August 23, 2017 (LifeSiteNews.com) – In May and June, Italian media sources began to report of the existence of a secret commission created by Pope Francis to bring about a “reinterpretation” of Pope Paul VI’s encyclical Humanae Vitae, which reiterates the Catholic Church’s perennial condemnation of artificial birth control.
After the story was first reported by Marco Tosatti on May 11 and soon given further confirmation by Maike Hickson at One Peter Five, the Vatican refused to verify or deny it for an entire month, prompting Tosatti to quip that the silence “could in itself be a sign.”
Finally, in mid-June, Italian journalist Roberto de Mattei further confirmed the story and even listed the members of the alleged commission, including its head, Fr. Gilfredo Marengo, a theologian at the Pontifical John Paul II Institute for Studies on Marriage and Family.
This led Archbishop Vincenzo Paglia, the grand chancellor of the institute, to finally break the Vatican’s silence with an ambiguous denial made in an interview with the Catholic News Agency (CNA), in which he claimed that “there is no pontifical commission called to re-read or to reinterpret Humanae vitae” but added that “we should look positively on all those initiatives, such as that of Professor Marengo of the John Paul II Institute, which aim at studying and deepening this document in view of the 50th anniversary of its publication.”
Marengo himself told CNA that stories about such a “commission” were nothing more than an “imaginative report” and assured the agency that “the issue of a conciliation between Amoris Laetitia and Humanae Vitae is not in the agenda.” He described his work as a “historical-critical investigation without any aim other than reconstructing as well as possible the whole process of composing the encyclical.”
Despite such attempts to dismiss reports about Marengo’s Humanae Vitae “commission,” concerns continued to be raised in Catholic media, and on July 25 Fr. Marengo gave an extensive interview to Vatican Radio in an apparent attempt to quell them. However, in the interview Marengo not only confirmed details given by de Mattei about his “commission” — which he calls a “study group” — but also drops a new bombshell, revealing that he has been given what appears to be exclusive access to the Vatican’s secret archives for the purpose of carrying out this Humanae Vitae “study.”
In the interview, published on the Vatican Radio website only in Italian, Marengo acknowledged that his “study group” consists of the same people named more than a month earlier by de Mattei: Pierangelo Sequeri, president of the Pontifical John Paul II Institute; Philippe Chenaux, a professor of Church history at the Pontifical Lateran University; and Angelo Maffeis, president of the Paul VI Institute of Brescia.
“From the point of view of historical-theological research, it will be very useful to reconstruct the process of composing [the encyclical], which developed in distinct phases from June 1966 to its publication, by examining the documentation kept in some archives of the Holy See,” Marengo told Vatican Radio. “Given the approaching date of this 50th anniversary [of publication of Humanae Vitae], I have received permission to begin searching the archives, alongside some prominent scholars, Professors Sequeri, Maffeis and Chenaux.”
The next day, Marengo reaffirmed to the Catholic News Service that, in the words of CNS, “he felt it was important to ask the Vatican to set aside rules that prevent scholars from accessing Vatican archival material for 70 years.” CNS goes on to quote Marengo saying, “The competent Vatican authorities accepted my request, permitting access particularly to the collections of the Vatican Secret Archives and the archive of the Congregation for the Doctrine of the Faith.”
The privilege of accessing the archives of this period is no small matter. The Vatican excludes scholars from virtually all material in the archives dating from the pontificate of Pope Pius XII to the present, and has done so for many years, citing the need to catalog and prepare the material before scholars can be permitted to view it. The Holy See has maintained this position for decades despite much pressure to open the archives arising from controversy over Pope Pius XII’s conduct during World War II.
The Vatican has long claimed that it is simply unable to accommodate requests for such material and continues to tell scholars that all material following the pontificate of Pius XI is unavailable to the public, except for documents relating to Vatican II. Only when the cataloguing process is complete will scholars be permitted to see documents from later periods, officials have repeatedly said, citing the principle that material in the archive should be opened to scholarly access only after 70 years.
Fr. Marengo and his “study group,” however, have been given exclusive access to this restricted section of the archives, something that other historians have been unable to achieve after decades of insistent requests. It is, to put it mildly, an unimaginable privilege for a group of scholars who wish to do nothing more than an historical recounting of the composition of an encyclical, a purely academic walk down memory lane. Such access had to be granted at the highest levels of authority in the Vatican. If this is not a “pontifical commission,” as Archbishop Paglia put it, it has privileges that certainly would seem to rival one.
Fr. Marengo’s curious project
The repeated attempts by Vatican officials to evade questions about this Humanae Vitae non-commission and to deny its significance, despite the unique privileges granted to it, raises an urgent question: What, precisely, does this exclusive Vatican “study group” intend to do?
In his interview with Catholic News Service, Marengo described the group’s activity as a “a work of historical-critical investigation without any aim other than reconstructing as well as possible the whole process of composing the encyclical,” in view of its upcoming 50th anniversary in 2018.
“Historical-critical” methods of textual interpretation are those that seek to understand texts by means of the processes that produced them as well as the social and cultural contexts in which they were written. With regard to the Bible, they have been used in doctrinally orthodox ways but have also been used to justify revisionist forms of interpretation that deny traditional understandings of Scriptural texts. This leads to claims that miracle stories, even those in the New Testament, are nothing more than literary devices, and even bringing into question such articles of the faith as the Virgin Birth of Christ and his resurrection from the dead.
Why, on the anniversary of an encyclical that was published within the living memory of a large percentage of the population, would the Vatican have need of an “historical-critical” analysis of the encyclical?
Although Fr. Marengo and Archbishop Paglia have protested much that no revision of the document is intended, Marengo himself seems already to be in the process of reinterpreting Humanae Vitae in troubling ways, telling Catholic News Service, in their words, that “procreation … was seen by many as the primary purpose of marriage, so Pope Paul’s insistence in ‘Humanae Vitae’ that sex within marriage is both procreative and unitive was something new, as was his declaration ‘without uncertainty that the exercise of responsible parenthood is an objective value for Christian families’ when done using natural methods.’” Marengo made similar statements during his Vatican Radio interview.
Both of these statements are, to put it bluntly, deeply erroneous interpretations of the encyclical. Pope Paul VI was no innovator in such matters; the canon law and moral theology of the Church has long understood the sexual act as the consummation of an absolutely indissoluble sacramental union between the spouses, whether or not it results in procreation. Both the catechisms of the Council of Trent and of Pope Pius X list the unity of the spouses and their mutual support as among the primary ends of marriage, and Pope Pius XI writes at length about the unitive purpose of the sexual act in his encyclical Casti Connubii. Moreover, the Vatican’s Apostolic Penitentiary began to publicly permit periodic abstinence to avoid conception in the late 19th century. In Humanae Vitae, Paul VI never contradicts the Church’s teaching that the primary purpose of the sexual act is procreation.
It’s true that Humanae Vitae lists the unitive purpose before the procreative, but this was nothing new — the Catechism of the Council of Trent, 400 years earlier, had done the same thing, listing the first purpose of marriage as the satisfaction of the urge toward the companionship of the opposite sex, and mutual support in old age, and the second being the desire for begetting and raising children for the purpose of educating them in the faith. This order did not necessarily refer to any ultimate teleological priority but to the temporal sequence of ends sought in marriage.
Marengo has laughed off the idea that he somehow wants to reconcile Humanae Vitae with Pope Francis’ confused apostolic exhortation Amoris Laetitia, but that is exactly what his recent scholarship has sought to do. Only a few months ago, Marengo wrote an article for Vatican Insider called “Humanae Vitae and Amoris Laetitia,” in which he belittles the Church’s condemnation of birth control, asking if “the polemical game – the pill yes – the pill no, like today’s — Communion to the divorced yes – Communion to the divorced no — is only an appearance of discomfort and strain, [which is] much more decisive in the fabric of ecclesial life.”
In the same article, Marengo parrots the reasoning of Amoris Laetitia that seeks to lower Catholic moral dogma to an often unattainable and purely abstract ideal. “Every time the Christian community falls into error and proposes models of life derived from too abstract and artificially constructed theological ideals, it conceives its pastoral action as the schematic application of a doctrinal paradigm,” said Marengo, and cited Amoris Laetitia in asserting, “We have presented a too abstract theological ideal on marriage, almost artificially constructed, far from the concrete situation and the effective possibilities of families as they really are. This excessive idealization, above all when we have reawakened trust in grace, has not made marriage more attractive and desirable, but quite the opposite.”
Archbishop Paglia, Fr. Marengo, and their media sympathizers have labored mightily to convince Catholic journalists to “move along,” because there’s nothing to see here. They accuse them of hatching “conspiracy theories,” and even go so far as to claim that Pope Francis has never hinted at changing Humanae Vitae. In fact, Pope Francis has made statements that contradict Humanae Vitae almost verbatim, claiming that contraception can be justified as a lesser evil (a claim expressly condemned in the same encyclical). His apparently offhanded statement, made to reporters during a flight, was reaffirmed by Vatican spokesman Fr. Federico Lombardi soon after.
Moreover, Pope Francis’ recent conduct with regard to the Church’s perennial doctrines on life and family has given Catholics much cause for suspicion. His administration and its allies engaged in deceptive tactics to manipulate two synods of bishops in order to justify the subversive novelties against the integrity of marriage contained in Amoris Laetitia. Chillingly, Francis has made statements about Humanae Vitae hinting that he has a similar agenda for the document on its 50th anniversary of publication.
In a 2014 interview with the Italian newspaper Corriere della Sera, Francis was specifically asked about “tak[ing] up again the topic of birth control” half a century after the publication of Humanae Vitae. “Your confrere, Cardinal [Carlo Maria] Martini [the late Archbishop of Milan] believed it was now time,” added the interviewer.
“It all depends on how the text of ‘Humanae Vitae’ is interpreted,” responded Francis. “Paul VI himself, towards the end, recommended to confessors much mercy and attention to concrete situations.” Francis then complimented Paul VI, calling him a “prophetic” genius, but added, “The object is not to change the doctrine, but it is a matter of going into the issue in depth and to ensure that the pastoral ministry takes into account the situations of each person and what that person can do.”
The Catholic faithful have heard this language from Pope Francis before – it is the rationale underlying Amoris Laetitia’s apparent acceptance of permitting adulterers to receive Holy Communion, which has become the cause of immense scandal regarding the sacrament of marriage, and the greatest doctrinal controversy connected to a pope for more than six centuries. It’s hardly a cause for optimism regarding Fr. Marengo’s curious non-commission, and its “historical-critical” review of Humanae Vitae.
September 7, 2017 (National Review) — This could be one of the biggest bioethics cases since Terri Schiavo.
A judge has ruled that the teenager, declared dead in California, may not be dead. From the East Bay Express story:
Jahi McMath, the Oakland teenager whose brain death case has sparked national debate, may not currently fit the criteria of death as defined by a state law written in conjunction with the medical establishment, a judge wrote in an order Tuesday.
In his ruling, Alameda County Superior Court Judge Stephen Pulido wrote that while the brain death determination in 2013 was made in accordance with medical standards, there remains a question of whether the teenager “satisfies the statutory definition of ‘dead’ under the Uniform Determination of Death Act.”
Bottom line, if she is not brain dead, then by definition, she’s alive. At the very least, there is enough doubt in this case based on Dr. Alan Shewmon’s testimony to induce the judge to issue his ruling:
Pulido heavily cited Dr. Alan Shewmon, who concluded in a court declaration that Jahi doesn’t currently fit the criteria for brain death after reviewing 49 videos of her moving specific fingers and other extremities when given commands to do so.
Shewmon, a professor emeritus of pediatrics and neurology at UCLA, wrote that Jahi “is a living, severely disabled young lady, who currently fulfills neither the standard diagnostic guidelines for brain death nor California’s statutory definition of death.” Shewmon also reviewed an MRI.
Full disclosure. I recently visited Jahi and her mother, along with Bobby Schindler.
That visit reinforced my view, previously written here, that this case demands a much deeper investigation than it has received heretofore, including impartial and thorough renewed medical examinations.
A terminally ill Michigan woman who sacrificed her life to save her unborn baby’s gave birth to her baby girl, Life Lynn, on Wednesday.
Carrie DeKlyen, of Wyoming, Michigan, was diagnosed with a terminal brain tumor in April. Not long after that, she and her husband, Nick, discovered that they were pregnant with their sixth child, Life Lynn.
WOOD TV reports Carrie refused to participate in a clinical trial that could have prolonged her life because doctors said she would have had to abort her unborn baby.
On Wednesday, Life Lynn was born weighing 1 pound, 4 ounces at University Hospital in Ann Arbor, Michigan, Mlive.com reports. She spent 24 weeks and 5 days in the womb.
Carrie, 37, suffered a massive stroke earlier this summer and has not regained consciousness. She gave birth while in a coma, according to the report.
As the family celebrates the tiny baby girl’s life, they are preparing for their wife and mother’s death. Carrie’s condition has deteriorated, and she no longer is even minimally responsive, according to the family.
The DeKlyens said Carrie was taken off life support after she gave birth to her daughter, and they believe her life is “in God’s hands until he calls her home.”
Her sister-in-law, Sonya Nelson, said Life Lynn is doing “as well as could be expected” for a baby born so prematurely. She said doctors decided to deliver her this week because they feared that she would die in the womb if they waited much longer.
Here’s more from the local news:
“The doctors ran tests (Wednesday) and extensive ultrasounds – she wasn’t even moving and was very sick,” Nelson said, noting that the baby was born at 24 weeks and 5 days. “My brother said the doctors are extremely pleased with how the baby is doing.”
… “We are now just trying to keep Carrie comfortable and keeping it in God’s hands,” Nelson said. “We are so proud of Carrie. She laid down her life for her child while refusing treatment for (herself). Her rewards are going to be great.”
Her husband, Nick, told People that he is so proud of Carrie, and he is certain that he will see her again one day in heaven.
“Not in this life, but after my time is up I’ll be with her again in Heaven,” he said. “She made the decision to give Life a chance at life. And I couldn’t be more proud.”
Carrie has glioblastoma, a terminal brain cancer. Since she was diagnosed in April, she has undergone several surgeries to remove the tumor from her brain, but each time the cancer returned, according to the report.
The mother of six refused to participate in an experimental treatment that could have prolonged her life because it would have meant aborting her unborn daughter.
“The doctor said if you don’t terminate this baby, Carrie, you will die,” her husband told People in August. “But it was Carrie’s decision and I said, ‘What do you want to do?’ She said, ‘We’re keeping it.’”
Over the summer, Carrie began chemotherapy while pregnant; but she later suffered a massive stroke that left her unconscious. Doctors tried to keep her comfortable and her unborn baby in the womb until she developed enough to survive outside it.
“We are a family of faith,” Nelson said previously. “And so we are just believing that God’s plan for Carrie is to be healed. And if he chooses to heal her here or in heaven, we will still trust in him.”
The family is asking people to pray for Carrie and baby Life Lynn. Nelson also set up a GoFundMe page where people can donate to help with the large family’s expenses.
By Jean Mackenzie and Jessica FurstBBC Victoria Derbyshire programme
A number of women are having to undergo hysterectomies to remove a sterilisation device used on the NHS, the Victoria Derbyshire show has found.
The Essure implant is used to permanently sterilise women, but can cause side effects and complications.
One woman – who later had her uterus removed – said she was left suicidal due to the “unbearable” pain, and felt she was a burden to her family.
The manufacturer says Essure is safe and the benefits outweigh the risks.
The sale of the implants in the EU was temporarily suspended this month.
Manufacturer Bayer has asked hospitals in the UK not to use the device during this time.
‘Painful to move’
Laura Linkson, who was fitted with the Essure device in 2013, said the pain left her suicidal.
“The device was sold to me as a simple and easy procedure. I was told that I’d be in and out of the doctor’s office in 10 minutes and that there’d be no recovery time.
“I went from being a mum who was doing everything with her children, to a mum that was stuck in bed unable to move without pain, at some points being suicidal.
“I felt like I was a burden on everyone around me,” she added.
The small coil implants, which are made of nickel and polyester (PET) fibres, are used as a sterilisation device to stop eggs reaching the womb.
They are inserted into the fallopian tubes where they trigger inflammation, causing scar tissue to build up and eventually block the tubes, known as a hysteroscopic sterilisation.
They can cause intense pain, and some women are thought to react badly to the nickel and plastic.
Because of the way the coils attach to the fallopian tubes, the only way to take them out is to remove a woman’s fallopian tubes and often her uterus.
In other cases the device has been found to perforate a fallopian tube and fallen out, embedding itself elsewhere in the body.
Victoria Dethier was implanted with Essure in 2012 and for three years could not work out why she felt so unwell.
“There were moments where I couldn’t get out of bed I was in so much pain. It felt like I was dying, like something was killing me from the inside,” she said.
She thinks her body was reacting to the PET fibres designed to cause inflammation.
She had a hysterectomy to remove the device in 2015.
“Straight away there was a difference, I’d experienced a horrible taste in my mouth and that had gone,” she explained.
“I’d lost a lot of hair and that came back within 12 months, it was incredible.”
‘We need acknowledgement’
The medicines and healthcare products regulatory agency (MHRA) has been criticised for not responding to the increasing evidence regarding the device.
In 2015, a study published in the British Medical Journal (BMJ) suggested that women who had a hysteroscopic sterilisation were 10 times more likely to need follow-up surgery than those who had a traditional sterilisation – 2.4% of those surveyed, as opposed to 0.2% amongst those having a standard sterilisation.
In the US more than 15,000 women have reported problems to the US Food and Drug Administration (FDA), including pain, allergic reactions and “migration of device”.
Carl Heneghan, from the Centre for Evidence-Based Medicine at Oxford University, has criticised the regulator’s failure to act on such findings.
“How much evidence do you need to say let’s withdraw this from the market?” he asked.
Victoria Dethier is angry that she and so many other women feel they have been ignored.
“No-one is listening to us,” she said.
“There are many women coming forward… we need to be acknowledged.”
‘No long-term evidence’
The full extent of the problem in the UK is not known.
The MHRA rejected the Victoria Derbyshire programme’s Freedom of Information request asking how many women have reported problems.
The NHS does not have figures for the total number of women who have been fitted with Essure, or who have had it removed.
However, the clinical trial that led to the device being approved has been criticised for not considering the long-term effects of the implants.
“The trial… only followed up women for one year, so nobody has a real understanding of what happens with this device after two years, three years, five years,” Mr Heneghan explained.
Image caption Consultant obstetrician Ben Peyton-Jones says Essure implants can be safe when used correctly
Some women who have experienced problems say they were not informed about the risks.
But Ben Peyton-Jones, a consultant obstetrician and gynaecologist, said the device should still be used in some instances.
“I think it has a place for women who can’t have keyhole surgery and who are explained the risks very carefully,” he said.
“When used correctly, according to the manufacturer’s guidance and in trained hands, it is safe.”
The sale of Essure implants in the EU has now been suspended for further investigation.
Hospitals have been asked by Bayer not to use their existing stocks during this time.
It is a voluntary request and up to individual trusts to decide what to do.
The company said that independent reviews of Essure had concluded that the benefits outweighed the risks.
“Patient safety and appropriate use of Essure are the greatest priorities for Bayer, and the company fully stands behind Essure as an appropriate choice for women who desire permanent contraception,” it added in a statement.
“Many women with Essure rely on this form of contraception without any side effects.”
The MHRA said it had no evidence to suggest this product was unsafe, and that the recent suspension did not suggest any increased risk to patient safety.
It said it was important for healthcare professionals to discuss the risks with patients before a procedure.
For the first time since Harvey made landfall in Houston last weekend, Meredith Phillips was able to take the time to enjoy a hot meal Thursday afternoon.
Coming on the heels of several days’ worth of adrenaline, and with weeks and months ahead of her to process the impact of the storm, it was a well-earned—if too brief—respite for Phillips, a Houston resident who helps operate a Christian housing ministry for pregnant moms called LifeHouse.
As the storm approached late last week, Phillips and her team had to evacuate their program’s residents from one of its three locations, relocating the expectant mothers away from the rising water.
Once the nine pregnant women, as well as LifeHouse staff members—one of whom had to be rescued from a rooftop—were safe and sound, Phillips turned her attention to reaching out to expectant moms scattered throughout area shelters.
Bringing Help to the Shelters
Her first stop was nearby Lakewood Church, which was maligned along with its pastor, Joel Osteen, earlier in the week when local residents accused the megachurch of refusing to take in residents displaced by the storm. That wasn’t the case by the time Phillips arrived to help Wednesday morning, however, as Lakewood was bustling with activity.
“They had created a shelter on one floor and were offering services on another floor,” Phillips said. “There were so many volunteers that came, they were turning away volunteers, but I came in because I wanted to offer LifeHouse as a resource to any displaced pregnant women.”
Introducing herself to a volunteer who was overseeing the medical station at Lakewood, Phillips told him what she was there to do, and in return, he asked her to stay and work the rest of the day.
By the end of the day Wednesday, Phillips had talked at length with five expectant mothers who had lost their homes and had nowhere to go. She was able to immediately place one of the women in LifeHouse, which has the capacity for as many as 18 moms at a time, while the team helped connect 10 more women to vital resources within the community.
“We really worry about that pregnant woman who has been in this kind of stress,” Phillips said. “We want to be able to give her an environment where she can rest physically and emotionally and be able to nurture the baby who is growing inside of her.”
One of the women Phillips met Wednesday is due this November with twins. She had just moved to Houston from Alabama to take a teaching position when the storm hit, washing away everything she had packed in the move.
With the woman’s family still in Alabama, Phillips was able to get her out of the shelter at Lakewood and into a bed at LifeHouse on Wednesday night.
“For someone who’s never been through the floods of Houston, and on top of that, one of the largest floods in history, then you add that she’s away from her family and pregnant with twins—that’s a lot,” Phillips said.
Philips and her team also reached out over social media and were able to recruit five social workers and five counselors to join them during the crisis, streamlining LifeHouse’s intake process and growing their ability to help expectant mothers through the crisis.
Meanwhile, LifeHouse reached out to maternity homes in a 300-mile radius of Houston via email Thursday to see if any of those ministries could house women affected by Harvey.
“We’re definitely in the mode of mobilizing and equipping our staff and any volunteers who are able to help,” Phillips said.
Life-Affirming Help in Harvey’s Wake
Along with LifeHouse, Heartbeat International is reporting that several of its affiliated and allied pro-life pregnancy help ministries are back up and running amidst the devastation caused by Harvey.
The downtown location and mobile ultrasound unit for Houston Pregnancy Help Center are both open as of Thursday, while the center’s Fifth Ward location sustained minimal damage and will need new carpeting before reopening.
In Lake Charles, La., New Life Counseling executive director Jeanne LeBato said her center was being used as “a place of refuge” in her community, distributing diapers, wipes and baby clothes to area shelters. Ark La Tex Learning Center in Shreveport, La., also checked in, reporting no damage from the storm.
In the midst of all the stress the past week has brought on—and with the many months and years of recovery ahead—Phillips said her team has bonded together like never before.
“We’re having to access strength from a place we’ve never had to access before,” Phillips said. “We’ve been able to run off of Scripture and encouragement from each other, being the hands and feet of Christ together. That’s how we were able to really get through it. Now, we’re in a place where we have to emotionally process it, and that will take a little bit longer.”
Heartbeat International is accepting donations to help offset the cost of damages for affected pregnancy help centers and maternity homes. Click here to give.
On Saturday, September 9, 2017, Citizens for a Pro-Life Society, Priests for Life and the Pro-Life Action League will co-sponsor the 5th annual National Day of Remembrance for Aborted Children, calling on pro-life Americans to honor the gravesites of our aborted brothers and sisters.
Solemn prayer vigils will be conducted at these gravesites, of which there are 51 across the United States, as well as at dozens of other sites dedicated in memory of aborted children.
Day of Rememberance 2016
The 4th annual National Day of Remembrance for Aborted Children was held on Saturday, September 10 at 165 locations throughout the United States, with over 5,000 in attendance. See photos from some of the memorial services below:
Why Visit the Gravesites of the Aborted Unborn?
When people become truly aware of the reality of abortion, they can more easily cut through the lies by which some try to justify it, and the natural apathy to which human nature is inclined. Even pro-life people are thrust into a higher level of commitment and activism.
Touching this reality happens in various ways: hearing a vivid description of the procedure, seeing diagrams of it or images of aborted children, hearing a woman’s personal testimony of regret over her abortion.
This impact, whereby abortion no longer remains an abstraction, can be brought to an even more profound level when experienced during an event, such as the funeral for an aborted baby.
Tens of thousands of these children have been retrieved and buried at gravesites across our country. The stories of how they were killed, how they were found, and how they were buried, along with the pictures and videos that document those events, are powerful tools to awaken the consciences of our fellow citizens.
But while a funeral and burial for an aborted baby may be a relatively rare event, the opportunity to visit the burial places and recall how those children got there does not have to be rare—in fact, it shouldn’t be.
Pro-lifers should be visiting these gravesites—and other memorial sites dedicated to aborted babies—as a regular part of their pro-life witness. That’s what the National Day of Remembrance for Aborted Children is all about.
An Annual Event—and More
The first National Day of Remembrance for Aborted Children was held in September 2013 on the 25th anniversay of the solemn burial of the earthly remains of some 1,500 abortion victims in Milwaukee, Wisconsin. Over 100 memorial services were held across the United States, and it was clear this should become an annual event.
The Day of Remembrance will be held annually on the second Saturday in September. Dates for upcoming Days of Remembrance are as follows:
Pro-lifers are also encouraged to carry on the spiritual mission of the Day of Remembrance througout the year by visiting a gravesite of aborted children or other memorial site to offer prayers of mourning for the victims of abortion. Find the site nearest you here.
During your visit, you may wish to pray one of the following prayers prepared for the National Day of Remembrance:
By participating in the National Day of Remembrance, visiting these solemn memorial places at other times of the year, and spreading the word about this prayer campaign, you are helping to humanize our aborted brothers and sisters and deepening your own commitment to ending the injustice of abortion.
There are the women whose waiting doesn’t matter. And then there are the women whose waiting is especially terrible and reported on at regular intervals.
The Canadian Press reported on August 15 that a 29-year-old whose birth control failed got the abortion she wanted. Except it wasn’t quite fast enough. She waited too long for her abortion, she says. She waited two months. This was reported in major media outlets across the country. “Abortion access in Nova Scotia among worst in Canada, advocates say,” read the headline.
Women always get their abortions—so far not one story of an abortion denied—but the agony of the waiting: that’s the story.
There are other women, waiting. They are waiting for pregnancies. Statistically, women are trying at older ages to have children. Time is not on their side. They still know of women who managed to get pregnant at 42 or 45, and it keeps them going. They take vitamins. They try acupuncture. They stimulate ovulation. They take hormonal supplements. They are poked and prodded. They change their diets. And they wait.
Merely two months of waiting would be a dream come true.
For some women, infertility is painful and every pregnancy announcement is like a stab in the side.
Abortion announcements, on the other hand, are much, much worse. A much-coveted conception, cast aside. One woman’s treasure is another woman’s imposition. Or disposition. Don’t you know, it’s all about personal choice? Don’t ask why, because any reason is a good reason. And don’t let those women wait. They can’t wait. The waiting makes them (so they say) feel shame. Not the abortion. The waiting.
Of course, waiting too long for an abortion has the terrible complication of delivering a baby. Early in the first trimester, one can more easily be deceived into wondering whether that is actually true. But every woman knows the end point is a baby and that is why abortions must be done quickly. At 12 weeks, for wanted pregnancies, eager mothers learn how the fingers of their babies are opening and closing, how the baby’s mouth makes sucking movements.
It’s better to get an abortion before the fingers start opening and closing. Before you know that the 12-week-old is making sucking movements.
When the Canadian Press reported that Nova Scotia is “among the worst in Canada, advocates say, for abortion access,” there should have been heavier emphasis on “advocates say.”
For advocates, there’s no abortion that shouldn’t be done sooner. Sometimes they get it wrong, publicly, as in the recent case in Newfoundland where a 12-year-old got a quick abortion and then another. It turns out her stepfather was abusing her. But there was no time to ask.
Advocates for abortion in Nova Scotia, it also turns out, have no data—something we learn in the fourth to last paragraph of the story: “Nova Scotia does not appear to keep statistics on how long it takes women to obtain an abortion after a referral.”
Still, the story sailed through under the headline about “worst in Canada” wait times for abortion. No editor batted an eye. A woman said she waited. And these women must not wait.
What abortion advocates want is to have their cake and eat it too. Abortion is such a hard decision, they say. Not at all easy, they say. Meanwhile, here, they want no time allotted to making that tough decision. No reflection. No waiting. This particular hard decision must be made quickly.
Melanie Mackenzie’s story was the lead for the Canadian Press article: “It was the worst two months of my life. The whole thing felt like a punishment,” she said.
That feeling of punishment is something some infertile women, feel too. Did I do something wrong? Why won’t pregnancy happen for me?
For women waiting for pregnancy, if they’ve had abortions in the past, that waiting is all the more a punishment.
It shouldn’t be. But one can forgive them for feeling that way.
Women get pregnant and they get abortions. Women wait for conceptions that they then track diligently through all gestational stages, holding their breath till a baby is born.
When women are waiting for pregnancy, they’re not allowed to say it hurts when reporters conjure up headlines about abortions that did happen, just not quite fast enough.
So many women in Canada waiting. But only one group has a loud lobby who will push non-stories to reporters.
The rest? They can wait.
Andrea Mrozek is Program Director of Cardus Family. Prior to joining Cardus, she was the Executive Director at the Institute of Marriage and Family Canada. This article is republished with permission from Convivium, the Cardus faith and community blog.
Nearly every day the news presents yet another article on sexbots, robots that are designed to take the place of women. This is the most obvious “objectification” of women that has followed upon the sexual revolution, the literal creation of an artificial object, a robotic woman, for the sexual pleasure of men degraded enough to prefer a machine to the real thing.
Note that I have not provided any links to such articles, the obvious reason being that they all very graphically depict the new and constantly “improving” sexbots. Readers do not need yet another near occasion for sin, and I don’t want to provide one, thereby racking up even more years for purgatory.
Just within the last few weeks articles report (with giddy excitement, the slightest touch of moral trepidation, and no sense of irony) that sexbots are getting ever more realistic all the time, meaning, we assume, more like an actual flesh and blood female. In other words, the ultimate aim of sexualized robotics is the creation of a new Eve, a machine so like a real woman that the two will become indistinguishable—except that sexbots aren’t actually alive and so don’t get pregnant.
That’s an important difference. The Pill promised men and woman that sexual pleasure could be technologically cut off from the inconvenience of the natural procreation of another human being. But the Pill initiated a sexual revolution that has ended up in cutting men off from women—women who, we suspect, are now considered by such men as just one more inconvenience from which technology has relieved them. First babies, now women.
As you might expect, with even a casual acquaintance with fallen humanity, the depravity only gets stranger and more perverse. Sexbot manufacturers now promise that you can have a sexbot made in the image of your dead wife, or your favorite female celebrity. But since robotic perversion follows the ruts of the already existing cultural perversions, manufacturers are also making female sexbots that express their enjoyment at being raped, and even further down the moral slide to hell, sexbot children for pedophiles.
That’s a pretty quick and abysmal moral tumble in the fifty years since the Pill hit the market. I assume that none of the “well-intentioned” advocates of the Pill then, would have been so optimistic if, by some miracle, they could have been given a quick vision of the future five decades hence.
Fifty years ago Pope Paul VI stood, almost alone, against the tide of those calling for the severing of sexual union from sexual procreation. In his famous encyclical, Humanae Vitae (1968), he states the following prophecy, which is now being fulfilled in far darker terms than even he envisioned. Read it again, very slowly, especially the part I’ve highlighted.
Responsible men can become more deeply convinced of the truth of the doctrine laid down by the Church on this issue if they reflect on the consequences of methods and plans for artificial birth control. Let them first consider how easily this course of action could open wide the way for marital infidelity and a general lowering of moral standards. Not much experience is needed to be fully aware of human weakness and to understand that human beings—and especially the young, who are so exposed to temptation—need incentives to keep the moral law, and it is an evil thing to make it easy for them to break that law. Another effect that gives cause for alarm is that a man who grows accustomed to the use of contraceptive methods may forget the reverence due to a woman, and, disregarding her physical and emotional equilibrium, reduce her to being a mere instrument for the satisfaction of his own desires, no longer considering her as his partner whom he should surround with care and affection.
Get it? See the horrid historical connection? Could Paul VI have possibly foreseen the full prophetic warning that a sexually liberated man would soon reduce a woman to being a mere instrument for the satisfaction of his own desires?
For some of the same reasons other well-done videos grab your attention: pace, music, and most of all the clear demonstration that fetal development is a natural progression, starting at fertilization and ending with the first cry. But there’s more.
For example, the video doubles back. You see that the baby has fully developed outer ears and then a little bit later the viewer sees a schematic (as it were) of the middle and inner ear. Message? Complexity.
You see examples of the behavior expectant parents can now see on 4-D ultrasounds: the smiles, the yawning, the swallowing of amniotic fluid, the nibbling on the toes, the movement to gain maneuvering room as the child grows larger.
I’m sure I’ve probably seen this before, but this video does a very nice job of conveying the last part of the baby’s journey: moving down through the birth canal.
One other thought: pro-lifers all know that the umbilical cord is the baby’s lifeline, connecting mom and baby, so that the little one can receive nutrients and oxygen. But “Life in the Womb (9 months in four minutes)” helps us appreciate what an endless source of fascination it must be to the baby.
When you have a free minute, be sure to go to youtube.com.
LifeNews.com Note: Dave Andrusko is the editor of National Right to Life News and an author and editor of several books on abortion topics. This post originally appeared in at National Right to Life News Today —- an online column on pro-life issues.
August 24, 2017 (LifeSiteNews) — Ten years after the elimination in 2006 of an allowance for “therapeutic abortion,” Nicaragua has dramatically decreased its maternal mortality rates. The decrease proved false those prophesies the pro-abortion activists made that “thousands of women would die from the criminalization of abortion.”
On May 30, the Ministry of Health (MINSA) disclosed the number of maternal deaths. In 2006, 93 women had died per 100,000 childbirths. That number was reduced to 59 deaths in 2011 and in 2016 to 38 women per 100,000 births.
Nicaragua also successfully achieved its millennium development goals thanks to a model of comprehensive health for pregnant women launched by the government. And in 2011 Nicaragua was also rewarded the World Health Organization’s “America Prize” for reducing maternal deaths.
It was no surprise that the decision to protect all life garnered energetic protest of the international pro-abortion powers, which immediately began threatening to remove economic aid. Many donor countries closed their embassies and external cooperation agencies in Nicaragua because they considered what was done a setback for “women’s rights.” Among them were Finland, Denmark, Sweden, and the Netherlands.
But even with the stellar drop in maternal mortality, the so-called defenders of women’s rights are not pleased. A bill called “Special law for interrupting pregnancy for health reasons” has been introduced before the Congress and advanced by the “Promoter Committee.” This committee is supported by IPAS (International Project Assistance Services), which manufactures and markets hand-held suctioning devices for abortions.
They use the slogan “Las Queremos Vivas” (“We want them alive”). The initiative was rejected by Congress, but the committee and other groups have stated that they will continue to insist until it is approved.
But Nicaraguans know that pro-abortion campaigns funded by powerful countries and agencies are permanent and sustained. The New World Order puppeteers consider poverty a destabilizing factor. They move powerful nations to establish policies that, instead of eliminating poverty through education and health, will eliminate the poor. Let’s not get caught in that trap. Let’s not go back to the past.
Recently Pope Francis tells of talking with his predecessor, Pope Benedict, who remarked that we are living in an “epoch of sins against God the Creator.” What did he mean? Evidently, other epochs had sins but they were not directed against the Creator. The sins we were to repent in the Redemption were not primarily directed against the Creator.
The Decalogue is divided into two parts: duties to God and duties to other human beings. Things like disobedience, murder, adultery, lying, stealing, and coveting constitute sins against others. Or to put it positively, these prohibitions are designed to protect others from the disorders in our own souls.
Most of these sins were recognized by classical philosophers from many different traditions. It really does not take a genius to see the point at issue in each sinful situation. No thief wants his own goods to be stolen. Liars do not enjoy being lied to. Clearly, Benedict had something other in mind than what we might call “ordinary sins”, the everyday kind to which most of us are tempted at one time or another.
A sin against God the Creator implies that we are not dealing with aberrations that arise from freedom in normal intercourse with others. We are dealing with what might be called “structural” sins. Even if God put us together in a certain way, He had it all wrong. Such a strange thing as a “gay marriage” is “structurally” as good as, if not better, than marriage as it has been handed down to us as the locus for preserving the human race.
Creation is a given thing. We do not participate in our own basic creation as a human being. The intricate design that distinguishes us from other finite beings was already there without our help. It is much too complicated for it ever to have just happened. It was meant to be the way it is. That is, its origin lies in an intelligence that is more than human.
We were, to be sure, required to “know ourselves” so that we might become what we ought to be. We had a hand in our own destiny. We were the rational beings who were to become what they ought to be. We had, as it were, a natural law in our very being. We were to live around four score years and ten, male and female we were created. Our future depended on begetting and families. One generation replaced another over the ages.
A sin against the Creator would thus be directed not at stealing or lying, but in denying that these issues had anything to do with what human life was about.
So we are not dealing here with a kind of Machiavellian notion of being able to use good or evil for our own purposes. Rather we are dealing with the rejection of what it is to be a man as originally constituted. The very design is said to be faulty. What was once wrong is in fact right. Our given-ness tells us nothing about what we should be.
It turns out, then, that we are faced not only with moral problems about how we ought to live, as depicted in the Decalogue, but with a metaphysical problem about what we are. We are not only asked to know and follow man’s moral good, but to affirm his existential or structural good as a being. We are asked to understand and know the original “being” as given to us is superior to anything that we might propose as an alternative.
However, the rejection of God as Creator means that we can now, to some considerable extent, reconfigure ourselves. We can propose birth without normal sexual relations in an environment of a family. We can infuse genes not our own into our offspring in order to “improve” their looks or intelligence. Whether we have multiple wives or husbands, whether we have wives or husbands at all, is up to us.
In the beginning Adam and Eve were asked not only to do good and avoid evil, but also to be what they were created to be. The full implications of this latter instruction did not become evident until we understood the very internal structures of our being, all the details of its biological and psychological structures.
Thus when Benedict said that what we are witnessing is something more basic than the issues of moral virtue, when he spoke of “sins against God the Creator”, he was exactly on target. The issue is not now whether we will accept the goodness inherent in our being, but whether we will accept the very order of our being through which we achieve our final goods.
The epoch we live in is the first one in human history that can pose this question. It has the wherewithal to reject actual creation in a way not previously known to our kind. We can go ahead and do these things — but we must live with the consequences. We should not be surprised if we create monsters in our pursuit of reconstructing what we were created to be.
Rev. James V. Schall SJ taught political science at Georgetown University for many years. He is the author of numerous books.
MICAIAH BILGER AUG 25, 2017 | 1:21PM WASHINGTON, DC
Aleks Patete simply could not abort her unborn son, despite her troubling cancer diagnosis. The 28-year-old Ohio mom said her unborn baby boy saved her life, and there was no way she was going to destroy his.
“I think about the things that could have happened and what could have gone wrong and there’s no other reason than the grace of God that everything worked out and we are both alive,” she told People. “I truly think God was watching over us.”
The Blaze reports Patete was diagnosed with ovarian cancer after her seven-week pregnancy ultrasound revealed that she had a cyst on her ovary.
Doctors suggested that she have an abortion so that she could begin chemotherapy, but Patete refused. She said her unborn son is the reason why doctors found her cancer.
“He saved my life,” Patete said. “Now it was my turn to save his life.
“It’s a miracle,” she continued. “The cancer could have progressed a lot further, and we would have had no idea if I wasn’t for my pregnancy. God sent DJ to save my life.”
Later in her pregnancy, Patete underwent chemotherapy at the University Hospital Cleveland. All the time, she said she worried that her cancer treatments might hurt her son.
“It was the hardest decision I’ve ever had to make,” she said. “But we had to weigh our options — if I didn’t do anything, I put my life at risk, if I did something, was I putting the baby at risk? It was extremely difficult.”
The expecting mom went through chemotherapy and continued to work full-time as a nurse, according to the report. She said she felt exhausted and sick a lot, but updates from her doctors comforted her with the knowledge that she and her unborn baby were doing ok.
On April 24, Patete gave birth to her son DJ – just three days after finishing chemotherapy. She later had surgery to remove her right ovary and fallopian tube, according to the report. Now, she said she is in remission.
Patete is thrilled to be DJ’s mother, and she hopes she will be able to have more children someday.
“It was just beautiful,” she said. “And he’s the sweetest baby, always smiling and just a joy.”
Research indicates that pregnant women who undergo cancer treatments later in their pregnancies do not put their unborn babies at significant risk. A 2015 study published in the highly reputable New England Journal of Medicine concluded, “Prenatal exposure to maternal cancer with or without treatment did not impair the cognitive, cardiac, or general development of children in early childhood.”
Lead researcher Professor Frédéric Amant said women should not abort their unborn babies based on fear that their cancer treatment could affect their child.
But doctors still suggest abortion frequently when pregnant moms are diagnosed with cancer.
British mom Chelsea Nally is another example. She was diagnosed with breast cancer early in her pregnancy. Nally said her doctors initially discussed abortion as an option for her unborn baby boy, Finley, but she refused. Later, when tests revealed that her cancer was limited to her left breast, the doctors did not push the idea, and Nally said she felt relieved.
She gave birth to a healthy baby boy on March 19. And like Patete, Nally also believes her son saved her life.
“Holding him in my arms for the first time I felt like my biggest battle was over,” she said. “I couldn’t believe we had both survived pregnancy and chemo. He is my hero, even before he was born he had saved my life.”
The Australian government is likely to provide a new version of the vaccine that is said to prevent cancer soon. Gardasil 9 would replace the original Gardasil — administered to young high school students in three doses – with a two-dose regime involving a stronger formula that is already used in New Zealand and the United States. The vaccine promises protection against the human papillomavirus (HPV), certain strains of which, it is generally accepted, can cause cervical cancer.
Like the original roll-out of the drug 10 years ago and promotions since, this one is being heralded by very optimistic messages: “New cervical cancer vaccine may almost eliminate disease, research shows,” ran a recent headline. “It’s truly ground-breaking,” the scientist who led the new research, Professor Julia Brotherton, told the ABC. “The possibility that we can now prevent our children being infected with this cancer-causing virus, I just think that’s amazing.”
But not everybody is so happy about Gardasil. In addition to the anti-vaccine camp, there are parents, women’s health activists and some doctors who question the way it was hustled into national health systems, its safety, and its claims.
One dissenter is Helen Lobato, author of an expose published recently by Australian feminist publisher Spinifex. In her introduction to Gardasil: Fast-Tracked and Flawed she says:
“Fast-tracked and poorly tested vaccines are now given to young girls and boys because of a link between the human papilloma virus and cervical cancer. … [T]hese vaccines are not only unproven but the vaccinated girls and boys can suffer devastating adverse effects that result in permanent ill-health and even death for some of them.”
Lobato, a former nurse, had her own brush with cervical cancer in 1985. This gives her a personal stake in the representation of the disease today. Like many other women, she may have been saved from full-blown cervical cancer by having a Pap smear (a test that dates back to the 1940s and has been offered through national screening programmes in more recent decades) that allowed timely (if somewhat brutal, in her experience) treatment for a pre-cancerous condition.
In fact, the effectiveness of cervical screening is a key argument in her case against the HPV vaccine. Others are: it was rushed onto the market after inadequate trials; it is associated with thousands of adverse reactions and some deaths; it is administered without adequate informed consent; there is no proof that it can prevent cervical cancer.
Is this vaccine really necessary?
When a lay person considers a vaccine they think in terms of being protected against a widespread contagious disease. HPV is, apparently, such a disease. It is said that around 80 percent of people who have sex at all will get this infection at some stage. But we are also told that 90 percent of the infections will clear within a year. So why vaccinate as many girls and boys as possible against it? Because 10 percent may be at risk of cancer?
But the incidence of cervical cancer in countries like Australia is nothing like 10 percent. It is less than 1 percent, Lobato reports. (P 81) There is no epidemic of cervical cancer in any developed country (it is a different story in developing countries).
Moreover deaths from this cancer in Western countries is even rarer – at the rate of 1.7 per 100,000 women in Australia, which in 2014 amounted to 223 deaths from the disease — compared with 2,844 deaths from breast cancer (a figure which is expected to rise). Cervical screening is said to have halved the number of deaths since 1991, though Lobato believes that improvements in living standards played a part.
Her reading of the history of the disease suggests that poverty (including poor nutrition and hygiene) played a large part in earlier times, and more recently the contraceptive pill (its effect on immunity), smoking and other lifestyle factors. She discounts early theories that linked cervical cancer to “sexual excesses and immorality” and regrets that the current focus on HPV has swung the pendulum back in this direction.
The race to provide a vaccine
The hypothesis that HPV and cervical cancer are linked goes back several decades, and the idea of a vaccine against the STD was first mooted in the 1970s. Research began in several centres but in the end it was an Australian team – Scottish-born Professor Ian Frazer, and Dr Jian Zhou, at the University of Queensland – that made the breakthrough by producing a synthetic version of the HPV virus in 1991.
From the late 1990s in Australia and internationally, Lobato says, “a relentless propaganda campaign” for the vaccine began to build. This reached its peak in 2006, when Frazer was hailed as a national hero (Zhou died in 1999) and he personally vaccinated the first woman at the Sydney launch. There were 947 pieces of media devoted to the Australian campaign, driven by PR giant Edelman.
US television hosts hailed the vaccine as “a triumph in science and medicine” and something that “could save your teenager’s life someday”. Based on a US television advertisement featuring health young girls, “One less” (victim of cervical cancer) became an international slogan – as though victims were dropping like flies.
“Gardasil was fast-tracked through the FDA [the US Food and Drug Administration], a process usually reserved for life threatening diseases to fill an unmet and urgent medical need,” says Lobato. For her, this was a coup for Big Pharma rather than women or even public health. The drug companies, which funded the trials, stood to gain huge revenues.
In November 2006 the vaccine was listed on Australia’s national immunisation register and on International Women’s Day 2007 the program was launched.
The vaccine is provided free through schools to girls aged 12 and 13, and to boys on the same basis since 2013. Up till now, three injections are given over six months. And yet Gardasil had been tested on fewer than 1200 girls under the age of 16 when the national program began. Cervarix, the other brand used in Australia and Europe, was also studied in a small number of young girls.
Lobato quotes Diane Harper, one of Merck’s HPV vaccine researchers “and now a whistleblower,” saying that the roll-out “went too fast, without any breaks.”
Adverse reactions, deaths: what’s in Gardasil?
That was in 2008 and Harper was commenting on the mounting toll of side effects being reported – the dominant concern of Lobato’s book. It begins with the case of Australian woman Krisitn Clulow, who received her first two shots of Gardasil in May and August 2008 and whose health thereafter collapsed owing to an inflammatory disease of the brain. With treatment she recovered by 2010. A homeopath who helped her recovery informed her that her body was high in aluminium.
“Aluminium is a neurotoxin,” says Lobato, and each dose of Gardasil contains 225 micrograms of it as an adjuvant – a booster of the essential ingredient. Gardasil 9, approved by the FDA in 2014 for the prevention of cervical, vulvar, vaginal and anal cancers will contain 500mcg of aluminium and a larger dose of antigens (the HPV LI proteins). Cervarix also contains the chemical in the form of aluminium hydroxide.
Lobato regards this as a major reason that “HPV vaccines are associated with more deaths, and serious adverse effects than other vaccines.” According to the World Health Organisation’s Vigibase, there are now over 73,000 recorded adverse events after HPV vaccination. Lobato says there have also been at least 324 deaths.
All vaccines have side effects, but the fact that an illness or death occurred after vaccination is not proof that it was caused by the vaccine. Also, the plausibility of the case against the HPV vaccine is influenced by one’s attitude to vaccines in general, and Lobato seems to lean to the anti-vaccination camp.
Nevertheless, the National Vaccine Information Center in the US published a Gardasil risk report in 2009 which found that death and serious adverse events are reported three to 30 times more often after Gardasil than after the meningococcal vaccination Menactra.
This data needs scientific study, but it will be difficult for interested scientists to get funding for such research in the current climate. Australian GP Deirdre Little has documented in medical journals three cases of premature ovarian failure (early menopause) in adolescent girls who had been vaccinated with Gardasil, and she has questions about the vaccine’s safety – and the manufacturer’s research — from that point of view.
No proof that HPV vaccination prevents cancer
“We can now prevent cancer.” Lobato says there is no proof that this is the case. This is because HPV vaccines have never been tested against cervical cancer outcomes only against surrogate endpoints: cervical intra-epithelial neoplasia (CIN) garde 2/3 lesions, and carcinoma in situ. These precursor lesions are common in women under 25 but rarely progress to cancer, according to Lobato.
To have allowed human test subjects to progress towards cancer in order to prove its efficacy at that point would be unethical, so there is nothing wrong with using surrogate endpoints, but the claims should be correspondingly modest. Instead, public messaging has harped on the cancer prevention potential of the vaccine – really, to maximise the number of young people receiving it. Basically, those young people are part of an experiment. A good experiment, perhaps, but shouldn’t parents and the wider public be informed that it has a downside?
Lobato concludes her book with an appeal to the media to do their job and give the public the fuller story about the HPV vaccine. You may not agree with her version of the story at all points, but she has shown Big Media some of the things they could be airing in the interests of informed debate.
For all the bluster about “choice,” “access,” and “reproductive health,” the abortion industry and its assorted fans in Hollywood, politics and the media have a remarkable tendency to swing for the fences and come up empty.
And that fact is becoming clearer to see every day.
Take, for instance, the recently failed “Expose Fake Clinics” campaign, starring Comedy Central and leftist icon Lizz Winstead and her abortion-extremist group, “Lady Parts Justice League.”
Seeking to “expose” pregnancy centers that offer women the help they need to make an informed choice of their own during an unexpected pregnancy, all Lady Parts Justice League exposed was its own ignorance of the facts.
That and the Left’s steely opposition to anything that could possibly make a dent in abortion’s cultural and financial stronghold. Cash flow and cultural currency—not “choice,” “access” or “reproductive health”—are at stake, and abortion profiteers know it.
The Left’s Science Deniers
Perhaps that’s why, in addition to organizing a spate of protests like Winstead’s at life-affirming pregnancy centers this summer, abortion absolutists have upped the ante (or is it “anti”?) in their fight against “Abortion Pill Reversal (APR),” a medical intervention that can halt a chemical abortion after a woman has taken the first of two pills involved in the RU-486 abortion pill regimen.
Even though the APR network now includes over 350 physicians who credit it with having saved the lives of 300 babies in the past 10 years, pro-abortion outlets like Rewire.com and DAME magazine, as well as mainstream outlets like The Washington Post and The Los Angeles Times continue to refer to it as “junk science.”
While the research on APR is still in its initial stages—APR researchers expect to release a major paper in the coming months—the abortion lobby’s knee-jerk resistance to the process says plenty about where “reproductive health” and “choice” rank on their hierarchy of values.
(Actually, the abortion industry’s decision to couch its lethal agenda as “reproductive health” breaks down far more easily than that: “Abortion is neither ‘reproductive’ nor ‘healthy.’” Discuss.)
Where Abortion and Access Collide
Meanwhile, when they’re not busy smearing the pro-life movement as closet racists or rapists, abortion-mongers like those at NARAL Pro-Choice America—an ironic name if ever there was one—are doing everything in their power to keep women headed for abortuaries from even interacting with a pro-lifer on the street.
In Chicago, pro-life advocates are continuing to fight for the right to speak with women outside of abortion mills—a fight that has gone on since 2009. Under a current city ordinance known as a “bubble zone,” no pro-life citizen can come within eight feet of any woman heading to an abortion clinic once she comes within 50 feet of the front door.
The ordinance, introduced under the “pro-choice” guise, effectively strips a woman of choice by trampling on her right to make the most informed decision possible about her own pregnancy. This strikes at the very heart of the “choice” and “access” abortion devotees claim to hold so dear.
In an Aug. 21 donor appeal, NARAL president Ilyse Hogue bemoaned the fact that Kentucky’s last remaining abortion mill, EMW Women’s Surgical Center in Louisville, may be on its way out of business.
Painting a rather drastic picture of a “mob of dozens of anti-choice fanatics trying to block the entrance” to the abortion business, Hogue later bewailed the fact that women could access a pro-life pregnancy center right next door instead of ending her child’s life through abortion at EMW Women’s Surgical Center.
In the fantasy world Hogue portrays, where peaceful protests and sidewalk counseling are depicted as a bread riot in the Soviet Union, reality holds no value.
And neither do “choice” or “access”—to anything other than abortion, that is.
Pro-Choice? Not So Much…
Because they couldn’t find anything productive to do with 10 days out of their summer, Winstead and Co. scoured the country to dig up as much dirt as they could on life-affirming pregnancy centers, which serve women with free ultrasounds, pregnancy tests, post-abortive counseling, peer counseling, parenting classes and material aid like diapers and car seats.
What we might call the “anti-anti-choice” crusade targeted over locally funded pregnancy help centers and ultrasound-equipped medical clinics across the country with online and on-site demonstrations, all focused on demonizing anyone with the gumption to offer an alternative to abortion.
Though the campaign—which one Cincinnati pregnancy center director called “underwhelming” after a handful of abortion fans picketed her center—identified over 4,000 centers on their hit list, only 40 locations were actually subjected to any sort of pro-abortion presence as part of the effort.
The crusade was doomed from the start. At its initial rally, a man and his toddler walked up on Lady Parts Justice League’s protest outside the very place where his son’s life had been rescued from abortion.
Confronting Winstead’s un-funny fiction, the man insisted that pro-abortion protesters take a look at his toddler and reckon with the fact that he was standing there because of the center’s work.
He wasn’t the only former pregnancy center client to speak up on behalf of the ministries under fire from “Expose Fake Clinics.” One mother, who chose life with the help of a Minnesota pregnancy center, actually thought the whole campaign was a joke before realizing that Winstead and her troupe actually meant business.
Running on Fumes
Another telling moment came as the campaign made a stop in Columbus, Ohio, at a pregnancy help medical clinic serving women just across a side street from a Planned Parenthood that aborts babies in a minority-heavy, low-income area.
When one pro-lifer, a pastor in Columbus, approached protesters and calmly asked why they were there and what they were hoping to accomplish, he was confronted with the same deluge of accusations against pregnancy centers that have poured forth from pro-abortion groups like NARAL for the past decade.
Rather than argue point-for-point, his response cut right to the heart of the issue. Far better to be accused of dishonesty than to be unashamedly committed to monetized killing.
“On one hand, you have someone supposedly lying and one hand you have someone killing,” he said. “If I had to [pick between] the two, I’d go with the lying.”
Winstead’s campaign was followed by another planned protest at a pregnancy center, this time in Atlanta, where 150 abortion absolutists showed up Aug. 12 to register their disdain for Cura Women’s Health Clinic—an ultrasound-equipped medical clinic that has saved 180 babies from abortion thus far in 2017.
Though 150 protesters may sound like quite the crowd, it’s really not all that impressive when you realize its organizers—including Lady Parts Justice League, Reproaction and SisterSong—were pulling from a Google and Facebook-backed “Netroots Nation” conference that gathered 3,000 leftists at a downtown hotel less than a mile away from the pregnancy center.
Coming just minutes after Massachusetts Sen. Elizabeth Warren urged the same crowd to stand unapologetically for abortion, the paltry Atlanta protest may be the best indicator yet of just how much ground abortion fanatics like Warren are losing even among their own constituency.
The old euphemisms just aren’t holding up, and there’s no candid way to defend an idea as ugly as abortion.
LifeNews Note: Jay Hobbs writes for PregnancyHelpNews, where this originally appeared.
MICAIAH BILGER AUG 21, 2017 | 11:42AM WASHINGTON, DC
For the second time in a year, a group of scientists managed to create an artificial womb that one day could save very premature babies’ lives.
Scientists in Philadelphia published promising research on artificial wombs using premature lambs earlier this year; and this week, a team of Australian scientists published their successful results of very similar research.
Science Daily reports the new study in the American Journal of Obstetrics and Gynecologythis week found that premature lambs at the equivalent of 22 to 23 weeks of human pregnancy developed well in the artificial womb. The Australian scientists observed the baby lambs for one week inside the ex-vivo uterine environment (EVE), or artificial womb. The lambs showed significant growth in the infection-free, womb-like environment, according to the report.
More very early preemies are surviving outside the womb thanks to modern medical technology, but the artificial womb could push back viability even earlier.
A Duke University study published in January found babies born at just 23 weeks gestation are surviving outside the womb at a greater rate than ever before, the Daily Mail reported. Research published in 2015 in the New England Journal of Medicine alsofound that 23 percent of premature infants are surviving birth as early as 22 weeks. The study also found that some hospitals are not giving babies treatment at this early age, despite talk about pushing back the standard viability line from 24 weeks to 23.
However, survival at 22-24 weeks remains low because the babies’ lungs are so underdeveloped.
Here’s more about the latest study:
Chief Investigator in Australia, Associate Professor Matt Kemp, said that with further development, EVE therapy could prevent the severe morbidity suffered by extremely premature infants by potentially offering a medical technology that does not currently exist.
“Designing treatment strategies for extremely preterm infants is a challenge,” he said.
“At this gestational age the lungs are often too structurally and functionally under-developed for the baby to breathe easily.”
The research team hypothesised that one means of improving outcomes for this group would be to treat them as a fetus rather than a small infant.
“At its core, our equipment is essentially is a high-tech amniotic fluid bath combined with an artificial placenta. Put those together, and with careful maintenance what you’ve got is an artificial womb,” Assoc Prof Kemp said.
Kemp said the ultimate goal is to create an environment where very premature human babies’ lungs can develop to a healthy stage. The scientists said more research must be done, but the artificial womb shows huge promise for helping very premature babies to survive and thrive.
The study came out of the Women and Infants Research Foundation at the University of Western Australia and Tohoku University Hospital in Japan.
The research is potentially life-saving, but it has abortion activists worried. In the July Gizmodo article “How New Technology Could Threaten a Woman’s Right to Abortion,” reporter Kristen V. Brown wrote, “[Artificial wombs] “complicate – and even jeopardize – the right to abortion in an America in which that right is predicated on whether a fetus is ‘viable.’”
If it becomes possible for the mother to abort with a method that leaves the baby alive and intact … can a mother then refuse to allow her baby to be put into an artificial womb where the child could further develop for a few more weeks and be “born” healthy?
Brown sketches out what is for abortion defenders a looming legal and ethical dilemma and notes how doctors, bioethicists, and lawyers “have long taken issue with viability as a standard for legality.”
This new technology just further exposes the problematic nature of their premises.
Micaiah Bilger Aug 18, 2017 | 11:50AM Reading, Pennsylvania
Parents and pro-life advocates urged a Pennsylvania school board Wednesday to reject a proposal to put a Planned Parenthood-run facility inside Reading High School.
The Reading Eagle reports the facility would not do abortions at the high school, but Planned Parenthood staffers would offer students sex education, counseling about reproductive health and referrals to their abortion facility in Reading.
Pro-lifers with Students for Life, the Pennsylvania Family Institute and others have been joining local parents to protest the proposal in the past few months. On June 21, about 80 pro-life advocates stood outside the Reading School District to urge the school board to oppose the Planned Parenthood-run center.
In addition, the center would be paid for by tax dollars, according to the Pennsylvania Family Institute.
According to the local news report:
Those who support the program advocate helping young people in Reading make more informed decisions about their own reproductive health, while those opposed bemoan the possibility of a Planned Parenthood staff member interacting with students.
The argument centers largely on abortion rights, though the program itself does not address that issue and simply seeks to provide optional counseling services to students with questions about reproductive health. For all services besides counseling and condoms, students would receive referrals to the Planned Parenthood location in Reading.
… AccessMatters, an organization based in Philadelphia, would oversee the program while Planned Parenthood Keystone would manage daily operations and assign a staff member to hold office hours in the school. Funding would come from the Pennsylvania Department of Health at no cost to the district.
The school board is scheduled to vote on the proposal on Aug. 23.
According to the NPR Michigan affiliate, Saline Area Schools asked local residents for their opinions about a proposal to allow Planned Parenthood-trained teens to teach sex education to students at its schools. In May, school officials said they abandoned the proposal because of the overwhelmingly negative responses they received from the public.
Planned Parenthood is the largest abortion provider in the United States, aborting more than 300,000 unborn babies every year. The abortion chain also teaches sex education in public schools across the country, and promotes risky sexual behavior to vulnerable young teens at its clinics.
In 2014, Live Action released an undercover video series showing Planned Parenthood employees encouraging young teens to participate in sado-masochistic sexual activities, including gagging, whipping, asphyxiation, shopping at sex stores and viewing pornography.
LifeNews also reported Planned Parenthood’s booklet for HIV-positive youth, “Healthy, Happy and Hot,” tells young people that it is their “human right” to not tell their partner that they have HIV.
The abortion giant also publishes multiple “resources” for children and teenagers concerning sexual activity. These materials claim to provide “age appropriate” sex education to children starting at age 4.
August 17, 2017 (LifeSiteNews) — Faced with gender ideology and the deliberate and methodical plan to destroy the traditional family, an “interior Vendée must arise in the heart of every family, of every Christian, of every man of good will!”
With this rousing call, Cardinal Robert Sarah, prefect of the Congregation for Divine Worship and the Discipline of Sacraments, has asked for a “revolt” against the new lies of the continuing revolution against God’s law. His call to prayer and action was made during a homily given during a Mass on August 12 in the foyer of the grandstand of France’s award-winning historical theme park, the Puy-du-Fou.
The Vendée is the region in Western France where an uprising took place during the Reign of Terror – the “Terreur” – in 1793 and 1794 when the leaders of the French Revolution conscripted ordinary men to serve in the revolutionary army and required Catholic priests to vow submission to the Civil Constitution of the Clergy and repudiate their commitment to obey the Pope.
For the faithful peasants of the Vendée, on whom the “missions” of Saint Louis-Marie Grignion de Montfort some 80 years back had left a profound mark, these requirements were unacceptable. They forced many nobles of the province to lead them into war with the new Republic, courageously fighting “for God and King” in an uneven battle that would culminate with the genocide of the Vendée. The Committee of Public Safety – the revolutionary government in Paris led by Robespierre – expressly ordered every man, woman and child from the province to be killed, their houses and villages to be destroyed, and the very earth of the province to be burned.
The reality of this fully-fledged genocide, truly a founding act of the French Revolution, was long negated in French politics and history books. The defeat of the Vendée would lead to its relegation in oblivion, or as French historian and specialist of the Vendée Reynald Secher puts it, to “memoricide.”
Cardinal Sarah’s visit to the diocese of Luçon in the Vendée, which this year celebrates the 700th anniversary of its founding, would not have been complete without a visit to the Puy-du-Fou theme park where Philippe de Villiers, former presidential candidate in France and visionary entrepreneur, created a profoundly original “sound and light show” 40 years ago presenting the history of a ruined castle in the form of a live cinematographic performance. Forty years later, the show has morphed into a spectacular embodiment of the history of the Vendée where several thousand volunteers act several times the week during the summer months, honoring the memory of the “Vendéens,” their forebears, especially in their uprising for their “God and King.”
The theme of the “Wars of the Vendée” is also present in the theme park that has grown into an international award-winning venture whose aim is to rekindle love for their homeland and for beauty in the hearts of the many millions of visitors who have come there over the years.
Cardinal Sarah certainly caught the spirit of the Puy-du-Fou in paying homage not only to those who have taken part in this unique cultural adventure but to the peasant warriors of the Vendée. Armed only with their “staffs, scythes, rosaries and the Sacred Heart” sewn on their coats, they stood up to fight and then, by their thousands, “died for their faith, for their churches and for their priests.”
“You give a voice to all those whom the ‘Terreu’ wanted to silence, because they refused the lie of atheistic ideology! You honor those whom it wanted to drown in oblivion, because they would not allow the liberty to believe and to offer Mass to be stripped from them!” the Cardinal said during his homily on Saturday evening.
“Your work is necessary! For our times seem to have been numbed! As we face the dictatorship of relativism, as we face a new thought terrorism that once again seeks to rip God from the hearts of children, we need to rediscover the freshness of mind, the joyful and fervent simplicity of these saints and these martyrs,” he preached, standing before the reliquary where the ring of Saint Joan of Arc reposes after having been providentially brought back from England last year by Philippe de Villiers to be honored in the Puy-du-Fou. Saint Joan’s ring had been taken to England in 1431 by Cardinal Henry Beaufort after she was burned at the stake in Rouen.
Cardinal Sarah insisted that even though death and martyrdom was the “Vendéens” lot, they were mysteriously victorious in that after the throes of the Revolution, Catholic priests in France were once again freely allowed to serve God without having to submit to the “lie of ideology” that had threatened to “reign supreme.”
He went on to speak of the present-day persecutions that stem from the atheistic “matrix” of the French Revolution, calling the all Christians and people of good will to accept and follow the heritage of the Vendée against new forms of totalitarianism.
“Even now, perhaps more than ever, the ideologues of the revolution want to annihilate the natural place for gift of self, of joyful generosity and of love! I am speaking of the family! Gender ideology, the contempt of fruitfulness and of fidelity are the new slogans of this revolution. Families have become the new Vendées to exterminate. Their disappearance is being methodically planned, as was that of the Vendée in the past,” said the African cardinal, particularly condemning modern-day attempts to force “sterilization, abortion, and contraception” on his home continent.
“These new revolutionaries are worried by the generosity of large families. They mock Christian families, because these embody everything that they hate. They are ready to attack Africa with new infernal columns in order to put pressure on families and to force on them sterilization, abortion and contraception. Africa, like the Vendée, will resist! Families everywhere must be the joyous spearheads of revolt against this new dictatorship of egoism! It is now in the heart of every family, of every Christian, of every man of goodwill that an interior Vendée must arise! Every Christian is, spiritually, a Vendéen!” said Cardinal Sarah, presenting today’s God-hating and man-hating ideology as every bit as violent and deadly as the violent killings of more than 200 years ago.
The Cardinal concluded that this uprising must be a peaceful one, founded in adoration and prayer and careful to uphold “forgiveness and mercy,” because “love only conquers the powers of death.”
ICELAND, August 15, 2017 (LifeSiteNews) – A new report from CBS News details how 100 percent of babies in Iceland who are diagnosed with Down syndrome prenatally are aborted.
This has “almost completely eliminated Down syndrome births since the test began in the early 2000s,” Elaine Quijano of CBS explained. She interviewed an abortion counselor, an Icelandic scientist, and the mothers of children with Down syndrome.
She also interviewed an Icelandic woman who has Down syndrome.
People “just see Downs. They don’t see me,” she told Quijano. “It doesn’t feel good. I want people to see that I am just like everybody else.”
In 2009, only three babies with Down syndrome were born in Iceland. Only one mom in the entire country has two children with Down syndrome. She lives in Hellissandur, on the northern coast.
“Yes, of course” some women express guilt at aborting their disabled babies, the abortion counselor told Quijano. The pro-abortion counselor showed her a prayer card with the footprints of an aborted baby. Parents can keep these footprints and prayer cards as a memento of their aborted child.
She said she tells women, “This is your life. You have the right to choose how your life will look like.”
“We don’t look at abortion as murder,” she continued. “We look at it as a thing that we ended. We ended a possible life that may have had huge complications.” It is “preventing suffering for the child and also the family.”
“The media sell this little three-year-old, nice cute one,” the abortion counselor continued. “But you have to look at Down syndrome as a spectrum. You have this little cute one who was Down syndrome … and then we have people who [have] Down syndrome plus lots of other complication[s].”
She said she sees life’s moral decisions as “gray” rather than “black and white.”
The Icelandic mother of a young child with Down syndrome asked Quijano, “What kind of society do you want to live in?”
One expectant mom told Quijano she decided to forgo the test because “it wouldn’t make a difference, actually.” She said she works with autistic children and has a brother-in-law who has Down syndrome. “I think it’s just horrible, the statistics.”
The CBS report pointed out that the country’s socialized healthcare system requires doctors to tell women about the option of prenatal testing for genetic defects.
There is “some truth” to the notion that informing women of this steers them toward abortion, a technician who does the prenatal tests said. “Obviously, if you didn’t mention it, then you wouldn’t be thinking about it.”
“My heart breaks for the innocent babies aborted in Iceland because society has deemed certain people undeserving of life,” Kristan Hawkins, president of Students for Life of America, told LifeSiteNews. “My children with genetic disabilities are loved and valued the same as my children without. I pray this report will wake up the people of Iceland to the discriminatory killing occurring amongst them. I pray they wake up before even more human beings fall victim to this disgusting mindset.”
Penny Nance, president and CEO of Concerned Women for America, the nation’s largest women’s public policy organization, said this is an example of eugenics.
“Iceland sounds like they are proud of the fact that they’ve killed nearly all unborn babies that had an in-utero diagnosis of Down syndrome. This is not a medical advancement,” said Nance. “This is eugenics and barbarianism at best. These individuals have no less worth than anyone else.”
“What is the next headline going to be?” asked Nance. “That a certain country has eradicated all females. Oh wait, China has already been down that road. There is no limit to this train of thought of devaluing human life.”
Actress Patricia Heaton blasted the notion that Iceland is eliminating Down syndrome, noting they’re just “killing” everyone who has it.
Popular blogger Matt Walsh called those perpetuating the abortion of Down syndrome babies “degenerate Nazis.”
Former U.S. presidential candidate Sen. Ted Cruz, R-Texas, weighed in, as did media critics and other pro-life activists.
The CBS report noted that Denmark trails Iceland with a 98 percent abortion rate for babies diagnosed with Down syndrome and that it is a trend throughout Europe. Abortion rates for Down syndrome babies in the U.S. are slightly lower but still well above 50 percent.
Hanna Klaus, February 8, 2017, Reproduced with Permission, Church Life Journal
Managing a couple’s fertility to regulate their family size does not require removing said fertility from the woman’s or the man’s body. This is not primarily a religious issue. Some years ago a psychologist from the National Institutes of Health (NIH) who had no religious affiliation came to me for instruction in the Billings Ovulation Method of natural family planning. She had already used mechanical and hormonal contraceptives, but, responding to a comment I had made at an NIH meeting, she decided to seek a natural method. After using the method for three months she told me, “This method is so different—now I can be all there, now I am not holding anything back.” The contrast between contraception and fertility acceptance methods has never been explained more simply.
Today, hormonal contraceptives and sterilization are marketed aggressively and exclusively. While the physical side effects of contraceptive steroids on every organ system have been described in the medical literature, the personal, social, and spiritual effects of contraceptive steroid hormones, in fact of any blocking of the total mutual self-giving which is the essence of the marriage act—has consequences. Until the publication of “The Association of Hormonal Contraception with Depression” in JAMA Psychiatry in September 2016[1], too many family planning providers either denied the link to depression or prescribed anti-depressive medications rather than stopping the cause of the depression.
Contraceptives as the status quo
Removing fertility from the healthy body is a lifestyle choice and, when done with contraceptive steroids or surgery, is far from risk-free. The regulations which our Department of Health and Human Services (DHHS) have issued only consider the end—reproduction-free sexual relations—as significant. Despite today’s contraceptive inundation, 54% of unplanned conceptions[2] begin in a cycle in which the woman used contraception, usually hormonal. She may not have used the drug correctly or consistently, or it may have failed.
Public health providers tend to think in terms of reaching the lowest common denominator. In the last five years LARCs—Long Acting Reversible Contraceptives—have been heavily promoted by public and private health care providers, especially to single teen mothers right after giving birth, and to single women “at risk” for pregnancy, especially teens. LARCs are either etonorgestrel or similar subdermal implants, levonorgestrel or copper IUDs, which are expected to remain in place for at least three years, or depoprovera injections which must be repeated every three months. While women report physical side effects such as patternless vaginal bleeding with both IUDs and implants, removal requires medical intervention and women are often persuaded that the symptoms will subside, and asked to try the devices a little longer. Between 80-85% of women still use the devices one year after insertion. Reports of side effects are limited to physical symptoms.
Apparently, no one has asked these predominantly low-income young women how they feel about being sexually available at all times, nor has anyone published figures for the occurrence or incidence of sexually transmitted infections among LARC users. However, a recent U.S. Public Health Service study of 15–19-year-old low-income girls found that half were sexually active.[3] According to the study, the overall incidence of the most common infections—chlamydia, human papilloma virus, herpes, and gonorrhea—was 26% for the total group. As only half the group was sexually active, it is reasonable to conclude that their disease burden was 50%. Their number of partners was not reported, so one can only speculate about the girls’ relationships or self-esteem. By 2015, the Center for Disease Control reports skyrocketing rates of sexually transmitted diseases, particularly high among 15–19-year-old women.
A healthier approach to sex education and family planning
There is a better approach to helping youths manage their emerging sexuality and fertility. We began Teen STAR in 1980. STAR stands for Sexuality Teaching in the context of Adult Responsibility. With parental permission, Teen STAR students explore and discuss the physical, emotional, social, intellectual, and spiritual aspects of sexuality and fertility. Girls learn to observe their fertility cycle, boys learn to understand their changing body and how to master its reactions. In religious settings the Theology of the Body is taught explicitly, but even in secular settings the sexual relationship is taught as part of procreation. Behavioral outcomes of program participants from the Americas, France, Uganda, and Ethiopia show excellent support for both primary and secondary abstinence.[4]
Indeed, natural means of recognition of times of fertility and infertility are available, reliable, and offer well-documented options that are free, both of side-effects and cost. Yet only a small number of couples follow any of these natural methods of family planning as they are seldom taught integrally to medical students. If the woman has the temerity to ask about natural methods, her physician either:
does not know much about them;
says they don’t work; (Most patient information inserts in contraceptive pill packages still cite a 25% failure rate for typical use of natural methods. This figure is the sum for modern NFP methods [described below], calendar rhythm, and “home methods.” The 2016 FDA-approved package inserts of contraceptive medications still cite the 25% failure rate. [See any contraceptives described in PDR Physicians Desk Reference 2016]. The American Congress of Obstetricians and Gynecologists only began to cite more contemporary figures in their April 2015 ‘FAQ’.)
belongs to a small select group who do know and advocate for fertility awareness based methods.
In 2013 the NIH offered $3,000,000 for proposals to produce non-hormonal contraceptives. (No active projects are on record—either no one applied, or none were funded.) But they need have looked no further, and saved taxpayer funds in the process.
Managing a couple’s fertility to regulate their family size can be achieved by understanding and heeding the physical sign(s) of a woman’s cyclic fertility. A man’s fertility begins at puberty and remains constant until age or disease reduce or remove it. A woman’s fertility begins at puberty and ends at menopause. As the egg cell matures in its follicle in each cycle, its rising estrogen causes the production of a changing mucus in her cervix which she can feel and see at the opening of her vagina. The discharge usually begins as a fairly dense material but becomes more fluid and slippery over the course of several days. The last day the mucus is slippery, clear and stringy is usually the day of ovulation. Couples who wish to conceive will ensure marital intercourse on the days of lubricative mucus; couples who wish to postpone conception will follow rules to avoid intercourse on the days of fertility, as it is known that sperm will survive for 3–5 days in the mucus which precedes ovulation.
Currently the Billings Ovulation Method, the Creighton Model, and Georgetown’s TwoDay Method rely on the mucus biomarker alone, while CCL (the Couple to Couple League) and Northwest Family Services add the postovulatory rise of the woman’s basal body temperature as well as a calendar calculation to determine the beginning and end of the couple’s fertile phase. The Marquette Model adds urinary testing for estrogen and luteinizing hormone (LH, the hormone which triggers ovulation) rise, as well as mucus and sometimes temperature observation, while LAM (Lactational Amenorrhea Method) and Georgetown’s SDM (Standard Days Method) rely on calendar calculations alone. All these methods have been professionally researched and need to be learned correctly from providers (or internet) and followed consistently to enable couples to manage their fertility reliably.
Fertility is not a disease.
The advent of non-coital methods of contraception gave rise to a highly lucrative industry which alters women’s bodies to remove their healthy fertility. Contraceptives are promoted aggressively and are now enshrined as a human “right” for which our government pays directly or by coercing third party payers.
The Affordable Care Act’s Contraceptive Mandate has limited the options for birth spacing to commodities approved by the FDA (Food and Drug Administration). Evidently the administration assumes that women want to include or exclude their fertility from any heterosexual encounter at will, and that they can do so without suffering any personal, physical, emotional, or spiritual sequelae.
By treating fertility as a disease, medicine today is close to coming full circle when it comes to ethics. Before Hippocrates, physicians might be either healers or killers. Hippocrates and his school taught that the function of the physician was to cure disease when possible, and relieve pain when cure was not possible. The physician-patient relationship was a fiduciary one, which obliged the practitioner to professional conduct irrespective of payment and to confidentiality. Altering or removing healthy organs was, and is, mutilation. Sadly, once this line was crossed with IVF (in vitro fertilization), manipulation and outright killing of embryos and fetuses became commonplace in Western medicine.
There is no need to remove fertility from the body of a woman or a man to allow them to have sexually fulfilling lives. What is needed is for men to understand the signs of the woman’s cyclic fertility and to behave in accordance with their family-building intentions.[5]
Featured Photo: Annabelle Shemer; CC-BY-NC-ND-2.0.
[1] Bradley, Sarah E.K., T.N. Croft and S.O. Rutstein. The impact of contraceptive failure on unintended births and induced abortions: Estimates and strategies for reduction. 2013. Demography and health division, ICF Macro, Calverton MD.
[2] Skovlund, C.W., Morch L.S, Kessing, L.V. Association of Hormonal Contraception with Depression. 2016 JAMA Psychiatry publ. online Sep. 28,2016. (doi:10.1001/jamapsychiatry.2016.2387)
[3] Forhan et. al. Prevalence of Sexually Transmitted Infections and Bacterial Vaginosis among Female Adolescents in the United States: Data from the National Health and Nutritional Examination Survey (NHANES) 2003–2004. MMWR Weekly. August 24, 2007/56(33); 852.
[4] See Cabezón C, Vigil P, Rojas I, Leiva ME, Riquelme R, Aranda W, García C. Adolescent pregnancy prevention: An abstinence-centered randomized controlled intervention in a Chilean public high school. J Adolesc Health. 2005 Jan; 36(1): 64–9; and
Jorge Alvarado and Hanna Klaus. The PEPFAR Program in Ethiopia and Uganda: Two and three year post program behavioral outcomes. Presented at NFP preconference, Catholic Medical Association, October 12, 2016.
[5] Information about natural family planning providers is widely available online. The USCCB natural family planning office within the office of Laity, Marriage, Family Life, and Youth offers a diocese-wide directory.
Hanna Klaus, MD
Hanna Klaus, MD, is a Medical Mission Sister and OB/GYN who directs the Natural Family Planning Center of Washington, D.C., and is co-founder of the TeenSTAR program. She has served in Pakistan and Bangladesh and on the faculties of Washington and St. Louis Universities in St. Louis, MO, and at the George Washington University Medical Center in Washington D.C.
SEATTLE, Washington, August 14, 2017 (LifeSiteNews) — When Claire Ryann’s mommy shows her a fetal heart monitor and suggests they try it out on Daddy, Claire Ryann is all for the idea — until she has a moment to reflect.
“No babies go in boys,” she says sternly.
“I think you’re probably right,” says her mother.
But good-humored Claire Ryann goes along with the game while her mother checks her father, her brother and Claire Ryann herself. Then, when Claire Ryann helps check Mommy, her face clouds with concentration, curiosity and finally astonishment.
“Is that a heartbeat?” she asks. “Is that a baby?”
“Yes,” her mother whispers.
“There’s a baby in there?” asks Claire Ryann with growing excitement.
“Yes!”
Claire Ryann laughs with joy.
“There’s a baby in there!” she shouts, and runs to tell her brother.
Claire Ryann Crosby is a four-year-old singing sensation whose YouTube videos have gone viral. She has appeared on NBC’s “Little Big Shots” and the “Ellen Degeneres Show.” Claire Ryann’s new little brother or sister is due to arrive in January.
Although a baby’s heart begins to beat around 21 days after conception, it is too small then to create audible sound waves. After eight weeks, however, it can be detected in an ultrasound, and after 12 weeks it can be picked up by a home fetal heart monitor.
Wesley Smith Aug 11, 2017 | 3:50PM Washington, DC http://www.lifenews.com
When I was a small boy, polio terrified me. Each year, it would strike thousands of children like me—and you never knew when or where it would hit next. In the 1952 epidemic, a very bad year, there were nearly 60,000 reported cases in the United States and more than 3,000 deaths.
Summer was the worst time, and I recall my parents’ tension as “polio season” approached. Most vividly, I remember my horror at the prospect of being encased in an iron lung. I had seen the photographs: hospital wards with children in iron lungs, only their heads visible outside the great metal beast, a mirror strategically angled so they could view their immediate surroundings.
That long-ago era came to mind the other day as the National Right to Life Committee’s executive director, Dr. David O’Steen, introduced me before a lecture on euthanasia. O’Steen described having polio as a youngster and wondered whether the same unequivocal commitment to recovery that he and his fellow patients experienced would continue to prevail in a health care system increasingly driven by utilitarian decision-making and cost-containment imperatives.
In those difficult days, there was never any question of letting a child with polio die based on a determination that his or her life would not be worth living. This included my late friend Mark O’Brien, who contracted a catastrophic polio infection at age 6 and spent most of his nearly 44 remaining years in an iron lung. Even so, Mark graduated from UC Berkeley, became a journalist, a published poet, a disability rights and anti-assisted-suicide activist. (He was the subject of the Academy Award-winning documentary Breathing Lessons and a motion picture, The Sessions.)
It’s comforting to believe today’s far more sophisticated health care system would swing into action should a similar decades-long epidemic leave tens of thousands of disabled children in its wake. To be sure, medicine’s full armamentarium would be deployed to treat the acutely ill and find a vaccine. But what about the Mark O’Briens—people whose lives might be saved with extended intensive interventions, albeit with a high probability of profound disability? Would they receive the same unequivocal commitment as during the polio epidemic, or would the greater impetus be toward letting them die—with “dignity,” of course?
And if the patients and their families insisted on continued care against medical advice, would hospitals and doctors force them off life-sustaining treatment—would care be deemed “futile” or “inappropriate,” to use the jargon already prevalent among bioethicists? Indeed, would seriously disabled patients such as Mark be considered candidates for the lethal “treatment” of euthanasia, as they are today in the Netherlands and Belgium?
I fear so. At the very least, I suspect that the unequivocal commitment to saving the life of every polio victim that so benefited America’s O’Steens and O’Briens in the 1950s is already a relic of the past. Today, people with disabilities often complain about being pressured by hospital personnel to sign “do not resuscitate” orders under circumstances in which able-bodied patients are not. Families of elderly patients and parents of children with developmental disabilities may meet similarly cold attitudes.
Victims of a contemporary polio-style epidemic might even be rationed out of receiving expensive treatment based on principles of “distributive justice.” This would especially be the case if the disease, unlike polio, affected their cognitive capacities. Thus, bioethicist Ezekiel Emanuel—an influential adviser on Obamacare—strongly implied in a 2009 Hastings Center Report column that care considered basic for most people should not be guaranteed for those “who are irreversibly prevented from being or becoming participating citizens. . . . An obvious example is not guaranteeing health services to patients with dementia.”
And how would people caught up in such an epidemic fare if we ever adopted the “quality-adjusted life year” (QALY) form of medical rationing, currently applied in the United Kingdom and popular among bioethicists? For example, the New England Journal of Medicine called (unsuccessfully) for QALYs to be deployed as a tool of Obamacare cost containment, saying “the best way to improve health and save money at the same time is often to redirect patient care resources from interventions with a high cost per QALY to those with a lower cost per QALY.”
What does that mean? QALY formulas can be complicated, but to illustrate the concept, consider a highly simplified hypothetical. Let’s say I have a serious illness and that Medicine A will give me two calendar years of life as an able-bodied man, or two QALYs. Now, let’s say that my friend and contemporary Mark O’Brien is sustained by an iron lung. Let’s say he has the same illness and Medicine A would also give him two calendar years of life. Because he is confined to the breathing contraption, his two remaining years might be deemed worthy of only a .5 QALY. His continued life would be deemed of less benefit than mine due to his disability.
Next, the cost of the treatment is measured against the perceived benefit. Let’s say the cost for each of us would be $200,000. Under a QALY rationing system, I would be more likely to be approved for the treatment than Mark because that expense would buy me 2 QALYs and in his case would buy a mere .5 QALYs.
In supporting such an invidious system, the authors of the NEJM article deploy an extreme example:
A ban on valuing life extension [via a QALY system] presents its own ethical dilemmas. Taken literally, it means that spending resources to extend by a month the life of a 100-year-old person who is in a vegetative state cannot be valued differently from spending resources to extend the life of a child by many healthy years.
For that matter, the QALY approach dictates that if the situation were reversed and the child had the severe cognitive disability, the child would be allowed to die while the older adult received support.
To say that one human life has greater value than another based on health prospects or disability is to declare the most weak and vulnerable among us, essentially, expendable. So David O’Steen was wise to worry. Many things have unquestionably improved in medicine since he came down with polio. But the introduction of a pernicious “quality of life” judgmentalism into the ethics of health care sure isn’t one of them.
LifeNews.com Note: Wesley J. Smith, J.D., is a special consultant to the Center for Bioethics and Culture and a bioethics attorney who blogs at Human Exeptionalism.
“The day that people lose their horror for abortion,” St. Padre Pio said, “will be the most terrible day for humanity. Abortion is not only a homicide but also a suicide.”
When the person he was speaking to expressed confusion at abortion being “suicide,” the saint explained: “The suicide of the human race will be understood by those who will see the earth populated by the elderly and depopulated of children: burnt as a desert.”
Indeed, according to the world bank, St. Padre Pio’s own home country, Italy, now has a fertility rate of 1.4, or about 33% below mere replacement fertility (2.1). The rate is actually currently up from its low of 1.18 in 1995. As a result, the medium age keeps rising. This is true throughout the developed world.
The Catholic Church has always opposed abortion and contraception, supports marriage, and sees large families as “a sign of God’s blessing.” (CCC 2373)
Here’s the full story:
“Today you denied absolution to a woman because she had voluntarily undergone an abortion. Why have you been so rigorous with this poor unfortunate?” (Padre Pio would sometimes refuse to give absolution to a penitent if they showed insufficient contrition; often they would return and he’d give absolution if they were sincere).
Padre Pio responded: “The day that people lose their horror for abortion will be the most terrible day for humanity. Abortion is not only a homicide but also a suicide. Shouldn’t we have the courage to manifest our faith before those who commit two crimes within one act?
“Suicide?,” asked Father Pellegrino.
“The suicide of the human race will be understood by those who will see the earth populated by the elderly and depopulated of children: burnt as a desert,” Padre Pio replied.
Ever since I was a kid, I’ve always wanted a ton of kids. My mother to this day laughs about how, even in my “too cool” teen years, babies would always melt my heart. I had no problem looking like a fool in front of my peers if it meant getting a laugh out of a child or having a chance to hold a baby. (If you’ve ever watched that scene in The Office where Michael Scott states that he tries to hold a baby every day, I can completely relate.) I can’t really explain why I’ve always had that fascination with children, but the best I can say is that they represent everything that is good in this world. Pure innocence meets curiosity meets a lack of any prejudice toward people, it’s the perfect place to experience what mankind ought to be. While the world is so bent on factions and argument, children just want you to play house or wrestle with them. While adults often question the motives of one another, children give it to you straight, even if that means they might say the “inappropriate” thing. Children are the light to a world so often wrapping itself in darkness.
There’s an odd narrative that has been continuously driven into the modern consciousness that having a ton of kids is supposed to leave you stressed, penniless, and in want of dreams that will never go fulfilled. Although I might be offering my simple subjective viewpoint, after three years of working with over sixty couples going through annulments, I can honestly say that I’ve experienced these symptoms more often with families who’ve had very few children by choice. Most often I find myself watching families with a gaggle of kids running around, as families full of joy. This doesn’t necessarily mean that they don’t also experience some of the troubles that many families face, but I think it does mean that within the chaos of a big family lies one virtue that often comes about from the alchemies of diaper changes, constant noise, and dealing with sibling fights; and that virtue is hope. Add that to the fact that children force adults to not take themselves so seriously and I would think that you’ve got a ripe situation for happiness.
My amazing wife is now expecting our sixth child, a little girl, and we couldn’t be happier and neither could our other five kids. While I wish I could say that having so many kids is an easy and carefree life, I can assure you it isn’t. But, what I can tell you is that having a gaggle of kids has taught me more about myself, the world, and the treasure trove of living life to the fullest. Sure, these little rug rats might be a lot of work, and you may never enjoy the comfort of sitting down for more than five minutes, but I find that there’s something incredibly freeing about taking care of them. I know my purpose and therefore I know what my day is meant to contain. Sure, most of my wife and I’s days are a bit monotonous; wake up, cook, clean, work, mow, change diapers, yell at one or all the kids to stop beating each other up indoors, work out, clean up all the spills from dinner, wrestle with the boys, play kitchen with my daughter, bath the kids, try to offer some semblance of virtue and prayer to the kids, spend about 30 minutes together talking about our days, pass out from exhaustion, repeat. My days might seem to reflect the same thing every day but to the untrained eye, it’s actually a glorious mix of madness and repetitiousness. Which, for a guy like me who could spend hours in my own mind fantasizing and philosophizing, healthily brings me back to reality daily.
G.K. Chesterton, who after years of marriage actually never had children, had a great love of kids and the way their minds work. (On a side note, I think both G.K. and Frances Chesterton ought to become the patron saints of couples struggling with fertility) He once noted how children don’t mind the repetitiveness of life. That, much like the sun rising every morning, children cry out, “do it again”. In my experience as a young parent, this is certainly true. It takes nothing for children to desire the same emotive response over and over again. So, when dealing with the seeming monotony of daily living as a busy parent with a large family, perhaps what we are partaking in is the very essence of God as Creator. He too, must constantly repeat His loving forgiveness and mercy. He too, must constantly keep the cosmos in order and repeat the needed consistencies to keep that order from turning in to chaos. As big families, we are given the daily task of forgiving each other daily. We are also given the daily task of keeping some semblance of order in the home before it turns into chaos.
This repetitive reality is something that many fear today. We are a culture that loves new experiences and gets bored very quickly with anything that might seem monotonous. However, it is in the repetitive actions of life that we grow as human beings. We learn what we are capable of doing each and every day. There is actually great beauty and wonder that comes along with the nature of repetitive action. The sun rises every morning and millions of people stare in amazement and wonder. The stars fix themselves in the sky in the same pattern which has led mankind to seek out and discover entire new worlds. Imagine then, the utter elation that is felt each and every time a new child is brought into the world, why would we not, in thoughtful consideration, say “do it again”? Anyone who has experienced the birth of a child, and the incredible journey of watching them grow, can attest to the incredible miracle that human life is. The curtain between the realms of spirit and the physical are ripped asunder and a new life is presented to the world which brings happiness and innocence into a world so badly in need of it. Sure, there are numerous instances when big families are a fearful thing, and that is why the Church has offered and recognized NFP as a viable, life-affirming opportunity for couples in different situations. But, honestly, for me, having a ton of kids has taught me that being pro-life and open to children is like riding the wave of one miracle after another.
In a recent address Archbishop Chaput offered what I think could be the greatest advice to young people today:
When young people ask me how to change the world, I tell them to love each other, get married, stay faithful to one another, have lots of children, and raise those children to be men and women of Christian character. Faith is a seed. It doesn’t flower overnight. It takes time and love and effort. Money is important, but it’s never the most important thing. The future belongs to people with children, not with things. Things rust and break. But every child is a universe of possibility that reaches into eternity, connecting our memories and our hopes in a sign of God’s love across the generations. That’s what matters. The soul of a child is forever.
What the world needs today is big, holy families. Families who embrace the seeming monotony of living for our lives for others. Families who’s ethos is solidly “My life is not about me.” If we find concerns in the harrowing numbers of the future of the Church, I firmly believe that it is in families who seek holiness with reckless abandon, among the difficulties and trials that come along with it, that not only will we find a change of heart of the desperate culture, but we will see a flowering of the virtue that comes with new life: hope.
During his first term on the Supreme Court, Justice Neil Gorsuch has in many ways shown himself to be a kindred spirit to the late Justice Antonin Scalia. Justice Gorsuch—like his predecessor—is an originalist, which means that he seeks to ascertain the original meaning of the constitutional text and to apply it faithfully. But one wonders: will Justice Gorsuch distinguish himself by being a more consistent originalist with respect to the constitutional status of abortion?
The late Justice Scalia wrote in his Planned Parenthood v. Casey opinion that “the Constitution says absolutely nothing about” abortion. In his view, the Fourteenth Amendment’s guarantees of due process and equal protection for all “persons” do not encompass prenatal life. Instead, the question of abortion should be decided state-by-state through the “political process” and “democratic choice.” In a 2008 interview, Justice Scalia opined:
There are anti-abortion people who think that the constitution requires a state to prohibit abortion. They say that the Equal Protection Clause requires that you treat a helpless human being that’s still in the womb the way you treat other human beings. I think that’s wrong. I think when the Constitution says that persons are entitled to equal protection of the laws, I think it clearly means walking-around persons.
Does the Constitution really only protect “walking-around persons” under an originalist interpretation? Or can one make a compelling originalist rejoinder by examining the original meaning of the term “person” as used in the Fourteenth Amendment? I attempt to do just that in my article, “Protecting Prenatal Persons: Does the Fourteenth Amendment Prohibit Abortion?” published in the Harvard Journal of Law and Public Policy.
The structure of the argument is simple: The Fourteenth Amendment’s use of the word “person” guarantees due process and equal protection to all members of the human species. The preborn are members of the human species from the moment of fertilization. Therefore, the Fourteenth Amendment protects the preborn. If one concedes the minor premise (that preborn humans are biological members of the human species), all that must be demonstrated is that the term “person,” in its original public meaning at the time of the Fourteenth Amendment’s adoption, applied to all members of the human species.
I draw on three strands of evidence to support that conclusion. First, dictionaries of common and legal usage at the time of the Fourteenth Amendment’s adoption defined the terms “person” and “human being” interchangeably. Thus, the original public meaning of the term “person” included every member of the human race. Second, centuries of common-law precedent and state practice leading up to the Fourteenth Amendment’s adoption in 1868 indicate that the unborn were considered legal persons. Third, the authors of the Fourteenth Amendment expected it to protect every human being—especially the weakest and most marginalized. This “original expected application” is indicative of the original public meaning and demonstrates that informed citizens believed that the text of the Fourteenth Amendment applied to every human without exception.
Starting with the Text
Dictionaries of common and legal usage at the time of the Fourteenth Amendment’s adoption treated the word “person” as interchangeable with “human being” or “man.” For example, the 1864 edition of Noah Webster’s Dictionary of the English Language defined the term “person” as relating “especially [to] a living human being; a man, woman, or child.” The entry for human includes those belonging to “the race of man.” No dictionary of the era referenced birth or the status of being born in its definition of “person,” “man,” or “human being.”
In legal usage, the term “person” had expansive scope. Alexander Burrill’s New Law Dictionary and Glossary defined “person” as “A human being, considered as the subject of rights, as distinguished from a thing.” This is consistent with Blackstone, for whom there was no distinction between biological human life and legal personhood. He considered every human being to be a “natural person.” Blackstone declared in his authoritative Commentaries that “life is . . . a right inherent by nature in every individual; and it begins in contemplation of law as soon as an infant is able to stir in the mother’s womb.” This mention of the preborn child’s stirring was intended to protect prenatal life as soon as it could be discerned, not to exclude human life from protection prior to that point. Thus, the principle can be derived from Blackstone and others that if human life could be shown to exist, legal personhood existed also.
Common Law Precedent and State Practice
The English common law tradition—which the United States inherited and developed after its independence—consistently treated abortion as the wrongful killing of a human being. Abortion was prohibited as soon as life in the womb could be detected. Prior to the advent of modern medical science, unborn life was detected at “quickening,” that is, at the first perceived fetal movement. This proved a useful evidentiary tool for determining whether the crime of abortion had occurred. Legal giants such as Lord Coke and Blackstone formalized the legal principles protecting prenatal life, which were eventually passed on to the American colonies and adopted into their state common law systems. When embryologists discovered that each human individual begins its life cycle at fertilization in the 1830s, the states rapidly discarded the obsolete quickening standard in favor of the new, medically accurate fertilization standard.
By the time the Fourteenth Amendment was ratified in 1868, the states widely recognized unborn children as persons. Twenty-three states and six territories referred to the fetus as a “child” in their anti-abortion statutes. Twenty-eight labeled abortion as an “offense[] against the person” or a functionally equivalent classification. Most strikingly, the same Ohio legislature that ratified the Fourteenth Amendment in January 1867 passed legislation criminalizing abortion at all stages in April. The committee that reviewed the bill, which was composed of several Senators who had voted for ratification of the amendment, declared in their report that abortion “at any stage of existence” is “child-murder.” Given the historical context, it is clear that the public meaning of the term “person” in 1868 included the preborn.
The Amendment’s Anticipated Application
The framers of the amendment themselves certainly thought their amendment required due process and equal protection of every human being. While the intentions of the drafters of the Fourteenth Amendment do not directly govern the meaning of the text, it is worth wondering whether the radically inclusive amendment can reasonably be interpreted to exclude a subset of individuals who were considered human beings at the time it was written.
The primary framer of the Fourteenth Amendment, Representative John Bingham, believed the Amendment prevented states from refusing “any of the rights which pertain . . . to common humanity.” Senator Jacob Howard, who sponsored the Amendment in the Senate, emphasized that the Amendment guaranteed even the lowest and “most despised” members of the human race equal protection of the laws. During congressional debates, Representative James Brown asked rhetorically: “Does the term ‘person’ carry with it anything further than a simple allusion to the existence of the individual?”
As Justice Hugo Black later put it, “the history of the [Fourteenth] Amendment proves that the people were told that its purpose was to protect weak and helpless human beings.” The drafters of the Amendment carefully crafted the text to include all human beings within its jurisdictional reach, regardless of their origin or circumstance. Their widely shared belief sheds light on the Amendment’s public meaning at the time of its adoption. The Fourteenth Amendment was meant to be a new birth of freedom for all human beings.
A Clear Case for Originalists
In his Roe v. Wade majority opinion, Justice Harry Blackmun acknowledged that if “personhood is established,” the case for a constitutional right to abortion “collapses, for the fetus’ right to life would then be guaranteed specifically by the [Fourteenth] Amendment.” Under an originalist interpretation of the Constitution, the edifice supporting Roe and its progeny crumbles.
Given the original public meaning of the term “person,” the contemporaneous anti-abortion statutes purposed to protect prenatal life, and the public explanations given by the framers of the Fourteenth Amendment as to its scope of meaning, protections should be extended to prenatal life on originalist grounds. If constitutional protections for the unborn were acknowledged, a state could not refuse to prosecute the intentional killing of the unborn while continuing to prosecute the killings of other classes of persons without violating the Equal Protection Clause.
A Path Forward
In light of the evidence, the Supreme Court should reverse course on abortion. But only two current Supreme Court Justices are identifiably originalist in their interpretive method: Justices Thomas and Gorsuch. Without a majority on the Court who might be persuaded by such arguments, what is the path forward for extending constitutional protections to the unborn?
Each branch and level of government has a role to play. Congress should act immediately under Section 5 of the Fourteenth Amendment to “enforce . . . by appropriate legislation” the Constitution’s protections for unborn persons, such as through the Life at Conception Act. The executive should assert his departmental authority to interpret and uphold the Constitution—rejecting the false doctrine of judicial supremacy and fulfilling his constitutional duty to “take Care that the Laws be faithfully executed.” Finally, the states retain the primary duty to protect the inalienable rights of all human beings within their jurisdictions, the foremost of which is the right to life. States have a responsibility to exercise their police powers (their powers to promote public health, safety, and morals) to prohibit abortion.
Until the Supreme Court, the people, or their elected representatives undo the caste system of separate and unequal treatment for unborn persons, there can be no true equal protection under the law. The legal regime that discriminates against preborn human beings should be abolished on originalist grounds, restoring the harmony between science and law in a manner consistent with the Constitution.
Josh Craddock is a student at Harvard Law School. He lives in Cambridge with his wife and two children.
“St. Augustine said it’s no use whining about the times because we are the times. So our actions matter, our choices matter, our lives matter,” Archbishop Chaput said in a July 27 opening address for the seventh annual Napa Institute Conference.
“It is through us that God acts in society and the Gospel of Jesus Christ is carried forward. So we need to own that mission, and only when we do will things change for the better,” Archbishop Chaput told the 500-plus people gathered for the four-day conference in Northern California’s wine country.
This is “really a privileged moment for Christians. My brothers and sisters, this is not a time to retreat from the world. We need to engage the world and convert it,” Archbishop Chaput said.
The conference this year was organized around the themes discussed by Archbishop Chaput in his 2017 book, “Strangers in a Strange Land: Living the Catholic Faith in a Post-Christian World.”
In urging both engagement and Christian hope, Archbishop Chaput did not sugarcoat American culture. He described it bleakly as one where one third of men and 40 percent of women will someday experience an anxiety disorder, where nearly half of men have contracted a sexually transmitted disease, and where “the birth control pill and the separation of sex from procreation have altered the fundamental meaning of sex.”
In the conflict between religious liberty defined by natural law and erotic liberty espoused by gay activists and many others, those who believe in biblical values of family and marriage are labeled bigots, he noted.
The rapid advances of technology are too much for most people to absorb and the practical American talent for getting things to work is carried to extremes, he said. “Technological man sees the world not as a gift of God — with its own purpose and meaning, to be treasured and stewarded — but as a collection of dead material to be organized and used.
“And that ‘utility attitude’ eventually spreads to the way we treat the environment, other living creatures, other people, and our own bodies and selves,” he added.
As an antidote to pessimism, he urged his audience to read Pope Francis’ “great text,” the apostolic exhortation “Evangelii Gaudium” (“The Joy of the Gospel”).
The pope “reminds us how vital it is to believe in Christ’s victory and to lift up our hearts. We need to see the world and its problems as they really are. Otherwise we can accomplish nothing. But we can’t let the weight of the world crush the joy that’s our birthright by our rebirth in Jesus Christ through baptism. If we cling to that joy, if we cling to God, then all things are possible,” Archbishop Chaput said.
“It’s part of our American DNA to want a well-crafted strategic plan to get the church back in the ‘influence game,’” Archbishop Chaput said. “There’s no quick fix for problems we behaved ourselves into, and the culture we have is a culture we helped make with our appetites, distractions and compromises.”
Archbishop Chaput said he advises young Catholics that the most important thing they can do is very basic.
“I tell them to love each other, get married, stay faithful to one another, have lots of children, and raise those children to be men and women of Christian character,” the Philadelphia archbishop said. “The future belongs to people with children, not with things. Things rust and break. But every child is a universe of possibility that reaches into eternity, connecting our memories and our hopes in a sign of God’s love across the generations. That’s what matters. The soul of a child is forever.”
And, Archbishop Chaput said, the “first task of modern life is to unplug. To make room for the conversation that the church has traditionally called prayer.”
“We do not see the full effects of what we do in this life,” Archbishop Chaput said, but one day we will.
“Have faith. Trust in the Lord. Love with all your hearts and believe in his love for you,” he said.
Schmalz is assistant editor of Catholic San Francisco, newspaper of the Archdiocese of San Francisco.
NASA has publicized the results of the related examination of Our Lady of Guadalupe.
It was established, with instruments of the eye-specialist, that in the picture, the eyes of Mary’s retinas, when exposed to light – similar to the human’s eye – expand and contract. The researchers have also concluded that the temperature of the cloth, where the image can be observed, is permanently 36.6 degrees, such as a healthy human’s body temperature. The image has also been examined with a stethoscope. The scientists have measured a pulse of 115 beats/min at Mary’s belt which corresponds with the number of a fetal heart rate.
NASA engineers have also stated the paint with which the image was made does not exist on Earth and has never existed – written by the Tsn.ua which is a news site on the internet. In the beginning of the 20th century a bomb was detonated next to the image. As a result of this, everything was destroyed in a large circular radius, the image, however, remained intact.
The Holy Virgin, according to records, appeared to an Indian, Juan Diego, in the winter of 1531, on the mountain of Tepeyac, near Mexico City to the north. The records shows that a woman appeared in a gold fog and called upon the man to “go to the bishop […] I want a church to be built on this place!” The bishop did not believe Juan Diego and the meeting repeated itself the next day. Diego went to the bishop for the second time. The bishop said that he would believe that the Blessed Mother had appeared if he brought a sign. Diego met again with the Blessed Mother who sent him up to the hilltop where he found blossoming roses despite the season. Juan Diegon gathered the roses into his simple rob and took them to Zumarraga bishop. The chief priest fell down to his knees before the sight: the poor clothing, a tilma (loose robe) of the indigenous man changed into the portrait of Our Lady. The Cathedral of Our Lady was built at that place where Diego’s tilma is still guarded today.
Aldofo Orozco, research physicist, reports that there is no scientific explanation for the still surviving tilma. Over 10 years similar cloths become ruined by the local moist, salty air. The copy, for example, which was made using the most advanced technology in 1789 was placed behind protective glass, totally faded over 8 years. In contrast to the original, unprotected tilma which has not been damaged after more than a hundred years by the UV-rays, the moist, salty air and the tens of thousands of lit candles near the image.The. original image attracts crowds of pilgrims: the basilica which guards the icon is said to be the most visited pilgrimage in the world. According to data of Mexico City, in 2004, ten million pilgrims were welcomed only between 9th December and 12th December. The numbers of the visitors reach twenty millions throughout the year. Source: karpatinfo.net
EDITOR’S NOTE: This article addresses a specific question regarding whether Catholic hospitals should administer Plan B in rape cases based on the scientific evidence regarding how the drug works. The discussion does not in any way imply that contraceptives are or can be morally licit. The Catholic Church teaches that “every action which, whether in anticipation of the conjugal act, or in its accomplishment, or in the development of its natural consequences, proposes, whether as an end or as a means, to render procreation impossible” is intrinsically evil (CCC 2370 quoting Humanae Vitae 14).
Plan B is the most popular brand of the drug levonorgestrel, which has been dubbed an “emergency contraceptive” that is popularly known as “the morning-after pill.”
Some Catholics, even actively pro-life Catholics, might be surprised to know that Plan B has for many years been considered acceptable by numerous bishops for use in rape cases. But there is growing evidence that Plan B may work in many instances as an abortifacient.
Dr. Chris Kahlenborn, a Pennsylvania-based physician, researcher, and member of the Catholic Medical Association, has made it his mission to spread the word about the moral and ethical ramifications of Plan B. However, he and his collaborators, who include Dr. Rebecca Peck and Dr. Walter Severs, are increasingly frustrated with the lack of response to their findings. After 20 years of investigating the topic, he is flabbergasted that the science is clear and yet so few bishops in the Unites States have acknowledged the problem. The same goes for most Catholic hospitals and influential organizations such as the National Catholic Bioethics Center.
A sketchy presumption
Hospitals, doctors, and crisis centers most commonly give Plan B to women after they have been raped. It’s believed that the drug, if taken before ovulation, acts to prevent ovulation, and therefore, pregnancy. That was the accepted science in 1995 when Bishop John J. Myers, then the head of the Catholic diocese in Peoria, Illinois, approved its use and established directives that became known as the Peoria Protocol. Many other bishops and Catholic hospitals now refer to these guidelines to justify using Plan B.
“That was the presumption at the time,” Dr. Kahlenborn said of Plan B’s contraceptive nature. “However, I must say, even then, the evidence in favor of that presumption was sketchy at best. I contacted Bishop Myers—the local ordinary of Newark, New Jersey, at the time— about 15 years ago to plead with him to retract the protocol but received a return letter calling me an alarmist.”
Essentially, Plan B is a high dose of progestin birth control pill taken in two separate doses that may cause the destruction of human life within five days of fertilization when given prior to ovulation. According to a study published in the Linacre Quarterly and available at www.Polycarp.org, Plan B prevents pregnancy as a contraceptive only in a minority of cases. Rather than being called an “emergency contraceptive,” a more accurate term for the drug is “emergency abortifacient.”
Father Christopher Kubat, the executive director for Catholic Social Services of Southern Nebraska in the diocese of Lincoln, was involved in Linacre Quarterly publication on Plan B. He confirmed that Plan B is not acceptable to use post-sexual assault.
“In short, Plan B can never be used even after ‘ovulation testing,’ because despite determining that a woman is in the pre-ovulatory period of her cycle, most of them ovulate despite giving Plan B,” Father Kubat said. “The levonorgestrel given in this instance then acts as an abortifacient.”
The dignity of persons (Dignitatis Personae)
Meanwhile, RU-486, which increasingly has come into use in the US and other countries during recent years as a chemical alternative to surgical abortion, is strictly an abortifacient.
While RU-486 is supposed to be banned by Catholic health providers, the United States Conference of Catholic Bishops has not issued a similar condemnation of Plan B. It’s unclear how many Catholic hospitals allow its use, but Dr. Kahlenborn estimates about 75 percent make the emergency contraceptive available.
“This is probably a low figure,” he said. “Studies have shown that about 50 percent of Catholic hospitals dispensed EC about 20 years ago, so the figure is probably higher today. Most bishops have little idea whether their local hospitals dispense EC. Only a handful of bishops have advocated against it.”
Bishops in California, Colorado, Connecticut, Massachusetts, New York, Washington, and Wisconsin allow hospitals in their dioceses to administer the morning-after pill to rape victims. Some hospitals around the country perform an ovulation test in addition to a simple pregnancy test before handing out the drug. Several states have laws requiring hospitals to offer the drug to rape victims.
The Vatican has indicated in the past that the Church should leave the decision to the scientists and researchers. But 10 years ago, when the Holy See issued the document Dignitatis Personae, it said the morning-after pill fell within the sin of abortion and was gravely immoral. A former head of the Pontifical Academy for Life once said there is no exception for Plan B to keep it from being gravely immoral. Another head of the Academy emphasized that the morning-after drug is acceptable as long as it’s classified as a contraceptive in the case of rape and does not terminate a pregnancy.
Under the US bishops’ “Ethical and Religious Directives for Catholic Health Care Services,” Catholic facilities are permitted to dispense emergency contraception to a rape victim but only to prevent ovulation or fertilization. Number 36 of “Ethical and Religious Directives” says it is not permissible to initiate or recommend procedures that destroy an already “fertilized ovum” (human being) or prevent implantation in the womb. In Catholic teaching, that is no longer contraception but abortion.
An abortion mechanism of action
The challenge for Dr. Kahlenborn and his collaborators is to convince the Church that, after administering Plan B, the human being could be destroyed. He is considering making a series of videos to explain the science and the need to examine more closely the ethical ramifications associated with “emergency contraception.” The scientific proof is there, through ultrasounds, to show Plan B fails to halt ovulation in the majority of instances when it is given within a few days prior to ovulation. “These two facts alone point strongly to an abortion mechanism of action, since if you have sperm (which Plan B does not impede) and an egg, you should be getting visibly pregnant, but you are not,” Dr. Kahlenborn said. From a moral perspective, researchers have determined that the drug cannot definitively prevent a pregnancy, and in fact, may terminate it by destroying a human being, which is illicit.
“The main argument that Plan B stops ovulation is not even an argument at this point,” Dr. Kahlenborn continued. “There’s no basis in research for that claim anymore.”
Since there is now legitimate evidence that the drug can cause a chemical abortion, the researchers are pleading that the bishops take the time to reevaluate the evidence and their position.
“The bishops refer to the theologians” for moral guidance, Dr. Kahlenborn explained. “But it really is a scientific question at this point.”
The Catholic Medical Association (CMA), the nation’s largest organization of Catholic healthcare professionals, has issued a position statement that Plan B distribution is unethical and that the Peoria Protocol is flawed because of the potential for abortion.
“Simply put, it’s pure hypocrisy to continue to allow Plan B to be dispensed,” Dr. Kahlenborn said. The CMA noted in their position statement that the Peoria Protocol cannot be safely followed because (Plan B) cannot be given prior to ovulation without having a possible post-fertilization effect on a new human life.
“The reasons for supporting the use of Plan B in the Peoria Protocol are now really excuses that result in the death of our embryonic brothers and sisters. The Catholic Medical Association has studied the science for years and would never have published their position paper unless the scientific evidence was compelling.”
In 2013, the USCCB condemned the government’s decision to allow Plan B to be sold over the counter, making it readily available to young teens. But there has not been any movement, at least publicly, by the bishops toward reassessing their stance. Celebrate Life Magazine contacted the USCCB to inquire whether the bishops plan to evaluate the latest evidence but did not receive a statement before publication.
Protocol and episcopal policies on Plan B need to change
Two years ago, a letter was sent to every US bishop with the latest research findings on Plan B, Dr. Kahlenborn said, “. . . and I didn’t hear from anybody. I was frustrated. What’s wrong? What’s the problem? Are they just all afraid?”
Planned Parenthood and other women’s abortion centers dispense Plan B at no cost and encourage women to “have some on hand in case you need it.” The Catholic Health Association, which has taken positions contrary to Church teaching on issues such as the Health and Human Services mandate on contraception coverage in Obamacare health insurance plans has stated that it does not consider Plan B an abortifacient but emergency contraception.
“Plan B should be challenged, especially given the pro-life stance of the current administration, since abortion pills should not be sold over the counter to anyone, especially teenagers,” Dr. Kahlenborn said.
Dr. Kahlenborn remains convinced that the influential National Catholic Bioethics Center based in Philadelphia has the influence to be the agent-of-change on the issue.
“The USCCB has made no movement to change their position on the Peoria Protocol, despite overwhelming medical evidence over the past few years,” Dr. Kahlenborn said. “It is my strong impression that the USCCB takes its cues from the National Catholic Bioethics Center. Unfortunately, the NCBC still endorses the antiquated and totally disproven hypothesis that Plan B stops ovulation. This hypothesis has been debunked even by pro-EC researchers. I addressed the NCBC directly last year and showed them the evidence and they still remain unconvinced. Very disheartening.” He concluded, “I am literally stunned that the NCBC, who are mainly composed of ethicists and theologians, are trying to argue the merits of the science, when the Catholic Medical Association has already stated that the scientific evidence is more than sufficient to now conclude that the Peoria Protocol is fatally flawed.”
Dr. Kahlenborn visited their headquarters to lay out the research, but its ethicists there have been unwilling to budge on their position.
“The National Catholic Bioethics Center remains concerned about the possibility of an abortifacient effect when using Plan B, but believes that with appropriate testing, the risk of such an event is sufficiently diminished to allow for the use of this drug in limited circumstances,” said Ted Furton, an ethicist and director of publications for The National Catholic Bioethics Center, (NCBC) in a statement to Celebrate Life Magazine.
The National Catholic Bioethics Quarterly has published numerous articles pro and con on Plan B and its use. These studies are often highly technical. Plan B clearly poses dangers if a woman has conceived. The embryo may not successfully implant in the uterus. Therefore, careful testing is necessary to ensure that there is little-to-no likelihood that a woman has recently conceived before using this drug.
“The National Catholic Bioethics Center regularly meets to discuss pressing moral issues in healthcare, including the so-called Peoria Protocol. The Center continues to review published material on this topic as it becomes available. As of yet, there has been no change in our views on this matter.” Dr. John Haas, president of the NCBC, added, “We’re constantly studying this. We just don’t think the evidence is there.”
Dr. Kahlenborn was stunned by the response from this influential organization. While ethicists argue that there is no moral certainty, he said the medical evidence in most recent years gives one more than enough cause to pause the current Peoria Protocol: a similar conclusion was reached by the Catholic Medical Association’s in 2015, as noted on their position statement on emergency contraception. Dr. Kahlenborn noted: “It’s simply incomprehensible that the NCBC remains in denial regarding the most recent evidence when one considers that all of the top world researchers on Plan B, such as Dr. Horacio Croxatto and Dr. James Trussell—both of whom support Planned Parenthood—openly publish that Plan B does not effectively stop ovulation!”
“The studies the NCBC claim to support” that fertilization is impossible “do not support it at all and now new animal research and a human in-vitro trail have both shown that fertilization occurs with absent (Luteinizing Hormone) levels, disproving their hypothesis.”
Until the protocol changes and more bishops revamp their policy on Plan B, more babies face the possibility of death by abortifacient.
Is it possible to talk about the pollution of sexuality in the same way that we can talk about the pollution of the air with sulfur dioxide belched out of smoke stacks or pollution of the water through industrial waste dumped in rivers?
If we can befoul nature by violating its intrinsic order and beauty, can we do the same to human nature and, in particular, human sexuality? If intemperance and greed destroy the natural environment, do they also destroy the sexual environment? Can we measure that destruction, so that it is scientifically verifiable?
Yes. Our sexual environment is about as polluted as China’s air, and the harm caused by such pollution is just as scientifically demonstrable.
Readers will forgive me, I hope, if I have to treat some rather delicate topics in what follows. Talking about the evil effects of dumping raw sewage into our streams is much less embarrassing than examining the evils of dumping the parallel equivalent of raw sewage into our sexuality. But the seriousness of contemporary sexual pollution demands some candor on my part.
There is, quite literally, a world-wide epidemic of erectile dysfunction (ED) among young men, men less than 40 years old. While it is quite natural to have problems of this sort in men over 40 (although it has been made worse by increasing obesity and the diabetes that often comes with it), a significant rise in the number of young men with ED is historically unprecedented. In one study, one in four men seeking treatment for ED was under 40 years old—setting off an alarm for clinicians. In another, a third of young men were suffering from sexual dysfunction. A study (in Italy) uncovered a doubling of ED in teenagers in just eight years (2005-2013). A study in Canada found that over 50% of male teens reported some ED symptoms, with half of those being severe.
There are several causal factors, including increased obesity in the young, as well as the use of illegal drugs. But one cause stands out with great clarity: the world-wide epidemic of ED is made possible by the world-wide availability of internet porn coupled with obsessive masturbation. The internet is the pipeline that dumps the raw sexual sewage into our sexual environment at a level unprecedented historically.
Pause here to consider this epidemic in an illuminating way. What if the world-wide population of pigeons, white-tailed deer, or dolphins were suddenly exhibiting just this kind of sexual dysfunction, thereby severely harming its reproductive capacities? Wouldn’t that be considered a kind of environmental crisis? Wouldn’t we be looking for causes, and attempting to help the poor creatures from sexual self-destruction?
ED isn’t the only verifiable effect of sexual pollution. The super-normal, intense nature of porn causes actual addiction, just like cocaine or any opioid, causing what researchers Jennifer Riemersma and Michael Sytsma, call “a toxic cocktail of contemporary addiction.”
As scientists now understand, addiction of any kind, including sexual addiction, “hijacks” the brain’s natural reward system, primarily by overworking the “pleasure” neurotransmitter dopamine. When our pleasure center is continually overstimulated, it responds by “dulling down” by producing less dopamine or eliminating dopamine receptors. That makes the addict continually look for a stronger “fix,” spending ever more time chasing ever more unnatural sexual stimuli. This is all scientifically verifiable, as part of the larger research done into addiction of all kinds and its measurable, deleterious effects on the human brain.
This cycle of addiction leads to further destruction of our sexuality and sexual environment. The first kind of destruction is social, or rather, it strikes at the very heart of the social order: marriage. The American Academy of Matrimonial Lawyers, the top 1600 lawyers dealing with divorce, report that 56% of divorces they deal with are the result of a spouse’s obsession with porn. If human marital love is the perfection of our sexual nature, then this is decidedly destructive and unnatural result. As sociologists and psychologist attest, destroyed families are a leading source of every kind of social disorder and pathology.
Again, step back and imagine an illuminating scenario, one based on actual scientific experiments. What if we found that the mating of adult male rhesus macaques in the wild was being significantly disrupted by prankster teenagers having hung pictures of female macaques’ hindquarters from the trees, which the titillated males soon preferred to the real thing? Wouldn’t we want to catch and punish the perpetrators and restore the macaques to sexual sanity?
In addition to the social harm of addiction to porn, we have a second kind of destruction that strikes at the naturalness of sexuality itself. If biologists look at any other creature in nature that reproduces through male and female sexual union, they will assure you that—amazingly!—sexuality is naturally designed for sexual procreation. By contrast, the cycle of sexual addiction drives human sexuality to the far limits of the unnatural, seeking a libidinous “fix” in anything but heterosexual intercourse.
Every sexual combination or variation is now available on the web, both creating and responding to the demands of the addicted: sex with any gender combination, including transgender; oral, anal, and masturbatory sex; sex with objects; sex with animals; sex involving participants wearing diapers; sex involving feces or urine; amputee sex; sex involving choking and vomiting; brutal sadism, torture, rape, and even murder; cartoon pornography and child pornography; sex with sexbots; and finally, computer generated virtual sex of any and every unnatural, and previously unimaginable kind.
Now think about this parallel as well. If any other animal exhibited this bizarre array of entirely unnatural sexual behaviors, every sane scientist would be looking for some destructive cause in the environment, some major haywiring of its DNA. But when it comes to human nature, somehow this scientific understanding of “natural” is dismissed without explanation.
We can map the downslide into the evermore unnatural in porn itself. As sociologist and researcher Dr. Natalie Purcell has shown in depressing, nauseating detail, porn movies over the last forty years have become increasingly violent and misogynist, with women being choked, suffocated, dragged by the hair, gang raped, slapped, punched, gagged through oral sex to the point of vomiting, and humiliated in other ways that I have not the courage or the stomach to report (much of it dealing with hideously disgusting variations of anal intercourse). The women either pretend to love it, the more abusive the better, or the women are shown actually suffering in their painful humiliation as real rape victims, both of which are meant to “turn on” porn addicts seeking new highs, both of which form the brains of porn viewers to associate their own sexual satisfaction with brutal and unnatural violations of women.
All of this, we now understand, “re-wires” the brain’s pleasure system in regard to sexual desire, literally twisting natural sexual desire into ever-more unnatural and self-destructive addictions. For the sexually malformed, only the unnatural is desirable. That’s the result of what addiction scientists call “tolerance,” the above-mentioned dulling down of the brain’s pleasure circuits, and the consequent need for ever greater stimulation.
That brings us to a third, related kind of destruction: moral destruction. The “tolerance” caused by dulling down the brain’s pleasure circuits causes ever-widening sexual “tolerance” in society. As the increasingly unnatural porn spreads throughout society, affecting more and more men and women, the sexually unnatural is normalized socially, as in radically redefining the sexual desires and hence the sexual morality of society. With anal sex the new “high” among, and the porn-addicted getting ever younger, is it a really a shock that young teenage girls now routinely complain of being forced to “perform” accordingly? With rape as the new turn-on, is it any wonder that young men increasingly associate sex with violence?
Perhaps adding a fourth kind of destruction might tip the scales: psychological and physical destruction. The number of porn addicted is so large, that the afflicted have started therapeutic chat sites for those trying to shake the addiction. And no wonder. Listen to the list of deleterious symptoms: along with ED, they experience irritability, fatigue, sleeplessness, trembling, inability to focus or concentrate, depression, completely deadened sexual desire for an actual person of the opposite sex, completely dead libido period, significant social awkwardness, loss of job or flunking in school, development of ever-more alarming sexual tastes, panic attacks, memory impairment, and thoughts of suicide. As the conversation among recovering porn addicts makes clear, they realized that the symptoms were porn-caused because the ill effects went away after they quit.
Now which of these symptoms doesn’t count as a scientifically, medically verifiable bad effect of porn addiction? If some other cause were bringing about such awful effects, we’d declare societal “war” on the causes. But you can’t declare war on malformed sexuality without calling into question the assumption of the sexual revolution that there is no such thing as malformed sexuality.
Given all that I’ve offered in the way of obvious, demonstrable ill effects on human nature, how could anyone deny that there is such a thing as sexual pollution? How much more destruction is needed? How much more harm can we sustain without social collapse? And finally, at what point will the sexual revolution admit defeat, and confess that the Catholic Church was right all along about sex.
FRANKFORT, Kentucky, August 1, 2017 (LifeSiteNews) — An obstetrician in Kentucky was waiting to give birth to her own baby when she came to the aid of another woman in the ward.
Dr. Amanda Hess, 38, had checked into the Frankfort Regional Medical Center to give birth to her second child through induced labor when she heard a woman crying in pain. Hess discovered that both the expectant mother and her unborn baby were in distress and that the on-call obstetrician had left the hospital on break before they arrived. Undressed and in an open-backed hospital gown, Hess tied on another gown to “cover up [her] backside” and came to the rescue.
Hess recognized the patient, Leah Halliday-Johnston, as she had performed her last prenatal examination earlier that week. The unborn baby’s heartbeat was dangerously low and her umbilical cord was loosely tied around her neck, so there was no time to wait for the on-call doctor, still 10 minutes away. Hess stayed to deliver the baby. The on-call doctor arrived shortly afterward and took it from there.
Leah Halliday-Johnston and her newborn
“You know I love doing what I do,” Hess told Kentucky’s WKYT news. “I love taking care of mothers and babies and … really a lot of doctors are always thinking of their patients even when they’re a patient themselves.”
“[Hess] was definitely in doctor mode,” Halliday-Johnson, also 38, later told NBC. “My husband noticed something was going on because she had on a hospital gown, but I didn’t notice that because I was on the delivery table. I was in my own world there.”
Halliday-Johnston gave birth to a baby girl, her fourth child. The next morning at 9:30, Hess gave birth to her own baby girl, whom she named Ellen Joyce.
The events unfolded on July 23-24. Since then, the story has caught the attention of American media, with publications as disparate as People and The Washington Post publishing their versions.
By Cardinal Daniel N. DiNardo, opinion contributor – 08/03/17 10:20 AM EDT
After meeting with President Trump in the Oval Office on May 4, I sat in the Rose Garden and listened as the president promised the Little Sisters of the Poor that their “long ordeal” with the government’s contraceptive mandate “would soon be over.” Yet here we are, nearly three months later, and the Health and Human Services (HHS) mandate still stands.
For four years, the Little Sisters and many other faith-based nonprofit groups have patiently asked the government to do the right thing and let them serve the poor. In a pluralistic society like ours, people should be free to serve the common good without compromising their moral or religious convictions. The HHS mandate, requiring employers to cover contraceptive and abortion-inducing drugs and devices, has tested this country’s commitment to a healthy pluralism.
President Trump asked some of the Little Sisters to stand next to him on May 4 while he signed an executive order “promoting free speech and religious liberty,” and he promised that “we are ending the attacks on your religious liberty.”
The HHS mandate tries to force faith-based employers — including religious charities, schools and pro-life advocacy organizations such as the March for Life — to facilitate the coverage of drugs and devices that go against our moral mandate to respect the dignity of every human person, born and unborn. If a solution is not reached, these nonprofit organizations could face millions of dollars in fines from the federal government for non-compliance with the HHS mandate.
The president’s promises were not just in his speeches. The text of the executive order itself directs the secretary of Health and Human Services to “consider issuing amended regulations, consistent with applicable law, to address conscience-based objections to the preventive-care mandate.”
Yet the onerous regulations that are still on the books have not been amended.
In a diverse society like ours, people will disagree on moral issues. A majority should not be able to impose its way of life on others by using the government to coerce people into violating their consciences. The Catholic Church teaches that religious freedom has to do with immunity from coercion. Immunity from government coercion is a right that all citizens in this country should enjoy. So in asking for an exemption to the HHS mandate to fully accommodate deeply held moral and religious beliefs, we are simply asking that the government give us the space to fully participate in American life.
Following the signing ceremony, I said that the executive order “begins a process.” It is now time for the administration to take the next steps in the process of ensuring that the Little Sisters, and all those who seek to abide by their religious beliefs or moral convictions, would be able to continue to serve their fellow citizens in accordance with their consciences.
Religious freedom is a fundamental right, not a political football. Freedom belongs to us by human nature, not by government dictate. A government that serves its citizens is one that respects the right to religious freedom.
President Trump suggested that he understood the stakes when he said, “Freedom is not a gift from government. Freedom is a gift from God.”
The HHS mandate puts an unnecessary burden on religious freedom, a burden that the administration has the power to lift, a burden that the administration has promised to lift. And yet the burden has not been lifted.
Mr. President, please lift this burden.
Cardinal Daniel N. DiNardo, archbishop of Galveston-Houston, is president of the United States Conference of Catholic Bishops.
NAPA, California, August 1, 2017 (LifeSiteNews) – Archbishop Charles Chaput delivered a searing analysis of problems facing the Western world and encouraged Catholics seeking to restore culture to get married, have children, and raise them in the faith.
Speaking at the Napa Institute conference, Chaput lamented the current cultural crisis in the United States.
“The nature and the pace of changes in our culture today have no precedent,” Chaput observed. “They’re extraordinarily fast. They’re also accelerating.”
Such changes are really “transformations — in our legal philosophy; our sexual mores; our demography; educational philosophy; economy and technology,” he said.
“The birth control pill and the separation of sex from procreation have altered the fundamental meaning of sex,” said Chaput. And same-sex “marriage” activism has moved from demanding not just acceptance but approval, he said.
“Same-sex activism now runs on a moral passion for gay rights and social acceptance,” he warned. “From a biblical point of view, that passion is deeply flawed. The arguments for religious liberty and erotic liberty stem from two very different ideas of who the human person is and what our sexuality means. But a moral passion, even when it’s wrong, is always powerful.”
“Thus, concessions to nominal gay equality are no longer enough,” he continued, noting that a major LGBT activist and donor, Tim Gill, recently said he wants to “punish” those who disagree.
Chaput praised Becket Law (formerly the Becket Fund for Religious Liberty) and Alliance Defending Freedom for their work protecting the rights of people to not be forced to violate their consciences.
‘Things rust and break. But every child is a universe of possibility that reaches into eternity’
“America is a much less biblically influenced nation than it was at its founding. And our moral vision of who we are and what our lives mean is much more fragmented,” said Chaput. “The only way to create new life in a culture is to live our lives joyfully and fruitfully, as individuals ruled by convictions greater than ourselves and shared with people we know and love. It’s a path that’s very simple and very hard at the same time. But it’s the only way to make a revolution that matters.”
He continued:
When young people ask me how to change the world, I tell them to love each other, get married, stay faithful to one another, have lots of children, and raise those children to be men and women of Christian character. Faith is a seed. It doesn’t flower overnight. It takes time and love and effort. Money is important, but it’s never the most important thing. The future belongs to people with children, not with things. Things rust and break. But every child is a universe of possibility that reaches into eternity, connecting our memories and our hopes in a sign of God’s love across the generations. That’s what matters. The soul of a child is forever.
If you want to see the face of Europe in 100 years, barring a miracle, look to the faces of young Muslim immigrants. Islam has a future because Islam believes in children. Without a transcendent faith that makes life worth living, there’s no reason to bear children. And where there are no children, there’s no imagination, no reason to sacrifice, and no future. At least six of Europe’s most senior national leaders have no children at all. Their world ends with them. It’s hard to avoid a sense that much of Europe is already dead or dying without knowing it.
Chaput cited Cardinal Robert Sarah and his acclaimed new book The Power of Silence.
“God renews the world by first renewing each precious, immortal individual person in the quiet of his or her soul,” he said. “God is not absent from the world. We just make it impossible to hear him. So the first task of the Christian life today is to unplug, carve out the silence that allows us to listen for God’s voice, and make room for the conversation we call prayer.”
Chaput said the Internet can be “a source of isolation.”
“The human spirit begins to gradually starve” when we only rely on technology, he said. “We use our tools, but our tools also use us. They shape the way we think, the way we act, and the way we see the world. Technological man sees the world not as a gift of God — with its own purpose and meaning, to be treasured and stewarded — but as a collection of dead material to be organized and used.”
Such an attitude “eventually spreads to the way we treat the environment, other living creatures, other people, and our own bodies and selves.”
God allows us to ‘add to the great story of His creation’
“We don’t see the full effects of the good we do in this life,” Chaput concluded, recalling how a friend once saw a tapestry that up close was just “hundreds of ugly knots and tangles of stray thread in a chaos of confused shapes that made very little sense.” It was the Tapestry of the Apocalypse of St. John, a famous European work of art.
“It’s one of the most stunning and beautiful expressions of medieval civilization, and among the greatest artistic achievements of the European heritage,” said Chaput. “So much of what we do seems a tangle of frustrations and failures. We don’t see — on this side of the tapestry — the pattern of meaning that our faith weaves.”
“But one day we’ll stand on the other side,” he said. “And on that day, we’ll see the beauty that God has allowed us to add to the great story of His creation, the revelation of his love that goes from age to age no matter how good or bad the times. And this is why our lives matter.”
I will never forget the night my life changed forever. That night, I woke up with a deep stabbing pain in my chest. Each breath felt like a thin knife in my lungs. Even today, I cannot understand how a completely healthy 25-year-old woman could suffer the blow I discovered that night. This is my story.
Libby and her husband Joel on their wedding day
When I was sixteen, I began having horrible cramps throughout my period. I would spend the day throwing up and passing out from the pain. My doctor told me that I had two options. I could take a pain pill a few days prior to starting my period or I could go on the Pill. Without regular cycles, I was unable to use pain pills successfully. So, as a young teen, my doctor put me on birth control pills.
I was on the Pill for ten years on and off. Each time that I tried to go off the Pill, I would have a few quiet months that would eventually culminate in debilitating pain and going back on the Pill. I couldn’t continue to live with the pain and passing out. Even after marrying my husband, I continued to take the Pill only for my pain. I would never have imagined that birth control pills would eventually cause me more pain than I had ever felt.
In October 2014, I went off the Pill hoping to get pregnant. Unfortunately, my body had forgotten how to regulate itself. When I went to my obstetrician for help, it was the first time someone told me that the pain I suffered with each period was probably endometriosis. I sought help from a fertility specialist and he put on the Pill for a second time while waiting for surgery.
One night as I snuggled with my husband and dog, I felt a deep pain in my chest. I could not understand why my chest hurt so much. I thought, I must have indigestion at best or at worst, I was having some sort of asthma attack. I took some Benadryl and went to sleep. At midnight I woke up coughing, gasping for air and in severe pain. So, I called my mom, a nurse, and asked what she thought I should do. She told me I should go to the hospital.
At the hospital, I was in so much pain that I could not lay flat without stabbing pains in my chest. The staff immediately stripped my clothes off, held me down and performed an EKG on my heart. Later, a CT scan confirmed that I had blood clots in both of my lungs. Pulmonary embolism. We were stunned. How does a healthy 25-year-old who does not smoke or have any other risk factors end up with blood clots?
The next day the doctors told me that I should never take artificial hormones again, including the birth control pill. I was put on blood thinners for four months. For months, I couldn’t sing, go outside, or walk long distances without getting tired or having pain. Not being able to take deep breaths without pain resulted in a low energy level. Chores around the house became a burden. At work, I had to sit while teaching. I could not lift or use any of my crisis prevention training. I had to rely on others for any difficulties at work. My young body suddenly felt old. Even after months of healing, I know I will never be the same.
Libby at the hospital after her blood clot
After going off of the blood thinners, genetic testing revealed I did not have Factor Five Leiden or any other genetic condition that would predispose me to blood clots. Doctors have not been able to give me a good explanation of why I joined the ranks of women who have been injured from the pill, but it happened.
Before this, I blissfully believed that the Pill was not dangerous. I never read the fine print that came with each of the packets I got from the pharmacy and do not remember ever being warned about the worst side effects. I know many who do read that fine print and think that they won’t be part of the small percentage of women who get hurt. After my experience, that small percentage feels a lot larger. I hope my story makes women think twice before taking a pill and thinking that it will solve all their problems.
July 18, 2017 (LifeSiteNews) — One thing that confuses at Mass today is just what the priest is doing at the altar/table up front. Depending on the prayers he chooses, he is either offering a sacrifice to God or preparing a communal meal: Which is it? Similarly, if the priest is booming prayers into a microphone, is he speaking to God (Who has perfect hearing) or is he really addressing the congregation? Meanwhile, if the modern Mass is such an improvement over the old (as we hear so often), why have most Catholics in the West stopped attending it? Such questions troubled me until I fell in love with the work of St. Thomas Aquinas and then, a few years later, discovered the Traditional Latin Mass (TLM) for myself.
Having thrown my Sunday lot in with the TLM, I began to peruse books about it. The best and most readable I have encountered is Noble Beauty, Transcendent Holiness: Why the Modern Age Needs the Mass of Ages by Peter Kwasniewski. As Kwasniewski is a traditionalist, he may feel embarrassed that I enjoyed his book more than the works of epochal Martin Mosebach (The Heresy of Formlessness), the masterful Michael Davies (Cranmer’s Godly Order, Pope Paul’s New Mass) and the excellent H.J.A. Sire (Phoenix for the Ashes). A good spiritual son to these fathers of the liturgical restoration, Kwasniewski has starred their works in his bibliography for our attention. Nevertheless, as a voice of the post-1970 generation, Kwasniewski gives old arguments new juice.
Dr. Kwasniewski (give it a shot — k’vas-n’YEF-ski is easier to pronounce than Wojtyła) is well-known in Catholic traditionalist circles for his writings on the New Liturgical Movement blog. He taught at the International Theological Institute in Gaming, Austria, and now he teaches at Wyoming Catholic College. If Kwasniewski teaches as well as he writes, his students are very lucky indeed.
Noble Beauty, Transcendent Holiness argues on several fronts that the Roman Catholic Church is in a spiritual crisis that can be resolved only by a return to the ancient, slowly and organically developed liturgy of the Latin Church. Given the “hemorrhaging” of adherents from that Church and the maelstrom of confusion among those who remain as to what the Church actually believes, Kwasniewski is on very strong ground.
One of his most convincing arguments involves the human longing for something challenging, complicated, and mysterious in the worship of God. (Note the 50-year craze in the West for East Asian meditations.) Kwasniewski considers the traditional liturgy not as much the work of human hands as one of the greatest gifts of God to humanity. He argues that the Traditional Latin Mass, alongside the Marian piety and Thomist theology inextricably linked to it, is one of the guardians of authentic Catholic faith.
Noble Beauty, Transcendent Holiness is itself a beautiful book, both in form and content. Each chapter begins with a meditative photograph, and most end with a heartfelt prayer. Like any organic development, the book grafts the new onto the old. It begins with a Forward written by Mosebach and ends with young Kwasniewski’s most personal reflections. Mosebach delves into the legacy of Pope Benedict, and Kwasniewski faces the challenges offered by Pope Francis. Meanwhile, Kwasniewski is so adept at writing simple yet gorgeous sentences that I broke my pencil several times underscoring them all.
Take, for example, Kwasniewski’s conclusion that it is better to suffer the knowledge of what the liturgy of 1970 replaced than to have remained in blissful ignorance:
My spiritual life would never have grown as it did, nor my grasp of sacred theology, had it not been for the beauty, reverence and profundity of the traditional liturgy that I discovered as a young man, fell in love with, and now long for ceaselessly. I would not today be a Benedictine oblate praying the Divine Office, which is a source of tremendous vitality, light and consolation to me. My situation is far from optimal, due to the irregular availability of the traditional liturgy in my community, but I do not regret bearing the cross of knowledge, which has opened to me a whole world of wonders to which I would otherwise be blind. It is a flowering cross, and I imagine the same is true for many who love traditional ways.
Many of Kwasniewski’s chapters were developed from essays, so he repeats himself a number of times throughout the book. This is not a weakness — repetitions enrich both the Traditional Rite and the Holy Rosary, after all — but it adds to necessity of reading the book slowly, chapter by chapter, instead of in one great 300-page gulp.
Meanwhile, although there is much meaty scholarship here, the book is accessible to the serious and curious reader — for the most part. Although I studied theology for five years, I could not remember what an “anaphora” was, and I was stumped by the phrase “hylomorphic composition” until I consulted a professor of linguistics. I conclude, therefore, that this excellent book would be even better if it included a glossary.
We have learned much from Baby Charlie’s tragedy, not only about the perils of government deciding who should live and who should die but also about the love and commitment of his dedicated parents and the importance of the worldwide support they received.
Now we know there is more hope for babies born with conditions like Baby Charlie’s because of the publicity and probably more parents will try to find alternatives when they are given a poor or fatal prognosis.
Here are two cases where the parents did just that and saved their children.
Congresswoman Beutler’s interest was also personal.
In 2013, she and her husband found out that their unborn baby Abigail had Potter’s Syndrome, a fatal condition where the kidneys are missing. She and her husband were told that no one ever survived this condition and abortion was offered more than once.
They looked for other options and found there was an experimental treatment given before birth for other conditions that might work on their Abigail. The parents contacted many different hospitals before Johns Hopkins finally agreed to try.
Today, Abigail is a healthy four year old and has a kidney donated by her father a year ago. She is the first known person to survive Potter’s Syndrome, thanks to her dedicated parents.
NOAH WALL, BORN WITH LESS THAN 2% OF HIS BRAIN
Also known as the “boy with no brain”, four year old Noah Wall was born in the UK with a rare complication of spina bifida that caused fluid to compress his brain down to an estimated less than 2% brain tissue.
The condition was discovered before birth and the parents were told that even if he survived birth, he would be severely mentally and physically disabled. Abortion was offed 5 times.
But Noah did survive birth and an immediate surgery was done for his spina bifida and a shunt was installed to drain excess fluid from his brain.
Thanks to the efforts of his devoted parents and sister to keep his brain stimulated, Noah has confounded the doctors by the regrowth of his brain. When a CT scan of his brain was done years later, doctors found that Noah now has 80% of his brain tissue. Even more amazing to the doctors, Noah has developed into a charming, expressive and empathetic little boy who now attends a local primary school, despite still having some physical and mental impairments.
This year, a documentary about Noah was made. I saw it myself a few weeks ago on TV and I highly recommend seeing it.
And as the UK’s Daily Mirror newspaper article wrote:
“Neurosurgeon Dr Nicholson sums up the larger importance of Noah’s incredible story:
‘He teaches the medical profession that you can’t ever know’.”
CONCLUSION
Over the years, medical progress has made great strides while medical and legal ethics have deteriorated because of a “quality of life” mentality.
This has led to medically discriminatory attitudes affecting people with disabilities as I personally found out when my daughter Karen was born with Down Syndrome and a severe heart condition.
All children with disabilities deserve both a welcome and a commitment to help them have the best life possible from not only their parents but also from the rest of us.
In a modern-day version of eugenics, inmates in White County, Tennessee are volunteering to receive vasectomies or birth control implants in exchange for credit toward their jail sentence.
It’s a dark program that the ACLU says is unconstitutional, and whether or not it is, it certainly hearkens back to similar cases in which inmates and mental patients, particularly racial minorities or other disenfranchised groups, were forced to obtain sterilization.
The program was begun on May 15 of this year when Judge Sam Benningfield signed an order to allow inmates to receive a credit of 30 days toward their outstanding jail sentence of they consent and obtain either a vasectomy for men, or a birth control implant for women.
For men, the procedure is technically reversible, though it is performed with the possibility of never being able to be reversed thanks to complications. For women, the choice to consent to a birth control implant requires that the implant be removed at a later date (up to 10 years in the future) with possible complications including the perforation of the uterine wall, rejection, and other dangerous side effects.
In both cases, the state is putting pressure on inmates to consent to invasive medical procedures in exchange for reduced jail sentences, a complicated process that can leave inmates vulnerable.
So far, 32 women have elected to participate in the program and have received the Nexplanon implant. 38 men are currently waiting to receive their vasectomies.
Though the judge who ordered the program believes he is giving the inmates an opportunity, the pressure for an inmate to submit to temporary or semi-permanent sterilization in exchange for freedom is troubling to say the least.
As the tragic case of British infant Charlie Gard nears a close, another family in the United States continues their fight for their severely ill daughter’s life.
Many LifeNews readers will remember Jahi McMath, the teenager who was declared brain dead three years ago after complications from a tonsillectomy. McMath remains alive at a New Jersey hospital where her family continues to fight for her rights.
Right now, McMath’s family is waiting for a court ruling on whether California, her home state, will revoke her death certificate, the AP reports. McMath was 13 when doctors declared her brain dead at Children’s Hospital in Oakland, California in late 2013, and state officials issued her a death certificate.
Here’s more from the report:
In court documents filed last month supporting the family’s lawsuit to have the death certificate revoked, retired neurologist Dr. Alan Shewmon said videos recorded by Jahi McMath’s family from 2014 to 2016 show the teen is still alive.
Shewmon is a longtime critic of how brain death is defined and has filed similar court papers supporting efforts by McMath’s family to undo the death certificate. The family has previously shown video clips of McMath twitching her fingers, which they said showed she still has brain function.
Shewmon is a world-renowned expert on the brain and a professor emeritus at UCLA.
Based on the materials provided to me so far, I can assert unequivocally that Jahi currently does not fulfill the diagnostic criteria for brain death. The materials include extensive medical records from St. Peter’s University Hospital, which I am still in the process of reviewing, videos of Jahi moving her hand and her foot in response to verbal requests by her mother, images from an EEG done in her apartment on 9/1/14, images of a brain MRI scan done at Rutgers on 9/26/20-14, and heart rate variability analysis by my colleague Dr. Calizto Machado based on the EKG channel from 9/1/14 EEG.
Her mother, Latasha Spears Winkfield, said they understand that Jahi’s brain is damaged, but they believe she still deserves a right to life.
Lawyers for the hospital say the videos do not necessarily prove that Jahi is not brain dead. They said Jahi’s movements could be “easily manipulated,” and the camera was located in a “convenient angle.”
A judge is expected to rule on Jahi’s life within the next two months, according to the report.
Bioethicist Wesley J. Smith, who has been following her case, wrote last year:
If Jahi is alive, either the earlier death determination was mistaken or–and this would be huge–something never seen before in this field will have happened, a brain dead person recovering sufficient brain function to be deemed again alive. If Jahi lives, it will send shock waves through the medical, scientific, and organ transplant communities. ….But that’s tough. Our duty to Jahi, the integrity of the system, and the needs of scientific understanding require that the truth will out.
The timing of your recent article, “Keeping Our Promise to 120 Million Women and Girls,” and the Global Family Planning Summit in London could not be better in light of the upcoming Natural Family Planning (NFP) Awareness Week. We are in agreement that, “the conversation around contraceptives is one of the most important conversations the world will have this year.” However we disagree on a fundamental level that the answer to a global epidemic of unplanned pregnancies is contraception.
While generally the Gates’ endeavors can be deemed admirable the tone and content of this most recent article outlining the Gates Foundation’s additional $375 million dollar contribution over the next three years to make family planning a global priority through the use of contraceptives leaves much to be desired—especially considering that $250 million or almost 70% of this money will be used to fund services for teenagers as recently noted in an article published in The Guardian.
Flippant distribution of contraceptives is a superficial Band-Aid which masks a social pandemic of responsibility free sex and poor education without curing the disease. What the teenagers of this world need is not free condoms or a pill that remove accountability—they need a society that does not commodify them. They need a world that does not tolerate sexual exploitation and violence, which does not ostracize the teen mother, and that does not paint the picture of the mother of many as the antagonist to a flourishing world.
You state in your article that, “contraceptives are an essential part of the healthier, more prosperous world we’re all working toward. When a woman has access to contraceptives, she tends to have fewer children. Families can devote more resources to each child’s nutrition, health, and education, setting them up for a better future.” How different would the conversation be if were instead concerned for the struggling mother and partnered with her to ensure her success campaigning for a social structure that empowers her to provide her children with nutrition, healthcare and equal opportunity for education? Within this article childbearing and rearing are portrayed as an inexplicable burden that limit a woman’s freedom to work, ability to earn an income, and contribute to the economy. In the United States the majority or 70% of mothers with children under the age of 18 participate in the labor force, working, and contributing to both their families and the economy according to the 2013 data published by the Department of Labor. Arguably stay at home mothers are also working and contributing to the economy as they painstakingly invest their time and energy in raising the next generation. Motherhood does not limit a woman’s capacity to contribute; it magnifies it in ways that she may never have realized.
The Center for Disease Control reported in 2013 Contraceptive Methods Women Have Ever Used: United States, 1982–2010 that, “Overall, 47% of women who have used at least one method of contraception have discontinued using a method due to dissatisfaction.” This is a sobering statistic considering the amount of money being raised in order to distribute contraceptives. Will women be able to receive follow-up care if their prescribed birth control sends them into a spiral of depression and they need to switch? It seems that distribution of contraceptives as propagated by the Global Family Planning Summit is not a wholistic approach for women. If it was wholistic the goal would extend beyond distribution, it would involve at a minimum fertility education. NFP methods allow for family planning in a way that honor the mind, body, spirit, and as an added bonus even the environment. Could we be so bold instead to consider that the answer to family planning is not in a prescription it is in education?
Fertility Awareness-Based Methods of Family Planning (FABM) are an excellent option for women in rural situations and under developed countries—it just takes a little investment of time and education. According to the American College of Obstetricians and Gynecologists FAQ 024 published in April 2015, “when used properly, fewer than 1–5 women out of 100 will become pregnant during the first year,” using FABM.
We are in agreement that the 1.2 billion adolescents in the world today, do need to be empowered with the right tools — but it seems unlikely that passing out contraceptives like candy to teenagers to prevent pregnancy will, “unlock unprecedented growth in the world’s poorest countries.” We need to change the conversation from treating the symptoms to attacking the disease. By promoting awareness of physiology, equipping our world’s mothers, and holding each individual responsible for the consequences of their decisions perhaps we all will have a chance at a brighter future.
Is the Church going to “revisit” its teachings against artificial contraception? That’s what Melinda Gates – wife of Microsoft founder and billionaire Bill Gates – hopes. In a recent interview with the BBC, Gates said she is “optimistic” that Pope Francis and the Vatican might do just that.
The Bill and Melinda Gates Foundation is one of the leading promoters and providers of contraception in the developing world. So it’s no surprise that Melinda, who dissents from Church teaching on contraception yet considers herself a Catholic, is excited and hopeful the Catholic Church – the last major holdout against the contraception revolution – will cave into the zeitgeist. Perhaps Melinda was reacting to rumors swirling among well-informed Vatican sources that there are efforts afoot within the Vatican to “reinterpret” Blessed Pope Paul VI’s famous encyclical Humanae Vitae.
Published on July 25, 1968, Humanae Vitae stunned the world by reiterating the Church’s perennial teachings against artificial contraception, at a time when many people – including many of Paul VI’s own advisors on the subject – expected and were urging him to do the exact opposite.
Given how prophetic Humanae Vitae turned out to be, and the vast path of destruction that has resulted from its widespread rejection by Catholics and the culture alike, one would think that the time is ripe for the Church to celebrate that great encyclical and launch a widespread effort at catechesis on its teachings. Instead, troubling reports emerged earlier this year about a secret Vatican “commission” tasked with reviewing Humanae Vitae. The existence of this commission has since been confirmed, although there are conflicting reports about its purpose, and to what extent it has formal Vatican recognition.
Either way, it is evident there is a great need to remind ourselves of just how prophetic Humanae Vitae was and why its teaching must be upheld, defended, and vigorously taught.
Perhaps the most famous sentence from Humane Vitae is found in section 17, where Paul VI describes the “consequences” of embracing artificial contraception. That great pope predicted:
A general lowering of moral standards throughout society; a rise in infidelity; a lessening of respect for women by men; and the coercive use of reproductive technologies by governments.
He added:
Another effect that gives cause for alarm is that a man who grows accustomed to the use of contraceptive methods may forget the reverence due to a woman, and, disregarding her physical and emotional equilibrium, reduce her to being a mere instrument for the satisfaction of his own desires, no longer considering her as his partner whom he should surround with care and affection.
It is heartbreaking now, 49 years later, to realize how painfully right Paul VI was. At the time many accused (and still accuse) Paul VI of being an alarmist. A quick survey of our culture reveals that, if anything, his predictions were understated.
Just last week, I wrote about how a leading magazine aimed at teen girls had published an article coaching those girls on how to engage in sodomy. That article is merely the tiniest tip of the iceberg of the vast and nearly unthinkable sexualization of our society – “a general lowering of moral standards” – in the past 49 years.
Since Humanae Vitae was published, we’ve seen the explosion of pornography, beginning with popular magazines like Playboy and Hustler, then VHS tapes, and now, on-demand streaming high definition Internet porn. The initial age of exposure to pornography is 12 years old, while a staggering percentage of teens – boys and girls – now watch hardcore porn as a matter of routine. Even many of our mainstream television shows and movies are now filled with sexuality so graphic that it is indiscernible from the stuff found on the porn sites.
Meanwhile, we now accept as “normal” public parades celebrating immoral lifestyles, in which nude men and women march down the street and simulate graphic sex acts. Millions of people attend these parades, and many of them bring their children.
After the advent of the Pill, divorce rates skyrocketed – “a rise in infidelity” – with as many as half of all marriages at one point ending in divorce. And while the divorce rates seem to have peaked, and possibly even fallen, sadly a large part of the reason is that many young adults aren’t even bothering to get married in the first place. They “cohabitate,” simulating married life.
The impact this has had on children is staggering. A 2012 study found that, among women under 30, more than one-half of all children are born out of wedlock. An unthinkable number of children have never known the fundamental good of a stable household or have never known one of their parents; moreover, many children are the innocent victims of ugly divorce proceedings and are passed around from household to household.
We have also seen massive government-sponsored programs of forced abortion and sterilization – “the coercive use of reproductive technologies by governments” – in countries like India and China. Many population alarmists, including Paul Ehrlich, the population controller who recently spoke at the Vatican, endorse government efforts to coerce couples into reducing how many children they have.
Meanwhile, new reproductive technologies, like IVF and surrogacy, have arisen that deliberately sever procreation from sex altogether. Children are bought like commodities. Prospective parents can even choose the characteristics of their child. Millions of excess human embryos are created and then left in a state of limbo in cryo-banks, or simply thawed and flushed down the drain like so much garbage. Wealthy couples and same-sex couples hire out impoverished women from third world countries to bear their children for them, and this is called “progress.”
I could go on and on.
Ultimately all of this unthinkable evil can be traced to one single thing: the severing of sexuality from the only place it belongs – marriage – and from its primary purpose – procreation.
After all, if we accept that it is moral to deliberately cut off sexuality from these two things, then sex becomes little more than a form of mutual masturbation. At that point, it also becomes practically impossible to make a cogent argument against other forms of non-procreative sex: mutual masturbation, sodomy, and other debased sexual activities.
In a post-Pill world, that most-powerful and fundamental force of human sexuality has now broken away from its mooring, no longer bound by the life-giving principles of the Christian worldview. Self-control, responsibility, and consequences are no longer deemed relevant. And set loose from these necessary constraints, sexuality becomes a ravening beast, consuming men, women and children.
Humanae Vitae is perhaps the most-hated and most-rejected encyclical in history. And yet, Paul VI himself knew that he was simply doing what any loving father does: helping his children understand and live within the life-giving laws that are the only path towards happiness and fulfillment. For as he wrote:
In preserving intact the whole moral law of marriage, the Church is convinced that she is contributing to the creation of a truly human civilization. She urges man not to betray his personal responsibilities by putting all his faith in technical expedients. In this way she defends the dignity of husband and wife. This course of action shows that the Church, loyal to the example and teaching of the divine Savior, is sincere and unselfish in her regard for men whom she strives to help even now during this earthly pilgrimage “to share God’s life as sons of the living God, the Father of all men.”
Leah Barkoukis Jul 21, 2017 | 9:53AM Washington, DC
Want to reduce climate change? You may want to think about having fewer children, a recent study out of Sweden finds.
That’s right—the biggest impact on reducing climate change is to limit the size of your family, according to the study. Other important ways to reduce one’s carbon footprint include ditching four wheels for two, not eating meat, and avoiding air travel.
We recommend four widely applicable high-impact (i.e. low emissions) actions with the potential to contribute to systemic change and substantially reduce annual personal emissions: having one fewer child (an average for developed countries of 58.6?tonnes CO2-equivalent (tCO2e) emission reductions per year), living car-free (2.4 tCO2e saved per year), avoiding airplane travel (1.6 tCO2e saved per roundtrip transatlantic flight) and eating a plant-based diet (0.8 tCO2e saved per year).
“I knew this was a sensitive topic to bring up,” the study’s co-author Kimberly Nicholas told NPR’s Morning Edition. “Certainly it’s not my place as a scientist to dictate choices for other people. But I do think it is my place to do the analysis and report it fairly.”
The researchers found these four lifestyle changes reduce CO2 gas emissions much more than recycling, use of energy efficient light bulbs, or hang drying clothing, for example.
These actions have much greater potential to reduce emissions than commonly promoted strategies like comprehensive recycling (four times less effective than a plant-based diet) or changing household lightbulbs (eight times less).
Nicholas did note, however, that the study’s findings aren’t meant to tell people how to plan their family.
“I think the decision to become a parent is a really personal decision,” she said. “I think the way people relate to it in terms of climate change depends on their view about climate change.”
July 23 marks the beginning of Natural Family Planning (NFP) Awareness Week in the United States. In this article Gerard Migeon, founder and CEO of Natural Womanhood, takes a look at some recent research on fertility awareness based methods and sets out 10 ways in which fertility awareness can improve a couple’s relationship.
When I first tell young couples that Fertility Awareness Based Methods improve sex and relationships, I sense a subtle skepticism in the room: “Wait, you’re saying that we have to abstain from sex eight days a month? How is that going to make our relationship better?”
But at the end of the talk, they say the strongest argument for fertility awareness comes from hearing the testimony of couples who have been practicing a method for several years and watching them interact: they can see the peace, the complicity, the passion they display. So what’s the difference and how does it play out?
These methods teach women to recognize the signs of their natural cycle so they will know when they are fertile and not fertile, usually, a six-day window per monthly cycle. With that information, they can work their partner to avoid or to achieve pregnancy effectively.
What studies say about fertility awareness and relationships
While more research needs to be done, several studies strongly suggest that FABMs often improve couples’ relationships.
A study co-authored by the Couple to Couple League and published this year in the journal Frontiers in Public Health was conducted online with 2,560 respondents who were using the Sympto-Thermal Method, referred to as NFP (natural family planning) in the report. These couples lived in several countries in Western Europe and in the US. The abstract of the study reported that:
“95% of women and 55% of men said using NFP has helped them to know their body better. Large majorities of men (74%) and women (64%) felt NFP helped to improve their relationship while less than 10% felt use of NFP had harmed their relationship. Most women (53%) and men (63%) felt using NFP improved their sex life while 32% of women and 24% of men felt it was unchanged from before they used NFP. 75% of women and 73% of men said they are either ‘satisfied’ or ‘very satisfied’ with their frequency of sexual intercourse.”
In a 2004 study published by the Journal of Nursing Scholarship, designed to gauge the effect of natural family planning on marital relationships, asked married couples practicing these methods a series of open-ended questions to. “Of the 2,287 coded comments, 1,765 (74%) were positive,” indicating that the majority of those practicing natural methods of family planning believed it had had a positive influence on their marriage.
10 ways fertility awareness improves your relationship
The second study mentioned above reviewed the key reasons why people reported that FABMs improved their relationship. It is in great part the source of the content below along with other research.
You know yourself and become a better you. Most psychologists will tell you that good relationships with others start with a good relationship with yourself. As we have written here and here, it’s more difficult to be oneself on the pill; the practice of charting allows women to know themselves better and gain self-confidence. We even found that “cycle mindfulness” helped teen girls become less influenced by peers and better able to plan their life: they became more mature and self–directed, they moved “from being victims of their hormones to being in control,” were more able to think ahead and to make decisions ahead of crisis.
Your partner knows you better. When you practice FABM, your man gets to know where you are in your cycle: post-period and not ovulating yet, getting close to ovulation, past ovulation. Each phase usually corresponds to different levels of energy for you: medium, higher energy, lower energy. A considerate man can then pay attention to these phases to adjust his expectations of how much activity the couple can tackle and the needs for rest.
You have better, deeper communication. Here is the test of your communication level right now: how often do you talk about your sex life as a couple? If you can talk about sex with one another you can talk about anything. Discussing sexual intercourse, fertility and starting or adding to a family are integral to using FABM successfully. Couples who use FABM become more open to talking about difficult topics and they are more in touch with each other’s feelings.
You show each other love in different ways. Users of FABMs are often led to understand their love relationship in a broader way: how can I love this person better rather than “what I am getting out of this?” It shows especially during the time of abstinence, as they are both challenged to go back to “dating time,” when they found creative ways to show love for each other in a non-sexual way.
You have a deeper relationship: for all the reasons above, FABMs creates a stronger bond including feeling less selfish and more sensitive to the spouse/partner’s needs, feeling greater love and more understanding of one another.
You have a better libido. The suppression of women’s libido by hormonal contraceptives is fairly common. You can have sex anytime when you’re on the pill, but many women report feeling emotionally flat and less interested in sex. Science shows that hormonal contraceptives affect the level of testosterone in women, which is the hormone responsible for sexual desire and arousal in women. While the woman’s drive to have sex is usually highest during the abstinence time (welcome to man’s world, which feels like that all or most of the time!), her enjoyment of sex can be just as high after ovulation. It all depends on your attitude.
You enjoy monthly honeymoons. The couple intending to avoid pregnancy has to wait to avoid sex during the fertile time. This is called periodic abstinence. Couples report that the time of waiting enhances their anticipation, thus increasing their enjoyment. As we mentioned above, that “dating period” also prepares them for the time they can have intercourse, which becomes the sequel of their romantic love, not simply a response to a personal physical need.
You have greater respect for one another. Because of the need for closer dialog about when sex happens, women report feeling more respected and less used by their spouse/partner. In turn, they also feel a greater respect for and pride in him for his ability to abstain and his self-control.
You experience gender equality. If a couple is avoiding pregnancy, they both have to know what days they’re taking a break from sex, and what day they can — happily — get back to it. It is no longer only the woman’s responsibility to avoid pregnancy. As a man, I think this is very important and value the idea that the choice to become pregnant or not is something that is the fruit of a partnership. It is too easy to forget about that crucial dimension of the relationship when relying on the pill. Not with FABMs.
You are better prepared for life’s unpredictable twists. Because of all the reasons listed above, couples are much better equipped to deal with serious incidents in their life. Friends of ours had the misfortune of losing a child, which very often leads to a separation or serious relationship difficulties. In their case, they reported that the relationship grew closer and they believed they were there for one another in a way they wouldn’t have been otherwise.
Fertility awareness changes your life as a couple
Practicing fertility awareness is not just using another method of birth control. It’s a shift in the way a couple thinks of their sex life. Suddenly, there is a rhythm to it, not “just whenever you want” (which is often when the man wants: the pill makes the woman always available for sex, which is unnatural for her).
It is crucial that couples who decide to use a FABM as a way to avoid pregnancy are aware of that change, and have a frank discussion about what they’re committing to. In the end, they will most often find it was worth it, but the change may take some work if they had a different approach before. Realistically, couples are already abstinent most of the time, as on average, they only have intercourse less than twice a week. However, a good understanding of expectations makes for a happy partnership.
They need to go into it with eyes wide open.
Gerard Migeon is the founder and CEO of Natural Womanhood, a MercatorNet partner site. The above article is a slightly abridged version of the original article published at Natural Womanhood.
Lauretta Brown Jul 18, 2017 | 4:26PM Washington, DC
Obianuju Ekeocha, a Nigerian-born biomedical scientist and the founder of Culture of Life Africa, a U.K.-based pro-life group, argued on BBC’s Sunday Morning Live that the Gates Foundation’s push for contraception in Africa might be “an insidious way of moving the agenda of population control” since in many African countries the “desired number of children is actually quite high.”
Melinda Gates announced last week that the Gates Foundation will commit an additional $375 million to family planning programs citing deep concerns “about the White House’s proposed budget cuts to global family planning efforts.” President Trump recently expanded a policy that bans taxpayer funds from going to programs that perform or promote abortion overseas.
“When a woman has access to contraceptives, she tends to have fewer children. Families can devote more resources to each child’s nutrition, health, and education, setting them up for a better future,” Gates said.
“I’m sure Melinda Gates means well,” Ekeocha began, “but you see the problem is there is an arrogance and something in what I see as questions not being asked in all the talk about contraception and helping women space their children is what exactly, speaking of Africa for example, what exactly do women want?”
“In most of the African countries you get to find and research continues to show all the time that African women you know in a lot of the countries desire or desired number of children is actually quite high when cultures where people for example value children or value big families what are you saying to the women if you continue to push their governments towards the so-called family planning projects?”
“Not that people are not spacing their children,” she added, “it’s that this might indeed be an insidious way of moving the agenda of population control.”
Ekeocha clarified that she was not saying family planning programs were “bad in and of themselves” but that “there is a real problem with a multi-billionaire from a Western country coming in to tell African governments what to do or how to control populations.”
Mairo Mandara, the Bill and Melinda Gates Foundation Country Representative for Nigeria, said at a World Population Day (WPD) event that “Family Planning should be declared a National Emergency,” adding, “it is not about stopping people from giving birth, but seeking to control the process. The WPD is meant to draw attention to population explosion in the coming years. In Nigeria, the WPD 2017 provides opportunity to discuss ways of checking possible population explosion.”
French President Emmanuel Macron drew criticism last week for saying that Africa has a “civilizational” problem and women are having “seven or eight children.”
Canadian Prime Minister Justin Trudeau’s Minister of International Development, Marie-Claude Bibeau, recently defended Canada’s increase in funds toward abortion and contraception overseas by calling abortion and contraception a “tool to end poverty.”
Professor Charles Tyler, reproductive physiologist and environmental biologist at the University of Exeter (United Kingdom), has found that chemicals from contraceptive pills and other household cleaning products are causing fresh-water male fish to develop female parts and even to lay eggs.
Tyler’s research has shown that oestrogen and other chemicals being washed down the drain are causing male fish to reduce “sperm quality and display less aggressive and competitive behaviour, usually associated with attracting females of the species, which make them less likely to breed successfully,” reported Exeter in a press release.
Tyler presented his research on July 3 in a keynote address at 50th Anniversary Symposium of the Fisheries Society in the British Isles, held at Exeter University. His lecture was titled “The Feminisation of Nature – an Unnatural History.”
In the lecture, he laid out data on the Roach fish in particular, and how estrogens are causing some males to develop ovaries and become an “intersex.”
(Screenshot of Slide 17)
One of Tyler’s research reports (which he sighted in his presentation) explained that “intersex” fish are male fish that “can have feminized reproductive ducts and/or developing oocytes within their testes (Nolan et al. 2001). They also “have abnormal concentrations of sex steroid hormones (Jobling et al. 2002a) and (often) elevated concentrations of the estrogen-dependent blood protein vitellogenin (VTG) in their blood (Jobling et al. 1998).”
This research also states that “fertility is reduced” in feminized fish.
(Screenshot of Slide 18)
“We are showing that some of these chemicals can have much wider health effects on fish that we expected. Using specially created transgenic fish that allow us to see responses to these chemicals in the bodies of fish in real time for example we have shown that oestrogens found in some plastics affect the valves in the heart, “ Tyler said in the Exeter press release.
He added, “Other research has shown that many other chemicals that are discharged through sewage treatment works can affect fish including antidepressant drugs that reduce the natural shyness of some fish species, including the way they react to predators.”
When CNSNews.com asked Tyler how long he has been doing research on transgender fish, Tyler responded in an email, “I have been working on sexual disruption in fish as a consequence of exposure to chemicals for years.”
Tyler also corrected the word “transgender” with regard to the fish, saying, “I think it may be better to call them intersex fish — as some people like to use the term transgender in the human context only.”
In his presentation, Tyler also mentioned that chemicals are having this effect on fish in other continents around the world: “Feminised Fish have been reported from sites across Europe, America, Canada ( Rainbow Darter – Etheostoma caeruleum, Percidae), Africa and Asia.”
(Screenshot of Slide 15)
On this topic, CNSNews asked Tyler, “Slide 15 mentions that fish are being ‘feminized’ in other continents around the globe. Is this a result of contraceptive chemicals as well? Or is it something else?”
Tyler responded, “The feminising effects on fish in other countries does indeed include effects from the contraceptive pill, but also from chemicals including industrial surfactants – detergents, plasticisers and bulk chemicals such as bisphenol A.”
It’s almost NFP Awareness week (July 23)! It’s easy to get swept away in NFP promotion and forget that it’s not always a breezy journey for everyone. So here we have laid out the guide to promoting Natural Family Planning without the rose-colored glasses. The three most important things to keep in mind when sharing your love of Natural Family Planning are sincerity in the struggles you have encountered, joy in the wonderful parts, and flexibility in allowing others to be where they are on their journey.
Sharing Your Struggles
NFP can be hard. I don’t think I’m the only person ever to say that. In seasons of difficult charting – like postpartum, perimenopause, times of stress, or hormonal imbalance, it can be hard to find the type of support you need. Sometimes finding NFP support period can be a challenge. Instructors usually are doing it pro-bono so they are fitting it into their already busy lives. While there are chat rooms and facebook groups and great literature on learning NFP, nothing replaces that one-on-one exchange.
Abstaining can be hard. Biology has other plans. Dealing with questions of whether or not your pregnancy was planned can be awkward at best, and downright offensive at worst. As I’ve written before, the decision to grow your family is not always an on/off switch. NFP is not, by definition, a wonder drug for your relationship. It will not solve pre-existing issues, it won’t make your in-laws any easier to deal with, and it certainly won’t clear up any financial debt.
Before I crush your spirits, this is not to say that NFP is dreadful, or even unfavorable. It’s just important to be honest about the struggles that can accompany the choice to use NFP. When one person speaks out about their challenge, another person says, “Hey, me too.” And another pipes up, “Yes! Same!” These voices deserve a place in the conversation. Otherwise, they don’t get heard and it becomes too easy to outcast them.
Sharing Joy
So if it’s not a wonder drug, then what it is it? NFP can be an amazing tool for couples and women. One of the reasons we hear so often that NFP has improved relationships and health is because it can. When couples are communicative, and open, and working through their challenges, NFP can open many wonderful doors. The empowerment a woman gains by learning her cycles is alone reason enough to get excited about sharing NFP! It’s important to share your joy. I love teaching women simply because it’s a joy to watch them grow in the self-discovery that they had never realized was possible.
Along with joy, (and empowerment and sheer awesomeness of knowing your cycles), there are the undeniable health benefits to steering clear of hormonal contraceptives. Some people are desperate to find an alternative for both managing hormonal health and family planning. It’s important for the risks of hormonal contraception to be considered, but emphasizing the health benefits of NFP is key, including an improved ability to figure out what hormonal imbalances may be behind symptoms and what to do about them.
Meeting People Where They Are
Lastly, and arguably the most important thing to keep in mind when promoting NFP is flexibility. Meet people where they are. Listen to their journey and don’t try to place them on yours. Maybe they’re not ready yet, maybe they don’t want to use an app, maybe they don’t want to learn X method, or maybe they want to blend a few methods. I always tell my clients the most effective method of NFP is the method they feel is sustainable for their lifestyle and fits in line with their family planning intentions. Maybe they don’t really care if they get pregnant so they don’t need a super strict set of rules. Or maybe they want as many biomarkers as possible. Or maybe they hate paper charting or can visualize better with a different style of chart.
The reason flexibility is so important is that people will never listen to you if you’re not first listening to them. You can plant the seed by sharing your joys and yes, your struggles, but then let them make the choice for themselves. I’ve had people ponder getting off the pill for months, even years before making the switch. But when they do, they are stoked to jump in and learn about their cycles.
So now that you have a guide for promoting NFP without the syrup, we want to know: how you are planning to celebrate NFP Awareness Week? Writing a blog piece? Giving a talk at a local library? The awesome thing about the NFP community is that most of us really do love it and just want to share the love. So here is a challenge for you: if you are interested in sharing your joys and struggles about NFP (and how you overcame them), send us your story. We’ll get as many as we can on our blog during NFP week. Not sure how to start? Use this short questionnaire.
Cassondra Moriarty is a filmmaker and fertility charting instructor in training based out of Brooklyn, New York, where she lives with her husband. She is currently screening Miscontraceptions around the city and working to promote Fertility Awareness. She has trained with the Couple to Couple League and is in the process of getting her FEMM certification.
https://thefederalist.com For many women, the decision to go on birth control is a normal part of womanhood. At well-woman checks and appointments after a baby’s birth doctors say it’s time to talk about birth control, and the general assumption is that you’ll use birth control until it’s the perfect time to have exactly as many kids as you want.
Birth control, especially the Pill, is interwoven with women’s health care, and access and funding for contraception has featured heavily in recent years with the debates on insurance policies and coverage. A new study has introduced a troubling concern for a medication so ubiquitous in most Western women’s lives, finding that the Pill might be putting women at significantly higher risk for breast cancers.
It’s hard to find a family in America that hasn’t been affected by breast cancer. It’s the most common cancer for women in the USA, and the rates of diagnosis are staggering. This year, more than 250,000 women will be diagnosed with invasive breast cancer, and tens of thousands more will be diagnosed with non-invasive breast cancer. Breast cancer is the second leading cause of cancer deaths for women. This makes the information in the new study particularly concerning.
When We Treat Fertility Like a Disease
Combining data from 12 previous studies looking at the health histories of American and European women from 19 to 40 years old, researchers from the University of Michigan discovered that some types of hormonal birth control increase women’s progestin levels fourfold. In addition, ethinyl estradiol, an artificial estrogen strongly correlated to breast cancer, was increased by 40 percent in women who use some forms of the Pill.
These two hormones work together normally to control a woman’s menstrual cycle and fertility. The synthetic versions are used in hormonal birth control to alter the normal monthly changes in a woman’s body to prevent pregnancy. Advocates of hormonal birth control frequently insist the risks of birth control are less than the risks of pregnancy for women.
When medications are widely prescribed without careful and deliberate attention paid to serious and potentially fatal side-effects, it’s a disservice to women. Birth control has been widely prescribed in America since 1960 when it became legal for contraceptive use, and with Griswold v. Connecticut in 1965 Supreme Court made it unconstitutional for the government to deny birth control to married couples. Instead of the legality or morality of birth control, the focus here is on product safety.
Generally, we take medications to improve our health, or to treat a condition that’s hurting us. Is the Pill, in its current formulations, really doing either of these things? Or is the Pill instead increasing cancer risks in normal, healthy women? How does that relate to the broader societal treatment of women’s fertility as a disease to control, despite the increasing list of negative health effects for women?
Cancer isn’t the only frightening risk of the Pill. Another recent study showed that blood clots, some of them serious enough to cause permanent injuries or death, could be far more common than originally thought, and doctors often do not discuss these risks with women. Other troubling risks include weight gain and mood disorders that can become serious enough to cause suicidal thoughts and urges. Add in that the Pill can wreak havoc with a woman’s sex drive, and it’s clear that the effects of the Pill are far-reaching for women and men who love them.
Women Deserve Better Research and Care
“Not enough has changed over the generations of these drugs, and given how many people take hormonal birth control worldwide—millions—the pharmaceutical industry shouldn’t rest on its laurels,” said Beverly Strassmann, one of the study’s authors. The pharmaceutical industry is a multi-billion-dollar American institution, and there’s no good reason for a widely used medication class to not be continually striving to improve safety.
Hormone Replacement Therapy or HRT, the hormone therapy used to decrease negative symptoms of menopause, changed radically after the Women’s Health Initiative study results in 2002, when they concluded the hormones used could increase cancer risks. Strassmann rightly noted that since the correlation between synthetic hormones and breast cancer isn’t new news to clinicians, it’s important to research if that link extends to birth control pills.
It’s especially important to consider these health concerns with the newer, often lesser-researched types of Long-Acting Reversible Contraception, which some are targeting at vulnerable young and poor women. Since screenings for breast cancer are more difficult to schedule, and mammograms less effective for young women, the breast cancer risks with hormonal contraception need to be taken seriously in these populations. Outside age, poverty is its own common barrier to timely cancer screenings.
With this study, we now know that there is a relationship between birth control pills and the hormonal changes associated with breast cancer. It’s time to seriously consider the health impact of the Pill on American women and families. Birth control is part of the modern American way of life. If that way of life increases the risk of life- altering cancer, those risks need to be clearly shared with women before they ever start taking the Pill, and regularly thereafter as knowledge increases.
More women may also wish to consider whether the social script of treating their body’s natural fertility like a disease is worth the noticeable spike in lifetime health risks numerous studies have now demonstrated, especially when studies often come years after thousands of women are irreversibly harmed. We’re more than 50 years after the Pill, and only just now finding out about the dramatic increases in breast cancer and other risks. What else will we know in another 40 years?
Holly Scheer is a writer and editor. She’s fascinated by politics, culture and theology. Follow her on Twitter @HScheer1580.
The Justin Trudeau Liberals will pour $241.5 million into providing and promoting contraception and abortion in developing nations — particularly in Africa — as part of their commitment to securing global access to “sexual and reproductive health and rights.”
International Development Minister Marie-Claude Bibeau made the announcement on Tuesday during the Family Planning Summit in London, England.
The money is part of the $650 million the Liberals pledged in March to promote global access to “sexual and reproductive health and rights,” as well the $840 million they’ve earmarked “for humanitarian assistance in response to the crises in Iraq and Syria,” according to a Liberal backgrounder.
About 65 percent of the $241.5 million targets Africa.
The backgrounder, entitled “Canada’s leadership on sexual and reproductive health and rights,” details that the Liberals will dole out money over five years to veteran abortion promoters.
These include the United Nations Population Fund, Marie Stopes, International Planned Parenthood Federation, and the World Bank.
The UNPF receives $45 million to provide “reproductive health and family planning services” in Iraq, Syria, and Afghanistan along with humanitarian aid.
The IPPF gets $5 million to promote abortion and provide contraception in South Sudan; Marie Stopes Tanzania $15 million to do the same in Tanzania; the Clinton Health Access Initiative $20 million to “improve access” to sexual and reproductive health choices through an “innovative approach” in Nigeria.
Pathfinder International gets $15 million to “support family planning and abortion services” in Mozambique, where abortion was legalized in December 2014.
Other African nations targeted are Ghana, Benin, Ethiopia, Democratic Republic of Congo, and Burkina Faso.
But African pro-life advocates are slamming the Liberals for “arrogance,” “hypocrisy,” and “cultural colonialism.”
“The Liberal government, by offering what Africans neither want nor need, shows its hunger to inherit the infamous throne of the ‘world abortion champions’ which the United States has abdicated,” Archbishop Emmanuel Badejo of Oyo, Nigeria, told LifeSiteNews in an email.
Communications director for the African bishops, Badejo excoriated the Trudeau government for “hypocrisy” in “pushing an imperialist agenda that undermine religious and cultural sensibilities and demean the cherished African respect for the life of the unborn.”
That was echoed by Obianuju Ekeocha, founder of the UK-based Culture of Life Africa.
“This new breed of Western leaders who want to impose an abortion-friendly ideology, if you will, by all means in Africa, one thing about them that they all have in common is that they are not listening to us,” she told LifeSiteNews.
“Most of the African cultures across the the different African countries consider abortion the destruction of human life, consider abortion as a way of death,” she said.
Moreover, Canada’s money will do a lot of damage in Africa when organizations such as Marie Stopes use it to lobby for abortion, Ekeocha said.
“In Africa, where there is a lot of corruption, some of it might go into bribery.”
And that will “involve terrible things,” Ekeocha said, because the “very fabric of that society is being shredded, put under pressure, first of all, by this kind of money, but also being shredded at the end of the day — by the time the money goes into buying favours, buying traditional rulers, buying community leaders, buying parliamentarians.”
The Liberals’ promotion of the sexual and reproductive rights agenda is “also terrible for the image of Canada,” hitherto highly regarded in Africa as “one of the few developed countries that was not a colonial master.”
Now under the Liberals, Canada in 2017 is “becoming a massive colonial master” as leader of what Ekeocha describes as the “neo-colonial” movement of the “reproductive rights agenda.”
Canada is not only “going and throwing all this money, it’s also trying to inspire other Western nations to do likewise,” she said.
“Even in their speeches, when you listen to them, you see that it’s kind of a clarion call, ‘we’re putting 650 million, what can you do, what would you do’,” she said. “They’re looking at other countries, and winking at other Western countries.”
The Trudeau government “has put itself right at the forefront of this unfortunate movement that is trying to colonize an Africa that has been decolonized a long ago,” Ekeocha said.
“But they are trying to colonize it in the worst way ever, they’re trying to colonize us culturally and ideologically.”
When Noah Wall was born, the doctors said he probably wouldn’t survive and if he did, he would be severely physically and developmentally disabled. Born with only 2 percent of his brain to a family in Cumbria, England, Noah had no hope — at least according to the doctors.
In utero, Noah had developed a rare complication of spina bifida where his skull filled with fluid, crushing his brain down into a “thin sliver of tissue,” according to the UK’s Mirror. His parents — Shelly and Rob — were advised to abort him on five occasions. They refused. After Noah’s birth, an open wound in his back was closed and a shunt was installed to drain the fluid from his brain.
Shelly and Rob picked out a baby coffin for Noah, but they also never stopped believing he was anything less than a great gift. They took him home and the entire family surrounded him constantly with love, affection, and 24-7 care. Noah’s brain began to grow. And grow. And grow some more.
When he was 3, a brain scan showed that his brain “had expanded to 80% of a normal brain.” Now a movie on Britain’s Channel 5 calledThe Boy Who Grew A Brain documents just how far Noah has come.
The family continues to keep Noah’s brain stimulated to aid his neurological growth. Dr. Claire Nicholson of Newcastle’s Great North Children’s Hospital in England — Noah’s neurosurgeon — calls him “a remarkable child with two remarkable parents.”
Noah, who’s always smiling and shows empathy and love in his words and deeds, is learning to read and write, can count, and attends school. His brain continues to develop beyond anyone’s wildest dreams and after some surgeries on his hips, Noah’s family believes he may actually walk one day. Given how this story has unfolded so far, you should probably bet on it
July 10, 2017 (HLI) – The case of baby Charlie Gard has the gravest consequences for the rights of parents and the autonomy of the family. This assault against the family and life stretches beyond the borders of the UK, and we should all be very concerned.
For those unfamiliar with the case in question, Charlie Gard was born in the UK in 2016 with mitochondrial DNA depletion syndrome, a severe condition that left him struggling for his life. This past March doctors told his parents that there was nothing more they could do. They recommended removing his ventilator and letting him die.
Undeterred, Chris Gard and Connie Yates searched for alternatives. They discovered an experimental treatment that offered the small possibility of a cure. The catch? It’s extremely expensive, and is only offered in the United States.
Still undeterred, Charlie’s parents launched an online crowd-funding campaign and received tens of thousands of donations. In all, the parents raised over 1.3 million British pounds (nearly $1.7 million U.S.) – more than enough to pay for the treatment.
For the first time, there was a glimmer of hope for Charlie.
Then, inexplicably, the hospital where Charlie is being kept – Great Ormond Street Hospital in London – refused to release Charlie. They said they had determined that the proposed treatment was unlikely to help the boy, and would only prolong his suffering.
Shocked, Charlie’s parents appealed that decision. A court ruled that Charlie should be permitted to “die with dignity” (a chilling phrase, for those familiar with pro-death rhetoric). They appealed the case all the way up to the UK Supreme Court. At every step, they lost. Then, last week, the parents’ last recourse – the European Court of Human Rights – refused to overrule the UK court.
With that decision, Charlie’s case exploded onto the international stage. A ferocious public debate ensued, with global figures including President Trump, Pope Francis and many others weighing in. Charlie remains on life support, but at any moment the hospital could decide to remove his ventilator.
Sadly, confusion has plagued the emotionally fraught case. Even some pro-lifers seem to have been misled by the rhetoric of the hospital and the court system, while the core issue – the natural rights of the parents to make this decision for their child – has been lost.
Moreover, many were shocked after an initial statement from the Vatican’s own Pontifical Academy for Life (PAV) seemed to side with the hospital, which was met with a fierce backlash from Charlie’s supporters. Thankfully, shortly thereafter Pope Francis issued his own statement. The Holy Father rightly pivoted the Vatican’s focus away from the complex and ultimately tangential issue of the nature of the proposed treatment, to the rights of Charlie’s parents. Speaking of the parents, the statement said: “For them [Pope Francis] prays, hoping that their desire to accompany and care for their own child to the end is not ignored.”
Equally as important, the Vatican followed up with concrete action: Bambino Gesu, the Vatican’s own hospital, offered to take Charlie and care for him, for free. This was a strong, and much-needed gesture.
It is important that we be 100 percent clear what this case is not ultimately about: the distinction between “aggressive” or “extraordinary” care, and ordinary care. The Catholic Church has always been very clear that there is no moral obligation to use what the Church labels “extraordinary” means – which can include artificial respiration – to prolong life. As Pope John Paul II wrote in Evangelium Vitae:
In such situations, when death is clearly imminent and inevitable, one can in conscience “refuse forms of treatment that would only secure a precarious and burdensome prolongation of life, so long as the normal care due to the sick person in similar cases is not interrupted”. … To forego extraordinary or disproportionate means is not the equivalent of suicide or euthanasia; it rather expresses acceptance of the human condition in the face of death.
However, at the same time, the Church has also never said that there is a moral obligation not to pursue extraordinary means. That must be evaluated on a case by case basis. More importantly, the decision about whether to pursue extraordinary care should rest with the rightful authority – in this case, clearly Charlie’s parents.
So what is the fundamental issue? One thing only: a struggle for power.
That is: The hospital, and the UK government, believe that the state, and not Charlie’s parents, should have the power to decide what is best for Charlie (and, presumably, others like him). And to drive that point home, they were willing to fight this case all the way to the EU Court of Human Rights.
If they succeed, what this means for parental rights is terrifying. As Phil Lawler at Catholic Culture summarized:
The injustice here is not that Charlie will be (maybe already has been) taken off his life-support system. The decision to turn off a ventilator is always painful, but sometimes justified.
The injustice is that Charlie will die when the hospital administration wants, and where the hospital administration wants. His parents have been deprived of their right to supervise his case. They could not take him the U.S. for experimental treatment. They could not take him home, to die in peace. As one of our readers observed, Charlie was essentially kidnapped, so that the authorities would be sure that he died on schedule.
The Catholic Church has always defended the primary rights of parents over the welfare and education of their children. Wherever those rights have been eroded, totalitarianism has not been far behind.
Indeed, it is no accident that Communism, Fascism, and other totalitarian ideologies have always sought first to sever the bond between parents and children. Once the family has been dismantled, it is an easy matter for the totalitarian state to fill the void.
The hospital and the courts may believe that they are doing what is best for Charlie. But in reality, their actions are at root totalitarian. They have robbed the parents of their natural rights, and set the state up instead as the final arbiter of life and death.
Rev. Patrick Mahoney, a U.S. pro-life activist who is spearheading protests in the UK on behalf of Charlie, warns that what is at stake in Charlie’s case is “universal.” The issue is, he says, “will parents be at the center of making decisions for their children? Or will those decisions be ripped from them by hospital officials, judges, and government bureaucrats?”
“This is not a liberal, conservative, or political issue at all. It’s a human rights issue,” he continued. “It’s the simple notion that parents should not be excluded and shut out from making critical decisions that impact the health and future of their children.”
The concerns and moral questions about this case will continue; meanwhile, Charlie and his parents deserve our steadfast support and prayer. Charlie’s parents have the best interests of their son at heart, and we must demand that the government respect their decision, as well as acknowledge and secure Charlie’s inherent dignity.
Micaiah Bilger Jul 7, 2017 | 10:45AM London, England
Claiming that birth control cuts abortion numbers is a favorite talking point of abortion groups like Planned Parenthood, but more and more studies are finding that this is not the case.
One of the latest reports comes from the abortion chain British Pregnancy Advisory Services (BPAS). According to the abortion group, half of the women who had abortions in 2016 in the UK were using contraception when they became pregnant, the Metro reports.
BPAS reports one in four of the women on birth control got pregnant while using methods considered to be the most effective, such as the birth control pill or the IUD.
Ann Furedi, CEO of BPAS and a late-term abortion advocate, claimed the data shows why women need easy access to abortions.
“Family planning is contraception and abortion. Abortion is birth control that women need when their regular method lets them down,” Furedi said. “When you encourage women to use contraception, you give them the sense that they can control their fertility – but if you do not provide safe abortion services when that contraception fails you are doing them a great disservice.”
The BPAS study involved its more than 60,000 abortion clients in 2016. In total, 51.2 percent of women said they were using at least one form of contraception when they became pregnant, according to the study. Of those women, a quarter said they were using a form of contraception considered to be at least 90-percent effective.
Previous studies have found similar results. A number of reports by the Guttmacher Institute, the former research arm of Planned Parenthood, also show that 55 percent to 60 percent of women having abortions were using contraception at the time.
And a ten-year study in Spain found that abortions increased as contraception use did:
[C]ontraception use increased by about 60%, the abortion rate doubled. In other words, even with an increase in contraception use, there weren’t fewer unwanted pregnancies, there were more.
Yet, Planned Parenthood leaders continue to claim their contraception work decreases abortions. Of course, their motivation in saying it is the hundreds of millions of tax dollars they receive each year.
Furedi at least was more honest about the data and her abortion goals. She said women deserve to know that contraception is not 100-percent effective, but she also touted abortion as the answer when contraception fails.
She wrote in the Telegraph: “The truth of the matter is that any society that values ‘planning families’ needs to value abortion services as part of the birth control package. Abortion is necessary as a supplement to contraception. If you have not been able to prevent a pregnancy, then you need to be able to end it – safely and easily.”
Killing a member of the family should never be a “value” promoted by society, though. Pro-lifers may have different opinions about the use of artificial contraception, but they all agree that family planning should never involve violence against another human being.
An abortion destroys a unique unborn baby’s life. By the time most women have abortions, their unborn baby’s hearts already are beating, and every unborn baby already has his or her unique DNA, unlike any other person’s in the world.
When I started nursing school 50 years ago, medical ethics was not a course but rather common sense principles incorporated into our education. There was no controversy about not harming patients, integrity, equality of treatment regardless of status, etc.
So, of course, abortion and euthanasia were unacceptable and even thinkable in those days.
I particularly remember one teacher who told us about the hypothetical situation of a child with Down Syndrome whose parents wanted to let their baby die and how we naturally had to put the interests of the child first. This kind of protection for patients was routine both ethically and legally in those days.
In 1982, I remembered that situation when Baby Doe, a newborn baby boy with an easily correctable hole between his esophagus (food pipe) and trachea (windpipe), was denied this lifesaving surgery by his parents and a judge because he also had Down Syndrome. Six days later, Baby Doe starved and dehydrated to death while his case was being appealed to the Supreme Court after the Indiana Supreme Court ruled 3-1 against saving him.
My husband, a doctor, and I were appalled when we first read about Baby Doe in the newspaper and my husband suggested that we adopt the baby ourselves and pay for the surgery.
I said yes but with some reluctance since I was already pregnant with our third child and our other children were just 5 and 3. But who else was better situated than us to care for a child with a disability who needed surgery?
In the end, we were too late to save Baby Doe. We found out that Baby Doe’s parents had already rejected the many other families who tried to adopt him.
Five months later, I gave birth to my daughter Karen who also happened to have Down Syndrome and a life-threatening condition that needed surgery. Karen was born with a complete endocardial cushion defect of the heart that the cardiologist told us was inoperable. We were told to just take her home and our baby would die within 2 weeks to 2 months.
I was heartbroken and cried for 3 days in the hospital before I finally got mad. My obstetrician never came back to check on me in the hospital even though I had a C-section and I demanded a second opinion on her heart condition in case the cardiologist was biased against children with Down Syndrome.
I insisted on leaving the hospital early with my daughter because I wanted as much time as possible with her and especially because I realized that I needed to research Karen’s heart condition to effectively advocate for her.
I joined the St. Louis Down Syndrome Association which helped me enormously, especially with my research and emotional support. Fortunately, it turned out that the initial prognosis was wrong and the cardiologist told us that Karen’s heart could be fixed with just one open-heart operation at age 6 months.
I was elated until the cardiologist told me that he would support my decision to operate “either way”, meaning I could refuse surgery just like Baby Doe’s parents.
I was furious and told him that the issue of Down Syndrome was irrelevant to Karen’s heart condition and that my daughter must be treated the same as any other child with this condition. I also added that if he were biased against people with Down Syndrome, he could not touch my daughter.
To his credit, this doctor recognized the injustice and because of Karen, he eventually became one of the strongest advocates for babies with Down Syndrome.
Unfortunately, I ran into other medical professionals caring for Karen who were not so accepting. One doctor actually told us that “people like you shouldn’t be saddled with a child like this” and another doctor secretly wrote a DNR (do not resuscitate) order against my instructions at the time. It was then that I realized that my so-called “choice” to save my daughter was really a fight.
Tragically, Karen died of complications of pneumonia when she was just 5 ½ months old and just before her scheduled open-heart surgery. I will always miss her but I am so grateful that I was her mother. Karen changed many lives for the better, especially mine.
I became active in the Down Syndrome Association, promoted President Reagan’s “Baby Doe” rules, provided babysitting/respite for many children with various disabilities, and even got a chance to talk to then Surgeon General C. Everett Koop about setting up a national hotline for new parents of children with disabilities to find resources.
But most importantly, I was determined to find out what had happened to medical ethics over the years since nursing school that resulted in the Baby Doe tragedy and hopefully help reverse the mindset that people with disabilities were “better off dead”.
What I discovered was a landmark 1979 book titled “Principles of Biomedical Ethics” written by Tom Beauchamp PhD, a professor of philosophy, and James Childress PhD, a theologian and also a professor of philosophy. Neither one had a medical degree.
Autonomy – The right for an individual to make his or her own choice.
Beneficence – The principle of acting with the best interest of the other in mind.
Non-maleficence – The principle that “above all, do no harm,” as stated in the Hippocratic Oath.
Justice – A concept that emphasizes fairness and equality among individuals.
Although all these principles were considered equal, it wasn’t long before autonomy became the cornerstone principle in ethics and law, ultimately leading not only to Baby Doe but also to the legalization of assisted suicide/euthanasia.
Ironically, all these principles have been used to justify cases like Baby Doe’s as well as assisted suicide/euthanasia.
Beneficence and non-maleficence have become a ways to see death as an actual blessing to real, perceived or potential suffering. Ominously, the justice principle has become the rationale for rationing under the guise of supposedly not wasting scarce healthcare resources .
CONCLUSION
35 years after Baby Doe, some things like medical technologies and education for people with disabilities are better but many things like assisted suicide/euthanasia have pushed the ethics of death even farther and are a threat to all of us and our loved ones.
The Baby Doe tragedy should have been a fire alarm for the evils we see today but it is never too late or impossible to try to promote a culture of respect for all lives.
Today marks the 25th anniversary of the Supreme Court’s decision in Planned Parenthood v. Casey. This case involved the constitutionality of several provisions in Pennsylvania’s Abortion Control Act and marked the only time that the Supreme Court formally reconsidered its holdings in Roe v. Wade. When the Supreme Court failed to reverse Roe in this case, it was a substantial setback for the pro-life movement. Still, the 25 years since Casey have been a story of substantial legislative, political, and legal progress for pro-lifers — progress that has occurred not only because of perseverance but also because the movement shrewdly used legal openings granted to them by the Casey decision.
The pro-life movement has devoted few resources to chronicling its own history, so not many people remember how much pro-lifers had invested in the Casey decision. During the early 1980s, pro-life political strategy shifted from enacting a constitutional amendment to changing the composition of the Supreme Court. At this time, a more conservative Supreme Court seemed almost inevitable, considering that Presidents Ronald Reagan and George H. W. Bush appointed a total of five new justices. As a result, a reversal of Roe v. Wade appeared not only plausible but even likely. That made the Supreme Court’s Casey decision particularly disappointing.
Following Casey, there were plenty more reasons for pessimism. The year 1992 saw the election of the first U.S. president publicly committed to keeping abortion legal. Annual abortion numbers had been gradually rising for much of the 1980s, and the number of abortions performed in 1990 surpassed 1.6 million. There was serious discussion about removing the anti-abortion plank from the Republican-party platform, and GOP governors who supported abortion rights — such as Christine Todd Whitman of New Jersey, William Weld of Massachusetts, and Pete Wilson of California — were heralded by many in the media as the future of the Republican party.
Even worse, in the early 1990s, pro-lifers were losing ground in the court of public opinion. Gallup surveys found that the percentage of people who felt that abortion should be “legal under any circumstances” had steadily increased since the 1970s. A 1995 Gallup survey found that only 33 percent of Americans identified as “pro-life.” Not even demographics appeared to offer much hope. Americans were becoming wealthier and better educated, both of which tended to correlate with “pro-choice” sentiment. All in all, there were good reasons to question the long-term political viability of the pro-life movement.
But the Casey decision contained a silver lining. Even though the Supreme Court did not overturn Roe v. Wade in Casey, it abandoned the trimester framework invented in Roe and instead adopted a doctrine of “undue burden.” This allowed for state regulation of abortion, as long as the regulation did not impose an “undue burden” on women seeking abortions. Under this new standard, the Casey decision upheld most of the provisions included in Pennsylvania’s Abortion Control Act, including the parental-consent provision, the reporting requirements, the waiting period, and the informed-consent language. Only the spousal-notification requirement was struck down.
The constitutional protection that Casey granted these laws, coupled with pro-life gains in numerous state legislatures since the 1990s, has led to a substantial increase in the number of state-level pro-life laws. Since 1992, the number of states with parental-involvement laws has increased from 20 to 37. The number of states with informed-consent laws pertaining to abortion has increased from 18 to 35. In recent years, 20 states have banned abortions that take place at or after 20 weeks’ gestation, based on the unborn child’s scientifically documented ability to feel pain. Even more important, after Casey, many states strengthened existing pro-life laws. In particular, several states improved their informed-consent laws by including more information about health risks, fetal development, and sources of support for single mothers.
The incremental strategy has paid dividends. Research shows that public-funding restrictions, parental-involvement laws, and informed-consent laws all reduce abortion rates.
This incremental strategy has paid a variety of dividends. A growing body of peer-reviewed research shows that public-funding restrictions, parental-involvement laws, and properly designed informed-consent laws all reduce abortion rates. Furthermore, the ongoing debates about these incremental laws — many of which enjoy broad public support — have succeeded in reframing the abortion debate in terms more favorable for pro-lifers. Indeed, many of the most worrisome trends of the early 1990s have reversed themselves. It is now Democrats who appear more conflicted over their party’s platform on abortion. The pro-choice Republican governors who were once thought to be the future of the party have largely vanished from the political scene.
Additionally, the pro-life position has been gaining public support. Seventeen of 18 Gallup polls from 1995 to 2008 showed a pro-choice plurality. But Gallup polls from both 2009 and 2012 found that a majority of Americans described themselves as “pro-life.” And those numbers are likely to grow even more in the future. During the 1970s and 1980s, many surveys showed that young adults were likely to favor abortion; since 2000, however, the General Social Survey (GSS) found that young adults are the age demographic most likely to oppose legal abortion.
Most important, the number of abortions is steadily declining. Since 1990, the number of abortions performed in the United States annually has declined by about 42 percent. The latest reported abortion rate from 2014 is half of what it was in 1980 and is even lower than it was in 1974, the year after the Roe v. Wade decision. Interestingly, the unintended-pregnancy rate has remained fairly constant over the long term. The decline in abortions is driven by the fact that a higher percentage of women facing unintended pregnancies are carrying those pregnancies to term. Clearly, pro-life legislative and educational efforts have succeeded in changing hearts and minds.
At some point, the Supreme Court will reconsider its holdings in both Roe and Casey. Predicting judicial rulings is far from an exact science. The Supreme Court may well decide to overturn Roe v. Wade. However, even if Roe is upheld, there is a good chance the Court will continue to allow for greater state-level regulation of abortion. It will be up to the next generation of activists to effectively use future legal openings to advance the culture of life.
Doctors in the United States cannot be forced to perform abortions or assist suicides. But that may soon change. Bioethicists and other medical elites have launched a frontal assault against doctors seeking to practice their professions under the values established by the Hippocratic Oath. The campaign’s goal? To force doctors, nurses, pharmacists, and others in the health field who hold pro-life or orthodox religious views to choose between their careers and their convictions.
Ethics opinions, legislation, and court filings seeking to deny “medical conscience” have proliferated as journals, legislative bodies, and the courts have taken up the cause. In the last year, these efforts have moved from the relative hinterlands of professional discussions into the center of establishment medical discourse. Most recently, preeminent bioethicist Ezekiel Emanuel—one of Obamacare’s principal architects—coauthored with Ronit Y. Stahl an attack on medical conscience in the New England Journal of Medicine, perhaps the world’s most prestigious medical journal. When advocacy of this kind is published by the NEJM, it is time to sound the air raid sirens.
The authors take an absolutist position, claiming that personal morality has no place in medical practice. Under the pretext of “patients’ rights” and a supposed obligation of doctors to adhere to the medical moral consensus—a tyranny of the majority, if you will—Emanuel and Stahl would prohibit doctors from conscientiously objecting to performing requested procedures on moral grounds. From “Physicians, Not Conscripts—Conscientious Objection in Health Care” (my emphasis):
Making the patient paramount means offering and providing accepted medical interventions in accordance with patients’ reasoned decisions. Thus, a health care professional cannot deny patients access to medications for mental health conditions, sexual dysfunction, or contraception on the basis of their conscience, since these drugs are professionally accepted as appropriate medical interventions.
This includes human life–taking actions such as abortion:
[A]bortion is politically and culturally contested, it is not medically controversial. It is a standard obstetrical practice. Health care professionals who conscientiously object to professionally contested interventions may avoid participating in them directly. … Conscientious objection still requires conveying accurate information and providing timely referrals to ensure patients receive care.
This would mean that a Catholic doctor who opposes contraception would have to prescribe it or find a doctor willing to fill out the prescription—even if she informs her patients before being retained that she practices medicine in accord with her church’s moral teachings. It would also require a pro-life OB/GYN who refuses to terminate a pregnancy to find an abortionist, thus becoming complicit in the act. The authors would still allow doctors to decline to assist suicides—for now—but only because that practice is not yet accepted generally within the medical community. If euthanasia ever does becomes generally accepted—as it is now in the Netherlands, Belgium, and Canada—under the Emanuel/Stahl rule, dissenting physicians would be required to participate in homicide.
Emanuel and Stahl would drive noncooperating doctors out of medicine (my emphasis):
Health care professionals who are unwilling to accept these limits have two choices: select an area of medicine, such as radiology, that will not put them in situations that conflict with their personal morality or, if there is no such area, leave the profession.
Shattering medical conscience rights would also dissuade those who hold officially unwanted values—orthodox Catholics and other Christians, Jews, Muslims, and pro-lifers—from entering medical school in the first place. There is a method to this madness: The goal is to cleanse healthcare of all those who would dare to practice medicine in accord with sanctity-of-life moral viewpoints.
The attacks on conscience have already moved beyond mere intellectual advocacy. The government of Ontario, Canada is on the verge of requiring doctors either to euthanize or to refer all legally qualified patients. In Victoria, Australia, all physicians must either perform an abortion when asked or find an abortionist for the patient. One doctor has been disciplined under the law for refusing to refer for a sex-selective abortion. In Washington, a small pharmacy chain owned by a Christian family failed in its attempt to be excused from a regulation requiring all legal prescriptions to be dispensed, with a specific provision precluding conscience exemptions. The chain now faces a requirement to fill prescriptions for the morning-after pill, against the owners’ religious beliefs. In Vermont, a regulation obligates all doctors to discuss assisted suicide with their terminally ill patients as an end-of-life option, even if they are morally opposed. Litigation to stay this forced speech has, so far, been unavailing.
The ACLU recently commenced a campaign of litigation against Catholic hospitals that adhere to the Church’s moral teaching. For example, it sued a Catholic hospital that refused to sterilize a woman in conjunction with her caesarian section. That lawsuit failed. Undaunted, the supposed guardians of civil liberties—except the free exercise of religion, it seems—recently brought a case against a Catholic hospital for refusing to permit doctors to perform an elective hysterectomy as part of a sex-reassignment surgery.
There is a reason that moral diversity is under attack in health care. When doctors refuse to abort a fetus, participate in assisted suicide, excise healthy organs, or otherwise follow their consciences about morally contentious matters, they send a powerful message: Just because a medical act is legal doesn’t make it right. Such a clarion witness is intolerable to those who want to weaponize medicine to impose secular individualistic and utilitarian values on all of society.
Wesley J. Smith is a senior fellow at the Discovery Institute’s Center on Human Exceptionalism. He is also a consultant to the Patients Rights Council.
If you’ve read any of my posts, you know that this is one of the questions that pervades my work. Do we really know what we think we know? More often than not, the answer is no. Upon examination, what we hold true falls short. In the field of pharmaceutical medicine, where money plays an enormous role in determining what is known about a particular drug, finding the real and honest truth about a medication is difficult and sometimes impossible. Hormonal contraception, because it has been on the market for decades and because as women we really want it to be safe and absent negative side effects, is one of those drugs where what we think we know and what we actually know are two entirely different things.
Over the last few years, we have been commission for a two studies on the safety of hormonal contraceptives. One study, the Real Risk project, ended early due to a loss of funding. As a result, Phase 2 data were never analyzed. (We decided to continue collecting data in the hopes of finding funding to complete the study at some point. We haven’t found the funding yet.) Nevertheless, we learned a lot and what we learned should be public. Slowly, some of that information is making its way into blog posts.
Below is a portion of the final report, covering the history of the pill, a sort of ‘what they knew when’ of side effects. Looking back at the history of the development of the pill and other forms of hormonal contraception, it becomes clear that the health and safety of the female population was not a primary objective. Indeed, more often than not, the serious side effects were ignored, particularly in the US, setting the precedent for the almost total acceptance of the drug’s safety that we see today. As a woman who used hormonal birth control and developed many of the side effects noted by early researchers, side effects that were ignored by my physicians, reading this is eye-opening. If I had known then what I know now, I would have never used this drug.
Early on, British researchers noted significant changes in blood clotting mechanisms in the women using oral contraceptives compared to those who did not, but also compared to pregnant women. Hormonal birth control, it appeared, increased several pro-clotting factors while simultaneously decreasing anti-clotting factors; changes in hemodynamics that were in many ways, though not entirely, akin to late pregnancy and early postpartum where blood clots are known risks. This was in addition to systemic vessel wall damage that simultaneously set the stage for both clotting and hemorrhage. They also found that clot risk increased over time and was compounded by other variables such as exercise and smoking. In 1967, based upon the results of three studies, the British Medical Research Council issued a preliminary communication that stated:
“The sum of the evidence, however, is so strong that there can be no reasonable doubt that some forms of thromboembolic disorder are associated with oral contraceptives. The association is particularly strong in the group of women with no known medical condition predisposing to thrombosis.”
Politics and Money Rewrite History
These findings, though clearly implicating hormonal contraceptives in thrombosis, became immediately controversial and were all-but-entirely dismissed by American medical societies who argued an inherent difference between British and American women (NPH pages 6222-6259); one that supposedly predisposed British women more strongly towards blood clots than their American counterparts.
Additionally, according to testimony made in the Nelson Pill Hearings, the American Medical Association allowed industry experts to write and publish the early safety statements while simultaneously refusing to publish research and case reports indicative of risk (NPH page 6113). G.D. Searle, one of the early manufacturers of oral contraceptives, went so far as to ‘vote away’ the risk of thrombosis at a medical conference (NPH pages 6108-6133). Sales and marketing materials were designed to dismiss the risk and obfuscate the research (NPH pages 6218-6296). This led American doctors, researchers, and the population as a whole, to presume falsely that the pill was safe and without risks. It bears noting that by failing to publish the evidence implicating the pill in thrombosis and by allowing industry experts to write and publish the safety reports, the American Medical Association set the precedent for what has now become a complete abrogation of scientific and medical ethics, not only regarding contraceptives, but also, for every other drug on the market.
Beyond Thrombosis: System Wide Side Effects
A persistent notion in contraceptive research is that progesterone and estradiol, the two hormones mimicked in contraceptives, are singularly involved with reproduction. What follows is a presumption that these hormones have no impact on other tissues and altering them affects nothing but the intended target. Contrary to this popular belief, these steroid hormones are not solely involved in reproduction. Hormone receptors are distributed throughout the brain and the body, on every organ, in every tissue, and in every fluid. Hormones, thus, regulate every physiological system. When synthetic hormones bind to endogenous or native hormone receptors, they effectively override the body’s natural regulatory functions in ways we have yet to comprehend fully. It is not unexpected then that the use of hormonal contraceptives would have broad based effects. Thus, in addition to the higher incidence of thrombotic events in otherwise healthy women, physicians and researchers testifying at the hearings noted clear associations between the use of hormonal contraceptives and a broad array of disease processes. Some of those effects are highlighted below.
Metabolic Disturbances
Perhaps some of the least well-recognized effects of these hormones include those to a woman’s general metabolism. Hormonal birth control induces wide ranging metabolic disturbances in insulin and glucose regulation, lipid control, and in heart rate, rhythm and pressure leading to weight gain, diabetes, high blood pressure, and cardiovascular disease. One researcher testified accordingly:
“There are more than 50 ways in which the metabolic functions of the body are modified, and to say therefore that normal physiological function has been demonstrated in the years of oral contraception is to overlook a very large amount of information (Dr. Victor Wynn, NPH page 6311).”
“When I say these changes occur, I mean they occur in everybody, more in some than in others, but no person entirely escapes from the metabolic influence of these compounds. It is merely that some manifest the changes more obviously than others (Dr. Victor Wynn, NPH page 6303).”
And yet another said:
“These alterations, which have been demonstrated, include changes in carbohydrate metabolism, fat metabolism, protein metabolism, and the endocrine, liver, nervous and vascular system, among others. The findings are straightforward and reproducible (Dr. Hilton Salhanick, NPH pages 6382).”
Impaired Reproductive Capacity
Impaired reproductive capacity, likely due to the pill’s effects on the pituitary gland and its ability to prevent ovulation was noted (Dr. James Whitelaw, NPH pages 6009-6019). Case studies presented by the physicians indicated use of hormonal birth control often delayed fertility while the body re-adjusted to its non-pill state. In at least 1-2% of the women who used the pill, however, it caused permanent infertility. Ovulation never resumed. Additionally, women who used the pill were more prone to miscarriage, stillbirth, and chromosomal abnormalities in the offspring; abnormalities that as one researcher indicated were:
Beyond the immediate effects to fertility and reproduction, early researchers postulated potential transgenerational effects. That is, when women use hormonal contraceptives, ovulation is suppressed unnaturally and germ cell damage to the ovarian follicles is possible: damage that may not only express itself in the first generation, but also in subsequent generations, e.g. in her grandchildren and great grandchildren.
“An unequivocal abnormality produced by estrogen-progestogen is the suppression of ovulation itself. It is only reasonable to consider the ultimate fate of the ovum that would have been normally released from the ovary. We do not know whether the ovum dies or survives. If it survives, is it altered in any way?”
Cancer
One of the most damning, but again disregarded and disputed, findings of the early researchers was the association between hormonal birth control and cancer. Researchers testifying at the Nelson Pill Hearings noted that cancer developed in all animal models tested when oral contraceptives were administered. In fact, the use of synthetic estrogens is banned in animal husbandry in Europe because it causes cancer in the animals and also in the workers. In the US, there is no such ban, owing partly to the decades delay in cancer onset but mostly to industry lobbying.
“I think here is the proper place to point out that when we talk about the pill being used by 18 million people in the prime of life throughout the world, we are in fact considering an internal pollution, the extent of which is not yet known, but the nature of which is indeed known. And we are threatening the destruction of a large segment of one of our most precious natural resources, the young women of our society (Dr. J. Harold Williams, NPH pages 6219).”
Liver
Liver function, because of its role in drug metabolism and detoxification, is inevitably altered by the use of any medication. To what extent the liver is impacted, is a key safety issue reviewed during drug approval considerations. As one might expect, hormonal contraceptives degrade liver function. At the hearings, researchers testified to four key changes in liver function.
A 40% reduction in the ability to clear sulfobromophatalein (a compound used to test liver function)
An increase in liver enzyme activity (a marker of liver damage) in 20% of the women who use hormonal contraceptives
Jaundice in 1 in 10,000 women that subsided after discontinuation of OC (Dr. Philip Corfman, NPH Pages 6391-6426)
Reduction in total plasma protein level (Dr. William Spellacy, NPH Pages 6426-6445)
Overall, the changes in liver function were summed up as follows:
“The immediate effects include the alteration of several of the laboratory tests used in medical diagnoses. Aggravation of existing liver disease, if present, to the point where jaundice may be seen has also been shown. There is no answer to the query of will permanent liver damage result from the use of the oral contraceptives.”
We have yet to answer the question of permanent damage, although a large study in 1997 suggests that liver damage abates upon cessation.
Disturbed Immune Function
One of the most commonly recognized but simultaneously disregarded effects of hormonal contraception include disturbances in immune function. Autoimmune diseases such as lupus and rheumatoid arthritis are significantly more common in women than men, especially in women who use hormonal contraceptives. Once again, the onset and increased incidence post-pill use was noted as soon as these medications hit the market, but because of the complexity of these diseases, all but disregarded. Early researchers noted that with new onset cases once contraceptive use ceased, symptoms resolved and most patients remained symptom free for at least the 2.5 years of the study period (Dr. Giles Boles, NPH pages 6086-6108). In recent years, awareness of this connection has increased somewhat.
“Over the past three years we have seen 22 young women who… after beginning oral contraceptives developed [arthritic symptoms]. The joint swelling was usually limited to the hands. On cessation of the oral contraceptive, the symptoms disappeared… We specifically inquire as to the use of oral contraceptives in all young women we see with rheumatic complaints…”
In addition to the increased incidence of autoimmune diseases associated with hormonal contraception, other immune system changes were noted, and again, dismissed.
“The Pill, by interfering with the natural secretions of the vagina, leaves women susceptible to a variety of infections, including syphilis and gonorrhea. Those who use the Pill develop VD, other sexually transmitted infections, and vaginitis twice as often as the female population as a whole.”
Perhaps one of the more disturbing findings regarding hormonal contraceptives is their role in new onset psychiatric illness and their capacity to induce suicide. In the original trials, at least one women committed suicide while taking the pill. Her case, along with at least 18 other deaths (Dr. Edmond Kassouf, NPH pages 6108-6133), was omitted in the reports filed to the FDA.
“There is considerable incidence of mild to moderate psychiatric morbidity [disease] associated with the use of combination oral contraceptive agents… In three of the four studies, there seems to be agreement that those who have required psychiatric care in the past will be more at risk for the development of morbidity, including psychosis. One study also suggests that there may be some increase in the depth of illness the longer the medication is taken (Dr. Francis Kane, NPH page 6457).”
“The emotional or psychiatric problems are the complications which seem to me to have the most serious potential danger. Three patients have stated that they were desperately afraid that they were going to kill themselves… After the pills were omitted, the depression and suicidal fears of the three patients disappeared, as did the depression of the other patients (Dr. John McCain, NPH page 6473).”
“It is disturbing to consider the patients on the pills whose depression may have ended in suicide and/or homicide with no recognition of any association with the contraceptive pills… Personality changes could be a factor in other conditions such as automobile accidents and divorces (Dr. John McCain, NPH page 6473).”
Despite the early research, connections between hormonal contraceptives and mental health have been largely ignored. In fact, since the nineties, hormonal contraceptives have been marketed specifically for depression and anxiety in direct opposition to the data suggesting these medications cause and/or exacerbated psychiatric illness. As recently as three years ago, an epidemiological study suggested,
“…a protective association between hormonal contraceptive use and depressive symptoms, as well as suicide attempts, in a population-based sample of young, sexually active US women.”
Fortunately, the tide appears to be changing. Fifty years after the release of these medications and after generations of women have complained of serious mental health issues while using hormonal contraceptives, a large study published definitive data indicating that hormonal contraceptives did indeed induce depression, especially in adolescents. No doubt, industry sponsored studies will surface shortly and contradict these findings.
That there are over 200 brands currently available on the market worldwide, suggests an abundance of options, but from a pharmacological standpoint, not much has changed in hormonal contraceptive technology over the last half century. The predominant estrogen used in contraceptives remains the same as was developed decades ago, a compound called ethinyl estradiol (EE2). With the exception of the fourth generation progestins, the progestins used in modern contraceptives involve only slight modifications to the original compounds. Even the ‘newer’ delivery methods, like the intrauterine device and the cervical ring, were developed decades ago, in the 1950s and 1960s. For all practical purposes, contraceptive technology remains as it was over half a century ago. Therefore, today’s contraceptives carry as many or more of the side effects and risks as their predecessors did.
Only now, our increased familiarity with these drugs has fostered a deeply ingrained but false sense of safety. Phrases suggesting that after 50 years on the market these are among ‘the most studied medications’ pepper the literature. When in fact, these medications were never studied properly before their release:
“Evidently, for whatever reasons, there is no sound body of scientific studies concerning these possible effects available today, a situation which I regard as scandalous. If we proceed in the future as we have in the past, we will continue to stumble from one tentative and inadequately supported conclusion to another, always relying on data which come to hand, and which were not designed for the purpose (Dr. Paul Meier, NPH pages 6548-6560).”
And they have not been studied conclusively since. For all intents and purposes, safety issues associated with hormonal birth control remain largely under-investigated and unrecognized. What research exists generally favors commercial interests, and if we’re honest, our interests as women. We want easy, safe and effective birth. We need it and so we ignore the side effects and ignore any research that confirms our suspicions. We allow ourselves to accept the risks. Maybe it’s time we didn’t. Maybe it’s time we dig in and find out what is really going on and then fix the problems.
The family is the most sexual of all organizations. But given the sexual chaos of modern times, new families who want to succeed in their task of child-raising must quickly find a community of other families of like mind. They are most likely to find such families at their place of worship if the sexuality taught there is a family and child centered sexuality.
The data show (see chart below) that central to family sexuality is an ethos of chastity, necessary for marital unity and stability and out of which flow myriad benefits. Without chastity the family is no more a thriving family than a monastery without celibacy is a monastery.
Chastity is now central to the public argument for religious freedom because such families need their freedom of association and freedom of action to raise the next generation to live the same strong family life. They need freedom to teach their own way of life: marriage till death do us part, and raising their children to do the same. Much as the Amish fought and won their freedom of association and way of life, so too other religious communities are now finding they too must fight and win a freedom which they had assumed was theirs without asking. It had been so. It is no longer.
If we want our religious freedom we have to be able to make the argument for teaching chastity as a way of life, not as a “risk reduction strategy”. Chaste family life is easy to defend in the public debate because it is far superior to all other ways, by any measure of human thriving. Teenagers (who have yet to experience life and learn its hard lessons by experience) need to understand that there are lifelong consequences for “sowing wild oats”, as the most important chart in all the social sciences makes clear:
They need to be very familiar with the data (with the lessons of life experience) that the totally monogamous couple (only sexual partner ever: their spouse) is the least likely to divorce – by far. And that one third of women who have had only one other sexual partner (normally before marriage) are likely to divorce within five years, and that those who had two such sexual partners (other than their husband – again most likely before marriage) have a fifty percent chance of divorce within five years — and that half of their children will be raised without their father present.
Chastity may be difficult but it is central to a family-centered life. And it is also central to justice for children. There is no free lunch on this issue, not for teenagers, adults nor for society itself.
If churches and parents do not make the strongest case possible for the chastity-based family (and on its fruits and benefits it is an easy case to make) they will not get their religious freedom.
The rest of society may think such families are weird (despite the data) but they will likely respect them for the path they have chosen.
The future of the First Amendment rests on the freedom to teach the centrality of chaste family life. We will not win I if we are ambivalent or shy.
Pat Fagan is the director of the Marriage and Religion Research Initiative at The Catholic University of America. He is publisher and editor of Marripedia.org. Republished from the MARRI blog with permission.
Secular Pro-Life’s conference booth was set up just a few yards away from our friends at Rehumanize International, with whom I also shared a hotel. Quick plug: their latest project is Create | Encounter, which wants your visual art, creative writing, musical works, etc. related to any and all life issues. Submissions are due July 31; details here.
Saturday
The program opened with Lacey Buchanan, who spoke about her experience as a mother. Her son, Christian, has an extremely rare disability. Among other things, his eyes never developed. She struggled with people who’ve stared at Christian, made insensitive comments, and even attacked her as a “bad mother” for not aborting him! But the family has persevered, and the more she publicly advocates for him, the better it’s gotten. She had a wonderful message about the inherent worth and dignity of every person.
Next up was a panel of women who had all received poor prenatal diagnoses. Some did indeed give birth to children with disabilities; in other cases, the doctors turned out to be wrong. All of them described immense pressure from their doctors to abort, even after repeated refusals. One asked for a note to be placed in her chart that she was keeping the baby and did not want to hear any more abortion talk, to no avail. The most moving story came from a woman who received a scary initial test result. She asked the doctor for more testing, and was told “The only test I’ll perform on your daughter is an autopsy.” After sharing this, she asked her daughter to please stand—she was there attending the conference, 19 years old and perfectly healthy!
After lunch, there was a panel of pro-life physicians. Much of the discussion focused on natural family planning (NFP): what it is, and what it isn’t. Specifically, it is not the rhythm method, and it is not just having a period tracker app on your phone! Effective natural family planning methods use personal indicators like cervical mucous and temperature readings to determine when you are ovulating, as opposed to when the “average” woman in an “average” cycle is ovulating. NFP allows women to either avoid pregnancy or try to conceive, and charting also offers doctors insight into underlying hormonal issues that may be treatable. The panelists were religious, and opposed hormonal birth control for a mix of medical and religious reasons, but noted that NFP can benefit women from all walks of life. This led to the memorable line “Atheists have cervical mucous too!” (Can confirm.)
Two breakout sessions were scheduled for the afternoon. All the speakers and topics looked interesting, and it was hard to pick. For the first session, I attended a presentation on pregnancy loss from a woman who had experienced seven miscarriages/stillbirths at various gestations. She shared that she was well supported when she lost a child later in pregnancy; people brought her meals and sent sympathy cards and listened. But that was not the case when she miscarried early, and that hurt. The pro-life community needs to step up in those situations, and we shouldn’t expect women’s grief to follow the classic linear “seven stages.” Life is much messier than that.
The second breakout session I attended focused on sex trafficking. The speaker was a social worker who shared (with names changed, of course) how her clients, often young teens, were recruited into prostitution rings through a combination of seemingly legitimate job opportunities, manipulation, and force or the threat of force. Helpful tip for pregnancy care centers: trafficked women and girls are often supervised by a handler, except when they are in the restroom. When a client goes to the ladies room to take a pregnancy test, give her the opportunity to tell you what is going on. This can be accomplished with a sign and a message box. Naturally the message box must be checked after each pregnancy test.
Sunday
The morning’s keynote speaker was Melissa Ohden, who shared her story of surviving a saline abortion, growing up in a loving adoptive home, and eventually reconnecting with her birth mother—who, as it turned out, had been coerced into the abortion by her mother, Melissa’s grandmother. You can read more about Melissa’s incredible journey here.
Next up was a panel entitled “Engaging the Black Community.” Much of it was church-focused, which is not surprising given the large role Black churches play in social and political life. But here’s an important takeaway for the pro-life movement in general: be mindful of Martin Luther King Day! It often falls on or near the anniversary of Roe v. Wade, when we have memorial events and rallies planned. But Planned Parenthood is attending the MLK events, and if we aren’t, we’re giving the abortion industry a free pass. Schedule accordingly.
The final event of the conference was also one of the most moving. Seven birth mothers shared their pregnancy and adoption stories. They were incredibly diverse; some never considered abortion, others wavered back and forth, and others were dead set on abortion until a pro-lifer changed their mind. One woman was incarcerated during her pregnancy and gave birth in shackles, a terribly inhumane practice that everyone, whether pro-life or pro-choice, should oppose. There were many adoptive parents and adoptees in the audience, and the Q&A was truly beautiful.
Throughout the weekend, I had the opportunity to network with like-minded women from all over the country, and I also got to hold three different babies. This is the most mom- and child-friendly conference on the planet. Whenever a mom needed a break, there was a line of people volunteering for a shift. If you want to see what pro-life means in practice, this is it! The date for the 2018 conference is TBD (I assume it will be sometime in the summer), but the location has been announced: St. Louis, MO. See you there!
LifeNews Note: Kelsey Hazzard is the head of Secular Pro-Life and this article originally appeared at its blog.
June 26, 2017 (HLI) — Most Catholics reject the Church’s teaching on contraception not because they’ve carefully considered it but because they’ve never had to do so.
When someone hears that the Catholic Church has a teaching about contraception, a common response is “Why?” Since this crucial teaching is so rarely given in venues where everyday Catholics can hear and consider it, there is widespread ignorance of, and therefore rejection of, the Church’s teaching.
This teaching dates back many centuries but was reiterated and expanded in Pope Paul VI’s Humanae Vitae in 1968. Following continued confusion and widespread rejection of this teaching, Pope John Paul II shed further light on this teaching in his encyclical Evangelium Vitae and a series of Wednesday audiences over several years, which has come to be known as The Theology of the Body. Here we offer a brief introduction to a beautiful teaching that we believe, when understood, will be embraced with great joy.
Why is the Church always saying ‘no?’
The Church has the solemn responsibility to uphold truth, and to do so with love. She has a vested interest in the good of both Catholics and non-Catholics, so she seeks the “common good” of all in society. Her teaching regarding contraception is made “in the light of an integral vision of man and of his vocation, not only his natural and earthly, but also his supernatural and eternal vocation” (Humanae Vitae 7).
We have been made by God and for God, and the Church proposes the truths necessary to aid men and women to live this life so that they might enjoy eternal life with Him. The Church teaches because she loves everyone who, as Scripture reminds us, is set free by the truth both in this life and for the next.
Despite what most people hear about Church teaching through other sources – that it is just a bunch of “nos” to good things – the Church’s teaching about contraception is based on her teaching about sexuality and marriage, which is primarily an affirmation of great goods to which the Church proclaims a resounding “Yes!”
The true meaning of marriage
Scripture affirms that marriage is not a man-made institution, but an institution of nature that has been divinely ordained by God. Marriage is a beautiful lifelong covenantal relationship between one man and one woman, and it is exclusive and open to new life. It is “the wise institution of the Creator to realize in mankind His design of love” and the marriage between the baptized has been raised by Christ to the dignity of a sacrament (HV 8).
Through marriage, spouses enrich one another’s lives through union in love, and so that their mutual love might give rise to new life. This is expressed beautifully in the Book of Genesis by Adam who, upon seeing Eve, exclaimed “at last this one is bone of my bone and flesh of my flesh;” and our understanding of marriage is enriched further by God’s first command to “be fruitful and multiply.” (Gen 1:28)
What does the Church teach about contraception?
The marital act is and must always remain open to new life, therefore the union of spouses through conjugal love must never be deliberately closed to life or love. As Pope Paul VI explained, “The Church … teaches that each and every marital act must of necessity retain its intrinsic relationship to the procreation of human life” (HV 12). In God’s divine plan, the marital act unites spouses in love and gives rise to new life. God has established an “inseparable connection” between these unitive and procreative purposes of marital love, so when a couple rejects one of these beautiful purposes of their sexual union they harm their spouse and their marriage, even if their intentions are good.
Contraceptive intercourse involves a choice against the possibility of new life so as to prevent pregnancy. It deliberately makes infertile a sexual act within marriage that should be fertile. The couple who freely and knowingly does this commits a mortal sin.
Contraception is “anti-life”
Contraception contributes to a culture of death by creating an environment in which children are treated as an unwelcome burden, an impediment to personal goals, or even worse, an enemy to be avoided at all costs. This negativity toward new life which is part and parcel of the “contraceptive mentality,” and is why so many children conceived are considered an “accident,” “unplanned,” or “unwanted.”
Blessed John Paul II noted that contraception and abortion are “fruits of the same tree.” “Indeed,” he writes, “the pro-abortion culture is especially strong precisely where the Church’s teaching on contraception is rejected” (Evangelium Vitae 13). Recent studies have confirmed something that may seem counterintuitive, but was actually predicted by the leadership of Planned Parenthood as contraception achieved wider acceptance: higher rates of contraception use do not reduce demand for abortion but rather lead to an increase in abortion because abortion becomes a sort of “Plan C” after a woman becomes unexpectedly pregnant following the type of behavior that naturally leads to pregnancy.(i) This self-ignorance affects women’s identity, and distorts male/female relationships as sex becomes detached from its natural end, becoming meaningless and leading toward an attitude of using the other person for one’s own enjoyment.
It’s not just about potential new life, but about love
Recall that Jesus revealed to us on the Cross that the true and full nature of love is that love is self-gift. Husbands and wives are called to foster love and unity within their marriage. Every couple seeks marriage precisely because they ardently desire to love deeply and fully. But love is more than a feeling: it is a choice and it is hard. Instead of facilitating love, contraception actually makes it more difficult to love.
In The Theology of the Body, Blessed John Paul II explains that we communicate with our bodies. Marital intercourse (without contraceptives) allows for spouses to fully give and receive one another – there are no barriers, there is no withholding of self from one’s beloved. With contraceptive intercourse, however couples reject one another’s fertility, protecting themselves from one another, and withholding a full gift of self. John Paul emphasized that “(W)hen the conjugal act is deprived of its inner truth because it is deprived artificially of its procreative capacity, it also ceases to be an act of love.” Contraceptive intercourse is incapable of the complete gift of self that married couples truly desire. Ultimately, contraception is opposed to love.
Does this mean we have to breed like rabbits?
Not at all. Following the teaching about “responsible parenthood” in Humanae Vitae and previous Church documents, John Paul stressed that, “unfortunately, Catholic thought is often misunderstood on this point, as if the Church supported an ideology of fertility at all costs, urging married couples to procreate indiscriminately and without thought for the future. But one need only study the pronouncements of the Magisterium to know that this is not so.” When couples have serious reasons to postpone having children they may do so by abstaining from intercourse periodically by using “Natural Family Planning” or “Fertility Awareness.”
Spouses must prayerfully and responsibly decide when to have children, while always maintaining a generous commitment to being open to new life and complete love.
(i) Malcolm Potts, M.D., Medical Director of the International Planned Parenthood Federation, in 1973. Quoted in Andrew Scholberg, “The Abortionists and Planned Parenthood: Familiar Bedfellows.” International Review of Natural Family Planning, Winter 1980, page 298.
June 22, 2017 (LifeSiteNews) — I was scrolling through the news on our publicly funded CBC website the other day and, when I clicked on one video for a story, I had to first watch a 15-second advertisement (this one funded by the government of Ontario). The ad may seem tame enough to the average viewer, but it was shocking to me and left me with many different questions and thoughts.
A few thoughts swimming through my head after watching the ad:
What in the world is a cash-strapped province doing advertising birth control? How much did they spend on creating and on airing this ad?
Why advertise one choice over another when it comes to having children? Why sell (which is what ads do) childlessness over having and nurturing children? (I’m not saying the government needs to do the latter, just questioning why they chose to do the former at the expense of the latter.)
Connected with selling childlessness, the attitude toward children in this ad is pretty deplorable. I can’t imagine anyone with children or hoping for children even dreaming up such an ad. Take it from a guy who, with my wife, desires to have more kids: this ad is pretty offensive. It plays to a terribly self-centered attitude of being able to mindlessly scroll your phone and sip your latte without a care in the world, and certainly without what this ad portrays as the annoyance and hassle of kids.
Not only is Ontario broke, its fertility rate is terribly low, well below the replacement level of 2.1 children per couple. The social and economic costs of this demographic trend are severe. It appears that the current government is either blind to these costs or willing to promote the trend despite the costs.
My colleague suggested I leave this one alone, but I do wonder: Why did they choose to portray the child as red-haired? This minority happens to suffer much higher rates of bullying than other kids. The casting of a ginger child struck me as an intentional choice to emphasize the point of the ad, which is: “You don’t want one of these!”
The message of the ad is pretty obvious: “Isn’t life gonna suck with a kid? Make sure you get your birth control!” Basically the opposite of “Behold, children are a heritage from the Lord, the fruit of the womb a reward” (Psalm 127).
I find the ad tasteless, a waste of money, displaying terrible moral judgment, and well outside the role of government. I hope we don’t see any more of these ads. If you agree, maybe send your Ontario MPP a respectful note.
DES MOINES, Iowa, June 21, 2016 (LifeSiteNews) — Katie Buck felt that any moment she was about to completely lose it as she sat in the hospital room listening to the devastating words of the doctor. The 29-year-old mother suddenly felt as if she was living somebody else’s life, or like she was having a bad dream from which she could not wake up. Her precious newborn baby was going to die. The baby she had carried within her womb for 37 weeks and who she had born into the world just days ago would no longer be there for her to hold, to love, to kiss. She felt her world come crashing down around her.
It was just three days prior to this that doctors had decided to induce Katie, even though it was three weeks before her due date. Scans had revealed that her little baby was not developing properly. He was too small. And to make matters worse, the flow of blood through his umbilical cord that delivered life-giving nourishment and oxygen was somehow restricted.
Alexander Buck shortly after his birth.
While the birth went well, Katie and her husband Ryan could immediately tell that not all was right with their little boy, whom they had named Alexander before he was born.
“He had some low-set ears. He had an extra thumb. The shape of his head was a little off,” Katie told LifeSiteNews. “You could just tell that something was going on.”
The parents had refused genetic testing earlier in the pregnancy on principle, believing it to be discriminatory against disabled people. They had decided to love and respect any baby that came to them, whether the baby had problems or not.
Blood tests were carried out on the tiny four-and-a-half pound Alexander, but the results were not fast coming. And then, three days after his December 8 birth, the doctor walked into Katie’s room to tell her what the tests had found.
‘Not in his best interest’
Alexander had Trisomy 18, a condition where there are three copies of chromosome 18 instead of the normal two. The condition often disrupts the baby’s normal pattern of development, often causing life-threatening problems including defects in the heart, lungs, kidneys as well as other developmental problems. A large majority of babies with this condition die within the first year.
As she sat now in the Des Moines hospital room listening to the doctor, Katie was having trouble taking it all in. Words became jumbled. It was all too surreal. She asked the doctor to wait until her husband arrived to finish what he had to say.
When Ryan arrived, he found his wife totally distraught. Katie pleaded with him to go with the doctor into another room to discuss Alexander’s condition. When Ryan asked the doctor if he could record what he was about to hear so that his wife could listen to it once she had calmed down, the doctor consented.
What Ryan caught the doctor saying on film six months ago when Alexander was born continues to anger him and his wife to this very day.
“He’s got increased risk of having significant heart defects…rib, kidney abnormalities, inter-abdominal tumors. All of those are not super important because some ninety percent of those kids don’t make it past the first month of age,” the doctor said.
Offering no help and giving no hope, but suggesting death as the only possible outcome for the baby, the doctor continued:
“We can look at his heart and run all kinds of tests, but no matter what his heart shows, heart surgery is not in his best interest, okay? Why put him through a big surgery, cause pain, discomfort, extend his stay if we can get him home? And, his life expectancy isn’t going to be lengthened by a heart surgery.”
Ryan, like his wife, was deeply shaken by the doctor’s words.
“Is there, like, a chance? Is it really that bleak?” he asked.
“It really is,” the doctor replied. “Ninety percent don’t make it through the first year. Most will die in the first month.”
The doctor then went on to tell the shaken father that it didn’t matter if Alexander ate or not, suggesting that if he didn’t eat, “that’s ok too.”
“There is, how do I say it, very little limiting you from going home tomorrow,” he said. “Bottle feed him, breast feed him. Whatever he takes, great. Whatever he doesn’t take, that’s ok too,” the doctor said.
When the dad asked about the possibility of a feeding tube, the doctor immediately questioned the move.
Not giving up
Despite the doctor’s bleak prognosis, the parents did not intend to give up on their baby so easily. They stayed in the hospital another two weeks so that Alexander could receive a feeding tube and so that other tests could be continued.
“He was going to have a full tummy, no matter what happened to him,” Katie said.
But at each new twist or turn, the couple found roadblocks to Alexander’s care. For instance, despite the baby having a heart murmur that was easily picked up during his constant monitoring, no one suggested that he undergo a heart scan to determine the extent of the problem. When Alexander was having trouble breathing, no one suggested that he be hooked up to the oxygen machine.
“Alex actually needed oxygen and they didn’t give him any. We didn’t realize he needed it. We assumed he was ok, that it was perhaps a normal variant for him being born so small. But later we learned that he actually suffered from not having enough oxygen in his blood,” Katie said.
Doctors even suggested that it would be pointless to treat the baby’s case of jaundice. The parents had to constantly argue for tests or treatment that would have been offered to babies with normal chromosomes. When the parents suggested certain tests that might be done on Alexander to determined the extent of his problems, the doctor would say to them, “I just wouldn’t.”
Despite many odds, Alexander was eventually stable enough to go home. But the doctor’s dire words about the boy’s inevitable death kept ringing in the parents’ ears. At every moment, they expected their son to leave them.
“The doctor was the expert,” Katie said. “I really believed him. I wasn’t in a state of denial. I really believed Alex was going to die.”
But Alexander didn’t die.
Days turned into weeks. Weeks turned into months. Time went by and Alexander kept on not only living and growing, but thriving beyond everyone’s expectations.
Alexander Buck full of smiles for the camera.
“It was scary at first because you live as if death is on your doorstep. We were very apprehensive. It was very hard to enjoy a lot of our time with him. We would often think whether or not this was the last time we were going to give him a bath, or was this the last time I was going to breast-feed him, or was this the last time he was going to play with his brother,” Katie said.
When Katie and Ryan saw that Alexander was staying put for the time being, they realized that they needed to stop living in the future of the “what if” and live in the present of the “here and now.”
“Alex has taught me so much about not worrying about tomorrow. All the Scriptures about not worrying about tomorrow, they are true,” said Katie.
It has now been over six months since Alexander returned home from the hospital. The parents have learned how to change his feeding tube, how to administer oxygen, and how to tend for their baby who needs a little more care than other babies.
But most of all, they have learn an important lesson from their son about the beauty of life itself, no matter what kind of package it comes in.
“He rolls, he coos, he smiles. He is very social. He makes a lot of eye contact,” Katie said.
One day the parents were bolstered by a surprise visit in their home from Sen. Rick Santorum, whose eight-year-old daughter Bella also has Trisomy 18. Santorum talked about what a joy Bella is to their family and encouraged Ryan and Katie by telling them that they were doing the right thing.
Sen. Rick Santorum visits the Buck family.
Santorum gave the family a copy of Bella’s Gift, a book published in 2014 that tells the story of life with their special-needs youngest child. In the book, he inscribed this message:
“To Alex – You are blessed to be born to a family that loves you unconditionally. May God continue to bless you as you bless others who cross your path. Your friend, Rick Santorum.”
Katie remembers being encouraged by Santorum’s visit and his words.
Rick Santorum’s note to Alexander Buck.
“Alex will continue to surprise you. No matter what happens, everything will be ok,” she remembers him saying.
Full of surprises
And Alexander continues to be full of surprises.
“To be honest, his future is still uncertain, but that is frankly true for any of us. But, there is nothing in his immediate future that is life-threatening,” Katie said.
Katie said that the experience has taught her to be more cautious about what the doctor says, especially when it involves the life of a baby with chromosomal abnormalities.
“There is a pattern of tactics that these doctors use to steer these babies towards death,” she said, adding, “But, they can’t predict the future. They don’t have crystal balls. They can’t say for sure whether your child will live or die.”
Katie was able to tell the doctor to his face what she thought about his attitude toward her son.
“I told him that he made me very uncomfortable when he recommended that we not feed Alex. And I told him that he should strongly consider giving parents all of the options and information, rather than his own opinion, because we are the ones who need to live with these decisions at the end of the day,” she recalled.
Katie and Ryan Buck with their two sons Alexander and Daniel.
Katie and Alex believe that the medical community needs to change its perceptive on babies who have extra chromosomes.
“The belief has been perpetuated that Trisomy 18 means that affected babies are ‘incompatible with life.’ And that is just not true,” said Katie.
“Even if they don’t survive for very long, that is the only life that they have, and it should be respected, treated with dignity, most of all loved, and given just as much care as any other baby would receive. Our children deserve no less,” she said.
Editor’s note: The Buck family has created a gofundme page here to help cover the cost of Alexander’s care. They have also created a facebook page.
CAMBRIDGE, Massachusetts, June 19, 2017 (LifeSiteNews) – “Unborn babies are constitutional persons,” the Harvard Journal of Law and Public Policy stated in a remarkable release last month.
The nation’s “leading forum for conservative and libertarian legal scholarship,” according to its website, said in its report that unborn children do in fact fall under the Fourteenth Amendment’s protections.
The Fourteenth Amendment, adopted in 1868, holds that no state shall “deprive any person of life, liberty, or property, without due process of law; nor deny to any person within its jurisdiction the equal protection of the laws.”
The question of whether “life” includes unborn life has been the crux of the pro-life debate carried out in the courtrooms for years.
Harvard Law student Joshua Craddock challenged the premises of both the pro-abortion and pro-life sides of the debate in the article.
Since Roe vs. Wade, the court’s abortion-friendly decisions have basically been predicated upon the assertion that it is unknown if the unborn child constitutes life, The Stream reported, so the court has typically said “no” it does not.
Similarly, Craddock’s argument also challenges the conservative – often originalist – position that the Constitution does not deal with the nature of the unborn person.
Craddock believes both are wrong and that the “original” meaning of the Constitution includes the unborn child’s right to life.
He argues through three premises that the amendment includes the unborn: What the word person meant when the Amendment was crafted, the anti-abortion laws of the time, and what the people who wrote the amendment said about it.
The article states in part:
One might look to dictionaries of legal and common usage, the context of the English common law tradition, and cases that attempted to construe the meaning of the text in a manner consistent with original meaning. Using this methodology, it is reasonable to construe the Fourteenth Amendment to include prenatal life. The structure of the argument is simple: The Fourteenth Amendment’s use of the word “person” guarantees due process and equal protection to all members of the human species. The preborn are members of the human species from the moment of fertilization. Therefore, the Fourteenth Amendment protects the preborn. If one concedes the minor premise (that preborn humans are members of the human species), all that must be demonstrated is that the term “person,” in its original public meaning at the time of the Fourteenth Amendment’s adoption, applied to all members of the human species.
Craddock concluded that states allowing abortions violate the Constitution and that a higher authority must act to protect the lives of the unborn.
If Craddock is correct, The Stream report said, the Supreme Court may finally base its rulings upon what the Constitution supposes about the unborn. “The Fourteenth Amendment,” Craddock stated in conclusion, “was to be a new birth of freedom for all human beings.”
June 2, 2017 (LifeSiteNews) – When I first became pro-life, the solution to ending abortion seemed fairly obvious: just give people condoms so that there won’t be accidental pregnancies.
I chuckle when I think about that now. But at the time it made perfect sense. I had yet to realize the deep relationship between the bioethical issues surrounding sex, procreation, and the human person.
The phrase “seamless garment” to most people means the “consistent life ethic,” a philosophy that equates moral issues like abortion and euthanasia with war and poverty.
I would like to propose a different kind of “seamless garment”: the garment by which abortion, contraception, pornography, and distortions of human sexuality are all woven together.
Typically, shortly after a country legalizes and spreads contraception, it legalizes abortion. Why? Contraception can fail, but it gives couples the impression that they’re “protected” from the natural result of sex, offspring. If contraception fails, abortion is a back-up.
Why are couples contracepting in the first place? Perhaps they’re unmarried and uninterested in a long-term future together.
Why are they hooking up? Well, why not? Perhaps their sex ed classes, or parents, or friends and favorite television shows and magazines and celebrities told them sex is rather meaningless. If you feel like it, just go ahead.
Of course, these lessons weren’t complete unless they included instructions on how to best eliminate the chances of pregnancy.
“Here’s how babies are made, but don’t worry, we’ve got a great way to prevent that from happening.”
Is it easy for anyone who’s undergone years of public (or sadly, perhaps “Catholic”) school sex education to even imagine sex that is “safe” unless it involves latex or hormonal distortion? No, of course not. And it’s not their fault. It’s something they were taught their entire lives, something reinforced by the media, the abortion industry, and many who think they’re doing good by promoting contraception.
It was difficult for me to fathom that there were actually people out there who had sex without some form of contraception on purpose. But, it turns out there are lots of those people (and I’m grateful to the one who argued with me about contraception long enough to eventually change my mind).
Such people have usually learned, either from a solid foundation, personal experience, or friend or loved one’s experience, the pain and emptiness that so often accompany such a sterile view of sex and the human person.
The world basically says:
Your mind and body are separate, and there’s no real meaning to your body.
It’s important that sex be procreation-free and consensual.
Contraception and abortion are necessary for a sexually active society.
No one is harmed if you watch a girl be subject to sex that would make E.L. James blush, because you’re just watching it on your computer. In fact, this is probably better than going out and trying that on someone in real life (and there’s no risk of an assault charge either).
Since your body has no meaning, it doesn’t matter if you castrate yourself or “marry” someone of the same sex.
Freedom means having the right to be able to do whatever you want.
All of these notions support each other, and each one persists because the others persist.
For example, contraception, which attempts to remove the procreative purpose of sex, fuels abortion, pornography, and same-sex unions. They all remove the procreative purpose of sex in one way or another. Pornography distorts sex, just like sodomy and contraception do.
Countless marriages have been wrecked, young children robbed of their innocence, girls and boys pressured to do things they don’t want to sexually, babies aborted, and souls deeply wounded due to this prevailing ideology.
The antidote to it is simple: the beautiful teachings of the Catholic Church and the healing power of the Sacraments.
To the world’s culture of death ideology, the Church responds by saying, essentially:
You are body and soul.
Sex is beautiful and awesome and so meaningful. You are made for love and to be loved, not to be used by someone or to use another. Your body was designed to be a gift to another. God made fertility for a reason; it doesn’t need to be suppressed. Of course sex needs to be consensual – in fact, it needs to be way more than that.
Abortion and contraception aren’t necessary for a sexually active society. But they certainly help make society miserable.
Turning in on oneself closes us off from God. You don’t need pornography to be happy.
Your ears are for hearing. Your feet are for walking. Your body is designed the way it was for a reason.
Freedom means the capacity and ability to choose what is good and right.
Coming to understand this “seamless garment” is a process. Many people begin this when they experience horror at the injustice of abortion, and then gradually come to agree with Church teaching on other issues. Anti-abortion beliefs are a gateway that can lead to chastity, greater respect for self and others, and authentic human freedom.
With God’s grace, may we realize that the Church teaches what it teaches because it’s true, and because it wants what’s best for humanity, and that the culture of death teaches lies because it wants the worst for humanity.
(Natural News) If you’ve ever spent time around a baby, you have probably noticed that he or she seemed fixated on your face. No one would blame you for assuming that babies develop this fascination as a result of early interactions and bonding experiences with their mothers, but new research has shown that babies might develop the ability to recognize human faces while they are still in the womb.
Researchers at Lancaster University shone dots of light through the uterine wall of expectant mothers when they were 34 weeks pregnant. When the dots were arranged in a formation that made them look like the eyes and the mouth of a human face, the babies turned their heads to face the light, but they did not have this reaction when the dots were arranged in another shape that did not resemble a face. The babies were seen moving their heads more in order to track the stimuli when the lights were shown in the face-like arrangement. Overall, the babies were four times more likely to show a response to the face-like pattern than other patterns.
The scientists used high-quality 4D ultrasounds to monitor the babies’ reaction to the light, and they used computer modeling to get an idea of how the light would change once it has passed through their mother’s abdomen. They used red light because previous studies showed that third-trimester fetuses are able to see light in this hue.
Babies have long shown a preference for looking at human faces over all other stimuli. Past studies have demonstrated that babies prefer to look at dots of light arranged in this manner after birth, and now it appears that this preference starts in the womb.
Study co-author Kirsty Dunn remarked that the babies’ response in the womb was very similar to that of infants. Moreover, the babies appeared to blink in the ultrasound scans despite the fact that it is believed that their eyes are normally closed for much of the time. She said it was the first time fetal vision had been explored in the womb, although other senses like smell, taste, hearing and touch have already been studied.
Scientific discoveries like this one continue to dispute the notion embraced by abortion activists that a fetus is an unfeeling and dispensable ball of tissue.
New insight into visual development
Professor Vincent Reid, the psychologist who led the study, theorizes that babies in the womb could already be hardwired to recognize human faces, but he believes it’s more likely that their experience while in the womb is what primes them to recognize face-like shapes. He thinks this preference could be triggered by the patterned light that babies are exposed to in the womb and is due to prenatal visual experiences. For example, he posits that their mother’s rib cage might create variation in the light that penetrates the womb, spurring this preference.
He also says the results imply that upper visual fields are more advanced developmentally and more sensitive than lower visual fields. This would mean that light exposure inside the womb might be just as important to human eye development as it is after birth. Nevertheless, Professor Reid advised expectant mothers against shining bright lights through their abdomens as they could inadvertently damage their baby’s eyes. He pointed out that the study used controlled conditions and a very low level of light.
Babies in the womb are already known to respond to sounds like music and the voice of their mothers, and this groundbreaking new study shows that they do have some visual abilities. The researchers believe this could lead to further discoveries about fetuses.
Reid has already used this technique in studies that suggest fetuses have the ability to differentiate between varying numbers of objects. Next, he’d like to find out if the fetuses have the ability to associate particular light patterns to other types of stimuli, like a specific nursery rhyme. This would provide some clues as to how early the brain can integrate information across senses.
I recently spoke with a bright college student fresh from her Gender Studies class who wanted to know why Christians were trying to “force their morality upon a secular society” by supporting traditional marriage. It’s a good question, and one that we should be ready to answer.
From a Christian perspective sex is relational, covenantal, intimate, fruitful, selfless, complex (involving the mind, soul, and body), complimentary and symbolic- that is, giving us a picture of the union of Christ and the church. But I’m certain she couldn’t care less about my well-churched rhetoric because from the secular perspective, sex is about fun.
From an evolutionary standpoint however, sex is for one thing and one thing only: baby-making. The problem is that this baby-making activity demands much more from women than men.
It is the woman whose body will be burdened and stretched (literally) for nine months of pregnancy. She will have to endure labor and delivery. She will be vulnerable and dependent as she recovers and meets the demands of a helpless and needy infant. Her availability to work and provide for herself and her child is hindered for several years as the child grows. Her anatomy demands that she be present for the birth of the baby. And after delivery, her brain and body are wired for infant attachment- making it highly unlikely that she’ll abandon her child.
The problem is that biology does not demand anything more of the man than, on average, a 2-3 minute contribution.
Every culture and religion throughout history has understood that when the father is absent, the child, the mother, and by extension all of society, suffers as a result. Whether in 200 B.C during the Han Dynasty or 2017 America, children who grow up fatherless (and their mothers) are more vulnerable to poverty and exploitation. They are more likely to be involved in criminal activity and less likely to become responsible citizens, not to mention a host of other risks. Therefore, every community throughout history has wrestled with the same problem: How do you require of men what biology makes optional?
Interestingly, nearly every religion has come up with the same answer: society-wide expectations that a man commit to a woman prior to sex and remain committed to her, and only her, throughout his life. And up until the last ten minutes of history, we have all called this “marriage.”
The five major religions of the world disagree about:
The nature of God
The nature of man
The problem in this world
The solution to this problem
The nature of the afterlife
And yet each faith encourages monogamy, complementary, and permanence in sexual relationships. Each faith independently developed these marital norms because they recognized that it was good not just for men, women and children, but for society at large.
What does that tell us? That marriage has much more to do with being human than it does with being Buddhist, Hindu, Muslim, Jewish or Christian. A Buddhist teen, a Hindu sixth-grader, a Sunni boy, a Jewish girl and a Lutheran adolescent may have little in common when it comes to their religious life. But I guarantee that if those kids are being raised by a single mother, they all have laid awake at night wondering “Where is my father?” and “Does he love me?” But don’t take my word for it. Why don’t you ask several fatherless children of various faiths that you know whether or not they wish they had a dad and let me know what they say.
Except you wouldn’t ask those questions because you know the answer will be one of pain and heartache, if they are able to choke words out at all. All the “sex-positive” cultural messaging is powerless in the face of a child who has had to pay for their parents belief that they had a “right” to sexual expression, freedom, and pleasure.
The issue of marriage, especially civil marriage, has less to do with religion and everything to do with biology. Primarily, the fact that children need both of their parents so that they can mature and thrive. But that means demanding that adults channel their sexual behavior into faithful life-long marriage. Without the society-wide expectation that men commit prior to sex, there is little protection for women from whom biology demands so much. And there is no provision, protection and involvement from the men for whom children so desperately long.
Cardinal Carlo Caffarra, archbishop emeritus of Bologna, Italy, has a key message to deliver: Great efforts must be made in Catholic education and catechesis if the Church is to combat today’s attacks on marriage, life and the family.
In a May 19 interview with the Register in Rome, the founding president of the Pontifical John Paul II Institute for Studies on Marriage and Family, also called on Catholics to be present in the public square and to call things by their real names. “Error is error,” he says. “There is no peace between truth and error.”
One of the four dubia cardinals, he preferred not to discuss that topic in the interview, but warned about a current trend in the Church of separating doctrine or theory from pastoral practice, ostensibly to be more pastoral and compassionate. “Theory without praxis is like a wheel without an axis,” he says. “Praxis without theory is a blind man on the road. To give primacy to praxis: First of all, this is theologically false.”
Your Eminence, much is said about the importance of the family. But what does the Church have to do to defend it against gender ideology and other attacks?
I think that the first choice has to be a very clear, very complete and very profound proclamation of the gospel of marriage and of the family, because the situation has now already reached the extreme point, even of putting into question the definition itself of marriage.
Humanity has always defined marriage as the legitimate union between a man and a woman, with a view to procreation and education. Today that definition has been put into question; some juridical laws have even put in place another definition of marriage. It was in this sense that I said that we have arrived at an extreme point. Therefore, the Church needs to say to man: “This is what God had in mind for marriage; this is what Christ has done — because marriage is a path to salvation for a man and a woman who marry.”
The gospel of marriage has two great chapters: The first is the good of marriage in creation; the second is the announcement of the salvation of marriage, which Jesus came to bring forth, both in words and behavior.
We must not forget that the first miracle brought about by Jesus was in favor of two spouses during the marriage banquet. So that is the first thing that the Church needs to do. The second thing, no less important, is the need for great efforts in educating the young generation, because the heart of every boy and every girl desires to love and be loved, in the truth. Otherwise, after a while, the thing becomes boring because it was not what the heart wanted.
So this desire, it is necessary to say, is inscribed, sculpted in the heart of every man and woman. Education is needed to liberate it from all that impedes it, so that this desire is fulfilled.
I’ll give you an example: If there is a stone covering a spring of water, the spring continues to exist, but the water doesn’t flow. I have to get rid of the stone; then the true spring gives all of its wealth of water. It’s as if a stone is covering this human desire, and the Church, with its educational work, needs to remove it.
How can the Church better resist the current crisis she is facing within?
I believe — I’ll say this right away — the point at which we have arrived is a station at the end of a long process. I am speaking of the West and a process that has lasted centuries. It would, therefore, be naïve to think that in a few years — at times, I think, in a few generations — one could correct this process, turn it around. This must be said as a premise. It’s not as if St. Benedict saw immediately the consequences of the communities he founded in the woods around Rome. It was necessary to have a whole process of civilization. We have to always remember this in order not to be naïve.
Coming now more precisely to address the question, I believe there is, above all, a swift-acting strategy, and it is this: We cannot continue to let ourselves get used to this real absence of lay Catholics from places where juridical norms, laws are formed. So there should be a strong presence of Catholics, for it’s not just a good for the Christian; on the contrary, it’s a good that pertains to creation, marriage and the family. However, laws by themselves don’t resolve the problem. Therefore, the more long-term strategy is to busy ourselves in a great educational work.
Third, St. Thomas, at the beginning of the Summa, says that antithesis cannot exist together. He gives an example: He says the doctor, by the fact that he wants the sick person to recover, fights against the illness. Wanting one [the person’s health] means he doesn’t want the other [the illness]. Thomas continues: The wise man seeks the first principle, God the creator; therefore, he fights the error which obscures the truth he is seeking.
Augustine is even stronger: For he says, love the one who errs, but persecute the error. The corresponding Latin verb is one grammarians call emphatic. It doesn’t mean tolerate the error, but tear it out and to show its insubstantiality.
Therefore, there are three things: laws, the presence of Christians in parliaments, public institutions; second, a great work of instruction; and, third, call things by their real names. Error is error. There is no peace between truth and error.
Is the problem today that people do not speak out strongly enough against sin?
Yes, in places of learning. Thomas’ strategy at the beginning of the Summa against the Gentiles [of calling out sin] is not followed. On the contrary, it is even belittled.
I also often saw this when I was the titular pastor in Bologna. In my opinion, in the places of learning, there’s also no education of true love of the truth anymore. On the contrary, many people teach the young that the search for the truth is a sad and useless passion that can breed only intolerance. At this point, the human person is lost and finds himself, the famous philosopher would say, before paths that don’t lead anywhere.
What is your view of Amoris Laetitia in this regard?
First of all, there is a whole chapter on education, which, for me, is very important. Second, the initial chapter is supposed to, through commenting on a Psalm, describe marriage and family life in the light of God’s plan. These are, with regard to Amoris Laetitia, the second part of Familiaris Consortio — all the great catechesis of John Paul II on marriage and the family.
We have a wealth [of teaching] that can help us at this difficult moment. But, says a great German poet, where the danger increases, there salvation increases
Looking back at your time with the Pontifical John Paul II Institute, what, according to you, should be its priorities?
With regard to the institute, I believe I can say it was one of the things dearest to John Paul II. I can show this with numerous proofs. The priorities, the motives, for the research are written in the apostolic constitution, which direct the institute.
Every great pastoral program for marriage and the family points to, and therefore requires, a true knowledge of marriage and the family. It is not the case that, in diminishing the doctrinal dimension, one becomes more pastoral. One becomes more ignorant. In medieval times, they said that theory without praxis is like a wheel without an axis. Praxis without theory is a blind man on the road. To give primacy to praxis: First of all, this is theologically false.
It’s a false compassion.
Yes, I’ll return to this afterward. Because every praxis presupposes an intellectual project. The second reason is that the basis of the Christian life is not charity; charity is the perfection of the Christian life. The foundation is the faith.
A Christian life without faith is like the house, which Jesus talks about, built on sand. It’s no longer built upon the word of God, so it doesn’t stand. To put charity before the faith through the category of compassion brings us to a street that does not have an exit, if you stop only with compassion. The Samaritan did not stop just to say: “Poor devil, look how they treated him,” and then went on his way. No. He who is truly compassionate takes care of the person, using the adequate instruments, or how do you take care of a person if you don’t know what a person really needs?
The result is disorder.
Yes, there we are. Certainly this is true. Aristotle said there is nothing greater than teaching a man philosophy. But if you come across a man who is hungry, don’t teach him philosophy first. Feed him first, and then teach him philosophy.
Thomas quotes this text approvingly. It’s evident that you need to feed a hunger, without which man is no longer a man — he loses his dignity. However, these are not the only needs of man. A great medieval theologian, St. Albert the Great, says that the needs of man are two: in dulcedine societatis inquirere veritatem — “in the sweetness of a good life with others, seek the truth.” This shows us the greatness of the man.
Is the problem that, in the Church, we have lost sight of heaven, that there’s too much attention paid to this world and not the next?
I would say when you speak of the Church you are speaking of such a vast reality. But I would say we’re running a risk of doing this; we are in danger of doing this, forgetting that the Church, at her base, is not an NGO or an emergency room of the International Red Cross. The Church exists, above all, to free man from sin and to accompany him into eternal life. This is the purpose of the Church.
Jesus taught us nevertheless that this implies, also, attention to the human person and his needs. Around Jesus, there were always sick people. Jesus cured them. Jesus found himself before a hungry crowd. Jesus multiplied the loaves. Jesus knew well who Zacchaeus was, that is, a collector of unjust taxes, because taxes can also be unjust.
But he cured him of this profound sickness of the heart. As I was saying before, this is the ultimate end of the Church.
June 12, 2017 (Priests for Life) — Millennials have a bad rap. They’re labeled as crybabies, snowflakes, fragile, spoiled, and entitled. They’re told they want safe spaces, participation trophies, and handouts. They’re accused of wanting the most benefits for the least work, and the list goes on and on. I feel kind of bad for them. I suspect that every new generation of young adults that pops up gets some flack, but I don’t ever remember having it as bad as Millennials. If there is one thing that gets most overlooked within their cohort, it’s that they are the most pro-life generation yet. And they deserve a thumbs up for that.
In the 2016 March for Life, the youth made up 80 percent of approximately the half-million marchers. The pro-life movement is mostly a youth movement. As the most tech savvy of all the generations, they are perhaps the least likely to be fooled by pro-abortion rhetoric. Their first baby pictures were most likely sonogram images or even 3D ultrasound pictures. They have access to YouTube, Snapchat, Tumblr, Twitter, VSCO, Instagram, etc. and they know how to use it. There is no topic they don’t know how to Google search within seconds for answers. They know what abortion is and they don’t like it.
It’s easy to understand why. This generation is not just standing up for babies in danger of being aborted — they are also standing up for themselves. They understand that they are survivors. They know that when they were in the womb, they were not protected. Millennials experience “survivor syndrome,” like soldiers back from the war in which their comrades were killed. In fact, during the gatherings of the Silent No More campaign (a project of Priests for Life and Anglicans for Life), we have a growing awareness of siblings holding signs that say, I mourn my aborted sibling.
The sense of being an abortion survivor is a big part of what motivates young pro-life activists today. In fact, when I am asked to encourage parishes and pro-life organizations to focus more on recruiting youth, it’s not a difficult task. Millennials understand the pro-life message better than older generations, and the most common response they give to the question, “Why are you involved in trying to stop abortion?” is “Because it could have been me.”
I often point out that our youth are not simply the “future leaders” of the pro-life movement. They are leaders here and now, in more ways than one. They have a lot to offer to their peers, as well as to the rest of us. Those of us who have been in the movement longer need to understand what will happen when we recruit more youth into the pro-life effort. They will challenge us. They will remind us of things that we have perhaps forgotten, and will even be able to teach us a new way of activism, and even a new way of thinking. We’ve all seen the edgy, in-your-face activism of Millennials. It’s void of any pretense. That’s refreshing.
Straightforwardness is a characteristic of young people when confronting fundamental moral issues like pro-life. They think in straight lines. Unaccustomed to the layers of complication that years of enduring resistance from opponents can bring, young people can frame certain questions with a simple and direct clarity. And while they always need to be open to learn from those with more experience, they also need to be listened to. We need to let them shape our own thinking.
When made aware that killing is taking place in the building down the street, they will ask, “Well, let’s go down there and stop it! We should go there and tell them we are not going to leave until the killing stops! If that’s where the babies are that we need to save, what are we doing here?” Or, when told that a particular candidate for office is in favor of keeping child-killing legal, our youth will declare, “Well, we have to tell people not to vote for that person!” When they understand the clarity of Gospel teaching about the sanctity of life, they will say, “All the pastors need to preach about this and sign their people up for pro-life activity! It’s more important than anything else!”
Is there not truth in this “straight-line thinking?” We can learn something from them and refocus our attention and energy on fundamental things which, in the end, simply have to be said and done. Maybe we’ve become too complicated and are too quick to say, “it’s not so simple.”
I rejoice in the pro-life commitment and involvement of our youth — so much so, in fact, that while I am committed to training them for the battle, I am not going to “hand the battle over to them.” The time to end abortion is now, not in another generation or two. Rather than “handing the baton” to our young people, let’s take their hands, and let’s march together into the promised land of victory for the unborn!
Fr. Frank Pavone is the national director of Priests for Life, the world’s largest Catholic organization focused exclusively on ending abortion.
BISHKEK, Kyrgyzstan, May 31, 2017 (LifeSiteNews) — The leader of Russia’s 150 million Orthodox Christians says homosexual “marriage” is unnatural and contrary to the conscience of every human being, which is why so many people resist its normalization for the same reason that people resisted fascism and apartheid.
In an interview at Kyrgyz-Russian Slavic University, His All-Holiness Kirill was asked about same-sex “marriage.” The Patriarch, who is well known for opposing sodomy, referred to legalized gay unions as false, “so-called” marriages. He then flatly stated that they are a threat to family values because homosexuality is a “complete break with the moral nature of man.”
The Russian government and its people have been under severe criticism from leaders in the West for standing against the normalization of homosexuality. “When laws are detached from morality, they cease being laws people can accept,” Kirill explained.
The Christian leader then said something immediately pounced upon by Western pro-gay mainstream media.
People resist the legalization of same-sex “marriage,” the Patriarch commented, “for the same reason that they resisted both fascist laws and the laws of apartheid — (because) such laws break with morality.”
Hence, the Western headlines:
Russian Orthodox Patriarch Says Gay Marriage is Like Nazism”
Same-Sex Marriage as Immoral as Nazi Laws: Russian Putin Ally Says“
Head of Orthodox Church Compares Homosexual Marriage to Nazism”
Russian Orthodox Leader: Gay Marriage Advocates, like Nazis, Promote Immoral Laws”
Head of Russian Orthodox Church Compares Same-Sex Marriage to Nazism“
“Patriarch Kirill’s statement will probably garner a lot of criticism with the gay pride folks,” Fr. Johannes Jacobse, founder of the American Orthodox Institute, told LifeSiteNews, “but he’s pointing out a fundamental truth: Gay ‘marriage’ is a creation of the state. Natural marriage, on the other hand, conforms to nature.”
“When the state affirms natural marriage, it merely recognizes that which already exists across cultures and time,” Fr. Jacobse explained. “When the state deems that homosexual marriage should exist as part of the social order, however, it declares that the state is source and judge of what qualifies as legitimate human relationships.”
“The state has assumed an authority it legitimately does not have and becomes the enforcer of a new social order,” Fr. Jacobse concluded.
“The moral code reflects the natural law, which is ingrained into our very being,” His Beatitude Metropolitan Jonah of the Russian Orthodox Church Outside of Russia explained.
“We have an innate sense of right and wrong, which is the voice of our conscience,” the Metropolitan continued. “Fascist, communist, and apartheid laws violate our fundamental sense of freedom.”
“The validation of gay ‘marriage,’ so-called, distorts the natural mode of relationship between the sexes,” His Beatitude said. “It fundamentally distorts the nature of the family. Thus, many people will reject it as unnatural.”
Kirill was presenting his book, Freedom and Responsibility: A Search for Harmony. The point His All-Holiness wanted to make was that homosexual behavior comes out of “an emphasis on freedom with complete disregard for moral responsibility.”
“The forced imposition of homosexual marriage will be met with resistance just like other contrived orderings enforced by state authority, like fascism and apartheid were,” Fr. Jacobse elaborated. “New social orderings that go against nature universally oppress the human spirit.”
“We see the early stages of this conflict with the state driving people out of business who resist the attempts to define homosexuality as a natural expression of human sexuality,” Jacobse pointed out. “Clear thinkers will discern the totalitarian spirit behind the enforcement and reject it, regardless of the reasoning used to justify it.”
In a 2016 interview, the Patriarch said same-sex “marriage” laws “are at odds with the moral nature of human beings” and are “a significant threat for the existence of the human race.”
In that interview, he compared pressure to normalize sodomy as “very reminiscent of what was happening under Soviet totalitarianism.”
In 2013, His All-Holiness said homosexual “marriage” was “self-destructive” and a “very dangerous and apocalyptic symptom” of the end times.
Last year, Kirill shared his view that many young men are drawn to Islamic radicalization because of the extremist, unnatural liberalization consuming the West. He speculated that some youth who join ISIS are misguided, “honest people” who join out of “truly religious grounds” because of the moral morass the West is sinking in.
“It’s not the same thing, of course, but we could compare this to an extent to the apartheid in Africa or Nazi laws – when the law went against inherent moral values, people rebelled,” he said. “They knew it wasn’t right; it was artificial; it was part of some ideology and not in sync with their moral nature.”
Kirill emphasized, however, that those who have fallen into the pernicious sin of same-sex attraction or homosexual behavior should not be criminally punished.
“The Church can never approve of this, but we don’t condemn people who have homosexual tendencies,” he said at a meeting with Council of Europe Secretary General Thorbjørn Jagland at the Cathedral of Christ the Savior in Moscow. “It’s on their conscience and it’s their business, but they shouldn’t be discriminated against or punished, as used to be common practice in some states.”
In 2013, Russia passed a law banning the distribution of gay propaganda to children and teen minors.
“You can sin if you want to, but you will answer to God,” the Patriarch said. “However, if you are trying to propagate your sin by seducing and degrading people, society must oppose it.”
Metropolitan Jonah reasoned that the church opposes the normalization of homosexual behavior out of love for the sinner.
“On a spiritual level, unnatural relationships are profoundly unhealthy,” he explained. “They isolate people rather than build a real community that will last.”
Robert Cardinal Sarah’s recent book The Power of Silence: Against the Dictatorship of Noiseexplores a number of themes both theological and spiritual, all centering around the unhappy role that noise has come to play in our culture and more specifically in the Church. His observations are most trenchant in regard to the liturgy, which should come as no great surprise, given his role as head of the Vatican Congregation devoted to liturgy and sacraments. As I read the sections of his book dealing with the importance of silence during Mass, I often found myself nodding vigorously.
I came of age in the period immediately following the Second Vatican Council, when an enormous stress was placed, quite legitimately, on the conciliar call for “full, conscious, and active participation” in the Mass. That famous phrase, derived from the ground-breaking work of the theologians of the liturgical movement of the early and mid twentieth century, was a clarion call to the laity to assume their rightful role as real actors in the liturgy and not mere spectators. But in its practical application this came too often to imply that the laity must be continually stimulated into action during the Mass: processing, standing, singing, responding, clapping, etc. It was as though the directors and leaders of the liturgy felt they must be constantly grabbing the congregation by the shoulders and shaking them into conscious participation.
Silence, accordingly, tended to be construed as the enemy, for it would lull the people into inattention and boredom. Hardly anyone in the post-conciliar liturgical establishment appreciated that silence could be a sign of heightened, even enraptured, attention on the part of the congregation, a deeply contemplative entry into the mystery of the Mass. And what several decades of this in turn has produced, especially among the young today, is the impression that the Mass is a sort of religiously-themed jamboree, during which our fellowship is celebrated and at which lots and lots of sound is indispensable. I will confess that during many years as a priest, and now as a bishop, I have often wondered whether our hyper-stimulated congregations know exactly what they are participating in. They know that they are active, but active precisely in what?
The Mass is the act by which the Son of God, in union with his mystical body, turns toward the Father in worship. Through our full, conscious, and active participation in this right praise, we become more rightly ordered, more completely configured to Christ and more thoroughly directed toward the Father. We do indeed experience heightened fellowship with one another during the Mass, but this is because we are realizing, not so much our mutual affection, but our common love of a transcendent third, to use Aristotle’s language.
In this regard, one of the most illuminating rubrics under which to read the Mass is that of call and response: Christ the head, through the priest who is acting in Christ’s person, calls out to the members of his mystical body, and they respond, somewhat in the manner of the lovers in the Song of Songs. At the very commencement of the liturgy, the priest (again, operating not in his own name but in persona Christi) says, “The Lord be with you,” and the people respond, “and with your spirit.” The spirit in question here is the power of Christ dwelling in the priest through the sacrament of Holy Orders. This exchange continues throughout the Mass, Head and members conversing with one another and solidifying their communion. Jesus speaks his Word in the Old Testament readings and in the Pauline epistles, and the members of his body sing back to him in the responsorial psalm; Jesus announces himself in the Gospel, and the people chant back, “Praise to you, Lord Jesus Christ;” Jesus breaks open the Word through the preaching of the priest, and the people respond with the Creed, a signal of their faith.
Having prepared the gifts (presented by the people), the priest says, “Pray, brothers and sisters, that my sacrifice and yours may be acceptable to God, the Father almighty.” This line is of great significance, for it signals the moment when Christ and the members of his body are turning toward the Father in order to perform an act of sacrifice and thanksgiving. How beautifully the Preface to the Eucharistic Prayer expresses this dynamic: “Lift up your hearts!” says Christ to his people; they respond, “We lift them up to the Lord,” and then Jesus, through his priest, says, “Let us give thanks to the Lord our God.” What follows is the magnificent Eucharistic Prayer, directed toward the Father and prayed by Head and members together, the latter’s many sacrifices—small and large—subsumed into the former’s definitive sacrifice on the cross. At the conclusion of the liturgy, Christ sends his mystical body, now more perfectly ordered to the Father, back into the world to effect its transformation.
Cardinal Sarah imitates his master Joseph Ratzinger in insisting that silence rightly asserts itself throughout this entire process. The silence of gathering, recollecting, listening, praying, offering, etc. There is plenty of sound in the Mass, but unless silence is cultivated therein as well, we can easily lose sight of what we are doing in this most sublime of prayers.
If a couple is having trouble conceiving after a year, or even as little as six months, they often head off to an IVF clinic.
However, as advocates of natural family planning have been saying for decades, the costly, emotionally draining and ethically contentious process of IVF many not be necessary.
And now the fertility industry could have another strong competitor. A cheap, simple, time-tested fertility remedy has been proved to be even more effective than IVF.
For a hundred years, doctors have checked whether a woman’s fallopian tubes are blocked by flushing them with iodised poppy seed oil. Although the test is purely diagnostic, many women claimed that it helped them to become pregnant.
And now a team of Dutch and Australian researchers has shown that it really does help.
A study published in the New England Journal of Medicine compared the benefits of flushing the fallopian tubes with either an oil-based or water-based solution in 1119 women.
The procedure, known as hysterosalpingography (HSG), is a dye test of the fallopian tubes conducted under X-ray. The procedure was first carried out in 1917, and since the 1950s both water-based and oil-based solutions have been used.
“Over the past century, pregnancy rates among infertile women reportedly increased after their tubes had been flushed with either water or oil during this X-ray procedure. Until now, it has been unclear whether the type of solution used in the procedure was influencing the change in fertility,” says Professor Ben Mol, a Dutch doctor at the University of Adelaide, in South Australia. He himself was conceived after his mother underwent such a procedure.
“Our results have been even more exciting than we could have predicted, helping to confirm that an age-old medical technique still has an important place in modern medicine,” he says. Almost 40 percent of infertile women in the oil group and 29 percent of infertile women in the water group achieved successful pregnancies within six months of the technique being performed.
“This is an important outcome for women who would have had no other course of action other than to seek IVF treatment. It offers new hope to infertile couples,” Professor Mol says. Writing in The Conversation, he noted that the technique has some big advantages over IVF:
Tubal flushing has several advantages over IVF, including that the benefit persists over time, while IVF only helps for the current cycle. Tubal flushing also helps achieve an otherwise natural conception, and its costs are around A$600, a fraction of the cost of a A$10,000 IVF cycle. IVF also has a heavy impact on emotional wellbeing and sometimes causes medical complications.
In our study, 40 percent of women undergoing HSG with an oil-based contrast achieved a successful pregnancy within six months. That’s 40 percent of couples with unexplained infertility who could avoid the huge financial and emotional costs associated with undergoing IVF treatment.
Until he embarked on this study, Professor Mol had no idea that he himself was the result of a successful pregnancy following such a procedure. In the 1960s, after being considered infertile for nine years, his mother underwent an HSG which, coincidentally, also used the poppy-seed oil. “It was only after I started researching this technique that my family told me what had happened,” Professor Mol says.
“My mother went from being infertile for many years to becoming pregnant, and I was born in 1965. I also have a younger brother. So it’s entirely possible – in fact, based on our team’s research, it’s highly likely – that my brother and I are both the result of this technique helping my mother to achieve fertility.”
A leading Australian IVF practitioner, Dr David Molloy, dismissed the news, saying that IVF patients have more complex fertility issues. “They are totally different populations of patients,” he told the ABC. “One is a low-risk group starting out at the very start of their infertility journey that have got virtually nothing wrong with them, and our IVF patients are a higher risk group.”
Scepticism about procedures which threaten the status (and profitability) of IVF is to be expected. But a big dollop of scepticism about IVF is needed, too.
IVF was adopted after the birth of Louise Brown in 1978 without the randomized control trials that doctors expect of nearly every other treatment. And ever since, according to research published earlier this year in a leading academic journal, Human Reproduction, “IVF patients are routinely offered and charged for a selection of adjunct treatments and tests or ‘add-ons’ that they are told may improve their chance of a live birth, despite there being no clinical evidence supporting the efficacy of the add-on.”
Fertility experts often exploit women’s longing for children by offering “new, improved” IVF techniques with little or no proof. One hundred years of proof backed up by formal research published in the world’s leading medical journal is worth investigating.
Michael Cook is editor of MercatorNet.
– See more at: https://www.mercatornet.com/features/view/will-flushing-fallopian-tubes-displace-ivf/19838#sthash.30Jgwhhm.dpuf
The dedication and legacy of a prodigious pro-life hero
When five-year-old Lilliana Dennis was born in February 2011 in Indianapolis, doctors informed her mom and dad that she suffered from a rare genetic condition that was “incompatible with life.” As Lilliana approaches her sixth birthday, she continues to defy the odds and prove conventional medical wisdom both wrong and wrongheaded.
Lilliana has Trisomy 18, also known as Edwards syndrome. As with Down syndrome, such babies are born with an extra chromosome, resulting in heart defects, respiratory problems, and finger and toe abnormalities. Most die before their first birthday, the doctors said, and there was little the Dennises could do to stop that eventual outcome.
Fortunately, the Dennises did some of their own research, which contradicted what they had been told. In fact, one child graduated from college and lived to the age of 42. The Dennises also befriended Dr. Paul Byrne, a retired neonatologist, longtime pro-life activist, and founder of the Life Guardian Foundation (LifeGuardianFoundation.org). He recommended heart surgery for Lilliana, along with other life-saving measures, and although the road has been difficult, Lilliana’s prognosis continues to improve.
Dr. Byrne is no stranger to death-and-dying issues and the challenges posed by both preemies and babies with congenital illnesses. In 1963, he established the neonatal intensive care unit at Cardinal Glennon Children’s Hospital in St. Louis. Though he no longer makes hospital rounds, he stays very, very busy working on behalf of the preborn, sick newborns, the disabled, the elderly, and people with illnesses deemed “terminal.”
“Not only do we have a culture of death in our society—it is a System of Death,” Dr. Byrne says. “We have to work hard to protect life from its beginning until true death. That’s why Life Guardian Foundation was founded.”
“I retired a few years ago after practicing medicine for 55 years,” Dr. Byrne adds. “Yet, instead of a retirement party, I asked my family to have a ‘redirection party.’ My work has not stopped—in fact, I’m busier than ever! People have a way of finding out that I can help them in the cause for life and in their own difficult situations.”
Small beginnings
To get a sense of how Dr. Byrne’s passion for saving lives all began, it’s helpful to go back to the very beginning, when he was a young doctor practicing at Cardinal Glennon Children’s Hospital in the mid- 1960s. There, Dr. Byrne established the hospital’s very first special care nursery for at-risk infants.
“Back then, there were no treatments for preemies and low-birthweight babies, the kinds of things we take for granted today,” he recalls. “I went to the administrator at Cardinal Glennon with the idea of creating a center where we could find ways to treat these babies. She said, ‘OK, let’s try it for a year.’”
After that first year, Dr. Byrne’s efforts had saved the lives of 30 babies. “How?” you might ask. For starters, he partnered with engineers working nearby on the space pro-gram. They had developed a plastic cuff to fit around the fingers of astronauts, enabling their blood pressure to be monitored during space missions. Together, they developed a spinoff that fit around the arm of a tiny baby: Before this invention, there was no way to monitor a baby’s blood pressure.
Dr. Byrne and his team also pioneered new techniques for feeding these babies intravenously as well as specially designed ventilators to augment their respiratory function. All were instrumental in helping such infants survive. Since preemies are so small, new, highly sensitive measurement protocols were also necessary to track their health.
“For instance, premature infants have very small total quantities of blood,” Dr. Byrne notes. “That required development of micro techniques to analyze blood for indicators of health or disease. These micro-techniques that were developed for sick babies are used for everyone. It was exciting for me to be able to participate in the development of what was then a brand-new field.”
Signs of life
It was also heartening for him to witness babies who had been deemed hopeless develop into healthy children and adults. The birth of Joseph in 1975—at a mere 24 weeks’ gestation— was one such miracle. “He had a flat electroencephalogram or EEG—in other words, no brainwaves,” Dr. Byrne recalls.
The EEG is a common method of measuring brain activity at any age. The flat EEG of Joseph was interpreted as “consistent with cerebral death.” “Nonetheless, Joseph went on to be a straight-A student in school, build a brilliant career, and he’s now married and the father of three kids.”
While considered breakthroughs in their day, many of these developments are now commonplace in both neonatal intensive care units and medical care as a whole. Plastic cuffs are routinely used to measure blood pressure of patients.
“My medical philosophy is that the best doctors are the ones who work the hardest on the people who are the sickest,” he says. “What you try to accomplish for those sickest people first will ultimately have a beneficial impact on the rest of humanity.”
Darker trends
During the early 1970s, Dr. Byrne witnessed a trend he found troubling: the increased acceptance of brainwave cessation as a legally acceptable marker of death. This occurred even before abortion became legally available in most states, and it owed in part to new ways to artificially resuscitate patients to keep a person’s heart beating with circulation and respiration. It also followed the world’s first heart transplant in 1967, after which organ transplants became common practice in a short amount of time.
“The push to accept ‘brain death’ has a lot do with the concurrent push for viable organs for transplants,” says Dr. Byrne. He noted that, following that first heart transplant, the medical community began lobbying elected officials for new laws that first codified “brain death” in the US.
This had practical reasons. Dr. Byrne points out that to transplant a heart or a liver, the donor’s heart, circulation and respiratory processes must be kept functioning for healthy vital organs to be removed. Organs from a cadaver are useless, he notes, because organs begin to decompose immediately after those functions cease.
“Now, when someone suffers a head injury or is deeply unconscious, there is a shift of emphasis from helping that patient to harvesting his or her organs for transplantation,” he says. The fact that viable organs are very valuable to the organ transplant industry can add a monetary incentive to the push to declare patients legally dead.
Forty-seven US states have passed the Uniform Anatomical Gift Act (UAGA) that presumes everyone is an organ donor. This is in addition to those who have willingly registered as organ donors on their drivers’ licenses. This often creates a conflict, when the same individuals have also filed advance DNR (do not resuscitate) directives. In such situations, that previous DNR order will be overruled and the patient will be resuscitated in order for their vital organs to be usable for transplantation.
It could happen . . . to anyone
This isn’t all just academic. In 2007, 19-year-old Gregory Jacobs sustained a severe head injury while skiing and died at a Pennsylvania hospital less than a week later. In a lawsuit, his parents maintained that their son “experienced neither a cessation of cardiac activity nor a cessation of brain activities when surgeons began the procedures for removing his vital organs.”
The Jacobs case was the subject of a CBS News report, and the elder Jacobses ultimately won a $1.2 million settlement in 2012. More recent is the case of the now-16-year-old Jahi McMath, who had severe sleep apnea and on which Dr. Byrne is a medical advisor.
Jahi underwent a tonsillectomy at a California hospital, which aimed to improve her ability to sleep at night. She later hemorrhaged and went into cardiac arrest. Physicians declared her to be “brain dead” and ordered the removal of life-support systems.
Jahi’s mom, Latasha Winkfield, disagreed and filed a lawsuit seeking to keep her on life support. A death certificate was issued for Jahi in California before she could be moved to a New Jersey hospital. She later was moved to an apartment with her mom, where she continues to live on life support.
Incidentally, Dr. Byrne was instrumental in getting a new law passed in that state, which gives parents or caregivers the ability to object conscientiously to such orders from a physician or hospital. A similar regulation, though not as strong, now exists in neighboring New York.
“Jahi McMath is very much alive . . . but a death certificate was issued in California!” exclaims Dr. Byrne. “She has had three birthdays since being declared legally dead.”
A broadened focus
Dr. Byrne is a steadfast pro-life advocate and supporter of American Life League (ALL). His knowledge and guidance shaped ALL’s policy on euthanasia and brain death; he is the author of our materials on the subject. Most recently, he played an important role in the development of a study guide on euthanasia for ALL’s Culture of Life Studies Program. In addition to supporting ALL and other organizations, Dr. Byrne saw a need for another organization focusing attention on end-of-life issues. That led to the founding of the Life Guardian Foundation in 2007.
The organization’s website offers a rich repository of resources that helps people understand the controversies that now surround the end of life. Besides the moral and ethical implications, there’s a lot of practical value as well. Many of us now must deal with the treatment of elderly parents, and the use of feeding tubes is often taken to mean that their lives are at the end. Not necessarily so, says Dr. Byrne.
“People on a feeding tube don’t always have to remain on a feeding tube,” Dr. Byrne says. Noting that it’s not always easy, there are ways to treat such patients that can improve their outlook and lead to a time where a feeding tube can be removed. Similarly, severe head injury often leads to a grim prognosis— yet treating the patient with thyroid medications can greatly improve patient prognosis.
Poke around a bit more on the website and you’ll uncover other fascinating information. There are more than 30 disparate sets of criteria. You can be declared “brain dead” by one but be alive by others. The Uniform Declaration of Death Act (UDDA) now on the books in all 50 states mandates that the determination be “in accordance with acceptable medical standards.” The patient who is declared “brain dead,” whichever criteria are used, always has a beating heart with circulation and respiration, albeit on a ventilator.
The procedure of an apnea test (not a test for sleep apnea) is part of every set of “brain death” criteria. The patient is taken off the ventilator for 10 minutes. Carbon dioxide and acids accumulate. This makes the brain swelling worse. Everyone must learn to instruct No! to the apnea test. It can only cause the patient to get worse.
“If you end up unconscious and on a ventilator, the doctors at the hospital treating you will declare that your death is imminent, and by law, they have to notify the Organ Procurement Organization (OPO),” says Dr. Byrne. If you don’t want that to happen, Dr. Byrne strongly urges you to explicitly document your refusal in writing.
The foundation website offers three key directives that can help you accomplish that objective: a healthcare power of attorney directive, a directive to protect and preserve life for a dependent minor or mentally incapacitated person, and an organ donation opt-out form that can be carried in your wallet or purse.
“Very often I work with parents of students who go away to college, get into a car accident, and end up at the mercies of a medical system that wants their organs for a transplant patient,” he notes. Since few people have taken the time to study the issue, and since parents are often bewildered and grief-stricken at such times, it can become a complex battle to receive any form of life-extending care for such patients.
A modest hero
Upon being reached by phone for an hour-long interview, Dr. Byrne was quick to shift the emphasis away from himself and to his large family. He’s the father of 12 children. He also has 33 grandchildren and five great-grandchildren. He’s proud that he has reared a pro-life family.
He’s especially proud of the pro-life poems that his son, Mark, wrote from his heart in the eighth grade—and as Providence would have it—his granddaughter Kaitlyn, Mark’s daughter, recently wrote from her heart in the eighth grade as well. Celebrate Life has happily agreed to publish each poem in its entirety!
More critically, he pointed out the clarity by which young people often view the world around them, and the crystal-clear viewpoints they often form on issues that bedevil their elders, provides a lesson for the rest of us. Both pieces speak right to the heart, he says.
“If you read Mark’s and Kaitlyn’s poems, you can see how they recognize just what is at stake: that we must value life,” Dr. Byrne says. “Most importantly, they show us what we need to do to think correctly about life.”
Poems
Temptation ruled like an evil dictator,
destroying the hope of everyone around,
clouding the decisions people make every day,
where is our dignity?
Adultery shatters a marriage like a plate dropping,
June 7, 2017 (LifeSiteNews) — My wife and I had trouble conceiving when we were first married in 2004. After our daughter came two years later we again had trouble conceiving. Being open to a larger family, we went to a healing service to ask the good Lord for his help.
It came our turn to be prayed over. We told the priest we were having trouble conceiving and wanted more children. As he was praying over us, he started smiling. Then he started laughing. I asked him what he was laughing about. “The Lord has much in store for you,” he said. “You have nothing to worry about.”
Shortly thereafter we conceived our second daughter. In less than a year after she was born we had our third. Then came our son, another daughter, another son, another son, and three miscarriages in between.
Yup, our fertility had clicked. It seemed that all I had to do was look at my wife and she became pregnant. Now I knew what the priest had been laughing about.
While my wife and I dearly love our seven living children and our three little blessings in heaven, we realized that we needed more space in between births. My dear wife needed time to recuperate and build up her body after the exhausting months of nursing day and night. The baby just born also needed time to be loved and nurtured before another baby became the priority. We saw these as serious reasons.
My wife and I don’t believe in using pills or plastic to block the gift of fertility. We actually see contracepted sex as morally evil. Yeah, I know, sounds crazy. Let me explain.
We believe God made sex for the purpose of making babies and bonding with your spouse. Contraception essentially poisons both of these. It blocks the baby-making purpose of sex by rejecting fertility. By rejecting fertility, one spouse is basically telling the other that there is a part of them that they want nothing to do with. And out the window goes that unconditional self-giving and receiving-of-the-other in love that marriage needs in order to survive.
So, my wife and I didn’t want to poison our love with any kind of contraception. Our only options to postpone pregnancy for a time were to completely abstain (a struggle for any man) or to only come together when my wife was not fertile.
So, we learned a fertility awareness method.
A rather significant problem arose when it turned out that my wife had various fertility signs during many days of her cycle, not just around the days of ovulation. Bummer. This meant waiting, and waiting, and waiting for the right signs that would permit us to come together during the infertile time. And added to this is that she sometimes has a cycle length that is longer than for most women.
Ok, I’ll be honest. I usually find these times of waiting a trial. And no, there can’t be any kind of cheating during this time. No masturbation, single or mutual, since the former is a selfish perversion of the sexual act, and the latter really amounts to contracepted sex (see above).
The only real option to safeguard the beauty and holiness of the sexual act during this time of abstinence was self-mastery. And yes, self-mastery is difficult, a big learning curve.
If I wasn’t going to wallow in self-misery or fantasyland during this time, I had to learn to control my impulses and desires. And this is where I would sometimes fail, pushing past a boundary that we had set so as to not reach the point of no return. Or, me anticipating so much the time when we could finally come together that I would fail to find joy in the time that we had together right here and now.
One thing that I’ve found is that abstinence during fertility signs becomes a kind of mirror that shows me things about myself that I don’t really like to see. Ugly things. Such as how selfish I can be. How little I can control my impulses and desires. And how easily I can lose focus on what’s really important in our relationship, like the fact that we’re together, that we’ve been faithful and true to one another all these years, and that we’re still crazy-mad in love with one another.
I can just imagine people scratching their heads, wondering why my wife and I put ourselves through this struggle when there are such easy alternatives out there that make it possible for a man to never have to deny himself.
I’ve thought about this very question long and hard. I probably don’t have the perfect answer yet, but I know it has something to do with love being about denying oneself for the sake of the one you love.
I truly do love my wife. I have no doubt that contraception would poison our love. So, if we’re going to space our children, we have to abstain during the fertile times. This means that love demands that I not only deny myself during fertile times, but that I learn to find peace and even joy in it. Yup, that’s a tall order for any man, but I really think it’s the whole truth and nothing but the truth.
Don’t laugh at this, but my wife suggested that we both make a little daily sacrifice with the intention of helping us be victorious during these times. I’ve found this has made a rather significant difference for me. It’s pretty amazing to know that I have my wife’s prayer support to back up my own (often pitiful) efforts at mastery of self.
Jesus said something about this denial thing too. He said that those who wish to be his followers must deny themselves and take up their cross. Sometimes prolific fertility can seem like a cross, but when I really think about it, I realize that it becomes an occasion during our child-spacing times to show my wife how much I really love her. And every man, including me, loves to show his wife how much he loves her.
Euthanasia and assisted suicide are only legal in a handful of countries, but their supporters are already thinking of creative ways to integrate them into the economy and social life. Doctors in Belgium and the Netherlands are using organs from people who time their euthanasia for organ donation programs, for instance.
And recently an American law journal has published a study of euthanasia for prisoners serving life sentences. This is not a new idea. Australian activist Dr Philip Nitschke described it in his book Killing Me Softly as the “last frontier in prison reform”.
The article in the latest issue of the Virginia Journal of Social Policy & the Law takes a serious look at the hurdles such a scheme would encounter in Europe and in the United States. The authors are an Estonian Fullbright Scholar, Kärt Pormeister, and two officials at Baylor Scott & White Health, the largest not-for-profit health care system in Texas and one of the largest in the US. They conclude that
Where there is no feasible chance of the prisoner regaining freedom during their lifetime, [physician-assisted suicide] as a means of mercy could provide relief to suffering prisoners and closure to victims’ loved ones, while also enabling more efficient allocation of resources.
The springboard for this frank discussion of the merits of allowing lifers to kill themselves is a case in Belgium, where euthanasia is legal. In 2014 a man convicted of rape and murder and sentenced to life imprisonment, Frank Van Den Bleeken, applied for euthanasia in accordance with the law. He was not ill, but he claimed that he was in a state of unbearable psychological anguish. He preferred to die with dignity rather than spend the rest of his life behind bars. A Belgian court granted his request, but at the last minute he was transferred to a more modern facility in the Netherlands where he could be better cared for.
Although Van Den Bleeken’s euthanasia never happened, his case was an instructive precedent for the authors. He was not seeking death as an end to unbearable physical pain, but as a “mercy”. Could this be incorporated into European and US legal systems?
It certainly is different from euthanasia for terminally ill patients. They typically ask for death because of a diminished quality of life. However, the whole point of prison is to diminish quality of life. Euthanasia is often described as the ultimate exercise of autonomy, but prison is an environment in which autonomy is severely limited in many ways, physical and psychological. In fact, the authors point out that “penal institutions might be inclined to maintain or even create harsher environments to encourage recourse to PAS” as a cost-saving measure.
So there are tricky legal issues to work through in both Europe and the US. In Europe prisoner euthanasia might be regarded as a revival of the death penalty, which is banned nearly everywhere. In the US, it might violate constitutional protections of people who are in the custody of the state, including self-inflicted harm. The victims and their relatives might think that escaping life imprisonment is unfair.
Although the difficulties in making a legal case for prisoner euthanasia are substantial, there are persuasive arguments for it, according to the authors.
The first are financial. There would be real benefits for society:
First, the choice of PAS as a means of mercy as an alternative to life in prison would eliminate costs of incarceration that accumulate during a prisoner’s lifetime … Second, allowing PAS as a means of mercy could influence society to move towards the abolition of the death penalty …
Thus, PAS as a means of mercy would enable tax revenue to be used in ways more beneficial to society than keeping someone in prison for their entire lifetime or executing them for retributive purposes. Instead, money could be reallocated to further help those prisoners who still stand a feasible chance of rehabilitation to become productive members of society again. Alternatively, such funds could be used to support the families of the perpetrator’s victims.
From another angle, it could be argued – as Frank Van Den Bleeker did – that a life sentence is a kind of torture.
considering the limited resources to offer proper psychiatric or other complex care to inmates, not offering PAS as a means of mercy to people serving life sentences could, in rare cases, constitute torture or cruel or inhuman treatment which is prohibited in both the U.S. and European human rights systems.
It’s not difficult to imagine courts accepting these arguments if euthanasia were already legal.
The conclusion reached by the authors is far from a ringing endorsement of prisoner euthanasia. They concede that there is a risk of coercion by prison officials and that drafting regulations would be difficult. But it could be “a viable option in rare cases”.
Coming from writers who are involved in shaping health care policy (Ms Pormeister works in the Ministry of Social Affairs in Estonia), the arguments in the journal article are alarming.
The experience in Belgium and the Netherlands is that supporters of euthanasia keep widening the boundaries. At the beginning, it was meant only for people who were terminally ill and in great pain. Now it is available for children of all ages in Belgium and for the mentally ill. Euthanasia for prisoners in a few exceptional cases is certain to expand to all prisoners who demand it. In the claustrophobic atmosphere of prison life, it could become an epidemic, like tattooing or drugs.
And the idea will have a seductive attraction for politicians who have already reconciled their consciences to euthanasia for free citizens – the dregs of society find relief and the state is relieved of the cost of their care. What’s not to like?
The answer is given in the paper: prisoners are amongst the most vulnerable people in society. Their crimes notwithstanding, they deserve to be treated with dignity and helped to discover a meaning in their lives – not helped to kill themselves.
Michael Cook is editor of MercatorNet.
– See more at: https://www.mercatornet.com/careful/view/whats-wrong-with-prisoner-euthanasia/19923#sthash.pJ0TWqX0.dpuf
Micaiah Bilger Jun 5, 2017 | 1:26PM London, England | LifeNews.com
Just one week after Chelsea Nally and her husband, Daniel, were married, the newlyweds discovered they were pregnant.
For some, the news may have brought thoughts of abortion, but the British couple said they were excited about their unplanned pregnancy. They did not know that several weeks later, a serious discussion about abortion would come up when Chelsea found a cancerous tumor in her left breast, The Sun reports.
The Nallys chose life for their baby boy, Finley, and today the mother and son are doing well. Chelsea said Finley saved her life because the pregnancy helped her find the cancer sooner.
“Finley saved me before he was even born,” she told The Sun. “He’ll always be so special to me for that reason.”
Chelsea Nally said she found a lump on her left breast about 10 days after they learned she was pregnant – barely a month after their wedding. A few weeks later, doctors confirmed that she had stage 3 breast cancer, according to the report.
“When I heard the words’ breast cancer’ I reeled,” Nally remembered. “In six weeks, I’d gotten married, found out I was pregnant and was diagnosed with cancer. Medics weren’t sure of the prognosis. They had no idea if the baby was at risk.
“The doctors told me that it was unusual for a lump to move in a breast, but said that had my breasts not changed with the pregnancy, I might never have found the lump,” she continued.
Initially, doctors discussed the possibility of Nally having an abortion; but when further testing revealed that her cancer was limited to her left breast, they did not push the idea, according to the report. Nally said she felt relieved because she did not want to abort her unborn son.
“I was determined to fight the disease for the both of us,” she said.
After undergoing surgery to have the tumor removed, Nally went through multiple rounds of chemotherapy. She said she constantly worried about how it would affect Finley.
“With every scan, Daniel and I would hold hands watching the monitor, desperately hoping to see a sign our baby was growing,” she said.
Here’s more from the report:
Medics told Chelsea the swelling of her breasts had moved the lump in her breast closer to the skin where it could be detected – saving her life.
Incredibly, on March 19 this year, baby Finley was born healthy, weighing 5lbs 3oz.
Speaking from her home in Woodbridge, Suffolk, she said: “Battling a deadly illness while growing new life inside of me was indescribable.
“The chemo was tough but it was nothing compared to the fear that my baby might not survive the treatment.
Nally said she felt so relieved when she heard Finley cry for the first time. Even more relief followed when doctors told her that Finley was healthy.
“Holding him in my arms for the first time I felt like my biggest battle was over,” she said. “I couldn’t believe we had both survived pregnancy and chemo. He is my hero, even before he was born he had saved my life.”
Recent studies indicate pregnant women who undergo cancer treatments do not put their unborn babies at significant risk. A 2015 study published in the highly reputable New England Journal of Medicine concluded, “Prenatal exposure to maternal cancer with or without treatment did not impair the cognitive, cardiac, or general development of children in early childhood.”
Based on these findings, lead researcher Professor Frédéric Amant said women should not abort their unborn babies based on fear that their cancer treatment could affect their child.
address was given by His Eminence Carlo Cardinal Caffarra on 19 May 2017 at the fourth annual Rome Life Forum, which is organised by Voice of the Family.
“When I am lifted up from the earth, I will draw all people to myself” [John 12, 32]. “The whole world is under the power of the Evil One” [1 John, 5, 19].
Reading these divine words gives us perfect awareness of what is really happening in the world, within the human story, considered in its depths. The human story is a confrontation between two forces: the force of attraction, whose source is in the wounded Heart of the Crucified-Risen One, and the power of Satan, who does not want to be ousted from his kingdom.
The area in which the confrontation takes place is the human heart, it is human liberty. And the confrontation has two dimensions: an interior dimension and an exterior dimension. We will briefly consider the one and the other.
At the trial before Pilate, the Governor asks Jesus whether he is a king; whether – which is the meaning of Pilate’s question – he has true and sovereign political power over a given territory. Jesus responds: “You say that I am a king. For this I was born, and for this I came into the world, to testify to the truth. Everyone who belongs to the truth listens to my voice” [John 18, 37]. ‘Jesus wants us to understand that his kingship is not that of the kings of this world, but consists of the obedience of his subjects to his word, to his truth. Although He reigns over his subjects, it is not through force or power, but through the truth of which he is witness, which “all who are from the truth” receive with faith’. [I. De La Potterie]. Thomas Aquinas puts the following words into the mouth of the Saviour: “As I myself manifest truth, so I am preparing a kingdom for myself”. Jesus on the Cross attracts everyone to Himself, because it is on the Cross that the Truth of which he is witness is resplendent.
Yet this force of attraction can only take effect on those who “are from the truth”. That is, on those who are profoundly available to the Truth, who love truth, who live in familiarity with it. Pascal writes: “You would not seek me if you had not already found me”.
He who holds the entire world under his sway, instead dominates through lies. Jesus says of Satan: “He was a murderer from the beginning and does not stand in the truth, because there is no truth in him. When he lies, he speaks according to his own nature, for he is a liar and the father of lies. [John 8, 44].
The wording is dramatic. The first proposition – “He was a murderer from the beginning” – is explained by the second: “and he does not stand in the truth”. The murder which the devil performs consists in his not standing in the truth, not dwelling in the truth. It is murder, because he is seeking to extinguish, to kill in the heart of man truth, the desire for truth. By inducing man to unbelief, he wants man to close himself to the light of the Divine Revelation, which is the Word incarnate. Therefore, these words of Jesus on Satan – as today the majority of exegetes believe – do not speak of the fall of the angels. They speak of something far more profound, something frightful: Satan constantly refuses the truth, and his action within human society consists in opposition to the truth. Satan is this refusal; he is this opposition.
The text continues: “because there is no truth in him”. The words of Jesus go to the deepest root of Satan’s work. He is in himself a lie. From his person truth is completely absent, and hence he is by definition the one who opposes truth. Jesus adds immediately afterwards: “When he lies, he speaks according to his own nature, for he is a liar and the father of lies”. When the Lord says “speaks according to his own nature”, he introduces us to the interiority of Satan, to his heart. A heart which lives in darkness, in shadows: a house without doors and without windows.
