham, Alabama and is Chancellor of the Diocese of Birmingham. He blogs at http://fatherjerabek.com.
Editor’s Note: In Part II, Fr. Jerabek discusses whose hands are consecrated for handling the Blessed Sacrament, what other priests and bishops think of the practice of receiving Holy Communion in the hand, and provides recommendations (and links) for further reading.
Art for this post on Communion on the Tongue: Partial restoration of San Carlo Borromeo comunica San Luigi Gonzaga (St. Charles Borromeo communicates St. Aloysius Gonzaga), tapestry by unknown artist, photographed by Giovanni Dall’Orto, June 22, 2007, copyright holder allows use for any purpose, provided copyright holder is properly attributed, Wikimedia Commons. Photograph of Fr. Bryan Jerabek used with permission.
A neuroscientist has found that at least 20 percent of people thought to be in a vegetative state are completely aware of what’s happening around them and to them, but they are unable to respond or move. This means that people thought to be in comas or a ‘vegetative state’ are suffering horrible abuses – being starved and murdered like Terri Schiavo – all while being completely aware of what’s being done to them.
Dr. Adrian Owen, the author of Into the Gray Zone, is a neuroscientist who has been studying how people who are thought to be unaware — often because they cannot answer commands such as “squeeze my hand” — are actually very aware. He asked the question, “could somebody command follow with their brain?”
By scanning the brains of conscious individuals and asking them yes or no questions, he took note of the areas of their brains that were activated with blood flow. Rather than answer yes or no, these healthy individuals were asked to think of playing a game of tennis if the answer to the question was yes and to think of moving through their own home if the answer was no. Each of those thoughts uses a different part of the brain and doctors could watch which part became activated when asking the questions.
Then Owen tried this with hundreds of people thought to be unresponsive and vegetative. What he found was astonishing. An astounding one in five people who were unable to physically respond to command prompts in the past were able to respond to them with their brains, proving that they were not unresponsive or unaware as previously believed.
“What we’re doing is returning the ability to communicate to some patients who seem to have lost that forever,” said Owen. “[…] I can still remember exactly what it felt like the first time we saw a patient that we thought was in a vegetative state activate their brain in the scanner. The patient’s name was Kate. Nobody would have predicted that we would have seen brain activity in response to asking a patient to do something and when we first saw it it was absolutely astonishing. Before we made that discovery, nobody bothered to look at any of these patients.”
What he discovered will change the way doctors and family members treat people who are living like Terri Schiavo did. Rather than pass them off as people who are unable to live or unworthy of living and assuming these people would rather die and then starving them to death, doctors will actually be able to ask people how they feel, if they are in pain, and what they want for their lives. They will no longer be locked inside their minds, forced to watch as well-meaning doctors and family members make life or death decisions for them. They will no longer have to sit in pain unable to express it. And the lives of people around the world who are currently written off as “vegetative” will be opened to a whole new way of living. Because that’s what they have always been – living human beings worthy of the best that medical care and love can give them.
40 years after her birth it is estimated that more than seven million babies have been born as a result of IVF and other assisted reproduction treatments. Around 2.4 million assisted reproductive technologies (ART) cycles are estimated to take place each year world-wide, with about 500,000 babies born as a result. If rates stay at current levels, then a million people alive at the end of the century will owe their lives to assisted reproductive technologies (1.4 percent of the global population).
40 years ago it was generally assumed that IVF would remain rare. However there has since been an explosion of assisted fertility services: intracytoplasmic sperm injection (ICSI), gamete and embryo freezing, gamete and embryo donation, embryo genetic diagnosis and surrogacy, to name some. The most common fertility treatment now is ICSI, accounting for around two-thirds of all treatments worldwide, with conventional IVF around one-third (proportions that vary across countries).
Infertility is deeply distressing and can affect every area of life for those struggling to conceive – as many as one in six couples. The Bible views childlessness as a painful, personal tragedy (Samuel’s mother Hannah’s anguished prayer illustrates the stress of infertility, as does Rachel in Genesis 30) while the Psalmist praises the God who ‘gives the barren woman a home, making her the joyous mother of children’ (Psalm 113:9).
IVF can provide couples with a child they desperately want. And it has brought many precious new lives into being, and real happiness to millions of parents.
Therefore, many now think IVF is the answer to infertility.
But it is not. While the IVF industry and media focus on and market the success stories, the average delivery rate from ART treatments are around just 19 percent per cycle – a global IVF cycle failure rate of around 80 percent. In the UK, the Human Fertilisation and Embryology Authority reports a ‘success’ rate of 26.5 percent . This ‘success’ rate actually means that 73.5 percent of cycles do not lead to a birth.
Success rates for IVF diminish rapidly after 35 years of age for women, largely because of loss of ovarian follicle reserve and oocyte quality with age. Even a woman under 35 years has less than a one in three chance of having a baby per embryo transferred, using her own eggs and partner’s sperm. A woman in her early 40s only has about a one in ten chance of having a baby per embryo transferred. And the success rate drops to a mere two percent for women over 44. This is highly relevant in a time when more and more women are delaying childbirth to concentrate on jobs and careers. When celebrities in their 50s become pregnant, what the media do not tell you is that it is almost always with a donor egg (indeed, 59 percent of women over 44 years used donor eggs in their treatment).
IVF heartbreak is real. IVF is no guarantee of success, despite all too often being touted as such. Added to this is the significant financial, emotional and physical toll that IVF can have on women.
Yet still, with one in six couples experiencing problems conceiving, the fertility industry is thriving. It is estimated to be worth over £600 million in the UK alone, with one cycle of IVF costing up to £5,000 or more.
There are some very troubling aspects of the fertility industry.
IVF has also opened what many regard as a Pandora ’s Box of genetic engineering, cloning, pre-implantation genetic diagnosis (screening out of embryos), embryonic stem cell harvesting, research on three parent babies and animal-human hybrids. Many IVF programmes involve the production of spare embryos, which are then used for research, disposed of, or frozen for future use. Between 1990 and 2013 over two million were allowed to perish, according to a Parliamentary answer. Now, over 170,000 IVF embryos perish every year. Embryos are experimented on, donated to other couples, frozen indefinitely … or even turned into jewellery.
The last 40 years of IVF and ART have given many couples happiness but even more couples, dashed hopes. The next 40 years will undoubtedly bring even more possibilities for the fertility industry, but what is possible is not always right.
A moral vision, especially one shaped by a Christian understanding of the person and family, has to be prepared to say ‘no’ to some exercises of human freedom and to turn away from technology that is possible but unwise. With fertility treatments, while we can and should use our God-given skills to help alleviate infertility we should also be prepared to acknowledge that there may be suffering we are free to end, but ought not to, that there are children who might be produced through artificial means, but maybe ought not to be.
Philippa Taylor is Head of Public Policy at the Christian Medical Fellowship in the UK. She has an MA in Bioethics from St Mary’s University College and a background in policy work on bioethics and family issues. This article has been abridged from the original post on the CMF blog. To read the original article, click here.
My friend, a 36-year-old man, sitting across from me at a popular Mexican eatery for a beer, is a tall, kind, and rather quiet type. A scientist, he is also a Catholic who wants to live the teachings of his faith about sexuality, which, if a couple would like to avoid pregnancy, requires the practice of Natural Family Planning (NFP) as opposed to the use of contraceptives.
“I get the ideology, the ideas behind it, and why it’s better than contraception. But in practice I hate it. I bet a lot of Catholic men feel the same but nobody talks about it.”
John’s situation may be somewhat uncommon, but it’s certainly not unique. His wife of 10 years got pregnant the first time they had intercourse without contraceptives. They now have two children, the youngest of whom is four. One of the reasons they don’t have more children is because they hardly have intercourse. Adding to the difficulty, his wife has a very anxious personality, in part from a hard upbringing.
John is angry. He feels a lot of rejection from her.
“I’ve tried everything to make it work for her. She turns me down most of the time; there is always a reason,” he said. “When we do it, it’s so stressful, she’s so tense that it’s not even enjoyable.”
What makes it even more challenging is that John feels he can’t tell anybody. There seems to be no place for men to speak about this issue. “There is a lot of shame,” he said.
The studies we’ve reported in past articles show that most women (53%) and men (63%) feel that using NFP improved their sex life while 32% of women and 24% of men felt it was unchanged from before they used NFP. But for 11% of men, it has made it worse (only 1% of women). And 5% of men and 3% of women were very unsatisfied with the frequency of their sex relations.
If you are in that 11% of men, or don’t think it’s worth the risk that you might fall into that 11%, I can see you jumping to conclusions from this data: NFP is not for me. Think again, because the level of dissatisfaction with frequency of sex is actually much higher in the general public: while 23% of women and 27% of men using NFP were dissatisfied or very dissatisfied with the frequency of sexual intercourse, the Relationships in America survey reports that the respective numbers for the greater population are 33% for women and 53% for men. Almost double!
This data tells us not only that NFP is not necessarily the source of sex-life dissatisfaction, but also that, clearly, other forms of family planning aren’t helping much either.
Still, there’s more to the story.
What men experience
Obviously, men are not the only ones who can feel frustrated with the lack of sex, but this article is focusing on how men can deal with this situation. It is likely a stronger physical burden for most of them by the mere fact that they don’t really have the cycles of desire that women go through around ovulation. Our hormones tend to be steady in that area. Our physical desire is sometimes compared to women’s desire for emotional affirmation and comfort.
So that women understand the difficulty a man experiences when he is repeatedly rejected sexually by his wife, or accepted with reluctance, I would venture to say it is likely as painful as if every time his wife started to show emotions and feelings, he would leave or disconnect from her. If she complained to him about it he would ignore her, dismiss her, or even mock her. Unfortunately, many women have likely experienced this and can see my point.
So we need to talk about it.
A Lack of Physical Intimacy As a Sign of Deeper Dysfunction
Sexuality, unless it’s purely selfish, cannot be taken out of the broader relational context. It is easy to imagine that the lack of physical relations in a marriage can lead to resentment and relationship difficulties. Conversely, intercourse is known to increase couples’ connection through the release of oxytocin, the same hormone that helps a mother and a baby connect through breastfeeding. Often, a dysfunctional sexual relationship is a sign of something deeper that is crying to be healed. Sex is impacted by the values of the couples, their own psyches, their physical health, and the quality of their relationship. The following suggestions barely touch on the subject but are starting points to explore.
Check your bodies.
Let’s start with the somewhat basic stuff. If one party is experiencing lower interest in sex than they used to, they might want to see a doctor about it. Urologist Joan Meaney, MD, explained to me in a recent interview that there are two major physical factors to difficult sexuality for women: painful intercourse and hormonal imbalance.
“Multiple physical and hormonal factors can contribute to difficult or painful intercourse,” she explained. “Painful intercourse finds its sources in both gynecologic and/or bladder problems.” The bladder and vaginal tissues share some nerve functions and are influenced by a woman’s hormonal balance.
Pelvic pain can be related to dysfunction and spasms of the muscles that support the pelvic floor organs: the bladder, bowel, and uterus. What makes it worse is that “the anticipation of pain can create a negative feedback loop that kills women’s libido,” Dr. Meaney noted.
Multiple approaches are available for women and their doctors to help with these problems, including pelvic floor physical therapy, behavioral therapies (stress is a factor), diet (reduce acid and caffeine), and medications to reduce nerve ending pain.
The lack of libido can also be related to stress, depression, and/or hormonal imbalances. Testosterone in both women and men is the hormone of desire.
“Unfortunately, hormonal contraceptives can have an effect on the body that is detrimental to the production of the normal hormonal balance, which can last even after stopping the contraceptives,” said Dr. Meany. Taking testosterone supplements may help.
Check your values.
The values you bring into the physical relationship matter a lot. For example, what is your position concerning family size? What religious beliefs do you share or not? Do you have deep-seated ideas that sex is dirty and shameful? Having a dialogue and coming together on these topics will help.
One area that may not often be discussed and is often difficult for men and women to talk about is the meaning of sexuality. Just like other physical gestures like facial expressions, touches, body postures, the sexual act has a deep meaning and is often unconsciously interpreted by your partner. People who are deeply engaged in use of pornography and non-relational sex habits come to this part at a huge disadvantage. It’s a bit like someone who has only been used to dancing alone who is trying to dance in a duo. It introduces the chance that he will only be looking for his own satisfaction and be less attentive the partner’s needs, rhythm, and signals.
It is crucial to seek healing in this area if you’d like to improve your relational life, because porn leads to unrealistic expectations of partners and less satisfaction with real-life partners. It’s certainly exciting and an easy way to get aroused, but not so good for dancing together. Porn and NFP don’t work well together because it can generate cravings that make the abstinence periods of NFP more difficult and lead to anger.
Check your psychological life.
We are all wounded persons in some respect, and these wounds can easily show up in our sex life. For some of us, shame and trauma played a role. Others are driven by examples of domination and power. For many, like John’s wife, deep seated anxiety and fears are a factor. If personal issues are not being resolved in the relationship, it is a responsible step to work on them with the support of a professional therapist. It is not different from a physical wound that can use treatment. It takes time, effort, and courage, but your relationship is worth it.
If your partner is struggling with such challenges but is not self-aware and/or unwilling to get help, you can’t force him or her. However, it is not uncommon that after years of experiencing this relationship, you may have developed enabling behaviors and can’t see it. Seeking therapy help for yourself will help untangle these complex relationship issues, set healthy boundaries, and begin better communication. You both will win.
Check your communication.
Much is written about communication these days that needs to be said. Although my wife and I have known and somewhat practiced methods, we both feel like beginners sometimes. Here are a couple of basics to get you started. Practice them for a month or two, and you will see changes.
One basic rule is listening—really listening to each other. Stop everything, including the running commentary in your head; hold off judgement, put away the phone, and the TV remote, sit down, look at each other, and listen. Then once you’ve heard her, repeat what you’ve heard in some way. Use your own words if you can, but mainly seek to really understand what the other person experiences, and even feel it. Ask your wife to describe how she feels when thus-and-so happened. And then stop. Here is my frequent mistake: I want to help, I suggest solutions, give advice, judge, and so on (especially if I am responsible for the feelings she experiences). Most of the time, all my wife wants and needs is to be heard, understood, and accepted.
When it’s your turn to share your own feelings, express them using “I statements”; as in, “I feel rejected when you don’t look at me when I get home.” Or, “I feel frustrated in the evenings when I try to be with you and the kids are still taking all your attention.” You can illustrate: “It feels like when the time I was bullied at school,” or “it feels like when I was a kid and my parents never took the time to listen to me.” You get the picture. It can get pretty deep and opens you to being vulnerable. Ask for the same listening treatment described above from your partner. If you model it for her, she will learn too.
Check your spiritual life.
Whatever your spiritual practice, sexual relationship difficulties are definitely something to bring into your quiet time. It touches us so deeply about our identity and our desires for fulfillment that we cannot deny its connection to our spiritual life. If you have a meditation or prayer practice, you will find that it helps you deal with negative feelings around the pain you may experience. It will likely help you regain confidence in who you are as a loved and important human person and regain hope. In these matters, you can also carefully choose a spiritual director, someone relatable but who also has a broad understanding of human sexuality as a relationship as opposed to a merely physical need.
With all this said, I have barely touched the tip of the iceberg. I see this article as an opportunity to invite other men to share about these experiences and about the way they have overcome these challenges so that we can have real conversations and help each other. You can use this link to write us confidentially and anonymously. I also want to encourage men to break the ice and find someone else to talk to about topics like these. Just having a conversation with someone who can listen will help blow off a lot of steam. That’s what John did when he talked to me, and I trust it will help many people as a result.
The #MeToo movement provides a sobering opportunity for deeper reflection on the meaning of sex and the nature of the sexual revolution. A core question is this: Do the experiences underlying #MeToo reveal the need to carry the sexual revolution still further, or do they reveal fundamental flaws in that revolution?
Some are treating the movement with suspicion, worrying that it is a pretext for promoting identity politics. Others, predictably, are doubling down on the logic of the sexual revolution, rushing to assure us that #MeToo is merely a correction toward kinder, more equitable, more explicitly consensual sexual milieu.
A growing number of people sense, often from painful personal experience, that “something is rotten” in the sexual revolution—something that no regime of affirmative consent codes is likely to fix. And although there have been compelling argumentschallenging the basic claims of the sexual revolution, experience may be the most powerful argument of all.
The personal experience of sex
Sometimes the things we most take for granted escape our notice precisely because they lie in plain sight. Start with the experience underlying the #MeToo movement. Large numbers of people, mostly women, report traumatic experiences of being coerced to engage in sexual activity with men.
Although Americans today are deeply divided about many things, the wrongfulness of sexual assault is not one of them. This is encouraging, but there is also something mysterious about it. Why do we treat sexual assault differently from other forms of assault, giving it a special and more serious legal classification?
Why is it that some people can require years of therapy after being touched on their genitals without their consent but can quickly forget a much more painful punch to the face? Why is it that if someone touches any other part of our body without our consent it is not usually traumatic, but if they touch our genitals without our consent we feel personally violated?
Or consider sexual shame, a characteristic unique to homo sapiens. Why is it that people do not generally object when pictures of them are circulated in public, but they feel personally violated when naked pictures of them are circulated? Why is covering the genitals in public a universal norm?
Why do people—even advocates of radical sexual autonomy—seek some privacy for their sexual activity, and why are public sexual activity and nakedness legally banned in most societies? Pornography is not an exception. Porn is not “public sex” but curious voyeurism that trades on the private fantasy that one is being given a privileged “peek” into the intimacy of others.
The meaning of sex
These experiences suggest that human sexuality is somehow bound up with the whole person in a unique way. It has a deeply personal meaning that we cannot simply construct for ourselves. If the meaning of sexuality is wholly conventional—if sex is merely a biological event—then the seriousness of sexual assault and ubiquity of sexual shame make no sense.
In fact, in human experience, the meaning of sexuality is closely connected with a particular desire, the desire for embodied union withanother person. (For the best account of the intentionality of sexual desire, and its distortions, see Roger Scruton’s marvelous book by this title). This desire is not simply reducible to biology, although it is certainly inseparable from it.
Each of our other organs can fulfill its complete organic function within our own bodies. The genitals alone, as reproductive organs, can be organically actualized only in sexual intercourse, when a man and a woman become a single, complete organism.
This reality suggests that sexual intercourse will always mean a wholly personal union, whatever the partners to that union may intend or think. In other words, sexuality has its own language, which human beings cannot completely change. They can only choose to live the truth of their bodies with integrity or to contradict and falsify that truth with their bodies, damaging their own integrity as well as that of their sexual partners. In sexual intercourse, the body uniquely says “I give my whole self to you, and I receive your whole self, which you are giving me.”
Certain moral norms follow from the personal meaning of sex. In the first place, there is a need for consent. Sexual contact without consent is a direct assault against the whole person. It is deeply depersonalizing. But sexual assault is only the most extreme kind of sexual depersonalization.
Every time a person is used for sexual gratification, he or she is depersonalized. This fact accounts for the true meaning of sexual modesty (and shame), not puritanical repression. It is our natural defense against the “objectifying” gaze, against being used for someone else’s gratification.
But not just any kind of consent is adequate to the intrinsic and personal language of sex, and thus to the dignity of the person. Because sex is an embodied union of the whole person, consent to sex without total commitment to the whole person contradicts the meaning and language of the body. It makes an act that speaks love between persons into an act of use of persons.
Sex is thus very different from other human activities. In some contexts, the mutual “use” of persons is morally acceptable. In typical market transactions, for example, the parties “use” one another for their own benefit. When someone purchases bread from the baker, each person is unproblematically looking to his or her own advantage, and (unless the transaction involves force or fraud) neither person feels “used.”
Why is it that “feeling used” is a common experience in sexual intercourse, even when it is consented to? And what conditions for sexual intercourse would prevent that feeling? While “affirmative consent” may at least avoid rape, most people have a sense that consent should be broader, that sex should at least be “a part of a relationship.”
But what kind of relationship is sufficient to prevent sex from being depersonalizing? A committed one? How committed? Experience leads us to the following conclusion: Nothing short of comprehensive personal consent—in other words, marriage—is adequate to the intrinsic language of sex or the vulnerability it necessarily entails.
Thus Karol Wojtyla, the future John Paul II, writes that “an actual sexual relationship between a man and a woman demands the institution of marriage as its natural setting, for the institution legitimates the actuality above all in the minds of the partners to the sexual relationship themselves.” The institution of marriage, Wojtyla makes clear, is not a means of legitimating the mutual use of one another’s bodies for sex (as Immanuel Kant describes it) but of expressing and facilitating the full meaning of conjugal love, which is reciprocal, total self-gift.
The Hook-Up Culture and #MeToo reveal the contradictions of the Sexual Revolution
These reflections help to highlight the deep contradiction at the heart of the sexual revolution, which trivializes sex while at the same time making it the very center of personal identity.
There is a deep tension between the premises of the sexual revolution and those of #MeToo. The sexual revolution promises greater availability and enjoyment of sexual pleasure without commitment or guilt. This promise can only be accomplished by the trivialization of the intrinsically personal meaning of sex. It is very difficult to see how we can simultaneously promote the trivialization of sex and treat sexual assault with the seriousness that it deserves.
But a powerful personal drive like sexual desire cannot really be trivialized, and its personal meaning cannot be completely denied. If sex ceases to be about love, it will necessarily be about war.
This is evident in the hook-up culture, which pushes the revolution’s core premise—sex without marital commitment, or “free love”—to its logical conclusion by elevating sex without any commitment at all. In the hook-up culture and its #MeToo reaction, we can see how sex without comprehensive commitment necessarily becomes predatory, thus paving the way for sexual assault.
In a powerful article called “I Thought Casual Sex Would Be Empowering, But It Wasn’t, Jennifer Joyner describes her initial attraction to hooking up: “The idea of the 21st century woman making her own sexual narrative sounded enticing,” she writes. “I wanted to be in control . . . and I didn’t want to be left out.” Joyner then recalls her experience the day after losing her virginity to a stranger in the back of a car:
He was concerned and called the next day to see if I was okay. I didn’t call back. I remember feeling smug about it, as if in successfully caring less than him I had somehow “won” the game. I proceeded to hook up with many more men in short order, chasing an elusive thrill.
As Joyner, Donna Freitas, and others have shown, the primary motive of those who “hook up” is not sexual pleasure, but power, or the achievement of victory over another. Victory is won by having sex without caring, without vulnerability.In other words, hooking up inverts the intrinsic meaning of sex, transforming eros, the desire for intimate embodied union with another person, with its attendant emotional and physical vulnerability, into thumos, the desire for domination, recognition, control, and independence.
The #MeToo movement has exposed the ugly and predatory underside of the revolution waged under the banner of radical feminism, and it highlights the ironic result that men have the upper hand in the new sexual marketplace.
This inversion of the personal meaning of sex in the hook-up culture reveals the deeper contradiction at the heart of the sexual revolution itself. Underlying the apparent trivialization of sex for the sake of more “love” or more widely available sexual pleasure is the pursuit of a much more radical personal agenda: sexual autonomy for its own sake.
Why sexual autonomy? If sex has a unique connection to our personhood and is also fundamentally erotic, an experience of going out of oneself, of potentially life-altering vulnerability and risk, then our sexuality is the most patent reminder that human beings are not radically autonomous.
This explains the otherwise mysterious fixation of modern liberals on sex. If human vulnerability and dependence are to be vanquished, the decisive battle must take place on the field of sex. It is precisely here that radical autonomy must prove itself, and why modern liberalism has made uncommitted sex the chief “liturgy” of its religion of personal identity (and why inebriation is its chief sacrament).
At the heart of the sexual revolution is the dogma that sex is the privileged arena where, in the words of the Supreme Court, I define and express my own “concept of existence, of meaning, of the universe, and of the mystery of human life” (Planned Parenthood v. Casey).
Making war, not love
In the harsh light of #MeToo, core assumptions and achievements of the sexual revolution don’t seem quite so attractive. In these latter days of Tinder and hooking up, all pretensions to the “love” part of “free love” have been shed, along with the naïvete of the hippie generation. We are left with just “free”—as in cheap—sex.
Perhaps all the sexual revolution can really deliver is a world where sex is a kind of weapon in the never-ending battle to continually create and achieve autonomous personal identity. No wonder asexuality has recently emerged as another strange feature of the modern sexual landscape. If sex is really about making war, not love, there are many who would rather opt out of such a destructive game.
Reflecting on the experiences behind #MeToo and the hook-up culture teaches us that something is deeply broken at the heart of the sexual revolution. The pathetic scramble to shore it up with consent speech codes only casts doubt on its key doctrines, bearing negative witness to the need for a comprehensive form of consent that is worthy of sex between persons—worthy of sexual love.
Nathan Schlueter is a professor of Philosophy and Religion at Hillsdale College. Elizabeth Schlueter, his wife, is a homemaker, homeschooler, mother of eight and a Michigan State Leader for CanaVox.Republished with permission from The Public Discourse
Think about the purity, holiness, and magnificence of the Blessed Virgin Mary. She was the only human being ever to be sinless and constantly in a state of grace. Because Mary was such a beautiful symbol of grace, her mother, St. Anne, must have also been a devout woman of God.
Though Anne’s name is not mentioned in the Bible, we can learn about her from tradition and legends. From these stories we learn that both Mary’s mother and father had a tremendous amount of faith.
Anne and her husband Joachim were an extremely pious couple, but they were unable to conceive a child. This burden weighed heavily on Joachim’s shoulders, so he spent much time fasting and in devout prayer pleading for God to bless him and Anne with a child.
According to tradition, Anne also became distraught. She went into her garden and prayed for God to bless her with a child, promising that the child would be dedicated to the service of the Lord. As Anne wept in prayer, an angel appeared and said to her, “The Lord has looked upon thy tears; thou shalt conceive and give birth and the fruit of thy womb shall be blessed by all the world.” Then the angel appeared to Joachim as well, and the couple rejoiced as they conceived a child, whom they named Mary.
For nine months Anne carried in her womb the future mother of Jesus Christ. She was such a pious daughter of God that she was chosen to bear a sinless child who is now the mother of all mankind. God most definitely answered her and Joachim’s prayers.
The story of St. Anne reminds us to continue to have faith in the Lord, even when things look impossible or hopeless. Anne never thought that she would be able to have a child, but she gave birth to the mother of Jesus Christ.
St. Anne understood that all children are a blessing from God and that God alone has the power to decide when the life of a person will begin and end. When God blesses us, it can be easy to merely accept the gift and move forward with our daily lives. But St. Anne did more than receive the gift of a child. She went a step further and trusted in the plan of God by promising her child to God’s service.
As we work to build a culture of life, we can easily become discouraged. But like St. Anne, we must put our faith and trust in God and His ultimate plan for our happiness. We can turn to God and pray for children, pray for an end to abortion, and pray for the gift of adoption. With God’s help, nothing is impossible.
Emily Brown graduated from Mount St. Mary’s University in May 2015. She began working for American Life League this summer and is the director of its new youth department, ALL Life Defenders. She plans on educating and collaborating with young adults all over the country to empower the new generation!
July 25, 2018 (LifeSiteNews) — The pro-life healthcare sharing ministry operating in unity with Catholic teaching will now pay for natural fertility healthcare and sterilization reversals for its members, it was announced on the 50th anniversary of Blessed Pope Paul VI’s 1968 encyclical Humanae Vitae.
Solidarity HealthShare informed members of the changes to its guidelines Wednesday, saying it will allow them to share the costs of medically proven procedures, including Natural Procreative Technology (NaPro Technology) and fertility awareness-based training and counseling, making the health share ministry the first to do so.
“Humanae Vitae, Pope Paul was emphatic about the need to defend every life at its beginning and to maintain the unitive and procreative integrity of the marital act,” said Bradley Hahn, CEO of Solidarity HealthShare. “But he also called on the medical community to continue to improve its understanding of fertility and develop natural fertility awareness methods that can help spouses be both generous and responsible with the gift of life.”
“While there have indeed been many advances that can help married couples to conceive or to postpone pregnancy if they have serious reasons to do so,” Hahn said, “Solidarity HealthShare will be the first to make this integral reproductive healthcare eligible for cost sharing for these couples, and we could not be more thrilled to share in the Church’s vision for authentic health care.”
“Solidarity HealthShare seeks to restore and rebuild an authentic Catholic healthcare system that will respect the Catholic Church’s teachings with regard to love, responsibility and the sanctity of all human life, while endeavoring to share the eligible medical expenses of our members,” according to the group’s website.
The addition of natural fertility healthcare and sterilization reversal is the next step in meeting the needs of those Catholic and Christian families.
Hahn said Solidarity’s members would share costs for the reversal of tubal ligation and vasectomy procedures, restoring the physical integrity of couples who want to be open to life.
The new member guidelines summarizing the policy change will go into effect on September 1.
Solidarity HealthShare noted specifics of the groundbreaking NaPro Technology and fertility awareness healthcare in its release announcing the guidelines.
NaPro Technology, based on 30 years of research, is “a new women’s health science that monitors and maintains a woman’s reproductive and gynecological health,” according its developers at the Pope Paul VI Institute for the Study of Human Reproduction in Omaha, Nebraska. “It provides medical and surgical treatments that cooperate completely with the reproductive system.”
There are several fertility awareness-based methods of achieving or postponing pregnancy that respect God’s design of our bodies and respect the marital act. These methods, often referred to as Natural Family Planning, will now be part of Solidarity’s health share plan.
Hahn also pointed out how the departure from God’s plan for sexuality and life has created damage in today’s culture.
“The gift of sexuality is integral to the human person, and in the marital act the married couple participates in the creative act of the Triune God,” Hahn said. “Our society is marred in innumerable ways by the many effects of the separation of the procreative and unitive ends of the sexual act, some of which Pope Paul predicted in Humanae Vitae.”
“If we at Solidarity HealthShare can play just a small role in helping spouses to live the life-giving teachings of the Church in an integral way,” he added, “we are fulfilling our mission of restoring Catholic healthcare while building community and serving families.”
For more information on Solidarity HealthShare and its offerings, click HERE.
July 25, 2018 (LifeSiteNews) – Today we commemorate the fiftieth anniversary of Humanae Vitae, Pope Paul VI’s most countercultural act of Christian fidelity to the law of God. This famous Encyclical continues to be attacked by a wide swath of modernizers, from top Vatican officials to the usual suspects at the National Catholic Reporter. In view of this determined resistance that shows every sign of continuing for another half-century, it would be appropriate to reflect on the deepest reasons why Christians must reject artificial contraception.
It is not merely because the practice of this vice leads to evil consequences, such as selfishness in relationships, unbridled lust, treating children as objects and possessions, and demeaning the personal dignity of the body by turning it into an object. No, it is because the fertility of man is a sublime gift, an imitation of God Himself, a way in which we participate in His act of creation and providence.
The greatest pagan philosophers already recognized this truth. Plato saw fertility as the expression sought by beauty: beautiful things naturally seek to multiply themselves. Proclus saw fertility as the metaphysical property of goodness: anything truly good spreads itself. Aristotle saw it as the way in which all things strive to partake of the divine fullness of life: if one cannot exist eternally, like God, one can echo that eternity through offspring.
It is no accident that ancient religions were characterized by cults, rites, and offerings focused on fertility. The central theme of wedding ceremonies was always fertility, begetting and bearing new life. Traditional initiation rites centered around the new and mysterious power of generation—boys became men, and girls women, because they could now exercise paternity or maternity, in common with their elders in society. And always, there was seen to be something godlike in this power of procreation, because it reflected the power of creation hidden in the depths of nature or in the heart of the creative God. Just as man was called upon to exercise “providence” or foresight in imitation of God, so, too, he was called upon to participate in the work of creation.
This is what pagans already perceived, still groping in the shadows of a world without revelation, unenlightened by the splendor of the Christian truth that God Himself lives a life of infinite fruitfulness in the relations of the Most Holy Trinity!
When man can dominate his ability to have children and uses this dominion to prevent children from coming into existence, this abusive power already shows a divorce between his life (a parcel of particular desires, ambitions, anxieties, etc.) and the goodness of life itself, which is endlessly sharable, as in the Blessed Trinity. In other words, even if a man or woman finds his or her own existence a good, being itself is not felt to be a good to be multiplied. Existence is either neutral or negative; one brings a child into the world calculating the net profits and losses.
Life is the first and most basic good, the one prior to and foundational of all others. We are talking here about an unconscious, prevoluntary attitude: the love of life simply speaking, and the innate desire to share it, produce it, foster it, rejoice in it. If ever children are not the focus of a young man’s or young woman’s desires in thinking ahead to marriage, both the individual and the society must be profoundly diseased. There has been an atrophying of the will to live; the most elemental love of all, love of being, has waned almost to the point of vanishing. Contraception therefore points to spiritual death, the death of the natural “love affair” with life.
Hence, what Paul VI was upholding with Humanae Vitae was not some kind of arbitrary “rule,” an enforced mortification of human desire. He was upholding the goodness of being, the beauty of creation, the godlike gift of procreation, the call to go beyond ourselves in love.
Since the advent of birth control more than 50 years ago, women have repeatedly been told that the drugs and devices being offered to help them avoid pregnancy are “safe and effective.” We’re told that the “small percentage” of women who experience adverse reactions is so minimal the risks simply don’t outweigh the benefits.
We believe all women’s lives matter, no matter how small the “percentage.” And we also believe women deserve the facts about the “safe and effective” drugs and devices they’re using, and why incidents of serious injury – even deaths – have been increasing in recent years with the introduction of a variety of trendy new birth control products.
The following is a list of some of the shocking and largely unreported details of a spate of major lawsuits that have been occurring in just the last decade.
• Although they say the number of serious illnesses resulting from birth control use is small, consider the 12,000 lawsuits currently pending against Bayer HealthCare Pharmaceuticals, Inc., the manufacturer of the trendy new Yasmin and Yaz pills. These pills, which contain the new “fourth generation” progestin known as drospirenone, have been linked to blood clots, gall bladder disease, stroke, heart attack and death in young women. (Source: Lawyers and Settlements.com) Note: If you’re wondering why we don’t hear about these cases, consider the fact that in 2008, Yaz accounted for 17.7% of the birth control market with sales of $616 million and Yasmin had 11% of the market with $382 million in sales. (Source: AboutLawsuits.com)
• Proponents like to point out that even though the pill was declared a Class 1 carcinogen by the World Health Organization in 2005 – which means it has been found to cause cancer in both laboratory and human studies – it has also been found to offer protection for certain types of cancers, such as ovarian and uterine. This is true, but the pill is also known to cause cancers, such as breast, cervical and liver cancers. (Source: American Cancer Society; Burkman R, Schlesselman JJ, Zieman M. Safety concerns and health benefits associated with oral contraception. American Journal of Obstetrics and Gynecology; 190(4 Suppl):S5–22.) In other words, you might not get ovarian or uterine cancer, but you could get breast, cervical or liver cancer. How safe is that?
• The British Medical Journal revealed that the pill also increases a woman’s risk of developing cerebrovascular disease (hypertension and stroke) by 1.9 times. A 25 year follow-up study with 46,000 British women also noted that the enhanced risk of death lasts for 10 years after women have stopped taking the pill. At particular risk are women who are overweight, sedentary, frequently take long plane flights, injure a leg, have had recent surgery, smoke, have a family history of blood clots, have high blood pressure (over 160/100mg) or suffer from migraines – a list that probably includes 80% of the adult female population of the U.S.
• Forms of artificial contraception that deliver hormones by means other than pill form have also been found to be dangerous, such as the Ortho-Evra patch, which delivers hormones through the skin by use of a patch. Johnson & Johnson and its subsidiary Ortho McNeil, manufacturer of the Ortho Evra Patch, has thus far paid $68.7 million to settle more than 4,000 state and federal lawsuits brought about by women who have suffered adverse side effects, from blood clots to heart attack and stroke. Ortho Evra has also been blamed for 20 deaths. (Source: Lawyers and Settlements. com)
• NuvaRing is no better. This is a vaginal ring that delivers hormones directly into the bloodstream, stopping ovulation by releasing a combination of the hormones estrogen and progestin into the body. This delivery causes what expert witnesses call hormone “spikes” that make women more susceptible to blood clots. In some cases, the blood clots were fatal. In 2014, the manufacturer, Merck, settled more than 1,700 lawsuits for a combined $100 million to litigants who claimed the active ingredient in the drug, etonogestrel, was inadequately tested before NuvaRing’s 2002 release. (Source: DrugWatch.com)
• Then there are the “devices” such as Essure, which consists of flexible metal coils that are inserted into the fallopian tubes. The coils create an infection which causes scar tissue to form, thus closing off the tubes and rendering the woman sterile. The problem is that the coils can dislodge and travel into the body where they have been known to lodge in, or perforate, organs. It has also been known to cause fetal disfigurement due to nickel poisoning. Chronic pain, exhaustion, bouts of depression and suicidal thoughts have also been reported by women who have used the device. After receiving thousands of reports of adverse effects from the device, Bayer AG, the manufacturer of the device, decided to halt sales in the U.S. effective December, 2018. Why did it take so long to ban this dangerous device? And why were calls for more testing answered by the same company that is profiting off the sale rather than independent researchers? And why weren’t these tests completed before the product was launched? This is what more than 27,000 injured women – known as the “E-sisters” – want to know. They banded together along with activist Erin Brokovitch and successfully got this product off the market. (Source: FDA , Essure Problems Facebook page)
• Mirena’s track record is just as bad. This IUD is manufactured by Bayer and is referred to as a “second generation” contraceptive because it contains levonorgestrel, a synthetic hormone that sometimes prevents ovulation. It has significant and very painful side effects, such as amenorrhea, intermenstrual bleeding and spotting, abdominal pain, pelvic pain, ovarian cysts, headache, migraines, acne, depression, and mood swings. Like Essure, the device has a tendency to migrate outside the uterus. According to AdverseEvents.com, the top three adverse events related to the use of Mirena were device expulsion, device dislocation and vaginal hemorrhage, with more than six percent of patients requiring hospitalization or surgery. In spite of this, Bayer continues to hawk this product, particularly to busy moms, even though the FDA scolded them in 2009 for overstating its efficacy and understating its risks. To date, the product remains on the market and rakes in more than a billion dollars a year for Bayer. (Source: Lawyers and Settlements.com)
• And let’s not forget the injectable contraceptives known as Depo-Provera. This contraceptive, which is a favorite of population controllers working in third world countries, comes with a black box warning stating that prolonged use of the drug may result in significant loss of bone density. The loss is greater the longer the drug is administered – and it may not be completely reversible after discontinuation of the drug. In addition, there are 45 other adverse effects women can experience from taking this drug. (Source: FindLaw.com) A 2010 study found that, after just two years of using Depo, almost half the women in the study (47.4 percent) had lost at least 5 percent of bone density at the spine or hip and continued to experience significant bone density losses in subsequent years of use. (Source: Rahman M, Berenson A, “Predictors of Higher Bone Mineral Density Loss and Use of Depot Medroxyprogesterone Acetate,” Obstetrics & Gynecology 2010: 115(1): 35-40)
In just the few examples documented here, it’s obvious that our bodies are being used as “laboratories” for the testing of dangerous drugs by the U.S. birth control industry which is expected to be worth $19 billion by 2020. They say the numbers of women injured are small, but because experts believe most adverse events are not reported, it’s safe to say we’re talking about millions of women who are experiencing problems with today’s birth control. For instance, if an estimated 37 million American women are currently using birth control, even five percent of that number is more than one million women! Maybe that’s not much compared to those who use it without problems, but those one million lives matter to the people who love them – and they matter to us.
So spread the word! No matter how small is the “percentage” of women harmed by these drugs and devices, every woman’s life matters!
In 1996 St. Pope John Paul II, speaking to a group of teachers of Natural Family Planning (NFP), boldly declared: “The moment has come for every parish and every structure of consultation and assistance to the familyand to the defense of life to have personnel available who can teach married couples how to use the natural methods.”
Meanwhile, this Wednesday we commemorate the 50th anniversary of Humanae Vitae. On this occasion we must pause and ask: How well have we implemented Pope Paul VI’s teachings, and how well have we lived up to St. Pope John Paul II’s hopes?
One article reports that according to a 2016 study by the U.S. bishops, “53 percent of dioceses spent less than $5,000 per year on NFP programs; 19 percent budgeted more than $30,000 a year for such programs. The study also found that 49 percent of NFP instructors in parish programs were unpaid volunteers.”
In the same article, a representative of the United States Catholic Conference of Bishops (USCCB) stated that more than half of U.S. dioceses have what the article termed “strong” NFP ministries. But if 53 percent of dioceses are spending less than $5,000 – scarcely enough to cover photocopying for the year, let alone to pay trained, full-time personnel – it’s hard to see how this could be possible. Even the $30,000 that just 19% of dioceses spend isn’t enough to cover the salary of a single full-time, trained staff member.
And if dioceses, many of which have budgets in the tens of millions of dollars, aren’t committing any meaningful resources to NFP programs, how many parishes are doing so?
Furthermore, if this is the situation in one of the wealthiest countries in the world, what is it like in poorer countries, where Catholic couples are far more likely to face difficulties like abject poverty and lack of access to basic health care, even as they are bombarded by foreign-funded pro-contraception propaganda.
One 2008 study gives a bleak look into the situation in at least one African country, Uganda. After surveying NFP training by the Catholic Church in one of the most densely-Catholic regions in Uganda, the study authors concluded: “There were no budgets, supplies, registers, teaching aids, and no records of NFP clients were kept. No space for NFP clinics was provided and there was no arrangement for continuous professional education (CPE) for NFP providers. Basic knowledge about NFP e.g. the role of breastfeeding and periodic abstinence was acquired from friends. Knowledge about NFP methods was insufficient among clients to the services and in some health workers.”
In many cases, the study’s findings directly match what we at Human Life International have seen over the past four decades of international missionary work. Because of our global footprint and experience we have witnessed firsthand the dearth of NFP programs and its negative consequences. We have also seen the positive impact when NFP is preached and taught as a good for spouses and married couples are given proper formation and education, supported and nurtured and there is continuous oversight and formation of training couples and teachers.
The study authors urged the Catholic Church “to provide political commitment to NFP, invest more in and reinvigorate the teaching of NFP methods through their structures” and to provide “support supervision on NFP access and use within [Catholic] health facilities.” Though the authors were clearly pro-contraception themselves, ironically, they placed higher expectations on the Church to live up to its teachings than even many Catholics. If the Catholic Church truly believes what it says it believes, then why – they rightly asked – is the Church doing so little to help Catholics in the pews learn NFP?
We’re Losing Souls
St. Pope John Paul II decried the fact that, due to misunderstandings and a tendency to treat NFP as a purely “functional” technique apart from the “ethical dimension,” some people had come to view NFP methods as just another form of contraception. “But this is certainly not the way they should be viewed or applied,” he said. Not only does NFP respect God’s moral law and foster growth in virtue when used according to the Church’s guidelines, but the Church always presents it as part of a broader message about the theological truth about marriage, the God-given purpose of sexuality, and generous openness to life.
Nevertheless, in its efforts to preach the truth about marriage and sexuality to Catholics, to a large extent the Church is in direct competition with the contraception industry. This vast, ubiquitous, and powerful industry, flush with cash and marketing savvy, is luring huge numbers of Catholics away from the truth about human sexuality with its deceptive, but slick message of easy, consequence-free sex. They’re in our schools, on our TV’s, in our magazines…everywhere.
And they’re winning. According to some statistics, well over 90% of self-professed Catholic women have used contraception at some point. One huge survey found that 79% of self-professed Catholics in the U.S. support contraception. Meanwhile, meaningful knowledge about NFP remains confined to a relatively tiny sub-set of faithful Catholics.
An Untenable Situation
If we truly believed that using contraception is a grave sin, as the Church teaches, then it seems self-evident that our priests and bishops would be preaching the message of Humanae Vitaefrom the pulpit regularly. And if we really believed that NFP is good for Catholic couples when used in accord with Church teaching, we would be pouring resources into developing sophisticated, evidence-based and faithful NFP-training materials and programs, translating them into numerous languages and implementing them in all dioceses and parishes around the world. Nor would we hesitate to invest time and money in studying the effectiveness of these programs using the best scientific and statistical techniques available.
We would be hiring highly trained NFP experts to serve in diocesan offices and parishes to provide individualized support to couples. We would be creating consistent, nationally recognized standards for training NFP teachers as well as national, easily searchable databases where couples could search for local NFP instructors. We would be advertising NFP-training resources in every parish bulletin, every week. We would be providing funding for low-income families who cannot afford the costs of NFP instruction, which in my opinion should be free. We would be holding regular and well-advertised NFP training sessions around the diocese to educate already-married couples and incorporating NFP into pre-marital preparation programs – and not just a one-hour course or weekend program.
We would be opening Catholic NFP clinics staffed with Catholic doctors and nurses. We would be hiring talented writers, designers and programmers to create attractive and user-friendly websites, apps, videos, hand-outs, booklets, advertising, and other teaching aids to make it as easy as possible for Catholics to learn about NFP. And last, and perhaps most importantly, we would be investing in new technologies and scientific research to refine our understanding of the science of fertility and to make it easier for couples to use NFP.
As St. Pope John Paul II exhorted: “It is necessary on the one hand to be committed in the medical field to disseminating knowledge of the scientific basis for the natural methods of fertility regulation, and on the other, to promoting study and research on the nature of the biochemical and biophysical events that accompany and indicate periods of fertility, leading to an easier and more reliable exercise of responsible parenthood.”
Much NFP Training Woefully Inadequate
I don’t at all mean to overlook the many Catholic organizations and individuals who already aredoing incredible work along these lines. Many of them are doing heroic work under difficult conditions: often with little or no funding or other resources. Many of the volunteers involved in NFP education heroically sacrifice enormous amounts of their time and resources, while even many paid NFP teachers work for a fraction of what they might make in the secular work force.
As the Pope of Life wrote in Evangelium Vitae: “The Church is grateful to those who, with personal sacrifice and often unacknowledged dedication, devote themselves to the study and spread of these methods, as well as to the promotion of education in the moral values which they presuppose.”
Nevertheless, we must be honest in taking stock of where we are. Clearly, we are leagues away from reaching St. Pope John Paul II’s dream of having well-trained personnel available to educate Catholics in every parish.
It seems to me that there are two obstacles to fulfilling St. Pope John Paul II’s wishes. The first is by far the most serious: the vast complacency and outright dissent against Humanae Vitae among some bishops, priests, theologians and Catholics in the pews. Many bishops and pastors invest nothing or very little in teaching Humanae Vitae and NFP. How this can be solved is another topic for another day.
The second obstacle is much subtler: it is that understandable concern among some faithful Catholics that by vigorously promoting NFP we may give the impression that we are promoting “Catholic contraception.” At times, indeed, this concern is thoroughly justified, as we discussed in last week’s column. In no way do I wish to diminish this concern. However, St. Pope John Paul II was absolutely clear that the solution to this concern is not to hide the Church’s teaching under a bushel, and to cede the field to Planned Parenthood and their ilk, who are more than happy to fill the void.
Instead, organizations and campaigns that promote contraception and its “utilitarian” worldview, he said, “must be answered with every initiative that can support scientifically and with correct information the validity of natural methods, in accordance with the Church’s constant teaching.”
The solution is to put serious thought, effort and resources into creating programs that fully and authentically transmit the whole of Church teaching. St. Pope John Paul II was clear that when he urged the Church to educate couples in NFP, he didn’t just want the Church to teach a certain set of physical techniques, but rather the whole theology of marriage, of which periodic abstinence to postpone pregnancy for grave a reason forms but one part. NFP, he said, must always be “taught and presented in a suitable anthropological and ethical context.”
As I have heard from so many couples, the NFP training in most parishes is woefully inadequate, if available at all. At best, engaged couples are given an hour or two of instruction, much of which is presented by eager, but untrained volunteers tasked with the impossible: convincing many already-cohabiting and contracepting couples to follow a teaching that they view as burdensome and which they have never heard compellingly preached or explained. Often, there is only enough time to give the basic talking points, which, as I observed last week, sometimes tend only to unrealistically emphasize how “easy” NFP can be, without addressing the deeper spiritual perspective or equipping couples to sort through the inevitable challenges.
The Church’s teaching on contraception and NFP is clear. It is time now for visionary Catholic leaders to step up to the plate to find ways to fulfill St. Pope John Paul II’s dream. The time is ripe for this effort. Increasingly, even many non-religious people are coming to view artificial contraception with suspicion. If only we were confident in proclaiming the truth taught to us by the Church, we could capture so many souls for Christ, deal a death-blow to the hedonistic, materialistic worldview of the population controllers, help strengthen marriages and families, encourage openness to life, and challenge couples to mutually pursue virtue.
Wanda Półtawska, a Polish doctor, is 97 years old. Her life and work is unknown outside her native Poland and some quarters of the Catholic Church, but her insights and influence have prospered the mission of the Church in defending the dignity of all human beings.
Equally unknown by most people is the long, close friendship she and her family enjoyed with Karol Wojtyla, later Pope John Paul II. In the 1960s, she advised him on family dynamics and sexual issues, including the newly developed contraceptive pill.
Through this relationship her views on artificial birth control are likely to have influenced Pope Paul VI in his writing of the encyclical Humanae Vitae, which ruled out family planning methods like the pill. Indeed, one biographer of John Paul II claims that not only her ideas but “in some cases her exact words can be found in the text.” (See note below)
The pill, in Dr Półtawska’s judgment, was no friend of married love and still less a healthy choice for women. She saw it as an assault on a woman’s dignity bringing not freedom, but a form of moral enslavement. It was a spoiler of love between spouses, an excuse for men to shirk their paternal responsibilities, and a straight path to abortion, pornography, sexual abuse and euthanasia. It was, in short, a destructive tool for the agendas of radical politics.
Having been herself a victim of the medical experimentation carried out by the Nazis during World War II, she also saw the pill as a tool of the eugenics movement for eliminating racially impure human beings.
Wanda Półtawska was just a slight teenage girl when she was dragged away to prison by four big men of the Gestapo. She spent most of the next four years in Ravensbrück concentration camp, where she, along with others, experienced the extreme of what was meant by eugenics. She endured having injections of bacteria into wounds deliberately created in order to observe the effect. This indescribably horrible and painful ordeal is recorded in her memoir, And I Am Afraid of My Dreams.
Before her incarceration, Wanda had been preparing to become a Classical scholar and teacher. But while in the hell of Ravensbrück she resolved that if she survived she would become a good doctor. Weak and disfigured in her legs, she did survive, went home and began her medical studies.
She married Dr Andrzej Półtawski in 1947, and they had four daughters. She completed her medical studies in 1951 at the Jagiellonian University, and in 1964 completed her doctorate in psychiatry, specializing in the care of sexual abuse victims and disorders of concentration camp survivors, whom she called her “Auschwitz children”.
By providential chance, sometime in the mid-1950s, Dr Półtawska took a pilgrimage with other Catholic doctors to the Shrine of Our Lady of Częstochowa, where she happened to meet Karol Wojtyla, assistant bishop of Krakow. She and her husband became close friends of the bishop, often discussing with him matters closest to their hearts and lives: chaste sexuality, marital relations, religion, theology, family life, marriage, celibacy, contraceptives, communism, philosophy and the changing times in the church and world.
Continuing pro-life work she had already begun with other women in the Krakow archdiocese before she met Bishop Wojtyla, she became his chief assistant in developing and managing programmes of marriage and sex counseling, as well as family and health care ministry there. This included a home for unwed mothers run by volunteers, which survived harassment by the communist authorities from 1957 to 1965, when it was forced to close.
She taught natural family planning, but took care to emphasize the possibility of conception and the importance of spouses remaining open to a child in their sexual relations, as Humanae Vitae was to reaffirm.
When, in 1962, Dr Półtawska was diagnosed with malignant colon cancer, Bishop Wojtyla – then in Rome for the opening of the second Vatican Council — wrote and asked for the prayers of the Italian mystic Padre Pio, with whom he was acquainted. In 1947, the newly ordained Fr. Wojtyla had been to visit the Capuchin friar and spent a week in San Giovanni Rotunda where they talked together. When, 15 years later, Padre Pio received Wojtyla’s hand-delivered letter with the urgent request, he agreed to honour the written plea. A few days later the Polish doctors prepared to operate on their colleague, but they found that the cancer had vanished; there was no tumor upon which to operate. This healing, which had no medical explanation, was cited as one of the miracles contributing to the canonization of Padre Pio in 2002.
With her strong understanding of family, Dr Półtawska contributed to Wojtyla’s book on romantic theology, Love and Responsibility, with its theme of sexual love between husband and wife. At a time when the topic of women’s sexual experience was not spoken of openly, but largely assumed to be the same as the male’s experience, she threw Freudian psychology on its ear by openly insisting that husbands get over their selfishness and train themselves to cherish their wives and caress them lovingly in slow and intimate ways so that their wives might know spousal love through female orgasm. At the same time she criticized “the myth of orgasm”, that is, the contemporary pursuit of pleasure for its own sake.
Wanda Półtawska’s faith, service, wisdom and love were forged through extreme suffering. Having experienced the vilest of indignities during the Second World War, she became a powerful witness for human dignity and for purity in intimate matters. Holiness in marriage and in the priesthood, decency and proper regard for the health of women were greatly needed in a critical moment of the dark 20th century.
Although the backwash of controversy following Humanae Vitae was violent and divisive, 50 years later there is a change, if not yet peace. The wisdom and sanity of that encyclical is beginning to be realized within and beyond the church and even, implicitly, in the secular world, where young women unhappy with hormonal contraception are turning to natural methods of family planning.
Indeed, the pill has been a bitter one, with many evil consequences, all foretold by this little known Polish doctor, wife, mother and concentration camp survivor.
Ruth Lasseter lives in a three generation household in St Paul, Minnesota. Mother of six and grandmother of 17, she contributed with her late husband Dr Rollin A. Lasseter to the Catholic School Textbook Project, and served in the Moreau Seminary (1983-84) as the “Voice of the Family”. Her article on contraception and sterilization, “Sensible Sex”, appeared in “Homiletic and Pastoral Review” and also in Why Humanae Vitae was Right (1993) by Dr Janet E. Smith.
ROME, July 19, 2018 (LifeSiteNews) — At the beginning of 2017, Pope Francis set up a “study commission” to prepare for the 50th anniversary of Humanae Vitae (July 25, 2018). The existence of this “secret” commission was brought to light some months after by two Catholic publications, Stilum Curae and Corrispondenza Romana.
The commission, coordinated by Msgr. Gilfredo Marengo, was tasked with finding in the Vatican Archives the documentation relating to the preparatory work on Humanae Vitae which took place during and after Vatican Council II.
The first fruit of this work is the volume by Monsignor Gilfredo Marengo, The birth of an Encyclical. Humanae Vitae in the light of the Vatican Archives [La nascita di un’Enciclica. Humanae Vitae alla luce degli Archivi Vaticani], published by the Vatican Publishing House. Other publications perhaps will follow, and other documents will presumably be submitted privately to Pope Francis.
Dr. Roberto de MatteiSteve Jalsevac / LifeSiteNews
From a historiographical point of view, Msgr. Marengo’s book is disappointing. Regarding the genesis and consequences of the encyclical Humanae Vitae within the context of the contraceptive revolution, the best book, to my opinion, is the one by Renzo Puccetti, The poison of contraception [I veleni della contraccezione] (Dominican Edizioni Studio, Bologna 2013).
Msgr. Marengo’s study does, however, contain some new elements. The most relevant is the publication of the complete text of an encyclical De nascendi prolis(pp. 215-238), which, after five years of tormented work, Paul VI approved on May 9, 1968, fixing the date of its promulgation on the Solemnity of the Ascension (May 23).
The encyclical, which Msgr. Marengo calls “a rigorous pronouncement of moral doctrine” (pg. 104), was already been printed in Latin when a surprising twist occurred. The two French translators, Msgr. Jacques Martin and Msgr. Paul Poupard, expressed serious reservations about the document’s overly “traditional” approach. Disturbed by the criticism, Paul VI worked personally on numerous modifications of the text, changing above all its pastoral tone, which became more “open” to the cultural and social demands of the contemporary world.
Two months later, De nascendi prolis was transformed into Humanae Vitae. The Pope’s concern was to ensure that this new encyclical “would be accepted in the least problematic way possible” (p. 121), thanks not only to the reformulation of its language, but also to the devaluation of its dogmatic character (p. 103).
Msgr. Marengo recalls that Paul VI did not accept the invitation of the Archbishop of Krakow, Karol Wojtyla, to issue a “pastoral instruction, reaffirming without uncertainty the authoritativeness of the doctrine of Humanae Vitae, in the face of the widespread protest movement against it” (p. 128).
The objective, or at least the outcome, of Msgr. Marengo’s book, seems to be to relativize the encyclical of Paul VI, which is presented as one phase in a complex historical path that does not end with the publication of Humanae Vitae, nor with the discussions that followed it. One cannot “claim to give a ‘definitive’ word and to close down, if ever there were need, the decades-long debates” (pg. 11).
On the basis of the historical reconstruction of Msgr. Marengo, the new theologians who refer to Amoris laetitia will say the teaching of Humanae Vitae has not changed, but must be understood as a whole, without limiting oneself to the condemnation of contraception, which is only one aspect of it. Pastoral care — it will be added — is the criterion for interpreting a document that reminds us about the Church’s doctrine on the regulation of births, but also of the need to apply it according to wise pastoral discernment. In the final analysis, it is a question of reading Humanae Vitae in the light of Amoris laetitia.
Humanae Vitae was a painful (as Paul VI himself called it) and certainly courageous encyclical. Indeed, the essence of the 1968 Revolution was captured in the saying “it is forbidden to forbid,” a slogan that expressed the rejection of every authority and every law, in the name of the liberation of instincts and desires.
Humanae Vitae, in reiterating its condemnation of abortion and contraception, recalled that not everything is allowed, that there is a natural law and a supreme authority — the Church — which has the right and the duty to protect it. Humanae Vitae, however, was not a “prophetic” encyclical. It would have been so, had it dared to oppose the false prophets of Neo-Malthusianism with the divine words “Increase and multiply.” (Genesis 1:28; 9:27).
Yet it did not do so, because Paul VI, in his fear of colliding with the world, accepted the myth of the demographic explosion, launched in 1968 by Paul Ehrlich’s book, The population bomb. In 2017, Ehrlich himself was invited by Msgr. Marcelo Sánchez Sorondo to reiterate his theories on overpopulation at the conference organized by the Pontifical Academy of Sciences. The conference was titled: Biological Extinction. How to save the natural world we depend on(February 27 – March 1, 2017).
In his book, the author described the catastrophic scenarios that the inhabitants of Earth would have to face if measures were not taken to contain population growth. What the encyclical rightly condemns is artificial contraception, but without rejecting the new “dogma” of the necessary reduction in births. Humanae Vitaereplaced Divine Providence, which up to that point had regulated births in Christian families, with the human calculation of “responsible parenthood.”
However, the Magisterium of the Church does dogmatically state that contraception is to be condemned not only because it is an un-natural method in itself, but also because it is directly opposed to the primary end of marriage, which is procreation. If one does not affirm that the procreative end prevails over the unitive one, one can maintain the thesis that contraception can be lawful when it undermines the “intima communitas” of the spouses.
John Paul II vigorously reaffirmed the teaching of Humanae Vitae, but the concept of conjugal love that spread under his pontificate is at the origin of many misunderstandings. In this regard, I refer to the precise observations of Don Pietro Leone, the pseudonym of an excellent contemporary theologian, in his book The Family Under Attack [La famiglia sotto attacco] (Solfanelli 2017).
In the last 50 years, due also to a misguided understanding of the ends of marriage, papal teachings were disregarded, and among Catholics the practice of contraception and abortion, extra-matrimonial cohabitations, and homosexuality have become widespread. The post-synodal Exhortation Amoris laetitia represents the result of an itinerary that has been a long time coming.
Repeating almost verbatim the words spoken on October 29, 1964, in the Council hall, by Cardinal Leo-Joseph Suenens: “It may be that we have accentuated the word of Scripture, ‘Increase and multiply,’ to the point of overshadowing the other divine word, ‘The two will be one flesh’,” Pope Francis said in Amoris laetitia. “We often present marriage in such a way that its unitive meaning, its call to grow in love and its ideal of mutual assistance are overshadowed by an almost exclusive insistence on the duty of procreation” (n. 36).
Reversing these words, we could say that in recent decades we have almost exclusively accentuated the biblical word, “The two will be one flesh,” to the point of overshadowing the other divine Word: “Increase and multiply.” It is also from this deeply meaningful Word that we must set out again towards not only a demographic, but also spiritual and moral, rebirth of Europe and the Christian West.
This article originally appeared in Italian at Corrispondenza Romana. This translation for LifeSite was done by Diane Montagna.
The American Board of Obsetrics and Gynecology wants a sub-specialty certification known as “Complex Family Planning” and it’s asking the American Board of Medical Specialties to approve it.
“But, see, the point of an abortion at that gestational age,” says Harrison, “is to make sure that the baby is dead. So it’s to produce a dead baby. It’s not to save a mother’s life.”
If that were the case, Harrison says the doctor would perform a C-section so the mother and child would have a chance at life.
The request for a medical specialty is a smokescreen for training doctors to do late-term abortions, and Harrison says there is no place in Hippocratic medicine to justify that.
“And there is no reason,” she tells OneNewsNow, “why there should be a board certification for doctors to be able to kill babies.”
“[U]sing the natural [family planning] methods requires and strengthens the harmony of the married couple, it helps and confirms the rediscovery of the marvelous gift of parenthood, it involves respect for nature and demands the responsibility of the individuals. According to many authoritative opinions, they also foster more completely that human ecology which is the harmony between the demands of nature and personal behavior.”
Pope Paul VI on the Benefits and Challenges of NFP
As numerous popes have made clear, couples who shun the temptation of contraception and follow the Church’s teachings on what St. Pope John Paul II called “responsible procreation,” open themselves up to a myriad of blessings. The most obvious is that couples who opt for natural family planning are far less likely to get divorced. Were this the one and only benefit, it would be sufficient reason to recommend the practice.
In Humanae Vitae, however, Pope Paul VI lists a host of other benefits. The use of periodic continence, he begins, has “the salutary effect of enabling husband and wife to develop to their personalities and to be enriched with spiritual blessings.” This practice, he said, “brings to family life abundant fruits of tranquility and peace.”
It also, he added, helps “in solving difficulties of other kinds. It fosters in husband and wife thoughtfulness and loving consideration for one another. It helps them to repel inordinate self-love, which is the opposite of charity. It arouses in them a consciousness of their responsibilities. And finally, it confers upon parents a deeper and more effective influence in the education of their children.”
Still, the pope also stressed the difficulties – “at times very great” – that couples face in striving to follow the Church’s teaching. “For them, as indeed for every one of us,” he added somewhat bleakly, “the gate is narrow, and the way is hard, that leads to life.” Acknowledging that some couples may become “deeply distressed” by the difficulties they face, and the real risk of failure on the part of some couples, he urged them never to “lose heart,” but to resort – “humble and persevering” – to the Sacrament of Penance.
A One-Sided Perspective
Unfortunately, in a well-intentioned, but misguided effort to lure couples away from contraception towards NFP, some teachers or preachers may occasionally paint an overly one-sided picture of NFP. In the very worst cases, this presentation can almost make NFP seem like a form of “Catholic contraception,” suggesting to couples that they can attain perfect control over their fertility at the expense of only the mildest inconveniences to their sex life or other plans.
Some teachers, for instance, may continuously emphasize how a few days a month couples might have to abstain from sex to postpone (avoid) pregnancy. Others will repeatedly point to statistics showing how reliable NFP can be, compared to contraception. Others might suggest that couples who use NFP often have more and better sex than their contracepting peers. Or they may wax eloquent on the “honeymoon effect” that can follow a period of abstinence.
None of these claims are wrong in themselves. However, without balance or a deeper perspective they can create an unrealistic and superficial picture of the Church’s teaching.
On a practical level, by creating overly rosy expectations, they set couples up for disappointment and failure. Not having been prepared for the inevitable difficulties of practicing NFP, such couples may feel tempted to give up after frustrating initial attempts, thinking they have been duped. Tragically, if their teachers have failed to transmit to such couples the rich spirituality of marriage and personal sanctity in which Pope Paul VI and other popes have always been careful to place this teaching, they will lack the tools they need to stay the course and reap its great benefits.
Why the Church Bias in Favor of Life
These couples may not, for instance, have been told about what we might call the Church’s “bias for life:” that is, the Church’s life-affirming teaching that procreation is the primary good of marriage. Indeed, so central is this teaching to the Church’s understanding of marriage, that She states that a couple that has the intention never to have children is incapable of contracting a valid sacramental marriage.
“Marriage and conjugal love are by their nature ordained toward the procreation and education of children,” states the Second Vatican Council. “Children are really the supreme gift of marriage and contribute in the highest degree to their parents’ welfare.”
This stands in stark contrast to the contraceptive mentality of our age, in which a couple typically enters a sexual relationship with the tacit understanding that children are only something to be discussed at a later date. Children thus become a mere accessory to a marriage, to be added on once a couple has discerned at excruciating length if they are “ready.”
Indeed, if couples only ever listened to worldly family planners, economists and other experts, they might think they never have a sufficiently stable relationship, enough money, a sufficiently promising clear career path, a big enough house, or access to good enough schools, to have a child.
Unfortunately, even many Catholic couples approach the altar having unintentionally absorbed this pessimistic, anti-child spirit of our age. Such as these may never have had the chance to learn what so many other Catholic couples have learned: that it is in trusting in God’s providence and taking reasonable “risks” by generously welcoming new life that they have been blessed with the greatest joys of their married lives.
For that reason, if NFP instruction only emphasizes perfect planning or pregnancy prevention (postponement) without challenging couples by speaking of the value of a generous openness to life, it deprives Catholic couples of an important part of the Church’s Good News about marriage.
Yes, NFP Can Be Difficult
Nevertheless, the Church is also clear that human beings also have a responsibility to exercise their reason while seeking the will of God in their lives, including in the area of procreation. If a couple prayerfully discerns that they have just reasons for postponing a child at this time, then (as numerous statements from popes have made clear) they may in good conscience have recourse to natural family planning.
It is true that some couples find practicing NFP relatively easy. Perhaps they have a knack for grasping the technical aspect of NFP, or the woman is blessed with regular, predictable cycles, or they have strong communication skills, etc. However, many other couples will not find things so easy. Such as these may experience NFP as a real cross.
They may, for instance, find the scientific principles of NFP confusing or difficult to apply to their circumstances. This can cause frustration and may lead to the need for long periods of abstinence. Or they may find that practicing NFP exposes a significant difference in libido between the spouses, so that one spouse feels that they are disproportionately shouldering the burden of abstinence. This can provoke feelings of emotional rejection and resentment, which may in turn lead to temptations to seek solace or sexual release in other, immoral ways (pornography, masturbation, etc.). On the other hand, the other spouse may feel unduly pressured to engage in sex, even when doing so might jeopardize the couple’s mutual agreement to postpone pregnancy for the time being.
Another common problem is that the woman may begin to resent that the couple’s sexual relations depends entirely on the patterns of her body. This can lead to a sense that NFP places undue pressure on her, or that she is at “fault” if her cycle is unpredictable or lengthy and requires difficult periods of abstinence. Furthermore, she may resent that it is typically when her sexual desire is at its height – the days leading up to ovulation – that the couple must abstain. The man, for his part, may feel uncertain to what extent or how he should be involved in the process of charting, etc., and can feel alienated or “out of the loop.” If the couple does not already have strong communication skills, they may find that practicing NFP exacerbates this problem, leading to painful miscommunications.
Finally, even when practiced perfectly (and it often isn’t), there is always the “risk” of an unplanned pregnancy when using NFP. If a couple was legitimately using NFP for just reasons, this will inevitably bring with it some degree of stress. Ironically, the hardest time to practice NFP is also in the woman’s post-partum phase, when her cycles are most unpredictable. Some couples will thus find that in addition to the challenges of a new baby, they must navigate the stress of long, uncertain periods of abstinence.
And these are only some of the challenges facing couples using NFP.
Such Difficulties As Some Experience Don’t Negate NFP
The first, and most important thing to note about these difficulties is that they are not a “bug” of NFP: they are a feature.
In reading the Church’s documents on periodic abstinence, you will nowhere find the popes promising couples an easy path. They do not promise lives planned with pinpoint accuracy to minimize suffering or uncertainty, or marriages characterized by an unlimited supply of pleasurable sex. On the contrary, they continuously emphasize that NFP requires the practice of self-denial. Furthermore, they insist, any benefits that NFP brings the couple are precisely because it requires self-denial.
As St. Pope John Paul II says in Evangelium Vitae, whether couples are currently open to life or seeking to postpone pregnancy, “The moral law obliges them in every case to control the impulse of instinct and passion, and to respect the biological laws inscribed in their person.” It is, says Pope Paul VI in Humanae Vitae, when the couple acquires “complete mastery over themselves and their emotions” that “the expression of love, essential to married life” will “conform to right order.” Then the couple will experience the “thoughtfulness,” “peace,” “tranquility,” and other benefits that Pope Paul VI promises.
Contrast this to the case of contraception. Whereas contraception promises couples endless pleasure and the security of the perfectly planned life with little or no sacrifice, instead it so often leads only to heartache, alienation and suffering. After all, if contraception were the panacea its advocates promise it to be, then why do so many contracepting couples feel sexually unfilled or emotionally alienated? Why do so many contracepting couples get divorced? Why does so much contracepted sex end in the abortion clinic?
Practicing NFP, on the other hand, can serve as a crucible, exposing the weaknesses of the couple as a couple, or as individuals: bad communication habits, emotional immaturity, a lack of self-control in areas of sexuality, a slavery to the spirit of the world, a weak prayer life or lack of trust in God, etc.
At these times, Catholic couples committed to faithfulness to the Church will find that they are instinctively driven to deeper prayer and to sacrifice. Complacency is no longer an option. The difficulties of NFP have exposed the ways that they urgently need to develop their personalities and their relationship. The couple has no option but to learn to communicate better. They must learn to pray together. They must deepen their concept of love, and learn other, non-sexual ways to express intimacy. They must learn to sacrifice immediate gratification for the sake of the long-term welfare of the other spouse and their family. They must begin to fast more in order to bring their passions under control. And thus, will they prove St. Paul right that “in weakness I am made strong.”
As Pope Paul VI exhorted couples struggling with this teaching: “let them implore the help of God with unremitting prayer and, most of all, let them draw grace and charity from that unfailing fount which is the Eucharist.” And to priests, the pope exhorted: “Teach married couples the necessary way of prayer and prepare them to approach more often with great faith the Sacraments of the Eucharist and of Penance.”
The reason that couples that practice NFP so rarely get divorced is not, I believe, because NFP removes any difficulties in their marriages. Rather, it is because: a) They already have a deep commitment to transcendent ideals about marriage, including an understanding of love as other-oriented and rooted in self-sacrifice, and b) The primary mechanism of NFP – self-denial – forces the couple to forthrightly address their weaknesses as a couple and as individuals, opens their hearts to a supernatural perspective, and drives them to a greater dependence on God’s grace.
Peace in this life is not found in indiscriminately following our passions. It is found in gaining mastery over our passions, and directing them towards a transcendent ideal, in accord with God’s law. The “complete mastery” over ourselves and our emotions that Pope Paul VI exhorts in Humanae Vitae is the work of a lifetime. Our efforts will be punctuated by failures and times of frustration. But in the end, the rewards are worth it: a growth in virtue, and a deepening of our relationship with our spouse and with God.
IT IS WAR! NO, ITS NOT POISON GAS THE ENEMY IS USING, IT IS ESTROGEN. IT IS IN THE TAP WATER. WHEN MY VOICE STARTED CHANGING FROM BASS TO TENOR I STARTED DRINKING DISTILLED WATER AND NOW I AM A BARITONE !!!
“I used to not pay too much attention to the whole gender-mix up issue because I know from my science training that there are a certain number of humans born with the sex chromosomes of both genders. They may be true hermaphrodites or just mosaics who look like one gender but feel the feelings of the other. I always felt sorry for them, knowing that the road they were about to go down would be difficult, confusing, and sad – not of their own making but rather a result of mixed-up genes. But they were, by far, in the minority.
So it’s with a lot of curiosity that I watch the unfolding of this issue in the media. Every day it seems we have another celebrity with a trans-child or a sad story of a person who falls under one of the letters of the LGBTQ (have I left any letters out?) acronym, the poor victim of heartless right-leaning (of course!) friends and family members. And I have to ask myself, are there really that many kids who struggle with this issue or is it just the latest “cause célèbre” of the more left-leaning of us? As this article points out, are we actually fostering the creation of MORE mixed-up kids in the attempt to be kind-hearted?
The thoughts in this article also fall into line with something my late husband used to complain about: the feminization of the American male. He was a medical researcher at a leading research institute, and even though this was not his area of investigation, he was quite concerned about it. When our first son, now in his 30’s, went to school and encountered a bully, the headmaster taught him how to box and told him that the only way to stop a bully was to stand up to him. My son did stand up to him and the bully backed down, leaving school, in fact. Good riddance! Two decades before, two other students with a long-standing feud were given boxing gloves and told to go settle their differences in the courtyard, with their parents’ blessing. It worked and they finished with bloody noses and a new-found respect for each other. Do you think that would EVER happen today. Never!
Our good friend, who worked for the state version of the EPA, concurred with my husband from a environmental point-of-view. She tested the water we drank and swam in and admitted that it was virtually impossible to remove all of the estrogen, that women urinated out after taking the Pill, from our drinking water . She looked at the amphibians in the streams and estuaries downstream from water treatment plants and found that they were either outright females or at least hermaphrodites. There were fewer and fewer males. I asked what will happen in the long-term when the levels of estrogen keep coming in above “safe” levels. She just shrugged and said, “Oh they’ll eventually just raise the level that’s considered “safe”. Do you really think the Big-Pharma PACs are going to allow the state to do anything to actually solve the problem?” I actually downloaded the last report of the water testing in my local area and the estrogen level was not even tested. It gave me the chills.
So folks, it’s only going to get worse. Our males are under attack, both societally and environmentally, and who knows what the outcome is going to mean for our nation?”
July 12, 2018 (LifeSiteNews) — I’m often told, when I address the transgender ideology, that it is an exaggeration to claim that trans activists actually wish to impart their ideology to children. Surely, people say, all trans activists really want to do is help teenagers who are grappling with genuine issues of gender identity and confusion—and thus to claim that trans activists wish to impart or apply their ideology to young children is simply fear-mongering. I wish that were the case, but a survey of the evidence indicates that this analysis is about facts, not fearmongering.
To illustrate just how radical the transgender ideology is, consider some advice given to parents at a 2016 conference (attended by over 400) people by Dr. Diane Ehrensaft, who is a developmental psychologist and the author of The Gender Creative Child. She is one of the key proponents of determining a child’s gender through careful observation, followed by affirmation of whatever the child says or acts upon—including very early transition, if that happens to be the case. She is a very influential figure within the trans movement, sitting on the board of directors of Gender Spectrum, a San Francisco trans advocacy organization, as well as serving as the director of the University of California-San Francisco children’s hospital gender clinic.
If you would like to understand what the transgender movement is all about, you can watch the 2016 Jon E. Nadherny/Calciano Memorial Youth Symposium in its entirety. The guest speakers bluntly lay out their agenda and explain how they are capturing the hearts and minds of the next generation, resulting in both sky-rocketing numbers of trans-identified youth as well as young people supportive of the trans ideology. One speaker showed a cartoon that had one parent asking another parent who was pushing a stroller whether her child was a boy or a girl. “I don’t know,” the mother replied. “It can’t talk yet.” It wasn’t meant as a joke.
After Ehrensaft’s presentation, one mother stood up to ask how best to “explain gender to a three, for, and five-year-old? My daughter asks a lot of questions about gender expression and identity without knowing what she’s asking, but I don’t quite have the language to talk to her about it…Is that a boy, is that a girl, what does it mean to be a boy, what does it mean to be a girl? Is it because they have a penis? Is it because they have a vagina? And I don’t quite know how to use language to talk about gender…” Dr. Diane Ehrensaft’s answer gives a clear picture of how trans activists wish to impart the ideology of gender fluidity to children:
First of all, in terms of the question is that a boy or is that a girl, I would say we don’t know—we’ll have to ask them. So that would be the start, that only they know for sure. Some people like to be asked and some people don’t. I’d say you know, some people think (because by three you’re learning) that if you have a penis you’re a boy and if you have a vagina or a vulva you’re a girl, but actually it’s not like that. It’s not like that at all. If you’re a boy it’s because your mind is telling you I’m a boy. If you’re a girl it’s because your mind is telling you you’re a girl. Some girls like to wear dresses and some girls like to dress as Darth Vader—that’s a people thing, but there are some people where we live who think one thing is a boy thing and one thing is a girl thing. So there is a teaching moment there. Kids by three know their culture. Remember I said gender socialization starts at two? So we have to sometimes unsocialize those messages with new messages. Then the next thing is: Some people think there is only two genders. But there is lots and lots of genders—it’s just like a rainbow. It has all different colors. And then I’d stop there because that’s almost way too many words already for a three-year-old.
There you have it, in her own words: Children must be “unsocialized” out of antiquated beliefs such as the idea that men have penises and women have vaginas, or that there are only two genders. Instead, children as young as three years old are to be told that you can be whatever you decide to be, regardless of biological reality. When children meet adults who have not yet relinquished common sense, they will be gently introduced to the concept of transphobia.
Ehrensaft’s views do not simply extend to children between the age of toddler and kindergarten, either. A father stood up to ask her another question: “A very strong message people have been talking about this morning is listening to the child, and letting them tell us. I’m just wondering if there are recommendations for pre-verbal children, so between the ages of one and two, suggestions for how to approach the topics that we’re talking about today?” Unsurprisingly, Ehrensaft had advice regarding “pre-verbal children” who can’t talk yet, too:
So the question is, what about the kids between one and two who are just developing language, or may not have it yet? They’re very action-oriented. This is where mirroring is very important, and listening to actions. So let me give you an example. I have a colleague who is transgender, and there is a video of him as a toddler—so he was assigned female at birth—there is a video of him as a toddler tearing barrettes out of then-her hair and throwing them on the ground and sobbing. That’s a gender message! And when it happens not just once or twice or three times, that’s a gender message. Sometimes kids between the age of one and two with beginning language will say “I boy!” when you say girl. Those two words: “I boy.” That’s not a pre-verbal, but an early verbal message. Sometimes there is a tendency to say, well honey, no, you’re a girl, because little girls have vaginas and you have a vagina so you’re a girl. And then when they get a little older you’ll hear them say: Did you not listen to me? I said I was a boy with a vagina. But they can’t say that between one and two, but they can show you by what they want to play with, and if they feel uncomfortable about how you are responding to them and their gender if you are misgendering them. So you look for those kinds of actions, like tearing a skirt off. There was one, I think this was in the Barbara Walters special, where this child wore the little onesies with snap-ups in between the legs, and at age one would unsnap them to make a dress and have the dress flow. This was a child who was assigned male. That’s a preverbal communication about gender, and the message back should not be to negate any of those expressions, but to go with them and see where they go. So that’s my sense about the one to two-year-olds. Children will know as early as the second year of life. They probably know before, but they’re pre-pre-verbal.
In Ehrensaft’s view, a child throwing a tantrum and pulling out her barrettes, or a boy opening his onesie, or children simply playing make-believe—these are all reasons to believe that your child may not be the gender they were “assigned.” Despite evidence telling us that up to 80% of children who genuinely do struggle with gender dysphoria will later grow out of it, and the incredible danger that physical and chemical mutilation poses to the physical and mental well-being of children who decide to transition at a young age (which is already giving birth to the phenomenon of “detransitioning”), Ehrensaft advises parents to be on the lookout for signs that their child might actually be of the opposite gender—or any of an assortment of different genders, some of them yet unnamed and presumably undiscovered.
Trans activists are especially focused on young people because they rightly feel that indoctrination is more effective at a younger age. The fact is that experts like Ehrensaft are the ones informing new sex-ed curriculum for schools, new governmental policies, and new social responses to the transgender ideology. In her view, her ideology applies even to children under the age of five, including those who are “preverbal.” Most parents are unaware of what activists like Ehrensaft believe and teach, but it is incredibly important for people to be aware of what this ideology constitutes, and to find out whether it has infiltrated the curriculum of your local schools, as well.
Trans activists are waging a war for the hearts and minds of the next generation. Don’t fool yourself: That means your children, too.
We are already seeing a great battle unfold over the Supreme Court in our land. At one level the battle is “all about abortion” which the left sees as almost a “sacrament” or sacred honor, and the right sees as the most immoral and legally flawed decision ever handed down by the court (Dred Scott notwithstanding).
Count me among the right in this matter. No one can reasonably refute the fact that Roe v. Wade has resulted in the death of over 50 million children. That anyone supports this right to kill cannot avoid withering contempt as a position. The medical evidence is clear: abortion is the killing of unique human persons. These infants have done nothing morally wrong, so they are innocent. There is simply no other reasonable conclusion. Abortion must be opposed for the lie and the evil it is.
But while abortion will head the list of concerns on both sides, it is also the symbol of a far wider agenda involving other issues such as euthanasia, marriage, family, sexuality and religious liberty.
But why has the Supreme Court become the locus of political battles? Of all three branches of our government, the judicial branch is supposed to be the least political. But, not only has it become politicized, I would argue it has become the actual center of political power in this land. Something is deeply wrong here, and all the storm and noise illustrates that almost nothing succeeds politically if the Supreme Court is opposed.
I am a Catholic priest. You do not read my offerings to learn of constitutional law or political science. But while I write of a concern over government, I also write of a Catholic principle: subsidiarity.
Subsidiarity as a Catholic principle is rendered:
The teaching of the Church has elaborated the principle of subsidiarity, according to which a community of a higher order should not interfere in the internal life of a community of a lower order, depriving the latter of its functions, but rather should support it in case of need and help to coordinate its activity with the activities of the rest of society, always with a view to the common good. (Catechism # 1883)
It seems clear that the balance of power set forth in our system has shifted steeply toward the judicial branch, and ultimately, to the Supreme Court. Hence the principle of subsidiarity, which should not be needed, now applies here. Yes, the executive and legislative branches have strangely ceded much of their power to the “High” Court and to the judicial branch in general. When a Supreme Court decision comes down, presidents and legislators and citizens either celebrate or bow their heads and say, “I guess this is now the ‘Law of the Land.’”
The legislative branch was supposed to be the branch tasked with making the “law of the Land.” Indeed, I am rather surprised that the legislative branch has not been more combative in resisting their increasingly subservient role to the nine unelected justices just across the street from the U.S. Capitol.
Something tells me that sloth is likely a big part of it. Crafting true legislation requires a lot of work, and the amassing of support and voter buy-in. There are compromises and trade-offs in the process. It is hard work, not only for members of congress, but also for the groups who seek to establish their views in law. Amending the Constitution is even more work, requiring whole states to agree to the amendment. It is a lot of work to be sure, and the outcome may be very uncertain, or the results very compromised. So even legislators and lobbyists seem willing to shed some of their power for the simpler route of convincing local judges or federal courts or even nine “supremes” of their views, and having them legislate by judicial fiat.
Legal and political experts tell me the rise of the nine Supremes can be traced to the Marbury v. Madison case of 1803 which established the principle of judicial review in the United States, so that American courts have the power to strike down laws, statutes and executive actions that contravene the U.S. Constitution. At some level judicial review seems like a good thing to an ordinary citizen like me. Congress or the president can overreach and suspend or violate our obvious constitutional rights. But I suppose, like many things, judicial review has become unbalanced and set its sights on less-than-obvious violations of constitutional rights. There is also the problem of the court simply establishing or inventing constitutional rights.
For example, the Roe v. Wade decision, finding no obviously constitutional right to kill a child in the womb, established one, claiming it was in the “penumbras and emanations” as set forth by the Griswold v. Connecticut case of 1965. Never mind that all this is very vague. This is where we are today at the federal level. Federal judges get to strike down laws and order actions. They do not merely remand the case to legislators for a fix — they often make the fix and order compliance.
If this were merely the case for arcane federal statutes, perhaps it might be tolerable. But instead it is also about some of the most wrenching and definitional issues of our culture: abortion, euthanasia, “gender,” health care and marriage. At lower federal levels one judge can compel recognition of groups and actions that offend the sincerely-held and once-ubiquitous beliefs of countless Americans.
And, if the Supreme Court deigns to hear appeals, nine unelected officials get to decide what marriage is, who can kill a child in the womb or engage in physician-assisted suicide, or compel women to admit biological males into their locker room merely because he says he identifies as female.
And in a way, it is even worse than that. It hasn’t really been nine justices who get to decide. In our currently divided court, it is really just one man, Justice Anthony Kennedy, who just announced his retirement. He has been arguably the most powerful man on the planet — more powerful than the president, more powerful than any member of congress or the whole congress itself. The four liberals and the four conservatives usually canceled each other out. It all came down to Anthony Kennedy. Yes, one man has called the shots for years.
All of this violates subsidiarity and accountability. We are in an era where the courts have largely eclipsed the legislative process.
The “high” court should not be the final legislator in this land. Judicial review would seem to be an assisting function, as the principle of subsidiarity above articulates. Determining that a proposed or existing law has constitutional concerns should be the opportunity to return the matter to legislators for adjustments, fixes, or elaboration and further review. Crafting law should be the work of elected officials who are accountable and must work in the existing public discourse, however divided or contentious it may be. This allows necessary debate, compromises and consensus to be reached. It also requires groups that demand sweeping social changes to effect it the old-fashioned way — by garnering public support for their views, rather than seeking to have it imposed by judicial fiat.
Currently there is panic on the left over the mere retirement of one justice. They see their entire world as dependent on one man. Just one. This is unhealthy for all of us. Nothing so serious in this land should depend on nine unelected people — and certainly not on a single person! But too often it does. The left knows this, as does the right. The Supreme Court increasingly looks like the pantheon, and the judges act like gods — getting to say who can live or die, what marriage is, and so forth.
I admit, I am glad that it is the left that is in agony this time. But it could just as easily have been the right. Either way, there are going to be some very ugly moments in the days and weeks ahead — perhaps even violence. It is all evidence of a system that is broken, tilted excessively toward the courts, and swaying in the winds of political discontent. We have increasingly surrendered our power to unelected judges and don’t know the way back out. We all play the game, and the game and the stakes have gotten higher.
To state the problem once more in terms of subsidiarity: “a community of a higher order routinely interferes in the internal life of a community of a lower order, depriving the latter of its functions.” The executive, legislative and judicial branches should be of equal power. But that is not realistically the case today. The judicial branch is of enormous and overriding power compared to the other two, and their functions are increasingly hindered. Further, federal law and policy too easily eclipses state and local law.
So subsidiarity matters. It is not merely an arcane Catholic or sociological principle. How to re-establish it in our broken land is well above my paygrade or ability. Meanwhile, this latest round of war commences. There is no option — we must fight hard for a pro-life justice to be appointed, and fight we will. But somewhere we should all remember that the intensity of this battle already begun comes from the unhealthy reality that too much depends on too little, and too few. Nine unelected officials have attained too much power.
ALBANY, July 10, 2018 (LifeSiteNews) – New York Democratic Gov. Andrew Cuomo announced an executive order Monday placing new mandates on insurance companies to subsidize contraception, in what he calls a preemptive measure to guard against a more conservative Supreme Court majority.
The order directs the state Department of Financial Services and Department of Health to force insurers to cover over-the-counter emergency contraception (which has the capacity to act as an abortifacient), voluntary sterilization, and other FDA-approved female contraceptive drugs or devices, as well as dispense a year’s worth of contraception at once, “all without co-insurance, co-pays or deductibles,” Cuomo’s office announced.
“A representative from the governor’s office clarified that copays are a subset of cost-sharing, so ‘no cost-sharing’ means that consumers pay no additional fees for the service,” AM New York added.
The announcement, made before the identity of President Donald Trump’s latest judicial nominee was revealed, said the measure was a safeguard against “an extreme conservative Supreme Court Justice who could roll back advancements in reproductive health care.”
“In the face of this federal assault, New York is going to protect itself because this state has always been the progressive capital of the nation. This is the time to fight back,” Cuomo declared. “This is the time to resist. This is the time to make your voice heard. This is the time where every New Yorker has to say, you’re not taking women’s right to reproductive rights away. We’re going to protect ourselves because this is the state that has always stood up for what’s right.”
Cuomo signed the order on Tuesday, and said at a pro-abortion rally at the Yonkers Public Library’s Will branch there was “no question” Judge Brett Kavanaugh “will overturn Roe v. Wade.” Kavanaugh’s views on the subject are not fully known, but pro-lifers see causes for both encouragement and concern in his record.
In addition, Cuomo called on the state Senate to vote on legislation codifying Roe v. Wade’s protection of abortion in state law. The state Assembly has passed the so-called Reproductive Health Act in each of the past six years, but the Senate has never voted on it. In the New York Legislature, Democrats enjoy an overwhelming 104-41 Assembly majority, but a razor-thin 32-31 Senate majority (the Senate currently has a Republican majority leader due to a power-sharing agreement between the Independent Democratic Conference and Senate Republicans).
“One of the reasons they opposed it, they said, ‘Well, we have Roe v. Wade in law. And there’s no way anybody would ever think of overturning Roe v. Wade,’” Cuomo said. “These were the Republican senators just a couple of years ago, telling me it’s unimaginable that anyone would try to overturn Roe v. Wade. Well, they elected someone who wants to do the unimaginable.”
Even though it remains unknown how Kavanaugh or all four current conservative justices will vote on Roe, the abortion lobby has begun taking several steps to insulate abortion-on-demand from a hypothetical case overturning it. Democrats in Massachusetts recently moved to repeal the state’s century-old, pre-Roe abortion ban (one of ten still on the books yet unenforced), while pro-life activist Rebecca Kiessling warns that pro-abortion groups in states like Iowa, North Dakota, and Minnesota are filing lawsuits claiming a “right” to abortion rooted in state constitutions rather than Roe v. Wade.
Cuomo’s announcement came accompanied with enthusiastic praise from state pro-abortion leaders, with Planned Parenthood Empire State CEO Robin Chappelle praising Cuomo for “standing up today to remind the nation that New York won’t go backwards,” while National Institute for Reproductive Health president Andrea Miller said the “best defense against a hostile Supreme Court and Trump-Pence Administration is a strong state-level offense.”
The move is the latest in a string of aggressively pro-abortion moves by the New York governor, who has previously embraced late-term abortion and called for mandatingthat abortions themselves be provided at no cost as well. In 2013 he promoted an women’s “bill of rights” that critics said would effectively allow abortion up until birth.
A year later, Cuomo landed in hot water for saying that “right-to-life” supporters “have no place in the state of New York, because that’s not who New Yorkers are.” He later walked back the attack by claiming he “respects” the pro-life position and meant only that it was a minority position that “cannot win statewide.”
The readings for the 14th Sunday of Ordinary Time (July 8) focus on prophets. The text from Ezekiel tells us that, whether people listen or not has nothing to do with the truth of the prophet’s message. The Gospel contains the famous line about “a prophet [being] not without honor, except in his native place.”
We need to make clear up front two things about prophets: (1) what the prophetic mission is and (2) why you should be a prophet.
First, what the prophetic mission is. The prophets make up a substantial part of the Old Testament and, in Jewish theology, they rank right after the Law (torah) in terms of significance.
The prophets were notfortune tellers. Granted, sometimes their message extended to what would happen in the future, but the primary focus of the Old Testament prophets’ attention was now, not the future. They took the Law, the basis of the covenant between God and His People, and demanded that Israel live up to it today, here and now. The prophet is concerned that Israel has fallen off the wagon and needs to get right with God now.
The prophets did agree that, because God is just and because He has acted (Exodus) and continues to act in history, the events of history could be understood as ways God called Israel and Judah to get back on track. In the Old Testament, the most obvious example was the progressive extermination of the Jewish people’s freedom, first of Israel’s by Assyria, then of Judah’s by Babylon. But the prophets were not so much interested in what might happen if the Chosen People persist in evil, but rather of averting what could happen by conversion today: “If today you hear his voice, harden not your hearts” (Psalm 95:7).
The other important thing to say about the prophet was that his message was not his. The prophet understood that the message he was conveying was God’s. “Thus says the Lord” is the usual refrain that precedes a prophet’s statement. Indeed, when we look at a reluctant prophet like Jeremiah, it’s very clear he’s not particularly happy bringing the message he had to Israel. But God did not ask the prophet whether he liked the message: he asked the prophet to deliver it intact. The reading from Ezekiel is clear: he is sent to the Jews and, whether they accept the message or not, “they shall know that a prophet has been among them.”
The next thing we should say about prophets is: Each of us is called to be one.
By virtue of Baptism, we have received a share in the threefold mission of Christ (triplex munere Christi): we are called to be priests, prophets and kings.
How do we exercise our prophetic vocation? St. John Paul II, who stressed the Christian’s share in the threefold office of Christ and the teaching of Vatican II (on being a prophet, see Lumen gentium, # 12) that underscored it, puts it simply: a Christian exercises his prophetic vocation when he lives and speaks the truth. Truth, after all, is God, comes from God, and is the Word of God – and a prophet’s job is to speak God’s word.
Being a Christian means living up to one’s Baptism and especially one’s Confirmation. It doesn’t mean being a “holy roller” or putting on extravagant demonstrations. It does mean: hewing to the truth, no matter what.
One area where the truth is very much under assault today—even by some who claim to be within the Church—is in the area of marriage and family life. In two weeks, the Church will mark the 50thanniversary of Bl. Paul VI’s encyclical, Humanae vitae.
Humanae vitae has been called in many quarters “prophetic,” and that’s true. Many of the things that Paul VI predicted would follow the widespread acceptance of contraception, such as the devaluation of women (see #17), the intrusion of the state into promotion of contraception (also #17) and, most especially, to the idea that, through technology, man can do anything he is capable of in the realm of life ethics (#18). Humanae vitae stood athwart the effort to separate sex from babies; in the ensuing 50 years, we now also have babies separated from sex, not just as the way they come into the world but also as a constitutive element of the families in which they grow up.
There will undoubtedly be voices in the next few weeks that announce the Humanae vitae was a failure and that “Catholics” have rejected it as pervasively as the larger world. Perhaps, although I would quibble with the definition of Catholic that puts itself at odds with the Teaching Church on so fundamental a moral question as relevant to so many people on a daily basis as: what does Catholic marriage and sexual life entail? My point is different. Perhaps many “Catholics” do not accept the encyclical. Ezekiel had an answer for that: “whether they heed or resist—for they are a rebellious house—they shall know that a prophet has been among them.”
Undoubtedly, in the next few weeks, somebody around you will mention “the Church sticking its nose into sex” and “how silly was Pope Paul VI.” Will you be enough of a prophet – will you live up to your Confirmation – and maybe gently suggest there’s something correct to the encyclical? Priests – will you say anything about the encyclical to help Catholics understand it, or will you maintain the vow of omertà when it comes to talking about the front line issue where human dignity and the truth of love is at stake?
Few of the prophets had an easy time in their vocation. The ultimate prophet, John the Baptist, even lost his head when the leader of his day lost his head over sex, a woman and a dancing girl. Plus ça change. … So, we should hardly be surprised that the prophetic Paul VI – and those who follow Humanae vitae – encounter resistance from a rebellious house. The prophet is told to proclaim the truth, but receives no guarantee he will prevail. The one thing of which he can be sure, however, is that what he says will prevail, because the word is not his but His.
Remember the Holy League of Nations that Pope St. Pius V formed in 1571, and the result of the battle they engaged in? Their victory at Lepanto on Oct. 7, 1571 was attributed to the Rosary, and the date became the Feast of Our Lady of the Holy Rosary.
The new Holy League of Nations is gearing up for another battle this Oct. 7 — using only one weapon — the Rosary.
The battleground is not Lepanto but this entire country. Plus other countries also joining in this international Allied effort. It’s not named Operation This or That, but very much to the point — the “U.S. Rosary Coast to Coast.”
Stirring the People
The website RosaryCoastToCoast.com opens with a powerful three-plus minute video that illustrates a stirring homily being given about this call to prayerful arms because so many are wounded in this spiritual battle now raging.
“We are at war. A war without borders. No one is exempt. The bloodless battle affects us all… No man is exempt. No woman excused. The fight has come full force.”
Now there is “a clarion call of the Holy Spirit to engage in spiritual warfare through prayer, fasting, and sacrifice.”
Our Lady gave a clarion call at Quito, LaSalette, Fatima and other apparitions.
We’re reminded that the “spark” from Poland in 2017 as people prayed at the borders for the country then ignited another in Ireland, then the British Isles. Ordinary people answered along with priests and bishops “physically surrounding their nations in active prayer.”
Now the United States is being called upon to do the same at this critical moment in history — to pray at rallies coast-to-coast on Oct. 7.
“We are being called upon to help turn our country back towards God. We must acknowledge as a people that we have turned away from God; we’ve allowed the kingdom of Satan to assault us, we must confess our errors, turn away from the darkness, and
Repair what we as a Church and as a nation, have wrought,” the homily continues.
“We will accomplish this through prayer which will change hearts, change families, change our communities, change our country and change the world.
“St. Padre Pio and St. Maximillian Kolbe both agree that there is no strong weapon in this spiritual battle than the Rosary.”
Padre Pio called the Rosary “The Weapon.”
The homily ends — “We hear the clarion call of the Holy Spirit, through the Immaculata, and each of us sounds the reply in the face of the battle around us: “I’m going in!”
Rallies Movement Quickly Growing
The Rosary Coast to Coast is ready to defend the “dignity of the Human person — Life, Marriage, Family, as well as Religious Liberty — praying at Rosary Rallies across the U.S. and the world on Oct. 7, the Feast of Our Lady of the Rosary. The New Holy League of Nations sees this as “a united front in worldwide spiritual battle, a ‘declaration of war’ not against flesh and blood; but against principalities and power, against the rulers of the world of this darkness, against the spirits of wickedness in the high places (Ephesians 6:12).”
“Together we are calling upon God, through the powerful intercession of Our Lady of the Rosary, to heal our countries and return them to Holiness,” announces their latest statement.
A reported 400 registered rallies span the United States — hopefully hundreds, really thousands more to come. Countries that inspired this Coast to Coast Rally will join the U.S. for this spiritual engagement. Others will too.
Already signed on and enlisted are Poland, the British Isles, Ireland, Canada, Australia, Lebanon, India, Mexico, Panama and some Central and South America countries. More are in the works to sign up in the next weeks.
An entry from St. Faustina’s Diary (1732) has been applied to St. John Paul II, considering him “the spark,” but in this case, considering where the idea came from, can “the spark” also apply to the Rosary Rallies? Jesus said to Faustina: “I bear a special love for Poland, and if she will be obedient to My will, I will exalt her in might and holiness. From her will come forth the spark that will prepare the world for My final coming.”
Possible Extra
A recommendation for the Coast to Coast Rally is coming from the U.S. Holy League of Nations where each country involved will be represented in this league. It’s encouraging that member nations also join in the 54-day Rosary Novena, beginning Aug. 15, Feast of the Assumption of the Blessed Virgin Mary, “for the intentions of reparation and petition for their countries.” The U.S. Novena for Our Nation begins Aug. 15. People can sign up for a daily reminder and reflection.
The Holy League reminded of the encouraging worlds from Bishop John Keenan of Paisley, Scotland after the Rosary on the Coasts in the British Isles this April. He said that “there was something changed in the Catholic Church, in the British Isles… it was as though Catholics are beginning to get the sense, the inspiration that all the problems of the world really can be solved by prayer. It was like a day of New Evangelization. It felt like a day of Grace for us. Therefore, I commend it to the Catholics in the United States.”
The Holy League also quoted Cardinal Raymond Burke: “Let us now turn to the powerful prayer of the Holy Rosary, asking Mary Immaculate to intercede with Our Lord to bring healing to our nation and to inspire in her citizens the holiness of life which alone can transform our nation…”
Watch for new developments and more information in an article later this summer.
In the meantime, obtain promotional materials to get prayer troops forming for the great Oct. 7 event.
Perhaps no other encyclical in the history of the Church has received so much ridicule and caused such controversy as Humanae Vitae. Even today, 50 years later, it still evokes heated discussions and debates, often from people (including some priests) who have never read the document. Yet when encouraged to read the encyclical, one quickly learns of its profound teaching and defense of God’s divine plan for human sexuality, marriage, family and life. The Church, in this encyclical, is preaching Good News and is pro-love and pro-life.
Pope Paul VI begins by highlighting an understanding of God as Love, and how this love overflows into new love and new life. The human persons God creates have an immutable dignity – being made in the image and likeness of a loving God – and have an immortal destiny. The beauty of Catholic Church teaching on human sexuality is based on the dignity of the human person. The gift of life is a most precious gift – to be cherished and respected – which enables us to anticipate and strive for eternal life, where there will be an everlasting enjoyment made possible by union with our loving Father.
God has bestowed upon spouses an “extremely important mission of transmitting human life” – the wondrous gift of being co-creators with Him in the creation of new persons. Having and raising children is an act of immense generosity and immeasurable responsibility; it enables human persons to participate in an act of inestimable value, assisting God in bringing a new immortal soul into existence.
To assist us in appreciating the magnanimity of God, Pope Paul VI emphasizes the importance of priests in their role as pastors of souls regarding the spiritual guidance of spouses. The priest is the first in the line of defense against the false language, philosophies and doctrines confusing spouses about their understanding of conjugal love, which is self-giving, self-donating love. He says to priests,
… speak with full confidence, beloved sons, convinced that while the Holy Spirit of God is present to the magisterium proclaiming sound doctrine, He also illumines from within the hearts of the faithful and invites their assent. Teach married couples the necessary way of prayer and prepare them to approach more often with great faith the Sacraments of the Eucharist and of Penance. Let them never lose heart because of their weakness. — Humanae Vitae, ¶29
What powerful words of encouragement from our soon-to-be saint! Yet I have sadly encountered far too many times the lack of zeal – for many reasons – of my brothers in preaching the full spectrum of Catholic teaching regarding marriage and human life.
If I were to receive five dollars every time I heard, “I never hear any homilies in my church about contraception, abortion, co-habitation, fornication or homosexuality,” or, “This is first time I heard a priest talk about these issues” or, “It seems our pastor is afraid to address any issues affecting Life and Family,” I would be a multi-millionaire.
In commemoration of Humanae Vitae’s 50th anniversary, I would like to highlight the priest as one who teaches, governs and sanctifies. He is irreplaceable in the defense of spouses and family life – in building a Culture of Life.
Who is the Priest?
Chaplain (Maj.) Chad Zielinski, the 354th Fighter Wing deputy wing chaplain, prostrates himself in front of praying bishops and a crowd during a ceremony ordaining him the bishop of the Fairbanks Catholic diocese Dec. 15, 2014, at the Carlson Center in Fairbanks, Alaska. The ordained lies prostrate symbolizing his unworthiness for the office to be assumed and his dependence upon God and the prayers of the community. (U.S. Air Force photo by Staff Sgt. Shawn Nickel/Released)
In the most profound way possible, the priestly ordination of a man creates a new man, one who, if genuinely living his vocation, can proclaim with St. Paul: It is no longer I who live, but Christ who lives in me. (Galatians 2:20). He is ordained to continue the Savior’s work of redemption until the end of time. He is transformed not because of what he can do, but because of what he has become – a priest of Jesus Christ. He is specially chosen, called to proclaim the Gospel of salvation and lead the faithful to their final destiny – Heaven and the Beatific Vision.
The bishop during the priestly ordination rite in his homily speaks about the nature of the priesthood and how the work of Christ the teacher, priest and shepherd continues through the ministerial priesthood. He also stresses to those to be ordained that they are to model their lives upon the Good Shepherd who did not come to be served but to serve and to give his life as a ransom for many. (Matthew 20:28)
My son, you are now to be advanced to the order of the presbyterate. You must apply your energies to the duty of preaching in the name of Christ, the Chief Teacher. Share with all mankind the word of God you have received in joy. Meditate on the law of God, believe what you read, teach what you believe, and put into practice what you teach. Let the doctrine you teach be true nourishment for the people of God. Let the example of your life attract the followers of the Christ, so that by word and action you may build up the house which is God’s Church. In the same way you must carry out your mission of sanctifying in the power of Christ. — Rites of the Catholic Church, Volume 2
The Catechism of the Catholic Church describes Holy Orders as: The sacrament through which the mission entrusted by Christ to his apostles continues to be exercised in the Church until the end of time. (CCC, ¶1536) The priest receives unique powers at ordination to preside at Mass, confer the Sacraments, absolve sinners, anoint the sick, proclaim and explain the Gospel and give blessings. His whole pastoral ministry and leadership of building up a local community of faith is ultimately to reconcile a sinful people with their God. Through the grace and authority entrusted to him through Holy Orders, he is not only to teach the truths of revelation but inspire his hearers and fellow believers to follow what he teaches, as he believes and lives. In collaboration with his bishop, he is to be the primary former and sustainer of a Christian community.
To Whom Else Can One Go?
A cultural war is in progress, and the Christian community has not been immune to the process of social and moral deterioration. Many are confused about the meaning of life, its fundamental choices and purpose. They question what the world is, where it comes from, where we are heading and no longer know from what and for what we have been made.
It is here, at this critical junction, where the priest, the one called to build and sustain the people of God, proclaims like St. Peter, Master, to whom shall we go? You have the words of eternal life. (John 6:28) With so many contrasting philosophies, it is the priest, entrusted with the Good News, the Master sends in His name to the nations: Go into the whole world and proclaim the gospel to every creature. Whoever believes and is baptized will be saved. (Mark 16:15)
The Word of God and its teaching is entrusted to him and serves as the anchor for his ministry. He is reminded by the bishop of what was said to him on the day of his diaconal ordination when the Book of Gospels was placed in his hands, “Receive the Gospel of Christ, whose herald you now are. Believe what you read, teach what you believe, and practice what you teach.”
The priest is never to forget that he is entrusted with the Gospel of Christ. He is not the Master but the steward. He does not teach his own ideas or a philosophy that he has invented or prefers; he does not speak of himself or for himself, to gain popularity, fortune or fame. He does not say his own thing. Being configured to Christ, he teaches in the name of Christ. He proposes the truth that is Christ himself, His word and His way of living who is the Way and the Truth and the Life. (John 14:6)
The priest’s life is to be completely identified with Christ the Head and High Priest and, in this manner, the Word that is not his own becomes a profoundly personal word. He accepts and seeks to live, as his own, all that the Lord Jesus taught and that the Church has passed on and incorporated into his own priestly ministry. The people of God want, need and have a right to hear from their priest the genuine Word of God and ecclesial doctrine through which they can renew their encounter with Christ who says, Follow Me.
In Persona Christi…
St John Vianney, the Curé of Ars, the patron saint of priests
Saint John Vianney, the patron saint of priests, understood the irreplaceable role of the priest and who he is:
O how great is the priest! If he realized what he is he would die… God obeys him: he utters a few words and the Lord descends from Heaven at his voice, to be contained within a small host. Without the Sacrament of Holy Orders, we would not have the Lord. Who put him there in the tabernacle? The priest. Who welcomed your soul at the beginning of life? The priest. Who feeds your soul and gives it strength for the journey? The priest. Who will prepare it to appear before God, bathing it one last time in the blood of Jesus Christ? The priest—always the priest. And if the soul should happen to die (as a result of sin) who will raise it up, who will restore its calm and peace? Again, the priest. After God, the priest is everything. Only in heaven will he fully realize what he is.
Rightfully, we look to our priests in their irreplaceable role in the service of Life and Family for assurance, moral guidance and leadership. It is no secret that priests too suffer in the struggle to live authentic discipleship. They, like the people they serve, are assaulted by a secular and violent culture determined to silence their influence and voice, especially in the West and de-Christianized countries.
I recall the words of a priest I recently met during an HLI conference, “Father, you would not believe the amount of hate mail and verbal abuse I receive when I preach Church teaching on Life and Family, particularly on contraception, fornication and homosexuality.” His experience is not uncommon and causes many priests [bishops] to shy away from addressing these issues. However difficult it may be, the priest is never excused of his role and duty to preach Christ and be persistent whether it is convenient or inconvenient. (2 Timothy 4:2) In the person of Christ, the priest makes present, in the confusion and bewilderment of our times, the light of God’s Word, the light that is Christ who said, I am with you always, until the end of the age. (Matthew 28:20) It does, however, help us better understand the challenges our shepherds face in the current global climate and pray far more earnestly for them.
Behold the Lamb of God
At the end of his encyclical Humanae Vitae, Pope Paul VI calls upon priests to fulfill their duty as pastors of souls by assisting married couples through authentic ecclesial doctrine:
And now, beloved sons, you who are priests, you who in virtue of your sacred office act as counselors and spiritual leaders both of individual men and women and of families—We turn to you filled with great confidence. For it is your principal duty—We are speaking especially to you who teach moral theology—to spell out clearly and completely the Church’s teaching on marriage. In the performance of your ministry you must be the first to give an example of that sincere obedience, inward as well as outward, which is due to the magisterium of the Church. — ¶28
Pope Paul VI reminds priests in every age that, through their ordination, they have received the charism of teaching and preaching. They should not be afraid to proclaim the truth of God’s plan for human love with firm but gentle clarity. In obedience to Truth and its proclamation, the priest helps liberate his flock (couples) from the false doctrines and philosophies that confuse them. Pastoral charity does not mean being silent in face of sin or error. The priest must be courageous in unmasking the language of our day, which disguises immorality, calling evil good and good evil. Christ never flinched from re-orienting souls toward truth and obedience to the Father’s will. As ministers in His name, a priest motivated by love should have the same fervor and zeal. Jesus exposed the lies, helping souls to see with clarity Truth and the demands of living the Christian life – in persona Christi, the priest does the same.
Pope Paul VI also reminds priests of their attitude and posture toward married couples, “Husbands and wives, therefore, when deeply distressed by reason of the difficulties of their life, must find stamped in the heart and voice of their priest the likeness of the voice and the love of our Redeemer.” — HV, ¶29
The priest, living his vocation and fulfilling the promise to practice what he preaches, approaches these difficult subjects and the wounded lives of his people with humility and meekness – recognizing in humility his own woundedness and daily need of the Lord’s grace, healing and mercy. From this vantage point, he patiently offers insight and understanding appropriate to the situation(s) and person(s). Perhaps the most important point he must get across is that the Church has an eminently positive approach to human love, sexuality and marriage.
Many within the Church have become disillusioned with the world and the situation of the Church, especially within de-Christianized environments. They feel there is no way to recapture the ground lost, so they compromise and tolerate evil. This is not our response. Like Jesus, we (priests) are to re-orient people toward Truth. The priest, a man configured to Christ, is the fulcrum being used to enliven the souls of the faithful and to enkindle hope and courage in the face of their struggles and know that grace abounds. The answer is not to turn away from Christ, but to turn toward Him – the Lamb of God.
LA CROSSE, Wisconsin, July 4, 2018 (LifeSiteNews) — National Rosary organizers from around the world are joining forces to create a new “Holy League.”
There have been a number of “Holy Leagues” in history, national allies coming together to protect Christendom from its political enemies. Now, inspired by the mass rosary prayer events of recent months, the organizers of the American “Rosary Coast to Coast” have invited Catholics around the world to join them in a worldwide 54 day novena beginning at 4 PM (Eastern Time) on August 15, the Feast of the Assumption of the Blessed Virgin Mary, and culminating in a rosary on October 7, the Feast of the Most Holy Rosary.
“The formation of the New Holy League of Nations declares a united front in the worldwide spiritual battle, defending the dignity of the human person–life, marriage, family, as well as religious liberty,” organizers of Rosary Coast to Coast stated in a press release on Tuesday.
Unlike the Holy Leagues of old, this army will not be using blades, arrows, or cannons.
“This ‘declaration of war’ is ‘not against flesh and blood; but against principalities and power, against the rulers of the world of this darkness, against the spirits of wickedness in the high places.” (Ephesians 6:12),” Rosary Coast-to-Coast explained. “Together we are calling upon God, through the powerful intercession of Our Lady of the Rosary, to heal our countries and return them to Holiness.”
Every group that participates is asked to choose intentions specific to their nation.
Representatives from the national rosaries recently held in the UK, Ireland, and Australia, and a spokeswoman from Canada, have all confirmed with LifeSiteNews that their groups are participating in the New Holy League of Nations.
Jane Chifley of the “Oz [Australia] Rosary” wrote that Australia, which is 15 hours ahead of New York, will “light the match” by starting the novena first.
“Our [national] intentions for the world rosary will be family, rekindling of faith and continued Godly protection,” she stated.
The Oz Rosary, which was held on May 13, was a great success, taking place in over 252 locations. Organizers estimated that between 20,000 to 35,000 Australians took part.
Jennifer Paufler of Canada’s new “Rosary on the Coasts and Border for Life and Faith” group told LifeSiteNews that she had wanted her northern nation to pray the Rosary for Life and Faith ever since she read about the events in Poland, Italy, Ireland, and the United Kingdom. Paufler contacted a “Holy League” spokeswoman when she first read of the global rosary plans.
“We’re hoping to receive support from our Canadian Bishops, and we are currently waiting to hear back from them,” she wrote.
New Holy League of Nations organizers say that, in addition to the above nations, they have representatives in Poland, Lebanon, India, Mexico, Panama, and other countries in Central and South America.
Preparations are well underway with over 400 related events registered across the United States alone.
One of the biggest complaints of those who visit their doctors is how the physician pays more attention to their computer screens than them. This treatment of a human being, at least implicitly, denies the needs of the soul. Things such as compassion and understanding, so helpful in the healing process, are often absent in these impersonal medical visits. Patients can be left with the feeling they are nothing but the sum of data entered into a spreadsheet.
However, there are physicians who take an intensely personal interest in their patients. Some even go so far as to recognize God’s role in the healing process and even recommend prayer as part of the remedy for their patient’s illness. If this sounds a bit surprising the reader will be consoled to find out that this type of doctor can be found right here in America.
To Be a Good Doctor: Pray an Hour a Day
This kind of treatment is what a fellow member of Tradition, Family and Property (TFP) experienced with his new doctor in York, Penn. This physician is a consecrated servant of Our Lady, according to the method of Saint Louis de Montfort, and attends Mass almost on a daily basis. The TFP member was impressed by the amount of personal attention he received. “When you are with him,” he said with an evident sigh of relief, “you feel you have all the time in the world.”
What makes this particular doctor so unique is that he not only holds himself to these high standards, but is shaping future physicians in the same mold. For example, his interns commonly ask him, “What is the most important thing I can do to become a better doctor?” His response: “Pray for one hour every day.” They frequently moan and groan at a suggestion they consider impracticable. “It’s not a matter of if you can find time,” he affirms, “It is a necessity. You have to do this, it’s not an option.”
“Spend Time in Front of the Blessed Sacrament”
This is what Mr. Dominick Galatolo found in Dr. Jose Fernandez, his general practitioner in Orlando, Fla. The consultations, he says, can last for over an hour, and that is not screen time, but rather face to face personal conversation.
The patient already perceives something different as he sits in the waiting room listening to a recorded message: “We know you are anxious when you come to see the doctor, the most important thing to do is relax.” Mr. Galatolo described how Dr. Fernandez is constantly instilling a sense of calm and confidence in his patients with frequent words of encouragement.
“He will look at you with certainty and say, ‘You are going to be fine, Our Lord is going to be with you.’” Mr. Galatolo, who was experiencing some blood pressure issues coupled with anxiety, explained how Dr. Fernandez expressed such a degree of empathy for what he was going through that this caring physician got teary-eyed. After prescribing appropriate medicine, he directed him towards the Divine Healer.
“What you really need is to spend time in front of the Blessed Sacrament,” said Dr. Fernandez. He then advised him to attend daily Mass and stop at the adoration chapel on the way home and spend as much time as possible. “In three months you are going to be a new man, because God wants you to be better.”
“If It Is God’s Will, You Are Going to Be Cured”
Jessie Walczak is a friend of Dr. Fernandez and explained how he was not always like this. She described the change which occurred when he was challenged by another physician who asked him if he was a “Catholic doctor.” Dr. Fernandez responded, “Of course! I am a Catholic and I am a doctor.” The other doctor then responded, “No, that is not what I mean.” He then explained for Dr. Fernandez what it meant to truly be a “Catholic doctor,” which essentially means seeing Christ in the patient.
With this, Dr. Fernandez had a eureka moment. He became both a better Catholic and an outstanding doctor. He now begins his day by praying with his staff which includes reading the Gospel of the day and providing reflections.
Mrs. Walczak is thankful for his spiritual transformation since she attributes his wisdom to not only saving her life but allowing her to have more children. After giving birth to her first child, she was diagnosed with lupus. Her previous doctor told her that she could not have more children and therefore needed to take birth control. When she refused, he said she would die. At this point, she was confused and did not know what to do. As a last resort, she went to see Dr. Fernandez.
She described how he gave her such hope. He kept repeating, “If it’s God’s will, you are going to be cured and you will have more children, but you have to do what I am going to tell you.” Besides putting her on a new diet, she says, he “prescribed” adoration. She laughingly explained how he literally wrote on a prescription pad, “you have to go to adoration twice a week. This is part of your protocol.”
Thanks to Dr. Fernandez, at the time of writing this article Jessie has given birth to her fourth child and is a picture of health.
Develop a Devotion to Saint Joseph
Such care is by no means confined to those who take care of the body but also those who care for the mind. This is where the godly touch is perhaps most needed. It is for this reason that a friend of mine expressed his unbounded appreciation for Dr. Richard Fitzgibbons, in Conshohocken, Penn. He had tried numerous other psychiatrists who were simply satisfied with prescribing medicine. With Dr. Fitzgibbons he found a psychiatrist that was as interested in finding out more about the “why” than the “what.”
In other words, he is concerned in getting to the root of the problem before or even if he must resort to medication. He specializes in marital healing, but also helps men who suffer from anxiety caused by, among other things, negative paternal modeling. It is for this reason that my friend was extremely consoled when Dr. Fitzgibbons, a very Catholic psychologist, counseled him to have more devotion to Saint Joseph. Dr. Fitzgibbons also makes it a point to end every consultation with a prayer.
Doctors Who Love God
This article is not meant to idealize our medical establishment, but merely to point out some examples—there are many others—of doctors who demonstrate a deep concern for their patients. Even if they don’t make it explicit, they seem to see clearly that a patient also has a soul, which has needs. Compassion and empathy may not heal a physical wound but they will do wonders to calm a disturbed soul.
Saint Jacinta Marto, the youngest seer of the Mother of God at Fatima, Portugal in 1917, is frequently quoted as saying that, “Doctors have lost the ability to cure because they have lost the love of God.” Well, according to Saint John, it is impossible to love God who we do not see, if we do not love our neighbor who we do see. That is what makes these doctors so refreshing, and it is the secret to their success. They are capable of curing people because they love God.
Writing in The Times, Dominic Lawson says there is something obscene about the ‘shortening’ of the lives of more than 450 patients who were staying in Gosport War Memorial Hospital. He is right.
The Gosport scandal concerns the ‘shortening’ of 456 patients’ lives through the excessive use of painkillers at the hospital in Hampshire between 1989 and 2000. An inquiry, the Gosport Independent Panel, says such ‘life-shortening’ had become virtually routine.
The use of the word shortening is striking. We might say that Jack the Ripper ‘shortened the lives’ of prostitutes in the East End of London. In fact, if we employ the rather ludicrous measurement of time left – QALYs, or quality-of-life years, as some experts say when referring to care for the elderly in particular – then the doctors who presided over the regime of ‘shortening’ lives in Gosport undoubtedly stole more time than the Ripper could ever have managed.
Even the term ‘patients’ in this discussion masks the real people involved, with their experiences, lives, loves, families, and, yes, hopes. The report into the scandal anonymised mothers, fathers, grandmothers, brave veterans, beloved teachers, aunts and uncles, friends and rivals, reporting as if they were victims of some foreign disaster rather than having been purposefully killed.
There are, admittedly, some situations – now thankfully rare – when a doctor must heavily sedate patients to prevent suffering in the last hours of life. But Gosport wasn’t like this. It appears that the killings took place because the people involved were ‘inconvenient’. This was revealed in a meeting between members of staff about an annoying patient, where the following alarming exchange took place: ‘We agreed that if he wasn’t careful he would “talk himself on to a syringe driver”.’ According to the report, that patient, who was able to walk, talk and dress himself, did have a syringe driver and died the next day. Many others were also seemingly despatched for being irritating. Fifty-five per cent of those who were given lethal doses of diamorphine were not in pain. In 29 per cent of cases, the notes give no justification at all for the lethal dose.
Much more than an event like the Grenfell disaster, the treatment of these individuals indicates how far a moral crisis besets this country. As expressed all too clearly in our language, human lives are no longer sacred. Another euphemism beloved by people like Polly Toynbee, who summoned her mother from the grave yet again to argue for legalised assisted suicide, is ‘choice’.
Everyone wants to have choice. ‘Compassion and Choices’ is the new, improved name for the Euthanasia Society of America. British lobbyists Dignity in Dying (formerly the Voluntary Euthanasia Society) want to ‘allow a dying person the choice to control their death’.
Let’s leave aside the fetishising of the moment of death when people seem to want their favourite music playing (hint: you won’t hear the end of the song). It is actually this misuse of the concept of ‘choice’ that led to the monstrous events in Gosport. The ‘choice’ referred to by pro-assisted dying organisations is actually suicide. But by calling it a choice, we remove all moral responsibility from the action. The culture of assisted dying reduces the most profound decision a human can make – whether to shuffle off this mortal coil – to a medicalised menu selection. The decision to execute a human being in the United States – even a horrific rapist/murderer – is at least attended with ritual and ceremony, as if something of huge moral importance is occurring. With assisted dying, suicide is given as a treatment option in a pamphlet. The message is ‘we won’t judge’ – that is, ‘we don’t care if you live or die’.
If such an ‘option’ is offered so casually to individuals, why would it be surprising that a doctor should treat human lives just as casually? If the act of suicide carries no real moral responsibility for the individual, why would killing a patient – or ‘shortening a life’ – carry any special moral responsibility for a doctor? We make it easy to wink and, as the Gosport report notes, tell the nurses to ‘Make the patient comfortable. I am happy for nursing staff to confirm death.’
Elderly people already find themselves resented for inconveniently continuing to exist, for voting for Brexit, for blocking beds, for taking up the time of harried NHS staff. Assisted suicide is always preferred for those who have little time left. In the country that has tolerated assisted death the longest – the Netherlands – plans are afoot to extend assisted death to all those over 70 who are ‘tired of life’. How many lonely elderly Dutch people will be despatched in a similar fashion to the patients at Gosport?
Hopefully someone will be found responsible for the crimes that took place in Gosport. But it is really an entire culture that supports assisted dying, that believes that life and death are nothing but menu selections, that must be changed if we are to avoid future scandals like this one.
Kevin Yuill teaches American studies at the University of Sunderland. His book, Assisted Suicide: The Liberal, Humanist Case Against Legalisation, is published by Palgrave Macmillan. (Buy this book from Amazon (UK).)
June 28, 2018 (American Thinker) – Africa’s burgeoning birth rate is expected to touch off more migration to its northern continental neighbor, as globalization and rising global temperatures both push desperate people to a place less ravished by crime and intolerable clime. European countries, in turn, have revolted against current migration trends and their expected increase by electing populist leaders who promise to stem the flow of foreigners to their land.
Out of this demographic upheaval, three policy experts want to revive an unfashionable doctrine: top-down population control.
Frances Kissling, president of the Center for Health, Ethics, and Social Policy; Jotham Musinguzi, director general of Uganda’s National Population Council; and Peter Singer, famed promoter of eugenics and infanticide, teamed up in The Washington Post to endorse an “ethical” means for hindering Africa’s robust fertility rate. Citing Paul Ehrlich’s The Population Bomb, they readily acknowledge the taboo nature of considering population control as a humane device.
But Africa’s population growth can’t be denied, nor can Europe’s slow suicide, with its birth rate falling below replacement level. So, bucking conventional wisdom, they grasp firmly the discomfiting notion of widespread population restriction, attempting to break the informal prohibition on even discussing the topic.
Their icebreaker statistic: 26 African countries are expected to double their population by 2050. More so, by 2100, “Angola, Burundi, Niger, Somalia, Tanzania and Zambia are expected to have five times as many people as they do today.”
It would be wise to consider what effect such an enormous population explosion will cause on global resources, particularly the laundry list of rights that the United Nations attests belong to all people. The trio’s solution isn’t all that radical once you get over the queasy idea of deliberate population curtailment: increase access to contraceptives and abortion. In other words, a Malthus-inspired abortion-on-demand initiative.
“We should not shy away from discussing what actions are ethically permissible to facilitate a stable level of population growth, nor should we leave this discussion in the hands of the affluent,” they write, imploring others from outside the upper strata of the world’s developed nations to take part in the dialogue. “The conversation about ethics, population and reproduction needs to shift from the perspective of white donor countries to the places and people most affected by poverty, climate change and environmental degradation.”
This is a curious proposition. It is only decadent societies that entertain the idea of curbing population growth. Poor but growing nations rely on high fertility rates to combat high levels of infant mortality. The few exceptions are communist countries like China, where central planning absorbs all facets of private life.
It’s no coincidence that the one-child policy – the quintessential model of population control – originated in Red China. As Robert Nisbet wrote in The Quest for Community, thinking in terms of “the masses” is not something a free people does. “The masses are fundamental to the establishment of a totalitarian society,” he observed. It is the totalitarian impulse that inspires the notion that reproduction must be controlled.
Similarly, population control advocates often make their case by atomizing individuals down to lifeless statistics. Rather than real flesh-and-blood people with hopes, dreams, desires, and fears, they become integers of utility, slaves to the god of gross domestic product. In what is the most vivid argument ever lodged against population control, L. Brent Bozell condemned the “sin of head counts” in the New York Times back in 1971. He starts by describing an impoverished boy in Bombay whose “stomach is swollen,” with only a single rag hanging “about his loins.” To God, he is loved as anyone else. But to social demographers, he is a net loss. Bozell writes:
There is a greater supply of him than there is demand. He disturbs the ecological balance. He is socially inconvenient. The demographic mind eyes him and observes it would be better had his father been sterilized, or his mother aborted him – or, better still, had he never been conceived.
The devaluing of human life in the future leads to the devaluing of human life in the present. And there is a difference between a personal decision to put off having children and a national campaign to delay procreation or discourage it completely. The former is an ineradicable part of spousal relations; the latter is license for a small band of bureaucrats to make that choice on behalf of millions.
Here’s a simple idea on how best to combat Africa’s explosive increase in births: control borders, not population. Better police the Mediterranean Sea for migrant flotillas. Apply strict criteria for those seeking asylum. Send migrants home who don’t qualify for sanctuary.
That doesn’t mean we turn a blind eye to Africa’s expected birth trends. Food and medical aid should still be provided. Missionaries should continue to bring the Christian word to the continent. Philanthropists and charitable corporations should continue to finance new endeavors, providing a path to a legal livelihood for many who want to escape poverty.
Surely, those are a more moral means to enable prosperity than devising and implementing a plan to de-incentivize the creation of human life. Africa’s fecundity doesn’t have to mean the future foretold in Camp of the Saints.
TYLER, Texas, June 27, 2018 (LifeSiteNews) — Bishop Joseph Strickland of Tyler, Texas, included a powerful message about the truth of God’s plan for human life in his homily Sunday on the Solemnity of the Nativity of St. John the Baptist.
We need God in every aspect of married life, he said, in the marital act and beyond, and that means being open to the gift of life.
Coupling the sacrifice that John the Baptist made for marriage with the perennial and prophetic teaching of Humanae Vitae in the lead-up to the document’s 50th anniversary, Bishop Strickland effectively articulated God’s call for chaste love and repentance when it’s not achieved.
Catholics who are contracepting must refrain from presenting themselves for Holy Communion, he said as well, until they align their lives to God’s plan.
“God’s mercy is always with us,” Bishop Strickland said, “but His mercy calls us away from falsehood and to embrace the truth however challenging it is for all of us to live chaste lives.”
St. John’s parents, Zechariah and Elizabeth, are ancient models for modern couples, the bishop said, because they listened to the voice of the Lord and not the world with regard to their marriage and their son.
“The world told Zechariah and Elizabeth they were crazy for doing God’s will in their marriage,” he said. “Sadly, the world today, much like the world of Zechariah and Elizabeth, tells Catholics they are crazy for doing God’s will in their marriage.”
Observing God’s Commandments in every aspect of married life is difficult and challenging, the bishop said, but it bears beautiful fruit.
When people ask why God must be part of the marriage act, they’ve unknowingly touched on the very heart of the issue, he added.
“It’s not that God needs to be part merely of the marriage embrace,” Bishop Strickland said. “Rather, God needs to be part of your whole marriage, 24/7.”
“You need God in your married life,” he said. “The marriage embrace is only a part of your life together as husband and wife. God is present and desires to lift up all aspects of your married life. And to many couples, He is shut out of their most intimate moments.”
Today, many people acknowledge that God should be in the marriage, he added, but they still close the door on the most important moments of their life together.
The marriage embrace uniting husband and wife in the closest intimacy also renders them capable of generating new life, of participating with God in his creation, said Bishop Strickland. “How beautiful that is.”
He then detailed how artificial contraception impedes God’s plan for life.
“A marital act which intentionally impairs the capacity to transmit life frustrates God’s holy design and beautiful plan,” the Texas bishop said.
Quoting Pope Paul VI’s groundbreaking document, promulgated July 25, 1968, Strickland shared how any action taken during sexual intercourse to prevent procreation is intrinsically wrong and immoral.
“Those are challenging words the world heard 50 years ago,” he said, “but they bring a beauty of what God desires to us for every married couple to every person.”
In the 50 years since Humanae Vitae was first issued, a long list of artificial contraception methods have been developed, the bishop explained, acknowledging that the Church has not done well in teaching Catholics about the corresponding evil with contraception.
“I must say they are all intrinsically evil and wrong and gravely sinful,” stated Strickland. “I’m well aware that the Church has failed to effectively teach this truth and as your bishop I’m committed to sharing this beautiful teaching for the world today.”
He expressed hope for Catholics to learn more about the beautiful truth the Church teaches and embrace it with open hearts.
“This is God’s plan for all humanity,” said Bishop Strickland. “As Catholics, we can lead the world in believing that we are guided by God’s revealed truth, the truth that bread and wine become the body and blood of the Son of God at this altar, and so many other doctrines and dogmas that are important for us to flourish in God’s plan.”
The bishop was then forthright about the need for Catholics using contraception to recognize and examine this sinful act, to repent and forgo receiving Communion until they do so.
“Catholic couples who continue to use the methods of artificial contraception need to examine their hearts and recognize that this is sinful,” he said. “They should not receive Holy Communion without going to Confession and until they discontinue the use of artificial contraception.”
The Church considers it responsible for couples to refrain the marital embrace when necessary through the means of Natural Family Planning, the bishop said, but they must do this while always ultimately seeking the will of God and embracing the children that God brings them as the greatest gift and the fruit of their love and the marriage.
“When making the decision to refrain because they find it necessary, there is a painful sting to this,” he noted. “It’s called a sacrifice. And they can offer this as the bread and wine are brought to the altar of sacrifice.”
Catholics can join this and all sacrifices to the bread and wine as it comes to the altar at Mass, said Bishop Strickland, the bread and wine then becoming the body and blood, soul and divinity of Jesus Christ, God’s divine Son.
“This supernatural truth is what nurtures us from the heart of our Catholic faith,” he said, “And we must proclaim it to the world.”
All Catholics are called to live a life of Christian purity, he said, included him as a celibate priest, and all unmarried people.
“We all live in a world where this is difficult, where continence and chastity is scoffed at,” stated Bishop Strickland. “But we know what God has revealed and we joyfully embrace that challenge.”
“Living Christian marriage is hard. It’s painful,” he acknowledged. “There are many sacrifices, but we know that really living Christ’s way is to take up our cross and follow Him, and to see that cross blossom into a staff of new life and hope.”
The sacrifice of Jesus Christ, His Passion and suffering is wondrously powerful, the bishop said, and called for Catholics to tap into that power for their lives.
“Human Life — Humanae vitae — is our most sacred and precious gift,” Bishop Strickland concluded. “Let us pray, brothers and sisters, that we might cooperate with God’s grace facing the cross facing the challenges and joyfully embracing His call of life.”
June 26, 2018 (LifeSiteNews) – One day in New Jersey, years ago, I was standing on a train platform waiting to catch a train into New York City. Seeing well-dressed young women waiting at the platform, on their way to work, I thought: How many of these women are committing themselves to a life of single-hearted devotion to Mammon, the god of the world, without reaping any of the benefits that would arise from a life dedicated to the true God?
They are celibate, after a fashion, but they are not virgins; they make sacrifices day after day, but reap no salvation from them, and bring no immortal souls into the world. They might have sex, but no children; thus, they lose the chief glory and merit of the married woman. Once they have a child, they then frequently hand over the burden of childcare to someone else, losing the greatest opportunity and privilege of all, that of nurturing and educating their own offspring.
So many modern women are a set of absolute contradictions: their lives are consecrated, but to a false god who takes away the blessings of virginal faith; they are lying down with their husbands, but choose barrenness; when they bear children they do not nurse and educate them. In a satire upon their own existence, they are unvirginal celibates, unfruitful wives, unfaithful mothers—and all this by choice.
In many of his sonnets, Shakespeare urges the recipient to beget children in order to pass on beauty, and not waste it on oneself. The sonnets assume that sexual intercourse is naturally and quite happily linked with the conception of children; that marriage, all things being normal, leads to family (to think otherwise just would not have made any sense to a person living in a traditional culture); that a spouse will not only bear but rear children with complete dedication.
What would Shakespeare have said to these women on the train platform? “You should get married”? But they are married, many of them, yet they have no children. “You should have children”? But some of them have—one or two, and they think this is “more than enough.” The whole structure of social relations, the most elementary moral responsibilities, the most basic human realities, have disappeared; Shakespeare would have almost no way of entering the minds of these people.
Let me emphasize that I am talking only about what might be called voluntary barrenness, the de facto sterility chosen by those who either do not want children or do not wish to shoulder the burden of commitment. Obviously those who deeply desire to have children and cannot must bear this cross with the help of God’s grace, for their infertility is certainly neither chosen nor blameworthy. Childlessness is in truth the deepest sorrow and burden for those who have a worthy conception of marriage and human life. The perversity of the modern attitude consists in viewing children as a losing proposition, as a throwing away of one’s life.
When the prophet Isaiah uses the metaphor of mother for God’s tender love, it relies upon the fact that the bond between mother and child is known and felt to be the strongest, the most sacred, the most intimate of all bonds. It is perhaps the noblest model of love available to us, and thus God can make use of it and expect to be immediately understood. No mother forgets her child; how then could God? When Scripture says, “Even if a mother should forget her child, I will not forget you, says the Lord,” it is making a reductio ad absurdum: no mother worthy of the name forgets her child, and, since this is true, how much more will God remember us, since He is our maker and sustains our very being?
Today, the very basis for making this comparison, the natural and beautiful bond of mother and child, is openly mocked and repudiated. We are, alas, very far away from the image in Isaiah the Prophet, where the yearning of the mother for her child serves as a vivid image for the tender mercies of God towards lost and wayward Israel.
Somewhere in the human heart, no matter how calloused and cynical, there is an ember of that yearning, a spark of that love. We need to breathe on those embers and throw tinder on those sparks as much as we can, by witnessing constantly to the great gift of human life, the beauty of motherly and fatherly love, and the hard-won but deeply satisfying joy of living outside of oneself, for the sake of another.
WASHINGTON, D.C., June 26, 2018 (LifeSiteNews) – The United States Supreme Court ruled 5-4 on Tuesday that California cannot force pro-life pregnancy centers in the state to advertise abortions.
National Institute of Family and Life Advocates v. Becerra concerned a 2015 law forcing pregnancy centers to provide written information advertising how to obtain abortions in the state at taxpayer expense, and requiring those without medical licenses to post disclaimers that they do not offer medical services. The National Institution of Family and Life Advocates (NIFLA) represented nearly 1,500 pro-life pregnancy centers opposed to the law.
California argued that the law was necessary to prevent “deceptive advertising” by pregnancy centers, echoing a false claim commonly leveled at pregnancy centers across the country by abortion advocates. Pro-lifers responded by calling the requirements “compelled speech” that violated the First Amendment, and which would have dramatic ramifications for free speech and religious liberty if they were allowed to stand.
In a majority opinion written by Justice Clarence Thomas, the court struck down the law as a violation of the First Amendment. Thomas rejected California’s argument that “professional speech” was a separate category from that covered in the Bill of Rights, noting that “[s]peech is not unprotected merely because it is uttered by ‘professionals.’”
“As with other kinds of speech, regulating the content of professionals’ speech ‘pose[s] the inherent risk that the Government seeks not to advance a legitimate regulatory goal, but to suppress unpopular ideas or information,’” Thomas continued, noting that “[t]hroughout history, governments have “manipulat[ed] the content of doctor-patient discourse” to increase state power and suppress minorities.”
Thomas also rejected the argument that the requirement was medically necessary, and observed that it singled out pregnancy centers without applying to other facilities that offer similar services.
“The notice does not facilitate informed consent to a medical procedure. In fact, it is not tied to a procedure at all. It applies to all interactions between a covered facility and its clients, regardless of whether a medical procedure is ever sought, offered, or performed,” he wrote. “If a covered facility does provide medical procedures, the notice provides no information about the risks or benefits of those procedures. Tellingly, many facilities that provide the exact same services as covered facilities […] are not required to provide the licensed notice.”
Lila Rose, founder and president of national pro-life organization Live Action, praised the court for striking down what she called an “unjust law.”
“Planned Parenthood and pro-abortion politicians in California manufactured this law specifically to target pro-life pregnancy centers. This unjust law was one of the worst offenses against First Amendment rights we’ve seen and shows the illegal lengths the abortion industry and its political allies are willing to go to suppress the pro-life viewpoint and promote the killing of children in the womb. We applaud the Supreme Court for upholding the free speech rights of these centers,” she said.
“Pro-life pregnancy centers are doing some of the most important work in our communities today. They are providing advocacy, education, baby supplies, parenting classes, and maternity care to women in need. In addition to helping women during pregnancy, they often provide support long after the baby is born,” she continued.
“Abortion facilities like Planned Parenthood already use millions of dollars from taxpayers to promote their abortion business. No one should be forced to provide free advertising for the abortion industry – least of all pro-life pregnancy centers who are working to promote life, not destroy it,” she added.
Oral arguments in the case took place in March, and can be listened to here and read here. Alliance Defending Freedom CEO Michael Farris served as NIFLA’s lead attorney before the court, and pro-lifers widely interpreted the justices’ questioning as a sign they would ultimately uphold the pregnancy centers’ speech rights.
SCOTUSblog’s Amy Howe interpreted Justices Elena Kagan and Anthony Kennedy’s questions as skeptical of the California law, despite their records of supporting abortion itself. Kagan suggested the state had “gerrymandered” the law’s exceptions to ensure it targeted only pregnancy centers, while Kennedy was concerned the disclaimer mandates constituted an “undue burden.”
Further reinforcing the sense that California had overplayed their hand was a brief by Institute for Justice attorneys Robert McNamara and Paul Sherman. The two support abortion but nevertheless sided with NIFLA, arguing that if allowed to stand, the law would enshrine a distinction between “professional” and “private speech” that would empower governments to “crack down on everything from everyday advice about healthy eating to private citizens’ testimony at public city-council hearings.”
Ultimately, the decision fell along predictable ideological lines. Thomas was joined by John Roberts, Anthony Kennedy, Samuel Alito, and Neil Gorsuch. Justices Ruth Bader Ginsburg, Sonia Sotomayor, and Elena Kagan joined a dissenting opinion penned by Justice Stephen Breyer
“In this case, the government used its power to force pro-life pregnancy centers to provide free advertising for abortion. The Supreme Court said that the government can’t do that, and that it must respect pro-life beliefs,” Alliance Defending Freedom head Michael Farris said. “Tolerance and respect for good-faith differences of opinion are essential in a diverse society like ours. They enable us to peacefully coexist with one another. If we want to have freedom for ourselves, we have to extend it to others.”
The ruling is likely to have significant ramifications for similar laws in Hawaii and Illinois.
Ruining Respectful Relationships Between the Sexes
“Husbands, love your wives, as Christ loved the Church… Even so husbands should love their wives as their own bodies. He who loves his wife loves himself. For no man ever hates his own flesh, but nourishes and cherishes it, as Christ does the Church… This is a great mystery, and I mean in reference to Christ and the Church; however, let each one of you love his wife as himself, and let the wife see that she respects her husband.”
— Ephesians 5:25-33
Towards the beginning of Humanae Vitae Pope Paul VI describes the four characteristics of married love – or rather, the characteristics that married love should have.
Firstly, married love must fully be “human.” That is, it must involve the whole person, the “compound of sense and spirit,” and cannot be merely “a question of natural instinct or emotional drive.” Thus, it must be an act of the “free will,” so deep that it can “survive the joys and sorrows of daily love” and also to grow, “so that husband and wife become in a way one heart and one soul, and together attain their human fulfillment.”
Secondly, married love must be “total.” It should be based on a deep “friendship” in which “husband and wife generously share everything.” Within this total love, one spouse does not love the other for what he “receives” but rather “for the partner’s own sake.”
Thirdly, married love must be “faithful and exclusive.” While at times this may be difficult, it is “always honorable and meritorious,” insists the pope. “The example of countless married couples proves not only that fidelity is in accord with the nature of marriage,” he added, “but also that it is the source of profound and enduring happiness.”
Finally, married love must be “fecund” – or, at least, open to the possibility of children. “It is not confined wholly to the loving interchange of husband and wife; it also contrives to go beyond this to bring new life into being.”
There are two striking elements about Pope Paul VI’s vision of married love. The first is that it is a vision of love that demands continual effort and sacrifice. It is not enough for a couple simply to feel “in love”; to attain this depth of love, both spouses must work hard for it. And, secondly, it is a love that presumes equality between the spouses, an equality that is fostered by the spirit of sacrifice mentioned above. Rather than adversaries in the “battle of the sexes,” husband and wife are friends, each seeking in their own way to give to the other, for the other’s own sake.
Pope Paul VI’s Third Prophecy and the #MeToo Movement
A marriage based upon a love of this kind clearly benefits both men and women. However, it is striking how monogamous, life-long marriage is uniquely suited to protecting women from the worst exploitative tendencies of men.
Pope Paul VI, writing in the late 1960s in Humanae Vitae, was gravely concerned about how societal changes undermining the Christian ideal of marriage and sex exposed women to exploitation. In the third famous prophesy of Humanae Vitae the pope expressed his “alarm” that “a man who grows accustomed to the use of contraceptive methods may forget the reverence due to a woman.” Instead, he warned, by “disregarding her physical and emotional equilibrium” a man might reduce a woman “to being a mere instrument for the satisfaction of his own desires, no longer considering her as his partner whom he should surround with care and affection.”
It hardly seems necessary to expend any effort “proving” that this prophesy has come true. Over the past year we have been inundated with stories of powerful men taking advantage of vulnerable women to satisfy their insatiable sexual appetites. At the height of the #MeToo movement, millions of ordinary women shared stories on social media of being sexually harassed or abused. As many commentators have noted, one of the most striking aspects of these stories is the degree to which the men involved seemed to feel that they were entitled to sexual favors from women they scarcely knew. It doesn’t even seem to occur to these men that the women involved are human beings, with their own desires and dignity.
Furthermore, one need only glance at our advertising and popular culture to see the systematic sexual exploitation of women. Pope Francis lamented this problem this week, pointing out in a homily how women are routinely “humiliated” in ads, shown “wearing no clothes,” simply to sell a product. “This is a sin against God the Creator,” said the pope, “rejecting women, because without her we men cannot be the image and likeness of God. …. how many times do young women have to sell themselves as disposable objects in order to get a job? How many times?”
Decrying the practice of prostitution and sex trafficking, Pope Francis added, “All this happens here in Rome. It happens in every city. Anonymous women. Women we can describe as ‘faceless,’ because shame covers their faces, women who do not know how to laugh and many of them do not know the joy of breastfeeding their baby and the experience of being a mother…A woman is trampled underfoot precisely because she is a woman!”
The Sexual Complementarity of Men and Women
If women have always been vulnerable to exploitation by men, the widespread use of contraception has made them doubly so, as Pope Paul VI rightly predicted. To understand why this is so, it is first necessary to understand some of the core sexual differences between men and women, and then to see how contraception exacerbates and highjacks these differences, at women’s expense.
To begin with, men (on average) have a much stronger sex drive than women. Their sexual desires are also often only tangentially related to a desire for relationship or procreation. Their sex drive is also largely visually-driven and non-specific, meaning that men can be (and often are) instantly attracted to total strangers. As a general rule, this makes men the sexual pursuers, rather than the pursued. While sexual pursuit is good – indeed, necessary – when oriented towards marriage and procreation, if unchecked the male sexual appetite can easily become exploitative. This is the central point of a famous letter by the famous Catholic author JRR Tolkien to his son Christopher (to which I will return later), in which Tolkien makes the somewhat startling claim that for most men, monogamy is not natural, but rather “a piece of ‘revealed’ ethic” – that is, something learned by faith.
A woman’s sex drive, on the other hand, is (on average) significantly less intense and more complex in its mechanisms. The science on this is quite clear: a woman’s libido tends to be significantly more relationally-oriented, and responds to an unpredictable mix of intangible factors such as feelings of personal security, a sense of emotional connection with her partner, a comfortable and undistracted environment, etc. If this complexity is sometimes a source of frustration for men, it also makes perfect sense biologically. Women are, after all, much closer to and bear the overwhelming burden for the natural biological outcome of sex. A woman’s monthly cycle is a continuous and often-painful reminder to her of the natural purpose of sex. Contrary to a man, a woman is often keenly aware of the fact (indeed, how could she forget it!) that the risk of having sex is that she may spend the next several years of her life nurturing a new human being with her own body. Furthermore, she knows that if her sexual partner is not invested in the relationship, she may spend her life raising that child alone. It is wholly unsurprising, therefore, that a woman’s sexual nature is oriented towards relationship and security.
Any man who has been married quickly learns that he cannot expect sex on demand; and if he is at all sensitive, he also learns that there are very good reasons for his wife’s caution. He learns that if he wishes to have a healthy and regular sex life with his wife, he must pay attention to and nurture the whole of their relationship. Furthermore, he cannot do so only in the cynical hope of more sex (she will quickly detect that ruse) but rather out of a legitimate concern for her welfare.
In this way, a woman’s sexual nature draws a man out of the narrowness of his indiscriminate sexual appetites. A man who responds to the challenge thus learns to integrate those appetites into a broader context of relationality and self-giving: only one of the many ways in which men and women complement one another. Even as Tolkien bluntly acknowledged the troubling tendencies of male sexuality in a world after Adam’s Fall, he also movingly affirmed the only appropriate response for men: to train their sexuality through self-sacrifice. Faithfulness in marriage, he told his son in the letter mentioned above, requires “great self-mortification.” “For a Christian man there is no escape,” he added.
Marriage may help to sanctify and direct to its proper object, his sexual desires; its grace may help him in the struggle; but the struggle remains. It will not satisfy him – as hunger may be kept off by regular meals. It will offer as many difficulties to the purity proper to that state, as it provides easements. No man, however truly he loved his betrothed and bride as a young man, has lived faithful to her as a wife in mind and body without deliberate conscious exercise of the will, without self-denial.
Contraception: De-sexing Sex
The problem with contraception is that it removes one of the primary incentives for a man to embrace this ethos of self-denial. It does this by “de-sexing” sex.
That is, contraception suppresses the one aspect of sex that is overwhelmingly associated with the feminine: procreation. The chemical suppression of the woman’s cycle and the removal of the possibility of procreation creates the illusion of rendering “moot” all that complex female reproductive business. It suggests to a man that he no longer has to worry about the “risks” of sex, or the demands that those risks make on him. As a consequence, a man risks viewing a woman as just another man, but with a woman’s body. If he is excited about having sex right now (as he often will be), and there is no longer any serious risk of an unwanted pregnancy, then why is she still hesitant? What more does she want?
Just because a woman is on contraception doesn’t mean that her nature has changed. She is as much a woman as before. In many respects, she remains just as sexually vulnerable as before. Her deep-seated need for the sense of security that comes from the knowledge that her husband truly loves her remains.
Within a marriage, the risks are two-fold: 1) That the woman will become resentful that she is being used as an instrument of pleasure for her husband, who no longer sees any reason to expend effort learning to understand and love her as a woman. This is only exacerbated in our pro-abortion and pro-contraception culture, since women are overwhelmingly expected to bear the burden of so-called “consequence-free” sex: for it is they who are expected to pay for and take the hormone-laden contraceptive pills every day, or to submit their bodies to the violence of abortion if a “mistake” happens. And, 2) That without the incentives to control his passions and deepen his concept of love, the man will fall prey to the illusions of his baser instincts, believing that the quality of his marriage is solely dependent on the extent to which he is attaining sexual fulfillment. As Tolkien warned his son: “When the glamour wears off, or merely works a bit thin, [men] think they have made a mistake, and that the real soul-mate is still to find. The real soul-mate too often proves to be the next sexually attractive person that comes along.” In both cases, the end result is divorce and disillusionment.
Within a culture, on the other hand, the risks are what we have seen above: The catastrophic collapse of respectful relationships between the sexes, to be replaced with a culture of casual sexual exploitation and resentment: i.e. the #MeToo generation. The solution is teaching found in Humanae Vitae. The solution is St. Paul’s inspired word: “Husbands, love your wives, as Christ loved the Church.” And as the Church has always taught, contraception has no place in a love like that.
“Incompatible with life.” Those words have pierced the hearts of parents around the world as doctors handed them devastating diagnoses for their preborn children. Karen Santorum, wife of former Senator Rick Santorum, is one of those parents. Doctors told them that their daughter Bella had Trisomy 18, a condition that is considered “incompatible with life.”
But there Bella was, safely in her mother’s womb, very much alive. The pro-life couple refused abortion… and now Bella has turned ten years old.
“[…] she is the happiest little girl in the world and is full of life,” said Karen Santorum in a Facebook post on April 30, 2018.
Santorum could not hold back her frustration when the case of Alfie Evans caused international uproar after his parents were denied the right to fight for his life. Along with Charlie Gard, Alfie was the second little boy in a year to die in a hospital in England because the hospital staff and courts believed that they knew best, despite other doctors in other countries expressing their willingness to try new treatments with the hope of saving the boys’ lives.
Doctors said Bella Santorum was incompatible with life, now she’s 10.
Watching Charlie and Alfie die woke up parents around the world to the fact that some people believe our children are not our own. And for parents of children with special health needs, this thought reaches frightening, life-threatening heights. It means these precious children are seen as invaluable and unwanted by a large portion of society. It causes the concern and fear that if our children are hospitalized, we may lose our parental rights. Santorum will not have it:
What kind of a country gives their infants and children no chance at life? What kind of a country holds parents hostage and gives them no rights over the care of their children? What kind of a country euthanizes their children without fully understanding the medical diagnosis and possible treatments? What kind of a country places armed guards outside hospital doors? What kind of a country denies parents the right to a priest and prayerful time at the bedside of their dying child? What kind of a country holds parents prisoner, and will not allow them to bring their sweet little boy home so he could die peacefully in their arms? What kind of a country will not carry the burdens of its weakest members?
Santorum, who canceled the planned family trip to England this summer after Alfie’s death, expressed shock at the lack of a statement from the Royal Family, especially Prince William and Kate, who recently welcomed their third child.
“Their silence” over Alfie’s life and death, “is deafening,” she said.
On May 13, Bella’s 10th birthday and Mother’s Day, Santorum took to Facebook to wish her daughter a happy birthday:
Ten years have gone by since your birth. Ten years more than the skeptical and scientific said you would live. 87,648 hours of life, unexplained and miraculous. 3,652 days of letting all the world know that you are beautifully and wonderfully made!
Santorum knows better than most that doctors can be wrong. After all, doctors predicted that Bella Santorum wouldn’t survive long enough to leave the hospital. Yet here she is, ten years later. No one can say for sure that Charlie or Alfie would have died if their doctors hadn’t been too prideful to allow other doctors to try and save them. Bella proves that a diagnosis of “incompatible with life” does not make anyone incompatible with hope.
June 19, 2018 (LifeSiteNews) – St. Benedict in his Rule tells the monk that all the possessions of the monastery are to be treated with the same care that a monk would give to the vessels of the altar. The monk owns nothing, not even his own body, or his own will, says the saint.
The human body is a liturgical vessel. It is part of the sacrificial offering we bring to God, not just at Mass but throughout our lives: “I beseech you, therefore, brethren, by the mercy of God, that you present your bodies as a living sacrifice, holy, pleasing unto God, your reasonable service” (Rom 12:1).
Now, what do we offer to God upon the altar of sacrifice? Moldy bread and sour wine? How could that be something suitable for consecration? But the same question should be asked of that which a husband or wife offers to the other. Is it some artificially segregated portion of ourselves, sexual functionality separated from its procreative purpose or from the person as a whole? A hungry selfishness? Will they offer themselves in the totality of their human nature, body and soul, together with the children who may come? “Let the little children come to me, and do not hinder them” (Mt 19:14)—let them come into being!
Will we offer the whole of creation, as the priests and rulers He has placed in this world? What is worthy of the Divine Liturgy? What is worthy of the cosmic liturgy? The bees, the grain, the grapes, the olives, are not selfish; they yield everything they are to man and to God. Consider the lilies of the field. They prodigally offer their scent and shape, giving glory to their maker and comfort to their beholder. They do not feel the need to hold back or to do this at their pleasure.
Each time a husband and wife embrace one another, it is a re-enactment of the sacrament of their marriage, as each Eucharist is a re-enactment of the sacrifice of the Cross. What do we offer God and each other in this act? In what condition is the matter we offer? “This holy and unspotted host,” “an umblemished lamb.” If God deserves gold and silver vessels for the Eucharist, and pure wine and bread, then at least we can say that husbands and wives deserve worthy intentions and honest fleshliness without chemicals or barriers.
Should not the giver of the most intimate gift give his or her best? What is best in man is not just his flesh or his “heart” but the whole man, body and soul, flesh and spirit, mind and will, the power to unite and the power to give life and receive it. We are not dualists: man is not two things but one. If he is to give himself, he must give all of himself, surrendering who and what he is to the beloved, that the union may be a complete and perfect union—not a business contract or a prostitution or a recreation, none of which has anything to do with true love of a person for the person’s own sake, for who he or she is in the fullness of his or her being.
Nature-defying, man-denying, God-hating nihilism is at the root of “recreational sex” as well as “sex ed.” People who do not love one another for who and what they are live in a world without realism, love, or hope. They learn the cynical arts of distraction and dissipation to forget the miserable isolation of their condition. If one has nothing worth giving up one’s life for, the only thing left is a ceaseless pursuit of pleasures or frenetic business. In this way one tries to escape the asking and answering of existential questions like: Who am I? Why am I here? What is the purpose of my life? What does death mean? The reason religion seems to be irrelevant to so many people today is that religion exists to ask and to answerthese questions. When people no longer ask them, religion has nothing to say to them.
The action of nuptial union carries with it immense meaning and responsibility, which is why it ought to be freely and consciously chosen with the full weight of one’s being and with an unspoken but vital awareness of what it is. The best of Christian customs and pious traditions surrounding marriage always underlined this truth; Christians today should thoughtfully retain or recover them as they plan and celebrate their weddings and embark on the pilgrimage of married life in Christ.
Those who are engaged or betrothed and not yet married do not really know what the Lord will ask of them, what the burden of joy and suffering will be, until it has come upon them. But when they receive humbly and trustingly the mysteries handed down from eternity to time, from one age to another, they also receive the grace to be broken and healed, to hold on and let go, to die and rise again. It is a lifelong initiation into the paschal mystery, and its fruit is perfect conformity to the Bridegroom and the Bride, the oneness of eternal life, and a family beyond all earthly families.
Note: Part one of Father Boquet’s series may be accessed here.
“Contraception Leads to Falsification, Deception…”
Released in 1968, at the height of the hippie revolution with its optimistic doctrines of “free love” and emancipation from tradition and authority, Pope Paul VI’s encyclical Humanae Vitae was widely dismissed as the proverbial killjoy at the greatest party the world had yet seen: the sexual revolution.
Blessed Paul VI’s four “prophesies” about what would happen if contraception became normalized – from an increase in marital infidelity to totalitarian implementations of forced birth control by governments – are certainly bleak. However, it is worth drawing attention to another set of predictions contained in Humanae Vitae, ones that get far less attention than they deserve.
Speaking of married couples who opt for self-control and periodic continence, rather than contraception, in order to plan their family, the pope wrote that this effort enables:
…husband and wife to develop to their personalities and to be enriched with spiritual blessings. For it brings to family life abundant fruits of tranquility and peace. It helps in solving difficulties of other kinds. It fosters in husband and wife thoughtfulness and loving consideration for one another. It helps them to repel inordinate self-love, which is the opposite of charity. It arouses in them a consciousness of their responsibilities. And finally, it confers upon parents a deeper and more effective influence in the education of their children. As their children grow up, they develop a right sense of values and achieve a serene and harmonious use of their mental and physical powers.
A husband and wife open to life and children carry with them in marriage untold selflessness and blessings.
“Tranquility,” “peace,” “charity,” “thoughtfulness,” “loving consideration,” “serene,” and “harmonious.” The language of this paragraph, and others like it in Humanae Vitae, suggest that Pope Paul VI was far less interested in forbidding certain behaviors, as seeking to protect something that he saw to be good, beautiful, and – at the time he was writing in the 1960s – extremely vulnerable.
Time and again, Pope Paul VI insists that he is not imposing some arbitrary standard, but instead pointing to an order that is woven into the fabric of the universe, and which humans transgress at their peril. Human beings are made in the image and likeness of God. Their sexual faculties, with their creative potential, are designed by God to be used in a certain way, mirroring God’s own self-giving love and creative fecundity. Human beings’ technical triumph in suppressing the creative potential of sexual intercourse does not, he warned, alter that underlying design. For that reason, the technological triumph is only apparent, a meaningless victory.
To those who were urging the pope to “change” the Church’s teaching on contraception, the pope could only throw up his hands and reply, “Since the Church did not make either of these laws, she cannot be their arbiter—only their guardian and interpreter…” By “respecting the laws of conception,” he said, a married person acknowledges that he is “not the master of the sources of life but rather the minister of the design established by God.” Were he to declare contraception moral, the pope would be proclaiming right something that “by its very nature, is always opposed to the true good of man.”
“In preserving intact, the whole moral law of marriage,” he added, “the Church is convinced that she is contributing to the creation of a truly human civilization. She urges man not to betray his personal responsibilities by putting all his faith in technical expedients. In this way she defends the dignity of husband and wife.”
..And a “General Lowering of Moral Standards”
A “truly human civilization” is the same as the “civilization of love” – a term popularized by St. John Paul II, but in fact coined by Blessed Paul VI himself. This is a civilization characterized, above all, by the loving regard that its citizens have for one another, a love that, as St. John Paul II so often insisted, must begin in the family, the schoolroom of virtue. This love is not the rapacious, violent love of those who are seeking to “get” whatever they can from another, but the peaceful love of those whose primary motivating goal is to “give” to the beloved.
Pope Paul VI was worried that contraception drives a wedge in the very heart of the heart of the civilization of love: the family. In so doing, it will have ripple effects far beyond the relationship between the husband and wife. It will start there, of course – hence his prophesy about an increase in marital infidelity, which we looked at last week. But spreading from the sanctum of the marital bedroom, contraception will, he warned (his second prophesy), lead to a “general lowering of moral standards.”
Granted, this prophesy is extremely broad. In some respects, it virtually contains the other three prophesies, which all predict some deterioration in moral standards in some particular area of life. But it also goes beyond them, suggesting a far more global threat, affecting all areas of human life, and not just sexual morals.
Pope Paul VI Proved Right
Nevertheless, it begins with a deterioration in standards of sexual morality. And who, looking around, can possibly deny that there has been a catastrophic deterioration on this front?
I thought of Pope Paul VI’s prophesy this week while watching this stomach-churning propaganda video, recently produced by the CBC, the government-owned Canadian media giant. In it, the chipper host, Jessi Cruikshank, waving a rainbow flag and surrounded by rainbow balloons, discusses “gay pride” with a group of little children. As if she knows what “gay pride” is, one little girl pipes up, “Gay pride is, like, where all the gay people, transgender, lesbian, bisexual people gather up and celebrate.” The low point of the video might be when Cruikshank happily recounts to the children how when she was a kid she repeatedly watched the film Nell, which features nude scenes with the actress Jodie Foster. Foster, she said, “made me question my sexuality when I was a child because I like her so much.”
At one time, Cruikshank’s decision to expose young children to explicit, and deviant sexual ideas, would have resulted in accusations of child abuse. In 2018, however, her video has been viewed millions of times, and earned her plaudits from across the echo chamber of the media.
Indeed, it sometimes seems that absolutely everywhere one turns, one is confronted with a perverse, in-your-face, and graphic sexuality.
Over the next month, for instance, dozens of “gay pride” parades will take place across North America and Europe. Millions of people – including many of our most prominent politicians – will attend these parades, often with their children in tow, to watch completely nude marchers, men in sado-masochistic paraphernalia, and floats with drag queens and gyrating men in underwear.
Another example: In recent years, a pornographic book about a manipulative sado-masochistic relationship between a controlling billionaire and a naive young woman became one of the best-selling books of all time, selling in excess of 125 million copies as of 2015. 50 Shades of Grey has been dubbed “mommy porn,” with the sales apparently being largely driven by married women looking to “spice up” their lives.
Meanwhile, studies have found that the average age of exposure to hardcore pornography is eleven. Gargantuan pornographic advertisements are splashed across entire apartment buildings in our cities. Porn shops line our freeways, with giant billboards enticing lonely truckers. The most mainstream of films and TV shows are routinely filled with the kind of graphic sexuality that were once kept in the seediest porn shops in the seediest parts of a seedy town. The “dancing” at most dance clubs has gradually degenerated into undisguised forms of simulated sex. Finally, (and it boggles the mind to think of) the strip club has become one of the commonest venues for the bachelor party.
It’s all so bleak, and tawdry, and degrading. And that’s just the tip of the iceberg. Is there no shame left?
The “Contraceptive Mentality”
In explaining why he expected this lowering of moral standards, Pope Paul VI wrote: “Not much experience is needed to be fully aware of human weakness and to understand that human beings—and especially the young, who are so exposed to temptation—need incentives to keep the moral law, and it is an evil thing to make it easy for them to break that law.” That, the pope is suggesting, is precisely what contraception does.
And he’s obviously correct. Contraception is routinely presented by our sex educators as making possible the enjoyment of the pleasures of sexual intercourse without any of the traditional “risks.” Young people who accept this message (as most do) are thus led to believe that they can have all the sex they want, without worrying about the consequences.
As is the case with all sinful behavior, however, these alluring promises are far more illusory than real. As Pope Paul VI warned, the natural law will not be subverted. Not only has readily available contraception not eradicated the risks of sex, it has led more or less directly to a staggering explosion in the rate of the transmission of sexually transmitted diseases.
As the pope feared, the (apparent) removal of the most obvious incentives to keeping the moral law regarding sexuality led to a huge increase in casual sex. More importantly, however, it has generated what has been called the “contraceptive mentality.”
At the basic level, the contraceptive mentality is a collective form of wishful thinking. Its essential (and catastrophically wrong-headed) premise is that sex and conceiving babies have no intrinsic connection. Sex is one thing, and baby-making is another. Maybe they once had something to do with one another. But technology has changed all that. Sex is primarily about pleasure, and perhaps (though not necessarily) forging a bond with another human being. If one wishes to connect sex with babies, one may do so. But that is a choice. Furthermore, and most wrong-headed of all, the contraceptive mentality holds that we have a right to expect that sex will not lead to babies, and that if “by accident” it does so, we have no responsibility to accept or deal with the consequences.
But the contraceptive mentality also has a much deeper, and even more pernicious principle: namely that it’s ok to use another person for our own benefit and pleasure. Sex (which, when used according to God’s plan is an expression of the highest, most sublime love of one human being for another) thus risks becoming at heart a selfish transaction.
When this principle is enthroned in the heart of the family, infecting the union between husband and wife, it is not likely to stay there. This, I think, is why Pope Paul VI warned about a “general lowering of moral standards,” and not just a lowering of sexual moral standards.
At its worst, the contraceptive mentality leads directly to murder: the wanton slaughter of untold millions of our unborn brothers and sisters, the “unwanted” products of sexual relations pursued without regard for the consequences. There are even valid arguments that the contraceptive mentality is also behind the rise in that other legalized form of murder – “euthanasia.” Many older people are reaching old age without any children to take care of them, or with children who have absorbed the principle of selfish self-seeking and who are therefore uninterested in caring for their parents. Euthanasia presents itself as the easy way out.
There are myriad of other deep connections that could be made – at least in part – between contraception and many of the woes in our society: The epidemic of fatherless households, for instance, which is in turn connected to violent and anti-social behavior in their children; a crisis in trust for children who have been victims of divorce, which tends to affect their own relations with their future spouses and children; a rise in a consumeristic mentality that puts selfish desires first; a widespread breakdown in trust between the sexes, etc. This is, however, an investigation for another day.
In the 1960s it seemed to many that the choice about whether or not to use contraception could not possibly have any significant consequences. We now know better. Which will we choose: the rapacious, violent, restless, sterile and numbing sexuality of our porn-saturated culture, or the tranquil, peaceful, thoughtful, loving, and fecund love of a husband and wife who have learned to control their passions, and to turn them outwards, in a loving act open to the possibility of procreation?
Next week we will look at Blessed Paul VI’s third prophesy in Humanae Vitae.
Alzheimer’s disease is a currently irreversible, progressive brain disorder that slowly destroys memory and thinking skills and, eventually, the ability to carry out the simplest tasks.
According to the Alzheimer’s Association , the term “preclinical” refers to “a newly defined stage of the disease reflecting current evidence that changes in the brain may occur years before symptoms affecting memory, thinking or behavior can be detected by affected individuals or their physicians”.
Although biomarkers are still being investigated and validated, this new study can be reassuring to many people worrying that, for example, forgetting where they left their car keys means the beginning of Alzheimer’s.
While the cause of Alzheimer’s is still a mystery, research on the disease is massive and ongoing. Currently, there are drug and non-drug treatmentsthat may help with both thinking and behavior symptoms. There is hope.
THE BAD NEWS
With the many negative stories in major media about Alzheimer’s, it is no wonder that people are so afraid of it.
“Alzheimer’s has been portrayed as the ‘disease of the century’ that is poised to have a near catastrophic impact on the world’s healthcare system as the population ages…
This representation of the disease—along with other often used terms such as ‘living dead’, a ‘funeral that never ends’ and a ‘fate worse than death’—places Alzheimer’s as a soft target in the euthanasia debate because it plays to people’s fears of developing the disease and what it symbolizes. It positions Alzheimer’s as something that requires a remedy; that remedy increasingly being pre-emptive and beneficent euthanasia.” (Emphasis added)
While countries like Belgium and Holland have long allowed lethal injections for people with Alzheimer’s , this is forbidden in the US-for now. However, assisted suicide groups are now trying new “living wills” stating that if or when the person is diagnosed “with Alzheimer’s or another incurable dementing disease”, he or she refuses not only a feeding tube but also even assistance with oral eating and drinking to end their lives.
So influential major media outlets like the New York Times often publish articles such as the May 30, 2018 article titled “Alzheimer’s? Your Paperwork May Not Be in Order”that quote Dr. Judith Schwarz:
“People should at least understand what the normal process of advanced dementia is about,” Dr. Schwarz said. “Feeding tubes are not the issue….Opening your mouth when a spoon approaches is a primitive reflex that persists long after you’ve lost the ability to swallow and know what to do with what’s put in your mouth.” (Emphasis added)
Dr. Schwarz’s advice?
“Complete her organization’s Advance Directive for Receiving Oral Food and Fluids in the Event of Dementia.”
But what Dr. Schwarz and others do not want to talk about is the often tragic reality of deliberate death by starvation and dehydration.
Although media articles portray VSED as a gentle, peaceful death, a 2018 Palliative Practice Pointers article in the Journal of the American Geriatric Society titled “Voluntary Stopping Eating and Drinking” states:
“VSED is an intense process fraught with new sources of somatic and emotional suffering for individuals and their caregivers…The most common symptoms encountered after starting VSED are extreme thirst, hunger, dysuria (painful urination due to concentrated urine NV), progressive disability, delirium, and somnolence.” (Emphasis added)
Most chillingly, the authors state:
“Because an individual with delirium may forget his or her intention and ask for drinks of water, caregivers will struggle with the need to remind the incapacitated individual of his or her own wishes. This possibility should be anticipated and discussed with the individual in advance. While reminding the individual of his or her prior intentions may feel like coercion, acquiescing to requests for water will prolong the dying process for someone who has clearly articulated the desire to hasten death.” (Emphasis added)
The authors also state that if the patient’s suffering becomes severe, “proportionate palliative sedation and admission to inpatient hospice should be considered”. This is not the so-called peaceful death at home within two weeks that people envision with VSED.
Lastly, on the legal requirement of a cause on the death certificate, the authors state:
“the clinician may consider including dehydration secondary to the principle illness that caused the individual’s intractable suffering. Although VSED is a self–willed death(as stopping life support might also be), use of the word “suicide” on death certificates in this context is discouraged because in incorrectly suggests that the decision for VSED stemmed from mental illness rather than intolerable suffering.” (Emphasis added)
So, like assisted suicide, the real cause of death is basically falsified with the rationale that the deliberate stopping of eating and drinking to hasten death is just another legalwithdrawal of treatment decision like a feeding tube.
CONCLUSION
Years ago, my mother told me that she never wanted to be a burden on her family.
I never told my children that-especially when they were teenagers and already thought I was a burden to their lifestyles! Instead, I told them that the “circle of life” includes caring for each other at all ages and stages. Such caring also eliminates future guilt and leaves a sense of pride that we did the best we could for each other during our lives.
When my mother developed Alzheimer’s in the late 1980s (and later terminal thyroid cancer), a friend asked if I was going to feed her. At the time, my mother was fully mobile and able to get ice cream out of the freezer and eat it. I was shocked and offended.
“Do you want me to tackle her?!” I asked my friend.
“Oh, no!”, he answered, “I was talking about a feeding tube later on.”
I told him that my mother would die of her disease, not from deliberate starvation and dehydration.
Near the end of her life, we did spoon feed my mother and she enjoyed it very much before dying peacefully in her sleep.
For decades now, I have enjoyed caring for many people with Alzheimer’s or other dementias both personally and professionally. I can attest that such people can be sweet and funny and as well as difficult at times.
Abortion, no matter the race, is a tragic loss of beauty and potential that kills over 1.2 million innocent human lives each year. The abortion industry has created a culture of abandonment. Responsibility has become someone else’s concern, and death the solution to this serious character flaw. Men have been empowered by Roe v. Wade to abandon their primary responsibility–protecting. They’ve either chosen to run away from their role or have been forced out by a brand of liberal feminism that spews gender animus in an effort to elevate women. No one is elevated by 41% of all U.S. children being born to unmarried mothers. In the black community, 72.3% of all children are born in homes without fathers (compared to 35.7% of white children). Fatherlessness is epidemic in our culture.
Where are the Men?
Fatherhood begins in the womb and doesn’t end until you enter the tomb. President Obama forcefully declared, in a Father’s Day speech, that “fatherhood doesn’t end at conception.” There is no excuse for men who’ve chosen to have sex, to then choose to avoid any and all responsibility, when the natural result of sexual activity brings forth Life. Our government, too, has failed miserably in protecting the rights of fathers to exercise that responsibility by stripping away any ability to protect ones own unborn child. Every man is completely powerless, thanks to the anti-family, anti-life Roe v. Wade decision, to defend the life he is 50% responsible for biologically, emotionally, materially, and spiritually. The ideal is that children are born following marriage. The reality is that we’ve got a lot of healing, education, and mentoring to happen to get there. So even if marriage is not chosen, children STILL need their fathers!
The CDC reports nearly 84% of all abortions are attributed to unmarried women. Guttmacher, the Planned Parenthood-funded “research” arm, in typical fashion tries to distract from this staggering statistic by adding a few words. They add ‘co-habitating’ with the statistic to drive down the number, thus claiming: “53% of women having abortions are unmarried and cohabitating.”
The Consequences
An unborn child without a father’s presence is most likely to…die. Abortion has taken the place of fathers. This devastation of the absence of fathers doesn’t stop there. Cohabitation harms children, too.
“Compared to children living with married biological parents, those whose single parent had a live-in partner had more than 8 times the rate of maltreatment overall, over 10 times the rate of abuse, and nearly 8 times the rate of neglect.” –Administration of Children & Families, Dept. of Health & Human Services, pg. 12, “Fourth National Incidence Study of Child Abuse and Neglect”, 2010
Let’s dispel this myth that all families are equal. Every piece of evidence shows that they are not. Although many single parents bravely do all they can do to raise and love their children, the simple truth is that single-parenthood is not the best situation for our children, for our future. The majority of social science studies prove that traditional marriage, between a man and a woman, provide the most stable environment for a child economically, emotionally, educationally, physically, and spiritually. Yet, Planned Parenthood and its abortion allies, have to denigrate marriage in order to sell their number one service: abortion. Despite their namesake, they do little to nothing to promote family or parenthood. Their latest annual report uses the term ‘abortion’ 35 times, while never ONCE using the terms ‘mother’ or ‘father’…or ‘parenthood’. They depend upon the denigration of family to inject their life-killing venom into communities most vulnerable, especially our inner-cities.
“The marriage bed is the most degenerative influence in the social order—Quote from “The Woman Rebel” written by Margaret Sanger, Founder of Planned Parenthood
Poverty
Children, without fathers in the home, are 5 times more likely to live in poverty than those raised by two married parents. Nearly one third of single female-led households live in poverty versus 16.9% of single male-led households and only 5.8% of two-parent married homes. Women are remarkable, resilient, and worthy of much praise for all they do. But single-parent led homes have not always been the norm. According to the U.S. Census Bureau, 78% of all black households were led by two-parent married homes in the 1950s. In 1970, prior to Roe v. Wade, only 68% were. Today, only 28.7% of homes in the black community are led by married parents. And fatherlessness is increasing in the majority population too, at a slower rate, but still putting children equally in danger through the abandonment or exclusion of much-needed fathers.
There are an incredible host of disparities and disastrous consequences of the breakdown of the family, especially in the black community. The CDC reports that infant mortality among children of unmarried women increases 78% compared to children in two-parent married homes. Children, without fathers in the homes, are twice as likely to drop out of school, at much higher risk of incarceration, drug use, teenage pregnancy, and continuing cycle of poverty. Perpetual welfare (there isn’t a welfare bill that Planned Parenthood hasn’t lobbied for), population control efforts (via abortion and birth control policies), and personal behavior (heavily influenced by media and public education) have resulted in an environment that is, too often, toxic for our children.
We need our fathers. Mothers should never be left to play both roles.
The moment a child is conceived, a father is born. What will we do, as a society, to help stop this destructive trend of abandonment?
ROME, June 13, 2018 (LifeSiteNews) — Failure to heed Blessed Paul VI’s “prophetic” teaching against contraception in Humanae Vitae has caused a damaging “mutation” in social relations, a prominent theologian argued last week.
Speaking on Saturday, June 9, at a conference on Humanae vitae heldin the northern Italian city of Brescia, Italian moral theologian Monsignor Livio Melina argued that Blessed Paul VI’s encyclical reaffirming the Church’s ban on contraception “does not concern only the private sphere of sexuality, but also the social and public dimension of life.”
Melina reaffirmed the teaching contained in Humanae vitae, and explained that the encyclical essentially sets forth the conditions under which sexual intercourse between husband and wife can be considered a fitting expression of marital love.
He also argued that those in favor of contraception ultimately will have “no arguments to oppose homosexual relationships.”
Msgr. Melina is a tenured Professor of Moral Theology at the Pontifical John Paul II Institute for Studies on Marriage and the Family, where he served as a President from 2006 till 2016.
The conference, marking the 50th anniversary of Paul VI’s 1968 encyclical, was themed ‘Humanae vitae: the truth that shines.’ Its keynote speaker was Cardinal Willem Jacobus Eijk, Archbishop of Utrecht, Netherlands, who recently made the news for his forceful response in defense of orthodoxy following the German bishops’ controversial intercommunion proposal.
In his talk, Msgr. Melina noted that for centuries the family has been under attack from radical secularists, including those in Rome, who fought in the 1960’s to reduce the population; and freemasons in France, who at the dawn of the sexual revolution sought to transform society by emancipating it from its “Judeo-Christian tradition” through a redefinition of the family.
Today — with the widespread use of contraception — families, communities and entire societies are experiencing the devastating effects of these attacks.
Love is not a relativistic reality, Melina argues. The love that flows from God is a gift for each of us, and it is shared according to our natural and supernatural vocation: to live the life of grace and make our way to heaven. Sexuality, then, is a gift for the individuals as well as the common good: and whoever misuses this gift introduces disorder into the world. Thus, homosexual “marriage” is at root contrary to a truly human ecology, which recognizes that the context of marriage is the male-female self-giving relationship always open to life and symbolizing Christ’s love for the Church.
Here below is a LifeSiteNews translation of Msgr. Livio Melina’s talk.
***
The meaning of Humanae vitae for social relations and the common good
by Livio Melina
The thesis that I would like to illustrate is the following: The encyclical of Blessed Paul VI does not concern only the private sphere of sexuality, but also the social and public dimension of life. It is a question of social morality and not only of individual ethics.
Indeed, the context in which Humanae Vitae was published fifty years ago, on July 25th of that fateful 1968, was marked by an obsessive alarm over an uncontrolled growth of the world’s population, a true “demographic bomb” launched by Aurelio Peccei’s “Club of Rome.” From the outset, therefore, political concerns were at the heart of the debate. This is echoed throughout the encyclical, which nonetheless has the courage to go against the tide, and indeed prophetically to recall the serious consequences of the introduction of contraception into social custom: a general lowering of morality, an increase in marital infidelity, a loss of the respect due to women, and an exposure to the arbitrariness of public authority, to the detriment of the poorest peoples (HV, 17).
Paul VI was a prophet — unfortunately, an unheeded one. And today we can see that not only these but even more radical consequences have resulted: the introduction of contraception has caused a real genetic mutation in fundamental social relations, with grave threat to the common good. This is what I would like to talk about.
1. Sexuality in the logic of gift: the teaching of Humanae Vitae
Let us start with the doctrinal heart of the document found in n. 11: “Every marital act must of necessity retain its intrinsic relationship to the procreation of human life,” by virtue of the “inseparable connection, established by God, which man on his own initiative may not break, between the unitive significance and the procreative significance which are both inherent to the marriage act” (HV 12).
This is not a general affirmation of an ideal which should then be applied to concrete situations according to the discernment of each person’s conscience, as is often said today, with deliberate forgery of the letter and the spirit of the Magisterium. In reality, Montini’s encyclical formulates a concrete moral norm that is valid for any conjugal act: “Similarly excluded is any action which either before, at the moment of, or after sexual intercourse, is specifically intended to prevent procreation—whether as an end or as a means.” (HV 14). And he specifies that contraception is an “intrinsically dishonest” act, which can never be justified either by the principle of the whole or by the principle of a lesser evil. In order to be a faithful interpreter of the objective moral order established by God, the conscience of the spouses cannot proceed arbitrarily and decide for itself what are the honest paths to follow (cf. HV 10).
The moral norm just mentioned is not a legalistic prescription of a despotic will, which just as it issued the norm could also change it. On the contrary, it is the expression of a truth about the good inscribed in human nature by creative Wisdom. There are, therefore, intelligible reasons for the moral norm. And it is precisely these anthropological, ethical and theological reasons that St John Paul II wanted to explore and to teach in his Catecheses on the “theology of the body.”
The body, as a witness of the Creator’s original love, is the place where relationships break the isolation of the individual to generate a person. In his encounter with the woman, the man discovers his own body’s spousal vocation to the gift of self. And it is only by respecting this logic of gift that the personal dignity of love is safeguarded in openness to a new life, who can thus be born not as a mere physiological effect but as a gift from a gift.
In summary, we could say that Humanae vitae formulates the conditions according to which a sexual act is an adequate expression of conjugal love. Only when it remains in itself open to the transmission of life is the sexual act between spouses an act of union between the two, in which the authentic gift of self is realized in the body. The link between the two meanings should not be located at the biological level, but rather at the intentional level: there can be an intentionally contraceptive act which, even if it is physiologically fruitful, contradicts the truth of self-giving (for example, an act in which artificial contraception fails); just as there can be an act that per se is open to life, even though it is physiologically sterile and known as such (as happens in the natural regulation of births).
An act rendered intentionally sterile denies at the same time the sincere openness to the gift of oneself and the full acceptance of the other: it is an act that turns in on itself. Although carried out with the consent and collaboration of one’s partner, the contraceptive act intentionally closed to procreation is an act aimed at the pursuit of individual pleasure, which does not differ from masturbation. For this reason, sexual difference does not play a qualifying role in such an act and it is therefore analogous to homosexual acts. The English philosopher G.E.M. Anscombe says that those in favor of contraception will have no arguments to oppose homosexual relationships. The Italian philosopher Augusto Del Noce went so far as to say that “today’s nihilism (which he calls gay nihilism) always intends love ‘homosexually’ even when upholding a man-woman relationship.” It has been rightly observed that the man-woman relationship was public from its origin with its openness to the generation of children, and that is why it is sanctioned by marriage, while the homosexual relationship is in se private and cannot be recognized as marriage.
2. Sexuality, relationships and the common good
At the dawn of the sexual revolution in the West, the grand master of French Freemasonry, Pierre Simon, published a disturbing book in which he set forth a global project to transform French society, which was to be emancipated from its Judeo-Christian tradition through a redefinition of family and its constitutive relationships. Medicine was indicated as the instrument that would allow this surgical operation on the social body to occur, first through contraception and then through abortion and euthanasia. How does this transformation take place?
Sexuality has to do with the relationships that determine the identity of the subject and his social position: relationships of origin and those that point to our future: our being sons and daughters, husbands and wives, fathers and mothers. The separation of procreation from sexuality necessarily implies a radical transformation of these relationships. The child who is wanted and procreated outside of sexuality is reduced to a “product” of a technically controlled and evaluated project. Sexuality that is closed to reproduction no longer opens up to the other and loses its social meaning: it is “privatized,” because it is deprived of the generative breath that inherently permeates it.
The social dimension present in a man-woman couple consists in procreation. Insofar as it is ordered to procreation, sex, in the order of nature, is the only activity performed in the body that connects us also with the common good of society. And it is an activity accomplished outwardly by the body which, through personal communion and procreative cooperation, makes us more like God; it makes us a reflection of the Trinity. Privatization restricts sexual experience to an individualistic sphere, and impoverishes it on the level of semantics and relationships. Closed to generation, sexual activity is also futureless and restricted to the moment. The emphasis on performance has led to an agony in eros. A serious reflection on the statistics of the “Italian case” shows that the so-called “sexual revolution” has led, contrary to popular belief, to a drastic reduction in sexual relations: “free” sex has become even more banal and unsatisfying.
The introduction of technology that separates sexuality and procreation distorts sexual relations and ultimately leads to a perversion in the relationship between the generations. Gratitude and the gift which is recognized, accepted and communicated, disappear from the sexual experience, and are replaced by the search for self-sufficient eroticism and anxiety over performance. Fathers and mothers no longer live for their children; rather, they want their children only and only when they fit into a project that satisfies them. The natural order is reversed: children are called to live for their parents.
The demographic desert that we have been facing for decades is only the consequence of a loss of the generative and generous logic of giving, of a privatization of sexuality that is excluded from the common good of society, of a perversion of the relationship between the generations.
Contraception corrodes the common good of society because it introduces an “un-political” (S. Fontana), indeed and perhaps even more apt, an “anti-political” factor into social relations: the principle of the individualism of individual beings close to one other and at the same time subjected to a despotic power that dominates them.
Privatized to the extreme, sexuality is also paradoxically put under the domain of public control, and handed over to an invasion of public, political and legal power. The purely contractual logic of post-modern democracy invades private life and transforms intimacy such that, in virtue of a utopian absolute autonomy of the individual, it formulates models of “pure relations” that are unhinged from any reference to nature and tradition. As Stefano Fontana rightly states, a sexual relationship is neither private nor public: it is personal and communal. Only if it is set forth, not in terms of contraception but of spousal union open to life, can it be freed from the grip of privatization and public control.
3. Symbol and transcendence
And thus do we reach an even deeper manipulation: the elimination of the symbolic dimension and of transcendence from the sexual relationship. Paul VI evoked the presence of God the Creator in Humanae vitae, as the guarantor of the unity between the unitive and procreative meanings of the conjugal act. If God has nothing to do with it, procreation becomes a simple reproduction of a specimen of the species. If God has nothing to do with it, sexual union loses its symbolic meaning of covenant and becomes a diabolical place of confusion and exploitation. Separated from any reference to God, the body becomes a simple manipulable object to be disposed of as one wishes. When reference to divine Providence disappears from the horizon of existence, life becomes a calculation of advantages and disadvantages, a utilitarian planning that closes itself off in fear to surprises which the future holds — a future which we claim to govern, but which ultimately we do not decide.
“This is a great mystery, and I mean in reference to Christ and the Church” (Eph5:32). The mystery of sexuality experienced in marriage is a great light for the life of the world. The elimination of the dimension of “mystery” from sexuality has accompanied the sexual revolution and its alleged emancipation from its inception. The Marquis De Sade, in his attempt at compulsory re-education in a purely hedonistic practice of sex, obsessively repeats the formula: “It is nothing more than” — a formula that is both reductive and violent, that wants to censor the indispensable question of meaning.
In one of his last brilliant addresses, on the occasion of his Christmas greetings to the Roman Curia, on December 21, 2012, Pope Benedict XVI sounded a cry of alarm on the theme of the family, which precisely since contraception was introduced, has been radically questioned in its natural shape, as a relationship founded on marriage as a stable bond between a man and a woman, ordered to the procreation and education of children. He reiterated that it is not only a particular social form that is at stake here, but man himself in his fundamental dignity: in fact, if this bond is rejected, “the key figures of human existence likewise vanish: father, mother, child – essential elements of the experience of being human are lost.”
An authentic human ecology, as Pope Francis has also mentioned in Laudato si’ (No. 155), should deal not only with the pollution of the natural environment but also with that of the human environment, with social relations, which enable man to be himself, by finding his identity and breathing in deeply the truth of love.
I can therefore conclude by saying that Paul VI’s encyclical Humanae vitae, precisely because it protects the truth regarding married love from a logic of domination of the body and the pollution of a hedonistic and individualistic mentality, is also an essential contribution to the common good of human society.
June 11, 2018 (LifeSiteNews) – The outgoing U.S. bishops’ pro-life chief Cardinal Timothy Dolan has said that the pro-life movement absolutely must make abortion illegal, rebuking Jesuit Father Thomas Reese’s recent suggestion that pro-lifers give up on that and promote contraception instead.
“Besides supporting programs to help mothers and children, the pro-life movement also has to support birth control as a means of avoiding unwanted pregnancies. Planned pregnancies do not get aborted; many unplanned pregnancies do,” the Jesuit wrote after Ireland voted to legalize abortion.
Contraception is the “lesser of two evils,” Reese argued.
“The contraceptive mandate of the Obama administration will do more to reduce the number of abortions than all of the legislative gimmicks of Republican legislators,” the elderly Jesuit wrote. “If European Catholic institutions can pay money into national health programs that perform abortions, then American Catholic employers can pay for insurance programs that pay for birth control.”
“If abortion is never going to be illegal, pro-lifers must consider voting for candidates, even pro-choice Democrats,” Reese wrote, claiming that Democrats “will reduce the number of abortions by supporting programs that help mothers and their children.”
One of Reese’s most troubling assertions is that contraception should be used to reduce abortions. In addition to rejecting the church’s teaching that contraception is itself morally flawed, and the fact that it can be medically harmful to women, his reasoning is questionable.
In reality, more than half of women seeking abortion were actually using contraception during the month they became pregnant, and studies have shown that once contraception is more widely available, abortion rates may actually rise!
Another reality is that some contraceptive drugs and devices may work by preventing the newly conceived embryo from implanting in the womb and surviving. It is difficult to claim that we can reduce abortions by promoting drugs that may sometimes induce an early abortion.
There is a host of evidence that suggests left-wing, big government policies do not reduce abortions. Rather, pro-life laws are very effective at cutting abortion numbers, as social scientist and professor Dr. Michael New has documented extensively.
Reese suggested that “increasing the minimum wage” and government handouts might be the best solution to child killing.
Reese’s article did not give credit to the thousands of non-government pro-life programs, resources, and organizations that help moms facing unplanned pregnancies.
“Pro-life voters must choose between Republican rhetoric and Democratic results,” Reese wrote.
The Democratic party’s 2016 platform advocated for taxpayer-funded abortions at home and abroad, overturning any state and federal restrictions on abortion, and called abortion “core” to people’s “health and well-being.”
It’s an “unnecessary dichotomy” to say the pro-life movement should give up “all efforts to legally protect unborn human life, and work only to reduce the number of abortions” through left-wing programs, Cardinal Dolan responded. “Catholic tradition and basic human rights teach us that every human being has an inalienable right to life that must be recognized and protected in law. While the law is not the only means of protecting life, it plays a key and decisive role in affecting both human behavior and thinking. We cannot give up!”
Dolan said he does agree with “some” of Reese’s suggestions for reducing abortions, but overall the Jesuit’s strategy is a “capitulation to the abortion culture, and a grave weakening of the powerful pro-life witness.”
Dolan also dismantled Reese’s claim that because certain polls indicate support for abortion, pro-life activists should essentially give up.
“Reese would rightly be disappointed, as would I, if pro-immigration reformers were to give up because polls discourage them,” Dolan noted. “We would lament if anti-capital punishment advocates in some states were to surrender because of polls showing their fellow citizens were not on their side. I expect he would laudably urge them to persevere. Why not pro-lifers?”
Reese also admitted, “while I would be happy to see Planned Parenthood put out of business, closing clinics that provide health care and birth control to women before replacements are up and running is irresponsible and counterproductive.”
In a groundbreaking conference held in Washington DC last month, some of the Church’s most influential women spoke about how the #MeToo movement proves the abject failure of the now 50-year-old sexual revolution that was supposed to liberate us and set us free.
Writing for The Stream, Carrie Gress attended the May 31 conference entitled, “The #MeToo Moment: Second Thoughts on the Sexual Revolution,” which was sponsored by The Catholic Women’s Forum along with the Ethics and Public Policy Center (EPPC) and the Notre Dame Center for Ethics and Culture and took place in Washington DC.
Moderated by Mary Rice Hasson of EPPC, she opened the conference by saying that the #MeToo movement, which sparked widespread outrage over sexual harassment and the culture that condones it, has “created space” for women to ask questions about how the sexual revolution might have contributed to the problem.
“We step into that space today to begin that larger conversation,” Hasson said.
Cardinal Donald W. Wuerl, Archbishop of the Diocese of Washington, spoke next, and addressed how the sexual revolution undermined the moral compass of life and led to increasingly acceptability of dissent from papal magisterium.
Mary Hassan
Mary Eberstadt of the Faith and Reason Institute spoke about the damages done by the pill and how its pioneers never foresaw the consequences even though some of their critics did, like Blessed Paul VI. In his document, Humanae Vitae, he warned that women would see their value “cheapened” and their dignity cast aside as a result of using artificial contraception.
Dr. Suzanne Nortier Hollman of the Institute for Psychological Sciences tackled the mental fall-out for women from casual (“hook-up”) sex..
As Gress reports, Hollman noted that women were much more damaged by it than men and that only 26 percent of females in one survey reported a positive emotional response to a hook up.
“Why do the other 74 percent take part? Many women report that they feel pressured into sex. That’s even if they end up consenting. It’s not just eager male partners at fault; many young women succumb to peer pressure. They feel that ‘hook-ups’ are simply expected of them.”
Dr. Marguerite Duane of Georgetown spoke about how the Pill has been classified as a Class One carcinogen like tobacco and asbestos and yet we continue to ignore the very real health issues stemming from it.
Monique Chireau, an OB/GYN at Duke University Medical Center, spoke about the dramatic rise in STDs since the 1960’s when the main concern was syphilis and chlamydia. Now we’re facing a pandemic of more than 25 types of common STD’s which are causing a rise in cancers, particularly those associated with the colon, mouth, and throat.
According to Chireau, more than 10 million women take it, which puts the industry at $4 billion a year – and yet we still see two million unintended pregnancies a year. Unfortunately, those who expect perfect control over their fertility are often the ones who turn to abortion as a backup.
Dr. Monique Chireau
“Planned Parenthood’s number one product is abortion,” Chireau said. “Their second product is contraception. Do you really think they would provide contraception if it was hurting their bottom line?”
Both Chireau and Duane believe oral contraception has caused feminism to become distorted. For example, instead of demanding that the workplace accommodate their biological realities, they resort to dangerous “medicine” to “beat biology into place,” Gress reports.
As Dr. Duane pointed out, the Pill has “stunted medicine” because it became a panacea for every gynecological ailment. “Instead of treating the root problem, a woman’s cycle is just disrupted,” she explained. “Women deserve better medicine than that.”
Another panel of experts discussed the commodification of women’s and children’s bodies.
Jennifer Lahl of The Center for Bioethics and Culture addressed surrogate motherhood and how it abuses women and treats children like commodities. Beneath the happy rhetoric of “helping would-be-parents,” women suffer a host of complications from the procedures involved.
“Egg donors suffer strokes and sterility. Surrogate mothers deal with manifold issues, since the womb was not designed to carry someone else’s child,” Gress reports.
Lahl also spoke about the tragic plight of nearly one million tiny humans who are languishing in the freezers in the U.S. alone – a place from which most will never be rescued.
Mary Leary of Catholic University’s law school, spoke about worldwide human trafficking which involves an estimated 27 million people, mostly women and children. This practice is spreading across the U.S. where traffickers are earning $200 million just in Atlanta.
“Their victims work as slave laborers in industries from domestic service to sweatshops to pornography,” Gress reports.
Dr. Mary Anne Layden
Mary Anne Layden of the University of Pennsylvania also addressed the epidemic of pornography and how users begin to think that aggressive, unwanted sexual advances are actually mutual and even invited – which could be how the #MeToo phenomenon got started.
Helen Alvare, George Mason Law Professor, wrapped up the day by explaining how the family has been under legal attack ever since the sexual revolution. Beginning with Roe v. Wade, which stripped the unborn of the right to life, the government is now promoting contraception even while protections for families and parental rights are slowly eroding.
“It really did take some decades to have this many qualified women” who lived through the sexual revolution, Alvare said. “We could not have had such a conference 30 years ago.”
As the Catholic News Service reports, Alvare expressed her hope that the conversation that began at this conference will begin “an honest dialogue based on well-sourced facts had by honest women.”
June 12, 2018 (LifeSiteNews) – Seven years ago, Alana and Rickard Newman set out to make a movie chronicling Alana’s very personal quest to find her biological father – an anonymous sperm donor.
The duo ended up producing something quite different – a sprawling, visually and intellectually engaging documentary to benefit the entire world.
Alana, a talented secular musician who gave up her musical career for life, family, and love, remains at the heart of the final product, sharing how through desperation to know her father she finds herself discovering the treasures of St. John Paul II’s Theology of the Body and Pope Paul VI’s encyclical Humanae Vitae, both on the topics of love and marriage.
And perhaps not surprisingly, Alana and Rickard’s search for truth led them to a place neither anticipated at the outset of their quest: Both experienced a dramatic conversion to Catholicism.
Sexual Revolution seeks to examine the effects of the free-love experiment of the hippie generation and the prophetic encyclical, Humanae Vitae, while closely examining the history of the parallel developments of the Pill and modern Natural Family Planning (NFP).
The film features interviews with leading thinkers Archbishop Charles J. Chaput, Dr. Janet Smith, Dr. Peter Kreeft, Dr. Robert P. George, Dr. Mark Regnerus, Steven Mosher, Mary Eberstadt and many more who are important voices reckoning the ongoing damage of the sexual revolution with the timeless wisdom of Church teaching.
The movie captures the mood of the era with its lush musical soundtrack featuring artists such as Joni Mitchell, The Byrds, Eric Clapton, Neil Diamond, Paul McCartney, and Crosby, Stills, Nash & Young.
LifeSiteNews reached out to Alana Newman in order to better understand how and why she and husband, Rickard, devoted seven years of their lives to this project.
LifeSiteNews: Alana, most of our readers don’t know your personal story regarding third party reproduction. Can you speak a little about that so our readers understand the deep yearning that compelled you to launch this project?
Alana: I have never met my biological father. And actually, neither has my mother. This is because my mother’s first husband was infertile and they decided to use an anonymous donor to conceive me.
My husband started filming me soon after we met and the original thought behind this film was that we were going to search for, discover and meet my father. The only thing I knew about this man who makes up half my genes is that he was ethnically Polish and raised Catholic—so in my efforts to learn more about my long lost Polish and Catholic heritage I picked up an interest in the most famous Polish Catholic man I was aware of, Pope John Paul II.
So in the more important sense, I did come to know and embrace my father during the making of this film—God, the Father. I am continually blown away by the wisdom the Church offers—it’s like discovering a well when you’ve been wandering in the desert by yourself for years.
LifeSiteNews: How did the movie take shape? The idea of pairing the sexual revolution with the Humanae Vitae, while also pairing the parallel developments of the Pill and modern Natural Family Planning (NFP) by telling the stories of Dr. Pincus and the Drs. Billings is awesome. How did that come together?
Alana: My husband began filming shortly after we met. It was going to be about my donor-conception story. Then at some point we became very interested in finding solutions to infertility. I realized that two major causes of infertility could be generalized as our toxic environment and our toxic behaviors. Hormonal contraceptives make massive, negative contributions to both our toxic environment (via synthetic estrogens) as well as our toxic behaviors (STD induced infertility, delayed childbearing, mistrust between genders, etc.). So I developed a passionate conviction that hormonal contraceptives were evil.
But as a woman in my 20’s and now early 30’s, I truly understand the fears and responsibilities associated with pregnancy and childrearing. It is very important to me to be able to enjoy intimacy, while confidently being able to manage and space my children. That is where my interest in Natural Family Planning took root.
Luckily, my husband stumbled upon The Billings Ovulation Method at a conference for Family Life Directors and we felt like God really loved us by revealing to us an NFP method that is so simple and intuitive. He bought a couple of books, one called The Billings Enigma, and previously having read The Birth of The Pill by Jonathan Eig he realized that there was an intense spiritual battle going on during the 50’s and 60’s. It was only a small group of people responsible for the invention of The Pill, and only a small group of people involved in discovering modern NFP—and if you examine their stories and the timeline you can really see God’s hand at work, His mercy, and creativity.
Alana NewmanSpringtime Productions / Youtube screen grab
I think viewers of this film will be struck with the level of investigative journalism that went into it—and when they learn about the differences in how these two different forms of family planning were developed, I imagine many people might have their faith strengthened significantly.
LifeSiteNews: You say that the experts you interviewed were not only instrumental in making the movie, but also helped you and Rickard on the way to your conversion to the Catholic Church. What happened?
Alana: People will see me in the film and think that I’m a regular conservative Catholic white lady with some kids living in the suburbs. What they don’t realize is that I used to be a militant feminist volunteer for NARAL that dated women and went to atheist club meetings at a German bar in San Francisco.
I discovered the marriage and family work of Elizabeth Marquardt and David Blankenhorn at The Institute for American Values. Then through them I met some incredible Catholic thinkers like Professor Robert George, Mark Regnerus, Mary Eberstadt, Jennifer Roback Morse, and others. Reading these people’s work, I was struck first by how well they seemed to articulate human nature. Secondly, they didn’t back off or back down when peer pressure became too intense.
It was the hardcore Catholics that showed backbone and courage under fire. Clear language and good ideas regarding marriage and family were the tools I needed to cultivate a family of my own. Thank you to all of you who stand fiercely behind Church wisdom on these topics. Your steadfastness matters.
LifeSiteNews: Our readers are highly engaged in pro-life, pro-marriage, and pro-family issues, often as local activists. How will your movie aid them in promoting a culture of life in their parishes and local communities?
Alana: Films are the preferred way of communicating ideas for most people today. With film you get the opportunity to communicate through not only words, but also body language, iconography, fashion, and music.
Film is communal. It starts conversations. And it can be an event—an excuse to gather. 500 people can sit side by side and watch a film and discuss it immediately afterwards.
Films are also difficult to make. A well done film that promotes Church teaching on human ecology is rare—so this is a great opportunity for parishes and pro-family organizations to share the wisdom the Church has revealed to us, in a popular and easy-to-digest format.
LifeSiteNews: What do you hope people will take away from your movie? What role do you think it can play to advance a culture of life?
Alana: I want people to see this film and want to learn NFP, or make the move to become an NFP instructor.
Natural Family Planning is the practical application of Theology of The Body. Learning how to chart is like learning how to read music, and it eventually offers total bliss from being able to take those notes on a page and make real music with your body.
NFP advances a culture of life because it reconnects sex and babies in people’s imagination. It means that every time a man approaches a woman for sex, he can’t help but recognize the power of her body to make new human beings. That recognition of power is the beginning of respect.
Like Jacob Marley, 13-year-old Trenton McKinley was dead. There is no doubt whatever about that. Or so the doctors said.
He had suffered seven skull fractures and traumatic brain injury in a freak vehicle accident last March. His mother reported on Facebook that during emergency surgery he “died four times,” which, I presume, means he flat-lined; “one time,” she said, “for 15 minutes.”
After his heart’s final injection with epinephrine, “he had no brain waves,” including apparently from his brain stem. His eyes were dry and solid black. The doctors concluded — andeverymediaoutletreported — that the boy was “brain-dead.”
When doctors say a patient is “brain-dead,” they mean the patient has suffered the complete and irreversible loss of all brain function, including of the brain stem. The condition is called “whole brain death.”
Ever since the publication of the so-called Harvard brain-death definition in 1968, clinicians the world over have taken brain death to mean human death; so that even if certain bodily functions continue, such as circulation and breathing aided by machines, the person, the living human being, John or Mary, is gone, and what remains is an elaborately functioning corpse the true state of which is being hidden by the effects of medical technology. These individuals are often even issued death certificates (see the case of Jahi McMath).
The doctors were so certain of their diagnosis that his mother signed the paperwork to have his vital organs harvested for donation. Now to qualify for such donation, an individual must have died; this is the meaning of the “dead-donor rule” that prevails in the United States: Only corpses supply vital organs, although somebioethicists in recent decades have called for the lifting of the dead-donor rule.
If, therefore, Trenton’s body was a corpse, removing his heart, lungs, liver, etc. would have been no violation of human dignity. If, however, he were still alive, taking his vital organs would constitute homicide.
Happily, before his organs were harvested, Trenton began to exhibit signs of life: Brain activity resumed; his eye color returned; he regained consciousness, speech and mobility; they took him off the ventilator; and, finally, he went home.
It’s being called a miracle. Perhaps. They certainly occur. But because this same report — “brain-dead” patient recovers consciousness — is increasingly common (see here, here and here), let’s doubt the miracle claim for the sake of argument and look at the situation empirically.
Was Trenton Dead?
One may reasonably ask whether the boy ever was dead. For if he was, then he rose from the dead. But without a miraculous intervention, people do not, indeed cannot, rise from the dead. This is because death by definition is irreversible.
Death is the definitive separation of the spiritual soul from the material body, not just a temporary separation, as seems to be the case in so-called “near-death” experiences. This causes the body to lose irretrievably the integrative functioning proper to a living organism. So the fact that a brain-dead individual wakes up means he was never dead to begin with.
Was Trenton Brain-Dead?
Now, this implies one of two things: Either Trenton was brain-dead but brain death isn’t human death, and brain tissue can regenerate itself even when its entire living substrate is destroyed, and Trenton’s regenerated itself, so dramatically that he is now not only conscious but carrying out fine motor skills like playing basketball; or Trenton was not brain-dead.
The second, it seems, has to be the case. Not because I am confident that all brain-dead individuals are humanly dead, or because I am a better diagnostician than his doctors, but because there is no evidence that brains can recover from total infarction (death).
Neurologists traditionally believed that damaged brain cells never regenerate; but recent studies indicate that some cell regeneration does take place in the human brain, especially in younger persons (under 40 years of age). Moreover, it has long been known that neural tissue has a high degree of “plasticity,” which means when certain regions are destroyed, the functions associated with those regions are not necessarily lost; the brain can reroute the neural connections in such a way that those functions begin to be carried out by other regions.
But there is no evidence whatsoever, at least none to my knowledge, that any brain has ever recovered from total death. So Trenton must not have been brain-dead.
Lessons Learned from Trenton’s Case
This raises an important educational point for all of us: Protocols (confirmatory tests) for diagnosing brain death can be unreliable. Since there are clinical states that mimic brain death, such as certain neurological diseases and metabolic disorders, even a conscientious application of corroborating tests can render a false positive, as obviously happened with Trenton McKinley.
There are two lessons to take away from this:
First, when dealing with a loved one who may be brain-dead, make sure you get multiple corroborating opinions from doctors who are practiced in diagnosing brain death.
Second, make certain the doctors are asking the question of whole brain death. Some clinicians conclude that patients are brain-dead even when there is evidence, however minimal, of brain activity. These patients donot meet the criteria for brain death, and so do not fulfill the commonly accepted conditions for human death. And yet, as soon as they are defined as brain-dead, they become possible candidates for vital organ transplantation, which certainly will result in their deaths.
Is Brain Death Human Death?
But there is one question left standing: Is brain death coextensive with human death? There is a lively debate among Catholic philosophers, scientists and clinicians about this. Someethicists are convinced that brain death is human death and that this has been officially taught by the Catholic Church.
But the doubters are many indeed and include faithful Catholic thinkers and clinicians, some quite eminent, such as Josef Seifert, Alan Shewmon, Robert Spaemann, Dominican Father Nicanor Austriaco, Alfonso Gómez-Lobo, David Albert Jones, Charles Camosy, Paul Byrne, Nancy Valko, etc. Each, after examining recent startling evidence suggesting that ventilated brain-dead individuals are living human beings — extremely disabled, to be sure, but not dead bodies — believe there are reasons for doubting the now 50-year-old Harvard definition.
Doubts about the traditional rationale also exist among non-Catholics, some of whom don’t share a Christian view of the dignity of the human body: e.g., Truog, Miller and Halpern, Halevy and Brody, Youngner and Arnold, Robert Veatch, Karen Gervais, John Lizza. They, too, doubt that functioning brain-dead bodies should be classified as corpses or dead organisms.
Err on the Side of Life
Listen to the words of the renowned Catholic physician, bioethicist, Georgetown professor and chairman of the G.W. Bush President’s Council on Bioethics, Edmund Pellegrino, who also expressed reasonable doubts, as he quotes the philosopher Hans Jonas, a man whose ideas have exercised a salutary but too-little influence on the development of bioethics in the West:
“Ultimately, the central ethical challenge for any transplantation protocol is to give the gift of life to one human being without taking life away from another. Until the uncertainties and imprecision of the life-death spectrum so clearly recognized by Hans Jonas are dispelled, his moral advice must be our guide for all transplant protocols”:
“We do not know with certainty the borderline between life and death, and a definition cannot substitute for knowledge. Moreover, we have sufficient grounds for suspecting that the artificially supported condition of the comatose [i.e., brain-dead] patient may still be one of life, however reduced — i.e., for doubting that, even with the brain function gone, he is completely dead. In this state of marginal ignorance and doubt the only course to take is to lean over backward toward the side of possible life” (Hans Jonas, “Against the Stream,” in in Philosophical Essays, emphasis added).
The conversation about whether brain death rightly diagnosed constitutes human death needs to make its way from the heady journals of medicine and bioethics to the pews. Catholics who face difficult questions about whether to submit themselves or their loved ones to transplant protocols based upon a judgment of death that’s grounded in a definition that many reasonable Catholic thinkers find doubtful have a right to inform themselves more fully on the question.
E. Christian Brugger is a senior fellow of ethics and the director of the fellows program at the Culture of Life Foundation in Washington, D.C.
Pope Paul VI Rejects Paradigm Shift, Re-Affirms Church Teaching on Inherent Dignity of Marriage
Two Opposing Views of Marriage and Human Sexuality and Their Consequences
“False teachers, many belonging to an intellectual elite in the worlds of science, culture and the media, present an anti-gospel…When you ask them, “What must I do?” their only certainty is that there is no definite truth, no sure path….Consciously or not, they advocate an approach to life that has led millions of young people into a sad loneliness, in which they are deprived of reasons for hope and are incapable of real love.”
These days, many people tend to interpret any prohibition whatsoever as a repressive encroachment upon their personal autonomy. Not only is this wrong-headed, but it is completely self-defeating. While some prohibitions can be unjust and repressive, many others are true and just. Not only are these not repressive, they are in fact liberating. Just as mastering the rules of perspective allowed Raphael to paint his masterpiece, The School of Athens, so too can mastering the moral laws allow us to create the ultimate masterpiece of a virtuous life. On the other hand, to contravene or seek to “transcend” those rules does not lead to more freedom: it leads only to anarchy and misery.
When Pope Paul VI issued the encyclical Humanae Vitae on July 25, 1968, the world immediately interpreted it as a gigantic “no.” At a time when the whole world was ecstatically embracing the new forms of artificial contraception – especially the seemingly miraculous birth control pill – many, including a large percentage of Catholics, looked to the Church to change its teachings to align with technological and so-called societal progress.
Instead, it seemed to many, that Pope Paul VI stubbornly turned his back on progress. According to this interpretation, Humanae Vitae is, quite simply, the encyclical that refused to allow Catholics the freedom to use contraception. Or more bluntly, it is the encyclical that has kept the Church in the “dark ages,” clinging to a gloomy view of sex, based upon arbitrary and authoritarian moralizing.
Humanae Vitae: An All-Encompassing “Yes” to a Love
But that’s not how Pope Paul VI understood what he was doing. On the contrary, he quite obviously believed that the “no” that he re-affirmed (the Church has been saying the same thing for 2000+ years) in Humanae Vitae was couched within a “yes” to something far greater and beautiful: an anthropology and theology of marriage that grant to marriage and married couples a dignity, value and calling far surpassing the understanding of the world.
Our age tends to view marriage as a temporary union of persons oriented towards the gratification of various more or less noble desires (personal fulfillment, companionship, sexual pleasure, etc.). Within this view, a marriage need only endure as long as it continues to serve those purposes. Children, also, are shoe-horned into this paradigm: something to be chosen under ideal circumstances as part of the couple’s “journey” of personal discovery and self-actualization.
Compare that view of marriage to the one expressed by Pope Paul VI in paragraph 9 of Humanae Vitae. Speaking of the love to which husband and wife are called, the pope wrote:
It is a love which is total—that very special form of personal friendship in which husband and wife generously share everything, allowing no unreasonable exceptions and not thinking solely of their own convenience. Whoever really loves his partner loves not only for what he receives, but loves that partner for the partner’s own sake, content to be able to enrich the other with the gift of himself.
“A love which is total.” A love like this, modeled on the wholly selfless love of God for us, cannot be self-contained. If, as the Gospel of John says, God is Love, then love is the creative force of the universe. Insofar as married couples mirror that love in their own lives, so too will their relationships participate in God’s creative powers. That greatest of human loves, that between a husband and wife, is also innately oriented outwards, towards creation. As Pope Paul VI wrote, married love “is fecund… it is not confined wholly to the loving interchange of husband and wife; it also contrives to go beyond this to bring new life into being.”
The problem of contraception, wrote Pope Paul VI, is that by separating the unitive and procreative ends of sexuality, couples “act as ‘arbiters’ of the divine plan and they ‘manipulate’ and degrade human sexuality – and with it themselves and their married partner – by altering its value of ‘total’ self-giving.” To love totally in marriage means not withholding the fertile part of being a man or woman; that is, the wife gives all of her femininity and the husband gives allof his masculinity. Should one or both resort to contraception (employing the contraceptive mentality), they would be withdrawing their fertility from the self-giving. They would not be giving their all to each other. Such an action not only makes procreation impossible – preventing cooperation with God in life-giving love – but also damages the bonds of love – harming the unitive, love-giving end.
It is no surprise that many marriages are weak because of the use of contraception. Every time that a married couple uses contraception they withhold love from one another. The marital embrace then becomes solely focused on gratification and is not the self-giving, unifying, and potentially fruitful act that God created it to be.
The Four Prophesies
Paragraph 17 of Humanae Vitae is perhaps the most famous paragraph. In this paragraph Pope Paul VI predicts the consequences for couples and society on the whole should contraception become normative. Many commentators have referred to these as the “four prophesies” of Humanae Vitae, all of which were dismissed as mere fear-mongering by most of the pope’s contemporaries, but all of which have come startlingly true.
Contraception would lead, said the pope, to:
an increase in marital infidelity
a “general lowering of morality”
men increasingly using women as “mere instruments of selfish enjoyment” rather than as cherished partners
an imposition of contraception by unscrupulous governments
Over the next few weeks, I will examine each of these prophesies in greater depth. Let us briefly look at the first.
An Increase in Marital Infidelity
At face value, verifying whether this first prophesy has come true is difficult: there simply don’t exist any reliable statistics on rates of marital infidelity, especially over time. This is hardly surprising. People, it turns out, are extremely reticent to admit being unfaithful to their spouses, even to researchers in an anonymous survey. This makes it difficult to correlate rates of contraception use with rates of marital infidelity.
But this difficulty is only apparent. Because, in fact, we have a mass of other information pointing to a catastrophic sea-change in the stability of marriages and the cultural normalization of adultery. Before the legalization of divorce in the 1960s, could any of us have imagined the creation of websites and services dedicated solely to facilitating adultery? Now, however, they are shamelessly advertised on street corners, public transit, and during commercial breaks on TV.
Furthermore, even if we did have reliable statistics about how many married people have been unfaithful over the past number of decades, those statistics would be hopelessly complicated by the fact that what was long been considered a clear case of “infidelity” – i.e. leaving one’s marriage and starting a new long-term sexual relationship with a person other than one’s spouse – is now just a common and socially acceptable practice. We call it “divorce.”
And we do have solid statistics on the rates of divorce in the U.S. As this graph shows, there was a spike in divorce rates beginning in the mid 1960s. That happens to coincide with the Supreme Court’s 1965 ruling that it was unconstitutional for government to prohibit married couples from using contraception. Divorce rates continued to climb up to the 1980s, as the ideology of the sexual revolution spread, and contraception use also increased. This brought in its wake a host of deleterious consequences, not least of which is that a huge number of children now grow up in single-parent households, or are shuffled around from one parent to another.
While people have pointed to a decrease in divorce rates since the mid-1980s as a sign of improvement, unfortunately they are missing the elephant in the living room: namely, that one significant reason for the decrease in divorce is that far fewer people are getting married in the first place. One graph mentioned above (click here) shows divorce rates and marriage rates falling in tandem, beginning in the early 1980s. That makes sense. If you never get married, you can’t get divorced. But this is hardly good news. It just means that the pornified, low-commitment, easy-sex culture has reached such a nadir that people see no need to even attempt a life-long, exclusive relationship. Instead of getting married, many couples opt for co-habiting. But on this front the statistics are also clear: co-habitation is inherently far more unstable than marriage, with many people engaging in serial co-habitation over time. Does such serial co-habitation constitute “infidelity”?
In the end, Pope Paul VI’s first prophesy came far truer than perhaps he himself knew it would: not only did marital infidelity significantly increase, but things have now gone so far that we have re-defined and institutionalized infidelity, removing the stigma and presenting it as just one acceptable option among many. There is no doubt in my mind that the redefinition of the purpose of sexuality created by easy access of contraception – away from sex as oriented towards procreation, to sex as primarily a means of self-gratification – has contributed mightily to the situation we find ourselves in. Next week, we will look at the second prophesy.
Same-sex couples and transgender-identifying individuals should be treated with respect and dignity, but there are moral issues with them entering into the life of the Church, the USCCB’s incoming pro-life chairsaid.
Archbishop Joseph Naumann of Kansas City, Kansas, said the first response is to communicate with each person that they’re made in the divine image of God and they should be treated with the respect and dignity of someone for whom Jesus gave His life on Calvary.
However, he said that does not entail accepting gender fluidity or same-sex “marriage,” because it would conflict with Church principles. He also said that loving people means being honest with them.
In an exclusive interview with LifeSiteNews, Archbishop Naumann said that when someone advocates publicly for something contrary to Church teaching, such as gay “marriage,” then it’s a clear contravention of the Church’s moral principles and priests are obliged to address the situation before permitting them to receive Holy Communion.
Asked by LifeSite editor-in-chief and co-founder John-Henry Westen how to deal pastorally with instances where a same-sex couple seeks to enter the Church and one is ‘transgender” or identifies as the opposite sex, the archbishop said there’s always an effort by the Church to communicate the dignity of the human person in any situation.
“But in the circumstances described, then I think we also have to be honest that there are some real moral issues there that would be a source of conflict for them to be able to really live authentically their Catholic faith,” he told LifeSiteNews. “And I think one would have to have a discussion with them that — this is not a marriage. If they consider themselves married, it’s not a marriage as the Church would understand it.”
“Nor can we change the gender that we’ve been given,” the archbishop added, “even a person who’s had surgery, that doesn’t change their basic identities.”
These situations present difficulties, Archbishop Naumann said, with implications of an impediment to the sacraments.
“So there are some real moral issues,” he said, “and for them to enter the Church, this is going to present some real obstacles for them to be able to be disposed to receive the sacraments and participate in the sacraments.”
Being truthful about the matter is the proper way to love people, said Archbishop Naumann, and the truth cannot be ignored.
“So I think we have to have an honest conversation,” he stated. “As much as we can to say we want to accompany them, and they’re trying to come to know Jesus, and to follow them with their lives — but also to be honest with them, because that’s how we love people. We can’t ignore the truth of the dilemma their situation.”
Asked whether priests or Communion distributors should withhold the Eucharist from individuals in an open homosexual relationship, the archbishop said it was difficult to always know for certain whether someone is in an active same-sex relationship, but in situations when someone publicly advocates that homosexual relationships are morally good, a definite issue exists.
“So I think if you have somebody that’s advocating in this way, contrary to the moral teaching of the Church, then you have somewhat a clear violation,” he said.
And this entails being upfront about the issue, he said, and offering fraternal correction.
“I think as a pastor we have an obligation to dialogue with an individual in that situation,” he added, “much as like with politicians that are conducting themselves in their public life any way contrary to the Catholic teachings, that we have an obligation to talk to them, help to make sure that they understand what they’re doing and why it’s wrong and the reason is that it’s wrong.”
The Church teaches the individuals experiencing same-sex attraction are to be treated with respect, compassion, and sensitivity (CCC 2358).
However, the Church holds that homosexual tendencies are objectively disordered (CCC 2358) and homosexual acts can never be approved as they are gravely depraved, intrinsically disordered and contrary to natural law (CCC 2357).
The Church says that men and women are to acknowledge and accept their God-given sexual identity (CCC 2333), and it does not identify humans by their sexual inclinations.
There are those who believe he should never have been allowed to be born.
He came into this world prematurely with severe spina bifida, Chiari II malformation, hydrocephalus, autonomic dysreflexia, central sleep apnea, dysphagia, hypotonia, and paralyzed vocal cords. He would develop chronic lung disease, anemia, kyphosis, knee contractures, osteopenia, and so much more.
In layman’s terms, he was paralyzed, except for partial movement of his arms. He couldn’t speak because his vocal cords were paralyzed, nor could he eat or even breathe on his own. His own family can’t remember how many times the ambulance raced him to the hospital to save his life. One doctor called this child “sometimes the sickest boy in America.”
His mind was supposed to be in a vegetative state – except it wasn’t. This little boy was bursting with life. He learned to spell, read, do basic math. He could even sign, a talent he employed, along with his beaming smile, to shower affection on the world. For eight years, against all odds, he persevered.
But then one night, Paulie fell ill and within 24 hours, he was suddenly gone. When the news came out, an entire community was shattered.
On a somber Thursday morning, hundreds arrived at the funeral home. Paulie had countless doctors and caregivers, some 40 nurses just at the house alone. Many came to pay their respects. So did the head of Special Needs care, his teachers and therapists; as did the firefighters, paramedics and the bus drivers; as did his neighbors and so many more who’d come to know this special lad. On their lapels many wore ribbons adorned with Sesame Street characters. Paul Ribbons, they called them.
The Make-a-Wish Foundation along with the Shawmut Construction company had built “Fort Paul,” a custom backyard playground for the child. Over 100 people had participated in the project. Many of these volunteers were there. Two crews from South Windsor Public Works arrived in massive dump trucks, lights blinking. Paulie liked dump trucks, you see.
Paulie’s parents regularly would take him to a street corner across from church so from his wheelchair he could smile and wave at passing motorists. They in turn would tap their horns and wave back. It came to be known as “Paul’s Corner.” At the funeral a young police officer recounted to Paulie’s grandmother how, when he was having “a bad day, or was feeling low,” he’d intentionally drive to Paul’s Corner just to catch the angelic smile.
There was another Connecticut State Trooper there that day. He lived near Paul and on his way from work would sometimes flash his lights, or turn on his siren, or call out his name over his loudspeaker. Paul liked that, too. He’d deputized Paulie last year, as had two other troopers from nearby towns.
After the funeral an endless trail of cars followed the hearse for the burial. One police car roared by and placed itself in front of the hearse, lights blazing. A second squad car zoomed past and pulled in behind it. Together they cradled the boy. Police cars blocked the intersections allowing the vast motorcade through. Construction crews on the side of the road stopped working while burly men stood at attention, heads bowed, hands clasped.
The motorcade passed Paul’s Corner and some people gasped. The boy’s wheelchair was there, adorned with balloons and flowers, with neighbors asking for a final tribute, holding a “Honk for Paul” sign, which of course they received. A policeman stood silently next to the chair, head bowed, hands clasped.
Hours later, after all had left Paul’s Corner, the wheelchair remained, still adorned with its decorations, but now on top, in silent tribute, a “CT State Trooper” hat.
“He was undersized but larger than life. He could not speak but had no trouble letting you know what he had to say. He couldn’t get around very well but had literally hundreds and hundreds of friends. He created immeasurable love and caused just as much trouble. So many people spent so much time and effort working on how to care for him. But it was Paul who taught us, nurtured us, ministered to us even. He made us our best selves.
“By worldly standards, he was the least among us. But by the standards that matter most, he was perfection. There was never a nastier, more rotten, disobedient, redheaded, innocent, angelic, gorgeous, kind, amazing boy.”
Those were the tender words spoken by Paul’s father at the funeral. Grown men wept.
TV and social media are reporting a wonderful story about Dr. Eric Voigt and Nicole McGuinness. Dr. Voigt, an ENT physician, was watching the “Beachfront Bargain Hunt” TV show (one of my own semi-guilty pleasures) when he noticed that a woman on the show named Nicole McGuiness seemed to have a suspicious lump in her neck. Alarmed, Dr. Voigt turned to Facebook find her and urge her to get the lump checked. Nicole had her lump checked and it was thyroid cancer. She will be starting treatment soon and is very grateful to Dr. Voigt for his sharp eye.
Ironically, Brittany Maynard was also 29 and had a glioblastoma brain cancer when she decided to move from California to Oregon, a state that legalized assisted suicide in 1997. She and her family moved to Oregon so that Brittany could commit physician-assisted suicide before her symptoms became more severe. The date she chose was November 1, 2014. Brittany also agreed to help Compassion and Choices (the former Hemlock Society) use her story to raise funds with the goal of legalizing physician-assisted suicide throughout the US.
After weeks of widespread and sympathetic media coverage, Brittany did take a doctor-prescribed lethal overdose on her planned date.
No one will never know if Brittany could have been one of the people this treatment could help.
CALIFORNIA AND PHYSICIAN-ASSISTED SUICIDE
The first target state for Compassion and Choices’ campaign for legalizing assisted suicide after Brittany’s assisted suicide was her home state of California. Both Brittany’s mother and husband went to California to support a physician-assisted suicide bill. Although the bill apparently died in committee, Governor Jerry Brown called a special legislative session to deal with healthcare spending where the assisted suicide bill was resurrected and passed. Governor Brown then signed it into law in October, 2015. Over 100 people died by assisted suicide in the first six months after the law took effect.
However just last month, a California judge overturned the law stating that the California Legislature violated the law by passing it outside of the scope of health care spending which was given as the reason for a special session and thus was unconstitutional.
Now Compassion and Choices has filed an appeal on behalf of a palliative care doctor and two terminally ill patients in California to get California’s law back into law.
Stay tuned for further developments.
CONCLUSION
As a former oncology and hospice nurse, I pray that Nicole has a speedy recovery from her thyroid cancer and I am still saddened by Brittany’s assisted suicide but assisted suicide is not a remedy for cancer.
I remember when just a few decades ago, AIDS was the poster disease for legalizing assisted suicide. Then it became terminal cancer after AIDS became treatable. Now the scary poster disease is Alzheimer’s.
And that’s how the slippery slope works.
Instead, we need realistic hope and real support for people and their families dealing with difficult situations rather than just offering the “solution” of death.
June 5, 2018 (LifeSiteNews) – Using contraception is an “intrinsic evil” in all circumstances because it “cuts off one of the goals of marriage which is an openness to life,” Kansas City Archbishop Joseph Naumann told LifeSiteNews.
Any question on this issue lies on the level of moral culpability for those who do use it, he added.
“Circumstances can affect the culpability, [but] it doesn’t affect the rightness or wrongness of the act,” he said.
Speaking exclusively with LifeSiteNews, the incoming chair for the U.S. Bishops’ pro-life committee said further that following the Church’s teaching on contraception is an attainable goal, and that people simply need good confessors to help them understand that fact.
“Good confessors can help and guide people through this, and, I think, help every individual realize that the moral good the moral law is attainable for all of us.”
LifeSiteNews Editor-in-chief and co-founder John-Henry Westen had asked Archbishop Naumann in the context of this year’s 50th anniversary of Humanae Vitae whether it was, in fact, the case — as some bishops suggesting at the time of the document’s release — that Catholic couples may still use contraception if they feel in conscience that they were justified, and if not, whether this would make them ineligible then to receive Holy Communion.
Archbishop Naumann confirmed the Church’s teaching on contraception as a moral evil, as well as Church teaching that each and every conjugal act must be open to life.
“I think objectively contraception, and we see this in the Catechism, it is clear about that, that there is an intrinsic evil to use it,” the archbishop said, “because it cuts off one of the goals of marriage, which is an openness to life.”
With contraception use typically conducted privately, the issue of a couple’s worthiness to receive Communion would be problematic to handle. But Archbishop Naumann said in cases where a person is publicly advocating for actions contrary to Church teaching, it is incumbent on the priest to address the situation with them.
“I think as a pastor we have an obligation to dialogue with an individual in that situation,” said Archbishop Naumann. “We have an obligation to talk to them, help to make sure that they understand what they’re doing and why it’s wrong and the reason is that it’s wrong.”
He recalled having had a long dialogue years ago with then-Kansas Governor Kathleen Sebelius prior to directing her to not receive Communion, saying he had no alternative.
Archbishop Naumannwas elected Chairman of U.S. Conference of Catholic Bishops’ Committee on Pro-Life Activities last November. He will be installed this November.
In June, the Church celebrates the Solemnity of the Sacred Heart of Jesus. Christ extends to us His flaming heart that has been lanced and pierced with thorns. It is a suffering heart. Christ loves us by saving our lives in exchange for His life. We, as the body of Christ, are called to do the same.
Fr. Frank Pavone
One way this love is embodied is in pro-life work. It is a work of self-giving love for children in the womb who don’t even know we are loving them. It is a lifesaving work that comes with a cost. The crown of thorns on the heart and the piercing with the lance symbolize the suffering that all those who defend the unborn will undergo; defend the unborn and you will be treated like them. Despite suffering, Christ’s heart keeps on beating inside His body. Similarly, we persevere within the Body of Christ.
And we worship the Sacred Heart of Jesus. His heart is part of His body, the body of God. Devotion to the Sacred Heart brings to the forefront the reality of the Incarnation. And so does pro-life work. Just as the heart is a physical organ, prolife work is a physical concern, not just a spiritual one. We must pray for the children in the womb, but we must also encounter them physically and defend them physically. We pray at the places where they are being killed, we counsel the moms in whose wombs they are nourished, we bury the bodies of those we could not save. We act, in the body, because we are moved by His love, which He shows us in His Body.
Jesus said He is meek and humble of heart, and this brings us to the heart of the pro-life movement. The attitude of humility is the opposite of prochoice, which asserts itself. Humility humbles itself and accepts the choices of God. It accepts that God’s will and plans are better than our own, even if they come unexpectedly.
Moreover, the passion of love in the Sacred Heart is also the passion of love by which we defend the baby in the womb; His heart of mercy is the mercy we extend to all who have been involved in abortion. Pro-lifers are often stereotyped as caring about the baby but not about the mother. This claim couldn’t be further from the truth. Our ministry at Priests for Life ministers to the baby’s mom, dad, and entire family. Under our umbrella, the world’s largest ministries for healing after abortion operate. Rachel’s Vineyard offers healing retreats for families broken by abortion. Silent No More gives them an opportunity to share their testimony of pain and healing, and thereby to inspire in others the hope that they too can be forgiven.
Close to the annual celebration of the Sacred Heart, of course, comes Father’s Day, and we are seeing more and more men come to our healing programs to grieve the children they have lost to abortion. Many repent of having consented to the abortion. But likewise, so many men didn’t even know about it. I have never seen a man more angry than a friend of mine who told me many years ago that his girlfriend had their baby killed without his knowledge. Men are hardwired to be protectors and providers. To be unable to save one’s own child, and to even be shut out of the possibility of doing so, is an insult to one’s manhood. This is why the men of our Silent No More campaign hold signs saying, “I Regret Lost Fatherhood.”
Father’s Day gives us an opportunity to renew our awareness of the pain of these fathers, and our efforts to reach them with the love and mercy of the Sacred Heart of Jesus, a heart which, like theirs, is wounded precisely because of Its love. For more information, visit www.FatherhoodForever.org.
FR. FRANK PAVONE is national director for Priests for Life – the largest ministry in the Catholic Church focused exclusively on ending abortion. Learn more at www.ProLifeCentral.com
Statue of Jesus of the Sacred Heart inside the church Fontana, Gozo, Malta
The devotion that Catholics have cultivated to the Sacred Heart of Jesus is fitting for several reasons.
First, when we revere the Sacred Heart we are recognizing the fullness of humanity in Christ. But we are doing more than just that: in ancient Israel, the heart was considered the seat of man’s being. In the Sacred Heart then, we are focusing our gaze upon Christ in the depths of His being.
Two other reasons have to do with the flames that are always associated with the heart. They signify the fact that the sacrifice on the cross was a spiritual holocaust, a burnt offering, even though physical flames were not present. And fire itself always symbolized the divine essence in the Old Testament. It is fitting then that the heart, as the essential core of man, be joined to the divine fire in the Incarnate God. In a way, the burning of the Sacred Heart becomes yet again a figure for both the humanity and divinity of Christ — the sacrifice and the God who consumes it.
However, there is yet one more reason devotion to the Sacred Heart is fitting and it is rooted in the Old Testament.
Two Old Testament passages connect the heart, word of God, and fire.
First, there is Psalm 39,
I said, “I will watch my ways,
lest I sin with my tongue;
I will keep a muzzle on my mouth.”
Mute and silent before the wicked,
I refrain from good things.
But my sorrow increases;
my heart smolders within me.
In my sighing a fire blazes up,
and I break into speech (vv. 2-4).
An intriguing parallel occurs in Jeremiah 20:
I say I will not mention him,
I will no longer speak in his name.
But then it is as if fire is burning in my heart,
imprisoned in my bones;
I grow weary holding back,
I cannot! (v. 9)
In both passages the desire for God is likened to a kind of fire. The metaphor is an apt one, as fire is representative of God — think of the burning bush that spoke to Moses, the consuming fire on Mt. Sinai, and the fire that devoured the sacrifice of Elijah.
In both cases, the fire is seated in the heart. The heart of the psalmist ‘smolders.’ Jeremiah feels as ‘if fire is burning in my heart.’ Desire for God is something that takes hold at the center of our being. It is not peripheral. It is not some mental itch or a passing passion.
In both the psalm and Jeremiah the speakers attempt to repress the fire. Both fail to do so. Here, the analogy of fire serves to explain why: just as fire cannot be contained but spreads and rises upwards, so also the desire for God overtakes both men.
And it does so in a most specific way: it issues forth in words addressed to God. Because these words are also recorded in the Bible they are Scripture — the word of God.
The psalmist had tried to ‘muzzle’ his mouth. Instead, his cry of anguish turns into a prayer. Jeremiah had also attempted to refrain from mentioning the name of God. But the fire in his heart spurs him to sing a song of praise to God. In both cases, the burning desire for God issues forth in words of prayer addressed to God.
The experience of the psalmist and Jeremiah point to a twofold way in which devotion to the Sacred Heart is fitting.
First, as perfect man, Christ experiences the desire for God more fully and expresses it more perfectly than any other. He shows us the way to stoke the fire of our heart so that it might rise up in sacrificial prayer.
Christ is not only an exemplar but also the cause, hence the second reason. His Sacred Heart — His Incarnation and sacrifice on our behalf — is what ought to light the fire of divine love in our hearts and fan the flames into prayer.
Heart of Jesus burning with love for us, inflame our hearts with love of thee!
“The little pill that gave women freedom.” That’s the way The Conversation bills a clutch of articles marking nearly six decades of what the birth control boffins call “effective” contraception. With the release of the pill from 1957 onwards, women “celebrated the new control they had over their fertility,” writes Bryony McNeill, a lecturer in reproductive physiology at Deakin University, in “A short history of the pill”.
Actually, women already had a basic control over their fertility – probably as much as the pill has given them considering that abortion has underwritten this technology almost from day one – only, the control they had was moral, not technical. By and large, they set the terms for sex: marriage, and co-responsibility for the children.
Chemical contraception plus abortion has certainly controlled the number of children the average woman has, but what kind of freedom has it given her? Given current trends, here’s a list of 10 things Ms Millennial is free to do with her sterilised body:
1. Enter the cheap sex market. That is, hook up, date or cohabit with a series of men who are only interested in sex, while she spends ten to twenty years looking for someone who is really interested in her.
2. Suffer sexual harassment at college and work from men who think that, since women now have bodies like men (can’t get pregnant), they also have the same mechanical attitude to sex. She may even be free for a relationship with an abuser like Eric Schneiderman.
3. Put up with the side-effects of ingesting completely unnecessary synthetic hormones: weight gain, headaches, depression, loss of libido – to say nothing of more serious effects.
4. Get pregnant anyway because she was careless about her contraception, or it just did not work this time (which happens) – and “have to” have an abortion.
5. Not get an abortion and become a solo mother, reducing further her chances of marrying, though not of being exploited by boyfriends.
6. Get a sexually transmitted infection that will not go away. If she missed out on the HPV vaccine it may mean she is “free” to develop cervical cancer.
7. Increase her risk of breast cancer — by an average of 20 percent, according to a recent study reported in the New York Times.
8. Listen to her biological clock ticking relentlessly while Mr Right fails to show up. Or find out, too late, that her fertility has a different time frame than his.
9 Cohabit with a man who does not love her enough to marry her. If lucky, eventually marry him; if not (more likely) then break up. Perhaps several times. The consequences of this freedom extend, of course, to any children they have.
10. Decide it’s time for a baby, married or not, only to find she is infertile. She is then free to pay a fortune for IVF or, in some countries, to wait on a public list. Or remain childless.
Pill advocates can no doubt come up with a list of wonderful things that women have achieved with the help of the pill – higher education, independent incomes, amazing careers, a lasting marriage, one or two carefully reared children… But this is much truer of the college educatedthan those down the social scale, and even among the most educated there are women struggling with some of these issues.
If this is freedom, it seems a very dubious exchange for the life of the average woman of the pre-pill era – the one stereotyped as chained to the kitchen sink and wondering, according to Betty Friedan, “Is this all?” There are many 30-year-olds today who, considering their health and happiness, could ask the same question.
The following post is by contributor Fr. Donald L. Kloster, a priest of the Diocese of Bridgeport. Fr. Kloster is the parochial vicar at St. Mary’s in Norwalk, Connecticut. He is also a graduate of St. Charles Borromeo Seminary Philadelphia, having completed his Master’s Thesis in Moral Theology. A native of Texas and a graduate of the University of Texas (Austin), Fr. Kloster also spent two years as a student (and then novice) at the 7th century Benedictine Abbey of Disentis, Switzerland.
It seems like the question keeps coming up and yet there seems to be little to no response from our Bishops. Every year since 1965, the priest to faithful ratio has gotten worse. There is not much more than hand wringing going on to solve the problem. The trend keeps spiraling downwards. The seminaries of yesteryear are almost all closed, consolidated, or operating at minimal capacities.
What about the elephant in the room that is the ratio of priests to faithful? Back in 1950, there was 1 priest to every 652 Catholics here in the USA. In 2010, it was 1 priest to every 1,653 Catholics. In 2016, the most recent numbers available, there was 1 priest to every 1,843 Catholics. So, we have about 3 times less priests to tend to the flock than we had 66 years ago who were serving the faithful. The priestly apostolate is being spread over ever thinning ranks.
There is one Diocese that should be the model. The Diocese of Lincoln is the only Diocese that has consistently been in the top 20 Dioceses producing vocations since the downward trend after 1965. Their ratio as of 2016 is 1 priest to 598 Catholics. Their numbers are just better than the 1950 ratio. Another noteworthy occurrence is that their number of male religious has nearly tripled since 1950 going from 35 to 96. That increased number of male religious is perhaps a singular occurrence in all of the USA Dioceses. Why other bishops aren’t implementing similar programs, speaks volumes. Perhaps the vast majority of USA bishops aren’t really interested in reviving vocations to the priesthood. You can’t keep on the same failed course and expect positive results or even a continuous positive trend.
In 2017, the Priestly Fraternity of St. Peter did an internal survey of priests to faithful in their parishes worldwide. As a Religious Order, they would make an above average size USA Diocese since they have around 287 priests. Their survey indicated that they are right at 1 priest to every 250 faithful or more than 2.5 times better than the 1950 USA priest to faithful ratio of 1 to 652.
There were many who clamored for fresh air to be let into the Church during and after the Second Vatican Council. Later, even Pope Paul VI admitted that the smoke of Satan had entered the Church. All of the leading spiritual indicators and sacramental numbers are down since the end of the Council and there are no real overall up trends within the Novus Ordo parishes. So where is the “renewal?”
I would submit that we stop looking in the direction of the Novus Ordo; the veritable “front door” of our attention. It is a distraction. We need to look at the “back door” and the side windows to see the true flowering of the Church. The Traditional Latin Mass only parishes are producing more fruit, more renewal, than even the pre-Conciliar Church. The Traditional Latin Mass parishes are beating all of the pre-Conciliar numbers. They are authoring a true springtime resplendent with ripe and succulent fruit. The Traditional Latin Mass parishes are only being let in the “back door” since there is so much resistance from the hierarchy. Of what are they so afraid? Why is the Traditional Latin Mass so threatening? I thought the idea was to renew the Church. Why do they turn their backs on authentic renewal? The bishops allow any language under the sun except for the language preferred by the Second Vatican Council!
The vibrant priest to faithful ratio among the Priestly Fraternity of St. Peter is only the tip of the iceberg. The National Survey on the Traditional Latin Mass parishes I am doing with the help of Mr. Brian Williams has astounding preliminary numbers (800+ samples so far). The National Survey will conclude on October 29, 2018. I want to dispel, in any fair minded individual, the notion that the society is responsible for the failing Church numbers. Come November, we’ll try to publicize the results of the Survey as widely as possible. It is a spiritual problem that can only be rectified by returning to what practically evangelized the whole world. The Novus Ordo and Traditional Latin Mass faithful live side by side. They have the same modern challenges. However, when you ask them about the faith, they give much different answers statistically.
My dear brethren in Christ, there is a very simple course to more vocations. Be friendly to the Traditional Latin Mass parishes. If you don’t want to promote it, at the very least, stop blocking it! There is absolutely no harm to the Church when we say the Mass that was said for 19 centuries as a universal practice. If we want vocations, we must be humble enough to admit the source and conduit; the Traditional Latin Mass. Our seminaries were full when we had the Traditional Latin Mass. They will fill up again if we allow the Traditional Latin Mass an unencumbered and a freely celebrated praxis.
The pro-choice movement in Ireland won as emphatic a victory on Friday as the pro-life movement did in 1983. What was the response of the pro-choice side to their heavy defeat back then? Was it to go away? It was not. Instead they took the long view and immediately began the work of repealing the 8th amendment.
It has taken them 35 years to get to this point, and we have to be as patient and as diligent as they were. The unborn child still has a moral right to life and we must work to restore that in law.
As I said in my Sunday Times column:
“It remains as much the case today as it was on Friday that the unborn child has a moral right to life; that it is one of us. If the referendum vote had been 99-1 in favour of repeal, that would still be so. The law acknowledges the fundamental rights that are ours by virtue of being human, but it does not create them. The law may fail to acknowledge and protect your rights, but they still exist, morally speaking. The size of a vote has absolutely no effect on this. It then becomes a matter of fighting to have your rights acknowledged in law once more.”
We now live in a society that values choice and “personal freedom” above all else. We are horrified at unchosen burdens and we have now created a legal right to eliminate the unwanted unborn. It is inevitable that we will now try to do the same to the old and infirm who have come to believe they are also burdensome.
No moral consensus lasts forever. This one will likely last for several decades, and we must be the ones who have the courage and perseverance to dissent from it and be the voice that says we must help those with burdens instead of ending the lives of the ‘burdensome’. That is the only humane and acceptable response.
We must continue to advocate for the right to life of the unborn as the pro-life movement has done, and is doing, in other countries. We must learn from them to be patient, confident that at some point in the future the law will once again protect the unborn members of the human family.
We own our unborn fellow human beings nothing less.
David Quinn is the director of the Iona Institute. The above is adapted from a press release of the Institute.
Individual Americans have enjoyed more personal freedom, individual rights, and collective liberty than most, if not all, other civilizations in history. Yet we are living in a time when freedom, rights, and liberty have been so thoroughly redefined and distorted that we struggle to communicate with each other. A faithful Catholic uses the same words as a secular progressive, but the meanings of the words we use are often different. We may as well be speaking a different language. Words like freedom, gender, identity, and healthcare are defined differently by progressives. Meanwhile, public relations firms and marketing professionals spend untold hours coming up with the perfect way to pitch the product and ideology of their client. Arguments are carefully framed to make sure all dissent sounds politically incorrect. The redefinitions are now being used to eliminate religious freedom, virtue, and the most basic building blocks of civilization: marriage and family.
Redefinitions have led to new laws regarding sexual orientation and gender identity, known as SOGI laws. Once adopted, SOGI laws are used to make public sacrifices out of dissenters such as Jack Phillips, Melissa and Aaron Klein, and Barronelle Stutzman. The intent is to send a warning to all who may dissent: comply or suffer the consequences. Brendan Eich suffered the consequences and he was not even dissenting; he was simply donating money to promote California’s constitutional amendment to define marriage as an institution in which one man is married to one woman. If the LGBT activists win the cases currently pending in the U.S. Supreme Court, it will take a century or more before the country can return to just laws. Many question whether the United States has another century.
Eich, Stutzman, Phillips, and the Kleins are the victims we know about. There are many anonymous victims as well. Their parents dress them in clothing which conflicts with their biological sex or give them hormone treatments to arrest their physical development, so they have time to decide which “gender” they want to be for the rest of their lives. We have victims of abortion as abortion workers laugh about the baby parts through which they sort, selecting which organs can be sold for scientific experimentation. Then there is the silent agony of the mothers who suffer deep regret for their abortions. How many people are ritually euthanized in their hospital beds in the name of economy and sympathy? Then there are our co-workers and colleagues who feel they must remain silent for fear of losing their jobs after Brendan Eich was publicly shamed into resigning.
How did things get so bad? There has always been a battle between good and evil, but just looking over the past 100 years in the United States, we can see a blueprint that comes right out of Antonio Gramsci’s Prison Notebooks and through the Frankfurt School of pre-WWII Germany. It was through these sources that came the “Long March,” which is Cultural Marxism’s way of overthrowing Western Civilization. Lenin’s style of Marxism required violence, oppression, and state-controlled propaganda. Gramsci’s Cultural Marxism simply required persistence, patience, and carefully manipulated definitions of existing words and phrases. Russia’s Marxism was a messy and violent process whereas the “Long March” of Cultural Marxism in America was accompanied by kind smiles, songs about sexual freedom, the aroma of marijuana, and the ringing of cash registers. We can blame those who introduced the Long March to the U.S., but in the end, we must simply accept the blame ourselves. We stood dumbfounded as Satan assaulted our culture and then our families, through six blatant attacks within the last 100 years. The first attack was artificial contraception, followed by no-fault divorce, abortion, hedonism and consumerism, same-sex “marriage,” and pornography. I do not think it is a coincidence that technology, from television to the internet to the smartphone, has played an increasingly significant role in these attacks.
Since this July we will celebrate the 50th anniversary of the publication of Humanae Vitae, we’ll focus on the first attack: artificial contraception.
You may know Margaret Sanger as the founder of Planned Parenthood, the abortion powerhouse, but her initial focus was artificial contraception. Sanger traveled the world trying to sell birth control to anyone who would listen. However, as she was scheming for the legalization of oral contraception in the U.S. from the 1920s into the 1960s, she kept running into a scientific roadblock. At that time, the medical and scientific fields agreed that pregnancy (and therefore, life) began at fertilization. Fertilization happens when a sperm unites with the egg. At that point, the two become one. The new life is called a zygote, a.k.a. a fetus, a.k.a. a baby. It is at fertilization that the new life form receives its own DNA and the sex of the child is determined.
Medical and scientific professionals knew that oral contraception would not prevent the fertilization of the egg on many occasions. When the pill fails to prevent ovulation, it can prevent the fertilized egg (now a distinct human being) from implanting into the wall of the uterus and therefore, the human life dies. Until the late 1950s, doctors, scientists, and others knew that to legalize the pill was to legalize abortion. Because of this, whenever Sanger and her supporters would promote artificial contraception, knowledgeable people knew they were talking about an abortion pill, and they almost always rejected contraception.
All this began to change in the late 1950s when some medical professionals began to say that life begins at implantation. A new definition of conception was in the making. Implantation occurs approximately five to seven days after fertilization. By 1960, the FDA had approved an oral contraception, an effort largely funded by Margaret Sanger and her supporters. As usual, changes in culture happen in small increments, but the legalization of contraception for married women was to be one of the most significant increments in the cultural change of the United States. A little change in a definition made this possible.
The floodgates opened in 1965 through word games in the courtroom and the medical field. First, the U.S. Supreme Court entered its decision in Griswold v. Connecticut, declaring birth control legal via prescription for married women. According to the Supreme Court, the right to birth control was found somewhere in the “penumbras” of the Bill of Rights. Are we to believe that the woman’s right to privacy was hiding in the shadows of the Bill of Rights for 184 years until five judges discovered it? The Supreme Court thought so. And if you wanted to advocate for the right to life, you were declared a nosy, foolish, religious fanatic who wanted to control women. Those words had a chilling effect on people who disagreed with the Supreme Court. Word games are not always fun.
Due to the Equal Protection Clause, the Griswold Court knew that by legalizing contraception for married women they were laying the foundation for legalization of contraception for all women. This occurred in 1972, in Eisenstadt v. Baird.
On the heels of the Griswold decision, the American College of Obstetricians and Gynecologists (ACOG) issued a bulletin redefining the term “conception.” The bulletin stated that conception occurred upon “the implantation of a fertilized ovum,” instead of fertilization. One wonders if the projected revenue generated by the legalized pill had anything to do with the new definition.
Regardless of laws and definitions, reality tells us that artificial contraception does not always prevent fertilization and frequently results in full-term pregnancy. The Guttmacher Institute says that over 50 percent of women who have an abortion report using contraception during the month they became pregnant. The U.S. has approximately 1.5 million unplanned pregnancies per year in which the woman was using some form of artificial contraception. The Shriver Report says that approximately 43 percent of these women choose to abort their child. Many doctors and abortion advocates believe that the ultimate backup plan for failed contraception is induced abortion, not adoption.
Remember those silent victims of the LGBT craze I mentioned earlier? Contraception has many millions more silent victims each year: women diagnosed with blood clots, those who wonder if their infertility or cancer is related to their use of hormonal contraception, and all those five to seven-day old humans who have their own DNA and sex, but die due to their inability to implant in the uterine wall. Contraception’s failure to prevent fertilization can result in an abortion long before anyone knows about the pregnancy. Contraception, including IUD’s, Depo-Provera, Ortho Evra, etc., commonly acts as an abortifacient (a drug or device which causes an abortion).
As of 2018, there have been over 60 million abortions in the United States since Roe v. Wade. But this only counts the abortions we know about after implantation. How many millions, if not billions of abortions have taken place because the artificial contraception did not prevent fertilization? This is not an easy question to consider, due to the widespread use of the pill among Christians, including Catholics, sometimes prescribed by Catholic doctors and distributed by Catholic pharmacists.
Scientific knowledge didn’t change in 1965, nor did human biology. Advocates of contraception changed the way they talked about it, and doctors and judges simply changed their minds. America has had to cope with the change in the definitions and verbiage. Most of us coped by going along with the word game. We simply used artificial contraception without wondering if we were aborting our child. After all, intelligent doctors and unelected judges told us not to worry about it. If anything happens without our knowledge, it is as if it never happened.
As faithful Catholics, we need to be more knowledgeable about the history of the legalization of contraception and we need to recognize that artificial contraception is the largest killer of human life in the United States. We need to teach this to our children, and we need to help our contemporaries understand this as well. Regardless of the word games, reasonable people do not want to kill people, much less their own children.
FROM THE National Center for Health Statistics came some disturbing news last week: The US birthrate, which has been on the skids for a decade, hit another record low.
About 3.85 million babies were born in the United States in 2017. That was down from 3.95 million births in 2016, which in turn was down from 3.98 million in 2015. For every 1,000 American women of childbearing age, there were just 60.2 births last year, the lowest birthrate ever recorded. A related yardstick is the fertility rate — the number of babies each woman, on average, will have over her lifetime. It takes a fertility rate of 2.1 just to keep a nation’s population stable, neither growing nor shrinking. Last year, the US rate dwindled to 1.76, a 40-year low.
Americans are less inclined than ever, it seems, to be fruitful and multiply. That should trouble anyone who hopes that America’s best days are yet to come. Nothing is more indispensable to the growth of any society than its human capital — the knowledge, skills, imagination, and energy of human beings. As the late, great economist Julian Simonfamously argued, people are the ultimate resource in any society, since human beings over time create more than they destroy.
When nations retreat from marriage and children, their outlook tends to become bleaker and less prosperous. Japan, which has one of the lowest fertility rates in the world, illustrates the phenomenon well. As Japanese births have dwindled, the working-age cohort has accounted for a smaller and smaller share of an older and older population. Economic decline has followed demographic decline. And with Japan’s labor force doomed to keep shrinking, the worst is yet to come.
There are many reasons for the plunge in fertility rates, and some of those reasons are unequivocal blessings. First and foremost is the near-eradication of infant mortality. In the 1850s, wrote Jonathan V. Last in his 2013 book What to Expect When No One’s Expecting, one-fifth of white American babies, and one-third of black babies, died during infancy. Today, by comparison, the infant mortality rate is minuscule: 5.8 deaths for every 1,000 live births. When children are more likely to survive, parents have fewer children.
Other positive changes have also helped bring down fertility rates. Among them: the explosive increase in women’s education, the availability of modern contraception, and the surge of women into the workforce. Added to those have been still other social transformations. The establishment of Social Security and Medicare eroded the need for children to support their parents in old age. The waning of religion in modern America has weakened the conviction that getting married and raising a family are moral imperatives. And the din by environmental alarmists about the dangers of “overpopulation” have convinced many people that childlessness is a virtue.
But it isn’t.
It should go without saying that Americans are perfectly free to delay getting married or having children, or to decide that they want no part of the expense, commitment, and restrictions of parenthood. This isn’t Margaret Atwood’s Gilead. Individual men and women who choose not to have kids are exercising a reproductive liberty that most of us regard as inviolable.
To opt out of having children is=to opt out of the most meaningful investment in the future.
Yet that doesn’t mean we’re obliged to close our eyes to the aggregate impact of those individual choices. A society that ceases to “be fruitful and multiply” is a society that sows the seeds of its own decay. The retreat from child-rearing, in columnist Ross Douthat’s words, is a form of “decadence” — an attitude that “privileges the present over the future, chooses stagnation over innovation, prefers what already exists over what might be.” A plummeting birthrate has ramifications that go beyond the economic burden of a swelling elderly population and fewer people of working age to bear that burden. To opt out of having children is to opt out of the most meaningful investment in the future — and to thereby make it more likely that America’s best days are not to come.
Government can’t make people have babies, and shouldn’t try to. But that doesn’t mean we shouldn’t encourage parenthood, or remind ourselves how important babies are to American success, enterprise, and optimism. America’s children are its most valuable asset, and a persistently sinking birthrate is a warning: That asset is being dangerously depleted. Life with kids is undoubtedly a challenge. But as America is on the verge of finding out, life without them will be more challenging by far.
(Jeff Jacoby is a columnist for The Boston Globe).
CHARTRES, France, May 25, 2018 (LifeSiteNews) – A leading Catholic churchman warned pilgrims at an iconic French cathedral that a Western society without God is like a “drunken boat in the night.”
Robert Cardinal Sarah, 72, made his remarks during a homily he gave on Monday at the Mass celebrating the conclusion of the annual Pentecost pilgrimage from the Cathedral of Notre Dame de Paris to the Cathedral of Notre Dame de Chartres. The African prelate invited the congregation to ponder the state of the Western world:
“Let’s look around us! Western society has chosen to establish itself without God. Witness how it is now delivered to the flashy and deceptive lights of a consumer society: to profit at all costs, and frenzied individualism,” he said.
“A world without God is a world of darkness, of lies and of selfishness,” the Cardinal continued.
“Without the light of God, Western society has become like a drunken boat in the night! She does not have enough love to take in children, to protect them beginning from their mother’s womb, to protect them from the aggression of pornography.”
The Cardinal said that Western society no longer knows how to respect the elderly, care properly for the sick and to welcome the poorest and weakest human beings.
“Society is abandoned to the darkness of fear, sadness and isolation. She has nothing to offer but emptiness and nothingness. It allows the proliferation of the maddest ideologies,” he warned.
Sarah observed that without God the West could become the “the cradle of an ethical and moral terrorism more virulent and more destructive than Islamist terrorism.”
The Cardinal also spoke out against plans to open the priesthood to married men. The Guinean prelate believes that an attempt to unmoor the priesthood from celibacy will rob it of its closeness to Christ.
Addressing the priests in a massive crowd that spilled out into the cathedral’s forecourt, the Guinean prelate begged them to remember the meaning of their celibacy:
“Dear fellow priests, always keep this certainty: to be with Christ on the Cross is what priestly celibacy proclaims to the world,” he said.
“The plan, again advanced by some, to detach celibacy from the priesthood by conferring the sacrament of the Order on married men (“viri probati”) for, they say, ‘pastoral reasons or necessities,’ would have serious consequences, in fact, to definitively break with the Apostolic Tradition,” he added.
Sarah intimated that ordaining married men would not “perpetuate” the priesthood of Christ.
“We would manufacture a priesthood according to our human dimension, but without perpetuating, without extending the priesthood of Christ, obedient, poor and chaste,” he said.
“Indeed, the priest is not only an “alter Christus”, but he is truly “ipse Christus”, he is Christ himself,” the Cardinal stated. “And that is why, following Christ and the Church, the priest will always be a sign of contradiction!”
Although the Catholic Church has allowed married Anglican ministers who have become Catholic to be ordained as priests, this has been a pastoral concession not intended to set a precedent for the western Church. Even in the Eastern Church, celibacy is considered a superior state for a priest, freeing him to serve his flock with a whole heart: married priests in the eastern Church are not, for example, chosen as bishops.
In the dearth of vocations following the Second Vatican Council, Pope Francis has stated that the church has to consider ordaining married men to the priesthood.
“We have to think about if the viri probati are a possibility,” Pope Francis told German newspaper Die Zeit. “Then we also have to discern which tasks they can take on, for example, in forlorn communities.”
“There is much talk about voluntary celibacy, especially there where the clergy is lacking,” the pope said. “But a voluntary celibacy is not a solution.”
In his Chartres homily yesterday, Cardinal Sarah entreated the crowds to distinguish between the world they must love — the world of people, especially the poor, to be served — and the world which they must not love–the world “as it became under the rule of Satan and sin.”
He warned in particular against “the world of ideologies that deny human nature and destroy the family.”
Editor’s note: The following address was given by Lepanto Institute President Michael Hichborn at the John Paul II Academy for Human Life and the Family conference on Human Life and the Family in Rome, May 21, 2018.
May 24, 2018 (LifeSiteNews) – I’ve been asked to give a few words, giving personal witness to the gift of Truth, Love, and Life.
It’s difficult to place nearly 16 years of marriage into a capsule as testimony to these things, but as I have reflected on my own marriage in light of the teachings of Holy Mother Church, one thing has become abundantly clear: The very essence of marriage is a reflection of the Holy Trinity through Divine Sacrificial Love.
It has taken me a long time to discover, understand and live by what my wife has personified from the very beginning of our marriage. True Love, which is the total giving of self to another without regard to the self, requires perpetual sacrifice.
While there are many different examples of a spirit of sacrifice … and a spirit of selfishness … that come and go through all marriages, there are two instances that stand out in my mind the most.
Yesterday, our 7-year-old daughter … the fourth of six children … Tatiana, received her first Holy Communion. I couldn’t be with her, obviously, but my heart was filled with a mixture of joy and gratitude by the pictures my wife sent to me. Joy, because of the beauty that comes with providing Our Lord with a pure, new bride. Gratitude because of the circumstances regarding her birth.
Seven years ago, just a mere 36 hours after Tatiana was born, my wife awakened me by crying out with intense pain. What I thought was an intense bout of postpartum cramps turned out to a ruptured aneurysm in her kidney. After staying up with her throughout the night, the midwives visited in the morning and told me that I had to get her to the hospital right away. When we got to the hospital, the triage nurse couldn’t register any blood pressure. And while the doctors wheeled her away for an MRI, I got on the phone and called for a priest.
Throughout what would be the most terrifying day of my life, nothing went right, and in fact, went from bad to worse. At about 3:00 in the afternoon … the Hour of Mercy … the first attempt to clam off the artery resulted in a vascular spasm, and the doctors became concerned that it resulted in arterial damage that would require them to amputate my wife’s leg.
It was at this time that I knew that the situation was entirely out of my hands. There was nothing I could do to fix this, and the very real possibility of having to go home to tell our other three kids that mommy was never coming home again pressed intensely on my heart.
But this is where I discovered what a marriage is made of.
I was alone, and with nowhere to turn, I fell to my knees and I prayed as Our Lord did in Gethsemane. I told Our Lord that I wanted my wife to live, but I had to be willing to let her go, if it was God’s wish. I said, “Lord, you know that I desire my wife to live. I beg you for her life. But I desire Your Will above all else. Even at the great cost of losing my wife, I give myself entirely over to Your Divine Will.”
Obviously, this story has a happy ending … in fact, despite the emergency surgery to remove her right kidney, the doctors were amazed at the speed of my wife’s recovery. After receiving 14 units of blood and having gone through the trauma of an emergency nephrectomy, she was expected to remain in the hospital for 2 weeks, but went home after only 5 days.
Another story …
4 years ago, our fifth child, Maria Faustina, was born. When Maria was four months old, my wife and I took her with us on our very first trip to Rome. Taking in the glory, beauty, and history of the Eternal City, we grew in awe as we went from church to church. By a happy accident, we happened to enter into Santa Maria Sopra Minerva on the feast of St. Catherine of Siena. The back of the altar was opened so pilgrims could actually touch the tomb of St. Catherine.
Kneeling in prayer, my wife and I placed our wedding rings on the tomb, we prayed for a strengthening of our marriage, and then we held our four-month-old daughter to the tomb as well. Afterward, my wife told me that what she prayed was this … she prayed to Our Lord for her willingness to give our children entirely to Him, whenever and in whatever capacity He may will. It was a beautiful prayer that I then shared with her, and then didn’t give another thought.
The very next day, she went to the Wednesday papal audience with our daughter while I was in a meeting. As it was customary for the pope to ride around among those present for the audience, the crowd pressed past her, and while she was juggling both the baby and her phone, trying to take a picture, the lady next to her gestured that she would hold the baby.
So, my wife handed her our daughter to the person in front of her, who passed the baby to the person in front of them, and on to the security detail surrounding the pope, who then passed her right up to the pope himself. He held our daughter, blessed her. Gave her a kiss, and then Maria Faustina was passed back down to my wife. In an amazing way, Our Lord has answered my wife’s prayer … He took our daughter from her hands, and then returned her with a blessing. As Scripture is very clear, Our Lord will not be outdone in generosity.
Pope Francis kissing baby Maria Faustina Hichborn in 2014.Supplied by Michael Hichborn
All marriages are called to live a sacrificial love.
As I was listening to Bishop Schneider speak at the Rome Life Forum last week, I was struck by the thought of the Holy Family being a reflection of the Trinity. God the Father is reflected in the image of St. Joseph. Our Lady represents her spouse, the Holy Spirit. And, Our Blessed Lord, Who has two natures, one Divine and one Human, is the bridge between the Trinity and the Holy Family.
In the Holy Family, we find the model for all families. All husbands are called to be the head of the family, representing God the Father to his wife and children, providing the law and right judgment. All mothers are called to follow the example of Our Lady, dispensing the goods of the home as Our Lady dispenses the Graces of the Holy Spirit. And all children are to follow the example of Our Blessed Lord, who, St. Luke tells us, was subject to … or obedient to … his parents.
The last mention of St. Joseph in the Gospel of St. Luke is made when Jesus disappeared from his parents for a period of three days. After that, we have no other mention of St. Joseph, and when Our Lord begins His public ministry, He is with Mary, but Joseph is not around. Venerable Mary of Agrida tells us that “Love was then the real cause of the death of Saint Joseph,” and according to Sister Mary Ephrem Neuzel, as part of the revelations of Our Lady of America, St. Joseph said:
My heart suffered with the Hearts of Jesus and Mary. Mine was a silent suffering, for it was my special vocation to hide and shield, as long as God willed, the Virgin Mother and Son from the malice and hatred of men.
The most painful of my sorrows was that I knew beforehand of their passion, yet would not be there to console them.
Venerable Mary of Agrida indicated that St. Joseph was thirty-three when he was espoused to the Blessed Virgin, lived with Her a little longer than twenty-seven years as her husband, and died at the age of sixty. If this is the case, then St. Joseph died just about three years prior to Our Lord’s public ministry.
What’s interesting is that Mark 15:33-34 indicates a period of three hours that the world was in darkness, at the end of which, Our Lord cried out, “My God, my God, why hast thou forsaken me?” If we think about the three years of St. Joseph’s death as a reflection of the three hours of God the Father being mystically shrouded from the Human Nature of the Son, we can also consider how the Father participated in the suffering of the Son.
Imagine the immense pain it would be for any husband and father to know that his family would endure the worst kind of suffering imaginable, and not be there to help, console, or die with them. Given the unity of the Blessed Trinity, the intimate participation of the Father in the Passion of the Son can be contemplated in the death of St. Joseph.
And just as Our Lady — whose Heart was pierced by a sword — is the Spouse of the Holy Spirit so, too the Holy Spirit would have shared in the same piercing wound in this Triune expression of Sacrificial Love.
The sacrificial love of the Trinity is found in the sacrificial love of the Holy Family. And all families are modeled on the Holy Family. But it doesn’t end there. Every individual, being made in the image and likeness of God, is called likewise to reflect the Trinity within themselves.
All humans in existence are the children of two parents, and so we are all called to the self-sacrifice found in the obedience exemplified by Our Blessed Lord. But also, all people are called to “bear fruit” in some respect, and so, in a sense, all people are called to be parents in one of two ways; physical parenthood and spiritual parenthood.
In physical parenthood, married couples bring new lives into the world. In spiritual parenthood, individuals bring souls to our Lord through prayer, sacrifice and witness to the Truth. And because all of us are called to bear fruit in one of these two ways, we are likewise all called to be spouses … spouses to either a bride or groom or spouses to the Church and our Lord.
For God so loved the world, as to give his only begotten Son … The love of the Trinity is Sacrifice, the Love of the Holy Family is Sacrifice, the love of all families is sacrifice, and the love of each of us is sacrifice.
The survival of the family, the glory of the family, the very life of the family relies entirely on the sacrificial love of husbands, wives, and children, for without sacrifice there is no love, there is no life, and there is no salvation.
WASHINGTON, D.C., May 22, 2018 (LifeSiteNews) — President Donald Trump affirmed the importance of the right to life and called on pro-life voters to help secure it Tuesday night, in his keynote address at the Susan B. Anthony List’s 11th annual Campaign for Life Gala.
In a speech bookended by lengthy applause, Trump began by acknowledging many of the pro-life activists and lawmakers in the audience, including House Majority Whip Steve Scalise, R-LA, Rep. Steve King, R-IA, Rep. Marsha Blackburn, R-TN, and Rep. Jim Jordan, R-OH. From there he transitioned to an overview of the current prognosis for the fall midterm elections, citing a new Reuters poll finding Republicans have taken the lead in the generic congressional ballot.
Yet there was still more work that needed to be done, the president said, to elect more lawmakers who “share our values, cherish our heritage, and proudly stand for life.”
Trump reminded the audience that he campaigned for president pledging to protect life, and he listed progress he’s made doing so thus far: reinstating the Mexico City policy barring overseas abortion funding, signing a law letting states defund abortion providers, appointing a record number of federal judges, protecting religious liberty, disqualifying abortion facilities from family planning subsidies, and championing a ban on abortions at 20 weeks, at which point preborn babies can feel pain.
Unfortunately, he lamented, Democrats are “doing everything in their power to block” the last measure, leaving it nine Senate votes short of the supermajority necessary to break a filibuster under current Senate rules.
Trump expressed optimism that Republicans could close that gap in this fall’s Senate races “if we work hard between now and November,” and singled out Democrat Sens. Jon Tester, Heidi Heitkamp, Claire McCaskill, and Debbie Stabenow for voting to continue late-term abortion.
The president then spent several minutes touting his economic policies, foreign policy decisions, and job creation record, and discussing illegal immigration, but soon brought the conversation back to his efforts to appeal to voters “who want a government that protects family, faith, and life.”
“We can’t be complacent. What happens historically, a tremendous percentage of the time, is that you win the election and become complacent,” Trump warned. “We sit back, the other side has energy, and they win.” But he said he doesn’t believe history will repeat itself this year.
“This organization bears the name of one of the biggest heroines of freedom, Susan B. Anthony,” Trump noted. “She fought to end slavery, restore women’s right to vote & respect the dignity of every person. Now we have a chance to honor her legacy and restore the first right in the Declaration of Independence. It’s called the right to life.”
The president then told the story of Lisa and Bruce Alexander, a couple in attendance who adopted their now-four-year-old daughter Katherine despite her being born with an opioid addiction. Trump invited the little girl on stage to warm applause.
“At the age of two, she memorized ‘America the Beautiful,’” Trump revealed. “She recites poetry, and recently she announced to her dad that when she grows up she wants to be a famous police officer, and then when she gets tired of that, she wants to become president.”
“We celebrate all lives, we celebrate the loving choice of adoption,” the president declared. “Katherine reminds us that every life is sacred, that every child is a loving gift from God.”
“When we stand for life, we stand for the true source of America’s greatness: it’s our people,” Trump declared. “It’s the people who grace our lives, who sustain our communities, and who make America a nation, a home, and this magnificent land we all love so much.”
The president concluded his remarks by calling on the audience to “vote for family, vote for love, vote for faith and values, vote for country, and vote for life.”
The United States just hit a 40-year low in its fertility rate, according to numbers just releasedby the Centers for Disease Control and Prevention. The 2017 provisional estimate of fertility for the entire U.S. indicates about 3.85 million births in 2017 and a total fertility rate of about 1.76 births per women. These are low numbers: births were as high as 4.31 million in 2007, and the total fertility rate was 2.08 kids back then. The United States has experienced a remarkable slump in fertility over the last several years, as I’ve explained elsewhere.
Since 2007, fertility has fallen the most for the youngest women, but in the last year, declines have set in for women in their 30s as well. Fertility declines increasingly seem to be about much more than just postponed fertility, or else these women must be planning to have some very fertile 40s.
At least through 2016, this trend appeared to be mostly driven by changes in marital status. Births to never-married women are down more than births to ever-married women: age-adjusted marital fertility is down 14% since 2007, while age-adjusted never-married fertility is down 21%, as of 2016. Preliminary data from several states suggest these trends are likely to continue in 2017.
When it comes to discussions about declining fertility, conservatives tend to “get it” right away: not having a next generation, or having a far smaller one, will cause problems down the line. In my experience, progressives tend to be more hesitant: is this a back-door argument to keep women out of the workplace? No; in fact, there’s robust empirical evidence most women want more kids. Is this some science-denying attempt to ignore climate change? Again, no; in fact, no plausible trajectory of U.S. fertility has any appreciable impact on carbon emissions. And, one question I find the most perplexing, is this some underhanded racist argument that white people need to pick up the pace of baby-making to out-compete minorities?
It’s true that some people in the right wing have flirted dangerously close to, and sometimes engaged in, the kind of racialized thinking that has tarred pro-fertility initiatives throughout the 20th century, complaining about “other peoples’ babies,” or quietly suggesting that if African Americans have fewer kids, maybe that’s a good thing.
At the end of the day, though, racists on the right are wrong (and comparatively few in number), but so are the progressives who assume that calls for more babies are racially driven.
That’s because the decline in fertility has been far greater among minorities than among non-Hispanic whites. If we take age-specific birth rates from the peak-fertility year of 2007 and apply them to each age cohort in 2008-2016, the most recent complete data, we can create a counterfactual scenario of how many babies would have been born if age-adjusted fertility rates had not fallen after 2007. From 2008 to 2016, the deficit turns out to be between 4.1 and 4.6 million missing babies: basically, an entire year’s worth or more of childbearing vanished.
The deficit varies across racial and ethnic groups. American Indians and Alaska Natives have it worst among racial groups, having lost a whopping 15% of expected fertility from 2008 to 2016, or about 83,000 births, with total fertility rates falling from 1.62 births per woman to a shockingly low 1.23. It’s unclear exactly why Native American fertility has fallen so quickly and why it is so low, but they are indisputably the hardest-hit race in the fertility declines of the last 10 years.
Then come African Americans, who are missing 9.6% of expected births, or about 700,000 births, which is only slightly more severe than whites, who are missing 9.3%, or about 3.2 million births. Black fertility declined from 2.15 births per woman to 1.89, while white fertility fell from 2.14 to 1.82. Asians experienced a less severe decline, but their fertility was somewhat lower to start with.
In racial or ethnic terms, America’s “Baby Bust” is kinda, sorta, a little bit racist: it’s hammered Native Americans and Hispanics particularly hard, and hit even African Americans harder than whites generally, and certainly harder than non-Hispanic whites.
But the “white” fertility figure is a bit misleading, as it includes most Hispanics, who have historically had much higher birth rates than non-Hispanic whites. Looking at all Hispanics together, these women are missing nearly 19% of the babies that would have been born from 2008-2016, or about 2.2 million births, as their age-adjusted fertility rates have fallen from 2.85 births per woman to just 2.1, and continue to decline. Meanwhile, non-Hispanic fertility has only declined from 1.95 births per woman to 1.72, yielding about 2.3 million missing births. Solidly half of the missing kids over the last decade would have been born to Hispanic mothers, despite the fact that Hispanics only make up about a quarter of fertility-age women.
Thus, in racial or ethnic terms, America’s “Baby Bust” is kinda, sorta, a little bit racist: it’s hammered Native Americans and Hispanics particularly hard, and hit even African Americans harder than whites generally, and certainly harder than non-Hispanic whites. The call to boost fertility is far from being a call for whites to keep up with minority fertility; rather, it’s an exhortation that we need to be listening to the fertility desires of women of racial and ethnic minorities, who are experiencing precipitous declines in fertility, largely unnoticed by the white-dominated world of mommy-blogs and late-in-life fertility treatments. Any serious pro-natal policy in America worth its salt would primarily result in birth gains among minority mothers, not white ones. Accelerating the national birth rate would also accelerate the pace at which the non-Hispanic white population share declines.
The effect is electorally significant, as well. These lost births are not distributed evenly around the country, as the figure below shows.
Some states have lost far more births than others, while lucky North Dakota has seen an increase in births. But even as declining fertility makes the country’s population whiter, it is making the country’s politics redder: on average, states won by Clinton in 2016 are missing 9% of their expected births since 2008, whereas states Trump won are missing just 7.8%. Within states, Hispanic-, Native American-, and African American-dominated places are seeing the steepest population growth underperformance as a result of missing births. During the 2020 Census apportionment and redistricting process, this will all combine to weaken the political power of minority-heavy areas. The map of declines in 2017 suggests that the observed decline in minority fertility through 2016 almost certainly continued in 2017.
In terms of change in age-adjusted fertility, the sharpest declines in births have been in Arizona, where fertility has fallen from 2.47 births per woman in 2007, to an estimated 1.81 in 2017. Provisional data from early 2018 suggests these declines are likely to continue. Arizona is double-whammied by two different racial or ethnic trends: steep declines among Hispanics and steep declines among Native Americans. Both groups make up a larger share of Arizona’s population than the national average. Both groups have seen steep declines within Arizona; steeper even than their peers in other states.
Other factors are at work, too. Fertility has fallen somewhat more for less educated than for more educated women. Age-adjusted fertility has fallen 15% for women with a bachelor’s degree or less, versus just 7% for women with graduate degrees. On the whole, births to women with no bachelor’s have totaled 12% below what would be expected if 2007 fertility rates had continued, yielding 3.1 million missing births, while births to women with a bachelor’s degree are down 10% for 1.1 million missing births, and births to women with a graduate degree are down just 7%, or 300,000.
In relative terms, these differences are smaller than differences by age or race, suggesting that socioeconomic class is not the biggest driver of changing fertility rates. This is borne out using other variables: Having insurance or not doesn’t seem to make any difference in fertility changes since 2007, and household income also has no clear, linear trend. With more covariates, these factors might have a stronger effect, but they aren’t the dominant story of declining fertility. There are plenty of other factors that could be looked at, but the basic conclusion is pretty straightforward.
Race, ethnicity, marital status, and geography are the best predictors of changes in fertility over the last decade. Fertility declines are most strongly associated with factors that are race- or region-specific, not broadly class-specific, as different economic classes appear to have quite similar trends. This doesn’t rule out all economic causes: there are important interactions between race and socioeconomic class. But this association does suggest two key takeaways to be kept in mind when discussing declining fertility: it is disproportionately landing on minority moms, births have fallen most for unmarried women, and economically-oriented solutions may only have modest direct effects.
Lyman Stone is a Research Fellow at the Institute for Family Studies, and an International Economist at the U.S. Department of Agriculture, where he forecasts cotton market conditions. He blogs about migration, population dynamics, and regional economics at In a State of Migration.
AUSTIN, Texas, May 21, 2018 (LifeSiteNews) – The Republican lieutenant governor of Texas cited abortion this weekend as one of several factors that have degraded America’s respect for human life, which he believes was one of the causes of the recent school shooting in his state.
A 17-year-old shot and killed eight students and two teachers at Santa Fe High School in Texas last Friday. He was subdued after a shootout with police, and is currently being held on murder and assault charges.
On Sunday, Lt. Gov. Dan Patrick appeared on ABC News’ “This Week” with George Stephanopoulos to discuss the case. The two debated a number of topics, including the availability of guns and school security procedures, but Patrick’s central thesis was that the problem is rooted in America’s “culture of violence.”
“We have devalued life, whether it’s through abortion, whether it’s the breakup of families, through violent movies, and particularly violent video games,” Patrick said.
“We can’t sit back and say, ‘It’s the gun.’ It’s us as a nation, George,” Patrick continued. “On this Sunday morning, when we all go to church and pray or go to synagogue or the mosque or wherever we go, let’s look inward at ourselves as a nation.”
Stephanopoulos pushed back on Patrick’s arguments about gun control and violent entertainment, but he notably declined to dispute his reference to abortion.
“We have 50 million abortions […] and we stand here and we wonder why this happens to certain students,” Patrick added Sunday in additional remarks reported by CNN.
Fred Guttenberg, who became a gun control activist after his 14-year-old daughter Jaime was murdered during February’s school shooting in Parkland, Florida, quickly denounced Patrick for “the most idiotic comments I’ve heard regarding gun safety” and demanded that he “be removed from office for his failure to want to protect the citizens of Texas.”
But while mass shootings typically happen due to a wide range of factors, from mental illness to children’s upbringing to overlooked warning signs, many have argued it’s no coincidence that a society which enshrines a “right” to kill preborn children has seen an uptick in killings of born children.
“If we have created a culture, in the words of one Catholic Deacon Greg Kandra, where human life is treated like trash, what do we expect here?” The American Spectator’s Jeffrey Lord has asked. He notes that “Wikipedia lists eight years of mass shootings in the United States between 1929 and 1972. That is a span of 43 years. Roe v. Wade was issued in 1973. Between 1973 and 2017 — a span of 44 years — the site lists 39 years of mass killings in the United States.”
It is said that Blessed Paul VI was so heart-broken by the outpouring of dissent to Humanae Vitae, he couldn’t bear to write another encyclical in the final decade of his pontificate. Certainly, one can feel the pope’s anguish in this homily, given just months before he died – already seeing many of his worst predictions about the consequences of the embrace of artificial contraception coming true.
“[Humanae vitae] was inspired by the immutable teaching of the Bible and the Gospel, which confirms the norms of the natural law and the irrepressible dictates of conscience regarding respect for life and its transmission by fathers and mothers who practice a responsible parenthood. The document has acquired new and urgent relevance in view of the wounds now being inflicted by civil laws on the holiness of the indissoluble marriage bond and the sacredness of human life even in the maternal womb. In face of saddening defections in the Church and society, We, like Peter, feel compelled to go to Him as the only source of salvation and cry out to Him: Lord, to whom shall we go? You have the words of eternal life.” — Blessed Paul VI, Homily on June 29, 1978 (available here in French, Italian and Spanish)
Yet even still, bishops, priests, and lay Catholics persist en masse in ridiculing and ignoring his warnings. In the face of the failures of so many pastors, and the apparent futility of his encyclical, Paul VI could only cry out with St. Peter: “Lord, to whom shall we go? You have the words of eternal life!”
Since our foundation, Human Life International has committed itself to emphasizing efforts to teach the truth about contraception. This approach is based upon the belief that the contraceptive mentality is the root cause of many of the greatest evils of our age: the abortion holocaust, the explosion of divorce, the epidemic of fatherless children, the legalization of same-sex “marriage,” the advent of brutally enforced population control programs, and more.
To many, this claim is still nothing short of absurd. The apparent “benefits” of contraception seem to them so obvious, and its connection to the above-mentioned evils so tenuous that they casually dismiss that prophetic encyclical as the backwards and repressive musings of an uninformed celibate who couldn’t possibly understand the “real” struggles and needs of ordinary, married men and women.
Despite the enormous amount of empirical data that has piled up in support of each of Paul VI’s predictions, it is astonishing how widespread this dissent to Humanae Vitae, despite fulfillment of predictions on what would happen if contraception became normalized. In other respects, however, it is perfectly understandable, if only we understand the truth about human nature, in particular the wounds that affect our nature after the Fall.
The Blindness of Concupiscence
Before the Fall, human beings possessed what theologians call the gift of “integrity.” What that means is that man’s lower passions completely obeyed his reason. Things changed after Adam’s sin, however, at which point humans became subject to concupiscence. That means that our lower passions are no longer subject to reason. We all experience this reality on a daily basis, when we desire things that we know to be harmful for us and contrary to God’s law.
Concupiscence means that we are constantly subjected to the restlessness of our own hearts, and the illusions of our passions. Sometimes, this restlessness results in obviously destructive and evil behaviors – the abuse of drugs or pornography, for instance, or violence towards other human beings. In the pursuit of happiness, we seize upon and relentlessly pursue the very things that make us most unhappy and that harm others.
But such is our brokenness, that we often misuse even things that are morally good in themselves. For instance, a man might be so anxious to support his family by working hard (a very good thing!), that he becomes a workaholic. If he is not rooted in God and His truths, his anxiety about the future, or need for affirmation from others, instead leads him to abuse a good thing (work), possibly without his even consciously realizing it.
Often, the temptation to pervert something good by misusing it is so subtle and convincing that it takes long experience, spiritual discernment, and the constant practice of self-denial. This is one reason we Catholics are so fortunate: in the pursuit of holiness, we have the wisdom of the Scriptures, 2,000 years of Church teaching, the Sacraments, and the support of a church community committed to God’s law.
There is, perhaps, no area of human life in which we are more subject to illusion, and more in need of divine wisdom, than sexuality. The Church teaches that sex is a great good – and so it is! (“The acts in marriage by which the intimate and chaste union of the spouses takes place are noble and honorable; the truly human performance of these acts fosters the self-giving they signify and enriches the spouses in joy and gratitude.” – Catechism, ¶2362) And yet, so virulent are our sexual passions, that we can easily fall prey to destructive illusions about sex. One need only take the briefest glance at the world around us to see the immeasurable pain and suffering caused by the many lies related to sex: so many broken hearts, broken bodies, and lost and hurting souls!
The Illusion of Contraception
To many people alive 50 years ago, contraception seemed the near-miraculous “solution” to much of the chaos caused by sex. One can easily understand why. For the first time in history, human beings had invented reliable, affordable, and seemingly harmless and non-invasive methods of birth control. For the first time in history married couples could (it seemed) enjoy the pleasures and intimacy of sexual intercourse, without having to worry about having babies they felt they weren’t prepared for or couldn’t afford. Contraception (it was said) – especially the pill – would thus strengthen marriages. Many even claimed contraception would eliminate the need for abortion and would reduce poverty.
To most people – including Blessed Paul VI’s own advisors at the Vatican – it seemed obvious what the Holy Father should do: he should get with the times and follow all the other Christian churches and teach that artificial contraception was morally permissible for married couples. It turned out the Church’s past condemnations of contraception were short-sighted. Technology had changed everything.
So, why didn’t Paul VI follow this seeming obvious path? Why did he alienate and anger so many Catholics and non-Catholics by issuing words that would provoke dissent to Humanae Vitae?
A Jesuit priest, Fr. John Ford, recounts a startling and revealing conversation he had with Paul VI, while the two were discussing the arguments put forward by the papal commission on birth control. Fr. Ford recounts: “[W]hen I said to Pope Paul, ‘Are you ready to say that Casti Connubii can be changed?’ Paul came alive and spoke with vehemence: ‘No!’ he said. He reacted exactly as though I was calling him a traitor to his Catholic belief.” Casti Connubii, of course, was the encyclical by Pope Pius XI, in which the pope had clearly reaffirmed Catholic teaching on Christian marriage and against artificial contraception.
In other words, for all the enormous pressure being placed on Paul VI to change Church teaching, he knew that teaching was there for a reason. Even if human reason could find all manner of arguments to prove that contraception was a blessing for humanity, the Divine Reason that inspires Church teaching saw further and deeper into the heart of things. For the papal advisors on the birth control commission, the promise of consequence-free sex was too powerful a temptation; it appeared to them to be an unmitigated good. As the Supreme Pontiff, however, it was Paul VI’s duty to see with the eyes of Divine Reason, and to do that, all he had to do was to look to the wisdom of the Church and the Scriptures.
And that is what he did. And what he saw chilled him to the bone: humanity, he saw, was obliviously careening straight towards a cliff. And as a Shepherd, he did what he had to do and proclaimed the truth – not because he viewed sex as evil, but because he understood its profound goodness and power.
“Lord, You have the words of eternal life!”
The wisdom of the Church’s teaching on contraception, in Humanae Vitae and elsewhere, is not always obvious, even to faithful Catholics determined to follow that teaching. During extended times of abstinence, or when an unplanned pregnancy occurs, the temptation to question that teaching may arise.
At such times, the answer is to remember the words of St. Peter, quoted by Paul VI. Because of His teaching on the Eucharist, many of Christ’s disciples were abandoning Him. They did not understand how they could eat His flesh. Neither, for that matter, did St. Peter. But when Christ asked him if he, too, would abandon Him, St. Peter’s heart welled forth with that great cry of faith: “Lord, to whom shall we go? You have the words of eternal life!”
We may not always understand. But as St. Pope John Paul II assured us, God never commands the impossible: “As the Tradition of the Church has constantly taught, God does not command the impossible, but every commandment also entails a gift of grace which helps human freedom to fulfill it.” “Yet,” he added, in order to follow the Church’s teachings on sexuality, “constant prayer, frequent recourse to the sacraments and the exercise of conjugal chastity are needed.” (John Paul II, Address to Participants in a Study Meeting on Responsible Procreation, June 5, 1987)
The world does not understand. It may never understand. But that must never stop us from proclaiming and living the truth. Divine wisdom sees deeper and further than we do. The world has been scarred by the lies of the sexual revolution, and men and women are starving for the truth about love and sexuality.
“Today,” said St. Pope John Paul II, “more than yesterday, man is again beginning to feel the need for truth and right reason in his daily experience. Always be ready to say, without ambiguity, the truth about the good and evil regarding man and the family.”
Most Rev. Alexander Sample, Archbishop of Portland
Tuesday, May 15, 2018 12:35 PM
My sister who lives here in Portland watched on EWTN the Mass I celebrated at the Basilica of the National Shrine of the Immaculate Conception on April 28. One of her comments (after she finished making fun of her younger brother!) was about how Holy Communion was received. She remembered with some real fondness how, when we were children, we always received Holy Communion at the Communion rail and on the tongue. No one dared touch the Holy Eucharist, except the priest.
Whatever anyone reading this thinks about the current practices regarding the distribution of Holy Communion, the rationale behind the former discipline was a profound sense of reverence and awe for the presence of our Lord in the Blessed Sacrament. It is not just a symbol or sign. Jesus Christ is truly present, body, blood, soul and divinity in the Holy Eucharist.
The Real Presence
That’s what Catholics believe. But our liturgical and sacramental practices far too often do not reflect that profound understanding and faith in the Real Presence. The story is told of a Protestant minister who was invited to attend Mass. Afterward he was questioned on what he thought. He replied that he did not think that the congregation really believed in the Real Presence. When asked why he thought this, he said that he personally did not believe in the Eucharist as Catholics do, but if he did, he would approach our Lord for Communion walking on his knees. He found the casusal and irreverent attitude at the time of Communion in that particular church very unconvincing.
As part of a new Liturgical Handbook for the Archdiocese of Portland to be released on the Solemnity of Corpus Christi (June 3), and after consultation, there are two changes in practice I am implementing with regard to our understanding and reverence for the Holy Eucharist. Please consider this a “teaching moment” for all of us. As shepherd and teacher of the faith, and as the one ultimately responsible for the liturgical life of the Archdiocese of Portland, my intent is to foster greater devotion to our Lord in the Blessed Eucharist and in the Holy Mass.
Showing reverence
We will return to the practice of kneeling after the Agnus Dei (Lamb of God). The current practice is to remain standing, which has been an exception to the universal norm of kneeling that has been perfectly legitimate and permitted by the liturgical norms. Nevertheless, returning to the practice of kneeling at this moment in the Mass will foster a greater reverence for our Lord.
The priest at that moment is about to hold up before the congregation our Blessed Lord in the Holy Eucharist and proclaim, “Behold the Lamb of God.” It seems most fitting that we be on our knees before the Lord for such a proclamation of faith. In the Book of Revelation, when the Lamb of God (Christ) is presented before the throng of heaven, all fall down in worship before him. The Mass is a participation in this heavenly liturgy.
On Communion and Holy Sacrifice of Mass
The second change coming is that, in the absence of a priest to offer Mass, the distribution of Holy Communion on weekdays in the parish church during a “Communion service” will no longer be permitted. This does not affect such Communion services in nursing homes, prisons, etc., where the people do not have the opportunity to attend Mass on Sunday in the parish.
There is an intimate and intrinsic link between three realities that is essential in this context. They are the offering of the Holy Sacrifice of the Mass, the priest who ministers in the person of Christ, and the distribution of Holy Communion. These are not to be separated except for serious reasons and pastoral need. As long as the faithful have the opportunity to participate in Mass and receive Holy Communion on Sunday, there is no such pastoral need to receive Holy Communion outside of Mass.
When we go to Mass, we are there to do much more than just receive Holy Communion. We participate actively and consciously in the offering of Christ, the Paschal Victim, through the hands of the priest, who ministers in the very person of Christ at the altar. From this sacramental offering, we receive the Body and Blood of the Lord, thus culminating our participation in the paschal mystery being celebrated. This is the way the Church has always viewed this. The Church never envisioned breaking them apart by distributing Communion outside of Mass. This is only done for the sick and those otherwise unable to participate in the Sunday Eucharist. To do otherwise is very poor sacramental and Eucharistic theology.
When Mass cannot be offered on a weekday in a particular church, parishioners are invited to experience the wider Church by attending daily Mass in a neighboring parish. The faithful can also gather for other forms of prayer, and our Office of Divine Worship has prepared a prayer service for such occasions that include parts of the Liturgy of the Hours with readings from the Mass of the day. This is a way to experience another form of the Church’s liturgical prayer.
These changes may take some time for adjustment, but I am confident that they will lead us to a more profound reverence for the most precious gift of the Holy Eucharist, and a more informed, conscious and active participation in the Holy Mass. And a greater love for our Lord in the Mass and in the Blessed Sacrament will lead to a greater love of neighbor and service to the poor.
WASHINGTON — The extraordinary form of the Mass is drawing young people with its sense of reverence and transcendence, Portland Archbishop Alexander Sample said during an April 28 homily in Washington, D.C.
“It has clearly been demonstrated that young persons, too, have discovered this liturgical form, felt its attraction, and found it a form of encounter with the mystery of the most holy Eucharist particularly suited to them,” Archbishop Sample said, quoting a 2007 letter from Pope Benedict XVI to the world’s bishops.
The archbishop made the remarks during his homily at the Basilica of the National Shrine of the Immaculate Conception here, where he was celebrating a pontifical high Mass to commemorate the 10th anniversary of Pope Benedict’s XVIs apostolic letter “Summorum Pontificum.” Archbishop Sample thanked Pope Benedict in his homily for allowing the older form of the Latin Mass to flourish in the new millennium.
“Let us thank the Lord for Pope Benedict’s gift to us — the greater celebration and availability of the usus antiquior [older use] of our common heritage in the Roman rite,” said the archbishop.
Close to 3,000 worshippers attended the Mass, including pilgrims from all over the country. It was broadcast worldwide on EWTN. Young people were in attendance, including the traditional young adult group Juventutem. The archbishop called the young people present a promising sign for the church in modern times.
“I have met a good number of you personally,” Archbishop Sample said to the assembled young adults. “You are a sign — a great sign — of encouragement and hope for the church tossed about these days on the troubled waters of secularism and relativism. As they say, you ‘get it.’”
Young people’s attraction should make church leaders question what is drawing them to the older form of the Mass, the archbishop said. Some priests and bishops, he explained, wonder what it is about the extraordinary form that attracts young people who didn’t grow up with it.
“That is exactly the question you should be asking,” Archbishop Sample said. “What is it that this form of the Roman rite provides for them that their own experience growing up with the ordinary form did not provide?”
The archbishop made it clear that he was not questioning the legitimacy or benefits of the reforms called for by the Second Vatican Council, but rather that their implementations had not always “borne good fruit.”
“Certainly, through liturgical abuses, other aberrations or simply a poor ars celebrandi [art of celebration], the ordinary form of the Roman rite has too often been disfigured and has been experienced as a rupture with our liturgical past,” he said.
Still, he said, quoting Pope Benedict, “There is no contradiction between the two editions of the Roman Missal.”
Both the extraordinary and ordinary forms serve to enrich each other, said Archbishop Sample. “There must be further liturgical growth and development along the lines of a hermeneutic of continuity with the past and any experience of rupture must come to an end,” he said.
After the Mass, Archbishop Sample spent time with many of the attendees, interacting and taking photos with them.
John Mayer, a member of St. Mary Parish in Mount Angel, made the six-hour drive from Franciscan University of Steubenville in Ohio, where he is studying, to attend the Mass and was able to meet with the archbishop. Being there, he said, reminded him that the sacred liturgy is something that can unify Catholics from all walks of life.
“Tradition in the liturgy unites people of all ages,” he said. “It was amazing to see so many people flock to Our Lady’s national shrine in our nation’s capital for this Mass, tied together by this ancient practice of the Roman rite.”
For Mother’s Day the US website Women Speak For Themselves ran a contest for women to write to other women about why not to fear motherhood. WSFT got 140 entries and the winning piece is here. The following is the third of three runners-up. The other two are here.
* * * * *
Dear Millennial Woman,
I did not think I would ever be a biological mother. This didn’t bother me; I was too busy anyway and much too afraid of the sheer pain of it all. I winced to hear the word “labor” in connection with childbirth. But love won me over.
It started with my need to be loved and cherished by someone. I know you have that need, too. A woman wants nothing quite as much as arms to hold her and a heart to lay her head on. Let’s be honest: this is at the root of some of our worst decisions, driven by passion, fueled by lust. We let ourselves be scorched by the heat of our hook-ups because we want someone to hold and harbor us and our fears. But it isn’t where we find love. My husband, however, knew how to love me unconditionally and it was in the comfort and security of his love that I found my true self.
But this letter isn’t about me, it’s about you. It’s about your desire for love. I want you to experience the strong, solid tethers of a true union, bound by marriage, within which love bears its most beautiful fruit — the birth of a child.
I gave birth to my first-born three months ago; a year ago she was conceived. And, yes, I labored, long and hard, to bring her into this world. But love once again won me over. Hers is like her father’s love, but even more so in its untainted innocence; she looks at me with a tender love that knows no limits. I am the first person she loved.
Every time she looks at me, she recognizes that I am unique – I am her mother – and she loves me uniquely. To be loved so fully and perfectly, to be embraced by her and know that to her, I am everything (for now), is a reward in itself.
Young woman, look no further for love than in the eyes of a child. They are like the eyes of God — in them you can see yourself anew and recognize that you are loved unconditionally. I can’t imagine now who I would be without my little daughter to teach me every day who I am. I can’t imagine how much love I would have lost without her.
Young woman, what is it worth to gain the world and not experience love? The love of a child is too beautiful to refuse. Choose life and you will find love. ~ Julia M. Dezelski
WASHINGTON, D.C., May 19, 2018 (LifeSiteNews) – President Donald Trump will announce today a long-awaited rule change that will forbid facilities that perform or refer for abortions from receiving Title X family planning funds. The move will come as a blow to abortion giant Planned Parenthood.
The move, reported by multiple media outlets, originated as a proposal by senior White House counselor Kellyanne Conway, to require facilities performing Title X services to be physically separate from those that perform or refer for abortions.
Under the current rules, Title X services and abortions may “co-locate” in the same center, as long as the abortions are privately funded. The money would be redirected to Women’s Qualified Health Centers that are not involved in abortions, which dramatically outnumber Planned Parenthood locations across the United States.
“This proposal does not necessarily defund Planned Parenthood, as long as they’re willing to disentangle taxpayer funds from abortion as a method of family planning, which is required by the Title X law,” a Trump administration official told CNN.
“Any grantees that perform, support, or refer for abortion have a choice — disentangle themselves from abortion or fund their activities with privately raised funds.” Such disentangling would entail requiring abortions to be performed at different facilities, and by different employees, than the one receiving Title X funds.
The majority of Planned Parenthood’s federal funding comes via Medicaid reimbursements and would not be affected, but the loss of more than $50 million per year would still be a significant blow to the abortion giant.
“Abortion advocates and Planned Parenthood’s allies will likely try to claim poverty if these regulations are passed,” March for Life Action president Tom McClusky wroteThursday in support of the change. “But during the 2013-2014 reporting year, Planned Parenthood reported $127 million in net income and $1.4 billion in held assets. They will likely claim that defunding them will increase the infant mortality rate (this claim was made after Texas defunded the abortion-giant, and was quickly found to be false.)”
Almost 200 Republican House and Senate members, as well as more than 80 pro-life leaders, have already sent the administration letters urging it to make the change, and those pro-life leaders are now celebrating the realization of their hopes.
“We thank President Trump for taking action to disentangle taxpayers from the abortion business,” Susan B. Anthony List President Marjorie Dannenfelser said. “Planned Parenthood, the nation’s largest abortion business, is responsible for more than 300,000 abortions a year and has been receiving $50-60 million in Title X taxpayer funds annually.”
“President Trump has shown decisive leadership, delivering on a key promise to pro-life voters who worked so hard to elect him,” she continued. “This is a major victory which will energize the grassroots as we head into the critical midterm elections.”
The move brings President Trump and the GOP-controlled Congress one step closer to fulfilling their campaign promises to defund the nation’s largest abortion provider, but Planned Parenthood’s overall taxpayer funding exceeds $500 million per year.
Previous efforts to defund the abortion industry through Obamacare repeal legislation failed last year, and in March the government enacted a budget that continues the abortion giant’s funding. Standalone defunding legislation has been introduced in Congress, but has yet to receive action.
Donald Trump ran his presidential campaign saying he is pro-life. He has proved time and again by his actions that he meant what he said.
This is what we face. According to the prevailing view, the love of a man and a woman is not an enduring commitment of the will to the true good of another person, but a feeling or an emotion. Essentially, then, what the culture calls matrimony is cohabitation with formalities. Like cohabiting couples — or cohabiting threesomes or what have you — a married couple may speak of having a committed relationship, but commitment in the traditional sense is just what they do not have. Sexual intercourse is not viewed as suggestive of the possibility of new life; neither is having children viewed as requiring intercourse, because these days there are labs for that. Though even in this day of plummeting birth rates, children may still be desired, adults tend to view them as a lifestyle enhancement, something like a home entertainment center, but more expensive. Though having a few children may still be regarded favorably, having more than a few is frowned upon, because children consume resources, use up disposable income, and require a great deal of care. A puzzled writer who is not quite so extreme as to condemn all childbearing says nevertheless, “I don’t have the answer to the origin of the longing for children that many experience. It’s almost certainly due to a complex mixture of biological and social factors. It might even be an evolutionary trick.”
Against this, we want to argue that the love between the husband and wife is an act of free will by which the spouses give themselves to each other mutually, totally, indissolubly, and exclusively, for the sake of God. Opening themselves to the possibility of bearing fruit is the most beautiful way that they do give themselves to each other, and the very basis of their love. By acknowledging that the sexual powers have a procreative purpose, we are not denying that we are ends in ourselves. Rather we are acknowledging what kinds of ends in ourselves we are. We are beings whose biological functions are not shackles, but constitutive properties of our embodied personhood. We do not diminish ourselves by honoring them. We would alienate ourselves by not honoring them.
All of this has roots in the doctrine of Thomas Aquinas. Now in one sense, matrimony is complicated, because it has a number of origins. He argues that natural law itself originates matrimony in matters concerned with having and raising children. Natural law after the Fall further shapes matrimony so that its natural purposes are not unraveled by the wound of sin, which tempts us to employ our sexual powers in ways that forestall the formation of families or undermine their good order. The civil law shapes matrimony with respect to such things as spousal support. The Gospel shapes matrimony by directing it to an additional purpose, for the union of husband and wife represents and makes present the mystery of Christ’s union with the Church.
We can say, then, that natural law institutes marriage in one way, the law of the Gospel institutes it in another, and civil law institutes it in still another. St. Thomas says that these various “institutions” or origins “are not of the same thing in the same respect.” However, they are all linked. Thus, for the civil law to treat marriage as something contrary to what it is by nature would be profoundly wrong; any such so-called civil marriage would not be marriage at all.
As I said, that is rather complicated. But in another sense, the basics of matrimony are simple, because as St. Thomas says, all of this involves only three matrimonial goods. The first good of matrimony, he says, is “the birth of children and the educating of them to the worship of God.” If I ask my students to identify the purpose of the sexual powers, they usually reply “pleasure.” If, on the other hand, I focus their attention on our natural teleology by asking them to identify the purpose of the eye, the purpose of the ear, the purpose of the capacity for anger, and so on, and then ask them to identify the purpose of the sexual powers, they say instead “reproduction,” which is not bad. However, procreation means much more. Reproduction merely means turning out new humans by one means or another. If this were the only purpose of the sexual powers, it wouldn’t matter whether the partners were united. In fact, it wouldn’t matter if there were any partners. We could dispense with parents altogether, gestating children in flasks and raising them in state-run institutions, as they do in Huxley’s Brave New World. Procreation, by contrast, is the loving act by which posterity is generated. It means conceiving children in the embrace of their father and mother; it means not only having them together, but nurturing them together, so that they can become virtuous adults; and it means forming families, thereby forging new links between dimmest antiquity and remotest futurity. Any guppy can reproduce. We have the privilege of procreating.
The second good of matrimony is the mutual faithfulness of the husband and wife. Here St. Thomas is using the figure of speech called metonymy, in which a part represents a whole, as when I say “the crown” to represent everything about the institution of monarchy. St. Thomas does not express his thought by saying that the second matrimonial good is the spouses’ union; rather he uses the most important aspect of their union to represent everything about their union. “After an injury inflicted upon a man in his own person,” St. Thomas says, “none is so grave as that which is inflicted upon a person with whom one is joined.” This, he says, is why the Decalogue prohibits adultery immediately after it prohibits murder.
If we view procreation and unity as entirely distinct goods of matrimony, we are making a profound mistake. Today one hears often hears couples say, “we are putting off children so that we can enjoy each other first.” But according to the inherited wisdom of the human race, if we seek to enhance matrimonial unity by refusing the gift of children, we are merely turning a pair of selfish MEs into a single selfish US.
The third good of matrimony is sacramental. As the man and woman are espoused, so Christ and the Church are espoused. Just because of the indivisible union of the husband and wife, it can represent and make present the indivisible union of Christ and His Church. And just as the union of their bodies makes the spouses biologically fruitful, so the sacrament makes their union spiritually fruitful, as they pass on their faith to their children and display it to the world.