To summarise, this therefore is what is happening in the heart of man: Jesus, the Revelation of the Father, exerts a strong attraction to Himself. Satan works against this, to neutralise the attractive force of the Crucified-Risen One. The force of truth which makes us free acts on the heart of man. It is the Satanic force of the lie which makes slaves of us.
Yet, not being pure spirit, the human person is not solely interiority. Human interiority is expressed and manifested in construction of the society in which he or she lives. Human interiority is expressed and manifested in culture, as an essential dimension of human life as such. Culture is the mode of living which is specifically human.
Given that man is positioned between two opposing forces, the condition in which he finds himself must necessarily give rise to two cultures: the culture of the truth and the culture of the lie.
There is a book in Holy Scripture, the last, the Apocalypse, which describes the final confrontation between the two kingdoms. In this book, the attraction of Christ takes the form of triumph over enemy powers commanded by Satan. It is a triumph which comes after lengthy combat. The first fruits of the victory are the martyrs. “The great Dragon, serpent of the primal age, he whom we call the devil, or Satan, seducer of the whole world, was flung down to earth… But they [= the martyrs] overcame him by the blood of the Lamb and by the word of the testimony of their martyrdom” [cfr. Ap. 12, 9.11].
In this second section, I would like to respond to the following question: in our Western culture, are there developments which reveal with particular clarity the confrontation between the attraction exerted over man by the Crucified-Risen One, and the culture of the lie constructed by Satan? My response is affirmative, and there are two developments in particular.
The first development is the transformation of a crime [termed by Vatican Council II nefandum crimen], abortion, into a right. Note well. I am not speaking of abortion as an act perpetrated by one person. I am speaking of the broader legitimation which can be perpetrated by a judicial system in a single act: to subsume it into the category of the subjective right, which is an ethical category. This signifies calling what is good, evil, what is light, shadow. “When he lies, he speaks according to his own nature, for he is a liar and the father of lies”. This is an attempt to produce an “anti-Revelation”.
What in fact is the logic which presides over the ennoblement of abortion? Firstly, it is the profoundest negation of the truth of man. As soon as Noah left the floodwaters, God said: “Whoever sheds the blood of a man, by a man shall that person’s blood be shed, for in his own image God made man” [Gen. 9, 6]. The reason why man should not shed the blood of man is that man is the image of God. Through man, God dwells in His creation. This creation is the temple of the Lord, because man inhabits it. To violate the intangibility of the human person is a sacrilegious act against the Sanctity of God. It is the Satanic attempt to generate an “anti-creation”. By ennobling the killing of humans, Satan has laid the foundations for his “creation”: to remove from creation the image of God, to obscure his presence therein.
St Ambrose writes: “The creation of the world was completed with formation of the masterpiece which is man, which… is in fact the culmination of creation, the supreme beauty of every created being” [Exam., Sixth day, Disc 9, 10.75; BA I, page 417]. At the moment at which the right of man to order the life and the death of another man is affirmed, God is expelled from his creation, because his original presence is denied, and his original dwelling-place within creation – the human person – is desecrated
The second development is the ennoblement of homosexuality. This in fact denies entirely the truth of marriage, the mind of God the Creator with regard to marriage.
The Divine Revelation has told us how God thinks of marriage: the lawful union of a man and woman, the source of life. In the mind of God, marriage has a permanent structure, based on the duality of the human mode of being: femininity and masculinity. Not two opposite poles, but the one with and for the other. Only thus does man escape his original solitude.
One of the fundamental laws through which God governs the universe is that He does not act alone. This is the law of human cooperation with the divine governance. The union between a man and woman, who become one flesh, is human cooperation in the creative act of God: every human person is created by God and begotten by its parents. God celebrates the liturgy of his creative act in the holy temple of conjugal love.
In summary. There are two pillars of creation: the human person in its irreducibility to the material universe, and the conjugal union between a man and woman, the place in which God creates new human persons “in His image and likeness”. The axiological elevation of abortion to a subjective right is the demolition of the first pillar. The ennoblement of a homosexual relationship, when equated to marriage, is the destruction of the second pillar.
At the root of this is the work of Satan, who wants to build an actual anti-creation. This is the ultimate and terrible challenge which Satan is hurling at God. “I am demonstrating to you that I am capable of constructing an alternative to your creation. And man will say: it is better in the alternative creation than in your creation”.
This is the frightful strategy of the lie, constructed around a profound contempt for man. Man is not capable of elevating himself to the splendour of the Truth. He is not capable of living within the paradox of an infinite desire for happiness. He is not able to find himself in the sincere gift of himself. And therefore – continues the Satanic discourse – we tell him banalities about man. We convince him that the Truth does not exist and that his search is therefore a sad and futile passion. We persuade him to shorten the measure of his desire in line with the measure of the transient moment. We place in his heart the suspicion that love is merely a mask of pleasure.
The Grand Inquisitor of Dostoevsky speaks thus to Jesus: “You judge of men too highly, for though rebels they be, they are born slaves …. I swear to you that man is weaker and lower than You have ever imagined him to be! Man is weak and cowardly.”
How should we dwell in this situation? In the third and final section of my reflection, I will seek to answer this question.
The reply is simple: within the confrontation between creation and anti-creation, we are called upon to TESTIFY. This testimony is our mode of being in the world.
The New Testament has an abundantly rich doctrine on this matter. I must confine myself to an indication of the three fundamental meanings which constitute testimony.
(i) Testimony means to say, to speak, to announce openly and publicly. Someone who does not testify in this way is like a soldier who flees at the decisive moment in a battle. We are no longer witnesses, but deserters, if we do not speak openly and publicly. The March for Life is therefore a great testimony.
(ii) Testimony means to say, to announce openly and publicly the divine Revelation, which involves the original evidence, discoverable only by reason, rightfully used. And to speak in particular of the Gospel of Life and Marriage.
(iii) Testimony means to say, to announce openly and publicly the Gospel of Life and Marriage as if in a trial [cfr. John 16, 8-11]. I will explain myself. I have spoken frequently of a confrontation. This confrontation is increasingly assuming the appearance of a trial, of a legal proceeding, in which the defendant is Jesus and his Gospel. As in every legal proceeding, there are also witnesses in favour: in favour of Jesus and his Gospel. Announcement of the Gospel of Marriage and of Life today takes place in a context of hostility, of challenge, of unbelief. The alternative is one of two options: either one remains silent on the Gospel, or one says something else. Obviously, what I have said should not be interpreted as meaning that Christians should render themselves… antipathetic to everyone.
St Thomas writes: “It is the same thing, when faced with two contraries, to pursue the one and reject the other. Medicine, for example, proposes the cure while excluding the illness. Hence, it belongs to the wise man to meditate on the truth, in particular with regard to the First Principle …and to refute the opposing falsehood.” [CG Book I, Chapter I, no. 6]. In the context of testimony to the Gospel, irenics and concordism must be excluded. On this Jesus has been explicit. It would be a terrible doctor who adopted an irenical attitude towards the disease. Augustine writes: “Love the sinner, but persecute the sin”. Note this well. The Latin word per-sequor is an intensifying verb. The meaning therefore is: “Hunt down the sin. Track it down in the hidden places of its lies, and condemn it, bringing to light its insubstantiality”.
I CONCLUDE with a quotation from a great confessor of the faith, the Russian Pavel A. Florenskij. “Christ is witness, in the extreme sense of the word, THE WITNESS.
At His crucifixion, the Jews and Romans believed they were only witnessing a historical event, but the event revealed itself as the Truth”. [The philosophy of religion, San Paolo ed., Milan 2017, page 512].
“WHEN I AM LIFTED UP FROM THE EARTH, I WILL DRAW ALL PEOPLE TO MYSELF” [John 12, 32].
The Brazilian priest Alexandre Awi Mello, the National Director of Brazil’s Schönstatt Movement, will serve as the new secretary for the the Dicastery for Laity, Family and Life. He was born Rio de Janeiro in 1971, and was ordained a priest in 2001.
Since 2002, he has been a professor of Pastoral Theology in several Brazilian universities. In 2007, he collaborated in the Aparecida Conference. He also directs the magazine “Tabor,” and has published several articles in magazines specialized in catechetical and pastoral works.
He studied Philosophy and Theology at the Pontifical Catholic University of Santiago de Chile and later moved to Germany to continue his studies.He holds a PhD in Mariology from the University of Dayton in the United States.
The Vatican announced the creation of the new Dicastery for Laity Family and Life in June 2016 and began operations on September 1 of the same year.
This new department absorbed the Pontifical Council for the Laity and the Pontifical Council for the Family, which ceased to function as of that date.
“The discourse is competent in those matters which belong to the Apostolic See for the promotion of life and the apostolate of the lay faithful for the pastoral care of the family and its mission, according to the design of God and forthe tutelage and the help of human life, “the Vatican reported on that occasion.
The effect of birth control and a contraceptive culture has altered our world in ways we could never have expected.
Think for a moment about the effect contraception has had on the number of vocations to the priesthood and religious life.
First of all, if a family has ten kids it is more likely that they are going to be happy for a few of them to pursue the priesthood or religious life. Mothers will quite happily send a few off to the seminary or monastery. If she has ten she can spare a few.
But if the neat and tidy suburban career woman only has two she is going to treasure them that much more. The idea that one would become a priest would be a shocking idea, but there is another more subtle attitude shift beneath this.
When mother and father decided to limit their family to two children by artificial means they usually do so in order for the woman to go back to work. The silent statement is, “What is most important to this family is to have as much income as possible.” and “The career. The career is everything! It comes first. Children? Meh.”
This attitude is then transmitted to the children who also put career first. Will there be any vocations from a home like that? Probably not.
Think further of the effects of this revolution in family life on the question of vocations. Before the invention and acceptance of artificial contraception a young man considering the priesthood would look around and weigh up his option.
Let’s say he lived in Philadelphia in the 1950s. He came from an Italian American family. He sees his Dad, his uncles, his grandfather. They are working class. They sweat in dangerous jobs to support their large families. They come home to a little house full of kids. Its a good life, but its a hard life.
The priest, on the other hand, doesn’t have his own wife and family, but he’s in Philadelphia. He gets sent to St Anthony of Padua parish. He’s surrounded by a big extended Italian family. He has status. He’s the priest. He gets an education. Maybe he travels to Rome. He lives in a big house with maybe three or four other priests. They have a nice Italian mama who cooks and cleans and looks after them.
The point I’m making is that, from a human point of view, the young man’s choice is fairer. With a wife and family he will have certain joys and certain sorrows and sacrifices. With the priesthood he will have certain joys and certain sorrows and sacrifices.
You pays your money and you makes your choice.
But think of the young man’s choice in today’s contraceptive culture. To be married and have a family doesn’t seem to require any sacrifices at all. Indeed, it seems like the passport to perfection. You get married. You eventually have two nice trophy children. Your wife continues her education and career. You’re both earning enough money to have everything. No sorrows. No sacrifice.
Of course I know it doesn’t always pan out that way, but that is what seems to be on offer.
On the other hand, for a young man to be a priest? He’s faced with a life of loneliness–stuck in Rectory by himself with onerous duties and little reward.
Again–I know it is not really like this, but this is what it may very well appear to be.
What’s to be done?
I happen to feel optimistic about the problem because I think the pendulum is going to swing back. I think an increasing number of young people are going to reject the contraceptive culture and choose a life giving alternative, and with that will be an increasing number of young men and women who choose a religious vocation, and they’ll be choosing for all the right reasons.
Why do I think this? Because a lie cannot sustain itself. All that is false eventually implodes. It can’t last.
On the other hand, all that is beautiful, good and true will always be attractive. Like fresh shoots on a tree that has been felled, it will spring back.
I am often asked to speak about sex to high school students. Many adults shudder at the thought of talking to kids about sex, but I love it. First, I have a captive audience, and second, I get to talk about two things that I am very passionate about: the dangers of teen sex and the joys of sex in marriage. Many adults worry that kids will be too shy to ask questions but on the contrary, I have found them eager to have ever their questions answered in an honest, upbeat manner.
I do not take the topic of teens and sex lightly. I have seen the pain of STDs in 13- and 14-year-old children in my office along with other serious health issues caused by sex.
Most people are aware of the physical repercussions of sex:
We now have 35 known STDs. In 1960, we only had two.
Teenagers make up one-third of the U.S. population, but they carry 50 percent of STDs.
One in four teens has an STD. (Over 80% of those infections have no symptoms, so they can go undetected, which is dangerous for the teen, their future sexual partners and their future children.)
You may be familiar with those numbers, but few are aware of the emotional repercussions teen sex can have.
For the thousands of teens I’ve treated and counseled, many of them—yes, teen boys too—have depression related to sexual activity. You rarely hear the correlation made, but I consider depression an STD with effects as devastating as HPV, chlamydia or any physical infection.
Depression related to teen sex can be as devastating as any STD
Consider these numbers:
In 2015, an estimated 3 million adolescents age 12 to 17 in the U.S. had at least one major depressive episode in the past year—that’s about 12.5% of all 12 to 17 year olds.
From 1999-2014, the suicide rate in girls age 10 to 14 tripled.
About 20% of teens will experience depression before they reach adulthood.
I believe it is no coincidence that as STDs have become an epidemic in teens, so has depression. The correlation is startling.
Depression in a teen occurs on a biochemical as well as psychological level and the two are linked. We know that the levels of specific hormones in the cerebral spinal fluid of depressed teens are different from those of non-depressed teens.
We know that depression occurs when a teen experiences un-grieved losses—hurts that have been buried in their psyche, festering like abscesses. When a teen doesn’t deal with a traumatic or hurtful event, he ends up stuffing it and the negative emotions come out sideways. He becomes angry, withdrawn and depressed.
Teenagers don’t have the maturity to handle sex
Think about a 17-year-old boy who has had multiple sexual partners (as most 17 year old boys these days are encouraged to do.) He has sex because he believes this is what he must do to be a “man”. However, not all of those sexual encounters go well. He is too ashamed to admit this to his friends and knows he can’t talk to his parents about it, so he pretends like everything is fine, stuffs his feelings and continues having multiple partners.
Or consider a 15-year-old girl who feels pressured to have sex with her boyfriend. She finally does and two weeks later, he breaks up with her. She can’t explain to her parents why the break-up is so upsetting (she may not even know why herself), so she tries to find consolation in the next boy she dates, starting an unhealthy cycle and not dealing with the grief and the loss.
Teenagers don’t have the psychological or cognitive maturity to handle sex, regardless of what adults in our culture say. And they certainly can’t handle sex with multiple partners. Depression occurs by un-grieved losses and the truth is, sex for teen boys and girls causes many losses on many levels.
The misconceptions many parents have about their teenagers are these: that teen boys are nothing more than vats of hormones, that girls want to be sexually active in high school and college because that’s what girls do, and that sex is really fine for kids if they use “precautions” and stay “safe.” I discuss the dangers of both of these misconceptions, as well as the link between teen sex and depression in a recent episode of my Parenting Great Kids podcast.
First, boys have minds, hearts and spirits and treating them otherwise is wrong. Second, most girls don’t want to be sexually active but have no one to counsel them how to postpone sex. Finally, terms like “precautions” and “safe” are meaningless. How is a teen to avoid hurt if he has sex, bonds to a girl and then breaks up? And studies show that condoms don’t protect equally against different diseases, so being “safe” is nonsense.
I can’t tell you how many 16- and 17-year-old boys come up to me after I’ve spoken at their school to talk about the emotional scars they have from sex.
Parents, make sure your teens understand the mental and emotional connection of sex
This is why simply talking to your child about “safe sex” (a phrase that even the CDC won’t use anymore) is not enough. It’s your job as your son or daughter’s parent to help set them up for a lifelong, monogamous relationship and to get them there as emotionally unscathed as possible; not to simply cross your fingers and hope your child doesn’t get one of the over 35 STDs.
Do more than teach your child about the physical harm that can result from sex. Talk to them about their feelings and make sure they understand the emotional and mental connection that sex has. You need to be the person to tell your child this and know that they want to hear what you have to say. Work very hard to protect their hearts and minds as much as their bodies because trust me, nobody else is going to help teach them what you will.
Dr Meg Meeker is a US pediatrician, mother and best-selling author of six books. She is a leading authority on parenting, teens and children’s health. This article is republished from her blog with permission. Refer to the original article for promotions and other information.
– See more at: https://www.mercatornet.com/family_edge/view/teenagers-and-the-std-nobody-is-talking-about/19892#sthash.bJ4bufSW.dpuf
ROME, May 18, 2017 (LifeSiteNews) — There is a need to “prioritize” procreation as the primary end of marriage today, because when this “distinctive” and “proper” purpose is questioned or doubted, the “marriage institution itself — and society thereafter — begins its slide down the slippery slope,” the head of Human Life International’s (HLI) Rome office told an international gathering of pro-life and family groups there today.
Father Francesco Giordano speaking at the 2017 Rome Life Forum.
Father Francesco Giordano, a professor in Rome who addressed the fourth annual Rome Life Forum today, said that a de-emphasis of procreation within marriage has not only resulted in legalized abortion, but homosexual “marriage.”
To illustrate his point, he presented the main argument behind the U.S. Supreme Court 2015 decision that legalized same-sex “marriage.”
We read in a Catholic World News article from the day: “Claiming that the institution of marriage has “evolved over time,” Justice Kennedy wrote that the essence of the marital bond is a sharing of intimacy, which does not require partners of opposite sexes. He argued that the plaintiffs in the Obergefell case were not undermining the institution of marriage, but showing their respect for that institution by seeking to participate in it. The majority opinion reasoned that the ability to marry would help to stabilize same-sex unions, and benefit the children raised by homosexual partners. Justice Kennedy explicitly rejected the notion that marriage is intrinsically oriented to procreation, writing: “An ability, desire, or promise to procreate is not and has not been a prerequisite for a valid marriage in any state.”” With the stress on the end or good of union, we are seeing these sorts of results, so it only confirms me in stressing the procreative end as the proprium of marriage.
Giordano noted how Pope Paul VI’s 1968 Encyclical Humanae Vitae, which outlined the moral evil of contraception, was a “novel” approach to conjugal relations in that it “placed the unitive end of marriage at par with the procreative end.”
He said that while the unitive purpose of the conjugal act “works with the procreative end in harmonizing the love between the parents” it is the procreative purpose which makes the act “unique” when compared to any other human act.
“The telos [purpose by nature] of the union between man and woman is generative. It is the proprium of marriage after all. It is the first end of the sexual act to be intimately united to the second end, but we have to prioritize the procreative end of marriage because it is the distinctive, proper and privative end of marriage,” he said.
He went on to quote the first account of Creation, including that God created man in his image, created them male and female, and told them: “Be fertile and multiply.”
“So it is clear that the first duty of the first family was to generate children,” he said.
Not only is this the Church’s teaching, he said, it is substantiated by natural law, not something we just follow in an abstract way.
“We adhere to a teaching because of its compelling truth,” Giordano said, “a truth which the Church naturally defends.”
Giordano’s presentation comes days after rumors began circulating in Rome of a secret committee set up by Pope Francis to study Humanae Vitae. Francis’ position on contraceptive practices — which the Church has always taught to be gravely immoral — remains sufficiently ambiguous to be interpreted as lending support to the use of contraception and condoms, in certain cases.
In a March 2014 interview with Corriere della Sera, Francis said that the question of birth control must be answered not by “changing the doctrine” but by “making pastoral (ministry) take into account the situations and that which it is possible for people to do.”
During a November 2015 press conference on his return flight from Africa, Francis, when asked if it was time for the Church to allow the use of condoms to prevent HIV agreed that condom use is “one of the methods,” but that it brought into conflict the fifth and sixth commandments.
And during his February 2016 return flight from Mexico, Francis said that contraception may be the “lesser of two evils” for parents wanting to avoid conceiving a child in areas affected by the Zika virus. Vatican spokesman Fr. Federico Lombardi confirmed the pope’s words the following day, stating: “The contraceptive or condom, in particular cases of emergency or gravity, could be the object of ‘discernment’ in a serious case of conscience. This is what the Pope said.”
Giordano also outlined a number of threats facing the family, including gender ideology and transhumanism.
“The end of man is the adoration of God. The end of gender ideology is the adoration of the body,” he said.
Giordano also discussed how the negative social changes resulting from the family’s decline, including the breakdown in the understanding of the human being as male or female, are now being advanced by a transhumanist mentality.
“Unlike animals, men can truly shape their lives, and this the transhumanists understand. However, what the transhumanists do not seem to understand is that there are limits posed by our nature on what we can do to shape our lives,” he said.
“In order to bring about the reduction of human identity to a freely chosen, mutable sexual orientation and avoid its formation in the countless influences besides sex, the elimination of these other influences—such as family, culture, and religion—are necessary [for the transhumanists,]” he said.
This mentality represents a sign of man’s demise, he said, “and the only response to all of these threats is found in strong traditional family units.”
Giordano went on to explain how the transhumanist movement is based on the belief that man is a failed experiment, and its assumption that man can come to salvation by knowing or doing something particular displays elements of the Gnostic-Pelagian heresies.
As man moves further away from human nature today, and we also see an increase in barbarous acts, it shows rejection of God and His law, said Giordano.
Conversely, he said, “When we search for that which is most elevated, dignified, and noble, we inevitably find God who is Truth, Beauty, and Goodness itself.”
“The Magisterium in the papal teachings on Marriage and the Family has been attentive to the family seeing it as a real jewel of a social institution to be protected for the greater common good of society and each man,” stated Giordano.
“If the family unit is hurt, man is ultimately hurt, and the results are evident all around us that there is indeed an abolition of man in course. If instead, the family unit is united and faithful to God, focused on Our Lord, then there is order in its life and that of its members,” he added.
From ‘us to ‘me’
In discussing the importance of marriage, Giordano said emphasis has shifted from the family to the individual since the time of the French Revolution.
The family is understood as an institution that is beyond social functions, however, the priest said. And he told the forum “the family is very much under attack, starting with the very sacrament that is its foundation: marriage.”
He explained how problems have emerged from the center of work being moved from the household to outside the home since the Industrial Revolution.
Further, divorce has come about from many social, economic and political issues. Giordano cited the sexual revolution, the move to an industrial society over the last 200 years, and the way governments have interfered in marriage, being agents of divorce.
“We know from our fight with the abortion industry just how important legalization of such matters is in influencing the mindset,” said Giordano.
A long time coming
A look at the works written by the popes since the 19th-century on the subjects of family and marriage show they were already addressing the crisis then, he continued, citing Benedict XIV, Pius IX and Leo XIII.
“The popes were very conscious of the fact that the Church’s role was to protect sacred matrimony from all sorts of confusion because both the Church and society as a whole would suffer,” Giordano stated.
“Marriage is not merely a convention which the State can decide upon at whim,” he said, quoting Pope Leo XIII’s Arcanum divinae Sapientiae. “Marriage was established by God after the creation of our first parents so that they would transmit the life that He had given to them.”
“Marriage sanctifies the union of man and woman, and in these two accounts we see two ends of marriage clearly identified: procreative and unitive,” explained Giordano. “Through marriage, there is a remedy in store for man’s wounded nature.”
He told the forum that the Congregation for Rites having inserted the Feast of the Holy Family in the Calendar of the Roman Rite in 1921 upon the directive of Pope Benedict XV, while not the beginning of the devotion to the Holy Family, displayed the deep concern of the Holy Father for the breakdown of the family.
“Each time I read documents from the early part of the 20th century I notice that many good Catholic writers were lamenting the breakdown of the family and society back then, and I wonder: what would they say today?” the priest queried for those in attendance. “In many ways, they predicted what is happening today.”
Regarding gender, Giordano discussed St. Thomas Aquinas’s definition of man as a composite of body and soul; the two are not separate.
He explained how a number of subsequent modern philosophies reject this. And also that disruption of the natural order of man’s make-up, whether material, physical, spiritual or psychological, can have devastating effects on the whole.
These can lead to gender confusion and transhumanism.
“In a time when nature itself is questioned,” Giordano said, “when its goodness is doubted and reproduction altered, when it is no longer considered enough in itself, and attempts are made to go beyond it in the realm of transhumanism, St. Thomas’ insights are now quite valuable to consider.”
“St. Thomas teaches that even in the state of being separate, the soul is inclined to being united to its specific body,” he told the forum. “It is in this union that we see how maleness and femaleness characterize the whole person, uniting the body’s biological structure to the soul.”
“Even if this can be a debated position,” said Giordano, “we affirm that the soul is itself not a gender, or else the distinction between men and women would make them different species. The gender is in the body, but the soul is not immune from its influence since it is so integrally united to the body.”
Further, he said, if gender deals with the whole person the way that the soul does, then sex-reassignment surgery really cannot change one’s gender.
According to St. Thomas, the common end between male and female is the procreative end, he said. The particular material ends between male and female, though, are complimentary, but different.
Editor’s note: Pete Baklinski contributed to this report.
Editor’s note: This address was delivered by His Excellency Bishop Athanasius Schneider, auxiliary bishop of Astana in Kazakhstan, on 19 May 2017 at the fourth annual Rome Life Forum, which is organised by Voice of the Family.
May 19, 2017 (LifeSiteNews) – The family has been created immediately by God, so the Magisterium of the Church teaches us.[1] Pope Leo XIII says in his magisterial encyclical on marriage and family: “Marriage has God for its Author, and was from the very beginning a kind of foreshadowing of the Incarnation of His Son; and therefore there abides in it something holy and religious; not extraneous, but innate; not derived from men, but implanted by nature. Innocent III, therefore, and Honorius III, our predecessors, affirmed not falsely nor rashly that a sacrament of marriage existed ever amongst the faithful and unbelievers.”[2]
“The family therefore holds directly from the Creator the mission and hence the right to educate the offspring, a right inalienable because inseparably joined to the strict obligation, a right anterior to any right whatever of civil society and of the State, and therefore inviolable on the part of any power on earth.”[3] Parents are therefore under a grave obligation to see to the religious and moral education of their children.[4]
Pope Leo XIII gave us a very concise explanation about the original and first duty of parents concerning the education of their children, and in the first place concerning the education in the Catholic faith. This duty has its foundation in the natural order of the Divine creation: “The common sense of mankind is in such complete accord, that they would be in open contradiction with it who dared maintain that the children belong to the State before they belong to the family, and that the State has an absolute right over their education. Untenable is the reason they adduce, namely that man is born a citizen and hence belongs primarily to the State, not bearing in mind that before being a citizen man must exist; and existence does not come from the State, but from the parents. The children are something of the father, and as it were an extension of the person of the father; and, to be perfectly accurate, they enter into and become part of civil society, not directly by themselves, but through the family in which they were born.”[5] “And therefore,” says the same Pope Leo XIII, “the father’s power is of such a nature that it cannot be destroyed or absorbed by the State; for it has the same origin as human life itself.”[6] Pope Leo XIII declares in another memorable encyclical, where he thus sums up the rights and duties of parents: “By nature parents have a right to the education of their children, but with this added duty that the education and instruction of the child be in accord with the end for which by God’s blessing it was begotten. Therefore it is the duty of parents to make every effort to prevent any invasion of their rights in this matter, and to make absolutely sure that the education of their children remain under their own control in keeping with their Christian duty, and above all to refuse to send them to those schools in which there is danger of imbibing the deadly poison of impiety.”[7]
Already more than seventy years ago Pope Pius XII made an appeal to the Christian families to be new crusaders in spreading and defending the true Catholic faith in midst of the general and heavy torpor into which the drugs of false ideas, widely diffused, have sunk the human family in the twentieth century. This diagnosis, which Pius XII made about the spiritual health of his time, is fully applicable to our times and it became even much worse. Pius XII said: “It is for the best and most distinguished members of the Christian family, filled with the enthusiasm of Crusaders, to unite in the spirit of truth, justice and love to the call; God wills it, ready to serve, to sacrifice themselves, like the Crusaders of old. If the issue was then the liberation of the land hallowed by the life of the Incarnate Word of God, the call today is, if We may so express Ourselves, to traverse the sea of errors of our day and to march on to free the holy land of the spirit, which is destined to sustain in its foundations the unchangeable norms and laws on which will rise a social construction of solid internal consistency.”[8]
The first and most holy goal and end of matrimony and family consists in giving birth to new citizens of heaven. Pope Leo XIII said: “By the command of Christ, it not only looks to the propagation of the human race, but to the bringing forth of children for the Church, ‘fellow citizens with the saints, and the domestics of God’;(Eph. 2:19) so that ‘a people might be born and brought up for the worship and religion of the true God and our Saviour Jesus Christ’ (Catechismus Romanus, cap. 8).”[9] The family is therefore the first and original place, where the integrity and the beauty of the Catholic faith should be taught to the children, and by this way handed over to the future generations. Indeed from this transmission of the faith depends the spiritual health of a nation as taught Pope Pius XII: “The family is holy. It is the cradle not only for the children, but the entire nations. Man and woman should pass on the torch of the physical and also spiritual, of the moral and of the Christian life to the future generations.”[10]
From the early centuries of Christianity the family was seen as the Church “in miniature,” and the Church itself was called the “family of God”, especially the Christian community gathered for the celebration of the sacred liturgy was called the “family of God”, as we can often read in the liturgical texts, so for example in the Canon of the Mass. It was especially the Second Vatican Council, which reminded us of this ancient truth. In the Dogmatic Constitution “Lumen gentium” the Council teaches: “The family is, so to speak, the domestic church. In it parents should, by their word and example, be the first preachers of the faith to their children; they should encourage them in the vocation which is proper to each of them, fostering with special care a vocation to a sacred state.”[11] Pope John Paul II, the Pope of the family, made this famous affirmation: “In the future, evangelization will depend largely on the domestic church.”[12] The same Pope said: “The future of humanity passes by way of the family.”[13]
So great and splendid is the educational ministry of Christian parents that Saint Thomas has no hesitation in comparing it with the ministry of priests: “Some only propagate and guard spiritual life by a spiritual ministry: this is the role of the sacrament of Orders; others do this for both corporal and spiritual life, and this is brought about by the sacrament of marriage, by which a man and a woman join in order to beget offspring and bring them up to worship God.”[14]
Pope John Paul II gives to the catechesis in family the priority over all other forms of catechesis, when he says: “Family catechesis, therefore, precedes, accompanies, and enriches all other forms of catechesis. Furthermore, in places where anti-religious legislation endeavors even to prevent education in the faith, and in places where widespread unbelief or invasive secularism makes real religious growth practically impossible, ‘the domestic church’ remains the one place where children and young people can receive an authentic catechesis. Thus, there cannot be too great an effort on the part of Christian parents to prepare for this ministry of being their own children’s catechists and to carry it out with tireless zeal. Encouragement must also be given to the individuals or institutions that, through person-to-person contacts, through meetings, and through all kinds of pedagogical means, help parents to perform their task: the service they are doing to catechesis is beyond price.”[15]
One of the main causes of the moral, spiritual and religious crisis of the current time consists in the religious ignorance, in ignoring the truths of the faith and in an erroneous knowledge of the faith. Pope Pius X very rightly observed this connection, saying: “The enemy has, indeed, long been prowling about the fold and attacking it with such subtle cunning that now, more than ever before, the prediction of the Apostle to the elders of the Church of Ephesus seems to be verified: ‘I know that . . . fierce wolves will get in among you, and will not spare the flock’ (Act 20:29). Those who still are zealous for the glory of God are seeking the causes and reasons for this decline in religion. Coming to a different explanation, each points out, according to his own view, a different plan for the protection and restoration of the kingdom of God on earth. But it seems to Us, that while we should not overlook other considerations. We are forced to agree with those who hold that the chief cause of the present indifference and, as it were, infirmity of soul, and the serious evils that result from it, is to be found above all in ignorance of things divine. This is fully in accord with what God Himself declared through the Prophet Osee: ‘And there is no knowledge of God in the land. Cursing and lying and killing and theft and adultery have overflowed: and blood hath touched blood. Thereafter shall the land mourn, and everyone that dwelleth in it shall languish’ (Osee 4:1-3).”[16] And Pope Benedict XIV wrote: “We declare that a great number of those who are condemned to eternal punishment suffer that everlasting calamity because of ignorance of those mysteries of faith which must be known and believed in order to be numbered among the elect.”[17] For this reason the same Pope Benedict XIV said: “There is nothing more effective than catechetical instruction to spread the glory of God and to secure the salvation of souls.”[18]
The beauty of the Catholic faith manifests itself in a special manner in large families. We possess one of the most striking and illuminating affirmations of the Magisterium on this theme in the following words of Pope Pius XII addressed to the Associations of Large Families: “Large families are the most splendid flower-beds in the garden of the Church. […] The brows of the fathers and mothers may be burdened with cares, but there is never a trace of that inner shadow that betrays anxiety of conscience or fear of an irreparable return to loneliness, Their youth never seems to fade away, as long as the sweet fragrance of a crib remains in the home, as long as the walls of the house echo to the silvery voices of children and grandchildren. Their heavy labors multiplied many times over, their redoubled sacrifices and their renunciation of costly amusements are generously rewarded even here below by the inexhaustible treasury of affection and tender hopes that dwell in their hearts without ever tiring them or bothering them. And the hopes soon become a reality when the eldest daughter begins to help her mother to take care of the baby and on the day the oldest son comes home with his face beaming with the first salary he has earned himself. […] Children in large families learn almost automatically to be careful of what they do and to assume responsibility for it, to have a respect for each other and help each other, to be open-hearted and generous. For them, the family is a little proving ground, before they move into the world outside, which will be harder on them and more demanding.”[19]
The beauty of the Catholic faith manifests itself in the fact that it is precisely the family which is the first breeding ground and the first seedbed for the priestly vocations. The Second Vatican Council spoke about the family as the first seminary in the process of fostering and training priestly vocations.[20] History has given proof that the majority of priestly vocations come from large families. Pope Pius XII highlighted this interrelationship saying: “With good reason, it has often been pointed out that large families have been in the forefront as the cradles of saints. We might cite, among others, the family of St. Louis, the King of France, made up of ten children, that of St. Catherine of Siena who came from a family of twenty-five, St. Robert Bellarmine from a family of twelve, and St. Pius X from a family of ten. Every vocation is a secret of Providence; but these cases prove that a large number of children does not prevent parents from giving them an outstanding and perfect upbringing; and they show that the number does not work out to the disadvantage of their quality, with regard to either physical or spiritual values.”[21]
The supernatural spirit of love and of self-sacrifice of the mother (and oftentimes of the mother of a large family) is the very foundation of a priestly vocation and of the fruitfulness of the priestly life of her son. The following moving example illustrates this truth in an impressive manner: “In the city of Zaborze in Upper Silesia is a grave which is frequently visited by pilgrims. Above the grave rises a Lourdes grotto. At the foot of the statue of the Immaculate Conception, in a little glass case, lies a myrtle wreath. Here is the story of the myrtle wreath. A priest is buried in the grave at the foot of the grotto. He was the youngest of ten children. As a young man he worked very hard to earn enough money to study for the priesthood, because his parents were poor. After his ordination he went as a missionary to India where he worked for many years. When he died they buried him in his home town of Zaborze and erected a grotto of Our Lady of Lourdes above his tomb because he had always fostered a special devotion to Mary Immaculate. Some time after the burial of this zealous priest, a little box was found among his possessions with a note pasted upon it: ‘To be opened after my death.’ The box contained a myrtle wreath and this note: ‘This is my mother’s bridal wreath. I have carried it with me to various countries, on my journeys over land and sea, in memory of that sacred moment when my mother vowed not only fidelity but also uprightness at the altar of God. She has kept that vow. She has had the courage to have me after the ninth child. Next to God I owe her my life and my vocation to the priesthood. If she had not wanted me, I would not have become a priest and a missionary; I would not have been able to work for the salvation of souls. Place this wreath, my mother’s bridal wreath, into my grave. This I ask of the one who finds it.’ When they found the wreath, the grave had already been closed, so they placed it at the foot of the statue of the Immaculate Mother to whom he dedicated his life.”[22]
As another example we could mention the mother of Saint Pius X, Margherita Sanson. She raised up ten children. She taught them to pray first thing in the morning, communicate with God throughout the day, and to end each day with prayer, bringing the family together for an examination of conscience. The well-known story of the wedding ring of his mother remains always inspiring: Following her son’s episcopal ordination and placement in Mantova, the future Pope Pius X visited his old mother to thank her. After kissing his episcopal ring, she showed him her wedding ring and said, “Your ring is very beautiful, Giuseppe, but you wouldn’t have it if I didn’t wore this my ring.” I know the following story: A priest came to the mother of a priest to congratulate her with the episcopal nomination of her son. To this congratulation the mother replied: “This does not mean this much. The most important thing is, that my son remain always faithful to Jesus”. And each time when this bishop phones his mother, before hanging up the telephone receiver, she says to her son: “You remain faithful to Jesus!” To remain faithful to Jesus, means to remain faithful to all of His commandments and to all of His Divine teachings, and to prefer temporal disadvantages and disdain, even on the part of ecclesiastical persons, rather than to make compromises regarding the teaching and the observance of His commandments and teachings.
When parents impart to their children a truly Catholic education in faith, they lay the foundation of the faith of the future priests and bishops. Usually the uncompromising and life-long fidelity to the integrity of the Catholic faith on behalf of a priest and of a bishop, is a fruit of the education which he got in his family from his father or from his mother or from both, or from his grandmother.
The truth which says that the family is the original place of the beauty of the Catholic Faith we can see also in the following edifying witness in the autobiography of Saint Therese of the Infant Jesus: “Feast days! Those words conjure up more wonderful memories! I did so love them and you were able to explain so well what they were all about. That again was a foretaste of Heaven. But the procession of the Blessed Sacrament was what I loved best, for I could scatter flowers beneath the feet of God! I used to throw them up high into the air before they fell and when my rose petals touched the monstrance my happiness was complete. The big feasts did not come along so often but there was one most dear to me, and it came every week – Sunday, Our Lord’s own day, a wonderful day, a day of rest. We all went to the High Mass, and when it was time for the sermon, I remember we had to leave our place because it was so far away from the pulpit and go all up the nave to find places nearer. This was not always easy to do, but everyone seemed quite ready to find room for little Thérèse and her father. Uncle, especially, seemed very happy when he saw us Coming; he used to call me his little ray of sunshine and say that the sight of this venerable patriarch hand in hand with his little daughter always touched his heart. The fact that all this drew attention to us never bothered me; I was far too interested in what the priest was saying. The first sermon I really understood was one on Our Lord’s Passion, and I was very much moved by it; that was when I was five and a half, and from then on I could take in and appreciate all that was said. If ever St. Teresa was mentioned, Father used to bend down toward me and whisper: “Listen, my Little Queen, he is talking about your Patron Saint.” Then I would really listen, but I am afraid I kept my eyes on Father far more than on the preacher because I could read such a lot in his noble face. Sometimes his eyes would fill with tears he could not keep back, and when he was listening to the eternal truths, he seemed to be already in another world and no longer in this. He was then a long way from his journey’s end, however; long, sad years had yet to pass before he opened his eyes on Heaven’s loveliness and Jesus wiped away His faithful servant’s tears” (Story of a soul).
In those times, the Eucharistic liturgy was not celebrated in the vernacular and without explanatory remarks and commentaries. However, Saint Therese of the Infant Jesus and her father Saint Louis Martin had a very intense active participation in the liturgy of the Holy Mass, an active participation, which was marked with silence, as recommended also by the Second Vatican Council.[23] Undoubtedly, their participation in the liturgy was more active, that means, more conscious, attentive and pious than that of many Catholics in our days, where the liturgy is celebrated entirely in vernacular and where active participation is realized in playing an exterior liturgical role, against the prescriptions of the Second Vatican Council.[24] Recently Cardinal Robert Sarah, the Prefect of the Congregation of Divine Worship, made the following apt observation on this issue: “Most of the faithful—including priests and bishops—do not know this teaching of the Council. […] As Benedict XVI often emphasized, at the root of the liturgy is adoration, and therefore God. Hence it is necessary to recognize that the serious, profound crisis that has affected the liturgy and the Church itself since the Council is due to the fact that its center is no longer God and the adoration of Him, but rather men and their alleged ability to ‘do’ something to keep themselves busy during the Eucharistic celebrations.”[25]
The present situation of the world and partly of the life of many Catholics and ministers of the Church could be characterized as a great apostasy, an apostasy from the faith in the true Divinity of Christ, from the faith in the unique way of salvation through Christ and an apostasy from the faith in the perennial validity of the Divine commandments. Such an apostasy signifies ultimately to renounce Christ and to accept the spirit of the world, diluting Christ in a gnostic manner into the materialistic, naturalistic and esoteric spirit of the world. Recently Cardinal Robert Sarah made the following striking statement on the real current spiritual situation inside the Church: “Political Europe is rebuked for abandoning or denying its Christian roots. But the first to have abandoned her Christian roots and past is indisputably the post-conciliar Catholic Church. […] While more and more voices of high-ranking prelates stubbornly affirm obvious doctrinal, moral and liturgical errors that have been condemned a hundred times and work to demolish the little faith remaining in the people of God, while the bark of the Church furrows the stormy sea of this decadent world and the waves crash down on the ship, so that it is already filling with water, a growing number of Church leaders and faithful shout: ‘Tout va très bien, Madame la Marquise!’ (‘Everything is just fine, Milady!’)”[26] These words reflect perfectly the analysis of the modern world made by Saint Pius X already a hundred years ago: “The great movement of apostasy being organized in every country for the establishment of a One-World Church which shall have neither dogmas, nor hierarchy, neither discipline for the mind, nor curb for the passions, and which, under the pretext of freedom and human dignity, would bring back to the world (if such a Church could overcome) the reign of legalized cunning and force, and the oppression of the weak, and of all those who toil and suffer. […] Indeed, the true friends of the people are neither revolutionaries, nor innovators: they are traditionalists.”[27]
The Catholic family is the original place of the experience of the beauty of the Catholic Faith. The Catholic family represents the first bulwark against the current great apostasy. The two most efficient weapons against the modern apostasy outside and inside the life of the Church are the purity and integrity of the faith and the purity of a chaste life. The admonition which Saint Louis IX, King of France, left to his son, remains always valid: “My dearest son, my first instruction is that you should love the Lord your God with all your heart and all your strength. Without this there is no salvation. Keep yourself, my son, from everything that you know displeases God, that is to say, from every mortal sin. You should permit yourself to be tormented by every kind of martyrdom before you would allow yourself to commit a mortal sin. […] Work to remove all sin from your land, particularly blasphemies and heresies” (Letter to his son).
Once a member of an anti-christian movement, who later converted to the Catholic Church, said to Fr. Mateo Crawley, the Apostle of the Enthronement of the Sacred Heart: “We have only one goal in mind: to dechristianise the family. We leave to the Catholics gladly the churches, the chapels, the cathedrals. For us it is enough to have the family in order to corrupt the society. If we have control over the family, our victory over the Church is guaranteed.”[28] True Catholic families – and desirably large families – will strengthen the Church of our days with the beauty of the Catholic Faith. From that faith will come out new Catholic fathers and mothers, and from them there will come out a new generation of zealous priests and intrepid bishops, who will be ready to give their life for Christ and for the salvation of the souls. Christianity was born out of the family, the Holy Family, so that the family may be born again out of Christianity. The first fruit of the redemption is the Holy Family, just as the first blessing of the Creator was given to the family. Indeed, what the current world and the Church mostly need, are true Catholic families, the original places of the beauty of the Catholic Faith.
[1] cf. Pius XI., Encyclical Divini illius magistri, 12.
[2] Encyclical Arcanum Divinae, n. 19, 10 February 1880. Concerning Innocent III, see Corpus juris canonici, cap. 8, De divort., ed. cit., Part 2, col. 723. Innocent III refers to 1 Cor. 7:13. Concerning Honorius III, see cap. ii, De transact., (op. cit., Part 2 col. 210).
[3] Pius XI, Encyclical Divini illius magistri, 32.
[25] Address to the Colloquium “The Source of the Future” on the occasion of the 10th anniversary of the publication of the Motu proprio Summorum Pontificum by Pope Benedict XVI, March 29 – April 1, 2017, Herzogenrath, Germany
[26] Address to the Colloquium “The Source of the Future” on the occasion of the 10th anniversary of the publication of the Motu proprio Summorum Pontificum by Pope Benedict XVI, March 29 – April 1, 2017, Herzogenrath, Germany
In an attempt to continue her desired “transition” from female to male, Evan Michael Minton was scheduled by her surgeon to undergo a hysterectomy at Dignity Health chain’s Catholic Mercy San Juan Medical Center in Carmichael, California last summer. The surgery was denied by the Catholic hospital’s policy. And, although Minton was able to have the surgery at another Dignity Health chain hospital in September, she told a reporter for the Sacramento Bee that she was “devastated” by the denial. Claiming that the hospital’s unwillingness to perform the surgery caused such “frustration and disappointment,” the American Civil Liberties Union has now stepped in to file a lawsuit against the hospital last week on his behalf.
Filed in San Francisco Superior Court, the ACLU lawsuit claims that Minton was “discriminated against” when she sought a hysterectomy as part of her transition from female to male. Spokeswoman Melissa Jue, of the Mercy San Juan Medical Center, told reporters that “sterilization procedures, such as hysterectomies or tubal ligations are permitted by Catholic hospitals only to cure or alleviate a serious pathology.” She pointed out that Dignity Health officials helped Minton obtain the hysterectomy the following month at one of Dignity’s non-Catholic hospitals, Methodist Hospital of Sacramento.
Minton’s surgeon, obstetrician gynecologist Dr. Lindsey Dawson, told reporters: “I don’t blame the administrators. I blame the (Catholic) doctrines.” Minton has already had a double mastectomy and a phalloplasty in her quest to become a male. The hysterectomy was the final step in Minton’s journey to “be able to be congruent with who I am.” Telling reporters that “When I got my complete body, the rest of my life starts here,” Minton added that: “I don’t want it to affect my transgender brothers and sisters the way it affected me…No one should have to go through that.” That is exactly what should concern all Catholic institutions—including Catholic colleges and universities—as they are all vulnerable to transgender discrimination lawsuits. Minton’s suit is a cautionary tale for Catholic institutions.
All of this is emerging from U.S. Department of Health and Human Services rule issued on September 8, 2015, by the Obama administration. The rule is really a new interpretation of Section 1557 of the Affordable Care Act (ACA) to extend Title IX’s definition of “sex” to include gender identity. The Rule was published as final on May 18, 2016, and it expanded the HHS definition of gender identity even further from the proposed definition to mean an individual’s internal sense of gender, which may be male, female, neither, or a combination of male and female. HHS stated in the new rule that “gender identity spectrum includes an array of possible gender identities beyond male and female,” and individuals with “non-binary gender identities are protected under the rule.” This means that doctors, hospitals and other healthcare providers—including those receiving nursing or medical training on Catholic college campuses—may not “deny or limit treatment” to those seeking sex reassignment procedures, even when those procedures run contrary to the provider’s religious beliefs and medical judgement.
Religious institutions have attempted to fight back. Last August, the Becket Fund for Religious Liberty filed a lawsuit in a Texas federal court on behalf of a coalition of religious healthcare providers, charging that Obama’s Health and Human Services Administration “overstepped its bounds” by requiring medical providers to participate in sex-reassignment procedures—including sex reassignment services and procedures on young children.
More recently, on November 7, 2016 the Beckett Fund filed yet another lawsuit—this time including a Catholic college in the lawsuit—against the federal government’s HHS mandates on behalf of the Religious Sisters of Mercy and the University of Mary. The State of North Dakota also joined Becket’s legal challenge. According to the complaint, Becket points out that the HHS mandate forces healthcare professionals and the University of Mary to violate their deeply held religious beliefs. One of the plaintiffs, the University of Mary, maintains that the Catholic school “infuses Benedictine values throughout its educational experience, including its premier nursing program,” yet will be forced to violate their deeply held religious beliefs by participating in what the Catholic Church teaches are “harmful medical transition procedures.” The regulation also requires that they pay for these same medical transition procedures in their health plans on pain of massive financial liability.
The Conference of Catholic Bishops opposed inclusion of gender identity in federal health care laws barring sexual discrimination. In a November 6, 2015 letter to the U.S. Department of Health and Human Services the bishops claimed that “that medical and surgical interventions that attempt to alter one’s sex are, in fact, detrimental to patients” and “are not properly viewed as health care because they do not cure or prevent disease or illness. Rather they reject a person’s nature at birth as male or female.”
As the Sisters of Mercy/University of Mary lawsuit points out, since the Sisters of Mercy Health System provides hysterectomies to some patients, such as those diagnosed with uterine cancer, the HHS Regulations force the Catholic health care providers to provide a hysterectomy and remove an otherwise healthy uterus for a medial transition—notwithstanding the serious potential harm to the patient, and the violation of the religious beliefs of the providers. The Becket complaint also points out that the Regulations require Plaintiffs to “compel the speech of healthcare professionals” (including Catholic university nursing students) in several ways—mandating revisions to healthcare professionals written policies, requiring them to promise to provide transition related procedures, and requires healthcare providers to use gender-transition affirming language in all situations regardless of circumstance.
Unless President Trump actually repeals the Affordable Care Act—including its religious liberty destroying mandates surrounding gender identity—the Catholic Church is likely in for a long battle. The Church cannot change her teachings on non-negotiable issues such as the nature of man and woman. Pope Francis has already joined his predecessor Pope Emeritus Benedict XVI in condemning contemporary gender theory as denying “the order of creation.” In a Christmas-time homily on December 23, 2008, Pope Benedict directly addressed transgender issues by cautioning Catholics about “destroying the very essence of the human creature through manipulating their God-given gender to suit their sexual choices.” Likewise, Pope Francis rejects the social constructionist view of gender as fluid and changeable, maintain that gender is God-given.
The Church understands that there are several dimensions to gender dysphoria—including a sociological dimension and a psychological dimension—that gender transitioning procedures cannot begin to treat. UCLA and the National Foundation for Suicide Prevention data reveal that more than 41 percent of those identifying as “transgender” or gender nonconforming have attempted suicide, compared with only 4.6 percent of the overall U. S. population who report a lifetime suicide attempt. It is also higher than the 10-20 percent of lesbian, gay and bisexual adults who report ever attempting suicide. This data come from the American Foundation for Suicide Prevention and UCLA’s Williams Institute, which analyzed results from the National Transgender Discrimination Survey. More than a dozen other studies since 2001 have found similar results for the alarmingly high rates of suicide for transgender individuals.
In 2013, a 44-year old Belgian female-to-male transsexual chose to die by euthanasia after expressing her unhappiness with her sex-change operation. Claiming that the surgery had turned her into a “monster,” doctors assisted her in ending her life on the grounds of “unbearable psychological suffering”. While progressives insist that the reason for the high suicide rates for the LGBT community is due to the stigma and discrimination they have historically faced, the reality is far more complex. In fact, the prevalence of suicide attempts is actually elevated among those transgendered individuals who are open about their transgender identity. Those who disclose to others that they are transgender have the highest rates of suicide (50%).
The Obama administration’s HHS mandate seems to ignore the documented evidence of the risks associated with medical transition procedures. Yet, as the November 2016 Becket Fund lawsuit points out, “HHS’s own medical experts recently wrote, ‘Based on a thorough review of the clinical evidence available at this time, there is not enough evidence to determine whether gender reassignment surgery improves health outcomes for Medicare beneficiaries with gender dysphoria.” Some of the best designed studies have reported serious harms.
Unless the Trump administration is willing to repeal the HHS mandates that violate the religious liberty of all Catholic institutions—including Catholic colleges and universities—these institutions will continue to be vulnerable to costly lawsuits for “discriminating” against transgendered individuals desiring transition procedures.
March 28, 2017 (LifeSiteNews) — I had always dreamed as a little girl of Prince Charming, castles, and fairytale endings. But what took place exactly one week before my birthday in September 2009 was no childhood dream, but an evil nightmare filled with pain and utter disbelief.
When I was violently raped by my fiancé, my dreams were dashed. My world came crashing down. That violent act shattered my very core.
I’m often asked when sharing my story how a fiancé could be guilty of rape.
What some people fail to understand is that when a girl says “No,” she means “No,” regardless of whether or not there is an intimate/sexual relationship. Yes, we were engaged, but this does not mean we were having sex. In fact, we weren’t. We had decided as followers of Jesus Christ that we would wait until we got married to have sex.
My fiancé had even said, “It will be difficult to wait, but it will be worth the wait!” I had no idea that the man who vowed to always protect me was capable of hurting me so much. How could the man who planned a future with me, who prayed with me every night for our future children, and who read and quoted scriptures to me be the same man who could cause me such harm?
It was through this situation that I had a true understanding of the meaning behind the phrase “a wolf in sheep’s clothing.” Not only had my body been violated, but also my heart had been betrayed.
I had been visiting him out of state. There was no family around. After he violated me, I called my sister and asked her what to do. I was in pain. She suggested I go to a hospital for urgent care, though I was still very much in denial with all that had just happened. My fiancé’s actions were, for the first time, the opposite of his words, and it was a lot to process.
After I relayed every harrowing detail of the traumatic event to the urgent care doctor, he sat on his spinning chair in front of me and told me by law he had to report it to authorities. He gave me the choice to make the call to the police and turn in my own fiancé for rape, or else he would.
All I could do was cry. I couldn’t believe this was happening.
The doctor said he would make the call and would come back once the police arrived. Meanwhile, my family and friends were hundreds of miles away as I sat by myself in the urgent care room, wondering how my happily ever after had turned so dark and violent. This was not at all how I expected to spend my weekend: Raped, then in urgent care with a doctor turning my fiancé in for rape, then having the rape kit (to collect evidence of sexual assault) performed on me as the police searched for my now ex-fiancé.
It was a woman’s worst nightmare. I went from being blissfully in love to feeling like the most unloved and alone woman in the world.
Most are unaware of the logistics of what a rape kit involves. It is horrifying to have it performed, but it is made even worse when you are so scared and facing so many unknowns. I found myself lying down in that hospital room as the Sexual Assault Response Team (SART) nurse performed the rape kit on me, all while a SART nurse-in-training looked on.
How did I get here? I was terrified and an emotional wreck. I couldn’t help but sob and feel so utterly alone, as my future now looked so bleak.
Now, I’ve been pro-life all my life. As the painful rape kit was performed on me, one thought that went through my mind was that I finally understood why some rape victims would be tempted to have an abortion. And that thought deeply disturbed me because of the strong pro-life beliefs I have always stood for. Yet, I could not bear the thought of becoming pregnant with the child of my rapist.
Just then the nurse asked me, “Do you think you could be pregnant?”
Her question made me want to crawl out of my skin and scream. The nurse discussed with me the timing of everything and determined that I was likely pregnant.
She then told me she was going to give me the “Morning-After” pill. I lay there crying, pleading with God to let me somehow die or escape this nightmare.
I knew the purpose of the Morning-After abortion pill was to terminate a pregnancy, to destroy the life of another human being. There are three ways the Morning-After Pill operates: 1) If a woman has not yet ovulated, it prevents ovulation. 2) If she has ovulated, but has not conceived, it prevents conception. 3) If she has conceived, it prevents the tiny baby (referred to as a “blastocyst”) from implanting in the uterine wall, which causes the baby to die because he or she cannot receive the nutrients needed to survive.
The SART team deceives a raped woman if they tell her that the Morning-After pill does not “terminate a pregnancy.” If she is pregnant, the pill does kill.
As I lay there crying and in pain, I knew in my heart that a life, no matter how it is conceived, is still a precious gift created by God. It is a gift that I knew I had no right to destroy, regardless of the trauma I was now experiencing. No pre-born child deserves capital punishment for the sins of the father. So, I knew, as I sobbed while they took the most graphic pictures of my injuries, that regardless of the future, I would choose life.
That night I not only declined the Morning-After pill, but I refused to take any of the STD emergency antibiotics, not sure which pills the SART nurse might slip in if I took any. So, I took the risks with my health and trusted God.
I have since learned that it is standard practice that while the rape kit is being performed, not only is the Morning-After pill given to victims of rape, but also emergency antibiotics to combat sexually transmitted diseases (STDs), including AIDS, just in case the victim has been exposed. All the pills are usually administered together. There is no way for a girl to know which pill is what.
Even though I had declined the abortion pill, the nurse continued to strongly advise that I take it, saying, “Who would want a baby out of rape?”
I was shocked and saddened by her comment. I felt very much like the nurse was trying to manipulate me into doing what she wanted me to do, not what was in the best interest for a potential pregnancy, or for me.
I eventually was released from the hospital and drove home throughout the night, not knowing what the future held. But I knew who held my future: my Lord and Savior, Jesus Christ.
The next few weeks were physically painful and ridden with anxiety as I waited to see if the pregnancy tests I took would either show one line or two. But the tests were only showing one line. I was surprised when a doctor confirmed that I was not pregnant.
Tests that I took six months later also showed that I had not been exposed to any type of STDs.
As I reflect on that low valley I walked through in 2009, I am able to say that, regardless of what the pregnancy tests revealed weeks after my rape, I did choose life under the most unthinkable and traumatic circumstances while facing a world of unknowns. It’s a choice I would make again.
Since my rape, I have forgiven my rapist. I have become an advocate for abuse victims, speaking about rape, choosing life, and domestic violence. I have found hope and healing through God. Today I am an advocate for the pre-born.
I refused the Morning-After pill after rape because I am pro-life. It is deeply woven within the very core of who I am. My choice for life has helped make me into the woman I am today.
Editor’s Note: Witlee Ethan’s story is used here by permission from the author. It has been edited. Witlee can be reached on twitter: @VoiceUrRights
When I get in touch with Rosa Pich by Skype during Holy Week, I discover that she is on holiday with 12 of her children in Torreciudad, a shrine dedicated to Our Lady in northern Spain. “We are trying to return to normal life,” she says, following the death of her husband, Chema, of liver cancer little more than a month earlier. “We have cried a lot, we have prayed a lot, but life continues,” she says. “I have come to see that when God gives you a cross to carry, he always gives you the grace you need to bear it.”
Rosa is a supernumerary member of Opus Dei and is the ninth of 16 siblings. Chema Postigo, who also belonged to Opus Dei, came from a family of 14. They got married young and aspired to have a family as large as those they came from. Their first child, however, was born with a congenital heart defect and was not expected to survive for long (although she actually lived till the age of 22). The second and third children died in infancy. It was then that a doctor advised the couple not to have any more children.
But after much prayer and discernment they decided against this advice. “Nobody other than the spouses should enter the marriage bed,” she explains, “not the doctor, or one’s mother or mother-in-law, or the priest.” Rosa and Chema resolved not to give up on their dream of a large family and went on to have 15 more children, all alive to this day, aged now from 25 down to seven. They became the parents of Spain’s largest family and have appeared in documentaries in several countries including one made by the BBC.
How did they manage? They lived in an apartment in Barcelona with five bedrooms: two for boys, two for girls and one for the couple. In one of the boys’ rooms, there is a four-level bunk bed and another two-level bunk bed with a spare bed for guests, since their children are positively encouraged to bring their friends home to play and to stay the night.
Each of the older children is assigned a younger sibling to look after, ensuring that they make their bed, eat enough, do their homework, clear their toys and get their clothes ready for the next day. Chores in the house are distributed monthly according to a schedule which is agreed by all. This allowed Chema to have a full-time job and Rosa to work part time in the mornings, while they spent many weekends travelling the world to help other couples make their families a success through a programme developed by the Family Development Foundation (FDF).
Rosa’s daily schedule entails getting up early to go to Mass, then on to work as a sales executive in a textile firm, getting back home for lunch. Meanwhile, the children help each other to get up, have breakfast, and travel to school and university.
Their dining table is round, with room for 20 people. This allows everyone to see and hear everyone else as the conversation around the dinner table is always very animated.
“We have three rules about our meals,” Rosa tells me. “First, you need to ensure the person to your right and to your left are served before you start eating. Secondly, when you get the tray of food, you should choose the worst for yourself, leaving the better portions for your siblings. And third, all of us, including mum and dad, should aim to do one small sacrifice in each meal.”
This sacrifice could be as simple as taking a bit more of what you don’t like or a bit less of what you like, or delaying drinking the glass of water till the end of the meal – something small that shows solidarity with those who don’t have enough to eat or are otherwise suffering.
These and many other experiences are collected in a book that Rosa wrote in 2013 and has now been translated into 10 languages, including Chinese. It was published in English by Scepter Publishers in New York this year, with the title Rosa, What’s Your Secret?: Raising a Large Family with Love.
But isn’t it very expensive to have such a large family? The Postigo-Pich family consumes 1,300 biscuits, 420 pints of milk and seven lots of a dozen eggs per month. But they are extremely careful where they buy their provisions, searching for the biggest discounts they can get. Every day one of the children walks to a bakery 15 minutes away from home because each loaf is 20 cents cheaper. This adds up to a saving of many euros per month. Sometimes the fridge becomes empty before the end of the month, so they have to skimp and make do with the basics until the next salary comes in.
In the last four months of Chema’s life the couple were able to travel to six countries in three different continents to promote FDF courses: South Korea, China, Ivory Coast, Portugal, Italy and Belarus. In the latter they had the distinct feeling they were being followed by KGB-type secret police who were about to deport them. But all was fine, and in fact they appeared in the main news programme in Minsk.
Chema felt ill during these months, losing almost two stone in weight. Eventually he went to hospital to have a number of tests. In late February, he was diagnosed with aggressive liver cancer with a metastasis in the lungs. Clearly he was not going to live much longer. He then called all his children together.
“Jesus is very good. He loves us a lot,” he told them. “He took Javi and Montse to himself when they were young and Carmina when she was 22. Now it is my turn.”
He then spoke to them one by one. Less than two weeks later he died.
The funeral was held in the largest church in Barcelona and was attended by more than 4,000 people from all over the world. At least 30 people told Rosa that Chema was their best friend. Each person who attended was given a rosary in a little pouch prepared by the children the day before. One of the people who came to the funeral said that “in the midst of the pain, these days we have touched heaven.”
Their son Gaby, 17, went to Rome for Holy Week and was able to greet Pope Francis personally after the Wednesday audience. Chema had written to the Pope, who had answered by sending his prayers and blessings. Gaby told the Holy Father that his father had died recently: would he have a message for his mother? Pope Francis said: “Tell your mother to always look up to heaven, as your father looks at her from there.”
How can Rosa cope as a young widow with so many children? Yet it is precisely having so many children which allows her to live surrounded by love. The week after the funeral there was a family meeting at which all the jobs done by Chema up to then were distributed among the family members. Rosa admits that dealing with banks is not her forte and is happy that one of the older children has taken that on. As she puts it: “In a large family, joys are multiplied and sorrows are divided.”
Recently she spotted her 10-year-old reading the newspaper, something he had never done before. When she asked him, he said that dad would always explain the news to him every night but that now he had to find it out by himself.
Rosa knows she will never be alone. “The problem today in developed societies is loneliness,” she says, “something we have never known in our families.” She adds that, although having small children takes a lot of time and effort, the years of looking after them pass quickly, and then you have around you “these wonderful human beings, who will exist forever, forever, forever”.
Each child was a gift of God and there was nothing like it: “I have many friends,” Rosa says, “who later in life have one regret: not having had more children.” She believes this is the best present parents can give to their older children.
At school, many of the boys and girls want to be friends with her children because they are used to being generous and sharing their lives with others. “I believe in this house they are getting the best possible training to run multinationals,” she says, “because they learn to negotiate, to spot the needs of others, to make the case for their suggested course of action, to give in when needed, to ask for forgiveness when they make a mistake.”
What is the most important thing in a family, I ask her as we are finishing our conversation. She does not hesitate: “That the mum and dad love each other. Everything else comes from that.”
Jack Valero is the press officer of Opus Dei UK and a founder of Catholic Voices
This article first appeared in the May 19 2017 issue of the Catholic Herald. To read the magazine in full, from anywhere in the world, go here
Within the next 10-20 years, a new and controversial fertility technology called in vitro gametogenesis could make it possible to manipulate skin cells into creating a human baby.
However, this groundbreaking research has caused push-back from some critics, like Fr. Tadeusz Pacholczyk, director of education at the National Catholic Bioethics Center, who says IVG would turn procreation into a transaction.
“IVG extends the faulty logic of IVF by introducing additional steps to the process of manipulating the origins of the human person, in order to satisfy the desires of customers and consumers,” Fr. Pacholczyk told EWTN News in an email interview.
“The technology also offers the possibility of introducing further fractures into parenthood, distancing children from their parents by multiplying the number of those involved in generating the child, so that 3-parent embryos, or even more parents, may become involved,” he continued.
IVG has been successfully tested by Japanese researchers on mice, which produced healthy babies derived from skin cells.
The process begins by taking the skin cells from the mouse’s tail and re-programing them to become induced pluripotent stem cells. These manipulated cells are able to grow different kinds of cells, and are then used to grow eggs and sperm, which are then fertilized in the lab. The resulting embryos are then implanted in a womb.
Although similar to in vitro fertilization, IVG eliminates the step of needing pre-existing egg and sperm, and instead creates these gametes
But many experts in the reproductive field are sceptical of its potential outcomes and ethical compromises.
“It gives me an unsettled feeling because we don’t know what this could lead to,” Paul Knoepfler, a stem cell researcher at the University of California, Davis, told the New York Times.
Knoepfler noted that some of the potential repercussions of IVG could turn into “cloning” or “designer babies.” Other dangers could include the “Brad Pitt scenario,” in which celebrity’s skin cells retrieved from random places, like hotel rooms, could be used to create a baby.
Potentially anyone’s skin cells could be used to create a baby, even without their knowledge or consent.
In an issue of Science Translational Medicine earlier this year, a trio of academics – a Harvard Law professor, the dean of Harvard Medical School, and a medical science professor at Brown – wrote that IVG “may raise the specter of ‘embryo farming’ on a scale currently unimagined, which might exacerbate concerns about the devaluation of human life.”
They added that “refining the science of IVG to the point of clinical use will involve the generation and likely destruction of large numbers of embryos from stem cell–derived gametes” and the process “may exacerbate concerns regarding human enhancement.”
Fr. Pacholczyk also pointed to further concerns, saying IVG disrupts the uniqueness of every individual’s sex cells.
“I.V.G raises additional concerns because of the way it manipulates human sex cells. Our sex cells, or gametes, are special cells. They uniquely identify us,” Fr. Pacholczyk stated.
“It is most unfortunate that overwhelming parental desires are being permitted to trump and distort the right order of transmitting human life,” he continued.
Fr. Pacholczyk said that processes like IVG “enable a consumerist mentality that holds that children are ‘projects’ to be realized through commercial transactions and laboratory techniques of gamete manipulation.”
The Catholic Church teaches that IVF and similar reproductive technologies are morally illicit for several reasons, including their separation of procreation from the conjugal act and the creation of embryos which are discarded.
Pope Francis recently spoke out against the destruction of human embryos, saying that no good result from research can justify the destruction of embryos.
“Some branches of research use human embryos, inevitably causing their destruction. But we know that no ends, even noble in themselves – such as a predicted utility for science, for other human beings or for society – can justify the destruction of human embryos,” the Holy Father said May 18.
Although IVG has proven successful in mice, there are still some wrinkles that need to be ironed out before it is tested on humans, and will entail years more of tedious bioengineering.
However, Fr. Pacholczyk hopes that potential parents will come to realize that children should not products that can be ordered or purchased by consumers, and should rather be seen as a gift.
“Turning commercial laboratories to create children on our behalf is an unethical step in the direction of treating our offspring as objects to be planned and created in the pursuit of parental gratification, rather than gifts received from the Lord.”
The message of Fatima is, in its basic nucleus, a call to conversion and repentance, as in the Gospel. This call was uttered at the beginning of the twentieth century, and it was addressed particularly to this present century. … The call to repentance is a motherly one, and at the same time it is strong and decisive. (Pope Saint John Paul II, homily given in Fatima on May 13, 1982)
May 15, 2017 (HLI) — On Saturday the universal Church remembered and celebrated the 100th Anniversary of the miraculous events at Fatima, recalling the wondrous appearance of Our Heavenly Mother and the life-giving message she brought. In considering the meaning of her message as it pertains to us today, I am reminded of something Sister Lucia wrote in a letter to Cardinal Caffarra:
[T]he final battle between the Lord and the reign of Satan will be about marriage and the family. Don’t be afraid, she added, because anyone who works for the sanctity of marriage and the family will always be fought and opposed in every way, because this is the decisive issue… however, Our Lady has already crushed its head.
In my many travels, I experience firsthand the prophetic words of Sister Lucia concerning marriage and the family. These sacred institutions are at the heart of the battle because they touch upon the very pillar of creation, which is the truth about the relationship between man and woman, who are made in the likeness and image of God. If these heavenly created institutions are compromised, then the entire building collapses.
We should not view the message of Fatima as merely a historic moment, but rather as a living message purposely spoken to this age. The moral crisis we see in the world demands continued prayers, penance and sacrifices. Our response to the perverse secular culture is our ongoing conversion and spiritual renewal. We are being called to holiness.
We are prompted by the example of the visionaries, Francisco, Jacinta and Lucia, to offer acts of mortification with heroic virtue. At the height of their innocence, the two younger children, Francisco and Jacinta, offered themselves as expiatory victims. Sister Lucia, told she would live a long life, would exhaust her life in the service of prayer and mortification for the salvation of souls. Lucia asked Our Lady if she would take them to heaven. Our Lady answered:
Yes, I will take Jacinta and Francisco soon. You, however, are to stay here a longer time. Jesus wants to use you to make me known and loved. He wants to establish the devotion to my Immaculate Heart in the world. I promise salvation to those who embrace it, and their souls will be loved by God as flowers placed by me before His throne.
When Lucia asked if she were going to be left alone, Our Lady responded:
No, my daughter. Does this cause you to suffer a great deal? I will never leave you, my Immaculate Heart will be your refuge and the way that will lead you to God.
Our Lady’s appeal for prayer and penance made to the children, to which the children responded with joy and complete obedience, also applies to us. Striving for holiness and mortifying our senses enables us to be fervent in prayer, gives us interior strength in resisting temptations, helps us to detach from worldly concerns, and unshackles our hearts from earthly vanities and attachments. Seeking holiness increases clarity of thought, making us more sensitive to the discernment of what is holy and what is abomination.
The evil one also knows the significance of marriage and the family. This is why he attacked our first parents and continues his assault today upon marriage and family. Marriage is the only institution that unites parents with their children, that recognizes the natural right of a child to have a mother and father. The family is the first cell of society, the domestic church, first government, first school, first hospital, first economy and the first mediating institution of society. Within this primary school, children learn moral and gospel values, which ultimately give shape to our cultures and societies. After all, society passes through the family, the first school.
Defending the truth about life, marriage and family is costly. The visionaries of Fatima suffered greatly because of the apparitions. Family and friends who failed to understand what the children received from Our Lady persecuted them. Newspapers waged a bitter campaign to discredit the apparitions and the visionaries. Despite all the ill treatment, the children bore it all with patience and charity, always mindful of Our Lady’s request to offer their sacrifices for the sake of poor sinners.
As we enter the good fight in the battle over marriage and family, we know that we too will be besieged by hatred and rejection. Our Lord reminds us, “If the world hates you, realize that it hated me first. If you belonged to the world, the world would love its own; but because you do not belong to the world, and I have chosen you out of the world, the world hates you” (John 15:18-19). We stand before two opposing views; one set upon a path of obedience and life and the other upon disobedience and death.
We also know that the attacks against God’s divine plan for marriage and family do not come only from outside the Church but also come from within – born of sins from disobedience, dissent and rejection. This is why the Church, the people of God, needs the message of Fatima to be a constant reminder as to the universal call for repentance conversion, and renewal. Only in this spirit, renewal of heart and soul, can we be the leaven in the dough. There is no fear in love, but perfect love drives out fear…(1 John 4:18) We draw strength and comfort from Our Lady of Fatima who reminded Sister Lucia that she was not alone in this great battle – in her Immaculate Heart we find refuge.
There is still much for us to learn from Our Lady of Fatima. Her message is a sign of hope to a world torn by strife and discord. The answer to the attacks on marriage, family and society is the same today as it was 100 years ago – repent and be obedient to the will of God.
There are some people — and I am one of them — who think that the most practical and important thing about a man is still his view of the universe. We think that for a landlady considering a lodger, it is important to know his income, but still more important to know his philosophy. We think that for a general about to fight an enemy, it is important to know the enemy’s numbers, but still more important to know the enemy’s philosophy. We think the question is not whether the theory of the cosmos affects matters, but whether in the long run, anything else affects them.
Chesterton is making the point that one’s general system of values is an all-important factor in the choices he makes. For example, someone who subscribes to Ayn Rand’s “philosophy of selfishness,” or to Peter Singer’s judgment that infanticide is permissible because of utilitarian values, or to Christopher Hitchens’s view that religion is the most dangerous thing on earth, or to theologian Rev. Richard McBrien’s claim that popes have no authority in morals, can be expected to act in certain ways and take certain positions when confronted with choices. If we know their world view, we do not have 100 percent certainty about particular choices they might make under particular circumstances — but we do have high probability.
The Catholic analytic philosopher G. E. M. Anscombe (1919-2001), whose 1958 article “Modern Moral Philosophy” instigated new movements in “virtue ethics” and renewed interest in natural law, astonished her academic colleagues at Cambridge University in 1979 by publishing Contraception and Chastity, a defense of the Catholic Church’s position on contraception. Anscombe’s influence is still being felt in the United States via the Anscombe Society at Princeton University.
Analytic philosophy is famous for investigating logical connections, even in ethics, and Anscombe draws out the inescapable deductions that can be made from a value system accepting contraception:
If contraceptive intercourse is permissible, then what objection could there be after all to mutual masturbation, or copulation in vase indebito, sodomy, buggery, when normal copulation is impossible or inadvisable (or in any case, according to taste)? … But if such things are all right, it becomes perfectly impossible to see anything wrong with homosexual intercourse, for example. I am not saying: if you think contraception all right you will do these other things; not at all. The habit of respectability persists and old prejudices die hard. But I am saying: you will have no solid reason against these things. You will have no answer to someone who proclaims as many do that they are good too. You cannot point to the known fact that Christianity drew people out of the pagan world, always saying no to these things. Because, if you are defending contraception, you will have rejected Christian tradition…. For in contraceptive intercourse you intend to perform a sexual act which, if it has a chance of being fertile, you render infertile. Qua your intentional action, then, what you do is something intrinsically unapt for generation (emphasis added).
In other words, Anscombe is saying that, if you believe you have a right to non-procreative sexual intercourse, you have no right to criticize non-procreative sex by others — for example, by a gay couple. You may justify your personal practices on the basis of your genuine mutual love and commitment to lifelong fidelity. But homosexuals may be even more intensely in love with each other and even more firmly committed to mutual fidelity. They may even be more open to procreation than you are, through adoption or through in vitro fertilization. To want to have sex without the possibility of offspring, and condemn others for similarly non-procreative sex, would be blatantly inconsistent.
According to polls, more than 80 percent of Catholic married couples are using various kinds of contraceptives in order to prevent or separate births. But there is no necessary connection between control of births and contraception. Natural family planning (NFP), which is approved by the Church and often used by couples who want to identify a woman’s fertile periods in order to have children, can also be used to space out births without contraceptives. NFP has been shown in various studies to be just as effective as the contraceptive pill. Systematic development and improvement of the Billings method of NFP over the years has been carried out at Creighton University. The Pope Paul VI institute at Creighton has a good history of assisting married and unmarried women with irregular cycles and other problems.
A variety of objections to gay marriage have been offered. Some oppose it because it arbitrarily redefines marriage, or because it is not suitable for children to have gay parents, or because it will involve greater taxpayer burdens for Medicare and Social Security down the line, and so forth. But if we are part of that 80 percent of Catholics who are also involved in non-procreative sex, we cannot take the “high road” and be opposed to gay marriage because of “immorality.” At the very least, Catholics who choose artificial contraceptive methods, in the interests of consistency, should modify their opposition to gay marriage. If and when they follow the Church’s teaching on contraception, which has not changed over two thousand years and was reiterated by Pope Paul VI in Humanae Vitae, they will have a more secure moral justification for their opposition.
Nexplanon, a contraceptive implant promoted as Long Acting Reversible Contraceptive, is a single-rod, progestogen-only implant measuring 4 cm in length and 2 mm in diameter. It is not biodegradable, and it contains 68 mg etonogestrel.
Nexplanon should be placed subdermally at the inner side of the upper nondominant arm.
Subdermal contraceptive implant embolism to a pulmonary artery is an emerging iatrogenic condition.
This case was reported in The Annals of Thoracic Surgery.
An 18-year old woman underwent a voluntary termination of pregnancy in July 2014 and had a concomitant subdermal contraceptive implant (Nexplanon) inside her left upper arm.
During the procedure, the performed an inappropriate movement of flexion of her elbow. Because the gynecologist could not feel for the device to ensure that was placed correctly, a nonhormonal birth control method was advised and upper arm roentgenography was prescribed to check the device location. As the patient presented with no symptoms, she did not attend the outpatient clinic until March 2015. At that time, she asked for the removal of the device because of unfavorable change in her menstrual bleeding pattern. Examination and roentgenology of the patient’s arm failed to localize the implant, and it was deduced that it had migrated elsewhere. Chest radiography and computed tomography confirmed that the device was lodged in a subsegmental branch of the left lower lobe pulmonary artery.
The implant was removed from the pulmonary artery thoracoscopically, thereby avoiding the need of thoracotomy or lung resection.
Maria Gallagher May 17, 2017 | 3:59PM Washington, DC
A champion of life—that title expertly captures the work and legacy of Pope John Paul II. More than a decade after his death, the author of Evangelium Vitae (The Gospel of Life) remains one of the greatest heroes of the pro-life movement, respected by people of all faiths and all walks of life.
The story of Pope John Paul II’s life is filled with suspense, heroism, and intrigue. What is particularly striking is the number of times during the course of his long life, he escaped death. His life hung in the balance when he was hit by a vehicle in his youth. His life was certainly at risk when the Nazis invaded Poland. In 1981, after assuming the Papacy, he nearly died from an assassin’s bullet.
In the new book The Pope and the President, author Paul Kengor paints an intriguing portrait of the lives of pro-life stalwarts Pope John Paul II and President Ronald Reagan. The two have been credited with playing key roles in the breaking down of the Berlin Wall, a long-standing symbol of Communism. The two also shared a passion for defending innocent human life and played hugely instrumental roles in combating what the Pope memorably described as a “culture of death.”
The Pope and the President notes that the future Pope’s life was at risk even before he was born. Kengor points to a report that the Pope’s mother “was in such precarious health that her doctor advised her not to continue her pregnancy.”
According to Kengor’s account, the doctor told Emilia Wojtyla, “You have to have an abortion.” The physician’s rationale was that Emilia’s life was at stake and that she should abort her child to preserve it. The Vatican Insider said of the incident, “John Paul II was in danger of not being born.”
But Emilia proved the doctor wrong. She came through the pregnancy and childbirth and delivered a baby Kengor described as “healthy and strong as an ox.” Emilia predicted that Karol Józef Wojtyła, who would become John Paul, would be “a great man someday.”
A great man who could have easily lost his life to abortion.
Ponder for a minute how different the world might be had this champion of life never entered into it.
His absence would have created a vacuum that no one else could fill—because no one else was quite like him.
And therein lies one of the great tragedies of abortion. It creates a dark abyss where our heroes might have stood.
With the birth of Karol Wojtyla, history changed—so very, very much for the better. May all of us, of all faith traditions, live out his legacy by defending mothers and their children from the scourge of abortion.
Cardinal Robert Sarah, prefect of the Congregation for Divine Worship and the Sacraments, is pictured at the Vatican in this Oct. 9, 2012, file photo (CNS); right: Monastère de la grande chartreuse, in the Chartreuse Mountains, France (Wikipedia)
About 365 miles south-east of Paris, high in France’s remote Chartreuse Mountains, lies one of the world’s most well-known monasteries. Since its foundation in 1084 by the religious order that would become known as the Carthusians, La Grande Chartreuse has been characterized by a daunting quietness. This was famously captured and brought to the world’s attention in the award-winning 2005 documentary Into Great Silence. The power of that silence forms the backdrop to a new book, La Force du Silence, by Cardinal Robert Sarah, the African-born Prefect of the Congregation for Divine Worship, who first came to the universal church’s attention with his best-selling God or Nothing (2015).
On many levels, this is a very different book to God or Nothing. The latter is about a journey of faith of a poor boy from an impoverished and obscure rural village in the then-colony of French Guinea to one of the highest offices at the Holy See. Cardinal Sarah’s new book, however, is a spiritual testimony to that faith: the type of witness that more of the Church’s prelates should—but often don’t—provide as successors of the Apostles. Working again with the distinguished French journalist Nicolas Diat, Sarah focuses the reader’s mind upon something easily trivialized in an age preoccupied with equality. And that is the sheer grandeur of God. To grasp this unfathomable depth, Sarah urges us to be mastered by a silence which liberates us from the Babel of distractions surrounding us.
Silence functions as a metaphor for many things in this book. It evokes the wonder that anyone should experience in God’s presence. But the silence of which Sarah speaks also embodies fidelity, humility, charity, and the clarifying light of reason. Noise, for Sarah, concerns the confusion and sentimentalism of unreason; the bombast of those who scorn the faith of the simple and the saints, and the unfaithfulness of those who would sell out the Church to the applause of the world—primarily a Western world—that tries to disguise its abandonment of God with the type of franticness that’s a sure sign of superficiality.
Pascal’s way
Having described the nature of the noise that surrounds us, Sarah illustrates how God’s silence speaks to humanity. He then turns to that most difficult of questions: God’s apparent silence in the face of unspeakable evil. The last chapter consists of a three-way exchange in which Diat poses questions to Sarah and the current prior of La Grande Chartreuse and minister-general of the Carthusian order, Dom Dysmas de Lassus. Sarah and de Lassus take turns to explore how silence reveals not only our need of God, but also sheds light on what isn’t essential as we seek this God who is beyond historical contingency and yet always with us.
Sarah’s approach throughout this book is reminiscent of the posthumously-published Pensées penned by the French scientist and philosopher Blaise Pascal (1623-1662). Like the Pensées, each numbered paragraph in La Force du silence may be read as a stand-alone counsel upon which readers can reflect. The similarities do not end there. Sarah references, for example, numerous Church Fathers and saints. Among others, these include Jerome, Ignatius of Antioch, Maximus the Confessor, John of the Cross, Teresa of Calcutta, Thomas More, and Thérèse of Lisieux. Yet, like Pascal, the life and thought of Saint Augustine looms large throughout Sarah’s reflections and Diat’s questions.
Pascal and Augustine were not shy about naming the problems they regarded as characterizing the Church of their respective times. Nor is Sarah. The noisy sophistry of many contemporary Western theologians (particularly that, some might add, presently emanating from the German-speaking Catholic world) is named for what it is: a prattle which reflects a lack of humility and a disinterest in truth. More generally, Sarah suggests that the propensity of many Christians to talk endlessly about that which is peripheral to the faith reflects their loss of a sense of who God is.
So too does a tendency that Sarah singles out for particular criticism: those forms of activism which marginalize the truths proclaimed by the Church and the life of prayer in the name of “relevance”. In this connection, Sarah points out that saints who were especially immersed in the hustle and bustle of the world, such as John Bosco, John Paul II, Thomas More, and Josemaría Escrivá, maintained especially intense prayer lives, much of which was characterized by silent adoration. This is a reminder that, without regularly immersing ourselves in quiet contemplation of Christ, God’s presence in any Christian’s life will inevitably fade. That is how a church starts collapsing into being just another activist group or NGO.
Into the Darkness
Addressing these contemporary matters, however, don’t preoccupy the bulk of Sarah’s reflections. Far more attention is expended on some of the hardest questions with which every person—Christian or non-Christian, believer or atheist—wrestles. Why was God silent, for example, in face of the genocide of European Jewry? Where was God when seven Trappist monks from the Tibhirine monastery in Algeria were beheaded by Islamists in 1996? How could God not save those who remain his Chosen People? Why did God not stay the hand of jihadist executors?
The problem of evil—not mere discomfort or inconvenience, but evil—has long preoccupied Jews and Christians. They have also produced answers that many find intellectually convincing and to which atheists don’t have especially convincing rebuttals. Yet these Jewish and Christian responses can’t provide by themselves immediate or even long-term release from bewilderment and pain. Intellectual certainty is one thing, the experience of suffering is quite another.
Like any good bishop, Sarah patiently outlines some of the theological and philosophical responses to the problem of evil. Here he draws upon Catholic and Protestant theologians such as Maurice Zundel (1897-1975) and Søren Kierkegaard (1813-1855) as well as the German Jewish philosopher Hans Jonas (1903-1993) and his famous 1968 essay, The Concept of God after Auschwitz. But, Sarah cautions, there is a limit. The existence of evil doesn’t disprove the existence of the rational and loving God revealed in the Scriptures. Nonetheless, Sarah warns, evil “is a mystery that humanity can never completely comprehend.” Part of the genius of Sarah’s meditation is how he uses the motif of silence to illuminate this darkness.
For Sarah, it is important that humans resist and combat evil. He himself had no hesitation in denouncing the crimes and terrorism of Sékou Touré’s Marxist regime in Guinea—the same Communist dictator who imprisoned Sarah’s predecessor as Archbishop of Conakry in a concentration camp for eight years and placed Sarah himself on a death-list. That said, Sarah states, we need to remember two things.
First, God’s silence reflects the truth that he is working through time to renew all things, often in ways that we often cannot understand, precisely because we are not God. That’s not a call to be passive. Rather, it’s a caution against imagining that we can master evil in a god-like fashion.
Second, we cannot contest evil, Sarah holds, unless we are willing to quieten ourselves, enter into God’s presence, and meet his silence. In this context, silence implies neither a deaf and mute God nor a master-watchmaker God who does nothing except set time in motion. Instead, God’s silence serves to shed light upon the truth and thus the nature of the injustice and the identity of its perpetrators. Christ himself, Sarah points out, is silent before his accusers. Yet Christ’s stillness discredits the false accusations made against him. More than any words, it convinces Pilate that he’s being asked to sentence an innocent man to death. Likewise Christ’s silence on the Cross testifies to God’s willingness to let himself be humiliated and sacrifice himself in reparation for the evils we have all done. Only the one true God could do this.
Silence and the interior path to God
Silence, however, concerns not only that which is exterior to us. For Sarah, it’s also indispensable if we really want to come to know the God who would allow himself to be nailed to a tree to atone for our sins.
Sarah recalls that as a young priest and archbishop, he often retreated into the Guinean desert to find the solitude and silence he needed to find God. In doing so, he sought to create what he calls “an interior desert”. The models Sarah has in mind are Biblical figures such as Moses, Elijah, John the Baptist, and Christ himself—all of whom took themselves into the wilderness to contemplate God. Entering into this silence, Sarah maintains, helps us to strip away those exteriorities that prevent us from encountering the hidden presence of God which Augustine discovered after his conversion to Christianity. Experiencing that presence, Sarah says, can be “terrifying” and “destabilizing”. Those who choose to embark on this path therefore need enormous courage to do so. Yet at the end of the quest, Sarah promises, we will find true life and true peace.
And that is ultimately where Cardinal Sarah’s at-times mystical reflections on silence are meant to take us: the place of true joy in which the silence no longer frightens us because we are alone with the God who is Love—the Love who is the only alternative to Nothing.
La Force du silence: Contre la dictature du Bruit
by Cardinal Robert Sarah with Nicolas Diat
Fayard, 2016
Paperback, 374 pages
Related at CWR:“Cardinal Robert Sarah on ‘The Strength of Silence’ and the Dictatorship of Noise”(Oct 3, 2016): An exclusive English translation of a wide-ranging interview by Cardinal Sarah with the French newspaper “La Nef”.
Culture is a society’s way of joyfully guiding itself into the future, a future made most visible in its ever-repeating cycle of celebrations.
When you cut to the quick on that future the child emerges. Looked at differently, our culture is our way of collectively guiding ourselves to guide our children along certain paths, as elegantly as we can, to ensure as good a future as we can for them.
Why the emphasis on elegance? Because culture is a common enjoyment. It is “beauty for everyone”.
Culture is a people giving themselves a little bit of heaven while here on earth: enjoying the beauty we have created for ourselves as a people. Thus special days are celebrated as beautifully as we can: birthdays, weddings especially — a high point of culture, as are all the key steps leading up to it: the patterns of romance and of engagement. So too are a peoples big festivals honoring its history as a people and so too are its big religious holidays made to be enjoyed (even the somber ones).
Thus we can also admire and vicariously enjoy other peoples’ cultures: the Italians as they celebrate in their very Italian way all sorts of feast days; Indians of India with very different religious feast days and holidays; Chinese in their ways, Japanese in theirs. And so it goes on, all around the world.
There are common elements in all cultures: birth, marriage, death and funerals, courtship, birthdays, high religious feast days. They exist all over the globe for all peoples in all places. Life has the same common “critical tasks” no matter what nation or people we are.
For us in the US the question today is “What do we celebrate together now?” With birth a suspect thing (thanks to abortion and out of wedlock births), with romance dying (given contraception and the hookup culture), with weddings only for some and far fewer, and with the afterlife non-existent for an increasing number, lots of the reasons for elegant celebration or mourning are gone. The building of elegance around these milestones in the life can no longer be a common project for present America. We do not have a culture war. Instead, through shared embarrassment, we have a culture starvation.
Some of our states have even eliminated death as a stage – it has now become a choice! But who can celebrate an assisted suicide. Can anyone envisage great art being inspired by such? A new Mozart Requiem that brings us deep within ourselves even as it brings us up to the heavens? For suicide?
We are a people who no longer have a common project of shepherding the child onto a life path that leads to the “good life” (or a “good enough” life) and finally into the afterlife. We no longer have such a common project to which to commit. Hence we can have no culture.
But the America that will survive will build its own new culture and it will come, it can only come, from those who love bringing new life into existence, for without the baby there is no cycle to repeat.
Out of the ashes of present post-modernity will spring the new American culture – probably already well underway but not visible through the mainstream media whose energies are fixated elsewhere. Our new America will be one with ways of moving through the stages of life with the elegance that “Joe the construction worker and his wife Jane” are quite capable of expressing when they get together with their families and friends at community celebrations.
I predict that the dominant color in the new patterns being woven into the cultural fabric of the new America, the one that not only lasts but thrives, will be the celebration of new life, and in the tapestry of this culture the thread of the Fatherhood of God will be visible. We will find an American way to do this. We will be a people who celebrate four beings, the new baby, the couple who co-created this new life, and God the creator. This is the culture that will emerge, likely already is emerging. The logic of reality makes it so.
We have lots to look forward to. Culture spotting will be the new enjoyment.
Pat Fagan is Senior Fellow and Director of the Marriage and Religion Research Institute (MARRI). This article is republished from the MARRI blog with permission.
Motherhood comes in all shapes and sizes. There’s the mom who sat through hours of blood tests, chart analyses, and waiting rooms. The one who saw countless negative pregnancy tests and was crestfallen every time. There’s the mom who only saw one positive pregnancy test, you know the one I’m talking about. The unexpected one. The test that made the room spin and her ears ring a little. The mom who tried, the mom who took her pill loyally every night by the bedside. There’s young moms, older moms, moms of many, and moms of one. Single moms, moms with little ones whose lives were lost far too soon, and moms who didn’t birth a child, but still give out love like it’s limitless.
Mother and child by Graham Crumb
Mother’s Day is a loaded holiday, that’s for sure. Everyone’s journey to motherhood looks a little different, but every mother holds a love like no other for her children. American culture frequently talks about entering motherhood and family planning as if it’s a play book. Each couple chooses their plays and goes about their life. But in actuality, family planning is about as fluid as…well, cervical fluid. Constantly changing. Constantly ebbing and flowing. Might be one thing one week and another, another week. Couples who use fertility awareness methods are generally more in tune with this ebb and flow. I mean literally, but also emotionally. Each cycle is a new chance to deliberate the playbook.
Fertility Awareness Methods are anything but set it and forget it. But that’s not necessarily a bad thing. It puts you in touch with your fertility every cycle, and quite intimately. I think that’s a really cool part about it. I get to make decisions, but also work with the many moving parts of deciding when or if to grow my family.
But we don’t always get a say – life sometimes has its own plans. Infertility, miscarriage, unplanned pregnancy, they happen. Family planning isn’t always so planned. And maybe that’s a beautiful thing. No matter how many childbirth ed classes you take, no matter how many parenting books your read, we can only control so much. I’m so grateful that using fertility awareness as a method of family planning allows me to be flexible.
So this Mother’s Day, we want to honor everyone’s journey to motherhood. It’s the most common and somehow unique job in the world. No two moms’ journeys are alike. What a shame that parenthood gets placed into two boxes, planned and unplanned. Sometimes life happens and sometimes we just need a support system to help us through. Be it miscarriage, infertility, unexpected pregnancy, and all the things that happen after birth that we simply can’t plan for.
To every mama, we see you and we are ever grateful for the tireless work, the sleepless nights, the early mornings, the playdates, the many doctor’s visits, and the tears (often your own). You’re rocking it.
Posted by Cassie Moriarty
Cassondra Moriarty is a filmmaker and fertility charting instructor in training based out of Brooklyn, New York, where she lives with her husband. She is currently screening Miscontraceptions around the city and working to promote Fertility Awareness. She has trained with the Couple to Couple League and is in the process of getting her FEMM certification.
Note: numbers before quoted paragraphs are as published in Cardinal Sarah’s book.
May 12, 2017 (LifeSiteNews) – Why have we seen such a dramatic increase in anxiety, fear, personal disorientation, irrational anger and forced imposition of political correctness over the past 50+ years in developed nations? Have you noticed how many now reject reason and sound arguments and accept only “facts”, “evidence” or “studies” that agree with what they desire – no matter how pathetically flawed their supporting items are? There is a surprising cause for most of this and an ages-old, surprising remedy.
We are in an age of increasing social madness. Cardinal Robert Sarah, in his new book, The Power of Silence, reveals this to be symptomatic of a widespread spiritual illness in modern Western culture. This illness, according to him, is largely caused by an absence of crucially needed, God and truth-revealing periods of silence of the ears, of the eyes and of the heart in the life of modern men and women.
Yes, silence. Sarah shows the way out of the tyranny of destructive external and internal noise and the incredible power and necessity of silence, which he proclaims is “more important than any other human work.”
Reading the comments under LifeSite’s well-researched and written reports, we are frequently struck by the inability of so many to calmly think and reason and to appreciate the implications of what the news reports reveal. Reason, facts, solid research – are all given much less importance, if any, these days than politically correct and especially emotional considerations. Modern man allows feelings and images to dominate and enslave him, much to his personal and social detriment.
Cardinal Sarah warns us that,
47. Humanity itself has returned to the sad prophecy of Isaiah, which was repeated by Jesus: “seeing they do not see, and hearing they do not hear, nor do they understand…. For this people’s heart has grown dull, and their ears are heavy of hearing and their eyes they have closed, lest they should perceive with their eyes, and hear with their ears, and understand with heart, and turn for me to heal them”. (Mt 13:13, 15) p.44
Because of all the noise experienced by our eyes, ears and hearts, modern man no longer hears, experiences and knows God. He is unable to comprehend the purpose and even the value of his life and the lives of others. Hence the acceptance of abortion, euthanasia, homosexuality, transgenerism and many other anti-human perversities. Today’s men and women and youth are lost and swirling in a downward spiral of self-destroying anxieties, fears, vulgarity, disorientation and violence.
Sarah goes so far as to proclaim that, “In killing silence, man assassinates God.” p.57
Modern civilization does not know how to be quiet
Let me further quote liberally from Cardinal Sarah and the astonishing insights in his book:
74. Our world no longer hears God because it is constantly speaking, at a devastating speed and volume, in order to say nothing. Modern civilization does not know how to be quiet. It holds fourth in an unending monologue. Postmodern society rejects the past and looks at the present as a cheap consumer object; it pictures the future in terms of an almost obsessive progress. It’s dream, which has become a sad reality, will have been to lock silence away in a damp, dark dungeon. Thus there is a dictatorship of speech, a dictatorship of verbal emphasis. In this theatre of shadows, nothing is left but a purulent wound of mechanical words, without perspective, without truth, and without foundation. Quite often “truth” is nothing more than the pure and misleading creation of the media, corroborated by fabricated images and testimonies.
When that happens the word of God fades away, inaccessible and inaudible. Postmodernity is an ongoing offence and aggression against the divine silence. From morning to evening, from evening to morning, silence no longer has any place at all; the noise tries to prevent God himself from speaking. In this hell of noise, man disintegrates and is lost; he is broken up into countless worries, fantasies, and fears. In order to get out of these depressing tunnels, he desperately awaits noise so that it will bring him a few consolations. Noise is a deceptive, addictive, and false tranquilizer. P. 56
Those are powerful, perceptive words! Much of the chaos that we report every day in LifeSite stories is reflected in those two preceding paragraphs. Cardinal Sarah does not “beat around the bush.” He gives it to us straight so that we might be able to fully understand and respond to our illness. That is what a genuine doctor of the soul must do. This is not facile “accompaniment,” but rather true shepherding and acceptance of the call to be a prophet for our time.
The silence of the eyes
Sarah carefully explains that the silence he is talking about involves much more that what enters the ears. Everything that enters the mind and heart through the senses, emotions and memories can create howling internal “noise” and greatly disturb our internal equilibrium, sense of being and relationship to our Creator.
I have never heard the term, “silence of the eyes,” but Cardinal Sarah explains it well, especially as it applies to our modern culture:
46. The silence of the eyes consists of being able to close one’s eyes in order to contemplate God who is in us, in the interior depths of our personal abyss. Images are drugs that we can no longer do without, because they are present everywhere and at every moment. Our eyes are sick, intoxicated, they can no longer close. It is necessary to stop one’s ears too, because there are sonic images that assault and violate our sense of hearing, our intellect, and our imagination. P.44
43. For some years now there has been a constant onslaught of images, lights, and colours that blind man. His interior dwelling is violated by the unhealthy, provocative images of pornography, bestial violence, and all sorts of worldly obscenities that assault purity of heart and infiltrate through the door of sight. P.42
44. The faculty of sight, which ought to see and contemplate the essential things, is turned aside to what is artificial. Our eyes confuse day and night because our whole lives are so immersed in a permanent light. In the cities that shine with a thousand lights, our eyes no longer find restful areas of darkness, and consciences no longer recognize sin.
Negative impact on the conscience
All this external and subsequent internal “noise” has had a profoundly negative impact on the consciences of modern men and women. Our otherwise natural perceptions of right and wrong are suppressed or confused. Modern man can’t comprehend the reality of moral absolutes and instead wallows in ever-changing, emotionally self-serving and personally destructive moral relativism.
Cardinal Sarah continues,
To a large extent, humanity has lost an awareness of the seriousness of sin and of the disorder that its presence has introduced into personal, ecclesial, and social life. More than 50 years ago, in his homily on September 20, 1964, Blessed Paul VI stated this tragedy in these terms:
In the language of respectable people today, in their books, in the things that they say about man, you will not find that dreadful word which, however, is very frequent in the religious world – our world – especially in close relation to God: the word is “sin”. In today’s way of thinking, people are no longer regarded as sinners. They’re categorized as being healthy, sick, good, strong, weak, rich, poor, wise, ignorant; but one never encounters the word sin. The human intellect having thus been detached from divine wisdom, this word “sin” does not recur because we have lost the concept of sin. One of the most penetrating and grave words of Pope Pius XII, of venerable memory, was, “the modern world has lost the sense of sin.” What is this if not the rupture of our relationship with, God, caused precisely by “sin”.
Those words were written by Paul VI in 1964, but so much has happened since then that we can confidently say that the word “sin” is no longer even “very frequent in the religious world.” Pastors, bishops and even the current Pope don’t like to inflict guilt on the flock, and especially on those engaged in immoral behaviours, by using the word “sin”. If any sin is mentioned at all it is often in relation to supposed “sins” against the environment or economic or other worldly issue “sins” or the sin of being too “rigid” and faithful.
Sarah next presents a poetic and powerful quote from Saint John Paul II in his Post-Synodal Apostolic Exhortation Reconciliatio et Paenitencia dated December 2, 1984 (no. 18).
45. Far from God and from the lights that spring from the true Light, man can no longer see the stars, cities have become such flashlights the dazzle our eyes. Modern life does not allow us to look calmly at things. Our eyelids remain open incessantly, but our eyes are forced to look at a sort of ongoing spectacle. The dictatorship of the image, which plunges our attention into a perpetual whirlpool, detests silence. Man feels obliged to seek ever new realities that give him an appetite to own things; but his eyes are red, haggard, and sick. The artificial spectacles and the screens glowing uninterruptedly try to bewitch the mind and the soul. In the brightly lit prisons of the modern world, man is separated from himself and from God. He is riveted to ephemeral things, farther and farther away from what is essential. P.43
I have so far only read up to page 56 in the The Power of Silence, but already Sarah has given a few prescriptions here and there on how to overcome this tyranny of noise.
He quotes Mother Teresa who wrote, “silence of speech, gesture, or activity finds its full meaning in the search for God. This search is truly possible only in a silent heart.” Sarah says that “This nun did not like to speak and fled the storms of worldly noise.”
“Silence needs meekness and humility”, writes Sarah, “and it also opens for us the way to these two qualities. The humblest, meekest, and most silent of all beings is God. Silence is the only means by which to enter into this great mystery of God… In silence, man is absorbed by the divine and the world’s movements no longer have any hold on his soul.” There is the solution.
I am very much looking forward to reading the rest of The Power of Silence. There is no doubt that many LifeSite readers would also benefit from obtaining and reading this timely, exceptionally insightful book.
Never like now a beautiful scene of a baby, his family and the experience of faith is conquering smiles and tenderness in social networks: the baptism of little Gustavo, a Brazilian baby who literally “found grace” in the middle of baptismal font!
During the ritual of baptism by immersion, the celebrant priest immerses the baby three times in the baptismal font while pronouncing the formula “I baptize you in the name of the Father and of the Son and of the Holy Spirit.” After the first partial immersion, Gustavo releases an enormous and spontaneous laughter, of the type that only the babies manage to give, infecting the whole church with his joy.
To complete this true feast, the new baptized clap his hands together with the assembly, who applauded him by welcoming him as a Catholic! The contagious joy of baptism, in a video that will not leave you indifferent.
May 9, 2017 (ALL) — The latest fashion news from Australia is truly demonic: “Human embryos left over from in vitro fertilization (IVF) procedures, as well as other bodily parts and fluids, can be transformed into jewelry.”
Baby Bee Hummingbirds, the company manufacturing these trinkets, is known for creating keepsakes containing such things such as breast milk and umbilical cords. Its latest product, the “leftover” human embryos from a couple’s IVF cycle, is, according to company founder Amy McGlade, a work of art. McGlade stated: “I don’t believe there is any other business in the world that creates jewelry from human embryos, and I firmly believe that we are pioneering the way in this sacred art, and opening the possibilities to families around the world.” McGlade says that this pioneering art of embryo jewelry is her way of giving couples “the everlasting tangible keepsake of a loved one that you can have forever.”
Naturally, many people find this disturbing. Writer Simcha Fisher is as disturbed about this latest Australian fad as we are, and in response to McGlade’s sentimental query “What a better way to celebrate your most treasured gift, your child, than through jewelry?” wrote:
Well, you could let him live, I suppose. You could allow him the basic dignity of spending time in the womb of his mother, to live or not, to grow or not, but at least to have a chance. You could celebrate the life of your child by giving him some small gift of warmth and softness, however brief, rather than letting him travel in an insulated pouch from lab to lab, frozen and sterile from beginning to end. You could conceive a child so as to give him life, and you could rise like a human should above the blind proliferation of biology.
Precisely!
Jennifer Lahl of the Center for Bioethics and Culture Networkexpressed her disgust as well: “It’s so undignified that these embryos have been destroyed to become jewelry. . . . I thought, ‘My gosh, it really has hit rock bottom.’”
But what many people apparently do not see is that the floor—or should I say the underside—of rock bottom where the synergies of evil reside is the practice of IVF itself. That is where the lack of respect for the dignity of human beings actually begins.
The Catholic Church has long held that, from a merely humane view of the child, we must realize that nobody has a right to a child. We must also understand that every child has the right to be procreated within a marriage and to have a stable family from the beginning. And certainly no child should ever be strung around someone’s neck in a piece of jewelry.
During the reign of Pope Benedict XVI, the Congregation for the Doctrine of the Faith issued the document Dignitas Personae in which it stated: “The Church moreover holds that it is ethically unacceptable to dissociate procreation from the integrally personal context of the conjugal act: human procreation is a personal act of a husband and wife, which is not capable of substitution. The blithe acceptance of the enormous number of abortions involved in the process of in vitro fertilization vividly illustrates how the replacement of the conjugal act by a technical procedure—in addition to being in contradiction with the respect that is due to procreation as something that cannot be reduced to mere reproduction—leads to a weakening of the respect owed to every human being.”
There is no doubt that the progeny of in vitro fertilization and other reproductive technologies has done nothing to restore respect for the dignity of the human person. On the contrary, it has contributed to a cultural attitude that the human embryonic child is a thing, a possession, and a biological sample that can be accepted, destroyed, or frozen in time in a piece of jewelry.
Business enterprises like Baby Bee Hummingbirds gain traction in society because the bearing of a child has become nothing more than a mechanical function. And that, my friends, has taken the jewelry business to a new hellish low.
May 4, 2017 (LifeSiteNews) — As I’ve been researching Fatima for several speaking engagements this year, I was confronted over and over again by Our Lady’s insistence on Russia’s consecration. That after it was done, as well as the practice of the First Five Saturdays of reparation, Our Lady promised Russia would be converted and a period of peace would be given to the world. If not, the Queen of Heaven warned, Russia “will spread her errors throughout the world, causing wars and persecutions of the Church.” She added, “The good will be martyred, the Holy Father will have much to suffer, various nations will be annihilated.”
“In the end, my Immaculate Heart will triumph,” she said. “The Holy Father will consecrate Russia to me, and she shall be converted, and a period of peace will be granted to the world.”
Of course, St. Pope John Paul II entrusted the world to the Immaculate Heart in 1984, but we still await that period of peace. We have seen more war, massacres, martyrs, and abortions in the last half century than ever before. Ominously, we have not yet seen the annihilation of various nations. But what does all this have to do with Russia?
Russia, in the minds of most people, is the originator of communism – thought mainly to be an economic system competing with capitalism. However, when we really comprehend communism, the spread of Russia’s errors becomes recognizable.
“The Naked Communist” is the most concise and straightforward source outlining communist goals and ideology. It was written by W. Cleon Skousen, a former FBI agent who used many original sources, and the best intelligence of the FBI during its investigation of communist infiltration into the United States. The book is recorded in the Congressional Record and President Ronald Reagan commented on it saying: “No one is better qualified to discuss the threat to this nation from communism.”
A selection of the goals of communism listed by Skousen serve to illustrate its spread to all nations, especially the West:
Eliminate all laws governing obscenity by calling them “censorship” and a violation of free speech and free press.
Break down cultural standards of morality by promoting pornography and obscenity in books, magazines, motion pictures, radio, and TV.
Present homosexuality, degeneracy, and promiscuity as “normal, natural, healthy.”
Infiltrate the churches and replace revealed religion with “social” religion.
Discredit the Bible and emphasize the need for intellectual maturity which does not need a “religious crutch.”
Eliminate prayer or any phase of religious expression in the schools on the ground that it violates the principle of “separation of church and state.”
Discredit the family as an institution. Encourage promiscuity, masturbation, and easy divorce.
Emphasize the need to raise children away from the negative influence of parents. Attribute ”prejudices, mental blocks, and retarding of children to suppressive influence of parents.”
Beyond communism, however, another of Russia’s errors has spread throughout the world – abortion. Abortion was first legalized in Russia in 1920. To this day, Russia has the highest abortion rate in the world per capita. With a population of 143 million, there are 1.2 million abortions per year.
There is no doubt Mary’s predictions and promises will come true. Our Lady of Fatima predicted the Second World War and even noted a warning sign that would precede it. She warned of the massive plague of impurity that has infested the planet. She gave the faithful tasks to fulfill in order to see the Triumph her Immaculate Heart and she will be faithful to those prophecies too.
So, as we honor our own mothers this month, let’s examine again the requests of Our Blessed Mother and put them into practice. She asked for prayer, particularly the Holy Rosary and the devotion of the Brown Scapular. She urged reparation for the sins and outrages perpetrated against God’s Grace and blasphemies against the Holy Hearts of Jesus and Mary, especially with the practice of the First Five Saturdays. And finally, she asked for consecration to the Immaculate Heart of Mary, both on a personal basis and, publicly, that of Russia by the Pope and all the world’s bishops.
Almost all of those matters are within our personal control. There is no better time than this year, especially during the season of the Resurrection, the season of Easter, to implement these practices in our lives. Let us take up the weapon of the rosary – our umbilical cord to Our Heavenly Mother. Let us make the First Five Saturdays devotion and teach them to our children. Let us consecrate ourselves to the Immaculate Heart as St. Louis de Montfort taught and St. John Paul called “indispensable to anyone who means to give himself without reserve to Christ and to the work of redemption.”
MICAIAH BILGER APR 27, 2017 | 11:42AM WASHINGTON, DC
When doctors told Chelsea Torres that she was carrying conjoined twins, they warned her that the babies probably would not survive past the first trimester.
Doctors encouraged Torres and her husband, Nick, of Blackfoot, Idaho, to consider having an abortion, The Daily Mail reports. They refused.
The Idaho parents now are so thankful that they did not listen to their doctors’ advice. Their twin girls, Callie and Carter, were born in January, and they are doing well, according to the report.
Here’s more from the report:
Callie and Carter are omphalo-ischiopagus twins, which make up less than five per cent of conjoined twins.
This means they have just two legs and one pelvis between them, but have two separate torsos that face each other.
The girls do not appear to share any vital organs.
Today, the girls are three months old and healthy. The family said Callie and Carter are doing so well that doctors do not recommend separating them.
Daily living is more difficult with conjoined twins. The twins require a lot of custom-made things, like car seats and clothes. Chelsea said she sews clothing together to fit the twins.
She said a few people stare when they see the twins, but most are very supportive.
“I’m so happy I didn’t terminate Callie and Carter, they are amazing,” their mother told the Mail. “I knew termination would not happen and I’m glad that little speck of thought I did have, I pushed away.”
Research from the University of Maryland indicates that between 40 percent and 60 percent of conjoined twins are stillborn.
But the length of a child’s life inside or outside the womb should not justify killing them. Too often, parents are pressured to abort their unborn babies because of a disability or a short lifespan.
In the case of Callie and Carter, the odds were against them; but because their parents chose life, they are alive and well today. Stories like the Torres family’s demonstrate why every unborn baby deserves a chance to live.
MICAIAH BILGER MAY 4, 2017 | 10:15AM MONTGOMERY, ALABAMA
Baby Dexter was not supposed to be.
His mother, Lucy Hellein of Fort Mitchell, Alabama, was using a supposedly highly effective birth control device when doctors believe she conceived Dexter, according to the Daily Mail.
And when Dexter was born on April 27, the IUD coil that was supposed to prevent his life from being conceived came out, too. A photo of the newborn grabbing the contraceptive device has been catching people’s eyes on the internet. More than 70,000 people have shared it on Facebook, the report states.
Mirena, the contraceptive coil, or IUD, that Hellein used, is advertised as 99-percent effective.
According to the Mayo Clinic: “A T-shaped plastic frame that releases a type of progestin, Mirena thickens the cervical mucus to prevent sperm from reaching or fertilizing an egg. Mirena also thins the lining of the uterus and partially suppresses ovulation.” Some think the IUD also may act as an abortifacient by preventing a newly-conceived unborn baby from attaching to the womb.
Hellein told the Metro that she had the Mirena inserted last August, and then discovered she was pregnant with Dexter in December. Doctors said she likely conceived him just a few days after she had the device inserted.
“I assumed I was only a few weeks along, but the ultrasound confirmed that I was already 18 weeks along,” she said. “My Mirena was nowhere to be found on ultrasound so my OB assumed that it had fallen out, but I wasn’t convinced.”
The news of an unplanned pregnancy often is followed by suggestions of abortion, but Hellein chose life for her son.
“Dexter was definitely meant to be,” she said. “Although he wasn’t planned, my family and I feel incredibly blessed.”
When Dexter was born last week, doctors found the IUD behind Hellein’s placenta, according to the report.
It is believed that nurses posed newborn Dexter with the contraceptive device in the hospital to highlight his unplanned — but not unwelcome — life. Hellein later shared the image on Facebook, where tens of thousands of people have viewed it.
Pro-lifers take varying positions on artificial contraception. Some argue that birth control can help reduce abortion rates by preventing unwanted pregnancies, while others argue that it leads down a slippery slope to abortion.
No matter what their position on birth control, pro-lifers agree that every baby’s life, planned or unplanned, is worth celebrating.
Some say it gives them mood swings, stress and even depression. Others insist it clears their skin and balances their emotions.
According to a new study, it could all boil down to your genes.
Although studies have long shown estrogen-heavy pills ease depression symptoms, researchers at the National Institutes of Health found it has the opposite effect in women who carry a certain gene variant.
Brain scans revealed modified activity was linked to changes in the sex hormone in women with the gene while they performed a working memory task (the ability to hold memories for a short time while performing a separate task).
The researchers say their findings not only shed light on individual differences in the menstrual cycle but also mechanisms underlying differences in the onset, severity, and course of mood and anxiety disorders.
A new study has revealed that the hormone estrogen – found in many oral contraceptives – alters a memory circuit in women with a gene variant, while performing a working memory task (the ability to hold memories for a short time while performing a separate task)
The authors, from the National Institutes of Mental Health in Maryland, say that prior to the study, there was little evidence from research that might account for individual differences in cognitive and behavioral effects of sex hormones.
‘Why do some women report that estrogen replacement improved their memory, whereas large studies of postmenopausal estrogen therapy show no overall improvement in memory performance?’ they wrote.
The study hypothesized that estrogen alters circuit function by interacting with a gene that codes for brain derived neurotrophic factor (BDNF).
BDNF is a key protein in brain plasticity and acts on certain neurons to help support the survival of existing neurons and promote the growth and development of new ones.
Researchers experimentally manipulated estrogen levels in healthy women with one or the other version of the BDNF gene over a period of months.
Brain scan showed activity in the hippocampus, or the brain’s memory hub, in response to estrogen in women performing a working memory task – if they carried the gene variant.
However, activity in this area is typically suppressed during working memory, causing the researchers to conclude that the gene-hormone interaction affects thinking and behavior.
There is mounting evidence that sex steroids, such as testosterone, estrogen and progesterone, play an important role in a number of serious mood disorders, such as depression, anxiety and schizophrenia.
Women who have episodes of depression associated with reproductive events (premenstrual or postpartum) are prone to them because of a heightened sensitivity to intense hormonal fluctuations.
While estrogen is an ‘upper’ when released naturally during the menstrual cycle, at high doses it has the opposite effect, according to Dr Deborah Sichel, a psychiatrist specializing in female mood disorders.
Estrogen induces side effects such as nausea, breast tenderness, headaches and lower libido.
‘Women may not notice their negative mood because they have been on the pill for so long, they don’t know what their mood would be like if they were off hormones,’ Dr Sichel told Shape.
‘These are all real biochemical disorders that can and should be treated.’
MICHAEL COOK MAY 2, 2017 | 5:45PM BRUSSELS, BELGIUM
One of the last substantial barriers to increasing the number of euthanasia cases for non-terminally-ill psychiatric patients in Belgium seems to have crumbled.
A religious order in the Catholic Church, the Brothers of Charity, is responsible for a large proportion of beds for psychiatric patients in Belgium – about 5,000 of them. The international head of the order, Brother René Stockman, is a Belgian who has been one of the leading opponents of euthanasia in recent years.
Nonetheless, in a surprise move this week, the board controlling the institutions of the Brothers of Charity announced that from now on, it will allow euthanasia to take place in their psychiatric hospitals.
In a statement posted on their website the Brothers of Charity explain the policy shift. “We take seriously unbearable and hopeless suffering and patients’ request for euthanasia. On the other hand, we do want to protect lives and ensure that euthanasia is performed only if there is no more possibility to provide a reasonable perspective to treat the patient.”
Euthanasia for psychiatric patients has already happened dozens of times in Belgium. But from now on it will probably be easier for people suffering from schizophrenia, personality
disorders, depression, autism, or loneliness to access it. In fact, it will be hard to find an institution in Belgium where euthanasia is not being offered as an option.
Brother Stockman was stunned. “We deplore this new vision,” he told the media.
Nursing homes and hospitals opposing euthanasia have been under even more pressure after a court fined a Catholic nursing home a total of €6,000 last year for blocking a resident from accessing euthanasia.
However, Stockman felt that this was not an open and shut case. “I am confident that we have the right to refuse euthanasia,” Stockman told De Morgen. “We want to take seriously the needs of the patients, but the inviolability of life is for us an absolute. We cannot accept that euthanasia is carried out within the walls of our institutions. “
The leading figure in Belgian euthanasia, Dr Wim Distelmans, was delighted. Fifteen years after legalisation, he wrote in a newspaper op-ed, the Brothers of Charity have finally admitted that they had excluded the democratically approved policy of euthanasia from their institutions and forbidden doctors to follow their conscience and professional judgement.
Rubbing it in further, a member of the Belgian Parliament, Jean-Jacques De Gucht, summed up the situation: “the last relics of the paternalism of the shepherd have been replaced by individual self-determination”.
The chairman of the board, Raf De Rycke, an economist who has worked with the Brothers of Charity for years, denied that the ethos of their hospitals had changed “We have not made a 180 degree turn,” he told De Morgen newspaper. “It is not that we used to be against euthanasia and now suddenly are for it. This is consistent with our existing criteria. We are making both possible routes for our patients: both a pro-life perspective and euthanasia.”
Although this seems odd for a Catholic group, especially when the Pope has been outspoken in denouncing euthanasia, De Rycke believes that the inspiration of the Belgian Brothers of Charity fundamentally remains the same. “We start from the same basic values: the inviolability of life is an important foundation, but for us it is not absolute. This is where we are on a different wavelength from Rome.”
MANCHESTER, England, April 27, 2016 (LifeSiteNews) — Maria Santa, a healthy and gifted 17 year-old ballerina from Romania, died unexpectedly from a blood clot that doctors believe was caused by taking oral contraceptives.
Maria, who was studying in England on a scholarship at Manchester’s famous Northern Ballet School, went to a walk-in medical facility complaining of severe headaches, her father Robert Santa explained. No testing was done to see what was wrong, and Maria was sent home with antibiotics.
But Maria only got worse “day by day,” her father said. A second visit to the doctor did not help, either.
Maria began vomiting every hour, without eating or drinking. Going to the healthcare center for the third time last fall, she said she found it difficult to stand or sit; all she wanted to do was lie down. She was again given pills and sent home.
Two days later, on November 11, Maria complained that it felt like her head was going to explode, and she couldn’t feel her right leg. She was taken to the hospital by ambulance.
Mr. Santa shared that when the doctor came into her hospital room, Maria “could speak, then when he came back and asked where the headache was, she couldn’t speak.”
“The doctor told us not to worry because she was tired,” Mr. Santa said. “She didn’t speak any more, and she needed help with everything.”
Later that morning, Maria’s boyfriend found her unconscious at their apartment.
Maria was rushed to Salford Royal Hospital, but never regained consciousness. She died two days later.
The doctor who treated Maria at the hospital, Dr. Jonathan Greenbaum, said, “She was a fit, young woman, and the only risk factor was being on the oral contraceptive pill.”
He explained that the risk of blood clots with oral contraception is “very low, but if you take the pill then your risk is slightly increased.” He said identifying a medical risk is difficult, “because it’s so rare and the symptoms can be non-specific.”
Maria’s case, he said, was “just unfortunate and bad luck.”
“In Greater Manchester, I would guess we would see three or four patients a year with this problem,” Dr. Greenbaum estimated.
Dr. Piyali Pal, a pathologist, said Maria’s cause of death was blood clots in the brain.
“Causes could be dehydration, malnutrition, blood clotting disorders or somebody who had taken oral contraception pills. There was no underlying pathological cause,” he said. “It’s very very rare for someone so young to have this condition. One woman who was a similar age was also on some form of oral contraception.”
Coroner Simon Nelson recorded Maria’s cause of death as “natural causes.”
In a society where preborn children are treated as disposable property, and disregarded in the name of cold, sterile, euphemisms such as “reproductive rights” and “choice,” it’s rare to find a mother who actually does the opposite of putting herself above her child.
But in April 27th’s episode of Grey’s Anatomy on ABC, we got to see that rarity played out in a heart-wrenching yet inspiring storyline.
Patient Veronica is in the ER at Grey-Sloan Memorial Hospital for back pain. She’s almost 35 weeks pregnant and her body is riddled with cancer. She decided to forgo cancer treatment because, as she put it, “I didn’t want to microwave the baby.”
The storyline is a continuation from earlier this season when Veronica refused to abort her baby despite pressure from Doctor Miranda Bailey (Chandra Wilson) to kill her child to begin treatments for her terminal pancreatic cancer. (See previous article for factual information on cancer during pregnancy as well, as this episode did not accurately reflect the truth on the effects of chemotherapy and radiation on a preborn baby.)
The prognosis isn’t good, as was expected, and as Veronica planned for. The doctors give her two months at best left to live, as the cancer has spread even further and is compressing her spinal cord. And they tell her that they must deliver the baby that day..
“All right. Let’s cheer up, everybody. We’re having a baby,” Veronica announces optimistically, looking forward to having two months to spend with her baby and the baby’s father.
But during the C-section, things take a turn for the worst:
Amelia: Heart rate’s up to 130. Veronica, how’s your breathing?
Veronica: It’s fi– um, it’s a little tough.
Jeremy: What’s happening? What’s going on?
Veronica: Hey, Jer, come on. Look at him. He has the sweetest eyes.
Arizona: Her sats are dropping. She’s persistently tachycardic.
Amelia: Let’s put her back on high-flow oxygen. It could be an embolus.
Veronica: Time to get him out of here.
Alex: Yeah, in a minute.
Arizona: If it’s an embolus, we don’t have a minute.
Alex: She did all this so she can meet the baby. Just give them another damn minute.
Veronica: Jer, can you take him?
Alex: He needs to go to the NICU now.
Jeremy: And, uh, what — what about Veronica?
Alex: She’s in good hands. She’ll be just fine. I’ll take good care of her.
Veronica: Jer, you stay with him. You promised. I’m counting on you.
Jeremy: But I don’t —
Veronica: Go on. Stay with him. I’ll see you in a little bit.
Amelia: Are we pushing heparin or going straight to thrombolytics?
Arizona: Thrombolytics are contraindicated. We need to do an embolectomy, and let’s get an ivc filter.
Amelia: Veronica, you’ve thrown a blood clot, and it’s traveled all the way to your lungs. It’s very serious. We need to remove it immediately, so we’re gonna need to put you under and open up your chest.
Veronica: Is that… Uh… Uh, will that work?
Amelia: The procedure will only last about a half an hour.
Veronica: Will it work?
Amelia: There’s no guarantee you’d survive it.
Veronica: And what if we didn’t do anything?
Arizona: Veronica, we need to do this procedure. If we don’t, you might not make it off this table today.
Amelia: Okay, pressure’s dropping. Get a cart ready!
Veronica: No. I signed that dnr for a reason.
Arizona: You can rescind. Let us help you.
Veronica: I did what I wanted. My baby’s…okay. It — I’m so tired.
Amelia: I know. I know.
Too bad Dr. Miranda Bailey wasn’t around to see that beautiful baby alive and well thanks to his mother not listening to her pro-abortive advice.
Later, we see Veronica in her last moments and realize even further what an amazing mother she was to give up her own life for her child’s:
Amelia: What do you want? What do you need right now?
Veronica: I’m so cold.
Amelia: I’ll get a warming blanket.
Veronica: No! No. Can you — Will you just hold me? We did good? The baby’s good?
Amelia: Baby’s good.
Yes, Veronica, you did good. And your baby is so very good because of your beautiful sacrifice.
The FDA received 5,016 medical device reports involving Essure in 2016, plus another 6,176 reports in 2015, and 30 reports of deaths. The deaths include four adult women, 18 pregnancy losses, two infants who died after they were born, and a possibly stillborn baby.
Many reports listed multiple side effects. The most common problems with Essure included:
Pain/abdominal pain (10,746)
Heavier menstrual bleeding or irregularities (5,377)
Headache (4,396)
Fatigue (3,560)
Weight changes (3,270)
Patient-device incompatibility, such as nickel allergy (2,402)
Pregnancy (1,113)
Migration of Essure (1,485)
Broken Essure (617)
Pregnancy losses, ectopic pregnancy, abortion, miscarriage (474)
Essure difficult to remove (304)
Malposition of Essure (261)
The FDA update also provides new details on an ongoing Essure safety study that will compare 1,400 women who are sterilized with Essure against 1,400 women who have a traditional “tube tying” sterilization.
So far, the study has not shown any new safety problems or an increased risk of problems since Essure was approved. The researchers are investigating side effects like chronic pain, abnormal uterine bleeding, allergic reactions, hypersensitivity to nickel in Essure, autoimmune diseases, follow-up surgery, pregnancy, and effectiveness.
However, other recent studies have already shown that women who choose Essure are 10-times more likely to need another surgery compared to women who have a laparoscopic tubal ligation.
Essure is a metal coil that is permanently implanted in a woman’s fallopian tubes, where it causes irritation and scar-tissue growth. Essure is supposed to block the fallopian tubes to prevent pregnancy. Instead, many women got pregnant or developed severe side effects.
In November 2016, the FDA added a “Black Box” warning label to Essure, which is the strongest label the FDA can require on a device. The FDA also created a checklist to better inform patients about the potential side effects.
The problem is that Essure is marketed as a 30-minute non-surgical outpatient procedure for busy women, with less pain and a faster recovery time than tubal ligation. Lawsuits have been filed by women who accuse manufacturers of downplaying risks and violating approval requirements to get Essure on the market without adequate safety studies.
Source: Reviewing Ongoing Clinical Study to Gather More Information on Essure Benefits and Risks
A new study has reinforced what many women have been saying for years – the oral contraceptive pill is associated with reduced quality of life and wellbeing in healthy women.
The double-blind, randomised, placebo-controlled trial found that healthy women reported reduced quality of life, mood, and physical wellbeing after taking a common birth control pill containing ethinylestradiol and levonorgestrel for three months.
But there was no significant evidence that the contraceptive increased depressive symptoms in the latest study… so, there’s that.
Surprisingly, this is one of the most rigorous studies to date to look into the impact of the pill on women’s quality of life.
“Despite the fact that an estimated 100 million women around the world use contraceptive pills we know surprisingly little today about the pill’s effect on women’s health,” said lead researcher Angelica Lindén Hirschberg from the Karolinska Institutet in Sweden.
“The scientific base is very limited as regards the contraceptive pill’s effect on quality of life and depression and there is a great need for randomised studies where it is compared with placebos.”
To fix that, her team took 340 healthy women aged between 18 and 35 and gave them either placebo pills, or contraceptive pills containing ethinylestradiol and levonorgestrel over a three-month period.
Ethinylestradiol and levonorgestrel-containing pills are among the most common form of combined oral contraceptive pills around the world because they’re the least associated with a risk of blood clots, and they include brand names such as Levlen, Microgynon, Portia, and Alesse.
The study was double blind, which meant that neither the researchers giving out the pills or the women taking them knew whether they were getting a placebo or not.
At the start of the study, the women had their general health measured, including weight, height, and blood pressure.
They then went through the same tests at the end of the three months so the researchers could compare the results.
The women who were given contraceptive pills reported that their quality of life was significantly lower at the end of the study than those who were given placebos.
This was true for general quality of life and also specific aspects of wellbeing, such as self control and energy levels.
No significant increase in depressive symptoms was observed.
While it’s an interesting first step towards better measuring the pills’ side effects, the researchers caution that the changes were relatively small so we can’t read too much into them just yet. And we can only apply these findings to ethinylestradiol and levonorgestrel-containg pills.
Also, the study only looked at women over three months – it will require longer monitoring to get a more accurate idea of how the contraceptive pill affects women.
“This possible degradation of quality of life should be paid attention to and taken into account in conjunction with prescribing of contraceptive pills and when choosing a method of contraception.”
More research is needed before we can identify more accurately how the pill impacts women, but these early results are reassuring for many women who’ve struggled with side effects while on the pill.
NEW YORK, April 24, 2017 (LifeSiteNews) — Cardinal Robert Sarah warned that the Church’s unity is being threatened by influential leaders within the Church who “insist” that national churches have the “capacity to decide for themselves” on doctrinal and moral matters.
“Without a common faith, the Church is threatened by confusion and then, progressively, she can slide into dispersion and schism,” he said.
“Today there is a grave risk of the fragmentation of the Church, of breaking up the Mystical Body of Christ by insisting on the national identities of the Churches and thus on their capacity to decide for themselves, above all in the so-crucial domain of doctrine and morals,” he added.
Catholics profess every Sunday in the Nicene Creed that the Church is “one, holy, Catholic, and Apostolic.” These are often called the four “marks” of the one true Church.
Sarah, who comes from Guinea, made the comments when asked in an April 18 interview with the charitable organization Aid to the Church in Need about the relationship between the “African Church” and the “Universal Church.”
The Cardinal, who is the Prefect of the Congregation for Divine Worship, said that, strictly speaking, there is no such reality as the “African Church.”
“The Universal Church is not a sort of federation of local churches,” he said. “The Universal Church is symbolized and represented by the Church of Rome, with the Pope at its head, the successor of Saint Peter and the head of the apostolic college; hence it is she who has given birth to all the local churches and she who sustains them in the unity of faith and love.”
Sarah’s remarks will be seen by some as opposing a push by Pope Francis to give bishops’ conferences in individual countries more power, even to settle doctrinal and moral disputes.
In his 2013 Exhortation Evangelii Gaudium, Pope Francis called for a “conversion of the papacy” that would help him “exercise” the Petrine ministry. He criticized in the same document “excessive centralization” of power in the office of Peter, suggesting that bishops’ conferences should be empowered with “genuine doctrinal authority.”
Francis also wrote about a decentralized Church in his 2016 Exhortation Amoris Laetitia. He wrote: “I would make it clear that not all discussions of doctrinal, moral or pastoral issues need to be settled by interventions of the magisterium…Each country or region, moreover, can seek solutions better suited to its culture and sensitive to its traditions and local needs.”
According to Archbishop Stanislaw Gadecki, president of the Polish bishops’ conference, the Pope told Polish bishops last year that a decentralized Church would be able to interpret papal encyclicals and to solve contentious issues, such as giving Communion to civilly divorced and remarried Catholics.
In the interview with Aid to the Church in Need, Cardinal Sarah said that the Church will grow throughout the world only if it is united by “our common faith and our fidelity to Christ and his Gospel, in union with the Pope.”
“As Pope Benedict XVI tells us: ‘It is clear that a Church does not grow by becoming individualised, by separating on a national level, by closing herself off within a specific cultural context, by giving herself an entirely cultural or national scope; instead the Church needs to have unity of faith, unity of doctrine, unity of moral teaching. She needs the primacy of the Pope, and his mission to confirm the faith of his brethren,’” he said.
Later in the interview, Sarah said the Church would be “gravely mistaken” to think that social justice issues such as combatting poverty and helping migrants were her real mission.
“The Church is gravely mistaken as to the nature of the real crisis if she thinks that her essential mission is to offer solutions to all the political problems relating to justice, peace, poverty, the reception of migrants, etc. while neglecting evangelisation,” he said.
The Cardinal said that while the Church “cannot disassociate herself from the human problems,” she will ultimately “fail in her mission” if she forgets her real purpose. Sarah then quoted Yahya Pallavicini, an Italian and former Catholic who converted to Islam, to drive home his point: “If the Church, with the obsession she has today with the values of justice, social rights and the struggle against poverty, ends up as a result by forgetting her contemplative soul, she will fail in her mission and she will be abandoned by a great many of her faithful, owing to the fact that they will no longer recognize in her what constitutes her specific mission.”
Although many in the media praise abortion, some Hollywood and sports stars are starting a new pro-life trend: celebrating their unborn babies on social media.
Serena Williams is the latest to join the team. On Monday, world-famous tennis player posted an Instagram picture of herself lounging at the beach. In the caption, the 35-year-old penned a heartfelt message to her unborn baby:
My Dearest Baby,
You gave me the strength I didn’t know I had. You taught me the true meaning of serenity and peace. I can’t wait to meet you. I can’t wait for you to join the players box next year. But most importantly, I am so happy to share being number one in the world with you…. once again today. On @alexisohanian bday. from the world’s oldest number one to the world’s youngest number one. -Your Mommy
By “@alexisohanian,” Williams meant her fiancé, Reddit cofounder Alexis Ohanian.
Last week, Williams revealed her 20-week pregnancy on social media platform Snapchat. As her fans calculated, that means Williams won the Australian Open while pregnant with baby number one.
(CNN) Students at UC Davis can now press A4 for Plan B.
A new vending machine in a University of California Davis study room traded the usual Hot Cheetos and Red Bull for condoms, tampons, pregnancy tests, Advil, and the morning after pill (or Plan B). They call it the “Wellness To Go” Machine.
Stocking contraception rather than caffeine may seem out of place in a study area, but to former UC Davis student Parteek Singh it makes total sense.
Although the Wellness To Go machine was installed in early April, Singh spent two years working to make it happen.
“The more skeptical and negativity I got from people like ‘oh it’s not going to happen,’ kind of pushed me more,” Singh told CNN affiliate KTXL.
Plan B and other contraceptive methods have had their ups and downs. In 2013, Plan B was made available to women without a prescription. But the Trump Administration has threatened funding for Planned Parenthood.
With a nation divided on the issue comes a campus divided as well.
“It is promoting like ‘Oh hey, go and have unsafe sex because then you have a backup option and it’s gonna be cheaper than if you just wanna go to a drug store,'” UC Davis student Jordan Herrera told the affiliate.
But other students come to its defense.
“It’s a great thing for women,” student KC Cui said.
CNN has reached out to UC Davis and is waiting on a response.
(Editor’s note: The following is a slightly edited version of the editorial of the April issue of LifeSite’s Faithful Insight magazine. Those interested in subscribing to the monthly Catholic news magazine may do so here.)
April 19, 2017 (LifeSiteNews) – Mayhem. That’s the only word to describe what is taking place in the Church today. Remember the archbishop who released a scandalous Vatican sex-ed program at World Youth Day in Krakow? He was appointed as the new head of the Pontifical Academy for Life and Rome’s John Paul II Institute for Marriage and Family. Both institutions have now been stripped bare – the Academy of all its members and the Institute of its most conservative faculty.
Archbishop Vincenzo Paglia recently gushed praise for one of Italy’s leading proponents of abortion, same-sex “marriage” and restriction on religious freedom. More than that, prior to his Vatican post he commissioned a homoerotic mural in his cathedral church in which he had included an image of himself.
Another Vatican bishop in charge of two Pontifical Academies is responsible for bringing into the Vatican, to speak at his conferences, some of the most anti-life, anti-family people in the world. Those supporting forced abortion and forced sterilization are finding themselves at home in a new Vatican where the lovers of life and family are increasingly alienated and ostracized. A Vatican where fear among the orthodox rules and in the words of retiring Archbishop Luigi Negri – the only Italian bishop to go to the Rome March for Life – those who are normally papal critics, “for a time have become hyper papists for their own ends.”
The only solution to this mess is Divine intervention. And in this year of the 100th anniversary of Fatima, it is time to beg for that intervention and to do what we can to bring it about.
Pope Emeritus Benedict XVI himself hoped that such an intervention would happen shortly. “May the seven years which separate us from the centenary of the apparitions hasten the fulfillment of the prophecy of the triumph of the Immaculate Heart of Mary, to the glory of the Most Holy Trinity,” he said in a homily on May 13, 2010. “We would be mistaken to think that Fatima’s prophetic mission is complete,” he said.
The October 13, 1917 Fatima miracle of the dance of the sun was witnessed by 70,000 people with coverage in all the secular papers at the time. It was the most spectacular public miracle of all time. What was it that heaven was trying to communicate with this stupendous event?
Our Lady showed the three shepherd children hell. “You have seen hell where the souls of poor sinners go,” she told them. “To save them, God wishes to establish in the world devotion to my Immaculate Heart. If what I say to you is done, many souls will be saved and there will be peace.”
What did Our Lady ask for to bring about the triumph of her Immaculate Heart? First prayer, most particularly the Holy Rosary, and the devotion of the Brown Scapular. Second, she called for us to make reparation for the sins and outrages perpetrated against God’s Grace and blasphemies against the Holy Hearts of Jesus and Mary. Thirdly, she asked for consecration to the Immaculate Heart of Mary, both on a personal basis and, publicly, that of Russia by the Pope and all the world’s bishops.
Our Lady warned that if Russia was not consecrated to her Immaculate Heart, Russia would spread its errors throughout the world. We have seen atheistic communism spread throughout the world. But most don’t realize that legalized abortion began in Russia and this global atrocity has cost more lives than all wars combined.
Our Lady warned specifically that if Russia was not consecrated there would be “wars and persecutions against the Church. The good will be martyred, the Holy Father will have much to suffer, various nations will be annihilated.”
She predicted the Second World War, and it happened. She predicted “fashions will be introduced that will offend Our Lord very much. Woe to women lacking in modesty.” And it happened like never before in the history of the world. She predicted wars, and there have been more wars in the last 30 years than ever before. We have not yet seen whole nations annihilated.
Many have said her wish for the consecration of Russia was accomplished in 1984 when Pope St. John Paul II entrusted the world to Our Lady. Let’s skip the debate over it and do it again, but this time mentioning Russia specifically, as was requested by Our Lady. Poland was blessed greatly each time they consecrated their nation to Our Lady.
“In the end, my Immaculate Heart will triumph,” she promised. “The Holy Father will consecrate Russia to me, which will be converted, and a period of peace will be granted to the world.” We await that peace eagerly both in the world and in the Church.
But Our Lord warned Sr. Lucia in a vision in 1931, expressing dismay that the Pope would not carry out the consecration of Russia as requested. “Like the King of France, they will repent of it, and they will do it, but it will be late. Russia will already have spread its errors in the world.” He added, “Make it known to My ministers, seeing that they follow the example of the King of France in delaying the execution of My demand, they will also have to follow him into misfortune.”
That warning has a severe implication for our days. The mention of the King of France by Our Lord refers to the request He made of St. Margaret Mary Alacoque. On June 17, 1689, He asked her to have the King of France consecrate France to the Sacred Heart. For 100 years, the Kings of France failed to make the consecration.
On June 17, 1789, 100 years to the day of the request, the King of France was stripped of his legislative authority and four years later executed.
Let us play our part in hastening the Triumph of the Immaculate Heart. Let us pray the Rosary, wear the Scapular, make the First Saturdays devotion and request the explicit consecration of Russia to the Immaculate Heart.
Physician assisted suicide legislation has been making the news recently. Legalized euthanasia in Canada, Netherlands, Belgium and other European nations have also generated headlines.
However, a silent, rampant killer is intentionally claiming lives of far more patients each day in America’s medical facilities.
This quiet, legal killer is taking the lives more Americans than all the assisted suicide deaths combined. It’s the withdrawal of food and water from patients whose lives are deemed “futile” by hospitals, nursing homes and hospices throughout the nation.
Food and water delivered by tube instead of mouth was once deemed “basic and ordinary care” but is now viewed as “extraordinary medical treatment.” Further, it’s legal in all 50 states to withhold food and water when it will directly result in the death of a patient.
Terri Schiavo was denied food and water. It too her 13 days to die.
So how many patients is this likely affecting? According to the American Hospital Association and the Centers for Disease Control, there are nearly 35,000 hospitals, nursing homes and hospices operating in the USA — 1.3 million patients in hospice alone. After doing the math it’s easy to assume that every day patients are being “put down” using an agonizingly cruel, drawn-out death sentence.
Bobby Schindler, president of the Terri Schiavo Life and Hope Network and brother to Terri Schiavo, saw this horror play out in a very personal way with his sister. It took her 13 excruciating days to die. A time period he appropriately describes as a nightmare for Terri and her family.
“My sister’s lips were horribly cracked to the point they were blistering. Her skin became jaundice with areas that turned different shades of blue. Terri’s breathing became rapid and uncontrollable. Her moaning, at times, was raucous, which indicated to us the insufferable pain she was experiencing. Terri’s face became skeletal, with blood pooling in her deeply sunken eyes and her teeth protruding forward. What will be forever seared in my memory is the look of utter horror on my sister’s face when my family visited her just after she died.”
Death with dignity?
How did a compassionate and progressive nation like ours resort to such a barbaric practice in the name of medicine? So-called bioethicist Daniel Callahan planted the seeds of what can be considered “medical cleansing” in 1983. “A denial of nutrition may in the long run become the only effective way to make certain that a large number of biologically tenacious patents actually die. . .it could well become a non-treatment of choice.”
Brutal and prophetic.
Don’t think you’re immune to the risk of death by dehydration. Laws in 46 states already allow the medical provider—not the patient or family—the right to refuse life-saving or sustaining treatments, including food and water.
Over the years laws have quietly been enacted that prioritize the financial standing of insurance companies and medical facilities over patient autonomy and well-being. Ending the life of a costly patient by dehydration and starvation is an economic no-brainer in this day and age of demanded profitability within medical care. Obamacare has expedited this process.
We have seen examples of patients like Stephanie Packer, California mother of four, denied life-saving treatment where physician assisted suicide is legal, while being offered coverage for a lethal prescription to end her life.
Hospital ethics committees routinely assume full decision-making authority over the treatment of patients when family members disagree on how to proceed. And medical facilities have effective methods of “treatment” for the biologically tenacious who simply refuse to die.
Ethicist Wesley Smith calls it “termination without request or consent.” It involves offing “futile” patients via the denial of food and water or by using terminal sedation, which administers a heavy dose of morphine or other pain killer, whether it’s needed or not, to slow respiration and cause an early death.
Bobby says the best way to protect yourself is to have a legally designated advocate as your power of attorney who will vigorously fight for you. Visit our website for free resources that can help protect you and your family.
Defending innocent human life,
Bradley Mattes
President, Life Issues Institute
Life Issues Institute is dedicated to changing hearts and minds of millions of people through education. For 25 years, organizations and individuals around the world have depended upon Life Issues Institute to provide the latest information and effective tools to protect innocent human life from womb to tomb.
April 10, 2017 (LifeSiteNews) — The Catholic Church under Pope Francis has not changed her teaching on the immorality of cohabitation, adultery, divorce, or homosexuality, and she has certainly not opened the door for civilly-divorced-and-remarried Catholics to receive Holy Communion, said Cardinal Gerhard Muller in a new book-length interview published April 1.
Muller, the head of the Vatican’s Congregation for the Doctrine of the Faith, said in the 240-page book, titled The Cardinal Muller Report, that Catholics must not fear “confessing our faith.” The book was dedicated to Pope Francis.
In the interview, conducted about a year ago but only made available in English this month, the Cardinal said that it would be a “false concept of God” as well as a “false interpretation of mercy” to allow civilly-divorced-and-remarried Catholics living in adultery to receive Communion.
In “immoral relationships” such as cohabitation and divorce-and-remarriage, he said, “the seeds of the Word [of God] do not abide in [these] sinful situations.” In these situations, he added, “despite the fact that it might seem otherwise, there can be no authentic dynamic of love but, rather, only a serious obstacle to the ability to grow in humanity.”
Muller said that the 2015 Synod on the Family insisted that “given the intimate nature of the sacraments and the character of the indissolubility of marriage as divine law, it is not possible to admit to the Eucharist divorced people who have remarried civilly.”
Any pastoral accompaniment for those in irregular situations, he said, must “always be rendered according to conscience and the teaching of the Church.”
“Saint John Paul II warned that being pastoral does not mean a compromise between the doctrine of the Church and the complex reality of daily life but, rather, leading individuals to Christ,” he added.
The Cardinal said that Pope Francis’ much used statement that the Eucharist “is not a prize for the perfect but a powerful medicine and nourishment for the weak,” is often mistakenly interpreted. He maintained that it does not mean that “anyone can come to receive the Eucharist even though he is not in grace and does not have the required state of mind, just because it is nourishment for the weak.”
He noted that access to the Eucharist comes with necessary preconditions.
“Certainly access to Eucharistic Communion presupposes a life of grace, presupposes communion in the Body of the Church, and also presupposes a life ordered in conformity with the Body of the Church so as to be able to say the ‘Amen’ to which you referred before. Saint Paul insists that whoever eats the bread or drinks the cup of the Lord in an unworthy manner will be guilty of profaning the Body and Blood of the Lord,” he said.
To go to Communion without being in the required state of grace and with the assumption that God “grants me privately the forgiveness of my sins” is a “false concept of God; this is tempting him,” he added.
Muller said that Pope Francis’ famous statement “Who am I to judge,” often repeated by those who are hoping to see a “change of direction” in the Church on homosexuality, does not mean the Church has suddenly become “less dogmatic” on the issue.
“The concept of the intrinsic disorder of homosexual acts, because they do not proceed from a genuine emotional and sexual complementarity, stems from Holy Scripture,” he said.
And yes, he said, the Church “with her Magisterium, has the power to judge the morality of specific situations,” such as sexual acts.
“This is an undisputed truth: God is the only judge who will judge us at the end times, and the pope and bishops have the obligation to present the revealed criteria for this Last Judgment which our moral conscience already anticipates. The Church has always said ‘this is true, this is false,’ and no one can live by his own subjectivist interpretation of God’s commandments,” he added.
The Cardinal warned against “new anti-family ideologies” that have arisen that “attempt to redefine what is human, based, not on the truth, but on individual feeling and social utility.”
He specifically mentioned the danger of “gender ideology.”
This ideology, he said, “does not respect the reality of things and that ultimately denies the Creator and man’s condition of having been created.” It “affirms that man’s identity does not depend on nature, with a body that is limited to a masculine or feminine sexuality” and “makes use of medical advances to use the body as an area of experimentation, viewing a change in sex as a simply biological operation,” he said.
Muller said that lurking behind gender ideology is the manmade “idol” of “our own liberty, of our own wish, proposing to be, ourselves, those who determine what is good and bad.”
“Was this not the substance of the first temptation of Adam and Eve? Is it possible to build a society without respecting the fundamental difference between a man and a woman?” he added.
The Cardinal concluded his interview by proposing how the Church can help modern man find “peace and reconciliation with himself.”
“There is only one way open to us: compunction or repentance for the evil committed. The Cross of Christ is the only path. There is no other path for evangelization today,” he said.
Other topics Cardinal Muller addressed in his interview (paragraphs not necessarily linked in original):
Islamist terrorism
More deeply, I believe that we have here a path out of the phenomenon of Islamist terrorism: we should not favor a separation of society as a whole from God, but should instead, on the contrary, harness the power of religion as a social relationship that reinforces living together, peace, and therefore progress for all.
Priestly celibacy
Priestly celibacy, which is being challenged so much today in certain ecclesiastical quarters, is rooted in the Gospels as an evangelical counsel, but it also is intrinsically related to the ministry of the priest.
We cannot break unilaterally from the series of declarations by a long line of popes and councils and from the steady and continuous adherence of the Catholic Church to the image of the celibate priest.
Women priests
This is not a legitimate issue, because it touches on a subject that has already been decided. Pope Francis has made it clear, as have his predecessors: in that connection, I remember that Saint John Paul II, in number 4 of his Apostolic Exhortation Ordinatio sacerdotalis of 1994, reinforced with the use of the royal “we” (“declaramus”), the only document in which that pope uses that verb form, that it is a definitive doctrine infallibly taught by the ordinary universal Magisterium (CIC, can. 750 §2) that the Church does not have the authority to admit women to the priesthood.
It is the province of the Magisterium to decide if a question is dogmatic or disciplinary: in this case, the Church has already decided that this proposition is dogmatic and that, because it is divine law, it cannot be changed or even reviewed.
[Male-only priesthood] can be supported with many reasons, such as fidelity to the example of the Lord or the normative nature of the centuries-old practice of the Church.
I would not want to leave it unsaid that there is an essential equality between male and female, in nature and also in the relationship with God through grace (see Gal 3:28). The priesthood, however, implies a sacramental symbolism of the relationship of Christ, the Head or husband, with the Church, the Body or wife.
Married priesthood (viri probati)
A vocational crisis cannot be dealt with by addressing only its symptoms and not its real cause. What has given rise to the vocational crisis? I believe I can say that it is a matter of a crisis of faith, which in turn is a result of a long secularization that has dried up what was once fertile soil and has scorched the earth.
Are we aware that a massive inclusion of viri probati, which is especially foreseeable in countries where Catholicism is expanding and there are not many priests, would unquestionably mean the end of celibacy?
We cannot solve such big problems through compromise solutions or half-measures.
Catholics and Protestants
Strictly speaking, we Catholics do not have any reason to celebrate October 31, 1517, the date that is considered to be the beginning of the Reformation that led to the rupture in Western Christianity. If we are convinced that revelation has been preserved, in its entirety and unchanged, through Scripture and tradition in the doctrine of the faith, in the sacraments, in the hierarchic constitution of the Church by divine right, founded on the sacrament of holy orders, we cannot accept that there are sufficient reasons to separate from the Church.
Indissolubility of Sacramental marriage
We therefore have to take as our premise that she will never have the authority to dispense with the divine commandments, in the name of a supposedly compassionate and loving vision, in situations that do not conform to the Word of God. She cannot, for example, grant a second marriage while a first spouse of a sacramental marriage, consummated or unconsummated, is still alive. In certain difficult family situations, the Church can allow an interruption of marital life together, but she cannot break the sacramental bond.
Population control
Anti-birth policies are nothing but another ideological proposal that hides the unmentionable: the attempt to maintain, unfairly, the privileged status of a few, at the expense of blocking access to wealth by broad layers of the population. Actually, as we have just explained, we know that hunger in the world is not at all the consequence of overpopulation and that abortion does nothing to contain population growth, serving only to satisfy our hedonism.
Based on catastrophic predictions that have never been borne out, rooted in neo-Malthusianism (for example, Paul Ehrlich, The Population Bomb), some international organizations have recently exacerbated the problem, proposing a “responsible parenthood” that implies reducing the birthrate, by whatever means, for a better distribution and optimal use of resources.
In that regard, we must clearly denounce as having no scientific basis the claim that the alleged current population explosion has caused global economic impoverishment: if two thousand years ago the world had an estimated two hundred million inhabitants, and it took fifteen centuries to double that population, in the last two centuries the world population has multiplied by six, surpassing six billion inhabitants, while real GDP worldwide has multiplied by fifty. It is no surprise, then, that the anti-birth theories based on the myth of population’s geometric progression while the means of subsistence have grown only in arithmetic progression (Thomas Robert Malthus, An Essay on the Principle of Population), should be more and more discredited among the scientific community, which now leans more and more to the conclusion that people, when they are seen clearly, unclouded by erroneous ideological distortions (Friedrich Hayek, The Fatal Conceit), end up resolving the problems themselves thanks to human creativity.
Anti-birth policies are nothing but another ideological proposal that hides the unmentionable: the attempt to maintain, unfairly, the privileged status of a few, at the expense of blocking access to wealth by broad layers of the population. Actually, as we have just explained, we know that hunger in the world is not at all the consequence of overpopulation and that abortion does nothing to contain population growth, serving only to satisfy our hedonism.
Large families
Large families are an expression of the superabundance of love. They are a great yes to life. Several children are a great gift not only for their parents but also for the Church and all of society. Lumen gentium (no. 11) speaks of Christian parents as those who in a certain way bestow their children on the Church.
Humanae Vitae / Contraception
The encyclical Humanae vitae had many difficulties in its reception, as much for its underlying anthropology— especially regarding its proposal on the experience of love and sexuality—as for its clarification of the intrinsic morality of the methods of birth control. The indiscriminate attacks to which it was subject from the outset caused it to be marginalized and forgotten, despite its richness in inventively and prophetically posing the reality of love, of marriage, and of the beauty of married life.
Today, almost fifty years later, we see much more clearly that Pope Paul VI was right in everything that at the time he had the courage to make clear. Ahead of his time, this humanist pope had the courage to offer this document to the Church and to society, denouncing with an accurate analysis what ended up happening. Are we not, indeed, witnessing a pandemic of divorce? Have we not, just as unmistakably, turned sex into a trivial reality devoid of feeling? And is it not as patently clear today that Western societies, having radically separated the unitive function from that of procreation, have a true problem in their birthrate? The situation is one of authentic demographic involution that carries grave consequences, considered both synchronically and diachronically, if we examine the present moment and the foreseeable possibilities for the near future.
But the problem, I repeat, is not only demographic but rather, above all, one of meaning: I mean the question of the identity and vitality of marriage. Perhaps five decades ago it was not so evident, since the institution of the family was still strong: in fact, it was not yet foreseen that there could be so many broken marriages in our own families, with so many children who could not enjoy a father and a mother living under the same roof or so many adolescents initiating themselves at a young age in a life of frivolous sex. Yes, we are much more able today to grasp the negative impact of a mistaken conception of sex, valued only for the gratification it brings and not for the gift that it makes possible. We understand better today the perverse effects of artificial birth control, as a simple means toward the worry-free enjoyment of sex, without wanting to see the consequences for physical, psychological, and spiritual health.
Moral problems demand moral solutions. We must humanize sexuality, which is at the service of the personal union of spouses, making it possible for each to be a gift to the other and not only a means for satisfying their desire. We must explain to new spouses the goodness, for example, of natural methods that, based on abstinence from sexual contact during the fertile days, foster dialogue, mutual respect, and understanding in the couple.
Divorce
In the East, for example, after the separation of those ecclesial communities from the Cathedra Petri, an increasingly liberal praxis or “right of consuetudinary origin” was accepted, under which—after a period of penitence—a second marriage was allowed, even in the case of a valid first marriage and with the first spouse still living, and participation in Communion, as a life preserver that enabled “salvation”, was allowed at the same time. As a result, the Orthodox Churches, by the principle of oikonomia or pastoral condescension (called the “pastoral approach of tolerance, clemency, and indulgence”) went on to justify a multitude of reasons for divorce. Considering the words of Jesus concerning the indissolubility of marriage, I do not see how this practice can be derived from the will of God.
The Church lives by God’s truth and therefore is responsible to man for it. She bears witness to it with humility and with the strength that the Lord gives her, without allowing herself to be cowed by the world’s accusations. On marriage and the sexual morality that she has received from God, she must remember the substantial unity of man in spirit, soul, and body, his relationship with the community, the truth about the totality of the gift required for sexuality to be human, the intergenerational responsibility, the identity as man and woman in their essential mutual reference.
These principles are not just an ideal, because love is never just an ideal, or even just a beautiful concept; it is instead a concrete dedication of life and the deep-rooted availability that opens the horizon of hope in individuals’ daily lives.
All of us know that we are sinners and that it is in the sphere of sexuality that human weakness obviously manifests itself. But this does not mean that the sexual morality taught by the Church is an unattainable ideal. The biggest scandal of which the Church is capable is not that there should be sinners in her, but that she should stop explicitly calling the difference between good and evil by name and that she should relativize that difference, stop explaining what sin is, or try to justify it by a supposedly greater closeness to and mercy toward the sinner.
We know, for example, that marriage is indissoluble, that the union of a man and a woman has “forever” as an essential and unforsakable characteristic, and that spousal love is therefore so deep and so beautiful. So in a traumatic situation where a woman has been abandoned by her husband, in the context of a sacramental marriage, whether consummated or unconsummated, it would not be permissible to say “let us be merciful and allow her to contract a new marriage with another man.” This would not be true mercy but, instead, a failure to take her personal travail seriously, besides favoring sin and mocking God and his commandments.
Sex-education / parental rights
Throughout my years of priestly ministry, however, I have been able to see that what young people want is precisely to discover the meaning of sex, its relationship to love, its opening to the future. For that reason, emotional-sexual education is a duty that begins at the first moment of the child’s life and that, unavoidably and definitively, falls on the parents. They can be supported, but they cannot be supplanted, by school and other educational institutions like the parish.
Mercy
I said before that mercy cannot consist in relativizing God’s commandments but must, rather, make possible the encounter with God’s love, which renews and changes our life. Mercy consists in recognizing that the truth, the truth of love, will make us free (see Jn 8:32).
All of us know that we are sinners and that it is in the sphere of sexuality that human weakness obviously manifests itself. But this does not mean that the sexual morality taught by the Church is an unattainable ideal. The biggest scandal of which the Church is capable is not that there should be sinners in her, but that she should stop explicitly calling the difference between good and evil by name and that she should relativize that difference, stop explaining what sin is, or try to justify it by a supposedly greater close- ness to and mercy toward the sinner.
I think, first, that sacramental confession is the most paradigmatic expression of God’s mercy.
Hell
Hell, certainly, is not just a rhetorical and pedagogical tool with which to frighten sinners: it is a real possibility.
The Cross
How can modern man find peace and reconciliation with himself ? There is only one way open to us: compunction or repentance for the evil committed. The Cross of Christ is the only path. There is no other path for evangelization today.
Eric Metaxas Apr 12, 2017 | 11:42AM Washington, DC
A funny thing happened on the way to our supposed brave new world of assisted suicide.
Proponents of assisted suicide would have us believe that legalized killing is an unstoppable freight train and that those who oppose it are going to get run over. And no wonder. Last year Colorado and the District of Columbia legalized it, while California enacted a bill that had been passed in 2015. They joined Oregon, Vermont, Washington, and Montana where this great evil is now legal.
That’s why I’m very pleased to tell you that reports of the demise of a culture of life have been, to borrow a phrase, greatly exaggerated. We’re starting to win again. No, this doesn’t mean we can relax, but it’s really good news—and frankly, we could use some.
Bills to legalize euthanasia “have done very poorly” in 2017, Rita Marker, executive director of the Patients Rights Council, told Baptist Press. “That has been a shock to those who are in favor of it because they thought that all of [a] sudden the dam had burst and everything would happen for them.”
So far, that has not happened. Bills to advance the idea that some lives aren’t worth living have gone down to defeat in Indiana, Mississippi, New Mexico and Tennessee. Also in New Mexico, the state senate voted 22-20 against a bill to legalize assisted suicide for people expected to die within six months. It was a bipartisan vote, with 7 Democrats joining 15 Republicans.
Similar bills stalled in Hawaii, Maryland, Utah, and Wyoming, Marker said, although it’s always possible they could be brought back. In Hawaii, a House of Representatives committee unanimously decided not to advance a proposal allowing physicians to prescribe lethal drugs on the same day a patient is diagnosed as terminally ill.
Eva Andrade of the Hawaii Family Forum said that Hawaiians should “say a prayer of thanksgiving” while remaining vigilant—because when it comes to assisted suicide bills, death is never final. “Although this may seem like the battle is over, please be advised that the battle is not over until the last day of session,” Andrade said. “And even then, the bill is still alive for next session. Even now, proponents are most likely regrouping.”
Dauneen Dolce, executive director of the Right to Life Committee of New Mexico, told the American Family Association that assisted suicide legislation likely will be introduced next year. Therefore, she said, those opposing the culture of death must remain “actively involved in some way,” by “educating yourself, or giving support to the organizations that are educating others, or [being] involved in the political arena. If you don’t do that,” she added, “you are handing over our state [and] our laws, and the culture of death will come to us—and that’ll be from apathy.”
The job is immense. According to a 2016 survey by LifeWay Research, 67 percent of Americans say it is morally acceptable for terminally ill patients to ask their physicians to help them end their lives. We must not only work to change—or block—laws in the political and legislative realms. We must also work—and pray—to change hearts and minds in our neighborhoods, in our social and work circles, and across society.
Apparently most Americans see pain and suffering as the ultimate evil and personal autonomy as the highest good. What I can only call this “sub-Christian worldview” completely misses the truth that God can and often does use the things we’d rather avoid in our lives—even at the end of life—to draw us closer to Himself.
Remember, when it comes to assisted suicide, apathy is deadly. So let’s educate our fellow Americans about the beauty and dignity of life, from the moment of conception to the moment of natural death. Remember as well: “If we live, we live for the Lord; and if we die, we die for the Lord. So, whether we live or die, we belong to the Lord.”
LifeNews Note: Eric Metaxas is best known for two biographies: Bonhoeffer: Pastor, Martyr, Prophet, Spy about Dietrich Bonhoeffer, and Amazing Grace: William Wilberforce and the Heroic Campaign to End Slavery about William Wilberforce. He also wrote books and videos for VeggieTales.
The pope convened all of the resident cardinals of Rome on Thursday to officially establish the canonization date for more than three dozen new saints, according to Rome Reports, including two of the three child seers of Fatima.
Cardinal Angelo Amato, Prefect of the Congregation for the Causes of Saints, recounted some aspects of the Fatima siblings’ lives for the gathering.
“They attended little school, and they were practically illiterate,” he said. “They learned the catechism at home, along with their cousin Lucia.”
Pope Francis announced the date of the canonization in Latin, as prescribed by ecclesiastical tradition.
“May the Blessed Francis and Jacinta Marta be canonized on May 13, 2017,” he said.
Pope Francis is scheduled to travel to the Fatima shrine in Portugal on May 12-13 for the centenary celebration of the 1917 apparitions of Our Lady.
The April 20 announcement took place in the course of an Ordinary Public Consistory, a meeting of the pope, cardinals and promoters of sainthood causes that formally concludes the sainthood process.
A year after the Fatima apparitions, both Marto siblings became ill during a European flu epidemic. Francisco died April 4, 1919, at age 10, and Jacinta died almost a year later on February 20, 1920, at age 9.
Francisco and Jacinta’s cousin, Lucia Santos, became a Carmelite nun and passed away in 2005 at age 97. The diocesan phase of her sainthood cause concluded in February and has advanced to the Vatican for study.
The pope also announced at Thursday’s consistory that he would canonize 34 others on October 15.
Among them are:
The 30 martyrs of Natal, Brazil, including Jesuit Father Andre Soveral; diocesan Father Ambrosio Francisco Ferro; and layman Mateus Moreira, along with 27 others murdered in 1645 by Dutch soldiers;
The child martyrs of Tlaxcala, the first martyrs of Mexico, named Cristóbal, Antonio and Juan, who died in 1527 and 1529;
The Spanish Piarist Faustino Miguez, who founded the Daughters of the Divine Shepherd Institute in 1855, a school for girls;
Religious priest Father Angelo da Acri (formerly known as Luca Antonio Falcone) of the Order of Friars Minor Capuchin.
Tightening of laws in other countries fuels U.S. market, but not all states are relaxing statutesNicholas W. SmithOSV Newsweekly
4/19/2017
Modern technology for nearly two decades has made it possible for infertile couples to use the wombs of other women, known as surrogates, to have their biological children. But cultural changes, a crackdown in international surrogacy and high-profile endorsements from celebrities experiencing fertility issues, including Kim Kardashian and Tyra Banks, have resulted in increased demand for surrogacy in the United States.
Surrogacy involves contracting with a woman to carry a child conceived through artificial means, such as artificial insemination or in vitro fertilization. Many fertility companies recommend gestational surrogacy, where couples have their own IVF-manufactured embryo implanted into a surrogate mother, in order to decrease her likelihood of forming an attachment to the child she carried.
Patchwork of laws
International surrogacy arrangements have been popular because of the inexpensiveness of the procedure, compared to the United States. Whereas a surrogate pregnancy can cost $100,000 or more in the United States, similar arrangements would cost a third or less in countries like India or Thailand. In 2012, an estimated 20,000 children were born through international commercial surrogacy.
But beginning in 2015, the most popular countries for international surrogacy banned the practice: Thailand, Nepal, India and Mexico all issued instructions to prevent foreigners from using their citizens as surrogates. As these countries enacted new regulations, though, other countries, like Cambodia, become hubs for surrogacy tourism.
But the uncertainty of international surrogacy has made the United States a more attractive location for couples, despite the high price tag for an American surrogate. Jennifer Lahl, president of the Center for Bioethics and Culture, told Our Sunday Visitor that the closure of other countries to international surrogacy has “most certainly” led to an increase of the industry in the United States, because “we have very favorable and friendly laws here.”
Church’s Concern For Those Seeking Parenthood
The suffering of unanticipated childlessness is real. Spouses may feel they have somehow failed, that they are inadequate in a basic aspect of their marital life. Their pain may even be aggravated by regret or guilt over past contraceptive use, sterilization, abortion, or other factors that can contribute to infertility. The sight of other couples’ children may make them yearn for a child all the more and add to their distress. Infertility can affect a couple’s sexual relationship and the stability of their marriage. It may even affect relationships with parents and in-laws who express disappointment at the absence of grandchildren. Catholic couples may feel this pain even more deeply as they hear the Church praise family life and teach that children are “the supreme gift of marriage” (Gaudium et Spes, No. 50).
— U.S. Conference of Catholic Bishops, “Life-Giving Love in an Age of Technology” (2009)
In addition, Obergefell v. Hodges, the 2015 U.S. Supreme Court decision guaranteeing a right to marriage for same-sex couples, has removed in many states the barriers to these couples being listed as legal parents of a child, and many fertility clinics target their services to gay men looking to hire a surrogate.
The domestic fertility market, which the investment bank Harris Williams & Co. estimated at a value of $3-4 billion, lacks a coherent legal framework in the United States. In contrast to other western nations, there is little federal or state oversight of the industry, and laws vary among states.
“The surrogacy laws around the country are kind of a patchwork quilt,” Jason Adkins, executive director for the Minnesota Catholic Conference, told OSV. While some states like Indiana or New York prohibit surrogacy agreements because they are contrary to the public good, others like California enjoy a booming business in surrogacy.
Other states have recently passed legislation allowing for gestational surrogacy. Last year Louisiana Gov. John Bel Edwards, who identifies as pro-life, signed legislation recognizing surrogacy contracts for married, heterosexual couples. New Hampshire has passed even less restrictive legislation, as has the District of Columbia.
Fertility clinics thrive in states where surrogacy agreements giving all parental rights to the contracting couple can be enforced in court. In such an arrangement, the contracting couple are listed as the parents on the birth certificate, and not the surrogate mother who delivered the child.
Pushing back on surrogacy
In states like Minnesota, where the law has not explicitly guaranteed the parental rights of a contracting couple, the fertility industry has repeatedly sought “enabling legislation, not regulations of surrogacy,” Adkins said.
If states “create a legal mechanism by which contracts are honored and enforced, it really creates a legal framework for the surrogacy market to flourish and grow.”
As states continue to pass legislation supportive of surrogacy, Minnesota represents a rare bright spot for those opposed to contracting women to carry children. Adkins credits the state’s success to stepping back from an emotionally fraught legislative environment.
“You’re not going to have rational discourse in the context of a heated legislative environment in which people need to take votes,” said Adkins.
The state created a bipartisan commission to hear evidence on the issue during several months of meetings, and it issued its report in December 2016. While a bill to enforce surrogacy contracts was sponsored in the 2017 legislative session, it died in committee.
Adkins told OSV that while “the moral teaching is clear” from the Church on surrogacy, the issue fails to attract the same attention or coordination of resources as abortion and assisted suicide do, even though abortion frequently plays a role in surrogacy, through selective reduction of implanted embryos or requests by parents to abort children with birth defects.
“Sometimes we overlook the key life and bioethics questions that aren’t directly related to abortion,” he said, “and that’s a significant deficit in the national Church.”
Pastoral care needed
The desire to have children propels the surrogacy industry, which presents the Church with the challenge to do more to recognize and address the particular role that infertile couples have. Timothy O’Malley, a theologian at the University of Notre Dame and founding editor of Church Life: A Journal for the New Evangelization, told OSV that the Church is not providing enough pastoral care in this area.
“If you’re infertile as a couple, the only advice you’re going to get is from your doctor. No one in the Church is there for you, except for a couple of resources you might find online,” he said.
For O’Malley, infertility can serve as a charism of authentic marriage because “in the Catholic imagination, marriage is not reducible to having children, but is really a conjugal bond of love shared between husband and wife.” While children are often a gift of that love, “there are a variety of gifts that are not reducible to having children, and the infertile can have these gifts whether or not they have children.” O’Malley said that parishes and dioceses can value the marriages of the infertile in the pulpit, but also address their needs through diocesan support groups.
“It’s not just saying, well, let’s fix it for you, it’s saying that not being able to have children can become a particular icon of love for the Church, and it can lead to adoption, it can lead to foster care, but it can also lead to other spiritual gifts and renewal that can take place.”
Vatican City, Apr 17, 2017 / 05:30 am (CNA/EWTN News).- On Easter Monday, Pope Francis stressed that Christ’s resurrection calls each of us to bring the message of Easter – a message of hope and life – to the world.
“There is life!” the Pope said April 17. Now, following the Resurrection, “we will be resurrection men and women, men and women of life.”
We are called to show solidarity, welcoming, and peace to people “in the midst of events that afflict the world – there are many today – in the midst of worldliness that is distant from God,” he said.
These are only human signs that we can give, he continued, but “inspired and sustained by faith in the Risen Lord,” we can gain effectiveness “well beyond our capacity.”
Pope Francis gave his message Easter Monday before leading pilgrims in the Regina Coeli prayer from a window overlooking St. Peter’s square.
It is customary for the Pope to lead this traditional Marian prayer on the Monday following Easter Sunday, also sometimes called the “Monday of the Angel” for the angel which announced Christ’s resurrection to the women at the tomb.
During the fifty days of Easter, the Regina Coeli will replace the usual recitation of the Angelus on Sundays.
In the message of the Angel to the women on Easter morning, “Go quickly and tell his disciples: ‘He has risen from the dead,’” we hear our directions as well, Pope Francis said. The angel invites us as well to “act quickly” and to go “proclaim to the men and women of our time this message of joy and hope.”
This message is hopeful because on the dawn of the third day, Jesus was risen from the dead, therefore “the last word is not death, but life! And this is our certainty. The last word is not the grave, is not death, it is life!”
And our Mother Mary can help us to live this out, Francis said.
“The Virgin Mary, silent witness of the death and resurrection of her son Jesus, helps us to be clear signs of the risen Christ among the events of the world.”
“Those who are in distress and difficulties,” he explained, can “find in us so many brothers and sisters who offer them support and consolation.”
“And this is so because Christ is alive and active in history through his Holy Spirit, redeems our miseries, reaches every human heart and gives hope to anyone who is oppressed and suffering,” he said.
“Our Mother, help us to believe strongly in the resurrection of Jesus: Jesus is risen, he is alive here, among us, and this is a wonderful mystery of salvation with the ability to transform hearts and lives,” he prayed.
“And intercede in a particular way for the Christian communities persecuted and oppressed as they are today, in many parts of the world, called to a difficult and courageous witness.”
A leading Catholic Cardinal says abortion is “the greatest tragedy of our time.”
The comments from Cardinal Robert Sarah came during an event commemorating the 23rd anniversary of the death of Dr. Jerome Lejeune. He was the physician responsible for discovering the genetic chromosome that leads to Down syndrome. Dr. Lejeune was a pro-life advocate who believed that life begin at conception and his opposition to aborting babies with Down Syndrome ultimately cost him a shot at a Nobel Prize.
Cal Catholic has more on Cardinal Sarah’s comments concerning abortion and how he calls it a life-and-death battle that pits the spiritual forces of God and Satan against each other.
Cardinal Robert Sarah says abortion is the “greatest tragedy of our time,” and the pro-life cause is “part of the final battle…between God and Satan.”
In the worldwide battle against abortion, what is at stake is the “survival of humanity itself,” Cardinal Sarah said.
“The ‘infernal red-fire dragon with seven heads’ — a prototype of the culture of death denounced by St. John Paul II in his teaching — stands before the pregnant woman, ready to devour her child at birth,” he said.
“Yes, it is a battle … of life or death,” he said.
He pointed out how the battle rages against even the smallest of human beings, the tiny embryo, an “innocent and defenseless” human life, that he said must be protected if civilization is not to revert to “barbarism.”
Loss of the “sacred respect of human life,” said the cardinal, coupled with advances in the science of genetics, has led man to the false notion that he is now the master of life who can “manipulate” it as he pleases.
DES MOINES, Iowa, April 7, 2017 (LifeSiteNews) – A poignant pro-life message from an unexpected source in a recent television commercial has grabbed some attention.
The one-minute “Graduation” spot from Principal Financial Group shows how an unexpected pregnancy doesn’t have to mean life isn’t worth living. It is moving and effective, and has more than a 1.5 million YouTube views.
The ad chronicles the story of a young couple that meets, start a relationship, become unexpectedly pregnant, and then make life changes to keep their baby. It quite successfully captures the struggles and joys of parenthood and life in 60 seconds.
https://youtu.be/SR2nA0PNp4I
A key component is the child’s father forgoing school to support the family. The commercial ends with a touching payoff for the viewer.
“Life doesn’t always go according to plan,” Principal’s ad states at the end. “We can help you plan for that.”
Incorporating a pro-life message in its marketing strategy isn’t hurting the global financial investment management company’s stock returns, Media Research Center’s NewsBusters pointed out in a recent article.
MRC links to a NASDAQ report on Des Moines, Iowa-based Principal shares having just under a 60 percent gain in the last year.
This isn’t the first time Principal has employed a pro-life message in its advertising.
Another Principal commercial released last year was titled “Adoption” and took a similar approach. That ad had also topped one million views.
For the second time in the past three months, Option Line—a 24-7 pregnancy helpline operated by Heartbeat International—is celebrating a high-water mark, having reached 28,414 women with life-affirming help in the month of March.
Far outpacing the previous single-month record of 24,000, set in 2008, over half the women and men who reached out to Option Line during March did so over the phone, connecting with a professionally trained consultant in real time.
In January, Option Line’s 23,660 contacts marked the highest single-month total since 2008 and what was then the second-busiest month in the helpline’s 14-year history.
While virtually everyone who contacts Option Line is encouraged to contact a specific pregnancy help center, medical clinic or nonprofit adoption agency near them, Option Line consultants were able to directly schedule appointments at local centers for over 300 women throughout the month.
“We celebrate each of those women and men who contact us for help” Nafisa Shamsher, Option Line’s director, said. “We have every confidence that they’ll be in the best position to make a true choice with the support Option Line and pregnancy help organizations in their own communities.”
One woman, “Sarah,” was in hysterics when she called Option Line’s toll free number (1-800-712-HELP) for help during her unexpected pregnancy in March. Sarah already has a son, and she’s recovering from drug addiction.
Though she’s remained sober since she was pregnant with her first son, the new pregnancy threw Sarah into a panic. By the time she called Option Line, she felt that abortion was her only option—particularly since she’s unemployed and having trouble making ends meet as it is.
On the phone, the Option Line consultant listened as Sarah said, between sobs, that she didn’t have the strength to go through another pregnancy. The Option Line consultant then reminded Sarah of all that she’d been through, pointing out that she’d already shown so much courage, and assuring her she was strong enough to overcome this new challenge and welcome a new child into the world.
Finally, the Option Line consultant referred Sarah to a local pregnancy center, where she was able to find the information, help and support she needed.
“An unexpected pregnancy is such a vulnerable, sensitive time in a young woman’s life,” Shamsher said. “What most women need, and what Option Line offers, is another person to help them sort through their thoughts to make a safe, healthy decision.”
Overall, more than 2.6 million women and men have contacted Option Line since 2003, while OptionLine.org has attracted upwards of 4 million visitors during that same timeframe.
Option Line is the first and only fully staffed 24-7 helpline in the U.S., and answers an average of 650 direct contacts each month.
It’s a tragedy for the Supreme Court and the American people that Supreme Court confirmation hearings have been so terribly skewed for 45 years by undue emphasis on one case, Roe v. Wade. We should hope that one day Roe v. Wade is overturned, and the abortion issue returned to the people, so that the range of important constitutional and federal issues can be given proper treatment in the assessment of Supreme Court nominees. But that is not where we are today.
In her opening statement on day one of the Supreme Court confirmation hearings for Judge Neil Gorsuch, Senator Dianne Feinstein (D-CA) singled out Roe v. Wade—the Supreme Court’s 1973 decision that legalized abortion for any reason, at any time, in every state—as the most important Supreme Court decision that she wanted the judge to keep, saying it was “super precedent” because it had been affirmed in 39 cases.
That false claim cobbles together cases in which Roe was merely cited or applied, not reaffirmed on the merits. (The actual number of decisions in which Roe was “reaffirmed” is 3, not 39.) More importantly, Senator Feinstein’s claim ignores many other factors that show that Roe is the most unsettled constitutional decision of the past 50 years.
Roe is unsettled by the Justices’ own inconsistency in their application of Roe’s abortion doctrine, and its detailed standards, over the past 44 years. That, in turn, has sown inconsistency and confusion among the lower federal courts.
In fact, Roe 1.0—the original opinion including the original rationale for Roe—is defunct, discarded in the Casey decision of 1992. The historical rationale for Roe—the legal justification for its connection to the Constitution—was replaced by a new sociological rationale created in Casey—the assumption that women have come to rely on abortion as a back-up to failed contraception.
Roe is unsettled because the original opinion and rationale have never been persuasive. The Court abandoned the original rationale by 1989. Abortion-rights activists have spent the past 44 years looking for a new constitutional hook for Roe—the equal protection clause? the Nineteenth Amendment that gave women the vote in 1920? Or (my favorite) the cruel and unusual punishment clause?
Roe is unsettled in public opinion. Public opinion polls periodically show majority “support” for Roe, but only when Roe is intentionally distorted and mischaracterized as only legalizing abortion in the first three months of pregnancy. A majority of Americans oppose abortion after the first trimester.
A February 2017 poll, commissioned by the Human Family Research Center and conducted by the Polling Company, found that Americans were almost evenly divided when they were told that overruling Roewould leave the abortion issue to the states (45% reconsider, 49% continue to follow, with 5% undecided).
The abortion rate, according to 2014 figures, has dropped to its lowest level since 1973. Women still seek approximately 900,000 abortions or less a year, but more than half of these are repeatabortions, and millions of women haven’t had an induced abortion and never will. If women “rely” on anything, it’s contraception, not abortion.
Roe is unsettled in medical practice. Ultrasound came on the commercial market a few years after Roe and permanently changed medical practice and public understanding.
Roe is unsettled because American doctors have abandoned abortion. Few will do it. Women go to an abortion provider for an abortion but another gynecologist for everything else. It’s long been a myth that abortion is “between a woman and her doctor.”
Roe is unsettled by its extremely narrow focus. It has nothing to do with contraception (which is independently protected by other decisions of the Court) or with women’s health care. It’s about a “right” to “terminate pregnancy” and nothing more.
Roe is unsettled by state protection for prenatal human beings in property, prenatal injury, wrongful death, and fetal homicide law. Despite Roe, the states have moved ahead with state legislation and judicial decisions that treat the unborn child as a human being from conception, creating considerable schizophrenia. Twenty-five states now have a fetal homicide law that treats the killing of an unborn child (outside the context of abortion) as a homicide—from conception.
Roe is unsettled by a growing body of international medical data finding increased risk of pre-term birth, mental trauma, and breast cancer after abortion. And, in recent years, statistical studies from Ireland and Chile have provided evidence that abortion prohibitions do not compromise women’s health and that legalizing abortion does not positively impact women’s health.
Roe is unsettled because the Justices cannot perform their self-appointed role as the national abortion control board, created when the Justices in Roe drafted a new, detailed national abortion law, which binds every state and local government in the country.
Roe is unsettled because other nations have not followed its sweep. The U.S. is one of only 4 nations of 195 across the globe which allows abortion for any reason after fetal viability, and one of only 7 that allows election abortion after 20 weeks.
The mere passage of time does not settle a Supreme Court decision. Roe is 44 years old. But Plessy v. Ferguson (1896) (which affirmed racial segregation) was 58 years old when it was overturned in Brown v. Board of Education (1954). Several other decisions were older when they were overturned.
Roe is unsettled in politics. One major party has opposed the decision in its party platform since the 1970s. And just last year, the nation elected a presidential and vice-presidential candidate who promised to appoint “pro-life” justices and to “overturn Roe v. Wade.”
Dozens of other decisions by the Supreme Court were not mentioned during the Gorsuch hearings because they are so unquestionably settled that no one needs to raise the question. To ask the question, “Is Roe settled?” is to answer it.
Clarke D. Forsythe is Acting President & Senior Counsel at Americans United for Life and author of Abuse of Discretion: The Inside Story of Roe v. Wade (Encounter Books 2013).
Micaiah Bilger Apr 5, 2017 | 10:55AM Washington, DC
New evidence about the Zika virus and the potential link to defects in unborn babies came out this week.
A new Centers for Disease Control report found about 10 percent of pregnant women who showed signs of the Zika virus had unborn babies with neurological defects linked to the virus.
The CDC tracked more than 1,200 cases involving pregnant women in the U.S. who showed signs of the virus. However, the cases with laboratory-confirmed evidence of Zika were much smaller.
The CDC confirmed 250 cases of a likely Zika infection with laboratory testing, and 10 percent, or 24 unborn babies, in those cases had birth defects.
Researcher said women infected with Zika during the first trimester of pregnancy appear to be at a greater risk of having a child with birth defects. In the cases of 60 babies whose mothers had confirmed evidence of Zika during the first trimester, 15 percent had birth defects, according to the CDC.
Almost all of the cases in the CDC report involved women who contracted the virus outside the United States.
The most common defect linked to Zika is microcephaly, a brain disorder that causes babies’ heads and brains to be abnormally small. The condition has a range of severity. Some people who have microcephaly require daily care, while others live independently and have jobs.
Some have speculated that other factors may be responsible for the disabilities, rather than the virus. Some research suggests the virus may not be to blame for the uptick in birth defects in certain areas of South America affected by Zika; however, research is on-going.
The Associated Press previously reported on various research estimating between 1 percent and 15 percent of pregnant women who contracted Zika in the first trimester had babies with birth defects.
The abortion chain has been heavily involved in Zika-related politics in the U.S. Last summer, Planned Parenthood sent staffers to knock on women’s doors in Miami, Florida to talk about the Zika virus, according to the Miami Herald. They also gave pregnant women “Zika kits” and informational fliers.
In a shocking case coming out of Tulsa, Oklahoma, a mother who consented to what she was told was a “field trip” discovered that her 16-year-old daughter had been taken — by representatives of a local clinic and with the consent of school officials — to receive the Norplant contraceptive implant.
The girl — whose name is being withheld because she is a minor — is a student at Langston Hughes Academy, an arts and technology charter school located in North Tulsa. Her mother, Miracle Foster, told FOX23 that she was blindsided when her daughter came home with the implant. “Had I known that this field trip was to get that done, I would not have allowed her to go,” Foster said, adding, “I just feel like my rights as a parent were violated.”
While it is obvious to any right-thinking person that Foster is correct in her assertion that her parental rights were violated, the overreaching federal guidelines in the Title X Family Planning Program serve to give Uncle Sam’s stamp of approval to that violation. Because of the overreach of the federal government — and the acquiescence of state governments addicted to federal monies — parental rights have come under increasing attacks in the past few decades. According to interpretations of Title X, children as young as 12 years old are allowed to receive contraceptives without a parent’s consent.
While the report from FOX News makes it appear this was a recent event, Foster’s daughter actually received the implant in November. When her daughter told her about it that evening, Foster cried. In an interview with The New American, Foster said, “It’s like they take the parental control away. These are children who cannot make decisions.” She added that children need their parents “to nurture them” and “to protect them.” She also said that by taking the place of the parent, the government school system deprives those children of that nurturing and protection.
At least one Oklahoma state legislator agrees with Foster. Dr. Mike Ritze spoke with The New American about the issues surrounding this case. Dr. Ritze is well qualified to speak to this issue. He is a family physician who has delivered around 2,000 babies. He is also the chairman of the Oklahoma House Public Health Committee and a ranking member of the Oklahoma House Public Safety Committee. He told The New American, “If the mother [had given her] permission, I would disagree with her, if she was not properly informed of the dangers of Norplant,” adding, “Norplant can cause strokes, blood clots, migraine headaches and other side effects.” But since Foster did not consent to her minor daughter receiving a hormonal implant, Dr. Ritze pointed out the duplicity in the way the law deals with this issue. “A school official cannot give a [minor] student an aspirin without the parent’s consent, but can take them out of school to get contraception.” Or an abortion.
Dr. Ritze said it may be “legally wrong” for the school to have allowed the student to be taken to the clinic to get the implant without her mother’s consent. He added that — either way — it is certainly morally wrong. “The government shouldn’t have anything to do with promoting anything but abstinence,” he said. He added that abstinence is not just the best method for avoiding pregnancy and sexually transmitted diseases; it is the only method that always works. But because government schools have been drinking at the poisoned well of of progressive liberalism, Dr. Ritze said the attitude of the government schools seems to be “We know students are going to be promiscuous — like monkeys — so let them go out there and use a condom or other birth control or get an abortion if they get pregnant.” He added, “The truth is that they (the students) are not monkeys; they are people, made in the image of God, and when they are given the right information about their choices and the consequences, they can make better choices — like abstinence.”
Those are some pretty serious risks for a 16-year-old girl to take — especially since it seems that she was never even made aware of them. Foster said her daughter was not given any information about the dangers of Norplant. She said her daughter told her “the lady told her about the different choices she had” but did not discuss side effects or risks.
Foster knows her daughter. Granted, her daughter made a decision without talking it over with her, but that seems to be a mark of teenagers. This writer asked Foster if she thought her daughter would have had any type of medical implant — for any reason, contraception or otherwise — that carried those risks if she had been educated about them. “No, no. She would not agree,” she said, “I think that would have scared her. I know for sure she would not have.” She added, “I wasn’t there, so I don’t know how much information they gave her. I don’t know if there was pressure there — I don’t know.”
And because the government school system and the clinic can hide behind Title X, Foster may never know. After all, the only reason she knows about the Norplant implant in the first place is because her daughter told her.
Laws are supposed to protect minors. Because society recognizes that young people do not always have the best judgment, they are protected from those who would prey on them. That is why minors cannot enter into many legal contracts without parental consent. For instance, minors in most states are protected from incurring debt by not being able to get credit cards. But the way Title X is interpreted, as soon as a child is at “reproductive age” (as young as 12), he or she can be exploited by the contraception industry.
Let that sink in: A person whose judgment is rightly considered underdeveloped to the point that he or she cannot make decisions about the ramifications of incurring debt is considered wise and experienced enough to make decisions about having sex, receiving contraception, or getting an abortion. The parent cannot object because the parent doesn’t even have to be told.
Oklahoma’s government school sex-education curricula (like all government school curricula in the state) has to be approved by the legislature. Currently, it favors an approach toward teaching abstinence. But as Dr. Ritze explained, “What is happening with the advent of Planned Parenthood and some of the other more progressive and liberal elements is that they have tried to introduce legislation year after year” to include what he called “how-to” education. “It’s like the failed DARE program [which ostensibly was a drug use prevention program] that turned out basically to be a ‘how-to’ course on drug experimentation — teaching kids how to use drugs.”
In fact, a bill “masquerading as a bill about HIV and STD prevention”— authored by Representative Emily Virgin — introduced this legislative session would have placed sex education curricula under the control of the State Department of Education. Dr. Ritze said, “several of us rose to the concern in the debate that that was morally wrong and something we couldn’t agree with because that is our job as legislators to spell out what they should do and not do in education on such a critical subject.” The progressive liberals in the legislature objected, saying that the legislature didn’t have the expertise to address those issues. “I rose again to remind them of my credentials — and there’s another physician in the House who has credentials on teaching all about HIV and other sexually transmitted diseases.”
Dr. Ritze said that while speaking out against the bill on the floor of the House, he asked Representative Virgin about what kinds of condoms she would want to recommend to students, since her bill would have allowed that to be taught as part of the “how-to” sex education class. He told The New American, “She said, ‘Well, that’s a very sensitive subject. I don’t think we should be discussing that.’ I said, ‘Wait a minute. You’re wanting to teach children — seventh graders and on — how to use condoms, but you don’t want to discuss that amongst adults on the floor of the House and let parents know what we’re going to be teaching?’ and she got embarrassed and didn’t want to go any further when she realized the bill was headed for defeat.” The bill was defeated, but it — or something much like it — will likely return.
Reintroducing bills — time and again — seems to be a favorite tactic of those whose agenda it is to reshape the very fabric of American society by attacking basic morality. And schools seem to be one of their favorite points of attack. Even as they seek legislation on the one hand, they rely on overreaching — and largely unknown or misunderstood — interpretations of federal guidelines on the other hand.
That can be illustrated by Foster’s experience. She told The New American, “The day it happened, I contacted the school.” She spoke to Assistant Principal Mario Choice. “He said he was going to contact the organization that picks up the children and that he would call me back.” Because this was the week of Thanksgiving break, she didn’t get that call until the next week. She said Choice told her that the representative at the clinic — Youth Services of Tulsa — that he spoke with said that because of Title X, “the kids didn’t have to have consent to get any type of birth control.” Foster added, “To me that just didn’t sound right, because I’ve never heard that before. Like I said it was a school field trip, so I didn’t know anything like this could happen. Had I known, I wouldn’t have given consent for her to go on the field trip.”
Foster said she thought the reason for the field trip to the clinic was to get information that her daughter could bring home for them to discuss as mother and daughter. “We have our own doctor. We have a relationship with our doctor.” She added that contraception is something she and her daughter have discussed. “In October we talked about birth control.” But because Foster — as a parent — wanted to be a part of that decision, she was shocked to hear that the school and the clinic had circumvented her parental authority and responsibility by removing her entirely from that decision-making process.
A statement released by the school echoes Choice’s words to Foster:
This was not a field trip. Youth Services of Tulsa does an annual in-service on Sex Education. They offer students an opportunity to contact them on their own for more information. The parent gave her child permission to leave the school. Under Title X once young people are at the clinic and are of reproductive age, they can make decisions on their own without parental consent. As you can understand this situation involves a minor and we do not release information about students. Nevertheless, the student was well within their rights of Title X which is a federal guideline that provides reduced cost family planning services to persons of all reproductive age.
Next, Foster reached out to the school board. She told us, “I went to the school board before I went to the news.” She added that the school board admitted to being ignorant of the situation. “The school board didn’t know about it.” She said the school board asked questions — such as “How did this happen?” and “Was the disclosure out there?” and “Who is this organization?” — of the school principal, Dr. Rodney L. Clark. She said the principal “didn’t know that this could be a possibility for them [the students] to get anything done” at the clinic.
But in the end, the only answer Foster got was that — because of Title X — no one had any obligation to get her consent or even to inform her. When asked how she feels about it even all these months later, she told The New American, “I’m p***ed! Quote that. I’m p***ed off.”
And, who can blame her?
Because the girl is a minor, the school is legally obligated not to “release information about” her. This magazine is not publishing the girl’s name out of a moral responsibility because of her age. It is a bizarre situation when everyone seems to agree that the girl — based solely on her age — deserves to be protected by not having her name and information published, but the school and school board cannot see that she needed protection from being exploited by the contraception industry.
Foster is not alone in her concern about the direction government schools are taking to supersede the authority of parents. Casey Polczynski, who lives in Central Virginia, is a mother of two children. Last year, her daughter — who, at the time, was in kindergarten and not yet six years old — came home and announced she wanted to marry her friend when she grows up. Her friend is also a girl. Polczynski asked her daughter why she thought she could do that. She said her daughter told her, “My teacher said boys can marry boys and girls can marry girls.” Polczynski explained to her daughter that the teacher was mistaken.
This year, because of that episode opening her eyes, Polczynski is taking a more proactive approach. While visiting the school last week, she asked the school nurse about any programs that may be coming up that she would need to know about. She told The New American, “I asked what programs I needed to know about to make sure my rights as a parent were being protected.” She said the nurse was taken aback by the question and answered that Polczynski’s son’s fifth grade class would be having the “boys talk” but there was nothing to worry about because “this is not the sex education talk, it’s just about things like hygiene and wet dreams.” If classroom discussion about “wet dreams” is not “the sex education talk,” one wonders what subject matter will be taught in sex education.
Polczynski told the nurse that she would not want her son in that class and was informed that a consent form would be sent to her and unless she signed it, he would not be in the class anyway. If that is true, it’s likely because her son is shy of his 12th birthday and not yet considered of “reproductive age” by the prevalent interpretation of Title X. Next year, Polczynski will probably not be involved in that decision. In fact, if the trend continues, her son may well be taken off campus to a contraception clinic and sent home with a box or three of condoms.
As the government school system continues down into the sewer, concerned parents who care about their children’s moral formation are seeking solutions. As Dr. Duke Pesta, Director of FreedomProject Academy, explained in an interview with The New American:
For years, we at FreedomProject Academy have been fighting this [the immoral agenda of the government school system]. I’ve given hundreds of talks all over the country about this. What’s happening here — and this is a symptom of a larger problem — the federal government has taken control over America’s public schools. And they have decided that the primary purpose of public schools is to serve as surrogate parents. It is not to educate your kids; it is not to make your kids college-ready; it is not to prepare your kids to be entrepreneurs or business owners. The primary purpose of America’s public schools now is social justice education. That means that teachers, school nurses, school administrators, are assuming almost every aspect of parental responsibility — from your kids’ health-care to your kids’ birth control choices to how young they’re going to teach your kids about sex and homosexuality.
Dr. Pesta added, “They are doing this whether you want them to or not.” When asked what parents whose children are in government schools can do to fix this, Dr. Pesta said, “There’s no way you’re going to fix this because control has now been ceded to the federal government.” As Foster’s story illustrates, Dr. Pesta is correct. Local, city, county, and state schools and school boards will simply hide behind Title X and keep on keeping on with the immoral agenda of — as Dr. Ritze said — treating kids like promiscuous monkeys.
BAKER CITY, Oregon, March 31, 2017 (LifeSiteNews) – Matt and Elsa Cunningham thought they’d lost their young son in a drowning accident earlier this month. But 22-month-old Matty made it through the terrible ordeal with no medical complications.
The toddler should not have survived. His case has defied the laws of nature and science. And the Oregon family wants to share the joy of their miraculous experience, which they attribute to the power of prayer.
“Our Catholic faith is at the center of our lives,” Matt Cunningham told LifeSiteNews. “But I never knew that we’d be blessed this richly. It’s more than we could have ever asked for.”
Elsa expressed confidence that her son’s survival is due to a miracle, and how his very presence every day is an even greater testament to the miracle of life than it was before.
“Because you know when you wake up and he’s alive,” she told LifeSiteNews.
It couldn’t happen without God
Many human hands helped to save Matty, and the Cunninghams are grateful to them.
But it was also a stream of apparent Divine Interventions that led to Matty’s survival.
They are grateful to God, to the venerable Archbishop Fulton Sheen and St. Joseph, Matt’s late mother and the Blessed Virgin Mary.
The couple prayed to God and His saints throughout Matty’s plight, but especially upon the horror of finding him in the water. And it was Archbishop Sheen, the revered pioneer of modern evangelization, that Matt thought to turn to at that moment.
“Archbishop Sheen was the one I screamed to,” Matt recounted in describing the 911 call, which was a mingling of his cries to Heaven to save his son and communicating with EMS.
The family had been praying a morning devotional with Archbishop Sheen each day in the month leading up to the accident. They were enamored of the prospective saint’s teaching. He has stood out among those they invoked to intercede on Matty’s behalf, and they think he had a hand in Matty’s survival.
“The Church is our life,” said Elsa. “If we could give credit to one saint, it would be Archbishop Sheen, but there were so many.”
“The crazy part is, Matty was dead, and now he’s perfect.”
Without knowing whether their situation would ever qualify for a miracle, the Cunninghams nevertheless now feel an affinity with the family whose child is at the center of the first approved miracle in the cause for Archbishop Sheen’s canonization. The stillborn baby was resuscitated after medical professionals worked on him for just over an hour.
“I feel for those parents who waited for 61 minutes for their child to come back,” Elsa said.
What happened that day
Thursday, March 9, was a mild late winter day that found the Cunninghams anticipating spring and working in the yard of their home seven miles from Baker City.
The homeschooling family had recently seen the first bluebird of the season, so Elsa was cleaning out a birdhouse for the birds to nest. The family had a litter of a couple-months-old puppies, and Matt was building an extension to their dog kennel.
Their oldest, Johnathan, 17, was inside working on school. Shane, 14, was not at home. The rest of the kids, Daniel, 11, Isabel, 9, and Abigail, 7, were outside helping their parents, along with Matty.
They don’t know when, but Matty wandered away on his own. They think he may have been following one of the puppies and fell into the pond about 100 yards from where they were working.
A string of miracles begins
But the pond is on a neighbor’s property behind a tightly spaced barbed wire fence that Matty shouldn’t have been able to get through. So it didn’t dawn on them at first to even check the pond, but as they realized he was missing, something took them there.
“The Holy Spirit led us, we believe,” Matt said.
The first miracle was not just that they were led to him, he said, but also that Matty was floating on the surface instead of sinking, despite his being dressed in a heavy winter coat and boots.
Elsa went through the barbed wire fence, tearing her clothes, and Matt went over the top.
“Whatever we had to do,” Matt told LifeSiteNews. “Elsa dove in with all her clothes on. Every second counted.”
Elsa started chest compressions and Matt performed mouth-to-mouth resuscitation.
A parent’s worst nightmare
No one knows how long he’d been in the water, but they thought for sure they’d lost him.
Matty was blue, unresponsive, not breathing.
“We thought he was dead,” Matt said. “There was no movement in his limbs. He looked like he’d been there all winter.”
“Every parent knows the terror we felt,” he said. “It was pure hell.”
Still, Matt said they would try to resuscitate him “until they pried him away from us.”
Matt screamed to the 911 dispatcher on the phone as they also cried out to God. The other children immediately fell on their knees and prayed, Cunningham told LifeSiteNews, and John called 911 too.
Archbishop Sheen was on the tip of Matt’s tongue when it came time to beseech God to save Matty. He can be heard invoking him on the 911 tape.
He is grateful for the family’s daily devotional to the venerable prelate.
“I believe that was the Lord’s way of preparing us for that morning,” said Matt.
He remembers jumping out of the way as soon as the EMTs touched his shoulder, knowing they needed to work.
They detected a faint heartbeat at the scene, but Matty was still not breathing.
A friend jumps to action
Local sheriff Travis Ash, a family friend, had arrived on the scene apart from EMS, having also heard the call.
Ash instinctively ran to the ambulance, ahead of everyone else running, and jumped in to drive. Matt Cunningham doesn’t know why, but it’s another thing he considers the foundation of a miracle.
Ash was compelled to action, taking the driver’s seat, and driving such that the EMTs told him to take it easy. Ash continued at top speed, and the ambulance made it across the nearby railroad tracks in time to avoid a train that would have cost them valuable time.
“His haste gave Matty precious moments of needed care in the hospital,” Matt said. “It was all hands on deck, something that restores your faith in humanity.”
When Matty got to the ER at St. Alphonsus Medical Center in Baker City, an estimated 17 minutes after the first 911 call was placed, his body temperature was 84 degrees.
Matty’s initial blood work was that of a dead baby in Baker City, Matt told LifeSiteNews.
The staff had to administer two bone IVs in his calves because he was too cold to get a regular IV started. They performed blood work and other tests to assess his condition, the implication being there would be permanent damage assuming Matty survived.
They intubated Matty with a mobile ventilator and tried to warm him.
As the staff worked, Elsa prayed quietly to herself, Matt said, “I just spent most of the time on my knees.”
During this time, he had an experience that convinced him that Bishop Sheen was interceding on their behalf for Matty.
As he prayed, Matty cried out every so often while the hospital staff tried to revive him.
“Every time I kept imploring Archbishop Sheen, those were the two or three times I heard him cry,” Matt said.
He’d been told it was likely just a physical reaction his son had been making. The sound had him alternating between hope and fear.
People that they knew, and many they didn’t, stood in prayer in the parking lot, Matt recalled.
Everyone who was either at the scene or in that hospital knew how hopeless and tragic the situation was, he said, “how it was sure to end later that day with the planning of our son’s funeral.”
Matty was then airlifted the 125 miles to St. Alphonsus Regional Medical Center in Boise and would later be transferred to St. Luke’s Children’s Hospital, also in Boise.
A mother’s plea to God
Elsa rode in the helicopter as Matty was life-flighted to Boise. Matt followed by car with a family friend.
“I had the 50-minute helicopter ride from hell,” she told LifeSiteNews.
It was raining, there was turbulence, and she needed an airsickness bag handy nearby.
“But I’m just praying,” Elsa said, praying that God will allow her to keep her son.
Elsa, like many women, has miscarried, in her case three times.
Naming one of her other babies, she told LifeSiteNews that she thought as she prayed, “He has Michael (and the others).”
She prayed to God in the helicopter, “I want this one. I don’t know if we can live through this” (losing Matty).
Another sort of miracle Matt described was when they raced past a highway patrolman on the normally two-plus-hour drive to Boise, the officer simply waved at them, despite their speed.
Care, with prayer
Then, the experience with first doctor they encountered out of the helicopter at St. Alphonsus, Dr. Adrian John Curnow, also seemed in line with their impending miracle.
Curnow was willing to pray for their son.
“He grabbed me by the shoulder and told me, “God loves your son more than you do, and he’s going to be OK,” said Matt.
Curnow wasn’t the only medical professional to pray.
“All along the way, person after person and physician after physician prayed with us, and over our son,” Matt said. “This doesn’t happen in a secular world, but again, God allows small miracles to form the foundation of one large miracle.”
The doctor explained to the Cunninghams how Matty’s temperature would come up and then could spike, which would be dangerous.
He had a line put in through Matty’s nose to the boy’s stomach, and with a large syringe, taking water in and out of the line, he moderated Matty’s core temperature.
Curnow then rode in the ambulance with the Cunninghams to St. Luke’s, continuing the water-cooling procedure and staying with them after they arrived at the new hospital.
Matty remained heavily sedated there, until he could have an MRI to determine damage from the accident.
As the family waited the few days for Matty’s MRI, fellow parishioners at the Cunninghams’ parish of St. Francis de Sales Cathedral in Baker City and many others prayed.
Their doctor at St. Luke’s was another beacon of faith, Matt told LifeSiteNews.
Between his manner, praying and using scripture with them, Dr. Derrick Dauplaise really embodied Christ to them, Matt said. He always came to them in a reassuring way, no matter what.
“He laid hands on Matty and prayed,” Matt recalled. “He then said God was going to take care of all of us.”
“He was the doctor to us just as much as Matty,” he said. “He was so loving, this man, we could just tell God was with us.”
An outcome with no medical explanation
The MRI took longer than expected, and likewise, the wait for results was difficult. The staff was taken aback by what they found. They wanted to be sure before they brought the Cunninghams the news.
Matty’s MRI results were absolutely normal, defying medical explanation.
When the Cunninghams were told there was no sign of brain damage, despite the specifics of Matty’s case, they couldn’t believe it.
“We just wept,” said Matt, “and I just fell on my knees and prayed to God. Thank you God, Archbishop Sheen and all the saints and angels.”
Prayer had been the key, prayer in the face of fear, and faith in God’s plan, no matter what, where or when.
At one point in the middle of the night during Matty’s hospital stay, Matt said, he wanted to pray the rosary, but he’d forgotten his rosary at home in the rush for the hospital.
So in the quiet of the night in Matty’s room, Matt used his son’s 10 toes in place of the 10 Hail Mary rosary beads to pray for the Blessed Mother’s intercession for his son.
“So I used his toes,” he said. “I just thought it was a great thing to do.”
After the MRI, things went quickly. Matty’s sedation was stopped and his breathing tube removed once he came to.
Within an hour, he knew who everyone was and called his siblings by name, Matt said. “He was just perfect.”
The first sound Matty actually made when he awoke was barking like a dog, as if nothing had happened.
“It was the greatest thing he could have said,” his father stated. Matty had been often mimicking their puppies before the accident. And this was just him picking up where he’d left off.
Matty didn’t skip a beat after waking up, Elsa recalled, and he was running around in no time.
Elsa stayed with him that night in the barred hospital crib before Matty was released the next day to go home.
Photos of Matty from the time of his waking show a healthy, happy child.
There’s more
The miraculous events didn’t end with Matty’s physical revival.
After they began to settle in at home, Matt and Elsa came together at one point, each wondering, “Have you noticed anything different about him?”
The couple had individually seen the same things; Matty’s eyes were brighter, almost as if they were bigger, and he was using bigger words.
Image
Matty heads home.
Matt said his son was always beautiful and bright-eyed, but now Matty is just more so. He doesn’t know how else to explain it.
“They’re just wider and brighter,” he said of Matty’s eyes. “He’s just wide-eyed and bright.”
Elsa can tell as a mother.
“You know when we’re smiling at him,” she said.
“We firmly believe it’s because he’s seen the Lord,” said Matt.
Matty was a late talker as compared with his siblings, they said, and since the accident he has been using phrases they’d never heard from him before.
An example of this, which also suggests a miracle, involves a photograph that hangs in their house of Matt’s mother, who died shortly before Matty was born.
Virginia Cunningham’s love for her children was unmatched, Matt said, and the example she gave through her suffering makes her the closest thing to a saint without a formal declaration. Matty only knows his grandmother from the picture and when they talk about her.
One day soon after he was home from the hospital, as they happened to be contemplating the picture of her in the hallway, they asked him, “Have you seen Grandma?”
Matty replied matter-of-factly, “Yes, I have.”
“He’s never said, Yes I have, ever,” Matt explained. “We firmly believe this has a miraculous explanation.”
Another instance involved an appointment the Cunninghams had scheduled before Matty’s accident with a buyer for one of their dogs. It had been set for soon after they returned home from Boise with Matty. Elsa said that despite the timing they went ahead and kept it since it would be easier to follow through than to cancel.
She explained to the wife of the couple who’d driven 2 1/2 hours to buy the dog how they’d been tied up with Matty’s situation and were just getting settled.
The woman shared that they had a similar experience with their son, who was now 10 and doing fine as well. She told Elsa she’d been thinking her husband didn’t need another dog and wanted to discourage the purchase.
But if she had done so, the two women would not have met.
The woman advised Elsa that it will take awhile for things to get back to normal for them. A happy miracle is not necessarily without some human fallout.
This paralleled the doctors’ advice, which cautioned the Cunninghams against being overprotective of Matty, and to monitor themselves for Post Traumatic Stress. It was especially powerful, though, coming from another family who had experienced it.
“God put her there for me,” Elsa told LifeSiteNews. “I know the stress is real, and I know Jesus will carry us through.”
“It’s a miracle”
Matty’s main doctors from the Boise facilities have said his case is a miracle.
Elsa recounts what Dauplaise told them the day they took Matty home.
“If you’re not open to the fact that it’s a miracle, then you can’t receive the gift,” he said.
Curnow called Elsa’s cell phone a little more than a week after they brought Matty home.
Elsa remembers, “He said, ‘Matty was beyond what we could do. This was a miracle. God must have great plans for him.’”
Curnow also told Elsa they should read Psalm 112, verses 1 and 2.
“He said that they remind him of our family,” she recalled.
The Scripture verses state:
“Praise the LORD. Blessed is the man who fears the LORD, who greatly delights in his commandments! His descendants will be mighty in the land; the generation of the upright will be blessed.”
Elsa found the implications with Matty’s experience to be powerful, stating, “It’s awesome and heart wrenching at the same time.”
Life goes on
The family continues to get back to normal. Matt has since spoken to a Catholic men’s group to share their experience. Elsa said Matt’s witness stirred the emotions of the men there.
Matty will turn two years old on April 26, 10 days after Easter.
The Lord’s death and resurrection will have additional significance this year for the Cunninghams.
The Baker City Herald ran a letter Matt wrote about Matty’s ordeal, which he titled “A love letter to the city with a heart of gold.”
In it, Matt wrote:
“Our son has been raised from the dead. Thanks be to God, and to all of you for begging and helping him on our behalf. He, in His mercy, heard and answered, and we will never be able to thank you enough.”
The family maintains their devotion to Archbishop Sheen and they are convicted in the belief he interceded on Matty’s behalf.
“I know he was involved,” Matt said. “I know it.”
“The Lord is the Lord of life, and life just perpetuates itself,” Matt continued. “God is bringing us more life with him than we could have hoped.”
“God is amazing,” Elsa told LifeSiteNews. “He’s so good.”
“The biggest thing is this wasn’t just a miracle just for us,” she said. “He answered everybody’s prayers.”
Yesterday the Planned Parenthood Federation of America arranged a Pink Out Day on social media to promote their brand in the face of calls to defund the organisation and an unsympathetic Trump administration. What impact their noon “thunderclap” had is not clear, but there is no doubt that PPFA has many supporters who defend its claim to be an important women’s reproductive health provider.
However, the literal meaning of “reproductive health” is incompatible with two of Planned Parenthood’s main activities: abortion and the provision of hormonal contraception. For at least two decades researchers have been tracing a link between these birth control methods and the rising incidence of breast cancer – a link denied or ignored by the scientific and medical establishment.
But the international evidence continues to mount. A new British study by Patrick S. Carroll and colleagues, using readily available data on breast cancer and abortion from British official sources, shows that the lifetime risk of breast cancer for women in the UK keeps increasing: it is now around 1 in 7 women for malignant tumours and 1 in 6 for in-situ lesions, which also need treatment and therefore should be planned for. And this increased risk cannot be explained by increased screening – the usual explanation — on its own.
Here is one reason: women do not enjoy being screened. It’s an uncomfortable business and there is always the thought in one’s mind that repeated x-rays may themselves cause trouble. So the raising of the cut-off age for screening from 65 to 75, as the UK has done, is unlikely, say the study authors, to increase the response rate among women who were screened between ages 50 and 65.
Another explanation of the risk trend is that childlessness has increased since the 1970s. It is widely acknowledged that a younger age at the birth of her first child reduces a woman’s risk of developing breast cancer, as do further full term pregnancies and longer breastfeeding of each of her infants. However, the authors find that neither childlessness nor increased age at first birth by themselves can predict breast cancer risk.
Baby boomer women and their daughters, of course, have had ways of delaying or avoiding childbirth that were not generally available to earlier cohorts, and these may bring their own risks. The authors state:
“Although still contested, there is significant literature that demonstrates that induced abortion, particularly of a woman’s first pregnancy, as well as hormonal contraceptives and HRT [hormone replacement therapy], also raise the risk of developing breast cancer.”
The reasons why this would be are now familiar. Abortion, especially of the first pregnancy, not only removes the protective maturing of the breasts during pregnancy and lactation, but actually leaves them in a more vulnerable state, while the estrogen in hormonal contraceptives increases cancer risk. A new study from Finland this month finds further evidence of a link between hormonal contraceptives (the IUD) and breast cancer.
British data, in fact, show a high positive correlation between abortion rates and breast cancer in women aged 50-54 (abortion was liberalised in the UK in 1967). This also seems to reflect the advent of hormonal contraception, say the authors. “When women were first having large numbers of induced abortions, their contemporaries were also starting to make extensive use of hormonal contraceptives.”
A remarkable social gradient
There is a further interesting angle on these links in the study – a “social gradient”. Data from the 1990s shows that women in the higher socio-economic groups have more breast cancer than those down the social scale. A possible explanation:
“Upper-class women and women who achieve upward social mobility are known to have children later and to make more use of hormonal contraceptives, and when they have pregnancies at a young age they are more likely to opt for nulliparous abortions. Lower-class single parents, who score highly as to deprivation, often have benefited from the breast cancer protection afforded by their first pregnancy taken to full term at a young age.”
No serious scientist is claiming that these factors are the only, or even the main cause of breast cancer, but the likelihood that they explain part of the largely unexplained current epidemic of the disease should at least receive some acknowledgement. Yet, as the authors point out, “While doctors are now more reluctant to prescribe HRT for reasons of the breast cancer risk they continue to prescribe hormonal contraceptive on a massive scale.”
It’s true that these doctors can cite some studies reporting no additional risk 10 years after a woman has ceased to use hormonal contraceptives. However, say Carroll and colleagues, “this risk is quite long-term and not apparent within such a time interval. Breast cancers discovered after age 50 are more reflective of these events in a woman’s reproductive history.”
The lack of official explanation for aspects of the epidemic such as the remarkable social gradient is a failure of public health education, of a piece with neglect of breast cancer prevention programmes, they conclude.
Indeed, women should be informed and the authorities should plan for an increasing breast cancer burden on the health system based on all known risk factors and not just politically correct ones.
Yet there is solid resistance to such moves in the UK. Patrick Carroll, who is neither a doctor nor a medical scientist but an actuary with the (UK) Pension and Population Research Institute, seems to have had no competition in using first class resources for a neglected, or rather, deliberately sidelined area of cancer research. However, getting his work published in medical journals is another matter.
Having failed on previous occasions, he submitted the paper discussed here to the (British) Journal of Epidemiology and Community Health last year. They sat on it for several months, he told MercatorNet, “offering no intelligent comments nor constructive criticism. They said they read it with great interest but found it unsuitable for their audience! They then suggested I try another of their journals, BMJ Open. Even though the editorial staff of the two journals are in the same building they did not offer a short process for submission to the second journal.”
Warned by another researcher that BMJ Open would inflict another delay of several months, he sent it to the independently minded Association of American Physicians and Surgeons (AAPS) who published it – as they had a previous paper — in their journal.
The reasons for the establishment’s defensive attitude is not difficult to discern. Carroll and colleagues describe the situation in the UK in their published paper:
“Each prescription for hormonal contraceptives has a doctor’s signature. Every abortion notification form (HSA1), as required by the 1967 Abortion Act, needs two doctors’ signatures. In the UK, claims under medical professional liability insurance are largely in the area of obstetrics and gynecology. If women who experience breast cancer could make claims against doctors for prescribing hormonal contraceptives or approving induced abortions, there would be many more claims. For this reason it is understandable that British medical journals are reluctant to publish papers that report a link of breast cancer to induced abortions.”
Meanwhile, back in the United States, Planned Parenthood has tried selling itself as the household name that millions of women “turn to” for — guess what? — mammograms. In fact PPFA does not do mammograms but refers a small percentage of its clients (less than one percent) to specialised services after doing simple, routine breast checks.
But the irony of its claim only increases with this latest evidence that, even if it did do mammograms, it would be largely as a result of making its own work through the much more lucrative lines of abortion and contraception. And that applies to a significant part of the health sector internationally.
It must be time for a class action suit on this front.
March 29, 2017 (LiveActionNews) — Being pro-life was always something that came easy for me. I was raised by a mother who was part of the generation that began protesting and praying outside of abortion clinics. As a teenager I wrote letters to my senators to end abortion. I volunteered at crisis pregnancy centers.
This is not to give myself a pat on the back by any means; I just did it because it was the right thing to do. These issues were so black and white to me.
The only “gray area” I struggled with were the exception cases: rape, incest, or to save the life of the mother. Politicians and the media told me these were the only situations in which abortion was necessary and needed. It was okay in those instances. Wasn’t it? It seemed heartless to argue otherwise.
So when I found myself in one of those situations, with a swollen belly full of tiny kicks and movement and a doctor telling me I would most likely die if I continued the pregnancy, I had to come to grips with what exactly I believed about those “gray areas.”
Eli as a newborn
I was 20 weeks pregnant with my son, Eli, when we got the news. We were there for a routine anatomy scan to find out the gender. One moment we were elated and hugging, rejoicing that we were going to have a second son, and the next our world came to a complete halt.
“Your son isn’t going to make it,” the doctor said.
We were told that Eli had a less than 1 percent chance of survival and they were surprised he was even alive at that point. He would most likely die within the next few days, we were told. Even if he did by some miracle survive, he would have a condition called triploidy. It was incompatible with life and most babies who made it to birth died immediately thereafter. So either way, we would lose our son.
My heart broke into a million pieces. My husband Chris and I just cried and held each other. We wanted this baby. We had already imagined him and his brother Rhett (who was 9 months old at the time) growing up and being best friends. We loved this baby.
Then the doctor continued speaking.
“My biggest concern is for your health right now.” She told me I was extremely at risk. I had a partial molar pregnancy and this meant that I had cancer in my placenta that would spread to my brain, lungs, and liver the longer I carried Eli. I was at risk for seizures and strokes, blindness and ultimately death. She warned me that my symptoms could happen quickly and without notice.
She recommended I terminate the pregnancy immediately and start chemotherapy as soon as I could.
I felt like I had no choice.
It made sense and it seemed like the only logical decision. And you know what? I considered it for a half second. Me, the pro-life guru.
All I could think about was not losing the things I had. My husband and I hadn’t even been married for two years, he was the man I wanted to grow old with. Would we not get that chance? I had a 9 month old son who I loved with all of my heart. I wanted to see his first steps, his first birthday, his graduation, his wedding, my grandchildren. It all kept playing over and over in my mind. I don’t want to lose this.
But then I remembered those tiny hands and feet I had just watched dance around on the ultrasound screen. I remembered the kicks and the movement. That was my son too.
The words of Psalm 139:16 came into my head: “Your eyes have seen my unformed substance, and in Your book were all written the days that were ordained for me when as yet there was not one of them.”
I knew the Lord had Eli’s days, however many they were to be, written in His book. Who was I to cut them short? My days were also in that book and nothing, not even cancer or a high risk pregnancy could end them unless the Lord allowed it.
I looked at my husband, he had the same determined look. We told the doctor, “No. That is not an option for us.”
The goal was to make it to 24 weeks. That was the earliest he would be considered viable at this hospital. Those 4 weeks felt like a lifetime. I was in the hospital at least 3 times a week for monitoring and blood tests. They ran out of places to draw blood because my arms were so bruised and my veins worn out.
It hurt when they wouldn’t acknowledge Eli as a baby. All they talked about was me and hardly ever referenced him. I know they probably did that to make it seem easier if I lost him, but it still hurt. I remember lying on an exam table, waiting on one of the doctors to come in and crying. “Lord, why does no one care about my son?! I feel like I am fighting alone here.” I felt His peace and was reminded that He, more than anyone else, cared about my son.
I made it to 24 weeks and they gave me steroid shots to help develop his lungs in preparation for his early arrival. I almost cried when one of the doctors finally mentioned the baby and how he needed to be monitored closely.
They did two ultrasounds a week and at each one they were amazed that Eli was growing normally and was still alive. But at 28 weeks they started to notice his growth was halting and that was due to the placenta slowly falling apart. I got another round of steroid shots and at 30 weeks his heart rate was dropping so we were scheduled for a c-section the next morning.
The doctor met with us that night to discuss the risks. We still didn’t know if Eli had triploidy because we didn’t want invasive tests to put him more at risk, and my fluid was so low anyway, we didn’t want to take any more out than necessary.
She told us she had blood ready for a transfusion because they had to cut through my placenta to get to Eli and I might bleed out. My placenta was 5 times the size of a normal one. I might have to have an immediate hysterectomy because there was a chance the placenta had grown through my uterine wall.
We went into the operating room, not knowing if these would be our last moments together.
On April 1st, of all days, our little Elijah Lewis Mitchell came into this world. He weighed 2 lbs 7 ounces and I was able to kiss his tiny little head that was covered in black hair before they took him back to the NICU.
My placenta came out easily and with no complications. It was sent off for testing. I remember crying and taking a deep breath for what felt like the first time in months. One of the nurses put her hand on my shoulder and said, “Just rest now, momma.”
When our doctor came into the recovery room, she told us, “I think we may have misdiagnosed you.” She said I was cancer free and a few weeks later Eli’s genetic tests came back NORMAL. We were both in the clear and healed completely! We were overwhelmed by all that the Lord had done.
Eli was released from the NICU 55 days later, weighing five pounds and drinking his bottles on his own.
Eli today
The reason I share our story with you today is because I think we really need to look at these exception cases, and figure out what we believe. Because you never know when you, or someone close to you might be faced with one of these situations. I have no doubt, if it was not for the Lord and knowing what I know about life in the womb, I would have aborted my son that day. Doctors that I respected were telling me to. It made sense to.
So I have a newfound compassion for women in these circumstances. It is a HARD decision. It feels impossible. But I want them to know, it can be done.
You can give your baby a chance at life. I promise you, it will be a choice you will never regret.
I have a daily reminder of my choice: a wobbly little two-year-old who has the sweetest smile, the bluest eyes, and the heart of a fighter. His life blesses mine every day and I am so thankful I gave him a chance to live.
With infertility more common than ever and birth rates around the world at a record low, a crucial first step for couples trying to get pregnant is to clearly understand exactly when they are fertile. Yet that is something just 13 per cent of women surveyed were able to identify according to a new study just published in the Australian and New Zealand Journal of Obstetrics and Gynaecology which surveyed over 1000 New Zealand women. That was despite a third of the women reporting that they monitored their ovulation.
The authors concluded that fertility knowledge needs to be better addressed among women intending to conceive. Professor Wayne Gillett, a researcher at the university’s Dunedin School of Medicine and medical director at Fertility Associates Dunedin commented:
“When a couple are trying to have a baby, problems like age, endometriosis and male problems are always touted – but no one ever considers knowledge, and that’s one of the things we often see,”
Gillett said there was one enduring myth that the best time in the menstrual cycle to conceive was during, or even after, ovulation, when the reality is that the fertile window is pre-ovulation. He expressed concern that even health professionals are not well-educated about a woman’s fertile window.
An article discussing infertility published in the New Zealand media this month comically writes “at high school we’re taught that if you so much as look at a girl strangely, she’ll get pregnant.” Sadly many indeed carry this idea into adulthood after years of only being told how not to get pregnant. However, given that interest in natural family planning continues to grow, it is hopeful that fertility knowledge will be better circulated, including the knowledge that fertility begins to reduce in a woman’s late twenties and more drastically after the age of 35.
One in six couples in Australia use IVF, and one in every 25 Australian children are now born as a result of IVF. In Denmark one in 15 children are IVF babies. Yet it is questionable whether people are first given good advice about the other more simple and inexpensive options available to them – including accurate knowledge about their exact fertile window which is normally only 6 days long if not shorter. To some, IVF services are a business and there is little incentive to first offer easier, cheaper options to couples.
John Aitken, Newcastle University laureate professor, Director of the University of Newcastle’s large 50-staff Priority Research Centre for Reproductive Science, and the 2012 NSW Scientist of the Year, recently commented:
“We should guard against recklessly marching into a future where we use too much assisted conception in order to compensate for our loss of fertility … It’s an inexorable upward trend. We are taking recourse to IVF in increasing numbers and the thing we have to remember as a society is that the more you use assisted conception in one generation, the more you’re going to need it in the next.”
March 23, 2017 (LiveActionNews) — In a village in the Philippines in 2014, a little girl was born without limbs. At six months old she was placed in an orphanage for children with special needs, where she waited for a family to adopt her.
In October of 2014, when she was nine months old, the Stewart family saw a picture of the little girl and decided to adopt her. It would take months of paperwork and a trip to the Philippines, but a year later, Adrianne and Jason Stewart were bringing little Maria home to join their family of five, including two biological daughters and an adopted son.
“When we found our daughter we did not think we were qualified or prepared enough to parent a child like her, a child born without arms and legs, but we knew that we could love her and that loving her was what mattered most,” Adrianne Stewart wrote in a post for Love What Matters.
At about two years old at the time of her adoption, CNN reports Maria was unable to hold up her head and her parents knew they had a lot of work ahead of them. She now receives speech and occupational therapy and attends preschool in an inclusive classroom.
“She has given us far more than we will ever give her,” Maria’s mother wrote on Facebook. “She is so full of joy and light, and is an inspiration to all who meet her. We put limits on her abilities and then we see her doing exactly what we thought she was not capable of.”
Since sharing their story in hopes of inspiring other families to adopt, the Stewarts have received a lot of positive notes. However, they have also heard from mothers who have chosen abortion when their preborn children were diagnosed with conditions similar to Maria’s. These women express to the Stewarts their abortion regret. Adrianne Stewart hopes that Maria will help other expectant mothers choose life when faced with similar prenatal diagnoses.
Let’s say you are 33 years old and got married a year ago. In the past ten years, you have been using a variety of hormonal birth control methods. Now you and your husband are looking forward to starting a family. You get off the pill, hopeful and a bit anxious as you know time is working against you. You try for eight months and nothing happens.
You start getting concerned, and you talk your doctor into putting you on Clomid, a drug to stimulate ovulation. This drug actually lowers your chances of conceiving, unbeknownst to you. A few months later, you get your first appointment at a fertility clinic where you discuss Intrauterine Insemination (IUI) and In-Vitro Fertilization (IVF), bracing yourself for several months of treatment and thousands of dollars in medical bills.
But could all that anxiety, doctor visits and interventions be completely unnecessary?
The pill may not cause long-term infertility after discontinuation, but it can delay fertility by up to a year. The delay is caused by the pill’s impact on the production of cervical fluid, an essential component of conception. The delay can be critical as women tend to start their family much later in life now than in earlier decades, and may lead them to engaging into unnecessary fertility treatment.
It takes three to get pregnant
We were all taught in high school biology or sex-ed that it took and a sperm and an egg (an ovule) to make pregnancy happen. What is often left out of this equation is the cervical fluid, aka cervical mucus.
In order for the sperm to survive more than a few hours in the vagina, and then have the energy reserves to travel through the uterus all the way to the fallopian tubes and maybe wait for the egg to arrive, it needs good quality fertile cervical fluid.
Cervical fluid is secreted by the cervix; it changes in aspect and properties as ovulation approaches. At the time of ovulation, it becomes stretchy, almost like raw egg whites, and allows the sperm to go through the cervix into the uterus. Before and after ovulation, the fluid is thick and blocks access to the uterus, a wonderful mechanism to protect the womb from infection. It also naturally prevents fertilization during a major part of the cycle.
Without sufficient, good quality mucus, no baby.
The way hormonal contraceptives work to stop pregnancy
Hormonal contraceptives, as generally documented in scientific literature, don’t work merely by suppressing ovulation. Another mechanism is the effect on the production of mucus, thickening it consistently throughout the cycle, providing a barrier in case ovulation still takes place (which does happen).
How does it work? The cervix normally follows the marching orders of hormones. With the use of contraceptives, the synthetic hormones take over the natural ones and run the cervix in a non-natural way to produce consistently this type of non-fertile mucus.
So far so good. What’s wrong with a secondary barrier to make sure pregnancy doesn’t happen when that’s the reason why the woman is on the pill in the first place?
Here is how things get more complicated.
The impact of the pill on the production of cervical fluid
Professor Erik Odeblad is one of the first scientists to use MRI technology for a medical purpose. A Swedish physician, professor and researcher born in 1922, he spent most of his life studying and explaining the secretion of cervical fluid: the various types of fluids at different stages in a woman’s cycle and in her life, and their role and composition.
One of his discoveries was to show that there are different types of mucus[i], which he called G, L, S. Each has different roles and is secreted from different cervical crypts (the pockets lining the cervix) at different times. For instance, right after puberty, a young woman has an abundance of S crypts, and as she ages, the number decreases and are replaced by L crypts. S mucus is the type of mucus that is essential to fertilization: it allows passage and then transports and nourishes sperm.
What Dr. Odeblad found was that “for each year the Pill is taken, the cervix ages by an extra year.” He explains that: “If a woman takes the Pill for 10-15 years and then ceases taking it in order to achieve pregnancy, she may encounter some difficulties.”
In simple terms, a 20-year-old woman who stays on the pill for 10 years can end up with the cervix of a 40 year-old with 20% of S crypts instead of 40-50%. It can take a long time after a woman stops the pill for her cervix, and especially the S crypts, to function again. Her cervix may never recover some of those lost capacities.
To make matters worse, if she gets on Clomid, thinking it will increase her chance of pregnancy, it will do the opposite: a known side effect of this drug is to reduce the production of cervical fluid. A thorough evaluation of both her ovulation and of her mucus production is needed.
Why it matters more today
Woman are waiting longer to start their families now that in the past. In 1970, most women had their first pregnancy in their early 20s. The average age of first child birth was 22. Today, it has risen to 26.4 years old. More women are delaying their first pregnancy past age 30. The percentage of first birth to women over 30 went from just one in ten in 1970 to almost one in three in 2014[ii].
If these women have been on the pill, as many have been, it’s no surprise that they would experience more difficulties getting pregnant. As the cervix may take up to a year to retrieve a functioning production of mucus, many couples may be directed to drastic medical procedures, such as IVF, a costly and emotionally difficult process. If they waited or found other ways to improve the production of their cervical mucus, they could resolve their problem. Some good news: a pregnancy will rejuvenate the cervix by 2 to 3 years.
Here is the scoop: as a result of being on the pill for an extended time, a woman may not be able to conceive for up to a year, leading her to think she’s infertile, when she’s not! Her fertility is certainly impaired, but medication to stimulate ovulation will actually aggravate the problem.
We find here yet another great reason why young women who are hoping to get pregnant one day should avoid hormonal birth control all together and use a Fertility Awareness Based Method. Not only will these methods preserve their fertility, but when the couple is ready to achieve a pregnancy, the knowledge gained through training in a FABM will help them reach that goal more quickly and easily.
[i] The Discovery of Different Types of Cervical Mucus and the Billings Ovulation Method, Erik Obledad, Emeritus Professor, Dept. of Medical Biophysics, University of Umeå, Sweden, Bulletin of the Ovulation Method Research and Reference Centre of Australia, 27 Alexandra Parade, North Fitzroy, Victoria 3068, Australia, Volume 21, Number 3, pages 3-35, September 1994.
Today, March 21, is World Down Syndrome Day. Why? Because it is the 21st day of the 3rd month. The numbers represent the triplication (trisomy) of the 21st chromosome which causes Down syndrome.
Unhapply, about 90% of women who learn that they will give birth to a child with Down syndrome have an abortion. This barbarity is not just the mother’s fault. They receive so little encouragement — even from their doctor – and they are under intense pressure just to make the problem disappear. Society takes a very dim view of disability.
Mary Le Rumeur writes from France about two young women with Down’s who have made a splash in the media as a model and as a weathergirl.
Two beautiful young girls – one in France and the other from Australia – are showing the world a new face of Down Syndrome.
Mélanie had a dream; she wanted to present the weather report on television. So last month, 21-year-old Mélanie Ségard posted a message on FaceBook: “If I get 100,000 likes, I can be the weather girl.”
Within 10 days Mélanie had 200,000 likes, and several television channels contacted her. The choice was made to accept the spot offered by France 2 on its main evening news programme.
Mélanie spent four days at the TV channel’s studios in Paris, under the tuition of former weather girl Catherine Laborde. She had to learn her text by heart because she can not read or write. The current weather girl Anaïs Baydemir took her under her wing and they worked as a team.
On March 14 the final preparations were made with Melanie choosing her clothes and make-up. Finally, at 8.35 pm, she was on screen, wearing a little black skirt, pretty pink top, chic earrings and a confident smile. Mélanie was telling the whole of France that Spring weather was arriving: “ Thursday, cloudy in the north, sunny near Marseille…. ”
And to finish, “Happy feastday tomorrow to all the Louises.” Anaïs and Mélanie hugged each other, a big happy smile on both faces.
This project was initiated to mark Down Syndrome Day, March 21. (The 21st of the third month represents the extra chromosome at the 21st pair that causes trisomy 21.) An association of families with DS children was looking for a way to overcome the “ invisibility ”of their children, especially on television. And they were very proud of Mélanie’s exploits.
“ Mélanie was natural and spontaneous. Her presentation was happy and confident. Mélanie gave the message that if society helps these young people, they can achieve many things, ” said the president of the association, Luc Gateau. “ We hope that schools will become more inclusive of children with handicaps, and the next generation will be more familiar with different handicaps and able to interact more easily. ”
Mélanie’s weather report gave France 2 a record audience of over 5 million and it was also watched more than 3 million times on internet. On Twitter, 12,000 people sent Melanie a message of congratulations.
Meanwhile in Los Angeles, Madeline Stuart was launching her own fashion label – in the Beverly Hills Hilton Hotel, no less ! Since 2015 Madeline has made a special place for herself in the fashion world, modelling in New York, Birmingham, Dubai, Paris, Los Angeles, Melbourne, and China.
“ Exuberance ” is the word for this 20-year-old Australian who watched a fashion parade one day in her home town of Brisbane, and said to her mother, “ Mum, me, model.” Her mother Rosanne took up the challenge, first helping her daughter to lose 20 kilos, by dancing and going to the gym. Maddie’s new silhouette inspired people around the world.
Then in September 2015 Madeline was on the catwalk for the first time, during the New York Fashion Week. You can see the video of her first parade, in a stunning black dress, on her website. Colours and zazzy patterns are the trademark of Madeline’s casual but chic ready-to-wear collection. Her label: “ 21 Reasons Why ”.
Madeline and her team assume with pride all her 21 chromosomes, and showcase a young woman who takes life full on, with her arms open wide, a toss of her long shiny hair, and a smile to reach your heart. In 2016 Madeline was nominated for the Pride of Australia and Young Australian of the Year.
In 2015 a United States group called Changing the Face of Beauty set out to find 15 retailers to commit to using models with disabilities in their advertisements – and wound up getting commitments from more than 100 companies. With television and fashion weeks coming to the party, the face of beauty is certainly changing.
Mary O’Neill Le Remeur writes from Angers in France.
– See more at: https://www.mercatornet.com/features/view/melanie-and-madeline-changing-the-face-of-beauty/19526#sthash.32pllWF4.dpuf
March 16, 2017 (LifeSiteNews) — A picture of a 26-week-old preemie reaching out to touch a nurse’s hand affirms the humanity of the most fragile human beings.
The Daily Mail published the photo, found on a website for medical staff called Figure 1. It shows a tiny baby girl, born at 26 weeks’ gestation and weighing less than one pound, “seeking the comfort of human touch.”
The baby girl’s whole hand was only 3/4 of an inch.
“I was changing her nappy and she just held onto my hand,” the nurse explained online. “I had to stop and just let her. Human touch is so important.”
Scientists believe skin-to-skin contact is crucial to a child’s physical and psychological development.
Birmingham City University’s head of psychology, Professor Craig Jackson, explained that babies need skin-to-skin contact. They crave the type of relational and physical closeness they experienced in the womb.
A mother’s skin contact with her baby is known to stimulate the production of breast milk. Such contact also releases oxytocin, known to create interpersonal bonding.
The Daily Mail reported on a 20-year Bogota, Columbia, study of 250 babies on the effects of skin-to-skin contact. The results were published in the December issue of the journal Pediatrics.
The study tested “Kangaroo Mother Care” for low-weight newborns, which replaced the cautious incubator approach for the most fragile human beings with “strapping the baby upright to the mother’s chest in skin-to-skin contact” and exclusively breast feeding.
The study found that babies who were given close skin-to-skin contact were calmer, less hyperactive, less aggressive, more faithful to school attendance, more sociable, slept better, and grew more brain matter.
A major review of 21 studies and more than 3,000 babies concluded that the maternal skin-to-skin contact “was preferable to conventional neonatal care.” Fathers making skin contact led to positive results as well.
The nurse reported that the fragile little girl in the picture is now a “happy, healthy, 14-pound nine-month-old.”
“Premature babies are the definition of a miracle,” she said. “I have the best job ever.”
Dave Andrusko of National Right to Life News opined, “If ever a picture was worth a thousand words, this is it.”
A Newcastle fertility clinic has been given a license by the Human Fertilization and Embryology Authority (HFEA) to carry out the controversial “three-parent baby” technique.
It is the first time such a license has been granted in the UK. The next step in the two-stage licensing process will be to consider the application relating to an individual patient.
Children as commodities
Dr Anthony McCarthy of SPUC and author of Cloning and Stem Cell Research explains the news, saying:
“This depressing but entirely foreseeable development puts into practice a technique known as ‘pro-nuclear transfer’. This technique involves the gutting and destruction of two embryos to create a third ‘combined’ embryo – a clone of one of the first two who will have no genetic parents in the ordinary sense. Early human beings are treated by scientists as mere commodities, and the would-be parents, with their encouragement, are more concerned with ensuring ‘quality’ in any child born than with reverence for the gift of human life.
Embryos used for spare parts
“As so often with such developments, safety concerns, which bodies such as the HFEA claim to be paramount, are set aside. Actual interference in the germ-line, which could affect countless future generations, is now permitted in this country, where so many other countries sensibly restrict it.
“The granting of this license entrenches the idea that eggs can be bought from women who will be cut off from the children to whom they also will have some genetic link. It worsens the situation for embryos, who are merely valued as sources of spare parts for ‘improved’ embryos ‘designed’ for would-be parents – who are in fact the full genetic parents of the embryo who is cloned and destroyed. And of course, such procedures do not even attempt to treat the mitochondrial problems some dishonestly claim they do.”
LifeNews Note: Courtesy of SPUC. The Society for the Protection of Unborn Children is a leading pro-life organization in the United Kingdom.
LIMA, Peru, March 14, 2017 (LifeSiteNews)—The pro-life movement in Peru has produced a video of startling vitality and youthful exuberance to promote what may be the world’s largest annual March for Life.
Staged as a flash mob in a spacious public square in downtown Lima, the video begins with a teenage girl doing a solo song and dance with “en la marcha por la vida” as its chorus. Soon the square is filled with hundreds of young men and women joining her in both the song and dance, with both closeups filmed at ground level and long shots taken from a drone. The video is followed by a second one that teaches the song’s four verses and accompanying movements.
The flash mob matches this year’s theme: “La Calle Es Nuestra: Defienda La Vida (The Street is Ours: Defend Life).” Not only are Peruvians the most pro-life population identified in a world survey conducted earlier this year by Ipsos, their yearly Marcha Por La Vida may be the world’s largest. It drew 500,000 in 2015 and 750,000 last year. The biggest U.S. march, in 2013, attracted 650,000.
Abortion is illegal in Peru except to save the life of the mother. An effort two years ago to extend decriminalization to abortions of unborn children conceived in rape failed.
This is the second in a series of videos. The first is available here.
March 13, 2017 (LifeSiteNews) — Campaign Life Coalition’s awareness campaign against Canada’s newest abortion drug, RU-486 or Mifegymiso, included a video posted on International Women’s Day warning women about the hypocrisy of radical feminists who put abortion access above women’s health.
So far, eight videos have been produced in the #Ru486RuCrazy campaign and are being released every few days. Marie-Claire Bissonnette, youth coordinator for Campaign Life Coalition, says more are in the works.
For more videos, check out Facebook, Twitter, or YouTube @CLCYouthProLife.
I don’t like to harp on about Bill and Melinda Gates, but, honestly, is propaganda for contraception the best they could do for International Women’s Day?
In my mail this morning (March 8, US time) was a newsletter headed “Talking contraceptives with mom and grandma”. You know, like, “Having scones and jam with mom and grandma,” or “Taking a walk in the park with mom and grandma.” As nice and feminine as that. Except that it isn’t nice and feminine.
Contraception is about sterilising yourself in different ways: overdosing on hormones or having a metal or plastic device poked inside you, for instance; practices designed to make your body like a man’s, unable to conceive, except for the times they fail and either destroy a new human life or present you with an unwanted pregnancy.
Now that would be something to discuss with grandma: “Dear Gran, if my contraception failed do you think I should go to Family Planning and get an abortion?” That’s if you wnt to completely spoil her day.
There’s a video with four grandmother-mom-daughter groups, but none of them had an abortion, although it would have been legal for a few of the younger women who had unplanned pregnancies. It makes you wonder why American women had to turn out in their hundreds of thousands in January to claim their abortion rights.
And the grandmothers are the only ones to talk about marriage and children in the same breath. Their daughters planned and used IUDs and things – and had the odd lapse (“my son was a big oops”). But for the youngest generation (still having unplanned babies occasionally) it’s all about education, careers, “being anything I want”, and, ideally, achieving all sorts of milestones, including home ownership, before children enter the picture. Being “in control” is big.
True, the stories start with an English grandma saying how wonderful it is to be a mother, “a privilege”, but the poor things really had no choice. And neither, according to Bill and Melinda, do 225 million women in developing countries who “want to time and space their pregnancies, but they don’t have access to modern contraceptives.”
(Really? That many? Did they ask them all?)
“Let’s work to give every woman the chance to lead a healthy and prosperous life,” say the Gateses. “When women can plan their futures, everyone benefits.”
No-one could disagree with that. But why, if contraception is the key to health, wealth and happiness – and goodness knows, it’s been around for 50 years –are there so many women in countries saturated with cheap, often free, “modern contraceptives” who are struggling in poverty to bring up kids on their own?
Has Melinda warned the women she talks to in Africa and India that this is what can happen? And does she tell them straight off that the backstop is abortion, advocated and/or provided by organisations that the Gates Foundation partners with through the Family Planning 2020 coalition?
That network, which up until now, at least, includes US and UK government aid organisations, also had something to advertise on IWD. It’s their own riff on international human rights agreements, although some of those “agreements” only exist in the reports of UN committees and not in international treaties.
Family Planning 2020: Rights and Empowerment Principles For Family Planning is an elaboration of the familiar “sexual and reproductive health” agenda. “Abortion rights” are implicit in projects like FP2020, which have an official aura about them, but are often boldly stated by groups like Planned Parenthood, which sponsored the Washington Women’s March.
Western governments are shelling out enormous amounts of money for this reproductive health crusade. Yesterday Canadian Prime Minister Justin Trudeau announced that it would be boosted by $650 million from his government – this, hot on the heels of a $20 million commitment to an international abortion fund.
As I’ve said before, Bill and Melinda do some great things – they also sent out yesterday a feature, Alive Under 5, highlighting the 50 percent drop in childhood mortality since 1990, which they have assisted. It’s a shame to spoil these achievements with a patronising and compromising role in the war on population.
If you want to understand why just one-in-five Americans self-identify as a feminist, look no further than today’s “Day Without A Woman” event.
The organizers already told about half of America’s women to get lost when they explicitly stated the preceding January’s Women’s March’s “platform is pro-choice” and “has been since day one” and participants will be “marching on behalf of individuals who share th(at) view.” Today is supposed to be the “part two,” if you will, to that event.
The Day Without A Woman website claims to stand for “the human rights of women,” and yet they side-step the reality that tens of millions of American women consider abortion to be an egregious human rights violation against hundreds of thousands of females annually and millions more globally.
Understandably, the organizers would probably prefer not to rename the event, “A Day Without Pro-Choice Women,” but even if they did, that would still be too broad. That still wouldn’t address the reality, for example, that poor women don’t have the same luxury as wealthy women of risking being fired in order to stand for left-wing ideologies, many of which help to keep women in oppression and poverty, such as advocating for legalized prostitution.
Advocating for legalized prostitution?
Yep. Amnesty International is a sponsor of the Day Without a Woman. Amnesty was last seen coming out in favor of decriminalizing prostitution, or “sex work” as they now call it. Amnesty’s policy shift comes at a time when the number of people living in human slavery, many of them as sex slaves, is at a record high. An estimated 35 million people today are living in slavery and one can easily draw a straight line between prostitution and the trafficking of human beings, most of them girls and women, for sex.
Planned Parenthood is also heavily invested in the Day Without A Woman. They were a sponsor of the Women’s March and are hosting various events across the country in conjunction with tomorrow’s events.
Planned Parenthood keeps trying to bill itself as a representative of women’s interests, but those efforts are sagging under constant exposes that suggest the abortion chain is more interested in its bottom line than it is in authentic women’s health. For starters, the organization has lobbied against even the most commonsense regulations on the abortion industry, such as higher safety standards for abortion centers or bills that would restrict late term abortion, bills that just so happen to have the support of the overwhelming majority of … women.
So you’ll forgive those of us women who opt out of an event that purports to be pro-woman, but feels instead quite out of step with the attitudes of plenty of women who don’t care to see our country legalize the sexual exploitation of women, kill our preborn daughters, or get us fired from our jobs and call it progress for women.
Sam and Rob Fatzinger, second and third from right, of Bowie, Md., have 13 children, including, from left, Barbara, Robert, Kolbe, Alex, Mary, Cecelia and Dominic. (April Greer/For The Washington Post)
Sam Fatzinger prowls the aisles of an Aldi grocery store with an engineer’s precision. Workers greet her, mostly by name.
She puts several trays of chicken into a huge cart. Then it’s on to fresh blueberries for $1.79 a pint, in February. And she recalls the time the no-frills store had a sale on potatoes: 10 pounds for 99 cents. She bought 60 pounds. Her husband loves them.
To get these best buys, “it’s just watching and waiting and knowing,” Sam says.“Every cent counts.”
At the cashier, her groceries fill every inch of the conveyor belt. My silent guess: $250 in all. The bill: $127, half of my estimate.
Very impressive. But not as impressive as this:
Rob and Sam Fatzinger, lifelong residents of Bowie, Md., lead a single-income family in one of the country’s most expensive regions. Rob’s income never topped $50,000 until he was 40; he’s now 51 and earns just north of $100,000 as a software tester.
They have 13 children. Which means they require things like a seven-bedroom house and a 15-passenger van. Four children have graduated from college, three are undergrads and six are on the runway.
Yet they paid off their mortgage early four years ago. They have no debt — never have, besides mortgages. And Rob is on track to retire by 62.
This family gets the gold medal for being frugal. This family is the Einstein of economical.
These days, frugality is not about clipping coupons. It’s about rethinking your finances, and maybe your life.
Rob’s philosophy: “Spend money on what makes you truly happy and on what you enjoy. … The thing that people need to understand is that we don’t feel deprived or poor. … We pick and choose carefully.”
The Fatzingers are getting it done.
Could you?
A Fatzinger family portrait with, from left, Caleb, Kolbe, Alex, Mary, Joey, Cecilia, Barbara, Dominic, Lizzie, Robert, Rob, Eric, Sam and Ray. Not pictured: Joshua. (April Greer/For The Washington Post)
Frugality is hardly new. In 1789, George Washington wrote to Marquis de Lafayette, the French military officer who fought for the American Revolution: “Nothing but harmony, honesty, industry and frugality are necessary to make us a great and happy people.” And we were a frugal people well into the 20th century. Then came the era of instant credit, rampant consumerism and record personal bankruptcies.
Recently, frugality has gotten a boost thanks to hundreds of personal-finance bloggers, and no thanks at all to the Great Recession of 2007-2009. Many focus on FIRE, an acronym for financial independence/retire early.
Aspirants often strive to save at least 25 percent of their take-home pay over the years, or even twice that — or more — to feel financially secure or to pursue a new career. Others yearn to quit their jobs for the long haul, even in their 30s.
One leading blogger grew up on food stamps. Others learned about money from their parents, for good or ill. The best are innovative, funny and surprisingly philosophical as they chart a course for change and places unknown.
They’re about ideas and possibilities, not suffering. And millions are listening. Until a couple of years ago, Rob Fatzinger had a blog called Sardonic Catholic Dad, focusing on family, faith and frugality. Two of his hits: “College on the Cheap — How the Sardonic Family Does It” and “How to Retire Early With 13 Kids,” which he wrote as a guest post on the FIRE site Mad Fientist.
Frugalism is often about math, determination and thinking a bit differently. A few key principles: How much you save, as a percentage of your paycheck, will foretell when you’ll be able to build your own business or retire. Small financial changes can make a big impact. And it’s not really about your income; it’s about your savings, says Pete Adeney, a lapsed engineer from outside Boulder, Colo., who created the popular Mr. Money Mustache blog.
And then there’s the “miracle” of compounding interest, the gift that keeps giving as your investment’s interest spawns its own interest, time and again.
Dinnertime can be hectic for the Fatzingers, although they’ve learned shortcuts to speed the process through sharing and passing silverware. (April Greer/For The Washington Post)
The Fatzingers would never claim to be financial magicians. But to outsiders, it might look that way.
After marrying 27 years ago, Sam and Rob started a small Christian bookstore in Crofton, Md., and soon had a daughter. Rob said the couple never earned more than $36,000 a year in the business. Still, they saved 10 to 15 percent of their earnings. By the time they shuttered the store in 2000, they had seven kids.
About 10 years ago, Rob got the job testing software. Earnings of $40,000 gave way to $60,000 and are now about $110,000, counting a few thousand from mowing neighbors’ lawns and other tasks.
Back in 2000, they bought a five-bedroom house out of foreclosure and later added three bedrooms. Nine children, including the youngest, who is 4, live there now.
The good news: The home cost $150,000. The Fatzingers paid down $50,000, saving interest on the 15-year mortgage.
The bad news: Sam said their priest, visiting to bless the new home, “walked in and said: ‘Should I do an exorcism on this house?’ ” The place was in serious disrepair.
“Relatives gutted it and made it livable,” Sam said. “Youth groups were over here, ripping up carpet, taking down walls.” Someone gave them a wood stove. A relative gifted them a used couch. Later, another couch was left on a curb for anyone to take. Score.
Years later, they enlarged the kitchen, using two zero-percent finance offers good for 12 months. Eleven months later, they paid off the loan, without paying any interest. The project cost $28,000, with family members doing much of the demolition, painting and decorating.
Now they have two refrigerators, two stoves, two dishwashers and a welcoming, comfortable home. (Even the clothes washer is a champ. Sam estimates that the family cleans 42 loads a week, but never on Sundays. The only children who don’t do the wash are the 4- and 6-year-olds.)
Since the mortgage was paid off in 2012, Rob and Sam have turbo-charged their savings rate, now investing about $3,000 a month. Even so, they don’t go without. Sam has a $10 monthly gym membership, and Rob and Sam go out for lunch on the 20th of each month, maybe at Red Robin Gourmet Burgers and Brews in Bowie, marking the day of the month they got married.
Occasionally, Sam and Rob are annoyed by strangers at the grocery store. “People still say, “Oh my God, you have so many kids!” said Sam, a devout Catholic, as is Rob. “I have this ‘Don’t mess with me’ reaction. I’m not your typical, quiet, passive woman.”
Rob, 51, is soft-spoken, a work-from-home dad and a former “American Idol” fan. A few years back, he finished a 50-mile trail run — and kept going to 54.
Sam, who is 48, home-schools the children through high school and is certified to do so. The kids also get outside tutoring. Her nonacademic lessons extend to the rules and responsibility of money.
“My kids all get jobs as soon as they’re old enough,” she says, and they “learn to discern between needs and wants. They pay for their cellphones, they pay for college, they pay for their own gas.” Allowances? Nope.
Daughter Barbara, 20, a rising senior at the University of Maryland Baltimore County, started babysitting at 11. She got her first “real job” at Rita’s Italian Ice. Babysitting, she noted, “paid way more than Rita’s.”
When she was 15, Barbara bought a 1994 Ford Escort with 30,000 miles for $2,600 from her savings. “It sat in the driveway until I got my driver’s permit,” she said. Five years later, “I still drive it.”
The family shops at sales or secondhand stores and checks out the Freecycle Network, a site for giving away belongings.
Friends and strangers also chip in. “We always have someone dropping off a bike,” Sam said. “We would get things and not even know where they came from.”
Someone stuck an anonymous $500 gift card on the Fatzingers’ front door. And a pair of size 3 white shoes for church wound up on the doorstep for a young daughter who could use them.
“Bowie just does that,” Sam said. A friend from church gave them a used car, and Sam’s sister gave her a used red Chevrolet Suburban. And later, an older white Suburban.
Fine. Except this is America. Surely the kids are seething cauldrons of Nike-deprived resentment.
Or maybe not. “I always had a ton of clothes,” Barbara said. “I would go with Grandma and buy any cute clothes I wanted.”
Older brother Caleb: “I can see how some people would think … we might have been deprived. It was never like that.” He played soccer at a small Christian school, was a counselor at a summer camp and swam at a community pool. The kids had cable TV and high-speed Internet. In community college, Caleb said, he “knew I didn’t have what some other kids had, but it was never out of control.”
As for the givers: Sam’s sister, Joan Salvagno, who is 11 years older than Sam in a family of nine, said her sister’s family “needed the car more than we did. … You don’t really think of them as gifts. … We’ve gotten more than we’ve given.”
The children head down the driveway for a family bike ride. (April Greer/For The Washington Post)
These days, even the childless can be terrified of college costs, so just imagine having 13 kids. But the Fatzingers have a strategy, and it’s working. The plan: Start in community college, don’t expect a handout from Mom and Dad, and graduate debt-free.
So far, Alexandria, the oldest at 26, graduated at 21 with a master’s degree in social work. Joshua, 25, graduated from the University of Maryland with a degree in kinesiology and became a missionary.
Caleb, 23, is in the last year of a doctoral program in physical therapy at the University of Maryland at Baltimore. And Lizzie, 21, graduated in May from the University of Maryland with a math major, while also cleaning houses and tutoring. All four graduated from college debt-free.
All five oldest Fatzingers have gone first to Anne Arundel Community College.
In Barbara’s first semester, her tuition, textbooks and gas money were covered by scholarships and other aid. In her second semester, she spent “probably $500” in tuition. The next year, she paid $700 to $1,000 per semester. After two years, she had paid about $2,500 at most. It came from savings and her job in a child-care center at a gym.
In September, Barbara started at UMBC, a public university with higher expenses. Her first year there cost about $15,000, after receiving a $5,800 scholarship based on grades and financial need. Money was tight. Again, she paid with her savings, which included money from a grandparent, who gives each child a one-time gift of $5,000 for college. Barbara used some of the gift money to stay in school, but she’s saving most of it.
She will soon begin her senior year at UMBC. She has a $7,500 stipend for tuition and five small scholarships “that will fill the holes.” In return for the stipend, she’ll work for a state child-welfare program.
Barbara has decided to live at home this year, which means she’ll be commuting and “won’t be spending at all,” she said in a text message. “And I WILL graduate debt-free.”
Next year, she’ll follow in oldest sister Alex’s footsteps, pursuing her master’s degree in social work at another school, which could take one or two years. A Maryland program will pay most of her tuition, and in exchange, she’ll work for a child-welfare agency for two or three years after she graduates.
In total, roughly speaking, Barbara has paid about $17,500 out of pocket for tuition, books, supplies and fees for four years of college.
Common mistakes you could be making for your retirement
The Washington Post’s Jonnelle Marte gives helpful tips to avoid frequent mistakes made by people while preparing for retirement. (Ashleigh Joplin, Jonnelle Marte/The Washington Post)
I asked if she had paid for all her expenses in her first year at UMBC. The $15,000, she said, “was all of my money that I’ve been saving since I was 8 years old!”
But even the Fatzingers can’t outrun the college-cost steamroller.
Caleb was fine in community college, where he paid “essentially nothing,” in part because of his good grades and aid. And he graduated debt-free at Towson University, a public state school, where he worked in the admissions office.
But when he began the doctoral program in physical therapy two years ago, he had to take out a loan. With aid more scarce in grad school, he said he’ll end up owing almost $90,000.
“I think about it a good amount,” said Caleb, who started working as a physical therapy technician at 18. “I try not to worry too much.” He hopes to pay off the loan in 10 years.
He has one more year to go. He works at the school gym some days at 5:30 a.m. and slips into class at 9:30. “I think I’ve done the best I can,” he says.
Barbara goofs off with Cecilia and Mary. The Fatzingers have a seven-bedroom house. (April Greer/For The Washington Post)
The Fatzingers’ recent challenge: Joshua, the oldest son, is getting married in November — in Arizona. Could they all get there?
There was considerable concern. With 13 kids, the need to be frugal never takes a vacation.
At the end, they got three plane tickets for free, using air miles. Then they bit the bullet and bought 10. They’ll all be at the wedding.
My advice: Never bet against the Fatzingers.
Erica Johnston, an editor at The Post, never knew she came from a “small” family of nine until she met the Fatzingers.
Last week the Swedish app Natural Cycles made international news coverage with their breakthrough European certification. Among others, the online magazine Business Insider reported the event in a fairly extensive article on the topic. However, the magazine, which is read by over 70 million individual readers every month, tainted the announcement with partial and uninformed views, to a point that can mislead many readers to question the viability of FABMs.
Natural Cycles is an app that was designed by two physicists, Elina Berglund and her husband Raoul Scherwzil. The app is based on the user’s daily basal temperature (lowest temperature of the day, first thing in the morning), and it calculates her fertile window using a proprietary algorithm. The user and her spouse/partner can choose to abstain during that period if they would like to avoid pregnancy, or to have intercourse if they are trying to achieve pregnancy. Currently over 150,000 women in 161 countries already use the app.
The app was clinically tested and approved by the Tüv Süd, a German inspection and certification agency, allowing the UK’s Medicines and Healthcare products Regulatory Agency (MHRA) to recognize the app as a medical product. This is good news for the FABM industry as a whole, as it gives a more official place to FABMs within the family planning and women’s health sector.
The manufacturer conducted two rounds of extensive clinical trials. The second study collected data from over 4,000 women aged 18-45 and showed a perfect use effectiveness rate of 99.5% and a typical use effectiveness of 93%, which is equivalent to the pill (99.7% and 92.5% according to the CDC).
Business Insider related the news and treated the industry as a whole with great skepticism. The general stance of the article is that, while the apps received a great report, the usefulness of FABMs and such apps is extremely limited: “Problem is, they (‘fertility awareness-based’ methods) aren’t always reliable, because human bodies aren’t always reliable.”
Here is their argument, and our response:
The effectiveness of Natural Cycles is “way better than traditional fertility-based awareness methods, which have an average failure rate of 24%, according to the CDC.”
It is true that the CDC officially cited this low effectiveness rate in a 2011 report. However, the report is based on a study that used a low quality research methodology[i]. In this retrospective survey, the research team asked pregnant women to recall the method of birth control they were using when they got pregnant. In a letter published in the American Family Physician, Dr. Marguerite Duane, co-founder of FACTS, explains that not only is recall a weak indicator, but any method that sounded like a periodic abstinence method, including the obsolete, ineffective rhythm method, was put in the “Fertility Awareness” group. “This lumping together of FABMs or NFP methods old and new masks important differences in their effectiveness” she writes. It’s as if they had put all physical devices like the IUD and the condom in the same category and classified them as having one lower effectiveness rate with typical use.
An article from the FACTS team published in May 2013 by the Osteopathic Family Physician Journal[ii] shows that the top three FABMs have a perfect use effectiveness of 98.1%-99.6% and a typical use rate between 90.5 to 97.8%. Those numbers are far from the 24% failure rate reported by the CDC.
The Natural Cycles app Photograph: Danijela Froki/Natural Cycles via The Guardian
“Natural Cycles is inarguably one of the best forms of fertility-based awareness birth control that exists.”
While Natural Cycles offers a well-researched option of FABM, we would argue that methods like Sympto-Thermal, Billings or Creighton, all methods with extensive clinical trial that have also been evaluated by international organizations such as the World Health Organization[iii], have similar effectiveness rates. These evidence-based methods are also beneficial in health literacy. Women learn not only to track their signs, but also to interpret the data in order to calculate the fertile window on their own. That knowledge is invaluable. These methods also have worldwide networks of instructors that can assist women in the interpretation of their charts.
“The length of a woman’s cycle can vary for several reasons, including stress. For many women, this variability is the only constant thing about their periods. In this case, fertility awareness-based methods are generally a bad option, according to Planned Parenthood.”
With the exception of the Standard Days Method, which is effective only for women whose cycles fall consistently within a range of 26-32 days, all evidence-based Fertility Awareness Based Methods’ effectiveness rates apply regardless of the cycle irregularity. The physical signs used by these methods (cervical fluid, temperature, and/or LH level) are present even when their cycle is longer or shorter than usual or than a normal cycle and still enable women to calculate their fertility window.
“Fertility awareness methods also aren’t advisable for women who have a sexually-transmitted infection (STI).”
This is not a limiting factor specific to FABMs. FABMs do not protect from STIs, but neither does the pill or most other contraceptives methods.
“And Planned Parenthood suggests these methods ’may not work‘ for women who have any of the following: more than one sex partner; a sex partner who ‘isn’t as committed to fertility awareness-based methods as you are’; trouble keeping close track of ’safe days’; trouble abstaining or using another method for at least 10 ‘unsafe days’ during each cycle; or for women who take medicine that may affect reading any of the signs of these methods.”
While it is true that the partner must cooperate in order to achieve the effectiveness rate of FABM, one can argue for example that a partner can be convinced to cooperate as he learns about the reasons and the benefits of doing so. Couples who are motivated to avoid pregnancy manage to abstain. Once a woman acquires the habit of tracking her cycles, keeping track of safe days is scarcely more difficult than remembering to take the pill every day. Evidence-based FABMs also have provisions for women who take medications that can impact their signs, so that the effectiveness rates remain high.
[i] Trussell J. Contraceptive Efficacy. In Hatcher RA, Trussell J, Nelson AL, Cates W, Kowal D, Policar M. Contraceptive Techology: Twentieth Revised Edition. New York NY: Ardent Media, 2011.
[ii] Manhart MD, Duane M, Lind A, et al. Fertility awareness-based methods of family planning: a review of effectiveness for avoiding pregnancy using SORT. Osteopathic Fam Physician. 2013;5(1):2–8.
[iii] Family Planning, A Global Handbook for Providers, World Health Organization, 2011 http://apps.who.int/iris/bitstream/10665/44028/1/9780978856373_eng.pdf
Anna Migeon is the co-founder of Natural Womanhood, a MercatorNet partner site.
– See more at: https://www.mercatornet.com/family_edge/view/a-fertility-awareness-app-gets-official-nod-and-fake-news-treatment/19415#sthash.KXAYLQVI.dpuf
The media never stops banging on about women’s health, particularly in the wake of the disgusting revelations about Planned Parenthood. They’re always telling us that “women’s bodies” and “women’s choices” should be paramount. But just how healthy are the solutions to unwanted pregnancy that they propose?
Ladies — I’d like you to imagine that you are Neo from the popular film franchise The Matrix. For the purposes of this thought experiment, I am Laurence Fishburne, except with really good hair, a charming personality, and of course I’m much blacker than he is.
In one hand I hold a pill that lets you see the truth, even if at it first it is very bitter. In the other I hold a pill that you have to take every day and it will keep you from getting pregnant at the low cost of turning you into a hideous monster.
Ask yourself before continuing: are you ready for the truth, or do you want to continue turning yourself into Gollum for the benefit of not having to practice any sexual responsibility at all? Okay, different movie franchise, but you get the idea.
God-fearing nutcases like me have long argued that birth control, like abortion (or “the murder of children,” if you prefer), is the work of the Devil. Like all things discouraged by the Bible, it leads only to misery and suffering — for young men as well as women.
Now, assuming you’ve chosen the right pill, I can prove with the power of science that religious folk were right all along and that science has a little-known but undeniable Roman Catholic bias.
BIRTH CONTROL MAKES YOU FAT
Let’s start with the grossest form: injectable birth control. IT MAKES YOU FAT. A 2009 study from the University of Texas found that women using DMPA gain an average of 11 pounds over three years, a 3-4 per cent increase.
Worse, this was abdominal fat, which is linked to cardiovascular disease, strokes and diabetes. 25 per cent of women on DMPA experienced “significant and potentially dangerous body composition changes.” Yes, that’s right. They became dangerously fat. On the bright side, they’re able to stop the injections at that point because being fat is the best form of birth control anyone could ask for.
So in other words, your birth control injection will add on pounds that will prevent the injection you really want — of man meat. This, in turn, will lead to depression and excessive ice-cream consumption, which adds on more pounds. Eventually, you’ll find yourself in what medical professionals call “a vicious cycle” but what I call FFAS, or “Female Forever Alone Syndrome.”
BIRTH CONTROL MAKES YOUR VOICE UNSEXY
It’s not just your body that will get less sexy. Your voice will lose its seductiveness too. Women sound most attractive to men when their estrogen levels are high, and their progesterone levels are low. Birth control lowers the former and raises the latter, making women sound as erotically appealing as Bruce Jenner giving a croaky acceptance speech.
If you think the man of your dreams will be eager to meet you after that first Skype call where you sound like a lumberjack, keep dreaming. Men trust their senses and will create a mental picture of you long before you meet. Do you really want to be labelled a pity lay, betrayed by your whacked-out hormones? No you do not.
BIRTH CONTROL MAKES YOU JIGGLE WRONG
Women on the Pill don’t look right and don’t talk right. What could be worse? Well, they can’t jiggle correctly either. A study from the University of Göttingen in 2012 gauged the attractiveness of female dancers. Men judged fertile women as more attractive dancers — and even walkers — than women in their non-fertile phase.
The researchers speculated that estrogen fluctuations during a woman’s fertile period can affect muscle, ligament and tendon strength, leading to subtle differences in movement. Fertile gals, in other words, have all the right moves.
The rougher elements in society will talk about a woman’s posterior — or mine — and describe the way a quarter might bounce off it. Birth control’s estrogen enroachment is liable to have that coin ricocheting off into someone’s eye or just slowly sinking in (see cottage cheese, below).
BIRTH CONTROL MAKES YOU CHOOSE THE WRONG MATES
It’s already established that going on the Pill makes you less attractive to men. But it also affects who you’re attracted to as well. Healthy, fertile women seek out men who are genetically different to them. Women on the Pill do the opposite, seeking out men who are closer to their own tribe. That’s right, ladies: the Pill turns you into Lannisters. I understand lusting after close relations might be a positive thing in some locations, such as West Virginia, or Norfolk, so YMMV on this one.
BIRTH CONTROL MAKES YOU UNSEXY ALL THE TIME
Don’t be fooled into thinking that birth control only makes you stupid and unattractive during your fertile periods. Although studies have found that female strippers make an average of $70 an hour during peak fertility, versus $35 while menstruating and $50 in between, women on the Pill averaged $37 — just two dollars more than a menstruating woman — and obviously had no performance peak for periods of fertility. To put it as one of my beloved rappers might: to make Wall Street, you gotta be in heat.
If you’re dropping hints to a man who doesn’t even know you exist, it might be because according to his brain, thanks to your birth control, you’re as attractive as a post-menopausal cat lady.
BIRTH CONTROL MAKES YOU A SLUT
It’s well established that women lust after rugged, manly men during their fertile cycles, and prefer baby-faced “provider” types outside this period. Indeed, this alternating pair of desires is the leading cause of female infidelity. However, imagine how accentuated this process is with women on the Pill.
A single month of it would be enough to have even the most loyal woman deliberately tripping attractive men and falling on top of them… regardless of affirmative consent. Be aware lads, if she’s on the Pill, you’re probably getting cucked — unless you’re dating a polyamorous third-wave feminist, in which case you’re getting cucked no matter what birth control method is being used (and let’s be honest, it’s probably abstinence).
BIRTH CONTROL MAKES MEN UNMANLY
Birth control has a knock-on effect on men, too. During ovulation, women are more likely to be critical of unsexy men. This, of course, is vital to the health of masculinity. Female nagging is, of course, 90 per cent pointless noise, but the 10 per cent that occurs during an ovulation cycle is what men should listen to, because it could help them be more manly. Of course, if your woman’s on the Pill, you won’t hear it at all.
(This one is a stretch, I know, but I’ve added it for the sake of completeness. As far as I can tell most women are hysterical hypercritical harpies towards their boyfriends and husbands the vast majority of the time. Man am I relieved to be a fag right now.)
BIRTH CONTROL GIVES YOU COTTAGE CHEESE THIGHS
Cellulite is the stuff of nightmares. It’s the ugly, dumpling-like ridges you see on the thighs of overweight women. It’s true some fellows like thick girls these days, but cellulite will slam the brakes on any guy’s lust.
But did you know that cellulite didn’t exist before the Pill? According to The Scientific American, pictures of women with cottage cheese thighs are almost impossible to find prior to the 1970s. That doesn’t necessarily mean the Pill is responsible, of course: other factors like increasingly sedentary lifestyles and the rise of fast food might have been responsible.
Might have been. But the Pill is the most likely culprit, because cellulite is linked to estrogen imbalances. What causes estrogen imbalances? The Pill!
THE PILL MAY HAVE DESTROYED THE INSTITUTION OF MARRIAGE
Take a look at the graph below. It’s divorce rates in the U.S., overlaid with the rise of the pill.
Exactly why there is such a close correlation between the rise of the Pill and the rise of divorce rates we can’t say with total certainty, but the relationship is stark. Possible explanations include: a lack of children leading to fewer reasons for couples to stay together, and… all of the items mentioned on the list above.
Of course, if your darling wife has been on the Pill for the last five years of your union, you’ve never actually met her in her true form. When she finally stops dosing, you will be faced with a woman who has spent the last half-decade not learning how to deal with the Twilight Zone insanity endemic to the female brain.
When she comes off the drugs, be prepared for all your worst nightmares to come true. You literally just asked an addict to go cold turkey.
Now, you may be asking what I would have women replace the Pill with, since it’s obviously so awful. Condoms? Vasectomies? The answer is: nothing. We need the kids if we’re to breed enough to keep the Muslim invaders at bay.
Tossing out birth control isn’t just kinder to women, it may be the only way to save civilization. Sorry, no offense, but it’s true. And hey! It’s what God wants, too.
Amid conflicting reports about whether or not the American Medical Association was going to consider a position of neutrality on physician assisted suicide, I was informed that the AMA’s Council on Ethical and Judicial Affairs was collecting data, position statements, etc. for consideration of assisted suicide and other topics before the June AMA Annual meeting. The deadline for submissions was February 15.
The following is my submission titled “Neutrality on physician assisted suicide also hurts nurses”
Dear AMA,
I have been a registered nurse since 1969. After working in critical care, hospice, home health, oncology, dialysis and other specialties for 45 years, I am currently working as a legal nurse consultant and volunteer as well as spokesperson for the National Association of Pro-Life Nurses. Over the years, I have cared for many suicidal people as well as people who attempt suicide.
I have served on medical and nursing ethics committees, served on disability and nursing boards. I have written and spoken on medical ethics-especially end of life issues-since 1984.
The dangers of the legalization of physician-assisted suicide are especially acute for us nurses. Unlike doctors, we nurses cannot refuse to care for a patient in a situation like assisted suicide unless another willing nurse can be found which can be impossible. If we do refuse, that is considered abandonment and cause for discipline and even termination. And we are necessarily involved when the assisted suicide act occurs in home health, hospice or health care facility even though the doctor is not required to be there.
As a nurse and the mother of a suicide victim (see picture above), I am alarmed by reports that the AMA is considering a position of neutrality on physician-assisted suicide. I beg you to uphold the legal and ethical standard that medical professionals must not kill their patients or help them kill themselves. Suicide is a tragedy to be prevented if possible, not a civil right.
MY DAUGHTER KILLED HERSELF USING AN ASSISTED SUICIDE TECHNIQUE
In 2009, I lost a beautiful, physically well 30-year-old daughter, Marie, to suicide after a 16-year battle with substance abuse and other issues. Her suicide was like an atom bomb dropped on our family, friends and even her therapists.
Despite all of our efforts to save her, my Marie told me that she learned how to kill herself from visiting suicide/assisted suicide websites and reading Derek Humphry’s book Final Exit. The medical examiner called Marie’s suicide technique “textbook final exit” but her death was neither dignified nor peaceful.
Marie was not mere collateral damage in the controversy over physician-assisted suicide. She was a victim of the physician-assisted suicide movement, seduced by the rhetoric of a painless exit from what she believed was a hopeless life of suffering.
SUICIDE CONTAGION
Adding to our family’s pain, at least two people close to Marie became suicidal not long after her suicide. Luckily, these two young people received help and were saved, but suicide contagion, better known as “copycat suicide”, is a well-documented phenomenon. Often media coverage or publicity around one death encourages other vulnerable people to commit suicide in the same way.
STUDY SHOWS LEGALIZING PHYSICIAN-ASSISTED SUICIDE IS ASSOCIATED WITH AN INCREASE RATE OF TOTAL SUICIDES
“Legalizing PAS has been associated with an increased rate of total suicides relative to other states and no decrease in nonassisted suicides. This suggests either that PAS does not inhibit (nor acts as an alternative to) nonassisted suicide, or that it acts in this way in some individuals but is associated with an increased inclination to suicide in other individuals.”
THE HEALTH AND ECONOMIC COSTS OF SUICIDE
My Marie was one of the almost 37,000 reported US suicides in 2009. In contrast, only about 800 assisted-suicide deaths have been reported in the past 16 years in Oregon, the first state to legalize physician-assisted suicide. According to the Centers for Disease Control (CDC) suicide was the 10th leading cause of death for Americans in 2012, with “More than 1 million people reported making a suicide attempt in the past year” and “More than 2 million adults reported thinking about suicide in the past year.” The CDC estimates that suicide “costs society approximately $34.6 billion a year in combined medical and work loss costs”, not to mention the emotional toll on families.
Obviously our real health-care crisis here is a staggering and increasing rate of suicides, not the lack of enough assisted suicides.
BRITTANY MAYNARD
There was a media frenzy in October 2014 when Brittany Maynard, a young newlywed woman with a brain tumor, announced plans to commit physician-assisted suicide on November 1 and raise money to have physician-assisted suicide legalized in all US states. There was an immediate and unprecedented media frenzy surrounding Ms. Maynard’s tragic story that routinely portrayed her pending assisted suicide as “heroic” and even counting down the days to her suicide. Personally, I thought this looked like a crowd on the street shouting for a suicidal person on a window ledge to jump.
In the end, Brittany hesitated for a day before she went through with her pledge to take the lethal overdose.
Now, assisted suicide supporters even deny that physician-assisted suicide is suicide, insisting that media stories use euphemisms like “aid-in-dying” and “death with dignity” in cases like Ms. Maynard’s to make assisted suicide more palatable to the public. However, this defies common sense when the definition of suicide is the intentional taking of one’s own life.
PHYSICIAN-ASSISTED SUICIDE AND MEDICAL DISCRIMINATION
I have been a registered nurse for 47 years, working in intensive care, oncology, hospice and home health among other specialties. Personally and professionally, I have cared for many people who attempt or consider killing themselves.
Some of these people were old, chronically ill or had disabilities. Some were young and physically healthy. A few were terminally ill. I cared for all of them to the best of my ability without discrimination as to their condition, age, socioeconomic status, race or gender. I will do anything to help my patients — except kill them or help them kill themselves.
Suicide prevention and treatment works, and the standards must not be changed just because some people insist their desire for physician-assisted suicide is rational and even a civil right.
An Iowa bill that would recognize unborn babies as people and protect them from abortion passed a state Senate committee on Monday amid heated debate.
Radio Iowa reports “a large and vocal crowd” attended the hearing on Monday to voice their support and opposition to the measure. The committee gave its initial approval of the bill, moving it to another Senate committee for consideration.
“The sovereign state of Iowa recognizes that life is valued and protected from the moment of conception,” the bill states.
The bill would recognize that human life begins at the moment of conception and ban abortions in the state. According to the Associated Press, it is unclear if the bill has enough support to pass the full state Senate.
Pro-life attorney Rebecca Keissling, who attended the hearing, was one of several pro-lifers who spoke up in support of the bill, according to the radio report.
“You’re providing the framework to recognize that the unborn child is a person and also to have a public policy that prefers childbirth over abortion,” Keissling said.
Abortion advocates criticized the legislation, claiming it pushes a “religious point of view” about when life begins, according to the report. Others indicated that there would be a lawsuit if the bill becomes law.
Because of the current make-up of the U.S. Supreme Court, the measure likely would be overturned in the courts. In 2012, the Oklahoma Supreme Court struck down a similar personhood bill as unconstitutional because it recognized unborn babies as human beings with a right to life.
Many pro-life groups think one of the keys to ending legalized abortion is to overturn Roe v. Wade, but the current Supreme Court justices are highly unlikely to do so, especially after the unexpected death of pro-life Justice Antonin Scalia. Three of the justices, Clarence Thomas, Samuel Alito and John Roberts, potentially would vote to overturn Roe and return abortion laws back to the authority of the states; but five of the other justices almost certainly would not. Scalia’s seat on the high court remains empty.
President Donald Trump promised to nominate “pro-life” justices to the high court, but he would need to nominate and the Senate would have to confirm several before there is a chance of Roe v. Wade being overturned.
Maureen Condic, Ph.D., is an Associate Professor of Neurobiology and Anatomy at the University of Utah. She has been a member of the Pontifical Academy for Life, a distinguished group of physicians, scientists, and theologians from the international community whose mission it is to study questions and issues regarding the promotion and defense of human life from an interdisciplinary perspective, since 2014. Dr. Condic is one of our nearly 40 associate scholars. In this interview, she discusses the beginning of human life and the moral status of the human being.
What can science tell us about when human life begins?
Condic: The question of when life begins has been addressed for a very long time by philosophers and religious thinkers—often without the benefit of detailed information regarding what actually happens during prenatal life. Consequently, this question has also been answered in a wide variety of ways, leading many to believe that the question simply cannot be answered.
The advantage of a scientific approach to the question of when life begins is that the answer is not based on opinion or personal values, but rather on direct observation. And in the modern age, we have very detailed observations, confirming beyond any reasonable doubt, that the cell produced by sperm-egg fusion (the zygote) is a human organism; i.e. a human being. We know this because immediately upon the binding and fusion of the gametes (a rapid event taking less than a quarter second to complete), the newly formed zygote enters into a sequence of molecular events that determine and direct its subsequent maturation and growth. The fact that the zygote autonomously initiates the process of embryonic development distinguishes it from a mere human cell and clearly indicates that it is a full and complete, albeit immature, member of the human species.
What can reason tell us about the moral status of the unique human being who comes into being at conception?
Condic: Similar to the question of when life begins, the question of when human beings have moral status and a right to life has also been answered in many ways. The three most common approaches are to confer rights based on 1) some aspect of form and/or function (ability), 2) social convention (or fiat) and 3) status as a human being (or nature).
Most of us reject linking rights to abilities as repugnant. It defies our basic sense of justice to envision a world where the strong, the beautiful, and the intelligent have a right to life, liberty, and the pursuit of happiness, while the weak, the plain, and the slow are enslaved or killed. Similarly, most of us find repulsive the idea that a simple plurality of opinion can decide, as it did in Nazi Germany, who has rights and who does not.
The principles of liberty and justice form the basis of all civilized societies. The only way of viewing human rights that does not offend these principles is that rights are inalienable for all human beings; i.e. that we have rights only and always because we are humans. And this would apply equally to humans at all stages of maturity, including the zygote stage.
Why is it important that the right to life of the human being from conception until natural death can be established by scientific and philosophical, rather than revelation-based, arguments? Does this mean that religious arguments are somehow unimportant or should be excluded from the public square?
Condic: I don’t believe that the right to life of the human being can be established by a scientific argument. Science is simply a useful system for making accurate and neutral observations. As such, it does not speak to abstract principles like human rights.
In contrast, reason and logic are common to both philosophy and science. And the conclusion that all human beings have human rights is a logical, not a scientific conclusion. This does not mean that the truths revealed by religion have no place in formulating moral judgments. But I would argue that religious truths must be consistent with both reason and observation. For example, a religion that denies rights to people of a particular gender, race, or faith would have to reconcile this belief with scientific fact and place it within a logically consistent framework.
Why should the state not fund or promote embryonic stem cell research, and what alternative research should the state support?
Condic: As a matter of justice, no state should support, or indeed tolerate, research that involves the destruction of a living human being. While embryonic stem cells are scientifically interesting, research on stem cells derived from ethical sources (for example; animal’s stem cells, stem cells from mature tissues, and stem cells produced by cell reprogramming) are viable alternatives to human embryonic stem cell research.
Why are you pro-life? If you had 60 seconds to explain to someone why you have pursued the work that you have throughout your career, what do you tell them?
Condic: I have pursued scientific research because I am fascinated by how things work. And human development is an enormously complex, and therefore enormously engaging intellectual problem. It is also an astonishingly beautiful process; an elegant, intricate, and yet quite robust molecular dance. It seems to me that anyone who appreciates the beauty of human development and who has paused long enough to think through the logical implications, would inevitably have a profound respect and admiration for the beauty of human life.
TORONTO, February 13, 2017 (LifeSiteNews) – A Calgary conscience rights group has joined Ontario Christian doctors in fighting a requirement that they refer patients for euthanasia and abortion — and perform both procedures in emergencies.
The Justice Centre for Constitutional Freedoms (JCCF) was granted intervenor status in a legal action launched by five Ontario Christian doctors, the Christian Medical and Dental Society of Canada (CMDS), and other doctors’ groups.
Their target is the College of Physicians and Surgeons of Ontario, which controls the profession with the power to licence and de-licence doctors. In June, the Christian doctors will go to court in an attempt to have two new college policies ruled unconstitutional.
The first policy, according to CMDS executive director Larry Worthen, requires doctors whose consciences prevent them from performing a procedure to provide an “effective referral” to another doctor who will do it.
The second requires the same protections specifically with euthanasia and assisted suicide.
The College of Physicians and Surgeon’s policy becomes even more morally problematic in an emergency. If there is no other doctor available, the objecting doctor objection must do it anyway, even if it is an abortion.
“Our members can’t do an effective referral,” Worthen told LifeSiteNews. An “effective referral” is what a doctor provides when he believes a treatment is required but cannot do it himself. But Worthen’s members do not believe that assisted suicide, euthanasia or abortion are morally or medically justified.
As for doing these procedures in emergencies, “There is no definition of emergency,” Worthen pointed out.
The CMDS will focus on how the college’s requirements violate provisions in the Constitution and the Charter of Rights and Freedoms protecting freedom of conscience. However, The Justice Centre will take a different tack.
John Carpay, director of the JCCF, said his group will attack the college’s basic premise that Canadians have a right to a specific treatment.
“We make the point that there is therefore no Charter right to healthcare” in general, nor any specific treatment, “including MAID,” Carpay stated.
“Further,” he added. “There is no right, Charter or otherwise, to demand that an individual doctor perform or provide an effective referral for a specific medical procedure or service that violates that doctor’s conscientious or religious beliefs.”
Other intervenors on the Christian doctors’ side include the Ontario Catholic Bishops Conference and the Evangelical Fellowship of Canada.
Seven other provinces have adopted ethical guidelines for euthanasia and assisted suicide that respect doctors’ freedom of conscience. Worthen said this should carry weight in court because it will undermine the defence expected from the college. It will contend its policy was the only one available to it to protect patients wanting so-called “medical assistance in dying” or abortion.
Europe and its contiguous lands were in a chaotic condition in 1240: the Mongols were destroying Kiev, the Novgorod army virtually wiped out the Swedes along the Neva River, and the Holy Roman Emperor, Frederick II, was pillaging the Papal States using Islamic Saracens as his mercenaries. Pope Gregory IX’s attempt to rally a Crusade against the invaders failed, and his good friend Saint Clare was virtually bedridden as the Saracens besieged her convent at San Damiano. Her beloved Francis of Assisi had died fourteen years before. In this emergency, she left her invalid couch, went to the window and exposed the Blessed Sacrament in a silver and ivory ciborium, and the alien troops fled.
In northern Mexico until just a few years ago, drug- and gang-related violence had made Ciudad Juarez one of the most dangerous cities in the world. Following the example of Saint Clare, missionaries turned to the Eucharistic Lord for help. A perpetual adoration chapel was opened in 2013 when the murder rate was forty people a day, with soldiers and policemen joining the gangs. Increasing numbers of devotees urged the soldiers to join them in Holy Hours. Few now dismiss as only coincidence the fact that within five years the annual murder rate dropped from 3,766 to 256.
That rate is far lower than many cities in the United States now. With dismaying insouciance,
statisticians in our nation over recent years have coldly taken for granted its moral decay. Besides graphic violence in the streets, there are over 500,000 abortions each year. In many places, births out of wedlock are the norm, teenage suicide has doubled in little more than a decade, 40% of all children live in broken homes, school diplomas and college degrees have generally become meaningless, marriage has been redefined into surreality, and freedom of religion has been intimidated by false readings of constitutional rights.
Recent political shifts in our nation offer a faint glimmer of genuine promise for a change in all this, as more people realize that in the past they had placed their confidence in gossamer hopes and tinsel messiahs. But the ballot box is no substitute for the Tabernacle. A well-known Pentecostal preacher surprisingly admitted that most miracles happen in the Catholic Church because “Catholic people revere the Eucharist.” If more Catholics themselves understood that, there would be more miracles. Now, miracles do not contradict nature: they are God’s will at work at high speed. Christ promised to be with us “until the end of the world.” Eucharistic adoration is simply the recognition of his presence. Saint Clare prayed, “My Lord, if it is your wish, protect this city which is sustained by your love.” The Lord answered, “It will have to undergo trials, but it will be defended by my protection.”
Eucharistic Adoration—Our hope for a Culture of Life in America
God told us: “Be fruitful and multiply. Fill the earth and govern it. ” Genesis 1:28. The latest birth rate numbers show we aren’t listening.
Instead, the U.S. fertility rate fell to the lowest point since the 1909 record keeping began, according to statistics released by the Centers for Disease Control and Prevention. In the first three months of 2016, for every 1,000 women, there are now only 59.6 births. During the Baby Boom in 1957, the fertility rate was 122.9 births per 1,000 women.
The future goes to those willing to populate it. Countries below replacement of 2.1 child per woman, are dying. We’ve joined that crowd since 2007, although perhaps “crowd” is a poor word choice. Right now, the rate in the U.S. is sitting at 1.87, as compared to Germany’s 1.38.
It’s noteworthy that there are sharp differences between religions. According Pew Research Center, the average Mormon family has 3.4 babies while Jews, Catholics, and most Protestantism denominations have fertility rates ranging from 2 to 2.5. Atheists average 1.6 kids, and agnostics, only 1.3.
Live Catholic!
As a Catholic, the one, holy, Catholic, and apostolic Church has all the truth. But relativism has gummed up the works. So has contraception. If my husband and I had not gotten on board with all the teachings of the Church, our family would be minus one reversal and less 4 biological kids. (We had 8, adopted 2 more.)
Although the Church accepts working with a woman’s natural fertility to limit children, it can be abused if used with a contraceptive mentality. The default marriage setting is to be open to the gift of life unless there are serious reasons dictating the contrary.
Early in his pontificate, Pope Francis encouraged married couples to be fruitful in our vocation of marriage. He said, “Fidelity, perseverance and fruitfulness are the three characteristics of God’s love for his Church and should be the same three pillars of a Christian marriage.”
The Pope scolded couples that intentionally choose worldly comforts over children as a lack of fruitfulness and something, “Jesus does not like.”
Bad Reasons Not to Have More Children
I know the excuses. But they are bad excuses. Mostly. Some couples have valid reasons for not being open to life, so my list only applies to the people to whom it applies. Check with God to find out if you are on his list to receive more precious bundles with eternal souls.
* Hooked on contraception. Read On Human Life: Humanae Vitae. It explains why Catholic teaching against contraception is in our best interest.
* I don’t want another baby. Be open to what God wants. How many times have you been pleasantly surprised in life?
* The world is a bad place to bring children into. It’s just temporary. Heaven is our final destination
* I gave away the maternity clothes. There are equally generous women out there.
* I’m not ready. Then don’t have sex.
* I’m too old. Menopause is the fertility finish line.
* I’m not patient enough. Practice makes perfect and prayer helps.
* Money. Mother Teresa used to say: “God has all the money in the world.” Read this story about a one-income family of 15, (until age 40, the father never made more than $50,000) debt free, their house is paid off and all their kids go to college—some have masters and one is working on a doctorate. And don’t put an earthly price tag an eternally priceless gift.
* Our house is too small. Get bunk beds. Re-evaluate your need for space.
* Overpopulation. It’s a major myth. Educate yourself. Here’s an hour-long video and good 10-minute explanation that there is no overpopulation problem.
* I don’t like babies. God does. Find out why you don’t like what God likes. That’s a disturbing state of mind.
* When is it going to be my time? No one begrudges you time and space for yourself, but practice moderation.
Be Open
Sadly, 40 percent of women actually want more children than they have. I say, have those desired babies. Since love begets love, your family’s heart can grow bigger and you might end up wanting even more.
Babies are precious, their souls are eternal, and they make you a better, holier person. Could you be closing yourself off to such a gift from God?
London, England, Feb 8, 2017 / 04:35 pm (CNA/EWTN News).- When the fetal ultrasound gained popularity in the 1970s, it was hailed as a “window to the womb.” But now, new technology could offer a much more in-depth view of babies before birth.
Courtesy of a new multimillion dollar project based out of London, some parents are able to see clear scans of every movement and organ of their babies in the womb starting as early as 20 weeks, using advanced MRI technology.
“There is nothing quite as emotional as seeing your unborn child moving inside you, and these MRI scans are taking images to the next level,” stated Cathy Ranson, the editor of ChannelMum.com, a website that is distributing videos of the MRI scans.
“They are truly breathtaking,” Ranson continued.
Traditionally, ultrasounds are used during pregnancy to check in on growing babies in the womb using high frequency sound waves. Although useful, ultrasounds usually produce limited visual scopes of the womb and can vary in quality depending on various factors, such as age, weight, and position.
However, a curious team of medics pushed the limits of the ultrasound to find out if there was a better way to get in-utero scans.
Top minds from Kings College London, St. Thomas’ Hospital, Imperial College London, University of Firenze, the Hospital for Sick Children in Toronto and Philips Health were given £10 million from the Wellcome Trust and Engineering and Physical Sciences Research Council to see if they could advance antenatal scans.
This team of medics composed a new series of algorithms and magnetic fields to go beyond the limits of the ultrasound. This new technology is allowing clear pictures of the entire womb, making details like a 20-week heart valve crystal clear.
A video, produced by the iFIND project, shows just how detailed the scans are: the baby is stretching, turning, and even playing with the umbilical cord. They also recorded the reverberations of the baby’s movements, which could be seen rippling through the mother’s belly.
In addition to creating the optimal scan, the MRI technology also has a mechanism that auto corrects any small movements to produce an overall smooth image.
Dr. David Lloyd, a Clinical Research Fellow at King’s College London, said the new MRI scans “can see the structures inside the body, regardless of whether there’s bone, muscle or fat in the way.”
“It is also one of the few imaging techniques that is safe to use in pregnancy,” Dr. Lloyd continued.
This new technology is more than just a great picture for excited parents to see. The MRI scans could also reveal complications or growth deficiencies earlier in the pregnancy, which could allow for advanced treatment even before the baby is born.
The MRI scans have already kicked up some debate, especially in the UK where abortion is legal up to 24 weeks. These new scans, showing how babies actively move around at 20 weeks, is making the current abortion limit even more questionable.
Moving forward, the iFIND project wants the MRI scans to become available for all pregnant women around the world.
By now, regular readers of Faith and Family Findings are familiar with the data on family structure and its impact on everything important to a functioning society. On every outcome measured, for adults and children, those in an intact family do best on all the positive outcomes we desire for ourselves and our children (education, income, savings, health, longevity, happiness, sexual enjoyment, intergenerational support) and have the least incidence of all the negatives we hope never afflict our children (crime, addictions, abuse both physical and sexual, poverty, illiteracy, exclusion, ill health, unhappiness, mental illness, lack of sexual fulfillment).
Thus family structure is exceedingly important to society and a return to intact marriage is a sine qua non for a nation or for families set on rebuilding themselves.
Given that, consider the implications of the following chart on the intactness of marriage at the end of the first five years of marriage:
What this chart shows is the probability of intactness of family after the first five years of marriage– given the number of sexual partners of the spouses have had in their lifetime. Using rounded numbers: 95% of those who are monogamous, that is only one sexual partner in their life time —i.e. only their spouse–95% are still in an intact marriage after the first five years. But for the woman (national average) who has had one extra sexual partner other than her husband (almost always prior to marriage) the percent drops to 62% and with two extra partners it drops almost to 50%. Thereafter it plateaus. For men it takes five sexual partners to reach the same level of breakup.
When I first saw this phenomenon in the 1995 data (the above is 2006-2010 data) my immediate reaction was “Those Mediterranean cultures that had chaperoning during courtship knew something about human nature, family life and intergenerational stability.” They ensured Mediterranean family was on the three-love diet.
Chastity and monogamy are foundational to the intact married family, and thus to the prosperity and success of a nation. Hence my conclusion that this chart is the most important chart in all of the social sciences.
A culture of monogamy is critical to a thriving nation or a thriving culture.
A culture of chastity is foundational to a culture of monogamy.
Thus the cultivation of chastity is central to a robust nation and a robust culture. Chastity is an old term but now out of favor even among Christians, given the impact of political correctness i.e. cultural Marxism. However it is the accurate label for the virtue or strength behind the data.
For the impact of monogamy at a more causative level check out the work of JD Teachman on Google Scholar or his CV and you will be able to thread the impact of monogamy in an admirable corpus of cumulative scholarship that is one of the great contributions to research on the family.
Though the above chart is purely correlational – it is demographically descriptive of America, of what is happening between our couples who get married. One chart cannot prove chastity is causative (go to Teachman and others to tease that out) but it sure indicates where causal strength (or weakness) can be found.
It was contraception that caused me to leave the Church as a teenager and it was contraception that brought me back into the Church in my 20s. I shared some of that story in my last blog. Here I want to share how discovering the predictions of some very prominent thinkers of the early 20th century helped open my eyes to what’s at stake.
I remember how surprised I was to learn that, until 1930, all Christian denominations were unanimous in their firm opposition to any attempt to sterilize sexual intercourse. That year, when the Anglican Church opened the door to contraception at its Lambeth Conference, it was the first Christian body to break with the continuous teaching of the early Church, the spiritual masters throughout the ages, and all the Reformers from Luther to Calvin and beyond. By the time the Pill debuted in the early 1960s, the historical Christian teaching, once universally held, had come to be seen by most of the modern world as archaic and absurd.
Only a few decades earlier, when Planned Parenthood founder Margaret Sanger first started her global campaigns for contraception, there was no shortage of predictions that embracing contraception would lead to the societal chaos in which we’re now immersed. You might be just as surprised as I was to read what the following prominent thinkers of the early 20th century had to say about contraception and what they predicted would happen if we embraced it.
Sigmund Freud, for example, while he was clearly no friend of religion, understood that the “abandonment of the reproductive function is the common feature of all perversions. We actually describe a sexual activity as perverse,” he said, “if it has given up the aim of reproduction and pursues the attainment of pleasure as an aim independent of it” (Introductory Lectures in Psychoanalysis, W. W. Norton and Company, 1966, p. 392).
Theodore Roosevelt condemned contraception as a serious threat against the welfare of the nation, describing it as “the one sin for which the penalty is national death, race death; a sin for which there is no atonement.” The “men and women guilty thereof,” he believed, exhibited a “dreadful” lack of character (State Papers as Governor and President, in Works XVII).
Mahatma Gandhi insisted that “there can be no two opinions about the necessity of birth-control. But the only [appropriate] method … is self-control,” which he described as “an infallibly sovereign remedy doing good to those who practice it.” On the other hand, “to seek to escape the consequences of one’s acts” with contraception is a remedy that “will prove to be worse than the disease.” Why? Because contraceptive methods are “like putting a premium on vice,” he said. “They make men and women reckless … Nature is relentless and will have full revenge for any such violation of her laws,” he predicted. “Moral results can only be produced by moral restraints.” Hence, if contraceptive methods “become the order of the day, nothing but moral degradation can be the result … As it is, man has sufficiently degraded woman for his lust, and [contraception], no matter how well meaning the advocates may be, will still further degrade her” (India of My Dreams, Mahatma Gandhi, Rajpal & Sons, edition: 2009, pp. 219-220).
When a committee of the Federal Council of Churches in America issued a report suggesting it follow the Anglican acceptance of contraception, The Washington Post published a stinging editorial with the following prophetic statement: “Carried to its logical conclusions, the committee’s report if carried into effect would sound the death knell of marriage as a holy institution by establishing degrading practices which would encourage indiscriminate immorality. The suggestion that the use of legalized contraceptives would be ‘careful and restrained’ is preposterous” (“Forgetting Religion,” The Washington Post,March 22, 1931).
Also in response to the Anglican break with Christian moral teaching, T.S. Eliot insisted that the church “is trying the experiment of attempting to form a civilized, but non-Christian, mentality. The experiment will fail; but we must be very patient in waiting its collapse; meanwhile redeeming the time so that the Faith may be preserved alive through the dark ages before us; to renew and rebuild civilization and save the world from suicide” (T. S. Eliot, Thoughts After Lambeth, Faber and Faber, 1931).
Perversity? National death? Moral degradation? The death of marriage as a holy institution? World suicide? Isn’t that a bit much to pin on contraception? It would certainly seem so, if it weren’t for the fact that so much of what these forecasters predicted has, indeed, come to pass. What did they understand that we have forgotten?
Feb. 7, 2017 (LiveActionNews) — 2016 was a year filled with shocking news, too many deaths, and plenty of surprises. However, we can’t let the year go without also stopping to celebrate the lives that were saved and the people who were loved this year. There’s more than we may ever know, but let’s meet 12 beautiful babies who were saved from abortion in 2016:
1. Esther’s baby
Esther came to the United States from Nigeria and soon discovered she was pregnant. She had already gone through two abortions back in her home country and thought she would make the same choice again. However, Esther found Her Choice Birmingham Women’s Center, and they gave her love, support, and the truth. At the center, Esther watched the Abortion Procedure videos made by Live Action (including the one below), where former abortionist Dr. Anthony Levatino describes what actually happens in various types of abortion. Esther was shocked and saddened, and after seeing an ultrasound of her own baby at the center, she chose life.
2. This baby whose abortion was canceled
Late in 2015, mother Ester Garcia shared amazing photos of her daughter, Hope, who was miscarried at 16 weeks, with Live Action News. The article continued to be read all throughout the year, and during the summer, one commenter wrote that she canceled her abortion after seeing Baby Hope.
It is very likely that this baby would have suffered through a D&E abortion if her mother had not changed her mind, as that is one of the most common abortion procedures in the U.S. at 16 weeks.
3. Over 100 babies saved through abortion pill reversal
In May 2016, Dr. Matthew Harrison of Abortion Pill Reversal (APR) revealed that 100 babies were due to be born this year after their mothers successfully chose to reverse their abortions. As APR’s doctors work all throughout the year, this number has now grown well past 100 for 2016. Here is Dr. Harrison with one of the babies who was born after a reversal:
For anyone seeking information on abortion reversal for medication abortion or abortions involving laminaria insertion, including pregnant mothers, doctors or pregnancy centers who want to help, or other pro-life volunteers who are willing to man the phone line:
There are over 300 doctors across the country who are ready and able to help women stop an abortion. There are also doctors trained in 14 other countries. Women looking for help to reverse their abortion can call the 24 hour hotline (1-877-558-0333) to talk with a nurse, or visit the website (abortionpillreversal.com).
4 and 5. These two babies saved when sidewalk counselors offered help in abusive situations (Click on “See More” in the Facebook post to read the whole stories.)
If you are a woman experiencing pressure to choose abortion, please see this guide for help. Here is another beautiful baby recently saved by Sidewalk Advocates for Life’s work:
6 and 7. These Christmas twins
Live Action writer and pregnancy center staffer, Christina Martin, was able to meet a beautiful set of twins she helped save from abortion in 2016. Their photo was spread all over social media, and thousands were able to rejoice that a new little brother and sister pair were here to celebrate Christmas.
Christina shared the story (in full here):
Sara told me that she had an ultrasound at her doctor’s office which revealed she was pregnant with twins. She had children at home and she felt she couldn’t have another baby, let alone twins. Her boyfriend had recently broken up with her and she was lacking significant family support.
Unbeknownst to me, she scheduled an abortion appointment on the weekend before she was scheduled to come to our pregnancy center. She had planned to go through with the abortion and we would have likely never seen her after that.
The morning of her appointment at the clinic, Sara felt an emotional weight upon her shoulders. She felt sick on the inside as she thought about her abortion. The intense feelings were a sign to her that she couldn’t abort her twins. In the quiet of her home, she made a decision to cancel her scheduled abortion. Sara told me as soon as she decided to cancel her abortion, a sense of relief washed over her. In an instant, all of the emotional weight was lifted off of her and she felt free.
The staff and volunteers at the ABC Women’s Center walked with Sara through her pregnancy. …
8. Michelle’s baby
In December, Live Action shared this story with some of its supporters in an email:
Your gift helps us save lives: Michelle is a young mother who almost aborted her child this year but chose life instead after learning the truth about abortion online. She wouldn’t have made that decision if it weren’t for Live Action’s Abortion Procedures videos showing the development of her preborn child and what abortion actually would do to kill that child.
Michelle just celebrated her son’s first Christmas all because YOU made those videos possible.
9. Baby Axton
Axton’s mom, Acacia, was planning on abortion when she walked into a pregnancy help medical clinic in Casper, Wyoming. Pregnancy Help News reports:
During the conversation, Acacia heard a life-changing statement.
“The advocate explained to me how God has a purpose for everybody, and a huge purpose of mine was to be alive if I was supposed to be dead a month before that [due to a terrible car wreck],” she said.
After learning her earlier positive pregnancy test was accurate, Acacia was given an ultrasound. She was too early to verify a viable pregnancy, so the clinic’s nurse scheduled her for a return appointment two weeks later.
That provided Acacia time to consider all her options, and to hear a message of life-changing hope.
“I sat there and listened and talked to her,” Acacia said. “She helped me realize that whatever I did choose would affect me the rest of my life, and that the obstacles I was facing at that time were temporary. She made me look at things from another point of view. I realized I did have a purpose, and even though I felt alone, I knew there would be other people there for me fully.”
Today, Acacia is living out that purpose. She decided to carry to term and parent, signing up for True Care’s long-term parenting program called Baby & Me. She met regularly with an advocate who helped guide her through parenting classes and has become a strong support throughout the first stages of Acacia’s motherhood.
In January 2017, Acacia brought Axton — who she says “saved my life” — to Washington, D.C., to participate in Babies Go to Congress.
10. Baby Jude
Baby Jude is not born yet, but his parents have already rejected abortion, despite doctors’ counsel to terminate their son’s life. Jude has a condition that impairs his kidneys and threatens his life, but instead of aborting him, his parents, Josh and Kelli, have connected with doctors who are willing to treat their son in utero. Through amnioinfusion, Baby Jude is being given a chance at life and also may pave the wave for other children like him to be saved in the future.
11 and 12. These twins whose mother walked out of an abortion facility
On her way to the abortion facility, this mom promised God that she would not have her scheduled abortion if she was pregnant with twins. To her surprise, the ultrasound showed two beating hearts and two little babies. She informed the staff that she changed her mind, but they reportedly locked her inside the facility for awhile and refused to refund all her money. You can read the rest of her harrowing account here, and if you or anyone you know is being pressured to go through with an abortion, see this guide here.
So, in 2017, how are you going to step out and save a life? How are you going to spread information, stories, and videos that will influence others to choose life and know there are support, love, and real facts available? Let’s do this together, and make 2017 the best year for LIFE yet!
In 1951, Dr. Mildred Jefferson was the first black woman to graduate from Harvard Medical School with 28 honorary degrees. She dedicated her life to caring for the sick and exposing the evil of Eugenics. She co-founded the National Right to Life and is credited to bringing Ronald Reagan into the Pro-Life Movement.
Thank you, Dr. Mildred Jefferson!
Your work has paved the way for the Pro-Life movement.
Pope Francis encouraged Catholics to pray for babies in danger of being aborted during a special pro-life message Sunday for the annual Day of Life in Italy
Breitbart reports the pope spoke, as he often does, about the dangers of what he calls the modern “throwaway culture” and its effects on human life.