We mentioned just now that matrimony is indissoluble, but why is it indissoluble? According to St. Thomas, there are two reasons. To understand the first one, consider our difference from the other animals. Among some of the beasts, the female is capable not only of giving birth to the offspring, but also of training them without help from the male. In such species, intercourse is “random and indiscriminate.” Among other beasts, the female needs assistance, so the male cooperates with the female in caring for them. This requires that he recognize the offspring, that he possess a natural inclination to care for them, and that a definite male be joined to a definite female. In such species, the male and female cooperate until the children are grown. Now since we are rational beings, not just beasts, this applies even more to us, because our children need nourishment not just for their bodies, but even more for their souls, and their attainment of maturity and virtue takes a long time.
The second reason is stronger. Even after the children have reached maturity and virtue, they still need the help of their parents to establish their own new families. “Hence it is of natural law,” says St. Thomas, “that parents should lay up for their children, and that children should be their parents’ heirs. Therefore, since the offspring is the common good of husband and wife, the dictate of the natural law requires the latter to live together for ever inseparably.”
According to a certain caricature, St. Thomas is quite interested in the procreative good but hardly interested at all in the unitive good. This is utterly false. True, the matrimonial friendship differs from other friendships because of its procreative purpose. On the other hand, everything that applies to loving union in general applies to the loving matrimonial union too. Taking this into account, St. Thomas actually says more about union than about procreation. For example, he says, the lovers experience confidence that what has begun well will get better; they experience glory because each one glories in the good of the other; they are consoled because through delight in the good they share, each one possesses a remedy against sadness, and they experience exuberant joy because not only is sadness absorbed, but their exuberance “overcomes every tribulation.”
It is quite amazing how far St. Thomas is willing to go in describing the quality of loving union. He says, for example, that the lover and the beloved mutually indwell each other. “The beloved is contained in the lover, by being impressed on his heart” and becoming the object of his affections; the lover, in turn, “is contained in the beloved, inasmuch as the lover penetrates, so to speak, into the beloved.” Or take the idea that the lover “loves to love.” In our day we associate such language with soupy sentimentalism and the lavish use of emojis, but St. Thomas gives diamond-hard meaning to it. The power of will, he explains, is directed to the good. Love is a spontaneous act of the will, directed to the good of the beloved. But since to will is itself a good, man can will himself to will. For this reason, love, by its own nature, “is capable of reflecting on itself.” “Wherefore,” says the Angelic Doctor, “from the moment a man loves, he loves himself to love.” This does not mean that he is infatuated with his feelings. It means that with all his heart, he concurs with the direction of his will. His attitude toward the beloved might be expressed, “I exult that you exist in this world, I seek all good for you, and I know it is good that I do.”
Another caricature is that St. Thomas frowns on sexual pleasure. On the contrary, he argues that had it not been for the Fall, the pleasure of sexual intercourse would have been even greater than it is now. What happened when we fell is not that our pleasure became stronger, but that our reason became weaker. If we had not fallen, then, our pleasures would have been even stronger, but they would not have disordered our thinking, as they do now. Our minds would obey God, and our passions and desires would obey our minds.
Still another caricature is that St. Thomas thinks the spouses should have intercourse only because they are trying to have children. Wrong again. He does say that sexual intercourse must always be rightly related to its procreative purpose, which means that the spouses must never do anything to make intercourse incapable of bringing about new life. However, they may also have intercourse simply to celebrate their procreative union.
To see this more clearly, we might think of eating. We eat because food is necessary, but as St. Thomas points out, necessity has several different meanings. In one sense we must eat because otherwise we cannot live. But in another sense we must eat because otherwise we cannot live becomingly. This is why we eat and drink more on festive occasions: Not to keep from starving, but to celebrate. Obviously God endorses this motive; after all, at the wedding feast in Cana, Jesus turned water into wine. Now even at feasts, eating and drinking must still be rightly ordered to life and health. It would be prejudicial to life and health if we ate as much as we could and then purged so that we could eat still more. But right order does not require that we eat and drink only for life and health. It is not prejudicial to life and health to toast the married couple with wine.
Now apply these distinctions to the enjoyment of sexual intercourse. In the first sense of necessity, sexual intercourse is necessary simply to be fruitful. But in the second sense, it is necessary so that the husband and wife may enjoy their partnership in the possibility of fruitfulness becomingly – so that they may celebrate it. Even celebratory intercourse must still be rightly ordered to procreation, but right order does not require that the spouses enjoy intercourse just for making babies. Rather it allows them to enjoy intercourse so long as they do nothing to thwart the procreative possibility of their action.
Here is another way to think of the matter. The husband and wife should cherish their procreative union as good in itself, not just as a tool for pleasure. But because their union is good in itself, it is also pleasurable, for pleasure, says St. Thomas, is the repose of the soul in what is good. And so desiring the pleasure of their union is exactly right. Notice here that pleasure is not the main thing; it is the enjoyment of the main thing. Pleasure it is not the good itself; it is the delight of experiencing the good.
Hedonists get this backward. Rather than viewing pleasure as repose in whatever is good, they view pleasure itself as the good – in fact, as the only good. From this point of view, one does not really cherish one’s wife for her own sake; he cherishes only the resulting pleasure. It follows from this theory that if there were a way to have the pleasure of one’s wife without one’s wife, then that would be just as good, or even better. Never mind marriage – let us just arrange to have electrodes implanted to stimulate the pleasure centers of our brains. Why experience pleasure indirectly, when we can experience it directly?
St. Thomas is pointing out that I should not treat my wife as that electrode. She herself is what I should cherish, experiencing the pleasure of that cherishing. What she and I enjoy, in both the procreative and unitive aspects of our marital friendship, is delightful. It is delightful to rest in the hope of new life; it is also delightful to rest in our mutual love, as partners in this hope. But if I say “never mind our hope of children, never mind our mutual love, I just want pleasure,” then I am missing the point. I understand neither children, nor love, nor delight.
J. Budziszewski is a Professor in the Departments of Government and Philosophy, University of Texas at Austin. This article has been republished with permission from his blog, The Underground Thomist.
Micaiah Bilger May 16, 2018 | 4:35PM Queensland, Australia
Mackinlee Anderson nearly died of severe brain injuries last September after her family was involved in a multiple-vehicle accident.
Anderson’s grandmother died, and the 6-year-old sustained major injuries. Doctors initially told her family that she was “99.8 percent brain dead” and would never walk, talk or eat on her own again – if she survived at all, the Daily Mail reports.
Now, she can do all three.
Her family and friends nicknamed her the “miracle girl.”
The Queensland, Australian girl recently took her first steps on her own after the accident, according to the blog Now To Love. She has come a long way.
In September, she and her family were visiting her grandparents when they were involved in a major vehicle crash on a highway in New South Wales, according to the report. Her grandmother died, and she, her brother and mother all were injured.
Mackinlee’s injuries almost claimed her life. Her family said she had a broken pelvis and femur, ruptured bladder, dislocated hip, paralysis and extensive brain injuries and brain trauma.
“We were pretty much in a place there where the doctors thought there was no hope for her,” her mother, Kylee Anderson, told nine.com.au.
But 32 days after the accident, she began to talk again. Mackinlee said “mom” that day, and later called her cousin to wish her a happy birthday, the family said on their GoFundMe page. Last week, her family said she took her first unaided steps since the accident.
“It is amazing, we are still just in shock,” her mother said. “Mackinlee amazes me every day with her determination. Every day the doctors say she can’t do something and the next day she can do it.”
The 6-year-old spent five and a half months in the hospital, but she now is home. Though Mackinlee still has a number of medical needs, her family said she is doing so much better than expected.
“She takes us by surprise every day. They told me that she wouldn’t be the same little girl. Well, she is the same little girl she was before the accident,” her mother said.
ASTANA, Kazakhstan, May 14, 2018 (LifeSiteNews) – Bishop Athanasius Schneider along with other bishops and ordinaries of the Catholic Church in Kazakhstan have released a pastoral letter to honor the “enduring importance” of Paul VI’s encyclical Humanae vitae.
This year marks the fiftieth anniversary of the famous pro-life, pro-family document. Pope Paul VI released Humanae vitae in 1968. He taught unequivocally that “each and every marriage act must remain open to the transmission of human life” and called the use of contraception “intrinsically wrong.”
“Blessed Paul VI confirmed the teaching of the constant Magisterium of the Church regarding the transmission of human life,” states the pastoral letter.
The letter quotes portions of the encyclical to highlight “main truths of the Magisterium of the Church with regard to the Christian marriage and the sanctity of human life from the moment of its conception.”
The reception of Humanae vitae exposed a rift between orthodox Catholics and would-be modernizers, including the architects of the infamous Winnipeg Statement. The Winnipeg Statement, promulgated by the Canadian bishops, suggested that Catholics could use contraception if the decision was made in “good conscience.”
Some priests who had led married Catholics to expect that the Church would overturn her teaching against the use of contraception within marriage continued to counsel the faithful to use it as their consciences directed. The average size of Catholic families in western countries plummeted, and the European birth-rate is now in freefall.
In their letter, the bishops and ordinaries of Kazakhstan not only highlight the “main truths” of Humanae vitae, but they also cite subsequent remarks by Paul VI, St John Paul II, and Benedict XVI.
They affirm that every marital act must retain its proper relationship to procreation, that no evil may be done to bring about a good, that the decision to call a human being into existence belongs to God alone, that none of God’s commandments are impossible, that truth does not change, and that Humanae vitae has new relevance thanks to years of “wounds” being inflicted by civil law against marriage and the unborn.
Pastoral letter on the occasion of the 50th anniversary of the encyclical Humanae vitae
Praised be Our Lord Jesus Christ! Dear brothers and sisters in Christ! The current year is marked by the memorable event of the 50th anniversary of the encyclical Humanae vitae, in which Blessed Paul VI confirmed the teaching of the constant Magisterium of the Church regarding the transmission of human life. The Bishops and Ordinaries of Kazakhstan want to take this favorable occasion in order to honor the memory and the enduring importance of this encyclical.
During the last meeting of all our priests and religious sisters in Almaty, there were thorough discussions on the theme of the preparation of young people to the sacrament of marriage. There was made the proposal to transmit to young people the main truths of the Magisterium of the Church with regard to the Christian marriage and the sanctity of human life from the moment of its conception.
We proclaim with the voice of the Magisterium of the Church as we can learn it in the encyclical Humanae vitae and in the documents of other Roman Pontiffs the following demanding truths of Christ’s “sweet yoke and light burden” (Math. 11:30):
“The Church in urging men to the observance of the precepts of the natural law, which it interprets by its constant doctrine, teaches that each and every marital act must of necessity retain its intrinsic relationship to the procreation of human life” (Paul VI, Encyclical Humanae vitae, 11).
“Excluded is any action which either before, at the moment of, or after sexual intercourse, is specifically intended to prevent procreation—whether as an end or as a means. Neither is it valid to argue, as a justification for sexual intercourse which is deliberately contraceptive, that a lesser evil is to be preferred to a greater one, or that such intercourse would merge with procreative acts of past and future to form a single entity, and so be qualified by exactly the same moral goodness as these. Though it is true that sometimes it is lawful to tolerate a lesser moral evil in order to avoid a greater evil or in order to promote a greater good,” it is never lawful, even for the gravest reasons, to do evil that good may come of it (cf. Rom 3. 8) — in other words, to intend directly something which of its very nature contradicts the moral order, and which must therefore be judged unworthy of man, even though the intention is to protect or promote the welfare of an individual, of a family or of society in general. Consequently, it is a serious error to think that a whole married life of otherwise normal relations can justify sexual intercourse which is deliberately contraceptive and so intrinsically wrong” (Paul VI, Encyclical Humanae Vitae, n. 14).
“When the spouses through contraception deprive the exercise of their conjugal sexuality of its potential procreative capacity, they attribute to themselves a power which belongs to God alone: the power to decide in the last instance the coming to existence of a human person. They attribute to themselves the qualification of being not the cooperators of the creative power of God, but the ultimate holders of the source of the human life. From this perspective, contraception is to be objectively judged to such an extent illicit, that it could never, for any reason, be justified. To think or to speak the contrary, equals to hold that in human life there could be given situations in which it would be licit not to recognize God as God” (John Paul II, Address to Participants of a Study Seminar on Responsible Procreation, September 17, 1983).
“Many think that the Christian teaching, although true, is nonetheless unfeasible, at least in some circumstances. As the Tradition of the Church has constantly taught, God does not command the impossible but every commandment also entails a gift of grace which helps human freedom to fulfill it. Yet constant prayer, frequent recourse to the sacraments and the exercise of conjugal chastity are needed. Today more than yesterday, man is again beginning to feel the need for truth and right reason in his daily experience. Always be ready to say, without ambiguity, the truth about the good and evil regarding man and the family” (John Paul II, Address to Participants in a Study Meeting on Responsible Procreation, June 5, 1987).
“Humanae Vitae reasserts the continuity of the Church’s doctrine and tradition. […] This teaching not only expresses the unchanged truth of Humanae Vitae, but also reveals the farsightedness with which the problem is treated. […] What was true yesterday, is true also today. The truth expressed in Humanae Vitae does not change; on the contrary, precisely in the light of the new scientific discoveries, its teaching becomes more timely and elicits reflection on the intrinsic value it possesses” (Benedict XVI, Address to Participants in the International Congress on the 40th Anniversary of the Encyclical Humanae vitae, May 10, 2008).
“This document, i.e. Humanae vitae, was inspired by the immutable teaching of the Bible and the Gospel, which confirms the norms of the natural law and the irrepressible dictates of conscience regarding respect for life and its transmission by fathers and mothers who practice a responsible parenthood. The document has acquired new and urgent relevance in view of the wounds now being inflicted by civil laws on the holiness of the indissoluble marriage bond and the sacredness of human life even in the maternal womb. In face of saddening defections in the Church and society, We, like Peter, feel compelled to go to Him as the only source of salvation and cry out to Him: Lord, to whom shall we go? You have the words of eternal life” (Paul VI, Homily on June 29, 1978).
The entire human history gave sufficient evidence for the fact that a true progress of society depends to a large extent on large families. This fact applies all the more to the life of the Church. Pope Francis reminds us of this truth: “It is a consolation and hope to see so many large families that welcome children as a true gift from God. They know that every child is a blessing” (Pope Francis, General Audience, January 21, 2015).
May the following words of Saint John Paul II, the pope of the family, by a light, a strength, a consolation and a joyful courage to all Christian couples and to the young men and young women, who prepare themselves for the life of a Christian marriage and family.
“We have the distinctive confirmation that the path of holiness lived together as a couple is possible, beautiful, extraordinarily fruitful, and fundamental for the good of the family, the Church and society. This prompts us to pray the Lord that there be many more married couples who can reveal in the holiness of their lives, the “great mystery” of spousal love, which originates in creation and is fulfilled in the union of Christ with his Church (cf. Eph. 5:22-33). Like every path of holiness, yours too, dear married couples, is not easy. We know how many families in these cases are tempted to discouragement. I am particularly referring to those who are going through the sad event of separation; I am thinking of those who must face illness and those who are suffering the premature death of their spouse or of a child. In these situations, one can bear a great witness to fidelity in love, which is purified by having to pass through the crucible of suffering. Dear married couples, do not be overcome by hardship: the grace of the Sacrament supports you and helps you constantly to raise your arms to heaven, like Moses. At the same time, I ask all families to hold up the arms of the Church, so that she may never fail in her mission of interceding, consoling, guiding and encouraging” (Homily in the Holy Mass of the Beatification of the couple Luigi Beltrame Quattrocchi and Maria Corsini, October 21, 2001).
“May the Virgin Mary, who is the Mother of the Church, also be the Mother of “the Church of the home.” Thanks to her motherly aid, may each Christian family really become a “little Church” in which the mystery of the Church of Christ is mirrored and given new life. May she, the Handmaid of the Lord, be an example of humble and generous acceptance of the will of God. May she, the Sorrowful Mother at the foot of the Cross, comfort the sufferings and dry the tears of those in distress because of the difficulties of their families. May Christ the Lord, the Universal King, the King of Families, be present in every Christian home as He was at Cana, bestowing light, joy, serenity and strength” (Apostolic Exhortation Familiaris consortio, 86).
Astana, May 13th 2018, Memory of the Blessed Virgin Mary of Fatima
Your Bishops and Ordinaries:
+ Jose Luis Mumbiela Sierra, Bishop of the diocese of Most Holy Trinity in Almaty and President of the Conference of the Catholic Bishops of Kazakhstan
+ Tomash Peta, Metropolitan Archbishop of the archdiocese of Saint Mary in Astana
+ Adelio Dell’Oro, Bishop of Karaganda
+ Athanasius Schneider, Auxiliary Bishop of the archdiocese of Saint Mary in Astana
Very Reverend Father Dariusz Buras, Apostolic Administrator of Atyrau
Very Reverend Mitred Archpriest Vasyl Hovera, Delegate of the Congregation for the Oriental Churches for the Greek-Catholic faithful in Kazakhstan and Central Asia
May 9, 2018 (LifeSiteNews) – This past weekend was the 200th anniversary of the birth of Karl Marx, who is widely recognized as the architect of the most brutal and bloodthirsty philosophy ever to scar the earth: Atheistic Communism. On the occasion of this infamous event, it was my intention to write an article about the horrors of Communism, the legacy of Karl Marx, the Marxist hatred of humanity, and even his connection with secret societies.
After countless attempts to write this article, committing well over 5,000 words and three days of chasing rabbit holes and rhetorical dead ends, two things became painfully obvious to me. The first is that the bitter fruits of Marx’s ideologies are self-evident, and the second is that I am not as clever as I thought.
On the verge of abandoning my article, my wife suggested that I take a walk and pray the Rosary, and since Our Lady has never failed to help me when I ask, I knew that this was inspired advice.
It didn’t take long into my Rosary to realize that the answer to the problem of Marx was resting in the very beads I held in my hand; each of the Joyful Mysteries I had been praying was an answer provided long before Marx’s birth to his philosophy of revolution.
The First Joyful Mystery: The Annunciation
Marx’s entire philosophy is built upon the tension between two vices; greed and envy. He accuses, not entirely wrongly, the upper class of the greedy enslavement of the lower classes. But rather than address the upper class and remind them of their duties through filial love to care for those who struggle to feed their families, he appeals to the suffering of the laborers and fans the flames of envy into an all-out rage. His demagoguery is built upon vice, encouraging a class warfare that leads directly to revolution.
In the first mystery of the Rosary, we meditate on the Annunciation of the Incarnate Word, given to Our Lady by the Angel Gabriel. St. Bernard of Clairvaux explained in his homily In Praise of the Virgin Mother:
“You have heard, O Virgin, that you will conceive and bear a son; you have heard that it will not be by man but by the Holy Spirit. The angel awaits an answer; it is time for him to return to God who sent him. We too are waiting, O Lady, for your word of compassion; the sentence of condemnation weighs heavily upon us.”
It was through Our Lady’s reply, “Thy will be done,” that she answers the war of vices proclaimed by Marx. Marx announced a revolution which he claimed would be the salvation of the working class, and it was a revolution predicated on grasping at power, wealth and control for the supremacy of the state. Yet, Gabriel announced the salvation of men’s souls through the shedding of Divine blood! All of Heaven awaited her answer because without her willful consent to God’s proposal, man was doomed to the material salvation offered by the likes of Karl Marx. Through meditation on this mystery, we give thanks to Almighty God for Our Lady’s consent to bring the Savior into the world.
The Second Joyful Mystery: The Visitation
As soon as Gabriel left Our Lady, Scripture tells us that she “made haste” to be with her cousin Elizabeth, who was then in her sixth month of pregnancy. Thus filled with the Holy Spirit, and carrying the Christ in her womb, Our Lady’s first desire was to help family and serve others. She is the very model of the corporal works of Mercy.
Marx, on the other hand, proposes a system that abolishes and ridicules the service of charity and seeks to impose a heavy-handed system of a labor-fed society. In Marx’s system, there is no love of neighbor, but only the service of all under the imposing gaze of the state.
The Third Joyful Mystery: The Birth of Christ
As we contemplate the Birth of the Savior of mankind, we have in mind the image of Joseph, Mary and the infant Christ Child lying in a manger. This image alone could fill volumes of contemplative meditations. Here, we see the image of the Holy Family as an Earthly representation of the Holy Trinity; Joseph the Father, Our Lady filled with the Grace of the Holy Spirit, and Our Blessed Lord bridging the gap between Trinity and Family. But in all the various ways we could contemplate this Mystery, what remains is the image of the family.
Marx’s revolutionary manifesto asked, “What will be the influence of communist society on the family?” His answer is to abolish it by destroying its very foundations:
It will transform the relations between the sexes into a purely private matter which concerns only the persons involved and into which society has no occasion to intervene. It can do this since it does away with private property and educates children on a communal basis, and in this way removes the two bases of traditional marriage – the dependence rooted in private property, of the women on the man, and of the children on the parents.
If the Holy Family is the model for all families, and the Holy Family is the reflection of the Holy Trinity, then Marx’s assault upon the family is no less an assault on God, which is why, at its very core, Communism is an atheist philosophy.
The Fourth Joyful Mystery: The Presentation of the Child Jesus in the Temple
When the priest Simeon received Our Lord from Our Lady, he prophesied: “Behold this child is set for the fall, and for the resurrection of many in Israel, and for a sign which shall be contradicted.” At this very moment, he foretold of the crucifixion of Our Lord, and in so doing, he told Our Lady that “thy own soul a sword shall pierce, that, out of many hearts, thoughts may be revealed.”
Here we can see the willingness to suffer and die out of love. Our Lady knows that because she shares in the great joy contained in Our Lord, that she will also share in His suffering. There is no man who has ever lived who knows suffering like Our Lady does. At the Annunciation, she knew that if all mankind would fall and suffer because of Eve’s rebellion against her husband and God, that all mankind would be saved because the Christ Child would take the sin and pain of all mankind to Himself, and it could only be accomplished by her consent. At the Visitation, she knew the joy the Divine Savior growing within her womb would bring to others. After His birth, she laid Him upon the dead wood of a manger, which is a food trough for animals … a manger that would prefigure the wood of His Cross as He became the food for all mankind. And while Simeon was prophesying the suffering Our Lady would share in her Son’s Passion, she embraced it all with humility.
In the second chapter of St. Paul’s letter to the Philippians, he said, “Jesus Christ, Who being in the form of God, thought it not robbery to be equal with God: But emptied himself, taking the form of a slave, being made in the likeness of men, and in habit found as a man. He humbled himself, becoming obedient unto death, even to the death of the cross.”
But Marx preaches a rejection of suffering and servitude. Rather than accepting one’s state in life, Marx preaches an anti-Gospel of envy, where the collective of workers cast off their servitude and rise against the upper class and GRASP what is not theirs.
The Fifth Joyful Mystery: The Finding of the Child Jesus Teaching in the Temple
In the final Joyful Mystery of the Rosary, we read the conversation between Our Lady and Our Lord, wherein Our Lady asks him to explain why He left them frantic for three days. At the end of the conversation, St. Luke tells us, “And he went down with them, and came to Nazareth, and was subject to them.”
The lesson to be had here is Holy Obedience. Our Lord delights in those who are obedient. Beginning with Adam and Eve and running throughout all of Scripture, we see a theme of the curses associated with disobedience and the blessings associated with obedience. When we are obedient to God and subject to proper authority, we are pleasing to Him. When we are disobedient and rebel against rightful authority, we incite His wrath.
The materialist philosophy of Marx’s Communist Manifesto is a blueprint for rebellion against God and rebellion against rightful authority. When one considers the state-sponsored executions, the state-generated famines, the wars, and the spread of abortion, its bitter fruits have resulted in the deaths of countless millions.
Even now, the horrors of Marx’s philosophies are infecting nearly every facet of human civilization. It comes in the form of contraception, abortion, homosexuality, on-going rebellious movements, and every other man-centered -ism that takes our minds away from the Four Last Things; death, judgment, Heaven and Hell.
As we can see, the Rosary provides the answer. The Mysteries we meditate upon provide for us an understanding that man is not made for this world, as Marx would have us believe … but that we are made for Love of God and Love of neighbor. But more than that, The Rosary is the remedy to Marx’s poison.
The Golden Legend tells us that St. Martha went to the Southern part of France, and while she was there, a horrible dragon had taken up residence in the River of Rhone. The locals, try as they may to defeat it, could do nothing to slay this beast. According to the Legend, the locals asked Martha for help, who went with them to find the dragon. They found it devouring a man, but St. Martha approached with the sign of the cross and cast holy water on it, at which point the creature became as docile as a sheep. She bound it with her own girdle and led it to the villagers, who then killed it with spears.
Through this image, we can see a foreshadowing of the prophesied Triumph of Our Lady’s Immaculate Heart. Our Lady asked us to pray the Rosary every day. If the dragon scourging us now is the philosophy of Marx, can we not see how the symbol of the cross and the girdle of St. Martha, which bound her dragon, make the loop of beads and the cross of the Rosaries we have today? The beast facing St. Martha could not resist her, and neither will the Marxist Dragon of today resist our Lady.
Neo-Marxist Rudi Dutschke’s “long march through the institutions of power” has reached the Roman Catholic College of Cardinals.
Cardinal Joseph Tobin welcomes openly gay Catholics to Holy Mass in his cathedral. Cardinal Walter Kasper supports giving Holy Communion to couples living in adultery. Cardinal Reinhard Marx protests against the crucifix being displayed in government buildings and endorses blessings for same-sex couples. Cardinal Jozef de Kesel declares that gay sexual experience should be a possibility in the Church. Cardinal Blase Cupich promotes a “New Paradigm” for Catholic morality and argues that active gays can receive Holy Communion if their conscience permits.
Cardinal Vincent Nichols is the latest recruit to the ranks of the men in red. The Archbishop of Westminster believes that the nanny state can usurp the rights of parents. He insists that suffocating a terminally ill child by yanking it off the ventilator is “an act of mercy.” He reveals that his interpretative framework for Catholic doctrine is “society’s common good.” He defends a children’s hospital notorious for harvesting organs from dead babies and failing to meet four out of five safety standards.
Most lamentably, Cdl. Nichols, President of the Catholic Bishops Conference of England and Wales, distorts Catholic teaching on palliative care in relation to the case of Alfie Evans. Nichols is right when he claims that “palliative care, which isn’t a denial of help, can be an act of mercy.” However, he is in serious danger of confusing palliative care with euthanasia by stealth.
The World Health Organization defines palliative care as “an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.”
The definition is unambiguously pro-life and in no way confuses palliative care with stealth euthanasia. Palliative care offers care when medicine cannot cure. Withdrawing life support and ventilation from Alfie Evans following a court order is emphatically not palliative care. It is, rather, a flagrant violation of magisterial teaching as laid down in the Catechism of the Catholic Church.
Even “an act or omission which, of itself or by intention, causes death in order to eliminate suffering constitutes a murder,” states the Catechism. It warns that the “error of judgment into which one can fall in good faith does not change the nature of this murderous act, which must always be forbidden and excluded.”
An act or omission which, of itself or by intention, causes death in order to eliminate suffering constitutes a murder’Tweet
Cardinal Nichols is right when he cites Church teaching stating that “we do not have a moral obligation to continue a severe therapy when it’s having no effect.” The Catechism permits the discontinuation of “over-zealous” treatment that is “burdensome, dangerous, extraordinary, or disproportionate to the expected outcome.” But it clarifies that the “ordinary care,” such as food and water, owed to a sick person cannot be legitimately interrupted “even if death is imminent.”
Alder Hey Children’s Hospital refused oxygen and water to Alfie for the first nine hours after his ventilator was removed, and starved him of food for 36 hours, greatly worsening his condition. Refusing nutrition, hydration and ventilation to a small child is not an act of mercy: It is a cruel and barbaric form of execution. Is Cdl. Nichols arguing that such an act, in effect euthanasia by stealth, is a form of palliative care?
The Catechism also specifies who is to make the decisions to discontinue treatment. If the patient is unable to make the decision, such decisions should be made by those who are “legally entitled to act for the patient” — in this case, Alfie’s parents — and their “reasonable will and legitimate interests must always be respected.” By what sleight of hand can Cdl. Nichols interpret this to mean that “a court must decide what’s best not for the parents, but for the child”?
The Catechism recognizes the significance of intention in bringing about a person’s death. Even if done “indirectly,” this violates the Fifth Commandment: “Thou shall not kill.” By withdrawing food and water, the medical staff intended for him to die, even though they knew he wasn’t going to live.
United States Supreme Court Justice Neil Gorsuch in his book The Future of Assisted Suicide and Euthanasia raises the question of “why omissions of care cannot sometimes, at least where an intention to kill is present, also qualify as acts of murder.” Hence, an omission of care undertaken with the intention of ending life crosses the fine line and may become a deliberate act intended to end life.
Three judges of the Second Circuit of the U.S. Court of Appeals, striking down parts of New York’s law against assisted suicide, ruled:
The withdrawal of nutrition brings on death by starvation, the withdrawal of hydration brings on death by dehydration, and the withdrawal of ventilation brings on respiratory failure. By ordering the discontinuance of these artificial life-sustaining processes or refusing to accept them in the first place, a patient hastens his death by means that are not natural in any sense. It certainly cannot be said that the death that immediately ensues is the natural result of the progression of the disease.
The conclusion is clear. When doctors and courts decide to withdraw basic care such as food and water, it is hard to claim “human choice doesn’t play any causal role in their deaths,” Gorsuch contends.
The U.S. Child Abuse Prevention and Treatment Act provides guidelines for when treatment may be withheld, for example, when “the infant is chronically and irreversibly comatose” or when “the provision of such treatment would merely prolong dying” or would “be virtually futile in terms of the survival of the infant.” Even in these circumstances, the physician is always required to provide nutrition and hydration, observes Gorsuch.
The cardinals wear red as a sign that they are willing to give themselves totally to the Church, even to the point of shedding their own blood for Her. With the neo-Marxist takeover of the Church, it seems that the cardinals’ vestments are a sign of their loyalty to the new “Red Army.”
The Rev. Dr. Jules Gomes, B.A., B.D., M.Th., Ph.D. (Cambridge) is columnist for The Conservative Woman. He writes regularly on his website at julesgomes.com.
LIVERPOOL, England (ChurchMilitant.com) – Troubling revelations are emerging about the last hours of Alfie Evans, the U.K. toddler who died after a protracted legal battle with Alder Hey Hospital.
According to Benedetta Frigerio, writing in Italian journal La Nuova Bussola Quotidiana, Alfie — suffering from an undiagnosed brain condition — was showing promising vital signs only two hours before death, but took a downturn after a cocktail of unknown drugs was administered by a hospital nurse.
Two hours before dying, the oxygen saturation was about 98 and Alfie’s [heart]beats were about 160, so much so that Thomas was convinced that they would let him go home soon (as the hospital administration told him on Friday afternoon). Before dying, while Thomas had gone out for a moment, leaving Kate half-awake and another family member in the room, a nurse entered and explained that he would give the baby four drugs (no one knows what) to treat him. After about 30 minutes the saturation dropped to 15. Two hours later Alfie was dead.
Although some have contradicted the account, Frigerio insists the account is accurate. She also claims the ventilator, on which Alfie had been relying for many months, was abruptly removed, causing major stress to his body.
“Being that his lungs were used to being dilated mechanically, the doctors would have to ‘wean him’ so as not to provoke his immediate death,” Frigerio wrote, “which, however, did not happen … .”
She reports that he immediately contracted “a lung infection” after the breathing tubes were removed, prompting his father Thomas to plead for antibiotics — denied by Alder Hey.
The account details the father’s frantic attempts to get oxygen and water to his child, repeatedly denied by the hospital until Thomas pointed out that the end-of-life plan approved by the courts nowhere included an order to deprive Alfie of oxygen or nutrition.
Alfie went without oxygen or water for nine hours before the hospital relented, and for a full 36 hours before being given milk — an exceptionally long time for a 23-month-old, whose bodily needs require food every 3–4 hours.
“Yes, Alfie was left without food for 36 hours, a very long time for such a small child, whose heart had already sustained a huge effort after the violent removal of ventilation without weaning,” Frigerio wrote.
Bruno Dalla Dallapiccola, scientific director of the Vatican-run Bambino Gesù Hospital, which was working to get Alfie transferred to their care, commented at the time that “little Alfie will not be able to last long without the supply of nutritional substances through a drip. Without the nutritional intake, in fact, survival can vary from a few hours to a few days.”
And Italian geneticist Angelo Selicorni remarked two days after Alfie’s breathing tubes were removed, “Detached from the machines the child has [resisted] for hours with no intention of dying,” which “raises some doubts about the ‘terminality’ of his state.”
Other reports reveal Alfie’s undiagnosed brain condition did not appear until after he was admitted to Alder Hey Hospital. David Catron writes in The American Spectator that the toddler’s “initial diagnosis involved a fairly common condition: ‘viral bronchiolitis and a possible prolonged febrile convulsion.’ The still-undiagnosed brain disease that allegedly killed Alfie didn’t appear until after he entered this dangerous hospital.”
Viral bronchiolitis is a common ailment among babies and toddlers, and involves cold-like symptoms, including stuffy nose and congestion, coughing and a fever. With basic care most children recover quickly.
Frigerio also notes Alder Hey failed to change Alfie’s breathing tubes frequently, leading to development of mold inside the tubes bringing oxygen to the child’s lungs.
She ends with a final lament:
This is what Alfie’s martyrdom did, as well as converting many hearts: It forced us to unite against a monster, to look at the brutality of a eugenics system disguised as democracy. A system with unlimited power over the person and considered a civil religion by English politics and justice. A power that crushes so many other fragile lives and spreads a utilitarian mentality that one must begin to fight if one does not want to do the same end.
PHILADELPHIA, Pennsylvania, April 25, 2018 (LifeSiteNews) – The fundamental truths about the nature of marriage are under a “diabolical” and “ferocious” attack today, Cardinal Raymond Burke told hundreds of Catholics at Philadelphia’s Cathedral of Saints Peter and Paul on Saturday.
The dubia cardinal, known internationally for his strong defense of Catholic orthodoxy and the pro-life cause, was the keynote speaker at a conference titled Matrimony: Rediscovering Its Truth. Catholics came from all over the east coast and as far as California to hear him speak.
Upon introducing Burke, the cathedral’s rector Father Dennis Gill said Archbishop Charles Chaput was “personally delighted that someone like Cardinal Burke can join us today,” although the archbishop was unable to come to the conference.
Cardinal Burke told the faithful in order to understand the crisis in the Church over marriage, they must consider the relationship between faith and culture, the true purpose of a synod of bishops, the limits of papal and Church power on annulments, the relationship between doctrine and discipline, and confusion about human sexuality.
“At the present moment in the Church there is perhaps no more critical issue for us to address than the truth about marriage,” said Burke. “In a world in which the institution of marriage [has been] under attack for decades, the Church has remained the faithful hero of the truth about God’s plan for man and woman in the faithful, indissoluble, and procreative union of marriage.”
But “in the present time, certainly under pressure from a totally secularized culture, a growing confusion and even error has entered [into] the Church, which would weaken seriously – if not totally compromise – the Church’s witness.” That would be “to the detriment of the whole of society.”
“Those who love the truth and therefore the Church are called as ‘co-workers of the truth’ and living members of the Body of Christ…to do all within their power to defend the authority of Christ [and his] Church. There could be no place for silence or for an attitude of defeat,” said Burke.
He explained that the “confusion and error” of some “became evident” for the world to see during the synods on the family that led up to Amoris Laetitia.
The assemblies ended up having to address “practices that contradict the Church’s constant teaching and practice regarding Holy Matrimony,” he said. “I refer to practices which would give access to the Sacraments to those who are living in a public state of adultery, and which would condone in some matter conjugal cohabitation in some manner outside the sacrament of matrimony, and genital relations between persons of the same sex.”
In 2014, the synod’s mid-point report “made strikingly clear the gravity of the situation” and did not adequately outline Church teaching.
“It was not a report; it was a manifesto, a kind of insight into a new approach of fundamental issues of human sexuality in the Church,” said Burke. This is “an approach which is revolutionary – that is, which is detached from what the Church has always taught and practiced.”
The cardinal recommended Catholics and people of goodwill read Remaining in the Truth of Christ, to which he contributed, which plainly explains why Communion may not be extended to the divorced and “remarried.”
He also emphasized that a synod cannot change Catholic teaching by a majority vote.
‘The Church has to call things by their proper names’
Recently, some have “declared that the Church must update its practice and above all its language in order to address herself effectively to a totally secularized culture,” Burke said as he discussed the relationship of faith and culture.
“Some have gone so far as to assert that the Church can no longer speak of the natural law, of intrinsically evil acts, of irregular unions, and so forth,” he began. “Their point is that the language itself already makes the culture hostile.”
Abandoning truthful language would be the Church giving “the impression of wanting to draw near to the culture without a clear identity of her own and of what she has to say to the culture. According to divine wisdom, the Church must always speak the truth with love.”
“Yes, the Church should go to the peripheries of today’s culture, but always secure in her identity, manifesting the greatest compassion which necessarily involves respect for the truth of the cultural situation which many times is marked by confusion and error regarding those fundamental truths of human life and its credo, which is the family,” he said.
“The Church has to call things by their proper names in order not to risk contributing to the confusion and error,” the cardinal continued. “Honest people who live in such a culture have a thirst for the truth and for its proclamation in charity. To encounter the protagonists of such a culture without manifesting the truth of Christ’s clear words would be a serious lack of charity. It is certainly a cause of grave scandal – that is, leading people to be confused or even leading them into error about what the Church actually teaches.”
Burke noted that Jesus was very compassionate toward the Samaritan woman at the well and the woman caught in adultery: “The Lord is full of understanding for their situations.”
Jesus pardoned them but also indicated “the necessity of leaving a life of sin, the necessity of sinning no more,” he explained.
“The Church should not lose its confidence in the natural law inscribed in every human heart and in its full expression in the saving work of Our Lord,” said Burke. Cultural confusion about the meaning of human sexuality leads to the breakup of marriage, “corruption of children and young people,” and ultimately self-destruction.
“Disordered sexual activity, sexual activity outside of marriage, and the media’s constant, powerful, and false messages regarding our identity as men and women are all signs of the urgent need of a new evangelization which begins in marriages and families, and through marriages reaches the entire culture,” he said.
Catholics must bear witness to the “distinct gifts of man and woman, who both dispose themselves to the service of Christ and His mystical body by means of a chaste life.”
Follow the examples of saints who died protecting marriage
Cardinal Burke also skewered certain false notions of tolerance and charity that persist in the Church and society.
“Today’s popular notion of tolerance is not securely grounded in the moral tradition,” he said. It often means “tolerating ways of thinking and acting which are diametrically opposed to the moral law revealed to us in nature and in sacred scriptures.”
“The approach at times becomes so relativistic and subjective that we do not even observe the fundamental logical principle of non-contradiction, that is that a thing cannot be and not be at the same time and in the same respect,” he cautioned. “In other words, certain actions cannot at the same time be both true to the moral law and not true to it.”
“In the context of charity, tolerance means unconditional love of the person who is involved in evil” but “complete abhorrence” of the evil in which the person is involved, he said.
Catholics should look to St. John Fisher, St. Thomas More, and St. John the Baptist – martyrs for the sanctity of marriage – for inspiration and ask for their intercession, Cardinal Burke advised.
“Let us follow their example and let us invoke their intercession so that the great gift of married life and love will be evermore revered in the Church and in society,” he said.
After Cardinal Burke spoke, conference participants held a Marian procession and prayed the rosary together. Father Dennis Gill, the rector of the cathedral, and popular EWTN guest canon lawyer Father Gerald Murray gave presentations in the afternoon.
Like other conference attendees, the cardinal ate a simple boxed lunch of a ham and cheese sandwich at the archdiocesan pastoral center.
The day ended with a Holy Hour, Confessions, and an Ordinary Form (Novus Ordo) Mass at which Cardinal Burke was the main celebrant.
On December 6, 1865, the 13th amendment to the U.S. Constitution was ratified, and with it came the formal abolition of slavery in this country. It states, “Neither slavery nor involuntary servitude…shall exist within the United States, or any place subject to their jurisdiction.” This amendment was especially significant considering that just eight years prior, in 1857, the Supreme Court ruled in Dred Scott v. Sandford that blacks were property and non-persons.
Even earlier than this, on July 1, 1854, Abraham Lincoln wrote this small fragment that seems to address some of the popular arguments put forward by slavery-choice advocates of his day. Should whites have the right to enslave blacks based on color, intellect, or interest? Lincoln responds:
You say A. is white, and B. is black. It is color, then; the lighter, having the right to enslave the darker? Take care. By this rule, you are to be slave to the first man you meet, with a fairer skin than your own.
You do not mean color exactly? You mean the whites are intellectually the superiors of the blacks, and, therefore have the right to enslave them? Take care again. By this rule, you are to be slave to the first man you meet, with an intellect superior to your own.
But, say you, it is a question of interest; and, if you can make it your interest, you have the right to enslave another. Very well. And if he can make it his interest, he has the right to enslave you.
The importance of Lincoln’s logic should not be overlooked. Lincoln understood that if you attempt to establish human rights or personhood by appealing to a set of arbitrary, degreed properties such as color and intellect, properties which carry no moral weight or significance and which none of us share equally, then you end up undermining human rights for everyone.
What slavery-choice advocates did in the past, abortion-choice advocates do today. Only, instead of arguing that blacks are non-persons based on color and intellect and can therefore be enslaved, they argue the unborn are non-persons based on size, development, and dependency and can therefore be killed.
But the reasoning of abortion-choice advocates today is just as flawed as that of the slavery-choice advocates then. If Lincoln were alive today and were to address the current abortion debate, he might say something like this:
You say A. is big and B. is small. It is size, then; the larger, having the right to kill the smaller? Take care. By this rule, you are to be victim to the first man you meet, with a larger body than your own.
You do not mean size exactly? You mean human persons are developmentally the superiors of the unborn, and, therefore have the right to kill them? Take care again. By this rule, you are to be victim to the first man you meet, with a development superior to your own.
But, say you, it is a question of interest; and, if you can make it your interest, you have the right to kill the unborn. Very well. And if another can make it his interest, he has the right to kill you.
Scott Klusendorf states in The Case for Life, “In the past, we used to discriminate on the basis of skin color and gender (and still do at times), but now, with elective abortion, we discriminate on the basis of size, level of development, location, and degree of dependency. We’ve simply swapped one form of bigotry for another” (p. 66).
In the past, slavery-choice advocates adopted an elitist view and sought to create a subclass of human beings who didn’t qualify as human persons. Today, abortion-choice advocates do the same. They argue that larger, more developed, and independent human beings can kill smaller, less developed, dependent human beings.
Contrast this with the pro-life movement, which is inclusive and wide-open to all. Pro-life advocates argue that all human beings (including the unborn) are valuable human persons simply in light of being what they are: human beings who possess a common human nature. And no arbitrary, degreed property or characteristic, whether it be color, intellect, size, development, or dependency, should disqualify any human being from the right to life and liberty.
Aaron Brake (@littlebrake) received his M.A. in Christian apologetics from Biola University. He is a speaker and apologist with Life Training Institute, a pro-life organization.
To many who can recall it, the on-going drama and death of Alfie Evans in the hospital in Liverpool recalls Burt Bacharach’s plaintiff song: ”What’s It All About, Alfie?” That is exactly the right question here. “What’s it all about, when you sort it out. Alfie?” Probably no single reality could bring together so many things that need sorting out. “To sort out” means to put things in order, to distinguish what is important, what relates to what. In sorting it out, Alfie, recalls for us almost the whole moral memory of our peoples.
The most obvious issue is this: “What is the meaning and value of a single human life?” It was a question that Dostoyevsky often asked. Can one kill an utterly useless and obnoxious human being with no consequences to himself. In the case of infants, who is to decide this question of their worth? The parents? The doctors? The health system? The Government? The Courts?
Why was not this question posed differently? A human life is worthy in itself; it already existed in Alfie. Parents, doctors, health systems, judges. and governments are at his service, not vice versa. Governments were established to secure human life.
In Alfie’s case, a young Catholic couple of no particular standing simply wanted their child at home or in the hands of other doctors. They even go to the Pope. The Italians were ready to do what they can. We wonder why the English Queen did not visit the child. Petitions were circulated that she should do so. Where was Theresa May?
Europe is famous for leaders who have no children. The Queen has children, grand-children, and great grand-children. She once visited the ravages of war. Alfie was the victim of another sort of war. The Queen is bound by law. She did not choose to break it. If she had asked her son, “Take me to the hospital in Liverpool”, the world would be quite different. The case now has world-wide attention. Alfie’s death will keep it so.
What makes this case so riveting? It touches many strands in our civilization’s history. There is something of Socrates in it. “It is never right to do wrong.” This is the very Socratic foundation of the civilization into which Alfie was born. He was jailed in a hospital because some, with Machiavelli, think at times it is right to do wrong.
Also, something of the death of Christ is here in these scenes. The High Priest said that it is better for one man to die than the nation parish. “We have no king but Caesar.” Alfie is kept a prisoner in a hospital to protect a government health system’s credibility. Alfie must die there rather than take a chance that he might live. An Italian hospital plane was there to take him away. He should die in the care of his parents. This line of reasoning takes us back to Genesis itself, to a natural law found in our being, in Alfie’s being.
With the visit to the Pope, we had something of the controversies of the Reformation. The English king is head of the church. Thomas More died over whether this local primacy was true. The silence of the Queen, herself a mother and a grandmother, implied that she had no independent voice. Parliament is supreme. All law is civil law. The parents in wanting their child home were breaking the law which decides who gets what care. No writ goes against the King. The King is in Parliament. No higher law exists in the land. Mrs May was silent. Alfie was isolated. Police enforced the law, whatever it is.
This case is also about the 1931 Lambeth Conference that justified for the first time contraception, a decision that led logically to abortion, same-sex marriages, and euthanasia, to a continent that is choosing not to reproduce itself. If it was all right to kill millions of failed contraceptions, Alfie did not have a chance. He was an expense. He had no legal right to live in his land. His life did not have enough “quality”.
When we “sort out” Alfie’s case, we find that it connects almost everything that is wrong and everything that is right in our culture. Alfie had parents who were willing to confront the Leviathan. In Leviathan theory, they are bound to lose. In losing, however, they will win. That was what your life was about Alfie. You did sort things out for many who otherwise pay little attention to the lethal meaning of many of our laws and customs.
April 27, 2018 (Population Research Institute) – The Great Recession in 2008 sent American birth rates into sharp decline. The total number of births has dropped below 4 million and stayed there. Now that economic growth is picking up again, birth rates should follow that same upward course, if history is any guide.
The forces arrayed against such an American renaissance are powerful, however. The radical feminist and radical environmental movements, for instance, have twisted the virtue of childbearing into the vice of overpopulation. Planned Parenthood–still funded with our tax dollars–sends hundreds of thousands of unborn children prematurely to their graves. The culture itself is predominately anti-natal. Christian parents know that children are blessings from God but, buffeted by these forces, they often need further encouragement to accept additional “blessings.”
We at Population Research Institute are happy to provide such encouragement. We believe that there are at least ten great reasons to have another child.
“Be fruitful and multiply”
Reason 1: Have another child to join with God in the creation of an immortal soul.
Parents are given the incredible opportunity to assist God in the creation of an immortal soul. As the late Cardinal Mindszenty said, even the angels have not been given such a grace.
“The most important person on earth is a mother. She cannot claim the honor of having built Notre Dame Cathedral. She need not. She has built something more magnificent than any cathedral—a dwelling for an immortal soul, the tiny perfection of her baby’s body. Even the angels have not been given such a grace! What is more glorious than this: to be a mother.”
— Joseph Cardinal Mindszenty
Reason 2: Have another child to bring joy into your life.
There is no joy like the joy of welcoming another child into your life. You will marvel anew at how perfectly formed your little one is, and over how quickly you will fall head over heels in love with him. You will be enchanted with every tiny aspect of her appearance. The color of her hair, the shape of her nose, and the winsomeness of her smile will occasion endless happy debates about from which side of the family (yours, of course) she got that adorable trait.
The birth of a child will bind you to God more tightly than ever before, in awed gratitude. “She was the most miraculous thing that had ever happened in my life,” Whitaker Chambers wrote about his new daughter in Witness. And in the lives of most of us.
I thought that one day
I would be a famous artist.
and create great works of art
Instead, God made me a mother,
and my children
are His masterpiece.
The design of their lives
will live on after me.
What is painted on their hearts
will last an eternity
—Anonymous
Reason 3: Have another child to grow in holiness and virtue
For those who marry and have families, children are the primary means God uses to help them grow in holiness and virtue. Children teach their parents patience, perseverance, charity, and humility. They give their parents the opportunity to practice the corporal and spiritual works of mercy. They come into the world naked, and we clothe them, hungry and we feed them. Thirsty, and we give them drink. All of the things that we are required to do for the “least of these our brothers,” we do first and foremost for our own children. St Catherine of Sienna once had a vision in which God took her to a roomful of crosses and told her to pick one. St Catherine went to the largest, heaviest cross in the room and would have chosen it. But God told her that it was not for her: That was reserved for the parents of large families.
“Mary gave birth to her first-born son and wrapped him in swaddling clothes.” Luke 2:7.
Reason 4: Have another child to help end abortion.
When Mother Teresa of Calcutta was asked by a young mother about the best way to proceed with pro-life work, she responded emphatically, “Have a big family. That is the best way to end abortion!”
How this works is not difficult to understand. As children become more rare due to contraception, sterilization and abortion, whole segments of society become less and less familiar with the sense of joy and hope that only babies and children can give. In this climate, contraception and abortion feeds on themselves, as the increasingly selfish few further reduce their number.
By having another child, you demonstrate once again to the world that children are God’s greatest gifts. “Children build up the life of the family and society,” as Pope John Paul II has said. “The child becomes a gift to its brothers and sisters, parents and entire family. Its entire life becomes a gift for the very people who were givers of life and who cannot help but feel its presence, its sharing in their life and its contribution to the common good and to the community of the family.”
The more children there are in society, the more pro-life that society will become, and the easier it will be for the great evil of abortion to be eradicated once and for all.
Reason 5(a): Have another child so your sons will have brothers and your daughters will have sisters.
Children who have siblings learn early to share. They learn to take turns and to put the needs of others before their own. The bond formed between brothers and sisters is lifelong, and stronger than the bond between the closest friends.
Reason 5(b): Have another child so your sons will have sisters and your daughters will have brothers.
Boys who have sisters learn the dignity of women. They learn to treat other girls and women with respect, as they consider how they would like their own sisters to be treated. Girls who have brothers learn that he complementarity of men and women, both fashioned in the image and likeness of God.
Reason 6: Have another child so you (and your parents) won’t be lonely in old age
People who have children don’t have to rely upon strangers to care for them in their old age. Children also become the parents of your grandchildren. Grandchildren bring joy, happiness, and laughter, while still allowing you to get a good night’s sleep!
Reason 7: Have another child because people are our greatest resource.
Humans are blessed with the gifts of an intellect and free will. It is human ingenuity that discovers creative solutions to the problems which confront us. People without children should remember that it will be someone else’s child who will become the doctor that performs their life-saving operations. Someone else’s child will become the firefighter that saves their house. Someone else’s child will become the railroad engineer.
Reason 8: Have another child to contribute to the economy.
Families with children are fuel to the economy, purchasing houses and cars and college educations. Without young people to enter the workforce, social security systems fail. Without children to attend school, teachers are jobless. A lot of industries, from fast food restaurants to toy stores, obviously rely heavily upon business from and for children to stay in business. But ultimately the whole economy does.
Reason 9: Have another child to counter the coming global population implosion
Anyone who has traveled from coast to coast in the United States and seen the vast empty spaces should know that America is not overpopulated. In fact, the entire population of the world could live in the state of Texas, in single-family dwellings with front and back yards.
Fertility rates are falling everywhere. The world’s population will never again double. If current trends continue, world population will peak by the middle of this century and then begin demographic freefall.
Our long-term problem is not too many children, but too few children. Having another child will help offset the coming population implosion.
Reason 10: Have another child to help populate heaven.
The child that you and your spouse have been generous in accepting from God was created to return to Him, after a life of love, service, and obedience on earth, to spend eternity with God in heaven.
Our Lord Himself said that there was plenty of room for those returning souls. There is no overpopulation problem in Heaven!
“There are many mansions in my Father’s house…” John 14:2
These reasons are inspired by the work and wisdom of Father Paul Marx, OSB of happy memory.
It’s been a titanic battle – UK’s Alder Hey Children’s Hospital versus a helpless 23-month-old boy.
Alfie Evans suffers from an undiagnosed neurological disorder. He is not terminal, but that hasn’t stopped the hospital’s aggressive attempts – which some have called perverse, heinous and obscene – to end Alfie’s life.
Lest you think we’re safe in America, our nation’s landscape is already littered with innocent victims.
Throughout a lengthy string of court actions, Alder Hey has opposed Alfie’s parents at every turn. The hospital refused to allow them to transfer Alfie to one of four other hospitals – two each in Germany and Italy – that have offered to take the young patient. Police were posted outside his room, and his parents have been threatened with arrest if they attempt to remove their son from his medical jail cell.
With the world watching, the last couple of days have become a dramatic human tug-of-war. Here are a few highlights:
Friday, April 20
The hospital set what they intended to be Alfie’s execution date: Monday at noon UK time.
Monday
The ventilator was removed, but Alfie continued to breath.
Italy granted Alfie citizenship to allow him to travel there for treatment. An air ambulance was at the ready outside the hospital to whisk him and his parents to a military transport, equipped with specialized medical personnel.
The hospital allowed Alfie to have supplemental oxygen and water while another appeal took place.
Tuesday
After another failed appeal, the hospital removed Alfie’s oxygen and refused the parents’ attempt to provide it themselves. Alfie’s father had to resort to giving his son mouth-to-mouth resuscitation when the boy’s lips would turn blue.
Pope Francis, Members of Parliament and a physician organization pleaded for the life of the defenseless patient.
Wednesday
Oxygen, food and water were restored during yet another appeal.
It’s a Global Battle
Americans are not immune to tragic situations like Alfie’s – in large part due to “futile care laws.” Medical institutions and associations have quietly lobbied state legislatures to strip parents and family members of their right to make critical healthcare decisions. According to Wesley Smith, consultant to the Patients Rights Council, the states have given these critical rights to “self-appointed, anonymous hospital ethics committees.”
A few examples demonstrate the tragic results.
After a severe asthma attack and cardiac arrest rendered two-year-old Israel Stinson mostly unresponsive, doctors declared him brain dead and recommended removing his ventilator against the wishes of his parents. The parents sought an injunction to prevent Children’s Hospital of Los Angeles from ending their son’s life. Immediately after a judge ruled on behalf of the hospital, they disconnected Israel from his lifeline without even stopping to explain the process to his distraught parents. Israel died.
Israel’s parents didn’t believe their son was brain dead. Why might there be room for doubt when a patient receives such a diagnosis? According to the American Academy of Neurology, the guidelines for brain death determination are “opinion-based.”
Another reason is Jahi McMath.
A routine surgery went horribly wrong at Children’s Hospital in Oakland, CA. Jahi suffered severe blood loss resulting in a cardiac arrest and interruption of oxygen to her brain. Days later the hospital declared Jahi brain dead and pressured her family to donate her organs.
Eventually Jahi was transported to New Jersey where, with expert help, her parents have provided ongoing care in an apartment. After nearly five years, this so-called brain dead patient has experienced puberty and menstruates, has moved upon request and achieved other important milestones which have persuaded doctors to conclude that her diagnosis was in error. Jahi’s parents are now forced to navigate the court system to have the brain death diagnosis lifted.
What empowered these healthcare facilities to act in such heavy-handed ways against the parents? A California futile care law states “a healthcare provider or healthcare institution may decline to comply with an individual healthcare instruction or healthcare decision that requires medically ineffective healthcare…” provided they believe they’re acting “in good faith” (emphasis mine). “Ineffective” and “in good faith” are left to the interpretation of healthcare providers.
Andrea Clark’s life was in immediate danger when an ethics committee at St. Luke’s Hospital in Houston, TX decided to remove her ventilator and other life support, even though she was conscious and appeared to want to live. A subsequent public battle between the hospital and Andrea’s family eventually persuaded St. Luke’s to continue her care until she peacefully died without a “push” from the institution.
What entitled St. Luke’s raw authority over her family’s wishes and resulted in an attempt to end Andrea’s life? A Texas futile care law which allowed hospitals to end life-sustaining care with an agonizingly short ten-day notice to find another healthcare facility. Thankfully, this law has been amended to significantly limit its danger to vulnerable patients.
We are living in dangerous times, so it’s necessary to be watchful and aware of threats around us. Having said this, many communities are blessed with life-affirming hospitals and healthcare facilities that work hard to defend their patients. We thank them.
I’ll leave you with two action items to help protect at-risk patients.
Please pray for Alfie Evans and his parents. At this writing, Alfie’s life literally hangs in the balance.
Second, find out if your state has passed a futile care law that strips your right to make critical healthcare decisions for a loved one and empowers healthcare facilities to impose life-and-death verdicts based on “quality of life” or “cost-ratio” indicators.
Visit our website to take advantage of free critical-care resources, including a two-part episode DVD of Facing Life Head-On called Surprising Realities of Brain Death and Organ Donation. We were shocked by the revelations uncovered during our research.
Be equipped and prepared to defend life.
LifeNews.com Note: Bradley Mattes is the President of Life Issues Institute, a national pro-life educational group.
MICAIAH BILGER APR 24, 2018 | 4:09PM WASHINGTON, DC
A New Hampshire father recently admitted to leaving a bullet at a Massachusetts abortion facility while his girlfriend was having their unborn baby aborted.
Salem News reports Joshua Paiva, 21, of New Hampshire, told police that he should not have done it, but he felt “sad” about his girlfriend’s decision.
The incident occurred on Feb. 14 (Valentine’s Day) at the Health Quarters abortion facility in Beverly, Massachusetts. According to the report, staff noticed the 9 mm bullet in the office lobby and immediately called police.
Later, a review of security tapes showed Paiva dropping something onto a tray under a window in the lobby while he was waiting for his girlfriend to come out from the abortion, the report states.
When contacted by police, Paiva admitted to leaving the bullet there and expressed regret about the action, according to police.
“I left the bullet there because they killed my baby,” he told police.
Paiva was arrested and charged with threatening to commit a crime, according to police. However, on Wednesday, he agreed to plead guilty to a lesser charge and serve one year of probation, authorities said. He also will undergo mental health counseling, according to authorities.
Here’s more from the report:
[Paiva’s attorney Patrick] Conway said his client had no history of protesting or making threats toward abortion clinics but on that day was upset about his girlfriend’s choice, even as he accompanied her to the facility inside the Cummings Center.
“He was sad,” Conway said. Paiva had only just learned he was going to be a father when his girlfriend told him of her decision. “He still wanted to be there for his girlfriend,” said the lawyer.
“By his own admission, he should have done some things differently,” Conway said.
Research indicates fathers often experience deep pain and regret when their unborn babies are aborted. One study that investigated the effects of abortion on men found more than 90 percent experienced grief and sadness after the abortion and 90 percent had persistent thoughts about their aborted child. Only about 1 percent of men said they would consider abortion again.
Even though biologically an unborn baby is just as much the father’s as the mother’s, fathers have no legal rights to protect their unborn baby’s life if the mother of their child decides to have an abortion.
The young man’s voice cracked as he pleaded, “Can you help me? ‘Kaylee’ is going to have an abortion, and I want my baby to live.”
He was not the first young father to come to us with this dilemma. Over my 10 years of pregnancy center work, I’ve spoken with a number of fathers who desperately wanted to rescue the life of their child—but the decision was not theirs to make.
In Humanae Vitae, Blessed Pope Paul VI made several predictions of what widespread use of contraceptives would lead to. These included an increase in marital infidelity, lowering of moral standards, men considering women as “a mere instrument for the satisfaction of his own desires” (e.g. Harvey Weinstein and many others) and the imposition of contraception by governmental authorities. These have all come to pass. How could he have been so accurate in his predictions? I think this is because the Blessed Pope had a firm grasp of the profound unity of spirit, mind and body that is the human person. The Catechism teaches us, “The unity of soul and body is so profound that one has to consider the soul to be the “form” of the body: i.e., it is because of its spiritual soul that the body made of matter becomes a living, human body; spirit and matter, in man, are not two natures united, but rather their union forms a single nature.” (CCC 365).
This union has consequences that effect the entire person. Thus, spiritual sickness (sins) and spiritual health (virtues) have physical/psychological and sociological consequences. Blessed Pope Paul VI saw this and was able to make accurate predictions (prophecies?) because of this understanding. He knew life begins with the marital act, and this act has unitive and procreative aspects which should not be separated. Indeed, how can the “two become one flesh” if there is a barrier between them, or if one of the partners withholds an essential part of themselves? This division of the one flesh union results in the consequences that Paul VI predicted. But the use of “oral contraceptives”, which are in fact potent steroid hormones that cause temporary sterility of the woman (sterilizing steroids), have additional moral and biological implications. It is a violation of the moral law to treat a normal, functioning, healthy body system as if it were a disease. Yet this is precisely what sterilizing steroids do. They treat the reproductive system of the woman as if it were a disease that needs to be fixed. So understandably, sterilizing steroids have additional side effects, beyond those of barrier methods of contraception.
If you read the package insert for “Yaz” (one of the most popular contraceptives), there you will see increased risk of:
Serious Cardiovascular Events and Stroke
Vascular Events
Venous thromboembolism
Liver Disease
Hepatic adenomas
Hepatocellular carcinoma
Gallbladder disease
Increased blood pressure
Adverse lipid changes
These only cover the “serious risks” of sterilizing steroids. Other side effects include headache/migraine, menstrual irregularities, nausea/vomiting, breast pain/tenderness and mood changes. But there are more side effects that are not listed. The estrogen in contraceptives has been classified as a carcinogen, and there is a clear association with the use of these sterilizing steroids and the risk of breast, cervical and liver cancer. In addition, although less widely known, there is a clear association of the use of sterilizing steroids with certain autoimmune diseases, including inflammatory bowel disease and systemic lupus erythematosus. This information, while available in the medical literature, is not widely known by the public. Why? Why should a medication which treats no disease, cures no pathology and provides little benefit to women with sometimes severe side effects be tolerated by our society? What does this say about us?
Certainly, we can point to concupiscence inherent in the human condition. We can point to the sexual addiction of our society. We can also point to the media who selectively report what they deem is newsworthy. But we, who know the truth about the human person, must bear some of the blame as well. We have failed to communicate the truth in love as our Lord instructed us. We live in a society of one-liners, twitter feeds and catchphrases. And I often hear Catholics complain that the truth of Catholic teaching is too complicated to communicate in one-liners. Yet that is exactly what Jesus did. “As I have loved you, so you also should love one another” (Jn 13:34). “Let he who is without sin cast the first stone” (Jn 8:7). “But I say to you, everyone who looks at a woman with lust has already committed adultery with her in his heart” (Mt 5:28). And on and on. Our problem is that we are losing the war of the one-liners, although if we truly follow Jesus we should be masters at it. So here are some pro-life one liners we should be using, developing, and improving.
Real men use NFP.
All family planning should be natural.
Love is life giving. Lust is sterile.
We should love people and use things, not use people and love things(Bishop Fulton Sheen).
Oral contraceptives are really sterilizing steroids.
But they are not performance enhancing, but performance inhibiting.
Good morals is good medicine! (Attributed to Bishop Robert Vasa)
Fetus is Latin for little one. (Remember Jesus said whatever you did for these little ones you did for me Mt 25:40).
True love holds nothing back.
Using someone is not loving them.
True love is free, total, faithful and fruitful.
In vitro fertilization reduces a human person to a commodity that can be bought and sold.
A child need not be planned, nor even wanted.
But they all must be welcomed with open hearts as gifts from God.
Fertility is not a disease to be treated but a blessing to cherish.
God gives us a choice between life giving love and sterile sex. Choose wisely. Choose life.
As disciples of Jesus, the Master of the one-liners, we need to learn our faith and how to communicate it quickly and simply. This is a starting list. Please add your own.
Deacon William V. Williams, M.D., husband of Lorraine, father of Ron, Christina and Jon, is a board-certified rheumatologist and a medical researcher. He served from 2009-2017 and the Editor-in-Chief of The Linacre Quarterly, the official journal of the Catholic Medical Association. He is an Adjunct Professor of Medicine at the University of Pennsylvania and is currently the President and CEO of BriaCell Therapeutics Corporation. He has helped to coordinate and participate in a series of comprehensive literature reviews of the medical, psychological, sociological and spiritual effects of contraceptives on women focusing on hormonal agents.
large Hispanic man holding and looking at tiny baby girl in arms
Bishops get a lot of unsolicited mail from strangers, some of it pleasant, some of it much less so. It goes with the job. But every once in a while a letter comes in that’s worth sharing with a wider audience.
Last month, in preparation for the October 2018 synod, roughly 300 young adults from around the world gathered in Rome to discuss their views of faith and the Church. The result was a valuable experience of dialogue and learning—so valuable that I think that continuing the process of listening to a wide range of young adult experiences is important. In that spirit, I offer a letter below, which I received just afterthe March pre-synod gathering. It was unsolicited and from a stranger—but hardly the first such letter to come my way. Though I’ve removed the author’s name and other identifiers, the content is unchanged and used with his permission. It deserves consideration as we seek a fuller understanding of the pastoral challenges facing young adults in a changing world.
I am 26 years old, a father of three young children, and I wish to offer my perspective, shared by many of my peers, on Rome’s upcoming synod [on “Young People, the Faith, and Vocational Discernment”].
Though the Church’s growing focus on evangelization of the “Nones” is encouraging, there have been recent discussions emanating from several prominent figures in Rome and throughout Church leadership regarding a so-called “paradigm shift” relative to doctrine, the supremacy of individual conscience, and pastoral accommodation. My wife and I find these developments disturbing and potentially disastrous for the evangelization of the young and the fallen-away.
We young people crave the truth and clarity of good teaching. On a secular level this is evidenced by the meteoric rise in popularity of Jordan Peterson. We crave the truth, no matter how blunt or difficult it is for us to swallow or for the shepherds of our flock to teach.
Our culture is roiled in confusion concerning the basic tenets of human nature: From a very young age, we’re deluged with propaganda that distorts basic scientific truths about gender, paints virtue and chivalry as “toxic masculinity,” denigrates the family, and desecrates the nature of sex and its fruits, especially the unborn child.
We urgently need the Church’s clarity and authoritative guidance on issues like abortion, homosexuality, gender dysphoria, the indissolubility of matrimony, the four last things, and the consequences of contraception (moral, anthropological, and abortifacient). My generation has never, or rarely, heard these truths winsomely taught in the parishes. Instead, we hear most forcefully and frequently from our bishops’ conference and our dioceses regarding the federal budget, border policy, net neutrality, gun control, and the environment.
Increasingly, we have noticed an appeasement of modern culture under the broad cloak of pastoral sensitivity, including cases of some high-profile clergy who deliberately blur the Church’s teaching regarding homosexuality and transgenderism in the name of “building bridges.” The dubia remain unanswered. Discussions of beauty in the liturgy and reverent reception of the Eucharist are mocked. Heads are scratched at decreasing Mass attendance, yet young people who look to tradition to recover our bearings are chided as “rigid.”
This shift away from clarity is demoralizing for young faithful Catholics, particularly those with a heart for the New Evangelization and my friends raising children against an ever-stronger cultural tide. Peers of mine who are converts or reverts have specifically cited teachings like Humanae Vitae, Familiaris Consortio, and Veritatis Splendor as beacons that set the Church and her wisdom apart from the world and other faiths. Now they’re hearing from some in the highest levels of the Church that these liberating teachings are unrealistic ideals, and that “conscience” should be the arbiter of truth.
Young Catholics crave the beauty that guided and inspired previous generations for nearly two millennia. Many of my generation received their upbringing surrounded by bland, ugly, and often downright counter-mystical modern church architecture, hidden tabernacles, and banal modern liturgical music more suitable to failed off-Broadway theater. The disastrous effect that Beige Catholicism (as Bishop Robert Barron aptly describes it) has had on my generation can’t be overstated. In a world of soulless modern vulgarity, we’re frustrated by the iconoclasm of the past 60 years.
In sum, many of us feel that we’re the rightful heirs of thousands of years of rich teaching, tradition, art, architecture, and music. We young Catholics increasingly recognize that these riches will be crucial for evangelizing our peers and passing on a thriving Church to our children. If the Church abandons her traditions of beauty and truth, she abandons us.
I offer these observations without bitterness or insult, but with love for my brothers and sisters who have not received the blessing, love, and formation God mysteriously granted to me and my friends. I am not alone. Though deeply troubled by the current state of affairs, we remain hopeful; and rooted in that confidence, we’re raising large families who will inherit the future of the Church. I sincerely hope this can be conveyed emphatically at the upcoming synod, and I thank every pastor and bishop who stands as a role model for evangelizing, preaching the truth, and promoting the beauty and richness our faith has to offer.
I can add little to that kind of witness. I’ll merely suggest the obvious: The future of the Catholic faith belongs to those who create it with their fidelity, their self-sacrifice, their commitment to bringing new life into the world and raising their children in truth, and their determination to walk Christ’s “narrow way” with joy. May God grant the 2018 synod fathers the grace and courage to lead young people on that path.
Charles J. Chaput, O.F.M. Cap., is the archbishop of Philadelphia.
Pope Saint John Paul II’s Evangelium vitae just about says it all when it comes to discussing the sanctity of human life, threats to life in the modern world, and the related Catholic Church’s teachings on the issues. In today’s culture – where the deciding factor of an action among young people tends to be “if it feels good, do it” – this encyclical should be added to the top of our student reading list.
Let me tell you why reading through the pages of The Gospel of Life is crucial.
If you’re a liberal arts major pondering the universe, Evangelium vitae covers moral issues from one end of the spectrum of human life to the other: abortion to euthanasia, embryonic research to the death penalty, contraception to in vitro fertilization, and so on. At our time in our lives we are confronted with so many challenges and we need to know how to defend human life in all its stages, right? And this encyclical covers so many threats to life humanity faces, we need to both know and understand what it says.
In Evangelium vitae, not only does John Paul condemn the immoral practices that destroy human life, but he also discusses the links between these and the rise of the “culture of death” – a culture that values self-gratification above everything else.
Two of the immoral practices condemned in this work are contraception and abortion. These inextricably linked evils are key to recognizing the culture of death throughout the world. A growing number of young people admit that abortion is wrong, but they’re not convicted contraception is also gravely immoral. Seeing images of the unborn via ultrasounds has greatly helped to expose the lie that an unborn child is just a “clump of cells.” Contraception seems “harmless” by comparison; it is as simple as using a condom, or taking a pill. And nobody gets killed, so we’re told (though numerous women have suffered fatal side effects from contraceptive use, and some are actually abortifacient).
But the Pope was wise, he understood all our struggles. Unlike the culture of death, Christianity is a love story. Remember all those thousands of confessions heheard? In Evangelium vitae he speaks to our hearts. Pope John Paul II reaffirms the immorality of contraception because it “contradicts the full truth of the sexual act as the proper expression of conjugal love” and promotes “a hedonistic mentality unwilling to accept responsibility in matters of sexuality” (13). The immorality of contraception is rooted in a violation of the nature of the sexual act, which is an act of total self-giving to one’s spouse. Yes, that means within marriage, it’s not just about “me.” I and my spouse need to be open to each other, to life and to children. Because of today’s contraceptive mindset, which sees the sexual act as solely a source of self-gratification, many sadly see procreation as a disease to be avoided.
Though “the close connection which exists…between the practice of contraception and that of abortion is becoming increasingly obvious” (13), in our over-sexualized culture it is unfortunately still not very clear to the average person. It’s just as important to tell those who think contraception is the best way to decrease abortions, claiming it prevents “unwanted pregnancies,” that it’s a lie and the numbers just don’t add up. In many countries where contraception is widely available, the abortion rate has also remained high, and sometimes even increased.
In the UK, the British government launched a “Teenage Pregnancy Strategy” program in 1999, which spent hundreds of millions of dollars to promote contraception in an attempt to lower the teenage pregnancy rate. But abortion rates among teenage girls in the UK are now higher than before the program started. Today over 60% of pregnant teens under 16 years of age abort their unborn baby.
You see, where contraception is everywhere, pregnancy is treated like a disease, an enemy: “The life which could result from a sexual encounter becomes an enemy to be avoided at all costs, and abortion becomes the only possible decisive response to failed contraception” (13). So when contraception fails – which it often does – abortion is seen as “necessary” and becomes widespread, as other assaults on life and human dignity naturally follow. The destruction of those who are inconvenient, whether it is an unborn child or a severely disabled person, gradually appears to be a reasonable and “enlightened” step to take.
Our pro-life generation needs to witness. Learn your Faith. Try to come annually to Marches for Life. Share prayer support and fellowship. Youth in the U.S. and around the world have to recognize and understand the tragic effects of contraception on our wider culture if we truly wish to abolish abortion and defend life.
So again, why not start with reading Evangelium vitae? We are the future; it’s increasingly important we understand its teachings so we can spread them far and wide, and finally free ourselves from this culture of death in which we live.
David Bereit, founder of the amazingly successful prayer-based pro-life organization 40 Days for Life, just entered the Catholic Church this Easter. When I mentioned this to a friend, they were surprised to hear that he wasn’t already Catholic.
Indeed, while evangelical Protestants generally vote pro-life, on-the-ground activism seems to be dominated by Catholics. Of course, lots of people who join the pro-life movement are not Catholic – but many don’t remain that way.
Bereit is just the latest leader in the pro-life movement to convert to Catholicism.
Lila Rose was raised in a devout evangelical protestant family. She founded the pro-life organization Live Action in 2003 when she was just 15 years old. By 2009, she had joined the Catholic Church.
Bryan Kemper was baptized Catholic but his family didn’t practice the faith. As an adult, he was a member of the Orthodox Presbyterian Church. In 2003, he founded a youth-oriented arm of Priests for Life called Stand True, and in 2011 he came back to the Catholic Church.
Abby Johnson was an Episcopalian Christian who ran a Planned Parenthood abortion clinic. After personally witnessing an abortion in 2009, she changed her mind on abortion and became pro-life (which she recounts in her book Unplanned). In 2012, she joined the Catholic Church.
And this is just the more recent crop of converts.
Dr. Bernard Nathanson founded NARAL and helped lead the push for legalized abortion in the late 1960s and early 1970s in the United States. He ran one of the largest abortion clinics in the world and personally performed thousands of abortions. But due to the advent of ultrasound technology, he changed his mind on abortion and joined the pro-life movement just a few years after Roe v. Wade, the infamous 1973 U.S. Supreme Court Decision that erroneously ruled that abortion was protected by the Constitution. In 1996, he was baptized Catholic by Cardinal John O’Connor himself in New York City’s St. Patrick Cathedral.
And then there’s the most amazing convert of them all.
Norma McCorvey had her crisis pregnancy situation exploited by pro-abortion activists and was thrust into American politics as “Jane Roe” in Roe v. Wade. In the 1980s, she revealed her identity and was hailed as a hero of the pro-choice movement. In the mid-1990s, she changed her mind through an unlikely friendship with the protestant Christian pro-life activist Flip Benham and was baptized a protestant Christian in 1995. Now active in the pro-life movement, she converted to Catholicism in 1998.
And there are certainly more examples.
The Catholic Church has been against abortion for two thousand years. While many non-Catholic Christians as well as non-Christians oppose abortion, the pro-life movement is full of Catholics. What this means is that when people start working in the pro-life movement, they end up working alongside Catholics and forming friendships they might not have had otherwise.
And when people are shown the beauty, consistency, and vitality of true Catholicism, in contrast to commonly held stereotypes, it seems many people end up wanting to join.
KRISTAN HAWKINS APR 17, 2018 | 1:02PM WASHINGTON, DC
In a strange twist of fate, leading athletics programs seem to be ignoring federal protections for women that went into effect the year before Roe v. Wade and Doe v. Boltoncreated almost unlimited abortion access. While the 1972 Title IX was created to protect female athletes from discrimination on the basis of sex, many athletes report that rather than their pregnancies being welcomed or accommodated, they are facing incredible pressure to abort, almost as though Roe’s 1973 abortion ruling trumped their rights.
Last year, Olympian Sanya Richards-Ross told Sports Illustrated, “I literally don’t know another female track and field athlete who hasn’t had an abortion.” Richards-Ross herself openly recounts her own abortion two weeks before the Olympic games in Beijing. She told Sports Illustrated that abortion is pervasive among college athletes because they are often misinformed about their own reproductive capacity and she said that she didn’t know all of her pregnancy options when she underwent her abortion. And Richards-Ross’ story is representative of countless others like her own.
Something is seriously amiss when students don’t know that they have choices other than abortion. At Students for Life, we see egregious failures like this all too often. We encounter students who have never been told that they are protected by law from being kicked off of a sports team or losing a scholarship if they become pregnant. We meet students who have had abortions because they believed it was their only choice.
The question is this: Why are the schools, coaches, staff, and professors in these students’ lives doing almost nothing to ensure that they are apprised of their rights under Title IX? Title IX of the Education Amendments of 1972 explicitly prohibits discrimination on the basis of sex in education programs or activities at schools that receive federal taxpayer funding. In other words, it is against the law for a student to lose her scholarship or be kicked off her sports team for being pregnant.
Still, problems persist. Through the Pregnant on Campus Initiative, Students for Life America staff and student leaders have responded to dozens of complaints from pregnant students who were told to drop out of school, were dropped from or failed out of classes, and even lost financial aid. In many cases, SFLA staff has had to explain to the students what the Title IX violation was so that they could then advocate for themselves because Title IX coordinators were not providing them the correct information, or were directly complicit in the action. Title IX questions are among the top concerns that our initiative responds to because most students are uninformed on the topic and are surprised to learn that the actions of administration and staff are illegal (e.g. encouraging them to drop out of class, failing to provide excused absences for childbirth and labor).
The Department of Justice states that Title IX’s objective is “to avoid the use of federal money to support sexual discrimination in educational programs and to provide individual citizens effective protections against those practices.” Yet, every year, female athletes seek abortions because they believe that carrying a child to term and giving birth will end their athletic careers.
This fact brings to light a second problem: If pregnant students are not being adequately informed by their schools that they’re protected by law under Title IX, shouldn’t this be disclosed in pre-abortion counseling? If a young woman goes to Planned Parenthood and tells the counselor that she is seeking an abortion because she will lose her scholarship if she continues her pregnancy, Planned Parenthood’s counseling and informed consent policies should include a disclosure that she is protected by Title IX and does not have to undergo an abortion to maintain her status or scholarship.
Informing students of their Title IX protections is a large component of Students for Life’s Pregnant on Campus Initiative. We must stop failing the young female students who comprise the biggest target of the abortion industry. We know that when students are not informed of their rights by school officials, we cannot count on the abortion industry to deliver this life-saving information, considering its history of exploitation and abuse.
No woman should be forced to choose between her pre-born child and her athletic and educational future. The law says they don’t have to pit one against the other. It’s time for those in charge of athletic programming to stop forcing a choice for abortion.
EDITORIAL: While the early Christians set themselves apart in their reverence for the body and for the spousal one-flesh union as a sign of Christ’s unconditional love for his Church, those who embrace the chemical corset scorn, perhaps unthinkingly, the body’s limits and the sacrifices that come with marriage and family life.
The Editors
Imagine the birth-control pill as a “chemical corset” that controls and reshapes a woman’s body so that it operates like a man’s.
It’s a strange, unsettling image, worthy of a feminist-inspired dystopian novel or film. In fact, when this chemical corset was first approved by the Food and Drug Administration in 1960, its arrival was heralded as a milestone of sorts. “It was the first medicine ever designed to be taken regularly by people who were not sick,” noted Time magazine.
Nevertheless, oral contraceptives were successfully marketed as a precondition for personal freedom, liberating women from the burden of fertility. And, today, artificial birth control and the various moral, political and legal arguments employed to justify its use are deeply entrenched in the culture.
Indeed, what’s even more disturbing is that artificial contraception use is so widespread, including among Catholics, that moral resistance seems at times impossible, even for some at the highest levels of the Church. A half-century after the release of Pope Paul VI’s groundbreaking encyclical, Humanae Vitae(The Regulation of Birth), the Vatican has commissioned a high-level review of the internal Church debate that preceded the encyclical’s release, and the encyclical’s supporters fear it will be consigned to the dustbin of history.
From the start, Humanae Vitae was greeted with considerable derision. Influential theologians argued that its endorsement of Christianity’s long-standing prohibition of contraception would undermine the Church’s credibility with the lay faithful, many of whom had begun to use artificial contraceptives in spite of Church teaching. This year, that line of argument will likely get more traction as the Vatican prepares for the upcoming Synod of Bishops on Youth scheduled for October. Last month, a “pre-synodal report,” which summarized the views of young participants in a wide-ranging Holy See-facilitated discussion, confirmed that Catholic teaching on contraception still sparks controversy.
No doubt, this is partly the legacy of a flawed catechetical effort that has largely ignored Humanae Vitae. It is also a poignant reminder that young Catholics have inherited a world transformed by the logic of the chemical corset.
But it is worth noting that the pre-synodal report also made clear that many participants embraced the Church’s teachings as “a source of joy” and urged the Church to “proclaim them with greater depth of teaching.”
What are we to make of this pivotal time and the mixed messages from the young?
This “is a very difficult but also very promising moment: difficult, because the language of Catholic moral wisdom is alien to many young people, who often leave the Church without ever really encountering her,” observed Archbishop Charles Chaput of Philadelphia in an April 4 address at The Catholic University of America that marked the 50th anniversary of the 1968 papal encyclical. He continued that it was “promising, because the most awake of those same young people want something better and more enduring than the emptiness and noise they now have.”
Archbishop Chaput introduced the image of the chemical corset — a term he heard from a friend, who is a wife and mother with an ironic humor — as he headlined a major conference, “Humanae Vitae (1968-2018): Embracing God’s Vision for Marriage, Love and Life.” The gathering brought together leading theologians and physicians, natural family planning specialists and legal scholars in a rousing celebration of the prophetic witness to the hidden dangers of artificial contraception and the healing power of Catholic teaching on marriage by Pope Paul VI, who is soon to be canonized (see related commentary). And while many active Catholics are familiar with Pope Paul VI’s foresight that artificial contraception would harm marriage and lessen the dignity of women, Archbishop Chaput observed that the adoption of the chemical corset has also tainted modern Christianity, shaking believers’ faith in God and in the gift of his creation.
In contrast, early Christians set themselves apart from the dominant pagan culture, rejecting all threats to nascent human life, including contraception, abortion and infanticide.
These distinctive practices persisted into the modern world but had not yet tainted Christianity. Then, in 1930, the Lambeth Conference of Anglican bishops determined that contraception could be permitted in certain cases “where there is such a clearly felt moral obligation to limit or avoid parenthood and where there is a morally sound reason for avoiding complete abstinence.”
But, over time, noted Archbishop Chaput, the entire teaching on contraception was reversed by many, and “reformers” employed similar arguments to modify or upend bans on abortion, premarital sex and homosexual relations.
As other Christian churches followed the Anglicans’ lead, the ensuing moral vacuum fostered the creation of “a new religion,” with its own distinctive social and sexual practices. While the early Christians set themselves apart in their reverence for the body and for the spousal one-flesh union as a sign of Christ’s unconditional love for his Church, those who embrace the chemical corset scorn, perhaps unthinkingly, the body’s limits and the sacrifices that come with marriage and family life.
“Much of the moral conflict, broken family life, social unraveling and gender confusion that seems so common today stems — directly or more subtly — from our disordered attitudes toward creation and our appetite to master, reshape and even deform nature to our wills,” said Archbishop Chaput. The fractured, angry state of American culture surely vindicates Humanae Vitae and its dire predictions. But the encyclical was even more ambitious, for it sought to advance a holistic vision of life and of married love, anchored in a profound respect for the dignity of the human person, body and soul. Further, the sacrifices that accompany marriage, including periodic abstinence to regulate births, are part of the Creator’s plan. The sacrifices can be painful, but we are called to embrace them with a glad heart, not to sweep them aside as a threat to our freedom.
Yes, the Catholic Church has failed to effectively transmit this difficult teaching in the face of an all-out assault on human dignity and God’s plan for sexuality. But that does not mean we should give up now. And it does not justify a repudiation of the teaching by Church authority, a move that will inevitably provoke a review of other inconvenient moral teachings.
The steady drumbeat of dissent, said Cardinal Joseph Ratzinger, then-prefect of the Congregation for the Doctrine of the Faith, confers “the aura of morality upon changed norms of behavior.” But it is nothing less than “a surrender of moral integrity.”
Cardinal Ratzinger issued this judgment 30 years ago, well before Catholics had begun to challenge Church teaching on same-sex “marriage” or questioned the ban on so-called sex reassignment surgery for people with gender dysphoria. And only the most prophetic of voices will correctly predict the future distortions first ushered in by the chemical corset. Nevertheless, the very first Christians have taught the faithful what they must do as they navigate this world and as they accompany the young on their journey.
“Our mission now, as always,” said Archbishop Chaput, “is not to surrender to the world as it is, but to feed and ennoble the deepest yearnings of the world — and thereby to lead it to Jesus Christ and his true freedom and joy.”
Students at hundreds of schools across America walked out of their classrooms Wednesday to protest the violence committed every day against babies in the womb.
The event originated with Sacramento, California high school student Brandon Gillespie after his history teacher was suspended for talking with students about whether pro-life students would get the same support for their human rights concerns as those who engaged in the walkout regarding gun violence earlier this spring, according to Students for Life of America.
It did not.
While students at hundreds of high schools and colleges across the country held walk-outs Wednesday, their efforts received very little media attention. Some also faced obstacles from school administrators regarding the 17-minute protest.
“One principal tried to intimidate a student out of promoting his pro-life walkout,” according to Students for Life. The student told them: “My principal has proposed a compromise, he wants me to meet with the FCA and do a ‘meet at the pole’ at 8:30 so that ‘we don’t disrupt instruction.’ He also told me it doesn’t need to go to the media (I’ve already made a press release and sent it to local press.”
Gillespie said he did not receive the same accommodations from his school that those protesting gun violence did several weeks ago.
“I really was not surprised when they told me that they were not going to give me the accommodations and that they were not going to sanction this walkout as they did the previous one,” he said prior to the event. “It just confirms for me that there is a political double standard, at least in my school district, but I’m still going to be out there.”
His school administrators contend the gun violence protest was “viewpoint neutral,” while Gillespie’s pro-life protest was not.
At Gillespie’s school, Rocklin High School, the Sacramento Bee estimated about 40 students participated. However, it also noted school officials refused to allow the media near the protest.
“I just want to spread awareness about the cruel things that are happening in Planned Parenthood clinics across the country, the cruel murder of these children who have done nothing wrong,” Gillespie said, previously.
More than 100 Mississippi students participated in the walk-out at Cathedral School, according to The Natchez Democrat. Their school was one of the few that supported the event. Many students carried signs urging lawmakers to defund the abortion business Planned Parenthood and end abortion.
Some of the walk-outs had hundreds of participants, while an Oregon walk-out had only one student. Large or small, each protest showed young adults’ passion for protecting unborn babies.
April 10, 2018 (LifeSiteNews) – The U.S. Food and Drug Administration has announced new restrictions on who can offer the birth control implant Essure, along with new requirements for informed consent to the device’s medical risks.
The agency announced Monday that the permanent implant must now carry a label that restricts its sale and distribution to providers that review a brochure entitled “Patient-Doctor Discussion Checklist – Acceptance of Risk and Informed Decision Acknowledgement” with patients beforehand. After reviewing the document, both the patient and the physician performing the implantation must sign an informed consent acknowledgment.
The pamphlet lists perforation of the uterus and/or fallopian tubes, migration of inserts to the abdominal or pelvic cavity, persistent pelvic pain, suspected allergic or hypersensitivity reactions, and ectopic pregnancy as potential side effects of Essure. It adds that some women have reported headaches, fatigue, weight changes, hair loss, and mood changes such as depression, though those symptoms’ link to Essure remains unconfirmed.
It further warns that Essure’s safety and effectiveness for women below age 21 and above age 45 remain unknown, as do the safety and effectiveness of reversing the procedure.
The FDA also says that through the end of 2017, there have been 10 reported instances of adult death related to Essure, 20 instances of miscarriage, and four instances of an infant dying after a live birth. It cautions that it cannot “determine whether the device caused the death with only the information provided in the report,” but Device Events founder Madris Tomes said Essure is actually responsible for as many as 303 fetal deaths.
The FDA expects Essure manufacturer Bayer to “immediately” implement the new rules and says it will monitor its actions for compliance.
These new rules follow a February 2016 decision ordering Bayer to conduct a review of their product’s safety and add a warning to its packaging. The FDAY says that since then, American sales of Essure have declined by about 70 percent.
“We’ve been closely evaluating new information on the use of Essure, and based on our review of a growing body of evidence, we believe this product requires additional, meaningful safeguards to ensure women are able to make informed decisions about risk when considering this option,” FDA Commissioner Scott Gottlieb said in the announcement. “We take the concerns of all women affected by Essure very seriously. I’ve personally had the opportunity to meet with several women and hear their important concerns about this product. Despite previous efforts to alert women to the potential complications of Essure, we know that some patients still aren’t receiving this important information.”
“That is simply unacceptable. Every single woman receiving this device should fully understand the associated risks,” Gottlieb added.
Bayer responded Monday that Essure is a “safe and effective medical device” whose benefit/risk profile “remains positive.” But CNN reported that the FDA registered more than 5,000 complaints about the implant from November 2002 to May 2015, and that 2017 saw a almost 12,000 “adverse event reports” concerning Essure. In itsmost recent financial statement, Bayer reported that more than 16,000 Essure users had filed lawsuits against Bayer for experiencing hysterectomies, perforations, depression, and weight gain.
In a 2016 study, researchers from Northwestern University concluded that the FDA originally approved Essure after examining only its short-term effects and left it on the market without performing adequate follow-up trials or observation. “There are much higher standards for the approval of new drugs, whether oral, injectable or even topical,” Dr. Steve Xu said. “The important question to ask is: Should we really be holding high-risk medical devices to a lower standard of evidence than drugs?”
In 2015, several women who participated in clinical trials for Essure testified that FDA researchers altered reports to hide their severe reactions to the device.
While this week’s development comes as welcome news to many pro-lifers, others believe the government should go further. Former Rep. Mike Fitzpatrick, R-Pennsylvania, introduced legislation to ban Essure entirely in 2015.
“The failures of Essure are well documented and wide-ranging,” Fitzpatrick said at the time. “Yet in the face of all these facts, this device remains on the market, certified with the FDA’s stamp of approval. That’s unacceptable to me and unacceptable to the tens of thousands of ‘Essure sisters’ who are living with this device’s effects.”
WASHINGTON, DC, April 9, 2018 (LifeSiteNews) – “The most globally reviled and widely misunderstood document of the last half-century — Humanae Vitae — is also the most prophetic and explanatory of our era,” Catholic author Mary Eberstadt told attendees at a conference on the topic of the 1968 encyclical.
“The beauty of Pope Paul VI’s Encyclical, shines forth in a new and continuously illuminating way,” said Eberstadt. “Humanae Vitae — and the two thousand years of teaching it represents — remains true in ways that all reasonable people can discern, if only they are supplied with the relevant evidence.”
Eberstadt was speaking at The Catholic University of America’s academic symposium commemorating the 50th anniversary of Humanae Vitae, Pope Paul VI’s landmark encyclical. Attendees came from around the country and as far away as Hong Kong.
Humanae Vitae’s “signature predictions have been ratified as few predictions ever are,” she explained, “in ways that its authors could not possibly have foreseen, including by information which did not exist when the document was written; by scholars and others with no interest whatever in Church teaching, and even inadvertently by proud public adversaries of the Catholic Church.”
Why Humanae Vitae resisted
“The reasons for the resistance to the teaching are obvious,” said Eberstadt. “The promise of sex on demand, unencumbered by constraint, may be the strongest collective temptation that humanity has ever encountered. And that’s why, since the invention of the birth control pill, resistance to traditional Christian teaching has been unremittingly ferocious. It is also why so many in the laity and clergy wish that this rule—among others—were less taxing. As the disciples of Jesus complained upon hearing his teaching about marriage, ‘these lessons are hard.’
“But to confuse ‘hard’ with ‘wrong’ is an elementary error, unworthy even of a layman, let alone a theologian or a philosopher.”
Eberstadt, speaking to a room packed with Catholic academics, scholars, clerics and prelates counted up self-evident realities vindicating Humanae Vitae.
Contraception increases abortion
“It is clear beyond a reasonable doubt that the increased use of contraception has also increased abortion,” said Eberstadt. “Fifty years ago, many people of good will defended contraception precisely because they thought it would render abortion obsolete. But the statistical record since the 1960s shows this commonly held logic to be wrong.”
“During the past several decades, studies have emanated from the social sciences trying to explain what secular wisdom regards as a puzzling fact. Far from preventing abortion and unplanned pregnancies, contraception’s effects ran quite the other way. Rates of contraception usage, abortion, and out-of-wedlock births all exploded simultaneously.”
Contraception absolved men of responsibility
Eberstadt said that contraception has led to more abortion because it eroded the idea that men had equal responsibility in case of an unplanned pregnancy.
Contraception, as even many secular economists have explained, “sharply reduced the incentive for men to marry—including marrying their pregnant girlfriends,” and explains why the phrase, ‘shotgun wedding,’ is now antiquarian.
“As a matter of historical fact, the mass use of contraception called forth the demand for more abortion,” because contraceptive use, “invites pregnancies that occur in situations where women do not feel ready to become pregnant.”
“We cannot pretend that fifty years of social science connecting contraception to abortion don’t exist,” said Eberstadt, adding, “It would seem that from now on, anyone inside or outside the Church who advocates expanding the use of contraception, needs also to explain why it is permissible to increase abortion.”
Eberstadt said that many non-Catholic Christians are increasingly valuing Humanae Vitae as prophetic.
“This is one of the least reported religious stories of our time, and has the potential to reconfigure the Christianity of the future, replacing disunity over birth control with a new unity. Observing what the sexual revolution has wrought, more and more Protestant and other non-Catholic voices now question yesterday’s nonchalance about contraception,” she said.
According to Eberstadt, a Mormon doctor conceded ten years ago that Contraception is a “heavy part of the fuel behind the sexual revolution and many of the problems in society we are facing. I think ‘Humanae Vitae’ is basically a prophetic statement.”
Africa’s rejection of contraception proves ‘strict churches are strong’
“It is in tradition-minded Africa that Christianity has grown explosively in the years since Humanae Vitae—as opposed to in those nations whose Christian leaders struggle still to change the rulebook,” noted Eberstadt, proving the maxim, “Strict churches are strong.” Concomitantly, “lax churches are weak.”
Eberstadt quoted Nigerian-born Obianuju Ekeocha, author of the new book Target Africa: Ideological Neo-Colonialism of the Twenty-first Century, who wrote an open letter to Melinda Gates, whose foundation dedicates impressive resources to spreading birth control among Africans:
“I see this $4.6 billion buying us misery. I see it buying us unfaithful husbands; I see it buying us streets devoid of the innocent chatter of children; and a retirement without the tender loving care of our children.”
Contraception has not made women happier
Evidence from social science suggests that female happiness across the United States and Europe has been declining over time, leading to the “growing worry among secular women that marriage has become impossible,” and so, “it is time to go it alone.”
“The technological shock of widespread contraception licensed predation,” said Eberstadt. “No longer does a man have to be a king or a master of the universe to prey upon women in unrelenting serial fashion. All he needs is a world in which women are assumed to use contraception—the world we’ve had since Humanae Vitae. The one that Humanae Vitae foresaw.”
Eberstadt noted how fifty years of contraception has created an epidemic of loneliness.
Five decades into the sexual revolution, “one of the most pressing and growing issues for social science researchers is not overpopulation,” said Eberstadt. “Properly understood, it is under-population.”
“A great many people, especially in the increasingly-barren, graying west, are suffering from what some call an ‘epidemic of loneliness,’” she said. “Fifty years after the embrace of the pill—and undeniably, because of the embrace of the pill—loneliness is spreading across the materially better-off countries of the planet.”
Eberstadt noted reports from around world. In Japan, where 4,000 elderly die “lonely deaths” each week, “an entire industry has grown up . . . which specializes in cleaning up the apartments where decomposing remains are found.” And in Germany, “One in four Germans over seventy receives a visit less than once a month from friends and acquaintances. And nearly one in ten is not visited by anyone anymore.”
“This epidemic of loneliness is a new form of human poverty, and it is abounding in societies awash in material wealth,” said Eberstadt. “It doesn’t take a demographer to connect the dots between the pill and elderly loneliness, any more than it takes a theologian to understand that contraception and abortion are joined at the root.”
The Catholic Church was right
“In this moment of watchfulness inside and outside the Church, a global fellowship that includes more and more non-Catholics, knows the truths of Humanae Vitae and related teachings as truths, however unwanted or hard. They are the latest pilgrims in a line stretching two thousand years back. They have sacrificed to stand where they do, and they sacrifice still—including by relinquishing the good opinion of a mocking world.”
“The Catholic Church was right to stand as a sign of contradiction to the devastation now surrounding us,” said Eberstadt, noting that accommodating the sexual revolution “has been an epic fail for the churches that have tried it.”
“Mocked and rejected in many places though it may be, [Humanae Vitae] got one of the biggest calls in history right.”
Archbishop Charles J. Chaput of Philadelphia speaks during a press conference with a delegation from Pennsylvania at the Vatican March 25. A delegation of government, religious and community leaders from Pennsylvania were meeting with Vatican officials to plan the Sept. 22-27, 2015, World Meeting of Families in Philadelphia. (CNS photo/Paul Haring) (March 25, 2014) See FAMILY-PHILADELPHIA March 25, 2014.
The Catholic Church’s teaching on marriage, abortion, human sexuality and contraception is rooted in the same respect for human dignity that guides its work for social justice and care for poor people, Philadelphia Archbishop Charles Chaput told a Catholic University of America audience.
It is imperative that the church make known why it upholds its teaching, as reiterated in Blessed Paul VI’s 1968 encyclical “Humanae Vitae” (“Of Human Life”), so that Catholics and the world understand God’s plan for humanity, the archbishop said during the April 4 opening session of a symposium marking the 50th anniversary of the papal teaching.
The encyclical is notably known for upholding church renouncement of contraception. It followed by eight years the 1960 U.S. Food and Drug Administration approval of the first birth control pill.
Blessed Paul convened a commission to examine whether the historic Christian rejection of contraceptives would apply to the new technology. Most commission members advised the pope that it would not, but Blessed Paul eventually disagreed, saying in the encyclical that the new technology was prohibited birth control.
Blessed Paul’s decision has been widely criticized, Archbishop Chaput acknowledged, with some Catholic clergy, theologians and laypeople refusing to accept it. “That resistance continues in our own day,” said the archbishop, who chairs the U.S. Conference of Catholic Bishops’ Committee on Laity, Marriage, Family Life and Youth. He made the comments in a 35-minute presentation to about 200 people.
“‘Humanae Vitae’ revealed deep wounds in the church about our understanding of the human person, the nature of sexuality and marriage as God created it,” he explained. “We still seek the cure for those wounds. But thanks to the witness of St. John Paul II, Pope Benedict, Pope Francis and many other faithful shepherds, the church has continued to preach the truth of Jesus Christ about who we are and what God desires for us.
“People willing to open their eyes and their hearts to the truth will see the hope that Catholic teaching represents and the power that comes when that truth makes us free,” he said.
The archbishop challenged widespread denunciation of the teaching on contraception by those who say church leaders spend too much time on “pelvic issues,” thus obscuring, they argue, the Gospel message of caring for poor people.
“As a bishop for 30 years in the dioceses where I served, that’s three of them, the church has put far more money, time and personnel into the care and education of the underprivileged than into programs related to sex,” he said.
“And it’s not that the critics don’t know this. Many don’t want to know it because facts interfere with their story line of a sexually repressed, body-denying institution locked in the past.”
Church teaching on contraception can be traced to the early days of Christianity, particularly in ancient Rome, where Christians emphasized upholding human dignity, he said.
Citing the work of Kyle Harper, provost at the University of Oklahoma and an expert in Roman history, the archbishop said the Romans “presumed that sex was just sex, one instinctual need among others” and that prostitutes and slaves were “safety valves” to satisfy such needs. But it was the early Christians who “welcomed all new life as something holy and a blessing,” teaching that each person was created in the image and likeness of God, he explained.
Christians also preached that God gave all people free will to act in accordance with God’s commands or against them, he said, continuing to cite Harper.
“Christianity embedded that notion of free will in human culture for the first time. Christian sexual morality was a key part of this understanding of free will. The body was a ‘consecrated space’ in which we could choose or reject God,” he said.
As a result, Christians began demanding “care for vulnerable bodies,” speaking out against slavery and supporting the needs of poor people, and that concern included opposition to contraception, he said.
Archbishop Chaput noted that Christian opposition to contraception continued until the 1930 Lambeth Conference of Anglican bishops, which determined that while the preferred method of avoiding birth should be sexual abstinence, other methods may be used to prevent pregnancy as long as they fell in line with Christian principles.
“Their minor tweak gradually turned into a full reversal on the issue of contraception. Other Christian leaders followed suit,” he said.
“Today this leaves the Catholic Church almost alone as a body of Christian believers whose leaders still maintain the historic Christian teaching on contraception,” he continued. “The church can thus look stubborn and out of touch for not adjusting her beliefs to the prevailing culture. But she’s simply remaining true to the faith she received from the apostles and can’t barter away.”
Since then, Archbishop Chaput said, “developed society has moved sharply away from Christian faith and morals, without shedding them completely.”
He echoed author G.K. Chesterton, who asserted that society is surrounded by “fragments of Christian ideas removed from their original framework and used in strange new ways. Human dignity and rights are still popular concepts, just don’t ask what their foundation is or whether human rights have any solid content beyond sentiment or personal preference.”
“Our culture isn’t reverting to the paganism of the past. It’s creating a new religion to replace Christianity. It’s that we understand that today’s new sexual mores are part of this larger change.”
The moral conflicts society faces, such as broken families, social unraveling and “gender confusion” stems “from our disordered attitudes toward creation and our appetite to master, reshape and even deform nature to our wills. We want the freedom to decide what reality is. And we insist on the power to make it so,” he said.
Such thinking is manifest in efforts to master the limitations of the human body and “attack the heart of our humanity,” the archbishop added.
Blessed Paul explains that “marriage is not just a social convention we’ve inherited, but the design of God himself. Christian couples are called to welcome the sacrifices that God’s design requires so they can enter into the joy it offers. This means that while husbands and wives may take advantage of periods of natural infertility to regulate the birth of their children, they can’t actively intervene to stamp out the fertility that’s natural to sexual love,” he said.
Because the church’s teaching often was not being followed prior to the encyclical, Archbishop Chaput said Blessed Paul offered four predictions if that trend continued: widespread infidelity and the general lowering of morality; loss of respect for women as they become viewed as instruments of selfish enjoyment rather than as beloved companions; public policies that advocate and implement birth control as a form of population policy; and humans thinking they had unlimited dominion over their own bodies, turning the person into the object of his or her own intrusive power.
“Half a century after ‘Humanae Vitae’ the church in the United States is at a very difficult but also very promising moment,” the archbishop said. “Difficult because the language of Catholic moral wisdom is alien to many young people, who often leave the church without every really encountering her. Promising because the most awake of those same young people want something better and more enduring than the emptiness and noise they now have.
“Our mission now, as always, is not to surrender to the world as it is, but to feed an ennoble the deepest yearnings of the world and thereby to lead it to Jesus Christ and his true freedom and joy.”
This is just one of the dozens of lawsuits facing The University Hospitals Fertility Clinic in Cleveland, after the failure in early March of a cryopreservation tank containing approximately 4,000 eggs and embryos belonging to at least 950 families.
The accidental destruction of these very young human beings is raising a host of ethical and legal questions, and highlighting some of the inherent problems of IVF.
Is an embryo a person?
In Cleveland, clinic patients Wendy and Rick Penniman’s attorney is “asking the court to declare that an embryo is a person and that life begins at conception”, allowing the couple to bring a wrongful death lawsuit. However, the Roe v Wade decision, which legalised abortion, holds that a foetus, let alone an embryo, is not a person.
Antonia Tully, Director of Campaigns for SPUC said: “Of course we hope that the judge in this case does recognise the humanity of the embryos. But at the same time we must be clear that manufacturing human beings to order, outside the womb by IVF is inherently wrong. We must also remember that many other tiny embryonic humans will have been discarded at the time that these embryos were selected for freezing.”
How do you put a figure on children?
Even without arguing that the embryo is a person, lawyers are struggling to determine what compensation is appropriate for what one affected patient calls “irreplaceable” – the loss of one’s children, or, as many see it, their only chance to become parents.
Adam Wolf, an attorney who is working on a number of these cases, tells MarieClaire.com that putting a figure on an accidentally destroyed embryo is one of the most challenging aspects of these lawsuits. “How to place a monetary value on an embryo is something I have struggled with for years. Because in some ways there isn’t enough a money in the world, and it is a little bit gross to think of monetary figure to represent the value of future children,” he says. “On the other hand, that is how the legal system compensates people.”
“It is really easy to quantify the amount of money that someone has spent on the process or treatment, and has paid in storage fees. It’s far more challenging to think: What is the price of parenthood? How much do you value the ability to have children?” he continues.
Experimenting on embryos
The case also highlights how the death of embryos is treated differently depending on the circumstances. Between 1978 and 2002 68,000 IVF babies have been born but in the process 1.2 million embryos created by IVF were frozen, destroyed or used in research. Embryos are not legally seen as persons, and are often deliberately destroyed or left frozen indefinitely.
SPUC has spoken out strongly against using embryonic human being for experimental purposes. Dr Anthony McCarthy criticised the proposal to extend the time limit on using embryos for experiments and made the point that parents do think of their embryos as children.
This is borne out by the distress to parents caused by the Cleveland fertility clinic malfunctions.
“I feel like I failed them”
Kathy and her husband, Ben had been planning on implanting one or more of their five frozen embryos this coming August, and were going to donate any remaining to another couple – a process controversially known as “embryo adoption”. “We wanted to do an open adoption, and keep in touch with the family. I realized that I needed to know that they were okay,” Kathy tells MarieClaire.com. But now none of this is possible, because their five embryos, stored at University Hospitals, are gone. “Even if it didn’t make sense for my husband and I to raise them, I was still their mother and I wanted to protect them and I feel like I failed them now.”
Antonia Tully said: “While our hearts go out to infertile couples, no one has an absolute right to have children. IVF turns children into a commodity, rather than a gift.”
Pope Paul VI’s legacy as a strong advocate for babies in the womb could be recognized in a special way when he is canonized as a saint later this year.
Known for overseeing the Second Vatican Council in the 1960s, Pope Paul VI is expected to be canonized in October. Among his most notable achievements, he published the important church document “Humanae Vitae” in 1968 about the value of human life.
“Paul VI might be invoked as the protector of unborn life,” Fr Antonio Marrazzo told CNA.
Here’s more from the report:
In both cases, the mother was never in mortal danger, it was not a first pregnancy, and could have ended in the child suffering severe deformities. Doctors also suggested abortion in both cases. However, the children were born healthy.
The former Pope, who reigned from 1963 to 1978, wrote in his famous encyclical Humanae Vitae that “the direct interruption of the generative process already begun and, above all, all direct abortion, even for therapeutic reasons, are to be absolutely excluded as lawful means of regulating the number of children.”
In February, cardinals approved the second miracle, involving an Italian mother who was urged to abort her unborn child.
The miracle attributed to the cause of Paul VI is the healing of an unborn child in the fifth month of pregnancy. The case was brought forward in 2014 for study.
The mother, originally from the province of Verona, Italy, had an illness that risked her own life and the life of her unborn child, and was advised to have an abortion.
A few days after the beatification of Paul VI on 19 Oct 2014, she went to pray to him at the Shrine of Holy Mary of Grace in the town of Brescia. The baby girl was later born in good health, and remains in good health today.
According to the report, another unborn baby in the 1990s in California also was healed after his mother entrusted her pregnancy to Pope Paul VI.
The unborn baby boy had a high risk of brain damage and his mother’s doctors encouraged her to abort him. However, she prayed for a miracle and asked for the pope’s intervention in her son’s life. He also was healed and now is a healthy young adult, according to the report.
A petition drive is underway to ask the United States Postal Service (USPS) to issue a special commemorative “Choose Life” stamp in honor of the sanctity of life.
The petition drive is being sponsored by the Population Research Institute (PRI), the International Organization for the Family (IOF), Human Life International, and Heartbeat International.
Each year, the USPS Citizens’ Stamp Advisory Committee accepts suggestions from citizens on subjects for commemorative stamps which usually honor special persons, events and subjects with national appeal. Thirty to 40 new stamps are selected each year celebrating celebrating love, peace and everything from Disney villains and “retro funny cats” to “frozen treats.”
“Imagine the impact a pro-life stamp would have,” says PRI President Steven Mosher, “It would serve as a reminder for all Americans that every person deserves a chance at life. It would signal to the rest of the world that the United States of America respects the right to life for all.”
Although the USPS has never issued a stamp in honor of the right to life, in 1972 the USPS issued a stamp commemorating family planning. As the petition explains, at a luncheon with 300 members of the Planned Parenthood Federation present, J.T. Ellison, USPS spokesman, described what he considered to be the significance of the stamp. “We hope… this stamp will serve as a reminder to all members of our society that a spiraling world population and the environmental and social ills that inevitably follow – is everyone’s concern,” he said at the time.
In other words, with the issuance of the family planning stamp, the USPS endorsed the Malthusian myth of over-population, which was so prevalent at the time thanks, in part, to book by Paul Ehrlich, The Population Bomb, which had been published just four years earlier.
If we could base a stamp on a theory that has now been proven wrong, “It seems only fitting that the right to life, the first right mentioned in the Declaration of Independence, should be celebrated by having its own commemorative stamp,” Mosher says.
A stamp of this nature would hardly be out of the mainstream with recent polls showing that a majority of Americans (56%) now believe that abortion to be morally wrong.
And public displays of the “Choose Life” slogan already have ample precedent. Currently, 32 states allow drivers to display “Choose Life” license plates on their vehicles. In fact, Russ Amerling, founder of the popular “Choose Life” license plate campaign, has endorsed the pro-life postage stamp initiative.
As the petition states: “We need a Choose Life stamp that will serve as a reminder that worldwide, fertility rates have been cut in half since the late 1960s (in the United States, the fertility rate in 2015 was 1.84, well below the replacement level of 2.1), that each year there are 56 million abortions worldwide (900,000 to 1 million in the U.S. alone) and that the Declaration of Independence proclaims the rights to ‘life, liberty and the pursuit of happiness’ among humanity’s inalienable rights.”
Click here to sign on to this important initiative!
Many women who’ve chosen abortion afterward immediately regret their decision. Though the abortion industry tells us otherwise, it’s true.
Until recently, women who began taking the chemical abortion pill, commonly known as RU 486, but had second thoughts had no way of stopping the abortion process once it began.
But a new medical breakthrough gives hope to women who want to save their unborn babies.
Dr. George Delgado just released a peer-reviewed study that shows women now have a safe, effective method of reversing chemical abortion.
Dr. Delgado is the medical director of Culture of Life Family Services, a non-profit medical facility in California dedicated to offering pregnant women a life-affirming alternative to abortion. He is passionate about saving babies’ lives and protecting mothers from the trauma and aftermath of abortion. Abortion not only kills a child, but it often harms the mother physically, psychologically and spiritually.
Since the FDA approved RU 486 in 2000, Dr. Delgado and others have worked tirelessly to find a method to reverse chemical abortion.
The latest issue of the medical journal Issues in Law and Medicine features a groundbreaking study by Dr. Delgado and his co-authors that gives babies and their mothers new hope. They find that the effects of mifepristone can be reversed by administering progesterone.
Progesterone is a hormone produced in the ovaries, placenta and adrenal glands that is essential to pregnancy. The administration of this hormone for at-risk pregnancies has been safely used for over forty years.
Mifepristone in the abortion pill blocks the woman’s progesterone receptors which essentially starves the baby to death, robbing him or her of vital nutrients. Then a second drug, misoprostol, is prescribed which causes the uterus to contract and expel the dead baby.
Dr. Delgado finds that “increasing the progesterone levels in a pregnant woman by giving supplemental progesterone” could in many cases “blunt the abortifacient effects of mifepristone.” In 547 cases when patients took progesterone after taking mifepristone but prior to taking misoprostol, 261 patients had successful mifepristone reversals.
Patients taking a high dose oral form of progesterone had a reversal rate of 68%. And those taking injected progesterone saw a reversal rate of 64%. These are remarkable numbers considering that just 25% of chemical abortions were reversed when no treatment was given.
What about dangerous side-effects for the baby? Contrary to what staff at abortion facilities often tell women, the study found no increased risks of pre-term births or birth defects. As Dr. Delgado concludes, “The reversal of the effects of mifepristone using progesterone is safe and effective.”
You can read more details in Dr. Delgado’s new research. Please share it widely. Women need to know that help is available.
In a special two-part edition of our TV program Facing Life Head-On, I interviewed Dr. Delgado, as well as Cynthia Galvan and Becky Buell, who now have beautiful babies they love and adore because of this revolutionary new protocol. As Dr. Delgado said, “Women who change their minds…have a second chance at choice.”
A woman who has begun the chemical abortion process but is now doubting her decision can get immediate help through the Abortion Reversal Hotline at (877) 558-0333. Nurse are available 24 hours a day, 7 days a week to find a doctor in her area who can assist.
Mothers facing unexpected pregnancies need our support and encouragement. We now have an additional tool to show them love and compassion as we work to protect life and help spread this important pro-life message.
LifeNews.com Note: Bradley Mattes is the President of Life Issues Institute, a national pro-life educational group.
CYPRUS, April 3, 2018 (LifeSiteNews) – On Good Friday, the parliament of the eastern Mediterranean island of Cyprus voted 33-8 to legalize abortion.
Five members of parliament abstained from voting.
The new law allows all babies to be aborted through the first 12 weeks of pregnancy, and babies conceived in rape to be aborted through 19 weeks of pregnancy.
The people of Cyprus are predominantly Greek Orthodox. Good Friday is the day that Christians around the world commemorate Jesus’ sacrifice on the cross where they believe he saved mankind from sin and opened heaven’s doors closed by the original sin of Adam and Eve.
“Akel MP Skevi Koukouma said the bill had been kept for years inside drawers at the House legal committee and didn’t move forward so party votes wouldn’t be lost and so as not to upset the Archbishop, who has been vociferously opposed to the law,” Cyprus-Mail.com reported.
In their arguments, lawmakers who pushed for the pro-abortion legislation used classic canards about illegal abortions and women having to leave the country to abort their babies. Abortion supporters in Ireland are making similar claims as they campaign to overturn the pro-life Eighth Amendment via referendum in May.
Cyprus MPs say that they now plan to introduce a bill that “would require mandatory advice from doctors to female patients” about contraception.
April 1, 2018 (LifeSiteNews) – Even though you are reading this on Easter, it is a challenge for me to write this now, while still in the midst of a Lent that has been quite the challenge both personally and professionally. Nevertheless, despite our hardships, even those severe ones, we know that in the end Christ is victorious. We know that the more difficult the cross, the greater the glory will come of it when offered in union with the ultimate sacrifice of Christ on Calvary.
From the greatest suffering ever experienced has come the redemption of all mankind. Our Lord’s choice of crosses for us to take up and follow Him are never going to be too much for us to bear, even if we feel like they are. The strength to bear them is ours for the asking. An army of prayer warriors in heaven, on earth, and in purgatory are there to assist us in attaining the necessary strength to persevere.
So too in the Church this Easter we look to the ultimate victory of Christ and His Truth. No matter how dark things get, His Victory is assured. Let us lift up our heads with Hope to the coming Resurrection – which is also the triumph of the Immaculate Heart of Mary. May She triumph even now in our souls to mold us in Her womb into the image of Her Son.
Remember the miracle of the Eucharist just discovered in Italy. It is a demonstration of God’s power and control so that we may maintain our faith in the midst of struggle. Just as Jesus showed His disciples His Transfiguration so they could endure the seeming total loss of the crucifixion, so too even now God demonstrates His Almighty power in miracles to boost our faith.
The main attack of this whole crisis in the Church is the Eucharistic Presence. The debates seem always to be about desecrating the Eucharist. Whether it is to allow for sacrilegious reception of Holy Communion or to forbid or disdain reception in a reverent manner (kneeling and on the tongue).
The whole attack on God-ordained marriage we’ve experienced for the last 60 years can itself be seen as an attack on the Eucharist. St. Paul compares the union of a husband and wife to Christ’s union with the Church – a union wherein the “two become one flesh.”
Let us together resolve to believe in the victory of Christ over sin and death despite the trials of this valley of tears. Let us follow Our Lady’s example of faith in the Resurrection in the face of the crucifixion. Let us say with Her “Amen, so be it” to all that Christ did during His earthly life, and “Amen, so be it” to all that Christ permits now on earth so that we may be able to sing “Amen, so be it” at the glorious resurrection of His Mystical Body the Church.
If sacrifices speak so much to us,” it’s because they “reveal a common foundation that is the ground on which one relies,” says French Catholic philosopher Martin Steffens: “As one relies on the ground, one doesn’t see it and yet it’s certainly there.”
Questioned by Olivier Bonnel on Vatican News, Steffens reflected on the sacrifice of Lieutenant Colonel Arnaud Beltrame who, to save lives, offered himself as hostage to the terrorist during the attacks perpetrated in L’Aude, France, on March 23, 2018. In a telegram of condolence for the victims, Pope Francis praised in particular “the generous and heroic gesture of Lieutenant Colonel Arnaud Beltrame, who gave his life to protect persons.”
“Sacrifice is the inverse system of murder,” stresses Martin Steffens. “On one hand, someone takes lives and on the other someone gives his life. And in this sense, one could almost speak . . . of a violence of goodness,’ ‘violence of love that one opposes to the crass stupidity of evil.”
Steffens believes that sacrifice is “born of Christ’s Passion”: in the Passion, evil is unleashed on the Son of God who seems to be handed over to its blows; and yet, each blow witnesses the love that God expresses for humanity,” he explains. It’s “somewhat the same thing with Arnaud Beltrame: finally what we are going to retain is evidently the stupidity of evil, but in addition, even more so, the trick of the good: it’s to add something to evil by inventing an issue that doesn’t belong to evil, namely, that one will evidently retain the heroic and holy act of Arnaud Beltrame,” he continues.
The philosopher hopes that the sacrifice of the French Lieutenant Colonel is an occasion “to rethink the way of how good can respond to evil without becoming that evil.” And all those personages who effected a sacrifice “are, finally, a source of inspiration to lead us back to that good that invents, in places of violence, something that resembles life,” he adds.
According to Martin Steffens, “the world can but be thankful for all those discreet, secret, intimate sacrifices that we make.” He mentioned the example of a mother expecting a child: “A mother that bears a child must evidently sacrifice a good part of her comfort the whole time of the pregnancy. To have children being born, it’s necessary that that crazy gift be there. If the world of our days still receives children, it’s that sacrifice is like the continuous, discreet base that supports the world.”
“Sacrifice forces respect,” adds the philosopher. “Sacrifice is at the same time something that one can’t prescribe morally, command morally, and <yet> . . . it’s something that is eminently moral, which arouses admiration and which is — I want to say — the source itself of all morality, which is a brimming love for life, a love such that one is ready to give one’s life for that of another.”
This statue is the three-dimensional representation in actual size of the Man of the Shroud, created following the precise measurements taken from the cloth in which the body of Christ was wrapped after the crucifixion,” explains Giulio Fanti, teacher of mechanical and thermal measurements at the University of Padua, who studies the Shroud. Based on his measurements, the professor has created a “carbon copy” in 3D which, he claims, allows him to affirm that these are the true features of the crucified Christ.
“Therefore, we believe that we finally have the precise image of what Jesus looked like on this earth. From now on, He may no longer be depicted without taking this work into account.” The professor granted exclusive coverage of his work to the weekly periodical Chi, to which he revealed: “According to our studies, Jesus was a man of extraordinary beauty. Long-limbed, but very robust, he was nearly 5 ft. 11 in. tall, whereas the average height at the time was around 5 ft. 5 in. And he had a regal and majestic expression.” (Vatican Insider)
Through the study and three-dimensional projection of the figure, Fanti was also able to count the numerous wounds on the body of the man of the Shroud:
“On the Shroud,” the professor explains, “I counted 370 wounds from the flagellation, without taking into account the wounds on his sides, which the Shroud doesn’t show because it only enveloped the back and front of the body. We can therefore hypothesize a total of at least 600 blows. In addition, the three-dimensional reconstruction has made it possible to discover that at the moment of his death, the man of the Shroud sagged down towards the right, because his right shoulder was dislocated so seriously as to injure the nerves.” (Il Mattino di Padova)
The questions surrounding the mystery of the Shroud are still intact; certainly, in that tortured man we see the signs of suffering in which we find also a piece of each one of ourselves, but also—seen by the eyes of faith—hope that this man was not just anyone, but the Man par excellence, that “Behold the Man” who appeared docilely before Pilate and who, after the terrible flagellation, was raised up on the cross as an innocent man; not only innocent, but taking upon himself the guilt of all people. While belief in the Shroud is not obligatory, even for Christians, the exceptionality of that piece of linen remains there to challenge our understanding and our certainties, almost like a certain Jesus of Nazareth, who challenged our certainties by loving his persecutors, forgiving them from the cross, and conquering death, 2,000 years ago …
This article first appeared in the Italian edition of Aleteia.
While we continue to hear about fallen-away Catholics, more than 30,000 will enter the Church during the Easter Vigil Masses in the U.S. this Saturday. That’s enough for a small city!
That number is based on 85 of the nearly 200 dioceses reporting to the United States Conference of Bishops, so there are certainly much more than just that. The Archdiocese of Los Angeles, will welcome nearly 3,000 people into the Church;1,700 catechumens and 1,127 candidates. In the Galveston-Houston archdiocese, more than 2,000 will become Catholic.
The Easter Vigil Mass is the first Mass of Easter on Saturday evening, celebrating the resurrection of Jesus Christ. Catechumens, who have never been baptized, will receive baptism, confirmation and first Communion and those already baptized in another Christian tradition recognized as valid by the Catholic Church, will enter the Church through a profession of faith and reception of confirmation and the Eucharist.
Although people can enter the Church throughout the year, it is customary during the Easter Vigil.
“Holy Baptism is the basis of the whole Christian life, the gateway to life in the Spirit (vitae spiritualis ianua), and the door which gives access to the other sacraments. Through Baptism we are freed from sin and reborn as sons of God; we become members of Christ, are incorporated into the Church and made sharers in her mission: “Baptism is the sacrament of regeneration through water in the word,” (CCC 1213 ).
Welcome Our Brothers and Sisters
We can make our new Catholic brothers and sisters feel at home in their new Church. Catholics have a bit of a reputation for keeping to themselves, so it might take a little push. If that’s the case, pray to God for the courage and inspiration for how best to welcome new Catholics in your parish. Here are some suggestions.
If you attend the Easter Vigil, go up and congratulate them after Mass. Continue to be friendly and greet them after other Masses or on the street.
Invite them to your prayer group or Bible study.
Do you have a favorite book to inspire a new Catholic? If you have the means, no one is going to be offended if you hand out such gifts to help celebrate.
Print out this form for a free 6-month subscription to the National Catholic Register. Anyone can take advantage of the offer, but what a great way for a new Catholic to become informed on news relevant to the Church.
Share the Good News! Every Catholic can benefit in a big way by starting the day with a short summary of the news from a Catholic perspective, along with inspiration, trivia, and a whole assortment of inspiration—all of it brief to fit easily into the day. Go here to sign them up, or yourself.
Give them a card to congratulate them with a short note. Include your phone number or email. You can also write down the websites for the 6-month National Catholic Register trial subscription or to sign up for the Good News letter.
Enroll them up for a year of Masses and give them a card. Call your parish office for the names. If the parish secretary doesn’t know you, you might have to verify that you are a parishioner and not some stalker. There are many orders who enroll people in memberships and parishes which will take names to have a Mass said.
Pray for them. They could use the prayers to stay the course.
Light a candle for for all the new Catholics.
Hand them a favorite holy card. Catholic books stores have them or order them online. It might be too late to arrive in time for the Easter Vigil, but you can hand them out later if you know who the new Catholics are or order them now to be ready for next year.
Let us praise God and pray for those entering the Church. “Dear Lord, we pray for all new Catholics. May they be strengthened and blessed in the faith and grow ever closer to you. Help us to support them through our prayers and friendships. And use us and them, according to your will to lead others home to the Church.”
Go to the USCCB website to see specific numbers for all the US dioceses.
March 28, 2018 (LifeSiteNews) – France is under the shock of its most recent Islamic terrorist attack in a small supermarket near the beautifully preserved medieval town of Carcassonne in the Southwest, where Muslim immigrants of North African descent form an ever-increasing part of the population.
But this attack has been very different from the previous shootings and bombings.
This time, the focus was on one of the victims who sacrificed his own life in order to allow the many customers and workers trapped in the little “Super U” of Trèbes to escape to freedom while he offered to take the place of a woman hostage held by the attacker.
She was able to go free; he would be viciously attacked, having his throat slit by the radical Muslim terrorist Radouane Ladkim who also shot him three times.
Arnaud Beltrame’s subsequent death shocked and moved a nation: celebrated as a hero, he has become a symbol of courage but also of faith.
Arnaud Beltrame, 44, was a lieutenant-colonel in the French gendarmerie, a military corps responsible for security in the smaller towns and rural areas. His career had been one of exceptional bravery and excellence: he had participated in special operations in Iraq, organized security for French nuclear sites and he was also one of the first French military to have joined the elite “GIGN” counter-terrorism and special protection unit.
He had recently taken a post as commanding officer of the gendarmerie in the Carcassonne area in order to join the woman he was to have married next June. Even more importantly, after having been brought up in a family that no longer practiced the Catholic faith, he had undergone a personal and profound conversion about 10 years ago, receiving Holy Communion for the first time and also the sacrament of confirmation.
He lived his Christian faith
His sacrifice was immediately compared to that of Saint Maximilian Kolbe who offered to take the place of a young father in the Nazi extermination camp of Auschwitz during the Second World War in a roundup of prisoners condemned to die of thirst. The saint died in his stead.
Beltrame was savagely assaulted by Ladkim at 2 p.m. on Passion Friday. Father Jean-Baptiste of the nearby abbey of Lagrasse, which shelters the Catholic community of the Canons Regular of the Mother of God, was able to visit the soldier in hospital that same evening, where he lay, heavily wounded and unconscious but capable of receiving the last rites: the sacrament of Extreme Unction which sometimes brings healing to the ill, and always comfort and pardon to the dying.
Father Jean-Baptiste knew the man well: it was he who was preparing him and his fiancée Marielle, with whom he was already engaged in a civil marriage, for his religious wedding. Marielle was present; she answered the prayers for the dying led by the young priest in the traditional Latin form in which the Canons of Lagrasse celebrate the liturgy.
At the Father’s request, a nurse fixed a Miraculous Medal to Beltrame’s shoulder with tape: in secularized France where most young people have lost the sense of the faith of their fathers the ministering of the Catholic priest was welcomed with respect and helpfulness.
Beltrame died in the early hours of Saturday morning and the news spread like a wildfire. His heroic act had been that of a deeply faithful man, a man who gave his life to save the life of others.
There could have been no starker contrast to the fanatical act of the radical Islamic terrorist who deliberately took the soldier’s life, and who had already in his infernal orgy of killing for Allah fatally shot the driver of the car he had hijacked hours before, as well as an employee of the “Super U” and a client, and wounded 17 others.
To Father Jean-Baptiste, it was obvious that Beltrame had been driven not only by his sense of duty as a soldier, but also by the charity that is proper to the Christian faith.
Ladkim, on the other hand, appeared as the worshipper of a lesser god, killing where Beltrame served life out of love. Beltrame’s fatal injury was characteristic of Islamic ritual killings: animals must be sacrificed by having their throat slashed and are then bled to death. Beltrame was slain like a dog – the impure animal and hated enemy of Islam – or like a lamb, that offers itself to the slaughterer’s knife.
Islam is the rising religion in secularist France: the killing of a devout French Catholic believer in such a manner is acting as a wake-up call as to the realities and values of the two religions.
But there is even more to this than meets the eye.
He saved a mother
Beltrame took the place of a female hostage, and certainly saved her life. Julie, 40, is married and has a young daughter, 2-and-a-half years old. She had recently lost her job as an engineer and had accepted a modest post as a cashier at her local supermarket.
So, he saved a woman and a mother. This is the order Christian civilization: “women and children first”, where men are expected to protect and defend the most fragile, and especially those who carry the future by bearing children and nurturing them.
In Islam, women are second-rate citizens, the objects of men’s desire who must be hidden from public view. It is Christianity that invented courtly love and gallantry. And gallantry means an attitude of courteous respect, but also bravery and valor.
This goes very much against the grain of gender ideology.
But so does the whole story. The mother of Arnaud Beltrame, Nicolle Nicolic-Beltrame, made a point of speaking to the press about her deceased son. From the moment she heard on the radio that a lieutenant-colonel of the gendarmes had substituted himself for a hostage, she knew it was he.
From a boy, he had wanted action, to be the best, to learn what could be learned to help the oppressed, she said.
His father, grandfather, and great-grandfather had all served in the army. And when he was small, Arnaud loved nothing better than to play with toy soldiers. No one thought of stopping him to avoid “gender stereotypes”. It was considered totally normal for him to join a military high school, and then military college and elite officer training where he graduated with the highest marks of his year. Virile courage is nurtured in the family, as his mother’s poise and dignity amply demonstrated.
Her son, she said, loved his parents and his brothers, but he always put “the fatherland first, his family afterwards”, freely accepting the risks of his perilous missions. “Knowing how much he hated mediocrity, you want his gesture to help others”, she said. “When people are attacked in the subway or on the train, if only people would get together to react and stopped being passive, things would probably be better.”
Beltrame will receive a solemn homage from the nation in Paris on Wednesday in the courtyard of the Invalides. His mother approves: “I want it mostly because of the symbol it will bring: in France, we have decided not to take things lying down, we are not running away, we are trying to face the risks of the day, in France and elsewhere.”
A lesson of courage, and a lesson of faith
Arnaud Beltrame had taken his conversion most seriously, going on a pilgrimage to the sanctuary of Saint Anne of Auray – the mother of the Virgin Mary – in Brittany in 2015 in order to find a good wife. That led to his meeting with Marielle, a young and radiant veterinary surgeon with a “profound and discreet Catholic faith”, said Father Jean-Baptiste in a statement. She also has a history of generosity, having done volunteer work with handicapped young people and manning a hotline for people with addictions. She spent three years as a volunteer with the Franciscans of the Bronx. Nothing could be further from the image of women in Islam.
Their engagement took place in the Breton abbey of Timadeuc in 2016; they were civilly married that same year so that Arnaud could obtain a posting in the South of France. They had spent many hours with Father Jean-Baptiste whom they had met by chance while visiting the beautiful medieval abbey of Lagrasse, preparing their religious marriage, which they took most seriously.
Speaking to the French weekly “La Vie”, Marielle said: “The funeral of my husband will take place during Holy Week, after his death on a Friday just before Palm Sunday, and this was not insignificant to my eyes. It is with a great deal of hope that I am waiting to celebrate the Easter Resurrection with him.”
“Arnaud will never have children according to the order of the flesh. But his striking heroism will encourage many imitators, I am sure, who will be ready to give the gift of self for France and for its Christian joy”, concluded Father Jean-Baptiste in his statement.
These words have been seen and shared thousands of times. They cannot but touch the heart of a whole people.
ROCKLIN, California, March 26, 2018 (LifeSiteNews) – A 17-year-old California student is planning a pro-life “walkout” to take place at schools across the country next month in imitation of the recent ‘gun-violence’ protests.
The aim of the event is to witness to the millions of lives destroyed by abortion. The event will also test if there’s a double standard from school administration when it comes to allowing students to protest against destroyers of life and the tools they use.
Rocklin High School student Brandon Gillespie is organizing a nationwide pro-life student demonstration to “honor all the lives of the millions of aborted babies every year.” He also wants to focus the nation’s attention on “cruel injustices taking place at Planned Parenthood.”
Every school in the United States is encouraged to participate in the pro-life walkout Wednesday, April 11, at 10:00 am EDT, for 17 minutes.
Brandon Gillespie@bgillie13
I have officially announced the pro-life walkout that i am organizing. It is going to take place on Wednesday, April 11th at 10:00 am. The walkout will last for 17 minutes. We encourage students across the country to participate in a stand for #life
Gillespie is also organizing the event after his history teacher was suspended for questioning the anti-gun walkout and commenting that such an event would likely not be tolerated had the protest been over abortion.
Gillespie’s walkout will put his school’s administration to the test to see if they will allow student protests standing for conservative values.
“I would like to see if there really is a double standard and what will come of that,” the pro-life walkout organizer said.
Students for Life of America president Kristan Hawkins said that pro-life students “deserve the same respect and accommodation that anti-gun student activists experienced.”
“Having opened the door to student-led walkouts as a way to express a political or cultural viewpoint, schools cannot shut that door to pro-life students who also are moved by the loss of life and horrific realities of the toll of abortion,” she added.
Gillespie says he was inspired by his history teacher, Julianne Benzel. Benzel was abruptly disciplined and not allowed back to school for two days when she initiated a class discussion about the partisan nature of “walkout” protests for stricter gun laws.
An estimated 3,000 public schools across the United States gave permission for students to walk out of classes on March 14, one month after the deadly shooting at Marjory Stoneman Douglas High School in Parkland, Florida.
Mrs. Benzel started the discussion in her history class about the then-upcoming anti-gun protests. “If schools across the country are going to allow one group of students to get up during class and walk out to protest one issue, would they still give the same courtesy to another group of students who wanted to protest…abortion?” she challenged.
“If you’re going to allow students to walk up and get out of class without penalty then you have to allow any group of students that wants to protest,” she later explained. “Are we going to allow this on the other side?”
Fox News
✔@FoxNews
Julianne Benzel: “Would they still give the same courtesy to another group of students who wanted to get up and walk out to protest?”
The 20-year veteran teacher at Rocklin was promptly given an official letter informing her that she was immediately on “administrative leave.” She was, in her words, “aghast.” She added that the way she was handled has created a “climate of fear” among Rocklin teachers.
Benzel, a mother of five, says she believes school officials only allowed her back after two days of being banned because of widespread backlash over her suspension.
Benzel heartily approves of Gillespie’s pro-life challenge to the school administration.
“I’m thrilled that he’s going to not only actively engage, but also that he’s going to challenge,” she said. “He literally is trying to answer my question.”
Gillespie admitted his planned 17-minute pro-life walkout is seeking to do just that: answer Mrs. Benzel’s question of the existence of a liberal double standard at Rocklin and at schools across the nation. He noted that in the past, Rocklin High blocked prolifers peacefully handing out pamphlets across the street from the school.
The student organizer told the National Review that his protest is not only for the sanctity of innocent human life but also “stands for all students’ right to freedoms of speech and assembly.” He is calling on Rocklin High administration to publicly apologize to the history teacher.
“Brandon Gillespie is a terrific example of the passion this pro-life generation has,” Hawkins said. “His courageous effort to draw attention to the reality that more lives have been lost in our generation to abortion than all other causes should be national news.”
Gillespie says he will go forward with the pro-life demonstration whether the school approves of it or not.
PROVIDENCE, Rhode Island, March 26, 2018 (LifeSiteNews) – After public pressure, the President of Providence College, Father Brian Shanley, OP, has finally condemned the gay rape cartoon threatening a pro-family student.
He also said the Dominican-run institution “always has, and always will, remain faithful to the teachings of the Catholic Church” but “our collective challenge is to find a way to be faithful to our Catholic identity and to be inclusive” of the “LGBTQ+ community.”
The pro-family student and Resident Advisor (RA) who has faced threats and harassment for defending Catholic teaching is Michael Smalanskas. Smalanskas told LifeSiteNews “there are still reasons for serious concern moving forward” after Fr. Shanley’s email.
The bulletin board was repeatedly vandalized. Smalanskas’ fellow RAs threateningly congregated outside his door, leading campus police to transport Smalanskas to a secure, undisclosed location in the middle of the night because they feared for his safety.
On March 14, a cartoon of Smalanskas being forcibly sodomized was posted in the bathroom of his residence hall. Later that day, Vice President of Student Affairs Kristine Goodwin sent student leaders an email encouraging them to attend the pro-LGBT march being organized in response to the Catholic bulletin board. It’s unclear whether she was aware of the sexual assault threat.
That pro-LGBT march, originally scheduled for March 21, was postponed to March 23 due to weather.
More than 2,500 people signed a LifeSiteNews-hosted petition demanding Fr. Shanley condemn the gay rape cartoon.
“I admire and commend your courage in stepping forward to proclaim the teachings of the Church about Holy Matrimony,” Tobin wrote.
“For the sake of the record, I want to say that the President of Providence College, Father Brian Shanley, O.P., continues to have my personal support,” the bishop continued. “He is a good man, a dedicated and faithful priest, and has proven to be an effective leader of Providence College.”
After praising Shanley, Tobin asked:
…it does seem to me that Providence College is standing at the crossroads and now has to make a conscious decision about which road to travel. Will it maintain, proudly, unapologetically and unambiguously, its Catholic heritage by preaching, teaching and living the Catholic Faith in all its beauty and richness? Or, like so many other institutions today, will it succumb to modernist trends and become just one more progressive, secular bastion of political correctness? Or, we might ask: Will it continue to be P.C. – the Providence College we’ve come to know and love; or simply be p.c. – politically correct, the pathetic, ephemeral fashion that has, in recent years, taken such an ironclad grip on our culture?
‘My office has been barraged with phone calls and e-mails’ because of ‘conservative media sites’
On the morning of March 26, Fr. Shanley sent an email to all of campus complaining that “the College has been the subject of much discussion and negative publicity, mostly on conservative social media sites.”
“Much of what has been reported is not accurate,” he asserted, but did not give any examples of any part of the scandal being inaccurately reported.
“I am distressed by the way Michael Smalanskas has been vilified and ostracized by many of his peers,” Fr. Shanley wrote. “While some might not agree with how he tried to express Church teaching, he is entitled to the same respect, charity, and protection that is due any student. There can be no place on our campus for bullying, harassment, or intimidation. The drawing of him that was posted in the St. Joseph Hall men’s room was odious and reprehensible.”
Fr. Shanley’s full email stated:
Dear Members of the Providence College Community:
I am writing to follow up on my communication of March 19 and to address again the controversy that is currently roiling our campus. Since I wrote my first message, the College has been the subject of much discussion and negative publicity, mostly on conservative social media sites. Much of what has been reported is not accurate. My office has been barraged with phone calls and e-mails that have been angry, accusatory, and ironically uncharitable. Many suggest that Providence College has abandoned its Catholic identity and fidelity to Church teachings, particularly with regard to the sanctity of Marriage, and has succumbed to “political correctness.” In order to address several of the issues that have surfaced, I would like to make the following points:
1. The College always has, and always will, remain faithful to the teachings of the Catholic Church. We will do everything in our power to proclaim and explain these teachings to our students from the pulpit, in the classroom, and in the day-to day life of our campus. We will, however, do this in a spirit of Christ-like charity and compassion. This is especially important and challenging in difficult matters related to human sexuality. For those who do not accept the premises of the Church’s teaching on marriage and human sexuality, the doctrine can appear to be hard to accept or even harsh. Our challenge is to dialogue respectfully with those who disagree with the Church. This is especially a challenge for those on our campus who are members of the LGBTQ+ community. What I hear from members of that community is not that they expect us to disavow the Church’s teaching, but rather to find a way to help them feel included in the light of our Catholic identity and in a way that recognizes their inherent dignity as created in the image and likeness of God. Our collective challenge is to find a way to be faithful to our Catholic identity and to be inclusive.
2. I am distressed by the way Michael Smalanskas has been vilified and ostracized by many of his peers. While some might not agree with how he tried to express Church teaching, he is entitled to the same respect, charity, and protection that is due any student. There can be no place on our campus for bullying, harassment, or intimidation. The drawing of him that was posted in the St. Joseph Hall men’s room was odious and reprehensible. The Providence Police were notified, and the Office of Public Safety is attempting to determine who was responsible. If you have any information about this, I would encourage you to contact Public Safety.
Let me conclude by saying that I believe that the challenge to be faithful to our Catholic and Dominican identity and to be inclusive appears daunting. It is a challenge on every Catholic campus and in the Church as a whole. We are not alone. I take heart in the belief that God’s providence will guide us through our challenges as a community. It is my hope and prayer for our community that as we enter into the Church’s holiest time of the year, we will find the gift of a Resurrection that brings healing, reconciliation, and peace.
Fr. Brian Shanley
President
“Many will champion this communication from Fr. Shanley as a victory for faithful Catholics. While I appreciate that he addressed the issue more thoroughly today, there are still reasons for serious concern moving forward,” Smalanskas told LifeSiteNews.
Fr. Shanley’s “hesitation to speak forcefully on the matter speaks volumes,” he continued. “It took the president over three weeks to try and do something that could have easily been addressed immediately. He seems to suggest that his only reason for doing so was in response to the negative publicity and criticism from concerned Catholics, once again insulting anyone who is concerned about Catholic identity as uncharitable and angry.”
Smalanskas concluded:
Fr. Shanley affirms that the college has always and will always be faithful to Church teaching, yet for the last three weeks [and much longer], people have been rightfully concerned that this is not the case.
He continues to pit Catholic teaching against efforts toward inclusion. There will always be such a tension for Fr. Shanley and others who have a vision of inclusion that seems to desire express affirmation of the very lifestyle choices and behavior of LGBTQ people. Instead of using the vast treasury of the Church’s knowledge to approach diversity and inclusion in a way that draws people in and toward a higher good that has been revealed by God and ordained in nature, he comes across as exhausted by a rigid Church that is in desperate need of a new way to approach these issues.
A couple of events over the past few weeks brought to mind two towering people who had a tremendous effect on the Archdiocese of New York and the U.S. more broadly. Their witness is worth remembering, especially in this political moment.
Last Saturday’s feast of St. Patrick, the patron saint of our cathedral and archdiocese, reminded me of Archbishop John Hughes. As the first archbishop of New York (1842-64), “Dagger John” displayed dramatic reverence for the dignity of Irish immigrants. Thousands arrived daily in New York—penniless, starving and sometimes ill—only to be met with hostility, bigotry and injustice.
Portrait of Archbishop John Hughes, c. 1840s.PHOTO: GETTY IMAGES
An immigrant himself, Hughes prophetically and vigorously defended their dignity. Because the schools at the time were hostile to these immigrants, he initiated Catholic schools to provide children with a good education sensitive to their religion and to prepare them as responsible, patriotic citizens. The schools worked. Many remain open to this day, their mission unchanged.
The second event was the recent funeral of a great African-American woman, Dolores Grier. A convert to Catholicism, she was named vice chancellor of the archdiocese three decades ago by Cardinal John O’Connor; she was the first layperson and first woman to hold the prestigious position. Grier was passionate about civil rights, especially the right to life of babies in the womb. She never missed an opportunity to defend, lovingly but forcefully, their right to life.
Grier attributed her pro-life sensitivity to the Rev. Jesse Jackson, who preached that abortion was an act of genocide against minorities. No wonder, she often observed, abortuaries were clustered in poor black and brown neighborhoods. The statistics today confirm her observation: In 2013 there were more black babies aborted in New York City (29,007) than were born here (24,758), according to a reportfrom the New York City Department of Health and Mental Hygiene.
The values Archbishop Hughes and Dolores Grier cherished—the dignity and sanctity of human life, the importance of Catholic schools, the defense of a baby’s civil rights—were, and still are, widely embraced by Catholics. This often led Catholics to become loyal Democrats. I remember my own grandmother whispering to me, “We Catholics don’t trust those Republicans.”
Such is no longer the case, a cause of sadness to many Catholics, me included. The two causes so vigorously promoted by Hughes and Grier—the needs of poor and middle-class children in Catholic schools, and the right to life of the baby in the womb—largely have been rejected by the party of our youth. An esteemed pro-life Democrat in Illinois, Rep. Dan Lipinski, effectively was blacklisted by his own party. Last year, Democratic National Committee Chairman Tom Perez insisted that pro-life candidates have no place in the modern Democratic Party.
It is particularly chilly for us here in the state Hughes and Grier proudly called their earthly home. In recent years, some Democrats in the New York state Assembly repeatedly blocked education tax credit legislation, which would have helped middle-class and low-income families make the choice to select Catholic or other nonpublic schools for their children. Opposing the bill reduces the ability of fine Catholic schools across the state to continue their mission of serving the poor, many of them immigrants.
More sobering, what is already the most radical abortion license in the country may soon be even more morbidly expanded. For instance, under the proposed Reproductive Health Act, doctors would not be required to care for a baby who survives an abortion. The newborn simply would be allowed to die without any legal implications. And abortions would be legal up to the moment of birth.
The “big tent” of the Democratic Party now seems a pup tent. Annafi Wahed, a former staffer to Hillary Clinton, recently wrote in this newspaper about her experience attending the Conservative Political Action Conference. She complimented the conservative attendees, pointing out that most made her feel welcome at their meeting. They listened attentively to her views—a courtesy, she had to admit, that would not be given to them at a meeting of political liberals.
I’m a pastor, not a politician, and I’ve certainly had spats and disappointments with politicians from both of America’s leading parties. But it saddens me, and weakens the democracy millions of Americans cherish, when the party that once embraced Catholics now slams the door on us.
To Archbishop Hughes, Dolores Grier, and Grandma Dolan, I’m sorry to have to write this. But not as sad as you are to know it is true.
WASHINGTON, D.C. – His Excellency, the Most Reverend Timothy P. Broglio, J.C.D., Archbishop for the Military Services, USA, issued the following statement today on President Trump’s decision to disqualify transgender individuals from military service:
“Saint Pope John Paul the Second wrote that, ‘Every individual, precisely by reason of the mystery of the Word of God who was made flesh (cf. Jn 1:14), is entrusted to the maternal care of the Church.’ This care extends from the time an individual is conceived, until natural death, and every point of life in between. It is offered regardless of personal choices or conditions, because Christ offers salvation to all people.
“Earlier this week, citing a detriment to military readiness and the cost associated with gender reassignment surgeries and therapies, President Trump banned individuals who identify as transgender from serving in the military in any capacity.
“Certainly military readiness is of utmost importance to our servicemen and women who selflessly risk personal safety to defend the values and freedoms of our Nation. The President’s announcement and the prevailing response, however, fail to address the essence of the issue – the dignity of the human person.
“The dignity of the human person is rooted in the fact that people are created in the image and likeness of God – God who in the fullness of his divinity assumed humanity to redeem the world. A recent conference, titled ‘Framing a Catholic Response to Gender Ideology’ held this past May at Saint John Vianney Theological Seminary in Denver, noted that gender ideology undermines basic Christian anthropology by defining the person as a disembodied mind and the body as a mere instrument. A Catholic response to gender ideology considers multiple insights including medical, psychological, philosophical, theological, pastoral, and legal perspectives. The Church honors human dignity by drawing near in order to accompany people.
“Sexual orientation and gender identity issues reflect a rapidly increasing and incorrect societal attitude that individual behaviors in life should pursue immediate and personal choices rather than eternal truth. In extending the maternal care of the Church to the faithful of this Archdiocese, it is opportune to reaffirm that personal choices in life, whether regarding the protection of the unborn, the sanctity of marriage and the family, or the acceptance of a person’s God-created biology, should be made not solely for a penultimate reality on this earth but in anticipation of the ultimate reality of sharing in the very life of God in heaven.”
Colloquium “The Source of the Future” (“Quelle der Zukunft”) on the occasion of the 10th anniversary of the publication of the Motu proprio Summorum Pontificum by Pope Benedict XVI
March 29 – April 1, 2017 Herzogenrath, near Aachen (Germany)
Introductory Message
First of all I wish to thank from the bottom of my heart the organizers of the Colloquium entitled “The Source of the Future” on the occasion of the tenth anniversary of the Motu proprio Summorum Pontificum by Pope Benedict XVI, in Herzogenrath, for allowing me to offer an introduction to your reflections on this subject, which is so important for the life of the Church and, more particularly, for the future of the Liturgy; I do so with great joy. I would like to greet very cordially all the participants in this Colloquium, particularly the members of the following associations whose names are mentioned on the invitation that you so kindly sent me, and I hope that I do not forget any: Una Voce Germany; The Catholic Circle of the Priests and Laity of the Archdioceses of Hamburg and Cologne; The Cardinal Newman Association; the Network of the priests of Saint Gertrude Parish in Herzogenrath. As I wrote to the Rev. Father Guido Rodheudt, pastor of Saint Gertrude Parish in Herzogenrath, I am very sorry that I had to forgo participating in your Colloquium because of obligations that came up unexpectedly and were added to a schedule that was already very busy. Nevertheless, be assured that I will be among you through prayer: it will accompany you every day, and of course you will all be present at the offertory of the daily Holy Mass that I will celebrate during the four days of your Colloquium, from March 29 to April 1. I will therefore start off your proceedings to the best of my ability with a brief reflection on the way that the Motu proprio Summorum Pontificumshould be applied in unity and peace.
As you know, what was called “the liturgical movement” in the early twentieth century was the intention of Pope Saint Pius X, expressed in another Motu proprio entitled Tra le sollicitudini (1903), to restore the liturgy so as to make its treasures more accessible, so that it might also become again the source of authentically Christian life. Hence the definition of the liturgy as “summit and source of the life and mission of the Church” found in the Constitution on the Sacred Liturgy Sacrosanctum Concilium of Vatican Council II (see n. 10). And it can never be repeated often enough that the Liturgy, as summit and source of the Church, has its foundation in Christ Himself. In fact, Our Lord Jesus Christ is the sole and definitive High Priest of the New and Eternal Covenant, since He offered Himself in sacrifice, and “by a single offering He has perfected for all time those whom He sanctifies” (cf. Heb 10:14). Thus as the Catechism of the Catholic Church declares, “It is this mystery of Christ that the Church proclaims and celebrates in her liturgy so that the faithful may live from it and bear witness to it in the world” (n. 1068). This “liturgical movement”, one of the finest fruits of which was the Constitution Sacrosanctum Concilium, is the context in which we ought to consider the Motu proprio Summorum Pontificum dated July 7, 2007; we are happy to celebrate this year with great joy and thanksgiving the tenth anniversary of its promulgation. We can say therefore that the “liturgical movement” initiated by Pope Saint Pius X was never interrupted, and that it still continues in our days following the new impetus given to it by Pope Benedict XVI. On this subject we might mention the particular care and personal attention that he showed in celebrating the Sacred Liturgy as Pope, and then the frequent references in his speeches to its centrality in the life of the Church, and finally his two Magisterial documents Sacramentum Caritatisand Summorum Pontificum. In other words, what is called liturgical aggiornamento1 was in a way completed by the Motu proprio Summorum Pontificum by Pope Benedict XVI. What was it about? The Pope emeritus made the distinction between two forms of the same Roman rite: a so-called “ordinary” form, referring to the liturgical texts of the Roman Missal as revised following the guidelines of Vatican Council II, and a form designated “extraordinary” that corresponds to the liturgy that was in use before the liturgical aggiornamento. Thus, presently, in the Roman or Latin rite, two missals are in force: that of Blessed Pope Paul VI, the third edition of which is dated 2002, and that of Saint Pius V, the last edition of which, promulgated by Saint John XXIII, goes back to 1962.