“Let us promote the culture of life in response to the logic of disposability and a declining population,” the pontiff said Sunday.
“Let us join together and pray for babies who are in danger of being aborted, as well as for people who are at the end of life. All life is sacred!” he continued. “Let no one be left alone and may love defend the meaning of life.”
The pope also recognized people who work and volunteer in pro-life causes, hoping that “they may be capable of building a society that is welcoming and worthy for every person.”
Pope Francis said he and the Italian bishops also jointly are calling for support of “bold educational action in favor of human life. Every life is sacred!”
In line with Catholic teachings, Pope Francis has been a strong advocate against abortion throughout the world. He repeatedly has condemned the modern “throwaway culture” that allows unborn babies to be killed in abortions.
Unfortunately, in our epoch, so rich in many accomplishments and hopes, there is no lack of powers and forces that end up producing a throwaway culture (cultura di scarto); and this threatens to become the dominant mentality. The victims of such a culture are precisely the weakest and most fragile human beings – the unborn, the poorest people, sick elderly people, gravely disabled people… who are in danger of being “thrown out,” expelled from a machine that must be efficient at all costs.
He also has been encouraging the Catholic Church to help individuals who are seeking forgiveness from a past abortion. In November, he encouraged priests to forgive the “grave sin” of abortion when people are repentant and seeking mercy.
“I wish to restate as firmly as I can that abortion is a grave sin, since it puts an end to an innocent life,” the pope wrote in the letter. “In the same way, however, I can and must state that there is no sin that God’s mercy cannot reach and wipe away when it finds a repentant heart seeking to be reconciled with the Father. May every priest, therefore, be a guide, support and comfort to penitents on this journey of special reconciliation.”
Doctors suggested that Hayley Lampshire may have to abort one of her unborn sons after they discovered the twins shared an amniotic sac and placenta.
The Daily Mail reports the twins’ rare condition put their lives in jeopardy; the survival rate is only about 50 percent. But selectively aborting one of them would have 100-percent denied one child a chance at life.
Lampshire and her husband said they were “heartbroken” when they heard the news, but their hopes were renewed when they saw an ultrasound image of their sons cuddling in the womb.
The British family chose life for their twin boys. Rowan and Blake were born on Aug. 25; they now are home and doing well, according to the report.
Lampshire said she learned about her Monoamniotic-Monochorionic twins when she was 12 weeks pregnant. The condition is rare, but it can be deadly for one or both of the twins.
“Because the boys were in the same amniotic sac, their cords could get tangled if they moved around, which would cut off their oxygen and food supply,” Lampshire explained. “If that did happen then it would be likely that we wouldn’t know, we couldn’t do anything to prevent it which was the scariest part.”
Doctors said the boys would have a better chance of survival if they stayed still, and they did, the family told the Mail.
Ultrasounds of the twins gave the family hope. Lampshire said the images often looked like the boys were holding hands or cuddling inside her womb. She said they also stayed pretty still, another sign that gave her hope.
At 34 weeks of pregnancy, Lampshire said her doctors told her she needed to give birth. If the boys grew any more, their lives could be in greater danger, she explained.
“The boys were born 36 seconds apart, Rowan weighed 2.12kg and Blake weighed 2.05kg, and were taken straight to special care,” she said. “They had fluid on their lungs and were struggling to breathe on their own.”
The twins stayed in the hospital for three weeks before they were allowed to go home, the report states.
“The boys are now doing really well and are growing so fast, and Charlie and I know how lucky we are to have them both here,” their mother said. “When they get older we will tell them how special their bond is.”
She said her boys still like to cuddle, too.
“So far they have been good at sharing, after all it saved their lives, but I’m sure it will be a different story when they get older,” she said.
Lampshire urged other families to not give up hope if their baby or babies have been diagnosed with a risky condition. Doctors say the survival rate is increasing for Monoamniotic-Monochorionic twins, thanks to modern medical advancements.
“Charlie and I were terrified at first, but we want to share our story to reassure others that there is hope, something that we struggled to find when doing our own research,” she said.
Kayla Gaytan, who gave birth to quadruplets and is fighting cancer.
A Tennessee military family received a huge outpouring of support recently after the mother was diagnosed with cancer while carrying quadruplets.
Sgt. Charles Gaytan and his wife, Kayla, welcomed the naturally conceived quadruplets into the world on Dec. 30, but their birth was bittersweet. Doctors delivered the babies early by cesarean section because their mother needed immediate cancer treatment.
The Daily Mail reports the Fort Campbell, Tennessee family is doing relatively well. Kayla currently is undergoing cancer treatments, and the four babies are in the neo-natal intensive care unit. Doctors said the four siblings should be well enough to go home in a few weeks.
Their story attracted national media attention, and a donation fund for the family has received more than $1 million to support them, according to the report.
“It renews my faith in humanity,” Kayla told People. “To know that people that don’t even know us just wanted to help our family is amazing.”
Before the quadruplets were conceived, Kayla was diagnosed with Hodgkin’s Lymphoma, according to the report. The young mother said she went through five months of chemotherapy and was in remission.
Not long after that, the couple was overjoyed to learn that they were pregnant – something doctors told Kayla might never happen. Not only that, but they had conceived quadruplets naturally. Later into her pregnancy, Kayla said she began noticing symptoms of cancer again. Doctors confirmed it, her Hodgkin’s lymphoma had returned.
Though relatively treatable, the cancer can be serious if it returns, according to the report. Doctors gave the Tennessee mother a 50-percent chance of living five years, she said.
“With four babies on the way, I just couldn’t wrap my head around how it could come back,” she said. “I thought I had beat it the first time.”
When she was 30 weeks pregnant, Kayla gave birth to her babies in an emergency C-section. The babies, Lillian, Victoria, Michael and Charles were born weighing between 2 pounds, 8 ounces and 3 pounds, 2 ounces, according to the report.
Doctors immediately began Kayla’s cancer treatment. She said she will have a stem cell treatment and a 16-month round of chemotherapy.
The Gaytan family said they are not giving up hope. With the quadruplets and two older children to care for, Kayla said she and her husband are trusting in God to handle the situation.
“We know that He’s gotta have a different plan up there for us, and surely everything’s gonna work out in the end,” Kayla said.
Earlier this week, the family posted a grateful message on their fundraiser page: “Words cant not even describe how thankful we are. Not even in our wildest dreams could we have ever phantom the amount of support we have received. God Bless everyone of you. From the bottom of our hearts thank you from all the Gaytan family.”
The year 2017 already is bringing strong hopes for future babies in the womb.
World News Service reports state legislators have introduced almost 50 pro-life bills already this year that would increase protections for unborn babies and moms. Pro-life leaders said the November election results kindled new hopes that these protections will pass state legislatures and be upheld in the courts.
“With the election of a pro-life president, with all of the gains that we made across the different states with last year’s election, I think we are very optimistic in passing laws that protect the unborn baby and their moms,” Ingrid Duran of the National Right to Life Committee told the news service.
LifeNews has reported on many of the new bills, including measures that would prohibit brutal dismemberment abortions and late-term abortions after 20 weeks when strong scientific evidence indicates babies can feel pain. Other bills would defund the abortion giant Planned Parenthood.
In Missouri alone, lawmakers introduced dozens of pro-life bills this year, including prohibitions on sales or donations of aborted babies’ body parts, according to the report.
Kentucky lawmakers used the first week of their legislative session to pass two pro-life bills into law. The two new laws prohibit abortions after 20 weeks of pregnancy and require women to receive an ultrasound and the opportunity to see it prior to having an abortion. The ACLU is challenging the ultrasound law.
Arkansas is another example. Gov. Asa Hutchinson signed a bill into law last week that bans brutal dismemberment abortions that rip apart babies in the womb and pull them out in pieces.
Some states previously had Democrat majorities in at least one house that blocked pro-life measures; but in November, that changed. Voters in Iowa and Kentucky, for example, elected new pro-life Republican majorities to both houses, which means pro-life bills are much more likely to pass.
Here’s more from the report:
Last year, lawmakers approved 60 new pro-life laws across the country, and leaders expect more of the same focus this year, simply with more energy.
Eric Scheidler, director of Pro-Life Action League, told me the surge of pro-life bills is a reaction to years of “elitist cultural bullying.” He pointed to President Donald Trump’s choice of pro-life advisers: Vice President Mike Pence, White House counselor Kellyanne Conway, and Attorney General nominee Jeff Sessions.
“It isn’t the person of Trump, but it’s the whole phenomenon and all the people around him and the people he’s appointed. That’s really what’s driving this optimism,” Scheidler said.
Denise Burke of Americans United for Life said there is a lot of hope that President Donald Trump will appoint U.S. Supreme Court justices who will uphold these laws.
“I think there’s increasing confidence among many pro-life allies and legislators that Hellerstedt [the recent Supreme Court decision that struck down Texas abortion clinic regulations] may have a limited shelf life with the potential new Supreme Court,” Burke said. “So we’re seeing a lot of what we’ve seen in the last couple of years, but just with renewed vigor and enthusiasm.”
“I will protect it and the biggest way to protect it is through the Supreme Court and putting people in the court — and actually the biggest way to protect is electing me as president,” he said.
STATE ERIN PARFET JAN 31, 2017 | 2:44PM BATON ROUGE, LOUISIANA
A cool, crisp morning did not stop thousands of pro-life advocates from flooding the streets of Shreveport, Louisiana in the second of three similar weekend events in the Pelican State, KSLA-12 News of Shreveport reported.
“We want to fight for the silent, the ones that can’t speak for themselves,” said Mary Britt, who supported the Louisiana Life March North.
The Shreveport event follows a similar event in Baton Rouge the weekend before, and there will be a third and final pro-life march in Alexandria this weekend. Some estimated the march drew as many as 9,000 pro-lifers to the streets to march in defense of unborn babies’ right to life.
However, abortion supporters also showed up at the event.
“The funny thing is that there are no babies involved in abortion,” stated Debbie Hollis, Vice President for Louisiana’s National Organization for Women, according to KSLA. “The fetus is not even viable until 24 weeks gestation. And we do have a ban at 20 weeks here in Louisiana. So, no one’s killing babies.”
But Hollis’s pro-abortion semantics hide the truth. Whether called a fetus or a baby, the human being in the womb is a totally unique, living human being who deserves a right to life.
A Journal of American Medical Association Pediatrics study demonstrates how premature babies born at 22 to 23 weeks LMP (20 weeks post-fertilization) are surviving at a greater rate than ever before. These very premature babies, when provided “active” care, survived 67 percent of the time until hospital discharge after active care, and 85 percent of them survived without severe complications.
At 20 weeks, a baby’s heart is beating and can feel pain. At 21 weeks, a baby is capable of swallowing, according to the Mayo Clinic. Hair becomes visible at week 22, and footprints and fingerprints at week 23, the Mayo Clinic continues.
“With intensive medical care, some babies born this week might be able to survive,” said the Mayo Clinic of babies born at 23 weeks.
Yet, babies at this stage still can be legally aborted for any reason in many states across the U.S.
“Women do die when they don’t have access to safe, legal abortion,” Hollis continued. “We all know the horror stories that our grandmothers told us before the ’70s.”
This also is a manipulation of the truth. Though the birth process has been the same since the beginning, standards of prenatal care and hygiene have improved since the days of our grandparents and great-grandparents. Blood loss and infection, childbed fever, and postpartum hemorrhage were more common causes of death in generations of yesteryear.
This isn’t to say that some women may not die during childbirth, with a rate of 24 deaths per 100,000 live births, up from 19 deaths out of 100,000 for the years 2000-2014, according to Time Magazine citing the medical journal, Obstetrics & Gynecology. However, the report continues in stating that the World Health Organization determined half of these deaths to be preventable.
There also is evidence that legalizing abortion does not reduce maternal mortality rates. In countries like Ireland and Poland that largely protect unborn babies from abortion, maternal mortality rates are lower than neighboring countries where abortion is legal. Ireland has one of the lowest maternal mortality rates in the world. A study from Chile also found that maternal mortality declined because of better access to health care, not changes in the country’s abortion laws.
In the case of abortion, a life is lost 100 percent of the time: that of the child.
“There’s just absolutely no need in it,” said Betsy Henderson who supported the pro-life march. “There’s other places a baby could go. There’s women that are hurting and they want to have babies.”
According to a Royal College of General Practitioners study, women using oral contraceptives have a five times greater risk of death from cardiovascular causes. 1
Five of the pill’s many deadly side effects are pulmonary embolism, cardiac arrest, hypertensive disease, heart failure and stroke.
In 2004, in the U.S., there were a total of:
3,565 recorded female deaths from pulmonary embolism;
8,065 recorded female deaths from cardiac arrest;
16,445 recorded female deaths from hypertensive diseases;
How many of these women were on the birth control pill? That’s a good question. By looking at the U.S. Standard Certificate of Death, it does not ask if the deceased was using any form of birth control. It does, however, ask if tobacco use contributed to death, so why not ask about the pill?
This is an example of what the U.S. Standard Certificate of Death should look like; currently it does not include a question about the pill being a cause of death. 2
There are serious problems that women face because of the pill, and we must TALK about it and DO SOMETHING about it!
If you are taking the birth control pill or other birth control products you may have…
Increased risk of heart disease
The Department of Biomedical Sciences and Technologies at the University of Udine, in Italy, conducted a study in 2008 that showed the pill increases the risk of heart disease. Women on the pill were over four times more likely to have high levels of CRP (C-reactive protein) and 3.9 times more likely to have levels of CRP high enough to cause an “intermediate risk” for heart disease. 3
Increased risk of breast cancer
In her talk on “A New Beginning” at the 2006 Humanae Vitae Conference, endocrinologist Dr. Maria Kraw discussed the pill’s serious side effects. “Looking at 54 studies of the pill, she observed that researchers found that it caused a 24 percent increased risk of breast cancer.” 4
Increased risk of cerbrovascular disease and cervical cancer
A woman taking the pill is 1.9 times more likely to die from cerebrovascular disease and 2.5 times more likely to die from cervical cancer. This came from a study that was published in 1999 in a British medical journal. “The 25 year follow-up study with 46,000 British women also notes that the enhanced risk of death lasts for 10 years after women have stopped taking the pill.” 5
Increased risk of plaque buildup in arteries
A study on 1,300 women aged 35 to 55 found that the women who take oral contraceptives may have more plaque buildup in their arteries. The study was done in Belgium by researchers at the University of Ghent. It was discovered that every 10 years of oral contraceptive use was connected with a 20–30 percent increase in plaque buildup. 6
Increased risk of raising your blood pressure
Studies done on 60,000 women, 35,000 of whom were taking birth control pills, showed that “a rise in blood pressure occurs in virtually all women who use OCs [oral contraceptives] for [six] months or longer.” The studies also showed an increase in heart attacks and strokes. 7
Increased risk of liver problems
Several cases of liver tumors were found in young women who had been taking oral contraceptives. These case studies took place in the U.S., Great Britain, Italy, South Africa and several developing countries, and they show a connection between tumors of the liver and the use of oral contraceptives. 8
On Friday January 27, well over half a million gathered in Washington to commemorate 44 years since Roe v. Wade made abortion legal nationwide. (2013 was 650,000 and regulars kept telling me this was the biggest crowd ever.)
Many people held printed signs with phrases like “I Am the Pro-Life Generation,” “Stop Abortion Now,” or “[Organization or Church] Supports Life.” But what always impresses me are the handwritten signs that show a personal conviction.
I spent much of the March taking pictures of homemade signs and posting them to Twitter. The morning after, I went through and found the best of those signs for this story.
Here are 29 that I think are totally LIT! Click any for full resolution.
Unplanned Pregnancies can do great things!
No excuse for killing a child
The loving option…
Real social justice!
Every group can be pro-life and this man is a great example of this. (And he shows intersectionality which is a very important concept now in social justice / rights.)
I’m with Both (mom & child).
Whole life pro-life ethic.
Another post with intersectionality pointing out the racist nature of current and historical abortion practice.
Take your chances on life!
Simple.
These people came all the way from Scotland to March with us.
Jesus loves everyone, but the Gospels show a special love for those who’ve fallen.
Love all women!
A Down Syndrome diagnosis should not be a death sentence.
Every life is worth saving… from someone who is vocally pro-abortion.
People are willing to adopt.
Total Nerd. This is from Dr Who (a show involving time travel) if you don’t get it.
We are all former fetuses.
Here’s a real Feminist!
Let’s be there for every mother.
Women deserve better.
Protect all.
Every person is a person… no matter the size.
I am a CHILD.
Chick-fil-A almost got a product placement.
The true safe space.
This should be what people mean when they say All Lives Matter.
Accept the gift.
A prayer from John Paul II
To conclude, I want to make a few notes:
I took every picture and I got permission for those of minors.
Every picture is run through an HDR filter.
You can reuse these pictures on a few conditions: you give me credit (@FrMatthewLC or Fr Matthew P. Schneider, LC), send me a link via social media, and if you want to sell it or use it for advertisement ask me 1st as I want a cut.
(LiveActionNews) – This month, Pampers released a new ad: “A Newborn Journey of Firsts.” Pampers has been known in the past for its beautiful, visually stirring ads that broadcast a pro-life message. A previous ad called babies miracles who “deserve protection” and referred to a baby on an ultrasound screen as a “he” instead of an “it.”
This time, Pampers’s ad — which has already received over 860,000 views on YouTube — opens as a mother lovingly caresses her pregnant belly. The scene switches to an incredible ultrasound where a baby is moving in the womb and, as Pampers puts it, is giving her “first hello.”
Below the video, Pampers writes:
From the first scan to the first cuddle, every first is significant no matter how small they seem. For both baby and mom, it’s a journey full of firsts. And there’s nothing more rewarding than experiencing each and every one together.
And indeed, even though the moment of a baby’s first existence — fertilization — is so small that it can’t be seen by the naked eye, it’s incredibly significant. From that moment, a new, unique, living human being has been created. That human being will never exist again in a different body. All he or she needs is the opportunity to grow and develop. This is the same opportunity that a newborn, a preschooler, and an adolescent need.
Even the liberal Huffington Post agrees, in an article featuring the Pampers ad, that “as soon as fertilization occurs, your baby will begin undergoing thousands of changes over the next 40 weeks.” Note that “fertilization” is named as “your baby’s” first stage of life.
Celebrate, with Pampers, the journey of a baby’s firsts. And see the beauty of human life at its various stages. As the Huffington Post sums it up, “new parents and their babies are in this thing together.”
Yes, from the very first “first moment” of fertilization.
https://youtu.be/p9csq_MujV8
– See more at: http://aleteia.org/2017/01/25/i-had-a-plan-and-a-baby-wasnt-in-it/#sthash.YTLsXSnU.dpuf
After 10 years of charting my cycles, I was a natural family planning fail. And I was furious.
I think I took five pregnancy tests that day. Looking back, it may actually have been seven.
I was chasing a toddler at Mass that bright Sunday morning when I was suddenly hit with the realization that I was off schedule. And by off schedule, I mean, way off schedule. My heart was instantly in my throat and I was in full panic mode by the time we gathered my little chickadees into the car and drove the mile and a half home from church. I didn’t even leave the car, hastily explaining to my husband that I needed to run a quick errand, and I was off to the first of three pharmacies I would descend upon that day.
Each time the test blared neon-light positive, I stared down in disbelief and took another. With each one I found myself more urgently pleading with God that the tests were a fluke, some crazy cosmic joke that would somehow have a different ending. When I was finally defeated, I sat on my bed and cried and cried and I continued to cry for the next few weeks.
I couldn’t have thought of worse timing. I was in the middle of applying for local jobs so I could stop my weekly Ohio-DC plane commute, which had become more and more of a burden to my marriage and children. We were financially strapped. I felt underwater with the kids that I had. And worst of all, six weeks earlier I had lost my beloved mother to a sudden and unexpected brain aneurism. Her death had left me reeling. Not only was I scrambling to secure the childcare she had provided, but I had lost my biggest fan. She was an irreplaceable support in the day-to-day responsibilities of raising a family as a working mother. What would I do with another baby?
This unplanned and unexpected pregnancy crushed me. I was confused. I was heartbroken. I felt let down by God. After 10 years of successfully monitoring and charting my cycles, I was a natural family planning fail. And I was furious.
So I moped. And I was cranky. And I cried. And I felt incredibly and insanely guilty because I knew I had nothing really to mope, cry, and be cranky about. Unlike others in unplanned pregnancy situations, I had a job with great benefits, a husband who was excited for another baby, a house full of baby accessories, and no health problems. And I felt guilty that I felt so terribly bitter about having a baby when I had so many close friends and loved ones who bore the heavy, heavy cross of infertility.
My darkness only lifted when someone finally had the guts to say to the moodiest pregnant woman in the world, “Why are you so upset about this? Isn’t this the point of natural family planning anyway — to leave room for God to work so that he can plan your family?”
And I realized it was true. This pregnancy blindsided me because according to my chart it was simply not possible. It wasn’t part of my plan for my life. But nothing is impossible with God and he knew what I needed. Without knowing it, what I needed was this baby.
My Zelie, now two years old, is my greatest source of joy. She has filled a void we didn’t even know existed and established a unique and irreplaceable place in my family. And I simply cannot imagine my life without her.
Through her, I learned that it’s OK to not be excited about an unexpected pregnancy. Because in the end, that pregnancy is not a “pregnancy”: it’s a bright, sweet, bouncing baby with a name.
Every night when I put Zelie to sleep I tell her the same story: Once my heart was broken and God loved me so much that he sent you to heal my heart and fill our home with joy and laughter. She smiles. And I smile too, content with the realization that God’s plan for my life will always surpass all of my expectations.
Maria Garabis Davis holds a Juris Doctor degree and a BA in theology. A former youth minister and now a practicing attorney, she is the founder and co-owner of the greeting card company Pio Prints (www.pioprints.com). Maria resides in Columbus, Ohio, with her husband and four children.
By Anna Douglas, William Douglas and Alex Daugherty
Star-Telegram Washington Bureau
WASHINGTON
Thousands of members of the anti-abortion movement gathered Friday for a triumphant rally on the National Mall, celebrating its growing clout and rejoicing at the end of the eight-year presidency of Barack Obama that participants said was dismissive of their views.
Vice President Mike Pence promised thousands of anti-abortion activists gathered for the March for Life that Donald Trump’s administration will keep its pledge to name a conservative to the Supreme Court.
Pence, the first sitting vice president in history to address this annual rally, said their movement was on the verge of victory with conservatives in control of both the White House and Congress. And soon a conservative will tilt the balance on the Supreme Court as well.
“Life is winning in America,” Pence said. “That is evident in the election of pro-life majorities in the Congress of the United States of America.”
The crowd erupted in cheers, reflecting what many described as a feeling that victory for the anti-abortion movement was in reach for the first time in more than a decade. Dozens of Texans made the trip to Washington for the march, but many stayed home because they plan to participate in Saturday’s companion march in Austin.
“It feels different. For the first time, the administration is on our side,” said Brenna Lewis, a 22-year-old from Lexington, Kentucky. The full-time employee with Students for Life of America — a national organization that provides training, resources and support for anti-abortion college and high school student groups — handed out “I Am the Pro-Life Generation” signs.
“This is like the Super Bowl for the pro-life movement,” she said
The march began at the Washington Monument following the musical rally and guest speakers, and concludes at the Supreme Court.
Pence called on the spirited crowd to carry out their rally and march with gentleness and to approach women who are pregnant “with generosity, not judgment.”
Lewis was particularly excited for another of the day’s headline speakers: top Trump adviser Kellyanne Conway. In years past, Republican presidents and senior officials have only called in to the conference.
On Friday morning, Trump tweeted that he’s in “full support” of the March for Life.
Trump wrote: “The #MarchForLife is so important. To all of you marching — you have my full support!”
Around the National Mall on Friday, police and security presence was light but March for Life organizers told attendees to expect “airport-like” security screenings near the rally point. Pence’s late-Thursday addition to the speaker lineup likely increased security precautions.
There were counter-protesters, too, as anti-Trump demonstrators tried to hold on to the momentum they built by amassing half a million people on the mall for the Women’s March on Washington the day after the inauguration.
Lewis said she had been confronted at that march last Saturday and was spit on.
“I’ve never heard `F-U’ directed at me so many times,” Lewis said of the experience.
Abortion rights activists were a core part of the coalition that organized the women’s march and sister rallies nationwide. Some Students for Life groups reported that they were not allowed to officially join the women’s march but sporadic “pro-life” signs were visible throughout the crowd.
‘Pro-life is pro-woman’
On Friday, March for Life President Jeanne Mancini said her organization viewed itself as “pro-women.”
“Pro-life is pro-woman. That voice might have been shut out last week,” she said.
Like the women’s march, the March for Life brings together people from around the country.
Steve Hoff, of Charlotte, North Carolina, brought 80 students from Charlotte Christian School. He said the 2017 March for Life was special because Trump and Pence had vowed to appoint a conservative Supreme Court justice who would overturn Roe v. Wade, the landmark case that originated in Texas.
“Donald Trump is on the verge of appointing a pro-life Supreme Court justice,” Hoff said. “So it is much more exciting for us to be here.”
Trump hasn’t been in office long but already he’s made the March for Life “a little more optimistic,” said Ted Hanman.
Hanman attended the event with the Benedictine College drum and flag corps. They entertained the crowd when music wasn’t playing on the stage. About 200 students on five buses made a 24-hour trip from Atchison, Kansas, to Washington for the March.
“It’s about life, man,” said Will Medina, 22, a drummer with the college group. “I feel it’s a little more positive out here today.”
He applauded Trump’s recent executive action bringing back the “Mexico City policy,” which bans foreign organizations that receive family planning aid from the United States from performing or promoting abortion. But, Medina said, “One person (Trump) isn’t enough to change everything.”
Texas voices
Kyleen Wright, president of the Texans for Life Coalition, said she was encouraged by the turnout — and the message delivered — at Friday’s march.
“You could just see the energy in the crowd,” said Wright, of Mansfield. “It’s obviously very exciting to have the president tweeting in support and the Vice President and Kellyanne Conway there.
“I’m gratified people turned out,” she said. “I think that what we needed to do today, we did. Now we keep marching.”
Wright will be among those attending a Texas Rally for Life Saturday in Austin. Participants will start gathering around noon at 18th Street and North Congress Avenue to march to the Capitol for a rally that begins at 2 p.m.
One local youth ministry group was lucky to attend the march after being attacked by a gang of teens earlier in the week. A group of nearly two dozen from St. Elizabeth Ann Seton in Keller was getting off the metro, on their way to the Assumption Catholic Church where they were staying, when they were attacked by a youth gang. The youths were uninjured but the two adults were attacked, one having his nose broken and eye socket possibly fractured.
All were able to attend the march and all are heading home Saturday, said Pat Svacina, a spokesman for the Catholic Diocese of Fort Worth.
Jason Spoolstra, a director of youth ministry with the Catholic Diocese of Fort Worth, led a column of 25 youth and chaperones through the streets of Washington at the March for Life on Friday. The 31-year-old is hopeful that next year he will be marching in celebration instead of protest.
“The size is very impressive this year,” Spoolstra said. “It’s the perfect storm, good weather, people who are passionate and a new administration.”
Spoolstra is hopeful that the Trump administration will overturn Roe v. Wade.
“Abortion is killing an innocent human being,” Spoolstra said, adding that he would show women “mercy” who have an abortion if it’s made illegal instead of punishing them like Trump proposed during the campaign.
“The March for Life is very specific, it’s one cause, and you’re going to get every race, religion, gender or creed out here,” Spoolstra said.
Spoolstra’s cohort of marchers were part of hundreds of thousands in attendance in Washington, and they began their trek to the Supreme Court at the Washington monument after hearing remarks from Pence and Conway. For a while, the group couldn’t move on Constitution Avenue on the National Mall because so many people were trying to march.
“We want to see all human life be protected,” Spoolstra said, adding that he does not support the death penalty and that he votes “Catholic” instead of Democratic or Republican.
One marcher from Texas in Washington, Isela Macias, told The New York Times that she marched in honor of her beliefs, and also as a counter to last weekend’s anti-Trump women’s marches, which she dismissed as just a group of angry people.
Read more here: http://www.star-telegram.com/news/nation-world/national/article129167314.html#storylink=cpy
January 25, 2017 (LifeSiteNews) — A billion is an almost impossible number to comprehend. It’s a thousand million, or a thousand, thousand-thousands. One mathematician speculated that if one billion children made a human tower, it would reach beyond the moon. Counting to a billion would take almost 100 years. A time-traveler going back about a billion minutes would find himself in the time of Jesus.
Researchers released a first-of-its-kind report today estimating that one billion babies have been killed by abortion worldwide in the past 100 years.
They say their findings reveal the “greatest genocide in history,” estimating that about 12.5 million babies continue to be exterminated every year by abortion.
“First motivated by the moral crisis and information shortage represented by abortion, the research quickly became a sobering and sacred task of tabulating how many babies have been exterminated in the greatest deliberate slaughter of human beings in history, far exceeding all wars and democides of what was already the bloodiest century in history,” the researchers state.
Titled “Abortion Worldwide Report: 100 Nations, 1 Century, 1 Billion Babies” the report is the fruit of years of tracking international abortion statistics by Dr. W. Robert Johnston, who began such tracking in 1983, and Mr. Thomas Jacobson, who began in 2002. The report begins with data from 1920 when the former Soviet Union became the first country in the world to legalize abortion. Data came from 136 nations that currently allow a mother to destroy life within her womb.
The report is extensive, covering the history of infanticide and abortion, national policies, a compilation of abortion data, methodologies for estimating missing year data, and fact-based abortion numbers.
Researcher Jacobson, who is the executive director of the Global Life Campaign, defended in a press conference today the use of the word “genocide” to describe the bloodshed against the preborn.
“This is targeting a specific group of people,” he said.
“It is time to end this genocide and become people and nations again who highly cherish and protect innocent human life, pre-born and born, girls and boys, pregnant mothers, and every person until natural death. It is time to change course from being death-loving cultures to life-giving cultures,” he added.
Researchers took issue with abortion estimates from the Guttmacher Institute, a pro-abortion research group and former arm of the abortion giant Planned Parenthood, that 56 million abortions occur worldwide annually. They said the numbers were far too high, and “lacking in credibility.”
Dr. Brian Clowes of Human Life International explained during a press conference today that abortion advocates deliberately inflate abortion numbers to compel leaders in developing countries to accept contraception handouts as a way to bring down abortion numbers.
“The money is not really in abortions,” he explained. It’s in big pharma companies doling out contraceptives to women in developing countries and making $500 a head, what amounts to a $60 billion industry, he said.
“We have to convince these countries using this weapon here, the Abortion Worldwide Report, [and] give them true and solid numbers on the numbers of abortions that are happening [so they won’t be pressured to accept contraception as a solution to a problem that doesn’t exist],” he said.
Among their “general findings” related to the abortion data, they show that:
contrary to claims that legalized abortion can be “safe, legal, and rare,” “once a government authorizes abortion, it never becomes rare, unless they again prohibit or highly restrict it;”
contrary to claims that morality surrounding abortion cannot be legislated to effect change, “government policies, including both laws themselves and the level of enforcement, profoundly affect the level of abortion;” and
the highest levels of abortion ever recorded occurred in communist atheistic countries. In fact, the majority (73%) of known abortions were committed in such countries.
Researchers say the report will be useful in a number of ways.
It will help “nations who prohibit abortion, giving them an abundance of reasons why they should preserve their good policies protecting human life, and not make the same mistake as the United States and most other nations.” It will also be useful for nations that allow abortion, allowing them to see the wisdom in “restor[ing] lawful protection of human life from the moment of conception.”
The researchers make a number of recommendations, aimed at individuals, clergy, churches and synagogues, pro-life organizations, and the governments of nations. Some of these include:
Anyone who cherishes human rights and justice for all, even the least, should “seek to ultimately end abortion for all reasons except to save the life of the mother.”
Individuals should “encourage women who are considering abortion to cherish the life of the child within them. Many women are victimized by abortion, and do not adequately comprehend, at least until afterwards, that they actually took the life of their baby. Choosing life requires addressing physical, emotional, and spiritual needs of women.”
Clergy should be “courageous to preach, teach, speak up, and stand for the sanctity of human life and for the protection of preborn children and pregnant mothers.” They should “deliver a sermon or message, or multiple ones, on these topics every year,” helping their “congregation to understand what the Bible says about the sanctity of life, the evil of abortion, [and] forgiveness available through Jesus Christ.”
Governments in nations banning abortion should “not yield to pressure from regional and international governmental organizations, and in every inter-governmental meeting, uphold the sanctity of human life and marriage whenever they are put to the challenge.”
Governments in nations allowing abortion should “recognize the innocent bloodshed on your land” and “reconsider your policy on abortion, abolish it, and restore your laws protecting human life [from] the moment of conception to natural death.”
Jacobson said that while it “may take many years, perhaps generations” to restore protection of preborn children and pregnant women in every nation, “that is the direction we should be moving.”
“The womb of a woman should be the safest place for a developing baby, not the most dangerous,” he added.
WASHINGTON, D.C., January 25, 2017 (LifeSiteNews) – President Trump’s newly reinstated ban on funding to foreign pro-abortion groups is not just a repeat of old Republican policy it turns out. In fact, it is vastly stronger.
The “Mexico City Policy” has been enacted by Republican presidents since Reagan, and subsequently overturned by Democratic presidents. It bars U.S. taxpayer funding to organizations abroad that perform or promote abortions.
But Trump’s version of the executive order goes even further. Not only does it ban funding to notorious abortion providers such as the International Planned Parenthood Federation and Marie Stopes International, but it could even be used to cut off the United Nations Population Fund (UNFPA).
Steve Mosher, president of the Population Research Institute and one of the world’s leading opponents of population control, said it is “absolutely” more comprehensive than its predecessors, for two main reasons:
It now applies to “global health assistance furnished by all departments or agencies”—i.e., not just USAID family planning programs; and
It now covers “involuntary sterilizations” in addition to abortion.
“It’s a wonderful policy,” Mosher said. “Trump is not just reverting to the policy of previous Republican administrations, but is actually going well beyond it.”
He said if properly implemented, the Trump policy will save more lives than past Mexico City Policies.
Mosher, more than any scholar in the West, has exposed the ravages of China’s forced “one-child” policy and the Communist regime’s forced sterilization of women. Both have been funded through international “family planning” agencies like the UNFPA (United Nations Population Fund), which in turn are funded in part by U.S. taxpayer dollars, especially during Democratic administrations.
International Planned Parenthood Federation (IPPF) and its member associations alone performed 964,325 chemical and surgical abortions worldwide in 2015, according to PRI research analyst Jonathan Abbamonte. He told LifeSiteNews that various abortion-friendly, international “family planning” agencies across the world “collectively received nearly $90 million from 2013-2015 in global health assistance funding from the U.S. Government.”
For its part, IPPF said yesterday that it “will lose $100 million USD” under the Trump policy, which it denigrates as a “Global Gag Rule.”
“Over the years USAID has been a huge supporter of family planning – with a budget of over $600 million per year. Reinstatement [of the Mexico City Policy] will mean that years of progress to increase access to essential services globally, will be lost,” said the IPPF statement.
Defunding more agencies means stopping more abortions
Mosher told LifeSiteNews that by expanding the Mexico City Policy to include all international “health assistance” programs, it becomes easier to stop funding of international groups pushing abortion and sterilization.
“So many health programs are compromised by ‘family planning,’” he said. He cited the theoretical example of an aid organization that offers to provide mosquito netting to a foreign country on the condition that its people take part in programs that incentivize sterilization or promote abortion as part of “family planning.” “Now we get the blanket prohibition on any program that promotes involuntary sterilization.”
PRI’s Abbamonte expanded on the significance of the more comprehensive Trump policy:
This means that the new [Mexico City Policy] not only applies to funding through USAID and the Department of State as it did under the Bush Administration but will now also include global health funding coming from other sources like PEPFAR (the U.S. President’s Emergency Plan for AIDS Relief)—which President Bush had exempted from the [Mexico City Policy]—and various government departments like the Department of Health and Human Services.”
Mosher is bullish about Trump’s “very strong” Mexico City Policy defunding UNFPA, which he says has clearly promoted abortion and “involuntary sterilization” overseas, in places such as China and El Salvador. The UN agency, formed in the 1960s, has evolved into the world’s leading organization promoting liberal population control policies, including abortion and coercive sterilization.
“The UNFPA is telling El Salvador that they need to legalize abortion,” Mosher said, noting that this will disqualify it from receiving U.S. funds under the new Trump executive order.
Mosher said the new policy will also help stop abortion in situations where an international organization claims it does not promote abortion as family planning–so it can receive U.S. funds–when it actually does, which happened in the past with International Planned Parenthood’s Western Hemisphere Region (IPPF/WHR).
“They would not get away with it now,” he predicted.
Say good-bye to UNFPA?
Mosher explained how the comprehensive Trump Mexico City executive order essentially incorporates all the efforts by Republicans over the last 35 years to stop American funding of anti-life policies overseas. One of those reforms is the Kemp-Kasten Amendment, authored in 1985 by pro-life conservative icon Rep. Jack Kemp, R-NY, and Sen. Bob Kasten, R-WI.
Kemp-Kasten was a pro-life reform that banned U.S. foreign aid to any organization operating abroad found to be involved in coercive abortion or involuntary sterilization. The amendment essentially sought to correct loopholes through which coercive abortion and sterilization were funded through U.S. taxpayer funds.
From 1973 on, the United States Agency for International Development (USAID) has followed the Helms Amendment named after the late conservative stalwart Sen. Jesse Helms (R-NC). It bans U.S. government funds for the use of providing abortions as a method of family planning worldwide.
Following the Clinton years, the George H.W. Bush administration determined that the UNFPA’s involvement with China’s abortion and sterilization practices under the Communist dictatorship’s “One Child” policy violated Kemp-Kasten, so Bush barred U.S. funding for UNFPA in 2002.
The renewed ban stood until Obama became president in 2009 and overturned the Bush policy, directing Congress to restore U.S. funding to the UNFPA.
But Trump’s beefed-up Mexico City Policy could end that funding, for at least four to eight more years.
“Kemp-Kasten [the 1985 pro-life appropriations amendment] is written into the [Trump] Mexico City policy,” Mosher said. “Now we have both in the same memorandum. I think this can be used to cut off [U.S.] funding to the UN Population Fund.”
He added, “The UN is involved in [involuntary] sterilization policies everywhere,” citing China, Vietnam and North Korea as examples.
Pro-abortion fury
IPPF/WHR joined a pro-abortion coalition of nearly 140 groups in protesting the Trump Mexico City Policy and essentially swearing off U.S. funds due to the new restrictions.
IPPF/WHC complained that the new Trump policy “prohibits international organizations from receiving U.S. funding for contraception if they provide, counsel, refer or advocate for abortion services. The Rule prohibits these activities even if organizations carry them out with their own non-U.S. funding, and even if abortion is legal in their own country.”
The reinstated Trump policy retains abortion exceptions for rape, incest and life of the mother, according to PRI and other observers familiar with the history of the on-again, off-again Mexico City Policy.
Marie Stopes International, the UK-based “family planning” organization that admittedly commits illegal abortions in numerous countries, claimed NGOs could now be defunded merely for informing women that abortion is legal. They stated:
The Mexico City Policy, re-enacted today on ‘Day One’ of President Trump’s term of office, demands that all non-US international organizations in receipt of US Government funding neither perform nor ‘actively promote’ abortion. This effectively means NGOs forfeit all US aid if they so much as tell a woman abortion is a legal option in her country, refer her to another provider or advocate for abortion rights with their own alternative resources.
According to the organization’s financial statement, Marie Stopes received $1.6 million in non-UK and non-Australian “grants” funding in 2014, and $1.5 million in such grants for 2013. But those are classified as “other overseas” funding and do not reveal how much comes from the U.S. government.
“Exciting times”
Mosher, who sits on Trump’s Catholic Advisory Committee, said part of the reason the new president is bolder than other GOP leaders is that “he’s not afraid of anything,” including the media.
“These are exciting times,” he said. “Trump is going to govern as Trump. Who can get to him?”
Other pro-life advocates celebrated the quick action by President Trump to protect human life abroad, and set their sights on further pro-life reforms under the new administration, after an eight-year draught of abortion-affirming policies under Obama.
“Almost immediately, the Trump administration set to work building a different kind of wall: the one between taxpayers and abortion-on-demand,” said Tony Perkins, president of the Family Research Council, based in Washington, D.C.
Perkins highlighted White House spokesman Sean Spicer’s strong pro-life remarks in his first press briefing. “Not only does this help tear down the financial stronghold that groups like Planned Parenthood have on other nations, but it also sends a message to the world that America recognizes that all human beings have inherent worth and dignity.”
On Monday, President Donald Trump signed an executive order reinstating the Mexico City Policy, which prohibits federal funding from going towards foreign nonprofit organizations that promote or commit abortions. The action comes just one day after the 44th anniversary of the devastating Roe v. Wade decision, which legalized abortion-on-demand in America.
The policy, which was implemented by President Ronald Reagan, will effectively defund International Planned Parenthood Federation and Marie Stopes International. Trump, who has made promises to defund Planned Parenthood and make permanent the Hyde Amendment, took an important step to halt America’s hand in bankrolling abortion overseas.
Rep. Michael Burgess, chairman of the House Subcommittee on Health, praised the move, calling it a crucial step in “advancing pro-life policies and protecting taxpayer dollars.”
“Life is a precious and sacred gift, and we must do all we can to protect it. I applaud President Trump for taking this important action and look forward to continuing to work together in advancing pro-life policies and protecting taxpayer dollars.”
Although nonprofit organizations can keep their funding by complying with the Mexico City Policy, International Planned Parenthood Federation gave up tax dollars when former President George W. Bush reinstated the policy.
Hospitals and clinics throughout Colorado are refusing to comply with Proposition 106, Colorado’s newly passed legalization of doctor-prescribed suicide, StatNews reported.
Medical, disability rights, pro-life and religious groups all campaigned against the deadly measure. The Archdiocese of Denver, Colorado actively campaigned against the initiative, a parallel of Oregon’s doctor-prescribed suicide law, spending upward of $1.6 million in their effort to protect lives, the report states.
However, in November, the suicide measure passed in the polls by a two-thirds to one-third vote, and “victory” was declared within an hour of polls closing, the report continued.
“We are deeply disappointed and concerned about Colorado legalizing doctor-assisted suicide,” Jeff Hunt, Vice President of Public Policy at Colorado Christian University, told the Denver Post. “The fight is not over.”
Indeed the fight isn’t over on the ground, for several of the largest healthcare systems in the state.
Centura Health, the largest hospital system in the Centennial State operated by a partnership between Catholic Health Initiatives and the Adventist Health System, stated it would “opt out” of performing assisted suicides, according to StatNews.
SCL Health, Colorado’s second largest hospital system and rooted in the Catholic faith, issued a statement that patients requesting physician assistance in suicide “will be offered an opportunity to transfer to another facility of the patient’s choice.”
HealthONE, which is not affiliated with any religious groups, also said it will not allow doctor-prescribed suicides in its eight hospitals, according to the report.
The Colorado legislation permits doctors, nurses and pharmacists to decline participation in assisted suicide, euthanasia and similar practices, based on an individual’s conscience, the report continued.
It is noted by StatNews that one third of Colorado’s acute care hospital beds are under the umbrella of various Catholic-based health systems.
UCHealth and Kaiser Permanente allow physician-assisted suicide in their practices and clinics as permitted by state law, the report continued.
“This is a historic day for all Coloradans, and an especially tremendous victory for terminally ill adults who worry about horrific suffering in their final days,” said Barbara Coombs Lee, Compassion and Choices Action Network President in a statement reported by 9News.
“We are delighted the significant investment paid off and are proud to have lent the expertise and resources to empower the voters of Colorado. We congratulate Colorado for becoming the sixth state where more people have peace of mind at the end of life and fewer suffer unnecessarily.”
However, Alan Rastrelli, medical director for Divine Mercy Supportive Care, a non-profit hospice service, expressed different sentiments in an editorial in the Denver Post.
“The harm of physician-assisted suicide to patients and the healing profession of medicine was lamented in 400 BC by the Greek philosopher and physician Hippocrates when he wrote: ‘The regimen I adopt shall be for the benefit of my patients … and not for their hurt or for any wrong. I will give no deadly drug to any, though it be asked of me, nor will I counsel such,’” Rastrelli wrote.
He continued: “The healing profession, with hospice and palliative care, is entrusted with the sacred privilege of assisting their patients compassionately through the dying process, ensuring that patients have the comfort and dignity they deserve. With ‘intensive caring’ we strive to ease their suffering, their fear of death — and their fear of living.”
Rastrelli emphasized that care, not killing, is the answer to help people who are suffering.
“Patients can chooseto forgo life-sustaining interventions that may excessively burden them or prolong the dying process,” he wrote. “They can choose to allow a natural death in the comfort of their home, surrounded by loving caregivers. This is the difference between blowing out the candle vs. allowing it to flicker out on its own. Physicians and nurses are to help the patients as their life is ending, not end their life by an unethical act.”
But overturning Roe would not immediately protect unborn babies from abortion; instead, it would return the power to legislate abortion to the states.
A new report from the abortion advocacy group NARAL predicts that 13 states immediately would ban abortions if the high court overturns Roe.
“This report paints a grim picture of the current status of reproductive freedom in the United States, and if Donald Trump succeeds in appointing Supreme Court justices who overturn Roe v. Wade, our data shows that women will be even worse off,” NARAL President Ilyse Hogue said in a statement.
The 50-state report points out that 11 states currently have laws on the books criminally banning abortion and two more have near-total criminal bans. That means if Roe is overturned after Trump puts an anti-choice justice on the bench, women seeking abortions in Alabama, Arizona, Arkansas, Delaware, Louisiana, Massachusetts, Michigan, Mississippi, New Mexico, North Dakota, Oklahoma, South Dakota, West Virginia could be criminally punished.
This is just an estimate. Analyses vary about state abortion laws post-Roe. Back in 2012, NARAL itself presented a different estimate. Its 2012 report predicted that 17 states would ban abortions if Roe was overturned.
Another estimate by the Center for Reproductive Rights predicted that 31 states and the District of Columbia would ban abortions if Roe were overturned. But a third analysis by attorney Paul Linton in the journal “Issues in Law and Medicine” in 2012 put the estimate at between eight and 11 states, according to research by Dr. Michael New, a political science professor at the University of Michigan–Dearborn.
Here’s more about the latest analysis:
Of course, the downfall of the law guaranteeing women have a right to abortion at least up until viability would drastically jeopardize women in every state’s access to the safe medical procedure, but these 13 states would be even worse. On top of just not being able to go to a clinic to end a pregnancy, women and doctors could literally be fined, go to jail, and/or have a criminal record if they attempt to get or perform the procedure.
This is only partially true. Historically, the pro-life movement and the U.S. legal system have not prosecuted women for abortions, even prior to Roe v. Wade.
While pro-life advocates yearn for the day when unborn children are protected under law and abortions are banned, the pro-life movement continuously has opposed punishing women who have abortions — instead focusing on holding abortion practitioners criminally accountable for the unborn children they kill in abortions. Current abortion bans, such as the ban on partial-birth abortions, do not punish women who have abortions.
The movement tends to view women, who frequently are pressured or coerced into having an abortion, as second victims of the abortion industry. That is how states viewed the issue prior to Roe v. Wade, too, according to research by Clarke D. Forsythe, senior legal counsel for Americans United for Life.
This political claim is not an abstract question that is left to speculation—there is a long record of states treating women as the second victim of abortion in the law that can be found and read. To state the policy in legal terms, the states prosecuted the principal (the abortionist) and did not prosecute someone who might be considered an accomplice (the woman) in order to more effectively enforce the law against the principal. And that will most certainly be the state policy if the abortion issue is returned to the states.
He noted that California and 19 other states had statutes that technically made it a crime for a woman to participate in her own abortion; however, these were not enforced, and even historians who support Roe v. Wade admit this to be true.
January 21, 2016 (LifeSiteNews) – You may have seen the viral photo on Facebook: a beautiful young couple with a baby that looks to be less than a year old, with the husband holding a sign that reads: “Our baby survived his abortion appointment.”
The photo was taken in 2014 at the West Coast Walk for Life, but went viral in the past few days on Facebook after LiveActionNews shared it on their Facebook.
Clearly there is a powerful story behind the photo. Who is that couple? And how exactly was their baby snatched from the jaws of death?
There aren’t a lot of details available online, but a search found a video shot during the 2014 Walk for Life, with a brief interview with the couple. (The interview begins at about 5:22.)
The baby’s name is Cassius. His father is named Caesar, and his mother Selfa.
Caesar briefly recounted the story for the camera. “People tried to convince my wife to have an abortion and she almost did it,” he explained.
“She set an appointment, and the date that he was scheduled for his execution, for him to be aborted, she decided no, she didn’t want to do it.”
“So we continued on, and here we are, against abortion,” concludes Caesar. “This is our family. And we thank God for all the miracles and all the blessings.”
I’d love to find out more details about how Selfa was brought to decide to choose life.
However, theirs is a simple and powerful story of redemption. It is clear that Caesar and Selfa love their child. The evil advice of others, and the easy availability of abortion, could easily have led to a completely different outcome – one that left a dead baby, and bereaved and broken parents.
Hopefully their testimony will give courage and hope to others in similar circumstances. Don’t give in to fear! Don’t listen to the evil advice of others! Choose life. Choose hope. And you won’t ever regret it.
As a labor and delivery nurse, there are countless times I’ve talked with women about the dragging side effects of hormonal contraception. They agree that hormonal contraception is not the best choice, stating, “Oh, I don’t use hormonal contraception. I have an IUD instead.”
Yet the most popular implanted intrauterine devices—commonly known as IUDs—are actually laden with synthetic hormones, similar to the pill, that disrupt the body’s normal hormonal equilibrium and continuum. Copper IUDs also greatly alter the interior workings of the reproductive system.Women who use IUDs may only have a narrow view of the larger picture. Here are five facts about IUDs to know before making a decision that will greatly affect your health.
01. IUDs secrete copper or synthetic hormones into the body.
Let’s start with the basics. An IUD is a small, T-shaped device that is placed into the uterus by a trained health professional during an office visit. It provides continuous birth control for several years depending on which one is chosen.
There are two classes of IUDs: Copper (Paragard) and Hormonal (Mirena, Skyla, Liletta and the new Kyleena). These fall within a larger class of long-acting reversible contraceptives (LARCs). According to the CDC, use of these contraceptives have increased five-fold in the past decade among women aged 15-44 from 1.5% in 2002 to 7.2% in 2013.
Paragard is the only 100% hormone-free IUD. But don’t jump too hastily at this being good news. It works by constantly secreting copper into the uterine cavity. Paragard states that “it interferes with sperm movement, egg fertilization, and possibly prevents implantation” by creating an inflammatory reaction within the endometrial cavity of the uterus. The typical failure rate of a copper IUD is 0.8%.
Hormonal IUDs have a typical failure rate of 0.2%. According to Mirena’s website, it is the No. 1 prescribed IUD in the U.S. It is synthetically coated with 52 mg of the hormone levonorgestrel, a much higher dosage amount than the less popular Skyla that contains 13.5 mg. The newly launched Kyleena IUD contains 19.5 mg levonorgestrel and was created for women who have never had a child before. All three have several mechanisms to prevent pregnancy: thickening of cervical mucus to inhibit sperm passage and survival, and alterations in the endometrium (the lining shed during menstruation). It’s worth noting that the majority of levonorgestrel IUD users are affected by the same hormonal influences as women on the pill.
02. It’s a foreign object.
Our culture is obsessed with what we put in our bodies. From Non-GMO to organic, we all want to be fit, feel well, and be free from the threats of additives. An IUD is a foreign object inserted into the uterine wall that releases foreign chemicals. Most objects placed into the body are there to aid the natural processes of the body, like a heart pacemaker. But an IUD hinders the natural processes of a woman’s body: ovulation, fertilization and sometimes implantation.
Many women report discomfort upon the implantation—for some, it is severe. Cramping is considered par for the course, but in some instances women have reported nausea and dizziness or have even fainted. Another risk of using an IUD is infection. If the infection goes too long undetected, it could cause permanent damage like sterilization.
03. It triples the risk of mental illness.
In women who have had a child, most IUDs are inserted by the 6 week postpartum office visit. Mirena, for instance, is a popular IUD deemed compatible with breastfeeding. Postpartum depression (PPD) can be debilitating for a woman and her family. According to the CDC, about 1 in 8 women experience PPD. Some women struggling with PPD may really be suffering from the side effects of their IUD and may not know it.
Non-postpartum women are also at increased risk for depression. A recent Danish study concluded that “compared with nonusers, users of hormonal contraception had a 40 percent increased risk of depression after six months of use. Some types of contraceptives carried even greater risk. Women who used progestin-only pills more than doubled their risk, for example, while those who used the levonorgestrel IUD (brand name Mirena) tripled their risk.”
04. It creates a loss of hormonal equilibrium.
When asked about noticeable differences with an IUD, one Mirena user shares, “I mostly do not have periods with my IUD. In the rare occasions when I get a period, they are much lighter and shorter when compared to the flow and duration of my periods without the IUD. Pre-menstrual cramps are also much lighter.” The majority of side effects with levonorgestrel-releasing IUDs include changes in uterine and vaginal bleeding which occur about 52% of the time and cessation of menstruation which occurs at least 24% of the time.
Endometrium shedding (i.e., bleeding), increasing estrogen, ovulation, and rising progesterone are all necessary to our overall health. Estrogen, for instance, promotes bone growth while progesterone promotes bone maintenance. If these hormones aren’t reaching their optimal levels each month, over time, lack of estrogen and progesterone can lead to osteoporosis in postmenopausal women.
05. The side effects of an IUD can mask underlying health concerns.
Sometimes IUDs are prescribed to “solve” heavy menstrual periods or debilitating cramps. But IUDs should not be the panacea for abnormalities because it doesn’t fix the underlying problems. Dr. Mary Kotob, a Board Certified OB-GYN in Newport Beach, California, specializes in gynecologic surgery. She has seen firsthand the side effects of IUDs in her patients.
Dr. Kotob notices the opposite outcome when using an IUD to alleviate period-related symptoms. She says “bleeding can increase and so can cramping with menses. I often see patients who have returned to their own doctor’s office requesting the IUD taken out only to be told by a nurse practitioner that they’re doing fine. No ultrasound is done. No labs. She is just advised to put up with it. The bleeding with an IUD can mask other problems such as pregnancy, thyroid disease, ovarian cysts, and precancerous lesions—further investigation is always warranted.” In fact, Human Reproductive Update found that many gynecologists concentrate on simply regularizing bleeding patterns without understanding the underlying hormonal environment.
A woman’s reproductive cycle is a collection of events that need sufficient quality and quantity to nurture and sustain her whole healthy self. It is interesting how gynecology is the only area of medicine where finding the root of the problem is the last answer and, instead, it is “cured” with unnatural remedies. All women deserve to know more about their cycle; only then will we be able to recover our health as it was intended.
In his letter The Gospel of Life, St. John Paul II’s “summa” of the Church’s prolife teaching, he took us to the root of the problem when he insisted that it “is an illusion to think we can build a true culture of human life if we do not … accept and experience sexuality and love and the whole of life according to their true meaning and their close inter-connection” (Gospel of Life 97).
In other words, it’s an illusion to think we will ever overcome the horror of abortion if we aren’t going to the root of the problem, and the root of the problem is that we simply have not “accepted and experienced” the true meaning of sexuality and love and how inter-connected they are with the whole of life.
At its root the abortion debate is not a debate about when life begins or the “rights” of women. At its root the abortion debate is a debate about the purpose and meaning of sex. The reason millions upon millions of children have had their lives ended in the womb is because we don’t understand the beauty and splendor of God’s plan for sex.
And I’m not just saying that the secular world “out there” doesn’t get it. The problem is right here in our own churches, in our own homes, in our own families, in our own lives. Polls of my audiences over nearly 20 years have shown only 1-2 percent of us have been raised with open, honest, normal, healthy conversation about God’s glorious, stupendous plan for sex. And when the hunger of our erotic desires is not fed from God’s banquet, we fill the void with junk food.
It’s time for a detox. It’s time for a new way of seeing, thinking and talking about sexuality. It’s time for healing and sexual redemption. This is why St. John Paul II gave us his Theology of the Body.
(NaturalNews) A new warning has emerged about the use of Gardasil, a vaccine for the human papilloma virus (HPV).
Gardasil (a four-strain HPV vaccine, or HPV4), is typically administered to both boys and girls as young as age 11 to prevent the sexually transmitted disease.
Developed by Merck, Gardasil received FDA approval in 2006. The disease did not become of concern until the 1980s, when research first suggested that there may be a connection between HPV and cervical cancer. However, whether this link actually exists has been a major point of contention. (RELATED: Learn more about the science fraud behind vaccine marketing at Vaccines.news)
As Natural News previously explained, the vaccine has reportedly been linked to severe complications such as cervical cysts, autoimmune diseases, and harm to women’s ovaries. Natural News has also detailed how one of the developers of the HPV vaccine has now disavowed the inoculation, given that that cervical cancer risk is extremely low in the U.S. and that 90 percent of all HPV apparently infections clear up on their own within two years.
The American College of Pediatricians apparently is apparently not so sure. In a statement primarily written by Scott S. Field, MD, the organization cautioned that there may be an association between the HPV vaccine and premature ovarian failure (POF), which is also known as premature menopause. The statement indicates that the POF cases are very rare, however.
“Since licensure of Gardasil in 2006, there have been about 213 VAERS reports…involving amenorrhea, POF or premature menopause, 88% of which have been associated with Gardasil,” the statement asserts. VAERS is the CDC’s Vaccine Adverse Event Reporting System.
Amenorrhea is the absence of menstruation.
The statement also points out that family doctors are probably unaware of the possible link between HPV and premature ovarian failure and therefore may be not be reporting such cases to the CDC’s VAERS network, which could mean that the condition is more widespread.
The pediatricians’ organization statement also calls attention to the issue that before the vaccine was brought to market, “long-term ovarian function was not assessed in either the original rat safety studies or in the human vaccine trials.”
Another issue with Gardasil is a possible flaw in the pre-release safety trials in that the vaccine and the placebo both contained polysorbate 80. The placebo also contained aluminum adjuvant. “Therefore, if such ingredients could cause ovarian dysfunction, an increase in amenorrhea probably would not have been detected in the placebo controlled trials. ”
The College also noted that many of the young girls in the trials were on birth control, “which can mask ovarian dysfunction including amenorrhea and ovarian failure. Thus, a causal relationship between human papillomavirus vaccines (if not Gardasil specifically) and ovarian dysfunction cannot be ruled out at this time.”
The ACP statement calls for additional studies of the effects of Gardasil on rats, further CCD review of the appropriate VAERS reports, and alerting primary care doctors of the possible linkage between HPV and amenorrhea. The feds say that are monitoring the situation and plan to conduct additional safety studies.
As part of the draining the swamp effort, President-elect Trump has named Robert F. Kennedy Jr., a vaccine skeptic, to a committee to study vaccine safety. The committee will have its hands full, in part because the mainstream media, or what Health Ranger Mike Adams calls the “fakestream media,” accepts everything from Big Pharma at face value.
Moreover, a movement appears to be underway for more states to require mandatory HPV vaccinations for pre-teens or teens. Against that backdrop, parents might be well advised to study the American College of Pediatricians statement and review the many articles here on the Natural News website to make an informed decision, along with their healthcare provider, as to what is best for their family.
The last time the CDC recorded a lower abortion rate was in 1971, two years before the U.S. Supreme Court’s Roe v. Wade decision that established a nationwide right for women to have abortions. Abortion was legal in some states at that time.
Boston, MA Women are used to being given a long list of side effects linked to their birth control, so hearing about alleged Implanon side effects is likely nothing new. Some birth control comes with alleged risks such as blood clots, others may increase the chances of pseudotumor cerebri, still others can increase the risk of depression. For its part, Implanon reportedly carries an increased risk of device migration. As a result, Implanon is just the latest birth control to face lawsuits alleging women were put at risk of serious side effects.
Implanon Lawsuits Allege Serious Birth Control Side Effects Because it is a birth control implant rather than an oral medication, Implanon’s alleged side effects are somewhat different from those linked to pills. According to lawsuits filed concerning Implanon, women who have the birth control implant are at an increased risk of having the device migrate, making it irretrievable. This is a problem because some women may use Implanon in the short term but decide to have children later and have the device taken out. Further, Implanon is only meant to be implanted for three years.
If the device cannot be found, it cannot be removed. That puts women not only at a risk of not being able to become pregnant for as long as the device releases progestin in their body, it also means those women could be at a higher risk of side effects linked to the extended exposure to progestin or linked to having a device moving through the body. Among those risks are a reported increased risk of ectopic pregnancy and a risk of vascular damage. Merck’s own Implanon documentation notes that implants have been found in blood vessels, “including a blood vessel in the lung.”
Other side effects linked to Implanon, according to Merck, are mood swings, weight gain, and depressed mood. The drug maker notes that some women may require surgery to remove the implant, if the implant is not found at the insertion site.
“If the implant is not removed, then the effects of IMPLANON will continue for a longer period of time,” the drug label notes.
Merck, maker of Implanon, faces a lawsuit filed by women who allege they were not properly warned about the risks associated with using Implanon. They further allege that Merck and Organon designed and manufactured a defective device, fraudulently misrepresented the birth control implant and breached their warranty.
“The soul is present the moment the active and passive principles of germination coalesce to form a definite entity. We therefore say that from the moment of conception, the soul is present. Our very doctrine of the Immaculate Conception of the Blessed Virgin Mary implies that doctrine. For we say that, from the moment of her conception, her soul was preserved immaculate, or free from any taint of original or inherited sin. Her soul, therefore, was created by God at the moment of her conception and long before human activity in the sense of discernible physical movement.”
“In St. Luke we read that, when our Blessed Lady visited Elizabeth, the latter cried, ‘for behold, when the voice of your greeting came to my ears, the child in my womb leaped for joy’ (Luke 1:44). Even before his birth, St. John the Baptist was able to know by revelation of the presence of the also yet-inborn Christ. And the souls of others are also created at the moment of their conception. The unborn child possesses an ‘earthly existence’ every bit as much as the child lying in a cradle or romping in the streets. It is a living human being from the moment of conception.”
— Fr. Leslie Rumble (1892-1975), pioneer Catholic radio apologist
Excerpt from Radio Replies: Classic Answers to Timeless Questions about the Catholic Faith
Most people don’t know that in order for the body to metabolize the pill, the liver requires extra amounts of the B-complex vitamins, vitamin C, magnesium and zinc. This means that if a woman has been on the pill for years at a time (as many American women are, starting in their 20s or even late teens), she is creating a situation where nutrient deficiency is more likely. Deficiencies, such as iron deficiency or magnesium deficiency, are some of the primary contributors to most disease (others being factors like diet, genetics, stress and toxicity). If you take the pill, consuming a nutrient-dense, healing diet is key for maintaining gut health and preventing deficiency side effects, like fatigue, indigestion, muscle pains and sleep troubles.
2. May Cause or Worsen Candida
While yeast (candida albicans) generally makes its home in the digestive tract, common lifestyle choices like use of birth control pills, taking antibiotics, a diet high in refined grains and sugar, and high stress levels often lead to a candida overgrowth that infiltrates other parts of the body and leads to candida symptoms.
According to the Healthy Women Organization’s website, yeast overgrowth has been closely linked to estrogen dominance in a woman’s body, which is highly influenced by taking the pill. Women who use hormonal birth control (not just the pill but also a patch or ring) may have more yeast infections than those who don’t. (6)
Toxins from yeast overgrowth can lead to a host of other problems, presenting themselves in a variety of manners far beyond the common vaginal infection. For example, symptoms like migraines, infertility, fibromyalgia, endometriosis, psoriasis, PMS, depression and digestive disorders have all been linked to candida yeast overgrowth. The evidence clearly shows that when you address the yeast overgrowth, the symptoms improve or subside. If you do choose to use birth control pills, try an oral contraceptive that’s a progestin-only pill, since these are linked with occurrence of fewer yeast infections. (7)
3. Often Causes Moodiness (Symptoms of Anxiety and Depression)
Does taking birth control pills cause depression or simply worsen moodiness and existing symptoms? There’s evidence that with estrogen and progesterone levels in the body out of their natural equilibrium due to taking the pill, the brain’s response system is consequently altered, leading many to experience psychological side effects. A proportion of women express concern about low sex drive, lack of appetite, helplessness, disinterest and an overall sad disposition while on birth control pills — yet often their doctors tell them, “It’s all in your head.”
A study conducted in Denmark involving more than 1 million women found a notable increase in depression rates among women taking birth control versus women who were not. Progestin-only pills, the transdermal patch and the vaginal ring were all especially tied to higher ratio of depression diagnoses and antidepressant prescriptions. (8) To be fair, however, other studies, such as one published in 2012 in the Archives of Gynecology and Obstetrics, have not found the same correlation, so there seems to be individual differences in terms of the pill’s psychological effects. (9) Some evidence now suggests that most of the side effects of hormonal contraception may actually be a result of a psychological stress response to the practice of contraception (wanting to prevent pregnancy despite having sex). (10)
4. May Increase Cancer Risk
The National Cancer Institute tells us that the risk of developing breast cancer is around one in eight for the general public. (11) But studies done by doctors, such as Chris Kahlenborn, M.D., from Altoona Hospital in Altoona, Penn., indicate that “women who took oral birth control before having their first child have a 44-percent increased risk of developing breast cancer.” If this is true, that would bring your risk of developing breast cancer to one in five, astaggeringly high risk.
According to the Breast Cancer Organization’s website: (12)
“There are concerns that because birth control pills use hormones to block pregnancy they may overstimulate breast cells, which can increase the risk of breast cancer. The concern is greater if you’re at high risk for breast cancer because of: a strong family history of the disease, past breast biopsies showing abnormal cells, or you or someone in your family has an abnormal breast cancer gene.”
There is lots of ongoing debate about the breast cancer-depression link. For example, one study published in Cancer Research found a higher risk for breast cancer among women takinghigh-dose estrogen birth control pills. A review of 54 studies in 1996 found that women have a slightly higher risk of breast cancer while they’re taking birth control pills that contain both estrogen and progestin and during the 10 years after they stop taking the pills. And results from the 2010 Nurses’ Health Study found that use slightly increased risk, especially among women taking triphasic pills, which alter doses of hormones over three stages of the monthly cycle.
Why doesn’t your doctor tell you about this? “There’s tremendous vested interested — drug companies with a lot of money, government agencies who give a lot of money for contraception. It doesn’t make people look good when a study like this comes out,” Dr. Kahlenborn said.
5. Increased Risk for Blood Clots (Pulmonary Problems, Embolism and Thrombosis)
The link between estrogen use and developing blood clots in the veins (called venous thromboembolism) was identified more than 20 years ago. Extensive literature has now been published describing how the risk for embolism increases as estrogen dosages increase. (13) When a clot forms in a deep vein, usually in the leg, it’s called a deep vein thrombosis, and if that clot breaks loose and travels to the lungs, it’s called a pulmonary embolism, which is a serious condition (10 percent to 15 percent of cases cause sudden death). (14) Estrogen seems to increase clotting factors in the blood, making clots more likely.
It’s been found that combination hormonal birth control pills that contain the progestin called desogestrel increase the risk of blood clots more than birth control pills that contain other types of progestin. Birth control pills containing drospirenone are some of the most popular types available and include such brand names as Yaz, Yasmin, Beyaz, Ocella and Zarah. (15)
Shortness of breath, chest pain (particularly with deep breathing), coughing up blood, persistent leg pain, or redness, swelling, or warmth in your lower legs are all signs of clots. The risk is highest among women with family histories of clots, those who smoke and those who are obese/sedentary — so if any of these apply to you, carefully discuss options with your doctor.
Concerned about the impact of rising population numbers, a British environmentalist group is urging United Kingdom residents to have fewer children.
Breitbart reports a new report from Population Matters argues that the predicted population growth in the UK in the next 15 years will put a heavy strain on the economy. According to the environmental group, the expected 5.5 million-person surge could cost the UK billions of dollars for roads, infrastructure and more.
One of the group’s proposed solutions is to promote abortions.
Here’s more from Breitbart:
They claim drivers will waste an extra 12 hours a year on average in traffic delays by 2030, costing the average household £600 [ about $730] a year in lost working time, additional fuel, and the higher cost of delivering goods.
The group is lobbying the government to pour more public money into “family planning” to curb the population boom, including easy access to contraception and abortion. …
Reacting to the report, Chris Packham, the broadcaster and a patron of Population Matters, wrote in The Times:
“In the UK we already have the choice of how many children we have. If we want them to enjoy the natural world — to have a thriving, supportive natural world they will need to survive — we have to recognize that the more of them we have, the more difficult it will be for them to do that.
“We all need breathing room: animals, plants, human beings. We shouldn’t have to compete for it, and we don’t have to.”
Overpopulation fears have been around for hundreds years, coupled with dire predictions about huge populations depleting the world’s resources. These predictions largely have been proved untrue, but they still are being used as excuses to push abortions. In 2015, the New York Times even published an article admitting that overpopulation fears were unfounded.
Steven Mosher of the Population Research Institute wrote at the time:
The article included a video interview with Paul Ehrlich, the author of “The Population Bomb.” He was the butterfly scientist from Stanford who scared tens of millions with the specter of overpopulation—and the population apocalypse that would supposedly result. He predicted that by the 1970’s the “population bomb” would explode—and hundreds of millions of people would starve to death in India and elsewhere. (India is still there, and doing quite well, thank you.)
But America’s “newspaper of record,” as it styles itself, failed to record the horrors themselves. It was woefully incomplete. There was no mention of the human costs when governments made population control a priority. No mention of the savage forced abortions and forced sterilizations that followed. No mention of the killing of baby girls through female infanticide and sex-selective abortion. No mention of the wasted money, the age and gender imbalances that continue to unfold and will take effect for years to come. No mention of how the overpopulation panic helped to fuel the rise of birth control use and abortion.
Even if overpopulation was a problem, killing innocent human beings should never be the answer. The United States and the UK do not allow born children to be killed because of environmental or economic concerns, and they should not let children in the womb be killed either.
WASHINGTON, D.C., January 10, 2016 (LifeSiteNews) — Oklahoma stands at the top and Washington ranks at the bottom of the Americans United for Life’s annual “Life List” released Tuesday that ranks the most pro-life and pro-abortion states in the U.S.
The rest of the top five behind Oklahoma, which was at the top for the second year in a row, in order, are Kansas, Louisiana, Arkansas, and Arizona.
Washington remained the least protective state for the unborn for the eighth consecutive year. They are followed by California, Vermont, New Jersey, and Oregon.
2016 was a record-breaking year for pro-life legislation, with 43 states proposing more than 360 abortion restrictions, including tax funding for women’s health centers that perform abortions, limits on late-term abortions of viable babies, informed consent and ultrasound requirements, outlawing abortions on handicapped babies, banning aborted baby tissue trafficking, and prohibitions on sex-selection or race-selection abortions.
In a press release announcing the “Life List,” AUL Vice President of Legal Affairs Denise Burke denounced the abortion industry for “fighting the kinds of common-sense regulations that protect women.”
The “Life List” and its state-by-state details can be found here.
Meanwhile, the Planned Parenthood-backed Guttmacher Institute gave a far more dismal year-end review. “2016 was a bad year for women’s health,” the Guttmacher report states, pointing out 50 new abortion restrictions in 18 states. “A total of 338 laws that restrict reproductive rights have been enacted since the Republicans took control of the majority of state governments in 2010.”
The Center for Reproductive Rights, while reporting on the pro-life gains, noted that the strongest pro-life bills were stopped by the courts. “State or federal courts ultimately blocked many of the onerous provisions, a circumstance that underscores how important the judiciary is in protecting women’s rights.”
The most devastating blow to pro-life laws in 2016 was the U.S. Supreme Court ruling that overturned Texas’ safety regulations for abortion clinics, requiring emergency access, and hospital admission privileges.
Burke says, however, that the high court’s ruling is not insurmountable. “When the Supreme Court rejected Texas’ abortion safety standards, abortion advocates celebrated, but they ignored the fine print,” she said. “In fact, the Court found that such laws could survive a legal challenge if well-supported by medical evidence.”
AUL is working to provide that evidence, creating research statistics and pro-life resources for lawmakers to successfully make their case and win in court. The organization’s new and unique report, entitled, “Unsafe,” documents substandard conditions in abortuaries across the country.
“This groundbreaking report will equip legislators as they argue for better and more comprehensive pro-life protections,” Burke explained. Additionally, AUL has formulated model legislation for states that addresses the Supreme Court’s reservations.
The “Unsafe” report documents 227 abortion businesses in 32 states that were cited for more than 1,400 health and safety violations between 2008 and 2016. “Unsafe” also exposes more than 750 significant violations of state laws regulating abortion.
“Legislators … will be empowered in 2017 with new and updated model legislation, new analysis in Unsafe, and new tools for exposing substandard abortion care and remedying it through better inspections and more comprehensive health and safety mandates,” Burke said. AUL has also drafted a model letter for lawmakers to call for inspections of abortion businesses in their states.
Ultimately, the tragic reality that abortion supporters will never view pro-life laws the same way those who value the sanctity of innocent human life do was summed up by Betty Cockrum, president and CEO of Planned Parenthood of Indiana and Kentucky:
“The law does not value life,” the pro-abortionist said, “it (only) values birth.”
CLACTON-ON-SEA, United Kingdom, January 7, 2016 (LifeSiteNews) – Bella Moore-Williams is being hailed as “a Christmas miracle” by the headline-hungry British press. There is no question that the two-year-old’s survival last July is an answer to fervent prayer and has confounded medical expertise.
Now Bella is far enough along in recovery for her mother Francesca to tell The Daily Mail, “She made our family complete and it’s great to see how well she is doing.” Pictures show Bella standing on her own with a wide grin on her face, and beaming just as much in her parents’ arms. “When she says ‘Mama’ it just melts my heart.”
Diagnosed with mitochondrial disease in July after showing a steady decline in energy and motor ability, the second child of Francesca and Lee Moore-Williams of Clacton-on-Sea was first treated for asthma. But after the girl declined further while on a family holiday, doctors at a Colchester hospital told the parents their daughter had the degenerative genetic disease that would shortly lead to her death.
But mitochondrial disease is hard to identify, and an alternative diagnosis was proposed by staff – a long shot, but one with hope – which was that Bella had biotinidase deficiency. Only two cases a year happen in all of the United Kingdom, the family were told, but fortunately, one of the cases six years earlier was at Colchester and presented similar symptoms. The disease prevents cell growth.
The treatment was simple: injections of Biotin, or Vitamin H. After a month Bella was taken off her ventilator but had immediately to be reconnected. The treatment had not worked, making staff think that their original diagnosis was correct. “We were told three times that she’s not likely to survive, so every day we sat at her bedside praying,” her mother recalls.
The couple agreed to take no heroic measures to sustain their daughter and set the date of July 21 with hospital staff to take her off life support. The extended family gathered to say goodbye, one by one. On the appointed day, the Moore-Williamses posed with son Bobby for one last picture at their daughter’s bedside before giving staff the go-ahead to shut off Bella’s ventilator.
Then came the answer to prayer. They thought they were watching her breathe her last breaths, and they wept. Instead, after 30 minutes, her oxygen levels were up to 100%, and she was doing it on her own. “It’s just amazing,” said Mrs. Moore-Williams. “It’s like we have won the lottery.”
The same hospital staff who had counseled them to prepare for Bella’s death now fought for her life. After three days, her energy was back to normal. After three weeks, she was ready to go home and after another nine to go off her infection-fighting medications. Now she takes four tablets of Biotin daily and will continue to do so, says her mother, “for the rest of her life.”
Bella now
“She’s now learning to talk,” Mrs. Moore-Williams says, “and her hair is growing back and she’s even walking. She’s about eight months behind where she should be but doctors are confident she will pick up quite quickly. She’s at nursery and to look at her you wouldn’t think she’s been through what she has.”
Congress approved legislation to defund the Planned Parenthood abortion business last year only to see pro-abortion President Barack Obama veto it. Today, a leading pro-life me member f the House of representatives introduced a bill to yank taxpayer funding from the nation’s biggest abortion company.
Pro-life Congresswoman a registered nurse and member of the recently concluded Select Investigative Panel on Infant Lives, reintroduced H.R. 354 today – the Defund Planned Parenthood Act of 2017.
The legislation would prioritize preventive healthcare over elective abortion by placing a one year moratorium on all federal funding for Planned Parenthood, including its affiliates and associated clinics, until such time as Planned Parenthood certifies that it will not perform elective abortions or give funding to entities that do. The bill was introduced with the support of 127 cosponsors.
The legislation would instead redirect federal dollars to the more than 13,500 community health centers nationwide that provide a broader range of healthcare services to women (e.g., mammograms) and do not perform abortions. The bill provides $235 million in funding for community health centers, in addition to the funding that would be reallocated from Planned Parenthood.
Black released the following statement: “Planned Parenthood’s grand deception is quickly collapsing. For too long, this organization has cashed in on our tax dollars – to the tune of more than $550 million a year – all while performing more than 320,000 abortions during the same length of time. Abortion is not healthcare, yet it is the centerpiece of Planned Parenthood’s mission. What’s more, legitimate questions persist about Planned Parenthood’s compliance with federal law and regulatory guidelines, as evidenced by the work of our Select Investigative Panel on Infant Lives and the Senate Judiciary Committee’s recent decision to refer Planned Parenthood to both the Department of Justice and the FBI,” said Congressman Diane Black. “Our unified pro-life government is proof that Americans have rejected Planned Parenthood’s callous extremism. Now, it is our time to act. Planned Parenthood President Cecile Richards should consider the introduction of this bill as her notice: the days of her organization receiving a free ride from taxpayers and a blind eye from Washington are coming to an end.”
Black added, “From my years on the frontlines of the pro-life movement, I know the scare tactics that Planned Parenthood will use when speaking about this bill, so let me be very clear: My legislation does not cut a single dime from public health funding. In fact, this bill provides an additional $235 million for our nation’s community health centers. For Planned Parenthood or others to claim that our legislation blocks access to preventive care is an outright lie. This is about promoting true women’s healthcare over elective abortion and honoring the conscience rights of American taxpayers who don’t want their tax dollars used to fund a scandal-ridden abortion enterprise.”
Leading pro-life groups that also support the reconciliation bill to de-fund Planned Parenthood include Susan B. Anthony List, National Right to Life, Family Research Council, March for Life, Concerned Women for America, Students for Life, Priests for Life, Operation Rescue, and American Life League, among others.
The expose’ videos catching Planned Parenthood officials selling the body parts of aborted babies have shocked the nation. Here is a list of all eleven:
In the first video: Dr. Deborah Nucatola of Planned Parenthood commented on baby-crushing: “We’ve been very good at getting heart, lung, liver, because we know that, so I’m not gonna crush that part, I’m gonna basically crush below, I’m gonna crush above, and I’m gonna see if I can get it all intact.”
In the second video: Planned Parenthood’s Dr. Mary Gatter joked, “I want a Lamborghini” as she negotiated the best price for baby parts.
In the third video: Holly O’Donnell, a former Stem Express employee who worked inside a Planned Parenthood clinic, detailed first-hand the unspeakable atrocities and how she fainted in horror over handling baby legs.
In the fourth video: Planned Parenthood’s Dr. Savita Ginde stated, “We don’t want to do just a flat-fee (per baby) of like, $200. A per-item thing works a little better, just because we can see how much we can get out of it.” She also laughed while looking at a plate of fetal kidneys that were “good to go.”
In the fifth video: Melissa Farrell of Planned Parenthood-Gulf Coast in Houston boasted of Planned Parenthood’s skill in obtaining “intact fetal cadavers” and how her “research” department “contributes so much to the bottom line of our organization here, you know we’re one of the largest affiliates, our Research Department is the largest in the United States.”
In the sixth video: Holly O’Donnell described technicians taking fetal parts without patient consent: “There were times when they would just take what they wanted. And these mothers don’t know. And there’s no way they would know.”
In the seventh and perhaps most disturbing video: Holly O’Donnell described the harvesting, or “procurement,” of organs from a nearly intact late-term fetus aborted at Planned Parenthood Mar Monte’s Alameda clinic in San Jose, CA. “‘You want to see something kind of cool,’” O’Donnell says her supervisor asked her. “And she just taps the heart, and it starts beating. And I’m sitting here and I’m looking at this fetus, and its heart is beating, and I don’t know what to think.”
In the eighth video: StemExpress CEO Cate Dyer admits Planned Parenthood sells “a lot of” fully intact aborted babies.
The ninth video: catches a Planned Parenthood medical director discussing how the abortion company sells fully intact aborted babies — including one who “just fell out” of the womb.
The 10th video: catches the nation’s biggest abortion business selling specific body parts — including the heart, eyes and “gonads” of unborn babies.The video also shows the shocking ways in which Planned Parenthood officials admit that they are breaking federal law by selling aborted baby body parts for profit.
Unreleased Videos: Unreleased videos from CMP show Deb Vanderhei of Planned Parenthood caught on tape talking about how Planned Parenthood abortion business affiliates may “want to increase revenue [from selling baby parts] but we can’t stop them…” Another video has a woman talking about the “financial incentives” of selling aborted baby body parts.
The 11th video: catches a texas Planned Parenthood abortionist planning to sell the intact heads of aborted babies for research. Amna Dermish is caught on tape describing an illegal partial-birth abortion procedure to terminate living, late-term unborn babies which she hopes will yield intact fetal heads for brain harvesting.
A newly-born baby boy was rescued by a Catholic church employee on Wednesday shortly before mass at the Cathedral of St. Paul in St. Paul, Minnesota, Fox9 News reports.
“I am profoundly grateful that this beautiful baby is healthy and safe and whomever dropped him off at the Cathedral felt that this was a safe place where he would receive the care he needs and deserves as a child of God.” Father John Ubel, leader of the cathedral, told local media.
The baby had been wrapped in a green fleece blanket and left in a plastic laundry basket in a hallway of the church, Fox9 News reported. His faint cries alerted a church employee to investigate the basket. The baby was subsequently transferred to the local children’s hospital, and will be released to country child welfare officials following his hospitalization.
While waiting for the police to arrive at the church, the child was christened “Nathan John” by the local congregation and baptized, according to the report.
Unfortunately, there is no database or organization tracking the number of babies surrendered via Safe Haven laws, according to Fusion. These laws allow parents who feel they cannot care for a newborn to leave the baby at a police station, fire house or hospital without fear of recourse.
However, grassroots activists and other volunteers estimate 3,000 babies have been saved since the inception of the law in Texas in 1999, which has since been ratified in varying forms in each of the remaining 49 states.
Indiana recently developed the concept of “baby boxes” where mothers can anonymously drop off their newborn children in approved locations at local fire stations as an extension of the already existing Safe Haven laws, according to NBC News. The boxes include protection from the climate and the surroundings, and allow the mother the opportunity to uphold the law without having direct conversation with emergency, hospital or law enforcement personnel.
The St. Paul Police state that no crime was committed in leaving the child at the cathedral, despite it not being a traditional drop off site under Minnesota’s Safe Haven laws, according to Fox9 News.
Furthermore, the St. Paul Police used the situation to remind and encourage parents to call 911 or go to the local hospital if there are any concerns with the ability to care for the welfare of their children.
This statement in support of Humanae Vitae, the Catholic Church’s traditional teaching on love, sexuality, and contraception, is entitled “Affirmation of the Church’s Teaching on the Gift of Sexuality.” It was released at a press conference at the Catholic University of America on September 20, 2016.
We, the undersigned scholars, affirm that the Catholic Church’s teachings on the gift of sexuality, on marriage, and on contraception are true and defensible on many grounds, among them the truths of reason and revelation concerning the dignity of the human person.
Scholarly support for the Church’s teachings on the gift of sexuality, on marriage, and on contraception has burgeoned in recent decades. Moreover, institutes and programs supporting that teaching have been established all over the world. Even some secular feminists and secular programs have begun to acknowledge the harms of contraception.
These facts, however, seem to have escaped the notice of the authors of “On the Ethics of Using Contraceptives” (hereafter, the Wijngaards Statement) which urges the Catholic Church to change its teaching and issue an “official magisterial document [that] should revoke the absolute ban on the use of ‘artificial’ contraceptives, and allow the use of modern non-abortifacient contraceptives for both prophylactic and family planning purposes.” The Wijngaards Statement, unfortunately, offers nothing new to discussions about the morality of contraception and, in fact, repeats the arguments that the Church has rejected and that numerous scholars have engaged and refuted since 1968.
The Wijngaards Statement seriously misrepresents the authentic position of the Catholic Church. Among the most erroneous claims made by the Wijngaards Statement is that neither Scripture nor natural law offers any support for the Church’s teaching that contraception is never compatible with God’s plan for sexuality and marriage. During the past half century, there has been an enormous amount of creative scholarly thinking around the Church’s teaching on contraception, thinking that includes profound reflections on the Theology of the Body, personalism, and natural law. In addition, there has been extensive research on and analysis of the negative impact of contraception on individuals, relationships, and culture.
The Wijngaards Statement, rather than engaging recent scholarship in support of the Church’s teaching, misdirects the conversation from the start by claiming that the argument against contraception in Humanae Vitae is based primarily on “biological laws.” Humanae Vitae instead focuses, as it should, on the person’s relationship to God and to other persons.
The points below briefly outline the true basis of the Church’s teaching that contraception is not in accord with God’s plan for sexuality and marriage. It also responds to some of the erroneous claims found in the Wijngaards Statement.
1. God is Love
The God who made this beautiful and ordered world is a loving and good God. All of His creation is a loving gift to humankind. Even after the Fall, God continued to reach out to His people, gradually revealing Himself and the depths of his love and mercy. God the Father’s gift of His Son Jesus, whose life was poured out on the Cross, was the ultimate and complete self-gift. This great and radical love is borne out in Scripture where the biblical authors in the Old Testament often speak of God in the image of husband and His people as His wife, and in the New Testament where Christ is described as the bridegroom and the Church as His bride. Throughout the history of the Church, many have seen this spousal imagery as a key to understanding God’s relationship to every human soul.
2. Made in God’s Image
Because God is Love – a communion of Divine Persons– He made men and women in His image: able to reason and to choose freely, with the capacity to love and to be in loving relationships.
3. Gift of Self
God invites all people to share in His love. Every person, therefore, is beloved by God and made to be in loving relationships; every person is created to make a gift of self to God and to others. The gift of self means living in a way that promotes the good of everyone, especially those with whom one is in close relationship.
4. Marriage: A Unique Communion of Persons
Marriage was designed by God to enable a man and a woman to live out humanity’s core identity as lovers and givers of life, to enable the two to become “one flesh” (Gen. 2:24) and for that one flesh to “be fruitful and multiply and fill the earth” (Gen. 1:28). Human sexual relations fulfill God’s intent only when they respect the procreative meaning of the sexual act and involve a complete gift of self between married partners.
5: God’s Law, not Man’s
“The doctrine that the Magisterium of the Church has often explained is this: there is an unbreakable connection between the unitive meaning and the procreative meaning [of the marital act], and both are inherent in the marital act. This connection was established by God and human beings are not permitted to break it through their own volition.” (HV12) The teaching that contraception is always against God’s plan for sexuality, marriage and happiness is not based on human law: “The teaching of the Church about the proper spacing of children is a promulgation of the divine law itself.” (HV 20)
6. Faith and Reason
God has revealed the truths about sexuality to human beings through the biblical vision of the human person and has also made it accessible to our reason. Several well-argued versions of “natural law” defenses support the Church’s teaching that contraception is not in accord with God’s plan for sexuality and marriage. Each begins with different basic truths and thus each constructs its arguments differently.
7. The Theology of the Body: Saint John Paul II’s Contribution
Saint John Paul II’s Man and Woman He Created Them: A Theology of the Body (virtually ignored by the Wijngaards Statement) provides a powerful defense of the view that contraception is not in accord with the understanding of the human person as conveyed by Scripture and sacred Catholic Tradition. He speaks of the “language of the body” and has shown that to violate the procreative meaning of the marital act is also to violate the unitive (the “commitment-expressing”) meaning of the marital act. There he demonstrates that our very bodies have a language and a “spousal meaning” — that they express the truth that we are to be in loving and fruitful relationships with others.
8. Humanae Vitae as Prophetic
Humanae Vitae speaks against the distorted view of human sexuality and intimate relationships that many in the modern world promote. Humanae Vitae was prophetic when it listed some of the harms that would result from the widespread use of contraception. Abundant studies show that contraception, such as hormonal contraceptives and intrauterine devices, can cause serious health problems for women. The widespread use of contraception appears to have contributed greatly to the increase of sex outside of marriage, to an increase of unwed pregnancies, abortion, single parenthood, cohabitation, divorce, poverty, the exploitation of women, to declining marriage rates as well as to declining population growth in many parts of the world. There is even growing evidence that chemical contraceptives harm the environment.
9. A Practical Help to Husbands and Wives–FABMs
In order to live God’s design for married love, husband and wife need moral family planning methods. Fertility Awareness Based Methods of Family Planning (or FABMs, i.e., the many forms of Natural Family Planning) respect the God-given spousal union and the potential to procreate. FABMs are fully consistent with the Church’s teaching on marital chastity. Couples using these methods make no attempt to thwart the power of acts that could result in the procreation of new human persons. They respect God’s design for sexuality; they help individuals grow in self-mastery; they have the potential to strengthen marriages and respect the physical and psychological health of women. Moreover, science demonstrates that they are highly effective both in helping couples limit their family size when necessary and conceive when appropriate.
10. Respect for Cultural Values, Freedom
International organizations and governments should respect the values and beliefs of families and cultures that see children as a gift, and, therefore, should not impose—on individuals, families, or cultures—practices antithetical to their values and beliefs about children and family planning. Governments and international organizations should make instruction in Fertility Awareness Based Methods (FABMs) of family planning a priority. FABMs are based on solid scientific understanding of a woman’s fertility cycle, are easily learned by women in developing countries, are virtually without cost, and promote respect for women.
11. Christ provides grace
Because of Original Sin, men and women became subject to temptations that sometimes seem insuperable. Christ came not just to restore our original goodness but to enable us to achieve holiness. The Catholic Church invites married couples to participate in the life of Christ, to participate in the sacraments, especially in Reconciliation and Holy Eucharist. The Church asks the faithful to deepen their relationship with the Lord God the Father, to be open to receive the direction of the Holy Spirit, and to ask Christ to provide the graces needed to live in accord with God’s will for their married lives, even the difficult moral truths.
We, the undersigned Catholic scholars, hold that the Church’s teaching on contraception is true and defensible on the basis of Scripture and reason. We hold that Catholic teaching respects the true dignity of the human person and is conducive to happiness.
Johanna Morton was 12 weeks pregnant when she went in for an ultrasound anticipating good news, only to find out her baby’s heart was malfunctioning, Catholic Online report.
“I was 12 weeks gestation when we were told something was wrong with my baby’s heart. I was told she will not survive. ‘You will miscarry.’ I left the office in tears and heart broken,” Morton said on Facebook. “My baby fought her way to 18 weeks as her heart beat slower and slower. With each new appointment seemed to come another diagnosis, another heartbreak and a waterfall of tears.”
Morton’s GoFundMe page elaborates on her daughter’s diagnosis: congenital heart defect (CHD) and heterotaxy syndrome including a full heart block, atrioventricular (AV) canal defect, and valve defects. The prognosis was poor, according to doctors, who did not expect the baby to live past 18-20 weeks gestation.
Congenital heart defects affect nearly 1 in 100 children, according to the John Hopkins Heart & Vascular Institute. Over 75% of babies with critical CHD prenatally will be “terminated for medical reasons,” The Federalist reports. The New York Times recently covered the story of a California mother justifying the late term abortion of her child missing half his heart.
As in many instances of pediatric heart defects, doctors pressured Morton to abort the child.
“I was told ‘She’s going to be stillborn, Save [sic] yourself the pain,” Morton said on Facebook.
“I wouldn’t be surprised if you come back next week, and have her stillborn.’ There was little to no hope for my baby. Even the number #1 children’s hospital, had not seen a heart like hers.”
Yet, Morton opted to give her baby a chance to live.
Baby Clara Ray Morton was born at 37 weeks, and underwent open heart surgery at Boston Children’s Hospital, Catholic Online reported. Clara was able to go home with her family soon after, and has been thriving.
Despite oxygen tubes taped to her face, many photographs circulating Facebook and the internet show Clara’s face smiling in delight as she enjoys the view of the snow falling outside the window.
“This is her seeing her first snowfall,” Morton wrote. “She absolutely loved it. I can’t explain the emotions we felt, as we watched that smile come across her face. Pure. Joy.”
Mexico City, Mexico, Dec 31, 2016 / 02:33 pm (CNA/EWTN News).- Sister Lucia dos Santos, one of the three children who witnessed the Marian apparitions at Fatima, died in 2005. But before her death, she predicted that the final battle between Christ and Satan would be over marriage and the family.
So says Cardinal Carlo Caffarra, who reports that the visionary sent him a letter with this prediction when he was Archbishop of Bologna, Italy.
This reported statement by Sister Lucia, expressed during the pontificate of Saint John Paul II, was revisited earlier this year by the Desde la Fe (From the Faith) weekly of the Archdiocese of Mexico, in the midst of the debate generated by President Enrique Pena Nieto, who announced his intention to promote gay marriage in this country.
The Mexican weekly recalled the statements that Cardinal Caffarra made to the Italian press in 2008, three years after the death of Sister Lucia.
On February 16, 2008, the Italian cardinal had celebrated a Mass at the tomb of Padre Pio, after which he gave an interview with Tele Radio Padre Pio. He was asked about the prophecy of Sister Lucia dos Santos that speaks about “the final battle between the Lord and the kingdom of Satan.”
Cardinal Caffarra explained that Saint John Paul II had commissioned him to plan and establish the Pontifical Institute for Studies on Marriage and Family. At the beginning of this work, the cardinal wrote a letter to Sister Lucia of Fatima through her bishop, since he could not do it directly.
“Inexplicably, since I did not expect a reply, seeing as I had only asked for her prayers, I received a long letter with her signature, which is now in the archives of the Institute,” the Italian cardinal said.
“In that letter we find written: ‘The final battle between the Lord and the kingdom of Satan will be about Marriage and the Family.’ Don’t be afraid, she added, because whoever works for the sanctity of Marriage and the Family will always be fought against and opposed in every way, because this is the decisive issue. Then she concluded: ‘nevertheless, Our Lady has already crushed his head’.”
Cardinal Caffarra added that “speaking again with John Paul II, you could feel that the family was the core, since it has to do with the supporting pillar of creation, the truth of the relationship between man and woman, between the generations. If the foundational pillar is damaged, the entire building collapses and we’re seeing this now, because we are right at this point and we know it.”
“And I am moved when I read the best biographies of Padre Pio,” the cardinal concluded, “about how this man was so attentive to the sanctity of marriage and the holiness of the spouses, even with justifiable rigor at times.”
Yesterday, the Catholic Benefits Association and the Diocese of Fargo filed a lawsuit challenging federal rules that require Catholic hospitals and healthcare providers to perform gender transition procedures and abortions contrary to their own medical judgment and Catholic values.
The new rules also require Catholic dioceses, religious orders, and other Catholic employers to cover gender transition surgeries and their group insurers to cover surgical abortions in their health plans. These rules are part of a multi-agency effort to redefine the term “sex” in federal antidiscrimination laws.
“For decades, Congress and the courts have understood the term ‘sex’ in federal law to mean biological sex – male and female,” explained Archbishop William Lori, Chairman of the Catholic Benefits Association (CBA). “By redefining ‘sex’ to mean both ‘gender identity’ and ‘termination of pregnancy,’ the Obama administration is not only trying to sidestep Congress and impose radical new healthcare mandates on hospitals and employers, it is creating a moral problem for Catholic employers that must be addressed.”
Pope Francis has reiterated Catholic teaching on both the sanctity of life for all—including the unborn—and on the theories stating that gender is mutable or fluid. Such “gender theory,” the Pope said last year, “does not recognize the order of creation.”
The lawsuit takes aim at regulations issued earlier this year by the Department of Health and Human Services requiring Catholic healthcare providers to ignore their own medical judgment and perform gender transition surgeries. Among the newly mandated procedures are a penectomy (removal of penis), metoidioplasty (creation of penis, using clitoris), vaginectomy (removal of vagina), and vulvectomy (removal of vulva).
“HHS’s own experts agree that these procedures can harm patients with gender dysphoria in ways that are often irreversible,” said Douglas Wilson, the CBA’s CEO, who spent decades in healthcare administration before joining the CBA last year. “So, even as HHS is requiring doctors to perform these surgeries, it has chosen not to mandate coverage of the same procedures in Medicare and Medicaid. This is blatant hypocrisy coupled with shoddy science.”
“Catholic hospitals provide compassionate care to everyone, regardless of status. Patients experiencing gender dysphoria deserve no less,” Wilson said. “The prime ethic of any healthcare provider is do no harm. These regulations do the opposite.”
Similar rules issued by HHS and the Equal Employment Opportunity Commission (EEOC) require employers to cover gender transition surgeries in their group health plans. None of the HHS or EEOC rules has a religious exemption or a grandfathered plan exemption. This means that institutions across the Catholic spectrum–dioceses, religious institutes, private schools, colleges, hospitals, and closely held businesses–-are required to perform or pay for medical procedures that directly contradict Catholic teachings.
“This continued assault on religious freedom by the Obama administration is mystifying,” remarked Martin Nussbaum of Lewis Roca Rothgerber Christie LLP, CBA’s General Counsel, who is also representing the CBA in the lawsuit. “Even assuming the government has a sound basis for these rules – and it doesn’t – it can accomplish its objectives in other ways. HHS and EEOC shouldn’t be conscripting the Catholic Church to advance their political agenda.”
In the lawsuit, the CBA seeks to invalidate HHS regulations issued under Section 1557 of the Affordance Care Act and EEOC rules purporting to interpret Title VII of the Civil Rights Act of 1964. The plaintiffs assert violations of the Administrative Procedure Act, the Religious Freedom Restoration Act, the First Amendment, and other federal laws. The lawsuit was filed in federal district court in North Dakota.
The Catholic Benefits Association is a group of employers committed to providing life-affirming health coverage consistent with Catholic teaching. Directed by seven archbishops and four laypersons, it consists of over 880 Catholic employers (including hospitals, colleges, religious orders, businesses, and over 60 archdioceses and dioceses,) plus over 5,000 parishes, together covering over 90,000 employees and their families.
Hearkening to the birth of Jesus Christ, Pope Francis used his Christmas message to urge Catholics worldwide to express compassion for those “not allowed to be born.”
Speaking to tens of thousands of Catholics in Saint Peter’s Square, the head of the Catholic Church asked worshipers to celebrate “the fragile simplicity of a small newborn.”
“Let us allow ourselves to be challenged by the children who are not allowed to be born, by those who cry because no one satiates their hunger, by those who do have not toys in their hands, but rather weapons,” he said.
Referring to the meaning of Jesus’ birth, Francis said: “Today this message goes out to the ends of the Earth to reach all peoples, especially those scarred by war and harsh conflicts that seem stronger than the yearning for peace.”
Earlier this year, the Pope told the Polish people that “life must always be welcomed and protected. These two things go together – welcome and protection, from conception to natural death.”
During the pope’s speech, addressed to government authorities, Pope Francis encouraged the state to reach out and help expectant mothers.
“All of us are called to respect life and care for it,” he said. “On the other hand, it is the responsibility of the State, the Church and society to accompany and concretely help all those who find themselves in serious difficulty, so that a child will never be seen as a burden but as a gift, and those who are most vulnerable and poor will not be abandoned.”
During his visit, Pope Francis continued to demonstrated his pro-life convictions. On Friday, Pope Francis visited a children’s hospital. He met with 50 patients, their families and medical personnel at the Prokocim University Pediatric Hospital, according to Patheos.
During his brief address, Pope Francis spoke on the importance of government working to protect and help the disadvantaged.
“This is the sign of true civility, human and Christian: to make those who are most disadvantaged the center of social and political concern,” he said.
“Sadly, our society is tainted by the culture of waste, which is the opposite of the culture of acceptance. And the victims of the culture of waste are those who are weakest and most frail; and this is indeed cruel.”
On the subject of abortion, the document states the church’s commitment to its anti-abortion stance, adding that no woman’s “right to choose” over what happens to their own body can “justify terminating a life”.
It also states that healthcare workers in [facilities that perform abortions] should exercise their right to conscientiously object to abortion.
Author anonymous due to workplace/patient confidentiality
I put my probe down, find the head, then slide down to the bum. Fortunately, the baby is in a good position. “It’s definitely a boy!” I tell the mom and dad, as they peer over my shoulder at the screen. I point out the very obviously displayed male anatomy. The dad’s face drops. “That sucks!” he exclaims. “I wanted to have a girl.” He continues to express his displeasure as I show them their child and take a couple more pictures for them to take home with them. He is still unhappy as I tell them I’m done and they can get the results from their doctor.
“Can we just end this and start over?” he says to his wife as they leave the room. She laughs nervously. He’s joking . . . I hope.
This is my both my least and most favorite part of my job as an ultrasound technologist. There is something indescribably beautiful about watching human life develop and grow at all of its stages. From the tiny flicker of the heartbeat at just six weeks’ gestation, to seeing the little bouncing 8-9 week old peanuts which (given a good scan) wave tiny little arms and legs. It only gets better from there on out as the baby gets bigger and is easier to see with my ultrasound equipment.
There are also the fun opportunities of telling good news and watching mothers’ faces beam as they get to see their child for the first time. Then there are the good news stories that warm your heart and put a smile on your face. There is nothing quite like telling the mother who thought she had a miscarriage several weeks ago that she is in fact still pregnant and has a bouncing, healthy twelve-week gestation baby. Not to mention finding live twins in a patient who had just had an ectopic pregnancy removed.
But this is only the happy side of the story. There is a sad side too. Like the countless miscarriages that we see day after day. Nothing is quite so disappointing as finding no heart heat and then trying to keep a neutral expression for the rest of the scan, knowing that when they get the results from their doctor their dreams and hopes will be disappointed.
Even that is still not the worst part of scanning pregnant females. The absolute worst is the unwanted children that you see. There is nothing so heart wrenching as the feeling of scanning and seeing little miracles that have been sentenced to die by the ones who are supposed to support and love them.
Scanning early pregnancies only so that some abortion provider knows how to best stop that little heart beat is one example. Another is guiding the needle in an amniocentesis procedure, knowing that the results of the test will be the determining factor of life or death for the baby whose heart rate is carefully recorded to see that they don’t show adverse effects from the procedure.
Then there was the young woman who was already more than twenty weeks pregnant but had decided not to continue the pregnancy. I had to scan her that same day so her doctor could still send her to a hospital that would do abortions up to twenty-four weeks (in the same building where NICU teams fight to save babies born earlier than that). Her baby was a little girl.
I have no words that I can say to my patients. I am not allowed to share my views or offer support. I can’t suggest pregnancy resource centers or tell them how wonderful adoption is. I am not allowed to explain to them exactly what abortion is or tell them about the struggles that other patients have told me that they have had afterwards.
I am not allowed to be a voice for the silent ones. I only have my machine. I can turn my screen and show them that little beating heart and those tiny little arms and legs, fingers and toes. I can show them and hope that they are seeing the same baby, the same human, the same life that I do.
Scanning pregnant ladies has taught me that children in our culture are conditionally loved and conditionally valued. If they are planned and expected or wanted, then I see excited parents and smiling faces. When things don’t go according to plan then I hear disappointment. There are still those that will face the unexpected and make it work, but there are so many who just get rid of the problem instead of accepting and working with it.
That’s why we need people on the streets. We need people to hear and see the truth of what abortion is and what it does. We need to show our culture that abortion does stop a beating heart and that it ends a life. I can only show one side of the story, but people need to know both.
This brings the Christmas message vividly and movingly to life. Patricia Heaton tweeted this Saturday, and it’s quickly going viral. Here’s a pro-life message to stir the heart.
Keep a Kleenex handy. You’ll need it.
– See more at: http://aleteia.org/blogs/deacon-greg-kandra/beautiful-see-christmas-as-never-before-in-a-pageant-of-children-with-down-syndrome/#sthash.6gZEFMcE.dpuf
After the general assembly sent two pro-life bills to Governor John Kasich last week, opponents of abortion and abortion promoters held their breath to see what he would do.
Today, they had their answer.
If the governor had done nothing, both bills (one banning abortion as soon as a fetal heartbeat could be detected, the other banning abortion at 20 weeks) would have become law.
Today Gov. Kasich signed the Pain Capable Unborn Child Act, the 20-week ban, and used his line-item veto authority to veto the Heartbeat Bill, which passed as an amendment to another bill.
Citing the probability of an expensive lawsuit over the Heartbeat Bill, Gov. Kasich wrote, “The State of Ohio will be the losing party in a lawsuit and, as the losing party, the State of Ohio will be forced to pay hundreds of thousands of taxpayer dollars to cover the legal fees for the pro-choice activists’ lawyers.
Furthermore, such a defeat invites additional challenges to Ohio’s strong legal protections for unborn life.”
December 13, 2016 (Stephanie Gray) — On November 21 of this year, I returned to the University of California, Berkeley, to explain the pro-life view to one hundred students who signed up for the course, “Public Health 198.” I would be presenting after their course’s sponsor teacher, Dr. Malcolm Potts (abortionist and first medical director of International Planned Parenthood Federation) gave his talk on why he believes abortion is right.
Having spoken to hundreds of his students the year prior, I listened to last year’s recording. And when I heard myself, I felt I had relied too much on the intellectual case and not enough on stories that reach the heart. So I began to pray about how I could better package the message this year. Kneeling in one of my favorite chapels in Vancouver, I prayed for inspiration, and sensed that my message should focus primarily on beauty.
Without my notebook, I grabbed the next best thing—notepad on my phone, and began to type ideas. I saw that on that same notepad entry, a couple weeks before while speaking in Guatemala, I had typed a note when I heard another speaker, Clay Olsen; he said, “Make it cool first and inform them second.” That’s what I would do—share stories of beauty, of those who authentically live the pro-life message to show it is possible to do so, and only then segue into pro-life apologetics.
A beautiful family I met several years ago while in Denver came to mind—Brianna Heldt and her husband Kevin (whose story I share below). I jotted that idea down. I wrote, “They need Jesus”—which was a deep conviction I had while speaking to the students a year ago as I sensed a very broken and hostile crowd. I further typed, “Give them Jesus in the faces of the Heldts, Ryan, Lianna.”
In my 14-plus years of travelling the world, I have met the most incredible pro-life people whose inspiring life choices would move you to tears. Having interacted with many hostile abortion supporters I have come to see that my experiences and theirs are very different. They have not met the people I’ve met, not seen the things I’ve seen, not experienced the love I’ve experienced. It is love and beauty that is at the heart of the pro-life message and this time at Berkeley I would introduce them to this other world.
After my opening, I addressed the “tough cases” people often raise to justify abortion. I began with poor prenatal diagnosis and poured out the beauty: I told my story of meeting limbless inspirational speaker Nick Vujicic back in 2010, and spending time with him along with a then-2-year-old girl, Brooke, who was born without arms. I talked about how Nick had contemplated suicide when he was younger, but he eventually realized that instead of focusing on what his disability prevented him from doing, he could focus on what it enabled him to do. As this documentary shows, Nick lives a full and satisfying life, inspiring and motivating people all around the world. I then told them about Brooke: her parents were offered an abortion when a routine ultrasound showed she had no arms. But they rejected that, got connected to Nick, and now Brooke has also learned how to turn an obstacle into an opportunity. Abortion doesn’t have to be the answer; we can choose a better way.
Nick and Brooke’s lived experiences are really about perspective—that we can choose our response to situations we haven’t chosen. So I then shared the story of photographer Rick Guidotti who devotes his time and talent to use “photography, film and narrative to transform public perceptions of people living with genetic, physical, intellectual and behavioral differences.” I played a clip from this documentary featuring him, to illustrate a better response than abortion to poor prenatal diagnosis.
“Lianna asked the doctor if abortion would help her forget the rape and ease her pain and suffering. When he replied ‘No,’ she realized that ending the baby’s life would not really benefit anybody.
“‘If abortion wasn’t going to heal anything, I didn’t see the point,’ she said.
“‘I just knew that I had somebody inside my body. I never thought about who her biological father was. She was my kid. She was inside of me. Just knowing that she needed me, and I needed her…it made me want to work, to get a job [to support her],’ she said.
“Rape caused Lianna’s life to become a living hell. No matter how many times she showered, she could not rid herself of feeling dirty. The idea of suicide seemed to offer the young girl instant release from so much misery, but she began to realize that she had to think not only about herself, but about the future of this little life that was blossoming within her body.”
I further told the students that Lianna says, “I saved my daughter’s life and she saved mine.”
But what if someone feels they can’t parent their child like Lianna did? That brings me back to Brianna and Kevin, the couple I met in Denver a few years ago. I infrequently speak about adoption, and decided to emphasize it in my talk at Berkeley. When the Heldt’s first child was only one year old, they adopted two children. They have since adopted two more children, both of whom have down syndrome and serious heart conditions, along with having 7 more biological kids (but tragically losing 3 of them to miscarriage). Brianna wrote, which I quoted for the students,
“When we adopted my sons, we went from being a family of three to a family of five. As one would expect, we got a lot of ‘Why are you doing that?’ and, when I became pregnant four months after my sons joined our family (taking us to a family of six), a lot of ‘Was this an accident?’ And when I answered no, a lot of dumbfounded looks. What struck me most back then (and still does today) is that people were incredulous not so much because of the number of children we had, but simply because we were saying yes. Being open. Allowing love to grow and exponentially multiply, which it always does when a family is graced with new life.
“Those early years of our marriage with four itty-bitty children were outright hilarious, but they were beautiful too. If I could go back for a time, I would. A three-year-old sister sneaking cookies from the pantry to distribute to two-year-old brothers. Sloppy kisses and chubby hands welcoming a new baby sister. Exhausted parents collapsing onto the couch at the day’s end, laughing at how ridiculously amusing our life was.
“But there was love. Always.”
I told the students that “suffering unleashes love” (one of my favourite quotes from St. John Paul II), and that while Dr. Potts is saying that the suffering in the world should unleash violence (i.e., abortion), I would like to propose—not impose, but propose (to borrow the phrase of the late Fr. Richard John Neuhaus who I discovered was simply borrowing more great words from St. John Paul II)—that suffering unleash love. I would like to propose that we follow in the footsteps of people who prove this is possible, people like the Heldt’s, Lianna, Nick, Brooke and her family, and Rick Guidotti.
There is much more that 50 minutes plus Q & A allowed me to share (that a brief blog post does not), but suffice it to say I sought to heed the words of Dostoevsky: “beauty will save the world.”
P.S., The good news? One of the course organizers e-mailed me, “Based on our evals (we run a short iClicker evaluation) students overwhelmingly enjoyed your presentation. Since we didn’t have discussion sections due to the holiday, we weren’t able to get a full idea of their feedback, but students were happy to talk to us after and were very receptive to your message.”
Ohio has become the Fifth State in the past few years to strengthen protections in law from assisted suicide.
The Ohio Senate voted on House Bill 470, a bill that would make assisting a suicide a felony in Ohio on Thursday December 8. HB 470 had previously passed in the Ohio House last May by a vote of 92 – 5.
Jeremy Pelzer, reported for Cleveland.com on November 7 before the vote that:
House Bill 470 … would make knowingly assisting in a suicide a third-degree felony in Ohio, punishable by up to five years in prison.
Currently, Ohio law only permits a court to issue an injunction against anyone helping other people to kill themselves.
If the Senate passes the bill on Thursday – expected to be the last day of the legislative session – it would head to Gov. John Kasich for his signature. The measure passed the Ohio House 92-5 last May.
State Sen. Bill Seitz, the Cincinnati Republican who authored HB 470, said the legislation mirrors Michigan’s 1998 ban on assisted suicide, which was passed in response to Dr. Jack Kevorkian’s well-publicized campaign.
In the past few years Georgia, Idaho, Louisiana, and Arizona have passed bills to strengthen protection from assisted suicide.
LifeNews.com Note: Alex Schadenberg is the executive director of the Euthanasia Prevention Coalition and you can read his blog here.
George Osborne’s ‘two-child policy’ made headlines this week, but it shows that a lot of people still don’t get why mums like me would choose to have more than 2 kids.
So, here’s my list of 11 reasons why large families are totally awesome:
1. You’ll all be healthier
Awesome fact #1: did you know that children with siblings have stronger immune systems? This means that your kids are better guarded against conditions like eczema and hay fever.
And medical research in recent years indicates that they may even be getting protection from food allergies, multiple sclerosis and some cancers!
2. Like, so much healthier
Major studies the world over show that children in a larger family grow up slimmer. That’s how to tackle child obesity! An US study even went so far as to calculate that each extra sibling meant that a child would be 14% less obese on average.
Likewise, children with brothers and sisters tend to enjoy better mental health. How cool is that?
3. Family team games are now a thing
Now you’ll always have enough people to play any game you want.
Football? Cricket? Touch rugby? Once you’re up to 4+ kids, suddenly all kinds of sports become possible.
4. It gets easier after the first one
Ok, so I’ll admit that having a baby for the first time can be tiring and stressful at times (although it’s definitely made up for by the new bundle of joy in your life)! But the weird thing you’ll find is that it gets easier for every new child you have.
After you have two children you’re already outnumbered, so why not go ahead and add a few more to the tribe?
In fact, as your kids grow up, it actually makes life easier – after all:
5. Many hands make light work
You’ll always have plenty of helpers around the house!
6. More birthdays = more parties!
And who doesn’t love a good party?
7. Learning to share
Let’s face it, when you grow up in a large family you have to learn how to share things from a very young age! All great training for later life – your kids will be perfect housemates at university.
8. Older children will learn to take care of their younger siblings
And that’s the coolest thing in the world.
9. You’ll never be bored again
Seriously, how could you ever be bored with jokers like these?
10. More children now = more taxpayers later
(That one’s just for you, George)
But most important of all:
11. You’ll always have friends
Reprinted with permission from Society for the Protection of the Unborn.
United Nations officials have set a noble goal “to end poverty in all its forms everywhere by 2030”—also known as Sustainable Development Goal #1. “Is this goal well intentioned? Indeed. Is it attainable? That depends on how one makes sense of the problem,” says Dr Timothy Rarick in this essay from the e-book Family Capital and the SDGs, produced for the World Congress of Families. The second in this series on MercatorNet.
According to the World Bank, in the year 2015 the extreme poverty rate (less than $2/day) around the world allegedly dropped below 10% for the first time.1 Although this is good progress, extreme poverty, for 702 million people, remains an international crisis. We know that women and children are deeply impacted socially and academically by living in poverty.
Politicians, economists and other organizations have many ideas for solving this crisis. United Nations officials, for example, have set a noble goal “to end poverty in all its forms everywhere by 2030”—also known as Sustainable Development Goal #1.2 Is this goal well intentioned? Indeed. Is it attainable? That depends on how one makes sense of the problem. Misdiagnosing the source of this poverty problem can lead to the wrong prescribed solution—no matter how well-intentioned.
Symptoms vs infections
When a person is suffering from cold or flu-like symptoms it can be very difficult to discern the cause of these debilitating effects. Bacterial and viral infections can manifest very similar symptoms such as: coughing, sneezing, fever, inflammation, etc.3 However, the method for treating these symptoms largely depends on whether this is a bacterial or viral infection. Whereas cold or flu medicine can only treat symptoms, thankfully, antibiotics can rid your body of the bacterial infection, taking care of both symptoms and the problem.
In a similar way, we can approach the plague of poverty by setting goals and prescribing ideas that primarily treat symptoms . . . or we can see the bigger picture and find ways to root out the source of the problem. Some ideas may include simply raising the minimum wage and creating more stable, well-paid jobs—but they can only go so far in treating the symptoms of poverty. Besides, we need competent, educated individuals who can qualify for such jobs. The deeper poverty problem (or infection) may be rooted in the state of the family.
The family: The cause and the solution
Renowned Russian developmental psychologist Urie Bronfenbrenner summarized his research, stating: “The family is the most powerful, the most humane, and by far the most economical system known for building competence and character.”4
Consider this powerful, evidence-based statement! Now consider how the current trends in out-of-wedlock childbearing, divorce and cohabitation are threatening the power of the family unit. Furthermore, each of these threats produces a common result: fatherlessness. These infections, along with many others, have decimated stable homes and families for millions of children worldwide. Until we address the breakdown of the family— particularly the absentee father problem—there will never be a sustainable alternative to eradicating poverty.
Fatherlessness
Current social science research powerfully asserts: “. . . there is a Father-Factor in our [world’s] worst social problems. In other words, for many of our most intractable social ills affecting children, father absence is to blame.”5 In the United States over 24 million children are growing up without their biological father; in the year 2014 nearly a quarter of children lived in father-absent homes.6 Dr. Pat Fagan writes: “The Index of Family Belonging for the United States is now just above 45%, which means that 45% of U.S. children on the cusp of adulthood have grown up in an intact married family.”7
This is, in large measure, due to the rise of divorce rates and out-of-wedlock births over the past 50 years. In 1960 only 6% of babies were born to unwed mothers in the United States.8 Thanks to the sexual revolution of the 1960’s and the passing of no-fault divorce laws in many countries, that number has risen to over 40% today and continues to increase. Similar trends can be seen in countries around the world. Creating a worldwide culture that teaches sex is a deserved commodity and marriage is based in adult desires and emotions has done more damage to the family structure than almost anything else.
In the overwhelming majority of divorce cases in many countries, custody of the children is given to the mother.9 Although children who are victims of divorce still have a father, the severing of their parents’ marriage often severs the consistent influence from the father. This has had devastating effects—especially in the economic realm, as we will see in the next section.
If one does not have a good grasp of economics and social science one might assume that poverty is driving the family breakdown rather than the other way around.
The vicious cycle of fatherlessness and poverty
The positive impact that committed fathers have on women, children and society is staggering. For example:10
Infant mortality rates are nearly two times higher for infants of unmarried mothers than for married mothers.
Boys in households with a father present had significantly lower odds of incarceration than those in single-mother families.
Fathers raise their daughters’ chances of success in academics, earning potential and relationships when they are present and involved.11
Father involvement in schools is associated with greater academic success and achievement for both boys and girls.
Children in father-absent homes are almost four times more likely to be poor. In 2011, 12% of children in married-couple families were living in poverty, compared to 44% of children in fatherless families.
Are we seeing the connection between fathers and poverty? Dads have the power to decrease the odds of poverty by over 30% and increase the earning potential for his children. One of the crippling effects of poverty is the cycle that is perpetuated throughout the generations.
This runs in parallel with the fatherless cycle. Just as children raised in poverty are likely to raise their own children in the same poor economic conditions, so it is with girls born to unwed mothers. Daughters born out-of-wedlock are much more likely to give birth to fatherless children.
The ‘Vicious Cycle’ diagram helps illustrate the connection between fatherlessness and poverty. Keep in mind, even though this cycle and its connections are based in research, it is important to note that none of these factors cause the others to happen. For example, a child who is born out of wedlock is not guaranteed to be poorly educated or live in poverty. Each preceding item simply makes the following factor much more likely to occur.
Education, skills and competence are keys to economic freedom and success. They are the antidote to poverty. A family headed by a married father and mother provides the best setting to not only succeed economically, but to raise confident, competent, well-educated children who can increase their earning potential and “promote inclusive and sustainable economic growth, . . . employment and decent work for all” (SDG #8). Social scientists claim:
An abundant social-science literature, as well as common sense, supports the claim that children are more likely to flourish, and to become productive adults, when they are raised in stable, married couple households. We know, for example, that children in the United States who are raised outside of an intact, married home are two to three times more likely to suffer from social and psychological problems, such as delinquency, depression, and dropping out of high school. They are also markedly less likely to attend college and be stably employed as young adults.12
Stable families will create a society and worldwide economy that is sustainable, because the intact family is the fundamental unit of society. As the families of the world thrive, so do the economies.
Rethinking our approach to poverty
The first Sustainable Development Goal calls for governments to “help create an enabling environment to generate productive employment and job opportunities for the poor and the marginalized. They can formulate strategies and fiscal policies that stimulate pro-poor growth and reduce poverty.”13
This approach to government policy is necessary, to be sure. Job creation and government subsidies can help alleviate the symptoms associated with poverty, yet they cannot revive and sustain the socioeconomic status of an individual family—let alone a nation’s economy. Furthermore, girls — and by extension women — are much more empowered by having involved fathers than by any government policy or sexual rights agenda attempting to free them from the home. In addition to the SDG#1 proposal, we need governments to view everything through a “family-impact” lens in order to be effective over time.
In her book, Family Policy Matters, Professor Karen Bogenshneider put it this way:
Most policymakers would not think of passing a law or enacting a rule without considering its economic or environmental impact, yet family considerations are seldom taken into account in the normal routine of policymaking…Policymakers explain that they do not have the staff or time to gather all the relevant data on the complex issues that confront them. As a result, they rely on information from lobbyists and special interest groups that is often fragmented, parochial, biased, and less focused on family issues.14
Including creating an enabling environment for families to thrive, here are several ways to bring back fatherhood and promote sustainable economic growth for all:
Teach community programs to promote involved, responsible fathering. Research has shown if these programs are taught well and are evidence-based, they increase a father’s (both married and divorced) involvement substantially.15
Create educational and skill-based opportunities for fathers (and mothers) to get the training to lift themselves out of the poverty cycle.
Improve services and education related to: sexuality, caregiving, violence and parenting for boys and men.
Generate a true shift in policy (more than lip service) to focus on teaching all children from a young age about the value of, and their opportunity to be, both caregivers and professionals.
Utilize mass and social media outlets to produce and share positive messages about dads, rather than as the incompetent fools many television shows and commercials show them to be.
Inform the public about research on the harmful effects of pornography addiction. Porn has the power to destroy our most cherished relationships, thus removing fathers emotionally, physically and financially from the family.
Perhaps the most important of all: Re-establish marriage!
Graph: Marriage Foundation UK
The institution of marriage acts as culture’s chief vehicle to bind men to their children. The marriage gap between rich and poor exists in all 20 of the European countries. As Figure 1.2 indicates, 84% of parents who are in the top fifth of household income are married, as opposed to 42% of parents in the bottom fifth of household income. Marriage matters for men, women, children, and economies. But how do we re-establish marriage in the various cultures of the world?
Employers: Create policies and work environments that respect and favor the marital commitment.
Social work: Within the limits of good practice, promote a culture of family formation.
Marriage counselors: Begin with a bias in favor of marriage. Avoid being “value-free.”
Teachers & education administrators: Minimize the implicit and frequently explicit anti-marriage bias prevalent in many schools’ curricula.16
Strong fathers, strong economies: An auspicious cycle
Whereas fatherless children and poverty create a vicious cycle that perpetuates downward (see figure 1.1), the married, intact family with a hard-working, involved father creates an auspicious cycle that moves upward (figure 1.3).
Along with his wife, a father has the power to promote or increase the financial, academic, professional, and relational competence in a child. Being a responsible person is a matter of character, which is best built in the home. At a young age, boys can and should be taught by both parents—and the predominant culture—to be responsible with: their money, their education, their work, their sex drive and their future children. Boys and men need to learn there is more to life than self-centered, pleasurable pursuits. The values of hard work, integrity and responsibility will be perpetuated throughout generations and society.
Will this take time? Absolutely! Just as cold medicine gives immediate, temporary relief to symptoms, an antibiotic brings gradual yet permanent healing. Only with this kind of approach can the economies—and families—of the world be truly sustainable.
Let us bring back fatherhood and heal the plague of poverty.
Timothy M. Rarick is Professor of Family Studies at Brigham Young University – Idaho. His essay is reproduced with his permission and that of the editor of Family Capital and the SDGS, Susan Roylance.
Endnotes
1. Kottasova, Ivana. “World Poverty Rate to Fall below 10% for the First Time.” CNNMoney. October 5, 2015. Accessed July 10, 2016. http://money.cnn.com/2015/10/05/news/economy/poverty-worldbank/.
2. “Poverty – United Nations Sustainable Development.” UN News Center. Accessed July 13, 2016. http://www.un.org/sustainabledevelopment/poverty/.
3. Ratini, Melinda. “Bacterial vs. Viral Infections: Causes and Treatments.” WebMD. April 10, 2015. Accessed July 13, 2016. http://www.webmd.com/a-to-z-guides/bacterial-and-viral-infections.
4. Bogenschneider, Karen. Family Policy Matters: How Policymaking Affects Families and What Professionals Can Do. 2nd ed. Mahwah, NJ: Lawrence Erlbaum Associates, 2006. page 52.
5. Mclanahan, Sara, Laura Tach, and Daniel Schneider, “The Causal Effects of Father Absence.” Annu. Rev. Sociol. Annual Review of Sociology 39, no. 1 (2013): 399-427. doi:10.1146/annurev-soc-071312- 145704.
6. Sanders, Ryan. “The Father Absence Crisis in America [Infographic].” The Father Absence Crisis in America. November 12, 2013. Accessed July 14, 2016. http://www.fatherhood.org/The-Father- Absence-Crisis-in-America. 7. Fagan, Patrick. “The Third Annual Index of Family Belonging & Rejection.” Marriage & Religion Research Institute. Accessed July 14, 2016. http://marri.us/index-2013.
8. U.S. Census Bureau, National Center for Health Statistics, 2011.
9. Grall, Timothy. “Custodial Mothers and Fathers and Their Child Support: 2011.” United States Census Bureau. October 2013. Accessed July 10, 2016. https://www.census.gov/prod/2013pubs/p60- 246.pdf.
10. “Statistics on the Father Absence Crisis in America.” Father Facts. Accessed July 14, 2016. http://www.fatherhood.org/father-absence-statistics.
11. Nielsen, Linda. Between Fathers & Daughters: Enriching and Rebuilding Your Adult Relationship. Nashville, TN: Cumberland House, 2008.
12. Longman, Phillip and Paul Corcuera, Laurie Derose, Marga Gonzalvo Cirac, Andres Salazar,Claudia Tarud Aravena and Antonio Torralby, “The Empty Cradle—How Contemporary Family Trends Undermine the Global Economy,” The Sustainable Demographic Dividend, Social Trends Institute, 2010. http://sustaindemographicdividend.org/wp-content/uploads/2012/07/SDD-2011-Final.pdf
13. “Poverty – United Nations Sustainable Development.” UN News Center. Accessed July 13, 2016. http://www.un.org/sustainabledevelopment/poverty/.
14. Bogenschneider, Karen. Family Policy Matters: How Policymaking Affects Families and What Professionals Can Do. 2nd ed. Mahwah, NJ: Lawrence Erlbaum Associates, 2006. page 4.
15. Cowan, Philip A., Carolyn Pape Cowan, Marsha Kline Pruett, Kyle Pruett, and Jessie J. Wong. “Promoting Fathers’ Engagement With Children: Preventive Interventions for Low-Income Families.” Journal of Marriage and Family 71, no. 3 (2009): 663-79. doi:10.1111/j.1741-3737.2009.00625.x.
16. Popenoe, David. Life without Father: Compelling New Evidence That Fatherhood and Marriage Are Indispensable for the Good of Children and Society. New York: Martin Kessler Books, 1996.
Micaiah Bilger Nov 28, 2016 | 7:22PM Washington, DC
The controversial infertility procedure in vitro fertilization may lead to a greater risk of infertility and cancer in children conceived through the procedure, an Australian researcher says.
University of Newcastle laureate professor John Aitken, a world-renowned expert on male fertility, warned about the negative effects of over-using in vitro fertilization, or IVF, to conceive, the Sydney Morning Herald reports.
In the past decade, couples experiencing infertility or waiting until later in life to get pregnant have increasingly turned to IVF to conceive. The procedure involves harvesting sperm and eggs and using them to create living, human embryos outside the womb; the embryos then are implanted in the woman’s womb.
One of the problems with the procedure is that most couples have more embryos created than they will use. Sometimes the leftover embryos are destroyed or donated to research. Others believe the procedure has commoditized human life.
Aitken said the children conceived through IVF and born also are being impacted. He said the infertility procedure, which is used by one in six couples in Australia, is producing a new generation of infertile children. He also pointed to research showing that male children conceived through IVF to aging fathers were more likely to get cancer.
“There is a negative pay-off,” Aitken said, citing new research in Belgium about male infertility. “If you have a son from this process, it is possible that he too will have the same pathology that you had.”
Aitken expressed serious concern at society’s heavy reliance on assisted conception through procedures like IVF. In Australia, one in 25 babies are now born after being conceived through in vitro fertilization, according to the report. The rate in which couples use IVF is increasing in the U.S., too. Aitken blamed the infertility industry for ignoring that male infertility problems often are to blame, and that IVF should not always be the solution.
“Its an inexorable upward trend. We are taking recourse to IVF in increasing numbers and the thing we have to remember as a society is that the more you use assisted conception in one generation, the more you’re going to need it in the next,” he said.
Another bioethics concern with IVF is the screening of eggs and embryos for health problems, as well as qualities desired by the couple. Some fear that couples are using the screening to pick and choose their child’s traits.
“For us to make real progress as a country, our interventions must target this group.”
— Ummy Mwalimu, Minister for Health, Community Development, Elderly and Children, speaking of the need to target adolescent girls with contraceptives, at the opening of the Family Planning 2020 “Progress Report” conference in Dar es Salaam, Tanzania, earlier this month.
Progress.
That is the word that the Honorable Ms. Mwalimu uses to outline the goal of getting Tanzanian girls under the age of 18 to start having sex and “protecting” themselves from its consequences with the drugs provided through the massive “Family Planning 2020” campaign. The stated goal of the Gates Foundation and its partners in this 2.6 billion dollar project is to get 120 million women in Africa and Asia to start using Depo Provera and other hormonal drugs. This, Ms. Gates told the New York Times again last week, will help women in developing nations “start to break the cycle of poverty.”
This is the technocratic case for “progress”: Get many millions of poor women with no doctors, no hospitals, no corner drug store, and little education and access to information to start using drugs that American women shun due to their serious health risks. And since Ms. Gates has such a knack for getting uncritical media coverage from such outlets as the New York Times, the Wall Street Journal, and even, sadly, the American Enterprise Institute, “FP2020” continues its philanthropic assault on millions of poor women who are literally being told that a shot in the arm is the key to getting out of poverty.
So FP 2020 is all about “progress” for poor women in poor countries. Hence, the great generosity of the Gates Foundation, Pfizer (the maker of Depo Provera, in which the Gates Foundation is a major stockholder), the United States and British governments, and a whole host of the usual suspects in the multibillion dollar “development” and “aid” industry. They’re here to help.
No doubt, Ms. Mwalimu does believe in the “health” initiative of FP 2020. But it is not her initiative. Nor was this massive project initiated in the dozens of other health ministries of African nations who have bought into this scheme. It was initiated in Seattle, New York City, Washington D.C., and London.
The New Colonialism
One of the great successes of the latest form of colonization lies in the redefinition of words like “progress” to mean something other than movement toward genuine human flourishing. Who could look at the last fifty years of “aid” to Africa and say that the goal was to secure genuine human flourishing? Who would dare say such a thing? No, if you want to see the goal of this “aid”, the “progress” it inflicted on Africa, look at the decrease in total fertility rate measurements over time, the only “success” of which this corrupt industry can boast.
To the “aid” industry, “progress” is getting Africans to internalize the corrupt values and priorities of powerful western elites, and lead their own people into further subjection, while thanking the donors for their generosity.
It is a massive export of the sexual revolution: get people to abandon traditional mores and have sex, supposedly without consequences. Break the natural, healthy, intrinsic link between sex and fertility and you have a people that are easy to control. Give them sex in their media, “comprehensive sex education” in schools that provide pornographic instruction with the façade of educational authority, and tell children they have the “right” to sexual pleasure. Then give them drugs and condoms to make them (here’s another word that has been redefined) “safe,” and when these things fail—as they do tens of millions of times per year around the world—you get a (demonic term) “unintended pregnancy.” Yes, their “education” leads to tens of millions of women every year to have “safe” sex and then wonder how they got pregnant and a sexually transmitted infection to boot.
Progress.
Strategies at Home and Abroad
That’s what marketers call the “pull” strategy—create a demand for your product. Then there is the “push strategy”. For African adolescent girls, that means your governments and health ministers become advocates for dangerous drugs without ever mentioning the serious physical and spiritual side effects. Next comes abortion—something these ministers never saw themselves promoting even a short time ago. But once contraception is widespread, abortion becomes the next step in “reproductive health,” since behaviors and mores change, leading to many, many more unintended pregnancies.
This isn’t only in Africa; it’s well advanced here, as we well know. Thanks to the “progress” promoted in our schools and media by the “progressive” elite, our kids are regressing in intellect and maturity, and are increasingly reliant on the government for their basic needs and even their ideas. But they sure know how to put a condom on a banana, and their only marketable skill is throwing a tantrum, which apparently is a part time job for some lucky millennials in today’s progressive America.
We’re Not Enemies
I don’t say this to demonize health ministers or billionaire philanthropists. They are not the enemy. People can have good intentions that lead to bad things. Ms. Gates is a Catholic, and by many accounts a kind and generous person. There is a good chance she never heard a word from the pulpit about the Church’s beautiful and life-giving teaching on marriage and sexuality.
These health ministers and billionaire philanthropists are acting, one can imagine, in accordance with their consciences. They can mean well, even if what they mean to do is not at all good—that is, their consciences have not been formed in the truth. The fact that they follow the exact modus operandi of the racist eugenicists of the early 20th century probably has not occurred to them, nor do they think of themselves as participants in a new colonialism.
Still, even billionaires would have questions to answer if we had a functioning media industry. When Family Planning 2020 was launched in July 2012 in London— exactly 100 years after the first London eugenics conference of 1912—Ms. Gates made it clear that Depo Provera was her preferred method of long-acting reversible contraceptive (LARC). She said this despite the fact that her foundation had just funded a Lancet-published research project that again found that Depo Provera use correlated with a twofold increase in HIV transmission among women. Despite knowing this, as Ms. Gates must have, she and her collaborators pressed ahead with FP 2020, with Depo Provera as the primary method on offer.
Unusual Allies
Within the last several months, after more studies have been published supporting the case against Depo Provera, many organizations have surprisingly begun to distance themselves from the dangerous drug and its promoters. Pro-abortion and pro-contraception women’s health advocates have even publicly criticized the World Health Organization (largest funder: the Gates Foundation), for lowering rather than increasing its risk assessment of Depo Provera due to the growing amount of research pointing to its risks.
Well, if some women’s health advocates are starting to wake up, then that may be a step toward real progress. Again, many of these folks mean well, but were educated in an academic environment where sexual “health” and pleasure are the highest values, and pregnancy is a dangerous disease. We hope that Ms. Mwalimu and her fellow African health ministers start to ask questions. Among these should be questions about the true meaning of progress, and about whether those pushing destructive drugs as the key to poverty reduction have really thought things through.
Bill & Melinda Gates received the Presidential Medal of Freedom, the nation’s highest civilian honor, from President Barack Obama, on 16 Nov 2016.
Rihanna Truman is a young woman who will give birth in just one week to her first child. What makes her unique is not only that she is 16-years-old, but that she is also battling cancer.
At just 12-years-old, Truman was diagnosed with adamantinoma, a rare and slow-growing bone cancer. So rare that it only accounts for less than one percent of all bone cancers. She had the tumor removed from her leg, but the cancer never left her body. It is now in her lungs as well.
“Chemotherapy, radiation isn’t proven to work, so they’re trying to find a new drug so I can hopefully beat it,” Truman told NewsHub.
When she first discovered that she was pregnant, family and friends told her that she should abort her baby or place him for adoption. They were scared that having a child could kill Truman.
“Everyone was telling me to abort or adopt it out, but for me that was just not an option that I was willing to choose,” she said.
“We got told that if I did have the baby that they don’t know what’s gonna happen to me by giving birth. So my family was quite scared that if I had this baby that I was gonna pass away. Ya know, I said that’s a risk I’m willing to take. I was scared, but now I’m not.”
Her baby has been growing as expected – a bit on the small side, likely due to his mother’s condition, but healthy. When he is born next week, he will have two parents who love him very much.
“If I die, I’m gonna die happy, and my son will hopefully be grateful that I chose to have him,” said Truman. “I want him to be proud of me as a mum.”
With the cancer having spread, Truman is living with holes in her lungs. In order to keep them from collapsing, her lungs have been essentially glued to her rib cage. Her fight to stay alive to raise her son is very real, but she is putting his life first.
“Before I was pregnant, every day I’d wake up and be like, ‘I don’t want to live here, I don’t want to be here,’” she said. “But ever since I’ve been pregnant, I knew that this baby was my reason for staying in this world.”
Baltimore, Md., Nov 16, 2016 / 05:05 pm (CNA/EWTN News).- Infidelity, divorce, sexual violence, pornography, hook-up culture – all things that have both increased en masse in society over the last few decades, and have seared pain into the lives of individual men and women.
So how do we even begin to address the problem? By people – especially the youth – choosing to live in true, authentic and virtuous community with one another, says Archbishop Chaput.
“We’re getting a culture that’s just hugely preoccupied with sexuality, and being restrained sexually is not considered a virtue anymore, apparently. I think that’s very hurtful to everyone,” Archbishop Charles Chaput of Philadelphia, who chairs the U.S. bishops’ working group on Amoris laetitia, told CNA on Monday.
The archbishop, who in a lecture in September noted a marked increase in the number and kind of sexual sins he had heard in the confessional throughout his priesthood, told CNA that young Catholics need virtuous relationships to live chastely in the midst of a promiscuous culture.
“I think it’s really important for us to encourage young people to form communities of young people, peers, who can give them support in the face of this culture of cheapening human relationships,” he insisted.
Archbishop Chaput spoke with CNA during the U.S. bishops’ fall general assembly in Baltimore Nov. 14. He chairs the U.S. bishops’ working group on Amoris laetitia, Pope Francis’ apostolic exhortation on love in the family.
The exhortation was the fruit of two synods on the family, which sparked controversy amid speculation over whether there would be a change in the Church’s practice that the divorced-and-remarried may not receive Communion.
Since Amoris laetitia was published, some of its vague language has inspired conflicting interpretations. Some have seen it as a break with the Church’s teaching tradition, others as not changing the Church’s teaching. Still others consider it a progression toward a new pastoral praxis, or that it need not be interpreted at all.
For his part, Archbishop Chaput noted in pastoral guidelines for his archdiocese that in putting Amoris laetitia into practice, “the Holy Father himself states clearly that neither Church teaching nor the canonical discipline concerning marriage has changed.”
Francis’ exhortation “should therefore be read in continuity with the great treasury of wisdom handed on by the Fathers and Doctors of the Church … and previous magisterial documents,” he said.
In his Sept. 15 Tocqueville Lecture at the University of Notre Dame, Archbishop Chaput had insisted that the task of rebuilding society comes from personal conversion, not politics. Even if presidential candidates might be unpopular and controversial, he noted, they came from a flawed culture and were nominated by the citizens.
As evidence of this cultural decline, he noted that over recent decades the number of sexual sins he heard in the Sacrament of Confession has increased, as well as their “scope,” “novelty,” “violence,” and “compulsiveness”:
“As a priest, what’s most striking to me about the last five decades is the huge spike in people – both men and women — confessing promiscuity, infidelity, sexual violence and sexual confusion as an ordinary part of life, and the massive role of pornography in wrecking marriages, families and even the vocations of clergy and religious.”
Even more women are now viewing pornography, he said.
All these sins “create human wreckage,” he added, and on a mass scale they bring about “a dysfunctional culture.” Thus, “as families and religious faith break down, the power of the state grows.”
However, given that President-elect Trump has said lewd and degrading things about women, how can the Church begin rebuilding the culture after this election season?
It starts with community, the archbishop said. “I don’t think anybody can be chaste alone, so you need to pick a spouse who helps you to be that way.”
These virtuous communities are “really what the Church should be,” he added. “It should be a community of people who think like Jesus and want to act like He calls us to act.”
“So in some ways, that’s the foundational purpose of the Church, to provide us companions in virtue and worship, and care for the poor. We’re supposed to be companions that call one another to all those things that are essentially part of being a Christian,” he added.
The government has a role in protecting this culture, he said, but has abandoned its duty to protect children and families from the effects of pornography by allowing it in the name of “personal freedom.”
Archbishop Chaput also discussed with CNA how Catholics should react to the recent presidential election – with both “gratitude” and “concern,” he said.
“One, gratitude to God for the opportunities it’s going to give us to protect the Church on religious freedom issues,” he said, noting anticipated changes to the HHS birth control mandate. “And also on the life issues, it seems like there’s openness to supporting the Church’s position on life that wasn’t present before.”
However, serious concerns persist on issues such as immigration, he added, with “the possible deportation of people that will undermine family life in a very serious way.”
“There are a lot of people in my diocese who are very much afraid because of the things they’re imagining that’s going to happen. And that can be hugely disruptive and destructive of the life of families,” he explained.
“Fear is not a good way to live your life. And intense fear for children is especially disruptive. So I think sometimes because of our excitement about the pro-life positive news, we can be naïve about the dangers that exist.”
Ultimately, Catholics should be open to working with the Trump administration on areas of agreement with Church teaching, but must also be vigilant for other areas of policy that oppose Catholic social teaching.
“I think it’s really important to do our best to give the new administration the chance to develop its plan and support it in the good things that it proposes, and to express our concerns about the things that are worrisome,” he said.
“But it’s important for us to pray for government officials. The Scriptures call us to do that.”
According to a recent report by Reuters, abortion in America has reached a new turning point: Nearly half—43 percent—of abortions at Planned Parenthood clinics are now medication-induced rather than surgical procedures. It’s a sharp increase since 2010, when Planned Parenthood ended 34 percent of pregnancies chemically. At some point, chemical abortions could exceed surgical ones nationally. They already do in Michigan, at 55 percent, and Iowa at a whopping 64 percent.
What precipitated this spike? In March 2016, the Food and Drug Administration caved to pressure from drug companies, changing prescription guidelines so that the abortion drug Mifeprex—use of which the FDA hadn’t permitted after seven weeks of pregnancy—could now be administered up to 10 weeks. The FDA loosened restrictions further by cutting the number of required medical visits and even allowing non-physicians to dispense the abortion pill.
“Of the more than 2.75 million U.S. women who have used abortion pills since they were approved in 2000, at least 1 million got them at Planned Parenthood,” Reuters reports. The number is likely to increase as a result of the new guidelines. This, “despite concerns about the drug’s medical risks, including blood, psychiatric, immune, respiratory, cardiac, reproductive, and more disorders, as well as a handful of deaths,” warns Live Action.
Add to the increase the fact that contraceptives such as the morning-after pill—also known as Plan B—and others act as abortifacients by inhibiting implantation of a newly conceived embryo in the womb. Countless abortions are therefore going unreported as it becomes easy for a woman to have an early abortion without going to a clinic or hospital.
Women on Web is a digital community where women from most parts of the world can order abortifacients Mifepristone and Misoprostol online. Reuters reports that Gynuity Health Projects, a private technical institute working in conjunction with clinics in New York and several other states, sends abortion pills by mail to pre-screened women.
Early this year, many pro-life advocates celebrated declining abortion rates in the U.S. But it is very possible that the decline is not as steep as has been reported. Not only because of the abortifacient nature of some contraception methods, and that women are now ordering their abortion pills online without ever going to a hospital, but also because several state health departments, including the most populous, California, do not even provide abortion data.
Talk about heartwarming! A video of a set of newborn twins being bathed by a nurse in France has taken Youtube by storm, earning over 4.2 million views in the space of just a few days.
The nurse, Sonia Rochel, says the babies were only a few days old when she gave them a type of immersive bath using warm water that she says causes babies to move as they would in the womb.
When these twins were immersed in the water, they clung to each other in a tight embrace, their eyes closed peacefully.
“They’re already born, but they might not know it yet,” wrote Today Moms, which interviewed the nurse.
The video has strongly resonated with viewers.
“Sweet baby Jesus. Words can’t even begin to explain the beauty in this video,” wrote one commenter.
“It breaks my heart when I watch this clip. It’s beautiful!” wrote another.
COLUMBUS, Ohio–In September, a hearing examiner at the Ohio Department of Health recommended that the license of a Dayton-area abortion facility be revoked for failure to meet the department’s health and safety standards. This followed a hearing in April in which the abortion facility, Women’s Med Center of Dayton, requested to maintain its license and stay open. In addition, in October, the Ohio Department of Health denied the facility’s request for a variance from the law for the fifth year in a row.
“The abortion industry’s repeated failure to meet basic health and safety standards is a concern that should alarm every Ohioan,” said Devin Scribner, executive director of Ohio Right to Life. “Last summer, this same abortion facility performed an abortion on an incapacitated woman who was unable to consent. Enough is enough. Women’s Med Center’s repeated offenses need to result in its swift closure.”
Ohio law requires that all ambulatory surgical facilities, including abortion facilities, secure a written transfer agreement with a local hospital. If unable to obtain an agreement, the facility may seek a variance from the law. In June 2015, Women’s Med Center submitted a variance request to ODH. It cited three back-up physicians who would provide care in the event of an emergency and indicated that Miami Valley Hospital would continue to treat the facility’s patients through its emergency room. That same month, a woman exhibiting signs of recreational drug use arrived at Women’s Med Center for an abortion appointment. She was unable to walk or hold a conversation. Women’s Med Center consulted Miami Valley Hospital by phone. Despite the woman’s inability to provide consent, Women’s Med Center performed the abortion. According to the Department of Health’s hearing examiner, the following month, in a letter to the Ohio Department of Health, the president of Miami Valley Hospital objected to the use of its name in the agreement and requested that all references to its name be removed.
“As the traditional medical community rejects affiliation with this abortion facility, it’s time Ohio does the same,” said Scribner. “Women’s Med Center has failed to meet the Department of Health’s expectations for five years. In that time span, thousands of human children have lost their lives and the health of thousands of women has been jeopardized at this facility. If we take women’s health seriously, we simply cannot afford to have this facility continue operating in this reckless manner.”
Women’s Med Center of Dayton is operated by abortionist Martin Haskell who is known for popularizing the now-banned partial-birth abortion technique.
To view the hearing examiner’s report and recommendation to the Ohio Department of Health, click here.
To view the Department of Health’s 2016 denial of variance request, click here.
Since the U.S. Food and Drug Administration first approved hormonal birth control in 1960, it has been touted by some as the best thing since sliced bread. But a new landmark study has concluded that hormonal birth control carries significant mental health risks to women.
Newspaper headline writers appear surprised by the study, but they should not be. Hormonal birth control also has established physical health risks. Given what we now know about the health dangers of hormonal birth control, making it available without a prescription is a troubling public health policy driven by politics, not science.
Recall the Big Recent Study in Denmark
A recent Danish study at the University of Copenhagen revealed that using hormonal contraceptives, including the pill, injections, patches, rings, implants, and intrauterine devices, is correlated with clinical depression. This longitudinal study was conducted over the course of 13 years. Its subjects included one million women aged 15 to 34, pre-screened for depression and other medical and psychiatric disorders. Women who had a pre-existing condition of depression or were using anti-depressants were excluded from the trials.
These women were tracked for hormonal birth control use and psychiatric health. Results showed that the women on hormonal birth control were almost twice as likely to develop depression and be given a prescription to combat these symptoms. Teenage women, in particular, were most susceptible to these effects. Women aged 14 to 19 were 80 percent more likely to be prescribed anti-depressants, especially if they were on the combined pill containing both artificial estrogen and progesterone.
Given the findings of this newest study showing the correlation between hormonal birth control and depression, women who are already susceptible to depression and who use hormonal birth control could put themselves at greater risk for self-harm or suicide. While correlation does not equal causation, these statistics are startling and should not be ignored, especially since 62 percent (11 million) of women of reproductive age in the United States use contraception.
We’ve Known about Negatives for Years
In addition to the mental health risks, hormonal birth control has various established health risks. Common side-effects include nausea, vomiting, cramps, weight gain, and acne, to name a few. Serious side-effects of hormonal birth control include blurred vision; severe stomach pain or headache; swelling or pain in the legs; chest pain; gallbladder disease; increased risk of blood clots cutting off blood flow to the heart or brain, increasing the risk of cardiovascular arterial disease, heart attack, or stroke; increased risk of liver tumors that can turn malignant; increased risk of cervical cancer; and increased risk of breast cancer.
Citing increased risk of cancer, the World Health Organization has classified hormonal contraception as a definite group-one carcinogen along with other harmful substances like asbestos, tobacco, mustard gas, engine exhaust, and outdoor air pollution.
In addition, hormonal contraception can cause an abortion when breakthrough ovulation happens and the egg is fertilized. Hormonal birth control changes the lining of the uterus and can act as an abortifacient if fertilization occurs, since the embryo would not be able to implant and receive nutrients. This is called a pre-implantation chemical abortion.
The new Danish study’s findings along with the previously established health risks must be taken into account when considering some Republicans’ legislative strategy to promote over-the-counter birth control in a misguided effort to fight the Left’s “war on women” narrative. Senators Kelly Ayotte and Cory Gardner proposed a bill (S.1438) with other Republican senators that would require the FDA to make hormonal birth control available over-the-counter for those over the age of 18.
This legislation will harm women. Women deserve to know the real health risks of hormonal birth control from their doctor in order to make an informed decision, not from a size-eight font warning label in the supermarket aisle.
Contraception Use Increases Abortion Rates
Some argue that decreasing the cost and increasing the accessibility of hormonal birth control would reduce abortions and unplanned pregnancies and help low-income women. However, studies such as this 2011 study in the journal Contraception show that contraceptive use correlates with an increase in unplanned pregnancies and an increase in the elective abortion rate.
Contraceptive use encourages sexual activity by setting up the false expectation that contraception makes one “safe” from pregnancy. When contraception fails, women who end up in unplanned pregnancies often get an abortion. In fact, the Guttmacher Institute reported that “more than half of women obtaining abortions in 2000 (54%) had been using a contraceptive method during the month they became pregnant.”
First, scientists are discovering health risks that suggest dangers to women’s health and safety. Second, there is the real concern that over-the-counter contraceptives will increase unplanned pregnancies and abortion. Third, making hormonal birth control available over the counter without the oversight and care of her doctor endangers a woman and deprives her of proper informed consent.
As part of informed consent, doctors should share the findings of these health risks with women who are considering hormonal birth control and share information about natural, healthier, organic alternatives in family planning. These include fertility-awareness based methods, alternatives that have been found to be equally or more effective than hormonal based birth control. These methods empower women to make more informed choices about family planning and to teach them how to monitor and understand their own reproductive health, instead of using harmful means to suppress it.
Our public servants should do all they can to protect women’s health and safety. Politicians who push for making hormonal contraception, a group-one carcinogen and a known abortifacient, available over the counter are playing Russian roulette with women’s health and safety for their own political gain. Women deserve better.
Former U.S. Ambassador to the Holy See, Jim Nicholson, says the President-elect has been a “very good listener” at meetings with a Catholic coalition of advisers.
Edward Pentin
President-elect Donald Trump has been a “very good listener” during meetings of a Catholic coalition group that he set up to advise him on the faith during his presidential campaign.
This is according to one of its members, former U.S. Ambassador to the Holy See, Jim Nicholson.
Nicholson told the Register Nov. 10 that the newly elected President is not only an “intent listener” who heeded their advice in the lead up to Tuesday’s ballot, but also “asks very good questions”. He therefore believes the group could have a “very positive effect on President-elect Trump”.
Trump formally set up the body of 34 respected Catholics in September in a bid to allay concerns about his candidacy among some in the Church, and to attract more Catholic voters. Part of the Trump Faith and Cultural Advisory Committee, it was viewed as evidence of his commitment to protecting religious freedom and moral values.
“I think we’ll have a good audience and a good chance to be heard and help shape his views about all things Catholic,” said Nicholson, who served as U.S. ambassador to the Holy See during President George W. Bush’s first term before being appointed Secretary of Veterans Affairs from 2005 to 2007.
Trump pledged to continue communication with its members if elected president.
Nicholson further pointed out that Trump “carries the Catholic vote which is a large number”, adding that he has “a lot of friends and associates who are Catholic — he grew up in New York City.”
Catholics were crucial to Trump’s election: he won 52% of the Catholic vote, compared to Hillary Clinton’s 45%.
In addition to Nicholson, the Catholic coalition group’s members include former US Senator and presidential candidate Rick Santorum; Ambassador Francis Rooney, Nicholson’s immediate successor as U.S. Ambassador to the Holy See and now newly elected congressman in Florida; and Austin Ruse, president of the Center for Family and Human Rights and tireless defender of life at the United Nations.
Also in his comments to the Register, Nicholson spoke about his hopes for relations between Trump, the Holy See and Pope Francis, despite clear differences.
Here below is the full text of Secretary Nicholson’s remarks to the Register:
“Secretary Nicholson, what are your expectations regarding Trump’s relationship with the Holy See?
I think it will be a good relationship. I’m delighted with the Trump victory because it’s a victory for working class people, for underemployed people and unemployed people — people for whom the Pope has great concern. So they have a great amount in common in their priorities.
The Pope has often spoken of his concerns about capitalism. Could this be a problem going forward in relations with a Trump administration?
They have differences in views but a great deal in common. They have a mutual concern for poor, a mutual concern for the foundation of the Catholic Church which is life. Trump is adamantly pro-life, as is the Pope. I think on matters like their view of capitalism and the free market and of course immigration, we should acknowledge differences.
That is going to depend a lot on how effective the ambassador that Trump selects to represent him at the Holy See will be. If he gets a very good, articulate interlocutor to explain what he wants to do and what his thinking is to the Holy See and to the Holy Father, it will go along way, because the Pope respects the rule of law, he respects sovereignty. So that’s a very important issue in the immigration debate.
The Pope is also concerned for the humanitarian aspects of people, migrant people, so those are issues that need to be discussed openly, a common set of foundational values about the dignity of people, their welfare.
Trump and I agree with him on this – that the best thing you can do is help people get a job, help them get on their feet, and get back to dignity of having a purpose in life. That has got to be very consistent with the Pope’s values at a human level. How that’s done on an economic level, they might not agree, so that has to be dealt with. I think Trump has a healthy respect for the Pope, he recognizes his moral authority, and I think it could be a very enduring relationship.
Regarding the Catholic coalition of advisors, how much effect and influence could it have going forward?
It can have a very positive effect on President-elect Trump. He carries the Catholic vote, it’s a large number and he has a lot of friends and associates who are Catholic — he grew up in New York City. I think we’ll have a good audience and a good chance to be heard and help shape his views about all things Catholic.
Was he listening to what the group had to say before the election?
He was. In fact he’s a very good listener. He had a lot of bravado regarding the external part of his presentation which served him well on the campaign but when he gets into a meeting with us, he’s a very intent listener and asks very good questions.
Does Trump respect the Pope’s authority do you think, given their clash earlier this year?
Trump had the dust up with the “wall” [when the Pope said on returning from Mexico that we should build bridges rather than walls and that anyone who wishes to build a wall “is not Christian”]. What I think the Holy Father should have said, more appropriately, was that’s not a Christian way to act, but instead he branded Trump as not being a Christian. Trump retorted pretty robustly to that. It’s a two way street. I think that both of the world leaders recognize the external challenges they have in common, growing secularism and terrorism. They’ll find they can do so much by working closely together, even though they may have certain differences.
As an example, George W. Bush, my president, and Pope St. John Paul II worked together in spite of a very stark difference over Iraq, but they had so much in common, a values system, life, taking care of people in Africa with disease and suffering, starvation. Bush visited the Vatican three times, the most times any president has visited a pope in Rome. I think they’re both smart men and they’ll realize that there’s a lot to be gained by them working closely together than by not doing so, by stressing the important priorities they have in common rather than some important things about which they don’t agree.”
VATICAN CITY —Cardinal Raymond Burke has said Donald Trump’s election Tuesday is a sign that the United States’ political leaders need to listen more to the people and return to safeguarding life, marriage, the family and religious liberty.
In an exclusive interview with the Register Nov. 9, the patron of the Sovereign Order of Malta said he was confident Trump would be able to help heal divisions in the country, that he has a “great disposition” to listen to the Church’s position on the moral law, and hopes he will “follow the principles and dictates of our Declaration of Independence and the Constitution.” However, aware of inevitable areas of divergence with Church teaching, Cardinal Burke stressed the importance of Catholics continuing to make objections known whenever necessary.
Your Eminence, what is your reaction to the news of Donald Trump’s election as U.S. president?
I think that it is a clear sign of the will of the people. I understand that the voter turnout was stronger than usual, and I think that the American people have awoken to the really serious situation in which the country finds itself with regard to the common good, the fundamental goods that constitute the common good, whether it be the protection of human life itself, the integrity of marriage and the family or religious liberty. That a candidate like Donald Trump — who was completely out of the normal system of politics — could be elected is an indication that our political leaders need to listen more carefully to the people and, in my judgment, return to those fundamental principles that safeguard the common good that were so clearly enunciated at the foundation of the country in the Declaration of Independence and in the Constitution.
You’d say the silent majority has spoken?
Yes, that’s clear.
Some are calling this a golden opportunity for the Church, particularly because of Trump’s position on life issues and religious freedom.
Exactly; what he has said about pro-life issues, family issues and also issues regarding religious freedom shows a great disposition to hear the Church on these matters and to understand that these are fundamentally questions of the moral law, not questions of religious confession. They are questions of the moral law, which religion in the country, as the Founding Fathers understood from the start, is meant to support and to sustain. The government needs the help of religious leadership in order to hold to an ethical norm.
Do you think he’s authentic when he talks about these issues? Recently, for example, some were concerned that he waved a pro-homosexual rainbow flag at a rally.
Of course, after any election, this is the big question: Will the candidate be true to his word, follow through? We have to hope and pray that he does that. One thing I heard about him is that he tends to associate himself with very sound advisers, and I would trust that he will do that.
He appointed 34 prominent Catholics during the campaign to advise him on Church issues.
Yes, some of them are well-known to me, and they are very fine people. It is a hopeful sign.
His election also means it’s practically inevitable that the contraceptive mandate that the Obama administration tried to impose on EWTN and other Catholic organizations will be overturned.
I certainly hope so, because that’s certainly a question of a fundamental right of conscience. I trust that he will address the many moral problems with the health care mandate that was pushed during these last eight years.
In the lead-up to the election, 35 prominent Catholics signed an open letter before he was nominated, saying that Trump is “manifestly unfit to be president of the United States.” They said: “His campaign has already driven our politics down to new levels of vulgarity. His appeals to racial and ethnic fears and prejudice are offensive to any genuinely Catholic sensibility. He promised to order U.S. military personnel to torture terrorist suspects and to kill terrorists’ families — actions condemned by the Church and policies that would bring shame upon our country.” Should Catholics still be wary of these concerns?
Certainly, we must be alert to them, as we would be to any U.S. president, and be attentive to insist on what’s morally right. But I think a Catholic could, in good conscience, vote for Donald Trump because, in all that he said, at least there was a hope of advancing in some way the common good of the nation. But on these objectionable issues, when one votes in conscience for a candidate with whom one doesn’t share all the same moral principles, but certainly very important ones, then one makes clear his or her objections on positions that the candidate may have that are not correct.
But on the key one, the life one, although there were some earlier concerns (he had been pro-abortion rights in the past), he seems to be right?
Yes, on the life issue, he’s right on the money.
What about immigration, where his views diverge with the common position taken by U.S. bishops? Pope Francis also said, in comments perceived as criticism of Trump’s plan to build a wall on the Mexican-U.S. border to keep out illegal immigrants, that we should build bridges rather than walls.
I don’t think the new president will be inspired by hatred in his treatment of the issue of immigration. These are prudential questions — of how much immigration a country can responsibly sustain, also what is the meaning of immigration, and if the immigrants are coming from one country — questions that principally address that country’s responsibility for its own citizens. Those are all questions that have to be addressed, and, certainly, the bishops of the United States have addressed them consistently, and I’m sure they will with him, too. He has these Catholic advisers; and at least some of them, I know, are very well aware of these questions, and I can’t imagine that they’re not speaking up.
A Christian cannot close his heart to a true refugee, this is an absolute principle, there’s no question about it, but it should be done with prudence and true charity. Charity is always intelligent; it demands to know: Exactly who are these immigrants? Are they really refugees, and what communities can sustain them?
What is your opinion regarding other accusations of divisiveness and lowering the tone of political debate and culture? Some, particularly in the Clinton campaign, blamed Trump for that.
I don’t think that at all. I think the campaign itself, and that means both parties, contributed to that, and I believe, from what I’ve heard him say, although I didn’t hear his acceptance speech, that he will work to unify the country. But it has to be a unity that’s on a solid foundation, namely those moral principles that have to guide the life of a nation. So I believe that he will do that. I mean, you have to imagine, he’s not a stupid man; he realizes that it’s one thing to run for president, but it’s another thing to become the president, and that will certainly be in his mind — the heavy responsibility that he has, that’s on his shoulders.
Another fear that arose during the campaign, heightened by Trump’s opponents, was that giving him the nuclear codes would be dangerous.
I’m not afraid of this. I think the new president, in the long tradition of American presidents, will follow the way of cooperation and communication with foreign powers, and I highly doubt he will be able to take any unilateral action that would endanger the world. I am convinced he will deal with other countries on a wider variety of foreign-policy issues.
Overall, what are your hopes for this new presidency?
I hope that Trump will follow the principles and dictates of our Declaration of Independence and the Constitution — certainly, that he will turn out to be a good president and heal the divisions in the country (in fact, he has already said that it is a time not to be divisive) and that, therefore, there will be unconditional understanding, that is, unity among all American citizens.
Edward Pentin is the Register’s Rome correspondent
In the United States, when abortion became legal in 1973, the Supreme Court basically declared that unborn people don’t have constitutional rights like those of us that are out of the womb do. In further denying the “personhood” of unborn children, proponents of abortion insist on referring to a child in the womb as a “fetus” rather than a “baby” or a “child.” One of the great challenges of the pro-life movement has been how to give back this personhood to the little ones inside their mother’s wombs who have no voice that can be audibly heard yet.
In the powerful video below, you’ll see a group of women in Chile figured out a way to do just that. The pro-life femininist group Reivindica Feminist Movement staged a protest in Octobr to call attention to the personhood of unborn babies, and to let others hear “The Voice of the Heart.”
These women strapped fetal heart monitors with speakers to their pregnant bellies, then marched the streets of Chile with megaphones up to the monitors so that their unborn babies’ heartbeats – “the voice of the heart” – could be heard loud and clear by all nearby. They did not chant, cheer, or even carry signs as they marched together toward government buildings. They simply let their children’s voices, through their heartbeats, send a lesson about LIFE.
Unborn babies don’t get to choose whether or not they live or die. Although that is a decision that should only be left up to God, hundreds of thousands of expectant mothers make the choice to end their child’s lives before they are born each year. I love the powerful way that these feminists for life have chosen to speak out and show the world that they are carrying PEOPLE inside their wombs, not just “products of conception.”
If you believe in being a voice for unborn children, I hope you’ll share this post on Facebook!
It has not been an easy decision. Many whose opinion I deeply respect have recommended strongly against my doing so. Not least among these are several members of my immediate family. My own children think that voting for Mr. Trump is, well, “deplorable.” Certainly, there are many reasons not to vote for Mr. Trump. I only wish that the man would not make a point of adding to them on an almost daily basis.
The option of either not voting at all or voting for a write in or for a third party candidate is a tempting alternative. Voting for a third party candidate or for any candidate that you truly respect is never “throwing your vote away.” It is a moral victory of one!
However, I have finally decided to vote for Mr. Trump on behalf of a special, undocumented American. She has not been in this country long enough to be allowed to vote. So I have decided to cast my ballot in her place.
Mr. Trump is, at his best, a very successful businessman and he certainly knows how to motivate a crowd. At his worst, he is huckster, a carnival sideshow barker. Hardly the ideal presidential candidate.
While Mr. Trump’s candidacy is dubious, Ms. Clinton’s presidency will be an unmitigated disaster. We have to choose between a clown and a cobra. As one pundit put it, “My trouble with Trump is that I do not know what he will do. The trouble with Clinton is that I know exactly what she will do!
Trump’s campaign consists largely of theoretical constructs. What he will actually do in Washington remains to be seen. Much of his rhetoric could be dismissed as bombast and vacuous campaign promises. On the other hand, there is nothing theoretical about the Clinton threat. The bloody reality of today is that 1.2 million abortions are now being performed in America every year. Ms. Clinton celebrates this reality and pledges to expand it to a spectacular extent. She envisions a single, federally mandated healthcare system in which tax funded abortion on demand will be freely provided universally. She has little patience with those in the healthcare system who have grave moral reservations. Physicians, nurses, pharmacists and other healthcare professionals we, too, will have a right to choose either.
Beyond the transformation of our country into a power house of abortion on demand, Clinton envisions worldwide dominance of the abortion culture. Through the UN and through multiple US overseas programs, Ms. Clinton will ensure that abortion on demand is forcefully promoted and funded throughout the world. The rights of Catholic nations will be trampled just as surely as the rights of Catholics in the US will be disregarded. No one will long stand in the path of the Clinton’s pro abortion juggernaut.
Ms. Clinton declares that “deep seated cultural codes, religious beliefs, and structural biases have to be changed.” The evil that President Clinton will achieve, even in four years, let alone in eight, will endure certainly past my lifetime. The appointment of pro abortion judges to the Supreme Court will insure that not even our Constitution will stand in the way.
The situation, with respect to the vice presidential candidate, is even starker from a Catholic standpoint. Mr. Pence is, by all measures, a soundly pro life Christian. Mr. Kaine is the worst of all possibilities. He is a proudly self declared Catholic and, at the same time, a 100% pro abortion advocate. He states that he is personally opposed to abortion. (However, it is not clear why he would be opposed “personally” to the exercise of an act that he believes to be a basic human right one which he now actively promotes as a US senator). More sadly still, Senator Kaine came into office as a prolife Democrat, but has since converted to the dark side. Planned Parenthood endorses his candidacy enthusiastically; he now has a 100% pro abortion voting record!
Senator Kaine was brought up as a Catholic and trained by Jesuits. He spent time working in a mission in Honduras. He took time out from that mission, in order to make a difficult pilgrimage to neighboring Nicaragua, where he met with a self declared Marxist priest, who was serving there as chaplain to a band of communist guerillas. Whatever inspiration Senator Kaine received from this Marxist guru, in terms of “liberation theology,” evidently did not extend to liberating from oppression the weakest and most defenseless of our little brothers and sisters those unborn children who are depending on us for protection in the wombs their mothers. It is bad enough to have an anti Catholic, such as Hillary Clinton, running for president. But to have a man, who claims to be a Catholic, teaming with her to turn America into an abortion powerhouse is truly deplorable. We have the possibility (albeit small) that Ms. Clinton would become the first president to be convicted of a felony. In any event, Vice President Kaine will be, for the next four years or more, one heartbeat away from becoming Commander in Chief. We would face the specter of a President who is, in this world, the most powerful Catholic on earth and, at the same time, the proud champion of the wholesale, murderous expansion of abortion on demand across America and throughout the entire world. Then we would face the possibility (albeit also very unlikely) of his becoming the first president ever to be excommunicated from the Catholic Church. Were that to happen, you could be sure that liberal Democrats and the media would lionize him for his courage the Patron Saint of Planned Parenthood. The Clinton/Kaine duo will truly mark our nation with the Sign of Kaine.
So there you have it. What a disaster for democracy this election seems to be! Two candidates for President of the United States in a mad race to the bottom! The goal for each of them seems to be, not so much to get their supporters to vote for them, as to convince supporters of their opponent to either stay home and not vote at all or to vote for a third candidate. The alternative is to “hold your nose” and vote for the less bad candidate. In ancient times, there was what was called the “War of Roses.” This election might be called the “War of Noses.
Well, I am not holding my nose. Rather, I am holding my breath in suspense and gasping at the thought of an America in which the Clinton presidency would cement and celebrate federally funded abortion on demand, worldwide, for the foreseeable future for the rest of my life and beyond. Whatever issues ‘The Donald’ has going against him, the issue of protecting all human life takes precedence. I guess you could So I am casting my vote for Mr. Trump for the sake of all America but especially for that undocumented American that I mentioned at the outset. Yes, as you have probably guessed, the undocumented young lady, on whose behalf I am voting, is a little unborn baby girl. Call me a radical, but I believe that dismembering her is wrong dead wrong! Where is the ‘women’s vote’ when this little lady really needs it? I am voting to safeguard for her a world in which being unwanted or inconvenient is no longer a death sentence, neither before nor after birth.
I will be casting my vote, not only for Mr. Trump, but also for all the other prolife candidates on the ballot. They will need support especially in this election. I will be voting, down the line, in full support of the Republican Party’s solidly prolife platform. Please join with me in doing the same.
We are the Borg. Lower your shields and surrender your ships. We will add your biological and technological distinctiveness to our own. Your culture will adapt to service us. Resistance is futile.
In the fictional universe of Star Trek, the Borg are a collection of species that have been turned into cybernetic organisms functioning as drones in “The Collective,” which acts in a hive mentality. They assimilate new species into the Collective thus adding the new acquisition’s intellect and abilities. As part of the Borg, those assimilated become a small part of The Collective, and lose all sense of individuality.
Sounds familiar? It should because this is the ultimate goal of the ideologies plaguing our culture today – individualism and cultural relativism.
The number of Catholics in the US hovers around 70 million. Many see the Catholic Church in the US as respected and influential precisely to the extent that we hobnob with the elite and get people to like us. That’s how we make ourselves relevant.
On this view, the goal is to “build bridges.” Anything distinctively Catholic and Christian can be set aside until later. Once we have enough influence and relevance, then we (someday) can bring Christ back into the conversation.
But after decades of this failed strategy, still many strive to blend into an increasingly hostile culture, and most Catholics have no idea what the Church believes anymore or what is distinctive about her. We have been assimilated, and our assimilation into “The American Collective” has been disastrous.
Supported by a steady and gradual death of conscience, Catholics in the US rationalize immoral behavior and the politics that flow from acceptance of this behavior that is contrary to the teaching of Jesus and His Church. And still many are afraid to offend, setting Christ and His teaching aside in the search for relevance.
Over the last few weeks we have seen a number of articles from Catholic leaders concerning the upcoming elections. This is welcome and entirely appropriate, despite what some say. Yet, sadly, we are left trying to do in a couple weeks what many have set aside for decades and it will likely have little effect. We have done very little to influence the pool of potential candidates – Catholic and non-Catholic. Although there have been faithful and countercultural examples of courageous leadership in the Church all along, and it seems that pockets of resistance continue to grow, as a whole we have failed to authentically teach the Faith and reject assimilation into the culture. In the last few decades, Catholics as a bloc have become indistinguishable from non-Catholics, voting for some of the vilest opponents of Catholic teaching, especially concerning the sanctity of human life. Most notable was Barack Obama, who received a majority of Catholic votes in both presidential elections.
Catholics in the US are radically divided on the doctrinal and moral issues of contraception, abortion, same-sex unions, sex education, and gender ideology. Political candidates and their respective parties exploit this reality. Further exasperating the problem, many Catholics who rise to public service, instead of incorporating Faith into their leadership duties, have caused scandal and confusion by their dissent from Church teaching and endorsement of secular culture: Joe Biden, Anthony Kennedy, John Kerry, Tim Kaine, and Nancy Pelosi, just to name a few.
As a Catholic am I supposed to endorse the immoral laws and behavior of this nation carte blanche because we live in an imperfect culture among an imperfect people? Am I to ignore my identity as Catholic – a disciple of Jesus Christ – because it offends others? Am I to remain silent to the injustice done to the most vulnerable of our society – the unborn child – because my government says it is legal to kill the baby? Am I am to accept and pretend that the redefinition of marriage and gender ideology is morally sound?
It may seem at times that our efforts do not bear fruit. We see some victories, but overall it is clear that God is granting our nation its collective desire for a false “freedom” cut off from Him. But, my friends, resistance to evil and a refusal to be assimilated is never futile!
Consider a married Catholic couple I recently met. They told me they changed their circle of friends because their friends’ immoral behavior was harmful to their family life, especially for their children. At first they tried to patiently influence their friends, but when all attempts failed, they had to decide what was best for their family.
A medical doctor I recently met abroad was being persecuted because he will not write a prescription for contraception. He is being threatened with the loss of his license and potential livelihood. After numerous failed attempts to defend his freedom of conscience, he now is forced to move his family and practice to a new country.
Did this couple and the doctor make the right choices? Should the doctor have compromised – assimilated – and continued to partner with those he did not agree with because he could still do good work as a doctor – helping people in need? Should the married couple have maintained their friendship – assimilated – hoping that change would occur over time while tolerating the negative impact upon their children?
Keep watch over your manner of life, dear people, and make sure that you are indeed the Lord’s laborers. Each person should take into account what he does and consider if he is laboring in the vineyard of the Lord. – St. Gregory the Great
The command of the Lord Jesus, “You too go into my vineyard” is a universal call that echoes in every generation and is addressed to every one of us. Catholics in the US are not exempt from this duty in Christ, but as with every generation of disciples, the Lord Jesus is sending us out to the byroads and marketplaces to proclaim the Good News – Jesus is Lord and by His cross He has defeated sin and death!
We will shortly know the consequences of the elections, but no mater their outcome the task and challenge before us is clear – let us recommit ourselves to true and heroic discipleship, while at the same time defending life, family, the most vulnerable, and our Faith. Such a commitment allows God to raise people of virtue, good moral character, and skills worthy of leadership.
We have nothing to fear as long as we live and act with courage and in Faith. Resistance to evil is never futile; on the contrary, it is necessary.
A new study shows that a hormonal birth-control shot for males could effectively prevent pregnancy in female partners, but further studies were cancelled after the men involved in the study experienced side effects, primarily depression. The decision to curtail the studies is ironic, considering the growing evidence that hormonal birth control has similarly negative side effects for women.
The latest example is a recent study of over one million women, which showed that the birth-control pill greatly increases women’s risk of depression, exponentially so among teenage girls. It’s generally accepted — especially after reviewing the evidence gathered over the 55 years since the pill was first approved — that 20 to 30 percent of women on hormonal birth control have experienced depression severe enough to require anti-depressants. Contraception bears negative consequences for a vast number of women, compared to the depression experienced by a mere three percent of the 320 men who received the trial birth-control shot.
And depression is not the only possible side effect for women who take hormonal birth control. A number of studies have shown that women on the pill have a higher risk for developing breast cancer; the World Health Organization has classified many hormonal contraceptives as class-one carcinogens. There are reports that Plan B One-Step, an emergency contraceptive that can function as an abortifacient, necessarily causes systemic side effects in every woman who takes the drug. Hormonal contraception clearly poses terrible risks to women’s health, risks much more serious those experienced by the men in this study.
“If anything, this may wake us up to finding out better hormonal contraceptives for women, right?” said Dr. Seth Cohen, a urologist at NYU Langone Medical Center. “Because certainly, I know that a lot of young women don’t get the type of counseling that maybe they deserve when it comes to contraception. Just a [prescription] and a visit to Duane Reade is all they get, and that may not be enough.”
It is disgraceful that the medical community would abandon male contraception due to mild side effects while at the same continuing to prescribe and advocate even more harmful methods of birth control for countless women. If feminists and “pro-woman” medical professionals actually cared about women’s health — as opposed to unequivocally defending Planned Parenthood, insisting upon abortion-on-demand, and advocating ubiquitous, government-funded contraceptives — they would expose this clear double standard that favors men’s health over women’s.
November 2, 2016 (LifeSiteNews) — In 1979 I arrived, elated yet diffident, in the Chinese village that would be my home for the next year. Within a few months of my arrival, pregnant mothers were being rounded up by local Communist officials and marched off to abortuaries. China’s one-child policy had begun.
As a visiting scholar from America, I insisted on being present when one of these sobbing mothers was forcibly aborted at 7 ½ months. It changed my life.
I was horrified to see the military doctors who had been brought in to perform this butchery actually cut open the mother’s body to get at the baby. The poor baby — I think she was a girl — was of course already dead, having been injected with poison in utero two days before. As the doctor reached in to pull out her corpse, I fled the scene.
But not soon enough.
The sight of the dead girl’s limp body being pulled from the ruined abdomen of her mother is burned into my mind. It is a nightmarish vision that I will carry with me to the grave. I have been uncompromisingly Pro-Life ever since.
I returned to the United States determined to fight for Life. I joined the ranks of the millions of Americans who had been selflessly giving of their time and treasure since 1973, when the Supreme had authorized this modern-day slaughter of the innocents. In my naiveté I anticipated a speedy victory. After all, we had the most pro-life president in modern American history, Ronald Reagan, in office and on our side.
I was wrong. Today, almost four decades later:
Abortion continues to be legal in the United States up to birth.
Planned Parenthood’s industrial-sized killing fields continue in operation.
Hundreds of millions of taxpayer dollars continue to flow into Planned Parenthood’s coffers.
The U.S. State Department continues to coerce foreign governments into legalizing abortion.
USAID continues to vigorously promote and fund population control programs.
To be sure, over the years we have won some victories. Thanks to President Reagan, in 1984 we were able to put in place the Mexico City Policy. This requires non-governmental organizations (NGOs) that receive federal funding to certify that they will not perform, promote, or lobby for the legalization of abortion in other countries.
A year later, again thanks to Reagan, we were able to defund the UN Population Fund, an agency that was — and is — heavily involved in China’s program of forced abortions and sterilizations. I was proud of this victory. I provided much of the evidence.
We also cut back spending on population control and reduced Planned Parenthood’s taxpayer subsidies.
Yet with each new Democrat administration — first Clinton, and then Obama — these advances were undone. The pro-life movement was never politically strong enough to write these gains into settled law.
Legislative victories were few and far between, although there have been a few. We were, in 2003, thanks to the tireless efforts of Senator Rick Santorum, able to prohibit a particularly horrific form of late-term abortion, partial birth abortion.
Moreover, we have been increasingly successful at the state level. After the Supreme Court in 1989 allowed states to pass reasonable restrictions on abortion, hundreds of pro-life laws have been passed by state legislatures. Dozens of states now mandate waiting periods, counseling, ultrasounds and, in the case of minors, parental consent. Underlining the humanity of the unborn, dozens of states have also put “fetal homicide” laws in place.
Still, abortion remains legal throughout all fifty states. Decade after decade, the lives of more than one million unborn Americans continue to be wrongly snuffed out each year. This is without a doubt the greatest continuing human tragedy in American history.
Why have we not been able to stop this tragedy, which violates the very principles that America was founded upon? Why have we not been able to keep the promise of The Declaration of Independence that every American is entitled to Life, Liberty, and the pursuit of Happiness?
The answer lies in the brilliantly designed system of checks and balances bequeathed to us by our Founders. Those who drafted the Constitution did not want to escape one tyrant only to fall into the hands of one of their own making, so they carefully divided power between three separate but equal branches of government. The legislature would pass laws, the chief executive would carry them out, and the judiciary would look over the shoulders of both, making sure that neither overstepped their bounds.
This worked pretty well for a couple of centuries, then the unexpected happened. An abortion case came before the U.S. Supreme Court. And a majority of justices decided that they would write their own prejudices into their ruling. Justice Harry Blackmun, who wrote the majority opinion, was careful to concoct a tissue of rationalizations to hide the fact that he and his colleagues were legislating from the bench. But it was clear to legal scholars what they were about. As my friend Judge Robert Bork often remarked, “Roe v. Wade was an act of raw judicial tyranny.”
This infamous act could have been overturned by the Congress and the President, or by the Supreme Court itself. This hasn’t happened, primarily because the American people, in their wisdom, rarely give the same political party control over the House, the Senate, and the White House. Since our two main political parties are on opposite sides of this issue — the Republicans are the Party of Life, while the Democrats are in lockstep on abortion — gridlock ensues.
In the Eighties the House Republicans were checked by the Senate Democrats, and little pro-life legislation wound up on President Reagan’s desk. In the nineties, the situation was reversed. The Republican House refused to go along with proposals that the Democratic Senate and a pro-abortion president, Bill Clinton, would have signed.
The Party of Abortion and the Party of Life have been in a political stalemate for almost four decades, preventing a legislative remedy to our national tragedy of abortion from emerging from the Congress and the White House.
The Supreme Court has been equally divided, due in no small part to the carelessness with which pro-life presidents have made their judicial nominations, and the carefulness with which pro-abortion presidents made theirs.
Since before World War II, the Democrats have consistently appointed only ideological soul mates to the Supreme Court. Their appointees, like Justices Sonia Sotomayor and Elena Kagan, invariably believe that the Constitution is a “living document” and that the law is a “social construct.” Thus they can be counted upon to reinterpret the Constitution at will to justify whatever behavior the liberal prejudices of the day approve of, including gay marriage, assisted suicide and, in this case, unrestricted abortion.
The Republican record on nominations is much more spotty. In addition to nominating brilliant conservative justices like Antonin Scalia and William Rehnquist, President Reagan also brought the unreliable Sandra Day O’Connor and notoriously quixotic Anthony Kennedy onto the Court. The first President Bush, himself a latecomer to the pro-life cause, had an equally mixed record. Clarence Thomas, one of Bush’s nominees, has been one of the great pro-life justices of all time. But he also gave us David Souter, who sailed through confirmation and promptly took up residence on the Court’s left wing, where he has been a reliable vote for abortion on demand ever since.
Not once in the last 43 years have we enjoyed a solid pro-life majority on the Supreme Court.
Not once in the past 43 years have we ever had a pro-life President and a solid pro-life majority in the Senate and the House at the same time. We have always fallen short in one respect or another.
That’s why this upcoming election is so important for pro-lifers.
On November 8th, for the first time in a generation, we have an opportunity to elect not just a pro-life House, and not just a pro-life Senate. We have an opportunity to elect a President who has promised to implement pro-life measures, and a Vice President with a solid and longstanding pro-life record.
If this happens, a number of very good things will happen quickly. Planned Parenthood will be defunded, and a bill banning abortions after 20 weeks will be passed and signed into law. U.S.-driven population control programs will be shut down, and the State Department will be told to get out of the business of trying to impose abortion and other aberrations on the rest of the world.
The Supreme Court will follow, albeit more slowly.
First the seat vacated by Antonin Scalia will be filled — the list of possible replacements has already been released. Then we must wait until another elderly justice or two steps down, at which time a solid pro-life majority will be created.
Then and only then, Roe v. Wade will be decisively overturned. The issue of abortion will be sent back to the states, most of which have laws protecting Life already on the books.
This happy scenario, of course, depends entirely on the outcome of the election.
By the morning of November 9th, we will know the fate of our movement. We will either be savoring our electoral victory and the prospect of pro-life victories in the Executive, in the Congress, and in the Supreme Court.
Or we will be hunkering down to fight a desperate rearguard action against the most rapidly pro-abortion administration America has ever seen.
One thing is absolutely certain: It took 43 long years for this historic opportunity to present itself.
If we let this opportunity slip by, it may not come again in our lifetimes.
In the meantime, millions of unborn Americans will die at the hands of Planned Parenthood’s abortionists. Overseas the death toll will be even higher. Tens of millions will perish, condemned to death by a U.S. foreign aid establishment that is hellbent on eliminating the poor.
Seize the moment. Vote Pro-Life.
The babies can’t wait.
Steven W. Mosher is the president of the Population Research Institute and the author of the forthcoming, The Bully of Asia (Regnery).
Less than a week before Americans cast their votes for president, Catholic bishops are urging their congregants to educate themselves about the candidates’ positions on abortion.
The next president could make a huge impact on the future of abortion in the U.S. through his or her nominees to the U.S. Supreme Court and other policies. And Democratic candidate Hillary Clinton specifically is touting a radical pro-abortion agenda that would force Americans to pay for abortions with their tax dollars.
On Sunday, Catholic Bishop William Murphy, head of the Diocese of Rockville Centre in Long Island, said in a letter at Masses that support for abortion “should disqualify any and every such candidate from receiving our vote,” Newsday reports.
Murphy encouraged Catholics not to participate in the “division,” “mean spiritedness” and “intolerance” surrounding the presidential election. He urged them to make serious, educated decisions about who they choose as our nation’s next leaders, and he emphasized that abortion is the most “crucial” issue of all.
Murphy continued:
The human person, made in the image and likeness of God, is the ultimate measure of what is good or bad, right or wrong. Every person is sacred and has inherent rights which political leaders must protect and serve. Those who do not are unworthy of our vote. Those who contradict themselves by saying one thing and doing another are unworthy of our vote.
Many issues are very important in our society today. But none of them can eclipse the centrality of human life, especially innocent human life in the womb or at the end of life. Above all and over all, the number one issue more fundamental and crucial than any other is abortion – that is the direct taking of innocent life, which is financed by government funds — the diversion of our tax dollars to abortionists like Planned Parenthood as well as government insistence that we Catholics like the Little Sisters of the Poor, violate our consciences to advance such programs.
Support of abortion by a candidate for public office, some of whom are Catholics, even if they use the fallacious and deeply offensive “personally opposed but . . .” line, is reason sufficient unto itself to disqualify any and every such candidate from receiving our vote. Let me repeat that: Support of abortion by a candidate for public office, some of whom are Catholics, even if they use the fallacious and deeply offensive “personally opposed but . . .” line, is reason sufficient unto itself to disqualify any and every such candidate from receiving our vote.
Murphy did not name names, but Clinton’s vice presidential running mate, Tim Kaine, is a Catholic who supports abortions while claiming to be “personally opposed.” Kaine has flip-flopped several times on whether he will support Clinton’s plan to repeal the Hyde Amendment and force taxpayers to fund abortions.
In an interview with CNN in July, Kaine said: “On Hyde my position is the same I support the Hyde amendment. I haven’t changed that. As the vice president I have to get comfortable with the notion that I can have my personal views but I’m going to support the president of the United States and I will.”
As a U.S. Senator, Kaine has voted against the pro-life position every chance he got. Kaine took his most extreme pro-abortion action yet with his recent co-sponsorship of the so-called “Women’s Health Protection Act” (S.217), known to pro-lifers as the “Abortion Without Limits Until Birth Act.”
Every year, more than 1 million unborn babies are killed in legal abortions in the U.S., and the nation’s largest abortion provider, Planned Parenthood, gets half a billion of our tax dollars. Pro-lifers of all faiths and no faith should weigh these facts heavily before casting their vote next Tuesday.
Contemporary culture is in a deep crisis regarding holy matrimony. Both the truth about the family and families themselves are being ripped a part by violent forces. Proponents of the Culture of Death know well the importance and centrality of the natural family; otherwise, why exhaust so much time, effort, and resources attacking it?
This doesn’t only weaken the family, it will weaken the nation. Indeed, throughout history, this has been a well known strategy for conquering opponents — attacking the most fundamental elements of language and culture. The renowned general, military strategist, and philosopher of ancient China, Sun Tzu (544-496 BC), laid out the strategy in The Art of War:
There is no art higher than to destroy your enemy without a fight by subverting anything of value in your enemy’s country.
Over time and with great diligence, promoters of sexual license, gender ideology, and the redefinition of marriage have radically changed the way we think of matrimony and family. Most no longer understand that basic truth that in its essence, marriage is one man and one woman in an indissoluble, exclusive, and fruitful union. Most people in our culture no longer understand the role of matrimony and family and are incapable of defending these sacred institutions, thus becoming easy prey to radical anti-marriage and family ideologies.
Of course we shouldn’t be surprised that marriage and family are at the crux of the battle.
The final battle between the Lord and the reign of Satan will be about marriage and the family. Don’t be afraid, she added, because anyone who works for the sanctity of marriage and the family will always be fought and opposed in every way, because this is the decisive issue. And then she concluded: however, Our Lady has already crushed its head. — Sister Lucia, Visionary of Fatima
It has been so for nearly a century. On October 13, 1917, while the three seers of Fatima were joined by tens of thousands who witnessed the Miracle of the Sun, Russia’s October Revolution was underway. Its leader, Vladimir Lenin, was open about his attack on the family, and as prophesied by the Virgin Mary, Russia’s errors spread throughout the world, their destruction accelerated in part by how they have found purchase here in the United State.
The current US presidential and congressional elections are but one example of how the war on these institutions continues. With poisonous eloquence, political candidates and pundits defend same-sex unions, perverted sex education programs, sex and reproductive rights — contraception and abortion — and gender role confusion. These modern day pipers play their melodious tunes, leading all who listen to cultural and societal demise.
The attack on the family would not have so much success, even among Christians, without the misrepresentation of the role of conscience. The catchphrase “Follow your conscience” is used to justify one’s ability to do almost anything one chooses or believes is good. This misunderstanding of freedom of conscience is an exceptionally clever way of ending all discussion on what is morally good from evil: “Who are you to tell me what I can or cannot do?”
Try telling a judge or jury that your conscience allowed you to steal from your neighbor or kill your boss because he wouldn’t give you a raise. Try convincing a police officer that you ran the red light because you were “following your conscience.” It sounds ridiculous because it is ridiculous!
The weapons of this battle on marriage and the family, and our ability to use our conscience to do good, are the tools of propaganda and illusion aimed at transforming the minds and hearts. They use television, radio, film, the internet, and music as their primary media to promote a radical and distorted worldview. They further their grasp through perverted sex education programs imposed upon our youth, beginning as early as grade school. I recently witnessed an example of this in Guatemala City. One of the speakers showed a video depicting girls ages 6 and 7 being taught how to place a condom on a phallus. The video also showed young adolescents how to masturbate and be open to experimentation with other boys and girls. Under the guise of “comprehensive sex education”, these programs desensitize our young and pervert the moral and religious values being taught by their parents.
HLI’s global leaders see this all over the world. Emil Hagamu and George Wirnkar, our regional directors in Africa, have seen such programs firsthand. On a recent trip to Africa, I saw a textbook being used in many African countries to teach sex education. It was filled with pornography and images of children experimenting with different types of sexual activities. It taught African children how to use condoms and promoted gender role confusion.
The US government’s war on matrimony and family is upheld in its foreign policy. These policies demand and assure that any funding is directly connected to population control and the promotion of sexual and reproductive rights — contraception, abortion, sterilization, sex education programs and legalization of same sex unions. Through USAID and the UN’s Population (Control) Fund (UNFPA), such programs and policies are implemented. This directly influences cultures and their understanding of matrimony and family. The US does not use weapons of mass destruction to carry out its battle plans, but the destruction and devastation is the same, and its affects are generational.
Our nation, founded on the rights to “life, liberty, and the pursuit of happiness” is itself in crisis. We are divided because we no longer uphold objective truth. In his brilliant book God or Nothing, Robert Cardinal Sarah sheds a different light — the light of faith – on these same realities.
Without God, man builds his hell on earth. Amusements and pleasures can become a true scourge for the soul when it sinks into pornography, drugs, violence, and all sorts of perversions. There is great sadness in claiming to want to indulge in limitless pleasures, whereas the most beautiful joy is to remain simply with God, allowing him to clothe us in light and purity.
Our faith and resolve to bring about a cultural transformation is being tested.
What is our response to this war? Return to the Creator’s plan. Matrimony and family are God’s design, and as divine institutions they are not open to renegotiation or revision — there are no substitutions. Fundamentally, our global cultures and societies need a moral counter-revolution to replace the Culture of Death.
Too bad. If united, Catholics could control the outcome of the election, protect the Church and move the country in a direction more attuned to the values of the Church. But we are split between Catholics who deem the sanctity of life as the pre-eminent issue (conservatives) and those for whom care for the poor, the vulnerable and the stranger among us is the more cogent concern (progressives). But there is an issue that should unite us. If ignored then both groups face persecution and neither will be free to carry out their mission.
CONSIDER THE FOLLOWING ACTUAL CASES
1) The Little Sisters of the Poor just want to take care of old people and practice their faith. Yet there are people in this country who would rather prevent them from doing the former than let them do the latter.
2) Catholic Social Services in Massachusetts took care of orphans for over one hundred years, but there are people who put them out of business rather than let them practice their faith which required not placing orphans with gay couples.
3) There are people who preferred to see Catholic Charities stop providing aid to refugees rather than let them do so without also providing contraception and abortion.
4) There are people who preferred to see a county clerk in Kentucky thrown in jail rather than figure out how to let her do her job in such a way as not to be cooperating with what she believed and what the Catholic Church teaches is grave sin.
5) There are people who have chosen to drive bakers in Washington out of business rather than allow them to commit the same “crime” of not cooperating with sin.
6) There are people who would rather see a military chaplain disciplined than let him provide spiritual advice that is not politically correct.
7) There are people who fired a football coach rather than let him pray voluntarily after a football game.
8) There are people who want men to be free to go into girls and women’s bathrooms and locker rooms.
9) And there are people who not only want to be free to kill babies until the moment of birth, and even during birth, but want all of us to pay for it.
A TWO PART PATTERN THAT’S HARD TO MISS
1) In each case above the Church and the faithful (both conservatives and progressives) are being prevented from carrying out their mission; and 2) The people who are taking away these freedoms all belong to the same political party. If you know which party that is, it proves the point.
Shouldn’t the issue of the freedom of the Church to carry out its mission and of the faithful to practice their religion in public be the preeminent concern for all Catholic voters and indeed all true Christians and Americans? We have every reason to unite in opposition to the easy to identify people who are perpetrating these injustices. If we don’t unite against these attacks by voting these people out of office, then we and our Church will soon no longer have the freedom to either battle the wanton destruction of human life called abortion, or to care for the poor, the vulnerable and the stranger among us.
YOU MIGHT NOT HAVE A CHURCH TO GO TO IF YOU DON’T VOTE THE RIGHT WAY IN NOVEMBER
Father Michael Orsi of St. Agnes Parish in Naples Florida and former chaplain of Ave Maria Law School, in reminding pastors that they are allowed to be political in church and in urging them to “speak truth to power”, told them, “You might not have a church to go to if you don’t vote the right way in November.” Was he exaggerating or was he right? Can we afford to vote the wrong way, or not vote at all, and find out?
Reggie Littlejohn, President of Women’s Rights Without Frontiers, stated, “With all her experience as former Secretary of State, it is untrue and deeply disappointing for Hillary Clinton to put the Chinese government’s practice of forced abortion in the past. If she thinks that China no longer forces women to abort babies, she should explain that to a couple, surnamed Zhong, who in August of this year were forced to choose between an abortion at eight months or the loss of both of their government jobs. Or she should inform He Liping, who was forced either to pay an impossible “terror fine” of $39,000 or face abortion at six months.
“Or perhaps she should read the May 4, 2016, BBC article entitled ‘Reinventing China’s Abortion Police,’ which discusses a small collaborative project by Stanford University and Shaanxi Normal University to repurpose 69 Family Planning Officials — apparently on the assumption that they are no longer needed now that China has moved to a two-child policy.” The article follows one Family Planning Official, Li Bo, who has been “reinvented” from “hunt[ing] down families suspected of violating the country’s draconian rules on how many children couples can have” into a rubber duckie squeezing, nursery rhyme singing “Chinese Father Christmas,” complete with “a bag full of toys and picture books.”
Has his job really been “reinvented,” or is he really a member of the womb police, masquerading as “Chinese Father Christmas” — the new face of China’s Family Planning Police? Buried deep in the article is the following account of the dark side of Li Bo’s job – an important piece of original reporting by the BBC:
Since the start of 2016, all Chinese couples have been allowed two children. But they can have no more than that unless they are from ethnic minorities – so Li Bo still spends some of his time working as a birth-control enforcer. In the town’s health clinic he is busy screening local women. All women of childbearing age have check-ups four times a year to ensure they’re healthy . . . and to see if they are pregnant. . . But Li is also a loyal Communist party official who believes the state knows best and society’s needs are greater than those of individuals. So he is matter-of-fact about the unpleasant task of telling women who couldn’t afford the fine to terminate their pregnancies. “People didn’t swear at us but they probably did behind our backs,” he says. “It’s natural because we were carrying out the law and they were breaking it so it is just like the clash between a policeman and a thief.” He adds that as long as restrictions are in place, such clashes will continue.
From these words, uttered by a Chinese Communist Family Planning Official, we learn that:
1) Coercive pregnancy screening continues. Under the Two-Child Policy, Family Planning Police continue to screen women of child-bearing age for pregnancy four times a year.
2) Forced abortion continues. It is still illegal for single women to have babies in China, and for couples to have third children. It appears that some may be given an opportunity to pay a fine, but Li Bo tells “those who couldn’t afford the fine to terminate their pregnancies.” In other words, if a woman is illegally pregnant and cannot pay the fine – which can be as much as ten times her annual salary – she is forced to abort. Forced abortion, therefore, continues under the Two-Child Policy.
3) Women pregnant without permission are considered criminals. Li Bo’s statement that women who are pregnant without permission “were breaking it [the law] so it is just like the clash between a policeman and a thief” demonstrates that such pregnancies are still considered illegal; and illegally pregnant women are regarded lawbreakers deserving of punishment, just like thieves.
4) Forced abortion continues to cause unrest. Li Bo is correct in adding that “as long as restrictions are in place, such clashes will continue.” This statement is an admission that these clashes – often resulting in forced abortion – continue to this day, due to the two-child restrictions.
Littlejohn concluded: “The Chinese Communist Party has not agreed to get out of the bedrooms of the Chinese people, and Presidential candidates should not be stating or implying that they have. We need to keep the international pressure on the Chinese Communist Party until all coercive population control is eradicated.”
Though he has local roots in the Kansas City area, I have never met vice presidential candidate, Senator Tim Kaine. From those who do know him, I understand that he is a very affable and likable person.
In the Oct. 4 vice presidential debate, Senator Kaine acknowledged he was blessed with great Irish Catholic parents and grew up in a wonderful faith-filled family. He also mentioned proudly that he is a graduate of Rockhurst High School, crediting the Jesuits with instilling within him a desire for public service and a commitment to advocate for the poor. I wish that was the end of the story.
It was painful to listen to Senator Kaine repeat the same tired and contorted reasoning to profess his personal opposition to abortion while justifying his commitment to keep it legal. He said all the usual made-for-modern-media sound bites: It is not proper to impose his religious beliefs upon all Americans. He trusts women to make good reproductive choices. And when all else fails, there is always: Do we really want to criminalize and fill our jails with post-abortive women?
With regard to the imposition of religious beliefs, Senator Kaine appears to have no qualms with his public positions conforming with his religious beliefs with regard to such issues as the church’s opposition to racism or our preferential option for the poor. He appears not to be conflicted with our public policies mirroring the Ten Commandments with regard to stealing, perjury, or forms of murder, other than abortion.
The founders of our nation actually dealt with this issue 240 years ago in the Declaration of Independence, in which they articulate certain self-evident and inalienable rights that government does not bestow but has a responsibility to protect. Our founders actually believed that the right to life is given to us by our Creator, not by the Supreme Court.
Of course, religion will speak about fundamental human rights issues. However, to understand that the government has a right to protect human life is not dependent on religious belief. As the founders’ stated, these are self-evident truths. They are accessible to everyone through the use of reason. They do not require faith.
Why is Senator Kaine personally opposed to abortion, if he does not believe that it is the taking of an innocent human life? I hope in his science classes at Rockhurst he learned that at the moment of fertilization a new human life has begun with his or her own distinct DNA — different from the genetic code of both the child’s mother and father.
It is difficult to imagine that Senator Kaine has not seen the ultrasound images of his children and grandchildren when they were in their mother’s womb. Is the senator unaware that abortion stopped the beating hearts of 60 million American children aborted legally since 1973?
If he knows these truths of biology, why would he believe that anyone has the right to authorize the killing of an unborn human being? This is where the reproductive choice euphemism breaks apart. Does anyone really have the choice to end another human being’s life? Our choices end where another individual’s more fundamental rights begin.
As far as Senator Kaine’s fear that if abortion is made illegal, our prisons will be teeming with post-abortive women, we actually have decades of legal history in our own country when this was certainly not the case.
Before the late 1960s when abortion was illegal in every state, except for the life-of-the-mother cases, it is difficult to find a single instance of a woman imprisoned for abortion. The laws were enforced against the abortionists. Our own legal experience shows clearly that it is possible to develop public policies aimed at protecting children, not punishing women.
Actually, I wish Senator Kaine would take the time to talk with some of the post–abortive women that are assisted by Project Rachel and other post-abortion ministries helping women and men find healing, hope and mercy after an abortion. Our current permissive abortion policies, placing the entire burden of responsibility for the abortion decision upon the mother, results in millions of women experiencing an inner imprisonment where the bars keeping them from freedom and happiness are the guilt and unresolved grief that inevitably ensues from abortion.
It is interesting that Senator Kaine expressed his personal anguish when as governor he enforced capital punishment sentences. He gave the impression that he attempted unsuccessfully to convince Virginians to abolish the death penalty. Yet, with regard to legalized abortion, I am not aware of Senator Kaine making a similar effort to convince his constituents to work for public policies that protect the lives of the unborn. Instead, he appears eager to champion not only maintaining the status quo, but actually expanding abortion rights.
It is ironic that Senator Kaine expressed such profound concern about imposing his religious beliefs on others, while supporting efforts: 1) to coerce the Little Sisters of the Poor and other faith-based ministries to violate their conscience by including abortifacients, contraceptives and sterilizations in their employee health plans; 2) to put small business owners (e.g., florists, bakers, photographers, etc.) out of business with crippling fines if they decline to participate in same-sex marriage ceremonies; and 3) to force every American taxpayer to help fund abortion.
This presidential election presents all Americans with a difficult choice. Both major political parties have nominated very flawed candidates. In making your decision as a voter, I encourage you to think not only of the candidate, but who they will appoint to key Cabinet and other powerful government positions if he or she becomes president. We are choosing not just a president, but an entire administration.
Finally, be wary of candidates who assume to take upon themselves the role of defining what Catholics believe or should believe. Unfortunately, the vice-presidential debate revealed that the Catholic running for the second highest office in our land is an orthodox member of his party, fully embracing his party’s platform, but a cafeteria Catholic, picking and choosing the teachings of the Catholic Church that are politically convenient.
WASHINGTON (Lepanto Institute) – An explosive new report by the Lepanto Institute reveals that the official overseas relief and development agency of the U.S. Conference of Catholic Bishops received and dispensed over 2.25 million units of abortifacient contraception and condoms for a government-funded project in Africa. From 2006–2010, Catholic Relief Services (CRS) was an implementing partner for a USAID project called Project AXxes, and according to inventory reports contained in quarterly and annual reports for the project, CRS received, stored and dispensed millions of contraceptives, including condoms, oral contraceptives, injectable contraceptives, intra-uterine devices, and even surgical sterilization kits.
“The implications of this report could have far-reaching consequences for CRS,” said Michael Hichborn, president of the Lepanto Institute. “For the last six years, CRS has been dodging around revelations of its impropriety by telling bishops and faithful Catholics that it ‘never’ promotes, distributes or facilitates the distribution of contraception. We now have proof that CRS’s claim is completely untrue.”
The report by Lepanto Institute references section 3.4.1 of the Administrative, Financial, and Operations Procedures Manual for Project AXxes on physical inventory. According to the procedures manual, visual inventory was to be conducted each quarter, by “the administrator/manager of the project, the logistician and another member of the team,” and signed by each, as well as “by the owner and the person responsible for the inventory.”
“The most disturbing thing we discovered about Project AXxes is that the promotion of contraception was integrated into nearly every aspect of the project, even to the point that natural family planning was identified as an entry to introducing contraception,” said Hichborn. “And what’s really sad is that CRSintroduced this program to a people who had no previous access to methods of birth control.”
In relation to the report, the Lepanto Institute has launched a petition to the bishops of the United States asking them to forbid CRS from participating in any future PEPFAR or USAID programs. The petition can be found here.
Read the report: “Catholic Relief Services and the Distribution of Abortifacient Contraception in the Congo.”
Many young women were understandably seduced by the once widely publicized message that if they chose to delay pregnancy and were then unable to conceive, they could still have babies through in vitro fertilization, also known as I.V.F.
Miriam Zoll was one of them. Married at age 35, she thought she had plenty of time to start a family. After all, she said, “My mother had me at 40, and since 1978, the fertility industry has been celebrating its ability to help women have children at older ages.”
When at 39 she and her husband decided to start a family, they discovered that nature refused to cooperate. Four emotionally and physically exhausting I.V.F. cycles (and two attempted donor egg cycles) later, they remained childless.
“What the industry didn’t say is that the success rate for older women is consistently low,” she said. “It focused on the 20 percent of women who succeed, not the 80 percent failure rate. The industry avoided saying that the technology hasn’t worked for an estimated 20 million women globally during the last 40 years.”
Women who did not have healthy babies with I.V.F. are far less likely to speak openly about the procedure than those for whom the technique was successful.
Shocked by what happened to her and realizing that so many other women faced similar disappointment, Ms. Zoll, who lives in Conway, Mass., decided to write a book, “Cracked Open: Liberty, Fertility, and the Pursuit of High-Tech Babies,” to put assisted reproduction on a more realistic footing and counter the rosy picture of I.V.F.
Her story prompted me to check the latest federally mandated statistics gathered by the Centers for Disease and Prevention from the nation’s nearly 500 fertility clinics on I.V.F. procedures done in 2013. Using fresh (that is, not frozen) eggs or embryos from women trying to conceive, at age 40 fewer than 30 percent undergoing I.V.F. became pregnant and fewer than 20 percent gave birth to live babies as a result.
The success rate was somewhat better when I.V.F. was done with frozen embryos from a woman’s own eggs: about 42 percent became pregnant and 30 percent delivered live babies.
Dr. Mark V. Sauer, former director of the I.V.F. clinic at Columbia Presbyterian Medical Center who has been using the technique for three decades, corroborated Ms. Zoll’s frustration with the industry’s self-promotion.
“Programs will brag that they are the best, with extraordinarily high rates of pregnancy even in women over 40,” Dr. Sauer said in an interview. “There’s hardly any age that the clinics now turn away.” He cited reports in both the lay and medical literature of even postmenopausal women giving birth through I.V.F.
On clinic websites, he said, “There’s a lot of massaging of the data, often combining data from several years to make the results look better. And clinical pregnancy rates do not necessarily reflect live birthrates. Live births are what really matter.”
Furthermore, he said, “The younger women are when they undergo I.V.F., the better the pregnancy rates,” adding that younger women are also more likely to have healthy pregnancies that end with the birth of healthy babies.
In a report he published last year in Fertility and Sterility, Dr. Sauer wrote that “advanced age” is a risk factor not only for female infertility, but also for “pregnancy loss, fetal anomalies, stillbirth, and obstetric complications.”
Although these risks have been known for centuries, “women are delaying childbearing to pursue educational and career goals in greater numbers than ever before,” he wrote. “Data from the United States demonstrate a dramatic rise in births to mothers once considered ‘elderly.’ This is particularly evident in women older than 40,” an age at which there is a significant rise in infertility, as well as higher rates of miscarriage among women who succeed in getting pregnant.
Dr. Sauer pleaded with doctors to “promote more realistic views” of the realities of pregnancy at advanced ages. He advised doctors to “actively educate both patients and the public that there is a real danger of childlessness if individuals choose to delay reproduction. It should be with guarded optimism that we promote delayed childbearing to our patients, because risks to both mother and child are invariably present; and because many failed attempts also occur, the risk of lifelong childlessness cannot be overstated.”
The doctor acknowledges the dilemma faced by women who seek higher education and want to become established in a career before attempting to start a family. And he realizes that “ideally pregnancy should also occur when they are settled with a life partner who will share the burden of raising offspring.”
Nonetheless, Dr. Sauer points out, the facts of biology are irrefutable. “Biologically speaking,” he wrote, “women are most fertile between the ages of 15 and 30.” Although from a career perspective, many are unwilling to start a family then, ages 35 to 45 represent the “terminal decline in normal fecundity,” as well as a greatly increased risk of producing eggs and embryos with chromosomal and other abnormalities.
Ms. Zoll’s devastating experience with I.V.F. changed her “from a trusting consumer into a person who now knows she has to do her own research — even before seeing the doctor — and has to ask lots of questions. I trusted what the doctors told me, and afterward was blown away by my own naïveté. Consumers should be saying, ‘Let me see the evidence.’”
After spending a significant amount of money (most, fortunately in her case, covered by insurance mandated by the state of Massachusetts) and seven years trying to have a baby, Ms. Zoll said she and her husband “moved very quickly into adoption, and within seven months of filing adoption papers, our son was placed with us.” She described their son, now 7, as “tenacious, smart and funny. I can’t imagine having anyone so close to my heart.”
This Sunday, the glitterati will celebrate the one hundredth anniversary of the Planned Parenthood Federation of America. Senate Democrats have introduced a resolution honoring PPFA. One hundred Hollywood stars have signed a congratulatory letter to the organization. Hillary Clinton herself has spoken repeatedly about how much she adores the abortion business’s founder, eugenicist Margaret Sanger. And, of course, we see in the media hundreds of fawning editorials singing the praises of the most corrupt business in the history of this nation.
If the proverbial Martian visited our planet right about now, he would assume from such coverage that Planned Parenthood is an organization composed entirely of saints whose lives are dedicated to the ideals of freedom, choice and human happiness while struggling valiantly against woman-hating terrorists.
However, if the Martian had the capacity for rational thought took the time to dig a little deeper, he would be horrified by what lies below the surface.
Margaret Sanger
Margaret Sanger
Margaret Sanger was not merely friendly to the idea of eugenics, she was a eugenicist to the core. She wrote that the mission of her organization was “To promote eugenic birth selection throughout the United States so that there may be more well‑born and fewer ill‑born children ― a stronger, healthier and more intelligent race.”[1] Sanger followed eugenic reasoning to its logical conclusion ― that charity is “dysgenic,” leading to a degradation of the human race:
We are now in a state where our charities, our compensation acts, our pensions, hospitals, and even our drainage and sanitary equipment all tend to keep alive the sickly and the weak, who are allowed to propagate and in turn produce a race of degenerates.[2]
Of course, then as now, if the lowly do not embrace the Utopian plans of the elite, they must be whipped into line by greater and greater degrees of coercion. Sanger herself said that “Possibly drastic and Spartan methods may be forced upon society if it continues complacently to encourage the chance and chaotic breeding that has resulted from our stupidly cruel sentimentalism.”[3]
Contributors to Sanger’s The Birth Control Review especially loathed the Catholic Church, but they had plenty of contempt left over for minorities. Julian Huxley, founder of the World Wildlife Fund, commented in a BCR article that “There is, first, the mere question of quantity of population, quantity of Americans in the world versus the quantity of Englishmen, versus the quantity of Africans, versus the quantity of Chinese. If you have one race whose population is going down and another whose population is going up, there is always the possibility of race suicide ….”[4]
In an article entitled “God’s Chillun” in the special “Negro Number” of The Birth Control Review, Walter Terpenning wrote that “Many of the colored citizens are fine specimens of humanity. A good share of them, however, constitute a large percentage of Kalamazoo’s human scrap‑pile … The dissemination of the information of birth control should have begun with this [Negro] class rather than with the upper social and economic classes of white citizens.”[5]
At least we cannot accuse the contributors to The Birth Control Review of being inconsistent in their racism, because they held everyone in contempt who did not measure up to their Nordic ideal.
On Puerto Ricans: “He lives literally in chronic starvation, crowding his filthy scarecrow body into a hut where his female counterpart and their numberless wretched children almost always share at least one of his diseases.”[6]
On Italians: “Look over ‘Who’s Who in America’ for Italian names. They are conspicuous by their absence. …”[7]
On the Polish: “Polish men are often immoral because they have been born of too young mothers or preceded by many born before.”[8]
On Southerners: “The southern woman is fifty years behind the rest of the women in the country. She has no mind, no individuality, no initiative, and without question accepts all the absurd conventionalities that hedge her about and keep her a charming and useless dependent on her husband.”[9]
The result is inevitable: A staggering one-third of African Americans have been aborted.[10]
The American Birth Control League led the way in the 1920s, and its successor, the Planned Parenthood Federation of America leads the way now. The organization’s highest award is named for its founder, and they defend her legacy without qualification to this day.
Planned Parenthood Today
Planned Parenthood has never lost sight of Sanger’s vision, pursuing it with a single-minded fanaticism that boggles the imagination even if the organization’s targeting of minorities is no longer so overt. PPFA’s clinics and affiliates now perform one out of three abortions in the United States. Its abortionists have snuffed out the lives of 7.6 million unborn American babies, disproportionately those of poor and minority women. To give this some idea of scale, this is the fourth largest genocide in modern history, ranking behind only Hitler, Stalin and Mao. PP’s income since 1999 has been 20 billion dollars, much of which has been our involuntary contribution through our tax dollars.
But these numbers, as stunning as they are, do not even begin to properly describe the true legacy of the Planned Parenthood Federation of America.
Its legacy is reflected in the desperate face of the teenage girl whose PP-supplied birth control failed her, an unfortunately common occurrence that, if many former PP employees are to believed, was part of a strategy to create abortion clients. It is in the face of the sex-addict furtively glancing both ways before opening the door of a run-down, tawdry “adult book and novelty shop.” It is in the face of the poor single mother who has embraced the Planned Parenthood gospel of free (but “responsible”) sex, who has had several abortions of children conceived by different men who abandoned her, and yet has not achieved “empowerment.” It is in the face of the homosexual man dying of AIDS at the age of forty because he took PP’s advice to “have as much sex as you want, but have it ‘responsibly.’”
It is no exaggeration to say that the “free sex” mantra of Planned Parenthood has destroyed and stunted millions of lives.
This, then, is the legacy of Planned Parenthood — not freedom for women, but slavery. Not happiness, but sorrow and guilt. Not choice, but coercion.
It has covered up for sex slavery. Its `counselors’ have told child molesters how to avoid detection. It has sold the body parts of its victims for profit. It has even produced a cartoon that shows pro-lifers being blown up, drowned and decapitated.[11]
The fact that Planned Parenthood is turning 100 is an indictment against our nation, not cause for celebration. Though babies, minorities, and women have been targeted most directly by its unrelenting assault on life, we have all been harmed by its being allowed to grow its grisly business funded by our tax dollars and allowed by our indifference. Let this anniversary be a reminder to all of us to increase our efforts in prayer and peaceful activism to end Planned Parenthood’s reign of destruction.
Endnotes
[1] Advertisement in the Birth Control Review, Volume I, Number 1 (New Series, October 1933), page 8. Another advertisement in this vein said that “THE AMERICAN BIRTH CONTROL LEAGUE. Its Aim: To promote eugenic birth selection throughout the United States so that there may be more well‑born and fewer ill‑born children ― a stronger, healthier, more intelligent race … and in order that those who are physically and mentally unsound may use birth control to have fewer or no children” [Membership advertisement for the American Birth Control League. Birth Control Review, Volume XVI, Number 12 (December 1932), page 319].
[2] Margaret Sanger. “Birth Control and Women’s Health.” Birth Control Review, Volume I, Number 12 (December 1917), page 7.
[3] Margaret Sanger. “The Eugenic Value of Birth Control Propaganda.” Birth Control Review, Volume V, Number 10 (October 1921), page 5.
[4] Julian Huxley. “Towards a Higher Civilization.” Birth Control Review, Volume XIV, Number 12 (December 1930), pages 342 to 345.
[5] Walter Terpenning. “God’s Chillun.” Birth Control Review, Volume XVI, Number 6 (June 1932, the “Negro Number”), pages 171 and 172.
[6] “Puerto Rico: Old Woman in a Shoe.” Birth Control Review, Volume IV, Number 5 (New Series, January 1937), page 6.
[7] Edward M. East. “The Fascisti on Birth Control; An Italian Problem: Reply to Count Cippico.” Birth Control Review, Volume IX, Number 9 (September 1925), pages 245 and 246.
[8] Rev. T.V. Jakimowitz. “A Priest on Birth Control.” Birth Control Review, Volume IV, Number 3 (March 1920), page 12.
[9] Bianca Van Beuren. “The Women of the South.” Birth Control Review, Volume II, Numbers 2 and 3 (February‑March 1918), page 7.
[10] For references and calculations, e-mail Brian Clowes at bclowes@hli.org and ask for Excel spreadsheet F-19-04.XLS, “Analysis of United States Abortion Statistics, 1967-2013.”
[11] See “A Superhero for Choice,” available on YouTube.
27th Sunday OT (Year C) – October 2, 2016
HAB 1:2-3; 2:2-4; PS 95:1-2, 6-7, 8-9; 2 TM 1:6-8, 13-14; LK 17:5-10
The Catholic Mass is broadcast live at 9 a.m. (Arizona time) each Sunday from
Ss. Simon and Jude Cathedral in Phoenix, Arizona
Homily- Fr. Lankeit
The Devil is a divider who will use almost any tactic to separate Christians from
Christ…except for one. He doesn’t typically come right out and say, “Deny Jesus
Christ!” because he knows that someone who loves Jesus would immediately reject
the suggestion. So, he tends to use more subtle means and subtle words. But more
on that later…
For now, let’s deal with something closer to home, and very much in the forefront of
many people’s minds: the 2016 presidential election. But let’s do so from a
Catholic perspective. Let’s consider the intersection of the practice of our Catholic
faith and the exercise of our civic duty, especially when it comes to voting.
Let’s first acknowledge that there has never been a political party in the United
States that is perfectly aligned with Catholic teaching on every issue. That does not
mean, however, that we are therefore automatically free to vote for either major
party, because one party can be much further from Catholic principles on the
most important issues than the other party. As a result of that, we are often faced
with the task of discerning which party and which policies are most in line with
Catholic teaching, and which ones aren’t.
So many issues are subject to the prudential judgment of Catholic voters. What
does that mean? It means that Catholics can legitimately disagree, for example, on
the best way to address issues such as racial injustice, education, the economy,
immigration and healthcare and still remain in good standing in the Church.
There are other issues, however, which touch on matters of intrinsic evil—actions
that can never, at any time, under any circumstances be committed, promoted or
even enabled by a faithful Catholic. But setting aside issues of intrinsic evil for
now, let’s consider some of the more common issues for which Catholics can
legitimately exercise prudential judgment.
One such issue is Affirmative Action. This program aims to eliminate perceived
disadvantages that minorities face when competing, for example, for admission to
college. In our nation, one party favors Affirmative Action to bring justice and
balance in our multiracial society. The other party holds that it penalizes high
achievers by giving limited spots in the college classroom to less qualified
candidates, while denying more qualified students access. One party sees affirmative
action as a matter of justice…while the other party sees it as injustice.
But, suppose a candidate for president promoted a policy that would make it legal
for someone to kill a black person if that black person created a hardship for them
getting the education they desired.
How many of you would be comfortable voting for that candidate?
Another issue that falls under the category of prudential judgment is immigration.
One of the major political parties seeks to allow immigration with very little
restriction. The other party is concerned that unrestricted immigration leads to,
among other things, non-citizens taking jobs that could be worked by citizens.
One party favors open borders—the other favors “law and order”.
Now, suppose a candidate for president promoted a policy that would make it legal
for someone to kill a Hispanic person if the presence of that Hispanic person made
it more difficult to pursue one’s career of choice.
How many of you would be comfortable voting for that candidate?
Thank God we don’t have a candidate from either party who says that they condone
such policies. Nobody in their right mind would say such a thing—that we could kill
blacks or Hispanics—or anyone else—just for the sake of protecting personal
economic or educational interests.
Nobody would say it, but, as you’ll see in a moment…
There is a candidate, in this 2016 race for president, who along with that candidate’s
political party does, in fact, sanction the killing of blacks and Hispanics in the
situations previously described…under one…particular…condition:
That the black person or the Hispanic person is still in his or her mother’s womb.
Now, this candidate and party certainly won’t say it that way, not publicly
anyway. Instead, they use words like “choice” or “reproductive rights” or
“women’s health” or other sanitized statements in order to cover up what abortion
is and what abortion does.
Now, before we go any further in discussing the extremely sensitive issue of
abortion…I want to say a word to any woman in this congregation here today—or among
those watching or listening on TV or radio—who has chosen abortion:
God’s mercy is bigger than your sin and your pain. In ten years of priesthood, I have
often been blessed to welcome a woman back to the merciful embrace of God the
Father after she has admitted to, and repented of, her abortion in the Sacrament of
Confession. A priest in such a situation has the privilege of assuring the woman that
she has never lost the love of God the Father, nor her dignity as his beloved
daughter, no matter what she did. And so I say to these women today: You do not
have to hide from God any longer. I know it’s exhausting to pretend that your pain
is not real, that your loss is not immense and that your choice was not
devastating. But when you experience God’s loving mercy even after the abortion,
you will really come to know and experience that God’s love in forgiving our most
serious sins is even greater than his love in creating us. Your Father has been
waiting for you for a very long time. It’s time for you to come home!
So, now, having shared that important word with grieving mothers let’s return to
the subject of our duty as Catholics in the public square.
When we consider that a woman can walk into Planned Parenthood and have her
baby put to death because she doesn’t want to jeopardize her education or career,
we must acknowlege that the shocking scenarios described previously are not only
possible…not only real…but also among the most common reasons for abortion in
America.
Even the word “abortion” has been drained of its meaning—we treat it like nothing
more than a term that starts a heated debate rather than a procedure that stops a
heartbeat. Many want to treat abortion as merely one issue among many—but that
requires that a person pretend not to know what abortion is and what abortion does.
So let’s stop beating around the bush with regard to the current presidential race:
• Do you know which candidate and party in this election promotes abortion and
even promises to expand its availability here at home as well as abroad?
• Do you know that this candidate and party intend to make you and me pay for
other people’s abortions with our tax dollars—something that has always been
illegal?
• Are you aware that this candidate and party, which until recently, said that
abortion should be “safe, legal and rare” no longer even bothers to say that it
should be rare—but rather, that it must be available any time, any place, even up
to the last moment that the fully formed, full-term baby remains in the womb?
If you do not know which candidate and party I’m referring to, then you should not
even consider voting until you do know! Ignorance in this area is unacceptable,
because ignorance in this area costs millions of babies their lives and jeopardizes the
souls of many Catholics voters.
On the other hand, if you DO know which candidate and party want to promote and
expand abortion, and you still intend to enable them to continue their war on the
unborn with the help of your vote, then it is my duty as a priest to tell you that
your soul will be in grave danger, especially if you present yourself for Holy
Communion after casting such a vote with the full knowledge of what you’re
doing.
Every election season, when a priest addresses such topics from the pulpit, a certain
portion of the population complains that he’s preaching politics:
“A priest has no business discussing politics in church!”
That’s what some people say.
But what does God say to the priest whom he has designated to be spiritual father for
the people entrusted to his care?
The same thing he said to the Prophet Ezekiel: “…I have made [you] a watchman
for the house of Israel; whenever you hear a word from my mouth, you shall give
them warning from me. If I say to the wicked, O wicked man, you shall surely die,
and you do not speak to warn the wicked to turn from his way, that wicked man
shall die in his [sin], but his blood I will require at your hand. But if you warn the
wicked to turn from his way, and he does not turn from his way; he shall die in his
[sin], but you will have saved your life. (Ez 33:7-9)
Another of the Devil’s tactics is to encourage us to make excuses for our
participation in really bad things by appealing to other good things that we support,
which we try to convince ourselves somehow “cancel out” the grave evil we enable.
Take capital punishment, for example. If you bring up abortion, some people will
say, “I’m against capital punishment…and if you’re against abortion, then you
should be against capital punishment!” Fair enough. What is the biggest
objection to capital punishment? That innocent people might be mistakenly put to
death. And it must be acknowledged that innocent people very well could be
unjustly executed due to the many flaws in our legal system.
And this very reason for opposing capital punishment is precisely the reason that
Catholics must never willingly support or even enable abortion with their vote.
Because, while some innocent people have no doubt been put to death mistakenly
through capital punishment, in abortion an innocent person is always put to death,
and never by mistake. It’s always chosen…always intended.
If a person is against capital punishment, then, they necessarily must be against
abortion because the intention of abortion is to knowingly and deliberately kill an
innocent boy or girl—each and every time.
What about war? People who vigorously oppose the wars in the Middle East, for
example, often quote statistics on the great number of innocent people accidentally
killed in the crossfire. “Collateral damage”—the innocent people killed in war—is,
perhaps the greatest tragedy of war. But if a person opposes the accidental killing
of innocent people in war, while enabling the intentional killing of the most
innocent human beings on the planet with their vote—well…this is hypocrisy of the
most extreme kind.
If a person opposes war because of the accidental, unintended deaths of innocent
people, they necessarily must oppose abortion because the killing in abortion is
neither accidental nor unintended, but always directly willed.
Sometimes we hear the stupendously deceptive claim that a candidate or party will
reduce abortions by improving economic or social conditions, while simultaneously
promoting abortion as a right worth protecting.
But let’s face facts: Abortion is not caused by economics or social conditions.
Economic and social factors are, no doubt, circumstances that affect a mother’s
decision in some cases, but they are not causes.
After all, if eliminating abortion were merely a matter of economics, or access to
healthcare, or other socioeconomic factors, then why do wealthy mothers also
abort their babies?
There are plenty of Catholics who, quite rightly, have criticized bishops and priests
in recent years for not having spoken out more forcefully against the sexual abuse
of children by priests.
Why, then, do many of these same Catholics want to silence bishops and priests
who speak out forcefully against killing innocent children?
Why is opposing sexual abuse of children a matter of justice, but opposing the
murder of children a matter of “preaching politics”?
Regardless of the resistance, a priest must follow the example of Peter and John in
the Acts of the Apostles when it comes to preaching difficult truths. To those who
sought to silence their proclamation of the Gospel these Apostles boldly responded:
“Whether it is right in the sight of God to listen to you rather than to God, you
must judge; for [I] cannot but speak of what [I] have seen and heard.” (Acts 4:19-
20)
A priest is not only protected by the 1st Amendment (at least for now).
He is also bound by the 5th Commandment—Thou Shalt Not Kill.
If a priest doesn’t speak up for those most vulnerable in our society, and if the
Catholic faithful don’t actively protect the most vulnerable in our society by
refusing to enable their deliberate destruction with their vote, then such Catholics
are condoning the killing by their cowardice.
And what did St. Paul say to Timothy about cowardice in today’s 2nd Reading?
God did not give us a spirit of cowardice but rather of power and love and selfcontrol.
So do not be ashamed of your testimony to our Lord…but bear your share
of hardship for the gospel with the strength that comes from God. (2 Tim 1:7-8)
Part of every Catholic’s share in the hardship for the Gospel is that we must repent
of our actions that are offensive to God and destructive to our brothers and
sisters. And we must oppose the threats to innocent life that are most real and most
urgent. Make no mistake! There is no single issue that threatens innocent human life
more directly, consistently and urgently than the deliberate killing of baby boys
and baby girls in their mother’s womb. No…issue!
In the time since this homily started, at least 30 children have been deliberately
executed in the womb in the United States—and that’s just the ones that are
reported.
Let me sum up with some very challenging words:
“We have a serious obligation to protect human life, and especially the lives of
the most innocent and vulnerable among us. Whoever fails to do this, when
otherwise able to do so, commits a serious sin of omission. They jeopardize their
own spiritual wellbeing and they are a source of scandal for others. Should they
be Catholics, they should not receive Holy Communion.” Catholics in the Public Square, 4th Ed., p. 25
Now, I hope you realize that it takes a lot of courage for a priest to communicate
such challenging words as these—reminding his people that some actions are so
gravely sinful that they render a Catholic unworthy to receive Holy Communion
until there is complete repentance.
A priest who is more concerned about the state of his people’s souls than they are
themselves, deserves the esteem of his people for his willingness to speak such
difficult truth to them with genuine love—to put the welfare of his people’s souls
ahead of his own reputation, popularity or comfort. Such a priest should receive
respect, admiration and support, rather than their resistance or criticism.
So please pray for, thank and encourage the spiritual father that God has appointed
for you and who loves you enough to tell you the truth.
Because the priest who said these particular words…is your bishop…and mine.
By Archbishop of Denver Samuel Aquila
Source: http://denvercatholic.org/voting-catholic-2016/
I have voted in every presidential election since 1972 and I have never experienced an election like this year’s. Both candidates are disliked, lack credibility, and have made comments that make the hair on the back of your neck stand up. The American public is fed up with politics as usual and with the establishment in both parties. So, what should Catholics do when we vote in November?
That question is one that I have been asked by the faithful more this year than in any previous election. Recently in a dinner discussion with a group of Catholics, the conversation turned to politics and became vigorous, as some at the table supported Clinton and some Trump. All eyes turned to me and one of them asked, “Archbishop, what do you think?”
First, I shared my aversion for both candidates. Then I said that they need to reflect on the platforms of both parties, with an emphasis on the human life issues. Everyone at the table knew well the teaching of the Church on life and the dignity of life. They knew that Catholics in good conscience cannot support candidates who will advance abortion. All pretty much agreed that, when it comes to life issues, Catholic politicians on both sides of the aisle have put party ideology before their faith and living their faith in the public square.
This is the most important guidance I can give: allow your ongoing personal encounter with Jesus Christ and the Church to guide your political decisions. I say this because we believe that the truth about ourselves and the world we live in is revealed in and through him. Our society suffers and has suffered for quite some time because too few people live an integrated life – one that does not divide “the personal” from “the public.”
This year there are some critical changes to the two major parties’ platforms that some at the dinner were not aware of. Most important is that this year the Democratic party platform calls for the overturning of the Hyde Amendment, a provision that both parties have voted to include in the federal budget and on other spending bills for 40 years. The Hyde Amendment prohibits federal taxpayer money from being used for abortion. The platform is aggressively pro-abortion, not only in funding matters, but in the appointment of only those judges who will support abortion and the repealing of the Helms Amendment, which prevents the U.S. from supporting abortion availability overseas. Conversely, the Republican party platform is supportive of the Hyde Amendment and just this year strengthened its support for life by calling for the defunding of Planned Parenthood, banning dismemberment abortion and opposing assisted suicide.
Our conversation then turned to the understanding of the freedom of religion, the freedom of conscience, and the ability for faith-based organizations like the Church to provide charity through shelters, hospitals, homes for the elderly, etc., without fear of government interference and the existence of a respect for religious values.
In that vein, the subject was raised of the Health and Human Services mandate. This regulation requires the provision of contraceptives, sterilizations and some abortifacients through employer’s health plans. Most surprising to me was that all at the table were practicing Catholics who are involved in their faith, and a couple of them had neither heard of the difficulty the Obama Administration has created for the Little Sisters of the Poor, nor the litigation that has occurred trying to force them to violate their consciences.
Catholic voters must make themselves aware of where the parties stand on these essential issues. The right to life is the most important and fundamental right, since life is necessary for any of the other rights to matter. There are some issues that can legitimately be debated by Christians, such as which policies are the most effective in caring for the poor, but the direct killing of innocent human life must be opposed at all times by every follower of Jesus Christ. There are no legitimate exceptions to this teaching.
The health of our nation depends on a deep respect for human life from the moment of conception until natural death, and the future of our society depends on how we protect that right. If we don’t, eventually we will go the way of Rome and Greece and other great civilizations that have risen and fallen.
Some, both in politics and in the Church, have stated that it is the Church that needs to change her teaching to include abortion, same-sex unions, and even euthanasia. Yet, in faithfulness to Jesus Christ, to the Gospel and to Sacred Tradition, the Church cannot change her teaching on these issues without denying Christ. She would cut herself from the vine and only wither away, as promised by Christ. The further we move away from Jesus Christ and his teachings, the more will our churches empty.
We are where we are today because too many Catholics and other people of faith have embraced the ways of the world and not the ways of Christ. They have not served as leaven that transforms society, but rather have condoned evil and the throw-away culture that Pope Francis frequently reminds us to reject.
When we fail to do this, the government will step in to fill the void. Indeed, the government will become “god” and impose its beliefs on the citizens. One only needs to look to the Health and Human Service contraceptive mandate, or the attempt by President Obama to force a transgender agenda onto public schools. We may even soon see the federal funding of abortion and the approval of physician-assisted suicide in Colorado. We are witnessing the dictatorship of relativism and the erosion of true freedom. And as Pope Francis often preaches, the devil gets in the mix quickly, especially when people no longer believe in God.
So my advice to Catholics in voting in this presidential election is to first look at who forms you and your conscience. Is it your personal encounter with Jesus Christ and the Church, the voice of God which cannot contradict the truth or revelation, or is it the ideology of some political party? Secondly, look at how you have been a leaven in society. How have you sought the common good and the values of the Gospel, especially by serving the poor, the needy, the unborn and the dying. If you truly live your Catholic faith, you will not find complete alignment with any political party, and that is okay. Thirdly, look at how each party platform supports human life from conception through natural death, the freedom of religion and the freedom of conscience, the family, and the poor. Finally, do vote, as every Catholic has an obligation to participate in the political process.
For many, the presidential election will involve a choice between the lesser of two evils. On the Colorado ballot, we will also face the evil of physician-assisted suicide, known as Proposition 106. In conforming our hearts and minds with the Gospel and its clear teaching on life, all Catholics are called to vote “no” on this issue. A “yes” vote only furthers the throw-away society, and the culture of death. You will be hearing much more on this in the days and weeks ahead. Let us keep our country and state in our daily prayers, praying for God’s protection and blessings in these challenging, difficult times in which we live. And let us in charity pray for the conversion of those who support a throw-away culture of death!
A newly published study from the University of Copenhagen has confirmed a link between hormonal contraceptives and depression. The largest of its kind, with one million Danish women between the ages of 15 and 34 tracked for a total of 13 years, it’s the kind of study that women such as me, who have experienced the side-effects of birth control-induced depression first hand, have been waiting for.
Researchers found that women taking the combined oral contraceptive were 23% more likely to be diagnosed with depression and those using progestin-only pills (also known as “the mini-pill”) were 34% more likely. Teens were at the greatest risk of depression, with an 80% increase when taking the combined pill, and that risk is two-fold with the progestin-only pill. In addition, other hormone-based methods commonly offered to women seeking an alternative to the pill – such as the hormonal IUS/coil, the patch and the ring – were shown to increase depression at a rate much higher than either kind of oral contraceptives.
In recent years we’ve seen efforts from the NHS and family planning organizations to encourage teens to use these so-called LARCs (long-acting reversible contraceptives), primarily because they eliminate the need to remember to take a pill every day, but also due to the fact they’re commonly believed to have less severe potential side-effects than the pill. The new research suggests this practice is misguided. We already know that those with pre-existing depression may find the pill worsens their symptoms, and if teens were at greater risk of depression, then continuing this practice would be negligent.
The researchers note that, because GPs are less likely to prescribe the pill to women who already have depression and because women who do experience depression on the pill are more likely to stop taking it, this study probably underestimates the potential negative affect that hormonal contraceptives can have on mental health.
Having spent the past eight years researching and writing on the emotional and psychological side-effects of hormonal birth control, I initially felt elated to read this study. Not just for myself, but for the hundreds of women I’ve interviewed over the years. Mood changes are one of the top reasons many women discontinue using the pill within the first year. Finally, here was the kind of large-scale, long-term study I’d been told was necessary before we could seriously talk about this issue or make a change in how we prescribe hormonal contraceptives.
However, I was naive, because it seems that no study will ever be good enough for the medical community to take women’s experiences seriously. As soon as this research dropped, the experts lined up to deliver their usual mix of gaslighting and paternalistic platitudes. We’re told not to be alarmed, concerned, or deterred from continuing to use our hormonal contraceptives, mostly by men who have never and will never take them themselves (partly because the long-term, large-scale study undertaken by WHO on the “acceptability” of the male pill revealed it would negatively impact their emotional wellbeing).
This “pillsplaining” is specific to discussions of research into the side-effects of hormonal birth control. Usually, when the research is on the pill alone, we’re quickly informed there are many other hormone-based methods to choose from, but unfortunately this new study says those alternatives are even worse. One expert even tried to dismiss the link with depression in pill-taking teens as more likely the result of “teen heartbreak”.
So, why is it that we’re not supposed to take this study seriously? Considering that women are fertile just six days per menstrual cycle and men are fertile every single day, that the burden of avoiding unwanted pregnancy falls to us, regardless of the burden that might have on our health and wellbeing, is nothing short of sexism.
Yet, we’re reminded with one medical professional’s response to this new research that “an unwanted pregnancy far outweighs all the other side effects that could occur from a contraceptive.” If that’s true, why bother researching the side-effects at all?
It is important to remember that women are twice as likely to experience depression as men, reportedly due to “the fluctuation of progesterone and estrogen levels”, in other words our biological femaleness. It’s apparently acceptable to blame women’s depression on the fact that they’re women, but it’s not OK to claim a powerful medication formulated from synthetic hormones could be at fault.
To me, and many other women, these Danish researchers are heroes and criticism of their methods (such as, they should have tracked those women using condoms or the copper IUD as well – even though these options were not available to them; or that women were likely depressed because of menstrual cramps – which the pill is supposed to prevent), only highlights the incredible knots the medical establishment will twist itself into in order to deny there’s a problem with the pill.
One of the study’s authors, Øjvind Lidegaard, professor of obstetrics and gynaecology, also brought attention in 2011 to the increased risk of blood clots associated with newer, and supposedly “improved” hormonal contraceptives such as the ring, the patch and drospirenone-containing pills. Lidegaard plans to focus next on researching the possible “association between taking hormonal birth control and attempting or committing suicide”. Researchers originally flagged up this potential link back in 1970 at the Nelson Pill Hearings, but the topic has not been touched since.
Depression and anxiety from hormonal contraceptives may not be the experience of every woman, but that doesn’t mean it’s not the experience of your friend, your daughter or your partner, and of many women out there, who, in reading about this could have their lives changed for the better.
Today marks 40 years since the life-saving Hyde Amendment was first enacted. This annual appropriations amendment stops taxpayer dollars from being used to fund most abortions and abortion coverage through government programs like Medicaid.
Thanks to new analysis by the Charlotte Lozier Institute we now know that as many as two million children — some much older now — are alive today because of the Hyde amendment.
Prior to enactment of Hyde, the Medicaid program paid for about 300,000 abortions annually. Research, including by the pro-abortion Guttmacher Institute, has long shown that stopping taxpayer-funded abortion reduces the abortion rate. In an analysis released just this week, the Charlotte Lozier Institute estimates that the Hyde amendment saves as many as 60,000 lives each year.
I remember the day several years ago when my friend and author of the amendment, Henry Hyde of Illinois, first learned that about one million children were alive because of his amendment. He was overcome with joy knowing that a million mothers were spared the agony of post abortion pain, a million children were alive and well, growing up, going to school, playing sports, dating, marrying and having kids of their own. Today that number is estimated at two million — all because abortion subsidies have been prohibited by this law. Since the first bitter and protracted battles over this policy, the Hyde amendment has generally, if begrudgingly, been accepted as the status quo. President Bill Clinton — who supported partial-birth abortion — and President Barack Obama — who pledged to veto a bill protecting children born alive after abortion, both consistently signed the Hyde amendment into law.
Yet Hillary Clinton represents a new era of pro-abortion extremism.
Not only does she fall in party line with her opposition to the Pain-Capable Unborn Child Protection Act, the ban on sex selection abortion, and the Born Alive Abortion Survivors Protection Act, she will have an abortion litmus-test for every judge and justice. And in a new assault on innocent human life, she has vowed to decimate the Hyde Amendment and fund abortion on demand using taxpayer dollars.
In 1980 the Hyde Amendment narrowly overcame a constitutional challenge in a 5-4 Supreme Court decision. If Hillary Clinton appoints just one justice, the Hyde amendment will be nullified.
Hillary Clinton is outside of the mainstream. Today, more Americans support the sanctity of life and oppose taxpayer funding for abortions than ever.
America has an ever-growing majority that believes our government should not fund abortion. A July 2016 Marist poll found that nearly two-thirds of Americans oppose taxpayer funding for abortion — including 45 percent of those who identify as “pro-choice.”
The Hyde Amendment is not extreme. Hillary Clinton is.
Hillary Clinton is so extreme and outside the mainstream that when MSNBC’s Chuck Todd asked her in an April 3 interview: “When, and if, does an unborn child have constitutional rights?” Hillary Clinton fired back: “unborn persons don’t have constitutional rights .” Mrs. Clinton acknowledges that unborn children are persons, but denies them their right to life and wants taxpayers to pay for their destruction.
When Hillary Clinton was awarded the Margaret Sanger award by Planned Parenthood in 2009, she said she was “in awe” of Margaret Sanger, the infamous founder of Planned Parenthood. Shockingly, its American affiliate alone claims responsibility for the death of over seven million babies.
In her 2009 speech Mrs. Clinton also said she admired Sanger for her vision and that Sanger’s work here in the United States and across the globe was not done. “Not done” means more abortions, paid for by the taxpayer, and an end to conscience rights for those who don’t agree.
If we lose the Hyde Amendment our country will be carrying out Sanger’s eugenic legacy — incentivizing the destruction of the poor and vulnerable by paying for their death.
There are nearly 60 million Americans missing from 43 years of legal abortion. That’s 60 million lives with potential that have been snuffed out by state-sanctioned killing.
Hillary Clinton poses an existential threat to the welfare and well-being of unborn children and their mothers in the United States and around the world. Rather than expand the culture of death and shred the Hyde amendment — as Hillary Clinton promises — women and men of conscience have a duty to protect the weakest and most vulnerable from the violence of abortion.
Chris Smith is an 18-term Republican congressman from New Jersey.
The Office of Readings for the feast of the Archangels, St. Michael, St. Gabriel and St. Raphael, offers a reflection by Saint Gregory, pope, “…Those who deliver messages of lesser importance are called angels; and those who proclaim messages of supreme importance are called archangels. Personal names are assigned to some to denote their ministry when they come among us. Thus, Michael means, “Who is like God?”; Gabriel is “The Strength of God”; Raphael is “God’s Remedy.”
We are beloved of God, and He provides us with angelic companions and protectors as the Catechism states, “The existence of the spiritual, non-corporeal beings that Sacred Scripture usually calls “angels” is a truth of the faith. The witness of Scripture is as clear as the unanimity of Tradition” (328).
The Archangel Michael
Pope Gregory continues, “Whenever some act of wondrous power must be performed, Michael is sent, so that his action and his name may make it clear that no one can do what God does by his superior power. So also our ancient foe desired in his pride to be like God, saying, I will ascend into heaven; I will exalt my throne above the stars of heaven; I will be like the Most High. He will be allowed to remain in power until the end of the world when he will be destroyed in the final punishment.”
St. Michael is known to be the warrior angel who fights Satan and his demons from the beginning, and throughout the epic Christian pilgrimage, St. Michael is the great defender of the Church on earth.
I’d like to share an anecdote related to St. Michael. As I was exiting St. Michael’s Norbertine Abbey Chapel after Mass, I noted 2 young boys standing in front of a nearby large white marble statute of St. Michael. I also stopped before the same statute to silently pray the St. Michael Prayer. I saw that the younger boy, approximately 5 years old, stood in awe of the impressive St. Michael statute as he inquisitively examined the details of the handsome sculpture. Suddenly he exclaimed to the older boy, approximately 12 years old, “Look, St. Michael is stepping on the head of the devil!” To which the older boy quickly replied, “Yes, that is what St. Michael does and he thrusts his sword into him too!” I thought to myself, “Bravo, St. Michael! Bravo, boys and bravo to your parents who taught you about the role of St. Michael!”
Since childhood, I have had a strong devotion to St. Michael, always perceiving myself under the protective canopy of his God-given power. So devoted am I to St. Michael that our first-born son was named after him and we enthusiastically encouraged him to have real devotion to his patron saint. In my new book I share how St. Michael dramatically helped to defend our family when all odds where stacked against us in a lawsuit by the F.B.I.—who lost their case. Recently when my car was broadsided by an eight-passenger van, I thought of St. Michael as I walked away without injury though my new sedan was totaled.
I often ponder how truly present and effective St. Michael is in the battle against the fallen angels who roam the earth seeking to tempt, vex, oppress or possess God’s children. During each official rite of exorcism that I have witnessed, the priest and team ardently summon the help of St. Michael throughout the ministry. St. Michael never fails to support the priest in his ministry of proclaiming Christ’s victory over evil. Victims attest that the evil spirits greatly fear St. Michael knowing that God has given him the power not only to expel them, but also to increase their torment. St. Michael is a reflection of God’s omnipotent love and His provision for the Church militant in all our struggles.
The Archangel Gabriel
Again, in the Office of Readings, Pope Gregory teaches, “…Gabriel, who is called God’s strength, was sent to Mary. He came to announce the One who appeared as a humble man to quell the cosmic powers. Thus, God’s strength announced the coming of the Lord of heavenly powers, mighty in battle.”
Just prior to the coming of Christ, the Archangel Gabriel is sent to announce to Zachariah the birth of a son, John the Baptist, who would prepare the way of the Lord. “I am Gabriel, who stand before God, and am sent to speak to you, and to bring you these good tidings.”
Probably the most joyful message ever given to an angel was the message brought by Archangel Gabriel to the Virgin Mary—the message of the Incarnation.
The Catholic Encyclopedia states:
It is the first time that a prince of the court of heaven greets an earthly child of God, a young woman, with a deference and respect a prince would show to his Queen. That Angel’s flight to the earth marked the dawn of a new day, the beginning of a new covenant, and the fulfillment of God’s promises to His people. …Gabriel must overcome Mary’s reaction of surprise at both his appearance and especially at his manner of salutation. He has to prepare and dispose her pure virginal mind to the idea of maternity, and obtain her consent to become the mother of the Son of God. Gabriel nobly fulfills this task: “Fear not, Mary, for you have found grace with God.” He calls her by her own name in order to inspire confidence and to show affection and solicitude for her perturbation. As a last word of encouragement and, at the same time, a most gratifying information, the Archangel reveals to Mary that her elderly and barren cousin Elizabeth is now an expectant mother in her sixth month of pregnancy. This final argument was offered in order “to prove that nothing can be impossible with God.”
Theologians think that Gabriel was probably given special charge of the Holy Family in Nazareth, and was probably the angel who brought good tidings of great joy to the shepherds keeping night watches over their flock on the night that Christ was born, and probably the angel who appeared to Joseph in his sleep to warn him against Herod and guide him to Egypt. Gabriel who is “the strength of God” may have been the angel in Luke’s gospel narrative of Christ’s agony in Gethsemane, “And there appeared to him an angel from heaven, strengthening him.” It seems fitting that the angel, who announced His birth, protected Him in infancy, and strengthened Him in the Garden, should be the first to announce his resurrection on Easter morning.
The Archangel Rafael
Pope Gregory’s homily continues, “Raphael means God’s remedy, for when he touched Tobit’s eyes in order to cure him, he banished the darkness of his blindness. Thus, since he is to heal, he is rightly called God’s remedy.”
The Catholic Encyclopedia states:
The history of Tobias, father and son, contains the grandest angelophany of the whole Bible, and it all revolves around the manifestation of the Archangel Raphael under the assumed name and form of a beautiful young man named Azarias. At the very end of his long mission the Archangel revealed his own identity and his real name, together with the actual purpose of his mission: “And now the Lord hath sent me to heal thee, and to deliver Sara thy son’s wife from the devil. For I am the angel Raphael, …who stand before the Lord.” In this angelophany, Saint Raphael reveals himself as a divine healer not only of physical infirmities, the blindness of old Tobias, but also of spiritual afflictions and diabolical vexations, as in the case of Sara, young Tobias’ wife. (Angelophany is a term used to describe the visible manifestation of angels to mankind.)
Raphael seems to have been at work at Jerusalem, in the days of Christ, in the pool called Bethsaida. In the five porticoes surrounding that pool there was a multitude of sick people, waiting for the action of the Angel upon the water of the pool: “An Angel of the Lord used to come down at certain times into the pool and the water was moved. And he that went down first into the pool after the motion of the water, was cured of whatever infirmity he had.”
Archangel Raphael’s healing ministry may still be seen in the miraculous cures that have taken place up to our own times in many of the sacred shrines throughout the Christian world.
Saints Michael, Gabriel and Raphael, mighty Archangels, graciously protect, guide and heal us on our journey to the Father’s house. Amen.
A shocking new report claims the world’s first three-parent baby (pictured above) has been born. Children born through ‘three-person IVF’ would contain some genetic material from each of three different people.
There are about 50 known mitochondrial diseases (MCDs), which are passed on in genes coded by mitochondrial (as opposed to nuclear) DNA. They range hugely in severity, but for most there is presently no cure and little other than supportive treatment. The goal behind creating “designer babies” with three parents is to eliminate such diseases.
But there are good reasons for pro-life people to be concerned about the process and the eugenics-based reasons behind it.
Here’s more on the infant born from three parents:
It’s a boy! A five-month-old boy is the first baby to be born using a new technique that incorporates DNA from three people, New Scientist can reveal. “This is great news and a huge deal,” says Dusko Ilic at King’s College London, who wasn’t involved in the work. “It’s revolutionary.”
The controversial technique, which allows parents with rare genetic mutations to have healthy babies, has only been legally approved in the UK. But the birth of the child, whose Jordanian parents were treated by a US-based team in Mexico, should fast-forward progress around the world, say embryologists.
The boy’s mother carries genes for Leigh syndrome, a fatal disorder that affects the developing nervous system. Genes for the disease reside in DNA in the mitochondria, which provide energy for our cells and carry just 37 genes that are passed down to us from our mothers. This is separate from the majority of our DNA, which is housed in each cell’s nucleus.
Around a quarter of her mitochondria have the disease-causing mutation. While she is healthy, Leigh syndrome was responsible for the deaths of her first two children. The couple sought out the help of John Zhang and his team at the New Hope Fertility Center in New York City.
Dr. Peter Saunders, a pro-life physician in England, has commented on the ethical problems with three-parent embryos:
This is not about finding a cure. It is about preventing people with MCD being born. We need first to be clear that these new technologies, even if they are eventually shown to work, will do nothing for the thousands of people already suffering from mitochondrial disease or for those who will be born with it in the future.
Is it safe? This is far from established. Each technique involves experimental reproductive cloning techniques and germline genetic engineering, both highly controversial and potentially very dangerous. Cloning by nuclear transfer has so far proved ineffective in humans and unsafe in other mammals with a large number of cloned individuals spontaneously aborting and many others suffering from physical abnormalities or limited lifespans. Also, any changes, or unpredicted genetic problems (mutations) will be passed to future generations. In general, the more manipulation needed, the higher the severity and frequency of problems in resulting embryos and fetuses.
Is it ethical? No, there are huge ethical issues. A large number of human eggs will be needed for the research, involving ‘harvesting’ that is both risky and invasive for women donors. How many debt-laden students or desperate infertile women will be exploited and incentivised by being offered money or free IVF treatment in return for their eggs? How many thousands of human embryos will be destroyed? If it ever works, what issues of identity confusion will arise in children with effectively three biological parents? What does preventing those with mitochondrial disease being born say about how we value people already living with the condition? Where will this selection end? Some mitochondrial diseases are much less serious than others. Once we have judged some affected babies not worthy of being conceived, where do we draw the line, and who should draw it?
In 2014, the American Academy of Pediatrics published its policy statement on contraception for adolescents, which provides, in effect, a mandate to temporarily sterilize all adolescents with long-acting reversible contraceptives for five to ten years. The author reviews the AAP guidelines and their effects on Catholic adolescents, their families, and adolescent health care providers. He then discusses medicolegal issues raised by the policy, outlines Catholic strategies for combating it, and proposes a diocese-based physician-led program for teaching and counseling elementary and high school students.
Click on the icon to read the entire article published on the National Catholic Bioethics Quarterly 16.1 (Spring 2016): 63–81.
Strange things happen in election years. That was clear to me last Monday morning as I opened the newspaper to a full-page ad from an organization called “Catholics for Choice” referring to “Abortion in Good Faith” and misrepresenting Catholic social teaching by claiming that “public funding for abortion is a Catholic social justice value.” This ad, with slight regional variations, appeared in newspapers across the country, and represented the latest in a series of public relations efforts by this organization to promote a pro-abortion agenda by attempting to counter the Church’s consistent and convincing proclamation of the Gospel of life.
You may remember Catholics for Choice from their failed efforts, for example, to challenge the Holy See’s permanent observer status at the United Nations. It’s the same group that put St. John Paul II at the top of its “enemies list” at the time of the U.N. Cairo Conference. Its long-time president, Frances Kissling, would go so far as to express her longing at times “for the destruction of the Catholic Church,” which she saw as a “fatally flawed” institution — quite a contrast from our Catholic understanding of the Church as the body of Christ. As an organization, there’s nothing Catholic about “Catholics for Choice.”
Unable to muffle the Church’s opposition to the culture of death, its most recent ad campaign seems to be an attempt to sow seeds of confusion concerning authentic Church teaching as we once again approach election time.
Judging from the phone calls and email messages that we received this week, however, the Catholic faithful of this archdiocese are too well-educated in the faith to be so easily misled. They know that Christ, in founding the Church upon the apostles, assured that through them and their successors she would always be blessed with authentic teachers endowed with his authority who, as taught at the Second Vatican Council, would “preach to the people committed to them the faith they must believe and put into practice” (Lumen Gentium 25). They also know that those authentic teachers have consistently taught that the value of human life needs to be respected and protected from conception to natural death.
In his most recent encyclical, “The Joy of Love,” Pope Francis, reiterating the teaching of his predecessors, could not be any clearer: “So great is the value of a human life, and so inalienable the right to life of an innocent child growing in the mother’s womb, that no alleged right to one’s own body can justify a decision to terminate that life.” Earlier this year, he called on all Christians to “a renewed esteem of the human person and a more adequate care of life, from conception to natural death.” That, brothers and sisters, is authentic Catholic social teaching.
I am not naïve enough to think that there are not individual Catholics who struggle with different aspects of Catholic teaching, even here in our local Church. I bristle as you do whenever I hear a politician begin a sentence with “I’m a devout Catholic, but … .” Living in a throwaway culture that at times values things more than people and convenience even more than life, it is all too easy to forget that the right to life is the first human right. As men and women of faith who have taken to heart the theme of this jubilee year, “Merciful like the Father,” our hearts have to move with compassion not only for new parents anxiously wondering how a child is going to fit into their lives, but also for their unborn children.
Indeed, in “The Joy of the Gospel,” Pope Francis noted that we need to have a special compassion for the unborn: “Among the vulnerable for whom the Church wishes to care with particular love and concern are unborn children, the most defenseless and innocent among us. Nowadays efforts are made to deny them their human dignity and to do with them whatever one pleases, taking their lives and passing laws preventing anyone from standing in the way of this … . Precisely because this involves the internal consistency of our message about the value of the human person, the Church cannot be expected to change her position on this question … . It’s not ‘progressive’ to try to resolve problems by eliminating a human life … .”
I am very proud that our Catholic community is so obviously committed to providing concrete support to new parents and families. I know that so many of you are supporting the many pregnancy resource centers in this region that offer practical assistance to pregnant women in need. I know as well the wonderful programs that are offered locally to enable young moms to be great parents, even when they are facing that responsibility alone or need to finish their education. I know the phenomenal work that Catholic Charities is doing to keep struggling families together. It is a blessing to be part of a Church that lives what it believes about the dignity of human life.
It seems to me that the recent ad from Catholics for Choice presents us as a local Church with a wonderful teachable moment. I hope that the priests and faithful of this archdiocese, who have been relentless in their defense of human life, will join me in looking for opportunities to lovingly and patiently bring the light of authentic Catholic social teaching into this discussion in the days and weeks ahead. May the Lord bring forth our efforts to preach his Gospel of life.
WASHINGTON, D.C., September 21, 2016 (LifeSiteNews) — More than 400 Catholic academics released a statement affirming the Catholic Church’s teaching on contraception and human sexuality in response to recent calls for the Church to change her teaching as the 50th anniversary of Humanae Vitae approaches. Opponents of Catholic teaching presented those calls Tuesday at the United Nations.
Humanae Vitae, Pope Paul VI’s landmark encyclical upholding the Catholic Church’s long-held teaching on human sexuality, was released in 1968. In preparation for its upcoming 50th anniversary, the Wijngaards Institute for Catholic Research released a statement titled On the Ethics of Using Contraceptives calling for the Church to accept the use of artificial contraception as moral.
It said the Church should issue an “official magisterial document … affirming that the use of non-abortifacient modern contraceptives for prophylactic purposes can be morally legitimate and even morally obligatory” and consider revising its teaching on in-vitro fertilization, homosexual activity, and masturbation.
To counter the so-called Wijngaards statement, the 400+ scholars released Affirmation of the Church’s Teaching on the Gift of Sexuality at a press conference at The Catholic University of America (CUA) yesterday. Numerous CUA faculty members, including President John H. Garvey, signed the statement.
Scholars: There is no Catholic argument for contraception
“The Wijngaards Statement seriously misrepresents the authentic position of the Catholic Church,” the scholars wrote. “Among the most erroneous claims made by the Wijngaards Statement is that neither Scripture nor natural law offers any support for the Church’s teaching that contraception is never compatible with God’s plan for sexuality and marriage. During the past half century, there has been an enormous amount of creative scholarly thinking around the Church’s teaching on contraception, thinking that includes profound reflections on the Theology of the Body, personalism, and natural law. In addition, there has been extensive research on and analysis of the negative impact of contraception on individuals, relationships, and culture.”
The Wijngaards Statement “offers nothing new to discussions about the morality of contraception and, in fact, repeats the arguments that the Church has rejected and that numerous scholars have engaged and refuted since 1968,” the document continued. One of the key inaccuracies of the Wijngaards Statement, the scholars assert, is its claim “that the argument against contraception in Humanae Vitae is based primarily on ‘biological laws.’ Humanae Vitae instead focuses, as it should, on the person’s relationship to God and to other persons.”
On the Ethics of Using Contraceptives “virtually ignored” Pope St. John Paul II’s Theology of the Body that defended Humanae Vitae, the scholars wrote.
Affirmation of the Church’s Teaching on the Gift of Sexuality outlined 11 points about the nature of God, the nature of marriage, and faith and reason that are the basis of the Church’s teaching that artificial contraception “is not in accord with God’s plan for sexuality and marriage.”
Humanae Vitae’s ‘prophetic’ warnings coming true
“Humanae Vitae was prophetic” when it predicted that contraception would lead to marital infidelity, a general lowering of morality, and abuse of women for sexual pleasure, the signers of the CUA statement agreed. “Abundant studies show that contraception, such as hormonal contraceptives and intrauterine devices, can cause serious health problems for women. The widespread use of contraception appears to have contributed greatly to the increase of sex outside of marriage, to an increase of unwed pregnancies, abortion, single parenthood, cohabitation, divorce, poverty, the exploitation of women, to declining marriage rates as well as to declining population growth in many parts of the world. There is even growing evidence that chemical contraceptives harm the environment.”
Pope Paul VI also predicted that contraception would begin to be imposed on people after its widespread acceptance. This prediction makes the Wijngaards Statement rather ironic given that it says the Church should label the use of artificial contraception “morally obligatory” in some cases.
Also in tune with Humanae Vitae’s predictions, the Wijngaards Statement recommended that the Church “seek the opinion of Christian theologians and experts in other relevant disciplines … on the other areas of Catholic sexual ethics which will likely be affected by a revision of the present teaching banning the use of contraceptives for family planning, namely the negative evaluation of masturbation, homosexual relationships, and in vitro fertilization.”
The CUA statement, however, calls for governments and international organizations to “make instruction in Fertility Awareness Based Methods (FABMs) of family planning a priority” because “FABMs are based on solid scientific understanding of a woman’s fertility cycle, are easily learned by women in developing countries, are virtually without cost, and promote respect for women.”
“International organizations and governments should respect the values and beliefs of families and cultures that see children as a gift, and, therefore, should not impose — on individuals, families, or cultures — practices antithetical to their values and beliefs about children and family planning,” the CUA statement said.
Notable signers of Affirmation of the Church’s Teaching on the Gift of Sexuality include:
Janet E. Smith, Ph.D, Father Michael J. McGivney Chair of Life Ethics, Sacred Heart Major Seminary; Author, Humanae Vitae: A Generation Later
John S. Grabowski, Ph.D, Associate Professor and Director of Moral Theology/Ethics, School of Theology & Religious Studies, The Catholic University of America, Board Member, The Academy of Catholic Theology; Author, Sex and Virtue: An Introduction to Sexual Ethics
Mary Rice Hasson, JD, Director, Catholic Women’s Forum, Ethics and Public Policy Center; Editor, Catholic Women Reflect on Feminism, Complementarity, and the Church
Helen M. Alvare, JD, Professor of Law, Scalia Law School at George Mason University; Editor: Breaking Through: Catholic Women Speak for Themselves
John H. Garvey, JD, President, The Catholic University of America
Richard J. Fehring, Ph.D, RN, FAAN, Professor Emeritus and Director, Marquette University’s Institute for Natural Family Planning
Angela Franks, Ph.D, Director of Theology Programs for the Theological Institute for the New Evangelization at St. John’s seminary in Massachusetts
John M. Haas, Ph.D, STL., MDiv, K.M. President, The National Catholic Bioethics Center
Mary Healy, PhD, Sacred Heart Major Seminary
Rev. Thomas Petri, O.P., STD, Vice President and Academic Dean, Pontifical Faculty of the Immaculate Conception at the Dominican House of Studies
Michael Waldstein, Max Seckler Professor of Theology, Ave Maria University, Florida, Translator of Man and Woman He Created Them: A Theology of the Body and author of Glory of the Logos in the Flesh: John Paul II’s Theology of the Body (forthcoming)
George Weigel, Distinguished Senior Fellow, Ethics and Public Policy Center, Washington, D.C.; author of the two-volume biography of Pope St. John Paul II, Witness to Hope and The End and the Beginning
The other signers included professors and intellectuals from around the world and Dominican and Jesuit religious.
Dominican Father Thomas Petri, one of the main signers of the CUA statement, noted that CUA’s sponsorship of the statement shows it has come a long way since the 1960s, when its theology department was known for heterodoxy and dissent from Catholic doctrine.
Five Jesuits and two Dominicans were signatories of the Wijngaards Statement, along with 140 others, some of whom are not Catholic.
The full Affirmation and list of signatories is available here.
The first child has died under a new law in Belgium allowing doctors to euthanize children.
In 2014, Belgium voted to extend euthanasia to children with disabilities, in a move pro-life advocates worldwide had been fearing would come and expand an already much-abused euthanasia law even further. The law allows minors to seek euthanasia under certain conditions and the measure also would extend the right to request euthanasia to adults with dementia. No age limit would be set, but the children who are euthanized would have “to possess the capacity of discernment.”
Euthanasia has been legal in Belgium since 2002 but has, since its enactment, been prohibited for patients under 18. While euthanasia is legal in a handful of countries in Europe, Belgium is the first country in the world to lift all age restrictions on the practice.
Professor Wim Distelmans, the head of Belgium’s Federal Control and Evaluation Committee on Euthanasia, issued a statement confirming that the first physician induced death of a minor was reported to the committee by a doctor last week.
Few details were released about the child’s condition.
Now, the first child has been killed:
A terminally ill minor has been helped to die in Belgium for the first time since the country did away with age restrictions on euthanasia two years ago, according to the senator who wrote the law.
Liberal Senator Jean-Jacques De Gucht confirmed the death of the sick juvenile to The Associated Press Saturday.
He said the minor was from Belgium’s Flemish region, but declined to provide any further details about the patient to protect the privacy of the grieving family.
Catholic teaching forbids euthanasia and the president of the Italian bishops conference on Saturday described the news of the euthanasia of a child as painful and worrisome.
“It pains us as Christians but it also pains us as persons,” Genoa Cardinal Angelo Bagnasco told Italian news agency ANSA.
Some have questioned whether children should be allowed to make the choice between life and death. In 2014, a group of doctors — including pediatricians — signed a group letter to voice opposition to the measure.
In 2012, Belgium recorded 1,432 cases of euthanasia – a 25% increase from 2011.
At the time the law was being debated in the Belgian Senate, euthanasia opponent decried the proposal.
“Currently the Belgian euthanasia law limits euthanasia to people who are at least 18 years old. This unprecedented bill would extend euthanasia to children with disabilities,” says Alex Schadenberg of the Euthanasia Prevention Coalition at the time. “The Belgian Socialist government is adamant that the euthanasia law needs to extend to minors and people with dementia even though there is significant examples of how the current law is being abused and the bracket creep of acceptable reasons for euthanasia continues to grow. The current practice of euthanasia in Belgium appears to have become an easy way to cover-up medical errors.”
“Regardless of disability, life should be valued. To pass legislation that allows termination of life for people with disabilities who are minors is unacceptable,” he added. “Instead we must make every effort to use the research provided to us to provide attentive care to relieve their physical suffering in a moral way.”
Dr Paul Saba of Physicians for Social Justice, was very concerned about the situation in Belgium.
“They are already euthanising people who are depressed or tired of life because they have taken the interpretations of saying physical and/or psychological suffering – you don’t have to have both, if you have one, why is that not enough? If you are suffering, it’s a personal experience and it would be discriminatory for someone to judge what a person is suffering,” he said during that time. “What this teaches us is that despite the government’s assurances that they will set very strict criteria, that won’t work.”
Professor Chris Van Geet of Leuven University asserted that the proposed law poses “an enormous ethical problem.” Following the vote on Thursday, Tom Mortier, a lecturer in chemistry at Leuven University and an anti-euthanasia campaigner, called the vote “insanity.” Professor Mortier’s own mother, who was suffering from chronic depression at the time, was euthanized in 2012.
“Her departure wasn’t the serene family gathering, full of peace and reconciliation, which euthanasia supporters gush about,” Mortier stated. “The University Hospital in Brussels phoned my wife the day after.”
The leaders of Belgium’s Christian, Muslim, and Jewish communities put out a joint statement opposing the vote’s outcome. The statement read, “We mark out opposition to this extension and express our trepidation in the face of the risk of a growing trivialization of such a grave reality.”
There is enormous concern about abuses under the expanded euthanasia law.
Research conducted by the Canadian Medical Association Journal (CMAJ) in 2010 found that 32% of euthanasia deaths in the Flanders region of Belgium occurred without an explicit request.
Meanwhile, according to Schadenberg:
The number of euthanasia deaths in Belgium is skyrocketing with an increase of 25% in 2012. Recent studies indicate that up to 47% of all assisted deaths are not being reported, 32% of all assisted deaths are being done without request and nurses are killing their patients, even though the law restricts euthanasia to doctors.
Some Belgian experts are supporting the extension of euthanasia to children with disabilities because they say that it is being done already. The same medical experts suggest that the extension of euthanasia will result in an increase of 10 to 100 euthanasia deaths each year.
The Belgian euthanasia law appears out-of-control. The Belgian Euthanasia Control and Evaluation Commission appear to be in a conflict of interest. The Commission supported the euthanasia deaths of: Nathan Verhelst (44) who was born as Nancy, Ann G who had Anorexia Nervosa and was sexually exploited by her psychiatrist, Mark & Eddy Verbessem, and at least one depressed woman. These are only the cases that we know about.
Dr Wim Distelmans, who is the leading euthanasia doctor in Belgium has also been the chairman of the Belgium euthanasia commission for more than 10 years, and the commission has been stacked with supporters of the euthanasia lobby.
The Netherlands already allows children over the age of 12 to request euthanasia with the consent of their parents.
September 13, 2016 (LifeSiteNews) — Voting isn’t about feeling good and there is no reason for Catholics to sit out the 2016 election, Father Frank Pavone told LifeSiteNews.
“We might feel like we’re uncomfortable voting for a particular person even if we know it’s the better of the two choices,” said Pavone, the national director of Priests for Life. “Voting is not about what’s good for me. It’s about the common good.”
“A vote is not about liking the person. … A vote is a transfer of power,” he said. “And we transfer the power to best of the viable alternatives.”
Pavone compared voting in the 2016 presidential election with changing a runaway train’s tracks in order to limit its damage.
“At the end of those two tracks, the damage is going to be done,” he said. “But what if you know that less damage is going to be done at the end of track B than at track A? It’s not that you intend any damage; you don’t. But it’s beyond your control. Wouldn’t you switch the train to track B, even if you couldn’t stop it? To lessen the damage, to reduce the harm? Of course you would.”
“People should never think that by not voting at all they escape responsibility for the outcome,” said Pavone, noting that Catholics at the beginning of Mass ask for forgiveness for “what I have done and what I have failed to do.”
Those who abstain from voting in a certain race or voting at all “still have responsibility for the [election’s] outcome, because if you don’t vote at all, that took away a vote from the better of the candidates,” the priest explained.
Pavone said Catholics should consider that when they vote for a candidate they are essentially voting for an entire administration.
“You are also putting someone in the office of the Secretary of State, the Surgeon General, the Attorney General, the Secretary of [Health and Human Services], and in fact thousands of positions in the federal administration — not to mention that you’re also putting a certain type of person on the Supreme Court, and on all the other federal courts that decide so many issues of public policy,” he said. “Who are the people the president brings with him into office?”
It is “critically important” for Catholic voters to recognize the significance of party platforms, Pavone said.
“You have to consider, what do the parties represent?” he asked. “The platform contains an entire philosophy, a set of policy preferences, a whole worldview, and the people … [on politicians’] staffs are going to be people who are … more or less consistent with the position, the philosophy, the worldview, of that particular party.”
“This is so much more than, ‘Oh, that candidate said something bad or this other one said this other thing,’” Pavone said. “It’s not about what they’re saying in a particular set of remarks. What are they representing? And we need to look at that closely.”
Only days after Baton Rouge Police Officer Matthew Gerald was buried, his three year-old daughter made a shocking announcement to his grieving widow – that Jesus said she had a baby boy in her tummy.
WAFB is reporting on the incredible story of Dechia Gerald whose 41 year-old husband was one of three officers slain during a July 17 ambush on police in Baton Rouge.
Dechia said both her daughters – Dawclyn,9 and Fynleigh, 3 – were strangely aware of her pregnancy even before she knew it herself.
Her first hint came while she was hunting for something to wear to her husband’s funeral and Dawclyn said, “Mommy, I don’t know why you’re complaining because you’re pregnant.”
Shocked, Dechia responded, “Girl, hush! Don’t say that kind of stuff.”
A few days later, while giving Fynleigh a bath, Dechia said that she was told the same thing. “However this time, she [Fynleigh] told me that Jesus told her that there was a baby boy in my tummy.”
A week later, just before attending a get together with family, she decided to buy a pregnancy test.
“I took it and within a second of that being done, the test read positive,” she said. “I wanted to cry but at the same time, it’s kind of exciting but then the flood of knowing all of the firsts that he would miss with that one.”
She immediately told her family and friends, including the wives of the two officers who died alongside her husband.
“For the most part, it’s a blessing. I mean obviously he left us a very special gift behind, but at the same time, all those days that I get overwhelmed, I ask how am I going to do this by myself without him,” Dechia said.
But everything happens for a reason, she believes.
“Did I ever think that we were going to have our time cut that short? No. Did I want to be a widow at 38 years old? No,” she said.
Looking back on it now, she’s surprised that in the midst of 12 hour work days, she had time alone with her husband on July 12, the night she believes she conceived, which was just five days before he died in the line of duty.
But she feels her husband’s presence all around her. For example, while driving to the doctor for her first ultrasound at four weeks, she heard their wedding song on the radio, something she had not heard in a while.
She also noticed something that looks like a wedding ring in the first ultrasound image of the child.
“I felt like when I saw that he was with us,” Dechia said.
All she’s hoping for now is to one day hold a little carbon copy of her husband in her arms, completed with the blue eyes that she fell for seven years ago.
“It’ll have the blue eyes. I’m sure the blonde hair although I’ve been praying for the red hair however I don’t know if that’ll happen,” Gerald said.
Now 10 weeks pregnant, she believes God will guide her through life.
“There’s no better gift that a husband could leave behind than a baby, a gift from God. There’s no better gift than that,” Gerald said.
“Even if a mother could forget her child, I will not forget you. I have carved you in the palm of my hand.” – Isaiah 49:15-16
Today is the National Day of Remembrance for Aborted Children, and across our country pro-lifers are honoring the memory of little boys and girls whose lives were violently ended at the hands of the very people who should have welcomed and loved them – their mothers and fathers. These precious little ones are victims of a culture and society growing increasingly more violent.
It is fitting that this day falls adjacent to September 11, the anniversary of the terrorist attacks in New York and Arlington, Virginia. Though the number of lives taken by abortion is much larger than that taken on that terrible day fifteen years ago, both acts of mass murder rely on the same evil, the denial of the humanity of others.
In the Culture of Death, the fundamental and immutable value of each human life is rejected to sustain a self-consumed culture that destroys more than one million unborn children every year in the United States and nearly 55 million globally. This irrational and immoral behavior contributes to the pervasive culture of violence escalating in our nation and in our world. Even using the word abortion shields us from its reality, keeping the humanity of the child distant and shadowed.
For these innocent children, there is no story to tell about their lives. There are no names to recollect or pictures to share. No birthdays or special occasions to celebrate. There are no “firsts” to remember – a first smile, first tooth, first walk or first day of school. There is no burial place among his family. For the majority, they are labeled “medical waste” and disposed of.
There is something tragically wrong when society ignores the humanity of the unborn child or worse yet, is indifferent toward the violence done to him/her. In 1994, Saint Teresa of Kolkata during the National Prayer Breakfast said:
Any country that accepts abortion is not teaching its people to love, but to use any violence to get what they want. This is why the greatest destroyer of love and peace is abortion…. I feel that the greatest destroyer of peace today is abortion, because it is a war against the child, a direct killing of the innocent child, murder by the mother herself. And if we accept that a mother can kill even her own child, how can we tell other people not to kill one another?
The argument in favor of legal abortion rests upon a deception—keeping the science obscure and language about the beginning of life ambiguous.
It’s not a baby… It’s just a blob of tissue. Or… It’s not a human person… It’s a potential human being.
Any distinction about the worth of the unborn child based on his stage of development is entirely arbitrary, and when abortion is the result of such distinctions, it is the cruelest form of discrimination. The unborn child in the womb is not a potential life, but a life with potential – a teenager, brother, sister, mother, father, doctor, lawyer, teacher.
It is interesting that an unborn child wanted by his/her parents is called a baby and given a name, but the same set of parents could decide that the same baby is a “fetus” unworthy of life because he is unwanted.
Life begins at the moment of conception/fertilization. There is no debate about the science, only denial from those for whom it is inconvenient. Human development begins when a male gamete unites with a female gamete to produce a single cell, a zygote. This highly specialized, totipotent cell marks the beginning of each of us as a unique individual with our own genetic code. The 23 chromosomes in the sperm join the 23 chromosomes in the ovum to make a genetically unique human being with 46 chromosomes. Since the baby is genetically unique at fertilization, it is inaccurate to say he/she is merely another part of his/her mother’s body. At fertilization our genetic make-up is complete including gender and eye and hair color. The heart begins to beat at 18 to 21 days after fertilization. There are brain waves at 6 weeks, and at 8 weeks all body systems are present, including the baby’s fingers and toes.
Most abortions take place after the 8th week of the pregnancy, about 5 weeks after the baby’s heart has started to beat. Abortion silences the beating heart and active brain waves of the individual maturing in the womb of his mother.
The Day of Remembrance is a chance to remember the humanity of the more than 55 million boys and girls whose lives were violently—and legally—ended.
To transform our culture and society from its perilous path, we must affirm and protect all life, especially the most vulnerable among us. Pope Saint John Paul II understood what was necessary to build a Culture of Life where the most vulnerable are defended, welcomed, and cared for:
The first and fundamental step towards this cultural transformation consists in forming consciences with regard to the incomparable and inviolable worth of every human life. It is of the greatest importance to re-establish the essential connection between life and freedom. These are inseparable goods: where one is violated, the other also ends up being violated. There is no true freedom where life is not welcomed and loved; and there is no fullness of life except in freedom. (Evangelium Vitae n. 96)
Today we remember those who have been killed and the survivors, those who have been harmed by abortion. Let us also renew our commitment to abolish abortion in law, eradicate the idea that it is acceptable in culture, and love those in our lives who mistakenly see it as a solution to a difficult situation. Let’s love them by telling them the truth and praying for and with them. Let’s continue to live and promote chastity as the life- and freedom-affirming virtue that it is.
In September 2015 the United Nations General Assembly adopted a series of goals and targets in order to eradicate poverty, eliminate inequality, and subdue climate change by 2030. These Sustainable Development Goals (SDGs), comprising 17 goals, 169 targets, and 230 indicators (to measure progress) replaced the eight Millennium Development Goals that had guided UN development policy thinking over the previous 15 years. Secretary-General Ban Ki-moon characterized the SDGs as heralding “an historic turning point for our world”; they will probably be the hallmark of his legacy as he ends his decade-long reign at the helm of the UN in December.
The SDGs, bannered “Transforming Our World: The 2030 Agenda for Sustainable Development,” are universal and thus apply to the entire UN membership of 193 nations. Through the UN’s online “The World We Want” campaign, millions of people the world over initially provided input on what they considered the most pressing global problems. The actual compilation and formulation of the SDGs lay in the hands of civil society through an Open Working Group of non-governmental organizations (NGOs) accredited to the Economic and Social Council of the UN. Some of the more powerful and better-financed NGOs exerted considerable influence in the process, which started in 2013 and ended after an all-day, all-night session in early July 2014. UN member-country delegations refined and tweaked the content for presentation to world leaders for their acclamation a year ago.
In their entirety, the goals are supposed to be a blueprint for development but not everyone can agree on the content. Unfortunately, the SDGs contain some controversial language that is disturbing to promoters of life. A major problem lies with “reproductive rights” language that was inserted into the document during the initial formulation period by powerful pro-choice NGOs, and which none of the country-delegations were subsequently able to remove. The controversial wording is found in targets 3.7 and 5.6, which many pro-life NGOs are now fighting battles over.
Goal 3 reads: “Ensure healthy lives and promote well-being for all at all ages.” While this is rather vague, target 3.7 is disconcertingly specific:[1]
3.7 By 2030, ensure universal access to sexual and reproductive health-care
services, including for family planning, information and education, and the
integration of reproductive health into national strategies and programmes
Goal 5 reads: “Achieve gender equality and empower all women and girls.” This may be laudable as it stands, but target 5.6 raises a red flag:
5.6 Ensure universal access to sexual and reproductive health and reproductive
rights as agreed in accordance with the Programme of Action of the International
Conference on Population and Development and the Beijing Platform for Action and
the outcome documents of their review conferences
The two targets have become the springboard for abortion promoters and providers to foist their credo on mostly poorer countries which, unlike nearly all developed countries, do not have abortion on demand. “Reproductive,” however modified—“rights,” “health,” “services,” “care,” “access”—is subject to varying interpretations according to the beliefs of the beholder. The word itself is almost never used in a procreative sense; rather the opposite. Given the importance and universality of the SDGs, this “reproductive” language is being used to support the agenda of population controllers.
The references in 5.6 relate to two major UN conferences: the 1994 Cairo International Conference on Population and Development and the 1995 Beijing World Conference on Women. The formulation of the Cairo outcome document witnessed a word struggle that yielded specific language important to pro-lifers and often repeated by them: namely, that family planning does not involve abortion. In the section covering women’s health and motherhood there is this in paragraph 8.25:
In no case should abortion be promoted as a method of family planning . . .. Any measures or changes related to abortion within the health system can only be determined at the national or local level according to the national legislative process. In circumstances where abortion is not against the law, such abortion should be safe.i
The Cairo document contained several references on abortion language. As is common with UN conferences, however, there have been periodic “reviews” which revisited the language of the document, each time pushing forward the abortion agenda. Therefore, the inclusion of the “reproductive” language in target 5.6 is problematic.
Statistical experts are now busy drafting a set of 230 indicators to hold governments accountable for implementation of the Sustainable Development Goals and to monitor progress. Given that the UN has a slogan “you measure what you treasure,” and vice versa, global statisticians have a herculean task ahead of them. There is supposed to be at least one indicator for each target but about 30% of identified indicators as of yet have no methodology and no data. So-called reproductive rights represent one challenge.
[1] For all interested in reading the entire SDG document, this is the source:
September 2, 2016 (Life Legal Defense Foundation) — Just days ago, two-year-old Israel Stinson was forcibly removed from life support at Children’s Hospital of Los Angeles. I was on the phone with Jonee Fonseca, Israel’s mother, when doctors disconnected his ventilator.
I could hear Jonee begging the doctors to wait just a few more hours until her family arrived to say goodbye to Israel. They refused. Then I heard her begging her son to breathe.
It was a horrific end to an ordeal that began over four months ago. Israel suffered an asthma attack and stopped breathing while being treated at a Sacramento hospital on April 2 of this year. He was resuscitated, but was placed on a ventilator.
Jonee called Life Legal for help when a second hospital declared Israel brain dead. Doctors at Kaiser Permanente Medical Center in Roseville, California said Israel’s condition would soon deteriorate and that his heart would stop beating even if he were kept on life support. They refused to feed Israel for over five weeks, saying that giving him a feeding tube would be “catastrophic.”
Life Legal attorneys were able to obtain court orders in state and federal court keeping Israel alive until arrangements could be made to care for Israel at home. In order for that to happen, Israel needed two minor procedures to provide him with a breathing tube and feeding tube. Kaiser refused to perform those procedures.
A Catholic hospital in Central America agreed to accept Israel as a patient to do the procedures. In May, Israel was transported by air ambulance to Guatemala. He had to leave a hospital with state-of-the-art healthcare and travel thousands of miles to a developing nation to get the care he needed to survive.
After the procedures, Israel’s condition improved markedly. Doctors did two EEGs, which showed active brain waves. Three separate doctors reported that Israel was not brain dead! Moreover, the doctors were so committed to saving Israel’s life that they agreed to treat Israel without cost during the last few weeks at the Guatemalan hospital.
Jonee then began the arduous process of finding a hospital that would accept Israel temporarily while she arranged for him to be cared for at home. Children’s Hospital of Los Angeles agreed to admit Israel after speaking with Israel’s doctors about his condition.
However, shortly after Israel arrived at Children’s Hospital, doctors threatened to end Israel’s life. They refused even to look at the EEGs or examine Israel’s movements in response to his mother’s voice. They did not consider that Israel’s condition in Guatemala had stabilized such that he needed no artificial means to maintain his heart rate, blood pressure, or body temperature. Jonee asked that a Los Angeles neurologist be permitted to examine Israel, as California’s brain death statute requires an independent exam. The hospital refused.
Ten days ago, Jonee called me saying the hospital was going to remove Israel’s ventilator the following day. I flew to Los Angeles to assist her in obtaining a court order. The judge ordered that Israel be kept on life support for three weeks to allow the neurologist to complete his exam. We also found a local attorney to work with Jonee going forward.
But the hospital immediately filed a motion asking the judge to dissolve the court order so they could terminate Israel’s life as soon as possible.
Again, Life Legal attorneys fought heroically alongside Jonee, but ultimately the fight for Israel’s life was lost.
So where do we go from here?
Last January, in a unanimous decision, the Nevada Supreme Court held that the state’s brain death guidelines should be reexamined after a young woman was declared brain dead even though several EEGs showed that she had active brain waves. In that case, the woman died because the hospital refused to feed or treat her.
We have no ethical obligation to fight nature every step of the way in the dying process. However, these cases continue a very disturbing trend of medical professionals actually facilitating a person’s death. Life Legal has represented people in several recent cases where hospitals and hospice facilities have tried to end the life of a patient with a brain injury because doctors or family members believed that person had no chance for recovery. In reality, however, the decision was made in haste, before the person’s brain had a chance to heal. In two cases, young women were sentenced to death who, just weeks later, were on their way to a full recovery. This should NEVER be permitted to happen!
Please join Life Legal as we press on in the fight to protect vulnerable human life.
September 1, 2016 (LifeSiteNews) — Cardinal Raymond Burke called it an “absolute contradiction” for poverty, immigration, and the environment to be placed by leading U.S. prelates on the same priority level as protecting and defending life and the family.
“All of these questions have moral importance, but there can be no question — also in the long tradition of not only the Church’s thinking but also of philosophical reason — that the fundamental question has to be the question of human life itself, the respect for the inviolable dignity of human life, and of its cradle, its source, in the union of a man and woman in marriage, which according to God’s plan, is the place where new human life is welcomed and nurtured,” he said during a teleconference on August 29 hosted by Carmel Communications to discuss his new book, Hope for the World.
Burke, responding to a question on the topic posed by LifeSiteNews, stated that he would be “very concerned” to see priorities shift.
“I would be very concerned that in any way the questions about the protection of human life, either at its beginning — here questions regarding abortion and other questions regarding the artificial creation of human life, etc. — or at its conclusion — questions regarding euthanasia — be in some way seen to be at the same level as questions regarding immigration and poverty,” he said.
Last year, a group of Pope Francis’ episcopal appointees and other like-minded prelates provoked an open clash at the U.S. Catholic bishops’ fall meeting when they pressed the conference to rewrite its election guide for 2016 to downplay the importance of the battle for life and family.
Bishop Robert McElroy, appointed as head of the Diocese of San Diego by Pope Francis, went as far as to argue that the proposed guide, with its emphasis on the evils of abortion and euthanasia, was out of step with Pope Francis’ priorities of combating poverty and protecting the environment.
“Pope Francis has, in certain aspects of the social doctrine of the Church, radically transformed the prioritization of Catholic social teaching and its elements,” McElroy urged the assembly at that time. “Not the truth of them, not the substance of them, but the prioritization of them, has radically transformed that, in articulating the claims that fall upon the citizen as believer and disciple of Jesus Christ.”
Burke, however, stated during the teleconference that the priority of life must not change if Catholics are to get the other issues such as poverty and immigration right.
“We have to give the first priority to the respect for human life and for the family in order to have the right orientation in addressing all of the other questions which are involved with poverty and immigration, the many challenges that any human being faces in life,” he said.
“But it doesn’t make any sense at all to be concerned about immigration or poverty if human life itself is not protected in society. It’s an absolute contradiction. The first justice accorded to any human being is to respect the gift of life itself, which is received from God. And so, that the unborn should be protected and at the same time those whose lives are burdened either by advanced years or special needs or some grave illness, their lives also are to be equally protected.”
When LifeSiteNews pressed the cardinal about how Catholics might go wrong on the fronts of poverty and immigration if they did not prioritize respect for life, he responded:
Well, for instance, it is not uncommon that some people’s idea of how to address the question of poverty is to eliminate a certain part of the population, so that there is less draw on the natural goods available, or to propagate a contraceptive mentality.
In the same way too, in the question of immigration, one has to respect the family, both the family of the country which is receiving the immigrants but also the families from which these immigrants are coming. If we don’t have this fundamental direction in our lives, it all can become a kind of social engineering and so forth, which can be, in the end, very harmful to society and therefore to the individuals.
Cardinal Burke is backed by St. Pope John Paul II in asserting the priority of life over other concerns. In his 1988 apostolic exhortation Christifideles Laici, John Paul II called the right to health, home, work, family, and culture “false and illusory if the right to life, the most basic and fundamental right and the condition of all other personal rights, is not defended with maximum determination.”
John Paul II said on another occasion that the promotion of the culture of life should be the “highest priority in our societies,” stating that if the “right to life is not defended decisively as a condition for all other rights of the person, all other references to human rights remain deceitful and illusory.”
Later during the call, John Allen from Crux asked Cardinal Burke to comment on Mother Teresa’s “obvious concern for the poor and an obvious concern for the unborn.”
Unsatisfied by Burke’s initial answer, Allen pressed: “Can I just pressure you, that was a beautiful answer, but I was hoping what you would also say is something about how for Mother Teresa and for Catholics who think with the mind of the Church that concern for the poor and concern for the unborn are two sides of the same coin.”
While Burke replied that the “matters are absolutely related one to the other,” he did so in a way that gives priority to respect for life.
He explained: “As I mentioned in response to one of the earlier questions, when someone asked, ‘Why is this teaching about abortion or about euthanasia, what importance does it have for addressing poverty?’ she [Mother Teresa] said frequently that the greatest poverty in the world is the fear of life, are those nations which seemingly are very rich which practice freely, for instance, the killing of unborn children in the womb and so forth as a response to social needs.”
“And so she is a brilliant teacher to us in addressing, whether it be questions of a difficult pregnancy, or questions of a difficult illness, whatever it may be, she teaches us that the way to address these issues is with respect for the individual human life and in that way no matter what the suffering is of the person, or no matter what great sacrifices have to be made, the person will find that happiness and fulfillment for which he or she is seeking,” Burke said.
NEW YORK, September 2 (C-Fam) Mother Teresa will be declared a Saint by Pope Francis in a special ceremony on Sunday at the Vatican. The pro-life heroine skillfully exploited her celebrity status to propel the pro-life cause internationally like no one else before her or since.
The four feet tall Albanian nun was never afraid to speak truth to power, even when it made the powerful of the world feel uncomfortable, and she never pandered to curry their favor. Draped in her iconic white sari, she traveled the globe condemning abortion even when doing so was inconvenient and unwelcome.
While lunching at the White House, First lady Hillary Clinton reportedly asked Mother Teresa why America had not yet elected a woman president. “She has probably been aborted,” Mother Teresa replied.
During her acceptance speech of the 1979 Nobel Peace Prize Mother Teresa first popularized her signature condemnation of abortion.
“The greatest destroyer of peace today is the cry of the innocent unborn child,” she told the crowd of nobles, politicians, and celebrities. After a moment of deathly silence Mother Teresa continued.
“For if a mother can murder her own child, in her own womb, what is left for you and for me? To kill each other.”
“Today millions of unborn children are being killed, but we say nothing.”
Then she raised her voice with alarm.
“To me the nations that have legalized abortion, they are the poorest nations. They are afraid of the little one! They are afraid of the unborn child! And the child must die. Because they don’t want to feed one more child! Because they don’t want to educate one more child! The child must die.”
She concluded her remarks about abortion with a plea.
“Let us make a strong resolution. We are going to save every little child. Every unborn child. Give them a chance to be born.”
Her plea was not heeded, and she continued to speak for the unborn unabashedly.
In 1985 she was a special invitee at the 40th anniversary of the founding of the United Nations during the height of the Cold War.
“We all want peace, and yet, and yet we are frightened of nuclears [weapons], we are frightened of this new disease [HIV/AIDS]. But we are not afraid to kill an innocent child, that little unborn child, who has been created for that same purpose: to love God and to love you and me.”
At the 1994 National Prayer Breakfast in Washington, she surprised Bill and Hillary Clinton with scathing remarks against abortion as they sat close to her. She called abortion “a war against the child, a direct killing of the innocent child, murder by the mother herself.”
“Any country that accepts abortion is not teaching its people to love, but to use any violence to get what they want. This is why the greatest destroyer of love and peace is abortion,” she said. President and First Lady remained quietly seated as the entire room erupted into a standing ovation after her speech
She also challenged those with a narrow view of feminism, such as when she said motherhood was “the gift of God to women” and that abortion destroyed it. “Those who want to make women and men the same are all in favor of abortion,” she stated in a message to the Fourth World Conference on Women in Beijing in 1995.
Sept. 1, 2016 (LifeSiteNews) – While euthanasia is being presented across North America as “compassionate” and a good way to end suffering by suicide activists, there is something chilling about the intimacy of these killings. As pro-life activist Gregg Cunningham noted, “Ours is the first generation that, having demanded the right to kill its children through elective abortion, is now demanding the right to kill its parents through doctor-assisted suicide.”
The closest of human relationships are rupturing under the sheer weight of the selfishness and narcissism of the Me Generation. The tagline “dying with dignity” is starting to very much sound like, “Now don’t make a fuss, off with you now.”
Consider this 2014 story in The Daily Mail:
An elderly husband and wife have announced their plans to die in the world’s first ‘couple’ euthanasia – despite neither of them being terminally ill.
Instead the pair fear loneliness if the other one dies first from natural causes.
Identified only by their first names, Francis, 89, and Anne, 86, they have the support of their three adult children who say they would be unable to care for either parent if they became widowed.
The children have even gone so far as to find a practitioner willing to carry out the double killings on the grounds that the couple’s mental anguish constituted the unbearable suffering needed to legally justify euthanasia…
The couple’s daughter has remarked that her parents are talking about their deaths as eagerly as if they were planning a holiday.
John Paul [their son] said the double euthanasia of his parents was the ‘best solution’.
‘If one of them should die, who would remain would be so sad and totally dependent on us,’ he said. ‘It would be impossible for us to come here every day, take care of our father or our mother.’
I wonder why no one considers the fact that the reason some elderly parents may experience “mental anguish” is that they have come to the sickening realization that their grown children would rather find an executioner to dispatch them than take on the responsibility of caring for their parents.
It is for precisely that reason that some scenes in the 2011 HBO euthanasia documentary How To Die In Oregon are so jarring. In one scene, an elderly father explains to the interviewer why he has procured death drugs that he plans to take in case of severe health problems. “I don’t want to be a burden,” he explains while his adult daughter nods approvingly, “It’s the decent thing to do. For once in my life I’ll do something decent.” There was no argument from his daughter.
Think about that for a minute. Would that not be real suffering? To come to the realization that the children you loved with all your heart would rather find someone to kill you than find someone to care for you? Or to care for you themselves? Would it not truly be suffering to realize that those very closest to you, those you loved the very most, would like you to kill yourself, or support your suicide?
Let me take this a step further. Suicidal people often reach out to others, often let someone know about their plans. By telling people they are contemplating suicide, they are letting out one last cry for help—I’m going to kill myself…are you going to stop me? Is it not possible that many elderly parents may be suggesting assisted suicide in the desperate hope that their children will reject such a situation out of hand? That their children will tell them how much they are loved, will promise to come see them, will offer to find them the care that they need? What if the suggestions of some elderly or sick people that suicide is the best option is not so much a suggestion as it is a question: How much do you love me?
Which leads to more questions: Love is not proven until it is tested. As those we love suffer illness and the many afflictions of old age, what is our responsibility towards them? A loved one with Alzheimer’s, for example. It is easy to love someone when they can love us back. But does our responsibility suddenly vanish when that person is not capable of loving us in the same way? Does mental illness, old age, or disease relieve us of our responsibility towards them, eliminate our duty to care for them, or change the fact that we love them? Too often the idea of euthanasia is not about releasing the suffering one from pain. It is about releasing those around him from their responsibility.
Another question: If assisted suicide is a right, do you ever have the responsibility to kill someone? Or rather, do we have the responsibility to protect people from themselves? Many of these questions are simply not surfacing in the debate on suicide. People are simply accepting euthanasia on the grounds that death is a solution to suffering, and are not asking questions that desperately need answers.
Perhaps I’m naïve, but the news stories of children happily arranging the suicide of their parents actually shocked me, and I’m not shocked by much these days. I simply could not fathom responding to fears or depression of parents or grandparents by agreeing to get them killed. In fact, if one of them told me that their life no longer had any meaning and that they wanted to die, I would take that very personally and very seriously. I love them, and it would be my responsibility to dispel their will to die, to convince them that they were precious, and necessary, and I wanted them in my life for as long as was possible.
A final question that I’d like you to think about, long and hard: Would hearing that those who you loved the most agreed that suicide was your best option cause you great suffering?
Washington, DC You may not have heard much about Implanon birth control previously. But you will, given the emergence of an Implanon birth control personal injury lawsuit that’s been filed as a class action. The issue in the current lawsuit is device migration. But there can be other issues as well.
First, a refresher as to exactly what Implanon is: an implantable birth control device, small and thin akin to the size of a toothpick, that’s inserted below the skin in the upper arm and designed to provide birth control protection through the measured release of the progestin etonogestrel for about three years before removal. Various advocates of the device claim that it can last as long as four years – but three years is the recommended window.
It’s one of the latest examples of the so-called ‘set-it-and-forget-it’ line of devices that does not require the ingestion of a daily birth control pill, or the management of a dermal patch that requires changing at regular intervals. For busy women prone to forget their birth control pill, the automatic dispensary option is viewed with some favor. The US Food and Drug Administration (FDA) approved Implanon, marketed by Merck & Co., in July of 2006.
After ten years on the market, it has been reported that some 500,000 women use the device for birth control.
However, lawsuits are beginning to emerge. Co-plaintiff Brook Reynolds, who joined the class action Implanon birth control personal injury lawsuit, alleges that the Implanon device she received in 2012 migrated away from the initial implantation site. In 2014, when Reynolds attended her doctor’s office to have the device removed, her physician was unable to locate it.
The toothpick-sized device had migrated away from the original implantation site. Other plaintiffs cite remarkably similar issues to those of Brook Reynolds. Co-plaintiffs Jenni Akins, Major Akins, Ruby Ginns, Robert Reynolds and Julie Reynolds allege that Merck & Co. and subsidiary Organon failed to warn of the potential for migration.
There is, indeed, little mention – if any – about the potential for device migration by way of information generally available to consumers. The Contraceptive Technology Update (06/01/16) carried a report that lauded the effectiveness of the implantable Implanon and its successor, Nexplanon, in terms of effectiveness. While common side effects were outlined, there was no mention of the potential for device migration.
In another example, Planned Parenthood on its website includes more common Implanon birth control side effects – as well as less-common side effects – but makes no mention with regard to the potential for device migration. Under the heading of ‘Serious Side Effects of the Birth Control Implant’ Planned Parenthood lists as the last item, “tell your health care provider immediately if the implant comes out or you have concerns about its location.” Device migration is not mentioned. Reference to ‘concerns about its location’ is subject to interpretation.
It is not until we look to Merck.com before we get any sense as to the possibility of device migration. In a downloadable pdf document intended for consumers, there is references made at the bottom of a bullet listing of common side effects – but is not part of the active list.
“Implants have been reported to be found in a blood vessel including a blood vessel in the lung.”
And,
“Implants have been found in the pulmonary artery (a blood vessel in the lung). If the implant cannot be found in the arm, your healthcare professional may use imaging methods on the chest. If the implant is located in the chest, surgery may be needed.”
Downloading a document intended for doctors and healthcare providers reveals more information – specifically with regard to guidance for the removal of a spent implant, which is normal after a few years. The Implanon is meant to be retrieved at the end of its useful life cycle:
“Confirm that the entire implant, which is 4 centimeters long, has been removed by measuring its length. There have been reports of broken implants while in the patient’s arm. In some cases, difficult removal of the broken implant has been reported.
“There have been reports of migration of the implant; usually this involves minor movement relative to the original position [see Warnings and Precautions (5.1)] (original reference), but may lead to the implant not being palpable in the location in which it was placed. An implant that has been deeply inserted or has migrated may not be palpable and therefore imaging procedures, as described below, may be required for localization.
“Exploratory surgery without knowledge of the exact location of the implant is strongly discouraged.”
This is a dilemma faced, in particular, by Brook Reynolds, according to the Implanon birth control consumer fraud lawsuit to which she belongs. When Reynolds attended her doctor to have the device removed, her physician was not able to locate it. Presumably, diagnostic imaging was unsuccessful in locating the device and thus, the location of the Implanon remains a mystery. As suggested by the manufacturer’s dissertation to doctors noted above, exploratory surgery is not recommended without first knowing where the device is. In Brook’s case, without knowing where the device is, surgery appears out of the question.Thus, the Implanon originally received by plaintiff Brook Reynolds appears to be irretrievable. The continued migration of the toothpick-sized object could subject her to Implanon birth control personal injury, including ectopic pregnancy and potential damage to her vascular system – not to mention her peace of mind, living daily without a clear picture of where this thing is.
TAMPA BAY, FL, August 26, 2015 (LifeSiteNews) — Their child might only live a few hours, but an NFL player and his wife say that prayer led them to not abort Layla Sky.
According to Evan Rodriguez, who was released by the Tampa Bay Buccaneers last week, his wife Olivia is due with their first child in December. Named Layla Sky, she was diagnosed with anencephaly, and is expected to be born with parts of her brain and skull missing — and to only live a few days.
“From that moment on, I’m like, what can we do?” Rodriguez told Tampa Bay’s ABC News affiliate about his reaction after the diagnosis. The doctor told the couple to “either terminate it or move forward with the process.”
The couple, which prays together each morning, spent a week making their decision. “God, show me what it is that you want to do through all of this. What’s the good to come out of it?” asked Olivia each morning.
“We decided to continue with the process because we felt like who are we to determine a baby’s life. So, we are going to leave it in God’s hands,” Rodriguez said.
In addition to preparing for the arrival of Layla, Olivia and Evan are raising awareness of anencephaly. At practices, Rodriguez wore a towel with his daughter’s name, and created the hashtag “The Fight for Layla Sky.” Their Facebook page has more than 2,600 followers. On Monday, Rodriguez posted that “most of the time we plan on teaching our child about the world never expecting you have to teach the world about your child.”
ABC reports Olivia and Evan are using the hashtag to advise women on how to avoid birth defects, and they are partnering with Duke University to study the disorder their child has. The CDC estimates that one in 4,859 babies are born with the disorder.
“It felt like it was our job to let other people know about this,” said Rodriguez, who said he knows he’ll see her again. “She’ll be waiting up there saying daddy. So, there’s a time and place for everything.”
Rodriguez said his daughter’s name came from how “I always zone out and look at the sky and wonder what else is out there.” He is hoping to be picked up by another NFL team.
In an abrupt, unexpected, and surprise decision, a Los Angeles Superior Court judge Thursday dissolved an injunction that prevented a local hospital from turning off 2-year-old Israel Stinson’s ventilator.
The adorable little boy, whose brain-dead diagnosis was fought on two continents by his parents, died shortly afterwards.
“They are devastated. I think still in shock,” family attorney Alexandra Snyder told reporters. “It’s not even my child; I am still in shock this could happen so quickly.”
Snyder is shocked by a judge’s decision because just last week the court gave her a temporary order to stop the hospital from removing the ventilator so they could get an opinion from another neurologist.
It all started last April, reports Michael E. Miller, “with an asthma attack.”
Israel Stinson was an adorable toddler with a sweet smile and unruly hair. But on April 1, he began having trouble breathing. After he was taken to a northern California hospital, the unthinkable happened: Israel suffered a heart attack. After 40 minutes of CPR, doctors were able to restart his heart. But nearly an hour without oxygen had left him brain dead, they determined.
That’s when the battle began.
In those nearly four months, the family had pulled out all the legal stops and moved Israel to Guatemala on May 22 just before Israel was to be taken off the ventilator. There, Snyder told the Post,
three Guatemalan doctors, including a neurologist, declared that the boy was not brain dead after all.
That diagnosis was based in part on EEG, or electroencephalogram, tests, used to measure electrical activity in the brain, she said.
Snyder declined to name the Guatemalan doctors or their hospital but dismissed the idea that their opinion weighed less than that of American doctors.
“We’re not talking voodoo here,” she told The Post. “They have access to the same equipment as American doctors. Many of them probably have degrees from American medical schools.”
Some three months later they returned to the United States, Miller wrote because, “Despite the pending death certificate, and possibly because of the EEG tests from Guatemala, he had been accepted as a patient at Children’s Hospital of Los Angeles.”