In his Letter to the Bishops that accompanied the Motu proprio, Pope Benedict XVI clearly explained that the purpose for his decision to have the two missals coexist was not only to satisfy the wishes of certain groups of the faithful who are attached to the liturgical forms prior to the Second Vatican Council, but also to allow for the mutual enrichment of the two forms of the same Roman rite, in other words, not only their peaceful coexistence but also the possibility of perfecting them by emphasizing the best features that characterize them. He wrote in particular that “the two Forms of the usage of the Roman rite can be mutually enriching: new Saints and some of the new Prefaces can and should be inserted in the old Missal…. The celebration of the Mass according to the Missal of Paul VI will be able to demonstrate, more powerfully than has been the case hitherto, the sacrality which attracts many people to the former usage.” These then are the terms in which the Pope emeritus expressed his desire to re-launch the “liturgical movement”. In parishes where it has been possible to implement the Motu proprio, pastors testify to the greater fervor both in the faithful and in the priests, as Father Rodheudt himself can bear witness. They have also noted a repercussion and a positive spiritual development in the way of experiencing Eucharistic liturgies according to the Ordinary Form, particularly the rediscovery of postures expressing adoration of the Blessed Sacrament: kneeling, genuflection, etc., and also greater recollection characterized by the sacred silence that should mark the important moments of the Holy Sacrifice of the Mass, so as to allow the priests and the faithful to interiorize the mystery of faith that is being celebrated. It is true also that liturgical and spiritual formation must be encouraged and promoted. Similarly, it will be necessary to promote a thoroughly revised pedagogy in order to get beyond an excessively formal “rubricism” in explaining the rites of the Tridentine Missal to those who are not yet familiar with it, or who are only partly acquainted with it…and sometimes not impartially. To do that, it is urgently necessary to finalize a bilingual Latin-vernacular missal to allow for full, conscious, intimate and more fruitful participation of the lay faithful in Eucharistic celebrations. It is also very important to emphasize the continuity between the two missals by appropriate liturgical catecheses…. Many priests testify that this is a stimulating task, because they are conscious of working for the liturgical renewal, of contributing their own efforts to the “liturgical movement” that we were just talking about, in other words, in reality, to this mystical and spiritual renewal that is therefore missionary in character, which was intended by the Second Vatican Council, to which Pope Francis is vigorously calling us. The liturgy must therefore always be reformed so as to be more faithful to its mystical essence. But most of the time, this “reform” that replaced the genuine “restoration” intended by the Second Vatican Council was carried out in a superficial spirit and on the basis of only one criterion: to suppress at all costs a heritage that must be perceived as totally negative and outmoded so as to excavate a gulf between the time before and the time after the Council. Now it is enough to pick up the Constitution on the Sacred Liturgy again and to read it honestly, without betraying its meaning, to see that the true purpose of the Second Vatican Council was not to start a reform that could become the occasion for a break with Tradition, but quite the contrary, to rediscover and to confirm Tradition in its deepest meaning. In fact, what is called “the reform of the reform”, which perhaps ought to be called more precisely “the mutual enrichment of the rites”, to use an expression from the Magisterium of Benedict XVI, is a primarily spiritual necessity. And it quite obviously concerns the two forms of the Roman rite. The particular care that should be brought to the liturgy, the urgency of holding it in high esteem and working for its beauty, its sacral character and keeping the right balance between fidelity to Tradition and legitimate development, and therefore rejecting absolutely and radically any hermeneutic of discontinuity or rupture: these essential elements are the heart of all authentic Christian liturgy. Cardinal Joseph Ratzinger tirelessly repeated that the crisis that has shaken the Church for fifty years, chiefly since Vatican Council II, is connected with the crisis of the liturgy, and therefore to the lack of respect, the desacralization and the leveling of the essential elements of divine worship. “I am convinced,” he writes, “that the crisis in the Church that we are experiencing today is to a large extent due to the disintegration of the liturgy.”2
Certainly, the Second Vatican Council wished to promote greater active participation by the people of God and to bring about progress day by day in the Christian life of the faithful (see Sacrosanctum Concilium, n. 1). Certainly, some fine initiatives were taken along these lines. However we cannot close our eyes to the disaster, the devastation and the schism that the modern promoters of a living liturgy caused by remodeling the Church’s liturgy according to their ideas. They forgot that the liturgical act is not just a PRAYER, but also and above all a MYSTERY in which something is accomplished for us that we cannot fully understand but that we must accept and receive in faith, love, obedience and adoring silence. And this is the real meaning of active participation of the faithful. It is not about exclusively external activity, the distribution of roles or of functions in the liturgy, but rather about an intensely active receptivity: this reception is, in Christ and with Christ, the humble offering of oneself in silent prayer and a thoroughly contemplative attitude. The serious crisis of faith, not only at the level of the Christian faithful but also and especially among many priests and bishops, has made us incapable of understanding the Eucharistic liturgy as a sacrifice, as identical to the act performed once and for all by Jesus Christ, making present the Sacrifice of the Cross in a non-bloody manner, throughout the Church, through different ages, places, peoples and nations. There is often a sacrilegious tendency to reduce the Holy Mass to a simple convivial meal, the celebration of a profane feast, the community’s celebration of itself, or even worse, a terrible diversion from the anguish of a life that no longer has meaning or from the fear of meeting God face to face, because His glance unveils and obliges us to look truly and unflinchingly at the ugliness of our interior life. But the Holy Mass is not a diversion. It is the living sacrifice of Christ who died on the cross to free us from sin and death, for the purpose of revealing the love and the glory of God the Father. Many Catholics do not know that the final purpose of every liturgical celebration is the glory and adoration of God, the salvation and sanctification of human beings, since in the liturgy “God is perfectly glorified and men are sanctified” (Sacrosanctum Concilium, n. 7). Most of the faithful—including priests and bishops—do not know this teaching of the Council. Just as they do not know that the true worshippers of God are not those who reform the liturgy according to their own ideas and creativity, to make it something pleasing to the world, but rather those who reform the world in depth with the Gospel so as to allow it access to a liturgy that is the reflection of the liturgy that is celebrated from all eternity in the heavenly Jerusalem. As Benedict XVI often emphasized, at the root of the liturgy is adoration, and therefore God. Hence it is necessary to recognize that the serious, profound crisis that has affected the liturgy and the Church itself since the Council is due to the fact that its CENTER is no longer God and the adoration of Him, but rather men and their alleged ability to “do” something to keep themselves busy during the Eucharistic celebrations. Even today, a significant number of Church leaders underestimate the serious crisis that the Church is going through: relativism in doctrinal, moral and disciplinary teaching, grave abuses, the desacralization and trivialization of the Sacred Liturgy, a merely social and horizontal view of the Church’s mission. Many believe and declare loud and long that Vatican Council II brought about a true springtime in the Church. Nevertheless, a growing number of Church leaders see this “springtime” as a rejection, a renunciation of her centuries-old heritage, or even as a radical questioning of her past and Tradition. Political Europe is rebuked for abandoning or denying its Christian roots. But the first to have abandoned her Christian roots and past is indisputably the post-conciliar Catholic Church. Some episcopal conferences even refuse to translate faithfully the original Latin text of the Roman Missal. Some claim that each local Church can translate the Roman Missal, not according to the sacred heritage of the Church, following the methods and principles indicated by Liturgiam authenticam, but according to the fantasies, ideologies and cultural expressions which, they say, can be understood and accepted by the people. But the people desire to be initiated into the sacred language of God. The Gospel and revelation themselves are “reinterpreted”, “contextualized” and adapted to decadent Western culture. In 1968, the Bishop of Metz, in France, wrote in his diocesan newsletter a horrible, outrageous thing that seemed like the desire for and expression of a complete break with the Church’s past. According to that bishop, today we must rethink the very concept of the salvation brought by Jesus Christ, because the apostolic Church and the Christian communities in the early centuries of Christianity had understood nothing of the Gospel. Only in our era has the plan of salvation brought by Jesus been understood. Here is the audacious, surprising statement by the Bishop of Metz:
The transformation of the world (change of civilization) teaches and demands a change in the very concept of the salvation brought by Jesus Christ; this transformation reveals to us that the Church’s thinking about God’s plan was, before the present change, insufficiently evangelical…. No era has been as capable as ours of understanding the evangelical ideal of fraternal life.3
With a vision like that, it is not surprising that devastation, destruction and wars have followed and persisted these days at the liturgical, doctrinal and moral level, because they claim that no era has been capable of understanding the “evangelical ideal” as well as ours. Many refuse to face up to the Church’s work of self-destruction through the deliberate demolition of her doctrinal, liturgical, moral and pastoral foundations. While more and more voices of high-ranking prelates stubbornly affirm obvious doctrinal, moral and liturgical errors that have been condemned a hundred times and work to demolish the little faith remaining in the people of God, while the bark of the Church furrows the stormy sea of this decadent world and the waves crash down on the ship, so that it is already filling with water, a growing number of Church leaders and faithful shout: “Tout va très bien, Madame la Marquise!” [“Everything is just fine, Milady,” the refrain of a popular comic song from the 1930’s, in which the employees of a noblewoman report to her a series of catastrophes]. But the reality is quite different: in fact, as Cardinal Ratzinger said:
What the Popes and the Council Fathers were expecting was a new Catholic unity, and instead one has encountered a dissension which—to use the words of Paul VI—seems to have passed over from self-criticism to self-destruction. There had been the expectation of a new enthusiasm, and instead too often it has ended in boredom and discouragement. There had been the expectation of a step forward, and instead one found oneself facing a progressive process of decadence that to a large measure has been unfolding under the sign of a summons to a presumed “spirit of the Council” and by so doing has actually and increasingly discredited it.4
“No one can seriously deny the critical manifestations” and liturgy wars that Vatican Council II led to.5Today they have gone on to fragment and demolish the sacred Missale Romanum by abandoning it to experiments in cultural diversity and compilers of liturgical texts. Here I am happy to congratulate the tremendous, marvelous work accomplished, through Vox Clara, by the English-language Episcopal Conferences, by the Spanish- and Korean-language Episcopal Conferences, etc., which have faithfully translated the Missale Romanum in perfect conformity with the guidelines and principles of Liturgiam authenticam, and the Congregation for Divine Worship and the Discipline of the Sacraments has granted them the recognitio [approval].
Following the publication of my book God or Nothing, people have asked me about the “liturgy wars” which for decades have too often divided Catholics. I stated that that is an aberration, because the liturgy is the field par excellence in which Catholics ought to experience unity in the truth, in faith and in love, and consequently that it is inconceivable to celebrate the liturgy while having in one’s heart feelings of fratricidal struggle and rancor. Besides, did Jesus not speak very demanding words about the need to go and be reconciled with one’s brother before presenting his own sacrifice at the altar? (See Mt 5:23-24.)
The liturgy in its turn moves the faithful, filled with “the paschal sacraments,” to be “one in holiness”6; it prays that “they may hold fast in their lives to what they have grasped by their faith”; the renewal in the Eucharist of the covenant between the Lord and man draws the faithful into the compelling love of Christ and sets them on fire. From the liturgy, therefore, and especially from the Eucharist, as from a font, grace is poured forth upon us; and the sanctification of men in Christ and the glorification of God, to which all other activities of the Church are directed as toward their end, is achieved in the most efficacious possible way. (Sacrosanctum Concilium, n. 10)
In this “face-to-face encounter” with God, which the liturgy is, our heart must be pure of all enmity, which presupposes that everyone must be respected with his own sensibility. This means concretely that, although it must be reaffirmed that Vatican Council II never asked to make tabula rasa of the past and therefore to abandon the Missal said to be of Saint Pius V, which produced so many saints, not to mention three such admirable priests as Saint John Vianney, the Curé of Ars, Saint Pius of Pietrelcina (Padre Pio) and Saint Josemaría Escrivá de Balaguer, at the same time it is essential to promote the liturgical renewal intended by that same Council, and therefore the liturgical books were updated following the Constitution Sacrosanctum Concilium, in particular the Missal said to be of Blessed Pope Paul VI. And I added that what is important above all, whether one is celebrating in the Ordinary or the Extraordinary Form, is to bring to the faithful something that they have a right to: the beauty of the liturgy, its sacrality, silence, recollection, the mystical dimension and adoration. The liturgy should put us face to face with God in a personal relationship of intense intimacy. It should plunge us into the inner life of the Most Holy Trinity. Speaking of the usus antiquior (the older form of the Mass) in his Letter that accompanies Summorum Pontificum, Pope Benedict XVI said that
Immediately after the Second Vatican Council it was presumed that requests for the use of the 1962 Missal would be limited to the older generation which had grown up with it, but in the meantime it has clearly been demonstrated that young persons too have discovered this liturgical form, felt its attraction and found in it a form of encounter with the Mystery of the Most Holy Eucharist, particularly suited to them.
This is an unavoidable reality, a true sign of our times. When young people are absent from the holy Liturgy, we must ask ourselves: Why? We must make sure that the celebrations according to the usus recentior (the newer form of the Mass) facilitate this encounter too, that they lead people on the path of the via pulchritudinis (the way of beauty) that leads through her sacred rites to the living Christ and to the work within His Church today. Indeed, the Eucharist is not a sort of “dinner among friends”, a convivial meal of the community, but rather a sacred Mystery, the great Mystery of our faith, the celebration of the Redemption accomplished by Our Lord Jesus Christ, the commemoration of the death of Jesus on the cross to free us from our sins. It is therefore appropriate to celebrate Holy Mass with the beauty and fervor of the saintly Curé of Ars, of Padre Pio or Saint Josemaría, and this is the sine qua non condition for arriving at a liturgical reconciliation “by the high road”, if I may put it that way.7 I vehemently refuse therefore to waste our time pitting one liturgy against another, or the Missal of Saint Pius V against that of Blessed Paul VI. Rather, it is a question of entering into the great silence of the liturgy, by allowing ourselves to be enriched by all the liturgical forms, whether they are Latin or Eastern. Indeed, without this mystical dimension of silence and without a contemplative spirit, the liturgy will remain an occasion for hateful divisions, ideological confrontations and the public humiliation of the weak by those who claim to hold some authority, instead of being the place of our unity and communion in the Lord. Thus, instead of being an occasion for confronting and hating each other, the liturgy should bring us all together to unity in the faith and to the true knowledge of the Son of God, to mature manhood, to the measure of the stature of the fullness of Christ… and, by living in the truth of love, we will grow into Christ so as to be raised up in all things to Him who is the Head (cf. Eph 4:13-15).8
As you know, the great German liturgist Msgr. Klaus Gamber (1919-1989) used the word Heimat to designate this common home or “little homeland” of Catholics gathered around the altar of the Holy Sacrifice. The sense of the sacred that imbues and irrigates the rites of the Church is the inseparable correlative of the liturgy. Now in recent decades, many, many of the faithful have been ill treated or profoundly troubled by celebrations marked with a superficial, devastating subjectivism, to the point where they did not recognize their Heimat, their common home, whereas the youngest among them had never known it! How many have tiptoed away, particularly the least significant and the poorest among them! They have become in a way “liturgically stateless persons”. The “liturgical movement”, with which the two forms (of the Latin rite) are associated, aims therefore to restore to them their Heimatand thus to bring them back into their common home, for we know very well that, in his works on sacramental theology, Joseph Cardinal Ratzinger, well before the publication of Summorum Pontificum, had pointed out that the crisis in the Church and therefore the crisis of the weakening of the faith comes in large measure from the way in which we treat the liturgy, according to the old adage: lex orandi, lex credendi(the law of faith is the law of prayer). In the preface that he wrote for the French edition of the magisterial volume by Msgr. Gamber, La réforme de la liturgie romaine [English edition: The Reform of the Roman Liturgy], the future Pope Benedict XVI said this, and I quote:
A young priest told me recently, “What we need today is a new liturgical movement.” This was an expression of a concern which nowadays only willfully superficial minds could ignore. What mattered to this priest was not winning new, daring liberties: what liberty has not been arrogantly taken already? He thought that we needed a new start coming from within the liturgy, just as the liturgical movement had intended when it was at the height of its true nature, when it was not a matter of fabricating texts or inventing actions and forms, but of rediscovering the living center, of penetrating into the tissue, strictly speaking, of the liturgy, so that the celebration thereof might proceed from its very substance. The liturgical reform, in its concrete implementation, has strayed ever farther from this origin. The result was not a revival but devastation. On the one hand, we have a liturgy that has degenerated into a show, in which one attempts to make religion interesting with the help of fashionable innovations and catchy moral platitudes, with short-lived successes within the guild of liturgical craftsmen, and an even more pronounced attitude of retreat from them on the part of those who seek in the liturgy not a spiritual “emcee”, but rather an encounter with the living God before Whom all “making” becomes meaningless, since that encounter alone is capable of giving us access to the true riches of being. On the other hand, there is the conservation of the ritual forms whose grandeur is always moving, but which, taken to the extreme, manifests a stubborn isolation and finally leaves nothing but sadness. Surely, between these two poles there are still all the priests and their parishioners who celebrate the new liturgy with respect and solemnity; but they are called into question by the contradiction between the two extremes, and the lack of internal unity in the Church finally makes their fidelity appear, wrongly in many cases, to be merely a personal brand of neo-conservatism. Because that is the situation, a new spiritual impulse is necessary if the liturgy is to be once more for us a communitarian activity of the Church and to be delivered from arbitrariness. One cannot “fabricate” a liturgical movement of that sort—any more than one can “fabricate” a living thing—but one can contribute to its development by striving to assimilate anew the spirit of the liturgy, and by defending publicly what one has received in this way.
I think that this long citation, which is so accurate and clear, should be of interest to you, at the beginning of this Colloquium, and also should help to start off your reflections on “the source of the future” (“die Quelle der Zukunft”) of the Motu proprio Summorum Pontificum. Indeed, allow me to communicate to you a conviction that I have held deeply for a long time: the Roman liturgy, reconciled in its two forms, which is itself the “fruit of a development”, as the great German liturgist Joseph Jungmann (1889-1975) put it, can initiate the decisive process of the “liturgical movement” that so many priests and faithful have awaited for so long. Where to begin? I take the liberty of proposing to you the three following paths, which I sum up in the three letters SAF: silence-adoration-formation in English and French, and in German: SAA, Stille-Anbetung-Ausbildung. First of all, sacred silence, without which we cannot encounter God. In my book The Power of Silence, [La Force du silence] I write: “In silence, a human being gains his nobility and his grandeur only if he is on his knees in order to hear and adore God” (n. 66). Next, adoration; in this regard I cite my spiritual experience in the same book, The Power of Silence:
For my part, I know that all the great moments of my day are found in the incomparable hours that I spend on my knees in darkness before the Most Blessed Sacrament of the Body and Blood of Our Lord Jesus Christ. I am so to speak swallowed up in God and surrounded on all sides by His presence. I would like to belong now to God alone and to plunge into the purity of His Love. And yet, I can tell how poor I am, how far from loving the Lord as He loved me to the point of giving Himself up for me. (n. 54)
Finally, liturgical formation based on a proclamation of the faith or catechesis that refers to the Catechism of the Catholic Church, which protects us from possible more-or-less learned ravings of some theologians who long for “novelties”. This is what I said in this connection in what is now commonly called, with some humor, the “London Discourse” of July 5, 2016, given during the Third International Conference of Sacra Liturgia:
The liturgical formation that is primary and essential is…one of immersion in the liturgy, in the deep mystery of God our loving Father. It is a question of living the liturgy in all its richness, so that having drunk deeply from its fount we always have a thirst for its delights, its order and beauty, its silence and contemplation, its exultation and adoration, its ability to connect us intimately with He who is at work in and through the Church’s sacred rites.9
In this global context, therefore, and in a spirit of faith and profound communion with Christ’s obedience on the cross, I humbly ask you to apply Summorum Pontificum very carefully; not as a negative, backward measure that looks toward the past, or as something that builds walls and creates a ghetto, but as an important and real contribution to the present and future liturgical life of the Church, and also to the liturgical movement of our era, from which more and more people, and particularly young people, are drawing so many things that are true, good and beautiful.
I would like to conclude this introduction with the luminous words of Benedict XVI at the end of the homily that he gave in 2008, on the Solemnity of Saints Peter and Paul: “When the world in all its parts has become a liturgy of God, when, in its reality, it has become adoration, then it will have reached its goal and will be safe and sound.”
I thank you for your kind attention. And may God bless you and fill your lives with His silent Presence!
Robert Cardinal Sarah
Prefect of the Congregation for Divine Worship and the Discipline of the Sacraments
(Translation from the French original by Michael J. Miller.)
Endnotes:
1“Aggiornamento” is an Italian term that means literally: “updating”. We celebrated the fiftieth anniversary of the Constitution on the Sacred Liturgy of Vatican Council II Sacrosanctum Concilium in 2013, since it was promulgated on December 4, 1963.
2 Joseph Ratzinger, Milestones: Memoirs: 1927-1977, translated by Erasmo Leiva-Merikakis (San Francisco: Ignatius Press, 1998), 148.
3 Cited by Jean Madiran, L’hérésie du XX siècle (Paris: Nouvelles Editions Latines [NEL], 1968), 166.
Father Tad Pacholczyk
Director of Education
The National Catholic Bioethics Center
A major study published on December 7 in the New England Journal of Medicine concludes that hormonal contraception increases the risk of breast cancer for women. The research used all of Denmark as its sample, following nearly 1.8 million Danish women of childbearing age for over a decade. The study, as described by the New York Times, “upends widely held assumptions about modern contraceptives for younger generations of women,” especially the view that “newer hormonal contraceptives are much safer than those taken by their mothers or grandmothers.” It also establishes that the risk to women increases with longer periods of use. Major media outlets have done their best to minimize the implications of the study and “soften the blow” for the millions who, for decades, have faithfully embraced a “contraceptive mentality.”
This mentality has promoted contraception, especially the Pill, as a path for women to move toward
equality with men by enabling them to reap the “benefits” of the sexual revolution. But Mary Rice Hasson, J.D., director of the Catholic Women’s Forum at the Ethics and Public Policy Center in Washington, D.C. notes that the reality for women is very different, and “our lived experience has shown that this is a false promise.” Countless women, she emphasizes, have ended up being vulnerable to, and harmed by, the sexual revolution and its promotion of contraception as “the solution.” They have been given a “bitter pill” in the form of the Pill.
In a remarkably prescient passage dating back to July, 1968, Pope Paul VI already foresaw this
in his encyclical Humanae Vitae, the momentous and beautiful document explaining not only the
moral problems with contraception, but also its devastating effects on men, families and women in particular. Contraception, he writes,opens a wide and easy road
“towards conjugal infidelity and the general lowering of morality. Not much experience is needed in order to know human weakness, and to understand that men–especially the young, who are so vulnerable on this point– have need of encouragement to be faithful to the moral law, so that they must not be offered some easy means of eluding its observance. It is also to be feared that the man, growing used to the employment of anti-conceptive practices, may finally lose respect for the woman and, no longer caring for her physical and psychological equilibrium, may come to the point of considering her as a mere instrument of selfish enjoyment, and no longer as his respected and beloved companion.”
Paul VI offers a profound, but unpopular, observation — that contraception is harmful to women, and
is, in fact, anti-woman. The widespread adoption of the “contraceptive mentality” has led inexorably to a new perspective on women, namely, that they should be more like men, and therefore they should, like men, become impregnable, through the ongoing practice of contraception. Very young women, sometimes just entering puberty, are now placed onto regimens of hormonal contraception that can continue for years or even decades. From this perspective, their ability to conceive life becomes tantamount to a malady needing to be remedied, a “defect” that renders them “unequal” to men. Strikingly, though, ever greater numbers of women are discovering an authentic and liberating form of feminism as they come to the awareness that, in the words of Hasson, “we don’t have a design flaw. Being a woman is good… and it’s a wonderful thing.” Wonderful, too, is that confident feminism and liberating sense of self-control that enables a woman to choose abstinence before marriage, rather than contraception, and, once married, to choose periodic abstinence in agreement with her husband if their circumstances indicate they ought to avoid a pregnancy.
Hormonal contraceptives, meanwhile, throw a wrench into the works on a number of different levels.
Beyond setting up a woman to be “used” by men, the Pill (and hormone-releasing IUD’s) cause significant alterations in her delicately-balanced physiology. These include restricting her ability to ovulate, altering her cycles and secretions, and modifying her uterine lining — in effect, forcing her body into a pseudo-pregnant state to exclude the possibility of a real pregnancy. Whenever a woman takes these kinds of steps to disrupt her natural fertility, it should come as little surprise that her body rebels in one fashion or another, including possible weight gain, headaches, depression, and the heightened and well-documented risk of thrombotic stroke, myocardial infarction (heart attack), and — as confirmed by the recent study — breast cancer. A woman’s body doesn’t stand in need of being “fixed” by these powerful drugs that wreak havoc on her biology.
The Church’s ageless but countercultural teaching on contraception respects and uplifts women. It supports them in an authentic feminism that affirms their uniquely important maternal role in family and society, and esteems their fruitfulness in marriage not as a defect, but as a real gift.
March 22, 2018, (LifeSiteNews) – A newly developed contraceptive pill for men, now in trials, works by reducing the presence of testosterone in adult males to levels typically found only in prepubescent boys and girls.
One of the side effects among some of test subjects is decreased libido, also a common side effect of female contraceptives.
Despite the drug’s side effects and impact on the male body, mainstream media outlets are hailing this as “a male birth control pill that is both safe and effective.”
The results of the study were presented Sunday at the annual Endocrine Society meeting in Chicago. The researchers found that the proposed hormone pill, called dimethandrolone undecanoate or DMAU, effectively reduced testosterone and other hormone levels responsible for sperm production without any serious side effects, according to Dr. Stephanie Page, an endocrinologist at the University of Washington School of Medicine and a lead author of the study.
“Our goal – and everyone’s goal in this field – is to develop a method for men that has minimal side effects, and the holy grail would be to develop something that also has a health benefit for men,” Page said.
Researchers studied 83 men between the ages of 18 and 50 who were divided into four groups. The first was a control group, and the remaining three groups received the drug in dosages of 100, 200, or 400 milligrams.
After men ingested the drug for 28 days, “testosterone in the blood dropped to castrate levels for all three doses,” according to the CNN report. “‘Castrate levels’ refers to the target range of testosterone in the blood after chemical or surgical castration and is usually defined as 50 nanograms per deciliter.”
Normal testosterone levels in adult males ranges from 350 to 1,100 nanograms per deciliter.
DMAU works by tricking the body into believing that testosterone levels are normal while reducing testosterone production, subsequently reducing sperm production.
The next round of DMAU trials will focus on sperm production levels, which weren’t actually observed during the first set of tests.
Growing boys and men require testosterone for building muscle mass, bone density, mental sharpness, and depression avoidance. It is also what produces male sexual desire.
The question that will no doubt face the manufacturers and marketers of DMAU is, “How do you get male customers to pay for a product that will chemically castrate them?”
SUMTER, South Carolina, March 22, 2018, (LifeSiteNews) – Kimberly Henderson is a musician who rose to prominence in 2014 thanks to a viral video of her singing to her baby daughter Vaida. And it would never have happened had God not convinced her to walk out of an abortion facility the year before.
On Monday, the Daily Wire revisited Henderson’s story, which she details in full on Facebook. “I sat in the abortion clinic for nearly 7 hours,” she writes. “I remember wearing a pink t shirt that was soaking wet from crying.” She had made the March 15, 2013 visit out of fear of having another child all alone, her outlook further worsened by a cheating boyfriend and fear of what others might think of her.
Despite part of her being desperate to justify the abortion and feeling she had no other choice, Henderson says a heavy heart kept her in conflict and desperate for a divine signal of what to do. “I prayed God would stop and give me a sign, give me the strength to get up and walk out of here,” she says…which is exactly what happened next.
When she was finally called to the front desk, Henderson says that fumbling through her wallet caused a card she had received the previous Saturday to fall out. It was a church card bearing Isaiah 41:10:
“Don’t be afraid, for I am with you. Don’t be discouraged, for I am your God. I will strengthen you and help you. I will hold you up with my victorious right hand.”
Henderson is convinced God was speaking to her through that card, which finally gave her the will to turn around.
On her way out the door, a girl Henderson estimates to be 19 years old lamented, “I wish I could be brave like you.” Henderson told her she could do the same thing, but the girl replied that unspecified “serious circumstances” left her with no other choice.
Before they parted, though, the girl told her, “When you see your baby’s face for the first time you’re gonna be so glad you walked out of here today.”
Today, Henderson is more than glad; she is fulfilled.
“My daughter Vaida Everly has a purpose. Her name means beautiful life. And lord she is just that,” Henderson writes, a source of inexplicable joy such that “if a war was going on outside I wouldn’t even know it.”
Just two months after that first video went viral, Henderson was contacted to professionally record a single, “Tiny Hearts,” based on her story. Her musical career has skyrocketed since, leading her to speak with multiple record labels and songwriters, acquire a business manager, and as of the time of this writing, amass more than nine million YouTube views.
Ultimately, Henderson believes the experience was God’s way of “showing me that HIS plan is and will always be greater and bigger than anything and everything I’ve ever known […] No matter what your circumstances are God doesn’t make mistakes and he is here for you.”
I still remember experiencing the wonder of walking up and down the aisles of Toys R Us as a child visiting America from New Zealand. To be honest I think my parents were as awed as I was at the rows and rows of Barbie dolls and Ninja turtles, especially coming from a country that did not yet have such a huge range of mass-produced toys available.
It was a time when the age of mass materialism was only just upon us and held wonder and magic. I ended up buying a Little Mermaid sheet set and giant, long, variously coloured ice-blocks which we savoured all that summer, though I do now question my parents’ use of suitcase space.
However, Toys R Us has obviously not managed to maintain the magic. As it prepares to close its doors, people are questioning what went wrong for the once mighty, culturally emblematic business. In its court filing, one of the factors Toys R Us itself has blamed is the world’s low birth rates:
The decrease of birthrates in countries where we operate could negatively affect our business. Most of our end-customers are newborns and children and, as a result, our revenue are dependent on the birthrates in countries where we operate. In recent years, many countries’ birthrates have dropped or stagnated as their population ages, and education and income levels increase. A continued and significant decline in the number of newborns and children in these countries could have a material adverse effect on our operating results.
Although online competition and bad financial and operational decisions must also surely be factors, the company claims in its annual report that its income is linked to birthrates, and it appears to be right. Fertility has declined worldwide to unprecedented levels since the 1970s and by 2011 total fertility was below 1.4 children per woman in about half of developed countries. As The Washington Post observes, the change in the number of children born in the previous 12 years tracks closely with the company’s changing annual revenue, as shown by the following graphs:
Some are wondering if Toys R Us is just the first of many businesses to feel the economic effects of the lower population growth which will eventually affect the whole economy. I have previously discussed some of the far-reaching economic ramifications of an aging population here and in numerous other posts.
The economic effects will be still greater when the world’s population actually starts to decline. There are differing long-range population projections and they depend on a range of assumptions. One Austrian Institute estimates that there is an 85 percent chance that the world’s population will stop growing before 2100, and it is in fact most likely that global population will start to shrink before that, around 2070. A recent comprehensive study by the International Institute for Applied Systems Analysis reached the same conclusion based on the input of over 550 experts.
So will be see more business failures blaming birth rates? Watch this space.
MICAIAH BILGER MAR 20, 2018 | 4:40PM WASHINGTON, DC
A group of mothers and their children with Down syndrome are wowing the internet with a powerful music video to the popular song “A Thousand Years.”
The video, launched a few days ahead of World Down Syndrome Day on March 21, already has about 1.3 million views as of the writing of this article.
As the name suggests, the “50 Mums, 50 Children, 1 Extra Chromosome” video features 50 mothers and young children with Down syndrome using Makaton sign language to sing “A Thousand Years” by Christina Perri.
Its Scottish creators described how the project came about: “The mums are all part of a Facebook group known as ‘Designer Genes’ created for parents who have a child with Down’s Syndrome born in 2013/14. They got together to show the world just how ordinary and fun life with the condition is and how they ‘Wouldn’t Change a Thing.’”
The Daily Record reports Kirsty Davidson and her son Ruairidh were one of the Scottish families who participated in the video.
“Ruairidh is the best thing that has happened to us. He makes us smile and laugh every day,” Davidson said. “We want to show everyone that an extra chromosome is nothing to be scared of or worried about and hope people will get involved in celebrating Down’s syndrome on March 21.”
Another mother and daughter on the video, Julie Britton and Connie Seabourne, of Morley, had no idea how popular the video would become.
“I wanted to get involved in the carpool karaoke to get more awareness out there,” Britton told LeedsLive. “We knew it was going to be shared on social media, but that’s as far as we thought it would go. Within the first hour there was around a thousand views and people were saying: ‘This is going to be quite big’.
“It’s just getting more and more momentum as it’s going. I don’t think any of us ever expected it would quite turn out like it has done,” she said.
Celebrities including James Corden and Christina Perri are supporting the video.
Children with Down syndrome and their families often face discrimination. But videos like this one help to demonstrate how precious and valuable every single child is, no matter what their abilities.
March 19, 2018 (Lepanto Institute) – Caritas Internationalis, which is the Vatican-run confederation of Catholic international aid and development agencies, is on the board of directors of The Sphere Project, whose central purpose is to promote a standard handbook for aid and development work. The handbook strongly advocates for the use of contraception, including so-called “emergency” contraceptives for victims of rape.
a voluntary initiative that brings a wide range of humanitarian agencies together around a common aim – to improve the quality of humanitarian assistance and the accountability of humanitarian actors to their constituents, donors and affected populations.
The Sphere Handbook, Humanitarian Charter and Minimum Standards in Humanitarian Response, is one of the most widely known and internationally recognized sets of common principles and universal minimum standards in life-saving areas of humanitarian response.
Listed among some of the more notorious pro-abortion and pro-contraception international aid agencies (like CARE, InterAction, International Medical Corps, Oxfam, Plan International, Save the Children and World Vision) Caritas Internationalis is a member of the Board of Directors.
In 1997, a small group of international aid and development agencies, including Caritas Internationalis, developed a set of minimum standards in core areas of humanitarian assistance. The primary outcome of the project was the publication of the handbook Humanitarian Charter and Minimum Standards in Disaster Response. From the earliest iterations of this handbook, it has always promoted the use of contraception and condoms. Although there is a note in each edition which indicates that Caritas Internationalis and its member organizations do not support those sections of the handbook which promote contraception, the fact that Caritas promotes the handbook and remains on the governing body of the Sphere Project makes the note completely disingenuous.
Page 40 of the 2004 edition of the Handbook, under “Guidance notes,” says:
Staff and field partners should know how to refer women, men and children seekingredress for human rights violations, and be familiar with procedures for referring survivors of rape and sexual violence for counselling, medical or contraceptive care.
Page 283 states clearly that access to condoms and instruction on condom use is “essential” in disaster relief.
In 2011, the Sphere Project’s Handbook underwent a revision, expanding the 344-page manual to 402 pages. Three major Catholic aid organizations participated in this revision: Caritas Internationalis, Catholic Relief Services, and Jesuit Refugee Service. Several pages of the handbook instruct the user to ensure access to contraception and condoms. For instance, beginning on page 325, under section 2.3, titled “Essential health services – sexual and reproductive health,” the Handbook states:
All individuals, including those living in disaster-affected areas, have the right to reproductive health (RH). To exercise this right, affected populations must have access to comprehensive RH information and services to make free and informed choices.
In support of this, the following three pages provide details on what this entails.
Page 326 not only states that contraception should be readily available, but that “comprehensive reproductive health services” (which include contraception) should be “integrated” into primary healthcare:
Page 327 explicitly calls for the provision of abortifacient emergency contraception for survivors of sexual violence:
And, on page 328, under a section titled “Essential health services – sexual and reproductive health standard 2: HIV and AIDS,” the Handbook establishes a “minimum set” of services and products during disasters. Included in this set are male and female condoms and “contraceptives”:
As with the previous edition, one page contains a footnote, which amounts to an empty gesture, stating that “Caritas Internationalis and its Members do not promote the use of, or distribute any form of, artificial birth control.”
In 2012, two members of Caritas Internationalis (Trocaire and Catholic Relief Services) funded a “trainer of trainers” (ToT) workshop intended bring Sphere Trainers up to date on the new 2011 edition. In the image from the front cover of CRS’s report on this workshop, you can clearly see CRS’s banner, Trocaire’s banner, and a host of trainers holding the 2011 edition of the handbook, which we just profiled.
While there is nothing in the report on this training workshop indicating the promotion of contraception in any way, the problem is that the handbook specifically instructs users to promote contraception and condom use. In other words, it is the promotion of the use of the handbook itself which is the problem, because the handbook establishes contraception as a “right.”
In addition to the 2012 training session, in 2014, CRS and several other organizations added the Sphere Handbook in Action e-learning course to their educational offerings. The Sphere Handbook in Action e-learning course aims to strengthen the effective use of the Sphere Handbook. Again, CRS’s training modules do not contain any promotion of contraception, but as with the 2012 training session, it is helping to promote a manual which contains gravely immoral matter.
As a member of Caritas Internationalis, Catholic Relief Services’ involvement in the production and promotion of the Sphere Project’s handbook isn’t surprising. In April of 2011, Caritas Internationalis co-hosted the launch of the Sphere Project’s 2011 edition of the Handbook in various locations around the world. Three months later, Alistair Dutton, Caritas’s Humanitarian Director, gave an interview about Caritas’ involvement with the Sphere Project. Dutton said:
Caritas was a founding member of the Sphere project and has always been a member of the Sphere board. Caritas helped draft the original standards and has been involved in every revision of the standards. The Sphere handbook is a normative document for all the member organisations of the Caritas confederation and we at Caritas Internationalis insist that all the Caritas members apply those standards.
Now with the new Sphere handbook, our next challenge will be to make sure that people within all the Caritas member organisations are trained and aware of the new standards.
This is just one more reason why it is so important for Catholic aid and development agencies to disentangle themselves from secular organizations that include contraception and abortion in their work. In a case such as this, it isn’t enough for Catholic agencies to claim in a footnote that they aren’t involved in the promotion or distribution of contraception when they not only had a hand in the creation of a handbook promoting such things, but also are involved in the promotion of the handbook itself. If Caritas Internationalis, Catholic Relief Services, and other Catholic aid organizations truly want to win back the trust and support of pew-sitting Catholics, they are going to have to make some hard decisions, beginning with ending their relationships with the enemies of Christ, children, and souls.
NEW YORK, March 15, 2018 (LifeSiteNews) – One of the consequences of mass contraception is the loneliness of the elderly in some of the richest countries in the world.
So concludes Mary Eberstadt in an excellent essay commemorating the fiftieth anniversary of the promulgation of Paul VI’s encyclical Humanae Vitae. Her article, “The Prophetic Power of Humanae Vitae: Documenting the Realities of the Sexual Revolution”, has appeared in the April 2018 issue of the scholarly Catholic journal First Things.
In her article, Eberstadt lists a number of realities that have come to pass in the world since the invention of hormonal contraception. They include the increase of abortion, which is inextricably tied to the increase of the use of contraception; a gradual Protestant backlash against contraception, especially in Africa; the downturn in female happiness and the rise of sadomasochism in pop culture; the implosion of the Anglican communion; and the greying of the western world.
“Fifty years into the sexual revolution, one of the most pressing…issues for researchers is not overpopulation,” Eberstadt writes, “but its opposite: under-population.”
The “overpopulation” hysteria of the late 1960s has proven to be an “ideological chimera”, she says. Originally very useful to those who wanted the Church to change her teaching on contraception, the overpopulation myth has led to what Eberstadt calls “an epidemic of loneliness”.
“This finding would not surprise Pope Francis, who in an interview with La Repubblica in 2013 called the “loneliness of the old” one of the worst “evils” in today’s world,” she writes. “Fifty years after the embrace of the pill—undeniably, because of the embrace of the pill—loneliness is spreading across the materially better-off countries of the planet.”
Birthrates have plummeted across the western world and Japan. The Pill has not led to women having three children instead of seven but to women having one child or two children, or none at all. And there are consequences.
According to the New York Times, four thousand elderly Japanese now die alone every week. In 2017, the Grey Lady reported that every year there are news stories in Japan of people who die alone in their homes. Often their deaths go unnoticed and unremarked for weeks or months, rent and utility payments silently flowing out of the deceased’s bank accounts, until finally neighbours complain about a bad smell.
There is now a Japanese business whose remit is to clean apartments after the corpses of “lonelies” are discovered in them.
Unremarked deaths and an increase in loneliness generally have also featured in news stories and studies in such European countries as France, Germany, Portugal, and Sweden. The new loneliness is often blamed on divorce and “family rupture.” Eberstadt notes with irony that one can “read through many ‘loneliness studies’ without seeing reference to children, a striking omission that says a good deal about our era.”
Although loneliness can strike anyone, it is the elderly who are most at risk. Apparently in Germany over 20% of people aged over 70 have regular contact with only one person or none. Over two million Germans aged over 80 live alone.
“One in four receives a visit less than once a month from friends and acquaintances, and nearly one in 10 is not visited by anyone anymore,” Der Spiegel reported in 2013.
The German newsmagazine bluntly said that loneliness among the elderly is expected to rise:
“…the fact that more and more people are opting not to have children threatens to worsen the isolation experienced by older people. Indeed, childlessness significantly increases the risk of loneliness. Likewise, since people are becoming more mobile and live less frequently near their aging parents, the older generation can no longer depend on their children to remain an integral part of their lives and look after them someday. Consequently, the risk of loneliness among older people could possibly rise in the future, says [German Center of Gerontology] director Clemens Tesch-Römer.
In Britain the issue of loneliness is so serious, said to affect nine million people in the UK, that the government has appointed a Minister for loneliness. And far from being a gentle melancholy, loneliness has serious repercussions for the health of elderly people, including cognitive decline.
Eberstadt contrasted such “human poverty” with the material wealth in those same greying societies. She also pointed out that what unites Japan and European countries culturally is the sexual revolution, which increased divorces rates, depressed marriage rates, and drove down the number of children.
March 16, 2018 (LifeSiteNews) – As recently as the year 2010, less than 10 years ago, Planned Parenthood had an enormous marketing advantage over pro-life Pregnancy Help Centers.
At that time, the only way a Pregnancy Help Center could get the word out about its services to a significant number of women aged 18 to 29 years old, the age group that accounts for 70% of all abortions in the U.S., was to use traditional mass market media channels like TV, radio, billboards, and print (magazines and newspapers).
For Pregnancy Help Centers on a limited budget, which compared to Planned Parenthood’s massive marketing budget would basically mean all Pregnancy Help Centers, mass media was, and still is, cost-prohibitive.
But a very important technology development started quickly working its way into our society a little after 2010, and is now so firmly entrenched within every demographic, and especially the millennial age group, that most of us probably don’t realize how big this change was.
What was the change? The adoption of smartphones and high bandwidth wireless plans by the vast majority of American consumers.
According to Pew Research, 100% of American millennials now own a cell phone, and importantly 94% of those cell phones are smartphones.
Why does this matter to the pro-life movement?
It matters because the old standard cell phone technology, combined with standard low bandwidth wireless plans, did not allow for a cost-effective way to reach consumers with advertising messages.
However, once affordable smartphones and high bandwidth wireless plans became the norm, especially within the millennial age group, it opened up an entirely new and very cost-effective way for marketers to reach them.
In place of expensive budget-busting mass media “broadcasting”, Pregnancy Help Centers now have the option to use very cost-effective “narrowcasting” to reach women in a specific geographic area using Google, YouTube, and Facebook.
No longer are Pregnancy Help Centers essentially “locked out” of reaching young women with advertising to make them aware about the help and hope available to them should they face an unexpected pregnancy.
No longer does Planned Parenthood have an overwhelming marketing advantage against Pregnancy Help Centers.
Technology innovation has helped level the playing field.
Here are two specific examples of how we at Heroic Media are reaching young women, redirecting them away from Planned Parenthood, and connecting them to local Pregnancy Help Centers.
First, for some women who discover that they are facing an unexpected pregnancy, they become afraid and believe that the only option available to them is an abortion. These women will do an internet search and when the search results appear, Heroic Media places a small advertisement that competes directly with Planned Parenthood’s advertisements. When women respond to our ad, they are redirected away from Planned Parenthood and into the compassionate care of a local pro-life Pregnancy Help Center in their area.
Second, many women who face an unexpected pregnancy already know about Planned Parenthood, and know where its office is located. Believing Planned Parenthood is their only option for dealing with an unexpected pregnancy, many women will go straight there.
This tragic occurrence is a result of decades of Planned Parenthood investing in building its brand in the minds of young women, and on the opposite side, a significant lack of investment by Pregnancy Help Centers in building awareness about the help and hope available to women should they face an unexpected pregnancy.
This result is understandable given the cost required to build brand awareness using expensive mass media.
But now we have the opportunity to change that.
In March of 2017, Heroic Media began running 30 second video advertisements on Facebook and YouTube targeted specifically for viewing by women 18 to 29 years old in the top 10 largest cities in the U.S. The goal of these videos is to raise awareness about the existence of Pregnancy Help Centers, and the hope and help they can offer to young women.
In just over 12 months these videos have reached approximately 735,000 women aged 18 to 29, and have been watched to completion over 1,300,000 times.
Both of these advertising programs are bringing more women into Pregnancy Help Centers, saving countless preborn babies lives from abortion, and putting Planned Parenthood on its heels.
On Heroic Media’s website at http://heroicmedia.org, we post a new save story every weekday. Please visit our site to see how Pregnancy Help Centers are turning women away from Planned Parenthood and saving lives from abortion every day.
WEST BLOOMFIELD, Michigan, March 14, 2018 (LifeSiteNews) – A judge sentenced five pro-life activists today to one year of reporting probation, eight days of community service, more than $1,000 in fines each, and forbade them from going within 500 feet of any abortion facility in the United States.
Several of them will likely serve jail time for refusing to pay the fines or perform community service. Some of them could end up being in jail for 120 days.
Their “crime”?
Entering an abortion facility on December 2, 2017, to distribute red roses to the mothers inside, peacefully begging them to choose life. They call this a “Red Rose Rescue.” For that, they were charged with and convicted of trespassing and obstructing a police officer.
The five pro-life activists are Monica Migliorino Miller of Citizens for a Pro-Life Society, Will Goodman, Patrice Woodworth, Matthew Connolly, and Robert “Doc” Kovaly. In February, a jury took 30 minutes to convict them.
They are also forbidden from associating with or communicating with each other for a year. They also can’t associate with anyone who is “engaged in breaking the law,” which potentially limits their contact with Red Rose Rescuers in other states.
“I’ll (agree to) go see a probation officer, but I’m not paying a fine, and I’m not gonna do community service,” Migliorino Miller told LifeSiteNews. “I am not guilty of a crime.”
“Even in the heyday of the Rescue movement, we never saw anything like this, really,” Miller said of their severe sentences. “I can only come to the conclusion that the judge is in favor of legalized abortion, that he saw that the Red Rose Rescue was a threat to the practice of abortion. Otherwise, we would have had a lenient sentence. … I don’t think any of us expected the harshness of this sentence.”
Migliorino Miller has 30 days to pay the fine, according to the judge, even though she already told him she refuses to do so. Some of the others have six months to pay, she told LifeSiteNews.
During the trial, Judge Marc Barron allowed the prosecutor’s request to never call the abortion facility that the rescuers entered – the “Women’s Center” operated by abortionist Jacob Kalo – an “abortion clinic.”
“The victims of abortion, namely the unborn, were kept hidden from the jury and the judge’s rules were designed to stifle any testimony having to do with the reality of abortion,” said Migliorino Miller.
Each of the pro-lifers was sentenced separately and read pre-sentencing statements. During hers, Migliorino Miller showed the judge and the abortion workers who came to watch the sentencing a photo of an aborted baby she herself took.
It showed a “severed hand and severed foot of a 20 week aborted baby that was taken out of a clinic trash dumpster here in Michigan,” she said. “They seemed uncomfortable” seeing it.
Migliorino Miller, who has been in the pro-life movement for decades, chronicled in her book Abandoned: The Untold Story of the Abortion Wars how she retrieved the bodies of babies from abortion center trash cans and gave them proper burials. She captured a number of well-known, heart wrenching photos of babies killed by abortion.
After they were found guilty, Barron ordered the rescuers to stay at least 150 feet away from every abortion facility in America before their sentencing. This was a “bond condition unprecedented in the history of legalized abortion,” according to Citizens for a Pro-Life Society.
Red Rose Rescues inspired by Mary Wagner
The Red Rose Rescues are in a sense a revival of the “rescue” days of the pro-life movement, when pro-lifers would enter abortion facilities and plead with moms inside to choose life.
During these “rescues” in the early days of the pro-life movement, pro-lifers would block the entrances to these facilities or chain themselves to abortion equipment, saving many lives.
In 1994, then-President Clinton signed the Freedom of Access to Clinic Entrances (FACE) Act, which makes it a federal crime to physically block women from obtaining abortions. FACE effectively ended the widespread use of normal rescue tactics.
But, inspired by Mary Wagner, the Red Rose Rescue movement focuses on distributing red roses to mothers inside abortion centers and urging them to choose life. No one involved in the Red Rose Rescue has been charged with violating FACE. The pro-lifers don’t block the entrances to the abortion centers, but simply refuse to leave in solidarity with the pre-born.
In Canada, Wagner is often jailed for refusing to comply with probation orders that she stay away from any abortion centers.
In Alexandria, Virginia, Red Rose Rescuers Lauren Handy and Linda Mueller will be tried for their December 2, 2017, rescue – conducted in conjunction with the Michigan rescue – on May 18. Their trial date, originally March 9, was postponed due to their lawyer’s illness.
Earlier this year, another Michigan judge sentenced Migliorino Miller, Goodman, Connolly and full-time college student Abby McIntyre to two years of non-reporting probation for convictions stemming from their September 15 arrest at a Sterling Heights abortion center.
‘The babies were worth the sacrifice’
“The babies were worth the sacrifice,” said Migliorino Miller. “The babies are worth this burden that’s been imposed on us and we’re gonna do our best to continue to witness to the sanctity of life and I hope that more Red Rose Rescues will happen.”
She said pro-lifers must “not be intimidated” and must perform “radical acts of love and that means radical acts of sacrifice.”
“We’re dealing with life and death here. How could (our actions) be any different?”
The Pope decided to publish the encyclical at a time when strong pressures existed from the pharmaceutical industry and activist groups that had dazzled a good number of judges, doctors’ associations, women’s groups, the US Food and Drug Administration and the World Health Organization. The sale of a product like the Pill to the healthy population, to be taken daily, would be a multi-million dollar business.
The key argument was a new definition of pregnancy. They were aware that this was essential to make the Pill acceptable (especially to Catholic women), because they knew that it was not possible to rule out, as one of its mechanisms, abortifacient effects before the embryo could be implanted.
Finally, arbitrarily, without any scientific evidence, the American College of Obstetricians and Gynecologists, decided that pregnancy begins with implantation and not at fertilization.
The final reports of the Pontifical Commission, noted above, kept a surprising silence; they did not inform the Pope that the Pill could, in some cases, destroy embryos during the initial phase of development. In addition, the Commission did not pursue an in-depth study of natural family planning methods, such as the Billings or the Symptothermal method, limiting themselves to criticizing the “rhythm” method as if it were the only natural option. This atmosphere of concealment and half-truths supports the notion that the Pope’s decision was indeed an inspiration, another gift of the Holy Spirit.
Pastoral response
The pastoral response to support the implementation of Humanae Vitae was immediate. Medical and Church associations around the world emerged to guide young people in the understanding of their affective-sexual dimension and to prepare themselves to put that basic human dimension at the service of personal giving and love. Actions were taken to guide marriages to help them integrate the teaching of Humanae Vitae in married life, to achieve responsible parenthood and thus enrich their relationship and their family life.
Fifty years ago, Humanae Vitae warned about the dangers of contraception. Many contemporary adolescent and marital affective and sexual problems – some in epidemic proportions — are directly related to not taking these into account. Humanae Vitae was prophetic.
In the 1980s the World Health Organization showed that illiterate women in developing countries were also able to learn to recognize their fertility after observing three cycles. Mother Teresa’s Missionaries of Charity even managed to prevent the government of India from carrying out forced sterilizations on men who could prove that they had learned the Symptothermal method of NFP that the sisters were teaching.
NFP methods and the instruction for persons in developing countries have improved markedly. NFP is now included in scientific and teaching projects by different universities around the world. Studies have been published in medical journals showing that modern NFP methods are five times more effective than condoms and as effective as the contraceptive pill. In addition, electronic devices and applications for Smartphones have been developed and help marriages to more easily interpret the cyclical changes of fertility in combination with their own graphs and observations.
This is the reality of many couples and us natural family planning educators. A visit to a selection of websites should suffice to realize how much progress has been made in this field (1). Hence, surprisingly perhaps, Humanae Vitae is being vindicated scientifically.
Today, millions of people have learned to recognize their fertility and use modern NFP methods. They are autonomously managing their fertility at low cost. They are free from the side effects of artificial contraception and live their sexuality without the interference of health professionals. NFP encourages communication between husband and wife and enhances living sexuality in a truly full way; both adapt their sexuality and thus share their decisions of avoiding, spacing or having a pregnancy.
Recognition of fertility indicators in NFP involves an educational process of empowerment of women and men to achieve a better knowledge and care of their fertility and even favors the efficient diagnosis of health problems if they arise. Humanae Vitae promotes a true sexual ecology.
Is Humane Vitae too demanding? Fifty years show otherwise.
It is clear that in the application of Humanae Vitae there may be difficult circumstances. As John Paul II said in Familiaris Consortio, the Church should keep close to couples who struggle with it. Sometimes discernment and guidance call for the invocation of the “law of gradualness”.
But this has not led us to believe that Humanae Vitae is an ideal that cannot be achieved. When difficulties exist (for example during breastfeeding or pre-menopause), there are solutions without resorting to artificial contraception. This supposed alternative causes serious problems.
Throughout the world we have accompanied couples with difficulties. Our focus has been “Humanae Vitae is also for you, and we will accompany you so that you too can benefit from its teaching”. Pope Francis guides us in this line, stressing the importance of guidance and the merciful discernment of spouses. As he writes in Amoris Laetitia (n.294): “It is necessary to face all these situations constructively, trying to transform them into an opportunity towards the fullness of marriage and of the family in the light of the Gospel. It is about welcoming them and accompanying them with patience and delicacy”.
But the richness of Humanae Vitae is not achieved without some effort. It is not a pill swallowed with a sip of water. From the outset, it is necessary that the couple learn to recognize and interpret their fertility. They must also learn to understand and live periodic continence as an additional opportunity to grow as a couple. It is not easy to prepare young people for conjugal love. However, we educators do it because we want them to be happier.
Problems with artificial contraception
Current versions of the contraceptive pill continue to have unacceptable mechanisms of action. When ovulation occurs in spite of the Pill, the early elimination of embryos by preventing their implantation in the uterus cannot be ruled out and remains one of its mechanisms of action. And this is not what women want. One study showed that a majority of European women said that they should be informed about the abortifacient effect.
The best epidemiological study to date on the pill-breast cancer association was published in December last year in the New England Journal of Medicine, based on data from 1.8 million women in Denmark. Without a doubt, the recent contraceptives, like the old ones, raise the risk of breast cancer. Contraceptives do reduce the risk of some types of cancers, but this possible benefit is not comparable to the risk of producing breast, liver and cervical cancer. In addition, current contraceptives increase the risk of myocardial infarction and stroke by 60 percent.
Taking into account the best and most current scientific evidence, from a public health point of view, not from a moral standpoint, NFP is preferable to contraceptives. If the advice of Humanae Vitae had been followed, countless deaths from these causes could have been avoided over the last 50 years.
There are other serious health issues. In the past two years, two high-quality studies have been published in JAMA Psychiatry and the American Journal of Psychiatry (the latter based on data from half a million women and followed for eight years), which confirm an increased risk of depression, suicides and suicide attempts in relation to the use of contraceptives.
The weight of scientific evidence, then, confirms that Humanae Vitae is also a public health promoter, just as exercise and good eating habits are healthier than pills for losing weight. But the pharmaceutical industry is more interested in pills.
Scepticism of Humanae Vitae or a focus on NFP’s supposed problems could lead us to one of the biggest public health scandals of all times. It would affect the health of millions of women. In addition, it would be an unprecedented victory for the pharmaceutical industry that seeks to silence the current scientific evidence on the contraceptive pill and continue increasing its business at the expense of women’s health (2).
In short, Humanae Vitae is a gift from the Holy Spirit. It is a prophetic, ecological and health-promoting document. And its message is being vindicated ever more strongly by scientific research. History will show that Paul VI was right.
Jokin de Irala MD MPH PhD is a member of the Pontifical Academy for Life and President of the Spanish Association of Natural Family Planning Teachers
ROME, March 8, 2018 (LifeSiteNews) — The Pope has no power to change or relax the Church’s ban on artificial contraception, just as he can never allow women to be ordained, Cardinal Gerhard Müller said on Wednesday.
The former prefect of the Congregation for the Doctrine for the Faith was speaking at a book launch at the Lateran University in Rome. The launch was hosted by the Pontifical John Paul II Institute and was attended by key Vatican figures.
His remarks on the infallibility of Humanae Vitae’s teaching were supported by comments made at the same event by Professor Livio Melina, who served as president of the John Paul II Institute in Rome from 2006-2016.
Prof. Melina said that while the Church’s ban on contraception has never been dogmatically defined ex cathedra, nonetheless the teaching “belongs to the universal ordinary magisterium,” and as such is infallible.
He also called media attempts to recast Karol Wojtyła (St. John Paul II) as a “rigid” traditionalist, in contrast to a “more open” Paul VI, “fake news.”
A never-before-published letter
The new book by Fr. Paweł Stanisław Gałuszka, entitled “Karol Wojtyła and Humanae vitae,” examines the contribution that Karol Wojtyła and the Polish bishops made to the editing and reception of Humanae Vitae when Wojtyła was Archbishop of Krakow. The book contains several never-before-published documents, including a letter that Wojtyła sent to Pope Paul VI in 1969, after numerous episcopates had spoken out critically of Humanae Vitae.
In the letter to Pope Montini, Wojtyła suggests that the Holy See “contemplate a series of provisions aimed at helping priests and laity” to resolve difficulties arising from “harmful” interpretations of the papal document.
To this end, Wojtyła includes with the letter several detailed proposals for an “instruction addressed to priests engaged in the ministry — above all confessors, catechists and to preachers.”
The Spin
In the lead up to Wednesday’s book launch, news reports circulated in Rome about the contents of the letter.
Avvenire’s editor-in-chief, Luciano Moia — a clear dissenter from Humanae vitae — said the “tone” of Wojtyła’s proposed guidelines represented a “substantial stiffening” [irrigidimento] with regard to what Paul VI wrote in Humanae vitae. He added that the guidelines were “explicitly” at odds with the thoughts expressed by “half the world’s bishops” at the time, which were characterized by “respect, welcoming and understanding.”
Moia said the “most surprising aspect of the letter” was that Wojtyła asked Paul VI to proclaim the “infallible and irreformable” character of the encyclical, even though Moia ignores the fact that the word “irreformabile” never appears in the letter.
“Is it possible that Wojtyła was unaware that Paul VI required Msgr. Ferdinando Lambruschini … to explain at the press conference presenting the encyclical that the text should not be considered either as infallible or irreformable?” Moia asked.
Moia has openly supported a relaxing of the Church’s ban on artificial contraception. Readers may also recall that Avvenire — the official newspaper of the Italian bishops — prominently featured and praised Fr. Maurizio Chiodi’s controversial public lecture in which he said that responsible parenthood can obligate married couples to use artificial contraception.
Fake News
During the question and answer session at the book launch, the panel was asked about the claims made in the Avvenire article. One gentleman asked: “If it’s true that Karol Wojtyla asked Pope Paul VI to declare Humanae vitae infallible, and Pope Paul VI did not grant his request, why didn’t he do it himself during his own 27-year pontificate?”
Prof. Melina welcomed the opportunity to clarify the matter, saying:
I think that all of this is what, today, is fashionably called “Fake News.” You just have to carefully and critically read the letter that the Archbishop of Krakow wrote to Paul VI in 1969 to realize that, in fact, he didn’t make this request.
The Archbishop of Krakow sharply distinguishes two things: he distinguishes a dogmatic definition ex cathedra which is not given in Humanae vitae, and the presence of a teaching that is affirmed in Humanae vitae with the authority of the ordinary universal magisterium.
And since the Archbishop of Krakow thinks, on the basis of what Humanae vitae itself states, that the moral teaching of the Church is not an arbitrary decision, that the Magisterium is not an exercise of power but is a service to the truth, the Archbishop of Krakow is convinced that the teaching of Humanae vitae expresses a truth about the good, which the Church does not have the right, does not have the presumption to define or to change, but of which she is simply the depository and witness.
In this sense, the letter of 1969 simply invites Pope Paul VI to reconfirm what the encyclical Humanae vitae says, that is, that the teaching belongs to the universal ordinary magisterium, which according to the teaching of the Second Vatican Council in Lumen Gentium, 25, is infallible. Therefore, not the definition ex cathedra of a new dogmatic truth according to the teaching of Vatican I, but rather the acknowledgment of the truth as ordinary universal magisterium of what is written in Humane vitae itself.
Furthermore, St. John Paul II, on various occasions, particularly in his address in June 1987, acknowledged that, after Humanae Vitae, the interventions of the bishops, the interventions at the Synod in 1980 and Familiaris Consortio, as well as the interventions of his own magisterium, had rendered that doctrine no longer — these are the precise words — an “object of possible theological discussion,” which is the formula according to which once can say that it belongs to the ordinary universal magisterium. Of course, this is not a definition ex cathedra but it is, we might say, an assessment that theologians can responsibly make regarding the theological note of this teaching.
Cardinal Müller endorsed Prof. Melina’s comments, saying “it is absolutely unnecessary to make an ex cathedra definition” about Humanae vitae’s ban on contraception.
“Materially it is infallible, because it belongs to Christian anthropology and revealed anthropology and natural anthropology,” Müller said. “God is the Creator and the parents are the servants of divine providence, which includes the existence of men,” he added.
“We have the same issue in Ordinatio Sacerdotalis, regarding the impossibility of the Church to administer the sacrament of ordination to a woman,” the former CDF prefect continued. “It’s clear… the Pope doesn’t have the power to change this doctrine.”
No one can change it
Also featured on the panel was Professor Stanisław Grygiel, a Polish layman who holds the Karol Wojtyła chair in philosophical anthropology at the JP II Institute in Rome. Prof. Grygiel was a close personal friend of Pope John Paul II and responded by recounting two events from his life and friendship with Wojtyła.
He said:
In the 1980s, on an evening when I was speaking to St. John Paul II, he showed me a letter written and addressed to him by a very well known moral theologian in Europe. In this letter, the theologian asked the Pope to change the moral teaching regarding sexual life in marriage, Humane vitae, because “we are losing the faithful.” It’s too difficult so we need to change — not because its false, no — because it’s too difficult. The Pope gave me this letter, and asked me what I thought. I read it immediately and a little imprudently a word popped out of my mouth. I said: “This letter is stupid.” And the Pope looked at me and said: “Yes, it’s true. But who will tell him.”
Prof. Grygiel recounted another event involving Pope St. John Paul II:
There was a priest who was telling him that people are leaving because it’s too difficult; they need condoms; they need the pill. What do we do? After a little pause of silence, the Pope said: “Dear Fr. [X], tell me, did I and Paul VI invent the doctrine contained in Humanae Vitae? I cannot change it. No one can change it. No one. Not even the Church, my dear priest. Think about this.”
“The priest didn’t respond. He bowed his head and the conversation ended. I think these two events give us something to think about,” Grygiel said.
Wednesday’s book launch was received by a packed hall. Among the attendees were key Vatican figures such as German Cardinal Walter Brandmüller, the Theologian of the Pontifical Household, Polish Dominican Wojciech Giertych, and former vice-president of the Pontifical Academy for Life, Bishop Jean Laffitte.
On a Saturday morning in early 2017, Katrina officially hit rock bottom. A day earlier, she had caved in—at her boyfriend’s insistence—and surrendered to abortion at a clinic in Alamonte Springs, Florida, near Orlando.
As guilty as she felt, there was just no turning back now as she sat across the table from Mercedes Henry at Life Choices Medical Clinic—a pro-life pregnancy center located right next door to the abortion clinic Katrina had visited the day before.
That’s how Katrina felt in the moment, at least. The dread of fear and shame over her pregnancy had given way to a settled, lifelong night of hopeless finality the moment she took the first of two pills in the chemical “abortion pill” regimen.
It would take a miracle to save her baby at this point, but perhaps something even more extraordinary to revive the hope that had died in her heart 24 hours earlier.
Even while Henry pleaded with her to try and rescue her baby with an off-label use of progesterone that’s been used since the 1950s to hold off early miscarriages, Katrina just couldn’t see the glimmer of light opening wide before her eyes.
After spending an hour with Katrina, begging her to take one more chance at life, Henry offered to pray with her, then left the room to get a drink of water.
By the time she came back, Katrina’s mind had changed. She was ready to give Abortion Pill Reversal a try.
“I don’t know what happened,” Katrina said. “I really don’t know what changed in me, but in those few moments she was gone, I just felt this overwhelming sense of peace. For the first time since I found out I was pregnant, I didn’t feel like I was living in fear.”
A Miracle in the Making
The fact the two women were talking at all was miraculous in and of itself. In the weeks leading up to her abortion next door, Katrina had been practically hijacked by fear and shame—not to mention constant manipulation from her boyfriend, who threatened to kill himself if she didn’t abort their child.
Enslaved by those dynamics, Katrina told her sister, a practicing Catholic, about her pregnancy at one point. On the day of her abortion, Katrina lied and told her sister she’d lost the baby in a miscarriage. She hadn’t dared to tell her parents, who were living in Jacksonville, but they realized she was pregnant when they found a Google search Katrina had run on their home computer over Christmas break.
Incredibly, Katrina’s parents put two and two together the very day of her abortion, and showed up unannounced in Orlando—a two-hour drive from their home. Katrina told them the truth, thinking that would be the end of it, but her mother started a Google search of her own.
Eventually, Katrina’s mother found the Abortion Pill Reversal network and hotline (AbortionPillReversal.com, 1-877-558-0333), which has helped over 400 mothers rescue their children after starting the two-step abortion pill process since 2007.
That’s what led the family to Life Choices Medical Clinic in Alamonte Springs—just steps away from the abortion clinic Katrina’s boyfriend drove her to the day before.
“I told my mom, ‘Hey, this isn’t the place,’” Katrina said. “‘I don’t know what it is, but this is the place I actually got the abortion.’ She started freaking out, but then I looked again and realized we were headed next door.
“It was just so welcoming inside. You feel relaxed and at ease—the total, complete opposite of when I was at the abortion clinic.”
A Choice of Her Own
The weeks leading up to that Saturday afternoon had taken a heavy emotional toll on Katrina, which made it an uphill climb for her parents and Henry to help her see she could still change her mind.
Before she found out she was pregnant, she’d been the president of her sorority and was looking ahead to her future career, just over the horizon of the upcoming spring semester. Now, it seemed, Katrina was at a crucial crossroads.
Katrina was raised as a Catholic, but college life had taken care of that. By the time she knew she was pregnant, Katrina’s nominal faith was no match for her boyfriend’s knee-jerk reaction and relentless pressure.
Still, the despair she felt after having taken mifepristone—the first pill in the chemical abortion pill process, known euphemistically as “medication abortion” or technically as RU-486—was as crushing as it was immediate.
“The second I got there, it didn’t feel right,” Galvez said. “It was just an eerie, chilling feeling once I walked in. I just felt completely lifeless. The second I actually took the pill, it hit me—‘I can’t believe that my selfishness is really getting the best of me and allowing me to murder an unborn child because of my own selfish reasons and because someone else is getting in my head.’”
At no point in the process did the abortion clinic staff so much as mention the possibility that Katrina could change her mind and stop the abortion once it was started. In the minds and ledgers of the abortion business, Katrina had already made her “choice,” and there was no turning back now.
It was another story altogether at the pregnancy center next door, however, where Henry answered Katrina’s doubts and fears to finally empower her to make her own decision.
Finally, when Henry came back into the room with a cup of cold water, she looked Katrina in the eye and said, “Let’s save your baby, Katrina.”
God’s Hand at Work
Within hours, Katrina was in the office of Life Choices’ medical director John Littell, MD, FAAFP, receiving emergency injections of progesterone to try and counter the effects of the first abortion pill. Later that spring—after weeks of regular progesterone treatment—Katrina gave birth to a healthy little boy she named Gabriel.
Along the way, Katrina finished up her college degree and landed a job in her hometown, where she and Gabriel live with her parents.
“Everything just seemed like it was God’s hand at work,” Katrina said. “We are so blessed to have this amazing kid, even though he wasn’t in our plans at all. He was just completely unexpected, but he’s been such a blessing to everyone who’s been part of this. It’s really brought us closer together in ways we couldn’t have imagined.”
While Katrina’s story is exceptional on multiple levels, women in her situation are exactly why Life Choices opened shop next door to the abortion business in the summer of 2015.
The center sees about 1,300 women per year, many of whom—just like Katrina—resort to abortion because they feel they have no other choice. As their name indicates, Life Choices is there to counter the very hopelessness that keeps abortion businesses like the one next door afloat financially.
In addition to free pregnancy tests, free ultrasounds and help with material goods, Life Choices offers ongoing parenting classes and support for women and men who regret a past abortion.
“Katrina has said from the beginning, ‘I never want to be a mom,’ but she’s now a great, very thankful mom,” Life Choices’ executive director Norma Stives said. “It is amazing what can happen when information and love are presented to these women who are under such great stress. Katrina is a great example of what happens when you’re empowered.”
Hormonal birth-control raises a woman’s risk of having an ischemic stroke
This occurs when an artery to the brain is blocked and makes up 85% of cases
Hormonal pills and patches do not increase the risk of bleeding in the brain
Certain birth-control pills appear to raise the risk by making blood clot easier
In the US, nearly 37% of women are currently using some form of birth control
Oral contraceptives increase the risk of women suffering from certain types of stroke, new research suggests.
Birth-control pills raise a woman’s likelihood of suffering from an ischemic stroke, which occurs when an artery to the brain is blocked and makes up around 85 percent of cases of the life-threatening condition, a study found.
The researchers, from Loyola University in Chicago, wrote: ‘[Among] women with other stroke risk factors, the risk seems higher and, in most cases, oral contraceptive use should be discouraged’.
Such contraceptives do not raise the risk of hemorrhagic strokes, which are caused by bleeding in the brain, the research adds.
Birth-control pills, patches and jabs are thought to rise the risk of artery blockages by making blood more likely to clot.
The researchers stress, however, the risk is low among women without any risk factors for clotting. These include high-blood pressure and smoking.
Most women have tried at least one hormonal contraceptive in their lives. In the US, nearly 37 percent of women are currently using birth control.
Stroke is the third leading cause of death in women in the US, with 55,000 more females suffering than men every year.
Results further suggest women are not being accurately screened for potential stroke risk-factors before being prescribed hormonal contraceptives.
Among women at risk of the medical emergency, only 15 percent recall being advised not to take birth-control pills, while just 36 percent have been told to stop taking the medication.
Some 15 percent of women carry on their birth-control course after being told to discontinue.
The researchers believe this highlights the need for effective doctor-patient communication.
Speaking of how women can reduce their stroke risk, the researchers wrote: ‘The ideal drug is one with the lowest estrogen and progestin doses that will be effective in preventing pregnancy while minimizing adverse effects.’
March 7, 2018 (Joseph Sciambra) – Editor’s note: Joseph Sciambra recovered, in part through the prayers of his father, from years immersed in a homosexual lifestyle and alienated from the Catholic Faith. He now writes extensively concerning the real-life issues of pornography, homosexuality, and the occult, particularly in the Church.
1. Pray
“Rejoice always, pray without ceasing, give thanks in all circumstances; for this is the will of God in Christ Jesus for you.“ – Thess. 5:16-18
Start every morning with a prayer of thanksgiving to God for the gift of your son. Ask God to keep him safe from harm. Throughout the day, even if they seem insignificant, offer up little prayers, hardships, and sacrifices to the Lord for your son’s protection. Remain joyful in everything you do. Many young men who identify as “gay,” in general, retain very negative perceptions of their fathers as well as Christianity, particularly Catholicism; in addition, these two forces are often seen as either incredibly harsh and condemning or all-accepting and tolerant. Therefore, the religious man can be one of only two things: an ally or an enemy. You must be neither, but a father. In this regard, you must pray for determination, empathy, and prudence. This is sometimes a difficult balancing act that requires humility through supplication to God’s will; Bishop Athanasius Schneider stated this very well when he said: “Genuine understanding and compassion” for a person’s true good certainly does not result “from concealing or weakening moral truth.”
2. Attend Mass (daily if possible) and frequently receive the Sacrament of Confession
“I believe that were it not for the Holy Mass, as of this moment the world would be in the abyss.“ – St. Leonard of Port Maurice
At Mass, offer up your reception of the Eucharist for the reparation of those sins committed by those who are confused or have been deceived about their sexual identity. Your prayers at Mass are critically important because a number of Catholics, especially those who are young, do not pray for the conversion of anyone involved in a same-sex relationship, because they do not believe that it’s wrong. You could be the only human being on the Earth who prays for your son, and no other prayer is as efficacious as those offered to heaven during the Sacrifice of the Mass.
3. Work on your own personal sanctification
“Day after day I was able to observe the austere way in which he lived. By profession he was a soldier and, after my mother’s death, his life became one of constant prayer. Sometimes I would wake up during the night and find my father on his knees, just as I would always see him kneeling in the parish church. We never spoke about a vocation to the priesthood, but his example was in a way my first seminary, a kind of domestic seminary.” – Saint John Paul II
Be an example of Catholic masculinity to your son. But what does that mean? Use as your model the foster father of Our Lord Jesus Christ – Saint Joseph. Many “gay” men, beginning in childhood, are attracted to the strong, silent type who is also a man of decisive action, as evidenced in the example of homoerotic male icons from James Dean to Channing Tatum. These are secular and sexualized versions of what Saint Joseph represents; everything in the “gay” community is a poor substitute for what is our hearts’ true longing. Of course, you cannot be something different from your own temperament, but you can be a resolute figure for your son – even if you were not in the past. That requires not being afraid or embarrassed to reveal your faith – and this can mean doing something as simple as making the sign of the cross and praying before meals. As in the case of the father of John Paul II, these small acts can be accomplished quietly and unobtrusively.
4. Develop a devotion to Saint Joseph
“The Holy Patriarch was not an old man, but a young, strong, upright man, a great lover of loyalty, a man with fortitude. Holy Scripture defines him with a single word: just (see Mt 1:20-21). Joseph was a just man, a man filled with all the virtues, as was fitting for the one who was to be God’s protector on earth.“ – Saint Josemaria Escrivá
In the Gospels, there are no recorded words spoken by Saint Joseph. Yet, except for the Blessed Virgin Mary, no other human being had such a great influence over Our Lord Jesus Christ. According to Scripture: “… he went down with them, and came to Nazareth, and was subject to them.” Therefore, ask Saint Joseph to intercede on behalf of your son; Our Lord will refuse nothing to the man who so bravely protected Him from Herod’s assassins. In the same manner, you must now go into battle to help save your own son. And, if you have to – offer up your own life for his salvation.
5. The family should be the center of your life
“The Catholic family represents the first bulwark against the current great apostasy. The two most efficient weapons against the modern apostasy outside and inside the life if the Church, are the purity and integrity of the faith and the purity of a chaste life.“ – Bishop Athanasius Schneider
The only hope for your son ever leaving homosexuality – is you. When the “prodigal son,” after his self-imposed evil in the decadent world of sexual liberty, found himself near death and sleeping among the pigs, what would have happened if he had no father waiting for him at home? When the prodigal son demanded that his father accept him for who he claimed to be, what if his father had done just that? Where would the boy go?
The sad truth – many parents, particularly mothers of “gay” sons, willingly accept those demands for instantaneous approval and recognition. Especially in those families with a history of abuse or neglect, it’s far easier to believe that someone was “born gay” than to go through the heartache and pain of self-examination in order to determine the underlying trauma that perhaps initiated the homosexuality.
Those in the LGBT community have many family members and friends who celebrate their sexual orientation, sometimes as a gift from God. But they have very few, or more likely no one, who love them enough to challenge some of their most dearly held assumptions. You can be that one person. This doesn’t mean that you should browbeat your son, but any relationship with him, no matter what transpired in the past, must now be based upon the truth. How he reacts to that truth will largely dictate his future perception of you. But, in order to preserve a place that he may return to one day, you have to allow him to get angry and walk away. Then, like the father of the prodigal son, all you can do is pray and wait.
6. Never accept the false ideology that your son was “born gay”
There is no evidence for a biological or genetic determinant for homosexuality; even the very gay-affirmative American Psychological Association cannot claim that anyone was “born gay.” According to the APA:
There is no consensus among scientists about the exact reasons that an individual develops a heterosexual, bisexual, gay or lesbian orientation. Although much research has examined the possible genetic, hormonal, developmental, social and cultural influences on sexual orientation, no findings have emerged that permit scientists to conclude that sexual orientation is determined by any particular factor or factors.
However, psychiatrists, psychologists, and counselors, and even some priests within the Catholic Church, will tell you that if you do not accept your son as “gay,” you will contribute to his eventual psychological destruction – even to the point of suicide. However, in nations with the longest recorded history of modern LGBT acceptance – namely, the Netherlands and Sweden – disparities in terms of mental illness still exist between homosexuals and heterosexuals, and even among same-sex “married” couples. In addition, drug use and STD rates remain higher among the LGBT population.
7. Promote healthy heterosexual relationships
“There is no greater force against evil in the world than the love of a man and a woman in marriage.“ – Cardinal Raymond Burke
Oftentimes, a boy who later comes out as “gay” experienced difficult circumstances in his own family. Whether these situations were due to domestic violence, abandonment issues, neglect, an overprotective mother and a disinterested father, molestation, or even bullying at school, these early experiences sometimes leave “gay” men with a profound sense of loss. In order to fill that void, they attempt to self-heal through sexual behavior with other men. It doesn’t work, hence the proclivity for multiple partners in the gay male community, even among those who are in a relationship.
The Catechism of the Catholic Church refers to the family as a “domestic church.” Consequently, observation of the family creates an innate appreciation for creation and the Creator. For every “gay” man seeks the same sort of harmony that is biologically possible in heterosexual couples but results in only a simulacrum when imitated by two men. And, instead of the potential for generating life, the all-male imitation of copulation brings forth only death – through the rise of the AIDS epidemic and a continuing scourge of rampant STDs among the gay male community. The total opposite of this disorder can be appreciated in Catholic men who are husbands and fathers as they mirror not only the tremendous courage and self-sacrifice of Saint Joseph, but the love of the Father, through the death of His Son, for all of humanity.
8. Talk to your son
“Jesus does not deny the existence of sin and sinners. This is obvious from the fact that he calls them ‘sick.’ On this point he is more rigorous than his adversaries. If they condemn actual adultery, Jesus condemns adultery already at the stage of desire; if the law says not to kill, Jesus says that we must not even hate or insult our brother. To the sinners who draw near to him, he says ‘Go and sin no more;’ he does not say: ‘Go and live as you were living before.‘” – Father Raneiro Cantalamessa
Never be afraid to initiate a conversation. The person your son most fervently disregards is also the person he most wants approval from; the person your son would rather not talk to is also the person he most desires to have a connection with. In fact, the majority of men who “come out” will do so first to their mothers, and sometimes not at all to their fathers. Therefore, it’s important that you begin the discussion. Usually, this will immediately elicit a response of avoidance, curiosity, or disdain. The conversation may end before it starts. But given the opportunity – the truth must be stated out loud. This may be your only chance. And there is a sense of urgency that always exists when approaching this topic with a young man who is about to become sexually active with other men or has just started. Because there exists a unique set of factors, including a large alienated population where sexual opportunities are plentiful, the presence of numerous psychological disorders and the absence of the moderating influence exerted by women, the gay male community creates an environment in which STDs often multiply completely out of control. Therefore, it’s better for someone to walk away upset, after hearing the truth, than remain in an oftentimes silent and tacitly facilitating relationship. You have to be willing to fully take on the role of the father to the prodigal son. And sometimes that means saying goodbye – staying behind, and praying as if your son’s life depends on it – because it does.
9. Eucharistic Adoration
“Every one of us needs a half an hour of prayer each day, except when we are busy – then we need an hour.“ – Saint Francis de Sales
Take time out of your day, about an hour, to adore Our Lord Jesus Christ in the form of the Blessed Sacrament. Find a quiet chapel, close your eyes, and ask God for His help. Thank Him for giving you the patience and strength to endure and for keeping your son alive, so that one day he may perhaps turn around and head back home – where you will be waiting.
10. Fast and penance
“All that we do without offering it to God is wasted.“ – St. John Vianney
Deny yourself little pleasures, such as a favorite meal, snack, or drink. Skip a lunchtime break and instead attend Mass or visit an Adoration Chapel. Oftentimes, when a loved one does something that we know is wrong for him, he is oblivious to the perilous situation he has placed himself in – and we are the people who suffer. But your suffering is not in vain – when combined with prayer, it will perhaps make the difference between life and death for your son. Never think, just because the two of you are not speaking – that what you are doing every day of your life is not having a direct impact on your son. The unappreciated and unnoticed prayers of my father, while I danced the night away in a San Francisco gay disco, although I didn’t know it, kept me from utterly destroying myself. The father I abandoned and despised – never abandoned me.
Two more, and they are the most important:
11. Pray the rosary
“The rosary is the ‘weapon’ for these times.“ – Saint Padre Pio
Every day, make it a habit to recite the rosary. Set aside a certain time that is dedicated to this prayer. If possible, pray the rosary with your wife, other family members, or alone. At first, like much of what you are doing on behalf of your son, it seems ineffectual and hidden, but if and when your son returns to his senses, the worth of those prayers and sacrifices will be revealed. Until that day arrives, you must remain vigilant; as Padre Pio remarked, the rosary is a “weapon” through which you will defend your son from the demonic forces of confusion and deceit. My father prayed the rosary daily for my conversion.
12. Never give up hope
“The father of the prodigal son who waited on the road suffered more than the prodigal son.“ – Archbishop Fulton Sheen
If you give up on your son – it’s almost over. When I was a kid, I tried to hide. I thought being artistic, effeminate, and shy made me “gay.” I was embarrassed. While I may have exhibited a natural aptitude toward creativity, the insular world of drawing and picture-making became a safe escape from what I wasn’t good at – namely, sports or any physical activity which required a modicum of hand-eye coordination and dexterity. Was I effeminate, or did I become reclusive and unsure of myself, soft-spoken, scared of other boys, but accepted by some girls? Did I begin to take on the outward expressions of my peer group? As a boy, when I was comfortable with my surroundings, especially around women – I was bouncy and exuberant; among men, I didn’t know what to do.
By my late teens, I didn’t care what anyone thought of me, including my father. As my attitude changed, so did my appearance. I was simultaneously trying to shock, gain attention, and test the loyalty of those closest to me. Not surprisingly, my father wasn’t pleased. His continued distance and silence signaled to me what I wanted to know. However, I pushed a little further. Finally, my father had to speak up, and he said what needed to be said. Of course, I didn’t take it well; even objective criticism, with my best interest at heart, I regarded as a personal attack. It was inevitable. Because this battle was never just about me, and it wasn’t about a scared kid against a homophobic world in the age of AIDS, and it wasn’t about finding myself in the arms of another man – it was always about me and my father. When I would curse him, I subconsciously believed that he was the one who sent me into every gay bar, bathhouse, and sex dungeon. I wasn’t ashamed of who I was or what I did, but I hated him for it. Maybe he wasn’t the father I wanted – or needed; maybe he didn’t give me the attention I wanted – or needed. But when all seemed lost, when it mattered most – he did the right thing. Looking back, it’s the ultimate irony that through his prayers – I was saved.
This past Saturday, I had the good fortune to join Doug Barry in giving a day of reflection for men. By and large, the day centered around being, as Doug calls it, “Battle Ready.”
As the day approached, I was working on my two talks … refining and tweaking. It was the day before our “Battle Ready” day that this news broke from CNN:
When Coral Springs police officers arrived at Marjory Stoneman Douglas High School in Parkland, Florida, on February 14 in the midst of the school shooting crisis, many officers were surprised to find not only that Broward County Sheriff’s Deputy Scot Peterson, the armed school resource officer, had not entered the building, but that three other Broward County Sheriff’s deputies were also outside the school and had not entered, Coral Springs sources tell CNN. The deputies had their pistols drawn and were behind their vehicles, the sources said, and not one of them had gone into the school.
You read that right … there were four armed officers outside the school. And none of them did anything, according to CNN.
With less than 24 hours before presenting to those men at that day of reflection, I completely “reframed” my talks. But, I didn’t change the essence of what I was going to talk about, because it could not have applied more squarely on what happen on that Ash Wednesday at the Florida school.
“You see?” (I told the men) … “those four officers, cowering behind their cars in the school parking lot, as they listened to the gunman kill one student after another, could not encapsulate more effectively what has gone on in our culture, especially in the past half century.”
A few years ago, Jeffrey Kuhner of the Washington Times wrote this …
“For the past 50 years, every major institution has been captured by the radical secular left. The media, Hollywood, TV, universities, public schools, theater, the arts, literature — they relentlessly promote the false gods of sexual hedonism and radical individualism. Conservatives have ceded the culture to the enemy. Tens of millions of unborn babies have been slaughtered; illegitimacy rates have soared; divorce has skyrocketed; pornography is rampant; drug use has exploded; sexually transmitted diseases such as AIDS have killed millions; birth control is a way of life; sex outside of wedlock has become the norm; countless children have been permanently damaged — their innocence lost forever — because of the proliferation of broken homes; and sodomy and homosexuality are celebrated openly. America has become the new Babylon.”
“My brothers,” I said to those men, “this was under our watch.” “Why did this happen? Because we allowed it. We crouched behind our proverbial cars in our proverbial school parking lots, while we allowed lives to be lost.”
At the very beginning of our great nation, Sir Edmund Burke said,
“The only thing necessary for the triumph of evil is for good men to do nothing.”
Venerable Fulton Sheen put it this way …
“The refusal to take sides on great moral issues is itself a decision. It is a silent acquiescence to evil. The tragedy of our time is that those who still believe in honesty lack fire and conviction, while those who believe in dishonesty are full of passionate conviction.”
In our Church …
… we’ve cowered behind our proverbial cars while “passionate modernist Deists” gutted out anything that pointed to the supernatural power of God. A woman was the only one who seemed to stand against these destroyers. One, Mother Angelica. While we cowered behind our cars, Mother Angelica was about the only one who stood and, in essence, said,
“I’M GOING IN!”
Here’s a sample (Oh, how the modernists hated this woman):
In our culture …
… just less than three years ago, we were “told” marriage no longer meant what it had for all of civilization. Now, it can mean whatever we want it to mean. And we hid behind our proverbial cars.
Not too long after that, we were “told” we must allow adult men to share a bathroom with our little girls. And we hid behind our proverbial cars.
It has now been 45 years since we were “told” that vulnerable babies in, what was once the safest place in the universe … our mothers’ wombs, no longer received those protections. No, we were now free to tear these babies apart, limb from limb. And, for all of these 45 years, the VAST MAJORITY of us have been hiding behind our proverbial cars in the proverbial school parking lot.
In today’s Gospel …
… Peter wanted to stay back and just live his days wallowing in the “mystical experience” he received by witnessing the Transfiguration. Jesus said, “No!” In essence, Jesus said, “Don’t be afraid … now, let’s move out, because …
“I’M GOING IN!”
How much do we want to make our faith “just” about getting the ooey-gooey feeling from going to Mass on Sunday? But, when we are called upon to engage the evils and/or needs of our culture (primarily through the collective force of our parishes), we stand outside behind our proverbial cars in our proverbial school parking lots, and wait for “someone else” to do it … we wait for someone else to say,
“I’M GOING IN!”
I get that those four officers were most likely thinking, “my family needs to see me walking through the door tonight. It is better that they have a dad who is alive and well.” Yes, but now those four families are looking at dads who had an opportunity to save some of the lives of those 17 students on that fateful day, and their dads chose to cower behind a car in the school parking lot.
I’m going to drive the point home here with …
… my dad, who was probably the most active in our parish, whether he brought us kids with him (when applicable) or not. This, while he found it very difficult to find other dads (who still brought their families to Mass on Sunday) who were willing to make that kind of sacrifice, in “going in.” Our family – with dad’s lead – were active at everything the parish asked for. Did we think dad neglected his family by this level of dedication? Never! What’s the fruit? While most of the children of those other dads’ families fell away from the practice of the faith, all of us seven kids (six now, since my brother died), are “practicing Catholics,” active in our parishes, while one of my sisters is a Catholic school principal, and I am a priest. Why? Because dad, like Abraham and Jesus, had his priorities straight … God, and His will, before anything or anyone else … and his children learned this from him. When God asked him to sacrifice, dad said …
“I’M GOING IN!”
The moral of the story is this:
Jesus was right … “just” staying on the mountain, wallowing in a mystical experience (akin to our “just going to Mass”), is not going to change the world. We cannot “hide on top of the mountain” (believing “going to Mass” is enough). No! We can surely receive the strength of that “mystical experience” (going to Mass), but we must understand the gifts God has given, receive the strength He gives to us, and we must head down the mountain … get out from behind our proverbial cars in our proverbial school parking lots … and “engage” evil, care for need and, in essence, say …
“I’M GOING IN!”
Then I heard the voice of the Lord saying, “Whom shall I send? And who will go for us?” And I said, “Here am I. Send me!” -Isaiah 6:8
NB: Doug Barry and I, along with the Knights of Columbus, are already in talks to develop a campaign entitled, “I’M GOING IN!” We feel this tragic event at the school in Florida, especially the cowardice of the officers who stayed outside, is a “wake up call” and speaks directly to the great need in our men today. Stay Tuned!
For the first time ever, Gerber has chosen a baby with Down syndrome as their official “Gerber baby.” Baby Lucas, whose infectious smile is certainly an attention grabber, was chosen from among 140,000 applicants. The position comes with a $50,000 prize, which Lucas’ parents say they intend to put towards his education.
PIcture: Gerber Newsroom
While Gerber’s decision may ultimately be motivated more by good marketing than the desire to do a good deed, I strongly applaud their decision. After all, if there’s anything that activists have learned over the decades, it’s that visibility matters. Part of the reason that as many as 90% of babies diagnosed with Down syndrome in utero are aborted, is because of the pervasive ignorance that surrounds the condition.
By beaming Lucas’ smiling face, and the self-evident love that his parents have for him, all around the world, Gerber is giving visibility to the dwindling Down syndrome community, and helping to correct the some of the many myths about Down’s – myths with literally murderous consequences.
Down Syndrome is Not a Life Sentence
The Down syndrome abortion holocaust is driven primarily by ignorance and fear. The antidote to fear is hope, and the antidote to ignorance, facts. And in the case of Down syndrome the facts strongly support hope.
The authors of one study, which I will never tire of citing, interviewed thousands of people with Down’s, as well as their parents and siblings. They found that 99% of people with Down’s describe themselves as “happy.” Meanwhile, 99% of parents said they love their child with Down’s, and only 4% said they regretted having their child.
This isn’t to say that there aren’t sometimes enormous challenges in raising a child with Down’s – but what it does say is that for the vast majority of people, the positives overwhelmingly outweigh the negatives. Unfortunately, many parents of children diagnosed with Down’s aren’t given the facts, and without the facts, are robbed of hope.
Famous actress Sally Phillips was one of these women. In 2016, she teamed up with the BBC to make a film arguing against the introduction of a new, non-invasive test that is purported to be 99% accurate in detecting Down syndrome in utero. In that film, Phillips describes the moment doctors told her that her son Olly had Down’s, shortly after Olly’s birth.
“The doctor said to us: ‘I’m sorry, I’m so sorry.’ The nurse on duty cried. I don’t think anyone said anything at all positive,” says Phillips, known for her role in the Bridget Jones Diary movies. “It wouldn’t have been any different if they’d told me my child wasn’t going to make it.”
Phillips was lucky, however, in that her son was already born. Had her son been diagnosed in utero, there’s every chance that she would have been strongly pressured into aborting. And given that she is pro-choice, she may well have given in. Phillips, instead, was given the chance to experience what life is actually like for a child with Down’s. And what she found didn’t at all measure up to the doom and gloom of medical professionals or the pity of her friends.
“I was told it was a tragedy and actually it’s a comedy,” she says. “It’s like a sitcom where something appears to go wrong but there’s nothing bad at the end of it.”
Another mother, Dr. Lise Poirier-Groulx, says that when her child was diagnosed in utero with the condition, it was simply “assumed” that she was going to abort. “Everywhere I went it was assumed.”
“I got mostly cold stares and silences – Is this doctor for real? What is she doing? – that kind of attitude. We had to constantly state it: No, we don’t want to terminate. There was none of this talk – the pros and cons, positives and negatives of having a handicapped child. We never got that. It was just negative, when do you want to do it (the termination) type of thing.”
This pervasive atmosphere of hopelessness in the medical community can have a profound impact on vulnerable mothers and fathers, preying upon their already existing fears of the future, and magnifying them outside of any due proportion. In the end, they are never given the chance to see Down syndrome for what it is – a part of their experience as parents, and one that comes with very real difficulties, but difficulties that are dwarfed by the physical reality of the beauty and dignity of their child.
Overwhelmed by their fears, many parents will simply opt to abort as the quickest way out of their predicament. They are thus robbed of the opportunity of facing those fears, and of finding the enormous joy and love that are on the other side.
As one mother who admits she was terrified and in a “dark place” for a long time after receiving the diagnosis says: “The only way out of grief is through it. You have to feel it. You have to cry. You have to get pissed off. But do all this with a hopeful heart. The love for your child just comes, whether you want it to or not.”
A Twisted Irony
Last year, a woman with Down syndrome, Charlotte “Charlie” Fien, gave a moving speech to the U.N. She was inspired to write the speech after seeing Phillips’ documentary. In her speech, Fien compared the systematic elimination of babies with Down syndrome to the Nazi’s targeted elimination of individuals with disabilities.
Charlotte Fien (L) with her parents at the U.N. Image courtesy of Pax Press Agency.
“I am not suffering,” Fien said told the U.N. delegates. “I am not ill. None of my friends who have Down’s syndrome are suffering either. We live happy lives.”
“We just have an extra chromosome,” she added. “We are still human beings. We are not monsters. Don’t be afraid of us. … Please don’t try to kill us all off.”
At the end of the speech Fien received a standing ovation.
There is a twisted irony in the positive reception of Fien’s speech, however. Many of the U.N. delegates who stood and applauded her likely support abortion on demand. While they might be willing to applaud a woman like Fien, and even appreciate her defense of the disabled, they would not have had any objection had Fien’s parents chosen to abort her.
One such UN delegate is Ben Achour, ironically a member of the U.N. Human Rights Committee. After he gave a speech defending aborting babies diagnosed with Down syndrome, Fien shot back with a video of her own.
In his speech, Achour had stated: “If you tell a woman your child has …Down syndrome. If you tell her that, or that he may have a handicap forever, for the rest of his life, it should be possible for her to resort to abortion to avoid the handicap [as] a preventive measure.”
Fien’s response to Achour was blunt. “It’s disgusting and evil,” she said. “You need to apologize for your horrible comments. You should also be removed from the Human Rights Committee as an expert. You are not an expert about Down syndrome. You sir, do not speak for my community. … I will fight for our right to exist for the rest of my life.”
This exchange between Fien and Achour exposes the twisted irony at the heart of our society – that we profess to be willing to bend over backward in order to accommodate the needs of people with disabilities, and yet that we have no problem with eliminating those very same people before birth. Even as we have a U.N. Convention on the Rights of Persons with Disabilities that lays out myriad ways that the rights of people with disabilities should be protected on a global scale, we also have members of the U.N. Human Rights Committee openly defending the slaughter of those same people
Gerber Baby “Shines Light”
The timing of Gerber’s decision couldn’t be perfect. March 21st is World Down Syndrome Day. It’s a great opportunity to raise awareness about Down syndrome – in particular by sharing the unsung positive reality of life with Down syndrome.
Lucas’s mom, Courtney, has expressed her hope that Gerber’s choice of her son as Gerber Baby “shines light to the special needs community, showing that they are just like you and me. They should be accepted, not based on their looks, but based on who they are.”
“My biggest concern always with Lucas was how people were going to treat him,” she told the Today Show.” I was always afraid he would be bullied or people would be scared of him. It’s never once changed how we felt about him. He was always our son.”
So why not mark March 21st on your calendars, and on take the opportunity that day to share some of the many, manypositive stories of Down syndrome? Our brothers and sisters with Down syndrome are under attack globally. The best way to stand up for their inherent dignity and right to life is by making them visible to the world. Gerber has lent a helping hand with their choice of Lucas. Now let’s all pitch in, and bring a message of hope, not fear, to any parents who may find out that their unborn child has Down syndrome
ERIC METAXAS & ANNE MORSE MAR 2, 2018 | 1:11PM WASHINGTON, DC
What would you have given to become an Olympic athlete? One famous Japanese figure skater knows what she wouldn’t give.
The skater is gliding gracefully across the ice in a bright red costume, holding her arms aloft. Skating backwards now, Miki Ando of Japan is preparing for a huge jump: A quadruple Salchow.
And she lands it!
The audience explodes with delight. But a few years later, the applause went silent when the two-time Olympian became pregnant—and refused to have an abortion.
Miki Ando landed that quadruple Salchow—the only female skater ever to do so in competition—at the Junior Grand Prix figure skating finals at The Hague in 2002. She took part in the Olympic Games in both Turin and in Vancouver, representing Japan—a country where figure skating is insanely popular. and she’s a two-time World Champion.
Four years ago, Ando was preparing for a spot on the Olympic team for the Sochi Games when she made a shocking discovery: She was pregnant. And now she had a hard decision to make. She considered having an abortion. Competitive skating was her life; having a baby meant missing months of practice. And in Japan it’s considered shameful to have a baby out of wedlock.
As Ando later recalled, “I could not make up my mind all the way, but I hate[d] to make a decision to say goodbye to the baby.”
In the end, she announced: “I have chosen the baby’s life over skating.”
When news broke of Miki’s pregnancy—and of her decision to give birth—the Japanese public was furious. Their quad-jumping champion was now told she was setting a bad example.
“Honestly,” Miki told Kristi Burton Brown at LiveAction.org, “98 percent of the people said I was so bad.”
But her critics were forgotten when, in April of 2013, Miki gave birth to a little girl she named Himawari, now an adorable almost-five-year-old in pigtails. Her mother takes her with her to skating events, and when she cannot, Himawari’s grandmother cares for her.
Would Miki have won a spot on the Japanese Olympic team four years ago if she had aborted her baby? It’s hard to tell; many factors are involved. In any case, she has no regrets. Miki is now a professional figure skater, coach, and television personality. And as she told a Japanese website, the sight of her daughter’s face makes her want to do her best.
Miki is sending a vital message to women of the Western world: that babies and careers are not mutually exclusive. Sadly, women are often told from early childhood how important it is to have a career—that they should put off childbearing until they have finished college and gotten a good start on their careers. Men, also, are told to put off marriage and fatherhood and focus on making money. But babies tend to show up when they want to, regardless of our plans, and couples are often put under pressure to abort.
Miki’s story is proof that life doesn’t end with the birth of a baby—and that their appearance, even if seemingly ill-timed, can become a great joy. And as Kristi Burton Brown pointed out at LiveAction.org, the message that women must choose between career and motherhood “is harmful.”
And as for the Olympic medal Miki might have won, she notes that “No one is guaranteed the successes they most covet—no matter how much or who they sacrifice in the name of the success they crave.”
More than three quarters of a century ago, an Olympic runner named Eric Liddell taught us that there are more important things in life than winning Olympic medals. Miki Ando has taught us the same lesson today.
LifeNews Note: Eric Metaxas is best known for two biographies: Bonhoeffer: Pastor, Martyr, Prophet, Spy about Dietrich Bonhoeffer, and Amazing Grace: William Wilberforce and the Heroic Campaign to End Slavery about William Wilberforce. He also wrote books and videos for VeggieTales. This column originally appeared at Breakpoint.
Demographic Intelligence’s senior advisor, Lyman Stone, comments on recent articles in The New York Times and Politico magazine providing four factors that are driving the recent fall in births.
Writing in The New York Times, the economist Lyman Stone predicts that U.S. births fell to 3.84 million births in 2017, down from about 3.95 million in 2016. Stone was drawing upon research from Demographic Intelligence’s new 2018 U.S. Fertility Forecast. Stone, who serves as an advisor to Demographic Intelligence, also noted that the U.S. total fertility rate fell to 1.77 lifetime births per woman in 2017. Such low fertility is below what women in the United States want. What’s driving the decline in United States births?
The team of demographers and family scholars at Demographic Intelligence identify four factors driving the recent fall in births:
1) The share of unmarried women using long-acting reversible contraceptives (LARC) is up, from 1.5 percent LARC usage in 2002 to 7.2 percent in 2011-2013.
2) Young adult sex in America is down. The share of young adults (18-30) who did not have sex in the last year rose from about 10 percent in the early 2000s to 18 percent in 2014-2016, according to a recent Politico article co-authored by DI President Samuel Sturgeon and Bradford Wilcox, also an advisor to Demographic Intelligence.
3) Marriage rates have been falling among adults, which is important because married women have higher fertility rates than unmarried women. The share of adults 18-64 who are married fell from 54.2 percent in 2010 to 48.6 percent in 2016.
4) Finally, immigration rates have been declining, especially in the wake of the 2016 presidential election and President Donald Trump’s policies. Demographic Intelligence analysis indicates that births are now down more among foreign-born women than native-born women.
“The decline in U.S. births since 2014 is surprising, given that the economy has been improving,” said Demographic Intelligence president Samuel Sturgeon. “But changes in young adult relationships, sexual practices, and contraception usage appear to be pushing births downwards. Moreover, the Trump Administration’s policies are also discouraging immigration, which has an impact on births.”
“The big question is: When will the decline in births come to an end?” added Sturgeon. “We address this question in the latest edition of The U.S. Fertility Forecast.”
For more on recent trends in U.S. births, see the Demographic Intelligence research cited in the following articles:
MICAIAH BILGER FEB 28, 2018 | 11:11AM WASHINGTON, DC
With hard work and perseverance, abortion will be abolished “in our time,” Vice President Mike Pence said Tuesday.
Pence encouraged pro-life advocates during the 2018 National Religious Broadcasters Convention in Tennessee. He was a keynote speaker at a luncheon organized by Susan B. Anthony List and Life Issues Institute, which recently merged.
“I truly do believe, if all of us do all that we can, that we will once again, in our time, restore the sanctity of life to the center of American law. But we have to do the work,” Pence said, according to Newsweek.
He said the passion and love demonstrated by young pro-life advocates brings him hope for the future.
“I mean, for all the progress since 1973, the resilience of this movement proceeding out of the heart of a compassionate nation, I just know in my heart of hearts that this will be the generation that restores life in America,” he said.
In contrast, he said abortion activists have become increasingly radical. They have abandoned moderates who oppose late-term abortions and taxpayer-funded abortions, and are openly embracing abortion on demand. Pence mentioned the 20-week abortion ban as evidence; it narrowly failed in the U.S. Senate after pro-abortion Democrats and two pro-abortion Republicans rejected the moderate abortion limit.
“The truth of matter is the other side, the other party, continues to go farther and farther to the left,” Pence said.
He called for the activists in the room to work ever harder to help “restore the sanctity of life to the center of American law.” He then made a stunning suggestion: that legal abortion could “once again” be banned in the U.S., and that it could happen “in our time.”
… the vice president announced that “life is winning in America once again,” before ticking off the many policies enacted under Trump aimed at limiting access to abortions.
Pence said Trump has kept his word about supporting pro-life policies, including the Mexico City Policy, which prohibits taxpayer funding to groups that promote or provide abortions overseas. Trump also signed a law that makes it easier for states to defund the abortion giant Planned Parenthood.
“From the very first day of this administration, President Trump has been keeping his word,” Pence said, according to the AP.
Pence is one of the most sincere and passionate pro-life advocates to ever serve in the White House. In 2017, he became the first vice president to address the March for Life. A former U.S. Congressman and governor of Indiana, Pence has a lengthy pro-life record that shows his dedication to protecting unborn babies and mothers from abortion.
February 26, 2018 (HLI) – The cobra knocks on John’s door and asks, “John please let me in. It is cold and damp outside. I promise I will do no harm to you or your family.” But John vigorously rejects – at first – the pleas of the cobra, knowing the imminent danger. Yet the cobra seductively repeats his plea, preying upon John’s compassion and concern, repeating, “John please let me in. It is cold and damp outside. I promise I will do no harm to you or your family.” John, believing the cobra is sincere, lets his guard down against his better judgment, giving way to the cobra’s plea. A few days pass without incident, and John becomes acceptant and indifferent towards his so-called guest. But one night while everyone is asleep, the cobra strikes, injecting his lethal poison and killing everyone.
John is to blame for not defending his family – stepping into the breach. We cannot be angry with the cobra; after all, the cobra could not deny its nature.
Modern Day Cobras
Though I have seen many atrocities against life and family during missions to nearly 80 countries, I have not seen or experienced such a comprehensive and concentrated affront to life and family as I saw in my recent mission to Uganda. More than 100 anti-life groups, death peddlers (cobras), unashamedly market their poisonous wares, under the guise of “health care.” And they are doing this among a people who love life and family and who struggle simply to obtain basic human necessities.
The leading organization actively involved in anti-life work down to the village level in Uganda is Marie Stopes International (MSI), which has admitted to doing illegal abortions all over the world and which operates 14 illegal abortion mills in the country. MSI is supported by the usual population control groups, including: AVERT, CEDPA, the Center for Reproductive Rights, DFiD, Family Health International, the Gates Foundation, Human Rights Watch, IPAS, IPPF, PATH, Pathfinder International, Population Action International, the Population Council, the Population Reference Bureau, Population Services International, USAID, and at least nine organs of the United Nations. Each group is working to convince Ugandans that their economic problems are the consequence of too many children – the average family size still being 5-6 children.
No matter where, in the nearly 1,200 miles I traveled, I saw sign after sign, of various sizes and colors, marketing perverse sexual behavior that undermines
Billboards in Uganda advertising contraception.
Ugandan culture and traditional life and family values. Alongside major highways, side roads, and even in some of the remotest villages, population controllers advertise their wares. Without conscience or shame and emboldened by the lack of resistance, poor education, economic need, and indifference, they display their evil goods openly. For example, the boulevards surrounding parliament, the seat of Ugandan government, are decorated with dozens of signs advertising contraception – injectables and condoms. Billboards advertise the need for lower numbers of children, which currently make up 55% of the total population.
Sadly, most parliamentarians and civil leaders are unfamiliar with the history of Marie Stopes or what each of the organizations actually has as its mission and strategy.
Ideological Colonization of the Mind and Desensitization
A people enters with an idea that has nothing, nothing to do with the nation. … And they colonize the people with an idea that changes, or wants to change, a mentality or a structure.
– Pope Francis, Jan. 19, 2015
There is more to life than material abundance. With our own families and culture collapsing around us, it seems odd that we in the West so easily consider our way of life superior; that we see our relationship to the poor and to poorer nations as one in which we have all the answers, and that they should listen to us.
Really?
Many seek to impose certain aspects of Western thinking – an “ideological colonization” – in response to the struggles affecting millions of people and families living in abject poverty. They advocate for lower birth rates, introducing contraception and abortion, because from their point of view children are an obstacle to progress and development. This violent attack on life and family in the developing world is part of the “development” efforts of Western elites and wealthy nations, whose objectives are carried out by large non-governmental organizations (NGOs), who promote and uphold their values.
More billboards in Uganda advertising contraception.
In Uganda, it is estimated that over 4 trillion Ugandan shillings a year are wasted by corruption. This act of injustice and violence against the Ugandan people is met with anger but also with indifference: “What can we do about it?” is the general response. The death peddlers exploit this situation and pour billions of dollars into the hands of corrupt government officials and locals willing to sell-out their fellow brothers and sisters, convincing them that they must do their part to decrease the size of Ugandan families in order to prosper as a nation.
This great lie does nothing to change the systemic reasons for abject poverty but only makes larger poorer families into smaller poorer families. The people are left with no improvement in their access to basic needs such as: clean water, sanitation, highways, medical care, schools, electrification and equipment for farming or resolving the maldistribution of goods.
Since 1996, over $170 billion has been spent in population control programs around the world, with over $70+ billion spent in Africa alone. Imagine what these funds could do authentically to change the standard of living for Africans? Instead, the death peddlers seek to keep Africa in poverty while exploiting its natural resources.
Why is Uganda’s life expectancy still 21 years short of the United Kingdom’s? Why do one in five Ugandans lack clean drinking water? Why do an incredible eighty percent of Ugandans not have access to sanitation facilities? Whatever happened to the empty promise that smaller families would lead to better and richer lives?
The ultimate goal of “ideological colonialism” is to abolish any sense of objective truth and limit all influence of Christianity – constructing a new world and vision of humanity. Among the poor nations, the West not only promotes contraception and abortion with a Malthusian approach, but we also see a gradual and steady increase in the promotion of euthanasia – seeking to eliminate the aged and the infirm. So, as demography sharply declines, people become lonely, depressed and isolated; as a consequence, they are more easily susceptible to the seduction of euthanasia.
Western colonialism tries to impose false morality and deceitful values like gender theory, comprehensive sex-education – so-called “sexual and reproductive values” – and the LGBT agenda. Such an agenda attempts, over time, to desensitize the conscience of people, pulling them from the truth. For example, gender ideology conveys a crude lie, denying the reality that a human being is a man or a woman, deconstructing the human person, and destroying family life and social order.
No Man is an Iceberg… Man needs God
We will never succeed in overcoming the challenges of the world by mere political and rational means. Man needs God. When a person’s strength is anchored and sustained by faith and nourished in prayer, he or she is unstoppable. This becomes the source of joy and serenity because it unites us to God, who is our strength – our anchor.
Life is a talent entrusted to us so that we can transform it and increase it, making it a gift to others. No man is an iceberg drifting on the ocean of history. Each one of us belongs to a great family, in which he has his own place and his own role to play. Selfishness makes people deaf and dumb; love opens eyes and hearts, enabling people to make that original and irreplaceable contribution which, together with the thousands of deeds of so many brothers and sisters, often distant and unknown, converges to form the mosaic of charity, which can change the tide of history.
– Pope St. John Paul II, World Youth Day 1996
What has aided the death peddlers’ success in promoting their anti-life agenda is that the laity’s knowledge of and adherence to moral Truth concerning life and the family is woefully inadequate. Many Ugandans have not been exposed to Church teaching, rendering them incapable of adequately responding to the growing trend of secularization and the aggressive and militant approach with which it is pushed. Components of this secular agenda are predominantly hostile to Church teaching, promoting instead homosexuality as a positive good, so-called homosexual “marriage,” and all means of attack on the most vulnerable life via contraception, abortion and euthanasia, as well as promoting promiscuity and other perverse sexual behaviors.
Where There is Hope There is Life…
Our brothers and sisters are ill-prepared to defend themselves against this onslaught and often fall prey to the illusionary language and destructive practices. There is hope, however, in developing nations where fidelity to the whole of the Catholic faith is present; there is hope where the Church is growing (Asia and Africa). Teaching the faith as an integral whole yields benefits in the crucial areas of life, family and society.
We presume that poor people in every part of the world want what the West has – material prosperity at any cost. There is much the West (and the world) can learn from many of the world’s poor about the meaning of life and family. Their strong family values are cherished by their cultures, whereas we have sacrificed these traditional values for radical individualism and so-called progress.
Most Africans love and respect life, welcoming it with gratitude to God. The family and family relationships are still very strong, and people live their lives in happiness and generosity, despite daunting challenges. They celebrate God’s abundance ― when a child is born, when the child is baptized, confirmed and married, at wedding anniversaries and graduations. Thinking about this makes me yearn for the time when we and the majority of the world held such values and treasures.
Though the majority of Western countries have followed the voice of the death peddlers instead of the Master of Life, we know that conversion is always possible and that lives, people and nations can be transformed – through repentance and amendment of life.
There is much we can learn from our brothers and sisters in Africa, especially the centrality of God, family and defense of human life. With increased faith and determination to regain what has been lost, perhaps both the developing and developed nations can, together, renew and reaffirm the great importance of life, marriage and family and authentically cultivate, build and sustain a Culture of Life and Civilization of Love – where the great commands of the Lord are expressed and fulfilled:
“You shall love the Lord, your God, with all your heart, with all your soul, and with all your mind. This is the greatest and the first commandment. The second is like it: You shall love your neighbor as yourself.” – Matthew 22:37-40
February 20, 2018 (The Public Discourse) – As we approach the fiftieth anniversary of Pope Paul VI’s prophetic affirmation (in Humanae vitae) of the Church’s perennial teaching that contraception is always morally wrong, it is perhaps fitting that contraception, notwithstanding its widespread acceptance even among Catholics, is much in the news. The news has mainly had to do with the Trump administration’s courageous decision to nullify the Obamacare “contraception” mandate, at least for those employers who conscientiously object to being made providers of drugs and devices including abortifacients, as well as the Pill, IUDs, and other simple contraceptives.
The administration’s new regulations provide a total exemption from any legal duty to pay for these drugs and devices or even to facilitate their use in a remote way. My employer, the University of Notre Dame, is eligible to take that exemption. In fact, along with many other religious institutions, Notre Dame sued the United States several years ago to secure precisely that relief. And note well: these institutions sued for total exemption, even though they were already beneficiaries of an Obama-era “accommodation” that relieved them of any duty to directly fund or distribute contraception or abortifacients.
In its lawsuit, Notre Dame cited chapter and verse of Church teaching. Its pleadings and supporting papers amounted to a sound, and at times moving, argument that it would betray the faith if it were to accept even the watered-down involvement of the “accommodation.” The University said, basically, that, to remain faithful to its beliefs, it could not be involved in any way whatsoever with a process designed to provide contraceptives to its employees, its students, or their dependents. Just so.
Yet, in spite of its sworn declarations that Catholic faith precludes doing so, the University announced in late 2017 that it would decline the proffered exemption and instead stay the course prescribed to it by the Obama administration. This decision surprised many observers (though, truth be told, not this one). Notre Dame’s choice came under withering public criticism, on and off campus, from (among others) the University Faculty for Life and the Sycamore Trust, an alumni group dedicated chiefly to encouraging Our Lady’s University to live up to its stated Catholic mission.
On February 7, the University changed course yet again. In a letter to the entire campus community, President John Jenkins, CSC, announced new “steps based on Catholic principles that nevertheless provide access to some of the coverage that members of our community seek.” In one “step” Notre Dame rightly repudiated any role in providing abortifacients (such as Plan B and ella) for, as Fr. Jenkins wrote, these things destroy “an innocent human life.”
Sadly, however, Fr. Jenkins chose to go all-in on contraceptives. He wrote: “the University will provide coverage in the University’s own insurance plans for simple contraceptives (i.e., drugs designed to prevent conception).” This “step” is really a giant leap into immorality. Under the Obama administration’s “accommodation,” Notre Dame did not directly fund contraception and was only peripherally involved in providing access to it. Now the University is to be sole funder and proprietor of a contraception giveaway, with only the logistics of it delegated by Notre Dame to its plan administrators. What it solemnly declared for years to be morally impossible is, suddenly, the substance of Notre Dame’s free choice.
Many on campus will congratulate Fr. Jenkins for a wise and even Solomonic decision. Many others will disagree, in silence. But there can be no doubt that Notre Dame, according to its own sworn declarations, has betrayed the Catholic faith. Fr. Jenkins and all others involved in making this fateful, gravely wrong choice should be rebuked. One expects that, now, the local bishop will have no choice but to publicly do so. Leave aside the prospect that anything Bishop Rhoades could do or say would cause Notre Dame yet again to change course. His duty to protect all the faithful in his care from this grave scandal will compel him to speak out.
Fr. Jenkins’s announcement is, however, worse than all that. The harm to so many persons’ minds, bodies, and souls unleashed by Notre Dame’s embrace of contraception is great, and perhaps incalculable. But, in the course of rationalizing his decision, Fr. Jenkins supplied a primer about how Catholics should make all sorts of morally important decisions that is not only mistaken, but catastrophic for the moral life.
Here is the relevant part of Fr. Jenkins’s announcement. First, he affirmed that contraception is “contrary to Catholic teaching.” But then he observed that “many [people on campus] conscientiously disagree with this particular teaching.” Fr. Jenkins wrote that Notre Dame “must be unwavering in our fidelity to our Catholic mission at Notre Dame, while we recognize that among the values in our Catholic tradition is a respect for other religious traditions and the conscientious decisions of members of our community.” He stated that a “tension exists between establishing policies in accord with Catholic teaching and respecting the religious traditions and decisions of the many members of our community.” This “tension” is particularly acute when it comes to healthcare. Fr. Jenkins also noted that, several years after submitting to the Obama accommodation, “some of those enrolled in our health plans – an increasingly diverse group – have come to rely on access to contraceptives through enrollment in our plans.” Ergo, according to the university president, Notre Dame will become a contraceptives distributor.
The grave and potentially disastrous error in Fr. Jenkins’s reasoning is that nothing in it has the slightest tendency to morally justify helping others – even people we respect deeply – to do what is morally wrong, even if they happen to believe otherwise. Our moral duty to respect others’ choices does not have anything to do with giving them the means to do evil. If the person working next to you shares his plan to, say, patronize a prostitute, it would be wrong to give him the cash to pay for it. There may be nothing you can do to stop a friend whom you generally respect from entering an adulterous relationship or from cooking the books of his small business. But surely one is morally bound not to give him the keys to one’s apartment for his assignations or to file a false tax return for him. Indeed, everything that Fr. Jenkins says about the campus community’s attitudes toward contraception would apply almost equally to abortifacients. Yet even he recognizes that paying for Plan B or ella would be wrong, no matter how much we might respect those who would take those drugs. The only reason Fr. Jenkins reversed course on February 7 was to eliminate the modest role Notre Dame played, per the Obamacare “accommodation,” in facilitating access to abortifacients. By that same measure of how much complicity in others’ immoral choices is too much, Notre Dame is much more obviously guilty of contraception than ever before.
In truth, one should not respect another’s specific immoral choice at all. Everyone’s immoral choices should be regretted, and their repetition discouraged, and their occurrences criticized appropriately. The word “respect” hardly leaps to mind to describe that complex of morally required responses. One can and should in general nonetheless respect the person whose immoral choice it is. Beyond that, speaking of “respecting” others’ immoral choices has to do with the moral and prudential limits on what one may, and may not, do to stop, or just to interfere in, their wrongdoing. Your adult brother might regularly use his laptop to access pornography. Anyone who respects him should remonstrate with him about his bad habit and dissuade him as best one can. It would be wrong, of course, out of “respect” to give him the web addresses where the sordid stuff he fancies can easily be found. But it would ordinarily be wrong, too, to take his laptop and throw it away. It would surely be wrong to lock him in his bedroom until he promised to stop.
As a matter of fact, Notre Dame’s practice until just a few years ago exhibited all the “respect” possibly due to those who want to contracept. Notre Dame rightly did nothing to make that immoral practice easier or cheaper. At the same time, Notre Dame did not discriminate in the workplace against those who chose to contracept. The University left everyone alone, if you will, to do as he or she wished in private.
The crucial mistake in Fr. Jenkins’s rationalization is to use the hazy fog generated by a sonorous phrase – “respecting” others – to cover up what he is really doing, which is to violate in and by his own deed the moral truth that he seems to affirm (that contraception is immoral). The central truth of the moral life is that everyone is invariably morally responsible for his or her own actions, no matter what others are doing or not doing. Neither Fr. Jenkins (nor I nor you) is permitted, much less obliged, by “respect” for any other persons to choose to aid their immoral plans, because doing so makes Fr. Jenkins (or me or you) guilty of that same immorality – just as Notre Dame itself alleged under oath in its lawsuit over the course of several years. Thus Fr. Jenkins has most regrettably muddied what it means to say that any norm of morality is, simply, true.
That Fr. Jenkins chose the other day to wrap his gross disservice to all who read his words in expressly Catholic refinements is especially scandalous. He wrote, earnestly, that this situation is one that demands discernment – something to which Pope Francis has called the Church in his various writings and addresses. Discernment, which has a long history in the Catholic spiritual tradition, is, of course, a process of weighing thoughtfully considerations for and against various courses of action. Yet it also demands prayerful attention to God’s guidance through the prompting of the Holy Spirit.
But the Holy Spirit is not a consequentialist. God does not want us to weigh up pros and cons of adhering to the moral truth. And the greatest respect we can show others is to bear faithful witness to that truth.
Gerard V. Bradley is Professor of Law at the University of Notre Dame Law School and a Senior Fellow of the Witherspoon Institute, where he is Chair of the Academic Committee of the Simon Center on Religion and the Constitution.
STEVEN ERTELT FEB 22, 2018 | 12:30PM WASHINGTON, DC
Pro-life Catholics who wish Catholic Church leaders would step up and deny communion to leading politicians who support abortion are getting good news today.
Bishop Thomas J. Paprocki of Springfield, Illinois says Durbin is “cooperating in evil” and persisting in “manifest grave sin” because of his abortion advocacy and must therefore “not be admitted to Holy Communion until he repents of his sin.”
In a statement on the Diocese of Springfield website, Bishop Paprocki said, “Fourteen Catholic senators voted against the bill that would have prohibited abortions starting at 20 weeks after fertilization, including Sen. Richard Durbin, whose residence is in the Diocese of Springfield in Illinois.”
The full statement reads:
I agree completely with His Eminence, Cardinal Timothy Dolan, Chairman of the United States Conference of Catholic Bishops’ (USCCB) Committee on Pro-Life Activities, who called the U.S. Senate’s failure to pass the Pain-Capable Unborn Child Protection Act “appalling.”
Fourteen Catholic senators voted against the bill that would have prohibited abortions starting at 20 weeks after fertilization, including Sen. Richard Durbin, whose residence is in the Diocese of Springfield in Illinois. In April 2004, Sen. Durbin’s pastor, then Msgr. Kevin Vann (now Bishop Kevin Vann of Orange, CA), said that he would be reticent to give Sen. Durbin Holy Communion because his pro-abortion position put him outside of communion or unity with the Church’s teachings on life. My predecessor, now Archbishop George Lucas of Omaha, said that he would support that decision. I have continued that position.
Canon 915 of the Catholic Church’s Code of Canon Law states that those “who obstinately persist in manifest grave sin are not to be admitted to Holy Communion.” In our 2004 Statement on Catholics in Political Life, the USCCB said, “Failing to protect the lives of innocent and defenseless members of the human race is to sin against justice. Those who formulate law therefore have an obligation in conscience to work toward correcting morally defective laws, lest they be guilty of cooperating in evil and in sinning against the common good.” Because his voting record in support of abortion over many years constitutes “obstinate persistence in manifest grave sin,” the determination continues that Sen. Durbin is not to be admitted to Holy Communion until he repents of this sin. This provision is intended not to punish, but to bring about a change of heart. Sen. Durbin was once pro-life. I sincerely pray that he will repent and return to being pro-life.
In the letter, Pope Francis directed the Argentinean bishops to govern the Church there following the Aparecida Document.
The text states, in part, “[people] cannot receive Holy Communion and at the same time act with deeds or words against the commandments, particularly when abortion, euthanasia, and other grave crimes against life and family are encouraged. This responsibility weighs particularly over legislators, heads of governments, and health professionals.”
“These are the guidelines we need for this time in history,” the pope wrote to the bishops.
Richard Heilman20180220APOPE ST. LEO XIII’S VISION
According to legend, exactly 33 years (span of our Lord’s life) to the day prior to the great Miracle of the Sun in Fatima, that is, on October 13, 1884, Pope Leo XIII had a remarkable vision. When the aged Pontiff had finished celebrating Mass in his private Vatican Chapel, attended by a few Cardinals and members of the Vatican staff, he suddenly stopped at the foot of the altar. He stood there for about 10 minutes, as if in a trance, his face ashen white. Then, going immediately from the Chapel to his office, he composed the prayer to St. Michael, with instructions it be said after all Low Masses everywhere. When asked what had happened, he explained that, as he was about to leave the foot of the altar, he suddenly heard voices – two voices, one kind and gentle, the other guttural and harsh. They seemed to come from near the tabernacle. As he listened, he heard the following conversation:
The guttural voice, the voice of Satan in his pride, boasted to Our Lord: “I can destroy your Church.”
The gentle voice of Our Lord: “You can? Then go ahead and do so.”
Satan: “To do so, I need more time and more power.”
Our Lord: “How much time? How much power?”
Satan: “75 to 100 years, and a greater power over those who will give themselves over to my service.”
Our Lord: “You have the time, you will have the power. Do with them what you will.”
Dietrich von Hildebrand, In Defense of Purity, Steubenville: Hildebrand Press, 2017.
It is 50 years since Paul VI, in Humanae Vitae, predicted four effects of the widespread use of contraception: first, “conjugal infidelity and the general lowering of morality” would become widespread; second, there would be a loss of respect for women; third, contraception would increasingly be wielded as a political weapon; and finally, that man would come to think he had utter dominion over his own body.
All this has come to pass.
The acceptance of same sex marriage is a capstone legitimization of sex without responsibility; the Weinstein scandal typifies the abusive sexual treatment doled out to women; the rise of demographic politics, typified in President Johnson’s famous remark, “I’m not going to piss away foreign aid in nations where they refuse to deal with their population problems” has expanded into government advocacy of abortion; and euthanasia has become a human right – the cult of the body now embraces the culture of death.
Those who coined the term “sexual revolution” in the 1920s could not have even fantasised about the degree to which our age would not only trivialise sex, but that it would anathematise any suggestion that self-indulgent sexual behaviour could just possibly be bad for us. We legislate laws to facilitate behaviours that, even a decade ago were, by consensus, immoral.
Moral behaviour and belief in God are deeply connected. Although morality is the product of reason it is devilishly difficult to argue the objectivity of moral norms once God is dismissed from man’s vision. Philosopher Hayden Ramsey stated in 2004 that “Every young person in our society is inducted into two ways of thinking – an ethic of autonomy and a relativistic view of morality”, approaches that are completely incompatible with recognition that human beings are created and have objective duties towards God and towards others.
With this thinking we have seen an acceleration in the breakdown of committed relationships and disengagement from religion.
Can such a way of living continue indefinitely? A society where women exist for men’s pleasure, where children are a problem to be avoided, and where sacrifice for others is no longer encouraged, is already disunited and so must disintegrate.
A newly released early work of philosopher Dietrich von Hildebrand, In Defense of Purity, is a stunning reminder of what sexual relationships can and should be. His astounding clarity of insight led to Pius XII describing him as “a 20th century Doctor of the Church”. One can see why. These 1927 reflections on purity and virginity are breathtaking in their grasp of the great calling of human beings to authentic sexual relationships and to love of God, and how the first is a path to the second.
Only such a positive vision of authentic sexual expression has the power to stop the ever widening devastation of marriage, family and society. Beautifully written and marked by acute philosophical analysis, this work has set in train a new way of thinking about sex that has the power to restore what has been lost. Together with his Marriage: The Mystery of Faithful Love (1929), In Defense of Purity constitutes an important source of John Paul II’s Love and Responsibility and theology of the body.
In Defense of Purity should be required reading for every marriage educator. It is founded on a deep appreciation of biological reality and of the psychological and existential needs of men and women.
Purity is neither prudery nor sexual repression. Von Hildebrand’s central premise is that man is fulfilled only through an orientation towards God with all his being. Purity sensitises us to this divine revelation and is primarily “an abiding in God’s presence”. It is a necessity for holiness, an essential virtue for a relationship of love with God. And hence it is a necessity for prayer. It is the virtue by which our impulses and selfishness are reformed in an orientation of one’s life to God.
Sex is great gift to man and woman. “Sex necessarily involves a revelation of the deepest personal intimacy;” and “to make the sexual surrender is to anchor oneself most firmly to the world and to enter into the closest union with one’s fellow creatures”.
But only in marriage and the virtue of purity can sexual activity become an expression of love. “Sex belongs in a special manner to God” and one may only make use of it “as explicitly sanctioned by him” in marriage where “each party seeks to share in the being of the other, not simply in his or her life and thoughts.” Because so much is at stake, true purity stands in contrast to the “fearful profanation” involved when sexual pleasure becomes an end itself, or is pursued outside the divine plan of marriage. Such impurity is degrading for the person involved, desecrating in that it is a misuse of God’s gift, and defiling, because it separates us from God in our very being.
Marriage is a great good. It teaches us to live for others, and this is a prerequisite for love of God. Physical sex may only be understood in wedded love, otherwise “we become blind to the mystery it contains”. Sexual activity, if pursued outside of the commitment of marriage, will lead to bestial use of others. But with humility, acknowledgement of the spiritual, there is no loss of self-possession in the sexual act. In the absence of humility, the sexual act is overcome by dominance and brutality.
At length too there is an exploration of the importance of tenderness and deep consideration for one’s spouse, where “every detail has become an expression of love”, if there is to be true and selfless love.
Marriage, he writes, is a true calling from God. “Sex is a domain which belongs in a special fashion to God. Only by the permission of the Master of life and death may he draw the curtain from its secret.” In marriage the full and free assent of the person “to belong perpetually to the other with the bond in the sight of God”, is decisive. This assent is crucial if the couple are to transcend the experience, transforming a sexual encounter into what von Hildebrand calls, “the actualisation of the spiritual person”. Love, a willed choice of a person loved as God loves them, “makes the physical event an expression of itself.”
Von Hildebrand was the first to distinguish and integrate the unitive and procreative ends of marriage, a notion that is now a given in Catholic theology. When one grasps this way of thinking, it is immediately obvious that true marriage can only exist between a man and a woman. Same sex marriage is incapable of integrating the unitive and procreative; it is a sterile parody of what should be a sharing in God’s very creativity. Instead of being a path of offering one’s very being, it becomes an exercise in shameful self-indulgence. The distinction between male and female “lie far deeper than the biological sphere,” writes von Hildebrand.
Humility before the creator of life is crucial. He stresses the privilege, in sexual activity, of cooperating in the very creative action of God. “The pure man perceives clearly the solemn import of the act ordained by God to give life to a new human being, and this aspect of the mystery must colour everything and intensify the reference to God, providing a further motive to remain in his presence. He will never lose sight of the marvelous creative significance attaching to this act … If this act is to be enabled to the measure of perfect purity love of the partner is insufficient not to mention the single purpose of propagation; an upward glance to God thankful and loving and abiding reverently in his sight is indispensable.”
Dietrich might leave us with three take-aways.
Husbands and wives, give thanks for this great calling you have received to live tenderly and in surrender to each other; it is a shortcut to love of God so let your daily joy be the proof of this gratitude.
Parents, be pure, otherwise you will not talk clearly to your children about purity – as the habit of managing our impulsive desires so that we can be united with God in all we do, “an abiding interior rejection of the negative values associated with sex as an end in itself.”
And let Christians remember that purity is a supernatural virtue and that our efforts must, at every step, be accompanied by the grace of sacraments. It is the “fruit of an entirely new life in the soul.”
Dr Andrew Mullins was the Headmaster of Redfield College and Wollemi Colleges in Sydney for 18 years. He is the author of Parenting for Character. He now works with university students in Melbourne.
Troubling rumors have been swirling around Rome for months now about an alleged papal commission tasked with undertaking an “historical review” of Blessed Pope Paul VI’s encyclical Humanae Vitae. Despite initial denials about the existence of the commission, it appears that a Vatican official has just confirmed that there is, in fact, such a commission at work.
Of course, it’s not inherently troubling that the Vatican should study the encyclical, which celebrates the 50th anniversary of its publication this June. Humanae Vitae, which reiterated Church teaching against artificial contraception, is both one of the most important, and also one of the most opposed, misunderstood, and least taught encyclicals in Church history.
The response to Humanae Vitae is one of the great tragedies of the 20th century Church, one which contributed mightily to ensuring the dominance of the Culture of Death. A Vatican-led study oriented towards strongly reaffirming Humanae Vitae and developing a strategy for how to better present its teaching to the faithful would be very welcome.
However, there are reasons to be concerned that this may not be the primary intent of the commission. It is no secret that ever since its publication, there has been an ongoing, concerted, and often successful campaign by many theologians and some high-level clergy and church officials to “reinterpret” Humanae Vitae.
This effort received its most dramatic backing in the “Winnipeg Statement,” the Canadian bishops’ official 1968 response to Humanae Vitae. In that statement the bishops conference gave an official wink and a nod to contraception, stating that if a couple “tried sincerely but without success to pursue a line of conduct in keeping with the given directives [of Humanae Vitae], they may be safely assured that, whoever honestly chooses that course which seems right to him does so in good conscience.”
The Winnipeg Statement, the most authoritative statement of dissent in the Church against Humanae Vitae, has never been retracted. In light of the news in Rome, many pro-life leaders are naturally nervous about what sorts of findings this new, and surprisingly secretive papal commission might arrive at. Any statement even remotely resembling the Winnipeg Statement coming from the Vatican would be disastrous for souls, families, and efforts to build a Culture of Life.
St. John Paul II’s prophetic (and timely) message
For this reason, the timing couldn’t be better for the recent publication in English, for the first time, of a prophetic speech by St. John Paul II, defending Humanae Vitae from its many detractors. I urge you to read the speech, which was delivered to a conference on “responsible procreation,” in its entirety.
John Paul II had stern words for those, including some “in the Christian community,” who would oppose the teaching of Humanae Vitae. “[T]hose who place themselves in open contrast with the law of God, authentically taught by the Church, guide spouses on a wrong path,” warned the pope. “What the Church teaches about contraception is not a matter of free discussion among theologians.”
In response to those who would argue that following Humanae Vitae in some cases is “unfeasible” for spouses, John Paul II called for greater efforts to support couples, and greater faith in the power of God’s grace. “The grace of Christ gives spouses the real capacity to fulfill the whole ‘truth,’ of their conjugal love,” he said. “As the Tradition of the Church has constantly taught, God does not command the impossible, but every commandment also entails a gift of grace which helps human freedom to fulfill it.”
The pope was sympathetic to the struggles of married couples, but also unwilling to extend to them a false compassion that was inconsistent with truth. Following the moral law can be challenging, he acknowledged. The solution is not for couples to give in to temptation or to listen to the myriad voices of the world, but rather to rise to the challenge, resorting to “constant prayer” and “frequent recourse to the sacraments and the exercise of conjugal chastity.”
“Today more than yesterday, man is again beginning to feel the need for truth and right reason in his daily experience,” the Holy Father concluded. “Always be ready to say, without ambiguity, the truth about the good and evil regarding man and the family.
In this speech the sainted pope was providing a template for authentically compassionate pastoral teaching: expressing understanding for the trials of Christians, but also standing firm in the truth, and challenging couples to holiness, rather than capitulation to the world.
Uganda’s sad experiment with contraception
Why is it that so many are so afraid of upholding the beauty of Church teaching? In these past five decades we have done little to nothing to assist young couples and families as they are assaulted by a sex-saturated, anti-marriage culture. Countless Catholics have never even heard Paul VI’s teaching about the dignity and meaning of conjugal love expressed to them with both clarity and compassion. Consequently, a large majority of Catholic couples openly reject that teaching in their conjugal relations. The practical consequences have been catastrophic.
I just experienced this in Uganda where contraception is being pushed mercilessly by powerful international NGO’s and foundations. Uganda was once a very, very rare success story in Africa in the fight against AIDS, experiencing a sharp reduction in AIDS rates throughout the 1990s. How did Uganda accomplish this extraordinary feat? By a public awareness campaign heavily stressing abstinence and faithful, monogamous relationships as the only reliable ways to avoid infection. Condoms were only presented as last resort.
This message prioritizing behavioral responsibility didn’t sit well with the sex-obsessed Western foundations and governments pouring their poisoned “aid” into the country. In response to pressure, Uganda gradually began putting a greater emphasis on sexual “freedom” and condom use for prevention. The result? The end of Uganda’s success in combating the disease, with Uganda joining the few countries seeing AIDS rates increase rather than decrease. What a tragedy!
And this is only one of the most obvious negative consequences of the decision to embrace contraception, rather than responsibility and virtue, as the answer to the complexities of human sexuality.
Contraception is not the answer
Every day the Church is being proved more right: Contraception is not an answer to poverty and economic difficulties in under developed countries; nor is it a solution to the frustrations that married couples naturally feel at times in their efforts to abide by the moral law and pursue responsible procreation.
While rejecting the truth may at times appear to offer a welcome solution to difficult or painful circumstances, experience shows the costs always outweigh the apparent benefits. Paul VI warned us of this in his encyclical. He predicted at least four significant negative consequences of embracing contraception, including: a) an increase in infidelity in marriage; b) “a general lowering of morality”; c) that men would increasingly treat women as “mere instruments of selfish enjoyment,” and; d) that governments would push coercive population control on their citizens.
Who can possibly deny that each of these consequences – and many more that even Paul VI may not have envisioned – has dramatically come true?
Where the Church should be acting as the vanguard, Her representatives too often have crumpled at the first sign of opposition, afraid of appearing not with the times or “uncompassionate.” Fortunately, however there are also courageous prelates who recognize the spiritual dangers of our contraceptive, sex-obsessed culture. One of these is Archbishop Samuel Aquila, the bishop of Denver, who recently released a pastoral letter urging priests to warn their flocks of the dangerous of contraception.
“While the 1968 reception of Humanae Vitae was mixed, the fulfillment of Blessed Paul VI’s prophetic wisdom is undeniable and points to the truth of the teaching contained in Humanae Vitae,” said the bishop. “Furthermore, those communities of faith which have gone the way of the world in their teaching on human sexuality have not filled their churches but only emptied them. As Jesus made clear in the Gospel, apart from him and his life-giving teachings, we cannot bear fruit.”
The archbishop concluded, urging his priests,”[D]o not be afraid to proclaim the truth of God’s plan for human love with gentle clarity and charity.”
Let us pray for all bishops and pastors that they may be filled with similar zeal for the truth, and love for their flock. And let us pray for the members of the Vatican’s commission, that they may strongly reaffirm Church teaching, and help the Church chart a courageous path forward, finding new ways to reach the human heart with Christ’s life-giving message of salvation, including in the contested area of human sexuality.
A New Jersey couple, who invested $25K and sacrificed the lives of four other embryos to insure they would have a baby girl, are just one example among many who see nothing wrong with a new trend called “family balancing.”
Breitbart is reporting on the story of Janine Tardibuono who told NJ101.5 that having her daughter, Gianna Rosalia, after having two boys, was a dream come true. But the way she went about having this little girl is raising alarms about the use of reproductive technology in a modern world.
As Tardibuono described, she and her husband went through in vitro fertilization (IVF) at North Hudson IVF in Englewood Cliffs. The procedure produced five embryos, one of which was female. This embryo was then implanted into Tardibuono’s uterus and, nine months later, their little girl was born.
What the story doesn’t mention, however, is that four little boys died in the process.
Typical of the mainstream media, there’s no mention of the embryos that were thrown away. Instead, it goes on to interview Dr. Jane Miller, medical director at the clinic, who refers to the sex selection procedure as “family balancing.” The doctor says that she is seeing an increase in the number of couples who are using IVF to choose the sex of their children.
“There’s been so much good, solid science that’s progressed what we can do in the embryo lab,” she told NJ 101.5.
She claims to often work with parents from cultures who “value male children” as if this is a good thing. Apparently, she hasn’t read the news about the demographic disaster being experienced in cultures where sex selection procedures have resulted in a lop-sided male to female ratio that is leaving many innocent young people without mates.
Tardibuono admitted to the station that their families were critical of what they were doing and accused them of “playing with God’s plans.”
She rebutted them by saying that “God created these doctors and these people that do the lab work. “So if God created them, then their work is good.”
Obviously, she never heard of free will and how a lot of people created by God use the personal freedom He gave them for evil purposes rather than for good – such as Hitler and Kim Jung Un and serial killers such as Ted Bundy and John Wayne Gacy.
This twisted reasoning is resulting in a new trend where the commodification of children is being raised to new heights.
For example, Breitbart cites a Daily Mailarticle in which Vice correspondent Isobel Yeung said she spoke to biologists who predict that within the next five decades “we are going to completely change the way we procreate, so having sex for procreation reasons is going to feel a bit old fashioned.”
It’s already starting.
The Fertility Institutes, which operate in the U.S., Mexico, and India allow couples to use preimplantation genetic diagnosis (PGD) to choose a child’s sex as well as screen them for genetic defects. In fact, they are currently encouraging couples to commit the ultimate discrimination by offering a “special sale” – a discounted fee of $14,880 for cycles with PGD gender determinations made until June 30, 2018.
As one couple told Yeung, they chose IVF for fertility problems, but then decided to select the sex of their child while they were at it. Because they both had strong women in their lives who they looked up, they decided they wanted a girl who they could raise to be a “strong feminist.”
Being a “strong feminist” has nothing to do with flouting God’s will for our lives and making other people suffer in the process – such as the millions of tiny human lives who are being flushed down the drain in fertility centers for no other reason than because they’re the “wrong” sex.
An authentic feminist does the exact opposite. As we read in Full of Grace: Woman and the Abundant Life, she celebrates who she is and the fact that she can be in loving union with God’s plans and thus “be a catalyst of His love in the lives of others.”
Isn’t that what the world needs – love and acceptance of all? Isn’t there enough intolerance in this world already?
Too many so-called feminists run around with their hair on fire over every slight, shouting “discrimination!” and “sexist!” and yet think nothing of committing the ultimate discrimination against the unborn babies they abort and the tiny embryos they toss down the drain because they were inconvenient or didn’t match their specifications.
We can only pray for those who resort to “family balancing” to get what they want. As history has proven over and over again, whether one is a believer or not, standing in opposition to God’s will never ends well – and that’s something technology will never change.
PYEONGCHANG, South Korea, February 7, 2018 (LifeSiteNews) — Both men and women Olympic athletes at the Winter Games in South Korea will be given an average of 37 condoms each.
Olympic officials are distributing 110,000 prophylactics in grab-as-many-as-you-want baskets at athlete bathrooms, apartments, medical clinics, media rooms, and wherever the competitors gather, according to the South China Morning Post.
CNN asked if Olympic organizers are “expecting the most promiscuous Winter Games in modern history?”
“Olympic athletes are some of the few remaining decent role models for our youth, demonstrating that hard work, diligence, drive and clean living can bring about higher levels of excellence,” Father John Peck, blogger and creator of Good Guys Wear Black, Preacher’s Institute, and Journey to Orthodoxy, told LifeSiteNews.
“The International Olympic Committee continues the push for sexual license in an Olympic Babylon,” Father Peck said. “Soon, the Committee will no doubt be pushing for mentally ill men to compete in women’s sports, showing that rules mean little, reality means nothing, and demonstrating to the world that they are morally and intellectually inferior to the very athletes they encourage to fornicate as often as they eat.”
“Surely there is a better use Olympic Committee money can be spent on,” Peck concluded. “Leave the social engineering off the docket.”
“Generous contributors to the U.S. Olympic Committee ought to know that their tax-deductible donations are directly supporting promiscuity and gross immorality,” Archpriest Alexander F.C. Webster, Ph.D, dean and professor of moral theology at Holy Trinity Seminary in Jordanville, New York, told LifeSiteNews. “That is assuredly not in keeping with the venerable Olympic ‘spirit.’”
The number of contraceptives breaks a Winter Olympics record: 10,000 more than in 2010 and 2014. It doesn’t come close, however, to the 2016 Summer Games in Rio de Janeiro, where 350,000 male condoms and 100,000 female condoms were distributed.
The South China Morning Post announcement has raised little public concern. Organizers say their motive is to encourage “safe sex.”
EliteDaily explains “the facade perpetuating nothing but wholesome happenings in the Olympic Village first began to crumble at the 1992 Games” when organizers ordered thousands of rubbers.
Some of the 2,925 athletes won’t take them. Many will be taken home.
One athlete estimated that 75 percent of the competitors engage in licentiousness.
Elitedaily.com reported that most of the condoms were donated by manufacturer Convenience Co. The company says it is trying to help “a successful hosting of the Winter Olympics and the prevention of the spread of the HIV virus.”
The International Olympic Committee began distributing contraceptives at the 1988 Olympics in Seoul, South Korea.
PARIS, France, February 6, 2018 (LifeSiteNews) – In what viewers are calling the “most powerful pro-life video…ever,” a new youtube video highlights abortion as a choice that destroys the most important relationship on earth, between a mother and her child. The minute-and-a-half video has over 61,000 views.
“À un Choix de te Perdre” [With a Choice to Lose You] begins with a young woman discovering she is pregnant. She then begins to imagine what life would be like with her new baby. She plays “hide and seek” with him. She teaches him to count with his fingers. She helps him take his first step.
Suddenly, the happy scene becomes overcast as the thought of aborting her baby enters the woman’s imagination.
The woman finds herself on an operating table with the instruments of abortion close at hand.
Flashing before her mind are images of her son who is recoiling from danger. She kneels before him, wanting to protect him.
Wounds appear on the boy’s face. Blood drips from his nose. It’s as if the boy is being destroyed by abortion right before her eyes.
He looks at her pleadingly to do something to stop it.
She tries to hug him, but he disappears from her arms. She is left alone and broken.
But the film ends with a message of hope.
“What would my life have been like, without you?” states a text that fills the screen.
The boy, now alive and well, is seen running to his smiling mother who hugs and kisses him. All is well.
She made the choice to protect her baby.
Another text fades into view: “Malchance” [Bad luck] turns into “Ma Chance” [My chance].
DENVER, Colorado, February 5, 2018 (LifeSiteNews) – As the 50th anniversary of Humanae Vitae approaches, the “liberating truth” of Church teaching on human sexuality must be proclaimed to the “increasingly confused” world, Archbishop Samuel Aquila of Denver wrote in a new pastoral letter.
In his pastoral letter, titled The Splendor of Love, Aquila wrote that although contraception has wrecked much of the culture and family life, not all is lost and there are great opportunities for people in every state of life to live and share Catholic teaching.
Catholics must have a “strong commitment” to defend authentic love, Aquila said, noting that Fatima visionary Sister Lucia said the final battle between God and Satan will be over “marriage and family”:
Indeed, Sr. Lucia, one of the visionaries from Our Lady’s apparition at Fatima, related that a “decisive battle between the kingdom of Christ and Satan will be over marriage and the family.” The family is the foundation of society, and when it is undermined, society itself is threatened with collapse. Therefore, it is crucial to reaffirm our commitment to the truth, goodness, and beauty of Christ’s teaching on marriage and sexuality.
Priests should “address” the 50th anniversary of Humanae Vitae in their parishes, wrote Aquila, urging them, “do not be afraid to proclaim the truth of God’s plan for human love with gentle clarity and charity.”
‘Undeniable’ that Paul VI’s predictions all came true
Some positive developments since Blessed Pope Paul VI’s encyclical upholding the Church’s perennial teaching against artificial contraception are the rise of Natural Family Planning (NFP) and Pope St. John Paul II’s Theology of the Body, Aquila wrote.
“Pope Saint John Paul II has deepened our understanding of the great gift of human sexuality, which requires nothing less from us than a complete gift of self,” Aquila explained. “In his reflections on the theology of the body, he teaches us that ‘The human body includes right from the beginning … the capacity of expressing love, that love in which the person becomes a gift – and by means of this gift – fulfills the meaning of his being and existence.’”
Aquila cited as another positive development Pope Emeritus Benedict XVI’s writings on marriage and how the love between husband and wife is a reflection of the love between God and His Church and the emphasis of Pope Francis on “the importance of fostering a culture of encounter within the family, so that the deeply social character of marriage is supported and spreads to society at large.”
Aquila cited chapters 3, 4, and 5 of the current pontiff’s controversial exhortation Amoris Laetitia. One of the portions of the document he quoted referenced St. John Paul II’s Familiaris Consortio.
“Unfortunately, Blessed Paul VI’s prophecies” about the effects of contraception “have all come true,” the archbishop wrote. He explained:
While advocates of contraception predicted that divorce rates and abortions would decrease with its use, they skyrocketed. Women have also greatly suffered from objectification, which is found in advertising and movies, but also takes on more extreme forms like pornography and sex trafficking. The Holy Father’s expectation that governments would impose contraception on people most recently came to fruition in the Obama administration’s Health and Human Services contraception mandate, but has also appeared in American and European government programs that provide contraception in developing countries.
While the 1968 reception of Humanae Vitae was mixed, the fulfillment of Blessed Paul VI’s prophetic wisdom is undeniable and points to the truth of the teaching contained in Humanae Vitae. Furthermore, those communities of faith which have gone the way of the world in their teaching on human sexuality have not filled their churches but only emptied them. As Jesus made clear in the Gospel, apart from him and his life-giving teachings, we cannot bear fruit.
Other “unique challenges” have arisen, “of which Blessed Paul VI could not have even dreamed,” Aquila lamented. “Rejecting the true nature of the sexual act has not led to increased happiness and fulfillment but to a distortion of the relationship between men and women. The effects of the sexual revolution have devastated our culture: large numbers of abortions, a sharp rise in STDs, divorce rates hovering near 50 percent, birth rates falling below replacement level, and a decline in people getting married.”
The prevalence of pornography has cheapened sex and led to “a decline in a rightly ordered sex drive, with a loss of libido and even a movement towards intercourse with robots, as reported in the media.”
Aquila observed that artificial contraception has had a negative impact on the planet.
“The predominant use of the pill, and endocrine-disrupting chemicals found in plastics and other products have flooded our water supplies with synthetic estrogens and endocrine-disrupting chemicals, causing a rise in infertility, an increased risk of cancer and hormonal changes for our children,” he wrote.
Catholic Church has the ‘antidote’ for today’s sexual brokenness
Citing the first book of the Bible, Genesis, Aquila told his flock that God created humans “male and female.”
“Our dignity comes from being made in his image and likeness,” he wrote. “God, the source of all life and love, planned from the beginning that the love between a man and a woman should image his own love and bring forth new life in the context of a family. The blessing of children was given to man and woman before their fall from grace, and it was not lost because of their sin.”
Family allows us a “glimpse” of “the joy of eternity” while on Earth. The family shows the reality of the two sexes and created in God’s image and loves new life into existence, Aquila explained, quoting homilies from Pope Benedict and Pope Francis.
Humanae Vitae and Theology of the Body are “vitally important teachings” that “convey these truths in a way that is both bold and pastorally aware of the challenges men and women encounter in the modern world.”
Family allows us a “glimpse” of “the joy of eternity” while on Earth.
They offer the “antidote” to “the widespread false ideas of freedom and the purpose of sexuality that so many are suffering from today.”
Total, faithful, fruitful
Citing Humanae Vitae, Aquila wrote that married love “needs to be fully human, total, faithful, and fruitful.”
He emphasized the importance of husbands and wives loving each other unconditionally. Marriage is “exclusive until death, reflecting God’s fidelity.”
Aquila recalled:
Within the last couple years, I met a couple who was living together and had conceived a child but also wanted to get married in the Church. Their situation was further complicated by the fact that the man had been married previously and had children from those marriages. The woman wanted to regularize their situation with the Church. He began the annulment process, their child was born, and they went through marriage preparation classes and NFP classes. The couple was so convicted by what they learned in NFP classes that they decided they should live as brother and sister for several months until I happily officiated their sacrament of marriage. Their love was profoundly deepened by encountering Jesus and his plan for sexuality and the family. Not only were they transformed, but their extended family and their friends heard about their experience too.
Children are “esteemed as marriage’s greatest gift,” not a burden and infertile couples can still have fruitful love “when they seek to serve the community around them.”
“Through marriage, the spouses are joined in their flesh, but also in their affections and spirit (fully human), in all the dimensions of their life (total), in their past and future (faithful and exclusive), and in the possibility of receiving the gift of a new life (fruitful),” the archbishop wrote. “Genuine married love has these four features.”
“Because God designed sex to have both a unitive and procreative dimension, man cannot separate them without causing real damage,” wrote Aquila. “Sex, too, is a part of ‘what God has joined together.’ It is a blessing! Like the wings of an eagle, these two meanings can only subsist together. If we try to separate them, we will lose both.”
He then outlined how the attempted sterilization of sex has led to procreation without sex:
That contraception attacks the procreative aspect of sex is readily apparent from its design. What is less apparent, though, is how it harms the unitive dimension of sex.
Saint John Paul II observed that our bodies were designed by God so that they speak a language. In the one-flesh union of husband and wife, that language communicates the total gift of self, including their fertility, without any limits or restrictions. But contraception introduces a falsehood into the language of the body. While the spouses indicate with their bodies that they are totally giving themselves, contracepted sex withholds one’s fertility and the chance to become a potential parent. Blessed Paul VI did not reject contraception because it is artificial but because it damages the conjugal act of the spouses, which lies at the heart of their intimacy and is the sanctuary of life. This makes contraceptive acts “repugnant to the nature of man and of woman” and contrary to God’s plan, as Humanae Vitae states.
Blessed Paul VI’s teaching also helps us understand the link between contraception and in vitro fertilization, that is, between sex without babies and producing babies without sex. While contraception involves removing the procreative dimension, in vitro fertilization jettisons the unitive dimension of sexual intimacy. Instead of conceiving a child in an act of love, the couple produces a child in a lab, which violates the child’s inherent dignity.
‘Take a stand against the gender ideology that is sweeping through our country’
The archbishop ended his pastoral letter with a call to action, imploring Catholics to share the beauty of the Church’s teaching.
Rather than being “a burden and a source of repression,” it helps people “overcome the many burdens and wounds that follow from our broken families and sexuality.”
“Our bodies were designed by God so that they speak a language.”