But, within days,
the new hospital also moved to take the boy off life support. Once again, the family sought an injunction. And on Aug. 11, they received a temporary restraining order blocking the hospital from taking Israel off his ventilator.
Then, on Thursday, came a final, sudden twist in the international medical saga.
A Los Angeles Superior Court judge removed the restraining order, saying the case had already been decided at state and federal level before the family traveled to Guatemala.
And with that, doctors turned off Israel’s ventilator.
“I heard them disconnect the ventilator and then heard, of course, a very grieving mother,” said Snyder, who was on the phone with Fonseca at the time.
Snyder told the Post, “What I really don’t understand is why this hospital agreed to take this little boy in the first place,” adding
the boy’s parents never would have brought Israel back to the United States if they had known the hospital was going to pull the plug. “They knew exactly what his condition was, what his treatment was, and they agreed to take him. But it appears they only accepted him as a patient to put him to death. …
“The irony is this little boy was cared for so much better in Guatemala than he was here,” she added.
LifeNews.com Note: Dave Andrusko is the editor of National Right to Life News and an author and editor of several books on abortion topics. This post originally appeared in atNational Right to Life News Today —- an online column on pro-life issues.
Just after you have a baby people ask all sorts of interesting questions. Questions about pooping and labor and the details of breastfeeding. By and large, however, one of the most common questions I field is, “So, are you guys going to have more kids?”
I laugh when asked this question. (well, in those first days I probably cried) I just endured/survived 9 months of sickness, hormones and stretching. Then I went through horrible pain during delivery and now I’m not sleeping. GIVE ME SOME TIME TO DEAL WITH THIS, PLEASE!
But this question, are you going to have more kids, is something my husband and I are thinking about.
And the answer is maybe–hopefully. Let’s wait and see.
Depending on the crowd I’m with this answer can seem strange, strange that we don’t have a plan for how many kids we want…or even a plan for the space we’d like between kids. We practice NFP. The “plan”, if you want to call it a plan, is to avoid for a while, if it feels right. We have several months of breastfeeding infertility to keep talking, thinking and praying about this, but yes, we do hope to have more kids. We currently have 3 kids, each 18 months apart, and although I spend some days going from one crying kid to another, we love our lives and feel blessed–and that blessing is thanks to the kids we have. We won’t turn our backs on more blessings.
I’ve spent a little bit of time reflecting on this choice–the choice to be open to life, open to a big family–and I think I can best explain this choice with these 3 facts:
1. I’m in love with the miracle of life
My husband and I got married in our late 20’s and hit ground running. We had a 3 month old baby on our first anniversary…another one 18 months later and another one 18 months after that. At the end of this month we will be celebrating our 4th anniversary with 3 kids.
Shortly after my daughter was born (#2) my husband said something that was profoundly true for both of us. We now had a boy and a girl. He was cradling our daughter in his arms and he said, “I would be so sad if I knew that this was the last baby we’d have.”
I feel the same way.
It is such a profound miracle–the conception of a baby, the pregnancy, the delivery… the whole process of welcoming a new human being into the world. My first weeks with my infants I can’t help but look at them and wonder, where did you come from? How are you possible? Even during pregnancy, each time I feel that baby kick or squirm I am humbled by the miracle I am part of.
I’m in love with this miracle of life. They way they change and learn and grow–it’s all a miracle.
So, yes, yes, I want to have more children. That’s the thing about miracles, they’re sort of like potato chips. Once you know how good they are, you are always going to want another. And another. And another.
2. I (really) have no idea what is good for me
I am so happily in love with my husband, but he is not the type of guy I thought I’d end up with. In fact I knew him a full year before I even considered dating him…he just isn’t want I thought I needed. Turns out he’s exactly what I needed, I’m just clueless.
The same is true with our family size. Despite this choice to be open to life I still catch myself thinking, I would love to just hurry up and get done having kids so that I can get back to MY life, get onto accomplishing MY goals. Once I don’t have these kids in my hair I can get this done, do that, have time for all of this…
You see, what I love above all other things is the ability to get things done–to check things off of the ole’ to-do list. I think I might be addicted to checking things off the list. But, my kids are always getting in the way of me accomplishing anything.
I get frustrated, but then the baby cries and I’m forced to pull myself away from the computer and sit down to nurse him. During those quiet moments, when the older two are sleeping and I’m rocking with a nursing baby, during those moments I can feel the hand of God on my shoulder. I can feel my feet touch ground and I just want to bask in the joy that is oh so real. In those moments the unfinished projects, the dirty house, none of those things matter. In those moments I actually KNOW what matters. I actually KNOW what will really make me happy.
Turns out that if left to my own devices and desires I’d end up chasing things that would leave me unhappy, unfulfilled and alone. Happiness and joy–I know these things when I see my kids dancing together, as I stand over a sink full of dirty dishes following a great family meal, when all three kids want to climb up on my lap at the same time… I know joy when I am accomplishing nothing.
Turns out that happiness is found through my children. Wanting to get this chapter of diapers and nursing and tantrums closed already so that I can focus on myself is probably not the surest path to happiness (or holiness).
3. The Gift of Siblings
I grew up in a family of 7–3 sister and 1 brother. Although not big by some standards, I loved the fact that my family was bigger than most. When I went off to school I already had friends there–my sisters. In the evenings we would all sit around the dinning room table and do homework together. We were on the swim team together. When we got older we were roommates, and travel companions and bridesmaids for each other.
Simply, my siblings are my best friends.
It was a sacrifice for my parents to have 5 kids, I’m sure. We didn’t have a lot of things that other kids had in terms of clothes and toys. I drove a aqua Astro Van to school and was always on the hook for picking up or dropping off this sibling or that. But I knew that my parents had as many kids as they could–and that is the greatest gift that they ever gave us.
This idea–that siblings are the greatest gift I can give my kids–is reinforced every time I see my kids play together. They certainly fight, but they also love each other.
I want my kids to be challenged and loved and molded in a way that only a sibling (or lots of siblings) can. Sure, kids are expensive, but I would rather cut back on all the STUFF and instead have a house full of kids.
And so there you have it. We are Catholic and we do embrace the teaching of the church on contraception–but our choice to be open to life, to welcome more children, is so much richer than just obedience.
ATLANTA, August 23, 2016 (LifeSiteNews) – Although homosexual men are a tiny sliver of the U.S. population, they account for the majority of all Americans living with HIV, the virus that causes AIDS, the Centers for Disease Control and Prevention (CDC) has announced.
Men who have sex with men (MSM) are two percent of the population but make up 55 percent of people who were HIV-positive in 2013, according to a CDC fact sheetreleased last Wednesday.
More than nine out of 10 new HIV diagnoses (92 percent) come from young gay and bisexual MSM, ages 13 to 24.
If these trends continue, one of every six men who has sex with men will be diagnosed with AIDS in his lifetime. Already, 15 percent of all HIV-positive homosexuals and bisexuals don’t know they are infected, the government agency said.
“Gay and bisexual men are also at increased risk for other STDs, like syphilis, gonorrhea, and chlamydia,” the CDC added.
“Two things never change when it comes to the U.S. government and homosexualism. First, the CDC is constantly providing evidence like this of the high risks associated with male homosexual behavior; and second, the CDC and pro-LGBT politicians never admit that the problem is unnatural homosexual behavior itself,” Peter LaBarbera, president of Americans for Truth, told LifeSiteNews.
“In a sane world, the CDC would encourage all men, but especially young men and teenage boys, to avoid homosexual sex,” LaBarbera said. “Instead, the CDC blames societal ‘homophobia’ and ‘stigma’ for the rising disease rates, even though the American public’s acceptance of homosexuality is at an all-time high.”
More Americans (60 percent) regard homosexual sex as moral than immoral, a 13 percent increase since 2001, according to a poll released in June. The number of Americans who favor same-sex “marriage” has virtually reversed since Gallup started polling the question in 2001, with 55 percent in favor and 37 percent opposed.
“Social conservatives in the United States and across the world should demand that, if sex education is taught to their children in school, it be taught accurately,” LaBarbera told LifeSiteNews. “Kids need to see these statistics to cut through the ubiquitous gay propaganda.”
The fertility rate, which is based on the number of babies born per thousand women aged 15-44, is 59.8 babies per 1,000. That’s a slight drop compared to the first quarter of 2015, when the rate was 60 babies per 1,000 women. According to researchers at the CDC, this is the lowest number on record. Note that fertility rate is slightly different than birth rate, which is based on the number of babies born compared to the entire U.S. population.
The numbers also reflect interesting demographic changes. Between 2015 and 2016, the fertility rate among teens dropped from 22.7 babies per thousand women to 20.8. For women aged 20-24, the drop was from 75.2 babies per thousand women to 72.5, and for women aged 25-29, the drop was from 100.3 to 98.4.
However, the rate actually rose slightly for women in their 30s and 40s. For example, the fertility rate for women aged 30-34 increased from 95.6 to 97.9. The numbers may reflect the trend of more women choosing to have children later in life, as well as an overall decrease in teen pregnancy. This correlates with an earlier study released by the CDC in January, finding that the average age of mothers when they have their first child has risen from 24.9 years old in 2000 to 26.3 years old in 2014.
August 18, 2016 (LiveActionNews) — When Michael and Megan Foster shared a video of the “Gotcha” moment when they adopted their daughter Fen from China, they never expected the reaction would be so overwhelming. Their new daughter was so excited to see her parents and siblings that her joy is contagious – and is felt around the world.
“She comes out from behind a curtain (our heart skips a beat), squints (she needs glasses), takes a couple steps, spots Meg, proclaims, ‘Mama? Mama!’ and runs and leaps into her arms,” writes her father, “and gives a huge hug while repeating ‘Mama.’ She says ‘I missed you.’ She finds dad and says ‘Baba’ and gives a big hug, then back to mom […]”
She continues to run around hugging her siblings before jumping up and down for joy. Her smile is so brilliant that other people in the room take notice.
The video has been viewed over 415,000 times in just two days. Mr. Foster calls it “completely mindblowing” that for 11 years this little girl went unnoticed by the world and now is being seen and loved by thousands.
“[…] this morning I’ve replied to messages from people from Minnesota to Moscow to everywhere in between all over the world,” wrote Mr. Foster after the video had been posted for one day. “The network of people moved to tears of joy from this video is as broad and diverse as the world itself – and yet we are brought together by the power of this LOUD LOVE! Love wins. Love unites. Love prevails. Love never fails! Thank you Jesus! We love you Fen!”
Fen will be back home in the United States soon, joining her new family – which includes five siblings. Her parents are aware that there will be challenges as they all adjust to their new life, but right now they are loving getting to know Fen and enjoying her “uncontainable joy.”
Adoption saves lives and should be the preferred option over abortion. In China, millions of baby girls have been aborted through gendercide. Knowing that fact, it makes Fen’s joy even more beautiful to watch.
In it, she wrote: “Nearly one in three American women will have an abortion by age 45. Why are we so afraid to talk about it—or to acknowledge that our lives would have been so much less than we hoped for without it? Why are we pressured to feel that we should regret our choice, and that there’s something wrong with us if we don’t?”
This kind of content had shaped my expectations. In fact, Abraham’s article could have been a perfect segue for the tale of an empowered woman who aborted the baby that got in the way of her Olympic dreams. Warily, I clicked on the link.
But what I got was a lovely surprise. The article detailed the inspirational story of Sarah Brown, an elite runner who discovered, while at the peak of her Olympic trials training, that she was pregnant—but she never even considered abortion.
“I was at top of my game and then, all the sudden, it was like I fell off a cliff. I felt so fatigued in my races, like I felt like I was running through sand. I couldn’t figure out what was wrong. By the time I found out I was pregnant, it was a lot of mixed emotions.” But she was excited too. “This is my first child and my husband and I did plan on having kids at some point, it just happened a bit earlier than we were expecting!” she told Elle’s Kristina Rodulfo.
In an interview with Alison Wade of Runner’s World, Brown revealed that she wanted to keep her child from the moment she heard the news. “It was one of those things where I wasn’t ready to have a kid, but also, as soon as I found out I was pregnant, I wasn’t ready for the thought of losing that kid. As terrifying as it was to become a mom, I knew that that was what I wanted,” she said.
In the ultimate display of true feminist choice, “she set her sights on both achieving her career goals and having her child,” Rodulfo wrote. The decision was a family affair. Brown’s husband and coach, Darren, was literally with her every step of the way. He often trained alongside Sarah, donning a weight vest to truly empathize. “I don’t know if I could have done a lot of the things I did if [my coach wasn’t my husband],” Sarah told Rodulfo, “just from a standpoint of him seeing me every day, working very closely with me, knowing how I’m feeling.”
What gave Brown these strong convictions and determination? Her bio on Athlete Biz gives a clue: “Sarah believes that her running talent is a gift from God and needs to be used for something more than her own personal gains.”
This summer, she had an opportunity to put her beliefs into practice. Although Brown was slated to place at the Rio Olympics, she never made it past the trials. But her inspirational reaction to the disappointment revealed her strong faith.
“Today wasn’t the fairytale ending you dream about. But then again, this journey never really was about an ending, it’s a beginning,” she posted on Instagram. “A new chapter as a family of three. Thanks for all the support ❤ & you can bet you will continue to see this mama run #runmamarun”
The time is now to call upon God, through the powerful intercession of Our Lady of the Rosary, to heal our country and return it to holiness.
This is a nationwide prayer campaign called the “Novena for Our Nation.” Everyone from around the nation is encouraged to join ranks as, united, we pray the very powerful 54 Day Rosary Novena from the Feast of the Assumption on August 15 to the Feast of Our Lady of the Rosary on October 7.
We are living in extraordinary times. Presidential executive actions, US congressional and state legislation as well as court rulings at all levels up to the Supreme Court are in conflict with God’s laws; especially the disregard for the rights of the unborn, elderly and weak in our society and the attacks on marriage and family values. At the same time society and government are becoming more intolerant towards biblically based religious belief and practice. In conflict with First Amendment constitutional rights, persecution of traditional religious expression has reached unprecedented levels. We are in a Spiritual Battle.
Extraordinary times call for extraordinary action. In this Jubilee Year of Mercy, and as we enter the centennial year of the apparitions of Our Lady of Fatima, we are called upon to help turn our country back towards God. We will accomplish that through prayer; prayer that can change hearts, change families, change our communities and change our country. There is no stronger weapon in this Spiritual Battle than the Rosary.
THE HOLY LEAGUE RISES AGAIN!
Pope St. Pius V formed the original Holy League in response to the dire situation in which Christian Europe found itself in 1571. Small bands of Catholic men and remnant armies from various nations came together under the spiritual leadership of the saintly pontiff and the military leadership of Don John of Austria. By prayer and fasting, they implored the help of God’s grace, through the intercession of the Mother of God, and, by the grace of Almighty God, on October 7, 1571, at the Battle of Lepanto; the Christian fleet won a crushing victory over the Ottoman Turks, saving Christendom and western civilization.
The new Holy League, under the spiritual guidance of Cardinal Raymond Burke is, .essentially, calling men to combat the forces of evil in today’s society. The Holy League strives to call men back to the state of grace and to transforming the culture through prayer (primarily Adoration and Confession) and training in holiness. You can read about this Catholic men’s movement (http://holyleague.com/).
The new Holy League is sponsoring this very necessary campaign because, at this particular moment in time, the Church finds itself in a similar situation to that of the Church in the late Sixteenth Century. However, instead of a physical enemy on the horizon, the Church and the family (the domestic Church) are threatened daily by relativism, secularism, impurity, and confusion regarding Church teaching.
The battle today “is not against human forces but against the principalities and powers, the rulers of this world of darkness, the evil spirits in the heavens” (Ephesians 6: 10-12).
PRAYER AND TRAINING!
This prayer campaign is also a Basic Training in Holiness. Each day, along with praying your rosary, holiness trainees will be provided with a 1-2 minute reflection on the qualities of excellence. The first 27 days, trainees will read from passages in scripture, quotes from saints and the catechism on one of the following: Theological Virtues, Cardinal Virtues, Gifts of the Holy Spirit, and the Fruits of the Holy Spirit. The second 27 days will be excerpts from the book entitled, Church Militant Field Manual: Special Forces Training for the Life in Christ.
The daily reflections for this prayer and training campaign can be found in multiple places.
1) If you would like a hard copy to carry with you, it is available in book form that is entitled, 54 Day Basic Training in Holiness. The 54 Day Rosary Novena prayers are included in this book. Order your book HERE(https://romancatholicgear. com/54-day-basic-training-in-holiness-pre-order.html). The books are also offered in bulk, at a reduced rate.
2) You can sign up to receive the daily reflection in your email. Sign up on the main page of novenaforournation.com
3) You can join the Novena for Our Nation Facebook group HERE(https://www.facebook. com/novenaforournation/), to receive the reflections each day.
NATIONAL ROSARY RALLY IN WASHINGTON DC
We are asking everyone to join us in Union Square in front of U.S. Capitol for a very special Rosary Rally on October 7. As the Year of Mercy recedes, and the Presidential election only days away, we want to call out to God in a very special way at the conclusion of our 54 Day Rosary Novena.
If you can join us, please do. If you cannot, please consider planning your own Rosary Rally in your area. Some suggestions for locations might a government facility or Planned Parenthood or your parish church or wherever you think would be best.
SPREAD THE WORD!
Finally, please do everything you can to get the word out about this very important and necessary prayer campaign for our nation, that begins on August 15, 2016! May God, through the powerful intercession of the Blessed Mother, truly pour out His grace upon the United State of America.
RIO DE JANEIRO, Brazil, August 10, 2016 (LifeSiteNews) — When three-time world champion gymnast Simone Biles flew to Rio de Janeiro for the Olympic Games, the 19-year-old carried a rosary her mother gave her and a St. Sebastian medal from her family’s spiritual home, St. James the Apostle Catholic Church in Spring, Texas.
Simone is already the most decorated woman gymnast in her sport’s history, winning golds at the world level in all-around and individual events. But as the young daughter of a fatherless home who was shunted between a drug-addicted mother and foster homes, her chances of excelling in any sport let alone one so intense as gymnastics seemed slim indeed.
Then her grandparents, Ron and Nellie Biles, stepped in, took her and three siblings into their home and then adopted Simone and her sister, while Ron’s sister adopted her two brothers. Simone grew up in a family of achievers, who were also devout Catholics, not incidentally, according the social science findings showing strong correlation between family stability, regular and frequent church attendance, and success.
According to this week’s story in Independent Journal Review, “Little Girl Abandoned by Father and Drug-Addict Mother Is Adopted by Christian Texas Family, Becomes Best Athlete in the World,” her faith plays an important role in her life and success.
“Her parents,” reporter Benny Johnson wrote, “also introduced Simone to her Christian faith. She attends mass [sic] with her family every Sunday when she is not competing. Simone prays regularly and carries a rosary that her mother gave her.”
Simone Biles goes to Mass with her family.
US Magazine has the details on the rosary, in a story on what Simone carries in her bag. “My mom, Nellie, got me a rosary at church. I don’t use it to pray before a competition. I’ll just pray normally to myself, but I have it there in case.”
Simone’s own innate talent and strong will are clearly crucial to her success. As Texas Monthly reports, when the girl came home from a day care field trip to a gymnastics school insisting on becoming its newest pupil, there was no denying her. “She’s always been headstrong,” said adoptive mother Nellie, the now-retired owner of a chain of nursing homes. “When she makes up her mind, it’s, like, oh, my gosh — the whole world could be upset and she’d still do it. My other kids would listen. Her, no. She makes her mind up and that’s it.”
Simone was six when she self-launched her gymnastics career, the same year Ron and Nellie adopted her and her sister Adria, and the two girls started calling them Dad and Mom.
Until then, the sisters called them Grandpa and Grandma. Then Nellie told the girls, “It’s up to you guys. If you want to, you can call us Mom and Dad.”
“I went upstairs,” Simone told the Texas Monthly, “and tried practicing it in the mirror — ‘Mom, Dad, Mom, Dad.’ Then I went downstairs, and she was in the kitchen. I looked up at her and I was like, ‘Mom?’ She said, ‘Yes!’ ”
Simone soon had a second mother in coach Aimee Boorman, who not only mentored Simone in gymnastics but babysat her and her sister when her father was out-of-state installing apparatus for the Federal Aviation Administration and her mother was away overseeing her nursing home network.
Completing the stability to which Simone returns when lands from her increasingly athletic and gravity-defying vaults and jumps is the family church, St. James the Apostle. Father Charles Semperi, the church’s pastor, describes the Biles as “very faithful Catholics who are always at Mass.”
Father Semperi told LifeSiteNews that the family frequently asks for the congregation and priests to pray for Simone in her efforts both during Mass and privately. “She was very good in Confirmation class,” he recalls. The family now concentrates on supporting Simone and building a world-class gymnastics training facility called World Champions Centre in Spring.
The parish sent Simone off with a St. Sebastian medal. “I told her not to wear it during her events,” Fr. Charles joked, “in case it flies up in her face.”
As of Tuesday, Simone had qualified for the finals individually for all events in her field and was well on her way to winning as many as five medals, perhaps all gold.
Explains the IJR story, “Biles is able, with ease, to pull off moves other gymnasts could only dream about in a world seemingly unbound by the laws of gravity. Her routines and dismounts are so complex and so rarely seen in competition, several are named for her.”
Though already established as the best in the world, Biles will need an Olympic victory, the news media make clear, to ensure the 19-year-old becomes a multi-millionaire through endorsements, as if that was the point of sports, or of the Olympics, or of hers and her family’s 13-year effort.
Success could also bring family troubles, they warn, such as the possible re-emergence in her life of her natural mother, who lives in Columbus, Ohio, and has reportedly been clean from drugs for several years, or even of the father who disappeared virtually at birth. Teammate Gabby Douglas faced similar embarrassment at the hands of her long-absent father, who showed up after her Olympic victory in 2012 seeking her signature on various sports memorabilia he wanted to sell.
However, Simone’s adoptive parents and family have done their best to shield her from a preoccupation with such outcomes and focus her efforts on her sport, family life, and faith.
This supports the scientific research conducted or collected by the Washington D.C.-based Marriage and Religion Research Institute, which it summarizes on its website: “Regular attendance at religious services is linked to healthy, stable family life, strong marriages, and well-behaved children.
“Religious worship also leads to a reduction in the incidence of domestic abuse, crime, substance abuse, and addiction. In addition, religious practice can increase physical and mental health, longevity, and education attainment. These effects are intergenerational, as grandparents and parents pass on the benefits to the next generation.”
August 3, 2016 (LifeSiteNews) – Think Millennials are the most sexually active generation in history? Think again, say the authors of a new study released on Monday.
The number of young adults born in the 1990s who report they are not having sex is more than twice as high as it was for the Baby Boomer generation, a sign they have learned from the fallout of the sexual revolution, experts tell LifeSiteNews.
The study found that 15 percent of Millenials aged 20-24 said they had not had sex since age 18, more than those born in the late 1960s (six percent), 1970s (11 percent) or 1980s (12 percent). That is lower than their fellow Millenials born in the previous decade.
The definition of “sex” is left up to the respondent to define. However, the number of women who were sexually abstinent as young adults tripled since the 1960s, while the number of men doubled, according to the study, which appeared in the Archive of Sexual Behavior.
“I think a lot of them are watching the adults around them and concluding that sex without limits is not making people happy,” particularly “parents with multiple marriages and divorces,” Dr. Jennifer Roback Morse of The Ruth Institute told LifeSiteNews.
The study concludes that “the new sexual revolution has apparently left behind a larger segment of the generation than first thought.”
“The idea that these kids are ‘left behind’ by the sexual revolution is quite strange, as if they’ve somehow been sealed in a bomb shelter and never knew it happened,” Rebecca Oas, Ph.D., the associate director of research for the Center for Family and Human Rights (C-Fam), told LifeSiteNews. “More likely, they’ve seen that experiment running its course and decided they’d rather learn from someone else’s mistakes instead of their own.”
The finding dovetails with CDC figures that show a majority of teenagers are choosing not to have sex. Only 41 percent of high school students reported sexual activity, a 13-point drop since 1991. Millenials also have a lower average number of sexual partners (eight) than either Baby Boomers (11) and Generation X (10).
Valerie Huber, the president of Ascend, told LifeSiteNews that her group – formerly the National Abstinence Education Association – “commissioned the Barna Group to survey 18 and 19 year olds and found similar results. The majority did not like the idea of ‘hooking up,’ and most of those who were not sexually experienced were waiting for a committed relationship.”
Some do not know what to make of the results. The Washington Postwrote, “Delaying sex is not necessarily bad, experts say.”
Numerous studies show having sex at a younger-than-average age leads to negative results, while delaying sexual activity and reducing the number of partners has positive outcomes.
Dana Haynie of Ohio State University found that early sexual activity increased delinquency by 20 percent. Experts have warned that earlier sexual activity can increase anxiety and negative psychological reactions, such as feeling used, especially for girls. A study in Pediatrics last year concluded that troubled children were more likely to begin having sex earlier in life, reinforcing the vicious circle.
Those who had sex later than average had higher incomes, educational achievement, and satisfaction in marriage, according to a 2012 report from Dr. Paige Harden of the University of Texas.
A 2014 report found that having multiple sexual partners and cohabitation before marriage decreased marital happiness after couples eventually tied the knot.
“We know that early sexual behavior tends to set a pattern for later behavior. The fact that more and more emerging adults are avoiding sex suggests they recognize that casual sex can compromise their life goals,” Huber told LifeSiteNews.
One young person toldThe Washington Post that, having seen so much sex depicted in pornography, “there really isn’t anything magical about it” anymore.
Those who attend religious services are more likely to be abstinent, as well. “There was a significant increase in sexual inactivity among those who attend religious services once a week or more compared with those who do not,” Oas noted.
Huber said the most common reasons young people reported to Ascend for delaying sex were personal values and a focus on attaining their goals. She encouraged schools teach Sexual Risk Avoidance (SRA) education – as opposed to Sexual Risk Reducation (SRR) or Comprehensive Sex Education, which present teen sexual activity as more normative.
The study notes, “abstinence-only sex education and virginity pledges became more popular (and federally funded) after the 1980s, especially between 1996 and 2009, when abstinence-only programs received large amounts of federal and state funding.” Studies have found that abstinence-based education reduces the overall teen sex rate.
“This new research suggests that our students have caught a positive and healthy vision for their futures,” she said. “It also means that we must, as a society, be more intentional on reinforcing this same healthy behavior for young, single adults.”
Editor’s note: The following address was given in a catechesis to youth at World Youth Day.
World Youth Day
July 28, 2016
(Church of the Conversion of St. Paul, Krakow, Poland)
Hugh Owen, Director, Kolbe Center for the Study of Creation
Dr. Thomas Seiler, Ph.D., Physics, Technical University of Munich
Your Excellency, Reverend Fathers, brothers and sisters, younger brothers and sisters in Christ, God is a loving Father, He is Mercy Itself. So, He always teaches us clearly the things that we need to know for our happiness here on Earth and in eternity. He doesn’t confuse us. In fact, He teaches us through the inspired, inerrant words of Holy Scripture that, “HE is NOT the Author of confusion.” He is the Father of Mercy who CLEARLY proclaims the Truth that saves us from the father of Lies, from Sin and from Death. And so that we would never be in doubt about the fundamental truths, the Dogmas, of the Catholic Faith, God has appointed the Holy Father and the Bishops to GUARD the Deposit of Faith that was handed down from the Apostles, so that all that was taught by the Apostles and defined by their successors through the centuries, will always be upheld in its original form, without any corruption or deviation. That is Divine Mercy in action.
Today, however, my younger brothers and sisters, there is great confusion among many Catholics, especially about what it means to be a man or a woman, and about God’s unchanging plan for Holy Marriage and for the Family. God is not the Author of this confusion. And no one who studies and abides by His teaching on this subject as it has been handed down from the Apostles will ever be confused.
Now what is this beautiful teaching on man and woman, on Holy Marriage and on the family that was handed down by all of the Apostles, Fathers, Doctors, Popes and Council Fathers in their authoritative teaching?
It is very simple and very clear.
It is that “In the beginning, God created ONE Man for ONE woman for LIFE.”
My scientist colleague Dr. Thomas Seiler and I are here to proclaim that sound theology, sound philosophy, and sound natural science ALL confirm this beautiful revelation from God that in the beginning He created Adam’s body from the material elements of the Earth and at one and the same time created his soul to be the form of that body; then He created EVE for Adam from Adam’s side; and placed them as the king and queen of the entire universe, a universe that was completely free not only from human death but from any kind of deformity or disease.
Less than 150 years ago, when the enemies of the Church launched the current war against Holy Marriage and the Family by trying to legalize divorce in Catholic countries where it was forbidden by law, Pope Leo XIII wrote an entire encyclical on Holy Marriage. In that encyclical Pope Leo directed the Bishops of the whole world to defend Holy Marriage on this foundation. He wrote—and please listen very carefully:
We recall what is known to all and cannot be denied by anyone that God on the sixth day of creation having created Adam from the dust of the Earth and breathed into him the breath of life gave him a companion whom He formed from his side miraculously while he was locked in sleep.
Now the Pope was certainly correct to direct the Bishops in this way — because if every Catholic young person in the world were taught that God created one man for one woman for life from the beginning, it wouldn’t be possible to be confused about the Church’s teaching on Holy Marriage, divorce, contraception, and sexual morality! When God created Eve, the first woman, for the first man, Adam, by creating Eve’s body from the body of Adam, He showed us CLEARLY that the union of man and woman in Holy Marriage is not something that comes up from the animals; it is something that comes down from the Heaven. And, therefore, any use of the gift of sexual intimacy outside of a Holy Marriage between one man and one woman committed to each other for life is not only a great sin but a sacrilege — because it takes a gift that God created specifically for man and woman in a permanent, holy, exclusive, and life-giving union and desecrates it.
That is why when Jesus was asked about divorce, He answered CLEARLY, “From the beginning of creation God made them male and female . . .” and of divorce He said to the Pharisees, “From the beginning it was not so . . .”
Now, my younger brothers and sisters, why is it that this beautiful doctrine which the Vicar of Christ on Earth said is “known to all and cannot be denied by any” is today known by so few of your generation and denied by so many of your teachers?
I think you all know the answer.
The reason why many young Catholics do not hear this beautiful Catholic teaching on the creation of Adam and Eve is because we are told that “science” — meaning natural and physical science — has proven that the bodies of the first human beings evolved from microbes over hundreds of millions of years through mutation and natural selection. And, so, we are told, what all of the Fathers, Doctors, Popes and Council Fathers in their authoritative teaching called the sacred HISTORY of Genesis—is actually a myth.
But is that true?
Did God allow His Church to teach a totally false account of the origins of man and the universe for almost two thousand years only to enlighten her through the wild speculations of godless men like Charles Lyell, Charles Darwin, and T. H. Huxley who hated the Church and wanted to destroy her?
At this point I would like to introduce a Catholic natural scientist who has dedicated much of his life to studying the scientific evidence for and against the hypothesis that molecules turned into human bodies over billions of years of the same kinds of natural processes that are going on now — Dr. Thomas Seiler. Dr. Seiler has a Ph.D. in Physics from the Technical University of Munich, Germany. He has lectured at Catholic universities, seminaries, schools, and parishes all over the world, demonstrating that all of the evidence in natural science harmonizes with the traditional Catholic teaching that all human beings on Earth today are descended from one man and one woman who were created in a state of genetic perfection less than ten thousand years ago, just as we are told in the sacred history of Genesis. Dr. Seiler . . .
Dr. Thomas Seiler:
Most of you may have heard the statement that chimpanzees and humans are having 99% of their genes in common. However, what you are usually not told is that this result was not based on comparing the entire DNA of man and ape but only on comparing a very small fraction of it (ca. 3 %). The function of the other 97% of the genetic code was not understood. Therefore, it was concluded that this DNA had no function at all and it was considered “leftover junk from evolution” and not taken into consideration for the comparison between man and ape. Meanwhile, modern genetics has demonstrated for almost the entire DNA that there is functionality in every genetic letter. And this has led to the collapse of the claim that man and chimpanzee have 99% of their DNA in common.
In 2007, the leading scientific journal Science therefore called the suggested 1% difference “a myth.” And from a publication in Nature in 2010 comparing the genes of our so-called Y-chromosome with those of the chimpanzee Y-chromosome we know now that 60% of human Y-chromosome is not contained in that of the chimpanzee. This represents a difference of one billion genetic letters, known as nucleotides.
And modern genetics has recently made another important discovery which was very unexpected. Researchers found that all of the different groups of humans on earth, wherever they live and whatever they look like, have 99.9% of their genes in common. This leads to a problem for the hypothesis of evolution because if humans really were descended from the apes, then how could it be that we only have 40% of our Y-chromosome in common with the apes but at the same time there is almost a complete genetic identity among all humans? If there had been an evolution from ape to man then it should still go on among men and reveal significant genetic differences. These recent discoveries therefore drastically widen the gap between man and the animals. And they confirm that there are in reality no such things as human “races”. Asians, Europeans, Africans and Indigenous people from America and Australia only have superficial differences like color of skin or shape of the nose but they are all extremely similar on the genetic level.
And these recent breakthrough discoveries even go further. Today, because of the extreme similarity of the human genome, it is considered a well-established fact among geneticists, that all humans living on earth now are descended from one single man and from one single woman. In order to convince yourself of this you only have to search in the internet for the terms “mitochondrial Eve” or “Y-chromosome Adam”. These names were given by evolutionists in an ironic sense but now many regret that choice of name because this discovery perfectly confirms the Catholic Doctrine of Creation which has taught for 2000 years that all humans are brothers and sisters descended from one single human couple, the real historical persons Adam and Eve, not from a multitude of subhuman primates.
Another evolution-related research field is embryology. Biologist Ernst Haeckel proposed his so-called “Biogenetic Law” according to which the embryonic development of vertebrates repeats the assumed history of their evolution from one-celled ancestors. This was formulated by Julian Huxley in the following way: “Embryology gives us the most striking proof of evolution. Many animals which are extremely different as adults are hard to tell apart as embryos. You yourself when you were a young embryo were very like the embryos of lizards, rabbits, chickens, dogfish, and other vertebrates. The only reasonable explanation is that we vertebrates are all related by common descent.” However, apart from the logical error of concluding from similarity to descent, the “evidence” for this proposed law only consisted in Haeckel’s skillful drawings of embryos belonging to different animals and man.
After 120 years, British embryologist Michael Richardson used modern microscopes and examined the embryos of humans and different animals at the same stage of development. His work has been published in the scientific literature and he summarized the significance of Haeckel’s influential drawings in an interview in The Times London in 1997: “This is one of the worst cases of scientific fraud. It’s shocking to find that somebody one thought was a great scientist was deliberately misleading. … What he [Haeckel] did was to take a human embryo and copy it, pretending that the salamander and the pig and all the others looked the same at the same stage of development. They don’t … These are fakes.”
A further field of research which is related to origins is anatomy. If evolution were true, we would expect to find many vestiges of the organic constructions produced in the course of evolutionary history. Anatomist Robert Wiedersheim presented about one hundred “rudimentary” or “vestigial” organs in humans, organs which have a reduced function or no function at all because they are left-overs from an earlier stage of evolution. Famous examples include the vermiform appendix and the tonsils. Wiedersheim and most of his peers did not understand the function of these organs and concluded from this that they have no function at all. Meanwhile, however, new scientific research has reached a different conclusion. For the appendix, for example, it was found that it has indeed a function in the immune system, especially during the first years of our life.
A similar conclusion has been reached in regard to the tonsils and also for almost all of the other organs functionality has meanwhile been discovered. Yet, even if there were still many organs whose function is unknown, we would never be allowed to conclude from our ignorance of a biological function that there is no function. This would be exactly the same logical error which has been made with the so-called “junk-DNA” for many years.
Now you may ask: But what about the Neanderthals? Have we not found much fossil evidence that there were once ape-men on earth which were our ancestors?
To say it briefly: All fossils which we have found finally turned out to be either fully human, like Neanderthals and others, or fully ape, like Australopithecines. Paleontologists could not find any ape-man fossils — which indicates that these creatures never existed.
The theory of evolution predicts that things change from less complex to more complex, from incompleteness to completeness and that we should find many failures, lost functions, wrong constructions and half-finished organs which are in the process of evolution. However, all the different areas of relevant research, such as genetics, embryology, anatomy and paleontology, over and over again confirm that all the different kinds of creatures began their existence as already perfect and fully formed. Indeed, we do not find any evolving, half-finished eye, ear, leg, or wing in nature, neither in the fossil record nor in today’s world. If such half-complete organs ever had existed then many of them should have survived until today since they were per definition more fit than their ancestors which did not have that organ at all and which are still existing, like the wing-less reptile which supposedly has turned into a bird or the land-mammal which should have turned into a whale.
Furthermore, all changes which we do actually observe in nature are never processes of genetic increase or perfection but always processes of genetic loss and degeneration. This certainly supports that in the beginning, everything must have been perfect and not vice versa. Geneticists observe an ongoing accumulation of harmful mutations in our genome instead of an ongoing perfection of our DNA. This observation is to be expected because the most fundamental natural law, the law of increasing entropy, demands that all natural processes can only proceed from order to disorder and never vice versa. Also so-called open systems cannot produce new constructional information, not in one single case. Therefore, assumed processes like changing a leg into a wing or an ape body into a human body by mutation and selection are excluded by natural law.
Let me conclude with an analogy: One could certainly change a refrigerator into a television by many small steps, replacing one small electrical or mechanical part by another one until one has got a TV. However, it is very improbable that each of these small changes towards the television would lead to a fridge which is a better one than its predecessor or the original one. However, that would be needed to make evolution via continuous selection possible.
For more information, you can visit www.originality-of-species.net.
Hugh Owen:
So, you see, my younger brothers and sisters, REAL NATURAL SCIENCE does not support the evolutionary mythology that human bodies resulted from hundreds of millions of years of genetic mistakes! It confirms the traditional Catholic teaching on the creation of Adam and Eve.
Some of you may be thinking, “Well, what difference does it make?”
I will show you that it makes a huge difference.
In the first place, this doctrine tells us that God really did create ONE man for ONE woman for LIFE from the beginning of creation, just as Jesus said.
So we can be sure that God will not bless any change in the Church’s teaching on Holy Marriage, divorce, contraception, or sexual morality.
We can be sure that your happiness and the happiness of your brothers and sisters all over the world depends on KNOWING and OBEYING this teaching — even if some of the professors and teachers in our Catholic institutions want to introduce something new.
Divine Mercy demands that we believe and proclaim this teaching to the whole world: that God created one man for one woman for life from the beginning of Creation.
By our words and by our lives, we must tell the whole world, loudly and clearly, “If you want to be happy, you must follow God’s plan for Holy Marriage.”
That is Divine Mercy.
St. Maximilian Kolbe, the great saint of Auschwitz, understood and defended this teaching against those like Adolf Hitler and Josef Stalin who abandoned the Christian doctrine of creation to embrace evolution. The last teaching that St. Maximilian gave before he went to the starvation bunker in Auschwitz was a defense of this beautiful doctrine. Let me share it with you in closing.
As most of you know, Our Blessed Mother visited Lourdes in the south of France in 1858 on the very eve of the publication of Charles Darwin’s book The Origin of Species in which he argued that humans had evolved from sub-human primates. At the request of her pastor, St. Bernadette asked Our Lady: “Who are You?” And the Blessed Mother answered
“I AM THE Immaculate Conception.”
St. Maximilian meditated on these words for decades and before he died he explained that with these words Our Blessed MOTHER defended the traditional Catholic teaching that God created ONE MAN body and soul for ONE WOMAN for LIFE from the beginning of creation and refuted Darwin’s claim of man’s descent from the apes.
Listen to his explanation.
“Adam,” St. Maximilian explained, “was not conceived in the womb of a parent. He was created body and soul.” “Eve,” St. Maximilian observed, “was not conceived in the womb of a mother; she was created by God from Adam’s side.”
“Our Lord’s Divine Personhood,” St. Maximilian continued, “was not conceived in the womb of the Blessed Virgin. As a Divine Person — the Second Person of the Most Holy Trinity — He existed from eternity.”
Therefore, St. Maximilian concluded, it is true: Our Blessed Mother is THE UNIQUE IMMACULATE CONCEPTION.
But, you see, if so-called theistic evolution is true, then Adam was conceived in the womb of a sub-human primate; so was Eve. And if that were true — since theistic evolutionists must hold that Adam and Eve were created without sin — then the Blessed Virgin would have said to St. Bernadette: “I am Immaculate Conception Number Three.”
But She didn’t say that.
Why?
Because She wanted to remind us that God CREATED ONE MAN (body and soul) for ONE WOMAN (formed from his side), FOR LIFE, from the beginning of Creation.
And that is why the Blessed Mother is the UNIQUE, ONE AND ONLY, IMMACULATE CONCEPTION.
Live, embrace and proclaim that Truth wherever you go, and you will be a powerful channel of Divine Mercy!
July 29, 2016 (LifeSiteNews) — Contraception is at the root of the culture of death and the defense of family is inseparable from the defense of life, Cardinal Raymond Burke says in a broad book-length interview.
In his lengthy interview with French journalist Guillaume d’Alançon, titled Hope for the World: To Unite All Things in Christ, the American cardinal calls gender theory “madness,” addresses the question of Communion for the divorced and remarried, and offers remedies for the crisis in the Church.
Burke is the patron of the Sovereign Military Order of Malta and the former Prefect of the Apostolic Signatura, the Vatican’s highest court.
“I do not see how it is possible to talk about the family without talking about the defense of human life,” Burke said. “It is fundamental. Contraception and abortion are two stages in the attack on conjugal love. In contraception there is a fear of new life, and this practice often leads to abortion. It is of fundamental importance to associate works on behalf of the family with pro-life works, because marriage is the source of new life.”
“The Lord created man and woman to love each other and to marry, and they express their love more fully in conjugal union, which is by nature procreative,” Burke explained.
“Gender theory” is an attack on this truth, he said.
“Gender theory is an invention, an artificial creation. It is impossible to have an identity that does not respect the proper nature of man and that of woman,” Burke said. “It is madness that will cause immense damage in society and in the lives of those who support this theory. With gender theory, it is impossible to live in society. Already today, in certain places in the United States, anyone at all can change identity and say, ‘Today I am a man; tomorrow I will be a woman.’ That is truly madness. Some men insist on going into the women’s rest rooms. That is inhuman. In the schools, you can imagine the confusion. … Nowadays there is enormous confusion, which is based on the false idea that there are practically an infinite number of possible sexual orientations. The twofold expression of the human person is not heterosexuality and homosexuality, but male and female. This is the authentic theology of anthropology: that God created man: ‘male and female he created them.’”
Burke warned that Christians must defend the natural law from legislative attacks that contradict what “is inscribed in the heart of man by the sovereign will of God.”
“Not to speak about the natural law is to deny reason,” he said.
Similarly, people who experience same-sex attraction deserve authentic pastoral care, Burke said, care that doesn’t cause them harm by encouraging them to follow “inclinations against the natural law.”
Homosexual acts ultimately cause suffering, he said, because they go against the natural “complementarity of the sexes and the sexual faculty’s potential for procreation.”
But the Church offers those with same-sex attraction the opportunity to “discover what authentic love means,” Burke said. He cited the teaching of the Catechism of the Catholic Church that people attracted to the same sex must be “accepted with respect, compassion, and sensitivity” (CCC 2358).
In addition to the dismantling of natural law, Burke said Islam’s inability to peacefully coexist with other religions and President Obama’s attacks on religious liberty pose threats to the Catholic Church.
“President Obama wants to push the Church back behind the walls of her church buildings and to prevent her from applying her law to her own hospitals and schools,” the cardinal cautioned. “He claims that the Church may not intervene on the question of abortion, of homosexuality, but that the State alone must manage these questions.”
The U.S. government “wants citizens to obey unjust laws,” he said, such as requirements that Catholic hospitals commit abortions and dispense contraceptives. “To that, I reply: We cannot do it,” because “there are situations in which the Christian must disobey when civil law commands an action contrary to the moral law.”
‘There is no justification for saying that a certain percentage of marriages are null’
“It is impossible to say anything other than what Saint John Paul II said” on the question of whether non-abstinent divorced and remarried couples may receive Holy Communion, Burke insisted.
He addressed the controversial topic that has been the source of a heated debate within the Catholic Church by quoting the late Pope’s exhortation Familiaris Consortio, which reiterated the Church’s longstanding teaching of not admitting to the Sacraments the divorced and civilly remarried unless they live as brother and sister.
“The state of life of divorced-and-remarried Catholics is not consistent with the mystery of the union of Christ and the Church,” Burke said.
Liberal prelates such as Cardinal Walter Kasper pushed for the Church to admit the divorced and remarried to Communion at two contentious synods on the family. Pope Francis brought up the topic in his April 2016 exhortation.
Many see Pope Francis’ exhortation Amoris Laetitia as having poured gasoline on this fire with its seeming suggestion that in some cases the Church will allow those living unrepentantly in situations it labels objectively sinful to receive Holy Communion.
“In the recent synod … the tendency was sometimes to dwell at length on all the problems of the family, at the risk of speaking only about that, giving me the impression that the family I knew as a child, that the [healthy] families I met during the first years of my priesthood no longer exist,” Burke said. “I can tell you that there are many magnificent families that function well!”
After the exhortation’s release, Burke wrote in the National Catholic Register that it must be read through the lens of Catholic doctrine.
No pope could change the Church’s moral teaching even if he wanted to, Burke told d’Alançon.
“It is impossible for the Church to change her teaching in matters concerning the indissolubility of marriage,” he said. “The Church, the Bride of Christ, obeys His words in chapter 19 of the Gospel of Saint Matthew, which are very clear insofar as they concern the nature of marriage. No one disputes the fact that these are the words of Christ Himself, and after the response of the Apostles, the import of these words for those who are called to married life is quite clear.”
As one of the Catholic Church’s most well-established canonists, Burke has spent a good part of his career in the Vatican working on cases of marriage validity. In other words, Burke has defended unions as being valid marriages and reviewed cases when the Church declared that a marriage never actually existed and thus is null.
Pope Francis made waves in June when he said that the “great majority” of Catholic marriages are “null.” The Vatican subsequently altered his remarks in their official transcript of his speech, and numerous canon lawyers and theologians responded that his remarks were incorrect.
Although d’Alançon did not mention the pontiff’s remarks explicitly, he asked Burke if “many marriages” are “actually null from the start.”
“It is difficult to say how many marriages are null from the moment when consent is exchanged. … There is no justification for saying that a certain percentage of marriages are null,” Burke said. “That would open the door to a mentality favoring divorce, which would dissolve some valid marriages because no one investigates whether there are grounds for the request for a declaration of nullity.” Poor catechesis and ‘unrecognizable’ liturgy have contributed to Church’s crisis
Throughout Hope for the World, Burke spoke warmly of the love for the Catholic faith that his parents instilled in him as a child.
He lamented the “invasive secularization of the culture” which he found had also “entered into the life of the Church” as the biggest obstacle to his ministry as a bishop.
Bad catechesis and changes to the liturgy falsely believed to have been sanctioned by the Second Vatican Council or the “spirit” of it have contributed to this crisis, Burke said.
“I remember that in the years after 1968, I attended liturgical celebrations that had retained almost nothing of what could be a Mass,” the cardinal recalled. “I had gone to the Netherlands, at that time, and witnessed a Mass in which the priest arrived in civilian clothing. The whole celebration was totally unrecognizable as a Holy Mass.”
“More and more man became his own idol, making his subjective impressions the judge of good and evil,” he said. “Very often he has forgotten or denied the sense of mystery, and therefore he has no longer been able to marvel at it. Along with mystery, the sense of the faith and of the sacred has gradually faded. At the same time, people have suffered cruelly from a lack of formation and, at best, have kept up a rootless formalism, whether in their human relations or in their liturgical practice.”
“Worship centered on man is a self-contradiction, and this is what led many people to stop attending Sunday Mass and other sacramental celebrations,” the cardinal noted.
Burke said he has noticed the younger generation craves more traditional forms of worship and are “thirsting to hear the truths of the faith.” Growing up in a secularized culture, rather than the Christian one in which the prelate was raised, has stifled and in many cases wounded young people. The divorce of parents, pornography, and “‘liberation’ from morality” contribute to these wounds, but many are still “looking for true love” and God nonetheless.
“I observe also that many of these young people, who live in this world from which God is excluded, feel a great attraction to a beautiful, holy liturgy that is celebrated with the dignity that befits the Holy Sacrifice, whether in the Extraordinary Form or in the Ordinary Form of the Roman Rite, provided that there is great devotion and the sense of transcendence that indicates that we are turned toward the Lord and that the sacrifice on Calvary is being renewed,” Burke said.
He also echoed the sentiment of Cardinal Robert Sarah, the Prefect for the Congregation for Divine Worship, that receiving Holy Communion kneeling and on the tongue fosters respect for the Eucharist, which the Catholic Church teaches is the literal body, blood, soul and divinity of Jesus Christ.
Post-abortive women ‘told me that at night they would hear the cries of their unborn child’
In addition to the restoration of the liturgy, Burke said people must reject “narcissistic individualism,” rediscover the meaning of family life, and promote virtue in order to fix the deep crises the modern world faces.
“Lack of moral life” is more grave than material poverty, Burke said, and he noted the “emotional frailty” that many young people experience after having multiple sexual partners.
“Emotional instability is a terrible form of poverty,” he said.
Burke encouraged Catholics to never cease defending life and family, and to look to the examples of soon-to-be-canonized Blessed Mother Teresa of Calcutta, Professor Jérôme Lejeune, and people like Bishop Austin Vaughan, an Auxiliary Bishop of New York, “who went to prison for their commitment to the service of life.”
“Calm and strong” pro-life witness “bears fruit,” Burke said, and pro-life activists would do well to look to converts to the pro-life cause like former abortionist Bernard Nathanson and Roe v. Wade plaintiff-turned pro-life activist Norma McCorvey.
And pro-life advocates can never forget to show compassion and mercy toward those who have participated in abortion, he said.
Burke said that throughout his priesthood he has encountered many people suffering from abortion and several post-abortive women “told me that at night they would hear the cries of their unborn child.”
“We must understand and listen to the great suffering of women who have experienced an abortion and stand beside them as witnesses of divine mercy, of the unfathomable love of Jesus, who opens the riches of His Heart to those who, despite their sin, dare to turn to Him with trust,” he said.
Burke also revealed in Hope for the World that a doctor pressured his mother to abort him after she became seriously ill while pregnant, but his parents believed that “Christ would give them the necessary help” and he was born in good health.
It was at a medical conference in Orlando, Florida, some years back when I decided I must write a book about, and for, women who have been victimized by the health care system. As a family physician practicing for more than twenty-five years, I’ve had countless women come through my doors with a myriad of gynecologic concerns. At this particular conference, I asked the lecturer—a prominent women’s health physician—to explain why he did not mention the connection between cervical cancer and the use of oral contraceptives in his talk on cervical cancer. He replied (before three hundred other physicians), “Let’s keep that to ourselves.”
Let’s keep that to ourselves? Keep information from patients?
The status quo, it seemed, was this: Let’s keep women in the dark about the risks associated with using the Pill. Women today are prescribed the Pill from a range of doctors—general practitioners, dermatologists, psychiatrists, OB-GYNs, and others. There is an overriding concern in the medical community across all disciplines of preventing unplanned pregnancy. I came to find this thinking problematic because in effect it presumes that women are incapable of making choices about their reproductive health care.
For a physician to think a woman must take a contraceptive pill to avoid pregnancy, especially when she isn’t seeing the doctor for that expressed concern, is for a physician to place his or her agenda ahead of the patient’s best interests. It makes sense for doctors to have an “agenda,” if by that we mean a predisposition to helping patients avoid diseases and inform them of it. But when it comes to the Pill, we’re talking about suppressing not an illness but healthy fertility. It may seem worthwhile in the name of preventing a woman from having an unexpected pregnancy, but it’s up to the woman to make the choice of whether that benefit is worth the risks of the medication.
Still, this “let’s keep information of the risks to ourselves” thinking isn’t isolated to one physician on a panel. Physicians in training during the past thirty years or so have been taught to find any reason to put women on some form of contraception—without mentioning any possible risk associated with these methods. Physicians in the United States may agree on the facts concerning the physical and physiologic side effects of hormonal contraception, yet the vast majority of them still prescribe any and all manners of artificial contraception with little visible hesitation.
So, you may ask, why doesn’t my family doctor, my OB-GYN, my dermatologist, my psychiatrist, and so on—why doesn’t anyone mention the risks? I’ll tell you why—because I used to be a physician who didn’t.
The reason for this peculiar contradiction is that while depression, cancer, stroke, heart disease, and increased risk of blood clots are most certainly problematic, most doctors are trained to see them less of a problem (for women as well as the rest of us) than the overarching “problem” of pregnancy.
For many in the medical community, pregnancy, especially in young women, is considered to be a disease. There’s somewhat of an indoctrination that all physicians receive as we go through seemingly endless years of medical training. I experienced it myself going through school. I was taught, as in intern in family medicine, that one of the first questions I needed to ask every woman within the first twenty-four hours of delivering her baby was, “What are you planning to use to prevent another pregnancy?” (Talk about timing—most women will accept any form of birth control after going through a difficult vaginal delivery.) I was instructed that women who have had two or more children should be strongly encouraged to consider permanent sterilization. And teenagers seen for pretty much any concern are to be encouraged to get started on long-acting forms of contraception—regardless of their level of or interest in sexual activity. If pregnancy was a disease, preemptive contraception was the vaccine.
Not only is medical school and residency highly structured and resistant to change, medical students and residents in training are in no position to question the views of their instructors, often for the real fear of losing all they have striven to achieve in a career in medicine.
As a trusting medical student, and then a faculty member who taught other doctors, it took me years to come to the realization that during those years I was blinded by a combination of stubbornness and ignorance.
This discussion surrounding female fertility and family planning is controversial, to say the least. There are many differing opinions, but my own experience has led me to a conclusion that, thirty years ago, I never would have believed.
All physicians have sacrificed a great deal to get to the point in time where they can actually provide healthcare to patients. During the majority of my near three decades in practice, if I was approached by someone trying to tell me that what I was taught to do by my preceptors was “bad medicine” or “harmful” to women, I would reject their criticism outright. I would figure they were just some overly zealous, ill-informed doctor who, though they meant well, was clueless as to how best to treat women. That was my attitude; no amount of factual data on the harms of the Pill, the shot, the implant, the ring, the patch, the IUD, or sterilization could change my mind about how to care for my female patients.
As is often the case in life, it wasn’t until it affected me personally that I changed my perspective.
Close to Home
After welcoming three beautiful daughters in the first five years of marriage, my wife and I had to make a decision to limit our family size using some form of birth control. That’s when the truth about female fertility really hit home for me. Since my wife’s mother had died at the age of 52 from a cerebral aneurysm, we knew that exposing my wife to artificial hormones would place her at increased risk of stroke. We were convinced for other reasons that permanent sterilization was not an option for us either.
Only in later years did I discover that one-third of women who chose Bilateral Tubal Ligation regretted this decision. Further research has also correlated other serious health issues with Bilateral Tubal Ligations, such as an increased occurrence of dysfunctional uterine bleeding.
At that time we were able to find other couples who were learning, and then teaching, natural methods of family planning. Kathleen and I learned of the Fertility Awareness Method (FAM) and ultimately chose to use the Billings Ovulation Method for the rest of our marriage.
The Billings Method allows couples to either avoid or pursue pregnancy by determining the body’s natural fertile and infertile periods, based on observing and charting vulva sensations and the discharge of cervical mucus. Couples using the Billings Method to avoid pregnancy then avoid sexual intercourse during the fertile days of the cycle. When we starting using the Billings Method in our marriage, it put the challenge on me as a husband to communicate about and cooperate with my wife’s fertility, rather than ending or altering her fertility with chemicals.
This allowed us to refrain from having kids for a number of years, and then when we returned to seeking pregnancy we had two more children—all while preserving my wife’s health. Because had we gone the route of the Pill, it’s exactly that—her overall health—that could have been compromised.
The fact is that the normal human estrogens, progesterone, and testosterone produced by the ovaries do far more than simply help a woman to achieve a normal reproductive cycle and pregnancy. The natural ovarian hormones act on practically every organ system in the woman’s body to ensure optimal functioning. Examples include improved mood (especially during elevated estrogen phases), reduced risk of heart disease and stroke (as compared to men), cleansing of the breast tissue with each normal reproductive cycle to reduce the woman’s risk of breast cancer, and improvements in bone mass to prevent osteoporosis and premature fractures. Not to mention improved libido and overall energy level.
Conversely, women using these artificial hormonal methods may be at increased risk of cardiovascular disease (largely due to the chemicals causing deficiencies of essential vitamins and minerals folic acid, magnesium, and B12). Depression is a common side effect, due to the folic acid deficiency as well as the relative lack of estrogen (a “feel good” hormone). Loss of libido, weight gain, and premature bone loss also frequently occur. One study found that breast cancer rates in women who have used the Pill for more than five years prior to first pregnancy are two to three times higher than in women who have never used the Pill. And women who have been on oral contraceptives for any length of time will find they are at an increased risk of miscarriage within several months of stopping the Pill.
Needless to say, what I experienced in choosing a method to protect my own family forever changed the way I saw my patients. It may sound obvious, but the notion became much more solidified in me: every patient’s life and health should be treated of equal value to my wife’s. But when I returned to my practice to start incorporating FAM and other fertility awareness methods in my work, I faced a well-established rhetoric that proved difficult to overcome.
The Pill That Rules Them All
The Pill was a game-changing technology when it was invented a half-century ago. During these past fifty-plus years since the discovery of the pill and its widespread embrace in the 1960s, many women have believed that artificial birth control made them more powerful than ever before. The ability to remove the possibility of pregnancy from the sexual act was seen as liberating event.
But the Pill didn’t just provide advancements in what medicine could do; it has also been treated differently than any other medication prescribed by physicians to patients. Unlike other medicines which are usually only prescribed when medically necessary, the Pill is prescribed routinely and by default.
Further, unlike other medications that are prescribed along with a warning of possible risk, the Pill is often prescribed without any sense of hesitation from the prescribing physician—stating risks is viewed as less important than encouraging the woman to take it.
One example of how common this thinking is in the medical world took place at a conference on migraine headaches that I attended. Upon being asked to discuss the increased risk of stroke among women who suffer from migraine headache and use oral contraceptives, the physician speaker answered, to a room of over a couple hundred physicians that it would seem impractical to ask women to discontinue the use of oral contraceptives so as to prevent stroke, for fear of pregnancy. While the facts are what they are, the primary goal of avoiding pregnancy takes precedence.
This thinking, that pregnancy reduction is more important than informing women of the risks of the Pill or other contraceptive medication, is pervasive in my field.
FAM, on the other hand, has been distorted in the medical textbooks, and most physicians still refer to it as the “rhythm method” of ages past. In fact, when taught and used correctly, modern methods of FAM have an effectiveness rate of 99 percent, which is as effective as the Pill for avoiding pregnancy.
Nonetheless, instead of pursuing the natural methods to avoid pregnancy, today’s medical community prefers to encourage prescribing stronger hormones and devices, even if it means lessening a patient’s agency over her fertility cycle. In recent years, ACOG (American Congress of Obstetricians and Gynecologists), the professional organization representing most of America’s OB-GYN docs, has encouraged women’s health providers to recommend to teenage girls in particular to utilize LARCs (long acting reversible contraceptives), which do a more effective job of preventing pregnancy—though at increased risk to her health. IUDs going by the pharmaceutical names of Mirena and Skyla have highly touted effectiveness, with less than 1 percent pregnancy rate per year of typical use; that high prevention rate, also seen in such implants as Nexplanon and Implanon, and the long acting injection, Depo-Provera, is what makes them so popular today.
The use of these long-acting methods of contraception for young women came to my attention in 1995 when my wife was working toward her master’s degree in maternal and child nursing. Kathleen came home one day from a rotation at a county health department in rural Georgia, where she saw many teenage black girls who were lining up by the dozens to receive their quarterly injection of Depo-Provera, which, while preventing ovulation also dramatically reduces estrogen levels to that of a postmenopausal woman and so creates a host of adverse effects in its users. In speaking with several girls, she found that many had not even experienced their first menstrual cycle, and the majority had never been sexually active—they were simply told by their parents, grandparents, teachers, or government agencies that they need these quarterly shots for their own good.
What the general public doesn’t know, and what I detailed in my recent book, The Hidden Truth: Deception in Women’s Health Care: A Physician’s Advice to Women and All Who Care for Them, is this: Each of these LARC methods dramatically alters the woman’s normal hormonal makeup and replaces it with a host of artificial/synthetic female hormones that, in turn, suppress the healthy function of the woman’s ovaries. Not only do LARCs produce many of the risks as the artificial hormone methods mentioned above, the LARC Depo-Provera for instance makes estrogen levels fall so low that calcium is no longer taken into the bones, creating decreased bone mineral density in many users, not to mention significant weight gain. IUDs, which are abortifacient in that they interfere with formed embryos from implanting to uterus lining, are associated with heavier, more painful menstruation in many women. And while the ACOG stresses that contraceptive implants and IUDs are removable, many young women tell me they are having a tough time convincing their doctors who put them in to take them out. Further, while it is quite an easy procedure, it is often billed very highly. These highly billed patient costs no doubt influence women’s decisions.
Changes Unforeseen
Today, I have listened to and served female patients as a physician for almost thirty years, providing prenatal and obstetric care, caring for their gynecologic needs, and caring for their families—their husbands, their children, their parents. This has been my privilege as their family physician. And today, more than ever, I listen to women as they tell me the many ways in which they are suffering—truly suffering—as a result of choices made not only by themselves, but by their parents, their husbands, and their physicians. I too used to be that physician.
But now, it saddens me to see the effects of the Pill at play in unsuspecting lives. How often have I seen one patient after another frustrated by what has come to be viewed as a “necessary evil” for all women, if they ever hope to be a good wife, a good girlfriend, a good sexual partner. What is so “liberating” or “empowering” about feeling miserable, depressed, increasing one’s risk of breast cancer, cervical cancer, blood clots, strokes, and heart disease, while the male partner has not a worry in the world?
Take for instance the young women on the Pill for acne who is struggling with depression, taking antidepressants at the same time, having never been told that the Pill is linked to depression.
Or the patient who came in my office who decided the side effects of depression and weight gain she had experienced after receiving Depo-Provera injections wasn’t worth the pregnancy-avoiding effects, and signed up to learn more about how to track her fertility naturally.
Or another who I met in the ER who suffered a blood clot in her lungs after being prescribed oral contraceptives. While the Pill carries increased risk of blood clots in all users, it was particularly dangerous for this young woman who, unbeknownst to her, had a condition known as thrombophilia. After treatment with blood thinners for several months and stopping the Pill, she became anxious to learn about natural ways to avoid pregnancy without putting her life at risk.
I’ve also heard from women struggling in their marriages, after the birth of their first child, wondering why after going on the Pill, they have lost energy and libido. Often their husbands do not recognize them as the same women they married. Indeed, the relative absence of normal levels of female hormones can change the woman’s moods and emotions greatly. Simply take a moment to review recent studies on the changes in the limbic system of the brain (the emotional center) in women on the Pill after only three months.
It’s fascinating stuff—yet sobering.
All this explains why, in the middle of a crazily busy family practice, not to mention family life, I chose to write a book about, and for, women. I have seen women, day in and day out, who have made enough sacrifices in life already. Asking these women to make healthcare choices that further compromise their overall well-being is bad health care.
I believe in serving the reproductive health care needs of all women, we should consider more natural alternatives that do not put women at an increased risk of disease and at the same time encourage their male partners to demonstrate equal level of responsibility with regard to the prevention of unwanted pregnancy. As I see it, true equality of the sexes in matters of family planning would not require women to bear the brunt of risks, but one that requires men demonstrate some level of sacrifice as well.
Many couples I meet, once they hear all the information about FAM, prefer to refrain from sexual activity for the seven days or so that the woman is fertile, rather than put the woman at risk with artificial hormones. Couples using natural methods of family planning find that the need to communicate more often about the changes in the woman’s body leads to an increased respect for the woman and increased self-control and maturity in the husband.
Which is why I ask all women—and the men in their lives—to come to a better understanding of who they are, in their natural state, with normally cycling female hormones and to learn natural ways to deal with issues such as family planning and other gynecologic concerns. Female empowerment comes from knowing all the options. When a woman has agency over her health decisions and feels comfortable discussing them with her doctor and her partner, that’s when we’re all better off. Turning blindly to the Pill is not a fix-all; in fact, it’s quite the opposite.
(NaturalNews) It has been on the U.S. drug market since the early 1990s, and population control organizations like Planned Parenthood continue to push it heavily on black women and other ethnic minorities as a form of contraception. But the injectable contraceptive drug Depo-Provera, manufactured by Pfizer, has an extensive track record of causing serious harm to women, including its tendency to trigger the development of cancer.
Most people are unaware of this and many of the other long-term side effects of Depo-Provera, because eugenics groups like Planned Parenthood erroneously claim the drug is “safe, effective and convenient.” But the non-profit Rebecca Project for Human Rights (RPHR) recently issued a groundbreaking report outlining the adverse effects of this insidious birth control shot, which currently bears a “black box warning” issued by the U.S. Food and Drug Administration (FDA) back in 2004.
This warning clearly states that women who receive Depo-Provera could develop significant and irreversible bone mineral density loss, for instance. The drug can also lead to blood clots in arms, legs, lungs and eyes and may also cause stroke, bleeding irregularities, weight gain, ectopic pregnancy and delayed return to fertility. In some cases, women who get jabbed with Depo-Provera become permanently sterile.
https://youtu.be/nk1f95sDna0
Perhaps most concerning is the fact that Depo-Provera has been shown to more than double a woman’s risk of developing breast cancer. A 2012 study out of the Fred Hutchinson Cancer Research Center in Seattle found that, compared to women who had never received a Depo-Provera shot, jabbed women were about 220 percent more likely to develop the disease, regardless of their family and medical histories.
But according to RPHR, none of these catastrophic risk factors has deterred groups like the Bill & Melinda Gates Foundation, the United States Agency for International Development (USAID), Columbia University and others from aggressively pushing this horrific jab on unsuspecting women both domestically and abroad. The group’s report draws attention to the fact that these organizations have committed medical violence against women, particularly in third-world countries, by administering the shot time and time again without informed consent.
“The story of Rebecca Project for Human Right’s struggle to unmask Depo Provera as a deadly contraceptive for women is important, because it demonstrates the deeply rooted cultural hegemony of population control and corporate profits put before humanity at any cost,” explains the report, entitled Depo-Provera: Deadly Reproductive Violence Against Women. It goes on to highlight numerous Depo-Provera experiments that have taken place against women in the U.S., Ghana and elsewhere.
Federal government continues to endorse Depo-Provera, despite deadly adverse effects
Though many foreign governments have since outlawed medical experimentation on women with Depo-Provera, the U.S. continues to embrace the drug, as well as distribute it to overseas health contractors, according to Turtle Bay and Beyond. And the Gates Foundation and others continue to invest hundreds of millions of dollars into the distribution of Depo-Provera across the globe.
“The Rebecca Project for Human Rights urges the U.S. government to enforce mandatory FDA Black Box patient counseling requirements, and for health providers to obtain valid informed consent before Depo-Provera is administered in the United States, Africa, the Caribbean, Latin America, Southern Asia and the rest of USAID’s program areas,” concludes RPHR.
For a full breakdown of the fraud and corruption behind Depo-Provera, and a detailed analysis of the many groups involved in perpetrating this cancer-causing contraceptive drug to unsuspecting women, be sure to read the full RPHR report: http://www.rebeccaproject.org.
July 21, 2016 (BreakPoint) — Those who’ve pushed condoms like candy in public schools have given us any number of rationales. They told us that young people “are going to do it anyway,” so more condoms would equal fewer pregnancies. They also said that more condoms would lead to fewer STDs, or sexually transmitted diseases. And as they proceeded to pass out condoms by the handful to our school-age children, they told us that religion and morality should be left out of it, in the name of public health and, of course, science.
New research, however, suggests these prophets of prophylactics were wrong—desperately wrong—and that it’s time for a fresh look at the issue.
A recently released study by University of Notre Dame researchers Kasey S. Buckles and Daniel M. Hungerman has found that access to condoms in schools actually increases teen pregnancies by about 10 percent—that’s right, increases it! Buckles and Hungerman selected 22 school districts in 12 states that started such programs back in the 1990s, including New York City, Los Angeles, and San Francisco. The study analyzed teen-fertility data from nearly 400 high-population counties over a span of 19 years.
Among the contributing factors Buckles and Hungerman cite is the possibility that condom-distribution programs can crowd out efforts to encourage young people to delay sexual activity. Condom-distribution programs may actually encourage more teenagers to have sex.
Is this really that surprising? If adults tell teens that the decision to engage in sex is theirs and give them condoms, what message do they receive?
It makes sense, especially given another finding of the study. Buckles and Hungerman found that sexual activity, along with STDs, increased in counties with condom-distribution programs. This puts a lie to all those lofty assurances from the Sexual Left that condoms would prevent all that. No, more likely, they encouraged it!
Michael J. New, an assistant professor of political science at the University of Michigan at Dearborn, notes that this ugly outcome likely is a result of increased sexual risk-taking as a result of condoms in the schools. All at taxpayers’ expense.
Now Buckles and Hungerman are quick to point out that they believe the effects of teen fertility would be less alarming if the condom-distribution programs were also accompanied by mandatory sex-ed counseling. But New says such education efforts would not totally offset the jump in teen fertility caused by condom distribution. There would still be more births to teenaged mothers, and presumably more teen STDs, than if there were no condoms in the schools in the first place.
“Overall,” says New, “the study adds to an impressive body of research which shows that efforts to encourage contraceptive use either through mandates, subsidies, or distribution are ineffective at best or counterproductive at worst. In many countries, increases in contraception use are correlated with increase in the abortion rate.”
Now it would be optimistic at best to assume that the folks who brought these condom-distribution programs to us, and their cheerleaders in the media, would own up to the conundrum they have created and work to make things right. But no, we’ll have to do that ourselves.
So the first step to changing what our schools do is to read the study and make sure that members of your local school boards have a copy. Just come to BreakPoint.org and click on this commentary for a link to it, along with more information to get you up to speed.
And second, we shouldn’t be surprised that non-Christians teach our sons and daughters a non-Christian worldview concerning the human body, the unitive act, or marriage. Teaching our own kids about sex and design and relationships and marriage, while pointing out and countering the lies about sex proclaimed in the culture, is first and foremost our job as parents and as Christian communities.
While I had a mostly positive attitude toward NFP from the beginning of my marriage, in hindsight I still thought of it as “Catholic Birth Control.” In other words, my husband and I would use it until we wanted to have a baby (which was very soon), and then we would stop, and boom, I would get pregnant.
So we stopped. But no “boom.” No baby. Month after month, year after year.
All the “birth control” in the world won’t give you an ounce of control when you want to have a baby, and you can’t. It was when I wanted to get pregnant and couldn’t that I experienced how very different Natural Family Planning is from artificial contraception.
NFP isn’t a blunt instrument for manipulating the reproductive system; it is rather a means of obtaining information about one’s own body, information which can serve a woman’s health in a variety of ways.
When I was diagnosed with infertility, the very same methods that we thought we were using to delay pregnancy were immediately turned toward the goal of conceiving a child. All the records that we had kept and all the knowledge that we had gained about our mutual reproductive system were put to the service of healing that system so that it could do what it was supposed to do: create new life.
And that is just one way that NFP is much bigger, and much better, than mere “birth control.” Natural Family Planning respects the whole reality of women’s bodies, including the goodness of healthy human reproduction. Natural Family Planning respects science, and uses the methods of medical science to understand more about how women’s bodies work and how to heal them when they don’t. And Natural Family Planning respects women (and men), by empowering us with the knowledge that we need, both for prudence in family planning and awareness of our own reproductive health.
Thanks to the knowledge we gained from Natural Family Planning, and the skilled assistance of medical professionals trained in NFP, we are now the parents of two beautiful daughters. Through NFP, we found real help, true healing and new life.
Kristen Grant is a wife, mother, graduate student, and an alumna of WSFT Media Training. She and her family live in St. Paul, Minnesota.
According to a 2016 study, the hormones released by oral contraceptives may influence women’s ability to process emotional situations—especially during their “pill-free” days.
The study, published in the European Neuropsychopharmacology, tested 73 women: 18 who do not take oral contraceptives (OC), 30 who were currently taking OC, and 25 who take OC but were on their pill-free week.
Scientists were interested in the three components of empathy—emotion recognition, perspective-taking, and affective (emotional) responsiveness—and whether OC influence women’s ability to empathize for better or worse. The research has significant implications for adult women.
“If OC use is linked to a reduced ability to recognize emotions, this might ultimately have negative consequences for relationship quality…by leading to more conflict,” said Sina Radke, corresponding author.
“In light of…the widespread use of OC across the globe, effects of OC are of interest to millions of users, their partners and society,” Radke continued.
Measuring Emotion Recognition
To measure emotion recognition, participants looked at images of faces (one at a time) on one side of a computer screen. On the other side was a list of several terms describing emotions. Participants were asked to choose which word corresponded with the given image.
Scientists found no significant differences between the three groups regarding emotion recognition. Though the women who do not take OC (no pill group) scored the highest in this area, the differences were slight.
Measuring Perspective-Taking
In this exercise, participants watched a simulated interaction between two people that displayed a basic emotion. One of the simulated faces was masked. Participants were then asked to choose which facial expression (corresponding to an emotion) would describe the masked face in the scene.
Again, the differences between the three groups were negligible and indicated that OC use or pill phase did not have an influence on perspective-taking.
Measuring Affective Responsiveness
To measure affective responsiveness, participants read one-sentence hypothetical scenarios designed to evoke a specific emotion. They then chose which emotion they would feel if they were in the situation in real life.
Data showed that women currently taking OC (“on pill” group) scored significantly higher than those on their pill free week (“off pill” group). They also scored higher than the “no pill” group, indicating that OC influenced participants’ ability to respond emotionally. Scientists attribute this difference to the increased levels of exogenous estrogen and progesterone in OC users.
The results point to a need for further research and more data to explain these effects.
“With regard to the prevalence of hormonal contraception across the world, determining its psychological and behavioral effects more thoroughly will not only improve our understanding of the non-contraceptive impact of OC use, but also allow women and clinicians to make more informed contraceptive decisions,” said Radke.
Miriam Harding Jul 20, 2016 | 2:51PM Washington, DC
A few weeks ago, I had an unshakable urge to reach out to a former classmate of mine from high school: Sarah. We had never been good friends, but I had recently noticed a Facebook post that Sarah gave birth to a son. I sent Sarah a short message, asking her if she’d like a meal and diapers. I received an emphatic “Yes!” and we agreed to meet.
When I visited Sarah, I was not aware of how God worked in her life over the previous months.
Surprisingly, in the middle of our conversation, Sarah said that she “could not believe she had ever considered other options.” When I inquired about what she meant, I found out Sarah was engaged to a man for several months, and just weeks after breaking off the engagement, she learned she was pregnant. Sarah was devastated, and what’s worse, her ex-fiancé told her he wanted nothing to do with Sarah and nothing to do with the baby. Her experience followed the cliché perfectly – he told her to “get rid of it.”
Sarah began considering when she should schedule her abortion. Then, she saw my posts on Facebook: the Planned Parenthood videos, ADF blogs and articles, and pictures from the Planned Parenthood protests. Each time Sarah was considering abortion, one of my posts came back to mind–a photo of me at a Planned Parenthood protest, holding a homemade poster of my son’s ultrasound next to a current photo of my son.
Sarah immediately pulled out her ultrasound, obtained just days earlier from a local pregnancy center. She stared at the tiny human in black and white and wondered what her child would look like in just a few short months. Did it really already have fingernails, like Juno said?
After 4 days of looking at the ultrasound, it was too much. Abortion-minded Sarah decided abortion was no longer an option. She chose to carry her baby to full term.
As her story concluded and I held the newborn in my arms, I gave thanks to God for this baby’s life. In a way, I felt like somehow I was partly responsible to take care of him for the rest of my life.
Sarah had never intended to reach out about her experience, and she certainly never expected me to reach out to her. But as Sarah was sitting in the hospital after delivering her baby, she received the message from me, the girl from high school whose posts help change her mind about abortion … someone she barely knew…. reaching out to her with an offer of dinner and diapers the day after her child was born.
Only our Heavenly Father could have orchestrated these events, and I’m so overwhelmed by the way God chooses to reveal His work through us. What an amazing reminder that we never know the impact our lives may be having on those around us.
I hope you will celebrate with me in this victory of life – a victory accomplished only by God’s grace.
It is quite remarkable to be living at a time when a Cardinal of the Roman Church and the Prefect of the Congregation for Divine Worship is publicly contradicted and humiliated. I do not know Cardinal Sarah personally, but from his writings, I suspect that he is using his humiliation in a spiritually profitable way. But one has to wonder at the absence of any sense of fatherly concern and mercy in the Year of Mercy.
It seems that there is no limit to the nonsense that Father Lombardi allows himself to spew forth in defense of the indefensible. We hope that once he lays aside this burden, as he will very soon, he can return to more spiritually profitable endeavors. The ideology that lies behind that repudiation of Cardinal Sarah’s exhortation to return to the Traditional posture of the priest at Mass rang out quite clearly in the Clarification. It is an ideology that has for so many years prevented the Church from restoring the liturgical life of the Church that is necessary for the mission of the Church to the world. It is an ideology that has no basis in Tradition and in fact is a break with Tradition. Anyone who still believes that the Mass of Paul VI is continuous with the Roman Rite of Catholic Tradition needs to get out into the fresh air more.
The heart of the ideology driving the post-Conciliar reform of the liturgical books is the destruction of the Traditional understanding of the Mass as a sacrifice, namely, the re-presentation of the Sacrifice of Calvary, the offering of the Son to the Father. Without the Roman Canon, which the reformers tried to get rid of entirely, that the Mass is a sacrifice is not evident in the three new Eucharistic prayers. What is at stake in the insistence on versus populum is the very nature of the Mass. What most Catholics believe today is that the Mass is a community meal and the priest’s job is to say the words that change the bread and wine to the Body and Blood of Christ for the purpose of Holy Communion. The Mass is for them. The priest facing the people engenders this understanding quite readily and enforces a heavily horizontal experience of the Mass. The almost universal practice of Communion in the hand standing in a line as if waiting for ham in a deli is the result of a deliberate repression of Communion on the tongue kneeling and telling the people that standing in the hand is the only way to receive Holy Communion after Vatican II. All nonsense. All ideology.
Fr. Lombardi’s defense of the celebration versus populum had no substance except for ideology. For him to use the General Instruction of the Roman Missal 299 as a basis for versus populum as the necessary norm is shameless. Much has been written on the meaning of the Latin in this section of the GIRM, quite apart from the translation into English. I speak as a Latin teacher of many years, and I would insist that there is no way to conclude from 299 that all celebrations of Mass must befacing the people. That famous “quod” that introduces the relative clause cannot possibly refer to the celebration of Mass versus populum.The English translation has been faulty from the beginning, or rather, from when that clause was added. In addition the Congregation for Divine Worship in September 2000 rejected the interpretation that 299 made a free -standing altar obligatory and therefore versum populum obligatory.
Furthermore, the very rubrics of the Paul VI missal assume that the priest is celebrating ad orientem. It is distressing to have to repeat all of this at this time, but the fact is that most of our bishops may have never read the rubrics in English let alone Latin. At the “Orate fratres”, the rubric reads: Stans postea in medio altaris,versus ad populum….The obvious and easy English translation is: Then, standing in the middle of the altar, turning to the people….Why should he turn to the people if he is already facing them? There are other examples where the rubric calls for the priest to turn to the people. And again, it is tiresome to have to go through these explanations once again. But after what happened in the slap down of Cardinal Sarah by the powers that still be, one has to rehearse certain facts and show how it is sheer ideology that has driven and continues to drive the intense hostility to the Traditional understanding of the Mass as the Holy Sacrifice (despite pious talk about the Holy Sacrifice).
So much of what is happening and why it is allowed to happen has to do with a papalatry gone wild. The irony is that the Second Vatican Council introduced and spoke so glowingly of collegiality vis a vis the bishops and the Pope, but the reality after the Council is that of a highly centralized papacy whose power seems to have no bounds. There seems to be a never ending speculation about Benedict XVI’s resignation. Perhaps he figured out that the power of the papacy and the authority of the papacy are two different things entirely, and that it is entirely possible to renounce the power and keep the authority, because, as someone has said, power comes from the office, authority is earned. Stuff to ponder. But in this context, to claim, as Fr. Lombardi stated, that the Extraordinary Form must never or can never replace the Ordinary Form has no basis in Summorum Pontificum, nor in rational thinking, nor in any magisterial document.
What can be done about this shameful episode? Nothing much except prayer. Prayer, yes. And a lot of it. But as for me and my flock, we will go on worshiping God at the Holy Sacrifice of the Mass not facing each other over a table but rather together facing the Lord.
[emphasis added]
Father Richard Cipolla pastors St Mary Parish in Norwalk CT.
Pope Francis met Cardinal Sarah to indicate that no liturgical directives will begin in Advent, according to Vatican spokesman
Cardinal Robert Sarah, prefect of the Vatican’s Congregation for Divine Worship and the Sacraments, urged priests and bishops at the Sacra Liturgia conference in London on July 5 to start celebrating Masses ad orientem, or facing away from the congregation, beginning on the first Sunday of Advent this year.
However, Jesuit Father Federico Lombardi, Vatican spokesman, issued a statement on July 11 indicating the Pope Francis met with Cardinal Sarah on July 9 to indicate no liturgical directives will begin in Advent.
“Cardinal Sarah is always rightly concerned with the dignity of the celebration of Mass, that it might adequately express an attachment of respect and adoration for the eucharistic mystery,” Fr Lombardi’s statement said.
“Some of his phrasing has been badly interpreted, as if he had announced new, different indications from those now given in liturgical norms and the words of the popes on celebration toward the people and the ordinary rite of the Mass,” the spokesman added.
He recalled that the General Instruction of the Roman Missal, which “remains fully in force,” indicated that the altar should be built away from the wall so “that Mass can be celebrated at it facing the people, which is desirable wherever possible.”
The statement also reminded people that when Pope Francis visited the offices of the congregation for divine worship, “he expressly recalled that the ‘ordinary’ form of the celebration of Mass is that foreseen by the missal promulgated by Paul VI,” and that the extraordinary form permitted by Benedict XVI “should not take the place of that ‘ordinary’ form.”
Fr Lombardi also said it would be better “to avoid the use of the expression ‘reform of the reform,’ referring to the liturgy, given that it’s sometimes the sources of misunderstandings.”
At the conference in London, Cardinal Sarah had asked that “wherever possible, with prudence and with the necessary catechesis, certainly, but also with a pastor’s confidence that this is something good for the church,” priests face east when celebrating the Liturgy of the Eucharist.
Several liturgical experts said Cardinal Sarah does not have the authority to impose a change but is simply encouraging a practice that liturgical law already permits.
“I think he’s just encouraging as anyone can encourage, but because of his position, his encouragement carries more weight. He’s not changing the legislation at all; he’s just giving his opinion that he thinks this would help people to pray better,” Fr Andrew Menke, associate director of the US Conference of Catholic Bishops’ divine worship office, told Catholic News Service on July 6.
Fr Menke also said that as new editions of the Roman Missal are released, liturgical law is bound to shift, but he doubts anything would happen regarding the direction the priest faces, except perhaps more encouragement of “ad orientem” Masses in future missal editions.
Others agreed, saying neither bishops nor Cardinal Sarah have the right to force priests to celebrate Mass “facing East” until there is an official change to the missal, the official liturgical law.
Cardinal Robert Sarah, prefect of the Congregation for Divine Worship and the Discipline of the Sacraments, offered the opening speech at the 2016 Sacra Liturgia conference in London. Below is the complete English translation of his address.
In the first place I wish to express my thanks to His Eminence, Vincent Cardinal Nichols, for his welcome to the Archdiocese of Westminster and for his kind words of greeting. So too I wish to thank His Excellency, Bishop Dominique Rey, Bishop of Fréjus-Toulon, for his invitation to be present with you at this, the third international “Sacra Liturgia” conference, and to present the opening address this evening. Your Excellency, I congratulate you on this international initiative to promote the study of the importance of liturgical formation and celebration in the life and mission of the Church.
In this address I wish to place before you some considerations on how the Western Church might move towards a more faithful implementation of Sacrosanctum Concilium. In doing so I propose to ask, “What did the Fathers of the Second Vatican Council intend in the liturgical reform?” Then I would like to consider how their intentions were implemented following the Council. Finally, I would like to put before you some suggestions for the liturgical life of the Church today, so that our liturgical practice might more faithfully reflect the intentions of the Council Fathers.
It is very clear, I think, that the Church teaches that Catholic liturgy is the singularly privileged locus of Christ’s saving action in our world today, by means of real participation in which we receive His grace and strength which is so necessary for our perseverance and growth in the Christian life. It is the divinely instituted place where we come to fulfill our duty of offering sacrifice to God, of offering the One True Sacrifice. It is where we realize our profound need to worship Almighty God. Catholic liturgy is something sacred, something which is holy by its very nature. Catholic liturgy is no ordinary human gathering.
I wish to underline a very important fact here: God, not man is at the center of Catholic liturgy. We come to worship Him. The liturgy is not about you and me; it is not where we celebrate our own identity or achievements or exalt or promote our own culture and local religious customs. The liturgy is first and foremost about God and what He has done for us. In His Divine Providence Almighty God founded the Church and instituted the Sacred Liturgy by means of which we are able to offer Him true worship in accordance with the New Covenant established by Christ. In doing this, in entering into the demands of the sacred rites developed in the tradition of the Church, we are given our true identity and meaning as sons and daughters of the Father.
It is essential that we understand this specificity of Catholic worship, for in recent decades we have seen many liturgical celebrations where people, personalities and human achievements have been too prominent, almost to the exclusion of God. As Cardinal Ratzinger once wrote: “If the liturgy appears first of all as the workshop for our activity, then what is essential is being forgotten: God. For the liturgy is not about us, but about God. Forgetting about God is the most imminent danger of our age.” (Joseph Ratzinger, “Theology of the Liturgy,” Collected Works vol. 11, Ignatius Press, San Francisco 2014, p. 593)
We must be utterly clear about the nature of Catholic worship if we are to read the Second Vatican Council’s Constitution on the Sacred Liturgy correctly and if we are to implement it faithfully. For many years before the Council, in missionary countries and also in the more developed ones, there had been much discussion about the possibility of increasing the use of the vernacular languages in the liturgy, principally for the readings from Sacred Scripture, also for some of the other parts of the first part of the Mass (which we now call the “Liturgy of the Word”) and for liturgical singing. The Holy See had already given many permissions for the use of the vernacular in the administration of the sacraments. This is the context in which the Fathers of the Council spoke of the possible positive ecumenical or missionary effects of liturgical reform. It is true that the vernacular has a positive place in the liturgy. The Fathers were seeking this, not authorizing the protestantization of the Sacred Liturgy or agreeing to it being subjected to a false inculturation.
I am an African. Let me say clearly: the liturgy is not the place to promote my culture. Rather, it is the place where my culture is baptized, where my culture is taken up into the divine. Through the Church’s liturgy (which missionaries have carried throughout the world) God speaks to us, He changes us and enables us to partake in His divine life. When someone becomes a Christian, when someone enters into full communion with the Catholic Church, they receive something more, something which changes them. Certainly, cultures and other Christians bring gifts with them into the Church—the liturgy of the Ordinariates of Anglicans now in full communion with the Church is a beautiful example of this. But they bring these gifts with humility, and the Church in her maternal wisdom makes use of them as she judges appropriate.
One of the clearest and most beautiful expressions of the intentions of the Council Fathers is found at the beginning of the second chapter of the Constitution, which considers the mystery of the Most Holy Eucharist. In article 48 we read:
The Church … earnestly desires that Christ’s faithful, when present at this mystery of faith, should not be there as strangers or silent spectators; on the contrary, through a good understanding of the rites and prayers they should take part in the sacred action conscious of what they are doing, with devotion and full collaboration. They should be instructed by God’s word and be nourished at the table of the Lord’s body; they should give thanks to God; by offering the Immaculate Victim, not only through the hands of the priest, but also with him, they should learn also to offer themselves; through Christ the Mediator they should be drawn day by day into ever more perfect union with God and with each other, so that finally God may be all in all.
My brothers and sisters, this is what the Council Fathers intended. Yes, certainly, they discussed and voted on specific ways of achieving their intentions. But let us be very clear: the ritual reforms proposed in the Constitution such as the restoration of the prayer of the faithful at Mass (n. 53), the extension of concelebration (n. 57) or some of its policies such as the simplification desired by articles 34 and 50, are all subordinate to the fundamental intentions of the Council Fathers I have just outlined. They are means to an end, and it is the end which we must achieve.
If we are to move towards a more authentic implementation of Sacrosanctum Concilium, it is these goals, these ends, which we must keep before us first and foremost. It may be that, if we study them with fresh eyes and with the benefit of the experience of the past five decades, we shall see some specific ritual reforms and certain liturgical policies in a different light. If, today, so as to “impart an ever increasing vigor to the Christian life of the faithful” and “help to call the whole of mankind into the household of the Church,” some of these need to be reconsidered, let us ask the Lord to give us the love and the humility and wisdom so to do.
I raise this possibility of looking again at the Constitution and at the reform which followed its promulgation because I do not think that we can honestly read even the first article of Sacrosanctum Concilium today and be content that we have achieved its aims. My brothers and sisters, where are the faithful of whom the Council Fathers spoke? Many of the faithful are now unfaithful: they do not come to the liturgy at all. To use the words of Pope Saint John Paul II: many Christians are living in a state of “silent apostasy;” they “live as if God does not exist” (Apostolic Exhortation “Ecclesia in Europa,” June 28, 2003, 9). Where is the unity the Council hoped to achieve? We have not yet reached it. Have we made real progress in calling the whole of mankind into the household of the Church? I do not think so. And yet we have done very much to the liturgy!
In my forty-seven years of life as a priest and after more than 36 years of episcopal ministry I can attest that many Catholic communities and individuals live and pray the liturgy as reformed following the Council with fervour and joy, deriving from it many, if not all, of the goods that the Council Fathers desired. This is a great fruit of the Council. But from my experience I also know — now also through my service as Prefect of the Congregation of the Congregation for Divine Worship and the Discipline of the Sacraments — that there are many distortions of the liturgy throughout the Church today, and there are many situations that could be improved so that the aims of the Council can be achieved. Before I reflect on some possible improvements, let us consider what happened following the promulgation of the Constitution on the Sacred Liturgy.
While the official work of reform was taking place some very serious misinterpretations of the liturgy emerged and took root in different places throughout the world. These abuses of the Sacred Liturgy grew up because of an erroneous understanding of the Council, resulting in liturgical celebrations that were subjective and which were more focused on the individual community’s desires than on the sacrificial worship of Almighty God. My predecessor as Prefect of the Congregation, Francis Cardinal Arinze, once called this sort of thing “the do-it-yourself Mass.”
The Magisterium’s commitment to proclaiming the Eucharistic mystery has been matched by interior growth within the Christian community. Certainly the liturgical reform inaugurated by the Council has greatly contributed to a more conscious, active and fruitful participation in the Holy Sacrifice of the Altar on the part of the faithful. In many places, adoration of the Blessed Sacrament is also an important daily practice and becomes an inexhaustible source of holiness. The devout participation of the faithful in the Eucharistic procession on the Solemnity of the Body and Blood of Christ is a grace from the Lord which yearly brings joy to those who take part in it. Other positive signs of Eucharistic faith and love might also be mentioned.
Unfortunately, alongside these lights, there are also shadows. In some places the practice of Eucharistic adoration has been almost completely abandoned. In various parts of the Church abuses have occurred, leading to confusion with regard to sound faith and Catholic doctrine concerning this wonderful sacrament. At times one encounters an extremely reductive understanding of the Eucharistic mystery. Stripped of its sacrificial meaning, it is celebrated as if it were simply a fraternal banquet. Furthermore, the necessity of the ministerial priesthood, grounded in apostolic succession, is at times obscured and the sacramental nature of the Eucharist is reduced to its mere effectiveness as a form of proclamation. This has led here and there to ecumenical initiatives which, albeit well-intentioned, indulge in Eucharistic practices contrary to the discipline by which the Church expresses her faith. How can we not express profound grief at all this? The Eucharist is too great a gift to tolerate ambiguity and depreciation. It is my hope that the present Encyclical Letter will effectively help to banish the dark clouds of unacceptable doctrine and practice, so that the Eucharist will continue to shine forth in all its radiant mystery (n. 10).
There was also a pastoral reality here: whether for good reasons or not, some people could or would not participate in the reformed rites. They stayed away, or only participated in the unreformed liturgy where they could find it, even when its celebration was not authorized. In this way the liturgy became an expression of divisions within the Church, rather than one of Catholic unity. The Council did not intend that the liturgy divide us one from another! St John Paul II worked to heal this division, aided by Cardinal Ratzinger who, as Pope Benedict XVI, sought to facilitate the necessary internal reconciliation in the Church by establishing in his Motu Proprio “Summorum Pontificum” (July 7, 2007) that the more ancient form of the Roman rite is to be available without restriction to those individuals and groups who wish to draw from its riches. In God’s Providence it is now possible to celebrate our Catholic unity whilst respecting, and even rejoicing in, a legitimate diversity of ritual practice.
We may have built a very new, modern liturgy in the vernacular, but if we have not laid the correct foundations — if our seminarians and clergy are not “thoroughly imbued with the spirit and power of the liturgy” as the Council required — then they themselves cannot form the people entrusted to their care. We need to take the words of the Council itself very seriously: it would be “futile” to hope for a liturgical renewal without a thorough liturgical formation. Without this essential formation clergy could even damage peoples’ faith in the Eucharistic mystery.
I do not wish to be thought of as being unduly pessimistic, and I say again: there are many, many faithful lay men and women, many clergy and religious for whom the liturgy as reformed after the Council is a source of much spiritual and apostolic fruit, and for that I thank Almighty God. But, even from my brief analysis just now, I think you will agree that we can do better so that the Sacred Liturgy truly becomes the source and summit of the life and mission of the Church now, at the beginning of the twenty-first century, as the Fathers of the Council so earnestly desired.
In the light of the fundamental desires of the Council Fathers and of the different situations that we have seen arise following the Council, I would like to present some practical considerations on how we can implement Sacrosanctum Concilium more faithfully today. Even though I serve as the Prefect of the Congregation for Divine Worship, I do so in all humility as a priest and a bishop in the hope that they will promote mature reflection and scholarship and good liturgical practice throughout the Church.
It will come as no surprise if I say that first of all we must examine the quality and depth of our liturgical formation, of how we imbue our clergy, religious and lay faithful with the spirit and power of the liturgy. Too often we assume that our candidates for ordination to the priesthood or the permanent diaconate “know” enough about the liturgy. But the Council was not insisting on knowledge here, though, of course, the Constitution stressed the importance of liturgical studies (see nn. 15–17). No, the liturgical formation that is primary and essential is more one of immersion in the liturgy, in the deep mystery of God our loving Father. It is a question of living the liturgy in all its richness, so that having drunk deeply from its fount we always have a thirst for its delights, its order and beauty, its silence and contemplation, its exaltation and adoration, its ability to connect us intimately with He who is at work in and through the Church’s sacred rites.
That is why those “in formation” for pastoral ministry should live the liturgy as fully as is possible in their seminaries or houses of formation. Candidates for the permanent diaconate should have an immersion in an intense liturgical life over a prolonged period also. And, I would add, that the full and rich celebration of the more ancient use of the Roman rite, the usus antiquior, should be an important part of liturgical formation for clergy, for how can we begin to comprehend or celebrate the reformed rites with a hermeneutic of continuity if we have never experienced the beauty of the liturgical tradition which the Fathers of the Council themselves knew?
If we attend to this, if our new priests and deacons truly thirst for the liturgy, they will themselves be able to form those entrusted to their care — even if the liturgical circumstances and possibilities of their ecclesial mission are more modest than those of the seminary or of a cathedral. I am aware of many priests in such circumstances who form their people in the spirit and power of the liturgy, and whose parishes are examples of great liturgical beauty. We should remember that dignified simplicity is not the same as reductive minimalism or a negligent and vulgar style. As our Holy Father, Pope Francis, teaches in his Apostolic Exhortation “Evangelii Gaudium“: “The Church evangelizes and is herself evangelized through the beauty of the liturgy, which is both a celebration of the task of evangelization and the source of her renewed self-giving” (n. 24).
Secondly, I think it is very important that we are clear about the nature of liturgical participation, of the participatio actuosa for which the Council called. There has been a lot of confusion here over recent decades. Article 48 of the Constitution states:
The Church … earnestly desires that Christ’s faithful, when present at this mystery of faith, should not be there as strangers or silent spectators; on the contrary, through a good understanding of the rites and prayers they should take part in the sacred action conscious of what they are doing, with devotion and full collaboration.
The Council sees participation as primarily internal, coming about “through a good understanding of the rites and prayers.” The Fathers called for the faithful to sing, to respond to the priest, to assume liturgical ministries that are rightfully theirs, certainly, but it insists that all should be “conscious of what they are doing, with devotion and full collaboration.”
If we understand the priority of internalizing our liturgical participation we will avoid the noisy and dangerous liturgical activism that has been too prominent in recent decades. We do not go to the liturgy so as to perform, to do things for others to see: we go to be connected with Christ’s action through an internalisation of the external liturgical rites, prayers, signs and symbols. It may be that we whose vocation is to minister liturgically need to remember this more than others! But we also need to form others, particularly our children and young people, in the true meaning of liturgical participation, in the true way to pray the liturgy.
Thirdly, I have spoken of the fact that some of the reforms introduced following the Council may have been put together according to the spirit of the times and that there has been an increasing amount of critical study by faithful sons and daughters of the Church asking whether what was in fact produced truly implemented the aims of the Constitution, or whether in reality they went beyond them. This discussion sometimes takes place under the title of a “reform of the reform,” and I am aware that Father Thomas Kocik presented a learned study on this question at the Sacra Liturgia conference in New York one year ago.
I do not think that we can dismiss the possibility or the desirability of an official reform of the liturgical reform, because its proponents make some important claims in their attempt to be faithful to the Council’s insistence in article 23 of the Constitution “that sound tradition … be retained, and yet the way remain open to legitimate progress” and that “there must be no innovations unless the good of the Church genuinely and certainly requires them; and care must be taken that any new forms adopted should in some way grow organically from forms already existing.”
Indeed, I can say that when I was received in audience by the Holy Father last April, Pope Francis asked me to study the question of a reform of a reform and of how to enrich the two forms of the Roman rite. This will be a delicate work and I ask for your patience and prayers. But if we are to implement Sacrosanctum Concilium more faithfully, if we are to achieve what the Council desired, this is a serious question which must be carefully studied and acted on with the necessary clarity and prudence.
We priests, we bishops bear a great responsibility. How our good example builds up good liturgical practice; how our carelessness or wrongdoing harms the Church and her Sacred Liturgy!
We priests must be worshippers first and foremost. Our people can see the difference between a priest who celebrates with faith and one who celebrates in a hurry, frequently looking at his watch, almost so as to say that he wants to get back to the television as quickly as possible! Fathers, we can do no more important thing than celebrate the sacred mysteries: let us beware of the temptation of liturgical sloth, because it is a temptation of the devil.
We must remember that we are not the authors of the liturgy, we are its humble ministers, subject to its discipline and laws. We are also responsible to form those who assist us in liturgical ministries in both the spirit and power of the liturgy and indeed its regulations. Sometimes I have seen priests step aside to allow extraordinary ministers distribute Holy Communion: this is wrong, it is a denial of the priestly ministry as well as a clericalization of the laity. When this happens it is a sign that formation has gone very wrong, and that it needs to be corrected.
I have also seen priests, and bishops, vested to celebrate Holy Mass, take out telephones and cameras and use them in the Sacred Liturgy. This is a terrible indictment of what they understand they are doing when they put on the liturgical vestments, which clothe us as an alter Christus — and much more, as ipse Christus, as Christ himself. To do this is a sacrilege. No bishop, priest or deacon vested for liturgical ministry or present in the sanctuary should be taking photographs, even at large-scale concelebrated Masses. That priests often do this at such Masses, or talk with each other and sit casually, is a sign, I think, that we need to rethink their appropriateness, especially if they lead priests into this sort of scandalous behaviour that is so unworthy of the mystery being celebrated, or if the sheer size of these concelebrations leads to a risk of the profanation of the Blessed Eucharist.
I want to make an appeal to all priests. You may have read my article in L’Osservatore Romano one year ago (June 12, 2015) or my interview with the journal Famille Chrétienne in May of this year. On both occasions I said that I believe that it is very important that we return as soon as possible to a common orientation, of priests and the faithful turned together in the same direction — eastwards or at least towards the apse — to the Lord who comes, in those parts of the liturgical rites when we are addressing God. This practice is permitted by current liturgical legislation. It is perfectly legitimate in the modern rite. Indeed, I think it is a very important step in ensuring that in our celebrations the Lord is truly at the center.
And so, dear Fathers, I ask you to implement this practice wherever possible, with prudence and with the necessary catechesis, certainly, but also with a pastor’s confidence that this is something good for the Church, something good for our people. Your own pastoral judgement will determine how and when this is possible, but perhaps beginning this on the first Sunday of Advent this year, when we attend ‘the Lord who will come’ and ‘who will not delay’ (see: Introit, Mass of Wednesday of the first week of Advent) may be a very good time to do this. Dear Fathers, we should listen again to the lament of God proclaimed by the prophet Jeremiah: “they have turned their back to me” (2:27). Let us turn again towards the Lord!
I would like to appeal also to my brother bishops: please lead your priests and people towards the Lord in this way, particularly at large celebrations in your dioceses and in your cathedral. Please form your seminarians in the reality that we are not called to the priesthood to be at the center of liturgical worship ourselves, but to lead Christ’s faithful to him as fellow worshippers. Please facilitate this simple but profound reform in your dioceses, your cathedrals, your parishes and your seminaries.
We Bishops have a great responsibility, and one day we shall have to answer to the Lord for our stewardship. We are the owners of nothing! As St. Paul teaches, we are merely “the servants of Christ and the stewards of the mysteries of God” (1 Cor. 4:1). We are responsible to ensure that the sacred realities of the liturgy are respected in our dioceses and that our priests and deacons not only observe the liturgical laws, but know the spirit and power of the liturgy from which they emerge. I was very encouraged to read the presentation on “The Bishop: Governor, Promoter and Guardian of the Liturgical Life of the Diocese” made to the 2013 Sacra Liturgia conference in Rome by Archbishop Alexander Sample of Portland in Oregon in the USA, and I fraternally encourage my brother bishops to study his considerations carefully.
At this point I repeat what I have said elsewhere, that Pope Francis has asked me to continue the liturgical work Pope Benedict began (see: Message to Sacra Liturgia USA 2015, New York City). Just because we have a new pope does not mean that his predecessor’s vision is now invalid. On the contrary, as we know, our Holy Father Pope Francis has the greatest respect for the liturgical vision and measures Pope Benedict implemented in utter fidelity to the intentions and aims of the Council Fathers.
Before I conclude, please permit me to mention some other small ways which can also contribute to a more faithful implementation of Sacrosanctum Concilium. One is that we must sing the liturgy, we must sing the liturgical texts, respecting the liturgical traditions of the Church and rejoicing in the treasury of sacred music that is ours, most especially that music proper to the Roman rite, Gregorian chant. We must sing sacred liturgical music not merely religious music, or worse, profane songs.
We must obtain the right balance between the vernacular languages and the use of Latin in the liturgy. The Council never intended that the Roman rite be exclusively celebrated in the vernacular. But it did intend to allow its increased use, particularly for the readings. Today it should be possible, especially with modern means of printing, to facilitate comprehension by all when Latin is used, perhaps for the liturgy of the Eucharist, and of course this is particularly appropriate at international gatherings where the local vernacular is not understood by many. And naturally, when the vernacular is used, it must be a faithful translation of the original Latin, as Pope Francis recently affirmed to me.
We must ensure that adoration is at the heart of our liturgical celebrations. Too often we do not move from celebration to adoration, but if we do not do that I worry that we may not have always participated in the liturgy fully, internally. Two bodily dispositions are helpful, indeed indispensable here. The first is silence. If I am never silent, if the liturgy gives me no space for silent prayer and contemplation, how can I adore Christ, how can I connect with him in my heart and soul? Silence is very important, and not only before and after the liturgy.
So too, kneeling at the consecration (unless I am sick) is essential. In the West this is an act of bodily adoration that humbles us before our Lord and God. It is itself an act of prayer. Where kneeling and genuflection have disappeared from the liturgy, they need to be restored, in particular for our reception of our Blessed Lord in Holy Communion. Dear Fathers, where possible and with the pastoral prudence of which I spoke earlier, form your people in this beautiful act of worship and love. Let us kneel in adoration and love before the Eucharistic Lord once again!
In speaking of the reception of Holy Communion kneeling I would like to recall the 2002 letter of the Congregation of Divine Worship and Discipline of the Sacraments which clarifies that “any refusal of Holy Communion to a member of the faithful on the basis of his or her kneeling posture [is] a grave violation of one of the most basic rights of the Christian faithful” (Letter, July 1, 2002, “Notitiae,” n. 436, Nov–Dec 2002, p. 583).
Correctly vesting all the liturgical ministers in the sanctuary, including lectors, is also very important if such ministries are to be considered authentic and if they are to be exercised with the decorum due to the Sacred Liturgy — also if the ministers themselves are to show the correct reverence for the mysteries they minister.
These are some suggestions: I am sure that many others could be made. I put them before you as possible ways of moving towards “the right way of celebrating the liturgy inwardly and outwardly,” which was of course the desire expressed by Cardinal Ratzinger at the beginning of his great work, The Spirit of the Liturgy. (Joseph Ratzinger, “Theology of the Liturgy,” Collected Works vol. 11, Ignatius Press, San Francisco 2014, p. 4). I encourage you to do all that you can to realise this goal, which is utterly consistent with that of the Second Vatican Council’s Constitution on the Sacred Liturgy.
‘Momma, all I want to be is a saint,’ Kara Jackson has told her mother. The family has visited 40 states already, so that Kara can fulfill her dream. They consider each trip a pilgrimage.
by TONIA BORSELLINO/CNA/EWTN NEWS 07/08/2016
DENVER — On July 1, Kara Jackson crossed the 40th state off her list.
The 18-year-old helped serve Mass at Immaculate Heart of Mary Catholic Church in Northglenn, Colo. Dressed in her own vestments and with a big smile on her face, Jackson served with the same passion she began her journey with in 2013.
This all started because “God told me to,” Jackson told CNA. She said God came to her in a dream one night, telling her to begin the quest of helping serve Mass in all 50 states.
Her mother questioned this mission, at first.
“I didn’t think it was a good idea,” Christina Jackson said. “It was a crazy idea.” The thought of traveling to unknown areas, without financial support, and Kara’s heath complications made her mother hesitant.
But Kara was persistent. Christina and her husband, Rick, took the idea to their local priests in Middletown, Ohio, for their opinion. The late Msgr. Paul Metzger encouraged Kara because he had traveled to every state celebrating Mass. Father John Civille, their pastor, told Kara he would be her personal chaplain in Alaska and Hawaii.
With their support, Kara’s mother looked to the closest state, Indiana, to “test the waters.” Kara, having a strong devotion to the Blessed Mother, suggested stopping at St. Mary Catholic Church in Richmond.
“I didn’t think there was a St. Mary’s,” her mother said, but, sure enough, “they have a St. Mary’s.”
The family said a prayer and sent a letter to the parish. That Friday, at 3pm, the pastor of the parish called back welcoming Kara. The evening before Divine Mercy Sunday, she stood with Father Kevin Morris and served Mass in her second state.
Since then, Kara and her parents have traveled across the nation during school breaks and family vacations.
“God leads us where we’re supposed to go,” Christina said. The family never has a specific parish in mind. Sometimes they end up at a small church in a strong Protestant area or a parish that has more than 12,000 parishioners, like Immaculate Heart of Mary in Colorado.
“We’ve seen it all,” the family says.
The family tells stories of churches with expansion plans and others where the pastor’s dog also attended Mass. They recalled the time Kara served with Archbishop Joseph Kurtz, president of the U.S. Conference of Catholic Bishops, in her sixth state of Kentucky. They even said their journey impacted the life of a hotel clerk, bringing him back to God.
“I don’t think of ourselves has evangelists,” Christina said, “but we really are evangelizing our faith.”
The family considers each trip a pilgrimage. Kara prays for the priests and their parishes before Mass begins. Regardless of where they travel, they say God is always with them.
Seeing the universal Church and all the Godly encounters “gives me great hope, and it has strengthened my faith,” Christina said.
“We are a vibrant Church,” she said. “We’ve survived over 2,000 years, and we will still be here.”
Kara’s notebook filled with messages from every priest she has met documents her journey. One priest wrote a message inviting Kara to serve Mass at his home parish in Ireland. She hopes to make the trip for her 21st birthday.
“It’s emotional to see this,” Christina said, with tears in her eyes.
After struggling with infertility for many years, Christina became pregnant. When doctors told Christina and Rick their daughter had Down syndrome, they said she would never lift her head or talk. The doctors even suggested “adopting her out.”
“We brought her home,” Christina said, and have been blessed ever since.
Kara wanted to take altar-serving lessons when she was 9 years old. Her parents said she was focused and attentive the entire time. She watched daily Mass on EWTN to learn how to ring the bells.
“She tells me, ‘Momma, all I want to be is a saint,’” Christina said.
While traveling, Kara has never gotten sick consuming Communion hosts with gluten, though she has Celiac disease.
The family will stop in six more states on this leg of their trip, leaving only Arizona, New Mexico, Hawaii and Alaska to come. Though they would love to complete their journey in the Year of Mercy, they said they will finish “when the money comes in.”
The family said people have suggested their story be turned into a book or movie. Either way, Kara said she would like to become an actress and writer one day.
Starting in August, she will attend the “Project 101 Program” for students with special needs at Butler Tech University.
No. 86 must be lucky for Marie Frey, who received the gift of her 86th great grandchild just days before her 86th birthday.
“It’s pretty good that she got to see her,” said Frey’s grandson Kenny Frey of Forest, Ohio. “Family and faith are her two biggest favorites. She’s a very strong woman.”
Blakely Grace Frey was born the morning of June 23.
Frey told ABC News that his father’s mother Marie, of Upper Sandusky, was born and raised in Ohio.
She and her late husband Gerald, who died in October 2009, had 15 children, with the oldest being 66 years old.
Marie also has 68 grandchildren, including two sets of twins, and six step-grandchildren. In addition to 86 biological great-grandchildren, Marie also has nine step-great-grandchildren.
Blakely is Frey’s fifth daughter. She was born at 7 pounds, 5 ounces at Blanchard Valley Hospital in Findlay, Ohio, three days prior to her great-grandma Marie’s 86th birthday, and her mother Holly’s 32nd birthday on June 26.
Although they have quite the crowd to keep up with, Frey said he and his grandmother enjoy being part of such a large clan.
“She came from large family and Grandpa did too,” he said. “My wife and I also wanted a big family.”
This year, Marie is expecting two more great-grandchildren, Nos. 87 and 88, from Frey’s sister and cousin, he said.
The first ever pro-life women’s conference took place on the weekend of June 24-26 in Dallas. Hosted by activist Abby Johnson of And Then There Were None, the conference attracted women from all over the country eager to hear from female leaders and connect with one another. Over 500 activists participated: pregnancy center and sidewalk counselors, doulas and nurses, writers, lawyers, and community organizers. There were 31 sponsors, among them Natural Womanhood, Sidewalk Advocates for Life, Save the 1, and International Helpline. Keynote speakers included Marilyn Musgrave of Susan B. Anthony List, and Star Parker from the Center for Urban Renewal and Education; break-out informational sessions and panel discussions featured other popular figures like abortion survivor Melissa Ohden and Secular Pro-Life’s Kelsey Hazzard.
A recurring conference theme was the need for the feminist movement to get away from claiming men and women are the same in order to gain equality—in the workplace, in schools, and in society at large. Speakers stressed that women are equal because our contributions, while distinctively different from those of men, are just as valuable. It was therefore fitting for Feminists for Life president Serrin Foster, who opened the conference Friday night and spoke again on Saturday, to call on attendees to embrace feminism: To be pro-woman is to be pro-life, she declared. Foster shared insights gained from her decades-long experience as a pro-life feminist and related heart-breaking stories she had heard from both women and men effected by abortion.
Leah Jacobson, founder of The Guiding Star Project, was both a keynote speaker and leader of one of the informational sessions. She addressed how our society continues to perpetuate the idea that the female body can be manipulated to fit a cultural norm. There are three things that are distinctive to being a woman, she explained, which a man cannot mimic: the ability to ovulate, gestate, and lactate. As natural as these functions are, throughout American history, Jacobson claimed, attempts have been made to manipulate or suppress them, reflecting a troubled culture that undermines femininity by sending women the message that they can’t trust their own bodies. She also addressed the devaluing of the bond between mother and child indicated by the lack of workplace accommodations for families with babies. And she made a good point about the hypocrisy of a culture that promotes a movement protesting GMOs and hormones in meat, while remaining generally complacent about the hormones and chemicals in birth control pills. High amounts of artificial drugs in these pills, she pointed out, have been found in groundwater supplies.
In addition to Jacobson’s, other breakout sessions included topics such as “Latinas and Abortion,” “Pregnancy Loss,” “Fertility Awareness Based Methods for Family Planning,” “Pro-Life Concerns about the Girl Scouts,” and “How to Start a Pro-life Group on Campus.”
The panel discussions featured first-hand accounts concerning political activism, adoption and birth mothers, and creating a culture of life to embrace even the hard cases—such as that of Rebecca Kiessling, a public speaker who was conceived in rape. Kiessling told the story of how her mother had sought to end her pregnancy, then reconsidered because she didn’t want to gamble her own life and health by resorting to a back-alley abortion. “I wasn’t lucky,” Kiessling said. “I was protected. Legality matters.”
There was also a session on activism from the millennials’ perspective. The young panelists acknowledged that imagery plays an important role when trying to reach abortion-minded women or to initiate dialogue with pro-choicers. But in their experience, the use of graphic images of bloody aborted baby parts makes pro-lifers appear unapproachable and extreme. Destiny Herndon-De La Rosa of the New Wave Feminists added that it can be effective to show the violence of abortion, but only after a person has expressed genuine openness to pro-life viewpoints. In her experience with her own crisis pregnancy, and as a sidewalk counselor, she found that abortion-minded women responded better to sidewalk counselors offering pamphlets with a happy, young mother smiling on the cover, rather than a picture of an aborted baby.
The Conference was a call for more and better action for women, by women. As we began to leave the hotel on Sunday to return to our respective hometowns, the general chatter was, “We’re doing this again next year, right?” and “I know what I need to do”—the beginning of a new phase of a collective and cohesive national women’s movement to reclaim the narrative about abortion and what women’s equality really means.
Pier Giorgio Frassati smiled and laughed so freely that he was called “an explosion of joy.” He whistled and sang loudly and hopelessly out of tune. He loved playful teasing and practical jokes. In his early 20’s, he was the picture of strength and health, leading groups of friends into the Alps to scale mountain peaks.
His ready laughter and adventurous spirit were fountains that sprang from a well of holiness. Pier Giorgio was so filled with virtue that Saint John Paul II, who beatified him in 1990, called him the “Man of the Beatitudes.” Joy of life and love of God coursed readily through his veins. Could anyone who knew him in the sunshine of his youth, in the early twentieth century in Turin, Italy, have believed that he would die before the age of 25?
In her beautiful memoir My Brother Pier Giorgio: His Last Days, Luciana Frassati—Pier Giorgio’s only sibling—tells the story of her brother’s final week on earth, and of the veil that was lifted from the eyes of his family as they discovered two truths about him that they had not dreamed possible: that he was dying, and that he lived a life of immense charity that touched thousands of lives.
His family never suspected these truths, because Pier Giorgio quietly and humbly hid both his suffering and his good works.
“We were still unaware, at his death watch, that he had been late for mealtimes because he had given his tram money to some poor person and his jacket to another,” writes Luciana.
Pier Giorgio’s wealthy father was an important senator and owned one of Italy’s most prestigious newspapers, but Pier Giorgio was always broke and often begged for money from his family and friends—not for himself, but for the poor, whom he visited and served daily, and to whom he gave every cent he could find.
To his family, he was merely an engineering student—an average one, who worked hard but for whom learning never came easily. They saw him come and go from their large estate, where the discord between his parents created an atmosphere of constricted love, and where no one fully knew or understood Pier Giorgio, and they never guessed where he actually went.
It was as if a veil had been placed over their eyes, and it remained there until his very last days on earth. Until his death from poliomyelitis—a disease he most likely contracted while serving the poor—at the age of 24.
When Pier Giorgio first began to feel sick, he tried hard to hide it. His grandmother was on her deathbed upstairs in the Frassati home, and he did not want to bother anyone with his own ailments. Every time he came in the door, he inquired about his grandmother and went to visit her room. As his sickness progressed, he became less and less able to move, yet he still pushed himself out of his bedroom and down the hall to pray at his grandmother’s bedside. One sleepless night followed another, as he stumbled down the hall and back again, unable to rest, unwilling to complain.
His family, consumed by his grandmother’s illness, believed he had the flu. A doctor who came to examine him diagnosed him with rheumatism; and so, the veil remained. While his grandmother approached her death, no one knew that a few doors away, death was coming for her grandson, too.
Pier Giorgio wouldn’t have wanted it any other way. He prayed his heart out for his grandmother, and exhorted others to pray, too. “Go to Grandmother,” he told Luciana. “Pray for her because her condition is very serious,”—and then he broke down and sobbed.
When his grandmother passed away, polio was ravaging Pier Giorgio’s body and beginning to paralyze him—yet every two hours throughout the night, he made his way to his grandmother’s room, where he stood and prayed, or knelt and prayed, each time appearing more exhausted, less able to rise again.
All the while, his family thought what an inconvenient time he had chosen to get sick.
“You’re letting yourself go,” his mother told him, not knowing that he would be dead two days later. “If you want to get well, you must get hold of yourself.”
The regret with which Luciana writes about her family’s dismissal of Pier Giorgio’s sickness is heartbreaking. She spent the rest of her life spreading her brother’s story, wishing they had understood sooner and cared for him better. And yet, his family’s blindness helped to conform him to the Person he most wanted to imitate. It gave him the opportunity to be more like Christ. For as Pier Giorgio—a daily communicant who strived to live the Gospel with every breath he took—was misunderstood by his loved ones as his death came near, so was his Lord misunderstood by His loved ones as His death approached, as well.
In Mark 10:32-34, Jesus tells his apostles something that should have shocked, saddened, and stunned them: “Behold, we are going up to Jerusalem; and the Son of man will be delivered to the chief priests and the scribes, and they will condemn him to death, and deliver him to the Gentiles; and they will mock him, and spit upon him, and scourge him, and kill him; and after three days he will rise.”
The apostles should have wept, right? Shouldn’t they have fallen to their knees in grief? That’s not what Mark says they did, though. He says that James and John came forward to Jesus—and asked Him to let them sit at His right and His left in His glory. He had just told them He was going to be murdered, and they responded with a request for special treatment in heaven.
I imagine James and John might have regretted that move later, when they looked back and understood, in hindsight, what Jesus had been saying. But for some reason, at the time of Jesus’ words, the veil remained. Like Pier Giorgio’s family, Jesus’ apostles did not appear to understand the gravity of the situation they were in. For reasons that might only be revealed in heaven, the veil was not lifted until later.
As Saint Paul says, the Lord “will bring to light the things now hidden in darkness and will disclose the purposes of the heart. Then every man will receive his commendations from God.” (1 Corinthians 4:5) For Pier Giorgio, the time to “bring to light the things now hidden” was approaching hand in hand with the end of his earthly life.
Two days after Pier Giorgio’s grandmother died, the doctor who had diagnosed him with rheumatism returned and, deeply grieved by what he found, called for a second doctor, who called for a third, to confirm the sad diagnosis: poliomyelitis.
His family reeled in shock and grasped for quickly unraveling threads of hope while the paralysis moved into his lungs. As they struggled to comprehend the first hidden truth—that he was dying—the second hidden truth came to the surface as well: that he had been surreptitiously serving the poor in the manner of a saint.
“During his life he had kept quiet about his poor,” writes Luciana, “but at this point, having sensed his imminent death, he was forced to reveal himself.” One of his last acts was to ask Luciana to retrieve some medicine and a pawn ticket from his study. With effort that Luciana calls “impossible to describe,” he scrawled a note to ensure the items would reach the poor people for whom he had kept them. This small glimpse of charity on his deathbed was only a hint of what would come to light after his death.
Pier Giorgio took his last breath on July 4, 1925. At his funeral, thousands of people from every part of the city flooded the streets.
“The letters we began to receive and even more what was said about Pier Giorgio by unknown friends and all the strangers who turned to us constituted a revelation so imposing and so sublime that it overwhelmed us at least as much as his death,” Luciana writes. Only then did his family realize the impact he had made and the lives he had touched in the name of Jesus. Only then did they begin to understand the truth about Pier Giorgio. Only then did the lifted veil reveal that they had been living with a person of extraordinary grace.
On his feast day, July 4, and always, let us ask Blessed Pier Giorgio to intercede for us, that we, too, may live and die in humility, charity, and holiness.
Natural family planning is an invitation to live God’s plan for love and marriage
EDITOR’S NOTE: Natural Family Planning Awareness Week, a national education campaign of the U.S. Conference of Catholic Bishops, will be observed July 24-30. For more information, visit usccb.org/nfp.
When learned well and embraced by a couple, natural family planning strengthens and protects the marital bond. As a pro-life physician who works with couples seeking to learn NFP, I have seen it bring both blessings and challenges. Like any worthwhile endeavor, it requires time and effort.
A husband and wife using NFP have a unique opportunity to learn more about the beauty of the female reproductive system. The intricate symphony involved in the monthly cycle is fascinating and illuminates God’s plan for procreation. A couple’s enhanced understanding should be an occasion to grow in love and respect for one another as they move forward in marriage.
Monitoring a woman’s natural fertile and infertile periods leads a couple to regularly communicate about such topics as family size, physical health, psychological outlook and the role of intimacy in their married life. They also are encouraged to pray together to discern God’s will.
Humanae Vitae, the prophetic 1968 encyclical on the regulation of birth by Blessed Paul VI, mentions four considerations couples may take into account in delaying conception: physical, economic, social and psychological. While Pope Paul VI outlined reasonable grounds for spacing births, he also warned against a mindset that would be closed to conception, calling children “the supreme gift of marriage [who] contribute in the highest degree to their parents’ welfare” (8).
Thus, though couples may use NFP to delay conception for legitimate reasons, when touting the “effectiveness” of NFP we should never forget that children are a blessing.
In all cases, NFP differs from contraception, for it does not separate the unitive and procreative meaning of marital intimacy. Not only that, but NFP avoids the risks and side effects of ingesting chemicals to suppress one’s natural fertility. Invariably, there is a marked improvement in the health and well-being of women who stop using hormonal contraceptives. When they stop and learn NFP, women feel the difference in their daily lives.
There are other health benefits as well. Doctors who advocate NFP instead of contraception can more easily diagnose and treat underlying causes of infertility, and they can help women with irregular cycles by using natural therapies.
There are also challenges, which can become blessings when faced openly and with faith. When a couple uses NFP to delay conception, periodic abstinence is required during fertile periods. It is not uncommon for me to speak with women who become frustrated because their charting can reveal they must remain abstinent for long periods of time. Other women express a strong desire to have another child, yet their husband is not supportive. Practicing NFP can be difficult if a husband and wife are not on the same page.
Nonetheless, NFP can help by encouraging communication between spouses as well as prayer. There is a very beautiful and beneficial interplay involved that can bring a couple closer together; even periodic abstinence can lead them to desire each other more, especially if they work toward the same goal regarding conception.
Although everyone is different, and there is no one-sizefits- all method, all married couples of childbearing age can benefit from NFP. As they turn toward one another in openness to life, and see the love of God reflected in each other, they make for stronger marriages and happier families.
ANTHONY J. CARUSO, M.D., is an obstetrician/gynecologist and a member of Father Boecker Council 6090 in Lombard, Ill.
This article appeared in the July/2016 issue of Columbia magazine and is reprinted with permission of the Knights of Columbus, New Haven, Conn.
Dr. Ligaya Acosta, Human Life International’s regional director of Asia and Oceania, gave an eye-opening talk at the tenth World Congress of Families in the Republic of Georgia in May. Her presentation on contraception was accompanied by HLI resources on the subject.
Dr. Acosta took her time deciding on a topic for this important conference. While reviewing the programs of previous WCFs, she noticed that the topic of contraception had not been given much attention. After talking with conference organizers about the need to discuss the demographic problems facing many Asian countries, she agreed to connect these issues with one of their most important causes, one often overlooked even by those who defend life. Dr. Acosta’s presentation moved the audience, many of whom considered contraceptives to be a safe way to prevent abortion. Contraception is Unhealthy and Unsafe for Women
Not only has the wide promotion of contraception not lowered abortion rates, Contraception is not safe. The World Health Organization classified contraceptives as carcinogenic in a September 2005 report. In spite of the carcinogenicity, WHO routinely makes the unsupported claim that “the health benefits clearly exceed the health risks.” Apparently the World Health Organization is not concerned that women are putting cancer-causing chemicals in the same category as cigarettes and asbestos in their bodies daily.
Side Effects of Contraception
What are the health risks that are supposedly outweighed by the benefits? Different forms of contraception from birth control pills to IUDs to vaginal rings share side effects ranging from headache to depression to death. None of these forms protect against HIV-AIDS or any other STDs, and some have been shown to substantially increase risk of HIV transmission in women. Deep vein thrombosis, or blood clots, is one of the more dangerous side effects, which can lead to strokes even in young women. Other serious side effects include breast and cervical cancer, total or partial blindness, ectopic pregnancy, gallbladder disease, and depression and suicidal thoughts. Less serious side effects include acne, dizziness, diarrhea, and/or vomiting, weight loss or gain, nervousness, rash, and excessive sweating or body odor. Copper T IUD can cause an increase in menstrual cramping and bleeding. Depo-Provera, an injectable contraceptive that is very popular among population control organizations, has been given a “black box warning” from the FDA due to the fact that it can cause a loss in bone marrow density.
Contraception Does Not Prevent Abortion
There are two ways in which hormonal contraceptives cause abortion rather than prevent it. First, the term “contraceptive” (contra (against)- conception) is not entirely accurate. Most hormonal methods have three effects, only two of which actually prevent contraception by thickening cervical mucus or by preventing ovulation. Most of these methods, however, also act as abortifacients, ending the life of the unborn child at his earliest stage by preventing his implantation in the uterus. This has been known for some time: over 25 years ago, Planned Parenthood lawyer Frank Susman said, “The most common forms of contraception today—IUDs, low dose birth control pills, which are the safest type of birth control pills available—act as abortifacients.”[1] This is true for almost all hormonal contraceptives—the pill, patches, vaginal rings, and long-acting methods. The only contraceptive methods sure to not cause early abortions are surgical sterilization and barrier methods, such as condoms. Of course, these methods have their own problems, and neither of them prevents the spread of STDs.
The second reason that contraceptives cause abortion rather than prevent it is because of their higher-than-expected failure rate. Birth control pills need to be taken at the same time every day for peak effectiveness. Condoms can slip, break, or leak. Depo-Provera has a 6% failure rate, and is not recommended for long-term use (more than two years) due to the increased health risks for prolonged use. The effectiveness of all of these methods also decreases with time. Once a woman’s birth control method fails, she is likely to want to end the unwanted pregnancy in abortion. Former Medical Director of the International Planned Parenthood Federation, Malcolm Potts, said in 1977, “As has been pointed out, those who use contraceptives are more likely than those who do not to resort to induced abortion.”[2]
According to former abortion mill owner Carol Everett, contraception failure is part of Planned Parenthood’s strategy to sell abortions. Everett has stated in several interviews that Planned Parenthood sells abortions to young girls by first giving them contraceptives that will eventually fail, such as birth control pills that need to be taken at the same time every day. “You know and I know, there’s not a teenager in the world who does everything the same time every day.” Once Planned Parenthood has girls using contraceptives, it is easier to get them to choose abortion.
HLI’s Fight against Contraception
Contraception has been sold as a “safe” alternative to abortion for over a century. In the December 1918 issue of Margaret Sanger’s “Birth Control Review”, the founder of Planned Parenthood states, “If [a woman] is denied the knowledge of the safe, harmless, scientific methods of Birth Control, she limits her family by abortion…the abnormal, often dangerous, surgical operation.”[3] This is interesting considering that Planned Parenthood performed 327,653 of these “abnormal, often dangerous, surgical operations” in 2013.
Human Life International, on the other hand, has been fighting the lie of “safe contraception” since our founding in 1981. When many in the wake of Roe v. Wade were claiming that birth control would decrease abortions, Father Paul Marx, HLI’s founder, was teaching (in agreement with Planned Parenthood’s Malcolm Potts) that increased demand for abortion is the result of the widespread use of contraception. “Abortion is the endpoint of the abuse of sex, which begins with the unleashing of the sexual urge by contraception,”[4] Fr. Marx writes in his book The Warehouse Priest.
It was the discovery of the truth about contraception that brought Dr. Acosta to the pro-life movement and to Human Life International. Dr. Acosta spent over 28 years promoting contraception and population control as an employee of the Department of Health in the Philippines. In 2004, she was assigned to be Program Manager for Natural Family Planning. As she began to learn more about NFP, she began to realize the miracle of reproduction. “I realized that God in all His wisdom and glory really placed a body clock inside the body of a woman, where you will know exactly when you are fertile and not fertile.” Through her research, she learned the horrible side effects of artificial birth control on a woman’s body, and the ultimate consequence for the child. She then spent a year studying the subject of contraception, reading material from HLI as well as others. “The more I read, the more I cried.” She realized that she had to quit her job. She has been working for HLI Asia since 2007, avidly opposing the movement she promoted for so long.
Continuing the Fight
Dr. Acosta’s commitment and dedication to the pro-life movement shone through her talk at the World Congress of Families. Several of those who heard her speak were deeply moved to oppose contraception, the root of the Culture of Death. After her talk, activists from both Belarus and London requested copies of the presentation to use in their countries. Dr. Acosta continues to give many talks weekly in her native Philippines and around Asia and Oceania, winning many to the cause of life and family.
[1] “Excerpts of Arguments Before Supreme Court on Missouri Abortion Law.” Washington Post, April 27, 1989, page A16.
[2] Malcolm Potts, Peter Diggory, and John Peel. Abortion [Cambridge: Cambridge University Press], 1977, pages 491, 496, 498 and 526.
[3] Sanger, Margaret. “Birth Control or Abortion?” Birth Control Review (New York City), December 1918. Page 3-4.
[4] Marx, Paul. The Warehouse Priest. Gaithersburg, MD: Human Life International, 1993. Page 307.
Posted in News & Commentary | Comments Off on Contraception: An Alternative to Abortion?
June 27, 2016 (LifeSiteNews) – A new academic program that can be integrated into any curriculum teaches students of all ages to understand and defend the sanctity of life, one of the program’s pioneers told LifeSiteNews in an exclusive video interview.
The American Life League’s Culture of Life Studies Program uses educational supplements to teach students in an age-appropriate way about the value of each human life. This equips them to respond to the culture of death, which “plays on their emotions,” the program’s Educational Outreach Coordinator Mary Flores said.
“Young people today are very empathetic,” and the culture of death takes advantage of this, especially in regard to euthanasia and physician-assisted suicide, Flores said.
“One of the most important studies that we released actually last December was our first unit study for high school students, and that is on the difficult topic of euthanasia,” said Flores. The study is called Euthanasia: An Introduction and is increasingly relevant as the practice is pushed across the United States and Canada and teenagers struggle to understand it, she said.
Flores told LifeSiteNews that even at pro-life conferences, she meets young people who are not well-educated on the issue.
Watch LifeSiteNews’ full interview with Mary Flores:
The euthanasia study is “very simple to follow” and it can make anyone “an instant expert” on the topic, Flores said.
The majority of the program’s creators are homeschooling mothers, Flores said, which has ensured that the content is age-appropriate and easy to incorporate into other curricula.
“The fact that we’re mothers gives us a really special angle,” said Flores. “We also work with pro-life experts from around the country to make sure that all of our unit studies, including the ones for younger children, are age-appropriate and also top-notch.”
Younger children learn about being made in the image and likeness of God “from the moment of creation” through the program’s beginning series of lessons, titled Life Primer. Middle school students “continue their studies of the basic principles of the gospel of life in the series Life Foundations by examining age-appropriate pro-life topics in literature, history, science, and religion,” according to program’s website.
And in high school, the program places more emphasis on evangelization and communication through critical thinking and hands-on activities in the final three series of studies: Life Quest, Life Lens, and Life Scope.
One of the studies for high school students includes a unit on Margaret Sanger, the founder of Planned Parenthood, and how she promoted artificial birth control across the country. The American Life League is currently hosting a kickstarter campaign to fund the delivery of this unit to supporters of the project.
One of the best things about the Culture of Life Studies Program is “that the materials can be easily worked into youth groups or religious education programs,” said Flores, which can reach public school students who typically do not receive this kind of information.
“I definitely see the Culture of Life Studies Program as an antidote to the many problems in our schools,” said Flores.
This week saw a rare victory in the international battle for truth and religious freedom. You may have heard that Antonio Cardinal Cañizares Llovera, archbishop of Valencia in Spain, had been threatened with legal action following a controversial homily he gave some months ago. In the homily, he criticized the extremely aggressive and overreaching “gay empire” that is attacking the family. He called Catholics to vigilance and prayer, calling for a defense of the family.
Attacking the bishop
As if only to prove him right, homosexual activists brought charges against Cardinal Cañizares for giving the homily. He was in a Catholic Church speaking to Catholics, yet he cannot (to listen to these activists) be allowed to defend Church teaching on marriage and challenge those who, well, threaten anyone who dare raise a voice in opposition.
We’re well past the point of “You can’t make this stuff up.” You don’t have to. The sense of entitlement the “gay empire” (to use the cardinal’s term) has to silence all opposition is limitless and is becoming totalitarian. They’ve had too many successes in just such cases, so it is heartening to see a victory for sanity.
Threatened with three years in prison, Cardinal Cañizares prevailed when a Spanish judge threw out the charges, finding truthfully enough that in the controversial homily in question, he was exercising his right to free speech and had no criminal intent or appeal to hatred or violence.
We have discussed many times in Spirit & Life how radical gender ideology has infected many institutions here and around the world, bringing its corrosive anti-reality and anti-God worldview to corners once thought immune to politics. Since the LGBT movement cannot defend its views with reason, it must appeal with raw emotion and project its own hatred onto its opponents and remove their rights to free speech, and increasingly, to any public endeavor whatsoever.
Bishops Standing Together
So to do what Cardinal Cañizares did takes courage and leadership, traits he shares with Bishop Juan Antonio Reig Pla, who also hails from Valencia but is now bishop of Alcala de Henares, Spain. HLI awarded Bishop Reig Pla the Cardinal von Galen award in 2013 for his courage in defending Christ and His Church. Spain has seen many hardships over the years, but with leaders like this they have greater hope.
Bishops should dedicate themselves to their apostolic office as witness of Christ before all men. They should not only look after those who already follow the Prince of Pastors but should also wholeheartedly devote themselves to those who have strayed in any way from the path of truth or are ignorant of the Gospel of Christ and His saving mercy until finally all men walk “in all goodness and justice and truth (Eph. 5:9)” (Christus Dominus n. 11).
There are many good bishops out there, and we need to acknowledge their courage when we see it. All of our beloved shepherds deserve our love and prayers, and frankly deserve encouragement when they step into the breach and really lead in a difficult time.
Sometimes the attack comes from inside
This is especially true since there is so much to confuse the faithful coming from bishops. Last week we heard a bishop insist that the Church is somehow responsible for attacks on persons who identify as LGBT, repeating a key talking point of those who attack the Church unjustly and are trying to change her teaching on sexuality. This is truly disgraceful and deserves clear condemnation-when the Church is already under attack from powerful sexual radicals it is devastating to have a shepherd of the Church give aid and comfort to the enemy.
Yet, just when some are tempted to despair by such betrayals, we hear from Los Angeles Archbishop Jose Gomez an eloquent defense of the Church’s teaching that life is the most important among many issues that concern Catholics in the public square. He has been a leader on many social justice issues for the Church, particularly on immigration, yet he knows that while some issues admit of a variety of solutions for faithful Catholics, life deserves a complete and unqualified defense in law, which is sorely lacking in the US and around the world today. And it is so for the exact same reason that a poor migrant family deserves our help: because every human person is made in the image of God, and deserves to live the life he already has been given as a gift.
In exercising their duty of teaching — which is conspicuous among the principal duties of bishops — they should announce the Gospel of Christ to men, calling them to a faith in the power of the Spirit or confirming them in a living faith. They should expound the whole mystery of Christ to them, namely, those truths the ignorance of which is ignorance of Christ. At the same time they should point out the divinely revealed way to give glory to God and thereby to attain to eternal happiness. (Christus Dominus n. 12)
Giving glory to God
Cardinal Cañizares and Archbishop Gomez are two of many within the Church doing the right thing by opposing the threat of gender ideology, and by pointing to the truth in Our Lord. So many in the Church are indifferent, which is almost an understandable tragedy given the many years of poor catechesis and compromise with a culture that is falling apart. We pray for the conversion of these brothers and sisters also, as the choices are made clearer by the hostility of the surrounding culture and a core group of faithful Catholics who remain strong and joyful. We pray every day that they will choose Christ and His Church and leave the untruths behind. We pray this for ourselves as well, since we don’t presume to have every answer. We just strive in love and truth to be faithful in small and large things.
Our shepherds and priests desperately need the prayers of the faithful. We need the strength to give ourselves anew to Christ through His Church every day. We can’t do it without your prayers.
Thank you for praying for me and for all priests and bishops, and for standing strong in the fight for life and family with us.
June is the month of the Sacred Heart of Jesus. Father’s Day also falls within the month, and spiritual fatherhood ties these two together.
The human heart always operates in two directions—the muscle contracts and then relaxes. If this rhythm is disrupted, you have earned a trip to either the ER or the undertaker. There is also a rhythm of Catholic fatherhood—the rhythm of loving, then challenging; of being tender, then tough. Disruption of this rhythm can create major problems for kids.
Soccer
Chad played soccer. His parents were highly successful professionals, trying to motivate Chad to pay attention and engage in the game with some intensity. They were turning the situation into a life lesson: “How do you expect to succeed if you can’t do this?” There was a lot of criticism and pressure to perform. Another team was using psych ops, trashing Chad and his team. The way they talked, I would have sworn this was a U.S. Olympic competition, but Chad was in fourth grade! The parents assured me their behavior was mild compared to other parents. Nevertheless, the results were predictable: Chad was anxious, highly critical of himself, and impulsive, almost explosive at times. He was performing to be loved, which left him only as good as his last performance. The rhythm of Catholic fatherhood was broken, and they were all frustrated.
Sacred Heart and Spiritual Fatherhood
Jesus’ Sacred Heart teaches men a lot about this rhythm of fatherhood. During his time on earth Jesus fathered no physical children (unless you believe the fiction writer Dan Brown). But he was a spiritual father—a leader, mentor, and coach (and much more), to the twelve apostles and his other disciples! He loved and challenged them. It was the Heart of Jesus that revealed how his Father’s heart was turned towards his children—us—in love and mercy. The Father’s heart is what we need to receive and what we are to give to others. Scripture confirms the giving part, “The hearts of fathers will be turned back to the children” (Mal 3:24, 4:6; Lk 1:17; Sir 48:10). Jesus actually became indignant, incensed, or irate at the disciples for hindering the little children from coming to him to be embraced, touched, and blessed by him (Mk. 10:13-16). He was tough on his disciples and tender towards the children in his spiritual fatherhood!
St. John Paul II reflected on the Sacred Heart quite a bit. In talking about the gift of the Holy Spirit called piety (reverence, devoutness), he says, “the Spirit heals our hearts of every form of hardness, and opens them to tenderness toward God and our brothers and sisters” (May 28, 1989). From our sonship, tenderness flows toward God and is expressed in prayer that arises from our own poverty and void of chasing after earthly things, and then turns toward him for “grace, help, and pardon.” It is piety which directs us to trust God as “a good and generous Father” and to call him Abba (Gal. 4:4-7)!
This tenderness is manifested in meekness, a familial openness, toward our neighbor. Meekness is not weakness! Meekness is having the power to act or destroy, but not using it. The Spirit infuses into us a new capacity to love others, making our “heart[s] participate in some manner in the very meekness of the Heart of Christ.” Our spiritual fatherhood is made complete we when see others as part of the family of God, treating them with tenderness and friendliness.
Back to Soccer
I worked with Chad’s father to create new liturgies (rituals and routines) in their domestic church that communicated love to Chad. He affirmed Chad as a son rather than just his performance. And we shifted the focus from results, which Chad could not control, to his efforts—so while he might not always score a goal, he could always choose to play hard. These changes made a huge difference. Chad paid more attention, became more self-motivated, and everyone noticed the change. In fact, in one game, he was playing hard, but they were losing badly. He had put his shorts on backwards, and though it was not obvious, a friend started to harass him about it. Normally Chad would have blown up, but instead he retorted, “Do you really think that’s the biggest problem we have here?” I was amazed and laughed, saying, “I can’t even get adults to do this!” Chad was feeling much more secure and loved. The rhythm was back in right order: love and challenge; tenderness and toughness. We had returned from Olympic tryouts to fourth grade soccer!
The Challenge
June is the month of the Sacred Heart. It includes Father’s Day, which celebrates physical fatherhood. But we must challenge allmen to follow the Sacred Heart and be spiritual fathers, turning their hearts towards all fatherless children in tenderness, challenging them to be the best versions of themselves. All men are called to reveal and relive the very fatherhood of God on Earth—this is spiritual fatherhood.
Last January, I was travelling on business, staying in a little hotel in a college town. I like to think I’m usually more aware of my surroundings, but it was so snowy and windy that I wouldn’t have heard his footsteps even if he had he been stomping. It happened so fast. I got the door open, turned around to close it, and he was there – a huge man. My first instinct wasn’t fear, just confusion. In an instant, he punched me in the face. I don’t remember being dragged from the room, but I was found in the stairwell. I don’t know why — maybe I was trying to go for help.
The rape kit came back negative for HIV, gonorrhea, chlamydia, syphilis, herpes, and dozens of other things I’d never heard of. God is gracious.
The following month, I was scheduled to work on a cruise ship. I was struck with dysentery on day two. But after not getting better with antibiotics, I was taken to what passes for a hospital when we docked in Cartagena, Colombia. Concerned about intestinal obstruction, I was given an ultrasound. And we saw the pea — my son. Happy Valentine’s Day.
Back on the ship, I told the doctors an abbreviated version of my story, which resulted in me being quarantined. Suicide watch? In danger of a psychotic break that will have me running naked across the shuffleboard courts? Who knows. What I know is that I spent the next week listening to a team of very well-meaning doctors and nurses console me with how “easy” it would be to “take care of it” – to kill the child. To start over. Easy?
There were a lot of things discussed over scratchy, tearful transatlantic phone calls home that week, but the possibility of “taking care of it” never came off my lips. Or my husband’s. When I told him I was pregnant, he said with his voice calm and steady, “Okay. Okay . . . all right . . . this is all right.” I asked him, “What do you MEAN this is all right?” “I mean we can do this. We’ll get through this. It’ll be okay.” And, “I love babies. We’re going to have another baby. Sweetheart, this is a gift. This is something wonderful from something terrible. We can DO this.” And I began to feel the stirrings of joy for the new life in my womb, blossoming under my heart. That new love that would grow so fierce it overwhelmed any trepidation or angst. And my husband was right. We could do it.
On my last morning aboard the ship, I said to this caring team, “If you ever think about this again, if you ever wonder what happened to me — I had a beautiful baby in October 2014.” Their reaction…the looks on their faces…the doctor who had pushed abortion more vehemently than the others — she had tears in her eyes. For the first time, I thought of how God can use this, this nightmare I’d endured. Use me.
I live in North Carolina. My OB who delivered my last two children was running in the Republican primary for U.S. Senate. He talks to people all the time who challenge him with the “What about in cases of rape?” question. What about them? My son will have a voice. Until he can use it, it’s my responsibility — my privilege — to speak for him. That’s my story.
During my pregnancy, I was in and out of the hospital for a couple of months – more in than out. I had preeclampsia, high blood pressure and uncontrolled seizures. It was terrifying at 26 weeks when they admitted me saying they might have to deliver that night — terrifying because I desperately wanted my son to live! We got past that fear. I had strict bed rest, but was home. Every week we made it further was awesome, knowing how glad I’d be once he got here safely in my arms. Emotionally, I was doing very well.
We were working with a really godly team of doctors. It’s just a matter of trusting utterly. This wasn’t new. I’d felt completely out of control since the assault in January — not that “control” is ever anything but an illusion, but, you know. Eight and a half months ago the world upended and hadn’t righted since — until my son was born. It’s not a bad thing. It keeps me on my knees, keeps me from my arrogant, self-reliant “It’s okay, God. I got this” attitude, which I’m so quick to adopt.
Our little boy may have been conceived in violence, but he is a gift from God — a delicious gift that filled the hole in our family that we never realized was there. He made us complete.
I’m so thankful to have been connected to other mothers who became pregnant by rape as well. We are survivors. Not victims. My son has healed me.
The pressure to abort from the medical community was extremely eye-opening to me. So many times I was told how “simple” it would be and how quickly I could just “get on with my life” once it was over. It was heartbreaking to have to repeatedly hear it. Even some friends thought keeping the baby was a mistake — that I wouldn’t be able to handle things emotionally. Every time we, as rape survivor mothers, share our stories, we are strengthened as we strengthen others….And who knows what lives might be spared?
Jennifer Christie is a wife and mother of 5, and a blogger for www.savethe1.com. She’s using her middle name in lieu of her surname in order to protect the identity of her family.
Fish struggle to fertilize eggs three generations after exposure to contraceptive hormone, raising questions about the effects on humans.
by CELESTE MCGOVERN
WASHINGTON — A recent report from the U.S. Geological Survey (USGS) found that birth-control hormones excreted by women, flushed into waterways and eventually into drinking water can also impact fish fertility up to three generations after exposure — raising questions about their effects on humans, who are consuming the drugs without even knowing it in each glass of water they drink.
The survey, published in March in the journal Scientific Reports, looked at the impact of the synthetic hormone 17α-ethinylestradiol (EE2), an ingredient of most contraceptive pills, in the water of Japanese medaka fish during the first week of their development.
While the exposed fish and their immediate offspring appeared unaffected, the second generation of fish struggled to fertilize eggs — with a 30% reduction in fertilization rates — and their embryos were less likely to survive. Even the third generation of fish had 20% impaired fertility and survival rates, though they were never directly exposed to the hormone.
“This study shows that even though endocrine disruptors may not affect the life of the exposed fish, it may negatively affect future generations,” said lead author of the study Ramji Bhandari, a USGS visiting scientist and University of Missouri assistant research professor. “If similar trends were observed in subsequent generations, a severe decline in overall population numbers might be expected by the F4 generation.”
Conducted by scientists at the USGS and the University of Missouri, the research also examined the effect of bisphenol A (BPA), a chemical found in plastics that has been implicated in breast cancer, which was similar to the contraceptive hormone.
The study adds to a growing body of evidence that man-made endocrine-disrupting chemicals — those that affect hormone systems and numerous body functions, including conception — are damaging wildlife, wreaking havoc on reproductive, immunological and nervous systems.
Widespread Contamination
Scientists have known for more than 15 years that humans are excreting their prescription drugs into American sewers and that water-purification systems are not equipped to filter the chemical effluents from drugs, including anything from birth-control pills and painkillers to psychiatric medicines.
In a landmark 1999-2000 USGS survey, 80% of water samples from 139 American rivers and streams in 30 states were found to be contaminated with drugs, ranging from antibiotics and antidepressants to contraceptives and hormone replacements.
But scientists are particularly concerned about the contraceptive chemical EE2 because of its ability to “feminize” male fishes and its association with plummeting fish fertility. A landmark 2007 study, for example, described a seven-year whole-lake experiment in northern Ontario, Canada, in which tiny amounts of EE2 induced “intersex” male minnows whose testicles contained eggs, as well as altered egg production in female fishes; this ultimately resulted in the “near extinction” of the species from the lake, as well as a threat to larger fish populations.
Numerous subsequent studies across the globe have linked birth-control hormones to impaired fertility, “transgender fish” and reduced fish populations. Minnesota pollution researchers looking for the endocrine disruptors found them even in remote lakes thought to be pristine; and when they lowered cages of male lab minnows into the lakes, most of them were feminized within three weeks.
By 2009, USGS scientists found that one-third of 111 American waterways they tested contained some intersex fish, particularly male bass. A year later, scientists were reporting that 80% of the fish in the Potomac River — whose water is pumped into the homes of 4 million people — showed “intersex” features.
Mammals Affected Too
The impact of EE2 has been demonstrated experimentally in mammals as well. In one 2009 study, for example, newborn rats exposed to the hormone in the first days of life developed small and abnormal penises and lowered sperm counts, and they struggled to reproduce.
The researchers compared EE2’s effects to those of diethylstilbestrol (DES) — a notorious endocrine-disrupting chemical given to pregnant women to prevent miscarriage. The women themselves had an elevated risk of breast cancer, but it was their children who developed rare vaginal and testicular cancers and other reproductive anomalies after they reached puberty; and those children were 40 times more likely to be sterile.
It’s a comparison that the current Scientific Reports study researchers make as well.
“EE2 use during pregnancy can cause the same type of disruption of development that the drug DES caused in millions of offspring of women given this drug during the 1940s to 1970, when it was banned for use during pregnancy,” Frederick vom Saal, professor in the Division of Biological Sciences at the University of Missouri and one of the authors of the study of medaka fish, told the Register.
“Also, male reproductive organs are sensitive to estrogens, which interfere with normal function — estrogens have a contraceptive effect in males.” EE2 has also been linked to testicular tumors.
Toxicologists have dismissed the comparisons of EE2 in the water supply to DES because the DES exposures were in larger doses. However, tiny doses of hormones can produce large effects.
“That this is considered controversial by toxicologists is considered laughable by endocrinologists,” said vom Saal. “EE2 can cause effects in human tissues at concentrations in blood below one part per trillion, so this is an extremely potent drug.”
The Canadian lake study, for example, saw near extinction of a fish species with EE2 given in “environmentally relevant” doses of five parts per trillion — the equivalent of five drops in 20 Olympic-size swimming pools.
Unabsorbed Contraceptives
About 50 million women worldwide are taking contraceptive pills, and it is the leading form of birth control in the U.S., consumed by about 10.5 million women annually, according to the Guttmacher Institute. Up to 68% of the contraceptive drugs being consumed are not absorbed, but excreted into sewage systems, according to the USGS study.
And according to one 2009 study of loss of fertility in rats due to EE2, about 3%- to 4% of women continue to take birth control inadvertently in the first trimester of pregnancy, raising concerns about their babies’ early exposure to endocrine disruptors, though it’s impossible to say how many babies and children are inadvertently exposed through drinking water and to what doses or what impact the hormones are having on adults, if any.
With unexplained soaring incidences of testicular cancer, infertility, childhood “gender dysphoria” in increasingly young children, who are confused about their sexual identity, and plummeting sperm counts, some scientists are asking if the fish in the study are like miners’ canaries: They are warning of a problem that has not yet been fully realized.
“Beyond the aquatic environment, the feminizing syndromes found in wildlife appeared to mirror reports of male infertility, genital abnormalities and testicular cancer observed in the human male population, collectively termed Testicular Dysgenesis Syndrome,” recounted Susan Jobling, director of the Institute of Environment, Health and Societies at Brunel University, London, in a 2013 paper for the European Environment Agency.
But in the absence of public awareness and outcry, little has been done about the problem in the U.S. or elsewhere. As long ago as 2004 the Environment Agency of England and Wales had accepted the evidence of the environmental harm from EE2 as significant enough to warrant consideration of risk management, Jobling recounted.
In 2012, the European Commission proposed to regulate EE2 as a European Union-wide “priority substance” for legislation, but the proposal was later amended — mostly due to a consideration of the cost of removing trace amounts of chemicals from water — and a decision on a regulatory “environmental quality standard” was delayed until at least 2016.
Evidence Ignored
The Catholic Church has always taught that pharmaceutical contraception to prevent pregnancy is “intrinsically evil” and “contrary to the good of the transmission of life” (Vade Mecum for Confessors 2:4, Feb. 12, 1997), even without considering its effects on the environment or public health.
The effects of BPA from plastics are well recognized, but the impact of birth control on the environment and fertility has been downplayed and dismissed — a reaction vom Saal thinks is not based on science. “Clear evidence for equal potency is ignored by the industry,” he said.
“It’s strange how even the most ardent environmentalists suddenly go silent when confronted with evidence of how birth-control pills harm aquatic ecosystems. Instead of angry calls for the regulation of a pollutant that is causing a ‘silent spring’ of hermaphroditic fish unable to breed, we hear nothing,” said Steven Mosher, president of the Population Research Institute. “The barren left is so wedded to contracepted sex that they will brook no criticism of the means they use to ensure their sterility, even though, as the science shows, they sterilize other species in the process. Environmentalism meets the sexual revolution, and the sexual revolution wins.”
Virginity gets very little press or screen time these days and that’s a shame. As a new American study confirms, a woman who enters marriage as a virgin has the best chance of still being married five years later – and probably beyond that. In fact, the odds of her marriage lasting have got better over the last 30 years, as divorce rates for such women have dropped from 11 percent in the 1980s to 6 percent in the 2000s.
The likely reason for that, says the author of the study, University of Utah sociologist Nicholas H. Wolfinger, is religion –that other uncool topic. His data, taken from three waves of the National Survey of Family Growth, shows that women who marry as virgins are far more likely to attend church at least once a week. Sadly, there are fewer and fewer of them. Four decades ago 21 percent of brides had no previous sexual partner, but by 2010 that figure had dropped to 5 percent, representing the most religious women.
(By now you may be asking, Hey, what about the men? Wolfinger explains that “the NSFG doesn’t have full data on men’s premarital sexual behaviour, and in any event they recall their own marital histories less reliably than do women.”)
As you might expect, the next most likely to last marriages are those of women who have had only one sex partner previously – in most cases their future husbands. Their numbers, however, have dropped from 43 percent in the 1970s to 22 percent in the current decade.
Source: NSFG, 2002-2013
The stats for the 1970s may surprise us, as they did Wolfinger. Even though the sexual revolution was well under way, he notes, almost two-thirds of brides had at most one sexual partner before getting married.
“Even in the 1980s, slightly over half of women had a maximum of one sex partner before walking down the aisle. Things looked very different at the start of the new millennium.”
By the 2010s,the number of brides who had had multiple sexual partners had climbed significantly. Those who’d had 10 or more partners had gone from 2 percent to 18 percent. As you would expect, this group has the highest five-year divorce rates – but only since the 2000s. Prior to that, women with two partners prior to marriage had the highest divorce rates – around 30 percent – compared to those with more partners.
This again is surprising, Wolfinger admits. He suggests a couple of reasons:
* Women with two previous partners may already have a child from another relationship when they marry, and this is known to have a “profound negative effect on marital happiness” as well as carry a higher risk of divorce.
* “Over-emphasised comparisons”:
“In most cases, a woman’s two premarital sex partners include her future husband and one other man. That second sex partner is first-hand proof of a sexual alternative to one’s husband. These sexual experiences convince women that sex outside of wedlock is indeed a possibility. The man involved was likely to have become a partner in the course of a serious relationship—women inclined to hook up will have had more than two premarital partners—thereby emphasizing the seriousness of the alternative. Of course, women learn about the viability of nonmarital sex if they have multiple premarital partners, but with multiple partners, each one represents a smaller part of a woman’s sexual and romantic biography. Having two partners may lead to uncertainty, but having a few more apparently leads to greater clarity about the right man to marry. The odds of divorce are lowest with zero or one premarital partners, but otherwise sowing one’s oats seems compatible with having a lasting marriage.”
Well, lasting five years, at least. But this ceases to be the case (statistically) beyond 10 partners: “a lot of partners means a lot of baggage, which makes a stable marriage less tenable.” Wolfinger speculates further about whether this correlation is true or spurious, and notes that the difference between this group and the women with two premarital partners when it comes to divorce is not significant.
Bottom line, however: “The odds of divorce are lowest with zero or one premarital partners.”
Finally, Wolfinger notes that these findings remain substantially true after controlling for the effects of other social and demographic characteristics of women. Some of these factors, however, explained more than others:
“Aside from religion, race and family of origin accounted for the largest portion of the sexual partners/divorce relationship. Caucasian and African American women had similar premarital sexual behavior, but Latinas and members of the “Other” population group had notably fewer sex partners and lower divorce rates than either whites or blacks. Similarly, people who grew up without both parents had more partners and divorced more. Detailed psychometric data would be necessary to further explain the relationship between numbers of sex partners and marital stability.”
Perhaps one could conclude that the race factor is itself largely explained by family structure. It makes sense that coming from an intact family gives a person some protection against divorce. And religious practice makes that protection even stronger. That is not surprising, even if other aspects of the study are.
Michael Cook Jun 15, 2016 | 11:45AM Brussels, Belgium
Since 2005 about 40 people in Belgium and the Netherlands have successfully combined euthanasia with organ donation, according to an article in the Journal of Medical Ethics by ethicists and transplant specialists.
The [five] doctors are so enthusiastic about the procedure that they have proposed legal changes which will speed up the procedure and maximize the number of donations. Although the numbers are still low, the idea is becoming more popular in both countries, according to the authors.
(Not everyone – in fact, only a small proportion – of people who request euthanasia are potential organ donors. Most requests come from patients with cancer, which makes them unsuitable donors. Most of the Belgians who have already participated in the programme appear to have suffered from strokes or multiple sclerosis.)
However there are some legal and ethical wrinkles to be ironed out to make the transition from euthanasia to organ donation seamless.
Some regulations and laws are supposed to be safeguards, but they “slow” the procedure down. For example, in the Netherlands, euthanasia is not regarded as a natural death and so permission must be sought from the public prosecutor to dispose of the body. In Belgium (where euthanasia is regarded as “natural”), three doctors need to sign off on the procedure. …
Another consideration is whether informing euthanasia patients about organ donation puts pressure on them to agree. The authors believe that it doesn’t, provided that it is done tactfully.
According to the principles of the Hippocratic Oath, the authors argue, doctors may even have an obligation to inform patients because they will be saving lives of organ recipients. They also point out that “The patient could be very relieved discovering the existence of this option and receiving the possibility to give meaning to his or her own suffering, by potentially relieving the suffering of others.”
Until now, transplant protocols have specified a strict separation between organ donation and euthanasia. However, if the patient is [willing], this is not necessary. “As long as all due diligence requirements are fulfilled, it should not be an obstacle if euthanasia and donation are not fully separated,” the authors argue.
Finally, the “dead donor” rule is frustratingly inconvenient for organ donor euthanasia. Since the patient has chosen to die anyway, why shouldn’t it be possible, the authors argue, to have “a ‘heart-beating organ donation euthanasia’ where a patient is sedated, after which his organs are being removed, causing death”?
The authors conclude:
“Combining euthanasia and organ donation in a so-called ‘donation after circulatory death’ procedure seems feasible on legal, ethical or medical grounds, and is increasingly gaining social acceptance in both Belgium and the Netherlands. Since current legislation does not specifically focus on the—when drafted unpractised—combination, future redrafting may be necessary in perspective of the contemporary developments regarding occurrence of such combined procedures”
LifeNews Note: Michael Cook is editor of MercatorNet where this story appeared.
CHICAGO, June 13, 2016 (LifeSiteNews) – Catholics are not alone in holding that birth control is a sin against God.
Father Patrick Henry Reardon, pastor of All Saints Antiochian Orthodox Christian Church in Chicago, who’s also an author and senior editor for the Christian magazine Touchstone, spoke in a recently published YouTube video of how throughout history until the 20th century all Christians, not just the Orthodox, but the Church fathers and Protestants as well, regarded birth control use as immoral and a sin.
“Now it’s lost,” he states in the video. “And the Church really must not go with the flow on this matter. Because this really is an insult to God.”
Watch Father Reardon deliver his sound message with clarity on God’s gift of life and the consequences of separating procreation with the marital act:
Woe to those who call evil good and good evil, who put darkness for light and light for darkness, who put bitter for sweet and sweet for bitter! (Isaiah 5:20)
How much more bizarre can our society get? It’s a question that many have been asking for a long time, but these days it’s hard to keep up with the answers, which change hourly.
In Alaska, a boy who thinks he’s a girl is allowed to participate in the girls’ track meet, and he wins. The girls are not happy, but are not quite sure how to express their protest since they don’t want to be branded as bigots for calling a boy a boy when that boy wants to be called a girl.
There are a growing number of reports that the man formerly known as Bruce Jenner, who now goes by the name “Caitlyn,” is having second thoughts about “transitioning” to womanhood and is contemplating returning to identifying himself as what he still actually is, a man. This regret is actually common for people who adopt the appearance and lifestyle of the opposite sex. These reports have not been confirmed, but were this to occur, does anyone really think that the fascistic LGBT movement will support such a transition?
A famous homosexual couple has adopted children (apparently two men cannot naturally conceive a child) and projected a carefully cultivated image as a “happily” “married” couple with the help of media who desperately want to tell such a story. Yet as it turns out, their private lives are more sordid than the story allows, and the couple is suing to silence media who would report certain ugly and inconvenient facts, so that their adopted children would be spared the pain of knowing what their adoptive parents actually do.
The idea that the LGBTQQ… movement is about to implode has been discussed recently, and there are signs of sanity coming from progressives who have been supportive of the movement but are starting to recognize its totalitarian and anti-human nature. Better late than never, I suppose.
How much more bizarre can it get? I’m not sure the question is meaningful anymore, since all bets are off. There are many conversations going on about how we arrived here, with a great deal of interesting histories of cultural Marxism, Communism, feminism, and other anti-Christian ideologies whose goal has been to “liberate” men and woman from the oppression of religion, marriage, traditional roles of men and women, etc.
I’m not sure the girls in Alaska, Mr. Jenner, or the famous couple and their children feel all that liberated.
When your revolution is based on a lie, it will certainly fall, but it can do a lot of damage to nations, lives and souls before it does. We “got here” because we turned our backs on God. We happen to be living through a deluge of degradation almost unimaginable even a few years ago.
Except that the Church did imagine this collapse. Specifically, Cardinal Ratzinger, later Pope Benedict XVI, said something that could have been written yesterday, in 1984’s The Ratzinger Report (summarized by Christopher West):
What we are living through in our day is the result of an ideology that has completely severed body and soul. And that’s the very definition of death. Barring a divine intervention, we must now endure the full consequences of the “uprooting of the human person in the depth of his nature” – an uprooting that stems from the fact that “sex has remained without a locus and has lost its point of reference” since the cultural embrace of contraception (The Ratzinger Report, p. 84).
By detaching sex from procreation, the essential meaning and natural orientation of the gender distinction is lost and one’s sex is eventually “viewed as a simple role, interchangeable at one’s pleasure,” Ratzinger observed. From there, people end up demanding the right of “escaping from the ‘slavery of nature,’ demanding the right to be male or female at one’s will or pleasure” (p. 95).
Call this an update of Humanae vitae 17, in which Blessed Pope Paul VI famously predicted — against the spirit of the age — that the wide embrace of contraception would have a host of negative consequences. Those who dismissed Pope Paul, and later Cardinal Ratzinger, simply couldn’t imagine what we are actually seeing happen today, when we call evil good, and good, evil. When we don’t know God, how can we know ourselves?
I love serving a Church that knows the true nature of man and woman because she knows the One in whose image we are made. I love serving a Church that knows what is true and good, a Church that knows Christ because she was founded by Him. I am grateful for her social and moral doctrine, which are rooted in Holy Scripture, and offer true liberation by guiding all people of good will to live in love and truth.
If you are looking around for a rock to hold onto as the flood waters rise and currents seem to pull you away, know that you have it in the One, Holy, Catholic Church. Avail yourself of God’s mercy in the Sacrament of Penance and in His body and blood, soul and divinity in the Blessed Sacrament. Choose from among the many devotions available to the faithful and make your faith central to your life, and invite others to do the same. Be an example of joyful and intelligent faith, and a source of strength for your family and all whom you meet.
Don’t be afraid! Live with courage, faith, hope and love.
June 10, 2016 (LiveActionNews) — Estudiantes De Caracas, a professional soccer team in Venezuela, wanted to encourage parents to enroll their children in their soccer academy, so they created the first ever soccer game to be played by preborn children.
The dads were on hand to watch the game and the parents celebrated the kicks and goals with cheers and excitement. They also showed disappointment when the other team scored. Estudiantes De Caracas calls it “the first football match played by kids who haven’t been born, yet.” And you can tell by the expressions on the parents’ faces that they are just as excited by this game as any game played by a child already born.
While babies are active through all nine months of pregnancy, right around the 20th week is when those kicks can be better felt to the mother and anyone who touches her belly. That makes the 28th week a great time to put these kicks to fun use, highlighting the humanity of the preborn – and what the team calls “the next generation of footballers.”
Preborn children the same age as the children in this video are targeted for abortion in this country, and groups like Planned Parenthood intend to keep the killing going. States across the country are moving to ban abortion after 20 weeks gestation based on the viability of children this age, as well as their ability to feel pain.
WASHINGTON, D.C., June 7, 2016 (LifeSiteNews) – Senate Democrats have introduced a bill that would impose crushing fines on pharmacists who refuse to personally dispense “emergency contraception,” a potential abortifacient, removing conscience protections from the law.
The “Access to Birth Control Act” (S. 2960), introduced on May 19 by Sen. Cory Booker of New Jersey, would require pharmacists to provide “any drug or device approved by the Food and Drug Administration to prevent pregnancy.”
But the bill’s text specifically mentions “emergency contraception” – which often refers to Plan B, the “morning after pill,” or Ella, the “week after pill.”
The text specifically states that the Religious Freedom Restoration Act does not apply.
“Access to legal contraception is a protected fundamental right in the United States and should not be impeded by one individual’s personal beliefs,” the bill states.
Violators will be fined $1,000 a day, or up to $100,000 “for all violations adjudicated in a single proceeding,” according to the bill.
Emergency contraception may act to prevent fertilization, but it also acts to make the uterine lining inhospitable and sometimes prevents a newly conceived child from implanting in the womb.
While the Roman Catholic Church teaches that all contraceptive use constitutes a grave sin, evangelical Protestants object to providing any form of potentially abortifacient device. A 2014 study conducted by the Charlotte Lozier Institute found that all forms of emergency contraception has the potential to cause an early chemical abortion. Plan B is more likely to induce an abortion than to prevent conception, according to a 2015 analysis co-authored by Dr. Christopher Kahlenborn for the Linacre Review.
A pharmacist may only refuse to fill a prescription based on his “professional clinical judgment,” not due to religious conviction.
If the customer’s preferred method is not in stock and the customer refuses to take a referral to another pharmacy (which is also mandatory for druggists per the bill), the pharmacist would be required to order it through “expedited ordering.”
A similar law in Washington state is being contested in court.
“No one should be forced out of her profession solely because of her religious beliefs,” said Luke Goodrich, deputy general counsel of the Becket Fund for Religious Liberty, the group challenging the statute.
But lawmakers seem unmoved by appeals to conscience. “A pharmacist is free in their own life to live the way they want,” Sen. Tim Kaine, D-VA, told local media.
Some pro-life advocates warn that pharmacists are all-too-eager to dispense Plan B, which is available without a prescription. Students for Life of America released a video showing a pharmacist selling the morning after pill to an adult male who said he was using the drug to cover up statutory rape.
Judie Brown, president of the American Life League, blamed the bill on cultural degeneration. “We live in an age when sex is a god and respect for religious liberty is gasping for its final breath,” Brown, who lives in Virginia, told LifeSiteNews. “Given these two facts we are not at all shocked that the infamous pro-abortion U. S. Senator Tim Kaine would find it perhaps obligatory to assault the conscience rights of pharmacists who put good health and ethics before political correctness.”
The bill, which has 18 Democratic co-sponsors, has been assigned to the Senate Health, Education, Labor, and Pensions Committee.
In December, the new Polish Government[1] decided to terminate State funding of the in-vitro fertilisation (IVF) programme with effect from mid-2016 (cf. Poland: the government announces cessation of IVF reimbursement). The Health Minister, Konstanty Radziwill, completed this announcement: He wishes to integrate a “national programme for procreation”. It will suggest NaProTech solutions “that don’t provoke as much controversy as in vitro fertilisation.
During a press conference, the Polish Health Minister gave more details concerning his projects: diagnosis, treatment of infertility, as well as preventive measures will be funded within the new programme announced. “Treating infertility cannot be limited to IVF, the government must be able to suggest other solutions, and fund them equally”. Konstanty Radziwill used the word “abuse” to qualify the fact of suggesting IVF to infertile couples without looking for the cause of their infertility. He wishes to develop NaProTech which is not only less expensive[2] and simpler but also more effective without bringing up ethical issues.
Short for Natural Procreative Technology, NaProTech was developed by the American Professor Thomas W. Hilgers, obstetrician-gynaecologist, specialist in reproductive medicine. While medically assisted fertilisation avoids the causes of infertility, NaProTech looks at treating the underlying causes of infertility and offers results that speak for themselves: women of about 35 years old who have been trying to conceive a child for 5 years have a probability of success between 40% and 50% thanks to this method. For couples experiencing repeated miscarriages, 80% can hope to carry their pregnancy to term.
[1] Elected in October 2015.
[2] The Minister for Health reminded the people that in Ireland, Slovenia, and Luxemburg IVF procedures are not reimbursed, although “these countries are richer than Poland”.
June 6, 2016 (LifeSiteNews) – A study conducted by one of the pioneers of natural family planning found that there are inexpensive, highly effective ways for couples to achieve pregnancy without artificial fertility treatments.
Mercedes Wilson, a fertility expert and the president and founder of Family of the Americas, conducted the study, called Natural, Scientific and Highly Effective Treatment for Infertility, with Family of the Americas staff. Wilson has presented the study’s findings at medical conferences and the Pontifical Academy for Life, of which she is a member.
The study was conducted from January 2010 to April 2014 and outlines the effectiveness and simplicity of what Wilson calls the Ovulation Method, which teaches women to recognize natural indicators of their fertility in order to achieve or avoid pregnancy. Wilson’s study found that an overwhelming 90.74 percent of couples struggling to conceive who used her method, which emphasizes nutrition and a holistic approach to the woman’s health, were able to achieve pregnancy.
Wilson studied 54 couples whose struggles with infertility ranged anywhere from 1-12 years. Over the course of just over four years, 50 of the couples achieved pregnancy. The study stresses that the methods it used are essentially free and easy to learn, making them ideal for couples with limited financial resources. The only cost to the method is its educational component.
By contrast, In Vitro Fertilization (IVF), an artificial method of combining egg and sperm in a Petri dish to create an embryo and then implanting it into the mother’s uterus, has a success rate of anywhere from 20 to 40 percent. IVF typically costs upwards of $15,000 per cycle. The procedure frequently results in the destruction of “extra,” unwanted human embryos or selective abortion if a woman becomes pregnant with multiple babies.
Natural, Scientific and Highly Effective Treatment for Infertility detailed how the Ovulation Method of natural family planning has been successful in helping couples conceive despite their sometimes past use of artificial contraception.
“Couples from low income brackets, particularly in the cities of poor nations around the world are not informed of the serious side effects of artificial methods of birth control, and its abortifacient effect,” the study notes. Low-income women are frequently pressured into using artificial contraception, the study says, which results in health problems and fertility issues.
One 33-year-old woman was “given the three month Depo-Provena injection after miscarriages, an unfortunate medical procedure.” The contraceptive injection caused her to bleed for 23 days. After taking vitamins and maintaining good nutritional intake, she ultimately was able to conceive and deliver a baby girl.
“Because the poor are humble, they are afraid to question the recommendation of the doctors who often do not instruct them on the serious side effects of such dangerous hormonal chemicals of birth control,” the study noted.
Another woman who had had one miscarriage and had never used artificial birth control was able to regulate her cycle by taking vitamins. She also conceived and delivered a baby.
The study outlines the positive effects on fertility that nutrition and decreased stress can have. Many times women who are overweight, underweight, excessively exercise, or excessively work have difficulty conceiving, the study said, and teaching them to naturally improve their health and monitor their bodies for signs of fertility is sometimes all that is necessary for them to conceive.
Although the study is small and will likely need to be replicated in order to solidify its authority to the medical community, the authors say it shows that artificial reproductive technologies and hormonal contraceptives are not the all-encompassing solution to infertility.
Once again common sense has been turned on its head in our culture, this time by transgender activists agitating for people to be able to use the bathroom that they feel corresponds emotionally to their self-identified gender rather than the anatomical gender of their biological sex. The issue has emerged prominently in recent national and local news.
In North Carolina, in response to an ordinance adopted in Charlotte that would have allowed transgender people to use whatever bathroom they wanted, the state legislature passed a law in March blocking local governments from enacting rules that grant such privileges to transgender people. A similar law recently passed in Mississippi allows people to withhold services from lesbian, gay, bisexual and transgender individuals on religious grounds. In response, President Barack Obama has said that these laws in North Carolina and Mississippi are “wrong” and “should be overturned.” The Obama administration used the Department of Justice to warn the state of North Carolina that its new law limiting bathroom access violated the civil rights of transgender people.
Here in Illinois, in response to a federal complaint, the Palatine-Schaumburg High School District 211 in suburban Chicago earlier this year granted a transgender student, who was born male but identifies as female, limited access to the girls locker room at Fremd High School. Similarly, a transgender student at a Wheaton Warrenville Unit District 200 school has been granted access to a locker room designated for the opposite sex. The Chicago Public Schools have announced that their students, teachers and staff could use whichever restroom matches their self-selected gender identity.
Nearby in central Illinois, a transgender student at Williamsville High School who was born with female anatomy but identifies as a male recently resolved a complaint filed in October with the Illinois Department of Human Rights. The school had previously provided a private bathroom for the transgender student, who complained that this was unacceptable, saying, “It made me feel like I was being treated differently and ostracized.” So now all transgender students at Williamsville High School will have access to the restroom and locker room facilities of the gender they identify with emotionally, not the biological gender that they were born with.
Earlier this month, a group of Illinois students and parents sued the Obama administration over its stance on transgender students’ access to school bathrooms and locker rooms, arguing that the U.S. Department of Education is illegally forcing local authorities to let children use facilities that correspond to their subjectively chosen gender identity. The complaint alleges that the federal government has violated students’ fundamental right to privacy and parents’ constitutional right to instill moral standards and values in their children.
The transgender activists would have you believe that their politically correct ideology is based on science; however, the American College of Pediatricians has pointed out that transgenderism is classified as a mental illness and therefore has warned legislators and educators that conditioning children to accept transgenderism as normal is child abuse. They advised, “When an otherwise healthy biological boy believes he is a girl, or an otherwise healthy biological girl believes she is a boy, an objective psychological problem exists that lies in the mind, not the body, and it should be treated as such.”
Dr. Paul McHugh, psychiatrist-in-chief at Johns Hopkins Hospital, was so concerned about the psychological origins of gender-identity disorder that he halted the practice of sex-reassignment surgery at his institution. He concluded that the research demonstrated that Johns Hopkins should no longer participate in what he called “unusual and radical treatment” for “mental disorders.”
The Catholic Church has some clear teachings on transgender issues. Catholics are called to treat everyone with compassion. Yet the church maintains that people may not change what Pope Benedict XVI called “their very essence.” In a speech at the Vatican on Dec. 23, 2008, Benedict directly addressed transgender issues by cautioning Catholics about “destroying the very essence of the human creature through manipulating their God-given gender to suit their sexual choices.”
Similarly, in his encyclical Laudato Si, issued last year on the environment, Pope Francis called for men and women to acknowledge their bodies as a gift from God which should not be manipulated. “The acceptance of our bodies as God’s gift is vital for welcoming and accepting the entire world as a gift from the Father and our common home,” the pope wrote, “whereas thinking that we enjoy absolute power over our own bodies turns, often subtly, into thinking that we enjoy absolute power over creation” (no. 155).
In his recent apostolic exhortation Amoris Laetitia (The Joy of Love), Pope Francis warns that gender ideology “denies the difference and reciprocity in nature of a man and a woman and envisages a society without sexual differences … It is one thing to be understanding of human weakness and the complexities of life, and another to accept ideologies that attempt to sunder what are inseparable aspects of reality. Let us not fall into the sin of trying to replace the Creator. We are creatures, and not omnipotent. Creation is prior to us and must be received as a gift. At the same time, we are called to protect our humanity, and this means, in the first place, accepting it and respecting it as it was created” (no. 56).
Here in the Diocese of Springfield in Illinois, we ask that people respect these teachings of the Catholic Church in their use of facilities in our churches and schools. People who are confused about their gender identity — especially children and adolescents — should be treated with compassion and provided counseling rather than being further confused by activists promoting their political ideology.
Bishop James Conley, Lincoln Nebraska, Tuesday, 17 May 2016
On Friday, May 13, the U.S. Department of Education and Department of Justice issued a joint instruction, which they called “significant guidance,” to public school districts across the country. The guidance stated that in order to receive federal funds for education, every public school district must provide services, restrooms, and “equal access” to all students according to their stated gender identity.
The federal government has ordered that when any student and his parents tell the school that his “gender identity” has changed—if he was born a boy, for example, but considers himself a girl—the school must treat him, in every possible way, like an actual girl. The government declared that the boy who says he is a girl must be permitted to change in locker rooms with girls, to stay in girls’ rooms on overnight trips, and, very often, to participate on girls’ sports teams.
This “guidance” is deeply disturbing. In fact, the administration’s action is simply wrong. It is wrong to deny the fundamental difference between men and women; and to teach children that our identity, at its very core, is arbitrary and self-determined. God created us male and female, and policies like this deny the basic beauty of God’s creation.
Boethius, the 6th century Roman senator and Christian philosopher, was a thoughtful critic of disturbing trends he saw in Roman society. In his classic work, the Consolation of Philosophy, Boethius criticized those evil spirits “who slay the rich and fruitful harvest of Reason with the barren thorns of Passion. They habituate men to their sickness of mind instead of curing them.”
We are living in a time when ordinary human reason is quickly being replaced by “the barren thorns of passion.” Our entire culture has been caught up in a kind of sentimentalized and relativized tyranny of tolerance: we vilify and condemn, ever more quickly, any sense of reasonable and ordered social policy. We have a vague sense that endorsing certain fashionable kinds of social and emotional disorders—including transgenderism—is a mandate of justice, or a victory for civil rights.
But the real victims of our culture of relativism are those who suffer from serious problems, and who need compassionate help. Pathological confusion about one’s own identity is a kind of illness. It brings tremendous personal and emotional difficulties. Transgenderism cries out for compassionate assistance. Pope Francis says that “acceptance of our bodies as God’s gift is vital,” and “valuing one’s own body in its femininity or masculinity is necessary” for authentic human freedom.
But, as Boethius wrote, we “habituate men to their sickness, instead of curing them.”
Children and parents in very difficult situations deserve compassion, sensitivity, and respect. The Church will continue to make every effort to assist those suffering gender dysphoria; in fact, we can improve our efforts in this regard in many ways. But the Church will not deny that God created us male and female. We will not confuse respect and compassion with capitulation to a tragic delusion. Our Catholic schools will continue to teach and live the truth, because of our care for every student. We can only help students grow in holiness when we help them to live in accord with the truth. We will continue to do that, no matter the cost.
The Obama administration’s directive is a sign of the brokenness of our culture; of our lost sense of the common good, of individual goodness, of true freedom, real rights, and authentic happiness. Nebraska’s Governor Pete Ricketts pointed out earlier this week that this directive is basically a kind of coercive opinion, which does not enjoy the authority of law. It is a form of bullying and, ultimately, it is a sad sign of how much we have lost our way; how little of the Gospel’s good news forms and shapes our culture.
This directive is a sign of a great tragedy. We are living in an atheocracy: a society determined to stamp out every vestige of God’s plan for mercy, and justice, and goodness. We are living in a society ensnared by the evil of relativism, to which human flourishing, in this life and the next, poses a threat.
The Gospel is a threat to the forces of this world. And in such a circumstance, there is a great temptation, for all of us, to withdraw into our families, into our Catholic community, into those places which we believe are safe, places in which we think we might be spared from the evil of this world.
But facing an evil world, Boethius wrote that “it is time for healing, not lamenting.” Boethius was right. Our culture is in need of healing. The victims of relativism’s dictatorship—those who are harmed by false compassion and tolerance for evil—need our help. Only we can be the leaders who stand up in the face of the storms. The Lord calls us to leadership, and so do the victims of the culture of death.
We are called to stand up—right now, we must be committed to carrying the healing mercy of Jesus Christ to this world. And the fight is not easy. We will not likely fight on a battlefield, in a glamorous blaze of glory. Instead we fight by claiming our nation for Christ, by forming Catholic culture that welcomes others to real freedom, by speaking—heart to heart—with those who are in need of Christ’s healing. We fight evil by praying, and hoping, to win every heart, every soul, every life, for Jesus Christ; as missionaries and disciples of mercy.
We also fight evil on our knees. We fight evil through the intercession of the Blessed Virgin Mary. We fight evil by invoking St. Michael the Archangel. We fight evil by consecrating our nation to the Sacred Heart of Jesus, the fount of true mercy, and true peace.
All of us can read the signs of the times. We are living through a great trial and a great tragedy. Real people, about whom we care very much, are gravely harmed by the infiltration of evil in our world. We know that Christ will be victorious in the end. But we also know how urgently Christ is needed in this world. Only we can entrust this nation to Jesus Christ—especially his Sacred Heart—in our prayers. And only we can choose, in response to the urgency of the moment, to be active, joyful, faithful missionaries of Jesus Christ—declaring the Gospel, and inviting the world to mercy.
We live in a grave and serious time in history. But now is time for healing, not for lamenting.
By Cardinal Robert Sarah, Prefect of the Congregation for Divine Worship and the Discipline of the Sacraments, June 15, 2015
Fifty years after its promulgation by Pope Paul VI, will the Second Vatican Council’s Constitution on the Sacred Liturgy finally be read? Sacrosanctum Concilium is actually not just a catalogue of “recipes” for reform, but a veritable Magna Carta of all liturgical action.
In it the Ecumenical Council gives us a magisterial lesson in methodology. Indeed, far from being content with a disciplinary, external approach to the liturgy, the Council wishes to have us contemplate what it is in its essence. The Church’s practice always results from what she receives and contemplates in revelation. Pastoral ministry cannot be detached from doctrine.
In the Church “action is directed to contemplation” (cf. no. 2). The conciliar Constitution invites us to rediscover the Trinitarian origin of the liturgical work. Indeed, the Council determines that there is a continuity between the mission of Christ the Redeemer and the liturgical mission of the Church. “Just as Christ was sent by the Father, so also He sent the apostles,” so that “by means of sacrifice and sacraments, around which the entire liturgical life revolves” they might “accomplish the work of salvation” (no. 6).
Carrying out the liturgy therefore is the same as accomplishing the work of Christ. The liturgy is essentially “actio Christi”: “the work of Christ the Lord in redeeming mankind and giving perfect glory to God” (no. 5). He is the great high priest, the true subject, the true protagonist of the liturgy (cf. no. 7). If this vitally important principle is not accepted in faith, we run the risk of making the liturgy a human work, the community’s celebration of itself.
On the contrary, the Church’s real work is to enter into Christ’s action, to join in the work for which He has been commissioned by the Father. Therefore “the fullness of divine worship was given to us,” because “His humanity, united with the person of the Word, was the instrument of our salvation” (no. 5). The Church, the Body of Christ, must therefore become in turn an instrument in the hands of the Word.
This is the ultimate meaning of the key concept of the conciliar Constitution: “participatio actuosa”. For the Church, this participation consists of becoming the instrument of Christ the Priest, for the purpose of participating in His Trinitarian mission. The Church actively participates in Christ’s liturgical work insofar as she is the instrument thereof. In this sense, language about the “celebrating community” has its ambiguities and requires true caution (cf. the Instruction Redemptoris sacramentum, no. 42). Therefore this “participatio actuosa” should not be understood as the need to do something. On this point the Council’s teaching has often been distorted. Instead it is a matter of letting Christ take us and associate us with His sacrifice.
Liturgical “participatio” must therefore be understood as a grace from Christ who “always associates the Church with Himself” (Sacrosanctum Concilium, 7). He is the one who has the initiative and the primacy. The Church “calls to her Lord, and through Him offers worship to the Eternal Father” (no. 7).
The priest must therefore become this instrument that allows Christ to shine through. As our Holy Father Pope Francis recalled recently, the celebrant is not the host of a show, he must not look for sympathy from the assembly by setting himself in front of it as its main speaker. To enter into the spirit of the Council means, on the contrary, to be self-effacing, to refuse to be the center of attention.
Contrary to what has sometimes been maintained, and quite in keeping with the conciliar Constitution, it is altogether appropriate, during the penitential rite, the singing of the Gloria, the orations and the Eucharistic prayer, that everyone, priest and faithful, turn together toward the East, so as to express their intention to participate in the work of worship and redemption accomplished by Christ. This way of celebrating could possibly be implemented in cathedrals, where the liturgical life must be exemplary (cf. no. 41).
Of course, there are other parts of the Mass in which the priest, acting “in persona Christi Capitis” [“in the person of Christ the Head”] enters into a nuptial dialogue with the assembly. But the only purpose of this face-to-face is to lead to a tête-À-tête with God which, through the grace of the Holy Spirit, will become a heart-to-heart conversation. The Council thus proposes other means of promoting participation: “acclamations, responses, psalmody, antiphons, and songs, as well as by actions, gestures, and bodily attitudes” (no. 30).
An over-hasty and all-too-human interpretation has led some to conclude that it was necessary to make sure that the faithful were constantly busy. The contemporary Western mentality, shaped by technology and fascinated by the media, tried to make the liturgy a work of effective, rewarding instruction. In this spirit, many have tried to make liturgical celebrations convivial. Liturgical ministers, prompted by pastoral motives, sometimes try to instruct by introducing profane, show-business elements into liturgical celebrations. Don’t we sometimes see a proliferation of testimonies, scenery and applause? They think that this will foster the participation of the faithful, whereas in fact it reduces the liturgy to a human game.
“Silence is not a virtue, noise is not a sin, it is true,” says Thomas Merton, “but the turmoil and confusion and constant noise of modern society,” or of some African Eucharistic liturgies, “are the expression of the ambiance of its greatest sins—its godlessness, its despair. A world of propaganda, of endless argument, vituperation, criticism, or simply of chatter, is a world without anything to live for…. Mass becomes racket and confusion; prayers—an exterior or interior noise” (Thomas Merton The Sign of Jonas [San Diego: Harcourt, Inc., 1953, 1981], passim).
We run the real risk of leaving no room for God in our celebrations. We fall into the temptation of the Hebrews in the desert. They sought to create for themselves a form of worship on their own scale and of their own stature, and let us not forget that they ended up prostrate before an idol, the golden calf.
It is time to start listening to the Council. The liturgy is “above all things the worship of the divine majesty” (no. 33). It has instructional value to the extent to which it is completely ordered to the glorification of God and to divine worship. Liturgy really places us in the presence of divine transcendence. True participation means renewing in ourselves that “amazement” that Saint John Paul II held in high regard (cf. Ecclesia de Eucharistia, no. 6). This sacred wonder, this joyful fear, requires our silence before the divine majesty. We often forget that sacred silence is one of the means noted by the Council for promoting participation.
If the liturgy is Christ’s work, is it necessary for the celebrant to interject his own comments? We should remember that, when the missal authorizes an intervention, this must not become a profane, human speech, a more or less subtle commentary on current events, or a worldly greeting to the persons present, but rather a very brief exhortation to enter into the mystery (cf. General Introduction of the Roman Missal, no. 50). As for the homily, in itself it is always a liturgical act that has its own rules. “Participatio actuosa” in Christ’s work presupposes that we leave the profane world so as to enter into the “sacred action surpassing all others” (Sacrosanctum Concilium, 7). In fact, “we claim somewhat arrogantly to remain in the human sphere so as to enter into the divine” (Robert Sarah, God or Nothing [San Francisco: Ignatius Press, 2015], chapter IV).
In this regard it is deplorable that the sanctuary in our churches is not a place strictly reserved for divine worship, that people enter it in worldly garb, and that the sacred space is not clearly delimited by the architecture. Since, as the Council teaches, Christ is present in His word when it is proclaimed, it is likewise harmful that lectors do not have proper attire that shows that they are not pronouncing human words but a divine word.
The liturgy is a fundamentally mystical, contemplative reality, and consequently beyond the reach of our human action; even our “participatio” is a grace from God. Therefore it presupposes on our part openness to the mystery being celebrated. Thus, the Constitution recommends the full understanding of the rites (cf. no. 34), and at the same time prescribes that “the faithful… be able to say or to sing together in Latin those parts of the Ordinary of the Mass which pertain to them” (no. 54).
Indeed, understanding the rite is not the work of unaided human reason, which would have to grasp everything, understand everything, master everything. The understanding of the sacred rites is that of the “sensus fidei”, which practices a living faith through the symbol and knows by being attuned more than through concepts. This understanding presupposes that one approaches the mystery with humility.
But will people have the courage to follow the Council this far? Such an interpretation, illuminated by the faith, is fundamental however for evangelization. Indeed, “the liturgy… shows forth the Church to those who are outside as a sign lifted up among the nations, under which the scattered children of God may be gathered together” (no. 2). It must stop being a place of disobedience to the Church’s prescriptions.
More specifically, it cannot be an occasion for divisions among Christians. Dialectical interpretations of Sacrosanctum Concilium, the hermeneutics of rupture in one direction or the other, are not the fruit of a spirit of faith. The Council did not intend to break with the liturgical forms inherited from Tradition, but rather intended to appreciate them in greater depth. The Constitution declares that “any new forms adopted should in some way grow organically from forms already existing” (no. 23).
In this regard, it is necessary that some should celebrate according to the “usus antiquior” [older usage] and should do so without any spirit of opposition, and therefore in the spirit of Sacrosanctum Concilium. Similarly, it would be a mistake to consider the Extraordinary Form of the Roman Rite as coming from some other theology which is not that of the reformed liturgy. It would also be desirable in a future edition of the Missal to insert the penitential rite and the offertory of the “usus antiquior” for the purpose of emphasizing that the two liturgical forms illuminate each other, in continuity and without opposition.
If we live in this spirit, then the liturgy will stop being a place of rivalries and critiques, so as finally to make us participate actively in that liturgy “which is celebrated in the holy city of Jerusalem toward which we journey as pilgrims, where Christ is sitting at the right hand of God, a minister of the holies and of the true tabernacle” (no. 8).
Blood clots. Mood swings. Low sex drive. Migraines.
The list goes on and on.
At this point, it’s not really a surprise that shoving mega-doses of synthetic hormones into our systems year after year comes at a price. But for many women, the Pill still seems like the only option.
For years, it’s felt like Catholics have held the best-kept secret in women’s health – Natural Family Planning. A highly effective method of fertility monitoring without the need to pump your body full of artificial chemicals, it also boasts earlier detection for a whole host of diseases and disorders, and an overall understanding of your own health and fertility. Not to mention Catholic teaching that it’s the only moral method of family planning and allows you to be open to God’s will in a way that contraception does not.
But now, what was once viewed as a weird Catholic thing is becoming more and more mainstream. As people become increasingly conscious of what they are putting into their bodies, they are also realizing what it actually means to manipulate your body’s chemistry to the point that a healthy reproductive system no longer functions.
Even Cosmo has acknowledged that the Pill is pretty awful for women, and that natural fertility awareness methods may offer a better option.
In an article a while back (which was originally published in Elle and later run by Cosmo), the author explores the myriad side effects of the Pill – ranging from inconvenient to potentially deadly – and questions the prevailing mantra that the Pill is the best thing to happen to women since the 19th Amendment.
A few highlights:
To Christiane Northrup, MD, author of Women’s Bodies, Women’s Wisdom, prescribing the Pill for debilitating menstrual conditions, such as the endometriosis I suffered from, only masks the problem. “It’s like a mechanic putting a piece of duct tape over the indicator light on your dashboard and claiming he’s fixed your car,” she says.
The “fertility awareness method,” once the sole province of religions that didn’t allow other forms of contraception, has been newly embraced by holistic women’s health experts such as Northrup, who says it can be at least 95 percent effective when used correctly. She says, however, this requires that “women interact consciously with their fertility, and the reality is that many women still don’t have conscious dominion over their fertility.”
You can find the whole article here. Fair warning: it’s Cosmo. Some of the ads and language on the site are what my editor would refer to as “lusty smut.”
Cardinal Robert Sarah made the comments in an exclusive interview with Famille Chrétienne The Vatican’s liturgy chief has called on priests to celebrate Mass facing east.
In an interview [http://www.famillechretienne.fr/vie-chretienne/liturgie/cardinal-sarah-comment-remettre-dieu-au-caeur-de-la-liturgie-194987#.V0bFpURrE2U.twitter] with the French Catholic magazine Famille Chrétienne, Cardinal Robert Sarah said that the Second Vatican Council did not require priests to celebrate Mass facing the people.
This way of celebrating Mass, he said, was “a possibility, but not an obligation”.
Readers and listeners should face each other during the Liturgy of the Word, he said.
“But as soon as we reach the moment when one addresses God – from the Offertory onward – it is essential that the priest and faithful look together towards the east. This corresponds exactly to what the Council Fathers wanted.”
Cardinal Sarah, prefect of the Cardinal Robert Sarah celebrates Mass in Haiti in 2010 (CNS) Congregation for Divine Worship and the Discipline of the Sacraments, rejected the argument that priests celebrating Mass facing east are turning their backs on the faithful “or against them”.
Rather, he said, all are “turned in the same direction: towards the Lord who comes”.
“It is legitimate and complies with the letter and spirit of the Council,” he said. “As prefect of the Congregation for Divine Worship and the Discipline of the Sacraments, I wish to recall that the celebration versus orientem [https://en.wikipedia.org/wiki/Ad_orientem] is authorized by the rubrics, which specify the times when the celebrant must turn to the people. It is therefore not necessary to have special permission to celebrate facing the Lord.”
Cardinal Sarah’s remarks echo an article [http://www.catholicworldreport.com/Item/3947/silent_ action_of_the_heart.aspx] he wrote a year ago for L’Osservatore Romano, in which he said it was “altogether appropriate, during the penitential rite, the singing of the Gloria, the orations and the Eucharistic prayer, that everyone, priest and faithful, turn together toward the East, so as to express their intention to participate in the work of worship and redemption accomplished by Christ.”
The cardinal added in the article that Mass facing east could be “implemented in cathedrals, where the liturgical life must be exemplary”.
It is my opinion that for priests to courageously preach and teach Catholic Church doctrine on contraception, they will need great Grace that can only come from the Source and Summit of the Christian Life—the Liturgy.
Furthermore, I think that this infinite source of Grace can only be tapped to a degree commensurate with the holiness of the Mass being offered, and that depends on many factors. Here we address only the orientation of the priest during the Liturgy of the Eucharist.
Father, why do you face the people when offering the Sacrifice to the Lord?”
“That is the way we were trained to say Mass in the seminary. I think it was initiated following Vatican Council II when many other changes were made, like removing the communion rail, and receiving Holy Communion in the hand while standing.” (Common responses)
Why were these changes made to the long tradition of the Church?
“I really don’t know; they were made really quickly.” “The Novus Ordo has completely disoriented Catholics. There needs to be a complete top to bottom re-catechizing on just what the Mass is about—worshipping God.” (Two priests)
Why are all the Advent Masses (2014 & 2015) at the Cathedral of the Risen Christ in Lincoln NE being said Ad Orientem? (Asked of Bishop James Conley)
“I was really introduced to the Novus Ordo, celebrated Ad Orientem (AO), in a monastery in France. That (AO) means towards the altar, towards the east. In this case it was actually toward the geographical east; many places it’s not. But the idea, more importantly, is not the direction of east, but that the priest is standing facing the altar, facing God with the people so that he is standing there at the altar, representing the people and offering the holy sacrifice to God, as was the orientation of the priest for centuries. It was really only after the Second Vatican Council that permission to celebrate the Mass towards the people was allowed. And it’s interesting if you read the document [General Instruction of the Roman Missal], you can tell it wasn’t intended to be the norm. And the council fathers didn’t intend it to be changed that way, it was just allowed. Well, it became the norm, as we know. Very rarely do you find a place that celebrates the holy sacrifice of the Mass Ad Orientem, or towards the altar.” (Bishop James Conley, Diocese of Lincoln Nebraska, Radiomaria.us/ questforlife/ December 09, 2014 – Bishop James Conley on Liturgy, Synods and the Diocese of Lincoln) Does Ad Orientem refocus the Mass on God and less on the people, and less on the celebrant?
“Well that’s it; I think that’s one of the reasons the orientation is so important not only for the people, but also for the priest himself. It’s less distracting for the priest, because he’s concentrating on the sacrifice and he does not have to keep eye contact with the people. Also for the people it’s sort of a signal to them that now we’re at the altar and in solidarity with the priest celebrant and we’re offering this sacrifice to God. It just seems to be more appropriate for that part of the Mass. And at that point in the Mass it just seems appropriate that we would all be standing together facing the Lord, and the priest representing the people, sacrificing at the altar, they would all be facing the same direction. I can really sense the power of the prayer of the people behind me as I’m offering the consecration for example. And I didn’t really sense that until I celebrated it.” (Bishop James Conley)
What did Cardinal Joseph Ratzinger say about Ad Orientem?
“On the other hand, a common turning to the east during the Eucharistic Prayer remains essential. This is not a case of something accidental, but of what is essential. Looking at the priest has no importance. What matters is looking together at the Lord. It is not now a question of dialogue but of common worship, of setting off toward the One who is to come. What corresponds to the reality of what is happening is not the closed circle but the common movement forward, expressed in a common direction for prayer.” (Joseph Cardinal Ratzinger, The Spirit of the Liturgy, p81, emphasis added)
There is anecdotal evidence that priests who say Mass Ad Orientem (and may have instituted other traditional practices) do proclaim Church teaching on contraceptive use and thus have vibrant parishes with many families and lots of kids.
“We’ll never have a Culture of Life if we don’t get the Liturgy right.”
(Dr Lorna Cvetkovich, MD, 1999) Msgr Ignatio Barreiro put theological flesh and bones on Dr Lorna’s statement with “Sacred Liturgy and the Defense of Human Life”, presented at Sacra Liturgia 2013 in Rome, proceedings published as Sacra Liturgia, 2013, Ignatius Press 2014.
Msgr Barreiro’s paper is reprinted by One More Soul, with permission, and available at https://onemoresoul.com/catalog /sacred-liturgy-and-the-defense-of-human-life-p1233.html .
SACRAMENTO, California, May 25, 2016 (LifeSiteNews) – The parents of a two-year-old California boy on life support have won a crucial interim victory in the fight to keep their son alive, the latest in a lengthy dispute over his condition and care.
Israel Stinson was airlifted to a hospital in an undisclosed location outside the United States on Saturday after weeks of searching for a facility that would provide him treatment in preparation for long-term care, in a case hinging on the contested issue of the legal definition of brain death.
The Sacramento-area Kaiser Permanente facility where Israel Stinson had been since mid-April had declared him brain dead shortly after his arrival, eschewing treatment since then and providing the child only minimal nutrition while acting to remove him from life support.
“Victory!” his Israel’s mother Jonee Fonseca said in a statement Sunday. “Israel Stinson was transferred out of Kaiser Permanente yesterday. He has been taken to another facility and is already receiving treatment.”
“It is remarkable that Israel was given more treatment in the first five hours at the new hospital than in more than five weeks at the Kaiser facility,” Life Legal Defense Fund (LLDF) Executive Director Alexandra Snyder told LifeSiteNews.
Fonseca said because of the sensitivity of her son’s case, the family is not yet prepared to release his location.
“But we can say this, in order for Israel to receive his badly needed care, he had to be transferred out of the United States,” Fonseca stated. “That’s right. After weeks and weeks of searching, no hospital facility in the United States would accept our son.”
The difficulty securing a facility to accept and treat Israel while the family sought long-term care stemmed from Kaiser’s doctors having declared him brain dead, despite the conflicting opinions of specialists retained by the family.
Snyder told LifeSiteNews that doctors at the facility where Israel is now have also said the boy is not brain dead.
“A neurologist and Israel’s pediatric specialist did an extensive examination and determined that Israel is not brain dead,” she said. “This doesn’t mean he is out of the woods, as he does have a severe brain injury. But at least he is being provided treatment and nutrition now.”
Israel’s mother celebrated the fact that her son is now being “treated like a patient” and receiving basic nutrition and care.
“Israel’s medical chart at Kaiser said he was deceased. But Israel is alive!” Fonseca said. “He is right now receiving nutrients and a treatment protocol for the first time in 6 weeks.”
Israel’s story began April 1 when he was brought to the Sacramento Mercy General ER with a severe asthma attack. After he was stabilized, Israel was moved to the pediatric unit at UC Davis Medical Center in Sacramento, where he suffered another attack resulting in cardiac arrest. The toddler was put on a ventilator, and then transferred April 12 to the Kaiser facility for treatment at the family’s request due to concern over the handling of his treatment during the second attack at UC Davis.
Less than 24 hours after his arrival at Kaiser, the hospital performed brain function testing on Israel, without the family’s full knowledge or consent and against their wishes, prompting Fonseca to contact LLDF for help.
The legal battle began with a temporary restraining order enjoining Kaiser from removing life support to allow the family to find an interim facility for Israel, the ultimate goal being long-term care. The family was looking at New Jersey for this since its state law does not allow for a declaration of brain death in cases where the family members believe that life continues until the heart stops beating.
Fonseca and Israel’s father Nate Stinson have maintained throughout that Israel has been responsive to their touch and voices, as well as music, and they have relied openly on their faith to get them through.
LLDF has worked with Pacific Justice Institute as the case has wound its way through the courts to the Ninth Circuit Court of Appeals, where it was again headed this past Monday before Israel’s transfer over the weekend from Kaiser.
While Israel’s situation has stabilized for the time being, his family’s Pacific Justice Institute attorneys say the little boy’s case broaches the issue of the state of California’s law regarding a determination of brain death.
“While an important goal of this case has been achieved, it has also raised serious questions about the constitutionality of the California Uniform Determination of Death Act,” Matt McReynolds stated in a report by The Sacramento Bee. “It has become clear that declarations of brain death do not always reflect medical consensus and do not comport with basic notions of due process. These legal claims have not been mooted, and we will be evaluating how best to pursue these important constitutional questions.”
Fonseca’s suit against Kaiser to prevent the facility from removing Israel from life support contended that the hospital’s declaration of brain death violated her constitutional rights of due process to determine her son’s care.
Pacific Justice Institute lead attorney Kevin Snider said the crisis in Israel’s case was over, but a reason and opportunity to challenge the law remains, and it will be up to Israel’s parents if they want to go forward with that.
After Israel’s transfer Saturday to a new hospital Fonseca thanked supporters on the family’s GoFundMe page, set up last month to help fund the toddler’s transfer to another facility. Donations on the page have reached $20,000, and Fonseca said that because of the support, “Israel was able to beat the odds and is now being cared for as a live human being.”
The prayers of supporters have “made all the difference,” Fonseca continued, giving her son the chance to recover. But with the quest to finally get him home still ongoing, she asked supporters to remain engaged in his case.
“We have a long road ahead,” Fonseca stated. “Our story is not yet over.”
ARLINGTON, VA (May 24, 2016) — A new four-minute viral video is causing over a third — 34 percent — of “pro-choice” women surveyed to view abortion “less favorably.” And 28 percent of pro-choice women who watched the video stated there should be more restrictions on abortion.
The women watched the D&E Abortion Procedures video, part of Live Action’s new “Abortion Procedures” video series, which features an OB/GYN and former abortionist using medically accurate animations to give viewers a window into the womb during an abortion and show how developed a baby is during the procedure. The videos were produced in conjunction with a team of OB/GYNs, former abortionists, and other physicians, and have been viewed over 42 million times to become the most-watched pro-life videos in history.
Live Action conducted an online video survey of 502 women ages 18-30 through independent polling company Survey Monkey, then analyzed the responses of a subgroup of 208 women who self-identified as “pro-choice” and watched the video. The results are below.
In addition to the survey, Live Action conducted a series of man-on-the-street interviews in Los Angeles, showing abortion supporters rejecting abortion after viewing the “Abortion Procedures” videos. The man-on-the-street video is here.
“Abortionists have worked for decades to keep women in the dark about how developed their preborn children in the womb are and what abortion procedures actually entail for both the mother and the child,” said Lila Rose, president and founder of Live Action. “The more people learn about abortion, the more they see how barbaric and inhumane it is — whether the abortion is committed by depriving a preborn child of nutrients for days until she dies, or by ripping her limbs apart while she’s still alive, or by injecting her with a drug to induce cardiac arrest.”
Almost half of the pro-choice women polled — 46 percent — felt that the medical animations should be shown to high school sex education classes, and 39 percent felt that pregnant women considering abortion should watch them.
“Pro-choice women told us that young people and women considering abortion should have access to these facts about abortion, not just to the pro-abortion spin that seems to dominate media, entertainment, and politics today. The Internet allows us to spread the truth about abortion faster and farther than ever before, and the fact that these videos have already been viewed over 42 million times to become the most-watched pro-life videos in history proves it,” said Rose.
The Survey
Live Action conducted an online video survey during the weeks of May 9th and 16th that asked 502 women ages 18-30 to watch its D&E Abortion Procedures video and respond to a series of questions. The women were randomly chosen by independent online polling firm Survey Monkey from its universe of women 18-30 who self-identified their political leanings as moderately liberal, slightly liberal, slightly conservative, or neither liberal nor conservative. Of those women who self-identified as “pro-choice,” 208 watched all or most of the video. After watching the video, the 208 pro-choice women were asked:
Q. Did the video change the way you view abortion?
9.1% I view abortion much less favorably
25.0% I view abortion somewhat less favorably
62.0% I view abortion the same as I had previously
1.4% I view abortion somewhat more favorably
2.4% I view abortion much more favorably
Q. Under federal law, abortion is legal up until birth for any reason. Some states have further restrictions. After watching the video, do you think there should be more or fewer restrictions on abortion?
28.4% More restrictions
29.3% Fewer restrictions
42.3% Leave the current restrictions as-is
Q. Who do you think should see this video? (Total >100% because respondents could check as many as they wanted.)
46.6% High school sex education classes
42.8% College students
39.4% Pregnant women considering abortion
38.9% General public
26.0% Elected officials
34.1% None of the above
WASHINGTON, D.C., May 17, 2016 (LifeSiteNews) – Cardinal Robert Sarah slammed gender ideology, same-sex “marriage,” and transgender bathroom policies at the National Catholic Prayer Breakfast on Tuesday, describing them all as demonic attacks on humanity.
Sarah, the prefect for the Congregation of Divine Worship and the Sacraments, was the keynote speaker at the annual prayer breakfast, where he joined Speaker of the House Paul Ryan and Sister Constance Veit, the director of communications for the Little Sisters of the Poor. Numerous Catholic bishops and members of Congress, including Apostolic Nuncio Archbishop Carlo Maria Vigano, were in attendance.
“The battle to preserve the roots of mankind is perhaps the greatest challenge our world has faced since its origins,” Sarah told the crowd of nearly a thousand people. Catholics should follow the “courageous” example of St. John the Baptist, a martyr for the sanctity of marriage, Sarah said.
“Do not be afraid to proclaim the truth with love, especially about marriage according to God’s plans,” said Sarah. “In the words of St. Catherine of Siena, ‘proclaim the truth and do not be silent through fear.’”
Sarah blasted gender ideology as “ideological colonization” and lamented the “insidious” dismantling of religious freedom in the United States.
“Every human being, like the person of the Trinity, has the capacity to be united with other persons in communion through the…bone of charity of the Holy Spirit,” said Sarah. “The family is natural preparation and anticipation of the communion that is possible when we are united with God…this is why the devil is so intent on destroying the family. If the family is destroyed, we lose our God-given anthropological foundations and so find it more difficult to welcome the saving good news of Jesus Christ: self-giving, fruitful love.”
He continued:
The rupture of the foundational relationships of someone’s life—through separation, divorce, or distorted impositions of the family, such as cohabitation or same sex unions—is a deep wound that closes the heart to self-giving love [unto] death, and even leads to cynicism and despair.
These situations cause damage to the little children through inflicting upon them a deep existential doubt about love. They are a scandal—a stumbling block—that prevent the most vulnerable from believing in such love, and a crushing burden that can prevent them from opening to the healing power of the Gospel.
Advanced societies, including, I regret, this nation, have done and continue to do everything possible to legalize such situations. But this can never be a truthful solution. It is like putting bandages on the infected wound. It will continue to poison the body until antibiotics are taken.
Sadly, the advent of artificial reproductive technologies, surrogacy, so-called homosexual ‘marriage,’ and other evils of gender ideology, will inflict even more wounds in the midst of generations we live with.
This is why it is so important to fight to protect the family, the first cell of the life of the Church and every society. It is not about abstract ideas. It is not an ideological war between competing ideas. This is about defending ourselves, children, and future generations from a demonic ideology that says children do not need mothers and fathers. It denies human nature and wants to cut off entire generations from God.
Sarah warned that “today we are witnessing the next stage and the consummation of the efforts to build a utopian paradise on earth without God,” a “turmoil” about which Pope St. John XXIII alerted the Church when he announced the Second Vatican Council in the Apostolic Constitution Humanae Salutis.
This effort is in the “stage of denying sin and the fall altogether,” according to Sarah, and its fruits are the suppression of goodness, beauty, truth, and love.
“Good becomes evil, beauty is ugly, love becomes the satisfaction of sexual primal instincts, and truths are all relative,” said Sarah.
“All manner of immorality is not only accepted and tolerated today in advanced societies, but even promoted as a social good,” he continued. “The result is hostility to Christians, and, increasingly, religious persecution. Nowhere is [this] clearer than in the threat that societies are visiting on the family through a demonic ‘gender ideology,’ a deadly impulse that is being experienced in a world increasingly cut off from God through ideological colonialism.”
“I encourage you to truly make use of the freedom willed by your founding fathers, lest you lose it,” the African cardinal advised the faithful. He cited international religious persecution against Christians and “political, ideological, and cultural” persecution that damages the Christian faith and leads souls astray.
“Do we not see signs of this insidious war in this great nation of the United States?” Sarah asked. “In the name of ‘tolerance,’ the Church’s teachings on marriage, sexuality, and the human person are dismantled. The legalization of same-sex marriage, the obligation to accept contraception within healthcare programs, and even ‘bathroom bills’ that allow men to use the women’s restroom and locker rooms. Should not a biological man use the men’s restroom? How simpler can that concept be?”
Sarah offered the faithful three suggestions: be prophetic, be faithful, and pray.
“I am confident that your efforts will no doubt contribute to protecting human life, strengthening the family, and safeguarding religious freedom not only here in these United States, but everywhere in the world,” he finished. “For in the end it is ‘God or nothing.’”
Paul Ryan: ‘Religious liberty is going to make a comeback’
In his address, House Speaker Paul Ryan told attendees, “We have an obligation to advocate for our faith.”
Although religious liberty in America is under assault, he said, “I actually think that religious liberty is going to make a comeback because there is a growing need for faith across this nation.”
Quoting St. Thomas Aquinas, the former vice presidential nominee said that no matter one’s circumstances, the ultimate purpose of human life is contemplation of God.
Ryan noted that during his many meetings with individuals struggling with drug addiction, he noticed they often seem to “feel a deep, gnawing pain inside,” a lot of which “stems from loneliness.”
“We all feel loneliness at some level,” said Ryan. “We all feel that distance from God” and it is turning to God that consoles and heals us, he said.
And “when faith itself is ruled out of bounds, then happiness itself is being placed out of reach.”
“There is a spiritual void that needs to be filled,” continued Ryan. “Perhaps poverty is God’s way of leading us to contemplate something higher. The fight against poverty and the need for religious liberty go hand-in-hand.”
It’s not just enough to raise people’s wages and give them jobs, Ryan said. The spiritual void must be filled.
“When you meet people who have beaten addiction,” he continued, “most of them say something like this, ‘it wasn’t me. It was God’. … Every good work is the work of God. It is his grace working inside of us” and realizing that causes a loss of pride and a loss of any sense of despair.”
“There is nothing more life-changing than coming to know the Lord,” said Ryan.
Little Sisters of the Poor: We don’t have a ‘contingency plan,’ we trust in God
Sister Constance encouraged Catholics to be joyful and to view persecutors and adversaries as Christ would.
“Hate crucified love incarnate,” Sister Constance told the packed room. “The forces of death killed the Lord of life. So let us not be Christians who communicate Lent without Easter, but believers who know how to speak the truth in joy and love.”
“Even our most cunning adversary is a person longing to love and be loved,” she said.
Sister Constance said that the Little Sisters of the Poor trust in God regardless of the outcome of their ongoing legal case against the Obama administration, which has been attempting to force them to violate their consciences by cooperating with actions that the Catholic Church considers intrinsically evil. On Monday, the Supreme Court chose not to rule on the case and punted the case to the U.S. Courts of Appeals. Pro-life groups declared this an initial victory.
“We have no contingency plan, because like [our foundress], we believe that God will never abandon us,” said Sister Constance. “I don’t say this because it’s a clever sound bite, but because I have deliberately chosen to believe it.”
On March 30 Planned Parenthood got a big gift from the Obama Administration.
That’s the day the FDA rewrote the label on chemical abortion drugs. Now, the FDA regulations conform to what had long been the common off-label use of the drugs by chemical-abortion providers.
If that sounds like the tail wagging the dog, well, it is. The abortion industry is now setting standards for medical practice.
And if, as the year wears on, Planned Parenthood et al become concerned that a pro-life candidate might be headed toward the White House, they will no doubt get their government friends to make more executive-level changes that favor the abortion business.
But first, the March 30 action: Remember RU-486, the abortion-causing pill from France? The pro-life movement fought to keep it out of the United States, but in 2000 the FDA approved its use in a fairly strict regimen that included taking a second drug, misoprostol.
Today RU-486 is known as mifepristone—brand name Mifeprex. Mifepristone is a drug that blocks progesterone, a hormone necessary to sustain pregnancy. Taken in conjunction with misoprostol, which causes contractions to the uterus, it results in miscarriage.
The latest FDA action alters the chemical-abortion regimen the agency established back in 2000 in significant ways:
•It is now considered to be effective through 10 weeks of pregnancy, up from 7 weeks in 2000;
•The dosage of mifepristone, which was 600 milligrams in 2000, has been reduced to 200 milligrams;
•Women can now receive misoprostol—which is to be taken 24 to 48 hours after taking mifepristone—at their first doctor visit;
•In 2000, a woman had to be examined by a doctor 14 days after taking mifepristone. Today, no post-abortion examination is required, only an “assessment” between 7 and 14 days afterwards, just to make sure the “pregnancy has passed from the uterus.”
Why the changes? What do you think?
They can couch it in rhetoric about “current available scientific evidence and best practices” all they want, but the bottom line is: More customers for Planned Parenthood, which now gets an additional three weeks to enable a woman to kill her baby in her own home—with only one medical exam and one post-abortion “assessment” (a phone call?) required. Much easier, and cheaper (for Planned Parenthood at least) this way.
“Medication-induced abortions,” reported the New York Times on March 30,
made up as much of a quarter of all abortions in 2011 according to the most recent figures from the Guttmacher Institute, which tracks women’s reproductive health issues. Planned Parenthood said as many as half of eligible women in its clinics requested medication-induced abortions.
It’s the medically approved do-it-yourself abortion—for the independent woman. Its very convenience is part of its cruelty.
It allows a woman who is already going through the torment of an unwanted pregnancy to go through the agony of an abortion all by herself. With no need for someone to accompany her when she has an appointment with a chemical-abortion provider, she has no pretext to reach out to another human being as she destroys the life within her. And therefore little opportunity to hear the concern and support that others would be willing and eager to give her.
According to the FDA, between 2000 and the end of 2011 the number of women who had chemical abortions using mifepristone and misoprostol was 1.52 million.
What has their experience been like?
Miserable.
From the FDA’s own flyer “Questions and Answers on Mifeprex”:
Cramping and vaginal bleeding are expected effects of the treatment regimen. In some cases very heavy vaginal bleeding will need to be stopped by a surgical procedure . . .
Other common side effects of the treatment regimen include nausea, weakness, fever/chills, vomiting, headache, diarrhea, and dizziness . . .
The FDA has received reports of serious adverse events in women who took Mifeprex and followed the regimen.
From the FDA’s Medication Guide:
Be sure to contact your healthcare provider right away if you bleed enough to soak through two thick full-size sanitary pads per hour for two consecutive hours or if you are concerned about heavy bleeding. In about 1 out of 100 women, bleeding can be so heavy that it requires a surgical procedure (surgical aspiration or D&C).
(One out of a hundred for 1.52 million = 15,200 more procedures. More business for a full-service Planned Parenthood clinic. Perhaps the anticipation of more of this kind of business could help explain why PP is shifting its business model to mega centers?)
If you have abdominal pain or discomfort, or you are “feeling sick,” including weakness, nausea, vomiting, or diarrhea, with or without fever, more than 24 hours after taking misoprostol, you should contact your healthcare provider without delay. These symptoms may be a sign of a serious infection or another problem (including an ectopic pregnancy, a pregnancy outside the womb).
In the days after treatment, if you have a fever of 100.4F or higher that lasts for more than 4 hours, you should contact your healthcare provider right away. Fever may be a symptom of a serious infection or another problem.
If you are still pregnant [after Mifeprex with misoprostol treatment], your healthcare provider will talk with you about a surgical procedure to end your pregnancy. … The chance of birth defects if the pregnancy is not ended is unknown.
Mifepristone does not end a pregnancy outside the uterus, that is, an ectopic pregnancy. Unless there’s an ultrasound requirement to confirm pregnancy in the uterus, how would a woman know that she continues to be pregnant after going through all that? Yet the “reproductive freedom” lobby resists initiatives to require confirmation of pregnancy by ultrasound in the states where such measures are introduced.
What happens to women who will obtain the drugs on the internet and not bother to see a doctor? What happens to the girl who has von Willebrand’s Syndrome or another blood disorder but doesn’t know it . . . until she is bleeding to death in the privacy of her own home?
The FDA’s own adverse effects report, covering September 2000 until April 30, 2011, provides some unhappy answers: 2,207 cases of women suffering adverse events; 612 hospitalized; 14 deaths; 339 transfusions required; 256 infections; 58 ectopic pregnancies.
And those statistics are based only on cases in which a woman told someone she had taken the abortion drugs and that person reported it to medical authorities.
Not a pretty sight, the way modern reproductive medicine treats its victims.
An Australian mother who gave birth to quintuplets in January has released a photo shoot of her five new babies.
It took Kim Tucci, 26, just two minutes to give birth to the massive set of new arrivals – four daughters and one son – who were conceived naturally.
Doctors had advised Kim to abort some of her five unborn children on health grounds but she refused, going on to give birth to all five babies.
Surprised by Five
Kim and her husband Vaughn, who live in Perth, already have a nine-year-old daughter and two sons aged two and four. Now their family has expanded with the arrival of Tiffany, Keith, Penelope, Beatrix and Allie!
The odds of conceiving quintuplets naturally is approximately one in 55 million. Kim documented the story of her pregnancy on her blog, Surprised by Five.
She also described how doctors had recommended that she undergo a ‘selective abortion’ – i.e. abort up to three of her unborn children in order to give the others a better chance of survival.
Refusing selective abortion
On 26 September, 2015, Kim wrote:
“After my initial ultrasound I was told I could consider the selection method [abortion] to give 2 babies the best chance in life … I watched a YouTube video on the procedure and I cried, I could never do that! Was I selfish for not giving two the chance of 100% survival?? All I knew is that I already love them and that every heart beat I heard I connect with them more.”
A team of 50 doctors and nurses assisted with the planned caesarean birth and all of the children were born healthy after spending 29 weeks in the womb.
Not always easy
Kim’s pregnancy with her quintuplets was often far from easy. She blogged about pain, extreme discomfort, sleepless nights, constant trips to the bathroom and a 6,000-calorie a day diet to sustain her five unborn babies.
But the mum-of-eight also said that all the aches and pains, the stretch marks and hospital stays were worth it, knowing that her babies are healthy. She also thanked her husband for his constant support through her pregnancy struggles.
Support
“My husband always reminds me I should wear my stripes with pride and that I should be proud of them and what my body has achieved. Without him I would have broken down a long time ago,” Kim wrote.
Now that the babies have come home, friends and family are organizing a fundraiser to help the Tuccis buy a car big enough to transport their entire family.
Photoshoot
Kim recently posted on her blog:
“50 fingers 50 toes, 6 hearts beating at once. My body fought the toughest of battles to get five babies here safely. Everything I did I did for them.”
Local business Erin Elizabeth Photography, which helped document Mrs Tucci’s pregnancy, organised a photoshoot for the quintuplets and their proud mum, which has since gone viral. You can see the rest of the pictures below:
By Vince Sacksteder III, One More Soul, April 15, 2016
Children are treasures.
Jason Adams, a One More Soul author and a friend of mine, once wrote: “Once I worried about what I would have to give up in having children; now I know there is nothing that I would not give up for my children. They are infinitely more valuable to me than anything I own.” My own experience confirms this. My children have proven to be more valuable than everything else I have. Children help us value the future.
Every child helps us look to the future.
Once we have a child, we start being concerned about how that child will be doing 5, 10, 20 years from now. We start making plans for the future, and we take steps to fulfill those plans. Children strengthen our hope for a great future.
Children open our hearts.
If we never concerned ourselves with mercy and compassion, or with trust and fidelity, suddenly these virtues become very important to us. Seeing our children grow up opens to us vistas of who we can be, vistas that were hidden before.
Children toughen us.
Maybe I was a whiner; maybe I couldn’t bear setbacks or obstacles; maybe I felt that life was too much for me. Now, with children, I have a motivation to just get over those things and press on with life. I have become a more solid citizen and more valuable to myself and to those around me.
Children show us new things.
Children have new eyes and new approaches to life. One of my daughters is an artist and is constantly finding new ways to make our home beautiful. One is a great organizer and frequently helps put family events together, to say nothing of organizing events of her own. Each has strengths that we as parents did not have and each contributes something fresh to the family.
Children help us treasure the present moment.
Little children live in the present and mirror to us just how valuable the present is. For them the thing they are doing right now is the most important thing in the world. What a lesson for us all.
Children become adults.
One of the most wonderful things about children is that they grow, and grow and grow. They become as large as we are and often larger and stronger, physically and spiritually as well. We learn to lean on them for many things we never could do, or can no longer do.
Children make wonderful friends.
A friend is glad to see us no matter what, and always glad to do something for us, if at all possible. Children are like that; they love us and are not afraid to show it.
Children teach us discipline.
When it comes to holding our temper, doing a task we really don’t want to do, or stretching ourselves a bit more than we would be inclined to, children excel, especially small children. New babies, particularly the first baby, make parents many times more patient, more loving, and more accommodating than they ever were before.
Children reflect God to us.
God’s presence shines from the eyes of newborns and radiates from the simplicity of small children. God is shared with us by the wisdom that comes to us from grown-up children, and also the wisdom that we share with them, wisdom that we didn’t know we had. God’s presence grows in the love that is shared between us and our children.
I received a number of emails from friends after Respect Life Sunday saying that they heard little, if anything, about life and family from the pulpit. It is as if some pastors are afraid of preaching the Gospel of Life, or have something more important to talk about even when it is chosen as the day to preach on precisely these issues.
The failure to preach the Gospel of Life is not only a U.S. problem. During HLI’s conferences, I hear the same comments from around the world. I bring this up when I speak to seminarians, priests, and bishops – many times the only message the faithful will hear about these incredibly urgent pastoral and moral questions is at Mass.
Generally, Catholics might hear a homily on abortion once a year. They might hear an occasional reference to euthanasia – a subject some deem easier to preach about – but most usually never hear references to contraception, homosexuality, promiscuity, pornography, cohabitation or divorce.
It is also not helpful when Church leaders accept the false caricature that “the Church is always talking about these issues,” so it’s about time we talked about something else. Apparently “the Church” has not sufficiently talked about issues in a way that helps the political party that now treats abortion as a “human right.”
When one cardinal said two years ago that those Catholics who were in second civil unions without annulment of their marriages should not be expected to be heroes by being celibate, many couples who had been abstaining from sex felt like they had been punched in the gut. What had they been sacrificing for? Such a position makes it sound like Jesus’ teaching on marriage is just too hard to follow. We know better than Jesus. We are more pastoral. It is even more hurtful when the cardinal’s superior also seems to accept and repeat this characterization of Church teaching as being uncompassionate.
It is true that priests and bishops are people too. When they preach in a way that displeases people not only might they lose parishioners, they may also lose collection revenue and invite nasty e-mails and face-to-face conversations after Mass. Most of us know the risks too well.
But, my brothers, we have given our lives to a Man who submitted to a gruesome and humiliating death! We follow Our Lord, who died on a cross for us! If we love those whom we are given to serve in our parishes – let me choose my words carefully here – how the hell are we helping them if we do not tell them the truth – the Good News – about sexuality and marriage? These are pastoral issues, and cannot be reduced to some obscure teaching that was meant for another time! Pope Saint John Paul II knew this well:
The Gospel of life is at the heart of Jesus’ message. Lovingly received day after day by the Church, it is to be preached with dauntless fidelity as “good news” to the people of every age and culture. (Evangelium vitae 1)
My God, my God, why have we forsaken you? How did we let ourselves come to the belief that you, Our Lord, meant for our lives to be as easy as possible? That Your Law — what You told us is what those who love you will follow — can only be held up when it happens to find agreement with our fallen culture?
Why are we not protecting married couples from the violence of contraception — the divorce of unitive and procreative aspects of the beautiful gift of sexuality? Why are we afraid of helping our brothers and sisters to live in truth, according to their dignity?
What is our role and duty in Christ – in truth and charity?
No one has said that we must only preach about life and family issues. Anyone who claims differently is ignorant or is trying to manipulate the listener. As priests we must prayerfully discern how to bring the Word of God directly to those we serve in a way that they can hear. We absolutely must remind the faithful of their obligation to serve in solidarity with those in need, to be generous with their material gifts. We owe it to our congregations to remind them of the goodness of Truth and Beauty – the goodness of life, of God’s creation and our responsibility to be stewards of what we’ve been given. We have to remind people that our faith cannot be reduced to rules, but is based on Love.
But we must never accept the false representation of Church teaching on life and marriage as lacking compassion, or pretend it was made for another time. We must not be afraid to tell the truth about life and family, as there are no more immediate or urgent pastoral issues that our families are dealing with at home or in the public square.
Preaching on these issues on Respect Life Sunday is a bare minimum – a starting point. We are forming hearts and minds so that the faithful can in freedom choose wisely and lovingly when the moment of heroism – even everyday heroism for those with great challenges – comes their way. It is not “pastoral” to ignore the loving doctrine we have been given and offer solutions that soothe and confuse. This is not love.
May 3, 2016 (LiveActionNews) — Abortion advocates often claim as a defense of abortion that no one can really, truly define the moment life begins. Without knowing that, they say, there’s no real argument against abortion. Consider, for example, Melissa Harris-Perry’s insistence that life begins “whenever you feel like it does.” Obama famously said that the question of when life begins was above his pay grade. While the science of embryology has long been settled, it’s still not good enough for abortion activists.
But a new scientific breakthrough might go a long way towards changing hearts and minds: scientists have been able to capture the moment life begins, with a bright flash of light as a new life is conceived…
Human life begins in bright flash of light as a sperm meets an egg, scientists have shown for the first time, after capturing the astonishing ‘fireworks’ on film.
An explosion of tiny sparks erupts from the egg at the exact moment of conception.
Scientists had seen the phenomenon occur in…animals but it is the first time is has been also shown to happen in humans.
The photos included were not of actual embryos being created — the scientists used a sperm enzyme to replicate the incredible moment that life begins.
Unfortunately, rather than using this discovery to defend life, scientists are using it to better discern which lives to destroy.
Researchers from Northwestern University, in Chicago, noticed that some of the eggs burn brighter than others, showing that they are more likely to produce a healthy baby.
… “This means if you can look at the zinc spark at the time of fertilization, you will know immediately which eggs are the good ones to transfer in in vitro fertilization.
“It’s a way of sorting egg quality in a way we’ve never been able to assess before. “All of biology starts at the time of fertilization, yet we know next to nothing about the events that occur in the human.”
So basically, the scientists are advocating for embryos to be created in order to facilitate IVF, and then destroyed if they don’t seem to be the healthiest, strongest embryos. The ones with a dimmer glow are deemed to be weaker, perhaps because of a genetic abnormality, and so after creating their unique lives, scientists plan to destroy them. This is even though science has also just confirmed that babies with abnormalities can self-correct while still in the womb. People who are undergoing IVF are often encouraged to destroy “defective” embryos, ending the lives that were just created, without giving the embryos any chance at all to grow and develop, and certainly without placing any value on the uniqueness of each human life.
As Secular Pro-Life pointed out:
[T]he article is refreshingly clear about conception being the point where life begins. There is no obfuscation. The very first line of the article is “Human life begins in bright flash of light as a sperm meets an egg, scientists have shown for the first time, after capturing the astonishing ‘fireworks’ on film.”
Which is why the rest of the article is so incredibly disturbing.
Agreed. It’s sad that such a life-affirming discovery is being used to further the culture of death.
April 26, 2016 (NationalReview) — There has been a huge and alarming increase in the U.S. suicide rate. From the CDC announcement:
From 1999 through 2014, the age-adjusted suicide rate in the United States increased 24%, from 10.5 to 13.0 per 100,000 population, with the pace of increase greater after 2006…
Suicide is increasing against the backdrop of generally declining mortality, and is currently one of the 10 leading causes of death overall and within each age group 10–64…
This report highlights increases in suicide mortality from 1999 through 2014 and shows that while the rate increased almost steadily over the period, the average annual percent increase was greater for the second half of this period (2006–2014) than for the first half (1999–2006).
Color me decidedly not surprised. We are becoming a pro-suicide culture.
I believe the assisted suicide movement bears partial responsibility. Suicides have increased at the very time the assisted suicide movement has been vigorously and prominently promoting self-killing as a proper means to alleviate suffering.
Moreover, assisted suicide is often portrayed sympathetically in popular entertainment and the media is completely on board the assisted suicide bandwagon. Don’t tell me that doesn’t give despairing people lethal ideas.
At the same time, suicide prevention campaigns usually ignore this toxic elephant in the room.
It is also noteworthy that the suicide rate increased faster after 2006–the very time when the assisted suicide movement has become the most vigorous and made its most dramatic advances.
There is no question that assisted suicide advocacy is not the only factor causing this alarming increase in suicides. But I am convinced that the correlation could also be at least a partial causation.
Look at it this way: If we say that suicide is okay in some circumstances–but not others–at best we are sending a mixed message, making it more difficult for the anti-suicide message to sink in.
In this regard it is like telling someone, “Don’t smoke, but if you do, use filter cigarettes.”
One study has already found a weak linkage. I would like to see a more concerted investigations that aren’t afraid of making a controversial connection.
The name Israel means he who prevails with God. Right now, there is an emergency calling for the performance of God’s love and work here on earth. In no uncertain terms, prevailing in this instance means life and losing results in death.
Israel Stinson is a beautiful two-year-old boy with baby soft caramel skin and big brown sparkling eyes, the kind that penetrate through your chest and make you feel as if part of your heart is smiling. Israel’s mom uses her graceful fingers to comb Israel’s dark curls into a pile on the top of his head that gently rests on a white pillow case at the Kaiser Permanente Medical Center in Roseville, California—the hospital determined to end Israel Stinson’s young life.
On Monday, May 2nd at 1:30pm, the parents of two-year-old Israel Stinson took the next steps in their battle against the hospital, currently housing their son, from carrying out its decision to end Israel’s life. Israel’s parents, with the help of their heroic attorneys from the Life Legal Defense Foundation, asked Judge Kimberly Mueller to restrain the hospital from unplugging Israel’s ventilator. A move, that the hospital knows, will kill two-year-old Israel by suffocation. The court gave Israel until May 11th.
Just one month ago on April 1st, Israel’s parents could not have imagined this fate. It was the week after Easter Sunday. Israel was running around like a normal, active two-year old. Israel was enjoying his role of responsible and loving older brother to his younger sister. Israel was laughing, sharing his contagious grin, and beaming with life and innocence. But then the protective shield a mother builds around her child was pierced as Israel’s mom found herself rushing into an emergency room. Israel was having trouble breathing; he suffered an asthma attack.
The physicians in the emergency room placed Israel on a breathing machine and took x-rays. Eventually, the physicians intubated Israel and transferred him to a different hospital with a pediatric unit. There, on the very next day, Israel’s tube was removed. The hospital declared Israel was stable and told Israel’s parents that they could probably go home the following day. This never happened.
About an hour and a half later, the relief of this news drained from the room as Israel began wheezing and gasping to breathe again. Instead of providing a breathing tube, physicians attempted other methods that proved unsuccessful. Israel’s body went limp, and the hospital eventually performed CPR to resuscitate Israel’s tiny body. Doctors placed Israel on life support but encouraged Israel’s parents that he was “going to make it.” Later, doctors shared that a possibility of brain damage existed due the lack of oxygen to Israel’s brain prior to connecting Israel to life support.
Three days later, on April 6th, doctors determined that Israel’s heart and lungs were functioning on their own. Then six days after that, doctors transferred Israel to yet another hospital, the Kaiser Permanente Medical Center. It is here, within 24 hours of receiving Israel, that the hospital told Israel’s parents that they would likely withdraw life support. Indeed, just two days after being transferred to Kaiser Permanente Medical Center, the hospital pronounced two-year Israel “brain dead.”
To the hospital, this pronouncement means that Israel’s parents no longer have the right to exercise any decision making authority regarding Israel’s placement on a ventilator. Simply put, the hospital can unplug the machine that is keeping Israel alive. Israel’s parents filed a petition with the state court, begging the court to order the hospital to continue treatment and give their son more time. The state court temporarily restrained the hospital from removing the ventilator for the family to make arrangements for their son to be transferred to another hospital.
Dr. Paul Byrne, a board certified neonatologist, pediatrician, and Clinical Professor, visited Israel and examined his medical records. Dr. Paul Byrne wants everyone to know: “Israel is alive.”
Dr. Paul Byrne is an expert in traumatic brain injury, like Israel’s. In 1975, Dr. Paul Byrne treated a young man that some physicians concluded was brain dead and was on a ventilator for 6 weeks. The young man eventually gained full consciousness and was weaned from the ventilator. The man went on to live a full life, is married, and has three children. Dr. Paul Byrne also treated Jahi McMath, whose parents also had to take hospital administrators to court in order to save the life of their child. Since being declared “brain dead,” Jahi has celebrated her 14th and 15th birthdays, and is constantly surrounded by the love of her family.
Dr. Paul Byrne discovered that the hospital was failing to give Israel the nutrients and treatments he needed to recover. The hospital refused to change their treatment at the request of Israel’s parents claiming that “they do not treat or feed brain dead patients” and that Israel’s parents no longer have the ability to make decisions over their son’s healthcare.
In the past week, Israel has shown improvement. Israel’s heart continues to beat on its own. Israel responds to his mother’s voice, took breaths on his own, and even lifted his arm. The hospital, however, refuses to back down and is fighting to remove Israel’s life support.
Israel’s family and legal counsel find themselves in a race against time. Unable to secure placement in a different facility before the expiration of the state court’s temporary restraining order, the family filed an emergency motion with the federal court last Friday to stop the hospital from ending Israel’s life and to obtain more time. Yesterday, the federal court restrained the hospital from removing life support until May 11th, giving Israel’s family a brief reprieve. The family hopes that May 11th does not come too soon.
Israel currently needs a hospital willing to accept him and a doctor who is board certified in California to perform a tracheotomy and insert a feeding tube for Israel to breathe and receive nutrients while in transport to a new hospital. Perhaps someone in a position to help might read this article and rise to the challenge of helping Israel.
Critics may say recovery is impossible. That Israel’s parents should just give up. But why should Israel’s parents be forced into blind obeisance to a hospital, especially when there are conflicting opinions about their son’s condition? And, above all, when doing so will result in the death of their beautiful, two-year old son? Both Israel’s legal challenges against the hospital and his physical recovery pose significant, seemingly insurmountable, battles. But maybe there are times in life when love and the will to live can decimate the impossible to nothing. And maybe the truly wise know that nothing—absolutely nothing—is impossible for God.
LifeNews Note: Erin Mersino is a pro-life attorney who has worked for the More Law Center and has been published by National Right to Life News, USA Today, Politico Magazine, American Thinker and others.
Mining the theology of the Body-inspired wealth of the post-synodal apostolic exhortation “The Joy of Love”
After nearly 18 months of speculation, the other shoe has dropped, and Pope Francis has finally issued his apostolic exhortation on the 2014-15 Synod of the Family. In true Francis fashion he has issued a document that he hopes will challenge everyone (para. 7). Against calls for “general rules” or “immoderate … change,” he instead articulates a philosophy of accompaniment, which depends not on rules but on relationships (para. 2). In particular he urges us to cherish the good in every family situation, no matter how irregular (paras. 77, 292).
Apart from sparking an inevitable firestorm of controversy around hot-button issues, Amoris Laetitia (The Joy of Love) also directs stirringly beautiful words of encouragement and inspiration to married couples in line with the teaching of Pope St. John Paul II. Commentators have long wondered and worried if the thoughts of John Paul II would be reflected in this newest Church pronouncement on the family. The reading guide for bishops, presented earlier this week, reassured clerics that Amoris Laetitia was heavily inspired by the Theology of the Body, the former pontiff’s groundbreaking discourses on marriage and sexuality.
Amoris Laetitia combines brilliant scriptural analysis akin to John Paul II’s with a healthy dash of Francis’ plain-spoken, homespun wisdom. Its praise of sexual and erotic love echoes Pope Benedict XVI in Deus Caritas Est (God is Love). Pope Francis’ chapter 1 on the biblical basis of marriage tracks the journey of Adam and Eve from solitude to togetherness, and then to suffering and finally redemption through Jesus Christ (paras. 9-22), just as John Paul II did in the opening addresses of the Theology of the Body.
The two “central chapters” of Amoris Laetitia, and the ones in which Pope Francis speaks most directly to married couples, are chapters 4 and 5 (paras. 6-7). Chapter 4 leads us line by line through St. Paul’s much-beloved Hymn to Love in 1 Corinthians 13, while chapter 5 focuses on the fruitful love that is “a symbol of God’s inner life” (para. 11). These chapters offer the following strikingly practical insights on how to live the married vocation to the fullest.
See each other (para. 128). “We often hear in families: ‘My husband does not look at me,’” or “‘My wife no longer looks at me; she only has eyes for our children,’” notes Pope Francis. Husbands and wives must not withhold a “look of appreciation,” a gaze of “contemplative love,” even when our spouse has become “infirm, elderly or physically unattractive,” he continues. “Much hurt and many problems result when we stop looking at one another.”
Listen to each other (paras. 100, 137, 139). “How often we hear complaints like: ‘He does not listen to me,’” adds Pope Francis. Husbands and wives show love when we “listen patiently and attentively,” exercising “the self-discipline of not speaking until the time is right.” Our ability to listen depends on whether we cultivate “interior silence” and an ability to acknowledge the worth of the other person and their perspective. “The combination of two different ways of thinking can lead to a synthesis that enriches both,” he wisely observes.
And when we finally speak, “words should be carefully chosen,” he says. “Those who love are capable of speaking words of comfort, strength, consolation, and encouragement … not words that demean, sadden, anger or show scorn.”
Touch each other (paras. 148, 157). Authentic married love will “welcome with sincere and joyful gratitude … a caress, an embrace, a kiss and sexual union,” says Francis. The search for sexual pleasure should not resemble an obsessive insatiability, however. “Excess, lack of control or obsession with a single form of pleasure can end up weakening and tainting that very pleasure and damaging family life,” the pope warns.
Let nothing rob you of the joy of parenthood (paras. 168, 171, 179). “Don’t let fears, worries, other people’s comments or problems lessen your joy,” Pope Francis encourages us. Children are a gift from God, and the conception of each child marks a moment when “the Creator’s eternal dream [of that child] comes true.” The pope urges married couples, particularly those who struggle with infertility, to adopt or provide foster care, “offering the gift of a family to someone who has none.”
These nuggets of practical wisdom are a small fraction of the treasures to be found in Amoris Laetitia. The broad sweep of the document covers theological issues like the sacramentality and indissolubility of marriage, economic issues like migration and unemployment, and pastoral issues like marriage preparation, the training of priests and care for the divorced and remarried. With reason, Pope Francis refers to the synod proceedings as a “multifaceted gem” and asks us to devote more than “a rushed reading” to his post-synodal exhortation (paras. 4, 7).
April 6, 2016 (LifeSiteNews) – Accounts of the Pill’s negative side effects have been trending on Twitter, with a stream of women coming forward to share their chemical contraception horror stories gaining notice in the unlikely forum of the feminist press.
Women’s magazines have long championed the birth control pill as a liberator of women, but the #MyPillStory hashtag detailing the Pill’s medical downside has gotten coverage from a number of such outlets in the U.S. and the UK, such as Glamour, Huffington Post, and Stylist Magazine.
Twitter accounts of devastation from the Pill began March 31 and have continued since, one sharing, “T1Diabetic and the pill messed up my sugar levels so bad I developed an abscess, my sight damaged and had to leave college.”
The story took off after UK journalist Holly Brockwell tweeted her frustration over fighting with England’s National Health Service’s (NHS) to sterilize her, according to Glamour. She wanted the procedure because the pill caused her dizziness, vomiting, skin problems, bleeding and pain. Brockwell had either been told to take the Pill or that her boyfriend could have a vasectomy.
“Do you know what it’s like to bleed for a month?” Brockwell challenged a male on social media who questioned her effort to be sterilized. “Have you spent mornings off work because you’re throwing up from hormones you don’t need in your body? Have you called the NHS direct because your leg feels weird and you’re worried your high-risk pill has given you a fatal blood clot?”
“One pill made me bleed so much for so long that I was on iron tablets for months afterwards,” she’d also stated.
“I can’t take the pill because it gives me migraines, mood swings & weight gain,” was the reply from Kate Bevan, who came up with the hashtag.
Brockwell was clear in her posts she is not anti-pill; instead she opposes people telling her dismissively to take the Pill, particularly men.
But the campaign opened the door to the difficulties caused by chemical contraception, one Twitter user offering, “One pill I took … not only made my body feel alien but then started making me violently sick once every hour.”
The physical complications from oral contraceptives are well-documented, such as risk of blood clots, hair loss, greater chance of Crohn’s Disease and brain shrinkage, breast cancer, hardening of the arteries, increased risk of glaucoma and cervical cancer.
Some of the #MyPillStory posts demonstrated this, one stating, “Headaches, severe mood swings, nausea, vomiting and the autoimmune issues I have were all gifted to me from hormonal bc.”
But many also showed how the Pill is related to mental and psychological maladies as well.
“#MyPillStory depressed, lethargic, dissociated. sleeping for over 12 hours a day and still exhausted. reluctant to ever try it again,” one stated.
“I dealt with crushing depression and suicidal ideation for days in a row not realizing what was happening,” came from another, and still another saying, “On pill for a year before I realised it was why I was experiencing crippling gender dysphoria. By then I’d already quit my job.”
The disturbing accounts continued, showing a pattern.
“Took the pill when I was 18 cried everyday for a year, high anxiety, no libido, no idea what was going on until I stopped,” one person tweeted. Another said, “It made me lose my mind. I wasn’t myself. Suicidal and scared. Seems I’m not alone.”
Brockwell recently learned she will get her sterilization from the British government in the next few months, but her personal campaign to avoid pregnancy ultimately shed light on the dangerous chemical option millions of women use to achieve the same.
“This whole thing is straight-up terrifying,” one of her tweets stated. “Can’t wait to get off the pill.”
The world is reeling from the massive terrorist attacks last week in Brussels and Pakistan that killed dozens and left hundreds more wounded. But a pregnant woman who survived the Belgium attack walked away with a glimmer of hope amid the grief and destruction: Her unborn baby was safe.
The Telegraph reports the story of Sneha Mehta, 28, and her husband, Sameep, who had just arrived at the Brussels Airport last Tuesday when Islamic terrorists set off two bombs in the terminal. Terrorists also bombed the city’s metro system.
The couple said they had just walked off their flight from the United Arab Emirates when the bombs went off. Seeing the ceiling starting to fall down toward their heads, the couple rushed out of the building, according CNN. Though unharmed, the Mehtas grabbed a taxi and went to a nearby hospital to make sure their unborn baby was OK, the report states.
There on the ultrasound screen, the couple saw their 16-week unborn baby looking perfectly content sucking its thumb and moving around, according to the report. They do not know if it is a boy or girl yet.
When the couple finally got home, Sneha wrote a letter to her unborn child about her experiences on that terrible day. It reads:
“Hi Sweetheart,
“I don’t know if we already acknowledged this with you in person, but when you were 16 weeks old, mum and dad were in an explosion at Brussels Airport.
“And no matter where humanity is today, I just want to tell you that life is a wonderful thing, and the world is really full of remarkable people.
“You didn’t just give mum and dad faith and reason to live, you gave the awareness and presence of mind like never before.
“I felt more alive than I ever have, and I knew I had to protect you, so I was calm, composed and fully aware that we will survive.
“When we reached Sint-Augustinus emergency, and we saw you oblivious and sucking at your thumb at the ultrasound, and doing your general acrobatics, all the mistrust, hate and angst for the terrorist attack vaporized.
“I do hope with all my heart that you are born into a better world, and if not, then you do absolute best to make it that.
“You are absolutely precious to us, and have already been a hero today. I guess the world has sent so much love and hope your way, you owe your life to reciprocating that goodness.
“May you always be brave and healthy. We love you beyond words.
“Mum and Dad”
The expecting mother said she “knew for sure” that she would survive the attack. Her confidence came from her desire to protect her unborn baby, she said.
CNN reports the death toll from the Brussels terrorist attack is now 35, and approximately 300 others were injured. Another terrorist attack, apparently the work of the Taliban, occurred on Easter Sunday in a park in Pakistan where children and families were gathered, according to ABC News. About 70 people were killed and more than 300 others were injured, according to the report.
Amid such horrible acts of death and destruction, it is difficult to find hope for the future. But Sneha’s touching letter is a reminder that hope is renewed every time a new human life begins.
You are hereby dared to watch this video and not smile at the clear delight His Holiness takes in greeting these two girls, and their happiness at being called to him. Hugs are exchanged, rosaries given. May these two young ladies wear those beads out; the prayers of the innocent are powerful, and people with Down syndrome — who are gifted with a huge, underappreciated capacity for love and nearly aborted into extinction — know how to pray with big, generous hearts.
Perhaps that’s why the Evil One would prefer not to see them born?
Dare I say that? Yes, I think I dare.
Peter walks — has always walked — among those whose “quality of life” seems dubious to the world, which wonders why some people are permitted to be born at all. He gives them a bit of time, a bit of “kindness therapy” and thus affirms to the world that they are indeed acceptable to God with the life they have; that the life they have is as valuable as anyone’s. Even the most beautiful and most celebrated.
In Mexico, as you can see above and here and here and here, Peter has been doing a lot of affirming.
THOUSAND OAKS, California, December 14, 2015 (LifeSiteNews) – Another surrogate carrier is fighting for the life of the child in her womb.
As LifeSiteNews reported, Melissa Cook in California is carrying triplets conceived by a Georgia man and a 20-year-old egg donor. Since all three survived and are growing in Cook’s womb, the Georgia man is threatening Cook with financial ruin if she does not abort at least one of the babies.
Now, surrogate carrier Brittneyrose Torres is being pressured to abort at least one of her triplets. She told The New York Post that the birth parents “knew from the beginning that we wouldn’t want to abort unless it was a life-and-death situation.”
Torres, 26, was initially implanted with two embryos in hopes that one of them would develop. It is the usual practice to implant more than one conceived baby because many do not survive the procedure. In Torres’s case, not only did both survive, a boy and a girl, but twinning occurred, giving Torres one girl and two twin boys.
Initially excited about triplets, the parental contractors later claimed increased risk of developmental disabilities and demanded that Torres abort the girl.
“I told her I couldn’t abort one of the children,” Torres told The Post. “I believe it will be killing this baby.” She even offered to adopt the girl, but the parental contractors refused.
“Reproductive technology has reduced each of the children in question to a commodity that can be traded, discarded, killed, or accepted, according to the whims of the parents who paid for the procedure,” Judie Brown, president of the American Life League, told LifeSiteNews.
“It is clear that such technology breeds cavalier attitudes toward children who result from such practices,” Ms. Brown concluded. “As a result, the dignity that each pre-born child possesses is too easily ignored.”
“Torres’s decision to choose life for the triplets she was asked to carry for another couple speaks volumes to what is wrong with reproductive technology, and why the Catholic Church has been wise to teach that each child has a right to be created within the context of a loving marriage between a man and a woman,” the pro-life leader told LifeSiteNews. “This is very sad, and it calls us to remember that building a culture of life begins with accepting God’s plan for the procreation of children.
“No one has a right to a child, and surely no one should have the right to instruct a third party, a surrogate mother, to kill babies that they engaged the surrogate to carry for them,” the American Life League co-founder stated. “Thankfully, Britney has chosen to ignore the instructions of her triplets’ parents, and she will carry them to term.”
In both the Torres and Cook cases, the contract signed included a provision giving the parental contractors the legal right to order an abortion. In both cases, the parental contractors are withholding payments until the surrogate carriers abort.
“I want other women not to be put in this situation,” Torres said. “They shouldn’t be forced to do something they don’t want to.”
March 8, 2016 (POP) — A new peer-reviewed study,1 conducted in collaboration with the Population Research Institute (PRI), shows that women who use Depo-Provera are significantly more likely to acquire HIV.
Due to funding from organizations like the Bill and Melinda Gates Foundation and agencies like the United Nations Population Fund (UNFPA), Depo-Provera is the most widely used form of birth control by women in Sub-Saharan Africa where HIV prevalence remains high.
The study found that Depo-Provera and other DMPA based injectable contraceptives increased women’s risk of acquiring HIV-1 by 49% compared to those not using hormonal contraception.
Depo-Provera, a pharmaceutical brand owned by Pfizer, Inc., is a long-term injectable contraceptive that prevents pregnancy for three months.
The active ingredient in Depo-Provera, and other injectable contraceptives like Depo Sub-Q Provera 104, is a progestin known as depot-medroxyprogesterone acetate (DMPA). DMPA based injectable contraceptives account for an estimated 70% of injectable contraceptives procured by non-governmental organizations (NGOs) and government agencies, like the UNFPA and the U.S. Agency for International Development (USAID).
The study involved a meta-analysis of 23 articles from peer-reviewed journals, making this study the largest of its kind to date. The authors found consistent evidence that women using DMPA acquired the HIV-1 virus at significantly higher rates than the general population. In total, 88% of cross-sectional studies and 75% of longitudinal studies demonstrated a higher risk among DMPA users.
Joel Brind, Professor of Biology and Endocrinology at the City University of New York, Steven Condly, Research Psychologist at the U.S. Military Academy, Steven W. Mosher, President of the Population Research Institute, Anne Morse, graduate student at Pennsylvania State University, and Jennifer Kimball, Adjunct Professor of Bioethics at the Ave Maria School of Law participated in the study.
The authors also delved into possible biological explanations for why DMPA increases the risk of HIV. Researchers found a number of studies showing that DMPA weakens the body’s immune system and thins natural epithelial barriers that prevent the HIV virus from infecting women.
While study after study has demonstrated a clear and strong association between HIV and DMPA, the World Health Organization (WHO), the Gates Foundation and other interested parties involved in procuring injectable contraceptives worldwide have been less keen on the issue.
The WHO’s failure to acknowledge the associated risk has caused a controversy that has spanned political persuasions on both the left and the right.
A controversial statement released by the WHO acknowledges the evidence of an increased HIV risk. Yet, in spite of the associated risks involved, the WHO recommends that:
There are no restrictions on the use of hormonal contraceptives, including DMPA for women at high risk of HIV (MEC Category 1)
While scientists are still not certain why women who used DMPA were more likely to acquire HIV, a number of studies have found significant evidence of possible causal associations between DMPA and HIV transmission.
Huijbreghts, et al. (2013),2 for example, found in in vitro experiments that MPA decreased immune cell’s production of cytokines and chemokines essentially to the immune system and reduced the proliferation of T-cells. Others like Govender, et al. (2014),3 have shown that MPA, unlike endogenous progesterone, represses inflammatory cytokines by acting as a glucocorticoid receptor agonist.
In spite of the evidence, the WHO claims:
There is no evidence of a causal association between DMPA use and an increase in women’s risk of HIV acquisition.
It is unclear why the WHO continues to ignore the evidence of the associated risk of HIV. Some have suggested that the WHO and the U.N. are catering to some their largest donors. Up to 10% of the WHO’s annual budget is financed by the Bill and Melinda Gates Foundation. DMPA injectables are often appealing for population control programs because they are not subject to “user-error” and remain effective for long periods of time.
The WHO could also be turning a blind eye to the issue in light of the recent release of Sayana Press, Pfizer’s one-time use DMPA injectable intended for self-injection, which has been strongly promoted with the support of the Gates Foundation, USAID, and others. Trial introductions of the injectable in Africa have not relied on doctors and nurses but rather largely on unlicensed community health workers for distribution. A stronger statement from the WHO on recommendations for DMPA use would necessarily hamper efforts to widely distribute the new injectable contraceptive.
Depo-Provera is also one of Pfizer’s fastest growing products by total sales, with an almost 30% increase in revenue from FY 2012-2013. In 2014, Pfizer took in over $200 million in revenues from Depo-Provera sales
With HIV prevalence rates exceeding 20% of the adult population in some African countries, the WHO offers condoms as a solution to any possible risk associated with the use of DMPA. According to the WHO:
Women and couples at high risk of HIV acquisition considering progestogen-only injectables should also be informed about and have access to HIV preventive measures, including male and female condoms.
As Brind, et al. (2015) includes both DMPA users who reported using and not using condoms, there is reason to doubt that the recommendation—that serodiscordant and high risk couples use barrier methods such as condoms for protection against HIV-1 transmission—will be effective. As condom failure rates for pregnancy prevention are 18-21% within the first year with typical use,4 failure rates for STI prevention are likely similar.
Areas where HIV prevalence is high are also areas where condom use is inconsistent and has high failure rates.
A large study in Uganda5 showed inconsistent condom use failed to protect against HIV acquisition. Inconsistent users were found to contract HIV at incidence rates higher than persons who reported not using condoms at all. Even as consistent usage was found to reduce the risk, almost four times as many persons who reported using condoms used them inconsistently rather than consistently. As Uganda ranked 10th in the world for HIV prevalence among adults of reproductive age in 2013, according WHO data, adopting a policy of recommending condom usage with DMPA could have disastrous consequences.
Conversely, Niger, a country with one of the lowest contraceptive prevalence rates in the world, has one of the lowest HIV prevalence rates in Sub-Saharan Africa. Prevalence of HIV among adults of reproductive age in Niger match those in Spain and are only 0.1% higher than HIV prevalence in the U.K. According to 2012 data from the U.N. Population Division, female contraceptive prevalence in the U.K. was second only to China.
It is not likely that advising women who use DMPA to also use condoms will have much effect. Even in the United States where contraceptive prevalence and education remains high, among couples who report using dual methods of contraception, over 40% reported using condoms incorrectly and half fail to use them on a consistent basis.6 As less than one-third of South African women using hormonal contraception reported using dual methods,7 it is irresponsible to counsel women to use condoms as an effective means of protection against HIV.
1. Joel Brind, Steven J. Condly, Steven W. Mosher, Anne R. Morse, and Jennifer Kimball, “Risk of HIV infection in depot-medroxyprogesterone acetate (DMPA) users: a systematic review and meta-analysis,” Issues in Law & Medicine, 2015; 30(2):129-139.
2. Huijbregts, Richard P. H., E. Scott Helton, Katherine G. Michel, Steffanie Sabbaj, Holly E. Richter, Paul A. Goepfert, Zdenek Hell, “Hormonal contraception and HIV-1 infection: medroxyprogesterone acetate suppresses innate and adaptive immune mechanisms,” Endocrinology, 2013; 154(3): 1282-1295, doi: 10.1210/en.2012-1850.
3. Govender, Yashini, Chanel Avenant, Nicolette J. D. Verhoog, Roslyn M. Ray, Nicholas J. Grantham, Donita Africander, Janet P. Hapgood, “The injectable-only contraceptive medroxyprogesterone acetate, unlike norethisterone acetate and progesterone, regulates inflammatory genes in endocervical cells via the glucocorticoid receptor,” PLOS ONE, 2014; 9(5), doi:10. 1371/journal.pone.0096497.
4. Lisa B. Haddad, Chelsea B. Polis, Anandi N. Sheth, Jennifer Brown, Athena P. Kourtis, Caroline King, Rana Chakraborty, Igho Ofotokun, “Contraceptive methods and risk of HIV acquisition or female-to-male transmission,” HHS public access author manuscript, published in: Current HIV/AIDS Reports, 2014; 11(4): 447–458, doi:10.1007/s11904-014-0236-6.
5. Saifuddin Ahmed, Tom Lutalo, Maria Wawer, David Serwadda, Nelson K. Sewankambo, Fred Nalugoda, Fred Makumbi, Fred Wabwire-Mangen, Noah Kiwanuka, Godfrey Kigozi, Mohamed Kiddugavu and Ron Gray, “HIV incidence and sexually transmitted disease prevalence associated with condom use: a population study in Rakai, Uganda,” AIDS, 2001; 15:2171-2179.
6. Jenny A. Higgins, Nicole K. Smith, Stephanie A. Sanders, Vanessa Schick, Debby Herbenick, Michael Reece, Brian Dodge, J. Dennis Fortenberry, “Dual method use at last sexual encounter: a nationally representative, episode-level analysis of US men and women,” HHS public access author manuscript, published in: Contraception, 2014; 90(4): 399–406, doi:10.1016/j.contraception.2014.06.003.
7. Catherine MacPhail, Audrey Pettifor, Sophie Pascoe, Helen Rees, “Predictors of dual method use for pregnancy and HIV prevention among adolescent South African women,” Contraception, 2007; 75(5): 383-389.
February 22, 2016 (LifeSiteNews) — Among the many reactions to Pope Francis’ interview on the return flight from Mexico last week are the thoughtful reflections of two female theologians of note. Both Professor Janet Smith, who holds the Father Michael J. McGivney Chair of Life Ethics at Sacred Heart Major Seminary in Detroit, and Dr. Monica Miller, a Ph.D. in Theology from Marquette University and Director of Citizens for a Pro-Life Society, took up Pope Francis’ answer to a question about the Zika virus, contraception, and the “lesser of two evils.”
When asked about the ‘avoiding pregnancy’ in areas at risk of Zika virus transmission, Pope Francis spoke of the supposed permission given by Pope Paul VI to nuns in Africa to use “contraceptives in cases of rape.”
“Don’t confuse the evil of avoiding pregnancy by itself, with abortion,” he said. “In certain cases, as in this one, or in the one I mentioned of Blessed Paul VI, it was clear.” The Pope also suggested that the question of “avoiding pregnancy” in Zika zones could involve a “conflict between the fifth and sixth commandment.”
Responding to a request from LifeSiteNews Dr. Monica Miller said:
It is interesting to note that the reporter never used the term “contraception”—only whether “avoiding pregnancy” was the “lesser evil.” First, of all it is not necessarily an evil at all to avoid a pregnancy—as couples can certainly abstain from sex, or use Natural Family Planning when there is a serious reason to avoid pregnancy. Thus if the pope simply meant to say that the Zika virus threat was such a serious reason for couples to avoid pregnancy – with recourse to methods that are morally licit – the pope did not teach that there are circumstances when the use of artificial contraceptives can be morally licit.
However, the pope’s response is confusing, unclear and certainly people can come away from it thinking that His Holiness did endorse exceptions to the Church’s ban on the use of artificial contraception. Why? Because, number one—the reporter characterized “avoiding pregnancy” as an “evil”—albeit a “lesser evil” and everyone knows that the Church considers contraceptive use as a moral evil, whether they agree with that position or not.
Then Pope Francis made the statement that there was or could be a conflict between the 5th and 6th commandment—thus giving the impression that there was some kind of a moral quandary or tension between moral goods that perhaps can only be resolved by compromising with recourse to a “lesser evil” in order to secure or protect the greater good—in this case the good of life. It was a rather odd statement, and Catholic moral theology does not speak in terms of commandments being in conflict with each other. Then—when the Pope used the situation of nuns in the Belgian Congo being permitted to use contraception to thwart the effects of rape—the Pope certainly gave more than the impression that in difficult, crisis situations persons may licitly use artificial contraception—when indeed the Church is quite clear that such use is never morally licit as contraception violates the meaning of the conjugal act.
The problem, as usual is the use of imprecise language, improper characterizations of moral issues that lead to serious confusion. One has to wonder why the Pope did not immediately launch into an endorsement of Natural Family Planning as soon as he heard the reporter ask about the licitness of “avoiding pregnancy.” A missed teaching moment descended into confusion. Hopefully Pope Francis prays that prayer to Mary, the un-doer of knots—as there are a lot of knots here that need to be undone.
Dr. Janet Smith, writing in the pages of Catholic World Report said similarly:
The (Principle of Choosing the Lesser Evil) PCLE does not justify a woman using contraception to prevent a pregnancy because she fears the child may suffer some harm during the pregnancy. Here a woman is choosing to do something immoral to prevent harm. This choice violates the fundamental principle that we must never do moral evil to achieve good. She would be intending to thwart the purpose and meaning of the sexual act in order to protect any child conceived from harm, but she is doing harm—to the marital act and her marital relationship—by using contraception to prevent a pregnancy.
There are all sorts of “harm” that spouses may wish to attempt to avoid by using contraception. In fact, one suspects that there is always some harm spouses are trying to avoid by using contraception—harms such as financial stress, inconvenience, threats to the mother’s health, sexual frustration, etc. The Church has never taught that if the harms are serious enough, it is permissible to use contraception, for that would be choosing to do moral evil to avoid harm.
To suggest that some “emergency” or “special situation” would permit a person in conscience to use contraception does not align with Catholic moral theology. For spouses to use contraception is always wrong. How can any emergency or special situation justify what is always wrong? It is an improper use of conscience to use it to discern that it is moral to do what is intrinsically wrong in special situations. One job of the conscience is precisely to enable a person to honor moral norms in special situations. In emergencies or special situations we are not permitted, for instance, directly to kill innocent human beings even if great good could come from that death. Martyrdom is precisely a result of the refusal to do something that is morally wrong in an “emergency” or “special situation.”
Conflict between the Fifth and Sixth Commandments
Let us also consider the claim that there might be a conflict between the Fifth (“thou shalt not kill”) and Sixth (“thou shalt not commit adultery”) Commandments that would justify the use of contraception. What is the risk of violating one of those commandments by honoring the other? Is the reasoning here that those who conceive, for instance, a child with microcephaly are responsible for a kind of “killing of the child”? That is, their honoring their marital fidelity by having sexual intercourse open to life puts them in a position of endangering the life of a child conceived (a violation of the Fifth Commandment?). Or, if they refrain from sexual intercourse in order to avoid putting the life of a child at risk, is there the suggestion that that refraining is a violation of some kind of the Sixth Commandment?
This “conflict” seems to imply that to use contraception (which violates the Sixth Commandment) is a lesser evil than violating the Fifth Commandment and that spouses should be permitted to use contraception to avoid conceiving a child with microcephaly—seen as a kind of murder. But this reasoning is not sound for several reasons. First, to conceive a child with microcephaly is not a form of murder; life is always a gift, and even life as a person with microcephaly is a gift. There are undoubtedly serious challenges and difficulties in living with microcephaly and caring for someone with microcephaly, but one has not harmed a person by giving him or her life.
Moreover, spouses are not under an obligation to have sexual intercourse. If they believe their intercourse might lead to a problematic situation for which they are not prepared, they are free to abstain completely from sexual intercourse or abstain periodically. Spouses abstain for all sorts of reasons—because of physical separation, illness, and even such trivial reasons as a desire to watch sports on TV or to do the laundry. To abstain to avoid exposing a child to the danger of microcephaly would seem a respectable reason for abstaining.
These are some of basic principles that need to be kept in mind when assessing proposals to help women who live in areas where children conceived might contract lethal or disfiguring diseases. Contraception is not a moral solution. Use of a method of natural family planning is.
Read Dr. Smith’s full essay at Catholic World Report here.
The American College of Pediatricians (the College), recently updated its stance on Gardasil, a vaccine for the Human Papillomavirus (HPV), in wake of recent research about the virus and vaccine. The College acknowledged that HPV vaccines have been possibly linked to premature ovarian failure (POF), but quickly back peddled by stating that such side effects are rare.
Human papillomavirus (HPV) is a common sexually transmitted virus. According to the press release, approximately 14 types of HPV are believed to cause multiple cancers. The most common cancer that has been causally attached to HPV is cervical cancer.
Multiple concerns over HPV vaccines
The statement notes that there are legitimate concerns about the HPV vaccine that need to be addressed, including:
Long term ovarian function was not assessed in either the original rat safety studies, or in the human vaccine trial.
Most primary care physicians are probably unaware of a possible association between HPV4 and POF and may not consider reporting POF cases or prolonged missing menstrual periods to the Vaccine Adverse Event Reporting System (VAERS).
Potential mechanisms of action have been postulated based on autoimmune associations with the aluminum adjuvant used and previously documented ovarian toxicity in rats from another component, polysorbate 80.
Since licensure of Gardasil in 2006, there have been about 213 VAERS reports involving amenorrhea, POF or premature menopause, 88 percent of which have been associated with Gardasil.
“A Vaccine Safety Datalink POF study is planned to address an association between these vaccines and POF, but it may be years before results will be determined. Plus, POF within a few years of vaccination could be the tip of the iceberg since ovarian dysfunction manifested by months of amenorrhea may later progress to POF,” the press release reads.
Three vaccines intended to prevent cervical cancer caused by the HPV vaccine, have been licensed since 2006. More than a dozen girls in Europe have recently come forth, claiming to have experienced ill side effects from the vaccine. Most HPV infections go away by themselves
But there are truths about Gardasil and HPV that the press release overlooks, including the fact that 70 percent of HPV infections in women will clear themselves in a year without treatment. In two years, approximately 90 percent of these infections will clear themselves. In three years, only ten 10 percent of women will have an HPV infection, half of which will have developed into a pre-cancerous legion.
The authors of the statement claim they have notified the makers of Gardasil, the Advisory Committee on Immunization Practices (ACIP), and the Food and Drug Administration (FDA) about their concerns. The College went on to press that HPV vaccines should not be mandated by regulatory authorities.
“The College is opposed to any legislation which requires HPV vaccination for school attendance. Excluding children from school over refusal to vaccinate for a disease spread only by sexual intercourse is a serious, precedent-setting action that trespasses on the right of parents to make medical decisions for their children.”
ORLANDO, Florida, February 12, 2016 (LifeSiteNews) — What was it that allowed St. Gianna Beretta Molla to choose the life of her child over her own life when faced with the decision? What allowed her to offer praise and thanks to God even though she would die days after delivering her healthy baby, leaving four young children and a loving husband?
The secret of St. Gianna’s holiness was revealed to LifeSiteNews in an interview with the very person the saint gave up her life for, her daughter Gianna Emanuela Molla.
https://youtu.be/tJqUakQXs0A
Gianna Emanuela, 54 years old, said that if her parents’ lives have taught her anything, it’s that the “way of the cross” is “certainly the right way” that Christians must follow if they are “to be able one day to enjoy paradise joy in the sight of God, forever.”
She is not talking about a sad and sorrowful living out of the Christian faith, but a kind of living that brings one to the deepest and most profound — and very often unexpected — joy. How to accomplish these two seemingly irreconcilable things — embracing the cross and finding joy — is the “secret.”
Gianna Emanuela explained that for Christians, the cross does not have the final word, but becomes the source for the greatest transformation.
“The way of the cross, humanly [speaking], is the most uncomfortable and the difficult way to follow. But it is the only way that allows us to [find] a full and complete meaning to our lives,” she said.
“The way of the cross, as you know, is connected to the resurrection, as our Jesus teaches us. And, as our heavenly mother teaches us, this way of the cross requires our ‘yes,’ our continuous ‘yes’ to God’s will, always, even when we don’t understand God’s will. We have to say our ‘yes’ to God,” she added.
Gianna Emanuela sees in the example of her parents’ lives the joy that comes from embracing the crosses they encountered daily throughout life.
“Mom and dad’s lives teach me also that the way of the cross is the way of the joy, as well. Which kind of joy? The most perfect joy, the most great joy, the prelude to the greatest joy – to be able one day to have the joy of paradise, of being in God’s sight, forever,” she said.
“It’s possible to walk along the way of the cross and to live in the joy, if we have Jesus in our heart, if we see everything happening to us in the light of faith. And so, if we live in this way, we feel [inspired] to thank God continuously, as did my dad, for everything, for each of our breaths. We have to thank God,” she added.
That freely choosing to embrace the crosses in one’s life as God’s will and finding peace and joy in that action comes directly from Jesus himself. It was he who said, “Whoever wants to be my disciple must deny themselves and take up their cross and follow me” (Matt. 16:24). In another place he says, “Take my yoke upon you and learn from me, for I am gentle and humble in heart, and you will find rest for your souls. For my yoke is easy and my burden is light” (Matt. 11:28-30) He also said, “I have told you this so that my joy may be in you and that your joy may be complete” (Jn. 15:11).
Gianna Emanuela will forever be grateful for her “Saint Mama” deciding to embrace the cross after discovering a life threatening disease while being pregnant.
Her mom, a pediatric doctor, was pregnant with Gianna Emanuela in 1961 when she learned she had a life-threatening tumor of the uterus. Doctors gave her three choices: an abortion, a complete hysterectomy (which would also kill her baby), or surgical removal of only the tumor (less chance of success). With the life of her precious daughter in mind, the mom opted for the removal of the tumor.
But complications persisted. Facing a difficult delivery, she told doctors, “If you must decide between me and the child, do not hesitate: choose the child – I insist on it. Save him.” She died seven days later on April 28, 1962, giving her life for her child, after repeatedly exclaiming, “Jesus, I love you. Jesus, I love you.” She was 39 years old.
Gianna Emanuela said that her Mom’s ‘yes’ to God amidst the complications and agonizing pain surrounding the pregnancy and delivery allowed God to raise up something beautiful from what most people would consider a hopeless situation.
“My Saint Mama saying her ‘yes’ to God allowed God to realize (bring to fruition) my own life in a complete way,” she said.
She said the key to successfully embracing the cross while turning it into a source of joy is to “continuously” thank God for everything, the good and the bad, that come one’s way.
“Mom and dad, both of them suffered a lot in their lives…And even if they suffered a lot, they had a great joy in their heart. They continuously thanked God, which was their secret. If we think that Jesus went on the cross, it is not possible to think of a different way for us [as Christians]. This way of the cross, is also the way of the joy,” she said.
A miracle attributed to the young Mexican martyr, Jose del Rio, has been approved by the Vatican, opening the door to his canonization.
Aleteia is reporting on the miracle which occurred in Sahuayo, Mexico to a baby girl named Ximena Guadalupe Magallan Gálvez – or “Lupis” as her family called her.
Lupis began fighting the odds even before she was born. Her mother, Paulina Galvez, had serious problems throughout the pregnancy, including placental abruption, a condition that can prove fatal to the unborn child.
It was during these early difficulties that Paulina began to pray to Blessed Jose Sanchez del Rio, known locally as “Joselito”, who was born in Sahuayo in 1913.
Lupis was born on September 8, 2008, on the Feast of the Nativity of Our Lady, while Paulina was living in Los Angeles. A month later, she returned to Sahuayo, and shortly thereafter, the baby contracted pneumonia and tuberculosis. At four months, Lupis suffered a stroke, contracted meningitis and began to have epileptic seizures.
Gravely ill, she was transferred to an intensive care unit in Aguascalientes and underwent therapy and a series of tests. In an effort to stop her continuous spasms, doctors induced a coma.
The baby continued to decline until doctors determined that 90 percent of the baby’s brain was dead. They recommended that life support be removed.
Paulina agreed, but asked if she could hold the child in her arms for the last time.
“At that time I put my baby in the hands of God and the intercession of Joselito,” Paulina told the official Mexican news agency, Notimex.
Just then, Lupis “opened her eyes and smiled, looked at the doctors and started to laugh,” Paulina said.
Doctors were astonished, especially after CT scans and an EEG proved that Lupis’ brain had returned to normal.
The priest who baptized Lupis contacted Antonio Berumen, vice postulator of the cause of canonization for Blessed Jose and began the process of documenting and verifying the miracle. Seven years later, the Vatican approved the miracle.
Although Pope Francis will be visiting Mexico from February 12-17, it has not been announced if he will canonize Blessed Jose while there.
Sahuayo was the birthplace of Blessed Jose, who was martyred for the faith on February 10, 1928. Devoted to the Blessed Sacrament and Our Lady of Guadalupe, he was only 15 years old when he joined the Cristeros, a rebel band of Catholics who were fighting the violent anti-Christian despot, Plutarco Calles. After relinquishing his horse to a General during a particularly fierce battle, he was captured and locked up in a church sacristy that had been made into a prison.
On February 10, 1928, his captors decided to make an example out of him by executing him. They marched him out to a local cemetery, whipping him with sharp machetes along the way. With each blow, Jose cried out, “Viva Cristo Rey!” which means “Long live Christ the King.” His captors also cut off the soles of his feet and forced him to walk on salt. Even though he screamed in pain, Jose would not give in to the soldier’s wishes that he forsake his God. When they demanded that he shout, “Death to Christ the King,” Jose shouted all the louder, “Long Live Christ the King! Long live Our Lady of Guadalupe!”
Enraged, the soldiers finally rushed upon him with their bayonets, piercing his body in multiple places, but he still would not be silenced. “Viva Cristo Rey!” were the last words he uttered on this earth before the commander pulled out a pistol and shot him to death.
He was declared a martyr for the faith and was beatified in 2005 by Pope Benedict XVI.
His feast day is February 10.
– See more at: http://www.womenofgrace.com/blog/?p=47121#sthash.9SebxyzP.dpuf
If you haven’t already heard, the Doritos ad in the Super Bowl yesterday caused quite a stir.
https://youtu.be/vH2LsFcWOFY
The ad – which focused on an unborn baby wildly chasing after a cheesy chip that was being dangled over Mom’s tummy – attracted some harsh criticism from the pro-abortion group NARAL, which accused it of “humanizing the fetus.”
@NARAL
#NotBuyingIt – that @Doritos ad using #antichoice tactic of humanizing fetuses & sexist tropes of dads as clueless & moms as uptight. #SB50
Many Twitter users were quick to respond that NARAL is a bit out-of-touch with reality. It’s totally normal to go into a third-trimester ultrasound appointment and hear the doc say, “There’s your beautiful baby,” and see an ultrasound image that is very clearly a human baby. It’s not “humanizing the fetus”…it’s just real life.
Turns out, the image is more than just realistic. It’s actually real. (With computer-generated movement, of course). On the Doritos’ Super Bowl campaign website, we find the backstory inspiring the creator, an Australian man named Peter:
“Peter recently had his second child, Freddy, who’s now nine months old. When he was with his wife getting an ultrasound during the pregnancy, an idea popped into his head – wouldn’t it be funny to have a little fun in the hospital room, where everyone is supposed to remain poised, calm and collected. The baby in the ultrasound image is Freddy himself – of course with the help of a little camera magic.”
So the fetus that NARAL accused the commercial of “humanizing” – that’s a little boy named Freddy.
“For Super Bowl 50 the NFL and Seal brought together some actual Super Bowl Babies to recreate one of the greatest love songs of all time to celebrate the greatest game of all time.” (Video via YouTube/NFL)
Some people go to Disney World after a big Super Bowl win. More of us head to the bedroom, at least according to the NFL. Though it doesn’t point to specific data, the NFL says winning Super Bowl cities see a baby boom about nine months after the big game. It spun that idea into a “Super Bowl Babies Choir” commercial that will run at the end of the third quarter in Sunday’s Panthers vs. Broncos match-up.
The already released spot breaks the mold in ESPN’s view, in that it’s actually “memorable”: It features groups of kids and adults—whose sheer existence is potentially attributable to their parents’ city’s win—singing a football-themed take on Seal’s “Kiss From a Rose.”
Fox59 notes adults who came into this world after the Packers’ 1967 win are included, as are Super Bowl babies who owe a little something to the Steelers (1976), 49ers (1989), Cowboys (1993/1994), Buccaneers (2003), Colts (2007), Giants (2012), and Seahawks (2014). That final group tugged on America’s heartstrings, per CNN: “The combination of the adorable 2014 Super Bowl babies and cute lyrics left viewers praising the commercial,” which also stars Seal himself.
The forces of death and misery of the pro-abortion industry are at it again, and they are doing their best to use a troubling item in the news to scare and intimidate strongly pro-woman and pro-child Latin American countries into loosening restrictions on abortion. The Zika virus scare is the tool du jour. In an interview on NPR’s “All Things Considered” published on January 30, 2016, reporter Lourdes Garcia-Navarro interviewed staff of a fertility clinic and abortion activists who decried the slowing down of in vitro fertilizations as women were afraid to become pregnant lest their child be born with birth defects and disabilities due to the Zika virus.
“The pro-abortion movement hasn’t been able to get much traction on the issue, and they’re hoping the debate around the suspected cases of Zika-related microcephaly will change that. Debora Diniz is a law professor and activist. She and other pro-abortion groups are going to petition the Brazilian Supreme Court,” recounts Garcia-Valls.
Never mind the facts. Any and all excuses are valid in the minds of the pro-abortion activists to push for their desired end, free and unencumbered abortion rights.
But, what are the facts? Is Zika, actually, a hideous virus that threatens to spread uncontrollably across the world creating an army of disabled children with tiny heads and low IQ’s? Or might this be a willful misinterpretation of the scarce data to manipulate public opinion and legislatures?
According to the CDC and the WHO, Zika is a mild virus that spreads exclusively through the bite of a specific variety of mosquito, the Aedes Aegypti. This insect is found in tropical climates and is rare in the United States, existing only in some areas of Southern Texas and Southern Florida. It is not transmitted from human to human except through a blood transfusion. It is possible that it may be transmitted sexually although the data regarding this mode of transition is scarce.
According to the WHO, “it causes mild fever and rash. Other symptoms include muscle pain, joint pain, headache, pain behind the eyes and conjunctivitis. Zika virus disease is usually mild, with symptoms lasting only a few days. ”
Many people, never even realize they have it. There are nearly no deaths associated with it, and the disease cannot brought into the colder climates by humans who are infected by the virus while travelling in affected countries.
The most potentially problematic side-effects appear to be to pregnant women. Zika virus infection had been linked with an increased number of miscarriages and cases of microcephaly. But, according to the CDC, “Zika virus infections have been confirmed in infants with microcephaly, and in the current outbreak in Brazil, a marked increase in the number of infants born with microcephaly has been reported. However, it is not known how many of the microcephaly cases are associated with Zika virus infection. Studies are under way to investigate the association of Zika virus infection and microcephaly, including the role of other contributory factors (e.g., prior or concurrent infection with other organisms, nutrition, and environment). The full spectrum of outcomes that might be associated with Zika virus infections during pregnancy is unknown and requires further investigation.”
Contrast the troubling, yet unproven, effect of the Zika virus on unborn children and the very mild effects of upon the pregnant mothers with the well documented lethal effects of the seasonal flu and it becomes very clear that the publicity surrounding this story has a very little to do with medicine and a lot to do with a convenient crisis that is being used by those pushing for the legalization of abortion around the world.
The CDC goes on to recommend that women who may be pregnant not travel in areas where there are known outbreaks of Zika, and that if they do, they take reasonable precautions such as wearing bug spray and light-colored, long-sleeved clothing.
The reasoned and calm directives from the CDC contrast sharply with the hysteria being fostered by the abortion industry lobbyists and their media accomplices… but that is not surprising.
A teenage girl who was on the contraceptive pill died from an ‘extremely rare’ blood clot after returning home from a family holiday, an inquest heard.
Sophie Murray, 16, had been prescribed the pill for around eight months by the time she returned from Gran Canaria last September.
But two weeks later, the “happy and healthy” teenager, from Accrington, started complaining of breathlessness and chest pain.
Blackburn Coroners Court heard how tests by her GP confirmed she was suffering from exercise induced asthma (EIA), the Accrington Observer reported .
She was prescribed an inhaler, however it was ineffective.
Mum Shelley Crichton told the hearing how Sophie woke up on November 8 last year saying she couldn’t breathe and shortly after had a ‘fit’ and her ‘lips turned blue’.
She was rushed to hospital however passed away later that day.
Dr Richard Prescott said Sophie died of a pulmonary embolism due to deep vein thrombosis (DVT) and a contributory factor was the oral contraceptive pill.
He told the hearing that the ‘large clot’ was 8mm in diameter and if it had been detected earlier she could have been given blood thinners and survived.
The inquest heard how Sophie was using the ‘common’ pill Microgynon and a leaflet accompanying the prescription warned how using it ‘increases the risk of developing a blood clot’ and in ‘very rare cases’ a blood clot can form but it is ‘very rarely fatal’.
Simon Dawson/Bloomberg via Getty Images
Contraceptive pill: Sophie had been taking Microgynon for around eight months
Joanne Birch, a specialist nurse in sudden and unexpected deaths, said only six out of every 10,000 women on the contraceptive pill develop DVT, compared to only two in 10,000 without the pill, and that fatalities are ‘extremely rare’.
Shelley told the hearing how Sophie’s breathing had got worse since returning from holiday and she was struggling to walk to school, dance or enjoy exercise DVDs and complained her body was ‘aching’.
The inquest heard how Shelley and Sophie visited Dr Paramundayil Joseph at the Dill Hall surgery in Accrington on October 15 after feeling like she was ‘breathing through a straw’.
The GP said he ordered tests which later confirmed EIA and Sophie was prescribed an inhaler.
However she later returned on November 5 – three days before her death – to say it ‘didn’t do anything’ and was prescribed a different inhaler and a tablet to help with her breathing before exercise.
Dr Joseph said how he didn’t consider the diagnosis of DVT as she was young, not overweight or a smoker, had no family history and didn’t have any swelling or tenderness in her leg.
He said her breathlessness, which is a symptom of a pulmonary embolism, could also be the symptom of ‘many diseases’ and ‘can be similar’ to EIA.
He told the inquest that risks associated with the contraceptive pill usually occur after ‘many years of taking the pill and also when a woman is a lot older’.
He said: “It’s the most common combined pill. I have prescribed it for the last 31 years and this has never happened until now.
“She was very active and it’s very rare and very unfortunate.”
Assistant coroner Derek Baker recorded a narrative verdict and said it was a ‘tragic case’.
He said: “This tragedy has brought overwhelming grief to Sophie’s family.
“She was a young girl when she died. The cause of death pulmonary embolism is common enough but I have never seen it involving someone as young as this with no other problems.
“These conditions in a girl of this age are rare but they are a recognised side effect of the pill she was prescribed and can also be caused by long flights and the immobility associated. It’s not my role to blame but I must say Sophie’s mum did everything that could reasonably have been done. There was no delay, she took medical advice as the symptoms displayed themselves.
“Sophie herself was very stoic about it and I think you were both hoping the symptoms were relatively minor and would pass.
“If it was diagnosed and treated earlier she would have had a very good prospect of recovery.
“I acknowledge a tragedy of this scale is going to result in crushing, all-consuming grief.”
Sophie was a pupil at Accrington Academy and dreamed of being a paramedic.
On Thursday, January 21st, 2016, youth and young adults from Chicago began an adventure of the rarest kind. The “Crusaders for Life” participate in the March for Life in Washington, D.C. every year, but this year would be different. In the days preceding the trip, Father Nathan Caswell made a few remarks to the Crusaders at a planning meeting. He encouraged the youth to “Be present in a special way,” on the trip, emphasizing that “…when we go all out, when we really die to ourselves, we allow others to come out of themselves, too.” From the beginning, he and the other leaders set this challenge before the Crusaders: “Whoever loses his life for My sake will save it” (Luke 9:24)
However, as the 165 participants prepared for the trip in the following days, news of winter storm Jonas began to spread. Would they be able to go? The weather warnings loomed, the storm threatened to dump as much as two feet of snow on Friday night. Word came from organizers in D.C.: “The March for Life will not be cancelled.” Projected departure for home seemed promising. They would be just ahead of the storm.
The decision was made to go ahead. On Thursday morning after early Mass, 2 priests, 2 brothers, 160 youth and young adults from St. John Cantius in Chicago, St. Peter in Volo, and Our Lady of the Sacred Heart Academy in Rockford loaded onto three buses.
Celebrating Mass in Barnesville, Maryland the morning of the March
Fr. Nathan Caswell, SJC prepares the Crusaders before the March for Life
More pictures and the beautiful continuing story —–>> http://www.cantius.org/go/news/detail/march_for_life_2016/
They are a one in 60 million chance, and their mother making huge sacrifices to ensure their health and safety.
They are the Tucci quintuplets from Perth, Australia, and though they have not been born yet, they already are famous online. Their mother, Kim (pictured above), has been blogging about her pregnancy on Facebook ever since she discovered that she was naturally pregnant with five babies in September 2015. Tens of thousands of people are following the family’s journey through the blog and waiting for the arrival of the rare quintuplets.
Tucci and her husband have two young daughters, and last summer, they decided to try for just one more child, maybe a boy, they told The Sydney Morning Herald.
Not long after discovering they were pregnant last summer, the couple received the surprise of their lives. Kim wrote on her blog “Surprised By Five” on Sept. 21, 2015:
After a long wait for the ultrasound we finally went in… the sonographer told me there was multiple gestational sack but she could only see a heart beat in two!! I WAS SO EXCITED!! TWINS!!!
I was moved to another machine for a clearer view and had the head doctor come in and double check the findings. she started to count ONE, TWO, THREE, FOUR , FIVE!!! did i hear that correctly?? FIVE?? My legs start to shake uncontrollably and all i can do is laugh.. The sonographer then told me the term for 5 is QUINTUPLETS!! Time to call my husband…
When i called him from the ultrasound room i don’t think he believed me at first, he quickly drove down to the ultrasound place. I could see the excitement in his face he told me ” We can do this”
The Tuccis learned that conceiving quintuplets naturally was a one in 60 million chance. However, as is often the case with multiples, some did not treat Kim’s extremely rare quintuplets as unique individuals. Doctors advised Kim to abort up to three of her unborn babies.
On September 26, 2015, she wrote about the experience:
After my initial ultrasound I was told I could consider the selection method [abortion] to give 2 babies the best chance in life… I watched a YouTube video on the procedure and I cried, I could never do that! Was I selfish for not giving two the chance of 100% survival?? All I knew is that I already love them and that every heart beat I heard I connect with them more.
For me life starts when a heart starts beating and all I know for sure is that I will do whatever it takes to bring them into this world healthy.
And it has taken a lot of sacrifice. Kim told the newspaper that she struggles just to walk and sleep. She said her skin is stretching and her belly feels “hot to touch.” At just 11 weeks pregnant, the mother said her stomach already looked like she was in the third trimester.
“Mummy guilt has kicked up a level! I’m trying to get through all the pain just on Panadol alone if I can help it, I can’t bare the thought of any drugs passing through to my babies,” she wrote on her blog on Jan. 17. “Sometimes my pelvis becomes so stiff I can barely walk and my hips feel like they are grinding away constantly.”
Doctors also recommend that she eat 6,000 calories every day just to sustain her five unborn babies, according to the report. The expecting mother said because her belly is so large and full already, she sometimes has to force herself to eat enough for her babies.
The Australian mom said all the aches and pains, the stretch marks and hospital stays are worth it, knowing that her unborn babies are healthy. She also thanked her husband for his constant support.
“My husband always reminds me I should wear my stripes with pride and that I should be proud of them and what my body has achieved. Without him I would have broken down a long time ago,” Kim wrote.
The babies’ due date is unclear, but some predict that Kim could give birth any day, according to the report. She is pregnant with four girls and a boy, the report states.
Elizabeth Hoskins, a local photographer who photographed Kim when she was 24 weeks pregnant, told the newspaper that the expecting mother looks radiant.
“She could not be more beautiful …” she said. “Her strength just shines through every image. A true goddess, indeed.”
As January is National Birth Defects Prevention Month, you may have seen articles like this one in Time Magazine claiming that birth control pills are not linked to birth defects. It’s because a recent large scale study from Denmark just came out with these conclusions. But this study is not telling the whole story and the news distracts us from the real problem. In fact, it’s missing the mark on serious effects of the Pill’s chemistry on the fetus. Here is the rest of the story: babies whose mothers have been on the Pill and are thus exposed to synthetic estrogen may not show the birth defects researched in the Danish study, like a congenital heart anomaly or a missing limb, but are likely to suffer longer term effects such as prostate cancer, breast cancer, or low sperm counts. Yet there is a deafening silence and lack of research on this inconvenient truth.
Three years ago, our daughter created a very clever animation video as part of a communications project where she made a statement that the Pill was linked to prostate cancer, which at first glance sounds like an odd concept. Last summer, this allegation was clarified for me when I attended the Contraceptive Conundrum Conference in Washington DC and heard a presentation by Frederick Vom Saal, PhD. Dr. Vom Saal is a developmental biologist and professor of biology at University of Missouri-Columbia, Miss. He is a fellow of the American Association for the Advancement of Science. The National Institute of Health funds his research. He was interviewed by PBS in 1998 on his research showing the relationship between estrogen found in the environment and prostate diseases.
What history and world health data tell us
We must learn from history. Vom Saal’s introduced his presentation by reminding us of the DES scandal. Between 1940 and 1971, millions of women were prescribed a drug called DES as a way to prevent miscarriages. In 1971, this drug was found to cause a 40-fold increase in risk of vaginal or cervical cancer in the teen or adult daughters of these women. A major lesson from these tragic events was that when pregnant women absorbed certain forms of estrogen, they exposed their fetus to small amounts of the hormone and it would have grave and irreversible health consequences for their baby. It also showed that these consequences would only show up much later in the child’s life.
What happened to these women had been previously demonstrated on mice. “There was data that was ignored because it was animal research that wasn’t relevant to human health,” reports Vom Saal. But the reality of the syndrome showed the contrary: the animal research was predictive of the human impact. “We know that mouse cells are essentially identical to human cells in the way that they respond to these hormones,“ said Vom Saal. Such biological evidence allows him to correlate the results observed in his research on mice and what we all observe in public health statistics.
Indeed, if we focus only on men’s health, which is Vom Saal’s research field, we find two areas are of major public health concern:
The prevalence of prostate cancer: prostate cancer is the second most common cancer in men, accounting for 15% of the cancers diagnosed in men, with almost 70% of the cases (759,000 per year) occurring in more developed regions (which are also the main users of the Pill).
The alarming rate of decreased of sperm count, a major cause of infertility. This article presents the dramatic, accelerating drop in sperm count reported in some studies: 50% since 1950 and 25% just in the past 20 years. (read here for more on this topic)
The science behind the facts
While traditional toxicology studies look at elevated levels of chemicals and their relationship to diseases during the lifetime of the person, Vom Saal research shows that in fact very small amounts of estrogen impact the fetus permanently, showing its effects during the rest of the person’s life, in ways that cannot be corrected. Further, he claims that such changes could be multi-generational.
Vom Saal observed that male mice from the same litter could experience very minor differences in estrogen hormone exposure during gestation that would lead to major differences in the fully developed mice: the size of the scrotum and the penis, the libido, and the size of the prostate were all clearly affected.
This discovery led to further research on mice. Vom Saal was able to show that by exposing the fetus to very small amounts of estradiol estrogen (also famously known as EE) at critical times of development, the resulting males’ prostates had doubled in size compared to the control sample. Later, when exposing the adults to normal hormonal changes due to age, 100% of these males got prostate cancer.
“We see dramatic change in the sprouting of glands within the fetal prostate. We see changes in testicular sperm production. We see changes in the structure of the endocrine control region in the brain, which is accompanied by changes in sex behavior, aggression, the way these animals behave towards infants, their whole social interaction, the way they age, the time that they enter puberty, the age at which they cease reproduction. It changes their entire life history, and these changes are capable of occurring at very low levels of hormones,” reports Vom Saal in his 1998 PBS interview about environmental EE. In this study published in the journal Human Reproduction, exposure to a small dose of EE (from 0.002 to 2 µg/kg/day) during the early phase of gestation led to an increase in the prostate weight, a change in its response to hormones, and a significant reduction in sperm count.
Vom Saal claims that the dose of EE in the Pill, which is about 0.3 µg/kg/day, has similar potential effects. Not only does it change the physiology of the person’s reproductive system, but it also affects the way the cells in the organs will respond to hormonal changes in the future. That’s where the higher risk of cancer comes from. That’s how the DES daughters syndrome happened. Could it be why prostate cancer is so prevalent or sperm count reaching crisis levels? Vom Saal along with other scientists[i] are certainly making a strong case for it.
What is the exposure with the Pill?
The big question for women on the Pill is when does it likely happen, so that one would know when to quit hormonal contraceptives to minimize the chance of exposure? The answer is quite broad: before, during and after conception. According to Dr. Vom Saal, the impact can start as soon as the egg starts developing in the ovaries, which is 2 ½ to 3 months before conception: “you are at a stage of development of the ovocite when it’s absolutely clear that hormonal insults to the mother can impact that process.” Exposure during conception is pretty common. About 9% of women on oral contraceptive pills get pregnant. In the US, it represents about 1 million babies a year. Worldwide about 10 million. To make matters worse, it takes at least a couple of weeks for a woman to know she is pregnant, and some women won’t realize they are pregnant for some time simply because the pill is already suppressing their periods, which will potentially extend the duration of the exposure.
Dr. Vom Saal’s focus is on the male reproductive system. There are other areas and organs that are very likely affected in a similar fashion. The same process applies to female breast tissues and their response to estrogen, which can lead to breast cancer later in the life of babies exposed.
The CDC provides a list of measures to prevent birth defects, from eating healthy and avoiding harmful chemical substances to taking folic acid supplements. But they don’t warn about EE exposure from birth control. There is a deafening silence on these questions. “If anybody was looking, which the medical community does not want anybody to do because there is just panic over this, you would see the same kind of data. There is a massive uncontrolled experiment going on and nobody is collecting this data,” stated Dr. Vom Saal. Before we hurry and say it’s safe, have we really made sure?
TOXICOLOGICAL SCIENCES 112(2), 331–343 (2009) Mal-Development of the Penis and Loss of Fertility in Male Rats Treated Neonatally with Female Contraceptive 17a-Ethinyl Estradiol: A Dose-Response Study and a Comparative Study with a Known Estrogenic Teratogen Diethylstilbestrol. Ensa Mathews et Al
BMJ Open 2011 Occupational & environmental medicine, Oral contraceptive use is associated with prostate cancer: an ecological study, by David Margel, Neil E Fleshner. See also the correction here
You’ve probably heard the basic story by now: busses full of students heading home from the March for Life in Washington D.C. got stuck on a highway because of a blizzard, and while they were waiting they constructed an altar out of snow and held Mass on the side of the highway. Amazing!
ChurchPOP tracked down the priest who presided over this historic Mass, Fr. Patrick Behm, and interviewed him about his experience.
“It was incredible,” Fr. Behm told ChurchPOP, “easily one of the highlights of my time as a priest.”
Fr. Behm is the parochial vicar of All Saints’ Parish in Le Mars, IA as well as parochial vicar of St. Patrick’s Parish in Akron, IA, and the chaplain of Gehlen Catholic High School in Le Mars. He was chaperoning five students from the high school.
According to Fr. Behm, his group plus several other big groups from other schools got stuck near the mile marker 133 on the Pennsylvania Turnpike. They were there for approximately 22 hours! The cause of the jam, Fr. Behm was told, was an accident involving two tractor-trailers that blocked all of the westbound lanes of traffic. In the time it took to clear this accident, the snow in turn rendered the road impassible and the vehicles immobile.
He couldn’t claim credit for the idea of having Mass: “I was the principal celebrant of the liturgy,” he said, “but credit for the idea, and credit for building the altar, and credit for going around to the various buses inviting people to join them belongs completely to the pilgrims from the Archdiocese of St. Paul and Minneapolis, particularly Mr. Bill Dill, their youth minister.”
It was those students from the Archdiocese of St. Paul and Minneapolis who built the snow altar: “Those Minnesotans apparently know how to build stuff out of snow!”
The now famous Mass was a powerful spiritual experience for Fr. Behm and everyone else involved.
“It left me with many impressions, but among them was the fact that Jesus enters into the storm. Jesus comes to us, in the storms of our life, and enters in to be with us. He desires to be with His people, and if we respond to this invitation to let Him in, then the message is profound hope and joy.”
Fr. Behm praised everyone for responding positively to such a hard situation: “Everyone on that turnpike had a choice: to respond with joy and a positive outlook, or to respond with negativity and anger. Neither approach would have gotten us out of there any faster. But, one approach at least made the waiting more bearable and tolerable.”
Further, he saw God reap spiritual fruit from the event: “God, in His providence, used this event to share the Gospel with scores of people who may never hear the Good News.”
Lastly, wanted to express an immense gratitude to all the workers who helped them: “the Pennsylvania National Guard, the Highway Patrol, the Pennsylvania DOT, local law enforcement, and the local fire department. It was a massive undertaking, and these first responders did a remarkable job.”
Q: Have you ever done this before? How did you get the idea to build a snow altar have Mass outside on the side of the highway?
No. This was definitely a first for me. And, it wasn’t my idea at all.
I’m kind of being attached to this story, as I was the principal celebrant of the liturgy, but credit for the idea, and credit for building the altar, and credit for going around to the various buses inviting people to join them belongs completely to the pilgrims from the Archdiocese of St. Paul and Minneapolis, particularly Mr. Bill Dill, their youth minister.
Q: Who built the altar? Was it just snow?
Pilgrims from the Archdiocese of St. Paul and Minneapolis. And yes, it was completely made out of snow. Those Minnesotans apparently know how to build stuff out of snow!
Q: Did only people from your group participate in the Mass, or did other people stuck on the turnpike also participate?
It was far more than our group. The groups that I know were in attendance were from Dioceses from Iowa, Nebraska, Minnesota, Missouri, North Dakota, South Dakota, Wisconsin, Ohio, and Pennsylvania. In addition, there may have been others who got out of their vehicles and joined us. I’m not sure about that though.
Q: How many people participated approximately?
The number I’m being told is approximately 500.
Q: Do you have any stories about how this positively affected people spiritually?
Overall, I’d say it certainly raised the spirits of all those in attendance. It brought the light of Christ to a very bleak situation, and helped continue to spread the message of the Gospel of Life, that all life is sacred.
Q: What was it like? What impression did the event leave you with?
It was incredible…easily one of the highlights of my time as a priest. It left me with many impressions, but among them was the fact that Jesus enters into the storm. Jesus comes to us, in the storms of our life, and enters in to be with us. He desires to be with His people, and if we respond to this invitation to let Him in, then the message is profound hope and joy.
Everyone on that turnpike had a choice: to respond with joy and a positive outlook, or to respond with negativity and anger. Neither approach would have gotten us out of there any faster. But, one approach at least made the waiting more bearable and tolerable.
Q: What’s been your reaction to the overwhelmingly positive reaction to the event on social media?
I’m stunned, actually. I’ve been trying to deflect credit and praise away from myself and on those who truly deserve it, Mr. Dill and the ASPM pilgrims. I never would have envisioned that it would receive the type of coverage it has.
But, God, in His providence, used this event to share the Gospel with scores of people who may never hear the Good News.
Q: Is there anything else you’d like to share about it?
Just to thank people for their prayers, and to thank everyone who helped us: the Pennsylvania National Guard, the Highway Patrol, the Pennsylvania DOT, local law enforcement, and the local fire department. It was a massive undertaking, and these first responders did a remarkable job.
Few take the marriage vows “in sickness and in health” as seriously as Bernadette Adams.
For the past three decades, she has dedicated her life to taking care of her husband, former French soccer player Jean-Pierre Adams, who is in a coma, according to the Catholic News Agency.
In 1982, Jean-Pierre had routine knee surgery to repair a sports-related injury, but never woke up from the anesthesia; he was 34 years old, according to the report. The family later won a lawsuit against the medical staff who botched the procedure, the report states.
Bernadette, now 72, spends every day by her husband’s side at the home in Nimes, France. Jean-Pierre will be 68 in March; and his wife refuses to put him in a nursing home, according to the report.
“I talk to him all the time — about TV, what’s in the mail, anything!” Bernadette told CNN. “There is always movement around him. He is always next to us.”
The report continues:
“I think he feels things. He must recognize the sound of my voice as well,” Bernadette told CNN in a recent interview, saying he can still breathe on his own but needs round-the-clock attention.
Bernadette and Jean-Pierre met at a dance in the 1960s. As an interracial couple, the two grew in resilience through the challenges they faced and married in 1969. Not long after, Jean-Pierre was playing first division side football as the “garde noire” alongside some of the best in the world.
“He was the ‘joie di vivre’ embodied in human form – a laugher and joker who liked to go out,” his wife told CNN.
That all changed on March 17, 1982 when the understaffed hospital botched Adams’ intubation, causing a heart attack, brain damage, and an eventual coma. The surgery was ruled as an “involuntary injury” and the medical workers were found guilty seven years after the incident.
Jean-Pierre, now 68, is cared for daily by his faithful wife Bernadette. She feeds him, talks to him, clothes him, and still buys presents for him to open on his birthday.