“Every Catholic has a mission to live and share the good news of God’s plan for human sexuality,” he declared. “This requires courage to stand against the prevailing cultural winds, but Jesus calls us to nothing less. Only living in the truth will give us true freedom, true love, and true happiness.”
Evangelizing the culture about the wisdom and truth of the Church’s teachings includes taking “a stand against the gender ideology that is sweeping through our country. Pointing people to the teaching of Jesus is not confrontational, but an act of love, helping them to find true happiness.”
Aquila offered suggestions for people in various states of life and professions to witness to the truth about human sexuality.
As children’s “primary educators,” parents have a special role in this regard, he said. They should guide their children to avoid pornography and casual sex and be prepared to equip them to “respond when dangerous situations present themselves.”
“Unfortunately, and sadly, our children are exposed at a young age to many confusing distortions of human sexuality,” he noted.
The archbishop said parents have told him about their four-year-olds coming “home from public schools where teachers have told them that they can be whatever gender they want and that people of the same sex can marry each other. Innocence is harmed and confusion is instilled by such teachings.”
So, “having conversations early, without destroying their innocence, will be important so that children know how to respond when dangerous situations present themselves,” he wrote.
Aquila offered inspiration for doctors and nurses, lawyers and politicians, those in media, teachers and catechists, NFP instructors, and engaged couples to continue living the Church’s teachings on sexuality.
“Jesus is the source of true love” and “the one who heals us of our sexual wounds,” he concluded. “Humanae Vitae serves as a great light in the midst of a dark and confused world when it comes to human sexual intimacy. We ask for the prayers of Blessed Paul VI as we look to his guidance for handing on and living according to the teachings of Christ in the world today.”
In our sexually obsessed culture, the virgin martyrs are our “cloud of witnesses” for sexual purity and chastity. Today is the feast of Saint Agatha who is famous for her iconographical depiction of her breasts – sometimes euphemistically referred to as “Saint Agatha’s Bells.”
I’ve assembled her life and story (along with the legendary significance of her breasts) below in seven points:
Dates. Saint Agatha (not be be confused with the virgin martyr Saint Agnes) was murdered as a consecrated virgin during the persecution of Decius (250–253) in Catania, Sicily.
Her Passion and Martyrdom. According to legend, Agatha was the daughter of a rich and noble family. She consecrated her virginity to our Lord Jesus at age 15. The Roman prefect Quintianus sought to either rape her or marry her and she refused his advances. In retaliation, he sent Agatha to a whorehouse under a madame named Aphrodisia. Agatha refused to serve as a prostitute and was sent back to Quintianus who had both of her breasts cut off (the so-called “bells of Agatha”) and sentenced her to be burned at the stake. An earthquake prevented this fate. Saint Peter appeared to her and healed her breasts. She died in at peace in prison. Painting: St Peter healing the breasts of Saint Agatha.
An Early Legend featuring Saint Peter. The legend is ancient because by AD 325, male bishops would not touch Christian females – so that deaconesses were employed for the baptism by immersion of females. This legend describes Saint Peter not only touching Agatha’s body, but touching her breasts to heal her – something quite scandalous by the fourth century. The story also reveals that Christians in the 200s had a deep understanding of the Communion of the Saints and believed that saints can and did intervene miraculously in the lives of Christians.
Her Relics. Agatha’s body is buried at the Badia di Sant’Agata in Catania, Sicily.
Agatha’s Church in Rome. Church of Saint Agnes of the Goths. The Church of Sant’Agata dei Goti (of the Goths) adapted to Arian Church of the Goths, hence its name “Saint Agatha of Goths.” It was re-consecrated as a Catholic Church by Saint Gregory the Great.
Agatha’s Iconography. Agatha is almost always depicted carrying her breasts on a tray as in the painting by Zurbarán (below). It is difficult to find a traditional image, statue, or icon that does not depict her breasts. The removal of her breasts is a sign of consecrated virginity. For centuries, this depiction of Agatha visibly depicted how Agatha sacrificed the ability to nurse children. The breasts are a sign of motherhood. Saint Agatha by Zurbarán
Her Patronage for Breast Cancer Patients. She is the first recorded woman to experience a full and radical mastectomy, and she naturally became the patroness of breast cancer patients. Traditionally, she is also the patroness of Sicily, wet nurses, bell-founders, bakers, earthquakes, and eruptions of Mount Etna.
Please share this with you friends on this feast of Saint Agatha. May she pray for us and inspire to prefer chastity and love for Christ above all the temptations of this life.
ADDRESS OF JOHN PAUL II TO PARTICIPANTS IN A STUDY MEETING ON RESPONSIBLE PROCREATION
Friday, June 5, 1987
Dear brothers and sisters,
1. I warmly greet you and thank you for your presence, and I am pleased with the “Study and Research Center for the Natural Regulation of Fertility” at the Catholic University of the Sacred Heart’s faculty of medicine, for having promoted a study meeting on issues related to responsible procreation.
Your commitment is inscribed in the mission of the Church and participates in it, owing to a pastoral concern which is among the most urgent and important. It is about ensuring that spouses live their marriage in a holy manner. You offer to help them on their journey towards holiness, for the full realization of their conjugal vocation.
It is well known that often — as the Second Vatican Council has also revealed (cf. Gaudium et Spes, 51,1) — one of the main anxieties that spouses face is constituted by the difficulty of realizing the ethical value of responsible procreation in their conjugal life. The same Council bases a just solution to this problem on the truth that there can be no contradiction between the divine law concerning the transmission of human life and true conjugal love (cf. Gaudium et Spes, 2). To speak of a “conflict of values or goods” and of the consequent need to “balance” them, choosing one and rejecting the other, is not morally correct and only generates confusion in the conscience of the spouses. The grace of Christ gives spouses the real capacity to fulfill the whole “truth” of their conjugal love. You desire to bear witness concretely to this possibility and thus give married couples an invaluable help: to live their conjugal communion in its fullness. Despite the difficulties you may encounter, it is necessary to continue with generous dedication.
2. The difficulties you encounter vary in nature. The first, and in a certain sense the most serious, is that also in the Christian community, voices have been heard and are heard that call into question the truth of the Church’s teaching. This teaching was expressed forcefully by Vatican II, by the encyclical Humanae Vitae, by the apostolic exhortation Familiaris Consortio, and by the recent instruction “The gift of life.” In this regard, a serious responsibility emerges: those who place themselves in open contrast with the law of God, authentically taught by the Church, guide spouses on a wrong path. What the Church teaches about contraception is not a matter of free discussion among theologians. Teaching the contrary is tantamount to inducing the moral conscience of the spouses into error.
The second difficulty is constituted by the fact that many think that the Christian teaching, although true, is nonetheless unfeasible, at least in some circumstances. As the Tradition of the Church has constantly taught, God does not command the impossible but every commandment also entails a gift of grace which helps human freedom to fulfill it. Yet constant prayer, frequent recourse to the sacraments and the exercise of conjugal chastity are needed. Your commitment, then, must not be limited to teaching only a method for controlling human fertility. This information should be inserted into the context of a complete educational plan, which addresses the person of the spouses, considered in their integrity. Without this anthropological context, what you propose would risk being misunderstood. You are clearly convinced of this, for you have always put a correct anthropological and ethical reflection at the foundation of your courses.
Today more than yesterday, man is again beginning to feel the need for truth and right reason in his daily experience. Always be ready to say, without ambiguity, the truth about the good and evil regarding man and the family.
With these sentiments I wish to encourage the unique service of apostolate that you seek to carry out in dioceses and family formation centers. In educating in responsible procreation, know how to encourage spouses to follow the moral principles inherent in the natural law and in a healthy Christian conscience. Teach them to seek and to love the will of God. Encourage them to respect and to fulfill the sublime vocation to spousal love and the gift of life.
Gladly do I bless you all, your loved ones and the initiatives of your apostolate.
WASHINGTON—Cardinal Timothy M. Dolan of New York, chair of the U.S. Conference of Catholic Bishops’ (USCCB) Committee on Pro-Life Activities called the Senate’s failure to pass the Pain-Capable Unborn Child Protection Act “appalling”. The bill proposes to ban abortions starting at 20 weeks after fertilization.
“The U.S. Senate’s failure to adopt the Pain-Capable Unborn Child Protection Act, prohibiting abortions at 20 weeks post-fertilization, is appalling. Abortions performed in the second half of pregnancy usually involve brutally dismembering a defenseless unborn child, while also posing serious dangers to his or her mother. The Senate’s rejection of this common-sense legislation is radically out of step with most Americans. Opinion polls consistently show that a strong majority of the public opposes late-term abortions—including those who self-identify as ‘pro-choice’. Furthermore, the United States is currently one of only seven countries that allows abortions beyond 20-weeks. The other six are North Korea, China, Vietnam, Singapore, Canada and the Netherlands. The Senate must rethink its extreme stance on late-term abortions. I call upon the public to tell the Senate that this vote is absolutely unacceptable.”
MICAIAH BILGER JAN 29, 2018 | 1:30PM LONDON, ENGLAND
In abortion activists’ minds, Beth Morton had many good reasons to have an abortion. She was young, unmarried and her birth control failed. What’s more, she was pregnant with triplets and completely unprepared to be a parent.
But the 26-year-old mother from Essex, England knew that her unborn babies were valuable human beings.
The Daily Mail reports Morton chose life for her non-identical triplets, Archie, Lola and Ralphie, and gave birth in June.
Morton said she had been taking the birth control pill for years, and was shocked last year to learn that they had failed. Her partner, Danny Bellamy, was supportive; but Morton said her family was worried about how she would handle the unplanned pregnancy.
“I’m only young and my family were worried about how I was going to take to it, but I’ve just taken it in my stride,” Morton said. “I’m very calm with the triplets and I love being a mom. So, even though it was a shock, I wouldn’t change it for anything.”
Morton experienced another shock during her 12-week ultrasound scan when the technician announced that she was having triplets.
“I thought the sonographer was joking …” she said. “She told me she wasn’t joking, and I could see the three sacs in there. I burst out crying. I couldn’t take it in. Danny was really happy, but it was still a real shock to me.”
The medical team even suggested that she have a “selective reduction,” an abortion that would have destroyed one or two of the triples’ lives.
Morton said no.
Here’s more from the report:
Non-identical triplets are rarely conceived without the use of IVF, and Miss Morton was offered a ‘selective reduction’ – in which doctors terminate one or two of the babies to make it a safer pregnancy.
But the couple refused. Miss Morton said: ‘There was no way that we would have ever considered a selective termination.
‘How could you possibly choose one baby’s life over another … we were determined to give all three of them the best possible chance. I know it was a risky pregnancy, but I trusted the doctors to look after us all.’
A year later, Morton said she is happy as a mother of three, and each of the triplets already is displaying his or her own personality.
“They may have been a surprise, but I can’t imagine life without them now,” Morton said.
In our culture’s current self-examination on sexual harassment and sexual abuse, we would also do well to ponder how the “contraceptive mentality” has contributed to the many sexually related problems of the day. This view insists that there is no necessary connection between sex and having children; it separates what God has joined. This has led to a whirlwind of confusion about the nature and purpose of sexual intimacy as well as about marriage and family. Many treat sex lightly and frivolously; they falsely think that sex can be without consequences. As we have seen played out in the recent news, many men no longer see women as wives, mothers, and persons to be respected, but as sexual objects to be exploited.
Two generations have passed since the publication of the boldly pastoral and prophetic encyclical Humanae Vitae, which upheld the ancient ban on the use of artificial contraception. Perhaps no teaching of the Church causes more scoffing (even from Catholics) than our teaching against artificial contraception: Unrealistic! Out of touch! Uncompassionate! Silly! You’ve got to be kidding!
The Lord Jesus had an answer to those who ridiculed Him in a similar way:
“To what can I compare this generation? They are like children sitting in the marketplaces and calling out to others: ‘We played the flute for you, and you did not dance; we sang a dirge and you did not mourn.’ For John came neither eating nor drinking, and they say, ‘He has a demon.’ The Son of Man came eating and drinking, and they say, ‘Here is a glutton and a drunkard, a friend of tax collectors and sinners.’ But time will prove where wisdom lies” (Matt 11:16-18).
Indeed, times does prove where wisdom lies. Some fifty years after acceptance of contraception set in, how are we doing? Perhaps it is best to review some of the “promises” that advocates of contraception made and then review the prophecies of Pope Paul VI. Then let’s review the record and note the “fruits” of contraception.
The Promises of the Contraception Advocates:
Happier marriages and a lower divorce rates, because couples will be able to have all the sex they wanted without the “fear” of pregnancy.
Lower abortion rates because there will be far fewer “unwanted” children.
Greater dignity for women because they will no longer be “bound” by their reproductive system.
A more recent promise: reduction in sexually transmitted diseases (STDs) and AIDS.
The concerns and predictions of Pope Paul VI (in Humanae Vitae):
Consider how easily this course of action could open wide the way for marital infidelity (HV # 17)
A general lowering of moral standards. Not much experience is needed to be fully aware of human weakness and to understand that human beings—and especially the young, who are so exposed to temptation—need incentives to keep the moral law, and it is an evil thing to make it easy for them to break that law. (HV # 17)
Another effect that gives cause for alarm is that a man who grows accustomed to the use of contraceptive methods may forget the reverence due to a woman, and, disregarding her physical and emotional equilibrium, reduce her to being a mere instrument for the satisfaction of his own desires, no longer considering her as his partner whom he should surround with care and affection. (HV # 17)
Who will prevent public authorities from…impos[ing] their use on everyone. (HV # 17)
So who had the wisdom to see? Was it the world or the Church? Let’s consider some of the data:
The divorce rate did not decline; it skyrocketed. Divorce rates soared through the 1970s and beyond until nearly 50 percent of marriages were failing. In recent years the divorce rate has dropped slightly, but this may be due more to the fact that far fewer people get married in the first place, preferring instead to cohabitate and engage in a kind of serial monogamy, drifting from one relationship to the next. The overall divorce rate currently hovers in the low 40 percent range. Advocates of contraception today claim that divorce is a complicated matter, which is certainly true, but they cannot have it both ways: at first claiming that contraception will be a “simple” fix to make marriages happier and then, when they are proved so horrifyingly wrong, claiming that divorce is “complicated.” Pope Paul VI, on the other hand, predicted rough sailing for marriage with the advent of contraception; it looks as if he was right.
Abortion rates did not decline; they skyrocketed as well. Within a few years, the pressure to make abortion more available led to its “legalization” in 1973. It has been well argued that far from decreasing the abortion rate, contraception actually increased it. Because contraception routinely fails, abortion has become the contraception of last resort. Further, just as the Pope predicted, sexual immorality has become widespread; this also has led to higher rates of abortion. It is hard to compare promiscuity rates between periods because people don’t tend to tell the truth when asked about such things. But one would have to be very myopic not to notice the huge increase in open promiscuity, cohabitation, pornography, and the like. All of this bad behavior, made more possible by contraceptives, also fuels abortion rates. Chalk up another one for the Pope’s and the Church’s foresight.
Women’s dignity is a difficult thing to measure, and different people have different yardsticks by which to measure it. Women do have greater career choices today, but is that the true source of a person’s dignity? Dignity certainly involves more than one’s economic and utilitarian capacity. Sadly, motherhood has taken a back seat in popular culture. And, as the Pope predicted, women have been hypersexualized as well. Their dignity as wives and mothers has been set aside in favor of the sexual pleasure they offer to men. Many modern men, no longer bound by marriage for sexual satisfaction, use women and discard them on a regular basis. Men “get what they want” and it seems that many women are willing to supply it rather freely. In this scenario, men win. Women are often left with STDs. They are often left with children they must support and raise alone. And as they get older and “less attractive” to men, they are often alone. I am not sure that this is dignity. Have women really benefited under this new morality, which contraception helped to usher in? I think the Pope wins this point as well.
As for preventing/reducing STDs and AIDS: again, big failure. STDs were not prevented, nor did they decrease. Infection rates skyrocketed through the 1970s and 1980s. AIDS, which appeared on the scene in the 1980s continues to show terribly high rates. Where is the promised deliverance? It seems that contraceptives do not prevent anything. Rather, they encourage the spread of these diseases by encouraging the bad behavior that causes them. Here, too, it looks as if the Church was right and the world was wrong.
Add to this list of effects the high rate of teenage pregnancy, the devastation experienced by single parent families, and even increasing poverty. The link to poverty may seem a stretch, but the bottom line is that single motherhood is the chief cause of poverty in this country. Contraception encourages promiscuity. Promiscuity often leads to pregnancy at a young age. Youthful pregnancy often leads to single motherhood (absent fathers). Single motherhood often leads to welfare dependence and poverty. In our inner cities today, over 80 percent of homes are headed by single mothers. It is the single best predictor of poverty.
Declining birth rates, fueled by contraception, are devastating cultures. Europe as we have known it is simply going out of existence. (I have written on that before here: Contraception is Cultural Suicide!). Europe’s future is as a Muslim continent; Muslims typically have much larger families. Likewise, here in the United State, the birth rate in white and African-American communities is below replacement level. Thankfully, our immigrants are largely Christian and share our American vision. For the Church, the declining birthrates are resulting in the closing of parishes and schools, and a reduction in vocations to the priesthood and religious life. We cannot sustain what we have on a population that is no longer replacing itself. Immigration has insulated the Church from this to some extent, but the decline in Mass attendance has eclipsed the growth from immigration and we are starting to shut down a lot of our operations.
Conclusion: Time will prove where wisdom lies. What have we learned over these decades of contraception? First, we have learned that it is a huge failure in meeting its promises; it has backfired, making things worse rather than better. Marriage, families, and children have all taken a huge hit. Bad behavior has been encouraged and all the bad consequences that flow from it are flourishing. Most people seem largely uninterested in this data. Hearts have become numb and minds have gone to sleep. I hope that you will consider this information thoughtfully and share it with others. Time has proven where wisdom lies. It is time to admit the obvious.
If St. John Paul II was right in Evangelium Vitae (and he most assuredly was), this has been a most remarkable week not just for life, but also for democracy, in the United States.
There were, of course, the hundreds of thousands of pro-lifers who showed up in D.C. to march in the bitter cold to defend the right to life of the unborn – one of the largest crowds I’ve ever seen. (Watch an astonishing time-lapse video of the march here.) But while their presence was expected (pro-lifers have been doing it for 45 years after all) there were a series of additional, and wholly welcome, surprises.
One such was the vote by the U.S. House of Representatives on the same day as the March to pass H.R. 4712, also known as the Born Alive Abortion Survivors Protection Act, by a vote of 241-183. The bill clarifies that any baby that survives a botched abortion must be given the same care as any other baby that is born alive.
Sadly, such a law is still needed. Too few people know that President Obama repeatedly and unapologetically voted against a similar bill when he was a senator in Illinois. This was despite eye-witness testimony from a nurse in Illinois that living, born babies were in fact being abandoned to die. And even now, gruesome reports routinely emerge of similar instances happening in abortion facilities across the country.
Then, of course, there was President Trump’s extremely encouraging speech to the March for Life. Not only did Trump urge Congress to pass another crucial pro-life bill – the Pain-Capable Unborn Child Protection Act – and put it on his desk, but he powerfully affirmed the fundamental goodness of the pro-life cause. “We are protecting the sanctity of life and the family as the foundation of our society,” Trump said, “but this movement can only succeed with the heart and the soul and the prayer of the people.”
Speaking directly to the pro-lifers gathered on the Mall, Trump stated: “Because of you tens of thousands of Americans have been born and reached their full God-given potential, because of you. You’re living witnesses of this year’s March for life theme, and that theme is, ‘Love Saves Lives.’”
Amen.
On the same day, in another thoroughly pro-life statement, Trump declared January 22 – the tragic anniversary of the Roe v. Wade decision – National Sanctity of Human Life Day. Trump lamented that “much of the greatest suffering in our Nation’s history” is due to “disgracefully misguided attempts to dehumanize whole classes of people…” Calling attention to the “irrefutable evidence” of the humanity of the unborn child, he stated: “We cannot let this shameful history repeat itself in new forms, and we must be particularly vigilant to safeguard the most vulnerable lives among us.”
Rounding off the week was Congress’ decision to confirm Alex Azar, Trump’s nominee for Secretary for the Department of Health and Human Services. Pro-life groups welcomed the appointment of Azar, who defended the conscience rights of Christians during his confirmation hearing, while pro-abortion organizations like NARAL slammed him as “anti-choice.”
We Must Go Deeper: Abortion and the Unholy Trinity
Yes, it has been a remarkable week for life, and hopefully the beginning of much more to come.
However, this past week I was also sent something that reminded me just how far we have yet to go…how much deeper we must dig if we are to strike at the heart of this infernal invention called abortion.
What I was sent was one pro-life activist’s recollection of a conversation he once had with the dynamic and uncompromising founder of the March for Life, Nellie Gray. This person recounted how Gray told him abortion would not end, “Until the pro-life movement is 100% pro-life: that is, 100% against contraception, 100% against same-sex marriage, 100% supportive of showing abortion images…”
It is good that so many Americans have awoken to the reality of abortion. But, then again, how could they not? In this day of ubiquitous ultrasounds, in utero photography, and advanced embryology, how can anyone still defend abortion? When the living, moving human person in the womb is right in front of our eyes, available for the world to see, how can so many still be blind to the inhuman violence of abortion?
Alas, even though polls show the number of people who describe themselves as “pro-life” is increasing, when pressed, many of those “pro-life” people still support abortion in some cases. The person who spoke with Gray recalled her saying, “You’d be surprised by the number of people who say they are pro-life but support using contraception; support abortion in cases of rape, incest and to save the life of the mother!”
The reason we still have abortion isn’t because the Supreme Court has refused to overturn Roe v. Wade; it isn’t because our president isn’t pro-life enough; it isn’t because the media is overwhelmingly pro-abortion. It goes way deeper than that. It goes to the very heart of our culture. It goes to the individualistic selfishness that so many of us have unthinkingly accepted as our most fundamental value, and which we mistakenly call “freedom”: a self-centeredness that has manifested itself most perniciously in the total inversion of sexual values since the sexual revolution.
Abortion is only one member of an unholy Trinity –– perverse sex-education, contraception and abortion. In order to end abortion, we must pluck it up by the root. That means we must address the primordial self-centeredness on which it feeds; we must put sexuality back on a firm footing, oriented not towards selfish, empty pleasure, but towards creating new life and building strong, faithful, and fruitful marriages.
“[T]he more you sow contraception, the more you reap sexual sins, family and social disorders, venereal diseases, and deadly AIDS,” said HLI Founder Father Paul Marx, “and the more you must make available ‘abortion services’ to take care of the ‘contraceptive failures’.”
Abortion: a threat to democracy and peace
Unless our country concertedly does this, we can only expect the gradual dissolution of our democracy, a gradual descent into disorder and even tyranny: for what social order can possibly survive the violent dehumanization of so many of its members? Such, at least, is what the popes have so clearly affirmed.
“Every crime against life is an attack on peace, especially if it strikes at the moral conduct of people,” stated Blessed Pope Paul VI. “But where human rights are truly professed and publicly recognized and defended, peace becomes the joyful and operative climate of life in society.”
St. John Paul stated categorically that it is impossible to promote the common good if the right to life is not recognized. “Only respect for life can be the foundation and guarantee of the most precious and essential goods of society, such as democracy and peace,” he said.
Or, as Mother Teresa put it so succinctly, “The greatest destroyer of love and peace is abortion, because it is a war against the child, a direct killing of the innocent child, murder by the mother herself. And if we accept that a mother can kill even her own child, how can we tell other people not to kill one another?”
To his credit, in his speech to the March for Life, President Trump echoed these sentiments. Speaking of the “gift of life,” Trump said, “That it is why we march. That is why we pray. And that is why we declare that America’s future will be filled with goodness, peace, joy, dignity, and life for every child of God.”
A few years ago, I spoke with a young man preparing to get married. His aunt told him that she thought he and his fiancée were too financially-strapped to have a child, and that it wouldn’t be fair to bring up a baby in poverty. Keenly aware of his joblessness and his minuscule bank account, he concluded she was probably right.
The young man and his fiancée were ready to tie the knot in a few months and they expected that she would be at the infertile phase of her cycle around the time of their honeymoon, so they would be able to consummate the marriage while avoiding bringing a child into the world. They agreed they would use Natural Family Planning (NFP) after that to avoid a pregnancy. A few years later when they felt financially secure, he told me, they would have their first child. He admitted, however, that he was conflicted about whether they were really being “open to life” in their marriage if they were going into it with this kind of forethought and intention of avoiding children.
In marriage, it can certainly be challenging to harmonize spousal love with the responsible transmission of life. Janet Smith and Christopher Kaczor, in an illuminating passage from one of their recent books, acknowledge this challenge and point to the need for a “spirit of generosity” when it comes to procreation:
“Pope John Paul II spoke of ‘responsible parenthood,’ in which a couple uses practical wisdom, prayer and a spirit of generosity in determining how many children they should have. Some Catholics believe that the Church permits the use of NFP only for reasons that verge on the truly desperate, such as a situation where a pregnancy would threaten a woman’s life or a family is living in dire poverty. Magisterial documents, however, state that spouses may have physical, psychological, economic or social reasons for needing to limit family size, using several different adjectives to describe those reasons: One can have ‘just’ reasons, ‘worthy’ reasons, ‘defensible’ reasons, ‘serious’ reasons and ‘weighty’ reasons. In short, the Magisterium teaches that spouses must have unselfish reasons for using NFP and limiting their family size.”
At times, then, our justifications for avoiding a pregnancy may merit further reflection and scrutiny on our part. When it comes to “poverty,” for example, would our poverty, in the true sense of the word, mean that the child would be malnourished and without warm clothing, or would it simply mean that he or she would forego some of the latest hi-tech gadgets that other children in the neighborhood might be enjoying?
I recall what a father of seven children on a tight budget once told me in a conversation: “Honestly, there’s always room around the table for one more, and with ‘hand me down’ clothing we always manage. And my goodness, isn’t it a momentous thing to receive that trust of preparing another soul for an eternal destiny with God?” His wife pointed out how the older children ended up helping with raising the younger ones, lessening the burdens on mom and dad, and turning it into a “team effort.”
“I’ve never seen the Lord send a child without also sending a lunch pail.”
The ancient Christian teaching on the two-fold purpose of marriage, namely, the “procreation and education of children,” and the “mutual help and sanctification of the spouses,” accurately summarizes the inner order of marriage. As the future John Paul II wrote in his great 1960 book ‘Love and Responsibility,’ radical personal openness to both of these purposes is essential to the success and meaning of any marriage. We should never enter into marriage with active opposition to the very ends for which it exists. If a couple is preparing to embark upon marriage with the immediate intention of avoiding offspring (even if they are using morally acceptable means such as NFP), they perhaps ought to consider delaying the exchange of their vows until they have resolved the various impediments, whether financial, career-related, or personal, that are leading them to be closed to the idea of having children.
I recall hearing about another family that had six children. They didn’t have two nickels to rub together. After the father came down with mental illness, the mother had to support the family single-handedly. A clear-thinking woman with an unflinching faith, now elderly and reflecting on her past, she memorably remarked to her neighbor: “I’ve never seen the Lord send a child without also sending a lunch pail.” God, who is the very source of the immortal souls of our children, is a provident God who invites us to examine the heart of our marriages. He invites us to entrust ourselves to him, so that we might be courageous and authentically open to the gift of life he sends us in the midst of the marital embrace.
The Church exists to lead us to happiness. Yet the world sees the Church as one of the primary obstacles to self-fulfillment. This conflict comes from two opposing views of what makes us happy. The Church points to self-giving love as the path (other-focused), while the world holds to the fulfillment of our desires (self-focused). The flashpoint of these opposing views centers on sexuality — either as a gift or an itch. And the battle has entered the Church.
When Jesus founded the Church, he gave us a blueprint of our mission: “Go, therefore, and make disciples of all nations, baptizing them in the name of the Father, and of the Son, and of the Holy Spirit, teaching them to observe all that I have commanded you” (Matthew 28:19-20).
The Church’s message is good news because it liberates our minds and desires from our selfish inclinations. The truth given to the Church by Christ fulfills and completes the order of the created world, inscribed within it by its Creator. The Gospel and the natural law bear common testimony to the will of God, which leads us to happiness.
The Church is the guardian of the natural law, a moral order that arises from the inherent purpose of our nature as body-soul unities. We have been created in the image of God, a reality reflected even by the human body.
Pope St. John Paul II taught in his theology of the body that we must recognize the truth written into our very beings: “Man and woman are called to express that mysterious language of their bodies in all the truth which is proper to it” (Aug. 22, 1984). The body, including our sexuality, has a truth that we must recognize and respect.
This year will see a prolonged family feud about the relevance and applicability of the Church’s teaching on contraception. Fifty years ago, Pope Blessed Paul VI issued a prophetic affirmation of the natural law and the Church’s timeless teaching in his encyclical Humanae Vitae (The Regulation of Birth). At the heart of encyclical, we find the message that “each and every marital act must of necessity retain its intrinsic relationship to the procreation of human life” (11).
This teaching does not come from an outmoded moral code, but the recognition of what sexuality is in itself: an expression of the unity and fruitfulness of married love. To contend for the legitimacy of contraception would entail a move from truth to unreality — a shift from the Church’s mission to a lie.
As we encounter hostility on the topic of contraception, from outside and even within the Church, we will have to ask ourselves: Are we ashamed of the truth of the Church’s teaching on contraception? Do we think contraception really will help people to be happy?
These questions stand at the heart of the battle for the legacy of Humane Vitae. Are we willing to stand for the truth, or will we accommodate the lies surrounding sexuality that dominate our culture?
Humanae Vitae recognizes that couples, while respecting the nature of the marital act, may “for serious reasons and with due respect to moral precepts, decide not to have additional children for either a certain or an indefinite period of time” (10).
Many ask how practicing natural family planning differs from contraception. It comes down to the key moral principle that “the end does not justify the means” (Catechism of the Catholic Church, 1753). A good intention to defer pregnancy for a legitimate cause does not justify the use of means that are “intrinsically wrong” and that distort the natural ordering of the act (Humanae Vitae, 14).
I have found that very many people indeed hold that a good end can justify the means. It seems that even some prominent Churchmen agree.
A newly appointed member of the Pontifical Academy for Life, Father Maurizio Chiodi, recently argued at a conference at the Gregorian University that “in situations when natural methods are impossible or unfeasible, other forms of responsibility need to be found. There are circumstances — I refer to Amoris Laetitia, Chapter 8 — that, precisely for the sake of responsibility, require contraception.”
The title of Father Chiodi’s lecture itself, “Rereading Humanae Vitae (1968) in Light of Amoris Laetitia (2016)” points us to the nature of the present attack on Humanae Vitae.
Some would like to use Pope Francis’ apostolic exhortation, Amoris Laetitia (The Joy of Love), to justify actions, like contraception, that are by their very nature and object “intrinsically wrong” (Humanae Vitae, 14). Pope St. John Paul II already foresaw the foundation of this strategy, in allowing conscience to interpret and arbitrate the teaching of the Church, and warned us against it:
“A separation, or even an opposition, is thus established in some cases between the teaching of the precept, which is valid in general, and the norm of the individual conscience, which would in fact make the final decision about what is good and what is evil. On this basis, an attempt is made to legitimize so-called ‘pastoral’ solutions contrary to the teaching of the magisterium and to justify a ‘creative’ hermeneutic according to which the moral conscience is in no way obliged, in every case, by a particular negative precept” (Veritatis Splendor, 56).
To allow conscience to trump the moral law, rather than apply it, undermines the moral life itself, descending into individualism and relativism.
Thankfully, the Catechism stands against this distortion:
“It is therefore an error to judge the morality of human acts by considering only the intention that inspires them or the circumstances (environment, social pressure, duress or emergency, etc.) which supply their context. There are acts which, in and of themselves, independently of circumstances and intentions, are always gravely illicit by reason of their object, such as blasphemy and perjury, murder and adultery. One may not do evil so that good may result from it” (1756).
Both Popes Paul and John Paul II definitively taught that contraception falls into this category of an intrinsically evil action.
The Church cannot cave in to the predominate relativism of our time. We have fallen into unreality about who we are as men and women and what will make us happy.
If the Church does not stand for the truth, who will? We must speak the truth in love, rather than affirming positions that lead people away from true happiness. In fact, the Gospel holds the antidote to the world’s misery, and we can’t hide it under a bushel basket! The Church can never lie to her people or to the world, but must answer the summons of the Master to teach what he has commanded.
The interpretation of Humanae Vitae comes down to whether or not we are willing to be honest about who we are as Catholics. We belong to the Body of Christ, having put on the mind of Christ, and have accepted his word above our own.
Jesus has given us the mission to share his Good News, rather than our own concerns and opinions. If we have faith in Christ and accept our Catholic identity, then we must teach and observe honestly and truthfully all that he has commanded us. God offers us the truth, and living it offers the only true path to happiness.
R. Jared Staudt, Ph.D., works in the Office of Evangelization
and Family Life Ministries of the Archdiocese of Denver.
A significant number of American women who have had an abortion have felt subtle, or even substantial, unwanted pressure to abort, a recent study has found.
The study, published recently in the Journal of American Physicians and Surgeons, found that nearly three-quarters (73.8%) of women with a history of abortion surveyed admitted that they experienced at least subtle forms of pressure to terminate their pregnancies.
More than half of the women reported that the perceived pressure was great enough to significantly influence their decision to abort. Of the 987 women surveyed, more than half (58.3%) indicated that they decided to abort in order to make others happy. Nearly 30% of survey respondents admitted that they were afraid that they would lose their partner if they failed to terminate their pregnancy.
Further underlining the fact that choosing abortion is contrary women’s natural instincts, the study also found that two-thirds of the women (66%) knew in their heart that abortion was wrong. Many women (67.5%) said that the decision to terminate their pregnancies was one of the hardest decisions of their lives.
“These findings are alarming,” says Population Research Institute President Steven Mosher. “They suggest that a substantial number of women in America today who supposedly ‘choose’ abortion are actually being pressured into it by their husbands, boyfriends, or family members.”
“If a man tells a woman in so many words that he will leave her if she does not get an abortion, that woman is being denied the right to freely choose her—and her unborn child’s fate. The threat of abandonment is a very strong inducement to the woman not to carry her child to term.”
The study, led by Priscilla K. Coleman, Professor of Human Development and Family Studies at Bowling Green State University, Ohio, included anonymous surveys from 987 women seeking post-abortion counseling services at crisis pregnancy centers nationwide. While the findings are not representative of all women in the U.S. who have had an abortion, they nevertheless reveal a significant real and widespread problem among many post-abortive women in America.
“Over the years, many women have come to me with stories of how they were—blatantly or subtly—coerced into abortion they did not want and will always regret,” says PRI President Steven Mosher. “Kudos to Professor Coleman for her brilliant study, which suggests that the magnitude of the problem is far greater than any of us suspected. We must all do more to help young women in crisis pregnancies.”
Coleman’s study used both quantitative and qualitative analysis to investigate how women perceive their past abortion(s), providing a profound insight into the perduring difficulties that women have in coping with a past abortion. Survey respondents were asked open-ended questions about what they perceived to be the biggest positives and negatives of their abortion decision.
Most women could not note anything positive about their past abortions. More than half of the respondents (53.6%) indicated no positive response or simply left the question blank. Most of the remaining women in the survey noted that their abortion experience eventually helped them to grow stronger spiritually, providing the impetus for their conversion to the Christian faith or to a deeper faith life. Others noted that it had motivated them to engage in pro-life or crisis pregnancy work.
As far as the negative consequences of their abortion experiences were concerned, many women cited serious symptoms, including symptoms often associated with poor psychological health. Women reported symptoms of depression (14.4%), guilt (14%), shame, regret, self-hatred, feelings of worthlessness, feelings of being unworthy of love, drug or alcohol addiction (9%), low self-esteem, anxiety, and thoughts or attempts of suicide (6.2%).
These findings are even more striking given that the vast majority of women included in the study were believed to have been psychologically healthy prior to their first abortion. Only 6.6% of women surveyed self-reported having used prescription medication for mental health reasons prior to their first abortion. Following their first abortion, however, over half of the women (51%) reported using such medication.
Pro-abortion activists have long claimed that abortion empowers women to make decisions about their fertility. But the findings of Professor Coleman’s study indicate that rather than feeling “empowered” by their decision to have an abortion, they were in fact pressured into a decision that was not in line with their values and wants. Worse still, the consequences of their abortions have been detrimental to their psychological and emotional health and well-being.
The findings suggest that coercive treatment of women by pressuring them to choose abortion is widespread and deeply ingrained in many communities across the country. It appears that many young women facing an unplanned pregnancy are not receiving adequate support from the people who matter most in their lives—whether they be parents, family members, boyfriends, or peers—to make decisions that are not only in accord with their conscience and values, but also in the best interest of their physical and psychological well-being.
Pro-abortion activists often frame abortion as a women’s rights issue, claiming that abortion access is necessary for women to have control over their fertility. This, they claim, empowers women to prioritize career, education, or lifestyle goals, evidently over the life of their unborn child. Despite claiming to be pro-woman, however, pro-abortion advocates rarely, if ever, mention the importance that remaining abstinent has in freeing women to pursue their life goals without the negative emotional and psychological drawbacks associated with abortion.
Indeed, research has shown that the fewer non-marital sexual partners a woman has, the less likely she is to have a sexually transmitted disease (STD) or an out-of-wedlock birth, to become a single mother or have an abortion, or to report feeling depressed. In fact, the fewer sexual partners an unmarried woman has, the more likely she is to feel happy and the less likely she is to experience divorce later in life.
Likewise, women who postpone sexual activity are more likely to report feeling happy in life, have fewer sexual partners over their lifetimes, are less likely to be single mothers, are less likely to live in poverty as adults, are more likely to have a stable marriage, and are less likely to have an abortion. Teens who are sexually active are also more likely to attempt suicide than their abstinent peers. High school teens who remain abstinent are more likely to graduate high school and were twice as likely to obtain a 4-year college degree.
A significant number of women cited their partner’s desires as reasons for deciding to undergo abortion. The fact that nearly 30% of women surveyed indicated that they chose abortion to prevent their partners from leaving them is particularly alarming. It is perhaps indicative of wider problems in American culture including the of over-sexualization of modern society, a lack of respect for women, and the breakdown of morality and traditional family structures.
Sadly, it seems that too many men are not willing to respect women enough to make lifestyle decisions in their best interest and are unwilling to take responsibility for the consequences of their own actions, abandoning women to deal with unplanned pregnancies by themselves. Likewise, too many women have abandoned traditional values, giving themselves up without the real commitment that comes with marriage.
“Ignoring these sobering facts, the so-called pro-choice movement continues to treat abortion as a panacea for all of the ills that accompany a hypersexualized society,” Mosher says, “They turn a blind eye to those who not only sexually exploit women but then also coerce women into an abortion that will leave her spirit wounded and in pain.”
Until the life and dignity of each and every person, particularly women and the unborn, are respected and valued, coercive treatment of women who find themselves in unplanned pregnancies will, sadly, continue.
WASHINGTON, D.C., January 23, 2018 (LifeSiteNews) – A pro-life Catholic priest electrified the crowd at the National Prayer Service on the day of the March for Life with his homily about the inevitable victory of the pro-life movement over abortion.
“We are marching for a certainty,” declared Father Frank Pavone, executive director of Priests for Life.
Pavone’s homily was inspired by Christ’s victory over the grave.
“Our starting point in this movement is the victory over death that Jesus Christ has already won,” he declared. “We would not be here, we would not be the Church, we would not be the Body of Christ, and we would not be the pro-life movement, if it were not true that He came out of His own tomb, having suffered death, having joined Himself to our death.”
“He rose, and in doing so did not only conquer His death,” Pavone continued, “He conquered ALL death. He overturned the kingdom of death. He robbed death of its power. He conquered your death and mine. He conquered the death of every unborn child killed by abortion […]. He has conquered. Death is overcome.”
Pavone stated that because Christ conquered death, the pro-life movement knows with “certainty” that it will one day win the battle for the unborn. The marchers are merely marching towards that goal.
“And it’s not only the certainty that we will rise at the day of victory for the unborn. It is a certainty that the power which now dismembers them and crushes them and throws them in the garbage is a power which at its root has already been defeated,” he said. “And that is why we march today with confidence.”
He boldly asserted that the March for Life would not end until the unborn are granted their “God-given” right to life.
“Some people wonder, ‘When are you people going to go away,’” Pavone observed. “They’ve got a lesson to learn. We aren’t going away at all! Because we don’t wonder if we’re going to overcome the Culture of Death. We stand up today, and we look it in the eye and we say, ‘You have already been overcome. Away with you, you have no more power, no more authority over the human family. We do not belong to death. We belong to Christ, and He is Life.’”
Pavone spoke eloquently about Martin Luther King, Jr. and the Civil Rights movement. Every year he attends a commemorative service for Dr. King on his memorial day with King’s niece Alveda King, who works full-time for Priests for Life, and her family.
“At that service, by the way, you always hear wonderful preaching about justice, equality, non-violence and fulfilling the creed of Dr. Martin Luther King, Jr. by extending to those who are oppressed today the same rights and dignity that we try to extend to everybody else,” said Pavone. “And you know what? Over all those years going to that service, you know what word you never hear? ‘Abortion. ‘You know what word you never hear? ‘Unborn.’ But this year they had me speak.”
The crowd burst into laughter, followed by applause.
“They heard the word ‘abortion,’” Pavone continued. “They heard the term ‘unborn child.’ They heard the fact that when we advocate for justice, and for equality, and for non-violence, that includes the children in the womb.”
“Non-violence is not non-violence if you still tolerate some violence. Equality is not equality if some are still not equal. And so we come here in this city, the same city to which the Civil Rights marchers came under the leadership of Dr. Martin Luther King, Jr., and remember what he said.”
‘You can’t have any other rights unless you’re alive’
Pavone celebrated the fact that, after years of being ignored by American presidents, the unborn were going to be acknowledged in a few hours by President Donald Trump. He also stated firmly that although he understood and applauded people who work for the inmates on death row, for immigrants, for the poor, hungry and homeless, he could not agree with them that their issues outweighed the importance of the right to life for the unborn.
“You can’t have any other rights unless you’re alive,” he said. “If you kill that baby in the womb, you didn’t only take away her life, you took away her education, her right to work, her right to vote. You took away her health care. You took away her right to immigrate. You took away her protection from terrorism. You took away every right that she had, not just her right to life, but everything else because if you take away the foundation, the house collapses.”
Pavone also celebrated that fact that Congress was about to sign the Born Alive Bill. He said that in protecting unborn babies in their latest stage, Congress was not “abandoning the effort to protect them earlier” but “implementing the effort”.
He revealed that Priests for Life had been calling legal abortion centers across the country to find out if they will indeed do late-term abortions. Abortion advocates, he said, have been trying to make the American public think that late-term abortions only happen to save the life of the mother or because the baby has a serious medical condition.
Pavone then played a recording of a woman asking for an appointment to abort her 30-week, healthy unborn baby. After establishing that the mother was in good health, the clinic’s receptionist booked her abortion for the next Tuesday.
“Thirty weeks,” said the priest grimly. “Healthy baby. Healthy mother. The doctor will take you, come in next week. We have 30 other calls like that. Twenty different states so far.”
He ended his homily on a rousing coda of hope. He held up Norma McCorvey, the original “Roe” in the Roe v. Wade case, as the epitome of abortion advocates who become pro-life. He encouraged marchers to speak to the men and women of “Silent No More,” an activist group of people who regret having participated in abortion and who witness on the steps of the Supreme Court during the March for Life. He likened their healing from their shame and guilt from their abortions by the power of Jesus Christ to a raising of the dead.
“The dead are rising every day,” said Pavone. “Let’s hear their voices. Let’s spread their testimonies. And let’s let their redemption encourage us in our new journey to the Lord.
“Let us march. Let us march to victory. Let us honor and proclaim the Lord of Life Whose name is Jesus Christ. Amen.”
***
Full text of Father Pavone’s homily at the National Prayer Service on January 19, 2018 in Washington, D.C.
We’re not just marching in defense of life, we are marching towards life.
Pastor Capizzi has proclaimed the Gospel word to us today in which our Lord said “The time is coming when the dead will hear the voice of the Son of God and those who are in tombs will come out.” God has conquered death.[Applause.]
We in this great movement say this all the time, and we want this to be a strong conviction as we go forth from this place to march. We say that we are not only working for victory, working towards victory, trying to accomplish a goal of victory; we are working FROM victory.
Our starting point in this movement is the victory over death that Jesus Christ has already won. We would not be here, we would not be the Church, we would not be the Body of Christ, and we would not be the Pro-Life Movement, if it were not true that He came out of His own tomb, having suffered death, having joined Himself to our death. He rose, and in doing so did not only conquer His death, He conquered ALL death. He overturned the kingdom of death. He robbed death of its power. He conquered your death and mine. He conquered the death of every unborn child killed by abortion, and everyone else killed by […]. He has conquered. Death is overcome.
Now this is a reality, brothers and sisters, that will be manifested fully on the last day, because we know that we still have tombs around. We still have cemeteries around. People have died, and their bodies are still in the ground. Those are human bodies.
Sadly the bodies of the children we speak up for today, killed by abortion, most of them don’t even have the dignity of having a tomb. They’ve been thrown down the sewers, in the medical waste, incinerated like garbage. But those are human bodies, too.
Brothers and sisters, the Good News that Jesus Christ has proclaimed to us in this Gospel passage is that the day will come when those tombs will be empty, and those bodies will rise again. Even of the unborn, scattered throughout the countryside, blood seeping into the ground like it did at the first murder of Abel by Cain. Those bodies, too, will be restored and will rise. What we will see on that day is the full unfolding of a victory that has already happened, that death has been conquered, which means it cannot have the last word over human beings.
Some people think that the human story is birth, life, and death. We proclaim differently here today. The human story is life, death, and resurrection. The grave cannot hold us. We were created for the heavens. We were created to be on the throne with Christ. The grave cannot hold us. It is not the place that God has destined us to. It is not our destination, of our march during life […]. No. It is the throne of the fullness of life.
That is why when we speak up for life, when we defend life, when we march for life, we are not saying, “Oh, we HOPE that these children will be free from the power of death.” And we are far from saying, “Oh, I wonder IF we can set these children free from death. I wonder IF we can overcome the power of abortion. I wonder IF we can defeat Planned Parenthood. I wonder IF we can change the laws of this country to finally protect these children.”
No, we’re not here today wondering IF. We are not here today wondering IF death has been conquered. We are not here today wondering IF Christ came out of His tomb. We’re not wondering IF the dead will rise on the last day. It is not a question mark; it is a certainty. It’s an exclamation point. That is why we are here, clergy, ordained. We’re not ordained to preach a question mark. You’re not commissioned to march for a question mark. We are marching for a certainty.
And it’s not only the certainty that we will rise at the day of victory for the unborn. It is a certainty that the power which now dismembers them and crushes them and throws them in the garbage is a power which at its root has already been defeated. [Applause.]And that is why we march today with confidence. That is why we have energy in this movement. That is why it’s the 45th Annual March for Life–although some people wonder, “When are you people going to go away?” They’ve got a lesson to learn. We aren’t going away at all! [Applause] Because we don’t wonder if we’re going to overcome the Culture of Death. We stand up today, and we look it in the eye and we say, “You have already been overcome. Away with you, you have no more power, no more authority over the human family. We do not belong to death. We belong to Christ, and He is Life. [Applause.]
And if we […] to have that victory, it’s because Christ Himself marches with us to a destination that He already holds in His hands. It is because of that, that we can speak the truth, in THIS city especially. There are marches around, taking place from coast to coast, in fact, not only across the United States but around the world. But, brothers and sisters, especially significant is that we are marching in this city of power, the power of government. Legitimate power.
We are not anarchists. We acknowledge the legitimate authority of the courts and of the Congress and of the President. But authority is legitimate only when it is submitted to the authority of God. Then, only then does it require our obedience, so therefore we can prophesy. We can correct it when it goes astray. And that’s a big part of this march today, not only proclaiming that death is conquered, not only proclaiming that we’re on the side of the children, not only proclaiming that death is conquered, not only proclaiming that they must be allowed to live, but we’re sending a message here to the government.
We’re coming here to do what was done in the Civil Rights movement. Just on Monday, this past Monday, the holiday of Martin Luther King, Jr., I was, as I always am on that day, with Alveda King, who works on our team, full-time with Priests for Life. And we were with the rest of her family at the Ebenezer Baptist Church in Atlanta, in a national commemorative service. At that service, by the way, you always hear wonderful preaching about justice, equality, non-violence and fulfilling the creed of Dr. Martin Luther King, Jr. by extending to those who are oppressed today the same rights and dignity that we try to extend to everybody else. And you know what? Over all those years going to that service, you know what word you never hear? ‘Abortion. ‘You know what word you never hear? ‘Unborn.’ But this year they had me speak. [Laughter, applause.]
They heard the word “abortion”. They heard the term “unborn child.” They heard the fact that when we advocate for justice, and for equality, and for non-violence, that includes the children in the womb. Non-violence is not non-violence if you still tolerate some violence. Equality is not equality if some are still not equal. And so we come here in this city, the same city to which the Civil Rights marchers came under the leadership of Dr. Martin Luther King, Jr., and remember what he said.
[King] said, “We come here to cash a check. This nation has said on paper that all are created equal. That we all have God-given rights, and that this government exists to secure those rights.” He said, “So we’ve come here to cash a check today because the tragedy, the evil we face, is that in regard to our African-American brothers and sisters, we’ve been given a returned check marked ‘Insufficient Funds’.” And he said, “We refuse to believe that, that the vaults of justice and equality and protection in America aren’t full enough, aren’t rich enough to include us.” So they marched to cash a check. To say to America, “Be true to what you said on paper. Give us that recognition of our dignity and equality.”
My friends, guess what we are here to do today. We are here to march, and we are demanding a check for the unborn that does no longer say ‘Insufficient Funds’, that no longer says, “We don’t have the ability to protect you. There’s not room in America to recognize you as persons.” We demand to cash in on the check promised in our Declaration of Independence that, yes, the unborn children, too, are equal in dignity, and their God-given rights must be protected and respected.
Now we had this prayer service so many years under a presidential administration that did not recognize that. I started going to this service and helping to lead it back in the day when in the White House sat a man named Bill Clinton. And he kept sending punk checks marked ‘Insufficient Funds’ to the unborn children during those 8 years. And then a man named Barack Obama sat in that Office, and the message continued to be, ‘Insufficient Funds’. But I heard about an election in 2016. [Cheers, applause.] I heard something about an inauguration in 2017. [Cheers, applause.] I heard something about a man named Donald Trump who’s now in the White House. [Cheers, applause.] And we’re all going to hear him speak today, himself, for the unborn children. [Cheers, applause.]
My brothers and sisters, let’s make something clear. People disagree on many issues. People even in the churches will stand up today and say, “We have got to get straight on capital punishment. We cannot kill these people even if they are guilty of capital crimes.” We’re going to have people standing up and saying, “We have to take care of the immigrants. That’s a human rights issue; that’s a [Civil Rights] issue. And we have to make sure they can cross the borders of this country in a way that respects their freedom and dignity.” And we’ll have people talking about how we’ve got to serve the poor and feed the hungry and shelter the homeless. And, brothers and sisters, we need applaud all those whose organizations and whose personal efforts are directed to serving people in all these situations.
However, we have something to proclaim today: that if one advocates for human rights and does not recognize the rights of these children in the womb to life, they are building on quicksand. They, in fact, contradict themselves. It’s not just a matter of saying that this issue of the Right to Life of the unborn is more important. I do say that. It’s more important because it’s […]. You can’t have any other rights unless you’re alive. If you kill that baby in the womb, you didn’t only take away her life, you took away her education, her right to work, her right to vote. You took away her health care. You took away her right to immigrate. You took away her protection from terrorism. You took away every right that she had, not just her right to life, but everything else because if you take away the foundation, the house collapses. [Applause.]
So I say to those, whether they are politicians or educators or pastors, those who will stand up and say “But it’s more important right now to be focussed on all these other rights”, I say, “Not only is it not more important, but when you stop advocating the rights of these children in the womb to be protected, you are NOT advocating for the poor, the immigrant, health care, or the death row prisoner. You’re not even advocating adequately for them. Because if you’re defending them, it’s only for one reason: their humanity, their human rights.”
“YOU don’t give the immigrant his or her rights. YOU don’t give the death row prisoner his or her rights. YOU don’t give the person in need of health care his or her rights. Any rights they have they have already. If you’re saying it’s because of their human dignity, isn’t it because they’re human? And when did they start being human? That’s the point: our humanity. The protection of our human rights must begin when our humanity begins. And that is when we are in the womb.”
Brothers and sisters, we’re never going to build a society that protects the guilty when we can’t protect the innocent. We’re never going to build a society that feeds the poor when we can’t feed our own flesh and blood in the womb. And we are never going to treat right those who want to cross the borders and into this country if we don’t treat right those who have crossed the border from the womb to birth. [Applause.]
[…] You realize, we’re in a moment now when our nation is beginning to wake up to the reality of late-term abortion. The actions–the President may mention it today, but the actions of the Congress right now are focussed in a particular way at protecting babies in those last stages, not because they’re abandoning the effort to protect them earlier, but because they’re implementing that effort.
We wake up people where things are most obvious. Eventually, I’m going to play for you a telephone call. This is one of about 30 calls we made at Priests for Life into legal abortion clinics around the country to demonstrate to the American public that you can get an abortion on a healthy mother carrying a healthy [baby] even at 30 weeks into the pregnancy. And the reason we’re trying to prove this, is that the other side tries to make the public think that these only happen to save the life of the mother, or [because of] terrible medical conditions of the baby. That’s nonsense. Listen for a moment to this call:
[Recording]
Receptionist: [….] How can I help you today?
Caller: Yes, I need to schedule an abortion.
Receptionist: Okay. Can you tell me the first day of your last normal period?
Caller: Yes, it was back on October 8, 2016.
Receptionist: And, um, have you had an ultrasound done?
Caller: Yes, I have.
Receptionist: Okay. Can you tell me if you have a […] measurement or a due date?
Caller: Uh, I have a due date. July 15.
Receptionist: So, yeah, almost 30. Thirty. Is there anything wrong with the fetus?
Caller: No, there’s not. There’s just [a lot] happening. My husband lost his job. We already have some kids, and I was planning to continue the pregnancy, but now with our world falling apart, we just felt like this was the best way out.
Receptionist: Do you yourself have anything going on medically, like asthma, diabetes, high blood pressure?
Caller: No.
Receptionist: Are you currently taking any medications for any reason?
Caller: No.
Receptionist: Well, uh, the doctor accepting you as a patient, um, will be scheduling you for Tuesday next week. Uhhh…
Thirty weeks. Healthy baby. Healthy mother. The doctor will take you, come in next week. We have 30 other calls like that. Twenty different states so far. And we’re continuing to do this.
We come today to cast a light in this darkness. We come to Washington today to cash a check for these babies. We will hear from a President today who is quite aware of this tragedy. He has no magic wand. He has his role to play. We have our role to play. We will not cease until these babies are protected. And we, furthermore, have every hope that those on the wrong side can see His light that we are shedding. And that is why in this service we also recall that the woman who was the Jane Roe of the Roe v. Wade Supreme Court decision that legalized abortion, Norma McCorvey, whom many of us here knew and ministered to personally, she, Jane Roe, who definitely won that case, became pro-life, rejected the case she won, became a Christian.
I had the privilege of receiving her into the Catholic Church in 1998. She spent the rest of her life working to end abortion, and she herself has been present at this service, and we are happy this morning, at various years at the March for Life and given witness for life. Norma McCorvey, who died last February, and who shows us all what happens when we’re willing to courageously take those steps that God indicates to us. The right steps. The just steps. The steps that lead to him.
It wasn’t easy for her. We’ll hear more about her when our friends the Benham Brothers speak in a little while. But we take that example of Norma as a sign of hope. We commend her again in this service to the Lord. We thank the Lord for the example of His Grace powerfully at work in her, and we say once again, “Lord Jesus Christ, You have conquered death. Just as you have promised that the dead will rise on the Last Day, so you promised that those dead in conscience can hear Your voice and rise from the dead now, that those in such despair that they’re going to turn to abortion can rise from despair now.” And as you will see later, my friends, at the conclusion of the March as we go in to the Supreme Court, stop there a moment as the March passes by and listen to the testimonies of the women and men of Silent No More, who have had abortions, many of whom have been crouched in a dark corner, burning [with] the shame and the sin and guilt of their abortion.
But today, because of the Jesus Christ you proclaim, you will see them, you will hear them in front of that Supreme Court, standing up and saying, “I don’t have to be crouched there in that corner in darkness, silence and shame. I’m standing up. Why? Because there is Someone Who is shedding His life on me right now. There is Someone Who is saving me, redeeming me, Who’s taking my hand, Who is lifting me up. His name is Jesus Christ, and He’s saying ‘Rise from this darkness. Be free of your sin, and proclaim that gift of life that I give you anew.’”
The dead are rising every day. Let’s hear their voices. Let’s spread their testimonies. And let’s let their redemption encourage us in our new journey to the Lord. Let us march. Let us march to victory. Let us honor and proclaim the Lord of Life Whose name is Jesus Christ. Amen. [Applause.]
MICAIAH BILGER JAN 22, 2018 | 2:43PM WASHINGTON, DC
Watching an unborn baby move around in the womb can be a life-changing experience.
Ultrasound and MRI scans now are providing this new window into the womb, giving society a glimpse of the humanity of the unborn child and abortion-minded mothers a chance to see what an abortion would destroy.
An astonishing new video circulating around the internet shows an MRI of a 20-week unborn baby. The video shows amazing details of the unborn baby’s movements as she turns her head, kicks, wiggles around and repositions herself in the cramped space. Looking closely, people also can see the baby’s heartbeat.
This is the most detailed MRI scan of a preborn baby. The amazing video shows a child at 20 weeks moving around, turning her head, and kicking. The child’s beating heart can also be seen.
The video comes from Channel Mum, a parenting blog in the UK. More than 300,000 people have watched it online so far.
The unborn baby’s image is especially significant right now as U.S. lawmakers debate a bill to prohibit abortions after 20 weeks. The Pain-Capable Unborn Child Protection Act passed the U.S. House last year and awaits action in the U.S. Senate. President Donald Trump promised to sign the bill.
By 20 weeks, strong scientific evidence indicates unborn babies can feel pain. Their major organs are functioning, and they have their own unique fingerprints. They can suck their thumbs, yawn and perform other motions much like a born baby. At this stage, unborn babies are almost fully formed and are approaching the point of viability. The youngest premature baby to survive was 21 weeks and 4 days, according to the journal Pediatrics.
Videos like this one are making a difference for life in America. Thanks to these modern medical advances, people are discovering that unborn babies are unique, valuable human beings who deserve to be protected.
STEVEN ERTELT JAN 19, 2018 | 4:17PM WASHINGTON, DC
President Donald Trump today told hundreds of thousands of pro-life Americans gathered for the March for Life that he will sign a bill the House passed today to protect babies born alive after abortions. He also bashed abortion policy in the United States that allows legal late-term abortions, even up to the point of birth in some states.
“For example, in the United States, it’s one of only seven countries to allow elective late-term abortions, along with China, North Korea, and others,” the president said. “Right now in a number of states, the laws allow a baby to be born from his or her mother’s womb in the ninth month. It is wrong. It has to change.”
“I strongly support the House of Representatives Pain-Capable bill, which would end painful, late-term abortions nationwide,” Trump said. “I call upon the Senate to pass this important law and send it to my desk for signing.”
As hundreds of thousands of pro-life people prepare to march in the March for Life, the House of Representatives voted to approve the Born Alive Abortion Survivors Protection Act — legislation protecting babies who survive abortions.
The Born-Alive Abortion Survivors Protection Act (H.R. 4712) passed 241-183. All Republicans voted for final passage, but only six Democrats voted in favor of it.
Now that the House has approved the bill, President Trump is asking the Senate to vote to approve it and several Republican senators are requesting a vote on a related bill that would ban abortions after an unborn baby is 20 weeks old. Five Republican senators on Friday urged Senate Majority Leader Mitch McConnell to schedule a vote on a bill that would ban abortion after 20 weeks of pregnancy.
The bill, the Pain-Capable Unborn Child Protection Act, is unlikely to pass because it will need at least 60 votes in the Senate and does not have enough votes even if all 51 Republicans were to support it. But anti-abortion activists have urged leaders for a vote because they want to have senators on the record with their vote ahead of the midterm elections.
“A vote would make our constituents immediately aware of the members of Congress who support elective late-term abortions and oppose extending legal protection to pain-capable unborn children nationwide,” senators wrote in their letter.
The letter was sent by Republican Sens. Lindsey Graham of South Carolina, James Lankford of Oklahoma, Joni Ernst of Iowa, Steve Daines of Montana and Roy Blunt of Missouri. They urged the bill to reach the floor close to the 45th annual March for Life on Friday, a rally in Washington that protests abortion.
“The United States is currently one of only seven countries in the world that permit elective abortion after 20 weeks,” the letter stated. “Polling numbers consistently show that the majority of Americans support a ban on abortion at this stage of pregnancy; these Americans no longer want to keep the company of countries like China and North Korea.”
The similar language makes it clear Trump and Senate Republicans are on the same page.
MICAIAH BILGER JAN 17, 2018 | 1:11PM WASHINGTON, DC
Baby Royer’s success story brings hope to families whose unborn babies have been diagnosed with spina bifida.
Royer was born last week in Texas with the debilitating condition; but because of a surgery he underwent in the womb in September, his outlook appears extremely good.
The New York Times reports Royer was born with a “feisty spirit,” kicking and screaming. Doctors told his parents, Lexi and Joshuwa Royer, that these were great signs for a child with spina bifida.
“It was so worth it,” Lexi Royer told the newspaper. “I’d do it again in a heartbeat. That’s for sure.”
Here’s more from the report:
He arrived pink and screaming on Friday at 5:35 a.m., two days before his official due date, weighing 8 pounds 8 ounces, and almost 20 inches long.
Within moments of his birth at Texas Children’s Hospital, he did what his parents and doctors had eagerly hoped to see: He moved his legs and feet, a sign that the operation may have prevented damage to the spinal nerves needed for walking.
Indeed, placed on his belly, he managed to pull a knee underneath himself and push off, as if he intended to crawl away from the nurses who were trying to swaddle him.
Dr. Larry Hollier, the surgeon-in-chief at the hospital, said he was very pleased with how baby Royer looked at birth.
“I’ve never seen a such a big defect successfully repaired, with the child moving his feet at birth,” Hollier said. “It’s unbelievable. If this is the cost of getting that closed — just having to do a little skin operation — it’s fantastic.”
In September, the little boy and his mother underwent an experimental fetal surgery while he was still in his mother’s womb. Doctors at Texas Children’s Hospital made small incisions in his mother’s uterus and used a camera and surgical tools to repair a gap in his spine.
Dr. Michael Belfort, a surgeon at Baylor in Houston, Texas, explained that the fetal surgery helps decrease the damage to the spine while the baby still is in the womb. He said the amniotic fluid eats away at the nerve tissue in the gap of the spine, so closing the gap before birth is important.
Belfort said they typically perform the surgery around 24 weeks because if something goes wrong, there is a good chance the baby will survive outside the womb.
Though the technique is new, doctors have been performing in-utero surgery for spina bifida and other ailments for years in the United States. In 2003, the National Institute of Health’s Management of Myelomeningocele Study (MOMS) found that closing the spinal defect in utero reduced the need for shunts after birth and boosted the child’s chances of walking independently. Doctors think the procedure may reduce the odds of learning disabilities as well.
In 2014, LifeNews reported British doctors performed the first in-utero surgery on an unborn baby girl with spina bifida. The surgery was a success, and by December 2016, 14-month-old Frankie was overcoming her disability and learning to walk, The Express reports.
Currently, at least 13 hospitals in the U.S. perform the fetal surgery on unborn babies with spina bifida.
Researchers estimate that 68 percent of unborn children who are diagnosed with spina bifida die from abortion. However, these new surgical procedures recognize that unborn babies are individual patients who deserve care, not death.
MINNESOTA, January 16, 2018 (LifeSiteNews) — Catholics throughout the United States have been invited to a very special spiritual event.
Inspired by the Polish Rosary to the Borders, the American Rosary to the Interior is the work of laypeople frightened by the state of the Church today. They are encouraging Catholics to ask priests to make their churches available for a public recitation of the Rosary for the purification of the Church.
The chosen day for the Rosary to the Interior is February 2. Traditionally known as Candlemas, the day marks the double Feast of the Presentation of the Lord and of the Purification of the Blessed Virgin Mary. (By going to the Temple to be purified, Mary was obeying Mosaic Law.) The hour of the Rosary is up to each individual group or interested parish priests.
The organizers stated on their website, “Recognizing that the Catholic Church alone in this world was blessed and commissioned with the Light of Christ necessary for triumph over the Darkness of sin and error, and that this Light has now been severely obscured by the sin and errors of its own members, this Rosary asks us to turn our eyes inward in order to effect that interior purification which alone can once again make Christ’s Light manifest in its fullness to the world.”
‘Darkness descending … especially over our nation’
“On February 2, 2018, we will be participating in a national event, titled Rosary To The Interior: For the Purification of the Church. I would ask all the Catholics of this parish, if it is at all possible, to journey here on this day at [insert time] in order that, in union with the rest of the Church, we might pray this Rosary for the Purification of the Church and the Triumph of Christ’s Light over the darkness that now appears to be descending at an accelerating pace over our world, and especially over our nation. The Church will be open all day, and into the evening, for those who cannot be present at the above time.”
A spokesman for the group, Hans Kroll, told LifeSiteNews that the reference to the darkness “especially” falling upon the U.S. has to do with the nation’s export of abortion funding and pornography to the rest of the world. He also mentioned the woeful state of the faith among American Catholics.
American Catholics have assimilated to secular culture
“There’ve been polls that have shown that almost 50 percent of American Catholics don’t believe in the True Presence,” Kroll said. And they haven’t remained untouched by American’s exported pop culture, either. “… A very high percentage of Catholics have assimilated to the (secular) culture so much,” he sighed.
The founders of the event wish to remain anonymous so as not to take the focus from Jesus Christ and His mother Mary. Kroll did, however, admit that the idea for the Rosary for the Interior came to life in the great state of Minnesota.
On their website, the organizers state that they are united by “a deep love and concern for the Church and a strong belief that only Our Lord and Our Lady (especially through her Rosary) can sort out all of this (scandal) in the Church, and supply the grace and power necessary for the purification of each one of us, and the Church as a whole.”
“Purification has to be on a personal level, in our own hearts,” their spokesman told LifeSiteNews. “We need to begin with the personal struggle while admitting to the darkness that has crept into the Church. We can’t just point fingers.”
Kroll spoke also of the pain the Church feels at the parish level when children grow up and suddenly stop going to church, or when parish families break apart. That’s why the Rosary for the Interior should be said in participants’ parish churches.
Perhaps fearful of creating further division, the organizers of “Rosary to the Interior” have not mentioned specific, recognizable scandals in the wider Church, such as decades of homosexual abuse of boys and young men by Catholic priests, the honoring of pro-abortion grandees by Catholic leaders and institutions, and flagrant violations of perennial teachings regarding the transmission of life as defended in Paul VI’s Humanae Vitae.
However, the organizers stated that in the Rosary they would place themselves and the whole Church within Our Lady’s Immaculate Heart and “allow her to reveal thoughts, crush heresy, expose injustice and error, purify us of our prostitutions to the world, heal wounds and usher in Light and true peace and unity to Her Church.”
‘It’s all about Our Lady doing the work’
“We’re hoping this will become an annual event,” Kroll told LifeSiteNews. He encourages everyone to read the “Rosary to the Interior” website so they will know what to do when they organize at their own local level. The set program includes a Holy Hour, with a Statement of Intention, the Nicene Creed, a recitation of the Beatitudes and the Rosary.
Whereas the organizers are happy to receive comments, there is no registration form on their site. Kroll told LifeSiteNews that they may never know how many people joined their movement, but they don’t mind.
“It’s all about Our Lady doing the work,” he said.
The website has had 9,000 views since it was founded just over a week ago. The team doesn’t take any credit for that.
“It’s all been a small effort here,” Kroll said. “Our Lord and Our Lady have been doing all the work.”
The Polish Rosary to the Borders, held on the Feast of the Holy Rosary, attracted more than a million Polish Catholics and many other Catholics around the world who prayed the rosary in communion with them. It inspired another border rosary in Italy, the Irish Rosary to the Coasts and the American Rosary on the Coasts and Borders.
The Jane Roe of ‘Roe vs Wade’ was really Norma McCorvey, but she can no longer be the poster child for the pro-abortion movement she once was, because she is a hallmark example — and given her role in the history of abortion law — an iconic example of God’s way of changing hearts.
McCorvey had a traumatic childhood. Her grandmother was a prostitute and her mother a violent alcoholic. When her parents divorced she was taken in and then raped by a relative. After an abusive marriage at age 16, McCorvey turned to alcohol and lesbian relationships. By the age of 21 she was pregnant for the third time and sought an abortion. However, state enforcement closed the abortion clinic before she could procure the abortion. This action became the basis for Roe vs. Wade because she had given birth when she did not want to. (She gave her baby up for adoption.) For the next twenty-three years she lived quietly with her lesbian partner, occasionally working in abortion clinics. A sympathetic interview with her, published in the New York Times on the occasion of her first book, ‘I am Roe’ (1994) gives a sense of those years, including death threats and shootings from ‘anti-abortion’ people.
The publication of the book occasioned her meeting an Evangelical pastor which led to her conversion to Christianity and a change of heart on abortion after seeing a poster which illustrated the stages of development of the fetus: “…something in that poster made me lose my breath. I kept seeing the picture of that tiny, 10-week-old embryo, and I said to myself, that’s a baby! It’s as if blinders just fell off my eyes and I suddenly understood the truth—that’s a baby!”
The rest of her story is one of a gradual deepening of faith and active prolife work. She appealed to the Supreme Court, based on standing, to overturn the outcome of Roe vs. Wade. After her conversion to evangelical Christianity she ceased her lesbian lifestyle and later sought entrance to the Catholic Church.
Her second book, ‘Won by Love’, (1997) retells the story from her new perspective on life. She died last February 18, 2017 at age 69.
MICAIAH BILGER JAN 12, 2018 | 4:37PM WASHINGTON, DC
An amazingly brave teenager gave birth to a baby girl last week in Philadelphia while battling a deadly brain cancer.
Dana Scatton, 17, of Pennsylvania, is doing fairly well undergoing rounds of radiation treatment, and her “miracle” baby, Aries Marie, is thriving. The past few months have been extremely difficult for Dana and her family, but they told The Advertiser that their faith is keeping them strong.
The first shock came during the summer when Dana discovered she was pregnant. Though afraid, Scatton chose life for her baby girl, and her parents Lenore and Robert Scatton supported her decision.
“In June, Dana found out she was pregnant,” her mother told the news outlet. “She had an orthodontist appointment to get braces that day – and I met her there. That’s when she told me. She got out of the car, grabbed me, hugged me, and told me in my ear that she was pregnant.”
Dana continued with her plans to attend college in the fall.
“I was shocked when I first found out I was having a baby, but I was happy,” she said. “I knew my life would change, I would grow up a little faster … but that gave me more motivation.”
But tragedy struck in December. Dana said she began to experience weird delays in her speech, and sometimes her legs did not respond correctly; she also felt extremely tired.
Her family took her to the emergency room where doctors ran a series of tests. According to the report, the doctors discovered a cancerous, 2.3 centimeter tumor on her brain. She later was diagnosed with a deadly, incurable form of brain cancer called DIPG (diffuse intrinsic pontine glioma), the report states.
That was on Dec. 10, and she was 7 months pregnant.
Dana decided to start radiation after she gave birth, fearing for her unborn daughter’s safety, but she quickly became sicker and sicker. She said she started struggling to breathe, and she could no longer walk up or down stairs.
On the day after Christmas, her doctors decided that Dana could not wait any longer. They began radiation, assuring her that her unborn baby would not be harmed.
“I feel like God just directed the doctors to help decide what I should do,” Dana said. “I wasn’t sure if I wanted to start radiation without having the baby because I didn’t want it to hurt her. But I couldn’t decide what to do – it was too hard.”
She gave birth to her daughter, Aries Marie, on Jan. 4. The tiny miracle weighed 4 pounds 6 ounces.
Dana and her family said they continue to trust God for the future.
“God has been taking care of so much,” Dana said. “Like with the whole radiation thing, I was so worried about the baby, but when I was in there, I felt like he was holding my belly. I feel like I am just going along with him. My choice is to trust God with everything.
“Getting death thrown in your face … it’s so real,” she continued. “It really shows you what’s true. This world doesn’t matter, it’s temporary, you know? When I found out, I immediately let the world go. It’s like, that doesn’t matter anymore. We have to look at the eternal life. We all think we have so much time … honestly, I feel thankful that I have this time to wake up and realize what’s right. And I want everybody to see that.”
She currently is undergoing radiation five days a week, according to the report. Her family said Aries still is in the hospital, but she is doing very well.The family set up a GoFundMe page to help raise money for Dana’s medical expenses and a possible clinical trial that is not covered by insurance. People also can follow the family’s journey on Facebook.
BALTIMORE, Maryland, January 10, 2018 (LifeSiteNews) – The Fourth Circuit Court of Appeals handed Baltimore pro-life pregnancy centers a major victory last week, telling them that no one can compel them to post abortion-related signs in their waiting rooms.
Pro-lifers are rejoicing in the victory and hope it will translate to other states as well.
A 2009 city ordinance sponsored by Stephanie Rawlings-Blake, who would become the city’s mayor in 2010, forced pro-life pregnancy help centers to post signs telling clients that they do not do abortions nor refer for abortions. Pro-abortion activists initiated the law, arguing that the pro-life pregnancy help centers were deceptive “fake clinics.”
But the Court of Appeals upheld a series of previous rulings in favor of Greater Baltimore Center for Pregnancy Concerns, the plaintiff who challenged the ordinance. The court ruled that such laws violate First Amendment freedom of speech.
The three-judge panel unanimously ruled the city ordinance was unconstitutional because it forced “a politically and religiously motivated group to convey a message fundamentally at odds with its core belief and mission.”
“This court has in the past struck down attempts to compel speech from abortion providers. And today we do the same with regard to compelling speech from abortion foes,” Judge J. Harvie Wilkinson III explained. “We do so in the belief that earnest advocates on all sides of this issue should not be forced by the state into a corner and required essentially to renounce and forswear what they have come as a matter of deepest conviction to believe.”
Pro-lifers hailed the ruling. “Life-affirming centers should not be forced to promote the abortion industry’s agenda in order to help women,” Americans United for Life (AUL) Director of Legal Communications Deanna Wallace stated in a press release.
Wallace said the city ordinance essentially “forced the pro-life community to push an abortion message.”
“Clearly, the abortion industry feels threatened by the ability of these dedicated pregnancy care centers to provide women with alternatives to abortion, and is trying to protect their profits by forcing pro-life pregnancy centers to promote abortion,” Wallace, whose organization filed a friend-of-the-court brief in the case, said. “AUL is extremely pleased that the Fourth Circuit unanimously recognized the free speech rights of these commendable pro-life centers.”
In 2010, the Greater Baltimore Center for Pregnancy Concerns, a Catholic charity, fought the city ordinance in the courts. In 2011, District Court Judge Marvin J. Garbis, a George W. Bush appointee, decided that forcing the abortion disclaimers violates pro-lifers’ free speech.
“Whether a provider of pregnancy-related services is ‘pro-life’ or ‘pro-choice,’ it is for the provider—not the government—to decide when and how to discuss abortion,” Judge Garbis explained. “The government cannot…require a ‘pro-life’ pregnancy-related service center to post a sign.”
In 2013, the Fourth Circuit Court of Appeals overturned Garbis’ ruling, sending it back to him for reconsideration. Judge Garbis remained in agreement with the pro-life centers.
Garbis reiterated that the city ordinance was unconstitutional because it “forces pregnancy centers to begin their conversations with a stark government disclaimer, divorced from the support offered by the Center and suggesting that abortion is available elsewhere and might be considered a good option by pregnant women—a message that the Center expressly finds morally offensive and would not otherwise provide.”
The case was again appealed and handed to the Fourth Circuit panel, this time along with St. Brigid Roman Catholic Congregation and Archbishop Edwin O’Brien as co-plaintiffs, and the court unanimously agreed with the pro-life centers because defenders of the city ordinance could not identify one incidence of deception.
“After seven years… the City does not identify a single example of a woman who entered the Greater Baltimore Center’s waiting room under the misimpression that she could obtain an abortion there,” Judge Harvie Wilkinson III, a Reagan appointee, wrote.
“What the record does show is affirmative advocacy of abortion alternatives by a lawful non-profit group,” Judge Wilkinson continued. “None of the public advocacy of alternatives, however, suggests that the Center would provide help or assistance in obtaining an abortion.” He concluded that “Truthful affirmative assertions are not…misleading.”
Greater Baltimore Center for Pregnancy Concerns Chairman Tom Schetelich told WHSV-TV that the Fourth Circuit’s ultimate ruling was “a victory for the First Amendment and for the women of Baltimore.”
Pro-lifers are hoping the case influences several other appeals of forced abortion speech. The U.S. Supreme Court is considering a California law forcing pro-life pregnancy help centers to advertise government-assisted abortion on large notices, and Catholic facilities to advertise state-paid contraceptives. Their decision is expected in June.
January 9, 2018 (LifeSiteNews.com) – Cardinal Juan Sandoval Íñiguez, Archbishop Emeritus of Guadalajara, Mexico, rejected the possibility of giving Holy Communion to people who commit the sins of homosexuality, contraception, and adultery, in an exclusive interview with LifeSiteNews.
He also called homosexuality a “psychological illness” that leads to the self-destruction of its practitioners. He accused the elite financial class of the Anglo-Saxon countries of seeking to impose gender ideology on developing countries.
Asked about proposals to give practicing homosexuals Holy Communion if they are in “good conscience” about their behavior, Sandoval responded, “They can’t be in good conscience. Chastity is a universal precept. All of us must maintain chastity.”
The cardinal added that chastity is not something required exclusively of those who suffer from homosexual impulses, but of everyone according to his particular situation.
“So just as those who have normal tendencies, and aren’t married, have to abstain, so those who have abnormal tendencies must also abstain,” said Sandoval, adding, “Even more so, knowing that homosexuality is a psychological illness which can be cured. Let them seek a cure, because homosexuality is never permitted.”
“That’s what Genesis is about. Gomorrah . . . what happened with Sodom and Gomorrah? What happened? They gave vent to their desires and were destroyed in that way,” said the Cardinal.
“There are many people who have the misfortune of being homosexual but who live chastely,” said Sandoval. “Those, yes, are going to enter into the kingdom of God. But those who practice it will not enter the kingdom of God. St. Paul says that. And homosexuality is condemned, totally condemned, in the Old Testament, in Genesis, and by St. Paul in the New Testament.”
Sandoval also rejected proposals to give Holy Communion to Catholics who use artificial birth control, noting that “contraception is decisively condemned, totally condemned, in Blessed Paul VI’s Humanae vitae. It’s totally condemned because it runs counter to human nature and against the plan of God. All forms of contraception.”
The Cardinal said that Pope Francis had been misunderstood regarding giving Holy Communion to those who are divorced and remarried, and pointed to Pope John Paul II’s apostolic exhortation Familiaris consortio, which gave “a series of very wise and very concrete conditions that were established by the Holy Father, John Paul II.”
“It’s necessary to return to them,” he said. “They give a response to the confusion over chapter eight of Amoris Laetitia.” He observed that Familiaris consortio requires that those who have divorced and invalidly remarried cannot receive Holy Communion unless they abstain from the sexual act.
Sandoval made his remarks in an interview with LifeSiteNews in late August of last year.
Many bishops lacking in courage
Cardinal Sandoval told LifeSiteNews (LSN) that the progress of the culture of death in Mexico is continuing, despite a “great exorcism” that was performed on the country in 2015. He put part of the blame on bishops whom he said often don’t have the courage to speak the truth.
Asked LifeSiteNews: “In 2015 you did a rite of ‘great exorcism’ . . . for all of Mexico in response to attacks against the value of human life in the country. How has the situation changed in the country since then? Is it better, worse, or the same in your opinion?”
Responded the Cardinal: “Yes, I did that exorcism in the cathedral of San Luis Potosi with the doors closed and with few people at the request of the archbishop of San Luis Potosí, who asked me to do the exorcism, fundamentally because he was having many problems with the local government with his priests, and with those of his priests who were out of control were being pursued by the authorities.”
“And I added also the supplication of our Lord for family and life. I added that it would be for all of Mexico so that God would aid us to enable us to fight against that current that seeks to destroy life and family. An exorcism is an act of supplication. It’s a supplication made to God to repulse evil, to repulse the devil who is working underneath all of these nefarious initiatives.”
“Your question is, ‘What is the state of things in Mexico now?’ It’s worse. I say that it’s worse. Well, why is it worse? Because God permits it to be so. Or because of our sins, because we haven’t known how to pray and act as we should.”
Asked LifeSiteNews: “So you also see this problem in part as a symptom of a lack of action on the part of some Catholic prelates?”
Responded the Cardinal: “Yes. I think that the need is, above all, for systematic and solid catechesis for the people, that is, to preach the Gospel, as St. Paul said, in season and out of season, to instruct the people regarding the importance of the family and the value of the family, regarding the nature of Christian morality that Our Lord Jesus Christ left to us and really, to form their consciences from childhood.”
“Yes, we have been lacking in that. And furthermore, when the government undertakes initiatives, in one state or another here in Mexico, well, it’s necessary to protest and it’s necessary to ask the people to oppose them. . . . And I think that there is a lack, in many bishops, of that ‘parrhesia,’ as St. Paul says, that courage to announce and to denounce.”
Anglo-Saxon elite seeking to establish ‘new order’ of anti-family, global government
Cardinal Sandoval said that the impetus for initiatives to create homosexual “marriage” and impose gender ideology in Latin America were coming from foreign powers, principally from wealthy and powerful interests in the Anglo-Saxon countries, who are seeking to impose a “new order” and a global government on the world.
“They are forcing this on countries here in Latin America, most of all, by means of the economy,” said Sandoval. “Our countries are underdeveloped, they need help, they’re in debt, they need loans, and they can be denied to them if they don’t implement these policies. They can raise the interest rates on the debts they have, things like that.”
“So, that policy comes — so say many — from an Anglo-Saxon elite that is very dominant over international organizations, like the UN and others, and they have this plan to arrive at the ‘new order.’ And the ‘new order’ is one global government, one economy, one culture, one religion by which they can eliminate the Christian faith, or confuse it with the others.”
“[They claim that] it’s necessary to eliminate the family in which men are formed with conscience and character, who defend themselves. And it’s necessary to eliminate national independence, so that everyone is subject to an international authority. So you see it as a plan carried out by rich and powerful countries to impose themselves,” said Sandoval.
Cardinal Sandoval is one of the strongest pro-life voices in Latin America and emeritus archbishop of Guadalajara, Mexico, where he took on anti-Catholic government officials and repeatedly defied attempts by politicians to attack the right to life and family values. Repeated attempts have been made by public officials and political pressure groups in Mexico to prosecute Sandoval in response to his pro-life activities, but to no avail.
The cardinal expressed similar sentiments in a recent public act of reparation for the sins of Mexicans against life and family, in which he said, “We have sinned by committing the worst, most grave, and most cruel crime of all, that of abortion, practiced throughout our country, sometimes with the consent of iniquitous laws and sometimes in secret, in hiding, but always with cruelty, with malice that takes advantage of the innocent and defenseless.”
“We have sinned, O Lord, accepting and promoting gender ideology, which with its package of perversions aggresses against family and life, with the unconfessed purpose of ruining societies, subjugating and plundering them,” he said.
***
Interview excerpts:
About the 2015 exorcism:
Cardinal Sandoval: Yes, I did that exorcism in the cathedral of San Luis Potosi with the doors closed and with few people at the request of the archbishop of San Luis Potosí, who asked me to do the exorcism fundamentally because he was having many problems with the local government regarding his priests, and with those of his priests who were out of control and who were being pursued by the authorities. And I added also the supplication of our Lord for family and life. I added that it would be for all of Mexico so that God would aid us to enable us to fight against that current that seeks to destroy life and family.
An exorcism is an act of supplication. It’s a supplication made to God to repulse evil, to repulse the devil who is working underneath all of these nefarious initiatives. So God knows if he hears us or does not hear us. Your question is, “What is the state of things in Mexico now?” It’s worse. I say that it’s worse. Well, why is it worse? Because God permits it to be so. Or because of our sins, because we haven’t known how to pray and act as we should. So you also see this problem in part as a symptom of a lack of action on the part of some Catholic prelates? They can do their own exorcisms or, additionally, preach the Gospel more forcefully, or how do you see it? Yes. I think that the need is, above all, for systematic and solid catechesis for the people.
That is, to preach the Gospel, as St. Paul said, in season and out of season, to instruct the people regarding the importance of the family and the value of the family, regarding the nature of Christian morality that Our Lord Jesus Christ left to us and really, to form their consciences from childhood.
Yes, we have been lacking in that.
And furthermore, when the government undertakes initiatives, in one state or another here in Mexico, well, it’s necessary to protest and it’s necessary to ask the people to oppose them. Because supposedly — supposedly — this is a democratic country. I think that democracy exists in very few countries. For the rest, they give them a false democracy. But we’re assuming the existence of a democracy, so there is the right here to protest the laws if one is not in agreement with the opinion of the majority of the citizens. And I think that there is a lack, in many bishops, of that “parresía,” as St. Paul says that courage to announce and to denounce.
About confusion over giving Holy Communion to adulterers:
Cardinal Sandoval: The confusion has come, above all, with the very understanding and kindly attitude of Pope Francis, which has been misinterpreted, and with chapter seven — no, chapter eight — of Amoris Laetitia, which speaks of having much understanding and mercy regarding particular situations, etc., in which those who have gotten married and divorced could or can receive Holy Communion — married and divorced who unite with someone else.
The thing that is very clear, the point that is very clear, in Familiaris Consortio, which is by the Holy Father who is now a saint, John Paul II, in Familiaris Consortio[paragraph] number 84 he speaks of three or four situations in which those who are divorced and remarried could be accepted in the sacraments of penance and communion (confession and communion).
I remember it, more or less, in this way: The Holy Father says that if one of them is gravely ill and doesn’t have anyone to care for them except the person with whom they are living they may stay by their side, living like siblings, — that is, without the use of the sexual act. Living like siblings. If they have children, various children, who would be neglected they could, perhaps, continue to live together, but always agreeing to live like brother and sister.
And furthermore, if it is known that they are divorced and have gotten remarried they would have to receive the sacraments somewhere else, where there wouldn’t be any scandal. So it was a series of very wise and very concrete conditions that were established by the Holy Father, John Paul II. It’s necessary to return to them. They give a response to the confusion over chapter eight of Amoris Laetitia.
LifeSiteNews: Have we forgotten today, in the Church, this issue of scandal regarding the sacraments? How do you view this?
Cardinal Sandoval: I think so. I think that sometimes people are more lax, that there are lower standards. They’re going to lose the notion of “sin.” If they don’t know the commandments, if they don’t know them any more, how are they going to keep them? So they are guilty of sin, but because they aren’t aware that they’re living a bad life although the natural law is written on the heart, they say, “Well, I’m not guilty of a grave sin, I can receive communion,” and they go up to receive communion. They’re in sin. Because of a lack of instruction, because they lack an enlightened conscience.
On contraception being acceptable or not:
Cardinal Sandoval: Contraception is decisively condemned, totally condemned, in Blessed Paul VI’s Humanae Vitae. It’s totally condemned because it runs counter to human nature and against the plan of God. All forms of contraception.
But, there is an option, there is an option for those who are married, and who are unable to have children or cannot do so without inconvenience. Because they’re very poor and they are no longer able to bring them up, because they might have transmissible diseases, as in this case, and other similar cases. So the Holy Father speaks of the natural method. He recommends the natural method [Natural Family Planning (NFP)], which is based on the providence of God, who made it that the woman is not always fertile. Within her cycle of 28 days, she has some days of infertility.
And now, with modern research, it can be known very well when the woman is fertile and when she’s not. So that the natural method may be used to avoid having children.
It’s not contraception. It’s simply using the reality that the woman is not fertile all the time.
So it’s not contraception. It’s the natural method.
I think that the best [form of it] that has been proposed is that of Billings, from Australia. So the Holy Father prohibited contraception, but indicated a way by which those who in their consciences, before God, can’t have children, have sexual relations but avoid having children. But it is always necessary to be submissive to the providence of God. A Christian is always submissive to the providence of God.
I was present for the funeral of Cardinal Prionio who was from Argentina, and was working in the Holy See. Cardinal Pironio was a great man. And John Paul II, who celebrated the mass in St. Peter’s Basilica, said that the mother of Cardinal Pironio, when she had her first child she appeared to be in very bad health, on the brink of death.
And the doctor told her, “You can’t have a family, because you’re going to die.”
And so the mother was very anguished because she wanted to have more children.
She went to the bishop in [the town of] La Plata, And she told him what the doctor had told her.
And he told her, “Daughter, that’s what the doctor says, but he who is in heaven is the one who decides.”
And after that, she had 21 children!
And the twenty-first was Cardinal Pironio. So it’s necessary to have faith — that’s what the pope said in the funeral mass of Cardinal Eduardo Pironio. It’s always necessary to have faith in the providence of God
LifeSiteNews: And also, today we are hearing that even those who are living in homosexual relationships can receive Holy Communion if they are [doing so] “in good conscience.”
Cardinal Sandoval: No. That’s an abuse also. They can’t be in good conscience. Chastity is a universal precept. All of us must maintain chastity.
For those who are married, there is conjugal chastity. Which is their fidelity to one another, between the husband and the wife, conjugal fidelity, conjugal chastity. In the case of singles, it is that they abstain, and those who are homosexuals, those who have attractions to the same sex, also abstaining. So just as those who have normal tendencies, and aren’t married, have to abstain, so those who have abnormal tendencies must also abstain.
Even more so, knowing that homosexuality is a psychological illness which can be cured. Let them seek a cure, because homosexuality is never permitted. That’s what Genesis is about. Gomorrah . . . what happened with Sodom and Gomorrah? What happened?
He destroyed them . . .
They gave vent to their desires and were destroyed in that way. And St. Paul says clearly, in one of his letters — where he gives a list of those who will not possess the kingdom of God —, he says that homosexuals will not enter into the kingdom of God.
This means those homosexuals who practice it, not those who control themselves and maintain a correct life, and there are many people who have the misfortune of being homosexual but who live chastely. Those, yes, are going to enter into the kingdom of God. But those who practice it will not enter the kingdom of God. St. Paul says that. And homosexuality is condemned, totally condemned, in the Old Testament, in Genesis, and by St. Paul in the New Testament.
On resisting temptation:
Cardinal Sandoval: All of us can resist temptations, all of us, no matter how great they are, by the grace of God. Alone, no, alone no. And the Council of Trent, when it spoke of the grace of God and of justification said that man cannot, by his efforts alone, keep the law of God. He needs the grace of God to keep [the law of God].
MICAIAH BILGER JAN 8, 2018 | 6:00PM LONDON, ENGLAND
A British mother criticized her doctors for encouraging her to abort her unborn daughter after tests indicated that the baby girl could have a disability.
Baby Kyla-Shae Anderson was born healthy 18 months ago, and her mother, Kamelia Walters, 25, of South London, is grateful that she is alive, The Sun reports.
Walters said she also feels angry because her daughter would not be alive today if she had taken her doctors’ advice.
The young mother of two received the bad news in January 2016 during her first pregnancy scan at St. George’s Hospital in Tooting, according to the report.
“The woman said, ‘Everything is perfect but I just need to call my consultant,’” Walters remembered. “The consultant came in and said her bones were fractured in the womb.”
A doctor told her that her unborn daughter probably had Osteogenesis Imperfecta Type III, or brittle bone disease, a genetic disorder characterized by fragile bones and other physical deformities. Type III is one of the more severe forms.
“I was so scared when I first got told,” Walters said. “They started telling me I could get an abortion. I was just petrified when I came home that day.”
She said she went home and cried to her mother. Later, she and her partner Lamar Anderson, 27, decided to choose life for their baby girl; they also refused further testing because of the risks it posed to their unborn child, the report states.
When Kyla-Shae was born, she did not show any symptoms of the disease. Her parents were overjoyed.
“I said, ‘she doesn’t look like there’s anything wrong with her’ and I just started crying,” Walters said. “I knew already somehow that there was nothing wrong with her and when she was born it just confirmed it.”
Walters said she still is haunted by the thought that doctors were willing to end her daughter’s life because of a possible disability.
In 2016, a Florida mom’s letter to her doctor went viral after she faced a situation similar to Walters’. Courtney Baker said her doctor pressured her to abort her unborn daughter with Down syndrome. She refused, and later she wrote a letter to her former doctor urging him to see how valuable her daughter’s life is and how wrong it is to urge anyone to have an abortion.
Discrimination against unborn babies with disabilities has prompted legislation in several states in America and in Poland to end the eugenic targeting.
This address was delivered on 28 October 2017 at Voice of the Family’s conference, “Humanae Vitae: Setting the Context” which marked the approach of the 50th anniversary year of the encyclical letter Humanae Vitae.
The theological importance of Humanae vitaeand its prophecy for our time
by Fr Serafino M. Lanzetta
1. Humanae vitae has faced acute problems
Humanae vitae (HV), Pope Paul VI’s Encyclical on the solemn duty of the transmission of human life, spoke loud and clear at a troubled historical and cultural moment. 25th June 1968, the day on which Paul VI signed the Encyclical, marked the beginning of a major controversy in the Church. One objection put to the Magisterium was that pronouncements could not be made on moral questions beyond the scope of Divine Revelation, for example the natural moral law, in particular artificial birth control, that is, contraception. However, HV 4 states from the outset that it is beyond dispute – as moreover taught by Paul VI’s predecessors –
“that Jesus Christ, when He communicated His divine power to Peter and the other Apostles and sent them to teach all nations His commandments, constituted them as the authentic guardians and interpreters of the whole moral law, not only, that is, of the law of the Gospel but also of the natural law. For the natural law, too, declares the will of God, and its faithful observance is necessary for men’s eternal salvation”.
Some theologians were also of the opinion that, if the principle of totality[1] (a part in relation to a larger whole) was extended to the moral sphere of matrimony, it could be claimed that the procreative purpose belongs to the entirety of conjugal life and is therefore unaffected by individual acts intended to prevent conception. Individual matrimonial acts would hence be sterilising in material terms, but fertile in formal terms, invoking right intention and separating fertility from an order defined as merely bodily and material, linking it instead to a rational, and hence superior, order. Reliance was in fact placed on a morality of effects and consequences combined with convenience, an approach whose grave repercussions continue to this day.
The doctrinal vision presented by HV rests on two principles, abused to favour artificial birth control, but explained by Paul VI in the light of the Revelation as a whole. These two principles are: a) human love and b) responsible parenthood.
a) It appeared in fact that human love, said by many to have been restricted by Casti Connubibecause it focused on marriage whose sole purpose was the transmission of life, was an alternative approach to a static notion of “nature”, favouring instead the dynamic of the “person” and “communion”. HV 8 teaches that “husband and wife, through that mutual gift of themselves, which is specific and exclusive to them alone, develop that union of two persons in which they perfect one another, cooperating with God in the generation and rearing of new lives
b) Responsible parenthood, however, was not to be defined merely as the predominance of right judgement in the couple’s openness to fertility, but also as a decision either to have additional children or “for serious reasons and with due respect to natural law, not to have additional children for either a certain or an indefinite period of time” (HV 10). Further clarifying the limits of responsible parenthood, HV 10 sheds new light on true human love which guides a couple, stating that parents:
“are not free to act as they choose in the service of transmitting life, as if it were wholly up to them to decide what is the right course to follow. On the contrary, they are bound to ensure that what they do corresponds to the will of God the Creator. The very nature of marriage and its use makes His will clear, while the constant teaching of the Church spells it out”.
True human love unites parents and hence makes them capable of transmitting the gift of life; the gift of life is in turn an expression of human love. This will be important in avoiding a division between union and procreation (a binomial which remains indigestible). In fact, Paul VI was to observe in HV 11 – a significant magisterial step forward, in particular from the Second Vatican Council and Gaudium et spes (here authentically interpreted) and holding fast to Pius XI’s Casti Connubi – that
“the Church […] in urging men to the observance of the precepts of the natural law, which it interprets by its constant doctrine, teaches that each and every marital act must of necessity retain its intrinsic relationship to the procreation of human life”[2].
Here, always with the primary aim of procreation, the truths of love and union are welded together. HV 12 further states, on the indivisibility of these two aspects, that:
“This particular doctrine, often expounded by the magisterium of the Church, is based on the inseparable connection, established by God, which man on his own initiative may not break, between the unitive significance and the procreative significance which are both inherent to the marriage act. […] And if each of these essential qualities, the unitive and the procreative, is preserved, the use of marriage fully retains its sense of true mutual love and its ordination to the supreme responsibility of parenthood to which man is called”.
This indivisibility leads us to reflect on the fact that the binomial – first expressed by Paul VI and linking Gaudium et spes to Casti Connubi as a result of a reappraisal of the important contribution of human and sacramental love to marriage – brings together union and procreation in the same moral principle, in fact showing it to be a procreative union. Marriage makes a couple one in love with the aim of begetting new life. Hence, the matrimonial union is intended for procreation and procreation perfects the union in a circular relationship of truth and love: the truth of the union finds its completion in love which begets new life and the fertility of love is in turn built on the indissoluble unity of the couple; if this were not the case, the love would be false, a deceit. As there is no procreation without union, so there is no union without procreation. So too love and fertility go hand in hand and are a reflection of love and unity.
As correctly noted by Stephan Goertz and Caroline Wittin in a recent book of collected essays entitled Amoris laetitia. Un punto di svolta per la teologia morale? (Amoris laetitia. A turning point for moral theology?), invoking HV 12, “contraception is no longer only contrary to nature, but also contrary to love”[3].
2. To what extent does HV interpret and authentically complete Gaudium et spes while holding fast to Casti Connubi?
To begin this brief excursus, we must refer to the doctrine of the blessings of marriage, formulated by Augustine, taken up by St. Thomas Aquinas[4] and proclaimed in Casti Connubi. “All these – says St. Augustine – are the blessings which make marriage good: procreation, faith and the sacrament”.[5] According to Pius XI, these three blessings constitute a splendid compendium of the entire doctrine on Christian marriage. However, Casti Connubi affirms that, of the three, procreation has prime place. Marriage is intended by the Creator and elevated by the Redeemer for the procreation of life and enrichment of the Holy Church through the begetting of new citizens, that is the procreation of “fellow citizens of the Saints and members of God’s household” (Eph 2:19).
The discourse on the blessings of marriage is joined and intertwined with the discourse on the purposes of marriage (and its properties): the primary purpose which is procreation and the secondary purpose which is mutual aid associated with the blessing of fidelity (bona fidei) and the allaying of concupiscence associated with the blessing of indissolubility (bona sacramenti). These precepts were originally formulated in the theology of Saint Isidore of Seville. The 1917 Code of Canon Law attaches importance to expression of the three purposes of marriage, primary and secondary (cf. Canon 1013, § 1), continuing a long-standing scholastic and controversialist tradition. The relevant theological works endorsed this approach adopted in Canon Law and formulated the discourse on the blessings of marriage on which Casti Connubi rests.
However, tension was frequently noted, having developed after Casti Connubi, between a vision of marriage as “an institution given by nature” and a vision of marriage as a “communion of persons” founded on conjugal love. This tension was said to have been triggered by the neoscholastic thinking which underlies Pius XI’s Encyclical on marriage, where the Encyclical states:
“This mutual molding of husband and wife, this determined effort to perfect each other, can in a very real sense, as the Roman Catechism teaches [ch. VIII, q. 13], be said to be the chief reason and purpose of matrimony, provided matrimony be looked at not in the restricted sense as instituted for the proper conception and education of the child, but more widely as the blending of life as a whole and the mutual interchange and sharing thereof”.[6]
At Vatican II, there was a confrontation between two different motivations in the writing of Gaudium et spes, one defined as institutionalist and the other as personalist. The former, bolstered by the hierarchy of the purposes of marriage, continuously invoked Holy Scripture, Tradition and the Magisterium, while the latter, rooted in the centrality of conjugal love, exhorted a broader interpretation of traditional and scriptural works on the three purposes of marriage, seeking the inclusion of love and sexuality in the original plan of the Creator, giving rise to the exigencies of marriage.
It is indeed opportune to note that, in Casti Connubi, Pius XI refers to the Catechism of the Council of Trent which, even at that date, placed an emphasis on love in marriage.[7] For Pius XI, the love in married life which permeates all functions of conjugal life “holds pride of place in Christian marriage”.[8] Indeed Casti Connubi perceives no opposition between nature and the communion of persons, that is between the natural/sacramental aspect of matrimony and the communion/personalist dimension. This division, arising from an absolutist interpretation of love, was deepened by the application of an unbalanced hermeneutic to Gaudium et spes (and the rejection of HV). However, it is equally true that the interpretation of the Constitution of the Church in the modern world in fact leans towards the personalism of love rather than the hierarchy of the purposes of marriage, placing greater emphasis on the former and neglecting the doctrine of the hierarchy of the purposes of marriage formulated at an earlier date.
In Gaudium et spes 47-52 one sees the clear imprint of the personalist position of the majority. An entire paragraph is dedicated to human love (47) and as, last but not least, noted by Goertz and Witting, “the category of ‘natural’ as an ethical criterion has been consciously dropped”.[9]Gaudium et spes 48 affirms that: “By their very nature, the institution of matrimony itself and conjugal love are ordained for the procreation and education of children, and find in them their ultimate crown”. This is reiterated in paragraph 50. While it is hence emphasised that the intrinsic purpose (not the primary purpose, but the purpose deriving from matrimony as an “intimate partnership of life and conjugal love”, GS 48 reiterated in the 1985 Code of Canon Law, Canon 1055, § 1), is procreation, there is no longer mention of the fact that each single conjugal act is, by its very nature, oriented towards procreation, as stated in HV, in express reiteration of Casti Connubi. Only in a footnote to paragraph 51 of Gaudium et spes is the reader referred to the doctrine of Casti Connubi on the rules on birth control. It is added, again in note form, that problems requiring further and more careful consideration had been referred to an ad hoc Commission for study of the population, the family and the birth rate. Hence the Conciliar Magisterium offered no concrete solutions on the matter of birth regulation. As we well know, the study carried out by the Commission was to be preparatory to Pope Paul VI’s Encyclical on human life.
What emerges from this brief excursus is significant: while HV fills the void left by Gaudium et spes, condemning contraception and establishing a proper understanding of the value of human love, associated with responsible parenthood and always open to the gift of life, it also harmoniously unites the two inseparable aspects of marriage, the unitive and the procreative (described in paragraph 291 of the Catechism of the Council of Trent as “reasons of the matrimonial union”, together with the remedium concupiscentiae). Therefore, the link between Gaudium et spes and Casti Connubi is restored, the virtualities of the latter are developed and the truth of conjugal love is planted in the soil of procreation in cooperation in the design of God, which is the purpose of each individual act of conjugal love. This therefore is once again aprocreative union. For this reason, it is also expedient, in a discourse on Christian marriage, not to neglect the hierarchical purposes of matrimony, purposes to be continuously embedded in the vital and supreme discourse of procreation, likened to the Creator and the fertile love of Christ for his Bride. The unity of love of husband and wife finds its completion in procreation, even where this is naturally absent because love – from a consistently spiritual and supernatural standpoint – is, or is simply not, fertile.
3. Amoris laetitia as a means of overtaking HV?
The Magisterial teaching of HV, which provides a clear definition of the immorality of all contraceptive practice, includes the following passage (paragraph 14):
“Similarly excluded is any action which either before, at the moment of, or after sexual intercourse, is specifically intended to prevent procreation—whether as an end or as a means. Neither is it valid to argue, as a justification for sexual intercourse which is deliberately contraceptive, that a lesser evil is to be preferred to a greater one, or that such intercourse would merge with procreative acts of past and future to form a single entity, and so be qualified by exactly the same moral goodness as these”.
The warning given to us by Paul VI is the risk of focusing – as we said at the outset – on a morality based on the “principle of totality” in order to reject the morality of each individual act, hence of the moral act as such. A morality of the person, understood to be in opposition to nature, in relation to the moral act in itself, in fact postulates the soundness of teleological ethical theories such as consequentialism and proportionalism, condemned by Veritatis splendour, but reappearing in force and gaining popularity.
HV could be overtaken in a context of teleological morality – referring to the ethical and moral content of Amoris laetitias (AL), as articulated by leading interpreters of that document – through the application of a consequentialist or proportionalist morality to the ends chosen, and hence to the intentions of anyone who elects to make a choice rather than refer to the moral object. In a world in which human actions are increasingly a blend of good and evil, the only means of adequately assessing the morality of an act is not based on the act itself, the end chosen, hence ascribed to the person choosing it, but instead on the aims desired based on a calculation of effects produced or a just proportion between the good to be thereby achieved and the evil to be thereby caused. As explained by John Paul II in Veritatis splendour 75:
“concrete kinds of behaviour could be described as ‘right’ or ‘wrong’, without it being thereby possible to judge as morally ‘good’ or ‘bad’ the will of the person choosing them. In this way, an act which, by contradicting a universal negative norm, directly violates goods considered as ‘pre-moral’ could be qualified as morally acceptable if the intention of the subject is focused, in accordance with a ‘responsible’ assessment of the goods involved in the concrete action, on the moral value judged to be decisive in the situation.
The evaluation of the consequences of the action, based on the proportion between the act and its effects and between the effects themselves, would regard only the pre-moral order. The moral specificity of acts, that is their goodness or evil, would be determined exclusively by the faithfulness of the person to the highest values of charity and prudence, without this faithfulness necessarily being incompatible with choices contrary to certain particular moral precepts”.
Let us consider a concrete example. From a standpoint of “situational ethics”, in a situation of adultery (a pre-moral good), if the cohabitants are obliged to remain together for the good of the children and hence live as husband and wife to safeguard a more important good (the motive being charity and hence a moral good), the moral action would be good because there would be a satisfactory proportionate relationship between the good attained and the wrongful act tolerated. For this reason, the intention of the agent could not be judged to be good or bad and it would therefore no longer be possible to judge the behaviour in itself, but merely in relation to the circumstances of the case. However, in a situation involving contraception, in which the moral good of the act in itself is eliminated due to the circumstances of that act (for example the need to safeguard the good of the family as a whole or other children), the moral action would be judged on the basis of a calculation of the effects produced or the proportionate relationship between the good effects and the bad effects, but in any event the morality of the act would no longer pertain to the person or persons choosing this behaviour, but derive from a calculation based on the end attained. If the end is good because the chosen good inherent in it is, for example, the good of the family, contraception would be morally acceptable and the intention of the agent would be considered neutral and hence not open to judgement. Therefore the objectivity of the moral act per se, and hence of the divine precepts, including those which impose prohibitions semper et pro semper, is disregarded as futile or immaterial.
A morality such as this, which favours the intention and consequences of the act only, to the exclusion of the act itself, falls into the acceptance of “intrinsic evil”; these are acts whose object cannot be ordered to God because they radically contradict the good of the person created in His image, violating what is stated clearly in the letter of Saint Paul to the Romans (3:8): “It is not licit to do evil that good may come of it”.[10]
A closer examination of AL reveals two paragraphs which lend themselves to interpretation in this direction. The first is AL 80, where it is affirmed that:
“no genital act of husband and wife can refuse this [generative] meaning [here reference to HV 11-12 is made], even when for various reasons it may not always in fact beget a new life”.
As noted by Goertz and Witting, “this is surely an ambiguous assertion because, from a ‘not licit’, one proceeds to a ‘not being able’. Is fertility of love to be understood here as transcending actual procreation?”.[11] These reasons are not identified, or even defined as “grave”, but merely as reasons, ultimately ascribable to the supreme reason of love which, in a more general interpretation, precedes, or is implicit in, procreation. There is however a further text which paves the way for the convenient positioning of an invoked “shift in moral paradigm”, namely AL 82 which, quoting the Relatio Synodi states that:
“We need to rediscover the message of the Encyclical Humanae Vitae of Blessed Pope Paul VI, which highlights the need to respect the dignity of the person in morally assessing methods of regulating birth…”.
In fact, nowhere in HV is any reference to the dignity of the person in an assessment of birth control methods to be found; instead it is said that the Church, in defending conjugal morality in its entirety and consistently condemning contraception as directly contrary to the unitive and procreative aspect of marriage, is thereby defending the dignity of husband and wife (cf. HV 18). However, quoting Gaudium et spes 50 in AL 222, Pope Francis underlines the dignity of the spouses, inviting them to form a right judgement before God regarding children to be brought into the world. He adds that the use of natural methods birth control is to be encouraged.
According to an influential moral theologian, Eberhard Schockenhoff[12] (theological adviser to a number of German prelates), who perceives in AL a “Paradigmenwechsel”, a “paradigm shift” (which has attracted many followers in Italy also), if we follow the exhortation of Pope Francis on love in the family, we would be “downplaying the sexuality” affirmed in recent centuries. The title chosen for AL invite us instead to gaze from on high at the playfulness, passion and ecstasy of love. In the opinion of Schockenhoff, AL 82 is particularly expressive of this shift in moral perspective. In his opinion, the text should be read in the light of the sceptical observations made by Pope Francis on the overestimation of a deductive moral theory which, from general principles, aims to arrive at a solution for all possible situations. From this Schockenhoff forms the impression that behind this text is “a tendency to relativize the teaching hitherto upheld of the absolute moral censure of artificial birth control”.
In other words, according to this German theologian, AL has paved the way for an overhaul of the moral doctrine on contraception, favouring a personalistic morality rather than the existing neo-scholastic or essentialist morality. Is this the guiding idea behind the new Commission, established to monitor the historical progress of HV and so identify possible links between this document andGaudium et spes against Casti Connubi? Are we again to be confronted with the invocation of an absolute Conciliar Magisterium, contrary to the Church’s unwavering tradition and moreover developed homogenously and definitively in its earliest beginnings by the Pontifical Magisterium of the last 50 years?
Furthermore, according to Schockenhoff, this would be a propitious moment to set aside a morality based upon the neo-scholastic moral act deriving from the ethics of St. Thomas Aquinas. From a morality of acts (and their object), we would proceed, as in AL, to a morality of the person. Hence the root of the problem of remarried divorced persons would be solved in a nutshell: if it ceases to be necessary to judge consciences, it then becomes necessary to ask whether the life shared by remarried divorced persons is loved in its moral value. If what matters is the communion and personalism aspect, then, in the view of the German theologian, even a civil union should be seen as a bond and an entirely personal community of life. Therefore, to refer to ‘rupture’ of the abandoned partner will be simply absurd. This is the extreme conclusion to which arrival at the “paradigm shift” invoked would lead, resulting in substantial repercussions on life and procreation within marriage. This would mean that the love formerly proclaimed is trampled upon.
4. Conclusion
Much effort is being exerted to generate an irreversible turnaround in moral theology, as encouraged by AL. It is hence suggested that AL should be read in the light of Gaudium et spes in order to disregard the (neo-scholastic and jusnaturalistic) norms set in stone in HV, which refer organically to Casti Connubi and the moral doctrine on marriage of the Tradition as a whole. It is proposed to disregard an ethic on the law or the norm to make reference to an ethic of the person or of love or of responsibility. The moment of this disregard is important and programmatic. It is fed by characteristic prolixity, which in turn becomes a pedagogical method. In the opinion of another German theologian, H.K. Pottmeyer, prolixity (or verbosity) is instrumental to a transition which it is desired to cause: “Through persuasive language, it is intended to obtain support for a new beginning, while at the same time demonstrating continuity”.[13]
We should therefore focus increasingly on an analysis of the language employed and its proper usage in theology. What is at risk as a result of this reckless shift in paradigm is not just the morality of marriage, but morality itself, which would be reduced to good intentions. However, our stance is such that the only words we utter are “Yes for Yes” or “No for No”. Whatever goes beyond this comes from evil. (cf. Mt 5:37).
[1] This principle was formulated with reference to the matter of organ transplants, as developed by Pius XII. According to this principle, respect should always be given to oneself and others, as members of the human community regarded as an organic unity of persons, distinct from one another.
[2] This is the central statement, after making reference to the natural law, whose rule is inserted in the doctrine revealed by God: «[…] quilibetmatrimonii usus ad vitam humanam procreandam per se destinatus permaneat». HV here holds fast to Casti Connubi: «[…] quemlibet matrimonii usum, in quo exercendo, actus, de industria hominum, naturali sua vitae procreandae vi destituatur, Dei et naturae legem infringere, et eos qui tale quid commiserint gravis noxae labe commaculari, AAS XXII (1930) 560.
[3] S. Goertz – C. Witting (edited by), Amoris laetitia: un punto di svolta per la teologia morale? San Paolo, Cinisello Balsamo 2017 (in German: Amoris laetitia – Wendepunkt für die Moraltheologie, Herder, Freiburg im Breisgau 2016), p. 27.
[4] Cf. St. Thomas, Summa Theologiae, Supplement, q. 49.
[5] St. Augustine, De bono coniug., chap. 24, no. 32.
[7] The Catechism of the Council of Trent (par. 290) gives the following definition of matrimony: “The conjugal union of man and woman, contracted between two qualified persons, which obliges them to live together throughout life”.
[8] In AAS XXII (1930) 547-548: «[…] ex coniugali scilicet amore, qui omnia coniugalis vitae officia pervadit et quemdam tenet in christiano coniugio principatum nobilitatis».
[9] S. Goertz – C. Witting (edited by), Amoris laetitia: un punto di svolta per la teologia morale?, cit. p. 25.
[10]Veritatis splendor 79 teaches: “One must therefore reject the thesis, characteristic of teleological and proportionalist theories, which holds that it is impossible to qualify as morally evil according to its species – its ‘object’ – the deliberate choice of certain kinds of behaviour or specific acts, apart from a consideration of the intention for which the choice is made or the totality of the foreseeable consequences of that act for all persons concerned”. Paragraph 81 adds: “In teaching the existence of intrinsically evil acts, the Church accepts the teaching of Sacred Scripture. The Apostle Paul emphatically states: ‘Do not be deceived: neither the immoral, nor idolaters, nor adulterers, nor sexual perverts, nor thieves, nor the greedy, nor drunkards, nor revilers, nor robbers will inherit the Kingdom of God’ (1 Cor 6:9-10)”. Lastly, Veritatis splendor 80 quotes HV 14, in so doing ratifying its magisterial authority on matter of intrinsic evil acts with direct reference to contraception. Therefore, the Encyclical Veritatis splendour, in reiterating the teaching of HV (in the light of the magisterial tradition as a whole) and invoking it as an authority on this matter, allows us to hold HV to be definitive magisterial teaching on contraception.
[11] S. Goertz – C. Witting (edited by), Amoris laetitia: un punto di svolta per la teologia morale?, cit. p. 57.
[12] See his essay Traditionsbruch oder notwendige Weiterbildung. Zwei Lesarten des Nachsynodalen Schreibens “Amoris laetitia”, published in «Stimme der Zeit» 3 (2017) 147-158. Also a digital version is available: www.stimmen-derzeit.de/zeitschrift/archiv/beitrag_details?k_beitrag=4797115&k_produkt=None. We will make reference to this essay in its digital version.
[13] H.J. Pottmeyer, «Von einer neuen Phase der Rezeption des Vaticanum II. Zwanzig Jahre Hermeneutick des Konzils», in H.J. Pottmeyer – G. Alberigo – J.P. Jossua (edited by), Die Rezeption des Zweiten Vatikanischen Konzils, Düsseldorf 1986, p. 48, cit. in S. Goertz – C. Witting (edited by), Amoris laetitia: un punto di svolta per la teologia morale?, p. 56.
Thirty years ago this January 14th, President Ronald Reagan published a Personhood Proclamation.
It is a beautiful proclamation declaring that personhood begins at the moment of conception and continues to natural death.
As a philosophical statement, it is a wonderfully worded affirmation of the value of human life.
But it had no teeth and no power and in the end – NO EFFECT!
What we needed then and what we need now is the President Ronald Reagan Personhood Proclamation attached to a President Donald Trump Executive Order!!!
Proclamation 5761 — National Sanctity of Human Life Day, 1988
January 14, 1988
By the President of the United States of America
A Proclamation
America has given a great gift to the world, a gift that drew upon the accumulated wisdom derived from centuries of experiments in self-government, a gift that has irrevocably changed humanity’s future. Our gift is twofold: the declaration, as a cardinal principle of all just law, of the God-given, unalienable rights possessed by every human being; and the example of our determination to secure those rights and to defend them against every challenge through the generations. Our declaration and defense of our rights have made us and kept us free and have sent a tide of hope and inspiration around the globe.
One of those unalienable rights, as the Declaration of Independence affirms so eloquently, is the right to life. In the 15 years since the Supreme Court’s decision in Roe v. Wade, however, America’s unborn have been denied their right to life. Among the tragic and unspeakable results in the past decade and a half have been the loss of life of 22 million infants before birth; the pressure and anguish of countless women and girls who are driven to abortion; and a cheapening of our respect for the human person and the sanctity of human life.
We are told that we may not interfere with abortion. We are told that we may not “impose our morality” on those who wish to allow or participate in the taking of the life of infants before birth; yet no one calls it “imposing morality” to prohibit the taking of life after people are born. We are told as well that there exists a “right” to end the lives of unborn children; yet no one can explain how such a right can exist in stark contradiction of each person’s fundamental right to life.
That right to life belongs equally to babies in the womb, babies born handicapped, and the elderly or infirm. That we have killed the unborn for 15 years does not nullify this right, nor could any number of killings ever do so. The unalienable right to life is found not only in the Declaration of Independence but also in the Constitution that every President is sworn to preserve, protect, and defend. Both the Fifth and Fourteenth Amendments guarantee that no person shall be deprived of life without due process of law.
All medical and scientific evidence increasingly affirms that children before birth share all the basic attributes of human personality — that they in fact are persons. Modern medicine treats unborn children as patients. Yet, as the Supreme Court itself has noted, the decision in Roe v. Wade rested upon an earlier state of medical technology. The law of the land in 1988 should recognize all of the medical evidence.
Our Nation cannot continue down the path of abortion, so radically at odds with our history, our heritage, and our concepts of justice. This sacred legacy, and the well-being and the future of our country, demand that protection of the innocents must be guaranteed and that the personhood of the unborn be declared and defended throughout our land. In legislation introduced at my request in the First Session of the 100th Congress, I have
asked the Legislative branch to declare the “humanity of the unborn child and the compelling interest of the several states to protect the life of each person before birth.” This duty to declare on so fundamental a matter falls to the Executive as well. By this Proclamation I hereby do so.
Now, Therefore, I, Ronald Reagan, President of the United States of America, by virtue of the authority vested in me by the Constitution and laws of the United States, do hereby proclaim and declare the unalienable personhood of every American, from the moment of conception until natural death, and I do proclaim, ordain, and declare that I will take care that the Constitution and laws of the United States are faithfully executed for the protection of America’s unborn children. Upon this act, sincerely believed to be an act of justice, warranted by the Constitution, I invoke the considerate judgment of mankind and the gracious favor of Almighty God. I also proclaim Sunday, January 17, 1988, as National Sanctity of Human Life Day. I call upon the citizens of this blessed land to gather on that day in their homes and places of worship to give thanks for the gift of life they enjoy and to reaffirm their commitment to the dignity of every human being and the sanctity of every human life.
In Witness Whereof, I have hereunto set my hand this 14th day of January, in the year of our Lord nineteen hundred and eighty-eight, and of the Independence of the United States of America the two hundred and twelfth.
Cardinal Donald Wuerl of Washington and the bishop of the neighboring Diocese of Arlington announced Wednesday that the Catholic faithful may obtain a plenary indulgence by participating in the 2018 March for Life.
Often misunderstood or simply unknown to many Catholics, an indulgence is a way to cut time off of Purgatory either for oneself or for a soul who has already died. Purgatory is the state in which souls are as they are purified to enter heaven.
“All who die in God’s grace and friendship, but still imperfectly purified, are indeed assured of their eternal salvation; but after death they undergo purification, so as to achieve the holiness necessary to enter the joy of heaven,” the Catechism of the Catholic Church teaches (CCC 1030).
Purgatory is “entirely different from the punishment of the damned,” the Catechism explains, and Catholic doctrine on Purgatory was formulated “especially at the Councils of Florence and Trent” (CCC 1031).
The tradition of the Church, by reference to certain texts of Scripture, speaks of a cleansing fire, the Catechism says (1 Cor 3:15 and 1 Pet 1:7).
A common analogy Catechists use to explain Catholic teaching on sin, Confession, purgatory, and indulgences involves sewing.
Serious sins are like thick, red thread sewn into a white handkerchief. Confession pulls those threads out, but the needle and thread have still left the holes on the handkerchief, making it imperfect. Purgatory is the filling of those holes – and so is the gaining of a plenary indulgence – so that the handkerchief can be completely whole and untainted again.
Catholic doctrine on Purgatory and indulgences reveals a major difference between Catholic and Protestant theology about whether one’s actions, assisted by grace, can remove temporal punishment due to sin.
The Catholic Church teaches that a plenary indulgence – the kind available to Catholics attending the 2018 March for Life – frees a person from all temporal punishment due to sin.
In other words, if a Catholic properly received the plenary indulgence at the 2018 March for Life and then immediately died, he would go straight to heaven rather than spend some time in Purgatory.
Cardinal Wuerl and Arlington Bishop Michael Burbidge told their fellow bishops on December 20 about the possibility of Catholic faithful gaining a plenary indulgence by participating in March for Life events on January 18 and 19.
“We bring this to your attention in the hope that you will share this information with those entrusted to your pastoral care, and who may be traveling to Washington, D.C. to participate in March for Life activities this January,” the bishops wrote. The March for Life activities take place in the Archdiocese of Washington, which encompasses the whole District of Columbia and nearby parts of Maryland, and the Diocese of Arlington in Northern Virginia.
“Tradition also teaches…that an indulgence can be attached to various works of private and public devotion,” The Handbook of Indulgences: Norms and Grants(published in 1986) says. “Therefore such works of charity and repentance which ought to be given greater emphasis in our times can be enriched with an indulgence.”
“The Christian faithful who are truly penitential and compelled by charity” can gain a plenary indulgence “if they take part in the sacred celebrations, along with the great assembly of people, throughout the whole course of the annual event that is called ‘March for Life,’” the bishops wrote.
The normal conditions for a plenary indulgence must be met in order for this March for Life indulgence to be granted. Those wishing to gain the plenary indulgence must be detached from sin (not desiring to sin). They must make a sacramental Confession, receive Holy Communion, and pray for the pope’s intentions within eight days of attending the March for Life events.
“The aged, sick and all those who due to grave reason are not able to leave home will be equally able to obtain a plenary Indulgence” if they unite themselves spiritually to the March for Life, the bishops decreed.
The homebound can do this by “having the disposition of detachment from any kind of sin with the intention of fulfilling, as soon as one is able, the three customary conditions.” They must also “spiritually join themselves to the holy ceremonies, while also having offered prayers and their sufferings or the ailments of their own life to the merciful God.”
“I am delighted to learn of the offer of the plenary indulgence on the occasion of the March for Life,” Father Frank Pavone, National Director of Priests for Life, told LifeSiteNews.
“The opportunity to gain the indulgence reflects the fact that those who march for life are making a sacrifice motivated by love for their unborn neighbors,” Pavone explained. “Moreover, it reflects the fact that the pro-life movement is not simply a response to Roe v. Wade; it is a response to Jesus Christ.”
“Our Lord taught that whatever we do to the least of His brothers and sisters, we do to Him,” he said. “In speaking up for the unborn we are truly speaking up for Christ and in defending the rights of the unborn we are also defending the rights of the One who created them.”
It’s possible for Catholics to gain partial or plenary indulgences from a host of activities, like visiting churches on certain holy days and praying certain prayers.
Wuerl and Burbidge expressed their hope that “the efforts of all across this great nation to lift up the value and dignity of each human life continue to bear fruit” and that all may “experience God’s blessings in this noble undertaking.”
It is a profound irony that as we allow even very late term fetuses to be aborted on one hand, scientists are finding radical nature-bending ways to assist people have babies–including methods that could shatter familial norms.
Speaking at the Progress Educational Trust annual conference in London this month, Azim Surani, director of germline and epigenetics research at the University of Cambridge’s Gurdon Institute, said he and colleagues had passed a significant milestone on the path to producing sperm in the laboratory.
The team is thought to be the first to have reached the halfway point on the developmental path from human stem cells to immature sperm.
The study hints that one day it may be possible to manufacture sperm and eggs from stem cells or even adult skin cells.
This could, at least in theory, permit men to become biological mothers, and with genetic engineering, women to become fathers:
Fertility clinics in Britain are currently banned from using artificial sperm or eggs to treat infertile couples. However, if scientists perfected the ability to produce germ cells in the lab – something Surani predicts is at least a decade away – regulators could face pressure to revise the law to reflect the new possibilities.
For instance, two men could potentially have a baby that was genetically related to both of them by using skin cells from one to make an egg and cells from the other to make the sperm.
Then, a woman would be hired or would volunteer to become a surrogate mother of a baby with two male biological parents.
Or, if some get their way, one of the men could have a uterus transplanted so that he could gestate and give birth via caesarean section. That has been seriously advocated by such bioethics luminaries as Joseph Fletcher.
Now, add in CRISPR gene editing, three-parent IVF techniques, and the “no limits” mentality of some in science and society, and the atomizing Brave New World possibilities become endless.
By the way, the (phony) ban mentioned in the article is typical of what we see in biotech all the time: Outlaw what can’t be done today to permit the research to be perfomed that will permit it to be done. Then, once that succeeds,, lift the ban–meaning the prohibition was really meant to give false assurance and public space to work out the technology.
This is recipe for the transhumanist dream of radical individualistic procreation, baby manufacture, and radical family restructuring. If that’s what we want–I don’t think it should be permitted, but I don’t have a monopoly on wisdom–it is what we want.
We should at least have a serious societal discussion before these things can be done, to determine–through democratic means–the breadth and scope of regulations that should govern these technologies. Otherwise, we are heading toward an anarchic procreative society.
LifeNews.com Note: Wesley J. Smith, J.D., is a special consultant to the Center for Bioethics and Culture and a bioethics attorney who blogs at Human Exeptionalism.
“The year opens in the name of the Mother,” Pope Francis said in his homily at Mass in St. Peter’s Basilica on January 1, 2018, the Solemnity of Mary, Mother of God. “Mother of God is the most important title of Our Lady”
The Holy Father reminded the congregation that the Church has declared that Mary is not only the Mother of Jesus but the Mother of God. That shows “a magnificent truth” that God “took on our humanity.”
“The word mother (mater) is related to the word matter,” the Pope continued. “In his Mother, the God of heaven, the infinite God, made himself small, he became matter, not only to be with us but also to be like us.”
Devotion to Mary is “a requirement of the Christian life…not spiritual etiquette,” Francis concluded. He noted that it is important to “leave behind all sorts of useless baggage” and look to Mary to find what really matters.
The Homily of the Holy Father
The year opens in the name of the Mother. Mother of God is the most important title of Our Lady. But we might ask why we say Mother of God and not Mother of Jesus. In the past, some wanted to be content simply with the latter, but the Church has declared that Mary is the Mother of God. We should be grateful because these words contain a magnificent truth about God and about ourselves. From the moment that our Lord became incarnate in Mary, and for all time, he took on our humanity. There is no longer God without man; the flesh Jesus took from his Mother is our own, now and for all eternity. To call Mary the Mother of God reminds us of this: God is close to humanity, even as a child is close to the mother who bears him in her womb.
The word mother (mater) is related to the word matter. In his Mother, the God of heaven, the infinite God, made himself small, he became matter, not only to be with us but also to be like us. This is the miracle, the great novelty! Man is no longer alone; no more an orphan, but forever a child. The year opens with this novelty. And we proclaim it by saying: Mother of God! Ours is the joy of knowing that our solitude has ended. It is the beauty of knowing that we are beloved children, of knowing that this childhood of ours can never be taken away from us. It is to see a reflection of ourselves in the frail and infant God resting in his mother’s arms and to realize that humanity is precious and sacred to the Lord. Henceforth, to serve human life is to serve God. All life, from life in the mother’s womb to that of the elderly, the suffering and the sick, and to that of the troublesome and even repellent, is to be welcomed, loved and helped.
Let us now be guided by today’s Gospel. Only one thing is said about the Mother of God: “Mary kept all these things, pondering them in her heart” (Lk 2:19). She kept them. She simply kept; Mary does not speak. The Gospel does not report a single word of hers in the entire account of Christmas. Here too, the Mother is one with her Son: Jesus is an “infant”, a child “unable to speak”. The Word of God, who “long ago spoke in many and various ways” (Heb 1:1), now, in the “fullness of time” (Gal 4:4), is silent. The God before whom all fall silent is himself a speechless child. His Majesty is without words; his mystery of love is revealed in lowliness. This silence and lowliness is the language of his kingship. His Mother joins her Son and keeps these things in silence.
That silence tells us that, if we would “keep” ourselves, we need silence. We need to remain silent as we gaze upon the crib. Pondering the crib, we discover anew that we are loved; we savor the real meaning of life. As we look on in silence, we let Jesus speak to our heart. His lowliness lays low our pride; his poverty challenges our outward display; his tender love touches our hardened hearts. To set aside a moment of silence each day to be with God is to “keep” our soul; it is to “keep” our freedom from being corroded by the banality of consumerism, the blare of commercials, the stream of empty words and the overpowering waves of empty chatter and loud shouting.
The Gospel goes on to say that Mary kept all these things, pondering them in her heart. What were these things? They were joys and sorrows. On the one hand, the birth of Jesus, the love of Joseph, the visit of the shepherds, that radiant night. But on the other, an uncertain future, homelessness “because there was no place for them in the inn” (Lk 2:7), the desolation of rejection, the disappointment of having to give birth to Jesus in a stable. Hopes and worries, light and darkness: all these things dwelt in the heart of Mary. What did she do? She pondered them, that is to say she dwelt on them, with God, in her heart. She held nothing back; she locked nothing within out of self-pity or resentment. Instead, she gave everything over to God. That is how she “kept” those things. We “keep” things when we hand them over: by not letting our lives become prey to fear, distress or superstition, by not closing our hearts or trying to forget, but by turning everything into a dialogue with God. God, who keeps us in his heart, then comes to dwell in our lives.
These, then, are the secrets of the Mother of God: silently treasuring all things and bringing them to God. And this took place, the Gospel concludes, in her heart. The heart makes us look to the core of the person, his or her affections, and life. At the beginning of the year, we too, as Christians on our pilgrim way, feel the need to set out anew from the center, to leave behind the burdens of the past and to start over from the things that really matter. Today, we have before us the point of departure: the Mother of God. For Mary is exactly what God wants us to be, what he wants his Church to be: a Mother who is tender and lowly, poor in material goods and rich in love, free of sin and united to Jesus, keeping God in our hearts and our neighbor in our lives. To set out anew, let us look to our Mother. In her heart beats the heart of the Church. Today’s feast tells us that if we want to go forward, we need to turn back: to begin anew from the crib, from the Mother who holds God in her arms.
Devotion to Mary is not spiritual etiquette; it is a requirement of the Christian life. Looking to the Mother, we are asked to leave behind all sorts of useless baggage and to rediscover what really matters. The gift of the Mother, the gift of every mother and every woman, is most precious for the Church, for she too is mother and woman. While a man often abstracts, affirms and imposes ideas, a woman, a mother, knows how to “keep”, to put things together in her heart, to give life. If our faith is not to be reduced merely to an idea or a doctrine, all of us need a mother’s heart, one which knows how to keep the tender love of God and to feel the heartbeat of all around us. May the Mother, God’s finest human creation, guard and keep this year, and bring the peace of her Son to our hearts and to our world.
The recent testimony of female celebrities and ordinary women who have been preyed upon sexually by powerful men has demanded a reckoning across many sectors of American life.
“We are finally becoming conscious of a vice that has been socially accepted,” said the actress Salma Hayek, who accused the famous Hollywood producer Harvey Weinstein of pressuring her to have sex in exchange for his help with an important film project. “In his eyes, I was not an artist. I wasn’t even a person. I was a thing: not a nobody, but a body.” According to her story in The New York Times, she didn’t, and Weinstein made her life unbearable.
These revelations have stirred a multitude of questions: In an age of growing gender equality, why have 30% of U.S. women experienced job-related sexual harassment? What cultural values fuel this scourge? And what will be the practical outcome — will women be safer?
Less than 20 years ago, the 2002 clergy sex-abuse crisis forced Catholics in the U.S. to face equally disturbing questions. The U.S. bishops implemented a policy of zero tolerance for abusers. Today, stringent reporting rules and background checks and screening for seminarians have reduced new allegations of clergy sexual abuse to a trickle.
Along the way, we have learned a number of lessons. Perhaps the most painful is that, even within our churches and among our pastors, sin and the power of evil are real and must be met with vigilance.
What lessons, then, should we take away from the Weinstein-inspired campaign to unmask powerful men who have abused women?
It is surely too soon to issue a comprehensive evaluation of this moment and its ripple effects across the culture. No doubt, partisan groups are looking for ways to channel anger about male sexual misconduct into a potent political force.
Such plans, however, will be complicated by the fact that influential figures from both parties, including the president of the United States, have been called out by women.
Meanwhile, Weinstein and his strain have already learned one lesson: Their power cannot match the collective witness of men and women who have found the courage to confront their tormentors. Yes, some have argued that this new movement, to remain credible and avoid overkill, must distinguish between boorish behavior and rape or other forms of sexual assault. Nevertheless, these influential men have been put on notice: If they use their power to abuse others, they will suffer the consequences.
Further, as the stories of mostly female victims are published in the media, we have also learned that differences regarding sex are real. They can’t be chalked up to social conditioning, as feminists long argued. “Recent revelations about sexual harassment, assault and abuse underscore certain blunt realities about men, women and sex,” said Mark Regnerus, a sociologist at the University of Texas at Austin who studies sexual behavior.
“Men’s sex drives are, on average, stronger and less discriminating than women’s. If this were not true, we would not be talking about this in the first place,” he noted in an article for The Public Discourse.
Women are more likely to “find themselves in situations of sexual risk,” Regnerus, the author of Cheap Sex: The Transformation of Men, Marriage and Monogamy, noted.
But now, he said, as women rise up together to expose and shame sexual predators, their joint effort marks a real turning point. And while many victims have placed their hopes in litigation that will punish and deter sexual misconduct, Regnerus says we should go much further.
We should begin to acknowledge that gender differences exist and need to be taken into account if we want to set high standards for behavior in the workplace. Such an approach could begin with a tough-minded review of modern social codes promoted by the sexual revolution and feminism, as Catholic authors — like Mary Eberstadt, a senior research fellow at the Faith & Reason Institute — have pressed for.
Both movements attacked the virtue of chastity as a patriarchal taboo that held women back. And once contraception and legal abortion became easily accessible, feminists envisioned a level playing field for women — in bed and at work. Their untested agenda challenged the governing principles of the old social order that tightly controlled courtship practices.
The old order opposed premarital and extramarital sex on religious, moral and practical grounds. This was a system largely policed by women, who leveraged what social researchers describe as a “cartel” of chastity to discourage and punish sexual misconduct.
In contrast, the new code of sexual behavior facilitated by contraception and legal abortion has penalized the chaste and rewarded the promiscuous. Men now expect to have sex by the third or fourth date, if not sooner, and women who don’t comply can feel like social outliers.
But if men don’t learn self-control during their formative years, why should we expect that they will exercise restraint later in life, when they have gained a measure of power and have access to more women?
The modern cartel of promiscuity, which hinges on a murky concept of “consent,” does a poor job of forming men who respect women. It also turns out that the hook-up culture also does a poor job of instilling self-respect in young women. That’s another lesson to be learned, as the national conversation broadens to include accusations of sexual assault as well as stories that bemoan the problematic elements of “consensual” sex. “This particular moment of cultural reckoning … gets at a crucial nuance that seems to have long been missing from the conversation around sexual harassment and assault: that consent isn’t always black and white,” said Jessica Bennett, The New York Times’ new “gender editor,” in a column for the paper.
“Sometimes ‘Yes’ means ‘No,’ simply because it is easier to go through with it than explain our way out of the situation. … And if you’re a man, that ‘No’ often means ‘just try harder’ — because, you know, persuasion is part of the game.”
Bennett expressed a sense of unease with her own willingness to acquiesce to pushy men who wanted sex.
Like the proverbial frog in the pot of boiling water, she appears to have grown used to such encounters, until the recent news made her stop and think.
Her story should inspire Catholics to respond in creative ways to this cultural moment. While our immediate goal should be a workplace that prohibits sexual harassment and fosters the respectful treatment of women, our long-term mission should be far more ambitious. More than ever, we need a new social movement inspired by the Church’s own teachings on sexuality and chastity — chastity not as a form of social control, but as the path to an interior freedom born of self-restraint. This freedom makes it possible for a man to see every woman, but especially the woman he loves, as a priceless gift, not as an object to be used. This freedom helps us recover the distinctive value of masculinity and of femininity and their unity in difference. And in marriage, this freedom creates the conditions for an authentic sexual relationship of mutual self-gift.
Let the Body of Christ be a beacon of chastity so that men and women can learn to trust each other again. This is the lesson we are called to teach a culture struggling to regain a sense of hope.
Ever since the 5th century the Church has commemorated a separate day in memory of the children killed by King Herod after Jesus’ birth. Matthew is the only one to record the event and the details surrounding it are slim.
Then Herod, when he saw that he had been tricked by the wise men, was in a furious rage, and he sent and killed all the male children in Bethlehem and in all that region who were two years old or under, according to the time which he had ascertained from the wise men. – Matthew 2:16
This type of senseless action was typical of Herod, a deranged ruler who also killed his wife and two sons during his lifetime. Herod’s immediate response to those who opposed him was to eliminate them.
The biblical episode is usually labeled a “massacre,” to emphasize the ruthless spilling of innocent blood. It was a terrible act, though it pales in comparison to the modern day killing of innocent children throughout the world.
According to the Catholic Encyclopedia, “The Greek Liturgy asserts that Herod killed 14,000 boys (ton hagion id chiliadon Nepion), the Syrians speak of 64,000, [and] many medieval authors of 144,000.” However, this number of children is greater than the entire population of Bethlehem at the time of Jesus’ birth.
Professor William F. Albright “estimates that the population of Bethlehem at the time of Jesus’ birth to be about 300 people. The number of male children, two years old or younger, would be about six or seven.” Other scholars claim the number was between 10 – 20 male children in Bethlehem and the surrounding area.
This low number of deaths is the likely explanation for why there exist no secular historical accounts of the massacre. Simply put, a handful of children killed by a local ruler was not “noteworthy” enough.
Regardless of how many children were killed, their deaths were a horrible atrocity, and Jesus could have been part of that number if Joseph had not been warned to flee beforehand.
The Church’s commemoration of the event reminds us of the sanctity of all human life. In the end it doesn’t matter how many children were killed. The Church honors their memory whether it was 100 children or a single child that was killed.
All life is precious, especially any innocent child killed at the beginning of life.
After beginning, “Conversations about abortion take place on many different levels, including medical, legal, political, and moral,” Flowers quickly runs through each of them. She shows how fragile (okay, bogus) is the case for abortion made on each of these grounds. For instance,
“Most lawyers would agree that the constitutional basis for legalized abortion is flawed, and that Roe v. Wade is the perfect example of the ends justifying the mind-numbing means. Justice Harry Blackmun… essentially created a right to a medical procedure out of penumbras. Not exactly a stellar moment in constitutional history.”
But her best and most thoughtful rebuttal is “in the moral realm where the most heated debates take place.”
Flowers writes,
“Abortion supporters learned long ago that it helps to talk about the rights of the woman and shift attention away from the child.”
More specifically, Flowers bluntly challenges the notion that “it takes ‘courage’ to have an abortion, as a writer for the New York Times opined.” We can disagree on many aspects of the debate over abortion, Flowers writes, but we cannot,
“delude ourselves into believing that it takes more courage to destroy a growing fetus than it does to allow that child to be born. We can’t pretend that it is more selfless to use abortion as birth control than it is to give birth and then gift that child to loving, adoptive parents.”
Flowers then does something that pro-lifers (as a matter of course) do which pro-abortionists (also as a matter of course) insist we don’t do: acknowledge that it “hard to be pregnant, especially if you don’t want to.”
As Flowers writes, “Living is sometimes hard,” a truth about the human condition with which we are intimately familiar. Most pro-lifers have either worked in Crisis Pregnancy Centers/Women Helping Centers, or been through an unplanned pregnancy themselves–or known someone who has. Some have even succumbed to despair and aborted their child.
We know the temptation to “take the easy way out.”
So we know it doesn’t take courage to kill an unborn child.
But it often does require courage to stand up to a boyfriend who is pushing a woman into having an abortion, through emotional or physical coercion.
It takes courage to keep going when your “friends” are advising you that it is stupid to continue a pregnancy that can be ended with a “simple” operation.
It takes courage when most everyone you know says, “Don’t be a fool. Be smart.”
LifeNews.com Note: Dave Andrusko is the editor of National Right to Life News and an author and editor of several books on abortion topics. This post originally appeared in at National Right to Life News Today —- an online column on pro-life issues.
COLUMBUS, Ohio, December 22, 2017 (LifeSiteNews) — Ohio’s Republican Governor John Kasich today signed a pro-life bill banning abortion of babies diagnosed in utero with probable Down syndrome.
The bill, which passed the Ohio Senate 20-12 and the Ohio House 63-30 last month, prohibits abortion when prenatal tests show the baby has Downs syndrome or is likely to have it.
An individual who commits an abortion in these circumstances could be charged with a fourth-degree felony, and doctors who do so could also lose their licenses, but the mother would not be accountable, according to CNN.
Kasich said in 2015 he would be “more than glad” to sign such a bill.
Mike Gonidakis, president of Ohio Right to Life, lauded the bill’s passing.
“Now that the Down Syndrome Non-Discrimination Act is law, unborn babies prenatally diagnosed with Down syndrome are given a shot at life,” he said.
“Ohio is and will continue to be a state that sees the lives of people with Down syndrome as lives worth living, thanks to this legislation.”
That was echoed by Ohio Rep. Sarah LaTourette, who introduced the bill in the House last month.
“I believe that life begins at conception and that abortion should never be considered an option,” she said earlier this month, as CNN reported.
“However, regardless of if you agree with me or not, I hope that you can see that this is not an issue about abortion; it is an issue of discrimination — discriminating against a person, not allowing them their God-given right to life, simply because they might have Down syndrome.”
The American Civil Liberties Union of Ohio denounced the legislation as interfering with women’s right to choose abortion, CNN reported.
Up to 90 percent of preborn babies diagnosed with Down Syndrome are aborted, even though the chromosomal abnormality has not stopped such people from living happy, fulfilling lives.
The medical journal Prenatal Diagnosis reports that up to 85 percent of pregnant women who receive a Downs diagnosis abort their child. The numbers are so high that the European Center for Law and Justice appealed to the United Nations’ Human Rights Council in an oral intervention, calling the practice a “contemporary form of eugenics and racism.”
One in 691 babies is conceived with Down syndrome. The cause is not known, but it can be detected in the womb or after birth to help the child therapeutically.
Live Action reports that parents are often misinformed about Downs.
“They are not informed of the advances in science and medicine that allow people with Down syndrome to lead successful lives. Today, people with Down syndrome receive equal education alongside their peers, and many live on their own, get married, and hold jobs.”
ROME, May 18, 2017 (LifeSiteNews) — There is a need to “prioritize” procreation as the primary end of marriage today, because when this “distinctive” and “proper” purpose is questioned or doubted, the “marriage institution itself — and society thereafter — begins its slide down the slippery slope,” the head of Human Life International’s (HLI) Rome office told an international gathering of pro-life and family groups there today.
Father Francesco Giordano, a professor in Rome who addressed the fourth annual Rome Life Forum today, said that a de-emphasis of procreation within marriage has not only resulted in legalized abortion, but homosexual “marriage.”
To illustrate his point, he presented the main argument behind the U.S. Supreme Court 2015 decision that legalized same-sex “marriage.”
We read in a Catholic World News article from the day: “Claiming that the institution of marriage has “evolved over time,” Justice Kennedy wrote that the essence of the marital bond is a sharing of intimacy, which does not require partners of opposite sexes. He argued that the plaintiffs in the Obergefell case were not undermining the institution of marriage, but showing their respect for that institution by seeking to participate in it. The majority opinion reasoned that the ability to marry would help to stabilize same-sex unions, and benefit the children raised by homosexual partners. Justice Kennedy explicitly rejected the notion that marriage is intrinsically oriented to procreation, writing: “An ability, desire, or promise to procreate is not and has not been a prerequisite for a valid marriage in any state.”” With the stress on the end or good of union, we are seeing these sorts of results, so it only confirms me in stressing the procreative end as the proprium of marriage.
Giordano noted how Pope Paul VI’s 1968 Encyclical Humanae Vitae, which outlined the moral evil of contraception, was a “novel” approach to conjugal relations in that it “placed the unitive end of marriage at par with the procreative end.”
He said that while the unitive purpose of the conjugal act “works with the procreative end in harmonizing the love between the parents” it is the procreative purpose which makes the act “unique” when compared to any other human act.
“The telos [purpose by nature] of the union between man and woman is generative. It is the proprium of marriage after all. It is the first end of the sexual act to be intimately united to the second end, but we have to prioritize the procreative end of marriage because it is the distinctive, proper and privative end of marriage,” he said.
He went on to quote the first account of Creation, including that God created man in his image, created them male and female, and told them: “Be fertile and multiply.”
“So it is clear that the first duty of the first family was to generate children,” he said.
Not only is this the Church’s teaching, he said, it is substantiated by natural law, not something we just follow in an abstract way.
“We adhere to a teaching because of its compelling truth,” Giordano said, “a truth which the Church naturally defends.”
Giordano’s presentation comes days after rumors began circulating in Rome of a secret committee set up by Pope Francis to study Humanae Vitae. Francis’ position on contraceptive practices — which the Church has always taught to be gravely immoral — remains sufficiently ambiguous to be interpreted as lending support to the use of contraception and condoms, in certain cases.
In a March 2014 interview with Corriere della Sera, Francis said that the question of birth control must be answered not by “changing the doctrine” but by “making pastoral (ministry) take into account the situations and that which it is possible for people to do.”
During a November 2015 press conference on his return flight from Africa, Francis, when asked if it was time for the Church to allow the use of condoms to prevent HIV agreed that condom use is “one of the methods,” but that it brought into conflict the fifth and sixth commandments.
And during his February 2016 return flight from Mexico, Francis said that contraception may be the “lesser of two evils” for parents wanting to avoid conceiving a child in areas affected by the Zika virus. Vatican spokesman Fr. Federico Lombardi confirmed the pope’s words the following day, stating: “The contraceptive or condom, in particular cases of emergency or gravity, could be the object of ‘discernment’ in a serious case of conscience. This is what the Pope said.”
Giordano also outlined a number of threats facing the family, including gender ideology and transhumanism.
“The end of man is the adoration of God. The end of gender ideology is the adoration of the body,” he said.
Giordano also discussed how the negative social changes resulting from the family’s decline, including the breakdown in the understanding of the human being as male or female, are now being advanced by a transhumanist mentality.
“Unlike animals, men can truly shape their lives, and this the transhumanists understand. However, what the transhumanists do not seem to understand is that there are limits posed by our nature on what we can do to shape our lives,” he said.
“In order to bring about the reduction of human identity to a freely chosen, mutable sexual orientation and avoid its formation in the countless influences besides sex, the elimination of these other influences—such as family, culture, and religion—are necessary [for the transhumanists,]” he said.
This mentality represents a sign of man’s demise, he said, “and the only response to all of these threats is found in strong traditional family units.”
Giordano went on to explain how the transhumanist movement is based on the belief that man is a failed experiment, and its assumption that man can come to salvation by knowing or doing something particular displays elements of the Gnostic-Pelagian heresies.
As man moves further away from human nature today, and we also see an increase in barbarous acts, it shows rejection of God and His law, said Giordano.
Conversely, he said, “When we search for that which is most elevated, dignified, and noble, we inevitably find God who is Truth, Beauty, and Goodness itself.”
“The Magisterium in the papal teachings on Marriage and the Family has been attentive to the family seeing it as a real jewel of a social institution to be protected for the greater common good of society and each man,” stated Giordano.
“If the family unit is hurt, man is ultimately hurt, and the results are evident all around us that there is indeed an abolition of man in course. If instead, the family unit is united and faithful to God, focused on Our Lord, then there is order in its life and that of its members,” he added.
Fr. Giordano’s full talk:
DOCUMENT
PAGES
Zoom
From ‘us to ‘me’
In discussing the importance of marriage, Giordano said emphasis has shifted from the family to the individual since the time of the French Revolution.
The family is understood as an institution that is beyond social functions, however, the priest said. And he told the forum “the family is very much under attack, starting with the very sacrament that is its foundation: marriage.”
He explained how problems have emerged from the center of work being moved from the household to outside the home since the Industrial Revolution.
Further, divorce has come about from many social, economic and political issues. Giordano cited the sexual revolution, the move to an industrial society over the last 200 years, and the way governments have interfered in marriage, being agents of divorce.
“We know from our fight with the abortion industry just how important legalization of such matters is in influencing the mindset,” said Giordano.
A long time coming
A look at the works written by the popes since the 19th-century on the subjects of family and marriage show they were already addressing the crisis then, he continued, citing Benedict XIV, Pius IX and Leo XIII.
“The popes were very conscious of the fact that the Church’s role was to protect sacred matrimony from all sorts of confusion because both the Church and society as a whole would suffer,” Giordano stated.
“Marriage is not merely a convention which the State can decide upon at whim,” he said, quoting Pope Leo XIII’s Arcanum divinae Sapientiae. “Marriage was established by God after the creation of our first parents so that they would transmit the life that He had given to them.”
“Marriage sanctifies the union of man and woman, and in these two accounts we see two ends of marriage clearly identified: procreative and unitive,” explained Giordano. “Through marriage, there is a remedy in store for man’s wounded nature.”
He told the forum that the Congregation for Rites having inserted the Feast of the Holy Family in the Calendar of the Roman Rite in 1921 upon the directive of Pope Benedict XV, while not the beginning of the devotion to the Holy Family, displayed the deep concern of the Holy Father for the breakdown of the family.
“Each time I read documents from the early part of the 20th century I notice that many good Catholic writers were lamenting the breakdown of the family and society back then, and I wonder: what would they say today?” the priest queried for those in attendance. “In many ways, they predicted what is happening today.”
Regarding gender, Giordano discussed St. Thomas Aquinas’s definition of man as a composite of body and soul; the two are not separate.
He explained how a number of subsequent modern philosophies reject this. And also that disruption of the natural order of man’s make-up, whether material, physical, spiritual or psychological, can have devastating effects on the whole.
These can lead to gender confusion and transhumanism.
“In a time when nature itself is questioned,” Giordano said, “when its goodness is doubted and reproduction altered, when it is no longer considered enough in itself, and attempts are made to go beyond it in the realm of transhumanism, St. Thomas’ insights are now quite valuable to consider.”
“St. Thomas teaches that even in the state of being separate, the soul is inclined to being united to its specific body,” he told the forum. “It is in this union that we see how maleness and femaleness characterize the whole person, uniting the body’s biological structure to the soul.”
“Even if this can be a debated position,” said Giordano, “we affirm that the soul is itself not a gender, or else the distinction between men and women would make them different species. The gender is in the body, but the soul is not immune from its influence since it is so integrally united to the body.”
Further, he said, if gender deals with the whole person the way that the soul does, then sex-reassignment surgery really cannot change one’s gender.
According to St. Thomas, the common end between male and female is the procreative end, he said. The particular material ends between male and female, though, are complimentary, but different.
Editor’s note: Pete Baklinski contributed to this report.
Speaking to the world’s growing underpopulation problem, Pope Francis described children as a “blessing” that the devil is trying to destroy.
“The devil wants infertility,” the pontiff said during his Tuesday homily at the Vatican, according to the Church Militant. “He does not want us to give life, be it physical or spiritual, to others.”
Pope Francis said God’s first commandment to man was “Fill the earth, be fruitful!”
“Where there is God, there is fruitfulness,” he sad. “Fruitfulness is always a blessing of God.”
Yet, today, women across the world are having fewer children. The birth rates in many countries have sunk below replacement level, prompting concerns about future economics and care of the elderly.
Countries whose birth rates are below or near replacement level include Australia, Brazil, Canada, China, Iran, Russia, Hong Kong, Macau, Singapore, South Korea and Taiwan, according to the report. Many European nations also are struggling with increasingly elderly populations and low birth rates.
The pope distinguished between those who choose not to have children for selfish reasons and those who chose to be celibate to serve others.