“I’ll buy things so that he can have a nice room, such as pretty sheets, or some scent. He used to wear Paco Rabanne but his favorite one stopped so now I buy Sauvage by Dior,” Bernadette told CNN.
The couple has been married for 46 years. The first few years of their marriage were filled with Jean-Pierre’s rise to fame as one of the first black players for the French national soccer team, according to the report.
“He was the ‘joie de vivre’ embodied in human form — a laugher and joker who liked to go out,” Bernadette said. “Really, a smile was always bursting out. He loved the good life and was loved by everybody as well.
Then the tragic incident occurred, leaving Jean-Pierre in a coma. Though some have suggested euthanasia, which is legal in several European countries, Bernadette refuses to consider it. She still believes Jean-Pierre’s life is valuable, and hopes that he could get better.
“What do you want me to do – deprive him of food? Let him die little by little? No, no, no,” she said. “If one day, medical science evolves, then why not? Will there be a day when they’ll know how to do something for him? I don’t know.”
CNN reports more about the couple’s life together now:
Bernadette looks after her husband with an unfailing love — dressing, feeding and bathing him, turning him over in his bed to avoid sores, and often losing her own sleep to ensure he gets his.
It’s a measure of their bond that on the rare occasions Bernadette spends a night away from home, Jean-Pierre’s carers notice his mood seems to change.
“He senses that it is not me feeding him and looking after him,” says his wife of 46 years. “It’s the nurses who tell me, saying he is not the same.
“I think he feels things. He must recognize the sound of my voice as well.”
Though many would have given up on Jean-Pierre long ago or even thrown away his life by euthanasia, Bernadette perseveres in caring for him each and every day. And that is a true love story.
Weeks ago, I walked into our crisis pregnancy center and witnessed a miracle. I have been volunteering as a counselor for over 7 years now and never before have I seen this. I was honored to see God’s handiwork up close—watching the face and eyes of the woman who received a redemptive gift.
If you aren’t familiar with the abortion pill RU-486, I would like to introduce you before going any further. RU-486 is not a contraceptive. RU-486 kills an unborn baby (typically within 5-7 weeks of conception) whose heart has already begun to beat.
RU-486 is an artificial steroid that interferes with the action of progesterone, a hormone crucial to the early progress of pregnancy. Progesterone stimulates the increased development of the uterine lining, which nourishes the developing child. It also suppresses normal uterine contractions, which could dislodge the child implanted and growing on the wall of the mother’s womb.
This abortion-inducing procedure RU-486 fills the chemical receptor sites normally reserved for progesterone and blocks the progesterone signal. Failing to receive that signal, a woman’s body shuts down the preparation of the uterus and initiates the menstrual process.
The pre-born child, deprived of necessary nutrients, starves to death.
The baby’s heart—which has already begun to beat at least since 4 weeks old—stops beating. This is the only purpose for which the sponsor of RU-486 ever sought U.S. government approval: the stopping of a human heart. The baby then detaches and is swept out of the body along with the decayed uterine lining.
But that’s not all. A chemical abortion via RU-486 involves a second drug, misoprostol. By itself, RU-486 is able to induce an abortion only between 64% and 85% of the time—a percentage abortifacient researchers consider inadequate for general clinical use.
So two days after taking RU-486, a woman takes a prostaglandin, usually misoprostol, to induce powerful uterine contractions to expel the baby’s shrunken corpse. What does this part of the two-part pill abortion mean to the woman’s body? You will have severely heavy bleeding, nausea, vomiting and painful uterine contractions before and after the baby exits the body.
TIME Magazinedescribes this as “A painful, messy, and protracted” process. In its trial testing, two percent of women hemorrhaged while more than 1 in 100 required hospitalization. And this was when RU-486 was under constant trial supervision. Complications greatly increase when the woman is given the pills at abortion centers and sent home with instructions—no supervision and no follow up.
Can they really call this health care? (Let it be noted: Surgical abortions, though completely different in procedure, are just as dangerous to undergo.)
Having explained RU-486 and its process, let’s move on to that incredible evening at the crisis pregnancy center. In walks a young woman who had discovered she was testing positive on her home pregnancy test. She came into our clinic to follow-up and make sure the tests were correct.
She thought she felt movement inside of her, but wasn’t so sure it wasn’t in her head. She explained she had taken an RU-486 abortion pill some months prior and thought she might be imagining a baby moving. We naturally assumed that perhaps she was pregnant again, as a woman’s chance of pregnancy after a womb-loss is high.
She was tested and, sure enough, she was positive for pregnancy. I prayed as we waited to find out what was going on. The nurse took her into the ultrasound room to check her womb, since her claims of movement had left us stunned. Long after the clinic hours were passed, they emerged from the ultrasound room.
Photo for illustration only: Daniel Hoherd / Flickr
In her hand were 5×4 photos; I had to hold back my tears. The smile on her face was hard to miss, and I asked her how it went. She joyfully told me that she was 21 weeks pregnant and then asked me if I wanted to see. Ummm, yes! I thought. Please let me lay eyes on this miracle baby and never forget. There the baby was, sucking on a thumb. Beautiful. Perfect. Saved.
She was relieved and began telling me her crazy journey the last few months and how this had to have happened for a reason. I echoed, “God protected your baby. This is a miracle from Him.”
The young woman, who had only a few months prior decided to end her baby’s life, was now telling me she was going to decide whether to give the gift of adoption or parent. And she added that she would tell everyone never to take RU-486—it was traumatic and painful.
Asking her about that experience, I learned that she had visited the Tuscaloosa abortion center: West Alabama Women’s Center, Inc. They had given her the RU-486 pills and sent her home. The only information they gave her was that “there would be some bleeding and cramping.” She experienced severe bleeding and pain for days.
Did I mention there was no follow-up or continued care given by West Alabama Women’s Center? None. Thankfully due to their procedural negligence, she went on with a miracle pregnancy. However, many women suffer near-death hospitalizations due to this same negligence.
I’ve prayed outside this same abortion center before. While we were praying there, a song my husband and I had written from Psalm 27:5-6 came to my mind. It was written from the perspective of the baby in the womb facing their death by abortion:
“For He will conceal me there when troubles come; He will hide me in His sanctuary. He will place me out of reach on a high rock. Then I will hold my head high above my enemies who surround me.”
That prayer and that song came to my mind as I meditated on God saving this miracle baby. I feel a confidence in my soul that God honored those prayers to Him outside that abortion center. And I was blessed to see the living fruit!
Another incredible part of this miracle was that the young woman came in with a friend, who was also testing positive for pregnancy and was abortion-minded. After seeing her friend’s live ultrasound, she decided to keep her baby! She said that she couldn’t wait to see her baby, too.
I am privileged and humbled to see God’s redemptive plan for these women, as I’ve never witnessed before. God’s plans for us and our families cannot be controlled like we so naively think. Ever so often, He will reach beyond our own limiting perspectives and fill our ill-thought-out decisions with His grace and mercy—His Sovereignty cannot be thwarted. I’m so thankful for a loving Heavenly Father who moves in the midst of our desperate sin.
Her smile was evidence of the healing power of life. Her smile was proof of relief. And her smile was a confirmation of the beautiful choices that are now brilliantly before her.
Note: If you have recently started the RU-486 process within the last 48 hours, there is an effective process for reversing the abortion. Medical professionals are standing by at (877) 558-0333 or find more information at AbortionPillReversal.com.
LifeNews Note: Natalie Brumfield, chapter leader of Bound4LIFE Birmingham, serves at local crisis pregnancy center Sav-A-Life and at her local church. This Bound4LIFE article has been reprinted with permission.
Ending contraception is the only way to end abortion.
It’s time once again for the annual March for Life in Washington, D.C., where hundreds of thousands of well-intentioned folks come to protest the slaughter of little children, demanding the law be changed. But how did it come to pass that killing children in the womb is now protected by the law?
Like everything, you have to go back to the beginning to get the full picture. Owing to massive movement of soldiers, the U.S. Civil War had given rise to the first large-scale beginnings of pornography as an industry. Pornographic materials and literature, such as they were in the post-Civil War era, had begun a lessening of morals.
In 1873, the U.S. Congress passed a law called the “Suppression of Trade in, and Circulation of, Obscene Literature and Articles of Immoral Use.” It was championed by Anthony Comstock and thereafter was called simply the Comstock Law.
It was a federal law, but over half the states adopted it as well. Among other things, Comstock outlawed abortifacients and contraceptives. Comstock was essentially the law of the land for nearly a century; but it began drawing heated opposition in the early 1900s from the burgeoning birth control movement largely spearheaded by women.
In 1961, Estelle Griswold opened a Planned Parenthood clinic in New Haven, Connecticut and was eventually convicted for dispensing birth control to married women. She lost every appeal of her conviction except the only one that mattered: the U.S. Supreme Court.
On June 7, 1965, four years after opening her clinic, in a 7-2 decision, the justices ruled that married couples have a constitutional right to contraception. They cited the Fifth, Ninth and Fourteenth amendments as the basis for their ruling.
In the majority opinion, Justice William O. Douglas said that a right to contraception among married couples exists owing to “penumbras” and “emanations” in the fabric of the Constitution. Those are legal terms meaning, in short, things you can assume and interpret in a manner that will allow more than the actual law says. The Griswold case also established a right to privacy — and now you can see where this is all going to arrive.
In 1972, in another Supreme Court case, Eisenstadt v. Baird, the case was argued and eventually won that it is a violation of the Equal Protection Clause of the Fourteenth Amendment to allow married couples to use contraception and deny that “right” to unmarried couples. The vote of the Justices was again 7-2.
Exactly 10 months to the day after the Eisenstadt ruling, the same justices voted — again 7-2 — that the same arguments to allow contraception also allow a woman to kill the baby in her womb.
Everything about abortion is about contraception. Almost half of women who get abortions do so because their contraception failed, a little-realized point that keeps Planned Parenthood and its allies constantly pushing contraception. Failed contraception leads to unintended pregnancy, which leads to abortion in half the cases.
Contraception establishes a thought process in the minds of people that sex doesn’t necessarily relate to conception — which is where the word contraception comes from. A person — especially a Catholic — cannot decry abortion while permitting, supporting or ignoring contraception.
Yet many people do, even those at the heart of the self-styled pro-life movement. If you are against abortion but permit contraception, then you are not pro-life. All you are is pro-birth. That is not Catholic, and no amount of pretense will make it so.
Tomorrow, a look at some of the bigger names that will be present at the March for Life on Friday, and how they do against this litmus test. Are they really pro-life? Or are they just pro-birth?
Father Fredy Angel, a native of Bogotá, Colombia, serves as pastor of Queen of Peace Parish in Lakeland and of the parish’s mission in nearby Ray City. In the Diocese of Savannah in southern Georgia, only 3 percent of the population is Catholic. When he began his term as pastor in 2008, there was only a small group of parishioners attending Mass. Today Sunday Masses in the Lakeland church draw so many area Catholics that the congregation is spilling out of the church and into the street. Originally founded to serve a small population of African-American Catholics, the parish today is racially diverse and serves whites, African-Americans and the growing Hispanic population in the area.
Despite many difficulties early on in his pastoral appointment—Father Fredy had to travel more than 150 miles each week to celebrate up to eight Masses in four different locations, and he had to live in a run-down rectory—he persevered and has poured his heart and soul into turning this previously struggling small Catholic parish into a thriving, dynamic and growing multi-ethnic community. He has established religious education programs that draw both children and adults to the parish. Many Catholics who had previously stopped attending church have come back to worship, not only because of his outreach and dedication to the community, but also because of his charismatic personality and passion for his ministry. He has also earned the respect and admiration of many Protestants in the two towns, who see him as a leader of their community.
Today there are 100 children enrolled in the religious education classes. In the seven and a half years of being their pastor, Father Fredy has celebrated 32 marriages. In the 19 years prior to his time there, only 19 were celebrated. He has brought 154 people to celebrate their first Communion, when in the past 29 years, a total of only 140 people did so. His flock continues to grow, and with Father Fredy as their shepherd, it is easy to see why.
He has led his parish by example, always the first to pick up a mop to clean the buildings or lend a hand in washing the dishes. His congregation has seen how he cares for the sick. They have seen how he has bridged the long-standing gap between English- and Spanish-speaking parishioners. They have seen how he has hosted potlucks after Mass. They have seen how he has worked outside of the church walls to help them with daily struggles such as family problems, counseling needs, social services and the many challenges the area’s young people are facing. This kind of devotion has brought more life back to the church, as well as people.
As the parish has continued to grow, Father Fredy has had to realize that a new and larger church needed to be built. He is now leading and involving his congregation in building that new church in a centralized location—within 20 minutes of driving for any of the parishioners from the three towns it will serve. The new parish, to be named St. Anthony of Padua, is scheduled to be dedicated in early 2016 and will have enough space for every religious education class to have a single classroom, rather than the current situation of combining groups in one classroom, or being forced to use the kitchen as a substitute classroom. In addition, it will include soccer fields and the parish also owns a property across the street where Father Fredy hopes to one day build a parish school.
Father Fredy is a priest in the Pope Francis mold, a shepherd who, in the pope’s memorable expression, is “living with the smell of his sheep.” His perseverance, commitment to his community, his leadership in bridging the various ethnic communities, and his close collaboration with Bishop Gregory Hartmayer to build a sustainable new church for the parish are just a few of the ways he is bringing the “light of Christ” to the people in the Diocese of Savannah, Georgia.
SAN FRANCISCO, California, January 18, 2016 (LifeSiteNews) – A San Francisco judge dealt a Catholic hospital a victory in its fight for religious conscience rights last week.
Forcing Mercy Medical Center to sterilize a female patient is a violation of its religious freedom, Superior Court Judge Ernest Goldsmith ruled last Thursday.
“Religious-based hospitals have an enshrined place in American history and its communities, and the religious beliefs reflected in their operation are not to be interfered with by courts at this moment in history,” his ruling said, according to a New Boston Post report.
Rebecca Chamorro, who was originally scheduled to have a C-section February 4, had requested a tubal ligation after her delivery at the Redding, CA hospital because she and her husband did not want more children.
The Catholic directive pertaining to sterilization states:
Direct sterilization of either men or women, whether permanent or temporary, is not permitted in a Catholic health care institution. Procedures that induce sterility are permitted when their direct effect is the cure or alleviation of a present and serious pathology and a simpler treatment is not available.
The American Civil Liberties Union (ACLU) filed suit in December on behalf of Chamorro and Physicians for Reproductive Health, challenging the hospital’s use of the ERDs to refuse tubal ligations, naming both the hospital and Dignity Health, its parent company and the state’s largest hospital provider.
The ACLU had alleged sex discrimination with the reasoning that prohibiting sterilization disproportionately impacts women, a report from The Guardian said, also claiming that Mercy arbitrarily allowed some women to be sterilized while refusing others.
However, Goldsmith discounted the ALCU claim in his decision, stating that the hospital’s sterilization policy applies equally to men and women.
“The religious beliefs reflected in their operation are not to be interfered with by courts,” Goldsmith said in a hearing January 14. “There’s no law that says that hospitals are mandated to perform sterilizations.”
Goldsmith also ruled that Chamorro could have the elective sterilization in another hospital and found insufficient evidence that Mercy permitted other female sterilizations strictly for contraceptive purposes.
The Centers for Disease Control and Prevention (CDC) estimates some 15-plus percent of U.S. women of child-bearing age use sterilization as birth control.
Chamorro, whose delivery is now scheduled for January 28, criticized the judge’s decision, saying, “It’s unbelievable that the hospital where my doctor has admitting privileges is denying him the ability to provide a safe, legal and common procedure, especially considering that Mercy is my only real option.”
Chamorro’s physician, Dr. Samuel Van Kirk, is also the OB-GYN for two other female plaintiffs for ACLU legal action against Mercy Redding.
Van Kirk stated in a court declaration that Mercy denied his request to perform sterilization on women an estimated 50 times in the last eight years.
Chamorro’s ACLU attorney is considering appeal.
“Catholic hospitals have been aggressively expanding over the past 15 years, and as our client is experiencing, they’re the only option for care in a lot of cases,” Elizabeth Gill stated.
Dignity Health’s counsel said Mercy Redding was within its rights to refuse the sterilization.
“This is a request for a Catholic hospital to forsake ethical and religious directive,” Barry Landsberg said. “This is a private Catholic hospital. It’s not the public library. It can make decisions about the services it provides.”
Landsberg also said Van Kirk should have anticipated the denial of Chamorro’s sterilization because he agreed to be bound by the ERDs when he applied for hospital privileges at Mercy.
Goldsmith recognized the implications of the ALCU’s action against the Catholic hospital as it relates to religious conscience.
“I’d have blinders on if I ignored the essence of this lawsuit,” he said last Thursday. “It’s about church and state. It’s about exercise of religion and to what extent it can be regulated by a court.”
The ACLU taking legal action against Catholic health care providers or other Catholic entities for upholding Catholic teaching is nothing new.
In December, the ACLU contacted drugstore chain Walgreens to express concern over its partnership with Providence Health, worried the store might no longer provide contraception and abortifacients, or euthanasia drugs in states where they’re legal, also questioning how Walgreens would treat LGBTQ customers in the wake of the partnership.
NORTH CHARLESTON, South Carolina, January 15, 2016 (LifeSiteNews) – Americans are allowing a generation of at-risk children to lose their chance at the American dream, because we are “too politically correct” to say that the intact, traditional family is best for society, Rick Santorum said at last night’s Republican presidential debate.
The undercard debate, which began at 6 p.m., featured Santorum, Mike Huckabee, and Carly Fiorina.
Moderator Trish Regan asked Santorum about the role “family formation” plays in economic development. Currently, 40 percent of all children are born out-of-wedlock. “That’s twice as high as reported back in 1980, and it’s 11 times as high as in 1940,” she said.
The former Pennsylvania senator said he has been surprised to direct his audiences to “a book written by a liberal Harvard” social science professor: Robert Putnam’s Our Kids.
“He wrote this book, I think, ostensibly to support the Democratic argument that the middle of America’s hollowing out, and income gap is widening, and rich are getting richer,” Santorum said.
But when Putnam “studied all the information…he realized that the biggest reason that we’re seeing the hollowing out of the middle of America is the breakdown of the American family.”
“The reality is that if you’re…a child of a single parent, and you grew up in a single parent family neighborhood…the chance of you ever, ever reaching the top 20 percent of income earners is three percent in America.” “That’s not good enough,” Santorum said passionately. “And we have been too politically correct in this country, because we don’t want to offend anybody, to fight for the lives of our children,” he concluded to applause.
A wealth of social data support his conclusion that being reared by both parents greatly increases the chances of success.
Growing up with both parents “is strongly associated with more education, work, and income among today’s young men and women,” a study conducted in October 2014 by W. Bradford Wilcox and Robert I. Lerman for the American Enterprise Institute concluded.
The two found the benefits trickle down through the generations. Being raised in an intact family “increases your odds of becoming highly educated, which in turn leads to higher odds of being married as an adult. Both the added education and marriage result in higher income levels,” they found.
“Indeed, men and women who were raised with both parents present and then go on to marry enjoy an especially high income as adults,” they wrote.
They found the “premium” of education and increased lifetime economic earnings applies to all ethnicities, as well.
Being raised by both parents also decreases numerous social pathologies. Sarah Torre of the Heritage Foundation found, “Teens from intact, married families are less likely to be sexually active and also less likely to abuse drugs and/or alcohol, exhibit poor social behaviors, or participate in violent crimes.”
Economically, an intact family saves society a hefty sum in social spending.
Torre wrote, “Of the more than $450 billion spent on means-tested welfare for low-income families with children, roughly three-quarters goes to households led by single parents.” A 2008 study found family breakdown cost taxpayers $112 billion a year, the equivalent of the GDP of New Zealand.
“The substitutes to the family are expensive and ineffective, and taxpayers end up paying the price,” said Dr. Jennifer Roback Morse of The Ruth Institute during a lecture at Acton University.
Not everyone would be happy to see traditional families flourish. NARAL Pro-Choice America tweeted:
National Right to Life revealed that 85 percent of all abortions are performed on single women in its third annual “State of Abortion in the United States” report, which was released on Thursday.
The flagging fortunes of the family is an issue close to Santorum’s heart. He raised the theme himself during the last Fox Business debate in November and introduced the notion to Mitt Romney in the 2012 campaign.
In addition to Putnam, AEI scholar Charles Murray came to similar conclusions about the importance of the intact family for social and economic advancement in his 2012 book, Coming Apart.
Wilcox and Nicholas Wolfinger will explore the theme further in their forthcoming book, Soul Mates: Religion, Sex, Love and Marriage Among African Americans and Latinos.
Dr. Jeremy Kalamarides, medical director of the Vitae Clinic in Austin, Texas, and a member of Father Michael J. McGivney Council 5967, is pictured with his wife, Heather, and their daughter. (Photo by Jody Horton Photography)
In the 1960s, legalized access to hormonal contraception promised to bring women freedom: freedom to limit family size and freedom to have sex without the “worry” of conception. Today, proponents promote another line: contraception as preventative health care, with some groups going so far as to pathologize women who don’t have access to contraception as “at risk for unintended pregnancy.”
According to the Centers for Disease Control and Prevention, nearly 62 percent of U.S. women ages 15-44 are currently using some form of contraception or sterilization. Though multiple forms of birth control exist, the pill remains the most popular, more than 55 years after it was introduced.
Absent from nearly all of the public campaigns in support of contraception, though, are its health risks, which can be life-threatening. Adding to the concern about side effects, some of which are more troubling than others, is the reality that most women are simply not informed.
“Women have a right to know,” said Vicki Thorn, who recently organized a conference titled “The Contraceptive Conundrum: Effects and Side Effects” at Georgetown University. The founder of Project Rachel and the National Office for Post-Abortion Reconciliation and Healing, Thorn has for years collected research about the detrimental effects of chemical contraception.
“Contraception is hardly benign,” Thorn said. “Most forms use steroidal hormones that impact the pituitary gland, which is the master gland in the body, and there’s much fallout in terms of health issues.”
CALCULATING RISKS
The side effects of the pill and other forms of hormonal contraception can range from blood clots, headaches, weight gain, nausea, and irregular or diminished periods, to mood swings, loss of libido, depression and other psychological repercussions. Some of these side effects can significantly alter a woman’s lifestyle — leaving her feeling helpless and confused at her inability to control her emotions and even her physical appearance.
Some potential side effects are particularly alarming. Studies dating back to the 1990s have shown increases in breast cancer related to the pill. A study published in the journal Cancer Research in August 2014 suggests that use of some types of oral contraception within the past year increases breast cancer risk by 50 percent. Pills containing higher doses of estrogen lead to even greater risk.
While some side effects are rare, many are not, explained Dr. Marguerite Duane, adjunct associate professor at Georgetown University and a family physician.
“You can go onto any Facebook page or any groups for birth control and see many women complaining about all the awful effects of the birth control pill: mood swings, weight gain and the psychological symptoms like depression and anxiety,” said Dr. Duane, who assisted with the “Contraceptive Conundrum” conference.
The purpose of the conference, which was hosted at Georgetown’s Edmund D. Pellegrino Center for Clinical Bioethics in August, was to educate attendees about contraception from a scientific perspective. Topics ranged from a pharmacist discussing nutrition deficiencies caused by the pill to a post-doctoral researcher discussing how contraception affects women’s brains. Other speakers noted that the side effects of contraception are not limited to women’s health; they include behavioral changes as well.
Participants included doctors, researchers, graduate students and even a number of parents of women who had died due to contraception. Among them were the parents of Erika Langhart, who died in 2011 at age 24 due to pulmonary embolisms caused by NuvaRing, one of the more recent and controversial forms of hormonal birth control.
Karen Langhart, Erika’s mother, told Vanity Fair in a January 2014 feature story that her daughter was meticulous about risks, but was unaware of the risks of this device. And her story is not unique. NuvaRing has been the subject of high profile class action lawsuits and cited as the cause of numerous women’s deaths.
The Huffington Post reported in 2013 that the Food and Drug Administration (FDA) had advised Organon, a pharmaceutical company manufacturing NuvaRing, to warn users of the drug’s serious risks.
“Organon executives adamantly opposed such a statement,” the article said. “An elevated [blood clot] warning label would have been a huge blow. Such a warning might have discouraged women from using NuvaRing and made doctors less inclined to prescribe it — significantly cutting into the potential return on investment.”
Pharmaceutical companies that produce contraception are financially motivated to influence medical education as well, explained Dr. Duane.
“The reality is,” she said, “if millions of women started learning how to chart their cycle and fertility, and stopped using hormonal contraceptives, pharmaceutical companies would stand to lose billions of dollars.”
According to Dr. Jeremy Kalamarides, medical director of the Vitae Clinic in Austin, Texas, women are often prescribed contraception instead of receiving the medical care they need.
“Over and over again, I find women frustrated with the fact that what they thought was being treated is actually not being treated at all by hormonal contraception,” Dr. Kalamarides said. “They come in and say, ‘Can you please give me something different?’”
For Dr. Kalamarides, a member of Father Michael J. McGivney Council 5967 in Austin, his interest in contraception alternatives started when he and his wife were preparing for marriage in 1994.
“I was thrown for a loop by the fact that [the reproductive system] is the only system in the human body that we turn off when it’s working correctly,” he said.
A biology student at the time, Kalamarides’ interest in the topic led him to become an OB-GYN. He then studied NaProTechnology at the Pope Paul VI Institute for the Study of Human Reproduction in Omaha, Neb., and established a medical practice that does not prescribe contraception.
AN EDUCATION IN FERTILITY
Beyond the potentially dangerous side effects related to women’s health, hormonal birth control has resulted in a number of sociological consequences as well.
“The pill was a technological shock that profoundly altered the mating market by lowering the ‘cost’ of sex,” explained Dr. Duane, pointing to research done by the Austin Institute for the Study of Family and Culture.
At the Austin Institute and elsewhere, sociologists have argued that sex has become a nearly universal precondition for being in a romantic relationship in modern society; contraception’s ability to “safeguard” against pregnancy has made it so.
“It’s been well documented in particular how women date and how men date because of contraception,” said Dr. Kalamarides. “It contributes to young people getting married later in life and social distortion in the premarital process.”
A growing body of research indicates that contraception even alters a woman’s ability to choose a more genetically suited spouse.
A 2011 Wall Street Journal article noted, “The type of man a woman is drawn to is known to change during her monthly cycle — when a woman is fertile, for instance, she might look for a man with more masculine features.”
But contraception suppresses fertility and its corresponding hormones, which can lead to a woman choosing a different spouse than she would otherwise. Conversely, a woman does not attract the same men when her fertility is suppressed.
“Women tend to exhibit subtle cues when they are ovulating, and men tend to find them more attractive at this time,” the WSJ article explained.
For years, Thorn has shared the findings of this research in talks to young people. “This is a big deal,” she said. “If you’re serious about marriage, then both men and women should know this.”
Of course, proponents of contraception do not think that any of these risks warrant giving it up — since unintended pregnancy is a “risk” to be avoided.
Still, no matter how “protected” people think they are from pregnancy, contraception is not foolproof. Since the legalization of birth control, the sexually permissive culture that contraception has facilitated has contributed to a rise in the nonmarital pregnancy rate from 5 percent in 1960 to 40 percent today. Additionally, more than 85 percent of abortions performed in the United States involve single mothers.
And not only does contraception facilitate relationships that make abortion more likely, but hormonal contraception itself can have an abortifacient effect; by thinning the lining of the uterus, it can prevent a newly conceived embryo from being implanted.
“Everyone knows that conception is the moment when sperm and egg unite, but for utilitarian purposes, some professional groups associate ‘pregnancy’ with implantation,” Dr. Kalamarides explained. “Many doctors don’t go over informed consent about how birth control works. But when women find out that it can potentially cause very early miscarriage, most are sincerely not interested anymore, or at least would like to try something else.”
Many are skeptical, however, that viable alternatives to hormonal contraception exist.
“The problem is,” Dr. Duane said, “there is this presumption that if you’re not on birth control, you will be pregnant.”
As a result, relatively few women ever learn how to read and understand when they are fertile. To help bridge the knowledge gap, Dr. Duane co-founded and serves as director of FACTS — Fertility Appreciation Collaborative to Teach the Science of fertility awareness-based methods.
“Our mission is to educate our medical colleagues about the evidence-based fertility awareness methods, because medical students, residents and physicians are not learning about them,” Dr. Duane said. “When women who are interested in these methods go to doctors who don’t have information, they stop talking to their doctors about this very important part of health care.”
Nonetheless, the science of fertility awareness, including NaProTechnology, continues to advance and become more widely known.
“Nationally and in the Church, we have not done enough to promote alternatives,” Dr. Kalmarides said. “But I see a lot of hope, because there is a growing number of doctors who are receiving training and using natural family planning in their practices.”
The fact remains, Dr. Kalmarides added, that teaching modern fertility awareness methods serves patients much better than both contraception and assisted reproductive technology.
“It is better, and it will help more people, whether you are avoiding pregnancy temporarily, trying to achieve pregnancy or treating underlying conditions,” he said. “And when women gain understanding of their fertility, they feel an enormous sense of relief and are empowered. That is what happens when you keep love and life together.”
MEG T. MCDONNELL is executive director of the Chiaroscuro Institute and a journalist in Washington, D.C.
As a young adult, Lisa Duffy experienced one heartbreak after another: miscarriage, infertility, divorce.
Married at 26, Duffy and her first husband lost three children to miscarriage, one at almost 20-weeks gestation. Later, she went through a surgery that was supposed to help her carry babies to term – but ended up reducing her chances of getting pregnant instead. Then, her husband divorced her.
The Catholic writer recently shared these early life struggles in a column for Aleteia. Duffy said she wants to encourage other women who have experienced loss that there is hope.
She wrote:
The doctors were never able to figure out what was causing these miscarriages until that final pregnancy. My uterus had widened enough for them to detect the problem, which was a malformation that made it impossible to carry a child to term.
My OB/GYN was hopeful. He said if I had come to him with this problem a few years before, he wouldn’t have been able to help me, but now there was a groundbreaking surgery that could correct my problem. So I signed up and went under the knife. The outcome was successful. Sort of.
The surgeons had been able to fix the problem as they’d hoped, but the procedure was so invasive, it left me sterile. In fact, the odds of my ever conceiving a child were now fewer than 1 percent. I was heartbroken and angry, to say the least. Then my husband left, never to return.
The next several years were dark with the weight of her grief. Duffy said she let her anger and pain become excuses to “behave badly at times” and gave up hope of ever having children.
Eventually, Duffy said she met her husband Jim, who helped pull her up out of her misery. She said she began to find hope and happiness again as she worked to repair her relationship with God.
A month after she was married, Duffy said she joined a group of women on a week-long silent retreat in Bethesda, Maryland. On the second day, she began to feel a terrible but familiar experience – morning sickness.
I wanted to jump up and run out to tell the other women — one of whom was my new mother-in-law— but I couldn’t. It was a silent retreat. I didn’t have a cell phone back then, so I couldn’t call Jim. And then it dawned on me, the brilliance of what God was doing. It almost felt deliberate that he was the only one I could share my joy with for the next four days. He wanted me to recognize the miracle he had brought about and how great his love for me was. Despite all the doctors had predicted, I was going to have a baby!
Weeks later, as I sat in my doctor’s office, she said to me, “I hope you realize what a miracle this is. Someone with your history should not be able to get pregnant.” She didn’t have to tell me, I knew better than anyone. And today, I have three healthy, happy miracles who are the joy of my life.
Duffy ended her story with words of hope and encouragement for women who are struggling. Though Duffy experienced losses through infertility and divorce, her words also could apply to women experiencing an unplanned pregnancy or grieving after an abortion.
“Stay close to [God] in your struggles, and trust him with your future,” Duffy said. “Your plans might look different from his, but he ultimately knows how to make you happy.”
In 2007, the Washington State Pharmacy Commission decided to make it illegal for pharmacists to live consistent with their religious beliefs by continuing to refer customers seeking abortion-inducing drugs, like Plan B, to other nearby pharmacies.
The burden of this unconstitutional law has been swift and severe for the Stormans Family—owners of Ralph’s Thriftway, a small local grocery store in Olympia, Washington. They, along with two other Washington-based pharmacists,
Margo Thelen and Rhonda Mesler,filed a lawsuit challenging the law, after facing formal complaints brought by the State and pro-abortion activists that threatened their pharmacy license.
Despite winning their case after 12-day federal trial when the court found that the state’s law was “aimed at” conscientious objectors, the Stormans Family has been embroiled in an 8-year legal battle for their freedom. Today, ADF asked the United States Supreme Court to hearthe Stormans’ case and uphold this family’s freedom and the freedom of all pharmacists in the state to live by their conscience, instead of forcing them to violate their beliefs.
Here are four reasons the Supreme Court should take their case:
1. Washington is the only state that doesn’t allow referrals to other pharmacies for conscience reasons
In 49 states in the U.S., it is standard practice to allow licensed pharmacists to refer a patient for all kinds of reasons—business, economic, convenience, and yes, religious or conscience-based reasons. In fact, major health organizations, such as the American Pharmacists Association, the Washington State Pharmacy Association, and over 30 other professional pharmacy groups, recognize and support these conscience-based referrals.
2. The state’s radical stance was driven by a controversial organization’s agenda
It raises the question: What made the state take such a radical stance on referrals? Why would the Washington State Pharmacy Commission choose to discriminate against religious pharmacists and their conscience-based reasons for deciding to refer customers to other local pharmacies for certain drugs?
Two words – Planned Parenthood.
Washington’s referral law is based on rules drafted by Planned Parenthood at the request of former Governor Christine Gregoire. In 2005, Planned Parenthood and Gregoire began pressuring the Commission to prohibit conscience-based referrals for Plan B, threatening the members with personal liability under anti-discrimination laws if they voted to allow conscience-based referrals.
After the state’s Pharmacy Commission voted unanimously against the law, Gregoire replaced two Commission members. In 2007, the Commission enacted the Governor’s rule requiring pharmacies to dispense Plan B and making conscience-based referrals illegal, despite continuing to allow pharmacies to refuse to stock it for other reasons.
3. The law is not only an extreme abuse of power by the State of Washington, but it completely disregards the established standard of care and the professionals who have dedicated their lives to improving patient health.
As the American Pharmacists Association, Washington State Pharmacy Association, and thirty-three other pharmacy organizations have explained, the regulations are “truly radical” and “grossly out of step with state regulatory practice.”
4. Allowing pharmacists to make conscience-based referrals does not impede women’s access to abortion-inducing drugs.
The State of Washington has even admitted this fact. But instead of honoring decades of settled pharmacy practice, they still chose to single out religiously-motivated pharmacists, at the urging of a billion dollar organization that kills over 300,000 unborn babies a year, and force them to participate in what they consider to be an abortion.
“The state allows pharmacies to refer for all kinds of reasons. In practice, it only bans religiously motivated referrals,” said Kevin Stormans. “With more than 30 pharmacies stocking the drug within five miles of our store, it is extremely disappointing that the state demands that we violate our conscience or jeopardize our family business. All we are asking is to be able to live out the beliefs that we hold, as Americans have always been able to do, and to be able to refer patients for religious reasons, as the medical and pharmaceutical associations overwhelmingly recommend.”
Please Keep the Stormans Family in your Prayers
Eight years is a long time, but the Stormans Family has remained steadfast, relying on their faith and each other in the midst of an intense legal battle. Please keep them in your prayers and be praying that the Supreme Court will hear their case.
Marissa Poulson writes for Alliance Defending Freedom.
[Please copy for your pharmacist, or forward this to him or her, or send the link—-> http://www.lifenews.com/2016/01/11/ planned-
After an imgur user posted an ultrasound photo this week that appears to show a demon looking over an unborn baby, a mom from Wales decided to balance the scales of good and evil a bit by sharing her own ultrasound image.
Lewis’ ultrasound, performed in 2012, showed an image of what appears to be an angel in her womb with her unborn child.
The image, shared first with The Mirror by 26-year-old mom Kelly Lewis, shows what looks like an angel, watching over Lewis’ baby, Harper, in utero.
Harper is now three years old, and Lewis told TODAY Parents that she didn’t notice the angelic presence when the image was initially captured in 2012.
“It was when I showed my friend later that day — he pointed it out to me. From then on, everyone has been fascinated with it,” said Lewis.
Lewis says her daughter, Harper, now three, is her little angel.
Lewis points out that Harper’s name means, “someone who plays the harp,” instruments often attributed to angels.
“Harper is a very well-behaved little girl,” said Lewis. “She has a warmhearted, caring, and helpful personality — always polite and kind, and very sweet and innocent. She also has the sweetest smile — it’s very angelic. I am truly blessed to have her.”
“She has a warmhearted, caring, and helpful personality,” said Lewis of her daughter. “Always polite and kind, and very sweet and innocent.”
So, does Lewis believe that an angelic being was visiting her unborn daughter on that day in 2012?
“Yes, I’d like to believe that this is an angel,” said Lewis “It’s a nice thing to believe and a lovely thing to have.”
I had been putting off this visit for quite some time. I guess I really didn’t want to even think about it, and figured that maybe if I ignored it, it would just go away. Unfortunately, that isn’t reality.
So I sat there on the exam table answering questions about our presidents, reading letters off a card to check my vision, and listing off my health history for the past five years (that was the last time I saw a neurologist).
Are you willing to lose your vision in order to prevent pregnancy? Are you willing to develop osteoporosis in your 20s because of your “need” to be on birth control? Are you willing to have a stroke at 30?
I got married to Doug in 2005. I knew that we wanted to delay having children for a while, and I had tried pretty much every hormonal birth control method under the sun. I had not, however, gotten the Depo Provera birth control injection. It seemed like a pretty worry-free method. You only have to get a shot once every three months and most women didn’t even have a period on it. It sounded pretty good to me. I received my first injection just a few months before our wedding date.
About a week after getting the first injection, I started getting these debilitating headaches. And I mean, they were really BAD. I could hardly work. It was interfering with my job, my sleep, pretty much everything. After about of week of this, I made an appointment with my family doctor. I told her about my symptoms and she totally blew me off, saying, “Well, some people just get bad headaches.” Um, no they don’t…not like this.
My mom suggested that maybe it had something to do with my vision. I made an appointment with an ophthalmologist looking for an answer. It was time for my annual eye checkup anyway, so I just kind of figured that my vision must have changed. As soon as he sat down and pulled his fancy eye looker machine up to my face, he backed away from it, switched the light on and asked, “Have you been having really bad headaches?” Why yes I have. I knew it. Mom was right. My vision must have changed.
Here’s how the rest of the conversation went:
Doctor: “Your optic nerves aren’t pulsing. You will need to be seen by a neurologist immediately.”
Me: “A neurologist? Why? Don’t I just need a different contact lens prescription?”
Doctor: “No. This has nothing to do with your vision really, except that if they continue to lay dormant, you can go blind. Many times this means that your spinal pressure is very high, which could mean that there is a tumor in the brain.”
Me: “A tumor?”
Doctor: blah, blah, muffled sound, blah, blah (I heard nothing he said after the word “tumor”).
I suddenly felt hot and sick to my stomach. A brain tumor? Possible brain surgery? They will have to shave my head. I will look terrible bald. Am I going to die from this?
About three days later I was sitting in a neurologist’s office. A couple days after that, I was getting my first lumbar puncture. About a week after that, I was getting my first MRI. Then came another lumbar puncture and another MRI.
The results were all in and they had a diagnosis: Pseudotumor Cerebri, otherwise known as Intercranial Hypertension. Basically, I have increased spinal fluid pressure because of swelling in my brain. I also have reduced vein size because of the swelling. I would be on medication the rest of my life. And if I wasn’t diligent about taking my medication, my spinal pressure would become high resulting in debilitating headaches…and/or I will go blind…or anything in between.
I thought for a long time that my headaches must have been related to my Depo Provera use, but I didn’t have that confirmation until I was diagnosed. My neurologist told me that he very often saw this condition manifest after women took hormonal birth control…particularly birth control containing progestin. So I had to deal with the fact that because I was so desperate not to get pregnant, I put something in my body that gave me a life-long disorder, and could make me go blind.
I MEDICATED A PROBLEM THAT WASN’T THERE AND NOW I TRULY DO LIVE WITH THAT CONSEQUENCE EVERYDAY.
Like I said in part two of this series, when we use birth control we are taking medication in order to “fix” something that isn’t broken. I had done just that and now I was living with putting the pieces back together. Now I do have something to fix…something I never would have dealt with if I had never taken hormonal birth control.
I live everyday with the reality that I could permanently lose my vision. I live with very serious headaches, even though I am on daily medication. A medication, by the way, that costs me almost $500.00 per month.
The sad part is that I am not alone. We know the risks of birth control and yet we continue to pump it into our system as if we have no choice. So here are my two questions, ladies.
IS IT WORTH IT? HOW MUCH ARE YOU WILLING TO RISK?
Are you willing to lose your vision in order to prevent pregnancy? Are you willing to develop osteoporosis in your 20s because of your “need” to be on birth control? Are you willing to have a stroke at 30? Are you willing to increase your risk of cancer by 30 percent? Are you willing to develop deadly blood clots because you just can’t be a mom right now? Are you willing to risk a hysterectomy because that IUD looks so appealing? Are you willing to have a heart attack just so you can “fix” your unbroken fertility? If you are a married woman, are you willing to completely lose the desire to have sex with your husband?
How much are you willing to risk? The good news is that you don’t have to risk a thing in order to space your children and avoid pregnancy. There are other, natural options available that give you control over your body. Birth control does exactly the opposite of what its name implies. It doesn’t control birth. It doesn’t control anything. It actually takes your control away.
If you want to truly stand up for women’s reproductive rights, then stand against birth control. Because nothing says anti-woman more than birth control. Any drug that is pushed upon women in order to simply prevent a natural part of a woman’s cycle is one that needs to be outright rejected.
For more information about your other fertility options, please visit www.iusenfp.com or www.naturalwomanhood.org.
If you have been diagnosed with PTC after taking hormonal birth control and would like to talk to an attorney about your situation, please visit http://www.schmidtlaw.com/pseudotumor-cerebri-lawsuit/. Getting these dangerous drugs off the market is one of the best things we can do for the safety of women. Thousands of women, including myself, have now come forward in hopes to do just that.
Porn. Fornication. Prostitution. Loving and leaving. Creating children and then abandoning them. Is this the greatness of men? The answer is a resounding ‘no’ according to a powerful short film titled “A Call to Battle” which was released yesterday by the Catholic bishop of Phoenix.
https://youtu.be/9mDzNm7cylw
The short film, created by Blackstone Films, outlines how an epic battle is being waged for the souls of men. At stake is love and relationships, the family, and the very survival of society itself.
Drawing upon his landmark letter issued last September on the same topic, Bishop Thomas Olmsted is specifically summoning the men of his diocese to become the men that God created them to be and to “stand in the breach” against a raging enemy seeking to destroy.
As a hospice nurse, Cori Salchert began to notice a heartbreaking practice. Some terminally ill babies were being abandoned by their families and left to die alone.
The Wisconsin mother of eight told the Sheboygan Press that she often would cradle terminally ill infants and children so “no one had to die alone.”
“There was no judgment on my part that the parents should just be able to deal with the circumstances,” Cori said. “But I thought, ‘Wow, I would really like to take those kiddos and care for them.’”
And that’s exactly what the Salchert family is doing. Cori and her husband, Mark, have taken in three terminally ill infants since they decided to pursue foster care less than five years ago, according to the report.
On Dec. 18, the family adopted a little boy named Charlie who has severe neurological impairments that force him to depend on a tracheostomy, ventilator and feeding tube, according to the report.
“He will die; there’s no changing that,” Cori said, brushing away a tear. “But, we can make a difference in how he lives, and the difference for Charlie is that he will be loved before he dies.”
“God is love, and He loves this little boy, and He loves us to love him,” Mark added. “Charlie is truly an amazing individual; he’s made us richer — more alive, in a sense.”
The Salcherts decided to begin fostering these vulnerable, sick infants after they experienced a tragedy of their own. Five years ago, Cori was diagnosed with an autoimmune disorder that caused gastrointestinal distress. Faced with multiple surgeries and constant illness, Cori left her job as a perinatal hospice nurse, according to the report.
“My prayer at that time was asking how God could possibly use this for good,” Cori said.
The news report continues:
As fate would have it, Cori’s circumstances opened up the time for her to pursue the Salcherts’ dream of becoming foster parents to hospice infants. They connected with Children’s Hospital of Wisconsin’s treatment foster care program, which matches families with children who have significant to severe behavioral or medical challenges.
The Salcherts brought home Emmalynn in August 2012. She did not have the left or right hemispheres of her brain, only the brain stem. She lived 50 days. Emmalynn passed away tucked into Cori’s fuzzy green robe “like a kangaroo” while foster mother and daughter sat alone at the kitchen table one night.
The Salcherts’ next foster child was Jayden, who was able to overcome his medical challenges to become a thriving toddler. He was ultimately adopted by a cousin of his biological parents.
With Emmalynn’s passing and Jayden leaving the home, the Salcherts were heartbroken. Cori recalls turning to Mark and saying she was done with treatment foster care, but her husband encouraged her that “this is what she was meant to do.”
With their biological children in full-support, Cori and Mark persevered. That’s when they received Charlie, who now is officially a member of their family.
The family said they enjoy cuddling, watching movies and taking walks with Charlie. Their local fire department also made Charlie an honorary fireman, the report states. Charlie’s life is making an impact on people in their community. His father said Charlie “really brings out the nobler parts of a community.”
This amazing family humbly told the newspaper that they are far from perfect. Cori refused to accept the label “supermom,” the report states. But the Salcherts truly are extraordinary people in a culture that often devalues terminally ill people by suggesting that their lives be destroyed by abortion or doctor-prescribed suicide.
“These children need nurses, but the overarching thing is, they need moms,” Cori said. “Too many people never do anything because they can’t do everything and can’t save everyone. For me, even though I can’t help every child, I’m happy to make a difference in the lives of a few.”
A week before a huge global family planning conference in Indonesia, the World Health Organization (WHO) issued a short statement reiterating its position that injectable contraceptives are safe – for any duration – even for adolescents despite being linked to progressive bone density loss and other harmful side effects.
It came shortly after the U.S. Food and Drug Administration (FDA), widely regarded as the “gold standard” on drug safety, rejected a petition to remove its strong “black box” warning label and reiterated its concerns about the contraceptives’ long-term effects on women’s health.
Women around the world who want to postpone or avoid pregnancy cite health risks as one of the most prevalent reasons for not using modern contraceptives.
Their concerns are backed by science. In this case, injectable contraceptives containing depot-medroxyprogesterone acetate (DMPA), also known as Depo-Provera, have been linked with decreased bone density, increased risk of certain cancers, and increased risk of HIV.
Last year the drug manufacturer Pfizer, the Gates Foundation, USAID and other groups announced a major collaboration to increase use of injectable contraceptives among poor women in developing countries using a single-use syringe called Sayana Press.
Mindful of the global push for Depo-Provera and the weight that FDA warnings carry, two doctors submitted a petition in 2013 urging the FDA to remove the “black box” warning, claiming that it “has harmed public health in the United States and around the world.” One doctor is a consultant for a company that markets Depo-Provera and the other is an outspoken abortion advocate who asserts that abortion is safer than childbirth.
The petition says the warning label is “inconsistent with the assessment of major medical and public health organizations around the world,” citing WHO in particular.
The FDA denied the petition in no uncertain terms. Dr. Janet Woodcock, director of drug evaluation and research, stressed that “[a]lthough FDA considers the opinions and analyses of other reputable health bodies, in the end FDA relies on its own independent review of the available data to make regulatory decisions.”
Woodcock strongly disputed the claim that FDA was harming global public health by highlighting the risks of Depo-Provera. If the warning label has led to decreased use of the drug, she wrote, “we believe lower prevalence of prolonged DMPA use is a public health benefit.”
The FDA expressed concern “about the fact that adolescent users were losing bone density at a time in life when they should be experiencing significant increases” and that recovery of bone density after discontinuing use of Depo-Provera was slow and may not fully occur at all.
The FDA stressed that since Depo-Provera has not been on the market long enough to determine its long-term effects on women past menopause, the time of life when women experience the most serious effects of osteoporosis, its most serious health risks may not yet be known. Given that the regions of the world targeted for the highest marketing and use of Depo-Provera are also areas with the least available data on osteoporosis – and the least access to medical care – the FDA’s warnings are particularly timely as aging emerges as an important issue worldwide.
Governments, UN agencies and family planning groups which are spending millions of dollars to distribute Depo-Provera in developing countries may ignore the FDA’s warnings and take cover from the WHO’s claims about its safety.
Wendy Puckrin admits that she may have been persuaded to abort her unborn son if she had known he had Down syndrome before he was born.
“On the day my little man was born, I was informed he had Down’s syndrome. I was not only surprised, I was shocked, scared – in fact basically terrified,” Puckrin told the Harrogate Advertiser.
“Had I found out while I was pregnant, there is a very good chance he would not be here today. It pains me to say that, but the negativity in the media, my own preconceptions and the way that a diagnosis can be handled by medical professionals would have left me feeling like I had little choice.”
Now, the British mother is on a mission to show people that her son, Elijah, 2, and others like him with Down syndrome are valuable human beings.
Puckrin said many people don’t question the negative connotations about the genetic condition in today’s culture and assume parents will have an abortion. She said some wrongly believe people with Down syndrome can’t lead normal lives.
“The phrase I hear most of all from parents with Down’s Syndrome is ‘if I knew then what I know now there would be no tears, no worries and no fears,’” she said.
The report continues: Wendy is particularly keen to dispel the myth that people with Down’s Syndrome won’t amount to anything.
She said: “That is simply not true. There are many who have gone on to become councillors, models, actors, business owners etc.
“With the right environment and the right encouragement, any child can accomplish their dreams.”
Next month Elijah will start nursery at Coppice Valley, where Wendy says he will be treated like any other child.
With support from staff, including his special educational needs co-ordinator, he will be encouraged to use sign
language designed for young children to help them communicate.
“Elijah already knows some signs, including cat, dog, milk, biscuit, food and bottle,” said Wendy.
“He’s doing really well developmentally and his childminder has scrapped the developmental chart for children with Down’s.
“The only thing he is behind with is walking, but he’s getting there, and his speech, although he can say the odd word like mummy and I’m not terribly concerned.”
Elijah also has a hectic social life and enjoys riding at Follifoot Park Disabled Riders Group and swimming.
A single mom, Puckrin is actively involved with the Down Syndrome Association. She set up a Facebook page, This is Elijah, to encourage other parents of babies with Down syndrome, and she also talks to student midwives at Leeds University about the condition, the report states.
When ever she can, the proud mother shares the special moments and memories that she and her son have together – like wrapping presents for Christmas. “My son is determined, intelligent, curious and downright beautiful,” she said. “He is my teacher, my inspiration and my guiding star. He is as perfect as I could have hoped for.”
Though Puckrin described herself as pro-choice, she expressed concern about the extremely high number of babies like her son who are aborted. Studies found that about 90 percent of unborn babies diagnosed with Down syndrome are aborted. She said these discriminatory abortions could rise even more now that a new non-invasive pregnancy screening test is available. Puckrin said she wants to make sure parents are fully informed about Down syndrome before they make a decision about aborting their unborn child.
“If you had told me three years ago I would single-handedly be raising a child with special needs I would have probably laughed. He’s not what I expected but he’s more than I deserve.
Did you know a baby develops hands and arms just 32 days after conception?
That’s just one of the amazing discoveries made by Alexander Tsiaras, founder of thevisualMD [http://www.thevisualmd.com/].
Tsiaras said the ultra-complex formation of a human being is full of mystery, magic and divinity. He was an associate professor of medicine and chief of scientific visualization at Yale University in the department of medicine when he had to write many of the algorithms and code for NASA to use for virtual surgery in preparation for the astronauts going deep into space using robotic pods. We’re talking more complex than rocket science.
“Using new kinds of scanning technology allowed us to see things about the body that just make you marvel,” said Tsiaras of his research. ”Even though
I’m a mathematician, I marvel as these instruction sets do not make mistakes as they build what is us.”
Here are some spectacular facts about the developing human body during birth:
24 hours: the baby’s first division
25 days: heart chamber is developing
32 days: arms and hands are developing
36 days: Most rapid development – if the baby continued to grow at this speed for the entire 9 months, it would be 1.5 tons at birth
45 days: baby’s heartbeat is twice as fast at the mother’s
52 days: developing retina, nose and fingers
The baby’s continual movement in the womb is necessary for muscular and skeletal growth
9 months: baby has 60,000 miles of vessels bringing nutrients and taking waste away
Birth: mystery, magic and miracle.
Tsiaras sums up the early stages of the pregnancy, as the baby’s development in its mother’s womb seems to say, “I’m here to stay; plant me.”
In the video below, Tsiaras uses art and technology to visualize the miracle of the unseen human body. True to the slogan of TEDTalks
http://www.ted.com/talks/alexander_tsiaras_conception_to_birth_visualized], this is definitely an idea worth spreading.
[Editorial Comment: As we await the virgin birth of Jesus, this video helps us visualize the wonder of God’s design of the human being, including Jesus the God-Man.]
(LifeSiteNews.com) – Amid all the joyful bustle of family preparations in anticipation of the holy day of Christ’s birth, Christmas time always brings to my mind the deep regret that I feel over the one child my wife and I lost due to miscarriage, because it reminds me that at the time I was like the Bethlehem innkeeper who said there was no more room.
I was having a lot of trouble accepting that my wife was pregnant with our ninth child.
It’s not that we were against having children – we had eight boys already – but when Theresa told me she was pregnant again, something inside me rebelled against the thought of another baby.
You know: “Oh no, another mouth to feed; our house is too small, and full to the rafters, literally, with kids; we’ll have to build an addition; we can’t afford this; I’m already the brunt of tacky jokes (don’t you folks in the country having anything else to do?); I can’t take this … there’s just no more room!”
You can see where this was going – from a lack of trust in God’s purposeful generosity, to a miserly outburst of selfishness.
Most of Theresa’s pregnancies were planned, some were surprises, and although much to my later shame I once added my name to a “zero population growth” petition while at university (ah, how foolish I was when I was young!), we welcomed each baby as he came along.
And when things got out of hand, as things with piles of children often do, I reminded myself that they were, after all, God’s children first, and given to us to look after the best we could for really only a short while, if you consider the reality of eternity.
But with this pregnancy something in me didn’t rejoice.
I worked myself up to such a state of negativity that I began saying “Why me Lord?” while I brooded over the new life that was growing in Theresa’s womb with misgiving rather than hopeful expectation. “Isn’t eight enough Lord? How could You do this to me?!”
Then without warning – Theresa was always so healthy when she was pregnant – I got a call while at work that Theresa was taken to the hospital, bleeding.
The next days were a blur of frantic prayer, tears, uncertainty and dread, and then the final reality that we had lost him. We named him Stephan.
In the midst of trying to be strong and supportive for Theresa in our grief, I was overwhelmed with guilt. It seemed to me that my lack of acceptance of Stephan was the cause of his death – like God saying, “you don’t want him? okay, I’ll take him back.”
We buried Stephan’s remains (there wasn’t much, he was in the first trimester) in a garden behind our home where we have a statue of Our Lady, and planted a rose bush over him.
Then God in His mercy let something change in me again.
Through the tears of sorrow and guilt I began to understand the reality of the wondrous, almost unimaginably generous gift from God that every child is.
A gift that is given to parents to love and nurture and enjoy, certainly, but also a gift to all of humanity in that the future is held in the tiny hands and minds and souls of the children that parents, with God’s help, bring into the world.
Of course with such an awesome gift also comes an awesome responsibility, and God never said raising children was supposed to be easy.
I sometimes ponder on God’s judgment of me when I die, and always come round to a scenario where the Lord looks at me with love and compassion, and then says, “Lets talk about how you did with the children I gave you … ”
I have come to a deeper understanding that God does in fact give us exactly what we need, just when we need it, to live out the responsibilities that we have. But implicit in this is TRUST.
The reality finally dawned on me that there is always room for one more child, because if we trust in God’s providence, then we trust that He will give us the grace we need to persevere. A wise man once described this as the “grace of state” we are freely given and can freely accept, simply by virtue of being parents, and trying to live out God’s will in our lives.
Every child conceived is loved into existence by God and wanted by God, even if we choose not to want that child.
What changed in me after Stephan’s death was that I felt a grateful joy the next time we were pregnant that was somehow so much more profound than anything I had experienced before. I knew our little Stephan was praying for me in heaven, and I knew that however many children God sent us, we would always have love and room for them.
After Stephan we were blessed with four more wonderful sons, and two absolutely gorgeous daughters. We are also now blessed by 32 grandchildren with one more on the way, so far …
So now when we gather for Christmas at home we are always packed to the rafters, but unlike the inn in Bethlehem, there is always room for one more.
Dear friends of LifeSiteNews, I wish you a very merry and blessed Christmas. May this joyous season of Jesus’ birth be a time of wonder and renewal for all of us.
May I offer you a Christmas gift of a prayer, adapted from “Blessing Prayers: Devotions for Growing in Faith” by Fr. Peter John Cameron, O.P., that speaks profoundly of Christ’s coming to us as a baby born in a stable and the Father’s love and care for us all:
O Emmanuel,
may the assurance of your unfailing Presence
be for me the source of unending peace.
May I never fear my weakness, my inadequacy, or my imperfection.
Rather, as I gaze with faith, hope, and love upon your incarnate littleness,
may I love my own littleness, for God is with us.
Endow my life with a holy wonder
that leads me ever more deeply into the Mystery of Redemption
and the meaning of my vocation and destiny.
May I make of my life a total gift of self.
May my humble worship of your Nativity
manifest how much I seek the Father’s Kingship
and his way of holiness.
The beauty of your holy face bears the promise
that your Father will provide for us in all things.
This Christmas, I renew my trust
in God’s goodness, compassion, and providence.
December 21, 2015 (LifeSiteNews) – To defend life and marriage in their integrity we have to uphold and believe in the immediate creation of man and all that is substantially taught to us by God in the first three chapters of the book of Genesis. That man was created by a special intervention of God in His image and likeness. We have to hold in accordance with the teachings of the Pontifical Biblical Commission in 1909 that the first three chapters of Genesis are primarily historical and are foundational of Christian doctrine; they are not a compilation of mythical narratives or only “true” in a vague “religious” sense. The Genesis account of the truth of creation is also expressed with growing vigor in the message of the prophets, the prayer of the psalms, the liturgy, and in the wisdom literature of the Old Testament (see the Catechism of the Catholic Church, 288). The Church in her Magisterium teaches that, “The truth about creation is so important for all of human life that God in his tenderness wanted to reveal to his People everything that is salutary to know on the subject” (CCC 287). So this important statement reinforces our belief in the historical nature of the Genesis account. With the beginning of creation God established a historical sequence of events. The first three chapters of Genesis have to be read “in the light of Christ, within the unity of Sacred Scripture and in the living Tradition of the Church, these texts remain the principal source for catechesis on the mysteries of the ‘beginning’: creation, fall, and promise of salvation” (CCC 289). Creation is the first gift of God, His primary miracle. First we have the creation of spiritual creatures, then the material world designed to serve mankind as our habitat, and finally He crowned His work with the creation of man and woman.
Man’s creation
All forms of evolutionary theory require a complete rejection of God’s revelation about the creation of Our First Parents. Genesis speaks of God forming Adam’s body from the slime of the earth and breathing into it the breath of life. It also speaks of God forming Eve’s body from Adam’s side and presenting her to him as his help-mate. The Fathers and Doctors of the Church held that God created the body of Adam together with his soul. Summarizing the patristic doctrine, St. John of Damascus wrote: “From the earth He formed his body and by His own inbreathing gave him a rational and understanding soul, which last we say is the divine image . . .” (St. John Damascene, On the Orthodox Faith 2:12). The Magisterium of the Church is very clear in affirming the common origin of all the human race, interpreting in a literal way the teaching of Acts, “from one ancestor [God] made all nations to inhabit the whole earth” (Acts. 17:26, C.C.C. 360-361). As a consequence this teaching totally rejects the theory of polygenism that proposes that man has many different ancestors. As St. John Chrysostom eloquently shows, man is at the center of creation at how for his redemption he did not spare His own Son (Cf. St. John Chrysostom, In Gen. sermo 2, 1: PG 54, 587D-588A).
The acceptance of the theory of evolution leads us to consider that the newly conceived human passes through different stages of development that parallel the ones of which are described by this theory as the evolution of living beings and only at the end of this process the human embryo becomes human. This position leads to the acceptance of abortion in the first months of pregnancy. It is totally unacceptable because Jesus Christ who was the model that Christ had in mind when he created Adam was fully human at the moment of His incarnation. St. Maximus the Confessor held (in II Ambigua 42) that Jesus was a man like us in all things but sin and that therefore His assumption of our humanity from the moment of the Annunciation signified that we, too, become fully human from the moment of our conception.
If the humanity of Christ was the model of our first parents that should lead us to set aside the opinion that the body of our first parents was the body of a primate that “evolved” in such a way that it could “receive” a human soul. It is far more reasonable to believe in accordance with the teaching of Genesis that God created a special body to receive the human soul. Man is radically different from animals. The fact that he shares some elements with them only serves to mark the abysmal differences. These differences and the superiority of man are underlined in Genesis when he is given dominion over all the creatures that populate the Earth (Gn. 1:26-27).
The First Vatican Council teaches that God creates to manifest His perfections through the benefits He bestows on His creatures. It is evident that the main beneficiary of creation is man, so through his experience of the perfections of creation he would raise in adoration to God so that one day he would join in the unending heavenly liturgy.
Marriage and Creation
In the Genesis text of marriage we have a basic revelation on the indissolubility of marriage. After presenting Eve to Adam and hearing His response the Lord states “That is why a man leaves his father and mother and clings to his wife, and the two of them become one body” (Gn. 2:24). Jesus will comment later on this text in an authoritative way against those who favored divorce, stating that, “Have you not read that from the beginning the Creator ‘made them male and female’ and said, ‘For this reason a man shall leave his father and mother and be joined to his wife,and the two shall become one flesh’? So they are no longer two, but one flesh. Therefore, what God has joined together, no human being must separate” (Mt. 19:4-6).
We have to understand well that marriage “is far from being the effect of chance or the result of the blind evolution of natural forces. It is in reality the wise and provident institution of God the Creator, whose purpose was to effect in man His loving design. As a consequence, husband and wife, through that mutual gift of themselves, which is specific and exclusive to them alone, develop that union of two persons in which they perfect one another, cooperating with God in the generation and rearing of new lives” (Humanae Vitae, 8, July 25th, 1968).
The Fall
It is important to understand the central nature of the foundational doctrine of the tragic fall of our first parents: “the Church, which has the mind of Christ, knows very well that we cannot tamper with the revelation of original sin without undermining the mystery of Christ” (CCC 389). In the same way we cannot tamper with the revelation that we have received on creation. Our First Parents were the first ones to fall into the trap of negative liberty, they ill used freedom to separate themselves from God’s loving plans. They desired to be like God, becoming the ones to determine what is good and evil, of what is just and what is unjust. This is perhaps one of the main problems of contemporary society which wishes to replace the objective law of God with a subjective approach to reality that calls good what is evil and unnatural. Modern liberty can defined as a Luciferian liberty, the liberty of the enemy of mankind that refused to serve God. But after the Fall God did not leave man with hope he promised a redeemer in Genesis 3:15 which is considered by the Fathers of the Church the first Gospel.
Conclusions
The effort to reach some sort of accommodation with evolution theories comes from a naturalistic approach that seeks to decrease the miraculous interventions of God in history. If the creation story is a myth compiled from different mythological stories and lacks a historical value, the main grounds to proclaim human dignity which is its creation on the image and likeness of God collapses. Also as consequence confusion over man’s origins leads to confusion over man’s destiny, undermining the whole edifice of the faith.
Destiny Herndon-De La Rosa
http://liveactionnews.org/my-crisis-pregnancy-is-15-today-and-he-saved-me/
The panic is temporary. The fear is temporary. The crisis is temporary. The days when you wake up thinking “how did I make such a huge mistake” are so few in retrospect.
You have nine months for all that, but then it gets good. Still difficult, don’t get me wrong, but so so good…
My “crisis pregnancy” turned 15 today. He’s just a year shy of the age I was when I got pregnant with him (a thought that terrifies me, trust). However, he’s anything but a mistake.
He’s the other half to all my inside jokes. He’s the best person I’ve ever known. He’s the one who binge watches Doctor Who with me and teaches me about robots and video games. He’s the reason I started New Wave Feminists. He’s the owner of a pure heart, swiper of my favorite CDs, and contributor of copious amounts of laundry. He’s the kid who still has me hanging around skateparks a decade and a half later. He’s often my (much needed) filter, because he’s a stereotypical naturally mature firstborn, and the last one to ever let me down. He’s the kid that I didn’t really raise at all, but instead grew up alongside. He’s my heart and soul.
I didn’t know it at the time, but choosing life for him would give me a life that I wouldn’t trade for the world.
See, you don’t realize how temporary the “crisis” is when it’s consuming your every waking moment, but as soon as you get beyond that… Such beauty can be born from that which we never planned.
Fear is temporary, but the courage you gain facing it lasts forever. Panic subsides, but the strength you find in the midst of the crisis endures. Perhaps the most amazing thing though is how the love you feel for this new life, whether it was intended or not, suddenly turns a “mistake” into a miracle.
I didn’t save my son by “choosing life.” He saved me.
Editor’s Note: This was first published on the New Wave Feminists’ Facebook page on December 13, 2015, and is reprinted here with permission.
WADENA, Minnesota, December 16, 2015 (LifeSiteNews) – After an atheist group forced one Minnesota city to take down its Nativity scene, residents took matters into their own hands, blanketing the town with nativity scenes in response…hundreds of them.
Wadena officials were forced to take down a Christmas display by the Freedom From Religion Foundation (FFRF), which threatened to sue the city. After forty years of displaying the Nativity scene, Wadena officials sold the figures to the Wadena Ministerial Association for $25, who displayed it on private property.
The Catholic League’s Bill Donohue commented, “It is entirely legal to put a manger scene on public property, as long as it is privately paid for and it is a public forum, i.e., an area that is open to art displays, concerts, rallies, and the like.”
“For the past twenty years, the Catholic League has erected a life-size nativity scene in Central Park,” Donohue noted. “The New York City Parks Department grants us a permit every year. All that needs to be done is to apply for a permit.”
Disappointed Christians responded to the Wadena city council decision in various ways. Brady Folkestad applied to use a bandstand in a city park that has been designated for public discourse for his family Christmas gathering, in which he would like to display Christmas decorations and a Nativity scene.
The city officials denied his request.
Folkestad then contacted the American Center for Law and Justice, which reviewed the city’s bandstand usage policy and gave advice about equal access to public facilities for religious use. He resubmitted his request, this time tailored to the city’s policy, which says nothing can be left overnight.
This time, city officials agreed to let him put up his display for his family gathering.
Others have followed suit, renting the bandstand for a day to put up their Nativity scene and take it down when evening comes.
The bandstand is now booked throughout the holidays.
Other folks began to buy and put up Nativity scenes on their yards and in their shop windows. Hundreds of them. There are four sets in a craft store window, three at a local café, two at the local bookstore. Some stores painted their display windows with the Nativity scene.
Wadena resident Dani Sworski started a Facebook page filled with pictures of the manger scenes all over town. “Let’s shower the town with Nativity scenes, let’s share our faith!” she declared.
Minneapolis’s Star Tribune reports, “Holy families are starting to outnumber the 4,000 residents of this central Minnesota railroad town.”
“The whole community has come out to support this,” An Open Book bookstore owner Gillette Kempf said. “It’s an expression of who we are as a community and what we believe. We believe in the Nativity.”
Mayor George Deiss said, “I’m hoping we lit a little spark and the rest of the nation will catch on.” Deiss himself has at least eight Nativity scenes on display outside his home, and he estimates that Wadena residents have put up at least one thousand.
Offers have come from as far as St. Paul, 160 miles away, to donate Manger sets to anyone willing to display them.
The American Center for Law and Justice told LifeSiteNews, “We’re very pleased that the residents of this Minnesota city are sharing the true meaning of Christmas through these displays, which are constitutionally protected speech.”
The Freedom From Religion group said they are fine with private Nativity scenes, as long as government does not sponsor them.
“Outlaw abortion and abortion won’t stop. Women will just do it illegally and women will die!”
Or so the argument goes… But facts are pesky things, and they show that the opposite is true in Chile.
According to new research from the MELISA Institute, since Chile’s ban on abortion, not only has maternal health improved but the number of women seeking illegal abortion has plummeted!
Since Chile banned abortion in 1989, the number of maternal deaths decreased from 41.3 to 12.7 per 100,000 women (69.2% reduction). That puts Chile in second place for the lowest maternal mortality rate in the Americas (that’s right, even better than the United States).
Prof. Elard Koch, a molecular epidemiologist and lead author of the study, says educating women enhanced their ability to access existing health care resources, and since those resources included skilled attendants for childbirth, that directly led to a reduction of maternal deaths during pregnancy and childbirth.
As Dr. Koch explains, “it is a unique natural experiment conducted in a developing country.” During the fifty-year period under study, the overall maternal mortality rate dramatically declined by 93.8%, from 270.7 to 18.2 deaths per 100,000 live births, making Chile a leader in maternal healthcare outcomes in the Americas.
But wait. If abortion is legally banned, wouldn’t we expect to see the number of women hospitalized due to illegal abortion procedures increase? Aren’t women just seeking abortions outside of proper healthcare facilities?
No. Not only is Chile one of the safest places in the world for women to give birth, but the number of women actually seeking abortion is also declining. According to data from the Chilean Ministry of Health, the country displays a continuous decreasing trend of hospital discharges due to complications of abortions suspected to be illegally induced at a rate of 2% per year since 2001. In contrast, a decreasing trend was not observed in hospital discharges due to miscarriage or ectopic pregnancy, which have remained constant during the same period.
Dr. Koch’s research also found that a large sample of abortion-minded women in Chile displayed a vulnerability profile marked by coercion and fear, which accounted for nearly 70% of the reasons women considered abortion. Moreover, the research indicated that support programs directed to vulnerable women can prevent most illegal abortions, with an outcome of live birth (with or without adoption) ranging between 69% and 94% depending on the risk group.
It’s not sheer coincidence that Malta, The Republic of Ireland, and Chile, all of which have prohibited abortion, have lower maternal mortality rates than the United States. In Africa, where 56% of all maternal mortalities occur, abortion-related maternal mortality is less than half what it is in developed countries. Yet there are more restrictions on abortion in Africa than in developed countries! So what’s the deal? In countries with higher abortion restrictions, fewer women have to seek treatment for “unsafe abortion” than in countries where abortion is “safe and legal.”
The result’s of Chile’s natural experiment is bad news for the pro-abortion lobby. But it’s great news for mothers and the unborn!
When St. Louis mother Cara Combs was diagnosed with stage IV melanoma while she was pregnant with her fourth child, she was given the choice of having treatment or saving her own life. She chose to save her baby. She decided to put off treatment in favor of giving birth at the 28th week to give her baby girl a chance to live.
Sadly, Combs died Tuesday morning — three days after giving birth.
I feel it’s time to post this because I know a lot of information is going around. Last week I was diagnosed with stage IV melanoma. I am also 25 weeks pregnant. I can’t begin treatment while pregnant so I have some tough decisions to make. Against the advice of my oncologist, I am choosing to delay my treatment for three weeks in order to get the baby to 28 weeks. There is no good decision here. We will both be fighting for our lives and I feel incredibly guiltily about that. I saw a dermatologist last year and she didn’t find anything concerning. Even my oncologist can’t find the source. At 38 you don’t expect to find out that you are dying. It definitely puts things into perspective. All I can say is enjoy every minute with your kids and don’t stress about little things. The baby will probably be born the first week of December and I will start treatment 48 hours later. I know we are in for some big upcoming battles. Thank you for all of the support we have received so far. It is very much appreciated!
Tragically, Roy Combs had to post the message on the family’s GoFundMe page this week about losing his wife:
I wanted to let everyone know that we lost Cara Walters Combs this morning. I don’t have to tell you how great of a person she was. She will be missed by all. I always knew she was destined for greater things. We all have a perfect angel looking over us. She was the strongest person I ever met and the best wife and mother. She sacrificed everything so her legacy could live on. Thank you all for your support and prayers. She was my everything and always will be.
In similar cases, doctors often suggest an abortion, but, as studies show, there is typically no need for women to destroy the life of their unborn child to save their own. Her story story confirms what research has shown: women who are pregnant and battling breast cancer don’t need to have an abortion.
LifeNews previously covered a collection of stories from The Lancet, a prominent British medical journal, showing pregnant women don’t need to have an abortion in order to get treatment for cancer. The information shows chemo treatment does not harm the unborn baby and mothers can treat themselves for cancer without worrying about effects on the unborn child.
In 2009, LifeNews.com reported on a new study showing doctors don’t need to suggest an abortion to pregnant women who want cancer treatment. The study involved a concept called pregnancy associated breast cancer — breast cancer that is diagnosed when a woman is pregnant or within a year after delivery.
The mainstream media highlighted the study as if it showed a new concept, somehow finally dismissing the notion that pregnant women undergoing breast cancer treatment should have an abortion. But Dr. Joel Brind, a Baruch College professor says studies have shown that for decades.
“Actually, this finding has been reported many times in the last 15 years,” Brind explained.
“Unfortunately, many doctors still recommend abortion for women diagnosed with breast cancer while pregnant, so that they can treat the cancer more aggressively. This is despite worldwide research going back as far as the 1930’s that shows that so-called ‘therapeutic abortion’ substantially shortens lifespan, whereas carrying the pregnancy to term makes long-term cure more likely,” he said.
Brind says that a 1976 review of all studies published to that point, conducted by French doctor P. Juret, reported that, “The futility of therapeutic abortion is now certain.”
Although the study isn’t the revelation the mainstream media claimed, Brind says it is quite useful.
“What the new story out of MD Anderson shows is that women in this particular situation — which are only about 3% of all breast cancers — have no worse a prognosis than women with the same stage of breast cancer who are not pregnant,” he said.
“But what is most important about the current report is the absence of any data about abortion, i.e., a difference in prognosis as a function of whether or not the pregnant patient aborts the baby,” he explained. “To their credit, doctors at MD Anderson have, for at least the last several years, been very good at treating both patients: Mom and her unborn child.”
“Hopefully, the current report will be yet another nail in the coffin of ‘therapeutic abortion,’” he told LifeNews.com.
December 11, 2015 (LifeSiteNews) — One of the greatest Christian communicators in American history was Archbishop Fulton J. Sheen. Trained in top level theology, he chose to use his talents to convey the complex truths and deep human insights of Catholic thought to a wide American public. In the 1950s, his prime-time TV religious show (imagine that!) “Life Is Worth Living” had higher ratings than its rival, “The Milton Berle Show,” a fact which Sheen attributed to his fine top-notch Jewish writers: Matthew, Mark, Luke, and John.
One of the most profound reflections Sheen ever offered was about the tragic gulf that exists between the person each of us should be, and the person we really are. As he wrote in The World’s First Love:
God, too, has within Himself blueprints of everything in the universe. As the architect has in his mind a plan of the house before the house is built, so God has in His Mind an archetypal idea of every flower, bird, tree, springtime, and melody….
But it is not so with persons. God has to have two pictures of us: one is what we are, and the other is what we ought to be. He has the model, and He has the reality: the blueprint and the edifice, the score of the music and the way we play it. God has to have these two pictures because in each and every one of us there is some disproportion and want of conformity between the original plan and the way we have worked it out. The image is blurred; the print is faded. For one thing, our personality is not complete in time; we need a renewed body. Then, too, our sins diminish our personality; our evil acts daub the canvas the Master Hand designed. Like unhatched eggs, some of us refuse to be warmed by the Divine Love, which is so necessary for incubation to a higher level. We are in constant need of repairs; our free acts do not coincide with the law of our being; we fall short of all God wants us to be. St. Paul tells us that we were predestined, before the foundations of the world were laid, to become the sons of God. But some of us will not fulfill that hope.
There is, actually, only one person in all humanity of whom God has one picture and in whom there is a perfect conformity between what He wanted her to be and what she is, and that is His Own Mother. Most of us are a minus sign, in the sense that we do not fulfill the high hopes the Heavenly Father has for us. But Mary is the equal sign. The Ideal that God had of her, that she is, and in the flesh. The model and the copy are perfect; she is all that was foreseen, planned, and dreamed.
Sheen speaks of Mary as she is seen in the Catholic and Orthodox traditions, free of any personal sin, perfectly pleasing to God in all the decisions she has made, through the saving grace of Christ. Hence Mary is simply the perfect Christian, the one merely human being whose earthly image is exactly what God had in mind for her. She is in that sense a window into the very mind of God.
And that window pours light out for the rest of us, stumbling in our uncertainties and sins. Over centuries, Catholics have believed that Jesus has sent His mother from time to time to appear to certain people, to offer encouragement, or a warning, or to call us to more fervent prayer. Typically, these “apparitions” have been to the poor, the weak, the forgotten in society, but the words of the mother of God have sometimes changed the fate of nations. That is what happened in Mexico, in early December 1531, when an Indian peasant named Juan Diego, one of the few who had followed the Spanish missionaries who had accompanied the conquistadors into that country, was climbing the hill of Tepeyac. At the top
he saw a brilliant light on the summit and heard the strains of celestial music. Filled with wonder, he stopped. Then he heard a feminine voice asking him to ascend. When he reached the top he saw the Blessed Virgin Mary standing in the midst of a glorious light, in heavenly splendor. The beauty of her youthful countenance and her look of loving kindness filled Juan Diego with unspeakable happiness as he listened to the words which she spoke to him in his native language. She told him she was the perfect and eternal Virgin Mary, Mother of the true God, and made known to him her desire that a shrine be built there where she could demonstrate her love, her compassion and her protection. “For I am your merciful Mother,” she said, “to you and to all mankind who love me and trust in me and invoke my help. Therefore, go to the dwelling of the Bishop in Mexico City and say that the Virgin Mary sent you to make known to him her great desire.”
Mary did not speak Spanish, or wear the courtly clothes of the conquerors. Instead she appeared as a woman whom Juan Diego might have seen in any village. But she spoke of the love of God for the Mexican people, in a way that no foreign friar could hope to do. So Juan Diego dutifully marched off to the bishop, Fray Juan de Zumarraga, who heard Juan Diego’s case, but did not believe him. Juan Diego returned to Tepeyac Hill to pray, and Mary sent back to bother the bishop. At the second meeting, the bishop suggested that Juan Diego ask for some sign of proof. A few days later, the Virgin appeared to Juan Diego and told him to gather roses and bring them to the bishop. Juan Diego was astonished to see, in the midst of winter, an explosion of unfamiliar flowers all around him. He gathered them in his humble tunic (called a “tilma”) and carried them to the bishop’s palace.
Bishop Zumarraga was stunned by the flowers, of a breed which grew only in his native region of Spain. He was even more taken aback by what had happened to Juan Diego’s tilma: It bore a magnificent, mysterious image of the Virgin Mary, pregnant with Jesus. He was convinced. So were the native people of Mexico, who hearkened to the story and flocked to the shrine that Bishop Zumarraga built in Guadalupe, which enshrined the mysterious tilma—an ordinary garment, made of cheap materials that typically decay in just a few years, which has never aged or lost its luster over the next 500 years.
The Image of the Image of God
That’s a lovely story. But it is much more than that. The image of Mary and Jesus that appeared on that tilma is in fact a kind of book—a theology text that teaches us critical lessons that modern man has forgotten. First of all, the image teaches about human dignity, and where it comes from. If Mary is a perfect reflection of God’s vision of her in his own mind, then in this supernatural portrait we have a picture of how God sees mankind: More important than all of nature, since Mary stands on top of the moon, is backlit by the sun, and clothed in the stars of heaven. The human person, which our Culture of Death treats as a means to pleasure and power, is in fact much more important than the rest of the created universe.
What gives us such dignity and importance? Only the grace of God. Mary’s head is not turned by her glory; in fact it is bowed in prayer. She knows that all her importance derives from her Son, that all her virtues are only the fruit of His grace. We only fully retain our dignity when we unite our will with God’s, and obey His plan for us. It is perfect obedience to the promptings of grace, not power, learning, or knowledge, that elevates a person. When we try like Satan to rise against God’s will, we degrade ourselves—as our culture today has diminished the sanctity of life and the value of self-sacrifice, pretending to elevate man while in fact reducing him to the level of just one more primate.
This message might seem abstract, or unconvincing to modern people. But remember the original audience to whom the Virgin appeared in Mexico: The Indian people of Mexico had for centuries been subject to the brutal regime of the Aztecs, who believed in a cult of dark and desperate gods, that could only keep themselves and the universe alive if they were fed by human sacrifice. When the bold Spanish explorer Cortes landed in Mexico, he found an Aztec nation engaged in its own culture of death. Every month, thousands of people from conquered tribes would be dragged up Mexican temples and have their hearts ripped out of their chest—to “feed” the gods and the Aztec upper class, who had come to rely on the sacrifices as a key source of protein. (We have still have some of their ghoulish recipes for cooked human flesh.) With only a few hundred troops of his own, Cortes turned to the tribes that fed the sacrifices, who allied with him to obliterate the Aztec kingdom and close its temples.
This was the pagan despair that lurked in the background when the Virgin appeared in Mexico. Few Indians had dared to accept the new and gentle creed of Christ, a God who accepts no sacrifices, but offers Himself for us. It seemed too good to be true. But when they saw clothed in their own garments and speaking their own language a Lady who reflected God’s love for them in particular, the Mexican people gained the courage to hope. The faith of the Mexican people in Christ can be traced to the tilma of Juan Diego, and it has never failed despite the fiercest persecutions.
In our own age of pagan despair, we look to icons of courage and grace to remind us that goodness is possible. We read the lives of men like Dietrich Bonhoeffer, of women like Mother Teresa, and we search out the people who today are standing for life in the face of death—especially those in the pro-life movement, who face down the law and the media, the courts and the social elites, to defend the weakest, most vulnerable images of God’s most precious creation.
In Nov. 19, 1997, the McCaughey Family made world history when their septuplets were born alive and healthy in Des Moines, Iowa.
Kenny and Bobbi McCaughey’s four boys and three girls became the first known set of surviving septuplets in the world.
The seven siblings defied the odds in more ways than one. Families like the McCaugheys are sometimes pressured to “selectively reduce,” or abort, babies who are multiples because doctors claim it can increase the chances that the other babies will be born healthy. The McCaugheys gave all of their babies a chance to live.
Today, all seven of the septuplets are seniors in high school and preparing for college. The siblings turned 18 on Nov. 19.
Many people saw the septuplets as babies on TV and the cover of Time magazine, but the family has been keeping a lower profile since then – no reality shows or on-going camera appearances for them. The family returned briefly to the spotlight this fall to celebrate the septuplets’ lives after they defied all odds.
“The memories, the joys, the heartaches that have happened, it’s very special,” their mom, Bobbi, added.
The family received a lot of help from family and friends after the septuplets were born – help with food, diapers, potty training and much more; but most of all, the family’s faith has helped them throughout the years, Bobbi said.
“We have a super-strong faith that is the rock we’ve had to stand on,” Bobbi said.
When asked about the worst part of being a septuplet, the teens couldn’t come up with an answer.
“I’ve enjoyed all of it,” said Kelsey, one of the sisters. “There hasn’t been a worst part.”
“[The best thing is] just having a big family, a lot of brothers and sisters to hang out with you,” said one of the brothers, Kenny. “You’re never alone. There’s always someone to talk to and hang out with. That’s what I think is the best.”
I am conflicted because I am FULL of JOY and SADNESS. Joy-filled for the pending birth of Jesus and the many blessings in my life—family, Faith, One More Soul, a slowly expanding Culture of Life—the list is endless. But my joy is tempered by sadness—also an endless list, including the growing Culture of Death. To say all I want to say would take many more pages than are available here.
I believe that One More Soul IS the leading edge of the Culture of Life. I have FAITH that more capable organizations will join us. I HOPE that what you find in this End-of-Year newsletter will warm your heart, challenge your thinking, and increase your pride in One More Soul as we step forward with new efforts to encourage new life.
Our cupboard is bare—REALLY bare. We really need your CHARITY. Please pray for us. Please order our resources and distribute them in your parish and at other opportunities. We have great materials to encourage purity and chastity, marriage and openness to children, and acceptance of God’s direction in our lives.
Thank you for your generosity. May God bless you, your family, and those who care for you.
I also have HOPE and FAITH that you will support us with your CHARITY. One More Soul is a charitable organization and tax-exempt under section 501(c)(3) of the Internal Revenue Code We are eligible to receive your tax-deductible contributions. Thanks!
Welcoming the Christ Child
Each Christmas we recall the birth of the Christ Child who came to dwell among us. At the same time the secular community enters a seasonal nostalgia of childhood in movies, plays, and productions. Although this is often for business purposes, it is an open door. Let’s seize that cultural moment of openness to children and joyfully promote the culture of life in simple, easy ways. First ask yourself, “What can I do to show my joy in the gift of children?” Well, how would you welcome the Christ Child? You’d smile, so smile at children and wave to them. Coo at babies; tell parents how beautiful their baby is. Encourage harried mothers with a good word and offer a helping hand, especially at the grocery.
Now look around, for nearly everyone of childbearing age is pressured by our culture to contracept. People simply don’t know the dreadful things contraceptives do to human bodies and relationships. How can you help? Sow seeds of truth and speak about the blessings of children. The light of your gentle witness is needed in our dark world. Build strong relationships with those around you and at the right moment, speak the truth in love. Our website has abundant life-affirming resources and OMS is glad to assist you in spreading truth.
Finally, look at organizations. Newspapers, churches, and schools offer wonderful opportunities to share the message that children are a gift and contraceptives cause harm. So whenever the newspaper runs a pro-contraceptive piece, write a rebuttal telling the truth. When the news reports the horror of a young mother abandoning or harming her child, write a letter recounting the supreme gift children are to all. Do what it takes to elect government officials who act according to truth, not whims. Support organizations such as Knights of Columbus and others who spread the message of life.
Yes, the task can be huge but an old adage applies: “Inch by inch life is a cinch, yard by yard it’s very hard.” There are many of us, and we are able to do many good deeds large and small. Inch by inch, and smile by encouraging word, we can all impact those around us. Through the grace of God we can sow seeds of truth and transform our culture to once again value children. So smile, and welcome the Christ Child in our midst.
To read more articles in our newsletter click below:
Micaiah Bilger Dec 2, 2015
Little baby Naomi captured the hearts of pro-lifers recently after the tiny preemie defied doctors’ dire predictions and lived.
Naomi Bakker was born 15 weeks premature, and doctors told her parents that her “chances of survival without health complications were less than one percent,” National Right to Life News reported recently. But the “feisty” baby girl fought for her life for five months in a Reno, Nevada hospital and now “Naomi is healthy and ready to graduate from the NICU with few complications,” according to Fox 28 reporter Elizabeth Faugl.
Live Action News reports more on the family’s story:
At 23 weeks gestation, Angela Bakker and her husband, Michael, were devastated to learn that their baby girl was not going to live. A routine ultrasound revealed that she was measuring much smaller than she should be, and she was diagnosed with intrauterine growth restriction. The placenta had not grown into the uterus properly and the little girl was not receiving adequate nutrition. The doctor told the heartbroken parents that their daughter would likely die in the womb.
Concerned for their daughter, the couple decided to get a second opinion, and they left their home in Reno, Nevada, to head to the University of California at San Francisco to meet with experts in their baby’s condition. Unfortunately, those doctors confirmed the diagnosis, and they told the Bakkers that there was the option to terminate.
Doctors repeatedly encouraged the Bakkers to abort Naomi, but they refused. They said if their daughter was going to die, they were going to let her die on her own time, according to the article.
“There were four hours left until the abortion cut off,” Angela said. “But they told us that in cases like ours they make exceptions. They said, ‘The law doesn’t even apply to you. That’s how bad your case is.’ She started kicking, and I thought, that’s her little voice. That’s all she can say.”
Just one week later, Angela’s life also was threatened by preeclampsia, and she was sent to the hospital for an emergency C-section. Baby Naomi was not expected to survive, but doctors agreed to try to help her if she did, the article states.
On July 1st, baby Naomi Joy was born, and miraculously she was breathing on her own, something the doctor said he had never seen happen with a baby that tiny.
She was so tiny, her eyes were still fused shut, and though she was born at 25 weeks, she was only the size of a 19 week preborn child. She weighed just 364 grams. According to the doctors, babies need to weigh at least 450 grams to survive.
Her tiny life kept stunning doctors. First, she had a procedure done twice to repair a hole in her bowels, and the incision healed on its own. Then, doctors feared she could have brain bleeds and gave her medication to help; she never experienced the problem. And although she has chronic lung disease, doctors believe it will heal within the next two years, Live Action News reports.
Naomi arrived home in time for Thanksgiving with her big brother, Nathaniel. Doctors and her family will continue to monitor her health and growth closely from home, according to the report.
“It’s been quite a journey and so far it’s had a good ending,” Angela said. “These babies don’t get a chance because parents do end up terminating a lot of the time. It’s not been easy. It’s been difficult and heart-wrenching, and every day you wonder if your baby is going to live. … It was a shock that this happened, but our faith and trusting that no matter what, it’s taken care of, is a big part of it.”
To read the full story, find the Bakkers’ on Facebook [https://www.facebook.com/NaomiJoyBakker].
Pope Francis’ Encyclical Laudato Si invites us to reflect on the beauty of God’s creation and reminds us of our responsibility to care for the environment. The Holy Father draws attention not only to current environmental issues but also human ecology issues such as abortion, population control, experimentation on embryos, and other offenses against the sanctity of life.
Although people are very concerned about protecting the environment and humans from genetically modified crops, pesticides, and other hazards, there is very little concern about contamination of the body and the environment with potent steroid hormones (such as those in birth control pills).
Where are the hormones coming from?
Xenoestrogen, or hormones that imitate estrogen contaminate the environment from many sources such as plastics, detergents, fertilizers, and phthalates. Ethinyl Estradiol (EE2) is a potent synthetic estrogen used for birth control pills, rings, shots, and patches. It is excreted through urine to sewage treatment plants and is contaminating tap water world wide. Comparing all sources of estrogen, EE2 activity poses the greater ecological risk.
According to the most recent data available, 9 per cent of women aged 15 to 49 use the pill. Countries with the highest prevalence of pill use—over 40 percent—include Algeria, Czech Republic, France, Morocco, the Netherlands, Portugal, and Zimbabwe. Researchers have found that synthetic hormones can be transported considerable distances from the source of pollution.
How estrogen affects humans and the environment?
Natural estrogens produced in the human endocrine system enter the cell and activate receptors triggering processes in the cells such as gene expression. Natural estrogens have a short life, do not accumulate in tissues, and are easily broken down in the liver. In contrast, synthetic hormones such as EE2 are more stable, remain in the body longer than natural estrogen, and tend to accumulate in the fat and tissues of animals and humans. Synthetic estrogens can disrupt the cell’s natural hormonal processing, mimicking, blocking or cancelling natural estrogen’s effects.
What are the effects on the human body and the environment?
Excess estrogen (natural or synthetic) in humans has been related to infertility, breast cancer, endometriosis, fibromyalgia, prostate cancer, and early puberty.
Genetic alterations caused by synthetic hormones present in the aquatic environment have also been found in wildlife. Researchers have found that caged adult trout exposed to synthetic estrogen were half as fertile as fish kept in clean water. Exposure of zebra fish to low doses of EE2 has produced persistent changes in their behavior and fertility. Even the next generation of fish not directly exposed to EE2 was affected by their parents’ exposure. Toxicologists have also found that the presence of synthetic hormones made the male species less male in frogs, river otters and fish, thus affecting their ability to reproduce.
What we can do?
Elimination of synthetic estrogen in water treatment plants is complicated and very expensive. Upgrades to the waste treatment plants in Britain to remove EE2 could cost up to $46 billion and another $960,000 per year to operate the system. A much easier and effective solution would be to educate everyone to stop polluting the water with hormones. Education on breastfeeding and fertility awareness methods for spacing children would help women appreciate their fertility and take good care of God’s creation.
“The natural environment is a collective good, the patrimony of all humanity and the responsibility of everyone. If we make something our own, it is only to administer it for the good of all.” Pope Francis
References:
Barel-Cohen, K., Shore, L. S., Shemesh, M., Wenzel, A., Mueller, J., & Kronfeld-Schor, N. (2006). Monitoring of natural and synthetic hormones in a polluted river. Journal of Environmental Management, 78(1), 16-23.
Maqbool, F., Mostafalou, S., Bahadar, H., & Abdollahi, M. (2015). Review of endocrine disorders associated with environmental toxicants and possible involved mechanisms.
Margel, D., & Fleshner, N. E. (2011). Oral contraceptive use is associated with prostate cancer: An ecological study. BMJ Open, 1(2), e000311-2011-000311.
Parry, W. (2012). Water pollution caused by birth control poses dilemma. Life Sciences
Tavares, R. S., Escada-Rebelo, S., Correia, M., Mota, P. C., & Ramalho-Santos, J. (2016). The non-genomic effects of endocrine-disrupting chemicals on mammalian sperm. Reproduction (Cambridge, England), 151(1), R1-R13.
Tompsett, A. R., Wiseman, S., Higley, E., Giesy, J. P., & Hecker, M. (2013). Effects of exposure to 17alpha-ethynylestradiol during larval development on growth, sexual differentiation, and abundances of transcripts in the liver of the wood frog (lithobates sylvaticus). Aquatic Toxicology (Amsterdam, Netherlands), 126, 42-51.
United Nations, Department of Economic Affairs Population Division
World contraceptive use (2011). Retrieved from http://www.un.org/esa/population/publications/contraceptive2011/wallchart_front.pdf
Volkova, K., Reyhanian Caspillo, N., Porseryd, T., Hallgren, S., Dinnetz, P., & Porsch-Hallstrom, I. (2015). Developmental exposure of zebrafish (danio rerio) to 17alpha-ethinylestradiol affects non-reproductive behavior and fertility as adults, and increases anxiety in unexposed progeny.
Hormones and Behavior, 73, 30-38.
As authorities sift through the rubble and bodies in Paris, many questions which need to be asked directly involving the attacks are being asked. But some questions are not being asked.
For example, is there something wrong with the thinking and actions, the attitudes ,on the part of western societies that might have contributed to this horror? This is not a “blame us” examination which the progressive elitist crowd always seems to trot out — you know, the “It’s our fault in the West because we have done such horrible things in the Middle East and should feel guilty” mindset, the logic there being: “We did it to ourselves because of our greed” — the same stuff that came flying out of the mouths of crazy liberals in America in the aftermath of 9-11, and like the idiotic liberal publication Salon did over the weekend. Typical.
No. This report is definitely not of that variety. But something does seriously have to be looked at regarding how Western societies live. Many of these types of killers come into Western nations, cross the borders, as part of a kind of open-door policy because Western nations need to shore up their flagging numbers. Their numbers are flagging because of low birth rates due to the widespread acceptance of contraception and abortion.
The same thing is happening here in the United States and still happens today. Sixty million Americans are not here today because the culture approved of their murders in the womb — many of them because the contraception failed. Who knows how many more tens of millions are not here because the contraception worked? A shrinking population — as is the case with various nations in Europe — actual declining numbers, as in, for example, next year there will be fewer Italians on the planet born in Italy then this year. Same in Greece and France and Spain and Portugal and Germany.
Shrinking populations like that mean governments have to step in and do something before the economic chaos sets in. Many of them have. Various European countries, led by Germany, are growing more desperate about the soon-to-be-felt fallout from their aging and shrinking native populations. So they have instituted a variety of laws actually paying for women and/or families to have children in the form of cash payouts, tax rebates and so forth. Part of their bag of tricks has also been to open up the borders and liberalize their immigration policies in an effort to stem the demographic winter so closely approaching.
France, for example, now boasts the largest Muslim population in all of Europe, and 20 percent of immigrants to the country each year come from countries with predominant Muslim populations. Germany, too, sees indications that pockets of Muslim immigrants — or the sons of Muslim immigrants, who, like in France, have not assimilated — also pose a threat to peace and security.
Regardless of the reasons of these increased numbers of violent scenes in London, Madrid, Paris, Germany and threats in Rome, immigration policies cannot be discounted as a precipitating factor. And the immigration policies were put in place because the Pill had become accepted. In the rush to have no restrictions on sexual license and no consequence for unintended pregnancies, Western societies forgot that there are consequences for unbridled sexual liaisons, particularly on such a huge scale as the cultures accepted and practiced it.
A wise old seminary professor once said something I’ve never forgotten. Monsignor William Smith — God rest his soul — of St. Joseph’s Seminary in New York once said, “God is forgiving, but nature isn’t.” The West happily accepted and advanced contraception and child murder as standard and has become awash, drowning in sexual immorality. This has resulted in a precipitous decline of the population and a now-dire threat to economic stability. To shore themselves up and avert such a demographic and economic disaster, these nations have thrown open their borders and invited in immigrants, some of whom are rightfully disgusted and repulsed by the sexual liberty that rules the day. Many of these immigrants directly or indirectly — and as we see, it doesn’t take many — feel perfectly fine about killing at will and creating mayhem in a culture they have no intention of assimilating into — quite the opposite; they are spurred on by terrorists in their ranks who inspire them to remain outside the culture of the Great Satan and overrun from within, by whatever means works the best — including mass homicide.
Anyone who thinks this kind of evil is going to lessen doesn’t understand the world situation. Christ will reign on the earth, either by His presence shown forth by His peace, or by His absence shown forth in chaos. Until the world comes to embrace God and bow under His mighty and loving hand and live by His decrees, men will continue to think that they have all the answers and can solve every problem — and the folly of man will be clear for all to see.
Let us pray for not only the souls of the dead in Paris, but most especially for the souls of nations and peoples everywhere. There is no peace without God — and God cannot co-exist with sin enshrined as law.
It is God’s law or man’s law. Just as in eternity there is no middle ground, so in the lead-up to eternity on this earth, there is no middle ground.
A few months back, I told my readers on my blog how to raise eight children without even trying. Today, I’m going to tell you why I never should have had eight children in the first place: had I listened to the devil and modern conventional wisdom, that is.
When I was a happy mother of four, seriously considering and deeply desiring another child, an odd feeling overcame me. Over several days, my excitement at the idea of a new little soul became mixed with feelings of discouragement and fear. It began to dawn on me that I was barely good enough “mommy material” for the four treasures I already had, and that any further parenting would be irresponsible. It came to a head one evening: I remember standing in my kitchen, full of fear and anxiety, telling myself that I had no business – no business! – having another baby. Not now, not ever.
All my shortcomings and sins came to the forefront of my mind, and I stood there reeling from the truth of it:
I can’t cook.
I can’t grocery shop.
I can’t bring the kids out alone without help.
I have nooooo patience.
I am not crafty in the least.
I can’t sew.
I can’t throw a party.
I’m not athletic or outdoorsy.
I don’t know how to make a pretty home.
I don’t know how to make anything fun.
I am lazy and a procrastinator.
I’m used to being served, not serving.
I am sarcastic and cranky.
I am a complainer.
I like to be alone.
I hate to be interrupted or inconvenienced.
I am not particularly good with children.
In that moment, I knew all of these things. And I was discouraged. Any one of these reasons could be enough for a woman to convince herself that it’s imprudent to have another child. In fact, you might just be saying to yourself now, “My gosh, that woman shouldn’t have one child, much less eight!”
But see, there’s the thing: Moms of big families are told constantly by other women that “I couldn’t do what you do!” or “You must have so much patience!” or “You must have a real way with children!” They think we were given a special gift or have a mutant gene that they do not possess. But they have no idea how much we are just like them. In fact, most of the women who say those things to me are better suited to raise a large family than I.
As I stood there in the kitchen that night, a moment of grace overtook the moment of discouragement. How many times had I told others, “Discouragement is not from Christ, as Christ only encourages. Discouragement is from the devil!” I remembered it then, and my fears and anxieties were banished. Only the devil himself, the one who hates human beings to his rotten core, would taunt me with the notion that my lack of gourmet skills should preclude new life in my marriage. I saw the evil of it then, and I called him out. I still cussed a lot back then, and I am pretty sure I told the devil what he could do with his putrid flood of discouraging thoughts. Yeah, that was a good moment.
Since that day, five eternal souls have been created in our family, four of whom my husband and I have the privilege of raising on this earth. And, while I can’t claim to have conquered all the deficiencies and vices on my list (not even close! drat!), the existence of all my children has moved me along the path of holiness. Because that’s how it works: The souls in your life are gifts, each of whom is meant to sanctify you in a particular way. My little sanctifiers are the artisans who change and mold me in all the ways God knows I need, and they are their father’s and their siblings’ artisans, too.
That my family exists as it does is living proof that “with God, all things are possible” – even Leila Miller mothering eight great kids.
Manchester, England, November 12, 2015, LifeSiteNews
A young cancer-stricken mother who refused to abort after receiving her pre-natal diagnosis has given birth to healthy twins.
Doctor’s identified Holley Tierney’s Non-Hodgkin’s Lymphoma when the Manchester, England, mom was 23 weeks pregnant. They advised her to abort and begin chemotherapy.
But at this point in her pregnancy the 25-year-old mom was able to feel the babies kick inside her womb, and even though facing cancer while pregnant was her worst nightmare, she said she simply couldn’t deny her unborn children life.
“I knew there was no way I could terminate my pregnancy when I felt them kick, my maternal instincts had already kicked in,” Tierney said. “It was the happiest day of my life when my babies were delivered safely, it was definitely a risk worth taking, all I cared about was their health.”
Tierney was resolute in postponing the drugs until after her babies were born, according to a Daily Mail report.
“Once doctors realized I wasn’t having a termination they kept pushing for them to be born premature but I wanted my twins to reach 30-weeks before I had a caesarean,” she said.
However, at 29 weeks doctors told her she shouldn’t wait any longer because the cancer could spread, resulting in Tierney’s son Harlow and daughter Havana arriving via C-section 11 weeks early.
“My babies were delivered safely in August and taken straight to intensive care, they weighed almost 3lbs each,” Tierney recounted. “Seeing them for the first time was the best feeling in the world, I couldn’t believe they were mine.”
When the twins were a week old she started chemotherapy, encountering its accompanying side effects, including nausea and losing her hair. And at the same time as her babies were embarking on an 11-week hospital stay, and she began her cancer fight, Tierney had to ponder the possibility of her children growing up without their mother.
“It was bittersweet as I kept thinking I would never have chance to watch them grow up,” she said.
The twins recently made it home and are settling in, and after five cycles of chemotherapy Tierney has just one left before starting radiotherapy after the New Year.
Before her initial diagnosis, Doctors had thought her chest and arm pain were due to a pulled muscle. So as she moves forward with motherhood and her cancer battle, Tierney is also speaking out about her situation in hopes that other pregnant moms will be aware of potential problem symptoms.
“It was heart breaking but I knew I needed to stay strong and positive for my babies,” said Tierney. “They had fought to stay alive and now I needed to fight for my life and that’s exactly what I’m doing.”
The contraceptive pill could damage fertility, according to new research.
The powerful hormones could upset the reproductive system for months – or even years – after women stop taking it.
Women who have used the Pill are twice as likely to have problems conceiving later.
The findings are the first to suggest a link between oral contraceptives and infertility, and come despite repeated assurances from manufacturers that there are no long-term effects.
Today fertility experts described the research as “highly significant” and said Pill users must be told about the possible risks. But family planning groups urged women not to panic – stressing that most women had no problem conceiving after they stopped taking it.
The link emerged in a study of more than 2,200 women attending UK antenatal clinics. More than 40 per cent had taken combined oral contraceptives – the most common form – while 19 per cent had used condoms.
Five per cent had used other types of Pill, 13 per cent had used no contraception at all, and the rest had used hormonal implants, coils, or other methods.
On average, the women had been using contraceptives for three and a half years before trying for a baby. Overall, two thirds became pregnant within six months.
On average, however, former Pill users took twice as long to conceive than those who had used condoms. The longer they had been on the Pill, the longer it took to conceive.
The study, led by gynaecologist Stephen Killick at Hull Royal Infirmary, says: “In all, 6.5 per cent of previous combined Pill users took more than two years to conceive, compared with 2.6 per cent of condom users.”
The risks appear to be even greater among women who are over 35, or obese, or suffer from irregular periods. Over-35s who had taken the Pill took two-and-a-half times as long to conceive as those in the same age bracket who had used condoms.
Although 70 per cent of former Pill users became pregnant within six months, the researchers believe the hormones may take time to wear off among some women, in whom they may stop the ovaries releasing eggs normally.
Around three million women in Britain are on the Pill, most taking the combined as opposed to the progesterone-only version. It appears the impact of the combined Pill on fertility wears off after two years at the most.
I love devotional Catholicism. By this I mean making pilgrimages to shrines and praying at the tombs of saints. I frequented the tomb of St. Mariam of Jesus Crucified, the Palestinian Carmelite, while I was in Bethlehem for three weeks in 2014. In January 2015, I prayed for my (then) upcoming ordination to the priesthood at the tomb of St. Damien of Molokai in Leuven, Belgium. I find these spiritual practices and devotions to be beneficial.
With that being said, I must confess that when I heard about the Pilgrimage of Mercy, in which the relics of St. Maria Goretti would travel throughout the United States, I thought it was weird. It struck me as Catholicism meets the Antiques Roadshow. Not only that, but my pessimism wondered whether or not the story of Maria Goretti would attract any interest among American Catholics.
My devotionalism and curiosity got the best of me. I was intrigued by St. Maria Goretti’s Pilgrimage of Mercy, and so on October 16, 2015, after going back and forth interiorly whether or not I should make my own pilgrimage to venerate her relics, I buckled into the driver’s seat of my Ford Fusion and hit the road toward Madison, to a parish named after the Church’s youngest saint. It was at this parish that Bishop Robert Morlino presided over a Mass honoring St. Maria Goretti at 7pm. In a filled to capacity, standing room only church, Mass commenced and by the Ite, Missa Est, the entire congregation came to know the story of St. Maria Goretti.
I remained in the church following Mass for about an hour to pray. During that hour people kept coming. And as I exited the Church, I was amazed to see that the line extended outside, into the frigid cold. As I headed home, I could not help but ask myself: Why were so many people drawn to the relics of Maria Goretti? After all, this form of devotionalism, is not expressed all that often in the States. But there was something about this teenage saint that drew massive amounts of people. I realized that America needed the story of Maria Goretti, her witness, and her prayers.
We Admire Her Chastity
Why were people drawn to Maria Goretti? It’s because we admire her chastity and purity. Maria Goretti’s story challenges our American culture to a greater appreciation of these virtues. It was Maria’s resistance against her attacker which brought about her death. She reminded Alessandro that what he was trying to do was a sin. Not only did she care about her purity, but she was concerned about the soul of her attacker.
We live in a time marked by sexual promiscuity. Why do thousands of people line up to see Maria Goretti? Because they want their hearts to be like the heart of Maria. They want to grow in chastity, and so they look to her story and ask for her prayers. They desire a pure heart.
All we have to do is turn on the television and our purity is assaulted. We watch television shows that glorify the very cause of Maria’s death. Our entertainment, be it television or movies, highlight rape, its victims, and the quest to solve these crimes. We live in a sexually indulgent culture because of the easy accessibility of contraception. Teenage pregnancies are on the rise. People “hook-up” in our culture and search for one night stands. Many turn to pornography as a way to fill a void of love in their life. Sexuality is no longer valued as a gift from God, mirroring the love of Christ and His Church, but rather as something to be taken advantage of, at any opportunity.
People form lines and pass by the relics of St. Maria Goretti because they are wounded by their sinfulness. Many are enslaved to sexual sins. They look to Maria Goretti and ask her to pray for them, so that they can turn to God, and like her, be a defender of that gift given to them by God.
We Admire Her Ability to Forgive
The story of Maria Goretti does not end with her defense of purity. After being stabbed fourteen times, Maria, while on her deathbed, forgave Alessandro. As an American people we admire Maria’s ability to forgive.
We struggle to forgive in our American culture. Not only can we not forgive ourselves for things we have done in our life (e.g. impurity), but we find it extremely difficult to forgive other people. Many people, including myself, are holding grudges against those who have offended us. It is hard to forgive other people. Even more, it is difficult to forget what people have done; the memories of hurtful words are actions remain. But our God calls us to forgive those who have hurt us. We must forgive our family, coworkers, and friends.
People form lines and pass by the relics of St. Maria Goretti because they know there are people in their lives they need to forgive and need divine assistance in doing so. As they touch the glass case, they ask Maria Goretti, who forgave the one who hurt her, to help them forgive the people in their lives. And they ask for the grace to forgive themselves because in time, Alessandro was even able to forgive himself, after Maria came to him in a dream and gave him 14 es.
A Saint for the Year of Mercy
Maria Goretti is an appropriate saint for the Year of Mercy. Her story challenges all sinners in their struggles with the flesh. She is one of their patrons and intercessors in whatever struggle they face. Like Alessandro who turned to God for mercy, we must seek out Christ’s mercy in the confessional. But even more so, Maria is a living witness of forgiving offences willingly, one of the spiritual works of mercy. Just as Maria forgave Alessandro, she inspires us to reach out and extend mercy, forgiveness to the people in our lives who have hurt us. After all, Jesus told us to petition the Father in this way, “forgive us our trespasses as we forgive those who trespass against us.” For whatever wrong the eleven year old Maria Goretti did, she surely experienced God’s forgiveness, for she heroically forgave the one who trespassed against her, who ended her life too soon, taking her from her impoverished family, her friends, and the Church. Now, as one of the blessed in Heaven, she intercedes for us, praying that her story can inspire us to a greater love of purity in our lives and lead us to forgive our family and friends.
Sarah Conly, a professor a ultraliberal Bowdoin College, where students shell out tens of thousands of dollars a year to be spoon-fed such poppycock, think families should have no more than one child.
A philosophy professor at Bowdoin College, Sarah Conly, really misses China’s One-Child policy. I mean, really misses it.
She even wrote a book called “One Child: Do We Have a Right to More” because I don’t want to financially support garbage like that. I’m not going to buy that book but she was kind enough to write a column in the Boston Globe putting her anti-human kookiness on display for everyone to see.
In it, she bemoans China ending it’s one-child policy and asks “Is this really a good thing?” She thinks not.
She writes, “the idea that people should limit the number of children they have to just one is not, I would argue, a bad one, for the Chinese or for the rest of us.”
Then you get a lot of blah blah blah nonsense about overpopulation and all that. But then you get to the moral case. She posits that YOU have no right to have more than one child.
Given the damage we are causing, and the suffering we foresee for all those who live after us, it is clear that having more than one child is just something that none of us — Chinese or American — has a moral right to do. We have no right to cause great harm to others when we can avoid this without great loss to ourselves.
At this point, uncontrolled fertility is likely to have worse consequences than the false cry of “fire!” Even having two children — the replacement value for the population — as the new Chinese policy allows is likely to be too many children. Due to what specialists call “demographic momentum,” the population will continue to grow for quite some time even if we all cut back now to two children. By the time the birthrate stabilizes, the global population will be at an unsustainable level. So, we don’t have a right to have so many children.
Why is it that some of the most wacky, hairbrained ideas come from the ivory tower elite — the folks who are supposed to be the smartest of the smartest. Perhaps because they are elite, some of them don’t want more people in the world challenging them or their nutty theories.
“…what God has joined together, no human being must separate.” Mk 10: 9
The Bible Says
“But from the beginning of creation, ‘God made them male and female. For this reason a man shall leave his father and mother [and be joined to his wife], and the two shall become one flesh.’ So they are no longer two but one flesh. Therefore what God has joined together, no human being must separate.” Mk 10:7-9
Jesus spoke these words in response to the Pharisees’ questions about divorce—in particular Moses’ allowance of a decree of divorce. The 40-50% divorce rate in the USA indicates that Jesus’ teaching that “no human being must separate” husband and wife is largely ignored.
“God created mankind in his image; in the image of God he created them; male and female he created them. God blessed them and God said to them: Be fertile and multiply; fill the earth and subdue it.” Gen 1: 27-28
“Let the children come to me. Do not prevent them.” Mk 10:14
The joining of love and life in marital sexual intercourse—the marriage act—is a second God-ordained joining not intended for Man to separate by contraception.
Divorce & Contraception Violate God’s Plan
US Catholics divorce and contracept at about the same rate as non-Catholics. Annulment application is commonly offered in response to divorce. For most Catholics, their teaching on contraception has been nil. It is estimated that 60-90% of annulments world-wide are granted in the USA. Also studies indicate that almost all Catholic couples contracept before and during some part of their marriage.
What the Chart Shows
The enclosed Total Fertility & Divorce Rates chart demonstrates a strong correlation between family size and divorce. Why did family size begin a steep decline in the mid-1800s? Andrea Tone, in Devices and Desires, A History of Contraceptives in America, describes how Charles Goodyear’s 1839 invention of rubber vulcanization transformed a small but thriving side-line to sausage making into a lucrative condom manufacturing industry that continues into the 21st Century. Contraceptive use is the only feasible explanation for the rapid decline in Total Fertility Rates (TFRs) during the 19th and 20th Centuries. Note that TFRs dropped by almost half in each Century, and they have hovered a little below 2 during the 21st Century.
The Pill Effect
The Divorce Rate increased 2.5 times following wide acceptance of the Birth Control Pill in the early 1960s. No-fault divorce laws and legalized abortion were further consequences of over 10 million women being on the BCP and millions more continuing to use barrier and other means to limit child-bearing.
Marital Sexual Intercourse
In God’s first words to us, He commanded us to “be fruitful, multiply and fill the earth”—a single command stated three times. He must have thought it pretty important. In humility and trust, He surrendered to His creatures the duty and power to initiate a new human life, while retaining His right to allow that initial effort to succeed. We call that sacred act of initiation “marital sexual intercourse”.
The “marital” adjective is important because it sets marriage as the legitimate condition for use of sexual intercourse. This is based on marital sexual intercourse’s essential purpose to populate Earth and Heaven—its procreative purpose. To guarantee that we would engage in marital sexual intercourse, God added a unitive second dimension by making marital sexual intercourse delightful, enjoyable, exciting and mysterious. The unifying dimension cleverly encourages the marital sexual intercourse-performing couple to stay together for their continuing pleasure AND for mutual support in raising their children—and also God’s. Thus a family is formed!!
Why Marriage
Marriage publicly identifies the family as an institution formed by a man and woman engaging in sexual intercourse, and children that result from their union. Thus marital sexual intercourse is referred to as the “marriage act” or the “procreation act”—recognizing its essential and unique purpose of creating new human life with God. It is these procreative and unitive ends that “God has joined together [and] no human being must separate”.
Why is this so?
If the act which is primarily intended for procreation is counterfeited (neutered) by contraception, the act cannot achieve its intended and natural purposes—neither procreative nor unitive. A holy act has been hollowed out and made intrinsically evil. It should be expected that contraceptive-using-couples will feel dissatisfied, incomplete and expectant of something more. That missing more may be sought in another relationship, pornography, or other addictions. The stage is thus set for divorce.
Conclusion
The cultural chaos caused by divorce is due in large part to the effect of contraception on marriage. Separating the unitive and procreative ends of sexual intercourse redefines and destabilizes marriage. In God’s perfect plan for us, there would be no contraception, the average family would include many children, and divorce would be rare.
Has there ever been a time in history (or a culture) when both contraception and divorce were absent? What was that society like? Can a contraceptive and divorce free society be created? Can we humbly set aside our plan, and accept God’s plan for love, marriage, sex and children?
Conclusions Suggested by the Chart:
1. The “natural” Total Fertility Rate (TFR) may be as high as 7. With limited availability of contraception, the average American woman of the early 1800s birthed 7 children. Is that what God planned for average family size? The corresponding “natural” divorce rate is essentially zero.
2. The vulcanization of rubber by Charles Goodyear in 1839 jump-started the contraceptives industry with condoms and diaphragms. As contraceptives began to be readily available in the mid-1800s, TFRs rapidly declined.
3. The low TFRs during WWII (1941-1945) were followed by a jump in TFRs as millions of soldiers returned to marry and start families in 1945-1960. High divorce rates during and after WWII may be a result of long separations and mental and physical health problems of returning soldiers.
4. The advent of the Birth Control Pill (BCP) in the early 1960s and the universal acceptance of all forms of birth control soon fixed TFRs at about 2 (or less) for the 40+ years from 1970 to 2014. Divorce rates increase as TFRs decrease.
5. Rapid acceptance of the BCP in the 1960s corresponds with divorce rates more than doubling in 10 years.
6. While TFRs have held steady near 2 for the past 40 years, divorce rates have steadily declined to 1960’s levels possibly due to slow economic growth, fewer marriages reducing the pool of potential divorces, and aging couples’ greater tolerance of a less than ideal marriage.
7. Contraceptive use destabilizes and redefines marriage.
Source divorce rate data: U.S. Census Bureau: Statistical Abstract of the United States for 2001 (Table 117), available online at www.census.gov/prod/www/abs/statab.html; Current Population Report for 2000 (Table 3), available online at www.census.gov/cps; Centers for Disease Control and Prevention: “Births, Marriages, Divorces, and Deaths: Provisional Data” for 2000 (in National Vital Statistics Report 49) and 2009 (in NVS Report 58) (Table 2), available online at www.cdc.gov/nchs/products/nvsr.htm
“Every mom I know in anencephaly groups who has carried to term has no regrets, while there are so many who regret early induction/ termination. It is truly amazing (and not distinctly related to the parent’s religion).”
-The mother of Baby Joseph
Best Choices for Families Dealing with Adverse Fetal Diagnosis
Discovering one’s child has a serious medical condition is always devastating, whether it occurs at twenty years old or twenty weeks gestation. Among the many disorders that usually shorten a child’s lifespan dramatically, causing death within the first few months of life, are various Trisomy conditions, Potter’s Syndrome, and anencephaly (a neural tube disorder). Many families confronted with an adverse prenatal diagnosis have experienced a lack of resources, information, and support, and often face unwelcome pressures as well, but those who carry to term usually find peace nonetheless.
Dum Vivimus Vivamus
“Dum vivimus vivamus…While we live, let us live” is a fitting motto for families who give their babies a chance to survive, contrasting sharply with many historical and current medical prac-tices. What follows are four stories from a limited geographical region (western Ohio) representing hundreds of regions across the country; your own communities; your own hospitals.
The life of Joseph
Diagnosed with anencephaly at 20 weeks; lived 37 weeks in the womb and 88 minutes after birth.
The ultrasound doctor who diagnosed anencephaly gave Joseph’s parents one option: “we could induce early (like next week!) and then we wouldn’t have to go through the rest of the pregnancy…I thought to myself: If my firstborn, was diagnosed with a terminal illness and had only 4 months to live, would I ask the doctors to end her life right now, or would I love and cherish every moment until God called her home? Thinking of it that way, the answer was clear. It was obvious it wasn’t a choice at all. I was incredibly sad and discouraged having to be in this position, but the only possible choice we could live with is to just love this baby as long as we can.” After their initial office visit, they were fortunate to experience the support of family and friends, as well as that of their trusted family physician, who “grieved with us, prayed with us.”
The life of James Thomas
Son of Ben and Lynn, diagnosed with Potter’s Syn-drome at 22 weeks; lived 36 weeks in the womb and 90 minutes after birth.
James’ mom shared their experence, “At the initial appointment [22 week check up] when we discov-ered the Potter’s Syndrome, the first words from the doctor’s mouth were: ‘If you choose to terminate, you need to do so by the end of the week.’ ” James’ parents were “surprised, angry and hurt by this recommendation.” So much so that, at their request, the ethics board of the hospital has changed their guidelines for doctors, instructing them to present, in a compassionate manner, a full range of options to clients. James’ parents wondered, “Why was this the first option given to us?” The only risk factor for James’ mom was a previous history of pregnancy hypertension unrelated to Potter’s Syndrome. It was treatable and only a concern closer to term when James would be viable outside the womb.
Fortunately family and close friends were very supportive. Yet “lots of other people questioned the decision. No one could give any rationale for terminating, but the gist was ‘why would you want to continue with the pregnancy [considering it an inconvenience] when you know he is going to die anyway?’ ” The response of James’ parents was, “Why not? Why not give him the best chance at life that we could?”
The lives of Elizabeth and Jacob
Children of Scott and Julie, both diagnosed with Potter’s Syndrome at around 20 weeks gestation, with different outcomes.
Elizabeth and Jacob’s parents had a significantly different experience with their first child diagnosed with Potter’s syndrome than with their second. Elizabeth and Jacob’s stories are a poignant illustra-tion of the contrast between two different decisions. With Elizabeth, their first child with Potter’s, they followed advice from doctors and other counselors, undergoing “early induction” at 23 weeks. Doctors had avoided the word “termination” so they didn’t realize the implications—until later—nor the deep regret that came with “early induction” of an essen-tially non-viable baby. Nor would they have chosen that route had they been better informed. When Jacob came along, diagnosed with the same condi-tion, they knew they didn’t have to “induce early.” This time, “we were more at peace because we had given him every chance to live.” Monitoring vital signs closely, they carried Jacob as close to term as possible, birthing him at 37 weeks after discovering he passed away in the womb. Their only living child was almost 3 as they said their goodbyes to Jacob at the birth. With both Elizabeth and Jacob, pictures from the day of birth are precious memories, even though the children had not survived. A deeper regret lingers, however, with regard to the short time leading up to Elizabeth’s last day of life: “We feel like we weren’t given time with Elizabeth like we were with Jacob between diagnosis and birth. With Elizabeth we had a week and a half to make a decision and prepare. That wasn’t enough time and made everything harder after.” They had hoped for a live birth with both children, even if the time with them alive would be limited. In both cases it was not as they had hoped, but with Jacob they were grateful for those extra 14 weeks they had with him alive in the womb. “Doctors are afraid of giving false hope,” they added, “but parents need hope. The hopes are not naive; they give parents the opportunity to try to do something to help their child.”
Safeguarding Women’s Health and Applying Moral Principles
The short lives of the children introduced in this brochure deeply touched their families, calling them to love. All of these families experienced many blessings from choosing to carry their babies to term. They were fortunate to have access to information beyond the limited options given at the hospital, and to have ample support for their decisions from friends and family. These life-lim-iting prenatal conditions primarily affect the babies, not posing serious risk to the mother.
The hypertension that doctors feared for James’ mom didn’t result from Potter’s Syndrome; she also developed it during other pregnancies. Joseph’s mom had concerns about polyhydramnios (swelling from excess amniotic fluid) but the primary concern with that (besides discomfort) is early labor or stillbirth, which again concerns the baby, not the mom. Elizabeth and Jacob’s mom did not experience complications, but was told infection could follow if the baby died in the womb. All of these complications are manageable; none are life threatening or permanently damaging to the mother. In cases such as these, some try to use the princi-ple of double effect to justify actions that end the baby’s life. But double effect can only be invoked when the primary intended effect is not morally wrong. The intended effect of “early induction” (or “termination”) is to shorten the pregnancy by birthing a non-viable child. It may be a well-mean-ing attempt to minimize the parents’ grief, but it actually does nothing to take away the pain of infant loss. Early induction does directly result in the baby dying earlier rather than later and this is the primary intended effect of the procedure, not merely an unfortunate secondary result.1 In this case, “early induction” is not the only conceivable means of relieving grief, and is mostly ineffective. In fact, there is ample evidence that abortion often causes additional emotional complications, both from the grief of loss and from disrupted hormonal balance.2 The drastic hormonal shifts have also been shown to cause dramatically increased risk for disease, notably breast cancer.3 In addition, there is evidence that termination of pregnancy (abortion) can have a traumatic effect on those involved, including medical personnel who participate or witness the event.4 In any case, what if the diagnosis was wrong, which has been known to happen?
Why Couldn’t We…?
It’s natural for parents to ask if there is anything they can do to help their child survive as long as possible. With anencephaly and Potter’s Syndrome, possibilities are extremely limited because vital organs are severely affected. Unfortunately, possibil-ities are further limited by the hopeless practice of early induction. Since Potter’s Syndrome involves inadequate amniotic fluid, most parents ask the obvious question: “Can’t we try to inject synthetic amniotic fluid into the womb as needed?” Parents are told, “No.” Yet in 2013, a US Congresswoman, Jamie Herrera Beutler, and her husband wouldn’t take no for an answer. They found a team of doctors willing to try the injections. Their daughter Abigail became the first known survivor of Potter’s Syndrome, receiving a standing ovation on the House floor a year after her birth. Abigail’s dad, Daniel, said in a Today Show interview, “There are no guaranteed solutions…for [Potter’s Syndrome], but don’t be satisfied with one opinion because there are a lot of intelligent doctors with different perspectives and experiences and opinions, so work to find one who will partner with you to find anything possible.”5
Citations
1. Principle of Double Effect, download at Catholics United for the Faith: www.cuf.org/FileDownloads/doubleeffect.pdf
2. Afterabortion.org lists physiological effects of abortion.
3. The Breast Cancer Prevention Inst. (bcpinstitute.org) presents the physiological explanation and statistical correlation of abortion to breast cancer.
4. Many former abortion providers share their stories at ProLifeAction.org/providers and ATTWN.org (And Then There Were None.)
5. Steven Ertelt, “Congresswoman’s Miracle Baby Still Doing Well After Doctors Said She’d Die,” LifeNews.com, September 6, 2013.
Text by Anne Schmiesing Right to Life—Shelby County, OH
This brochure is not intended as a resource for medical information about the conditions mentioned. Note that although Down Syndrome is included in the list (as Trisomy 21), children with Down Syndrome have a much higher chance of survival than children with the other conditions named in this brochure. The life expectancy for all of these prenatal conditions increases with advances in medical knowledge and technology.
Information for stories was collected from personal interviews and with permission from a blog about Joseph. More information from the interviews is available at ShelbyCountyRTL.org. For additional stories and resources, see PrenatalPartnersForLife.org and SufficientGraceMinistries.org.
The book, I Will Carry Youby Angie Smith chronicles the creative ways one family found to spend time with their child in her short life. This is a helpful resource for families faced with a life-limiting prenatal diagnosis.
Benjamin Hartings, father of James Thomas, has written a book about his experience.Return to the Altar: A Sacred Journey through Grief and Joy is the story of a family’s loss, a death of a son, and how it transformed their view of the world. What brought the family back to the Altar was not an experience that was expected, but one that was accepted as God’s plan.
With all of the depressing news about abortion and the shocking things the Planned Parenthood abortion business does to sell aborted babies and their body parts, there’s a palpable need for good news that is uplifting.
Today, a British newspaper is reporting on a little boy who doctors said was “incompatible with life.” Because his courageous mother didn’t give up on him when doctors said he would die immediately after birth, little Aaron just turned two and said “Mommy” for the first time.
When she was pregnant, 24-year-old Emma Murray heard from doctors about her son’s condition. Aaron was diagnosed with rare health disorder called holoprosencephaly and he was born with a brain stem so can move and breathe but not a full brain. Physicians told Murrary Aaron could die in minutes and helped arrange a baptism for him.
Now, two years later, Aaron has amazed doctors – and has spoken his first word. Aaron is not only alive but enjoys giggling and clapping his hands with his big brother, Jack, aged three.
As the London Daily Mail reports:
Emma said: ‘When Aaron was first born, I was told there was no way he could survive. I was told he might live for three minutes, three hours or three days.
‘The doctors told me if it had been any of his other organs which had failed to grow, they would have been able to do something but they couldn’t grow him another brain.
‘But right from the very beginning, Aaron proved he is a real fighter.
‘And I was saying “mummy” to him recently and clapping my hands and he was giggling away.
‘He looked at me, and said “mummy”. I couldn’t believe it. I’d been told my son would only live for a few minutes, but now here he was saying ‘mummy’ which is something I never thought I would ever hear.’
That good news is a stark contrast to what happened after he was born.
Emma said: ‘I was absolutely heartbroken. He was hooked up to every machine and had a hat over his head so we couldn’t see the size of it. I just sat by his cot rubbing his little hand. I was in total shock.
‘Everything had happened so fast – I didn’t even know I was pregnant, I’d given birth and been told my baby was going to die all in the same 24 hours.’
Hospital staff helped Emma organise a baptism for her son, but within hours, Aaron’s condition started to improve and they realised he could even breathe unaided.
Emma said: ‘For the first few days of Aaron’s life, it felt like everyone was just waiting for something bad to happen but Aaron had other ideas.
Thankfully, Emma and her little boy are moving forward and focusing on embracing life a day at a time.
She said: ‘Some days, we take one step forward and two steps back – but since he turned one, we have been taking more steps forward than back.’
And the most emotional moment came just six weeks ago when Aaron amazed Emma by saying ‘mummy’ for the first time.
She said: ‘I was just playing with him in my front room. He was lying on his back on the carpet and I was leaning over him clapping my hands, and saying “mummy” to him over and over, really drawing out the sounds.
‘He was giggling, and then he said “mummy”. He had literally copied what I was saying. I just stared at him in shock, and then I just burst into tears. It was such an emotional moment.
Do you remember what it was like to be a 10 year old? I remember being an unabashed tomboy concerned with playing outside and acing 5th grade.
But life isn’t so innocent and carefree for some 10 years old in Washington State. This summer a report came out claiming that some schools in Washington were giving free birth control implants to children as young as 10 years old! These birth control devices are implanted in a girl’s uterus, and all of this can be done without a parent’s consent!
And now a public records request by Judicial Watch has confirmed the details of what is happening in Washington.
JW filed a public records request with the Washington Health Care Authority after reading a disturbing article in a pro-life news site over the summer about a Seattle high school that offers different forms of birth control without parental knowledge or consent. This includes implanting an intrauterine device (IUD) in a girl’s uterus free of cost. It’s part of an initiative offered by Medicaid, the joint federal and state insurance program for the poor. The article points out the irony that a teen in Seattle can’t get a sugary soft drink in high school but can have a device implanted into her uterus.
The data obtained by JW reflect increasing numbers of kids in all age groups receiving these birth control implants from 2013 to 2014. Figures can’t be compared for 2015 because the full year’s data is not yet available, but the records show that in 2014 and at least part of 2015, girls as young as 10 received the implants. The largest group of minors that got the birth control implants was 17 years old, according to the data, but girls much younger also received them. Four 11-year-olds got birth control from the state during the 2 ½- year period and so did more than 100 girls between the ages of 12 and 13. The numbers go up as the girls get older with 364 girls age 14 getting the implants and 744 15-year-olds. The records show that 2,336 girls ages 16 to 17 were given implants during this period.
It is crazy that the government is offering a controversial form of birth control that can have serious life-long side effects to 10-year-old CHILDREN, but then to do all of this behind a parent’s back is simply outrageous!
By Cheryl Sullenger, Operation Rescue, October 16, 2015
David Daleiden is the Director of the Center for Medical Progress, an organization that was known only to a handful of people prior to July 14, 2015, when he released the first of 10 summary videos that were part of his jaw-dropping 30-month undercover investigation into Planned Parenthood’s participation in the illegal sale of aborted baby body parts that has dramatically changed the abortion debate in America.
Recently, David was interviewed on camera by The Blaze’s Glenn Beck, who posted a fascinating clip from that interview. In that clip, Beck asks David about whether he ever realized the powerful evil that with which he had embedded himself.
“At some point, you guys had to have walked out of those [meetings] just shaking and thinking, A: ‘I can’t believe the evil I just faced,’ and B: people die for stuff like this. I mean, we’re going up against evil, and very powerful evil. Did that ever hit you while you were doing these things?”
David then related his encounter with late-term abortionist Shelley Sella, an abortionist conducting the latest of abortions throughout all nine months of pregnancy who currently works at Southwestern Women’s Options in Albuquerque, New Mexico. At the time of David’s encounter with her, she was a contract abortion provider with Planned Parenthood in Concord, California.
David described a meeting where he was laughing and joking with Sella after a showing of the independent film, “After Tiller.” But for a moment, their eyes locked, and he saw a change come over her.
“All of a sudden, her eyes looked really hard and mean and aggressive, and for the first time during this entire project, I felt really afraid – like an actual fear — fight or flight kind of response,” David related. “I felt very exposed, felt like she knew everything about me.”
But then her face changed again and she was back to laughing and joking with him.
“I talked to several people about that afterwards, and some people have kind of a spiritual interpretation of that event and there’s a more subtle interpretation. But on some level, we feel like that was the predator — the predator look or the predator instinct that you see in someone who is accustomed to killing people. This is a late-term abortion doctor who has terminated many, many, many big babies over the years,” Daleiden told Glenn Beck, who sat enthralled by the power of the moment.
Spiritual battle
I completely understood. For me, it was a real “Lord of the Rings” moment. I could imagine David as J.R.R. Tolkien’s Frodo laid bare before the all-searching Eye, with only the thinnest of veils keeping him from being discovered by the wicked Sauron, who was bent on the destruction of man-kind.
My faith informs me that there is a spiritual battle that interacts with our realm of reality, where angels and demons continuously fight for supremacy until the Final Day. Had David caught a glimpse of a demonic force that somehow sensed something about him for a brief moment in a similar way that Tolkien’s Ring Wraiths sensed the presence of Frodo, the Ring Bearer?
I am very familiar with this particular abortionist since she was one of three that were employed by the infamous George Tiller at his late-term abortion mill in Wichita, Kansas, who has aborted hundreds, if not thousands, of babies in the late second and third trimesters of pregnancy.
While my relationship with Sella has been more adversarial than David’s over the years, I have felt that same sense of evil, especially one day in June, 2008, when a licensed practical nurse walked into our office and unburdened her heart about her experiences working at Tiller’s abortion clinic. A story she related to us about Sella was one of those surreal moments when the evil hits home.
35-week born alive baby
Tina David was a slender older woman with short-cropped blonde hair who had worked assisting Tiller’s abortionists with the very late-term abortions for which he was so famous. But the work tormented her. She found it difficult to sleep at night. She began losing a dangerous amount of weight and ground her teeth down to the point that she required extensive dental work to correct.
Tina and I sat down in Troy Newman’s office with a digital audio recorder running. As Troy began to question her, Tina began to open up.
One day, she said, she was assisting Sella with the abortion of a 35-week baby.
“Well, my job was to hold the [woman’s] leg and count the parts, if it was in pieces,” she said. “And this was, um, maybe 35 weeks?”
“That’s a pretty big baby!” I responded.
“It was a big baby,” she affirmed. “And the baby came out and it was moving. I don’t know if it was alive or if it was nerves? I have no clue. But Dr. Sella looked up right away at me and took a utensil and stabbed it right here and twisted. And then it didn’t move anymore.”
Tina pointed to her right-side, just under the rib cage to show where there baby was stabbed.
It’s shocking to hear someone describing a murder. It’s almost like you can’t believe what you are hearing and it takes a few moments for the reality to sink in. There was no reason to doubt her story. We were also able to verify other information she gave us, giving her account of this baby’s death even more credibility.
When a 35-week baby comes out moving, that isn’t an abortion. It’s a live birth. I consulted an attorney friend of mine in California, and was advised that Troy and I had an obligation to report the matter to local law enforcement.
We turned over the raw, unedited audio file to the police. Detectives with the Wichita Police Department immediately picked up Tina and questioned her.
As much as David Daleiden reminded me of the Ring bearer, Frodo, Tina reminded me of another Tolkien character, a creature with a double-personality who was nearly consumed by darkness as Gollum, but in which there remained a nagging shred of conscience that manifested infrequently as Smeagol.
It was her “Smeagol” persona who shared with us in Troy’s office, but it was the “Gollum” part of her that was interviewed by police. Tina squirmed under questioning and recanted her ever-changing story, telling police she didn’t want to get involved. She sought to save herself from any implication in that cold-blooded murder.
There wasn’t much the police could do. Tina was an unreliable witness. The physical evidence held in the remains of the nearly full-term murder victim had been destroyed in the industrial crematorium that Tiller had installed in his clinic many years before.
Still unaccountable
I have often thought that if Pennsylvania’s late-term abortionist, Kermit Gosnell, who was convicted of first degree murder for stabbing babies born alive at his “House of Horrors” abortion mill, had owned such an incinerator, he would still be on his serial-killing spree today. It was the bodies of his victims that testified against him every bit as much as the witnesses that took the stand.
Unfortunately, Sella was never held accountable. Just months after the stabbing incident, Sella cancelled her Kansas medical license and relocated her late-term abortion practice to Albuquerque, New Mexico, where there are no laws to restrict abortion even until the day of a baby’s expected birth.
I continued to work with pro-life activists Tara and Bud Shaver, who once served as interns at our Wichita headquarters. Tara had obtained a number of 911 calls originating from Southwest Women’s Options.
One stood about above the others.
On May 12, 2011, a 911 call was placed by an employee of Southwest Women’s Options seeking emergency transport for a late-term abortion patient.
“The doctor’s concerned that we have a uterine rupture during a late-term abortion procedure. A patient with a previous C-Section. The patient’s stable at the moment, but. . .” the caller’s voice trailed off.
Documents revealed that Sella had indeed ruptured the uterus of a 26-year old patient who was 35 weeks pregnant – the same age of gestation as the baby that Sella stabbed in Wichita five years earlier — and that the clinic was ill-equipped to handle the life-threatening medical emergencies that can and do take place during risky late-term abortions.
Tara and I both filed complaints against Sella with the New Mexico Medical Board, which initially charged her with four counts of gross negligence. Medical boards rarely bring such charges if they are not positive they can prove the malfeasance. I had though we finally had Sella. She may have gotten away with that baby’s murder in Wichita, but she would not get away this time.
But unfortunately, the New Mexico Medical Board voted to absolve Sella, buying her specious argument that obstetrical standards of patient care should not be applied to late-term abortions, and that a much lower standard should be acceptable.
Today, Sella continues to conduct the latest of abortions in Albuquerque and has become famous as one of the most experienced late-term abortionists in America. According to a consent form obtained by the Shavers, the remains of babies aborted at Southwestern Women’s Options, are automatically used in research. Since the “consent” for research is buried in the same consent form for the abortion, it is doubtful many women even realize their babies are being turned into fodder for laboratory experimentation.
Changing times
Now, thanks to David Daleiden’s brave undercover journalistic study, a new day has dawned in American’s abortion wars where the public is finally confronted with the evil of child-killing in a way that has never been done before – in a way that could finally, eventually, lead to an end of the evil of abortion.
As Gandalf, another of Tolkien’s amazing characters, once said, “Dawn is ever the hope of man.”
The month of October is Breast Cancer Awareness Month. This is an annual campaign that began in 1991 to raise awareness about this disease. Although the campaign promotes regular self-breast exams, doctor visits, annual mammograms, and provides data on recurrence, preventable risk factors for breast cancer are not emphasized.
What are the risk factors for breast cancer?
According to the National Cancer Institute, the risk factors for breast cancer include: older age, genetic abnormalities, hormonal therapy, radiation therapy to the chest, alcohol and obesity. Although it has been demonstrated that hormonal contraceptive use increases breast cancer risk, this risk factor is virtually ignored during the campaign.
Synthetic estrogen was classified by the World Health Organization in 2005 as “Group 1 carcinogen”. Hormonal contraceptives contain synthetic estrogen and increase the risk of not only breast cancer, but also liver and cervical cancer. According to a meta-analysis published in the Mayo Clinic journal, women who have used hormonal contraceptives for four years before first full-term pregnancy, have an increase of 52% in breast cancer risk.
Another study funded by the National Institutes of Health found that the use of oral contraceptives for one year or more was associated with a 4.2-fold increased risk of triple-negative breast cancer for women 40 and under.
Another preventable risk factor that is not mentioned in the breast cancer awareness campaign is that due to induced abortion. Recent studies published in India and Bangladesh; report that induced abortion increases the risk of breast cancer 6-20 times in these populations. Although 53 studies (out of 73 worldwide) confirm the association between breast cancer and induced abortion, medical and government organizations continue to claim otherwise.
It is known that induced abortion in the first trimester of pregnancy alters the maturation of cells in the breast, which may trigger the development of cancer cells. Full term birth and lactation, mature breast cells and help to protect women from breast cancer.
How common is the problem of Breast Cancer?
Breast cancer is the most common cancer in women worldwide. In the U.S, 1 in 8 women have the chance of developing this cancer. According to statistics reported by the CDC, 211,731 women were diagnosed with breast cancer in the United States during 2011. Of those women 40,676 women died from this cancer resulting in one death for every five cases diagnosed. In some countries, this cancer survival ratio is lower. For example in India, 115,000 new cases of breast cancer were reported along with 53,000 deaths from this cause in 2008. In this case, there was one death for two newly-diagnosed cases.
Can breast cancer be prevented?
There are some breast cancer risk factors that you cannot modify such as age, being a female and the genetic predisposition. Some lifestyle changes could reduce the breast cancer risk. Regular exercise, healthy diet, and avoiding smoking, alcohol consumption, and radiation therapy on the chest may reduce the risk of the disease.
Another important measure to decrease the breast cancer risk is to avoid the use of potent steroids in hormonal birth control and hormonal replacement therapy (HRT). Natural family planning is a safe, healthy, and effective way to plan your family. Having children, and breastfeeding them offer an additional protection against breast cancer. There are alternatives to HRT such as bio-identical hormones and natural therapies. For single women, abstinence is the only way to prevent unwanted pregnancies and abortion.
One More Soul joins Breast Cancer Awareness Campaign to educate women and girls about the link between hormonal contraception, abortion and breast cancer. Visit our online store to see the wonderful resources we have on this subject. Please consider ordering some of our brochures and books for yourself or to share with your family, doctors, and friends about these preventable risk factors for a disease that is becoming epidemic.
Breast Cancer, Abortion and the Pill booklet presents the summary, conclusions, and recommendations from Chapter 17 of Dr. Kahlenborn’s book Breast Cancer, Its Link to Abortion and the Birth Control Pill. This is a great resource for explaining just how dangerous abortion and contraceptive pills are.
This pamphlet presents information from the book Breast Cancer, It’s Link to Abortion and the Birth Control Pill, in a short and highly persuasive format. From the time it was first published we have received letters and phone calls about babies saved from abortion when their mothers read this pamphlet and the number continues to grow. Praise God!!. – See more at: https://onemoresoul.com/catalog/breast-cancer-risk-from-abortion-p321.html
Based on six years of study and a meticulous analysis of hundreds of scientific papers and other sources, Dr. Chris Kahlenborn documents the effect that abortion and hormonal contraception have on breast cancer, as well as uterine, cervical, liver, and other cancers, and even the transmission of AIDS! Hormonal contraceptive use before first full term pregnancy is found to increase risk of breast cancer by at least 40%. The book gives special attention to black women, to various populations of the world, and to effective steps for prevention. This is a very timely and powerful work. –
Revised and updated. How the Pill increases the risk of breast cancer, and effective strategies for prevention. Women who take contraceptive pills before their first full pregnancy are 44% more likely to develop breast cancer before menopause. This is a real eye opener for people who thought the Pill was harmless. – See more at: https://onemoresoul.com/catalog/the-pill-and-breast-cancer-p711.html
Here’s something we missed in August: large families are the happiest, according to an Australian study.
Dr Bronwyn Harman of Edith Cowan University spent five years interviewing hundreds of parents from a range of family set-ups to ascertain what life is like for different families, and how resilience, social support and self-esteem contribute to parents’ happiness.
Parents with four or more children were the most satisfied with their lot, enjoying, rather than feeling overwhelmed by, the chaos of a big family.
Although they said they have to deal with comments such as “are they all yours?” or “do they all have the same father?”, large families benefit from lots of support from each other, and are rarely bored. Children learn responsibility from an early age, and older ones help out with their younger siblings.
“[The parents] usually say they always wanted a large family, it was planned that way, and it was a lifestyle they’d chosen,” Dr Harman said.
The study found that same-sex parents were the next happiest, and that single dads were the least happy, which is not surprising, given that they are usually separated from their children.
Dr Harman talked about her findings to the Sydney Morning Herald, but it appears that the details of the study have not yet been published. It will be interesting to read more about it in due course.
A black mark for the SMH, though, which ran a tasteless, not to say offensive cartoon with their report. Evidently the results were not to the editor’s liking.
In 1999, my son and I were blessed to have traveled to Medjugorje and then to Rome. When we went to the Wednesday audience with Pope John Paul II, I took some of the religious items I had bought in Medjugorje so that they could be blessed by the Pope. Of course I did not know at the time that in less than fifteen years, he would be canonized a saint, but I did think the medals of Our Lady of Medjugorje, blessed by Pope John Paul II, were special.
Over the years, I was pretty selective of the recipients of these special medals, so in April of 2014, when Pope John Paul II was canonized, I still had some left. I decided that I would give each of the members of our mailing staff a medal to thank them for their long hours of dedication each month. They thought it was so special to have a medal blessed by a saint!
One of our helpers, Diane, has a niece, Theresa, who wanted to have a child, but had been told she would never be able to conceive a baby, due to scar tissue left by a serious disease and its treatment. The doctors gave Theresa and her husband, Brett, the options of in vitro fertilization or adoption. Just like many Catholics, Theresa and Brett were not aware of the teachings of the Catholic Church on in vitro (usccb.org/upload/lifegiving-love-age-technology-2009.pdf), so they chose that option. Twenty-one weeks later, in March of 2014, Theresa miscarried two girls and a boy. Theresa herself almost died at the time, due to an infection. Diane wrote, “They were devastated! There really are no words to console a couple who has gone through so much. Prayer is all that really got us through.”
Carter
Diane gave Theresa her medal blessed by St. John Paul II, on May 30, with the following instructions: “I am lending you this blessed medal of Our Lady of Medjugorje, and you are to return it to me at the Baptism of your baby next year.”
Diane said, “These words were Spirit-driven – they were not the words I had in mind. All I wanted to do was to give her something to just make her feel a little better and give her a little hope.”
Diane was so excited a few months later when she told me that Our Lady and St. John Paul II had interceded and Theresa had conceived naturally! Diane related, “The doctor told her this is a high-risk pregnancy and they would do everything possible to get her to at least 24 weeks gestation. Then the baby would have a chance of survival.” She later added, “When 24 weeks came, they gave her steroid injections to help the baby’s lungs develop. The baby was doing well and so was Theresa. 28 weeks came and the doctor said, ‘Any day now.’ Theresa and the baby were showing some signs of early stress. 32 weeks came and the pregnancy continued. Because of losing the triplets less than a year ago, the doctor was sure Theresa wouldn’t be able to carry this baby longer than 36 weeks. But she did! At 39 weeks gestation, the doctor told her he would induce labor on his scheduled day for deliveries.”
Joseph
Carter was born on March 25, 2015. Diane was ecstatic that he was born on the feast of the Annunciation. She exclaimed, “This was confirmation from Mary that Carter is a gift from the Lord by Her intercession and that of St. John Paul II, who had a great devotion to the Blessed Mother and interceded many times on behalf of couples who were not able to conceive and have children on their own.”
Another member of our mailing crew, Kathy, gave her special medal to her daughter, Ashley. In January of 2014, Ashley had had an ectopic pregnancy. Ashley wrote, “After having the ectopic, we had to postpone attempting pregnancy for a while, in order to heal and have testing done. We were then devastated to find that I had lost a tube, due to damage from the ectopic. The doctors scheduled surgery, but gave me one more month to try.”
Around the same time that Kathy gave Ashley the medal, one of Ashley’s friends, who had just returned from Medjugorje, gave her a prayer cloth that she brought back. Ashley slept with the prayer cloth on her lower belly/ pelvis area. Ashley said, “I used the medal and cloth, then found out I was pregnant the week before I was scheduled for surgery!” Joseph Daniel was born during the Easter Octave, on April 7, 2015. “We feel so blessed,” Ashley beamed.
Maggie
In the meantime, I had been in touch with my cousin, Mary Jo, whose daughter-in-law had had multiple miscarriages since their first child was born seven years ago. Jenn and her husband, Chris, longed to have a second child. Whenever Jenn would get pregnant, Mary Jo would call me for prayers. But, it didn’t seem long before Mary Jo would be telling me that Jenn had miscarried again.
In August of 2014, my aunt, who is Mary Jo’s mother, told me that Chris and Jenn had decided to adopt. I wrote to Mary Jo and told her that was wonderful that they had decided to adopt, but I also shared that I had just read in the book, Saint John Paul the Great – His Five Loves by Jason Evert, that “one of the most common themes of the letters [regarding the intercession of St. John Paul II] is thanksgiving from couples who were previously unable to have children.” I offered her the last available medal I had, to give to Jenn.
About a month or so later, Mary Jo called me to say that Jenn was pregnant again. Mary Jo called me a couple of months later and told me that Jenn had made it through the risky time when she usually lost the babies, and wore the medal to her first sonogram. Mary Jo kept me updated as the pregnancy advanced.
Jenn was scheduled for a C-section on June 3, but God had other plans. Margaret (called Maggie) was born on May 31, 2015, the feast of the Most Holy Trinity. But, May 31 is a Marian feast when it does not fall on a Sunday – the feast of the Visitation – when Mary went to visit her cousin who had had trouble conceiving! What an awesome day to be born!
“Today I call you to place more blessed objects in your homes and that everyone put some blessed objects on their person” (Our Lady, July 18, 1985).
We thank Our Lady of Medjugorje and St. John Paul II for their intercession for these three beautiful babies.
Pope Francis has completed his visit to the United States. He came as a pastor for the whole church and a prophet for the whole world, and therefore his message and his ministry are far reaching, embracing a wide variety of needs and issues confronting the human family. Here I want to comment on the impact of his visit on one of those needs and issues which is at the foundation of all the rest.
How did the Pope’s visit help this greatest human rights cause of all time?
1. The Pope encouraged families, which are the sanctuaries of life.
The original purpose and reason for the Holy Father’s visit was to be part of the World Meeting of Families, an event sponsored by the Vatican’s Pontifical Council for the Family every three years. Having worked for the Pontifical Council for the Family, I helped to organize the Second World Meeting of Families in Rio back in 1997. The vision for these meetings, initiated by Pope Saint John Paul II, embraces and extols the interrelated themes of family and life. The family, by definition, is “the sanctuary of life.”
This was reflected in the theme of this year’s World Meeting of Families: Love is our Mission: The Family Fully Alive. As the Pro-life Symposium which Priests for Life sponsored as part of the World Meeting emphasized, the family cannot be fully alive unless all its members are protected.
The affirmation of life, therefore, is integral to understanding the very reason the Pope came.
One of many babies kissed by Pope Francis on his trip to the United States.
One of many babies kissed by Pope Francis on his trip to the United States.
2. The Pope’s words announced the foundation of the pro-life message.
When Pope Francis speaks about the pro-life cause and the issue of abortion, he does so in a way that emphasizes how it is integrally connected with every other issue of human rights. He speaks to the foundation, both of human rights and of the Faith, so that nobody can come away with the impression that the church’s opposition to abortion is simply a temporary, changeable, or accidental appendage to her life, teachings, and mission.
Consider his words at the White House that we must build a society that is that is “truly tolerant and inclusive to safeguarding the rights of individuals and communities, and to reject every form of injustice and discrimination.” A nation that holds the “the word person…does not include the unborn” (Roe vs. Wade) has ceased to be tolerant and inclusive and has embraced instead a deadly form of injustice and discrimination against its youngest children.
Again at the United Nations, the Pope warned against “a relentless process of exclusion.”
150926-pope-philadelphia-child-mn-1115_db03287935dba90190790162ee9607ed.nbcnews-fp-1200-800
Pope Francis kisses Michael Keating.
3. The Pope again displayed the spirituality of being with the vulnerable.
Pope Francis showed once again his desire to be with those who are disadvantaged in various ways, as he went out of his way to embrace the disabled boy at the airport, and visited an inner city school and a correctional facility. This conveys a spirituality and approach that strengthens the pro-life cause, which maintains that abortion is not an abstract issue, but involves real people who suffer physically, and with whom we are called to be present in their need. Our presence at abortion facilities, where these children are carried to their death, is an expression of this very same spirituality.
4. The Pope told the bishops not to be silent.
Few concerns within the pro-life cause are expressed more frequently than the need for leadership among the clergy. To the U.S. bishops gathered in Saint Matthew’s Cathedral, the Pope listed, again, a wide range of victims, including “the innocent victim of abortion,” and declared, “It is wrong, then, to look the other way or to remain silent.”
5. The Pope rejected the narrow territorialism that so often interferes with pro-life work in the Church.
In his final homily in Philadelphia, the Pope said,
Kristin Keating cries as Pope Francis blesses her son, Michael Keating, who has Cerebral palsy, upon the pontiff’s arrival at Philadelphia International Airport.
Kristin Keating, mother of Michael Keating, her son with cerebral palsy.
“Joshua tells Moses that two members of the people are prophesying, speaking God’s word, without a mandate. In the Gospel, John tells Jesus that the disciples had stopped someone from casting out evil spirits in the name of Jesus. Here is the surprise: Moses and Jesus both rebuke those closest to them for being so narrow! . . . The temptation to be scandalized by the freedom of God, who sends rain on the righteous and the unrighteous alike (Mt 5:45), bypassing bureaucracy, officialdom and inner circles, threatens the authenticity of faith. Hence it must be vigorously rejected . . . Jesus says, “Do not hold back anything that is good, instead help it to grow!” To raise doubts about the working of the Spirit, to give the impression that it cannot take place in those who are not “part of our group,” who are not “like us,” is a dangerous temptation. Not only does it block conversion to the faith; it is a perversion of faith!”
So many initiatives in the pro-life cause are stifled due to precisely this narrowness, to turf wars, and to the temptation within the institutional Church to think we are self-sufficient and do not need “outside groups.”
May the example, teaching, and spirit of Pope Francis continue to bless America and the pro-life cause!
Jesus says, “Do not hold back anything that is good, instead help it to grow!”
Editor’s note: Gina and Joseph Loehr were part of a panel presentation, “How Precious is the Family: Advice from Pope Francis on How to Love,” at the World Meeting of Families in Philadelphia on Sept. 25.
“It was like Catholic Disneyland.”
That’s how my friend, Rachel Bond, described the exhibitor plaza at the World Meeting of Families which she attended with her husband and two young daughters.
Nearly 500 Catholic organizations, ministries, companies and communities set up booths at the Philadelphia Convention Center. Some 20,000 attendees visited these vendors between the densely packed schedule of Masses, keynote addresses and breakout sessions – close to 100 talks in the course of four days.
It was a whirlwind week of Catholic formation and celebration that culminated in the visit of Pope Francis to the Festival of Families Saturday night.
My husband, Joe, and I missed out on most of this. With a delayed flight that didn’t get in until Thursday night, our panel presentation during the final Congress session on Friday morning, and our flight home Saturday afternoon, we were only able to attend one talk.
We didn’t even get to step into the exhibitor plaza, which the Secret Service suddenly shut down just before we arrived, nearly 24 hours ahead of schedule.
We did get our World Meeting of Families “pilgrim packs,” complete with program booklet, hat, poncho, water bottle and a ton of advertisements and brochures. We also went through a lot of security measures as we moved among hotel, meeting spaces and the city center.
We even got to catch a glimpse of the Holy Father from about 30 yards away when he arrived at the Basilica of Saints Peter and Paul on Saturday morning. However, we missed the chance to participate in most of the week’s events.
But that didn’t seem to matter.
Just being there amid thousands of Catholic pilgrims, just experiencing the jubilant and faith-filled atmosphere, just witnessing the coming and going of so many families from so many places was worth as much as hearing any inspiring talk or participating in any special activity.
We were among friends – strangers, yes, but also friends. There was a spirit of fraternity and camaraderie among people that was like a little foretaste of heaven. Here we were together, the church universal, with all of our diversity beautifully melding into a true unity.
As the parents of five young children, Joe and I sometimes feel a bit countercultural. When I’m out and about with the kids, people are forever making wry comments about how I have my “hands full.” (“Full hands, full heart,” I like to reply.)
But in this crowd, nobody was astonished or exasperated by the sight of multiple siblings being together. On the contrary, even though not all the families present were “big,” even though many attendees were priests or nuns or interested adults on their own, the love and appreciation everyone had for the gift of family life was tangible.
Simply put, it was encouraging to be in Philadelphia. It was refreshing to be in the company of tens of thousands of people who agree with Pope Francis’ comments Saturday night that “the family is a factory of hope,” and that children “are the future, the strength that moves us forward.”
Perhaps the best part of the trip was coming home. The time we spent in the presence of our global Catholic family helped me to appreciate our little domestic family
Here in our home, we have the privilege of living out the noble mission of Catholic family life.
“How precious is the family,” says Pope Francis.
Indeed, being part of a family is one of the greatest blessings that God the Father gives to us, his beloved children.
(Joseph and Gina Loehr, parents of five children, are members of Shepherd of the Hills Parish, Eden. Joseph is partner-owner of Loehr Dairy, LLC, a 700-acre dairy farm that has been in his family for 130 years and Gina is an instructor of theology at Marian University of Wisconsin. A freelance author and speaker on topics including marriage, women’s issues, and spirituality, she has also served as a delegate for the Pontifical Council for the Laity’s recent study seminar during which she met Pope Francis.)
‘This is a sign, obviously, of support’ for the nuns’ HHS mandate court case, papal spokesman Father Federico Lombardi affirmed at an evening press conference.
by MATT HADRO/CNA/EWTN NEWS 09/23/2015
Pope Francis converses Sept. 23 with Sister Marie Mathilde, a 102-year-old member of the Little Sisters of the Poor’s community in Washington.
– Courtesy Little Sisters of the Poor
WASHINGTON — Pope Francis paid a short visit to the Little Sisters of the Poor community in Washington on Wednesday to support them in their court case over the contraception mandate, the Vatican’s spokesman revealed.
It was a “short visit that was not in the program,” Father Federico Lombardi, director of the Holy See Press Office, said at an evening press conference during the papal visit to the nation’s capital.
“This is a sign, obviously, of support for them” in their court case, he affirmed.
The sisters had filed a lawsuit against the Obama administration for its 2012 mandate that employers provide insurance coverage for birth control, sterilizations and drugs that can cause abortions employee health plans. The sisters have maintained that to provide this coverage would violate their religious beliefs.
After the Obama administration modified the rules as an “accommodation” for objecting organizations, the sisters held that even under the revised rules they would have to violate their consciences.
The majority of a three-judge panel for the 10th Circuit Court of Appeals ruled in July that the Little Sisters of the Poor did not establish that the mandate was a “substantial burden” on their free exercise of religion, and thus ruled they still had to abide by the mandate.
“The Holy Father spoke to each of us individually, from the youngest postulant to our centenarian, and then he spoke to all of us about the importance of our ministry to the elderly,” Sister Constance Veit, communications director for the Little Sisters of the Poor, said following the visit. “We were deeply moved by his encouraging words.”
Mark Rienzi, senior counsel at the Becket Fund for Religious Liberty, which is representing the Little Sisters of the Poor in their court challenge against the mandate, said in a email statement, “Today, after Mass at the basilica, the Pope made an unscheduled visit to the Little Sisters of the Poor, where he spoke to each of the sisters privately and encouraged them in their vocation to serve the elderly and the poor. Earlier in the day, at the White House, the Pope expressed his support for religious liberty when he stated: [We] all are called to be vigilant, precisely as good citizens, to preserve and defend that freedom from everything that would threaten or compromise it.”
‘An Important Meaning’
The papal visit was not on the official schedule for Pope Francis’ Washington visit, which included Wednesday visits to the White House, a midday prayer service with the U.S. bishops at St. Matthew’s Cathedral and the canonization Mass for St. Junipero Serra at the Basilica of the National Shrine of the Immaculate Conception.
It was a “little addition to the program, but I think it has an important meaning,” Father Lombardi said.
He added that the visit “is connected” to “the words that the Pope has said in support of the position of the bishops of the United States in the speech to President Obama and also in the speech to the bishops.”
Pope Francis, with President Obama at the White House, called religious freedom “one of America’s most precious possessions” and hearkened to the U.S. bishops’ defense of religious freedom. “All are called to be vigilant, precisely as good citizens, to preserve and defend that freedom from everything that would threaten or compromise it,” he had said.
In response to the news of the visit with the sisters, Archbishop Joseph Kurtz of Louisville, Ky., president of the U.S. Conference of Catholics Bishops, said that he was “so pleased” to hear of the visit.
“As you know, the last thing the Little Sisters of the Poor want to do is sue somebody. They don’t want to sue in court,” he insisted. “They simply want to serve people who are poor and elderly, and they want to do it in a way that doesn’t conflict with their beliefs.”
The archbishop had previously warned against “interpreting freedom of religion in a very narrow way” in the press conference and emphasized that religion is not something practiced just for an hour on Sunday, but something lived out. To prove his point, he used the Little Sisters as an example.
Added Archbishop Kurtz, “We need to make room within our nation for people who have deeply held religious beliefs not to be forced to do that.”
Lynn Cassidy has no other words to explain what happened to her 3-month-old daughter Ave. Ave was born with Down syndrome, eye problems and hearing complications. Most concerning were the two holes in her heart.
“It seems like it was really meant to happen,” Lynn said. “And it’s as close to a miracle as we’ll ever see, I’m sure.”
In Easter of 2014, the family planned a Rome trip to see Pope Francis in person during the canonization of John Paul II and John XXIII.
“It was raining,” Lynn said. “We were told that if we stood on a barricade in St. Peter’s Square, the metal fences in front, the Pope would come by in his ‘Pope’-mobile.”
The Cassidy family waited for hours at the barricade. When the motorcade turned into the square, Lynn’s husband Scott held Ave up in the air.
“It was like the Lion King,” Lynn said. “The secret service person, Johnny, stopped and took her from Scott and held her up to the Pope. The Pope asked my husband, ‘How old is she? What’s her name?’ He told (the Pope) she has two holes in her heart. When we got home in May, we went back to the cardiologist for a check-up. One of the holes was completely closed and one was half the size.”
CONCORD, North Carolina, September 23, 2015 (LifeSiteNews) – Shelly Cawley, a nursing student, and husband Jeremy Cawley, a YMCA director, weren’t trying to get pregnant, but they weren’t trying not to.
When Shelly found out she was pregnant with their first child, she and husband Jeremy were very excited. “Having a child with the person you love is such a big deal,” Shelly said.
The couple planned a natural delivery, and they attended weekly classes on natural childbirth. “We knew what we were going to do,” Shelly explained, but “then, all of the sudden that plan was taken away from me.”
At eight months’ gestation, doctors discovered a blood clot in Shelly’s leg, so they began giving Shelly blood thinners.
Eventually, Shelly’s water broke, and Jeremy took her to the hospital. But labor did not progress.
Shelly had preeclampsia, a disorder characterized by high blood pressure and too much protein in the urine. Preeclampsia, if untreated, can lead to liver and kidney dysfunction, and fluid in the lungs. Shelly was also diagnosed with HELLP syndrome, a life-threatening condition involving the rupture of red blood cells, elevated liver enzymes, and a low platelet count.
Doctors told Shelly her baby had to be delivered immediately by emergency C-section.
Going in for an emergency delivery, Shelly had “a premonition.” “I was telling the doctors that I was scared I wasn’t going to wake up,” she said.
She didn’t.
The C-section was successful, and Rylan Grace Cawley was born. But Shelly failed to recover. As Jeremy was holding his newborn daughter, doctors informed him that Shelly’s lungs were filling with fluid and she was having trouble breathing on her own.
Eventually, Shelly fell into a coma. Physicians later discovered that the baby inside her womb had been holding Shelly’s blood clot in place and, when Rylan was delivered, the clot migrated to Shelly’s lung, causing a pulmonary embolism.
Shelly’s blood pressure was 60/40, and her heart rate was over 180 beats a minute. She was hooked up to what doctors called “the last-chance ventilator,” pumping air into her lungs so violently that it rattled her hospital bed, husband Jeremy said.
Doctors were convinced they could only wait and see if Shelly would wake up from the coma. “The doctors had done all they could and it was clear, they absolutely thought they were losing her at this point,” Jeremy said.
That was when the doctors decided to bring the family together. “We didn’t know how she was going to make it,” nurse Ashley Manus told the Washington Post.
The medical staff at Carolinas HealthCare System Northeast use the “skin-to-skin” method to strengthen the mother-baby bond. The physical touch stimulates the newborn’s brain development, stabilizes heart rate, and helps maintain body temperature. Nurse Manus suggested to lay little Rylan on Shelly’s chest. “If that was going to be it for her, we wanted to be able to tell the baby: ‘Your mom held you,'” she reasoned.
“Maybe somewhere in Shelly’s subconscious, she would hear her baby was calling out to her,” Manus said. “We just thought, it can’t hurt, [so we] might as well give it a try.”
Nurses brought little newborn Rylan into Shelly’s room. “I was hoping somewhere deep down, Shelly was still there and could feel her baby, hear her baby and her mother’s instincts would come out,” Manus anticipated.
Jeremy explained that the “hope was that if Shelly could smell the baby, feel the baby, hear the baby – even in the coma – it would give her a reason to fight. They needed her to start to fight.”
They put the newborn on her mother’s chest, but tiny Rylan went right to sleep. “We pinched Rylan and tickled her a little bit so that Shelly would hear her cry,” Jeremy shared.
And then, little Rylan – on her mommy’s chest – cried.
As soon as her baby cried, Shelly’s vitals jumped.
Jeremy said Rylan made the difference in saving her mother’s life. “All the doctors said there’s no way they would have gotten to that point if Shelly hadn’t made it through [that] night,” he said.
Doctors kept Shelly in her coma so that she could get the care she needed, including 21 units of blood, ventilators, and a heart-and-lung bypass machine. As the week-long ordeal continued, Jeremy put Rylan in a t-shirt of Shelly’s, so Rylan could smell her mother. He even learned how to pump his wife’s breast milk. “It was such an emotional and spiritual journey for our family while she was gone,” Jeremy said. “God’s hand was all over everything.”
Finally, Shelly awakened. Jeremy first asked her “if she knew who I was…, if she knew my name – and with the most breathy voice she said my name,” Jeremy Cawley said. “It was just such a huge thing.”
Then, Jeremy brought one-week-old Rylan in to her mother. Shelly “still couldn’t move,” Jeremy explained, “but you could see her eyes – as soon as I brought in Rylan, her eyes locked on Rylan. She just stared at her. And I laid Rylan on her chest.”
As the Washington Post reports, Jeremy brushed the hair from Shelly’s forehead and asked her a question: “Are you happy?”
September 16, 2015 (LifeSiteNews) — If you still have your children in a public school, you might want to have a talk with your child about the true meaning of “sustainability.”
Or you may want to call your kids who are off at college. Will any of those university courses on their “green” campuses assign students a project to evaluate the carbon footprint of a “gay pride” parade? Or an abortion clinic?
As Obama continues to exalt the climate change agenda above actual global crises, the tragedy is that sexual anarchy will never be objectively measured for its profound contribution to human rights abuses.
You know this word, “sustainable.” The Common Core school framework is full of sacrosanct “sustainable” propaganda, much of it built on the unsustainable quicksand of shifting politics, Marxist economic redistribution schemes, and population control.
But one lesson that’s omitted is the high-risk and low-return of homosexuality, gender-switching and sexual promiscuity. Sexual sin, it turns out, is an unsustainable human activity of the first order.
The reality is, the sexual anarchy movement is unsustainable.
Real humans are damaged and destroyed. Disease, emotional trauma, mutilation, family division, domestic violence and self-harm follow in the wake of “LGBTQetc.” identities and “reproductive rights.” There’s no way to disguise or adequately manage the wreckage left in the wake of these unnatural, life-rejecting behaviors.
And this global movement demands the revocation of freedom, productivity and sustainability for anyone who doesn’t cooperate. Think of the people out of work because of “gay” bullying– Kim Davis (for a few days– and who knows what the future holds?). Oregon bakers Aaron and Melissa Klein. Craig James. The list is expanding.
Anyone care to estimate the environmental waste of the entire “gay rights” political movement, from lobbying for harmful laws to parent school protests, to unneeded media coverage? The list goes on.
The Centers for Disease Control Youth Risk Behavior Survey reveals alarming sexual trends among youth. For instance, nearly 6% of students surveyed reported sex before age 13. Yet also deeply troubling, there is no indication these children were asked the obvious follow-up questions: “Who did you have sex with? What was the age and relationship?” Our sexualized culture surveys kids, then tosses them aside without addressing their actual needs. And we wonder why they begin to exhibit odd, even dangerous behavior?
And sinful sexual conduct is unnecessary, avoidable, and changeable, not healthy for children and other living things and we should be discouraging it in policies and programs.
A recent article in USA Today entitled, “Transgender People Face High Risk of Suicide” describes several gender-confused people who, when faced with taunts and rejection, attempted suicide. Of course, this is especially tragic among youth. But self-harm doesn’t just “happen” to people. While we must diligently teach kindness, a truly sustainable culture would also guide children away from adopting bizarre and self-destructive identities.
Still, your kids are being taught to be global citizens in a collectivist, sexually reckless, “sustainable” world.
Impossible.
What “sustainable” means is something that lasts, that can be maintained over time at a certain positive level. Christianity actually fosters that kind of culture, one we experienced in America until leftist revolutionaries gained positions of authority and began a long-term campaign of human destruction, using the rhetoric of freedom to cover the reality of bondage.
Department of Education Secretary Arne Duncan said at a 2010 Sustainability Summit: “A well educated citizen knows that we must not act in this generation in ways that endanger the next.”
Then why on earth is the USDOE pushing “transgenderism” on local schools, where kids are sold the idea of mutilating healthy bodies to satisfy a mental delusion? And why is the USDOE equating the embrace of sodomy as an aspect of school “safety” despite the CDC’s findings that 94% of HIV among American youth under age 24 involves male homosexual sex?
If “LGBT” behaviors were self-evidently glorious, our kids back at school would be happily opening their restrooms, locker rooms and showers to the opposite sex.
Of course, this is the fantasy world of leftist change agents, some of whom are school administrators. Most girls are actually outraged by boys invading their restrooms, and good for them.
AT Hillsboro High School in Missouri, over 150 students protested Lila Perry’s demand to use the girls’ restroom. “Lila” is a guy who angrily told the media “she”[he] thinks their protest is all about bigotry, pure and simple.
No, it’s actually about common sense, pure and simple. Sex masquerades, like boys trying to morph into girls, are not sensible, are impossible and therefore, not sustainable.
There’s also that privacy thing. And that selfishness thing. Being concerned only about your own irrational “rights” is totally unsustainable. Where’s the community, the tolerance? Where’s the embrace of the authentic instead of the phony?
Where is truth? Lies are not sustainable, either.
Human sexual excess consumes vast amounts of energy. And what’s the return? Once we account for the clean-up, the management, the waste, our culture’s current embrace of sexual license is an environmental disaster. The Gulf Oil spill is pond scum in comparison.
Sexually transmitted infections are at epidemic levels among American youth, the “gay” positive, hook-up generation. Only later does the tragic outcome become evident: disfigurement, infertility, sometimes death. Related health costs alone are unsustainable.
Just think about the lost human potential of aborted babies. And infertility means population reduction, less human capital, a less productive society…. waste.
And pornography? It’s the kerosene on this smoldering fire, a hidden public health crisis everyone pretends is not destroying families and children.
Devolution, not evolution. Regress, not progress. It’s ancient tribalism with Twitter and I-Phones, instead of the careful but rewarding outcome of real, enduring –“sustainable”– relationships.
There’s one other element critical to actual progress, actual sustainability —- doing the will of God.
What has God said about sexuality? It’s reserved for man/woman marriage, and that’s the framework for the most sustainable human relationship of all time.
Linda Harvey is founder and president of Mission America, is a radio talk show host in Ohio and a weekly columnist for WND.com.
(NaturalNews) In the age of authoritarian political correctness, it has come to the point where even threats of legal action are enough to cause targeted entities to surrender basic beliefs and values, even at the cost of violating centuries-old tradition.
As reported by The Daily Caller, the American Civil Liberties Union has managed to compel a Catholic hospital in California to sterilize a woman with just the threat of a lawsuit, even though such procedures contravene church teachings about the preservation and sanctity of life.
The hospital, Mercy Medical, located in the liberal bastion of San Francisco, is operated as a subsidiary of Dignity Health, California’s largest private health care provider. Rachel Miller, a woman who is scheduled to give birth by C-section in late September, also wanted her doctor to perform a tubal ligation following her birth, a procedure that would render her infertile.
However, Mercy hospital staff initially refused, explaining that as a Catholic institution, such a procedure violates centuries of belief and tradition.
It should also be noted that under the Constitution’s First Amendment protection of religious liberty, the hospital – like most other Catholic hospitals around the country – has a right to act on its beliefs. Catholic dogma teaches that sterilization and other forms of birth control are sinful because they deliberately sabotage the procreative aspect of human sexuality, which is a violation of natural law.
Religious freedom doesn’t apply any more
In addition, the hospital’s policies reflect the Catholic Church’s teachings; doctors there are not permitted to perform abortions and do not engage in in vitro fertilization.
None of this mattered to Miller or the ACLU, which is supposedly a legal organization that supports constitutional rights.
Miller says that without Mercy’s authorization for the sterilization procedure, she would be forced to travel 160 miles in order to get it. Instead, she sought the ACLU’s intervention; in a letter to the hospital, ACLU attorney Elizabeth Gill argued that denying Miller’s procedure was a violation of California law (sex discrimination) and as such, the organization was prepared to file a lawsuit against Mercy for refusing to provide “pregnancy-related care.”
It should be noted that in most cases, women (and men) opt for sterilization procedures after the birth of their children because they have decided that they don’t want to have any more kids. There is no “medical necessity” there in the real sense of the term (as in “to save a life”). Moreover, in the modern era, Catholic institutions’ decisions to not provide sterilization and abortion services dates back a hundred years. Why is such a refusal on religious grounds now “illegal?”
We may never know the answers because the hospital has caved to the threat of a suit rather than opting to stand up for its principles. As noted by The Daily Caller:
In a post on the group’s website, ACLU attorney Elizabeth Gill said she’s happy the hospital will comply with Miller’s request, but that the group won’t be satisfied until all hospitals are forced to stop following Catholic doctrine.
“Rachel is lucky — she stood up for herself, and she is getting the health care that she and her doctor have decided is best for her,” Gill said. “But as long as Catholic hospitals are allowed to apply the ethical and religious directives, many women will be denied care because Catholic bishops are telling medical professionals how to operate.”
Culture of depopulation and death
Actually, the centuries-old Catholic doctrine guides such decisions; bishops are merely the human conduit through which doctrine is administered and preserved.
None of this matters to the liberals, who continually seek to deny some Americans fundamental rights they don’t agree with using the color of law, the courts, or a presidential executive order while claiming to be upholding the fundamental rights of others.
The fact that the issues of sterilization and abortion excite liberals does not come as any surprise, however, given the Left’s vehement support of Planned Parenthood’s grotesque, Nazi-like exploitation of aborted human babies; it’s as though liberal dogma includes the concept of depopulation.
For example, as Natural News editor Mike Adams, the Health Ranger, reported in November 2014, the Kenya Catholic Doctors Association, a pro-vaccine organization, found that tetanus vaccines given to millions of young women in Kenya had been confirmed by laboratories to contain a sterilization chemical that causes miscarriages.
Abortion and sterilization on demand. Waging war on Christian religious faith and doctrine. Violating centuries of dogma and the U.S. Constitution in pursuit of narrow liberal pro-death policies.
Does this sound like the America our founders fought and died to create?
VATICAN CITY, September 11, 2015 (ChurchMilitant.com) – The family “as God wants it” is under attack. That’s the warning from the Holy Father yesterday to the international marriage group Equipes Notre Dame (END), or Teams of Our Lady.
Pope Francis told the END couples to defend traditional marriage. He said that today’ “the family — as God wants it, composed of a man and a woman for the good of the spouses and also the generation and education of children — is deformed by powerful contrary projects supported by ideological colonization.”
Equipes Notre Dame was formally established in 1947 by Fr. Henri Caffarel in order to help married couples achieve holiness by “belonging to a team within a Christian community.” Today, they exist in 48 different countries around the globe according to the Pontifical Council for the Laity. The Pope encouraged END couples to live the spirituality of their movement, stressing that married fidelity is a gift from God.
Pope Francis warned that amid the modern, busy, individualistic world, spouses must go against the current and take the time to “sit down” and talk with each other to strengthen their marriage. He also stressed the central role of prayer within the family, describing it as “a beautiful and necessary tradition that has always supported the faith and hope of Christians, and unfortunately abandoned in many regions of the world.”
Besides maintaining their own integrity, His Holiness said that families must reach out to other families, particularly those who are wounded and vulnerable through personal and social problems. “We must have the courage to enter into contact with these families in a discreet but generous way.”
His Holiness noted that the END group’s visit to Rome comes just before the Synod on the Family. Calling the family the “vital cell of our societies,” he said that Christian couples must strengthen and encourage other families by announcing Jesus to them. He told the END couples that families must witness and announce the joy that the Lord enables families to experience “so that others may take the same path.”
“It is necessary, therefore, that you bring your witness and your experience to help Christian communities to discern the real situations in which these people find themselves, to welcome them with their wounds, and to help them to journey in faith and in truth,” he admonished them. “Nor must you forget the unspeakable suffering of the children who experience these painful family situations: you can give a lot to them.”
Children born after Artificial Reproductive Treatments have a greater risk of preterm birth, low birth weight, and extended newborn hospital stay according to a recent study of perinatal outcomes.
Dr Joseph Stanford, MD, from University of Utah, with his colleagues, analyzed the adverse perinatal outcomes associated with Artificial Reproductive Technologies compared to outcomes from spontaneous pregnancies in Florida, Maryland and Utah.
The authors analyzed data from a population-based surveillance system designed by the Centers for Disease Control and Prevention to identify and monitor maternal health and perinatal outcomes.
The study represented 1,022,597 women with live births between 2004 and 2008. Women who received treatment with assisted reproductive technology (ART), intrauterine insemination with ovulation stimulation (IUI), and ovulation stimulation alone (OS) were compared to women who never used fertility treatment and subfertile women who conceived without any treatment.
The authors of the study found that premature birth, very premature birth and low birth weight are six times greater amongst women who undergo ART in the conception cycle compared to all women trying to conceive in the population of the study. Also the newborn hospitals stay of 1 week or longer were three times higher for all ART pregnancies compared with women who never used fertility treatment.
Indeed, it was discussed that much of this risk comes from multiple gestation pregnancies, but even singleton pregnancies achieved by ART had higher risk of complications. Among births of a single baby, and compared with women who never used fertility treatments, women who conceived with ART were three times more likely to experience preterm birth (<37 weeks the due date)
Another finding of the study was that the use of intrauterine insemination (IUI) and ovarian stimulation increased 2 times the risk of prematurity (<34 weeks before the due date) compared with women who never used fertility treatments.
Although preterm birth and low birthweight, were associated with ART, subfertility status itself was significantly associated with very low birthweight.
The authors explained that in contrast, there was a protective association of ‘other various’ fertility treatment on very low birthweight, compared with subfertile women who conceived without treatment. Subfertile couples could achieve pregnancy using fertility treatment protocols, such as Naprotechnology, that are less likely to result in adverse perinatal outcomes that cause long hospital stay for the newborn such as preterm birth or low birthweight.
A recent study may have found a biological explanation for why certain types of injectable and oral contraceptives can put women at increased risk of HIV infections. The study suggests these medications may suppress the vaginal immune response in certain women, a finding which sheds new light on the possible impact hormonal contraceptive methods can have on the vaginal environment.
Over the years, different studies have produced conflicting results on whether or not a relationship between hormonal contraceptives and HIV infection risk actually exists. However, the new study, published in the journal mBio, will hopefully set the record straight. According to lead author Dr. Raina Fichorova in a recent statement, the link does exist and the reason for previous inconsistencies in research “lies in the microbial communities of the reproductive tract.”
For the study, Fichorova and her fellow researchers analyzed cervical swabs and data from 823 HIV-negative women between the ages of 18 and 35 who had been enrolled in family planning clinics in Uganda and Zimbabwe. The women were divided into three groups: those who used injectable contraceptive depot medroxyprogesterone acetate (Depo-Provera or DMPA), those who used estrogen-progesterone oral contraceptives, and those who used no hormonal contraceptives. By the end of the project, around 200 of the original group of women had contracted HIV. The medical history of those who contracted the virus has given important insight into the role that hormonal contraceptives play in a women’s natural immunity.
An individual’s risk of contracting HIV heavily depends on their method of exposure. Blood transfusions have the highest risk of HIV transmission followed by receiving anal sex. According to the Centers for Disease Control and Prevention, the transmission risk for women who have vaginal intercourse with an HIV-positive man is about eight every 10,000 exposures. Of course, this number does not take into account factors that may increase transmission risk (such as already having an STD) or those that may decrease the risk (such as using a condom, which reduces the risk by up to 80 percent). Part of the reason why a woman is not guaranteed to contract HIV after exposure is because the vagina’s immune system provides a natural defense against infections and helps to form a protective barrier of mucous between a woman and potential pathogens.
The study’s results revealed that both DMPAs and oral contraceptives inhibited the vagina’s natural defense and thus put the women at an increased risk of contracting the viral and bacterial pathogens. However, this risk increase does not extend to all women taking these forms of contraceptives. According to the authors, the effects of hormonal contraceptives on cervical immunity “depend on the genital tract microenvironment,” and “a weakened mucosal barrier against HIV” may result from the combination of both hormonal contraceptive use and pre-existing infections.
Women who had vaginal infections such as bacterial vaginosis or disturbed microbial environments in their vagina were observed as being most at-risk for HIV infections. For example, results showed that women who had herpes or disturbed vaginal microbiota and took levonorgestrel-containing oral contraceptives were more likely to have increased levels of proteins that attract HIV host cells. Also, DMPA appeared to suppress a woman’s immune responses to Trichomonas vaginalis, a widespread parasite that aids HIV infection.
Along with clarifying the link between contraceptive use and HIV, the findings also highlight the importance of further investigating the possible effects that hormonal contraceptives can have on female reproductive health.
“Studies of new contraceptive methods should evaluate how they impact the microbial environment and how they act in concert with preexisting, treatable microbial disturbances, to weaken the mucosal barrier against HIV and other infections,” Fichorova explained in a statement.
According to Fichorova, the ultimate goal is to prevent the unwanted side effects of available hormonal contraceptives and improve the lives of millions of women throughout the world. “Women deserve to know more so that they can make informed choices about birth control.
Source: Fichorova RN, Chen P, Morrison CS, et al. The Contribution of Cervicovaginal Infections to the Immunomodulatory Effects of Hormonal Contraception. Mbio. 2015.
September 6, 2015 (Voice of the Family) – A new book, The Rigging of a Vatican Synod?: An Investigation into Alleged Manipulation at the Extraordinary Synod on the Family, will shed much light on allegations that the Extraordinary Synod, held in Rome last October, was subject to manipulation. The book has been written by highly respected Vatican journalist Edward Pentin and carries the endorsement of Wilfrid Fox Cardinal Napier, Archbishop of Durban. Cardinal Napier is one of the fifteen members of the permanent council of cardinals and bishops overseeing the Synod of Bishops, he attended the Extraordinary Synod and was a member of the committee that drafted the final relatio synodi of that Synod.
In this brief review we would like to draw attention to a few of the key examples of the manipulation that is alleged to have taken place at the Extraordinary Synod. We encourage readers to consult the book itself to make themselves aware of the full extent of the concerns raised and of the serious questions that now need to be asked in light of the upcoming Ordinary Synod on the Family. Voice of the Family has already drawn attention to the instrumentum laborisof that Synod, which, our analysis asserts, “threatens the entire structure of Catholic teaching on marriage, the family and human sexuality.”
Cardinal Napier told Edward Pentin that a few months before the Extraordinary Synod an official at the Synod Secretariat had come to see him to share serious concerns. The official told Napier that he was “very disturbed” by what he had witnessed and commented that “this thing is being manipulated, it’s being engineered. [They] want a certain result.”
Vatican journalist Ed Pentin
The Synod Secretariat is managed by the General Secretary of the Synod, Lorenzo Cardinal Baldisseri (pictured above). The organisation of the both Synods on the Family has been the responsibility of Cardinal Baldisseri, though the cardinal has stressed the close involvement of Pope Francis at every stage of the process. In an interview given in January 2015 he said:
“Pay attention, as this is something one really should know. The pope is the president of the synod of bishops. I am the secretary general, but I don’t have anyone else above me, such as a prefect of a congregation or a president of a council. I don’t have anyone else above me, only the pope. The pope presided over all of the council meetings of the secretariat. He presides. I am the secretary. And so the documents were all seen and approved by the pope, with the approval of his presence. Even the documents during the synod, such as the Relatio ante disceptationem, the Relatio post disceptationem, and the Relatio synodi were seen by him before they were published.”
Cardinal Baldisseri was publicly implicated in the manipulation of the synod on September 20 2014, in accusations made by Vaticanist Marco Tossati in La Stampa, which alleged that a cardinal had been heard explaining how he would manipulate the synod fathers. Pentin’s book identifies that cardinal as Baldisseri.
The manipulation seems already to have been well advanced by this date. Pentin recounts that some months before the Extraordinary Synod the Synod Secretariat had contacted the Pontifical John Paul II Institute for Studies on Marriage and the Family, known for its fidelity to Catholic moral teaching, to recommend experts to participate in the Synod. The Secretariat had made the same request to certain institutes of the Roman Curia. In the event none of the experts recommended by these institutes was invited participate in the Synod. A high-level Vatican source has stated that the opinion of these institutes was sought in order that the Secretariat could ensure that orthodox experts could be excluded from participating in the synod. It is also alleged that an official of the Synod Secretariat was told to go through a list of potential experts and exclude all those who were “conservative” and retain all those who were “progressive”.
The manipulation of the synod came to public attention following the release on 13th October 2014 of the interim relatio post disceptationem. This document, which purported to represent the contributions of the synod fathers, is alleged to have seriously misrepresented the views of the assembly. Cardinal Pell called it “tendentious, skewed” and said that “it didn’t represent accurately the feelings of the synod fathers”. Cardinal Napier alleges that the document contained opinions that were never expressed by any of the synod fathers. Pentin writes:
Cardinal Napier remembers a synod father saying he had put his name to the document, but it was not what he had written. “Others asked: How then could this be stated as coming from the synod when the synod hasn’t even discussed it yet?”
Another synod participant added his voice of concern, saying, “there are things said there about the synod saying this, that, and the other, but nobody ever said them. So that’s when it became plain that there was some engineering going on”, the South African cardinal recalled.
The document caused great controversy because it undermined Catholic teaching on key points of doctrine, including the indissolubility of marriage, cohabitation and homosexual unions. The manipulation surrounding the creation of this interim report is discussed at length in the book. More surprising, because previously unreported, is the manipulation involved in the drafting of the final report.
Pentin sheds light on other controversial events that took place during the synod, giving a detailed narrative of events surrounding the removal of a book co-authored by, among others, five Cardinals, from the mail boxes of the synod fathers in the synod hall. Pentin reports that Cardinal Baldisseri said that the sending of the books was not “opportune”. Many readers will ask: how could the mailing of books upholding Catholic teaching on the very point of doctrine under discussion not be considered “opportune”? Only, it would seem, if anything which would derail the previously laid plan for the synod was considered inopportune.
The Rigging of a Vatican Synod? provides a great deal of insight into the theological views of Cardinal Baldisseri. Pentin writes that:
“a sense of alarm was experienced among many holders of traditional Church doctrine and practice in May 2014, when, in an interview with Belgian Church newspaper Tertio, Cardinal Baldisseri said it was time to update the Church’s doctrine on marriage—for example, in connection with divorce and the situation of divorced persons and those who are in civil partnerships. ‘The Church is not timeless, she lives amid the vicissitudes of history, and the Gospel must be known and experienced by people today’, Cardinal Baldisseri said. ‘The message should be in the present, with all respect for the integrity of the one who receives that message. We now have two synods to treat this complex theme of the family, and I believe that these dynamics in two movements will allow a more adequate response to the expectations of the people.’”
In January Cardinal Baldisseri told a conference organised by Pontifical Council for the Family that “there’s no reason to be scandalized that there is a cardinal or a theologian saying something that’s different from the so-called ‘common doctrine’”. “This doesn’t imply a going against” he said, rather “it means reflecting, because dogma has its own evolution; that is a development, not a change.” He added: “Everything that we know today is a mystery, and since we are standing before a mystery and a mystery is not immediately known, we advance in our understanding. We need to keep this in mind. And so [Kasper’s proposal] should be welcomed as a contribution.” These comments were made in despite of the fact that Cardinal Kasper’s proposal directly contradicts the teaching of the Church as expressed most recently by John Paul II in Familiaris Consortioin 1981 and in official documents of the Congregation for the Doctrine of the Faith in 1994 and 1998.
There is good reason to believe that Cardinal Baldisseri’s theological views have had a very great influence on the synodal texts. One of the most shocking passages in Pentin’s book is an account of Baldisseri’s attempts to alter the content of the pre-synod report, by placing pressure on Cardinal Erdö. These revelations alone would be enough to make the book one of the most important contributions in the lead-up to the next Synod.
Voice of the Family has drawn attention to the “many problematic texts on the subject of the natural law” in the instrumentum laborisof the Extraordinary Synod and the omission of any reference to natural law in the relatio synodiof that Synod. It would seem, in the light of information presented by Pentin in the book, that this may be another example of Cardinal Baldisseri’s damaging influence.
The Extraordinary Synod on the Family, under Cardinal Baldisseri’s leadership, produced documents that undermined Catholic teaching on a whole range of issues relating to human sexuality, marriage and the family. The instrumentum laboris of the Ordinary Synod extends the assault on Catholic doctrine to an even wider number of areas. The Synod Secretariat’s grave failures have real implications for real families, struggling as they are in a society ever more hostile to authentic moral principles and the teachings of the Catholic Church.
Catholics at all levels of the Church should be extremely concerned both by Cardinal Baldisseri’s theological opinions and by the well-grounded accusations of manipulation contained in this book. It is difficult to see how Catholics can have any confidence in the synodal process while he remains General Secretary of the Synod. This article was originally published on Voice of the Family and is re-published with permission.
In light of the recent Planned Parenthood videos, I’ve been thinking about a group of pro-life friends who don’t fit the Catholic categories. These are staunchly pro-life Christians who believe sex should be saved for marriage, that marriage is a lifelong, exclusive union between one man and one woman, but who take contraception as the ‘default mode’ for marital relations, and sterilization as an acceptable way to avoid pregnancy indefinitely.
There are variations within that broad definition, but that’s the gist of it.
When Catholics talk about the connection between contraception and abortion, these couples do not quite fit the pattern. They use contraception (or sterilization) the way Catholics use NFP: If a pregnancy should result despite the couple’s attempt to avoid conceiving, they chalk it up to the will of God and joyfully accept the bundle of surprise happiness.
Why do these couples contracept? Because they’ve been told to, mostly. Keep in mind that even Catholics virtually never speak of the question, and we have Humanae Vitae. Christians of all brands tend to assume that if there is vast pastoral silence on a matter, then whatever the culture is saying must be right.
Thus these couples take what their pastors do have to say about love and marriage and sex, then fit the cultural norms into the gaps.
Do we have a problem?
I am not writing here a full argument against contraception. You can get started on that here, or here, or here. What I want to talk about is the one weird trick contraception plays on marriage, and how that trickles down to everyone else.
When we talk about contraception, especially methods with no abortifacient potential, people tend to say, “Well, NFP is the same thing. You’re preventing births. You’re just using time, rather than a physical barrier, as your thing to avoid pregnancy.”
This gets a little comical half a second later, when you say, “Gosh, if they are the same thing, then there’s no reason you shouldn’t switch.”
They are most definitely not the same thing. Choosing to abstain is radically different from choosing to have sex. It is much harder to play Scrabble while having sex, for one thing.
The whole point of contraception is that you intend to have sex but don’t want the consequences that might follow. The whole point of NFP is that because you are concerned about the consequence, you choose not to have sex.
What does this do to you as a person? To you as a couple? To you as a member of society?
The thing that contraception does is that it turns sex into something you are convinced that you need.
This is a problem because it is a lie, and a deadly one.
How To Kill A Marriage Quick
I’m a fan of the marital act. Not only can I show the goods to back up that claim, but longtime readers can attest that one of my intermittent themes is airing my suspicions about that handful of Catholics who fear that someone, somewhere, is abstaining for the pure pleasure of it.
The precise manner and frequency of intercourse is something each married couple has to work out for themselves, but two things tend to screw up a marriage fast. The first is a spouse who is resentful of the other person’s interest in them (a real problem for some, but not the topic of this post). The second is a spouse who is resentful of the reality that even married people can’t just drop their pants any time they want.
Related posts you might want to pause and peruse right now:
I am under no illusion that abstinence is easy, see “fan of the marital act,” above. Contraception first slid into the Christian world in response to that challenge: Maybe there’s a way that couples can make necessary abstinence easier by, you know, not abstaining.
We could argue that this (immoral) shift was merely a case of looking for a way to mitigate a difficult situation. Christians, after all, do like to relieve suffering when we can.
Perhaps so. But since that time, the availability and widespread use of contraception has persuaded couples that the devices aren’t merely a convenience but a necessity. We have become convinced that because abstinence is difficult, it is dangerous. We have become convinced that abstinence is a threat to our happiness, and thereby a threat to marriage. We are persuaded that if there exists a sexual drive, that drive must be satisfied. Self-denial is the new cyanide.
Marriage Really Is the Bedrock of Society
If abstinence is deadly to married people, the logic follows, then it must be bad for everyone.
Whereas NFP always reminds you that abstinence is a part of life we must make peace with, contraception says no, don’t make that peace. Very quickly we become persuaded we must have this thing that we want, because it is a necessity.
Thus the spiritual fruit of marriage extends outward to the wider society: If married people have to indulge-or-bust, then surely the same applies to engaged couples? To people dating seriously? To those who are just lonely and want some affection? To those who have no prospect of marriage, but have a sexual drive all the same?
After all, there is nothing different, biologically or psychologically, between a married person and everyone else. If a married person is going to combust for lack of intercourse, it follows that others might too. If a married person is incapable of maintaining healthy, balanced, rewarding relationships unless the sex drive is perpetually sated, it follows that others have the same need for satiation.
And if the married person, who has the advantage of a dear friend on hand for companionship and assistance and warmth and kindness, is unable to experience depth and emotional intimacy and chaste physical touch unless sex be a part of that relationship, it follows that others desiring close human connections have no hope — unless they, too, get the sexual gratification that is apparently necessary if there is to be any happiness.
These are lies of course. You won’t combust for lack of sex. You can have close, warm, satisfying relationships without having to include the sexual act in those relationships.
But these are the lies that contraception teaches us, whether we are intending to learn them or not.
Now that the definition of marriage as the union between one man and one woman has been arrogantly dismissed by the Supreme Court, other groups are looking to have their unions included in the “marriage” category. One such example is polygamists, led by the reality stars from the series ‘Sister Wives.’ The Blaze reports that these ‘Sister Wives’ stars are invoking same-sex marriage legalization in an attempt to overturn Utah’s polygamy ban.
Brown and his wives, Robyn, Christine, Janelle and Meri — the stars of “Sister Wives” — are asking judges to reject an appeal by Utah of a judge’s 2013 decision to strike a portion of the state’s ban on polyamorous relationships, KSTU-TV reported.
U.S. District Judge Clark Waddoups ruled that the law’s ban on cohabitation among individuals who are not married runs in contrast to the First and 14th Amendments, and essentially violates Brown’s religious freedom.
“From the rejection of morality legislation in Lawrence to the expansion of the protections of liberty interests in Obergefell, it is clear that states can no longer use criminal codes to coerce or punish those who choose to live in consensual but unpopular unions,” Jonathan Turley, an attorney for Brown, wrote to the 10th U.S. Circuit Court in Denver. ”This case is about criminalization of consensual relations and there are 21st century cases rather than 19th century cases that control.”
Brown has maintained that the legal battle is not about forcing acceptance of bigamy or challenging the rights of states to preclude individuals from holding multiple marriage licenses, but that it is, instead, about battling back against criminalization.
The state, though, maintains that polyamorous relationships are harmful to women and children.
“By only striking the cohabitation provision, the District Court left Utah with the same law maintained by most states in the Union prohibiting bigamy,” Turley wrote. “What was lost to the state is precisely what is denied to all states: the right to impose criminal morality codes on citizens, compelling them to live their lives in accordance with the religious or social values of the majority of citizens.”
When marriage is no longer protected as the union between one man and one woman, society opens itself up to harmful unions that not only further damage the institution, but also work to destroy the family.
Given that the family is the building block of society, our government should be looking to protect marriage and the family — not redefine and destroy it.
VATICAN CITY (CNS) — In an extraordinary gesture for the Year of Mercy, Pope Francis has extended to priests worldwide the authority to absolve women for the sin of abortion and has decreed the full validity during the year of the sacrament of confession celebrated by priests of the traditionalist Society of St. Pius X.
“This jubilee Year of Mercy excludes no one,” the pope wrote in a letter to Archbishop Rino Fisichella, president of the Pontifical Council for the Promotion of New Evangelization, the office organizing events for the holy year, which opens Dec. 8.
Pope Francis said one of the most serious problems facing people today is a “widespread and insensitive mentality” toward the sacredness of human life.
“The tragedy of abortion is experienced by some with a superficial awareness, as if not realizing the extreme harm that such an act entails,” while many other women believe that “they have no other option” but to have an abortion, the pope wrote in the letter, released Sept. 1 by the Vatican.
The pressures exerted on many women to abort lead to “an existential and moral ordeal,” Pope Francis said. “I have met so many women who bear in their heart the scar of this agonizing and painful decision.”
When such a woman has repented and seeks absolution in the sacrament of confession, he said, “the forgiveness of God cannot be denied.”
Although church law generally requires a priest to have special permission, called faculties, from his bishop to grant absolution to a person who has procured or helped another to procure an abortion, the pope said he decided “to concede to all priests for the jubilee year the discretion to absolve of the sin of abortion those who have procured it and who, with contrite heart, seek forgiveness for it.”
Pope Francis urged priests to welcome to the sacrament women who have had an abortion, explain “the gravity of the sin committed” and indicate to them “a path of authentic conversion by which to obtain the true and generous forgiveness of the Father who renews all with his presence.”
Jesuit Father Federico Lombardi, Vatican spokesman, told reporters the pope’s letter “highlights the wideness of God’s mercy” and is “not in any way minimizing the gravity of the sin” of abortion.
In his letter, Pope Francis also granted another exception to church rules out of concern for “those faithful who for various reasons choose to attend churches officiated by priests” belonging to the traditionalist Society of St Pius X. Although the society is no longer considered to be in schism and the excommunication of its bishops was lifted in 2009, questions remain over whether the sacraments they celebrate are valid and licit.
The pope’s decision was “taken with the faithful in mind” and is limited to the holy year, which runs through Nov. 20, 2016, Father Lombardi said.
The spokesman also confirmed that the Vatican’s contacts with leaders of the Society of St. Pius X have continued. Pope Francis wrote in his letter that he hoped “in the near future solutions may be found to recover full communion with the priests and superiors of the fraternity.”
Pope Francis’ letter also explained expanded opportunities for obtaining the indulgences that are a normal part of the celebration of a holy year. An indulgence is the remission of the temporal punishment a person is due because of his or her sins. In a holy year, it is offered to pilgrims who cross the threshold of the Holy Door at the Vatican or in their local diocese, confess their sins, receive the Eucharist and pray for the pope’s intentions.
The celebration of God’s mercy, he said, is “linked, first and foremost, to the sacrament of reconciliation and to the celebration of the holy Eucharist with a reflection on mercy. It will be necessary to accompany these celebrations with the profession of faith and with prayer for me and for the intentions that I bear in my heart for the good of the church and of the entire world.”
Those who are confined to their homes can obtain the indulgence by offering up their sickness and suffering, he said.
Pope Francis also included special consideration for people who are incarcerated, touching on the Old Testament tradition of a jubilee year as a time for granting prisoners amnesty.
Those who, “despite deserving punishment, have become conscious of the injustice they committed,” may receive the indulgence with prayers and the reception of the sacraments in their prison chapel, he wrote.
“May the gesture of directing their thought and prayer to the Father each time they cross the threshold of their cell signify for them their passage through the Holy Door, because the mercy of God is able to transform hearts, and is also able to transform bars into an experience of freedom,” he wrote.
WASHINGTON, September 1, 2015 (Dr. Susan Berry) – A federal court Monday decided in favor of pro-life organization March for Life, ruling that the government cannot force the group to act contrary to its pro-life beliefs by enforcing a mandate that the group provide abortion-inducing drugs to employees.
The court’s order in March for Life v. Burwell permanently bars the Obama administration from enforcing its mandate in Obamacare that requires employers to provide abortion-inducing drugs to employees through health insurance plans. Failure to comply with the mandate would result in IRS penalties for March for Life.
“If the purpose of the religious employer exemption is, as HHS states, to respect the anti-abortifacient tenets of an employment relationship, then it makes no rational sense – indeed, no sense whatsoever to deny March for Life that same respect,” the court said in its decision.
A press release states the order is the first “to be granted in favor of an organization opposed to the mandate for pro-life reasons based on science and moral convictions rather than religion.”
March for Life was represented by Alliance Defending Freedom, which requested a permanent injunction against the mandate.
“We are delighted that the court has ruled in our favor on this crucially important case,” March for Life Education and Defense Fund president Jeanne Mancini said regarding the ruling. “The government should not be allowed to force organizations like the March for Life to have health insurance with drugs and devices that can cause an abortion.”
MISSISSAUGA, ON, August 27, 2015 (LifeSiteNews) – Talking to their children about sex is “anxiety provoking to say the least,” for parents, says American sex-ed expert, Dr. Miriam Grossman.
“Some people just can’t even do it, and that’s okay,” the New York-based psychiatrist told the crowd of 1,000 who packed a Mississauga conference hall August 18 to hear her critique of the Ontario Liberal government’s controversial sex-ed curriculum.
After Grossman explained how the Liberal sex-ed curriculum is dangerously flawed and ideologically driven, she used the question-and-answer session to give parents much appreciated and sometimes humorous practical advice on how to teach their children about “the birds and the bees.”
“If you feel you can’t do it, maybe there’s someone else in the family or in the constellation of people that you know you can trust that could do it,” said Grossman, author of “You’re teaching my child WHAT?” and an internationally sought-after speaker on sex education.
A child, adolescent and adult psychiatrist with 12 years’ clinical experience treating students at the University of California, Los Angeles (UCLA) clinic, Grossman said explaining sexuality and procreation to children is “a process,” that “shouldn’t ideally happen all at once. A child is not a miniature adult, and absorbs…new information differently than adults do.”
And parents need to be sure just what their child wants to know.
To illustrate this, Grossman referred to her earlier story about a father who gave his son every detail on human procreation after the boy asked him, “Dad, where do I come from?”
After the father finished, his son replied, “Well, that’s funny, because Johnny told me that he came from Montreal.”
“Try to find out what your child is really getting at, and, don’t give it all at once,” Grossman said. “You start with a little bit at a time…and you know, there’s so many variables here, and people have their own traditions and their own ways of explaining things, and something that might be right for my family might not be right for your family.”
She also advised that, when confronted with a four, five, six or seven-year-old asking about a pregnant woman, or where babies come, a parent can ask, “What a good question that is. What do you think?”
And parents can also legitimately put off the discussion when appropriate, telling the child, “That’s really not something you need to know about right now.”
“Wow, what a novel idea: Telling a child that they could wait until they’re older to discuss that subject,” Grossman said, adding that parents wouldn’t brook a six- or even fifteen-year-old child asking how much money they made or had in the bank. “Excuse me? Not every subject has to be an open book.”
However, the time will come when a child needs to know “about how her body’s going to change, about reproduction, about how a new life is created.”
That time, Grossman advised, is puberty, or “as puberty is beginning,” and this is especially so for girls, who, if unprepared for the surprise onset of menstruation “might think [they’re] dying.”
“The actual nitty-gritty about the birds and the bees and intercourse” can “be told in bits and pieces, or it can be told all at once, if you feel it’s necessary,” she said, adding that it’s beneficial if the parent acknowledges his or her awkwardness, because the child will think: “This must be such an important subject that my mother or my father is sitting there squirming, but he’s doing it anyway. I’m really loved.”
“And the children need to understand that as you grow up, you change a lot, not only physically but emotionally,” Grossman said, “and what may seem odd or disgusting when you’re ten years old, or whatever age, it becomes something very special and beautiful when you’re older and you’ll understand it later. You don’t have to understand it now.”
Know your child and guard your home
But as an essential foundation for this discussion, parents must both know their children and guard their home from the encroachments of a culture that Grossman described as “very, very sexualized” and “really horrible.”
“Children need parents who are loving but are also firm and authoritative,” she asserted. “They don’t need best friends. They need us to guide them, to know what they’re doing, to be on top of what they’re doing.
So parents need to be aware of whom their child is “hanging around with, and what kind of movies are they watching…what’s going on with your child.”
“You need to know that anyway, even if it’s not about sex education,” she pointed out. “Try and know your child. Every child is different.”
And Grossman emphasized that it is “extremely important to be careful about what your child is exposed to in the home, in terms of television and Internet, obviously.”
Children need to understand that “just like you have garbage you take out of the house, you put it in the garbage bin, it’s dirty, it smells…there are other things that also don’t belong in the house.”
And children learn quickly what is, and is not, permissible inside the home, Grossman said. “Me, I keep kosher…If I go into a store, my kids know from a very young age, we don’t eat that.”
So they are used to the idea of “the world outside and the inside world, of inside your home, and inside your heart as well.”
Parents can also convey this by telling their children that “the world is an upside-down place, and sometimes the most special, holy subjects are…just thrown in the gutter. And that’s a bad thing. In our family, in our tradition, we don’t do that.”
“Sexuality is one of the subjects that in this upside-down world, it is sometimes just in the gutter,” she said. “And so I want you to tell your child to come to me when you have questions, I will give you the straight story about it.”
Grossman herself is “not even sure,” as she stated in her seminar, that sex education should be in the schools: “I believe sex education should be at home for those parents that want to do it.”
She also noted that parents “can make mistakes. We all make lots of mistakes but it’s okay, you can always come back and do it differently,” adding that this is “another wonderful message for your child. You know what, it’s okay to make mistakes, you can always go back and try and fix it.”
Grossman urged parents to visit her Facebook page, website and blog. “I have so much information you can get there that you’ll find useful,” and added that she will be publishing books for children, and has posted her critique of New York City’s sex-ed curriculum, which is similar to Ontario’s.
The parental backlash to that sex-ed curriculum, set to roll out in the province’s publicly funded schools this September, has been “amazing” Grossman noted.
Grossman’s seminar was sponsored by Mississauga-based HOWA Voice of Change along with the Canadian Families Alliance, an umbrella group representing more than 25 associations and 200,000 Ontarians opposed to the curriculum. The report on her devastating critique of the sex-ed curriculum can be found here, and the video here.
SPRINGFIELD, IL, August 26, 2015 (LifeSiteNews) — The Catholic bishop of Springfield, Illinois, is urging America to repent for massively funding Planned Parenthood despite its eugenic roots.
“Let us ask forgiveness for our nation giving half a billion dollars every year of taxpayer money to Planned Parenthood,” said Bishop Thomas Paprocki, “founded by Margaret Sanger, a proponent of eugenics who urged Americans to ‘restrict the propagation of those physically, mentally and socially inadequate’ and said that the ‘most merciful thing that a large family does to one of its infant members is to kill it.’”
Bishop Paprocki likened America today and its current prevalent disregard for unborn life to the period in history with slavery in force when President Abraham Lincoln issued a proclamation calling for a Day of National Humiliation, Fasting, and Prayer.
“President Lincoln lived in a time when many people thought that African-Americans were not fully human. The United States Supreme Court in fact declared as much in its infamously erroneous Dred Scott decision of 1857,” he said. “But in our own time the Supreme Court continues to make wrongful decisions, as it did in 1973 in Roe v. Wade in deciding that unborn babies do not deserve the protection of the law, as well as this past June in attempting to redefine marriage contrary to the plan of God as described in the Book of Genesis.”
“As a result, our nation is in need of ‘national humiliation, fasting and prayer’ now as it was in the time of President Lincoln’s Proclamation,” the bishop continued.
Bishop Paprocki quoted Lincoln throughout his August 23 message, stating that we as a country have forgotten God.
“Let us humble ourselves and pray to Almighty God to forgive our sins, especially the sins of abortion, sins of racism, sins against the divine and natural law of marriage, sins of greed, gluttony, anger, envy, lust, laziness and pride.”
The Springfield prelate also quoted Ephesians 5:15, when St. Paul warned them in his letter to “watch carefully how you live.”
“He does this not because he wants to control their lives, dictating what they can and cannot do,” he said. “Rather, he provides this guidance to them so that they can experience the joy of living a Gospel-centered life.”
“St. Paul knew well that those to whom he was writing were living in a culture that was not rooted in Christian values” Bishop Paprocki continued. “The message that they were receiving from the world around them, the popular opinion if you will, is the same message being promoted today in our secular culture: to live for themselves, to strive for those things which will maximize their satisfaction and happiness. But that happiness is rooted in the things of the world, and not on those of God, which promise true and lasting joy.”
He closed his message on the country’s need for forgiveness with another passage from Ephesians (5:17), where St. Paul encourages people to “try to understand what is the will of the Lord,” so “set aside what so-called worldly knowledge and understanding propose as truth, and seek to see things from the perspective of God and his loving design for the world and human life.”
Bishop Paprocki has been a devotedsupporter of life and marriage, condemning the Obama administration’s silence in the Planned Parenthood human remains trafficking scandal, conducting a public exorcism over the state of Illinois’s 2013 decision to redefine marriage and running a marathon in 2011 to raise awareness and support for life.
As we witness the horrific atrocities committed by Planned Parenthood, as documented in the many videos released by the pro-life Center for Medical Progress, it is time to stop the culture of death! And the best way, is to replace it with The Culture of Life! This is exactly what is happening! As part of this growth, another pro-life Gianna clinic has opened in Louisiana.
Click here to read about the beautiful event lead by Archbishop Gregory Aymond of New Orleans and the director of the new clinic, Dr. Christine Hamphill. St. Gianna Physicians Guild, an initiative of Catholic Action for Faith and Family, conducted an enshrinement ceremony of an image of St. Gianna Molla. An important step of the enshrinement witnessed Dr. Hamphill officially read and sign the Catholic Hippocratic Oath promoted by St. Gianna Physicians Guild. It is so uplifting to see such wonderful and sincere care provided for women and for babies at the Gianna clinics. I hope you take a moment to read this important report.
St. Gianna Physicians Guild continues to do its part to help spread the Culture of Life! In order to make this happen, we need your help! Please sign petition to tell the US Congress to defund Planned Parenthood and use the money to fund the thousands of pro-life clinics, like the Gianna centers, throughout America. If you have already signed, please get your friends and family to do so also. Just forward this link to them: Defund Planned Parenthood!
There is absolutely no excuse for taxpayer’s dollars to be used to fund the butchery and the evil perpetrated by Planned Parenthood and the culture of death. Let’s continue together to do everything we can to stop the culture of death and to spread the Culture of Life!
May God bless you and your family for your efforts! And may St. Gianna look down with love upon you and your loved ones. Sincerely yours in Christ, Thomas J. McKenna
Founder and President
When Pablo and Véronique Gaeta met and fell in love, they both knew it was a love connection that was meant to last a lifetime. And, from the start, this couple shared far more than just a loving bond; as devout Catholics, they also embraced the same outlook on faith and family, and before their “I do’s” they made the joint decision to make Natural Family Planning part of their marital and spiritual lives.
Today, more than 18 years after exchanging wedding vows at their home parish, Our Lady of Grace Church in Encino, the happy couple now has three children — Céline, 15, Emilie, 11, and six-year-old Gabriel — and they regularly discuss the “blessing” of Natural Family Planning (NFP) with engaged and married couples through their teaching ministry at Our Lady of Grace and across the archdiocese.
“Natural Family Planning has been such a blessing for our marriage that we wanted to share this gift with others,” Véronique told The Tidings. In 2002, the Gaetas became certified to teach the sympto-thermal method (one of several NFP methods endorsed by the Catholic Church), and since then, they have presented NFP information and resources with parish priests at various diocesan deanery meetings; via parish health fairs; to high school students; as part of marriage preparation classes; and with parishioners at the end of Mass at several parishes.
“We are always humbled by couples that come to our classes reluctantly, and after hearing what NFP can offer them, become advocates of the methods,” said Pablo.
“On several occasions, NFP has also served as an ecumenical tool — several couples have come to our class from different faith denominations, because their own church did not offer NFP. These couples were grateful that the Catholic Church had classes where they could learn about NFP, and they were also surprised to learn the beauty of the Church’s teaching on human sexuality.”
According to the Gaetas, the Church has always taught that artificial contraception “undermines God’s original plan for marriage between a man and a woman,” because marriage “needs to be free, total, faithful and fruitful.” Any method of family planning should respect these four traits, they explained.
“Every time a married couple has relations, the act itself must be open to the transmission of life, whether or not the act results in pregnancy,” said Pablo. “Artificial forms of contraception act as a barrier to the transmission of life. … Some forms suppress or alter a normal functioning part of the woman’s body.”
By contrast, he added, Natural Family Planning is 100 percent safe and free of any side effects, because it “works with a woman’s fertility, and not against it.”
Because the Church understands that couples may have just reasons to postpone a pregnancy, NFP offers “a morally acceptable way of family planning,” by utilizing methods that “respect the dignity of marriage as a sacrament.”
“In making any decision about family planning, however, a couple should prayerfully discern whether or not God is asking them to cooperate with him in bringing another child into the world,” explained Pablo.
The three primary NFP methods endorsed by the Church — all of which can be used either to help achieve or avoid pregnancy — are sympto-thermal (which relies on a combination of physical fertility signs, including body temperature, cervical mucus and cervical position), the Billings Ovulation and Creighton Fertility Care Model methods (both of which rely solely on mucus signs).
“They’re all equally effective,” said Véronique, adding that selecting a particular method comes down to preference, though she noted that the Creighton method is “especially useful for couples who may be having medical issues” that can impact fertility, such as PMS, endometriosis or polycystic ovary syndrome (PCOS).
According to Pablo, questions and misunderstandings are plentiful during classes among couples who are learning about NFP for the very first time.
“It is important to understand that NFP is not the ‘Calendar Rhythm Method’ of the 1930’s,” he said. “Modern methods of Natural Family Planning are more accurate and precise. … And all women, regardless of whether or not they have regular menstrual cycles, can use NFP successfully.”
However, said Véronique, the real root of the problem is not in such misunderstandings, but, rather the fact that, based on their experiences over the last 13 years, a significant “percentage of married couples do not even know NFP exists.”
“We strongly believe that a lot more couples would choose to embrace NFP in their marriages if they were better informed,” she said. “Married couples need multiple exposures at both the diocesan and parish levels … and engaged couples would benefit greatly from mentor couples that are open and honest about practicing NFP in their marriages.”
Which is exactly what the Gaetas try to do, with each class they teach: act as mentors and teach by example by sharing the beauty of NFP in their own family.
“Practicing NFP in our marriage has enabled us to come to a deeper understanding of God’s plan for us,” said Pablo. “Over the years, we have grown in our love for each other because NFP is not just a method of family planning; it is a way of life. Through NFP, we have learned to respect each other’s dignity.”
Thanks to NFP, the Gaetas have also experienced improved communication as a couple, because “Natural Family Planning is a shared responsibility that requires us to communicate candidly with each other on a regular basis,” said Véronique.
And, she continued, although practicing NFP “can be challenging at times — and it may even seem restrictive to some — we have found that it affords us a certain freedom that can only be properly understood by those who experience it.”
This is a wonderful respite from the regular news of the day. But it does put all the other stories into perspective. These children, through their God-given natural innocence, reveal more than many books in the world about the wonder and goodness of every new life. View here:
It is a powerful anti-Planned Parenthood video. I have viewed it three times so far and marveled as much each time. There is a message here for all of humanity and especially for the anti-life developed cultures of the world in this simple, short experience of these children’s responses to their parents’ good news. The parents as well are wonderful examples of parenthood as it should be.
CHICAGO, Aug. 20, 2015 /Christian Newswire/ – On Saturday, August 22 public protests of Planned Parenthood (PP) abortion clinics and facilities will take place all over the United States. Thousands are expected to attend these protests with the purpose of creating awareness of the barbaric practice of abortion and the sale of aborted baby body parts – a scandal that has erupted in recent weeks due to undercover videos released by the Center for Medical Progress. Currently, there are over 300 cities in 47 states and 5 countries represented in the nationwide protest.
What: Protest PP’s disrespect for human life, harvesting and selling of aborted baby parts
Where: Over 300 Planned Parenthood facilities across America. (See cities)
When: August 22, 2015 from 9:00am-11:00am
For more information or to locate a protest in your area, please go to ProtestPP.com
Recently released videos have shown the results of Planned Parenthood’s barbarous trade of killing babies and harvesting and selling their body parts.
Mark Harrington, Created Equal’s National Director:
“We don’t just want to defund Planned Parenthood; we want to defeat Planned Parenthood. We cannot only look to Washington, DC and our state governments to end the killing. It is up to each of us individually to take ownership over our own neighborhoods to stop Planned Parenthood and end abortion altogether.”
#ProtestPP is the largest demonstration against Planned Parenthood in their 99 year history.
Eric Scheidler of Pro-Life Action League:
“These videos are exposing the American people to the truth about Planned Parenthood and the truth about abortion. How can you deny the humanity of a tiny person whose body parts are being harvested for medical use? Worse yet, how can you make jokes about it, like the Planned Parenthood doctors do in these videos? It’s time to cease all taxpayer funding of this corrupt organization.”
#ProtestPP involves prayer, speakers and holding signs that read #PPSellSBabyParts.
Monica M. Miller of Citizens for a Pro-Life Society comments:
“When PP technicians are scavenging through the body parts of aborted babies to find tissue that they hope to sell, this adds a whole new gruesome and ghoulish layer to the already highly controversial practice of abortion in America. It’s bad enough that Planned Parenthood is profiting from abortions-but on top of that they exploit the bodies of their murder victims for additional revenue. It is the abortion providers themselves who describe what they do as violence.”
August 18, 2015 (VoiceoftheFamily) — John Smeaton, Chief Executive of the Society for the Protection of Unborn Children, and co-founder of the international coalition Voice of the Family, spoke on 7th August at a two day pro-life conference organised by the bishops of Ghana. The conference was entitled “Protecting Life and Family Values in the continuing Culture of Death”.
In his talk to the conference Mr Smeaton outlined the threat posed to Africa by the international population control movement. He also drew attention to the collaboration between leading figures in that movement and important Vatican departments. He went on to give an overview of the threat posed to families, in Africa and around the world, by the instrumentum laboris of the Ordinary Synod, to be held in Rome in October this year. His full talk can be read below:
I begin by drawing your attention to National Security Study Memorandum 200 (NSSM 200). The National Security Council of the United States completed a study in 1974 entitled Implications of the Worldwide Population Growth for US Security and Overseas Interests known in short as NSSM 200.
NSSM 200, promoted and endorsed by Dr Henry Kissinger, President Nixon’s National Security Adviser, expressed the gravest fears that the political consequences of current population factors in the less developed countries might create “political or even national security problems for the US”.
A 1977 annual report on the implementation of NSSM 200 emphasises the strategic importance of using “intermediaries” such as the United Nations Fund for Population Activities (UNFPA), the World Bank and the International Planned Parenthood Federation (IPPF), since they could operate in countries where the United States “are not now acceptable” thus avoiding the accusation of imperialism.
This is exactly what Marie Stopes International (MSI) and International Planned Parenthood Federation (IPPF) and others are doing in Ghana today. According to the IPPF website, Planned Parenthood Association Ghana, IPPF’s subsidiary, delivered in Ghana in the year 2011:
5.8 million condoms
330,000 contraceptive services
526,000 other sexual and reproductive health services
606,000 services to young people under 25 years
When International Planned Parenthood Federation refer to “reproductive health” they are referring to access to contraception and abortion – according to the definition of “reproductive health” used by the UNFPA and other UN bodies, governments such the current US administration and international anti-life NGOs such as IPPF and MSI.
On 26th March 2014 in New York, the International Planned Parenthood Federation co-hosted an event, particularly targeting African nations, to “present a declaration calling for universal access to safe and legal abortion”.
Let me say a little here about President Obama because his policies affect all of us, not least the people of Ghana. On October 12th 2009 the Obama administration confirmed at the UN that it would be promoting legalised abortion throughout the world, targeting adolescents in a worldwide abortion drive.
British Prime Minister, David Cameron has threatened to withhold UK aid from poor countries that do not conform and I quote: “British aid should have more strings attached”. David Cameron was speaking here in particular of the UK government’s homosexual rights agenda.
The homosexual rights agenda in my nation and in so many other nations represents a massive attack on the sanctity of human life for many reasons. For example, as you know, same-sex couples are now demanding the right to have children– making it even more difficult for pro-life groups effectively to oppose surrogacy and in vitro fertilisation. According to peer-reviewed research, for every baby born by IVF, 23 are either discarded, or frozen, or used in destructive experiments, or miscarry. Defending the right to life of unborn children will increasingly be viewed as an attack on the rights of homosexual couples.
Morever, the homosexual rights’ agenda is a top priority for Planned Parenthood working here in Ghana.
Make no mistake, Planned Parenthood, hugely funded by the US government, the British government and the overwhelming majority of nations worldwide, are the enemy of Ghana’s children. In 2011, at the Commission on the Status of Women at the UN in New York, the International Planned Parenthood Federation, the Population Council and other pro-abortion groups held a meeting to launch worldwide a massive programme of so-called comprehensive sex education entitled: “It’s All One Curriculum”.
The curriculum shows itself to be nakedly polemical rather than educational. It states:
“People can support or join movements for social change at the global level. For example: …youth-led networks for sexual and reproductive rights and services.” (p.231)
And on page 61 of their curriculum guidelines they advise educators: “Certain social movements promote greater equality and dignity within marriage. These include: movements to legalize same-sex marriage”.
In the same document, International Planned Parenthood Federation tell teachers of young children that sexual self-abuse is a human right. They say:
“Sexuality may be expressed by oneself … Sexuality — expressed alone…can be a source of pleasure and meaning in life. (p.84) “ … Masturbation is an important way that people learn about their bodies and sexuality … Masturbation is a safe sexual behavior. It is neither physically nor mentally harmful.” (p.99)]
This is the kind of thing which Planned Parenthood is delivering to your children here in Ghana. In their “Access, Services and Knowledge (ASK) programme” which IPPF describes as a “‘ what young people want, what young people need’ programme” they target your 10 – 24 year-olds including underserved groups: The specific focus – an uptake of sexual and reproductive health (SRH) services. The 3 year programme targets African young people in Kenya, Uganda, Ethiopia, Ghana and Senegal.”
IPPF Africa Region says: “ASK aims to ensure that young people … receive direct information on sexual and reproductive health and rights so that they can make independent informed decisions.” For a full appreciation of IPPF’s concept of sexual rights I urge you to study Sexual Rights: an IPPF Declaration.
Moreover, yesterday, a story in The Ghanaian Times reports that the Norweigan Development Agency is targeting thousands of your 15 – 25 year-old young women in poor and urban and peri-urban areas of Ghana to introduce them, amongst other things, to sexual and reproductive health – a term meaning access to contraception and abortion.
Powerful Western forces as I speak are seeking to control your population by corrupting your nation’s values, in particular by targeting the innocence of your children and young people.
In a book entitled Adam and Eve after the Pill – Paradoxes of the Sexual Revolution, Mary Eberstadt, research fellow at the Hoover Institution, describes the teaching of Pope Paul VI inHumanae Vitae on regulation of birth, published on July 25, 1968, as “perhaps the most unfashionable, unwanted, and ubiquitously deplored moral teaching on earth”. She then goes on to show that the teaching of Humanae Vitae is in fact the “most thoroughly vindicated” moral teaching on earth “by the accumulation of secular, empirical, post-revolutionary fact”. In this connection, Mary Eberstadt cites Nobel-Prize winning economist George Akerlof. In a 1996 article in the Quarterly Journal of Economics, Akerlof explains “why the sexual revolution, contrary to common prediction, especially those in and out of the church who wanted the teaching on birth control changed, had led to an increase in illegitimacy and abortion.” Mary Eberstadt continues: “In another work published in the Economic Journal in 1998, Akerlof traced the empirical connections between the decrease in marriage and married fatherhood for men – both clear consequences of the contraceptive revolution – and the simultaneous increase in behaviours to which single men appear more prone: substance abuse, incarceration, and arrests, to name just three.”
Mary Eberstadt in Adam and Eve and the Pill also says: “The years since Humanae Vitae have … vindicated the encyclical’s fear that government would use the new contraceptive technology coercively”.
In this connection, who can seriously doubt the effectiveness of powerful western nations and NGOs in promoting anti-life sex education programmes which seek to eliminate the role of parents as the primary educators and protectors of their children? This is a form of coercion on families which is resulting worldwide, not least in the UK my own country, in schoolchildren being given access to contraception and abortion without the knowledge of their parents, including in Catholic schools.
Thank God for the Catholic Bishops’ Conference of Ghana for your witness on these fundamental matters. In particular, I congratulate and thank you for your Communiqué last November in which you said: “We also deplore in no uncertain terms a radical and faceless culture of death which promotes among other things the supply and use of the condom in our schools, the in vitro fertilization and the contraception agenda of some national and international institutions in Ghana … we urge those who represent Ghana at the United Nations and other such bodies to realise that these practices are culturally abominable and morally and spiritually reprehensible …”
Above all, as Pope John Paul II pointed out in his encyclical, Evangelium Vitae, there is a close interconnection between contraception and abortion. According to the manufacturers, one of the contraceptive pill’s modes of action is to cause an early abortion. Thus the use of contraception undermines respect for the sanctity of human life from conception and makes the possibility of abortion an option.
As a pro-life leader for four decades and as a Catholic layman, a father and grandfather, I believe that it is urgent and overdue that the Church reaffirm the unchangeable teaching of Humanae Vitae on the separation of the procreative and unitive dimensions of the sexual act by the use of contraceptive methods. The separation of the procreative and unitive dimensions of the sexual act which is intrinsic to the use of contraception has acted as major catalyst of the culture of death. I am certain that until the core teaching of Humanae Vitae is constantly proclaimed throughout the Church and at the highest level of authority, the pro-life movement will not prevail.
In this connection, I am grateful to His Eminence Cardinal Turkson for sensitising our pro-life conference today to the pressures on church leaders which are constantly being brought to bear to change the Church’s unchanging and unchangeable teaching on contraception and abortion.
Particularly in relation to population control in Africa, I want to draw attention to the activities of Dr Jeffrey Sachs, the special adviser to UN Secretary General Ban Ki-Moon.
Jeffrey Sachs heads the Sustainable Solutions Network, which was responsible for producing a draft for the Sustainable Development Goals, which call for increased access to abortion and contraception worldwide.
Jeffrey Sachs made a plea for legalizing abortion as a cost-effective way to eliminate “unwanted children” when contraception fails in his 2008 book Commonwealth: Economics for a Crowded Planet.
In his book The Age of Sustainable Development, published last March, Jeffrey Sachs states quite clearly that the birth rate in Africa must be reduced.
Sachs proposes three methods of fertility rate reduction, the third of which is that governments must encourage their populations to lower family size by promoting birth control and providing access to free or low-cost contraception and family planning.
In 2011 Sachs expressed his horror at Nigeria’s rising population and called for the Nigerian government “to work towards attaining a maximum of three children.”
In June this year he called for the UN to provide 1 million healthcare workers for Africa. That is 1 million UN workers travelling through Africa promoting abortion and contraception.
Sachs will be in the Vatican in November to take part in a workshop organised by the Pontifical Academy of Sciences which will discuss how to “use children as agents of change” in pursuing sustainable development and the environmental agenda.
The Pontifical Academy of Sciences’ workshop explicitly cites the papal encyclical Laudato Si, as the basis for its work.
I repeat: the subject of the Vatican Workshop in November us “using children as agents of change” in pursuing sustainable development and the environmental agenda.
Not only in this context, as a parent and grandparent, I am deeply concerned that Laudato Si makes no reference to parents as the primary educators of their children. Using children as agents of change in pursuing sustainable development and the environmental agenda will very soon become a required part of school curricula throughout the world. Have no doubt that the worldwide population control powers-that-be, led by people like Jeffrey Sachs, will make their influence well and truly felt in shaping those school curricula.
It is extremely disturbing that at the very moment when the Society for the Protection of Unborn Children, the organization which I lead, and other pro-life organisations, have been fighting tooth-and-nail at the United Nations to protect developing countries from the pro-abortion, pro-contraception, anti-parent elements written into the sustainable development goals, that the Holy See has been seeking Jeffrey Sachs’s advice and permitting him to help shape the Holy See’s policies on sustainable development.
Jeffrey Sachs has played a leading role at Vatican conferences and workshops on these matters no less than six times in the last couple of years and has had a personal audience with Pope Francis.
I note here with great foreboding that the omission of any reference to Church teaching on the use of contraception in the papal encyclical in the environment leaves Catholics ill-prepared to resist the international population control agenda. The encyclical calls for increased international environmental action in paragraphs 173-175, while neglecting to prepare Catholics for what such action will undoubtedly involve: renewed attempts to further impose contraception and abortion on the developing world. There is now a grave danger that our children will be exposed to this agenda under the guise of education on environmental concerns. The proposed plans of the Pontifical Academy of Sciences, and the lack of clear teaching on these dangers in the encyclical, put us on our guard. Catholic parents must resist all attacks on our children, even when they emanate from within the Vatican.
Even more disturbing in relation to contraception is the recently published instrumentum laboris, the working document for the forthcoming Family Synod. The instrumentum laboris, clearly undermines the teaching of the encyclical letter Humanae Vitae. Paragraph 137 effectively seeks to nullify the central teaching of Humanae Vitae which declared morally inadmissable “any action which either before, at the moment of, or after sexual intercourse, [which] is specifically intended to prevent procreation—whether as an end or as a means.”
Paragraph 137 of the instrumentum laboris, without in any way restating this fundamental teaching of Humanae Vitae, suggests that a balance must be reached between the “role of conscience” and the “objective moral norm” under “the regular guidance of a competent and spiritual guide”. The implication of the whole passage is that contraceptive acts may sometimes be permitted. Let me conclude this section of my talk by quoting again the timeless teaching of Pope Paul VI in Humanae Vitae:
“Though it is true that sometimes it is lawful to tolerate a lesser moral evil in order to avoid a greater evil or in order to promote a greater good, it is never lawful, even for the gravest reasons, to do evil that good may come of it … even though the intention is to protect or promote the welfare of an individual, of a family or of society in general.”
Furthermore, Paragraph 86 of the instrumentum laboris contains a direct attack on the rights of parents. The paragraph states that “the family, while maintaining its privileged spot in education, cannot be the only place for teaching sexuality.” This statement is directly contrary to Catholic teaching which affirms the right and duty of parents to be the first and foremost providers of education to their children in sexual matters. Parents are entirely capable of performing this task by themselves and it is entirely their choice if they wish to involve others. Paragraph 86 of the instrumentum laboris leaves Ghanaian children, and my grandchildren, at the mercy of the International Planned Parenthood Federation.
There are other major terrible and terrifying passages for families throughout the world, Catholic and non-Catholic families, in the instrumentum laboris on which I don’t have the time to comment today – but I will leave copies of an analysis of this disturbing document for your attention.
I say these things to you today to fulfil my responsibility outlined in Canon 212 of the Code of Canon Law:
According to the knowledge, competence, and prestige which they possess, they [the Christian faithful] have the right and even at times the duty to manifest to the sacred pastors their opinion on matters which pertain to the good of the Church and to make their opinion known to the rest of the Christian faithful, without prejudice to the integrity of faith and morals, with reverence toward their pastors, and attentive to common advantage and the dignity of persons.
The crisis in the Church is quite possibly unparalleled. So let us say a prayer for Pope Francis. May the Lord preserve him and give him life and make him blessed upon the earth, and deliver him not up to the will of his enemies.
In June this year, a consultative meeting of African prelates was held in Accra, Ghana, which culminated in the 45 bishops and 5 cardinals representing episcopal conferences across the continent expressing their intention to present a united determination to defend Church teaching about marriage and family at the upcoming Synod of Bishops on the Family.
In the closing communique of the meeting in Accra, the bishops of Africa said that at the upcoming Synod on the Family they would offer “a clear affirmation of family and marriage values according to the Word of God and the doctrine of the Church.”
Thank God for the African bishops. My family and families throughout the world will be praying for you in the coming months – that you continue to be courageous apostles of the unchanging and unchangeable Gospel of Jesus Christ, the Gospel of the family, the Gospel of life.
August 13, 2015 (LifeSiteNews) — Voice of the Family, an international lay coalition of major pro-life and pro-family organizations, has warned that the Vatican’s preparatory document for the October Synod on the Family “threatens the entire structure of Catholic teaching on marriage, the family and human sexuality.” In an extensive analysis of the Vatican’s 77-page document called the Instrumentum Laboris,
The game plan of introducing ambiguity into the texts was revealed by Cardinal Walter Kasper, the central figure of the Synod who launched the controversy with his proposals for communion for divorced and remarried Catholics. In an interview with EWTN’s Raymond Arroyo in June he divulged an approach to overcome growing opposition to his heterodox plans.
“I get a lot of agreements, but also a lot of critiques, and there are tensions there,” Kasper acknowledged. “Now I propose to those who prepare the Synod to prepare a text which can get the agreement of the whole, of the great majority. It’s the same method also we had in the Council.” He later repeated, “My suggestion is to find now a formula where the great majority can adhere.”
The Second Vatican Council was also faced with challenges to traditional Catholic doctrine and practice, which were opposed by large numbers of bishops. Despite this opposition, many items on the agenda of the ultra-liberal bishops were accomplished by the use of often vague, ambiguous and even apparently conflicting language that seem to have appeased both sides. These expressions were later referred to as “time bombs” which some theologians were able to exploit following the council for the purpose of undermining the Church’s traditional teachings.
The Voice of the Family analysis explains “it is clear that the instrumentum laboris fails to clearly affirm Catholic doctrine, but rather, through the use of ambiguous terms, seriously undermines it.”
John Smeaton, co-founder of Voice of the Family, said, “The document undermines the doctrine of Humanae Vitae on contraception.” The 19-page critical analysis of the Instrumentum Laboris written by Voice of the Family’s Matthew McCusker notes that that Vatican preparatory document for the Synod “refuses to use the word ‘contraception’ or make any direct reference to any contraceptive method, despite the devastating consequences of the use of contraceptives in many areas of human life, not least the killing of unborn children by abortifacient methods.”
More than that, the Instrumentum Laboris misrepresents Humanae Vitae by leaving out the fact that it condemns contraception. The Synod document states that the “two principal points” of the encyclical are first about the role of conscience and second “an objective moral norm” without ever defining that moral norm – namely Humanae Vitae declares morally inadmissible “any action which either before, at the moment of, or after sexual intercourse, is specifically intended to prevent procreation—whether as an end or as a means.”
“The Instrumentum Laboris also resurrects the discredited Kasper proposals for Holy Communion for unrepentant adulterers, reduces the indissolubility of marriage to a mere ‘ideal’, and undermines the position of parents as their children’s primary educators,” added Smeaton.
With regard to the Church’s teaching that parents are the primary educators of children, the Instrumentum Laboris suggests otherwise. Paragraph 86 states that “the family, while maintaining its privileged spot in education, cannot be the only place for teaching sexuality.” The Voice of the Family analysis notes the “statement is directly contrary to Catholic teaching,” citing the teaching of St. Pope John Paul II in his Apostolic Exhortation Familiaris Consortio, where the pope leaves open the possibility that sex education can be done solely in the home. He wrote: “Sex education, which is a basic right and duty of parents, must always be carried out under their attentive guidance, whether at home or in educational centres chosen and controlled by them.”
“Voice of the Family urges Catholics not to be complacent or give in to a false sense of obedience, in the face of attacks on the fundamental principles of the natural law,” concluded Smeaton. “Catholics have a duty to oppose the direction being taken at the Synod. If that direction is not reversed, the greatest victims will be those who are most vulnerable, especially children, born and unborn.”
We are pleased to present a new interview, which has been granted to Catholic Voice newspaper by Bishop Athanasius Schneider, auxiliary bishop of Astana in Kazakhstan. Catholic Voice is one of 24 organisations that form the Voice of the Family coalition. Bishop Athanasius Schneider has risen to prominence because of his clear defence of Catholic teaching. In this interview the Bishop discusses the major threats to the family posed by the instrumentum laboris of the synod and by the actions of senior prelates who operate from within the official structures of the Church. Voice of the Family has produced an in-depth analysis of the instrumentum laboris.
Q. Your Excellency, the Instrumentum Laboris for the 2015 Synod states that there is a “common accord” [c’è un comune accordo] in favour of a “penitential way” for the divorced and remarried ” under the authority of the Bishop, for the faithful (who have been) divorced and remarried civilly, who find themselves in a situation of irreversible cohabitation.” Is it accurate to suggest there is a “common accord” ?
Bishop Schneider: The affirmation that there is a “common accord” on the “penitential way” is not correct. The only one public document that would permit to determine the effective opinion of the bishops on this topic, is the “Relatio Synodi” of 2014. There it is documented that 40% of the members of the Synod rejected such a “penitential way”. When faced with such a result, one can hardly speak of a “common accord”. Furthermore, there is no specification as to a concrete definition of such a “penitential way”.
Q. In light of this use of the phrase “c’è un comune accordo” is the credibility of the Instrumentum Laboris threatened? One could even conclude there is an attempt to impose communion for the divorced and remarried at the Synod despite opposition. Do you have any comment on this?
Bishop Schneider: In the light of a careful analysis of the facts, one is left with the suspicion that the authors of the Instrumentum Laboris try to push forward the agenda of a certain clerical pressure group in order to change the Divine law of the non-admission the divorced and remarried to Holy Communion.
Q. Commenting on the Synod, Archbishop Forte has said one of the priorities should be a discussion of allowing those who have divorced and remarried outside the Church to become “godfathers or godmothers, catechists, extraordinary ministers of the Eucharist.” What do you think of this idea?
Bishop Schneider: Firstly, it is necessary to remember the significance of godparents according to the constant teaching and practice of the Church: A sponsor (godfather or godmother) must help the baptized person to lead a Christian life in keeping with baptism and to fulfill faithfully the obligations inherent in it. To be permitted to take on the function of sponsor a person must be a Catholic who leads a life of faith in keeping with the function to be taken on (cf. Canons 872 and 874 § 1, 3). Sponsors and those who take the place of parents are obliged to form the children by word and example in faith and in the practice of Christian life (cf. Canon 774, § 2). When a godfather or a godmother or a catechist conducts a lifestyle that publicly contradicts the Sixth Commandment and the indissolubility of the Christian marriage, then he or she surely cannot be an example of a life of faith. The same is valid for extraordinary ministers of the Eucharist. The advocacy for the admission of divorced and remarried to the task ofgodparents and catechists cannot ultimately be for the true spiritual good of the children, but turns out to be an instrumentalization of a specific ideological agenda. This is a dishonesty and a mockery of the institution of godparents and catechists who by means of a public promise took on the task of educators of the faith. In the case of godparents or catechists who are divorced and remarried, their life however, continuously contradicts their words, and so they have to face the admonition of the Holy Spirit through the mouth of the Apostle Saint James: “But be doers of the word, and not hearers only, deceiving yourselves” (James 1: 22).
Q. Excellency, in the ongoing debate over same sex “marriage” some Catholic groups have become open to the notion of recognizing that same sex pairs can have long term loving relationships thus they conclude that it is possible to recognize same sex civil partnerships. It is evident that even a few bishops support this idea but could this ever be an authentic Catholic position?
Bishop Schneider: This can never be an authentic Catholic position because it contradicts directly the words of God, which says that homosexual acts and the homosexual lifestyle are a grievous offense of the will of God (cf. Gen 18:20; Lev 18:22; 20:13; Is 3:9; Rom 1:26-27; 1 Cor 6:10; 1 Tim 1:10; Jud 7). Committing evil in a long-term and even loving relationship cannot transform the same evil into good. Only true repentance that includes contrition and the firm intention to avoid the evil cancels with the grace of God the evil. It would be absurd to affirm that alcoholism will gain a positive recognition because of the long-term and loving relationship of two persons who established this relationship on the base of their propensity to alcohol. The same absurdity contains the above-mentioned affirmation about same sex unions.
Q. There also appears to be a push towards a “new language” with some saying that using the phrases “homosexual tendencies” and “intrinsically disordered” should be avoided less offence is caused – what do you make of this drive to use politically correct language?
Bishop Schneider: We have to call things by their real names; otherwise, we will deceive the others and ourselves. To call the things by their names does not mean an intention to create discrimination, provided we speak with respect and pedagogical wisdom. There exist some deficiency symptoms of a bodily or spiritual nature such as fear of heights, claustrophobia, seasickness, shortsightedness etc. No person of common sense will be indignant when we name such phenomena as a deficiency. In fact, the homosexual attraction is in itself a sexual-psychological deficiency symptom, which all civilized human history has considered as a deficiency and called by its name. Under pressure from the new gender ideology, which has its roots in the Marxist ideology, in the 1970s homosexuality was excluded from the International Handbook of Psychological diseases. In such a way, persons who suffer with homosexual attraction were taken hostages of a radical ideology, inasmuch as they are denied the opportunity to receive healing or improvement of their psychologically defective situation. To have a deficiency is not a shame, but it is a fact. Those who effectively encourage deficient persons, in our case persons who are feeling a homosexual attraction, to abuse their deficiency in order to become more deficient and to consequently become addicts, commit a grave injustice towards these persons who need and want to receive help in their spiritual and psychological deficiency.
Q. Your Excellency, since the legalisation of abortion in Ireland in 2013, Catholic hospitals such as the Mater Misericordiae University Hospital, Dublin, have issued statements indicating that they will comply with the new abortion laws. In these circumstances, what is the duty of an archbishop or bishop in whose jurisdiction these hospitals reside?
Bishop Schneider: The duty of a Catholic bishop in such a case is to deprive the hospital the title “Catholic” and remind his faithful that accomplices of the horrible crime of abortion commit a grave sin and are threatened with excommunication. The punishment of excommunication is a medicinal measure in order to prevent the guilty person from committing further crimes and so to ensure his eternal salvation. This was the method of God Himself (the preaching of judgement and punishment through the Prophets), of Our Lord Jesus Christ (the speech of excommunication in Mt 18: 15-18) and of the Apostles (the excommunication realized by Saint Paul, cf. 1 Cor 5: 4-5) and so it has to be also the method of the Church. When the Church desists of this Divine method, she will be no more faithful to God, she will be no more a real mother who punishes her child in order to save it. On the contrary, such a church will be a false mother who disastrously pampers the child to its damage or a stepmother who is indifferent about the child’s salvation. The following words of excommunication pronounced by Saint Paul and inspired by the Holy Spirit, remain valid for all periods of the Church’s history inclusively for our days: “With the power of our Lord Jesus we deliver this man to Satan for the destruction of the flesh, so that his spirit may be saved in the day of the Lord” (1 Cor 5: 4-5).
Q. During the same sex “marriage” debate in Ireland, one bishop stated that Catholics could in good conscience vote for this proposal and admonished them not to vote against it out of hate. In addition, many clergy used the media to also encourage voters to redefine marriage. This situation is repeated throughout the western world – what do you think has happened to the clergy in this respect and what should be done to correct matters?
Bishop Schneider: Those clerics who encouraged the faithful to vote for same sex marriage revealed themselves by this same fact as false prophets, as those who pervert the Word of God. They revealed themselves as public liars, to whom are fully applicable these words of Holy Scripture: “Woe to those who call evil good and good evil, who put darkness for light and light for darkness, who put bitter for sweet and sweet for bitter” (Is 5:20) and: “Your prophets have seen for you false and deceptive visions; they have not exposed your iniquity to restore your fortunes, but have seen for you oracles that are false and misleading” (Lam 2: 14). To such priests and bishops the Apostle Paul without any doubt would say today these words: “Such men are false apostles, deceitful workmen, disguising themselves as apostles of Christ” (2 Cor 11:13). In order to remedy this situation it is firstly necessary that faithful Bishops teach clearly and unambiguously the truth of Christ and correct explicitly the teaching of these false prophets.
Q. Excellency, in a number of interviews you have mentioned attempts to manipulate the proceedings of the 2014 Synod. Many faithful around the world are anxious that attempts are being made to manipulate the 2015 Synod. What can be done to stop such manipulation? What can those not directly involved in the Synod do if evidence emerges of renewed manipulation?
Bishop Schneider: In order to stop such manipulations we must first of all, implore fervently Divine and heavenly intervention, so that the following words of God may be realized in our days during the upcoming Synod: “God frustrates the devices of the crafty, so that their hands achieve no success.He catches the wise in their own craftiness, and the schemes of the wily are brought to a quick end” (Job 5: 12-13).
Furthermore, we have to expose and defend the Divine truth about marriage and family in written and oral forms, exercising hereby the service of the truth as an important gesture of our love for our neighbour. When there exists sure elements of proof one should try to unmask the machinations of the false prophets inside the Church. Saint Peter, the first Pope, wrote in his second Encyclical Letter the following words, which are applicable to those priests and bishops who teach in our days the goodness of the homosexual lifestyle and the legitimacy of receiving Holy Communion by those who live publicly in an adulterous partnership: “There will be false teachers among you, who will secretly bring in destructive heresies, even denying the Lord who redeemed them, bringing upon themselves swift destruction. And many will follow their sensuality, and because of them the way of truth will be blasphemed. And in their greed they will exploit you with false words. Their condemnation from long ago is not idle, and their destruction is not asleep.” (2 Peter 2: 1-3).
Q. Your Excellency, during this time of unprecedented confusion and disorientation in the Church are there any saints or spiritual writings to which you turn for consolation and encouragement? Could you share with our readers any sayings or insights that will encourage us?
Bishop Schneider: We have to look on those Saints who shone out as lights in particularly confused periods of the Church History. Among the clergy, I would name Saint Athanasius his sufferings and his writings about the history of the Arians; Saint Gregory VII, who intrepidly defended chastity (against clerical concubinage and sodomy) and liberty (against the interference of the civil power in spiritual affairs) of the Church, the Spouse of Christ; Saint John Fisher, who at the cost of his life was the only one English bishop of his time defended the indissolubility of the marriage and the primacy of the Pope; Saint Pius X who was in his words and his deeds extraordinarily clear and courageous and never bowed to the pressure of political correctness neither inside nor outside the Church.
Among the laity one can mention particularly: Saint Catherine of Siena, Saint Thomas More, Gabriel Garcia Moreno, the eminently pious and courageous President of Ecuador, who was assassinated in 1875 in “odium fidei” immediately when he came out of the church where he spent one hour in Eucharistic adoration. The servant of God Jerome Lejeune (+ 1994): he was ostracized by the medical, academic and political elite because of his strong position against abortion; he did not receive an increase in salary for nearly 20 years; his research grants were withdrawn and he was forced to close his laboratory.
It would be a great spiritual help for us in our days in midst of the persecution from outside the Church and the marginalization from inside the Church to read the biographies and writings of the above-mentioned saints and servants of God and especially the life of the martyrs. I read somewhere once this phrase, which can encourage us: “It is not important what people say about us today, but what they will say about us hundred years after our death”.
By Cardinal Robert Sarah, Prefect of the Congregation for Divine Worship and the Discipline of the Sacraments
Editor’s note: This article appeared in the Italian edition of L’Osservatore Romano on June 12, 2015. (English translation by Michael J. Miller for CWR.)
Fifty years after its promulgation by Pope Paul VI, will the Second Vatican Council’s Constitution on the Sacred Liturgy finally be read? Sacrosanctum Concilium is actually not just a catalogue of “recipes” for reform, but a veritable Magna Carta of all liturgical action.
In it the Ecumenical Council gives us a magisterial lesson in methodology. Indeed, far from being content with a disciplinary, external approach to the liturgy, the Council wishes to have us contemplate what it is in its essence. The Church’s practice always results from what she receives and contemplates in revelation. Pastoral ministry cannot be detached from doctrine.
In the Church “action is directed to contemplation” (cf. no. 2). The conciliar Constitution invites us to rediscover the Trinitarian origin of the liturgical work. Indeed, the Council determines that there is a continuity between the mission of Christ the Redeemer and the liturgical mission of the Church. “Just as Christ was sent by the Father, so also He sent the apostles,” so that “by means of sacrifice and sacraments, around which the entire liturgical life revolves” they might “accomplish the work of salvation” (no. 6).
Carrying out the liturgy therefore is the same as accomplishing the work of Christ. The liturgy is essentially “actio Christi”: “the work of Christ the Lord in redeeming mankind and giving perfect glory to God” (no. 5). He is the great high priest, the true subject, the true protagonist of the liturgy (cf. no. 7). If this vitally important principle is not accepted in faith, we run the risk of making the liturgy a human work, the community’s celebration of itself.
On the contrary, the Church’s real work is to enter into Christ’s action, to join in the work for which He has been commissioned by the Father. Therefore “the fullness of divine worship was given to us,” because “His humanity, united with the person of the Word, was the instrument of our salvation” (no. 5). The Church, the Body of Christ, must therefore become in turn an instrument in the hands of the Word.
This is the ultimate meaning of the key concept of the conciliar Constitution: “participatio actuosa”. For the Church, this participation consists of becoming the instrument of Christ the Priest, for the purpose of participating in His Trinitarian mission. The Church actively participates in Christ’s liturgical work insofar as she is the instrument thereof. In this sense, language about the “celebrating community” has its ambiguities and requires true caution (cf. the Instruction Redemptoris sacramentum, no. 42). Therefore this “participatio actuosa” should not be understood as the need to do something. On this point the Council’s teaching has often been distorted. Instead it is a matter of letting Christ take us and associate us with His sacrifice.
Liturgical “participatio” must therefore be understood as a grace from Christ who “always associates the Church with Himself” (Sacrosanctum Concilium, 7). He is the one who has the initiative and the primacy. The Church “calls to her Lord, and through Him offers worship to the Eternal Father” (no. 7).
The priest must therefore become this instrument that allows Christ to shine through. As our Holy Father Pope Francis recalled recently, the celebrant is not the host of a show, he must not look for sympathy from the assembly by setting himself in front of it as its main speaker. To enter into the spirit of the Council means, on the contrary, to be self-effacing, to refuse to be the center of attention.
Contrary to what has sometimes been maintained, and quite in keeping with the conciliar Constitution, it is altogether appropriate, during the penitential rite, the singing of the Gloria, the orations and the Eucharistic prayer, that everyone, priest and faithful, turn together toward the East, so as to express their intention to participate in the work of worship and redemption accomplished by Christ. This way of celebrating could possibly be implemented in cathedrals, where the liturgical life must be exemplary (cf. no. 41).
Of course, there are other parts of the Mass in which the priest, acting “in persona Christi Capitis” [“in the person of Christ the Head”] enters into a nuptial dialogue with the assembly. But the only purpose of this face-to-face is to lead to a tête-À-tête with God which, through the grace of the Holy Spirit, will become a heart-to-heart conversation. The Council thus proposes other means of promoting participation: “acclamations, responses, psalmody, antiphons, and songs, as well as by actions, gestures, and bodily attitudes” (no. 30).
An over-hasty and all-too-human interpretation has led some to conclude that it was necessary to make sure that the faithful were constantly busy. The contemporary Western mentality, shaped by technology and fascinated by the media, tried to make the liturgy a work of effective, rewarding instruction. In this spirit, many have tried to make liturgical celebrations convivial. Liturgical ministers, prompted by pastoral motives, sometimes try to instruct by introducing profane, show-business elements into liturgical celebrations. Don’t we sometimes see a proliferation of testimonies, scenery and applause? They think that this will foster the participation of the faithful, whereas in fact it reduces the liturgy to a human game.
“Silence is not a virtue, noise is not a sin, it is true,” says Thomas Merton, “but the turmoil and confusion and constant noise of modern society,” or of some African Eucharistic liturgies, “are the expression of the ambiance of its greatest sins—its godlessness, its despair. A world of propaganda, of endless argument, vituperation, criticism, or simply of chatter, is a world without anything to live for…. Mass becomes racket and confusion; prayers—an exterior or interior noise” (Thomas Merton The Sign of Jonas [San Diego: Harcourt, Inc., 1953, 1981], passim).
We run the real risk of leaving no room for God in our celebrations. We fall into the temptation of the Hebrews in the desert. They sought to create for themselves a form of worship on their own scale and of their own stature, and let us not forget that they ended up prostrate before an idol, the golden calf.
It is time to start listening to the Council. The liturgy is “above all things the worship of the divine majesty” (no. 33). It has instructional value to the extent to which it is completely ordered to the glorification of God and to divine worship. Liturgy really places us in the presence of divine transcendence. True participation means renewing in ourselves that “amazement” that Saint John Paul II held in high regard (cf. Ecclesia de Eucharistia, no. 6). This sacred wonder, this joyful fear, requires our silence before the divine majesty. We often forget that sacred silence is one of the means noted by the Council for promoting participation.
If the liturgy is Christ’s work, is it necessary for the celebrant to interject his own comments? We should remember that, when the missal authorizes an intervention, this must not become a profane, human speech, a more or less subtle commentary on current events, or a worldly greeting to the persons present, but rather a very brief exhortation to enter into the mystery (cf. General Introduction of the Roman Missal, no. 50). As for the homily, in itself it is always a liturgical act that has its own rules. “Participatio actuosa” in Christ’s work presupposes that we leave the profane world so as to enter into the “sacred action surpassing all others” (Sacrosanctum Concilium, 7). In fact, “we claim somewhat arrogantly to remain in the human sphere so as to enter into the divine” (Robert Sarah, God or Nothing [San Francisco: Ignatius Press, 2015], chapter IV).
In this regard it is deplorable that the sanctuary in our churches is not a place strictly reserved for divine worship, that people enter it in worldly garb, and that the sacred space is not clearly delimited by the architecture. Since, as the Council teaches, Christ is present in His word when it is proclaimed, it is likewise harmful that lectors do not have proper attire that shows that they are not pronouncing human words but a divine word.
The liturgy is a fundamentally mystical, contemplative reality, and consequently beyond the reach of our human action; even our “participatio” is a grace from God. Therefore it presupposes on our part openness to the mystery being celebrated. Thus, the Constitution recommends the full understanding of the rites (cf. no. 34), and at the same time prescribes that “the faithful… be able to say or to sing together in Latin those parts of the Ordinary of the Mass which pertain to them” (no. 54).
Indeed, understanding the rite is not the work of unaided human reason, which would have to grasp everything, understand everything, master everything. The understanding of the sacred rites is that of the “sensus fidei”, which practices a living faith through the symbol and knows by being attuned more than through concepts. This understanding presupposes that one approaches the mystery with humility.
But will people have the courage to follow the Council this far? Such an interpretation, illuminated by the faith, is fundamental however for evangelization. Indeed, “the liturgy… shows forth the Church to those who are outside as a sign lifted up among the nations, under which the scattered children of God may be gathered together” (no. 2). It must stop being a place of disobedience to the Church’s prescriptions.
More specifically, it cannot be an occasion for divisions among Christians. Dialectical interpretations of Sacrosanctum Concilium, the hermeneutics of rupture in one direction or the other, are not the fruit of a spirit of faith. The Council did not intend to break with the liturgical forms inherited from Tradition, but rather intended to appreciate them in greater depth. The Constitution declares that “any new forms adopted should in some way grow organically from forms already existing” (no. 23).
In this regard, it is necessary that some should celebrate according to the “usus antiquior” [older usage] and should do so without any spirit of opposition, and therefore in the spirit of Sacrosanctum Concilium. Similarly, it would be a mistake to consider the Extraordinary Form of the Roman Rite as coming from some other theology which is not that of the reformed liturgy. It would also be desirable in a future edition of the Missal to insert the penitential rite and the offertory of the “usus antiquior” for the purpose of emphasizing that the two liturgical forms illuminate each other, in continuity and without opposition.
If we live in this spirit, then the liturgy will stop being a place of rivalries and critiques, so as finally to make us participate actively in that liturgy “which is celebrated in the holy city of Jerusalem toward which we journey as pilgrims, where Christ is sitting at the right hand of God, a minister of the holies and of the true tabernacle” (no. 8).
Depleted nutrient absorption. Long-term alterations in brain activity and ability to interact with the world. Changes in choice of mate. If a commonly prescribed drug has these side effects, should it really be commonly prescribed?
That was the question raised at an Aug. 8 symposium at Georgetown University in Washington, D.C. Researchers and medical professionals from across the United States and overseas gathered together to discuss the little-known risks of the birth control pill.
Entitled “Contraceptive Conundrum,” the symposium explored the consequences of hormonal birth control, many of which are unknown by women and doctors alike.
Dr. S. Craig Roberts, a researcher who specializes in mate preferences, stressed that the pill can alter the chemistry of attraction.
Under normal circumstances, he said, “women express preferences for genetically-dissimilar, masculine-faced men. But the pill seems to alter these preferences.”
“Women on the pill tend to choose male partners who appear more feminine (and who are) more genetically similar to them.”
Children born from unions of genetically similar parents may have greater health risks. Furthermore, when women come off the pill – often when they decide to have kids – they may revert to their natural attraction patterns, which their partner whom they met on the pill no longer fits.
Dr. Roberts noted that “women who met their partner when on the pill are more likely to initiate divorce.”
Women’s choice of partner while using hormonal contraception is part of a larger concern – the impact of hormones in the pill on the human brain.
According to Dr. Nicole Peterson, a researcher at UCLA’s Semel Institute for Neuroscience and Human Behavior, the full extent of this impact is not yet clear, and research is still being done. But there is already ample evidence that the pill creates changes that may make permanent alterations to brain pathways.
“In women on the pill the amygdala – memory making part of brain – responds less to emotional stimuli,” she explained.
This can have some desirable results, such as lower rates of post-traumatic stress disorder among rape victims. However, it also drastically changes how women on the pill make choices and interact with the world around them.
Even more alarming, the pill’s effects on brain wiring can still be seen at least four months after a woman has stopped using the pill.
“If a woman is on oral contraceptives for long enough, she has a different kind of brain… there’s no guarantee that your brain remembers what the baseline is,” stressed Dr. Melissa Farmer, a post-doctoral fellow at Northwestern University’s Feinberg School of Medicine.
She said that she finds the long-term nature of these brain changes particularly troubling.
Endocrine changes due to the pill can also have long-lasting effects, with consequences that last after a woman is no longer on hormonal contraception.
For example, if a woman stops taking the pill in order to become pregnant, the hormonal changes left over from the pill can affect her child.
“Very small changes in hormones in critical periods of fetal development can have lifelong consequences,” explained Dr. Frederick vom Saal, a researcher in developmental biology at the University of Missouri.
Another potentially long-term effect of the pill: nutrient depletion, which is associated with a whole host of other health problems.
“Oral contraceptives deplete nutrients more than any other kind of commonly prescribed drug,” said cancer researcher and nutritionist Ross Pelton. This includes depletions in all B vitamins, vitamin C, folic acid, zinc and several others.
While the onset tends to be gradual, these depletions can last even after the cessation of pill use, he noted. The result can be a negative impact on sexual health and increase risk for other problems, including heart issues.
With such serious potential side effects, some symposium participants questioned the widespread, almost automatic use of hormonal birth control.
Dr. Stacy Trasancos, PhD
http://www.catholicstand.com
Recently the investigative journalism conducted by David Daleiden who started the Center for Medical Progress has provided a raw look into the minds of the people involved in the “human capital” abortion industry. As the videos continue to come out and lawsuits are filed threatening to suppress free speech and journalism, perhaps this is a good time to look more broadly at the sale and use of aborted fetuses in scientific research.
One does not need to conduct an undercover investigation to discover “human capital.” The facts are in the academic record, and they offer cold hard evidence that what Daleiden is revealing is not only true, but spans far, deep, and wide across time and locale.
The following information is just one example pieced together to demonstrate how ingrained this type of research is in the global scientific and industrial communities. Scientists are expected to provide meticulous accounts of their work for the sake of reproducibility and posterity. The language is thus very technical. Knowing how to read scientific literature means knowing how to decipher the scientific language. Please note: Because of the detail, however, the information in this case is also disturbing.
Let’s step through the facts.
Fetuses Presented a Special Test Case
In 1972, Pediatric Research journal published a paper submitted by researchers from the Department of Pediatric Research at New York State and Mount Sinai School of Medicine of the City University of New York in collaboration with a researcher from the Departments of Medical Chemistry and Obstetrics and Gynecology of the University of Helsinki in Finland. The paper was titled, “Development of Mammalian Sulfur Metabolism: Absence of Cystathionase in Human Fetal Tissues.” The fact that they used fetuses is stated right in the title. The researchers “examined the development of the transsulfuration pathway in 58 human fetuses obtained at therapeutic abortion during approximately the 2nd-6th month of gestation” as well as in premature and full term infants who died shortly after birth. They were trying to determine whether cysteine is an essential amino acid in “immature humans,” so they needed to analyze kidneys and brains at different developmental stages.
The fetuses presented a special test case. Since the fetuses were still alive at the beginning of the experiment in their mothers’ wombs, “in vivo” experiments were possible. This phrase “in vivo” is Latin and means “within the living.” With already deceased specimens, they could only measure the presence of amino acids after death. This type of analysis is an “in vitro” (in the glass, think in vitro fertilization) procedure. With the still-living fetuses, they could actually inject a known amount of amino acids, S-L-methionine and S-L-cysteine, “in vivo” into a living fetus and test how much of these substances were incorporated into fetal organs via the biological machinery of life over a set amount of time. The researchers therefore conducted the “in vivo” experiments by surgically cutting open the uterus of the mother, lifting out the living fetus with the umbilical cord still attached, and injecting the amino acids into the umbilical vein.
Then they waited 10 minutes with the heart still beating and the fetus still moving to allow the body to distribute and metabolize the amino acids. After 10 minutes, they cut the umbilical cord, dissected the brain and liver from the body of the fetus, and dropped the organs into liquid nitrogen to await analysis.
Here is the relevant description from the Methods and Materials section:
For “in vivo” experiments, each fetus immediately after removal from the uterus was injected with approximately 100 uCi of either 35S-L-methionine (specific activity 515 mCi/mmole) or 35S-L-cysteine (specific activity 31.3 mCi/mmole) contained in 0.5 ml of a 0.9% solution of NaCl at pH 7.0. In some experiments, unlabeled cysteine (2.0 /xmoles L-cysteine in 0.2 ml 0.9% NaCl, pH 7.0) as well as 35S-L-methionine were injected. All injections were made into the umbilical vein through a short Teflon catheter which was then rinsed with 0.2 ml 0.9% NaCl; the whole cord was clamped on the fetal side of the point of entry of the catheter to prevent blood loss during the experiment. After 10 min (elsewhere in the paper, “in all cases the heart continued to beat during the 10-min period and spontaneous movement was seen”), the cord was severed close to the fetus, and as much blood as possible was collected into a tube which contained heparin as anticoagulant. The fetal organs were quickly removed and dropped into liquid nitrogen.
The research was funded by the Lalor Foundation in Boston, Massachusetts, the New York State Department of Mental Hygiene, and the Association for Aid of Crippled Children also in New York. The abortions appear to have been done at the Central University Hospital and Borja Womens Hospital in Helsinki, Finland because an end note offers thanks to the staffs there. A shorter communication of this work was also published in Science journal, “Absence of Cystathionase in Human Fetal Liver: Is Cystine Essential?” Science journal is arguably the most prestigious journal to have your work published in because it is not specialized in any one area and only publishes the best work across all scientific disciplines. The Mothers and Hysterotomies
Among the details in the paper was the anesthesia procedure for the women. “Preoperative medications included Pethidine, 50-75 mg; Phenergan, 25 mg; and atropine, 0.5-0.8 mg intramuscularly. Anaesthesia was induced with 250-440 mg Pentothal intravenously and was maintained with N2O2.”
Not all the details regarding the women were recorded though. According to the Pediatric Research paper, the “mothers” (the authors called them “mothers”) were in good health but sought abortion for “social or psychological reasons.” The “mothers” apparently agreed to undergo “hysterotomies,” which seems odd. A hysterotomy is a surgery where an incision is made in the uterus, usually done for Cesarean birth or fetal surgery. A hysterotomy is a much more invasive procedure than a suction-aspiration procedure, which was certainly available in the 1970’s. Safe abortions (for the mother) are ones that reduce the risk of perforating the uterus as much as possible and reduce the risk of infection. It does not make sense to unnecessarily cut open the uterus and leave it open for an extended period of time if the safety of the mother is the first concern.
The research paper did not mention whether the mothers gave consent or were informed of the procedure. One might wonder if the mothers were told that, while they were unconscious with their abdomens laid open, their unwanted children were used as living biological machines in the only 10 minutes they would live outside the womb. It is hard to imagine that any woman would agree to such an experiment regardless of how much she did not want to be pregnant or raise a child.
Fetuses And Infant Formula
The goal of this 1972 paper was to demonstrate that cysteine is an essential amino acid in human fetuses and in infants for some time after birth. The end use of this work was to provide information about feeding newborns. In the conclusion, the authors noted that “infants of low birth weight who are fed a formula with the same quality of protein as that in human milk should grow as well.” (Proteins are large biomolecules made of long chains of amino acids.) The experiment was part of a broader set of experiments to understand the kind of protein newborns need to be fed in milk formulas. By understanding the differences in how fetuses process amino acids compared to infants and children, the researchers sought to better design infant formula especially for prematurely born infants.
The two researchers from the New York, John A. Sturman and Gerald E. Gaull, continued their work in the coming years using fetal brains, sometimes whole. Their work was funded, in part, by the National Institute of Health Clinical Genetics Grant and the New York State Department of Mental Hygiene. In 1974, they published “Polyamine Biosynthesis in Human Fetal Liver and Brain” in Pediatric Research. In that study they used many of the same samples used in the previous study. Their interests were neurological.
The Finnish researcher who was interested in infant nutrition, Niels C. R. Räihä, published “Phenylalanine Hydoxylase in Human Liver during Development” in 1973 using the livers of 18 human fetuses from 2nd-6th month of gestation. Räihä continued his work until 1985, collaborating with 55 other co-authors from around the world and publishing some 41 papers, according to internet sources.
In 1993, Räihä served as Editor of the proceedings from the Nestlé Nutrition Workshop Series held that year in South Africa by the Nestlé Corporation. The collection of chapters, which was published in 1994 and titled Protein Metabolism During Infancy (Nestle Nutrition Workshop Series: Pediatric Program), reviewed the “protein requirements of low-birthweight, very-low-birthweight, and small-for-gestational-age infants and the essential amino acid requirements of infants with inborn errors of metabolism.” The book also focused on the quality of protein in human milk and formulas, the digestibility and absorption of protein in infants, and the role of essential and nonessential amino acids in neonatal nutrition. Hence, the experimental procedures describe above have a connection to the Nestlé Corporation and development of infant formula.
Fetuses: The Value Chain Is Much Larger
If the language of the Planned Parenthood and biotech executives discussing the demand for fetal body parts over wine and salad for lunch is disgusting, perhaps one will find the experimental methods tied to the history of the development of infant formula equally, if not more so, disgusting. These facts have been in the academic record for over 40 years. Was there no outcry? No controversy? What? Did people just trust the academics blindly? I do not know. A million questions can be asked about why anyone thought this kind of research was remotely acceptable. Yet, here we are in 2015 in shock as if all of this behavior began overnight, speculating about whether it is all really true or not. It is true. Those “in vivo” experimental procedures are not speculation, indication, or accusation. They are as true as if the researchers confessed the activities to the public in their own handwriting—because they did.
If the published works in refereed journals are to be believed, then abortion clinics have indeed provided whole live fetuses for research, even live ones handed over to be used, killed, and dissected as a part of an experiment that feeds an industry. Apparently for decades the use of fetal material has been a research tactic that is 1) considered ethical and legal, 2) coordinated across continents if necessary, 3) funded by governments and private foundations, 4) demanded by industry, and 5) applauded by the scientific community. Planned Parenthood could shut down completely tomorrow, but the use of aborted fetuses and fetal body parts will not stop.
The value-chain, so to speak, is much longer and affects more aspects of modern life than any of us may yet realize, and Planned Parenthood is but one link. Again, this is only one example. There is more. So while the Center for Medical Progress continues to expose Planned Parenthood’s involvement, I will continue to back it up by exposing what is in the scientific literature.
Black pastors are asking the Smithsonian to remove Sanger from its “Champions of Justice” exhibit
by Miles Swigart
NORFOLK, August 10, 2015 (ChurchMilitant.com) – Black pastors are demanding the Smithsonian Museum remove a bust of Margaret Sanger.
The display is part of the museum’s “Struggle for Justice” exhibit, which features various historical figures considered champions of justice. The group of pastors, known as Ministers Taking a Stand (MTS), said in their letter to the museum that Margaret Sanger was a racist and eugenicist who is on record as saying she desired the extermination of “the Negro population.” Part of her plan was to contracept, sterilize and abort them out of existence, and the ministers claim these plans are still being carried out to this day.
“Perhaps the Gallery is unaware that Ms. Sanger supported black eugenics, a racist attitude toward black and other minority babies, an elitist attitude toward those she regarded as ‘the feeble-minded’; speaking at a rally of Ku Klux Klan women; and communications with Hitler sympathizers,” the letter states.
The letter mentions the recent Planned Parenthood exposés showing high-level employees trafficking in the sale of aborted babies’ organs, saying, “The fact is that the behavior of these abortionists, their callous and cavalier attitude toward these babies, is completely in keeping with Sanger’s perverse vision for America.”
The letter also links to a map showing that 70 percent of Planned Parenthood clinics are in minority neighborhoods in order to provide evidence that Planned Parenthood is targeting minorities.
During her life, Margaret Sanger was an outspoken proponent of the eugenics movement, calling for the forced government sterilization of black people and those deemed unfit for reproduction. The pastors cited a letter written by Sanger that stated, “We do not want word to get out that we want to exterminate the Negro population and the minister is the man who can straighten out the idea if it ever occurs to any of their more rebellious members.”
It seems Sanger’s vision is coming to fruition: A recent study revealed that more African American babies in New York City are being aborted than born. And nationwide, although African American women comprise only 13 percent of the population, they comprise nearly 40 percent of all U.S. abortions.
The dark history of racial population politics and eugenics that led to federal funding of Sanger’s organization is undeniable, and these pastors are insulted that the bust of Margaret Sanger is being housed in the same room as black civil rights leaders like Malcolm X and Martin Luther King, Jr. “How can a person like Sanger, who found common cause with the racial agenda of the Ku Klux Klan, be ranked among true champions of ‘justice’?”
From diversified revenue streams to intact late-term fetal cadavers, Planned Parenthood says, “We can make that happen.”
By Cheryl Sullenger
Houston, TX — A fifth video was released today by the Center for Medical Progress, this one discussing Planned Parenthood’s willingness alter abortion procedures to procure intact late-term aborted fetal cadavers form babies that could have been born alive. This information adds a shocking new layer of insight into Planned Parenthood’s participation in the illegal sale of fetal body parts.
Today’s video focuses on Planned Parenthood’s Center for Choice Surgical Center, located on Gulf Freeway in Houston, Texas.
CMP actors posing as representatives of an organ procurement company engaged in conversation with Melisa Farrell, Planned Parenthood’s Director of Research, who explained that abortion procedures are being altered to produce “intact specimens” when orders require it. “We can make that happen,” she said.
The discussion centered on the desire for aborted baby remains, particularly intact cadavers that were in the 16 to 22 week range. If such babies were birthed intact, the possibility exists that they could be born alive during the abortions, which is illegal.
“And we have had studies in which the company, and or in this case, investigator, has a specific need for certain portions of the parts of conception and we base that into our contract and our protocol that we follow this, so we deviate from our standard in order to do that,” Farrell said, (emphasis added).
Altering a medical procedure to ensure organs are better suited for harvesting is illegal. It is also dangerous. If a woman were to be injured or die during a procedure that was altered to ensure marketable organs, it would be grossly unethical and would represent huge liabilities to Planned Parenthood.
The Houston Planned Parenthood facility has been the site of multiple documented medical emergencies, including four incidents in less than 30 days that took place in January and February, 2015. Operation Rescue obtained 911 records that show a February 6 medical emergency involved a patient with a ruptured uterus during an abortion that required emergency transport to a nearby hospital.
“Whether any of those injuries were done during altered abortions is a matter for investigators to determine,” said Newman.
The Houston Planned Parenthood employs six abortion providers that do abortions “beyond 16 weeks.” The “buyers” were reassured that the abortionists have experience conducting abortion procedures “in a way that they get the best specimens, so we know that can happen,” according to XXX.
In a startling revelation, Farrell mentioned that Planned Parenthood abortion providers in Houston have been personally engaged in their own experiments using fetal body parts from abortions they perform. In addition, Farrell shared that research group wanted Planned Parenthood to provide a large amount of fetal tissue. In this case, the research lab was requesting 120 samples, including brain, thymus, liver, spleen, femur, bone marrow, and stem cells from 14 to 22 weeks gestation. The conclusion was reached that intact fetal cadavers were preferred for sale to the lab since so much of the body was required.
“The admission that Planned Parenthood abortionists manipulate procedures in order to better harvest organs or even late-term intact fetal cadavers for human experimentation purposes conjures images of H.G. Wells’ Dr. Moreau. It is all clearly illegal,” said Troy Newman, President of Operation Rescue. “Are ethical standards adhered to during these private experiments? Given Planned Parenthood’s propensity for unethical, above-the-law arrogance, it is doubtful.”
Newman also serves on the Board of the Center for Medical Progress, and acted in an advisory capacity during the nearly three-year long investigation.
Farrell’s contribution to the Planned Parenthood organization, both locally and nationally is “diversification of the revenue stream.” She goes on to agree that organ procurement can be a “gold mine” that financially benefits her clinic.
“I’m glad that you have that background so you can see the financial benefits,” noted one of the “buyers” as the Planned Parenthood executive nodded her head continually in agreement.
“I think everyone realizes, especially because my department contributes so much to the bottom line of our organization here, even though we are one of the largest affiliates, our research department is the largest in the United States, larger than any of the other affiliates combined,” Farrell said.
“Yeah, so if we alter a process and we are able to obtain intact fetal cadavers, then we can make it part of the budget, that any dissections are this, and spitting the specimens into different shipments is this, I mean, that’s – it’s all just a matter of line items.” The scene shifts to the “POC Room” where the fetal remains, also known as the ‘products of conception’ are sorted and stored in a freezer or simply comingled in a large biohazard bag for later collection and incineration.
One technician produced from a freezer a bag of remains from an 18-20 week old fetus that was aborted earlier that day. She poured the tissue in a colander and rinsed it, then dumped the chunky lumps of flesh into a glass pan.
There, the baby’s dismembered remains were inspected. Arms with hands attached and legs with feet were clearly observed, as well as eyeballs still within the orbital pockets.
The abortionist lifted a drippy clump, noting that this was the intestines.
Planned Parenthood employees at the Houston clinic packaged the specimens for shipment, which was a different procedure that at other Planned Parenthood affiliates where organ procurement technicians employed by biotech companies usually do that work.
The abortionist and Farrell discussed an upcoming National Abortion Federation meeting where Planned Parenthood Medical Director Deborah Nucatola was to present on the varying laws on fetal tissue procurement from state to state. Another Planned Parenthood abortion provider was set to present on “fetal collection,” they said.
“This information implicates the National Abortion Federation in the illegal selling of fetal organs,” said Newman.
Evidence of alleged NAF involvement comes one day after a San Francisco judge extended a temporary restraining order on videos taken during secretive NAF national meetings, citing NAF’s arguments that their meetings are confidential and attendees must sign non-disclosure agreements.
“The NAF knows that if the public understood what really is discussed behind closed doors that there is no public relations firm in existence that could spin that in a favorable light. In order for abortion to continue, the veil of secrecy that conceals horrifying acts from the public must be maintained at any cost,” said Newman, who was named in the suit along with the Center for Medical Progress and its Director, David Daleiden. “We will continue to fight to protect our Freedom of Speech and Freedom of the Press. The truth will ultimately come out, no matter how hard the Abortion Cartel tries to hide it.”
Planned Parenthood is under fire for organ trafficking admissions made by its senior executives in a series of undercover videos released over the last month. The videos, four of which have been released so far, show numerous top Planned Parenthood officials acknowledging the purchase and sale of aborted baby parts and haggling over their prices.
Planned Parenthood, the nation’s top abortion provider, swears up and down that notwithstanding the numerous admissions made on tape by its top officials, the organization doesn’t buy or sell organs and body parts harvested from aborted babies. Then, in order to defend its reputation, Planned Parenthood points to other medical procedures performed by the group that don’t result in body counts. One of its top rhetorical gimmicks is to reference all the mammograms that women can receive by visiting Planned Parenthood:
Planned Parenthood helps women nationwide get access to mammograms, as part of the range of health care Planned Parenthood health centers provide to nearly three million people a year.
There’s only one problem: Planned Parenthood does not manage a single licensed mammography facility in the U.S. Not one. Of the 8,735 licensed mammography facilities in America, Planned Parenthood operates exactly zero.
How do we know this? Because the U.S. Food and Drug Administration keeps a list of every licensed facility in the country. It updates this list weekly. And the most recent list of the more than 8,700 licensed mammogram facilities in the U.S. shows that not one is operated by Planned Parenthood. The following graphic from Alliance Defending Freedom shows just how little breast cancer screening is done by Planned Parenthood, especially compared to other non-abortion providers throughout the country:
Planned Parenthood has even intimated that if its spigot of federal funding is turned off, women will have nowhere to turn for vital health care and cancer screenings. But that’s also a lie, as Mollie Hemingway explains. It turns out that Planned Parenthood only qualifies as the nation’s largest health care provider for women if you think abortion — the deliberate taking of an innocent human life — counts as health care.
SENATOR MARCO RUBIO AUG 3, 2015 | 9:19AM WASHINGTON, DC
As Americans we live in a nation founded on the idea that our rights and freedoms are God-given and that government’s fundamental role is to protect them. But our government today falls tragically short of this duty by failing to protect the rights of the most defenseless in our society: unborn children. Each year, over half a billion dollars in taxpayer money is given to Planned Parenthood, an organization responsible for over 300,000 abortions each year. While the provision of taxpayer money to such an organization has drawn its share of criticism over the years, the most recent revelations of Planned Parenthood’s actions reveal a new low for the organization.
Millions of Americans, myself included, have been outraged by the recently released videos showing Planned Parenthood officials matter of factly describing the harvesting and sale of limbs and organs from unborn babies in graphic detail and with a callous and cruel disregard for human life. The videos also raise serious questions about potentially criminal and unethical practices at Planned Parenthood clinics. The videos clearly indicate that these practices are not contained, but endemic to the organization.
SIGN THE PETITION! Congress Must De-Fund Planned
Parenthood Immediately http://www.gopetition.com/petitions/congress-must-de-fund-planned-parenthood-immediately.html It should be noted that Planned Parenthood’s callousness does not extend merely to the unborn. The videos also reveal that Planned Parenthood views the women that they purport to serve as nothing more than profit centers for their macabre business. One of the videos shows a senior Planned Parenthood official speaking casually about the tactics she employs in order to deceive patients so that their unborn children can be better utilized for organ and limb harvesting. This is a violation of the rights of their patients. The videos are tough to watch and tough to fathom, especially for parents. It’s not something any of us want to have to discuss. And yet like many other uncomfortable topics confronting our nation, we have an obligation to not avert our eyes.
There is more than enough evidence to push forward with a serious and independent investigation into Planned Parenthood and its practices, like Governor Rick Scott has called for in our home state of Florida. I have asked the Secretary of Health and Human Services to do, but am not holding my breath for the Obama Administration to act. Congress should bring Planned Parenthood’s senior officials to testify under oath before the American people.
There can be no denying that Planned Parenthood is a morally bankrupt organization. Americans of conscience might disagree on the legality of abortion. It is a contentious issue that elicits deep passions. But as a country, we should at least be able to find common ground on acknowledging and respecting the humanity and basic dignity of both the mother and the unborn child. It is clear from the videos that Planned Parenthood long ago stopped acknowledging either. At Planned Parenthood, women are treated as paying clients, not patients. Unborn children are treated as cells and tissues, not human beings. The organs and limbs of babies are treated as commodities, for sale to the highest bidder on an open market. And taxpayers are forced to fund this.
There are countless organizations in America that provide health care, including reproductive health care, to women in need. None of them receive the undeserved political protection and taxpayer funding from the federal government that Planned Parenthood has enjoyed for decades. A purported health care organization that has allowed itself to become this callous and dismissive of the human dignity of their patients and unborn life cannot be redeemed. We must defund Planned Parenthood and make sure that taxpayer dollars are never spent on abortions or organizations that demonstrate such a callous disregard for basic human dignity. America is the freest and most powerful nation on earth, and we have done more to advance the rights of all human beings in our brief history than any society before or since. The Planned Parenthood videos, and the behavior and culture they reveal, are anathema to our very identity as a nation and run counter to the great sacrifices generations of Americans have made in the defense of human dignity here and abroad. We cannot fulfill our promise as a nation by simply turning the other way when we are confronted with difficult realities. Planned Parenthood should never receive another dime from American taxpayers.
LifeNews Note: This exclusive column is written by Senator Marco Rubio, a pro-life Florida Republican and presidential candidate.
Urgent: Sign the petition urging Congress to investigate and defund Planned Parenthood. Click here.
WASHINGTON, D.C., August 3, 2015 (LifeSiteNews) — Pro-life activists are urging moderate Democrats and Republicans in the Senate to vote to eliminate federal funding for Planned Parenthood in the vote scheduled for Monday night.
But even their support may not be enough to ensure that the measure passes, with nearly all Democrats opposed to S.1881 and a veto promised by President Obama. A defunding bill would require 60 votes in the Senate for passage, and 66 to override a veto.
Pressure from the pro-life movement to defund Planned Parenthood has intensified in light of the release of four videos showing senior Planned Parenthood officials describing how the organization harvests fetal parts, and illegally modifies abortions to guarantee the receipt of fetal parts.
Three committees are investigating Planned Parenthood, but pro-life Members of Congress and their allies are pushing for Congress to defund Planned Parenthood before the investigations are complete.
Despite the videos and intense pressure from pro-life groups, several of the Senate’s 54 Republicans are expected to not support S. 1881, which has the backing of GOP leadership and some of the pro-life community’s top senators.
Senators Lisa Murkowski of Alaska has remained silent — her office told LifeSiteNews that a statement would be released at approximately the same time as tonight’s vote — and Susan Collins of Maine, and Mark Kirk of Illinois have expressed outright opposition to defunding Planned Parenthood.
Murkowski supported federal funding for Planned Parenthood in 2011, the last time the issue was front-and-center in Congress.
On the Democratic side, Senators Joe Donnelly of Indiana, Bob Casey of Pennsylvania, and North Dakota’s Heidi Heitkamp are targets for pro-life pressure.
Also on the original target list was Senator Joe Manchin of West Virginia, who has since confirmed that he will support the defunding measure.
A pro-life leader told LifeSiteNews that “the seven targets are ‘swing’ votes who we think are most gettable. Of course, all 100 Senators need pressure. But the seven laid out are either on the fence or close to it.”
Five of the seven Senators are unlikely to vote to defund, said the activist. “We are not going to get 60 votes on this. Right now, I think our floor is 50 and our ceiling is 54 [votes]. The two who are the real wild cards are Donnelly and Murkowski.”
“But keep in mind that last time we had a vote on this in the Senate in 2011, we only got 42 votes. So if we can get to 51, it’s a victory in that the majority of the U.S. Senate voted to defund PP.”
Some pro-lifers are frustrated that the GOP-controlled Senate did not include the defunding legislation in a “must-pass” bill, such as the transportation bill that passed the Senate. The theory is that this would put pressure on Democrats to pass the bigger bill in order to keep parts of the government funded.
This was a strategy implemented in 2011, when the new GOP majority in the House wanted to defund Planned Parenthood in a Continuing Resolution to keep the government running. That effort failed when President Obama called the GOP’s bluff, joining Senate Democrats in being willing to shut down the government in order to keep Planned Parenthood’s funding intact.
The pro-life activist told LifeSiteNews that a similar strategy is under discussion for the new effort to defund Planned Parenthood. “There is already talk about defunding [Planned Parenthood] being a major issue in the [Continuing Resolution]. So I don’t see stand-alone versus must-pass an either/or. We can do both.”
Donnelly’s office said that it was unlikely that the senator, who supports a congressional investigation of Planned Parenthood, would be releasing further statements today on where he will vote tonight.
Senator Joe Manchin put out a statement today affirming that he would support the measure.
“Like many West Virginians, I am very troubled by the callous behavior of Planned Parenthood staff in recently released videos, which casually discuss the sale, possibly for profit, of fetal tissue after an abortion,” he said in a statement.
“Until these allegations have been answered and resolved, I do not believe that taxpayer money should be used to fund this organization; instead those funds should be sent to other health care providers, including community health centers, which provide important women’s healthcare services. While my vote is one that will prevent taxpayers dollars from going to Planned Parenthood, I will remain committed to ensuring that all women in West Virginia and America receive the health care services they need.”
Last week, Manchin and Collins said they were working on legislation that could defund only Planned Parenthood clinics that engage in fetal harvesting. Collins told National Journal she was worried about health access for women.
The bill currently before the full Senate, which was introduced by Senator Joni Ernst of Iowa, would shift Planned Parenthood funding to other providers.
July 30, 2015 (LifeSiteNews) – Workers in a lab are seen sorting through body parts on a dish: a heart, stomach, kidney, and legs.
And then a medical assistant suddenly announces: “It’s another boy!”
This is just a little of the macabre and heart-wrenching footage in the newest undercover video showing alleged harvesting and sale of body parts from aborted babies by Planned Parenthood, released Thursday morning.
The newest video also shows a Planned Parenthood medical director negotiating a fetal body parts deal while agreeing to prices for harvested parts, and suggesting ways to avoid legal consequences.
“For anyone with a conscience, the video’s entire fetal organ scene is wrenching — to the gut as well as the heart. It hearkens us back to the days of Joseph Mengele or Kermit Gosnell, who both coldly killed and dissected children without remorse,” said Operation Rescue President Troy Newman, in a press release.
The video takes the viewer into Planned Parenthood of the Rocky Mountains, where Vice President and Medical Director Dr. Savita Ginde discusses with actors posing as representatives from a human biologics company a potential partnership to harvest fetal organs.
When one of the actors posing as a buyer asks the doctor if “compensation could be specific to the specimen?” Ginde agrees. As the camera travels to the abortion clinic’s pathological laboratory to reveal the aftermath of a real abortion of a baby boy, Ginde tells the buyer that the abortion clinic would rather receive payment per body part harvested, rather than a standard flat fee for the entire case.
“I think a per-item thing works a little better, just because we can see how much we can get out of it,” she is heard saying on the video.
Planned Parenthood hit national headlines last month after undercover videos released by the pro-life group Center for Medical Progress (CMP) showed top officials
from the nation’s largest abortion provider discussing the sale of body parts harvested from babies aborted at their facilities. Those behind the undercover videos say that selling the body parts for profit is a violation of federal law.
Yesterday, the California Superior Court issued a narrow temporary restraining order preventing CMP from releasing further undercover video footage involving top-level staff of StemExpress, the company that purchases the body parts from Planned Parenthood.
Project Lead David Daleiden is using the fourth video to call for an immediate ending to Planned Parenthood’s funding.
“Elected officials need to listen to the public outcry for an immediate moratorium on Planned Parenthood’s taxpayer funding while the 10 state investigations and 3
Congressional committees determine the full extent of Planned Parenthood’s sale of baby parts.”
“Planned Parenthood’s recent call for the NIH to convene an expert panel to ‘study’ fetal experimentation is absurd after suggestions from Planned Parenthood’s Dr. Ginde that ‘research’ can be used as a catch-all to cover-up baby parts sales. The biggest problem is bad actors like Planned Parenthood who hold themselves above the law in order to harvest and make money off of aborted fetal brains, hearts, and livers,” he said.
On CNN this morning (3 August 15), Center for Medical Progress leader David Daleiden explained exactly why StemExpress is seeking to block release of secretly recorded video from a meeting he had with its top executives in May:
“In a meeting with their top leadership where their leadership admitted that they sometimes get fully intact fetuses shipped to their laboratory from the abortion clinics they work with, and that could be prima facie evidence of born alive infants. And so that’s why they’re trying to suppress that videotape and they’re very scared of it.”
WASHINGTON, D.C. – A long decline in the percentage of American teens who are sexually active has leveled off, and an increasing number of teen girls are using the morning after birth control pill on a regular basis, according to the findings of a recently published study.
None of that surprises Valerie Huber, president and CEO of the National Abstinence Education Association.
She says sex education in public schools in recent years has been focused on the assumption that all or most kids are sexually active, which puts pressure on more teens to meet that expectation.
That drowns out the main message students should be hearing – that the best way to avoid pregnancy and sexually transmitted disease is to put sex on hold during the middle school and high school years, Huber said.
“The recent stall in declines is precisely correlated to the Obama administration’s change in the kind of sex education being given to America’s youth,” Huber wrote to EAGnews in an email.
“A real emphasis should be renewed on sexual delay because it removes all the possible consequences of teen sex, including those that are not the ones people usually think of – pregnancy and STDs. Teens could greatly benefit from messages reinforcing the healthiest choice of waiting for sex.”
Huber was reacting to a new survey on teen sex from the Centers for Disease Control and Prevention. The survey is based on interviews with about 2,000 teens between the ages of 15 and 19, conducted between 2011 and 2013.
The survey revealed that 1 in 5 sexually active teen girls have used the morning-after pill, which was a huge increase from 10 years ago, when the statistic was 1 on 12, according to a news report from the Associated Press.
The most obvious reason for the increase is that the morning-after pill is now obtainable for girls and women of all ages, without a prescription.
Huber cited a lot of facts about the morning-after pill, and she wonders if the many teens who use it are aware of the potential pratfalls.
“Do teens think they are ‘safe’ as long as they use the morning after pill?” Huber wrote. “Do they know that Plan B offers NO protection against the epidemic of sexually transmitted diseases among young adults?
“Do they think that if they use emergency contraceptions, they are protected from pregnancy? A March, 2015 Princeton meta-analysis showed EC has effectiveness ranging from 62-85 percent, which is far from 100 percent.
“Do they know that if they have a high body mass index, EC may have a decreased or no effect on preventing pregnancy?
“Do they know that the CDC and EC providers warn that Plan B is not intended for use as a routine form of birth control and should not be used in this manner?”
The CDC report also showed that there is no statistical change in the percentage of teens who are sexually active, compared to a decade ago, the news report said. About 45 percent of boys and girls who participated in the study reported being sexually active.
The percentage of teens who were sexually active dropped steadily between the late 1980s and early 2000, but that trend appears to have ended.
Today’s “comprehensive” sex education is responsible for the new wave of sexual activity, according to Huber.
“Is it any surprise that when the predominant message is ‘have sex but use contraception’ that we are beginning to see sexual delay is stalled and even slightly decreasing and multiple partners in teens are increasing?” she wrote.
“Rather than normalizing teen sex, our sex education should promote information and skills that promote optimal sexual health. That means normalizing teen sexual delay.”
Undercover investigators in recent weeks have added to the evidence that we already had that the abortion industry, and Planned Parenthood in particular, sells the body parts of the babies it kills
As one of those who is close to this project through my partnership with Operation Rescue, and who knows the key players in this investigation, I have been asked by some reporters whether these videos represent a new strategy that replaces for the pro-life movement some of the older strategies like showing graphic pictures of aborted babies.
My answer: not at all. On the contrary, these videos fit into a coherent strategy that I and other pro-life leaders have taught for decades and that is rooted in the history of social reform: social injustices thrive when they are hidden; therefore, you expose them.
Planned Parenthood sells baby body parts. That is undeniable, and Congress as well as the individual states will now play their role in investigating the extent to which Planned Parenthood has broken the law. But whatever direction those investigations take, another investigation has also begun: the American people are being given a chance to look abortion in the eye.
I have always said that America will not reject abortion until America sees abortion. The abortion debate is too abstract; words lose their meaning, and an abundance of words can justify anything.
But when instead of abstract philosophical and legal debates about freedom, choice, and the Constitution, you talk about selling hearts, livers and brains, or see the pictures of them, you cut through the rationalizations and confront the reality of the injustice. That is exactly how the anti-slavery movement, the child labor reform movement, and the civil rights movement accomplished their goals.
It is how the pro-life movement will accomplish its goal, too. Expose abortion.
This is done in three distinct ways, in which the undercover videos fit in two places.
The first way we expose abortion is through images and descriptions of the procedure itself and what it does to the baby. Read articles and speeches defending abortion, and you will practically never read any description of the procedure. You will hear about choice and rights, but not about the body parts. But when the procedure is exposed in all its gory details, defending the practice becomes virtually impossible.
The second way to expose abortion is to expose what it does to those who undergo the procedure. The testimonies of mothers who have aborted their children reveal the devastation it brings to them — the suicidal thoughts and actions, the despair and loss of self-esteem, the nightmares and broken relationships, and more. When people hear these testimonies, as shared, for instance, through our Silent No More Campaign, they see abortion exposed — not as a solution to a problem, but as an action that creates more problems.
The third way we expose abortion is by lifting the veil from the abortion clinics themselves and looking at how corrupt the abortion industry is. This is accomplished in three ways: through dialogue with practicing abortionists and clinic workers, through the testimony of former abortionists and clinic workers, and through undercover conversations, recordings, and videos.
There is a distinction between two different groups of abortion advocates, the propagandists on the one hand and the practitioners on the other. The practitioners see the women crying and screaming. They deal with the bloody parts of little babies. They cope with the literal stench of death.
Of the two groups, the propagandists succeed more readily in the rationalizing necessary to support legal abortion. The reason is simple: they don’t see abortions. Nor do they deal with devastating results for child and parents. The practitioners, on the other hand, see the concrete evidence every day, and it is harder for them to deny. That is why they are more willing to talk with us on the pro-life side. They know we see what they see.
But for the propagandists things are a lot cleaner and simpler: they send out press releases; hold press conferences; prepare reports in cushy offices; and talk about freedom, rights, and choices. One thing the propagandists rarely discuss, however, is what an abortion actually is. For them it’s about viewpoints, not victims; it’s about beliefs, not bloodshed.
We are living in a world proud to turn a blind eye to the obvious. That great blind spot in our culture covers the children in the womb. Our mission is to shine light on that darkness.
One of the most helpful words in the English language is empathy, the feeling that we understand and share another person’s experiences and emotions. William Wilberforce, the catalyst in Britain’s abolition of the slave trade, gave the “Abolition Speech” to Parliament in 1789, and in that speech revealed a human imperative that took hold of him and made his commitment to abolition absolute:
As soon as ever I had arrived thus far in my investigation of the slave trade, I confess to you sir, so enormous, so dreadful, so irremediable did its wickedness appear that my own mind was completely made up for the abolition. A trade founded in iniquity, and carried on as this was, must be abolished, let the policy be what it might, let the consequences be what they would, I from this time determined that I would never rest till I had effected its abolition.
Observe how Wilberforce’s commitment is rooted not in some abstract “nuance,” but in a concrete, human connection with the victims. This connection did not lead Wilberforce to despair but rather a determination that he “would never rest.”
Exposing abortion leads to that same determination to stop its damaging effects. The undercover videos do not replace that strategy; they embody it.
Our Lord and His Blessed Mother Mary visited with Precious Blood Sister Mary Ephrem on several occasions from the 1940s until at least 1959 and probably until Sister’s death in 2000. Mary identified herself as the Immaculate Conception, and also as “Our Lady of America, the Immaculate Virgin”.
On September 25th, 1956, Our Lady promised that greater miracles than those granted at Lourdes and Fatima would be granted here in America, the United States in particular, if we would do as she desires. Our Lady indicated that this promise was not for miracles of the body, but of the soul. The following morning, Mary spoke ‘very solemnly and distinctly’: “I am Our Lady of America. I desire that my children honor me, especially by the purity of their lives.”
“Our Lady made three requests:
* That a medal be cast that bore her image as Our Lady of America, with these words around it: “By your Holy and Immaculate Conception, O Mary, deliver us from evil.” The Coat of Arms of the Christian Family is on the other side of the medal and includes a representation of the Divine Indwelling.
* That a statue be made according to the description she gave to Sister Mary Ephrem, and
* That this statue be placed, after being solemnly carried in procession, in the Shrine of The Immaculate Conception in Washington, DC. She wishes to be honored there in a special way as Our Lady of America, the Immaculate Virgin. (Nov 15, 1956)
Her first two requests have been accomplished and her statue is very near to the Shrine. Her third request-made over 58 years ago-has still not been granted. In three separate messages during 1959 (February, July, and December), Our Lady made it clear that she had run out of patience and could no longer stop the persecution that Her Son promised if her requests were not granted.
Could it be that the threatened persecution actually began the following year-1960-with the introduction of the revolutionary Birth Control Pill?1 Can this persecution be stopped by granting Mary’s third request?
Pope Francis will be at the Shrine of the Immaculate Conception on Wednesday September 23rd to canonize Fr Junipero Serra.
This may be a graced opportunity for having Our Lady’s remaining request granted. You can help make that happen by writing to Pope Francis.
Here is how to do that.
Ask Pope Francis to Advocate for, and Join in, that Solemn Procession
Write a letter to Pope Francis in which you ask His Holiness to endorse personally the devotion to Our Lady of America and to invite the United States Catholic Bishops to join Him in the Solemn Procession and permanent placement of the statue of Our Lady of America into the Basilica of the National Shrine of The Immaculate Conception at Washington, DC when he visits that shrine church in September.
You should address your letter or postcard, as follows:
His Holiness, Pope Francis c/o Archbishop Carlo Maria Viganò Apostolic Nuncio to the U.S.A. 3339 Massachusetts Avenue, N.W. Washington, D.C. 20008-3610
[EXAMPLE POST CARD MESSAGE]
Re: Our Lady of America, Her unique request here in the USA
Dear Pope Francis,
When you come to the USA in September 2015, please encourage the United States bishops to join you in a solemn procession and the permanent placement of the Our Lady of America statue into the National Shrine
Basilica of The Immaculate Conception in Washington, DC.
1. Our nation’s laws chronicle the shifts our culture has taken:
a) Prayer in public schools determined to be illegal-1962
b) Laws against distribution of birth control overturned-1965
c) First no-fault divorce law (CA)-1969
d) Title X provides free contraceptives to low-income women-1970
e) Laws against distribution of birth control to single people overturned-1972
f) All laws against abortion declared unconstitutional-1973
g) Supreme Court reaffirms Roe vs Wade, admits that abortion is necessary for failed contraception, and gives people the right to organize intimate relationships and make choices that define their views of themselves and their places in society-1992
h) First physician assisted suicide law approved in Oregon-1992
i)Supreme Court decides Texas Law banning sodomy is unconstitutional and thus eliminates all state laws against sodomy-2003
j) Legality of same-sex “marriage” established nation-wide-2015.
July 23, 2015 (CardinalNewmanSociety) — All Catholic colleges should be teaching students about the scientifically documented dangers of birth control, in addition to Catholic teaching against it, argued Vicki Thorn, founder of Project Rachel and organizer of an upcoming symposium set to discuss the biological case for avoiding contraception.
In an interview with The Cardinal Newman Society, Thorn explained that events such as these should set the pace for Catholic colleges to help students and young people understand the health risks of taking oral contraceptives.
The symposium, “Contraceptive Conundrum: Effects and Side Effects”, will be held August 8th, in conjunction with the Edmund D. Pellegrino Center for Clinical Bioethics at Georgetown University in Washington, D.C. Topics of discussion will include the brain’s relationship with hormones, oral contraceptives’ adverse effects on the unborn, and contraception’s impact on partner selection and relationship satisfaction.
“The more you learn about the biological processes, the more you see that what the Church has taught about sex is right,” said Thorn. The symposium is “about opening the door to the research that’s out there,” Thorn explained. “Women have been poorly informed. We’re told that the pill is wonderful and fixes everything, but there are real physical consequences to these chemicals.”
Thorn told the Society that her motivation for getting involved was the untimely death of one of her daughter’s friends, who suffered from fatal blood clots as a result of contraceptive use. “The pill ages a woman’s ovum, causes nutritional deficiencies, hormonal changes, increased cancer risk, strokes and blood clots,” said Thorn. “Women and men have a right to know this.”
Catholic colleges, she argued, need to put these facts, as well as Catholic teaching, in front of students. “We need to engage our young people and our students with this understanding of biology and couple it with theology,” Thorn urged.
“We live in a society where sex has become a recreational activity. We’ve become disembodied,” said Thorn. Moreover, “young people may struggle to embrace the moral teachings on contraception and the theology of the body if they’re coming from a broken sexual past,” she warned.
[T]he innate language that expresses the total reciprocal self-giving of husband and wife is overlaid, through contraception, by an objectively contradictory language, namely, that of not giving oneself totally to the other. This leads not only to a positive refusal to be open to life but also to a falsification of the inner truth of conjugal love, which is called upon to give itself in personal totality.
Thorn encouraged Catholic colleges to invite couples who are living a faithful, contraception-free marriage to come to campuses to discuss these issues and “to honestly reflect on what it means to be married” and to explain the sacramental nature of marriage as “a triune relationship with God.”
Thorn noted that young people often appear “so competent, but there may be a semi-truck full of wounds in their soul.” It is a Catholic college’s responsibility to “recognize those wounds, give them permission to talk about them and give young people the possibility of an ideal—of a committed marriage that is fruitful, wherein children are a gift.”
These are messages that “are not out there” in the mainstream college world, said Thorn.
Just because everyone is doing it doesn’t mean it’s right.
Generations of parents have known, understood, and parroted this fact to teenagers with raging hormones who didn’t want to hear the old adage one more time.
But for some reason, when it comes to hormones in 10-year-old girls, doctors aren’t getting it.
They decided that since everyone was doing it, it must be “normal” and simply redefined what’s acceptable (source) rather than digging into find out what’s wrong with a generation of young children. Even other researchers disagree (source).
If your daughter or granddaughter becomes one of the increasingly common 6-8-year-old girls growing pubic hair and breast buds (source), you might feel worried.
And you should be!
But your reaction should not be this: I know the problem! It is the hormones in the chicken!
When I posted an article about earlier puberty in girls on Facebook, I was dismayed to see the high percentage of commenters with that knee-jerk reaction. They clearly did not click through to actually read the article (there should be a disease name for that, like “title-is-enough-for-me-osis” or “don’t-need-to-know-the-whole-story-ism”).