“He who lives for himself produces selfishness, pride, vanity, greasing the soul without living for others,” he said.
Here’s more from the report:
Pointing to the Old Testament, Francis noted children were considered a blessing and childlessness a curse.
“Infertility was a disgrace; not being able to bear children, not being able to have descendants,” he noted.
But today, the pontiff observed, a corrosive mindset has taken hold of societies across the world: the notion that barrenness is a benefit — even virtuous.
Many couples are choosing childlessness to maintain their own “economic well-being.”
The endpoint of this self-absorption, the pope conveyed is “countries empty of children.” Having “chosen the path of sterility,” they “suffer from that grave disease … a demographic winter.”
Underpopulation is not merely a concern of the religious. A 2012 United Nations study warned that the “most serious impact of aging populations would be in developing countries without safety nets or adequate legal protection in place for older people,” and pushed for reforms of Social Security-type programs and “national pensions” for the elderly.
“Informal support systems for older persons are increasingly coming under stress, as a consequence, among others, of lower fertility, out-migration of the young, and women working outside the home,” the UN report states.
Legalized abortion also has destroyed millions of unborn babies across the world each year who otherwise may have lived fruitful lives.
MARK MELLINGER DEC 19, 2017 | 5:55PM KNOXVILLE, TN
A woman living in East Tennessee has delivered the longest-frozen embryo to successfully come to birth. Emma Wren was born to Benjamin and Tina Gibson on Saturday, November 25, 2017, weighing 6 lbs. 8 oz. and measuring 20 inches long.
Prior to being transferred into Tina’s uterus at the National Embryo Donation Center (NEDC) in Knoxville earlier this year, Emma had been cryopreserved for more than 24 years. According to research staff at the University of Tennessee Preston Medical Library, baby Emma now holds the all-time record for the longest-frozen embryo to come to birth.
Emma was frozen on October 14, 1992 and thawed by NEDC Lab Director Carol Sommerfelt on March 13, 2017. Tina became pregnant with Emma as the result of a frozen embryo transfer (FET) performed by NEDC Medical Director Dr. Jeffrey Keenan on March 15, 2017. Tina, 26, spent her pregnancy carrying an embryo conceived just 1.5 years after her own birth. “Emma is such a sweet miracle,” proud papa Benjamin said. “I think she looks pretty perfect to have been frozen all those years ago.”
“The NEDC has been privileged to work with the Gibsons to help them realize their dreams of becoming parents,” said Dr. Keenan. “We hope this story is a clarion call to all couples who have embryos in long-term storage to consider this life-affirming option for their embryos.”
“It is deeply moving and highly rewarding to see that embryos frozen 24.5 years ago using the old, early cryopreservation techniques of slow freezing on day one of development at the pronuclear stage can result in 100 percent survival of the embryos with a 100 percent continued proper development to the day-3 embryo stage,” said Sommerfelt. “I will always remember what the Gibsons said when presented with the picture of their embryos at the time of transfer: ‘These embryos could have been my best friends,’ as Tina herself was only 25 at the time of transfer.”
The faith-based NEDC has gained distinction as the world’s leading comprehensive embryo adoption program, with more pregnancies (nearly 700) through embryo adoption than any other organization or clinic. Its dual purpose is to protect the lives and dignity of frozen embryos that would not be used by their genetic parents and to help other couples build the families they have longed for via donated embryos. Embryos have been donated to the NEDC from all 50 states and couples have traveled to Knoxville from all over the United States as well as some foreign countries for their embryo transfers. Our website is www.embryodonation.org.
It’s the result of creative thinking about how to be of help and service to people in need, women in abortion clinics.
Throughout December, Christmas carolers will gather outside abortion facilities across America, to draw attention to the unborn children at risk of abortion. The Pro-Life Action League’s nationwide caroling event, Peace in the Womb brings the Christmas message of peace and joy to the darkness of abortion clinics at over 80 locations in 30 states.
“It’s particularly sad to think of someone getting an abortion during the Christmas season, when we celebrate a new dawn of hope and joy coming into the world with the birth of a child,” explained Eric Scheidler, Executive Director of the Pro-Life Action League. “With our Christmas carols, we seek to remind those entering abortion facilities, and the entire community, that the Christmas message of salvation came through an unplanned pregnancy.”
The Pro-Life Action League calls for pro-life advocates to gather outside of abortion facilities across America throughout December to sing Christmas carols. Peace in the Womb caroling events take place nationwide, with multiple events and locations in some metro areas, including Chicago, Omaha and Philadelphia. December 2017 marks the fifteenth year that the Pro-Life Action League has coordinated caroling outside of abortion clinics.
Scheidler remarked, “The message of the Christmas angels is, Be not afraid. This is the same message our carolers are sharing with abortion-minded mothers. Whatever fear might be bringing them to the abortion clinic, we want to help, in any way that we can.” Scheidler noted that pro-life carolers throughout the country will be prepared to refer women to pregnancy assistance centers that offer a wide range of assistance to help women choose life for their babies.
I talked with Eric Scheidler on radio this week, and learned from him that many women have decided against abortion after hearing the pro-life carolers over the years. At least nine babies were saved from abortion during the 2016 nationwide caroling event alone. Women, girls, left the clinics after changing their minds. Some were smiling, one saying ‘We’re having a baby! We changed our minds!” The father thanked the carolers, saying, “Good job!
Scheidler added
All they’d done was sing Christmas carols, and a life was saved.
JOHN STONESTREET DEC 18, 2017 | 12:51PM WASHINGTON, DC
America is shrinking. I don’t mean we’re getting shorter, I mean that we aren’t having enough babies. Here’s why that’s bad news.
An old Far Side cartoon by Gary Larson portrays an average American couple welcoming visitors to their home. In the corner of the living room sits a little boy watching TV and next to him, is half of another little boy. “Come on in!” exclaim the couple, “Have you met Russel and Bill, our 1.5 children?”
Larson’s attempt to make fun of the American average, unfortunately, wasn’t that far off. In fact, America’s fertility rate may be hitting a historic low.
Lyman Stone, an economist at the U.S. Department of Agriculture, writes at Medium about what he’s calling “the great baby bust of 2017.”
The latest official estimate—taken from two-year-old data—puts the U.S. fertility rate at 1.84. In other words, the average American woman will have just under two children in her lifetime. This is well below the replacement rate, or the average number of children necessary to keep a country’s population from declining.
But as Stone argues, this estimate is already hopelessly out-of-date. Using monthly birth data from 2016 and 2017, he suggests the birth rate in America has plummeted to somewhere near 1.77 births on average. His graph of American fertility since 2008 looks like a double diamond ski slope.
Whatever the reason, young adults are choosing to keep their nests mostly empty. And this is bad news for our economy, our culture, and our future as a nation.
As Weekly Standard digital editor Jonathan Last writes in his book, “What to Expect When No One’s Expecting,” countries where citizens aren’t having enough babies can look forward to long-term economic stagnation and social deterioration. “There is no economy that has managed to knock out gangbuster growth with a declining population,” he told The Atlantic, recently.
Journalist Philip Longman explains that “As governments raise taxes on a dwindling working-age population to cover the growing burdens of supporting the elderly, young couples may conclude they are even less able to afford children…” This creates a vicious cycle of childlessness, overwork, and despair, as seen in graying, shrinking countries like Japan, or in Europe, where some governments actually pay couples to get pregnant.
Also, children, because they are tomorrow’s labor force and consumers, are also the economic engines of the future. And on an individual level, the regret of having fewer children is verifiable. According to a Pew poll in 2014, a whopping 40 percent of mothers nearing the end of their childbearing years say they have fewer kids than they would have liked.
But that’s not all: a declining population also hurts us in ways that are harder to quantify in dollars and cents.
Babies, in a unique way, tend to make adults care about the future that’s beyond their own lifetimes. They’re often the reason people save, invest, make sacrifices, and most importantly defer gratification. When children become scarce, people are less apt to do these things and therefore they stop thinking about a future that’s beyond themselves.
And tomorrow on BreakPoint, my colleague Eric Metaxas will offer a glimpse into what that kind of future will look like, if the birth dearth continues. Please tune in.
December 18, 2017 (LifeSiteNews) – This month, two women from two different states contacted our office because the “intended parents” were now demanding that the women abort the “defective” children they were carrying as part of a surrogacy arrangement. One woman succumbed to the pressure, killing triplets. The other woman miscarried, undoubtedly, in part, because of the unrelenting stress being placed upon her. Her stillborn twin babies were hugging each other. This is the untold underside of the inherently immoral but deceptively alluring practice of “gestational surrogacy.”
Many staunchly pro-life people see only beautiful babies, innocent and precious. They want to celebrate the gift of life, and so they casually embrace surrogacy. Those treasured babies, however, should not be created through this abhorrent practice.
There are many reasons to oppose the practice of surrogacy – including its innate exploitation of women and purposeful destruction of the sanctity of the mother-child relationship – but it should be especially morally repugnant to those who are pro-life.
Here are three reasons why every pro-life person must be anti-surrogacy:
surrogacy affirms that children are disposable;
most of the embryos created are destroyed; and
surrogacy contracts contain provisions making abortion mandatory.
First, and most obviously, surrogacy is the manufacture of children to be sold. Although the industry speaks in terms of “renting a womb” or “gestational services,” it is manifest that the purchaser is buying a child, because that is the very object of the contract. Clearly, the purchasing party would not pay a woman for the use of her womb if they were not given exclusive ownership of a baby at the end. When we reduce children into products, we cheapen their value and dehumanize the child. This is the very antithesis of the pro-life dogma of the intrinsic dignity and value of every person. Once created for sale, they can be destroyed at the purchaser’s whim. And that is exactly what is happening.
Second, most of the embryos created by surrogacy arrangements will not be allowed to live. In so-called “traditional surrogacy” the mother who carries the child is also genetically related to the child, because she provides the egg to be fertilized. In so-called “gestational surrogacy,” in contrast, the mother who carries the child has no genetic relationship with the child because the fertilized eggs transferred into her uterus are from an anonymous donor. To improve the chances of contract enforceability, the surrogacy industry favors the use of anonymous egg donors. Therefore, all “gestational surrogacy” arrangements require the use of IVF, where the egg and sperm are joined in a laboratory to create a living human being for transfer into another woman’s uterus.
Although IVF can be done so that all fertilized eggs will be used, most surrogacy participants create multiple embryos which will be destroyed or indefinitely frozen (cryopreserved). It is not uncommon for IVF arrangements to involve the creation of 10-20 embryos, where only 2-3 are used. Because of these practices, hundreds of thousands of embryos are in a state of suspended animation. Countless more have simply been killed.
Third, nearly all surrogacy contracts contain “selective reduction” provisions that allow the purchaser of the child to demand that the mother have an abortion. Here’s an example of how it works. The purchaser creates 15 embryos, which are then screened for genetic anomalies and selected by gender. To ensure that at least one embryo successfully implants (the fail rate can be as high as 50% in women under age 35), two or three of the desired embryos are transferred into the mother’s uterus. If all three embryos implant, triplets would be born, so a purchaser who wants only twins will demand that one child is aborted. These clauses, although not legally enforceable, are used to mislead and pressure vulnerable mothers to have abortions – whether they want one or not.
Surrogacy manufactures children for sale, creates human beings for intentional destruction, and permits children to live only at the expediency of their purchasers. It will, if left undeterred, irrevocably alter human civilization to the detriment of women, children, and the culture at large.
Surrogacy is not “giving the gift of life” – it is part of the culture of death.
Joseph R. Zakhary is an attorney at The Cassidy Law Firm in Shrewsbury, NJ which specializes in public interest litigation and is considered among the leading authorities on surrogacy and abortion law.
December 14, 2017 (LifeIssues.org) – A recent study analyzed the safety and efficiency of chemical abortion pills that are available online.
The drugs are better known as RU 486 (mifepristone) and Cytotec (misoprostol). Chemical abortion is a two-drug process; first mifepristone kills the tiny developing baby and then misoprostol causes uterine cramping to expel the dead preborn child. The FDA has expanded approval of the two-drug approach through the tenth week of pregnancy. The World Health Organization (WHO) believes they can be safely administered after 12 weeks, which is wholly unsupported.
The study was conducted by Gynuity Health Projects. According to their website, they work “globally to ensure that reproductive health technologies are widely available.” By “reproductive health” they mean abortion. Gynuity’s particular focus is on poor nations and cultures.
Gynuity’s “findings” were published in the journal Contraception, the flagship journal of Planned Parenthood Federation of America and its allies. The very same day a summary of findings was posted in an online article by Rewire, which states it is committed to “evidence-based news, analysis, commentary, and investigative reporting on reproductive and sexual health, rights and justice.”
Again, reproductive health means abortion. Do you note a trend?
Gynuity ordered mifepristone and/or misoprostol from 20 websites. They then analyzed a small percentage of the pills to see if they would be effective in killing an unborn child. These pro-abortion entities must still be dizzy from spinning the results to support their political agenda. “Our study found no evidence that…mifepristone and misoprostol products sold online were dangerous or ineffective.”
Further, the researchers appeared to encourage abortion providers and advocates to utilize the internet “for enhancing access to safe and effective abortion in the United States…”
Charles Donovan, president of the Charlotte Lozier Institute and Donna Harrison, MD, executive director of the American Association of Pro-Life Obstetricians and Gynecologists, did an analysis of their own based on the published study and resultant Rewire article. It’s safe to say that they came to a far different conclusion. Here are some highlights.
All of the chemical abortion drugs were obtained without the requirement of a prescription, proof of pregnancy or confirmation that the pregnancy was not an intrauterine (such as a tubal) pregnancy. Another key safety factor was lacking—a requirement to provide the gestational age of the baby, which is crucial regarding the abortion pills’ effectiveness and safety.
The mifepristone pills that Gynuity’s analyzed were within eight percent of WHO’s unsupported recommendation of safety after 12 weeks. Misoprostol, the secondary drug, “varied more considerably.” That’s a whopper of an understatement. The pills were labeled 200 mcg but the actual amount of drug in them ranged from 34.1 mcg to 201.4 mcg.
25 percent of the pills contained less than half of the recommended dose!
Compounding the risk to women, the researchers suggested this wide variation didn’t “necessarily render a product ineffective for terminating a pregnancy.” And according to Rewire, the doses “would still be effective in causing an abortion.” These statements are neither unbiased nor based on established fact.
Of paramount importance was that none of the providers of these online chemical abortion drugs provided patient directions on how to administer them. Patient safety informationprovided to women in the US includes 19 pages of directions and cautions for mifepristone (marketed as Mifeprex).
Additional problems with the research revealed:
After the orders were placed, some of the websites soon disappeared from the web.
Gynuity investigated only twenty percent of available online websites identified by the Charlotte Lozier Institute this summer—hardly representative of the potential dangers to women and their babies.
Nearly half (45 percent) of the shipped packages arrived damaged or did not arrive at all, thus further compromising the online process.
Nothing in the ordering process afforded protections for women from nefarious third-party purchases such as disgruntled boyfriends or sex traffickers.
Time is of the essence when using chemical abortion drugs, yet many of the orders arrived up to three weeks after placing and paying for the orders.
Instead of declaring online orders of chemical abortion drugs safe, if these abortion advocates truly cared about women’s health, they’d be warning women to avoid them. In the context of securing a safe abortion, these questionable drugs are more akin to a chemical coat hanger than they are to a safe, private abortion experience.
This is an extreme case of buyer beware.
This article was originally published by the Life Issues Institute and it re-published with permission.
Little Vanellope Hope Wilkins would not be alive today if her mother had listened to her doctors’ repeated urgings to have an abortion.
At just nine weeks of pregnancy, Vanellope was diagnosed with ectopia cordis, a condition where the heart grows outside of the chest, the Daily Mail reports. Doctors advised Naomi Findlay, of Nottingham, England, to abort her unborn daughter after they said Vanellope had “next to zero” chance of survival.
Wilkins refused, despite repeated pressure to consider abortion; and today, baby Vanellope is alive and getting better every day.
“We were told our best bet was to terminate and my whole world just fell to bits,” said Dean Wilkins, Vanellope’s father.
Findlay described the pressure that they were under to choose abortion.
“All the way through it, it was ‘the chances of survival are next to none, the only option is to terminate, we can offer counselling’, and things like that,” she said. “In the end, I just said that termination is not an option for me. If [death] was to happen naturally, then so be it.”
Several weeks later, the British family found a glimmer of hope for their daughter. Scans conducted at 13 and 16 weeks of pregnancy revealed that Vanellope “appeared essentially normal,” except for her heart, according to the report.
Dr. Frances Bu’Lock, consultant pediatric cardiologist at Glenfield Hospital, Leicester, led the team that worked to save Vanellope’s life.
“It was decided that delivery by caesarean section would be best to reduce the risks of infection, risks of trauma or squashing of the heart during delivery, and that surgery to provide some sort of covering to the heart would be needed immediately after baby was delivered,” Bu’Lock said.
On Nov. 22, a month before her due date, Vanellope was born by cesarean section and immediately rushed to surgery.
Findlay said she felt so relieved when Vanellope came out of the womb crying. She did not have much time to see her newborn daughter, though. Vanellope was rushed to surgery where a team of 50 doctors, nurses and midwives worked to save her life, according to the report.
If you are involved in the pro-life movement for any length of time, you will encounter the image of Our Lady of Guadalupe. There are many connections between this particular image of Our Lady and the pro-life cause.
On December 12, 1531, the Blessed Virgin Mary appeared to an Indian named Juan Diego and requested that a shrine be built and dedicated to her on the Hill of Tepeyac. Juan Diego, upon reporting this event to the bishop, was disappointed because the bishop didn’t seem to believe him. Juan returned to the place of the apparition where Our Lady again appeared. She told him to return the next morning when she would give him a sign that would convince the bishop of the truth of her appearance and her request.
The following morning Our Lady told Juan to go to the top of the hill and gather Castilian roses that he would find there. Although he knew that only cactus grew there, he obeyed, and his simple faith was rewarded by the sight of beautiful roses growing where she had told him they would be. He gathered them and showed them to Our Lady who rearranged them for him. Juan returned to the bishop. As he opened his tilma (a type of pancho), the roses fell to the floor. All who were present were startled to see an image of Our Lady on the tilma. Today this image is still preserved on Juan Diego’s tilma, which hangs over the main altar in the basilica at the foot of Tepeyac Hill just outside of Mexico City. In the image, Our Lady is pregnant, carrying the Son of God in her womb. Her head is bowed in homage, indicating that she is not the Goddess, but rather the one who bears and at the same time worships the one true God. Many articles have been written on dozens of other theological lessons drawn from the details of the image.
When asked who the lady was, Juan replied in his Aztec dialect, “Te Coatlaxopeuh,” which means “she who crush the stone serpent.” His answer recalls Gen. 3:15 and the depictions of Mary as the Immaculate Conception, her heel on the serpent’s head. The devil exalts himself above God and above God’s law (see Isaiah 14:12-15), whereas Mary submits to God (see Luke 1:38). Some promote abortion as a “choice.” Self-will is exalted. We reject abortion because we, like Mary, submit all our choices to God. That spirit of obedience crushes evil and sin. Our Lady’s image reminds us to live in that obedience each day.
Human Sacrifice Then and Now
Some nine million Aztecs were converted to Christ by the power of the image of Our Lady of Guadalupe. At that time, the Aztec peoples were practicing human sacrifice. As a result of the image’s presence among the people, their hearts were converted to the true God and the practice of human sacrifice was abolished. A key theological dynamic operating here is that Our Lady turned the Aztecs from a worldview of despair to one of hope, from a conviction that the gods were against them to a conviction that God was so much for them that He became one of them.
We can listen to stories of Aztecs cutting out their victims’ hearts or placing their heads on poles and say, “Oh, how terrible that was!” But America is not doing any better, as the hearts and heads of innocent babies are destroyed by abortion! The image is therefore being used again to change the hearts of our people.
A Theology of Despair
The Aztects had a complicated mythology-theology. The universe for them was essentially unstable, and in that universe humans played a very small role. This view led to pessimism, and a fear that they needed to always appease the deities. Their view was that the present world was the “Fifth world,” made by the “Feathered Serpent.” The previous four worlds had been destroyed by gods who turned people into monkeys or dogs. The present world, they thought, would be destroyed by an earthquake, as a result of which skeleton creatures would come out of the ground to destroy the surviving inhabitants of earth.
This is a theology of despair. Whatever moral aversion they may have had to human sacrifice, their despair made them feel they had no choice but to practice it.
The dynamics behind abortion are essentially the same. While there may not be a mythology of feathered serpents and skeletons, there is real despair. People do not get abortions because of “freedom of choice”; they get them because they feel they have no freedom and no choice. They feel trapped, abandoned, desperate, and afraid. The thousands of case-studies that Priests for Life has collected from post-abortive women are permeated by the theme expressed by the woman who said, “My friends told me I had no other option. The clinic did not offer me any alternative, and I was almost crying out for one.” As author Frederica Mathewes-Green has said, a woman does not choose an abortion like she chooses a Porsche or an ice-cream — rather, she chooses it like an animal caught in a trap chooses to gnaw off its own leg. Her experience is that she either chooses to end the life of this baby, or her own life will end. “I cannot handle it, I can’t do it, nobody will support me, it’s impossible.”
The rationalizations offered for abortion are also full of despair for the child. “Why bring a child into this world, into these circumstances, where he/she will have to suffer so much?”
From Despair to Hope
How does the image of Our Lady of Guadalupe answer the theology of despair, both for the Aztecs and for the Americas?
Our Lady is carrying God within her womb. The God of the Universe has now become a human being. No longer is there any question as to whether God is on our side. He is not a God who will destroy us; He is a God who has become our brother. He is not a God far away who waits to be appeased by blood. He is a God who shares our own flesh and blood, and is as close to the human family as an unborn child to his mother.
In this framework, human beings no longer play a small part in the universe. On the contrary, as the Second Vatican Council proclaimed, “By his incarnation the Son of God has united himself in some fashion with every human being” (Pastoral Constitution on the Church in the Modern World Gaudium et Spes, 22). The result of that is the promise of Revelation 3:21, “I will give the victor the right to sit with me on my throne.”
The universe into which Our Lady of Guadalupe invites us is no longer an unstable universe. God clearly reveals Himself as the only God, who is and shares both love and life. This truth brings hope. There is no longer need for human sacrifice, whether on pagan altars or in abortion clinics, because both the present and the future are in the hands of a God who is “God with us.”
The Image and the Pro-life Movement
The image of Our Lady of Guadalupe which converted the Aztecs has been replicated and travels the United States on an explicit mission to end abortion. It is carried into Churches and it is brought in front of abortion clinics nationwide. I have been with the image many times in these settings. In one instance in Florida, a Catholic girl who was already in the clinic’s waiting room looked outside and saw us praying, and decided to cancel her abortion. She came out to talk to us. We arranged for all the assistance she needed, and later that year I had the joy of baptizing her baby, whom she named “Guadalupe.”
The image speaks to these girls a message of hope. It also speaks to the pro-life people a message about the task before us. We who fight abortion do not see abortion walking down the street. Instead, we see a girl, frightened and in the grip of despair. We, the Church, are to reach out to her in what is the most critical pastoral mission of our day.
That mission is illustrated by the Annunciation and the Visitation. When Mary is told she will be the Mother of Christ, she does not get wrapped up in herself, thinking about what has just been said and isolating herself from others in order to absorb some unique spiritual experience. Rather, she seems to pay more attention to what Gabriel said about Elisabeth, Mary’s cousin, that about Mary! She runs in haste into the hill country and tends to Elisabeth’s needs during her pregnancy. The message for us is that authentic religious experience and true worship never turn us in on ourselves. Rather, the more real our encounter is with God, the more attentive and responsive we are to the needs of our brothers and sisters.
Our Lady of Guadalupe has been declared the “Patroness of the Unborn.” They will be saved by the message of hope she brings, and by the message of concrete charity with which she challenges the Church. Among the many and varied groups that carry out this pro-life mission, one of special note in this context is “Indians for Life.” The outreach department of the National Right to Life Committee, as well as Priests for Life, have fostered and encouraged the growth of this yet small organization, coordinated by Clementine “Little Hawk” Hernandez. Archbishop Charles Chaput, OFM Cap., has been among the strong supporters of this effort, which gives concrete expression to the reverence of Native Americans for the gift of life.
Conclusion: For the little ones, for us
When Our Lady appeared to Juan Diego, she addressed him as “Juanito” (signifying the weakest or smallest member of the family), and as “Son”, and spoke of herself as both his “Mother” and the “Mother of the One, True living God.” All of this indicates another reason why Our Lady of Guadalupe should be entrusted with the unborn.
Today she addresses to us who defend life the same words she addressed to Juan Diego:
“Hear and let it penetrate your hearts, my dear little ones. Let nothing discourage you, nothing depress you; let nothing alter your heart or your countenance. Do not fear vexation, anxiety or pain. Am I not here, your Mother? Are you not in the folds of my mantle, in the crossing of my arms? Is there anything else that you need?”
Last week, the New England Journal of Medicinepublished a study finding that hormonal contraceptives increase the risk of breast cancer. It is among the first studies to specifically analyze the effect of newer, low-dosage methods of contraception. The study is both thorough and comprehensive, as it analyzes nearly 1.8 million women over a span of 17 years using Denmark’s comprehensive medical registry. The study has been covered by a number of mainstream media outlets including the New York Times, USA Today, Slate, NPR, and Time.
A significant body of public-health research finds that contraceptives with high doses of estrogen increase the risk of breast cancer. For instance, a 1996 meta-study in The Lancet analyzed data from 54 studies surveying 25 countries and found solid statistical evidence that both current and recent users of oral contraceptives were at an increased risk for breast cancer. Many public-health researchers believed that newer methods of contraception with lower doses of estrogen would eliminate these risks. In fact, a relatively small 2014 study of Seattle-area women arrived at this exact conclusion.
But this latest study — which analyzes a larger, more comprehensive data set over a longer period of time — is among the first to provide statistical evidence showing that even low-dosage hormonal contraceptives increase the risk of breast cancer. The study also contains enough data to analyze the effects of various types of low-dosage contraceptives. It finds that long-term use of each of seven different types of low-dosage contraceptives significantly increases the risk of contracting breast cancer.
The media’s coverage of this study has been surprisingly accurate. Most outlets tend to downplay research finding that either abortion or contraception poses health risks. For instance, in 1997 the New England Journal of Medicine published study methodologically similar to this latest one, which also used data from Denmark’s health registry to analyze the abortion–breast cancer link. When covering that study, outlets claimed that induced abortion does not increase the likelihood of developing breast cancer, when in fact, the study found that abortions performed after 18 weeks gestation significantly increased the risk of breast cancer.
However, despite the fact that this new research reports that low-dosage contraceptives increase the risk of breast cancer, the increase in that risk is relatively slight, and the media have emphasized this finding in their coverage. Additionally, in the days after the study was released, many commentators were quick to tout the purported health benefits of oral contraceptives. That said, in an era of exceptionally politicized news coverage, it is heartening to see the mainstream media cover research on a potentially controversial public-health topic in a reasonable manner.
LifeNews Note: Michael J. New is an Associate Professor of Economics at Ave Maria University and an Associate Scholar at the Charlotte Lozier Institute. He is a former political science professor at the University of Michigan–Dearborn and holds a Ph.D. from Stanford University. He is a fellow at Witherspoon Institute in Princeton, New Jersey.
In an interview with Catholic World Report Monday, Naumann explained why the sanctity of human life from conception to natural death is a priority in his ministry and why other priests should make it a priority, too.
“… if the Church is silent on the destruction of life, we’re being negligent, and leaving our young people vulnerable to making this tragic decision,” Naumann said.
When he preaches about abortion, Naumann said he tries to be sensitive that people in the pews may have had experiences with abortion. He said he often mentions post-abortion healing programs such as Project Rachel.
“I say to such people that they know better than anyone else what a tragedy abortion is, and ask them to pray for me in my work that I can help others to know about the pain they’re experiencing,” he said.
He urged priests to talk about abortion more often because of its massive destruction of unborn children and families. He said more needs to be done to teach young people about the sanctity of human life.
“I’d also like to say to our priests: we can’t fail to talk to our people about these real sins that affect the lives of our people. If we talk about sins they don’t commit, of what good is that?” Naumann challenged.
A few people may walk out, as they have when he preaches about abortion, but the truth must be shared, he said.
“I pray for those who walk away, as I’ve obviously hit a difficult chord with them. But most people who hear me are supportive,” he continued.
He feels the first reaction from bishops should be to presume the politician in question is ignorant or poorly-catechized and then must explain the Church’s position to him.
But, Naumann argues, if a politician uses his Catholic name to try to convince other Catholics to betray the Faith, that is a grave danger to souls.
He blasted so-called “pro-choice Catholics,” saying, “Tim Kaine, a U.S. Senator and former vice presidential candidate, is another example of a politician who flaunted his Catholic background but spewed a lot of pro-choice rhetoric. When they do this, they’re taking on a teaching role and misleading our people.”
Naumann, who regularly attends the March for Life in Washington, D.C., also shared why the pro-life cause means so much to him personally:
“My own father was murdered before I was born. It was in December 1948, and I was just three months along inside my mother’s womb. So, I was part of a crisis pregnancy, in a sense, even though it was a different culture at the time. As the issue evolved and became an issue in our culture today, my personal background gave me a greater sensitivity to women facing a pregnancy under traumatic circumstances.”
Naumann will begin serving in the new position in about a year. He will replace New York Cardinal Timothy Dolan who currently leads the pro-life committee.
December 1, 2017 (LifeSiteNews) — The continually unfolding epidemic of sexual harassment and sexual abuse is owed in part to the proliferation of contraception, Wall Street Journal columnist Peggy Noonan wrote last week.
Noonan explained in a Wall Street Journal opinion piece what popes have predicted and practicing Catholics have witnessed over the last four decades of exploding acceptance of the birth control pill – that when sexual intercourse is separated from its life-giving aspect, men will objectify women, making abuse inevitable.
“Once you separate sex from its seriousness, once you separate it from its life-changing, life-giving potential,” Noonan said, “men will come to see it as just another want, a desire like any other.”
“Once they think that, then they’ll see sexual violations as less serious, less charged, less full of weight,” she wrote. “They’ll be more able to rationalize. It’s only petty theft, a pack of chewing gum on the counter, and I took it.”
In her Thanksgiving op-ed, Noonan explored the sex abuse crisis that’s been rocking Hollywood, Washington, D.C., and places beyond for months.
In it, she said she was thankful that investigative reporting trends have resulted in more background in the varying accusations being unearthed, allowing for deeper insight than a simple “he said/she said” assessment.
Noonan also posited that some good journalistic work is being done in both uncovering instances of sexual abuse and examining response to them. She also examined how responses can vary depending on who is accused.
Sexual harassment is nothing new, Noonan noted, citing quarter-century-old scenarios, and a recent Quinnipiac poll said nearly two-thirds of U.S. women have experienced it.
More recent testimonies suggest it is perhaps “weirder, stranger, more brutish” than before, she said, but ultimately it’s merely how things play out that has changed.
She also pointed out that sexual harassment is the product of human sin.
“Sexual harassment is not over because sin is not over,” she wrote, adding, “The devil has been busy!” a journalist friend said this week as another story broke.”
Noonan referenced a recent conversation she had illustrating the damage wrought by the contraceptive divorce of sex from its purpose as God intends.
“An aging Catholic priest suggested to a friend that all this was inevitable,” wrote Noonan. “Contraception degenerates men,” he said, as does abortion.”
The Catholic Church teaches that the purpose of the marital act is procreative and unitive. When those two aspects are intentionally separated, as with artificial contraception, the openness to life is blocked and God is removed from the embrace, demeaning both husband and wife.
Blessed Pope Paul VI predicted in Humanae Vitae that acceptance of contraception would “lead to conjugal infidelity and the general lowering of morality.”
“Another effect that gives cause for alarm is that a man who grows accustomed to the use of contraceptive methods may forget the reverence due to a woman, and, disregarding her physical and emotional equilibrium, reduce her to being a mere instrument for the satisfaction of his own desires, no longer considering her as his partner whom he should surround with care and affection.”
Pope Pius XI also forecast in 1930 in his encyclicalCasti Connubii that moral decay would result from separating sex from God’s plan:
“ … The Catholic Church, to whom God has entrusted the defense of the integrity and purity of morals, standing erect in the midst of the moral ruin which surrounds her, in order that she may preserve the chastity of the nuptial union from being defiled by this foul stain, raises her voice in token of her divine ambassadorship and through Our mouth proclaims anew: any use whatsoever of matrimony exercised in such a way that the act is deliberately frustrated in its natural power to generate life is an offense against the law of God and of nature, and those who indulge in such are branded with the guilt of a grave sin.”
Pro-life and family advocates and others have chronicled for years specifics of how the late popes’ predictions have come to pass, citing domestic violence, human trafficking, pornography, sexual harassment, assault, abuse, divorce, government coercion of population control, and the overall demeaning of women.
Paul VI’s 1968 Humanae Vitae was promulgated just as the birth control pill was coming into prominence in the U.S. in the 1960s.
As contraception spread, so did fornication, adultery and divorce, a Church Militant report said.
Another byproduct of the moral decline brought on by contraception — abortion — was ramping up during the advent of contraception, with more than a dozen U.S. states legalizing abortion between 1967 and 1972. Since the 1973 Roe vs. Wade decision, some 60 million lives have been ended in the womb via abortion.
Former Planned Parenthood president Alan Guttmacher summed it up aptly a 1968 symposium.
“We find that when an abortion is easily obtainable, contraception is neither actively nor diligently used,” Guttmacher said. “Abortion on demand relieves the husband of all possible responsibility; he simply becomes a coital animal.”
Noonan added to her analogy of men viewing sexual harassment as petty theft of gum. “In time this will seem true not only to men, but to women.”
That further degradation of women was another reason she said she was thankful for the collective “no” signified by all of the allegations coming to light.
“This is important,” Noonan said. “It is serious.”
Have you been given this scenario to justify abortion before?
“What about a baby whose mother is addicted to crack cocaine and will be born with an addiction to crack? Would you rather that baby suffer horribly and have a terrible life?”
How do you respond? Usually, I reply with something like the following:
“No, of course I wouldn’t rather have the baby suffer. No one wants a baby to suffer. However, I wouldn’t kill a child as a solution to her potential suffering. Shouldn’t we always seek to eliminate suffering- not the person who is suffering?” Or “Do you think there are ways we could help the baby without killing her?”
We help people in need, not kill people in need.
I often hear the crack baby scenario from high school students, leading me to wonder where they encounter all these poor children born to mothers with terrible addictions. I was surprised to learn from an article in the Globe and Mail that this scenario, popular in the imaginations of today’s teenagers, came from a myth promulgated in the 1980’s.
In that decade, there was public outcry about the devastating situation of babies born to crack addicted mothers. Pictures of teeny, “crack-babies” undergoing withdrawal-like symptoms after birth were widespread. The fate of these children was deemed void of hope.
This prediction is now recognized as a myth because it turns out the fate of the children born in this situation is not a life full of unimaginable suffering. Relatively recently, a researcher at the University of Maryland had a review published in Pediatrics which summarized the findings of 27 different studies following the lives of these “crack-babies” into their teenage years. The studies did not find any severe outcomes for children whose mothers had used cocaine during their pregnancy, although it seemed that they sometimes functioned slightly lower than their peers as an adolescent, for example, achieving slightly lower test scores. Their development and well-being was much more affected by their family environment, which is something we actually can help to improve. The worries about their futures were largely exaggerated and not based on good evidence.
Many children do start off disadvantaged in life and this is a tragedy, but it is no argument for killing children. The seed of potential rests within these disadvantaged children, and given proper care, any child can overcome the challenges placed on their path towards thriving. Our society wouldn’t tolerate the slaughter of children in foster care who are struggling with the effects of their parent’s poor choices, so why would we kill those same children simply because they still reside in the womb?
The myth of the crack babies just underlines the point pro-lifers have been trying to make for years—the circumstances of your conception and birth do not have to seal your fate. People have an amazing ability to overcome significant obstacles and achieve things that smaller-minded people declare impossible. Even if things look grim, we can never predict what will or will not happen in someone’s future. A child born in desperate circumstances can live a happy, productive life as an adult—unless we kill her before she gets a chance.
The current declaration is still a noble attempt to affirm that doctors have duties towards their patients and towards society; they are not just profit-maximising entrepreneurs with an expertise in human physiology.
However, it has drifted from the urgency that doctors felt in 1948, just after World War II. Before and during the War a number of eminent German doctors had betrayed their profession by experimenting on unwilling concentration camp inmates, exploiting their helplessness to further scientific knowledge (often it was bogus). Some participated in involuntary euthanasia; others in mass murder. Amongst the trials of Nazis after the War was a trial of 23 doctors. Seven of them were hanged. Japanese doctors also participated in medical atrocities.
So a personal commitment not to harm patients was clearly serious business. In 2017 perhaps the danger of becoming an enemy of mankind instead of its servant seems less pressing. The changes in the 2017 code reflect a more bureacratised, more legalistic view of medicine.
First of all, the “Declaration of Geneva” is to be called, not an “oath”, but a “pledge”. An oath is a solemn promise, often invoking a divinity as a witness. In an increasingly secularised society, the WMA apparently feels that subtly introducing the idea of God and God-given laws is an anachronism.
Or even a natural law. In the 1948 version doctors declared that “even under threat, I will not use my medical knowledge contrary to the laws of humanity”. The “laws of humanity” has been replaced by “human rights and civil liberties”. In other words, the idea of innate right and wrong has been displaced by positive law. In some circumstances, at least, right and wrong may be defined by the government.
The most striking change implicitly allows abortion. In 1948, doctors were to declare that “I will maintain the utmost respect for human life from the time of conception.” In other words, the nigh-universal prohibition of abortion was fully backed by the medical profession. By 2017, this had been watered down to “I will maintain the utmost respect for human life”. In as much as some ethicists maintain that an embryo is life, but not a human life, this is an escape clause for abortion.
There is some pressure on the WMA to alter its position on end-of-life issues, although it seems resolutely opposed at the moment. But at this rate, it could change. Will doctors someday pledge to “maintain the utmost respect for freely chosen autonomous human life”?
Another important amendment is the emphasis on patient autonomy. A clause has been inserted into the 2017 version which says, “I will respect the autonomy and dignity of my patient”. While this sounds noble, the priority given to autonomy is ominous. Does that mean that a doctor must do whatever patients ask – whether it is performing abortions, giving adolescents a sex change, or helping them to commit suicide?
A somewhat unusual new clause requires doctors to look after their own health: “I will attend to my own health, well-being, and abilities in order to provide care of the highest standard”. Perhaps this is meant to exclude doctors whose age has outstripped their medical knowledge. But it also suggests that there is less emphasis on medicine as a confraternity, a guild ready to share knowledge. The 1948 version declared that “my colleagues will be my brothers”. In 2017, is this still true? What are the consequences of doctors abandoning the notion of profession?
The current Declaration of Geneva is used across the world by physicians. In many countries it is actually part of the medical professional code and in some it is legally binding. However, in other countries it is either not used at all or has been adapted. The revised pledge is supposed to be a global ethical code for all physicians. WMA President Dr Yoshitake Yokokura, of Japan, said:
“The life of physicians today is completely different to what it was in 1948 when the original Declaration of Geneva was adopted. Since then, the Declaration has become a core document of medical ethics and a modern version of the 2,500-year old Hippocratic Oath. We hope that the Declaration approved today will be used by all physicians around the world to strengthen the profession’s determination to maintain the highest standard of health care for patients.”
As you can read below, the Declaration of Geneva does not open the floodgates to a utilitarian view of health care. But in some key points – the value of human life, especially – it is far from clear.
I SOLEMNLY PLEDGE to dedicate my life to the service of humanity;
THE HEALTH AND WELL-BEING OF MY PATIENT will be my first consideration;
I WILL RESPECT the autonomy and dignity of my patient;
I WILL MAINTAIN the utmost respect for human life;
I WILL NOT PERMIT considerations of age, disease or disability, creed, ethnic origin, gender, nationality, political affiliation, race, sexual orientation, social standing, or any other factor to intervene between my duty and my patient;
I WILL RESPECT the secrets that are confided in me, even after the patient has died;
I WILL PRACTISE my profession with conscience and dignity and in accordance with good medical practice;
I WILL FOSTER the honour and noble traditions of the medical profession;
I WILL GIVE to my teachers, colleagues, and students the respect and gratitude that is their due;
I WILL SHARE my medical knowledge for the benefit of the patient and the advancement of healthcare;
I WILL ATTEND TO my own health, well-being, and abilities in order to provide care of the highest standard;
I WILL NOT USE my medical knowledge to violate human rights and civil liberties, even under threat;
I MAKE THESE PROMISES solemnly, freely, and upon my honour.
November 27, 2017 (LifeSiteNews) – Using hormonal contraceptives increases a woman’s risk of suicide, sometimes even tripling it, a new study published in the American Journal of Psychiatry revealed.
The study, Association of Hormonal Contraception With Suicide Attempts and Suicides, was conducted by Danish researchers.
“The patch,” a thin bandage-like piece of plastic that delivers hormones to users, was the method of birth control linked to the highest increase in suicide or suicide attempts. Intrauterine devices (IUDs), the vaginal ring, and then the birth control pill followed.
“Adolescent women are more sensitive than older women to the influence of hormonal contraceptive on risk of a first suicide attempt,” the study says.
Hormonal contraception is “likely to enhance the influence of any additional factor that might cause mood disturbances,” the authors wrote.
Because “adolescence is a period characterized by endogenous sex hormone changes and changing external cultural and social demands,” teen girls will be even more strongly affected by hormonal contraception.
The researchers’ sample “included only girls from the age of 15 who had no prior use of hormonal contraception.”
The study noted that the initiation of a sexual relationship for these women could be considered a factor that led to the suicidality. However, it eventually concluded “sexual activity does not seem to be an important confounder for the relationship between use of hormonal contraception and suicide attempt or suicide.”
The study suggested the hormone changes brought on by the contraceptives are what led to increased suicide attempts.
“Hormonal contraception may have a direct influence on the neurotransmitter and hypothalamic-pituitary-adrenal system involved in stress regulation and the neurobiology of suicidal behavior,” the authors wrote. The data they collected “demonstrates a rapid increase in first suicide attempt after initiation of hormonal contraception.”
Hormonal contraception also increases users’ risk of blood clots. Its other side effects include weight gain, decreased libido, and even changes in attraction.
The Little Sisters of the Poor are heading back to court to defend themselves against the Obama administration’s Health and Human Services mandate to provide contraception, yet again. In an unusual political move, Pennsylvania and California sued the Little Sisters, demanding the same group who won at the Supreme Court in Zubik v. Burwell provide contraceptives in their state.
In early October, HHS issued a new rule that protects religious non-profits like the Little Sisters of the Poor from providing anything like contraception that would violate their religious beliefs. In a press release, Mark Rienzi, senior counsel at Becket and lead attorney for the Little Sisters of the Poor, said: “Sadly Josh Shapiro and Xavier Becerra [attorneys general in Pennsylvania and California, respectively] think attacking nuns is a way to score political points. These men may think their campaign donors want them to sue nuns, but our guess is most taxpayers disagree. No one needs nuns in order to get contraceptives, and no one needs these guys reigniting the last administration’s divisive and unnecessary culture war.”
In a phone call to media, Rienzi took the time to further explain the situation, saying that once Little Sisters won their right to be excepted from the mandate in Burwell, “That should have been the end of a long and unnecessary and divisive culture war. We have a lot of problems, but figuring out how to deliver contraceptives without nuns should not be one of them. … Even the federal government, under the Obama administration, openly admitted they had many other ways to deliver contraceptives without nuns, and they didn’t need every employer to do it.”
On the call, I asked how the states were even able to sue the organization, given the Supreme Court’s ruling on the matter. Rienzi said it was merely “political grandstanding.” In a follow-up email, Rienzi explained “This is a pretty unusual situation. It’s similar to a collateral attack — filing a second lawsuit to challenge what has already been decided elsewhere. The protection is, and should be, to let the people from the old lawsuit intervene and defend their rights in the new one.”
Let’s hope for the Little Sisters’ sake, these frivolous lawsuits end swiftly and decisively so they can continue their good work.
In an early draft of its next strategic plan, the Department of Health and Human Services has described its mission as “serving and protecting Americans at every stage of life, beginning at conception” [emphasis added]. In an op-ed in the Los Angeles Times, Dr. Richard Paulson—a professor of obstetrics and gynecology and an infertility specialist—vehemently objects to HHS’s affirmation that life begins at conception. Paulson claims that this affirmation is based on religion rather than science, and that HHS should remove it from the report, because the agency’s endorsement of a religious view of human life violates the constitutional separation of church and state.
We heartily agree with Paulson that the HHS should define human life on the basis of “science and data, not faith-based belief.” But on the question of when the life of a new member of the human species comes to be, the scientific facts squarely support the position of HHS, not of Dr. Paulson. How he can be unaware of the pertinent facts is befuddling.
The standard science texts as well as scholarly articles in the fields of embryology, developmental biology, and microbiology assert the very position that Paulson says is merely faith-based and unscientific.
The Science of Embryology
The following are typical examples—only three of the many, many we could cite. These are from standard texts by embryologists, developmental biologists, and microbiologists:
“Human life begins at fertilization, the process during which a male gamete or sperm unites with a female gamete or oocyte (ovum) to form a single cell called a zygote. This highly specialized, totipotent cell marked the beginning of each of us as a unique individual.” “A zygote is the beginning of a new human being (i.e., an embryo).” Keith L. Moore, The Developing Human: Clinically Oriented Embryology, 7th edition.
“Although life is a continuous process, fertilization (which, incidentally, is not a ‘moment’) is a critical landmark because, under ordinary circumstances, a new, genetically distinct human organism is formed when the chromosomes of the male and female pronuclei blend in the oocyte” (emphasis added; Ronan O’Rahilly and Fabiola Mueller, Human Embryology and Teratology, 3rd edition.
Many other examples could be cited, some of which may be found here.
These authorities all agree because the underlying science is clear. At fertilization—or, more precisely, when the sperm (a male sex cell) fuses with the oocyte (a female sex cell, more commonly referred to as an egg)—each of them ceases to be, and a new entity, one that is both genetically and functionally distinct from either parent, is generated. This new entity, initially a single totipotent cell, then divides into two cells, then (asynchronously) three, then four, eight, and so on, enclosed all the while by a membrane inherited from the oocyte (the zona pellucida), which then dissolves during implantation, allowing for continued growth in the direction of maturity as a member of the species. Even prior to implantation, however, these cells and membrane function as parts of a whole that regularly and predictably develops into the more mature stages of a complex human body.
How do we know that the result of sperm-oocyte fusion is a new entity, rather than a continuation of the oocyte? We know that a new entity exists because, once the sperm penetrates the oocyte, a completely new trajectory of biological development commences. The biological activity of an oocyte is directed toward successful fertilization; the biological activity of sperm is directed toward penetration of an oocyte. The biological activity of the new entity that results when sperm and oocyte fuse, however, is directed toward nothing less than the development of a mature human organism, distinct from either parent. Further, this new entity’s activities are directed not by instructions from the mother’s body, as some people wrongly suppose, but by its own unique set of instructions, especially the blueprint for development contained in its unique genetic material. The mother’s body recognizes the zygote and then the embryo as an entity distinct from itself. In fact, the embryo must send out chemical signals to prevent the mother’s immune system from attacking it. The embryo also emits chemical signals that induce changes in the lining of the mother’s uterus to enable successful implantation.
If this embryo is provided a suitable environment, nutrition, and protection from deliberate attack, serious injury, or disease, it will develop to the mature stage of a human organism. Thus, from the zygote stage onward this distinct, new organism has all of the internal resources—in its genetic and epigenetic structure—needed to develop itself (or, rather, himself or herself, since in the human sex is determined from the very beginning) to the mature stage of a human organism. At no point after fertilization—implantation, gastrulation, birth, puberty, etc.—does a fundamental change in biological trajectory occur. These subsequent stages of development are simply the unfolding of the zygote’s inherent dynamism toward human organismal maturity. This shows that the zygote already is a human organism—a member of the species Homo sapiens—albeit at an early stage of his or her development.
Paulson’s Arguments
But perhaps Dr. Paulson objects to HHS’s claim that life begins at conception not because it contradicts the overwhelming scientific consensus, but because he has decisive arguments against that view? We can’t rule that out a priori, so let’s examine his arguments.
First, Paulson claims that no new life is formed at fertilization because the egg and the sperm were already alive: “The human egg is a single living cell and it becomes a one-cell embryo if it successfully combines with a live sperm. No new life is formed — the egg and the sperm were already alive — and fertilization is not instantaneous.” This argument, however, rests on utter confusion.
No one after the work of Louis Pasteur has maintained that life comes from anything other than life. Ofcourse there was life before fertilization (the egg and the sperm). There were living entities—living cells—from which the new living being came to be. But with fertilization there is a new life—that is, there is a new organism, a member of the same species as the parents and no mere part of either of them (as the male or female sex cells were)—an entity that was not there before.
If Paulson’s argument were sound, it would show that no new cells ever come to be, even in the asexual reproduction of cells—for example, within our bodies in cellular growth or repair. In such cases, the parent cell was alive before the reproduction, but of course the two daughter cells really do come to be. Thus, the continuum of life—which Paulson mentions again later in his piece—provides no evidence against the standard scientific view that a new human life comes to be at conception (fertilization).
Second, Paulson suggests that, because fertilization is a process, it can’t be the point at which a new human being comes to be. He writes: “fertilization is not instantaneous. Nearly 48 hours pass from the time sperm first bind to the outside of the zona pellucida, the human eggshell, until the first cell division of the fertilized egg.” But this argument too is stunningly weak. A radical change—in this case the coming to be of a new organism, marked by a radical change in the trajectory of the entity’s biological activity—can be caused by a coordinated series of smaller changes. Many smaller changes—such as the movement of sperm through the uterine tube and then through the outer protective structures of the oocyte—precede the radical change that occurs when one sperm cell penetrates the oocyte and its membrane fuses with the oocyte’s membrane to form a new, genetically distinct, single dynamic structure. As all the works of modern human embryology and developmental biology attest, this radical change marks the coming to be of a new human individual. A series of very small changes—a continuum—is no evidence at all against a discontinuity at the end of that series.
Note also that if Paulson’s argument were sound it would refute his own position as well. A human life can’t begin at conception, he says, because conception is an extended process. So, when does it occur? His answer: later during gestation, possibly with implantation. But of course, implantation too occurs by several small steps. The only point at which there is truly a radical change in biological trajectory—and so the only logical point to locate the generation of the new organism—is fertilization, with the ceasing to be of the male and female sex cells and the simultaneous coming to be of the self-directing new organism.
Third, Paulson claims that prior to implantation the human embryo is merely “a collection of stem cells, each of which has the capacity to grow into any part of the placenta, as well as fetal tissues and organs, but it is not itself a new human life.” But this ignores the internally coordinated collaboration of these cells. The embryo is of course composed of a multitude of cells (though not, it should be pointed out to Paulson, all of them stem cells). And the cells in the part of the embryo called the inner cell mass, when extracted from the human embryo, do qualify as pluripotent cells—that is, once extracted, they can be coaxed to become any type of human cell—but none of this shows that the embryo is a mere mass of undifferentiated cells rather than what it obviously is: an internally integrated organism. Again, all the scientific works acknowledge this fact.
Indeed, cell differentiation begins with the very first cell division. Unless something (such as twinning, discussed below) interferes with their trajectory, one of these two cells will develop into the future body, multiplying itself to form a cluster of cells at one end of the embryo called the inner cell mass. The other will develop into the placenta and other supporting structures, multiplying itself to form a ring of cells that lines the inside of the zona pellucida, leaving a large cavity in the middle of the embryo that is called the blastocoele. Thus, far from being an undifferentiated and unorganized mass, the embryo’s cells communicate and function together as parts of a complex whole in a regular and predictable manner, each new step preparing for the next along a developmental trajectory that, if all goes well, eventually by a continuous and gapless process results in a sixteen-year-old’s asking for the car keys.
Fourth, Paulson suggests that the possibility that an early embryo may give rise to twins (monozygotic) shows that they are not yet individuals: “It is also potentially more than one individual, since identical twins are the result of a single implantation.” However, from the fact that A can split into B and C, it simply does not follow, nor does the fact at all suggest, that A was not an individual before the division. Conceivably, A might cease to be and give rise to B and C, or A might be identical with B or with C. When a flatworm is sliced, the result is two living flatworms. It is obvious that a new individual is generated by the division of parts from a single whole. The fact that the division of a flatworm produces two flatworms in no way shows that prior to that division there was not actually a single flatworm. The evidence indicates that this same type of event occurs with most monozygotic twinning in human beings. That is, in most monozygotic twinning a single embryonic human being exists until the splitting of some cells from this first embryo, and this division generates a second embryo. Thus, monozygotic twinning casts no doubt at all on the fact that the human embryo is a distinct, whole, albeit immature, human organism from conception (fertilization) on.
In short, Dr. Paulson accuses the HHS of presenting a faith-based affirmation as if it were a scientific position. But it turns out that his denial of the claim that life begins at conception contradicts the standard scientific position, and his arguments against that claim are fallacious (sometimes egregiously so) and inaccurate. Ironically, it is Dr. Paulson, not the HHS, who seems to be basing his views about the beginning of human life on something other than scientific facts.
Patrick Lee is Phttps://onemoresoul.com/wp-admin/post-new.phprofessor of Philosophy and John N. and Jamie D. McAleer Professor of Bioethics at the Franciscan University of Steubenville. Melissa Moschella is an assistant professor of medical ethics at Columbia University.
Hours after the results of Australia’s plebiscite on same-sex marriage were released, Family Edge’sVeronika Winkels sat down with German sociologist and Catholic convert Gabriele Kubyto hear her thoughts on the effects this social development will have on Australians.. Ms Kuby, author of The Global Sexual Revolution, was on a speaking tour of Australia at the invitation of Parousia Media. The following is an edited excerpt from a videoed interview.
FE: In light of the majority yes vote, what advice do you have for Australians who voted no?
GK: We are living in an age of a global attack on marriage and family, and this result only comes about through very severe manipulation of the minds of people. I have been told many instances of how severe [the yes campaign] was, as it was in Ireland. Our opponents receive billions of money from the global network of international organizations, the UN, EU, together with the billionaire foundations: Rockefeller, Bill Gates, George Soros. They are all behind this strategy and they put their billions into this struggle around the world — along with the media and national governments.
Also, we have a deep human desire to be part of the pack. I think this must be something very deep in us because, in the history of human societies, you had to be part of it or you wouldn’t survive So we want to move with the mainstream, we want to be accepted.
This instinct is manipulated by an ideology that uses concepts that sound good: human rights, equality, justice, non-discrimination, tolerance, and we are all for that, of course, we are all for that.
So it is very hard to resist this battle. It is fought on a very sophisticated level of social science — how you change the attitudes of people — and this is the result. In states of the US where campaigns like this didn’t take place, most voted against same-sex marriage.
FE: How are Europeans dealing with this?
GK: In many east European countries there are big movements to carry out referendums for marriage to be as it always has been. In Europe, especially in Eastern Europe, there are something like 13 nations that have actually managed to put protections into the constitution to have marriage remain what it is: the union of man and woman.
Now this is being overturned, but many people are aware this trend is becoming totalitarian. I think many have noticed this in Australia.
We are proud of our democracy, but now we see a strained relationship between democracy and the constitutional freedom to act in accordance with our conscience: religious freedom, freedom of speech, of expression, of business, of education of our children — we see all this contested. All this is at stake at the moment, and the battle will continue, and the battle for these freedoms must continue.
I just hope there’s an awakening in Australia; that these 38 percent who voted against it become strong and continue this fight.
FE: How do Christian parents explain this cultural upheaval to their children?
GK: I am a mother of grown up children, you have small children. How do we bring up our children in this society? It is very, very difficult, because this society actually steals children from their parents. There was a time when Muslim invaders stole children from Christian families, in the 16th century or so. They stole the children and trained them to become fighters against Christianity.
This, in a way, is happening today. Children are stolen from their families, not with weapons, but by the media, by pornography, by the smart phone. There is huge pressure on our children — they must have a smart phone. Everyone else has a smart phone. If they do not have one, they are ridiculed.
Once they have a smart phone, pornography gets to them in just a few clicks. And when they see pornography, if that is the first information they receive about sexuality, that is terrible. It is traumatizing to see that, traumatizing. And it destroys the vision of what sexuality, and love, and marriage and family is about. This is what we are up against.
FE: So what can we do?
GE: Firstly, we Christians have to live our faith. If we live our faith, we are joyful. We are the village on the hill, we are the light on the stand, we are the salt of this earth. And people will see, “They have a quality which we actually desire- we desire love in our heart, and they are people who have that.”
And for children of broken families, they are a real apostolate for intact families. Invite children of broken families into your family, so they experience that this can be family: a father and a mother and love in the family.
This is number one: live your faith truly. If that lives in a family, there will be light in that family, and if others see that, if children come into that family they will think, “how wonderful it is here.”
It is a political achievement in our time to cultivate our Christian family life and have the love and joy this imparts to us. Then of course we have to struggle and we have to have a real, loving relationship with our children, who trust us. We trust the people who truly love us.
Children today have to be so strong. A mother spoke up today after my talk and said her daughter’s teacher, not in accordance with what she should actually do, asked the class for a show of hands for pro- and no votes- and her daughter was the only one to vote no. How brave!
How do we strengthen them? Very early on they see they have a mission in this life, and they need all the strength of their family, their parents, behind them
MICAIAH BILGER NOV 21, 2017 | 11:53AM WASHINGTON, DC
Every time Manda Grover received a pregnancy scan, the expecting mom felt pressured to abort her unborn baby boy.
Grover said the pressure began when a test revealed that one or both of her unborn twins may have Down syndrome. In an article at the Daily Mail, Grover and her husband, Richard, of Horsham, West Sussex, explained how they had to continuously defend their decision to choose life for their unborn son, no matter what his condition was.
Today, twins Jack and Jessica Grover are 2 years old, and doing well. Jack has Down syndrome, Jessica does not. Their mother said they are “just as perfect as each other.”
“It’s hard to believe that if I’d taken the advice of many people along the line, my beautiful boy would not be here today,” Manda said.
The Grovers said they tried to conceive a child for six years before turning to in vitro fertilization. Two attempts failed, but on the third, Manda became pregnant with twins, according to the report.
When she was 12 weeks along, Manda had a screening test that revealed that the twins may have Down syndrome. After more testing, doctors told the Grovers that their unborn daughter had a one in 80 chance of having Down syndrome, and their unborn son had a one in eight chance.
“I was 14 weeks pregnant and my mind was instantly made up, Down’s syndrome or not – I was having my babies,” Manda said. “I had waited so long for my babies. The thought that I would be getting rid of one, or even risk losing both was just not an option.”
Despite her determination, Manda said she continued to feel pressured to abort her son.
“At every scan after that – and I was given more than normal because of my age and the fact that I was having twins – I was asked about whether I was happy to continue with the pregnancy,” Manda said.
“Needless to say, of course I was but the question became hurtful and tedious. Nothing had ever been confirmed 100 per cent that he had DS, but Richard and I had accepted that he did and started reading up on the syndrome,” she continued.
On Oct. 10, 2015, the twins arrived. When the Grovers looked at their son, they knew for sure that he had Down syndrome, but it did not make any difference to them. They were happy to finally have the children that they had longed for.
Their doctor did not have the same attitude.
“I remember that after telling us about Jack, the doctor actually apologized,” Manda remembered. “I couldn’t understand what for. I explained that we have two beautiful babies, both healthy that we’d waited six years to come into our lives. They were a miracle – no one should feel sorry about that.”
The discriminatory attitudes that the Grovers faced are not uncommon anymore in the medical community. Parents whose unborn babies have Down syndrome or other disabilities frequently report feeling pressure to abort them.
Last year, a Florida mom’s letter to her doctor went viral after she exposed how the doctor pressured her to abort her unborn daughter with Down syndrome. Courtney Baker said she wanted her former doctor to see how valuable her daughter’s life is and how wrong it is to pressure anyone to have an abortion.
Research published in the Journal of the American Medical Association suggests that many women are not receiving adequate counseling about prenatal testing for Down syndrome and other disorders.
As a result, studies indicate unborn babies with Down syndrome are targeted for abortions at very high rates. A CBS News report earlier this year shocked the nation by reporting that Iceland has an almost 100-percent abortion rate for unborn babies with the genetic disorder. Other studies put the rate in the United States somewhere between 60 percent and 90 percent.
This has prompted legislation in several states in America and in Poland to end the deadly discrimination against unborn babies with Down syndrome.
The Grovers said they worry about the discrimination that their son could face as he grows, but they have no regrets whatsoever about choosing life for him.
“Two babies that in my eyes are just as perfect as one another,” Manda said. “Looking at Jack, it’s hard to believe that if I’d taken the advice of many people along the line, my beautiful, happy and healthy boy would not be here today, and the world would be a sadder place for it.”
TORONTO, November 20, 2017 (LifeSiteNews) — Euthanasia has been legal in Canada for just over a year and pediatricians are already “increasingly” being asked by parents to euthanize disabled or dying children and infants, a survey by the Canadian Paediatric Society (CPS) has found.
American anti-euthanasia activist Wesley Smith said the results of the survey prove the morally slippery slope that a nation slides down when it agrees that “killing is an acceptable answer to human suffering.”
“Once euthanasia consciousness is unleashed, it never stops expanding,” he wrote in the National Review.
“I guess Robert Latimer–a Canadian farmer who murdered his daughter because she had cerebral palsy–was a visionary,” he added.
The CPS surveyed its members in light of the possibility Canada will expand euthanasia to children.
Indeed, Justin Trudeau’s Liberal government wrote that possibility into the law it passed in June 2016.
Bill C-14 permits voluntary euthanasia for individuals of at least 18 years of age assessed to be suffering intolerably from a grievous and irremediable medical condition, and with natural death reasonably foreseeable.
But the Commons Justice Committee added an amendment to the bill directing the federal government to review expanding euthanasia on three further grounds: for children, or “mature” minors; solely for mental illness; and allowing advance directives in the case of those with degenerative diseases such as dementia.
The Liberals have asked the Council of Canadian Academics to research these questions, and report to Parliament by the end of 2018.
The CPS surveyed 1050 pediatricians on their experiences with “medical aid in dying” or MAID, and released a report at the end of October.
Forty-five doctors reported receiving explicit requests from parents to euthanize 91 children, it said. More than half of these requests were for “neonates or infants under a year old.”
A further 118 pediatricians had “exploratory” discussions about euthanasia with parents of 419 children.
As for requests from the children themselves, 35 paediatricians reported discussing euthanasia with 60 minors. Nine reported receiving direct requests for euthanasia from 17 minors.
While “such consultations may be rare, minors in Canada are contemplating MAID-related concepts and approaching health care providers with MAID-related questions,” noted the CPS survey.
“Given the evolving legislative landscape, it is reasonable to anticipate that such questions will increase in the near future.”
The CPS also conducted an attitude survey on euthanasia, with 574 of a possible 1,979 members, or 29 percent, responding.
Of these, 46 percent supported euthanizing mature minors who have “progressive or terminal illness or intractable pain.”
Thirty-three percent opposed euthanizing mature minors for any reason.
Mature minors are children who are allegedly capable of understanding the nature and consequences of treatment, and so judged competent to request death by lethal injection.
The CPS study suggested non-voluntary euthanasia for non-competent dying “and/or severely disabled” children is not far off.
Canada’s federal law, and Quebec’s law currently prohibit involuntary euthanasia for anyone, it said, adding:
However, given the human rights framework advanced in Carter v. Canada, the parents of a dying and/or severely disabled child who is deemed to be suffering may, in the near future, be looking to the courts to support a right to end their child’s life. Decision-making for treatment of never-competent children is based on the “best interest standard”: choosing among options that reasonable persons, acting in good faith on another’s behalf, would consider acceptable in similar circumstances.
“All this is very problematic,” says Alex Schadenberg, executive director of the Euthanasia Prevention Coalition.
Euthanasia lobbyists shift the argument for legalizing the killing of children by lethal injection from the autonomy of the individual to “why do you want to allow them to suffer,” he told LifeSiteNews.
“So the idea is, well, this isn’t fair, the law has an inequality because you’re allowing adults who are capable of requesting this, but not children or mature minors.”
Parents and guardians in Canada currently can authorize no treatment or the withdrawal of treatment for non-competent minors, Schadenberg added.
“If you had a child with a significant disability, then the question at birth would be, do you want that child to receive treatment or not, and you would have the right to say yes or no,” he said.
“So the argument is well, because we already have that, therefore, what’s the difference between that” and euthanasia.
Schadenberg echoed Smith’s warning that once euthanasia is allowed, the grounds for legally killing people keep expanding, as has been demonstrated in other jurisdictions.
It gives doctors impunity to lethally inject disabled infants, such as those spinal bifida or hydrocephalus.
The CPS study “shows us that the parents were the ones to ask about euthanasia. Rarely did the mature minor or child consider euthanasia,” Schadenberg said.
“The concept of euthanasia for children should be simply rejected based on the fact that children cannot consent.”
ALEXANDRIA, Virginia, November 20, 2017 (LifeSiteNews) – Six pro-life activists, including two Catholic priests, walked free today after facing obstruction of justice and trespassing charges for refusing to leave an abortion facility waiting room.
The pro-life activists were found guilty of trespassing and each given a $500 suspended fine. If they don’t trespass inside the abortion facility for the next year and maintain good behavior, the fine will be waived. They were found not guilty of obstruction of justice.
Inside that waiting room on September 15, 2017, they gave pregnant women roses and encouraged them to choose life. Police removed the activists from the facility, Alexandria Women’s Health Clinic, as they passively resisted arrest. The activists called this a “Red Rose Rescue.” It was because they passively resisted arrest, requiring wheelchairs to haul them out of the abortuary, that the pro-life activists were charged with obstruction of justice.
One of the priests, Father Fidelis Moscinski of the Franciscan Friars of the Renewal (CFR), told presiding Judge Donald Paddock that he would not pay any fines because he considers them unjust, and would similarly consider any jail time to which he was sentenced “illegal.”
“I consider this Court’s judgement of me as guilty invalid and therefore any subsequent incarceration illegal,” he said.
Appearing in Alexandria General District Court alongside Fr. Fidelis were his co-rescuers, Father Stephen Imbarrato of Priests for Life, Joan Andrews Bell, Julia Haag, Bonnie Borel Donahue, and Joan McKee.
Fr. Fidelis is a soft-spoken, gentle, serene friar who wears sandals without socks year-round as part of his religious habit.
Fr. Imbarrato is known as the “protest priest” and participates in pro-life activism around the country. He has offered Masses on EWTN and is a post-abortive father himself.
Haag, Donahue, and McKee were described as “seniors” during the trial. Haag and Donahue sometimes pray outside Planned Parenthood’s Washington, D.C. flagship abortion facility.
Bell is a seasoned pro-life activist who has participated in dozens of rescue-style operations across the country. The prosecutor only listed some of Bell’s previous convictions as she argued for Bell and others who have done past rescues to be punished more harshly.
Lauren Handy of Mercy Missions told LifeSiteNews this was likely because it would have taken too long to list all of Bell’s life-saving rescues.
Paddock did not sentence Bell more harshly than the others.
Canadian pro-life activist Mary Wagner, who has conducted similar rescues in her own country and served jail time for them, was present in court today to observe the trial.
“I’m glad we did what we did,” McKee told LifeSiteNews. “The babies just matter so much…I hope we can keep up and eliminate the killing of pre-born babies and help to educate people to love their children.”
“I’m very hesitant to rejoice in victory – so to speak – because I don’t think there’s really any victories or rejoicing until pre-born child killing comes to an end,” Fr. Imbarrato told LifeSiteNews. “This is just a small hurdle that we got past.”
“I think it shows that God wants us to continue discerning and praying about Red Rose Rescues and surely that’s what…my conscience has come to” make me believe, the priest concluded.
Employees hesitant to say Alexandria Women’s Health Clinic is an abortion facility
Judge Paddock allowed defense attorney Chris Kachouroff to argue that what the six activists did on September 15 was necessary to save the lives of other humans. He ultimately said the argument wasn’t applicable to the trespassing charge.
During his cross-examination of Alexandria Women’s Health Clinic receptionist Jerilyn, Kachouroff asked her to specify what types of services the facility offers. She was extremely hesitant to admit that the “services” her employer commits are abortions.
Of the defendants, Jerilyn was only able to identify Fr. Fidelis.
Kachouroff put Catherine Flandez, the facility’s head nurse and assistant administrator, on the spot during her cross-examination as he asked her if the “services” being provided were for the mother or the fetus.
Such questions “inherently assume a view of the world” not compatible with the witness’s worldview, said Judge Paddock. But he allowed Kachouroff to press Flandez on the issue slightly.
Police officer lives in apartments that house abortion facility
Alexandria Women’s Health Center is located in Landmark Towers, which has some businesses on its lower floors and apartments on the upper levels.
The building’s “resident manager,” Cecilia Gondor, and Alexandria City Police Officer Matthew Bramhall testified about an unusual arrangement they have.
Bramhall is given discounted rent in exchange for helping with building security when he is off duty as a police officer. It was suggested that it’s his job to “enforce the law” there while off duty.
Bramhall was in full uniform on his way to testify in another court case when he received a call about the Red Rose Rescue. He was off duty.
Returning home to deal with the rescuers on behalf of his landlord caused him to be “slightly delayed” for his other court appearance, he testified. Bramhall waited inside the abortion facility lobby telling the pro-lifers to leave for about 20 minutes before on-duty officers arrived.
Kachouroff pressed him on whether he actually remembered the six defendants given that he encounters hundreds of people because of his job.
“It’s probably something I’ll remember forever” because of the Catholic priests, the officer testified.
Gondor refused to admit whether she knows the facility to which her company leases space commits abortions. She would only call it “women’s services.”
Kachouroff asked that just as a landlord would likely know that a dentist works on teeth, wouldn’t Gondor be aware of the speciality of any doctors in her building? Gondor seemed to be annoyed by this question and questions about how closely she has actually read the lease.
Some of the Virginia “Red Rose Rescuers” with their attorneyClaire Chretien / LifeSiteNews
“Women’s Health Clinic, Inc. is proud to be the first choice in gynecology and abortion services for women in the Virginia, Maryland, Washington, D.C. and West Virginia area,” its website, which prominently advertises abortion, says.
Officer Jonathan Lopez, one of the responding officers, said that he repeatedly told the six pro-lifers they “needed to vacate the premises.” He testified that they told him they wouldn’t leave unless the facility closed for the day and stopped “killing babies.”
Lopez was the officer who took Fr. Imbarrato into custody.
‘We heard that at Nuremberg’
Kachouroff’s closing statement focused on Virginia’s fetal homicide law and how the six pro-lifers were acting in necessity to defend others from being killed.
Section 18.2-32.2 of the Virginia state code of law prohibits fetal homicide and allows those who kill a fetus to be charged with doing so.
Judge Paddock didn’t think it was an unfair argument, although he said general district court was an unusual place for this kind of debate to take place. But these cases have to start somewhere, he said, so he was willing to entertain the argument.
Kachouroff noted that no officers intervened on behalf of the pre-born humans even though the pro-life activists told them babies were being killed.
“We heard that at Nuremberg,” he said.
Kachouroff argued that civil authorities have a duty to protect the lives of their fellow humans. He said that the judge would have to say that a fetus is not a person if he were to reject such arguments.
The Virginia “Red Rose Rescuers” and their attorneyClaire Chretien / LifeSiteNews
Kachouroff then quoted Martin Luther King, Jr., who said that there can be a “moral responsibility” to disobey unjust laws. The six red rose rescuers don’t think laws against trespassing are unjust, he explained, but rather think that laws allowing other human beings to be killed through abortion are unjust.
“My clients were expressing the highest respect for the law,” he said. They were there not to trespass but to “stop the killings of babies.”
Praying, distributing roses, and giving abortion-minded women pamphlets is “not what’s encompassed by defense of others,” the prosecutor argued. She said an example of the “defense of others” would be if someone acted to stop another who had pulled out a knife.
AbortionProcedures.com explains that in a second trimester dilation and evacuation (“D&E”) abortion
the abortionist uses a sopher clamp — a grasping instrument with rows of sharp “teeth” — to grasp and pull the baby’s arms and legs, tearing the limbs from the child’s body. The abortionist continues to grasp intestines, spine, heart, lungs, and any other limbs or body parts. The most difficult part of the procedure is usually finding, grasping and crushing the baby’s head. After removing pieces of the child’s skull, the abortionist uses a curette to scrape the uterus and remove the placenta and any remaining parts of the baby.
It explains a first trimester abortion this way:
A suction, or aspiration, D&C abortion is a procedure in which a suction catheter is inserted into the mother’s uterus to extract the preborn baby. Tools are then used to scrape the lining of the uterus to remove any remaining parts.
‘As a Catholic priest, I must say to this Court that abortion is murder’
Judge Paddock said that the law the pro-lifers were charged with violating was not a segregation law, but rather was “the law that prohibits people remaining on the land of another” after being asked to leave.
“The defense of others I find is inapplicable in the case at hand,” he said. “I’m in no way attempting to…adjudicate the claims of the defendants.”
Judge Paddock said he simply saw it as a trespassing case and would treat it as such.
“I think there needs to be punishment, your honor,” the prosecutor said.
Judge Paddock then ordered the six pro-lifers to reappear in court on November 20, 2018. Provided they don’t enter the Alexandria abortion facility again, at that time their $500 fines will be rescinded.
“Your Honor, a unique human individual begins to exist at the moment of conception,” Fr. Fidelis told Judge Paddock in a prepared statement. “In a sane, civilized society that new human being would have his or her right to life clearly recognized in the law.”
“But we do not live in a sane, civilized society,” he said. “Since Roe v. Wade in 1973, we live in a nation, Your Honor, that has permitted the legal destruction of millions of innocent children.”
“As a Catholic priest, I must say to this Court that abortion is murder and no law or court decision can make legitimate what is intrinsically evil,” Fr. Fidelis continued. “Legalized abortion is an abomination in the eyes of God.”
Speaking louder but still in his signature gentle manner, Fr. Fidelis said, “now is the time for all of us to repent of our complicity in this national evil.”
“It is time to seek forgiveness from God, in the name of His Son, Jesus Christ,” he said. “It is not too late to turn away from sin and begin to respect the gift of life and the laws of God.”
“In finding me guilty, this Court has refused to recognize the humanity and value of pre-born children,” Fr. Fidelis concluded. “Since I stand here in solidarity with them, may God give me the grace to bear witness on their behalf.”
November 14, 2017 (LifeSiteNews) — Last week, we looked at how Lucifer, by refusing to serve the God of fruitfulness and sacrificial love, merited his own everlasting isolation and barrenness, and how he ever seeks to draw human souls into his realm of selfishness. In particular, the refusal to subordinate the natural to the supernatural is his defining trait, and explains why he hates celibacy and virginity more than anything else in the world.
Satan hates marriage for much the same reason: it, too, is a life of self-sacrifice made possible only by divine blessing, a state ordered to the multiplication of children of God who will have the potential to receive supernatural elevation by grace and to enjoy heavenly glory, of which the devil deprived himself. The power of generation in man — how mysterious it is! To be invited into partnership with the Author of life! To stand, in procreation, at the origin of being ex nihilo: this is a power no angelic spirit has. It is a direct participation in God’s creative act. As the great Thomist theologian Scheeben explains, if Adam and Eve had not fallen, they would have transmitted not only natural life to their offspring, but also the condition of supernatural life: their children would have been conceived and born in a state of grace. This is why the devil so hated Adam and Eve, resplendent in grace as they were: he knew that from their loins would spring an entire race of beings destined for immortal glory with the angels. Even though we are now fallen and no longer conceive “sons of God,” the privilege of procreation and the freedom to cooperate with Christ in the sanctification of our children remain ours. As Pope Pius XI eloquently testifies in the greatest papal document ever written on marriage and family:
How great a boon of God this (good of offspring) is, and how great a blessing of matrimony is clear from a consideration of man’s dignity and of his sublime end. For man surpasses all other visible creatures by the superiority of his rational nature alone. Besides, God wishes men to be born not only that they should live and fill the earth, but much more that they may be worshippers of God, that they may know Him and love Him and finally enjoy Him forever in heaven; and this end, since man is raised by God in a marvelous way to the supernatural order, surpasses all that eye hath seen, and ear heard, and all that hath entered into the heart of man. From which it is easily seen how great a gift of divine goodness and how remarkable a fruit of marriage are children born by the omnipotent power of God through the cooperation of those bound in wedlock.
For although Christian spouses even if sanctified themselves cannot transmit sanctification to their progeny, nay, although the very natural process of generating life has become the way of death by which original sin is passed on to posterity, nevertheless, they share to some extent in the blessings of that primeval marriage of Paradise, since it is theirs to offer their offspring to the Church in order that by this most fruitful Mother of the children of God they may be regenerated through the laver of baptism unto supernatural justice and finally be made living members of Christ, partakers of immortal life, and heirs of that eternal glory to which we all aspire from our inmost heart. (Encyclical Casti Connubii, no. 12)
Satan did what he could to thwart this plan — and so he does with each of us, if we let him. The devil opposes natural as well as supernatural generation: he seeks to prevent men and women from using the gift of their sexuality to bring more life into the world; he seeks to prevail upon them to kill the fruit they bear; he seeks to lead them away from the source of immortality in the sacraments of the Church. Hating procreation, he has bent all his efforts toward either preventing it through contraception or destroying its fruits through abortion. Contraception is an abomination of desolation in the midst of the temple, which is the human body sanctified by the Holy Spirit: through contraception, the Lord and Giver of Life is cast out as if He were an evil spirit, and in his place is welcomed the spirit of lust and avarice, to make its home in the barren womb, like a church with no tabernacle and no Real Presence.
Contrary to the demonic spirit of selfishness, spouses give up their right of self-determination over their own bodies when they vow their faithful love to each other until death, come what may. Christ, too, is faithful to His Church, come what may, and never gives up on her sinful members until all who are destined for glory have reached the fatherland. In light of God’s faithfulness to sinful Israel and Christ’s faithfulness to His still-imperfect Church, divorce is an unredeemable fiction, adultery an abomination, and Eucharistic communion for those who are “remarried” an act of sacrilege by which the Savior is spat upon, scourged, crowned with thorns, and crucified in His Sacrament.
Let us make no mistake about it: Lucifer, with the pseudo-patience of an immortal spirit, has slowly built up an anti-religion, a counterfeit Catholicism, that has for its purpose the eternal damnation of men, just as the Catholic religion has for its purpose their eternal salvation. Divorce, and with it, adultery, is the anti-sacrament of Marriage; contraception, and from it, abortion, is the anti-sacrament of Baptism; the self-indulgence of masturbation and homosexual activity is the anti-sacrament of Confirmation, which produces self-control and fortitude; euthanasia is the anti-sacrament of Extreme Unction. In place of holy orders, there is negligent fatherhood and man-hating feminism; in place of penance, there is the hedonistic satisfaction of every bodily appetite; in place of the Eucharist, there is idolatry of the world, the flesh, and the devil.
It is far from coincidental that the sacred liturgy had to fall into ruins first before the devil could carry out his attack on virginity and celibacy. These latter have no meaning, no purpose, apart from the wedding feast of the Lamb to which the liturgy gives us access. When the liturgy is drained of adoration, beauty, and contemplation, it can no longer awaken, nourish, and direct an all-consuming hunger and thirst for God’s kingdom. It will no longer stir up priestly and religious vocations or sustain them to the end. The Mass and the Divine Office had to be brought low before celibacy and virginity could be felled. The so-called “irreversible liturgical reform” had to predate the supposedly irreversible decline in “traditional models of ministry and service.”
In reality, the Church’s authentic liturgy, in all its depth and splendor, always summons forth abundant vocations to the priesthood and the religious life. This, again, is why the devil hates the usus antiquior with such implacable fury. Wherever the traditional liturgy returns, celibacy and virginity blossom anew — as do marriages in which husband and wife sacrificially welcome many children. Satan hates it all and is at work, sleeplessly, to fight against it, using every means at his disposal.
We are now in a better position to see the connection between Sr. Lucia’s statement that “the final battle between the Lord and the reign of Satan will be about marriage and the family” and Pope Siricius’ castigation of Jovinian for denying the superiority of the celibate or virginal life dedicated to God. False teachings on marriage and the “relaxation” of the required discipline of clerical celibacy are two flanks of a single army laying siege to the City of God on earth. Any word, any action against the sanctity of marriage, the good of the family, or the exalted vocations of clerical and religious life finds its origin in the General of this army, the Enemy of mankind. As we endure the worst doctrinal confusion, moral laxity, and liturgical uprootedness the Church has ever suffered, may the Lord, mighty in battle (Ps 23:8), save His people and bless His inheritance (Ps 27:9).
At church, Catholics should spend their time in silence before Mass, preparing “to meet with Jesus” instead of engaging in “chitchat,” the pope said Nov. 15 during his weekly general audience.
“Silence is so important,” he said. “Remember what I told you last time: we are not going to a show. Silence prepares us and accompanies us.”
The pope continued his new series of audience talks on the Mass, reflecting on the Eucharist as a form of prayer that is “the highest, the most sublime and, at the same time, the most concrete” way of encountering God’s love.
“This is the greatest grace: to experience that the Eucharist is the privileged moment to be with Jesus and, through him, with God and with our brothers and sisters,” the pope said.
In the Gospels, he continued, Jesus teaches his disciples that the first thing needed to pray “is to know how to say ‘father’” and to trust in God with the humility of a child.
Christians also must allow themselves to be “surprised by the living encounter with the Lord,” he said, and not simply “talk to God like a parrot,” repeating the words of prayers without thinking.
“The encounter with God is a living encounter,” the pope said departing from his prepared remarks. “It is not an encounter of a museum, it is a living encounter. And we go to Mass, not a museum! We go to a living encounter with the Lord.”
Pope Francis said the Mass is also a gift and a consolation where Christians discover that God’s greatest surprise is that he “loves us even in our weakness.”
“The Lord encounters our frailty,” the pope said. “This is the environment of the Eucharist. This is prayer.”
MICAIAH BILGER NOV 13, 2017 | 5:15PM WASHINGTON, DC
The San Francisco 49ers’ win on Sunday was marked by a player’s heartbreaking tribute to his baby who died too soon.
Wide receiver Marquise Goodwin, who scored a touchdown from an 83-yard pass in one of the biggest plays of the game, honored his baby son with a skyward kiss and what appeared to be a moment kneeling in prayer in the end zone, Yahoo Sports reports.
After the game, Goodwin revealed that he and his wife, Morgan, lost their very premature baby son early Sunday morning due to pregnancy complications.
Morgan Goodwin posted a photo of their son’s tiny hand Sunday on Instagram to mark his early death. She said they lost their son after she went into preterm labor in a failed struggle “to keep our healthy baby safe in my womb.”
Marquise said he scored the touchdown Sunday for his son.
According to the news report:
Goodwin had Giants’ corner Janoris Jenkins beat, and ran the last 20 or so yards to the end zone alone. Before he crossed the goal line, Goodwin blew a kiss skyward, and once he was in the end zone, he dropped to one knee, and then two.
He appeared to cross himself and then cradled the ball.
It was an emotional moment.
On Sunday night, Goodwin revealed just why he responded the way he did to his first touchdown as a member of the 49ers.
He explained: “Although we are hurt, I am grateful for the experience and grateful that God blessed me with a wife as courageous and resilient as Morgan. The pain (physically, mentally, & emotionally) that she has endured is unbelievable. Please Pray for the Goodwin family.”
Marquise’s post also included a photo of their son’s tiny hand against what appears to be his own.It is not clear how far along in the pregnancy their son was, but what is clear is that the Goodwins believe their son’s life was valuable. It did not matter how old he was or how long he lived, baby Goodwin’s life was precious and important.
When I was 18, I was prescribed birth control for some dubious reason … dubious primarily because I can’t even remember what the reason was. I wasn’t sexually active and didn’t have PCOS or unpleasant periods, but I went to the doctor for some reason and walked away with the pill.
It didn’t take long to figure out that it wasn’t really medicine at all. It made me feel terrible, weepy and unhinged, and I rapidly gained 10 pounds. More alarmingly for a college freshman, I found my thinking muddled and my schoolwork suffering. I didn’t even finish the first month before I stopped taking them altogether.
Years later, accepting Church teaching on contraception was part of the hurdle of converting. I’ll admit I struggled with the rejection of contraception as a whole for a while, but it took me no time at all to reject the pill, particularly. By that time I had my first child and I knew exactly what symptoms the pill mimicked — the weepy, crazy, cloudy days of early pregnancy. No way would I do that unless there was an actual baby on the other end … even though I was pretty sure that without the pill, there would be.
Turns out that I’m not alone in my easy rejection of the pill for reasons other than faith. Many Millennial women are rejecting the pill for various reasons, according to this month’s Vogue.
In fact, younger women are turning away from the pill in droves — an NHS study found that the number of women in contact with sexual and reproductive health services who used user-dependent contraception, including the pill, had dropped by more than 13 per cent between 2005 and 2015. It’s hardly surprising: a quick Google search chums up some alarming reports, from articles on possible links between the pill and cancer to claims that are outright bizarre, such as “contraceptive pills flushed down the toilet are turning fish transgender.”
Despite Vogue’s easy dismissal of reports as “alarmist,” the pill has been known for years to be carcinogenic. The World Health Organization classifies birth control pills as a Group 1 carcinogen, along with things like asbestos and tobacco. So it’s no wonder that women are finally saying enough is enough and finding alternate methods of pregnancy prevention.
Although alternate methods are denigrated as the “rhythm method” in popular media, Catholic women have been using them for years. Vogue features an app designed by a female particle physicist that tracks basal body temperature. Otherwise known as natural family planning, this is a method of pregnancy planning that Catholics have been using for decades. In fact, it’s the first method I learned when I converted 10 years ago.
As its creator mentions, this method doesn’t work for everyone. It didn’t work for me — but again, Catholics are ahead of the game. There are at least a half-dozen different methods that combine various symptom tracking, including the Marquette method that uses the ClearBlue Easy fertility monitor. And as technology has improved, so has fertility tracking; there’s an app for whichever method you choose.
So whatever the reasons might be for Millennial women’s rejection of the pill, they’re lucky that fertility tracking is easier and more accurate than ever — thanks, in large part, to the work Catholics have been doing all along.
MICAIAH BILGER NOV 10, 2017 | 5:14PM BRASILIA, BRAZIL
A Brazilian legislative committee passed a bill to protect unborn babies from abortion in all cases Wednesday, despite pressure on the South American country to expand its abortion laws.
The Daily Caller reports the bill passed by an overwhelming majority in an 18-1 vote. It would amend the constitution and recognize unborn babies’ right to life.
“To defend abortion, like it or not, is a Satanic, diabolical and destructive act,” Evangelical Congressman Pastor Eurico told the committee as he showed a model of a 12-week unborn baby.
In Brazil, abortion is legal in cases involving rape, incest and risks to the mother’s life; the country’s high court also ruled in 2012 that unborn babies with certain types of fatal anomalies also may be aborted, according to the report.
The bill would prohibit abortions in all cases and protect unborn babies’ right to life.
The committee vote is just a small hurdle. To become part of the constitution, the bill must pass both congressional bodies by a two-thirds majority.
Reuters speculated that the legislation may have a chance of passing: “The measure could clear those hurdles as part of a trade-off for other legislation the governing coalition seeks to pass, such as pension reform needed to plug a gaping budget deficit.”
But a poll at the time by the Datafolha Institute in Brazil found that 58 percent of Brazilians reject abortion in cases where pregnant women are infected with the Zika virus, according to the Catholic News Agency. According to the poll, 32 percent think the woman should be allowed to have an abortion and 10 percent had no opinion.
Brazilians also rejected abortion in cases where the unborn baby is diagnosed with microcephaly, with 51 percent opposed and 39 percent in favor, according to the report.
November 7, 2017 (LifeSiteNews) – The American College of Pediatricians is alerting parents to a dangerous new mobile phone app called Nurx. Dubbed the “Uber for birth control,” Nurx enables teens as young as age 12 to obtain contraceptive and abortive medications including the pill, vaginal ring, Plan B and Ella without parental knowledge or local physician oversight.
Sexual activity in adolescence is associated with harmful emotional and physical consequences including depression, suicide, sexually transmitted infections (STIs), and sexual exploitation at the hands of abusive boyfriends or sex traffickers. Easy access to contraceptives that bypasses parents and a physician visit, as Nurx does, increases the likelihood of teens experiencing these bad outcomes.
Adolescents are cognitively and emotionally immature. They need parental wisdom and oversight to compensate for their emotional impulsivity and their limited capacity to assess risk. All hormone based contraception has serious potential side effects including stroke and cancer; some increase the chance of contracting an STI. Plan B is embryocidal at certain points in a girl’s menstrual cycle, and Ella works the same way as the abortion pill. All women, especially adolescent women, benefit from a face-to-face encounter with a physician to discuss these risks.
Dr. Patricia Lee June of the American College of Pediatricians Board of Directors warns,
Nurx wrongly excludes those who know the child and her health history best — her parents and her physician, and places the full responsibility for a life-changing healthcare decision on a girl’s shoulders. When it comes to achieving optimal teen health, connected parents – not Smartphones – are paramount.
Fr Stephen Imbarrato of Priests for Life speaks about the impact of the Eucharist on his life and the power the Eucharist brings to the Pro-life Movement in America.
Planned Parenthood is marshalling women to #Fight4BirthControl, because apparently allowing those with moral objections to opt-out of the Obamacare contraception mandate is disastrous for women’s health. I wonder if the women using this hashtag understand how the contraception mandate works. Or how insurance works. Or birth control itself, for that matter.
To recap, the Obama administration’s contraception mandate directed employers to provide insurance coverage for contraception, including embryocidal methods, at no direct cost to employees. Several lawsuits challenged the mandate for violating the religious freedom of religious employers who object to providing birth control, including methods that may result in the loss of an embryo. So the Trump administration released a rule that allows any employer—publicly traded, nonprofit, or otherwise—to opt out of the mandate for religious or moral reasons.
Anyone who has followed the mandate controversy closely know this rollback will likely only affect a small percentage of employers. Birth control is so ingrained in our culture and medical community that the majority of employers already chose to pay for birth control prior to the mandate.
But there is another important conversation to have beyond what the mandate did or didn’t do: whether birth control is “necessary” for women’s health, and whether it should therefore be “free.” As a woman who has taken contraception for health-related reasons and suffers a chronic, life-threatening medical condition, and as a physician with a particular focus on fertility awareness and women’s health, I think the hysteria concerning the contraception opt-out is dishonest about the real answers to these questions.
Birth Control Doesn’t Treat Reproductive Problems Well
I know from personal experience and my medical practice that birth control is not the only, or even the best, way to treat the reproductive issues women experience. I also know as an adult who has paid for health insurance that no insurance is ever expected to cover all aspects of personal health care, even for life-threatening conditions. The treatment I need for my life-threatening asthma requires a substantial co-pay from me, which no “mandate” has been provided to alleviate.
Two medical emergencies in college revealed this tension, which I think deserves more weight in our conversation about the contraception mandate, and what is considered “necessary” in health care. Like many young women, in high school and college I suffered from debilitating menstrual cramps once a month. The pain was intense and seemed to drain me of all my energy such that I couldn’t get out of bed for at least one or two days.
The doctor I saw at the student health center was very kind and eager to help. She decided the best course of action would be to take the birth control pill. The doctor explained that the pill worked by suppressing my normal hormones almost entirely, preventing me from having true menstrual bleeds. Since I wasn’t sexually active, my cramps lasted only a couple days a month, and I worried about the side effects of the pill, I asked if I could take anything else that would eliminate the pain but not interfere with my natural cycle.
Not really, she explained, unless I had a crystal ball and could predict when I would get the cramps again—then, maybe, I could pre-medicate with an anti-inflammatory medication. So I started taking the pill. Thankfully, I did notice a difference right away. However, when my hair started to fall out, to the point that I had a huge bald spot, I decided to stop taking the pill. There had to be a better way!
I later discovered that if I tracked my menstrual cycle, I could better predict when my period would begin, and if I took ibuprofen a day or two before, my period was not nearly as painful. For me, the solution was simple, but I have a close family member who experienced even more severe pain with her periods. So, she started charting too, and consulted with a physician trained in NaPro Technology who discovered endometriosis.
Rather than temporarily suppress symptoms with the pill, the doctor performed the surgery necessary to truly eliminate the disease. My family member and I experienced real relief when charting allowed us to identify and treat the root causes of our pain, all without taking the pill. And the good news is, charting our cycles costs very little and has no harmful side effects.
We Should Focus Resources on Truly Critical Medication
This brings me to my second medical emergency: an asthma attack during a time I could not afford preventive medications.
When I was in college, my medications and doctors’ visits were covered under the student health insurance plan. Yet I still had to pay a significant medication co-pay for my steroid asthma inhalers. So often at the beginning of the school year, after paying tuition and purchasing a semester’s worth of textbooks, I didn’t always have the money to refill my asthma medications, especially for the steroid inhaler designed to prevent asthma attacks.
On one cold fall day in early October, this almost led to my demise. I was literally running late to my English writing seminar. The air was much colder than I expected, and as a result it triggered a severe asthma attack. I was halfway to class and my rescue inhaler did not seem to be working. I decided to walk the rest of the way to my classroom and did my best to not draw attention to my late arrival, but it was obvious I was in severe respiratory distress.
Thankfully, somebody had already called 911. When paramedics placed an oxygen mask over my face, I could feel the relief like a person walking in the desert for days taking her first sip of cold water. The air never tasted so good. And I promised myself that, no matter the cost, even if it meant eating Ramen noodles for a month, I would make sure to purchase my preventive asthma medication.
When I see the hysteria regarding the cost of birth control and women having to pay those fees, I think of that moment. I nearly died because there was no “mandate” that covered the cost of my preventive asthma medicine.
Women deserve relief from the conditions that disrupt their reproductive systems. As a physician with a particular interest in fertility and women’s health, I strongly believe women can learn to better monitor and manage reproductive health issues by charting their cycles and working with physicians trained to use those charts to aid in diagnosing and managing the true underlying causes of gynecological ailments.
As an added bonus, when couples learn to chart from a trained instructor, they can use this information to prevent pregnancy or even plan to have a baby. The birth control pill cannot “cure” anything, from acne to cramps to endometriosis; it simply masks symptoms of underlying hormonal issues. While it can help prevent pregnancy and then only some of the time, it does so by suppressing the normal function of the woman’s reproductive system.
Furthermore, as a patient who suffers from a chronic disease, I would rather see our health care dollars be spent to ensure people like me have access to medications that can truly prevent life-threatening complications. Why do we “fight for birth control,” but not drugs that allow people to breathe?
German Cardinal Walter Brandmuller greets Professor Josef Seifert at a conference on Blessed Paul VI’s 1968 encyclical, “Humanae Vitae,” in Rome Oct. 28. The conference was organized by Voice of the Family, a coalition of pro-life and pro-family groups. (CNS photo/Paul Haring) See HUMANAE-VITAE-CONFERENCE Oct. 30, 2017.
ROME (CNS) — The acceptance of artificial contraception by some Christian churches and communities beginning in the 1930s has led “to the monstrosity of what is today known as procreative medicine,” which includes abortion, said German Cardinal Walter Brandmuller.
Inaugurating an Oct. 28 conference anticipating the 50th anniversary of Blessed Paul VI’s encyclical “Humanae Vitae,” Cardinal Brandmuller told participants that in ignoring traditional church teaching men and women today have seated themselves “on the throne of the Creator.”
In “Humanae Vitae,” published in 1968, Pope Paul underlined the responsibility that goes with human sexuality and marriage. While he taught that couples can space the birth of their children for valid reasons, they must use only natural methods of avoiding fertility. Birth control, he said, causes an “artificial separation” of the unitive and procreative aspects of married love.
In his speech at the Rome conference, Cardinal Brandmuller said that after the Second Vatican Council, the church faced significant pressure — including from within its own ranks — to endorse contraception as “morally justifiable” just as the Anglican Church had done at the 1930 Lambeth Conference and the U.S. Federal Council of Churches, the precursor of the National Council of Churches, did in 1961.
Nevertheless, he added, Blessed Paul defended the sanctity of life and brought “temporary closure to a series of doctrinal affirmations on the matter of contraception.”
“Humanae Vitae” proves that ultimately, it is the Holy Spirit that guides the process of “paradosis,” or teaching based on church tradition, and “ensures that the faith of the church develops in the course of time” while remaining faithful to Christ’s teachings, Cardinal Brandmuller said.
He prayed that the document would continue to “irradiate the ‘splendor veritatis’ (‘the splendor of the truth’), capable of illuminating the current darkness of minds and hearts.”
Cardinal Brandmuller, former president of the Pontifical Commission for Historical Sciences, was one of four cardinals who formally asked Pope Francis to clarify his teaching on Communion for the divorced and civilly remarried. When the four prelates did not receive a response, they released the letter — commonly referred to as the “dubia” — to the press.
Reprinted below is part of the article FACTS co-founder Dr. Marguerite Duane authored in response to the recent Newsweek article perpetuating misinformation about fertility awareness based methods (FABMs).
October 24, 2017
by Marguerite Duane, MD
Newsweek is sounding the alarm that “The Trump administration wants to replace reliable birth control methods with ‘fertility awareness,’ a dubious family planning method that fails nearly a quarter of women every year.” Claiming that fertility awareness based methods are the same as the “rhythm method”, they imply that women with irregular periods or young girls can’t learn to chart their cycle, and that this could be a “disaster for women’s health.”
However, Newsweek is wrong on all accounts.
Fertility awareness is nota family planning method equivalent to the “rhythm method.” Fertility awareness based methods, or FABMs, refer to a group of family planning methods that work by teaching a woman how to track specific signs to identify when she may be fertile, and when she is not. Unlike the rhythm method, which was developed in the 1930s and is based on retrospective calendar calculations to predict future fertility, modern fertility awareness based methods allow women to use daily observable physical signs to identify her potential fertility in real time.
More importantly, these methods are based on solid scientific research and women may not only use them to prevent pregnancy, but also to achieve pregnancy, as well as monitor their health.
With ovulation based methods, including the Billings Ovulation Method and the Creighton Model, a woman tracks cervical fluid sensation and/or observations only, following certain guidelines to identify her fertile period or the 3 – 6 day window when she is capable of getting pregnant. With the sympto-thermal method, a woman tracks both cervical fluid and basal body temperature and uses these observations to identify her potential days of fertility. With the sympto-hormonal or Marquette Method, a woman tracks cervical fluid and/or urinary hormones to identify her fertile window.
This widely quoted figure is based on retrospective surveys from 1995 and 2002 in which women with unintended pregnancies were asked to recall which family planning method they were using at the time of conception. From this number, the rates for all natural or fertility awareness based methods were combined and one estimated unintended pregnancy rate was generated.
However, lumping together effectiveness rates for the 86% of women who reported using the outdated calendar rhythm method with a minority of women using newer methods masks the true effectiveness rates of modern FABMs. Modern FABMs incorporate different signs and guidelines for use, so reporting one combined rate for all natural methods, based on an overwhelming majority of women who reported using the rhythm method misrepresents the actual effectiveness of individual modern FABMs.
The real effectiveness rates of modern FABMs with correct use range between 95.2 and 99.6%, based on the highest quality published medical research. Even with typical use, the unintended pregnancy rates range from 2-14% per year, which are comparable to most commonly used forms of birth control. However, unlike conventional birth control methods, the World Health Organization recognizes FABMs as the only family planning methods that have no medical side effects.
Newsweek claims that “the calendar method asks a lot of young girls, who often learn little about sex and reproduction.” Fortunately, with fertility awareness based methods— again NOT the calendar-rhythm method—the goal is to teach women of all reproductive ages to monitor their cycle to better understand their health and more importantly identify their ovulatory pattern and window of fertility.
This information is sorely lacking even among adult women, as a 2014 study showed that 40 percent of women between the ages of 18 and 40 were not familiar with the ovulatory cycle and their time of fertility. Yet a study of 235 girls, aged 15 – 17 years trained in the Billings ovulation method, “proved that teen-age women can distinguish patterns of ovulation and anovulation by self-detection of cervical mucus.”
More importantly, another study showed a significant decrease in teen pregnancy rates with the implementation of TeenSTAR, a sex education program that aims to help youths manage their emerging sexuality and fertility through charting their cycle with the Billings method. Pregnancy rates for girls in the TeenSTAR program ranged from 3.3 – 4.4 percent, which was significantly less than those in the control group, where pregnancy rates ranged from 18.9 – 22.6 percent.
Dawn Laguens, an executive vice-president for Planned Parenthood, states that the Trump administration’s encouragement of fertility awareness “reveals not only a disdain for women’s health and lives, but a lack of understanding of the basics of sexual and reproductive health.”
Actually, the opposite is true. Teaching all women to understand and monitor their fertility through the use of fertility awareness-based methods, shows a high level of respect for women.
It recognizes that women, even teenagers, can learn to monitor and manage their fertility without resorting to drugs and devices that suppress the normal function of their reproductive health system. It offers relief from birth control drugs and devices that often have numerous side effects—side effects which women are exposed to 365 days a year, even though science shows us women are only capable of getting pregnant 70-80 days a year. It gives women the tools they need to understand their bodies and take control of their health based on solid scientific evidence.
What could be more empowering?
Marguerite Duane is a contributor to the Washington Examiner’s Beltway Confidential blog. She is a board-certified family physician and adjunct associate professor at Georgetown University. She is also co-founder and executive director of FACTS (the Fertility Appreciation Collaborative to Teach the Science). She is a member of Women Speak for Themselves.
As reported earlier this year, the United Nations Human Rights Committee has been attempting to redefine an important international human rights treaty by claiming that the “right to life” means that states should legalize abortion under expansive terms.
This past July, the committee released a document called General Comment No. 36 which seeks to reinterpret the International Covenant on Civil and Political Rights (ICCPR) to say that states “must” provide access to abortion, and permit states to legalize assisted suicide and euthanasia.
However, the ICCPR never mentions abortion or euthanasia. On contrary, the treaty explicitly recognizes that “Every human being has the inherent right to life.”[1]
In response, the Population Research Institute (PRI), in concert with other pro-life organizations and academics around the world, has called upon the Human Rights Committee to protect the right to life at all stages of development.
We made clear to the committee that neither the ICCPR nor the customary norms of international law obligate any state to legalize abortion. We further endeavoured to debunk some widely held myths pro-abortion advocates commonly use in justifying an invention of a “right” to abortion. My full written comment on behalf of PRI to the Human Rights Committee can be viewed here.
Several countries have also responded to General Comment No. 36, condemning the committee’s pro-abortion activism.
While the Human Rights Committee has gained a reputation for routinely subjecting countries to rebuke for their pro-life laws, General Comment No. 36 would permit the committee to place considerably more pressure on states to legalize abortion.
The quasi-official document states that countries “must provide” access to abortion in cases of health, rape, incest, fetal disability and “in situations in which carrying a pregnancy to term would cause the woman substantial pain or suffering.”[2]
The same document also calls on independent states to remove criminal sanctions for abortionists that break the law, and to repeal laws which place “humiliating or unreasonably burdensome requirements on women seeking to undergo abortion.”[3]
There would be much at stake if the comment is adopted.
The ICCPR is one of the oldest, most revered and widely adopted United Nations human rights treaties. States that have adopted the ICCPR (i.e. “state parties”) are bound by international law to faithfully observe the treaty’s terms. The United States, as a state party to the ICCPR, is bound by the U.S. Constitution to abide by the treaty.
General comments are essentially official statements by the committee on how they interpret the treaty.
And while their legal status is subject to much debate among international law scholars, most observers agree that general comments are highly esteemed, authoritative, quasi-juridical statements that play an ever increasingly important role in the development of “soft” law.[4] They have been invoked by various international courts including the European Court of Human Rights (ECtHR) and the Inter-American Court of Human Rights, and have, on occasion, even been cited in decisions by domestic courts, including a federal district court in the United States.[5],[6]
While states are free to ignore the parts of general comments that do not accord with their obligations under the ICCPR, they are widely recognized as authoritative and can place increased pressure on state parties to comply.
The Human Right Committee is tasked with monitoring the implementation of the ICCPR, with writing general comments, and with offering non-binding recommendations to state parties on fulfilling their obligations under the treaty.
But, as we were keen to point out, the committee has no authority to create new obligations or to reinterpret the treaty in manner contrary to the text of the ICCPR.
According to the Vienna Convention on the Law of Treaties (VCLT), treaties must be interpreted “in good faith” and according to “the ordinary meaning” of the text in its “context and in light of its object and purpose.”[7] Many of the framers of the ICCPR understood this well and carefully crafted the language of the treaty under the assumption that the treaty would “not admit of progressive implementation of its provisions.”[8]
As mentioned already, article 6(1) of the ICCPR explicitly recognizes the right to life of “every human being” and that this right should be “protected by law.”[9] Article 2 of the covenant declares that this right should respected “without distinction of any kind” including by “birth or other status.”[10] Article 7 further prohibits anyone to be subjected to “torture or to cruel, inhuman or degrading treatment or punishment.” Abortion procedures crush, poison, or dismember the unborn child, many of whom are able to feel pain, and clearly constitute the most cruel, inhumane, and degrading treatment imaginable.
Article 6(5) even specifically recognizes the right to life of the unborn child as distinct from the life of its mother. Article 6(5) prohibits the death penalty to be carried out on a pregnant woman:
“Sentence of death shall not be imposed for crimes committed by persons below eighteen years of age and shall not be carried out on pregnant women.”[11]
During the drafting process for the ICCPR, state parties made it clear that article 6(5) was included in the treaty precisely to protect the life of the unborn child. The Official Record of the proceedings of the 819thmeeting of the Third Committee summarized the comments of the Israeli delegation as follows:
“…the authors of the original text had specified that sentence of death should not be carried out on a pregnant woman principally in order to save the life of an innocent unborn child.”[12]
The Japanese delegation echoed this sentiment at the following meeting, saying to the effect, “the main reason for inserting the provision concerning pregnant women was to avoid involving in the death penalty a person who was not connected with the crime.”[13] It is thus impossible to read any “right” to abortion into the ICCPR.
Moreover, international law does not create any obligation on states to legalize abortion. The U.N. Charter seeks to promote “respect for human rights and for fundamental freedoms for all without distinction.”[14]The Convention on the Rights of the Child recognizes that “every child has the inherent right to life”[15] and that the “child, by reason of his physical and mental immaturity, needs special safeguards and care, including appropriate legal protection, before as well as after birth.”[16] The Universal Declaration of Human Rights, while not in and of itself constituting a customary norm in whole or in part, is nevertheless highly esteemed and provided the inspiration for the ICCPR. Article 3 of the Universal Declaration of Human Rights proclaims without qualification that “everyone has the right to life.”[17]
It is impossible for the Human Rights Committee to claim that states are obligated to legalize abortion under customary international law. A significant number of countries protect the right to life for the unborn child by law, several of them from the moment of conception. In fact, a majority of U.N.-recognized states (56%) have not legalized abortion under even the minimum cases the committee is now demanding that they be provided.[18]
It is clear that no so-called “right” to abortion exists in either the ICCPR or in states’ obligations under international law. On the contrary, the ICCPR recognizes the right to life for “every human being,” including the unborn child, the sick, the elderly, and the disabled.
The Human Rights Committee must abide by its mandate and must cease its attempts to reinterpret the covenant in a manner never intended by state parties.
Jonathan Abbamonte is a research analyst at the Population Research Institute.
While we need a variety of pro-life groups hacking away at the anti-life monster, it is enormously futile and indeed grossly shortsighted to overlook the chief source of baby-killing, which is contraception. – Father Paul Marx, OSB
I’ve written before about the link between contraception and abortion: that is, statistically contraception use actually increases, rather than decreases the abortion rate. For some reason, this claim is still met with shock and disbelief, even though top pro-abortion leaders have been admitting this truth – self-evident to anyone who examines the facts – since the 1960s.
However, a pair of new studies from the British Pregnancy Advisory Service (BPAS), a leading UK abortion provider, has given us a new, and even more horrific understanding of the infernal symbiosis that unites contraception and abortion.
The first study found that over half (51.2%) of the 60,000+ women who came to their facilities for an abortion in 2016 were using at least one form of contraception at the time they become pregnant. This first finding is not surprising. In fact, the only shocking thing is that it was “only” 51% – other recent BPAS studies have found that as many as 66% of women seeking an abortion at their facilities were using contraception.
So much for “safe, cheap, and effective”!
However, the second study is the one that truly makes the stomach turn. Surprised by the fact that the number of women seeking abortions after 20 weeks (i.e. when the baby is essentially fully-formed, and might even be able to survive outside the womb) has not decreased over the past decade, BPAS launched a study to find out why women were waiting that long before aborting. The answer? You guessed it: contraception.
It turns out that when women are on contraception, they are significantly less likely to recognize the signs of pregnancy until extremely late. In the first place, BPAS observes, hormonal contraception disrupts a woman’s menstrual cycle, removing one of the most obvious indicators of pregnancy. More importantly, however, because women are constantly told how “effective” contraception is, they simply assume it is “impossible” that they could be pregnant. Consequently, when they experience indicators that they’re pregnant, they either overlook or misinterpret those signs.
Contraception and Murderous Despair
The BPAS report says that when the women on contraception found out they were pregnant they were “shocked” and “devastated.”
Think about that for a moment! I understand that pregnancy can be a vulnerable time, even for women who were trying to become pregnant. And yet, how horrible that the news of the existence of a new human being – objectively an extraordinary and beautiful miracle – should be greeted not with joy by the mother, but despair! And not just any kind of despair: a despair that is so all-consuming, so dark, so bleak, that the response is to try to destroy the child.
This is what the lie of contraception has done to us: it has robbed us of a precious part of our humanity. By creating the false expectation of sexual pleasure free from the natural consequences of sexual intercourse, it has primed mothers and fathers to greet the existence of their own children not with joy, but dark, murderous despair!
The BPAS study includes some heart-rending details. Speaking of one woman, named “Catriona,” who was seeking a late abortion, BPAS states: “She is upset as she can now feel the pregnancy but feels abortion is the best for her.”
“Catriona” is “upset” because she can “feel the pregnancy.” “The pregnancy”! What she is feeling are the little fingers and toes of her child brushing against the sides of her womb. She is feeling her fully-formed, growing, healthy child stretching out its body, exercising its new-found strength, filling in the shrinking space in her womb with fleshy limbs, pressing its precious head up against her ribs, kicking his legs.
“For you formed my inward parts; you knitted me together in my mother’s womb” (Psalm 139:13).
Contraceptive Failure: Far More Common than You Think
To BPAS’s very limited credit, they are one of the very few pro-abortion organizations that are honest about how pro-contraception propaganda creates deadly false expectations. In their latest report, BPAS laments that, despite the fact that all current contraception fails some of the time, “public discourse and some family planning initiatives frequently imply that abortion can always be avoided through the use of contraception.”
This is far from true. As BPAS points out, “each year 9 in every 100 women using the contraceptive pill, the most popular method of contraception in the UK, 6 in every 100 using the contraceptive injection, and nearly 1 in every 100 using the IUD (copper coil), will become pregnant.”
I want you to stop and think about that statistic very carefully. Because it is a lot worse than most people realize at first.
Men and women are constantly told, from the time they’re in elementary school, that the best (and even only) way to avoid an unplanned pregnancy is to use contraception. In reality, as many as 9% of sexually active women on the pill will become pregnant…every year! That means that if a woman relies on hormonal contraception to avoid pregnancy throughout her 31-35 fertile years (on average), the chances she will experience an unplanned pregnancy at some point are not “slim.” In fact, it’s practically certain that she will!
And when that unplanned pregnancy happens? What will she do? That’s where BPAS’s diabolical logic enters in. “The answer to unsafe abortion is not contraception, it is safe abortion,” says BPAS Chief Executive Ann Furedi in the recent study.
The Great Contraceptive Lie
Before the invention of artificial contraception, everyone understood that there was only one infallible way to avoid an unwanted pregnancy: to avoid engaging in baby-making activities with anyone with whom you were not prepared to have a baby.
This is not to say that everyone followed this principle. The human race hardly invented fornication and adultery in the 20th century! And yet, the point stands: everybody knew the consequences of having sex, even if they still sometimes chose to risk the consequence nonetheless. The vast majority of people chose not to take the risk, unless they were in a stable, long-term relationship – i.e. marriage – and prepared to welcome a child into the world. If they did take the risk with someone with whom they did not intend to have a baby, and subsequently found out they were pregnant, while they might be disappointed or even terrified, they would not have been surprised. They knew that biology worked, even if they didn’t fully understand how it worked.
We “advanced” moderns, however, have spun for ourselves an elaborate fable: a fable of our limitless capacity to control nature using technology, and therefore to conduct ourselves sexually however we want, without any consequences. Decades ago Human Life International Founder Father Paul Marx identified this lie, and he spent his life trying to warn the world of its deadly consequences. In his book, The Death Peddlers, he warned:
The foolproof contraceptive does not exist, and sociological studies have shown, almost without exception, that intensive contraceptive programs, by emphasizing the prevention of unwanted pregnancies, also reinforce an intention not to bear an unwanted child under any circumstances; that is, there is a greater likelihood that women experiencing contraceptive failures will resort to abortion.
Elsewhere he wrote, even more poignantly:
… the more you sow contraception, the more you reap sexual sins, family and social disorders, venereal diseases, and deadly AIDS — and the more you must make available “abortion services” to take care of the “contraceptive failures”.
The truth is, we will never end the violence of abortion until we eradicate the underlying cause: i.e. the contraceptive mentality, which is the foundation for the entire sexual revolution. As Father Marx repeatedly said, no matter how good the intentions and efforts to stop abortion are, unless, we address the systemic root cause, contraception and its selfish mentality, everything is an exercise in futility.
Last Friday marked 50 years since the passing of the UK’s Abortion Act, 1967, which permitted abortion on very wide grounds. In these last five decades nearly 9 million unborn babies have been aborted in England, Scotland and Wales.
That figure has, of course, also impacted the lives of 9 million women, some of whom are celebrating this anniversary of the Act while many will instead remember and regret their abortion(s) and the harm each one brings to both mother and child.
While I strongly believe there are two victims for every abortion, for now I deliberately focus on the unborn victims, not the women, and the almost incomprehensible scale of destruction of innocent lives.
Nine million lives lost is a truly staggering figure.
On current abortion rates, every year we lose more lives than could fill three London Olympic Stadiums(approximately 200,000 per year).
Every month we lose the equivalent of 11 Titanics (over 16,000 per month, since 1992).
We lose many more than the number of people who died in the 9/11 attacks every week in England, Wales and Scotland (3840 per week).
And every day the number of unborn babies who are aborted would completely fill an Airbus A380(approximately 550 per day).
These are illustrations of the numbers of lives lost. Imagine the difference in England and Wales if those were all alive today? Which brings me to Northern Ireland where, in a poignant and striking contrast, there are an estimated 100,000 people who are alive today because they do not have the 1967 Abortion Act, but have a different law.
In other words, one in ten people under fifty in Northern Ireland are alive because of the more restrictive law on abortion there.
This number could fill their national football stadium five times over. Each one a precious, valuable human being who is alive today but would have never have had the chance of life in the rest of the UK.
An anniversary is a time for stopping to remember something very special or something very sad. It is either a celebration, such as of a marriage or a special birthday, or it is a time to commemorate a tragic event, such as a death.
I for one know which this 50th anniversary will signify: 9 million innocent lives lost. For me it is a time for commemoration of 9 million unborn children who have silently disappeared.
Please take a minute or two to stop and remember, by watching this short video we have put together at CMF to mark the Anniversary.
Philippa Taylor is Head of Public Policy at Christian Medical Fellowship. She has an MA in Bioethics from St Mary’s University College and a background in policy work on bioethics and family issues. Republished from the CMF blog with permission.
ROME, October 28, 2017 (LifeSiteNews) — The Church’s teaching against contraception as expressed in Humanae Vitae is an “extraordinary example” of how the “truth of faith” deepens and develops while “continuing to be identical to itself,” Cardinal Walter Brandmüller stated at a conference in Rome today.
Brandmüller made his remarks as he opened a conference titled Humanae Vitae at 50: Setting the Context that was organized by Voice of the Family. The conference took place at the Pontifical University of St. Thomas Aquinas.
Cardinal Brandmüller addressing the ‘Humanae Vitae at 50’ conference in Rome, Oct. 28, 2017.Diane Montagna / LifeSiteNews
German Cardinal Brandmüller is a world renowned-scholar of church history, having published numerous books on the Crusades, the Spanish Inquisition, and the Reformation. He holds a doctorate in theology and is the former President of the Pontifical Commission for Historical Sciences. He is one of the four Cardinals who signed the dubia [questions] to Pope Francis asking if the Pope’s 2016 exhortation Amoris Laetitia conforms to perennial Catholic teaching.
Pope Paul VI’s Encyclical Humanae Vitae [Of Human Life] celebrates its 50th anniversary next year. Catholic academics including Josef Seifert and Father George Woodall have outlined how Pope Francis’s teaching on marriage and family, especially as expressed in Amoris Laetitia [Joy of Love], could be used to overturn Catholic teaching against contraception.
Brandmüller told conference attendees that it is “impossible” for the Catholic Church to change it’s teaching in Humanae Vitae, what he referred to as a “doctrinal document” that was “truly prophetic.”
The Encyclical states that “each and every marriage act must remain open to the transmission of human life” and calls the use of contraception (including the pill, condom, withdrawal, and other methods) “intrinsically wrong.”
“Humanae Vitae provides an extraordinary example of the workings of the process of parodosis, which means transmission of the doctrine of the Church. When the truth of faith is received, adopted and transmitted, what happens is that what is received, when adopted and transmitted, responds with deeper understanding and more precise expression to the needs of the respective present, while continuing to be identical to itself,” he said.
“In all of this, contradiction between yesterday and today is impossible: it is the Holy Spirit who acts in the Church of Jesus Christ to guide this process of paradosis. It is the Holy Spirit who ensures that the faith of the Church develops in the course of time, just as an adult person continues to be identical to the infant it was in the past, an intuition formulated by Vincent of Lérins as early as 430 and elaborated upon by Blessed John Henry Newman,” he added.
The Cardinal said that the Catholic Church must withstand pressures from Protestant churches and from the world that want to see the Church use “situation ethics” to accept contraception as morally legitimate.
Instead, he said, “tribute should be paid” to the “doctrinal document whose prophetic nature has, over time, also been acknowledged by leading non-catholic thinkers.”
“In this Encyclical, Paul VI brought temporary closure to a series of doctrinal affirmations on the matter of contraception, instigated by Pius XI in Casti connubiiand continued by Pius XII and John XXIII. These were ultimately taken up, developed and deepened by John Paul II,” he said.
“The Conference inaugurated today has called for this renewed reception, adoption and more profound transmission of the truly prophetic teaching of Paul VI in the year 2017,” he added.
SUSANNE MAYNES OCT 26, 2017 | 1:21AM WASHINGTON, DC
Imagine standing on the shores of a dark, stormy sea. As you peer over perilous waters, you hear voices cry out. Horrified, you realize people are struggling out there in the tempest, about to sink beneath the angry waves.
Suddenly a rescue boat appears. Workers make their way quickly to the victims, tossing life preservers toward them. The boat makes its way back to shore.
At first you feel relief—but then you realize something is wrong. Only a few people disembark. The rescuers shake their heads, muttering, “They just don’t grab the life preservers anymore. How are we supposed to help them?”
And then you hear them—a multitude still crying out, fighting to keep their heads above the dark waters.
Here’s the point of the illustration: we live in a day and age of unprecedented sexual brokenness. The only world our youth have ever known is a world of legalized abortion, homosexual marriage, common divorce and cohabitation, as well as gender confusion. They are indoctrinated that “not judging” others means it’s wrong to say that some behaviors are sinful.
Porn is just a click away. Peer pressure is intense.
This is the world’s religion, where sex is god. This is where sexual “liberation” has taken us. And a generation cries out, drowning in a raging sea of life-and-soul-threatening choices.
Before we attempt a rescue, though, we need to know something about that sea. We need to discover why people don’t always trust the methods we may want to use to help them.
We must understand their frame of reference before we can speak into their lives.
This is where it’s so helpful to volunteer or work at a pregnancy help center. Our thorough training helps us understand culture so we can minister effectively to those whose idea of “normal” is anything but.
“Today’s sexual landscape is chaotic and bewildering. In the name of freedom, we’ve opened the door to a kind of sexual feeding frenzy that leaves victims strewn in its wake.
College students come to PRCs for pregnancy tests shortly after they land on campus as freshmen, or six weeks after attending the latest sex educator’s lecture, or after a weekend hookup with a friend-with-benefits (a relationship based on casual sex with no strings attached). A teenage girl goes to a party, gets so drunk she passes out, and later has no idea which of the boys who raped her is the father of her baby.
… Of course, unplanned pregnancies often result from the mess and heartache of using sex as a meaningless commodity. Abortion presents itself as the answer to this dilemma. Many times, the issue is that the baby’s father is the “wrong guy,” because the mother was involved with two or more men around the same time and fears being found out.”
Things have changed drastically, even in the last few years.
Last month, I had the privilege of addressing ReGenerate, an on-campus student ministry at our local state college, on the topic of “Stewarding Your Sacred Human Sexuality.”
The ministry leaders had told me beforehand that one student had just become a Christian two weeks before after living in homosexual sin. Another female student was struggling with same-sex temptation as well. A number of girls in the group had been sexually abused. Other students had been wounded by the shame that comes from a toxic mix of living outside God’s plan for our sexuality and encountering Christians seemingly more interested in record-keeping than forgiveness.
I could have simply reminded these students about God’s moral boundaries concerning sex, and then invited them to sign abstinence pledge cards, but that would have been inadequate at best, and harmful at worst.
These students didn’t need to hear that saving sex for marriage guarantees having the best sex ever (maybe, maybe not). They didn’t need a message about how sexual purity somehow rivals salvation in its importance. They didn’t need to try harder in their own strength.
As young singles navigating a war zone, they needed the hope of the gospel as it applies to their sexuality.
They needed conversion, not merely to heterosexuality or abstinence, but to total belief, trust and obedience to Christ in every area of life, including their sexuality.
The message these students needed was a biblically sound, logical, hopeful message about stewarding their sexuality—a message including God’s moral boundaries, but also His grace for those who have transgressed those boundaries.
So I apologized for the church’s mixed message about sex, and assured the students that sex is one of God’s very best gifts—a gift He wants them to look forward to and enjoy for a lifetime. I talked about their value as image-bearers of God. I described sex as a treasure worth guarding.
I explained the brain science behind bonding hormones, and how God wired humans this way so that married couples can stick together for a lifetime—but that this ability is impaired when used improperly. I described the emotional, relational and spiritual benefits of sex within a marriage covenant, and the serious damage done by sex outside of marriage.
I told them the real definition of “unprotected sex” is sex outside of a marriage covenant.
Finally, I assured them Jesus takes fragmented hearts and makes them whole again.
The topic was heavy, but the students were engaged. A number of good discussions were prompted. To use our stormy sea analogy, these young people were grabbing life preservers and hanging on.
Here’s the thing: our rescue operations must be well-strategized. If we are to reach this post-truth generation, including Christians influenced by the world, we must gain their trust.
We must understand the pressure they face daily. We must ask good questions about their relationships, hopes and dreams. We must help them see how the gospel relates to human sexuality.
A multitude cries out from the dangerous waters of unrestrained sex. Will we toss them a simplistic message about rules and self-effort—or will we offer them the hope of the gospel?
The resurgence of the dangerous “seamless garment” mentality should cause us grave concern. In its most pernicious form, this philosophy holds that grave intrinsic evils like contraception, abortion and euthanasia and social problems like poverty, immigration, health care and the environment are morally equivalent. It is dangerous because it distracts the Church from recognizing the intrinsic evil (“wrongness”) of certain moral acts and their deadly consequences, leading souls astray and paralyzing our ability to respond effectively.
The “seamless garment” philosophy also diverts attention from individual sin and culpability by focusing more on “collective” than personal sin. Under its influence, instead of a prophetic voice “crying out in the wilderness,” the Church becomes just another non-governmental organization (NGO), striving for “social justice” via a socially acceptable version of social reform eviscerated of the Gospel message of repentance.
Jesus came to Galilee proclaiming the gospel of God… Repent, and believe in the gospel. – Mark 1:14-15
‘Seamless Garment’ a Smokescreen
While the Church teaches that there are moral and social issues that are of greater gravity than others, the “seamless garment” mentality is a form of moral relativism that bulldozes these crucial moral distinctions. It is a philosophy that provides the death peddlers with the tools for deflecting attention from the abhorrent evils plaguing humanity and our cultures.
Perhaps unsurprisingly, those who advocate this philosophy tend to concentrate the heat of their outrage on the “collective” social ills (poverty, environmental degradation, etc.), while giving (at best) lip service to grave contemporary intrinsic evils like abortion or the demolition of marriage. To quote George Orwell, for proponents of the “seamless garment,” it sometimes seems that some moral issues are “more equal” than others. Usually the issues deemed “more equal” also happen to be more socially acceptable, and don’t demand deep personal conversion of heart.
Pope John Paul II clearly identified the inherent contradiction of this philosophy, when he wrote:
Above all, the common outcry, which is justly made on behalf of human rights – for example, the right to health, to home, to work, to family, to culture – is false and illusory if the right to life, the most basic and fundamental right and the condition for all other personal rights, is not defended with maximum determination. – Christifideles Laici, ¶38
Sadly, the influence of this mentality has stifled the courageous and unwavering preaching of the Gospel of Life from pulpits and classrooms for decades. John Paul II directly confronted this mentality with numerous Church documents like Evangelium Vitae and Veritatis Splendor. To see its ugly head reemerge is unsettling.
This mentality has aided in numbing the moral conscience of Catholics around the world. Priests are afraid to preach the Gospel of Life because of the backlash they will receive if they reference the evils of contraception, abortion, homosexual acts, fornication and euthanasia, instead preaching about fashionable issues that are far less controversial (i.e. the environment) – ignoring the violent assault on human life and its dignity, marriage and the family.
However, within Catholic social teaching there is a hierarchy of truths. Abortion and euthanasia, for example, are clearly condemned as direct assaults against innocent and vulnerable human life. They are among some of the greatest atrocities and injustices affecting humanity. To place these evils on equal par with other social issues – unemployment, poverty, homelessness – fails to represent the full spectrum of the Church’s moral and social teaching.
Some Evils are Intrinsic Evils
Indeed, the crucial distinction that advocates of the “seamless garment” often carelessly fail to make is that between acts which are evil by their very nature (intrinsic evils), and therefore always sinful if carried out with knowledge, and more complex social problems. These latter, while at times posing serious threats to the dignity of human beings, are nevertheless caused by a variety of causes, with human sin only playing one part.
Fortunately, on this complicated issue the Church guides us and offers us counsel in the formation of our consciences and moral lives. She teaches that there are three elements of morality, which every moral act consists of: the objective act – what we do; the subjective goal or intention – why we do the act; and the concrete situation or circumstances in which we perform the act. In order to have a morally good act, all three must be good.
There are acts, which in and of themselves, independently of circumstances and intentions, are always gravely illicit by reason of their object: such as blasphemy and perjury, murder and adultery. One may not do evil so that good may result from it. –– Catechism of the Catholic Church, ¶1756
Intrinsically evil acts are those that fundamentally conflict with the moral law – in other words, their moral object is evil. They can never be performed under any circumstances, and it is a serious sin to deliberately endorse or promote any of these actions. For instance, the Catechism of the Catholic Church makes it poignantly clear that an intrinsically evil act cannot be justified simply because the person performing it intended good to come of it, or because of the surrounding circumstances.
Consequently, circumstances or intentions can never transform an act, intrinsically evil by virtue of its object, into an act ‘subjectively’ good or defensible as a choice. – Veritatis Splendor, ¶81
The US Catholic Conference of Bishops in their pastoral Forming Consciences for Faithful Citizenship also makes it abundantly clear that not all issues are equal:
Our focus is not on party affiliation, ideology, economics, or even competence and capacity to perform duties, as important as such issues are. Rather, we focus on what protects or threatens the dignity of every human life… Not all issues are equal… Some involve intrinsically evil acts, which can never be approved. Others involve affirmative obligations to seek the common good (¶92).
In the case of abortion, the moral object is the intentional termination of innocent human life. As such, it is an intrinsic evil, and can never be justified. Homosexual acts and same-sex unions are also intrinsically evil and always gravely immoral due to an evil moral object – the deprivation of the marital act, which is unitive and procreative.
Church Leaders Giving Confusing Messages
Sadly, we live in a world in which countless millions of unborn babies are slaughtered every single year, direct attacks on the elderly and the vulnerable are growing daily, and powerful forces are concertedly seeking to undermine the truth about sexuality and the family. In light of this, the Church’s role ought to be blindingly clear – to preach the truth of the Gospel and the Church’s moral teachings, no matter the cost.
Instead, we are seeing a growing number of Church leaders giving confusing messages about the moral evils of contraception, abortion, euthanasia, homosexual acts and “same-sex marriage.” Instead of helping inform the conscience of their flocks and protect individual souls and the common good from the consequences of such evils, they minimize these atrocities by comparing them to other social problems. They refuse to explicitly identify these evils for what they fundamentally are: grave, intrinsic evils, which pose the most serious danger to the salvation of souls and the future of humanity.
The “seamless garment” mentality turns our attention away from the persons murdered by the violence of abortion and euthanasia and tries to focus our gaze upon institutions and social structures, which are always secondary. Like so many other culture of death tactics, the “seamless garment” is meant to divert attention from its evil acts and diffuse our efforts, making us ineffective. We mustn’t allow ourselves to be fooled.
Nexplanon, an artificial birth control arm implant, launched a recent ad campaign using the slogan “Armor Up.” It shows pictures of attractive young women with battle ready faces, flexing one bicep while pointing to the implant. The ad reads: “Pregnancy protection for up to 3 years. Over 99% effective. Your life. Your way.” This ad campaign merely takes the common phrasing of birth control as “protection” to its logical extreme. Against whom are women to “armor up?” Well, babies, it would seem. According to Nexplanon, a baby would be an invader, an enemy even.
This marketing technique promotes and plays into women’s fears that children mean the end of life. It perpetuates the idea that becoming pregnant is something to fear, unless it is meticulously planned. But protection, of course, comes at a cost. The risks and side effects include the possibility of blood clots, stroke, and death. More common, the website reports that 10 percent of women stopped using Nexplanon because it caused “an unfavorable change in their bleeding pattern.” The implant is only one of many varieties of hormonal birth control medications that pose similar risks.
There is an irony in the contraceptive mentality, as it purports to give women ultimate control over their bodies and reproduction. In reality though, women become dependent on pharmaceutical drugs that can cause a range of side effects, some of which are a nuisance, to those that threaten lives. In the end, the sense of “control” is an illusion. A pharmaceutical company recently recalled packets of birth control pills because of a packaging error that placed placebos where active pills should have been. This is not a lone incident. In 2015, 100 women filed a lawsuit against multiple pharmaceutical companies they held responsible for their pregnancies after another placebo pill mix up.
It is not uncommon to find women who become pregnant while using contraceptives. Yet the prevailing message is that if you “protect yourself,” you have nothing to fear. “99% effective,” proclaims the Nexplanon ad. That means some women will become pregnant while using the implant. How shocked will they be? Will they embrace this baby they were protecting themselves against, or seek an abortion?
Despite the messaging, artificial contraception takes control away from women in at least two ways. First, most forms suppress a woman’s natural hormones and cycle which give her important information about her reproductive and overall health. Second, they make women dependent on the pharmaceutical companies that make them, and government programs or insurance companies to pay for them.
Fortunately, there is a better way to avoid pregnancy when it’s not the right time for a baby. The dramatic language of the Nexplanon marketing campaign highlights the stark differences between Natural Family Planning (NFP) and artificial birth control. Birth control promotes the idea that babies are something to fear. They will derail your life so you don’t want to take any chances. “Armor up,” suppress your natural hormones, and accept side effects as the cost of this security. NFP recognizes that there are times when conceiving would not be wise. But instead of telling women that their bodies’ natural cycles are a threat and something to thwart, NFP gives women more information about what is going on with their bodies to allow for informed choices each cycle. NFP offers women an arsenal of information about fertility, hormonal health, and more. It educates women about their own bodies, which makes women stronger, independent, and more empowered than an implant or pill ever could.
October is Down Syndrome Awareness Month and one mom’s viral video is raising awareness indeed.
Oakley Peterson, mom of Welles, who has Down syndrome, worked with Jane.com’s #StrongLikeYou series to create a video telling the story of Welles’ birth and the joy he brings to his family. The video has been viewed more than 1 million times on Facebook alone since it was posted Sunday. Jane.com shared the video with ABC News.
Peterson also writes the blog Nothing Down About It. On it, she wrote, “Every time [the Jane.com filmmakers] sent me the latest edits, my heart re-opens the flood door and all of emotions rush back like a tidal wave. And I am so happy to have this video forever. I never want to forget those early days, even if they bring a touch of guilt for the heaviness that I felt.”
I’ve said it before, and I’ll say it again: it almost always starts with an emotional story.
The latest situation is an embryo custody battle in Arizona. It highlights the depth of real human emotions connected to having children and building a family, and the ways in which human lives are affected by a justice system that seeks to do what is right in the midst of a true ethical mess. As with all embryo custody battles, there are never any winners. There are plenty of losers, though, and the embryos have the most to lose by far.
This case, of course, tugs at our heartstrings. In 2014, at the age of thirty-three, Ruby Torres was diagnosed with triple negative breast cancer—a very aggressive breast cancer that has the lowest five-year survival rate of all breast cancers. Torres was engaged at the time of her diagnosis. Because her cancer treatments might leave her infertile, she and her then-fiancé, Joseph Terrell, made the decision to undergo IVF to create embryos and freeze them for later use. A contract was signed stipulating that neither Torres nor Terrell “could use the embryos without the written permission of the other person.” Soon after, they were married.
In August 2016, Terrell filed for divorce and told the court that he did not want to have children with Torres. The case is now in the courts of Arizona, where there is no case law on the disposition of surplus embryos once they have been created. On one side, Torres, who is now infertile, is fighting for her “right to have her own biological children.” Terrell, on the other side, is fighting for his “right not to parent.”
A Maricopa County Family Court judge recently ruled that the embryos must be donated to a couple seeking embryo adoption or to a fertility clinic since Torres and Terrell are not in agreement. Torres has filed a notice of intent to appeal the ruling to the Arizona Court of Appeals.
There Ought to Be a Law
How can we keep cases like this from happening in the future? Perhaps the simplest way would be for the United States to adopt a policy similar to Germany’s. The law there prohibits the creation of so-called surplus human embryos. In Germany, only three embryos can be created in one IVF cycle, and they must all be transferred into the mother’s womb.
But embryo donation and adoption is big business in the United States. Current estimates are that there are nearly three-quarters of a million frozen embryos here. In addition, approximately 28 million federal dollars are funding embryo donation programs, thus creating a whole new industry, which shows no signs of being interested in putting itself out of business.
Our country is a long way from passing a law like Germany’s, in part because we are so far down the path of embracing embryo adoption. We are gripped by the emotional stories of “snowflake” children. Recall the George W. Bush-era embryo battles over surplus human embryos being either destroyed for cures or adopted into loving homes. Almost no one pushed for a law banning the creation and freezing of human embryos then—and almost no one is pushing for it now—which is one of the reasons why this case in Arizona is so troublesome for the courts.
Souls on Ice
At the height of those embryo battles, Liza Mundy wrote in Mother Jones about “Souls on Ice.” That was 2006, when the count of frozen embryos was “only” about half a million. Mundy raised the question of embryo disposition after speaking with a California couple who had fourteen surplus frozen embryos. What should they do with them? Should they “Give them away to another couple, to gestate and bear? Her own children’s full biological siblings—raised in a different family? Donate them to scientific research? Let them . . . finally . . . lapse?”
That was eleven years ago. Now the number of souls on ice is rapidly approaching three-quarters of a million.
Human life was not meant to be created in the lab, put on ice, and left for years and years. Many frozen embryos do not survive the thawing process. As Paul Ramsey explained back in 1972, freezing human embryos would “constitute unethical medical experimentation on possible future human beings, and therefore it is subject to absolute moral prohibition.” Though the medical community failed to heed his warning, Ramsey’s words are still true:
My only point as an ethicist is that none of these researchers can exclude the possibility that they will do irreparable damage to the child-to-be. And my conclusion is that they cannot morally proceed to their first ostensibly successful achievement of the results they seek, since they cannot assuredly preclude all damage.
In other words, it is thought to be safe to freeze, thaw, and transfer human embryos into wombs, but the truth is that we are performing a highly experimental procedure on human beings who cannot in any way consent to the procedure they are undergoing. In fact, research is being done on these children, following them over the course of their lives to see how they fare. In what other circumstance would such treatment not be considered horrific?
How can we clean up this mess?
Parents, Come Get Your Children!
As I mentioned above, a good place to start is by legally limiting the number of embryos that can be created and prohibiting the freezing of embryos, as Germany does. But what about the embryos currently in cryopreservation storage? We need a policy that would require the people who created the embryos to make a decision. They can choose to transfer the embryos into their mother’s body, donate them to an embryo adoption agency, or allow them to thaw and die. I am open to discussions of ways to incentivize transferring the embryos into the mother—this, in my view, is what should happen, or being donated for embryo adoption—but I am not open to having the embryos donated to scientific research where they will be destroyed, killed.
The human embryos who are currently abandoned in freezers were created for the purpose of building families. The simple answer is for parents to come and get their children. If you choose to abandon your embryos—that is, your children—you can opt to “donate” them to someone who is willing to bear and raise your child.
Embryo adoption, though, is fraught with its own set of ethical issues. Anyone choosing to donate their unwanted embryos or to adopt such embryos must enter into such a decision with a clear mind about the problems that are likely to arise.
Children created in this way will face many difficult and troubling realities as they come to know and understand their conception stories. They must come to terms with the fact that they were created, abandoned, seen as surplus and unwanted, and ultimately given away by their biological parents. This can be an enormous burden for a child to carry. Given my extensive work on issues around third-party conception—egg donation, sperm donation, and surrogacy—I know all too well how likely it is that these children will grow up longing to know their biological parents, siblings, and larger family while at the same time feeling abandoned and perhaps even unloved.
Who Has Moral Obligations to Frozen Embryos?
Finally, I hold that we, the general public, have no moral obligation to rescue abandoned frozen embryos, just as we have no obligation to donate a kidney. Such acts—supererogatory acts—are those that are good but not morally required. I do believe, as I mentioned above, that the parents who created the embryos have a moral obligation to reclaim their embryos and have them transferred into the mother’s uterus. But that obligation does not extend beyond the parents who brought them into being. Physicians who assisted in creating and freezing embryos have broken with the Hippocratic roots of medicine, inevitably harming some embryos—that is, the ones that do not survive the freezing and thawing process.
Depending on where you are on the religious spectrum, you will find variations on the exact nature of our moral duty to abandoned embryos and their right to life. My own recommendation is to follow a pattern that Lutheran theologian Gilbert Meilaender, Senior Research Professor at Valparaiso University and Scholar at The Paul Ramsey Institute, recommends in his most recent book, Not by Nature but by Grace. He writes,
What Christians, at least, should want [with respect to abandoned embryos] is a brief religious ritual to accompany their dying, a liturgy in which we commend these weakest of human beings to God, though perhaps also a liturgy in which with the psalmists we ask God how long his providence will permit this to continue. . . . We demonstrate our humanity by accompanying frozen embryos to their death and committing them liturgically to God’s care.
But we must recognize, as the Catholic encyclical Donum vitae states,
In consequence of the fact that they have been produced in vitro, those embryos which are not transferred into the body of the mother and are called “spare” are exposed to an absurd fate, with no possibility of their being offered safe means of survival which can be licitly pursued.
Never to know the nurturing environment of their mothers’ wombs and never to be lovingly raised by their mothers and fathers, such embryos suffer an absurd—and tragic—fate indeed.
Jennifer Lahl is the Founder and President of the Center for Bioethics and Culture and producer of the documentary films,Eggsploitation, Anonymous Father’s Day, Breeders: A Subclass of Women?and Maggie’s Story, which tells of a ten-time egg donor and her battle with stage-four cancer.
October 18, 2017 (LifeSiteNews) — The U.S. government’s foreign aid development programs are often “a weapon for population control, hidden as a tool to fight poverty,” the organizer of an ongoing international symposium on population control said Tuesday.
And as a U.S. government relief contractor that receives millions of dollars each year in federal aid grants, the U.S. Catholic Church has had a hand in facilitating contraception and population control in developing nations.
Lepanto Institute president Michael Hichborn detailed specifics on the issue Tuesday for some 1,000 conference attendees from across the world for the International Conference on Population Control.
Hichborn was among four presenters for the opening day of the first-of-its-kind symposium running October 17-19 and offering 12 expert presentations in the area of population control online and free of charge to registrants.
In his address, “Foreign Aid as the Engine Behind Population Control,” Hichborn used data straight from the pertinent agencies to demonstrate how U.S. government programs “use foreign assistance and development work as a Trojan horse.”
“You tell people that you’re helping them get out of poverty, and use it as a vehicle to spread contraception and other programs for reducing fertility rates is essentially the goal,” Hichborn said.
He likewise explained how accepting grant money for relief programs involving abortion and contraception in conflict with Catholic teaching compromises Catholic identity.
The U.S. Congress created the United States Agency for International Development (USAID) through the Foreign Assistance Act of 1961. Since the beginning, Hichborn said, one of the primary goals of USAID was population control, offering chronological examples from throughout the agency’s early years.
“Today, USAID is the largest contraception donor in the entire world,” said Hichborn.
He also presented current data from the USAID website demonstrating its “family planning” goals in the world’s poorest countries, and touting how contraceptive use in the 27 countries with the largest USAID-supported programs has increased, resulting in a drop in the number of children per family in those areas.
“There can be absolutely no doubt that USAID is a population-control agency,” said Hichborn, “hiding its activities under the banner of fighting poverty.”
A Catholic tie to USAID
“So the question now is, why, then, does the United States Conference of Catholic Bishops (USCCB) and its own international aid and development organization called Catholic Relief Services (CRS) consistently ask Congress to take Catholic American tax money and use it to supply this population control giant?” he asked.
At least as far back as 2010, both the USCCB and CRS have sent letters to Congress in support of congressional funding for USAID, he said.
He referenced a Lepanto Institute report that showed how the two agencies for which the USCCB and CRS were asking Congress to provide funding – USAID and the President’s Emergency Plan for AIDS Relief (PEPFAR) — promote the use of condoms and artificial contraception.
Further, Hichborn pointed out, the USCCB sent another letter to Congress asking for this same funding just this past March.
“What happening here is the USCCB is lobbying Congress to maintain large amounts of funding for CRS and PEPFAR,” he stated. “They are essentially lobbying for their own paychecks.”
“What this really is about is the USCCB lobbying Congress to maintain large amounts of funding to PEPFAR and USAID so that it’s project, CRS, can continue to receive large government grants,” he said.
Big money in international relief
CRS is nearly a $1 billion organization, said Hichborn.
Approximately two-thirds of that money comes from grants through the U.S. government like USAID and PEPFAR, he said, and private foundations like the Bill and Melinda Gates Foundation.
“So, by lobbying Congress for continued funding to USAID and PEPFAR, CRS is actually just lobbying Congress for its own slice of the pie.”
This can’t be, they must not know
“When I first started investigating Catholic Relief Services, I was naïve enough to believe that the bishops must not have known about the organizations that CRS was partnering with and giving money to,” Hichborn told conference attendees. “I thought that if I met with the bishop in charge of Catholic Relief Services, he would at least be somewhat shocked by what I had found and would take some action to correct the matter. That was six years ago.”
He then recounted how an eye-opening conversation in 2011 with then-CRS chairman, Tucson Bishop Gerald Kicanas, had Kicanas dismissive of Hichborn’s findings on CRS. This included the relief group providing funding to organizations that were distributing abortifacient contraception, performing sterilizations and committing abortions, and CRS being part of several coalitions that promoted these as well. Further, the bishop wasn’t rattled by mention of CRS’ membership in a coalition promoting something called “safe abortion.”
Hichborn said the exchange was “chilling” and demonstrated an ends-justifies-the-means mentality coming from the USCCB and many of its associations.
A more recent case
A seven-month Lepanto investigation of Catholic Relief Services’ participation in a project in the Democratic Republic of Congo called Project AXxes showed that from 2006 to 2010 CRS was an implementing partner with AXxes, meaning the U.S. bishops’ relief agency was provided funds by the lead organization to implement the overall project in its particular region.
As such, “Catholic Relief Services received units of Depo-Provera, which is an injectable contraceptive,” Hichborn said, “along with Lo Femminal and Overette, which are oral contraceptives, IUDs, and condoms.”
“On other inventory reports,” he added, “we discovered that CRS had received and distributed surgical sterilization kits as well.”
He also recounted how CRS’ own medical coordinator explained in a video interview, while wearing a polo shirt displaying CRS and USAID logos, that the first component of Project AXxes included family planning.
Project AXxes reporting showed that Natural Family Planning programs had been vehicles for other methods of unnatural family planning; something of which Hichborn said CRS was not ignorant.
“There is no way CRS didn’t know what this project intended to do when it agreed to join in,” he said. “Given the stated intention to incorporate contraception into literally every aspect of the entire project, CRS may as well have partnered up with Planned Parenthood.”
An overseas instance
With the international nature of the population control conference, Hichborn also provided data showing that CORDAID, the international aid and development agency of the Catholic bishops of the Netherlands, has promoted contraception and sex education.
“Bear in mind,” Hichborn said, “that Cordaid is supposed to be a Catholic organization run by the Catholic bishops of the Netherlands.”
“Perhaps more disturbing than its own distribution of contraception,” continued Hichborn, citing Cordaid data with specifics spanning several years, “is the fact that Cordaid has partnered with several affiliates of the Catholic Church’s number one public enemy — Planned Parenthood.”
Other Catholic agencies that Hichborn knows of that have been engaged in the spread of contraception or contraception messaging include the Salesian Missions, Development and Peace in Canada, the Catholic Medical Mission Board, and Malteser International.
“The fact of the matter is that the problem is systemic,” Hichborn said. “The more money these Catholic agencies receive from population control groups, and the more they work with them, the more they begin to resemble and emulate them.”
“Our Blessed Lord was very clear when He said that we cannot serve both God and mammon,” he added. “And when you accept money from the devil, you cannot serve God.”
The International Population Control Conference runs through October 19, convening from noon to 4 p.m. Eastern time online.
When choosing a partner to have children with, it is only natural to desire “Prince Charming” or “Cinderella,” who may pass on their beneficial genetic qualities to future kids. Given that better genes increase the offspring’s survival and reproduction chances, mechanisms that detect “genetic quality” should have evolved to lead people to be sexually attracted to “knights in shining genes.”
One such cue for mate suitability is odor, which signals compatibility between potential mates’ immune systems. Specifically, odor indicates the extent of overlapping between potential mates’ immune systems, such that more attractive odor signals less overlap between mates’ immune systems. The larger the dissimilarity between mates’ immune systems, the more threats the immune system can combat.
Offspring would thus benefit the most from having parents with dissimilar immune systems, which results in an enhanced immune system. Accordingly, women have evolved to be sexually attracted to men with a dissimilar immune system, primarily during high-fertility cycle phases. Using the “sweaty T-shirts paradigm”, in which female participants sniff T-shirts recently worn by males, studies have demonstrated that women indeed tend to prefer the scent of partners with dissimilar immune system over that of partners with similar immune system1.
Unfortunately, contraceptive pill use interferes with mate selection and reverses the natural preference for mates with dissimilar immune system, such that women prefer the odor of partners with similar immune system over that of partners with dissimilar immune system while on contraceptive pills2. This shift in preferences corresponds to the one occurring across the menstrual cycle. In particular, naturally cycling women experience male preference shift throughout their menstrual cycle that helps them obtain resources relevant to their current fertility status (fertile versus infertile). During the fertile phase of the menstrual cycle, women seek genetic benefits for their offspring and are thus more attracted to men whose features indicate such benefits (e.g., masculine faces, bodies, and voice). In contrast, during the infertile phase of the cycle, women seek cues of high investment in parenting and partnership, which are typically associated with fewer masculine features3.
Women tend to prefer immune system similarity during the infertile phase for similar reasons: Its association with the smell of genetic relatives who may assist them during pregnancy. Because contraceptive pills introduce hormones that prevent ovulation and lead to temporary loss of fertility, women’s natural preference fixates on similarity as in natural infertile phases of the cycle. In particular, normally cycling women (women who are not using contraceptive agents) tend to rate men with dissimilar immune system as more physically attractive, whereas women using contraceptive pills tend to rate men with similar immune system as more physically attractive2.
The shift in women’s mate preferences, which occurs because of contraceptive pill use, and involves switching to preferring poorly-fitting partners, may adversely affect the adaptability of their children’s immune system. A recent study4 examined whether children born to couples who met during regular contraceptive pill use would display more symptoms associated with a weaker immune system (e.g., being infection-prone, needing more medical care) in comparison with children whose parents met when the mother was not using contraceptive pills.
One-hundred-ninety-two women aged 22 to 48 (M = 33.51, SD = 5.21) participated in the study. All participants reported being the biological mother of a child 1-8 years old. This age range was selected because children in their early years are frequent users of health services. Sixty-one women reported that they met their children’s father while using contraceptive pill, whereas 119 women reported that they were not using contraceptive pill while they met their children’s father. The participants provided information about their child’s health, including their children’s tendency to get sick, their overall health, overall relative health (in comparison with other children their age), child’s relative speed of recovery when sick, number of visits to a medical institute to receive medical treatment, and number of hospitalizations.
Results have revealed that children to mothers who were on the pill are more infection-prone, require more medical care, suffer from a higher frequency of common sicknesses, and are perceived as generally less healthy than children whose parents met on non-pill circumstances. These findings indicate that a key factor in securing children’s future might be traced to a choice people made years before their children were born: the decision to use a contraceptive pill.
The implications of these findings are profound as the use of contraceptive pills is widespread and still growing. Sixty-two percent of all US women in their reproductive ages are currently using a contraceptive method. The aftermath of these numbers is gloomy: The immune system of current-generation children might be more fragile than that of our ancestors, leaving the current and future generations more susceptible to pathogens and more dependent on medical care as its effective line of defense.
1. Saphire-Bernstein, S., Larson, C. M., Gildersleeve, K. A., Fales, M. R., Pillsworth, E. G., & Haselton, M. G. (2017). Genetic compatibility in long-term intimate relationships: partner similarity at major histocompatibility complex (MHC) genes may reduce in-pair attraction. Evolution and Human Behavior, 38(2), 190-196.
2. Wedekind, C., Seebeck, T., Bettens, F., & Paepke, A. J. (1995). MHC-dependent mate preferences in humans. Proceedings of the Royal Society of London B: Biological Sciences, 260(1359), 245-249.
3. Thornhill, R., & Gangestad, S. W. (2008). The evolutionary biology of human female sexuality: Oxford University Press.
4. Birnbaum, S., Birnbaum, G. E., & Ein-Dor, T. (2017). Can contraceptive pill affect future offspring’s health? The implications of using hormonal birth control for human evolution. Evolutionary Psychological Science, 3(2), 89-96.
Exactly 100 years ago, the sun danced. Nowadays you might read people like atheist Richard Dawkins dismissing the miracle in Fatima as a “mass hysteria.” Far more likely, however, you won’t hear about it at all. Or if you do, the media will be sure to give you only half the story.
And yet, the historical record is clear. The sun danced. And up to 70,000 people saw it. Secular newspapers reported it. Skeptical journalists and scientists who were present affirmed what they deemed to be impossible: the sun danced.
There has been nothing even remotely like it in modern history. At Fatima, Our Lady had a message for the world that was so urgent that she resorted to extraordinary means to grab our attention. And when people failed still to heed that message, the dreadful consequences she warned of followed close behind: another great war, persecutions, the annihilation of nations, and the spreading of the errors of Russia.
But what, exactly, was that message?
The Message of Fatima
To find out, let’s go back to that rainy morning of October 13, 1917, as three young peasant children gathered on a hillside in the countryside of Portugal. Throughout the morning tens of thousands of people arrived on foot, by car, and by train, from towns and cities far and near, drawn by the rumor of some great miracle to occur.
Shortly after noon, Our Lady appeared to the three children as she had promised, and as she had done five times before. During a brief conversation with them, she promised that the current war (World War I) would soon end, and revealed that she was the “Lady of the Rosary.”
And then she added: “People must amend their lives and ask pardon for their sins. They must not offend our Lord any more, for He is already too much offended!”
One of the children then asked: “And is that all you have to ask?” Our Lady affirmed: “There is nothing more.”
That’s it: Amend our lives, and ask pardon for our sins! Surely this is the self-same message preached by her Son, in the hills of Galilee, the voice crying in the wilderness, 2000 years ago: “Repent, for the kingdom of God is near!” (Matt. 4:17)
Fatima and the Attack on Morality
I have written about Fatima several times this year. I am writing about it one more time, because: we need the message of Fatima more than ever, a message that speaks directly to this dire fight to defend Life, Marriage, and Family.
I have written before about visionary Sr. Lucia’s warning to Cardinal Caffarra that the “final battle” between God and Satan would be the battle over marriage, and her assurance that “Our Lady has already crushed its head.” What I have not so far mentioned are the messages later given privately to some of the visionaries, which show that Our Lady was deeply concerned with the attack against morality, the consequences of which touch directly on the family.
“More souls go to Hell because of sins of the flesh than for any other reason,” she later told Jacinta. She also warned that “Certain fashions will be introduced that will offend Our Lord very much.” And she also issued a direct warning to women, saying: “Woe to women lacking in modesty.” And also: “Let men avoid greed, lies, envy, blasphemy, impurity.”
Alas! Even to mention a lack of “modesty” these days is to risk wrath. People become enraged upon being told that the way they dress and behave may be leading others to sin: they feel that their freedom is under attack. Often, too, women feel that they are being unfairly singled out, while men get a free pass. But this is only because at times we have adopted a far-too-narrow definition of “modesty” or “fashion.”
The Catechism of the Catholic Church has this to say about modesty:
Modesty protects the mystery of persons and their love. It encourages patience and moderation in loving relationships; it requires that the conditions for the definitive giving and commitment of man and woman to one another be fulfilled. Modesty is decency. It inspires one’s choice of clothing. It keeps silence or reserve where there is evident risk of unhealthy curiosity. It is discreet. – CCC, ¶ 2522
A friend of mine once told me how, a number of years ago, he visited a nightclub with several friends, including one who was a strikingly beautiful woman. The whole night, men who were strangers kept approaching this woman on the dance floor, attempting to behave with her in ways that I won’t describe. In this case, the woman wasn’t even provocatively dressed. It was the men who were displaying the lack of modesty, not in the way they dressed perhaps, but by their behavior.
Where in their behavior was the “patience” and “moderation” becoming of a gentleman? Where was the decency? Sadly, this has become the norm among many men, in part fueled by the ready availability of pornography.
Deadly Lack of Modesty
When we read that the Blessed Mother at Fatima condemned “certain fashions,” we are perhaps too apt only to think of certain fashions in women’s dress. And Our Lady very likely did have this in mind. But the word “fashion” is broader, referring not only to our choice of clothing, but also our behavior.
What would Our Lady think of the current “fashion” of men to squander hours every week lusting over pornographic images that are utterly degrading to women? Or what about the “fashion” of men to use social media apps to “swipe” to find no-commitment “hookups,” or the fashion of men to cohabitate with their girlfriends, with no intention of ever offering them the commitment and stability of marriage?
Or what about the “fashion” of school administrators and teachers to teach “sex-ed” classes to mixed classes that include the most obscene and graphic details about sexuality, without any reference to marriage or morality? Or what about the “fashion” of our politicians who support and march in public parades that celebrate nudity and graphic obscenity? Or the “fashion” of parents to bring their children to these parades, utterly destroying their innocence?
Though it may seem hyperbolic to say, it is provably true that our world is being literally torn apart at the seams by what might be termed a crisis of modesty, or “sins of the flesh.” Families are being torn apart by infidelity; women used, abused and abandoned for entertainment; children viewed as ‘inconveniences’ to be prevented with contraception; babies conceived in loveless, commitment-less relationships, and then aborted; children’s innocence stolen by pornography, and confusion about their sexuality sown at the youngest ages.
Our Lady warned us about this. And she warned of the consequences, not only in this world, but also in the next.
And yet, she did not leave us helpless or hopeless. For 100 years ago, the sun danced. And the promise that Our Lady made that summer to Lucia and the children is the same promise she makes to us: “I will be with you always, and my Immaculate Heart will be your comfort and the way which will lead you to God.”
It is only up to us to heed Our Lady’s message at Fatima, and to put it into effect in our lives. “Pray, pray a great deal,” Our Lady told the three children, “and make many sacrifices, for many souls go to Hell because they have no one to make sacrifices and to pray for them.”
Pope Francis has been a consistent pro-life advocate since becoming the leader of the Catholic Church and he is once again speaking out against abortion and in favor of protecting unborn children.
In a tweet that has been liked by tens of thousands of people across the world, Pope Francis said people should protect human life from conception until natural death. His tweet condemns both abortion as well as euthanasia and assisted suicide.
“We are called to defend and safeguard human life, especially in the mother’s womb, in infancy, old age and physical or mental disability,” he said.
We are called to defend and safeguard human life, especially in the mother’s womb, in infancy, old age and physical or mental disability.
A new book released last month contains thoughts and commentary from Pope Francis based on a series of interviews has the leader of the Catholic Church. The book makes it clear Pope Francis believes there should be no compromise on the longstanding pro-life teachings of the Catholic Church.
The Pope makes it clear that the Catholic Church takes two heartfelt positions when it comes to abortion. First the church takes a clear cut stance in opposition to abortion itself as the destruction of human life. Pope Francis, 80, minced no words when it came to abortion, but did offer a gentle sentiment to women who have opted to abort their unborn children.
“[Abortion is the] murder of an innocent person,” Francis said. “But if there is sin, forgiveness must be facilitated.”
Secondly the Catholic Church also believes in restoration for women who have had abortions.
As the Bible plainly teaches, there is no sin too big for God to forgive via the redemption found in the life-saving death and resurrection of his son Jesus Christ. Both Catholic and Protestant organizations have spent decades reaching out to post-abortive women and offering Bible studies and counseling to help repair their relationship with God and provide them emotional and spiritual support.
Francis stressed those themes of Mercy, Grace and forgiveness during the conversations he had in the interview. He added that many women are emotionally and spiritually scarred before finding God’s forgiveness for her sin.
“Think of a woman who has physical memory of her child, which oftentimes happens, and who cries, who cries for years without the courage to go to see a priest,” the pope explained. “Do you realize how many people can finally breathe?” he asked, reminding people that forgiveness is there for those who seek it.
Pope Francis said that while women who abort their children need to seek and accept the Lord’s forgiveness, it is imperative that they never commit the sin again.
LONDON, England, October 16, 2017 (LifeSiteNews) — UK scientists are experimenting on seven-day old humans to learn how to “edit” DNA before killing them and discarding them.
A team from the Francis Crick Institute is using “excess” living human embryos for their experiments who were frozen for in-vitro fertilization (IVF). They then “edit” the human DNA by taking out a vital gene from “healthy, normal” embryos.
States the BBC:
Breakthroughs in manipulating DNA have allowed the team at the Crick to turn off a gene – a genetic instruction – suspected to be of vital importance. The easiest way of working out how something works is to remove it and see what happens. So the researchers used the gene-editing tool Crispr-Cas9 to scour the billions of letters of genetic code, find their genetic target and break the DNA to effectively disable it.
They were targeting a gene. You are unlikely to have heard of it, but OCT4 is a superstar in early embryo development. Its complete role is not understood but it acts like an army general issuing commands to keep development on track. The researchers used 41 embryos that had been donated by couples who no longer needed them for IVF. After performing the genetic modification, the team could watch how the embryos developed without OCT4…But without OCT4 the blastocyst cannot form. It tries – but implodes in on itself.
From the embryo’s perspective it is a disaster but for scientists it has given unprecedented insight.
Pro-lifers oppose destructive human embryonic experimentation because it’s a human life that’s being destroyed at his or her earliest beginning.
Governor Sam Brownback, whom President Trump nominated for Ambassador At Large for International Religious Freedom, put it this way: “What lies at the heart of this debate is our view of the human embryo. The central question in this debate is simple: Is the human embryo a person or a piece of property?”
“If unborn persons are living beings, they have dignity and worth, and they deserve protection under the law from harm and destruction. If, however, unborn persons are a piece of property, then they can be destroyed with the consent of their owner,” he said.
Christians have always affirmed that men and woman are created in the image of God from the very first moment of their existence. Since the embryo is a living human being and not just a clump of cells, experimentation involves the willful taking of human life and can only be judged as morally and ethically wrong in every instance.
This isn’t just a matter of rules, but a matter of respecting “persons.”
At no point is one person, no matter what size or what state of development — be they zygote, preborn, infant, toddler, child, teen, adult, senior — of less value or less of a person than another human being.
As Dr. Seuss put it, “A person’s a person, no matter how small.”
One’s degree of biological development is irrelevant to the fact that a new being comes into existence when sperm meets egg, a person who must be valued and respected as a member of the human family who is a bearer of God’s image.
The embryonic DNA manipulation performed by the UK scientists deliberately targets and kills human beings. Experimenting on people and then killing them, even with the good intention of using the knowledge gained to help others, is simply wrong. No matter what good follows from it, it is always evil to directly murder someone.
The world was horrified when it learned about the horrors of Nazi experiments on those in concentration/death camps. With equal fervor, anyone who stands for human rights and justice ought to be equally horrified with human embryonic destructive experimentation.
Human embryos are people. Experimenting on them is morally equivalent to experimenting on any other human, like you or me.
Pro-life pioneer Dr. J. Willke put it this way: “You can’t have it both ways. You can’t profess to be pro-life and support experimentation on these tiny children that will result in their deaths.”
In other words, the end does not justify the means.
“Common sense tells us that no one has the right to kill another human being, no matter how much good they claim will come from that act. Most people instinctively reject the notion that doctors are qualified to decide who should live and who should die ‘for the greater good.’ That is why doctors have for centuries taken an oath declaring their first duty not to harm, let alone kill, anyone in their care,” said family advocate Gary Bauer.
The manipulation and destruction of human life at any stage have no humility, no reverence, no place for God.
From the perspective of human rights and justice, the issue is clear: The lives of preborn children must be defended from the earliest, smallest, and most fragile stages of development. Killing innocent human life for experimentation, or for any other reason, must be opposed.
I am on the road this week speaking to groups and doing radio interviews. So here is an article published in Voices magazine (a Catholic women’s’ magazine) in 2003 with an update in 2005. In the intervening years, the problems have grown worse but I originally wrote this article when almost no one had heard of futility policies. Here is the article.
When I first saw “Jack” last September (2002), he was lying unconscious in an ICU with a ventilator to help him breathe. It had been two weeks since a truck struck the 60 year-old and his injuries were devastating — including broken bones, blunt-force trauma and a severe head injury.
When Jack’s family contacted me about seeing him, they were desperate. The doctors told them that he would never come out of the coma and the issue of withdrawal of treatment was raised. The wife refused.
As an ICU nurse myself, I could see that some of the staff felt that taking care of Jack was a waste of time. So I was not surprised when the family was soon told that nothing more could be done. But it was shocking when the hospital told the family that Jack’s ventilator was going to be removed regardless of their wishes. The family was given a deadline to find another health facility to take him.
By that time, Jack was opening his eyes and his family thought he could squeeze their hands at times. The medical and nursing staff assured them that this was just a “reflex”.
After some frantic phone calls, Jack was transferred to a long care facility that took patients on ventilators. Soon after the transfer, his condition became critical again and the family insisted he be treated. Jack was transferred to a hospital ICU. When the staff found out I was a nurse, some of them asked me what the family’s rationale was for continuing treatment. It was obvious that they too felt Jack was a hopeless case.
But over time, Jack improved and was finally able to breathe on his own without a ventilator so he was transferred to a regular hospital bed. Eventually it became evident to all that Jack was starting to respond to commands but it took pressure to get rehab services for him.
Just before Thanksgiving — a little more than two months after his accident — Jack became fully awake. He is now in a rehabilitation facility near his home in Illinois where the staff is working to strengthen his arms and legs, which were broken in the accident. Now, no one meeting him would ever guess that he had had a brain injury.
Even doctors and nurses who ordinarily disdain religion often call cases like Jack’s “miracles”. Of course, for many in healthcare, it’s easier to believe in miracles than to accept that they were wrong and a life could have been unnecessarily or prematurely lost.
But while Jack’s story has a happy ending, many similar cases do not. Families often automatically accept or are even pressured into accepting a doctor’s grim prognosis for their loved one and withdraw treatment after a patient’s brain is injured by trauma or other conditions like a stroke. Usually, the patient then dies.
Unfortunately, families like Jack’s who choose to continue treatment despite a “hopeless” prognosis are increasingly being denied that choice because of “futile care” policies being adopted in many hospitals throughout the country.
And such “futile care” principles have so permeated much of medicine today that there are even cases of elderly or terminally ill patients expected to have months of life remaining whose doctors didn’t want to prescribe medications such as antibiotics because the person was going to die sooner or later anyway.
Futile Care Policies and “Choice”
Most people assume that either they or their families will have the right to decide about medical treatment when they become seriously or critically ill. The biggest problem, people are told, is that they or their loved one will be tethered to a machine forever if they do not sign a “living will” or other health care directive. The “right to die” movement has convinced most people and medical personnel that the ability to refuse treatment is one of the most important aspects of medical care to prevent patients and families from needless suffering. Indeed, poll after poll shows that most people say they would rather die than be a “vegetable”. And many people automatically assume that they would never want their lives prolonged if they had a terminal illness, were paralyzed or senile, etc. Most people assume that refusing treatment, like assisted suicide (the other goal of the “right to die” movement), means choice and control.
But a funny thing happened on the way to this supposed “right to die” nirvana.
Some families and patients did not “get with the program” and insisted that medical treatment be continued for themselves or their loved ones despite a “hopeless” prognosis and the recommendations of doctors and/or ethicists to stop treatment. Many doctors and ethicists were appalled that their expertise would be challenged and they theorized that such families or patients were unrealistic, “in denial” about the prognosis or were mired in dysfunctional family relationships. (In contrast, families who agree to withdraw treatment are almost always referred to as “loving” and their motives are spared such scrutiny.)
At a 1994 pediatric ethics conference I attended, one participant was even applauded when he suggested that parents who refused to withdraw treatment from their “vegetative” children were being “cruel” and even “abusive” by not “allowing” their children to die. In some cases, doctors and ethicists have even gone to court to force withdrawal of treatment over a family’s objections. These ethicists and doctors were stunned when judges were often reluctant to overrule the families.
Yet over the years and unknown to most of the public, many ethicists have still refused to concede the choice of a right to live and instead have developed a new theory that doctors cannot be forced to provide “inappropriate” or “futile” care and treatment to patients deemed “hopeless”. This theory has now evolved into “futile care” policies at hospitals in Houston, Des Moines, California and many other areas. Even Catholic hospitals are now becoming involved.
In the July-August 2000 issue of the Catholic Health Association’s magazine Health Progress, Catherine M. Mikus and Reverend Peter Clark — a lawyer and an ethicist — argue that it is “time for a formalized medical futility policy” in Catholic hospitals. Like many such articles in secular ethics journals, the authors refrain from being too specific about what conditions and which patients would be subject to such a policy. The authors concede that even the American Medical Association says that medical futility is a concept that “cannot be meaningfully defined” and is a “subjective judgment” on which there is no widespread agreement.
Mikus and Clark make it clear that they are not talking about treatments that are “harmful, ineffective, or impossible”, the traditional concept of medical futility that, of course, is not ethically obligatory. For example, no doctor would honor a family’s request for a kidney transplant for a person who is imminently dying. Instead, the authors argue for a new definition of futility to overrule patients and/or families on a case-by-case basis based on the doctor’s and/or ethicist’s determination of the “patient’s best interest”. Ironically, the “right to die” movement was founded on the premise that patients and/or families are the best judges of when it is time to die. Now, however, we are being told that doctors and/or ethicists are really the best judges of when we should die. This is reminiscent of the imperious statement attributed to Henry Ford that his Model T customers could “paint it any color, so long as it’s black”. Thus the “right to die” becomes the “duty to die”, with futile care policies offering death as the only “choice”.
But despite the lack of consensus on what constitutes futile care, these Catholic authors are passionate about why such policies should be adopted and insist that their policies are “firmly rooted in the Catholic tradition”:
“Proper stewardship of these resources entails not wasting them on treatments that are futile and inappropriate. They must be rationally allocated; to waste them is ethically irresponsible and morally objectionable”. (Emphasis added)
In other words, a social justice-style argument is being made to save money.
Unfortunately, when it comes to Mikus and Clark’s opinions, not only is a sense of humility lacking but also a sense of God’s jurisdiction:
“In assessing whether a treatment is medically futile, physicians must consider carefully not only the values and goals of the patient/surrogate, but also those of the community, the institution, and society as a whole”. (Emphasis added)
This not only ignores God’s ultimate role in life and death but also turns the Hippocratic oath on its head. While the Hippocratic oath is no longer routinely used with medical students, its enduring legacy has always been the sacredness of the commitment of the doctor to his individual patient. Now, new doctors are often told that their ultimate commitment instead resides with the health and welfare of society.
It is appalling that Catholic doctors are now also being encouraged to adopt the secular and utilitarian concept of the greatest good for the greatest number rather than a spiritual commitment to each individual for whom they care. Under this new standard, Jesus the great Healer must be considered a failure for tenderly concerning Himself with healing such “little” lives during His ministry rather than constructing a more “politically correct” health system.
Where Do We Go from Here?
Just a generation ago, doctors and nurses were ethically prohibited from hastening or causing death. Family disputes and ethically gray situations occurred, but certain actions (such as withdrawing medically assisted food and water from a severely brain-injured but non-dying person) were considered illegitimate no matter who was making the decision.
But with the rise of the modern bioethics movement, life is no longer assumed to have the intrinsic value it once did, and “quality of life” has become the overriding consideration. Over time, the ethical question “what is right?” became “who decides?” — which now has devolved into “what is legally allowed?”
Thus, it is not surprising that the Health Progress article on futility policies is subtitled “Mercy Health System’s Procedures Will Help Free Its Physicians from Legal Concerns”. This is no afterthought, but rather the greatest fear of the authors that families may sue.
Doctors are understandably afraid of civil or malpractice lawsuits. In this article, Mikus and Clark attempt to convince doctors that a written futility policy — no matter how vague — is necessary. Then doctors would use the power of an ethics committee to back up their decisions in any legal proceeding in order to prove that the determination of futility meets the hospital’s standard of care.
Even more ominously, there have been efforts to incorporate futile care policy into state and federal law. For example, Senator Arlen Specter introduced the Health Care Assurance Act of 2001 that, while aimed at improving health care for children and the disabled, nevertheless contains a provision that there is no obligation:
“to require that any individual be offered, or to state that any individual may demand, medical treatment which the health care provider does not have available, or which is, under prevailing medical standards, either futile or otherwise not medically indicated”. [Emphasis added.]
The first step in solving a problem is to recognize it. We cannot always rely on a mainstream media that would rather exhaustively cover a star’s shoplifting charge than alert us to thorny ethical problems. Legislation and policies are often developed without public knowledge or comment. Health insurance can no longer be counted on to pay for all needed treatment in many situations.
This is why publications such as Voices and many other Catholic periodicals, pro-life news services and the Internet are so important, especially in the area of ethics. We in the Church are also blessed with encyclicals, Vatican documents and the writings of the doctors of the Church, which give clear principles that are still just as valid and useful as ever in a world of increasing technology and seductive decadence.
If we truly want to protect lives, save souls and fight injustice, we cannot remain silent in the face of an ever-expanding “culture of death”.
Postscript (2005): A couple of years after this was published, Jack was home and doing well when I was contacted by a documentary team from the UK who were making a film about Jack’s experience. I was asked to be a part of this.
I spent a lot of time with the British team and they told me how giving up on someone like Jack would not happen in the UK, despite their government-run National Health Service.
SAN FRANCISCO, California, October 11, 2017 (LifeSiteNews) — Those who doubt the existence of hell, despite Our Lady of Fatima showing its horrors to three Portuguese shepherd children 100 years ago, can nevertheless see a “living reflection of hell” in abortion, euthanasia, and homosexuality, said San Francisco Archbishop Salvatore Cordileone.
Archbishop Cordileone made his remarks during a homily last weekend as he consecrated his Archdiocese to the Immaculate Heart of Mary.
He recalled during his October 7 homily the great evils witnessed in the past 100 years, including the great world wars, death camps, numerous genocides, and Christian persecution.
“Who would dare to say that such barbarity is not a mocking of God?” he asked.
Cordileone listed legal abortion as one of the many genocides.
“And then there is the attack on innocent human life: Our own land has been soiled by the blood of innocent children in what has become a deadly epidemic tantamount to a genocide on life in the womb,” he said.
“And now we are increasingly witnessing the abandonment of our suffering brothers and sisters at the other end of life’s journey,” he added, in a reference to euthanasia and assisted suicide of the elderly.
The Archbishop went on to list legal homosexual “marriage,” and made a reference to Pride Parades, as ways in which God is mocked.
“And even in our own city of St. Francis, we see … the celebration and even exaltation of the vulgar and the blasphemous, mocking God’s beautiful plan in how He created us, in our very bodies, for communion with one another and Himself,” he said.
“God is roundly mocked in our very streets, and it is met with approval and applause in our community – and yet, we remain silent,” he added.
Friday, October 13, marks the 100th anniversary of Fatima’s “miracle of the sun.” The day commemorates the last apparition of Our Lady of Fatima to the three children and the fulfillment of the promised “sign.” Tens of thousands of people, including atheists and those who had come to mock the children, witnessed the sun dancing and emitting radiant colors in the sky.
Cordileone said that today, 100 years after the Fatima apparition, shows itself to be “in so many ways … a living reflection of hell, one that on so many fronts has roundly mocked God.”
“If we think about what has transpired in these last 100 years,” the Archbishop said, “does it not tell us that the century through which we have just passed was nothing other than an experience of hell?”
“The century since the Fatima apparitions now ending has mocked God, but God will not be mocked: not because He delights in wreaking vengeance on us, but because turning our backs on God only bounces back to us, leading to our own self-destruction,” he said.
Heeding the message
The Archbishop said that now, more than ever, people must “heed the message of Fatima in imploring God for mercy,” especially through her request of “prayer, penance and adoration.”
He asked every Catholic in the Archdiocese to honor Our Lady’s request by praying the Rosary “every day.”
“I ask every Catholic in the Archdiocese of San Francisco, if you are not doing so already, to pray the Rosary every day. And I ask all families to pray the Rosary together at least once a week,” he said.
He also asked Catholics in his diocese to do penance on every Friday of the year.
“I ask every Catholic in the Archdiocese of San Francisco to dedicate Friday as a day of penance in honor of the day that our Lord died for us, selecting one concrete form of bodily fasting to observe on this day, whether that be abstaining from meat or another type of food or from some type of drink they normally enjoy, or omitting a meal altogether,” he said.
Finally, he asked Catholics to honor Our Lady’s request by praying before God in adoration once a week.
“I ask every Catholic in the Archdiocese of San Francisco to dedicate some time each week to pray before the Blessed Sacrament. If it is not possible during the week, take some time before or after Sunday Mass to pray on your knees before our Lord present in the tabernacle. At least some time every week praying before the presence of our Lord in the Blessed Sacrament – Body, Blood, Soul and Divinity – will fulfill his desire that we ask him for mercy,” he said.
He also asked that Catholics observe the devotion of the First Five Saturdays once a year.
“The devotion consists of attending Mass and receiving Communion in reparation for sins on five consecutive first Saturdays of the month shortly after or before going to Confession, and spending a quarter of an hour praying five decades of the Rosary,” he said.
Cordileone said that if Catholics honor the requests of Our Lady, it will hasten the fulfillment of her promise that “In the end, my Immaculate Heart will triumph.”
“Let us heed her message, let us grant her requests, in order to hasten that triumph, that triumph which is that of her Son over death, for she is inseparably linked to her Son, who came to win for us our eternal salvation,” he said.
“Her Immaculate Heart is the door that opens up for us entrance into that triumph. It is through that door that we walk from the darkness of sin and death to the light of Christ’s truth and mercy. There it is, on the other side of that door, a glorious, vast, light-filled paradise that is heaven. Her heart is the gate of heaven,” he added.
The U.S. Department of Health and Human Services released a draft of its new strategic plan for 2018-2022, and with the addition of a few small words, it’s clear that there is a major change.
Formerly, the document stated the following in its introductory information:
HHS accomplishes its mission through programs and initiatives that cover a wide spectrum of activities, serving Americans at every stage of life.
HHS accomplishes its mission through programs and initiatives that cover a wide spectrum of activities, serving and protecting Americans at every stage of life, beginning at conception.
8 weeks from conception
The change might be five little words, but its meaning is deep. It signifies that at the U.S. Department of Health and Human Services knows and accepts the truth, that life begins at conception (fertilization). Pro-life activists have said it for decades, scientists have proved it, and abortion supporters have denied and flat-out ignored it, but it’s true: life begins the moment a new human life is created – at fertilization. HHS is committed to protecting those lives.
In addition to this change, HHS’ first strategic goal is to “Reform, Strengthen, and Modernize the Nation’s Health Care.” In the introductory paragraph, it is made clear that there is a mission to improve health care in the United States for all Americans, including those still in the womb. It states:
HHS is dedicated to reforming, strengthening, and modernizing the Nation’s health care system. By promoting greater affordability and balancing spending, strengthening health care quality and patient safety, improving access and expanding choices, and investing in the health care workforce, HHS seeks to improve health care outcomes for people we serve. While we may refer to the people we serve as beneficiaries, enrollees, patients, or consumers, our ultimate goal is to improve healthcare outcomes for all people, including the unborn, across healthcare settings.
Another addition is noticeable in the third strategic goal, which states that the HHS works to “Strengthen the Economic and Social Well-Being of Americans across the Lifespan.” HHS clearly states that not only does life begin at conception, but it should end at “natural death”:
A core component of the HHS mission is our dedication to serve all Americans from conception to natural death, but especially those individuals and populations facing or at high risk for economic and social well-being challenges, through effective human services.
The changes are welcome moves for those who advocate for the protection of preborn humans in a country where preborn eagles currently have more rights. It’s a small step, but it is a step in the right direction, acknowledging that life exists inside the womb.
While former HHS Secretary Tom Price recently resigned from his position, pro-life Teresa Manningserves as deputy assistant secretary for population affairs, overseeing the federal funding for family planning programs, and Charmaine Yoest, former president of Americans United for Life, serves as assistant secretary of public affairs.
After the Trump administration’s rollback of the controversial and heavily litigated contraceptive mandate from the Affordable Care Act, everyone from Cecile Richards to Nancy Pelosi to Hollywood stars are crying foul.
When the mandate was put into effect in 2010, it was touted as “necessary” for women’s health and access to contraception. We have now had seven years to see whether the Mandate is actually “necessary” for women to access contraceptives. Short answer: it’s not. Research from the reproductive rights think tank, Guttmacher Institute, found that since the Affordable Care Act and the Mandate began, there has been no change in sexually active women’s use of contraception.
This is not surprising. Before the mandate began, a Centers for Disease Control (CDC) studyfound that among the 11 percent of women who do not use contraception, cost was not even a “frequently cited reason” for not using birth control (2). Guttmacher found that only 3.7 percent of women obtaining an abortion cited cost as a barrier to using contraception.
The 11 percent of women who do not use contraception have good reason to avoid it. It has been shown that some of the “birth control access” that we have pushed is correlated with an increase in casual sex, and in some cases, STD rates. Birth control has other serious health consequences for many women that are often not adequately communicated to them — nor the alternatives for spacing births or treating hormonal conditions. Saying birth control is essential healthcare for women can do them a disservice.
Birth control and skyrocketing STD rates
Many advocates of the HHS mandate support it because it ensures that all women will have free provision of long acting reversible contraceptives (LARCs). LARCs, which include intra-uterine devices, implants or hormonal injections, help keep women effectively sterile. LARCs are associated with increased rates of casual sex among teen girls, likely in part because they foster the illusion that sex can be “consequence free”. LARC users are more than twice as likely to have two or more sexual partners in the previous three months, and twice as likely to have four or more lifetime partners, than those who did not use LARCs”. An especially popular LARC, Depo Provera, is also associated with an increased rate of HIV transmission.
The defense of the contraceptive mandate comes at the same time that the CDC released its annual report on the status of Sexually Transmitted Diseases in the United States in 2016. The figures are staggering. The United States has reached record high rates of gonorrhea, syphilis and Chlamydia, with over 2 million new diagnoses. Especially heartbreaking is the CDC’s assertion that over half of 20 million new diagnoses of all STD’s occur in individuals aged 15-24. Interestingly, LARCs are currently being pushed to this exact population.
Birth control can harm women’s health
In addition to STD rates, contraceptives have other risks that have been largely ignored in this push for free birth control access because “women’s health” supposedly depends upon it. Hormonal contraceptives have been designated as a “known carcinogen” by the World Health Organization, and also carry an increased risk of blood clots which can result in heart attacks, pulmonary emboli or strokes. For example, Merck, the maker of the IUD, NuvaRing, paid out $100 million to settle 3,800 lawsuits related to blood clots. Bayer paid out almost $1.6 billion to settle suits related to Yaz and Yazmin birth control pill complications, which had led to heart attacks and strokes.
If our goal is really to support women’s essential health needs, then we need to start with a basic tenet of solid medical practice-informed consent, specifically in this case, actually informing women of the risks of these medications and devices. As a nurse, I have given presentations to college-aged women about contraceptives. The majority of these educated young women have little to no knowledge about these risks, or even about how contraceptives function in their bodies. I’ve heard these young women exclaim, “Why aren’t we told about this?”
It is disingenuous and simplistic to pretend that women as a group “need” hormonal birth control for their health, and that there are no alternatives for avoiding or achieving pregnancy, or treating hormonal conditions. Many hormonal conditions can be more effectively treated with targeted hormone therapies, rather than a daily contraceptive pill which only masks the underlying disease rather than actually treating it. I personally struggled with pelvic pain and irregular menstrual cycles and many physicians recommended the birth control pill; advice I didn’t take, due to both medical and moral concerns. Instead, I have found reproductive health through progesterone treatment during a limited, specific part of my cycle.
Further, women looking to space pregnancies have alternatives to birth control that are side-effect free and cost-free in the long run. Fertility awareness based methods empower women with knowledge about their cycles that they can use for a lifetime to avoid or achieve pregnancy, no hormonal manipulation necessary.
As a healthcare provider, I am ashamed that we have reached the point that we make women, both young and not-so-young, feel as if they “need” contraceptives to be healthy, or to succeed in life, and that we must force anyone and everyone to pay for it. Consequently, in that quest for access to free birth control, in the effort to paint BC as necessary for women’s health, we have failed to educate women about risks and alternatives.
Janet Garcia writes from Minnesota. She is a wife, mother and registered nurse. Janet is a member of Women Speak For Themselves.
AUMSVILLE, Oregon, October 11, 2017 (LifeSiteNews) — Assisted suicide advocates call their cause “death with dignity,” but they never saw the likes of Esther Ybarra.
Stricken with Stage 4 cancer just as life was blossoming at age 19, Esther exemplified what a true “death with dignity” is.
She died in July after two years of degenerating from a 5-foot-10, 175-pound college scholarship athlete and female athlete of the year to a frail and broken 100-pound hospital patient struggling to breathe. But those she left behind say Esther was the strongest person they’ve ever known, whose enduring, ultimate trial-tested faith in Jesus Christ changed their lives.
Esther had always been athletic and competitive. The oldest of seven, she loved gymnastics, dancing, and kicking. Ron and Teresa Suelzle told World Magazine that at two years old their daughter used cabinet drawers to climb up to the bathroom sink to brush her teeth.
“I’m capable,” the toddler with the beaming smile told her dad.
As she grew and joined extracurricular sports, Esther was driven to compete. On the ceiling above her bed she taped, “Pain is weakness leaving the body.” “No excuses.” “If I want to WIN, I will work harder.”
Finishing high school at the peak of health and athletic prowess, Esther even as a high school junior could squat 225 pounds and bench-press 155. Corban University gave her a scholarship to play volleyball.
Though she was raised in a Christian home, at one point the star athlete felt so strong that she didn’t need God anymore. That would soon change.
Two months into college, Esther’s life was turned upside down. When her back unexpectedly gave out, a biopsy near her fractured vertebra proved malignant. She was diagnosed with Stage 4 Alveolar Rhabdomyosarcoma, a deadly soft tissue cancer.
Everything changed at that moment. For the better.
While her homemaker mom later recalled “My head was swimming” at her daughter’s hopeless diagnosis and her high school teacher dad “felt like we had hit bottom,” Esther paused, then shook her doctors’ hands.
“I want to thank you for telling me,” Esther said. “That must have been difficult for you.”
For the next two years, Esther became the Rock of Gibraltar. It is astounding how one woman’s faith can unite and sustain an entire family — even an entire community. When Esther faced the gravest diagnosis known to man, she calmly thanked her doctors. When her boyfriend broke up with her, she never lost faith in Jesus. When she lost her hair to chemotherapy, she never blamed God.
Sure, she asked, “Why?” And there were plenty of tears. Esther was not a stranger to anxiety or fear, either. But by having lost it all, she somehow gained something. Something priceless.
“God took away everything that was important to me,” Esther explained. “He took away my ability to play volleyball, work out, go to school, and my hair. All I have left is God, my family, and my friends. And I’ve never been better.”
There was a period of remission. The whole family clung to fragile hope as Esther’s cancer treatment seemed to help. During that time, Esther met Jacob Ybarra, a track and field athlete at Corban.
When he took her out on Valentine’s Day, Esther was bald as a cue ball. She was also, understandably, somewhat guarded.
“She was a scared girl with a really, really strong shell,” Jacob told World’s Sophia Lee. “She acted like she was real tough and can do everything by herself, but she really needed help.”
Eventually, Jacob and Esther fell in love. When he asked her to marry him, Esther thought her life had turned around.
But not long after Jacob and Esther’s engagement, they got the crushing news that new cancer had formed and grown in her lungs.
Defying conventional wisdom, the two lovebirds wed in October 2016. Lee, who spent an entire day with the family recently, explained that when one was weak, the other provided strength.
“At times, Jacob returned home to find Esther in tears because she couldn’t finish the housework, and he taught her it was OK to rest. Other times, he came home to find his wife deep in prayer, and he sought to enjoy such intimacy with God as well,” Lee wrote.
“Esther’s greatest strength was her relationship with Jesus,” Jacob summarized. “Jesus was the only reason she could still sing, still fight.”
Esther and Jacob Ybarra with their stillborn son
The couple became unexpectedly pregnant, but at three months along Esther hemorrhaged, and tiny, perfectly-formed Thaddeus was stillborn.
Cancer treatments no longer helped as Esther grew dramatically worse. The fluid building up in her lungs made it progressively harder to breathe. Jacob helped ease the fluid buildup.
Oregon legalized assisted suicide in 1997, and if anybody qualified, it was Esther. But instead of killing herself, even when in great pain, Esther sang.
One of her favorite hymns to sing was “What a Friend We Have in Jesus,” and she didn’t care if others heard her. Hospital staff described her as the most joyful person in the room.
So often Esther would listen to someone’s troubles, lying on her deathbed herself, wiping away their tears and offering to pray for them. And any time she could, Esther would talk about Jesus with doctors, nurses, aides, and just about anyone.
“They were concerned about saving her life, but she was trying to save their souls,” Jacob told Lee.
Instead of killing herself, Esther saved souls. Of that, her family and relatives testify.
“She fully trusted what was supposed to happen, and that was the most beautiful thing I had ever seen,” her cousin, Kim Klaus, shared.
“She learned how to be instead of always doing,” her sister, Elizabeth, 20, said.
“Just by the way she lived, giving up everything for Christ, she really inspired me,” sister Marilyn, 13, said.
On July 24, 2017, Esther opened her eyes for the last time, in the loving presence of her family. After an all-too-brief goodbye glance, she was gone.
Last month, a “Celebration of Life” was held in Esther’s honor. Six hundred people gave thanks to God for the life and for the death of Esther Ybarra. Many gave testimony of the spiritual paradigm shift they experienced just by knowing the woman who truly “died with dignity.”
There’s more in Lee’s beautiful account of how Jacob and the family are now coping, but one lesson — among many — stands out.
Esther’s tragic plight has a lot in common with others who ultimately decide to kill themselves, with society’s legal blessing. Another vivacious woman stricken with cancer way too young, Brittany Maynard, became the poster-child for assisted suicide in 2014.
Lee points out that both Esther and Brittany may have had a common tragedy, but their responses were as different as life and death.
Brittany aggressively decided to fight for the right to kill herself, considering suicide as her “death with dignity,” and the state government blessed her death wish. She justified it as best for her family, because her suffering would be a “nightmare” for them. She sought to avoid “fear and uncertainty” by taking her own life.
In contrast, Esther sought to live what time she had left “to the glory of God.” While death has no dignity, Esther prized the days and used them to draw closer to Christ and to her family. In her suffering, she comforted those around her. She truly lived the hymn, “I Surrender All,” submitting her unknown future to her Lord.
As a result, Esther’s death, though tragically sad, inspired her family and countless others to see what truly matters in life. And as a result, her death brought eternal life to those around her.
“Her legacy is not one of despair,” one person said at Esther’s memorial. Instead, Esther’s awesome example encouraged all who came near her to “choose joy every day.”
“For the joy set before Him, He endured the Cross, despising the shame, and is now seated at the Right Hand of God the Father.” (Hebrews 12)
October 5, 2017 (Population Research Institute) – The last year of the Obama administration saw the fertility rate fall to an all-time low.
According to recent data from the CDC’s National Center for Health Statistics (NCHS), the U.S. fertility rate sank to a record low of 62.0 births per 1,000 women of reproductive age in 2016.
This was a slight decrease from the 2015 fertility rate which stood at 62.5. The downward trend is not showing signs of stopping either. According to NCHS preliminary estimates, fertility slumped even lower to 61.5 in the first quarter of 2017.
The U.S. birth rate—a slightly different measure of fertility—also fell among younger women, 15-29 years of age. A small increase in births among women 30 years of age and older was not enough to make up for the decline among younger women.
The Great Depression led to a staggering drop in fertility rates.
The current fertility decline is similarly driven by the still-lingering effects of the Great Recession of 2007.
Studies have shown that unemployment[1],[2] and employment uncertainty[3] adversely affect the birth rate overall and lead young people to postpone marriage. Both for male and female unemployment affects fertility, though the effect remains stronger for male unemployment.[4] Fertility is also more likely to decline in developed countries when Gross Domestic Product (GDP) contracts.[5]
A decline in the birth rate has also been found to be linked with other economic indicators such as per capita GDP, per capita income, the number of first-time unemployment claims, and consumer confidence.[6]
The Great Recession has fallen particularly hard on young adults who play a major role in contributing to the overall fertility rate. Following the 2007-16 Great Recession (which is more accurately referred to as a second Great Depression), many young adults have struggled to enter the workforce, to find affordable housing, and to accumulate wealth, prerequisites necessary in contemporary American society for partnership and family formation.
The Great Recession has also fallen particularly hard on Hispanics, a demographic that, for the past few decades, has helped boost the fertility rate in the U.S. While non-Hispanic black and non-Hispanic white women have seen a modest decrease in fertility by 7.3 and 1.7 births per 1,000 women of reproductive age from 2007-2015 respectively, Hispanic women have seen a precipitous decline of 25.7 births per 1,000 women over the same time period.[7]
According to NCHS, the total fertility rate in the U.S. in 2015 was 1.84. This rate sits below the replacement fertility rate, the rate of births necessary for population replacement. According to the United Nations Department of Economic and Social Affairs, replacement fertility in the U.S. is estimated to average 2.07 from 2015-2020.
If birth rates continue to decline, and immigration drops off, the impact on the U.S. economy could be significant. Population growth, or more specifically, an increase in the labor force, is a key determinant of economic growth. Economists estimate that as much as one third of economic growth is attributable to workers being added to the labor force every year.
Low birth rates correspond to aging population. The U.S. is facing a substantial increase in its dependency ratio as the Baby Boomers retire, and working-age adults must replace the productivity thus lost and pay for entitlement programs like Social Security and Medicare.
To maintain productivity, one solution is to work longer hours or to postpone retirement. But, given there are only so many hours in a day and only so many additional years the elderly can be expected to work, there is only so much lost productivity that can be compensated for in this way. Barring a major technological breakthrough to boost productivity and efficiency, demographic decline will almost certainly have a net drag effect on the economy.
Will birth rates rebound? As the Great Recession recedes into memory, and as the Trump economic policies stimulate growth, birth rates will likely increase again. They did, after all, following the Great Depression.
But the demographic recovery this time around is unlikely to be nearly as robust as it was during the Baby Boom. American society has changed. Fertility rates are unlikely to reach former levels because desired fertility goals in the U.S. overall have declined.
In recent decades, however, women have increasingly opted to postpone childbearing. The shift has been so consistent across the U.S. that the birth rate for women in the 30-34 age group has now surpassed the 20-24 age group. There are far fewer teenage brides than in years past, and more and more young women are choosing college over childbearing.
A more educated population is, of course, vital to continued economic growth. But so is a healthy birth rate. Are young couples merely postponing childbearing until they are older and have completed their education. Or are they foregoing it altogether?
It may be too soon to tell which way fertility will trend, post-Great Recession. While many couples initially seemed to merely postpone having children as when the downturn hit, recent fertility data seems to indicate that, as the Obama recession dragged on year after year, many ultimately revised their fertility goals downward. Couples who postponed births have generally yet to make-up for the loss, proving once again that fertility delayed is fertility denied.
The solution, in our opinion, is an expansion of the Child Tax Credit (CTC). Senator Marco Rubio has long advocated increasing the maximum credit from $1,000 to $2,500, as well as making it fully refundable. A fully refundable CTC would reduce the taxes of working families across the board. This in turn would be a powerful inducement for them to have another child. After all, children are the only future a family—or a nation—has.
[1] D’Addio AC, d’Ercole MM. Trends and determinants of fertility rates: The role of policies. OECD Publishing; 2005 Sep 2.
[2] Schmitt C. Gender-specific effects of unemployment on family formation: a cross-national perspective 2008; SOEPpaper No. 127; DIW Berlin Discussion Paper No. 841.
[3] Sobotka T, Skirbekk V, Philipov D. Economic recession and fertility in the developed world. Population and Development Review 2011; 37(2): 267-306.
[4] According to observation made by: Sobotka (2011).
[5] Relationship dissipates in multivariate model, however. See Sobotka (2011).
[6] Fokkema T, de Valk H, De Beer J, van Duin C. The Netherlands: Childbearing within the context of a “Poldermodel” society. Demographic Research 2008; 19(21): 743-794.
[7] Calculated using data from: Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, Mathews TJ, Division of Vital Statistics. Births: Final data for 2015. National vital statistics reports. Hyattsville, MD: National Center for Health Statistics 2017; 66(1): 32-33.
Editor’s note: Reprinted by permission from Population Research Institute.
MARIA GALLAGHER OCT 9, 2017 | 12:33PM WASHINGTON, DC
It is entirely possible to adopt a pro-life position based solely on reason. After all, science shows us that the baby’s heart starts beating at 24 days after conception; brain waves can be detected 43 days after fertilization.
Since every being in creation has a beginning, conception is the logical marker for determining the initiation of life. And, once a human life is initiated, the boy or girl should be protected. No religious creed is required to subscribe to that position.
Still, some look to faith to answer the question of when life begins, or to validate their position on abortion.
To me, one of the most telling verses in the Bible comes from the Gospel of St. Matthew, Chapter 25: “Amen, I say what you did not do for one of these least ones, you did not do for Me.”
The least among us are preborn children. They have no money, no voice of their own. They are small in stature and, under the tragic U.S. Supreme Court decision Roe v. Wade, they are largely unprotected under the law.
But according to Christian Scripture, whatever is done, or left undone, for these little ones is done, or not done, for Jesus, the Son of God.
Therefore, a Biblical imperative exists to defend the lives of preborn children. In honoring them, Christians honor God.
Again, one can come to a pro-life position entirely based on scientific evidence. But for those who look to the Bible for direction, the right to life is as clear as the waters of Baptism.
LifeNews.com Note: Maria Gallagher is the Legislative Director and Political Action Committee Director for the Pennsylvania Pro-Life Federation and she has written and reported for various broadcast and print media outlets, including National Public Radio, CBS Radio, and AP Radio.
WASHINGTON, D.C., October 6, 2017 (LifeSiteNews) – The Trump administration issued an order today ending the federal requirement that employers violate their consciences to participate in the provision of employees’ contraceptives and abortifacient drugs.
The Obama administration’s Department of Health and Human Services (HHS) began this mandate, often called the HHS contraceptive mandate. The Little Sisters of the Poor, pro-life nuns who care for the elderly, along with Hobby Lobby and other religious entities, refused to comply. The Little Sisters of the Poor providing contraceptive and life-ending drugs and devices would explicitly contradict their mission of respecting the dignity of every human life.
“HHS has issued a balanced rule that respects all sides– it keeps the contraceptive mandate in place for most employers and now provides a religious exemption,” said Mark Rienzi, senior counsel at Becket and lead attorney for the Little Sisters of the Poor. “The Little Sisters still need to get final relief in court, which should be easy now that the government admits it broke the law.”
The new rules, which are nearly 300 pages in total, prevent the Little Sisters of the Poor and other conscientious objectors from litigation.
“The United States has a long history of providing conscience protections in the regulation of health care for entities and individuals with objections based on religious beliefs or moral convictions,” the new rules state. “These rules do not alter multiple other Federal programs that provide free or subsidized contraceptives for women at risk of unintended pregnancy.”
The Supreme Court offered relief from the burdensome mandate to Hobby Lobby and other for-profit corporations in its 5-4 ruling in Burwell v. Hobby Lobby Stores, Inc.
“No American should be forced to choose between the dictates of the federal government and the tenants of their faith,” Trump said when he signed this order in the White House Rose Garden. He called the Little Sisters of the Poor up to the stage with him.
The New York Times reported that Matt Bowman, a pro-life attorney who worked for Alliance Defending Freedom (ADF) before joining the Trump administration’s HHS, is the “principal author of the rules.”
ADF has been one of the mandate’s strongest critics.
According to The New York Times, the new regulation cites some of the many health risks of contraception as well as its availability likely promoting teen sexual promiscuity. The June leaked version of this new regulation mentioned that as well.
The rule released today allows employers with religious and moral objections to contraception to not participate in its provision. This would exempt groups like the March for Life, which have expressed moral opposition to cooperating.
“The new exemptions will be available to colleges and universities that provide health insurance to students as well as employees,” according to TheNew York Times.
“After eight years of the federal government’s relentless assault on the First Amendment, the Trump administration has taken concrete steps today that will once again erect a bulwark of protection around American’s First Freedom – religious freedom,” said Tony Perkins, President of the Family Research Council.
“President Trump is demonstrating his commitment to undoing the anti-faith policies of the previous administration and restoring true religious freedom,” said Perkins. “Last May, the president ordered the federal government to vigorously promote and protect religious liberty.”
HHS is “moving to make that order a reality,” he said.
October 5, 2017, (Voice Of The Family) – 13 October 2017 will be the centenary of the Miracle of Sun and the final apparition of Our Lady of Fatima. Despite being essential for understanding the period of history that we are now living through, the details of these remarkable events are far too little known, including amongst Catholics. In this article, we wish to draw attention to the much-neglected role of St Joseph during that momentous event.
Following the Miracle of Sun, and at the culmination of Our Lady’s final apparition, St Joseph also appeared to the three young seers. Father John de Marchi, in his book The True Story of Fatima, describes it as follows:
To the left of the sun, Saint Joseph appeared holding in his left arm the Child Jesus. Saint Joseph emerged from the bright clouds only to his chest, sufficient to allow him to raise his right hand and make, together with the Child Jesus, the Sign of the Cross three times over the world. As Saint Joseph did this, Our Lady stood in all Her brilliancy to the right of the sun, dressed in the blue and white robes of Our Lady of the Rosary. Meanwhile, Francisco and Jacinta were bathed in the marvelous colors and signs of the sun, and Lucia was privileged to gaze upon Our Lord dressed in red as the Divine Redeemer, blessing the world, as Our Lady had foretold. Like Saint Joseph, He was seen only from His chest up. Beside Him stood Our Lady, dressed now in the purple robes of Our Lady of Sorrows, but without the sword. Finally, the Blessed Virgin appeared again to Lucia in all Her ethereal brightness, clothed in the simple brown robes of Mount Carmel.
This final apparition at Fatima points us towards three particular forms of devotion towards Our Lady that we are called to practice during this “final battle” against Satan. These are devotion to:
her Sorrowful and Immaculate Heart
the Holy Rosary
the Brown Scapular.
However, it is of the greatest importance to note that the final apparition of Fatima also directs us towards the intercession of St Joseph, whom Our Lord intimately associated with Himself in his blessing of the world.
Father de Marchi wrote:
Our Lord, already so much offended by the sins of mankind and particularly by the mistreatment of the children by the officials of the county, could easily have destroyed the world on that eventful day. However, Our Lord did not come to destroy, but to save. He saved the world that day through the blessing of good Saint Joseph and the love of the Immaculate Heart of Mary for Her children on earth. Our Lord would have stopped the great World War then raging and given peace to the world through Saint Joseph, Jacinta later declared, if the children had not been arrested and taken to Ourém.
On the Feast of the Immaculate Conception, 8 December 1870, Blessed Pope Pius IX, following appeals received from bishops worldwide, had declared St Joseph to be Patron of the Universal Church, “in this most sorrowful time” when “the Church herself is beset by enemies on every side and oppressed by heavy calamities, so that impious men imagine that the gates of Hell are at length prevailing against her.”
Pope Leo XIII, to whom it was revealed in 1884 that Satan would be given, for a time, increased power to work for the destruction the Church, instituted a new devotion to St Joseph in his encyclical letter Quamquam pluries, promulgated on the Feast of the Assumption, 15 August 1889. The Supreme Pontiff wrote:
During periods of stress and trial – chiefly when every lawlessness of act seems permitted to the powers of darkness – it has been the custom in the Church to plead with special fervour and perseverance to God, her author and protector, by recourse to the intercession of the saints – and chiefly of the Blessed Virgin, Mother of God – whose patronage has ever been the most efficacious.
He further explained:
We see faith, the root of all the Christian virtues, lessening in many souls; we see charity growing cold; the young generation daily growing in depravity of morals and views; the Church of Jesus Christ attacked on every side by open force or by craft; a relentless war waged against the Sovereign Pontiff; and the very foundations of religion undermined with a boldness which waxes daily in intensity. These things are, indeed, so much a matter of notoriety that it is needless for Us to expatiate on the depths to which society has sunk in these days, or on the designs which now agitate the minds of men. In circumstances so unhappy and troublous, human remedies are insufficient, and it becomes necessary, as a sole resource, to beg for assistance from the Divine power.
More than a century after the promulgation of this encyclical the evils identified by Pope Leo XIII have intensified to a degree that would have been inconceivable to most people in 1889. Thousands of innocent children are slaughtered every day with the approval of the governments that ought to be defending them, the sanctity of marriage is defiled by divorce, adultery and contraception, and the bonds between parents and their children are being deliberately targeted for destruction by the most powerful states and institutions in the world. Worst of all, the Pope himself is responsible for the spread of heresies which are leading the flock away from Christ and towards eternal damnation.
Pope Leo XIII urged the faithful, just as Our Lady would do twenty-eight years later at Fatima, to combat these evils through the prayer of the Holy Rosary:
At this proximity of the month of October, which We have already consecrated to the Virgin Mary, under the title of Our Lady of the Rosary, We earnestly exhort the faithful to perform the exercises of this month with, if possible, even more piety and constancy than heretofore. We know that there is sure help in the maternal goodness of the Virgin, and We are very certain that We shall never vainly place Our trust in her. If, on innumerable occasions, she has displayed her power in aid of the Christian world, why should We doubt that she will now renew the assistance of her power and favour, if humble and constant prayers are offered up on all sides to her? Nay, We rather believe that her intervention will be the more marvellous as she has permitted Us to pray to her, for so long a time, with special appeals.
But then, once more anticipating Fatima, he directed the faithful also towards St Joseph:
But We entertain another object, which, according to your wont, Venerable Brethren, you will advance with fervour. That God may be more favourable to Our prayers, and that He may come with bounty and promptitude to the aid of His Church, We judge it of deep utility for the Christian people, continually to invoke with great piety and trust, together with the Virgin-Mother of God, her chaste Spouse, the Blessed Joseph; and We regard it as most certain that this will be most pleasing to the Virgin herself.
He further explained:
the divine house which Joseph ruled with the authority of a father, contained within its limits the scarce-born Church. From the same fact that the most holy Virgin is the mother of Jesus Christ is she the mother of all Christians whom she bore on Mount Calvary amid the supreme throes of the Redemption; Jesus Christ is, in a manner, the first-born of Christians, who by the adoption and Redemption are his brothers. And for such reasons the Blessed Patriarch looks upon the multitude of Christians who make up the Church as confided specially to his trust – this limitless family spread over the earth, over which, because he is the spouse of Mary and the Father of Jesus Christ he holds, as it were, a paternal authority. It is, then, natural and worthy that as the Blessed Joseph ministered to all the needs of the family at Nazareth and girt it about with his protection, he should now cover with the cloak of his heavenly patronage and defend the Church of Jesus Christ.
Therefore the Holy Father instituted a new prayer to said after the Holy Rosary throughout the month of October. He intended this prayer to be said, not just in October 1889, but in October every year. As we prepare for the centenary of the Miracle of Sun, let us learn the lesson of St Joseph’s apparition at Fatima, and turn to him for help and protection.
St Joseph, terror of demons, pray for us!
Reminder: This coming Friday and Saturday are the First Friday and First Saturday of October.
***
Prayer of Pope Leo XIII to St Joseph after the Holy Rosary for the month of October
To thee, O blessed Joseph, do we have recourse in our tribulation, and having implored the help of thy thrice holy Spouse, we confidently invoke thy patronage also. By that charity wherewith thou wast united to the Immaculate Virgin Mother of God, and by that fatherly affection with which thou didst embrace the Child Jesus, we beseech thee and we humbly pray, that thou wouldst look graciously upon the inheritance which Jesus Christ hath purchased by His Blood, and assist us in our needs by thy power and strength.
Most watchful Guardian of the Holy Family, protect the chosen people of Jesus Christ; keep far from us, most loving father, all blight of error and corruption: mercifully assist us from heaven, most mighty defender, in this our conflict with the powers of darkness; and, even as of old thou didst rescue the Child Jesus from the supreme peril of his life, so now defend God’s Holy Church from the snares of the enemy and from all adversity; keep us one and all under thy continual protection, that we may be supported by thine example and thine assistance, may be enabled to lead a holy life, die a happy death and come at last to the possession of everlasting blessedness in heaven. Amen.
Litany of St Joseph
Lord, have mercy
Lord, have mercy
Christ, have mercy
Christ, have mercy
Lord, have mercy
Lord, have mercy
Christ, hear us
Christ, graciously hear us
God the Father of Heaven have mercy on us
God the Son, Redeemer of the world
God the Holy Spirit
Holy Trinity, one God
Holy Mary pray for us
Saint Joseph
Renowned offspring of David
Light of patriarchs
Spouse of the Mother of God
Chaste guardian of the Virgin
Foster-father of the Son of God
Diligent protector of Christ
Head of the holy family
Joseph most just
Joseph most chaste
Joseph most prudent
Joseph most brave
Joseph most obedient
Joseph most faithful
Mirror of patience
Lover of poverty
Model of artisans
Glory of home life
Guardian of virgins
Pillar of families
Solace of the wretched
Hope of the sick
Patron of the dying
Terror of demons
Protector of the holy Church
Lamb of God, who takes away the sins of the world, spare us, O Lord
Lamb of God, who takes away the sins of the world, graciously hear us, O Lord
Lamb of God, who takes away the sins of the world, have mercy on us
V. He made him lord of His House
R. And ruler of all His possessions
Let us pray
O God, Who, in Thine ineffable Providence didst vouchsafe to choose blessed Joseph to be the Spouse of Thy most holy Mother; grant, we beseech Thee, that we may be worthy to have him for our intercessor in Heaven whom, on earth, we venerate as our protector. Who livest and reignest world without end. Amen.
Editor’s note: Reprinted by permission from Voice of the Family.
MICAIAH BILGER OCT 4, 2017 | 1:39PM WASHINGTON, DC
A Hawaii abortion activist is suing the federal government in a case that could force every pharmacy in America to sell dangerous abortion drugs.
Dr. Graham Chelius, an ob-gyn in Waimea, Hawaii, is suing the FDA and the U.S. Department of Health and Human Services with the help of the American Civil Liberties Union.
In the lawsuit filed Tuesday, the ACLU argues that the FDA is restricting women’s access to abortion by requiring that the abortion drug be dispensed at a medical facility under the supervision of a certified provider (not necessarily even a doctor), KHON News 2 reports.
Chelius and the pro-abortion legal group want the FDA to allow pharmacies to give out the abortion drug mifeprex, also known as mifepristone or RU-486.
The abortion drug works by blocking the hormone progesterone, causing the uterine wall to break down and basically suffocating the unborn baby. A second abortion drug, misoprostol, typically is taken a day or two later to induce contractions to expel the dead baby’s body.
Because of the high failure rate and the risks involved with the abortion drug in later pregnancies, the FDA limited approval for use only in the first 49 days from the start of a woman’s last menstrual period. However, last year under pro-abortion President Barack Obama’s administration, the FDA changed its guidelines for the drug, allowing it to be used later in pregnancy and in smaller doses.
Now, abortion activists are pushing for even fewer regulations.
The suit, filed Tuesday in federal court in Hawaii, challenges a longstanding U.S. Food and Drug Administration regulation allowing the abortion pill, Mifeprex, to be dispensed only at a medical facility under the care of a certified provider. Among other requirements, those providers must pre-register with the drug manufacturer, keep the medication in stock, and be capable of providing a surgical abortion if complications arise.
Chelius argues those rules are unnecessary and cumbersome. Hawaii has one of the nation’s highest poverty rates, and the delays and expenses are sometimes insurmountable barriers, Chelius said. The case could have implications beyond Hawaii.
“The FDA restrictions create delays that often push medication abortion out of reach of my patients,” he said. “And some of my patients are simply unable to make this trip and instead have been forced to carry a pregnancy to term against their will.
Dr. Donna Harrison, executive director of the American Association of Pro-life Obstetricians and Gynecologists, told NPR that Chelius’ proposal really is very dangerous for women.
“Is the pharmacist going to answer her call at 5 in the morning when she’s suffering or needs some help? The pharmacist is not going to be there,” Harrison said.
Despite what abortion activists claim, the abortion drug is dangerous to women as well as their unborn babies, especially unsupervised. Mifepristone is responsible for killing millions of unborn babies in the United States and at least 14 women. In 2012, a U.S. Food and Drug Administration report indicated that 14 women in the United States alone died from using the mifepristone abortion drug and 2,207 women were injured by it.
Increasingly, abortion activists have been pushing for legal access to dangerous, do-it-yourself abortions, as well as abortions performed by nurses and midwives.
“All these things make it easier for the [abortion] clinic … but don’t necessarily make it safer for the woman,” said Randall O’Bannon with the National Right to Life Committee earlier this summer. “We’re seeing a full-blown promotion of do-it-yourself abortions.”
O’Bannon said some prominent pro-abortion researchers have been suggesting that abortion drugs be offered over the counter. And right now, a pro-abortion research group is offering women abortion drugs by mail as part of a study, he said.
The University of California, Berkeley has a Self-Induced Abortion Legal Team, a nonprofit group that “envisions a world” where abortion drugs are as easy to buy as the morning-after pill, according to the Christian Science Monitor.
Americans United for Life spokeswoman Kristi Hamrick told the Washington Post this spring: “These drugs are dangerous. They are deadly. If they are mishandled, they result in serious injury. To just distribute them and put them in an automatic dispenser like a can of soda is absolutely medical malpractice.”
CCLI is excited to announce the upcoming family conference titled “Families, become what you are!: Celebrating Humanae Vitae as the bedrock of family life.” The event is open to everyone and will be held on July 6-7, 2018, at the Sharonville Convention Center in Cincinnati, Ohio.
Co-sponsored by the Archdiocese of Cincinnati, this celebration comes just weeks before Humanae Vitae’s (HV) 50th anniversary and is designed to be a joyful way to thank God for the gifts of marriage, family life and the blessings that have come from the prophetic encyclical. The conference will inspire families to shine their light by strengthening them as a unit, and equipping them to be sent forth as missionary disciples in the world.
The two-day event will include well-loved speakers such as Janet E. Smith, Christopher West, Ben Nguyen and Eric Sammons; a Spanish track complete with all-Spanish workshops; daily Mass and adoration; a family-friendly concert; and — perhaps most anticipated of all — a 5-hour “Family Fun” session, set aside for families to create memories together on the town by exploring the Cincinnati’s Zoo, the Newport Aquarium, or another of many other attractions in our beautiful city!
While there will be many HV events throughout 2018 — HV’s 50th year — many will be philosophical, theological and academic. These are all very important facets of the anniversary to explore, but we decided to host a joyful celebration of lives lived according to HV and to thank the Church for consistently defending God’s loving will for the family and all of the blessings that flow from it.
In addition to the program on Friday and Saturday, there will be a pre-conference day on Thursday, July 5, reserved specifically for CCL volunteers from across the nation to enjoy valuable continuing education.
This special weekend will include keynote talks delivered by Janet E. Smith and Christopher West.
Janet E. Smith is a professor of moral theology at the Sacred Heart Major Seminary in Detroit, Michigan. She is currently serving a third term as a consultor to the Pontifical Council on the Family, and regularly speaks on the Church’s teaching regarding sexuality and bioethics. She has participated in many EWTN series and is no stranger to Catholic media. At our HV conference, Smith will discuss how the family acts as a path to holiness.
Christopher West is best known for his work making St. John Paul II’s Theology of the Body (TOB) available and accessible to all ages. He’s the founder of the COR Project and travels internationally to share the Church’s life-changing teaching on marriage, sex and the family. West will expound upon how HV and TOB are closely linked.
Friday and Saturday workshops include a variety of themes, including discussions on the feminine genius, Catholic manhood, TOB for children, the domestic church and much more.
The two-day conference is open to all families across the nation, and includes a childcare program for ages 3 to 18. Children two and under will remain with their parents. We’ve already extended invitations to 43 dioceses in nine surrounding states, including Illinois, Indiana, Michigan, Ohio, Pennsylvania, Kentucky, West Virginia, North Carolina and Kansas. If you’d like to spread the word in your own area, feel free to contact Angela Exner at aexner@ccli.org. We’d love to see all 50 states represented!
The conference center has a hotel attached and there are at least four other hotels on the same street. The Sharonville Convention Center is located less than 30 minutes north of downtown Cincinnati.
Keep an eye out on our social media for more information regarding registration and full conference details. Follow us on Facebook, Twitter, Instagram, or through our Family Foundations magazine.
— Forest Hempen Marketing and Communications Associate
An egregious surrogacy case has been filed with America’s highest court. Today, the Supreme Court is expected to announce whether or not it will hear the case of M.C. v. C.M.
The importance of this case cannot be overstated. If the Court decides to hear it, this will signal that the country’s highest judicial body recognizes that surrogacy raises serious ethical and constitutional issues. Its decision could be a game changer, with both national and international implications.
Currently, there are no national laws, regulations, or policies regarding surrogacy. Surrogacy is dealt with by the states, and there is no uniformity or consistency among their approaches. Whether by statute or case law, surrogacy has been moving inexorably toward legalization; 92 percent of US states allow surrogacy with varying levels of regulation. Only four states ban commercial surrogacy (Michigan, Indiana, New York and New Jersey). To make things even more complicated, state laws as written often differ dramatically from how they are actually enforced.
The United States’ Role in the Global Surrogacy Market
Most Americans probably do not know that the US is driving the surrogacy industry globally, on both the supply and demand sides. On the supply side, the US is second worldwide only to India in the supply of surrogates, many of whom are military wives. Among those who study the issue, it is estimated that between 40 and 50 percent of surrogate pregnancies in the US are commissioned by foreign buyers. There is a good reason for this: of the top commercial surrogacy markets in the world, only the US and Ukraine have not passed prohibitory legislation on it.
On the demand side, many American buyers go to India, Nepal, Mexico, Vietnam, Kenya, or Cambodia because surrogacy is far cheaper there than it is in the US. The cost of surrogacy in the United States ranges from $90,000 to $150,000. In India, it averages between $12,000 and $25,000. In fact, the US government via the State Department, in conjunction with the fertility industry, has been trying to get an international treaty passed at The Hague that would facilitate the global surrogacy industry. No wonder—surrogacy is a thriving, profit-driven international business worth approximately $6 billion.
In such a bustling global marketplace, it becomes easy to dehumanize the women and babies involved. It’s all too tempting to ignore the very real effects surrogacy has on the lives of the women who sell their bodies and the children who are bought and sold. The case petitioners have asked the Supreme Court to hear reveals the inherently exploitative nature of surrogacy, which clearly violates both constitutional and human rights.
The Story Behind the Case
Hollywood screenwriters couldn’t have invented a fictional story to match this very real case of M.C. v. C.M. The surrogate in question is a California resident who gave birth to triplets via emergency Caesarian section two months prematurely in February 2016. The buyer is a fifty-year-old single deaf and mute postal worker from Georgia who lives with his elderly parents. His mother is bedridden and requires daily nursing care. His father, who owns the house, stated before the children were born that he would not allow babies into his home.
The buyer demanded that the child he was ordering be male. Using his sperm, thirteen embryos were created with purchased eggs from anonymous sellers, and three were successfully implanted in the surrogate. When all three proved healthy and viable, the buyer initially accepted that there would be three children instead of one. Later, he changed his mind and demanded that the surrogate abort one child and put another up for adoption, admitting that he was incapable of caring for all three. The surrogate refused to abort and offered to take the undesired children. The buyer refused her offer, and his attorney, Robert Walmsley, threatened to sue the surrogate—an obvious scare tactic designed to intimidate the surrogate mother into complying with his client’s wishes. As a lawyer, Walmsley would have known that no US court would ever force a woman to have an abortion. Although it is common for surrogacy contracts to contain clauses requiring the surrogate to have an abortion (called “selective reduction” in the Orwellian language of the surrogacy world) if the buyer(s) demands it, the clauses are not legally enforceable.
In addition to acting as the buyer’s attorney, Walmsley also owns the surrogacy brokerage, Surrogacy International, that handled the transaction. No home visit and study—which routinely occur in adoption cases—were conducted to determine whether the buyer was a suitable potential parent. Walmsley wrote to Lesa Slaughter, an attorney who was supposed to represent the surrogate, “Triplets for a married couple is hard enough. Triplets for a single parent would be excruciating. Triplets for a single parent who is deaf is – well beyond contemplation.” Slaughter agreed.
Slaughter’s representation of the surrogate was neither competent nor independent. Slaughter was selected by Walmsley to represent the surrogate, and her fees were paid by the buyer. She wrote to the surrogate and incorrectly advised her that the buyer had a right to demand an abortion and that the surrogate would be legally liable if she refused.
Triplet pregnancies are very high-risk, requiring constant medical care and monitoring. Nevertheless, the buyer wanted to reduce the surrogate’s weekly clinic visits because he complained that they cost him too much money.
Throughout the pregnancy, the surrogate bonded with the children, and they bonded with her. Numerous studies have documented not only the bond that develops during pregnancy between mother and child but that their DNA is exchanged through the permeable placenta. As medical sociologist Barbara Katz Rothman puts it: “If you are pregnant with a baby, you are the mother of the baby that you’re carrying. End of discussion. The nutrients, the blood supply, the sounds, the sweep of the body. That’s not somebody standing in for somebody else to that baby. That’s the only mother that baby has.” Although the DNA linking the child to the woman whose egg provides half of his or her genetic code is clearly significant, the emerging science of epigenetics shows that the woman carrying the child also shapes his or her identity in permanent, deeply significant ways. To assert that a pregnant woman is not at all the mother of the child or children she is creating with her own body—regardless of whether the egg was hers—is a flat denial of biological reality.
A Surrogacy Nightmare
This surrogacy nightmare only became worse as time went on. On February 9, 2016, the Superior Court of California entered a judgment based upon a petition from the buyer’s attorney claiming to be uncontested, containing sworn statements that the surrogate wanted her rights terminated, when they knew that to be false. When the surrogate gave birth on February 22, the personnel at Kaiser Hospital in Panorama City took it upon themselves to enforce the state’s court order. They would not allow her to breastfeed the babies, know their condition, or even see them. They stationed security guards at the door of her hospital room and policed everyone who came to see her, demanding identification as if she were a prison inmate at a criminal incarceration facility.
The newborns were in the Neonatal Intensive Care Unit (NICU) for two months. This is another fact about surrogate births that is silenced by the industry. Since it is common to implant multiple embryos in surrogates to increase the chance of a surviving, healthy baby (there are no caps to the number of embryos that can be implanted in the US), twins and triplets frequently result. This vastly increases the probability that they will be born prematurely. The costs of NICU treatment are astronomical. The average cost for infants hospitalized in NICUs is around $3,000 per day. While the average cost of a healthy baby born at full term is $2,830, the average cost for a premature baby is $41,610.
When she was released from the hospital, the surrogate refused the remaining $19,000 payment she was owed. She had filed an appeal before the babies were born, and at the end of March she filed a petition for a writ of supersedeas, which suspends the authority of a court to execute a judgment in a case that is being appealed. The writ was stayed, yet Kaiser Hospital continued refusing to allow her to see the babies. In April, the appeals court denied the writ and vacated the stay order. The California courts refused to consider the surrogate’s complaints and refused to give her a hearing.
In January 2016, the surrogate had filed a civil complaint in the Superior Court seeking a declaration that California’s Gestational Surrogacy Statute—Family Code 7962—was an unconstitutional violation of her rights and the rights of the children. She sought custody of the children based on their best interests. She also filed a complaint in federal district court.
California’s Surrogacy Law Violates the Fourteenth Amendment
The main legal issue is the denial of Due Process and Equal Protection rights under the Fourteenth Amendment.
California’s surrogacy law violates the substantive due process rights of the children, their fundamental liberty interest to maintain their relationship with their mother, and their due process liberty interest to be free from commodification and state-sanctioned and enforced purchase of family rights. Under California’s law, children are purchased and placed with adults regardless of whether those adults are capable of properly raising or caring for children, whether such placement is in the children’s best interest, or whether the surrogate mothers desire to and are better able to care for the children.
The law also violates children’s equal protection rights. California refuses to place children created through surrogacy based on what is in their best interests, as it does forall other children inall other disputed custody situations.Judicial rulings completely disregard whether or not child buyers may be harmful to the child; all that matters is the contract.
In other words, property (in this instance, children) takes precedence over all—the child’s health and welfare, human rights, identity, biological and genetic relationships, and on and on. According to California’s surrogacy law, the best interests of the child cannot be considered, because he or she is a purchased commodity subject to property and contract law.
The case also presents serious federal constitutional issues concerning the surrogate mother’s fundamental due process rights in maintaining her relationship with the children she created, and in not being exploited.
A Stunning Denial of Due Process
What ensued in this case was a stunning denial of any semblance of due process. Judge Amy Pellman of the Superior Court of Los Angeles County denied the surrogate’s application for a continuance. She summarily ruled that the buyer was entitled to a judgment terminating the relationship between the surrogate mother and the children. She proceeded as if the petition was uncontested and barred the surrogate from producing any evidence. When the surrogate’s attorney brought up the buyer’s inability to take care of the children, Judge Pellman stated, “There’s no need for home study. There’s no need for representation of the children.” When counsel asked whether the well-being of the children was going to be considered by the court, Judge Pellman replied: “What is going to happen to these children once they are handed over to C.M. [the buyer], that’s none of my business.” The court observed that a best interest determination is required in other actions but surrogacy is an “exception.”
The summary disposition of the entire case, without discovery, evidence, the opportunity to present the surrogate’s case, and without the buyer being required to answer the allegations of the Answer and Counterclaim is an outrageous insult to any concept of “justice” and respect for the constitutional rights of US citizens.
As this case horrifyingly demonstrates, surrogacy is out of control in the United States. All those who care about justice, the Constitution, and human rights must fervently hope that the Supreme Court will decide to hear this case.
Surrogacy is creating a generation of children severed from biological and genetic identity and a breeder class of marginalized women. Both are being transformed into commodities for sale on the global marketplace. This can only be accepted and condoned by a society untethered from any sense of ethics, human rights, dignity, or moral values. When the primal bond—as ancient as humankind itself—between mother and child is destroyed, what will be left?
Kathleen Sloan is a former member of the board of directors of the National Organization for Women (NOW), Executive Director of Connecticut NOW, a consultant on third-party reproduction issues, and co-author of the book Race and the Genetic Revolution: Science, Myth and Culture. She has a master’s degree in International Relations and has traveled the world advocating women’s rights, including at the UN Human Rights Council in Geneva and the UN Commission on the Status of Women in New York. She co-authored a brief for fifteen feminist academics and advocates as amici curiae in support of the petitioner (the surrogate) in the case discussed above.
On Tuesday, the members of the House of Representatives will assemble in the U.S. Capitol Building to cast their votes yea or nay on the Pain-Capable Unborn Child Protection Act–H.R. 36.
The two-fold organizing principle that undergirds the pro-abortion playbook will be on display in force: an appeal to authority and rhetorical sleight of hand. We will hear how the Medical Establishment is firm in its preordained conviction that a 20-week old unborn child can’t experience horrific pain as she is ripped apart. Indeed some go so far as to insist the child can’t experience pain until the 29th week–or perhaps not until birth!
But as National Right to Life has explained
By 20 weeks after fertilization, all the physical structures necessary to experience pain have developed. Unborn children at 20 weeks fetal age react to painful stimuli, and their hormonal reactions consistent with pain can be measured. For the purposes of surgery on unborn children, fetal anesthesia is routinely administered and is associated with a decrease in stress hormones compared to their level when painful stimuli are applied without such anesthesia.
Supplementing this is the insistence that abortions at 20 weeks (and beyond!) are as rare as births at Planned Parenthood. But, of course, these abortions aren’t “rare” at all.
Based purely on published surveys, there are about 275 sites that provide abortions past the 20-week fetal age (22 weeks LMP) line contained in H.R. 36. But there are reasons to believe that such surveys under-estimate the prevalence of late abortions. There is growing evidence
Remember that abortionists have zero incentive to accurately date how old the baby is and that many of the states that abort the most babies have no reporting requirements! So whatever number is tossed out tomorrow will radically underestimate the number of abortions performed at 20 weeks and beyond.
An additional point. NRL News Today has written a small library worth of stories about convicted murderer, Philadelphia abortionist Kermit Gosnell. We quoted most of a 200+ page Grand Jury on a man eventually convicted of three counts of first-degree murder and one count of involuntary manslaughter.
On page 171, we read that for the years 200-2010, Gosnell reported one second-trimester abortion.
Yet it appears (pp. 26-27, 88) that Gosnell probably performed thousands of second-trimester and third-trimester abortions during that decade. Multiple other practitioners who perform large volumes of late abortions have also failed to report or not been required to report.
Conclusion is the same: an untold but large number of second and third trimester abortions are not reported.
We will have more to say, both later today, and tomorrow. Just do not allow yourself to be fooled by the pro-abortion propaganda line that will be reflexively, uncritically, and with enthusiasm reported by the Establishment Media.
This is a very important vote, a stepping stone to ending an atrocity of astonishing proportions.
LifeNews.com Note: Dave Andrusko is the editor of National Right to Life News and an author and editor of several books on abortion topics. This post originally appeared in at National Right to Life News Today —- an online column on pro-life issues.
LYON, France, October 2, 2017 (LifeSiteNews) — No human being is ever a “vegetable,” but the phrase “Permanent Vegetative State” certainly described “Jack.”
If someone falls into a “Persistent Vegetative State” (PVS), being completely unaware and unresponsive for a whole year, their condition is diagnosed as permanent.
Colloquially speaking, Jack (a pseudonym) looked awake, but he “wasn’t there.” Now, French doctors have shattered that medical conviction by reviving the 35-year-old man who spent 15 unresponsive years after a severe car accident.
Doctors implanted a device to stimulate Jack’s vagus nerve, the longest of the involuntary nerves that runs from the base of the brain to the abdomen. Besides helping regulate heart, lungs, and digestive tract, the nerve has a lot to do with wakefulness and attention.
They artificially stimulated Jack’s vagus nerve every day for a month. The results produced a medical science breakthrough perhaps greater than the discovery of penicillin.
Their subject responded for the first time in 15 years.
Jack didn’t gain full awareness, but he responded to simple requests. He followed objects with his eyes. He could turn his head when asked. He stayed awake listening to a therapist read a book. His eyes opened wide when someone suddenly got in his face.
In medical terms, he went from a “permanent vegetative state” to a minimally conscious state. “He cannot talk, but he can respond. Now he is more aware,” study leader Angela Sirigu of the Institute of Cognitive Science in Lyon said.
His dramatic change was documented in brain scan “before” and “after” comparisons. (PIC of brain scan comparison)
To the pro-life layman, this is a major vindication.
“Ever since Terri Schiavo, writing about the wrongness of removing feeding tubes from patients diagnosed with persistent unconsciousness (PVS) … is like spitting in the wind,” columnist Wesley J. Smith wrote. “Patients in this condition are often dehydrated to death by having their feeding tubes removed, which takes up to two weeks. … People with minimal awareness are legally dehydrated in all 50 states.”
“This should be good news that should cause us to pause in removing feeding tubes from the unconscious,” Smith advised. “Some bioethicists even want such removals to become standard” after a year or two, he warned.
Some still defend starving or painfully dehydrating patients “because they may be in horror at their impaired condition or otherwise suffering.” But Smith said a major study of patients who appeared completely unconscious but proved later to actually be awake and aware “shows that most are ‘happy,’ and majorities would not want euthanasia.”
“Let’s care for these seriously disabled patients — both apparently unconscious and conscious — as full and equal members of the moral community,” Smith concluded. “And let’s think twice before removing sustaining treatment that can only have one result: a protracted and perhaps painful death.”
Smith noted that 40 percent of PVS diagnoses are wrong, but it now seems possible, at least thinkable, that some who actually do fall into such a state may be revivable.
Jack’s results were published in the journal “Current Biology.”
Niels Birbaumer of the University of Tübingen pointed out that “many of these patients may and will have been neglected, and passive euthanasia may happen often in a vegetative state.” Jack’s example, Birbaumer said, “is a warning to all those believing that this state is hopeless after a year.”
National Geographic’s Karen Weintraub speculated that “if the method is shown to work in a broader population, vagal nerve stimulation could give people with limited consciousness at least a bit of free will and the ability to communicate.”
Hannah Devlin of The Guardian wrote that Jack’s success “offer(s) hope to the families of patients in PVS that it may one day be possible to re-establish some basic form of communication.”
University of Birmingham cognitive neuroscientist Damian Cruse called Jack’s story “pretty exciting.” “If you can just push the patient over the threshold so they can start responding to external stimulation you can maybe help them follow speech therapy and get them to a level where they can start to communicate,” he said.
In recent years, a brain-computer interface has been developed that facilitates paralyzed patients previously thought in a “vegetative state” to communicate basic “yes” or “no” answers to let loved ones know what they want, feel and need.
Vagal nerve stimulation has been used with epileptics, those with neurological disorders, and those suffering from recent brain injury.
Smith exhorts pro-lifers to “never call (human beings) ‘vegetables,’ a term as denigrating and dehumanizing as a racial epithet.”
Cardinal Carlo Caffarra – who died just a few weeks ago – revealed in 2008 that shortly after Pope John Paul II charged him with founding the Pontifical Institute for the Studies on Marriage and the Family he had written to Fatima visionary, Sr. Lucia, asking for her prayers. To his surprise, a few days later he received a lengthy response from Sr. Lucia. Included in her letter was this startling statement:
The final battle between the Lord and the reign of Satan will be about marriage and the family.
However, Sr. Lucia also offered words of encouragement to Cardinal Caffarra, who had just stepped into the front ranks of this battle, adding: Don’t be afraid, because anyone who works for the sanctity of marriage and the family will always be fought and opposed in every way, because this is the decisive issue.
Sr. Lucia concluded: However, Our Lady has already crushed its head.
How can we not be overwhelmed by these words, simultaneously troubling and comforting, when we look around and see that not only our secular culture but even Holy Mother Church is being convulsed with dissension precisely in relation to fundamental questions surrounding marriage and the family?
The enemies of Christ have long set their eyes on the family, recognizing that the family, as the domestic church, first government, first school, first hospital, first economy and the first mediating institution of society, is the primary obstacle to their moral revolution.
Indeed, in many respects the history of this past century is the history of the attack by the anti-Christ on the family – an effort which appears only now to be reaching its true climax, as we witness divorce, contraception, pornography, cohabitation, and even so-called same-sex “marriage,” and transgenderism becoming the nearly unquestioned societal norm!
Because of short-sightedness, many think that the assault on marriage began with the attempt to legalize same-sex “marriage.” Nothing could be further from the truth! What we are witnessing now is but the culmination of a revolution launched many, many decades ago, long before most of us even heard of same-sex “marriage”!
When people hear that Our Lady warned at Fatima that the “errors of Russia” would spread around the world “raising up wars and persecutions of the Church,” they naturally think of the communists’ revolutionary economic and political ideology; which, indeed, caused innumerable wars, and led to the violent deaths of untold millions. But we must not forget that Marx’s ideas – which the Russian revolutionaries put into practical effect and exported globally – were not merely political.
In The Communist Manifesto, Marx was clear that he believed the nuclear family was a tool of the capitalist bourgeoisie, and must be abolished to pave way for his revolution. Marx believed the family should be replaced with a “community of women” – i.e. a radical form of “free love” – and that children should be held in common and educated by the state.
Attacking the family was one of the very first things Vladimir Lenin and the other communists did after they seized power in Russia: replacing religious marriage with civil marriage, legalizing practically on-demand divorce, and handing over all education to the state.
In 1926, a reporter for The Atlantic visited the Soviet Union, and exposed the horrific impact of these innovations: a catastrophic rise in divorces – in many cases initiated by men who serially abandoned young and vulnerable women – as well as abortions (a previously nearly unheard-of crime in Russia), and the number of abandoned children. The article in The Atlantic is difficult to read, not only because of how it depicts the suffering of the Russian people at that time, but because of the disturbing parallels it bears to our current age.
Ironically, the Soviet Union was soon forced to abandon and even completely reverse many of their anti-family policies. The social and financial costs of the breakdown of the family were drastically weakening the state, threatening its very existence! Thus, the Soviet Union learned the hard way the truth summed up so pithily in the Catechism of the Catholic Church, namely: The well being of the individual person and of both human and Christian society is closely bound up with the healthy state of conjugal and family life. [CCC, 1603]
But the Communist-Marxist hatred of the family did not go away. On the contrary, Marx’s radical ideas were seized upon and expanded upon by the so-called “cultural Marxists”: a loose-knit group of ideologues who have inherited the Communist loathing of “bourgeois” Judeo-Christian Western civilization and revolutionary zeal, but who have recognized that the real revolution has to take place at the cultural level, especially in regards to sexual morality.
In many respects, where the Communists failed in 1918, the sexual revolutionaries of the 1960s have succeeded: overturning the old moral order, and embedding Marx’s ideas about the family so deeply within law and culture that it is hard to imagine how their revolution might be reversed.
So many of the ills of the modern world can be traced to this demolition of sexual mores and of the family – not least of which is the mass apostasy of the West from its Christian faith, a phenomenon which is only accelerating. After all, with the wholesale destruction of the family, the domestic church, the “seedbed of faith,” what hope does the Church Herself have to impart and nourish a faith that is thwarted at every step from the moment a child comes into the world?
That of course was the goal of the atheistic revolutionaries from the very first. The destruction of the family itself was never the final goal, but rather only the means: the most assured path of eradicating the Kingdom of God, and setting up the kingdom of this world.
And yet, rather than despair, we must call to mind the words of Sr. Lucia, who reminded Cardinal Caffarra that Our Lady has already crushed its head. In other words, victory in this war is assured.
And yet, that does not mean that there is not much work (and suffering) to do in the meantime. Listen to Our Lady’s words at Fatima, so simple, so direct, and so powerful:
I have come to warn the faithful to amend their lives and ask for pardon for their sins. They must not offend Our Lord any more, for He is already too grievously offended by the sins of men. People must say the Rosary. Let them continue saying it every day.
And
Sacrifice yourselves for sinners and say often, especially when you make some sacrifice, ‘O my Jesus, this is for love of You, for the conversion of sinners, and in reparation for the offenses committed against the Immaculate Heart of Mary.
Right now the Church’s mission – and our mission – is to defend Christ’s crystal-clear teaching about the nature of and indissolubility of marriage, not as an oppressive imposition on our freedom, but rather as the only route to true freedom: the only path towards creating a true culture of love!
But the only sure path forward is to listen to our Blessed Mother’s requests: to repent, to pray (especially the Rosary), and to sacrifice for the salvation of sinners. If we do these three things, not only will our own families be strengthened, but the tide will turn, and the enemies of the family will begin to retreat.
In this 100th anniversary year of Fatima, let us pray: Our Lady of Fatima. Pray for us!
Read more at: http://www.nationalreview.com/article/451955/hugh-hefner-playboy-legacy-despair-pornography-marriage-family
Hugh Hefner didn’t invent pornography, and it would no doubt be thriving today even if he hadn’t founded Playboy magazine those many years ago. After all, man is fallen, and somebody would have filled that depraved niche in American life. Hefner, however, played his part, and the part he played was immensely destructive to our nation’s cultural, moral, and spiritual fabric. Hefner mainstreamed porn, he put it in millions of homes, and he even glamorized it — recasting one of America’s most pathetic industries as the playground of the sophisticated rich. He then grew to a ripe old age, consorting with women young enough to be his granddaughters. He was America’s most famous dirty old man.
And now he’s dead. May God have mercy on his soul.
It’s hard to calculate the damage he did, but the cultural rubble is all around us. My generation is perhaps the first to grow up with easily accessible porn. Every one of us knew whose father had a Playboy subscription (only the scary pervs subscribed to Penthouse or Hustler), and their kids knew exactly where dad kept his stash. They’d sneak out old issues, bring them to school, and pass them around. Before teens could rent porn on tape, they could see porn on the page, and once they saw it, they were hooked.
The effects have lasted a lifetime. Boys grew up believing they were entitled to sex on demand, and the sex would always be amazing. They learned to grow bored of the “same old thing” and instead to seek new adventures. They learned that monogamy was confining, that promiscuity was liberating, and that women should always be hot. The normal female form was no longer enough. It had to be enhanced, sculpted, and waxed.
Though that kind of reality can’t exist for the vast majority of men, that didn’t stop the desire. So, they did and do the pitiful thing — retreated to bathrooms and bedrooms and masturbated nonstop to the women they could never have and the life they’d never live.
How many families have broken to pieces when a wife discovers her husband’s secret addiction and realizes that she’s not enough — that she’s never been enough — and he spends much of his life fantasizing about thousands of others? How many men have grown to hate themselves for their psychological dependence on the saddest of habits? The testimonies from porn nation are devastating.
“I watched so much porn that I can’t really enjoy sex with my wife.”
“He wants me to be something I can’t. I’ll never be as good as the girl on the screen.”
“I can’t imagine being content with just one woman. I’ve had sex with thousands in my mind.”
To see men become addicted to porn is to watch character formation in reverse. Their integrity and fidelity unwind before your eyes. They lie habitually to cover the extent of their habit, even when their wives are allegedly “open” and sexually liberated. After all, if she knew how much he watched or exactly what he looked at, even she would be shocked. The screen alone is never enough, the wife is never enough, and the addict so often seeks mistresses, prostitutes, or both.
Another family breaks. More lives fall into despair.
To see a man become addicted to porn is to watch character formation in reverse. All this is known. Everyone has seen it happen in their churches, in their neighborhoods, and in their families. This cycle has likely happened to thousands of men who’ll read this column. And yet, the secular, progressive guardians of our public morality — you know, the people who think you’re a horrible person if you don’t recycle or if you use the wrong pronouns — all so often don’t just tolerate but celebrate the sexual “liberation” that is part and parcel of porn nation.
So many A-list celebrities spent time at the Playboy Mansion, especially at its peak, that there was a time when one could wonder who hadn’t embraced Hef or the magazine he made. Our president has. The evidence is on his office wall. These were the people setting the tone for American culture. These were the people mocking the values that kept families strong. These were the people who were teaching a nation that fulfillment could be found in sex, and that the joy of sex was worth more than marriage itself.
They were wrong, and the cultural harm done outweighs the cost of botched presidential elections, bad congressmen, or a judiciary riddled with knaves and fools. The cultural harm done is even now ripping kids from parents and husbands from wives. When I think of Hugh Hefner, yes I mourn, but I mourn because the bitter fruit of his life’s work has helped poison the families of people I know and love. He is gone, but his legacy lives on. And his is a legacy of despair.
Shawn Carney and David Brando Sep 27, 2017 | 1:03PM Washington, DC
The biggest 40 Days for Life campaign yet is finally here! And we need YOU to step forward in faith to pray and fast for an end to abortion!
40 Days for Life begins TODAY — and continues through November 5 — in more than 375 locations across the United States and 24 other countries … including multiple locations in nations such as Canada, Colombia, Croatia, Mexico, Romania and the United Kingdom!
It’s important to prepare your heart for the campaign — this is, after all, a spiritual battle we are entering — so that’s the topic of this week’s edition of the 40 Days for Life podcast
It is because of your prayers that God has provided so many blessings — with 13,305 lives that have been saved from abortion … 154 abortion workers who’ve experienced conversions and left their jobs … and 90 abortion centers that have closed forever after 40 Days for Life vigils outside their doors.
Greenland, New Hampshire
We’re used to seeing pictures of snow at the 40 Days for Life vigil in Greenland.
But Jackie in Greenland says this campaign kicked off “on a sweltering, humid sunny day with temperatures rising to unseasonable upper 80s.”
So … folks gravitated towards “the bit of shade we could find.”
The rally focused on assistance available to women in unplanned pregnancies — “many options available free of charge in our local pregnancy resource centers,” Jackie said.
“We added the abortion pill reversal hotline to our list of resources,” she said, and an upcoming post-abortion healing retreat was highlighted.
“The majority of cars passing buy gave positive waves and thumbs up signs,” Jackie added, “which is always encouraging!”
Colorado Springs, Colorado
“We are off to a good start!” said Michele in Colorado Springs, which is beginning its 18th 40 Days for Life campaign.
“At our kickoff, we were in competition with a cement mixer that was pouring a new sidewalk,” she said. “We had a bullhorn, so we prevailed over the noise.”
On the way home, one rally participant saw a pregnant woman with a sign asking for help. The volunteer told the woman about the local pregnancy center and other forms of assistance that are available locally.
“It is a reminder to be aware at all times of people who are in need of help,” Michele said. “Perhaps the best help isn’t giving them money, but leading them to a place in the community where they can receive ongoing support.”
LifeNews.com Note: Shawn Carney is the campaign director for the 40 Days for Life pro-life prayer campaign against abortion.
A Catholic Church leader urged the United Nations on Monday to recognize that the right to life is the most fundamental of all human rights.
Archbishop Paul R. Gallagher, the Vatican’s Secretary for Relations with States addressed the UN in New York with a strong message about religious liberty and the right to life for all human beings, from conception to natural death, Breitbart reports.
“Putting people always first means protecting, at every stage and in every circumstance, the dignity of the person, and its human rights and fundamental freedoms,” Gallagher said, “and in a specific way, the rights to life and to freedom of religion from which all other rights flow and which are therefore the common foundation of the pillars of peace and security and integral human development.”
Gallagher emphasized how fundamental these two rights are to everything else in society.
“These two human rights are indivisible from those other rights and fundamental freedoms relating to a dignified spiritual, material and intellectual life for each citizen and for their families – among others, the right to food, the right to water, the right for housing, the right to a safe environment and the right to work,” he said.
Here’s more from the report:
The Vatican’s insistence on the primary importance of the right to life and the right to religious freedom comes just as news is spreading of grave violations of these very rights.
As Breitbart News reported Tuesday, China is tightening its control over religious organizations in the country, as President Xi Jinping moves toward a situation of “total religious control.”
Church officials fear that new norms regulating religious activities, set to go into effect on Feb 1, 2018, will be used to “further suppress religious activities” rather than pursuing their stated aim of protecting national security.
At the same time, abortion giant Planned Parenthood continues to combat all restrictions on the abortion industry, including laws that would ban sex-selective abortions and those aimed at eliminating children with Down syndrome.
The United Nations frequently pushes a pro-abortion agenda across the world. However, vocal advocates from pro-life countries, religious groups and others have been standing up to the international agency and demanding that it recognize every human being’s rights.
September 25, 2017 (HLI) — There are two very important upcoming Vatican meetings we should pay close attention to: the Pontifical Academy for Life (PAV) on October 5-7 and the Pontifical Academy of Sciences (PAS) on November 2-4.
This will be the first time the PAV meets since Pope Francis inaugurated the Academy’s new statues in October 2016 and appointed a fresh slate of members. Meanwhile, in its second meeting of the year, the PAS once again will focus on the controversial subjects of population control and climate change: “Health of People, Health of Planet and Our Responsibility: Climate Change, Air Pollution and Health”.
As you may be aware, there is growing concern among pro-life and family leaders right now about a seeming lack of focus by the two Academies upon the most directassaults against human life [and the family] by anti-life governments, academic institutions, the United Nations and its agencies, NGOs, and international corporations.
In other words, while there are numerous crucial issues affecting human life and the family that demand discussion – i.e. climate, pollution, governmental corruption, immigration, war, peace, health care, etc. – there can be no authentic progress on any of these issues until we recognize the need to protect the right to life of everyhuman life, born and unborn. All other issues hinge upon this fundamental and inarguable truth. And clearly this must be the unwavering starting point for any discussion within the Church.
Saint [Mother] Teresa of Calcutta, who exposed the heinous attack on the dignity of all human persons, especially the marginalized, poor, sick, vulnerable, and abandoned, fully understood the consequences when Life is treated with indifference:
We must not be surprised when we hear of murders, of killings, of wars, of hatred. If a mother can kill her own child, what is left but for us to kill each other.
But as we confront the death peddlers and their “religious” campaign against Life and Family, some Catholics and pro-life activists are anxious over the apparent lack of leadership from some members within the Church to stand in the breach and uphold Church teaching on Life and Family, without compromise. This is certainly true regarding the PAS’s approach to addressing population questions, which has seen the PAS recently invite notorious population controllers like Steve Ehrlich to address PAS conferences, largely without any authentic Catholic voice to counteract their claims and agenda.
We often hear from population doomsayers that “the population of the world is doubling every 35 years” and “we have 90 million new mouths to feed every year.” In reality, the rate of world population increase has been declining steeply since 1970, when it was 2.05 percent per year, to the current rate of 1.09 percent per year.
According to the United Nations Population Information Network, if current population rates hold steady the population of the world will stop growing between 2050 and 2075. At that point, the world population will begin to rapidly decline. For the doomsayers, this is welcome news; yet, we are already seeing the negative consequences of a declining population. Look at Europe where the continent is actually losing more than one million people per year, and will lose nearly half of its population by the year 2100.
What will be the consequences and ramifications of this demographic winter? The political and economic situation in Greece offers frightening insight.
Overpopulation doomsayers and death peddlers love to point toward larger overpopulated urban centers like Manila, Mexico City, New Delhi, and Nairobi, but never expose the real reason for such migration of peoples.
They would have us – the Church – believe and accept as doctrine that overpopulation is humanity’s greatest plague. Don’t be duped. It is not overpopulation that threatens humanity, but something with a more sinister origin – population maldistribution. This maldistribution has been facilitated by political and governmental corruption, misguided national and international policies, lack of authentic economic and social development, and armed conflicts – in other words, sin. This has caused millions to flee from their homes and countries, seeking places where they can find safety and provide for their families.
Consider, for example, the large migrant populations of Macau, Taiwan, and Dubai. What draws tens of thousands of Africans, Indians, and Filipinos to these areas? It is the need for work and basic necessities. Because of lack of development and corruption in their own nations, many are forced to leave their homes and families in search of opportunity – merely to survive.
This migration of peoples has also negatively affected the family. Among these peoples we have seen a steady growth in infidelity, divorce, promiscuity (fornication), abortion, and pornography addiction caused by long-term separation from their support structures and families. Yet, very few are talking about this deadly reality – even within the Church.
The agenda of population controllers and their solution to humanity’s struggles is to provide greater access to contraception and abortion – especially with the goal of diminishing growing populations in the developing world. However, their agendas and methods do not resolve corruption, poverty, or maldistribution. They do nothing to further the goals and potential of a nation or its peoples – they merely make larger poor families smaller poor families.
Emil Hagamu of Dar es Salaam, HLI’s Regional Director for Anglophone Africa, says it quite poignantly:
Africans need assistance with infrastructure. We need to have good roads. We need to have good hospitals and medicines. We need to have good schools. We don’t need condoms. We don’t need contraception. We don’t need abortion.
Since 1996 the United States and other developed nations have spent over $65 billion on anti-life programs in Africa – $150 billion in countries around the world – with little to show for it except paternalism, exploitation, and violation of peoples and cultures.
The real task at hand is to help developing countries to invest in their own nation and people and to foster laws, policies, and culture that value the dignity of every person, protect private property and entrepreneurship, and prioritize educational opportunities.
A person who is deprived of something he can call “his own”, and of the possibility of earning a living through his own initiative, comes to depend on the social machine and on those who control it. This makes it much more difficult for him to recognize his dignity as a person, and hinders progress towards the building up of an authentic human community. – Saint Pope John Paul II, Centesimus Annus, ¶ 13
Of course, in our anti-life culture [Culture of Death] anyone holding this unwavering position about the dignity of human life and duty to defend it is immediately labeled as radical, close-minded, and rigid – marginalized from any legitimate conversation and debate.
But my hope is that the two Vatican agencies mentioned at the beginning of this article will give a heroic, counter-cultural witness to truth about Life and Family. This is the Church’s duty: to uphold truth, point out injustice, and defend the vulnerable. She must denounce all violence against human dignity, beginning with the assault on the unborn.
May these agencies, who have the power to make a difference in this debate, begin with this fundamental principle: every human person is made in God’s image, is called to share in His creative effort to transform the world, and is destined for eternal life with Him.
There can be no authentic development of peoples, nations, and cultures as long as Life and Family are threatened.
In a recent piece for the Wall Street Journal (paywall), Bill and Melinda Gates wrote about their support for continued health investments as a way to reduce poverty in developing countries. They identified the President’s budget recommendation to stop funding contraception as a major concern, despite Congress’ likely continuation of contraceptive funding. The essay raises awareness about the much-needed aid to some of the poorest countries in the world but misses the mark on what women and families in these countries really need and want.
Senegalese women
Why aren’t more Senegalese women using contraceptives?
The Gates recount efforts to improve contraception access and awareness in Senegal as a success story for foreign aid. The Senegalese government has clearly made contraceptive provision a priority, but it’s not at all clear that Senegalese women agree. According to the article, only 10% of women of reproductive age in Senegal were taking birth control in 2011. Yet, despite a “massive public awareness campaign” and drastically reducing shortages, five years later the number of women using contraceptives is still only around 15% (described in the article as a percentage increase of “more than half”).
The article indicates that women’s choices are limited by cultural factors, and that may be part of it. But there is also good evidence that “culture” isn’t the whole story. A 2016 report published by the Guttmacher Institute, a strong supporter of increasing contraception use, found that most women in the sub-Saharan African countries surveyed knew about contraceptives and could access them (p. 28). The report presented itself as an answer to “unmet need for contraception,” a figure calculated by the number of fertile women who are sexually active, want to delay pregnancy, but aren’t using “modern methods of contraception.” This number is often used to justify increasing funding to improve contraceptive access.
Yet most of the women surveyed had reasons that increasing access won’t address. These included infrequent sex, not having returned to fertility following pregnancy, and sub-fecundity (p. 35). A quarter of married women also cited personal objections to contraceptive use, and of those women, three in five said they personally opposed using contraceptives (id.). Among unmarried women, very few cited cost or lack of awareness for non-use, but over a quarter of unmarried women in the African countries in the study said they were concerned about side effects, health risks, or inconvenience (p. 37). These figures are reflected to a greater or lesser extent in other developing countries, too, where many women discontinue or switch contraceptive methods due to side effects.
Why are we telling women they’re wrong about their choices and priorities?
As the above report discussed, many women in developing countries (like their counterparts in developed nations) have both health and ethical concerns. Many women have experienced side effects due to contraceptive use. Informational campaigns may address those concerns, but full information about how hormonal birth control works may also raise new questions. Moreover, transposing our medicated approach of family planning to countries where basic medical support and options are scarce fails to address the most pressing health needs. Preventing pregnancy is only one aspect of reproductive health care; perfect contraception access is not a substitute for skilled birth attendants, prenatal care, or adequately stocked clinics for childbirth.
Ethical values deserve no less consideration than concerns about side effects; in fact, as rights of conscience are enshrined in international human rights law, they deserve more. When women tell us they aren’t interested in contraceptives, we should find ways to help them achieve their family planning goals and meet their health needs in ways that are acceptable to them, rather than pressure them to conform to certain values and ideologies.
Any campaign to promote a particular health commodity must respect patients’ dignity and autonomy. A bedrock principle of this imperative is informed consent. Knowing that a contraceptive method will prevent pregnancy, an explanation of the side effects and potential health risks, such as blood clots, and instructions to manage or stop treatment are essential to realizing the human right to the highest attainable standard of health. Developed countries often fail to ensure women have the information they need to make an informed choice; we should not export this problem to developing countries.
Bill and Melinda Gates
How can we meet women’s needs?
We have to meet people where they are, cognizant of their values, cultures, priorities, and environment. Culture- and values-sensitive information is the best way to ensure that women and couples make the best choices for themselves. Fertility literacy ensures that women (and men) understand how their bodies work, the health-hormone connection, and how various methods of family planning affect their health and hormonal levels.
Fertility awareness methods of family planning often provide this essential information, have a proven track record of sustainable use in poor countries, and are consistent with the cultural norms of local populations. These programs teach women and couples about their hormonal health and about the ovulatory cycle, what a healthy cycle looks like, when to get medical help for hormonal imbalances, and how to use this knowledge to achieve or avoid pregnancy. Many women and couples find this knowledge empowering and helpful, and whatever decisions they make afterward are truly informed. Media campaigns promoting contraceptive use simply cannot compete with actual patient knowledge and understanding in terms of informed decision-making and better health and education outcomes.
Informed patients not only make informed choices; they get better healthcare because they know when they need it. The birth control pill has been used as a treatment for a wide variety of health concerns, from debilitating pain to persistent acne, without much attention to what is causing the problems. While the pill can manage symptoms, suppressing natural hormonal activity does not treat hormonal imbalances. Diagnosing and treating the specific hormonal imbalances is the only way to actually restore health.
When we take the focus off the pill and put it onto women, where it belongs, it becomes clear that the real shortage is of knowledge. By educating women and doctors about hormonal health, we can help women improve their health and achieve their fertility goals. That, Mr. and Mrs. Gates, is something worth investing in.
Nadja Wolfe, JD, is the Director of Advocacy for World Youth Alliance and a policy consultant for Fertility Education & Medical Management (FEMM)
TEXAS RIGHT TO LIFE SEP 22, 2017 | 3:15PM WASHINGTON, DC
Pro-Life Texans have long known the danger of giving hospital administrators power over life and death decisions. Under the anti-Life Texas 10-Day-Law, countless vulnerable Texans have been denied life-sustaining treatment against their written or spoken wishes or the wishes of their medical surrogate. Patients like Chris Dunn have been denied their rights when a hospital panel decides their cases are “futile.”
The story of the Way family shows why protecting a family’s right to make medical decisions for an ailing loved one in the face of medical uncertainty is so important. Doctors and hospital administrators may not be invested in giving that patient a chance at life, and sometimes that chance leads to nothing short of a miracle. Six years ago, Alexander Way suddenly had to make a medical decision for his wife Beatrice after she had a stroke and heart attack in their home in the United Kingdom. The Daily Mail reportsthat Beatrice slipped into a coma, and Alexander was “stunned” when doctors were ready to give up on her care, remove her from life support, and donate her organs.
A tense confrontation between Alexander and Beatrice’s medical team ensued. Alexander told the Daily Mail, “The doctors insisted Beatrice had very little brain response and that there was no way she could ever improve.” Doctors insisted that if she did wake from the coma, she would be largely unresponsive and she would be blind. Nonetheless, Alexander continued to speak on his wife’s behalf: “In no uncertain terms I told them, ‘Don’t switch off my wife’s life support.’”
Like many families facing the draconian Texas 10-Day-Law, Alexander was in disbelief that the people who were supposed to be helping Beatrice had so quickly given up on her, deeming her “quality of life” too inferior to continue treatment. He said, “I was stunned, angry, and felt they were ending my wife’s life without considering further treatment. I was adamant that more could be done.” With Alexander’s persistence, more was done. Beatrice was transferred to the care of specialists, and four weeks later she woke from the coma. Her path to recovery was long and difficult, including intensive physical therapy to overcome paralysis induced by the stroke.
Beatrice’s recovery was enough to shock doctors, but then last year Beatrice gave birth to a daughter, Rosemary. Beatrice told the Daily Mail, “[Rosemary] has blossomed into a beautiful, healthy infant. Every day is a reminder of how lucky we are.” She also said, “I am so grateful to Alexander for questioning the doctors who thought my life was over. He saved my life.” If Alexander had not fought for his wife’s continued care, she, and their beloved daughter Rosemary, would not be here today. Their journey has made them passionate advocates for seeking more information before making life and death decisions.
The Ways’ story is a powerful reminder of the grave injustice in Texas law. Once a hospital in Texas invokes the 10-Day-Law, there is nothing families can do if a transfer to another hospital willing to treat the patient cannot be arranged. The decision cannot be appealed. The ongoing fight for justice in the case of Chris Dunn shows how all Texas families are threatened by the Texas 10-Day-Law. Live Action notes that the lack of care shown to patients like Beatrice and Chris is part of a larger anti-Life worldview: “In a culture of death, hard medical cases have become easy to dismiss as throwaway lives.” As Pro-Lifers, we recognize the sanctity of every human Life. For this reason, the law must change.
Ten years ago, one in 35 Australian babies were born as a result of IVF treatment. Today, that number has tracked to one in 25 babies. In the Netherlands, one in 15 births is as a result of IVF treatment. Now, world-renowned Dr John Aitken, the University of Newcastle laureate professor, the director of the University’s Priority Research Centre for Reproductive Science and the 2012 New South Wales Scientist of the Year, is warning us of the dangers of overreliance on IVF.
It seems that male children born of IVF procedures are themselves more likely to require IVF to reproduce. As Aitken notes:
“It’s an inexorable upward trend. We are taking recourse to IVF in increasing numbers and the thing we have to remember as a society is that the more you use assisted conception in one generation, the more you are going to need it in the next…There’s a negative pay-off. If you have a son from this process it is possible that he too will have the same pathology that you had.”
The trouble is that already, without interference, the human male is not very fertile: one in twenty males are infertile. Dr Aitken criticises the IVF industry for ignoring the fact that failure to conceive stemmed largely from male infertility problems. And aside from the increased incidence of infertility, male IVF children are also at greater risk of cancer if their fathers smoked and used assisted conception techniques.
But, as Aitken notes, society is now out of kilter with human biology. Women are at their most fertile at around 19 or 20 years’ old, but at that stage of life most are halfway through university and nowhere near starting a family. Instead, many are putting off having children, getting financially secure and then having to resort to IVF in their late 30s when they cannot conceive.
“The average age of women in IVF is 36/7 years. If you’re contemplating a family when you’re close to the edge, IVF cannot fix you up. IVF live birth rates decline from 35 to 42 exactly the same way in naturally conceived population.”
Do we really think that we can keep on relying on technology and scientific breakthroughs to mask the deficiencies of our current lifestyles? Do we really think that doing so won’t result in something having to give in the future? Perhaps not in the next generation, but perhaps the one after that, or the one after that when more and more of us rely on IVF to “fix” our problems that are either caused by us delaying having a family, or because our parents had us through IVF… Now imagine a society where not only are our birthrates failing to keep up to hte level required to keep the population stable, but where more and more men are naturally infertile. Where we rely on IVF more, and thus perpetuate the cycle.
WOOMB International projects offer innovative policies and programmes for families, indigenous communities and youth. A recent project in Timore Leste addressed five Sustainable Development Goals as follows:Goal # 3 Good health and well-being; Goal #4 Quality education; Goal #5 Gender equality; Goal # 11 Sustainable communities; Goal #17 Partnerships.
WOOMB International Ltd has affiliates in forty countries around the world. All these affiliates offer education in the Billings Ovulation Method® of natural fertility regulation which enables women to plan their pregnancies or avoid pregnancy, without drugs or devices.This method is inexpensive and has proven to be more than 99% effective in avoiding pregnancy and 78% effective in achieving pregnancy in women who have previously had difficulty conceiving.
Knowledge of their bodies and their fertility empowers young women to avoid teenage pregnancy, complete their education and seek meaningful employment. Women living in poverty are able to avoid pregnancy without expensive, harmful contraception. Indigenous women are offered education programs in their own communities and in their own language.
Women living in societies where respect depends on their ability to have children can successfully achieve pregnancy, and even improve their chances of having a child of a particular gender, by timing intercourse using the Billings Ovulation Method® to improve these outcomes.
Success Story An example of the success of our programs is in Timore Leste where women live in poverty with limited access to education and health care, often having to travel for days across rough terrain to seek assistance. With the help of WOOMB International Ltd our local affiliate was able to build a simple office where they conduct education programs for women. They also acquired a vehicle so that instructors can travel to rural areas to reach women who cannot get to the office.
Maria’s Story Maria came to the office soon after it was opened.She had made the three day trek from the mountains on foot, sleeping beside the track each night. She was desperate to get help for the sake of her family and her health. Maria is the mother of seven young children. She had been visited in the village two years previously by a passing health worker who convinced her to have an IUD inserted.The health worker left and the bleeding started. Previously Maria had been poor but she had been able to work in the fields and care for her children.Now she was weak and always tired.
When she arrived at our office in Dili she was welcomed and looked after by our caring staff. She was given instruction in the Billings Ovulation Method® and an appointment was made for her to have the IUD removed at a local medical clinic. After a couple of days of rest she felt strong enough to make the return journey to her village. When visited at home by her Billings Ovulation Method® teacher a month later she was managing well.The bleeding had stopped and she was charting accurately. Over the next six months the teacher remained in contact with Maria and was delighted to report that she continued to use the Method successfully to avoid pregnancy, had returned to work and was able to look after her family.She and her husband have been glowing in their praise of the help given to them and she is now helping other women in the village, with the support of her teacher, to understand their fertility and plan their families naturally without drugs or devices.
In another case, a woman called Amivi, whose husband was told by his family that he must leave her if she could not give him children, was able to achieve a pregnancy successfully with knowledge of when she was ovulating according to the Billings Ovulation Method®.
Several women who have been able to apply the Method successfully themselves, have then sought training as instructors and taken this information back to their own communities to help other women. In this way communities benefit, partnerships to empower women are forged and the word spreads.
Lessons Learned This project has reinforced what we already know – that if knowledge of their fertility is delivered to women in their own communities, by other women who speak the same language, positive outcomes result for women, girls and their families. WOOMB International will continue to deliver health education projects to communities throughout the world, especially those communities where poverty, injustice and gender inequality exist.
For more information about the Billings Ovulation Method® see www.billings.life
If you believe that “all kids need is love” then these donor-conceived children should be perfectly happy. But they’re not.
Turns out that even if kids have one or two loving parents, many donor-conceived kids strugglewith the reality that they will never know half of their heritage. In addition, the fact that the decision to deny them a relationship with one of their biological parents was intentional– made by the very parent(s) with whom they are living- often leads these kids to feel guilty, angry, ashamed and… commodified.
So, do not continue reading unless you are ready for your “all kids need is love” paradigm to be challenged:
Well, my father is a anonymous sperm donor. If you had asked me a year ago how I felt about him, I would have felt mild curiosity and excitement. I wasn’t really concerned about him at all. But now I miss him like crazy. It sounds weird I know, how can you miss someone you never knew? But I feel it all the same. I’m also furious (and I know this sounds bad) at my mother. How dare she willingly deny me the right to know him? And my half brothers and sisters. I’ve tried talking to her about it but she just gets a face like a smashed plate every time in mention it. Sometimes I really hate her.
34 years ago my mother decided that it was time for her to have a child. With her biological clock ticking and no long term relationship in sight, she turned to an anonymous sperm donor. She probably thought like most women would: “I’ll give my baby enough love for two”. I was indeed a loved baby…but baby must grow… It was only recently That i truly realized that I’ll most probably never know anything about half of my heritage. I love my mother but often I find myself despising her for doing this to me, for being so selfish. I, myself, as a woman approaching the big 3.5, I know what it feels like to truly want a child but NEVER would I knowingly take away a child’s right to have a father and a family. Not only has my mother deprived me from having a father but also sisters, brothers, cousins, grandparents…. https://anonymousus.org/gift-life-gift-solitude/
I’ve only wanted one thing in this life that I have been missing: paternal love. ….All I ever wanted is to be loved by you. The reality is that you were some college aged student who needed money, so you chose to donate. I just want you to know that your selfish actions indeed have consequences. My mother tells me that I’m better off without a father than with a father who doesn’t love me. The issue with that statement is that in the latter situation, at least I would know who my father is, regardless of his love for me. In the first statement, I do not know if my father loves me or not, which causes this tornado of thoughts in my mind, but even worse: I feel like an entire half of my life is missing thanks to my mother’s decision. As much as mother depicts herself as the hero, she may be a villain in disguise. Perhaps, she does not even understand the impact of her selfish deeds. Did she ever think about how this could impact a child? How it keeps her daughter up at night, knowing that there is yet another man in this world who does not love her.
I am 22 years old and I just found out that I was conceived through sperm donation. This information was withheld from me for my entire life until now.I was born into a loving, happy family. My parents have had a strong admirable marriage for nearly 25 years. I never would have imagined that my father was not the biological male who contributed to my existence…However, I have since felt a shameful sadness about this news. In a single day, I went from looking at my appearance without second thought, to looking at a stranger…I feel sad, alone, confused, and lost at times, while other times I feel nothing at all. I am on a roller coaster of emotions and I am not even sure why. I don’t like that I am suddenly grieving a person that I do not know or care to ever know. More importantly, I feel as though I am grieving myself….In addition to not completely understanding why I feel this way, I feel guilty for feeling anything at all. I am afraid to tell my parents how this makes me feel out of the fear that they will misunderstand my confusion and curiosity for something that it isn’t. …I am uncomfortable knowing that this person exists out there (or doesn’t, I don’t know if he has died). I am equally uncomfortable knowing that this person out there knows that he might have genetic offspring in the world that he will never get to meet. I feel weirdly betrayed by this person. It makes me sick to admit that.
I am egg donor conceived. Male. I found out when I was 16… now in my mid 20’s. Years and years later I still wonder and ponder, “who is my REAL Mother”… where is she? Is she even alive? Would she accept me for who I am? My current Mother… well growing up never accepted me… or even really cared to grow a bond with me (favortizes my 3 sisters; yes I’m a Quadruplet). It makes sense why now. There is a massive dIsconnection due to IVF. My relationship with my father has always been the greater of the two. I wish to one day meet her. Talk with her, even if it’s for 5 minutes. You know who you are…. God has blessed my wife & I in being able to have children naturally, and it has been the most wonderful experience so far. I WILL give my children what I never had growing up and still am suffering with. Hurt. Wounds. Depression. Anxiety. And the “unknown” of my identity.
Today I’m overwhelmed with sadness. It is Thanksgiving. I’ve spent the days surrounded by sweet people who love me. My family. The ones who helped raise me. The ones who will claim me. I love them. I’m thankful to be with them. We’re having a lovely time. But I miss my biological dad. I wish I could call him today. I wish I knew him well. I wish I could hug my bio brother, or send a quick, silly text to him. What is he doing today? I look around the room at boys who look just like their daddies. Fathers and children who all have the same smirky giggle. I’ll never sit in the same room with him and know if we walk the same. I didn’t get to grow up reading the books he loves, or hearing his calming voice when I’m tired, or sharing a love for the way his mother, my grandmother, cooks. I cannot ever know these things. In the name of generosity, he gave me away.
My mother told him that she “knew” I was his child. [My dad] literally took that on faith, that “a mother knows”. I believe him, he is a trusting individual and I believe that he believes this to be true. However he had doubts or he would not share this with me at such a critical juncture. My first thoughts were “Are you expletive! kidding me?” Followed by thoughts that I shouldn’t exist, then followed by immense respect for my dad, who is most likely not my bio dad. He coached my baseball teams, taught me everything, was the best dad to me, and my friends that I have ever seen. Much better as a father than I am by leaps and bounds. He did everything for me. I could not look less like him. I look exactly like a male version of my mother. I have come to the realization that although I may want to know, he probably does not want to know, for certain, if I am his or not. He cares, but most likely would be devastated if he found out, like all my medical knowledge (am doctor) suggests that I am not his child. I have decided not to test at this time (somehow, it’s killing me), and upon his passing, reevaluate my desire to know. He told me the donor was a medical student. I am the first in my family, either side, in the medical profession. So many things seem different now, I am still processing, and am trying not to let it throw me off my game as a father myself, or even keep it inside and not tell everyone I know what I have just found out. I feel like running this by everyone I know because it alters my perception of my life so deeply. People have asked me already what is troubling me. I may need professional help to sort this through, and I will seek it out if my current mental state continues.
When my friends talk about their fathers they talk about their first fishing trip together and how he would always bait the hook for him, or when he didn’t like a significant other they brought home. When I talk about my father I don’t have any memories to reminisce on or a specific image that pops into my head, I am just filled with bitterness. Not just because you donated, and not because you did it anonymously, but that fact my single mother wanted it that way. She chose for me to never even have the chance to meet my real father. But I hate feeling this way because, how do I tell my mom she wasn’t enough, that her love doesn’t fill a hole that she created. Every time I even mention my biological father around her, I feel like I am betraying her in some way. But if I never bring you up, no one will. So many people say my mom and I look alike, and I hate hearing that, not because my mom is ugly, but because it just gives her more reason to just sweep you under the rug and ignore you exist. I wish I had the power to ignore you exist, but some nights I just can’t. stop. thinking. No matter how hard I try I just can’t. I try to muffle my cries because I can’t let my mom hear, because it will only hurt her. Then I get angry because I didn’t get any protection in this decision. I was put into this masturbated race without any rights or a voice at all. You get to hide behind your anonymity, and I can’t have my mom seeing that I am angry or sad because I don’t want her to get buyer’s remorse.
Biological connection matters to kids. These children had to discover that the hard way- by missing out on it.
September 12, 2017 (PregnancyHelpNews) — If there was any doubt about California’s status as the nation’s standard-bearer for abortion, a letter sent September 5 by the state’s Board of Registered Nursing should clear that up in a jiffy.
Acting at the behest of abortion activists in the state legislature and online media, the Board of Nursing reversed its decision from just a month prior, sending Heartbeat International a letter to demand that the pro-life pregnancy help network “cease and desist” offering nurses continuing education units (CEUs) for Abortion Pill Reversal classes.
Over 350 doctors nationally have joined the Abortion Pill Reversal network, while 300 mothers have successfully rescued their children from abortion through the medical intervention (see here and here for examples), which introduces an emergency and ongoing progesterone treatment to counteract the first of two pills in the chemical abortion (RU-486) process.
The Board’s sudden reversal seems a direct effort to deny a woman access to her own choice during an unexpected pregnancy, Heartbeat International president Jor-El Godsey said Monday.
“This is a naked political assault on a procedure that is the very essence of choice,” Godsey said. “To oppose Abortion Pill Reversal is not only to deny the science and reality that there are children living today because of it, but it’s to materially keep a woman from even so much as knowing she has the option to potentially stop a chemical abortion once it has begun. This is the abortion lobby taking choices away from women.”
Playing politics with women, children and nurses
The letter, postmarked September 5 and received September 11, gives Heartbeat International five days from receipt of the letter to remove CEU credit from its online courses, offered online through the Heartbeat Academy.
It also marks a 180-degree shift from a letter the same Board sent Heartbeat International and sister pro-life network, National Institute of Family and Life Advocates (NIFLA), approving both organizations’ status as a continuing education providers.
The original letter, sent July 28, 2017, followed a 17-month period where the Board reviewed hundreds of pages of submitted documentation starting in February 2016. No subsequent paperwork or filing of any kind was requested prior to or cited in the most recent letter.
The Board had originally questioned Heartbeat International’s inclusion of Abortion Pill Reversal courses during the audit process, but then agreed to reinstate the courses after Heartbeat International responded with a multi-point statement demonstrating the courses’ relevance to nursing practices.
While Heartbeat International is complying with the letter’s demand to remove CEU credit from its online Abortion Pill Reversal courses, the courses will still be activated while the organization appeals the Board’s latest decree.
“How the Board of Nursing can play politics with the lives of women and children is beyond me,” Godsey said. “If there were any hint of noncompliance on our part, it’s clear a 17-month audit would have uncovered it. What could possibly have changed in one month’s time?
“Meanwhile, nurses across California and the nation could be presented with patients who want to reverse their abortion decision before it is too late, and this new mandate prevents nurses from being prepared to serve their own patients.”
A hunt for non-compliance
Meanwhile, radically pro-abortion media source Rewire.com reported September 8 — three days before Heartbeat International received the letter — that the letter had been sent. The site had originally influenced San Francisco Bay Area state senator Jerry Hill to call for the audit of Heartbeat International and others in early 2016.
After pushing the Board to audit Heartbeat International — a nonprofit that serves 2,200 affiliates worldwide and operates a 24-7 pregnancy helpline, Option Line — Hill then proposed legislation that was eventually adopted by the state and signed into law in 2016 by Gov. Jerry Brown that beefed up the requirements for nursing CEU providers.
That law, however — which mandated that courses rely only on “generally accepted scientific principles” — was insufficient to wield against the Abortion Pill Reversal courses. Instead, the Board cited California Code of Regulations (CCR) Section 1456 in its demand letter to Heartbeat International.
Curiously, the section cited by the Board pertains only to the need for courses to be “relevant to the practice of nursing,” differentiating between courses that deal with patient care (direct and indirect) and those which, “deal with self-improvement, changes in attitude, financial gain, and those courses designed for lay people … ”
Fitting that definition, Heartbeat International only offers CEU credit to nurses for Abortion Pill Reversal courses it offers online and at its annual conference.
Heartbeat International has been a California-approved CEU provider since 2012, opting to go through California because the state’s CEUs are generally accepted throughout the U.S. Since 2015, Heartbeat International has issued nursing CEUs to well over 400 nurses.
A coordinated effort to steal choices
The Board’s flip-flop fits into a larger pattern of the state of California’s targeting of political opponents who pose an alternative to abortion or otherwise threaten the abortion industry’s marketplace stranglehold.
In addition to pursuing charges against David Daleiden and Sandra Merritt in response to their three-year undercover work of exposing Planned Parenthood and others’ complicity in the trafficking of body parts harvested from aborted babies, the state of California also launched an assault on community-funded pro-life pregnancy centers and medical clinics with a 2015 law that could be challenged at the Supreme Court as early as this month.
Earlier this month, a federal judge dismissed a lawsuit filed by several California churches that are challenging the state’s Department of Managed Health Care requirement that all insurance companies cover the cost of their employees’ abortions.
“At this point, it’s hard to say we’re surprised by any effort to prop up the failing abortion industry,” Godsey said. “But this is a direct effort to steal a mother’s choice right out from under her. Women and men become nurses to help and serve others, but politically driven moves like this keep them from accomplishing their compassionate, God-given mission.”
Reprinted with permission from Pregnancy Help News.
On May 9, 1985, President Ronald Reagan gave a rousing speech before the Assembly of the Republic of Portugal in Lisbon. In this speech he spoke of the historic greatness of the nation of Portugal. He also mentioned the Holy Father and, indirectly, the apparitions of Our Lady of Fatima.
Reagan declared that the example of Pope St. John Paul II (“No one has done more to remind the world of the truth of human dignity, as well as the truth that peace and justice begins with each of us”) and the prayers of simple people everywhere—like that of the children of Fatima (Lucia, Francisco, and Jacinta)—are more powerful than the greatest armies and politicians of the world. Read the excerpt and watch the full speech below.
PRESIDENT REAGAN’S 1985 LISBON SPEECH
. . . This belief in human dignity suggests the final truth upon which democracy is based—a belief that human beings are not just another part of the material universe, not just mere bundles of atoms. We believe in another dimension—a spiritual side to man. We find a transcendent source for our claims to human freedom, our suggestion that inalienable rights come from one greater than ourselves.
No one has done more to remind the world of the truth of human dignity, as well as the truth that peace and justice begins with each of us, than the special man who came to Portugal a few years ago after a terrible attempt on his life. He came here to Fatima, the site of your great religious shrine, to fulfill his special devotion to Mary, to plead for forgiveness and compassion among men, to pray for peace and the recognition of human dignity throughout the world.
When I met Pope John Paul II a year ago in Alaska, I thanked him for his life and his apostolate. And I dared to suggest to him the example of men like himself and in the prayers of simple people everywhere, simple people like the children of Fatima, there resides more power than in all the great armies and statesmen of the world.
This, too, is something the Portugese can teach the world. For your nation’s greatness, like that of any nation, is found in your people. It can be seen in their daily lives, in their communities and towns, and especially in those simple churches that dot your countryside and speak of a faith that justifies all of humanity’s claims to dignity, to freedom.
I would suggest to you that here is power, here is the final realization of life’s meaning and history’s purpose, and here is the foundation for a revolutionary idea—the idea that human beings have a right to determine their own destiny. . . .
LOS ANGELES, California, July 31, 2017 (LifeSiteNews) – When billionaire Elon Musk tweeted about population growth earlier this month, some of his more than 10 million Twitter followers assumed he was lamenting “overpopulation.”
The Tesla CEO and SpaceX founder has funded research in Mars colonization and artificial intelligence, and he is regarded as an enlightened and enterprising entrepreneur.
So given that and the fact his tweet contained the words “population” and “collapse,” it was not a stretch to suppose he’d be tweeting about the planet having too many people.
However, Musk’s message was that some of the world’s countries are not replacing themselves in population and they are in danger of demographic collapse.
In saying so, he inadvertently communicated to his sizable audience what the pro-life movement has said for years: The problem is NOT that we’re having too many kids.
“The world’s population is accelerating towards collapse, but few seem to notice or care,” Musk’s tweet said.
He was commenting on a November 2016 New Scientist article titled “The world in 2076: The population bomb has imploded.” The article projected a measured decline of global population over the next 60 years, because half of the countries in the world have fertility rates below the replacement rate.
Replacement fertility is around 2.1 children per woman. Most developed countries are not achieving this. Population Research Institute confirms that half the world’s population has below-replacement fertility.
Musk’s tweet in its intended context was then covered by a number of media outlets, albeit with the awkward task of how to package the narrative atypical of current accepted anti-population ideology.
But Musk has made similar comments before.
“We should be concerned about demographic implosion,” he told CNNMoney in a March interview.
“So if you look at countries like Japan, most of Europe, China,” Musk said, “and you look at the birth rates, in a lot of those places it is only at about half of the sustaining rate.”
Musk went on to describe an inverted demographic pyramid for CNN’s correspondent, where more people in older age groups are on top and how this is not sustainable.
“So it will sort of fall over,” he said, “it will not stand.”
“What we’ll actually have in those countries is a very high dependency ratio, where the number of people who are retired is very high relative to the number of who are net producers,” he said. “And so the social safety net will not hold.”
Musk’s analysis focused on the productivity of people in their respective demographics — not a measure of the value of life — but it does factor concretely into civic planning. Societies need future generations to logistically sustain themselves. Musk mentioned as well how immigration is not a feasible method of population replacement.
Musk may be an unlikely dispatcher of a pro-life message.
Indeed, in the CNN interview, he spoke of how we “sort of evolved to just procreate and there wasn’t birth control or anything,” as though this worldview is something from the past.
And he spoke of China’s one-child policy only in terms of its role in rendering the nation to its current state of non-replacement, with no mention of the horrible forced abortion element.
But his grasp of the economics and sizable platform enabled him to deliver the message that having too many kids is not the issue, and population control is not working.
“The full gravity of this is not well understood,” Musk said, “but will become a severe issue in the next few decades.”
Faith and reason are like two wings on which the human spirit rises to the contemplation of truth; and God has placed in the human heart the desire to know truth – in a word, to know himself – so that by knowing and loving God, men and women can come to the fullness of the truth about themselves.
– St. Pope John Paul II, Fides et Ratio, ¶ 1
September 11, 2017 (Human Life International) – Truth is known through a combination of faith and reason. The absence of either one diminishes the ability to know oneself, the world, and God. Human reason seeks truth; however, the ultimate truth about the meaning of life cannot be found by reason alone.
Sadly, the philosophy of relativism has poisoned our culture, which holds that all points of view are equally valid, and that all truth is relative to the individual. All moral positions, religious systems, political movements, etc., are truths that are relative to the individual. According to this philosophy, no system of truth is more valid than another. It rejects God – particularly Christianity – as well as objective truth and ethics (right and wrong).
Our pluralistic society wants us to abandon any idea of right and wrong. Those things once considered morally unacceptable – fornication, infidelity, pornography, and homosexual behavior – are now deemed permissible and even virtuous.
Skepticism about one’s ability to know truth has dire consequences both to the individual and society. The human person, left to human weakness and unbridled passions, inevitably walks down a path of tragedy – left adrift in a turbulent sea of uncertainty and hopelessness. The alternative is to walk in accordance with a moral compass, which guides, counsels, and provides shape to one’s behavior in daily life.
The unprecedented and relentless assault on the sanctity of human life, on marriage and human sexuality, and religious freedom will continue unless there is a genuine spiritual resurgence – faith and reason working in perfect harmony.
Christianity is not just about social action, or feeling good about one’s life, or working out one’s own salvation, or practicing one’s faith when convenient or opportunistic. Faith in Christ is about an unwavering commitment to Jesus, His mission, commands, and Church – to the truth about the human person.
Faith, then, must make a more substantial effort to become the “helper of reason”, so that reason can fully recover its own nature and competence.
Our Lord, in the parable of the Ten Bridesmaids, stresses to His disciples the need for greater vigilance and intensity of faith in response to the Christian vocation, as well as the sort of attitude we should have towards His coming – our posture remaining ever watchful, our love alert, and our daily lives filled with His Spirit.
It is not enough just to have started out on the journey that leads to Christ; we must be constant in our desire to remain on the narrow path and vigilant because the natural tendency of every person, due to a wounded nature, is to lower the level of self-giving that the Christian vocation demands.
Almost without realizing it, the disciple gradually – if he is unwatchful – gives way to the pressures of daily life and has the tendency to make Christ’s call compatible with a comfortable existence.
Saint Paul exhorted the early Church to be on guard against such a tendency:
I urge you therefore, brothers, by the mercies of God, to offer your bodies as a living sacrifice, holy and pleasing to God, your spiritual worship. Do not conform yourselves to this age but be transformed by the renewal of your mind, that you may discern what is the will of God, what is good and pleasing and perfect. – Romans 12:1-2
In the midst of this great campaign for life and family, it is easy to forget that the battle is primarily a spiritual one waged between principalities – with two diametrically opposing views about human life.
The spirit of the Culture of Death does not discriminate. It has set its will against the Heavenly Father and His eternal plan for humanity. The unborn, family, elderly, handicapped, sick, and poor are of no concern and are easily discarded. The Christian view of the human person and his eternal vocation is readily rejected and replaced with the modern day golden isms – materialism, hedonism, individualism, secularism, and relativism. The vile and profane are welcomed guests at this banquet, but all who forsake these self-madegods are banished and labeled as judgmental, intolerant, and discriminatory.
Even predominantly Catholic/Christian cultures – Western and Central Europe – having compromised their heritage in Christ, are suffering and are on the verge of collapse. Our families are victimized by ideologies and political agendas and aggrieved by a litany of afflictions: separation, divorce, pornography, infidelity, drug and alcohol abuse, suicides, domestic and societal violence, poverty, religious persecution and secularism – to name but a few.
A soul that chooses the comfortable path becomes lazy and weary, ignoring the call to pick up your cross and follow Me. Spiritual blindness is thus the only outcome for a soul that loses the attitude of vigilance, giving way instead to vice (sin) – allowing the flame of friendship with the Lord to flicker and die.
There is no doubt, therefore, that a ‘Kingdom of God’ accomplished without God — a kingdom therefore of man alone — inevitably ends up on the perverse end. – Benedict XVI, Spe Salvi, ¶ 23
History has taught us repeatedly that no civilization or nation has survived a moral collapse. Because of compromise, complacency, and the rejection of truth there is widespread spiritual blindness. After all, how can we not see the unborn child as a human being? How can we not see the plight of the elderly, poor, and persecuted? How can we not see the flagrant assault upon marriage? How can we not see our youth victimized and stalked by a perverse sex-saturated culture?
Simple. Spiritual blindness! Diminished faith! Rejection of truth!
What then is our response to such evil, hardheartedness, and spiritual blindness? The answer is holiness, vigilance, and perseverance. As we hear in the parable of the Ten Bridesmaids, five of the maidens were sterile – ill prepared and caught off guard – while; in contrast, the foresightedness of the five prepared maidens produced a far different outcome. With flasks of oil and with their lamps lit they welcomed the groom and entered the wedding feast.
The decision to follow Christ is born from being loved first and responding generously in Love. In Love one finds comfort, consolation, nourishment, assurance, guidance, and fortitude – a steady readiness to do all He tells you to do.
If we are to combat the Culture of Death and its self-serving ploys, we must be sincere with our Savior and remain close to Him at all times – we must be vigilant, faith-filled, and seek truth crying out, strengthen my faith, O Lord!
Being transformed by Christ is the fulcrum for a radical transformation of our cultures. To the extent to which we answer the call to personal holiness, to the extent to which it is the Holy Spirit living the Life of Christ in us, we will transform the world around us and build a Culture of Life.
On July 31 Smithonian.com published an article condemning other media sources for spreading “bad science” across the internet. These media sources claimed that women’s oral contraceptives are the cause of an endemic feminization of male fish around the world.
According to the Smithsonian, we don’t know that the Pill is responsible. The institute referred to a study that looked at sources of chemicals in water ways and concluded: “So theoretically, any of those chemicals could be having a far greater impact than EE2,” which is the powerful chemical contained in a number of hormonal contraceptives.
Is that the case?
Not according to Dr. Charles Tyler, a reproductive physiologist and eco-toxicologist, and Deputy Head of Biosciences at the University of Exeter, England. For the past 20 years, Tyler has devoted his research to studying the effects of chemicals that impact the hormonal systems of wildlife, mainly fish. I interviewed him in July and corresponded with him more recently about the Smithsonian article.
“There are lots of chemicals that are estrogenic, but nothing as exquisitely potent as EE2,” he told me. “If you look at the evidence objectively then it is pretty much overwhelming that this is a key player in the feminization of fish in English rivers—and likely more widely.
“My honest view is that even though I was interview by the Smithsonian, the writer of this article did not pay that much attention and had already formulated what she wanted to write and the angle of the story,” he added.
Natural Womanhood understands that it’s not fair to make women on the pill feel responsible for such a dramatic ecologic change, and that is not our goal. Smithonian.org, however, seems to be covering up for the pharmaceutical industry, with the effect of masking a major problem. It looks like they are trying to change the narrative and make it about many other causes when, in reality, hormonal contraceptives are the main culprit.
The European Commission recognized that fact when they proposed to regulate EE2 in 2012 (1). When one considers how common hormonal contraceptives are in Europe, it is difficult to imagine that they would have taken that stand lightly.
I asked James Murphy, a recognized United States expert in water law and policy, and he agreed: “Precisely no one in the water supply or water quality sectors of my business would disagree with that statement. The common knowledge is that pharmaceuticals are a problem for the treatment of wastewater as current treatment protocols do not include categorical limits for pharmaceuticals. There is universal agreement that we don’t have EPA limits for pharma because, among the many that are filtering through our municipal wastewater treatment plants, the largest component is by far estrogen from feminine birth control. Anti-depressants, etc., are ‘out there’ and environmental activists would like to address this problem; however, the birth control pill is, quite simply, sacred and off limits.”
My July interview with Dr Tyler (pictured, right) follows.
Gerard Migeon: In the past 10-15 years, you and other scientists have started raising concerns about the presence of endocrine disruptors in fresh waters and its impact on fish populations. Studies have been conducted in various parts of the world with a limited number of different species. Can you help us understand the scale of this problem today?
Charles Tyler: If we look at feminization of fish, it is widespread in the UK rivers, as up to 25 percent of male fish are affected. Feminization has been shown to occur in wildlife on every continent. While fish are perhaps amongst the most affected, it also occurs among many other species: amphibians, birds, reptiles, and even mammals like otters, seals, and whales.
GM: Can you please explain to us in lay terms and from start to finish, the key mechanisms of how EE2 ends up in fresh water and affects the biology of fish populations?
CT: Feminization of males refers to when males produce a yolk protein normally produced only by females, and/or an effect on the developing gonad, which may be the formation of a feminized reproductive duct and/or the presence of developing eggs (oocytes) in the male testes.
The fish suck a lot of the chemicals from the water and when we test what is in their body tissues, especially in the liver, we find a chemical blueprint of what we throw away down the toilets: natural steroids, contraceptive chemicals and in particular Estradiol Estrogen (EE); equine estrogen used for hormone therapy, and a series of industrial chemicals, including pesticides. There are 40,000 chemicals ….1,000 have endocrine ….200 have estrogen activity.
GM:Why is EE2 from the pill a major culprit? Are other chemicals equally responsible?
CT: EE is especially critical because it is designed to be more potent than natural steroids, and harder to degrade. It is very potent at low dosage. In addition, the receptor system of fish is very similar to that of vertebrates.
GM: Do you think that there is a potential for similar disruption among mammals, and even humans?
CT: EE2 would be effective in males if they were exposed. Drinking water is less likely to contain EE2, but has other chemicals, especially plasticizers. However, there is also a possibility of maternal transfer. We know that maternal transfer is a key root of exposure and that during development the fetus is very vulnerable so there is a greater chance of impact. However, this area is still under-researched.
(In other words, while there is currently no affordable method to clean all waste waters that go into our rivers, our drinking water is processed through filtration systems that remove toxins. The risk that Dr. Tyler refers to concerns women who get pregnant while they are on the pill; this can expose their fetus to small but potent amounts of EE. We reviewed research about this topic here. — GM)
Gerard Migeon is the founder and CEO of Natural Womanhood, a MercatorNet partner site. This article is republished from the NW blog.
1. “Ethinyl Oestradiol in the Aquatic Environment Late Lessons from Early Warnings: Science, Precaution, Innovation” 279 Emerging Lessons from Ecosystems | Ethinyl Oestradiol in the Aquatic Environment. Susan Jobling, Richard Owen 2013: “In 2012, nearly 75 years after its synthesis, the European Commission proposed to regulate EE2 as a EU-wide ‘priority substance’ under the Water Framework Directive (the primary legislation for protecting and conserving European water bodies).”
(Editor’s Note: His Eminence Raymond Leo Cardinal Burke, Patron of the Sovereign Military Order of Malta and Founder of the Shrine of Our Lady of Guadalupe in La Crosse, Wis., graciously took time out of his busy schedule to grant The Wanderer a wide-ranging interview during a recent visit to the Shrine. Included among the topics for which he provided his illuminating insights are the Message of Our Lady of Fatima, an appraisal of the situation in which the Church finds herself in contemporary times, and the celebration of the Sacred Liturgy.
(This interview has appeared in three parts in The Wanderer. This part is the conclusion.)
+ + +
Part 3
Q. Recently, Robert Cardinal Sarah again called for a serious implementation of a “reform of the reform” (RoftR) as it relates to the postconciliar Roman Rite. But most pastors (and diocesan worship directors), if they are sympathetic to the Cardinal’s suggestions, are eager to gradually implement these suggestions, recognizing that for many in the pews, a rapid implementation would be too much, and in fact would cause the same type of confusion and frustration many experienced after the Second Vatican Council.
So, which reforms suggested by the Cardinal should we focus on first, acknowledging that each parish and diocese is unique in its needs? Are there elements of the RoftR that are more important than others and should be focused on first?
A. Certainly I think the correction of all the liturgical abuses that were identified in Redemptionis Sacramentum [2004 Instruction issued by the Congregation for Divine Worship and the Discipline of the Sacraments] is critical. At the end of his pontificate, Pope St. John Paul II concentrated on trying to correct liturgical abuses. In a positive way, the two suggestions that Cardinal Sarah has made give us a good direction.
First, he encouraged offering the Mass with everyone facing the Lord [ad orientem]. This will help so much to restore the sense of worship and to show that the Mass is not some kind of social event between the priest and parishioners, or the parishioners among themselves. Rather, it is an action of the whole community with the priest at the head acting in the person of Christ [in persona Christi], of “worshipping the Father in spirit and truth” (John 4:23) as our Lord said to the Samaritan woman at the well. I think this would be a very good place to begin.
Cardinal Sarah explains this very well in an article he published in L’Osservatore Romano on June 12th of 2015 and then again in his presentation at the Sacra Liturgia Conference in London on July 5th of 2016.
Cardinal Sarah addressed a second area of reform at the 2017 Sacra Liturgia Conference in Milan when he asked once again for consideration of receiving Holy Communion kneeling and on the tongue. I think those are two areas to address that would be very effective.
Of course, we also have the whole reform that needs to take place with regard to the disposition of the Church. For example, in so many places the tabernacles were removed from the sanctuary of the Church as the result of a false interpretation of the Second Vatican Council. Likewise, other things were done that disturbed the image of worship, such as the sacred music that is employed.
I think the matter of orientation of all towards the Lord with the priest at the head (toward the East if possible, unless it is physically impossible because of the geographical location of the church) and the manner of receiving Holy Communion reverently on one’s knees and on the tongue are important places to start.
Interesting to note is that here at the Shrine it has become the custom to receive Holy Communion on the tongue while kneeling. People have gladly embraced this practice, and I have never once received any hate mail or any criticism in its regard. Also, as Cardinal Sarah requested, we implemented the liturgical practice of ad orientem observance of Mass this past Advent and people have commented on what a greater beauty this has brought to the celebration of the Holy Mass.
Q. Asked recently by The Wanderer if Pope Emeritus Benedict XVI’s influence on the liturgy continues, Dr. William Mahrt, president of the Church Music Association of America, said: “It’s still with us, absolutely, yes,” and continued on to state: “He had this notion of ars celebrandi, the art of celebrating the liturgy.” Dr. Mahrt added, “His writings on the liturgy are still being read, and we instituted many things upon his inspiration, which will continue.”
Your Eminence, do you concur with Dr. Mahrt’s assessment of Benedict’s ongoing influence on the liturgy? Can you add any personal observations on what you think his enduring legacy on liturgical worship will be?
A. Yes, I know Dr. Mahrt — he is a wonderful man. There is no question in my mind that the most splendid contribution of the pontificate of Pope Benedict XVI was in the area of restoring the correct order and beauty to the Sacred Liturgy. The art of celebrating (the ars celebrandi to which Dr. Mahrt refers) not only was exemplified in the manner of Benedict’s offering of Holy Mass, but also that by his teaching he helped so many priests to see that the priest gives over his body to Our Lord. It is the Lord Who offers the sacrifice and thus, the priest’s whole concentration should be on letting Our Lord act through him. In that way we avoid self-referential actions that have nothing to do with the Sacred Liturgy.
I believe that Pope Benedict XVI’s teaching was so profound because he had the courage to issue Summorum Pontificum [apostolic letter issued moto proprio in 2007]. The teaching contained in that document will certainly endure in its effects. Another enduring contribution was his magnificent book entitled Spirit of the Liturgy.
Q. Over the past few months, according the various news reports, you have stated that you do not believe that Muslims and Christians worship the same God. It has been suggested that this is inconsistent with the teachings of Vatican Council II (e.g., Lumen Gentium, n. 16; Nostra Aetate, n. 3) and public statements made by Pope St. John Paul II (e.g., Address to Young Muslims, Morocco, August 19, 1985). Your Eminence, can you provide clarity regarding this apparent contradiction?
A. In the Council documents and in Pope St. John Paul II’s writings, it is stressed that Islam, like Judaism and Christianity, teaches us that there is only one God, the Creator of the universe. So we are united in the belief that there is only one God. However, the God described in the documents of Islam as well as the actions of the very aggressive and violent Muslims do not portray Allah as a God of love. Love is the principal quality of God according to our Christian faith, for as St. John the Evangelist writes, “God is love” (1 John 4:8, 16).
The Muslims of some countries, in fact, have objected to Catholics using the word “Allah” (the Arabic word for God). They protested by saying, “Your God is not our God.” What is needed here is simply a realistic recognition of the teaching on God in Islam. I believe it will indicate that the Islamic understanding of the one God is in contradiction to the Christian teaching on the one God.
Q. It seems as if pro-life and pro-family apostolates are being viewed more favorably by the majority of the populace as a result of scientific advances conclusively proving when life begins, disclosure of the abhorrent practice of selling baby parts from aborted fetuses, and many other factors. It seemed unlikely just a few short years ago that defunding Planned Parenthood would even be discussed. In light of our new administration and the changing opinions of our country’s citizenry, what is your assessment of the progress being made by pro-life and pro-family movements in the United States?
A. I feel strongly that real progress has been made. For example, the annual March for Life and all the efforts on the part of individuals and groups who have the promoted respect for human life by such practices as providing free ultrasounds for women who are expecting a baby, giving witness at abortion clinics, praying the Rosary, giving help to young women by counseling them, and providing assistance to women who are having difficult pregnancies are producing good effects.
At the same time, the horrible evil of destroying an innocent, defenseless human life is becoming even clearer to people.
We now have a president, who, from all indications based on concrete actions he has taken, is pro-life himself. I personally have not studied this, but it is said that in the past this was not always so. The past does not make a difference; what matters is that now he seems to understand. I believe what is important now is that we make even stronger our pro-life and pro-family movements and build on the momentum that has been generated. The worst thing that could happen would be to rest on our laurels; we could then lose all this progress that has been made.
It is a constant battle. Satan hates human life: “He was a murderer from the beginning” (John 8:44). We know that the Evil One is constantly about the work of promoting the lack of respect of human life. So we really need to persevere and be vigilant in our continued promotion of a “culture of life.”
Q. Your continued perseverance and faithfulness to the Gospel message despite the many changes and the ill treatment you have experienced over the past few years have been an inspiration to countless faithful Catholics. It is truly amazing how you are able to maintain your rigorous travel and speaking schedule, which must be very physically taxing. What is the most important lesson you have learned during this time?
A. I believe the most important lesson I have learned is that I must abandon myself totally to defending Christ and His Church out of true love for Him and for His Mystical Body. We can always be confident that God will assist us with the grace we need, even in matters of physical strength and of being able to endure very difficult situations. I have discovered this more and more because there have been times when things that have been said about me are very painful. Just the physical demands of extensive traveling and of preparing, in the best way possible, presentations of the Church’s teaching have made this realization ever more evident to me.
At times, what seemed impossible to me has been accomplished if I remain serene in carrying out this work to the best of my ability. I know the strength comes from Our Lord because I do not have it in myself.
From my childhood, I have been rather sensitive to being criticized by other people — it is not something I enjoy. But I have found that the recent, somewhat harsh criticism does not deter me from doing what Our Lord asks of me and that I am very much at peace.
Support This Endeavor
Q. An ambitious and praiseworthy project that I know is near and dear to your heart is the effort you initiated in 2016, through the formation of a “Memorare Army of Prayer,” to raise funds for the construction of the “Father John A. Hardon, S.J., Marian Catechist Apostolate Center and Retreat House” at the Shrine of Our Lady of Guadalupe in La Crosse, Wis. What progress has been made thus far and have any definitive timelines yet been established? What can readers of The Wanderer do to help?
A. Towards the goal of saying the Memorare 500,000 times, a total of 377,023 have been prayed to date. From a financial perspective, we have raised over eleven million dollars towards the goal of thirteen million dollars. We were hoping that we could go well over the thirteen million dollar goal in order to build more of the Father John A. Hardon, S.J., Marian Catechist Apostolate Center and Retreat House.
Moreover, in order to secure the financial situation of the Shrine, seven million dollars of the funds that are raised go immediately into the Endowment Trust, in order to bring its holdings to ten million dollars. The Endowment Trust will then generate significant annual earnings to go towards the ongoing work of the Shrine.
We have not yet gone into the general phase of the capital campaign. Right now, we are simply approaching individual donors to get an initial substantial amount that would then encourage others to be generous. We should be bringing that to a conclusion by the Fall and then will make a general appeal to the public. So it is coming along well, but we hope to do even better.
In "Prove it God" Patty Schneier speaks as a Catholic woman and mother in our modern times. She tells her personal story of how God worked in her heart to turn her away from contraception and toward Natural Family Planning.
Patty Schneier's "Prove It, God" ...And He Did is available to listen to for free! Order it!
Stephen Patton M.A., J.D.
Stephen Patton's "Why Contraception Matters" talk is available to listen to for free! Read it!Order it!
La charla de Stephen Patton "Porque Importa la Anticoncepción" esta disponible aqui para que la escuchen gratis! Leela!Ordenala!