“It’s the meat! The dairy! The huge-breasted chickens! What are we doing to our food these days?!?”
Lo and behold, educated by their skill in reading titles of articles on the Internet, they knew exactly the problem.
Surprise, surprise: They’re wrong.
Chickens, Cattle, and Hormones, Oh My!
Chickens don’t even need growth hormones, steroids, or supplemental estrogen or testosterone of any kind.
It’s been illegal for decades.
Beef cattle are allowed to be treated with hormones (6 of them, 3 natural, 3 synthetic), but that can’t be the whole story. Dairy cattle are allowed to be treated with the infamous rBST or rBGH, but due to popular consumer demand, most farms no longer use it, as evidenced on the majority of milk jugs anyone can read in the store.
But even with that hormonal influence on our environment and our food supply via cattle farming, the problem of earlier puberty is not just about food, and in fact, only a small percentage of orally consumed hormones make it through the digestive system according to research done by Parodi (2012) and Hartmann et. al (1998).
It’s a much bigger issue than that.
Is this more than your average Facebook scroller and post title reader can handle?
I’m going to do my best to keep it brief and digestible…promise.
The beginning of the story is this:
The average age of onset of menstruation was 16 in 1860, 14 in 1920, and 12.5 today.
In the last 30-40 years, those numbers have moved down 6 months – which feels significant for such a short time.
The very start of puberty – breast development – has dropped two full years in those same four decades. So puberty is lasting longer, which may point to external sources of estrogen that our girls’ bodies are reacting to by beginning breast development.
The question to pursue is: Where is environmental estrogen found in larger quantities over the last century?
There is Estrogen in Meat…and Some Other Stuff
All animals create hormones as part of their normal growth and development, and the testosterone and estrogen in animals is the same substance as in humans.
So every time we eat meat, we’re going to consume that animal’s hormones.
There are also six hormones approved for use in cattle: 3 natural, 3 synthetic. However, the residue in the meat is extremely small, less than that of natural hormones in some instances, and remember that research that showed that consumed hormones don’t make it through our digestive system all that efficiently.
That doesn’t mean I’m a fan of hormone therapy for animals, and it doesn’t mean there are no ill effects from it – similar to the problems in fish from hormonal birth control excreted into the water supply, aquatic ecosystems downstream from cattle farms demonstrate major fertility problems. The males are feminized and the females are masculinized. The hormones are at least somewhat persistent in the environment.
Besides that, the fact remains that “A 2009 study found that children who consumed the most protein from animal sources entered puberty about seven months earlier than those who consumed the least.” (source)
But correlation does not equal causation, and it’s not necessarily about the hormones – Marcia Herman-Giddens, lead author of a 1997 study on early puberty in girls, rang in on the 2009 study for the Huffington Post:
“It’s more likely that meat, milk, and similar foods help trigger earlier puberty because they are rich in protein, calories, and nutrients.”
You can poo-poo that comment all you want, but check this out: many vegetables have more estrogen than hormone-therapy-implanted beef:
But – have these vegetables changed in estrogen quantity over the last century? Not likely. In the case of soy, we are certainly eating a massively larger quantity than the 1800s, and it’s possible we simply eat more meat because food in general is in greater abundance: easier to purchase, easier to prepare since it’s all done for you.
Why Chickens Get so Big so Fast
Yes, it’s true that the chicken breasts you buy in the store seem impossibly huge.
Yes, it’s true that today’s conventionally farmed meat chickens have massive amounts of breast meat.
Yes, it’s true that those poor chickens get so big in front that they often have trouble walking and may even break their own legs simply by the weight of their chests.
But it’s not added hormones in their feed (that wouldn’t work anyway).
It’s not injected hormones (they’d have to inject them multiple times per day for very little result).
It’s not any supplementation at all.
Big-breasted chickens are so because of three practices:
Breeding for growth
Feeding for growth
Growing for growth (their environment)
Are these things good for the chicken?
No.
But they make big meat.
Add to that the up to 30% filler that can be pumped into the chicken meat after it is slaughtered (salt, water, sugars, broth, preservatives), and you’ve got a recipe for impossibly fat, juicy chicken breasts.
The complexities of the human body are so vast that it’s impossible to pin a general downward trend in onset of puberty on one thing. However, scientists and doctors have quite a few researched theories:
Pharmaceuticals in tap water: How many millions of women take birth control and hormone replacement therapy these days? All that extra estrogen is excreted into the sewage system, cannot be filtered by water treatment, and ends up in our water supply. There’s no way this only effect girls. (sources: 1, 2)
Estrogen-like endocrine disrupting chemicals (EEDC) – they’re everywhere, and this is definitely new in the last century.
Not enough exercise: Getting exercise is one of the few actions research-proven to help avoid early puberty. (sources: 1, 2)
Fat accumulation/obesity: One theory is that because hormones collect in fatty tissue, additional fat may cause higher levels of hormones that spark the onset of puberty earlier. (sources: 1, 2, 3, 4, 5, 6, 7)
Familial make-up: Girls without dad in the home are twice as likely to enter puberty early. (sources: 1, 2)
Stress, especially severe and early in life. (sources: 1, 2)
Sleep patterns being interrupted: Poor sleep decreases melatonin levels, an important hormone. Artificial lighting and screens after natural daylight ends impact this greatly. (sources: 1, 2, 3)
Now we have to remember that research has only shown that all those elements may be related to early onset of puberty, in girls in particular (obesity, for example, actually works exactly the opposite in boys).
Correlation does not equal causation.
The problems above may in some cases be the result of early puberty or even completely unrelated.
Or perhaps they’re related to each other, like this one:
You’re Not Fat Because You Eat Too Much
Similar to the popular quick answer to the early puberty question, most people respond to the problem of obesity in one of three ways:
We eat too much!
Too much fat and sugar!
Not enough exercise!
Research over the last decade has begun to point to the possibility that endocrine disruptors in our environment – from the personal products we use to the containers for our food and drink – may be a major culprit in the obesity epidemic. (source)
Those same endocrine disruptors are also correlated with early puberty.
So it really isn’t all about the chicken.
The bottom line is this – you can’t just avoid early puberty in girls (or messed up reproductive systems for anyone) by becoming a vegan.
Nothing is that simple.
But rather than be overwhelmed by another fearful article, be encouraged – you’re probably already avoiding a lot of the things responsible for reproductive malfunctions already, and if you’re not, take some baby steps today.
15 Ways to Improve Your Family’s Chances for Healthy Reproductive Systems
Seek out natural personal products – I have a huge list of everything I use in our home RIGHT HERE. At the very least, familiarize yourself with the top chemicals to avoid, including any word that ends in “paraben.” From my interview with a biochemist, chemical sunscreens would be a big one to avoid, too. (See the interview here: “Have Some Hormone Replacement Therapy with your Bikini“)
Any organic food you can afford is a great idea since chemical pesticides are pegged in a whole host of issues including endocrine system woes.
Any whole foods you can eat vs. processed foods is a good step – you’ll avoid BPA in packaging and help your families’ bodies stay as healthy as possible and at a healthy weight. I can help you teach your kids to cook and enjoy real food – and if you’re a rookie yourself, you might pick up some skills in the process.
Avoid birth control in your home and advocate others to do the same. NFP is a fantastic alternative to chemical birth control. Unfortunately, there is no filter on the market that I know of that can remove pharmaceuticals and estrogen from the water supply, so in this case, you’re mostly at the mercy of other people’s decisions.
Exercise. It’s one of the few interventions known to help prevent early puberty. (source)
It’s Natural Family Planning Awareness Week and I didn’t really think I’d have much to add to the conversation. The Catholic blogging world is already saturated with posts about NFP this week and I’ve read many, many wonderful posts on every angle of the topic in the past. My experiences are unique (aren’t ours all?) but not necessarily anything completely new or different. But to do my part, I wrote this post on Facebook yesterday to share my perspective and as I was writing it, for the first in my life it occurred to me exactly why NFP is so difficult – because it was never part of God’s original plan.
You see, in the perfect world God intended – the world without sin or suffering – NFP doesn’t have a place. The situations that make postponing a pregnancy necessary – physical and mental health issues, financial concerns, marital problems, lack of support system, etc. – they wouldn’t exist. And fertility problems that require couples use NFP to become pregnant, they wouldn’t exist either. There simply would be no need for Natural Family Planning. It’s not the default for human beings as God designed us. But it’s there because we live in a flawed world; not the natural order of things but a gift given to us by God to help us cope with our imperfect situations in an imperfect existence.
Many people need NFP for one reason or another, and I am incredibly grateful that it exists for those situations. For most of our marriage, we’ve used NFP. When we got pregnant with Lucia in 2011, my husband and I had hoped we’d never use NFP again. We looked forward to the idea of our family planned completely on God’s timing, of never looking at a chart again, of being genuinely surprised (but not too surprised) by a new pregnancy. But then we went through a period of unemployment. Followed by miscarriage after miscarriage. And then my current bout of prenatal depression and anxiety (yes, it’s back). And it seems that for the rest of our childbearing years we’ll always have one reason or another to use NFP to either avoid pregnancy or help us decrease chances of future miscarriage. That’s a tough pill to swallow.
Yes, the day to day practice of NFP can be difficult. But the emotional strain is even harder because it reminds us of the brokenness of our world (and my body). My chart is a symbol of how far we are from Eden.For all that people talk about how wonderful NFP is for marriage and communication and knowing your body and (fill in the blank), the truth is that if all were as it should be, we simply wouldn’t need it.
NFP strikes me as similar to a cancer treatment, let’s say chemotherapy. Of course, it’s not poisonous or painful like chemotherapy (NFP is green! And completely natural! No physical side effects!), but bear with me. The only reason chemotherapy exists is to combat cancer. Those who have cancer (and their loved ones) are grateful it gives them the opportunity to fight the cancer, but they’d rather they didn’t need it in the first place. My family has had several extra years (and hopefully many more) with my 84 year old grandfather because of two rounds of chemotherapy. But the chemo itself took its toll on him and is a reminder of the brokenness of his body, the unnaturalness of the cancer that necessitated it in the first place. I wish there was no chemo because I wish there was no cancer. Actually, I suppose that’s how we feel about most medication. I’m grateful to God for well-trained doctors and medical researchers who allow us to combat the illnesses of the mind and body, but I’m still sad and bitter that we even have illnesses we have to treat.
So too with NFP. I wish we didn’t need it. I wish we lived in a perfect world where the circumstances were always perfect for more children to be welcomed and everyone had perfect, healthy, functioning fertility. Since there is a need for NFP, I’m grateful it’s there. But even if I appreciate it, I don’t have to like it. It’s ok if it doesn’t feel natural and beautiful and effortless, because it’s simply not how it was meant to be.
I don’t usually post my homilies for a variety of reasons. But several people asked me for this one, and this is the quickest way I have of distributing it. For those who weren’t able to make the Mass — or would like to better understand where the church is coming from on contraception — I invite you to give it a read.
Forty-Seventh Anniversary of Humanae Vitae
Feast of St. Bridget of Sweden
Tonight, we gather to give thanks for Blessed Paul VI and his prophetic teaching 47 years ago on the dignity of human life and the beauty of marital love. We gather on this Feast of St. Bridget of Sweden, who with her husband, Ulf, were God’s human instrument of giving life to eight children.
Bridget and Ulf understood that their role and responsibility as parents did not end, but began with conceiving their children. The aim and ambition of all Christian mothers and fathers are to rear their children to know and to love God in this world and to encourage them to live in such a way that they will live with God forever in heaven.
One of their children, Karin, is also venerated as a Saint – St. Catherine of Sweden. Catherine, like her Mother, was a young widow. She accompanied her Mother to Rome and on a Pilgrimage to the Holy Land. After St. Bridget’s death, she became the Abbess of the Monastery her Mother had founded.
We ask for St. Bridget’s and St. Catherine’s intercession tonight that that our Church today might be an effective defender of the beauty and importance of Christian marriage and family life.
II
Gifts from God
Yesterday, as I was preparing this homily at the Office in my Residence, there was a man making some repairs on the air-conditioning system. He asked me what I was reading. At the time, I was reading a meditation by St. Bridget.
He told me that he was raised a Methodist and had met his wife, who had been raised Catholic, at an Evangelical Protestant Church. He told me that he loved to read the Bible. He considered Himself, more Catholic than Protestant, in part because he believes in the Real Presence of Jesus in the Eucharist. He also considers himself practically Catholic because he has 10 children. Early in their marriage he and his wife decided that they wanted to have as many children as God wanted them to have. He could not imagine life without his youngest child, a daughter, or any of the other nine children. It was obvious that he treasured each of his children as a precious gift from God. He reminded me of St. Augustine who gave to his illegitimate child the name – Adeodatus, gift from God.
III
Paul VI, a Modern Prophet
I told this man that I was working on this homily for tonight, commemorating the 47th anniversary of Pope Paul VI’s teach on the dignity of Human Life and the beauty of Christian married life. I shared with him that Paul VI foresaw the terrible consequences of the sexual revolution, of the separation of life-giving component from the love-giving component of sexual love.
Paul VI had predicted that the widespread use of contraception would result in marital infidelity, a dramatic increase in divorce, and a general lowering of morality. Paul VI was particularly concerned about the vulnerability of men, particularly young men, who in the Pope’s words: “… have need of encouragement to be faithful to the moral law, so that they must not be offered some easy means of eluding its observance. It is also to be feared that the man, growing used to the employment of anticonceptive practices, may finally lose respect for woman and, no longer caring for her physical and psychological equilibrium, may come to the point of considering her as a mere instrument of selfish enjoyment, and no longer as his respected and beloved companion.”
Paul VI was prophetic in describing what we now would call the hook-up culture so rampant on college campuses and amidst young adults. It is a culture where so many young people have sexual encounters barely knowing the other person, much less having a committed and loving relationship. Is it any wonder that we have an epidemic of date rape? We see a culture today, where so many young men and young women, have lost respect for each other.
Paul VI appealed to public leaders of his time to protect young and old from “every form of pornography and licentious performances.” The Holy Father instead urged them to create a culture that fosters the virtue of chastity. He warned public officials of the danger of permitting toxic materials to infect the young under the pretense of a false freedom or artistic expression. Mercifully, Paul VI did not live to see what is common fare today on cable and even network television.
My AC Repairman marveled at the blessing for the Church to have someone who could see so clearly the consequences of contraception and the sexual revolution it fueled. Today, if we but have the eyes to see, we are surrounded by the casualties of the sexual revolution, e.g. the high number of single parents, the number of children that do not have a father in their home, the epidemic of sexually transmitted diseases, the millions that have died from AIDS, pornography as the largest internet industry and pornographic addiction at epidemic proportions. These victims also include more than a million unborn children aborted in our country alone, the large number of teen pregnancies, and the distressing number of victims of child abuse. Our modern culture is adept at providing access to every conceivable form of pleasure, but mystified at the incredible number of individuals suffering from depression. Millions of adults and children find authentic and enduring joy elusive.
Paul VI even foresaw governments like our own in its domestic policy promoting contraception and abortion as part of preventive health care as well as providing massive amounts of federal funding to Planned Parenthood, the nation’s largest abortion provider, and at the same time making foreign aid grants to third world nations, contingent on their subjecting their people to family planning and abortion propaganda. Similarly, he predicted government’s like China coercing women to have abortion and limiting the number of children married couples are permitted to bring into the world.
IV
Much That Was Not Foreseen
As much foresight as Paul VI had there were many aspects of our contemporary culture that he did not envision. He did not foresee abortion conglomerates selling fetal body parts for profit. He did not conceive of a society so confused that it would redefine marriage – no longer recognizing that essential to the marital covenant was complementary love of a man and a woman and that essential to marriage was the biological possibility of creating new life. Paul VI was unable to see the Brave New World of children being manufactured in laboratories. He did not foresee the Church being denied the ability to facilitate adoptions, because of our refusal to place children with same-sex couples. He did not imagine a new industry of what some call mommy porn as evidence with the popularity of books and movies like Fifty Shades of Gray. Paul VI did not foresee the gender question, resulting in iconic organizations like the Girl Scouts, permitting boys who want to be girls to become Brownies!
V
Everyone Has a Part in Reclaiming our Culture
Paul VI in Humanae Vitae identified the role and responsibility of many different groups to support authentic marriage and family life.
He challenged Bishops to be strong and courageous teachers of the Truth about love, sexuality, marriage and family life. He called upon priests to nourish with the Word of God and the Sacraments married couples and parents so that they could live well their beautiful, if challenging vocation.
Our late Holy Father called upon scientists to help couples find moral ways to address some of the challenges that made them vulnerable to resorting to contraception. Paul VI would have been so pleased by the advancements in Natural Family Planning. He would have been gratified by the Institute in Omaha named in his honor, where the best of medical science helps couples use moral means to exercise stewardship over their fertility and assists infertile couples to be able to conceive new life. The Holy Father called upon medical doctors, not only to refuse to perform abortions, but to assist couples by giving patients care that conforms to time honored moral principles as well as the best medical practice.
He challenged government leaders to enact public policies that protect the innocent and the vulnerable.
Paul VI called upon everyone (priests, religious, singles, married couples) to strive to live a life of virtue particularly the virtue of chastity, even when that required heroic sacrifice and a willingness to be counter-cultural.
VI
Vibrant Marriages and Families are the Vaccine and the Cure
However, the vaccine and the cure for healing our society and reclaiming our culture are present in this Church tonight. It is strong marriages and vibrant families.
Christian marriage is a call to heroic love. It is a call to lay down one’s life for another in love. It is a summons to seek the happiness and eternal welfare of one’s spouse before one’s own wants and desires. It is a call to make the self-sacrificing love of Jesus real and tangible to one’s spouse and children.
Christian parenthood is a call to lose your life, as you knew it, to embark upon the most important work for our culture, society, nation and the church, namely the formation of children – the next generation of leaders, citizens and parishioners. In the words of St. John Paul uttered in his 1999 pastoral visit to St. Louis: “As the family goes so goes the nation!”
It is difficult as married couples and as parents to realize the importance of the seemingly inconsequential decisions that you make each and every day to sacrifice for the good of your spouse and your children. It is the cumulative impact of these seemingly small choices made day after day over a lifetime that impact the good of society and the good of the Church so profoundly.
VII
The Entire Church and our Archdiocese Are Focused on Marriage and Family
The entire Church at this moment is focused upon the importance of marriage and family life. Last October, the Synod of Bishops, representing the Catholic Bishops of the entire world, met for several weeks identifying the challenges confronting married couples and families today. This coming October another Synod will meet in Rome to develop a pastoral strategies to guide the Church in its efforts to support better marriage and family life.
Pope Francis will make his first visit to the United States this September. The principal reason for his visit is to participate in the World Gathering of Families in Philadelphia. St. John Paul initiated the World Gathering of Families more than 20 years, in order to hold up to the world the importance of marriage and family life as the foundation for culture and civilization.
In our Archdiocese in the next few weeks, I will promulgate a Vision for the next decade in the Archdiocese. Among three Key Initiatives that give direction to this vision is one to strengthen the vocation of marriage and family life.
Part of this Key Initiative will be to invite married couples to give priority to strengthening their love for each other. We hope to help couples realize that one of the most important things they can do to change the world and help the Church is to invest in their marital relationship. Moreover, we want to find ways to help parents to live their vocation of being the first and most important teachers of their children in the Faith.
The Christian Family is to be a School of Faith and Virtue. It is the Christian Family that is the tool that God has ordained to pass the Faith from one generation to the next. Christian Parents are called to be teachers of the Faith by their words, but even more importantly by their example. They are called to create the environment in their home where the Faith is caught by their children. Christian families should be Saint Factories!
Parents are called to be Spiritual Directors for their Children, introducing them to a life of prayer and helping them from their earliest days to communicate sincerely, faithfully, and authentically with God. I want our Archdiocesan Church to do everything possible to help parents fulfill this critically important and awesome mission.
VIII
The Source of Complete Joy
In our first reading tonight from Galatians, St. Paul says the he lives “by Faith in the Son of God who has loved me and given himself up for me.” Paul knew well the profound joy that comes from knowing he was loved by His Creator, the Creator of the universe.
Paul knew, however, that there was even a more sublime joy that experiencing the love of the only one who can fulfill the deepest longings of our heart. Paul knew what it was like to allow Christ to live in Him and then through him to be the human instrument of bringing the joy and the peace of God’s love to others. To bring another to know the love of God revealed in His Son, Jesus Christ, is to experience what Jesus terms as “Complete Joy.”
Jesus instructs His Disciples that they must be connected to Him, the Vine. The disciples must allow the very life of Jesus to pulse through them so that they can be fruitful. Dear Parents, your children are the fruit of you love. They are your love with a name, like Grace or Jacob or Joey or Emily.
IX
Mass Intention
Tonight, I offer this Mass for all married couples that your love will not atrophy and grow dimmer with the passing of time, but instead it will grow stronger and deeper and more passionate. I offer this Mass for Parents that you will discover that complete joy Our Lord desires for you in devoting yourself to the most important of all human tasks, the giving and the nurturing of human life. I pray that you will do everything possible, not just so that your children can succeed and prosper in this world, but so that they will become Saints and achieve their destiny to live with God forever.
Thus we invoke some of the great Saints to intercede for us:
St. Bridget and St. Catherine – Wives and Mothers, Pray for Us
St. Thomas More – Defender of True Marriage, Pray for Us
St. Gianna Molla, who willing gave her life for her daughter, Pray for Us
St. Maximilian Kolbe, who offered his life to rescue a husband and father, Pray for us
St. Therese of Lisieux and your Holy Parents – Louis and Zelie Martin, Pray for us.
(NaturalNews) When Bill Gates, along with Paul Allen, began a little tech venture called “Microsoft” in a garage in 1975, he couldn’t possibly have imagined that the company would grow into the largest personal computer company and most widely used PC operating system on the planet.
Or make him the richest man in the known galaxy.
But all of that happened, of course, and for the last two decades Gates, through his Bill and Melinda Gates Foundation, have been involved in socially engineering the world to be a place they want to mold in an image they have devised.
In recent months Gates has taken his vision a step further, with the development of computer chip technology that will essentially serve as one element of his quest for population control and reduction.
As reported by the Activist Post’s Heather Callaghan, soon medical microchip implants will be introduced to the general population, which will serve as “the new face of medicine that polygamously marries Big Pharma, biotech, nanotech and wireless remote technology.”
“Maybe hooking oneself into the Internet of Things will be an additional app, although this sounds like a passive form of medicine where someone else gets to call the shots, so to speak,” she added.
From ‘pro-choice’ to ‘no-choice’
Perhaps not surprisingly – given its propensity to favor technology that reduces planetary human presence – the same developers who are bringing wireless, remote-controlled implants are currently focused on a product that is the cornerstone of future efforts: Gates Foundation-funded birth control microchip implants.
Callaghan notes that wireless technology allows the remotely controlled chips to essentially activate a woman’s ability to conceive, or prevent it, at will, which amounts to temporary sterilization (if a decision is made, say by an all-powerful government agency, to prevent a woman from bearing a child). Government in the U.S. would instantly transform itself from “pro-choice” (through the permission of abortion) to no choice.
The writer also observed:
Of course with remote technology funded by eugenics depopulation fanatics, the first questions should always be, “the ability to conceive by whose will?” This would be the complete antithesis of female empowerment or a “woman’s right to choose” – would it not?
What’s more, the chips are encrypted, so no hacking – not by cyber criminals or by technologically clever souls who are simply trying to bypass a government’s oppression.
The microchip is implantable into arms, hips or somewhere on a woman’s back. The development of the chip was kept under wraps while researchers and scientists worked to complete work the past couple of years. But the existence of the chip was finally confirmed publicly as beta testing of the technology is scheduled to begin towards the end of 2015, when volunteers will be sought.
If poor women are the target, why encrypt the chips?
As reported by TWCN:
The birth control chip is the brain child of a professor, Robert Langer, from Massachusetts Institute of Technology. The Bill Gates and Melinda Foundation has funded the research and the prototype is ready for human testing. The chips will be ready for sale by the year 2018 according to Robert Langer. The institute’s Chip Foundation and Bill Gates’ Foundation have been working on the birth control chip for past three years.
The safety tests would begin by the end of year 2015 and Robert Langer is confident that the chips will hit market sometime in 2018. The main target of these chips are women in third world who are often subject to pain and risks of death during early pregnancies.
That report noted that the chip is expected to remain viable for at least 16 years once implanted.
While the “target” population is poor, third-world women, such technology is, of course, ripe for abuse. After all, think about it: If that demographic is the primary target, why would the chips need to be encrypted? How many third-world populations have within their midst the technological capability or the power to resist?
When he began Microsoft, Bill Gates likely never thought he’d become rich enough to hold the power of life in his hands. Talk about your “evil corporations.”
July 21, 2015 (PregnancyHelpNews) — Now is as good a time as any to mention a factoid about the average salary for a Planned Parenthood regional CEO: just a cut below $200,000.
In other words, about one Lamborghini a year. And that’s before you consider the bonus potential of wheeling and dealing with aborted baby parts distributors.
Yessir, the sky’s the limit when you sign on to work for America’s most profitable non-profit—experts at exploiting existing revenue streams like taxpayer dollars and paid baby dismemberment, and veritable creative geniuses when it comes to pioneering innovative business lines like the resale of livers, kidneys and lungs.
Of course, climbing Big Abortion’s corporate ladder does have its downside.
For instance, you might need to crank up the music in your posh ride to drown out the voices in your head that call you a grave robber, or compare you to Dr. Frankenstein’s lab assistant.
Plus, business can get a little slow when you’ve only got 800 abortions per year at the “much smaller affiliate” of Planned Parenthood you might find yourself overseeing.
At that rate, it can almost feel like you’re not making a big enough contribution to the 327,166 abortions per year your parent company is “performing”—always a strange verb to use, since there’s generally no applause to follow the monetized snuffing out of a life.
Again, these thoughts can be drowned out pretty simply by the turning of a dial and the roar of your 641 horsepower machine—brought to you every year thanks to the American taxpayer, women overwhelmed by the shock of an unexpected pregnancy, and the retail of various body parts of aborted babies.
Let’s be fair, Planned Parenthood’s Medical Director’s Council President Dr. Mary Gatter was clearly joking when she said she wanted a Lamborghini in today’s video, released by The Center for Medical Progress.
It was tongue-in-cheek, and we need not take it out of context or blow it out of proportion. To do so would be dishonest and deceptive, and we need to remember that it’s Big Abortion—specifically Planned Parenthood—alone who has something to hide.
But, as the wheels continue to fall off Planned Parenthood’s hearse, let’s not miss the truth the latest evidence puts on a platter for us: Abortion is a profit game. Always has been. Always will be.
Which raises an interesting contrast. Every single day, while “doctors”—again, I’m searching for a better noun here—all across the United States are putting our hard-earned tax dollars to work by preying on roughly 3,500 desperate women, robbing these moms of motherhood and aborting their innocent children, there’s an alternative army of healers at work.
The 2,500 healers who make up this group bring home an average of $43,144 per year, and run their organizations on an annual budget the size of 3/4 of the cost of a Lamborghini. Like the highly paid practitioners and facilitators of abortion, this group wakes up every morning with a singular goal in mind.
It so happens that those who belong to this group have the same client in mind as their counterparts at Planned Parenthood: a woman facing an unexpected pregnancy.
It’s just that there’s a major difference between these two opposing schools of thought: You might even call it a life and death difference.
Who is this alternative force? It’s the leaders of a counter-movement that is responsible for reaching and rescuing over 3,000 lives every week from the violence of abortion.
It’s the leaders of the pregnancy help community, which traces its roots to the pre-Roe days of the late 1960s, when abortion on-demand became legalized in Colorado, California, and New York.
Seeing the need for a woman faced with an unexpected pregnancy to be surrounded by loving and compassionate support, fully equipped to make the healthiest decision for everyone involved, people began opening their homes, their lives, and their pocketbooks to see that every mother felt loved and supported during her pregnancy.
On their own dime, these life-minded individuals began to organize themselves in the early 1970s, when a doctor named John Hillabrand partnered with a Holocaust survivor named Lore Maier to form what would come to be known as Heartbeat International—now the largest, most expansive network of pregnancy help centers, medical clinics, maternity homes and non-profit adoption agencies.
Unlike highly profitable abortion businesses, pregnancy help organizations keep their lights on by raising their own money with local fundraisers like crab feeds and wedding dress resale shops—which offers a mind-blowing contrast to what Planned Parenthood is in the business of reselling.
The people who run these organizations actually believe that every life has inestimable value—like, wait for it, more value than a Lamborghini.
From start to finish, the motivation of the pregnancy help community’s pioneers, its 24-7 pregnancy helpline,Option Line, and all the way down to the smallest pregnancy center in Podunk, U.S.A., is a simple one: to reach and rescue as many lives as possible.
That’s it. Rescuing lives.
That kind of thinking won’t get you a Lamborghini, but, as the old saying goes, “The benefits are out of this world.”
Pastor of St. Mary of the Immaculate Conception in Greenville, Wisconsin Given on the 13th Sunday of Ordinary Time, June 28, 2015
“To sin by silence when they should protest makes cowards out of men.” – Abraham Lincoln
My dear parishioners, I had hoped I would not have to give this homily. But as your pastor and shepherd, I must speak today, lest I sin by silence and act in cowardice. This past Friday, June 26, 2015 by a 5-4 decision, the US Supreme Court has told us that our entire nation must accept the redefinition of marriage. The decision is being hailed by many as a victory for love. Our President’s twitter account acclaimed the decision as victory for freedom with the signature #LoveWins. It is no secret that the Catholic Church opposes this decision, and so it would seem to many in this confused cultural moment that we are now part of a church that is opposed to love, and is in fact a church that proclaims hatred by its teaching. For a long time now our society has been being prepared to celebrate and affirm this decision as a victory for love – the press, the entertainment media, our schools, the medical profession, business associations, the military – every aspect of our society has very aggressively been told that to oppose this decision is to be against the free expression of love. Why would we withhold the right to happiness and love from fellow citizens? Why would we tell others they cannot fulfill themselves in the way they choose to? Everyone is now forced to accept this redefinition by means of judicial rewriting of the law. And – here is the crux of the issue for us as the church – if we will not accept this redefinition, we are expected to be silent. And it is in this light that I wish to take President Lincoln’s challenging words – “To sin by silence when they should protest makes cowards out of men” – and ask how we may respond courageously and joyfully to the present challenging cultural moment.
Let’s be clear about what happened on Friday in terms of the big picture of the history of Western Civilization. I’ve brought a few books along for dramatic effect. Let’s see… Socrates…out the window. Plato…out the window. Aristotle…out the window. Roman law…out the window. Notice we haven’t gotten to Christian sources of law and culture yet. The Old Testament – Genesis 19, out the window. The New Testament – Romans 1 – read it, it is so clear! “While claiming to be wise they became fools…God handed them over to their undiscerning mind to do what is improper” – out the window. St. Augustine, out the window. Thomas Aquinas, out the window. The entire legal precedent of the United States up to 2003, out the window. The implication of course is that all of these sources of our law had a blind spot of prejudice when it came to the definition of marriage. All of these wise men were unenlightened, and it is only as of June 26, 2015, that we can say that we truly live in a free and loving society.
What was the reason for all of these foundational sources of our culture condemning the behavior associated with the redefinition of marriage, for calling such behavior a sin and a crime? Let’s say this very simply – with great wisdom, they understood that such behavior is destructive. It is destructive of the human body because it goes against human nature – it causes disease and death, and no less importantly it is destructive of the human soul. It leads to depression, anxiety, loneliness, mental illness, and even suicide. It is destructive of families and of children’s happiness. This was the established consensus of the American Psychiatric Association (APA), until 1973, when it removed such behavior from its lists of mental disorders in a change that had absolutely no scientific or medical basis but was pushed through by pressure from a small group of activists.
Now, however, we are told that the entire society must legally accept the redefinition of marriage and thus affirm the rationalization that what is bad and destructive is actually good and fulfilling. My dear people, let’s say this simply and clearly – to call what is bad good is a lie. And the redefinition of marriage into some thing other than a permanent covenant between a man and a woman for the purpose of raising a family is a lie. Why would we be opposed to Friday’s decision? The simple answer is- because it is based on a lie. If someone would ask us, “Why is it a lie?” we need to be able to connect the dots as to how we got here. There is a very simple thread of logic running through the Supreme Court’s decisions since 1966 concerning, first contraception, then abortion, and finally the redefinition of marriage. All three issues are intertwined, and ultimately to embrace one as a right is to embrace the others. We need to be able to understand that logic so as to refute it.
First, in 1961 Planned Parenthood sued the State of Connecticut for the right to distribute contraceptives, which was at that time against the law. In 1966 in Griswold v. Connecticut, the US Supreme Court defined the right to contracept as part of the “right to privacy” it claimed to find in the Constitution. This decision was then invoked in the decision with which we are all familiar,
Roe v. Wade in 1973, which legalized the right to abortion as part of the “right to privacy.’ It made logical sense. If children intrude upon our right to privacy, we need to have a way to eliminate them. To fully embrace the use of contraceptives, many of which act as abortifacients by killing the developing embryo in the mother’s womb, is to affirm abortion, which is the ultimate act of contraception. The Church’s beautiful teaching has always seen this connection and proclaimed it, even as our culture has scoffed. This brings us to 2015. Friday’s decision was entirely consistent with the precedent of Griswold and Roe. If we as a culture have sterilized married love by legalizing contraception and abortion, it is logically consistent that we would redefine marriage so that it no longer has any necessary connection with procreation, based on the “right to privacy.” A culture where everyone is contracepting and in which anyone can get an abortion, must, to be consistent, redefine marriage. Our Supreme Court acted consistently on Friday. It invoked its own language defending the right to abortion: “At the heart of liberty is the right to define one’s own concept of existence, of meaning, of the universe, and of the mystery of human life” (Planned Parenthood v Casey, 1992). Justice Kennedy’s opening sentence in Friday’s decision reaffirms this definition of liberty: “Liberty includes the right to define and express one’s own identity.” This is the heart of the lie. But there can be no freedom divorced from the truth of God’s law, which is also the law of human nature. In ignoring the natural law, our Supreme Court has proclaimed that we must all accept a lie.
What is to be our response as disciples of Jesus Christ to the lie? It is the same joyful witness that we always give: living lives of poverty, chastity, and obedience and mercifully inviting others, with us, to heed the first words of Jesus in the Gospel, “Reform your lives, and believe in the Gospel!” (Mark 1:15). Our witness needs to be joyful and compassionate, convicted and committed. No less than we are convicted that we would never let our little ones play with matches, because they are potentially destructive, so we must be convinced that the redefinition of marriage is destructive to individual people and to our entire society. If we are so convinced, we will joyfully invite others as fellow sinners to turn to the Merciful Jesus and know his healing grace as the woman with the hemorrhage did in today’s Gospel.
We can turn more than ever to the intercession of some of the great martyrs of our faith who were called on to witness to the truth of God’s law in the face of legal redefinition of the truth. I am thinking of the joyful witness of St. Thomas More and the Martyrs of England in the 1500’s. When King Henry VIII wished to deny the truth of his marriage, he ordered Parliament to pass the Act of Supremacy, which proclaimed Henry head of the Church and thus able to redefine marriage. The vast majority of bishops in England acquiesced to Henry’s demand. The law was changed and persecution followed for those who did not remain silent. The courageous martyrs of that storied moment in English history are interceding for us. They stood firm as they were accused of hating their King and hating their country. St. Edmund Campion’s powerful words ring clear – at his sentencing to execution, he said simply, “In condemning us, you condemn all of your own ancestors, all that was once the glory of England.” The present redefinition of marriage has indeed condemned all the great figures in American history as having been fundamentally opposed to freedom and rights in their understanding of marriage as a God-given gift between a man and a woman.
I am thinking of the joyful witness of Dietrich Bonhoeffer and the martyrs of the Third Reich. All of the reforms of the 1930’s were accomplished legally as the German nation was told to embrace a lie about the human person – that the Jews were not truly persons. As long as people were silent, the lie had room to grow. Anyone who loved Germany was expected to support the Fuhrer. The law was changed and persecution followed for those who did not remain silent. Those who spoke out paid the ultimate price. Bonhoeffer, a Lutheran pastor who dared to speak out in protest and to resist, wrote before his execution, “Silence in the face of evil is itself evil: God will not hold us guiltless. Not to speak is to speak. Not to act is to act.”
I am thinking, lastly, and perhaps most powerfully, of the courageous witness of John the Baptist, whose birth the Church just celebrated this past week. Face to face with King Herod, who had redefined marriage by taking his brother’s wife to be his own wife, John spoke the truth about marriage: “It is not lawful for you to have your brother’s wife” (Mark 6:18). John chose not to remain silent, and persecution followed. Because he spoke the truth about marriage, John was beheaded.
“To sin by silence when they should protest makes cowards out of men.” My dear people, all we have to do today is to remain silent in the face of the lie and we will be able to remain comfortable. May this comfortable silence never be our response. In the words of the great Russian dissident Alexander Solzhenitsyn, “Let the lie come into the world, let it even triumph. But not through me.” The Church in America in 2015 needs to call upon the intercession of all of these holy martyrs, asking them to obtain for our bishops and priests and for all of us the courage to bear witness to the truth about marriage.
So many are confused and hurting in their search for love today – they are searching for Christ without even knowing it. It falls to us at this moment to show forth Jesus by our witness of poverty, chastity, and obedience. This witness will mean having the courage to face whatever persecution, large and small, will come to us as a result of our refusal to remain silent. It will mean enduring accusations that we are opposed to love and hateful of those who celebrate and promote the redefinition of marriage. Let’s be confident that the Holy Spirit is with us and is raising up a great generation of witnesses loving, compassionate, merciful, courageous witnesses. I am confident that I am looking at those witnesses as I preach to you today.
Saint John the Baptist, pray for us.
St. Thomas More, Edmund Campion, and the martyrs of England, pray for us. Dietrich Bonhoeffer and the martyrs of the Third Re ich, pray for us. Amen.
Opponents of legalized same-sex marriage say they’re trying to protect a beleaguered institution, but they’re a little late. The walls of traditional marriage were breached 40 years ago; what we are witnessing now is the storming of the last bastion.
Marriage is primarily a social institution, not a religious one. That is, marriage is a universal phenomenon of human cultures in all times and places, regardless of the religion of the people concerned, and has taken the same basic form in all those cultures. Marriage existed long before Abraham, Jesus or any other religious figure. The institution of marriage is literally prehistoric.
The three monotheistic faiths (Judaism, Christianity and Islam) actually recognize this explicitly in their holy writings. The book of Genesis ascribes the foundation of marriage in the very acts of God himself in the creation of the world: “It is not good that man should be alone; I will make him a helper comparable to him. . . . A man shall leave his father and mother and be joined to his wife, and they shall become one flesh” (Genesis 2:18, 24).
The three great religions base their definition of marriage on these verses and others that echo them. In Christian theological terms, the definition of marriage is part of the natural law of the creation; therefore, the definition may not be changed by human will except in peril to the health of human community.
Psychobiologists argue that marriage evolved as a way of mediating the conflicting reproductive interests of men and women. It was the means by which a woman could guarantee to a specific man that the children she bore were his. In biological terms, men can sire hundreds of children in their lives, but this biological ability is limited by the fact that no one woman can keep pace.
Siring kids by multiple women is the only way men can achieve high levels of reproduction, but there is no adaptive advantage for women in bearing children by men who are simply trying to sire as many children as possible. For a mother, carrying and raising a child is a resource-intensive, years-long business. Doing it alone is a marked adaptive disadvantage for single mothers and their children.
So the economics of sex evolved into a win-win deal. Women agreed to give men exclusive sexual rights and guaranteed paternity in exchange for their sexual loyalty and enduring assistance with childbearing and -rearing. The man’s promise of sexual loyalty meant that he would expend his labor and resources supporting her children, not another woman’s. For the man, this arrangement lessens the number of potential children he can sire, but it ensures that her kids are his kids. Guaranteed sex with one woman also enabled him to conserve his resources and energies for other pursuits than repetitive courtship, which consumes both greatly.
Weddings ceremoniously legitimated the sexual union of a particular man and woman under the guidance of the greater community. In granting this license, society also promised structures beneficial to children arising from the marriage and ensuring their well-being.
Society’s stake in marriage as an institution is nothing less than the perpetuation of the society itself, a matter of much greater than merely private concern. Yet society cannot compel men and women to bring forth their replacements. Marriage as conventionally defined is still the ordinary practice in Europe, yet the birthrate in most of Europe is now less than the replacement rate, which will have all sorts of dire consequences for its future.
Today, though, sexual intercourse is delinked from procreation. Since the invention of the Pill some 40 years ago, human beings have for the first time been able to control reproduction with a very high degree of assurance. That led to what our grandparents would have called rampant promiscuity. The causal relationships between sex, pregnancy and marriage were severed in a fundamental way. The impulse toward premarital chastity for women was always the fear of bearing a child alone. The Pill removed this fear. Along with it went the need of men to commit themselves exclusively to one woman in order to enjoy sexual relations at all. Over the past four decades, women have trained men that marriage is no longer necessary for sex. But women have also sadly discovered that they can’t reliably gain men’s sexual and emotional commitment to them by giving them sex before marriage.
Nationwide, the marriage rate has plunged 43% since 1960. Instead of getting married, men and women are just living together, cohabitation having increased tenfold in the same period. According to a University of Chicago study, cohabitation has become the norm. More than half the men and women who do get married have already lived together.
The widespread social acceptance of these changes is impelling the move toward homosexual marriage. Men and women living together and having sexual relations “without benefit of clergy,” as the old phrasing goes, became not merely an accepted lifestyle, but the dominant lifestyle in the under-30 demographic within the past few years. Because they are able to control their reproductive abilities–that is, have sex without sex’s results–the arguments against homosexual consanguinity began to wilt.
When society decided–and we have decided, this fight is over–that society would no longer decide the legitimacy of sexual relations between particular men and women, weddings became basically symbolic rather than substantive, and have come for most couples the shortcut way to make the legal compact regarding property rights, inheritance and certain other regulatory benefits. But what weddings do not do any longer is give to a man and a woman society’s permission to have sex and procreate.
Sex, childbearing and marriage now have no necessary connection to one another, because the biological connection between sex and childbearing is controllable. The fundamental basis for marriage has thus been technologically obviated. Pair that development with rampant, easy divorce without social stigma, and talk in 2004 of “saving marriage” is pretty specious. There’s little there left to save. Men and women today who have successful, enduring marriages till death do them part do so in spite of society, not because of it.
If society has abandoned regulating heterosexual conduct of men and women, what right does it have to regulate homosexual conduct, including the regulation of their legal and property relationship with one another to mirror exactly that of hetero, married couples?
I believe that this state of affairs is contrary to the will of God. But traditionalists, especially Christian traditionalists (in whose ranks I include myself) need to get a clue about what has really been going on and face the fact that same-sex marriage, if it comes about, will not cause the degeneration of the institution of marriage; it is the result of it.
Rev. Sensing is pastor of the Trinity United Methodist Church in Franklin, Tenn. He writes at DonaldSensing.com.
An undercover video of a lunch meeting between Planned Parenthood official, Deborah Nucatola, M.D., and a man and a woman posing as buyers for a biologics company shows a discussion of how a dismemberment abortion is modified to meet customers’ needs, states AAPS executive director Jane M. Orient, M.D., who viewed the recording.
“The abortionist uses ultrasound to guide placement of forceps so as not to crush the organs to be procured,” Orient says. “According to Nucatola, who does abortions herself, livers and hearts are in great demand. Lungs and legs are also being requested.”
The fetus may be rotated into a breech position to facilitate recovery of an intact calvarium (head), the largest part, as cervical dilation increases during the procedure, Nucatola said.
The team “huddles” before the day’s work begins, Nucatola explained, to plan the most efficient way to meet demand for parts.
Allegations about trafficking in fetal body parts have been around for years, Orient said. Concerns were raised by Life Dynamics in 2000, but the practice apparently was just driven further underground.
American Life League states that the sale of human body parts is illegal throughout the U.S. It called for an investigation and immediate suspension of the $400 million in funding that Planned Parenthood receives annually from Medicaid.
“Developing human beings, capable of feeling pain, are apparently being torn apart and sold piece by piece,” Orient stated. “The truth about this practice needs to be exposed. Lawbreakers need to be prosecuted, and all public funding needs to be withdrawn from any entities connected in any way with this horrendous enterprise.”
The Association of American Physicians and Surgeons (AAPS) is a national organization representing physicians in all specialties, founded in 1943 to preserve private medicine and the patient-physician relationship.
Ruling to force nuns to violate faith or pay massive IRS penalties
By Denver Catholic
July 14, 2015
In a departure from the U.S. Supreme Court’s protection of the Little Sisters of the Poor last year, the 10th U.S. Circuit Court of Appeals ruled that the Little Sisters must comply with the government’s contraceptive mandate.
The federal Health and Human Services (HHS) mandate forces religious ministries to violate their faith or pay massive IRS penalties.
Sister Loraine Marie Maguire, Mother Provincial of the Little Sisters of the Poor, stated, “As Little Sisters of the Poor, we simply cannot choose between our care for the elderly poor and our faith. And we should not have to make that choice, because it violates our nation’s commitment to ensuring that people from diverse faiths can freely follow God’s calling in their lives.”
The Little Sisters have served the neediest in society across the world with dignity for more than 175 years.
“All we ask is to be able to continue our religious vocation free from government intrusion,” she said.
Attorneys from The Becket Fund for Religious Freedom presented the nuns’ case in a lawsuit challenging the mandate, a part of the Affordable Care Act also known as Obamacare. The nuns argued the government is forcing them to act against their religious beliefs because of its requirement to provide free contraceptives and abortion-inducing drugs to employees, or pay steep fines.
Churches are exempt from the mandate, but charitable organizations like the Little Sisters are not.
Mother Patricia Mary Metzgar, l.s.p., who oversees the Little Sisters’ Mullen Home for the Aged in Denver, has attended some of the court hearings with other nuns. The Little Sisters of Denver employ about 67 full-time employees.
Mark Rienzi, senior attorney of the Becket Fund for Religious Liberty and lead attorney for the Little Sisters, reacted to the ruling saying he was disappointed.
“After losing repeatedly at the Supreme Court, the government continues its unrelenting pursuit of the Little Sisters of the Poor,” he said in a statement. “It is a national embarrassment that the world’s most powerful government insists that, instead of providing contraceptives through its own existing exchanges and programs, it must crush the Little Sisters’ faith and force them to participate. Untold millions of people have managed to get contraceptives without involving nuns, and there is no reason the government cannot run its programs without hijacking the Little Sisters and their health plan.”
Before the court’s ruling, the nuns filed an appeal Feb. 2014 in Denver federal court and were granted a temporary injunction, which shielded them from the HHS mandate and its fines. At issue is a waiver form the sisters could sign to receive an exemption from the mandate, but the appeal states that it “would make them morally complicit in sin, would contradict their public witness to the value of life, and would immorally run the risk of misleading others.” The form in fact would authorize a third-party to provide the services they find morally objectionable.
The appeal argued the HHS mandate violates the Religious Freedom Restoration Act and the First Amendment that guarantee freedom of religion. The court heard oral arguments in the case in December, when Sister Maguire delivered her first public statement.
On July 14, the 10th Circuit ruled that the government can force the Little Sisters to adhere to the mandate. It said that participating in the HHS mandate is “as easy as obtaining a parade permit, filing a simple tax form, or registering to vote.” It also ruled that although the nuns argued it would make “them complicit in the overall delivery scheme,” the court “ultimately rejects the merits of this claim” because the court believes the exemption “relieves [the Little Sisters] from complicity.”
The Little Sisters and their attorneys are reviewing the court’s decision and will decide whether to bring their case to the Supreme Court, according to the Becket Fund.
“We will keep on fighting for the Little Sisters, even if that means having to go all the way to the Supreme Court,” Daniel Blomberg, attorney at the Becket Fund, said in a statement.
The court’s order also impacts the Christian Brothers Services and Christian Brothers Employee Benefit Trust, the Catholic ministries through which the Little Sisters obtain their health coverage.
WASHINGTON, D.C., July 13, 2015 (LifeSiteNews) – The Obama administration released new, finalized rules on Friday on the controversial HHS mandate – rules that critics say expose religious orders like the Little Sisters of the Poor to massive fines for following their conscience.
They also say the rule ignores the victory for religious freedom won by the Supreme Court with last year’s Hobby Lobby decision.
The HHS mandate requires all employers to furnish their employees with contraceptives, sterilization, and abortifacient drugs at no co-pay as part of the Affordable Care Act, conventionally known as ObamaCare. The provision led to a national backlash, saying it tramples upon the conscience rights of religious business owners, effectively forcing them to choose between their livelihood and their faith.
The Obama administration’s latest “accommodation” states that closely held corporations – in which the stock is held by five or fewer families – may opt out of the provision by signing the self-certification form (form 700) and sending it to its insurance company. This letter triggers the insurance company to provide women with birth control for “free.” Religious employers objected that this still violated their faith, as it required their material participation in sin by granting a de facto authorization.
They also protest having the services provided by their own insurance companies.
Under the new regulation, closely held corporations with religious objections to contraception or abortion-inducing drugs must pass a resolution stating their objection, then write a letter either to their insurers or to the Department of Health and Human Services (HHS). The HHS will then contact their insurers to insist upon the “free” contraceptives.
If found guilty, the Obama administration will impose fines of $100 per employee per day.
Opponents say the “accommodation” is an accounting gimmick that does not respect the First Amendment’s free exercise clause.
“The government keeps digging the hole deeper,” said Adèle Auxier Keim, Legal Counsel at the Becket Fund for Religious Liberty. “Just last week the Supreme Court ordered HHS not to enforce the exact rules they finalized today. But the government still won’t give up on its quest to force nuns and other religious employers to distribute contraceptives.”
“It’s small comfort to know that the government mandates a violation of a religious entity’s moral beliefs, and then offers to carry out the violation,” agreed Family Research Council President Tony Perkins. “Even more incredible, HHS is now applying this scheme to family-owned businesses such as Hobby Lobby and Conestoga Wood Specialties, which already won relief from the government mandate by the Supreme Court. The Obama administration is disregarding the Court’s ruling declaring this mandate a violation of the family owned business’s religious freedoms.”
Yet the administration’s supporters cheered the move, specifically because it undermined the High Court’s decision.
“While these new rules don’t do anything to push back against the dangerous precedent set by the Court — that corporations engaged in secular activity such as purchasing health insurance can claim the same religious protections normally reserved for private individuals — they mitigate the negative effects initially brought on by the court’s ruling,” wrote Jon Green at the liberal Americablog.
Perkins says the rule harms nuns, conscience, and the liberty of the American people at large.
“Crushing federal mandates of this kind don’t belong in a free country,” he said.
July 13, 2015 (POP) — On July 11th, the United Nations celebrated its 26th World Population Day. The point of this annual exercise is to raise money to promote abortion, sterilization and contraception among poor and vulnerable women by alarming us about the dangers of global population growth.
The problem with this narrative is that, in many regions of the world, the population is declining, not growing. About half the world’s population lives in “low-fertility” countries, where women have fewer than 2.1 children on average over their lifetimes. Low-fertility countries now include all of Europe (except Iceland), the Americas (17 countries), and most of Asia (19 countries). The list of low-fertility countries include China, the United States, Brazil, the Russian Federation, Japan and Viet Nam.
In other words, growth rates have dramatically declined from the late 1960s when the global population grew at a rate of 2.1% each year. That rate is now about 1% a year. The UN’s low variant projection (historically the most accurate) indicates that it will peak at around 8.3 billion in 2050. Even the medium variant projection shows population growth slowing to 0.1% by the century’s end, and turning negative beyond 2100. In either case, the population of the world will never double again.
Image
As these numbers suggest, fertility rates have dipped to all-time lows. The U.N.’s medium variant projection estimates that women are now averaging 2.45 children over their reproductive lifetime, while the low variant pegs this at only 2.05. The global average was 4.97 just 60 years ago. Under either variant, this number will be well under replacement by century’s end. After all, global replacement fertility—the rate needed to replace the current generation and prevent population decline—is 2.23 children per woman over her reproductive lifetime.
Many developed nations are already suffering from the effects of population decline. Populations in many areas are rapidly aging as younger cohorts are becoming smaller. Social safety nets are being strained to the breaking point as fewer workers are struggling to support increasing numbers of elderly.
In Japan, increasing urbanization in conjunction with falling fertility rates have resulted in a drastic depopulation of many rural towns and villages. Economic growth is being compromised as workers are in increasingly short supply. The elderly are being abandoned as their only children go on to have no children at all. There are simply too few members of the younger generation to care for them.
Europe is also reeling from the effects of declining populations. In Italy, Portugal, Poland, Russia and throughout most of Southern and Eastern Europe, crude death rates exceed crude birth rates. The fertility rate for all of Europe is 1.58, well off the 2.09 replacement fertility rate, and recipe for demographic disaster.
Growth rates have also slowed in many developing nations. Thailand, Myanmar, and Tunisia are all below replacement level fertility. Even once-fertile Bangladesh is projected to fall below the replacement threshold 2020. The U.N.’s medium variant projection predicts that the population of Bangladesh will begin to contract after 2060, sooner under the low variant.
China’s Planned Birth policy (one child in the cities; two in the countryside) has driven its fertility rate down to an unsustainable 1.66, far below the estimated 2.22 it needs to stabilize its population. Little girls continue to be aborted or killed at birth in shocking numbers. There are 116 boys born in China for every 100 girls, one of the most skewed sex ratios in the world. Millions of Chinese men will never marry.
In spite of this dismal picture, population alarmists continue to push for population control programs.
Under the Obama administration, population control remains a key foreign aid objective. Various agencies of the U.S. government spent a whopping of $2.77 billion on “family planning and reproductive health” in 2014, a sum of money that dwarfs spending on all other health-related assistance, such as nutrition, water supply and sanitation, malaria, pandemic diseases, and general health care.
Only HIV/AIDS received more funding at $3.42 billion, and much of this money also went to population control organizations for population control purposes. The same devices that supposedly stop the spread of AIDS also stop the “spread” of pregnancy.
Expenditures for maternal and child health care, on the other hand, came to a paltry $497 million. Yet the surest way to lower fertility is to lower infant and child mortality rates.
USAID does not exaggerate when it says that it “has been the leading donor in international family planning for more than 40 years…in most years making up 40–50% of all donor funds.”
Given that birth rates are falling farther and faster than anyone imagined possible a couple of decades ago, what’s the U.N. to do to galvanize the U.S. and the world to continue putting this kind of money into the overpopulation pot?
Change the subject, that’s what.
The theme for this year’s World Population Day is not “Overpopulation,” but rather “Vulnerable Populations in Emergencies.” This is nothing more than an attempt to exploit the tragic and desperate conditions of the millions displaced or threatened by war, disaster or violent extremism to raise funds for population control.
Of course, it is true that the UNFPA has no qualms with pushing contraception and abortion on vulnerable populations in their time of greatest need. In its own words: “UNFPA works in emergency settings around the globe to respond to…the needs of women and girls…restoring their access to sexual and reproductive health care.”
Refugees are in desperate need of almost everything. They generally lack shelter, food, access to clean drinking water, health care—the list goes on and on.
And, for this year’s World Population Day, the U.N. wants to give them … birth control.
Reprinted with permission from Population Research Institute.
San Diego, CA, July 9, 2015 (Operation Rescue) — A quietly-handled wrongful termination lawsuit brought in San Diego, California, against Planned Parenthood of the Pacific Southwest gives insight into Planned Parenthood’s defensive mechanisms that kick into full throttle when employees fail to march in lockstep.
But more disturbingly, it reveals something sinister about Planned Parenthood’s unethical treatment of at least one minor girl and its aggressive eagerness to cannibalize one of their own rather than admit there might be serious internal problems.
The 2014 suit was explained in a well-written piece that appeared in the San Diego Reader, a quirky, alternative newspaper that focuses on the trendy – and often gritty – cultural side of San Diego. Amid the bright promotions of local events, flashy concert advertisements, restaurant reviews and personal ads, one can find some of the best investigative reporting anywhere. The Reader dares to go where mainstream media will not, including behind the veil of obfuscation that usually characterizes abortion rhetoric that is force-fed to the public.
The case is Murray v. Planned Parenthood of the Pacific Southwest. It was brought by Carla M. Murray, nurse practitioner with an exemplary employment record who worked for Planned Parenthood for over ten years.
Murray worked at Planned Parenthood’s Chula Vista clinic, which offers abortion pills, birth control, STD testing, and other services to the primarily Hispanic community near the border with Mexico.
Murray’s problems began in mid-2012 when she reported to the clinic manager, Thelma Mendoza, that employees were accessing the clinic’s drug cabinet and dispensing drugs to patients without proper authorization in violation of California law.
Murray’s suit contends that Mendoza began to retaliate against her by writing her up for exaggerated and blatantly fabricated infractions. Murray alleges that Mendoza went so far as to sabotage her attempt to move to another Planned Parenthood clinic.
The final straw came on March 8, 2013, when a woman brought her minor step-daughter to the Chula Vista Planned Parenthood clinic for birth control. The young girl indicated to Murray that she did not want the Depo-Provera birth control shot. It became apparent to Murray that her young patient was being forced by her step-mother into taking a birth control injection that she did not want and apparently did not need.
Instead, after receiving guidance from Janeen Bullison, Planned Parenthood’s Quality Assurance Manager, Murray gave the minor girl “emergency contraception, condoms, and educational handouts” in lieu of the Depo-Provera shot.
Afterwards, the step-mother became irate and could be heard “screaming” at staff and demanding that her step-daughter be given a birth control injection. Murray contacted Mendoza’s supervisor, Julia Jura, for additional guidance but was told by Jura to allow Mendoza to handle the situation.
According to Murray’s suit, a medical assistant was illegally ordered by Mendoza to give the minor girl the Depo-Provera injection, even though Mendoza is unlicensed and not qualified to authorize drugs to patients.
This action violated Planned Parenthood’s own Mission Statement, which asserts that patients should be allowed to “manage their own fertility” regardless of their age. Could it be that such statements are merely window-dressing for a gullible public?
“It is clearly illegal and unethical to force a birth control injection on anyone against their will. Yet, Planned Parenthood seemed unbothered by the effects on their young patient, both physically and emotionally,” said Operation Rescue President Troy Newman. “It seems that if a parent is in opposition to a child receiving an abortion or birth control, they have no rights. However, if the parent is the one coercing a child into an unwanted abortion or forced birth control, then it is their wishes that prevail. We have to wonder how many girls there are out there that have been forced into ‘reproductive services’ such as abortion and birth control against their will and bear the emotional scars today. It’s probably more than we think.”
Murray reported the incident and lodged a complaint against Mendoza for practicing medicine without a license. She was promised an investigation, but days later, she was told that there had been no wrong-doing on Mendoza’s part.
It appears that there was an orchestrated conspiracy inside Planned Parenthood of the Pacific Southwest at the highest levels to protect Mendoza from the consequences of illegal actions that she committed and allowed, while vilifying the one that attempted to set things right.
Four days later, on March 30, 2013, Murray was terminated in an act that she believes was in retaliation for blowing the whistle on Mendoza.
After months of legal motions and maneuvers, the case was set for trial on August 14, 2015. However, it now seems that the facts will never see the inside of a courtroom.
On June 30, Planned Parenthood settled the suit with Murray and the case was dismissed.
Who knows what other information would have come out in open trial? Now we will never know.
“It would have served the public to allow this case to go to trial, but it would not have served Planned Parenthood’s interests. Now, the full reality of apparently illegal activity that led to the abuse and violation of a minor girl will never be told in court,” said Newman. “This only guarantees that the abuses will continue at Planned Parenthood and that employees that witness them will be too intimidated to speak out.”
The San Diego Reader asked, “Who’s giving injections at Planned Parenthood?”
The answer is something Planned Parenthood has gone to great lengths – and expense — to hide. In the meantime, a young girl has been violated by those who were entrusted with her care and protection.
She and others like her are the true losers in this case.
WASHINGTON, D.C., July 9, 2015 (LifeSiteNews) – After the Supreme Court’s ruling that same-sex “marriage” is a constitutionally guaranteed right, many Americans have asked, “How did we get here?” Last month’s opinion tells us the road stretches back more than 50 years.
Justice Anthony Kennedy’s ruling in Obergefell v. Hodges gave additional proof that the legal basis for same-sex “marriage” is inextricably tied up with abortion-on-demand and other aspects of the sexual revolution.
In his 5-4 decision, Justice Kennedy says the newly discovered constitutional right to enter into a homosexual “marriage” is granted, in part, by the “right to privacy.”
That right, first propounded by the court in 1965’s Griswold v. Connecticut ruling, also conferred a woman’s right to abortion-on-demand, according to the 1973 Roe v. Wade decision.
“Same-sex couples have the same right as opposite-sex couples to enjoy intimate association,” Justice Kennedy wrote last month, in an opinion that quoted Griswold. “Like choices concerning contraception, family relationships, procreation, and child-rearing, all of which are protected by the Constitution, decisions concerning marriage are among the most intimate that an individual can make.”
“As far as the right to life is concerned, that is the most troubling line in the opinion,” wrote Kelsey Hazzard, a pro-life lawyer, in an analysis of the decision posted at the Secular Pro-Life blog. That sentence “can be read as polite legalese for killing preborn children.”
But Kennedy actually put the same-sex “marriage” case on stronger ground even than abortion. “Justice Kennedy was smart,” Hazzard wrote. “By writing an opinion that does not cite any abortion cases, he has assured that Obergefell will withstand the reversal of Roe and Casey.”
Instead, he based his argument in part on the case that granted Americans the right to use contraception.
That lawsuit was brought by Estelle Griswold, the former executive director of Planned Parenthood in New Haven, against the state of Connecticut. Lawmakers had passed a law forbidding anyone, married or unmarried, from using contraception. Planned Parenthood challenged the law all the way to the U.S. Supreme Court.
On June 7, 1965, Planned Parenthood prevailed.
Justice William O. Douglas wrote that, while the “right to privacy” is not explicitly mentioned in the Constitution – much less the right to birth control – the idea flows from ideas embedded in the Constitution.
“Specific guarantees in the Bill of Rights have penumbras, formed by emanations from those guarantees that help give them life and substance,” he wrote.
For the state to determine whether married couples used contraception would require an invasion of their privacy, Douglas wrote; thus, couples had an inalienable right to contraception.
“Griswold took a major leap for women’s health by removing state interference with one of the most important and private decisions an individual considers: whether and when to have a child,” wrote Elizabeth G. Taylor, the executive director of the National Health Law Program (NHeLP).
That ruling applied only to married couples. The right to privacy was then extended for unmarried individuals to use contraception in the High Court’s Eisenstadt v. Baird decision in 1972.
And one year later, the right to privacy emanated further, to grant women the “right to choose” an abortion.
Over the last 50 years, the “right to privacy” has been used to cover every form of sexual practice, displacing the public’s right to object on moral grounds – something contained in Kennedy’s 2003 Lawrence v. Texas ruling.
Finally, last month, that right – granted in Griswold and expanded in Eisenstadt, Roe, and Casey – demanded a nationwide legal recognition of homosexual relationships on par with heterosexual marriages.
Thus, Lauren Barbato could write in Bustle that “marriage equality may very well not be here on June 27, 2015, without Estelle Griswold and her fight to provide birth control to New Haven couples.”
July 8, 2015 (IMFCanada) — Across North America today, there are calls to make the birth control pill accessible over the counter. The Pill, we are told, is part of comprehensive health care and it is an insult that women should need a doctor’s prescription to use it. Recently, a columnist at the National Post complained that it is easier to get the Pill in Abu Dhabi than in Calgary or Toronto.
Most calls for the Pill to be made more broadly accessible—ideally free and without a prescription—all share the same subtext. Denying access to the Pill isn’t merely denying health care, it’s denying women’s rights.
Yet this is not about the right to get the Pill but rather, the right to not get pregnant.
This stems from the modern idea that men and women are only equal in dignity when we are exactly the same. As a result, we think that if men can have sex without the responsibility of childbearing, then women should too. This is why some feel so strongly that it is wrong for women to not have access to the Pill—one of the most effective contraceptives the world knows today.
Why, however, should pregnancy diminish a woman’s dignity or her rights in the world? And if this is indeed the case, why is it the woman who must remain child free in order to thrive?
Barring fertility from the workforce?
For starters, it remains a matter of opinion, not fact, that total control over fertility improves women’s rights.
This is a creation of the later waves of the feminist movement, over which there has never been complete agreement. Early feminists were better able to accept, embrace and celebrate motherhood, while simultaneously demanding that others rise up to support this unique and beautiful aspect of women’s lives.
A first wave feminist might ask that work conditions be altered to suit a woman who is pregnant—the opposing view, very much supported by modern contraception, demands that a woman not get pregnant in order to continue working.
The Pill does not advance women’s rights. It normalizes the idea that women shouldn’t be fertile, let alone pregnant. As evidence, see how major corporations like Apple and Facebook have the chutzpah today to offer women egg freezing as a job “perk.” In reality, this highlights how little we are willing to incorporate pregnancy into the working world.
The Pill: Stridently pitched as being in favour of women’s rights, it simultaneously puts women into a disadvantaged position. Women who want to have children must negotiate this desire at work with their employers and at home with their partners who are often comfortably uninterested. Then there’s the negotiation you never win with the biological realities of Mother Nature. Extended education and job training most often mean women are left to conjure up pregnancy at an age when it is far more difficult or impossible. The bitterness of the Pill is that almost universally, women don’t care about age-induced infertility until they are experiencing it.
A tainted medical legacy
Even if we all accepted that not getting pregnant makes women more equal, thereby bestowing greater rights—it is not clear that the Pill is the best way to do this. The Pill has health risks, has been declared to be carcinogenic by the World Health Organization and there’s that pesky class action suit against Yaz and Yasmin. The death of 23 women in Canada taking those birth control pills would not be so blithely overlooked were the cause of death something different.
Beyond catastrophic health events, however, the Pill denies women valuable information about their health. The body sends us clues about how we are doing. For women, this includes the daily ups and downs of our reproductive cycles. Women who are in the know can better monitor their own health unaltered by a daily dose of hormones. It’s empowering.
For the vast majority, the Pill is not medicine in any meaningful sense of the word. To designate it as such castigates pregnancy as a disease. It is no surprise, then, that this is how we treat pregnancy today, as a clinical problem, not a beautiful miracle.
All this said, yes, please do make the Pill over the counter. Perhaps when it sits beside Tylenol on a drugstore shelf, advocacy groups will stop yammering on about how the Pill is a major component of women’s rights. Or that it is patronizing when doctors show concern. Perhaps then we will stop targeting excellent doctors who won’t prescribe it for very good reasons.
And about the Pill being more freely available in Abu Dhabi? Just shout out if you want to move there, as a Canadian or American woman today.
Andrea Mrozek is the Executive Director of the Institute of Marriage and Family Canada (www.imfcanada.org). She is currently co-authoring a book about the effects of the sexual revolution in women’s lives. Reprinted with permission from IMFC.
TEXAS RIGHT TO LIFE JUL 7, 2015 | 8:19AM WASHINGTON, DC
The U.K.’s Alliance of Pro-Life Students (APS) released an eye-opening perspective piece written by a pregnancy center volunteer who has interacted with hundreds of women seeking abortions. Her experience shatters common perceptions painted by the abortion movement, which suggest that virtually all women who undergo abortions do so as an exercise of their own free will and rights. On the contrary, according to APS’s anonymous guest blogger, “the word ‘choice’ is often the last word a woman in a crisis pregnancy feels applies to her when she’s looking for an abortion.” The volunteer enumerates the many reasons that motivate women to seek abortion. Indeed compelling, the reasons indicate that these women are certainly in crisis. But not, the volunteer explains, because they are pregnant.
Rather, the crisis is the reaction of those closest in their lives to the news. “The crisis,” she says, “is the fact that her workplace is prejudiced against pregnant women, or that she feels she has to do what her partner says, or that she is not financially stable, or that her boyfriend won’t commit, or that she is in an abusive relationship, or that she is being threatened with homelessness.” Pregnancy magnifies these tragedies in the woman’s life, and the natural conclusion for many is that by eliminating the preborn child, the crisis will go away. In reality, the crisis remains without the child who seems to be exacerbating her ordeal. The writer shares the story of a woman who was utterly under the control of her child’s father. He had the power to have her deported or ejected penniless onto the streets. “She was completely dependent on him and he was physically and emotionally abusive,” the volunteer shared.
But forcing the woman to abort her child proved to be an effortless endeavor for the abusive man; he took her from the pregnancy center to the abortion mill, and the child was dead within hours of their encounter. Abortion is portrayed as a woman’s right – an inviolable badge of her autonomy and freedom. And yet, every day countless women are forced and coerced into unwanted abortions, and the abortionists who operate under the auspices of “women’s rights” do absolutely nothing to counteract these disasters. “Silent complicity with abusive boyfriends is not what feminism has fought for,” said the volunteer.
While U.S. pregnancy resource centers have come under intense attack by the anti-Life movement in recent years, they are needed now more than ever. If this is the era of feminism – equality of the sexes – pregnancy resource centers are the hallmark of that age. Pregnancy centers are a singular refuge offering real compassion and concern without Big Abortion’s profit-driven tactics, which only come to fruition in the suctioning of children from their mothers’ wombs. “Women in the 21st Century should not feel they have to enter this secret world where ‘their mistake’ can be ‘fixed’, no questions asked,” the volunteer concludes. “They should feel that those who are putting pressure on them will be held accountable and that they have control over their lives.”
LifeNews Note: Reprinted with permission from Texas Right to Life.”
Read this open letter to the Gay Community from a loving daughter.
She wonders why there isn’t more attention on the rest of this story, namely the children raised by two mothers or two fathers.
Same-sex marriage and parenting withholds either a mother or father from a child while telling him or her that it doesn’t matter. That it’s all the same. But it’s not. A lot of us, a lot of your kids, are hurting. My father’s absence created a huge hole in me, and I ached every day for a dad. I loved my mom’s partner, but another mom could never have replaced the father I lost.
I grew up surrounded by women who said they didn’t need or want a man. Yet, as a little girl, I so desperately wanted a daddy. It is a strange and confusing thing to walk around with this deep-down unquenchable ache for a father, for a man, in a community that says that men are unnecessary…
I’m not saying that you can’t be good parents. You can. I had one of the best. I’m also not saying that being raised by straight parents means everything will turn out okay. We know there are so many different ways that the family unit can break down and cause kids to suffer: divorce, abandonment, infidelity, abuse, death, etc. But by and large, the best and most successful family structure is one in which kids are being raised by both their mother and father.
And she wonders why gay people’s kids can’t be honest in talking about the realities, for them, of gay marriage.
It promotes and normalizes a family structure that necessarily denies us something precious and foundational. It denies us something we need and long for, while at the same time tells us that we don’t need what we naturally crave. That we will be okay. But we’re not. We’re hurting.
She notes that children of divorced parents, adopted children of biological parents they never knew, are “allowed” to speak out about their pain, suffering, longing, feelings.
But children of same-sex parents haven’t been given the same voice. It’s not just me. There are so many of us.
One of the first to publish such an account was Robert Lopez, and his account of being ‘raised by two moms’ clearly reveals his love for his mother, but also the long term impact that home life had on him. It opened the door for many other children of same-sex parents who were afraid to speak up because they loved them and didn’t want to hurt them.
In the past couple of days, that link has become inaccessible, and the online journal that published it has been dealing with technical issues. Which may or may not be related to the silencing Heather Barwick referred to in her honest, open letter.
If we say we are hurting because we were raised by same-sex parents, we are either ignored or labeled a hater.
This isn’t about hate at all. I know you understand the pain of a label that doesn’t fit and the pain of a label that is used to malign or silence you. And I know that you really have been hated and that you really have been hurt. I was there, at the marches, when they held up signs that said, “God hates fags” and “AIDS cures homosexuality.” I cried and turned hot with anger right there in the street with you. But that’s not me. That’s not us.
That’s not most of us. It’s the extreme left and right doing the most outright condemnation. Most of us who are trying to engage at all, are trying to do so reasonably and charitably. Many of us make efforts to speak clearly and listen closely, with the courage of conviction and respect for the dignity of those who challenge and even try to silence our beliefs, beliefs which at core witness to human dignity.
So Heather Barwick closes her letter to the Gay Community in which she was raised, with which she identified most of her life, who she understands with great compassion, and appeals to now as a children’s rights activist, with this:
I know this is a hard conversation. But we need to talk about it. If anyone can talk about hard things, it’s us. You taught me that.
AUCKLAND, NZ, July 3, 2015 (LifeSiteNews) – Every girl in New Zealand will be put on long-acting reversible contraceptive drugs, delivered through implants or patches, before they become sexually active, if a group of health researchers at New Zealand’s Otago University gets its way.
“I would imagine, off the top of my head, that it would happen a bit like vaccinations happen,” Neil Pickering, a senior bioethics lecturer at the university, told Radio New Zealand report. “It would be a routine thing, and being done through schools would be an obvious way.”
Helen Paterson, of the University of Otago’s department of women’s and children’s health, suggested that a contraceptive called Jadelle, which is a drug-laden plastic rod that is implanted into the girl’s upper arm by a doctor, would be a good choice and should be available to the teens free of charge.
“What we want to do is make something that’s universally available,” Paterson said, “so that adolescents can easily access good care in terms of their contraception that’s provided to them.”
The Otago University group is aware that their suggestion is controversial, with Dr. Pickering noting that he “would expect there to be a reaction against this because it’s a fairly new suggestion that people perhaps haven’t thought about previously.”
He added that “obviously” the girls’ “parents and the children themselves would need to be informed that this is going to happen, and informed that they have the option not to take part if they don’t wish to.”
“The idea of giving young people, teens, medication which you might say they don’t need and can’t benefit from,” Pickering said, “all these things would no doubt come into people’s minds and in addition to that people might have fears such as, ‘Oh, won’t that mean they’ll start going out and having sex willy-nilly with everybody’.”
The call for universal contraception for young girls has met with strong criticism from groups on opposite sides of the issue.
Jackie Edmond, the director of “reproductive health” services provider Family Planning NZ said the proposal is “overkill” and goes further than necessary to reduce teen pregnancy, which is already declining.
“We’re overkilling it, putting implants in people who aren’t intending to or aren’t having sex,” Edmond told NZ Newswire.
Dave Ayling, clinical director of a youth health and counseling service in Palmerston North said, “Contraception is not a one-off task that involves sticking some rods in an arm.” He warned that adverse effects of the drugs could pose a potential health risk that young girls are not prepared for.
“I also worry about ongoing costs associated with LARCs [long-acting reversible contraception] for managing potential side-effects that a lot will not be able to afford, so focusing on a sustainable equitable contraception service is more where the emphasis should go,” Ayling said.
School guidance counselors are “horrified” at the idea of universal contraception, according to a report by Newstalk ZB.
“I think often it’s hard enough for young women to say no to sexual advances, but if a lot of young men know that they’re already on contraception, I wonder how that will be for them to actually say no,” said Sarah Maindonald of the New Zealand Association of Counselors.
Pro-life group Family First NZ called the scheme a “flawed, morally bankrupt” approach that will do more harm than good.
“The decreasing proportion of teens wanting to be sexually active need parental involvement and good advice,” said Bob McCoskrie, National Director of Family First NZ.
“Contraception deals with unwanted pregnancy, but there’s no mention of the danger of sexually transmitted infections and increased sexual activity. Making it free and even more accessible is going to continue to alienate parents from the role they should be involved in. What we should be asking is, why are young teenagers becoming sexually active, what messages are teens receiving about sexual involvement, and what messages do parents actually want their children to receive,” McCoskrie said.
Noting that rates of teen abortions have fallen significantly recently, McCoskrie pointed out that “this has nothing to do with contraception, and everything to do with decreased sexual activity, and education, and awareness for teens on the actual consequences” of early sexual activity.
Family First NZ stresses that a U.S. study found increased access to emergency contraception actually increases the rates of sexually transmitted diseases, risk taking and a false sense of security while doing nothing to reduce the number of abortions, and that the side effects specific to Jadelle implants, which contain levonorgestrel, include irregular menstrual bleeding, application site reactions, dizziness, headache, vaginal discharge, breast pain, nausea, pelvic pain, urinary tract symptoms, vaginitis, and weight gain.
Levonorgestrel is also linked to increased risk of liver dysfunction and potentially deadly blood clots.
All LARCs potentially act as abortifacients, rather than contraceptives, as well.
“Teen girls deserve to be informed of the serious consequences of early sexual activity including the impact on emotional and mental welfare and academic performance, rather than given a false sense of security and being encouraged to take risks by adults who should know better,” Bob McCoskrie said.
He added that British researchers found that greater use of contraceptive implants and drugs had an almost statistically insignificant effect on teenage pregnancy rates.
“Ironically, getting a good education could be the best form of contraception for teenagers, according to a recent UK study.”
WASHINGTON, D.C., July 1, 2015 (LifeSiteNews) – As ObamaCare enters its second year, the program is changing the way Americans use health care. More Americans used contraception this year compared to last year, while fewer asked for prescription drugs, according to a new study.
In the first quarter of this year, the use of oral contraceptives increased by 29 percent compared to the same period in 2014.
But the number of people using a prescription drug dropped 18 percent by comparison, according to a study by Express Scripts.
A controversial provision of the Obama administration’s health care law, known as the HHS mandate, requires employers to provide all women with contraceptives, abortifacients, and sterilization services with no co-pay.
In October 2012, Barack Obama told an audience at George Mason University that college-aged females should not “have to choose between text books” and “preventive care” – a euphemism for birth control. “That’s why we passed this law. And I am proud of it. It was the right thing to do.”
The study’s authors say the paradox is “likely due to the younger average age of exchange enrollees” in 2015 over 2014. “We may be seeing the start of a new chapter with this program, where healthier Americans who use fewer prescription medications are engaging with these plans, helping plans achieve a more balanced risk pool, which will help them sustain benefit offerings in the future.”
However, there may be another explanation: Fewer Americans are getting their prescriptions filled due to soaring deductibles.
Analysts say the creeping out-of-pocket expenses come as people search for a way to escape the skyrocketing cost of insurance premiums since the passage of the Affordable Care Act, conventionally known as ObamaCare.
Insurance premiums rose 41 percent the first year of the program, and insurers are asking for double-digit increases again this year.
To avoid the pinch, consumers are seeking plans with lower monthly costs but that entail higher deductibles and less coverage.
The number of Americans whose deductible is now at least $1,000 has more than quadrupled since 2006.
Worse, many of these plans do not cover the drugs patients need. “Simply put, many drugs may not be covered at all, and the costs patients incur by buying them with cash won’t count against out of pocket caps,” wrote Scott Gottlieb at Forbes.
As a result, many people are simply doing without their medicine. Holly Wilson of Denver did not take her high blood pressure medication for three months, despite suffering from congestive heart failure. She resumed taking the pills after her doctor told her that she risked having a stroke – but she gets the drugs by asking her doctor for free samples and purchasing only a few pills at a time, according to USA Today.
In 2012, 15 percent of Americans who had a prescription drug benefit said they could not afford their medical bills, according to Consumer Reports.
This message is an expansion of the previous message of June 3, 2015 [Feast of Saint Kevin of Glendalough]. We ask that you consider doing the following three (3) things:
1. Continue to Pray
Until further notice, please simply join in praying The Rosary daily (and if you can, the Chaplet of Divine Mercy) for the U.S. Catholic Bishops to join with Pope Francis and have that solemn procession and permanent placement of the statue of Our Lady of America (depicted above) in the National Shrine of the Immaculate Conception at Washington, D.C. this September (2015) when Pope Francis visits there.
2. Form an Our Lady of America Prayer Group
Pray and consult other Christians interested in this approved devotion to The Blessed Virgin Mary about forming a regular prayer group. Simply organize a prayer group to meet weekly (e.g., one evening, Saturday Morning after the Parish Mass, Sunday after Mass): Read one message each week and then recite The Rosary (either the daily Mystery or an entire 20-Decade Rosary); end with a period of conviviality and further discussion of the messages in light of current events, such as anti-abortion activities; upholding purity by traditional marriage, NFP, etc. . You may also wish to advise your pastor or bishop about the prayer group, or involve another holy priest in it.
3. Ask Pope Francis to Advocate and to Join in that Solemn Procession
Write a letter to Pope Francis in which you ask His Holiness to endorse personally the devotion to Our Lady of America and to invite the United States Catholic Bishops to join Him in the Solemn Procession and permanent placement of the statue of Our Lady of America into the Basilica of the National Shrine of The Immaculate Conception at Washington, D.C. when He visits that shrine church in September of this year (2015).
You should address your letter or postcard, as follows:
His Holiness, Pope Francis
c/o Archbishop Carlo Maria Viganò
Apostolic Nuncio to the U.S.A.
3339 Massachusetts Avenue, N.W.
Washington, D.C. 20008-3610
Ideas: Possible Points to Make in Your Letter or Postcard to His Holiness
(Please use your own thoughts and words; please do not just copy one of these!)
DRAFT #1 OF IDEAS (POINTS TO MAKE)—
Your Holiness (OR My dearest Pope Francis),
● Thank you for your ministry in the person of Our Lord Jesus Christ and for His Catholic Church.
● While I oppose the attack on the Christian family by the distortion of same-sex unions, abortion, artificial contraception, and other sinful manifestations of vice, I know that the path of Our Lord Jesus proceeds by way of conversion from sin and through prayer and the grace of virtuous human acts.
● Appearing as “Our Lady of America” here in the United States, The Blessed Virgin Mary has promised the grace of a nearly universal infusion of the Christian virtue of purity.
● To obtain this grace of purity for the people of the United States and of the whole world, Our Lady of America asked that the United States Catholic bishops carry Her statue in a solemn procession into the national Marian shrine at Washington, D.C. .
● This Christian virtue of purity is one of the most important invisible realities in the Catholic Church, among other spiritual realities like sin, other virtues and eternal life.
● This devotion to Our Lady of America received proper ecclesiastical approvals through Cincinnati Archbishop Paul Francis Leibold (1914-1972) here in the United States.
● Although I do understand that the Catholic bishops here in the United States of America have the primary responsibility to hold this solemn procession and permanent placement of the Our Lady of America statue, I am asking Your Holiness to use your leadership and take the personal initiative yourself to encourage these American bishops to join you directly in doing this public act when Your Holiness is also present at that National Marian Shrine in Washington, D.C.. Please take the lead and urge the U. S. Bishops to do this.
● Please encourage all of the United States Catholic bishops to join Your Holiness in this procession and placement of the statue of Our Lady of America during your visit this September at Washington, D.C..
With prayers and love for Your Holiness, Most respectfully,
DRAFT #2 OF IDEAS (POINTS TO MAKE)—
● A secular world nearly driven by lust and perversion has yielded many evils, including abortion, sodomite unions, and un-holy Eucharistic communions. We very much need chastity and self-control, especially among so many young people bereft of moral and religious formation. Without the Christian virtue of purity, many souls will not have chastity or self-control and they will be lost forever.
● However, before his death in 1972, the Catholic Archbishop of Cincinnati, The Most Reverend Paul F. Leibold, offered an answer to this problem by approving a devotion to The Blessed Virgin Mary under the title of “Our Lady of America” as described on the EWTN internet site: http://www.ewtn.com/library/BISHOPS/burkeolamer.HTM .
● Our Lady of America promised an outpouring of the grace of purity if the Catholic Bishops of the United States of America would, after a solemn procession, place her special image holding a Lily of Purity into that national Marian shrine at Washington, D.C.
● Since Your Holiness will be at this National Shrine of The Immaculate Conception in Washington, D.C. this September, please encourage the U.S. Bishops to have that procession and placement of the statue take place with you when you visit.
● Although I do understand that the Catholic bishops here in the United States of America have the primary responsibility to hold this solemn procession and permanent placement of the Our Lady of America statue, I am asking Your Holiness to use your leadership and take the personal initiative yourself to encourage these American bishops to join you directly in doing this public act when Your Holiness is also present at that National Marian Shrine in Washington, D.C.. Please urge the U. S. Bishops to do this.
● We pray for Your Holiness daily and we will now pray especially hard that Your Holiness has the good sense to encourage the American bishops to accomplish this solemn procession of the Our Lady of America statue while you can participate this September at Washington, D.C. .
Most respectfully,
DRAFT #3 OF IDEAS (POINTS TO MAKE)—
● Thank you for your ministry in the person of Our Lord Jesus Christ and for His Catholic Church.
● The secular world now confronts the Catholic Church with an array of heathen amoral values, including the distortion of human sexuality, marriage and normal family life. God gave us these beautiful gifts, even after The Fall of Adam and Eve—“Male and Female He made them.”
● I oppose the attack on the Christian family by the distortion of same-sex unions, abortion, artificial contraception, and other sinful manifestations of vice, and I know that the path of Our Lord Jesus proceeds by way of conversion from sin and through prayer and the grace of virtuous human acts.
● Realities are important, especially those “things visible and invisible” as we pray in the Credo at Mass. Actually, the most important religious “realities” are those which are invisible to us humans, including “The Holy Trinity” and “virtue”.
● The Christian virtue of purity is one of the most important invisible realities in the Catholic Church. Without it, the human race cannot restore regular order to marriage and family life, or recognize the indwelling Trinity in others very well.
● The Blessed Virgin Mary appeared as “Our Lady of America” here in the United States, and She has promised the grace of a nearly universal infusion of the Christian virtue of purity, if the United States Catholic bishops carry Her particular statue in which She holds lily in a solemn procession into the national Marian shrine at Washington, D.C. .
● This devotion to Our Lady of America received proper ecclesiastical approvals through Cincinnati (Ohio) Archbishop Paul Francis Leibold (1914-1972) here in the United States.
● Although I do understand that the Catholic bishops here in the United States of America have the primary responsibility to hold this solemn procession and permanent placement of the Our Lady of America statue, I am asking Your Holiness to use your leadership and take the personal initiative yourself to encourage these American bishops to join you directly in doing this public act when Your Holiness is also present at that National Marian Shrine in Washington, D.C.. Please take the lead in the procession and urge the U. S. Bishops to do this.
With prayers and love for Your Holiness,
Most respectfully,
DRAFT #4 OF IDEAS (POINTS TO MAKE)—
● The Church and the World need the Christian virtue of purity, a reality which we can obtain through a special intercession of Our Lady of America.
● Under this title (Our Lady of America), The Blessed Mother Mary asked for a solemn procession with her special statue by the U. S. bishops into our National Marian Shrine at Washington, D.C. .
● Although I do understand that the Catholic bishops here in the United States of America have the primary responsibility to hold this solemn procession and permanent placement of the Our Lady of America statue, I am asking Your Holiness to use your leadership and take the personal initiative yourself to encourage these American bishops to join you directly in doing this public act when Your Holiness is also present at that National Marian Shrine in Washington, D.C.. Please urge the U. S. Bishops to do this.
● Your Holiness should lead this procession and deposit of the statue of Our Lady of America when you come to that Shrine of The Immaculate Conception in September 2015.
● Thank you and know that I will be praying for you and your intentions.
● Hoping to see Your Holiness in that procession of the Our Lady of America statue,
With the utmost respect,
DRAFT #5 OF IDEAS (POINTS TO MAKE)—
● Thank you, Your Holiness, for all the hard work you have done since you became Pope. We pray that you will please Jesus with the help of Mother Mary.
● The Blessed Virgin Mary is important to the invisible reality of Christian purity which has some similarity to her character as The Immaculate.
● She appeared to an Austrian-American nun in 1956 as Our Lady of America and the Archbishop of Cincinnati approved this devotion.
● The Blessed Mother wants that special statue which shows both Her Immaculate Heart and Her holding a Lily of Purity carried by the U.S. Bishops in a solemn procession and put permanently in the National Shrine of the Immaculate Conception at Washington, D.C. .
● Although I do understand that the Catholic bishops here in the United States of America have the primary responsibility to hold this solemn procession and permanent placement of the Our Lady of America statue, I am asking Your Holiness to use your leadership and take the personal initiative yourself to encourage these American bishops to join you directly in doing this public act when Your Holiness is also present at that National Marian Shrine in Washington, D.C. in September 2015.
● Please get this procession and putting the statue into our Marian Shrine done along with all the U.S. Bishops when you visit there this September.
By Thy Holy & Immaculate Conception, O Mary, deliver us from evil!
B.V.M. Our Lady of America
C/O Langsenkamp Family Apostolate
9100 Purdue Rd #400
Indianapolis, IN 46268-1180
B.V.M. Our Lady of America is a not-for-profit activity of the BVM Foundation, Inc. Batesville, IN 47006
BVM Foundation, Inc. is a not-for-profit corporation.
I am composing this memo just hours after the US Supreme Court in a 5 to 4 decision—led by so-called Catholic Justice Anthony Kennedy—ruled that all 50 states must recognize gay so-called “marriage” as marriage according to the rights guaranteed by the 14th Amendment of the Constitution.
Let me say right out—there’s ultimately only one thing wrong with the Court’s decision and it’s this: Gay marriage is not marriage. What has just happened is that 5 mere human beings have completely re-defined marriage and thus have imposed a kind of madness on our society—madness in the sense that an immoral form of sexual behavior is called the equivalent of conjugal nuptial love—and to treat such unions as the moral equivalent of marriage is madness. Welcome to the insane asylum—that’s where you are now.
What happened today is the second to the last scene in a four act sad cultural drama—indeed a tragedy. The first act was the beginnings of acceptance of contraception by society and the Christian churches, the second act, the advent of the Birth Control Pill in the 1950s, the third act, the continued breakdown of marriage in the last 40 years (sex without marriage, couples living together, divorce, no-fault divorce, artificial reproduction, and of course abortion, all among heterosexuals) and the fourth and final act, the rise of the gay rights movement and its triumph
today—that unnatural sexual unions must be regarded the same as marriage.
Why is this gay “marriage” victory only the second to the last scene in our tragic social drama, and not the last scene itself? The last scene of the tragedy is the persecution of those who do not accept the madness.
It makes little difference that the Anthony written-opinion contains rhetoric to the effect that the Constitution protects the right of people to voice their views and advocate their views that gay “marriage” is not marriage. Such rhetoric will not matter. Now that the high court has said that what gays do in the bedroom is a matter of human rights and human dignity, and has cut off the political process on this issue, a cultural, social chill is created against those who do not agree with the Court—against those who refuse to be dragged into this cultural madness.
Those who do not accept so-called gay “marriage” are already viewed as ethically backwards, intolerant, and steeped in a narrow-minded religious bigotry. It will only get worse for those of us who actually believe that marriage means something—that it is a God-designed institution.
Today the court foisted upon America a completely subjectivist, relativistic view of human sexuality. Marriage is not regarded as an objective social/moral covenant that provides culture with innate order and structure and takes civilization into the future. Marriage is completely—and I need to emphasize this—completely relegated to emotions, feelings, romance—
and that’s essentially it! Indeed, one lesbian interviewed on WWJ radio said: “I want to be married for my own reasons.” This is a good statement on what marriage has come to mean, not just for gays, but for just about everyone—as if marriage had no objective moral or social meaning. Rather it’s just something I do for myself.
Today there is much celebrating going on, with social pundits and political figures like Obama himself congratulating the gay rights movement for never giving up in the advancement of their cause!
But let’s be very clear, it’s not the gay rights movement that should be congratulated. Rather it’s the heterosexual community that deserves the most credit for this gay rights victory. The success of the gay rights movement has only been possible due to the fact that the heterosexual community paved the way for it—as much of the sexual activity practiced by the heterosexual community cannot be called marriage either! Please see a link below to my article that provides one of the most cogent arguments on the difference between gay sexual unions and marriage.
When the Court made its decision I was at Mass praying that the Court would not make the decision that it did make. When I emerged from Mass, I entered a different world. My urge was to dash home, read my emails, listen to my voice mail messages—maybe there were requests from the media for interviews (there were a few) and make some kind of response. It took a huge of exertion of will to refuse that compulsion as I thought I should instead pray the Stations of the Cross.
Thus I forced myself to drive to my husband’s Catholic School where there are outdoor (somewhat neglected) Stations. I prayed them, walking from one station to the other up the hill behind the school. When I came to the Fifth Station—Simon Helps Jesus Carry His Cross—I was struck with the realization that this is what God is asking of me now—perhaps asking of all of us—as if He was saying: “Help me now to carry this cross.” So in this time of darkness and madness—our Lord on the Via Dolorosa—where God Himself was deemed a criminal in the eyes of the world— asks us to help Him carry the Cross—
and this is what we must do.
Do not despair and do not be afraid. For love of Christ—let us carry the Cross of love and truth.
While the last scene of the drama is persecution—another play is being written. It is the drama in which we reclaim the culture by a new evangelization. This is our holy task. Let us go forward. The God of the Resurrection is calling us.
One final note—we can lay the blame for the Court’s decision at the door step of the Church. The weakness of Christian witness from bishops down to the last man in the pew is the reason why we are facing this moral dissolution. And yet –the light is still there—as it is really only the Church that has the ability to reverse this time of darkness.
Lincoln, Neb., Jun 25, 2014 / 02:37 pm (CNA/EWTN News).- Nebraska Bishop James D. Conley’s pastoral letter “The Language of Love” has had an international impact in the first three months since it was published.
“Sacrifice is the language of love,” Bishop Conley’s pastoral letter reads. “Love is spoken in the sacrifice of Jesus Christ, who poured out his life for us on the cross. Love is spoken in the sacrifice of the Christian life, sharing in Christ’s life, death, and resurrection. And love is spoken in the sacrifice of parents, and pastors, and friends.”
The pastoral letter, published March 25, discusses topics like marriage and the reasons behind Catholic rejection of contraception and sterilization. It is addressed to the Catholic families and healthcare providers of the diocese of Lincoln, Neb.
The letter was reprinted in several outlets in the U.S. and in other countries. In Germany, the Bishop of Regensburg cited the letter in a homily and a German-language translation was published on the popular website Kath.net.
A Danish translation of the letter was published at the website of the Denmark-based magazine Katolsk. It has also been published in the Philippines.
Last week in London, Bishop Conley spoke about “The Language of Love” at St. Patrick’s Evangelization School, a formation program for young adults aged 20-30 based at the parish of St. Patrick in London’s SoHo neighborhood.
At the time of its release, the pastoral letter was delivered to every Catholic family registered in the Diocese of Lincoln. It was also made available as a podcast on the diocese’s website.
Bishop Conley’s letter says that American culture rejects “the gift of new life,” and therefore rejects love, through the use of contraception, which “gravely and seriously disrupts the sacrificial, holy and loving meaning of marriage itself.”
Marriage is a call to “loving as God loves… freely, creatively and generously.”
The letter also exhorts Catholic physicians, pharmacists and other health care professionals to pursue the “art of healing.” It notes that contraception and sterilization “denigrate and degrade the body’s very purpose.”
In March, Bishop Conley told CNA that Catholics who reject or ignore the immorality of contraception should look to the Church and to the teachings of Christ as “a message of love and mercy,” a message proclaimed by Pope Francis.
Denver, Colo., Jun 28, 2015 / 04:39 pm (CNA/EWTN News).- After receiving thousands of complaints about the adverse effects of the birth control implant Essure, the FDA announced late Wednesday that it has updated the list of risks and complications associated with the device, and that a public hearing would be held Sept. 24 to evaluate the product.
Essure is a permanent type of birth control in the form of tiny metal coils inserted into women’s Fallopian tubes. When the coils are implanted they are supposed to stay in the Fallopian tubes, where they create a chronic infection that will cause scar tissue to form around the coils, effectively closing the tubes and rendering the woman sterile.
Until this week, possible side effects of Essure listed on the product’s website included: “mild to moderate pain and/or cramping, vaginal bleeding, and pelvic or back discomfort for a few days. Some women experienced nausea and/or vomiting or fainting. In rare instances, an Essure insert may be expelled from the body.”
Angela Desa-Lynch, an administrator for the Facebook group “Essure Problems”, which protests the device, told CNA in February that the thousands of women in the group had experienced these problems to the extreme.
“Whatever they’ve put on the label, multiply it by 200,” she told CNA in February.
At least five deaths of women, and five deaths of fetuses in women who’ve been implanted with Essure, have been reported. Other side effects many of the “Essure Problems” women have experienced include perforated organs, coils lodged in colons, fetal disfigurement due to nickel poisoning, chronic pain, exhaustion, bouts of depression, and suicidal thoughts.
The group, which grew from about 14,000 to over 18,000 just since February, seeks to inform and save every woman they can from getting Essure implants. In a statement on their website, the group said they feel encouraged by the FDA’s announcement.
“We feel like the FDA has really been listening to us, to our group, and is taking some steps in the right direction to address the serious complications and problems with this device,” it reads.
“Having a large government agency paying attention to a group of women harmed by a medical device, and making arrangements to review information and allowing our voices to be heard, is huge,” the group said.
“We plan to bring with us as many of the original clinical trial participants as we can get there, along with our supporting physicians. We need every women harmed by Essure to get to this meeting. We need every media outlet there. All are welcome. Let’s fill the room and pour into the hallways. Let your faces be seen, and let your pain serve a purpose. Not one more woman harmed by Essure.”
The device was first manufactured by the group Conceptus and was pre-approved by the FDA before hitting the markets in 2002. In June 2014, Conceptus was bought by Bayer, which has continued to manufacture and distribute Essure.
In a statement released Thursday, Bayer said: “Patient safety is Bayer’s top priority. Given there has been a great deal of interest in the safety of Essure among some patients, we welcome this open dialogue with healthcare providers, patients, researchers, representatives from professional societies, and other members of the public to review and discuss available data regarding the benefits and risks associated with Essure.”
“Bayer is strongly committed to women having access to safe and effective birth control options. The only FDA-approved non-surgical option for women who have completed their families and want permanent contraception, Essure is supported by more than a decade of science and real world clinical experience.”
The announcement by the FDA and the promise of the September meeting is a step forward for the Essure Problems group, which has enlisted the help of environmental lawyer Erin Brockovich (yes, that one) in a few pending lawsuits to get Essure taken off the market.
The end of the statement from the group, which refers to their fellow members as “E-sisters”, reads: “Bound by pain, we will never stop until Essure is off the market.”
Got a big family? Then you already know that you’re crazy, a traitor to feminism, and a slave to the patriarchy; you’re neglecting most of your kids and robbing the rest of their childhood; you’re a burden on the system in general, and you probably don’t own a TV.
But wait, there’s more! Don’t forget, you’re also destroying the earth.
It’s become fashionable, in the name of the planet, to denounce large families as irresponsible, even selfish. Some politicians and a good many combox blabbermouths even say that it should be illegal for people to have more than one or two “replacement” children. Illegal!
And yet, if we can get beyond the inflammatory rhetoric, do radical environmentalists have a point? Should we slow down a little? It almost seems like common sense, especially when you’re having one of those days when you do feel a little crowded by the swarms of ravening locusts — uh, I mean, treasured offspring who share your last name.
After all, aren’t Catholics supposed to be good stewards of the earth? Isn’t it true that we “lotsas” are using more than our share of natural resources, burning more than our share of carbon, and just plain taking up too much space?
Probably not. Moms of many already know that the work of caring for, for instance, seven children is not the same as caring for one child times seven. In some ways, it’s easier. In the same way, many large families actually have a smaller carbon footprint than a typical family with one or two kids. A household of nine is not like a household of three times three. It just doesn’t work that way.
Moreover, when larger families do have an environmentally friendly profile, it often occurs naturally as a result of the family’s large size, not despite it. It’s not the numbers that count; it’s the lifestyle.
As Pope Francis says in Laudato Si,
To blame population growth instead of extreme and selective consumerism on the part of some, is one way of refusing to face the issues. It is an attempt to legitimize the present model of distribution, where a minority believes that it has the right to consume in a way which can never be universalized, since the planet could not even contain the waste products of such consumption. Besides, we know that approximately a third of all food produced is discarded, and “whenever food is thrown out it is as if it were stolen from the table of the poor.”
By necessity or for convenience, big families tend to naturally fall into patterns of behavior that would make Pope Francis proud.
How? Here are a few ways:
Cars Count
Let’s start with that enormous van we drive — could it be eco-friendly? Sure. It’s certainly not fuel efficient; it’s just that it’s usually parked in the driveway. With ten kids in tow, I leave the house as close to zero times as possible, bringing our weekly mileage to far less than the national average (and if you’re calculating PMPG or “people miles per gallon” – that is, how many people get moved per gallon of gas — large families look even greener). My husband has a smaller, more fuel-efficient car, which we use if only a few kids are on board.
And how often do we fly? Well, the stewardess is still in therapy from the last time our family boarded a plane together, about twelve years ago. We’d rather get our kicks at the beach down the road than go through the agony of air travel, which the New York Times called the “biggest carbon sin.”
Economy Size
How about electricity? Do twelve people use more than three or four? Not necessarily. Six kids playing Dinosaur Wedding do it by the light of a single light bulb, just like one or two kids would. Two or three kids fit in a bathtub at a time, and there aren’t enough hours in the day for all of us to shower daily. The oven stays on 350 degrees for 45 minutes, no matter how big the meatloaf.
Cozy Quarters
Most large families I know don’t live in energy-hogging giganto-mansions. They live in normal houses, they’re a little crowded, and they have lots of bunk beds. (They do, however, tend to go for big yards, lots of trees, and gardens. Natural wildlife preserves, you might say.)
Reduce and Re-use
Many large families also live with tight budgets. We happily trade a second or third income for another armful of babies. The quick and easy methods of saving the environment that make the news daily are hardly news to cash-strapped families: Turn down the heat, insulate, avoid anything disposable, buy in bulk, cook from scratch, breastfeed, don’t eat out, don’t waste this, don’t buy that. Turn out the light, close the door, unplug it, wash in cold water, make it do or do without. And if it does not get eaten for dinner, we serve it for lunch.
Even if we have plenty of money, the sheer clutter forces us to try and live simply and learn to do without excess stuff.
What a revelation! And so good for the earth.
Make Do
How about consumption of goods? My family and many Catholic families I know are almost complete failures as consumers. Our house is mostly furnished, from the couch to the car to the pots and pans and coffee cups, with used goods. We are not, for the most part, consuming new products, with all their attendant carbon costs in manufacture and transport. By taking in used things, we’re also preventing an entire houseful of stuff from clogging up the landfills.
Pregnancy is green
Babies perform a service to the world before they’re even born: they excuse their moms from using (and sending to landfills) pads and tampons for nine months — longer, if they breastfeed enough for lactational amenorrhea. And what about birth control pills? Catholics who refuse to use them are also refusing to excrete endocrine-disrupting hormones into the water supply.
Pass It On
Large families tend to buy used clothes, books, and toys, and we hang onto them, passing them down from child to child, even to the next generation. The thermal onesie on my baby last winter? It started life keeping my oldest nephew warm, then went on to clothe every one of my ten kids so far.
Not convinced? Still feeling some eco-guilt as you survey all the little consumers you’ve produced? Go ahead and plug your own family’s stats into one of the many carbon calculators available online (try SafeClimate.net). You may be surprised at how “be fruitful and multiply” translates quite naturally into treading lightly on mother earth.
Last time I took my family’s numbers and plugged them into the first three carbon calculators that Google turned up, we consumed and emitted less than the national average for a family of three. And we were just trying to get through the week.
But what about the future?
This is all very well, some will say, as long as your many children all live with you in your little green shoe. You may be very thrifty today, but what about when they all grow up and move out? More people is more people, no matter how you slice it.
For this argument, I have two answers.
First is that grown children of large families tend to be what you might call natural conservationists. Children who grow up as one of many are likely to have learned that they’ll survive without buying stuff, that it’s okay to share, that material things come and go, and that, like it or not, we all depend on each other for survival.
So who will I be sending out into the world? A small crowd of perfect environmentalists.
Second, children of families that are open to life also know something much more important, something that rabidly utilitarian environmentalists still don’t seem to realize: A human soul is more than the sum of how many kilowatts he consumes. This is what it comes down to. Human beings are a gift to the world.
What can we say to people who do not realize that the human family is the very seat of love, and that procreation is the ultimate human imitation of the action of the Holy Trinity? What can you say to people who somehow truly believe that everything humanity does is something to be apologized for — that the only good human is a human who was never born?
There is nothing you can say. Satisfy yourself that you’re not being wasteful, and then answer not the fool according to his folly. Love your children, and teach them to love each other; and if you and your brood feel like a sign of contradiction, then that’s a good sign.
The call of Laudato Si is nothing new. The Catholic Church has been teaching this lifestyle for thousands of years: a lifestyle of welcoming children while being careful and generous with the way we live. There is no contradiction between loving and caring for the earth and supplying it with inhabitants: We are commanded to do both.
Was it short-sighted when God the Father explained these things to Adam? Was it hyperbole when Christ asked, “What does it profit a man, if he gain the whole world, but suffer the loss of his own soul?”
‘A Great Big Yes’
Our beloved Benedict XVI said of big families:
“Their Yes to one another in the patience of the journey and in the strength of the sacrament with which Christ had bound them together, had become a great Yes to themselves, their children, to God the Creator and to the Redeemer, Jesus Christ. Thus, from the witness of these families a wave of joy reached us, not a superficial and scant gaiety that is all too soon dispelled, but a joy that developed also in suffering, a joy that reaches down to the depths and truly redeems man.”
Of course it’s Catholic to be an environmentalist. Of course it’s our job to care for the earth. But even more, it’s our job to remember, and to teach our children, that this world will not last, and to live accordingly.
“All flesh is as grass, and all its glory as the flower of grass; the grass withered, and the flower has fallen — but the word of the Lord endures forever” (Isaiah 40:6).
How will it endure, if there is no one to hear it? Let us answer the “No” of child-fearing radicals with a joyful and ancient “Yes.” The world needs big families.
June 24, 2015 (LifeSiteNews) — For the first time in seven years, the U.S. birth rate has risen, according to recorded U.S. birth certificates.
The number of births rose to 3.98 million babies born alive in 2014. It’s the most births since 2010, and the first time since 2007 that the number of annual births have risen.
Births rose during the late 1990s and hit an all-time high of over 4.3 million in 2007. But they began to plunge during the economic downturn caused by the Great Recession and the weakest economic “recovery” in memory. LifeSiteNews has noted the alarming trend of falling U.S. birth rates over the past several years.
Carl Haub of the Population Reference Bureau said rising birth rate is because of an improving economy. Laura Lindberg, researcher at Planned Parenthood’s Guttmacher Institute, said, “I think as people feel their paycheck is more stable, it feels like a safe environment to have a child in.”
Pro-life leaders, however, see other factors in the rising birth rate. Dr. Michael New, political science professor at the University of Michigan–Dearborn, explains, “A lower percentage of women facing unintended pregnancies are choosing abortion…Pro-life educational and service efforts, such as pregnancy-resource centers, have likely played a role.”
Steve Mosher, president of the Population Research Institute, has explained the rise in birth rates, “Pro-life sentiment in this country is gradually increasing,” he says, ” people who are pro-life tend to be open to life.”
Meanwhile, the report from the U.S. Centers for Disease Control and Prevention also found that birth rates for U.S. teens fell to an historic low, with 24.2 births per 1,000 –a nine percent drop. “What we have seen is quite remarkable,” said Bill Albert of the National Campaign to Prevent Teen and Unplanned Pregnancy.
Again, secularists attribute this to one thing, while pro-lifers attribute it to another. Lindberg said the lower teen fertility rate could be attributed to better access of sex information, though she cautions, “There remains room for improvement to help teens be in charge of their own fertility.”
Pro-life leaders say their efforts in teaching abstinence before marriage has helped. Albert admitted that the decline in teen births can be attributed to to a range of factors, including abstinence.
Researcher Brady Hamilton’s balanced the widely varying opinions by noting that researchers did not collect data on why pregnant mothers and biological fathers made the choice to give life, saying that such decisions are likely due to a “cacophony of factors.”
The birth rate among unmarried women also fell one percent last year.
June 19, 2015 (LifeSiteNews) — Carolyn Woo, President and CEO of Catholic Relief Services (CRS), spoke yesterday at the Vatican as a member of the panel that presented the papal encyclicalLaudato Si to the world’s media. Woo was invited by the Vatican despite longstanding and frequently expressed concerns that the CRS is involved in funding contraception and abortion worldwide.
Research carried out by the American Life League (ALL) alleges that “86 percent of CRS’ grants to domestic groups in 2012 went to groups that promote contraceptives, in addition to, in some cases, other evils such as abortion, the abortifacient ‘morning-after pill,’ and homosexuality. In 2013, the Catholic aid organization gave a $2.7 million grant to Population Services International, which markets a ‘Safe Abort Kit’ in developing countries.” (Source)
The evidence supports that the problems are real and exhibit a clear and present danger of grave scandal. According to CRS’ IRS Form 990 for FY 2012, CRS granted over $75 million to 47 different organizations based in the United States. This report documents that $64,656,809 went to 23 organizations that promote practices and policies contrary to Catholic moral teaching. This represents 86 percent of CRS’ domestic grants for 2012. These offenses include:
• the facilitation, promotion, and in some cases, direct commission of abortion;
• dispensing and promoting all forms of modern contraception, including abortifacient drugs and devices;
• facilitating, promoting, and in some cases, direct commission of male and female sterilization.
To be clear, CRS is providing funding and partnering with organizations that directly subvert Catholic moral teaching. The activities of the CRS grantees detailed in this report are not due to coalitions, associations, or tenuous relationships—they are performed directly by CRS grantees. In all cases, these activities represent the focus of these agencies, and in many instances, they are the preponderance of the grantees’ work. This large collection of evidence demonstrates systemic problems at Catholic Relief Services.
The vice-president of CRS responsible for overseas finance entered into a “marriage” with his male partner in April 2013. When asked about the “civil gay marriage,” Woo is reported to have said that CRS is “working through this” and that so-called same-sex marriage is a “very complex issue.”
The presence of Woo at the press conference further highlights the danger noted yesterday by Voice of the Familythat the lack of a clear defense of Catholic teaching on contraception in the new papal encyclical leaves Catholics vulnerable in the face of renewed efforts to control or reduce population growth, despite brief references in the document rejecting population control as a means of tackling environmental problems (c.f Laudato Si, No. 50).
In his 2009 encyclical Caritas in Veritate Pope Benedict XVI stressed the central importance of the Church’s understanding of human sexuality to her social doctrine. He wrote in paragraph 15:
The Encyclical Humanae Vitae emphasizes both the unitive and the procreative meaning of sexuality, thereby locating at the foundation of society the married couple, man and woman, who accept one another mutually, in distinction and in complementarity: a couple, therefore, that is open to life. This is not a question of purely individual morality: Humanae Vitae indicates the strong links between life ethics and social ethics, ushering in a new area of magisterial teaching that has gradually been articulated in a series of documents, most recently John Paul II’s Encyclical Evangelium Vitae. The Church forcefully maintains this link between life ethics and social ethics, fully aware that ‘a society lacks solid foundations when, on the one hand, it asserts values such as the dignity of the person, justice and peace, but then, on the other hand, radically acts to the contrary by allowing or tolerating a variety of ways in which human life is devalued and violated, especially where it is weak or marginalized.’
A workshop will be held in the Vatican from 13-15 November 2015 this year to discuss deploying “children as agents of change” in pursuit of “sustainable development”. Some of these workshops will be run by leading opponents of Catholic teaching, such as Jeffrey Sachs, drafter of pro-abortion sustainable development goals. These draft goals, which pose a serious threat to vulnerable human life worldwide, are under consideration by the United Nations at the same time as Sachs plays an increasingly prominent role in the Vatican.
In the light of such developments a clear restatement of the unchangeable teaching of the Church on contraception and the nature of the sexual act, as found in the encyclical letter Humanae Vitae, has never been more necessary.
“Therefore We base Our words on the first principles of a human and Christian doctrine of marriage when We are obliged once more to declare that the direct interruption of the generative process already begun and, above all, all direct abortion, even for therapeutic reasons, are to be absolutely excluded as lawful means of regulating the number of children. Equally to be condemned, as the magisterium of the Church has affirmed on many occasions, is direct sterilization, whether of the man or of the woman, whether permanent or temporary.
Similarly excluded is any action which either before, at the moment of, or after sexual intercourse, is specifically intended to prevent procreation—whether as an end or as a means.”
June 15, 2015 (LifeSiteNews) – A new study shows that certain birth control pills may impair sleep and raise the level of stress hormones in women who take them.
The study examined women and girls who use combined hormonal contraceptives (CHCs) to treat acne.
To ascertain the quality of subjects’ sleep, researchers used the Pittsburgh Sleep Quality Index, a questionnaire filled out by the subject that “scores” sleep attributes including sleep duration, sleep disturbances, and daytime dysfunction.
Comparing these subjects to a group using only a topical gel for acne treatment, the study revealed that, not only did CHC-takers sleep less, but there is also an increase in the concentration of the hormone cortisol in their bodies.
Cortisol has a reputation in medical circles as a “stress hormone”; at high levels, it is associated with anxiety, depression, heart disease, weight gain, and sleep problems, among other ailments.
Only the hormone’s relationship with sleep problems was examined in the São Paolo study.
Rachel G. Albuquerque, the primary author of the study, considered the findings worthy of a warning to consumers. “Although combined oral contraceptive…is a very effective treatment for adult female acne,” she said, “it can also increase cortisol concentrations and even impair sleep. These factors impact welfare and quality of life.”
What Albuquerque called a “very effective treatment for acne” has caused multiple deaths and injuries. Complications from Yasmin and Yaz in particular, both of which utilize the chemicals tested in the São Paolo study, have brought a plethora of lawsuits against Bayer, the pharmaceutical company that distributes the drugs. For example, Yasmin killed a 24-year-old Australian woman in 2008 who was taking it for acne and caused a stroke in a British beauty queen using it for the same reason. Other hormonal contraceptives marketed as acne treatment have yielded similar results.
More generally, many studies over the years have associated various forms of hormonal birth control with a myriad of ailments, including glaucoma, breast cancer, and shrinking of the brain. Women come forward regularly with stories of deleterious birth control side-effects; one young woman was left completely paralyzed, while another had her career destroyed by “blood clots everywhere” in her lungs. Additionally, the intrauterine device Mirena, like Yasmin/Yaz, has killed and injured enough women to incur multiple lawsuits.
Yet overall, she said the study found no difference overall in sleep quality between the CHC group and the topical gel group, notwithstanding findings of reduced subjective sleep duration in the former. She said that “all patients did not exhibit a difference on sleep quality,” and “these two different approaches [CHCs and the topical treatment] did not affect sleep quality in these patients.”
Albuquerque added that while “cortisol was higher in the patients treated with the combined oral contraceptives,” the hormone’s concentration in those subjects was also “on the normal range.”
The study – a six-month customized, comparative single-blind trial by researchers at the Universidade Federal de São Paolo in Brazil – focused on CHCs containing ethinyl estradiol and drospirenone. Brand-name drugs that comprise these chemicals include Yasmin and its sister drug Yaz (the subject of a plethora of lawsuits – see below), Ocella, Zarah, Safyral, and Syeda.
The Chemical and Veterinary Investigation Institute in Stuttgart said on Friday it had found the carcinogen N-Nitrosamine in 29 of 32 types of condoms it tested in simulated conditions.
The condoms, which were kept in a solution with artificial sweat, exuded huge amounts of cancer-causing N-Nitrosamine from its rubber coating. Researchers measured amounts of N-Nitrosamine, that were way above the prescribed limits for other rubber products such as baby pacifiers.
“N-Nitrosamine is one of the most carcinogenic substances,” the study’s authors said. “There is a pressing need for manufacturers to tackle this problem.”
The study said that the carcinogen is thought to be present in a substance used to improve condom elasticity. When the rubber material comes in contact with human bodily fluids, it can release traces of N-Nitrosamine.
No immediate health risk
But since there are no prescribed limits of N-Nitrosamine for condoms, the study hasn’t caused panic among manufacturers or mass-recalling of the products from counters.
Local government officials said condom users should not stop using rubber contraceptives based on the results of the study because N-Nitrosamine does not present an immediate health risk.
The Baden-Würtemmberg Social Ministry said it didn’t think “it posed a risk.” Authorities are also withholding the name of the affected manufacturers for fear of litigation.
Manufacturers should use alternative substances
But Germany’s Federal Institute for Risk Assessment said that daily condom use exposed users to N-Nitrosamine levels up to three times higher than levels naturally present in food.
Werner Altkofer, head of the Stuttgart-based Chemical and Veterinary Investigation Institute said that though the production of rubber usually uses chemicals that can exude N-Nitrosamine, condom manufacturers could bypass it by using more expensive alternative substances available on the market that didn’t form the carcinogen.
“We believe that it’s up to the manufacturers to use other production processes so that no N-Nitrosamine is formed in condoms,” Altkofer said.
He added that the latter was technically possible going by the fact that products of some manufacturers didn’t show traces of the carcinogen during the testing.
Beate Uhse taking no chances
Germany’s biggest erotica compnay Beate Uhse however, has decided to play it safe.
Shortly after the results of the study were introduced on Friday, the group banned chocolate-flavored condoms from its range. That was because the study had show that condoms laced with a chocolate flavoring had overwhelming high levels of N-Nitrosamine.
The Basilica of the National Shrine of the Immaculate Conception is pleased to confirm that Pope Francis will visit our nation’s preeminent
Marian shrine and patronal church on Wednesday, September 23, 2015.
Monsignor Walter R. Rossi, rector of the National Shrine, states, “We are truly delighted that Pope Francis is following in the footsteps of his predecessors Saint Pope John Paul II and Pope Benedict XVI in visiting the Basilica of the National Shrine of the Immaculate Conception during his apostolic visit to the United States. We are honored that the Holy Father will celebrate the Holy Sacrifice of the Mass and canonize Blessed Junipero Serra, the first-ever canonization to take place on American soil.”
No further details of the Holy Father’s visit are available at this time. To receive Papal Visit updates as they become available, please click here to sign up for email alerts. Updates will also be posted on this page, on our Facebook page and on Twitter @MarysShrine.
Please join us in praying for Pope Francis and his upcoming Apostolic Visit to the United States and to Mary’s Shrine.
CHAPEL HILL, NC, June 9, 2015 (LifeSiteNews) – A new study recommends that doctors implant IUDs into new mothers’ wombs while they are still in the hospital for childbirth, in an effort to increase the number of American women fitted with the abortifacient device.
Previously, new mothers were told to wait six months after birth to have an intrauterine device implanted. But a new study published in Obstetrics and Gynecology says too often women do not return to have an IUD implanted, and as a result, get pregnant.
Patients at North Carolina Women’s Hospital in Chapel Hill were studied and researchers found that women who received IUDs during cesarean sections were more likely to have them six months later than women who were told to return to the doctor’s office to receive one.
So, the professionals say, implant IUDs at childbirth.
The American Life League considers the North Carolina study’s recommendations medically irresponsible, because women who have just given birth are far more vulnerable, physically and emotionally, than after waiting six months to consider a major life decision like surgically implanted “contraception.”
“Medically speaking, this push to implant IUDs immediately after delivery is a travesty,” Rita Diller, the national director of the American Life League’s Stop Planned Parenthood Project, told LifeSiteNews. “Abnormal bleeding, one of the signs of uterine perforation, could be missed in the days following delivery, since women are already bleeding at that point.”
“It is extremely disturbing that mothers who have just delivered their babies are being encouraged to accept IUDs,” Diller said. “Uterine walls can be softer than usual in postpartum women, increasing the risk of uterine perforation and even resultant IUD migration to other parts of the body, which can cause additional internal injuries.”
The complications with surgical implantation of IUDs are magnified when implantation takes place at a new mother’s childbirth.
“IUDs also increase the risk of ectopic pregnancies and contribute to infections like pelvic inflammatory disease. More than 70,000 Mirena IUD complications have been reported to the FDA since 2000,” Diller elaborated. “In New York and New Jersey alone, there are over 1,000 lawsuits on file for IUD injuries.”
No mention was made in the study of the fact that an IUD is not “contraception” at all, but is an abortifacient. The IUD stops implantation, not just conception, up to 95 percent of the time, according to the Life Issue Institute, based in Cincinnati.
The IUD destroys the ability of the already fertilized egg – the “conceptus” – to implant in the uterine wall. Because s/he cannot implant in the mother’s womb, the conceived child dies.
“IUDs are intended to close off all hope of life developing in the womb, and take away a woman’s ability to be open to life, and to snuff out the life of any child who may begin developing while the device is in place,” Diller explained. “The womb is intended by God to be a place of life, not a tomb.”
The Obama administration’s Department of Health and Human Services admitted that intrauterine devices cause early abortions. IUDs can inflame the lining of the uterus, making implantation of a newly conceived child impossible, inducing abortion.
A government report put out by the Center for Disease Control singles out the use of IUDs, calling them “as effective as sterilization.” Brian Clowes of Human Life International puts it clearly: “All of the longer-acting methods sometimes act as abortifacients…which will actually lead to an increase, not a decrease, in total abortions,” he told LifeSiteNews.
The new North Carolina study’s recommendation follows similar recommendations from the World Health Organization (WHO), which encourages the use of abortion-inducing “contraception” for new mothers around the world.
Along with the new study, the publication printed an editorial by Dr. Lisa M. Goldthwaite, who wrote, “We are meeting a woman’s needs better when they get their contraception at the time of delivery.”
Dr. Erika E. Levi, assistant professor of obstetrics and gynecology at Albert Einstein College of Medicine in the Bronx, explained, “We need to make it easier for women to get access to the kind of contraception they want as new mothers.”
In 2010, the Cochrane Database of Systematic Reviews found that four times as many women who get an IUD implanted at childbirth expel the device (eight percent), compared with those placed later (two percent).
Diller concluded, “It is unconscionable for medical personnel to pressure women, when they are extremely vulnerable following a delivery, to be implanted with devices that may have very negative long-term consequences on their health and actually take the decision to be open to life out of their hands.”
A 26-year-old woman in Los Angeles nearly died last month because of a blood clot in her brain. The cause? An oral contraceptive (OC).
A 21-year-old woman in England, Fallan Kurek, did die last week after taking an oral contraceptive for only 25 days. It had been prescribed by her doctor to “regulate her periods.”
That drug was Rigevidon, a blend of ethinyl estradiol and levonorgestrel, manufactured in Hungary. It’s one of a new generation of OC’s utilizing synthetic hormones. The British Medical Journal reports that these new mixes are two to three times deadlier than the previous generation of OCs made from levonorgestrel.
When Enovid, the first OC, was licensed by the FDA in 1957, it was with the warning that no woman should take it for more than 24 months.
By now, millions of women have been on oral contraceptives for billions of woman-years.
And now there are multi-year contraceptives, which are implanted under the skin and require a physician to remove them. In the June issue of Vogue (that reveals who the target market is) there is a one-page ad with three (!!!) pages of disclaimers for Nexplanon. The pages warn against everything from depression to acne to ectopic pregnancy to serious blood clots.
Probably most women in England—as in America—are conscious about what they eat. They worry about pesticides in their salad and hormones in their meat. They seek out organic foods because they don’t want foreign chemicals messing up their bodies. They deplore athletes who use performance-enhancing drugs.
So why don’t they have the same concerns about the bodily effects of contraceptives? Why would a 21-year-old dose herself with ethinyl estradiol and levonorgestrel and other unpronounceable hormones and steroids?
For some—as was the case with poor Fallon Kurek—it is because a (perhaps lazy, perhaps overworked) doctor said it would solve the problem of irregular periods.
For others, it may be because a doctor said it would treat acne. That’s what happened to my college roommate. Once she was on the Pill she started to have sex, since she knew there would be no consequences.
That, of course, is why most women turn their bodies into toxic waste dumps. They cannot face life without being able to have sex “any time the moment is right,” as the ads put it. Which means they can’t imagine life without OC’s.
This creates a problem for unborn babies. Because if the goal is consequence-free sex, and a little consequence gets implanted in a womb anyhow, there’s only one way to eliminate it, and that’s called abortion.
Wouldn’t it be easier for adult females to live with their natural fertility intact?
Nobody asks that question because of the lifestyle changes it might imply.
B—b—b—but . . . you can’t mean . . . you can’t be talking about—chastity?
The very sound of that word conjures up images of crones wagging their fingers at sweet young things who just want to have fun. “Chastity” has a serious brand-identity problem: It is perceived as the antithesis of “fun,” which is equated with “sex.”
Dawn Eden used to practice that equation, and she has nailed the problem with that lifestyle: “The disconnected feelings that result from sexual intercourse outside of marriage can be emotionally disastrous,” she writes in her book The Thrill of the Chaste.
Eden played the game for years. “Thinking back on dating experiences that had seemed so spontaneous and passionate,” she came to see them “for what they were: cold, clinical couplings. They weren’t really about excitement. They were about control.”
In her sexual relationships, she knew “the pain of separation would come, but it wouldn’t hit me so deeply, because I’d see it coming.” Not only was she a sex object, she was making her partner a sex object too. He was using her, and she was using him.
Telling herself from the very beginning that the relationship wouldn’t last was the way she numbed her emotions.
She had to numb herself—because casual sex works against the way men and women are hard-wired. Recent research suggests some hormones associated with sexual arousal are also associated with bonding. Perhaps Nature intends for sexual relations to be permanent relationships?
But casual coupling doesn’t seek permanent relationships. It compels women to become sterile, to pump their bodies full of potentially dangerous chemicals so that they can be available for sex but not for motherhood.
Is this any way to live? What’s the alternative?
To love fully and completely in every relationship, in the manner that is appropriate to the relationship, says Eden.
Love fully and completely? Now there’s a brand statement with potential! Who can be against loving fully and completely in an appropriate manner?
It is Eden’s definition of chastity. It sounds like a natural alternative to synthetic hormones and other unpronounceable chemicals. Organic even.
* * * * *
Connie Marshner organized her first pro-life meeting in 1971, among Capitol Hill staffers who sensed a drift toward legalizing abortion. She’s worked in the movement in one capacity or another ever since.
Of all the gestures, actions, decisions, operations, motions in the life of the human person, by far the greatest (beyond comparison) is to receive Jesus, the Lord and God into the very depths of your soul in the greatest of all Sacraments: Holy Communion.
The Bread of Life, the Bread of the Angels, Corpus Christi, food for the journey, energy and strength on the Highway to holiness, Our Comfort, Friend, Guide, Light, Support and fortitude, spiritual manna, Our eternal life—all of these and many more can be mentioned are short names, titles or descriptions for Jesus, truly present in Mass in Holy Communion. We can call it the “Sacrament of Sacraments.”
Nobody on earth could ever compare one Holy Communion to any other created reality. However, reflect on this: the entire created universe from the stars, planets, immense oceans, and lofty mountains, and starry skies, as well as all of the fish in the seas and animals populating the earth cannot equal even one, just one Holy Communion.
Why?
The reason is simple but very sublime: Holy Communion is God himself! Holy Communion is not some vague or abstract symbol, as non-Catholic religions assert! No one Holy Communion is God Himself. God is the origin of all that exists and the purpose of our existence! God created all of us out of love, to love Him in this life so as to be with Him and to love Him for all eternity in Heaven!
How humble God is that he becomes one of us. By Mary’s “Yes” the second Person of the Blessed Trinity became like us; He became man. He became like us in all things except sin. Still more, Jesus the Son of Mary, after leaving this earth in His glorified Body, wanted to stay with us always even until the end of time.
The last words of Jesus in the Gospel Matthew were: “And behold I will be with you always even until the end of time.” (Mt. 28: 20 ) If Jesus went up to heaven then how can He still be with us and even until the end of time, until the end of the world? The response: in His Mystical Body which is the Church that He established as the primary Sacrament of salvation.
However of all of the Sacraments the greatest of all of the Sacraments is the most Holy Eucharist. Why? Because the most Holy Eucharist is really God; it is really Jesus Christ the Bread of life. The Holy Eucharist is truly and substantially the Body, Blood, Soul, and Divinity of Jesus Christ! Even the smallest consecrated Host, even half of the Host, even a small particle of the consecrated Host is still Jesus the Lord, Kind and God of the universe!
Ten Suggestions to Improve Your Reception of the Eucharist
The success of a party depends on the prior preparation; sports success depends on the prep and warm-up and mental attitude and discipline; a good and loving courtship terminates in a loving and permanent marriage. The same can be applied to a fervent and worthy reception of Our Lord and Savior Jesus Christ in Holy Communion.
Another analogy is receiving a guest There are very many different ways that we can receive a guest into our home. Here are a few! You could receive a guest against your will—sometimes due to circumstances, this is the case. Or you could receive a guest with resistance and begrudgingly. Then you can receive a guest willingly with the doors of your home wide open! Still more you could receive a guest by preparing the night before, with great joy, to receive such a guest you really long to have in your home and share a meal with. Finally, upon the knowledge of a special guest coming, you clean the whole home the day before, prepare the food and the meal that you know your guest enjoys most; put on the back-ground music that the guest enjoys listening to; and finally, decorate the home with balloons and attractive and joyful banners. We have portrayed a whole series of ways or manners that a guest could possibly be received—from the worst imaginable scenario to the best of bests!
This analogy of receiving a guest into one’s home can easily be applied to receiving Jesus into our souls. Examine your conscience now: what type of reception do you give the Eucharistic Lord Jesus when you receive Him into your home/soul when you receive Him in Holy Communion? How is He received? Accept the challenge to examine your Eucharistic reception. Why? As was said earlier, this is the most important action that you can possibly do in your life. This being the truth, we should all make a concerted effort to improve and upgrade the efficacy of our reception of the Eucharistic Lord. How then can we apply this principle to receiving the Lord of the universe into the inner recesses of our soul? Following are ten practical suggestions that can be of immense help!
FAITH. How easy it is for our faith to decline, to get weak, or even to disappear. Sad to say that the biggest religious group in USA are non-practicing Catholics! Let us pray with fervor: “Lord I do believe but strengthen my faith!” Faith is like a seed planted in the ground. May our faith grow, blossom and flourish until we reach heaven!
APPRECIATION. In relationships, especially in marriages, one of the greatest perennial dangers is to start to take the spouse for granted. This can be lethal to any marriage. The same thing can insinuate itself into our relationship with the Eucharistic Lord: we can become accustomed or used to Mass and Holy Communion—even among daily communicants- and start to take the Lord for granted. In the Diary of Mercy in my soul, by Saint Faustina, Jesus complains that there are souls that receive Him with no love, but rather as if He were a mere object. Jesus states that He would prefer not to be received than to be received like a mere object and out of mere routine, to be received mechanically! There is a plack with these words in many sacristies, which serves as a reminder to priests to celebrate every Mass with faith and fervor: “Priest, man of God celebrate this Mass as if it were your first Mass, last Mass and only Mass.” We should receive every Holy Communion as if it were our first, last and only Holy Communion.
CLEAN THE HOUSE. Make a good sacramental Confession. The saints and the church teach us that the cleaner and more pure the soul the more abundant the graces in receiving Holy Communion. If you like, a dirty glass pane prevents the sun from entering the room fully. Likewise, a dirtied or sullied soul will block the full and powerful presence of the Eucharistic Lord in His entirety from inundating the soul!
COME EARLY. It is doubtful that we would show up late for the last game in the World Series, or a graduation ceremony, or even an expensive and exquisite meal in a glamorous restaurant. Should we not then be early to welcome the King of Kings and the Lord of Lords into our hearts? What do you think? Coming late for Mass disturbs others, disturbs the priest and dampens one’s over-all participation in the Mass. Let us avoid cutting corners and selling God cheap!
REVERENCE. Moses was commanded to take off his sandals before the burning bush that was a mere symbol of the Eucharistic Presence. Isaiah complained that he was impure in the midst of an impure people. His lips had to be purified by the burning coal. How much more reverence we should manifest in front of the Real Presence and the Eucharistic Lord. He is not a symbol but a Real Person! If a King merits the greatest reverence and respect, what about the King of the universe the Eucharistic Lord?
INTENTIONS! The Parish priest usually has his specific intentions in every Mass. This does not negate the fact that you cannot have your own private intentions. Three suggestion to help you to live the Mass more fully : 1) Offer Mass for a deceased person that might be detained in Purgatory, for his quick release or at least alleviation of his suffering. 2) Conversion of sinners. We all have in mind family members, relatives, friends, fellow-workers who seem to have forgotten about God or are angry at God and have for many different reasons drifted away from the Church. Offer your Holy Mass and Holy Communion so that they will return. These lost sheep may return to the Good Shepherd if you take the effort to pray for them and place them on the altar in Holy Mass. 3) Personal conversion. We all struggle with the flesh; we all struggle with our own demons; we all struggle with the seduction of the world and its deception and many allurements. In Holy Communion why not beg the Lord Jesus that He would grant you the grace of a true HEART TRANSPLANT!!! Indeed you do receive the Body, and Blood of Jesus. That means you receive His total Body and that includes His Heart. Ask Jesus to give you His Sacred Heart and beg His Sacred Heart overflowing with the flames of love to consume all that which is in your heart which is displeasing to Him. Fervent and frequent Holy Communion is the short-cut to holiness!!!
PARTICIPATE. In Mass we are not called to be passive observers as if it were a play, a show or an opera. On the contrary we are called to participate fully, actively, and consciously. (Vatican II, Sacrosanctum Concilium, Dogmatic Constitution on the Liturgy) We are called to listen attentively to the Word of God, respond to the Word, and to sing with all our hearts in praise and worship of the Lord. When silence is called for we enter into profound silence where we will meet the Lord. As the prophet reminds: “Be silent and know that I am the Lord.”
MARY’S HEART AND YOURS. While approaching Holy Communion we should humbly beg the Blessed Virgin Mary—as Blessed Mother Teresa of Calcutta reminds us—to lend us her Immaculate Heart so that we can receive Jesus with the utmost purity, humility and burning love. This is truly a key to upgrade and improve our Holy Communions—to receive Holy Communion through the Heart of Mary. St. Pope John Paul II makes a beautiful parallel. He compares Our Lady’s “Yes” or fiat in the Annunciation to our “Amen” when we receive Jesus in Holy Communion. The result is the same: receiving Jesus into the heart. Our Lady’s yes resulted in the conception of Jesus in her womb. Our “Amen” in Holy Communion results in Jesus’ Eucharistic Presence taking root in our heart, mind and soul!
THANKSGIVING! After Holy Communion we should spend some time in rendering thanks to Jesus for this greatest of all gifts—His Body, Blood, Soul, and Divinity in Holy Communion. There is no greater gift! In a home visitation and a friendly meal, a guest who has even the least of manners will thank the hosts for having invited him. Should we not abound in thanksgiving to Jesus for humbling Himself to descend into our miserable interior home that we call our soul? Let us join our hearts, minds and voices with the Psalmist and acclaim: “Give thanks to the Lord for He is good, for His mercy endures forever.” Indeed God rejoices in a grateful heart. Let us cultivate and attitude of gratitude!
EUCHARISTIC APOSTLE. Given that you have encountered the greatest treasure in your life, the pearl of infinite value, you should be motivated to the fullest extent possible to bring Jesus to others and to bring others to Jesus! Take Our Lady as an example! After conceiving Jesus in her womb in the Annunciation, she went in haste to bring Jesus to her cousin Elizabeth who in her old age was with child. Mary hurried to bring Jesus to others. After you have received Jesus in Holy Communion and given Him a worthy thanksgiving, now it is time to become a fiery Apostle and to bring the Lord Jesus to others. Preach by your example but also by your word. Invite others to Church, to confession, to Mass and Holy Communion. Become a missionary! The harvest is rich but the laborers are few. You right now are called to work in the vineyard with the Lord; you are called to go fishing with the Lord and to save souls. One of the most efficacious tools to save souls is to help the wandering sheep, the stray Catholics, to come back to Church, make a good Sacramental Confession and then to receive the Lord Jesus in Holy Communion. Venerable Archbishop Fulton Seen expresses it this way: “First come and then go!” First we should come and receive Jesus with great fervor, faith and love; then we go out to the whole world to bring this good news of salvation to every living being!
In conclusion, we should be overflowing with joy and gratitude for the most sublime gift of the Holy Eucharist. The Holy Eucharist is truly and substantially the Body and Blood of the Lord Jesus. There is no greater action we can possibly do while we live on earth than to receive the Eucharist worthily. Jesus’ promise for receiving Him frequently and worthily should fill all of us with immense joy. Jesus consoles us with these words: “I am the Bread of life. Whoever eats my Body and drinks my Blood will have everlasting life and I will raise Him up on the last day.” (Bread of Life discourse: Jn. 6: 22-71) Heaven is ours if we receive Jesus here on earth with faith and burning love!
“One cannot encounter God, my brothers and sisters, without trembling, without awe, without profound respect and holy fear.”
The following Message from Cardinal Sarah, Prefect of the Congregation for Divine
Worship and the Discipline of the Sacraments, was sent to participants of the “Sacra Liturgia 2015” event in New York City, held this past week, from June 1-4. A reproduction of the Message was posted on the Sacra Liturgia USA Facebook page and has been reproduced here by kind permission of Dom Alcuin Reid, international organizer of the Sacra Liturgia events (see CWR’s May 2015 interview with Dom Reid about the New York event).
——————-
MESSAGE OF HIS EMINENCE, ROBERT CARDINAL SARAH PREFECT OF THE CONGREGATION FOR
DIVINE WORSHIP AND DISCIPLINE OF THE SACRAMENTS
TO THE CONFERENCE “SACRA LITURGlA USA 2015”
NEW YORK CITY, 1-4 JUNE 2015
1. It is my pleasure to greet all of you, gathered in New York City, for the inaugural conference of Sacra Liturgia in the United State of America. In particular, I greet His Eminence, Timothy Cardinal Dolan, the Archbishop of New York, and thank him for his interest in and support of this event underlining the essential role of liturgical formation and celebration in the life and mission of the Church.
I was very pleased to be present at the launch of the Italian and English editions of the proceedings of Sacra Liturgia 2013 in Rome last November, and congratulate Bishop Dominique Rey and all who work with him on making this happy initiative a reality, now also in the United Stales of America.
I greet His Eminence, Raymond Leo Cardinal Burke, who will present the keynote address. And I greet all the bishops, priests and religious and learned lay men and women who will make presentations as well as those who will celebrate the Sacred Liturgy and preach in the coming days. Your apostolate in promoting the Sacred Liturgy is a most important one in our time: I thank you for all that you do.
2. Because the Sacred Liturgy is truly the font from which all the Church’s power flows, as the Second Vatican Council insists (cf.Sacrosanctum Concilium , 10), we must do everything we can to put the Sacred Liturgy back at the very heart of the relationship between God and man, recognizing the primacy of Almighty God in this privileged and unique forum in which we, individually and ecclesially, encounter God at work in our world. One cannot encounter God, my brothers and sisters, without trembling, without awe, without profound respect and holy fear. This is why we must rank what Cardinal Ratzinger called “the right way of celebrating the Liturgy, inwardly and outwardly” first amongst our concerns (Joseph Cardinal Ratzinger, The Spirit of the Liturgy, Ignatius Press, San Francisco 2000, p. 9).
3. When The Holy Father, Pope Francis, asked me to accept the ministry of Prefect of the Congregation for Divine Worship and Discipline of the Sacraments, I asked: “Your Holiness, how do you want me to exercise this ministry? What do you want me to do as Prefect of this Congregation?” The Holy Father’s reply was clear. “I want you to continue to implement the liturgical reform of the Second Vatican Council,” he said, “and I want you to continue the good work in the liturgy begun by Pope Benedict XVI.”
My friends, I want you to help me in this task. I ask you to continue to work towards achieving the liturgical aims of the Second Vatican Council (cf.Sacrosanctum Concilium, I) and to work to continue the liturgical renewal promoted by Pope Benedict XVI, especially through the Post-Synodal Apostolic Exhortation Sacrosanctum Caritatis of 22 February 2007 and the Motu Proprio Summorum Pontificum of 7 July 2007. I ask you to be wise like the householder in St Matthew’s Gospel, who knows when to bring out of his treasure things both new and old (cf. Mtt 13:52), so that the Sacred Liturgy as it is celebrated and lived today may lose nothing of the estimable riches of the Church’s liturgical tradition, whilst always being open to legitimate development (cf.Sacrosanctum Concilium, 23).
4. You have many days in which to consider these questions in depth. I would like to suggest two critical areas in which authentic liturgical renewal in the twenty-first century can be furthered. The first is by being utterly clear what Catholic liturgy is: it is the worship of Almighty God, the place where mankind encounters God alive and at work in His Church today. Please—never underestimate the importance of this. The liturgy is not some social occasion or meeting where we come first, where what is most important is that we express our identity. No: God comes first. As Cardinal Ratzinger wrote in 2004:
If the Liturgy appears first of all as the workshop for our activity, then what is essential is being forgotten: God. For the Liturgy is not about us, but about God. Forgetting about God is the most imminent danger of our age. As against this, the Liturgy should be setting up a sign of God’s presence. (Joseph Cardinal Ratzinger, Collected Works: The Theology of t he Liturgy, Ignatius Press, San Francisco, 2015, p. 593).
The Church’s liturgy is given to us in tradition—it is not for us to make up the rites we celebrate or to change them to suit ourselves or our own ideas beyond the legitimate options permitted by the liturgical books. That is why we must celebrate the Sacred Liturgy faithfully, with that reverence and awe of which I spoke earlier.
5. The second area in which I ask you to give of your time and expertise is in the promotion of sound liturgical formation. The Council’s Constitution on the Sacred Liturgy went so far as to say that “it would be futile to entertain any hopes of realizing” the liturgical renewal it desired “unless the pastors themselves, in the first place, become thoroughly imbued with the spirit and power of the liturgy, and undertake to give instruction about it” (n. 14). We cannot truly participate in the Sacred Liturgy, we cannot drink deeply from the source of the Christian life, if we have not been formed in the spirit and power of the liturgy. As our Holy Father, Pope Francis, said last year:
Much remains to be done for a correct and complete assimilation of the Constitution on the Sacred Liturgy on the part of the baptized and by ecclesial communities. I refer in particular to a strong and organic invitation and liturgical formation of the lay faithful as well as the clergy and consecrated persons (Message to the participants of the Roman symposium on Sacrosanctum Concilium, 18 February 2014)
I hope and I pray that the different initiatives of Sacra Liturgia can do much to meet this urgent and crucial need.
5. Dear brothers in the episcopate, dear priests, deacons and religious, dear lay men and women, your participation in this conference is a sign that you are already aware of the importance of the Sacred Liturgy in the life of the Church. I thank you for you willingness to give of your time to study and consider this reality further. I pray that these days may increase your wisdom and knowledge, that they will help you grow in holiness and that they will make you ever more zealous in promoting authentic liturgical renewal in the Church.
I hope I will be able to join you for the new Sacra Liturgia Meeting of July 2015 in London.
Please pray for me that I may faithfully execute the service to which I have been called. May God bless you always!
Robert Cardinal Sarah
Prefect, Congregation for Divine Worship and the Discipline of the Sacraments
CAMBRIDGE, MA, June 5, 2015 (LifeSiteNews) – Oscar-winning actress Natalie Portman has announced that taking oral contraceptives caused depression that plunged her into some “dark moments” as a teenage college student.
The actress, best known for her portrayal as Padme in the popular big screen “Star Wars” saga, spoke to graduates of her alma mater, Harvard University, last Wednesday.
Portman admitted she had a difficult first and second year during her the keynote speech at Harvard College’s Class Day ceremony.
“Some combination of being 19, dealing with my first heartbreak, taking birth control pills that have since been taken off the market for their depressive side effects, and spending too much time missing daylight during winter months, led me to some pretty dark moments,” she said.
Portman’s admission that taking birth control pills contributed to ill health should not come as a surprise. Oral and injectable contraceptives have a well-documented history of negative effects on women, whether mental or, more often, physical. The risk for blood clots, which can cause stroke, heart attack, blindness, brain damage, and death, is three-to five times higher in women taking birth control pills.
In 2011, the Food and Drug Administration (FDA) admitted that “all birth control pills pose a risk of blood clots.” At the time, the FDA was looking into specific “low dose” contraceptives manufactured by Bayer. Two British medical studies contended that Bayer’s contraceptives containing drospirenone posed two to three times a greater risk of dangerous blood clots than other contraceptives.
An investigation found that pharmacists suspected the deaths of 23 Canadian women were attributable to two “low-dose” contraception pills, Yaz and Yasmin. Birth control pill manufacturer faces 7000 Yaz-related lawsuits, and has paid out over $1 billion to settle thousands of lawsuits in the United States.
Oral contraceptives also can contribute to blindness. One study examined the Center for Disease Control’s National Health and Nutrition Examination Survey, and found that women who used birth control pills for three years had doubled their chances of having glaucoma.
Birth control pills decrease the amount of antioxidants and vitamins in a woman’s blood. A study carried out by the Albert Einstein College of Medicine at Bronx-Lebanon Hospital found that women who use hormonal contraceptives have significantly lower levels of essential vitamins and antioxidants compared to women who do not use the drugs.
Despite these and many other studies, most people do not know the dangerous health effects of birth control pills.
“Thousands [of women] are experiencing life-threatening, health-destroying side-effects, such as blindness, depression, and pulmonary embolism,” Elizabeth Kissling wrote in Ms. Magazine. Kissling then told the stories of young, otherwise healthy women who had suffered each of these consequences.
In time, Portman recovered from the negative mental side effects of her contraceptive use.
In her Harvard speech, Portman admitted, “When I came in as a freshman in 1999, I felt like there had been some mistake.”
“I feared people would assume I had gotten in just for being famous, and not worthy of the intellectual rigor here,” Portman said, admitting the allegation had a great deal of merit. “When I came here, I had never written a 10-page paper before. I’m not sure I had written a five-page paper.”
“I had some difficult times,” she stated.
In her Harvard speech, Natalie Portman also admitted that as a famous actress at the Ivy League school, she received grades she didn’t deserve. “I should have failed both [of two difficult freshman year classes]. For your information, I got a B in both.”
Portman graduated Harvard in 2003 with a degree in psychology.
The 33-year-old, who is an outspoken supporter of abortion-on-demand, said in her 2010 Academy Award acceptance speech that motherhood is the “my most important role of my life.”
On another occasion, Portman said the Bible changed her view of her Best Actress Oscar statue, which she accepted in 2010 for her role in the movie “Black Swan.”
“I was reading the story of Abraham to my child, and talking about not worshiping false idols. And this is literally like gold men,” she said, explaining she keeps her Oscar statue in her safe, but not on display. “This is literally worshiping gold idols — if you worship it. That’s why it’s not displayed on the wall. It’s a false idol.”
May 29, 2015 (LifeSiteNews.com) — “So are you hoping for a boy or a girl?”
“It doesn’t matter as long as the baby is healthy.” This is the conversation that I listened to as I stood next to my special needs sister.
I bet you have heard this line before; or possibly even said it yourself.Most people do not seem to think through this statement, so I am going to bring up a few things that you may have not thought about.
My biggest question for those who say this is, “What if the baby isn’t healthy?” My sister was born with Trisomy 18. “Edwards syndrome (also known as trisomy 18 [T18]) is a chromosomal disorder caused by the presence of all, or part of, an extra 18th chromosome. This genetic condition almost always results from nondisjunction during meiosis. It is named after John Hilton Edwards, who first described the syndrome in 1960. It is the second-most common autosomal trisomy, after Down syndrome, that carries to term.
Half of the infants with this condition do not survive beyond the first week of life. The median lifespan is five to 15 days. About 8% of infants survive longer than 1 year. One percent of children live to age 10, typically in less severe cases of the mosaic Edwards syndrome.”
I apologize for the lengthy description, but I thought that it was important to show how serious my sister’s “disability” is, so you don’t think that I am some random person commenting on this topic with little to no personal experience.
And my sister clearly is not what most people consider a “healthy baby.”
I want to explain what I believe is the mindset behind the statement, “…as long as the baby is healthy.” Please keep in mind that this seems to be a society mindset; not necessarily the mindset of every individual.Ninety percent of babies who have Trisomy 18 are aborted. Ninety percent!
Our culture tells us that children who are different and require more help are not worthy of life. In a culture where “normal” people are constantly told to be “unique” and “be yourself” we do not want to accept those whose “normal” is unique.
In my sister’s case, unique meaning 1 in every 5,000 live-births.Society has told us that if there is a problem just “get rid of it.” That there is no need to “fix” something if you can get a new one with minimum trouble.
“Abortion is an ‘easy’ answer to solving the issue of a special needs child.”
“You do not want to make yourself or the child suffer.”
“You can get pregnant again and it will be a healthy child.”
I have said it before, but I will say it again. I have more compassion, love, understanding, and hope because of my sister than I would ever have without her. She lights up my life, and even when life is rough and it feels like we are going to hit rock bottom that little face will look up at you with the biggest smile and so much admiration in her eyes, for you, that you know all will be well in the end.
It breaks my heart every time someone says, “…as long as the baby is healthy,” mainly because my sister is not.
It hurts so much to hear someone say that, especially when they know that my sister is disabled.
They know that I have a sister, who I love very much by the way, who has special needs, and yet, they say to my face that they do not want a child like her. They basically say that they will take anyone, but a child like her.
I used to get extremely upset over this and it will still hurt sometimes, but I have come to the point where my mindset is, “If they do not get to experience the wonderful love of kids like my sister, they are the ones missing out.”
Please keep in mind that I did not put any of this to condemn anyone but to show them how simple phrases that are used all the time can be hurtful and that there is
May 29, 2015 (LifeSiteNews.com) — The grave effects of Ireland’s May 22 referendum in favor of same-sex “marriages,” not only for the secular world, but also especially for the Catholic Church, are showing themselves already.
None other than the leading cardinal who has promoted the liberal agenda for the two-part Synod of Bishops on the Family, Cardinal Walter Kasper, has now come out publicly and with force, telling the Italian newspaper Corriere della Sera that the Church needs to address more fully the question of same-sex couples. This topic was at the last Synod “only a marginal topic, but now it becomes central,” Kasper said on Wednesday.
Kasper also defended the vote of the Irish in favor of homosexual “marriages,” saying: “A democratic state has the duty to respect the will of the people; and it seems clear that, if the majority of the people wants such homosexual unions, the state has a duty to recognize such rights.” He also said that the Irish referendum is “emblematic for the situation in which we find ourselves, not only in Europe, but in the whole West.” Kasper also said: “The postmodern concept – following which everything is equal – stands in contrast to the doctrine of the Church.”
Cardinal Kasper made a link between the events in Ireland and the doctrine of the Catholic Church, when he said it now becomes harder for the Church to explain its own moral position to others in the question of homosexuality. “We have to find a new language,” he said. “We have to overcome [unjust] discrimination, which has a long tradition in our culture.” It is important in his view to honor those long-lasting same-sex relationships, which contain “elements of the good,” even though the Church cannot change its fundamental attitude toward them since they are themselves against the teaching of the Gospels.
Many observers have long expected Cardinal Kasper’s more explicit public support for the homosexual agenda, saying that the “opening” toward “remarried” couples was only the first step toward the widening of the revolutionary agenda, to include approval of same-sex relationships.
The other reason for this expectation is that Cardinal Walter Kasper had recently published his own book about Pope Francis, entitled “Pope Francis’ Revolution of Tenderness and Love”, and it was produced by Paulist Press. Father Mark-David Janus, president and publisher of Paulist Press, was present when Cardinal Kasper gave Pope Francis himself a copy of this new book on March 17. At a private audience later on the same day, Father Janus presented the pope with a promotional film on “LGBT Catholics,” called “Owning Our Faith,” which he himself had helped to bring about. These facts – which may be seen on the website of the St. Philip Neri Catholic Church – administered by the same Paulist Fathers – speak for themselves.
This current initiative of Cardinal Kasper comes, however, also right after a somewhat concealed May 25 “Day of Study” at the Gregorian University in Rome, which was organized by the three presidents of the Swiss, French, and German Bishops’ Conferences – Bishop Markus Büchel, Archbishop Georges Pontier, and Cardinal Reinhard Marx – who met with 50 participants: “partakers of the Synod, professors of theology, members of the Roman Curia, as well as journalists,” according to the press release of the German Bishops’ Conference of May 26. The general theme of this confidential gathering was the upcoming Synod of Bishops on the family, and the substance of the presentations was also to be kept confidential. The participants were even asked to preserve a silence after the Day of Study was over. As Catholic News Agency reports:
One of the speakers, who asked to be kept anonymous, refused to comment on the purpose of the conference and the tone of the discussion, as “it is unfortunately forbidden to us by the organizers to give any interview or explanation about yesterday’s conference.”
The well-respected Vatican reporter Edward Pentin spoke with Cardinal Marx after he exited the confidential meeting. Pentin reports:
Speaking to the Register as he left the meeting, Cardinal Marx insisted the study day wasn’t secret. But he became irritated when pressed about why it wasn’t advertised,saying he had simply come to Rome in a “private capacity” and that he had every right to do so. Close to Pope Francis and part of his nine-member council of cardinals, the cardinal is known to be especially eager to reform the Church’s approach to homosexuals.
During his Pentecost homily last Sunday, Cardinal Marx called for a “welcoming culture” in the Church for homosexuals, saying it’s “not the differences that count, but what unites us.”
As different media outlets have subsequently been able to report, the following themes were discussed favorably at this Rome meeting, all of which items indicate a liberalizing tendency:
a new “theology of love”: sexuality as a precious gift of God, as itself an expression of love
the Church’s acceptance of homosexual unions
the Church’s listening to the voice of the Baptized in moral questions
a Catholic Hermeneutic of the Bible on the basis of the words of Jesus about divorce
the change of moral patterns in a pluralistic society
admittance of “remarried” couples to the sacraments
a second marriage as an “authentic union”
the indissolubility of marriage as “an ideal or ‘utopia’”
the importance of the human sex drive
sexuality as basis for a long-lasting relationship
with the lengthening of lifespans, the borders of fidelity are also changed
the development of Church doctrine and discipline over time The spokesman for this one-day meeting, Matthias Kopp, told Catholic News Service on May 27, after some criticisms had arisen: “I reject the thesis that the bishops have an agenda to change church teaching.” In spite of this denial, many Catholics are indignant and suspicious about the procedure and tendency of this meeting, since many of the bishops, who are meant to be represented by the presidents of their own national bishops’ conferences, were not even informed about the confidential meeting, let alone invited.
Manfred Spieker, a German layman and professor emeritus of Christian social studies of the University of Osnabrück, wrote on May 28 on the German-speaking website kath.net about the fact that the other bishops were not even informed about the meeting, as organized by the three presidents of their bishops’ conferences: “This is close to an abuse of their office as moderators of the Bishops’ Conference, because their proper role as a president of a bishops’ conference is not much more than being a moderator.” He insists that their methods are undermining the explicit intent of the Synod of Bishops, which calls for and promises openness and fairness:
A conference that resembles more a secretive gathering than an academic, and therewith open event stands in opposition to the proclaimed openness and fairness. It is divisive. The three bishops [Presidents of the Bishops’ Conferences] also did not invite those journalists who are known experts on the subject, but only those who share their views and are able to intensify the public pressure which this whole meeting is supposed to place upon the Synod in October.
Professor Spieker compares this conduct with some of the methods that were used during the last Synod of Bishops, saying: “The attempts at manipulation which had reached – already during the extraordinary Synod of Bishops of 2014 – an until-now-unknown level in the Church, have now reached a new stage with this conference at the Gregoriana.” The German professor also comments, as follows, on the above-mentioned themes and on the statements made at the meeting which have now been leaked: “It will certainly not escape the notice of the Presidents of the three Bishops’ Conferences, what schismatic potential is to be found in such expressed views.”
May 29, 2015 (LifeSiteNews.com) – Women who use modern contraceptives have at least a 50 percent greater chance of having potentially deadly blood clots, according to a new study published in the British Journal of Medicine.
The study — which examines women aged 15-49 over the last 13 years — used two different United Kingdom databases to examine how frequently women developed blood clots while using new combined contraceptives, as compared to older contraceptives.
“Risks for women using newer pills were around 1.5-1.8 times higher than for women using older pills,” according to a press release announcing the study’s results. “In absolute terms, the number of extra [blood clot] cases per year per 10,000 treated women was lowest for levonorgestrel and norgestimate (six extra cases), and highest for desogestrel and cyproterone (14 extra cases).”
A BJM editorial about the study noted that the results showed “newer contraceptives increased risks by around 3.6- to 4.3-fold compared with non-use, and by around twofold compared with oral contraceptives containing levonorgestrel, norethisterone, or norgestimate.”
“Combined, the results provide compelling evidence that these newer oral contraceptives are associated with a higher risk of venous thromboembolism than older options, despite attempts to develop safer hormonal contraceptives for women,” concluded the BJM editorial.
The report’s lead author, University of Nottingham Research Fellow Yana Vinogradova, told LifeSiteNews in an email that “the risk [of blood clots] is 2.4-2.5 times higher in women taking old contraceptives compared with no use.”
The author told LifeSiteNews that “in each database, there were about 3 million women 15-49 years old, and more than 5,000 of them had [a blood clot].” The study said that 28 percent of women in the United Kingdom use contraceptives.
Despite the higher risk, the release also says that “the authors stress that oral contraceptives are remarkably safe, and…the reported three-times increased risk of VTE in women using oral contraceptives in their study is still lower than the up to 10-fold increased risk of VTE in pregnant women.”
The study is just the latest to find significant potential harm from using modern contraceptives. Last year, a study found that high-dose estrogen pills “increased breast cancer risk 2.7-fold,” while “those containing moderate-dose estrogen increased the risk 1.6-fold.”
Likewise, a 2014 Centers for Disease Control (CDC) study found a possible link between hormonal contraceptives and gestational diabetes, and a 2013 CDC study found a possible connection between use of the birth control pill and glaucoma.
Despite the higher risks of blood clots among women who use contraceptives, especially newer forms, Vinogradova defended the study’s finding that “this is an observational study so no definitive conclusions can be drawn about cause and effect.”
“Definite conclusions can be drawn only from a randomized controlled trial where patients with known and unknown risk factors are randomly allocated into the arms,” she wrote. “Conducting a randomized controlled trial in these circumstances is not feasible, therefore only observational studies can be performed. In observational studies, exposed and non-exposed participants may have different risk factors for outcome.”
“Although we considered all available from the databases risk factors, there may be other unknown or not-available ones. So the estimates of risks associated with different types of contraceptive pills provided by our study are the most accurate to date.”
BY STOYAN ZAIMOV , CHRISTIAN POST REPORTER, May 7, 2015
Pope Francis has said that Roman Catholic priests can begin pardoning women who’ve had abortions and doctors who have performed the procedure starting in 2016, changing long-standing Catholic practice. The Vatican insisted, however, that it continues to look at abortion as a sin.
Archbishop Rino Fisichella, the president of the Pontifical Council for the New Evangelisation, announced Francis’ decision earlier this week, and said: “The missionaries of mercy are priests sent out by the Holy Father at the beginning of Lent. The Pope is sending them out [to dioceses and parishes] as a tangible sign of how a priest should be a man of pardon, close to everyone …”
The Irish Times pointed out that Catholic tradition only allows bishops or the pope himself to absolve women of having an abortion, which is a sin that leads to excommunication from the Church.
The Catholic “Holy Year of Mercy” runs from Dec. 8 through Nov. 20, 2016, and will allow specially appointed priests “the authority to pardon even those sins reserved to the Holy See.”
The special year will also mark several individual jubilee days, such as for the Roman Curia, catechists, teenagers and prisoners.
Archbishop Fisichella clarified in an interview with Italian news agency ANSA that priests will also be able to offer absolution not only to women who’ve had abortions, but also to the doctors that performed them.
The Daily Mail reported that the Vatican has previously faced criticism from the United Nations for excommunicating the mother and doctor of a 9-year-old girl in Brazil who underwent an abortion in 2009 after she was raped by her stepfather and became pregnant with twins.
Italian Cardinal Velasio De Paolis, who has published a book alongside four other cardinals called Remaining In The Truth Of Christ, which defends marriage and Catholic tradition, insisted that the Catholic stance against abortion will not waver, however.
De Paolis said: “Regardless of this decision by the Pope, the Church will continue to consider abortion a sin. I hope it does not cause confusion.”
Francis has affirmed on a number of occasions his opposition to abortion, a well as to euthanasia, stem-cell research, and other attempts to end life.
Back in November 2014, the pontiff dismissed the notion that abortion is good for women, or that euthanasia is “an act of dignity,” or “a scientific breakthrough to ‘produce’ a child (who is) considered a right instead of accepted as a gift.” Francis also denounced “(the) use of human life as laboratory mice supposedly to save others.”
The Vatican has set up an official Jubilee of Mercy website which talks more about the tradition and the planned events.
“I have decided to announce an Extraordinary Jubilee which has at its centre the mercy of God. It will be a Holy Year of Mercy. We want to live in the light of the Word of the Lord: ‘Be merciful, even as your Father is merciful’ (Luke 6:36). And this especially applies to confessors! So much mercy!” Francis said when announcing the Holy Year.
BY STOYAN ZAIMOV , CHRISTIAN POST REPORTER, May 7, 2015
Ann Marie Lapkowicz is a friend of mine. Her daughter is now an international celebrity.
The story begins when Ann Marie’s daughter Mary was in 4th grade. As PennLive.com reports, her friend Ben Moser worked hard to make sure that Mary was included in the games the other fourth graders would play.
His act of kindness was significant because
Mary has Down Syndrome. But to Ben, Mary was not a statistic—she was a friend.
Ben informed his mother that, when he was old enough, he would invite Mary to the high school prom.
But Ben and Mary ended up attending different high schools. As fate would have it, their paths crossed one day, and Ben decided to make good on his long-ago promise. As he told PennLive.com, “We got balloons and I wrote ‘prom’ on it. I presented her with the balloons and asked her to go to prom with me.”
But the fairy tale did not end there. News of the quarterback who asked his Down Syndrome friend to the prom has gone viral. The pair even appeared on the cable program “Fox & Friends.” Ben told the
Fox News anchor, “Mary’s the coolest person ever!”
He also said his mother has never been prouder of him.
Mary’s mother, my friend Ann Marie, told me she was wondering if allowing PennLive to publicize the story was the right thing to do. After all, she is protective of her children, and is even reluctant to post pictures of them on Facebook.
But she had heard that such positive stories can save the lives of Down Syndrome children (It has been estimated that 90 percent of Down Syndrome babies are aborted.). If it could save one life, she figured the discomfort of the spotlight would be worth it.
I have watched Mary grow up into a beautiful young woman. I have known her to rise very early to attend church with her family on weekday mornings. She is a very special girl, and it is heartwarming that the world has come to recognize that through the “prom-promise” made by an equally special young man.
Ben and Mary’s friendship should provide a lesson to us all.
May 28, 2015 (BreakPoint.org) — For five years, Dr. Abigail Rine has been teaching a course on gender theory at George Fox University, an evangelical school in the Quaker tradition.
At the beginning of the semester, she tells her students that “they are guaranteed to read something they will find disagreeable, probably even offensive.”
Writing at FirstThings.com recently, she related how five years ago it was easy to find readings that challenged and even offended the evangelical college students “considering the secular bent of contemporary gender studies.” But today, things are different. “Students now,” she says, “arrive in my class thoroughly versed in the language and categories of identity politics; they are reticent to disagree with anything for fear of seeming intolerant—except, of course, what they perceive to be intolerant.”
And what do they find “intolerant”? Well, in her class, an essay entitled “What is Marriage?” by Sherif Girgis, Robert George, and Ryan Anderson, which was the beginning of the book “What Is Marriage?: Man and Woman: A Defense.” In their article, Girgis, George, and Anderson defend what they call the conjugal view of marriage. “Marriage,” they write, “is the union of a man and a woman who make a permanent and exclusive commitment to each other … that is naturally fulfilled by bearing and rearing children together.” They defend this view against what they call the “revisionist view” of marriage, which redefines marriage to include, among other things, same-sex couples.
“My students hate it,” Dr. Rine wrote. They “lambast the article.” “They also,” she adds, “seem unable to fully understand the argument.” And again, these are evangelical students at an evangelical school.
The only argument for conjugal marriage they’ve ever encountered has been the wooden proof-texting from the Bible. And besides, wrote Rine, “What the article names as a ‘revisionist’ idea of marriage—marriage as an emotional, romantic, sexual bond between two people—does not seem ‘new’ to my students at all, because this is the view of marriage they were raised with, albeit with a scriptural, heterosexual gloss.”
As Rine points out “the redefinition of marriage began decades ago” when “the link between sexuality and procreation was severed in our cultural imagination.”
And if marriage “has only an arbitrary relationship to reproduction,” then it seems mean-spirited to Rine’s students to argue that marriage by its very nature excludes same-sex couples.
And where do students get the idea that marriage “has only an arbitrary relationship to reproduction”? Well, everywhere—television, church, school, their homes, in youth groups.
Rine writes, “As I consider my own upbringing and the various ‘sex talks’ I encountered in evangelical church settings over the past twenty years, I realize that the view of marital sex presented there was primarily revisionist.” In other words, once you say, “I do,” you get “the gift” of sex which is presented as “a ‘gift’ largely due to its [erotic], unitive properties, rather than its intrinsic capacity to create life.” Even in the Church, children have become an optional add-on to married life rather than its primary purpose.
What can we do to win back our children, our churches, and the culture? In our recent book “Same Sex Marriage,” Sean McDowell and I lay out a game plan. We offer strategies for the short-term and the long-term, with the ultimate goal: re-shaping the cultural imagination towards what God intended marriage to be, starting with the church. Come to BreakPoint.org to pick up your copy.
As Chuck Colson once said in a BreakPoint commentary about marriage, “We Christians are very good at saying ‘No.’ But we’ve got to get better at saying ‘Yes’: showing how God’s plan for humanity is a blessing. That His ways, including faithful, life-giving marriage between one man and one woman, lead to human flourishing physically, emotionally, and spiritually.”
“There is an old prophecy that the Faith in Ireland will nearly die out, but will reignite and turn the nation into a bonfire of Catholicism.”
Father Tom Forde, OFM Cap, is a Chaplain at the University of Cork. In this deeply serious interview, he unflinchingly discusses the agony of Irish Catholicism today —and points to an unexpected light on Ireland’s dark horizon.
Q. What do you think is the greatest myth about Ireland today?
A. That we are still the old Ireland, a country filled with green hills and sheep. The reality is that out of a total of about 6 million people in Ireland — 4.5 in the Republic and 1.5 in Northern Ireland– 1.5 million live in or near Dublin alone, with over 500,000 living in Belfast and another 250,000 in Cork. Therefore a sizable portion of the population is urbanized and that alone has an impact on religious practice. Most of the immigrants to Ireland have come from ‘Catholic’ countries but that has not significantly impacted on the practice rates. The Poles especially tend to stick together and intend to return to Poland.
Q. Could you provide some insight on what’s happening to the Faith in Ireland today?
A. The Faith runs deep. Human beings are naturally religious and the Irish are no different. Mary Kenny (an Irish Catholic journalist) has a book where she argues that the faith and interests of the laity of one generation determines the faith and interests of the clergy of the next. When the people were pro-British we had generations of clergy who were also pro-British but when the people turned against the British the clergy did too. The exception, she believes, were the religious who were often counter-cultural. It’s an interesting argument.
Q. What have been the major trends contributing to the lack of religious practice in Ireland today?
A. There is a connection between the decline in the practice of the Faith in Ireland and the swing away from traditional values, between a skepticism about nationalism, an increasing devotion to consumerism and above all the widespread embracing of contraception. On the latter point if one could chart the decline in Mass attendance and the increase in contraceptive availability/sales (especially after legalization in 1979) I think there would be a clear correlation.
Q. This is not unique to Ireland, of course.
A. Yes. The same rebellious spirit that swept the Church, especially in Europe and the States, swept Ireland too but it took a little longer to have its effect. Ireland looks much more to the States than to probably any other country largely due to the sheer numbers of emigrants who have gone there.
Q. Has this affected the Irish clergy?
A. The Irish Church is no different (than the people). America has long been the country of choice for religious and clergy to study since travel there became cheaper and easier. That swing away from Europe towards the U.S. has meant that the liberalism that has dominated the American Church has also dominated the Irish if in a more toned-down form. The clerical promoters of the morality of contraception seem to have received little resistance within the Irish Church in the 70’s or since.
Q. And what about today?
A. The bishops say the right things but do little it seems to correct abuses until they are public scandals. One Irish priest Fr. Iggy O’Donovan, a religious, was deprived of faculties in the Archdiocese of Armagh after he had publically celebrated Mass with a Protestant minister as concelebrant and carried out invalid baptisms. He was granted faculties in another diocese (Limerick). That was last year!
There is not much confidence in the Irish bishops – they are not very inspiring. Apart from Child Protection (at which the Irish Church now excels) the dioceses of Ireland are not known for doing anything well. Even the Eucharistic Congress in 2011 was like a throwback to the 80’s! Unfortunately despite Pope Francis’ warnings against careerism it still thrives. There are also dark rumours of some of the filth that Pope Benedict spoke about. The devil has not gone away.
Q. To what do you attribute this?
A. I think that the Irish Church, like the Irish nation, is largely in decline due to the embracing of contraception. Contraception is the technology by which the net fertility rate has declined to as low as 1.8 (should be at the replacement rate – a minimum of 2.1) and although it has temporarily jumped up a little it is still below 2.1. It has been below the replacement rate since the late 80’s. Our nation like the rest of the West and much of the civilized world is in decline.
Q. Contraception is a technology that is used by non-Catholics as well, of course.
A. Yes, but for the Church this is a double blow. The people who contracept are largely Catholic and this places them in conflict with the Church’s official teaching and God’s plan. Even if they are reassured by some clergy, in their hearts they know the two are irreconcilable. With a refusal to co-operate with God’s plan for human sexuality and fertility – a moral problem – there comes the spiritual problem that faith does not thrive under disobedience and this means an interior conflict. That interior conflict leads to either repentance or exterior rebellion – they walk away. It also means that not only will vocations not thrive in such an atmosphere but a contracepting people will not conceive enough babies to support their own future let alone the priesthood and the future of the Church.
Q. Certainly contraception is not the only reason why the Irish have turned away from their Church?
A. Of course not. Neither can it be denied that the abuse of children by clergy and religious both in institutions and in private has done immense damage to the Faith in Ireland.
It has done immense damage to the victims and their families. It has been a body blow to faithful clergy, religious and laity. It has reassured some that it is right to walk away. It has erected walls across the path to the Faith for others. It has handed the enemies of the Faith and the Church a weapon with which to scourge and torture.
Q. Yes, Catholics in many countries are familiar with this agony — and with the fury it generates.
A. Today, it is not easy to be Catholic in public in Ireland. But the Church and the Faith were in decline even before the scandals broke. Some suggest that the abuse of children and vulnerable adults by clergy, religious and laity are signs that something had gone profoundly wrong in Ireland (as it obviously had in other countries e.g. Holland). The rot was already there spreading beneath the veneer of Irish Catholicism.
Q. These are dark days indeed for the Faith in Ireland.
A. Nevertheless, there are signs of hope. There is an old prophecy that the Faith in Ireland will nearly die out but will re-ignite and turn the nation into a bonfire of Catholicism.
There are small groups of young people ardent for the Faith all over the country. They are already like veterans so toughened by opposition that they take it for granted. You have to have a thick skin to be Catholic in many parts of Ireland. Eventually some of them will make it not only into the clergy but into the episcopacy and perhaps then we will see a change.
In the meantime there are clergy who are loyal to the Faith and who want to see it flourish. They are quietly organizing and working to reinforce and to rebuild what they can.
The Irish Church has a long dark road still ahead of her but she is not alone – she never was.
In Illinois, Leo and Ruth Zanger are celebrating 59 years of marriage and the birth of their 100thgrandchild. Leo said, “The good Lord has just kept sending them. We could start our own town.” The Daily Mail reports that the couple has 12 children, 53 grandchildren, 46 great-grandchildren and one great-great-grandchild. Ruth added, “There’s always room for one more.”
The couple’s oldest child, Linda, is 58-year-old and their youngest is Joe, who is 31-years-old. In between are Debbie, Donna, David, Greg, Daniel, Mike, Steve, Chuck, Matt, and Ernie. On April 8th, the couple’s grandson, Austin, welcomed his second
child and the couple’s hundredth grandchild into the world, Jaxton.
For family get-togethers, the Zangers usually rent out a church hall and share the responsibilities regarding food preparation. Leo and0 Ruth’s daughter, Donna, said, “Everyone takes their turn (in helping with food),
and they all try and outdo each other. We are always getting together for something.”
Donna’s also been named the family historian because she keeps track of all the birth records, phone numbers and anniversaries in the family. She said,”(Other family members) always say, ‘Since you already have all of the phone numbers, can you just text (or call) them and let them know about whatever the event is?’ ”
Although the Zangers say they have plenty of excuses to gather, unofficial ‘mandatory’ gatherings are Thanksgiving, Christmas, Easter, Mother’s Day, and Father’s Day. ‘We’re all really close. We get together a lot,’ Austin told the Whig.
‘There’s always a lot of interaction. We spend a lot of time with each other. I know there are a lot of families half of our size who only get together maybe once or twice a year.’
Austin said that he and his wife didn’t know that Jaxton would be the 100th grandchild until Donna, the unofficial family historian, told them.
‘It’s pretty special — 100 grandkids, that’s a big deal,’ Austin told the Whig.
Ashleigh said she is extremely proud of being the mother of grandchild No.100.
The Zangers describe themselves as close-knit with, all of the grandchildren knowing Ruth and Leo and much of the family living in or near Quincy.
A family gathering usually consists of 50 pounds of ham or 10 turkeys, according to NBC. But the family has had a lot of time to hone a routine for supplies and duties.
‘It’s a very busy family, and we enjoy being around each other,’ Daniel told the Whig. ‘There’s never a dull moment. We always had a lot of fun growing up.’
The Orthodox Church has historically taken a powerful stand against birth control.
Saints and Early Church Fathers put contraception on the same level as homicide. St. John Chrysostom, St. Ambrose, St. Augustine, St. John IV Nesteutes (St. John the Faster), St. Clement of Alexandria, St. Epiphanius of Salamis, and St. Caesarius of Arles are among the holy Fathers who condemned contraception in the strongest imaginable terms.
St. John Chrysostom goes so far as to call it “murder before conception”.
Why is this the historic position of the Orthodox Church?
Why do the Saints say that birth control is equivalent to murder?
Murder in the Heart
Imagine that your next-door neighbor hates you. He does not merely dislike you;
He wants you dead. He does not merely want you out of town, or out of the country.
He wants you off the planet.
His desire is for you to not exist.
According to Christ, this person is guilty of murder. God not only judges outward sins;
He also judges sins of the heart. Just as lust makes a person guilty of adultery,
hatred and anger make a person guilty of murder.
Murder by Time-Travel
Now suppose your neighbor hatches a wild plan. He attempts to invent a real working time-machine, so that he can use it to get rid of you. He does not want to kill you, because that would make a big mess, and he does not want to dispose of your body. He simply plans to go back in time, and provide your parents with birth control during the month you were conceived, so that you would never exist in the first place.
Does this new plan make you feel better about your neighbor?
Of course not. Planning to avoid your existence is no better than murdering you. Either way, he is showing hatred for you, regardless of the fact that you are a real human being, created in the image of God. Even with his “time travel” plan, he is still a murderer at heart.
Now consider a slightly different scenario. Instead of using a time-machine to go backward, you use it to go forward in time. You and your spouse travel 12 months into the future, to see what your life will look like a year from now. After making the trip, you find out that you will have a new little baby boy named “Johnny”. He is a precious child, created in the image of God.
But you and your spouse do not want Johnny. You don’t like him, and you would prefer that he never exist. But you don’t really want to kill him. You don’t want to dispose of his body. So you just use your time machine to return to this present time. Then your family doctor provides a prescription for birth-control pills. That way Johnny will never be conceived in the first place. Thanks to you, Johnny will never exist.
If you do this, are you not showing hatred for Johnny? Are you not a murderer at heart?
Yet millions of people make this sort of decision daily. With their current sexual practices, they know that a pregnancy is likely to occur within the next 12-24 months. They have good reason to believe that a precious little “Johnny” is on the way. And with this likelihood in mind, they intentionally try to stamp out Johnny’s existence. They use contraception, for no other reason than to avoid the existence of a precious child, created in the image of God. In their minds, it would be better for Johnny to never exist.
They think about Johnny. They hate him. They seek to deprive him of existence.
By using birth control, they reveal themselves to be murderers at heart.
A child is a blessing, a human being created in the image of God. It is an act of hatred–an act of murder–to intentionally avoid that blessing, whether the avoidance is done before the fact (via birth control) or after the fact (via abortion or infanticide).
Birth Control in the History of the Church
For 1,900 years, every church in the world opposed birth control. Throughout history, the Greek Orthodox, Russian Orthodox, Serbian Orthodox, and every other Orthodox jurisdiction condemned the use of birth control. Not only that, but the Catholic and Protestant churches prohibited birth control as well. Prior to the 20th century, there was not a single “Christian” group that approved of contraception.
The Early Church Fathers did not merely call birth control a sin. They called it murder.
One of the most respected saints in the history of the Church is St. John Chrysostom. The most frequently used Orthodox divine liturgy is named after him. He was the archbishop of Constantinople, and he left us with many volumes of solid Orthodox teaching. Here is what he had to say about birth control, otherwise known as “medicines of sterility”:
“Why do you sow where the field is eager to destroy the fruit, where there are medicines of sterility [oral contraceptives], where there is murder before conception? You do not even let a harlot remain only a harlot, but you make her a murderess as well. . . . Indeed, it is something worse than murder, and I do not know what to call it; for she does not kill what is formed but prevents its formation. What then? Do you condemn the gift of God and fight with His [natural] laws? . . . Yet such turpitude . . . the matter still seems indifferent to many men–even to many men having wives. In this indifference of the married men there is greater evil filth; for then poisons are prepared, not against the womb of a prostitute, but against your injured wife. Against her are these innumerable tricks”
~ St. John Chrysostom (Homilies on Romans 24 [A.D. 391]).
Another well-known early Father is St. Ambrose, bishop of Milan. In his commentary on Genesis, this saint commented on the contraceptive drugs which many people procured during his time. He lamented that people using birth control,
“lest their patrimony be divided among several, deny their own fetus in their uterus and by a parricidal potion extinguish the pledges of their womb in their genital belly, and life is taken away before it is transmitted.’”
~ St. Ambrose (Hexameron 5.18.58 [CSEL 32: 184])
According to St. Ambrose, it was dreadfully sinful for people to limit the number of offspring, merely so they could avoid dividing their inheritance “among several”. When considering their children’s inheritance, they mistakenly believed that money and land would make a better heritage than brothers and sisters.
When the Fifth Ecumenical Council singled out twelve “Holy Fathers” as being worthy of particular attention and veneration, St. Augustine was included as one of the twelve. (This list of 12 Fathers also included St. John Chrysostom and St. Ambrose, already quoted above.) In one of his letters, St. Augustine strongly condemns the use of birth control:
“I am supposing that then, although you are not lying for the sake of procreating offspring, you are not for the sake of lust obstructing their procreation by an evil prayer or an evil deed. Those who do this, although they are called husband and wife, are not; nor do they retain any reality of marriage, but with a respectable name cover a shame. They give themselves away, indeed, when they go so far as to expose their children who are born to them against their will; for they hate to nourish or to have those whom they feared to bear. Therefore a dark iniquity rages against those whom they have unwillingly borne, and with open iniquity this comes to light; a hidden shame is demonstrated by manifest cruelty. Sometimes this lustful cruelty, or cruel lust, comes to this, that they even procure poisons of sterility, and, if these do not work, extinguish and destroy the fetus in some way in the womb, preferring that their offspring die before it lives, or if it was already alive in the womb to kill it before it was born. Assuredly if both husband and wife are like this, they are not married, and if they were like this from the beginning they come together not joined in matrimony but in seduction. If both are not like this, I dare to say that either the wife is in a fashion the harlot of her husband or he is an adulterer with his own wife.”
~ St. Augustine (Marriage and Concupiscence 1.15.17, CSEL 42:229-230)
In St. Augustine’s understanding, there is very little difference between contraception and abortion. Either way, the spouses are avoiding the blessing of God, and are intentionally stopping a real human being from walking on earth. Birth control renders sexual relations illicit, even within a marriage. By default, the marriage bed is holy and undefiled. But according to this saint of the Church, birth control reduces the marital act to the level of fornication and adultery, satisfying one’s fleshly lust as with a whore.
St. John IV Nesteutes (St. John the Faster), a 6th century Patriarch of Constantinople, had the following to say regarding birth control:
“If someone to satisfy his lust or in deliberate hatred does something to a man or woman so that no children be born of him or her, or gives them to drink (pharmakon), so that he cannot generate or she conceive, let it be held as homicide.”
Many other Saints and Fathers of the Church have spoken likewise against contraception.
For example:
“Because of its divine institution for the propagation of man, the seed is not to be vainly ejaculated, nor is it to be damaged, nor is it to be wasted”.
~ St. Clement of Alexandria
“They [heretics] exercise genital acts, yet prevent the conceiving of children. Not in order to produce offspring, but to satisfy lust, are they eager for corruption”.
~ St. Epiphanius of Salamis
“Who is he who cannot warn that no woman may take a potion [an oral contraceptive] so that she is unable to conceive or condemns in herself the nature which God willed to be fecund? As often as she could have conceived or given birth, of that many homicides she will be held guilty, and, unless she undergoes suitable penance, she will be damned by eternal death in hell. If a woman does not wish to have children, let her enter into a religious agreement with her husband; for chastity is the sole sterility of a Christian woman.”
~ St. Caesarius of Arles
Marital Abstinence is Permitted
This last comment by St. Caesarius is noteworthy. While he agrees with the patristic consensus that artificial birth control is equivalent to homicide, he nevertheless observes that “chastity is the sole sterility of a Christian woman.” It would be wrong for a married couple to have sex, while using birth control to prevent conception. But it is OK to avoid sex itself. A married Christian couple is not required to copulate daily, in order to have as many children as possible.
St. Paul himself notes that marital abstinence is acceptable, as long as it is for the purpose of deepening the spiritual life of the couple:
Do not deprive one another except with consent for a time,
that you may give yourselves to fasting and prayer; and come together again so that Satan does not tempt you because of your lack of self-control. (1 Corinthians 7:5).
It is acceptable for a husband and wife to avoid sexual relations for a time, so they can focus on prayer. It is also acceptable for a husband and wife to have normal sexual relations, with a willingness to conceive children. But it is sinful to intentionally separate sex and conception from one another. It is sinful to have sexual relations, while intending to avoid the conception of children.
Consensus Through Recent Times
As recently as 1963, in his book, The Orthodox Church, Bishop Kallistos (Timothy) Ware states clearly and without qualification:
“Artificial methods of birth control are forbidden in the Orthodox Church.”
(Timothy Ware, The Orthodox Church, Penguin, 1963, p. 302.)
Similarly, after the Humanae Vitae encyclical letter was released in 1968, reaffirming Rome’s rejection of contraception, the Ecumenical Patriarch Athenagoras of Constantinople reviewed it and then wrote a letter to the Roman Pontiff, affirming the Orthodox Church’s “total agreement” with the contents of the encyclical:
“We assure you that we remain close to you, above all in these recent days when you have taken the good step of publishing the encyclical Humanae Vitae. We are in total agreement with you, and wish you all God’s help to continue your mission in the world.”
(Patriarch Athenagoras telegram to Pope Paul VI, 9 August 1968, reprinted in Towards the Healing of Schism, ed. & trans. E.J. Stormon, 1987, p. 197.)
For nearly 2000 years, the Orthodox Church has spoken with one voice.
Contraception is a sin. Artificial birth control is unacceptable.
If it was wrong for the Saints and the Early Church Fathers,
then it is wrong for us.
If it was wrong from the first century until the year 1968,
then it is still wrong today.
From the first century through the 1960s, I do not know of any Orthodox sources which advocate artificial birth control. The first hint of doctrinal innovation came in 1974 with
the article, “Morality of Contraception: An Eastern Orthodox Opinion”, written by Chrysostom Zaphiris and published in the Journal of Ecumenical Studies. Interestingly, this article ignores 1900 years of Orthodox consensus on this topic, and fails to address any of the pertinent quotes from St. John Chrysostom, St. Ambrose, St. John the Faster, St. Clement, St. Epiphanius, etc. Instead, Zaphiris invents a new “Orthodox” opinion out of thin air, without relying on the historic teachings of the Orthodox Church and its saints.
Thankfully, people like CJS Hayward, Taras Baytsar, and a number of other Orthodox Christians are remaining faithful to the historic teachings of the Orthodox Church.
Contraception is not a Christian option.
As St. John Chrysostom said, birth control is “murder before conception”.
This is the second in a series on Evangelium vitae. Find the whole series here.
Twenty years ago, Pope Saint John Paul II denounced the moral impoverishment, particularly abortion and euthanasia, that devalues human life in his encyclical Evangelium vitae. He described Christ’s central message that we “may have life, and have it abundantly,” which is the eternal life He came to bring that also gives “full significance” to “all aspects and stages of human life” (1). John Paul rails against a false notion of freedom and autonomy that is used to justify crimes against life, but actually inverts freedom and leads to the opposite of human good. An authentic understanding of freedom, freedom for excellence, is much needed in our culture to explain the goodness of life and opposition of abortion.
John Paul II does not wholly blame the individuals who face “difficult or even tragic situations” when facing abortion, and notes that such circumstances can “mitigate…subjective responsibility.” Rather, he locates the problem “at the cultural, social and political level” where legalized abortion is disturbingly interpreted as “legitimate expressions of individual freedom” (18). As he goes onto explain, this notion of freedom is fundamentally backwards and opposed to true democracy.
True freedom is the ability of every human being to seek their own good and potential; it is an expression of their intrinsic worth as made in the image of God and naturally harmonizes with the good for humanity as a whole and therefore does not involve killing or harming the human person. Law naturally recognizes this in the case of adults; we have a prohibition against murder, assault, and even illicit drug use that harms the individual himself and thus the wider social community of which he is an inseparable part.
John Paul praises the development of “human rights” in the Western tradition as the basis for constitutions and government.He says that “the various declarations of human rights and the many initiatives inspired by these declarations show … there is a growing moral sensitivity” that acknowledges the “dignity of every individual as a human being, without any distinction of race, nationality, religion, political opinion or social class” (18).
Yet the practical denial of the value of every human life in abortion and other crimes, he says, “is still more distressing…precisely because it is occurring in a society which makes the affirmation and protection of human rights its primary objective and its boast” (18). The United States and Western Europe posit our flagship virtue as the virtue of securing rights for all. America’s Declaration of Independence famously and rightly recognizes the foundation of society as affirmation of the rights of all humanity to “life, liberty and the pursuit of happiness.” And how tragic the contradiction when we say that some humans are not persons or do not have lives worthy of living simply because their end is likely to be swift.
John Paul excoriates the mentality which equates personal dignity with the “capacity for verbal and explicit, or at least perceptible communication” (19). In such a biased approach, the dignity of the unborn and the dying is rejected. In contrast, their dignity exists simply on the grounds of being human, of being made in the image of God. Even without an explicitly religious context, this dignity is what all declarations of human rights recognize. They are “human” rights, not rights of “humans who can communicate.” While secular democracies now abridge the rights of “fetuses” and the elderly, saying that they are not “persons,” it would be absurd to deny their humanity, which begs the question of the legitimacy of distinguished between “human” and “person”.
Actual human rights would recognize the freedom of these weak members of the human community, though they are “completely at the mercy of others and radically dependent on them, and can only communicate through the silent language of a profound sharing of affection” (19). Protection and love for these weak ones is the only authentic expression of human value; to dispense with them because of their weakness is to act as though we are fundamentally positioned competitively against or other members of our human family rather than in solidarity with them.
This atomistic view of self becomes a “promotion of the self,” that “is understood in terms of absolute autonomy,” and when this happens, “people inevitably reach the point of rejecting one another. Everyone else is considered an enemy from whom one has to defend oneself” (20). This defensive form of freedom is nothing more than the freedom of ‘the strong’ against the weak who have no choice but to submit” (19). John Paul II continues that this is tragically “the exact opposite of what a State ruled by law” is supposed to be. Governments, in classical philosophy, are meant to end the anarchy of the strong against the weak by enshrining protections for the weakest members. The culture of death, he says, “is a threat capable, in the end, of jeopardizing the very meaning of democratic coexistence: rather than societies of ‘people living together’, our cities risk becoming societies of people who are rejected, marginalized, uprooted and oppressed” (19).
“God entrusts us to one another. And it is also in view of this entrusting that God gives everyone freedom, a freedom which possesses an inherently relational dimension” (19). This solidarity, relational freedom, ties us to the broader human community and sees individual growth and development as linked to the growth and development of all. In this way, a use of freedom that harms others is no true freedom.
Consider that forbidding murder does not make American citizens less free; on the contrary, it makes citizens free to thrive in a peaceful environment. Likewise, a prohibition on abortion does not abridge anyone’s rights or make anyone less free. On the contrary, it recognizes with love the humanity of the growing child and demands help for a struggling mother from the wider human community. Abortion, in contrast, leaves a woman alone and hurting when faced with an unplanned pregnancy.
St. Thomas Aquinas argues that man’s freedom is found precisely in his ability to act for an end goal. “Since man especially knows the end of his work, and moves himself, in his acts especially is the voluntary to be found” (Summa Theologica II-I, 6, 1). Man’s truest freedom is when he acts for the true good and highest end, which is eternal beatitude with God and on earth a life of flourishing, not merely his own pleasure. All acts of the will, or choices, are made for a perceived good. Though those who seek abortion seek it for an illusory good, the woman is more free when she chooses the higher end, which would be the life of the child and solidarity with that child. True freedom, then, expresses not mere power or compulsory force of the agent, but rather a formative knowledge of the good to be sought in human life—that is to say, as we make choices for the good, we actually become better. So freedom is not an indifferent principle, but a force for human development.
Our nation, every nation, would only benefit from promoting authentic freedom and a culture of life that values the development of all its citizens, not just the strong ones.
Stephanie Pacheco is a writer, blogger, and speaker in Northern Virginia. She earned a M.A. in Theological Studies, summa cum laude, from Christendom College and holds a B.A. from the University of Virginia in Religious Studies with a minor in Government and Political Theory. She has presented at a conference of the American Catholic Historical Association and for Christian Women in Action. She lives with her husband and two young children.
Half of all pregnancies in the United States are unintended. One might therefore assume that making the morning-after pill (MAP) more widely accessible would cut the unplanned pregnancy rate.
Not so.
A new recent US study is the first to estimate the impact of making the morning-after pill available over the counter without prescription on abortions and risky sexual behaviour as measured by sexually transmitted infection (STI) rates.
Dr Karen Mulligan, associate professor of economics and finance at Middle Tennessee State University, found that providing individuals with over-the-counter access to emergency contraception (EC) leads to increased STI rates and has no effect on abortion rates.
Moreover, risky sexual behaviour such as engaging in unprotected sex and number of sexual encounters increases as a result of over-the-counter access to EC.
Mulligan’s analysis estimated that over the counter access increases STI rates by approximately 12% for women aged 15-44 and 9% for teenagers; these numbers are also consistent with the 12-17% increase in gonorrhea rates found in Washington as a result of expanded access.
She concluded that switching EC to over the counter status has three main effects on behaviour: individuals are more likely to have sex, they have a higher number of sexual encounters, and are less likely to use condoms.
The FDA approved access to emergency contraception, or Plan B (equivalent to Levonelle in the UK), through US pharmacies without a prescription in 2012 nationally. This followed pilot programmes in several states starting with Washington in 1998.
But the US’s persistence with this unproven strategy is apparently driven more by ideology than evidence.
In the light of Mulligan’s research, Dr David Paton, professor of industrial economics at Nottingham University Business School, today called on local and national governments in the UK to review their current policy of aggressive promotion of emergency contraception (EC) to young people in schools, pharmacies and sexual health centres.
‘It is very interesting to see further confirmation that access to emergency birth control (EBC) does not seem to reduce abortions but leads to higher rates of STIs. This paper is one of the first to explore the mechanisms whereby EBC affects STIs, finding that both rates of ‘unprotected’ sex and numbers of partners increase in response to over-the-counter EBC. Although this paper uses US data, it is consistent with evidence from the UK’, he said.
A previous 2012 American study showed that making emergency contraception available free over the counter without prescription leads to an increase in rates of sexually transmitted infections and does not decrease pregnancy or abortion rates.
Christine Durrance, Assistant Professor of Public Policy at the University of North Carolina, Chapel Hill, used county-level data as well as specific timing of changes in pharmacy access to consider the intended and unintended consequences of pharmacy access to emergency contraception in Washington.
This research, by professors Sourafel Girma and David Paton of Nottingham University, compared areas of England where the scheme was introduced with others that declined to provide emergency contraception free from chemists.
The academics found that rates of pregnancy among girls under 16 remained the same, but that rates of sexually transmitted infections increased by 12%.
In fact, in a systematic review published in 2007, twenty-three studies published between 1998 and 2006, and analyzed by James Trussell’s team at Princeton University, measured the effect of increased EC access on EC use, unintended pregnancy, and abortion. Not a single study among the 23 found a reduction in unintended pregnancies or abortions following increased access to emergency contraception (see also fact sheet here).
The phenomenon whereby applying a prevention measure results in an increase in the very thing it is trying to prevent is known as ‘risk compensation’.
The term has been applied to the fact that the wearing of seatbelts does not decrease the level of some forms of road traffic injuries since drivers are thereby encouraged to drive more recklessly.
In the same way it has been argued that making condoms readily available actually increases rather than decreases rates of pregnancy and sexually transmitted infections because condoms encourage teenagers to take more sexual risks in the false belief that they will not suffer harm.
Whilst condoms offer some protection against sexually transmitted infections the morning-after pill offers none.
Britain has the highest rate of teenage pregnancy in Western Europe. But international research has consistently failed to find any evidence that emergency birth control schemes achieve a reduction in teenage conception and abortion rates.
Now there is growing evidence showing that not only are such schemes failing to do any good, but they may in fact be doing harm.
Making the emergency contraceptive pill available over the counter free, without prescription, is sadly an ill-conceived knee-jerk response to Britain’s spiralling epidemic of unplanned pregnancy, abortion and sexually transmitted disease amongst teenagers. It is also not evidence-based.
The best way to counter the epidemic of unplanned pregnancy and sexually transmitted disease is to promote real behaviour change. The government would be well advised to enter into dialogue with leaders of communities in Britain where rates of sexually transmitted diseases and unplanned pregnancy are low, especially Christian faith communities, to learn about what actually works.
LifeNews.com Note: Dr. Peter Saunders is a doctor and the CEO of Christian Medical Fellowship, a British organization with 4,500 doctors and 1,000 medical students as members. This article originally appeared on his blog.He is also associated with the Care Not Killing Alliance in the UK.
May 7, 2015 (STOPP.org) — The young newlywed put herself at risk for collapse, stroke, heart attack, and death every day when she popped her birth control pill. Tragically, she had no idea there was any danger. Even medical personnel thought her symptoms were no big deal, and on more than one occasion chalked her symptoms up to dehydration. They never told her it could be that her contraception was causing blood clots.
Her name was Kate. She was a 28-year-old business woman whose story is told in “What Every Woman Needs to Know about Blood Clots” posted on the National Blood Clot Alliance “Stop the Clot” website. Kate’s symptoms started while she was in Hawaii on her honeymoon. She suffered pain in her calf that was so intense it woke her up at night. She went to an orthopedic surgeon, who ordered scans, found no problems, and dismissed her. She forgot about it. Seven months later she passed out in an airport following a flight. Medical personnel said she was dehydrated.
Completely unknown to her, Kate had developed deep vein thrombosis in her calf. From there, blood clots began breaking off and going to her lungs. These blood clots in the lungs, called pulmonary emboli, “can be life-threatening and in 10-15 percent of cases, cause sudden death,” according to Dr. Jack Ansell. Dr. Ansell is a hematologist and member of the National Blood Clot Alliance’s Medical & Scientific Advisory Board. The Alliance website goes on to quote Dr. Ansell: “The first sign of a PE can be death.”
Thanks to Kate’s mother, a nurse, who suggested that she might have pulmonary emboli, Kate got help and did not die. She caught it before it killed her. Many other women are not so lucky. They don’t learn the truth until it is too late.
The truth is that the birth control pill increases a woman’s relative risk for developing blood clots 300- to 500-fold—blood clots that can cause stroke, heart attack, blindness, brain damage, and death. Still, women are not warned about the risk of blood clots with their daily steroidal hormone pill. This is serious and senseless deception and negligence.
According to a Canadian Broadcasting Company report in June 2013, birth control pill manufacturer Bayer paid out in excess of $1 billion to settle thousands of birth control pill lawsuits in the United States. Those settlements were all related to two low-dose contraception pills, Yaz and Yasmin. At the same time, an investigation by the CBC revealed that pharmacists suspected the deaths of 23 Canadian women were attributable to those two same pills.
Miranda Scott, only 18, was working out at the University of British Columbia gym when she fell over backward and died. Her autopsy showed that she died of blood clots throughout her body. She was taking Yasmin at the time of her death. Her mother is now part of a Canadian class action lawsuit against the drug manufacturer, along with hundreds of family members and women who have been harmed or killed by the pill.
Yet, even as Bayer pays out huge settlements, it says it “stands by” its birth control products. Even Elizabeth Kissling, writing for the radical feminist magazine Ms, is troubled by the cover-up and lack of education and testing women are given before being prescribed the pill.
“Today . . . young women are again dying from something purported to help them, something that affects mostly women. Thousands more are experiencing life-threatening, health-destroying side-effects, such as blindness, depression, and pulmonary embolism,” Kissling said, citing accounts of young women who had suffered all these consequences.
She referenced a first-person account posted on xojane.com, that highlighted this shocking quote by a young woman who almost died from pulmonary embolism caused by her birth control pill. “‘Isn’t this bizarre?’ [the young woman] asked doctors in the hospital. They shook their heads and informed me that they regularly encountered otherwise healthy young women with blood clots, almost all caused by birth control.”
The pill kills truth. It exists and is prescribed to women amid a swirl of chaos; amidst contradictions and lies; and amidst dead, blind, and profoundly injured women. Prescribing doctors tell women birth control is perfectly safe if they don’t smoke. Emergency room doctors tell women they “regularly encounter otherwise healthy young women with blood clots, almost all caused by birth control.” Billions of dollars are paid out by drug companies to settle lawsuits, while they say they still stand by their contraceptive pills.
Women need to know. Join American Life League and a host of sponsors around the nation on June 6 to expose the lies and shine the light on the truth about the pill. For more information, visit our website, thepillkills.org. To sign up to sponsor the National Day of Action and/or organize a local event, click here.
Summary of Fr John Hollowell’s sermon on sexuality
* We representatives of the Church have failed to talk about sexual issues either because we are embarrassed or because we lack the courage.
* Public school sex education focuses on fear of pregnancy or of STDs, with the cure to both being one form or another of contraception.
* The accusation is made that the Church is obsessed with sex. The fact is that we have the obsession with sex and the Church is trying to help us deal with this obsession.
* We are told that the Church teaches us to feel bad about sex. The fact is that in 31 years he has never heard a sermon about saving yourself for marriage, about the problems with sex before marriage, about the joys and beauty of sex in its proper place, or about contraception.
* He has, however, dealt with people in the confessional who are devastated by the effects of pre-marital sex. Sex before or outside of marriage is Satanic communion; it is a Satanic sacrilege.
* Cohabitation endangers you soul.
* Contraception is sexual bulimia. Sterilization and contraception take God’s offer to co-create human beings with God and say: thanks, pal, for the offer, but I have my own ideas in mind.
* He sees the pain all the time from these sins.
* When we seek sex for pleasure, we are using the other person.
* If you have had sex, it is possible to start over.
* It takes heroic virtue to be chaste in this world.
Whether the mainstream media chooses to cover it or not, Pope Francis’ General Audience yesterday (http://www.zenit.org/en/articles/general-audience-on-man-and-woman) confirmed once again that he upholds the Church’s teaching on marriage. In fact, he unabashedly challenges us saying that it is the “great responsibility of the Church, of all believers, and first of all of believing families, to rediscover the beauty of the creative design that inscribes the
image of God also in the alliance between man and woman.” There are those who would dismiss Pope Francis’s previous statements that he is a “son of the Church” when it comes to traditional, sacramental marriage. I’ve heard it claimed that he is just biding his time, waiting to introduce a more “tolerant”, more “accepting” teaching when it comes to marriage.
But those who are hoping that the Church will open the door to homosexual “marriage” and other unions will surely be disappointed. He says, “I wonder, for example, if the so-called gender theory is not also an expression of a frustration and of a resignation, which aims to cancel the sexual difference because it no longer knows how to address it.” He goes on to lament that intellectuals have—for the most part—ceased to explore the importance of family and marriage bonds because they wish to pursue what they see as a more “free” and more “just” society.
God is the author of marriage and the author of the family. This fact, the Pope explains, can not be underestimated: “God has entrusted the earth to the alliance of man and of woman: its failure makes the world arid of affections and darkens the sky of hope.”
The Pope encourages us to fight against this tendency in society to forget (or even to attempt to erase) the difference between sexes. The first action he suggests highlights one of the traits I like best about the Pope. He is unafraid to look at reality and Church teaching in a way that may not fit people’s stereotypes of him and of the Church. In this audience, he encourages us to give more weight to women’s voices. He draws our attention to the way that Jesus treated women and reminds us that “We have not yet understood in depth what things the feminine genius can give us, which woman can give to society and also to us.”
What I love about this statement, though, is that while some might be tempted to label Pope Francis as a progressive, he is not buying in to that agenda. He points out that recognizing this feminine genius is not an end in itself. Rather, he argues “we must do much more in favor of woman if we want to give back more strength to the reciprocity between men and women.” Giving more recognition to the unique talents and
gifts of women should not make women the same as men, but instead add to the richness of human society by recognizing the essential difference and complementarity of men and women.
His second recommendation reflects centuries of Church teaching, but applies it to our modern understanding of “marriage”. He points out that the union between man and woman is supposed to reflect communion with God. “The loss of trust in the celestial Father generates division and conflict between man and woman,” the pontiff said.
He urges us to more fully recognize the unique gifts of each sex, the way in which they complement each other. Further still, the only successful unions are ones that are first entrusted to God. He gives us hope, saying, “The earth is filled with harmony and trust when the alliance between man and woman is lived well.”
With these words, Pope Francis looks not only at theology or the world as a whole, but at each person, marriage and family. As usual, he speaks directly to the hearts of each one of us. We are reminded that we can make a difference in the world by the way we strengthen our relationship with God, living out our lives as a man or woman created in His image.
Caitlin Bootsma is the editor of
Human Life International’s Truth and Charity Forum. Mrs. Bootsma received a Licentiate in Catholic Social Communications at the
Pontifical University of the Holy Cross in Rome as well as a Master’s of Systematic Theology from Notre Dame Graduate School of Christendom College. She lives in Richmond, Virginia with her husband and two sons.
Beloved, see what love the Father has bestowed on us that we may be called the children of God. Yet so we are. The reason the world does not know us is that it did not know him.Beloved, we are God’s children now; what we shall be has not yet been revealed. We do know that when it is revealed we shall be like him, for we shall see him as he is.Everyone who has this hope based on him makes himself pure, as he is pure. I John 3:1-3
We were in Los Angeles over Easter because our brother-in-law was received into the Church. It was so wonderful, so happy, so holy! We went to lunch one day with the family and I asked my niece’s son if he know who he was. I told him he was “God’s child.” It’s true!
I told Marcia’s sister and other Brother-in-law that I always ask the grandchildren who they are and they answer “God’s child” and I tell them to never forget it. I told them that through their Baptism they were God’s children too. It’s true!
At Easter Dinner I thanked my brother-in-law for allowing Marcia and I to be his Godparents. I told him to remember who he is through Baptism he is “God’s Child” and will be forever. It’s true!
We had dinner the other night with some old friends we hadn’t seen for years and in our conversation I told them the story of our grandchildren and about reminding them every chance I get that they are “God’s children.” They liked it and I let them know that they are too. It’s true!
At the “Growing Our Faith” meeting, a church group, I asked one of the members if she was a saint and she said yes because I had told her once, and praise the Holy Spirit who nudged me and caused her to believe it. I then asked everyone at the meeting if they were saints and they said yes. It is through there baptism that they are saints and “God’s children.” It’s true!
At Saturday night Mass Father reminded us that everyone is “Gods Children.’ It’s true!
Not only is it true it is our responsibility to remind each other often of this great gift of being God’s sons and daughters which makes us brothers and sisters. We have a responsibility to “Love one another” and help each other get to heaven.
Jesus commands us to be “Perfect as our heavenly father is Perfect.” Only Satan tells us we can’t … HE IS WRONG … HE IS A LIER!!
I’m telling all of you, especially my children, that they are “God’s children and never forget it.” Tell yours today because it’s true.
I often come across persons who attempt to justify forced abortion, sterilization, and contraception because “We (that is, human beings) are destroying the planet”. They view people as pollution, and argue that it is necessary to violate reproductive rights to protect the planet from the beings who are despoiling it. Yet that logic is intrinsically flawed.
Let us put it this way. Which of these do not belong: nitrous oxide, methane, Homo sapiens, or carbon dioxide?
The obvious answer is : “Homo sapiens.”
Pregnant women do not produce nitrous oxide. Childbirth does not generate methane. A newborn baby does breathe out carbon dioxide, but this is not a “pollutant” at all but a trace gas on which most life depends.
Yes, any given infant may grow up to be a notorious polluter, just as he may grow up to, say, recklessly endanger the lives of others by driving drunk. But such behaviors are not foregone conclusions. Unlike nitrous oxide, methane, or carbon dioxide, human beings have free will.
It is simply not true that more people equals more pollution. We have twice as many people living in the United States as we did in the early seventies, yet the skies over our major cities are clearer now than they were a half century ago. This is because the internal combustion engines that power our motor vehicles are no longer spewing out thousands of tons of particulate matter, sulfur dioxide, and other pollutants into the atmosphere as we drive. And this in turn is because we made a conscious decision to switch to cleaner burning fuels and install catalytic converters downstream from our engines.
As this example suggests, pollution is created by particular human behaviors such as the incomplete combustion of fossil fuels or the indiscriminate spraying of harmful pesticides. It can be corrected by altering that same behavior. Reducing the number of babies born will not solve these and other environmental problems.
No one would suggest that every baby born into a tech-savvy household will indubitably mature into a cyber-terrorist. Yet there are those who seem to believe that every baby human born will mature into a waste-creating, polar-bear-murdering, earth-destroying eco-terrorist. This is completely unreasonable. To be sure, some infants will grow up to secretly dump raw sewage into fragile estuaries, but many others will start compost piles and grow their own vegetables in backyard gardens.
No one can guarantee that any given infant will grow up to be a good conservationist, any more than anyone can guarantee that any given infant will grow up into a happy well-adjusted adult. Everyone, as we noted above, enjoys free will.
But it is true that—thanks to technological advances, reasonable environmental regulations, and education that emphasizes good stewardship—we have made great strides in recent decades. Very large populations can actually have a much smaller
environmental footprint than a much smaller population did a century or two ago. Population control has no part to play in these successes.
Sadly, not everyone has gotten this message. The anti-people argumentation continues to insist that babies equal pollution. The population control movement continues to receive billions of dollars in funding each year. Women’s fertility continues to be attacked in the name of the environment and “sustainable
development.”
The United Nations Population Fund (UNFPA) continues to cheerlead China’s one-child policy, ignoring the forced abortions and forced sterilizations that follow. The UNFPA continues to distribute 40 million doses of Depo-provera each year to unsuspecting women—despite the fact that this product is so unsafe that the FDA recommends against its use.
India still sterilizes over 4 million women annually under a system of statewide sterilization targets, ignoring the rising death toll of women who have died in such campaigns. And the developed nations—chief among them the United States—still continue to fund these programs in the name of achieving a mythical “sustainable population,” all the while ignoring the massive human rights abuses that they entail.
We agree that pollution sometimes constitutes an offense against other human beings. Those who wantonly and grossly pollute the water we drink and the air that we breathe endanger the rest of us, both those who are alive now and those who will come later.
But we also insist that forced abortion, forced sterilization, and forced contraception always constitute a grave violation of human rights. These actions are never justified, least of all by irrationally claiming that they are necessary to “protect the environment.”
We look forward to a future where our children and grandchildren enjoy a planet with clean air, clean water, and luxuriant greenery. We have already, in the U.S. and elsewhere, made great strides towards the realization of this future.
But we also hope and pray that our children and grandchildren grow up in a world without population control. We are working towards the day when they are valued for themselves, and are not seen by many in the environmental movement as a threat to their dream of a world without people.
After all, as Shakespeare remarked, “The world must be peopled.”
PRI is hosting an “Earth is for People Day” event on Wednesday the 22nd where people can ask the president of PRI questions about the environment and population. PRI will be answering your questions from 10 am to 4 pm EST on Earth Day.
Rome, Italy, Apr 21, 2015 / 02:44 am (CNA/EWTN News).- A Nigerian bishop says that he has seen Christ in a vision and now knows that the rosary is the key to ridding the country of the Islamist terrorist organization Boko Haram.
Bishop Oliver Dashe Doeme says he is being driven by a God-given mandate to lead others in praying the rosary until the extremist group disappears.
“Towards the end of last year
I was in my chapel before the Blessed Sacrament… praying the rosary, and then suddenly the Lord appeared,” Bishop Dashe told CNA April 18.
In the vision, the prelate said, Jesus didn’t say anything at first, but extended a sword toward him, and he in turn reached out for it.
“As soon as I received the sword, it turned into a rosary,” the bishop said, adding that Jesus then told him three times: “Boko Haram is gone.”
“I didn’t need any prophet to give me the explanation,” he said. “It was clear that with the rosary we would be able to expel Boko Haram.”
The bishop said he didn’t want to tell anyone, but “felt that the Holy Spirit was pushing him to do so.”
He started with the priests of his diocese, and then told participants in the April 17-19 #WeAreN2015 congress in Madrid, Spain. The event is being sponsored by the Spanish Catholic sister groups hazteoir.org and CitizenGo to gather ideas on how to preserve the Christian presence in nations where they are most persecuted.
Bishop Dashe leads the Diocese of Maiduguri, in northeastern Nigeria’s Borno State. In 2009, there were around 125,000 Catholics under his guidance. After a surge in violence from the Islamist extremist group called Boko Haram, today “there are only 50 to 60 thousand left,” he said.
Most of those who fled sought safer areas in other parts of Nigeria, he said. Some of the same families are now returning home as armed forces from Nigeria, Chad and Cameroon liberate their homes.
In 2014, Boko Haram became known worldwide when members kidnapped nearly 300 girls from a school in Borno State. On March 7, 2015, five suicide bombers killed 54 and wounded nearly three times as many in the capital city of Maidaguri, where the bishop lives and works.
The group has killed 1,000 people across Nigeria in the first three months of 2015, according to Human Rights Watch, which reports that more than 6,000 have died in Boko Haram-led violence since 2009.
Just last month, the group pledged its allegiance to ISIS – also known as the Islamic State – which launched a bloody campaign in Iraq and Syria last summer.
Meanwhile, Bishop Dashe has just completed a “consolation tour” to communities in his diocese, promoting forgiveness and continued faith. He believes he was asked by Jesus to spread devotion to the rosary in order to aid them as they do so.
“Maybe that’s why he did it,” said the bishop, referring to Jesus in his vision.
Bishop Dashe said he has a strong devotion to Christ’s mother, and that “I never joke with ‘Mamma Mary.’ I know she is here with us.”
And he is not the only Nigerian bishop putting the future of the country in the hands of Mary. The nation’s bishops’ conference has consecrated the country to her twice in recent years.
Bishop Dashe believes that one day his diocese will completely recover and grow thanks to her intercession.
“These terrorists… think that by burning our churches, burning our structures, they will destroy Christanity. Never,” Bishop Dashe told several hundred people from the dais of the #WeAreN2015 congress.
“It may take a few months or a few years … but ‘Boko Haram is gone.’”
He later told CNA that “prayer, particularly the prayer of the rosary, is (what) will deliver us from the claws of this demon, the demon of terrorism. And of course, it is working.”
IBADAN, April 17 (C-Fam) “We had to limit the number of people in each diocese who could come,” said one organizer of a pro-life and pro-family conference in Ibadan, Nigeria. Over 1,500 filled the auditorium, and even then people spilled outside.
One region with a small Christian population extended invitations to their Muslim neighbors who gladly attended. Bishops in this city near Lagos hosted the forum – and the joyful team of bishops and the archbishop led or participated in all the activities.
“We could never get so many bishops” at a pro-life event in Europe, exclaimed one British speaker.
Archbishop Gabriel Abegunrin explained his enthusiasm for putting on the two-day event.
New technology, attitudes and lobbies backed by powerful interests “challenge traditional beliefs, established faith and conventional practices,” he said. “We can together with experienced people from around the world identify contemporary challenges to human life, marriage and family and educate our people better on how to recognize and surmount those challenges in order to live integral, credible Christian lives.” “The icing on the cake was the march,” said Jerry
Okwuosa, a pro-life activist for 20 years. Marchers sang, “Yes, yes to life. No, no to death,” a song written for the conference as people in an outdoor market cheered them on and joined the march.
One nurse who attended used to work for Pathfinder, an international group that promotes abortion and sexual rights by weakening moral beliefs, especially of health care providers. Her son would play with the hordes of excess condoms at their house, more than could be distributed. Later he challenged her on Pathfinder’s work, and she resigned. Now he is a priest and helped organize the conference.
Most of the speakers were Nigerian professionals and religious leaders, covering topics like engaging in social media, trends in assisted reproductive techniques, sexuality education, secular humanism, domestic violence, and understanding legislation. Speakers from the UK, US and Ghana described international pressures to spread abortion and sexual license, and ways to counter them.
It “surpassed my expectations,” said
Obianuju Ekeocha, who the Archbishop credited with inspiring the conference. It was the fourth event the Nigerian scientist and founder of Culture of Life Africa helped
plan by inviting speakers to cover topics spanning abortion, strengthening family life and resisting harmful trends.
Teachers, nurses, students and religious leaders – “people from all walks of life” – who filled the conference hall are “so important because they serve the poorest of poor – like teaching and health care in communities that other doctors will not go,” Obianuju said.
The speakers “sensitized people” to “pro-abortion organizations with innocuous names like Planned Parenthood that they never knew before were anti-life,” said Obianuju. “UN agencies, associated with morally objectionable projects will be treated with suspicion because people now know their hidden agendas and track records.
One jovial bishop – who has competed in “You’ve Got Talent” televised shows – frequently burst into song to warm up the crowd, changing the words of popular music to address God while keeping the catchy tunes.
“Just call my name,” sang Bishop Adetoyese Bedejoe to the Michael Jackson tune, “and He’ll be there.” At a private dinner to cap off the event, he told the leaders, “God mixing with man can do powerful things.”
April 15, 2015 (LifeSiteNews.com) – Women who use the birth control pill may be shrinking their brains and increasing their chances of developing Crohn’s disease, two new studies have found.
Neuroscientists from the University of California, Los Angeles found that the two main regions of the brain controlling emotion and decision-making are thinner in women who take the pill.
A study published April 2 in the journal Human Brain Mapping reports that the pill’s chemicals block the body’s natural hormones, altering the brain’s structure and function.
The study concluded that oral contraceptive use “was associated with significantly lower cortical thickness measurements in the lateral orbitofrontal cortex and the posterior cingulate cortex.”
The orbitofrontal cortex controls decision-making and the posterior cingulate manages emotions. And among the, both of these two areas were smaller than average in those taking the pill.
The UCLA scientists – who studied 90 women, 44 who were on the pill and 46 who were not – found that the pill can shrink parts of the brain but stated their data pointed to no conclusive results about the effects of chemical contraceptives on female behavior.
The researchers also did not determine whether this brain shrinkage is permanent, and indicated more research is needed.
“Future studies can investigate the time course of these effects. It is currently not known whether these effects appear immediately after initiating OC use, or gradually accumulate and increase over time,” they said. “Further, it is not known how long these effects persist after OC discontinuation.”
Another report released in March says the pill triples the chance of developing the incurable digestive condition known as Crohn’s disease.
Harvard gastroenterologist Doctor Hamed Kha conducted a study of 230,000 American women who had used the pill for at least five years, finding that the synthetic hormones contained in the contraceptives can
weaken the digestive system, creating ideal conditions for Crohn’s development.
The study also concluded that the abortifacient “morning after” pill, which carries a higher dose of synthetic hormones, can also increase the likelihood of developing Crohn’s.
British researchers also found a link between chemical contraceptives and Crohn’s in 2009.
Kha said it was not likely the pill alone would cause Crohn’s, and that genetics also came into play. But he told The Telegraph that he expects women genetically predisposed to Crohn’s to be warned soon to avoid the pill.
A doctor in the UK was already doing so.
“If you have a family history of Crohn’s I would advise against starting on the pill,”
said Doctor Simon Anderson, a consultant gastroenterologist at London Bridge hospital.
Hormonal contraceptives, especially the birth control pill, have a well-documented history of physically harming the women who take them.
In 2005 a division of the World Health Organization declared chemical contraceptives to be a Group 1 Carcinogen, the highest classification of carcinogenicity, used only when there is sufficient evidence of carcinogenicity in humans.
The birth control pill has been linked to social ills and many medical problems, such as breast cancer, hair loss, increased risk of glaucoma and blood clots, hardening of the arteries and cervical cancer.
A 2014 study found the pill negatively affected women’s attraction to men, and a 2011 study linked the pill to reduction in women’s memory.
A specific type of hormone pill meant to treat acne and excessive hair growth in women which has often been used off-label as a contraceptive, was implicated in the deaths of 27 women in the Netherlands in 2013.
Researchers at the University of Missouri at Columbia found in 2005 that boys exposed certain synthetic hormones in the pill had a greater risk of prostate cancer and other urinary tract problems later in life.
Chemical contraceptives finding their way into water systems have adversely affected wildlife as well, mutating the gender of some species of fish and nearly causing extinction of others.
At the Indiana State House as the original bill was being debated.
The recent surrender on the “Religious Freedom Restoration Act” (RFRA) bills by the Governors of Indiana and Arkansas can be directly tied to the myriad bad decisions and compromises by well-meaning pro-family groups and individuals, who are sorely overmatched by the homosexual lobby in strategy, tactics, and funding.
RFRA Recap: Arizona, Indiana, Arkansas
Last month the Indiana legislature passed a rather bland RFRA bill, similar to many around the country, which was then signed by Republican Governor Mike Pence. The original bill would have allowed businesses to defend themselves in court if forced by a law to violate their religious beliefs — and the government would have to show a compelling state interest before a religious-belief defense could be rejected. (Read that original bill HERE.)
In Feb. 2014, in a preview of what was to occur in Indiana, the Arizona legislature passed a similar RFRA bill to protect Christian owners of small businesses. Republican Governor Jan Brewer was about to sign it when the homosexual lobby got its big corporate friends to pressure her. The NFL even threatened to take the Super Bowl out of Arizona. Gov. Brewer caved and vetoed the bill.
So it wasn’t too surprising when the homosexual movement decided to make another example of Indiana, unleashing its full fury against the state last month. A blizzard of major corporations and activist groups (along with the national liberal media) descended on Gov. Pence and the legislature, claiming that simply to allow a wedding photographer or caterer to defend himself in court (for refusing service) would be “discrimination” and reason for corporate America to boycott the state.
The pro-family movement’s response was a flood of articles analyzing and complaining about the situation. RFRA bills had been around for decades, they pointed out. The homosexual activists and their allies were decried as hypocrites and bullies. A parade of conservatives swore they were not “anti-gay,” would never discriminate against homosexuals, but did want their religious freedom. Most of the focus was on defending the freedom of religion, assuming that was the key to controlling the monstrous expansion of LGBT censorship and control.
After several days of pressure, Gov. Pence finally gave up and directed the legislature to draft a bill that would make sure business owners could not legally fight charges of “discrimination” based on sexual orientation or gender identity – even on religious grounds. In fact, the new bill , which Pence quickly signed, is basically a “gay rights” bill.
Days later, the same scenario played out in Arkansas. That state legislature passed a similar RFRA bill on April 1. The homosexual lobby and corporate allies (including gigantic Wal-Mart) pounced. Republican Governor Asa Hutchinson rolled over without a fight and had the bill modified to sufficiently appease the homosexual activists.
The immediate pro-family problem: politicians left dangling in storm
These were shameful surrenders. On the other hand, given the state of the national GOP, expecting any Republican politician to stand up for a pro-family principle under pressure is unrealistic.
To be fair to the politicians, the pro-family movement hasn’t offered them much support. The Governors needed a public outcry from thousands of angry conservatives pointing out that “religious freedom” means having the right to decide what is immoral, unnatural, perverse, and destructive – and can be openly opposed. And the Governors needed to be forced to think hard about giving special protections to people on the basis of undefined “sexual orientations” while demonizing citizens holding traditional moral values.
Instead, in each of these three states, when the homosexual media blitzkrieg marched in, the Governors were basically left on their own, untutored, swearing they opposed “discrimination” – while the pro-family movement mostly sat back and wrote commentaries. So of course our side got creamed. And now the surrender message is out there, so the same collapse will likely happen again.
The longer-term problems
As we noted in our previous article, the real problems go back a couple of decades. The seeds of disaster were planted long ago by leftists, but allowed to go unchallenged and even accepted by conservatives (including most pro-family leaders). Here are the major issues they have failed to address:
1. Conceding to the LGBT movement’s ideological concepts, language, and demands.
The concepts of “sexual orientation” and “gender identity” (and the umbrella acronym “LGBT” – lesbian/gay/bisexual/transgender) are completely phony ideas invented by the sexual radicals to conjure an identity out of sexual and psychological dysfunction. Further, the phrase “sexual orientation” has never (to our knowledge) been defined in federal or state law, so it’s poised to be put to unimaginably horrible new uses in the future. Similarly, homophobia, civil unions, tolerance, and (supposed threats to) safety are all part of the propaganda. Sadly, most in the pro-family movement have shied away from challenging these concepts, so we continue to lose court cases and legislative battles that deal with them.
2. Refusal to fight passage of LGBT anti-discrimination laws and local ordinances, or demand their repeal.
Starting in the 1990s, the homosexual movement worked tirelessly, spending enormous funds, to get state and local governments to amend their anti-discrimination laws covering public accommodations, employment, housing, public education, etc., to include “sexual orientation.” In recent years there’s been a push to include “gender identity” (cross-dressing, transgenderism, transsexuality) also.
There’s a big strategic reason for that. As Dr. Scott Lively has pointed out for years, these updated laws are the starting point for the whole, brutal legal jihad against Christians and others holding traditional values. Every outrage we’re now seeing — including the LGBT activism in the schools, targeting of businesses, men using women’s restrooms, sado-masochist/”swinger” conventions in hotels, etc. — emanates from these laws.
But pro-family people have only recently started to wake up on this. They instinctively realize that citizens should be able to discriminate and refuse to promote or celebrate perversion and “gay” marriage. But these anti-discrimination laws now make it a crime to do so.
This group of men dressed as women threateaned a restaurant in Massachusetts that refused to let them in after patrons became upset at their use of the restrooms. (See our report.)
Moreover, because of the emotional force of such laws and the shrewd way they’re portrayed by the opposition as a continuation of the Civil Rights struggle, we now see Republican Governors and conservative commentators swearing they oppose discrimination on the basis of homosexuality or gender identity. Their acquiescence on these laws has set up the very conflict with religious freedom they’re now agonizing over.
Clearly, the targeting of conservative private businesses is part of a strategy to silence all opposition to the LGBT agenda, not because there is any shortage of businesses who will accommodate them. In fact, they publish glossy directories of such “welcoming” companies that are distributed all over the country.
At the same time that the homosexual movement is using the legal system to bludgeon Christian businesses that “discriminate,” they have meticulously published glossy booklets listing “welcoming” pro-homosexual businesses across the country– especially weddings and flowers.This booklet was passed out at the Spokane, WA airport. See their online presence here.
Why are we not surprised? This “Pride Weddings” ad is bordered by two advertisements for HIV/AIDS programs. Only in the “LGBT” community.
3. Over-focusing on “religious freedom” protections as the solution to this culture clash.
The pro-family focus on “religious freedom” as a protection against the LGBT onslaught is basically a defensive strategy that will eventually be completely eroded.
Certainly, religious freedom is constitutionally guaranteed. But who is to define what is or is not a valid “religious objection”? Or whether a person’s religious objections are due to “sincerely held” beliefs? The RFRA’s leave that up to the court system, and government prosecutors can make strong cases for a “compelling interest” to overpower one’s religious argument.
Take the parents’ rights case of father David Parker and the Lexington, Mass. schools. The federal court dismissed Mr. Parker’s demand (on the basis of his deeply held religious beliefs) to opt his young son out of classroom activities dealing with homosexuality and transgenderism. Why? Because (the court said) since “gay marriage was legal” in Massachusetts, the state needed to instruct all young children to accept homosexuality and “gay marriage” as normal … a “compelling state interest.” This will continue to happen across the country.
More important, falling back on “religious freedom” becomes an excuse to avoid confronting the other side’s destructive concepts and propaganda.
4. “The Church of Nice” versus the Destruction of Society.
If we have to listen to “Love the sinner, hate the sin, ” etc., one more time while the LGBT movement marches through our elementary schools and private businesses, we’re going to jump out the window. If you truly “hate the sin,” you’ll fight against “gay” clubs in the schools, “sexual orientation” non-discrimination laws, and public accommodations protections for LGBT persons. We don’t see that happening.
The bloody Chinese dictator Mao Tse-tung once said that “A revolution is not a tea party.” Well, it’s not a Sunday School class, either.
5. Refusal to be aggressive.
Too many of our people are deathly afraid of being called names (e.g., “bigot”). So they won’t even talk about the well-documented medical, psychological, and emotional dangers of the LGBT lifestyles for fear of offending someone. They want to appear nice and polite, hoping this will win points. They fall back on intellectual arguments. (But few are listening to reason anymore.) They use a “feel-good” political strategy while the other side uses the real thing.
Liberals and LGBT activists are vicious, bullying, lying, hypocritical, angry, and fanatically dedicated. Such a large-scale denial of reality requires it. They have no interest in fairness – only force. Yes, one of their favorite tactics is to attack and brutally libel anyone who disagrees with them. Much of this also has to do with their own self-centeredness and need to feel superior.
Homosexual activists in Indiana. We can all see where the real “hate” comes from.
We need to take the gloves off and stop being sissies.
6. Not confronting corporations or politicians supporting the LGBT agenda.
Anyone who has been around people in high levels of corporate America can appreciate how loathsome and amoral (and pro-Obama) most of them are these days. It wasn’t always that way. But it is now. So the next logical step for them is aggressively supporting the LGBT agenda against conservative Americans.
Unfortunately, our side has rarely reacted to that, except for an occasional boycott. So it’s an easy choice for corporate leaders. Politicians, even Republicans, have gotten the message that there’s no downside for siding with evil.
And wealthy conservative donors, seeing all this, are afraid to donate to groups fighting this battle. Our side has a lot of work to do.
Angie’s List is one of the companies that threatened to boycott Indiana after Gov. Pence signed the original bill. So American Family Assn. and others are boycotting Angie’s List. We support the boycott. Let’s hope it’s effective!
And if all that is not bad enough …
7. Too much talk, not enough action.
We have often said that the Internet has been a crippling factor for the conservative movement. It allows thousands of individuals to sit back and write endless commentary, and regurgitate and re-send the latest bad news to other conservatives, under the delusion that they are doing something meaningful. Meanwhile, the Left is organized and actually going out and causing real change (for the worse, of course).
Amidst the bad news, a ray of hope
They haven’t silenced everyone yet!
There is a handful of conservative pro-family voices (besides MassResistance) who are fighting this destructive trend and are at least telling the truth. This includes Scott Lively, Bryan Fischer, Laurie Higgins, Peter LaBarbera, John Biver, Stella Morabito, Cliff Kincaid, Gina Miller, Robert Knight, Peter Sprigg, Linda Harvey, Robert R. Reilly, Michael Voris, and others. We hope it’s a growing trend.
Telling the truth loudly and clearly is an absolute necessity in a battle like this. But as we’ve pointed out, it’s just the beginning.
It’s almost become a part of the weekly news cycle: American citizens publicly tarred and feathered for professing their sincerely held religious beliefs.
Just this month, we watched a family-owned pizzeria close its doors after its owners received hate mail and death threats from around the country. Their offense? Giving the wrong answer to a question about whether they’d cater a gay wedding. Keep in mind that the restaurant had never actually turned down a gay customer. They were hammered for holding the wrong beliefs about a hypothetical scenario!
Major corporations are getting into the bullying act, as well. At least two state governments have now backed down or modified religious freedom legislation in response to pressure from companies like Walmart and Salesforce. Keep that in mind next time you think about shopping at Walmart.
And this culture-wide search-and-destroy mission is only accelerating. As Princeton’s Robby George writes in First Things, activists for the new sexual orthodoxy are “giddy with success and urged on by a compliant and even gleeful media.”
The message is clear: not only should Christians remain silent about gay marriage if we know what’s good for us, but we must be made to agree with and even celebrate what Scripture calls sin. As Ana Marie Cox recently said of Christians on MSNBC, “you’re going to have to force [them] to do things they don’t want to do.”
But gay columnist Frank Bruni recently took it to the next level in the New York Times, writing that it’s time Christians get with the program and “take homosexuality off the sin list.” The lived experience of same-sex couples ought to trump what he calls the “scattered passages of ancient texts” condemning his lifestyle. Wow.
As for freedom of religion, Bruni suggests a new definition: “freeing . . . religious people from prejudices that they . . . can indeed jettison, much as they’ve jettisoned other aspects of their faith’s history, rightly bowing to the enlightenments of modernity.”
Yes, he actually wrote “rightly bowing.”
I’m reminded of a scene from C. S. Lewis’ “The Last Battle,” in which Shift the Ape explains to the poor creatures of Narnia why they’re being shipped off to the Calormene salt mines.
“You think freedom means doing what you like,” says Shift. “Well, you’re wrong. That isn’t true freedom. True freedom means doing what I tell you.”
Writing at National Review, Yuval Levin says what we’re witnessing isn’t so much the suppression of free exercise of religion as it is the establishment of a new national religion; the religion of secular liberalism. And dissenters must be forced to worship at its altar and affirm its creed of anything-goes sexuality.
Given the likely outcome of this summer’s Supreme Court case on same-sex marriage, Rod Dreher asks what will it be like to be a Christian in our brave, new society—and what will become of orthodox Christianity now that the price of professing it could be our credibility and livelihoods.
The answer, Dreher says, will depend a great deal on us. Will we hold fast to biblical teaching and refuse, in a manner of speaking, to burn incense to Caesar?
Friends, the fight for religious liberty is far from over. And as John Stonestreet and I have been saying again and again, it’s time for the Church to wake up, to pray, and to publicly defend our religious rights and our brothers and sisters under assault for their beliefs.
Josh Danis is the Archdiocese of Cincinnati Family and Respect Life Office Coordinator for the Northern Area of the diocese. In that position he has authored an exciting new program for helping all Christians appreciate the dignity of each human brother and sister. His program draws our attention to Jesus the God-fetus during the 9 months He lived within Mary.
*A “Dear Jesus of the Womb” prayer card with a depiction of Jesus in the womb on the other side. How can you recognize the baby as Jesus? (See PS for the answer.)
*A monthly reflection on Jesus’ physical development tied to a Biblical story and a current situation where the dignity of human life is not universally accepted.
*A brief bulletin announcement for each week of the month.
Parishes are encouraged to purchase the prayer cards and distribute them at every opportunity, publish the Monthly Reflection one weekend of the month, and include the bulletin announcement each week. The primary purpose of this Respect Life Campaign is to foster prayer for a universal appreciation of the dignity of life at all stages and conditions.
NEW YORK, April 10, 2015 (C-Fam.org) — As the UN puts polishing touches on their ambitious global plan to curb poverty, attention shifts from the political to the technical: how to measure progress and ensure targets are clearly defined?
The new Sustainable Development Goals (SDGs) provide an opportunity to reassess the “indicators” or benchmarks for reaching the expiring Millennium Development Goals (MDGs) and make changes where appropriate. One outgoing indicator—“unmet need” for family planning—was controversial when it was first adopted and has gotten even more controversial in the hands of activists.
The concept of “unmet need” emerged in the wake of horrific population control programs that forcibly sterilized and aborted the children of poor women. “Unmet need” was an attempt to find common ground between women’s rights advocates and population control groups. As defined in the MDGs, “unmet need” described women who were married, presumably fertile, expressed a preference not to have a child in the next two years, and who were not currently using modern contraception.
Critics pointed out that such a definition was inadequate since it excluded women who had health, religious or other objections to using contraception. Others complained that the definition of modern methods excluded natural fertility-awareness-based methods despite their high level of accuracy and user satisfaction.
A closer look at the method used to measure “unmet need” is quite revealing.
While women’s attitudes toward childbearing and contraceptive use may be related, they are by no means equivalent. Before 2003, surveyed women expressing a desire to space births were asked a follow-up question about how strongly they wanted to avoid becoming pregnant.
Many of them said it would be a small problem or no problem at all if they found out they were pregnant in the next few weeks. That survey question is no longer asked, reducing a complex matter to a simple yes or no.
When women classified as having “unmet need” were asked why they did not use contraceptives, many were concerned about side effects, opposed using them for religious or other reasons, or cited breastfeeding or infrequent sex as the reason. In fact, only 4-8% of married women with “unmet need” in developing countries said they could not access modern contraceptives.
It is widely reported that 225 million women globally have an “unmet need” for family planning. A recent report from the pro-abortion Guttmacher Institute and the United Nations Population Fund calls for $9.4 billion dollars annually to meet that “need.” This request is based on the assumption that “all women with unmet need would use modern contraceptives”—despite strong evidence that many of these women have no intention of doing so.
“Unmet need” does not measure women’s access to or desire for contraceptives. But most of the top organizations promoting family planning use “unmet need” synonymously with “lack of access” to contraception.
Planned Parenthood even ran a billboard in New York’s busy Times Square claiming, “Over 200 million women want access to contraception but can’t get it.”
Despite this dubious history, a proposed indicator to measure the success of the UN’s new goals is “met demand” for family planning. This perpetuates the same underlying problem as “unmet need”: it presumes that delaying childbearing is equivalent to wanting contraception.
And it will channel billions of dollars toward family planning advocates and providers to reach an elusive goal – that every targeted women, whether she wants to or not – use contraception.
April 2, 2015 (CrisisMagazine.com) — When was the last time anyone heard a sermon that condemned the evils of fornication, or adultery, or cohabitation, or divorce, or bearing children outside wedlock (let alone homosexuality)? Controlling these sins is a core Christian value. At one time a preacher could be expected to devote extended attention to these sins. And he could be expected to condemn them unequivocally. Yet today, even as the social and economic fallout from precisely these practices becomes ever more glaring and serious, pastors and priests seem ever more determined to avoid discussing them.
Of course, the dowdy old parson long ago became the stuff of caricature, ranting on about unspecified “wickedness.” And since no pastor wants to be seen as old-fashioned, and most want to be modern and appeal to the ubiquitous cult of youth, one never hears much today about the sins of illicit sex. Indeed, churches that consider themselves highly orthodox or biblical or traditional or conservative or evangelical—those described by themselves and others as “fundamentalist”—even these churches avoid the problem of runaway sexual freedom. Most Christian magazines and newspapers do not publish articles about it and gatherings of clergy do not discuss how to control it. No church today would dream of admonishing or reproving, let alone excommunicating a member because of sexual misconduct.
Yet ever more conspicuously, it is precisely these sins that are wreaking havoc throughout our society.
All around us we can see—if we are willing to open our eyes—the social consequences of uncontrolled sex. The sexual decadence of popular culture—in music, television, and videos—is only the most obvious manifestation, providing material for endless and often pointless moralizing.
But beyond the lamenting and bemoaning are consequences that are concrete and serious. The vast proliferation of single-parent homes is having devastating consequences on our society, economy, and politics. The epidemics of cohabitation and runaway divorce have left millions of fatherless children on the exploding welfare and foster care rolls and spread crime and substance abuse and truancy throughout our communities. These problems are now bankrupting taxpayers and future generations with a “financial crisis” that is attributable almost in its entirety to welfare spending and its multiplier effects in crime and social anomie, while driving governments to ever more authoritarian measures to slake their insatiable thirst for revenue.
Our universities and schools have become little more than orgies, with a “hook-up” culture that dominates campus life almost to the exclusion of learning. Indeed, it now dominates the learning too, with indoctrination in not only sex education but sexual political ideology through faux-disciplines like “women’s studies,” and “queer studies,” that recast all knowledge as sexual-political grievances.
The tyrannical side of this orgiastic culture is now becoming too glaring to ignore, despite years of denial. For the inevitable corollary to licentious indulgence is authoritarianism. This is now plainly manifested in a political agenda pushed by the same sexual radicals who promote the hook-up culture: Young men are now routinely railroaded before campus kangaroo courts on obviously fabricated accusations of “rape,” “sexual assault,” “sexual harassment,” “sexual misconduct” (no clear distinctions separate these vague terms), sexual this and sexual that. In the regular courts, men are imprisoned for decades on rape accusations that are known to be false. Parents regularly lose their children through spurious accusations of “child abuse” that are never proven in any court. Fathers are incarcerated without trial by divorce courts for patently trumped-up accusations of “domestic violence,” or for simply trying to see their own children, or for criticizing judges.
The response of the churches to all this has been silence. Christians, by and large, do not know what to make of this authoritarianism. They are afraid to question accusations of sex crimes, but they also know that this agenda is not theirs. Terrified of being seen to defend “rapists,” “child abusers,” “wife beaters,” and “deadbeat dads,” the church sits mute in the face of what is claimed to be a vast epidemic of sex crimes. Tempted to play it safe by perfunctorily endorsing the purveyors of the new indulgence, the church sides with falsehood against truth.
Now in turn, Christians find themselves being accused of “hatred” and “bigotry” and threatened with punishment for criticizing the homosexual agenda by the same lobby of radicals. As Martin Niemoeller warned of a similar ideology, no one speaks out for us because we did not speak out for others.
Truly diabolical is how this neglect turns back on us and corrupts us too. Because we fail to control the sin, the sin controls us. By refusing to confront the sin on God’s terms, and instead relabeling it with terms we find easier and safer to confront, we allow the sin to enlist us as its agents. This takes the form of cheap moralizing and self-righteous posturing: refusing to confront the guilty, we join witch hunts against the innocent.
For what the radicals have done is to redefine sin. Rather than the biblical definition set forth in clear biblical language, we now have ideologically redefined, government-approved definitions formulated in politicized jargon. Sexual indulgence is no longer a sin against God; it is now a crime against the leviathan state.
Pastors nowadays are much more likely to couch sexual sins in the form that has been redefined and politicized by radical secular ideology. To disguise their own irrelevance, they join the mob to register their politically correct outrage at “sexual harassment” and “domestic violence.” (I have never heard a pastor preach at any length against the “hook-up” culture, but they will endorse the fabricated and discredited feminist claims of a “rape culture,” only to leave themselves looking foolish when the charges invariably prove false.)
Pastors who parrot this jargon cannot possibly know what these terms mean, because no one knows what they mean. I have been studying them for two decades and published articles on these topics in refereed academic journals, and I do not know what they mean, because it is precisely the purpose of these terms to be so vague as to mean anything. They are devised intentionally to circumvent the clear language that the law uses to define criminal assault and safeguard the innocent with vagaries whose only possible purpose is to criminalize heterosexual men and Christians with flexible accusations that no one really understands but everyone is terrified to question.
By contrast, pastors should know precisely what constitutes fornication and adultery, because the Bible tells them. But it is safer to preach about “sexual harassment” than about fornication, because clergy are often more frightened of feminists and functionaries than they are of God.
Thus Christian faith itself is gradually transformed from theology and morality into political ideology. “Fornication” and “adultery” were biblically defined sins committed by two people and punished by God and the moral sanctions of the community. “Sexual harassment” and “sexual abuse” are quasi-crimes committed only by the man and punished by the state gendarmerie. The preachers know whom it is safe to criticize.
The effect is to transform them from preachers of God’s Word into adjunct political prosecutors.
Christian scholars churn out pointless tracts on ever more esoteric points of theology and philosophy. But the church’s crisis today is not imprecise or unsound doctrine. The church’s failing now is lacking the courage to apply its doctrine in the face of a defiant and politicized sexual immorality.
Why do pastors now evade the basic sins that plague every congregation and the most critical sins that threaten to overwhelm our society? Why do they stand mute at the very suggestion that they should do so or mumble unconvincing excuses and evasive weasel words, before nervously changing the subject or walking away? (Try it.)
The answer is that they are frightened. No pastor or priest wants to touch the subject of sexual sin, because it will anger the liberal women who control most congregations. This is not meant as condemnation; simply a recognition of reality. The same dynamic produces similar silence from our other watchdogs and gadflies: journalists and university faculty members.
Sexual freedom is the inevitable corollary to the feminization of the church because radicals understand that sexual freedom transfers power to those who can use a sexual identity as leverage: politicized women and homosexuals. “My generation let all of this nonsense of sexual confusion, radical feminism, and the breakdown of the family go on, not realizing that we … have gravely wounded the current generations,” says Cardinal Leo Burke. “The Church has not effectively reacted to these destructive cultural forces” and has instead “become too influenced by radical feminism.”
And the first casualty of feminization is courage, the courage that is demanded foremost of men, including clergy. This is why Christian faith and radical sexual ideology are today on a direct collision course, and why the radicals believe Christian faith must lose.
In The American Conservative, Rod Dreher openly questions whether Western Christianity itself can survive the revolution in sexuality, as does the former Archbishop of Canterbury in the Daily Telegraph. The question demands an answer one way or the other.
We need to ask what remains that is still Christian not only about Western institutions—that seems clear—but about the rest of us.
If we have lost our will to enforce sexual morality in our congregations, if pastors will not defend the very marriages that they themselves have consecrated—and the rest of us the marriages we ourselves have witnessed—against involuntary divorce or enforce the discipline on cohabiting couples, then in what sense does Christian faith still have any practical meaning in our common lives? We complain that Christianity is being “banished from the public square,” but we can hardly be surprised when we ourselves have lost the stomach to defend our own parishioners, congregations, and communities against violations of God’s law, whether emanating from our ecclesiastical or secular polities.
For the rest of us are no more courageous than the clergy. Few of us will express moral disapproval when we find friends cohabiting or committing adultery or inflicting unilateral, involuntary divorce on their spouses and children. And therefore few of us speak out when the state gendarmerie, filling the vacuum that we have left, imposes the order that we refuse to enforce in its own way, by taking away our brothers and sisters in handcuffs.
“Religion is central to sexual regulation in almost all societies,” writes homosexualist scholar Dennis Altman. “Indeed, it may well be that the primary social function of religion is to control sexuality.” Abdicating this responsibility to regulate it in the name of God leaves us vulnerable not only to social anomie, but also to those who will step in and regulate it for their own purposes, imposing criminal penalties and rationalizing their measures by invoking various alternative, usually politicized theologies. “Ironically, those countries which rejected religion in the name of Communism tended to adopt their own version of sexual puritanism, which often matched those of the religions they assailed.” Today’s sexual revolutionaries are simply refining the Bolsheviks’ experiment.
Perhaps it is time that we have the courage to admit that the dowdy old parson who preached against illicit sex was a wise and sensible man all along and a more faithful Christian than those of us who made endless fun of him. Perhaps we should start encouraging the self-control that he demanded and the courage he displayed. Perhaps it is also time to regain some respect for the wisdom of elders and forsake the Pinocchio world where youth (along with its urges) is worshipped as an achievement in itself, while elders, whom the Bible sets as authority figures, are expected to hold their tongues.
Perhaps it is also time to discard the politically obligatory weasel words (“No one wants to return to the bad old days when…”) and accept that open-ended sexual freedom puts us on a trajectory that will only spread chaos, ruin more lives, destroy our freedom, and weaken our civilization, until we summon the courage to speak the truth.
In short, perhaps it is time to accept that, here too, the church does not have to change with the times and that it needs to be the “rock” that Christ mandated it to be.
On this day over 2 billion Christians around the world are celebrating Jesus’ resurrection and the great joy and hope the Easter season brings. It is a hope which transcends world circumstances, such as the killing of Christians in Kenya, that we find ourselves struggling to comprehend.
On the 10th anniversary of his death (2nd April), Saint John Paul II reminds us still of the great hope Christians have. Facing dehumanizing political systems and much resignation in the Church, the great Pontiff said “Do not abandon yourselves to despair. We are the Easter people and hallelujah is our song.”
Each new child that enters a family is also both a gift and a new miracle, bringing with it hope for what that child’s life is and might be. We thought we would celebrate Easter Sunday on our blog with this clip which celebrates the miracle each new life is – a great miracle so many of us have been privileged to experience firsthand and a great reason for hope:
Catholic Bishop of the Diocese of Lincoln, Nebraska.
Last week, a young friend of mine attempted to defend the truth about marriage among a group of peers at a secular university. She presented a meaningful argument about families, social stability, and gender complementarity. None of her classmates refuted her arguments. Instead, they accused her of being a bigot and a homophobe, called her intolerant, and changed the topic to something less intellectually taxing.
My friend’s experience is practically a cliché. Americans who offer traditional viewpoints on moral issues in the public square have become accustomed to calumny. They know that reasoned arguments will rarely receive reasoned refutation.
In California, Archbishop Salvatore Cordileone has become the victim of a well-funded smear campaign because he expects that Catholic teachers shouldn’t publicly undermine Catholic beliefs. Last month, a philosophy professor was suspended from a Catholic university for criticizing heterodox instruction. Even non-believers suffer this fate. Fashion house Dolce and Gabbana is being boycotted because its owners believe that children deserve mothers and fathers.
In the cultural conversation about moral issues, reasoned arguments seem increasingly drowned out by personal attacks. And twenty years ago today, Pope St. John Paul II predicted this would happen.
Today marks the twentieth anniversary of John Paul’s Evangelium Vitae, his encyclical on the mission of the Gospel of Life. Evangelium Vitae is probably the most comprehensive and compelling encyclical on moral issues I have ever read. It addresses the evils of abortion, contraception, and euthanasia. But the encyclical is fundamentally concerned with the relationships between love, truth, freedom, and justice. Twenty years after its promulgation, we must return to Evangelium Vitae. Its message becomes more relevant each year.
If we want to reverse our culture’s descent into socially accepted hedonism, we need to understand the connection between relativism, contraception, and abortion. The danger of contraception, Evangelium Vitae said, is that it fosters a “hedonistic mentality,” a “self-centered concept of freedom,” which places personal fulfillment at the center of life’s meaning and purpose. Abortion is the radical choice for personal fulfillment, convenience, or “freedom,” even at the immediate expense of another’s life. Together, contraception and abortion have contributed to a culture that believes that personal happiness is the highest possible human aim, and that it ought to be pursued by all possible means.
The consequences of contraception’s denial of the truth about human sexuality, said John Paul, have put “freedom” on the path of self-destruction. John Paul II cautioned:
freedom negates and destroys itself, and becomes a factor leading to the destruction of others, when it no longer recognizes and respects its essential link with the truth. When freedom, out of a desire to emancipate itself from all forms of tradition and authority, shuts out even the most obvious evidence of an objective and universal truth, which is the foundation of personal and social life, then the person ends up by no longer taking as the sole and indisputable point of reference for his own choices the truth about good and evil, but only his subjective and changeable opinion or, indeed, his selfish interest and whim.
Evangelium Vitae argued that contraception leads inevitably to the rejection of every rational opposition to unfettered sexual license. The line between our contraceptive mentality and our fights over marriage is direct, and obvious. But the social consequences of contraception go beyond even the confines of sexuality.
John Paul II said that a self-referential, subjective understanding of freedom builds cultures where “any reference to common values and to a truth absolutely binding on everyone is lost, and social life ventures on to the shifting sands of complete relativism.” Inevitably relativism leads to “the supremacy of the strong over the weak.”
We are witnesses to the supremacy of the strong over the weak. The tyranny of evil is shrouded today in trappings of “democratic consensus.” We equate moral goodness with popular consensus. We’re shamed into tolerance of evil.
And because truth seems to have little to do with our sense of freedom, we watch the unborn be eradicated for the sake of convenience. We watch the elderly and terminally ill be coerced into suicide. We watch the rights of children be trampled to satisfy the pleasures and preferences of adults. The homes and cities of the West are built on the “shifting sands of relativism,” and we pretend, too often, that popular consensus makes goodness from evil.
Last week, Archbishop Charles Chaput of Philadelphia explained that divorcing freedom from truth puts believers in grave danger. He pointed out that across the globe, the rights and safety of religious people are trampled by hedonism and greed, veiled beneath the language of human rights and civic tolerance. Evangelium Vitae‘s point was that contraception fosters the attitudes that lead to religious oppression and persecution. And thwarting that persecution requires exposing the lies of the contraceptive mentality.
In short, we can’t address the great cultural unraveling we’re experiencing if we do not address the consequences of contraception and abortion. “It is precisely the issue of respect for life” according to John Paul, “which shows what misunderstandings and contradictions, accompanied by terrible practical consequences, are concealed” in positions of positivistic relativism.
We have not successfully convinced most Catholics, or anyone else for that matter, that contraception has grave social consequences. Nor have we yet convinced enough Americans that abortion is a real social injustice. Until we do that, we can expect to see the contraceptive mentality continue to foster and encourage libertine social tyranny, religious persecution, and family disintegration.
But relativism is not immediately overcome by rational conversation in the public square. Rational conversation is important. But among the effects of relativism is a popular culture increasingly less capable—and less willing—to engage in rational discourse at all.
Evangelium Vitae made clear that the dignity of human life is best understood by disciples of Jesus Christ. The Holy Father’s proposal for eradicating the social evils of abortion and contraception—and their profound social consequences—is evangelization.
The Gospel of Life is the Christian gospel. John Paul said that we only understand human dignity in this life if we understand the human potential for eternal life.
I remember vividly John Paul II’s homily in Denver, at World Youth Day in 1993, less than two years before he wrote Evangelium Vitae. I was a young priest who had traveled there with pilgrims from Wichita, Kansas. John Paul outlined the culture of death’s grave social dangers. And he proposed this solution:
Do not be afraid to go out on the streets and into public places, like the first Apostles who preached Christ and the Good News of salvation in the squares of cities, towns and villages. This is no time to be ashamed of the Gospel. It is the time to preach it from the rooftops!
Evangelium Vitae proposed the urgency of transforming human hearts—and human culture—through the Gospel of Life. Cultural transformation will take time. It is likely that successive generations will be called upon to re-Christianize the western cultural tradition. But restoring Christian culture must begin by restoring hearts—through transformative, kerygmatic encounters with Jesus Christ. Recognizing that fact was the truest genius of Evangelium Vitae.
It is time to preach the Gospel from the rooftops. The culture of death still gains ground, and the weakest among us suffer. Their suffering will be relieved when courageous men and women proclaim Jesus Christ, and witness to the real dignity of human lives made for eternity with Him.
April 1, 2015 (LifeSiteNews.com) — After thousands of injuries and several deaths of women implanted with the Essure sterilization device – touted as a safer, less invasive alternative to surgical tubal ligation – the Food and Drug Administration (FDA) is finally taking action.
In response to a petition signed by more than 2,100 women urging the agency to remove Essure from the U.S. market, the FDA announced last week that it will launch an investigation into the allegations made by the petition’s signers.
The Essure device consists of a pair of metal coils designed to be implanted in a woman’s fallopian tubes, where they induce sterility by irritating the sensitive lining, causing a buildup of scar tissue that blocks passage of sperm and ova between the ovaries and the womb. The device was given conditional pre-market approval (PMA) by the FDA in 2002, a process that grants the manufacturer lifetime immunity from lawsuits related to the device, as long as the company upholds the terms of the approval.
The FDA says this practice – known as “preemption” – is fair because the scrutiny manufacturers must undergo to qualify for PMA is so rigorous that any significant risks would be caught long before the device ever hit the market. But the petitioners say Essure’s PMA process was unusually rushed, and ultimately rendered invalid by the numerous lies and cover-ups its manufacturer used to fool the FDA into thinking the device was safe.
According to the petitioners, Essure’s original manufacturers, Conceptus, Inc., falsified data during clinical trials in order to hide adverse reactions and injuries caused by the device. Multiple cases of uterine perforation – caused by coils drifting out of place and resulting in hysterectomies for the victims – were allegedly completely hidden from the FDA. Women who reported severe pain had their medical records altered to say that they were happy with the device and had no trouble at all. Later, in the interest of boosting sales, the company would successfully convince the FDA to allow the removal of a safety notice warning women with nickel allergies – up to 15 percent of the female population – not to use the device, which is made of a nickel-titanium alloy.
Conceptus is also accused of violating not only the terms of the PMA, but federal law by using unapproved materials to manufacture the Essure devices at unlicensed facilities, and by failing to notify the government of more than 16,000 complaints from women injured by the device, as well as several deaths.
Pharmaceutical giant Bayer bought out Conceptus in 2013, but according to the petitioners, the lies continued. The petition accuses Bayer of knowingly misleading its customers by promoting Essure as safe and “worry-free” while concealing numerous life-threatening injuries suffered by women during Conceptus’ clinical trials. It also accuses Bayer of exaggerating the device’s effectiveness, claiming that “no pregnancy can occur” with Essure even though the company’s own records show that between 1997 and 2005, 64 women became pregnant after having the device implanted. Today, the total number of Essure pregnancies stands at more than 700 – including former celebrity spokeswoman Picabo Street, who lost her endorsement contract after becoming pregnant.
Essure pregnancies are dangerous to both baby and mother, and doctors often urge women who become pregnant after Essure implantation to abort. For women who choose to give their unplanned babies a chance at life, the journey they face is fraught with peril. Adverse events reported by Essure moms include miscarriage, ectopic pregnancies, premature birth due to membranes ruptured by loose coils, and birth defects caused by nickel poisoning.
“Full disclosure is a necessity when deciding to implant a foreign device into one’s body,” wrote the petition’s authors. “Bayer should not be able to market and sell a medical device that was approved by the FDA on fraudulent results of its clinical trial and altered medical records. This puts the public in grave danger.”
“How can the public expect Essure to be safe and effective when … there is evidence of fraud in the preapproval process; … adverse events are not being reported; … complaints are not being considered in Essure’s risk analysis; … CAPA activities are not being documented; … Essure’s risk analysis is incomplete; … quality assurance forms, used for tracking non-conforming product, were not used; and … Essure violated its own PMA Order and federal law?” the signers asked.
The petitioners are asking that the FDA revoke Bayer’s PMA, opening the door for victims of complications from Essure to sue the company. Additionally, they want the FDA to order the company to publicly disclose all the adverse events it hid from the government and consumers. In the meantime, they say, the FDA should either recall Essure or require a black box warning on all packaging notifying consumers of the fraudulent safety data until Bayer carries out a new round of studies, this time factual and non-doctored.
The FDA said it has referred the case to its “Office of Compliance,” which will “investigate the complaint” and “pursue actions as deemed necessary.”
Honolulu, HI — The University of Hawaii is recruiting patients as young as 14 for second-trimester abortions to determine how much they bleed during the procedure. The controversial study is already underway at the Kapiolani Medical Center in Honolulu, led by Bliss Kaneshiro, MD and Kate Whitehouse, DO.
In the randomized trial, researchers experiment by either providing or denying intravenous oxytocin to abortion patients. Oxytocin is commonly used to minimize blood loss and decrease the risk of hemorrhage. However, some doctors are concerned that denying oxytocin during surgery may put patients, especially teen girls, at risk.
“This study is reminiscent of Nazi concentration camp experiments. I pity the poor women who are being treated like lab rats, especially those who are denied the drug to reduce hemorrhaging,” said Troy Newman, President of Operation Rescue. “I have read too many autopsy reports of women who bled to death during abortions to think this is anything but immoral and ghoulish.”
The abortion study is entitled “Effects of Oxytocin on Bleeding Outcomes During Dilation and Evacuation.” Abortion patients must be from 18-24 weeks gestation and from 14-50 years old. Researchers will measure how much each patient bleeds during her abortion, based on whether or not intravenous oxytocin is provided to her.
Dilation and evacuation abortions are grisly 2-3 day procedures that involve dismembering the pre-born baby with forceps and other instruments in order to remove him or her from the womb.
The study is still seeking up to 166 test subjects and is expected to conclude in July 2015. So far no study results have been released.
In a flyer recruiting a research associate to assist with the study, one of the “Factors for Success” in the position was “Comfort with observation of surgical procedures and abortion-related healthcare.” In other words, the applicant must be comfortable watching dismemberment abortions. (Click to view a dismemberment abortion. Warning, extremely graphic content.)
The University of Hawaii has done little to publicize the hospital-based abortions outside the medical community, perhaps fearing a public backlash. The Kapiolani Medical Center for Women and Children, where the abortion study is based, does not advertise abortions on its website.
“Abortionists are continually conducting abortion experimentation on women. That’s how the D&E abortion process and other abortion methods were invented, for example,” said Newman. “It is appalling to read the details of this particular experiment especially considering that they are using test subjects as young as 14 years old. It’s just heartbreaking.”
The study is being done by the University of Hawaii in collaboration with Society of Family Planning and the University of Washington.
The Society of Family Planning provides millions of dollars in grant money for abortion and contraception-related studies. Other example of studies funded by the Society of Family Planning include:
• Studying outcomes of very early surgical and medication abortions.
• Experimenting with the dosage of Misoprostol, a uterine contracting agent, prior to surgical abortions at 13-18 weeks.
• Exploring umbilical cord injections to produce fetal death prior to late-term abortions.
• A study called “Responding to Crisis” that evaluates how abortion providers are responding to abortion restrictions in their states.
“We completely oppose this gruesome abortion experimentation on women, especially minor girls who cannot legally give their consent,” said Newman. “Abortion experimentation is something that should have gone out with Josef Mengle. It has no place in a civilized, compassionate society. Those that really want to help women should put their efforts into ending abortion, not inventing new grisly ways to kill babies and exploit women.”
Ideas for observing Holy Week as a family adapted from the faith formation team of St. Edward in Bloomington.
General suggestions
Give up technology from Good Friday until Easter Sunday morning.
Sit down as a family (or group) each night of Holy Week and plan a spring party for April or May for those of all ages.
Daily Bible study. (It’s easy for only one week!)
Attend Triduum liturgies, going each day to a different parish.
Check Pinterest and blogs for online ideas for crafts for each day and display (See crown of thorns bread recipe below.)
Holy Thursday
1. Host an at-home foot washing ceremony. It is really powerful to wash someone else’s feet, and especially for children to wash their parents’ feet and each other’s. Use the account of the Lord’s supper in John 13:1-11.
2. To connect with the Last Supper and Jesus’ blessing of bread and his offering it to the Apostles as his body, bake bread for Holy Thursday’s evening meal. Follow the simple recipe on this page. (Even though it contains a rising element — the baking powder — it does not contain yeast, the leavening agent, in accordance with the Passover.) The bread can be used in prayer or just as a snack with honey or butter.
Good Friday
1. Create your own crown of thorns. Use the same bread recipe, but instead of forming a loaf, cut the dough into three 18-inch ropes and braid them into a circle. Add toothpicks and bake per the recipe on this page. Use the crown of thorns as a centerpiece for prayer.
2. Host a movie night. Watch “The Passion of the Christ” starring Jim Caviezel as Jesus.
3. With a group or family members, create “freeze-frame” Stations of the Cross. Form small groups and ask each to create a scene that illustrates a certain part of the Passion. Once groups are ready, have someone read the Passion narrative, allowing groups to do their freeze frame during the appropriate part of the story.
4. Have pretzels for dinner or snack and share the history of the symbolism of the pretzel as representing the Trinity.
5. Make a simple cross from two sticks gathered in the yard and tied with leather straps or twine and use for prayer.
Easter
1. Put religious items such as small books and gifts in the Easter basket, not just candy.
2. Read “The Legend of the Easter Egg” by Lori Walburg (Zondervan, 2011), which presents the egg as a symbol of new life and the resurrection.
3. Search online for activities, crafts and games that help children focus on the meaning of Easter.
Recipe for unleavened bread
1/2 cup of white flour
3/4 cup whole wheat flour
3/8 tsp salt
3/8 tsp baking powder
3 tbsp vegetable oil
3/8 cup warm water
2-3 tbsp honey
Mix all ingredients together in a bowl. Do not over stir.
Pat dough into a circle on a greased cookie sheet, about 3/8 inch thick, about 5 inches round.
Score top of loaf. (Cut lightly into eight sections, not all the way through.)
Bake about 15 minutes at 400 degrees.
Courtesy of Sue Fast, director of faith formation, St. Peter, Forest Lake
March 27, 2015 (ALL.org) — March Madness! It’s that time of year again when college basketball teams are vying for the national title and almost everyone gets involved. Discussions turn to “brackets,” and the hype can be felt everywhere. Even the president of the United States created his own bracket and is following the action.
And urologists across the country are gearing up for the madness!
Wait a minute. Urologists? Why would this group of medical professionals care about an annual sporting event?
Newspapers and media stories have recently reported a disturbing trend—a trend that began with a urology clinic in Oregon. One of the major surgeries performed at the clinic is vasectomies—a permanent form of contraception, and a surgery performed on an estimated half-a-million men annually in the United States. According to bizjournals.com,
College basketball and vasectomies didn’t always go together, but an enterprising urology business in Oregon changed that in 2008.
That year, the Oregon Urology Institute ran a promotion encouraging men to get vasectomies during the NCAA men’s basketball tournament, and within a matter of weeks the story had gained the clinic national attention.
If a college-basketball-loving man wants to get a vasectomy, why not schedule it for the Wednesday before the tournament begins, giving him an excuse to take a couple of sick days, lay [sic] on the couch . . . and watch basketball non-stop for the next four days?
Since that time, the number of men electing to get vasectomies has increased. In 2014, ESPN reported: “In the last several years, urologists across the country have reported increases of as much as 50 percent in the number of vasectomies scheduled in the days leading to the NCAA tournament.”
This discussion perfectly illustrates the total collapse of the culture in America. While no one is suggesting that these men are destroying their ability to have children just to watch a basketball game, it is clear that, once they’ve considered the decision to end their fertility, a simple basketball promotion can push them the final step.
Over the last century, there has been a concerted effort to convince the American public in general—and young people in particular—that babies are not to be wanted. In 1934, Planned Parenthood’s founder, Margaret Sanger, wrote an article in the American Weekly Magazine. The article, “America’s Baby Code,” was a call to limit the number of babies being born—especially to those parents Sanger considered “unfit.” This was followed by decades of propaganda trying to convince poor people that the only reason they were poor was because they had too many children. In 1986, Planned Parenthood’s affiliate in Minnesota expanded that to everyone as it ran an advertisement proclaiming “Babies are loud, smelly and expensive. Unless you want one.”
In school, our young people have been bombarded with cutesy projects using Baby Think it Over® dolls and raw eggs with the specific intent of convincing them to look at children as a burden. Most who advocate these programs do so under a misguided attempt to convince teenagers not to get pregnant while they are in school. But what they fail to understand is that there is no magic switch thrown when the young people receive their diplomas. The mindset that has been driven into them by these exercises—to avoid having children—continues into adulthood.
The results are predictable and devastating. Americans are not having children. The latest statistics show that the fertility rate in the United States has fallen from 2.1 in 2007 to 1.86 in 2013. Since it is generally agreed that a fertility rate of at least 2.1 is needed for a country to replace itself, the United States has become a dying nation.
As long as our society continually portrays babies as burdens and advertises ways to be “free” of them, we have a long road ahead of us. Yet, not all of our youth are convinced that children are a totally bad thing. With education and a good example, these young people can come to the understanding that a child is never a burden and that they should always remain open to the beauty of life. But, we must set the example. To do this, we must first change the mindset. We must show these young people that all human beings are made in the image and likeness of God. We must cherish all human beings. And we must start being vocal champions for large families.
This past week has seen the outrage generated by parents of donor and invitro-fertilization children following a now-infamous Panorama magazine interview conducted with the fashion designers Dolce & Gabbana, wherein Domenico Dolce proclaimed, “You are born to a mother and a father — or at least that’s how it should be. I call children of chemistry, synthetic children.” Immediately, Elton John advocated a boycott of the designers’ products in retaliation for the perceived offense against his two sons, who were conceived via an egg donor and surrogate mother.
Speaking as two donor-conceived young women—alive because of reproductive technologies—we felt an urgent need to respond…in support of Dolce and Gabbana.
John’s children were commissioned in partnership with his spouse, David Furnish, and it is not yet public information which man is the biological father, or if they both are and the children are not fully genetically related. The hashtags #BoycottDolceGabbana as well as #BoycottEltonJohn are trending on Twitter, with a multitude of parents defending IVF and their “beautiful children.” Many users are posting pictures of infants with captions such as:
It is important to note, however, that infants, toddlers, and all of these “miracle” beings are too young to protest their own objectification. We however, are now of age and in a position to speak for ourselves. “Synthetic” indeed is a harsh and inaccurate description of us offspring born by third-party reproduction. Dolce’s word choice was a mistake. But there is much underlying truth in what he said: “life [does] have a natural flow, there are things that should not be changed.” Emphasis ours.
Those of us conceived non-traditionally are full human beings with equal capacity in every regard—no one need question our humanity. It is not our individual, case-by-case worth as humans that is debatable; rather, it is how we value human beings in general that warrants discussion. Has anyone asked John for how much he purchased his kids? How much money he and Furnish paid the boy’s genetic and birth mother for their absence and invisibility?
Has anyone asked Elton John for how much he purchased his kids?
I (Alana) remember when I was in school and I told my then-best friend the truth about my conception. When our friendship frayed, as tween friendships do, she released my secret as gossip—invisible, quiet, and as poisonous as carbon monoxide fumes—and I became the “test-tube girl.” The label was humiliating.
Later, in a college English class we studied “Brave New World,” and it immediately became one of my favorite works of fiction, up there with “Gattaca.” What we were essentially studying was what it means to be human. My classroom was located in Cupertino, California, and even in my liberal environment the teacher and students took heed at Huxley’s warning against manufactured people and the “outdated” nature of mothers. The class was angry at the possibility of such a world—they felt that their humanity and most important relationships (like the one with their mothers and fathers) were being threatened. The din got to a point where I had to raise my hand and speak up. I was 17 years old. I barely understood myself, let alone the world, and I said simply and defensively, “I was conceived with reproductive technologies.”
The class was silent for a very long time. Finally, a boy sitting next to me offered solemnly, “Well, she seems like a perfectly fine human being—maybe we shouldn’t be so hysteric.”
I am indeed a human being. My liver, heart, hair, and enzymes all work the same. I’ve discovered it is my psychology that is different and not-quite-right, due to my conception. It’s not a matter for doctors to fix; it’s a spiritual problem. My father accepted money, and promised to have nothing to do with me. My mother was wonderful and I have always loved her deeply, as she has loved me. But my journey is a battle against the void left by my father’s absence, and a particular disability in understanding the difference between sacred and commercial, exploitation and cooperation. Those torments for me far outweigh any social stigma or momentarily painful gossip I’ve endured from ignorant people.
For children whose genetic or birth mother’s absence has been commissioned, they will ask, “Where is my mother?” Like this young author at The Anonymous Us Project:
I’m 14 and live with my father. He always told me that my mom died when I was very young. Recently I was going through some files and found out that I was actually born by a person who donated their egg and I was born through a surrogate mother in Virginia. This led me to believe that my father was never married. I’m also very sure my dad was never married because I discovered that he is gay. Why would my dad keep this all from me?
Implicitly stated in this post is that the author’s father considered a dead mother to be better, healthier than an egg donor or surrogate mother.
My father accepted money, and promised to have nothing to do with me.
And I (Hattie) have undergone a strikingly similar experience; my mother informed me of my true parentage when I was 14, and it was, as they say, irrevocable. My mother’s then-husband had waited until they divorced to permit her to tell me, and the revelation of his not being my biological father clarified an overwhelming amount of issues between us. For a multitude of reasons—his background, my personality and beliefs, our lack of biological connection—the cards were stacked against our having a conventional, loving father-daughter relationship. And we didn’t.
One of the greatest tragedies of donor conception is the loss of belonging: to family, to a culture. Essentially, one becomes malleable like an infant. I crave a home. I see myself as I travel in many directions—doing anything in order to find one.
Through the storytelling of other donor-conceived individuals, and scientific research pertaining to third-party reproduction and genetics, I have discovered that my situation is by no means unique, and I now understand the scientific explanations as to why my social father and I—up to a certain point—were unable to bond. It is natural for me to desire my father, for evolution has blessed those that secure such a bond with better survival rates.
The lack of my biological father’s presence is a devastating reality, a burden I will likely bare my entire existence. And now, knowing the truth of my conception, when I remember my past I remember everything that was absent from it.
Team Elton is literally promoting the obliteration of mothers—not through vilification, but by pretending they don’t even exist.
Team Elton, and the media that surround them, seem to think that this discussion is about gay parents. Team Dolce and Gabbana are instead trying to draw attention to missing parents. And to what should be the horror of millions, Team Elton is literally promoting the obliteration of mothers—not through vilification, but by pretending they don’t even exist.
Dolce and Gabbana, on the other hand, have recently unveiled two campaigns celebrating women and motherhood. And while this emphasis is unprecedented in the world of fashion, it seems a most rational tribute; these men spend hours designing garments made specifically to compliment women’s bodies; their hands—measuring and configuring—are constantly in proximity to a female figure. While fitting bustiers to real women’s bodies the last 30 years, perhaps Stefano or Domenico once considered to themselves, “Hmm, I wonder what these breast things are for?”
“I’m Sicilian and I grew up in a traditional family, made up of a mother, a father and children. I am very well aware that there are other types of families and they are as legitimate as the one I’ve known,” says Dolce, attempting consolation amid the uproar against he and his business partner. Currently, the family dynamic that has proved the healthiest and most successful has been the traditional one, and that of Dolce’s experience: A mother, a father, and ensuing offspring from the sexual and social union of the two sexually complimentary parents.
In the study “My Daddy’s Name Is Donor,” it was found that, “Regarding troubling outcomes, even with controls, the offspring of lesbian couples who used a sperm donor to conceive appear more than twice as likely as those raised by their biological parents to report struggling with substance abuse,” an alarming result displaying the reality of being raised without both genetic parents.
In order to obey the desires of one parent we must agree to the obliteration of the other.
Some suggest that spending more money on making children means that they are more loved. Our children are definitively wanted, they say.
“The baby doesn’t care anything about the money,” says marriage and family therapist Nancy Verrier, regarding the issues surrounding surrogacy. “That’s not what hurts the baby. The baby is hurt by the separation, by the loss of that mother that it knows.” This ever-present realization of loss remains with both mother and child throughout their lives. Nature has ensured that mothers and children attach to one another, as it is a trait necessary to our survival; without motivation to love or instinctively care for her child, why would a mother protect her children from potential danger? She wouldn’t, and that would have heralded the end of our species. With this biological connection so immediate and meaningful, why doesn’t society view maintenance of that connection as more imperative?
Dolce and Gabbana are realists whose daily work consumes their time with raw natural materials. They work hard to understand the practical applications and limitations of tangible things—silks, leathers, jewels, studs. As masters of their art, they know what is possible, and what is foolish to attempt. They owe their success to their understanding, appreciation, and honoring of the human body.
Growing up donor-conceived, it has been a great struggle to comply with the commandment “Honor thy mother and thy father,” because in order to obey the desires of one parent we must agree to the obliteration of the other. We plead, we beg: let us honor both our mothers and fathers as essential and irreplaceable.
Thank you, Domenico and Stefano, for your bravery.
The pill. Freedom in a tablet. The cause célèbre of the women’s rights movement. Particularly in the wake of the Supreme Court’s Hobby Lobby decision in 2014 and the uncertain future of the Affordable Care Act, no other issue, perhaps barring campus sexual assault, has dominated the contemporary feminist agenda as much as birth control.
Despite this focus, the history of this relative freedom is something about which many advocates seem ignorant. More women (27.5%, according to recent data from the Guttmacher Institute) rely on the pill than any other type of contraception, yet public discourse suggests that most, on the pill or not, have no idea about its past anchored in eugenics, sexism and racism.
The irony of the pill is that it was tested on women, specifically women of color — many of whom were forced to undergo sterilization — before later being marketed predominately to white women in America as a symbol of independence.
“The pill has functioned as a technique not only for controlling reproduction but also for producing and controlling gender and race,” scholar Beatriz Preciado writes in her book about gender in the age of pharmacology, Testo Junkie. Indeed, Dr. Gregory Pincus and Dr. John Rock — two of Eig’s “crusaders,” funded by Planned Parenthood founder Margaret Sanger — effectively sterilized hundreds of women, from non-consenting psychiatric patients at the Worcester State Hospital to destitute Puerto Rican women living in the housing projects of Rio Piedras, by testing variations of the pill on them.
“Guinea pigs”: There were a handful of reasons why Puerto Rico became “the ideal setting for pill trials, which were the largest series of clinical tests ever performed,” Preciado writes. As PBS reports, government “officials supported birth control as a form of population control in the hopes that it would stem Puerto Rico’s endemic poverty.” In 1937, the passage of Law 136 legally sanctioned sterilization of Puerto Rican women for such purposes. What’s more, the pill trials that later began in Puerto Rico in the 1950s also expanded to other “pseudo-colonial locations” like Haiti and Mexico, Iris Ofelia López points out in her book Matters of Choice: Puerto Rican Women’s Struggle for Reproductive Freedom.
The real kicker? Women of color continued to be used as “guinea pigs” because the FDA, Preciado writes, “felt it threw doubt on the femininity of American women by suppressing their periods altogether.”
As a result “one-third of ever-married women aged 20-49 had been sterilized” in Puerto Rico by 1965, with “two-fifths of them before the age of 25,” according to an article by sociology professor Harriet B. Presser.
“Black genocide”: Sanger has been canonized as the founder of Planned Parenthood, but she also advocated for the creation of the pill because she believed in eugenics as an effective form of birth control. (To be fair, some contend that attention to Sanger’s championing of eugenics is perhaps exaggerated, and that eugenics was par for the course for those in the early 20th century concerned with population control. Then again, Sanger is on record as having given at least one speech to a KKK group in New Jersey.)
“Some African-American leaders were especially critical of the pill,” Megan Gibson writes in her concise history of birth control for Time, “claiming that it was being peddled in their community for the purpose of a ‘black genocide.'” The eugenics objective of the pill was thus arguably targeted at all non-white individuals who posed a threat to the (white) face of America.
Remembering our history: This history, though deeply troubling, seemed to be forgotten the moment the pill was marketed to women living in the continental U.S. Ads for the pill promoted the product by touting women’s liberation — already hot topic of discussion in the early 1960s, and which largely enabled the Sexual Revolution of that decade, as Nancy L. Cohen has pointed out at AlterNet. The pill remains statistically the most popular form of birth control for women to date. “Within five years [of the pill’s legalization in 1960], 6 million American women” were on it, Cohen notes. By 2012, that number had jumped to 10.6 million.
History in general isn’t pretty — and it’s no different for the pill. But by being cognizant of the pill’s past, advocates for reproductive justice and for women’s rights in general can form a more nuanced, and more ideologically diverse, politics for our collective future.
March 16, 2015 (LifeSiteNews.com) – A new US study has found that a huge increase in Crohn’s disease cases in women in the past fifty years corresponds to the introduction and widespread use of oral contraceptive pills since the 1960s.
Crohn’s disease is an incurable ailment affecting the digestive system characterized by abdominal pain, severe diarrhea, fever, fatigue, weight loss and malnutrition.
Harvard gastroenterologist Dr Hamed Kha’s study of 230,000 American women found that those who had used the pill for five years or more had a 300 percent higher risk of developing Crohn’s disease than those who had never used it.
Dr Kha explained that while oral contraceptive drugs do not directly cause Crohn’s disease, the synthetic hormones have side effects that contribute to the higher risk he identified.
These side effects include thinning of the lining of the gut making it less able to properly hold in digestive waste, a reduction of beneficial intestinal bacteria, and a negative effect on the immune system.
“What’s very clear is that Crohn’s is not caused by oral contraceptive use by itself. It’s a combination of oral contraceptive use among individuals with a strong genetic predisposition to Crohn’s,” Kha told the Daily Mail.
“It’s an interaction between these two that significantly increases the risk of an individual developing it,” he said.
Dr Kha added that his study did not look at users of the so-called morning-after pill, but he expected that super-doses of the same types of drugs used in normal oral contraceptives would increase the risk of Crohn’s disease even further.
He said that genetic screening could dissuade women who have a genetic predisposition to Crohn’s from using the drugs.
The widespread availability of the morning-after pill, over the counter and without any medical consultation, could put many more women at risk.
The US Food and Drug Administration allowed non-prescription sales of the morning-after pill in 2006.
When the FDA approved the “Ella” brand of morning after pill in 2010 it allowed the drug to be marketed as an “occasional” emergency contraception, to be taken by a woman up to five days after sexual intercourse.
The FDA warned, however, that it was unsafe for women to use Ella more than occasionally, as they had no data on its safety over the long term.
Twenty years ago this month, on the solemnity of the Annunciation, St. John Paul II published Evangelium Vitae (The Gospel of Life). It was the 17th year of his pontificate. He was 75 years old.
The idea for an encyclical on the dignity of human life was first suggested to the pope after a consistory of cardinals convened in Rome in 1991 to discuss threats to human life in the modern world. The cardinals urged him to “reaffirm with the authority of the Successor of Peter” the Church’s well-trod teaching on human life. A discussion ensued at the Vatican as to whether its development should mirror the process used in the development of his influential Familiaris Consortio on the family published a decade earlier: namely, convene a Synod of Bishops on the topic, and then develop an Apostolic Exhortation from the Synodal Statement. John Paul II decided against the idea of a synod. He chose to use the authority of his own office—what George Weigel refers to as “the world’s most authoritative pulpit”—to publish a more doctrinally-weighty document, an encyclical. After consulting in writing every bishop in the world for input on its preparation, he drafted Evangelium Vitae (EV). Although theological experts usually assist in the drafting of papal documents, EV so clearly bears the imprint of the saint’s personality and set of concerns, that it’s likely he drafted the encyclical himself. Five years after its publication, he said that EV was “central to the whole Magisterium of my Pontificate.”
The Random House edition subtitles the document: “The encyclical letter on abortion, euthanasia and the death penalty in today’s world.” But the official Vatican subtitle, “On the value and inviolability of human life,” tells us more about the working thesis of the text. Whether addressing the connection between contraception and abortion (no. 13), in vitro fertilization, prenatal diagnosis, embryo destruction and infanticide (no. 14), threats to the incurably ill and dying (no. 15), or anti-birth policies imposed on developing nations (no. 16), the pope insists that the inviolability of human life, and the rights to which it gives rise, must be the basis of our moral analysis. The concepts are especially active in the encyclical’s three solemn condemnations: the intentional killing of the innocent, abortion and euthanasia, respectively (see nos. 57, 62, 65).
But EV’s most novel comments are reserved for the death penalty. The document reconceives the killing in capital punishment as a kind of societal self-defense. While, the practical implications of such have been felt the last twenty years in the Church’s worldwide turn towards abolition, the doctrinal implications are yet to be unpacked. By conceiving the killing of criminals in terms of norms traditionally limiting lawful killing in self-defense, we see that what the pope defends in cases of “absolute necessity” is no longer retributive killing, but death as an unintended side effect of a proportionate act of self defense aimed at rendering aggressors incapable of causing harm.
George Weigel suggests that EV should be read as the “third panel” in a “triptych” of encyclicals, together with Centesimus Annus (1991) and Veritatis Splendor (1993), all concerned with the moral foundations of a free and virtuous society (Witness to Hope, p. 757). And it’s true that the message of EV can be seen as an extended urgent warning that “democracy stands or falls” with the values it embodies and that “without an objective moral grounding” it will be incapable of ensuring a stable peace (no. 70).
But EV should also be read in conjunction with Ut Unum Sint, published two months after the encyclical (in May 2005), on the imperative of Christian unity. Those who have witnessed the advance of the culture of death since EV’s publication have experienced first hand the fearsome truth of what Pope Benedict XVI repeated so often, namely, that outside the context of faith, morality “weakens and then dies” (Christianity and the Crisis of Cultures, 71). All believers in revealed religion, therefore, and especially in the Gospel of Life, must tirelessly strive for unity if we are to give the strongest witness possible to the dignity of human life.
Among the innumerable fruitful initiatives surrounding, and proceeding from, the publication of the great encyclical, two in particular stand out.
A year before EV’s publication, Saint John Paul erected the Pontifical Academy for Life and installed at its helm the heroic French Catholic geneticist Jérôme Lejeune. EV can be seen as the unofficial mission statement and manifesto of the august new Academy.
And exactly two years after its publication, in March of 1997, the Culture of Life Foundation was formed, receiving the direct apostolic blessing of the pope.
March 4, 2015 (LifeSiteNews.com) — Although there has always been contraception, its acceptance and practice by society as a whole is a relatively new phenomenon. In the first part of the 20th century barrier methods became through mass production increasingly used. However, with the advent of the hormonal contraceptive pill in the 1960s the contraceptive era, ushering in the sexual revolution, really took off.
The term “revolution” is by no means exaggerated, for the result was a fundamental change in the understanding of human sexuality in society. With the pill, people thought, nothing can happen, i.e. no child could be conceived. Inhibitions broke down, so that there was an increase in adultery, living together before marriage and living together with no thought of marriage. Amoral sex education with the message, “You can do anything you like so long as your partner agrees and you use contraception. If there is an accident, have an abortion,” promoted sexual promiscuity from puberty onwards. Sexual activity has been degraded into a form of entertainment.
The immediate consequences of promiscuity starting in adolescence are obvious: the rampant increase of sexually transmitted diseases, infertility and the incapability of forming long-term relationships through frequent changes of partners and repeated disappointments.
The assumption that “nothing can happen” is erroneous, because contraceptives are by no means 100% effective. Children are conceived, and such “errors” must be corrected – the child is aborted.[1] The result has been devastating: the number of babies killed by abortion every year is about the same as the total number of deaths in the whole of World War II.
Apart from the carnage, enormous havoc is created in the relationship of the parents, whether married or not, very often leading to its breakdown. It would also be naive to imagine that Catholic women never resort to abortion.
The situation of couples practising NFP however is quite different. They are aware every day of the state of their fertility, asking themselves whether the marriage act on that day would result in conception; they do not lose sight of the child who could be conceived. They do not forget the fundamental purpose of the act. An unplanned child is therefore usually accepted.
The widespread practice of abortion leads to euthanasia. If it is acceptable to kill one category of people, then it is logically acceptable to kill others, specifically the ill, the handicapped and the old, for human life is no longer sacred. A chilling example of this kind of development can be seen in the National Socialist regime in Germany.
The pill “culture” leads to the rejection of children, small families, and a demographic winter. In the long-term it will be impossible to pay pensions. For couples practising NFP however, the child is neither an error nor a threat. Their natural love of children is not destroyed. They have larger families. The 15 teaching couples in our organisation, for example, have 62 children so far, an average of 4.1 per family.
The separation of sexual activity from child-bearing leads to the acceptance of the production of children through assisted reproduction without recourse to the marital act in the case of infertility. Through IVF society is being led, inspired by Aldous Huxley’s Brave New World, to the acceptance of controlled reproduction. Human beings are reduced to products. They are mass produced, selected, rejected, frozen or used in experiments. They are treated as material goods, in short, as slaves.
Slavery has been formally reintroduced into society. A doctor, whether mixing sperm and eggs in a Petri dish or injecting a sperm into an egg, is playing God. The arrogance of it! Surely this modern sin should be listed amongst those which cry to heaven.
When the practice of sterilised sexual intercourse is accepted, it leads logically to the acceptance of all practices leading to orgasm: oral, anal, homosexual acts, etc. The whole homosexual movement has become possible only through the general acceptance of contraceptive practice and the reduction of sexuality to a source of entertainment.
The practice of contraception within marriage contains within itself the mutual rejection of the spouses. It leads to the destruction of love. It belongs to the nature of love to give oneself, even to the point of sacrifice, seen eminently in the self-sacrifice of Christ on the cross. Even in our ordinary life a mother’s sacrifice of herself for her child is by no means exceptional. A mother will naturally go to great lengths to help her child, exceptionally even giving up her own life. The marriage act is meant to be an act of mutual love. The natural fruit of that love is the child. The spouses give and receive each other mutually completely. Even during the naturally infertile days of the cycle they give each other all they have at that time – their mutual love.
But if they use contraception they say to each other subconsciously, “I do give myself to you, but without my fertility, and I don’t want your fertility either.” Is that love? The act which in its nature expresses the total self-giving and receiving of the spouses contains an element of rejection, and therefore becomes a lie. When this act of rejection is systematically and continually repeated, love dies. The marriage is at least burdened. Many marriages break down.
Couples who use NFP do not practise this subconscious, systematic rejection. From personal experience and observation of our clients we see that such marriages are more stable. This is also shown in studies. Greater stability is evident even in those without religious practice. [2]
Contraception, which leads logically to other evils as described above, is destroying society. There are too few children and nations are dying out. It leads to abortion, as those who promote it concede. The combination of promoting promiscuity through Godless sex education, the long-term use of hormonal contraception with back-up abortions and the postponement of child-bearing leads to increased infertility.
The solution offered is not a true therapy of infertility, but assisted reproduction which bypasses the normal process of transmission of life through the marriage act. The long-term purpose of this policy could well be the desire to subject reproduction to state control, which would allow only those children to be born who pass quality control. At present this is illusory, but the tendency can be seen. It would appear that an elite group wishes to create a society of virtual slaves obedient to their desires. A new totalitarianism is being formed.
To this end it is necessary to destroy or at least weaken marriage and the family. For this purpose contraception, especially the convenient hormonal forms, is eminently suitable. And those who pour their millions into the homosexual movement and the gender ideology are not concerned with helping homosexuals and those with problems of sexual identity. Rather they are using these people to extend the concept of marriage and ultimately to widen its meaning so much as to make it meaningless.
[2] Wilson, M.A.: The Practice of Natural Family Planning versu the Use of Artificial Birth Control: Family, Sexual and Moral Issues, Catholic Social Sceince Review, Volume VII, November 2002.
The majority of Canada’s palliative care specialists don’t want to participate in assisted suicide, according to a survey recently conducted by the country’s Society of Palliative Care Physicians (CSPCP). The survey – discussed in the latest edition of the Canadian Medical Association Journal – revealed that only 25% of CSPCP members would be open to helping patients end their lives.
75% of respondents said assisted suicide fell outside the purview of palliative care (even when one adopts the World Health Organization’s definition of palliative care).*
Although some palliative care doctors may choose to assist patients in ending their lives once that becomes legal, others believe that who should actually administer lethal doses of medication is still an open question.
“There’s a huge misconception out there that that’s what palliative care is —it’s all about death”, remarked CSPCP president Dr. Susan McDonald. “No. The great majority of it is about life and living life as best as you possibly can”.
“[Assisted suicide] It’s not part of our practice and we don’t anticipate it will become part of our practice,” says Dr. Doris Barwich, the Society’s past president and current executive director of the British Columbia Centre for Palliative Care.
In a landmark decision on the 6th of February, the Supreme Court of Canada ruled that prohibiting assisted suicide is unconstitutional and a violation of the country’s Charter of Rights and Freedoms. Various healthcare organisations and representative bodies are currently debating the practicalities of the new law.
*Subsequent to the publication of this story on the 7th of March, the CMAJ have made a correction to their original article. The CSPCP study found that not 56% but rather 75% of respondents didn’t think they should provide assisted suicide or euthanasia. The CMAJ had originally reported 56%
Jennifer Brinker | jbrinker@archstl.org | twitter: @jenniferbrinker
A bill proposed in the Missouri House would prohibit health care facilities and others from withholding life-sustaining procedures from a minor patient without the written consent of a parent or legal guardian.
Sponsored by Rep. Bill Kidd, R-Kansas City, HB 113 also would require health care facilities, nursing homes and physicians to disclose in writing any policies that relate to a patient’s care, including life-sustaining or non-beneficial treatments.
The bill is nicknamed “Simon’s Law” after Simon Crosier, who was born in 2010 with Trisomy 18, a genetic disorder that includes an extra chromosome 18. Simon lived three months.
His mother, Sheryl Crosier, a member of Annunciation Parish in Webster Groves, wrote a book in 2012, called “I am Not a Syndrome — My Name is Simon.” In the early stages of her research, Crosier was going through Simon’s medical records and discovered that doctors had placed a “do not resuscitate” order in her son’s records without her knowledge, she said. He also was ordered to receive nutrition as a comfort measure only. Turns out, the hospital had in place a futility policy, which allows physicians to withdraw medical treatments deemed to be “futile.”
“They took the road they wanted to go,” said Sheryl Crosier. “They started taking away, stripping him of everything. They would say, things like ‘not for Simon,’ or ‘incompatible with life.’ It was very dehumanizing.”
In 2013, the Crosiers met with a film producer who was working on a documentary on families with children who have special needs. The Crosiers discovered they were not alone. Several others families shared stories of not being informed whether the hospital had a futility policy and what rights they had as parents in making decisions for their children.
Last fall, Crosier shared her story at a Missouri Right to Life event in Kansas City. There, she met Kidd, who was moved by her story.
“This should not even occur,” said Kidd. “Removing life-sustaining treatment (without permission) is punishable by law, but it’s being done and off the books, from my understanding. Morally and ethically they should inform the parents and that’s not always happening. This is about parental rights. If treatment is going to be withheld, then the parents have to have it in writing.”
The bill has been assigned to the Health and Mental Health Policy Committee; a hearing has not yet been scheduled.
Dr. Peter Morrow, president of the Catholic Medical Association, noted that not all health care facilities have futility policies in place, and there isn’t a uniform application among those that do. A 2007 position paper by the CMA noted that the concept of medical “futility” emerged in the 1990s, when medical and bioethics began promoting the idea connected to cases where patients or family members insisted on treatment over the objections of physicians and/or health care institutions.
The CMA, which does not endorse the concept of “medical futility,” included in its position paper a Catholic framework for addressing claims by families of inappropriate treatment. While not all health care facilities have futility policies, most have ethics committees, said Morrow, which also address issues related to patient care.
Crosier urges people to contact legislators in support of the bill. “If people feel strongly about their parental rights … it’s very important to have this law,” she said. “If we had Simon’s Law, this would not have happened, because we would have been the ones making the decisions — even if it would have been to put the DNR, we would have been the ones making the decision.”
• Futility policies have been adopted in several cities and states that rely on procedural grounds rather than widely accepted definitions of “futility.” These policies permit unilateral decisions by physicians/hospitals to withdraw medical treatment deemed to be “futile.”
• Beginning in the 1990s, the concept of medical “futility” was advanced in the medical and bioethics literature in connection with cases in which patients or family members insisted on treatment over the objections of physicians and/or health care institutions.
• Over the next ten years, a variety of definitions and categories (e.g., quantitative and qualitative) of “futility” were proposed; none achieved widespread support. Rather, there was general agreement that consensus on definitions and on individual cases was unlikely, if not impossible.
• There has been widespread agreement that the development and implementation of futility policies is fraught with dangers — that conflicts between patients/families and physicians/hospitals are best avoided in the first place or addressed in a non-confrontational manner once they arise.
From “Guidelines on Resolving Conflicts About Treatment Deemed ‘Futile,'” Catholic Medical Association, 2007.
March 2, 2015 (LifeSiteNews.com) — An article in the Frontiers journal of medicine is sounding the alarm about the possible effects of hormonal contraception on the human brain, suggesting that the effects may be much more profound than previously thought and calling on the scientific community to devote more research to the topic.
“Hormonal contraceptives are on the market for more than 50 years and used by 100 million women worldwide,” wrote Belinda A. Pletzer and Hubert H. Kerschbaum, a pair of Austrian neuropsychologists from the Paris-Lodron-University Salzburg. “However, while endogenous steroids have been convincingly associated with change in brain structure, function and cognitive performance, the effects of synthetic steroids contained in hormonal contraceptives on brain and cognition have barely been investigated.”
Based on what little scientific data exists tracking behavioral and neurological changes in users of hormonal contraceptives, the authors asserted that “synthetic steroids may contribute to masculinizing as well as feminizing effects on brain and behavior.”
“We conclude that there is a strong need for more systematic studies, especially on brain structural, functional and cognitive changes due to hormonal contraceptive use,” wrote Pletzer and Kerschbaum.
“Changes in brain structure and chemistry cause changes in cognition, emotion and personality and consequently in observable behaviors,” the pair continued. “If a majority of women use hormonal contraception, such behavioral changes could cause a shift in society dynamics. Since the pill is the major tool for population control, it is time to find out what it does to our brain.”
Pletzer and Kerschbaum called hormonal contraception a “global experiment” and noted that while the intake of steroids and hormones by athletes is considered “doping” and condemned by society, the same behavior by women and girls who wish to reduce the risk of pregnancy is not only tolerated but encouraged, and from increasingly younger ages, despite the lack of scientific data regarding the safety of such an approach.
“Adolescent girls start taking hormonal contraceptives earlier and earlier, often shortly after onset of puberty,” the duo wrote. “However, the majority of research on steroid actions in the brain focuses on post-menopausal hormone replacement therapy.”
Of particular concern to Pletzer and Kershbaum was the fact that the majority of neurological studies do not take into account whether female subjects are on hormonal birth control.
“Traditionally, medical as well as psychological research focused on male participants, because hormone fluctuations throughout the menstrual cycle were suspected to affect the results—rightly, as it turned out,” they wrote. “Nowadays, numerous women participate in scientific studies. However, while participants on medication are excluded, studies hardly control for the use of hormonal contraception.”
Upon reviewing available data regarding the cognitive impact of hormonal contraceptives, the scientists found evidence that the drugs fundamentally alter the way women process and react to information. Citing a handful of studies showing differences in contraceptive users’ verbal communication, memories, emotional recall, and even choice of mates, they concluded that it is possible that the drugs “cause a structural re-organization of the brain.” They also noted that some studies have linked hormonal contraception to chemically based mood disorders like depression, anxiety, fatigue, neurotic symptoms, compulsion and anger.
In light of the seriousness of the evidence shown by a relatively limited amount of data, Pletzer and Kershbaum called for more thorough investigation of the effects of hormonal contraceptives on girls and women, and for medical researchers in all fields to be sure to account for this common variable.
“First and foremost, we conclude that there is a strong demand for additional studies on how hormonal contraceptives affect the brain from the molecular to the behavioral level,” the authors wrote. “Thus, future studies aiming to investigate ‘normal’ brain functioning, should control for the use of hormonal contraceptives among their participants.”
“As the number of women using oral contraceptives constantly increases, while the age of first contraceptive use constantly decreases,” the authors concluded, “the associated changes in personality and social behavior imply significant consequences for society.”
It’s not easy swimming against the tide. I am sorry to admit that “pro-life activist” is not always my first response to the cocktail party question.
And standing by your belief in man-woman marriage sometimes feels like holding up a “punch me” sign.
But San Francisco Archbishop Salvatore Cordileone has shown again and again that he is made of the strongest stuff.
Here’s the tick-tock on his latest battle to protect Catholic teaching in Catholic schools:
February 3: The Archdiocese of San Francisco announces proposed changes in teacher contracts telling applicants that if they’d like a job teaching children at one of their schools, they will be expected to uphold and not publicly contradict Catholic moral teaching. In the view of the Archdiocese, this simply codifies the long-established expectation for school employees.
February 17: A group of legislators, all Democrats, writes a letter to Cordileone urging him to stand down, arguing that his plan would discriminate against the teachers and violate their civil rights to “choose who to love and marry, how to plan a family, and what causes or beliefs to support.”
February 19: The archbishop replies. Here is the meat of his letter:
First of all, I always believe that it is important, before making a judgment on a situation or anyone’s action, that one first obtain as complete and accurate information as possible. To this end, a number of documents and videos giving accurate and more complete information about this contentious issue are available on the website of our Archdiocese. I would encourage you to avail yourselves of these resources, as they will help to clear up a lot of misinformation being circulated about it (such as, for example, the falsehood that the morality clauses apply to the teachers’ private life).
The next thing I would like to mention is actually a question: would you hire a campaign manager who advocates policies contrary to those that you stand for, and who shows disrespect toward you and the Democratic Party in general? On the other hand, if you knew a brilliant campaign manager who, although a Republican, was willing to work for you and not speak or act in public contrary to you or your party — would you hire such a person? If your answer to the first question is “no,” and to the second question is “yes,” then we are actually in agreement on the principal point in debate here.
Now let’s say that this campaign manager you hired, despite promises to the contrary, starts speaking critically of your party and favorably of your running opponent, and so you decide to fire the person. Would you have done this because you hate all Republicans outright, or because this individual, who happens to be a Republican, violated the trust given to you and acted contrary to your mission? If the latter, then we are again in agreement on this principle.
My point is: I respect your right to employ or not employ whomever you wish to advance your mission. I simply ask the same respect from you.
This is how you do it. Bravo Archbishop Cordileone!
As the Archdiocesan announcement said: “Catholic schools exist to affirm and proclaim the Gospel of Jesus Christ.” Amen. Let them take their best shot at that goal, and complaining legislators stand aside.
ROME, February 26, 2015 (LifeSiteNews.com) – Allegations have surfaced this week that the lead organizer of the Vatican’s controversial Synod on the Family in October personally intervened to block the distribution of a book distributed by high-ranking cardinals, including Cardinal Raymond Burke, that defended the Church’s teachings on marriage.
Cardinal Lorenzo Baldisseri, general secretary for the Synod of Bishops, who became the focus of much criticism from bishops at the Synod for allegedly “manipulating” the process, is reported to have ordered that the books be seized, despite them having been posted through the official Vatican City State postal service.
The highly respected Vaticanist Edward Pentin, writing for NewsMax on Wednesday, said “reliable and high level sources” had confirmed that the book, “Remaining in the Truth of Christ,” was “intercepted” on the orders of Cardinal Baldisseri on the grounds that it would “interfere with the synod.” Baldisseri was also said to have been “furious” at the attempt to distribute them.
Cardinal Baldisseri reportedly claimed the books were confiscated because they had been distributed “improperly.” Those entrusted with ensuring the books made it into the hands of the Synod bishops, however, insisted that the books had gone through the regular Vatican postal service, and were therefore legally protected material, Pentin reports.
The book includes a set of essays defending and explaining the Catholic teaching on the indissoluble nature of marriage and was intended by its authors as a means of clarifying the discussion.
The book was organized and authored by a group of the Church’s highest-ranking prelates – including Cardinal Raymond Burke, then-head of the Vatican’s highest court, and Cardinal Gerhard Müller, prefect of the Congregation for the Doctrine of the Faith – who were gravely alarmed not only at the “proposal” by Cardinal Walter Kasper but at its positive reception among bishops and Catholic laity.
Cardinal Kasper had shocked the Catholic world at last year’s consistory of cardinals by his “suggestion” that the Church change its practice of withholding Communion from people in “irregular unions,” and by his claim that the pope had approved the proposal. The so-called “Kasper proposal” has since become the focal point of a nearly open civil war in the Church in which decades-long divisions between the “liberal/progressives” and orthodox prelates has been revealed by the world’s press.
At the Rome launch on October 6 of a different book opposing Kasper’s proposal, Cardinal George Pell, a member of Pope Francis’ Council of Nine, said that changing the practice or teaching of the Church would be “disastrous.”
Pentin writes, “Those responsible for mailing the books meticulously tried to avoid interception, ensuring the copies were sent through the proper channels within the Italian and Vatican postal systems.” Pentin added that his sources had “strongly” refuted the claim by the Synod’s secretariat that the books had been distributed “irregularly,” saying they had used the normal postal service that is governed according to Vatican state and international law and is known in Rome for its superior service to the Italian postal system.
Throughout the Synod, rumors circulated broadly among the assembled corps of journalists that the highly anticipated books had failed to reach the bishops and had in fact been confiscated on the orders of the Synod’s leadership. At the time, although this strange story had spread widely, none of the principal parties involved in the book’s publication or distribution were willing to come forward.
That rule of silence appears to still be in place; today none of the book’s authors or editors were willing to speak with LifeSiteNews “on the record” to confirm what had happened, and attempts to reach the Synod office went unanswered. It is public knowledge, however, that only a handful of bishops had been able to obtain a copy during the Synod itself.
Edward Pentin reported yesterday that the story has not stopped circulating in Rome since the Synod, despite having been dismissed at a December press conference by Vatican spokesman Fr. Federico Lombardi. “Since then the allegations have become more widely known and have been corroborated at the highest levels of the church,” Pentin writes, saying that his sources believe the seized books were likely destroyed.
It is notable that the accusation could have a potential of a criminal liability for unlawful seizure of posted materials. The Vatican City State postal service is a member of the Universal Postal Union, a body under the auspices of the UN, which regulates the postal service practice of 192 member states. One Vatican source told LifeSiteNews today that a first attempt had been made to stop the books being sent by the Vatican Post Office, but that the postal workers had refused to cooperate, saying that it would be “unethical” to tamper with the mail.
Baldisseri, appointed as a permanent Secretary of the Synod of Bishops by Pope Francis, has become a public spokesman for the Kasper Proposal and he was heavily criticized during the Synod by many of the bishops themselves, who complained that the process was being strictly controlled to produce a particular outcome.
At a conference in Rome last month, Baldisseri told delegates that “dogma can evolve” and that the purpose of the Synod was not merely to restate Catholic teaching. He also confirmed that the documents of the Synod, including the highly contested “mid-term Relatio” that had called for the Church to “accept and value” the “homosexual orientation” had been read and approved for publication by Pope Francis.
Advancements in science and medical technology have proven to be great gifts to the pro-life movement time and time again. Doctors are able to routinely deliver premature babies at earlier and earlier stages of development. Innovations in sonogram imaging have provided a window to the womb enabling expectant mothers to see their unborn children face to face. We also have the ability to hear the unborn baby’s tiny heartbeat.
These glimpses at the baby’s humanity have inspired countless numbers of mothers to reject abortion and choose life. However, until now, once a pregnant woman selected a chemically-induced abortion, there was little hope that the unborn child would survive.
Now, a new medical advancement is saving lives in a previously unimaginable way. Dr. George Delgado, medical director at the Culture of Life Family Health Care in San Diego, California, has been instrumental in developing a technique to reverse what was the inevitably fatal effect of the RU-486 abortion pill.
Dr. Delgado’s story began when he received a call from a friend in El Paso, Texas, who informed him about a woman who had taken the abortion pill but immediately regretted the decision.
At the 2015 American Association of Pro-Life Obstetricians and Gynecologists (AAPLOG) conference, Dr. Delgado told attendees, “I started thinking about my years of experience with progesterone, and how I’d used progesterone to try to prevent miscarriage.” The protocol calls for taking the injectable progesterone as soon as possible after taking the mifepristone.
Dr. Mary Davenport, another pro-life physician at the forefront of this new innovation, explained how chemical abortions involve two drugs:
“Medical [chemical] abortion is actually performed in early pregnancy with TWO pills, the first – RU-486 – mifepristone or Mifeprex, antagonizes the hormone progesterone, which is necessary for pregnancy. This cuts off the nutritional supply to the pregnancy, ending in the unborn baby’s death. One or two days later the woman takes a second pill, misoprostol or Cytotec, which causes uterine contractions and expels the pregnancy. Medical abortion is frequently a horrible experience for the women, lasting up to 2-4 weeks with nausea, vomiting, diarrhea, hemorrhage, and intense pain.”
The reversal attempts to counteract the first drug, mifepristone, before the second one, misoprostol, is ever given.
Progesterone is a critical hormone during pregnancy, said Delgado. It helps nourish the placenta, keeps the cervix closed, and inhibits contractions. Mifepristone, a progesterone receptor antagonist, acts like a “false key” binding with the progesterone receptor and blocking its activity. This action softens the cervix, makes the uterine wall more vulnerable to contractions, and attacks the placenta, Delgado said.
At a press conference held at the National Press Club, AAPLOG physicians reported that as of the end of 2014, 78 babies have been born after abortion reversal treatment, with 45 women still pregnant, a 57% success rate out of 223 attempted reversals.
Instead of taking the second pill the next day, which would induce contractions, she began to look into ways to stop the death of her unborn child. Not surprisingly, the abortion center staff was no help. A local hospital informed her that if she carried the baby to term, he would face severe health issues.
“Obviously women are changing their minds and interested in options,” said Delgado.
As noted, Dr. Delgado’s innovations have already saved 78 young lives. And that is just the beginning! AAPLOG recently unveiled a new “Emergency Abortion Pill Reversal Kit,” which they would like to see placed in emergency rooms and urgent care clinics nationwide.
Dr. George Delgado will address the National Right to Life Convention this summer in New Orleans, Louisiana. The event will run July 9-11 and also feature keynote speakers Louisiana Governor Bobby Jindal, John McCormack of the Weekly Standard, NRLC President Carol Tobias, and many more.
Brilliant! The same Canadian doctors who are apparently very poorly trained in palliative care, have been given a license to kill by the recent radical ruling of the country’s Supreme Court.
This medical and potentially humanitarian mess is sorted through in a good column in the Toronto Star by Harvey Max Chochinov. From, “Canada Failing on Palliative Care:”
Despite the impressive strides that palliative care has taken — in areas such as pain and symptom management, and sensitivities to the psychosocial, existential and spiritual challenges facing dying patients and their families — at their time of licensure, physicians have been taught less about pain management than those graduating from veterinary medicine.
Once in practice, most physicians have knowledge deficiencies that can significantly impair their ability to manage cancer pain.
Doctors are also not generally well-trained to engage in end-of-life conversations, meaning that goals of care often remain unclear; and patients may not receive the care they want or the opportunity to live out their final days in the place they would want to die…
For 70 to 80 per cent of Canadians, palliative care is not available and hence, not a real choice.
Yikes! And remember, the Supreme Court case legalized both assisted suicide and euthanasia to the dying, disabled, and mentally ill!
This means that doctors who can’t adequately care, will be allowed to kill–assuming they don’t botch it, which can definitely happen:
In the future, how might this kind of scenario play itself out in the many Canadian settings that do not have adequate palliative care? There, the choices will come down to settling for sub-optimal care; dislocating from friends and family to seek out better care elsewhere; or, if one is so inclined, considering medically hastened death.
We are about to become a country that extends patients the right to a hastened death, but offers no legislative guarantees or assurances that they will be well looked after until they die.
George Friedman is the Chairman of Stratfor and his (free) Geopolitical Weekly articles often appear in Mercatornet. I always enjoy reading them. He has recently written on demography and the long term implications of a declining world population. “Global Decline and the Great Economic Reversal” is an interesting read and I strongly recommend that you have a look at it. The key points that Friedman makes are the following:
1. Population decline is happening and it is happening around the globe:
In fact, the entire global population explosion is ending. In virtually all societies, from the poorest to the wealthiest, the birthrate among women has been declining.
By the end of this century, Friedman predicts, all countries will be at 2.1 births per woman or below (that is, at or below the rate of replacement).
2. Population decline is irreversible and inevitable:
It is primarily a matter of urbanization. In agricultural and low-level industrial societies, children are a productive asset. Children can be put to work at the age of 6 doing agricultural work or simple workshop labor. Children become a source of income, and the more you have the better. Just as important, since there is no retirement plan other than family in such societies, a large family can more easily support parents in old age. In a mature urban society, the economic value of children declines. In fact, children turn from instruments of production into objects of massive consumption…Children cost a tremendous amount of money with limited return, if any, for parents. Thus, people have fewer children.
3. There is an argument that there will be massive economic dislocation due to a rapidly ageing population (an argument that we’ve made on this blog before):
But the argument is that the contraction of the population, particularly during the transitional period before the older generations die off, will leave a relatively small number of workers supporting a very large group of retirees, particularly as life expectancy in advanced industrial countries increases. In addition, the debts incurred by the older generation would be left to the smaller, younger generation to pay off.
4. The obvious answer to this problem is immigration from countries that still have surplus population. The problem is that for some countries, mainly in Europe and Japan, there is no history of successfully assimilating immigrants.
5. Friedman predicts that as populations contract, GDP per capita will rise, as he believes that GDP will not fall as quickly as productivity will increase:
The capital base of society, its productive plant as broadly understood, will not dissolve as population declines. Moreover, assume that population fell but GDP fell less — or even grew. Per capita GDP would rise and, by that measure, the population would be more prosperous than before.
6. Friedman also emphasises the unprecedented nature of the current reversal of population growth. This is the first time in 500 years that the population will not be growing. As he notes, this will have a massive impact on our economies. In short, he believes that the cost of labour will increase while the cost of capital will decline. He also believes that declining populations will result in declining land values and therefore the decline in the value of housing:
For the first time in 500 years, this situation is reversing itself. First, fewer humans are being born, which means the labor force will contract and the price of all sorts of labor will increase. This has never happened before in the history of industrial man…That would mean that in addition to rising per capita GDP, the actual distribution of wealth would shift…If the cost of money declined and the price of labor increased, the wide disparities would shift, and the historical logic of industrial capitalism would be, if not turned on its head, certainly reformulated.
7. He concludes that the “path to rough equilibrium will be rocky and fraught with financial crisis” and that some countries will fare much worse than others. He ends on a positive note however:
The argument I am making here is that population decline will significantly transform the functioning of economies, but in the advanced industrial world it will not represent a catastrophe — quite the contrary. Perhaps the most important change will be that where for the past 500 years bankers and financiers have held the upper hand, in a labor-scarce society having pools of labor to broker will be the key.
Those are only some of the salient points of what is, overall, an excellent and interesting article. I would like to share some ideas that came to me as I read the piece:
Why can’t rich societies “afford” children? It is interesting that it is an economic inevitability that we have fewer children now because they are no longer economically valuable. Western societies that have lower birth rates are far, far richer societies than they were when birth rates were much higher. You would think that that would make it easier now for us economically to have larger families than our peasant forebears. It would also be interesting to compare the average family size of rural workers against urban dwellers and the upper classes in earlier societies to see if the latter two groups (which had less of an economic imperative for big families) had fewer children. (As a tangential aside, Shannon noted last week it seems to be the wealthier families that have fewer children in New Zealand suggesting it’s not all economic imperative…)
Urbanisation and house prices. The argument that homes will get cheaper with a lower population is not necessarily true if urbanisation keeps on intensifying and a declining population wants to live in the same place. Land as a whole might get cheaper but demand for housing in some places might increase. (I’m thinking of Auckland, New Zealand as an example of this.)
We are entering unknown territory. Friedman assumes that we will reach some population and economic equilibrium in the future (maybe by the end of the century). However, he does not state why this is so. If fertility rates go below replacement rate as they are in so many countries nowadays, is there any guarantee that they will climb to the magic replacement rate of 2.1 children per woman? Not only is the reversal of population growth unprecedented in the last 500 years, I would argue that global population decline is unprecedented throughout recorded history. Before the last 500 years the population may have remained stable as mortality kept pace with large families, but we simply do not know what the result of the world’s population declining. Once people get used to smaller and smaller families, why will this below replacement fertility rate reverse? Friedman suggests a population decline of 20% as an example, but places like Japan are looking at a much greater decline than that.
Loss of the family as the basic unit of society: Allied to this last point, there is a greater loss that is not mentioned in Friedman’s article, the decline of the extended family unit. The end of having numerous cousins, brothers, sisters, aunties and uncles. The rise of “little emperors” or single children not knowing the joy (and difficulties) of having a sibling. As families grow smaller, will their importance as the building blocks of civil society also decline? If so, what will take their place?
How will the aged be supported? Finally, the article does not give an answer for the problem of an ageing, top heavy population. Who will pay for the pensions, healthcare etc of an elderly population? Even if per capita GDP is to rise, taxes will have to significantly rise to pay for the current social welfare schemes. Will the younger, working population agree to that? I think that the problem of an inverse population pyramid will be one of the rocks on the path to a smaller global population in the 22ndcentury.
Whether we reach population equilibrium in that century is, I think, unclear. What such a world means for family life is also unclear.
The following questions and answers are based on the recent article on Plan B in the February, 2015 issue of the Linacre Quarterly. Feel free to contact the main author, Dr. Chris Kahlenborn with additional questions at drchrisk@polycarp.org
1. Would you say Plan B ever functions as a contraceptive (i.e., prevents sperm from fertilizing egg)?
Ideally, Plan B should be named emergency abortion/contraception instead of emergency contraception, because it has high potential of working as an abortifacient when given prior to ovulation. We noted in our recent paper (Linacre Quarterly, February, 2015), that when given prior to ovulation, Plan B frequently allows ovulation to occur and has no major impact on sperm flow or quality, yet one does not see any evidence of clinical pregnancy. If both sperm and an egg are present and one does not see evidence of clinical pregnancy, then abortion is the most likely mechanism of action. In the minority of cases, when Plan B truly stops ovulation, it likely works via a contraceptive method.
2. Plan B is supposed to “work” if taken within 72 hours of unprotected sex. But your paper says if Plan B is taken on the day of ovulation or thereafter, it does not appear to impact a pregnancy. Thus, would you say Plan B is (useless) if taken during or after ovulation?
Yes, it appears to be useless or actually may increase a woman’s risk of getting pregnant when taken on or after the day of ovulation, according to the data presented by Dr. Noe in her 2010 and 2011 studies (Contraception). Other leading researchers such as Dr. Trussell and Davidoff also raise this very real possibility: “it even raises the counter-intuitive but undocumented possibility that Plan B used after ovulation might actually prevent the loss of at least some of the 40% of fertilized ova that ordinarily fail spontaneously to implant or to survive after implantation.” (JAMA, October, 2006). In practical terms this means that while Plan B likely often works by abortion if given prior to ovulation, it has either no efficacy or actually could have a pregnancy enhancing effect if given on the day of ovulation or after.
3. Would you say Plan B also appears to be (useless) if taken by women whose BMI is 30 or higher?
It’s almost useless: Dr. Glasier noted in 2011 (Contraception) that women with BMI’s over 30 who take Plan B have a 400% higher failure rate than women of normal weight.
4. For these and other reasons, are you saying the efficacy of Plan B is inflated (the ACOG efficacy rate of 85 percent is unsupported? and the Noe study estimate of 68 percent could also be too high?)
According to the Noe paper, Plan B is almost 100% effective in stopping clinical pregnancy if given prior to ovulation and 0% effective when given on or after the day of ovulation. This means that the efficacy of Plan B is likely determined by the parameters of the particular study. If researchers place the majority of women in the preovulatory group, then efficacy will be high: conversely, if they place the majority of women in the postovulatory group, efficacy will be low. We can see evidence of this phenomenon in the Noe study where 103 women were placed in the preovulatory group and 45 in the postovulatory group which corresponds almost exactly to their stated efficacy rate of 68% (ie, almost 103/148 or 69.6%).
5. What are implications for rape-crisis centers to hear that Plan B only works if the victim hasn’t ovulated yet?
The Noe study has huge implications for women who have been raped who are told that Plan B makes it harder to become pregnant. The reality is, that most emergency rooms test for pregnancy, but rarely if ever test women’s ovulatory status (ie, by measuring Luteinizing Hormone and progesterone levels). As we noted earlier, top researchers who strongly advocate for Plan B, have noted that Plan B has either no effect or may actually be increasing the risk of pregnancy in cases where a woman has begun or already has ovulated. This has serious implications both ethically and medically. Rape centers who continue to give Plan B without checking ovulation status, are subjecting many woman to a hormonal drug that may actually be increasing their risk of pregnancy all the while claiming that Plan B has an efficacy rate of 85%!
6. What are implications for Catholic hospitals, who believe that Plan B acts like a contraception, when in fact, your paper recommends Plan B be renamed as “emergency abortion/contraception”?
In 1995, then Bishop Myers, accepted what is known today as the Peoria Protocol which in a nutshell states that it is okay to give Plan B to women who have been raped if it is given prior to ovulation, since it is based upon the assumption that Plan B consistently stops ovulation in this phase. Many Bishops have accepted this protocol while other have remained skeptical. Unfortunately, we now know from several large studies such as that of Dr. Croxatto (Contraception, 2004), that Plan B does not consistently stop ovulation. Therefore, the entire Peoria Protocol is based on a faulty premise.
This has immediate and serious implications for Catholic Hospitals because if Plan B is given prior to ovulation it is likely working via an abortive mechanism of action much of the time. Catholic Hospitals who currently use this faulty protocol are likely allowing abortions to occur in their facilities.
7. What are implications of redefining Plan B as an effective abortifacient (versus contraceptive) for purposes of healthcare battles, such as Hobby Lobby/others who do not want to pay for “abortion-causing drugs” in their insurance policies. (In other words, does your study strengthen the hand of Hobby Lobby, et. al.)
Plan B should be redefined as emergency abortion/contraception if given prior to ovulation since abortion appears to be its’ dominant method of action. Women should be informed of this method of action and people who value human life in the earliest stages should not be coerced to give or pay for this type of hormonal abortion.
8. Proponents who claim that Plan B works only as a contraceptive claim that it has little effect upon the endometrium, so therefore it could not cause an abortion? Is this true?
No. Proponents of Plan B often note that Plan B does not appear to have an effect on the endometrium on a histological level. However, we noted in our Linacre paper that when Plan B is taken prior to ovulation, it causes endometrial bleeding within 7 days about 30% of the time, which is gross anatomical evidence of an unstable endometrium. In addition, we noted that there is theoretical evidence that Plan B may cause slowing of tubal transport of the zygote, which theoretically could delay the timing and efficacy of implantation. While there are many different ways in which Plan B may be causing abortion, at this stage it is difficult to determine the exact mechanism of action due to current technological constraints. However, as we noted in our Linacre article, in the future one will probably be able to quantify how frequently Plan B causes abortion by employing the use of sophisticated hormonal assays (ie, Early Pregnancy Factor) which can often detect the presence of pregnancy within 48 hours of fertilization.
Continuing his series of Wednesday general audiences on the family, Pope Francis spoke on February 11 about children.
“Children are the joy of family and society,” he said. “They are not a problem of reproductive biology, or one of many ways to realize oneself in life, let alone their parents’ possession. Children are a gift.”
“Each is unique and each is unrepeatable; and yet unmistakably tied to his or her roots,” he continued. “You love your child because he is a child, not because he is beautiful, healthy, and good; not because he thinks like me, or embodies my desires.”
The Pope said that the “experience of being a son or daughter allows us to discover the most gratuitous dimension of love, which never ceases to amaze us. It is the beauty of being loved before … Before we have done anything to deserve it, before we can speak or think, even before coming into the world.”
Expanding upon this theme, he added that “being a child is the fundamental condition to know God’s love, which is the ultimate source of this real miracle. In the soul of every child, not matter how vulnerable, God puts the seal of this love, which is the basis of his or her personal dignity, a dignity that nothing and no one can destroy.”
Reflecting on the Fourth Commandment, he said that
a society of children who do not honor their parents is a society without honor, when you do not honor your parents you lose your honor! It is a society destined to fill itself with arid and greedy young. However, even a society with a greedy generation, that doesn’t want to surround itself with children, that considers them above all worrisome, a weight, a risk, is a depressed society.
Just think of the many societies we know here in Europe. They are depressed societies because they don’t want children, they don’t have children. The birth rate doesn’t even reach 1%, why? Everyone should think about that and answer it personally.
The Pope added:
As the encyclical Humanae Vitae of Blessed Pope Paul VI teaches, having more children cannot be automatically viewed as an irresponsible choice. The choice to not have children is selfish. Life rejuvenates and acquires energy when it multiplies: It is enriched, not impoverished! Children learn to take charge of their family, they mature in the sharing of sacrifices, and they grow in appreciation of its gifts. The experience of joyful fraternity animates the respect and care of parents, who are due our gratitude.
A major scientific review by Christopher Kahlenborn, MD, et al, published last week in the Linacre Quarterly, found that levonorgestrel emergency contraception, also known as Plan B, has “significant potential of working via abortion.” The review also revealed that arguments claiming Plan B is not an abortifacient are not scientifically defensible.
The review states:
Physicians who dispense LNG-EC [Plan B] to rape victims in the preovulatory period . . . are giving LNG-EC at a time in a woman’s menstrual cycle when it has significant potential to work via the death of the embryo. Physicians who dispense LNG-EC in the postovulatory period may be increasing a woman’s risk of becoming clinically pregnant.
“Catholic bishops have been assured, by Plan B proponents, that the drug does not cause an abortion,” stated Judie Brown, president of American Life League. “We now know this is not true. There is a grave risk that preborn human lives are being killed by Plan B, and Catholic hospitals need to immediately halt dispensing these drugs and review their policies.”
The authors of the review concluded that “Catholic hospitals that allow the dispensing of LNG-EC [Plan B] prior to ovulation-especially when given within 48 hours of ovulation-are permitting the use of a drug which has a significant potential of working via abortion. . . . If given prior to ovulation, LNG-EC should be labeled as emergency abortion/contraception.”
Carl Djerassi, widely dubbed “the father of the Pill”, has died at his home in San Francisco at the age of 91. Though best known for synthesizing the hormone that became the key ingredient of the contraceptive pill, the eminent Stanford University professor emeritus made a number of significant contributions to science and technology.
He was also well-known for his books, plays, art collection and cultivation of artists. Another contraceptive scientist this week called him “a true Renaissance man and scholar”. Stanford President John Hennessy hailed him “first and foremost a great scientist” who with his colleagues “transformed the world by making oral contraception effective.”
In an interview about his latest play last year Dr Djerassi told the San Francisco Chronicle that he was “sick and tired of talking about the pill”, and after 60 years who wouldn’t be? Perhaps also he had lived long enough to be disenchanted with the revolution he helped set in motion, or at least have some doubts about the social changes it fuelled.
As an Austrian-born Jew fleeing Hitler, Carl Djerassi arrived in America in 1939, with his mother, at the age of 16. His parents, both doctors, had divorced when he was six, although they remarried to assist the flight of mother and son from Austria. The marriage was annulled soon after, and the elder Dr Djerassi only emigrated to the US in 1949. Penniless in 1939, young Carl wrote to Eleanor Roosevelt to ask for help and received it in the form of a college scholarship.
He excelled in chemistry and after graduating from the University of Wisconsin with a doctorate in 1945 (still in his early twenties) went to work for the Swiss pharmaceutical company Ciba in New Jersey, where he developed the first commercial antihistamine.
In 1949 he was recruited to work for Syntex, a company established in Mexico by American chemist Russell E Marker to synthesize the pregnancy hormone progesterone from the Mexican wild yam. Marker, who pioneered this particular technique, left the company after a dispute with his partners who then hired George Rosenkranz to carry on the programme. It was Rozenkranz who hired the young Dr Djerassi and others.
Djerassi at first successfully led a programme to convert the steroid derived from the yam – diosgenin — into cortisone, then a new drug working wonders for sufferers from rheumatoid arthritis.
Syntex also competed with other drug companies in the hunt for an effective oral contraceptive, their researchers focusing on a synthetic form of progesterone, the hormone which prevents ovulation during pregnancy. This was linked with research on treatments for severe menstrual disorders, infertility and cervical cancer.
In 1951 Djerassi’s group made their breakthrough, synthesising norethindrone, the active ingredient in the first practical (economical and effective) oral contraceptive. Although G.D. Searle and Co actually marketed the first “pill” – following FDA approval in 1960 — Syntex’s product accounted for more than half the oral contraceptive market by the 1970s. In 1951 Fortune magazine headlined: “Syntex makes the biggest technological boom ever heard south of the border.”
Djerassi maintained his connections with the company, becoming president of Syntex Laboratories in Mexico City and Palo Alto, California, and growing wealthy on the strength of his shares in the company. He famously bought 1200 acres near Palo Alto, where he started a cattle ranch, began collecting art, and eventually made half the property over into an artist’s colony in memory of his only daughter, Pamela, an artist who took her own life in 1978.
At the same time he pursued an academic career, joining the faculty of chemistry at Stanford in 1959. Between then and his full retirement in 2002 he published more than 1,200 scientific papers, a rare achievement even by today’s standards, notes the Stanford obituary. It notes also his seminal contributions to molecular research and early computer modelling. In 1968 he founded Zoecon, a company that developed insect controls using modified insect growth hormones.
As a public figure, he was above all an apologist for the pill, travelling widely to promote it and also to defend it against the likes of Germaine Greer — “always a vociferous opponent of the pill,” he noted in a 2007 interview with The Guardian — and Barbara Seaman, whose 1969 book The Doctor’s Case Against the Pill exposed side effects including the risk of blood clots, heart attack, stroke, depression, weight gain and loss of libido.
He was dismissive of such claims – “everything has side effects” – and countered the feminist critique (Why not a male pill?”) by arguing that feminists, above all, should know that women could not trust men to take a pill. Scientifically, he told the Guardian, there was no difficulty; they knew how to make a male pill. But sharing the burden of contraception would take away women’s control over their own fertility, and potentially all the political gains of the previous 50 years.
It’s a comment that sheds quite a lot of light on the effects of the contraceptive revolution. The pill’s “guarantee” of sex without children is also the death of trust between spouses or partners, and between men and women generally. Sex from now on is about negotiation between two people who are (theoretically) equal in power, though equally uncertain of each other’s motives and feelings. And society is reduced to competing camps.
Djerassi’s own life experience perhaps helps to explain why such a miserable state of affairs would seem acceptable. His childhood experience of divorce was echoed in his own two divorces and three marriages. Each divorce was preceded by an affair with another woman – the first arranged when he announced that the woman who would become his second wife was pregnant with Pamela, his first child. (He is survived by her brother, Dale.) These ruptures suggest one reason why “effective contraception” would make good sense not only in terms of the population control for which it was mainly intended but also as a remedy for the social chaos it would cause.
Djerassi conceded that the pill had its downside for women. Its very “effectiveness” (did he ever acknowledge the massive abortion industry it spawned?), he told the Guardian, led men to take it for granted and not bother with condoms – “it is yet another thing that is put on women’s shoulders.” And although it facilitated women’s entry into more professions, it also meant that they postponed childbearing – with all the problems of infertility and unfulfilled dreams that go with that.
We read that in his books and plays he explored the ethical, political and interpersonal dilemmas resulting from science and technology — what really amounts, in the case of the pill, to social engineering. But nothing seems to have shaken his faith in science to provide answers and politics to make use of them. A deeper philosophical or moral perspective is lacking.
In the Guardian interview he said that the flipside of sex without children – that is, children without sex – was the way of the future: we would freeze our sperm and eggs , get sterilised (as he did after his two children were born, as his daughter did at the age of 25 and without children) and check out gametes from the bank when we wanted them later. “Then you might as well forget about contraception. I am absolutely convinced that is the direction in which we’re going in the long run in the Western world.”
Perhaps he was only playing the “agent provocateur” as he liked to style himself, but one would have liked to hear such a clever man, with the hindsight of so many years –not excluding personal tragedy – talk about what was wrong with that direction. What was soul destroying and inhuman about it. It would be too much to expect a confession that the pill itself was a wrong turn, but it is hard to believe that the idea did not occur to him. At least once.
Even during the wildest times of my youth, I would never have wanted to be the cause of an abortion. Yet, there is a possibility that I have been responsible for one, unaware. How? Because of contraceptive methods that my wife and I used before we knew about the natural methods.
While women’s positions on the legal and moral question of abortion vary, most would agree that full disclosure of the risk of abortion is a basic right of women using contraceptive drugs.
However, studies conducted among women 18-49 in the US[i] and in six European countries[ii] showed that about 8 out of 10 women do not know about the potential of some contraceptives to cause abortion.
The same studies shows that 75 percent of them would want to be informed about any reasonable possibility of this happening, and 3 out of 10 women would choose not to use a contraceptive that would risk causing an abortion.
Let’s look at the facts.
The right to informed consent
Being fully informed by the provider about a drug as potent as hormonal contraceptives is a basic and well recognized right of patients. The World Health Organization recommends that patient information about birth control methods include effectiveness, mechanisms of action, side effects, health risks and benefits, correct use and reversibility. In practice, it doesn’t happen. In general, physicians frequently don’t take the time to inform patients even of the side effects of medication they prescribe[iii], let alone the mechanisms of these powerful drugs.
Preventing implantation of an embryo
In order to reach high effectiveness rates, hormonal contraceptives rely on two main mechanisms: prevention of the fertilization of a woman’s egg (prefertilization effect), and prevention of the implantation of an embryo by the modification of the lining of the uterus (postfertilization effect). The second mechanism is what we’re concerned with here. If ovulation occurs and if the egg is fertilized by a sperm, which sometimes happens, especially with today’s low-dose pills[iv], the resulting embryo will travel to the uterus and attempt implantation. However, scientific literature shows that oral contraceptives, implants, the shot, the patch[v] and IUDs make the lining of the uterus inhospitable to it. It is also clearly stated in the labels of these contraceptive methods[vi].
Is this an abortion?
You may not agree that human life starts at conception, but rather at implantation, when the embryo attaches to the lining of the uterus about six days after conception. In which case, you wouldn’t consider the process described above an abortion. Some studies show that a majority of people believe it does start at conception. But it’s not actually a matter of opinion or belief. In a remarkable scientific paper[vii], Maureen L. Condic, Associate Professor of Neurobiology and Anatomy at the University of Utah School of Medicine, writes:
The scientific evidence supports the conclusion that a zygote is a human organism and that the life of a new human being commences at a scientifically well defined ‘moment of conception.’ This conclusion is objective, consistent with the factual evidence, and independent of any specific ethical, moral, political, or religious view of human life or of human embryos.
Because abortion is legal, this conclusion leaves the user of contraceptives with a personal moral choice about what may happen to the embryo once it is created as a result of the relatively small, yet real, possibility of the failure of a contraceptive’s first mechanism, the prevention of fertilization. But in order to freely exercise this moral choice, a woman has to be informed.
Lack of information
Full disclosure to all women about this possibility seems essential to ensure proper informed consent. Yet women don’t know about these risks, as the table below tells us[viii]. Women in the US are the most informed and only 22 percent of them know. In France (my homeland), it’s only 7 percent. Yet, 72 percent of US women want to know, as in most other countries. And the reality is that if women knew, not all, but a large number of them would not use methods that have a risk of postfertilization effect or abortion.
These facts are important for medical professional to know because they point to a real disconnect between them and their patients. It is also important for our readers to know so that they may be able to make a choice consistent with their moral beliefs.
What to do
If you’re currently using a contraceptive method described above and are concerned with the risk of abortion, here is what you can do:
Check the label of you current contraceptive method
Have a conversation with your spouse/partner
Have a conversation with your doctor about alternatives that guarantee no postfertilization effect
Consider learning about natural methods, which avoid this risk (learn about them here)
Share this article with the hashtag #DiscloseAbortionRisks
Back 25 years ago, my wife would have never used the Pill had she known about these risks. It comforts us both, though, to know that with this article we may help others avoid the same mistake.
Gerard Migeon is the editor of Natural Womanhood, a non-profit that promotes fertility charting so that women know their bodies, and enjoy good health, sexual intimacy, and effective family planning. This article first appeared on Natural Womanhood, a MercatorNet partner site.
Author’s note: I want to thank the following medical professionals for conducting this research and sharing their conclusions with Natural Womanhood: Jokin de Irala, MD, PhD, MPH. University of Navarra, Spain; Cristina Lopez-del Burgo, MD, PhD. University of Navarra, Spain; Joseph B. Stanford, MD, MSPH. University of Utah, USA. For more information about the research, they can be contacted at jdeirala@unav.es, cldelburgo@unav.es ;jstanford@dfpm.utah.edu.
Footnotes:
[i] Clinical sample in Utah and Oklahoma: Dye et al. BMC Womens Health 2005;5:11. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1325031/
[ii] European national representative samples: Lopez-del Burgo et al, Contraception 2012;85:69-77 and Lopez-del Burgo et al, J Clinical Nursing 2013 http://dadun.unav.edu/handle/10171/34346 Spain: Lopez-del Burgo et al, Eur J Obstet Gynecol Reprod Biol 2010;15:56-61.http://dadun.unav.edu/handle/10171/19107
[iii] SOURCES: Tarn, D.M. Archives of Internal Medicine, Sept. 25, 2006; vol 166: pp 1855-1862. Derjung M. Tarn, MD, PhD, assistant professor of medicine, department of family medicine, David Geffen School of Medicine, University of California, Los Angeles.http://www.webmd.com/news/20060925/study-doctors-dont-explain-rx-drugs
[v] Hormonal contraception is available in oral contraceptive pills and in newer formulations, including the transdermal patch, the vaginal ring, subcutaneous implants, and IM injections. Prevention of pregnancy is achieved by inhibiting ovulation, fertilization, and/or implantation of an egg. http://www.ncbi.nlm.nih.gov/pubmed/16567739
[vii] When does human life begin, A Scientific Perspective, Maureen L. Condic, http://bdfund.org/wordpress/wp-content/uploads/2012/06/wi_whitepaper_life_print.pdf
– See more at: http://www.mercatornet.com/family_edge/view/15508#sthash.Pd2LRWij.dpuf
Original article from: http://www.cancernetwork.com
A history of hormonal contraceptive use in younger women for 5 years or more was found to be associated with a possible increased risk of glioma, a rare type of brain tumor. The findings of the study were published in the British Journal of Clinical Pharmacology.
Prior studies have shown that female sex hormones, the active ingredients of hormonal contraceptives, may increase the risk of some cancers while reducing the risk of other cancers. This was the starting point of the study for author David Gaist, MD, PhD, of the Odense University Hospital in Southern Denmark, and colleagues.
Exposure to a hormonal contraceptive was categorized based on the hormone type: estrogen-progesterone or progesterone only, and by duration of use (less than 1 year, 1 year to 5 years, and more than 5 years).
Ever use of hormonal contraceptives was associated with a 50% relative increased risk of glioma, while those who used contraceptives for more than 5 years had a 90% relative increased risk. The women who used progesterone-only contraceptives had a greater risk compared with those on an estrogen-progesterone contraceptive. Those who were current hormonal contraceptive users had a 70% relative increased risk of glioma compared with past users, who had a 20% relative increased risk.
Analyzing the results by histological types of glioma, there was a slightly higher risk of glioblastoma multiforme.
Gaist and colleagues used data from Denmark’s national administrative and health registries. The authors identified women between the ages of 15 and 49 and a diagnosis of glioma between 2000 and 2009. Each of the 317 cases of glioma were compared with 2,126 age-matched women with no glioma diagnosis—8 for every case.
Of the 317 cases, 114 occurred in women between the ages of 15 and 34, 115 occurred in women between the ages of 35 and 44, and 88 occurred in women between 45 and 49 years of age.
Previous case-control and cohort studies either found no association, a weak inverse association, or an increased risk between glioma incidence and hormonal contraceptive use, but several of these studies only analyzed former hormone contraceptive users over the age of 50.
“In a population of women in the reproductive age, including those who use hormonal contraceptives, you would anticipate seeing 5 in 100,000 people develop a glioma annually, according to the nationwide Danish Cancer Registry,” said Gaist.
According to Gaist, tracking women who use contraceptives long term is needed to further assess the risk. The authors noted that there may be confounding factors such as the tendency of women who take contraceptives to get more regular checkups. Still, “considering the extensive use of hormonal contraceptives our finding merits further investigation,” stated the authors.
The tagline of our film Eggsploitation is “The infertility industry has a dirty little secret.” In the film we seek to expose the many facets of the market for human eggs, which very few people are aware of. These dirty little secrets include:
Egg donors aren’t tracked over their lifetimes, so we have no idea what the long-term effects on young women’s health are.
No major peer-reviewed studies have been done on the long-term effects of super ovulation on this donor population.
Eggs aren’t tracked, so once they leave a human body it’s difficult to know where they end up, which sometimes literally means they can be halfway around the world.
Many of the drugs used with egg donors carry risks of cancers, and some drugs have never been safety approved for this sort of use.
Children born via egg donation often aren’t told of their conception story, and they often don’t have access to important information about their genetic mother.
Because of what might arguably be described as a cavalier attitude toward young women, their eggs, and their reproductive health, a great deal of important information is never recorded as part of their medical records. I often wonder how many women receiving a cancer diagnosis have in their history the fact they sold or donated their eggs. How many women struggling to conceive today were egg donors during college, for example? Since the egg donor is not considered a patient, often her primary care physician doesn’t know to ask or to include this information in her health history. Women may not even think that the fact that they donated their eggs is relevant to include in their medical histories and thus may not inform their physicians.
Take, for example, the recent case of Brittany Maynard. Brittany is remembered mostly because of her decision to take her own life after receiving a tragic diagnosis of terminal brain cancer, glioblastoma. What most people don’t know about Brittany’s medical history is that she was an egg “donor.” A year ago, a close family friend of Brittany’s, who has asked to remain anonymous, contacted me. This friend knew about my work exposing the risks to egg donors, and was worried, wondering if Brittany’s decision to sell her eggs and expose herself to potentially harmful fertility drugs might have any connection with her cancer diagnosis.
This important part of Brittany’s health profile does not appear to be part of her medical history, and it certainly was not part of the larger, very public conversation that followed once she made the decision to end her life.
As with many egg donors, it’s often a secret that only a few know. I’ve interviewed countless women who sold their eggs, and this is rarely on the top of their list of things to talk about. Often it is only when an egg donor suffers health-related problems that this information becomes known to others.
What do we know about glioblastomas, and might there be any connection with hormone use in egg donation? Glioblastomas are more common in men than women. This tumor is more common in older people than in younger people, primarily striking those between the ages of 45-70. One reason it is less common in women is because of the protective effect estrogen has for women. Some research suggests that there is evidence that hormonal factors might influence glioma risk. This clue initially came from the fact that women are significantly less likely to get such tumors. Then researchers discovered that exposure to estrogen due to early age at menarche may act to protect against DNA damage to glial cells. This is discussed in a prospective study by Silvera, et al., (2006:1322). In other words, estrogens appear to be neuroprotective.
Is it possible that, during the Lupron phase of egg donation when estrogen production is blocked and the woman is put into a medically induced menopause, the woman is exposed to risks from which she would otherwise be protected? What might the repeated effect of this be for women, like Brittany, who donated her eggs more than once?
I wonder about the children born from Brittany’s eggs who should know about their biological mother’s health history and diagnosis of glioblastoma. What, if anything, will they ever be told?
When will we will finally track and monitor women who donate and sell their eggs? When will we do the studies necessary to ensure their health is protected?
Of course, I wish that policies would change so that women wouldn’t be targeted for their eggs and that this practice would be stopped altogether.
But the bottom line in Brittany’s case is that she had repeated exposure to a medley of hormone altering substances during her young and all too short life.
As I was finalizing this piece for publication, Brittany’s husband, Dan Diaz, announced he is going to work to expand the legalization of assisted suicide. This effort is deeply mistaken on many levels.
My point here is this: eggsploitation is real. I will continue to work to expose the dirty little secrets of the practice. And I wish, for the sake of the health of egg donors like Brittany, that her husband would join me and put his efforts into protecting women like his wife.
So, how do y’all like that Associated Press headline?
In case you might have missed it, Pope Francis’ recent return flight from his visit to the Philippines featured an in-flight press conference in which he was asked (according to a widely published translation):
A Filipino woman gives birth to an average of three children in her life, and the Catholic position concerning contraception seem to be one of the few questions on which a big number of people in the Philippines do not agree with the Church. What do you think about that?
This is Pope Francis’ reply:
I think the number of three children per family that you mentioned — it makes me suffer- I think it is the number experts say is important to keep the population going. Three per couple. When this decreases, the other extreme happens, like what is happening in Italy. I have heard, I do not know if it is true, that in 2024 there will be no money to pay pensioners because of the fall in population. Therefore, the key word, to give you an answer, and the one the Church uses all the time, and I do too, is responsible parenthood. How do we do this? With dialogue. Each person with his pastor seeks how to carry out responsible parenthood.
That example I mentioned shortly before about that woman who was expecting her eighth child and already had seven who were born with caesareans. That is an irresponsibility. That woman might say ‘No, I trust in God.’ But, look, God gives you means to be responsible. Some think that — excuse the language — that in order to be good Catholics, we have to be like rabbits. [NOTE: he never says “breed” here!] No. Responsible parenthood. This is clear and that is why in the Church there are marriage groups, there are experts in this matter, there are pastors, one can search; and I know so many ways that are licit and that have helped this. You did well to ask me this.
Purveyors of media hype, start your engines! As if to prove Pope Francis’ assertion that some observers of the Catholic Church actually think that Catholic couples are all supposed to “be like rabbits”—as in, have as many children as is humanly possible—worldwide reports made it sound like no one ever in the history of the Church had ever before thought of this notion of “responsible parenthood”!
Well, let’s just say that the secular surprise factor is about fifty years too late! That’s if your point of reference is the Second Vatican Council’s clearly stated teaching on “responsible parenthood” (see Gaudium et Spes, paragraph 50). But even fifty years is too recent when one traces the rise of contraception alongside the emergence of the art and science of “natural family planning” from its roots in the 1920s all the way to our contemporary 21st-Century approaches to it.
Suffice it to say that we Catholics have always embraced an authentically “responsible” approach to parenthood. We’ve never been taught otherwise by the Magisterium of the Catholic Church. We’ve been very blessed to have understood that there is no imperative, as the Holy Father indicates, for parents to have as many babies as time allows (!). Rather, non-Catholic observers have, forever it seems, misunderstood the Church’s long-held (and still-held) emphasis on children as the “supreme gift” of marriage.
The truth is that the Catholic Church holds that the objective “primary purpose” of Matrimony is the “procreation and education of children.” While this isn’t the only “end” or “purpose” of marriage, it’s considered “primary” precisely because the “stable union” of the married couple functions as the fundamental cell of society, in which we realize God’s primordial command to “be fruitful and multiply.” God’s plan for us as married couples is to be utterly open to the transmission of human life (that means babies!). Pope Paul VI, in the very first sentence of his 1968 encyclical “Humanae Vitae,” calls this a most serious “mission” for the married couple.
Being utterly open to transmitting life, though, does not necessarily mean being relentlessly in pursuit of it! Married couples sometimes have tangible and just reasons for postponing pregnancy. Indeed, it’s this “old-school” reference to the primary end of “procreation and education” of children that makes it perfectly clear that parents often need to balance those two aspects of the primary end—being able to raise (educate) our born children alongside our openness to transmitting new life (procreate) in the “now” of married life.
It is this kind of discernment that Pope Francis has in mind when he picks up the phrase “responsible parenthood” from the teaching documents of the Church. Even so, the Holy Father also says something much less widely reported but vitally important about the abundant blessing of every child born into the family:
Another curious thing in relation to this is that for most poor people, a child is a treasure. It is true that you have to be prudent here too, but for them a child is a treasure. Some would say ‘God knows how to help me’ and perhaps some of them are not prudent, this is true. Responsible paternity, but let us also look at the generosity of that father and mother who see a treasure in every child.
So it’s clear that Pope Francis speaks from the heart of the Church on “responsible parenthood” and on the beautiful blessing of children. Had the secular media been on the ball both fifty years ago and on the plane to Rome this week, we’d all be breathing—and “breeding”—a little easier.
Below is an excerpt from an address given by Pope Pius XII to the Directors of the Associations for Large Families of Rome and Italy in January 20, 1958, the nineteenth (and final) year of his papacy. Throughout the address the Holy Father eloquently speaks of the joy, sacrifice and generosity so prevalent amongst those families who God has abundantly blessed with the gift of children.
“Large families are the most splendid flower-beds in the garden of the Church; happiness flowers in them and sanctity ripens in favorable soil. Every family group, even the smallest, was meant by God to be an oasis of spiritual peace. But there is a tremendous difference: where the number of children is not much more than one, that serene intimacy that gives value to life has a touch of melancholy or of pallor about it; it does not last as long, it may be more uncertain, it is often clouded by secret fears and remorse.”
Happiness in a large family
“It is very different from the serenity of spirit to be found in parents who are surrounded by a rich abundance of young lives. The joy that comes from the plentiful blessings of God breaks out in a thousand different ways and there is no fear that it will end. The brows of these fathers and mothers may be burdened with cares, but there is never a trace of that inner shadow that betrays anxiety of conscience or fear of an irreparable return to loneliness, Their youth never seems to fade away, as long as the sweet fragrance of a crib remains in the home, as long as the walls of the house echo to the silvery voices of children and grandchildren.
“Their heavy labors multiplied many times over, their redoubled sacrifices and their renunciation of costly amusements are generously rewarded even here below by the inexhaustible treasury of affection and tender hopes that dwell in their hearts without ever tiring them or bothering them.
“And the hopes soon become a reality when the eldest daughter begins to help her mother to take care of the baby and on the day the oldest son comes home with his face beaming with the first salary he has earned himself. That day will be a particularly happy one for parents, for it will make the spectre of an old age spent in misery disappear, and they will feel assured of a reward for their sacrifices.
“When there are many children, the youngsters are spared the boredom of loneliness and the discomfort of having to live in the midst of adults all the time. It is true that they may sometimes become so lively as to get on your nerves, and their disagreements may seem like small riots; but even their arguments play an effective role in the formation of character, as long as they are brief and superficial. Children in large families learn almost automatically to be careful of what they do and to assume responsibility for it, to have a respect for each other and help each other, to be open-hearted and generous. For them, the family is a little proving ground, before they move into the world outside, which will be harder on them and more demanding.”
Vocations
“All of these precious benefits will be more solid and permanent, more intense and more fruitful if the large family takes the supernatural spirit of the Gospel, which spiritualizes everything and makes it eternal, as its own particular guiding rule and basis. Experience shows that in these cases, God often goes beyond the ordinary gifts of Providence, such as joy and peace, to bestow on it a special call — a vocation to the priesthood, to the religious life, to the highest sanctity.
“With good reason, it has often been pointed out that large families have been in the forefront as the cradles of saints. We might cite, among others, the family of St. Louis, the King of France, made up of ten children, that of St. Catherine of Siena who came from a family of twenty-five, St. Robert Bellarmine from a family of twelve, and St. Pius X from a family of ten.
“Every vocation is a secret of Providence; but these cases prove that a large number of children does not prevent parents from giving them an outstanding and perfect upbringing; and they show that the number does not work out to the disadvantage of their quality, with regard to either physical or spiritual values.”
Martin Pistorius fell into a mysterious coma when he was a vibrant 12-year-old boy in the 1980s.
He found himself locked inside his own body – unable to speak, make eye contact or even move his own limbs.
Martin’s doctors told his parents, Rodney and Joan Pistorius, that the boy had cryptococci meningitis. They said Martin should be taken home to die in peace.
But Martin would live 12 years in that vegetative state.Joan said, “Martin just kept going, just kept going.”
According to NPR, Martin’s father would wake up every day at 5 a.m., dress the boy, put him in the car and drive him to a special care center.“Eight hours later, I’d pick him up, bathe him, feed him, put him in bed, set my alarm for two hours so that I’d wake up to turn him so that he didn’t get bedsores,” Rodney recalled. And during those 12 years, according to the Pistorius family, there was never any indication that Martin’s condition was improving.One day, Joan, in a state of hopelessness, told her son, “I hope you die.”She never imagined that Martin would have understood those dreadful words.
But by the time he was 14 or 15 years old, Martin began to awaken.“Yes, I was there, not from the very beginning, but about two years into my vegetative state, I began to wake up,” Martin recalls. “I was aware of everything, just like any normal person. Everyone was so used to me not being there that they didn’t notice when I began to be present again. The stark reality hit me that I was going to spend the rest of my life like that – totally alone.”Martin had even heard his mother’s cruel words.
“You don’t really think about anything,” he said. “You simply exist. It’s a very dark place to find yourself because, in a sense, you are allowing yourself to vanish.”Martin added, “As time passed, I gradually learned to understand my mother’s desperation. Every time she looked at me, she could see only a cruel parody of the once-healthy child she had loved so much.”At the care center every day, Martin’s caregivers played “Barney” reruns. They too believed he was a vegetable.He said, “I cannot even express to you how much I hated Barney.”
Now Martin, 39, is in full control of his body. He’s married and lives a normal life in Harlow, England.
In his book “Ghost Boy,” he writes, “My mind was trapped inside a useless body, my arms and legs weren’t mine to control and my voice was mute. I couldn’t make a sign or sounds to let anyone know I’d become aware again. I was invisible – the ghost boy.”
LOS ANGELES, CA (Catholic Online) – During the wedding ceremony of the son of one of his close allies, Mustafa Kefeli, Erdogan stood up and addressed the bride and groom.
“One or two (children) is not enough. To make our nation stronger, we need a more dynamic and younger population. We need this to take Turkey above the level of modern civilizations,” exclaimed Erdogan.
Contraception risks causing a whole generation to dry up, according to Erdogan.
“Lineage is very important both economically and spiritually,” he said in comments reported by the Dogan news agency. “I have faith in you.”
Aside from lecturing on the dangers of contraception, Erdogan praised marriage saying, “Marriage is a long journey. There are good days and bad days. Good days become more frequent as we share them and bad days finally bring happiness if we are patient.”
“Marriage is more than a civil contract; it is a lifelong covenant of love between a man and a woman,” states the United States Conference of Catholic Bishops teachings on Married Love and the Gift of Life.
This love differs from any other kind in the world. Two people are joining together as one.
While couples share good and bad days, laughs and tears, “the power to create a new life with God is at the heart of what spouses share with each other.”
Erdogan has previously been criticized for his proposals against abortions, the morning-after pill and Caesarian sections, but declaring contraceptive use as treason appears to be his strongest attack.
The Catholic church teaches “suppressing fertility by using contraception denies part of the inherent meaning of married sexuality and does harm to the couple’s unity.”
Although contraceptive use may not entirely be treason, the Catholic church teaches it is against God’s will.
Many have found that living by this teaching contributes to a more intimate, open and honest marriage allowing for couples to feel truly fulfilled.
Alliance Defending Freedom, the Charlotte Lozier Institute, and the Family Research Council voiced concern to the U.S. Department of Health and Human Services and the U.S. Office of Personnel Management Monday over proposed rules that continue to allow the cover-up of abortion surcharges in Obamacare.
Although federal law prohibits taxpayer subsidies for elective abortions, regulations under the Affordable Care Act prevent disclosure of the abortion surcharge to customers, who then unknowingly pay the fee to cover elective abortions.
“No one should be forced to pay a secret fee to cover other people’s elective abortions,” said ADF Senior Counsel Casey Mattox. “The Obama administration needs to stop deceiving the American people and coercing them to fund abortion. No matter where a person stands on abortion itself, everyone should be able to agree that this type of intentional and illegal deception is wrong and should stop.”
The ADF comment filed with HHS and OPM explains that the proposed rules fail to protect consumers because they continue “to permit insurance companies to confuse abortion coverage and conceal the abortion premium surcharge.”
“If Americans are to be forced off their existing, chosen insurance plans and into the ACA insurance exchanges regulated by your agencies, they should at least be entitled to full disclosure of the contents of the plans on those exchanges and what they are paying for,” the comment states. “Unfortunately, the proposed rules do not protect consumers, and in fact may continue to mislead them into enrolling in abortion-including plans and paying for others’ abortions in violation of their conscience.”
“Whatever one’s views of abortion, the current exchanges and plans regulated by your agencies do not protect any ‘right to choose’ abortion coverage,” the comment continues. “In fact, they leave many Americans without a choice that fits both their health needs and respects their right of conscience. They deceive and compel Americans to pay for others’ elective abortions. This is unconscionable and within your power to correct.”
The Charlotte Lozier Institute and Family Research Council have collaborated on a new website that allows citizens to find out whether their Obamacare plans cover elective abortions and thus require the hidden abortion surcharge.
by Sarah Zagorski | Washington, DC | LifeNews.com | 12/30/14 12:52 PM
ill Duggar, daughter of Bob and Michelle Duggar from the reality show, 19 Kids and Counting, celebrated Christmas with her family and shared with the world that she and her husband, Derrick are thankful for their baby that’s on the way.
On Christmas Day, Jill, 23, posted a photo on Instagram of her baby bump wrapped up like a present. Jill’s wrapped baby bump had a note that read: “To: Jill & Derrick, From: God.”
Jill captioned the photo on Instagram, “Merry Christmas from the Dillard’s! As we rejoice in the celebrations around the birth of Jesus Christ, we thank God for our precious little gift! “For unto us a child is born, unto us a son is given: and the government shall be upon his shoulder: and his name shall be called Wonderful, Counselor, The Mighty God, The Everlasting Father, The Prince of Peace.”
On June 21st, Jill and Derrick got married in Springdale, Arkansas in front of 1,000 guests, including family and friends. Jill and Derrick met through Jill’s father, Bob Duggar and announced earlier this year that they’re expecting their first baby, a boy, in March 2015.
This past year the Duggar family has been the subject of much controversy because of their pro-life and Christian views. In fact, in November the liberal website Change.org organized a petition to pressure TLC to cancel “19 Kids and Counting” and gathered over 180,000 names. They accused the Duggar family of “using their fame to promote discrimination, hate, and fear-mongering” and criticized JessaDuggar’s comment on Instagram comparing abortion to the Holocaust.
However, their petition to cancel the popular reality show was unsuccessful and Jim Bob Duggar said it just gave them “more exposure.” As LifeNews previously reported, this isn’t the first time a Duggar has spoken out against the abortion holocaust. In 2013, during the Family Research Council’s Values Voter Summit, Jim Bob Duggar said, “We have since 1973 (when Roe v. Wade was decided) had 55 million abortions, so what we have going on is a baby holocaust.”
Babies who are 23 weeks into pregnancy qualify for legal abortions in Britain and other nations around the world, but doctors did their best to save Baby Connor when he was born prematurely.
Now, his parents say the abortion limits in Great Britain should be lowered so babies who are old enough to live outside the womb are not killed in abortions.
Before birth, scans revealed the baby had a heartbeat and she and her partner Craig Walkow told doctors they wanted them to save him. But they were told Connor would be treated as a miscarriage. If they wanted to save their son they were told to find a specialist hospital, so Connor parents fought for him to be moved 39 miles from Milton Keynes to Oxford.
A day later Connor was born at 23 weeks and two days weighing 1lb2oz.
When he was born, Connor was covered from the neck down in the liquid-filled freezer bag to improve his chances of surviving. Doctors told his mother they would act if he showed signs of life and he did. So they put the little guy in a polythene sleeping bag to mimic being in the womb so he would have a better chance at growing and his heath improving in those early hours, days and weeks after delivery.
Eventually, Connor had three operations for a perforated bowel, suffered from fungal meningitis, chronic lung disease and a bleed to the brain. He also needed laser eye surgery after his eyes failed to develop properly.
But, Connor is doing better now and has celebrated his first birthday. And his parents say it’s time to re-evaluate the legality of abortions done on premature babies.
Rachel Crockett, 25, and partner Craig Walkow, 38, of Wing, Bucks, now want this cut-off point and the abortion limit – also 24 weeks – cut to 20 weeks.
Rachel said: “We were told to say goodbye to Connor and that we wouldn’t see him again. It felt like the end of the world, we were numb.
“We just had to sit there and wait for the nurse to say the worst, there was such relief when they told us he was OK.
“Later on the consultant came by and looked in on him – he could not believe Connor looked so well.”
Rachel added: “I think the cut off point and abortion limit should be lowered to 20 weeks – especially considering what happened with Connor. “By then they are a person.”
An unborn child is a person long before that — their unique humanness begins at conception — but her point is well taken that abortions on babies, especially at this stage of pregnancy, are inhumane.
by Carole Novielli | Washington, DC | LifeNews.com | 12/30/14 12:00 PM
CNN’s Poppy Harlow interviewed Milwaukee Sheriff David Clarke about the recent protests that some in the Black Community have sparked after the police related deaths of Michael Brown and Eric Garner.
Harlow asked the Sheriff, who has been on several news shows on Fox and others, about a tweet he sent out implying that if Black lives mattered the protesters would be outside abortion clinics because of the high numbers of black babies killed by abortion.
The tweet sent by Sheriff Clarke, a black man himself, was sent to Mitch Smith, Journalist in the Chicago bureau of The New York Times and read, “If only these faux protesters were asked by media about all the black on black killing or black babies aborted in US every year.“
Poppy asked the Sheriff if he sent the tweet, “Yes I did,” Sheriff Clark responded.
He continued, “When I hear these things that Black lives matter, the only people who really believe that statement are American police officers who go into American ghettos every day to keep people from killing each other. Alright, so, yes I did say that and I meant it. Look, the abortions? If Black lives – if they really mattered, that’s where the outrage would be that’s where we’d see protests…”
This blog has proven time and again that abortion targets the Black community. Stats released by the CDC again prove that minorities are killed by abortion in disproportionate numbers. In fact, according to the most recent numbers, 36.2% of the total number of abortions recorded for race or ethnicity were reported on Black women.
Mississippi, which currently has only one abortion clinic in the state, had the highest number of abortions reported on Black women coming in at 63.4%.
Alabama, reported that 58.7% of their abortions were on Blacks while in Georgia they reported 52.1% abortions on Black.
Tennessee performed 49.9% of their abortions on Black women and Virginia performed 43.9% on Black women, while Michigan’s Black abortion percentage was 47.9%.
New York City alone performed 46.1% of their abortions on Black women and 41.1% of Black abortions was reported in Missouri.
It is a known fact that a majority of abortions are performed by Planned Parenthood.
So that begs the question, initiated by Sheriff Clark, if Black Lives Matter, and they certainly do, why is it that the one place known for killing off black babies and a black woman is not being protested?
LifeNews Note: Carole Novielli is the author of the blog Saynsumthn, where this article originally appeared.
Joe and Christine began their marriage willing to accept every child God would send them, and trusting totally in His spiritual and material support in that generous decision. They surely knew that if God responds with equal generosity, there will be great joy, many twists and turns, some sadness, and a substantial need for sacrifice. Christine tells their story!
MISSION Most Wonderful, Our testimony of trust
Nov 6, 2014
Each married couple is called into a cooperative mission with GOD. It is up to them to discover what that mission is. It has been such a blessing for my husband and me to receive 11 gifts of life. We always believed that being open to life was healthy and that God would help us feed, clothe and provide for as many children as we received. This agreement/commitment from the beginning of our marriage removed a ton of fear, doubt, over thinking, and stress from our life. Our mission was to grow a healthy family.
We could never have predicted the crazy turns and tests we would face as we joyfully seemed to announce a new family member every two years or so. Occasionally I cried with a new pregnancy just because I wasn’t surrounded by supportive people, but my husband assured me it was all good and “we could do it”! “WE” being the operative word! Each birth was a real celebration! I got bolder with do-gooders who dropped their jaws or gasped when they found out how many children we had. We learned to laugh a lot!!
After a miscarriage with our 9th blessing we clung to our faith and realized how fragile life was. We weren’t sure if there would be any more babies? We didn’t “need another child” but we assured each other and God that we were still open and willing to trust HIS timing. Our little MaryClaire came into the world in August of 2006. Joe and I were 42. Our oldest son was 20. Turns out we did need another child and God knew it!
In 2007 we began discerning moving our family to a new town—to live in, and help run a homeless mission. We let go of all job and insurance security and Joe became the Executive Director of a shelter, free clinic and food bank. ALL of us, 9 kids and parents, worked together serving the needs of others. This was a very positive experience. We loved it. Our family thrived and blossomed.
Boom! 2012 my husband’s minor health issues snowballed into major health issues. In March 2014 he’s finally diagnosed with Lyme disease. We all pitched in to keep the mission running. He begins aggressive treatments, becoming bedridden, riddled with pain, and loses his ability to focus or concentrate.
My mother becomes very ill in April, and dies in June. She was our champion, prayer warrior and full time cheerleader!
Another challenge to face. In July 2014, Joe sees some windows of health with IV therapy. We have some positive moments and become optimistic. Not to last though as he develops blood clots, has to come off Lyme treatment, essentially starting over. Strong oral meds caused Liver and Kidney problems. Come on GOD…what’s up with all of this?!!
Boom! At 50 years old and being sure it’s a not-so-funny menopausal trick, we have a positive pregnancy test!!! Second test….still positive. I announce pregnancy during a family game of Pictionary/Charades…my husband is rendered speechless!!! Images of Zechariah dance in my head. We are over the moon afraid to get too excited, but bursting with joy!! In the midst of suffering God has permitted new life and celebration!!!! …What’s up with all of this?!!
Boom! On August 19, 2014, Joe is fired–no warning, discussions or transition—due to his health, it appears. Given six hours’ notice, we have 30 days to relocate with no income, a desperately sick husband, fragile pregnancy, no money….and I mean NO savings or cash flow. We lived simply like those we served for 8 years, trusting God every day. Now we have become homeless and needy. Hey God, what’s up with this!?
Our parish gave us an empty rectory; friends and strangers have provided a steady flow of support. Meals, food, clothing, transportation, appliances, gift cards and all kinds of tokens of love have made their way to our door. God is loving us through His people! Our children are blanketed with goodness, kindness, and learning to receive many blessings. We are learning to forgive and persevere.
We know that many in this world would shake their finger and say you shouldn’t have had so many children; you shouldn’t be having another; you shouldn’t have given up security to give your lives to a non-profit serving others; etc, etc… But, in our Catholic world we don’t hear those words; we seek affirmation; we express trust, love and faith in our God who has it all under “control”. We go about our life, living without fear, allowing others to see our human imperfections and allowing the world to see our joy.
We share all of this to affirm couples! With age comes wisdom. Sometimes with age comes baby! “Trust in the Lord with all of your heart and lean not on your own understanding.”(Proverbs 3:5) Pray for all families to find their mission and thrive in peace and love!!
I love you. You know I love you dearly. I pray and fast for you every single day. But why don’t you ever give homilies on sex?
It’s a good question!
I am 34 years old and I have never, ever, not once, heard a priest talk about sex – either in or out of the pulpit. My mum is in her 70’s and she cannot recall ever hearing sex mentioned in church AT ALL throughout her entire life.
I have been thinking about why this could be:
1. This is Britain, and we don’t talk about that sort of thing. 2. Priests are celibate and don’t feel confident talking about sex. 3. There could be children in the congregation. 4. It’s embarrassing. 5. Telling people that artificial contraception is bad would be a very unpopular homily.
It’s a shame because it is becoming more and more obvious that the Catholic teaching on sex is one of THE biggest tools of evangelization in the modern age. The Catholic teaching on chastity, sex and marriage is completely and utterly counter-cultural. It teaches life in our ‘culture of death’. It is so radical that even you, the Priests don’t want to talk about it. (BTW, please don’t use ridiculous terms like ‘nuptial union’ and ‘conjugal act’!!! Instead use terms such as ‘make love’ and ‘have sex’, or if there are lots of children present say ‘be together’ or ‘be intimate’.)
From my own limited observations, I am confident to say that most people inside and outside of the church have absolutely no idea what the Catholic teaching on sex actually is. The vast majority have never read, or even heard of Humanae Vitae or Theology of the Body. They don’t know about NFP, Billings, Creighton or Napro technology which offers a natural alternative to IVF. They have no clue as to the damage artificial contraception is having on their bodies, their relationships or their souls. Because of this (and I use this word respectfully)… ignorance, they cannot understand why the church opposes gay marriage.
There is call now from liberal Catholics and dissident groups such as ‘A Call To Action’ to publish the results from the recent Vatican survey. They are of course hoping to highlight the fact that most Catholics ignore the church teaching on artificial contraception – and then get the teaching on sex officially ‘modernised’.
It is time for you, Priests, to start teaching your congregations what sex and marriage IS not just what it isn’t. Because if you don’t speak about it, who will? I’ll tell you… the extremely vocal gay lobby. The sex saturated media. The secularist lefty politicians. The money-making contraception and abortion industry (yes, it is an industry, with sales targets and bonuses and advertising campaigns.)
Please, Priests, do us a favour… learn Theology of the Body and Humanae Vitae like your life depends on it. Give it to us, your congregations in bite sized chunks each week. Trust me, the second you mention the word sex, you will have every eye and ear in the whole place focused on you. No one will be reading the newsletter or checking their Facebook status through that homily!
Visit 1flesh.org and catholicmarriagecentre.org.uk and the Couple to Couple League for tons of info. Explain the awful truth about the history of artificial contraception and its links to eugenics from people like Marie Stopes and Margaret Sanger. Find out who your local NFP teacher is and invite them to your parish. Start the conversation within your own parish and keep it going. Because if you don’t preach the beauty of Gods design on sex and marriage, no one will. Please don’t leave us to fight this battle on our own…
I had a thoroughly good time this morning. A nice young man from BBC Radio 4 came round to interview me for like 2 hours on how people view Pope Francis. He was very interested to hear that i identify as a totally orthodox catholic but i am also totally pro Francis. I will post the interview here when it airs at the beginning of October (please pray that they edit it fairly!).
I have had many discussions online recently regarding Pope Francis where the tone has been rather negative to say the least. It seems that my orthodox buddies just don’t get Francis. At best people think he is sloppy at his job and at worst they think he is single handedly going to destroy the catholic church!
There are several reasons for this:
1. He is not Benedict.
Benedict was just the most wonderful pope for the orthodox catholic community. He sorted out the liturgy, he loved and embraced the ‘traditional’ parts of Catholicism in a very visible way, he was a master theologian. He was old skool and rock steady. Orthodox catholic’s were extremely comfortable under Benedict.
Francis on the other hand has shunned many ‘traditional’ things ie. the red shoes, the papal apartment, the pomp and the highly bejewelled vestments ect… He has a completely different, simplistic style. He breaks with tradition in a big way.
I think there is a temptation to misunderstand Francis here. He is only breaking with tradition on superficial matters. If you take the time to really listen to his homilies and read Evangelii Gaudium (or a summary of it – it is 51,000 words long!) you immediately see that he is a completely orthodox pope. The man knows he is not God. He is not trying to change doctrine or re-write the 10 commandments or ‘loosen the rules’. What colour the man’s shoes are makes no difference to his capability to lead the people of God for goodness sake!
2. He uses ambiguous language.
Many orthodox catholic’s i have spoken to have described Francis’ ‘conversational’ style to be wishy-washy at best, and open to wrong interpretation at worst. Personally I think this style of speaking to be extremely clever. I believe he uses ambiguous language on purpose. It is difficult for the fringe catholic to immediately reject something that he/she might agree with in part… Francis understands modern western culture. He understands modern man’s lack of respect and suspicion of authority. He understands the moral relativist media style we have all become so accustomed to hearing. In fact the style Francis uses is actually very biblical in nature. Jesus spoke in parables which people could easily understand and interpret in different ways – the core element of the teaching is still the same, but the interpretation of how it actually effects your life is individually relevant to each listener on a personal level. Francis’ style actually encourages the reader to look within themselves and apply what is being said to their own lives.
The ugly side to this of course is that people on both sides of the fence can take ‘some’ of the information and misunderstand what has really been said ie the “who am i to judge” comment.
3. He challenges the Orthodox catholic to evangelise.
Something i have certainly been guilty of in the past has been to sit up nice and tall on my theological and moral high horse. Even though i still am in no doubt that I AM RIGHT, high-horsing is never going to work in terms of evangelisation.
Francis is a man of great humility. Just as Christ did, Francis meets people where they are on their journey of conversion. He doesn’t point the finger or condemn, but instead sees the person behind the sin and encourages them into a deeper relationship with Christ. This requires sensitivity, kindness, compassion and patience.
By his example, Francis challenges us to evangelise in the same way. Essentially the Gospel is a message of mercy and forgiveness. Christ died for every single human being who has ever lived out of total pure love including all members of ISIS and Adolf Hitler and paedophiles. He loves and values every human being the same as he loves you. This is the radical message of Christianity. Introducing people to this love, to this person – Jesus Christ – is the first step.
We are called not only to preach love, but to be love to others. For those of us who are secure and solid in our faith the weight of responsibility is much, much heavier regarding evangelisation. If we don’t get out there and start proclaiming the truth, other will (and their version of the truth is well, not true!) But it is how we approach our brothers and sisters that is key. Calling someone ‘a homosexual’ or ‘a muslim’ or a this or that in a negative tone, dilutes their humanity. This makes the person defensive. This is not bringing Christ to them. Im not saying sweep all the other stuff under the carpet – not at all, what i am saying is that they will never understand and accept the doctrine without first having a relationship with Christ. You have to BE Christ to them as you build bridges of trust, and respect where they are on their journey of conversion.
Pope Francis understands this. He is out there doing it. And you might, just might, have totally misunderstood what he is doing.
I’m just going to go ahead and let you know that this article is going to probably anger a lot of people. But I am a truth teller, and sometimes truth hurts. And as pro-lifers, this is information that we simply can’t ignore…no matter how much it affects our current lifestyle.
This is the first of a three-part piece on hormonal contraception. I hope you will read all three parts and share this factual information with people who may not know these truths.
The pro-life mantra has always been “Life Begins at Conception.” But do we really believe that? Do we really believe that life begins at that amazing moment of conception? Or do we actually believe that it begins at implantation? You may think that is a silly question. ‘Of COURSE pro-lifers believe that life begins at conception! Hello?! We have been saying that for years!’
Well, then here’s the kicker. If you believe that life begins at conception, then you MUST unequivocally oppose hormonal contraception. Here’s why. Hormonal contraception does not always prevent ovulation. In fact, many studies done by the birth control manufacturers themselves state that only about half of women using their methods actually cease ovulating.
Hmm. So how do these methods work if you are still ovulating at least half the time? Simple. These methods have a backup plan. Hormonal methods also work to thin the lining of the endometrium (uterine wall) so that a newly conceived human being (life begins at conception, right?) cannot implant on the uterine wall. Because the baby has nowhere to implant, they are spontaneously aborted.
Don’t believe me? View the screenshots of the information that comes directly from the manufacturers, or follow the links:
Will sexually active women abort their babies every cycle? Probably not. But you may. You don’t know, and that’s the scary (and morally troubling) part.
Let’s say that a demolition company was going to use a wrecking ball to destroy an old school. When the supervisor of the company asks the principal if they made sure to clear the building, the principal says, “We most likely did. We aren’t 100% sure, but we are pretty confident.” Would that be acceptable? Would you be willing to push that button that releases that wrecking ball? Would you be willing to risk that there may or may not be life in that building?
If you take hormonal contraception and you are sexually active, then you are releasing that wrecking ball every month.
Luckily, there is a way to space pregnancies without the potential loss of life. It’s called Natural Family Planning. There are MANY different methods and sometimes it takes trying a couple before you find the right one for you. I recommend visiting www.iusenfp.com to explore the various methods out there.
And just in case you are one of those people who say, “I have to take birth control because of xyz health condition,” you actually don’t. I’m going to write another article on this, but I will tell you that by taking birth control, you are masking the problem, not solving it. NFP and NaPro technology can actually FIX the problem. You can find more information at www.fertilitycare.org.
Ladies, we have been force fed the idea that we must fix our unbroken fertility…and that our fertility solely falls on our shoulders. But here’s the reality. Fertility should be shared between a husband and wife. You don’t get pregnant on your own. NFP is a beautiful way to help you share in that gift. It’s worth your time to check it out.
1. There will never be a meal where everyone is happy with the food.
2. Getting a table at a restaurant will take at least half an hour no matter where you go.
3. Car trips to far away places are more crammed than Target on Black Friday.
4. Someone is always around to watch a movie.
5. Someone will always being talking during that movie.
6. If they are close to your age and size, clothing is communal.
7. The youngest will be the favorite child.
8. There will be alliances within the siblings and you better make sure you have a buddy.
9. Everyone has their spot on the couch and will not be afraid to throw a couple elbows your way to defend it.
10. Everyone will refer to so you as “so and so’s older/ younger sibling” instead of your actual name.
11. Sneaking extra people into a hotel room will be a normal vacation activity.
12. Sharing a room is just something you will have to do forever.
13. When mom and dad get in a cleaning mood it is best to round up the troops and take a sibling trip to anywhere but home.
14. Someone will always do the least amount of work and somehow get away with it.
15. Holidays are never a bore because someone is always in for some shenanigans.
16. You have a brother or sister to suffer through awkward family moments.
17. There will always be someone who catches your movie references because they have seen “School of Rock” just as many times as you have.
18. Your cheering section for your soccer games is always larger than everyone else’s.
19. Getting a picture where everyone actually looks like a human is near too impossible.
20. Group chats will mostly consist of people asking who is on the Netflix and to please get off so you can watch your show.
21. You will be called every other person in your family’s name before your mom actually calls you the right one.
22. Board games will never end well because someone is cheating and someone else is a sore loser.
23. If you complain about your siblings it’s fine, but the second anyone else does all hell breaks loose.
24. People will get confused when you start talking the shorthand that your siblings and you have crafted over the years.
25. Even the family size option of a good cereal will be gone in a single day.
It’s not always easy having a lot of siblings. There will be days when you wonder why your parents thought your siblings were a good idea at all. There will be days when you literally cannot be in the same room as them. The thing is though, there will also be days were you and your siblings all belt the words to “Do You Know” by Enrique Iglesias together. There will be days that you all sit around talking and laughing about the horrible restaurant your dad made you go to in the Everglades. And when all else fails, they will indeed bail you out of anything, even jail.
It has long been known that the American way of life is being greatly threatened by the fragmentation of the family. A recent book featuring experts of all kinds who bemoan this phenomenon is Mitch Pearlstein’s Broken Bonds: What Family Fragmentation Means for America’s Future.
Jonathan Last, in a review of Pearlstein’s book, states, “The social capital created by traditional families is what undergirds the rest of our society. Sociologists and economists now understand that when this social capital is diminished, it causes all sorts of other problems. The crises of the welfare state, wage stagnation, income inequality, unemployment, the prison-industrial complex — all of these, and much more, can be traced to the breakdown of the family.”
The “fragmented family” refers to more than just the 50% of marriages that end in divorce, but also to the fact that many children never really have a family, since they are raised by mothers who have never married. It is not easy to come up with a precise number, but it is certainly true that, of the children who escape being aborted in the United States, the majority will not be raised by their married biological parents; one parent is likely to be missing, and it is usually the father.
The experts don’t know what to do, I would guess, largely because they can’t identify the causes. In fact, this book is not designed to propose solutions; its purpose is to get scholars, politicians and activists to realize that family fragmentation is a problem.
We in the Church are way ahead of the experts and activists. We have known for a very long time that to destroy the family is to destroy a culture. We also know a major reason for the destruction — and a workable solution.
We know that the major cause of the “sexual revolution” was the invention of the pill (even secularists such as Francis Fukuyama have written on the disruptive influence of the pill). When people remove the baby-making power from the sexual act, all hell breaks loose.
The fact that sex can result in a pregnancy has been the most powerful reason historically that minimally responsible people have waited until marriage to have sex. When that possibility is negated, people have sex outside of marriage, babies are born outside of marriage, people prepare poorly for marriage, and marriages break up, etc. Women — children and men, too — are more likely to be poor in this scenario.
To connect all of the dots would take a book (Mary Eberstadt connects the dots in her book, Adam and Eve After the Pill), but perhaps these dots are sufficient: The “sexual revolution” has led to too many children for several generations being raised without fathers; those children do not learn how to manage life well, and the cycle perpetuates itself. Many people who have not matured are raising the next generation, and the possibility of them maturing is negligible.
The other reason for not having sex outside of marriage is that to do so is a violation of God’s plan for sexuality. Religious people, especially Christians — especially Catholic Christians — should know how wrong and harmful sex is outside of marriage.
But the culture and the availability of contraception have clouded people’s intellects and weakened their wills, to the point that many Christians, Catholic Christians as well, conduct their sexual lives as foolishly as the rest of the culture.
Now, it is not likely that experts, scholars, politicians and activists are soon going to connect the dots. After all, they are just catching onto the fact that there is a problem.
But, as was said previously, those of us truly shaped by the Christian understanding of human nature and of reality are not in the dark about what the real problem is and what the real solution is. Even more than that, we have developed quite an abundance of good materials to get the job done.
Again, what is the job? The job is convincing people that sex outside of marriage is stupid, wrong and against their happiness and the well-being of their children. That requires that we teach them that contraception is stupid, wrong and against their happiness and the well-being of their children.
Do we have any hope of doing that?
Well, possibly yes, if it is done in the context of the New Evangelization. The New Evangelization means that we must help those who have been baptized Catholic to fall in love with Jesus and the truths that he teaches through his Church.
Many people, especially those from divorced households or those raised by unmarried mothers and parents, have a lot of misery in their being. We must introduce them to Jesus, the Divine Healer, and to the Church, aptly called by Pope Francis a “field hospital.”
Our priests need to speak to those wounds from the pulpit: Are you broken and confused? We have what you need: Jesus. He will give you graces to cope with the madness of this world that has seeped into your lives.
Jesus gives us grace through the sacraments and instruction through the various teaching mechanisms of the Church. Take advantage of these gifts. Sit in front of the Blessed Sacrament. Ask Jesus to heal you with his love.
All of us who wish to bring people out of darkness into light and out of misery into joy must be radical disciples of Christ himself. We must keep working to cut any compromise with comfort-seeking out of our lives.
The fact that the beatification of Blessed Pope Paul VI took place during the closing ceremony of the Extraordinary Synod of Bishops on the Family was interpreted by some of us as a manifest sign that the synod would closely ally itself with Humanae Vitae. That did not happen for the first part of the synod, which, as the interim report indicated, seemed preoccupied with how to deal with the question of the reception of the Eucharist by those who have been divorced and remarried without benefit of an annulment and with the proper pastoral response to those with same-sex attractions.
The final report, however, rang a positive note about Humanae Vitae, so we can have some hope that the Ordinary Synod of Bishops on the Family, to be held in 2015, will pay significant attention to Humanae Vitae and how the failure of bishops and priests to preach and teach the truths of Blessed Paul VI’s 1968 encyclical has been seriously detrimental to the family.
We can hope that, between now and next fall, the participants in the synod will come to realize what gold we have in St. John Paul II’s theology of the body, which he wrote to defend the truths of Humanae Vitae. The many programs for youth, for the engaged and married based on the theology of the body are a true work of the New Evangelization.
There is one institution on the face of the earth that has the answers to the problems we face; if it does not use the resources available to it, the family will continue to fragment — and then woe be to us all.
Bishop James D. Conley has announced that many of the faithful in the Diocese of Lincoln will see something significantly different when they go to Mass this Advent. From the bishop’s column in this week’s Southern Nebraska Register:
“In the season of Advent, as we recall Christ’s Incarnation at Christmas, we are reminded to be prepared for Christ’s coming. In the Gospel for the First Sunday of Advent this year, Nov. 30, Christ tells us his disciples “to be on the watch.”
“We remember that Christ is coming whenever we celebrate the Holy Sacrifice of the Mass. In the Holy Mass we are made present to the sacrifice at Calvary, and to the joy of Christ’s glory in heaven. But we also remember that Christ will return, and we remember to watch, to be vigilant, to wait for him, and to be prepared.
“The Mass is rich with symbolism. The vestments of the priest remind us of the dignity of Christ the King. We strike our breasts, and bow our heads, and bend our knees to remember our sinfulness, God’s mercy, and his glory. In the Mass, the ways we stand, and sit, and kneel, remind us of God’s eternal plan for us.
“Since ancient times, Christians have faced the east during the Holy Sacrifice of the Mass to remember to keep watch for Christ. Together, the priest and the people faced the east together, waiting and watching for Christ. Even in Churches that did not face the east, the priest and people stood together in the Mass, gazing at Christ on the crucifix, on the altar, and in the tabernacle, to recall the importance of watching for his return. The symbolism of the priest and people facing ad orientem—to the east—is an ancient reminder of the coming of Christ.”
“But the symbolism of facing together, and awaiting Christ, is rich, time-honored and important. Especially during Advent, as we await the coming of the Lord, facing the east together—even symbolically facing Christ together at the altar and on the crucifix—is a powerful witness to Christ’s imminent return. Today, at a time when it is easy to forget that Christ is coming—and easy to be complacent in our spiritual lives and in the work of evangelization—we need reminders that Christ will come.
“During the Sundays of Advent, the priests in the Cathedral of the Risen Christ will celebrate the Mass ad orientem. With the People of God, the priest will stand facing the altar, and facing the crucifix. When I celebrate midnight Mass on Christmas, I will celebrate ad orientem as well. This may take place in other parishes across the Diocese of Lincoln as well.“
Make no mistake about it, this is big news. In many ways the near total disappearance of mass offered facing the altar has been the liturgical story of the past fifty years. While not required by the Second Vatican Council, versus populum has become the de facto norm in the Ordinary Form. For the faithful more often than not these days, it is only in the Extraordinary Form that the priest offers the mass ad orientem.
In his seminal work The Spirit of the Liturgy, Joseph Cardinal Ratzinger discussed the ramifications of the post-conciliar change in liturgical orientation:
“The turning of the priest towards the people has turned the community into a self-enclosed circle. In its outward form, it no longer opens out on what lies ahead and above, but is closed in on itself…For just as the congregation in the synagogue looked together toward Jerusalem, so in the Christian liturgy the congregation looked together “towards the Lord.” As one of the Fathers of Vatican II’s Constitution on the Liturgy, J. A. Jungmann, put it, it was much more a question of priest and people facing in the same direction, knowing that together they were in a procession towards the Lord. They did not close themselves into a circle, they did not gaze at one another, but as the pilgrim People of God they set off for the Oriens, for the Christ who comes to meet us.”
Bishop Conley expresses a similar view in his column when he explains:
“In the ad orientem posture at Mass, the priest will not be facing away from the people. He will be with them—among them, and leading them—facing Christ, and waiting for His return.”
Sincerely pray for more bishops to step forward and also offer such a courageous example to the priests and laity of their dioceses. May they recognize that by offering the mass ad orientem during Advent, Bishop Conley will be catechizing the faithful while restoring authenticity and continuity to the liturgy.
I would like to tell a story of pro-life victory, a story of life. A young woman named Diana told the following story on the “Stories from the Sidewalk” series.
“I’ll never forget the day I found out I was pregnant. It was October 7, 2012. I had just returned from a retreat when I took a pregnancy test. I couldn’t believe it. I was active at Texas State’s Catholic Center and was a member of the Catholic sorority. I couldn’t let anyone find out I was pregnant – what would they say?
The baby’s father didn’t want a child and said he would pay for an abortion. Without his support, afraid of what others would say, and since I was expecting to graduate in just a few months, I scheduled an abortion.
I was the only person in the waiting room. I was really scared. The doctor had me sign some papers that he went through quickly. The examining room was dim and cold. There weren’t any pictures or posters like most doctor’s offices. He couldn’t confirm the pregnancy, so he asked me to reschedule.
The next few days, I tried to live life as usual, but kept thinking of that little person inside me. Fortunately, one of my sorority sisters told me about [The John Paul II Life Center]. I didn’t want to go, but eventually, I did.
The JPII Life Center was very different from the abortion facility. It was warm… welcoming. Instead of doing the sonogram to determine how much they would charge me, they gave me one for free. I’ll never forget that sonogram. The doctor told me to lay very still. Then, he showed me the most breathtaking sight I had ever seen – a tiny pulse of red and blue. My baby’s heartbeat! I was only about 5 weeks pregnant, but my baby’s heart was already beating. I knew I couldn’t abort my child.
But later, reality hit. My mom made it very clear that she wanted nothing to do with me or my baby. If I didn’t have an abortion, I would lose my cell phone, my car, my tuition, my apartment. Without the help of my parents, there was no way I could finish school or support myself. How could I take care of a baby?
I choked back tears as I made an appointment at another abortion clinic. Thankfully, God placed the right person at exactly the right time in exactly the right place. As I drove up to [the abortion clinic], I saw a familiar face praying outside the clinic. Then, I heard my name. “Diana, what are you doing here?”
It was Judy [a Sidewalk Counselor and also a counselor] from The JPII Life Center. I ran up to her and was greeted with a warm embrace. I told her my situation and she welcomed me into her home. Within a few hours, she, her husband and The JPII Life Center found me a place to stay and help with tuition. I didn’t know it at the time, but while this was going on, Drew Mariani and the listeners at Relevant Radio were also praying the Chaplet of Divine Mercy for me and my parents.
When I finally worked up the courage to tell my father, he reacted completely different from what I expected. He said he would stand behind my decision. And, he insisted that my mother do the same. After that day, I knew everything would be ok. Since then, I have graduated from Texas State and gave birth to Enrique, who is loved by me and his grandparents.
Without The JPII Life Center, [Relevant Radio and the Coalition for Life], I would not have my baby’s life – or even my own. You see, if I’d gone through with that abortion, not only would it have ended my son’s life, I would have taken my own life. [They] saved us both… and I am forever grateful.”
Diana’s story shows how even a religious person can have an abortion when the stress of an unplanned pregnancy becomes overwhelming. Her story is a good reason why priests and pastors should talk about abortion and educate their congregations not just about abortion facts but also about places then can go if they become pregnant.
Religious pregnant women often have the added stress of fearing what their congregation will think if they have a baby. This leads many frightened Christians to have abortions. With abortion such an easy option, always available, people panic. Always support mothers, whether or not they are married. They have made a brave choice.
LifeNews.com Note: Sarah Terzo is a pro-life liberal who runs ClinicQuotes.com, a web site devoted to exposing the abortion industry. She is a member of the pro-life groups PLAGAL and Secular Pro-Life. Follower her on Twitter.
A young mother is speaking out after her contraceptive pill caused her to have a catastrophic stroke, leaving her as helpless as her 5-month-old baby girl.
Donna Watson was just 26 when she began taking Rigevidon, an oral contraceptive, following the birth of her daughter Millie. “I thought I was doing a good thing by taking the Pill,” Watson told the U.K.’s Daily Mail. But within two months of starting on the drug, she suffered a massive stroke, which her doctors said was caused by her hormonal birth control, which had raised her blood pressure and caused two large blood clots to form in her brain stem.
“Although the risk of stroke in young women is generally low, pregnancy and contraceptive pills are both significant stroke risk factors,” a spokesman for the U.K.’s Stroke Association told the Daily Mail.
“[The hormones in the Pill] … increase the likelihood of the blood clotting and this may increase your risk of stroke,” the spokesman said. “Stroke can hit you out of nowhere and rob you of your speech, your ability to walk, your memory, your independence and your dignity.”
Noted the spokesman, “This devastating condition kills three times as many women as breast cancer every year.”
According to the American Stroke Association, “Women who take even a low-estrogen birth control pill may be twice as likely to have a stroke than those who don’t, and the risk may increase if other risk factors are present.” The group says that 100,000 women in the United States will have a stroke this year.
Watson, now 28, was at home with her young family when she heard a popping sound in her ears and began vomiting. She was rushed to the University Hospital of Hartlepool, where she slipped into a coma. When she awoke, she found herself unable to speak or move.
“The doctors said I would never walk again and I would probably leave the hospital after six months,” Watson told the Daily Mail. She said hospital staff told her fiancé and parents to be prepared for a lifetime of caring for her every need, as they did not expect her to recover.
But the determined young mother blew away her doctors’ expectations, recovering sufficiently to return home after just three months in the hospital. Once home, she began relearning how to walk, talk and eat solid foods – right alongside her daughter, who was by then eight months old.
“I was having physio sessions everyday and I started being able to move my arms,” Watson told the Daily Mail. “I learned to walk again by watching Millie gain her balance.”
Still, the stroke has had lasting consequences, leaving Watson unsteady on her feet with limited mobility, and unable to use her right hand. As a result, she now requires supervision when watching Millie, who is now an active 2-year-old.
“I still need people to accompany me when I am looking after Millie as I can not run after her if she runs away,” Watson explained. But she says she hasn’t given up. “I am hoping for a full recovery and to be to look after her like other mums do,” Watson said.
As for her feelings about the contraceptive pills that led to her stroke, Watson says she believes the medical industry needs to be more open about the risks of hormonal birth control.
“I had no idea something like this would happen to me – I wasn’t made aware,” Watson said. “I think nurses should tell people more about the risks and effects the Pill can have. They should monitor your cholesterol while you are taking it. I really regretted taking that one little tablet.”
We have Thanksgiving Day for giving thanks. We have two days for getting deals. Now, we have “#GivingTuesday”, a global day dedicated to giving back. On Tuesday, December 2, 2014, charities, families, businesses, community centers, and students around the world will come together for one common purpose: to celebrate generosity and to give.
Giving Tuesday, is an idea that encourages people to give back instead of concentrating on getting more for ourselves or our own families, Giving Tuesday calls us to foster organizations in our communities and to keep the spirit of true love during the Christmas season. It’s a national day and a global movement to “give back”.
One More Soul will participate in Giving Tuesday. One More Soul (OMS) is an organization founded and maintained by people committed to their Catholic Faith. We have realized that abortion and contraception are intrinsically intertwined evils, with contraception being the root cause for abortion. We have many educational resources to foster the culture of life around the world.
Please join us December 2nd and be a part of a global celebration of a new tradition of generosity.
What can you do?
There are many ways to support One More Soul on #GivingTuesday:
Pray
The single most important action in working to change the culture of death is really quite simple: Prayer.
Sharing:
Spreading the word is fast and cost-free, yet can potentially make the biggest difference!
Please use your facebook, twitter, or other social media outlets to tell your family and friends about our ministry. Please use 1MORESOUL and the hashtag #Giving Tuesday.
One More Soul could receive donations through the AmazonSmile program. Since we are a nonprofit, who has met AmazonSmile’s eligibility criteria, you, our faithful Pro Life supporter, will be able to donate a portion of your purchase price to One More Soul.
Amazon donates 0.5% of the price of your eligible AmazonSmile purchases. Support One More Soul by taking advantage of this special opportunity when shopping at: https://smile.amazon.com
You’re about to read the story of eleven million women and men who were forcibly sterilized in India. And be forewarned: This is very unpleasant reading!
Entire villages rounded up
In the Indian village of Uttawar, for instance, residents were roused from their sleep by loudspeakers and ordered to gather on the main road. There, police forcibly seized all males age 15 and over and herded them to sterilization centers.
The horror that happened in the village of Uttawar is just one example of how population controllers inflicted forced sterilization. When the forced mutilations were over, eleven million men and women had been sterilized against their will.
Assembly line sterilization
These millions of men and women were forcibly sterilized in conditions that were appallingly unsanitary. No follow-up care was offered. Many died from subsequent infections. 1,800 families filed wrongful death suits, but that number is thought to merely scratch the surface of the number of deaths inflicted as a result of forced, unhygenic sterilization.
Are you asking yourself these two questions? . . .
“Forced sterilization in India was a one-time tragedy, wasn’t it? It couldn’t happen again, could it?”
Wrong! Forced sterilization has happened again since this nightmare in India. It’s happened in Peru . . . Vietnam . . . and Indonesia. And it’s happening right now – on a truly massive scale – in China!
In fact, India’s coercive system of sterilization quotas and targets creates a climate ripe for human rights abuses in what amounts to mass sterilization camps. Just this November, Chhattisgarh, India, saw their own version of these abuses as 15 women died in one such mass sterilization camp under what appears to be the pressure of government quotas.
With officials seemingly obsessed with population control, health and sanitation take a secondary role to the priority of meeting sterilization targets. This abuse of power cannot go on.
by Steven Ertelt | London, England | LifeNews.com | 11/17/14
When their baby was 20 weeks along, doctors diagnosed Gina Beddoe and Dan Lavis’s unborn baby daughter with spina bifida. Sadly a high percentage of babies diagnosed with the medical condition while in the womb become victims of abortion — but not little Frankie Lavis.
The couple said the thought of aborting her never crossed their minds and Beddoe read online about a new pioneering operation to repair baby Frankie’s spine in the womb. The government-run health care pogram agreed to fund the surgery and the couple travelled to Belgium to one of four hospitals in the world offering the operation.
It took two hours and 22 surgical staff to close the gap in Frankie’s spine and she was born in August at 35 weeks — and to her parents’ delight she was moving and kicking her tiny legs in the air. It is too early to tell if Frankie is free of any signs of the condition but the fact she can move her legs means her nervous system is working.
‘We didn’t even have to ask each other whether we would continue with the pregnancy,’Mr Lavis said.
‘We have very good support from friends and family and we felt we could cope with another child if she or he had extra needs,’ added Ms Beddoe.
It was shortly after diagnosis that Ms Beddoe read online about a new operation to repair spina bifida while the baby is in the womb. She discovered that Dr Welch, a former president of the International Fetal Medicine and Surgery Society, had close links with Professor Jan Deprest at Leuven Teaching Hospital in Belgium.
Professor Deprest was one of the first surgeons to undertake the operation and leads one of only four centres in Europe that currently perform it.
At present, surgery to close the spinal column is usually carried out just after birth, by which time damage to the nerves may already be established.
Three years ago, a seminal U.S. trial of the new surgery, which was developed by surgeons at the Children’s Hospital in Philadelphia where it has now been performed 200 times, showed it halved the rate of disability in spina bifida babies, compared with surgery after birth.
The report – published in the New England Journal of Medicine in 2011 – found that 40 per cent of babies operated on in utero needed a hydrocephalus shunt by the time they were 12 months old, compared with 82 per cent of babies who had surgery after they were born.
Of the 64 babies in the trial who had the new surgery, 42 per cent were walking at 30 months compared with 21 per cent of the 70 babies who had surgery after birth.
Although closing the spinal cord will not repair nerve damage which has already occurred, it is thought to avoid further damage and prevent the build up of cerebrospinal fluid.
‘The idea is that closing the spinal lesion in utero avoids secondary damage to the nerves and reverses the malformation,’ says Dr Welch.
After counselling, the couple opted for the new operation.
This past February was one of the coldest on record, and South Toledo residents Adam and Melinda Hernandez, both 32, said it was so frigid they didn’t venture outside much. Now, nearly nine months later, the couple just welcomed a new addition, Adam Hernandez, Jr., to their family of five children.
When little Adam, just 5-days-old, grows up his parents plan to tell him, “You were the result of a bad winter. The polar vortex gave me a son,” Mr. Hernandez said.
The baby arrived a little early. Ms. Hernandez’s original due date was Nov. 18, but her doctor decided to bring Adam into the world ahead of time at ProMedica Flower Hospital to avoid some potential complications.
October, November, and December appear to be the peak months for what some area doctors are calling a small baby boom. Toledo-area obstetricians are expecting to deliver record numbers of babies this fall, because of the Arctic blast experienced in northwest Ohio last winter.
The Weather Channel called Toledo’s winter of 2013-14 the worst of any major city in the United States. Toledo broke five daily low temperature records and tied three others, with the coldest reading of -15 on Jan. 6 being the 10th-lowest temperature measured here, according to the National Weather Service.
Those temperatures combined with record levels of snowfall — nearly 40 inches in January alone — were attributed to a large pocket of very cold air sitting over the region.
Dr. Mychelle Owen of Mercy Ob/Gyn Associates in Perrysburg said she delivered nearly 20 babies in one week in October, which is typically the number of babies she delivers in one month.
“I said to [my patients], it’s been a busy time because of all the level-three snowstorms, and apparently there was nothing better for people to do,” Dr. Owen said. She added the expectant parents usually just laugh when she alludes to their babies being the result of a cold winter.
Officials at Mercy St. Vincent Medical Center said there’s been a slew of activity on the maternity floor this fall. The average number of births at the hospital increased from about 20 per week in October, 2013, to about 29 per week in October, 2014.
“Given the increases we’ve seen this fall, we anticipate total deliveries for 2014 to be about 200 more than we had in 2013,” said Sarah Bednarski, a Mercy spokesman.
Mercy St. Charles Hospital has also seen a major uptick in deliveries compared to last year at this time. There were 47 babies delivered there in October, compared to 25 in October, 2013.
Officials at ProMedica said things have not quite picked up yet on the maternity floor at Toledo Hospital. ProMedica St. Luke’s Hospital, however, had a big spike in September with 25 additional deliveries when compared to 2013, said hospital spokesman Serena Smith.
While the baby rush started as early as September for some, other local doctors report they are planning for a wave of deliveries in November and December.
“It’s gonna get crazy for us in December. We will have the busiest December that we have had in 10 years”, said ProMedica physician Dr. Terry Gibbs.
“All that snow that just kept coming last year, so people even in March kept hibernating or something,” Dr. Gibbs said.
Dr. Gibbs said he had to turn away some expectant mothers because he knows that he and his midwife are already at capacity for the number of babies they will have to deliver in November and December.
“I will be delivering double the normal numbers,” he said.
ProMedica obstetrician Dr. Sarah Puckett said she is also expecting a “50 to 75 percent increase in what we normally see this time of year. I think it is weather-related. People not being able to get out as much. People are inside, and it’s cozy and warm.”
She also thinks that for some parents having health insurance for the first time through the Affordable Care Act may have encouraged them to start thinking about babies.
Some are wondering what the coming winter might bring, and at least one local doctor is welcoming the same possibility over again.
“Snowstorms are great for business, and I hear it’s going to be another bad winter, so I’m probably looking at another busy year next year, Dr. Owen said.
As for the Hernandez family, this will be their last winter baby. Mrs. Hernandez said even though she always wanted a big family, no matter what the weather this winter, six children are enough.
Contact Marlene Harris-Taylor at: mtaylor@theblade.com or 419-724-6091.
[Note: In the early 1800s, the average American woman birthed 7 children; today the average is less than 2. In that same 200 year span, the divorce rate went from essentially zero to 18 per 1000 marriages.]
Joy DeFelice R.N., B.S.N., P.H.N. Director, Natural Family Planning ProgramProvidence Sacred Heart Medical Center, Spokane, WA 99220-2555 USA
Presentation and French translation. Françoise Soler
Light Elimination Therapy for the Treatment of Infertility (LET)
ABSTRACT: Infertility remains a common and often unresolved condition afflicting certain couples. Numerous animal studies have demonstrated that alterations in the light-dark cycle can affect reproduction as mediated by the pineal gland and its hormone, melatonin. To examine whether a similar disruption could affect human fertility, a pilot study was conducted with infertile women enrolled in a Natural Family Planning program.
OBJECTIVE: To examine the association between illumination present during sleep, abnormal menstrual cycle parameters, and infertility. STUDY DESIGN 1: Forty-eight women were studied over a 10-year period. They were taught to chart their menstrual cycle following standard Natural Family Planning methods on three consecutive cycles. At the last class, subjects were informed about the hypothesized effects of ambient light on their reproductive hormones. They were provided with a list of light sources and a rating system to gauge intensity, allowing each subject’s total light score to be calculated.
Subjects were then instructed to decrease their score as much as possible for six consecutive cycles. Their menstrual cycles were examined before and after light minimization looking at 6 parameters: menstrual flow; pre-follicular; follicular phase; ovulation; luteal phase; cycle length.
RESULTS: Initially, none (0%) of the subjects had all parameters within normal range in any of three consecutive cycles. An abnormal follicular phase was found in 96% of the women, followed by luteal (64%) and ovulation (58%) phase abnormalities. The mean light score was 37.5. Establishment of a darkened sleeping environment was associated with a significant reduction in abnormal parameters within 6 cycles. Twenty-six (54%) of the women became pregnant within that same time frame, a rate equivalent to a fertile non-contracepting population.
Two of these women had a history of habitual miscarriages, and both completed the pregnancy.
The mean light score at time of conception was 4.6, representing a reduction of over 87%. 15 conceived during the first 3 cycles of darkness; 11 others during cycles 4 to 6 of darkness. 11 were < 30 years old; and 15 > 30 years old. 8 pregnancies occurred during the months of April to September, and 18 between October and March. Darkness was maintained during the pregnancies. All had a healthy delivery. 30 women (62.5%) had previous physician fertility consultation. 25 then had infertility procedures, but it was after LET that 13 (52%) conceived.
Among the 12 men with abnormal tests before LET, 6 conceived after LET.
DISCUSSION: It is known that the brain (specifically the hypothalamus and pituitary glands) is the cycling center for the hormones that govern the menstrual cycle. In early 1978, Joy gained particular insight into why and how these light influences might work within the brain from research conducted on laboratory rats by R.J Wurtman, and particularly two papers1, 2. “The pineal gland has undergone extraordinary changes with evolution. It has developed into an unusual kind of gland, a neuro-endocrine transducer. This means that this gland can take an
outward stimulus (light) which is relayed through a special optic (eye) nerve route to the pineal gland, which can then convert this light impulse to hormonal output (melatonin)”. Joy postulates that melatonin is stored in the hypothalamus and from that location influences the woman’s reproductive hormones. “Therefore, if the definite 24 hour rhythm of melatonin (normally low during the day and high during the night), is disrupted, then the normal progression of hormonal events of the menstrual cycle can also become disrupted.” Joy has collated formal details to evaluate the sleeping environment for light sources3.
a) Artificial light sources located in the bedroom (with different scores if the light is white, green, blue, or red).
b) Contributing factors that increase the level of light in the sleeping area (as thin window shades, large windows, mirrors, snow on the ground…) by artificial or natural light sources.
c) Inside artificial light source reflecting into the bedroom (as a light on all night in the hallway or reflecting from another room…)
d) Outside artificial light source reflecting into the bedroom (as streetlights or neighbor’s….) Eliminate the light source itself for the best results. In situations where the light cannot be eliminated entirely, darker window coverings; or a sleep mask; or folded cool material placed snugly across the nose and eyes will block out the light. Other helpful ideas are available.
CONCLUSION: The presence of ambient light during sleep can have a fundamental and independent effect on a woman’s reproductive function. A simple regimen of adequate light exclusion can be an effective, economical and non-invasive treatment of a certain subset of infertile couples. Well-controlled studies are required to validate these results, including assays of reproductive hormones and melatonin to delineate the physiologic mechanisms involved. Couples can correctly identify their days of potential fertility in each cycle through STM instruction. A sufficient level of darkness during sleep, and then maintaining that darkness, helps to stabilize all the hormonal phases of the menstrual cycle. These phases can be observed in the woman’s STM charted patterns. Couples also report greatly improved sleep after darkening.
REFERENCES
1. Wurtman RJ The pineal and endocrine function Hospital Practice 1969;4:32-7
2. Wurtman RJ. The effects of light on the human body. Scientific American 1975;227:60-77
3. DeFelice J. Eleventh Edition (2009).The effects of light on the menstrual cycle: also infertility.Before and after clinical observations of light elimination therapy joydefelice@comcast.net
Les effets de la lumière sur la glaire cervicale dans le cycle menstruel, observations cliniques by SERENA info@serena.ca.
Questionnaire pour évaluer la pollution par la lumière Françoise Soler acodiplan@telefonica.net
On November 17-19, 2014, the Congregation for the Doctrine of the Faith will host a colloquium in Vatican City, in cooperation with the Pontifical Council for the Family, the Pontifical Council for Interreligious Dialogue, and the Pontifical Council for Promoting Christian Unity, on the subject of the Complementarity of Man and Woman in Marriage. It is a global, interreligious meeting featuring representatives from 14 religious traditions and 23 countries. The colloquium will be opened by Pope Francis.
Sessions will be opened successively by the leadership of each of the cooperating Vatican offices, followed by the presentations and witness testimonies of leading religious figures and scholars.
Watch this official Humanum video featuring Peter Kreeft:
Each session will also premiere one of six short films treating men and women and marriage the world over (see trailer above). Each film features a variety of illuminating interviews with young and old, single and married, women and men, lay and religious, from many cultures, continents and religions. Topics range from the beauty of the union between the man and the woman, to the loss of confidence in marital permanence, to the cultural and economic woes that follow upon the disappearance of marriage.
The colloquy website is http://www.humanum.it. It contains information about the agenda, the presenters, the films, and media credentialing.
by Bobby Schindler, Brad Mattes | Washington, DC | LifeNews.com | 9/26/14 6:51 PM
A silent and deadly epidemic is moving across America. No one is broadcasting it. No one is writing about it. Almost no one is even talking about it. But every day in hospitals, nursing homes and hospices across the country, more and more of our medically vulnerable loved ones are being euthanized.
Indeed, some physicians have admitted to this behavior. A 1998 article from the Journal of the American Medical Association (JAMA) reported that hastening death is occurring and is not rare.
In a survey of 355 oncologists, “(15.8%) reported participating in euthanasia or physician assisted suicide,” and “38 of 53 (72%) oncologists described clearly defined cases of euthanasia or physician assisted suicide.1
These decisions are being made by paid medical professionals. And loved ones, to their horror, are finding they’re not even part of the discussion.
The patients’ crimes? They’re charged with having insufficient quality of life, being too expensive to keep alive, and being beyond the reach of medical science and therefore beyond hope.
Such judgments may lie behind what seems to be an increase in the “brain death” diagnosis. The difficulty of making a pinpoint diagnosis in such complex neurological matters—and the lucrative financial incentives to harvest organs—will ultimately propel this issue into the forefront of public consciousness and discourse.
Not surprisingly, the current procurement market for human tissues and organs in the United States is booming, driven by insufficient supply and heavy demand.
According to The Milliman Report (see page 4), if all 11 tissues and organs could be harvested from a single patient declared brain-dead, however unlikely, the going rate for procurement would exceed half a million dollars.
If all costs related to those 11 transplants are counted—preparation, physicians’ services, post-op care and the like—the money involved exceeds $5.5 million.2
It’s crucial to shed a bright light on this menacing darkness, but we need your help.
Here are four ways you can assist:
First, we need to hear from healthcare workers and professionals. If you’ve witnessed this happening in your work environment, please come forward and share your observations with us.Perhaps you or someone you know has inside knowledge of the organ donation process as it relates to a situation of euthanasia.
Second, we need your personal stories. We’re also looking for family members willing to share healthcare experiences involving a loved one that are similar to what we’ve conveyed in this letter. Please trust that if you request your identity be held in confidence, that confidentiality will not be violated.
The program reaches tens of millions of American households, so imagine the number of people whose eyes could be opened. America will be told what is happening to the elderly, the chronically sick and the cognitively disabled. If necessary, we can keep the identity of our TV guests confidential.
Finally, we need your prayers. This is, first and foremost, a battle against powers and principalities. We cannot hope to win on our own. Only the power of prayer will permit us to expose this hideous and inhumane attack on precious human life. If you prefer not to be on television, we still need you.
Our ultimate goal is to build a network of people who can speak publicly about these issues to educate others regarding this horrific, unnoticed practice. This may entail speaking to pro-life groups or others sympathetic to protecting innocent human life; addressing a state legislative committee regarding pending legislation; or speaking to a hospital ethics committee as they struggle with a challenging situation or policy.
Our goal is to develop a network of experienced experts who can speak directly to the issues at hand. This is literally a life-and-death matter. And we who are blessed to have life and a voice must intervene to help those who are in danger of having life taken from them. We hope to hear from you soon. Reach us by e-mail or visit the Euthanasia page on the Life Issues Institute website.
For more information about this troubling issue, visit www.lifeissues.org and www.lifeandhope.com. Sincerely for the vulnerable among us, Bradley Mattes Bobby Schindler Executive Director Executive Director Life Issues Institute Terri Schiavo Life & Hope Network
In another legal victory against the HHS mandate, a court has ruled a Catholic college doesn’t have to obey the mandate, which compels it to pay for abortion-causing drugs for its employees.
A federal court issued a decision Tuesday in Ave Maria School of Law v. Sebelius that stops enforcement of the Obama administration’s abortion pill mandate against Ave Maria School of Law, a Catholic law school.
Alliance Defending Freedom Senior Legal Counsel Matt Bowman told LifeNews: “Faith-based educational institutions should be free to live and operate according to the faith they teach and espouse. The court was right to uphold the religious freedom of institutions that value the sanctity of life. If the government can force Ave Maria School of Law to violate its faith in order to exist, then the government can do the same or worse to others.”
The lawsuit challenges the constitutionality of the administration’s mandate that religious employers provide insurance coverage for abortifacients, sterilization, and contraception to employees regardless of religious or moral objections.
Facing millions of dollars of fines that would have taken effect this weekend, Ave Maria University stood up against the government and won an injunction this morning protecting its right to stay true to its beliefs. This is the first order enjoining the government’s latest attempt to coerce religious organizations via an “augmented rule” that it issued last August.
“After dozens of court rulings, the government still doesn’t seem to get that it can’t force faith institutions to violate their beliefs,” said Eric Baxter, Senior Counsel of the Becket Fund for Religious Liberty. “Fortunately, the courts continue to see through the government’s attempts to disguise the Mandate’s religious coercion. We congratulate Ave Maria for its courage, even under the threat of crippling fines.”
Ave Maria’s renewed lawsuit was filed last August in the U.S. District Court for the Middle District of Florida. To date, approximately 90% of the courts addressing the contraception mandate—including the Supreme Court in three separate lawsuits—have protected religious ministries.
“I am elated to announce that our Preliminary Injunction in Ave Maria School of Law’s case against the federal government’s mandate of abortifacient and contraceptive coverage in the Affordable Care Act was granted today. This allows us to practice our faith without being forced by the federal government to compromise our beliefs by providing contraceptive and abortifacient coverage for employees,” said Kevin Cieply, President and Dean of Ave Maria School of Law. “We are also especially proud of the fact that our attorney on this case from Alliance Defending Freedom, Matt Bowman, is a 2003 Ave Maria School of Law graduate.”
Ave Maria School of Law was founded in 1999 to provide a legal education that is publicly faithful to the authoritative teachings of the Catholic Church. The school’s sincere religious beliefs forbid it from facilitating the provision of abortion-inducing drugs, contraception, or sterilization through health insurance coverage it offers to its employees.
“The question is whether the government can pick and choose what faith is, who the faithful are, and when and where they can exercise that faith,” added Senior Counsel Kevin Theriot. “The cost of religious freedom for Americans and organizations across the country that face this mandate is severe. The potential for massive fines and lawsuits could shut down religious educational institutions as well as private employers with similar religious convictions.”
The lawsuit, Ave Maria School of Law v. Sebelius, filed with the U.S. District Court for the Middle District of Florida, argues that the mandate violates the Religious Freedom Restoration Act as well as the First and Fifth Amendments to the U.S. Constitution. Roger Gannam, one of nearly 2,300 attorneys allied with Alliance Defending Fre
by Sarah Zagorski | Houston, TX | LifeNews.com | 10/28/14 5:12 PM
In February 2013, a child known as Baby Chloe was abandoned outside an apartment complex in Texas.
She was left to die inside a Walmart plastic bag; however, a dog walker found her shortly after she was abandoned. The baby was discovered by a woman walking her dogs innorthwest Harris County when the animals became interested in a Wal-Mart bag on the perimeter of the Stonegate Villas Apartments.
About 3 inches of the child’s umbilical cord was still attached. She was a distinct infant – born with one bottom tooth – who weighed 4 pounds and 12 ounces.
Medical officials determined that she was a late preterm baby delivered at 36 to 37 weeks’ gestation. She was named Chloe by the Texas Children’s Hospital staff.
“She was perfectly healthy,” Olguin said. “No injuries, no health issues. No hypothermia. She was out there in February. She didn’t suffer any consequences from being left out in the elements.”
Despite releasing sketches depicting what the biological mother and father might look like and offering a rare opportunity for the media to photograph an abandoned child, officials have been unable to locate Chloe’s parents.
When the pictures were released, CPS received calls from across the United States and abroad. A few people were tested for a DNA match to the child, “but we didn’t come up with any leads,” Olguin said.”
Now, Chloe’s in foster care and her foster parents are planning to adopt her. The authorities have been unable to locate her biological parents and their parental rights have been terminated.
Amazingly, in the video below Chloe is all smiles despite her rough start in the world.
http://www.chron.com/news/houston-texas/houston/article/Baby-Chloe-moves-closer-to-adoption-4540388.php#photo-4261929
Vatican City, Oct 26, 2014 / 12:52 pm (CNA/EWTN News).- In an audience with members of an international Marian movement, Pope Francis warned that the sacrament of marriage has been reduced to a mere association, and urged participants to be witnesses in a secular world.
“The family is being hit, the family is being struck and the family is being bastardized,” the Pope told those in attendance at the Oct. 25 audience.
He warned against the common view in society that “you can call everything family, right?” “What is being proposed is not marriage, it’s an association. But it’s not marriage!
It’s necessary to say these things very clearly and we have to say it!” Pope Francis stressed.
He lamented that there are so many “new forms” of unions which are “totally destructive and limiting the greatness of the love of marriage.”
Noting that there are many who cohabitate, or are separated or divorced, he explained that the “key” to helping is a pastoral care of “close combat” that assists and patiently accompanies the couple.
Pope Francis offered his words in a question-and-answer format during his audience with members of the Schoenstatt movement, held in celebration of the 100th anniversary of its founding in Germany.
Roughly 7,500 members of the international Marian and apostolic organization, both lay and clerics from dozens of nations around the world, were present in the Vatican’s Paul VI Hall for the audience.
In his answers to questions regarding marriage, Pope Francis explained that contemporary society has “devalued” the sacrament by turning it into a social rite, removing the most essential element, which is union with God. “So many families are divided, so many marriages broken, (there is) such relativism in the concept of the Sacrament of Marriage,” he said, noting that from a sociological and Christian point of view “there is a crisis in the family because it’s beat up from all sides and left very wounded!”
In regard to Mary, the Roman Pontiff said that her visit to her cousin Elizabeth is a strong symbol for the movement’s mission, and emphasized how no Christians can call themselves orphans because they have a mother who continues to give them life. Pope Francis recalled this history of the movement’s foundation, noting how it was started by Fr. Joseph Kentenich during the First World War. It was after his time in a concentration camp during World War II, the Pope noted, that the priest traveled to the peripheries of the world in order to preach the Gospel.
Witness is key to spreading the Gospel, he said, explaining that true witness means living “in such a way that the will to live as we live is born in the heart of others…Living in a way (so that) others are interested and ask: ‘why?’” However, the Bishop of Rome emphasized that although we are called to give this witness, “we are not the saviors of anyone,” but rather are the transmitters of Jesus, who is the one that already saved us all.
True witness propels us out of ourselves and into the streets of the world, the Pope continued, repeating his common declaration that a Church, movement or community that doesn’t go out of itself “becomes sick.”
“A movement, a Church or a community that doesn’t go out, is mistaken,” he said. “Don’t be afraid! Go out in mission, go out on the road. We are walkers.”
In answer to questions regarding how he can be defined as “reckless,” the Roman Pontiff admitted that although he can be considered “a little reckless,” he still surrenders himself to prayer, saying that it helps him to place Jesus at the center, rather than himself.
“There is only one center: Jesus Christ – who rather looks at things from the periphery, no? Where he sees things more clearly,” the Pope observed, saying that when closed inside the small worlds of a parish, a community and even the Roman Curia, “then you do not grasp the truth.”
He explained how reality is always seen better from the peripheries rather than the center, and noted how he has seen some episcopal conferences who charge for almost every small thing, where “nothing escapes.”
“Everything is working well, everything is well organized,” the pontiff observed, but they could do with less “functionalism and more apostolic zeal, more interior freedom, more prayer, (and) this interior freedom is the courage to go out.”
When asked about his process of reforming the Roman Curia, Pope Francis explained that often renewal is understood as making small changes here or there, or even making changes out of the necessity of adapting to the times.
But this isn’t true renewal, he said, noting that while there are people every day who say that he needs to renew the Vatican Bank or the Curia, “It’s strange (that) no one speaks of the reform of the heart.”
“They don’t understand anything of what the renewal of the heart means: which is holiness, renewing one’s (own) heart,” the Pope observed, saying that a renewed heart is able of going beyond disagreements such as family conflicts, war and those that arise out of the “culture of the provisional.”
He concluded by blessing the missionary crosses of those present, who are called to missionaries in the five continents of the world, and recalled how some time ago he was given an image of the Mother of Schoenstatt, who prays and is always present.
The movement’s encounter with Pope Francis came on the second day of their visit to Rome, which culminated with a Mass in St. Peter’s Basilica presided over by Cardinal Francisco Javier Errazuriz.
It has been widely assumed that the issue of same-sex marriage is essentially a civil-rights issue. Therefore, any objection to it, no matter how reasonable, is construed as a form of discrimination or even bigotry.
The fundamental issue, however, has nothing to do with civil rights, but with whether a same-sex arrangement is truly a marriage. What has been summarily set aside is the nature of marriage.
Those looking for a clear, reasonable and objective presentation of the nature of marriage could do little better than read Robert George et al.’s “What Is Marriage” that appears in the Harvard Journal of Law & Public Policy. The authors state, “Marriage is the union of a man and a woman who make a permanent and exclusive commitment to each other of the type that is naturally (inherently) fulfilled by bearing and rearing children together. The spouses seal (consummate) and renew their union by conjugal acts — acts that constitute the behavioral part of the process of reproduction, thus uniting them as a reproductive unit.”
This working definition contains several elements that have been rejected, not by the Catholic Church, but by many individual Catholics and the secular world in general. The notion of a “permanent” union has been rejected by the widespread acceptance of divorce. That the union should be “exclusive” is violated in our permissive society by the frequency of marital infidelity.
Abortion is inimical to the “bearing” of children. Finally, contraception and sterilization are inconsistent with the conjugal act by which the spouses “seal” or “consummate” their union.
Divorce, infidelity, abortion, contraception and sterilization have carved out a sizeable hole in the nature of marriage, leaving it a relatively empty shell and making it susceptible to being taken over by an arrangement that is not marriage. By analogy, it is very much like the hermit crab, which occupies a vacant shell to provide itself with a protective home. The crab has no natural home of its own and seizes the opportunity to occupy the former home of an animal whose home has become hollow. When Rome lost its inner moral strength, it was invaded and occupied by barbarians.
Society has lost a sense of what marriage is in its essence, having misinterpreted it according to how it is commonly practiced. Thus, the misrepresentation has beclouded the authentic representation. It is a phenomenon akin to Gresham’s Law in economics, where bad money drives out good money. A particular Christian may be a poor example of Christ, but he should not be seen as his adequate representative.
An essential way to restore the authentic image of marriage is through the example of spouses who truly reflect its nature. The Catholic Church realizes both the importance and the difficulty involved in helping to bring this about. Trying to make marriage “easier” for spouses by emulating secular values, however, will prove to be counterproductive. Yet there is hardly anything more important to the good of society than restoring what is basic to it — marriage and the family, in their authenticity.
Marriage is something that a man and a woman enter into. It is something that precedes them. It is not an arrangement that proceeds from them, according to their private preferences. It is a covenant more than a contract.
Two prevailing philosophies are pernicious to marriage in its authenticity. One is relativism, which holds that the value of anything is not inherent in the object but consists in how it relates to me. Hence, marriage can be re-conceptualized to suit how it relates to my preferences. The second is deconstructionism, which maintains that notions such as “man,” “woman” and “marriage” have been arbitrarily constructed and therefore can just as easily be deconstructed and re-constructed.
These two philosophies, however, have much broader implications than how they negatively affect marriage. Losing sight of the objective nature of things, and tearing everything down on the mistaken belief that they were falsely constructed in the first place, has dire implications for society as a whole. These twin philosophies pave a two-lane highway to nihilism.
The importance of authentic marriage to society is well expressed by Edmund Burke: “The Christian religion, by confining marriage to pairs, and rendering the relation indissoluble, has by these two things done more toward the peace, happiness, settlement and civilization of the world than by any other part in this whole scheme of divine wisdom.”
Donald DeMarco is a senior fellow of Human Life International,
professor emeritus at St. Jerome’s University in Waterloo, Ontario,
and an adjunct professor at Holy Apostles College and Seminary in Cromwell, Connecticut.
(Vatican Radio) The concerns and the challenges of the family in Southern Africa have been brought to the Synod arena by the Archbishop of Cape Town, Stephen Brislin, who is also the President of the Southern African Catholic Bishops Conference (SACBC).
Pointing out how hard Synod participants are working, with long and intense sessions that require much concentration and focus, Archbishop Brislin said the Synod is a wonderful opportunity to listen to first-hand accounts of different realities across the globe with the aim of finding ways of giving pastoral help to families in crisis. “Getting away from judging and condemning” he said “we have to find ways to give support” by finding and taking “what is good, and building upon that”.
Speaking to Vatican Radio’s Linda Bordoni, Archbishop Brislin said the social and family reality he and his brother bishops are faced with in Southern Africa is quite particular as, according to recent research, in South Africa there is no “typical” family…
On behalf of the SACBC Brislin says he presented the input and concerns about the pastoral concerns of families, noting that in his geographical area there is no such thing as a “typical” family in the sense that only 27 % of African children grow up in families where both biological parents are present.
That – he says – is just an example: “there are many broken families, many families experience abuse, conflict and violence, and we do realize that many children are growing up in families that are characterized by trauma and violence”.
Pointing to the fact that at the opening of the Synod Pope Francis invited all participants to speak freely and to listen carefully to the input of others – and Brislin says that it is his impression that everyone is doing just that, Brislin says “There is nobody pushing a particular ideology or a particular standpoint”.
Of course – he said – people are bringing up their concerns and there is a great diversity, but he says he believes people are listening and trying to understand the particular local circumstances brought to the forum.
Brislin says that because of its history and political past, the situation in Southern Africa is quite different to the situation in other Sub Saharan African Nations, but he notes, there are common threads – not only in Africa but throughout the world.
He points to the issue of divorce and separation which is a growing problem in Africa as it is in the rest of the world. But the example of polygamy – brought up by some of the other African Bishops – is a first for a Synod and he says it is a very interesting question.
Brislin agrees that inter-religious marriage and coexistence presents issues that are, generally speaking, not a problem in Southern Africa where – he says – there is a respect for the other. And in his experience the issues that come to the surface in mixed marriages are issues that can be sorted out pretty peacefully.
The Archbishop of Cape Town speaks very positively of the testimonies provided by the couples who have been invited to speak to the Synod Fathers of their thoughts and experiences which he says have been very helpful: “we should never forget this is a pastoral synod that recognizes that there are many families in pain, many families that are failing, that are seeking help, solace, comfort and consolation”.
What we are saying – Archbishop Brislin said – is that the Church does and must teach about marriage “but this is not about laying down the law, it is about how can we reach out to people? How can we recognize that in all the imperfections of our humanity and all the imperfections that exist in families, how can we take what is good and what is positive and try to develop that even better?”
Brislin says the issue of the effects of forced migration on families is a huge one at the Synod and it is coming out from a number of countries. South Africa – he says – deals with this problem because of the legacy of apartheid where so many families were forced apart, mainly because of work (men who worked on the mines were forced to leave their families for years at a time), and he says this continues today where people have to leave their families to seek work in the cities, and from this many problems derive with a huge impact on Southern African families.
“The whole Synod in a sense is going further than family life itself in it that it is asking itself: what sort of a Church should we be?” he said. “
We should be a church that is reaching out to people, a Church that is caring, a Church that is compassionate, a Church that is not judging or condemning people, but a Church that is welcoming and accepting” he said.
And finally, asked what he will be taking back with him once the Synod comes to a close Brislin said : “What I will be taking back to Cape Town and to South Africa is the urgency about having to find ways of giving pastoral help to families in crisis”.
“We have to get away from judging and condemning and to say how can we give support? How can we build? How can we take what is good and build upon that?” he said.
And if that message can get across and into our Parish communities then I think we really will become a better Church” he said.
The Prefect of the Supreme Tribunal of the Apostolic Signatura says that a statement from Pope Francis “is long overdue”
Yesterday’s presentation of the mid-term report (Relatio post disceptationem) of the Extraordinary Synod of Bishops on the Family was met with a remarkable level of interest among both Catholic and non-Catholic media outlets. The Vatican Radio site, in its introduction to the document, stated in part:
In the mid-term report the Synod Fathers speak of how it’s the task of the Church to recognize those seeds of the Word that have spread beyond its visible and sacramental boundaries. They appeal to the “law of graduality,” as a reflection of the way God reached out to humanity and led His people forward step by step.
Reaction to the report ranged from positive declarations of “a shift in tone toward gays and divorce” (New York Times) to more pessimistic assessments. Mary Jo Anderson, reporting for Catholic World Report from Rome, remarked, “The Extraordinary Synod on the Family is at its midpoint and certain degrees of separation are clear: There is a divorce over divorce, remarriage, and Communion.”
Cardinal Raymond Burke, prefect of the Supreme Tribunal of the Apostolic Signatura and a contributor with four other cardinals (and four additional scholars) to the new book, Remaining in the Truth of Christ: Marriage and Communion in the Catholic Church (Ignatius Press), has expressed concern over several aspects of the Synod, including the push for changes in the handling of Communion for divorced and remarried Catholics and the way that information about the Synod is being, in his words, “manipulated.”
Cardinal Burke responded late yesterday to questions from Carl E. Olson, editor of Catholic World Report, about his concerns, his view of the mid-term report, and why he thinks a statement from Pope Francis is “long overdue.”
CWR: In what way is information about what is happening in the Synod being either manipulated or only partially reported and made public?
Cardinal Burke: The interventions of the individual Synod Fathers are not made available to the public, as has been the case in the past. All of the information regarding the Synod is controlled by the General Secretariat of the Synod which clearly has favored from the beginning the positions expressed in the Relatio post disceptationem of yesterday morning.
While the individual interventions of the Synod Fathers are not published, yesterday’s Relatio, which is merely a discussion document, was published immediately and, I am told, even broadcast live. You do not have to be a rocket scientist to see the approach at work, which is certainly not of the Church.
CWR: How is that reflected in the Synod’s midterm document, released yesterday, which is being criticized by many for its appeal to a so-called “law of graduality”?
Cardinal Burke: While the document in question (Relatio post disceptationem) purports to report only the discussion which took place among the Synod Fathers, it, in fact, advances positions which many Synod Fathers do not accept and, I would say, as faithful shepherds of the flock cannot accept. Clearly, the response to the document in the discussion which immediately followed its presentation manifested that a great number of the Synod Fathers found it objectionable.
The document lacks a solid foundation in the Sacred Scriptures and the Magisterium. In a matter on which the Church has a very rich and clear teaching, it gives the impression of inventing a totally new, what one Synod Father called “revolutionary” teaching on marriage and the family. It invokes repeatedly, and in a confused manner, principles which are not defined, for example, the law of graduality.
CWR: How important is it, do you think, that Pope Francis make a statement soon in order to address the growing sense—among many in the media and in the pews—that the Church is on the cusp of changing her teaching on various essential points regarding marriage, “remarriage,” reception of Communion, and even the place of “unions” among homosexuals?
Cardinal Burke: In my judgment, such a statement is long overdue. The debate on these questions has been going forward now for almost nine months, especially in the secular media but also through the speeches and interviews of Cardinal Walter Kasper and others who support his position.
The faithful and their good shepherds are looking to the Vicar of Christ for the confirmation of the Catholic faith and practice regarding marriage which is the first cell of the life of the Church.
ROME – A New Zealand archbishop has said on his blog that he was one of the speakers at the Extraordinary Synod on the Family yesterday to call on the Church to drop traditional language describing sin, such as the term “disordered.”
Archbishop John Dew of Wellington, New Zealand, wrote today that his intervention “seemed to be well received by most.”
“I basically said that we have to change the language which is used in various Church documents so that people do not see and hear the Church judging or condemning, passing out rules and laws, but rather showing concern and compassion and reaching out to help people discover God in their lives,” he wrote.
“I quoted St John Paul and the Catechism of the Church and two interventions after me another archbishop gave almost exactly the same intervention and used the same quotes. So at least two of us think the same,” he added.
Dew wrote that “there has been a huge variety” of speeches, “some very pastoral and with good suggestions” and “some defensive and saying that this cannot change at any cost.”
“Whenever someone speaks from his heart and from a very real pastoral experience it is almost possible to feel the change as a real life experience is spoken about, the compassion, concern, love and support for those in difficult pastoral situations is easily felt,” the archbishop added.
The call for the Church to cease using traditional language deemed offensive has been repeatedly frequently in recent decades. Cardinal Walter Kasper, whose intervention at February’s Consistory of Cardinals has largely framed the Synod in the public mind, gave an interview last week where he again called for the Church to drop its use of the term “adultery” when describing those who have divorced and entered into a second union, saying they find it “very offensive.”
In the video interview, released last week by
Catholic News Service, Kasper said there are “elements” of indissolubility in the second “new situation of marriage.” Kasper, whose ideas were described by Pope Francis at the Consistory as “serene,” rejected the Church’s teaching that within such relationships “every sexual act is sinful,” and added, “There is love, there is commitment, there is exclusivity, it is forever.”
“To tell them that’s adultery, permanent adultery, I think they would feel insulted and offended,” he said.
Although the organizers of the Vatican’s ongoing Synod of Bishops on the Family have decided not to make the bishops’ interventions public, opting instead to summarize the discussions without providing names, they have not placed any restrictions on bishops speaking to the press or writing about their interventions in the Synod hall.
Monday’s decision by the Supreme Court not to take up numerous state appeals regarding same-sex unions pretty much signals that the secular redefinition is here to stay. This is really no surprise given the rather deep confusion about sexuality and marriage in our culture. The polygamists and any number of other groups demanding recognition for their aberrant notions of marriage are sure to follow with all due haste. And what is to stop them, legally, at this point? The word “marriage” is now largely meaningless since, if marriage can mean anything, marriage means nothing, in the linguistic sense. At my parish, we celebrate the Sacrament of Holy Matrimony and are retooling our documents with this new designation wherever possible.
While Jesus did not directly address the issue of same-sex “marriage” (since such a bizarre notion would not even have occurred to anyone in the Jewish world of his day), he did address the notion of illicit or unchaste unions. He did this in the “Matthean exception” (Matt 19 and Matt 5). While Jesus forbade divorce, He set aside or excluded certain unions that were illicit or unchaste and indicated that these were not unions to which one should cling. In effect, He said that they are not marriages at all so the term “divorce” does not apply to them and they should be set aside.
Consider the text from Matthew 19. Let me first present the text itself and then provide some background and interpretation. (I am using the Catholic NABRE translation.)
[Jesus said],I say to you, whoever div orces his wife (unless the marriage is unlawful) and marries another commits adultery (Matt 19:9).
The RSV (Catholic Edition) translates the passage this way: whoever divorces his wife, except for unchastity, and marries another, commits adultery.
Now the phrases, “unless the marriage is unlawful” and “except for unchastity,” are translations of the Greek phrase μὴ ἐπὶ πορνείᾳ (me epi porneia). The usual meaning of the word porneia is “fornication” (i.e., sex between two unmarried people). However, depending on the context, porneia can also refer to other forms of sexual contact that are illicit or irregular by biblical standards. For example, many Greek lexicons (e.g., Strongs and Thayer & Smith) define porneia broadly as “illicit sexual intercourse” and then go on to define porneia to include fornication, homosexual activity, lesbian activity, sexual intercourse with animals, sexual intercourse with close relatives (as spelled out in Leviticus 18), or sexual intercourse with a divorced man or woman. Protestants tend to include adultery in the definition of porneia more so than do Catholics.
The reason that Catholics in general do not is that there is another Greek word specifically for adultery: μοιχᾶται (moichatai). Therefore we do not consider adultery to be grounds for divorce based on either Matt 19 or Matt 5.So, fundamentally, porneia most often means fornication (pre-marital sex) but can mean other illicit things as well.
Why then does Jesus utter this “exception” to the otherwise air-tight prohibition of divorce? The answer would seem to lie in the influence of certain Gentile notions, which the Lord wanted to be clear to exclude, at least in the settings Matthew recalled. The Gentile world was a very sexually confused—even depraved—world. All sorts of strange sexual practices were tolerated and even tied into some of the pagan religious practices. Gentile notions of marriage were often at wide variance with Jewish ones. Gentiles often called “marriage” what Judeo-Christians would call incest. There were also difficulties encountered with homosexual behavior and other sexual liaisons that the Christian Church could not and would not recognize as legitimate or anything but sinful. (The most thorough discussion of this background can be found in the Navarre Biblical Commentary.)
So, in effect, Jesus is declaring that certain so-called marriages that featured porneia (some form of illicit sexual union) were not marriages at all, and that His forbiddance of divorce should not be seen as applying to these illicit unions. The implication is that since such unions were not considered marriage at all, one could and should leave them without being guilty of divorce. The bottom line is this: there was a defined understanding of marriage that Jesus insisted upon, and He freely declared that just because someone called something a “marriage” didn’t make it a marriage.
Many today want to redefine marriage into something other than one man and one women in a fruitful (child-bearing) relationship until death do them part. I have little doubt, based on biblical evidence alone, that Jesus would declare such unions as “not marriages at all,” since He clearly set aside certain unions of His day by calling them unlawful, or more specifically, unchaste.
To those who would argue that Jesus did not specifically mention homosexual unions, I would point out, as already noted, that the term porneia can and does include all forms of illicit sexual unions: incest, fornication, and homosexual acts. Hence His use of the word here does include an exclusion of unions based on this form of unchastity.
As an aside, many today argue that Jesus never explicitly mentioned homosexual acts (though I’d like to point out that he also didn’t explicitly say “Don’t beat your wife,” either) and they seek to conclude from His “silence” that He therefore would approve of homosexual acts. But of course Jesus does address the sinfulness of homosexual acts—through His appointed spokesmen, the Apostles, to whom He said, “He who hears you hears me” (Luke 10:16). The New Testament teachings of the apostles, who speak for Jesus, clearly describe homosexual acts as sinful (e.g., Rom 1:18ff, 1 Cor 6:9; 1 Tim 1:8-11) and contrary to nature (paraphysin– Romans 1:26).
Hence, the term porneia (here understood widely as unchastity) surely does include homosexual acts (as any Greek dictionary will affirm). In the Matthean exception or exclusion, Jesus thus sets aside unchaste or illicit unions since they are not true marriages at all. Divorce does not apply to them and such unions should be discontinued since they are unchaste.
The Vatican’s Synod of Bishops on the Family, taking place in Rome from October 5-19, will not be successful unless it addresses the failure of clergy to preach the Catholic teaching on sexuality found in Humanae Vitae, says a U.S. Catholic priest of 56 years.
Father Daniel McCaffrey, from the Archdiocese of Oklahoma City, served as a military chaplain in Korea, Pakistan and during the Vietnam conflict and now travels throughout the country preaching God’s truth on sexuality, marriage, and family-life. He spoke to LifeSiteNews by telephone.
Listen here: https://soundcloud.com/lifesitenews/a-very-cold-dark-winter-lifesitenews-interviews-fr-daniel-mccaffrey “For four decades and more, the people have not heard the message of the Church on marriage,” McCaffrey said. If the Synod does not address this problem, “we’re going to have a very cold dark winter ahead of the Church,” he predicted.
Father McCaffrey, who works with Natural Family Planning Outreach [http://www.nfpoutreach.org/] may sound like a fire-and-brimstone kind-a preacher, but his message about the Church’s clear teaching on marriage and sexuality is one of love, compassion, forgiveness, and hope.
“I don’t come on in such a way that I’m talking down to the people or criticizing them. I come on as a shepherd. I tell the people that I’m here not to criticize or put them down or condemn, but that I’m here to enlighten them about a truth that’s going to make their life happy here and hereafter,” he said. “Once they know you’re there because you love them, they listen.”
Father McCaffrey’s main message given to parishes and colleges nationwide as well as in Canada is that “contraception is a cancer destroying our Church today.”
The Catholic Church teaches that God created marriage between a man and woman to be “fruitful” in imitation of God’s own Trinitarian life, wherein God is Father, Son, and Holy Spirit through the mystery of the “divine processions.” Seeing openness to life as an essential part of the sexual act, the Church teaches that each and every marital act must remain open to the transmission of new life.
Pope Paul VI warned in his 1968 watershed encyclical Humanae Vitae that a wide social acceptance of closing the sexual act to the gift of life would increase rates of infidelity, lower morality, and lead to a loss of respect for women. Many note that his warnings have proven to be totally accurate.
Father McCaffrey said that contrary to the expectations of parish priests and religious coordinators—who invite him to speak with apprehension, fearing a loss of parishioners—when people hear what the Church actually teaches about marriage and sexuality, they love it. It is very common for listeners to erupt into spontaneous applause at various points during the delivery of his talk.
“You can’t tell me that this is not a teachable subject and a preachable message,” he said.
Father McCaffrey puts the blame squarely on the shoulders of bishops and priests for the laity being largely unaware of this teaching. He lamented that contraception and divorce rates within the Church are practically identical with those outside the Church.
“The horrible thing today is people have not heard this teaching of Humanae Vitae explained clearly and in a loving way. That’s the real problem,” he said.
“And that’s why I say to this Synod: ‘Please send a questionnaire out to all of the bishops, priests, and deacons of the world, asking them why they are not getting the message of Humanae Vitae and [Saint John Paul II’s] Theology of the Body out to the people in the pews.”
Father McCaffrey called the social acceptance of contraception the “root of the problem” facing the Church today regarding the issues of marriage, divorce, and homosexuality. “It’s the root cause, in my opinion, for much of the heartache that the Church has today with regard to marriage.”
Homosexuality is “part and parcel of the whole thing,” he said, adding: “Once you separate the unitive from the procreative, you can do anything. You can perform any perverted act that you want. And that’s why this is a root issue.”
“That’s why I’m so adamant about proclaiming this, because, if we don’t settle this matter clearly, I don’t see the Synod doing very much in this area of evangelization in the married life.”
“It’s very sad, and it breaks my heart that we have the light, the truth, and why don’t we share it with the people forcefully and lovingly? We are the last hope of the world. Why don’t we get up and bring the message of God to the people?” he asked.
Hear Father McCaffrey preach a homily on openness to life at: http://www.nfpoutreach.org/media/ Underlying%20Moral%20Precepts-96.mp3
by Gayle Atteberry | Salem, OR | LifeNews.com | 10/7/14
I wanted to take a few minutes to address all that pink you’ve been seeing in stores, on athletes and on your TV screen. October is Breast Cancer Awareness month and it has never hit home harder for me than this year.
“We did find cancer cells in your breast biopsy,” said the doctor matter-of-factly.
Cancer!!! I was stunned, shocked senseless with words I never thought I would hear!
Cancer happens to other people, not to me! The doctor’s words were droning on: ”…we need to start treatment right away; do you have a surgeon, or would you like me to recommend one?” Treatment! Am I going to die? My mind raced.
The thought of heaven was a peaceful one in this sin-filled, trouble-wracked world. But am I ready to leave my family just now? How could I find someone to take my job quickly? My mind darted to all of the things I needed to do before I die. The doctor’s voice was assuring me that she would have the surgeon call and set up an appointment quickly. I hung up the phone.
My mind bounced from thought to thought, but before much time elapsed, anger welled up inside of me…anger at abortion! While I knew that abortion was not the cause of my cancer (ten years of hormonal replacement therapy is a likely culprit), it is a fact that women choosing abortion have a significantly higher chance of cancer than women who do not. My anger grew as I next thought of Planned Parenthood, who vehemently denies the abortion-breast cancer link, all the while pocketing millions of dollars annually as the nation’s largest abortion-provider.
My mind focused next on a gentleman who sat in front of my desk two years previously as a result of an article I wrote condemning the Susan G. Komen Foundation for giving donations to Planned Parenthood affiliates around the nation. As head of the Oregon affiliate of the Komen Foundation, he was asking me to relent of my words.
Even though the Oregon affiliate had not given to Planned Parenthood, he could give me no promise, no policy, no principle, that would prevent it from giving to Planned Parenthood in the future. He even attempted to defend the practice. I told him I found it unconscionable that an organization whose sole purpose was to find a cure for breast cancer would donate to an organization whose main action was one that could cause the cancer they were trying to heal.
Over 60 epidemiological studies conducted in countries throughout the world show an increased risk of breast cancer in women who have had abortions. Patrick Caroll, Director of Research for the UK Pension and Population Research Institute, says “legally induced abortion is found to be the best predictor of British breast cancer trends.”
Dr. Janet Daling, pro-choice researcher with Fred Hutchinson Cancer Research Center in Seattle found in a 1994 study that “among women who had been pregnant at least once, the risk of breast cancer in those who had experienced an induced abortion was 50% higher than among other women.” Daling also found that “teenagers under age 18 and women over 29 years of age who procure an abortion increase their breast cancer risk by more than 100%.”
Her most alarming find was that “teenagers with a family history of breast cancer who procure an abortion face a risk of breast cancer that is incalculably high. All 12 women in her study with this history were diagnosed with breast cancer by the age of 45″. [Janet R. Daling et al., “Risk of Breast Cancer Among Young Women: Relationship to Induced Abortion,” 86 Journal of the National Cancer Institute; (1994);1584]
My breast surgery in late September revealed the cancer has spread. Fear, uncertainty, chemo treatments. I do not wish these things on any woman. Breast cancer is the second leading cause of cancer deaths among women. Over 232,000 women are expected to be diagnosed with invasive breast cancer in 2014, and 40,000 women are projected to die of it. Many factors put women at risk for breast cancer, most of which women are beginning to be made aware of. However, the abortion-breast cancer link is the one risk factor that is covered over for “politically correct” reasons. It must be added to list so that women choosing abortion will have full knowledge ahead of time. Women who have had abortions must be more alert and diligent to get regular mammograms.
Abortion has become a “sacred right,” protected by abortion advocacy groups who would rather protect abortion rights than the women they claim to represent. Women are suffering a tremendous disservice in order to protect the pocket books of abortion providers. We are living in an age proud of its “full disclosure” for every decision. Shouldn’t every woman contemplating an abortion be given all the information she needs to make an informed choice? We certainly owe her that much.
Consider making a donation to help towards the end breast cancer to: The Breast Cancer Prevention Institute. Please, schedule your mammogram appointment today! For more information on the ABC link, see www.abortionbreastcancer.com.
I know and deeply respect Dr. Alan Shewmon, professor emeritus in neurology at UCLA. He is a world renowned expert on the brain, particularly dealing with pediatrics.
A source has sent me a declaration under penalty of perjury that Shewmon signed on October 3, 2014, testifying that Jahi McMath is not only alive, but now also awake! From his declaration (my emphases):
Based on the materials provided to me so far, I can assert unequivocally that Jahi currently does not fulfill the diagnostic criteria for brain death. The materials include extensive medical records from St. Peter’s University Hospital, which I am still in the process of reviewing, videos of Jahi moving her hand and her foot in response to verbal requests by her mother, images from an EEG done in her apartment on 9/1/14, images of a brain MRI scan done at Rutgers on 9/26/2014, and heart rate variability analysis by my colleague Dr. Calizto Machado based on the EKG channel from 9/1/14 EEG.
Wait, there’s more: Jahi does not currently fulfill criteria for brain death on several grounds.
First and foremost, the videos and the personal testimonies to me of several trustworthy witnesses of her motor responsiveness (yourself [lawyer Nolan], Drs. DeFina and Machado) leave no doubt that Jahi is conscious and can not only hear but even understand simple verbal requests (“move your hand,” “Move your foot,” even, “move your thumb.”)
Thus, the very first of the “three cardinal findings in brain death,” according to the American Academy of Neurology’s Practice Parameters for Determining Brain Death in Adults (and all other diagnostic criteria for brain death that have ever been proposed, for that matter)–namely “coma or unresponsiveness”–is not fulfilled.
More, Jahi now has periods: Corpses do not menstruate. Neither to corpses undergo sexual maturation. Neither is there any precedent in the medical literature of a brain-dead body beginning menarche and having regular menstrual periods.
The MRI: Jahi’s recent MRI scan shows vast areas of structural preserved brain, particularly the cerebral cortex, basal ganglia and cerebellum. There is major damage to the corpus callosum and the brainstem, particularly the pons…corresponding to the severe brainstem dysfunction that has been documented in her progress notes from St. Peter’s.
By contrast, the relative integrity of the cerebral cortex no doubt underlies her ability to understand language and to make voluntary motor responses.
Shewmon doesn’t blame the original diagnosing doctors. Clearly, Jahi is not currently brain dead. Yet, I have no doubt that at the time of her original diagnosis, she fulfilled the AAN diagnostic criteria, correctly and rigorously applied by the several doctors who independently made the diagnosis then…
She is an extremely disabled but very much alive teenage girl. Shewmon doesn’t believe in brain death–not from a religious but a scientific perspective. That is a heterodox position, with which I disagree when the condition is accurately diagnosed.
But no matter. He is not an advocate but medical doctor and scientist with an excellent worldwide reputation.
This is the kind of evidence I said was necessary for this case to go forward. The heft of Shewmon and Machado’s reputation compel the case be reopened.
Sometimes, we would be better heeding family observations than smugly assuming–as I have often seen in these kinds of cases–that they are only seeing what they want to see.
Good for Jahi’s family. Good for Bobby Schindler and the Terri Schiavo Life and Hope Network that went to their aid. And good for attorney Chris Dolan, who took a very unpopular case. Standing up to widespread scorn and derision is never easy–but so worth doing in the cause of what you see to be right.
To view video of Jahi moving hand and foot on command, go to original reference [http://www.nationalreview. com/human-exceptionalism/389564/ucla-neurologist-jahi-alive-awake-wesley-j-smith
Shawn Carney, 40 Days for Life Campaign Director, Oct 6, 2014
We’re almost two weeks into this 40 Days for Life campaign and we have more good news to share. So far … there have been 86 babies saved from abortion – that we know of.
Praise God!
MEMPHIS, TENNESSEE
Kathy in Memphis sent a quick note with great news: “Three babies saved!” A volunteer spoke to a young couple who were on their way into Planned Parenthood.
They listened, but kept on going into the building. Before too long, though, they came back out. “We took the young couple into the mobile unit, and they saw the ultrasound,” Kathy said … and the baby was saved.
vigil participant said she had just arrived for her prayer shift when a woman walked out of Planned Parenthood and announced that she would not be going through with the abortion. A short time later, volunteers reported a third woman also decided to turn away from Planned Parenthood.
WILMINGTON, DELAWARE
“I am happy to report,” Julie said, “that two little lives have been saved from abortion at the Planned Parenthood in Wilmington!”
One woman told counselors she had to abort her baby for the sake of her other two children – she didn’t think she could handle another. The volunteers gave her information about a nearby pregnancy center … and bus fare to get her there. She seemed quite relieved. “Thank you for being here,” she said. “I’m not going to do it!”
Volunteers drove another woman to the pregnancy center after telling her she had better options. “She was under a lot of pressure to abort,” Julie said, “and said if she could just get some help she would choose life for her baby”
A young man who joined the vigil confided that during a previous campaign, his wife was having pregnancy complications and made an appointment for an abortion – and she threatened to call the police if he tried to stop her.
So he prayed, asking the Lord to show his wife a sign at the abortion center that would change her mind.
Of course, when she got there, she saw people praying and realized that she was about to make a terrible “choice.” Their son is now 10 months old.
“He was so grateful that we had been there,” Julie said. “He wanted to join us and perhaps help save someone else’s child.”
GERMANTOWN, MARYLAND
A young man rode up on a bicycle and stopped to talk to a volunteer. He said that when he and his wife were expecting their third child, and had seriously discussed the idea of abortion because of family finances.
He said that they saw people standing in prayer outside the abortion center, and that made them think about what they were about to do. Their baby girl is now one month old.
“You never know what impact you will have,” said Andrew in Germantown. “The simple act of standing on the sidewalk and praying for an end to abortion can save a life.”
Posted by Eric Scheidler (September 30, 2014 at 3:02 pm)
Yesterday the American Academy of Pediatrics issued a new recommendation [http://pediatrics.aappublications.org/content/early/2014/09/24/peds.2014-2299.full.pdf] that physicians promote the progestin implant and the intrauterine device (IUD) for teen girls. As the father of six girls—including three teenagers—I find this new recommendation particularly disturbing.
It’s not just that I bristle at the thought of a doctor asking my daughters a battery of questions about sex, as the AAP recommends. It’s that I know how upset they would be to hear sexual acts they’ve never given a thought to presented as perfectly normal, or even expected of them.
Some might accuse me of being naïve, but they don’t know my girls. And that points to the first of four reasons the new AAP recommendations are wrong-headed:
1. They undermine the role of parents.
In the new AAP recommendation, doctors are strongly discouraged from involving parents in their daughters’ contraceptive use, even in states where the law doesn’t require such “confidentiality.” Though a nod is given to abstinence, moral questions about sex have no place in this private discussion between doctors and young girls, according to the AAP.
The message to teen girls is that—contrary to what their parents, church community and even their own well-formed consciences may have told them—there is no moral choice involved in whether or not to have sex. Sadly, it should come as no surprise that this AAP recommendation would undermine the role of parents.
One of the authors, Gina Sucato, is a member of the pro-abortion group Physicians for Reproductive Health, and testified against a parental notification bill in Washington State. Such measures are overwhelmingly supported by the public.
2. They weaken teens’ choice not to have sex.
Though you wouldn’t know it looking at our entertainment and news media, teen sex has actually been on the decline for over two decades—13% since 1991. How much more might it have declined in the absence of the constant barrage of messages teens are exposed to, telling them that everybody’s doing it and you’re kind of weird if you’re not?
Now add to that your own family doctor, with the door closed to your mom and dad, suggesting that you might want to have progestin implanted in your arm or an IUD inserted so you can have sex without worrying about pregnancy for years on end. The message is clear: You can’t be counted on to make good choices.
First, you can’t be counted on to take a pill every day (which is why the AAP is pushing implants and IUDs). Nor can you be counted on to decide not to have sex, despite all the reasons it’s not a good idea. Yet, somehow, you can be counted on to use a condom to prevent STDs. Sort of. The AAP’s attitude towards condoms is particularly puzzling.
In defending the new preference for implants and IUDs, they point out how inadequate condoms are for preventing pregnancy—both because teens often don’t want to use them, and even when used they have at least an 18% failure rate. But then, they insist that condoms are absolutely necessary, each and every time a girl has sex, lest she get an STD.
Back to the implants and IUDs, as one of my adult sons asked, what kind of impact will it have on a girl should it become known around school that she’s using one of these long-term methods of birth control?
Finally, the headlines accompanying the new AAP recommendations are discouraging both to teens who are abstaining form sex and the parents, pastors and educators who want to encourage that choice. What, instead, might Abe the impact of headlines announcing the AAP’s support for abstinence as the best choice for teens?
3. They set a double standard on adolescent health.
Even as parents and coaches are trying to discourage the boys on the football team from using steroids to improve athletic performance, the AAP is encouraging the girls on the cheerleading squad—or the volleyball team—to have steroid-releasing devices implanted in their bodies.
That’s what the artificial hormones in these devices are: steroids. Why the double standard? Shouldn’t we be protecting both our sons and daughters from artificial steroids, and the health risks associated with them? One of the long-term birth control methods being recommended by the AAP doesn’t release hormones: the copper IUD. However, it may be more problematic for my final objection:
4. They ignore the abortifacient potential of the IUD.
It was because the IUD has the potential to cause an early abortion that Hobby Lobby objected to providing the devices without copay in their high-profile lawsuit against the HHS Mandate. The U.S. Supreme Court ruled that the owners of such closely-held corporations cannot be forced to violate their moral objection to abortion by being required by the government to include abortion-inducing drugs in their health plans.
But the AAP has no problem promoting the IUD to teen girls without disclosing its abortifacient potential, which is completely ignored in the new birth control recommendations to doctors—despite the fact that teen girls might choose differently if they knew the IUD could cause an early abortion.
We already know that one of the co-authors of the new recommendations is a radical abortion advocate. Not only did she speak out against parental notification, she signed an amicus brief with the Supreme Court in opposition to the federal ban on partial birth abortion—again, a position at odds with the moral judgment of most Americans.
But however strongly Gina Sucato supports abortion, shouldn’t she and her colleagues at the AAP seek to respect the pro-life views of their patients? Don’t they have an ethical responsibility to disclose the fact that an IUD may prevent a newly-conceived human being at its embryonic stage of life from implanting in its mother’s uterus? In these new recommendations on birth control for teen girls, the AAP has adopted a cavalier attitude not only towards girls’ best interests and parents’ relationships with their daughters, but to the value of life itself.
I encourage parents to contact the AAP [ http://www2.aap.org/guestbook/ contactus-form.cfm ] to respectfully voice your objections to the new recommendation and call on them to emphasize abstinence as the only good choice for our daughters. – See more at: http://prolifeaction.org/hotline/2014/aapiud/#sthash.EA2vJFaH.dpuf
The American Academy of Pediatrics (AAP) has updated their policy guidelines (PDF) concerning contraceptives for children under 18, recommending that the first line of defense against pregnancy for adolescent girls should be implantable contraception such as an IUD or a sub-dermal hormonal implant.
The AAP says that because young girls cannot be trusted to remain abstinent, reliably take a daily birth control pill, or use condoms, the best way to ensure they do not become pregnant is to fit them with a “long-acting reversible contraceptive” – a device that, once installed, will either provide a continuous dose of hormones designed to prevent ovulation, or prevent a fertilized egg from implanting, causing an early abortion. The group says that even very young girls who are not yet sexually active can be fitted with the devices, as a preventive measure.
The recommendations were co-authored by Gina Sucato, a member of Physicians for Choice. Upon their public release on Monday, they were met with mixed reactions.
“I’m so happy about this,” said Ana Radovic, a doctor at the Center for Adolescent and Young Adult Health, a sex clinic for children and young adults ages 12 to 21. Her organization provides IUDs and other contraceptives to children as young as 12, without requiring parental notification or consent. It also offers similar “confidential care” through the nearby Magee-Women’s Hospital, which performs abortions.
Radovic told the Pittsburgh Post-Gazette she was eager to see more doctors implanting young children with IUDs. “This will give primary care physicians and pediatricians the much needed information that this is a safe procedure, even for young girls who have never had intercourse,” she said.
“The AAP’s recommendations will be a great help,” Heather Boonstra, director of public policy for the Guttmacher Institute – a pro-abortion think tank with links to Planned Parenthood – told the Post-Gazette. “This is about trying to change the minds of the provider community, more of who are recognizing that adolescents are appropriate users for the IUD.”
But child safety advocates and pro-life observers said the AAP recommendations send a dangerous message, and could even lead to lifelong health problems.
“As a father myself, I’m particularly horrified that this recommendation would come from this physicians’ group,” said Eric Scheidler, executive director of the Pro-Life Action League, in an interview with LifeSiteNews. “Everybody knows that teen sex is a bad idea, and a recommendation like this sends a mixed message. On the one hand, we’re trying to encourage teens to be abstinent, and on the other, we’re giving them the tools not to be.”
“We know that the biggest concern teens have about teen sex isn’t STDs, it isn’t the heartbreak that comes from it, it isn’t damaging their ability to bond later in life. The big concern they’re going to have is getting pregnant. Take that [concern] away, and teens are inevitably going to make less responsible choices.”
Scheidler said he was also concerned about the AAP’s heavy focus on “confidentiality,” which he said was really about “keeping parents in the dark” about their kids’ activities.
“The [AAP] recommendation not-so-obliquely suggests that even in states where [doctors] are not forbidden to talk to parents, [that they] not do so anyway,” he said.
Scheidler worries that giving children under the age of consent unfettered access to contraceptives could make it easier for rapists to hide their sexual abuse of minors.
“It’s just one more example of the mixed message and the contradiction here,” Scheidler said. “You know, the first contradiction is … we don’t want teens to be sexually active, that we should encourage them to be abstinent, but then we’ll discourage them from being abstinent by giving them birth control. Similarly, we say to physicians, you’re required to report sexual abuse of minors, but you’re also required not to tell parents about their minor children’s sexual activity – which in many cases, might by definition be criminal.”
Aside from the moral implications of fitting kids with long-term contraceptive devices, Scheidler said he was also disturbed from a safety standpoint.
There are two types of IUDs currently on the market in the U.S. – hormonal and copper. The hormonal IUD, marketed under the brand names Mirena and Skyla, releases a constant dose of hormones to fool the body into thinking it is already pregnant, so it won’t release an egg. Failing that, the device makes the uterus inhospitable to a growing life, causing an early abortion. Mirena lasts for five years; Skyla, which is targeted at younger girls, lasts for three. Skyla is new to the market, but its big sister Mirena has been the target of thousands of lawsuits by users who suffered catastrophic complications, and is now the subject of a class-action suit.
The damaging effects of the Mirena IUD are numerous, but the primary risk is puncture of the uterine wall, which can occur in up to 1 out of every 1000 installations, according to its manufacturer, Bayer. Uterine perforation can lead to intestinal, bladder, bowel, or other organ damage; infections; scarring; infertility and even death from sepsis. Additionally, the chemicals released by the device have been classified by the World Health Organization as class 1 carcinogens, or cancer-causing agents.
As for the copper IUD, it carries the same risks of uterine perforation as its hormonal counterparts, but without the increased risk of cancer and other side effects caused by the chemical component. However, the trade-off is that it doesn’t work until a woman or girl is already pregnant – it effectively works as a tiny “abortion machine,” ensuring that no fertilized egg can attach to the uterine wall.
None of the implantable devices being promoted by the AAP offer any protection from sexually transmitted diseases.
“You know, I have three teen daughters myself,” Scheidler told LifeSiteNews. “The thought of them being counseled by a physician to consider the IUD or one of the implantable contraceptives is pretty shocking.”
In previous years, the IUD lacked in popularity due to its expense – a single device costs between $800 to $1,000. However, since ObamaCare became law, all insurance providers must now provide the IUD free of charge to their female patients upon request.
Additionally, federally-funded reproductive clinics provide the devices free to girls under 18, even if they are covered by their parents’ insurance, in order to help them avoid disclosing their sexual activity to their parents.
From South Korea comes a startling prediction that, if current population trends continue, the country will “go extinct” in 2750. The study, based on a computer simulation conducted by that country’s National Assembly Research Service (NARS), also identifies the culprit: not a high death rate or emigration rate, but one of the lowest fertility rates in the world.
Of course, a world without South Koreans lies centuries in the future, and a lot can change in 700-plus years. But even the near-term demographic future of the southern half of the Korean Peninsula looks grim. Assuming that the current low-low fertility rate of 1.19 children per woman continues indefinitely, as NARS did, the population of South Korea will dwindle to less than half its current size by the end of the 21st century. It will go from 50 million down to 20 million, losing 60% of its population in less than 100 years.
South Korea is not alone in undergoing rapid depopulation. A similar simulation was conducted by Japan in 2012, and reached the conclusion that Japan would go extinct in the next millennium if current demographic trends continue. One Japanese university has created a kind of doomsday clock that counts down the declining number of Japanese children in real time.
On the other side of the globe, Europe has similarly low fertility rates and is experiencing a similar dramatic demographic decline. Today,half of the world lives in a country with below-replacement fertility. For the first time in human history, otherwise prosperous and thriving societies appear to be bent on their own destruction.
Total human extinction is a cheery thought for the radical fringe of the population control movement, which can’t wait for us to vacate the planet. But it is not something that normal people welcome. The depopulation sought by some population control advocates will bring in train its own unique forms of destruction and anarchy. Will sharply declining working age populations willingly support a huge and growing elderly population without complaint, even as their earnings are sucked away? Unlikely. The end won’t be pretty – but suicide, whether it be demographic and economic, never is.
South Korea’s low fertility is in large part the result of American efforts to combat “overpopulation” by exporting so-called “family planning” programs around the world. In South Korea, as in so many other countries, these efforts had a coercive element as families who dared to have more than two children were punished in various ways.[1]
Population control efforts in South Korea proved all too successful, and South Korean fertility rates plummeted from around 6 in 1960 down to a shockingly anemic 1.2 children in 2004. Even after overt anti-natal policies were discontinued in 1996, the fertility rate did not recover, but continued to drop. The South Korean government is currently trying to implement pro-natal policies to counteract the anti-natal policies that caused the disaster in the first place.
It is one thing to use government power to force people to stop reproducing; it is quite another to try and bribe people into having children they don’t want. South Korea is learning the hard way what Europe already knows: namely, that small financial perks simplyaren’t enough to restore the birth rate to healthy levels after a people’s fertility has been systematically undercut by anti-people policies and propaganda.
[1] Mosher, Steven W. “The Crisis of the Empty Cradle.” Population Control: Real Costs, Illusory Benefits. New Brunswick, NJ: Transaction, 2008. 20-25. Print.
Despite a promise President Obama made to lawmakers and the American public in a special joint session of Congress on healthcare reform that “under our plan, no federal dollars will be used to fund abortion” a new report released by the non-partisan Government Accountability Office (GAO) today documents massive new public funding of abortion in the President’s healthcare law.
“In an 11th hour ploy to garner a remnant of pro-life congressional Democrats absolutely needed for passage of ObamaCare, the President issued an executive order on March 24, 2010 that said: ‘the Act maintains current Hyde Amendment restrictions governing abortion policy and extends those restrictions to newly created health insurance exchanges’,” said Smith, co-chairman of the Bipartisan Congressional Pro-Life Caucus. “It turns out that those ironclad promises made by the President himself are absolutely untrue.”
A significant majority of Americans oppose public funding of abortion. Under current law, the Hyde Amendment prohibits funding for abortion, and funding for any insurance plan that includes abortion except in the case of rape, incest or to save the life of the mother.
GAO has found that in 2014, taxpayers are funding over a thousand Obamacare health plans that subsidize abortion on demand—even late-term abortion—in defiance of the Hyde Amendment the President publicly said he would honor.
Among GAO’s findings:
every ObamaCare taxpayer subsidized health insurance plan in New Jersey, Connecticut, Vermont, Rhode Island and Hawaii pays for abortion on demand
in New York a 405 out of 426 ObamaCare plans subsidize abortion on demand
in California—86 of 90
in Massachusetts—109 0f 111
in Oregon—92 of 102
in Washington, DC—23 of 34
According to the Congressional Budget Office (CBO) April 2014 estimate, between 2014 and 2024, taxpayer subsidies to buy ObamaCare health plans will total $855 billion, making taxpayers unwittingly complicit in abortion.
GAO found that even an accounting trick embedded in ObamaCare requiring premium payers to be accessed a separate monthly abortion surcharge is being completely ignored. The surcharge would have added some modicum of transparency so individuals would know whether they are purchasing a pro-life or pro-abortion health insurance plan if faithfully implemented. Sen. Ben Nelson of Nebraska summed up the plain meaning of the law: “you have to write two checks.” According to GAO, none of the 18 insurance companies they interviewed are collecting the abortion surcharge separately.
While the Democrat Leader famously said “We have to pass the bill to find out what’s in it,” during the debate on ObamaCare, now it turns out that consumers have to buy a plan to find out if abortion is in it—a complete lack of transparency. The majority of health insurance policy issuers interviewed by GAO reported that the consumers do not have access to information about whether the plan covers abortion.
Last year members of Congress and some staff were barred from any further participation in the Federal Employees Health Benefits Plan (FEHB) and compelled onto the ObamaCare exchanges. For instance, after months of misinformation, obfuscation and delay, Smith learned that of the 112 health plans offered on the exchange for his family, 103 paid for abortion on demand—a clear violation of the law, specifically of the Smith Amendment, a Hyde-like abortion funding ban Smith first sponsored in 1983.
“Americans throughout the country have raised serious concerns that they find it nearly impossible to determine whether the plan they purchase finances the killing of unborn children—there is little or no transparency—hence the request by several members of Congress including Speaker Boehner that GAO investigate,” Smith said.
To end President Obama’s new massive funding of abortion on demand, last January the House of Representatives passed a bill authored by Smith—the “No Taxpayers Funding for Abortion and Abortion Insurance Full Disclosure Act,” HR7.
“When Senator Harry Reid was a member of the House he was as pro-life as Henry Hyde,” Smith said. “Now, as Senate Majority Leader, he has refused to even allow a vote on HR 7.”
LLDF and ADF represent seven employees who do not want a plan covering elective abortions and allege that DMHC’s coercion of abortion coverage violates federal law.
In August, LLDF and ADF lodged a letter with DMHC warning it of its violation of federal law. DMHC responded by affirming its decision to force all plans to cover all abortions, without explaining how that decision squares with a federal law insisting otherwise.
“Forcing a Christian university to facilitate elective abortion is an assault on our most fundamental American freedoms,” said ADF Senior Counsel Casey Mattox. “California is violating the federal law that protects employers and employees from being strong-armed into having abortion in their health insurance plans. No state can ignore federal law and continue to unlawfully receive taxpayer money. So California has a choice: Stop forcing these employers to cover abortion or forfeit the tens of billions of dollars it receives under the condition that it follow the law.”
The LLDF and ADF letter explains that, because of the federal Weldon Amendment, “This directive of the DMHC constitutes unlawful discrimination against a health care entity…. Nothing in California law or the state’s constitution requires private health plans to cover abortions.”
“Under federal law, pro-life employers have the freedom to choose health insurance plans that do not conflict with their beliefs on the dignity of human life,” said LLDF Legal Director Catherine Short. “Already under Obamacare’s mandates, employers and individuals are required to purchase health insurance coverage they may not need or want. California cannot be allowed to discriminate against health plans that don’t cover elective abortions and force people to purchase coverage that conflicts with their convictions.”
by Steven Ertelt | Washington, DC | LifeNews.com | 9/9/14 5:12 PM
Bowen isn’t perfect, which could have made him a prime candidate for an abortion. But the story of this little Serbian boy ends differently — much differently.
Devon Toomey couldn’t take her eyes off of Bowen when she first met him — not because he was disfigured or ghastly, but because he was simply a little boy who needed the love of adoptive parents. Helpless and alone in his crib, Bowen just needed the same thing any 18-month-old needed: someone to love and take care of him.
“I couldn’t take my eyes off of him. I just loved him the moment I saw him,” adoptive mother Devon Toomey told KTVB-TV. “I just knew, I just knew he was our son when I saw him.”
“He wasn’t moving at all, he couldn’t sit up, he couldn’t roll over,” Devon said. “He didn’t know how to eat or to chew.”
I have honestly felt that when the time was right, our child would find us. I truly felt we would be brought together in one way or another. So for the last few years, when people would ask where we wanted to adopt, what age, etc. I would simply state “We’re not really sure. We want to leave our options open so our child can find us.” Well, on October 1, 2009 this is precisely what happened. After having an adoption conversation with two of my good friends, I came home and looked on Reece’s Rainbow. Now, this was nothing new for me. I have been looking at Reece’s Rainbow for years. I would always find amazing kids on there but I never felt that push to pursue a specific child because as I know now, my child had not even been born yet. On that beautiful October day however, everything changed! Our lives changed forever that day and for that we are so grateful.
Now Bowen has started kindergarten, he enjoys swimming and playing on the trampoline, and is doing just great.
“Within a couple of months, he was rolling over, sitting, doing all sorts of stuff.”
You can tell how proud his brothers are of him. They are his biggest fans.
“He can go up the stairs,” brags big brother Heath. “He can eat, we have this band that has hole and you can put the spoon in it and he can dip it in the bowl.”
He also bounces on the trampoline, writes, and reads books.
“Heath has always been very protective of him, as you can imagine when we’re out and about you get a lot of double takes,” said Jeremy. “If they say anything mean, Heath’s all over them.”
Bowen’s family exposes him to everything, but swimming is his favorite activity.
“I think (the pool) is the one place he doesn’t feel a lot of limitations,” said Devon.
Shortly after John J. O’Connor became Archbishop of New York in March 1984, he found himself in a battle with the state’s governor, Mario M. Cuomo, which not only made national headlines but also had a profound impact on the abortion debate in America.
It began when the archbishop said during a press conference: “I do not see how a Catholic, in good conscience, can vote for an individual expressing himself or herself as favoring abortion.” That didn’t sit well with Cuomo.
The governor, who in the early 1970s had been publicly pro-life, changed his position after losing a primary for lieutenant governor in 1973 and then a race for mayor in 1977. To advance his career, Cuomo adopted the now familiar line that, as a Catholic, he was personally opposed to abortion. But as an elected official it would be wrong for him to impose his religious beliefs on the general public. He went on the offensive about O’Connor’s comment, telling the New York Times:
The Church has never been this aggressively involved [in politics]. Now you have the Archbishop of New York saying that no Catholic can vote for Ed Koch [the N.Y.C. mayor], no Catholic can vote for [City Comptroller] Jay Goldin, for [City Council President] Carol Bellamy, for [U.S. Senator] Pat Moynihan or Mario Cuomo—anybody who disagrees with him on abortion. . . .The Archbishop says, “You Mario, are a Catholic who agrees with me that abortion is an evil”. . . . The Archbishop says, “OK, now I want you to insist that everybody believe what we believe.
Cuomo did not stop there; he described to Newsday what he believed were the potential implications of O’Connor’s remark:
So I’m a Catholic governor. I’m going to make you all Catholics—no birth control, you have to go to church on Sunday, no abortion. . . . What happens when an atheist wins? Then what do I do? Then they’re going to start drawing and quartering me.
At first, O’Connor appeared to back off. He told the Brooklyn Tablet that he had never said, “anywhere, at any time, that ‘no Catholic can vote for Ed Koch.’ . . . My sole responsibility is to present . . . the formal official teaching of the Catholic Church. I leave to those interested in such teachings [to judge how] the public statements of officeholders and candidates” match up.
In a New York magazine interview, he further explained:
I think there’s a deep disquiet in the national consciousness about this issue. People know it’s wrong. They know we’re killing. It’s not a matter of arguing the precise moment when a fetus becomes a baby—people know that thousands of real life human babies are being killed every day . . . and they don’t know what to do. They’re confused, upset about it. To me, that anguish is the only reasonable explanation of why I can utter a simple statement, a simple answer to a simple question—I don’t see how a Catholic in good conscience can vote for a politician who explicitly favors abortion—and immediately it becomes enormous news.
So O’Connor wasn’t backing off at all, and for him the debate was far from over.
After the Democratic National Convention nominated the first woman vice-presidential candidate, Congresswoman Geraldine Ferraro of Queens—a so-called pro-choice Catholic—O’Connor publicly criticized her for saying “things about abortion relevant to Catholic teaching which are not true”:
The only thing I know about her is that she has given the world to understand that Catholic teaching is divided on the subject of abortion. . . . As an officially approved teacher of the Catholic Church, all I can judge is that what has been said about Catholic teaching is wrong. . . . I have absolutely nothing against Geraldine Ferraro; I will not tell anybody in the United States you should vote for or against [her] or anybody else. . . . She has given the world to understand that Catholic teaching is divided on the subject of abortion [when there is] no variance, no flexibility, no leeway.
When the Congresswoman denied she had ever misinterpreted Church teaching, O’Connor released a copy of a letter Ferraro had signed and sent two years earlier to fifty Catholic members of Congress concerning a group called “Catholics For a Free Choice.” In it, she wrote that Catholics for a Free Choice “shows us that the Catholic position on abortion is not monolithic and that there can be a range of personal and political responses to the issue.”
This led to a 25-minute phone conversation between Ferraro and O’Connor during which the archbishop reemphasized that there is “simply no room for a ‘free choice’ on the matter of abortion . . . [T]he Second Vatican Council, Pope Paul VI, Pope John Paul II, and the bishops of the United States [have] made that abundantly clear.”
Mrs. Ferraro termed the conversation “cordial, direct and helpful,” but then she added, aping Cuomo, that:
when bishops speak out they are doing their duty as Church officials . . . .[W]hen I speak out I am doing my duty as a public official and my foremost duty as a public official is to uphold the United States Constitution, which guarantees freedom of religion. I cannot fulfill that duty if I seek to impose my own religion on other American citizens. And I am determined to do my duty as a public official.
The liberal establishment was appalled by what it viewed as O’Connor’s meddling. The New York Times pontificated:
It might as well be said bluntly. . .[the] effort to impose a religious test on the performance of Catholic politicians threatens the hard-won understanding that finally brought America to elect a Catholic President a generation ago.
Senator Ted Kennedy accused O’Connor of “blatant sectarian appeals” and argued that not “every moral command could become law.”
Mario Cuomo refused to sit on the sidelines. On September 13, 1984, he flew to America’s best known Catholic university, Notre Dame, to answer O’Connor in a talk titled “Religious Belief and Public Morality: A Catholic Governor’s Perspective.” Cuomo described himself to his audience, as “an old-fashioned Catholic who sins, regrets, struggles, worries, gets confused, and most of the time feels better after confession.”
“The Catholic Church,” Cuomo said, “is my spiritual home.” He added, “I accept the Church’s teaching on abortion,” but then asked, “Must I insist you do?”:
Our public morality then—the moral standards we maintain for everyone, not just the ones we insist on in our private lives—depends on a consensus view of right and wrong. The values derived from religious belief will not and should not be accepted as part of the public morality unless they are shared by the pluralistic community at large by consensus.
He evoked Cardinal Joseph Bernardin’s “seamless garment” argument, saying that abortion “has a unique significance but not a preemptive significance . . .[and] will always be a central concern of Catholics. But so will nuclear weapons. And hunger and homelessness and joblessness, all the forces diminishing human life and threatening to destroy it.”
And arguing that a consensus to ban abortion simply did not exist, Cuomo concluded:
I believe that legal interdicting of all abortions by either the federal government or the individual states is not a plausible possibility and, even if it could be obtained, it wouldn’t work. Given present attitudes, it would be Prohibition revisited, legislating what couldn’t be enforced and in the process creating a disrespect for law in general.
As historian Richard Brookhiser has written, “Cuomo had found, in consensus and prudence, a way of having religion when he wanted it to not having it when he didn’t.” The consensus argument was even too much for the very liberal Bishop of Albany, Howard Hubbard:
While I support wholeheartedly the governor’s position on capital punishment, there is no consensus in our state or nation on this matter. Quite the contrary. The polls show that 60 percent to 70 percent of the population favors the death penalty.
Also polls indicate that the vast majority of the citizens in New York are opposed to recent legislation about the mandatory usage of seat belts. Yet contrary to citizen consensus, the governor supports such legislation because it would save several hundred lives a year. Why not a similar concern about saving the thousands of human lives which are terminated annually through abortion on demand?
And the renowned theologian, Msgr. William B. Smith, dean of St. Joseph’s Seminary, agreed:
The governor’s style was smooth and slick, but the content was specious and misleading. He is obviously a competent man, but a couple of points were horrendous, one being the complete ignoring of the human rights issue. Human rights do not rest on consensus. Respect for the human rights of blacks, Jewish people—any minority—does not rest on consensus. This is why we call them inalienable rights. He relied on the 15-year old rhetoric of Planned Parenthood [that] we’re trying to impose our morality on others. The Supreme Court didn’t establish a consensus; it destroyed one. The laws in the 50 states weren’t there because the Catholic Church put them there.
A month later Archbishop O’Connor gave a speech before a Catholic Medical Group—with Mother Teresa sitting on the stage—in which he challenged the Cuomo thesis: “You have to uphold the law, the Constitution says. It does not say that you must agree with the law, or that you cannot work to change the law.”
There are those who argue that we cannot legislate morality. The reality is that we do legislate behavior every day. . . . It is obvious that law is not the entire answer to abortion. Nor is it the entire answer to theft, arson, child abuse, or shooting police officers. Everybody knows that. But who would suggest that we repeal the laws against such crimes because the law is so often broken.
He ended by reasserting his original public stance.
I have the responsibility of spelling out. . .with accuracy and clarity what the Church officially teaches. . . . I have simultaneously the obligation to try to dispel confusion about such teaching wherever it exists, however it has been generated, regardless of who may have generated it. . . . I recognize the dilemma confronted by some Catholics in political life. I cannot resolve that dilemma for them. As I see it, their disagreement, if they do disagree, is not simply with me [but] with the teaching of the Catholic Church.
For many Catholics, John O’Connor became a national hero. After years of bishops sitting on the sidelines, finally here was someone standing up and challenging whether Catholic politicians could separate their personal convictions from their public stance on abortion and still remain Catholic.
“I think,” said Patrick Ahern, an auxiliary bishop of New York, “John O’Connor upped the ante on abortion all by himself. He started the ball rolling, and the other bishops have been forced to follow along. I think, too, that it is an act of great courage, because they’re going to flay him over this before he’s finished.”
Flay him they did. The media consensus was that he was shilling for Ronald Reagan’s re-election. O’Connor remained unruffled. He told New York magazine reporter Joe Klein that he was “surprised by all the fuss,” and pointed out that was only saying what he’d always said:
In fact, when I was consecrated a bishop in Rome. . . . I vowed publicly that from that day on there would be some reference to the dignity of the human person and, in particular, to the defense of the most vulnerable—the unborn—in every public address I made. I have done that scrupulously since the day I became a bishop. I am not saying anything new. If that’s the case, why all the fuss?
O’Connor told Klein that other social issues also concerned him. For instance, during a September 1984 hospital strike, he said something that received very little press coverage, namely that no “Catholic Hospital could hire substitutes for the striking workers or threaten them in anyway.”
Nonetheless, he rejected the so-called seamless-garment approach. “I simply don’t see the rationale in saying that a politician is for better housing, a lower rate of unemployment, a more rational foreign policy—and the only thing wrong is that he supports abortion, so it’s okay to vote for him. You have to go back to the basic question: What is abortion? Do you think it’s the taking of innocent human life or don’t you? If you do, then translate it: How can we talk about a rational foreign policy or the horrors of nuclear war if we hold the position that you can take innocent human life?”
In January 1986, in a letter read at all Masses in the archdiocese on the anniversary of the Roe v. Wade decision, O’Connor described that day in 1973 as one of “national infamy.” From the pulpit in St. Patrick’s Cathedral, he told the faithful, “In 1984, when I talked strongly on the issues, I was accused of doing so because the national election campaign was in progress. I said then, ‘I’ll be talking about this in 1985 and 1986 and until the day I die.’” And so he did.
And O’Connor continued to critique the thin-skinned Mario Cuomo. In February 1986, he said, “I flat out think [Cuomo’s] wrong. I don’t think that makes him evil. It makes him wrong. He makes a serious effort to theologize his way through it and I think he’s been unsuccessful.” O’Connor was referring to Cuomo’s argument, repeated ad nauseam, that as an elected official he should not impose his religious views on the electorate.
The cardinal said that while Cuomo “has a great deal to offer on other issues, he [is] misguided about abortion.” O’Connor specifically criticized Cuomo for supporting Medicaid funding for abortion “without any constitutional requirement to do so.”
The public envelope was pushed further in August 1986 when a routine newsletter signed by the vicar general, Bishop Joseph O’Keefe, arrived at 410 parishes containing this paragraph, which was directed towards pro-abortion politicians and spokesmen:
Great care and prudence must be exercised in extending invitations to individuals to speak at parish-sponsored events, e.g., Communion breakfasts, graduations, meetings of parish societies, etc. It is not only inappropriate, it is unacceptable and inconsistent with diocesan policy to invite individuals to speak at such events whose public position is contrary to and in opposition to the clear, unambiguous teaching of the Church. This policy applies, as well, to all Archdiocesan owned or sponsored institutions and organizations.
The pro-abortion crowd and New York’s liberal establishment became unhinged over the announcement. Catholics for a Free Choice protested that the archdiocese had “nailed [the door] shut to prevent its members from being heard.”
A New York Times editorial described the directive as a “revival” of the argument between O’Connor and Cuomo “about how fervently Catholics in public office must oppose abortion.”
Initially, Governor Cuomo declined to comment, saying he had not read the statement. But a member of his press office coyly said that it “doesn’t seem to apply to the Governor” who “is totally within the confines of Church teaching.”
Defending the policy, Bishop O’Keefe said he was not denying free speech. “I’m not saying we shouldn’t listen. I’m not afraid to listen to anybody’s opinion. But when you are bringing together a church society, it is inappropriate to invite people who divide your community.” The bishop added that when he decided to issue the directive, “I never even thought of the Governor.”
On September 4, Cuomo, who was in the midst of a re-election campaign, went on the offensive. “We lay people have a right to be heard,” he declared. “It is very difficult to see how this [directive] would be implemented.” In typical Cuomo fashion he raised a host of questions to confuse the issue. “From what I’m told, it applies to Church teaching. But what is Church teaching? When are you teaching infallibly and when aren’t you? What people, which people will decide who agrees with Church teaching? Will you have ecclesiastical courts?”
Reacting, Monsignor Peter Finn, Director of Communications for the archdiocese, dismissed Cuomo’s comments, saying they were “nonsense.” “I hardly think,” Finn continued, “our local synagogue would be about to invite a P.L.O. [member] to their seder any more than a church in Harlem would invite Mr. Botha [the president of South Africa] to their supper. So I don’t understand. What’s the problem? In a response to a request from many people about what the guidelines should be for inviting people for speaking, a guideline was given. Period. . . . I think it’s very clear as far as the Church is concerned, what it means by ‘differing with the Church’s teachings.’”
Bishop O’Keefe joined the fray, ridiculing Cuomo’s Notre Dame speech as “the encyclical by Mario.” He also said that “under no circumstances would I invite [Cuomo] to speak to young people at a graduation” because “he would confuse young people.”
Cuomo did, however, concede to a Times reporter that “The Church has the right to make rules for itself, there’s no doubt about that. The Church has the right to make rules. It can say ‘If you want to belong these are the rules.’ But depending on what the rule was, one can say whether it was wise or whether it was unwise.”
The September 11 issue of Catholic New York published the cardinal’s response to Church critics in a column titled “A Matter of Common Sense.” O’Connor threw down the gauntlet, asking “how much further are the nonsensical allegations going to go on?”
Imitating Cuomo’s rapid-fire approach, the cardinal asked,
“So what is all this furor about? What is all this fuss about? What is the nonsense I read about squelching ‘free speech’? Where is the deep, dark sinister political motivation that some choose to see? When did common sense, or a sense of appropriateness, become unconstitutional or un-American? Why the hysterics that leads a columnist to speak of the ‘thought police’ of the Archdiocese of New York? (A rather nasty Nazi-like implication there, wouldn’t you say?)”
The cardinal also addressed Cuomo’s inquires as to who decides who will be heard: “Who is supposed to make the judgment in such matters? Our pastors, with the guidance of our Vicar General, are charged by Church law and by my delegation to provide guidance. Are we to have a Church in which everyone’s judgment is equal to everyone else’s? That’s not a Church, it’s chaos.”
The cardinal’s column was not his final word on the subject.
In November 1989, the cardinal took two active steps in support of his words. First, he became chairman of the U.S. Bishops’ Committee for Pro-Life Activities. That same month he urged the founding of a new order of nuns, the Sisters of Life, who would take an additional vow to defend human life against abortion and euthanasia. Nine women took up his challenge in June 1991 and co-founded the order, which thrives to this day.
On January 31, 1990, O’Connor defended his auxiliary bishop, the vicar of Orange County, Austin Vaughan, who had spent ten days in an Albany jail for protesting in front of an abortion clinic. While incarcerated, Vaughan stated that Governor Cuomo was “in serious risk of going to hell” because of his “active support of abortion rights and government financing of abortion.”
In his Catholic New York column, the cardinal, describing Vaughan as “one of the finest theologians I know,” continued:
I read in the newspapers that His Excellency, the Auxiliary Bishop of New York, had “’cursed” His Excellency, the Governor of New York, “’to hell.”’ Indeed, the Governor is quoted as saying: “I get condemned to hell for not agreeing [on abortion].”
“Not so,” Bishop Vaughan told me, “very much not so,” when I spoke with him after his release from prison. He went on to say that he is well aware that he has no power whatsoever to condemn anyone to hell. He would agree with the Governor completely that such an unpleasant task is exclusively the prerogative of a much higher and wiser power.
He told me, too, that despite the newspaper reports, he had never suggested for a moment that he would be happy to see me refuse the Governor Holy Communion. In fact, he says he was asked by the press whether he, Bishop Vaughan, would excommunicate the Governor, and replied that he had no authority to do so and would not think it a good idea anyway.
That out of the way, would anyone deny that the Bishop has the right and even the obligation to warn any Catholic that his soul is at risk if he should die while deliberately pursuing any gravely evil course of action, and that such would certainly include advocating publicly, as the Bishop puts it, “the right of a woman to kill a child.” What the Bishop told me he actually said was that the Governor is “quite possibly contributing to the loss of his soul.” To me that sounds significantly different from “cursing” or “condemning” the Governor to hell. . . .
I do have one major concern, however, and it’s not the highly confused report on who said what in the newspaper stories. It’s that such stories tend to distract from the real issue, that abortion, as the Second Vatican Council puts it, is an “abominable crime.” That, neither political fortunes nor ecclesiastical sanctions, is the bottom line.
Reacting to O’Connor’s column, Cuomo had a terse reply: “The Cardinal says the Bishop was misquoted, I’m glad.”
A June 14, 1990, special edition of Catholic New York contained a twenty-thousand-word Q&A written by O’Connor that addressed almost every conceivable subject concerning abortion, including suggestions to doctors, lawyers, educators, and parents “to advance the cause of life.”
What caused headlines was this statement:
Where Catholics are perceived not only as treating Church teaching on abortion with contempt, but helping to multiply abortions by advocating legislation supporting abortion or by making public funds available for abortion, bishops may decide that . . . such Catholics must be warned that they are at risk of excommunication. If such actions persist, bishops may consider excommunication the only option.
O’Connor went on to state that, at the same time, “the Church does not want to make ‘martyrs’ of individuals by punishing them. It is up to the local bishop to use his best judgment concerning particular cases.”
Of the “personally opposed” position, O’Connor stated that it “says, in effect, ‘In public life I will act indistinguishably from someone who sees abortion as a positive social good, but please know that I will do so with personal regret.’ This regret is hardly effective, since it serves the agenda of those who actively favor abortion.”
While the archdiocese’s communications director, Joe Zwilling, said that O’Connor’s Q&A was “not written with anyone in mind,” the New York Timesreported that Governor Cuomo “appeared to take it personally.” Cuomo told the Times, “It is difficult to discuss it. It is upsetting. I don’t like to hear it. How could you? This is something very fundamental to our family.”
Cardinal O’Connor kept up the battle on abortion for the rest of his life. And when O’Connor lay dying in 2000, his old adversary, Mario Cuomo, conceded in a New York Times op-ed piece that the archbishop “was an extraordinary prince of the Church who has always been a priest first.”
America could do with such another.
George J. Marlin is the author/editor of eleven books including The American Catholic Voter: Two Hundred Years of Political Impact. This essay was excerpted from his forthcoming book, co-authored with Brad Miner, The Sons of St. Patrick’s: A History of the Archbishops of New York.
By Jonathon Von Maren, Mon Sep 8, 2014 – 1:54 pm EST
From the front lines of the culture wars
For too long we have been lied to about the sexual revolution. But now the mask is coming off, and the younger generations are recognizing that they have been sold a pack of lies.
It’s sobering and frustrating to consider that each and every time social conservatives raised the cultural alarm throughout the last five decades, pointing out that each new manifestation of the Sexual Revolution would lead to devastating consequences, they were written off with derisive laughter. They were accused of “provoking a moral panic,” or being “stuck in the past” or “too prudish.” The “slippery-slope” arguments of aging moralists were simply dogmatic hysterics to be ignored, if not mocked.
Unfortunately, the briefest of cultural overviews reveals that those who sounded the alarm were not crackpots, but prophets.
More than 25 new categories of sexually transmitted diseases (now referred to as “sexually transmitted infections” in order to make them sound less permanent)?Check.
Regular, government-funded nude and sexually explicit frolics in the streets of our biggest cities? Check (and if you don’t go, you’re a bigot).
Soaring rates of pornography addiction that has now ensnared the majority of our population and is creating an insidious new rape culture emanating from the screens of our computers and smartphones? Check.
Millions upon millions of tiny human beings suctioned, shredded, dismembered, and burned to death in the name of “freedom”—the human cost of allowing us to copulate without consequence? Check.
While there are many depressing trends that we need to fight, one trend that it is encouraging is the number of people who have realized that the Sexual Revolution sold them a pack of lies.
And I could go on. But these sobering facts beg a very good question—how can the pro-life movement expect to impact, much less change, a culture that has gone so far?
The answer to that question, as I’ve seen in hundreds of personal conversations with high school students and university students, is that the truth eventually seeps in. There’s a reason that the current hyper-cynical, often nihilistic “Family Guy generation” responds so well to the pro-life message when we arrive at their high schools: When we tell them they’ve been lied to, they already know that. They’re just not sure how.
This is a generation that has never known what came before the Sexual Revolution. They weren’t part of the massive cultural shifts that resulted in the mainstreaming of pornography, hook-up culture, and abortion. It was simply bequeathed to them as their dubious inheritance.
And I say “dubious” for a reason—when you talk to a girl who had an abortion at 13 and was told by her mother or school nurse that it was “no big deal,” she knows she was lied to. When you tell a guy who has been hooked on porn since he was 10 and has never had a sexual experience that was not defined by that addiction that he’s been lied to, and that porn has changed him, he knows you’re telling the truth.
Teenagers dislike being lied to by adults, and when we confront them with reality, they realize very quickly that much of what they believed was nothing less than a failed cultural experiment.
Even mainstream media publications are slowly but surely admitting what social conservatives have said all along. Publications fromThe Atlantic to The New York Times to The Daily Mail are all admitting that pornography is warping the minds of the youth, creating situations in which girls are being coerced into sex acts they do not want to perform, impacting the ability of boys and girls to emotionally bond, and, bizarrely, rendering many boys and men sexually impotent.
The anti-porn movement has now driven an enormous wedge between those feminists and secularists who are honest about the damage porn has caused, and the Sexual Revolutionaries who are determined to defend every insidious and excessive manifestation of sexual “freedom.” After all, once we admit that certain behaviours are damaging and wrong, what’s stopping us from re-examining the whole bloody experiment?
The same goes for hook-up culture. Hannah Rosin of Slate, while ostensibly supportive of hook-up culture, was forced to admit in her recent book The End of Men that what many sexually-experienced university students wanted at the end of the day was just to go out on a romantic dinner date—an “experiment” that some of them had never tried.
TIME magazine released an article some time ago titled “The Hook-Up Culture Hurts Boys, Too”—tacitly admitting that the reality of hook-up culture hurting girls now just goes without saying. And while the Sexual Revolutionaries accuse social conservatives of being “anti-sex,” it is their ideology that has profoundly undervalued, debased, and degraded this most intimate of human experiences.
In fact, when a professor named Chap Clark set out to find the story behind the statistics of sex in high schools, he was shocked by what he found: “I was surprised to realize that for most mid-adolescents the issue of sex had lost its mystique and has become almost commonplace. They have been conditioned to expect so much from sex and have been so tainted by overexposure… as one student told me, ‘sex is a game and a toy, nothing more.’”
While there are many depressing trends that we need to fight, one trend that it is encouraging is the number of people who have realized that the Sexual Revolution sold them a pack of lies. The controversial actor and comedian Gavin McInnis, for instance, realized that everything he’d been told about abortion was wrong when he saw his wife give birth. I interviewed him some time ago, and he told me that he’s not the only one:
I think that the liberal world is realizing that, as I did, that it just doesn’t add up. And I think the world is catching on. You can check the internet, but that’s because the only place these liberal graduates, these liberalized graduates have to go, is the internet. So they spill out, and lost logic is seeping in. I was just at a conference, in Palm Beach this weekend, called Restoration, and there was a lot of old conservatives, and they were really negative, and they’ve given up. And I just kept saying to them, ‘Guys, the truth is seeping in. And the children in the information age, the really young kids, they don’t believe all this.’ And I also noticed it with abortion. Like you have punks for the first time carrying pro-life signs, and you have bands like Flat Foot 56 being ‘Be a man, don’t be a quitter, just because the child’s within her.’ And I think that it’s changing.
In many ways, it is. When we approach the youth of our culture today, we’re not telling them what might happen as the result of the Sexual Revolution, we’re telling them what has happened—and how to avoid those consequences themselves. We now know that the free love utopia promised by hedonistic academics and drugged-up hippies was as illusory as their narcotic-induced hallucinations. All we have to do is show them the half-century report card and ask them questions—ask them if porn and hook-up culture and abortion has made them happy. Our society has confused pleasure with happiness for too long, and now that we’ve gotten a good look at the fall-out, many people are rediscovering age-old truths that our culture abandoned on the ill-fated whim of those who thought to justify their own desires.
And yet, the truth seeps in. I know I’ve quoted this poem before, but Arthur Hugh Clough says it so beautifully:
For while the tired waves, vainly breaking, Seem here no painful inch to gain, Far back, through creeks and inlets making, Comes silent, flooding in, the main.
By Caitlin Bootsma, Mon Sep 8, 2014 – 11:30 am EST
Do you ever wonder why Hollywood stopped producing movies like It’s a Wonderful Life, Meet Me in St. Louis, or The Wizard of Oz? These were films that you could enjoy viewing by yourself, but also watch with your children or parents without skipping scandalous scenes or feeling like you were just wasting time. These movies are more than just pieces of nostalgia; they are value-based films that address universal questions about family, the meaning of life, and where one can call home.
When I started watching The Identical (to be released in theaters this September), I wondered if I would be in for two hours of a movie that, yes, would be value-based, but also would be nowhere near Hollywood standards. You know the movies I mean: the ones that are full of life lessons, but the characters fall flat and the plot just is not engaging.
Instead what I found was a movie for which I would grab some popcorn, watch with my kids, and enjoy the catchy rock-n-roll music and the lessons woven throughout the film.
The movie follows the story of twin boys born to a young couple during the Depression. Despite their love for both boys, they make a hard decision to let one be adopted by a pastor and his wife so that both boys will be provided for. We soon see that though the boys are separated by circumstance, they have the same extraordinary talent for music. The music sets the background for the entire film—even my two year old loved it, dancing at a dizzying pace around our living room.
The son who remained with his birth parents catapulted into fame; so well known he could be another Elvis. The adopted son, not knowing that he is adopted, develops his own love of music. Here, the life questions begin. The son, Ryan, is caught between his passion for music and his pastor father’s desire to have Ryan follow him into ministry. The question is: what does God want for his life?
I won’t give too much away, but as the twins’ talent grows, so do Ryan’s questions about his family and where he comes from. His questions about his vocation are very closely tied to his understanding of his identity and his relationship with his family, both birth and adoptive. Plot twists and confrontations between family members remind me of the many growing pains we all go through to find our way in life.
At the beginning of the film, I’ll admit I had some hesitations that this was going to be a thinly-disguised homily or sermon. Instead, I found myself wondering why more films couldn’t address similar themes that are relevant to everyone, regardless of background or creed.
To me, The Identical is a hopeful sign that we may be able to rebuild a culture that celebrates family, life and love through the arts. If we can teach these values in our homes and live them out in our own life, why shouldn’t we also see them on screen? Instead of watching a movie that is full of tired-out bathroom humor, flimsy relationships or gratuitous sex scenes, we could be enjoying entertainment that leaves one feeling joyful, introspective and perhaps even singing a new rock-n-roll song or two.
Reprinted with permission from our good friends atInsideCatholic.com, the leading online journal of Catholic faith, culture, and politics.
Contraception is the elephant in the living room of contemporary Catholicism: Everybody knows it’s there, but few people care to acknowledge the fact. Meanwhile, the accumulating pastoral damage that results from this state of collective denial is painfully real.
Partly it arises from the circumstance that even churchgoing Catholics today live in a state of make-believe. “We’re all one big happy family, aren’t we?” On the matter of contraception we most certainly aren’t, and the strain of pretending otherwise saps energies and weakens the bonds of ecclesial communion.
It gets worse. According to poll data, 75 percent of Catholics in the United States receive the sacrament of penance – go to confession, that is – less than once a year. In many cases, that’s never.
There are many reasons for this, but contraception obviously is one. Contracepting Catholics don’t wish to confess contraception, because they’re afraid of being told it’s wrong and have no intention of giving it up. But they don’t wish not to confess it, because they know the Church rejects it and not confessing it would be dishonest. Their non-solution to this dilemma is to stay away from confession entirely.
What to do about this state of affairs? Would a comprehensive public airing of the problem help?
Note that I raise this question as someone who supports the Church’s teaching on contraception and has publicly defended it many times. I support the teaching on two grounds: first, the firm and constant teaching of the Magisterium over many centuries; second, the powerful and sophisticated rational argument against contraception developed by Germain Grisez and his colleagues in the “New Natural Law Theory” school.
But – to repeat – would public discussion of the issue at this time actually help? That’s not so clear. The most recent experience in this line suggests the answer may be no.
I refer to the furor that erupted two months ago over Pope Benedict XVI’s remarks on condom use to prevent the spread of HIV-AIDS. The pope’s comments (in a book-length interview with German journalist Peter Seewald called Light of the World) were highly limited in scope and did not concern sexual relations within marriage; the focus instead was on relations outside the marital context in which one of the partners is HIV-infected.
Benedict made the following points: Sex outside marriage is itself wrong; condom use to prevent the transmission of HIV is not “a real or moral solution” to the AIDS problem; still, if people are determined to do what is wrong, using a condom could at least be a “first step” toward a responsible approach to sex that recognizes responsibility for the other party.
For the pope to say this was indeed something new, although it was hardly an earth-shaking utterance that turned the contraception debate on its head. In view of the flap that followed, however, you could be excused for not understanding that.
The blame for this confusion is widely shared. Acting with authorization from the Vatican publishing house (yes, you heard that right – the Vatican publishing house), the Vatican newspaper, L’Osservatore Romano, got the media frenzy rolling by breaking the embargo on the pope’s remarks and compounded the problem by leaving out a key passage that made his meaning clear. Here was another reminder, if one is needed, that Vatican communications are a shambles.
Secular journalists, unaccustomed to having to think rationally about issues of morality, rushed to serve up sensationalized coverage. Nothing new about that, either. The journalists received little or no help from the Holy See, but were aided and abetted by a bevy of Catholic commentators ready and willing to shoot from the hip. Then, to complete the foul-up, some of these latter, on the conservative side, fell to belaboring one another for having voiced a new idea or two. Some went so far as to take the pope to task.
The result: A month later, the Vatican was still issuing clarifications of something that should have been clear at the start.
If this messy episode did nothing else, at least it made it clear that the elephant in the Church’s living room – contraception, that is – is still there. In doing so, it raised the question of what, if anything, can be done about it.
An Austrian bishop named Klaus Kung suggested the time may have come when a papal encyclical on sexual morality would help. But he spoiled it by adding the thought that an international commission should be established to help prepare such a document. The suggestion contains undertones of the “papal birth-control commission” that did so much to tilt the playing field against Pope Paul VI’s anti-contraception encyclical Humanae Vitae even before it appeared. Do we really want to go through that again?
But can we just sit and wait, hoping against hope that sooner or later something or other – heaven knows what – will turn up to change things for the better?
I have no evidence, just a sneaking suspicion, that Benedict might have been asking himself that question when he floated his little trial balloon with Seewald. If so, he now has a lot more data to mull. One thing is for sure: If you leave an elephant in the living room long enough, eventually you’ll have an awful mess to clean up.
As detailed in the book Physicians Healed1, I began my OB-GYN training doing contraception. As time went on I saw that most contraceptives were actually abortifacient. But there were other bad humors in my contraceptive practice as well. By putting all fourteen-year-olds on birth control pills, it seemed like we were unleashing an epidemic of sexually transmitted diseases, including cervical dysplasia and cervical cancer. It seemed like there was a generalized loss of respect for patients. Not only did we trivialize the patients, but also our profession. We thought of ourselves as plumbers of the reproductive tract. Tubal ligation was a short, common and seemingly trivial operation.
Later I began to rethink things. In my genetic fellowship it began to dawn on me that Mary was the Ark of the Covenant. Her womb was thus a sanctuary, or Holy of Holies which contained the baby Jesus. I gained greater respect for the vocation of motherhood. I began to have much greater respect for the womb. It’s not just a hollow muscular organ. It is where women cooperate with God in developing a new human life.
Later I learned to become a natural family planning doctor. I began to see that rather than being a plumber of the reproductive tract, I could be the doctor to a marriage. I learned the contraceptive doctor unleashed more than 10 plagues on society. These may include teen pregnancy, abortion, divorce, fatherless children, gang violence, men’s loss of respect for women and many more. And I heard about a confessor in Yugoslavia who could read the minds of penitents. After they thought they had confessed everything, he would insist they had forgotten one. “Oh that!” they said. He told them that their fallopian tubes were “a river of love and life.” Their anatomic integrity was essential to love, marriage, family, and society. In distal fallopian tube was where the sperm, egg and God met for the individual act of creation.
Couples preparing for a new marriage often want tubal reversal. They sense that anatomic integrity of the fallopian tube is essential to love and marriage. They sense that being open to new life is integral to their marital relationship. Many are called to reverse tubal ligation but few actually do it. It requires faith, determination and some money. While I always encourage women to do it, I have great admiration for those who see it through to competition.
Some factors can be helpful in preparation. An X-ray of the uterus and tubes (hysterosalpingogram) is helpful.
One would hope to eventually have a fallopian tube which is at least 4 cm long. The operative report of the tubal ligation can be helpful at times, although it is not always reliable or complete. The surgeon doing the tubal ligation sometimes does more damage than necessary. Doing more damage at the time of the tubal ligation makes the tubal ligation less likely to fail, but could create more difficulties for reconstruction. There can be other factors as well, such as endometriosis, scarring, fibroids, ovarian cysts, etc. In the final analysis, one cannot be guaranteed full knowledge ahead of time.
It is a technically challenging operation. The structures are very small. The operation is usually done with high magnification by an operating microscope. It usually takes several hours of careful work.
Those who desire tubal reversal are usually older than those who got their tubes tied. Successful reconnection of the tubes does not guarantee pregnancy. Age has an influence on fertility, after this operation and in general. The chronological age cannot be changed. A program to decrease toxins, increase nutrients and exercise, and balance hormones may reduce biological age. It could be helpful to anyone preparing for a successful pregnancy.
Thus, I usually recommended tubal reversal for anyone who has been sterilized. It is not trivial, either for patient or doctor. I admire those women who have courage and determination to complete it. And they seem to be glad they did it, whether they get pregnant or not. It is an honor to be able to care for such heroic women.
Sound Choice Pharmaceutical Institute Website: www.soundchoice.org
Contact: Katie Doan 206-906-9922 PST Email: kdoan@soundchoice.org
For Immediate Release: 09/08/14, (Seattle)
A new study published in the September 2014 volume of the Journal of Public Health and Epidemiology reveals a significant correlation between autism disorder (AD) and MMR, Varicella (chickenpox) and Hepatitis-A vaccines.
Using statistical analysis and data from the US Government, UK, Denmark and Western Australia, scientists at Sound Choice Pharmaceutical Institute (SCPI) found that increases in autistic disorder correspond with the introduction of vaccines using human fetal cell lines and retroviral contaminants.
Even more alarming, Dr Theresa Deisher, lead scientist and SCPI founder noted that, “Not only are the human fetal contaminated vaccines associated with autistic disorder throughout the world, but also with epidemic childhood leukemia and lymphomas.”
Their study comes on the heels of recent breaking news that the CDC deliberately withheld evidence of the significant increase in autism among African-American boys who were vaccinated prior to 36 months of age.
So it should come as no surprise that the FDA has known for decades about the dangers of insertional mutagenesis by using the human fetal cell lines and yet, they chose to ignore it. Instead of conducting safety studies they regulated the amount of human DNA that could be present in a vaccine to no greater than 10ng.
Unfortunately, Dr. Deisher’s team discovered that the fetal DNA levels ranged anywhere from 142ng – 2000ng per dose, way beyond the so-called “safe” level.
“There are a large number of publications about the presence of HERV (human endogenous retrovirus – the only re-activatable endogenous retrovirus) and its association with childhood lymphoma,” noted Dr Deisher. “The MMR II and chickenpox vaccines and indeed all vaccines that were propagated or manufactured using the fetal cell line WI-38 are contaminated with this retrovirus. And both parents and physicians have a right to know this!”
Certainly these discoveries by SCPI should generate an immediate investigation by FDA officials, if not an outright ban on the use of aborted fetal cell lines as substrates for vaccine production. There are numerous other non-human FDA-approved cell lines that can and should be used.
Dr. Theresa Deisher is a PhD in Molecular and Cellular Physiology from Stanford University with over 20 years in commercial biotechnology, prior to founding AVM Biotechnology and Sound Choice Pharmaceutical Institute. As an inventor of 23 issued US patents she is world-renowned for her work in adult stem cell research and the first to discover adult cardiac derived stem cells. Dr. Deisher was a plaintiff in the US federal lawsuit to prohibit the use of taxpayer dollars for embryo destructive research, which resulted in steering science towards adult stem cell research and 14 US FDA approved adult stem cell products.
“Universal destination” may sound like a fancy way of saying where we’re all headed, but this odd expression happens to be the name for a central principle of Catholic social teaching. It follows therefore that it is also central to Pope Francis’ much-discussed apostolic exhortation,Evangelii Gaudium (The Joy of the Gospel).
The point is important particularly in light of the announcement that the Pope and President Obama will meet in late March in Rome to talk—according to the president—about their shared concern over economic inequality. It’s a matter on which they see eye to eye. Or do they?
Even friendly critics of the apostolic exhortation have seemed often to miss its central thrust, with perhaps some reason. The document is long, rambling, and studded with overly broad generalizations, and the flaws make it easy for well-disposed readers to become distracted and lose track of what its economic sections are actually saying.
Begin with the crucial fact that, like other social justice documents of the Magisterium, Evangelii Gaudium doesn’t deal in policies and programs but principles. The most important of these is the universal destination of goods, understood as an existential basis for an equitable sharing of the world’s wealth. (Worth recalling as America marks the 50th anniversary of the War on Poverty.)
Pope Francis, looking at the global scene, puts it like this: “We must never forget that the planet belongs to all mankind and is meant for all mankind; the mere fact that some people are born in places with fewer resource or less development does not justify the fact that they are living with less dignity” (Evangelii Gaudium, 190). With necessary adjustments, that applies to the national and local levels too.
The Pope isn’t saying anything new. Other popes have made the same point. But apparently it’s new to some. In conversation with several well-educated Catholic laymen a while back, I mentioned the universal destination of goods and
was met with blank disbelief: Surely the Church never said anything like that. Evidently there’s work to do getting the word around.
It’s a simple enough principle. God created the world for everyone to live in and cultivate and enjoy, and that should govern the distribution of its fruits. The right to private ownership, also affirmed by the Church, remains undisturbed in this view. But it isn’t absolute, and the principle shaping its exercise is “universal destination.” Francis says: “The private ownership of goods is justified by the need to protect and increase them, so that they can better serve the common good” (Evangelii Gaudium, 189).
This points to the moral imperative of some form of redistribution of wealth. Here many critics lose their cool, assuming this means heavy-handed statist intervention in the economy, ruinous taxation of individuals and private enterprises that discourages initiative, and the rest of the neo-liberal chamber of horrors. Francis’ remedy is different: it’s moral change—conversion.
Activists of the left and the right commonly proceed as if structures—government programs, free markets, or some combination of both—were sufficient to ensure justice and prosperity for all. But structures must be supported by change of heart. One without the other won’t do the job. Structural changes are needed, Francis says, but also more: “We are called to find Christ in [the poor], to lend our voice to their causes…to be their friends” (Evangelii Gaudium, 198).
Some people will reasonably ask: Is that realistic? To which the answer is: Maybe not, but the Church must keep saying it, or it never will be.
Russell Shaw is a freelance writer from Washington, D.C. You can email him at RShaw10290@aol.com.
If the United States wants to stop the wave of minors and young adults flooding across its southern border from Central America, it should help Hispanic women in those countries abort their children. That’s the thesis of a “featured article” posted August 19 in YaleGlobal Online, a publication of Yale University.
Marisol Ruiz, a past Fox International Fellow at Yale, proposes that Congress “should attach specific conditions” to emergency aid packages designed to stop crime in Central America, “ensuring the money will implement policies focused on gender mainstreaming, highlighting the importance of transforming gender relations.”
“Gender mainstreaming” in the heavily Catholic region would “entail investing in maternal and newborn health, as well as investing in family planning and reproductive health.”
He was particularly concerned the region lacks “access to safe and legal abortions.”
“Central America is home to two of the seven countries in the world where abortion is banned in all cases,” El Salvador and Honduras, Ruiz noted. “The consequences of total criminalization of abortion” include “high maternal mortality.”
Pro-life policies and organizations instituted by Republican presidents are singled out as a cause of the current border crisis.
“U.S. partisan politics and aid policies have been complicit by discouraging family-planning resources for impoverished nations” by adopting the Mexico City Policy. The “Global Gag Rule,” as Ruiz called it, “sporadically applied since the 1980s by conservative administrations, prohibited foreign organizations receiving US economic aid the right to use non-US funding to provide information for legal abortion or advocate for the legalization of abortion in their country.”
President Ronald Reagan instituted the ban, which remained policy until President Bill Clinton repealed it. President George W. Bush reinstituted the policy in 2001, but it was against repealed by President Barack Obama.
Ruiz wrote that abortion must be promoted in the region to “avoid facing an ongoing humanitarian crisis and address its real concerns about demographics and security.”
He views the push for abortion and contraception as a template to be exported to other nations, particularly poor nations with a transient population seeking employment or fleeing violence. “If implementation of such policies is successful, the lessons could be applied to every other region in the world with treacherous influxes of immigration,” he wrote.
That description could apply, for instance, to the Christian minority fleeing war-torn Iraq.
The website that published Ruiz’s article, YaleGlobal Online is a publication of the Ivy League school’s Whitney and Betty MacMillan Center for International and Area Studies. The center is dedicated to “globalization,” which it defines as the “increasing integration of the world’ based on its “interconnectedness and interdependence.” The center’s scholars acknowledge that deeply contested values like culture, the economic stability of the middle class, and national security – “issues like the growing anti-immigrant sentiment in Europe, the West’s farm subsidies and intellectual property rights concerns, and the tightened visa policies of the U.S. since Sept. 11” – could “could throw a wrench into the engines of” internationalists.
But they feel “the historical process of reconnecting the human community” into a one world government “is here to stay and increasingly visible.”
One year to the day since a team of 20 social workers, police officers, and special agents stormed a homeschooling family’s residence near Darmstadt, Germany, and forcibly removed all four of the family’s children, aged 7 to 14, a state appeals court has returned custody of the children to their parents.
The reason given for the removal was that parents Dirk and Petra Wunderlich continued to homeschool their children in defiance of a German ban on home education.
The children were returned three weeks after being taken, following an international outcry spearheaded by the Home School Legal Defense Association.
However, a lower court imposed the condition on the parents that their children were required to attend state schools in order for them to be released, and took legal custody of the children in order to prevent the family from leaving the country.
In a decision that was still highly critical of the parents and of homeschooling, the appeals court decided that the action of the lower court in putting the children in the custody of the state was “disproportional” and ordered complete custody returned to the parents, according to a statement by the HSLDA.
The Wunderlichs, who began homeschooling again when the court signaled it would rule this way, said they were very pleased with the result, but noted that the court’s harsh words about homeschooling indicated that their battle was far from over.
“We have won custody and we are glad about that,” Dirk said.
“The court said that taking our children away was not proportionate—only because the authorities should apply very high fines and criminal prosecution instead. But this decision upholds the absurd idea that homeschooling is child endangerment and an abuse of parental authority.”
The Wunderlichs are now free to emigrate to another country where homeschooling is legal, if they choose, but they said they intend to remain in Germany and work for educational freedom.
“While we no longer fear that our children will be taken away as long as we are living in Hessen, it can still happen to other people in Germany,” Dirk said. “Now we fear crushing fines up to $75,000 and jail. This should not be tolerated in a civilized country.”
Petra Wunderlich said, “We could not do this without the help of HSLDA,” but cautioned that, “No family can fight the powerful German state—it is too much, too expensive.”
“If it were not for HSLDA and their support, I am afraid our children would still be in state custody. We are so grateful and
thank all homeschoolers who have helped us by helping HSLDA.”
HSLDA’s Director for Global Outreach, Michael Donnelly, said he welcomed the ruling but was concerned about the court’s troubling language.
“We welcome this ruling that overturns what was an outrageous abuse of judicial power,” he said.
“The lower court decision to take away legal custody of the children essentially imprisoned the Wunderlich family in Germany. But this decision does not go far enough. The court has only grudgingly given back custody and has further signaled to local authorities that they should still go after the Wunderlichs with criminal charges or fines.”
Donnelly pointed out that such behavior in a democratic country is problematic.
“Imprisonment and fines for
homeschooling are outside the bounds of what free societies that respect fundamental human rights should tolerate,” he explained.
“Freedom and fundamental human rights norms demand respect for parental decision making in education. Germany’s state and national policies that permit banning home education must be changed.
“Such policies from a leading European democracy not only threaten the rights of tens of thousands of German families but establish a dangerous example that other countries may be tempted to follow,” Donnelly warned.
HSLDA Chairman Michael Farris said that acting on behalf of the Wunderlichs was an important stand for freedom.
“The Wunderlichs are a good and decent family whose basic human rights were violated and are still threatened,” Farris said.
“Their fight is our fight,” Farris stressed, “and we will continue to support those who stand against German policy banning homeschooling that violates international legal norms. Free people cannot tolerate such oppression and we will do whatever we can to fight for families like the Wunderlichs both here in the United States and abroad. We must stand up to this kind of persecution where it occurs or we risk seeing own freedom weakened.”
Visit the HSLDA website dedicated to helping the Wunderlich family
and other German homeschoolers http://www.hslda.org/LandingPages/Wunderlich Contact the German embassy in the U.S.
Ben Johnson recently wrote a great article about the damaging effects of the Gardasil (HPV) vaccine. In his article, he talks about women who have died, 96 to be exact. And those are just the ones that have been reported. He talks about women who have lost their fertility after receiving the highly regarded HPV vaccine. But the main focus of the article is how the Gardasil vaccine is being heavily promoted to the African-American community through ad placement on BET (Black Entertainment Television). When I read his article, my conspiracy alarms went off. Now, I’m not a conspiracy theorist (although I find people who are quite entertaining). But when I heard about these ads, my memory was triggered. Of course Planned Parenthood is trying to target minorities with this vaccine…they are getting big reimbursement for injecting their low income patients with this dangerous drug! Then I knew I had to write this article about my own experience inside Planned Parenthood regarding Gardasil. When Gardasil came out, Planned Parenthood was PUMPED. “Such a wonderful way to serve women,” they said. “This will help prevent cancer for so many young women,” one of my coworkers raved. But then I heard the real reason behind the excitement, “We are going to make so much money off of this vaccine.” Bingo. Of course they were excited. Each injection was going to cost around $200, and women have to get three to be “fully protected.” Six hundred dollars for a vaccine. That was a lot of money. But then I thought to myself, “Our clients don’t have $600 for a vaccine. This is going to be a huge flop.” What I didn’t know about at that time was the “Merck Vaccine Assistance Program.” Merck is the manufacturer of Gardasil. This program would pay 100% for the cost of the vaccine itself. Our patients would just have to pay a little $30 “injection fee” per vaccine. Ninety dollars versus six hundred was definitely doable. Next we were instructed to offer Gardasil to EVERY woman age 11-26 who walked through our doors. “Oh, you are here for a vaginal infection? How about a vaccine, too?” “Oh, I see you marked that you had Herpes and need treatment. Well, you better get this vaccine so you won’t get genital warts, too.” These may seem funny, but it was seriously how we were told to sell this vaccine to our clients. So, we started signing people up by the dozens. We faxed off countless applications for the “Vaccine Assistance Program.” Almost everyone was approved (most of our clients were low income). We were running out of vaccines. Those little bottles were flying off our refrigerator shelves at around $170 a piece, for which Planned Parenthood was being reimbursed by the Merck program. I’ve never been of the belief that Planned Parenthood operates solely out of racism, but strictly sees money-making opportunities and goes for them…unfortunately, that is usually at the expense of minority women. I don’t know if any of these women came back in with complications. I don’t know if they presented to the ER with problems. It’s not like we did any follow up. Heck, I don’t even know if they got all three doses. My gut tells me that 80% of them did not. Back to the conspiracy idea. Planned Parenthood just ran a series of ads promoting Gardasil on BET (Black Entertainment Television). Ninety-six women have died, several have experienced sterility, and yet Planned Parenthood launches a big campaign targeting the African-American community? The pro-life movement has talked for years about how Planned Parenthood targets our minority community in the United States. And even if we totally scrap the fact that the founder of Planned Parenthood, Margaret Sanger, was a raging racist we can still look and find racism inside of the organization. I’ve written before about the document that we were NOT to talk about inside of Planned Parenthood…the “Jaffe Memo.” Here is my article about that memo and what it entailed. This document was written in the late ’60s by a high level official with Planned Parenthood. You will notice some really interesting ideas in the document. “Fertility control agents in water supply” “Eliminate Welfare payments after first 2 children” “Encourage increased homosexuality” “Compulsory sterilization of all who have two children except for a few who would be allowed three” “Payments to encourage abortion” The document was proposed to the Population Council (a eugenics-based population control organization led by its first president, Frederick Osborn, who also served as the President of the American Eugenics Society). This was one of Planned Parenthood’s first attempts (after Margaret Sanger’s shenanigans) to reduce the minority population. We also know that currently over 70% of Planned Parenthood facilities are located in low income, high minority communities. We know that more than 50% of African-American pregnancies end in abortion. We know that Planned Parenthood has dumped tons of money into “Promotora” programs that go into Latino communities and convince them that Planned Parenthood is the ONLY place they can go for health care. And now, they are targeting these same communities for the dangerous Gardasil vaccine. I mean, am I crazy? How is it that rational people can’t see what Planned Parenthood is doing here? I’ve never been of the belief that Planned Parenthood operates solely out of racism, but strictly sees money-making opportunities and goes for them…unfortunately, that is usually at the expense of minority women. And the bottom line is that this will continue to happen until these minority communities wake up to the realization that Planned Parenthood is USING them to pad their bottom line. They don’t care about health care for minorities. They care about making money off of you! This won’t stop until people stand up to this abortion giant and say “NO MORE.” What will it take for these Black and Hispanic women to simply say, “We will not be used. We will not be your pawns. We will no longer be lied to. We are better than Planned Parenthood.” Kris Ford, an African-American woman who runs Women’s Health and Justice Initiative, said it better than I can. “Planned Parenthood has ignored the voices of women of color and the organizations that women of color lead for years. Planned Parenthood continues to raise large sums of money off of issues of reproductive justice while framing the issues as a binary that leaves out the experiences of women and communities of color.” It’s time to do something about it. Stop buying the lie.
U.S. Rep. Christopher Smith speaks at the Rally for Religious Freedom held in front of the U.S. Court of Appeals for the D.C. Circuit on May 8, 2014.
The nation’s political leaders – including one of the most outspoken pro-life leaders in Congress – have dismissed the new HHS mandate revision as the latest attempt to coerce religious non-profits and closely held corporations into paying for abortifacient drugs, contraception, and sterilization that violate their deeply held religious beliefs.
The latest change allows religious non-profits to contact the government with their religious objection to the HHS mandate, and the government in turn will notify the non-profit’s insurance provider of the need to furnish women with the offending drugs “free of charge.”
The penalty for entities that fail to comply is still $100 a day, or $36,500 a year, for each employee.
Congressman Chris Smith of New Jersey, co-chair of the Bipartisan Congressional Pro-Life Caucus called the new rule “just another highly coercive regulation — a direct, obnoxious, unprecedented government attack on the conscience rights of religious entities and anyone else who for moral reasons cannot and will not include potentially abortion-causing drugs — such as ella — or contraception and sterilization procedures in their private insurance plans.”
Arina Grossu, director for the Center for Human Dignity at the Family Research Council, said the revised procedure “remains an insulting accounting gimmick does not protect the rights of Americans with sincere conscientious objections.”
The new proposal also seeks to find a way to force closely held corporations into a similar procedure, in response to the Supreme Court’s Hobby Lobby decision.
Grossu sees this as an attempt to violate the religious liberty of closely held corporations and a power-grab around the Supreme Court’s Hobby Lobby decision.
Grossu says the Obama administration is still “soliciting comment on new ways to force family businesses to violate their deeply held moral and religious convictions due to the HHS mandate in an attempt to address and skirt the recent Supreme Court ruling. However, the government’s actions here still force family businesses to be complicit in what they view as morally wrong.”
“This overreach by the Obama administration is intended only to ensnare family businesses back into the web of the mandate,” Rep. Smith said.
Grossu added, “The Family Research Council urges the administration to offer a full exemption from the mandate to charities and non-profits that have sincere conscientious objections and to respect the Supreme Court’s ruling regarding family businesses like Hobby Lobby and Conestoga Wood Specialties.”
Meanwhile, Cecile Richards of Planned Parenthood objected that critics’ objections are based in fanaticism.
“Once again, we’re reminded of the great lengths opponents are willing to go to put barriers between women and their birth control,” she said. “While the Obama administration is working hard to protect women’s access to birth control in the face of harmful Supreme Court decisions, today’s notice also serves as a stark reminder of what is at stake for women in this country when it comes to affordable basic health care.”
But religious leaders say both religion and the Constitution rebuff the revision.
Dr. Russell Moore, president of the Ethics and Religious Liberty Commission of the Southern Baptist Convention, said, “When it comes to these contentious issues I don’t necessarily expect those who disagree with us to ask ‘What Would Jesus Do?’ But, in this case, asking ‘What Would Jefferson Do?’ would be a good start.”
OKLAHOMA CITY (Aug. 21, 2014) – Archbishop Coakley announced Thursday that the consecrated Host at the center of a lawsuit filed in Oklahoma County District Court has been returned.
An attorney representing the head of the satanic group presented the Host to a Catholic priest Thursday afternoon. The lawsuit sought return of the Host following multiple public statements by the head of the local satanic group that they planned to defile and desecrate the consecrated Host during a satanic ‘black mass’ scheduled next month in Oklahoma City.
With the return of the Host and an accompanying signed statement from the satanic group leader that the group no longer possesses a consecrated Host, nor will they use a consecrated Host in their rituals, the archbishop agreed to dismiss the lawsuit with prejudice.
“I am relieved that we have been able to secure the return of the sacred Host, and that we have prevented its desecration as part of a planned satanic ritual,” said Archbishop Paul Coakley of the Archdiocese of Oklahoma City. “I remain concerned about the dark powers that this satanic worship invites into our community and the spiritual danger that this poses to all who are involved in it, directly or indirectly.”
Archbishop Coakley has made repeated requests for the city’s leaders to cancel the satanic ritual in a publicly funded facility.
“I have raised my concerns … and pointed out how deeply offensive this proposed sacrilegious act is to Christians and especially to the more than 250,000 Catholics who live in Oklahoma.”
On Sept. 21, the day the satanic ritual has been scheduled, the archbishop invites the Catholic community as well as all Christians and people of good will to join him in prayer for a Eucharistic Holy Hour at 3 p.m. at St. Francis of Assisi Church, 1901 NW 18, followed by an outdoor Procession and Benediction.
“For more than 1 billion Catholics worldwide, the Mass is the most sacred of religious rituals,” the archbishop said. “It is the center of Catholic worship and celebrates Jesus Christ’s redemption of the world by his death and resurrection.
We are grateful for the gift of the Eucharist and pray that this threatened sacrilege will heighten our appreciation and deepen our faith in the Lord’s Eucharistic presence among us.”
SPECIAL NOTE: Jesus called us to be as wise as serpents, innocent as doves. In this case, my friend Michael Caspino might be wiser than the serpents. Please read this important guest message from the attorney representing Archbishop Coakley in the fight over the planned Black Mass in Oklahoma.
Brian Burch
Dear Friend of CatholicVote,
Have you heard about the “Black Mass” that a Satanist group has planned for next month in Oklahoma City?
The fake mass mocking our Faith is bad enough. But the Satanic group behind it has bragged that they have a consecrated host and intend to use it.
This must be stopped.
My own prayer and consultation with legal friends prompted an idea. So today I filed a lawsuit on behalf of Oklahoma City Archbishop Paul Coakley demanding that that consecrated host be returned to the Church immediately.
The lawsuit is simple: a consecrated host only comes from the Catholic Church. Satanists acquired the host by theft or fraud – both of which are illegal ways of acquiring property. That means that the Satanists have a legal obligation to return the stolen property.
And guess what…
The judge has ordered the Satanists not to destroy the host.
Furthermore, the lawsuit demands that the Satanists return the consecrated host to Archbishop Coakley in 5 days — or the judge may order them to do so.
In our lawsuit, Archbishop Coakley explains that not only is the consecrated host the rightful property of the Catholic Church, it is literally priceless. No value can be placed on the body, blood, soul and divinity of Christ.
So this is where you come in…
I’m willing to fight these black mass efforts with the law anywhere and everywhere they pop up.
But I also know there’s one thing that Archbishop Coakley would want you to do: Pray.
The Saint Michael prayer is the prayer he has asked Catholics everywhere to pray to win this fight. Will you join me in praying this prayer for the next 5 days?
St. Michael the Archangel, defend us in battle. Be our defense against the wickedness and snares of the Devil. May God rebuke him, we humbly pray, and do thou, O Prince of the heavenly hosts, by the power of God, thrust into hell Satan, and all the evil spirits, who prowl about the world seeking the ruin of souls. Amen.
Comment “yes” or simply “Like” this on Facebook to tell the CatholicVote.org team that you are praying.
I will let the Archbishop know that you are praying for him, and the Church in Oklahoma City.
For the Faith,
Michael W. Caspino, J.D.
by Steven Ertelt | Seoul, South Korea | LifeNews.com | 8/18/14
Over the weekend, Pope Francis visited a memorial in South Korea dedicated to remembering babies who have been victimized by abortions.
The leader of the Catholic Church is inspired by something done in and around The Vatican shortly after the death of Jesus Christ. Dug into the walls of the ancient Christian catacombs in the outskirts of Rome are countless small tombs, only a foot or two across. These are the burial places of infants cast out of their pagan homes and left to die of starvation and exposure—a common practice of that time. Members of the Early Church, charged by Christ to love all their neighbors, offered these tiny victims of Roman cruelty the only act of love they could: to bury their little bodies and mourn for them in prayer.
The abortion memorial, located at the Kkottongnae home for the sick about 120 miles from Seoul, is a field dotted with white crosses and statues of Joseph, Mary, and Jesus as a child. Francis paused briefly at the site, bowed his head and folded his hand in prayer, the Boston Globe reports.
Jung Kwang-ryul of the Kkottongnae community, described the site as a “one-of-a-kind memorial,” saying the Pope’s stop is “a clear testimony of his defense of life.”
“It is necessary to reiterate the strongest opposition to any direct attack on life, especially innocent and defenseless, and her unborn child in the womb is the innocent par excellence,” the pope said in April.
The Kkttongnae Home, located in the Diocese of Cheongju, was created in 1976 by Father John Oh, the founder of the Kkottongnae Brothers and Sisters of Jesus. The priest was inspired by a beggar named Choi Gwi Dong to feed 18 other sick beggars despite his own physical handicaps.
It offers assistance to the homeless, disabled individuals and alcohol addicts. Currently it can serve around 5,000 people.
The Cemetery for Aborted Children is located behind the home and includes a statue of the Holy Family surrounded by cross representing the unborn.
During the National Day of Remembrance for Aborted Children next month in the United States, mourners across the country will visit the gravesites of aborted children, whose broken bodies were recovered from trash dumpsters and pathology labs and solemnly buried over the four decades of legal abortion in the United States
There is intense social pressure to avoid even bringing up any controversial moral issues, and doing so can result in ire, accusations, and marginalization.
The year of our Lord 2014 finds us in a much different era than even a few short decades ago. The belief that a corrupt and decadent cabal of academics, politicians, and celebrities are trumpeting trends that the average hard-working, moral citizen – the “moral majority” – despises, has long since crumbled.
Presidential candidate George McGovern was widely mocked in 1972 as running on a platform of “acid, amnesty, and abortion.”
The Obama Democrats in 2012 called that a winning strategy.
The Sexual Revolution has made a clean sweep. Any pretense North Americans might have of living in “godly” nations look almost humorously naive. As the moral majority fades to a distinctly despised minority, how can Christians articulate their now-despised views on anything from marriage to abortion to the hook-up culture?
There is intense social pressure to avoid even bringing up any of these topics, and doing so can result in ire, accusations, and marginalization.
The biblical book of Proverbs informs us, “A soft answer turneth away wrath.” Better advice in our current culture wars could not possibly be given.
I remember one awkward moment back in university, when I attended a Fraser Institute dinner featuring George W. Bush’s right-hand man, Karl Rove. After he finished his analysis of the 2008 election campaigns, Rove took questions from the audience. One wealthy attendee, probably assuming that it was a safe joke, made some comment about a certain Democrat—I can’t recall which—having a string of wives. Rove’s short, terse response killed every snicker in the room: “I’ve been divorced.” I sympathized with the hapless businessman. I began my own university career hopelessly unequipped to deal with any discussions articulating my Christian beliefs. I realized very quickly that the principles I had taken for granted, coming as I did from a loving home with parents married for life and with my views untainted by the sexual nihilism promoted by the television shows they did not permit in the house, were not at all the consensus. Some disagreed with these principles because they were inconvenient. Others, because they were moral relativists. Others, because they thought religion was stupid. Many of these people were my classmates. Some of them became my friends. And as I navigated the shrilly left-wing landscape of modern university, I learned a few ways of defending my principles without automatically alienating those I was debating.
1. Always ask questions. Anyone who has taken a pro-life training course will not be surprised to hear that the Socratic Method is always the best. When I was confronted by university friends and peers on some of my perspectives that they found downright incredible, questions were always helpful. One friend demanded to know why I wasn’t sleeping around. I responded with a question: “How many of the people that you were with do you wish you hadn’t hooked up with?” After a pause, the thoughtful response: “Most of them, I guess. Maybe even all of them.” Another classmate demanded to know how I could call myself “a dude” if I wasn’t “sleeping with chicks.” I simply asked him whether it took more of a man to keep one woman happy for a lifetime or dozens for ten minutes. To that one, I got an arched eyebrow, an appreciative chuckle, and no follow-up questioning. In none of these cases and many others did I end up in a verbal brawl over sexual ethics. Instead, they thought about their own views, and gained a bit of respect for mine.
2. Always see whoever you’re debating with as a person first. I know it seems trite and perhaps a bit precious, but it’s absolutely true. I remember watching a documentary on the battle over Proposition 8 in California, where gay marriage proponents and opponents screamed at each other in the streets, unstoppable force meeting immovable object. It brings to mind a few lines from Matthew Arnold’s poem “Dover Beach,” in which he explains that the world: Hath really neither joy, nor love, nor light, Nor certitude, nor peace, nor help for pain; And we are here as on a darkling plain Swept with confused alarms of struggle and flight, Where ignorant armies clash by night. However, when you discuss things with people instead of placards, it’s amazing how the relationships that form can help others question some of their perspectives. We see this all the time debating abortion—once people realize that you’re not going to yell at them, that you just want to chat, and that you’re not judgmental monsters who are there to condemn them, they calm down. One pro-choice protestor screamed at me for ten minutes. Eventually, however, we had a three hour conversation that resulted in her tearing up her own sign. Once I was no longer a protestor but a person, she had to take me more seriously. She just had to realize that pro-lifers were people before she could grasp that pre-born children, are, too. Another time I was chatting with one of my friends, who happens to be gay, with whom I have extensively debated cultural issues. He started to talk about how support for traditional marriage is bigoted. But I interrupted him with a question: “Would you call me homophobic?” He barely paused. “I’d call you a friend,” he said, and carried on with the conversation.
3. Don’t get angry. Trust me, I know this one is difficult sometimes. At university, I failed this one multiple times. But if you choose to engage—and you should—on cultural issues like abortion or pornography or sexual ethics in general, where people’s views are often rooted in their own experiences and those of people that they love, staying calm is essential. As defensive as you might be when your principles are under attack, always remember that the people you are discussing or arguing with are probably just as defensive as you are. The biblical book of Proverbs informs us, “A soft answer turneth away wrath.” Better advice in our current culture wars could not possibly be given. That doesn’t mean we compromise on truth, and it doesn’t mean that there isn’t a time for “righteous indignation” in defence of our beliefs. But in the context of a one-on-one conversation with a university peer, many of whom will try to bait you, this advice is essential. I was involved in all sorts of campus rabble-rousing at university, and while I, being the loudmouth that I am, thoroughly enjoyed vociferous encounters, one of the lessons I learned and have learned time and time again since is that we often need less heat and more light. Keep your cool, and you might be surprised at how productive your conversations will turn out.
In summation, I always think of my discussions with university peers in the terms of one of Aesop’s Fables. The Wind and the Sun were debating as to which was the strongest, and decided to have a contest to resolve the issue. They decided to see which one of them could cause a man walking down the road to take off his cloak. The Wind howled and blew and whipped around the man, who only clung to his cloak all the harder and pulled it around him, until the Wind finally gave up in despair. The Sun simply shone brighter and warmer until the man relinquished his cloak and took it off. We have a chance on campuses to have real, meaningful discussions with our peers on the issues that matter the most. And we should
One of the duties we take most seriously at LifeSiteNews is fidelity to the Church’s teachings. We’ve reported on the priest abuse scandal, held Catholic Relief Services responsible for its partnerships with abortion groups, and noted Catholic politicians who publicly oppose Church teachings on life and marriage.
We also report on news that is less sexy, but no less important when it comes to upholding the Church’s teachings. For example, a few weeks ago, we reported on the firing of a choir director at a Chicago parish. The man was fired over his “engagement” to another man. How do all of these stories relate? They are all about fidelity to the Church by Catholics, but they also attempt to explain to Catholics and non-Catholics alike what the Church teaches — not what dissident individuals or media interpretations pretend the Church says.
It is with this in mind that I would like to address what appear to be a few misunderstandings by hundreds of Catholics in Chicago who believe the aforementioned choir director was unjustly fired.
First, to make sure we’re all on the same page, here is what the Catechism of the Catholic Church teaches on the morality of homosexual relationships:
Basing itself on Sacred Scripture, which presents homosexual acts as acts of grave depravity,141 tradition has always declared that “homosexual acts are intrinsically disordered.”142 They are contrary to the natural law. They close the sexual act to the gift of life. They do not proceed from a genuine affective and sexual complementarity. Under no circumstances can they be approved. The number of men and women who have deep-seated homosexual tendencies is not negligible. This inclination, which is objectively disordered, constitutes for most of them a trial. They must be accepted with respect, compassion, and sensitivity. Every sign of unjust discrimination in their regard should be avoided. These persons are called to fulfill God’s will in their lives and, if they are Christians, to unite to the sacrifice of the Lord’s Cross the difficulties they may encounter from their condition. Homosexual persons are called to chastity. By the virtues of self-mastery that teach them inner freedom, at times by the support of disinterested friendship, by prayer and sacramental grace, they can and should gradually and resolutely approach Christian perfection.
In Chicago, it appears that Colin Collete — the former choir director — does not understand that this is the Church’s teaching. In our piece on his firing, we quoted Collete: “I said, ‘I’m not going to resign. God brought me to this moment and God is saying this is why I created you. You are here to live and love,’” Collette told the Chicago Sun-Times. Likewise, the Chicago Tribune notes that Collete “received a standing ovation” when he walked into a meeting of approximately 700 people who wanted to discuss his firing.
So it appears that hundreds of local parishioners also don’t understand the Church’s teaching. Now that we’ve defined what the Catholic Church’s view of morality is, as it relates to homosexual relationships, it is important to ask why the parish fired him.
It appears that Collete’s relationship was accepted by local parishioners, as well as the priest. But when Cardinal Francis George found out that Collete got “engaged” to a man, his employment was ended.
Why did this happen?
First, to quote LifeSiteNews co-founder John-Henry Westen, “It is important that a choir director be able to sing and direct other musicians. But it’s more important that a choir directors be in line with the Church’s teachings both for their own sakes and for those in the Church who look up to them.”
In other words, the first and most important qualification to be a choir director at a Catholic Church isn’t skill at the material skill, but rather the ability to be an effective advocate and leader for the Church.
Second, the firing happened because Collete posted a picture of himself and his partner on Facebook, and that picture was brought to the attention of the cardinal. Now, not only was Collete violating the Church’s teachings in his private relationship — putting his body and soul at great risk — but he was publicly disagreeing with a core teaching of the Church. To put it another way: By promoting his relationship on Facebook, Collete was causing scandal for the Church.
A few excerpts from the Catechism, with emphasis added: Scandal is an attitude or behavior which leads another to do evil. The person who gives scandal becomes his neighbor’s tempter. He damages virtue and integrity; he may even draw his brother into spiritual death. Scandal is a grave offense if by deed or omission another is deliberately led into a grave offense. Scandal takes on a particular gravity by reason of the authority of those who cause it or the weakness of those who are scandalized. It prompted our Lord to utter this curse: “Whoever causes one of these little ones who believe in me to sin, it would be better for him to have a great millstone fastened round his neck and to be drowned in the depth of the sea.”86 Scandal is grave when given by those who by nature or office are obliged to teach and educate others. Jesus reproaches the scribes and Pharisees on this account: he likens them to wolves in sheep’s clothing.87 Anyone who uses the power at his disposal in such a way that it leads others to do wrong becomes guilty of scandal and responsible for the evil that he has directly or indirectly encouraged. “Temptations to sin are sure to come; but woe to him by whom they come!”90
Did Collete cause scandal, as a leader in his parish who was violating the Church’s teachings on sexuality and marriage?
The answer is undoubtedly “yes,” and thus the Church could not employ someone who would lead others to mortal sin and/or a rejection of the Church’s teachings.
Lastly, Collete was quoted as talking about “love.” What is love? I could quote St. Paul, who talked about what love is and is not, but I like the definition I came up with for my own understanding: Love is putting the needs of others first, even — and, perhaps, especially — when it’s difficult.
What does that mean with regards to Collete? Like a parent who does not let his or her child do something against the child’s best interests, those who uphold the Church’s teachings on sexuality must show love to those in the Church, and to God, by holding all members of the Church accountable.
Likewise, out of love, Collete must be made aware of the sins he is committing — scandal, pride, and sexual relations — so that he can realize them and change his life accordingly.
Love is not an emotion one feels for another, which Collete’s quote indicates. It is about doing what is best for the other — even if the short-term consequences are unpleasant.
Unfortunately, Collete’s situation is not the only one facing various parishes and dioceses. Some have seen lawsuits filed, even though the Church is merely acting within the tenets of its faith. Unlike businesses — which rightly look at the bottom line as a most critical factor in making hiring decisions — the Church has a higher calling: To bring all people to Christ. And while individuals in it regularly fail — e.g. the priest scandal — that does not take away from the importance of putting God, and His Church, first.
This video begins with a young girl and her brother looking at ultrasound pictures of the latest addition to their family. But they can’t quite make out what these pictures are until Dad announces that Mommy has a new baby brother or sister in her tummy. The response is magical, especially for the daughter who appears to be about 5 or 6 years old. Children seem to have an innate love for a newborn sibling, even before birth. Mom and Dad will certainly have lots of help caring for and entertaining this precious gift from God. What material gift can compare? Give the gift that keeps on giving–for eternity!
Staff Report
On Wednesday, August 6, the Sixth Circuit Court of Appeals, based in Cincinnati, will review challenges to laws upholding traditional marriage in four states — Ohio, Kentucky, Michigan and Tennessee. The court will review all the cases together.
A report by the Associated Press called Wednesday “one of the most important days yet in the wave of legal efforts around the country to overturn marriage bans.”
With such an important legal moment on the horizon, Archbishop of Cincinnati Dennis M. Schnurr released a statement urging prayer for the court, that it will act correctly to uphold traditional marriage.
“The law in our state was a constitutional amendment strongly supported by Ohio’s bishops in 2004, and for good reason,” Archbishop Schnurr wrote. “Traditional marriage, the union of one man and one woman for life, is the cradle of the family, which is the basic building block of society.”
Ohio Right to Life shared Archbishop Schnurr’s statement with their media release list along with an invitation to join others on Wednesday, from 12:30 p.m. to 2:30 p.m., outside the courthouse in prayer. The Potter Stewart Courthouse is located at 200 East Fifth Street, Cincinnati, Ohio 45202.
Below is the full text of Archbishop Schnurr’s statement and accompanying prayer.
“On August 6, the U.S. Sixth Circuit Court of Appeals in Cincinnati will be hearing arguments on efforts to strike down laws against “same-sex marriage” in four states, including Ohio. The law in our state was a constitutional amendment strongly supported by Ohio’s bishops in 2004, and for good reason.
Traditional marriage, the union of one man and one woman for life, is the cradle of the family, which is the basic building block of society. And at the same time, as Pope Francis said last April: “The image of God is a married couple, man and woman, not only man, not only woman, but rather both. This is the image of God: love, God’s alliance with us is represented in the alliance between man and woman.” Please join me in praying that the federal appeals court will act wisely to uphold traditional marriage. One appropriate prayer would be the USCCB’s “Prayer in Defense of Marriage.”
Prayer in Defense of Marriage
God our Father, we give you thanks
for the gift of marriage: the bond of life and love,
and the font of the family.
The love of husband and wife enriches your Church with children,
fills the world with a multitude of spiritual fruitfulness and service,
and is the sign of the love of your Son, Jesus Christ, for his Church.
The grace of Jesus flowed forth at Cana at the
request of the Blessed Mother. May your Son,
through the intercession of Mary, pour out upon us
a new measure of the Gifts of the Holy Spirit
as we join with all people of good will
to promote and protect the unique beauty of marriage.
May your Holy Spirit enlighten our society
to treasure the heroic love of husband and wife,
and guide our leaders to sustain and protect
the singular place of mothers and fathers
in the lives of their children.
Father, we ask that our prayers
be joined to those of the Virgin Mary,
that your Word may transform our service
so as to safeguard the incomparable splendor of marriage.
We ask all these things through Christ our Lord,
Amen.
VATICAN, July 26, 2005 (CWNews.com /LifeSiteNews.com) – Although the Pontifical Academy for Life has strongly condemned the development of vaccines from fetal tissues, the president of that Academy notes that parents may still be justified in having their children inoculated with such vaccines.
Bishop Elio Sgreccia, in a July 23 interview with Vatican Radio, clarified the position taken by the Pontifical Academy for Life, in response to an inquiry from an American pro-life group. The bishop said that pharmaceutical manufacturers have a grave moral obligation to provide vaccines that do not use fetal tissues. But parents whose children may risk serious disease without inoculation may still choose vaccination, he said.
Bishop Sgreccia said that the Vatican had sent a two-part message to the American pro-life group. “On the one hand,” he said, “in a particular context such as that in the United States, it is licit to use these vaccines, because there are no others actually available.” The bishop explained that parents have a serious obligation to protect their children from disease whenever possible, and in doing so they are not signaling their approval for aborton.
On the other hand, Bishop Sgreccia continued, drug manufacturers have the choice to provide vaccines that do not use fetal tissue, so their continued use of the “tainted” vaccines does involve formal cooperation in abortion. He said that government should press the pharmaceutical companies to make other vaccines available, using morally licit means such as the use of animal tissue, and Catholic families should join actively in that pressure campaign.
In a paper published in Medicina e Morale , a journal published by Rome’s University of the Sacred Heart, the Pontifical Academy had argued that parents might have the right to refuse vaccinations. The paper argued even more strongly that parents have an obligation—and government an even stronger obligation—to press for the development of vaccines that are not developed from fetal tissues.
The Vatican document—which was made public last week by the American group, Children of God for Life—said that different actors have different degrees of moral involvement in the use of fetal tissues. While drug manufacturers are “culpable of cooperation” in abortion, the parents who are under pressure to use vaccines have only a “very remote material cooperation” in the immoral act, the paper argues.
Even if they do accept vaccination for their children, the Vatican statement argued, parents remain obligated to press for the ethical development of other vaccines.
The statement from the Pontifical Academy for Life was approved by the Congregation for the Doctrine of the Faith.
See related LifeSiteNews.com coverage:
Vatican Condemns Vaccines Made with Tissue Obtained by Abortion
http://www.lifesite.net/ldn/2005/jul/05071801.html
Vatican Condemns Vaccines Made with Tissue Obtained by Abortion
LARGO, FL, July 18, 2005 (LifeSiteNews.com) – The Pontifical Academy for Life under the direction of the Congregation for the Doctrine of the Faith has issued an “approved” study regarding vaccines derived from aborted fetal cell lines. The study was undertaken in response to a US group called Children of God for Life, which has for years fought for the creation of ethical vaccines which are not ‘tainted’ by abortion.
In the document published in Medicina e Morale by the Center for Bioethics of Catholic University in Rome and titled, Moral Reflections On Vaccines Prepared From Cells Derived From Aborted Human Foetuses, Vatican officials put the burden of guilt 100% on the pharmaceutical industry, comparing their moral complicity to that of the abortionists themselves.
The 8-page document, which has been anxiously awaited for several years by pro-life parents and physicians nationwide states that, doctors and families “have a duty to take recourse to alternatives, putting pressure on political authorities and health systems…They should use conscientious objection and oppose by all means ” in writing, through various associations, mass media, etc, – the vaccines which do not yet have morally acceptable alternatives, creating pressure so that alternative vaccines are prepared, which are not connected with the abortion of a human foetus…”
The document, which can be viewed in full athttp://www.cogforlife.org/vaticanresponse.htm also supports parents who refuse to use the vaccines, citing that those who have been forced to vaccinate experience “a moral coercion of the conscience … an unjust alternative choice which must be eliminated as soon as possible.”
Debi Vinnedge, Executive Director of Children of God for Life Executive Director, who has battled this issue for years and received the document and letter directly from Bishop Elio Sgreccia, President of the Pontifical Academy for Life.
“We brought the matter to Canon lawyers at the St. Joseph Foundation prior to sending an appeal on to the Vatican,” Vinnedge said. “There is a serious problem when parents are denied the right to abstain from these vaccines in accord with State law, simply because there was nothing from the Vatican directly addressing it.”
Vinnedge says the Vatican document, which calls for “rigorous legal control of the pharmaceutical industry producers” should also spur action on their Fair Labeling and Informed Consent Act, introduced to members of Congress earlier this year. The legislation requires that pharmaceutical companies give full disclosure whenever aborted fetal or embryonic cell lines are used in their products.
Dr Steven White, President of the Catholic Medical Association agreed. “We must demand that the pharmaceutical industry provide accurate information on the origin of all vaccines so that we are able to make informed decisions in accord with our moral conscience – and we must mobilize to support development of ethical alternatives,” he said.
A study of 1,102 women has found that use of several kinds of birth control pills was linked to greater chances of developing breast cancer.
In a press release provided to LifeSiteNews by the American Association for Cancer Research (AARC), the study’s authors found that high-dose estrogen pills “increased breast cancer risk 2.7-fold,” while “those containing moderate-dose estrogen increased the risk 1.6-fold.”
Likewise, “pills containing ethynodiol diacetate” – such as Zovia and Demulen – “increased the risk 2.6-fold, and triphasic combination pills” – like Ortho Tri-Cyclen, Tri-Levien, and Triphasi – “containing an average of 0.75 milligrams of norethindrone increased the risk 3.1-fold.”
Pills with low doses of estrogen were not found to increase the risk of breast cancer.
The study found that recent use of oral contraceptives increased the risk of breast cancer by 50 percent when compared with those who have never used the birth control pills or are no longer using them.
Unlike a majority of other studies of the link between birth control pills and breast cancer, Beaber and her fellow authors did not rely on self-reporting or recall by women about their use of birth control. Instead, they used electronic pharmacy records to gather detailed information on the study participants.
The study, which was funded by the National Cancer Institute, is just the latest linking birth control pills to cancer and other ills. A report earlier this year found that chemicals in contraceptives are causing the feminization of male fish in Spain.
In 2013, a study found that using birth control for at least three years led to a greater chance of getting glaucoma. Teen girls who use contraceptives were found to have increased blood pressure in an Australian study done in 2012, and a Denmark study released earlier this year found birth control pills may damage the fertility of women who use them.
The AARC study, which was published by Cancer Research, a journal of the American Association for Cancer Research (AARC), studied women who were at Group Health Cooperative in the Seattle area and received cancer diagnoses between 1990 and 2009. It had 21,952 controls.
According to the press release, “about 24 percent, 78 percent, and less than 1 percent of study controls who were recent oral contraceptive users filled at least one prescription in the past year for low-, moderate-, and/or high-estrogen dose oral contraceptives, respectively.”
In other words, women rarely filled prescriptions for the most dangerous of the pills — those with high estrogen doses. The odds of breast cancer across the nation are approximately 1.5 percent at age 40.
However, one of the AARC study’s authors cautioned that the study’s “results require confirmation.”
One of the favorite claims of the population control movement is that the world is running out of resources: food, energy, and space. “There is plenty of evidence to suggest that humanity is already exceeding the planet’s limits and that we are reducing the earth’s capacity to support life, including human life,” purported Robert Walker, the president of the Population Institute, in a recent debate with our own Steven Mosher.
These—and similar dire predictions—have been bandied about for over two hundred years. The overpopulation drum-beaters repeatedly claim the imminent end of humanity, perpetually predicting earth-ending disaster just around the corner. These predictions, unsurprisingly, have not come to pass.
One, of course, might be tempted to dismiss the claims of population alarmists as the warnings of well-funded but harmless cranks. One might be tempted to wave them away with a rather cynical sort of amusement if government officials did not take their claims as dark gospel—and if their vision of population control was not exported to poorer countries, often by force.
It is therefore important to understand why their relentless claims of impending disaster never come to fruition. Population controllers falsely assume an arbitrarily static model of technological growth, coupled with an endlessly growing population—a “population bomb” without any advances to sustain ever-growing hordes.
In a certain sense, they are correct—if society did not advance technologically, and the population grew indefinitely, then the human race would not be able to provide enough necessities for its continued survival.
But that has never happened. The pace of technological advance has grown faster over time, making larger populations possible. In fact, the pace of advance has grown faster than the pace of population growth. Today, the world population is the largest it has ever been, yet the proportion of humans living in absolute poverty is the lowest it has ever been. This remarkable reality derives from the fact that human beings produce, as well as consume.
Because humans alone have the beautiful capacity to innovate, population control policies harm the very people they claim to help. Technological advance always comes from humans; it can never spring up from any other form of economic capital other than human capital. Alas, many in the corridors of power have bought into the claims that undesirable people (by which they often mean poor people in developing countries) must be reduced, or else the world will end in a sea of asphalt.
In short, the population control movement will create the very future it fears if its policies are adopted: a society stuck in economic stagnation, relying on the ever-diminishing resource of human ingenuity. By thinning the human population, you destroy the future. Humans are the world’s greatest resource.
by Steven Ertelt | Washington, DC | LifeNews.com | 7/22/14 3:07 PM
Here is a powerful video with a pro-life theme that you should spend two minutes watching.
Dave Andrusko of the National Right to Life Committee tells us why this video is so amazing:
It’s been a long, long time since I was a first-time dad trying frantically to figure out what to do (in the absence of my wife) when our newborn daughter would cry, seemingly inconsolable.
This afternoon, thanks to pro-life blogger Chelsea Zimmerman, I was vividly reminded of the rush of emotions lo those many years ago. She linked to a video whose closing line for the two-minute long video is “Technology can never replace love.”
First shot: a little baby is crying her lungs out and a young dad leaps from his chair (where he was probably sleeping) and races to the crib. What to do? What else? Uses his smart phone to call mom, who is shopping.
What should I do, he asks, she won’t stop crying? Maybe she’s hungry. In a hilarious moment, he takes a quick look down, realizes he isn’t carrying the necessary equipment (so to speak). What else? Well, use the phone to show her the dancing penguins. Nope, no dice, she cries louder.
by Steven Ertelt | Washington, DC | LifeNews.com | 7/22/14 2:52 PM
Here’s a unique way pregnant women are celebrating life! Women are commissioning an artist in England to paint their swollen bellies with unique and child-based images that are vivid and full of imagination.
Here is more and some of the amazing drawings—->
http://twentytwowords.com/women-celebrate-an-imminent-baby-with-paintings-on-their-pregnant-bellies-20-pics/?
In addition to doing more typical commissioned paintings, English artist My Little Sweet-pea is available for “Bump Painting.” Dozens of women have hired her to create temporary body art for their pregnant bellies.
Some women choose children’s stories as their theme; others pick an image that signifies the life growing within them; and some just want a beautiful picture. Here are some examples…
by Rebecca Taylor | Washington, DC | LifeNews.com | 7/22/14 2:50 PM
There is one argument against the Hobby Lobby decision that is driving me crazy maybe because it is going unchallenged on Facebook pages and comboxes all over.
It goes like this: if Hobby Lobby can deny health insurance coverage for birth control, then what will stop a company owned by other religious nut jobs from denying blood transfusions, chemotherapy, or inhalers for asthma?
This one seems to make sense and I am sure many people do not see where it falls short. I am not expert on Constitutional Law or on health insurance in general but this seems pretty obvious to me.
Blood transfusions, chemotherapy, and inhalers are medicine. They are therapeutic in nature needed for those who are sick. These are exactly the kinds of things health insurance is supposed to pay for. Any employer religious or otherwise is going to have a very tough time having a legitimate claim for not including well-known therapeutic measures for their employees because these are actually “health care.”
Birth control is different. Of course there are cases where the pill is prescribed for medical reasons, but I speak only about birth control for the prevention of pregnancy. In this case birth control is not medicine nor is it therapeutic.
Birth control actually takes something that is normal, fertility, and makes it not work properly. Birth control is not even remotely in the same class as blood transfusions, chemotherapy or inhalers.
Really birth control is something that allows people to engage in baby-making behavior without making babies.
That is not medicine; it is a life style choice no different from condoms, other barrier methods or even permanent sterilizations. Employers are not required to cover life style choices like condoms in their policies because they are not something health insurance should cover.
I have not heard a single man shouting about how his employer is denying him access to his condoms. Why? Probably because when it comes to men’s reproductive systems we can still engage in calm and clear reasoning without hysterical hyperbole.
If a man wants to engage in baby-making behavior without making a baby we make him pay for it.
Ladies, we want equality do we not? Or is this really about getting more than “health care” and making someone else pay for it?
Two obituaries published this weekend show how little progress America has made on abortion in the last several decades.
The death of actor James Garner saddened fans across the country. Born James Scott Bumgarner, the 86-year-old Rockford Files star overcame mental and physical abuse from his stepmother – who would regularly beat him with whatever was handy and force him to wear dresses as a form of emasculation – to become one of the most beloved stars of his day.
In his autobiography, The Garner Files, he revealed that he had no memory of his birth mother, who died when he was four years old.
“It wasn’t until I was fifteen that my cousin Betty told me my mother died of uremic poisoning after a botched abortion,” he wrote. “I have no idea whether my father was involved in the decision to have the abortion or whether he blamed himself for her death. We never talked about it in the family.”
After 1973, the back alley abortionists simply came out of the shadows, hung out a shingle, and continued business as usual.
Reading between the lines, Garner seems to have wondered whether his years of harrowing abuse could have been avoided if his father had intervened. (He also mentions the fact that his mother was a Christian Scientist and, thus, shunned conventional medical treatment.)
The same day Garner died, the St. Louis Post-Dispatch ran the obituary of Dr. Michael Freiman. Born Seymour Milton Freiman, the 85-year-old became infamous for performing the first legal abortion in Missouri after Roe v. Wade.
The obituary says Freiman referred women to abortionists in places where the procedure was legal before Roe, then pushed to open an abortion facility as soon as possible after the 1973 decision.
He celebrated its grand opening by performing seven abortions in one day.
He, too, had a backstory:
Michael Freiman was a teenager when his cousin had an abortion. It was the 1940s, and abortions were illegal. His cousin had found one of those clandestine places women sought out when they couldn’t find a willing doctor. The operation was botched. The cousin died, and the abortionist dumped her body on the parking lot in front of an emergency room.
His cousin’s tragedy continues to occur too frequently in his chosen industry, with doctors sometimes arranging for injured women to be transported to the ER in their employees’ cars to divert attention from their incompetence.
When they call an ambulance, they often withhold vital information that costs time – or someone’s life – as in the case of Tonya Reaves, the 24-year-old Chicago woman who died from a botched abortion in 2012. Planned Parenthood let her bleed for five-and-a-half hours in its facility, then sent her to the emergency room without telling the physicians the cause of her symptoms. Instead of administering life-saving treatment, doctors had to waste precious time determining the cause of the injuries for themselves. In the end, Reaves died of an incomplete abortion, perforated uterus, and needless delay.
The Thomas More Society filed a complaint charging that Planned Parenthood’s “abandonment of a patient” led to Tonya Reaves’ death.
Unfortunately, abandonment is standard operating procedure in Big Abortion. Dr. James C. Anderson, M.D., said not a single abortionist ever told him of the cause of the medical problems he had to fix when caring for butchered post-abortive women in his 30 years of practice.
The well-funded industry is now fighting against bills requiring abortionists to have admitting privileges at local hospitals, a move lawmakers hope will reduce patient abandonment of the sort that killed the late Dr. Freiman’s cousin.
Their callous decision to place money over the lives of others, pre- or post-natal, should surprise no one. Before Roe v. Wade, abortions were not typically performed by carnival barkers but by bottom-feeding physicians out to make a quick buck. After 1973, the back alley abortionists simply came out of the shadows, hung out a shingle, and continued business as usual.
Meanwhile, the death toll mounts. Participants at the 2013 National Memorial Service for the Preborn, just before the March for Life, read a litany of names of women who had died from legal abortion, led by Reaves. The list was both necessarily incomplete and interminably long.
With these two obituaries, we may add two more.
And the victimized women, the tears of family members, the profits of the abortion industry, and the deaths of innocent children will continue to multiply until each one of us decides that there have been enough obituaries, written and unwritten, caused by abortion.
A study from the Centers for Disease Control (CDC) released Tuesday found that there are far fewer who people who identify as homosexual and bisexual in America than many think. The study also found that self-identified homosexuals lead less healthy lives.
According to the study, which was based upon data from the 2013 National Health Interview Survey (NHIS), 2.3 percent of Americans identify as gay, lesbian, or bisexual. The study also found that “health behaviors,” “health conditions,” and “health care access and utilization” were statistically worse among what the CDC calls “sexual minorities.”
The NHIS survey interviewed 34,557 adults aged 18 and older. This was the first time the survey has ever examined sexual orientation.
The CDC’s calculation of the percentage of Americans who are homosexual is lower than many previous studies. According to The Washington Post, other surveys have found estimates closer to four percent.
Larger estimates include that of researcher Alfred Kinsey, whose assertion in 1948 that 10 percent of Americans were homosexual has shaped the common view. However, according to Professor Judith Reisman, “the point of [Kinsey’s] exaggerated numbers was to change perception and thus laws to cater to the large population and to normalize homosexuality.”
Kinsey’s research has been shown to have numerous flaws. Among them, he focused much of his research on prison populations and pro-homosexual groups, something a former director of the Kinsey Institute described as “opportunistic collection.” He also appears to have focused his study on specific regions of the nation, rather than the country as a whole, and interviewed male prostitutes and sexually abused children, claiming that these demographics represent average Americans.
The CDC study also found dramatically different health behaviors in the homosexual population. Over one-quarter of gay and lesbian Americans over the age of 18 currently smoke, the study found, while fewer than 20 percent of heterosexual Americans do the same. And homosexuals were far more likely to have had five or more alcoholic drinks in one night in the past year than their heterosexual and bisexual counterparts, though heterosexual men drank almost as much as the highest-risk women — bisexuals.
Over 50 percent of bisexual men had drunk at least five beverages in one night, compared with 31 percent of heterosexual men and 34 percent of bisexual women.
Homosexuals were more likely to have met the federal guidelines for aerobic exercise, and to have had flu shots, however.
Bob Witeck, president of Witeck Communications and a LGBT-issues consultant, argued that the CDC’s results are skewed. “The gay population sampled very likely skews younger on average than non-gay adults in the sample” because older homosexuals “are more likely not to disclose and remain closeted,” he told LifeSiteNews.
“Younger gay people also tend to socialize, meet and connect with others in gay bars, parties and other social venues. In all of these venues, smoking and drinking are prevalent – not rare. To visit and enjoy a bar’s social setting, for most adults is to choose to drink and smoke. If the data was controlled for age and behaviors about socializing, then the difference between the gay and non-gay adult might be closer.”
Kevin Naff, editor of the Washington Blade, a homosexual newspaper, told LifeSiteNews that while “it’s a terrific milestone that the government is finally gathering data about lesbian, gay and bisexual people, the actual number of gay Americans is routinely undercounted due to the reluctance of many to self-identify as gay.”
Witeck said another major factor in the health differentials were related to how “many gay people do feel more stress in their lives – not about their same-sex attraction or identity, but about the degree of alienation or hostility or disdain they may feel from their family, co-workers or their faith if they feel like outsiders.”
“They must have coping mechanisms that allow them to deal with all forms of stigma, and it’s not at all unusual for people feeling like outsiders to depend more on substances like alcohol and cigarettes,” Witeck said. “Again, that is not because of their sexual orientation. It is because of the way they are judged or alienated by others.”
According to Americans for Truth President Peter LaBarbera, however, “while it’s convenient for gay activists to blame homophobia or other outside sources for the ill health of homosexuals, the evidence shows that disease rates and other harms are represented disproportionately among homosexuals.”
“A good example is a study done 12 years after Denmark allowed same-sex domestic partnerships, which found that suicide among men in same-sex partnerships ‘was nearly eight times greater than for men with positive histories of heterosexual marriage,’” he continued.
“Certainly,” said LaBarbera, “nobody thinks of Denmark as a bastion of homophobia.”
Likewise, Focus on the Family Issues Analyst Jeff Johnston told LifeSiteNews,”Many studies have shown that lesbian-, gay-, or bisexual-identified people have greater health problems in a wide variety of areas, including behaviors, mental health issues and physical conditions. It’s significant that the CDC study would find similar outcomes.”
Last year, a CDC study of gay men in America found that approximately two-thirds of gay men who have HIV/AIDS engage in sex without using a condom. Earlier in 2013, the director of the CDC’s division of HIV/AIDS prevention said that “gay and bisexual men remain at the epicenter of the HIV/AIDS epidemic.”
Johnston also said that “the study just confirms what we already knew” about the population size of homosexuals. “What’s interesting,” according to Johnston, “is comparing that number with public perception. The average person thinks the percentage is much higher, probably because of the high profile that entertainment, news media and other influential sources have given homosexuality in recent years.”
In the understandable excitement so many of us felt two weeks ago over the wonderfully welcome and important U.S. Supreme Court decision regarding the Conestoga / Hobby Lobby case, I have delayed celebrating another high court decision in another Alliance Defending Freedom supported-case – one with its own enormous implications for your family’s First Amendment-protected freedom of speech. And, even more importantly, for the defense of life in the womb.
On June 26, the nation’s highest court unanimously struck down a Massachusetts law creating a 35-foot Gospel-free “buffer zone” around abortion facilities. These zones’ express purpose was to block advocates for life from speaking with women on their way into these buildings to have an abortion. (The law imposed up to two-and-a-half years in jail for its violation.) The court ruled that those who would gracefully make the case for life face-to-face are legally entitled to do so, up until the moment a woman enters the abortion facility’s property.
“It is no accident that public streets and sidewalks have developed as venues for the exchange of ideas,” the court wrote in its opinion. “Even today, they remain one of the few places where a speaker can be confident that he is not simply preaching to the choir. … In light of the First Amendment’s purpose ‘to preserve an uninhibited marketplace of ideas in which truth will ultimately prevail…,’ this aspect of traditional public fora is a virtue, not a vice.”
“Peaceful pro-life citizens should be able to freely share their message with mothers in vital need without being forced to shout from outside an anti-speech zone,” says ADF Senior Counsel Steven H. Aden. “As the Supreme Court found, Massachusetts had no constitutional basis for creating speech-restricted zones that exist to hinder a particular point of view.”
“Americans have the freedom to talk to whomever they please on public sidewalks,” says allied attorney Michael DePrimo, co-counsel on the case, which was argued before the court in January. “That includes peaceful pro-lifers who just want to offer information and help to women who would like it. The Supreme Court has affirmed a critical freedom that has been an essential part of American life since the nation’s founding.”
The ruling will impact other cases across the nation, including Reddy v. Foster, an ADF lawsuit challenging a similar anti-speech zone law in New Hampshire. The case will be heard later this month in federal court; last week, though, a temporary restraining order took effect, suspending enforcement of the zones pending a ruling in the case, and allowing pro-life speech there.
“The government has no sound justification for banning free speech on public sidewalks, as the U.S. Supreme Court recently affirmed,” says ADF Senior Legal Counsel Matt Bowman. “Censorship zones in such places are about as clear a violation of the First Amendment as it gets. This is especially true when the government allows some pro-abortion voices to speak within a zone but censors all pro-life speech there. While it’s good that the law has been temporarily suspended, we will continue to work toward ensuring that New Hampshire’s law is permanently halted in light of the Supreme Court’s decision that struck down such laws.”
Truly, we are blessed by this recent surge in support at the high court for your religious liberty, freedom of speech, and the sanctity of life. Please join me in giving thanks – and in praying for our attorneys as they continue to defend a host of cases, coast-to-coast, that involve these vital aspects of American life.
Reprinted with permission from Alliance Defending Freedom.
Thiago Silva is one of the top stars in Brazil’s national soccer team. So important was he to this year’s team that many sports commentators blamed the country’s first and only loss in the semifinals of this year’s world cup to the fact that Thiago was prevented from playing that game. But what people just recently learned inthis mini-documentary about Thiago’s life, is that abortion nearly took Thiago’s life before he ever had a chance to take a breath, much less kick a soccer ball.
Thiago Silva now lives the gilded life a soccer star playing in the big leagues in Europe. He lives in Paris and plays for the French champions, Paris Saint Germaine. In addition to his great skill as a defensive back, Thiago Silva’s deep Christian faith before and after the matches, when he is often seen praying, is evident.
As C.S. Lewis wrote “there are no ordinary people” and Thiago Silva is a great example.
Although Thiago Silva was born to a desperately poor family that lived near a dangerous shantytown in the city of Rio de Janeiro, he was able to overcome these hardships and achieve great success in the eyes of the world.
As a professional soccer player, Thiago Silva has won many prizes, including being named as one of the top 11 players in Europe for three consecutive years. But surely none of his professional achievements would have meant anything without the most amazing gift of all, the respect that his mother and grandfather had for Thiago’s God given right to life.
A report made by Globo TV Channel, the largest TV station in Brazil, revealed that Thiego’s mother, Angela, already had two children – a boy and a girl – when she became pregnant with Thiago. She was convinced she couldn’t afford to raise another child, and despite feeling terrible pain at the thought of aborting her baby, she was convinced she had no other option.
“I was sitting on my father’s lap and I cried a lot. I didn’t want to have an abortion but I couldn’t bear another child,” she said. Angela’s father, however, convinced her not to abort the baby. “My father did not allow me to commit this sin,” recalled Angela.
Poverty and illness loomed large in Thiago’s childhood. When he was 14, he suffered from tuberculosis. “It was the greatest battle of my life. I had to stay in the hospital for 6 months until I recovered.”
Living a mere 50 meters away from one of Rio’s infamous shantytowns, the famous soccer center back could have easily turned to a life of crime. “We would always hear shootings. The cops would come to the borough where I lived often. When I got home I would thank God for getting home safe.” But instead, Thiago chose to follow God and pursue his dream of becoming a professional soccer player.
Life had never been easy for Thiago and his professional life was no different. Thiago failed to get onto local Brazilian teams at first and ended up in a second rate local team from a poor area of Rio de Janeiro. But with hard work and discipline his initial failures soon turned to success. He finally got his chance to be seen in Europe when he was signed by a Russian team. He was eventually signed to play for the French powerhouse Paris Saint German. He now earns annual salary of $16 million/year.
Thiago’s story of courage and determination is an example of why we should never give in to the temptation of determining another human being’s potential in life, especially that of an unborn child. Thiago could have been aborted, but he wasn’t. He could have chosen a life of crime, but he didn’t. He could have given up his dream, but he persevered. Now, he is one of the best center backs in the world and an inspiring reminder that every life is worth living.
A person’s worth should never be measured by what they achieve, and therein lies the greatness of Thiago’s mother’s decision. She knew the chances that the world would give a child from a poor family growing up in the Brazilian slums surrounded by disease and crime. The fact that Thiago didn’t succumb to his environment is as much a credit to God as it is to Thiago and his family. This is the miracle of a Christian life which allows God the opportunity to transform every single person from the lowest depths to the greatest heights.
In the wake of the 5-4 Supreme Court decision acknowledging the rights ofHobby Lobby and other closely-held private companies to refuse to provide coverage for abortifacients to their employees and dependents on religious grounds, a group of atheists has accused the Court’s justices of participating in a “Catholic conspiracy” to deny women birth control.
In a full-page ad that ran in the New York Times July 3, just three days after the ruling, the Freedom From Religion Foundation slammed the “all-male, all-Roman Catholic majority” on the Supreme Court for putting “religious wrongs over women’s rights.” Alongside the text of the ad was a huge portrait of Planned Parenthood founder Margaret Sanger, whose motto, the group claims, was “No Gods — No Masters.”
“Dogma should not trump our civil liberties,” the ad said.
The group called on Congress to repeal the Religious Freedom Restoration Act (RFRA) of 1993. This is the law the Supreme Court cited in ruling that the Obama administration cannot force businesses that object to provide coverage for abortifacient drugs in employees’ health insurance plans.
“We must next ask whether the HHS contraceptive mandate ‘substantially burden[s]’ the exercise of religion,” the majority wrote. “We have little trouble concluding that it does.”
Hobby Lobby’s owners are protestant Christians, not Catholics, but all five justices who sided with the company are members of the Catholic faith. One of the four dissenting justicesnis also Catholic. (The other three are Jewish.)
“Allowing employers to decide what kind of birth control an employee can use is not, as the Supreme Court ruled, an ‘exercise of religion.’ It is an exercise of tyranny. Employers should have no right to impose their religious beliefs upon workers,” the ad said.
Cardinal Timothy Dolan, the archbishop of New York, responded to the ad with a sarcastic thank you note published in the Catholic New York newspaper, calling FFRF’s rhetoric “drippingly bigoted.”
“I simply want to welcome the grey, full-page ad, and thank the anonymous militiamen at FFRF for giving me yet another handout for my students when I give my next talk on ‘Anti-Catholic Bigotry in the United States,’” the cardinal wrote. “Now, don’t get me wrong: a robust examination of [the] Supreme Court decision, even one that disagrees with the ruling, is expected, welcome, and helpful in a Republic that prizes such give-and-take, indeed, protects it. But, as the professors of logic, rhetoric, and speech taught us in college, arguments attacking a person—instead of an idea, viewpoint, or opinion—are the weakest and most vicious of arguments…although, sadly, rather effective in firing up a mob.”
Mob tactics, Dolan suggested, are exactly what FFRF are engaging in, perhaps due to a lack of factual arguments with which to make their point.
“An ad soberly criticizing the decision would have been part of the discourse that makes us such a durable democracy…and there have been such ads,” Dolan wrote. “But the FFRF, perhaps knowing that their legal arguments fall flat, instead attacks the people on the court, and implies that their Catholic faith makes it impossible for them to protect the cherished Constitution they have sworn on a Bible to uphold.”
Dolan asked whether the FFRF would publish a similar ad saying a Jewish politician could not vote on Israel, or a Mormon judge tackle the issue of marriage.
“Of course not!” he said. “But, in keeping with a long, shadowy, legacy of antipathy, justices who happen to be Catholics—never mind their past frequent votes hardly consonant with the public teaching of their faith—are branded and bullied by a group who only succeed in providing the latest example of a prejudice that has haunted us for centuries.”
Bill Donohue of the Catholic League also condemned the FFRF ad as “hate speech” against Catholics.
“All the Jewish judges on the high court voted in the minority,” Donohue pointed out, “but only an anti-Semite would conclude that their Jewishness determined their vote. Similarly, only an anti-Catholic would conclude that those who voted in the majority did so because of their Catholicity.”
Added Donohue, “From the middle of the nineteenth century to the middle of the twentieth century, Catholics had to deal with the Ku Klux Klan. Now they must deal with more sophisticated bigots. What unites the Klan and FFRF is their maliciousness. Unfortunately, as we have seen this week, anti-Catholic bigotry has erupted in many quarters, all of them urbane.”
In a follow-up post on the FFRF blog Friday, staff attorney Andrew Seidel doubled down on the Catholic conspiracy theory.
“There is excellent cause to question the impartiality of any truly devout Catholic justice on an issue such as access to birth control,” Seidel wrote.
“When [Catholic] Justice Sotomayor dissented in Hobby Lobby, she violated the teachings of her church, and I respect her all the more for that,” Seidel wrote. “She held her civil duty (and in all probability her womanhood) above the out-dated and barbaric teachings of the Catholic Church.”
While praising Sotomayor for her “scruples” in voting to force religious people to act against their conscience, Seidel called on Justices Scalia, Alito, Kennedy, Roberts, and Thomas to either leave their faith at the courthouse door or resign.
Fr. Frank Pavone, National Director, Priests for Life, July 2014
Tax law says that Churches may not intervene in political campaigns. But the definition and boundaries of such intervention are vague and confusing. In its attempt at guidance, the IRS says “all the facts and circumstances” have to be examined. From one point of view, this standard itself is not a standard at all, but a mere statement of the obvious. After all, if a person, in making any kind of judgment, does not consider “facts and circumstances,” what, after all, does he or she consider — crystal balls, astrological signs, dreams and hallucinations?
From another point of view, how can one possibly consider all facts and circumstances of any action or decision? In real day to day life, we consider those facts and circumstances of which we are aware in the amount of time we have to make the decision, and which seem important enough to influence the decision. It’s a normal fact of life that, looking back on decisions we have made, we come to see facts and circumstances we did not have the time or ability to weigh at the time of the decision.
Obviously, a consideration of “all the surrounding facts and circumstances” if it can ever happen at all can only happen after the action has been taken, and perhaps a long time after, or indeed never.
The Congressional Research Service has reported, “In many situations, the activity is permissible unless it is structured or conducted in a way that shows bias towards or against a candidate. Some biases can be subtle and whether an act-ivity is campaign intervention will depend on the facts and circumstances of each case.” (Lunder & Whitkaker at 3.)
A question obviously arises here. Unless we are to say that Churches have no freedom to teach on issues that also happen to correspond to political debates, how are they protected from the accusation of being “partisan” simply because the position of the organization, or the teaching of the Church or the Gospel, corresponds to the position that one particular political party or candidate has, and is diametrically opposed to that of their opposing party or candidate?
The Church opposes abortion and stands up for the rights of the unborn. The Republican Party platform takes a similar position. The Democratic Party platform, on the other hand, supports abortion as a right. So now, is the Church’s pro-life position partisan, and therefore illegal to assert?
That would be both absurd and intolerable.
Erik Stanley states, “The predictable outcome of this state of affairs has been massive self-censorship among churches and pastors.” Even the Supreme Court, on more than one occasion, has noted with concern what happens when people aren’t given a clear, bright line regarding what speech and activity is forbidden and what is not. “Uncertain meanings inevitably lead citizens to ‘steer far wider of the unlawful zone . . . than if the boundaries of the forbidden areas were clearly marked.’”(Grayned v. City of Rockford, 408 U.S. 104, 109 (1972) (quoting Baggett v. Bullitt, 377 U.S. 360, 372 (1964)).
We at Priests for Life believe there is a solution to all this. We believe it’s time to stop censoring ourselves by the risk-averse mentality, often fostered by legal advisors, that wants to not only avoid breaking the law, but also avoid both the accusation and the appearance of breaking the law. This lack of willingness to fight leads to sterility and paralysis, keeping the Church’s mission from being fulfilled.
Instead, we should rely on legal counsel who are willing to interpret the IRS guidelines in a way that does not stifle our mission, and have the readiness to defend that interpretation. We need to conduct non-partisan activities in a way that common sense judges as non-partisan: no candidate or party is endorsed, and the activity is open to all. And we should push for legislation that provides a “bright line” test for Churches and tax exempt organizations so that they know ahead of time, by a clear, reasonable, andily discernible standard,what does and does not constitute prohibited political intervention. A perfect example of this is provided in the Buckley vs. Valeo Supreme Court decision which, in another context, indicated the bright line to be defined by whether or not one uses “explicit words of advocacy of election or defeat of a candidate.” The Court gave examples of such words and phrases: ‘vote for,’ ‘elect,’ ‘support,’ ‘cast your ballot for,’ ‘Smith for congress,’ ‘vote against,’ ‘defeat,’ ‘reject.’
It is time to apply a clear standard like this in order to interpret the political intervention prohibition on Churches.
According to a recent study, vasectomy, a surgical procedure for male sterilization, not only damages the vas deferens, but poses a higher risk of prostate cancer, especially advanced or fatal prostate cancer.
The effect appears to be stronger among men who had a vasectomy at a young age, according to the study. The results support the hypothesis that vasectomy is associated with an increased risk of advanced or fatal prostate cancer.
The researchers mentioned that this study is follow up of an initial publication on vasectomy and prostate cancer in 1993, with 19 additional years of follow-up and ten times as many cases. Data from 49,405 North American men in the Health Professionals Follow-up Study, who were followed for 24 years from 1986-2010 were analyzed.
The results showed an increased risk of prostate cancer overall by 10 percent in men who had a vasectomy. Vasectomy was not significantly associated with the risk of low-grade cancer, but was associated with a stronger risk of advanced prostate cancer and lethal prostate cancer, with an increased risk of 20 percent and 19 percent, respectively.
Among men who received regular examinations, the relative increase in the risk of lethal prostate cancer was 56 percent.
The researchers found that the association remained even among men who received regular examinations, suggesting an increased risk of fatal cancer cannot be explained by diagnostic bias. Neither the results were not influenced by differences in the levels of sex hormones, sexually transmitted infections, or cancer treatment.
ABUJA, Nigeria — The Catholic Bishops of Nigeria have called for the Church to be “more courageous and consistent in Pro-Life activities in favour of human life, marriage and the family as counter-cultural antidotes to anti-life ideologies and practices.”
The call came in a communiqué issued following an international pro-life march and conference organized by the Catholic Bishops’ Conference of Nigeria and held in Abuja from June 5-7.
“The relentless promotion by some international organizations of ‘sexual and reproductive rights’, a euphemism for abortion, is deceptive and unacceptable,” the communiqué asserts.
The bishops’ demand that “legislation for abortion, which is the intentional killing of innocent babies in the womb, be denounced and abrogated,” and promise that they “remain resolved in our efforts to ensure that abortion is never legalized in our country.”
The content of the communiqué echoes speeches made by bishops at the conference, which was attended by approximately 1,500 delegates and speakers from across Africa, Europe, and North America.
In a stirring speech, Archbishop Anthony Obinna of Owerri told the conference, “We have become aware of aggressive, ideological and practical assaults on human life, sexuality, marriage and the family.”
“By publicly repudiating the aberration of same-sex ‘marriage’ and prohibiting it in law, to the anger of several anti-life European/American governments and agencies, Nigeria, through its current President, Goodluck Jonathan, has placed itself in the position of a global defender of life and proper family values,” said the archbishop.
These points were emphasized by Archbishop Ignatius Kaigama, president of the Bishops’ Conference of Nigeria, who told the conference, “We cannot be terrorized into doing anything to diminish life and the family. … We don’t want an abortion industry. We want industries which produce food, roads, transport systems and other practical things which people need.”
The threat posed by international governments and agencies was stressed in a speech John Smeaton, chief executive of the UK’s Society for the Protection of Unborn Children, delivered to the Nigerian Bishops Conference on the eve of the two day event.
Smeaton warned the bishops that “the most powerful politicians and pro-abortion organizations in the world are absolutely determined that Nigeria should follow Britain, America, and other powerful western nations by legalizing abortion and by destroying the moral welfare and happiness of your children.”
Smeaton told the bishops that compared to the West, Nigeria was a “wealthy nation.” In Britain, he told them, children are given access to abortion at school and are subjected to pornographic anti-life sex education. Many teachers were receiving training from Stonewall, a militant homosexual “rights” group. All these things, Smeaton stressed, were taking place in Catholic schools with the co-operation of the Catholic authorities.
The assembled bishops responded to his honest and forthright speech with a standing ovation.
Smeaton told LifeSiteNews, “Archbishop Kaigama, and his fellow Nigerian bishops, are at the centre of the global defence of life and moral values. Bishops around the world should follow their lead and speak out for strong policies against the subversion of the truth and meaning of human sexuality.”
The Nigerian bishops’ communiqué can be read here: https://s3.amazonaws.com/lifesite/BUILDING_A_CULTURE_OF_LIFE_4.pdf.
John Smeaton’s full speech can be found here: https://s3.amazonaws.com/lifesite/Address_given_by_John_Smeaton_to_the_bishops_of_Nigeria_5th_June_2014.pdf.
Last week, every harried and hysterical abortion activist with the ability to type and access to a WordPress blog went completely crazy. You see, the United States Supreme Court ruled in a 5-4 decision on Monday that no, companies owned by people who dislike abortion don’t actually have to pay for abortion drugs or drugs that could result in killing an already existing human being.
This, of course, is totally unacceptable to the abortion crowd, who would like us all to soar to new heights of delusion and pretend that ending a pregnancy chemically is, in fact, “health care,” and that it’s none of our business what happens to tiny human beings, and that also we have to pay for the whole bloody process, because feminism, that’s why. The sheer number of stupid arguments being howled loudly in protest of this decision is mind-boggling.
The Supreme Court Justices voting in favor of Hobby Lobby were all male! Uh, so were the justices who legalized abortion—and I wasn’t aware that arguments had genitals? The pills we want don’t always cause abortions or hardly ever so who cares! Well, if there might be a human being sitting in the bushes, I think it most prudent not to fire a gun in that direction, because we value human life. Why do stupid pro-lifers want me to have hundreds of babies?! We’re not talking about preventing a human life, we’re talking about ending one that already exists. This is really basic stuff.
And I could go on (and on and on.) But I want to take a look at the three “arguments” that I’ve seen the most frequently, and have irritated me the most.
1. This ruling is an attack on American women!
Depending on what poll you take a look at, almost half of American women consider themselves pro-life. A majority support abortion restrictions. Sorry, abortion fans, but you don’t get to call yourselves the representatives of American women, as if half of them should stay out of the debate and vacuum their living rooms while you loudly and repulsively claim that for women to be free, they have to be able to have their children vacuumed out of their uteruses. In fact, instead of looking for real solutions to genuine threats to women, feminists pretend that abortion is the one-size-fits-all Band-Aid solution to every problem there is. Sexual assault? Give her an abortion. Abusive relationship? She needs an abortion. Poverty-stricken? Kill her fetus, that’ll do the trick! Abortion activists do nothing to actually address real problems, and it’s really tiring to read their constant babbling about how the fictitious right to chemically poison, suction, dismember, or otherwise kill pre-born children is essential to their identity as women.
2. Christians just want us to stop having all the sex we want!
Okay, look. Back in the day, the Sexual Revolutionaries told the State to get out of their bedrooms. And they did. But now, they want everyone back in the bedroom—approving of whatever sexual expression is taking place and paying for pills and rubbers to ensure that all the sex they’re having stays nice and sterile. If we don’t want to pay for such things and make the apparently offensive suggestion that the women who desire them are independent enough to obtain these products for themselves, we get berated by women like Jessica Valenti of the The Guardian, who gravely informs her readers that, “The Hobby Lobby ruling proves men of the law still can’t get over ‘immoral’ women having sex.” Uh, no. Actually, it proves that people like Jessica Valenti can’t get over the idea that she has to fund her own sex life.
3. Contraception and abortion are essential healthcare!
I know a million other people have made this point, but apparently abortion activists just don’t hear it. Pregnancy is not a disease. Unnaturally ending a pregnancy due to a bizarre cannibalistic ideology that says killing tiny humans is okay is not healthcare. And while people might decide that they want to avoid pregnancy, that’s still not healthcare. It’s not addressing some medical condition (unless, of course, fertility is a medical condition that we need to bombard with as many pharmaceuticals as we can so as to render it unhealthy.) A number of feminists have claimed that the Hobby Lobby ruling “threatens women’s lives and health.” This claim would be hilarious if it weren’t so dangerously asinine. It’s about time that they stop insulting women by claiming that their ability to get pregnant is a medical condition to be treated.
There have been more arguments, especially legal ones, bandied about since the ruling on Monday. But fortunately for religious freedom, for people who respect human life throughout all stages, and for those who possess a worldview that allows for rational discourse, Hobby Lobby won their case against the feminist fascists of the Sexual Revolution.
And it’s about time, too.
Jonathon Van Maren is a writer and pro-life speaker who has given presentations across North America on abortion and pro-life strategy. Jonathon graduated from Simon Fraser University in 2010 with a Bachelor of Arts Degree in History. He is the communications director for the Canadian Centre for Bio-Ethical Reform.
On June 30, the Supreme Court issued its decision in the Hobby Lobby case (Burwell v. Hobby Lobby Stores, Inc.), siding with Hobby Lobby. It was a 5-4 decision, with Justice Alito writing the opinion (Justice Kennedy, who joined the majority, also wrote a concurring opinion). The Court’s decision, holding that the HHS Mandate violates Hobby Lobby’s religious freedom, has already been seriously misunderstood. So let’s set the record straight on four major issues:
1. Is This Case About Scalia and Other Court Conservatives Imposing Their Religion?
No: something nearer the opposite, really. This whole case involves a law called the Religious Freedom Restoration Act (RFRA), a law that exists because of a controversial 1990 Supreme Court case called Employment Division v. Smith.
Here’s what happened: Alfred Smith and Galen Black worked at a rehab clinic, but were fired for using peyote, and denied unemployment benefits. They sued, claiming that they were using peyote for religious reasons, because they were members of the Native American Church. In a 5-4 decision authored by Justice Scalia, the Court held that a facially-neutral law could be applied across the board, even if it had the effect of hindering religious rituals.
The case was explosive. In his dissent from Smith, Justice Blackmun noted that the “respondents’ use of peyote seems closely analogous to the sacramental use of wine by the Roman Catholic Church.” Thus, the Smith decision seemed like it might allow the government to pass facially-neutral laws (like prohibiting peyote or wine) that effectively outlawed a particular religion.
Unsurprisingly, both conservatives and liberals were startled by Smith. Rep. Charles Schumer (D-NY) and 170 co-sponsors (122 Democrats, 47 Republicans, and an Independent) introduced RFRA. It quickly passed 435-0 in the House and 97-3 in the Senate. As the Court noted in its decision today, RFRA “prohibits the Federal Government from taking any action that substantially burdens the exercise of religion unless that action constitutes the least restrictive means of serving a compelling government interest.”
That’s the whole point of the law: to make it harder for a federal law to trample the exercise of religion, without a compelling government interest. In other words, Congress was concerned that Scalia and the other conservatives on the Supreme Court didn’t take a broad enough view of religious freedom. Which is probably the opposite of what you’ve heard.
2. Isn’t this Case just About Contraception?
No. While there are plenty of parties suing who are against contraception, Hobby Lobby isn’t amongst them. Their objection was just to paying for abortions.
Four of the twenty drugs involved in this case are believed, not just to prevent conception (which would make them contraceptive, as the name implies), but to prevent the implantation of an embryo into the uterine wall. Interfering with the natural development of an embryo in order to bring about its death is an abortion.
At the heart of this, there’s a semantic debate over when pregnancy begins, because two definitions are used. Some obstetricians use an early definition: pregnancy begins once the sperm fertilizes the egg, resulted in an embryo (an organism genetically distinct from both its parents). Other obstetricians use a late definition: that pregnancy doesn’t begin until the fertilized egg implants into the uterine wall.
Of these, the early definition is better. Imagine that, one day, scientists are able to fuse sperm and egg in a laboratory setting, and bring the child full term in an artificial womb (or some other laboratory conditions). According to the late definition, we would have to conclude that this person was never conceived. That’s an absurd result, easily avoided by holding to the early definition.
But regardless of the semantic debate, the fact remains: even amongst those people who are fine with contraception, many still disagree with killing a fertilized embryo (or being forced to pay for others to do so). The owners of Hobby Lobby are just such people. As the Court noted in today’s opinion:
The owners of the businesses have religious objections to abortion, and according to their religious beliefs the four contraceptive methods at issue are abortifacients. If the owners comply with the HHS mandate, they believe they will be facilitating abortions, and if they do not comply, they will pay a very heavy price—as much as $1.3 million per day, or about $475 million per year, in the case of one of the companies. If these conseq uences do not amount to a substantial burden, it is hard to see what would.
3. Did the Supreme Court Just Declare That Corporations are People?
Rick Ungar at Forbes responded to the Hobby Lobby decision by writing an article entitled “Founding Fathers Spinning In Their Graves As SCOTUS Rules That Corporations Are People Too.” This is a surprisingly frequent allegation, given how hilariously wrong it is.
Do you know who decided that corporations are people, too? Congress.To see that, you don’t need to read any further than 1 U.S.C. §1, the very first law on the books. It reads: “In determining the meaning of any Act of Congress, unless the context indicates otherwise […] the words “person” and “whoever” include corporations, companies, associations, firms, partnerships, societies, and joint stock companies, as well as individuals.”
And guess what? That’s the whole point of a corporation. They enter into contracts, as if they’re people. They’re allowed to own property, as if they’re people. They have to pay income tax, as if they’re people. If you got rid of these rights and duties, you would be eliminating the entire purpose of corporations existing, which is why no one who understands corporate law seriously proposes changing this part of 1 U.S.C. §1.
But having said that, corporations aren’t really people, and there are some rights that they don’t enjoy (for example, the right to vote). So the task of the Supreme Court was to figure out whether the religious freedom protections of RFRA is one of those rights. In today’s decision, they determined that it was, at least for a closely-held corporation (that is, a corporation in which 5 or fewer people control a majority of the shares).
4. Did Either Side Deny that Corporations are People Under RFRA?
No, which is why the panicky reactions of Ungar, et al, are so surreal. The HHS admitted that a nonprofit corporation can be a “person” under RFRA. But the HHS’ position was that a nonprofit corporation could exercise religion, but that a for-profit corporation couldn’t. So if you’re a Christian non-profit, you can exercise religion, but if you’re a for-profit Christian bookstore, you can’t.
As the Supreme Court noted, such a distinction makes no sense. That position also would make it very hard for activist corporations to exist: the HHS’ position amounts to saying that for-profit corporations can only exist for the sake of profit. The Court noted that:
This argument flies in the face of modern corporate law. […] While it is certainly true that a central objective of for profit corporations is to make money, modern corporate law does not require for-profit corporations to pursue profit at the expense of everything else, and many do not do so. For-profit corporations, with ownership approval, support a wide variety of charitable causes, and it is not at all uncommon for such corporations to further humanitarian and other altruistic objectives. Many examples come readily to mind. So long as its owners agree, a for-profit corporation may take costly pollution-control and energy conservation measures that go beyond what the law requires. A for-profit corporation that operates facilities in other countries may exceed the requirements of local law regarding working conditions and benefits. If for-profit corporations may pursue such worthy objectives, there is no apparent reason why they may not further religious objectives as well. […]
Not all corporations that decline to organize as nonprofits do so in order to maximize profit. For example, organizations with religious and charitable aims might organize as for-profit corporations because of the potential advantages of that corporate form, such as the freedom to participate in lobbying for legislation or campaigning for political candidates who promote their religious or charitable goals.
As an example of such a for-profit corporation, the Court pointed to Google.org, which ““advance[s] its charitable goals” while operating as a for-profit corporation to be able to“invest in for-profit endeavors, lobby for policies that support its philanthropic goals, and tap Google’s innovative technology and workforce.”” So it’s not just religious organizations that the HHS’ position would have undermined, but all manner of socially-conscious companies. The government was prepared to undermine all for-profit corporations’ ability to be socially conscious, just because they happened to dislike the particular kind of social activism that Hobby Lobby engaged in.
So regardless of your views on contraception or abortion, if you’re a person who wants for-profit corporations to be able to act ethically – to be able to concern themselves with something more than fattening their shareholders’ wallets – today’s decision is a very good thing.
Joe Heschmeyer is a seminarian for the Archdiocese of Kansas City, Kansas, a former attorney, a Royals fan, and a Catholic blogger (at Shameless Popery). God willing, he’ll be ordained a priest in 2018.
“The anti-life mandate the Obama Administration tried to impose on these families is evidence of Big Abortion’s manipulative agenda, as they move from choice to coercion,” said AUL’s Dr. Charmaine Yoest.
WASHINGTON, D.C. (06-30-14) – “Today’s decision is a victory for common-sense as pro-life Americans do not lose their First Amendment freedoms when they open a family business or when they value unborn life,” commented Americans United for Life President and CEO Dr. Charmaine Yoest, upon hearing news that the Court ruled in favor of the Green and Hahn families in two cases challenging Obamacare’s coercive HHS Mandate. “These cases underscore the critical need for laws protecting Americans’ freedom of conscience. The anti-life mandate the Obama Administration tried to impose on these families is evidence of Big Abortion’s manipulative agenda, as they move from choice to coercion.”
In a 5-4 decision in Conestoga Wood Specialties v. Burwell (formerly Sebelius) and Burwell v. Hobby Lobby Stores, the U.S. Supreme Court held that closely held corporations (such as the Green and Hahn family businesses) cannot be required to provide “contraception” coverage. The Court held that the Obama Administration failed to show that its coercive Mandate was the least restrictive means of advancing its claimed interest.
Including these cases, Americans United for Life has filed 18 amicus curiae briefs in challenges to Obamacare’s HHS Mandate which includes requiring employers to offer life-ending drugs and devices in health insurance policies. AUL’s briefs presented analysis and arguments defending the constitutional rights of all Americans when it comes to healthcare purchases.
Conestoga Wood Specialties is owned by Christians and operated according to the owners’ Mennonite Christian beliefs. Hobby Lobby is an Oklahoma-based national arts and crafts retailer founded and run by David Green and his family, and their Christian faith has remained an integral part of the business. Both Conestoga Wood and Hobby Lobby do not oppose all contraception, but only those drugs and devices that have been labeled as “contraception” by the FDA even though they are known to have life-ending effects.
In its briefs before the Supreme Court, AUL demonstrated that the life of a new human being begins at fertilization (conception), that so-called “emergency contraception” has a post-fertilization effect that can prevent a new human being from implanting in the uterus, and that forcing employers to provide coverage for such drugs violates their constitutionally protected freedom of conscience.
The briefs were filed by an all-woman team of four AUL attorneys on behalf of the Association of American Physicians and Surgeons, American Association of Pro-Life Obstetricians & Gynecologists, Christian Medical Association, National Catholic Bioethics Center, Physicians for Life, and National Association of Pro Life Nurses.
“Real healthcare respects life,” noted Dr. Yoest. “Whether the issue is punishing Americans for their beliefs, pushing life-ending drugs that have been deceptively labeled as contraception, or creating new income streams for the abortion industry, the anti-life implications of Obamacare are far reaching.”
Abortion is woven into the healthcare law at multiple levels, making repeal of the law a pro-life necessity. The abortion-related provisions of Obamacare, include:
• Failing to prohibit the use of federal tax dollars for abortion, abortion coverage, and abortion-inducing drugs and devices.
• Pretending that the Hyde Amendment protections were enough to prohibit direct payment for abortions.
• Permitting federally subsidized Qualified Health Plans (QHPs) to provide abortion coverage through the state insurance exchanges required in all 50 states.
• Failing to prohibit all multi-state qualified health plans from providing coverage for abortion.
• Including a “preventive care” mandate that is being used to force coverage of drugs and devices known to end life.
• Failing to provide comprehensive First Amendment conscience protections for individuals, employers, and insurance companies that have religious or moral objections to abortion.
Americans United for Life continues to work at the state and federal level to enact comprehensive statutory protections that guard against Big Abortion’s coercive agenda.
ALBANY, NY – Albany’s new bishop led about 1,000 pro-life activists in a Walk for Life around New York’s state capitol building June 17. Catholics from the diocese, which had been directed for nearly four decades by a bishop known for his progressivism, see the new bishop as a “springboard of new energy” for the pro-life movement in the city.
“It’s just wonderful to have someone in our corner who is committed to the cause.”
Organized by local Catholics Jason and Teri Kippen, and assisted by the New York State Council of the Knights of Columbus, the Walk was led by Bishop Edward Scharfenberger, who succeeded Bishop Howard Hubbard in February.
Scharfenberger, who also led a prayer service prior to the walk, told LifeSiteNews that he participated “because the issue was important. They invited me and so I joined. It was wonderful to participate in this.”
Theresa Schweigert, Respect Life Coordinator at St. Madeleine Sophie Church, said she was “so grateful to our new bishop for leading us in such a beautiful prayer service and procession.”
“Bishop Scharfenberger’s initiative reminds us once again that we Catholic Christians must be a visible witness of the Gospel of Life,” said Schweigert. “By taking our Catholic Faith out into the streets, and as in this case a Rosary Procession past the seats of government for both the City of Albany and the State of New York, we become the salt and light that Jesus taught about in the Sermon on the Mount.”
Bishop Edward Scharfenberger delivers the homily at the prayer service before the Walk for Life.Michael Schweigert / Citizens Concerned for Human Life
Teri Kippen told The Evangelist, the Albany diocese’s newspaper, that the pro-life movement in the diocese has been “a little lackluster” but she believes Bishop Scharfenberger’s involvement in their efforts can be “a springboard of new energy.”
“It’s just wonderful to have someone in our corner who is committed to the cause,” she said.
Scharfenberger visited an abortion clinic in April, and has engaged in Facebook discussions with pro-life activists.
Bishop Edward Scharfenberger leads Albany’s Walk for Life.Michael Schweigert / Citizens Concerned for Human Life
Bishop Hubbard famously held a Mass in 2011 for the Catholic Association for Lesbian & Gay Ministry, a Catholic organization that had been banned from meeting in other dicoeses because it dissents from Catholic teaching on same-sex relationships. That year, he also said it would not be “appropriate” to deny New York Gov. Andrew Cuomo Communion over his pro-abortion stance.
Additionally, Albany’s first female mayor, Kathy Sheehan, who publicly supportssame-sex “marriage” and abortion, served as the diocese’s communications director under Hubbard.
At the same time, in the 1980s Hubbard took the state of New York to court over its licensing of two Planned Parenthood abortion clinics.
Scharfenberger’s family has a history of pro-life activism. His nephew, Jon, worked for Students for Life of America before his untimely death, and ran the Students for Life group when he attended Ave Maria University.
Jason Kippen told LifeSiteNews that the Knights of Columbus played an enormous role in the Walk’s success. Not only did they pay $800 in fees to help get the Walk going, Kippen says the Knights “sponsored the event, got the permit, and paid for a million-dollar insurance policy for the Walk itself.”
ROME – The Vatican’s preparatory document for the upcoming Synod on the Family, released Thursday, includes as a major theme the fact that in many places ordinary Catholics, clergy and laity, either do not know or do not accept their Church’s teaching on sex, marriage, life, and family. This situation of general ignorance has come about, it says, because of a failure to clearly present the Church’s teachings to Catholics.
In some places “many Christians, for various reasons, are found to be unaware of the very existence of this teaching [on marriage and family],” states the document, known as the “Instrumentum Laboris” or working text.
“The People of God’s knowledge of conciliar and post-conciliar documents on the Magisterium of the family seems to be rather wanting,” the document notes. “The documents … do not seem to have taken a foothold in the Faithfull’s mentality.”
This remark will be considered the understatement of the century for most Catholics who have been involved in the pro-life and pro-family struggle. The entire pro-life movement has insisted for decades that one of their greatest obstacles is that the majority of Catholics have rarely, if ever, heard homilies or other instruction from the Church on sexual morality, procreation, abortion, marriage, homosexuality, contraception, divorce and remarriage, and cohabitation.
The Vatican’s document, titled “The Pastoral Challenges of the Family in the Context of Evangelization,” (*) was created after officials examined the results of a questionnaire sent out not only to bishops and theologians, but to the laity in parishes around the world. Whatever the outcome of the Synod, the first session of which is set for this coming October, this document can be taken as a general summary of the current situation of the Church, which some members of the hierarchy have already acknowledged is grim.
The document notes that many responses said it is not only laity who suffer from a general ignorance of Catholic teaching. “Some observations attribute the responsibility for this lack of knowledge to the clergy, who, in the judgment of some of the faithful, are not sufficiently familiar with the documentation on marriage and the family, nor do they seem to have the resources for development in these areas,” it states.
“Some observations inferred that the clergy sometimes feel so unsuited and ill-prepared to treat issues regarding sexuality, fertility and procreation that they often choose to remain silent,” it continues. “Some responses also voice a certain dissatisfaction with some members of the clergy who appear indifferent to some moral teachings.”
“Their divergence from Church doctrine leads to confusion among the People of God,” it adds. “Consequently, some responses ask that the clergy be better prepared and exercise a sense of responsibility in explaining the Word of God and presenting the documents of the Church on marriage and the family.”
In the months following the distribution of the questionnaire, various Episcopal conferences reported a dire lack of knowledge among the faithful of the Church’s teachings on marriage and family. The German and Swiss bishops went so far as to say that the near-total ignorance of Catholic teaching by the laity was an indication that it ought to be changed, or even abandoned.
This refrain was taken up by others, including the Vatican’s own head of the Synod, Cardinal Lorenzo Baldisseri, who suggested that the time has come to “update” Church teaching. (The cardinal later clarified that the update he was calling for was in the spirit of Pope St. John XXIII’s call at the Second Vatican Council, rather than a demand that the Church abandon her teachings.)
But the document offers a clear-cut and much more obvious solution: get busy teaching those doctrines.
“In places with a vibrant Christian tradition and a well-organized pastoral programme, people are responsive to the Christian doctrine on marriage and the family,” it says. “When the teaching of the Church is clearly communicated in its authentic, human and Christian beauty, it is enthusiastically received for the most part by the faithful.”(Part I, Chapter II (8))
Today the 10th Circuit Court of Appeals issued an important ruling on Utah’s marriage amendment. This is the first time a circuit court has ruled on marriage since the U.S. Supreme Court’s ruling on the federal Defense of Marriage Act (DOMA) this time last year. In a 2-1 split decision, the 10th circuit ruled that Utah’s marriage amendment defining marriage as the union of a man and a woman violates the 14th Amendment of the U.S. Constitution.
The majority held that “the Fourteenth Amendment protects the fundamental right to marry” and that “a state may not deny the issuance of a marriage license to two persons, or refuse to recognize their marriage, based solely upon the sex of the persons in the marriage union.” The decision will almost certainly be appealed.
Of course the Fourteenth Amendment protects the fundamental right to marry—but the Supreme Court decisions that established a fundamental right to marry understood marriage as the union of a man and a woman. In issuing today’s ruling, the court implicitly supplied its own, new answer to the central question in this debate: what is marriage?
The only way the 10th Circuit could reach its decision today was to smuggle in a view of marriage that sees it as an essentially genderless institution and then declare that the Constitution requires that the States (re)define marriage in such a way.
But our Constitution is silent on what marriage is. And there are good arguments on both sides of this debate. Judges should not insert their own policy preferences about marriage and declare them to be required by the Constitution.
Indeed, this is the message that Judge Paul Kelly delivered in his dissenting opinion in today’s case. Quoting Supreme Court Justice Samuel Alito, Judge Kelly explains: “‘Same-sex marriage presents a highly emotional and important question of public policy—but not a difficult question of constitutional law,’ at least when it comes to the States’ right to enact laws preserving or altering the traditional composition of marriage.”
Kelly continued:
The Constitution is silent on the regulation of marriage; accordingly, that power is reserved to the States, albeit consistent with federal constitutional guarantees. And while the Court has recognized a fundamental right to marriage, every decision vindicating that right has involved two persons of the opposite gender.
Kelly explained that we need not seek from the courts a single 50-state answer: “If the States are the laboratories of democracy, requiring every state to recognize same-gender unions—contrary to the views of its electorate and representatives—turns the notion of a limited national government on its head.”
In citing Justice Alito, Judge Kelly hit on an important point—that there are competing policy arguments on the definition of marriage and that in a system of limited constitutional self-government, the people and their elected representatives should be making these decisions.
Justice Alito’s opinion on DOMA cited my book, What Is Marriage? Man and Woman: A Defense, as an example of one view of marriage: a “comprehensive, exclusive, permanent union that is intrinsically ordered to producing new life.” And he cited Jonathan Rauch as a proponent of the idea that marriage is a commitment marked by emotional union.
Alito explained that the Constitution is silent on which of these substantive visions of marriage is correct. The Court, he explained, should defer to democratic debate.
Indeed, whatever any individual American thinks about marriage, the courts shouldn’t redefine it. Marriage policy should be worked out through the democratic process, not dictated by unelected judges. The courts should uphold the freedom of the American people and their elected representatives to make marriage policy.
Last summer, when the Supreme Court struck down DOMA, Chief Justice John Roberts emphasized the limits of the majority’s opinion. He made clear that neither the holding nor its logic required redefining state marriage laws. The states remain free to define marriage as the union of one man and one woman.
If marriage ends up back at the Supreme Court again next year, the Court will be less likely to usurp the authority of citizens if it is obvious that citizens are engaged in this democratic debate and care about the future of marriage.
We must rally in support of our constitutional authority to pass laws defining marriage. We must make clear that court-imposed same-sex marriage via a Roe v. Wade-style decision will not settle the marriage debate any better than it has settled the abortion debate.
We must insist, with Judge Kelly, that judges “should resist the temptation to become philosopher-kings, imposing [their] views under the guise of constitutional interpretation of the Fourteenth Amendment.”
Reprinted with permission from The Daily Signal. —
A Ministry of Forming Faithful Families http://www.formingfaithfulfamilies.com/ a non-profit public charity under section 501(c) (3) of the Internal Revenue Code.
Every baby is a magnificent treasure, an awe-inspiring gift, a precious gem! Is God calling you to take up this beautiful opportunity to trust Jesus, to triumph over this fear driven culture that is afraid of children, and to be open to having One More Baby for Jesus? Are you willing to live in the moment without suffering unnecessary anxiety about the future which you don’t control? God is truly in control.