 Dr. Susan Caldwell
Dr. Susan Caldwell






































































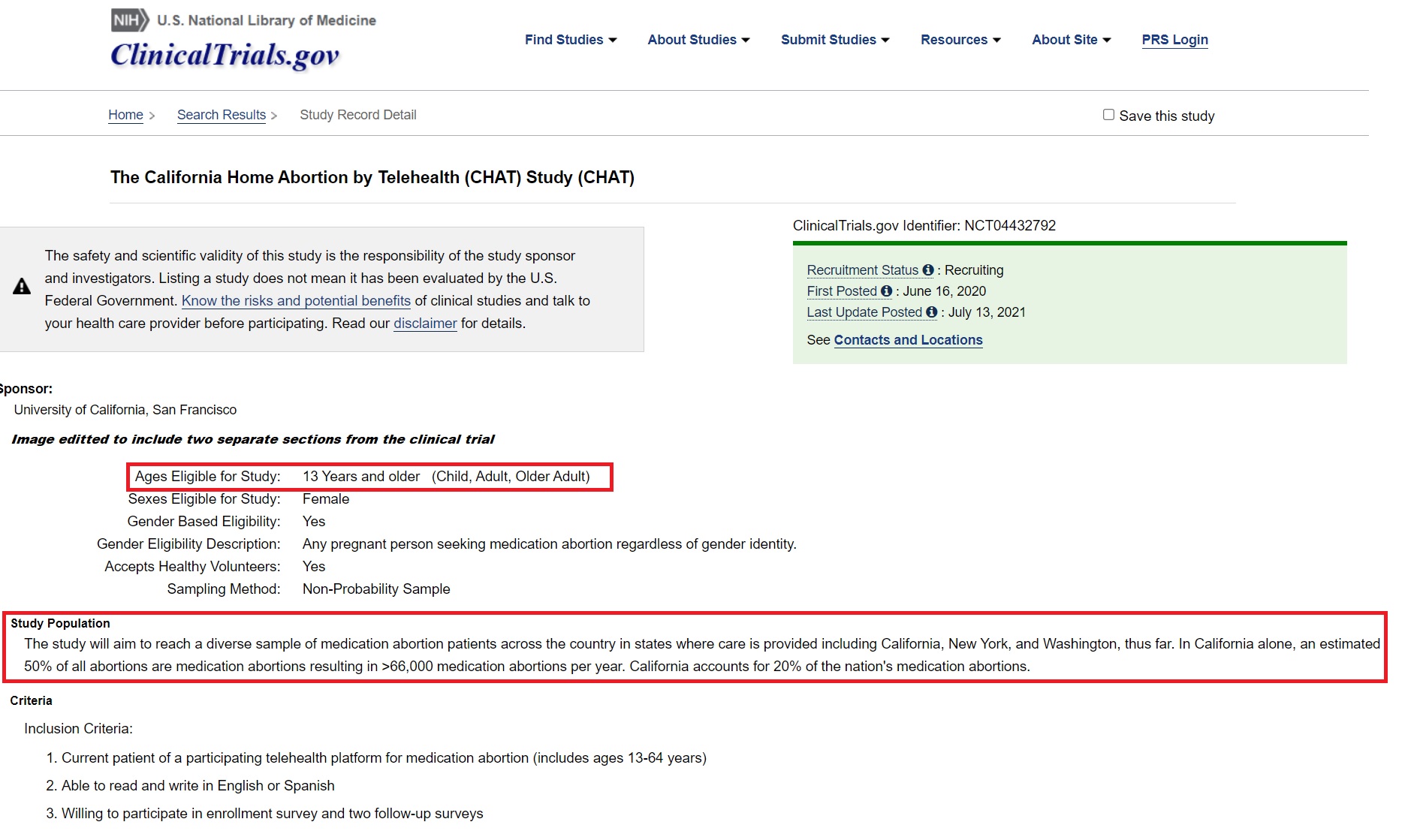

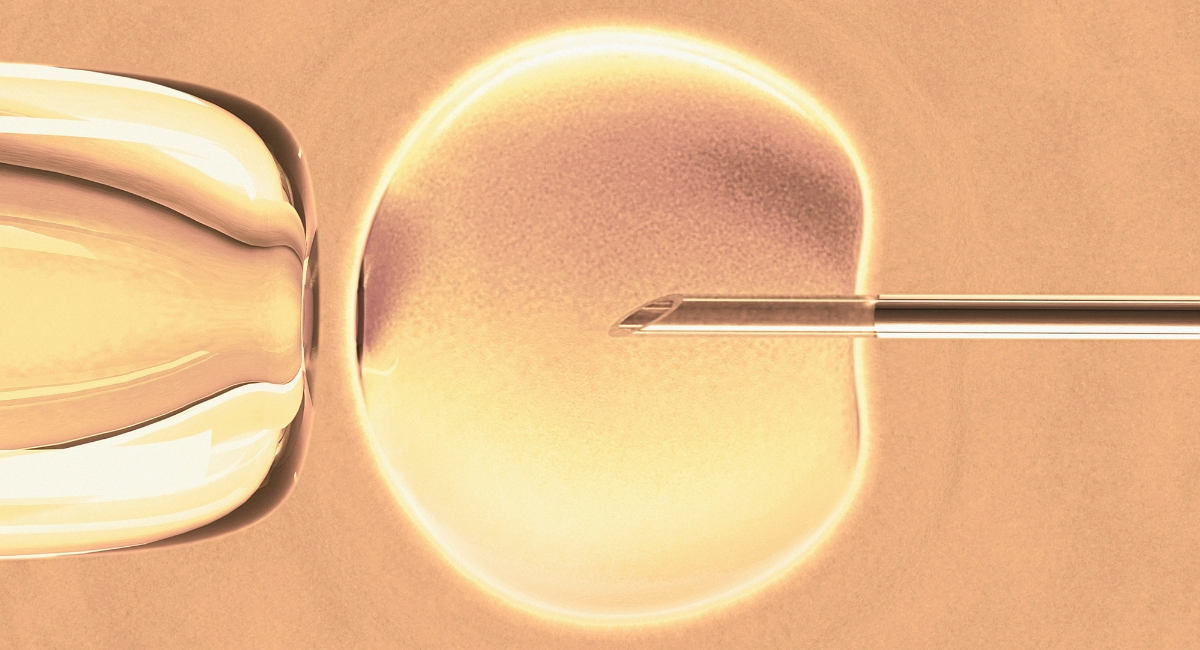











 I am a French mother whose teenage daughter recently announced to me that she was gender dysphoric and wanted hormones. Being left-wing politically oriented, a feminist, and sensitive to the rights of minorities, I first thought my daughter had to be supported in the difficult path to transition.
I am a French mother whose teenage daughter recently announced to me that she was gender dysphoric and wanted hormones. Being left-wing politically oriented, a feminist, and sensitive to the rights of minorities, I first thought my daughter had to be supported in the difficult path to transition.






























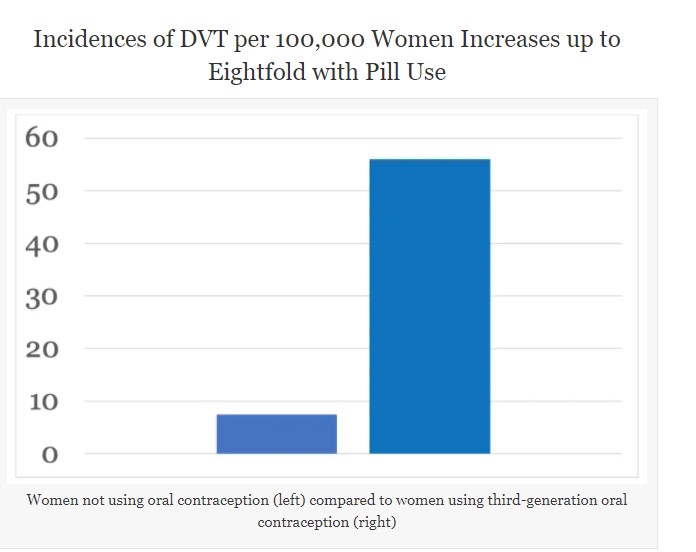















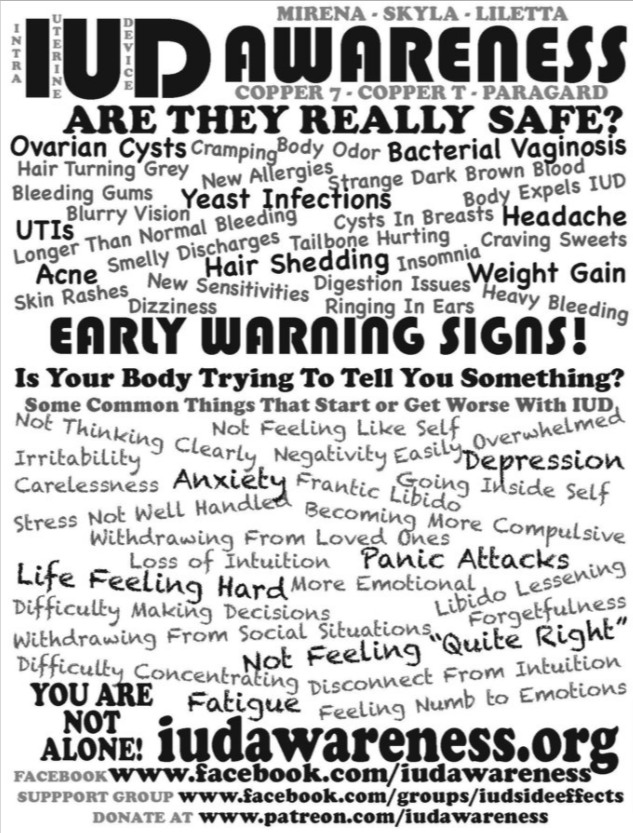


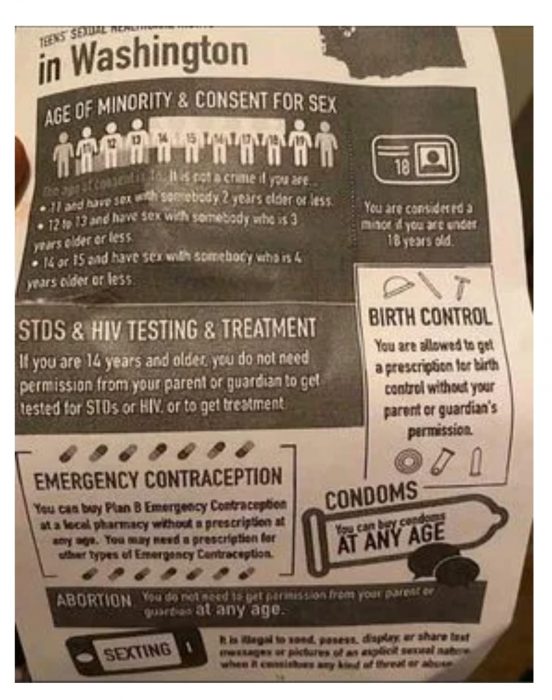


























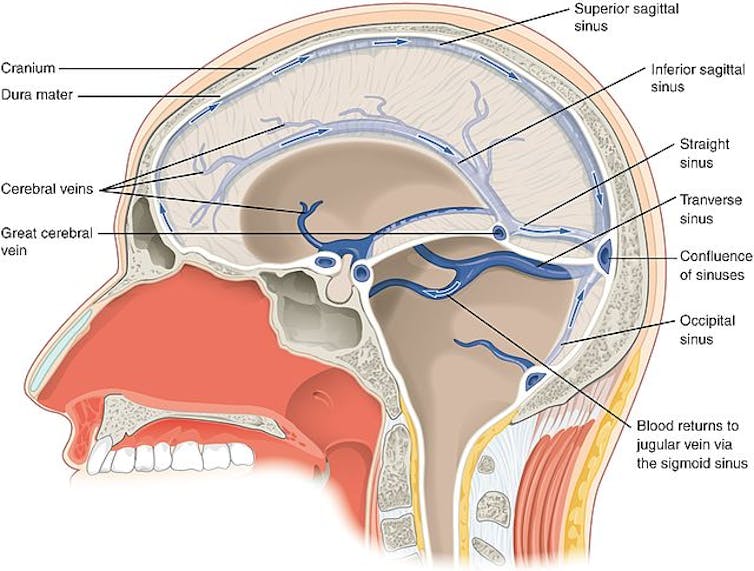








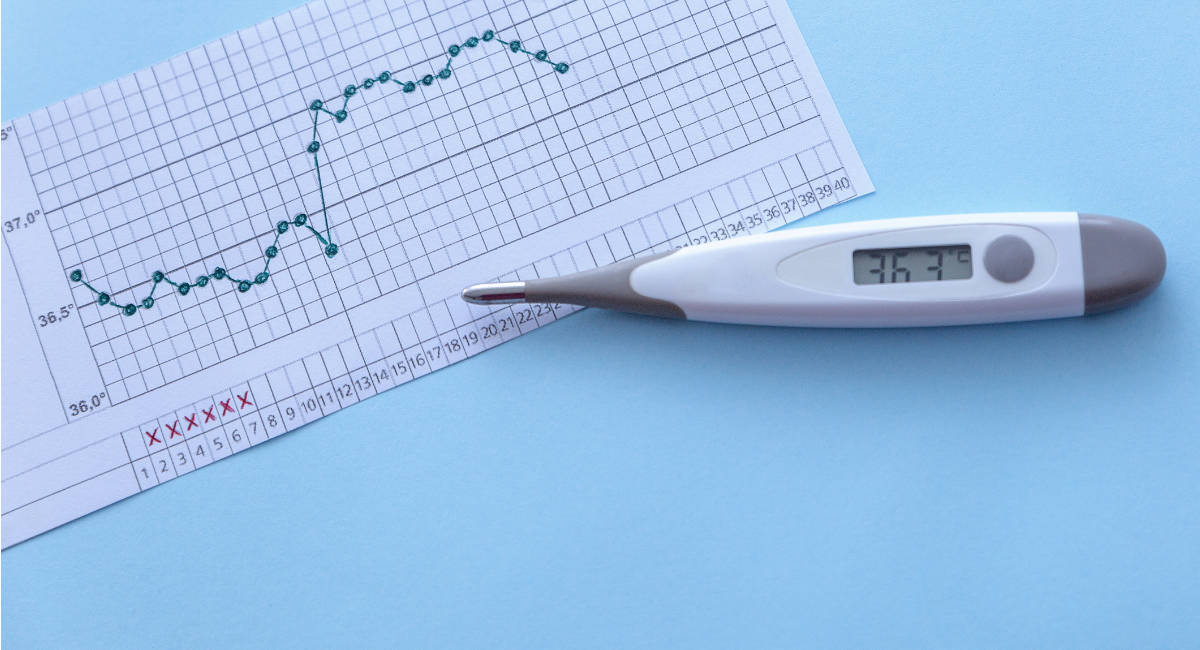




























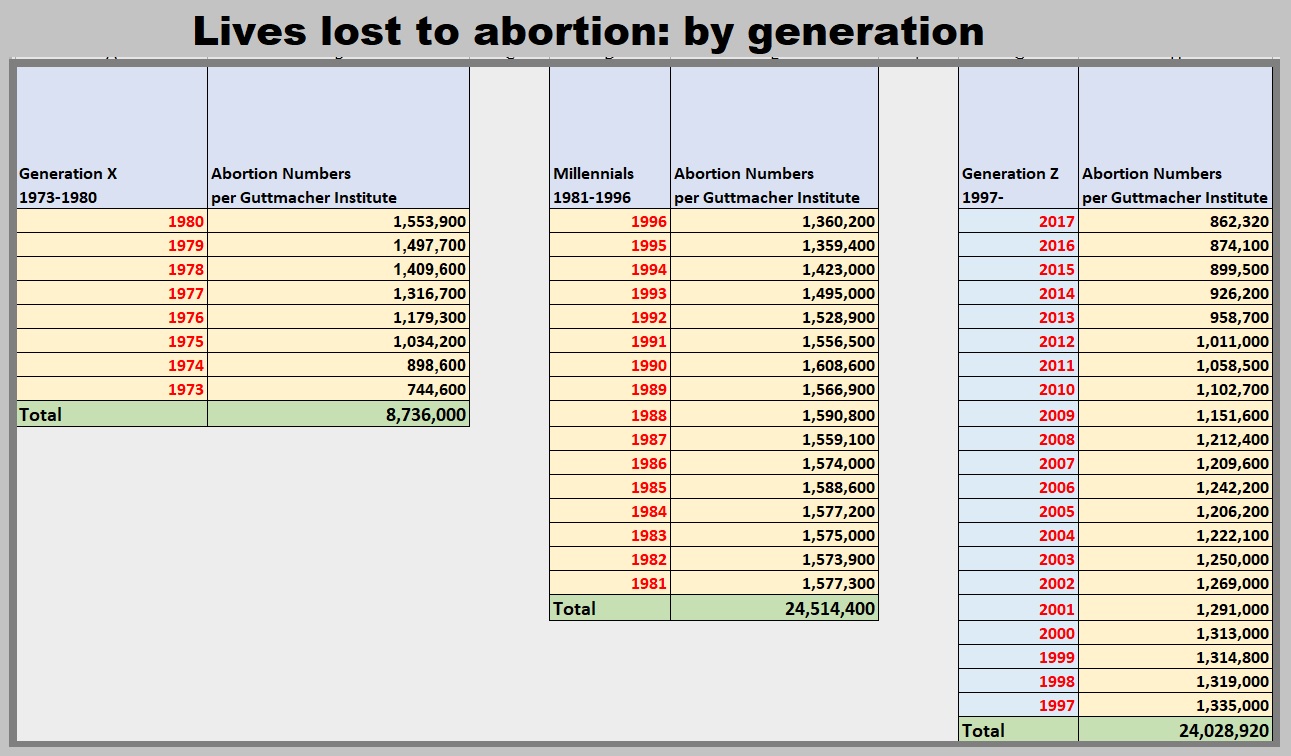











 It’s not the kind of thing one ever forgets, but this time of year our liturgical calendar resurrects the memory in a very poignant way.
It’s not the kind of thing one ever forgets, but this time of year our liturgical calendar resurrects the memory in a very poignant way.





















 We see an example of this at the Battle of Lepanto. During the 1400 and 1500s, the Muslims and Christians were locked in battle, as Christians attempted to block increasing expansion of the Ottoman Empire. The decisive turning point came in 1571, when Pope Pius V sent a fleet comprised of Catholic European states to fight off the Muslims and protect the Mediterranean. He requested all the faithful say the Rosary, asking all to invoke our Blessed Mother’s intercession.
We see an example of this at the Battle of Lepanto. During the 1400 and 1500s, the Muslims and Christians were locked in battle, as Christians attempted to block increasing expansion of the Ottoman Empire. The decisive turning point came in 1571, when Pope Pius V sent a fleet comprised of Catholic European states to fight off the Muslims and protect the Mediterranean. He requested all the faithful say the Rosary, asking all to invoke our Blessed Mother’s intercession.








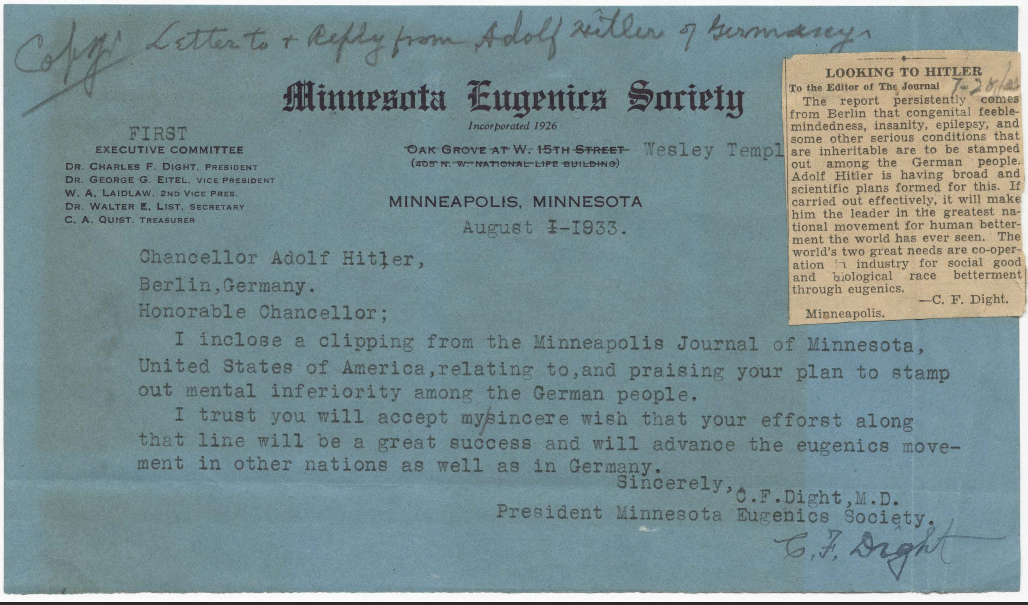
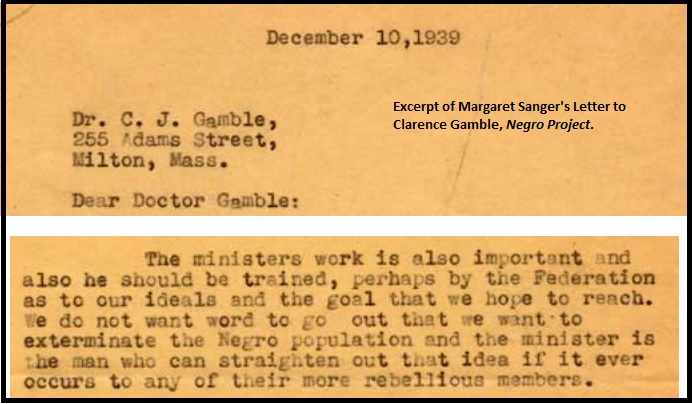
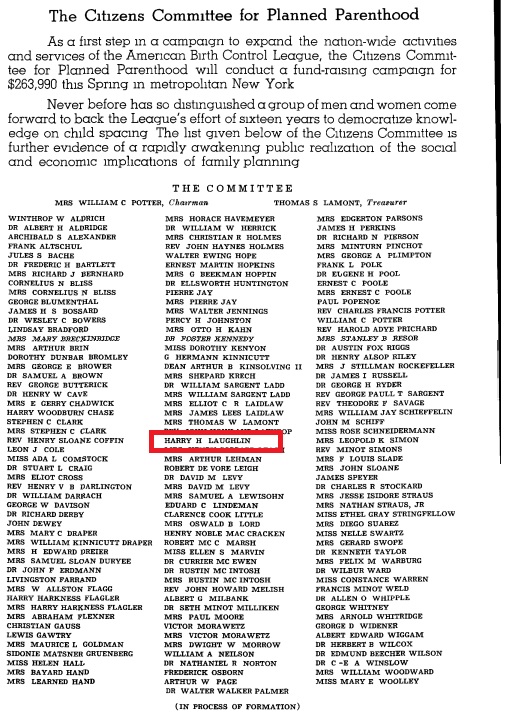




























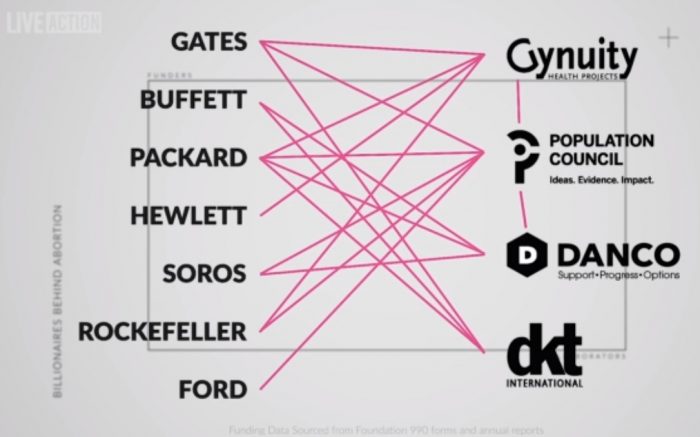

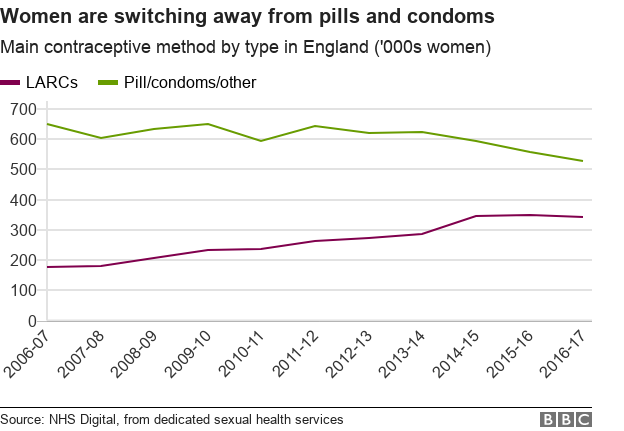























 As these hormones have an effect on our brain, bones, libido, and moods, it should come as no surprise that even our heart is affected by them, too.
As these hormones have an effect on our brain, bones, libido, and moods, it should come as no surprise that even our heart is affected by them, too.













































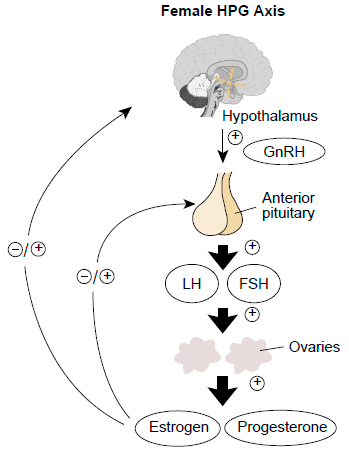













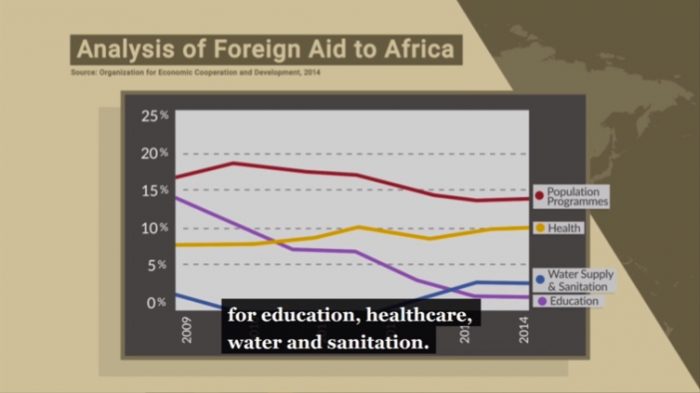


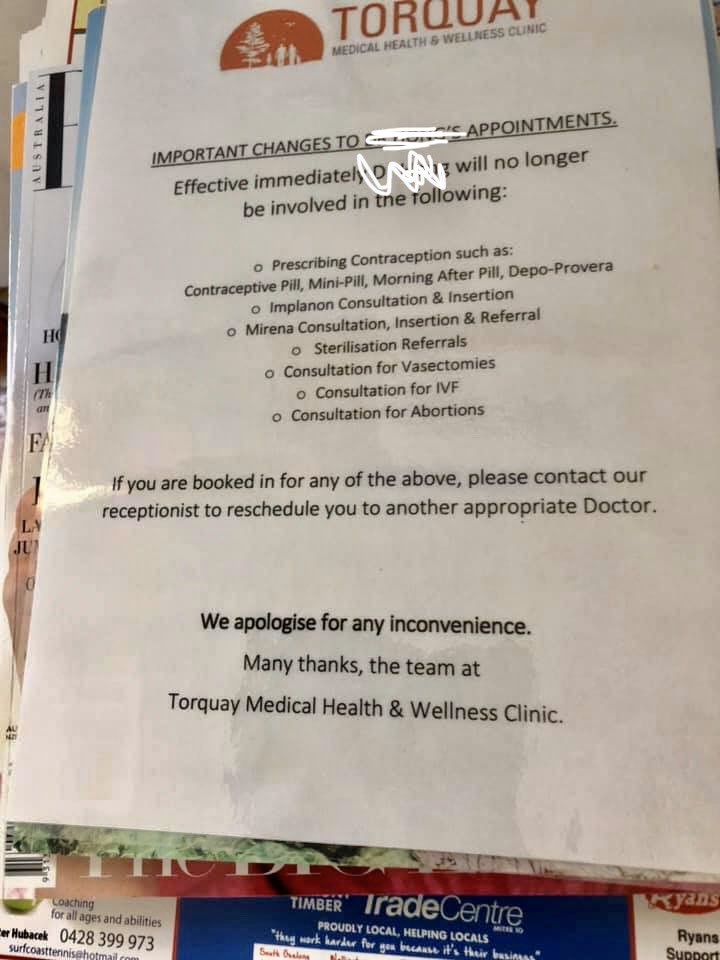


















































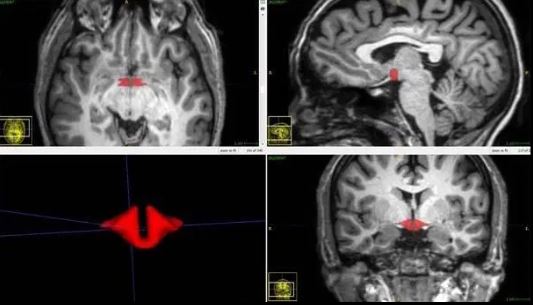









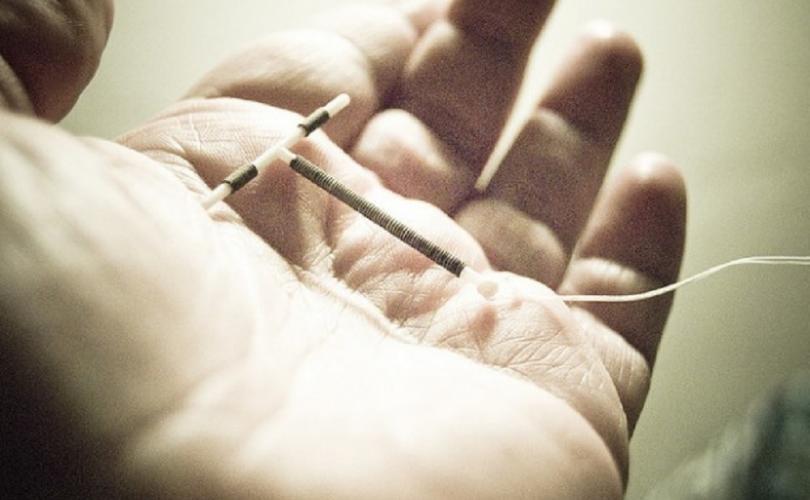

 “Thank you so much for your article. I had a close encounter with death just this afternoon.” Cheyenne then shared her story. She ended her note with these words: “Thank you for your website, which saved my life. I’m forever grateful.”
“Thank you so much for your article. I had a close encounter with death just this afternoon.” Cheyenne then shared her story. She ended her note with these words: “Thank you for your website, which saved my life. I’m forever grateful.”

















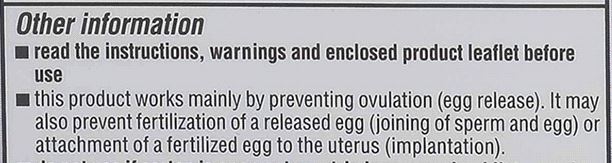






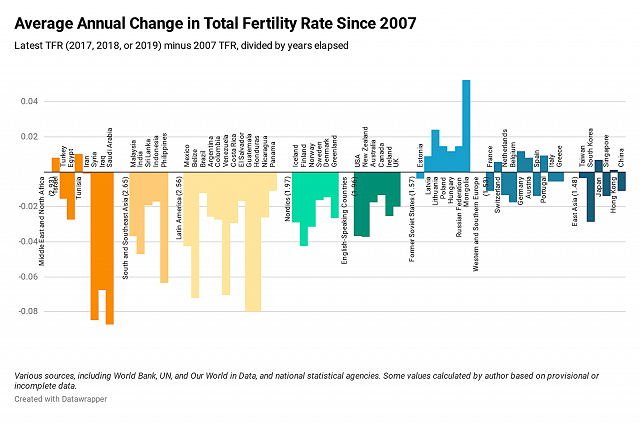
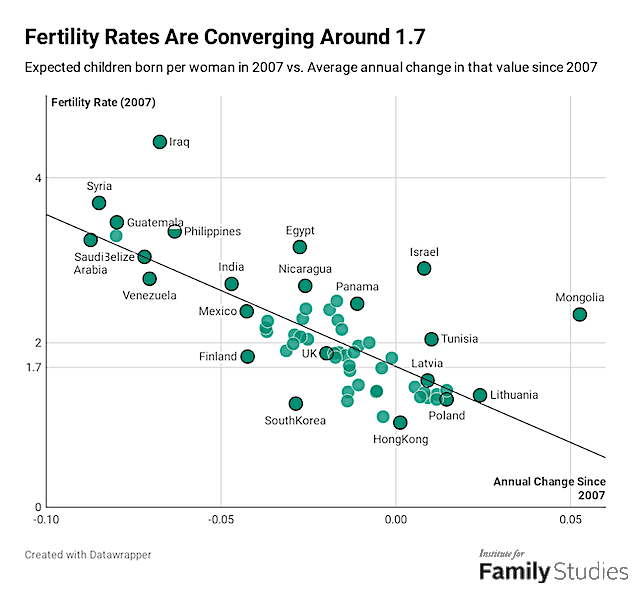
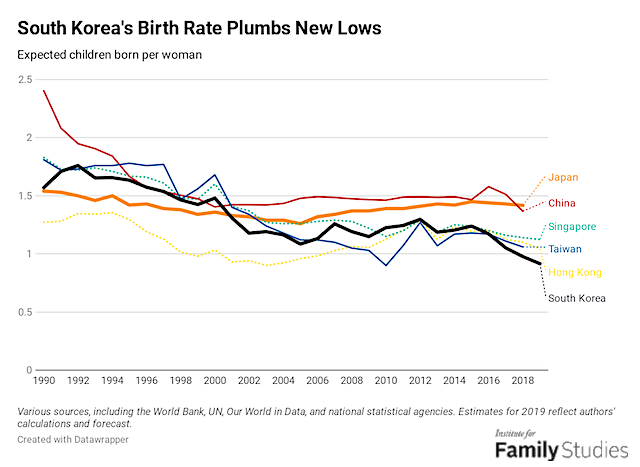
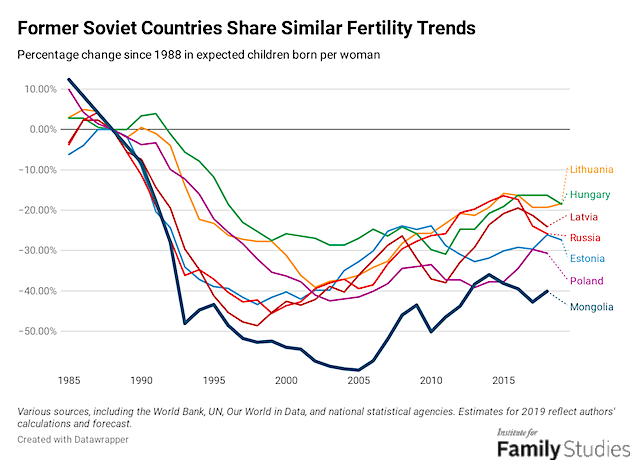
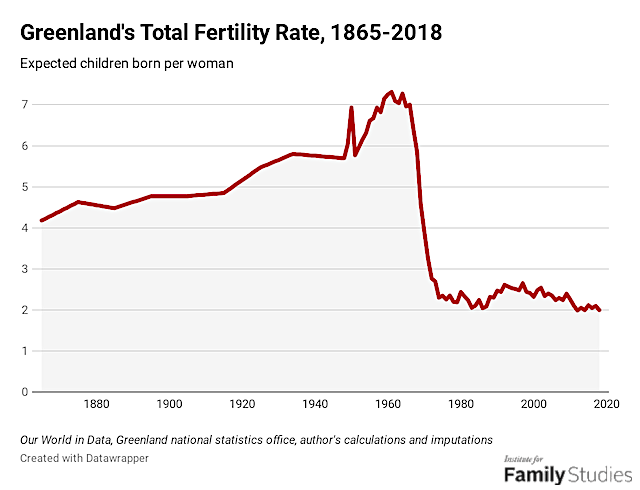
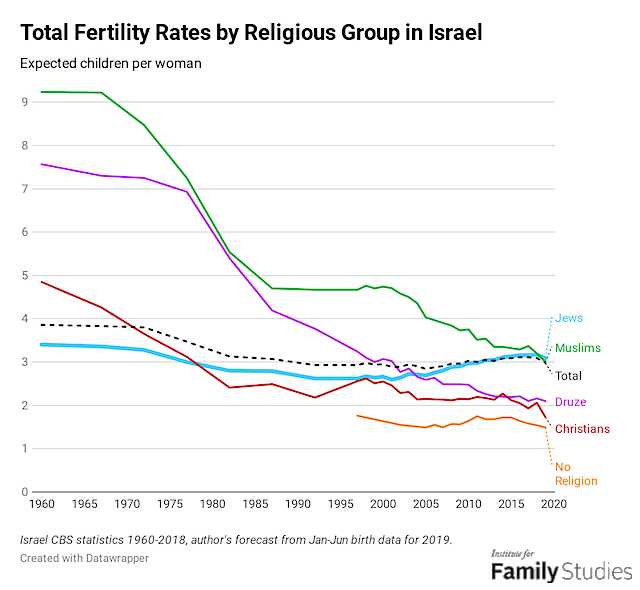



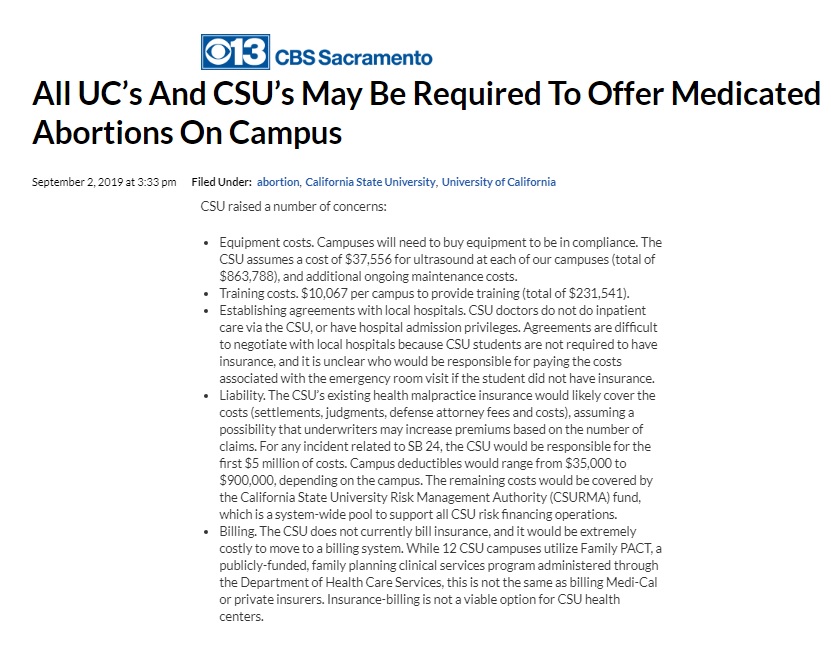
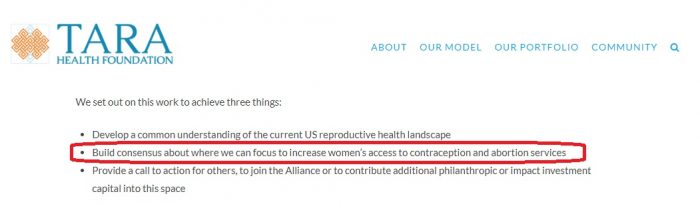
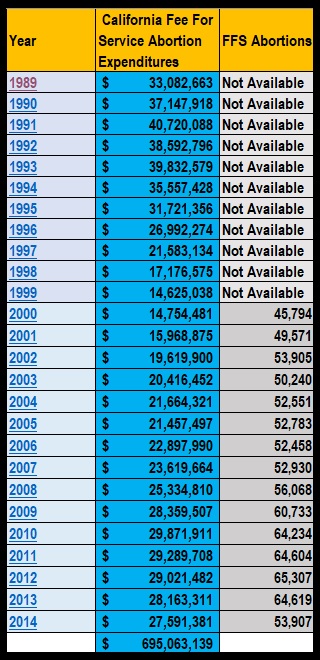





























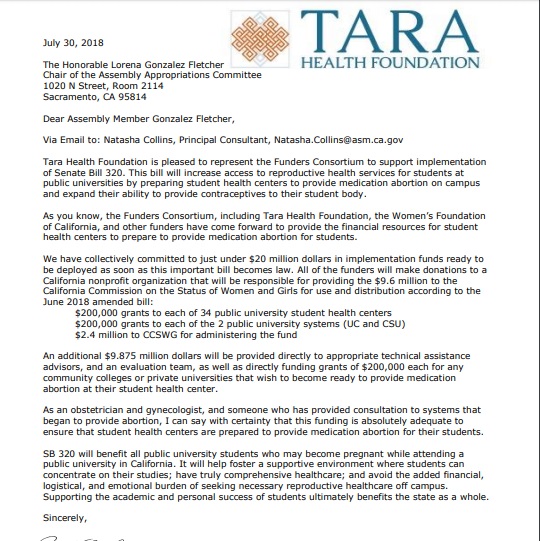























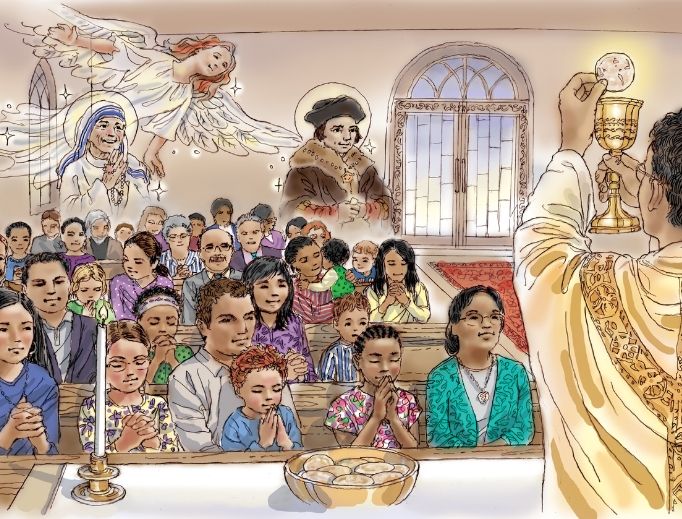

















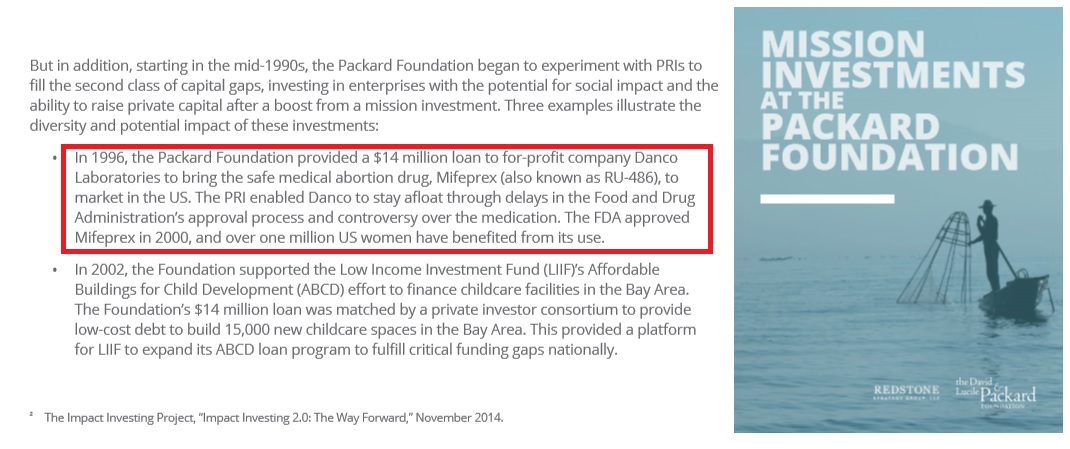

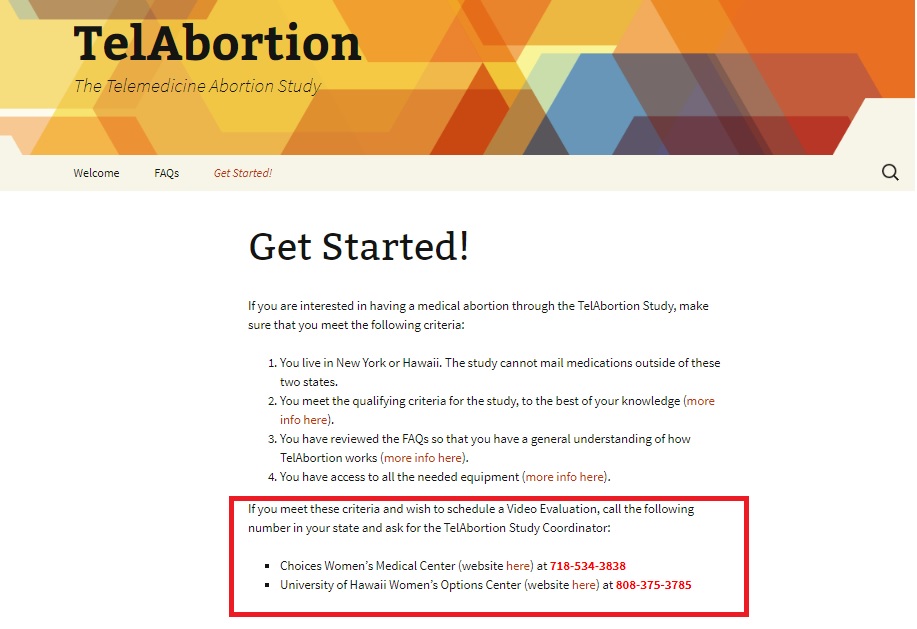
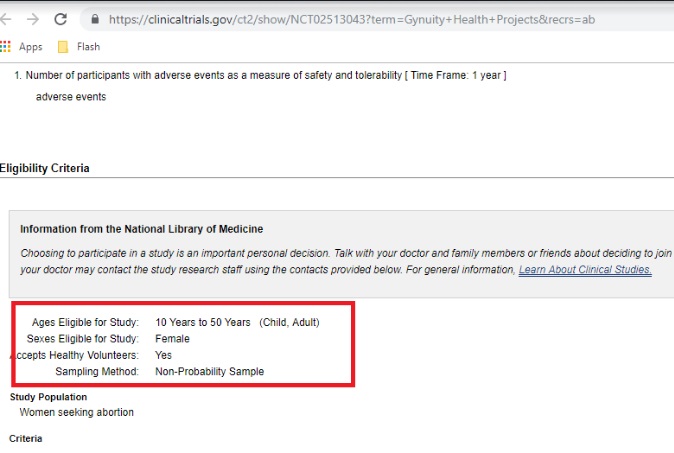
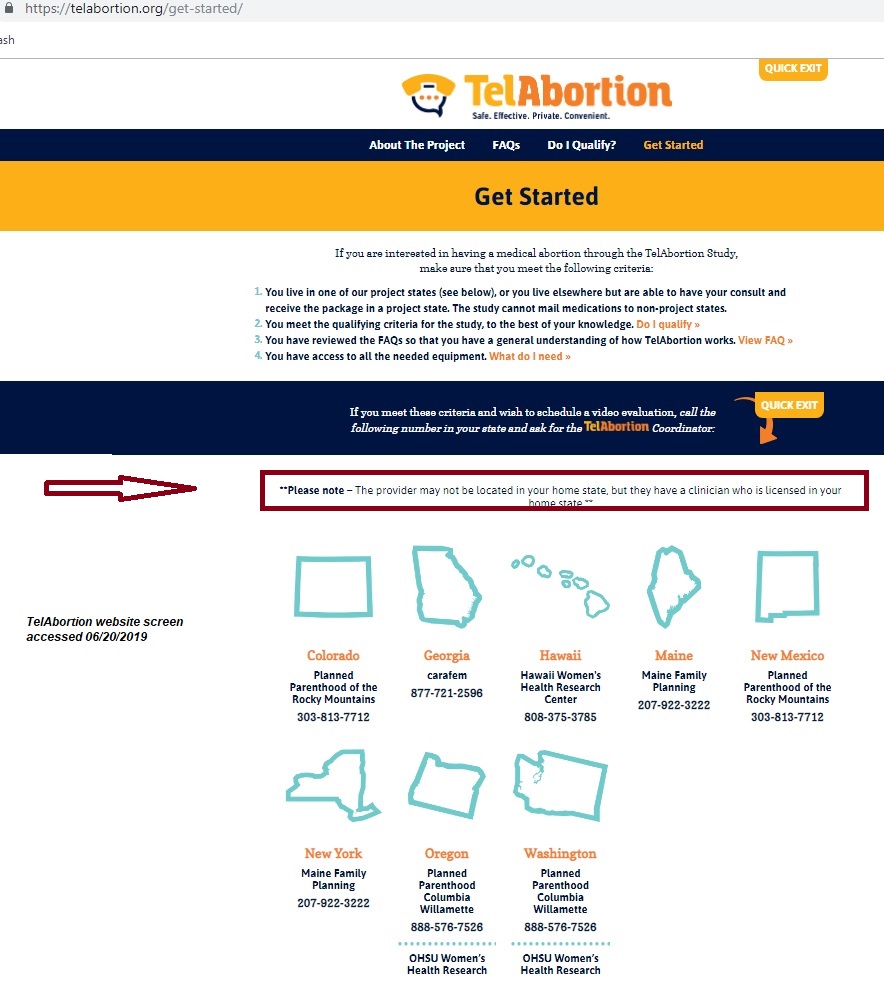


































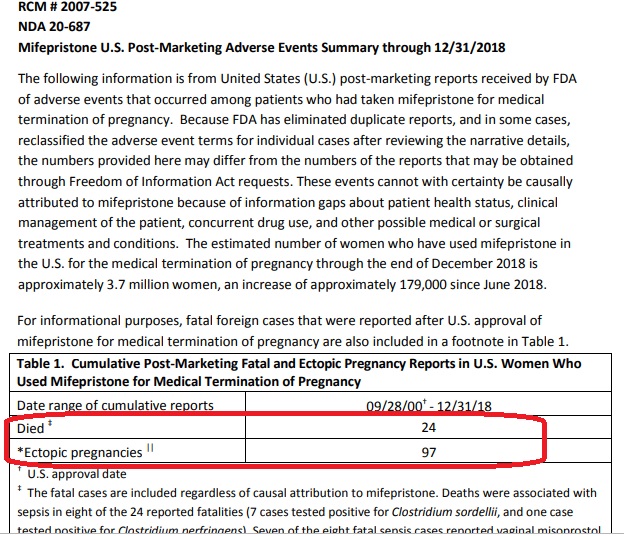

 Shannon Roberts
Shannon Roberts



 At the launch of the campaign,
At the launch of the campaign, 





























 Our latest report on a CRS project (
Our latest report on a CRS project (

 The primary goal of the project is to increase the use of primary healthcare services to local community and the adoption of health enhancing behavior. The project relies on human capital to achieve this goal. The establishment of CSLF or Cosen Savings and Loans funds, which are savings groups of community health volunteers is one way to achieve this. The CSLF presents an opportunity for community health volunteers to have access to financial opportunities such as credit and savings. This practice also enables them to develop their social capital into the community health volunteer’s professional network.
The primary goal of the project is to increase the use of primary healthcare services to local community and the adoption of health enhancing behavior. The project relies on human capital to achieve this goal. The establishment of CSLF or Cosen Savings and Loans funds, which are savings groups of community health volunteers is one way to achieve this. The CSLF presents an opportunity for community health volunteers to have access to financial opportunities such as credit and savings. This practice also enables them to develop their social capital into the community health volunteer’s professional network.





























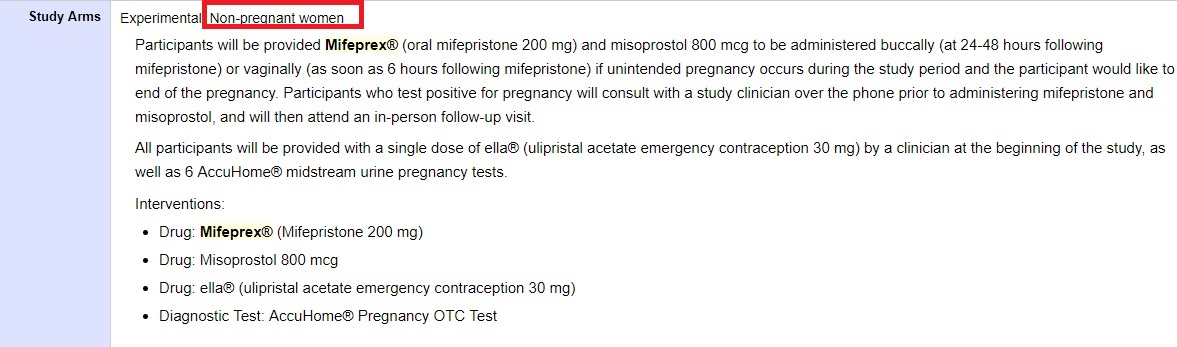

































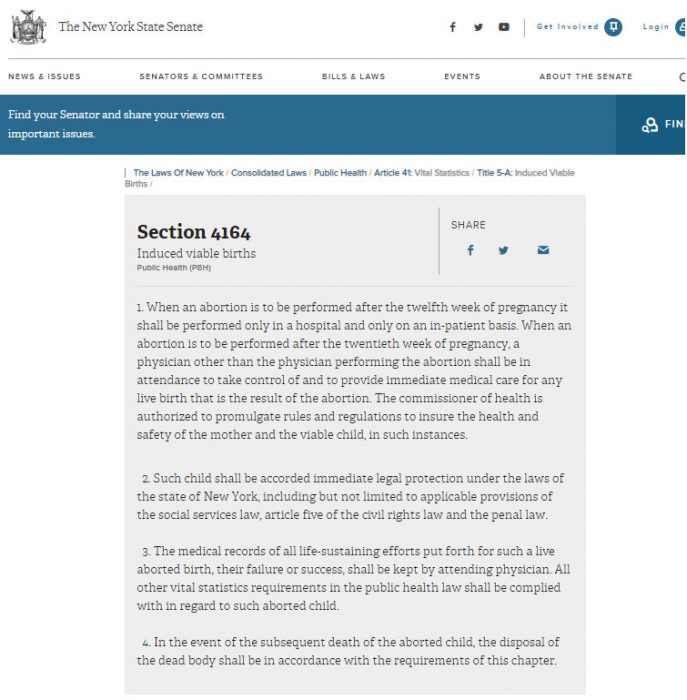




 Pro-abortion advocates want everyone to believe that abortion is a highly “complex” matter rife with shades of grey. But it’s not. Ultimately it comes down to one, simple, scientifically-answerable question: is the unborn child human or not?
Pro-abortion advocates want everyone to believe that abortion is a highly “complex” matter rife with shades of grey. But it’s not. Ultimately it comes down to one, simple, scientifically-answerable question: is the unborn child human or not?























































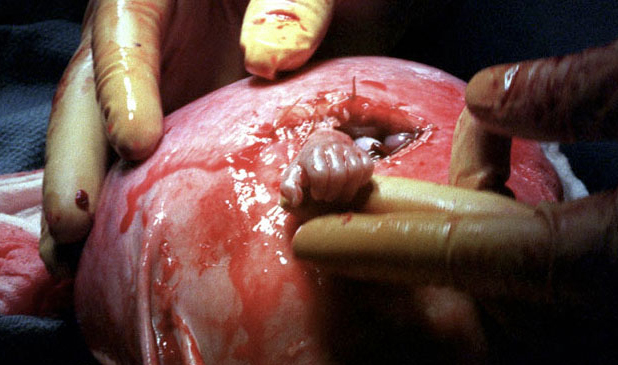
























































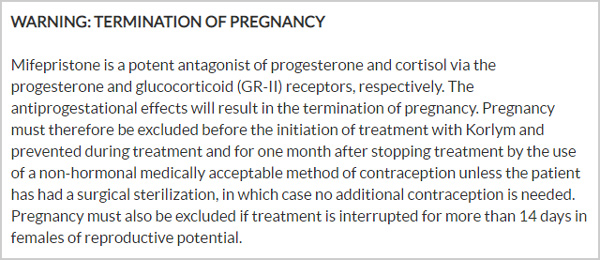
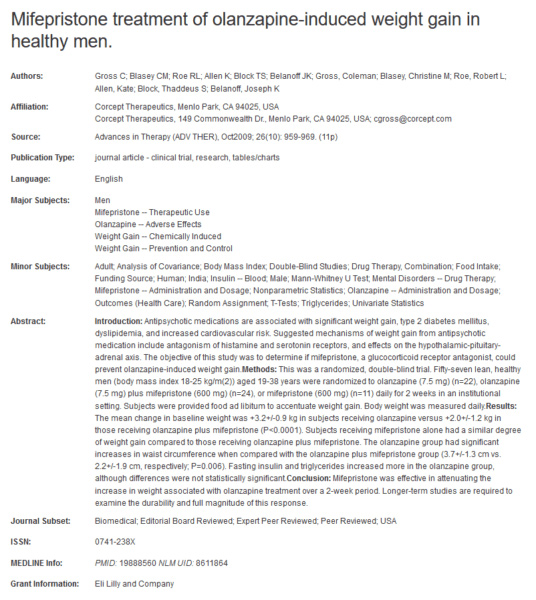



 The attached 1991 Inaugural Address by Dr John J. Ring, M.D. as President of the American Medical Association, includes the following statement:
The attached 1991 Inaugural Address by Dr John J. Ring, M.D. as President of the American Medical Association, includes the following statement:










































 I have had many relatives and friends who lived in nursing homes and, especially as a nurse, I am always saddened by how few of the other residents had any visitors, even family members. I have even heard relatives say they would just prefer to remember their relative “the way they were”.
I have had many relatives and friends who lived in nursing homes and, especially as a nurse, I am always saddened by how few of the other residents had any visitors, even family members. I have even heard relatives say they would just prefer to remember their relative “the way they were”. This week I have been swamped with messages from loyal Catholics who have been shaken and disgusted by the latest eruption of the continuing sex-abuse scandal in the Church. I wish I saw some sign that our bishops recognized the rising tide of anger—righteous anger—among the most active lay Catholics.
This week I have been swamped with messages from loyal Catholics who have been shaken and disgusted by the latest eruption of the continuing sex-abuse scandal in the Church. I wish I saw some sign that our bishops recognized the rising tide of anger—righteous anger—among the most active lay Catholics. When I was a child and preparing to receive my First Holy Communion, I remember being taught to do so the traditional way: on the tongue. In fact, if memory serves, we received Holy Communion via intinction that first time i.e. the priest carefully dipped the host in the Precious Blood before placing it on our tongues. (We were further instructed to allow the host to dissolve and not chew it; I believe this was very practical advice, for if we chewed it particles might have gotten caught in our teeth, which could then fly out if we coughed, sneezed, or just talked.)
When I was a child and preparing to receive my First Holy Communion, I remember being taught to do so the traditional way: on the tongue. In fact, if memory serves, we received Holy Communion via intinction that first time i.e. the priest carefully dipped the host in the Precious Blood before placing it on our tongues. (We were further instructed to allow the host to dissolve and not chew it; I believe this was very practical advice, for if we chewed it particles might have gotten caught in our teeth, which could then fly out if we coughed, sneezed, or just talked.)
 A neuroscientist has found that at least 20 percent of people thought to be in a vegetative state are completely aware of what’s happening around them and to them, but they are unable to respond or move. This means that people thought to be in comas or a ‘vegetative state’ are suffering horrible abuses – being starved and murdered like
A neuroscientist has found that at least 20 percent of people thought to be in a vegetative state are completely aware of what’s happening around them and to them, but they are unable to respond or move. This means that people thought to be in comas or a ‘vegetative state’ are suffering horrible abuses – being starved and murdered like  On July 25 Louise Brown, the world’s
On July 25 Louise Brown, the world’s 
 The #MeToo movement provides a sobering opportunity for deeper reflection on the meaning of sex and the nature of the sexual revolution. A core question is this: Do the experiences underlying #MeToo reveal the need to carry the sexual revolution still further, or do they reveal fundamental flaws in that revolution?
The #MeToo movement provides a sobering opportunity for deeper reflection on the meaning of sex and the nature of the sexual revolution. A core question is this: Do the experiences underlying #MeToo reveal the need to carry the sexual revolution still further, or do they reveal fundamental flaws in that revolution? Think about the purity, holiness, and magnificence of the Blessed Virgin Mary. She was the only human being ever to be sinless and constantly in a state of grace. Because Mary was such a beautiful symbol of grace, her mother, St. Anne, must have also been a devout woman of God.
Think about the purity, holiness, and magnificence of the Blessed Virgin Mary. She was the only human being ever to be sinless and constantly in a state of grace. Because Mary was such a beautiful symbol of grace, her mother, St. Anne, must have also been a devout woman of God. July 25, 2018 (
July 25, 2018 ( July 25, 2018 (
July 25, 2018 ( Since the advent of birth control more than 50 years ago, women have repeatedly been told that the drugs and devices being offered to help them avoid pregnancy are “safe and effective.” We’re told that the “small percentage” of women who experience adverse reactions is so minimal the risks simply don’t outweigh the benefits.
Since the advent of birth control more than 50 years ago, women have repeatedly been told that the drugs and devices being offered to help them avoid pregnancy are “safe and effective.” We’re told that the “small percentage” of women who experience adverse reactions is so minimal the risks simply don’t outweigh the benefits.

 We would be hiring highly trained NFP experts to serve in diocesan offices and parishes to provide individualized support to couples. We would be creating consistent, nationally recognized standards for training NFP teachers as well as national, easily searchable databases where couples could search for local NFP instructors. We would be advertising NFP-training resources in every parish bulletin, every week. We would be providing funding for low-income families who cannot afford the costs of NFP instruction, which in my opinion should be free. We would be holding regular and well-advertised NFP training sessions around the diocese to educate already-married couples and incorporating NFP into pre-marital preparation programs – and not just a one-hour course or weekend program.
We would be hiring highly trained NFP experts to serve in diocesan offices and parishes to provide individualized support to couples. We would be creating consistent, nationally recognized standards for training NFP teachers as well as national, easily searchable databases where couples could search for local NFP instructors. We would be advertising NFP-training resources in every parish bulletin, every week. We would be providing funding for low-income families who cannot afford the costs of NFP instruction, which in my opinion should be free. We would be holding regular and well-advertised NFP training sessions around the diocese to educate already-married couples and incorporating NFP into pre-marital preparation programs – and not just a one-hour course or weekend program.
 Wanda Półtawska, a Polish doctor, is 97 years old. Her life and work is unknown outside her native Poland and some quarters of the Catholic Church, but her insights and influence have prospered the mission of the Church in defending the dignity of all human beings.
Wanda Półtawska, a Polish doctor, is 97 years old. Her life and work is unknown outside her native Poland and some quarters of the Catholic Church, but her insights and influence have prospered the mission of the Church in defending the dignity of all human beings.
 “But, see, the point of an abortion at that gestational age,” says Harrison, “is to make sure that the baby is dead. So it’s to produce a dead baby. It’s not to save a mother’s life.”
“But, see, the point of an abortion at that gestational age,” says Harrison, “is to make sure that the baby is dead. So it’s to produce a dead baby. It’s not to save a mother’s life.”

 IT IS WAR! NO, ITS NOT POISON GAS THE ENEMY IS USING, IT IS ESTROGEN. IT IS IN THE TAP WATER. WHEN MY VOICE STARTED CHANGING FROM BASS TO TENOR I STARTED DRINKING DISTILLED WATER AND NOW I AM A BARITONE !!!
IT IS WAR! NO, ITS NOT POISON GAS THE ENEMY IS USING, IT IS ESTROGEN. IT IS IN THE TAP WATER. WHEN MY VOICE STARTED CHANGING FROM BASS TO TENOR I STARTED DRINKING DISTILLED WATER AND NOW I AM A BARITONE !!! July 12, 2018 (
July 12, 2018 ( We are already seeing a great battle unfold over the Supreme Court in our land. At one level the battle is “all about abortion” which the left sees as almost a “sacrament” or sacred honor, and the right sees as the most immoral and legally flawed decision ever handed down by the court (Dred Scott notwithstanding).
We are already seeing a great battle unfold over the Supreme Court in our land. At one level the battle is “all about abortion” which the left sees as almost a “sacrament” or sacred honor, and the right sees as the most immoral and legally flawed decision ever handed down by the court (Dred Scott notwithstanding). ALBANY, July 10, 2018 (
ALBANY, July 10, 2018 ( The readings for the 14th Sunday of Ordinary Time (July 8) focus on prophets. The text from Ezekiel tells us that, whether people listen or not has nothing to do with the truth of the prophet’s message. The Gospel contains the famous line about “a prophet [being] not without honor, except in his native place.”
The readings for the 14th Sunday of Ordinary Time (July 8) focus on prophets. The text from Ezekiel tells us that, whether people listen or not has nothing to do with the truth of the prophet’s message. The Gospel contains the famous line about “a prophet [being] not without honor, except in his native place.” Remember the Holy League of Nations that Pope St. Pius V formed in 1571, and the result of the battle they engaged in? Their victory at Lepanto on Oct. 7, 1571 was attributed to the Rosary, and the date became the Feast of Our Lady of the Holy Rosary.
Remember the Holy League of Nations that Pope St. Pius V formed in 1571, and the result of the battle they engaged in? Their victory at Lepanto on Oct. 7, 1571 was attributed to the Rosary, and the date became the Feast of Our Lady of the Holy Rosary.
 LA CROSSE, Wisconsin, July 4, 2018 (
LA CROSSE, Wisconsin, July 4, 2018 ( One of the biggest complaints of those who visit their doctors is how the physician pays more attention to their computer screens than them. This treatment of a human being, at least implicitly, denies the needs of the soul. Things such as compassion and understanding, so helpful in the healing process, are often absent in these impersonal medical visits. Patients can be left with the feeling they are nothing but the sum of data entered into a spreadsheet.
One of the biggest complaints of those who visit their doctors is how the physician pays more attention to their computer screens than them. This treatment of a human being, at least implicitly, denies the needs of the soul. Things such as compassion and understanding, so helpful in the healing process, are often absent in these impersonal medical visits. Patients can be left with the feeling they are nothing but the sum of data entered into a spreadsheet. Writing in The Times, Dominic Lawson says there is something obscene about the ‘shortening’ of the lives of more than 450 patients who were staying in Gosport War Memorial Hospital. He is right.
Writing in The Times, Dominic Lawson says there is something obscene about the ‘shortening’ of the lives of more than 450 patients who were staying in Gosport War Memorial Hospital. He is right. June 28, 2018 (
June 28, 2018 ( TYLER, Texas, June 27, 2018 (
TYLER, Texas, June 27, 2018 ( June 26, 2018 (
June 26, 2018 ( WASHINGTON, D.C., June 26, 2018 (
WASHINGTON, D.C., June 26, 2018 (


 Peter Kwasniewski
Peter Kwasniewski
 Over the next month, for instance, dozens of “gay pride” parades will take place across North America and Europe. Millions of people – including many of our most prominent politicians – will attend these parades, often with their children in tow, to watch completely nude marchers, men in sado-masochistic paraphernalia, and floats with drag queens and gyrating men in underwear.
Over the next month, for instance, dozens of “gay pride” parades will take place across North America and Europe. Millions of people – including many of our most prominent politicians – will attend these parades, often with their children in tow, to watch completely nude marchers, men in sado-masochistic paraphernalia, and floats with drag queens and gyrating men in underwear. Abortion, no matter the race, is a tragic loss of beauty and potential that kills over 1.2 million innocent human lives each year. The abortion industry has created a culture of abandonment. Responsibility has become someone else’s concern, and death the solution to this serious character flaw. Men have been empowered by Roe v. Wade to abandon their primary responsibility–protecting. They’ve either chosen to run away from their role or have been forced out by a brand of liberal feminism that spews gender animus in an effort to elevate women. No one is elevated by 41% of all U.S. children being born to unmarried mothers. In the black community, 72.3% of all children are born in homes without fathers (compared to 35.7% of white children). Fatherlessness is epidemic in our culture.
Abortion, no matter the race, is a tragic loss of beauty and potential that kills over 1.2 million innocent human lives each year. The abortion industry has created a culture of abandonment. Responsibility has become someone else’s concern, and death the solution to this serious character flaw. Men have been empowered by Roe v. Wade to abandon their primary responsibility–protecting. They’ve either chosen to run away from their role or have been forced out by a brand of liberal feminism that spews gender animus in an effort to elevate women. No one is elevated by 41% of all U.S. children being born to unmarried mothers. In the black community, 72.3% of all children are born in homes without fathers (compared to 35.7% of white children). Fatherlessness is epidemic in our culture.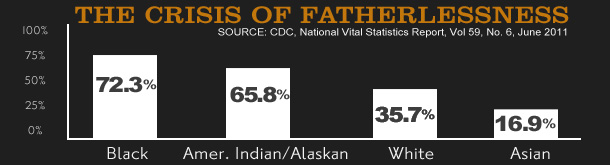
 children are born following marriage. The reality is that we’ve got a lot of healing, education, and mentoring to happen to get there. So even if marriage is not chosen, children STILL need their fathers!
children are born following marriage. The reality is that we’ve got a lot of healing, education, and mentoring to happen to get there. So even if marriage is not chosen, children STILL need their fathers! ROME, June 13, 2018 (
ROME, June 13, 2018 ( June 11, 2018 (
June 11, 2018 ( In a groundbreaking conference held in Washington DC last month, some of the Church’s most influential women spoke about how the #MeToo movement proves the abject failure of the now 50-year-old sexual revolution that was supposed to liberate us and set us free.
In a groundbreaking conference held in Washington DC last month, some of the Church’s most influential women spoke about how the #MeToo movement proves the abject failure of the now 50-year-old sexual revolution that was supposed to liberate us and set us free.





 E. Christian Brugger
E. Christian Brugger When Pope Paul VI issued the encyclical Humanae Vitae on July 25, 1968, the world immediately interpreted it as a gigantic “no.” At a time when the whole world was ecstatically embracing the new forms of artificial contraception – especially the seemingly miraculous birth control pill – many, including a large percentage of Catholics, looked to the Church to change its teachings to align with technological and so-called societal progress.
When Pope Paul VI issued the encyclical Humanae Vitae on July 25, 1968, the world immediately interpreted it as a gigantic “no.” At a time when the whole world was ecstatically embracing the new forms of artificial contraception – especially the seemingly miraculous birth control pill – many, including a large percentage of Catholics, looked to the Church to change its teachings to align with technological and so-called societal progress. June 6, 2018 (
June 6, 2018 ( There are those who believe he should never have been allowed to be born.
There are those who believe he should never have been allowed to be born. June 5, 2018 (
June 5, 2018 (

 “The little pill that gave women freedom.” That’s the way The Conversation bills a clutch of articles marking nearly six decades of what the birth control boffins call “effective” contraception. With the release of the pill from 1957 onwards, women “celebrated the new control they had over their fertility,” writes Bryony McNeill, a lecturer in reproductive physiology at Deakin University, in “
“The little pill that gave women freedom.” That’s the way The Conversation bills a clutch of articles marking nearly six decades of what the birth control boffins call “effective” contraception. With the release of the pill from 1957 onwards, women “celebrated the new control they had over their fertility,” writes Bryony McNeill, a lecturer in reproductive physiology at Deakin University, in “ It seems like the question keeps coming up and yet there seems to be little to no response from our Bishops. Every year since 1965, the priest to faithful ratio has gotten worse. There is not much more than hand wringing going on to solve the problem. The trend keeps spiraling downwards. The seminaries of yesteryear are almost all closed, consolidated, or operating at minimal capacities.
It seems like the question keeps coming up and yet there seems to be little to no response from our Bishops. Every year since 1965, the priest to faithful ratio has gotten worse. There is not much more than hand wringing going on to solve the problem. The trend keeps spiraling downwards. The seminaries of yesteryear are almost all closed, consolidated, or operating at minimal capacities. The pro-choice movement in Ireland won as emphatic a victory on Friday as the pro-life movement did in 1983. What was the response of the pro-choice side to their heavy defeat back then? Was it to go away? It was not. Instead they took the long view and immediately began the work of repealing the 8th amendment.
The pro-choice movement in Ireland won as emphatic a victory on Friday as the pro-life movement did in 1983. What was the response of the pro-choice side to their heavy defeat back then? Was it to go away? It was not. Instead they took the long view and immediately began the work of repealing the 8th amendment. Individual Americans have enjoyed more personal freedom, individual rights, and collective liberty than most, if not all, other civilizations in history. Yet we are living in a time when freedom, rights, and liberty have been so thoroughly redefined and distorted that we struggle to communicate with each other. A faithful Catholic uses the same words as a secular progressive, but the meanings of the words we use are often different. We may as well be speaking a different language. Words like freedom, gender, identity, and healthcare are defined differently by progressives. Meanwhile, public relations firms and marketing professionals spend untold hours coming up with the perfect way to pitch the product and ideology of their client. Arguments are carefully framed to make sure all dissent sounds politically incorrect. The redefinitions are now being used to eliminate religious freedom, virtue, and the most basic building blocks of civilization: marriage and family.
Individual Americans have enjoyed more personal freedom, individual rights, and collective liberty than most, if not all, other civilizations in history. Yet we are living in a time when freedom, rights, and liberty have been so thoroughly redefined and distorted that we struggle to communicate with each other. A faithful Catholic uses the same words as a secular progressive, but the meanings of the words we use are often different. We may as well be speaking a different language. Words like freedom, gender, identity, and healthcare are defined differently by progressives. Meanwhile, public relations firms and marketing professionals spend untold hours coming up with the perfect way to pitch the product and ideology of their client. Arguments are carefully framed to make sure all dissent sounds politically incorrect. The redefinitions are now being used to eliminate religious freedom, virtue, and the most basic building blocks of civilization: marriage and family. FROM THE National Center for Health Statistics came some disturbing news last week: The US birthrate, which has been on the skids for a decade,
FROM THE National Center for Health Statistics came some disturbing news last week: The US birthrate, which has been on the skids for a decade, 
 CHARTRES, France, May 25, 2018 (
CHARTRES, France, May 25, 2018 ( Editor’s note: The following address was given by Lepanto Institute President Michael Hichborn at the
Editor’s note: The following address was given by Lepanto Institute President Michael Hichborn at the 

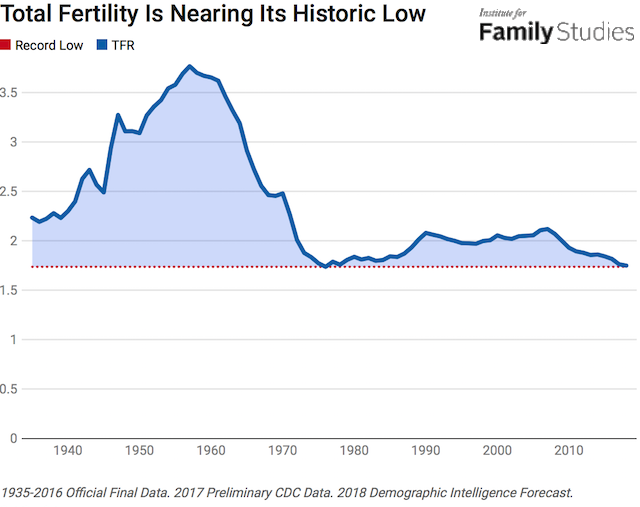
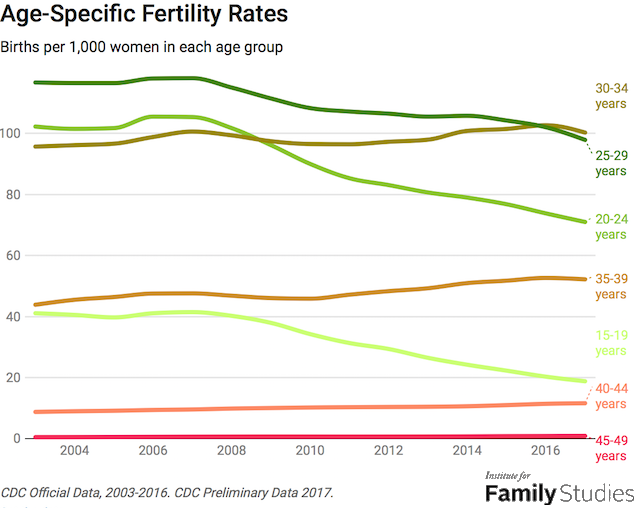
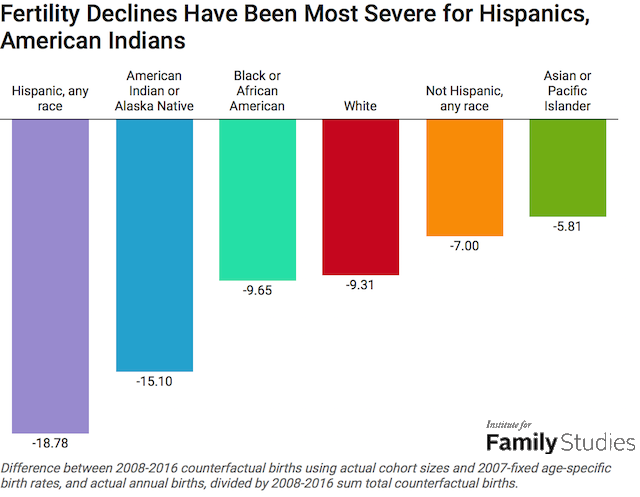
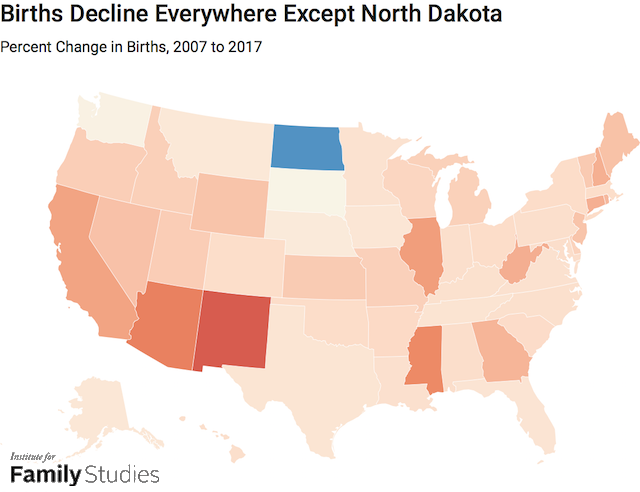
 Since our foundation, Human Life International has committed itself to emphasizing efforts
Since our foundation, Human Life International has committed itself to emphasizing efforts  My sister who lives here in Portland watched on EWTN the Mass I celebrated at the Basilica of the National Shrine of the Immaculate Conception on April 28. One of her comments (after she finished making fun of her younger brother!) was about how Holy Communion was received. She remembered with some real fondness how, when we were children, we always received Holy Communion at the Communion rail and on the tongue. No one dared touch the Holy Eucharist, except the priest.
My sister who lives here in Portland watched on EWTN the Mass I celebrated at the Basilica of the National Shrine of the Immaculate Conception on April 28. One of her comments (after she finished making fun of her younger brother!) was about how Holy Communion was received. She remembered with some real fondness how, when we were children, we always received Holy Communion at the Communion rail and on the tongue. No one dared touch the Holy Eucharist, except the priest. WASHINGTON — The extraordinary form of the Mass is drawing young people with its sense of reverence and transcendence, Portland Archbishop Alexander Sample said during an April 28 homily in Washington, D.C.
WASHINGTON — The extraordinary form of the Mass is drawing young people with its sense of reverence and transcendence, Portland Archbishop Alexander Sample said during an April 28 homily in Washington, D.C. For Mother’s Day the US website
For Mother’s Day the US website  This is what we face. According to the prevailing view, the love of a man and a woman is not an enduring commitment of the will to the true good of another person, but a feeling or an emotion. Essentially, then, what the culture calls matrimony is cohabitation with formalities. Like cohabiting couples — or cohabiting threesomes or what have you — a married couple may speak of having a committed relationship, but commitment in the traditional sense is just what they do not have. Sexual intercourse is not viewed as suggestive of the possibility of new life; neither is having children viewed as requiring intercourse, because these days there are labs for that. Though even in this day of plummeting birth rates, children may still be desired, adults tend to view them as a lifestyle enhancement, something like a home entertainment center, but more expensive. Though having a few children may still be regarded favorably, having more than a few is frowned upon, because children consume resources, use up disposable income, and require a great deal of care. A puzzled writer who is not quite so extreme as to condemn all childbearing says nevertheless, “I don’t have the answer to the origin of the longing for children that many experience. It’s almost certainly due to a complex mixture of biological and social factors. It might even be an evolutionary trick.”
This is what we face. According to the prevailing view, the love of a man and a woman is not an enduring commitment of the will to the true good of another person, but a feeling or an emotion. Essentially, then, what the culture calls matrimony is cohabitation with formalities. Like cohabiting couples — or cohabiting threesomes or what have you — a married couple may speak of having a committed relationship, but commitment in the traditional sense is just what they do not have. Sexual intercourse is not viewed as suggestive of the possibility of new life; neither is having children viewed as requiring intercourse, because these days there are labs for that. Though even in this day of plummeting birth rates, children may still be desired, adults tend to view them as a lifestyle enhancement, something like a home entertainment center, but more expensive. Though having a few children may still be regarded favorably, having more than a few is frowned upon, because children consume resources, use up disposable income, and require a great deal of care. A puzzled writer who is not quite so extreme as to condemn all childbearing says nevertheless, “I don’t have the answer to the origin of the longing for children that many experience. It’s almost certainly due to a complex mixture of biological and social factors. It might even be an evolutionary trick.”







 It’s been a titanic battle – UK’s Alder Hey Children’s Hospital versus a helpless 23-month-old boy.
It’s been a titanic battle – UK’s Alder Hey Children’s Hospital versus a helpless 23-month-old boy. A New Hampshire father recently admitted to leaving a bullet at a Massachusetts abortion facility while his girlfriend was having their unborn baby aborted.
A New Hampshire father recently admitted to leaving a bullet at a Massachusetts abortion facility while his girlfriend was having their unborn baby aborted. In Humanae Vitae, Blessed Pope Paul VI made several predictions of what widespread use of contraceptives would lead to. These included an increase in marital infidelity, lowering of moral standards, men considering women as “a mere instrument for the satisfaction of his own desires” (e.g. Harvey Weinstein and many others) and the imposition of contraception by governmental authorities. These have all come to pass. How could he have been so accurate in his predictions? I think this is because the Blessed Pope had a firm grasp of the profound unity of spirit, mind and body that is the human person. The Catechism teaches us, “The unity of soul and body is so profound that one has to consider the soul to be the “form” of the body: i.e., it is because of its spiritual soul that the body made of matter becomes a living, human body; spirit and matter, in man, are not two natures united, but rather their union forms a single nature.” (CCC 365).
In Humanae Vitae, Blessed Pope Paul VI made several predictions of what widespread use of contraceptives would lead to. These included an increase in marital infidelity, lowering of moral standards, men considering women as “a mere instrument for the satisfaction of his own desires” (e.g. Harvey Weinstein and many others) and the imposition of contraception by governmental authorities. These have all come to pass. How could he have been so accurate in his predictions? I think this is because the Blessed Pope had a firm grasp of the profound unity of spirit, mind and body that is the human person. The Catechism teaches us, “The unity of soul and body is so profound that one has to consider the soul to be the “form” of the body: i.e., it is because of its spiritual soul that the body made of matter becomes a living, human body; spirit and matter, in man, are not two natures united, but rather their union forms a single nature.” (CCC 365).
 Pope Saint John Paul II’s
Pope Saint John Paul II’s  It happened again.
It happened again. In a strange twist of fate, leading athletics programs seem to be ignoring federal protections for women that went into effect the year before Roe v. Wade and Doe v. Boltoncreated almost unlimited abortion access. While the 1972 Title IX was created to protect female athletes from
In a strange twist of fate, leading athletics programs seem to be ignoring federal protections for women that went into effect the year before Roe v. Wade and Doe v. Boltoncreated almost unlimited abortion access. While the 1972 Title IX was created to protect female athletes from  EDITORIAL: While the early Christians set themselves apart in their reverence for the body and for the spousal one-flesh union as a sign of Christ’s unconditional love for his Church, those who embrace the chemical corset scorn, perhaps unthinkingly, the body’s limits and the sacrifices that come with marriage and family life.
EDITORIAL: While the early Christians set themselves apart in their reverence for the body and for the spousal one-flesh union as a sign of Christ’s unconditional love for his Church, those who embrace the chemical corset scorn, perhaps unthinkingly, the body’s limits and the sacrifices that come with marriage and family life.












 April 10, 2018 (
April 10, 2018 ( WASHINGTON, DC, April 9, 2018 (
WASHINGTON, DC, April 9, 2018 (
 April 6, 2018 (
April 6, 2018 (
 Many women who’ve chosen abortion afterward immediately regret their decision. Though the abortion industry tells us otherwise, it’s true.
Many women who’ve chosen abortion afterward immediately regret their decision. Though the abortion industry tells us otherwise, it’s true.
 April 1, 2018 (
April 1, 2018 ( If sacrifices speak so much to us,” it’s because they “reveal a common foundation that is the ground on which one relies,” says French Catholic philosopher Martin Steffens: “As one relies on the ground, one doesn’t see it and yet it’s certainly there.”
If sacrifices speak so much to us,” it’s because they “reveal a common foundation that is the ground on which one relies,” says French Catholic philosopher Martin Steffens: “As one relies on the ground, one doesn’t see it and yet it’s certainly there.”

 http://www.pattimaguirearmstrong.com/2018/03/how-to-welcome-new-catholics-30000.html?
http://www.pattimaguirearmstrong.com/2018/03/how-to-welcome-new-catholics-30000.html? March 28, 2018 (
March 28, 2018 (
 PROVIDENCE, Rhode Island, March 26, 2018 (
PROVIDENCE, Rhode Island, March 26, 2018 (
 WASHINGTON, D.C. – His Excellency, the Most Reverend
WASHINGTON, D.C. – His Excellency, the Most Reverend  Introductory Message
Introductory Message A major study published on December 7 in the New England Journal of Medicine concludes that hormonal contraception increases the risk of breast cancer for women. The research used all of Denmark as its sample, following nearly 1.8 million Danish women of childbearing age for over a decade. The study, as described by the New York Times, “upends widely held assumptions about modern contraceptives for younger generations of women,” especially the view that “newer hormonal contraceptives are much safer than those taken by their mothers or grandmothers.” It also establishes that the risk to women increases with longer periods of use. Major media outlets have done their best to minimize the implications of the study and “soften the blow” for the millions who, for decades, have faithfully embraced a “contraceptive mentality.”
A major study published on December 7 in the New England Journal of Medicine concludes that hormonal contraception increases the risk of breast cancer for women. The research used all of Denmark as its sample, following nearly 1.8 million Danish women of childbearing age for over a decade. The study, as described by the New York Times, “upends widely held assumptions about modern contraceptives for younger generations of women,” especially the view that “newer hormonal contraceptives are much safer than those taken by their mothers or grandmothers.” It also establishes that the risk to women increases with longer periods of use. Major media outlets have done their best to minimize the implications of the study and “soften the blow” for the millions who, for decades, have faithfully embraced a “contraceptive mentality.” March 22, 2018, (
March 22, 2018, ( SUMTER, South Carolina, March 22, 2018, (
SUMTER, South Carolina, March 22, 2018, (
 A group of mothers and their children with Down syndrome are wowing the internet with a powerful music video to the popular song “A Thousand Years.”
A group of mothers and their children with Down syndrome are wowing the internet with a powerful music video to the popular song “A Thousand Years.”
 Page 40 of the 2004 edition of the Handbook, under “Guidance notes,” says:
Page 40 of the 2004 edition of the Handbook, under “Guidance notes,” says:




 NEW YORK, March 15, 2018 (
NEW YORK, March 15, 2018 ( March 16, 2018 (
March 16, 2018 ( WEST BLOOMFIELD, Michigan, March 14, 2018 (
WEST BLOOMFIELD, Michigan, March 14, 2018 ( This year marks the 50th anniversary of the publication of Humanae Vitae, Pope Paul VI’s controversial statement condemning artificial birth control. In July 1968, he published the encyclical even though an overwhelming majority of the
This year marks the 50th anniversary of the publication of Humanae Vitae, Pope Paul VI’s controversial statement condemning artificial birth control. In July 1968, he published the encyclical even though an overwhelming majority of the  ROME, March 8, 2018 (
ROME, March 8, 2018 ( Oral contraceptives increase the risk of women suffering from certain types of stroke, new research suggests.
Oral contraceptives increase the risk of women suffering from certain types of stroke, new research suggests. March 7, 2018 (
March 7, 2018 (


 What would you have given to become an Olympic athlete? One famous Japanese figure skater knows what she wouldn’t give.
What would you have given to become an Olympic athlete? One famous Japanese figure skater knows what she wouldn’t give. Demographic Intelligence’s senior advisor, Lyman Stone, comments on recent articles in The New York Times and Politico magazine providing four factors that are driving the recent fall in births.
Demographic Intelligence’s senior advisor, Lyman Stone, comments on recent articles in The New York Times and Politico magazine providing four factors that are driving the recent fall in births.


 February 20, 2018 (
February 20, 2018 ( Pro-life Catholics who wish Catholic Church leaders would step up and deny communion to leading politicians who support abortion are getting good news today.
Pro-life Catholics who wish Catholic Church leaders would step up and deny communion to leading politicians who support abortion are getting good news today. POPE ST. LEO XIII’S VISION
POPE ST. LEO XIII’S VISION
 PYEONGCHANG, South Korea, February 7, 2018 (
PYEONGCHANG, South Korea, February 7, 2018 ( PARIS, France, February 6, 2018 (
PARIS, France, February 6, 2018 ( DENVER, Colorado, February 5, 2018 (
DENVER, Colorado, February 5, 2018 ( Painting: St Peter healing the breasts of Saint Agatha.
Painting: St Peter healing the breasts of Saint Agatha. Saint Agatha by Zurbarán
Saint Agatha by Zurbarán Friday, June 5, 1987
Friday, June 5, 1987 WASHINGTON—Cardinal Timothy M. Dolan of New York, chair of the U.S. Conference of Catholic Bishops’ (USCCB) Committee on Pro-Life Activities called the Senate’s failure to pass the Pain-Capable Unborn Child Protection Act “appalling”. The bill proposes to ban abortions starting at 20 weeks after fertilization.
WASHINGTON—Cardinal Timothy M. Dolan of New York, chair of the U.S. Conference of Catholic Bishops’ (USCCB) Committee on Pro-Life Activities called the Senate’s failure to pass the Pain-Capable Unborn Child Protection Act “appalling”. The bill proposes to ban abortions starting at 20 weeks after fertilization.

 https://www.catholiceducation.org/en/science/ethical-issues/nickels-dimes-and-family-size.html
https://www.catholiceducation.org/en/science/ethical-issues/nickels-dimes-and-family-size.html R. Jared Staudt
R. Jared Staudt WASHINGTON, D.C., January 23, 2018 (
WASHINGTON, D.C., January 23, 2018 ( Watching an unborn baby move around in the womb can be a life-changing experience.
Watching an unborn baby move around in the womb can be a life-changing experience. President Donald Trump today told hundreds of thousands of pro-life Americans gathered for the March for Life that he will sign
President Donald Trump today told hundreds of thousands of pro-life Americans gathered for the March for Life that he will sign  Baby Royer’s success story brings hope to families whose unborn babies have been diagnosed with spina bifida.
Baby Royer’s success story brings hope to families whose unborn babies have been diagnosed with spina bifida. MINNESOTA, January 16, 2018 (
MINNESOTA, January 16, 2018 ( An amazingly brave teenager gave birth to a baby girl last week in Philadelphia while battling a deadly brain cancer.
An amazingly brave teenager gave birth to a baby girl last week in Philadelphia while battling a deadly brain cancer. BALTIMORE, Maryland, January 10, 2018 (
BALTIMORE, Maryland, January 10, 2018 ( January 9, 2018 (
January 9, 2018 ( A British mother criticized her doctors for encouraging her to abort her unborn daughter after tests indicated that the baby girl could have a disability.
A British mother criticized her doctors for encouraging her to abort her unborn daughter after tests indicated that the baby girl could have a disability. by Fr Serafino M. Lanzetta
by Fr Serafino M. Lanzetta Thirty years ago this January 14th, President Ronald Reagan published a Personhood Proclamation.
Thirty years ago this January 14th, President Ronald Reagan published a Personhood Proclamation.
 It is a profound irony that as we allow even very late term fetuses to be aborted on one hand, scientists are finding radical nature-bending ways to assist people have babies–including methods that could shatter familial norms.
It is a profound irony that as we allow even very late term fetuses to be aborted on one hand, scientists are finding radical nature-bending ways to assist people have babies–including methods that could shatter familial norms. The year opens in the name of the Mother. Mother of God is the most important title of Our Lady. But we might ask why we say Mother of God and not Mother of Jesus. In the past, some wanted to be content simply with the latter, but the Church has declared that Mary is the Mother of God. We should be grateful because these words contain a magnificent truth about God and about ourselves. From the moment that our Lord became incarnate in Mary, and for all time, he took on our humanity. There is no longer God without man; the flesh Jesus took from his Mother is our own, now and for all eternity. To call Mary the Mother of God reminds us of this: God is close to humanity, even as a child is close to the mother who bears him in her womb.
The year opens in the name of the Mother. Mother of God is the most important title of Our Lady. But we might ask why we say Mother of God and not Mother of Jesus. In the past, some wanted to be content simply with the latter, but the Church has declared that Mary is the Mother of God. We should be grateful because these words contain a magnificent truth about God and about ourselves. From the moment that our Lord became incarnate in Mary, and for all time, he took on our humanity. There is no longer God without man; the flesh Jesus took from his Mother is our own, now and for all eternity. To call Mary the Mother of God reminds us of this: God is close to humanity, even as a child is close to the mother who bears him in her womb. The recent testimony of female celebrities and ordinary women who have been preyed upon sexually by powerful men has demanded a reckoning across many sectors of American life.
The recent testimony of female celebrities and ordinary women who have been preyed upon sexually by powerful men has demanded a reckoning across many sectors of American life. Ever since the 5th century the Church has commemorated a separate day in memory of the children killed by King Herod after Jesus’ birth. Matthew is the only one to record the event and the details surrounding it are slim.
Ever since the 5th century the Church has commemorated a separate day in memory of the children killed by King Herod after Jesus’ birth. Matthew is the only one to record the event and the details surrounding it are slim.
 COLUMBUS, Ohio, December 22, 2017 (
COLUMBUS, Ohio, December 22, 2017 (

 A woman living in East Tennessee has delivered the longest-frozen embryo to successfully come to birth. Emma Wren was born to Benjamin and Tina Gibson on Saturday, November 25, 2017, weighing 6 lbs. 8 oz. and measuring 20 inches long.
A woman living in East Tennessee has delivered the longest-frozen embryo to successfully come to birth. Emma Wren was born to Benjamin and Tina Gibson on Saturday, November 25, 2017, weighing 6 lbs. 8 oz. and measuring 20 inches long.

 December 18, 2017 (
December 18, 2017 ( December 14, 2017 (
December 14, 2017 ( Little Vanellope Hope Wilkins would not be alive today if her mother had listened to her doctors’ repeated urgings to have an abortion.
Little Vanellope Hope Wilkins would not be alive today if her mother had listened to her doctors’ repeated urgings to have an abortion.
 Last week, the New England Journal of Medicine
Last week, the New England Journal of Medicine  Catholic Archbishop Joseph F. Naumann of Kansas City soon will become an even more influential pro-life leader in the United States.
Catholic Archbishop Joseph F. Naumann of Kansas City soon will become an even more influential pro-life leader in the United States. December 1, 2017 (
December 1, 2017 ( Have you been given this scenario to justify abortion before?
Have you been given this scenario to justify abortion before? A modern successor to the Hippocratic Oath
A modern successor to the Hippocratic Oath  November 27, 2017 (LifeSiteNews) – Using hormonal contraceptives increases a woman’s risk of suicide, sometimes even tripling it, a new study published in the American Journal of Psychiatry revealed.
November 27, 2017 (LifeSiteNews) – Using hormonal contraceptives increases a woman’s risk of suicide, sometimes even tripling it, a new study published in the American Journal of Psychiatry revealed. The Little Sisters of the Poor are heading back to court to defend themselves against the Obama administration’s Health and Human Services mandate to provide contraception, yet again. In an unusual political move, Pennsylvania and California sued the Little Sisters, demanding the same group who won at the Supreme Court in Zubik v. Burwell provide contraceptives in their state.
The Little Sisters of the Poor are heading back to court to defend themselves against the Obama administration’s Health and Human Services mandate to provide contraception, yet again. In an unusual political move, Pennsylvania and California sued the Little Sisters, demanding the same group who won at the Supreme Court in Zubik v. Burwell provide contraceptives in their state.
 Hours after the results of Australia’s plebiscite on same-sex marriage were released, Family Edge’s Veronika Winkels sat down with German sociologist and Catholic convert
Hours after the results of Australia’s plebiscite on same-sex marriage were released, Family Edge’s Veronika Winkels sat down with German sociologist and Catholic convert  Every time Manda Grover received a pregnancy scan, the expecting mom felt pressured to abort her unborn baby boy.
Every time Manda Grover received a pregnancy scan, the expecting mom felt pressured to abort her unborn baby boy. TORONTO, November 20, 2017 (
TORONTO, November 20, 2017 ( ALEXANDRIA, Virginia, November 20, 2017 (
ALEXANDRIA, Virginia, November 20, 2017 (

 November 14, 2017
November 14, 2017  At church, Catholics should spend their time in silence before Mass, preparing “to meet with Jesus” instead of engaging in “chitchat,” the pope said Nov. 15 during his weekly general audience.
At church, Catholics should spend their time in silence before Mass, preparing “to meet with Jesus” instead of engaging in “chitchat,” the pope said Nov. 15 during his weekly general audience.


 When I was 18, I was prescribed birth control for some dubious reason … dubious primarily because I can’t even remember what the reason was. I wasn’t sexually active and didn’t have PCOS or unpleasant periods, but I went to the doctor for some reason and walked away with the pill.
When I was 18, I was prescribed birth control for some dubious reason … dubious primarily because I can’t even remember what the reason was. I wasn’t sexually active and didn’t have PCOS or unpleasant periods, but I went to the doctor for some reason and walked away with the pill. Assessing the grim toll of the massacre in Sutherland Springs, Tex., sheriff’s deputies found 22 of the bodies inside the First Baptist Church, but by their reasoning, one more victim died there — inside the womb of Crystal Holcombe, who was killed in the pews along with three of her five children.
Assessing the grim toll of the massacre in Sutherland Springs, Tex., sheriff’s deputies found 22 of the bodies inside the First Baptist Church, but by their reasoning, one more victim died there — inside the womb of Crystal Holcombe, who was killed in the pews along with three of her five children. A Brazilian legislative committee passed a bill to protect unborn babies from abortion in all cases Wednesday, despite pressure on the South American country to expand its abortion laws.
A Brazilian legislative committee passed a bill to protect unborn babies from abortion in all cases Wednesday, despite pressure on the South American country to expand its abortion laws. November 7, 2017 (
November 7, 2017 (



 As reported
As reported (
( Last Friday marked 50 years since the passing of the UK’s
Last Friday marked 50 years since the passing of the UK’s 
 Imagine standing on the shores of a dark, stormy sea. As you peer over perilous waters, you hear voices cry out. Horrified, you realize people are struggling out there in the tempest, about to sink beneath the angry waves.
Imagine standing on the shores of a dark, stormy sea. As you peer over perilous waters, you hear voices cry out. Horrified, you realize people are struggling out there in the tempest, about to sink beneath the angry waves.
 by
by 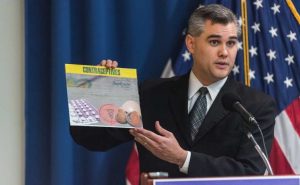
 When choosing a partner to have children with, it is only natural to desire “Prince Charming” or “Cinderella,” who may pass on their beneficial genetic qualities to future kids. Given that better
When choosing a partner to have children with, it is only natural to desire “Prince Charming” or “Cinderella,” who may pass on their beneficial genetic qualities to future kids. Given that better 
 Pope Francis has been a consistent pro-life advocate since becoming the leader of the Catholic Church and he is once again speaking out against abortion and in favor of protecting unborn children.
Pope Francis has been a consistent pro-life advocate since becoming the leader of the Catholic Church and he is once again speaking out against abortion and in favor of protecting unborn children. LONDON, England, October 16, 2017 (
LONDON, England, October 16, 2017 ( SAN FRANCISCO, California, October 11, 2017 (
SAN FRANCISCO, California, October 11, 2017 (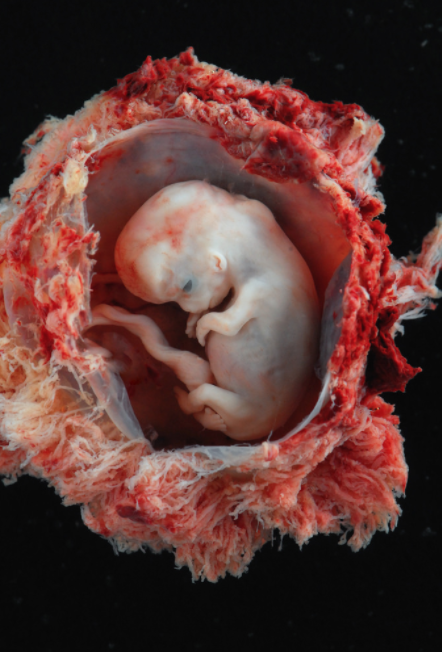
 After the Trump administration’s rollback of the controversial and heavily
After the Trump administration’s rollback of the controversial and heavily  AUMSVILLE, Oregon, October 11, 2017 (
AUMSVILLE, Oregon, October 11, 2017 (


 It is entirely possible to adopt a pro-life position based solely on reason. After all, science shows us that the baby’s heart starts beating at 24 days after conception; brain waves can be detected 43 days after fertilization.
It is entirely possible to adopt a pro-life position based solely on reason. After all, science shows us that the baby’s heart starts beating at 24 days after conception; brain waves can be detected 43 days after fertilization. WASHINGTON, D.C., October 6, 2017 (
WASHINGTON, D.C., October 6, 2017 ( A Hawaii abortion activist is suing the federal government in a case that could force every pharmacy in America to sell dangerous abortion drugs.
A Hawaii abortion activist is suing the federal government in a case that could force every pharmacy in America to sell dangerous abortion drugs.
 CCLI is excited to announce the upcoming family conference titled “Families, become what you are!: Celebrating Humanae Vitae as the bedrock of family life.” The event is open to everyone and will be held on July 6-7, 2018, at the Sharonville Convention Center in Cincinnati, Ohio.
CCLI is excited to announce the upcoming family conference titled “Families, become what you are!: Celebrating Humanae Vitae as the bedrock of family life.” The event is open to everyone and will be held on July 6-7, 2018, at the Sharonville Convention Center in Cincinnati, Ohio.

 An egregious surrogacy case has been filed with America’s highest court. Today, the Supreme Court is expected to announce whether or not it will hear the case of
An egregious surrogacy case has been filed with America’s highest court. Today, the Supreme Court is expected to announce whether or not it will hear the case of  On Tuesday, the members of the House of Representatives will assemble in the U.S. Capitol Building to cast their votes yea or nay on the Pain-Capable Unborn Child Protection Act–H.R. 36.
On Tuesday, the members of the House of Representatives will assemble in the U.S. Capitol Building to cast their votes yea or nay on the Pain-Capable Unborn Child Protection Act–H.R. 36. LYON, France, October 2, 2017 (
LYON, France, October 2, 2017 (




 Micaiah Bilger Sep 26, 2017 | 6:22PM New York, NY
Micaiah Bilger Sep 26, 2017 | 6:22PM New York, NY

 Pro-Life Texans have long known the danger of giving hospital administrators power over life and death decisions. Under the anti-Life
Pro-Life Texans have long known the danger of giving hospital administrators power over life and death decisions. Under the anti-Life  Ten years ago, one in 35 Australian babies were born as a result of IVF treatment. Today, that number has tracked to one in 25 babies. In the Netherlands, one in 15 births is as a result of IVF treatment. Now, world-renowned Dr John Aitken, the University of Newcastle laureate professor, the director of the University’s Priority Research Centre for Reproductive Science and the 2012 New South Wales Scientist of the Year, is
Ten years ago, one in 35 Australian babies were born as a result of IVF treatment. Today, that number has tracked to one in 25 babies. In the Netherlands, one in 15 births is as a result of IVF treatment. Now, world-renowned Dr John Aitken, the University of Newcastle laureate professor, the director of the University’s Priority Research Centre for Reproductive Science and the 2012 New South Wales Scientist of the Year, is  If you believe that “all kids need is love” then these
If you believe that “all kids need is love” then these 
 LOS ANGELES, California, July 31, 2017 (
LOS ANGELES, California, July 31, 2017 ( September 11, 2017 (
September 11, 2017 (
 My July interview with Dr Tyler (pictured, right) follows.
My July interview with Dr Tyler (pictured, right) follows.







{kind=link}
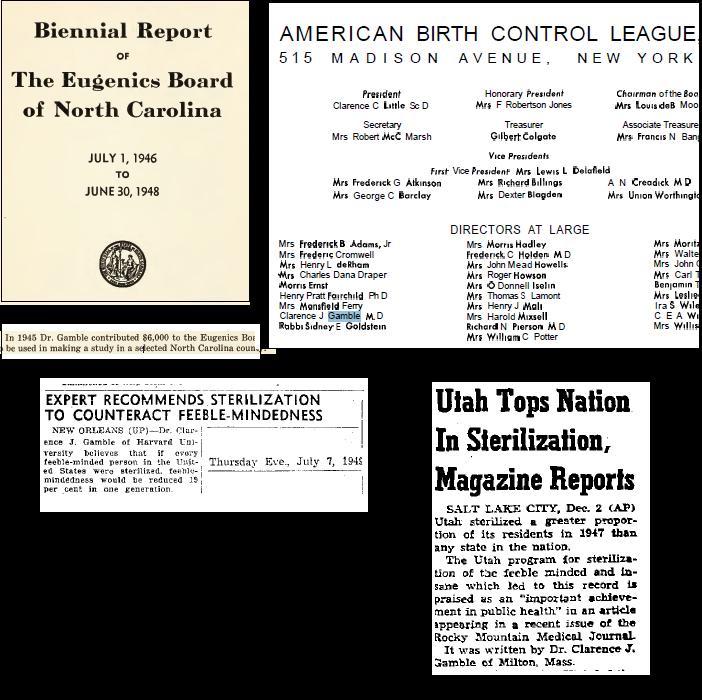{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A CBS News story earlier this week sounded a recurring alarm about the record decline of birth rates in the U.S.
The news agency obtained records from health departments in more than two dozen states showing a 7% drop in births in December 2020 — nine months after the first lockdowns began.
As the Pew graph below illustrates, the overall drop in birth rates actually began in 2006.
Baffled “experts” blame everything from social media to the economy. But they overlooked one obvious possible explanation: the Gardasil HPV vaccine, which the Centers for Disease Control (CDC) and Prevention’ Advisory Committee on Immunization Practices recommended for every American girl between the ages of 9 and 26 — beginning in 2006.
Clinical trial researchers for Merck, Gardasil’s manufacturer, reported an explosion of reproductive injuries among the 20,000 trial volunteers. An astronomical 15% – 17% of trial participants experienced a range of reproductive harms, including premature ovarian failure.
CDC’s own graph shows that the steepest drops in births have occurred among teens — the age group most likely to have received the vaccine. Among this group, birth rates dropped a breathtaking 46% between 2007 and 2015. There were no changes in birth control or abortion rates that would explain this drop.
Gardasil contains three ingredients, L-histidine, polysorbate 80 and sodium borate that are all associated with reproductive disorders. The U.S. Food and Drug Administration has banned sodium borate in foods in the U.S., partially because of its strong association with premature ovarian failure. Merck nevertheless includes it in Gardasil.
During our Gardasil litigation, we have spoken to hundreds of girls suffering premature ovarian failure and a range of other reproductive problems. Gardasil victims and their mothers frequently tell us of girls who cease menstruating after receiving the Gardasil vaccine.
Merck knew that it was orchestrating a population-wide fertility experiment when it persuaded the CDC to effectively mandate Gardasil for every American teenager. Merck’s pre-licensing studies predicted the current national drops in fertility.
If Gardasil injured you, and you want to know your rights, call me at 844-RFK-HPV1.
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children’s Health Defense.