Jesus tells us: “Do not worry about tomorrow; tomorrow will take care of itself” (Matthew 6:34, NABRE).
Be part of the antidote for the prevailing culture that tends to seriously undervalue life. We at One More Baby for Jesus are in awe of life! Join us!
By One More Baby for Jesus we don’t mean one last baby, but one more baby for now if God in His most perfect providence grants this remarkable gift.
We are creating awareness and bringing the Catholic Church’s beautiful and true teachings on openness to life and the sanctity of life down to a simple concrete application in the present moment which is really the only place we can ever act from, and that is to be supportive of, or earnestly discern being open to having One More Baby for Jesus. This is not an imposition, but the sharing of a gift, an invitation.
We want to help people to reflect upon the true breathtaking nature and value of a child versus the various, sometimes mediocre reasons, that often inhibit us from being open to new life.
Even setting theology aside for a moment, we are going to be audacious in countering the prevalent culture that is so afraid of life and say: if you are blessed with potential fertility, why not strongly consider being open to having another baby if God so blesses you? Go for it!
Google One More Baby for Jesus or visit: http://www.formingfaithfulfamilies.com/one_more_baby_for_jesus
Explore our website http://www.formingfaithfulfamilies.com/ for many helpful resources including books, articles, and audios relative to openness to life within marriage and blessed family life and for education, hope and encouragement from a Catholic Christian view.
COLORADO SPRINGS, Colo. (BP) — How many computers or cars do you think Toshiba and Toyota would sell if they didn’t let you test them out first? Who in their right mind would make a big commitment of purchase without trying it out first?
But don’t we do the same with marriage? We ask young people to make one of the biggest commitments of their lives — rivaled only by their decision to become parents — without any prior experience of what marriage is actually like.
More than 60 percent of marriages today are preceded by some form of cohabitation. And 75 percent of current cohabitors enter these relationships with some plans toward marriage, even seeing this live-in relationship as a smart move toward marriage. But does the experience of cohabiting teach couples things that help make them better spouses once they do marry? Does cohabitation contribute to stronger, happier marriages?
Unfortunately, it does not. Not even close!
This is a rare instance where there’s a Grand Canyon sized chasm between what many young adults believe and the proven reality of their experience. And it is not the moralizing preachers and traditionalists saying so. A massive body of robust, diverse and conclusive scientific research on this question leaves no doubt about whether cohabiting is helpful to marriage. Graduate and postdoctoral seminars in sociology are held on this topic, and this is what they learn.
Sociologists investigating this question — working from two leading schools of sociology, the Universities of Chicago and Michigan — tell us clearly that the “expectation of a positive relationship between cohabitation and marital stability … has been shattered in recent years by studies conducted in several Western countries, including Canada, Sweden, New Zealand, and the United States.”
Their data indicates that people with cohabiting experience who marry have a 50 to 80 percent higher likelihood of divorcing than married couples who never cohabited. A Canadian sociologist explains:
“Contrary to conventional wisdom that living together before marriage will screen out poor matches and therefore improve subsequent marital stability, there is considerable empirical evidence demonstrating that premarital cohabitation is associated with lowered marital stability.”
After surveying the data on this question, another leading scholar contends that the only conclusion one could honestly reach was to wholesale “reject the argument” that cohabitation contributes to stronger marriages.
In fact, if a couple wanted to substantially increase their likelihood of divorcing, there are few things they could do to so efficiently guarantee such an outcome than live together before marriage. In fact, this is such a consistent finding in the social science research that scholars have coined a term for it: “the cohabitational effect.”
This finding has become a truism partly because the process of cohabiting itself is shown to influence couples to learn to communicate, negotiate and settle differences in ways that are less healthy and honest than do couples who didn’t cohabit before marriage. This is probably because without a clearly defined relationship, the cohabiting couple can learn to be more controlling and manipulative with each other. And this leads to relational resentment and mistrust.
And this has nothing to do with social acceptance or rejection of living together. Doctors Claire Kamp-Dush and Paul Amato conducted a unique investigation that tracked two groups of cohabitors who eventually married: one that married between 1964 and 1980 and another that did so between 1981 and 1997. This allowed them to see if there were any changes in the cohabitation effect as cohabitation became more common and more accepted by society.
But they found “there was little evidence that the negative consequences of cohabitation dissipated over time as cohabitation became more prevalent.” Even after controlling for various social and economic factors that could account for such a difference, they discovered premarital cohabitors in both groups were significantly more likely to have lower levels of marital happiness, more marital conflict, and higher levels of divorce.
“One of the most clearly defined correlates of cohabitation is an increased risk of marital dissolution,” says professor Jay Teachman of Western Washington University. In a more recent examination of cohabitation’s impact, he calls cohabitation one of the most “robust predictors of marital dissolution” — making living together first one of the worst things you can do for your marriage. Teachman also warns that even premarital sex by itself is associated with an increased risk of marital disruption, though at lower rates than living together before marriage.
A 2010 “meta-analysis” looked at 26 peer-reviewed, published studies that followed various couples over time. This analysis found that marrieds who had cohabiting pasts were more likely to face divorce, and that “noncohabitors seem to have more confidence in the future of their relationship, and have less accepting attitudes toward divorce.”
And as with other studies, the married couples with no cohabiting past are less likely to engage in aggressive and negative interactions, experience more overtly positive interactions, and enjoy more positive communications. These researchers conclude, based on their review of the best studies to date:
“The major practical implication of this review is that psychologists can inform the public, that despite popular belief, cohabitation is generally associated with negative outcomes both in terms of marital quality and marital stability….”
You see, marriage is not a consumer product that you give a try to see how it suits you. Marriage is a leaving of all other relationships to give yourself completely to your beloved. Cohabitation says, “I’m not sure about you. Can I give you test-drive to see what I think?” Melts your hearts doesn’t it, ladies? Marriage says, “I want all of you and I want to give all of myself to you!” This is why cohabitation and marriage are such very different kinds of relationships. It is why the social sciences have come to the conclusions they have about living together before marriage being a poor and unhealthy idea.
–30–
This is an edited excerpt from Glenn T. Stanton’s book, “The Ring Makes all the Difference: The Hidden Consequences of Cohabitation and the Strong Benefits of Marriage.” Stanton is the director for family formation studies at Focus on the Family in Colorado Springs, Colo.
Contents
• What Is Our Conscience?
• Formation of Conscience
• Christian Marriage
• Humanae Vitae
• The Winnipeg Statement
• Follow-up Statement on Conscience by Canadian Bishops
• God Decides What Is Right and Wrong
• God Gives Moral Law To The Church
• The Church As Divine Institution and The Holy Father
As Vicar Of Christ
• Pastoral Obligation To Preach The Truth
• Papal Directives To Do More
What Is our Conscience?
“Deep within his conscience man discovers a law which he has not laid upon himself but which he must obey. Its voice, ever calling him to love and to do what is good and to avoid evil, sounds in his heart at the right moment” (GS 16) [1].
“Conscience is a judgment of reason whereby the human person recognizes the moral quality of a concrete act… In all that he says and does, man is obliged to follow faithfully what he knows to be just and right” (CCC 1778) [2].
“The dignity of the human person implies and requires uprightness of moral conscience. Conscience includes 1) the perception of the principles of morality (synderesis); 2) their application in the given circumstances by practical discernment of reasons and goods; and 3) finally judgment about concrete acts yet to be performed or already performed…” (CCC 1780) [3].
“Man has the right to act in conscience and in freedom so as personally to make moral decisions. ‘He must not be forced to act contrary to his conscience. Nor must he be prevented from acting according to his conscience, especially in religious matters’” (CCC 1782) [4].
Formation of Conscience
Now we deal with shaping, educating, and forming the conscience. Forming our conscience is a continuous conversion to what is true and to what is good (VS 63b) [5]. Recall the three components of conscience. First, we must learn the basic moral principles as known through the natural moral law, through Divine Revelation and by the teachings of the Magisterium. Part III of the CCC is very useful here. Second, we must learn how to do moral reasoning, how the moral principles apply to various situations in life. We must understand why a good moral principle is objective, consistent, with universal application. We see how they apply even to “hard cases.” Third, when making moral judgments about this particular human act, we are to use good reasoning in conformity with the truth and in pursuit of the good. All three components of the conscience require education, training, practice, and experience.
Very often we do not know what is good for us. Sinful surroundings and our own fallen nature, more prone to sin than to virtue, encourage us to dismiss teaching authority and prefer our own judgment. Formation of conscience helps us see the contrast between our culture and our faith. The faith is to shape the culture, not vice versa (CCC 1793) [6].
Education of the conscience is a lifelong task. It does not stop after Confirmation, or even after graduation from a Catholic college. Life takes us through different stages, all of which are more complex and rich in the mystery of life. New problems arise which require deeper and better applications of the basic moral principles. Papal encyclical and apostolic exhortations are often addressed to the morality of new problems, e.g. Humanae Vitae, Familiaris Consortio, Evanglium Vitae, Veritatis Splendor. These were written for everyone, not just clerics.
Education of the conscience will also emphasize the role of the virtues and their opposite vices. Human virtues are firm attitudes, stable dispositions, habitual perfections of intellect and will that govern our actions, order our passions, and guide our conduct according to reason and faith. They make possible ease, self-mastery, and joy in leading a morally good life. The virtuous man is he who freely practices the good. Human vices surface in the absence of virtue. The seven capital sins provide us with a rich insight into the inclinations of our fallen human nature, the dark side of human nature (CCC 1783) [7].
There are still other components for the formation of conscience. The Word of God is central. God reveals His plan for the human universe through the Sacred Scriptures. We are to interiorize the Gospels and allow them to help guide our choices and acts. We are to put on the mind of Christ, appreciate the beauty of the good, honor the splendor of the truth. Jesus is the Way, the Life and the Truth (Jn 14:6). The Cross is another component of the formation. The only way we overcome the ravages of sin in our lives is through the Cross, the instrument of our redemption. We must accept our share of redemptive suffering, our share of the work of our salvation. The moral life, the Christian life, demands self-denial, self-discipline, moral exercise. Still other components are: the gifts of the Holy Spirit, and the witness and advice of reliable moral guides.
In the Vatican document on Religious Liberty the Church teaches: “In forming their consciences the faithful must pay careful attention to the sacred and certain teaching of the Church. For the Catholic Church is by the will of Christ the teacher of truth. It is her duty to proclaim and teach with authority the truth which is Christ and, at the same time, to declare and confirm by her authority the principles of the moral order which spring from human nature itself” (DH 14) (CCC 1785) [8].
Christian Marriage
God has a plan for marriage. It is a very good plan. Our prophetic/teaching task is to teach God’s plan to our people.
“The intimate partnership of life and the love which constitutes the married state has been established by the creator and endowed by him with its own proper laws; it is rooted in the contract of its partners that is, in their irrevocable personal consent…. This sacred bond no longer depends on human decision alone” (GS 48a) [9].
“Married people should realize that in their behavior they may not simply follow their own fancy but must be ruled by conscience – and conscience ought to be in accord with the law of God and the teaching authority of the Church, which is the authentic interpreter of divine law. For the divine law throws light on the meaning of married love, protects it and leads it to truly human fulfillment” (GS 50a) [10].
“But marriage was not instituted solely for the procreation of children: its nature as an indissoluble covenant between two people and the good of the children demand that the mutual love of the partners be properly expressed, that it should grow and mature” (GS 50b) [11].
“Some of the proposed solutions to these problems are shameful and some people have not hesitated to suggest the taking of life: the Church wishes to emphasize that there can be no conflict between the divine laws governing the transmission of life and the fostering of authentic married love” (GS 51a) [12].
“When it is a question of harmonizing married love with the responsible transmission of life it is not enough to take only the good intention and the evaluation of motives into account: objective criteria must be used, criteria drawn from the nature of the human person and human action, criteria which respect the total meaning of mutual self-giving and human procreation in the context of true love; all this is possible only if the virtue of married chastity is seriously practiced. In questions of birth regulation the sons and daughters of the Church, faithful to these principles, are forbidden to used methods disapproved of by the teaching authority of the Church in its interpretation of the divine law” (GS 51b)[13].
Since Gaudium et Spes (1965) and Humanae Vitae (1968), much good writing has been done on the themes of 1) making the gift of self (Law of the Gift), 2) communion of persons, 3) theology of the body, and 4) a Christian personalism. These provide rich veins of insight for priests to mine as they search for better and more penetrating ways to explain the beauty of God’s plan for marriage and spousal love.
Sources:
• Gaudium et Spes 48, 50, 51
• Familiaris Consortio
• Theology of the Body: Human Love in the Divine Plan, John Paul II (Daughters of St. Paul, Boston: 1997).
• Crossing the Threshold of Love: A New Vision of Marriage, Mary Shivanandam (Catholic University of America Press, Washington, D.C.: 1999).
• Why Humanae Vitae was Right: A Reader, edited by Janet Smith (Ignatius Press, San Francisco, 1993).
Humanae Vitae
Humanae Vitae presents us with God’s plan for love, life, marriage and family.
Is contraception, sterilization and abortion right or wrong? If wrong, why is it wrong? If seriously wrong, intrinsically evil, then why? We have here a moral absolute, for which there are no exceptions.
“Especially to be rejected is direct abortion – even if done for reasons of health.
“Furthermore, as the Magisterium of the Church has taught repeatedly, direct sterilization of the male or female, whether permanent or temporary, is equally to be condemned.”
“Similarly there must be a rejection of all acts that attempt to impede procreation, both those chosen as means to an end and those chosen as ends. This includes acts that precede intercourse, acts that accompany intercourse, and acts that are directed to the natural consequences of intercourse” (HV 14) [14] (FC 32) [15].
The Winnipeg Statement
Compare this with what the Canadian bishops said in their Winnipeg statement of 27 September 1968:
“#26 Counselors may meet others who, accepting the teaching of the Holy Father, find that because of particular circumstances they are involved in what seems to them a clear conflict of duties, e.g., the reconciling of conjugal love and responsible parenthood with the education of children already born or with the health of the mother. In accord with the accepted principle of moral theology, if these persons have tried sincerely but without success to pursue a line of conduct in keeping with the given directives, they may be safely assured that, whoever honestly chooses that course which seems right to him does so in good conscience.”
The Church teaches that the prohibition against artificial contraception is a moral absolute. The Canadian bishops, on the other hand, say that there are circumstances in which the parties may use contraceptives. It is precisely as though they had said, “Canadian Catholics may in some circumstances commit fornication or adultery or sodomy.”
“Seems right to him…” We must seek the truth. We do not determine the rightness or wrongness of contraception, sterilization, homosexual acts, fornication or adultery. Only God determines moral principles. Where there is clear teaching by the Church, we must accept that teaching and inform our conscience with that teaching. It is only in gray areas, where there is no clear position taken by the Church, that we must honestly choose the course which seems right, as best we can determine the right.
The way #26 reads, anyone can decide for himself the morality of an act, and then do the act in good conscience. This is not following a well-informed conscience. This is making up my own mind and telling the conscience to accept my decision and come along. This is what Adam and Eve did. But conscience is never a teacher; it is always a pupil.
An erroneous conscience is an erroneous conscience. It is not a correct conscience. There is no moral equivalence between the two. There is no moral equivalence between truth and error, good and evil. A willfully erroneous conscience, where ignorance is not invincible, is objectively wrong and culpable.
If a person tries to keep a moral principle, or moral norm, but fails because of human weakness, we can praise his efforts to keep the moral principle. But we cannot praise his failing, or his offending against the moral principle. Murder is always wrong. Fornication is always wrong. Homosexual acts are always wrong. Contraception is also always wrong.
We do not help a person by attempting to change the moral principles. Rather than lowering the bar of moral standards, we are to encourage others, and ourselves, to measure up to the standard. Moral standards are good for us, not harmful. Physical exercise may be painful and vexing; but it is objectively good for us. Similarly, all moral standards are good for us; troublesome, yes; sometimes difficult, but always good for us.
Source: A Search for the Truth: Did Pope Paul VI Approve the Winnipeg Statement? by Msgr. Vincent Foy (Toronto, Life Ethics Information Centre: 1997)
Follow-up Statement on Conscience by Canadian Bishops
On 12 December 1973 the Canadian Catholic Conference issued their “Statement on the Formation of Conscience.” They gave clarifications and, in effect, moved away from the Winnipeg Statement. However, they have not formally rejected the Winnipeg Statement. A few excerpts of the 1973 document will illustrate their distancing themselves from their 1968 document.
In section #8 there is a recognition of God as a law-giver: “For anyone to accept the idea of conscience, as we here present it, he must begin by agreeing that man is not lord of the universe and that man is subject to a law-giver who is greater than he is. In a word, we must begin with that very first basis of any moral life … the acceptance of God.”
The document lists three types of conscience: 1) complacent, or lazy in seeking the reasons behind moral norms; 2) excessively dynamic and revolutionary and 3) the Christian conscience. The excessively dynamic conscience is described as “the person who has totally misread the idea that everyone must ultimately be the judge, before God, of his actions and that in the ultimate decision he must make up his own mind. The persons in this category have distorted an appeal to intelligent decision into a destruction of law, objective structures, and have arrived at the conclusion that no one can tell them what to do, including the Church. It is seldom stated this way but it is where this type of exaggerated subjectivism necessarily leads” (# 21).
The ideal Christian conscience “leads us to have a responsible attitude to someone, to Jesus, to the community, to the Church, etc. Every person who fits into this category feels a responsibility for a progressive search and striving to live out a life ideal according to the mind of Christ” (# 22).
With regard to the Magisterium, “to ‘follow one’s conscience’ and to remain a Catholic, one must take into account first and foremost the teaching of the Magisterium. When doubt arises due to a conflict of ‘my’ views and those of the Magisterium, the presumption of truth lies on the part of the Magisterium. ‘In matters of faith and morals, the bishops speak in the name of Christ and the faithful are to accept their teaching and adhere to it with a religious assent of soul. This religious submission of will and of mind must be shown in a special way to the authentic teaching authority of the Roman Pontiff, even when he is not speaking ex cathedra’ (LG 25) [16] . And this must be carefully distinguished from the teaching of individual theologians or individual priests, however intelligent or persuasive” (# 41).
Source: Statement on the FORMATION OF CONSCIENCE, issued by the Canadian Bishops (Daughters of St. Paul: 1974).
God Decides What Is Right and Wrong (Veritatis Splendor)
Human freedom is recognized as vitally important for human dignity and human acts. But there are limits to freedom, and these limits are set by the truth. Veritatis splendor [17] explains certain novel interpretations of the relationship of freedom to the moral law, to human nature and to conscience. In the section “Freedom and Law” we find the teaching that only God determines what is right and wrong.
“In the Book of Genesis we read: ‘The Lord God commanded the man, saying, You may eat freely of every tree of the garden; but of the tree of the knowledge of good and evil you shall not eat, for in the day that you eat of it you shall die ‘ (Gen 2:16-17).
“With this imagery, Revelation teaches that the power to decide what is good and what is evil does not belong to man, but to God alone. The man is certainly free, inasmuch as he can understand and accept God’s commands. And he possesses an extremely far-reaching freedom, since he can eat ‘of every tree of the garden.’ But his freedom is not unlimited: it must halt before the ‘tree of the knowledge of good and evil,’ for it is called to accept the moral law given by God. In fact, human freedom finds its authentic and complete fulfillment precisely in the acceptance of that law. God, who alone is good, knows perfectly what is good for man, and by virtue of his very love proposes this good to man in the commandments” (VS 35) [18].
“In fact, genuine understanding and compassion must mean love for the person, for his true good, for his authentic freedom. And this does not result, certainly, from concealing or weakening moral truth, but rather from proposing it in its most profound meaning as an outpouring of God’s eternal Wisdom, which we have received in Christ, and as a service to man, to the growth of his freedom and to the attainment of his happiness (cf. FC 33-4) [19] ” (VS 95b) [20].
God Gives Moral Law to the Church
Christ established the Church to continue His work. The Church is a “sacrament (sign and instrument) of intimate communion with God and of the unity of the entire human race” (LG 1) [21]. The Church is both a mother and a teacher.
“As Teacher, she never tires of proclaiming the moral norm that must guide the responsible transmission of life. The Church is in no way the author or the arbiter of this norm. In obedience to the truth which is Christ, whose image is reflected in the nature and dignity of the human person, the Church interprets the moral norm and proposes it to all people of good will, without concealing its demands of radicalness and perfection” (FC 33a) [22].
“As Mother, the Church is close to the many married couples who find themselves in difficulty over this important point of the moral life: she knows well their situation, which is often very arduous and at times truly tormented by difficulties of every kind, not only individual difficulties but social ones as well. She knows that many couples encounter difficulties not only in the concrete fulfillment of the moral norm but even in understanding its inherent values” (FC 33b) [23].
“But it is one and the same Church that is both Teacher and Mother. And so the Church never ceases to exhort and encourage all to resolve whatever conjugal difficulties may arise without ever falsifying or compromising the truth. She is convinced that there can be no true contradiction between the divine law on transmitting life and that on fostering authentic married love (GS 51) [24]. Accordingly, the concrete pedagogy of the Church must always remain linked with her doctrine and never be separated from it. With the same conviction as my predecessor, I therefore repeat: ‘To diminish in no way the saving teaching of Christ constitutes an eminent form of charity for souls’ (HV 29)” [25] (FC 33c)[26].
The Church as Divine Institution and the Holy Father as Vicar of Christ
We look to the teaching Church for moral guidance. The Church was established by Christ to speak (evangelize) and teach (moral principles) on His behalf. The Church must teach the mind and teachings of Christ. She cannot change, or hide them.
The authority to teach within the Church comes from God. “All authority in heaven and on earth has been given to me. Go therefore and make disciples of all nations… teaching them to observe all that I have commanded you; and I am with you always, to the close of the age” (Mt 28:18).
The Church teaches with authority in matters of faith and morals. The Faith deals with the twelve articles of the Creed and related matters (Part I of the CCC). Morality deals with the Ten Commandments and related matters (part III of the CCC). Faith pertains to what we believe; morals pertain to what we choose and what we do.
Teaching authority is vested most especially in Peter and his successors. “You are Peter, and upon this rock I will build my Church. Whatsoever you bind on earth will be bound in Heaven…” (Mt 16:18-19). “He who hears you, hears me. He who rejects you, rejects me. And he who rejects me, rejects him who sent me” (Lk 10:16). Peter does not act or teach on his own authority, but on that of Christ. Peter does not establish the moral law; only Christ can do that. Peter does not add to or subtract from the moral law. He can only teach what he knows to be true, as taught and revealed to him by the Holy Spirit.
The Magisterium, both ordinary and extraordinary, is a great blessing for us. By it we know that we are informing our conscience with true moral principles. We can put on the mind of Christ. We can know the good and do it. We can recognize evil and resist it.
Pastoral Obligation to Preach the Truth
“It is your great and manifest mission, and we address especially those of you who are moral theologians – to promote completely and clearly the teachings of the Church concerning marriage. … It is of the utmost importance for safeguarding the peace of souls and the unity of the Christian people, that in moral as in dogmatic matters, all should obey the Magisterium of the Church and should speak with one voice. … We call upon you again with whole heart: ‘I beg you brothers through the name of our Lord Jesus Christ: that you might all speak as one and that there might be no division among you: that you may be united in the same mind and the same judgment’ (1 Cor 1:10)” (HV 28a) [27].
“Refusal to compromise anything concerning the saving doctrine of Christ is an outstanding act of charity to souls; yet at the same time it is necessary always to combine this with tolerance and charity. … Therefore, let spouses in their times of trouble find in the speech and hearts of their priests the image of the voice and love of our Redeemer” (HV 29a) [28].
“So, beloved Sons, preach with full confidence and be certain that the Holy Spirit of God, who guides the Magisterium in its teaching, will illuminate the hearts of the faithful and invite them to give their assent. Teach spouses the indispensability of prayer; instruct them properly so that they may come regularly and with great faith to the sacraments of the Eucharist and of penance and that they may never become discouraged because of their weakness” (HV 29c) [29].
Papal Directives to Do More
On 2 October 1999 Pope John Paul II addressed U.S. Bishops from California, Nevada and Hawaii who were making their ad limina visit to Rome. He encouraged them in these words: “As bishops, together with your priests, deacons, seminarians and other pastoral personnel, you must find the right language and imagery to present the teaching of Humanae Vitae in a comprehensive and compelling way.”
The context of this statement is the following: “Give couples the Church’s full teaching on procreation.”
“We are coming to the end of a century which began with confidence in humanity’s prospects of almost unlimited progress, but which is now ending in widespread fear and moral confusion. If we want a springtime of the human spirit, we must rediscover the foundations of hope. Above all, society must learn to embrace once more the great gift of life, to cherish it, to protect it and to defend it against the culture of death, itself an expression of the great fear that stalks our times. One of your most noble tasks as Bishops is to stand firmly on the side of life, encouraging those who defend it and building with them a genuine culture of life.
“The Second Vatican Council was quite aware of the forces shaping contemporary society when it spoke out clearly in defense of human life against the many threats facing it (cf. GS 27) [30]. The Council also made a priceless contribution to the culture of life by its eloquent presentation of the full meaning of married love (cf. GS 48-51)[31]. Following the lead of the Council and expounding its teaching, Pope Paul VI wrote the prophetic encyclical Humanae Vitae, in which he addressed the moral implications of the power to co-operate with the Creator in bringing new life into the world. The Creator has made man and woman to complement one another in love, and their union is no less a sharing in the creative power of God himself. Conjugal love serves life not only insofar as it generates new life but also because, rightly understood as the total gift of spouses to one another, it shapes the loving and caring context in which new life is wholeheartedly welcomed as a gift of incomparable value.
“Thirty years after Humanae Vitae, we see that mistaken ideas about the individual’s moral autonomy continue to inflict wounds on the consciences of many people and on the life of society. Paul VI pointed out some of the consequences of separating the unitive aspect of conjugal love from its procreative dimension: a gradual weakening of moral discipline; a trivialization of human sexuality; the demeaning of women; marital infidelity, often leading to broken families; State sponsored programs of population control based on imposed contraception and sterilization (HV 17) [32]; the introduction of legalized abortion and euthanasia, ever increasing recourse to in vitro fertilization, and certain forms of genetic manipulation and embryo experimentation are also closely related in law and public policy, as well as in contemporary culture, to the idea of unlimited dominion over one’s body and life.
“The teaching of Humanae Vitae honors married love, promotes the dignity of women and helps couples grow in understanding the truth of their particular path to holiness. It is also a response to contemporary society’s temptation to reduce life to a commodity. As bishops, together with your priests, deacons, seminarians and other pastoral personnel, you must find the right language and imagery to present the teaching of Humanae Vitae in a comprehensive and compelling way. Marriage preparation programs should include an honest and complete presentation of the Church’s teaching on responsible procreation, and should explain the natural methods of regulating fertility, the legitimacy of which is based on respect for the human meaning of sexual intimacy. Couples who have embraced the teaching of Pope Paul VI have discovered that it is truly a source of profound unity and joy, nourished by their increased mutual understanding and respect; they should be invited to share their experience with engaged couples taking part in marriage preparation programs.”
Source: L’Osservatore Romano, English Edition, 7 October 1998, p.5
References
[1] Vatican Council II, Pastoral Constitution on the Church in the Modern World, Gaudium et Spes, 16
[2] Catechism of the Catholic Church, Part 3, Article 6, “Moral Conscience,” par. 1778.
[3] Catechism of the Catholic Church, Part 3, Article 6, “Moral Conscience,” par. 1780.
[4] Catechism of the Catholic Church, Part 3, Article 6, “Moral Conscience,” par. 1782.
[5] Papal Encyclical, Veritatis Splendor, 63b, John Paul II, Rome August 6, 1993, 63b.
[6] Catechism of the Catholic Church, Part 3, Article 6, “Moral Conscience,” par. 1793.
[7] Catechism of the Catholic Church, Part 3, Article 6, “Moral Conscience,” par. 1783.
[8]Catechism of the Catholic Church, Part 3, Article 6, “Moral Conscience,” par. 1785.
[9] Vatican Council II, Pastoral Constitution on the Church in the Modern World, Gaudium et Spes 48a.
[10] Vatican Council II, Pastoral Constitution on the Church in the Modern World, Gaudium et Spes 50a.
[11] Vatican Council II, Pastoral Constitution on the Church in the Modern World, Gaudium et Spes 50b.
[12] Vatican Council II, Pastoral Constitution on the Church in the Modern World, Gaudium et Spes 51a.
[13] Vatican Council II, Pastoral Constitution on the Church in the Modern World, Gaudium et Spes 51b
[14] Papal Encyclical, Humanae Vitae, Paul VI, Rome, July 25, 1968, 14.
[15] Papal Encyclical, Familiaris Consortio, John Paul II, Rome, Nov 22, 1981, 32.
[16] Council of Vatican II, Dogmatic Constitution on the Church, Lumen Gentium, Rome, Nov 21, 1964, 25.
[17] Papal Encyclical, Veritatis Splendor, John Paul II, Rome, August 6, 1993.
[18] Papal Encyclical, Veritatis Splendor, John Paul II, Rome, August 6, 1993, 35.
[19] Papal Encyclical, Familiaris Consortio, John Paul II, Rome, Nov 22, 1981, 33-4.
[20] Papal Encyclical, Veritatis Splendor, John Paul II, Rome, August 6, 1993, 95b.
[21] Council of Vatican II, Dogmatic Constitution on the Church, Lumen Gentium, Rome, Nov 21, 1964, 1.
[22] Papal Encyclical, Familiaris Consortio, John Paul II, Rome, Nov 22, 1981, 33a.
[23] Papal Encyclical, Familiaris Consortio, John Paul II, Rome, Nov 22, 1981, 33b.
[24] Vatican Council II, Pastoral Constitution on the Church in the Modern World, Gaudium et Spes 51
[25] Papal Encyclical, Humanae Vitae, Paul VI, Rome, July 25, 1968, 29.
[26] Papal Encyclical, Familiaris Consortio, John Paul II, Rome, Nov 22, 1981, 33c.
[27] Papal Encyclical, Humanae Vitae, Paul VI, Rome, July 25, 1968, 28a.
[28] Papal Encyclical, Humanae Vitae, Paul VI, Rome, July 25, 1968, 29a.
[29] Papal Encyclical, Humanae Vitae, Paul VI, Rome, July 25, 1968, 29c.
[30] Vatican Council II, Pastoral Constitution on the Church in the Modern World, Gaudium et Spes 27.
[31] Vatican Council II, Pastoral Constitution on the Church in the Modern World, Gaudium et Spes 48-51.
[32] Papal Encyclical, Humanae Vitae, Paul VI, Rome, July 25, 1968, 17.
One of my favorite gospels, one of my favorite reality checks, is in the Gospel according to Mark 4:35-41, NAB. It is the story about the disciples crossing the lake with Jesus asleep in the stern. “On that day, as evening drew on, Jesus said to them, ‘Let us cross over to the other side.’” Yes, he wants us all to cross to the other side. But, there is a risk involved. There is a mystery involved. Perhaps it is evening; perhaps it is late. Maybe we are tired, but He wants us to cross to the other side.
“Leaving the crowd behind, they took him, just as he was in the boat.” Yes, leaving the crowd. Leaving the opinion polls, political correctness, the dominant culture, the culture that says one or two children should be enough, acquire more things and you will be happy; the culture that insanely makes a god, an idol, a savior, a religion, an obsession out of politics; the dominant culture that says it’s all about power, prestige, early retirement, spending your final years playing golf, taking it easy, and waiting to die. Then what?
We tend to want to be in control. We want all our ducks to be in a row before we venture out to give God what He wants in our lives. “Lord, let us win the lottery first!” “Let us have all our finances locked in to supposedly be secure that our current children and our possible next child have their private college education fully paid for, and then we will be open to life.” Certainly we can apply prudence in our lives where prudence belongs, but what is often lacking in today’s western culture is faith, and faith entails risk.
Surrendering our comfort zone to our Blessed Lord Jesus includes pain and purification, but for our good. We can not reduce the value of a human life to an illusory sense of control and assurance that we will be able to provide that child a college education and all the “things” we think he needs to be happy and fulfilled.
After all, we do not co-create with God persons who will be totally dependent and useless consumers. No, every person comes into the world with unique gifts to contribute for his own good and for the good of others, and that includes every person, even those with so-called disabilities and illnesses. It is supreme arrogance and lunacy to think that we parents alone somehow possess our children, and are responsible for them all on our own. We must give God His infinite due!
God wants to reach us with His truth and encouragement, even through examples that nature provides around us. What if the majestic trees of the forest were to say, “let us grow in greenhouses as potted plants where we will be safe and comfortable?” They would never mature. Their potential, their mission would never be fulfilled. No, they risk to let their seeds fall where they will and die. Those seeds then take root in the earth where there is dirt, vermin, death, pain, and darkness. Eventually the trees sprout up and reach up for the sun, to the life-giving sun and to the heavens. In order to reach for the sun, there must be a willingness to embrace the inescapable risks and challenges; and while they are reaching up and developing their full potential, fierce storms are mixed in with the sunny tranquil days.
Life is tremendously short. We need to step out, put out into the deep (see Luke 5:4), and make the most of this great gift. God is asking us to be generous in some way according to our possibilities. What is He asking of you? For many could He be asking your openness to having another child, if He so blesses you? You don’t have to have fourteen today. Our Blessed Lord is just asking us to be open, to trust, to be open to having perhaps one more child for now, to make the best of the circumstances and opportunities He is blessing us with today; then to discern the possibility of having yet another child down the road, but never to shut God out of our decision making process, to never definitively marginalize His will. We must always be open to His will. He does not want us to be potted plants.
“They took him with them in the boat just as he was.” We need to take Jesus with us. We need to be with the Lord, and we need to take Jesus just as He is, the Jesus Who loves us, the Jesus Who is Mercy incarnate; and the Jesus who is demanding, who wants the best for us, Who wants us to live life to the fullest without fear.
Our Blessed Lord wants us to put Him first, to be open to the children He wants to bless us with, to put Him and our families above things, above power, above prestige.
“And other boats were with him.” And when we strive to fulfill our mission and gallantly venture out, putting God and His will first, others will be invigorated and emboldened. They will look to our example and find courage to take a risk themselves, to leave fear behind, and to begin to live their lives to the full.
“A violent squall came up and waves were breaking over the boat, so that it was already filling up.” Sure, it can seem difficult to take risks, like a violent squall, to do God’s will, to be open to having a larger family, to die to ourselves, to put our spouse and children before our own pleasure, things, and fears. But these are all opportunities to grow in faith, to grow in love, to exercise and augment our spiritual muscles.
None of us live selflessness perfectly, and my wife, Kathleen and I unquestionably don’t; but God wants us to give our best effort each day, even though we fall short. The growth and love is in the effort and struggle. How could we ever love if there were no opportunities for difficulty or sacrifice? This is God’s work. He is always there to help us.
“Jesus was in the stern, asleep on a cushion.” Sometimes when we follow the Lord and make an effort to do His will it will seem like He is not there, as if He has abandoned us, left us to ourselves, as if He is unaware of our dire situation. But the truth is, He is always there, aware of and supremely interested in every detail of our lives, always caring, and always in absolute command, even when He is asleep. Venerable Archbishop Luis Martinez wrote a beautiful, extensive meditation on this very gospel passage. It has been printed in English under the title When Jesus Sleeps. It is a beautiful book, a beautiful meditation. I hope you will get a copy.
“They woke him and said to him, ‘Teacher, do you not care that we are perishing?’” Yes, He cares, but He permits situations in our lives that take us out of our comfort zones. These are opportunities for us to grow in love, faith, hope, and virtue; to be transformed more into Jesus. God is our infinitely loving Father. A good parent will not continue to hold his child’s hand to cross the street as the child grows into his teens, twenties, thirties, and forties. A good parent knows when it is time to encourage the child to venture forth on his own.
When a parent teaches his child to swim, will the child not complain, “Don’t let go. I’m afraid! I’ll drown! “ But, the parent helps and encourages the child to take the risk, and when the child discovers he can stay afloat on the water through his trepid, but gallant efforts, he is proud as can be! All along the parent was there to save the child if he went under, although the child could not perhaps perceive it at the time, being so preoccupied with his fears, challenges, and efforts at hand. The child would never develop, never mature, never be capable of any grand accomplishments unless the parent permitted him to take risks, to step out of his comfort zone, his bubble, to accomplish something.
Our Heavenly Father is like this with us because He loves us, and is willing to do what is best for us regardless of our protests, thanks be to God. If it was up to us we would stay forever in our comfort zone, but God loves us too much for that; so He is always encouraging us through providential circumstances, events, disasters, and people in our lives to trust Him more, to take risks, to accept, and embrace difficulties and even tragedies in our lives, so we can grow and mature, and make the most of our lives.
“He woke up, rebuked the wind, and said to the sea, ‘Quiet! Be still!’ The wind ceased and there was great calm.” Yes, the Lord, with a word can quiet a storm on a lake. And if we permit him, He can calm the worst storm, the Category 5 Hurricane that rages in our interior when we don’t have Jesus in the boat of our soul. Do you think there are storms in your life that are currently raging or yet to come that are beyond our blessed Lord’s power? Be convinced, there is nothing that will ever happen or can ever happen that is beyond the power and control of our loving and merciful God. Listen, we are invincible when we take Jesus into our boat. Nothing can harm us when Jesus is in our boat, nothing! Don’t doubt. Count on this!
“Then he asked them, ‘Why are you terrified? Do you not yet have faith?’”
Why do we not yet have faith, a real faith that is relevant to our daily lives? Why not yet? Why don’t we sufficiently trust and believe in God? If we take the time to reflect, we will see the innumerable times that our merciful Father has cared for and protected us. We only need a little supernatural eyesight that is enhanced through prayer, and the sacraments, in order to be able to grasp this reality. How many times does our Blessed Lord have to intervene for us, to provide for us, to show His love for us, before we will stop the interior storm of being terrified, before we will truly have faith, a living deep faith that continuously permeates every aspect of our lives, before we will be free to live our life to its fullest joyful potential?
We need to ask God, to give Him permission to bequest us with an unshakeable faith. This is God’s work, but we must offer Him our consent, and cooperate with His graces. When much is given, much is expected (see Luke 12:48). With this kind of faith built on rock (see Luke 6:48), we are capable of living our mission in life to the full for our good and the good of others. We leave impotent mediocrity behind. What a magnificent adventure our life becomes when we leave fear behind and have faith.
“They were filled with great awe and said to one another, ‘Who then is this whom even wind and sea obey?’” Who is this? It is Jesus, our Lord, our Creator, our Savior, and He is in command. He knows what will become of us. He always wants our good, and will always arrange things for our benefit.
There is really only one power that can stand in the way of God’s will. What is that power? What could we say is the power that is virtually equal to God himself? It is the power of a gift He has given us. This is an awesome, but fearsome power. And it is so powerful because it is so absolute. It is absolute because God himself has given it to us and He will never revoke His gifts. He is faithful and true. (see: Revelation 19: 1) And this gift, that will never be revoked, this gift that is so awesome and fearsome, is the gift of our free will.
This is why we must pray, and pray some more, for the grace of God’s help to exercise this power, this free will in accordance with Almighty God’s will. His will is always for our good and the good of others. And in order to exercise our free will in line with God’s transcendent will, we must be a courageous, faith filled, grace filled people.
Really the safest way, the most efficacious way, to exercise this awesome and fearsome gift of free will is to surrender and abandon ourselves to God’s most holy will. Then God will providentially, lovingly rattle us out of our confusion and fear. He will empower us to take risks for the good. He will give us His supernatural vision to fall in line with His perfect hierarchy of values, to put God and His things first, then our spouse, then our children, then our work and service. We have to die to our old selves and to be risen with Christ so we can live Christ. (see Philippians 1:21)
Kathleen and I have many times been challenged about the size of our family by people, even by relatives, who were often concerned and perhaps had the best of intentions. One of the greatest means of persuasion to help them understand that our choice to have a large family was right and good and in accordance with God’s will would be to take out a picture of our complete family, or to point the children out if they are near by. Then I would ask which of these children should have been our last? Where should we have stopped? Which of these children should not have been born? Which of these children do you think has been brought into existence in opposition to God’s will? I will ask this in a charitable tone. Although I have seldom, if ever, experienced the person who has challenged the size of my family declare that they were wrong, and that they were now in full agreement with our radical openness to life and trust in God, I believe my challenging premise does put things into perspective and cause the person to reflect more deeply on the subject.
I have yet to have someone answer this question by maintaining that Kathleen and I should have stopped at a particular child. This has never happened because of the grave reality that such a response would imply. By virtue of their failure to answer this question by selecting particular beautiful and unique children to have never existed, implies that the challenge to our family’s size does not hold merit. To select a point at which we should have ceased the prayerful discernment and living of God’s will in regard to openness to life in our marriage, would be to imply that the children born after that point would have been better off not existing, and that the world is better off without them. How could anyone sincerely and in good conscience make such a statement?
The whole idea of overpopulation is a myth. Anyone who has flown in a plane or taken a drive in the country can clearly see that densely populated areas are minuscule compared to the vast, open, sparsely inhabited land. Look at the grave damage done to so many countries, especially in the western world, where the average completed family size is well below the replacement rate of 2.1 children. There are grave societal and economic consequences of this. The consequences being currently experienced are only the tip of the iceberg compared with those potentially to come.
One example is the growing percentage of elderly compared to younger working adults producing and paying taxes. There is an ever increasing motive in society to attempt to rationalize euthanasia. The prevalent culture of death, the abortion and contraception mentality, breeds more and more selfishness and self-centeredness in the individual and in society, which results in increased fear. This is a volatile and disordered recipe for evils such as abortion, euthanasia, and wars to flourish. Take this as certain.
When a culture pushes God’s gifts and His will aside, it pushes God aside. When we are left to ourselves, we encounter disaster. God does not impose himself on us as He completely respects our free will, but we are made free in order to choose to do what we ought, to choose God and His will and truth. We cannot remain locked up in our fears and self-centeredness and expect to live happy and fulfilled lives. Although it can seem challenging and difficult to trust God, to take risks, to step out of our comfort zone, to do God’s will, this is what truly brings us happiness, fulfillment, and peace.
I recognize that many parents who are trying very hard complain that they are struggling with perhaps one, two, or three young children, and are therefore very concerned about having another. I have nothing but compassion and love for them in their struggles and concerns. But I care about what is best for them, and I like to encourage these parents with the reality check that their young children will not always be little. The little ones do grow and become more mature, becoming more capable of helping around the house and with the new little ones to come. God really has thought all these things out in His great and generous plan for life. We have found also that as we have grown older, having less energy than when we were younger, God has blessed us with older children now who can appreciably help with responsibilities around the house and with the children.
How did we end up having nineteen children? Well I can assure you of one thing. We never would have had this many if it were not for the gift of our faith in God, a God who always provides what is truly necessary, a God who tells us not to worry: “Set your hearts on his kingdom first, and on his righteousness, and all these other things will be given you as well. So do not worry about tomorrow: tomorrow will take care of itself. Each day has enough trouble of its own.” (Matthew 6:16, JB)
by Joseph Meaney, POSTED ON JUN 18, 2014
The beautiful port city of Corpus Christi in Texas will have a special celebration of its feast day this weekend. For the first time in 37 years there will be no facilities committing abortions in the city!
At one time in Corpus Christi there were three abortion mills in operation and nine abortionists in this city of over 300,000 people. But the last of these deadly offices, that of Eduardo Aquino, is now closed.
Catholic pro-lifers credit the Mother of God for this triumph of life over the culture of death, along with innumerable prayers over the years. Corpus Christi Bishop Emeritus Rene H. Gracida was particularly touched that the facility’s closure came on his birthday, June 9. Bishop Gracida, who was a national leader in the fight against abortion, came to pray with the icon of Our Lady of Czestochowa in front of the abortion center when she visited Corpus Christi earlier this year. It is also true that Christians of various denominations have been praying with Catholics for these clinics to shut down for decades – this is truly a team effort of prayer and trust in God’s grace.
Human Life International’s Father Peter West led a special prayer with the icon outside Aquino’s office during the hours in which abortions were committed there. There was a dramatic confrontation with Aquino and his staff and over forty mothers there for abortions. Two women turned away and did not go into the abortion center, but others screamed and raged against the pro-lifers.
This is not the first time that pro-lifers in Corpus Christi credit Our Lady with shutting a local abortion mill down. Over ten years ago the pilgrim image of Our Lady of Guadalupe was brought to Corpus Christi by pro-lifers and the faithful prayed with her outside another abortion business with a special intention that the place would close its doors forever. Exactly one year later they brought Our Lady of Guadalupe back and discovered that the office had been sold and no further abortions would take place there.
Dr. Francette Meaney, who has led pro-life efforts in Corpus Christi for almost four decades, rejoiced saying, “We thank Mother Mary in her icon of Our Lady of Czestochowa for this blessing. Dr. Aquino performed 2,000 abortions a year here and now the city named for the Body of Christ will be a place where all children have a chance to have a birthday.”
In fact, with this closure there are no abortion centers south of San Antonio, meaning 300 miles of South Texas are abortion-free. This is part of a dramatic trend.
Since December 2010 the number of abortion businesses in Texas has dropped from 41 to 22. The Texas state government has passed a series of laws in recent years which have made a big impact on the availability of abortion. Women seeking abortion in Texas must now be given a sonogram and information about the development of their preborn child, as well as the full facts about the risks associated with abortion.
Offices that commit abortions must also now meet the same safety standards that normal ambulatory surgical centers are required to possess, and abortionists now need admitting privileges in a hospital within 30 miles of their abortion business.
With consistent peaceful, prayerful witness at abortion facilities, and a strong pro-life majority with the political will and ability act, good things can happen. As the saying goes: Work as if everything depends on you, pray as if everything depends on God.
But as we know, the fight to stop abortion does not end merely with shutting down offices – we must also help women who have unexpected pregnancies and don’t know where to turn.
There are several centers in Corpus Christi that help mothers with crisis pregnancies. Some pro-lifers there are hoping to buy the property where the last abortion facility in Corpus Christi was located and turn it into a pro-life memorial center that will also conduct pro-life counseling. Human Life International’s affiliate in Austria did something similar a few years ago: opening a crisis pregnancy center with a chapel in a former abortion facility – one they helped to close in Vienna with prayers and sidewalk counseling.
Pro-lifers in Corpus Christi plan to place a large statue of Our Lady on the roof of the new center with prayers of reparation for the thousands of children who were killed there.
Please continue to pray through the intercession of Our Lady (http://www.hli.org/hli_campaigns/ocean-ocean-pilgrimage/) for the end of abortion around the world!
LONDON, June 12, 2014 (LifeSiteNews.com) – The Catholic Church is living through a “great crisis” of belief and practice, facing a “new paganism” comparable to the first centuries of the Church, and in which many priests and bishops are actively collaborating, Bishop Athanasius Schneider, auxiliary bishop of Astana in Kazakhstan, said in an interview during a trip to the UK.
The bishop said the crisis has particularly manifested itself in the erosion of belief in the Real Presence of Jesus Christ in the Eucharist, which he says has a “causal connection” to the denial of the Church’s teachings on sex and marriage.
“This is the deepest evil,” says Schneider, “man, or the clergy, putting themselves in the centre when they are celebrating liturgy and when they change the revealed truth of God, for instance, concerning the Sixth Commandment and human sexuality.”
The bishop’s interview was conducted by Sarah Atkinson andpublished June 6 in the Catholic Herald. Atkinson is also editor of Mass of Ages, the magazine published by the Latin Mass Society of England and Wales, which published the full transcript.
“We are living in an un-Christian society, in a new paganism,” Schneider told Atkinson. “The temptation today for the clergy is to adapt to the new world to the new paganism, to be collaborationists. We are in a similar situation to the first centuries, when the majority of the society was pagan, and Christianity was discriminated against.”
He warned that Christians will likely be faced again with the choice of apostasy, offered to those in the early Church, to pinch “one grain of incense into a fire in front of the statue of the emperor.” This ultimatum may even be supported from within the Church.
It seems possible that Catholics who remain faithful “may, for a time, be persecuted or discriminated even on behalf of those who [have] power in the exterior structures of the Church,” he said.
“Unfortunately there were in the first century members of the clergy and even bishops who put grains of incense in front of the statue of the Emperor or of a pagan idol or who delivered the books of the Holy Scripture to be burned.”
In our times, he said, clergy and bishops are not being asked to pinch incense to the emperor, but “to collaborate with the pagan world today in this dissolution of the Sixth Commandment and in the revision of the way God created man and woman.” These clergy, he said, would be “traitors of the Faith; they are participating ultimately in pagan sacrifice.”
Asked whether he foresaw “a split coming in the Church,” he responded, “Unfortunately, for some decades some clergy have accepted these ideas of the world. Now however they are following them publicly.”
“When these things continue, I think, there will be an interior split in the Church of those who are faithful to the faith of their baptism and of the integrity of the Catholic faith.” This split, he said, will be between those who remain faithful “to the unchangeable Catholic truth” and those “who are assuming the spirit of this world and there will be a clear split, I think.”
“I can presume that such a separation will affect each level of the Catholics: lay people and even not excluding the high clergy.”
Bishop Schneider had particularly strong words for the prelates supporting the proposal by Cardinal Walter Kasper to admit divorced and remarried Catholics to Communion “after a period of penance.” These, he said, “operate with a false concept of mercy.” He compared it to a doctor prescribing sugar for a diabetic “although he knows it will kill him. But the soul is more important than the body.”
“If the bishops admit the divorced and remarried to Holy Communion, then they are confirming them in their errors in the sight of God. They will even close down the voice of their conscience. They will push them more into the irregular situation only for the sake of this temporal life, forgetting that after this life, though, there is the judgment of God.”
“I hope the majority of the bishops [at the Synod] still have so much Catholic spirit and faith that they will reject the above mentioned proposal and not accept this.”
“I think this issue of the reception of Holy Communion by the remarried will blow up and show the real crisis in the Church,” said Schneider.
“The real crisis of the Church is anthropocentrism, forgetting the Christocentrism.” It comes “when we place ourselves, including the priests, at the centre and when God is put in the corner and this is happening also materially.”
“Our first duty as human beings is to adore God, not us, but Him. Unfortunately, the liturgical practice of the last 40 years has been very anthropocentric,” he said.
“The gates of the hell, i.e. of the heresy,” he said, will ultimately be defeated by “the Supreme Magisterium” of the Church, which “will surely issue an unequivocal doctrinal statement, rejecting any collaboration with the neo-pagan ideas of changing e.g. the Sixth Commandment of God, the meaning of sexuality and of family.” Those who have opposed the true teaching of the Church, he added, would then leave and no longer call themselves Catholic.
He said that he was encouraged by the “purity” of the faith of some of the Catholic students he addressed at Oxford University on his trip, saying that these “little ones” of the Church, though they have been “let down and neglected” are the ones who have the “real power” granted to them by Christ Himself.
“I am not worried about the future,” he said. “The soul of the Church is the Holy Spirit and He is powerful. However we are now experiencing a deep crisis in the Church as it happened several times in two thousand years.”
“We will see the rising of a renewed Church,” he predicted. “This is already preparing. Then this liberal clerical edifice will crash down because they have roots and no fruits.”
Posted in News & Commentary | Comments Off on Bishop Schneider: Church faces ‘great crisis’ as she’s tempted to conform to the ‘new paganism’
By James V. Schall, S.J., June 08, 2014
Charles E. Rice’s new book argues that once absolute relativism is established as the state “religion” there is no limit to what the state can and will do
“There are many paths to total state control of life—fascism, totalitarianism, communism. In the United States the path is labeled protection of individual human rights.”
— Charles E. Rice, Contraception & Persecution (2014), 86.
I.
Contraception & Persecution is a brief, blunt analysis of our polity. It presents a clear line of thought to explain, to those who will listen, the totalitarian nature of our present regime. This regime no longer follows the basic moral and philosophic premises of its founding. Nor does it acknowledge the basic human good by which any regime is limited. Indeed, Rice argues that the American founding itself, for all its genius, was flawed. It recognized no authentic interpreter of the natural law that was presupposed from Christian and classic sources by those who established this republic.
Eventually, this lack of an authoritative interpreter meant that the state itself would become the sole arbitrator of what was the human good. The state itself came to be the highest law. It would recognize no other authority but itself; no one could appeal to a higher law. As a people we are reluctant to admit that things could go so wrong. We are comfortable and hate to think things have so radically deviated from any true human good. The result is that we do not take seriously the intellectual nature of our obvious decline into an increasingly anti-human state.
Through the interpretation of the courts, the lack of understanding or resistance by Congress, and the multiplicity of arbitrary decrees now stemming from the Executive, this founding flaw has solidified itself as the ruling doctrine of the public order—“whatever the prince wills is the law”—to cite the classic Roman Law dictum designating the state with no limits.
Basically, we have established absolute relativism as the state “religion.”
Of its very nature, this state brooks no opposition. It has no authority higher than itself. It is now in the process of overturning all the tenets of classical familial and the public order stemming from it. Step by step, this all-powerful state disallows and subjects to punishment any criticism of its agenda or scope. All of this absolutism is imposed on the citizens, often with their consent, in the name of “rights”. The avenue by which these “rights” have gained full control of the civil power in all its branches is through an unproven and unprovable denial. That is, it arbitrarily affirms that no order exists in nature that would or could indicate what we, as human beings, really are, and how we ought to live and act for our own good.
In this light, the title of Rice’s book will at first seem odd—Contraception & Persecution—what, pray tell, has contraception to do with persecution? As it turns out, everything. In a book that serves as a companion and corroboration of Robert R. Reilly’s Making Gay Okay (see my review essay, “Homosexuality and the Logic of a Disordered Polity”), Professor Rice spells out both the legal and philosophical steps by which the limits that were intended to protect us from the absolute state and its “ruling classes” have now been mostly eliminated. We live in an almost unrecognizable polity in which no limits can be assigned to the government. No area of life exists over which the state at any level cannot and does not claim immediate jurisdiction and coercive power. Even our very words are increasingly controlled by “hate language” laws that the state imposes to guarantee its version of “rights”.
But this democratic acceptance of totalitarian principles is not the cause of our problem. It is rather the result of disorders of soul. Rice is quite frank—he recognizes the widespread and often defining participation of Catholics voices and leaders in this new polity. They are not only judges and politicians, but also bishops and even elements in the Vatican. They have failed to provide intellectual and moral leadership; they did not (or would not) foresee what eventually is at stake in our culture, even though it was in the logic of civil disorder from the beginning. We find a great lack of the intellectual courage of which Plato spoke so highly.
It will, no doubt, be thought absurd by many that issues of morality could undermine a republic, even though classical authors have held this possibility from the beginning of our culture. Rice begins with the obvious fact that we have mostly replaced the legal and moral idea that the purpose of marriage between a man and a woman is to form a family in which children can be begotten, born, and raised by their own parents for the continuation of our kind in this world. The love of spouses goes along with this purpose; it must remain open to human life at the cost of undermining love itself. Rice argues that, historically, most of the Christian people and their institutions understood this connection. But with the entrance of birth control approval by the Anglican Lambeth Conference in 1930, a fatal separation of love and children was established. What we have seen in the eighty years after this conference is a carrying out of its logical consequences in our customs and laws.
If there is no necessary connection between children and the marital relation of a man and a woman in their relation to each other, what follows is that any sort of relationship, whether fertile or not, becomes legitimate. For the very act of contraception, in whatever form it takes, establishes the principle that sex need not be related to children in any way. This naturally and necessarily infertile condition is intrinsic to the homosexual relation. The kind of legal “marriage” it now claims as a “right” is at best a settlement about property. It can never provide what children really want and need, that is, a father and a mother in a stable relationship of caring for one another. But next we allow, as we have allowed, the basic begetting to be ruled by scientists and technicians. Children are begotten and designed outside the womb. The care of such children becomes highly ambiguous. Are they but subjects of the state?
If children are a product, not of the relation of a man and a woman, but of control of their ova and sperm by technicians, the latter, in the name of science, can “experiment”. Perhaps, as even Plato speculated, they can produce better human beings if they have no direct relation to their proper father and mother. Much of what we are seeing, of course, was anticipated by Plato and in the last century by Aldus Huxley in his Brave New World, published in 1932. But these men were aware of the dangers such practices entailed. We, however, seem oblivious.
II.
Rice is very good at showing how finely things put together by God and nature belong together. What we know as human nature itself is not some arbitrary collection of parts. It is an intricately woven person with a body, and a soul that vivifies it. Through the soul it has intellection to see what it is and how to guide it. Moreover, as both the fine Introduction and Preface of this book point out, the full understanding of what human life is—its relation to God and family—has not been well preached or understood. There has been a strange reluctance to challenge the on-going ethos of our time, an ethos that has been undermining what it is that men and women really are, want, and need.
Perhaps the main point of Rice’s book is the realization that each conceived human person, whether allowed to live or not, is created for eternal life, though in his life and deeds he can reject that for which he exists. This purpose of man’s being will not change. In this context, those responsible for undermining the conditions or life of actual human beings are the focus of both the divine mercy and the divine judgment.
Again, the disorder of polity follows from disorder of soul. But once we set our foot on a deviant step away from the human good, we will find that the next and more deviant step immediately confronts us until we have, in the name of our “rights,” succeeded to undermine the whole moral and political order. The arguments and positions by which courts, legislators, and executives use to justify their new “rights” to divorce, contraception, abortion, homosexuality, gay marriage, and human experimentation are all posed in the name of something noble: individual rights. But they actually each lead to a greater disorder in the human body and soul, in the body politic.
“Rights”, of course, are the modern heritage of Hobbes and Locke. At first, they look like another way to express human dignity. But they begin by postulating a lone individual, not an actual individual who is born into a family. “Rights” are still proposed in the name of the individual good even when they include abortion and the deprivation of children of proper homes and parents.
“Rights”, then, are what are “due” to me. No one but me can tell what is due to me. Therefore, society and state have a duty to support me in what I want for myself, since that is my “right”. And if I have a “right” to something, it is ultimately the state that must guarantee that “right” to me. But when the state is the ultimate guarantor of my rights, it is also the one that decides which of my “rights” it will enforce. That is, it rules me by my “rights”.
In this context, there is only one “wrong”—the claim that some objective order exists to which and on which true human dignity and happiness exist. This claim is now looked upon as fanatic or totalitarian. It forms the basis on which the state now increasingly proposes to control religion and philosophy, which become themselves functions of the state and its purposes.
Rice argues that the real issue is the first commandment, whether we will first worship God or ourselves. He sees that efforts to replace marriage are themselves implicitly attacks on the Godhead from whom order exists in things, including human things. This view probably explains why religion must be reduced to a function of the state. Religion must be only a kind of subjective private activity that goes on in out of the way places we call “churches”.
We no longer care what goes on in the places of worship we allow to exist. But nothing that goes on there can have any effect in the public order. No religion can be exempt from what the law requires men to do or hold. Conscience is at best purely subjective.
What does not conform to what the state decrees has no “rights”. This is the effect, as Rice shows, of the HHS mandate. Rice rightly sees these thought processes and laws as the context of increasing persecution by the state of religion. The only caveat I would make with this thesis is that it is not really an issue of religion but of reason. It is no accident that the main line of defense of reason in the world today is the Catholic Church in so far as it remains loyal to its own tradition, which many Catholics have chosen to not do. But it is the Catholic tradition that has been the protector of not just revelation but of reason.
In this sense, the contribution of John Paul II and Benedict XVI to reason itself has been unprecedented. The defenders of religion have first to defend man as he is. It is precisely because the advocates of various forms of “rights” want to have another form of human being that they have zeroed in on the Church as it stands for reason.
And it is in the logic of disorder of soul that the state cannot and will not stop its aggrandizing mission until it has eliminated all opposition. This elimination is the context of the persecution that Rice sees everywhere on our immediate horizon. That is, it is already taking place. We do not readily admit that it is the legacy of our own refusal to see the logic of contraception itself and its corroding effects on every institution of society. But the effect of this logic is what animates our public order today. This is what Charles Rice is at pains to point out.
Contraception & Persecution
by Charles E. Rice
St. Augustine’s Press (South Bend), 2014
Hardcover, 128 pages
James V. Schall, S.J. taught political philosophy at Georgetown University until recently retiring. He is the author of numerous books and countless essays on philosophy, theology, education, morality, and other topics. His most recent book is Reasonable Pleasures: The Strange Coherences of Catholicism (Ignatius Press). Visit his site, “Another Sort of Learning”, for more about his writings and work.
Posted in News & Commentary | Comments Off on Contraception, Rights, and Total State Control
“The American family is falling apart. Consider two grim trends.
The U.S. marriage rate has plunged 57% since 1970, according to ‘The State of Our Unions’ for 2012. Two-thirds of Americans over age 15 used to be married. Now it is only 48%.
The unwed birth rate was only 5% in 1960 and 10.7% in 1970. However, that figure has soared to 40.8% in 2010. In fact, 53% of all births to women under age 30 were to unmarried women.
Ohio’s’s unwed births are higher at 44% and our marriages plunged 34% in 21 years (1990-2011).
What’s gone wrong? ‘Uncle Sugar,’ as Mike Huckabee puts it, is the culprit.
Here’s the standard scenario. Susan gives birth -a happy occasion. An official will ask her: ‘Are you married? Who is the father?’ If the answer is No, the second question is important to government. Bill’s full name and address will be taken down, because he will be assessed for child support.
However, Uncle Sugar has good news for Susan. Her medical expenses of the birth will be covered by Medicaid – as well as future health care for her child for 18 years and for herself. She will begin getting welfare (Temporary Assistance to Needy Families) plus food stamps and possibly housing subsidies. If she goes back to work, she’ll get an Earned Income Tax Credit and subsidized day care.
However, if Susan marries Bill, they will lose about $25,000 of benefits.
So guess what? Fewer couples marry and marriage rates fall. More babies are born out of wedlock and government costs soar. The government gets what it pays for.
However, our question is simple: Why is government subsidizing couples to live together rather than to marry? This makes no sense to anyone – to the couple, their child, or to taxpayers who foot the bill.
The cost to taxpayers is immense. One study estimated 41% of cohabiting couples have children – almost the same as 46% of married couples. There were 8 million cohabiting couples in 2013, or about 293,000 in Ohio. If 41% have kids, that’s 120,000.
The cost? A staggering $3 billion to Ohio taxpayers. If they have only one child each.
There were about 4 million births in 2011, 44% of whom were to Ohio’s unmarried parents. Or 60,700 unwed births here at a one-year cost of $1.5 billion.
It is time for Cohabitation Reform. It comes in two parts.
First, the official who asks the unwed mother about the father, must add another question: ‘Are you cohabiting with him? BTW, we need his address and Social Security number. If he has the same address as you, you have access to his income as if you were married. Therefore, you are not eligible for the same benefits given to a single woman.’
What about the 3.3 million cohabiting couples who are already getting those benefits?
If we were running for governor this year in Ohio, California, Texas, New York, or 30 other states, we would pledge ‘Cohabitation Reform’ with a triple goal of increasing marriages, reducing unwed births and slashing government costs.
‘One reason our marriage rate has been dropping and unwed births are rising is that the state subsidizes couples to live together – but not to marry,’ a candidate might say. ‘This makes no sense to anyone. Therefore, if I am elected governor, this state will subsidize unwed couples with children to marry – rather than to cohabit.’
‘Currently, if a cohabiting couple with a child marries, they lose $25,000 of benefits. However, if I am Governor, I will make those couples an offer: if you marry, we will not cut your benefits for two years. After two years, the benefits will taper off over three more years. Married men earn more than cohabiting men, and subsidies are not needed.’
‘However, everyone will be better off. Couples who marry are healthier, wealthier, have more sex and better sex than singles. They even live longer – ten more years for married men, and four years longer for women. Their children do better in school, are far less delinquent or apt to commit suicide and will also live five years longer than children of unmarried parents.’
‘The percentage of Americans who are married will rise. Unwed births will fall – as will the costs of government, by billions of dollars.’
Cohabitation Reform makes everyone a winner – including innovative candidates for governor!
–Mike McManus is President of Marriage Savers
Posted in News & Commentary | Comments Off on Why Is Marriage Plunging & Unwed Births Soaring?
June 12, 2014 (POP) – Long, long ago, when Anne’s parents were in college (sorry, mom and dad), demographers made an observation: they saw that for most of human history, even though couples were having far more than two children, mortality was also very high. The result was that populations either stayed the same or grew very slowly.
Then, with the advent of modern medicine, our life expectancy doubled, and then doubled again. And, not unexpectedly, our population doubled, and then doubled again, as well.
Population alarmists saw this doubling as the harbinger of catastrophe: “The world is ending!” “We’ll breed ourselves to death!” “Famine!” “No more personal space!”
But demographers developed a theory: since fertility and mortality had complimented each other for most of human history, and demographers predicted that they would one day soon do so again. Mortality would fall first, and then fertility would follow. After a while, things would be back in balance.
For a while, this theory of the “demographic transition” seemed to work just fine. Countries modernized, mortality fell, and fertility, after a lag, followed the same downward path.
But instead of stabilizing at 2.1 children per couple or so—zero population growth—as the demographers expected, fertility continued to fall.
A growing number countries—Romania, Greece, Japan, Taiwan, and the Ukraine among them—now have fertility rates hovering between 1.1 and 1.4 children per woman.
For the first time in human history, otherwise prosperous and secure societies see their numbers shrinking: Russia is losing 750 people per day. Germany is losing over 600 people per day. Japan is losing 450 per day.
Demographers call this “lowest low” fertility, but they have no idea how “low” it will actually go. Nobody does.
Among the factors driving fertility downward is the radical redefining of human sexuality that has occurred over the past half-century. Don’t blame the demographers for failing to see this coming: it is something new in human history.
Over the last half century, the pill and the sexual revolution have changed the sexual dynamic so dramatically that previous paradigms no longer apply. Economic security and mortality, which once dominated reproductive decisions, now only play small, tertiary roles.
Once upon a time sex produced children—unless you acted to prevent conception. Now, intercourse is expected to be sterile, unless you choose to deviate from the norm and stop contracepting. As Ron Lesthaeghe wrote in the 2010 Population and Development Review “during the first transition, couples chose to adopt contraception in order to avoid pregnancies; during the second, the basic decision is [whether or not] to stop contraception in order to start a pregnancy.”
Sterile sex is the new baseline. In countries going through this second demographic transition, having children is increasingly viewed as aberrant social behavior. This is especially true if a couple is having their second or third child.
The reasoning behind when to have children and how many children to have has changed as well. Couples once asked themselves: “Do we need to space our children right now?” or “How many children can we care for right now?”
This concern about the well-being of one’s present and future children has been replaced by an emphasis on self. As Lesthaeghe wrote, reproduction mainly occurs after, “a prolonged ‘process of self-questioning and self-confrontation by prospective parents. . .in which the pair will weigh a great many issues, including direct costs and opportunity costs, but their guiding light will be the outcome of self-confrontation. Would a conception and having a child be self-fulfilling?”
The population controllers—who are still obsessed with the numbers—are now attempting to impose this indubitably flawed model of sex onto the women of less-developed countries. Perhaps if they gave an honest look at another set of numbers (namely, that half of the world lives in a society with below-replacement fertility) they would acknowledge it as a serious symptom of a larger social change.
Instead, they continue to force this flawed part of our culture on less developed countries. They are undermining marriage, harming children, and compromising the long-term health of society as a result.
Don’t get us wrong. We are not concerned with imploding fertility because we are obsessed with population numbers. In fact, we are bemused as governments attempt to bribe women into having children without realizing that the whole calculus of having children has changed.
We are concerned because imploding fertility has consequences far beyond the number of workers a country may or may not have in a certain year. It reflects a revolutionary sexual and social dynamic that changes everything, not just the number of children borne.
This new dynamic changes the age at which we have kids, whom we have them with, and our relationships with them. It changes the calculus of the long-term monogamous relationships that we call marriage; it means that ever greater percentages of children will grow up without one or more of their biological parents in the house; it isolates more and more people in one-person households; and it leads to more and more divorce.
We have not just lowered our birth rate or changed the way we view sex, we have, in a very real sense, dissolved the glue that holds society together.
That is to say, the family.
Reprinted with permission from POP
Posted in News & Commentary | Comments Off on Why normal people should care about ‘baby busts’
HALIFAX, Nova Scotia, June 10, 2014 (LifeSiteNews.com) – Robin Cyr, 34, was experiencing a birthing mother’s worst possible nightmare. Her baby girl who had done so well during nine months of pregnancy was, after a painful and complicated labor, stillborn.
The tiny baby had been officially declared dead after laying motionless for 25 minutes in the IWK Health Centre in Halifax, Nova Scotia. Robin laid in bed, heartbroken that her baby was gone.
But then something utterly unexpected happened.
Excited nurses came rushing back into the room, breathlessly announcing that the baby had started breathing again.
“Another nurse came over, two minutes later. … She couldn’t talk. She was speechless, and another nurse came over and said, ‘Your baby’s breathing,’” Robin said, reported Metro Halifax.
Doctors could give the mother no explanation for the baby’s recovery.
“He said it’s a miracle,” Robin recounted. “He said, ‘I’m very sorry I gave up on your baby when I did, because I turned around and she’s breathing on her own.”
Now three months later, Robin says that her little Mireya is “doing everything on time.”
“She holds her head up, she turns to your voice, she smiles,” she told Metro Halifax last week.
Robin’s aunt Pearleen Shephard believes that God was in the delivery room that day.
“It’s a miracle, and God is doing his work,” she said. “The doctors took their hands off her. They called it. She was gone. So she truly, truly is a miracle.”
Posted in News & Commentary | Comments Off on Stillborn baby declared ‘dead’ revives 25 minutes later, now 3 months old
June 10, 2014 (The Daily Signal) – Miss Pennsylvania Valerie Gatto, a contestant on last night’s Miss USA pageant, described herself as a “product of rape” in an interview with TODAY.com. Gatto revealed she was conceived after her mother was raped at knifepoint by a stranger.
Gatto is using her experience and status to educate women about sexual assault and to provide an example of someone who rose above her situation to achieve success.
“I believe God put me here for a reason,” Gatto told TODAY.com. “To inspire people, to encourage them, to give them hope that everything is possible and you can’t let your circumstances define your life.”
Gatto’s mother originally hid the pregnancy from her family and intended on putting her up for adoption, but was dissuaded the night Gatto was born.
“Valerie’s mom told her family about her adoption plans,” Gatto’s biography reads. “But Valerie’s great-grandmother said – God doesn’t give you more than you can handle. Her mother listened and decided to raise Valerie with the help of God and her family.”
Gatto acknowledged that most people would view her situation as negative, but she claims that her close family never “looked at it as something negative.”
“Being a voice is life-changing,” she said. “I’m not sharing this story for publicity. I’m not doing this for any selfish reasons. I truly am doing this to change the world and make a difference.”
Reprinted with permission from The Daily Signal
Posted in News & Commentary | Comments Off on Miss USA contestant says she was conceived in rape
Premarital sex, embryonic stem cell research, euthanasia growing in acceptance
by Rebecca Riffkin, May 30, 2014
WASHINGTON, D.C. — The American public has become more tolerant on a number of moral issues, including premarital sex, embryonic stem cell research, and euthanasia. On a list of 19 major moral issues of the day, Americans express levels of moral acceptance that are as high or higher than in the past on 12 of them, a group that also encompasses social mores such as polygamy, having a child out of wedlock, and divorce.
These 19 issues fall into five groups, ranging from highly acceptable to highly unacceptable. Overall, 11 of the 19 are considered morally acceptable by more than half of Americans. Ninety percent of Americans believe birth control is morally acceptable, putting it into the “highly acceptable” category, which has little moral opposition — the only such issue among the 19. Nine of the other 10 issues with majority acceptance can be put into a “largely acceptable” category, as they have smaller majorities considering them morally acceptable and sizable minorities that consider them morally wrong. Moral agreement with doctor-assisted suicide, though at the majority level this year, is separated from disagreement by fewer than 10 percentage points, and so this issue is considered “contentious.”
Solid majorities of Americans consider seven of the issues morally wrong. Four of these — extramarital affairs, cloning humans, polygamy, and suicide — are considered morally wrong by more than 70% of Americans and fall into the “highly unacceptable” group. Three other issues fall into the “largely unacceptable” category, as smaller majorities of Americans consider them morally wrong, and at least three in 10 consider them morally acceptable.
Abortion receives neither majority support nor majority disapproval, making it the most contentious issue of the 19 tested. The current split is similar to what Gallup measured last year, but is a more even division than the four prior years when at least half said it was morally wrong.
Gallup has tracked Americans’ views on the moral acceptability of 12 of these issues annually since 2001 and the rest annually since 2002 or later. These data are from an overall question asked each year as part of Gallup’s Values and Beliefs poll, the latest of which was conducted May 8-11, 2014.
Americans’ views on the morality of many of these issues have undergone significant changes over time. For example, acceptance of gay and lesbian relations has swelled from 38% in 2002 to majority support since 2010. Fifty-three percent of Americans in 2001 and 2002 said sex between an unmarried man and woman was morally acceptable, but this year it is among the most widely accepted issues, at 66%. Similarly, fewer than half of Americans in 2002 considered having a baby outside of wedlock morally acceptable, but in the past two years, acceptance has been at or near 60%.
Additionally, a few widely condemned actions, such as polygamy, have become slightly less taboo. Five percent of Americans viewed polygamy as morally acceptable in 2006, but that is now at 14%. The rise could be attributed to polygamist families being the subject of television shows — with the HBO TV show “Big Love” one example — thus removing some of the stigma.
Republicans and Democrats Divided on Moral Acceptability of Several Issues
Republicans, Independents, and Democrats have differing views of the morality of several issues. Democrats are more likely than Republicans to consider issues like divorce, gambling, medical research using embryos, and having a baby outside of wedlock morally acceptable. But Republicans are more likely than Democrats to see wearing fur, the death penalty, and medical testing on animals as morally acceptable. Independents tend to fall in the middle of the two groups.
In the 12 years Gallup has asked this overall question, Democrats have become significantly more tolerant on many issues, while independents generally show a smaller shift in the same direction and Republicans’ views have changed little. The percentage of Democrats who say an issue is morally acceptable has increased for 10 issues, including abortion, sex between an unmarried man and woman, extramarital affairs, cloning humans, divorce, cloning animals, suicide, research using stem cells from human embryos, polygamy, and gay and lesbian relations.
In some cases, the change among Democrats has been substantial. For example, in 2003, 52% of Democrats said having a baby outside of wedlock was morally acceptable, and 40% of Republicans and 61% of independents agreed. This year, 72% of Democrats, a 20-percentage-point increase, say it is morally acceptable. Meanwhile, Republicans have seen no change, with 40% still saying it is morally acceptable, although a higher 50% viewed it as morally acceptable last year. Independents have also not seen a change, with 60% saying having a baby out of wedlock is morally acceptable this year.
Republicans are slightly more accepting of gay and lesbian relations, sex between an unmarried man and woman, and divorce than they were in 2001, when these questions were first asked. Independents’ views on the first two issues (but not divorce) also have seen small shifts, but neither group has seen changes as drastic as those among Democrats.
Bottom Line
Americans largely agree about the morality of several issues. Most say birth control is acceptable but that extramarital affairs are wrong. However, other issues show clear, substantial divides. These differences are largely explained by party identification, but previous research has shown that age also plays a factor.
Attitudes about the morality of these behaviors have in many instances changed over the past 13 years, especially among Democrats, and Americans are
CLACKAMAS, OR, June 4, 2014 (LifeSiteNews.com) – A Planned Parenthood affiliate has announced that, in order to remain financially viable, it is closing three offices in the Pacific Northwest and laying off employees at its remaining locations.
Stacy Cross, CEO of Planned Parenthood Columbia Willamette, which covers Oregon and part of Washington State, said in a press release that the action is “necessary in order to maintain a fiscally solvent operation that continues to keep our doors open to patients in our region for the long-term.”
The organization has closed its centers in Clackamas and Gresham, Oregon, as well as its office in Salmon Creek, Washington.
Dan Kennedy of Human Life of Washington told LifeSiteNews, “Human Life is delighted that the killing business is losing ‘customers.’”
“As the nation becomes more pro-life, we anticipate seeing more of this,” he said. “This is good news for women, men, and children in the womb.”
Oregon Right to Life said on its Facebook page that the closures would save babies’ lives. “Considering those areas are already serviced by crisis pregnancy centers, we are confident that life will be chosen by Oregon women even more than ever!”
The group’s executive director, Gayle Attebury, told The Oregonian the closure was “a pleasant surprise” necessitated by the fact that the abortion providers “aren’t getting the business they’d like.”
Following the recent trend of Planned Parenthood closures and mergers, the closed facilities offered abortion referrals and the morning after pill but did not perform abortions themselves.
According to the Guttmacher Institute, which was long institutionally tied to Planned Parenthood,abortion rates fell in 2011 to their lowest level since Roe v. Wade.
Cross said some employees at the affiliate’s six remaining offices – in Beaverton, Bend, Salem, Vancouver, and two offices in Portland – will be fired for economic reasons.
“We are confident that with this realignment of resources, we can evolve our health care practices to create a sustainable model for patients today and the future,” Cross said.
Posted in News & Commentary | Comments Off on Three Planned Parenthood offices to close in Oregon and Washington
WARSAW, Poland, June 5, 2014 (LifeSiteNews.com) –– The Vatican’s Secretary of State has urged Poles to trust Divine Providence and welcome the “children whom God wants to give you.”
Cardinal Pietro Parolin, who was in Poland to mark its twenty-five years of freedom from communist rule, challenged the nation’s people to embrace St. John Paul II’s teachings on the family.
In remarks reported by the Polish Catholic weekly Niedziela, the cardinal said: “Courage! God does not take away anything, but fills us with grace if we trust him. I encourage you to entrust yourselves to Divine Providence and not be afraid of accepting [the] children whom God wants to give to you.”
“Let your nation still give birth to new saints. They will decide about the fate of your homeland! They are also needed by the Church and the world,” he said.
Parolin’s comments were reminiscent of strong words from Pope Francis in a homily he delivered on Monday to fifteen couples celebrating wedding anniversaries. The pope said that the practice of rejecting fertility by choice for the sake of comfort is something that “Jesus does not like.”
“Marriages, in which the spouses do not want children, in which the spouses want to remain without fertility. This culture of well-being from ten years ago convinced us: ‘It’s better not to have children! It’s better! You can go explore the world, go on holiday, you can have a villa in the countryside, you can be care-free,” the pope said. “It is not fruitful, it does not do what Jesus does with his Church: He makes His Church fruitful.”
Parolin’s visit to Poland also commemorated twenty-five years of renewed diplomatic relations between the Vatican and Poland. He used the occasion to urge the faithful to remember the example and teaching of two great figures of the 20th century: St. John Paul II and Cardinal Stefan Wyszyński. Wyszyński served as primate of Poland from 1948 to 1981.
Parolin’s remarks come at a time when Poland faces significant demographic problems. Although it is one of the most Catholic countries in the world, Poland has one of the lowest fertility rates in the world – 1.33 children born per woman, according to the CIA World Factbook.
The cardinal referred to the occasion as “the 25th anniversary of the revival of your Homeland,” and linked this renewal to the family specifically. “Dear friends, dear families, do not be afraid of holiness! How important it is today for the Christian families to be holy. Let them be a place, where one can experience God’s love to all people. I am aware that in Poland there are many testimonies of holy families, faithful to Christ and Church,” he said.
The cardinal added that he “is aware of difficulties which are faced by families, which want to open up to life and remain faithful to the marital covenant till the end. The last word does not belong to those who proclaim the end of the traditional family, but to Divine Providence which realizes its plans through the family.”
The Catechism of the Catholic Church teaches in paragraph 1652 that, “By its very nature the institution of marriage and married love is ordered to the procreation and education of the offspring and it is in them that it finds its crowning glory.”
It also states in paragraph 1653 that “the fundamental task of marriage and family is to be at the service of life.”
In paragraph 2373, the Catechism states: “Sacred Scripture and the Church’s traditional practice see in large families a sign of God’s blessing and the parents’ generosity.”
Posted in News & Commentary | Comments Off on Vatican Secretary of State: Welcome the ‘children whom God wants to give to you’
On May 13, 2014, Americans United for Life’s President & CEO Dr. Charmaine Yoest, and General Counsel Ovide M. Lamontagne, J.D. spoke alongside legal and medical experts at an panel hosted by The Heritage Foundation on the one-year anniversary of the conviction of late-term abortionist, Kermit Gosnell. Other speakers included Byron Calhoun, M.D., Professor and Vice-Chair, Department of Obstetrics and Gynecology, West Virginia University-Charleston; Angelina Baglini, J.D., Fellow, Charlotte Lozier Institute; and Teresa Collett, J.D., Professor, University of St. Thomas School of Law. The panel was moderated by Sarah Torre, a policy analyst at The Heritage Foundation.
5/19/2014 11:41:00 AM
By Laurie Higgins -Illinois Family Institute
Last week, Princeton University law professor Robert P. George delivered the following speech titled “Ashamed of the Gospel?” at the National Catholic Prayer Breakfast. Every faithful follower of Christ-Catholic and Protestant-should read this speech. Pastors and priests should read it from the pulpit. Adult, college, high school, and middle school Sunday school classes should read and discuss it. Give copies of it to your pastors, priests, elders-even if doing so is uncomfortable.
Anyone who claims they don’t have time to read it, should give up one television program, skip reading one newspaper, or abbreviate one workout session this week to read it. It is that important.
After reading it, think deeply and talk about what you are prepared to give up in order to be a servant of Christ who willingly chose a brutal death so that you could have eternal life.
Ashamed of the Gospel?
By Robert P George
The days of socially acceptable Christianity are over. The days of comfortable Catholicism are past. It is no longer easy to be a faithful Christian, a good Catholic, an authentic witness to the truths of the Gospel. A price is demanded and must be paid. There are costs of discipleship-heavy costs, costs that are burdensome and painful to bear.
Of course, one can still safely identify oneself as a “Catholic,” and even be seen going to mass. That is because the guardians of those norms of cultural orthodoxy that we have come to call “political correctness” do not assume that identifying as “Catholic” or going to mass necessarily means that one actually believes what the Church teaches on issues such as marriage and sexual morality and the sanctity of human life.
And if one in fact does not believe what the Church teaches, or, for now at least, even if one does believe those teachings but is prepared to be completely silent about them, one is safe-one can still be a comfortable Catholic. In other words, a tame Catholic, a Catholic who is ashamed of the Gospel-or who is willing to act publicly as if he or she were ashamed-is still socially acceptable. But a Catholic who makes it clear that he or she is not ashamed is in for a rough go-he or she must be prepared to take risks and make sacrifices. “If,” Jesus said, “anyone wants to be my disciple, let him take up his cross and follow me.” We American Catholics, having become comfortable, had forgotten, or ignored, that timeless Gospel truth. There will be no ignoring it now.
The question we face
The question each of us today must face is this: Am I ashamed of the Gospel?And that question opens others: Am I prepared to pay the price that will be demanded if I refuse to be ashamed, if, in other words, I am prepared to give public witness to the massive politically incorrect truths of the Gospel, truths that the mandarins of an elite culture shaped by the dogmas of expressive individualism and me-generation liberalism do not wish to hear spoken? Or, put more simply, am I willing, or am I, in the end, unwilling, to take up my cross and follow Christ?
Powerful forces and currents in our society press us to be ashamed of the Gospel-ashamed of the good, ashamed of our faith’s teachings on the sanctity of human life in all stages and conditions, ashamed of our faith’s teachings on marriage as the conjugal union of husband and wife. These forces insist that the Church’s teachings are out of date, retrograde, insensitive, uncompassionate, illiberal, bigoted-even hateful. These currents bring pressure on all of us-and on young Catholics in particular-to yield to this insistence. They threaten us with consequences if we refuse to call what is good evil, and what is evil good. They command us to conform our thinking to their orthodoxy, or else say nothing at all.
Do you believe, as I believe, that every member of the human family, irrespective of age or size or stage of development or condition of dependency, is the bearer of inherent dignity and an equal right to life? Do you hold that the precious child in the womb, as a creature made in the very image and likeness of God, deserves respect and protection? Then, powerful people and institutions say, you are a misogynist-a hater of women, someone who poses a threat to people’s privacy, an enemy of women’s “reproductive freedom.” You ought to be ashamed!
Do you believe, as I believe, that the core social function of marriage is to unite a man and woman as husband and wife to be mother and father to children born of their union? Do you hold, as I hold, that the norms that shape marriage as a truly conjugal partnership are grounded in its procreative nature-its singular aptness for the project of child-rearing? Do you understand marriage as the uniquely comprehensive type of bond-comprehensive in that it unites spouses in a bodily way and not merely at the level of hearts and minds-that is oriented to and would naturally be fulfilled by their conceiving and rearing children together? Then these same forces say you are a homophobe, a bigot, someone who doesn’t believe in equality. You even represent a threat to people’s safety. You ought to be ashamed!
But, of course, what you believe, if you believe these things, is a crucial part of the Gospel. You believe the truth-in its fullness-about the dignity of the human person and the nature of marriage and sexual morality as proclaimed by the Church-our only secure source of understanding the Gospel message. So when you are invited to distance yourself from these teachings or go silent about them, when you are threatened with opprobrium or the loss of professional opportunities or social standing if you do not, you are being pressured to be ashamed of the Gospel-which means to give up faith in the Lordship of Christ and hope in the triumph of goodness, righteousness, and love in and through Him.
Heavy costs
To be a witness to the Gospel today is to make oneself a marked man or woman. It is to expose oneself to scorn and reproach. To unashamedly proclaim the Gospel in its fullness is to place in jeopardy one’s security, one’s personal aspirations and ambitions, the peace and tranquility one enjoys, one’s standing in polite society. One may in consequence of one’s public witness be discriminated against and denied educational opportunities and the prestigious credentials they may offer; one may lose valuable opportunities for employment and professional advancement; one may be excluded from worldly recognition and honors of various sorts; one’s witness may even cost one treasured friendships. It may produce familial discord and even alienation from family members. Yes, there are costs of discipleship-heavy costs.
There was a time, not long ago, when things were quite different….Biblical and natural law beliefs about morality were culturally normative; they were not challenges to cultural norms. But those days are gone. What was once normative is now regarded as heretical-the moral and cultural equivalent of treason. And so, here we are.
You see, for us, as for our faithful Evangelical friends, it is now Good Friday. The memory of Jesus’s triumphal entry into Jerusalem has faded. Yes, he had been greeted-and not long ago-by throngs of people waving palm branches and shouting “Hosanna to the Son of David.” He rode into the Jerusalem of Europe and the Jerusalem of the Americas and was proclaimed Lord and King. But all that is now in the past. Friday has come. The love affair with Jesus and his Gospel and his Church is over. Elite sectors of the cultures of Europe and North America no longer welcome his message. “Away with him,” they shout. “Give us Barabbas!”
The days of comfortable Catholicism are past
So for us there is no avoiding the question: Am I ashamed of the Gospel? Am I unwilling to stand with Christ by proclaiming His truths? Oh, things were easy on Palm Sunday. Standing with Jesus and His truths was the in thing to do. Everybody was shouting “Hosanna.” But now it’s Friday, and the days of acceptable Christianity are over. The days of comfortable Catholicism are past. Jesus is before Pilate. The crowds are shouting “crucify him.” The Lord is being led to Calvary. Jesus is being nailed to the cross.
And where are we? Where are you and I? Are we afraid to be known as his disciples? Are we ashamed of the Gospel?
Will we muster the strength, the courage, the faith to be like Mary the Mother of Jesus, and like John, the apostle whom Jesus loved, and stand faithfully at the foot of the cross? Or will we, like all the other disciples, flee in terror? Fearing to place in jeopardy the wealth we have piled up, the businesses we have built, the professional and social standing we have earned, the security and tranquility we enjoy, the opportunities for worldly advancement we cherish, the connections we have cultivated, the relationships we treasure, will we silently acquiesce to the destruction of innocent human lives or the demolition of marriage? Will we seek to “fit in,” to be accepted, to live comfortably in the new Babylon? If so, our silence will speak. Its words will be the words of Peter, warming himself by the fire: “Jesus the Nazorean? I tell you, I do not know the man.”
Perhaps I should make explicit what you have no doubt perceived as implicit in my remarks. The saving message of the Gospel of Jesus Christ includes, integrally, the teachings of His church on the profound and inherent dignity of the human person and the nature of marriage as a conjugal bond-a one-flesh union. The question of faith and fidelity that is put to us today is not in the form it was put to Peter-“surely you are you this man’s disciple”-it is, rather, do you stand for the sanctity of human life and the dignity of marriage as the union of husband and wife? These teachings are not the whole Gospel-Christianity requires much more than their affirmation. But they are integral to the Gospel-they are not optional or dispensable. To be an authentic witness to the Gospel is to proclaim these truths among the rest. The Gospel is, as St. John Paul the Great said, a Gospel of Life. And it is a Gospel of family life, too. And it is these integral dimensions of the Gospel that powerful cultural forces and currents today demand that we deny or suppress.
History is not our judge
These forces tell us that our defeat in the causes of marriage and human life are inevitable. They warn us that we are on the “wrong side of history.” They insist that we will be judged by future generations the way we today judge those who championed racial injustice in the Jim Crow South. But history does not have sides. It is an impersonal and contingent sequence of events, events that are determined in decisive ways by human deliberation, judgment, choice, and action. The future of marriage and of countless human lives can and will be determined by our judgments and choices-our willingness or unwillingness to bear faithful witness, our acts of courage or cowardice. Nor is history, or future generations, a judge invested with god-like powers to decide, much less dictate, who was right and who was wrong. The idea of a “judgment of history” is secularism’s vain, meaningless, hopeless, and pathetic attempt to devise a substitute for what the great Abrahamic traditions of faith know is the final judgment of Almighty God. History is not God. God is God. History is not our judge. God is our judge.
One day we will give an account of all we have done and failed to do. Let no one suppose that we will make this accounting to some impersonal sequence of events possessing no more power to judge than a golden calf or a carved and painted totem pole. It is before God-the God of truth, the Lord of history-that we will stand. And as we tremble in His presence it will be no use for any of us to claim that we did everything in our power to put ourselves on “the right side of history.”
One thing alone will matter: Was I a faithful witness to the Gospel? Did I do everything in my power to place myself on the side of truth? The one whose only begotten Son tells us that he, and he alone, is “the way, the truth, and the life” will want to know from each of us whether we sought the truth with a pure and sincere heart, whether we sought to live by the truth authentically and with integrity, and-let me say this with maximum clarity-whether we stood up for the truth, speaking it out loud and in public, bearing the costs of discipleship that are inevitably imposed on faithful witnesses to truth by cultures that turn away from God and his law. Or were we ashamed of the Gospel?
The Gospel is true. The whole Gospel is true. Its teachings about life and marriage are true-even its hardest sayings, such as Christ’s clear teaching about the indissolubility of what God has united and about the adulterous nature of any sexual relation outside that bond.
“I do not know the man”
If we deny truths of the Gospel, we really are like Peter, avowing that “I do not know the man.” If we go silent about them, we really are like the other apostles, fleeing in fear. But when we proclaim the truths of the Gospel, we really do stand at the foot of the cross with Mary the Mother of Jesus and John the disciple whom Jesus loved. We show by our faithfulness that we are notashamed of the Gospel. We prove that we are truly Jesus’s disciples, willing to take up his cross and follow him-even to Calvary.
And we bear witness by our fidelity to the greatest truth of all, namely, that the story does not end at Golgotha. Evil and death do not triumph. Yes, it is Good Friday, but the one who became like us in all things but sin conquers death to redeem us from our transgressions and give us a full share in eternal life-the divine life of the most blessed Trinity. The cross cannot defeat him. The sepulcher cannot hold him. His heavenly Father will not abandon him. The psalm that begins in despair, Eloi, Eloi lama sabachtani, ends in hope and joy. Easter is coming. The crucified Christ will be raised from the dead. The chains of sin will be broken. “Oh death, where is thy victory? Oh death, where is thy sting?”
I grew up as a Catholic in a Protestant culture. The Protestants of my boyhood were what we today call Evangelicals. In those days, the religious differences between us seemed vast, though today the personal and spiritual bonds we have formed in bearing common witness to marriage and the sanctity of human life have relativized, though, of course, not eliminated, those differences. We now know that Evangelical Protestants are truly our brothers and sisters in Christ-separated from us in certain ways, to be sure, but bound together with us nevertheless in spiritual fellowship. Growing up, I admired the strength of their faith, and their willingness openly to profess it. And I loved their hymns. One of the most familiar ones contains a vital message for us Catholics today. You will recognize the first verse:
On a hill faraway, stood an old rugged cross,
The emblem of suffering and shame;
I love that old cross, where the dearest and best,
For a world of lost sinners was slain.
And the chorus goes:
I will cherish the old rugged cross,
Till my trophies at last I lay down.
I will cling to the old rugged cross,
And exchange it someday for a crown.
Yes, there’s the story. Christ must endure the sufferings of Good Friday to fulfill his salvific mission. But Easter is coming. And we, who cherish his cross, and are willing to bear his suffering and shame, will share in his glorious resurrection. We who cling to that old rugged cross will exchange it someday for a crown.
And then comes the next verse, and how perfectly it captures the attitude we must adopt, the stance we must take, the witness we must give, in these times of trial if we are to be true disciples of Jesus:
To the old rugged cross, I will ever be true,
Its shame and reproach gladly bear,
Till he calls me someday, to my home far away,
Where forever his glory I’ll share.
Yes.
And I’ll cherish that old rugged cross,
Till my trophies at last I lay down.
I will cling to the old rugged cross,
And exchange it someday for a crown.
Yes, for us Catholics and all who seek to be faithful, it’s Good Friday. We are no longer acceptable. We can no longer be comfortable. It is for us a time of trial, a time of testing by adversity. But lest we fail the test, as perhaps many will do, let us remember that Easter is coming. Jesus will vanquish sin and death. We will experience fear, just as the apostles did-that is inevitable. Like Jesus himself in Gethsemane, we would prefer not to drink this cup. We would much rather be acceptable Christians, comfortable Catholics. But our trust in him, our hope in his resurrection, our faith in the sovereignty of his heavenly Father can conquer fear. By the grace of Almighty God, Easter is indeed coming. Do not be ashamed of the Gospel. Never be ashamed of the Gospel.
Robert Peter George is McCormick Professor of Jurisprudence at Princeton University, where he lectures on constitutional interpretation, civil liberties and philosophy of law. He also serves as the director of the James Madison Program.
To listen, beginning at about 20 minutes:
Note:
Carlo Maria Vigano, Apostolic Nuncio to the Untied States, read a prayer by Pope Francis as the closing prayer for the National Catholic Prayer Breakfast, 2014. The Pope’s prayer ended this way:
“Our Lady of America, pray for us. Amen.”
Vatican City, Apr 25, 2014 / 02:48 pm (CNA/EWTN News).- Pope Francis on April 25 stressed the need for bishops and priests to give a “consistent witness” to Christian moral teaching, including the lifelong nature of Christian marriage, and to teach these truths “with great compassion.”
“The holiness and indissolubility of Christian matrimony, often disintegrating under tremendous pressure from the secular world, must be deepened by clear doctrine and supported by the witness of committed married couples,” Pope Francis said.
“Christian matrimony is a lifelong covenant of love between one man and one woman; it entails real sacrifices in order to turn away from illusory notions of sexual freedom and in order to foster conjugal fidelity.”
The Pope’s remarks came in a meeting with bishops from South Africa, Zimbabwe and Swaziland, who were making their routine ad limina visit to the Holy Father, Vatican Radio reports.
Pope Francis noted the pastoral challenges presented by marital separation and divorce, even in Christian families, and the lack of a stable home for many children.
“We also observe with great concern, and can only deplore, an increase in violence against women and children,” he continued. “All these realities threaten the sanctity of marriage, the stability of life in the home and consequently the life of society as a whole.”
He stressed the need to continue “indispensable” marriage preparation programs that give “new hope” to young people for their futures as husbands, wives, fathers and mothers.
Pope Francis’ comments follow media reports about the contents of a recent phone call he allegedly made to a remarried divorced woman in Argentina. The woman claimed that the Pope told her she could receive Holy Communion.
Catholic teaching recognizes the nature of matrimony as indissoluble, so a new marriage can only be contracted if the first union was found to be invalid. Those who have entered a new union without a recognition of annulment may not be admitted to Communion.
On April 24, Vatican spokesman Father Federico Lombardi said that the media coverage of the woman cannot be confirmed as reliable and is “a source of misunderstanding and confusion.”
In his comments to the southern African bishops, Pope Francis also noted the damage caused by abortion and an attitude of disrespect for life.
“Abortion compounds the grief of many women who now carry with them deep physical and spiritual wounds after succumbing to the pressures of a secular culture which devalues God’s gift of sexuality and the right to life of the unborn,” he said.
In addition, the Holy Father acknowledged the bishops’ reports that some Catholics are turning away from the Church to other groups, as well as a decline in family size that is affecting the number of vocations to the priesthood and religious life.
“In this sea of difficulties, we bishops and priests must give a consistent witness to the moral teaching of the Gospel,” he said. “I am confident that you will not weaken in your resolve to teach the truth ‘in season and out of season’ (2 Tim 4), sustained by prayer and discernment, and always with great compassion.”
The Pope also recognized several other concerns of the southern Africa bishops, including the plight of refugees and migrants, dishonesty and corruption in society, and unemployment.
“Most of your people can identify at once with Jesus who was poor and marginalized, who had no place to lay his head,” he observed. “In addressing these pastoral needs, I ask you to offer, in addition to the material support which you provide, the greater support of spiritual assistance and sound moral guidance, remembering that the absence of Christ is the greatest poverty of all.”
Despite the challenges facing the bishops, the Pope praised their “flourishing parishes” and their efforts to train permanent deacons and lay catechists. He praised African clergy and vowed religious who served “God’s most vulnerable sons and daughters,” including widows, single mothers, the divorced, children at risk, and the region’s several million AIDS orphans.
“Truly the richness and joy of the Gospel is being lived and shared by Catholics with others around them,” the Pope said. “I pray that they will continue to persevere in building up the Lord’s Kingdom with their lives that testify to the truth, and with the work of their hands that ease the sufferings of so many.”
He encouraged the bishops to “rekindle the precious gift of faith so as to renew your dedicated service to God’s people!”
“May the saints of Africa sustain you by their intercession. May Our Lady of Africa be always at your side, and may she guide you as you share in the teaching, sanctifying and governing mission of Christ,” he concluded.”
Aware of the U.N.’s contrary positions on many life issues, Pope Francis today challenged 29 heads of U.N. agencies to resist the “throwaway culture” and the “culture of death” which, he said, “nowadays sadly risk becoming passively accepted.”
It is one of the few times – if not the first – that Francis has used the term “culture of death” which was first coined by St. John Paul II in his 1995 encyclical Evangelium Vitae. John Paul defined the term as the “war of the powerful against the weak”, characterized by a society that lacks solidarity, and fostered by “powerful cultural, economic and political currents which encourage an idea of society excessively concerned with efficiency.” He included within this culture many current social evils such as procured abortion, modern slaveries such as pornography and drug addiction, disdain for the poor, and euthanasia.
In today’s private audience at the Vatican with the United Nations Chief Executives Board and Secretary General Ban Ki-Moon, the Pope said that “an awareness of the dignity of each of our brothers and sisters whose life is sacred and inviolable from conception to natural death must lead us to share with complete freedom the goods which God’s providence has placed in our hands.”
As in his speech at the World Economic Forum in Davos earlier this year, the Holy Father also underlined the “indispensable” cooperation of the private sector in working alongside state initiatives for the common good.
Quoting St. John Paul II’s encyclicals Sollicitudo Rei Socialis, Centesimus Annus, and Benedict XVI’s Caritas in Veritate, he stressed that “equitable economic and social progress can only be attained by joining scientific and technical abilities with an unfailing commitment to solidarity accompanied by a generous and disinterested spirit of gratuitousness at every level.
“A contribution to this equitable development will also be made both by international activity aimed at the integral human development of all the world’s peoples and by the legitimate redistribution of economic benefits by the State, as well as indispensable cooperation between the private sector and civil society,” he added.
He closed by urging the UN leaders to “work together in promoting a true, worldwide ethical mobilization which, beyond all differences of religious or political convictions, will spread and put into practice a shared ideal of fraternity and solidarity, especially with regard to the poorest and those most excluded.”
Here below is his speech in full:
***
Mr Secretary General,
Ladies and Gentlemen,
I am pleased to welcome you, Mr Secretary-General and the leading executive officers of the Agencies, Funds and Programmes of the United Nations and specialized Organizations, as you gather in Rome for the biannual meeting for strategic coordination of the United Nations System Chief Executives Board.
It is significant that today’s meeting takes place shortly after the solemn canonization of my predecessors, Popes John XXIII and John Paul II. The new saints inspire us by their passionate concern for integral human development and for understanding between peoples. This concern was concretely expressed by the numerous visits of John Paul II to the Organizations headquartered in Rome and by his travels to New York, Geneva, Vienna, Nairobi and The Hague.
I thank you, Mr Secretary-General, for your cordial words of introduction. I thank all of you, who are primarily responsible for the international system, for the great efforts being made to ensure world peace, respect for human dignity, the protection of persons, especially the poorest and most vulnerable, and harmonious economic and social development.
The results of the Millennium Development Goals, especially in terms of education and the decrease in extreme poverty, confirm the value of the work of coordination carried out by this Chief Executives Board. At the same time, it must be kept in mind that the world’s peoples deserve and expect even greater results.
An essential principle of management is the refusal to be satisfied with current results and to press forward, in the conviction that those gains are only consolidated by working to achieve even more. In the case of global political and economic organization, much more needs to be achieved, since an important part of humanity does not share in the benefits of progress and is in fact relegated to the status of second-class citizens. Future Sustainable Development Goals must therefore be formulated and carried out with generosity and courage, so that they can have a real impact on the structural causes of poverty and hunger, attain more substantial results in protecting the environment, ensure dignified and productive labor for all, and provide appropriate protection for the family, which is an essential element in sustainable human and social development. Specifically, this involves challenging all forms of injustice and resisting the “economy of exclusion”, the “throwaway culture” and the “culture of death” which nowadays sadly risk becoming passively accepted.
With this in mind, I would like to remind you, as representatives of the chief agencies of global cooperation, of an incident which took place two thousand years ago and is recounted in the Gospel of Saint Luke (19:1-10). It is the encounter between Jesus Christ and the rich tax collector Zacchaeus, as a result of which Zacchaeus made a radical decision of sharing and justice, because his conscience had been awakened by the gaze of Jesus. This same spirit should be at the beginning and end of all political and economic activity. The gaze, often silent, of that part of the human family which is cast off, left behind, ought to awaken the conscience of political and economic agents and lead them to generous and courageous decisions with immediate results, like the decision of Zacchaeus. Does this spirit of solidarity and sharing guide all our thoughts and actions?
Today, in concrete terms, an awareness of the dignity of each of our brothers and sisters whose life is sacred and inviolable from conception to natural death must lead us to share with complete freedom the goods which God’s providence has placed in our hands, material goods but also intellectual and spiritual ones, and to give back generously and lavishly whatever we may have earlier unjustly refused to others.
The account of Jesus and Zacchaeus teaches us that above and beyond economic and social systems and theories, there will always be a need to promote generous, effective and practical openness to the needs of others. Jesus does not ask Zacchaeus to change jobs nor does he condemn his financial activity; he simply inspires him to put everything, freely yet immediately and indisputably, at the service of others. Consequently, I do not hesitate to state, as did my predecessors (cf. JOHN PAUL II, Sollicitudo Rei Socialis, 42-43; Centesimus Annus, 43; BENEDICT XVI, Caritas in Veritate, 6; 24-40), that equitable economic and social progress can only be attained by joining scientific and technical abilities with an unfailing commitment to solidarity accompanied by a generous and disinterested spirit of gratuitousness at every level. A contribution to this equitable development will also be made both by international activity aimed at the integral human development of all the world’s peoples and by the legitimate redistribution of economic benefits by the State, as well as indispensable cooperation between the private sector and civil society.
Consequently, while encouraging you in your continuing efforts to coordinate the activity of the international agencies, which represents a service to all humanity, I urge you to work together in promoting a true, worldwide ethical mobilization which, beyond all differences of religious or political convictions, will spread and put into practice a shared ideal of fraternity and solidarity, especially with regard to the poorest and those most excluded.
Invoking divine guidance on the work of your Board, I also implore God’s special blessing for you, Mr Secretary-General, for the Presidents, Directors and Secretaries General present among us, and for all the personnel of the United Nations and the other international Agencies and Bodies, and their respective families.
My Dear Auntie,
You know what a weirdo I am! Here again is another case where I am afraid you might find me weird, weird, weird!! You asked if I plan to have the prenatal bunch of tests and I replied, “no”. I am sure that sounded strange.
Being pregnant at 46 is a little out of fashion, that is unless I focused on a career first and waited to have children until later- which many women do these days.
I do not plan to have the recommended invasive, expensive and dangerous barrage of tests because there is not much they can do if they discover a problem. An ultrasound and blood test would give us any heads up we or the baby would need at delivery if a medical issue was discovered. I also know that if they do discover something wrong, they will likely counsel us to have an abortion, which, of course, we would not do (reminds me of Nazi Germany- this whole contemporary, neurotic emphasis on perfection). If they did counsel us for an abortion, things might get very ugly and I am certain some regretful strong and pointed words would come out of my mouth.
From the time I was 35, the medical community (and society) has tried to instill terror into me (not only in me but in others as well) about having more children. Consider this though, since time immemorial women were having babies into their 40’s. They had babies until their biological clock stopped ticking, until their fertility came to it’s end and God shut the door. The door opens and it shuts—very big fact of life. There was never a time when we had to artificially determine, “Ok, I am X age, so therefore we should not have any more children”.
Anyway, in regards to a healthy baby- you will think me even weirder now—I actually told God that if He wanted to bless us with a baby with Down’s (for example), we would be very pleased and blessed. Children with Down’s are such a blessing to everyone. They are innocent and sweet and walking saints among us. They teach us to love and to give more freely, joyfully and sacrificially.
If we did have a baby with extraordinary health challenges, of course like anyone, I would be frightened. I would be frightened that I could not get over my own selfishness enough to really give our child all the love and attention needed. For this, I would have to pray and ask God who, I know (but have to learn over and over) would give me the necessary Graces.
The Church teaches that every life is worth living. God is especially close to the poor and the suffering and what would it matter ultimately if a person suffered due to ill health, lack of beauty, poverty if in the end they won the happiness of eternal life? I do not think they would remember it in eternity with God. I see people with perfect health, beauty and wealth suffer in ways harder to treat than illness or disfigurement; they suffer from greed, selfishness, lust, depression, boredom, dissatisfaction, etc., etc. Shoot, I suffer from some of those too at times.
I have a childhood friend who is married and very successful in her career—both she and her husband each earn 6 figures. She told me she does not want to have children because of the way she sees teens behave these days, the turbulent political climate and because of the general lowering of morality so apparent in the media. I was very sad to hear this and did not have a good way to answer her concerns. In my work teaching about God’s thrilling plan for love and marriage (aka moral family planning and NFP), I am always seeking ways to more effectively communicate this plan to couples who have mostly been catechized by the world and hold its values. It’s tough because it is a very counter-cultural message- but one that brings true happiness and satisfaction. I often go to the encyclicals and Church teaching pertaining to marriage and family for help and inspiration: Humanae Vitae (ever read this? It’s really good!), Evangelium Vitae, Familiaris Consortio and Theology of the Body.
I stumbled upon a quote that gave me the answer I needed to encourage my friend in Familiaris Consortio:
“Scientific and technical progress…not only offers the hope of creating a new and better humanity, but also causes ever greater anxiety regarding the future. Some ask themselves if it is a good thing to be alive or if it would be better never to have been born; they doubt therefore if it is right to bring others into life when perhaps they will curse their existence in a cruel world with unforeseeable terrors.
But the Church firmly believes that human life, even if weak and suffering is always a splendid gift of God’s goodness. Against the pessimism and selfishness which cast a shadow over the world, the Church stands for life: in each human life she sees the splendor of that “Yes,” that “Amen,” who is Christ Himself.”(84) (emphasis mine)
A very beautiful attitude!! And also VERY counter-cultural. Our culture tells us the only lives worth living are those that have health, wealth and beauty and that these hold the keys to happiness. Of course, it’s not true. Some of the most miserable people I have known have ‘it all’. I understand that we are all constantly bombarded by this ‘culture of death’, as Saint JPII put it, and it’s eugenic mania and also by the population control freaks who would like us to believe that the solution to the world’s ills is found in the elimination of human beings. These erroneous philosophies and ideas continually bombard us. It’s no wonder we fall prey. Without the Church we are rather helpless.
I am not making assumptions about your views (which were not out of the ordinary), but rather addressing modern trends I notice, especially because I am the mother of 7. The comments I receive are interesting- you might imagine- and I find it fun to think up loving one liner comebacks to hopefully induce a change in perspective. My husband, Ed, also has some good ones- In response to a co worker’s sarcastic, “Don’t you know what causes that?” He in good humor has replied, “Yeah, but can I help it if we are good at it!?”
Anyway, I hope this letter sheds some light on my decisions and choices. And hopefully takes away at least a little of my ‘weirdness’ :)
Thanks for your love and support and interest. Muah!!!!!
Happiest of Easters!!!
Love,
Your Little Niece
KC Schnitker is the Executive Director of
Family of the Americas Foundation and a
speaker and instructor of natural family planning
for the Archdiocese of Washington.
info@FamilyNFP.com
By Professor John S. Grabowski, Department of Theology, Catholic University of America
http://www.foryourmarriage.org/
When John Paul II was elevated to the papacy, he unveiled a series of reflections on which he had worked for some time. He gave these in the form of weekly general audiences between 1979 and 1984. These talks became known as “The Theology of the Body” and have had a growing impact on Christian thinking about what it means to be embodied as male or female.
Reflecting on the Genesis accounts of creation, Pope John Paul II underscored the way in which the body reflects or expresses the person. The human person discovers his dignity through his body and its capacity to express his ability to think and to choose, unlike the animals, who lack this ability. (See Genesis 2:19-21.)
Yet humanity is radically lacking in its expression in only one sex. The full meaning of the body and hence the human person is revealed only when the man stands over against another unique way of being human–woman. This distinctive way of being a person and a gift for others, male and female, reflects what the late pope called “the nuptial meaning of the body.” Coming together in the profound partnership of marriage, man and woman live for the other in mutual love and deference. This union is expressed concretely in the couple’s bodily gift of themselves to one another in sexual intercourse. Here they speak a profound language of total self-gift and unconditional fidelity.
The late pope understood the impact of sin on the human person. The Fall brings about a series of ruptures within the person, radically diminishing the body’s capacity to express reason and freedom. It introduces alienation and a struggle for control into the relationship of male and female, distorting their relationships in marriage and in human society (cf. Genesis 3:16). And it devastates the human sexual drive, redirecting it from an impulse toward life-giving interpersonal union between covenantal partners to a desire to use and exploit others for personal satisfaction.
Yet with the death and resurrection of Christ, sin does not have the last word on the condition of the body. The grace that flows from the cross and resurrection effects a “redemption of the body,” not just in heaven but here and now. Through the healing effects of Christian prayer and sacramental worship, the body is enabled to express the person and his or her ability to think and freely choose.
The grace of Christ also enables men and women to overcome their mutual conflict and live together in marriage in the exercise of “mutual submission out of reverence for Christ” (cf. Ephesians 5:21; Mulieris Dignitatem, no. 24). This transforming grace enables the body in its maleness and femaleness to be offered as the expression of the “sincere gift of self” in a way reflective of the person’s vocation– as single, married, or a consecrated celibate.
The human person as a unique embodied subject is thus understood through the three panels (or triptych) of the Christian mysteries of creation, sin, and redemption. The result is what John Paul II himself modestly referred to as an “adequate” understanding of the person. This vision enables us to recognize and affirm that the body and the gift of sexuality are good. At the same time it highlights why this gift is falsified by extramarital or contraceptive sex that sever sexual union from its inherent meanings of unconditional fidelity and life-giving fruitfulness.
The mystery of the human person is continually confronted by new issues and challenges. For example, much of the reflection on the body and its relation to the person within Christian tradition has been undertaken by men. During his pontificate John Paul II called for a “new feminism” that would better account for the distinctive insights, experiences, and gifts of women.
In addition, issues of the relationship between the body and the person take on new urgency in light of expanding scientific and medical technology that has raised questions at both the beginning of life (reproductive technologies, the status of cryo-preserved embryos, stem cell research, and attempts to clone human beings) and its end (the personhood of the persistently comatose, the meaning of suffering, and how to define the moment of death). To continue to affirm the fundamental biblical conviction of the goodness of the embodied person created in the image of God while addressing such pressing questions is the task for the further refinement of the “adequate anthropology” of John Paul II’s “Theology of the Body.”
Original article from:http://www.lawyersandsettlements.com
Chicago, IL: Women who claim they have suffered from Beyaz side effects might be watching Yasmin litigation closely, especially after a jury awarded a plaintiff $14 million in her lawsuit concerning Yasmin. Beyaz birth control is similar to Yasmin and carries similar warnings. So far, however, the focus of litigation has been on Yasmin and Yaz.
Yasmin Lawsuit Nets Million Award; Will It Affect Beyaz Lawsuits?In Yasmin litigation, a jury in Chicago recently awarded a woman $14 million in her lawsuit against her doctor, who recommended she take Yasmin. Thirteen days after she started the medication, Mariola Zapalski suffered a stroke. She survived, but was paralyzed on her left side and has a permanent brain injury, and requires round-the-clock care from her husband, who had to quit his job, according to The Associated Press (4/20/14).
The medical malpractice lawsuit against the doctor alleged that the physician did not tell Zapalski about the risks associated with Yasmin and should not have placed her on the drug because Zapalski had underlying risk factors. A lawsuit filed against Resurrection Medical Center, which referred Zapalski to her doctor, was reportedly settled for $2.5 million.
Many lawsuits concerning fourth-generation birth control such as Yasmin and Yaz allege that the drugs’ manufacturer knew or should have known about the risk of blood clot and stroke but did not adequately warm women about those risks. Zapalski’s lawsuit is different because it alleged the doctor did not inform her of the risks.
Yasmin, Yaz and Beyaz all contain drospirenone, a synthetic progestin. Beyaz is slightly different from the other fourth-generation birth control pills because it also contains folate. Drospirenone has been linked in studies to an increased risk of blood clots and stroke. In 2011, the US Food and Drug Administration (FDA) issued a warning that birth control medications containing drospirenone could potentially carry a higher risk of blood clots than other forms of birth control.
Preliminary results of an FDA study into drospirenone-containing birth control suggests that women who take such birth control are at 1.5 times the risk of blood clots as women who take other hormonal birth control. Despite critics arguing that there are safer forms of birth control that are just as effective, the FDA has not removed Yasmin, Yaz or Beyaz from the market.
Bayer, maker of Yasmin, Yaz and Beyaz, has settled some lawsuits involving allegations about Yasmin and Yaz.
AUCKLAND, New Zealand, April 11, 2014 (LifeSiteNews.com) Six week old, baby Liam is being dubbed a “miracle baby” after his parents were told he was dying in utero and they should abort him.
Liam’s parents, Marinda Brits and Norman Holleman, were told that the routine mid-pregnancy anatomy scan showed low amniotic fluid around the baby. Doctors told them the baby was dying and that an abortion would need to be arranged.
But the couple refused the abortion.
“We knew our baby was fighting for his life and we were going to fight with him,” related Holleman.
A visit to the Woman’s Assessment Unit at Auckland City Hospital a day later brought a small glimmer of hope. During a consultation there they were told that it is possible for a baby to be born with little fluid, although the risk of the brain, lungs and kidneys not developing properly was high.
An amnio infusion of 600 miltres of saline was given at 23 weeks, allowing doctors to see if there was a leakage or further complications.
At 24 weeks a further scan showed that Liam’s kidneys were not developing correctly. Brits and Holleman were told that it was likely he would die soon after birth.
Then, the news that Liam’s parents had hoped for came. A scan on New Year’s Eve revealed properly functioning kidneys. They were told to go home and prepare for the birth of a healthy baby.
Baby Liam has four siblings and shares his birthdate with his two-year-old brother Jayden.
“Everyone says their baby is a miracle but Liam really is ours,” says the proud father.
Brianna Heldt was 20 years-old when she first started taking the birth control pill. As an Evangelical Protestant, she believed in saving sex for marriage, but the young college student was planning her wedding and wanted to delay having children for a few years.
Like many young women, Heldt visited her college’s campus health clinic and got a prescription.
What followed was an unexpected and “horribly difficult” time for Heldt and her husband.
“From the time I began taking it I had severe headaches,” she recounted. “I was constantly bloated and hungry, and worst of all, I became an emotional wreck. Things that would never have bothered me before made me cry uncontrollably. Kevin (my husband) and I had always gotten along so well but we began arguing, and I was perpetually frustrated with him.”
“Intercourse was painful,” she added. “I even saw an OB/GYN about this problem who never once connected those dots for me, and just tried to tell me that it was some sort of psychological problem. But it was not.”
It turns out that Heldt’s experience was not unique. This January, 90s talk show host Ricki Lake opted to make a documentary exploring the dangers of hormonal contraceptives.
Based on Holly Grigg-Spall’s book, “Sweetening The Pill: or How We Became Hooked On Hormonal Birth Control,” the full-length film will consider the dangers of the birth control pill, as well as other contraceptives such as Yaz and Nuvaring.
“In the 50 years since its release, the pill has become synonymous with women’s liberation and has been thought of as some sort of miracle drug,” said Lake and her co-producer, Abby Epstein. “But now it’s making women sick and so our goal with this film is to wake women up to the unexposed side effects of these powerful medications and the unforeseen consequences of repressing women’s natural cycles.”
Perhaps Lake’s forthcoming documentary will not only “wake women up” but speak for those who have experienced some of the negative side effects of hormonal contraception.
Mara Kofoed – who writes the popular blog, “A Blog About Love,” with her husband Danny – recently wrote a post confessing her loathing of the birth control pill.
“You guys, I hate the birth control pill. I mean, I really, really hate it. I know it’s ‘supposed’ to be liberating to women, but I am convinced this pill is actually harming a lot of women – and therefore society at large including marriages, relationships, friendships, families, and work places,” she wrote on Feb. 26.
The Kofoeds are professed Mormons who have no moral objection to the hormonal contraceptives. Instead, Mara listed a series of side effects she had experienced, including physical symptoms such as “severe, acute pains in my heart,” as well as more general ones like a “lack of intuition & creativity,” and “numbed spirituality.”
Although the responses to Mara’s post were mixed, many women shared similar experiences, and one commenter noted her desire to avoid ingesting a substance classified as a group 1 carcinogenic by the World Health Organization, the “same group as asbestos.”
Heldt said the many side effects of the pill were reason enough to quit. “I had begun taking the pill a few months before our wedding to make sure it was working properly by the time I needed it. And only a couple of months after our wedding, I threw the prescription into the trash.”
“I decided I’d rather be a sane, healthy mother than a miserable, insane woman without children. I wasn’t sure what we’d use going forward but I knew I couldn’t continue with the pill.”
As many women begin to share a desire to avoid hormonal contraceptives, this growing trend has led to a rise in new technologies for “natural” methods of dealing with fertility, both in avoiding and achieving pregnancy.
William and Katherine Sacks, husband and wife co-founders of the new iPhone app, Kindara, recently told Business Insider, “we founded the company because we were looking for effective birth control that wasn’t the pill.”
“Kati had been on the pill for 10 years and she didn’t like the side effects. She introduced me to the fertility awareness method and I was blown away by how little I understood about female fertility,” William Sacks explained.
For those who do want to have a baby, Kindara now boasts that it has helped 10,000 women conceive.
The Kindara app is one among many of the latest technologies in offering women an opportunity to know their own fertility.
MyFertilityMD and MyFertilityCycle.com claim to be “tools designed for women by doctors and researches. At the apex of research and technology stands an organic way for women to reclaim their fertility without birth control or dangerous hormones.”
Other app options such as My Fertility Friend and Glow offer “advanced ovulation charts” and “fertility predictors.”
Many years later, Heldt and her husband are the parents of eight children through biology and adoption, noting that becoming parents has “changed our lives in the most beautiful and profound ways.”
Heldt says that now although she knows her cycle, they “don’t use any sort of formal fertility tracking.” She’s glad that more women are now talking about the problems with hormonal contraceptives.
“I’ve met many ladies who’ve had negative experiences with the pill just like me, but even if their personal experience wasn’t bad, there is a tension there for sure. Many women sense that there’s a problem with the fact that fertility is treated like a disease to be managed.”
“Some are concerned that the pill allows women to be used by men. And we should all be alarmed by the physical dangers inherent in using hormonal contraception, especially over a long period of years – an increased risk of blood clots, stroke, and certain types of cancer.”
“There is no doubt that women deserve better choices than the ones we’re being handed in our present society.
MONTGOMERY, AL, April 22, 2014 (LifeSiteNews.com) –– Children in the womb should have the same legal standing as other children, the Supreme Court of Alabama ruled Friday.
The decision upheld the prior conviction of Sarah Janie Hicks for “the chemical endangerment of her child,” when she exposed her unborn baby to cocaine. The boy, referred to as “JD,” was born testing positive for cocaine.
The 8-1 decision reaffirmed the Alabama Supreme Court’sruling in a similar case last year that the word “child” includes “unborn child.”
Friday’s decision was a review of the lower Court of Criminal Appeals’ conviction of Hicks.
According to Justice Tom Parker, who wrote the majoritydecision, “It is impossible for an unborn child to be a separate and distinct person at a particular point in time in one respect and not to be a separate and distinct person at the same point in time but in another respect. Because an unborn child has an inalienable right to life from its earliest stages of development, it is entitled not only to a life free from the harmful effects of chemicals at all stages of development but also to life itself at all stages of development. Treating an unborn child as a separate and distinct person in only select respects defies logic and our deepest sense of morality.”
Fr. Pavone, national director of Priests for Life, referred to the decision as a unique instance of “common sense and logical consistency.”
“In ruling that a child is a child whether born or unborn, the Alabama justices have cut through decades of tortured, twisted rationales and issued a national call for courts to recognize the obvious – all humans have the right to life.”
Justice Parker said, “Courts do not have the luxury of hiding behind ipse dixit assertions,” which means that courts cannot rule simply to uphold the legal status quo but must, in this case, “allow the law of non-contradiction” to come into play, in order to “recognize a child’s inalienable right to life at all stages of development.”
Until this is the case, the judge added, “our grief is not for the Constitution alone; we also grieve for the millions of children who have not been afforded equal value, love, and protection since Roe.”
“In contrast to the reasoning of Roe and Casey, Alabama’s reliance upon objective principles has led this court to consistently recognize the inalienable right to life inherently possessed by every human being and to dispel the shroud of doubt cast by the United States Supreme Court’s violation of the law of non-contradiction,” said Parker.
“Utterly amazing” are the words Pennsylvania Governor Tom Corbett used to describe what it was like to meet Pope Francis face-to-face before a crowd of 100,000 onlookers in Saint Peter’s Square in Rome. “I’ve met presidents. Those meetings were quite impressive,” he said, “but meeting the Pope blows that away!”
Governor Corbett is a life-long Catholic, baptized at Our Lady of Lourdes, Overbrook, in the Archdiocese of Philadelphia. As a former altar boy and past president of the Parent/Teacher Guild at St. Mary of the Assumption Parish and School in the Diocese of Pittsburgh, meeting the Pope was something Corbett never dreamed he would do. Last month, he had his chance.
Corbett’s conversation with Pope Francis was brief and in English. The governor and his wife shook Pope Francis’ hand, which Corbett described as strong, “like a farmer’s hands.” The Corbetts thanked him for his ministry to the Catholic Church and to the people of the world. The Pope replied, “Pray for me.”
As governor of Pennsylvania, Corbett was in Rome to plan for the World Meeting of Families, which will be held in Philadelphia in September 2015. He also wanted to personally invite Pope Francis to attend the meeting and visit Pennsylvania. Corbett told the Pope that the people of Pennsylvania “would really enjoy it if you came to see us.” The governor’s conversation with the Pope left him feeling “very optimistic” that Pope Francis will come to Philadelphia next year. It is expected that the decision about the Pope’s attendance will be announced approximately six months in advance of the event.
Governor Corbett was part of a special leadership delegation for the World Meeting of Families also led by Archbishop Charles J. Chaput, O.F.M. Cap., and Philadelphia Mayor Michael A. Nutter. The delegation included corporate and civic leaders who travelled to Rome to learn more about the logistics of the global event. The World Meeting of Families takes place every three years and is sponsored by the Holy See’s Pontifical Council for the Family.
The World Meeting of Families is expected to bring tens of thousands of people to Philadelphia from more than 100 different countries. People of all faiths will come together to talk about the common challenges that families face all over the globe.
Corbett thinks Philadelphia, with its roots in religious tolerance, is the perfect place to do that. “William Penn’s holy experiment is still ongoing,” he said. “Many issues stem from families not being together. How can we strengthen families through faith in God?” This important question will be part of the conversation at the World Meeting of Families.
Registration details will be posted at www.worldmeeting2015.org. Meanwhile, Governor Corbett has advice we can all follow to strengthen families – pray, volunteer in the Church and other ministries that keep families together, and get involved with public policy advocacy. “Those of us in (public) office have tough jobs,” said Corbett. “We have to make tough decisions. Your prayers are appreciated.”
For more information about current affairs that affect families and other Catholic concerns, visit www.pacatholic.org. For more information about the World Meeting of Families, visit www.worldmeeting2015.org.
– See more at: http://www.pacatholic.org/meeting-the-pope/#sthash.1DefbvKf.dpuf
April 23, 2014 (LifeSiteNews.com) – For decades, Dick and Rick Hoyt have served as living symbols of father-son love, the value that a life with disabilities can have, and of the power of pure, determined grit.
Together the pair have completed some 70 marathons, six Ironman competitions, and countless other endurance events. In each of these, Dick, now 74, has pushed his son in a special-made wheelchair, or pulled him in a raft or carried him on a seat on his bicycle.
Rick was diagnosed with cerebral palsy after birth, the result of oxygen deprivation during birth.
But now an era has come to a close, as Team Hoyt, as they called themselves, ran their last marathon in Boston this past weekend.
In fact, Dick was supposed to have hung up his running shoes after last year’s Boston Marathon. However, the tragic bombing at the finish line prevented the pair from completing the race, and they decided to give it one last go.
“We’re running in honor of the people who got killed and injured,” Dick said this past weekend. “Boston is so much stronger than it was a year ago.”
The pair’s best time in a marathon was 2:48. On Sunday they crossed the finish line in over seven and a half hours.
The main reason for the end of Team Hoyt’s career is Dick’s back problems, which have made it painful for him to compete.
Rick, however, who is now over 50 himself, intends to continue participating in events, with the help of other supporters.
The father-son team began competing in endurance events after Rick told his dad at the age of 15 that he wanted to participate in a 5-mile race to help a teen who had been paralyzed as the result of an accident.
His dad wasn’t a runner at the time, but rose to the challenge. That night, after the race, Rick told his father: “Dad, when I’m running, it feels like I’m not handicapped.”
That was enough motivation to push Dick to carry on. And since then they have never stopped running.
The charity that they founded, The Hoyt Foundation, seeks, in its own words, “to build the individual character, self-confidence and self-esteem of America’s disabled young people through inclusion in all facets of daily life; including in family and community activities, especially sports, at home, in schools, and in the workplace.”
Amazingly, despite the dire predictions of doctors that he would never be able to do much, Rick graduated from Boston University in 1993. He began communicating with the help of a computer in 1972.
NEW YORK, April 25 (C-FAM) Reporters called one program “x-rated.” Another was dubbed “kindergarten sex ed.” A World Health Organization version led to a spectacular defeat in the European Parliament. UN delegates reject it as an assault on their culture.
Comprehensive sexuality education often goes unchallenged – until people discover what it teaches. Now a new paper explains the politics behind the curricula and why so many people are upset.
A team of experts led by Professor Jokin de Irala found the self-described “evidence-based” comprehensive sexuality education to be riddled with ideology and opinions masquerading as facts. And outright disrespect for parents, with one program declaring sexual autonomy an “entitlement” that “strengthens the individual against intrusions by the family or society.”
“The Politics of ‘Comprehensive Sexuality Education‘” looks at the tactics of what the authors call the Sex Education Establishment, a collection of powerful organizations such as the UN Population Fund, the World Health Organization, USAID and Planned Parenthood.
The Sex Education Establishment creates policy guidelines and funds efforts to carry them out, presenting their product as neutral “best practices.” But the Establishment’s recommendations fail to distinguish facts from opinion, and its track record is questionable. Terms that appear innocuous, like “gender” and “evolving capacity,” disguise dubious teachings and practices.
In 2004, the journal Lancet published a joint statement by experts describing the ABC strategy – Abstinence, Be Faithful, and use a Condom – as the best ways for avoiding risk.
Yet the Sex Education Establishment does not “take seriously that the implementation of A or B is possible,” and seldom acknowledges that sexual activity is a risk for adolescents, note the authors.
“The Sex Education Establishment tends to assume that most minors are sexually active, and their programs do very little to protect the majority of non-sexually-initiated youth,” they write.
Recently, a UN Population Fund official exhibited this flawed thinking. When speaking to cadres of activists at a UN conference, Kate Gilmore was overheard more than once ridiculing the idea of abstinence.
Yet the vast majority of youth under 18 are not sexually active, report the authors. Promoting condoms as safe sex may “actually foster a false sense of security in youth and lead, paradoxically, to increased risk-taking behavior,” a behavioral phenomenon known as “risk compensation.”
Professor de Irala’s team found abstinence-centered programs are effective, presenting facts and presuming adolescents’ ability to make ideal decisions, not patronizing youth by presuming they will engage in risky sexual activity.
Sexuality education cannot be entirely evidence-based because many important concepts and terms are debatable, and get their meaning from the context they are used – such as the word “love.”
The authors argue that sex education programs, especially when publicly funded, should empower parents to be the educators, and in any case should not advance an agenda that is incompatible with the values of the communities in which they are implemented.
The authors advise sex experts to seek input from – and reflect the values of – the people who know and love their children the most: parents. They are most responsible for their children’s education and well-being, are sensitive to their child’s evolving maturity, and should have the legal right to protect their youngsters from harmful messages.
Other studies back up the paper’s conclusions, reporting that adolescent girls whose parents provide limits and supervision wait longer before having sex, regardless of socioeconomic factors like their neighborhood.
It’s Earth Day again, an occasion on which to reflect on our sins against the environment and make resolutions to clean up our act. We are familiar with the usual suspects: overpopulation, oil companies, overpopulation, chocolate, cattle farmers, the coal industry… and did I mention overpopulation?
Well, forget all that. Here’s our top 10 eco-villains, most of them getting away with ecological murder to date.
1. Underpopulation. Driven by the myth of overpopulation birth rates around the world, with very few exceptions are falling. Only three Western countries have total fertility rates around 2 per woman (“replacement”) and many developing countries are also below that figure. Several countries in Eastern Europe and Asia have a TFR of less than1.4. Nobody knows how to bring the birth rate back to 2 once it has fallen so low. Is this good for the environment? No. Here’s why.
2. Big cities. Small families and childless people crowd together in big cities, which gobble up open land and forest, destroy animal habitats, pollute the air and waterways, and create huge waste disposal problems requiring energy intensive solutions. Even where these things are under control, as in the big western capitals, continued growth demands massive infrastructure projects – tunnels, bridges, airports, public transport systems, sewerage… which demand equally massive amounts of raw materials and energy, and have to be periodically renewed. And you only have to look at China and its heavily polluted mega cities to see what the effects of population reduction policies are in the “developing” world.
3. Consumerism. Populations adhering to the small family norm consume more per person. People have more disposable income, which they spend on luxury goods with big environmental impacts: air travel, more powerful cars (because no-one takes the train all the time), multiple household appliances, electronic devices including touchscreens which require rare earth minerals mined from the earth or the ocean floor. People can afford to buy more than they need and they waste more, including food. Even when individuals or families are relatively poor they often emulate the habits of richer citizens and will gamble and go into debt to increase their spending on luxury goods.
4. Solo living. Divorce, delayed marriage and single living have all increased in the era of population explosion panic and widespread birth control. In Europe the number of people living alone has risen by 80 percent over the past 15 years. Widowed older people make up a significant section of singletons but they are perhaps less likely to move in with adult children living in small city dwellings, especially if the family is unstable.
Men and women find it harder to commit to each other or to remain committed, and women’s increasing financial independence has facilitated break-ups. Also cohabiting couples are more likely to break up than married. Marital or cohabiting break-ups increase the number of people living alone, at least temporarily, and therefore the demand for more housing units and household goods and services. One-person households are the biggest consumers of energy, land and household goods.
5. Big government. Small families and singletons living in big cities are more likely than their more fertile, community-oriented forebears to depend on government to support them in times of difficulty or dependency and to provide for their educational, health and retirement needs. The growth of the welfare state brings with it a vast bureaucracy of people travelling to their offices every day to pull the levers of whatever programme they are administering. Think of their carbon footprint as they commute daily by train or car, and of the meetings and conferences the managerial layer fly to on a regular basis.
6. Coffee. As you can see from the above, there is one original sin, one basic source of villainy against the ecosystem in our era, and it would not be difficult to demonstrate more downstream effects. However, I will mention just one more before turning to other culprits. In the West at least, coffee consumption has increased in inverse proportion to average family size. Besides directly reducing fertility, the daily fix at the cafe is one of the most common things that people throw their spare cash away on when they have two or less little mouths to feed.
It is no surprise, then, that this liquid gold is the world’s second most tradable commodity after oil (and we know how bad that stuff is), leading to clearing of swathes of forests for the cultivation of sun grown coffee. Sun-cultivation involves deforestation, water pollution, agro-chemical usage, huge amounts of waste, and impoverishment of soils. You could reduce your coffee footprint by looking for a café using the shade-grown variety. Good luck with that.
Now here are some other candidates for the 10 top eco-villains list, submitted by MercatorNet contributors:
7. Weather in the United States. According to the U.S. National Oceanic and Atmospheric Administration, February 2014 ranks 37th for coldest February on record nationwide. Despite the arrival of spring, the icy grip of winter still retains a stranglehold on much of the Midwest and Northeast. The 2013-14 winter season is one of the coldest winters in 20 years. How on earth are we going to make global warming a non-debatable issue when the weather keeps messing up the narrative?! ~ Matthew Mehan, in Washington
8. People who don’t like being cold (and that’s most of us). My candidate for eco-villains are people who don’t understand the fundamental basis of population density, and therefore rant about the “problem” that hot countries are crowded and polluted, and all the stuff “we” should do to thin out the crowd. We? Here are a bunch of human population density maps of the world. My country is the big, empty grey area at the top left. Now here is an average annual temperature range map of the world. My country is the big blue blob at the top left, the unmelted ice cube in your drink. Coincidence?
However humans came to exist, one timeless fact is that we like it hot. And humid. We say we don’t, but we obviously do. Eco-villains, even things out. Move to northern Canada. Embrace the frozenness. The Chamber of Commerce of Snowdrifts, Yukon Territory, will welcome you with open arms. He loves you. He forgives you. He is really tired of being all alone up there. ~ Denyse O’Leary is a Canadian journalist, author, and blogger.
9. Facebook. The electric use of all data centres for the information-communications-technology (ICT) ecosystem ranks– if it were a country –12th in the world. Three years ago, it would have only ranked 22. Every one of your posts on Facebook, every one of your searches on Google, uses power. And since much of that power comes from coal, you are adding to greenhouse gases. Even Facebook admits that only 19 percent of its energy mix in 2012 came from clean and renewable sources. How about your mobile phone? Sure, the handset doesn’t use much energy, but creating the infrastructure for mobile networks does. Total mobile traffic has risen more than 400-fold since 2007, with no sign of stopping. If you are really sincere about reducing greenhouse gases, pledge to one post a day, one search a day, one phone call a day. Come on! Do it now! ~ Michael Cook
10. Al Gore. A year ago, Google sponsored a summit on “How Green Is The Internet?” Al Gore was the keynote speaker. What was the carbon footprint of flying Al Gore to Mountain View, California? In fact, the inconvenient question is why is anyone flying Al Gore anywhere? Why not watch him on Skype? At a time when we are desperately seeking to reduce emissions from the internet’s data centres, it seems almost obscene to increase them in order to hear the man who invented it. ~ Michael Cook
– See more at: http://www.mercatornet.com/articles/view/earth_day_eco_villains_our_top_10#sthash.2tlxcEdD.dpuf
Posted By Vince Coglianese On 11:00 PM 04/15/2014 In President Barack Obama is attempting to lower the rate of “births”—and separately, pregnancies—among blacks and Latinos.
The Centers for Disease Control and Prevention lists reducing “births” as one of the top goals of Obama’s “Teen Pregnancy Prevention Initiative.”
The language on the CDC’s website makes clear that the program seeks to reduce the rate of both pregnancies and “births” among minorities.
Specifically, the CDC says the “purpose of this program is to demonstrate the effectiveness of innovative, multicomponent, communitywide initiatives in reducing rates of teen pregnancy and births in communities with the highest rates, with a focus on reaching African American and Latino/Hispanic youth aged 15–19 years.”
Eighteen-and 19-year olds are technically adults, but Obama’s program aims to reduce births among women that age as well.
The Daily Caller discovered the abortion-suggesting language during a routine analysis of government publications.
The CDC says the distinction is one without a difference.
“On the website for the initiative there is no distinction between the two,” CDC spokeswoman Renee Brown-Bryant wrote in an email to TheDC.
Although the CDC site explaining the program makes no mention of the word “abortion,” the $110 million program—as funded for FY2010—bankrolls a range of featured “partners,” some of whom readily encourage abortion.
The Obama administration has set a goal that those partners reduce teen births in the “target community” by 10% by next year.
Advocates for Youth, for instance, is one of the program’s five “national partners.” The group, which took in over $1.5 million in government funding in fiscal year 2013 according to its annual report, advocates that teenagers consider abortion when they become pregnant.
“Young women need the right to safe and legal abortion,” the government-funded group writes, saying that a young woman shouldn’t be forced to “carry a pregnancy she didn’t want to term.”
Advocates for Youth lists ending “the stigma and shame women are made to feel about abortion” among its goals.
Hartford, Conn.’s city government received a $900,000 slice of the CDC funding alone. According to that program’s website, Planned Parenthood of Southern New England serves as a partner in their initiative. Local teens can use the city’s site to locate nearby abortion providers and arrange appointments.
Obama has made no secret of his support for abortion and how he views its role in society, marking the 41st anniversary of Roe v. Wade in January by applauding “reproductive freedom.”
“And we resolve to reduce the number of unintended pregnancies,” Obama said in the statement, saying that abortions afford women the “freedom and opportunities to fulfill their dreams.”
Even before the president’s program came into existence, teen birth rates in the U.S. had been substantially declining. The CDC notes that by 2011, teen births had dropped to a record low, with 329,797 babies born to women aged 15-19. The CDC claims that “the reasons for the declines are not clear,” but pro-life site LifeNews.com attributed the drop to a mixture of teen abstinence and an uptick in the abortion rate.
While reducing teen pregnancies receives bipartisan support, abortions have had a deep impact on blacks and Hispanics in the United States.
The New York City Department of Health and Mental Hygiene recently reported that more black women in that city aborted their pregnancies (31,328) than gave birth (24,758) in 2012.
There were 22,917 abortions among Hispanic New Yorkers in the same time frame. In all, CNS News notes, black and Hispanic abortions accounted for 73 percent of the city’s total abortions that year.
The CDC is not yet prepared to share any results of the president’s Teen Pregnancy Prevention Initiative. “At the conclusion of the project, in September 2015, data will be analyzed and evaluated,” Brown-Bryant told TheDC.
URL to article: http://dailycaller.com/2014/04/15/obama-program-aims-to-reduce-births-among-blacks-latinos/
Vatican City, Apr 7, 2014 / 04:29 am (CNA).- Pope Francis recently gave an interview at the Vatican to some youth from Flanders, Belgium, accompanied by the Bishop of Ghent, Luc Van Looy. The Holy See Press office has released the text of the March 31 interview in Italian. The young people posed their questions in English and the Pope responded in Italian.
Below is Catholic News Agency’s translation, done by the agency’s Alan Holdren and Kerri Lenartowick.
They are part of a group of young people that began during World Youth Day in Rio, because in Rio they wished to communicate also to the other young Flemish what they had done there; and they are a group of 12 – the others are here outside, by the way – they also came with…
Well I would like to say hello to them, the others, afterwards, yes!
Well we can organize that … And they are truly carrying out this task of entering, penetrating into media as young people, starting with their Christian inspiration. It is also in that sense that they would like to pose some questions to you. She, on the other hand, is not a believer – they are thus four from that group – she is not a believer, but it seemed important to us also, because we are a very secular society in Flanders, and we know that we have a message for everyone. So, she was very happy…
I like it! We are all brothers and sisters!
Truly, indeed. The first question is: Thank you for having accepted our request, but why did you do so?
When I hear that a young man or woman is restless, I feel that it is my duty to serve these young people, to give a service to this restlessness, because this restlessness is like a seed, and later it will go on a give fruit. And, in this moment I feel that with you I am doing a service to that which is most precious, in this moment, which is your restlessness.
(Boy) Everyone in the world seeks to be happy. But we asked ourselves, are you happy? And, why?
Absolutely, absolutely, I am happy. I’m happy because … I don’t know why … maybe because I have a job, I am not unemployed, I have work, a job as a shepherd! I am happy because I found my path in life and walking this path makes me happy. And it is also a serene happiness, because at this age it is not the same happiness as that of a young person, there is a difference. A certain interior peace, a great peace, a happiness that also comes with age. And also with a journey that has always had problems, even now there are problems, but this happiness doesn’t go away with the problems, no. It sees the problems, it suffers them and then moves on. It does something to resolve them and moves ahead. But in the depths of the heart, there is this peace and this happiness. It is a grace of God, for me, truly. It is a grace. I don’t deserve it at all.
(Boy) You have shown your great love of the poor and the wounded in many ways. Why is this so important for you?
Because this is the heart of the Gospel. I am a believer. I believe in God. I believe in Jesus Christ and his Gospel. And, the core of the Gospel is the proclamation to the poor. When you read the Beatitudes, for example, or you read Matthew 25, you see there how Jesus is clear in this. The core of the Gospel is this. And Jesus says of himself, “I came to announce to the poor, freedom, health, the grace of God…” To the poor. Those who need salvation, that need to be welcomed in society. Then, if you read the Gospel, you see that Jesus had a certain preference for the marginalized. The lepers, the widows, orphaned children, the blind… marginalized people. And also the great sinners… and this is my consolation! Yes, because He is not even scared of sin! When he came across a person like Zaccheus, who was a thief, or like Matthew, who was a traitor to his heritage (patria) for money, He was not afraid! He looked at the them and he chose them. Also this is a poverty: the poverty of sin. For me, the heart of the Gospel is of the poor. I heard two months ago that someone said, for this reason (he is) speaking of the poor, because of this preference: “This Pope is a communist.” No! This is a banner of the Gospel, not of Communism: of the Gospel! But poverty without ideology, poverty… And for this reason I believe that the poor are at the center of the proclamation of Jesus. It’s enough just to read it. The problem is that then this attitude toward the poor sometimes, in history, has been ideologized. No, it is not like that: ideology is another thing. It is like this in the Gospel: it is simple, very simple. Also in the Old Testament, you see this. And it’s for this reason that I always place it at the center.
(Girl) I don’t believe in God, but your actions and your ideals inspire me. Perhaps you have a message for all of us, for the young Christians, for people who don’t believe or have other beliefs or believe in a different way?
For me, one must seek, in a way of speaking, authenticity. And for me, authenticity is this: I am speaking with my brothers. We are all brothers. Believers, non-believers, or those of one religious confession or another, Jews, Muslims… we are all brothers. Man is at the center of history, and this for me is very important: man is at the center. In this moment of history, man has been thrown out of the center, he has slipped out towards the periphery, and at the center – at least at this point – is power, money. And we must work for people, for man and woman, who are the image of God. Why young people? Because the young – I go back to what I said at the beginning – are the seed that will bear fruit along the path. But also in relation to that which I was saying now: in this world, where at the center is power, money, young people are chased away. Children are chased away – we don’t want kids, we want fewer of them, small families. Children aren’t wanted. The elderly are chased away. So many elderly die by way of a hidden euthanasia, because they are not cared for and they die. And now young people are chased away. Think that in Italy, for example, youth unemployment from 25 years or younger is almost 50 percent. In Spain, it is 60 percent. And, in Andalusia, in the south of Spain, it is nearly 70 percent… I don’t know what the unemployment rate in Belgium might be…
… a bit less: 5-10 percent.
That’s small. It is small, thanks be to God. But you think about what a generation of young people who don’t have work means! You can say to me, “But they can eat, because their society feeds them.” Yes, but this is not sufficient, because they don’t have the experience of the dignity of bringing bread home. And this is the moment of the “passion of the youth.” We have entered into a culture of waste. That which does not serve this globalization is discarded. The elderly, children, young people. But in this way one discards the future of a people, because in the children and youth and elderly is the future of a people. The children and the young people, because they will carry history forward: the elderly are those who must give us the memory of a people, how the path of a people has gone. If they are discarded, we will have a group of people without strength, because they will not have many young people and children, and (they will be) without memory. And, this is very grave! And, for this I believe that we must help young people so that they might have the role in society that in this difficult historical moment is needed.
But do you have a specific, very concrete message for us, so that we – perhaps – might inspire other people as you do? Even people who don’t believe?
You’ve said a very important word: “concrete.” It is an extremely important word, because in the concreteness of life you move forward. With ideas alone, you don’t move forward! This is very important. And, I believe that you young people must move forward with this concreteness in life. Often also with actions tied to situations, because you must take this, this… but also with strategies… I will tell you something. I have spoken, for my work, also in Buenos Aires, with so many young politicians who came by to say hello to me. And I am happy because they – whether from the left or the right – they spoke a new music, a new style of politics. And, this gives me hope. And, I believe that youth, in this moment, must take the tempo and move ahead. Be courageous! This gives me hope. I don’t know if I responded: concreteness in actions.
(Boy) When I read the newspapers, when I look around, I ask myself if the human race is truly capable of taking care of this world and of the human race itself. Do you share my doubt? (Translator) … We discard, as you said. Do you also feel sometimes, like doubting and saying to yourself, “But, where is God in all of this?”
I ask myself two questions about this question: Where is God and where is man? It’s the first question that, in the Gospel account God poses to man, “Adam, where are you?” It is the first question to man. And, also I ask myself now, “You, man of the 21st century, where are you?” And, this makes me think of another question, “You, God, where are you?” When man finds himself, he seeks God. Maybe he is unable to find him, but walks on a path of honesty, seeking truth, on a path of goodness and a path of beauty. For me, a young person who loves truth and seeks it, love goodness and is good, is a good person, and seeks and loves beauty, is on the good path and will surely find God! Sooner or later, he will find him! But the path is long and some people do not find it, in life. They don’t find it in a conscious way. But they are so true and honest with themselves, so good and so loving of beauty that in the end they have a very mature personality, capable of an encounter with God, which is always a grace. Because the encounter with God is a grace. We cannot make the path… Some find it in other persons… It is a path to take up… Everyone must find it personally. God is not found by being heard of (from a distance) nor can you pay to find God. It is a personal path. We must find him this way. I don’t know if I have responded to your question…
We are all human and we make errors. What have your errors taught you?
I have erred, erred… In the Bible, it says, in the Book of Wisdom, that the most just man errs seven times a day! … That is to say that everyone errs… They say that man is the only animal that falls twice in the same place, but he doesn’t learn immediately from his errors. One can say, “ I don’t err,” but he doesn’t improve. This takes you to vanity, arrogance, pride… I think that the errors also in my life have been and are great teachers of life. Great teachers: they teach you so much. They humiliate you also because you can think yourself to be a superman, a superwoman, and then you make a mistake, and this humiliates you and puts you in your place. I wouldn’t say that from all of my mistakes I have learned. No, I believe that from some I haven’t learned because I am stubborn, and it isn’t easy to learn. But from so many errors I have learned, and this has done me good. It has done me good. And also recognizing errors is important. I erred here, I erred there, I err there… And also being attentive not to return to the same error, to the same water-well… It is a good thing, the dialogue with our own errors, because they teach us. And the important thing is that they help you to become a bit more humble, humility does so much good, so much good to people, to us, it does us good. I don’t know if this was the answer…
(Translator) Do you have a concrete example of how you learned from an error? She (the girl who asked the question) ventures…
No, I will tell you. I wrote it in a book, it is public. For example, in guiding the life of the Church. I was appointed superior very young, and I made so many errors with authoritarianism, for example. I was too authoritarian, at 36 years old… And then I learned that one must dialogue, you must listen to what the others think… But you don’t learn once and for all, no. It is a long road. This is a concrete example. And, I learned from my slightly authoritarian attitude, as a religious superior, to find a path to not be so much like that, or to be more… but I still err! Is she happy?… Does she want to venture to say something else?
(Girl) I see God in others. Where do you see God?
I seek – seek! – to find him in all of life’s circumstances. I seek… I find him in the reading of the Bible, I find him in the celebration of the Sacraments, in prayer and also in my work I seek to find him, in the people, in different people… Most of all, I find him in the sick. The sick do me good, because I ask myself, when I am with a sick person, why this one yes and me no? And with those in prison I find him. Why is this person incarcerated and not me? And I speak with God, “You always make injustices, why to this person and not to me?” And, I find God in this, but always in dialogue. It does me good to look for him during the entire day. I am unable to do it, but I try to do this, to be in dialogue. I am not able to do it precisely like that. The saints did this well, I still don’t … but I am on the path.
(Girl) Since I don’t believe in God, I am unable to understand how you pray or why you pray. Can you explain how you pray, in your role as Pontiff, and why you pray? The most concrete way possible…
How I pray… Often I take the Bible, I read it a bit, then I leave it and I let myself be looked at by the Lord. That is the most common idea in my prayer. I allow myself to be looked at by Him. And I feel – but it isn’t sentimentalism – I feel deeply the things that the Lord tells me. Sometimes he doesn’t speak… nothing, empty, empty, empty… but patiently I am there, and I pray this way… I am seated, I pray seated, because it hurts me to kneel, and sometimes I fall asleep in prayer… It is also a way of praying, as a son with the Father, and this is important. I feel like a son with the Father. And why do I pray? “Why” as a cause or for whom do I pray?
Both…
I pray, because I need to. This I feel, which pushes me, as if God called me to speak. The first thing. And I pray for people, when I meet people that strike me because they are sick or have problems, or there are problems that… for example, war… Today I was with the Nuncio of Syria, and he showed me photographs… and I’m sure that this afternoon I will pray for this, for those people… I was shown photographs of those who have died of hunger, their bones were like this… at this time, I cannot understand this, when we have (everything) necessary to feed the entire world, that there are people dying of hunger- for me it’s terrible! And this makes me pray, precisely for these people.
I have my fears.
What are you afraid of?
Of myself! Fear… Look, in the Gospel, Jesus repeats often, “Do not be afraid! Do not be afraid!” So many time he says it. And, why? Because he knows that fear is a, I would say, normal thing. We are fearful of life, we are afraid before the challenges, we are afraid before God… All of us are afraid, everyone. You should not be worried about being afraid. You must feel this but not be afraid and then think, “Why am I scared?” And, before God and before yourself, seek to clarify the situation or ask help of another. Fear is not a good counselor, because it gives you bad advice. It pushes you onto a path that is not right. For this reason, Jesus said so often, “Do not be afraid! Do not be afraid!” Then, we must know ourselves, all of us. Everyone must know himself and seek where the zone is in which we may err the most, and have a bit of fear of that area, because there is bad fear and good fear. Good fear is like prudence. It is a prudent attitude. “Look, you are weak in this, this and this, be prudent and don’t fall.” Bad fear is that which you say and which nullifies you a bit, erases you. It nullifies you, it doesn’t allow you to do something. This is bad and it must be thrown out.
(Translator) She (the girl) has posed this question because sometimes it is not easy in Belgium, for example, to speak of one’s own faith. This was for her also a way, because so many don’t believe, and she said, “I want to pose this question because I also want to have the strength to bear witness.”
There it is, now I understand the root of the question. Bearing witness with simplicity. Because if you go with your faith as a flag, like the crusades, and you go out and proselytize, that doesn’t work. The best way is testimony, but humble, “I am like this,” with humility, without triumphalism. That is another sin of ours, another bad attitude, triumphalism. Jesus was not triumphalist and also history teaches us not to be triumphalist, because the great triumphalists were defeated. Testimony: this is a key, this question. I give it with humility, without proselytizing. I offer it. It is so. And this is not scary. You are not going on the crusades.
(Translator) There is a final question…
The last one? It is the terrible one, the last one, always…
Our last question, do you have a question for us?
The question I want to ask you is not original. I take it from the Gospel. But I think that after hearing it, maybe it will be the right one for you in the this moment. Where is your treasure? This is the question. Where does your heart rest? On what treasure does your heart rest? Because there where your treasure is will be your life. The heart is attached to the treasure, to a treasure that all of us have: power, money, pride, so many… or goodness, beauty, the will to do good… There can be so many treasures. Where is your treasure? This is the question I would like to ask you, but you will have to give the response yourselves, alone! At your home…
They will let you know by letter…
Have them give it to the bishop… Thanks! Thank you, thanks! And pray for me.
By Kerri LenartowicRome, Italy, Apr 8, 2014 (CNA/EWTN News)
Brianna Heldt was 20 years-old when she first started taking the birth control pill. As an Evangelical Protestant, she believed in saving sex for marriage, but the young college student was planning her wedding and wanted to delay having children for a few years.
Like many young women, Heldt visited her college’s campus health clinic and got a prescription.
What followed was an unexpected and “horribly difficult” time for Heldt and her husband.
“From the time I began taking it I had severe headaches,” she recounted. “I was constantly bloated and hungry, and worst of all, I became an emotional wreck. Things that would never have bothered me before made me cry uncontrollably. Kevin (my husband) and I had always gotten along so well but we began arguing, and I was perpetually frustrated with him.”
“Intercourse was painful,” she added. “I even saw an OB/GYN about this problem who never once connected those dots for me, and just tried to tell me that it was some sort of psychological problem. But it was not.”
It turns out that Heldt’s experience was not unique. This January, 90s talk show host Ricki Lake opted to make a documentary exploring the dangers of hormonal contraceptives.
Based on Holly Grigg-Spall’s book, “Sweetening The Pill: or How We Became Hooked On Hormonal Birth Control,” the full-length film will consider the dangers of the birth control pill, as well as other contraceptives such as Yaz and Nuvaring.
“In the 50 years since its release, the pill has become synonymous with women’s liberation and has been thought of as some sort of miracle drug,” said Lake and her co-producer, Abby Epstein. “But now it’s making women sick and so our goal with this film is to wake women up to the unexposed side effects of these powerful medications and the unforeseen consequences of repressing women’s natural cycles.”
Perhaps Lake’s forthcoming documentary will not only “wake women up” but speak for those who have experienced some of the negative side effects of hormonal contraception.
Mara Kofoed – who writes the popular blog, “A Blog About Love,” with her husband Danny – recently wrote a post confessing her loathing of the birth control pill.
“You guys, I hate the birth control pill. I mean, I really, really hate it. I know it’s ‘supposed’ to be liberating to women, but I am convinced this pill is actually harming a lot of women – and therefore society at large including marriages, relationships, friendships, families, and work places,” she wrote on Feb. 26.
The Kofoeds are professed Mormons who have no moral objection to the hormonal contraceptives. Instead, Mara listed a series of side effects she had experienced, including physical symptoms such as “severe, acute pains in my heart,” as well as more general ones like a “lack of intuition & creativity,” and “numbed spirituality.”
Although the responses to Mara’s post were mixed, many women shared similar experiences, and one commenter noted her desire to avoid ingesting a substance classified as a group 1 carcinogenic by the World Health Organization, the “same group as asbestos.”
Heldt said the many side effects of the pill were reason enough to quit. “I had begun taking the pill a few months before our wedding to make sure it was working properly by the time I needed it. And only a couple of months after our wedding, I threw the prescription into the trash.”
“I decided I’d rather be a sane, healthy mother than a miserable, insane woman without children. I wasn’t sure what we’d use going forward but I knew I couldn’t continue with the pill.”
As many women begin to share a desire to avoid hormonal contraceptives, this growing trend has led to a rise in new technologies for “natural” methods of dealing with fertility, both in avoiding and achieving pregnancy.
William and Katherine Sacks, husband and wife co-founders of the new iPhone app, Kindara, recently told Business Insider, “we founded the company because we were looking for effective birth control that wasn’t the pill.”
“Kati had been on the pill for 10 years and she didn’t like the side effects. She introduced me to the fertility awareness method and I was blown away by how little I understood about female fertility,” William Sacks explained.
For those who do want to have a baby, Kindara now boasts that it has helped 10,000 women conceive.
The Kindara app is one among many of the latest technologies in offering women an opportunity to know their own fertility.
MyFertilityMD and MyFertilityCycle.com claim to be “tools designed for women by doctors and researches. At the apex of research and technology stands an organic way for women to reclaim their fertility without birth control or dangerous hormones.”
Other app options such as My Fertility Friend and Glow offer “advanced ovulation charts” and “fertility predictors.”
Many years later, Heldt and her husband are the parents of eight children through biology and adoption, noting that becoming parents has “changed our lives in the most beautiful and profound ways.”
Heldt says that now although she knows her cycle, they “don’t use any sort of formal fertility tracking.” She’s glad that more women are now talking about the problems with hormonal contraceptives.
“I’ve met many ladies who’ve had negative experiences with the pill just like me, but even if their personal experience wasn’t bad, there is a tension there for sure. Many women sense that there’s a problem with the fact that fertility is treated like a disease to be managed.”
“Some are concerned that the pill allows women to be used by men. And we should all be alarmed by the physical dangers inherent in using hormonal contraception, especially over a long period of years – an increased risk of blood clots, stroke, and certain types of cancer.”
“There is no doubt that women deserve better choices than the ones we’re being handed in our present society.
NEW YORK – House Democratic Leader Nancy Pelosi called pro-lifers ‘dumb’ during her acceptance speech this week as she received the Margaret Sanger Award from the nation’s largest abortion provider.
“When you see how closed their minds are or oblivious or whatever it is—dumb—then you know what the fight is about,” Pelosi declared on Thursday at Planned Parenthood’s annual gala. “Whatever happens with the court …we must remember these battles will not be the end of the fight.”
Pelosi was speaking about the personhood laws that have been presented in various states and the corporate opposition to the Obamacare abortion pill mandate.
As previously reported, the Planned Parenthood Federation of America recognized Pelosi with the Margaret Sanger Award for “her leadership, excellence, and outstanding contributions to the reproductive health and rights movement over the course of her career.” Sanger founded Planned Parenthood in 1921, which was originally known as the American Birth Control League. She later changed the name as some found it offensive.
“We are paying for, and even submitting to, the dictates of an ever-increasing, unceasingly spawning class of human beings who never should have been born at all,” Sanger once said, who was reportedly a staunch advocate of eugenics. “The most merciful thing that a family does to one of its infant members is to kill it.”
Sanger was also the publisher of the newspaper The Woman Rebel, which she subtitled “No Gods, no masters.”
“I accept this honor tonight on behalf of my colleagues, who have fought the fight for and with you,” Pelosi said upon receipt of the award. “The aim of smart public policy in our country is to advocate for opportunity and freedom—the opportunity to lead healthy lives and the freedom of Americans to make their own choices.”
New York City Mayor Michael Bloomberg was also present at the gala, receiving the Planned Parenthood Global Citizen Award, as well as “minister” William Barber II, who leads a homosexual advocacy and social justice organization called “Moral Mondays” in North Carolina.
“We must build a movement knowing that those against Planned Parenthood are also against voting rights, labor rights, and immigration reform,” Barber told those gathered. “The same people trying to gut voting rights are the same people trying to remove southern states from [Medicaid] coverage, and are the same people trying to remove women’s rights. We are stronger together when we fight these injustices together.”
Bradley Bredeweg of the ABC Family show The Fosters, a sitcom that centers on children being raised by lesbians, also spoke at the event.
“Our family represents the new, loving and modern family,” he stated. “Two incredibly smart and passionate biracial lesbian women raising a family made up of a multicultural mix of biological, adopted, and foster kids. A family that is allowed to make their own choices, to decide what is best for their own family. With all of the prejudice and discrimination that we still have to fight as gays and lesbians, as women, as different races—the last thing we should be fighting for are our own bodies.”
Others present at Planned Parenthood’s gala included singer Mavis Staples, comedian Tig Notaro and BET’s Vice President of Public Affairs Sonya Lockett.
by Becca Aaronson, The Texas Tribune, March 27, 2014
The 5th Circuit Court of Appeals on Thursday upheld the new abortion regulations that were passed in July by the Republican-led Texas Legislature.
The plaintiffs, who represent the majority of abortion providers in Texas, including four Planned Parenthood affiliates, Whole Woman’s Health and other independent abortion providers, challenged the constitutionality of two requirements that the state implemented Nov. 1: that physicians obtain hospital admitting privileges within 30 miles of an abortion facility, and that they follow the U.S. Food and Drug Administration’s protocol for drug-induced abortions, rather than a common, evidence-based protocol.
In a unanimous opinion by a three-judge panel, the court sided with the state, which argued that the rules should be deemed constitutional by the federal court because the state’s objective was to protect women’s health, and that there isn’t enough evidence to suggest that the rules create an undue burden on the majority of Texas women attempting to access abortion.
The author of the opinion, Chief Justice Edith Jones, wrote that the state’s “articulation of rational legislative objectives, which was backed by evidence placed before the state legislature, easily supplied a connection between the admitting-privileges rule and the desirable protection of abortion patients’ health.”
Jones also authored the 2012 opinion affirming Texas’ abortion sonogram law. The other justices, Jennifer Elrod and Catharina Haynes, served on another three-judge panel that reversed a lower court’s injunction on the law in October, which allowed the rules to take effect.
Meanwhile, an attorney for the Center for Reproductive Rights, who argued on behalf of the majority of abortion providers in the state, asserted that the new rules are unconstitutional because some abortion facilities can no longer perform the procedure and women in South Texas, the Panhandle and other areas of the state are being forced to travel long distances to seek abortions.
Cecile Richards, president of Planned Parenthood Federation of America, said in a statement that the group would continue to fight the law. “We will combat these laws in the courts, and our separate political arm will mobilize voters to replace lawmakers who champion these dangerous laws in the first place,” she said.
If this case continues through the court system, the plaintiffs would need to appeal to the U.S. Supreme Court. In November, the Supreme Court justices rejected an earlier request by abortion providers to intervene in their lawsuit by reversing the 5th Circuit’s decision to lift an injunction on the rules by a lower court.
“The people of Texas have spoken through their elected leaders and in support of protecting the culture of life in our state,” Gov. Rick Perry said in a statement. “Today’s court decision is good news for Texas women and the unborn, and we will continue to fight for the protection of life and women’s health in Texas.”
Additional rules that require all abortions to be performed in ambulatory surgical centers starting in September and that ban abortions at 20 weeks of gestation remain unchallenged.
Since November, abortion facilities in South Texas, Beaumont and the Panhandle have closed as a result of the new abortion regulations. In August, before the rules took effect, there were 40 licensed abortion providers in Texas. Now there are 28 licensed abortion providers, only 24 of which still perform the procedure. When additional rules take effect in September that require abortion clinics to meet the same standards as ambulatory surgical centers, the number of abortion facilities will probably drop to six.
“Texas women deserve better than to have extremist politicians endanger their health and safety by preventing them from accessing safe and legal abortion,” Brigitte Amiri, a senior staff attorney at the ACLU Reproductive Freedom Project, said in a statement. “The law is having a devastating impact on women in Texas.
People care about keeping tax dollars out of the hands of the abortion industry, but in the future will they be able to talk about how their legislators voted on this topic? Life Legal Defense Foundation joined the Bioethics Defense Fund and the Alliance Defending Freedom in filing an amicus brief on this very question.
As the Affordable Care Act (ACA) has been implemented, it has become painfully clear that it increases federal funding of abortion in unprecedented ways. For example, consider the following: the ACA authorizes taxpayer funded abortion in newly created High Risk Pool and Community Health Center funding. It authorizes taxpayer subsidies for insurance exchange plans that cover elective abortion, and in fact applies an “abortion premium surcharge” to some of the plans offered on the exchanges.
Despite this clear evidence of expanded taxpayer funding of abortion, the outcome of two lawsuits turns on the issue of whether the ACA does in fact expand taxpayer funded abortion.
In 2009 when Congress was debating the ACA, a group of 20 Pro-Life Congressmen were set to support an amendment to the law that would provide permanent bill-wide prohibitions on taxpayer funding for elective abortion. Among this group were Congressmen Bart Stupak (D-MI) and Steve Driehaus (D-OH). Caving to political pressure from within their party, and the promise of an executive order on the topic, most of these Congressmen abandoned their resistance and voted to send the bill to the President for signature without limiting language.
Pro-life groups made it very clear that, in the absence of significant limiting language, a vote for the ACA equaled a vote for taxpayer funded abortion. During the 2010 midterm elections, the Susan B. Anthony List—a pro-life group dedicated to electing pro-life candidates—launched its Votes Have Consequences program to hold these so-called “pro-life” Democrats accountable for their votes, votes that opened the flood gates for unprecedented taxpayer funding of abortion. SBA’s efforts helped defeat 15 out of 20 of the Democrats who failed to hold firm on their pro-life principles during the vote on the ACA.
Congressman Steve Driehaus (D-Ohio) cited SBA’s efforts as the reason for his defeat, and went so far as to sue SBA for defamation. In the lawsuit, Driehaus alleges that the SBA cost him his job and a “loss of livelihood” by educating constituents about his vote in favor of the ACA. One of their efforts consisted of erecting billboards in his district in 2010 stating that by voting for the ACA, Driehaus voted for taxpayer funded abortion. Currently this suit is at the Sixth Circuit Court of Appeals on the issue of whether SBA’s actions constitute defamation.
LLDF’s Amicus brief filed Friday, March 21, 2014 argues that SBA’s statements were truthful and were protected speech and thus should not be censored by any application of the law.
“This brief lays out the numerous ways in which the ACA provides taxpayer funding for abortion,” states Dana Cody, LLDF’s President and Executive Director. “As such, SBA’s political advertisements were objectively true, and this lawsuit is exposed for what it really is—an attack on pro-life speech.”
In a related case, SBA has gone on the offensive challenging an Ohio election law that allows the Ohio Elections Commission to decide the truth or falsity of some political advertisements. The law makes it a crime to publish false statements. Here again, the truth of the statements that SBA sought to publish can be objectively established both by the legislative record and by the events that have transpired since the passage of the ACA. This case is currently being appealed by writ of Certiorari to the United States Supreme Court.
“It violates the law for a pro-life political organization to speak the truth about a Congressman’s voting record?” questions Dana Cody. “What has happened to free speech and the marketplace of ideas? We trust that this misguided Ohio law will be overturned and that SBA and others will be free to speak the truth without fear.”
by Julie Filby | Washington, DC | LifeNews.com | 3/17/14
Washington, DC (LiveActionNews) — Kim, 32, was frantic when she left the Planned Parenthood clinic in Fort Collins Saturday afternoon. As soon as she took the first dose of the abortion pill, she knew she’d made a mistake. She pulled over in a nearby church parking lot.
“I started trying to throw up right away,” she said, struggling to speak as she recalled the traumatic day last September when she was grappling with how to proceed with her pregnancy. “I just kept forcing myself to throw up until I couldn’t taste the pill anymore.”
At the same time, she searched the Internet for “abortion reversal” on her smartphone. That search landed her at www.abortionpillreversal.com and their 24-7 hotline. Her call ultimately connected her with Dr. Edwin Anselmi, a physician with Our Lady of Hope Medical Clinic in Centennial.
Anselmi advised her to come directly to the clinic. About two hours had elapsed from the time she took the pill when she arrived at his office. There he examined her, did an ultrasound—including listening to the baby’s heartbeat—and immediately began a protocol to reverse the effects of the drug.
How it works
Kim had taken mifepristone, also known as the abortion pill. It has been available in the United States as an oral tablet since 2000 and is also referred to as RU-486 and the brand name Mifiprex. According to the Food and Drug Administration, it can be used to terminate a pregnancy up to 49 days after the first day of the last menstrual period.
Kim was about nine weeks along when she took it. The drug is administered under supervision in a medical facility, in her case at Planned Parenthood; and it induces abortion by counteracting the hormone progesterone needed to maintain a pregnancy. Without progesterone, placenta—a structure that develops in the uterus during pregnancy—fails, cutting off oxygen and nutrition to an embryo.
“When I went in they were still giving me the option of the pill or the machine,” she said. “They were really pushing the machine saying ‘We all agree we’d do the machine, it’s less emotional.’”
“The machine” is a suction device that empties the uterus, commonly called aspiration or vacuum aspiration. Planned Parenthood personnel recommended it as a way to “get it over-with,” “get it done fast,” she said.
However Kim chose the pill, rationalizing that it wasn’t really an abortion.
“It will just look like a miscarriage,” she told herself. “I knew in my heart it was wrong. … I was praying the whole time.”
Just in time
God answered her prayers by connecting her with Anselmi before she continued to the next step of the abortion pill process. Following mifepristone, a second drug, misoprostol, is taken 36 to 72 hours later. Misoprostol causes contractions to expel the fetus, a process that can range from a few hours to a few days.
To block the effects of mifepristone, Anselmi launched a protocol developed by Doctors George Delgado and Mary Davenport described in their case study “Progesterone Use to Reverse the Effects of Mifepristone” published in “The Annals of Pharmacotherapy” December 2012. It involves progesterone injections for three consecutive days, followed by an injection every other day for two weeks, then continued progesterone twice a week until the end of the first trimester.
“He was amazing,” Kim said of Anselmi. “He was so kind and loving and gentle. He’s really an exceptional person.”
Anslemi, a parishioner of Our Lady of Mount Carmel Latin Rite Church in Littleton, has been practicing pro-life family medicine for 20 years since graduating from Columbia University in New York in 1994. He is currently the only doctor in the Denver-metro area providing the progesterone protocol to reverse the abortion pill, though he would like to see more join the network started by Delgado that currently stands at 140 doctors across the country.
“If you’re pro-life,” he said. “Here’s something you can do directly. I don’t know what the outcome would’ve been (with Kim) if we didn’t give her progesterone.”
What the future holds
Kim, now 32 weeks pregnant, is excited to welcome her son in early May, along with his father. The couple plans to marry next summer. When facing the reality of an unexpected pregnancy last August, she was between jobs, had no health insurance, and was considering moving from Denver. Today she is employed full-time, secure in her relationship and “at peace.”
“I’ve had a lot of anxiety,” she said. “But at the same time I know God is the one with the ultimate say here. So far, he’s done nothing but carry me and carry the baby. … It took me a while to get here, but now I’m really excited, I’m really happy.”
Anselmi has been contacted by two other women: in one case he successfully reversed the abortion pill two days after the patient ingested mifepristone; and the other woman called with questions but in the end, did not receive treatment.
Since the website was established in January 2013, 330 women have called the hotline seeking abortion reversal counseling, 100 of them received the progesterone protocol, and 60 of those pregnancies continued.
“We have 18 living babies and 42 pregnant moms right now,” according to Debbie Bradel, coordinator of the program.
“If there’s any way to help a woman that wants to keep her pregnancy, I want to do it,” said Anselmi, who provides the progesterone at no charge. “Babies are so precious.”
For more information, visit www.abortionpillreversal.com or call 877-558-0333.
LifeNews Note: This article was first published at the Denver Catholic Register on March 13, 2014, and is reprinted here by permission. Reprinted with permission from LiveActionNews.
One physicist calls researchers’ work ‘a grand slam.’
By Malcolm Ritter
Associated Press
Researchers say they have spotted evidence that a split-second after the Big Bang, the newly formed universe ballooned out at a pace so astonishing that it left behind ripples in the fabric of the cosmos.
If confirmed, experts said, the discovery would be a major advance in the understanding of the early universe. Although many scientists already believed that an initial, extremely rapid growth spurt happened, they have long sought the type of evidence cited in the new study.
The results reported Monday emerged after researchers peered into the faint light that remains from the Big Bang of nearly 14 billion years ago.
The discovery “gives us a window on the universe at the very beginning,” when it was far less than one-trillionth of a second old, said theoretical physicist Lawrence Krauss of Arizona State University, who was not involved in the work.
“It’s just amazing,” Krauss said. “You can see back to the beginning of time.”
Marc Kamionkowski, a theoretical physicist at Johns Hopkins University who did not participate in the research, said the finding is “not just a home run. It’s a grand slam.”
He and other experts said the results must be confirmed by other observations, a standard caveat in science.
Right after the Big Bang, the universe was a hot soup of particles. It took about 380,000 years to cool enough that the particles could form atoms, then stars and galaxies. Billions of years later, planets formed from gas and dust that were orbiting stars. The universe has continued to spread out.
Krauss said he thinks the new results could rank among the greatest breakthroughs in astrophysics over the last 25 years, such as the Nobel prize-winning discovery that the universe’s expansion is accelerating.
Monday’s findings were announced by a collaboration that included researchers from the Harvard-Smithsonian Center for Astrophysics, the University of Minnesota, Stanford University, the California Institute of Technology and NASA’s Jet Propulsion Laboratory.
The team plans to submit its conclusions to a scientific journal this week, said its leader, John Kovac of Harvard.
Scientists Clem Pryke (from left), Jamie Bock, Chao-Lin Kuo and John Kovac smile during a news conference at the Harvard-Smithsonian Center for Astrophysics in Cambridge, Mass., on Monday regarding their new findings on the early expansion of the universe. Experts called the discovery a major advance if confirmed. ELISE AMENDOLA / ASSOCIATED PRESS
VATICAN CITY (CBS St. Louis) — The Vatican’s chief justice feels that President Barack Obama’s policies have been hostile toward Christians.
In an interview with Polonia Christiana magazine –and transcribed by Life Site News — Cardinal Raymond Burke said that Obama “promotes anti-life and anti-family policies.”
“It is true that the policies of the president of the United States have become progressively more hostile toward Christian civilization. He appears to be a totally secularized man who aggressively promotes anti-life and anti-family policies,” Burke told the magazine.
The former archbishop of St. Louis stated that Obama is trying to “restrict” religion.
“Now he wants to restrict the exercise of the freedom of religion to freedom of worship, that is, he holds that one is free to act according to his conscience within the confines of his place of worship but that, once the person leaves the place of worship, the government can constrain him to act against his rightly-formed conscience, even in the most serious of moral questions,” Burke said.
Burke took a swipe against Obama’s Affordable Care Act over the law’s birth control mandate, saying “such policies would have been unimaginable in the United States even 40 years ago.”
“In a democracy, such a lack of awareness is deadly,” Burke told the magazine. “It leads to the loss of the freedom which a democratic government exists to protect. It is my hope that more and more of my fellow citizens, as they realize what is happening, will insist on electing leaders who respect the truth of the moral law as it is respected in the founding principles of our nation.”
Burke also believes there is hope that abortion will be overturned in the U.S.
“There is hope that the evil anti-life laws of the United States can be overthrown and that the anti-life movement which urges yet more of such legislation can be resisted,” Burke said. “The pro-life movement in the United States has been working since 1973 to reverse the unjust decision of the Supreme Court which struck down state laws prohibiting procured abortion. It is true that the Supreme Court decision stands, but it is also true that the pro-life movement has grown ever stronger in the United States, that is, that more and more citizens, especially young citizens, have been awakened to the truth about the grave evil of procured abortion.”
Pope Francis removed Burke from the Congregation for Bishops last December.
Obama will be meeting Pope Francis for the first time at the Vatican on Thursday.
by Dave Andrusko | Des Moines, IA | LifeNews.com | 3/17/14
While their chances were slim and none, nine Iowa Republican state Senators nonetheless held a press conference today to ask their pro-abortion Democratic colleagues who control the chamber to permit a vote on a bill that would require abortionists to meet with patients in-person before providing them with abortion-inducing drugs. The Republican senators said that the public is strongly behind the initiative and that webcam abortions pose a danger to women’s health.
However, “The GOP initiative was immediately rebuffed by majority Senate Democrats, who contend the practice is no threat to women’s health and point out that a lawsuit over the issue is pending in Iowa’s courts,” according to the Des Moines Register’s William Petroski.
Sen. David Johnson (R) spoke at a Statehouse news conference in front of a large stack of petitions signed by thousands of Iowans opposed to “web-cam abortions,” Petroski wrote.
“This bill has huge support across the state. Iowans have weighed in,” said Johnson. Johnson cited two statewide polls which found a large majority of Iowans are opposed to telemedicine [webcam] abortions.
As NRL News Today last week, a Des Moines Register Iowa Poll found that a whopping 66% of Iowans oppose so-called “telemedicine abortions” to only 27% who support them.
No subgroup favored webcam abortions, which eliminates the presence of the abortionist altogether. Instead it relies on a computer hookup which allows a pregnant woman in some remote location to electronically interact with an abortionist back in Des Moines. A review of some medical records, a couple of questions, and the abortionist merely clicks a button to release a drawer at her location containing the abortifacient pills. The woman is given a hotline number to call if she has problems.
Last week House File 2175 failed to meet the deadline to advance in the Senate. “However, under Senate rules, legislative leaders have authority to revive the legislation and allow a vote,” Petroski explained.
But Democrats were not interested in allowing a vote on a bill that is supported by 2/3rds of the public.
Board of Medicine opposes webcam abortions
On August 30, the Iowa Board of Medicine voted 8-2 in favor of new rules requiring that abortionists prescribing the abortion pill conduct a physical examination of the woman, be physically present when the drug is provided, and schedule a follow up to confirm completion of the abortion and evaluate the woman’s medical condition.
As for assertions that webcam abortions are safe, even under normal, circumstances (with the abortionist present), the chemical abortion process is generally painful, bloody, and protracted. Women taking these drugs have been hospitalized for hemorrhage, ruptured ectopic pregnancies, and infections, some of which have proven fatal. A number of women end up in surgery when the chemical method fails. And with webcam abortions, the abortionist can be anywhere but where the pregnant woman is.
As NRL News has reported, Iowa birthed webcam abortions. Since 2008 Planned Parenthood of the Heartland (PPH), which is expanding elsewhere in the country, has aborted over 5,000 women using the webcam abortion technique.
In just its first year offering web-cam abortions, the number of chemical abortions performed at PPH grew to exceed the number of surgical abortions by 2,582 to 2,210. Many of the new web-cam abortions were surely a part of that sad statistic.
NEWCASTLE, UK, March 14, 2014 (LifeSiteNews.com) – Five weeks before her due date, doctors advised the parents of Ella-Jai Harvey to abort their child because she was found to have hydrocephalus, or water on the brain. Now, six months after Ella-Jai was born, her parents are grateful they ignored the recommendation.
“It doesn’t bear thinking about what would have happened if we had decided on the termination,” Ella-Jai’s mother, Toni-Louise Hubbart, told The Sheilds Gazette. She and Daniel Harvey saw their daughter arrive on September 16, 2013. And while she did indeed have hydrocephalus, Hubbart reports now that “Ella-Jai is doing fantastic, she’s meeting all the markers she should be, and she’s great.”
“It doesn’t bear thinking about what would have happened if we had decided on the termination,” says Ella-Jai’s mother, Toni-Louise Hubbart.
A routine scan found Ella-Jai suffered from the condition, which is caused by spinal fluid build-up, and doctors told the couple abortion was an option. They refused, instead opting to give their child necessary medical care once she was born. Two days after birth, a shunt was placed in Ella-Jai’s head, to drain fluid. She also receives physiotherapy on her neck, and has a pressure gauge in her head that will use a tube to drain fluid from her head to her stomach.
As a way of thanking the medical staff of Royal Victoria Infirmary for taking care of their infant, the couple has decided to fundraise for the Infirmary’s “Tiny Lives” fund. The charity provides assistance to sick newborns and premature babies, as well as their families, who are in the hospital’s special care baby unit.
According to the National Institutes of Health, (NIH) hydrocephalus is a disorder that can occur in children and adults. No direct cause is known. NIH says that while death can occur if treatment is not sought, “some people recover almost completely after treatment and have a good quality of life.” It is found in a very small number of babies – the Children’s Hospital of Philadelphia says a maximum estimate of one-fourth of one percent of “live birth babies” have the disorder.
March 6 New York Times article, “Abortion law pushes Texas clinics to close doors,” included a slide show, “Last day for last abortion clinic in the Rio Grande,” referring to one of two Texas abortion mills that closed that day.
According to Think Progress, the number of abortion clinics is Texas is down to 19, from 44 as recently as 2011. By September 1 there could be as few as six abortion clinics in the state that meet the new ambulatory surgical center guidelines, hence a “state of emergency” for the lack of access to murder babies.
But the phenomenon of shuttering abortion clinics isn’t confined to the Lone Star State. As I wrote in a previous post, abortion clinics have been dropping like flies everywhere. Ninety-three clinics closed in 2013 alone, bringing the total number down to 759 from a high in 1991 of 2,176. According to Operation Rescue, an additional eight abortion clinics in four states have announced they are closing thus far in 2014.
A March 5 American Prospect article lamenting another recent pro-life tactic – stacking state boards of health with like-minded believers – included a rather amazing chart…
Disregard the fact that Guttmacher blames “anti-choice insurgents” for frightening abortionists out of the business. As even left-leaning Bloomberg News admitted, there are a number of factors – some self-imposed – but none of them fear.
Look instead at the changing abortion landscape. It’s quite something.
Pro-lifers and the rest of the world are slowly seeing the reverse of a perverse social experiment in likely the most watched, influential, and volatile pro-abortion country on the planet. Nowhere else is legalized abortion fought as much as it is here. What happens here on abortion is not only critical here but has a ripple effect.
Particularly in the last three years, pro-lifers have made significant gains throughout the states. Seethis Guttmacher chart (http://www.guttmacher.org/ media/inthenews/2014/01/02/index.html), the title of which says it all: “More abortion restrictions were enacted in 2011-2013 than in the entire previous decade.”
The sudden “clinic crash” in Texas serves as a reminder that pro-lifers must stand ready to meet the need. Fortunately, there are four times as many pregnancy care centers in the U.S. as there are abortion clinics, and there is also a church in almost every neighborhood.
If it’s true that “nobody likes abortion, dammit,” which I hear all the time, this becomes the time for abortion supporters to join forces with pro-lifers to truly help pregnant mothers in crisis, rather than merely direct them to a place that does what they say they don’t like – because there are fewer and fewer of them.
Rather than complain that the drive to kill one’s child is becoming impossibly long and increasingly expensive, or is shifting to a scary place like Mexico, pro-choicers could work with pro-lifers to stop crisis pregnancies before they start.
We pretty much know exactly who stumbles into a crisis pregnancy. According to About.com, “The majority of women with unplanned pregnancies do not live with their partners or have committed relationships. These women realize that in all likelihood they will be raising their child as a single mother.”
Abortion proponents should join pro-lifers in encouraging single women to respect themselves more than to have sex if they are not ready to parent a baby, particularly with a creep who will abandon them if they get pregnant.
That’s how they could do the most good, expend meaningful, productive energy.
CINCINNATI, OH, March 10, 2014 (LifeSiteNews.com) – In a move designed to protect itself from lawsuits, the Catholic Archdiocese of Cincinnati has expanded its morality clause to specifically bar Catholic school employees from publicly supporting positions that clash with Catholic doctrine.
According to local news, in contracts sent to 94 principals covering over 2,000 employees, the archdiocese spelled out specific policies on public behavior and personal lifestyles. The contract prohibits the “public support of” out-of-wedlock sexual activity, “homosexual lifestyle,” abortion, surrogacy, in vitro fertilization, and – among other prohibited behaviors – “flagrant deceit or dishonesty.”
It also strictly bans employees from engaging in any of the behaviors listed above, as well as others.
The specific layout of the restrictions appear to be related to conflicts over the last five years. In 2010, the Archdiocese fired a teacher who, unmarried, was impregnated through artificial insemination. A court ruled in 2013 that the Archdiocese owed her $171,000 for improperly firing her.
Other issues include a teacher being fired after she wrote a letter in favor of a nun suspended for supporting female priests in the public eye.
The archdiocese, which did not return a request for comment, expanded its current contract from three to six pages to accommodate the new specific restrictions.
Not everyone is happy with the new contracts. One local lay leader, Tom Miele, said the list “seems awfully intrusive and it all seems unfair.”
Miele also said, “Some of the things they put on that list are not a reflection of what has happened in our society. It’s more about protecting their schools from a lawsuit.”
An archdiocese spokesperson told Cincinnati.com, “There aren’t any new expectations of our teachers in the 2014-2015 contracts. The revised wording is just more explicit in that it lists examples of behaviors that are unacceptable as contrary to church teaching.” Dan Andriacco said the archdiocese believes “that’s fairer to the teachers and a help to them.”
“Our contract for many years has reflected that by including a moral conduct clause,” said Andriacco. “Last year we made that clause more explicit by mentioning the Catechism of the Catholic Church, and this year we’ve added examples of unacceptable behaviors.”
PHILADELPHIA, PA, February 28, 2014 (LifeSiteNews.com) – A new study has found that women who use the contraceptive pill may be as much as 50 percent more likely to develop multiple sclerosis.
The study was conducted by the Kaiser Permanente Southern California medical group, under the leadership of Dr. Kerstin Hellwig, and contradicts previous research that had suggested that use of the pill reduces its likelihood.
According to the press release issued by the American Academy of Neurology, “Women who had used hormonal contraceptives were 35 percent more likely to develop MS than those who did not use them. Those who had used the contraceptives but had stopped at least one month before symptoms started were 50 percent more likely to develop MS.”
“A total of 29 percent of the women with MS and 24 percent of those without MS had used hormonal contraceptives for at least three months in the three years before symptoms began. The majority used estrogen/progestin combinations.”
“These findings suggest that using hormonal contraceptives may be contributing at least in part to the rise in the rate of MS among women,” said Hellwig.
Although there are a number of factors that need to be considered, according to the World Health Organization, incidences of MS are much higher in wealthier parts of the world, especially among wealthier segments of those societies, which would also coincide with heavier contraceptive pill use. In Europe and North America the incidence of MS is approximately 80 in 100,000, and occurs most often in women between ages 20 and 40. Women are twice as likely to get it as men.
The new research will be presented at the American Academy of Neurology’s annual meeting in Philadelphia at the end of April and yet it is doubtful that the findings will greatly influence pill use.
Even Hellwig was herself dismissive of the implications of her study for everyday behaviour. “There may be some environmental factor that we have not been able to allow for, we are not telling women to stop using the pill,” she said.
According to the Guttmacher Institute, in 2010, approximately 17 percent of women aged 15-44 were using the pill, while about 80 percent of sexually-active women have used it at some point.
February 27, 2014 (MercatorNet) – On the morning of January 29 this year, a 25-year-old married woman went to Care-Medics Medical Centres in Ottawa, a walk-in clinic that she had frequented for about two years. She wanted a prescription for birth control pills.
After giving her health number to the receptionist, she sat down and waited until she was called. When she told the receptionist why she was there, she was advised that it was not possible to have the prescription filled. The young woman was surprised and asked why. The receptionist pointed to “a stack of letters” on the desk. The woman picked one up and began to read it.
Dear Patient:
Please be advised that because of reasons of my own medical judgment as well as professional ethical concerns and religious values, I only provide one form of birth control, Natural Family Planning. In addition, I do not refer for vasectomies, abortions, nor prescribe the morning after pill or any other artificial contraception. If you are interested in the latter, please be aware that you may approach your own family doctor or request to be seen by another physician…
Although she had attended the clinic for two years, this was the first time that this had happened, and she was understandably surprised. The receptionist told her that she could return the next day and see a different physician, but the woman explained that she could not do so because she was working. The receptionist advised her that she would have to go elsewhere if she wanted the prescription filled, as the physician was the only one available that day.
The patient described her reaction on a blog:
It almost felt like I was doing something wrong. I felt truly embarrassed having to leave in front of a group of people because of something that someone thinks is shameful and not right.
I had to go out of my way and find another clinic. Luckily for me, there was one not too far away. I still couldn’t even believe what happened. I even mentioned it to the receptionist at the other clinic, and she was just as shocked as I was.
The “other clinic” was the Sunrise Medical Centre in the Loblaws Store across the street on Merivale Road – a two minute drive. There was a pharmacy in the store, so presumably she had the prescription filled there. In brief, a young woman was refused a birth control prescription at one clinic, but obtained the prescription and pills at another clinic and pharmacy two minutes away.
A crusade on social media was started against the physician and two colleagues with the same views. Crusaders argued that in a “secular” state health care system, physicians should be forbidden to act on their moral or religious beliefs.
Outraged Facebookers called the physician a “jerk,” a “complete anachronism”, “disgusting”, incompetent, “unethical and unprofessional”, a “worthless piece of ____”, a “crummy doctor”, “an idiot”, and described him as judgemental. “Goofballs like this,” wrote one, “are the best walking arguments for the birth control they don’t believe in.” “He should move to the States, or maybe Dubai, where he will be among his own kind.”
Physicians who refuse to prescribe contraceptives face a difficult challenge, since aggressive contraceptive promotion has left most people unaware of alternatives. Further, the social progress of women is widely attributed to contraceptives, so that failure to provide them risks an adverse reaction.
Nonetheless, based on a respectful understanding of female fertility cycles and other factors, plausible reasons can be given to justify refusal to prescribe contraceptives and recommendation of Natural Family Planning.
The Supreme Court of Canada has acknowledged that secularists are believers, no less persons with religious beliefs. There is no legal warrant for the idea that a secular state must be purged of the expression of religious belief. The claim that a secular state or health care system is “faith-free” is radically false. Both religious belief and secularism can result in narrow dogmatism and intolerance, as demonstrated by the crusade against the physicians.
Since the practice of medicine is an inescapably moral enterprise, every decision concerning treatment is a moral decision. Since the practice of morality is a human enterprise, the secular public square is populated by people with many moral viewpoints. To discriminate against religious belief is a distortion of liberal principles. Moreover, if religious believers can be forced to do what they believe to be wrong, so can non-religious believers. This would establish a destructive and dangerous “duty to do what is wrong”.
It is essential to maintain the integrity of physicians and well-being of patients. After abortion was legalized, a difficult compromise emerged that safeguards both, while protecting the community against a purported “duty to do what is wrong”.
Nonetheless, some people are trying to entrench that duty in medical practice, moving from a purported duty to provide or facilitate abortion to a duty to kill or facilitate the killing of patients by euthanasia. It is unacceptable to compel people to commit or even to facilitate what they see as murder, and punish or penalize them if they refuse. It is equally unacceptable to insist that physicians must not act upon beliefs, because it is impossible; one cannot act morally without reference to beliefs. Such policies are inconsistent with the central place occupied by individual conscience and judgment in a liberal democracy.
Freedom of conscience can be adequately accommodated in a society characterized by a plurality of moral and political viewpoints if appropriate distinctions are made.
The first of these is the distinction between the exercise of perfective freedom of conscience: pursuing an apparent good – and preservative freedom of conscience: refusing to participate in wrongdoing. The state can sometimes legitimately limit perfective freedom of conscience by preventing people from doing what they believe to be good, but it does not follow that it is equally free to suppress preservative freedom of conscience by forcing them to do what they believe to be wrong.
To force people to do something they believe to be wrong is always an assault on their personal dignity and essential humanity, and it always has negative implications for society. It is a policy fundamentally opposed to civic friendship, which grounds and sustains political community and provides the strongest motive for justice. It is inconsistent with the best traditions and aspirations of liberal democracy, since it instils attitudes more suited to totalitarian regimes than to the demands of responsible freedom.
Even the strict approach taken to limiting other fundamental rights and freedoms is not sufficiently refined to be safely applied to limit freedom of conscience in its preservative form. Like the use of potentially deadly force, if the restriction of preservative freedom of conscience can be justified at all, it will only be as a last resort and only in the most exceptional circumstances.
That a young woman had to drive around the block to fill a birth control prescription does not meet this standard.
Sean Murphy is the administrator of the Canada-based Protection of Conscience Project. This article has been excerpted from a long essay on this case. For more detail and documentation, visit the site: http://www.consciencelaws.org/background/procedures/birth002-contents.aspx
I have five kids. I thought I was sane, but apparently, I’m living a crazy alternative lifestyle.
Freestyle halfpipe skier David Wise won gold at Sochi. NBC, rather than being impressed with his world-class athleticism, focused on his “alternative lifestyle.” You see, Wise is married to Alexandra, and they have a young son. Wise is also considering becoming a pastor.
San Diego Chargers quarterback Phillip Rivers has had his critics in terms of his play, but there are also critics of his “alternative lifestyle”: he and his wife, Tiffany, have six kids (they recently had a seventh child.) ESPN noted with this comment: Six kids? Regardless of your profession, it’s impossible to be a good parent to six kids. Not enough hours in the day.
One headline even read: “Phillip Rivers Is An Intense Weirdo,” and blamed his “weirdness” on the fact that there were “eight people running around his house.”
Why is our society so afraid of families and children? Why is there a backlash against women being fertile and men raising their own children? Mollie Hemingway at The Federalist has some thoughts.
The media remind us regularly that the most important cultural value relative to family life is what’s euphemistically called “choice.” The choice of whether to have kids or not is held so sacrosanct that our laws permit the decision to be made many months after a new human life begins. Some even advocate extending the choice to a period of time after birth. So why the weird reaction to people receiving children as a blessing instead of fighting them tooth and nail with hormones, chemicals, surgery and scissors? Do we need some remedial courses in how babies are made? It’s entirely natural, of course, for babies to be conceived when men and women have sex. Treating the entirely expected procreation of children as something to be avoided at all costs — and an unspeakable atrocity if one has, say, three children already — would be weird even if our culture weren’t obsessed with sex at all times, in all places, in every context, at every moment.
Hemingway goes on to point out that the press seems to give a pass to scoundrels like former Denver Bronco Travis Henry, who has eleven children with ten different women or NBA player J. J. Reddick, who made sure he wasn’t going to be responsible for any children. She tells:
…a supremely weird and horrifying tale of a 2007 contract drawn up by lawyers representing NBA player J.J. Redick and his then-pregnant ex-girlfriend Vanessa Lopez. The document discusses how Lopez’s abortion of an unborn child should be handled, including that Redick was not admitting paternity.
Another guy living the crazy alternative lifestyle of marriage and children is comedian Jim Gaffigan.Let’s give him the last word–http://www.catholicworldreport.com/Blog/2312/jim_gaffigan_on_big_families_well_why_not.aspx#.Uw-CJeNdWsN
–on why he and his wife live this way:
Well, why not? I guess the reasons against having more children always seemed uninspiring and superficial. What exactly am I missing out on? Money? A few more hours of sleep? A more peaceful meal? More hair? These are nothing compared to what I get from these five monsters who rule my life … each one of them has been a pump of light into my shriveled black heart.
REPORT & REFLECTIONS on NFP PROMOTIONAL TRIP In Hong Kong, 9-21 Jan 14
Fr. Matthew Habiger OSB
OUTLINE:
Intro
The Initiators: John and Yrene Lewis
Background on Hong Kong
The Speaking Tour
Some Results and Hopes
Introduction
If you make yourself available to promote God’s plan for Marriage, Spousal Love and Family, you never know where you might be called to go next. Recently I returned from Hong Kong where I spent 11 days (9-20 Jan) promoting Natural Family Planning to a wide variety of audiences. Why Hong Kong?
The Initiators: John and Yrene Lewis
Last September (2013) John Lewis emailed Fr. Dan McCaffrey and me, suggesting that we come to Hong Kong and help promote NFP. John is a private pilot, stationed now in HK, from where he flies businessmen by private jet all over Asia, and all over the world. We met in 2002 when he, his wife Yrene, and two sons (now there is four) lived in Wichita, Kansas. John and Yrene are NFP teachers, and are very active in whatever parish they are in. John is a convert. He and Yrene have studied their Faith in depth, and are committed to living it. They see the devastation that contraception and sterilization have brought to the marriages of their friends, and they understand how NFP accords so well with God’s plan for marriage and family. Having lived two years in HK, they recognized the great blessings that a stronger program in NFP could bring to the Catholic parishes in HK, as well as elsewhere in Asia.
John and Yrene are the ideal “persons of contact on location” that NFP Outreach is looking for. They know the area they live in, and are known to the major players in the local Church. They are able to set up a busy speaking tour that maximizes Fr. Dan McCaffrey or my time while we are there. They know how to network, how to find the people who can best support the promotional effort, and where to find the talent (e.g. making attractive fliers). In HK, people everywhere are using their cell phones and smart phones. Likewise, during most every free moment, John and Yrene were reading or texting emails, or making live calls to their network of friends. Add four sons, 13 years of age and younger, to the mix and you get a picture of their “connectedness” with the local culture.
Background on Hong Kong
Hong Kong is located off the southern coast of mainland China and in many ways is a gateway to China. 7 million people live there. That is three times as many people as live in Kansas, my home state. The Heritage Foundation rates it as the world’s freest economy. It is the financial capital of all Asia, and one of the great cities of the world. Everything bustles there with economic activity. Every five minutes a 747 airbus, or an air cargo jumbo jet, takes off from the Hong Kong International airport. This airport has the largest air cargo traffic in the world. It is also built on reclaimed land.
I spent my first two days in the Lewis’ apartment, on the 55th floor of Tower 5, south of the airport. From there I could observe the constant activity of the gigantic airplanes at the airport, and also one of the harbors where large container cargo ships and ocean liners were in abundance.
Hong Kong is the world’s most vertical city, where office buildings and apartment towers go upwards to compensate for scarce space. The standard of living there is very high. Real estate is very high. Public transportation provides 90% of the local travel, and it is very efficient. The subway system, the double-decker buses, cabs and ferries are very clean. A $5,000 fine is posted for littering (8 HK dollars = 1 US dollar). This city probably has the greatest number of elevators in the world, and most elevators are sanitized every four hours.
Everything here speaks of competence and resourceful planning. The opportunities which accompany economic freedom have drawn great talent into the city. Old buildings have been replaced with modern and attractive high structures. The architectural designs for the exterior and interior of major buildings are first class. The bridges, tunnels and roads are aesthetically pleasing and very functional. During rush hour, Central Station is a marvel to see as hundreds of thousands of people make their connections with the MTR (Mass Transit Railway). Photos of the city’s skyline would impress anyone. Here is a great Chinese success story.
Hong Kong also has the lowest fertility rate in the world: 1.1 babies per woman. Many women put off having their one baby until they are in their 40s, and then discover they have many infertility problems. You don’t see many pregnant woman or babies. You do see lots of dogs and pets. HK has a high rate of contraception usage: 75%. China has 84%.
The Chinese people are very lean and healthy. You hardly see one that is over weight. That is because people here walk abundantly, and eat moderately. Perhaps using chopsticks contributes to slower eating! 90% of all foods are imported; for example, the milk I used for breakfast cereal came from Switzerland.
The United Kingdom took over HK as a colony after the First Opium War in 1842, and transferred ownership of HK back to the Chinese government in 1997. The English infrastructure is very evident, and is a major contribution to the HK success story. Chinese officials would like to have full control over this economic powerhouse, but it is cautious with how it handles the “goose that lays golden eggs.” The official policy is: “One government with two systems.” HK residents defend their freedoms from outside intrusion with robust firmness. Economists think that Mainland China has adopted some of the traits of democratic capitalism found to be so successful in Japan, South Korea, Taiwan, HK and Singapore. That is why China today has the second largest economy, right under the USA. With growing economic freedoms, greater political freedoms usually follow. It is reasonable to think that if the Chinese leaders adapted HK’s democratic capitalism for the mainland, China would now be the world’s foremost superpower. Under Communist pretensions, it is fortunate that they are not the leading superpower.
But all of this economic prosperity in China would be of no avail if there were only weak marriages and forced small families. The one child policy, enforced with mandatory abortion for a second pregnancy, has recently been softened a trifle, but the demography of China still has serious problems. 50 million men will never have wives, because of Chinese leaders’ social engineering. The distribution of age groups is problematic. 12.5% of China is over 60. By the year 2030 that percentage will double. There are already too few workers and young people. That will have serious economic consequences. If baby girls can be aborted at will by parents who want a son in preference to a daughter, then consider what that does for the advancement of women.
Mainland China has 50 thousand trained NFP teachers. The Chinese government invited Drs. John and Evelyn Billings to come to China many times to teach the Billings method. This was an attempt to soften the brutal one child policy enforced by mandatory abortion.
What China needs is to discover God’s plan for Marriage, Spousal Love and Family. For too many years Communist China has tried to weaken the family and redirect all attention to the State. State propaganda, re-education centers, and a one-child policy have done great damage to marriage and family life in China. God’s plan for marriage, spousal love and family is a magnificent plan. It applies to all cultures, and to every generation. Strong marriages lead to healthy families. Healthy families produce young productive citizens, who have been led into the various natural and civic virtues that a stable citizenship requires. Marriage and family predate any government. The State exists for marriage and the family, not the other way around.
Teaching God’s plan for Marriage, Spousal Love and Family is the work of the Church, which was established by God to do this. NFP is part of the picture because couples must have an effective, and completely morally good, means of spacing their pregnancies. The good exercise of sexuality and a prudent use of fertility is a vital part of God’s plan. NFP is part of the big picture. Contraception and sterilization frustrate God’s plan, and have brought serious damage to anyone who uses them.
The Speaking Tour
The week was packed with events. I celebrated Mass and preached at one Sunday Mass at the Cathedral, and also one Mass on Friday at St. Joseph’s Church (near the Cathedral) to 300 Filipinos, and at two other locations during the week. The second weekend I preached at three Masses at Epiphany parish centers in Tung Chung, and after each Mass, John and Yrene gave a personal testimony to the many values of NFP in their marriage.
The Hong Kong Catholic Marriage Advisory Council made arrangements for these presentations:
Monday evening 7-9 PM I spoke to 22 permanent Deacons at the Pastoral Center on the theme: How to Preach God’s Plan for M, SL and F.
Tuesday evening 7-9 PM I spoke to 15 NFP teachers at the Grand Millennium Plaza on the themes: The Spirituality of NFP, and How to Encourage People to Discover NFP.
Friday evening 7-9:30 PM Dr. Lek-Lim Chan and I addressed 4 Catholic medical doctors, two social workers and other medical personnel at the HK Catholic Marriage Advisory Council on the theme: The Vital Role of NFP trained Doctors in Promoting Marriage and Family.
Sunday afternoon 2:30-4:30 there was a Conference at Epiphany Parish Catholic Secondary School in Tung Chung on the topic, God’s Plan for Love & Life. 75 attendees came, many of whom were parish leaders. At this Conference, I spoke on the beauty of God’s plan for marriage, family and spousal love, which NFP enriches and contraception injures and degrades. The Lewises gave an expanded personal testimony of the many values that NFP has brought to their marriage and their relationship. Then Dr. Lek-Lim Chan gave a PowerPoint presentation on how the various contraceptives harm a woman’s reproductive system, followed by a case by case presentation of how charting can be used to diagnose hidden problems within a woman’s fertility, and then find a natural cure for them.
Dr. Chan lives in Malaysia, is trained in the Billings Method, treats patients, trains teachers and promotes NFP at every opportunity in Southeast Asia, Australia, the UK, USA and elsewhere. When he heard about the Conference in HK, he immediately volunteered his services.
The diocesan paper, the Sunday Examiner carried advertisements on the Conference. A beautiful flier on the Conference was widely circulated.
Some Results and Hopes
Christians are 12% of the HK population, or 830,000, and the ratio between Protestants and Catholics is 4:3. I am told that there are 240,000 Filipinos there. Many Filipina women work as domestic helpers, and others perform as musicians. The Chinese Catholics that I met impressed me with the strength of their Faith. Perhaps they understand what religious persecution means.
What is the greatest contribution that the Catholics in Hong Kong can make to their country? The Catholic faith stresses the basics of humanity: a deep relationship with God, integral human fulfillment, strong marriages, healthy and happy families, education, health care, productivity, patriotism and culture. Catholics make a great contribution to whatever country and culture they live in. Perhaps the greatest contribution Catholics can make in HK is to foster all these qualities, especially strong marriages and healthy families, open to the gift of life. The Chinese people naturally respond to these values. Perhaps the Mainland leaders will come to appreciate these values and not consider Catholicism as a threat to their authority. Education and health care have always been strong Catholic assets, and the native people always request them.
In promoting religious freedom, the Catholic Church is really defending human dignity and human rights against an otherwise unchallenged government. Governments are totally incompetent in granting, or withdrawing, human dignity and human rights, or defining marriage and the family. If a country is to flourish, then there must be a just political order, which provides all the necessary services that a society requires.
We can hope that this speaking tour made a contribution to building stronger marriages and healthy, happy families. The contraceptive culture is entrenched in HK and on the mainland. The birth dearth and the fear of the child is a major problem in China. We can hope that many couples will discern God’s plan for their families. Many will be called to become trained teachers of NFP. Some Catholic doctors may become trained as NFP physicians. Perhaps this speaking tour will lead to others in Southeast Asia and in Southwest Asia. The perfect venue for this mission is working through diocesan structures and the parishes.
On a personal note, I celebrated my 72nd birthday on Sunday, Jan 19. This is one birthday I will not forget. After all Masses and the afternoon Conference, Fr. Henry SVD, the pastor of Epiphany Parish, took all the speakers to a Thai restaurant near the airport. Andrew Kong from Singapore, who had just given a two-day seminar on the Theology of the Body in Kennedy Town, HK, and several friends, joined us for a delightful evening. Truly, there are many enjoyable benefits that come with a speaking tour.
A shorter report by John Lewis:
HONG KONG — “We can learn NFP – God’s way and nature’s way of spacing the pregnancies naturally. NFP is in accord with God’s plan. It is 99% effective. It does not place powerful chemicals in a woman’s body. It is a responsibility shared by both husband and wife. It is inexpensive. It builds strong marriages, and healthy happy families,” preached NFP Outreach missionary Fr. Matthew Habiger, OSB, at “God’s Plan for Love & Life” seminar and Masses at Epiphany parish in Tung Chung on Sunday, January 19, 2014. Other speakers included Dr. Lek-Lim Chan of Malaysia, an expert in the Billings Ovulation Method of NFP, and John and Yrene Lewis, a couple who formerly lived in Wichita, KS, and taught NFP for the Couple to Couple League International and who now live in Hong Kong.
“There is widespread contraception and sterilization. This is a serious abuse of God’s plan for spousal love. Each marital act is to be open to 1) the goodness of love and, 2) the goodness of life. The two dimensions are inseparable,” said Fr. Matthew.
This seminar concluded Fr. Matthew’s 10-day preaching tour throughout Hong Kong, which included preaching NFP at Masses at the Cathedral of the Immaculate Conception (chair of Cardinal John Tong and home of relics of Blessed John Paul II) as well at churches in Discovery Bay, Central, and Mui Wo. Other venues included talks given to doctors, permanent deacons, and NFP teachers, arranged by the Hong Kong Marriage Advisory Council.
“Every couple, and every young adult should learn NFP. They should learn God’s plan for marriage, spousal love and family,” said Fr. Matthew, who mentioned that Hong Kong has one of the lowest fertility rates in the world at only 1.1 children per woman (whereas 2.1 children per woman is the minimum required just for a society’s replacement).
“NFP is good medicine!” Fr. Matthew told doctors and nurses during a talk where he and Dr. Chan explained the good bioethics of NFP for couples in contrast to the very harmful bioethical consequences of contraception.
Quotes from Dr. Chan:
“Intra-uterine devices work as abortifacients by preventing implantation of embryos and the oral contraceptive pill works part of the time in the same way.”
“Married couples who truly love each other know in their hearts that sexual relationship is meant to be a beautiful experience and not to be degraded with condoms, withdrawal or other artificial interference.”
” In 2005, the International Agency for Research on Cancer of WHO has stated that combined oral contraceptive pill is highly carcinogenic to humans based on review of scientific publications.”
” Modern natural family planning methods are based on science and have a reliability of over 99 % for avoiding pregnancy and up to 70 % for helping to achieve pregnancy in couples facing difficulty conceiving.”
“Billings Ovulation Method in which I am specialized can be used monitoring follicular activity and ovulation and thus serves as a tool for diagnosis of disorders. And once a disorder is identified and treatment commenced, the Method can be used to monitor recovery.”
Quote from Lewis:
“NFP is more than just a method, it’s a way of life, a language of love!” said John and Yrene Lewis during their couple testimony, “We like to use the acronym LOVE to describe what we believe to be the best four benefits of NFP: 1) Listen; it has taught us to Listen better to each other, our bodies, and to God. 2) Other-centered; it has helped us to focus on the other instead of selfishly only on ourselves. 3) Very low divorce rate; in fact, NFP couples have the lowest divorce rate in the world of around 4% and why some call it their “marriage insurance.” 4) Effective; NFP has been 100% effective for us at both postponing and achieving pregnancy over our 15 years of marriage and we have been blessed with four wonderful sons, each planned with NFP.”
Other…
“Cardinal John Tong wants to promote NFP to help married couples,” said Joseph Tang Cho Fai, a reporter who interviewed Fr. Habiger for The Examiner diocesan newspaper.
I have heard it said that people don’t change their minds on important issues that people need to make up their minds for themselves, that we can’t change people through facts and logical discussions. By the grace of God, I know this to be false; because I am not the man I was six years ago. Six years ago I was an avowed Protestant and mildly pro-life. I used to tell my wife that I would never become Catholic.
All that changed when my brother-in-law and mother-in-law began to be active in the pro-life movement. They would speak with powerful arguments that we know from science that the unborn are human beings, and we know from philosophy that they are not different in any way that justifies taking their lives by abortion. I found these arguments to be both compelling and consistent. If the unborn are human, shouldn’t something be done to protect them? What happened next was a call to action: 40 Days for Life.
My mother-in-law announced that she planned to pray for a full day at the abortion facility in Kettering. I decided to spend the day with her – I was a bit worried of what might happen out on the sidewalk, and I was a bit curious as well.
What I found on the sidewalk that day is the side of the pro-life movement that most people don’t see. There on the sidewalk, you witness life and death. In the parking lot you find mothers and fathers who are heading to an appointment for an abortion, many times out of fear and a lack of love. And what you find on the sidewalk is the call of life, the outpouring of love and prayers for the child, the mother, the father, the abortionist, and all those involved in the act of abortion. That is what 40 Days for Life is all about: prayer and fasting, peaceful vigil, and community outreach. It is about showing the love of Jesus Christ where love is so badly needed.
That day propelled me from mildly pro-life to passionately pro-life. The other thing it did was cause me to question everything that I believed about God. Just like abortion, I had reasons for what I believed about my Protestant faith, and I thought they were good ones. But were they true? This moment opened my mind to the Catholic faith. Within a few months of study, speaking with friends, and looking very closely at the Bible, I realized I was in trouble again! The priesthood, the Pope, the 7 Sacraments, Catholic teaching on morality, the saints, the Eucharist – you can find all of these in the Bible, and you find that the Catholic Church has been miraculously consistent for 2000 years.
That sealed the deal for me, and I joyously joined the Catholic Church at the Easter Vigil five years ago. If I had to pinpoint one moment that changed my life, it was that day on the sidewalk outside the abortion clinic almost six years ago. There is another 40 Days for Life starting this spring on March 5. Come out to see what it is all about, and perhaps your life will be changed as well. I’ll see you there.
JOS, Nigeria, February 14, 2014 (LifeSiteNews.com) – The president of the Catholic Bishops Conference of Nigeria says the Catholic Church’s position on sexual ethics and the defense of life cannot be compromised to placate Western governments, and said critics of Catholic moral teaching are prejudiced and ignorant.
“The Catholic Church has been criticized over her stance on such issues as abortion, condoms, homosexuality, cloning, stem cell research, etc.,” Archbishop Ignatius Ayau Kaigama of Jos told a recent meeting of Catholic doctors, nurses and health workers, according a report by the Catholic News Service of Nigeria.
“The Catholic Church is often judged by people who do not care to know what we really believe. Prejudices inherited from one generation to another have blinded critics of the Catholic Church so much that they cannot be objective about Catholic beliefs and traditions,” the archbishop said in his opening remarks at a seminar titled “The practice of health care and the social teachings of the Catholic Church.”
He urged health care providers to resist the influence of Western governments and international organizations who want to force their debased moral and cultural values on the continent of Africa and especially Nigeria.
“We must not be swallowed up by the tyrannical imposition of some governments or international non-governmental organizations who wish to dictate the moral trend of the world based on their secular values,” the archbishop said.
“In Africa, whether it is about population control, use of condoms, homosexuality, etc sometimes, the views of the West are forced down the throats of Africans through financial inducement. Africans must not be copy cats, believing that whatever comes from the West is ideal,” he warned.
The archbishop stressed that Nigerians and all Africans must look at the impact of Western coercion with “cultural or intellectual discernment … or else we run the risk of losing our values and becoming neither Africans nor Westerners.”
“We must be faithful to our religious heritage even at a time when some of the people who introduced Christianity to us have become its ardent critics and some of them nurture a pathological hatred for Church directives or moral judgments,” he pointed out.
While reminding Catholic doctors, nurses and other health workers that their work is not only a career but a vocation, Archbishop Kaigama urged them to delve deeply into the social teachings of the Church to enable them to render their services “according to sound moral and ethical principles.”
He also used the occasion to praise Catholic doctors who have stood in defense of life in conformity with the teaching of the Church. “They do not trade their faith for anything, no matter the economic inducements or physical threats,” the archbishop said.
February is “American Heart Month”. The campaign is designed to raise awareness about risks factors for heart disease and stroke and how to stay “heart healthy” for yourself and your loved ones.
The campaign mentions cardiovascular risk factors such as hypertension, diabetes, smoking, obesity and sedentary lifestyle, but little or no emphasis is given to an important preventable risk factor for heart disease: the use of hormonal birth control.
Recent research studies indicate that hormones in birth control are linked to an increased risk of cardiovascular disease and strokes. Although the risk of heart attack is rare in young women, the use of birth control doubles the risk. Women younger than 35 years who smoke and use birth control hormones have a 10-fold increased risk of heart attack. The risk is much higher for women over 35 years.1 One study found that women who smoked more than 15 cigarettes a day and used oral contraceptives had an increased risk of dying from heart disease.2
Researchers have analyzed the risk of heart attack among women who use oral contraceptives and have additional risk factors. They found that the risk of heart attack increased 6.1 times for oral contraceptive users suffering hypertension, 13.6 times for smokers, 17.4 times for diabetics, 24.7 times for oral contraceptive users who have high cholesterol.3
You can spread this message to your family, friends, and colleagues. See our info graphics and share them on Facebook, Twitter, or your favorite social network. Tell us if you or someone you know has suffered heart disease while using birth control pills. This testimony could help your friend, sister, cousin or somebody else to save their life.
by Steven Ertelt | Washington, DC | LifeNews.com | 2/17/14
Kimberly Fugate was expecting identical triplets. After a grueling labor process and the birth of three children, Fugate was ready for some much-needed rest. But rest would have to wait as the doctor shouted, “More feet!”
“They had got the three out and they said, ‘More feet,’” the Mississippi mother said. Fugate is now the proud mother of a statistical improbability – four identical newborn babies.
A fourth identical quadruplet had somehow been missed by numerous ultrasounds, managing to keep her existence hidden until she popped out behind three of her identical sisters last week at the University of Mississippi Medical Center.
“It’s one surprise after another,” Fugate said.
The Fugate four, named Kenleigh Rosa, Kristen Sue, Kayleigh Pearl and Kelsey Roxanne after family members, arrived three months earlier than expected, and just a day before their mother’s 42nd birthday.
All four are currently doing well in neonatal intensive care after being born nearly 13 weeks premature. The girls will need to remain in observation, but Kimberly says she hopes to have them out by early May, on their original due date.
“I haven’t been able to hold them yet,” Fugate said. “It will be very exciting to get to take them home and love them.”
Dr. James Bofill, a professor of maternal fetal medicine at the hospital said the odds of conceiving identical quadruplets is astonishingly rare, especially in a case like Fugate’s, where she became pregnant without the use of fertilization drugs or treatments.
“The odds of spontaneous quadruplets is one in every 729,000 live births,” Bofill said. “The chances of having identical quadruplets [are] almost incalculable.”
Kimberly Fugate and her husband Craig are also parents to another daughter Katelyn, 10. The pair have set up a Facebook page to keep relatives updated on the quadruplets’ progress.
Many in the pro-life community are reflecting on two tragic stories with very different outcomes: the Munoz situation in Texas and the Benson situation in Canada. In both, the wife and mother was declared brain dead. In the Benson story, Iver Benson, son of Dylan Benson and his now deceased wife, Robyn, has been allowed to live. Read more on the still-developing story at, http://www.lifenews.com/2014/02/11/son-is-born-after-husband-keeps-brain-dead-pregnant-wife-alive-to-give-birth/
In the Munoz situation, the result was the heartbreaking loss of both mother and child. We offer our sincere condolences to both families faced with these tragic situations.
Texas Attorney Jeff Turner is a long-time friend of Life Legal Defense Foundation (LLDF) who has supported our work over the years. His reflection on the tragedy of the Baby Munoz situation is compelling and he has allowed LLDF to share it.
On Friday, January 24, the 96th District Courtroom in Tarrant County, Texas was the stage for a tragic tale, not told by idiots, but still one “full of sound and fury, signifying nothing.” And by nothing, I mean a profound absence. The tale is one that will be retold more often as medical technology advances to keep people alive, in this case, Marlise Munoz, who in November 2013 suffered a pulmonary embolism when she was fourteen weeks into her pregnancy. Her husband and her parents asked John Peter Smith Hospital to discontinue all life-sustaining treatment for her, which action indirectly would cause the death of her (and his) child in utero. They contend that the very doctors treating her reported that she was brain dead and recommended the withdrawal of such treatment. The hospital did not oblige their request, relying solely on a provision of the Texas Health & Safety Code that provides that a “person may not withdraw or withhold life-sustaining treatmentunder this subchapter from a pregnant woman.” (emphasis added).
Absent from the courtroom, however, was any mention of God as the Author of all human life, including that of Baby Munoz. The mystery of God’s purpose in permitting this tale to unfold will remain that—an impenetrable mystery. What can be known is that He willed Baby Munoz’ life into existence and that fact deserves some weight. It is congruent with America’s Judeo-Christian heritage that God be included in her judicial determinations. The United States Supreme Court still opens each session with “God save the United States and this honorable court.” Edith Jones, Chief Judge of the U.S. Court of Appeals for the Fifth Circuit, placed a replicated Harlan Bible (named after Justice John Marshall Harlan’s personal Bible which he donated to the U.S. Supreme Court in 1906) prominently in her chambers “as a reminder to all who visit that we … remember our judgments are ultimately subject to a Divine standard.” The “Divine standard” is love: love of God and of neighbor, and love sometimes requires sacrifice of one’s own rights, interests, and desires for the benefit of another, like Baby Munoz. Love sometimes requires one to “wait for the Lord with courage.” Psalms 27:14. There was no mention of this “Divine standard” in the 96th District Court in determining the fate of Baby Munoz.
Also absent was any advocate for Mrs. Munoz or for Baby Munoz. Larry Thompson, the Assistant District Attorney who represented JPS Hospital, informed this writer that the appointment of an attorney ad litem or guardian ad litem had been considered; however, no such appointment was sought. This decision was a glaring error. An attorney appointed to zealously represent each party would have forced Mr. Munoz’ attorneys to prove his case. For example, does Mrs. Munoz’s medical condition satisfy the legal definition for “death?” The same Health & Safety Code states that a person is dead “when, according to ordinary standards of medical practice, there is irreversible cessation of the person’s spontaneous respiratory and circulatory functions.” It further states that “if artificial means of support preclude a determination that a person’s spontaneous respiratory and circulatory functions have ceased, the person is dead when, in the announced opinion of a physician, according to ordinary standards of medical practice, there is irreversible cessation of all spontaneous brain function. Death occurs when the relevant functions cease.” Death must be pronounced before a doctor can discontinue artificial or mechanical means of supporting a person’s respiratory and circulatory systems. Because artificial means of support had been initiated when Mrs. Munoz first arrived at JPS Hospital, the fact whether “all” of her spontaneous brain function had stopped became a critical issue.
“Brain death” was introduced in 1968 by an ad hoc committee of the Harvard Medical School in the Journal of the American Medical Association. It was introduced mainly to facilitate “organ harvesting” and to reallocate resources away from patients whose prognosis was unfavorable. Unfortunately, after three decades of clinical implementation, this standard has proven to be “conceptually flawed,” according to medical ethicist Dan Wikler of the University of Wisconsin at Madison, a member of a 1981 presidential commission that recommended a uniform law defining death. There is no reliable way to determine “irreversible cessation of all spontaneous brain function” unless and until the entire brain has been destroyed; but, in order for this destruction to occur, the respiratory and circulatory functions must stop. Cases have occurred in which the patient met the test for “brain death” because an EEG could not detect electrical activity on his brain’s surface, but the patient clearly had functioning of the mid-brain and brain stem, and maybe even of the cortex. The brain may not be the exclusive central organizing organ of the human person. Doctors have reported over thirty cases of protracted survival of “brain dead” patients, ranging from one week to fourteen years.
No expert witness was called to testify on behalf of Mrs. Munoz. Instead, the assistant district attorney, representing the state and not Mrs. Munoz or Baby Munoz, simply stipulated that the mother was “brain dead.” That stipulation practically decided the case.
An advocate for Baby Munoz not only would have challenged the allegation of “brain death” but also would have raised the equally crucial question of whether his client was viable. Viability refers to the gestational age at which a child in utero has a 50% chance to survive outside the womb. Most doctors believe viability is reached around 24 weeks of gestation. However, there is no hard and fast rule. Amillia Taylor, for example, was born in 2006 at 21 weeks, 6 days of gestation (but under 20 weeks from fertilization). At nine inches and 10 ounces, she faced digestive and respiratory issues and a brain hemorrhage. Today, “she runs, she plays, she does things she’s not supposed to do.” But, again, the assistant district attorney essentially threw the case by stipulating that Baby Munoz was not viable.
Another gaping absence was any discussion of medical ethics. As soon as a woman becomes pregnant, there are two patients. The first rule of medical ethics is: Do no harm. Removing the ventilator (which supports but does not substitute for the respiratory system) from Mrs. Munoz obviously caused harm to Baby Munoz. He died. The second rule is: Take all reasonable action to give the patient a fair chance to live. All that Baby Munoz needed was 3 to 4 more weeks. This would not have been the first time a brain-dead pregnant woman delivered a baby. In 2012, in Michigan, Christine Bolden delivered twins before her respirator was removed. Dr. Cosmas Vandeven, a specialist in high-risk pregnancies at University of Michigan hospital, said that an important ethical issue in such cases is whether a brain-dead woman would suffer by being kept on a respirator and undergoing a C-section. “Almost every parent would give their life for their child,” Dr. Vandeven opined. “But you need to get truly independent opinions: Are we sure we’re not causing harm to the mom?” Ms. Bolden’s brother said, “I know she wants the babies to be with us. This has brought our family together.”
In contrast, the Texas courtroom stage was filled with provocative commentary on Mrs. Munoz’ allegedly decaying corpse and the “smell of death.” Mr. Munoz’ attorneys pursued a backhanded ad hominem attack against JPS Hospital employees by accusing them of engaging in a scientific experiment with Mrs. Munoz’ body, thus questioning their motives. The defense failed to offer any alternative argument to its insistence that the Texas Health & Safety Code applies to a pregnant woman, whom it already had stipulated was dead, when the relevant subchapter at issue concerns only “qualified patient[s]” who have been diagnosed with a terminal or irreversible condition, Implicitly, it does not apply to a dead patient.
This writer does not question the motive of either the hospital employees or Mr. Munoz. This writer does question whether Mrs. Munoz or Baby Munoz received a fair hearing and whether all available legal and ethical arguments were presented.
In Shakespeare’s play, Macbeth found no meaning or purpose in life after his wife’s death. Let us pray that Mr. Munoz will find meaning and purpose after the death of his wife and child. Let us pray further that our culture, including our judiciary, will strive to meet the Divine standard by which we all will be judged.
Over 100 young adults held a press conference Tuesday at Indiana’s state House calling for an amendment protecting true marriage.
INDIANAPOLIS, IN, February 13, 2014 (LifeSiteNews.com) – “The media claims we don’t exist. Freedom Indiana claims there are none of us left. But as young Hoosiers, we are here today.”
Those were the words of Shane Weist, 33, who along with a group of more than 100 other young adults, held a press conference Tuesday in which they sought to prove that – despite media reports to the contrary – not every young person in America backs legally-sanctioned same-sex “marriage.”
Weist and his companions make up Young Hoosiers for Marriage, an Indiana-based group fighting for passage of HJR-3, an amendment to the state constitution defining marriage as a union between one man and one woman.
Also at issue in Indiana are so-called “civil unions,” which give many of the legal benefits of marriage without the name or federal recognition.
The House passed a version of the marriage amendment that stripped a provision banning civil unions, but the Senate must now debate whether to add the provision back in. A vote on the issue was expected late Thursday. If the two houses can come to an agreement on wording, the final version will appear on the general election ballot in November for approval by voters.
Weist told reporters that Young Hoosiers for Marriage support the amendment as it was originally conceived. He urged the Senate to add the language banning civil unions back in the bill.
“The Senate should restore the second sentence because without it, marriage remains vulnerable to redefinition and will more likely face prolonged litigation in court,” Weist explained.
“We are committed to rebuilding culture to ensure that children are not intentionally deprived of a mother and a father,” he added.
The Young Hoosiers’ public debut was met with mockery and derision by homosexual activists, who quickly launched a competing Facebook page called “Young Hoosiers 4 Marriage” serving up personal attacks on Weist and his allies, whom they dubbed “Stepford Kidz.”
Jennifer Wagner, spokeswoman for Freedom Indiana, a gay activist group fighting the proposed ban, accused the Young Hoosiers of “astroturfing,” or pretending to be grassroots when they are not. “Where have they been the last six months?” Wagner asked the Fort Wayne Journal Gazette. “Some of the national groups … have realized their voice has been lacking.”
In an interview with LifeSiteNews Thursday, Isaac Cramer, 24, said neither he nor his fellow Young Hoosiers have any connections with national organizations, and if they are late to the party it is due to their very lack of organization or funding.
“It is never too late to take a stand for something you believe in,” Cramer told LifeSiteNews. “Right now Indiana is in the middle of this debate. We are the only State this year that would have a marriage amendment potentially on the ballot. Everyone is looking at Indiana. We want to show that there is a strong contingent of young Hoosiers who believe in preserving the truth about marriage.”
“It’s really hard with a grassroots, kind of organic coalition to thrive without funding and without any kind of networking outside of the people we know and the people they know, which is kind of how we grew,” Cramer said. “We knew people who knew people, and we kind of just kept forming by word of mouth. Before we knew it, we had people contacting us, saying ‘Hey, can I participate in your group?’”
Cramer says he believes the real number of young people who oppose redefining marriage is much higher than media reports would have people believe, but that the controversy over the issue is so intense that many are afraid to speak up. Even Cramer himself was hesitant to speak on the record for this article, citing concerns about how his employers might react. But ultimately – stressing that his personal beliefs are his own, and should not be taken as representing his employers’ – he said he decided to go on the record because “it’s important to be willing to stand up.”
While the Young Hoosiers for Marriage are currently focused on getting the marriage amendment passed, they believe that is just the first battle in a larger war for the future of the culture. After the vote, they plan to expand their activism from the State House to Indiana’s college campuses and church youth groups, giving talks on the importance of traditional marriage and participating in debates with supporters of same-sex “marriage.”
Cramer said he hopes that by publicizing the fact that young people who support traditional marriage do exist, Young Hoosiers for Marriage will give others the courage to stand up, too.
“I think any time there is an issue that seems controversial, other people are going to be a little bit hesitant to speak out about it,” Cramer said. “I think that it takes somebody to be bold, and somebody to be courageous to take a stand for something, and … other people see that and they realize that, ‘You know what, I can join forces.’ There’s always strength in numbers.”
Cramer told LifeSiteNews that since Tuesday’s press conference, their group – which includes the 100+ young people at the press conference, plus “around another 100 who couldn’t make it because they worked or had class” – has received many more requests from other young people in Indiana wanting to join. Most of them are in their early 20s, juniors and seniors in college.
Asked what he would say to young people who oppose gay “marriage” but are afraid to speak out, Cramer said, “It takes courage to stand up for something you believe in. Sometimes you’re going to receive negative backlash for a stance you take, but that shouldn’t discourage you from taking a stand.”
Cramer encouraged young people who want the safety in numbers provided by Young Hoosiers for Marriage to start their own groups.
“You know friends, you know people in your community, you know kids in school, or college classmates who would be on your side, and that’s how you start,” he said. “You talk to people and you get their opinions, and a lot of times, your friends will share the same positions as you. You start small, and then you grow. It seems like it would be really hard, but really, you find that small group, and you just kind of build from there. That’s how we came together.”
This year National Marriage Week is celebrated in the United States from February 7-14.
National Marriage Week
The idea to celebrate National Marriage Week’s originated with a group of couples who made the World Marriage Weekend in Louisiana in 1983, and later established the International Marriage Week. This is a collaborative campaign to strengthen individual marriages, reduce the divorce rate, and build a stronger marriage culture, which in turn helps curtail poverty and benefits children. Marriage works. It makes people happier, live longer, and build more economic security. Children with married parents perform better in school.
One More Soul joins this collaborative to celebrate the blessing of marriage and to support engaged and married couples.
Please visit our online store to find some resources that can help you celebrate marriage.
On the Feast of the Baptism of the Lord Pope Francis baptized 32 babies in the Sistine Chapel. He encouraged the new mothers to breastfeed their babies right then and there if the infants were hungry. This isn’t the first time Pope Francis has promoted public breastfeeding. He recently invited a mother who was waiting to meet him, to please nurse her hungry baby.
The Holy Father told those gathered at the baptism, “Today the choir sings, but the most beautiful choir is [the choir] of children…Some are crying, because they are uncomfortable, or because they are hungry. If they are hungry, mothers, give them something to eat…”
The sound of a crying baby might not be objectively beautiful. However, in our modern culture of death, it should fall on our ears differently, as more precious and dear than ever before. Pope Francis’ words reminded me of British author P.D. James’ dystopian novel, Children of Men, in which mass infertility has prevented procreation and the youngest members of the human race are adults inhabiting a bleak and dying world. Against all odds, one woman becomes pregnant and the idea of a new life is a shocking and miraculous prospect. In the film adaption, there is a scene in which the newborn child begins to cry and the characters on-screen look as if the whole world has stopped–it is a sound that defiantly screams “Life!” in a world of death and darkness.
Our world is not as troubled as James’ fictional future, but tragically, modern society views children as inconveniences to be avoided rather than gifts of life and hope from God. We are fed lies that make contraception the norm and abortion a common “solution” to a pregnancy. In our culture of death, the cry of a baby takes on new meaning. The crying is the sound of the parents’ faithfulness to avoid contraception and the courage of a mother who carries her child to term. It is the sound of a woman who has rejected the cacophony of lies and has bravely whispered, “fiat!” instead. Could there be a more beautiful sound?
In light of this, we must consider what it really means to be pro-life. Is it merely a bumper sticker or a vote on a ballot? We must examine how our culture’s idolization of efficiency, convenience, and peace and quiet have warped us into seeking out “child-free” restaurants, airplane flights, and lives. If we truly reject the culture of death and seek to honor life, our actions will speak louder than our words. We must be reminded that a crying baby and the sight of a mother breastfeeding her child are the blessed fruits of the culture of life–and yes, that includes when that baby and mother are sitting beside you in Mass. It is wildly inconsistent to fight for the right of the unborn child and then give that child’s mother the stink eye when he has been born and she nurses him in the pew next to you.
We cannot allow the lies of a contraceptive culture to seep into our churches and sour us against the whispering toddler and the fussy baby who are also there to receive grace. We must see children as more than inconveniences or distractions. We must give thanks for the noise of life in a world of death.
I recently discovered the sad truth that the presence of children in Mass is still a heated debate when I wrote about the great blessing our parish family is to us and how they support young families. I was shocked and alarmed with not only the claims that children should be left at home so that the grown-ups could worship in peace, but more disturbingly, the anger some of the commenters expressed over the presence of infants and children at their Mass. One commenter even expressed outrage about a young mother nursing her child near his pew, an act he found repulsive and perverse.
But it seems that the Holy Father doesn’t see it that way. In fact, not only does he tolerate public breastfeeding, he openly encourages it (yes! even in church). Why? Because meeting the needs of infants demonstrates that they are important and precious, not only to their immediate family, but their larger family, the Church. By refusing to elevate convenience over life by such a tiny act as supporting public breastfeeding, you can promote the culture of life in a selfish world that sees children as inconveniences to be avoided, or worse, problems that can be solved by abortion.
Indeed we’re so immersed in this poisoned mindset that it makes the news when the Pope says the sound of babies crying is more beautiful than the music of the choir singing and urges mother to feed their babies if they are hungry. The Holy Father’s words are a startling reminder that those squawks and cries are precious sounds to Our Lord and should be the same to all of us. They remind us that we should rejoice that our churches are filled with life and encourage parents to care for those children, not show young families the door because they’re bugging us.
Whether we realize it or not, our attitude at Mass can serve or hinder a culture of life. If we hear a fussy baby in Mass and groan and fume because she’s bothering us, we must re-evaluate our priorities. If we are infuriated because a new mother nurses during the Consecration, we should remember that we are ourselves helpless infants preparing to receive the grace of Our Lord. If you seek to further the culture of life, I urge you to consider how you can love and encourage young families at your parish and beyond. A revolutionary stand for life in the culture of death might begin with something so simple as a pat on the shoulder and a “we’re so glad you’re here today.”
Haley Stewart lives in the deep south with her bearded husband, three kids, and seven backyard chickens. She went to a Baptist college and surprised herself by coming home Catholic. When she gets a moment to herself, she loves to read Austen, Waugh, and O’Connor with a strong cup of coffee in hand. Haley muses about cultivating a Catholic family through literature, liturgical living, and urban homesteading at her blogCarrots for Michaelmasand just released her first ebook: Feast! Real Food, Reflections, and Simple Living for the Christian Year.
by Steven Ertelt | Washington, DC | LifeNews.com | 1/28/14
While President Barack Obama defended Obamacare, which has taxpayer-funding of abortion and has rationed health care already by canceling Americans’ health care plans, Congresswoman Cathy McMorris Rodgers gave a compassionate pro-life response.
Rodgers, representing the State of Washington, is another high-profile mother in the political realm, who also chose to give life to her son with Down Syndrome. Cole was born in the spring of 2007. She talked about him when she said that children are a gift from God.
I was single when I was elected – but it wasn’t long before I met Brian, a retired Navy commander, and now we have three beautiful children, one who was born just eight weeks ago. Like all parents, we have high hopes and dreams for our children, but we also know what it’s like to face challenges. Three days after we gave birth to our son, Cole, we got news no parent expects.
Cole was diagnosed with Down syndrome. The doctors told us he could have endless complications, heart defects, even early Alzheimer’s. They told us all the problems. But when we looked at our son, we saw only possibilities. We saw a gift from God.
Today we see a 6-year old boy who dances to Bruce Springsteen; who reads above grade level; and who is the best big brother in the world. We see all the things he can do, not those he can’t. Cole, and his sisters, Grace and Brynn, have only made me more determined to see the potential in every human life – that whether we are born with an extra twenty-first chromosome or without a dollar to our name – we are not defined by our limits, but by our potential.
Tomorrow, I’ll watch my son Cole get on the school bus; others will wait in the doctor’s office or interview for that first job. Some of us will celebrate new beginnings… Others will face great challenges… But all of us will wake up and do what is uniquely American… We will look forward to the boundless potential that lies ahead. We will give thanks to the brave men and women who have answered America’s call to freedom, like Sgt. Jacob Hess from Spokane, who recently gave his life to protect all of ours.
So, tonight, I simply offer a prayer… A prayer for Sgt. Hess’s family, your family, and for our larger American family. That, with the guidance of God, we may prove worthy of His blessings of life … liberty … and the pursuit of happiness. For when we embrace these gifts, we are each doing our part to form a more perfect union. May God guide you and our President, and may God continue to bless the United States of America.
by Melissa Ohden | Washington, DC | LifeNews.com | 1/29/14
“There are other people who are haunted by
abortion, too. Nurses and doctors.”
No sooner had the woman in the crowd after a recent event quietly spoken these words to me, when the tears began to fall down her face. Without even saying another word, I knew that she was speaking from personal experience.
As the woman wept and I held onto her forearm, in an attempt to let her know I was listening to and supporting her, I was both grief-stricken for her and simultaneously shocked to hear her story. Sadly, I have met many nurses, in particular, who have been put in the position to complete an abortion, whether knowingly or unbeknownst to them initially, but this was the first nurse that I have met who had admittedly completed one at the very same hospital where I was aborted and survived.
“If I would have been there in 1977, you can be sure I would have been one of those nurses fighting to save you,” she shared. As I thanked this pro-life nurse, wife and mother for her commitment to lives like mine, I learned that although she has always been pro-life, she had a very good reason to have wanted to try and save me: because she had been put in the position to leave a child to die after a failed abortion just one year prior to when I survived.
If anyone reading this doubts for a second that abortion affects us all and silently haunts millions, including medical professionals and former clinic workers, I would encourage you to read the testimony of Dr. Bernard Nathanson or watch the film The Voice of John, which shares the story of a nurse much like this one that I spoke with recently. As hard as it is for me to live with the truth of what was done to me in the abortion and after it was discovered that I had survived, these former abortionists and nurses, along with so many like them around the world, have to live with the memories of what they’ve seen, heard, and done. And it stays with them and changes them. By this nurse’s own account, it certainly changed her to not only attend to the delivery of a baby after a saline infusion abortion, but in it, to come face to face with a child who survived.
Sadly, it was reaffirming for me to hear about this little boy who had survived the same type of abortion procedure, at the very same hospital, that I did. It was reaffirming simply to hear that I was not alone in my survival there. My affirmation was short-lived, however, as the nurse’s tears continued to fall and I found the nerve to ask her what had happened to the baby boy that she helped deliver.
I should have known. I should have known by her emotional state that she hadn’t just assisted in the delivery of an aborted baby; she hadn’t just come face to face with a survivor; she had witnessed first hand what often happens when a child survives.
“Where did you take him? Where were the surviving children taken?” I asked her, both anxiously awaiting her response and dreading it at the same time. Before she responded, I knew. I knew that I already knew where that little boy was taken.
“The utility closet.” In my mind’s eye, I could picture what that closet must have looked like, and I shuddered at the thought. “There was a bucket on the shelf there, filled with formaldehyde,” she continued.
Despite my knowledge of such practices, I had to force myself not to grimace. Once again, all of this was hitting far too close to home for me.
“You wrote the last name on the bucket, and you left them there to be picked up later, as, you know, waste,” the nurse finished, visibly lost in the memory of what she had experienced. “All these years later, I remember him. I remember everything that happened that day.”
Like so many nurses in similar shoes, this nurse’s experience that fateful day in 1976 forever changed her, and she has worked for the protection of lives ever since.
After meeting this nurse and hearing of the fate of this little boy at the very same hospital where I survived, I have no doubt this nurse would have done whatever she could to save my life. And I have no doubt that God had on hand exactly who He knew would do just that on the day that I survived. To say that I am thankful for all of that would be an understatement. Today and everyday, I offer my sincerest thanks to the nurses who rallied for me so that I wasn’t just another survivor left in a bucket to die.
MOSCOW, January 29, 2014 (LifeSiteNews.com) – In its continuing effort to boost its birth rate, the Russian government is looking at setting up crisis pregnancy centers to help dissuade women from abortion.
“The Health Ministry supports the creation of crisis centers for pregnant women, where they can get professional counseling from social workers. We think that this is the most promising and humane way of reducing the number of abortions,” said Elena Baibarina, the head of the Health Ministry’s Department for Health Care for Children and Obstetric Aid, according to a RIA Novosti report.
“The number of abortions in Russia is going down. The 2008 figure was 1.2 million, while in 2012 it dropped down to 935,000. But it is still too high, which also contributes to infertility issues,” Baibarina said.
Prominent Russian demographer Veniamin Bashlachev toldRossiyskaya Gazeta that Russia’s population loss through abortion in the decades leading up to the fall of communism was two and a half times the number of lives Russia lost in the First World War, the Russian Revolution and the Second World War combined. Abortions in the 1960s to the end of the 1980s averaged more than 4.5 million a year.
By 2011 the Russian population stood at 143 million people, down by 5.7 million since the break-up of the Soviet Union in 1991.
To combat the abortion epidemic, the Russian government has proposed legislation that would ban free abortions at government-run health clinics, require prescriptions for the ‘morning-after’ pill, require parental consent for teenagers and a husband’s consent for married women, and mandate a one-week waiting period before an abortion is performed.
Other proposals have included increasing the 2,000 ruble ($70) monthly government subsidy offered to pregnant women.
Late last year Russian President Vladimir Putin signed a law banning abortion advertising.
The abortion ad ban was part of broader changes to Russia’s Federal Law on Advertising that tightened up many aspects of advertising seen as having a negative impact on the population, such as campaigns offering free drug samples if these samples contain narcotic or psychotropic substances, and restrictions on the advertising of traditional “folk medicine” practices.
Steven Mosher, President of the Population Research Institute, pointed out that despite government incentives such as a baby bonus that offers the equivalent of $9,000 upon the birth of every child after the first, and calls from President Putin for families to have at least three children, abortion is still occurring in epidemic proportions.
“As long as society fails to recognize the value of human life, and wantonly destroys it in large numbers, it will be difficult to establish a new three-child norm. Abortion must cease being a way of life in Russia if her people are to survive,” Mosher said.
Pro-life legislation aimed at rolling back Russia’s abortion culture has been strongly supported by the Russian Orthodox Church.
Patriarch Kirill of Moscow and All Russia proposed a series of measures on the Moscow Patriarchate’s website, urging the Ministry of Health and Social Development to make “preservation of pregnancy a priority task for the doctor” and discourage incentives for abortion.
The Russian patriarch also advocated state support for pro-motherhood media campaigns, and early on suggested setting up crisis pregnancy centers in every maternity hospital to help “lonely mothers in difficult life situations. ”
“Adoption is real–and it’s forever.”, – Dr. Bill Platypus, Mister Rogers’ Neighborhood: Season 16, Episode 4: “Families”
Jan. 29, 2013 (JewelsGreen) – I’ll talk to anyone. No, really. I chat up the other shoppers in line at the grocery store, then carry on a conversation with the cashier and the fella bagging the groceries. I’m Facebook friends with a couple I met on the four-hour bus ride home from last year’s March for Life. So it was this year.
I’ve only taken the train a couple of times, so I must have been visibly befuddled at the Amtrak kiosk, holding my eTicket printout and staring at the screen waiting for it to tell me what to do. (Insert joke about me being over 40 here.) A pretty young woman offered to help me. She showed me how to scan my paper and voila! my boarding passes printed out. I thanked her and glanced at her boarding pass and noticed she was also headed to Washington, DC. This was my chance! I’ve done this in line at the bus terminal many times when traveling alone. I start a conversation with a woman and then ask her if we can sit together “so neither of us has to sit next to a big sweaty man” for the trip. It works every time. (THANK GOODNESS.)
“Oh, I see you’re going to DC, too!”
“Yes, I am.”
“Would you like to sit together so neither of us has to sit next to a big sweaty man?” (cue: laughter)
“OK.”
“Great! My name’s Jewels.”
That’s how it started.
This lovely young lady (I’ll call her Angela) was 19 years old and going to D.C. to visit with a friend she hadn’t seen since summer. I told her I was bound for the March for Life and some of the attendant conferences, as well as meeting up with friends I hadn’t seen in some time. Her friend had participated in LIFE Runners last year. Smiles, nods, and we both went back to checking our phones and arranging our coats and handbags.
The silence between us didn’t last very long. She looked out the window and beaming said, “I just love snow!” ME TOO! This instantly kicked off a delightful conversation about how everyone else seems to be complaining about the cold and the snow and how much we both just love it. There wasn’t any silence after that (I hope we weren’t in the Quiet Car!)
She is the middle of a year off from college to work as an adoption advocate. She told me that she was adopted and wanted to help others as a way of expressing gratitude for her own life. How cool is that? She told me about her parents, and how just a couple of years ago she and her mom went together to meet her birthmother, half-siblings, and assorted extended family. She told me about her favorite success story from her work in a private adoption firm, and shared a bit of the downsides, too. Clearly proud, she clicked on her phone and brandished a photo of a smiling happy family she had helped through the adoption process. She was planning to continue working through college because she disliked the idea of piling up debt. I was so impressed by her realistic attitude and how far-sighted her goals were. She was sensible and determined, with a level of self-possession and insight rarely found in people her age (indeed, rarely found in people my age!). I admired her.
She clicked her phone again and I asked if the picture of a brand new baby girl (pink hat, it was a girl) was another of her “success stories” from work. She smiled and shook her head, but said nothing at first.
“I don’t tell people this, I haven’t even told my grandpa yet, but I’m also a birthmom.”
(cue: tears)
She showed me photo after photo of this gorgeous little baby girl (just born in December!), then a shot of her hugging the adoptive parents while she was hugely pregnant, all smiling in the sunlight. I cried.
For the final months of her pregnancy, she’d moved to the state where the adoptive parents live, and invited them into the delivery room for the birth of their daughter. She didn’t want pain medication right away, because she said she “wanted to remember what it was like to go through this,” so she wouldn’t put herself in that position again until she was married. Moments after this precious baby took her first breath she was placed into the arms of her adoptive mother, skin-to-skin.
I cried.
(I’m still crying. )
We arrived. The train came to a stop and I nearly fell over myself hugging her. We walked into the station together and her friend spotted her right away – her friend who hadn’t seen her since she’d moved away, pregnant – and they hugged each other fiercely.
What a gift life is! What a gift that pretty young woman gave that baby girl and her parents. What a gift she gave me by sharing it all.
I walked away and realized Angela wasn’t pretty, she was beautiful.
Editor’s Note: Jewels Green is a post-abortive mother of three who worked in an abortion clinic before becoming pro-life. Read her original testimonyhttp://www.lifesitenews.com/news/former-abortion-clinic-worker-speaks-out-for-life. This article is reprinted with permission fromher blog.
(Vatican Radio) Pope Francis baptized 32 children on Sunday, the Feast of the Baptism of the Lord. The celebration took place, as is customary, in the Sistine Chapel.
Included among those baptized by the Holy Father were primarily the new-born children of Vatican employees.
In his homily at the Mass, Pope Francis noted that Jesus Himself had no need of Baptism, but that with His Divinity, united to His human body, Jesus blessed the waters and gave them the ability to be used in Baptism. Ascending into Heaven, the Lord commanded His followers to go into the world to baptize – a command that the Church fulfils even to the current day.
The children baptized today, he said, are a link in the chain; in time, they will return to have their own children baptized. This implies a duty on the part of parents, the duty of transmitting the Faith to their children, so that they in turn can pass it along to their children.
The Holy Father concluded his homily with a special word of affection for the newly baptized children. “Today the choir sings,” he said, “but the most beautiful choir is [the choir] of children” making noise. He continued, “Some are crying, because they are uncomfortable, or because they are hungry. If they are hungry, mothers, give them something to eat… they are the central figures, the protagonists [of this celebration].” It was with this “awareness of being the transmitters of faith” that Pope Francis continued on to the ceremony of Baptism.
Jesus did not need to be baptized, but the first theologians say that, with His body, with His divinity, in the Baptism He blessed all the waters, so that water would have the power to give baptism. And then, before ascending to Heaven, Jesus told us to go into all the world to baptize. And from that day until the present day, this has been an unbroken chain: they baptized their children, and their children [baptized] their children, and their children [and so on]… And even today this chain continues.
These children are a link in a chain. You parents have the baby boy or girl to be baptized, but in a few years it will be they who will have a baby to be baptized, or a grandchild… And so goes the chain of faith! What does this mean? I would just tell you this: you are the ones that transmit the faith, the transmitters, you have a duty to pass on the faith to these children. It ‘s the most beautiful legacy that you leave to them: the faith! Only this. Today, take this thought home with you. We must be transmitters of the faith. Think about this, always think of how to transmit the faith to the children.
Today the choir is singing; but the most beautiful choir is that of the children, who are making noise… Some cry because they are not comfortable, or because they are hungry: if they are hungry, moms, give them something to eat, calmly, because they are the central figures, the protagonists [of this celebration]. And now, with this awareness of being transmitters of the faith, let us continue the ceremony of Baptism.
Jesus did not need to be baptized, but the first theologians say that, with his body, with his divinity, in baptism he blessed all the waters, so that the waters would have the power to confer baptism. And then, before ascending to Heaven, Jesus told us to go into all the world to baptize. And from that day forward up until today, this has been an uninterrupted chain: they baptized their children, and their children their own, and those children… And also today this chain continues.
These children are a link in a chain. You parents have a baby boy or girl to baptize, but in some years they will have a child to baptize, or a grandchild… Such is the chain of faith! What does this mean? I would like to tell you only this: you are those who transmit the faith, the transmitters; you have a duty to hand on the faith to these children. It is the most beautiful inheritance you will leave to them: the faith! Only this. Today, take this thought home with you. We must be transmitters of the faith. Think about this, always think about how to hand on the faith to your children.
Today the choir sings, but the most beautiful choir is the children making noise… Some of them will cry, because they are uncomfortable or because they are hungry: if they are hungry, mothers, feed them with ease, because they are the most important ones here. And now, with this awareness of being transmitters of the faith, let us continue with the rite of Baptism.
This past week we seated our jury on Tuesday Morning. Opening statements were made in the afternoon and Kevin McCarthy was on the stand for the remainder of the week for direct examination. Cross examination will start tomorrow afternoon.
Anyone thinking of attending the proceedings on Monday morning, please be advised that the trail has been postponed until 1:00 PM due to weather.
God Bless you and keep praying that truth prevails in all of these proceedings.
_Al–317-713-8633 (O), 317-946-0495 (C)
BACKGROUND 1/19/2014
Dear Friends and Family,
Once again, please allow me to ask for your prayers.
Starting this past Tuesday, January 21, I have been in a Federal Court Trial (as a Plaintiff) that revolves around the question: does a certain person own a devotion to the Blessed Virgin Mary. This trial has certain constitutional and religious issues which have already set legal precedent (and may set more) concerning separation of Church and State issues. The fundamental question however is does the defendant own copyrights and trademarks concerning the Devotion to the Blessed Virgin Mary under the title of Our Lady of America.
Many of you know that I have been dedicated to promoting this devotion to The Blessed Virgin Mary under the title of Our Lady of America. This devotion originates with appearances of the Blessed Virgin as Our Lady of America to a Sister Mary Ephrem, C.PP.S. (8/2/1916-1/10/2000) in 1956 in Rome City, Indiana and continuing until 1960 in other locations. The devotion was approved by the Archbishop of Cincinnati, Paul Francis Leibold.
The messages are a call to purity for our county. There are certain requests made by Our Lady of us individually and of our Church collectively. If we respond, she has promised graces greater than those given at Fatima and Lourdes. During the course of these apparitions Jesus, St. Joseph, Our Lady, and St. Michael all appeared. You can learn more about the devotion and additionally download the messages atwww.ourladyofamerica.org.
In late 2005 Kevin B. McCarthy (a friend of mine) was asked by two U.S. bishops to find out why this devotion had fallen into dormancy and to “Get it going”. Terry and I discerned that we should help in this charge by the Bishops.
Starting in late 2005 we started collaborating with a Sr. Mary Joseph Therese, C.I.T. (Patricia Fuller) from Fostoria, OH. She was in the cloister of the Precious Blood Sister with the visionary. In the late 70’s the Precious Blood Sisters closed the cloister and the visionary left the Order. Sr. Joseph represented that a new Order was founded called the Contemplative Sisters of the Indwelling Trinity that she and the visionary went to after leaving the Precious Blood Cloister and that she was the last living member of that Order. She claimed copyrights and trademarks concerning the messages and devotionals. Unfortunately, I never met the visionary.
Kevin & I collaborated with Sr. Mary Joseph Therese and many things were accomplished to promote the devotion from 2006-2007. The statue of Our Lady of America attended the U.S.C.C.B. Conference in 2006. It was displayed in the Archdioceses of New Your, Galveston-Houston, St. Louis, Newark, Indianapolis and Milwaukee. Additionally, many Dioceses also promoted the devotion to some level. While it was a struggle working with her, we continued our collaboration until late 2007 when the relationship broke down and we simultaneously learned that Sr. Mary Joseph Therese was not recognized as a Catholic Religious by the Holy Roman Catholic Church and did not live in a convent. Subsequently, we also learned that Sr. Mary Joseph Therese was dismissed from religious life in 1982 for “incorrigible disobedience”. In other words she misrepresented her status and in essence who she was.
This caused a serious threat to the devotion. As a nun under a vow of poverty, Sr. Mary Joseph Therese could own trademarks and copyrights in her name that would through the operation of a vow of poverty belong to the Church. However, as a lay person, if those copyright and trademarks were allowed to stand then a lay person would own, under the laws of the United States, what may be one of the greatest gifts of grace available through the intercession of the Blessed Virgin.
In 2005, Kevin McCarthy, BVM Foundation, Inc and I filed a lawsuit in Federal Court, primarily seeking to overturn these copyrights and trademarks arguing that they were either owned by the Catholic Church or were in the public domain. Patricia Fuller and her co-defendant countersued with anything they could imagine producing a laundry list of illegal and immoral activities with which the created claims in the lawsuit.
This case has spanned over 5 years and has involved statements from 2 Bishops, the Congregation for Institutes of Consecrated Life and Societies of Apostolic Life, a diplomatic note from the Apostolic Nunciature, an Amicus Curie brief from the Vatican and a successful appeal to the Seventh Circuit Court of Appeals. Truly this has been a battle of “Powers and Principalities”.
The trial will last 4-6 weeks and is being held in the courtroom of William T. Lawrence at the U.S. Courthouse in downtown Indianapolis.
Terry and I sincerely implore your prayers that truth will prevail in this trial and that the evil one will be prevented from influencing anything about this trial resulting in a devotion which is free for the faithful and the bishops to practice.
The trial is open to the public. Should you be able to attend and pray silently during the proceedings, it would certainly be appreciated? If you are not able to attend, please offer your prayers for our success. The trial is expected to last for the next 3 weeks or beyond.
We need prayer warriors, so feel free to forward this message or post it.
May Jesus bless you and Our Lady of America intercede for you!
I want to tell you a story—one that this pro-life activist leader finds incredible—one which I believe was guided by the providence of God.
On Saturday, Jan. 18th I traveled by plane from Detroit, MI to Omaha, NE to deliver the keynote address at the Nebraskans United for Life banquet. A young twenty-three year-old female college student sat next to me on the flight. She asked me why I was traveling to Omaha and I told her that I was going to give a speech at a pro-life event. I had hoped to share with her a promotional card for my book Abandoned—The Untold Story of the Abortion Wars—as a way to evangelize on the issue of abortion—but I failed to put any of those cards in my coat pocket—and was kicking myself for missing the opportunity to give one to her.
When I was at the banquet I made a point of holding one card back from the table upon which my books were displayed and put it in my coat pocket—just in case I would meet someone on the flight back to Detroit to whom I could give the card. Well—not only did I have the card ready to take back—but two books remained unsold and I said to my Nebraskan host, Ann Marie Bowen (a great lady!) “Let me just take these books back with me since there are only two that will easily fit in my suitcase.”
During the banquet I met great pro-lifers and many of my conversations with them centered on the nationally-known notorious late-term abortionist Leroy Carhart who operates an abortion clinic in Omaha. I spoke with pro-lifers such as Larry Donlan, who are dedicated to keeping a heroic pro-life witness outside of his clinic. Carhart also does late term abortions in Germantown, MD at his clinic Germantown Reproductive Health Services. Not only does Carhart kill the unborn but at least 2 women have died due to complications from the abortions they received from him: Jennifer Morbelli and Christin Gilbert. See link at end of this memo or click here.
The next day I arrived at the Omaha airport for my 8am flight. The airport was de-populated and very quiet, the atmosphere relaxed on this Sunday morning. Eventually my Delta flight to Detroit was called and I got into line for “zone 3” boarding. Suddenly I noticed a gentleman get in line for “zone 2” and my heart nearly burst out of my chest. The man was none other than Leroy Carhart! I said to myself: “Oh, my gosh, I am about to share a flight with one of the most notorious, committed abortionists on planet earth—this is a golden opportunity to say something to him!”
We boarded the plane. Carhart was seated 4 rows behind me on the other side of the aisle. A woman, about the same age sat next to him.
All through the 90 minute flight I prayed that God would give me courage to approach him and that Carhart would be open to listening to me. I rehearsed in my mind what I would say—and now, unlike the flight to Omaha, I was ready—not only with a card about my book—but with actual copies of the book itself! This was no accident. This, as the late Fr. Norm Weslin was fond of saying, was a “divine set up”!
The plane landed. Since I was 4 rows ahead of Carhart I got off the plane before him. Once inside the concourse I quickly unzipped my suitcase, grabbed one of those “unsold” copies of Abandoned—took the promo card waiting in my pocket, slipped it into the book and watched the gate for Carhart to emerge. In a matter of minutes he was entering the concourse with the woman seated next to him on the plane now walking at his side.
He passed right in front of me and I asked stepping forward: “Are you Dr. Carhart?” He immediately stopped. “Yes, I am,” he answered. “Hello, I’m Monica Miller.” Carhart held out his hand to shake mine—and we shook hands. “I want to give you my book.” I handed it to him and he took it without a bit of hesitation. Indeed, it seemed I had caught him completely off guard.
Then I said, “Please Leroy, I want to urge that you leave the business of abortion.”
“Yeah, you and about ten thousand other people.”
We began to walk down the concourse together. It became apparent that the woman with him was none other than Mrs. Carhart. Together Leroy and I entered the moving walkway standing side by side.
“Leroy you can change—I believe you have a heart and a soul that can be reached.”
“Yes, I do, and I believe in God and I am doing his will.”
“Ok, Leroy, I want to understand—I want to understand why you think abortion is justified. I want to understand your view.”
“The fetus is not human until birth,” was his answer.
“So you’re saying that the unborn child has no human or moral status until the baby is born?”
“That’s right.”
The moving walk way ended and we together entered the next one—with his wife tagging behind.
He asked me: “Why do you think the fetus is human?”
“I think science demonstrates to us that the fetus is human—a full human being. What is your basis for believing otherwise?”
“Everything,” was his short non-answer.
“Leroy—when you kill the unborn you are involved in terrible violence and injustice—you need to get out.”
At that point he tried to give me back my book. Indeed, by now what was happening to Carhart had to be an abortionist’s worst nightmare, un-expectantly being confronted by a pro-lifer at an airport—and one who has given him a book no less!
I said, “No, please keep that book, it’s for you. Put it in your suitcase.”
Then I turned to his wife. “You need to encourage your husband to stop killing the unborn—that’s your place, you need to influence him.”
Then Carhart said to me: “You are the definition of insanity.”
At first I wasn’t quite sure to what he was referring. Was I insane because I believed abortion was the killing of innocent human beings? But then I quickly understood his meaning.
“You mean to say that I am the definition of insanity because an insane person keeps doing the same thing over and over again even when there is no result—such as pro-lifers trying to talk you out of doing abortions.”
“That’s right. You’re insane.”
“No. I am not insane. It is not insane for someone to encourage another person to do the right thing.”
Then his wife said to me: “We are more committed to our position than you are to yours.”
I said: “I don’t think so.”
And then—with my book still in his hand, Leroy and his wife ducked into the Delta Sky Club—and disappeared—but not before I was able to tell him: “I am praying for you.”
I remain amazed that this encounter with one of the most notorious abortionists took place. I believe that it was divinely arranged. I find it funny that I was intent on being prepared for a pro-life exchange, 35 thousand feet above the earth—with maybe just another college student. But, instead I would share the divinely arranged flight to Detroit with none other than Leroy Carhart, I would have a copy of my book available to give to him and I actually GAVE IT TO HIM. It seems like a dream.
I pray that he did not simply toss my book into the nearest trash receptacle at the Detroit Metro Airport. Something tells me he didn’t. If for no other reason he kept it out of curiosity. Furthermore, I believe God arranged that I would have a copy of the book to give to this abortionist—and so whatever good may come of my airport meeting with Carhart it is in God’s hands.
I ponder some of the statements that Carhart made to me—such as “The fetus is not human until birth.” I don’t believe Carhart does not know that the unborn are human. What I think he was really saying is that as long as the “fetus” remains in the womb of the mother the “fetus” has no rights. But let’s keep in mind this is a man who once committed partial birth abortions, thus even by his own definition these babies were at least “partially human”!
And indeed, if Carhart who sees up close every day the broken bodies of the innocent unborn really does deny that they are human-then he is the one who suffers from insanity.
Now—you may be wondering why Carhart was on that flight to Detroit. I am absolutely sure, and after talking to pro-life activists in Germantown, MD, that he and his wife, who aids him in the abortion practice, were simply catching a connecting flight to D.C. with their final destination that Germantown abortion center. That Sunday night Carhart would already be prepping his female clients for their late-term abortions.
Most likely Carhart is on that 8am flight out of Omaha, NE every Sunday morning with a stop-over at the Detroit Metro Airport.
Pray for him. And let’s also pray and make sure that Carhart’s wife’s remark is NOT true—“We are more committed to our position than you are to yours.”
by Kelsey Harris | Washington, DC | LifeNews.com | 1/22/14
Today, tens of thousands of people from around the country will gather in Washington to brave the cold for a cause they believe in. Some are marching for the first time, and others have been traveling to the nation’s capital since the Roe v. Wade decision in 1973. For the 41st year, they’ll meet again for the same reason — the sanctity of life.
We’re also celebrating life today, and we hope you will, too. Here are 19 moving reminders of the beauty of new life:
Learn more: “How to Speak Up for Life,” produced by Heritage in collaboration with Alliance Defending Freedom, Americans United for Life, Concerned Women for America, Focus on the Family, March for Life Education and Defense Fund, and the Susan B. Anthony List Education Fund
Yesterday hundreds of thousands marched on Washington DC for the Right to Life in the United States. This year marks the 41st anniversary of the Roe v. Wade Supreme Court decision to legalize abortion in every state in the United States. Since Roe v. Wade went into effect on January 22nd, 1973, more than 56 million human beings have been killed by abortion in the United States.
In the United States today, there are…
1.382 million Abortions every year
115,167 Abortions every month
26,577 Abortions every week
3,786 Abortions every day
157 Abortions every hour
2.6 Abortions every minute
The Pro-Life movement has not yet succeeded in reversing Roe v. Wade, but the Pro-Life movement is stronger than ever, even 41 years later.
This year One More Soul gave some people who attended the March for Life a short questionnaire. We wanted to know their personal reasons for attending the march in their own words. We will post their answers here and report how the annual March for Life changes lives.
Our mission is to encourage people to welcome “One More Soul”. Please consider to make a donation to One More Soul to continue to be a voice for the culture of life.
Wednesday, 22 January 2014, marks the 41st anniversary of the Supreme Court’s Roe vs Wade and Doe vs Bolton decisions legalizing the killing of pre-born children in America. Trent Horn is an appropriate Guest for this week’s “The Quest for a Culture of Life in America” program.
Trent holds a Master’s degree in Theology from the Franciscan University of Steubenville and is currently an apologist and speaker for Catholic Answers. He specializes in training pro-lifers to intelligently and compassionately engage pro-choice advocates in genuine dialogue. He is the author of Answering Atheism and Making the Case for Life (DVD), both published by Catholic Answers.
Making the Case for Life is a very valuable teaching tool for transforming any abortion debate into a fruitful conversation–one that opens minds and hearts to the humanity of the pre-born child while maintaining a non-confrontational environment. Trent’s approach has been developed by refining ideas of seasoned pro-life leaders and applying them with hundreds of college students. Please listen at NOON ET, 9:00 am PT, at radiomaria.us or on your local Radio Maria station. You will be better prepared to engage–without rage–family, friends and strangers in discussing America’s most divisive issue.
Blessings to all.
Steve Koob,
Director One More Soul, and Host for
“The Quest for a Culture of Life”
PS I thank all of our listeners who made end-of-year donations to Radio Maria and One More Soul. You have given us a running start on the New Year. We are very grateful!
Every month, we will post a quote about why babies, children, and new lives are a wonderful, beautiful blessing. We hope that, one positive quote at a time, we can change our society’s attitude towards children. If you like the quote, please post it on facebook, tweet it, pin it, or email it to your friends and family. We hope that, one message at a time, we can change peoples’ attitude towards having another child and children in general.
‘It’s a beautiful time’: 9-months-pregnant ballerina is breathtaking
Dec. 19, 2013 at 3:31 PM ET
At nine months pregnant, Mary Helen Bowers is dancing a lovely pas de deux with her unborn baby.
The former ballerina glows in photos and videos showing her twirling, stretching and moving to the music, her baby bump along for the ride. She has chronicled her growing body on her Instagram account, balletbeautiful.
“I just love knowing that when I’m dancing, the baby is dancing,” Bowers, 33, told TODAY Moms. “It’s just been awesome to know there’s this little life that’s sharing in everything you do every day.”
With her doctor’s approval, Bowers has been dancing and working out right until the last days of her pregnancy. She’s due to give birth next week.
Noting she’s been lucky to have a very healthy and comfortable pregnancy, Bowers said the most important thing she has done is listen to her body throughout the process. During her first trimester, she still felt like she could do almost everything, but she soon started to modify her dancing to accommodate her growing belly.
How does she balance with all that extra weight in the front?
“It’s not everything that it was,” Bowers admitted with a laugh. But she said she’s always paid great attention to having a good posture and focusing on her core, which has allowed her to maintain lots of control over her body.
“I feel like that’s really helped me with my balance and helped prevent back pain and a lot of other aches and pains that are really common with pregnancy.”
Bowers spends most of her day in a leotard and tights. “I’ve really been amazed by how active I’ve been able to be and how much my body has been able to do,” she says.
The dancer has also embraced watching her body change, noting she spends most of her days in a leotard and tights so there’s really no hiding a bump.
Bowers, who danced with the New York City Ballet for 10 years and helped train Natalie Portman for her role in “Black Swan,” now owns Ballet Beautiful, a New York fitness company designed to help regular women get a dancer’s lean and toned physique.
She’s also developed a prenatal workout, which she hopes will help women in the same way her dancing routine has helped her. “I’ve really been amazed by how active I’ve been able to be and how much my body has been able to do,” Bowers said.
“It’s a beautiful time. You feel connected to your body on a level like never before.”
by Steven Ertelt | Oakland, CA | LifeNews.com | 12/30/13 8:39 PM
The judge who is adjudicating the case of Jahi McMath has granted an extension for life support after a legal request from her family’s attorney.
A county judge extended the order for Oakland-based Children’s Hospital to keep Jahi McMath on life support until 5 p.m. on January 7. Her mother and family say she is alive following a tonsillectomy gone awry that has left her in an incapacitated state since early December.
“The family has located a licensed facility in the state of New York which has agreed to take Jahi,” Jahi’s uncle, Omari Sealey, said Monday afternoon, only about an hour before an Alameda County judge’s order keeping the girl on a ventilator was set to expire. “We have contracted with an air ambulance willing to take her from door to door. We have a doctor here in California who will be with her throughout the transfer.”
Sealey said Jahi has been responsive to her mother’s voice.
“Jahi is moving when her mother speaks,” he said. “We have video our attorneys have just produced it to the hospital’s attorney. We have a pediatrician who has seen Jahi who has sworn that she is not dead. We are hopeful that one of these (legal) actions will forestall the hospital’s rush to extinguish Jahi’s chance at life.”
Meanwhile, just three hours before the deadline today for removing her life support, the girl’s grandmother, Sandra Chapman spoke to the media and suggested Jahi was moving her body, saying there was leg and body movement as well as response to touch and voice.
“I know one’s [an alternative care facility] gonna come through. I know it. I feel it. Jahi’s moving. If she’s moving, the doctor should pay attention to that,” she said.
Jahi McMath’s family had found a new care facility that will continue her medical care and treatment. But the hospital she is at now won’t cooperate to move her.
A judge had ruled that a hospital in Oakland, California can remove life support from Jahi McMath, 13, who has been declared brain-dead days after undergoing surgery to have her tonsils removed. Her family is already devastated enough but has had to fight the hospital, which wanted to take her off life support against their wishes.
On Thursday, the lawyer for the family, Christopher Dolan, asked Children’s Hospital of Oakland to cooperate by performing a few procedures needed to move Jahi McMath. The hospital said no.
The Los Angeles-area long-term care facility that had been willing to accept Jahi has withdrawn its offer, leaving a New York hospital as the only apparent option for. That is happening as a deadline of 5 p.m. today reaches, whereby the hospital will officially cut offer her life support.
“I just found out that the facility my daughter was supposed to be going to has backed out! Children’s hospital has once again interfered with the placement of my daughter we still have a chance at 1 more facility so let us all pray,” family member Latasha Nailah Winkfield said.
The San Jose newspaper has more on this teenager’s case:
“I just found out that the facility my daughter was supposed to be going to has backed out,” Jahi’s mother, Nailah Winkfield, wrote on the family’s fundraising website early Sunday. “My family and I are still striving to find a location that will accept her in her current condition.”
That leaves an unnamed New York hospital “as our last, last hope,” Jahi’s lawyer, Christopher Dolan, said. The facility is run by an “organization that believes in life,” Dolan told The Associated Press.
But in a statement issued Sunday, a spokeswoman for Children’s Hospital Oakland said its doctors said no one from any other medical organization has been in contact with it to discuss a transfer of the 13-year-old.
“Our physicians have yet to receive a single call or message from the facility under consideration,” Cynthia Chiarappa wrote. “We have been waiting since Friday — when we were first told by the family lawyer of a potential facility that might accept the body of Jahi — for a call from a physician to discuss with our medical staff what may be necessary to transfer the deceased.”
Dolan said the unnamed Los Angeles-area facility withdrew its offer because it didn’t want media attention or to jeopardize its relationship with its doctors, who refused to treat someone who’s been declared brain dead.
As Jahi’s family prepared for a Sunday afternoon fundraiser at an Oakland church to help pay for a possible airlift, it remained unclear what will happen in the hours ahead.
Doctors at Children’s Hospital have refused to perform a tracheotomy for breathing and insert a gastric tube for feeding, procedures that are needed in order to transfer Jahi, saying it is unethical to perform surgery on a deceased person.
Jahi arrived at the hospital on a Monday and was supposed to be released Tuesday, the family said.
A member of Jahi’s family , a veteran nurse at Kaiser Permanente in Oakland, noticed her granddaughter was bleeding from her mouth and nose. She later went into cardiac arrest. Jahi spent Tuesday on a ventilator. By 2 a.m. Wednesday, doctors said she had swelling in her brain, and Thursday, she was declared legally brain-dead, family members said.
Judge Evelio Grillo ruled that Jahi must be kept on the breathing machine until at least 5 p.m. December 30. The verdict came after hearing testimony from two doctors, one an independent expert appointed by the judge on Monday and the other a 30-year veteran of the hospital. Both testified that the teen is brain-dead and that her body is alive only because of a ventilator hooked up to her since December 12.
The family has appealed the decision but pro-life attorney Wesley Smith said it is unlikely they will prevail.
“The judge gave the family, still fighting the determination, until Monday to appeal or adjust to the tragic reality,” he said. “I hope the family spends the remaining time loving Jahi and making preparations, as there is zero chance in my view that the court’s ruling will be overturned on appeal. If a miracle is to happen, it will have to be when the breathing assistance is removed. People who are brain dead have no ability to breathe on their own.”
“It’s also a shame the hospital has handled the tragedy so maladroitly. I was speaking about this to a former pediatric nurse who used to work in Children’s Hospital Oakland’s ICU. She said the facility has a real calling to serving the African-American community, and this has hurt trust. That’s why I was upset to hear a hospital spokesman say he was “gratified” that the court validated the hospital’s diagnosis,” Smith continued. “No, the proper and decent thing would have been to say that they were sorry the original diagnosis was affirmed. Good grief.”
by Rebecca Taylor | Washington, DC | LifeNews.com | 1/1/14
This e-mail from a reader broke my heart. It is a cry for help from a young IVF-conceived woman who mourns the loss of her siblings that didn’t make it. It is also a look at the darker-side of IVF that no one wants to talk about: the massive loss of life inherent in the IVF process.
She writes:
I was wondering if you knew of any websites or resources that support people struggling after being conceived using IVF. I’ve been searching and searching online, and I’ve been unable to find a single source of advice.
I was one of three embryos created in the process, but I was the only one who survived. I mourn my siblings every single day. I can’t talk about them with my parents, because bringing the subject up inevitably causes fights, and they don’t feel the way I do. They don’t regret what they did, they don’t see anything wrong with IVF, and they don’t count my siblings as members of the family.
They never bring them up in conversation, and when I talk about them, they’ll concede that they are my siblings, but it’s only to make me feel better. I don’t think they really believe it. If they did, they’d regret what they did. When people asked how many children they had, they’d say three. They’d talk about them as members of the family, and say how much they wished they could be there at Christmas and birthdays. My mum would light candles for them at church and have Masses said for them. But it’s just me. I’m the only one who seems to care about them.
It hurts me every time I see in the news something about IVF, because the media treats it as if it’s okay. There’s never any mention that people die during the process. I don’t even know if there’s anyone else out there who feels the same way I do. If there is, I’ve never met them. Sometimes, I feel like a freak. The only person I’ve found who understands me at all is my local priest, who I’ve spoken to about everything, but I can’t be bothering him all the time! It’d be nice to have someone else who understood.
The support groups I know of are for those conceived with donor gametes. I do not know of any support groups for those conceived with IVF without donor sperm or egg.
Does anyone know of a group that could help this young woman? Her pain is very real and she needs others who can understand what she is feeling.
Contact Rebecca: rhtaylor@marymeetsdolly.com
ROME, December 30, 2013 (LifeSiteNews.com) – Pope Francis piqued the curiosity of many members of the faithful in his November 24th exhortation, Evangelii Gaudium, when he said national bishops’ conferences should be granted “genuine doctrinal authority” as part of his effort to reform the papacy and decentralize authority in the Church.
The idea raised concern for many Catholics, including those active in the battle for life and family, who expressed misgivings about giving more authority to institutions that, in many countries, have often been used to undermine the Church’s teachings on life and family issues.
Now the Pope’s prefect of the Congregation for the Doctrine of the Faith has weighed in on the issue. Archbishop Gerhard Ludwig Müller says that while the conferences can exercise a certain doctrinal authority – in preparing local catechisms, for example – they exist to serve individual bishops and will never act as an intermediary between bishop and pope.
In an interview with the Italian daily Corriere della Serapublished December 22nd, Archbishop Müller said there is no such thing as “national churches,” and the president of a bishops’ conference cannot be a “vice-pope.”
“Some interpret Evangelii Gaudium as if the Holy Father wants to promote a certain autonomy of the local churches, the tendency to distance themselves from Rome,” he said. “But this is not possible. Particularism, like centralism, is a heresy. It would be the first step towards autocephaly.”
The papacy and the role of bishop are “by divine right, instituted by Christ,” but the bishops’ conference, he said, “both historically and today, belong only to the ecclesiastical law,” which he noted is a “human” creation.
“The presidents of the episcopal conferences, while important, are coordinators, nothing more, not vicepopes!” he said. “Each bishop has a direct and immediate relationship with the Pope.”
A “decentralization” of power to the conferences would only create a new centralization, he said, in which the conference president “has all the information and the bishops are inundated with documents without time to prepare.”
In a paragraph of his exhortation, Pope Francis spoke of the need for a “conversion of the papacy” and the way in which papal primacy is exercised. In particular, he said there was a need to better elaborate “a juridical status of episcopal conferences which would see them as subjects of specific attributions, including genuine doctrinal authority.”
“Excessive centralization, rather than proving helpful, complicates the Church’s life and her missionary outreach,” he added.
However, bishops conferences have often been criticized for harboring dissidents or being used to try to silence strong episcopal voices in the name of ‘collegiality,’ and producing statements that are vague, confusing, or even misleading.
One of the most famous examples is the Canadian Conference of Catholic Bishops’ 1968 Winnipeg Statement, which dissented from Humanae Vitae’s prohibition of contraception by claiming that Catholics could use contraception in “good conscience” provided they had “tried sincerely” to obey Church teaching.
Most recently, the German bishops’ conference has been embroiled in controversy after signaling that they would allow Communion for some Catholics who are “remarried” despite an existing Catholic marriage.
Many fear that increasing power at the conferences could undermine the efforts of outspoken bishops within their dioceses, and increase the tendency for bishops to yield their proper authority to the conference.
In the lead-up to the 2008 U.S. election, Bishop Joseph Martino, then the ordinary in Scranton, was forced to intervene when a liberal Catholic group at a parish used some vague lines from the USCCB document Forming Consciences for Faithful Citizenship to justify voting for a pro-abortion candidate. “No USCCB document is relevant in this diocese,” the bishop said, noting that he had produced his own pastoral letter insisting that Catholics must vote pro-life.
Perhaps the most incisive criticism of modern bishops’ conferences was offered by Pope Benedict XVI himself before his election.
In The Ratzinger Report, his 1985 book-length interview with journalist Vittorio Messori, Cardinal Ratzinger explained that while the Second Vatican Council sought to restore the role of individual bishops, in practice the post-Conciliar period saw a reduction of their role because of the greater emphasis on the conferences.
“The decisive new emphasis on the role of the bishops is in reality restrained or actually risks being smothered by the insertion of bishops into episcopal conferences that are ever more organized, often with burdensome bureaucratic structures,” he said.
Echoing Müller’s observation that the conferences are of human origin, Cardinal Ratzinger said they “have no theological basis, they do not belong to the structure of the Church, as willed by Christ, that cannot be eliminated; they have only a practical, concrete function.”
“No episcopal conference, as such, has a teaching mission: its documents have no weight of their own save that of the consent given to them by the individual bishops,” Cardinal Ratzinger added.
To what extent Müller’s view reflects that of Pope Francis, and to what extent it will impact the discussion going forward, is unclear.
The prefect made similar remarks at the end of September, days after Pope Francis confirmed him in his post.
Bishops’ conferences lack “a teaching competency over and above the authority of individual bishops,” he said, according to The Tablet. “They are not a third authority between the Pope and the bishops. So I don’t think we will see a sort of federalist reform similar to that in the Federal Republic [of Germany] where key competences are relayed from the central state to the individual states. That is not how the Church is constituted!”
COMBERMERE, December 25, 2013 (LifeSiteNews.com)–Amid all the joyful bustle of family preparations in anticipation of the holy day of Christ’s birth, Christmas time always brings to my mind the deep regret that I feel over the one child my wife and I lost due to miscarriage, because it reminds me that at the time I was like the Bethlehem innkeeper who said there was no more room.
I was having a lot of trouble accepting that my wife was pregnant with our ninth child. It’s not that we were against having children–we had eight boys already–but when Theresa told me she was pregnant again, something inside me rebelled against the thought of another baby.
You know: “Oh no, another mouth to feed; our house is too small, and full to the rafters, literally, with kids; we’ll have to build an addition; we can’t afford this; I’m already the brunt of tacky jokes (don’t you folks in the country having anything else to do?); I can’t take this…there’s just no more room!”
You can see where this was going–from a lack of trust in God’s purposeful generosity, to a miserly outburst of selfishness.
Most of Theresa’s pregnancies were planned, some were surprises, and although much to my later shame I once added my name to a “zero population growth” petition while at university (ah, how foolish I was when I was young!), we welcomed each baby as he came along.
And when things got out of hand, as things with piles of children often do, I reminded myself that they were, after all, God’s children first, and given to us to look after the best we could for really only a short while, if you consider the reality of eternity.
But with this pregnancy something in me didn’t rejoice.
I worked myself up to such a state of negativity that I began saying “Why me Lord?” while I brooded over the new life that was growing in Theresa’s womb with misgiving rather than hopeful expectation. “Isn’t eight enough Lord? How could You do this to me?!”
Then without warning–Theresa was always so healthy when she was pregnant–I got a call while at work that Theresa was taken to the hospital, bleeding.
The next days were a blur of frantic prayer, tears, uncertainty and dread, and then the final reality that we had lost him. We named him Stephan.
In the midst of trying to be strong and supportive for Theresa in our grief, I was overwhelmed with guilt. It seemed to me that my lack of acceptance of Stephan was the cause of his death–like God saying, “You don’t want him? Okay, I’ll take him back.”
We buried Stephan’s remains (there wasn’t much, he was in the first trimester) in a garden behind our home where we have a statue of Our Lady, and planted a rose bush over him.
Then God in His mercy let something change in me again.
Through the tears of sorrow and guilt I began to understand the reality of the wondrous, almost unimaginably generous gift from God that every child is.
A gift that is given to parents to love and nurture and enjoy, certainly, but also a gift to all of humanity in that the future is held in the tiny hands and minds and souls of the children that parents, with God’s help, bring into the world.
Of course with such an awesome gift also comes an awesome responsibility, and God never said raising children was supposed to be easy.
I sometimes ponder on God’s judgement of me when I die, and always come round to a scenario where the Lord looks at me with love and compassion, and then says, “Lets talk about how you did with the children I gave you…”
I have come to a deeper understanding that God does in fact give us exactly what we need, just when we need it, to live out the responsibilities that we have. But implicit in this is TRUST.
The reality finally dawned on me that there is always room for one more child, because if we trust in God’s providence, then we trust that He will give us the grace we need to persevere. A wise man once described this as the “grace of state” we are freely given and can freely accept, simply by virtue of being parents, and trying to live out God’s will in our lives.
Every child conceived is loved into existence by God and wanted by God, even if we choose not to want that child.
What changed in me after Stephan’s death was that I felt a grateful joy the next time we were pregnant that was somehow so much more profound than anything I had experienced before. I knew our little Stephan was praying for me in heaven, and I knew that however many children God sent us, we would always have love and room for them.
After Stephan we were blessed with four more wonderful sons, and two absolutely gorgeous daughters. We are also now blessed by 32 grandchildren with one more on the way, so far…
So now when we gather for Christmas at home we are always packed to the rafters, but unlike the inn in Bethlehem, there is always room for one more.
Dear friends of LifeSiteNews, I wish you a very merry and blessed Christmas. May this joyous season of Jesus’ birth be a time of wonder and renewal for all of us.
May I offer you a Christmas gift of a prayer, adapted from “Blessing Prayers: Devotions for Growing in Faith” by Fr. Peter John Cameron, O.P., that speaks profoundly of Christ’s coming to us as a baby born in a stable and the Father’s love and care for us all:
O Emmanuel,
may the assurance of your unfailing Presence
be for me the source of unending peace.
May I never fear my weakness, my inadequacy, or my imperfection.
Rather, as I gaze with faith, hope, and love upon your incarnate littleness,
may I love my own littleness, for God is with us.
Endow my life with a holy wonder
that leads me ever more deeply into the Mystery of Redemption and the meaning of my vocation and destiny.
May I make of my life a total gift of self.
May my humble worship of your Nativity
manifest how much I seek the Father’s Kingship
and his way of holiness.
The beauty of your holy face bears the promise
that your Father will provide for us in all things.
This Christmas, I renew my trust
in God’s goodness, compassion, and providence.
Ted Baklinski is a Canadian-based reporter for LifeSiteNews.com.
Steven W. Mosher, Weekly Briefing, 23 December 2013
Last week, Russian President Vladimir Putin signed a law banning abortion advertising. Some members of the Duma (the Russian state assembly), are talking about going even further and banning the procedure itself. The Russian Orthodox Church, whose numbers are swelling with converts and “reverts,” is weighing in as well. One Orthodox prelate called abortion a “mutiny against God.” I couldn’t have put it better myself.
This is an amazing turn about in a country which has long been known for its tragically high abortion rate. Until recently, the average woman in Russia could expect to have seven abortions over her lifetime. Even The New York Times, no bastion of pro-life sentiment, has been compelled to acknowledge that Russia’s high abortion rate was damaging the health and fertility of Russian women. As the paper noted in a 2003 editorial, “Now the Russian government is attempting to slow the abortion rate. It is an admirable goal, given the toll that multiple abortions have taken on the health and fertility of Russia’s women.” Not to mention the toll that abortion has taken on the unborn, and on the population as a whole.
Abortion was forced on the Russian people by the Bolsheviks (the Russian communist party under Lenin), who upon coming to power in 1920 legalized abortion up to birth without any restrictions. Their goal was to destroy the family by encouraging women to get abortions, get out of the home and into the workforce. Russia was the first country in the world to declare war on the unborn in this way. Of course, with its purges, mass executions, and Gulag it warred on the unborn in other ways as well.
In fact, it was the early Bolsheviks who developed the suction abortion machine that is still in use in abortion clinics today. They actually developed two versions. The first was the electric suction abortion machine used in abortion clinics in the U.S. and other countries. The second was the manual vacuum aspirator, a hand-held and operated abortion machine that is used in less developed countries in places where no electric power is available.
PRI has played a role in helping to turn Russia back to life. I participated in the first Demographic Summit at the Russian State Social University in Moscow in May, 2011. We talked with senior Russian leaders about the need to protect life. Not long thereafter, a law was passed banning abortion of unborn babies older than 12 weeks. It also mandated a waiting period of 2-7 days for those wanting an abortion, and required that anyone advertising abortion services include a warning to the effect that “abortion is hazardous to a woman’s health.” Now, of course, advertising of any kind has been banned.
Taken individually, each of the laws put in place by the Russian government has a fairly small demographic impact. The Russian government, for example, pays a one-time baby bonus of $13,000 to the parents of every newborn. According to Russian demographer Igor Beloborodov, however, this generous bonus has only convinced 8 percent of couples of reproductive age to consider having another child.
The cumulative effect of all of the pro-life, pro-natal policies taken to date is far more significant. While there are still, according to the Russian Health Ministry, 1.7 abortions for every live birth in the country, that ratio is shrinking as the birth rate climbs and abortion becomes gradually less common.
As a result of the adoption of enlightened policies to protect the sanctity of human life, Russia’s population decline has been virtually halted, and the country has been put on a more stable demographic course.
Russia’s demographic winter is not yet over, but there are signs of a spring thaw.
VATICAN CITY, December 16, 2013 (LifeSiteNews.com) – The extraordinary healing of a baby inside his mother’s womb has been declared medically “unexplainable” by top Vatican doctors, putting Pope Paul VI one step closer to being declared a saint by the Catholic Church.
Seventeen years ago, doctors in California offered a woman abortion as the only possible solution for the abnormality detected in her unborn baby, whom they diagnosed with serious problems that they said would result in severe brain damage, Vatican Insider reports.
Instead, the woman chose life, entrusting herself and her baby to God through the intercession of Paul VI, whose papacy ended with his death in 1978.
Pope Paul VI, born Giovanni Battista Montini, is most famous for his 1968 watershed document Humanae Vitae that upheld the long-standing Christian teaching against contraception. In the same document he also condemned “willed and procured abortion” for any reason.
To the doctors’ amazement, the woman’s baby not only made it to term, but was born without a single one of the predicted health problems.
The family was told to wait until their child was 16 – having passed puberty – before a confirmation of complete healing could be given. The child, now 17, is completely healthy.
The Medical Commission of the Congregation for the Causes of Saints, chaired by Dr. Patrizio Polisca – Benedict XVI and Francis’ personal doctor – has declared the healing authentic and inexplicable.
Benedict XVI approved the “heroic virtue” of Paul VI a year ago on December 20, the first of three steps in the canonical process of declaring someone a saint.
Fr. Antonio Marrazzo, C.Ss.R., who heads Paul VI’s cause, told Vatican Radio last year that all the evidence of the baby’s healing in utero points to a “truly extraordinary and supernatural event”.
“This healing fits in with Montini’s way of thinking,” he said.
LifeSiteNews.com contacted Marrazzo for comment but did not hear back by press time.
If the alleged miracle passes the scrutiny of theologians, cardinals, and the pope, then Paul VI will become beatified and recognized as a Blessed. A second miracle is required before he can be canonized (declared a Saint).
Paul VI’s beatification is expected within months, reports Vatican Insider.
“An unjust man is an abomination to the righteous, but one whose way is straight is an abomination to the wicked.” Proverbs 29:27 ESV
Webster defines the word “abominable” to mean “causing moral revulsion.” Yesterday I had an opportunity to sit down during a lunch break, one-on-one, with Peter Singer the DeCamp Professor of Bioethics at Princeton University and one of President Obama’s elite advisors for Obama Care. He is someone who openly declares the Christian worldview to be “abominable”. In fact I have spent my weekend with an entire body of scholars and left leaning world leaders in public policy . . . who openly declare Christianity to be the single most pervasive problem they face. I was not prepared for the number of presenters at an animal rights symposium who spoke to the theological underpinnings of my own “abominable” worldview.
I am here at Yale University for the last day of the “Beyond Human Personhood” Symposium. As National Field Director for Personhood USA, I was asked by my superiors to attend to see if I could garner any insight in how a leftist worldview approaches the effort of convincing our culture to accept personhood for non-human actors such as: elephants, dolphins, great apes, artificial intelligences and extra-terrestrials.
I was a little surprised to find a modicum of common ground as I observed their intense passion to promote their worldview. I can admire their sacrifice and commitment to what they hold as the true nature of things. I was wholly unprepared for the moral revulsion I felt as they described their overall agenda. They openly admitted that their goal is to “animalize” mankind as just another animal in the zoo we call earth. Their godless evolutionary pre-suppositions demand this. “Speciesism” was mentioned quite often—rightly accusing the Christian worldview of elevating all mankind as being “created in the image of God” and setting man apart from the other creatures of earth by placing all of God’s creation under mankind to act as steward “over the garden”. Countless speakers decried human exceptionalism” and Christianity’s role in promoting a worldview that demoted animals to a status under man’s “dominion.” As I mentioned earlier, I was struck by the sheer number of references to the early church fathers and various quotes from Christian theologians. This was a crowd who knew their church history and had made a conscious decision to reject the good news of Christ’s incarnation, death and resurrection for our soul’s sakes. And yes . . . there was a discussion on ensoulment and the fact that Christians denied ensoulment to non-humans. Again, I want to emphasized how unprepared I was to encounter such a high level of theological content, not to mention that it was all directed at me.
At first I thought that surely there were those in the audience that might question some of the presuppositions that were being openly proclaimed, perhaps a philosophy student with an inquiring mind who could connect the dots—particularly in the area of relegating man to the same level as other animals, thereby denigrating human life and dignity. Sadly, I didn’t find a single individual in a crowd of a 100, who spoke out against the obvious policy implications that these ideas proposed.
Singer delivered the keynote in the opening session of the symposium. In it he stated that there were a number of innate characteristics that were inherent in any being who was a candidate for attaining personhood.
They include:
Cognitive or phenomenal capacity (ie. Can it experience pain?)
Intentionality of action (free will)
The capacity to plan for the future
Self-awareness
Self-recognition
Self-interest
It should be obvious from this list that many classes of human life do not meet all of these criteria. For instance, those who are temporarily comatose or misdiagnosed as being in a persistent vegetative state, those who have temporary or progressive stages of dementia, Alzheimer patients, some with mental or developmental disabilities, the pre-born, post birth children suffering a congenital anomaly, and yes . . . even perfectly normal children thru 18 months post-birth. These classes were not inferred, they were openly acknowledged! They allege that personhood can NOT be assigned to these classes of human life.
This will have a profound impact on public policy, particularly in the area of denial of healthcare under Obama Care. The presenters in the symposium were not just “post-Christian” they were “anti-Christian” in their formulation of a future utilitarian philosophy that would deliver “the greatest good to the greatest number” by eliminating what Germany in the 1920’s labeled “useless eaters”.
I have always wondered if our side wasn’t succumbing to a certain amount of hysteria when it came to denouncing our pro-death opponents by ascribing to them certain extreme positions. I had the perfect opportunity to find out for myself. I approached Peter Singer after the very large crowd of his admirers had left with signed copies of his books. I note that he is well-loved and acknowledged by all academically as the “father” of the animal rights movement. He is a noted world leader in bioethics. The sheer presence of so many academic heavyweights was very intimidating. I introduced myself as the National Field Director for the largest Christian “Speciest” pro-personhood group in the nation . . . Personhood USA. I had his immediate attention. I asked if we could sit down at some point in the conference . . . I wanted to ask him a few questions. He was very gracious and said he would like to. He understood that I did not intend to debate his position, rather I wanted to verify his policy objectives firsthand. He suggested we meet the following day during the lunch break, somewhere private, so that we could discuss our positions freely.
Given the same opportunity, what questions would you ask Peter Singer? I prayerfully asked God’s leading in this matter. I am not at all certain that I succeeded.
Due to another conversation with the head of the Trans-humanist movement in America, I came into the lunch area a little late. Singer was already seated at a table with a large number of admirers who were seeking his wisdom and encouragement. I ate my lunch alone. He saw me standing over against the wall, and good to his word, he excused himself from the group and made his way over to where I was standing. He said, “Daniel let’s go find somewhere where we can talk.” As we were seated, I thanked him for granting me this opportunity to get beyond the myth to the man himself. I began by restating his criteria for personhood from the previous evening’s talk and asked him if he was intentional in excluding certain classes of human life. He said he was. He reemphasized that mankind is not exceptional. I stated that the ultimate goal of Personhood USA was the legal recognition of human personhood and asked, “Was not the legal recognition of non-human personhood ultimately the goal of his movement”? He agreed that it was. I stated that “Ideas have consequences”, and he replied, They certainly do.” I continued, “Would you agree that your definition of personhood diminishes and devalues human life and dignity and could have profound implications on healthcare policy? That it might lead to rationing and denial of service for those classes he has identified as non-persons under Obama Care?” His response was that it is already occurring and that reform is needed all across the healthcare system. That his definition of personhood would provide a consistent universal ethic for all of earth’s animals.
My final question was that given human nature, my greatest fear was that even if I granted him his definition of personhood with its immediate healthcare policy implications, what would prevent those classes of human life being extended to other classes – the traditional slippery slope argument. He said, “Our open society would self-police the issue and I am fine with the process.” He thought that our democratic process would prevent abuse. I then invoked history. I said, “A decade before the Nazis came to power, Germany’s open society advocated for some of the same ends that you have advocated. Within a decade the litany of killing useless eaters had expanded to the mentally ill, blind deaf and dumb children, gypsies, Christian leaders and Jews.” At that point Godwin’s law kicked in. Godwin’s law states that whoever brings Nazism into a discussion is automatically conceding their point in desperation . . . no matter how appropriate the analogy is. He strenuously objected and replied that the society in Germany was not a free society and couldn’t be responsible for Nazism’s extremes. I replied that it was free enough. That the parents of blind children who were exterminated under the guise “of the best medical care Germany could offer”—these same parents who received an urn of ashes when their children were said to have suddenly succumbed to some deadly disease—rose in public outrage against Hitler and put enough public pressure on him to end the “T4 Action” program in 1941. I stated that this was my greatest fear with his position and that once the sanctity of life was demolished as a cultural anchor that the legal protections of personhood, being redefined and lowered to include animals, would deliver a new human holocaust. He didn’t disagree, he merely restated his position with all of its implications.
My goal at the symposium was to stay under the radar and observe where these non-human personhood proponents were coming from—to discern their underlying presuppositions and to see them as persons and not the enemy. I was not there to argue because scripture indicates that you “answer not a fool according to his folly, lest you be like him.” Alas I failed. For probably the first time in my life it was not my mouth which got me in trouble . . . it was my feet! I had noticed a large number of tennis shoes among this otherwise very well dressed crowd, but had just assumed that it was the standard uniform for preppy liberals. My feet were shod in black “cow’s skin”! It was a dead give-away. I (and my footwear) was an abomination in their midst.
Dan Becker is President of Georgia Right to Life and Field Director for Personhood USA
See more at: http://www.grtl.org/?q=node/449#sthash.dTJtJWHp.dpuf
por Dr. Rebecca Peck, Dr. Benjamin Peck
Fr. Juan R. Vélez, MD (Ex Internista)
Actualizado por Liliana Cote de Bejarano, MD, MPH
Los anticonceptivos orales (y todos los demás anticonceptivos hormonales para el control de la natalidad) son utilizados habitualmente para prevenir el embarazo, aunque a veces se prescriben para tratar otras condiciones médicas. Los anticonceptivos hormonales pueden causar muchos posibles efectos adversos de tipo médico, social y espiritual. La gran mayoría de las recetas de anticonceptivos hormonales son dadas por los médicos a mujeres sanas, a veces a adolescentes sin enfermedad conocida. A algunas mujeres se les prescriben anticonceptivos hormonales para el control de la natalidad, por una sencilla razón—para impedir una condición completamente normal: el embarazo.
Dado que todos los medicamentos tienen potencialmente efectos secundarios no deseados, algunos de ellos graves, es importante que los médicos sopesen los riesgos y beneficios cuando se prescribe algún medicamento. De ello se deduce que no es ético exponer mujeres sanas a riesgos para la salud a fin de evitar una situación normal. El error de exponer las mujeres a estos riesgos es todavía peor dado el hecho de que otros métodos de planificación familiar existen, como la Planificación Natural de la Familia (PNF), los cuales no tienen efectos secundarios.
Como médicos, nosotros no prescribimos anticonceptivos hormonales para el control de la natalidad. Las razones médicas para esta decisión son las siguientes:
Los anticonceptivos hormonales tratan la fertilidad de la mujer y la maternidad como una enfermedad
Aunque puede haber razones legítimas de índole médica y personal para evitar el embarazo, la fertilidad femenina y la posibilidad del embarazo en sí no son una enfermedad, y por tanto no necesitan “tratamiento” con una pastilla (un parche, una inyección, o un DIU).
Los anticonceptivos hormonales causan abortos
Cuando los anticonceptivos orales no suprimen la ovulación en una mujer sexualmente activa y otros mecanismos que impiden la fertilización fallan, puede ocurrir la concepción. Los anticonceptivos hormonales interfieren con la implantación de un nuevo ser humano mediante la reducción del grosor del revestimiento del útero, y alterando moléculas y factores relacionados con la implantación. 1
Las dosis bajas de anticonceptivos hormonales impiden la liberación del óvulo femenino solamente en un 65-75% de los ciclos. 2,3 Por esta razón, si una mujer tiene relaciones sexuales en su periodo fertil es posible que en aproximadamente un 30% de sus ciclos suceda un embarazo y posteriormente un aborto químico.
Los anticonceptivos hormonales contribuyen a una mentalidad anti-vida
Los anticonceptivos hormonales como la Píldora, el parche, el DIU o la Inyección, sustentan la práctica del aborto. La gente inconscientemente concluye: “Si fracasa el control de la natalidad, el aborto es la solución.” Una encuesta a nivel nacional en los Estados Unidos indicó que el 54% de las mujeres que tuvieron un aborto estaban utilizando anticonceptivos el mes anterior.4
Los anticonceptivos hormonales aumentan el riesgo de cáncer de seno
Las mujeres se enfrentan a un mayor riesgo de desarrollar cáncer de seno, cuando usan anticonceptivos hormonales, y este riesgo continua por lo menos diez años después de que dejan de usar hormonas anticonceptivas. Según un estudio publicado en la revista New England Journal of Medicine el uso de anticonceptivos hormonales durante 10 años aumenta el riesgo de cáncer de mama en un 38%. Además, el estudio mostró que los DIU que liberan hormonas también aumentan el riesgo de cáncer de mama.5 Si la Píldora se toma por cuatro años antes de que la mujer de a luz por primera vez, hay un incremento del 52% en el riesgo de cáncer de seno.6
Un análisis de múltiples estudios señaló que 21 de 23 estudios retrospectivos mostraron un mayor riesgo de cáncer de seno premenopáusico en mujeres que tomaron anticonceptivos orales antes del nacimiento de su primer hijo.7
Los anticonceptivos hormonales aumentan el riesgo de trombo-embolismo pulmonar
Un estudio de 1524 pacientes en los Países Bajos, llegó a la conclusión de que los anticonceptivos hormonales aumentan el riesgo de trombosis venosa cinco veces comparado con el no uso.8 El riesgo es mayor para las mujeres que utilizan anticonceptivos hormonales y que tienen sobrepeso, fuman, o son mayores de 35 años.9
Una revisión sistemática reciente informó que el uso de los anticonceptivos orales combinados aumentaron el riesgo de trombosis cuatro veces comparado con las mujeres que nunca usaron anticonceptivos orales.10
Los anticonceptivos hormonales Incrementan el riesgo de suicidio y provocan un cambio continuo en el metabolismo saludable del cuerpo
Un estudio de casi medio millón de mujeres danesas (2017) con un seguimiento promedio de 8.3 años concluyó que había un riesgo casi dos veces mayor de intentos de suicidio en mujeres que usan anticonceptivos hormonales. También hubo un aumento de tres veces en el riesgo de suicidio en mujeres que usan anticonceptivos hormonales en comparación con mujeres que nunca usaron anticonceptivos.11
Un estudio reciente reportó que el uso de anticonceptivos hormonales vía oral, vaginal o transdérmica, produjo un aumento de los marcadores de inflamación crónica que es un factor de riesgo para la enfermedad cardiovascular. También, el uso de anticonceptivos combinados deterioró la sensibilidad a la insulina en mujeres jóvenes y sanas, el cual es un factor de riesgo para diabetes mellitus.12
Además, el uso de anticonceptivos hormonales puede producir dolores de cabeza tipo migraña, aumento de peso, cambios en el humor, y pérdida de la libido. Tambien contribuyen a un aumento prematuro de la perdida de masa osea.13 El uso de anticonceptivos hormonales asocia con infertilidad tras un uso prolongado, e incluso en cierta medida con el uso a corto plazo.
Los anticonceptivos hormonales aumentan la incidencia de cáncer de los organos reproductivos
Existe una asociación entre el uso de anticonceptivos hormonales y un aumento significativo del cáncer de cuello uterino.14 Es probable que esto sea causado por la infección con el virus del papiloma humano (VPH), el cual es transmitido sexualmente.
Los anticonceptivos hormonales aumentan el riesgo de tumores hepáticos
Hay alguna evidencia de que los anticonceptivos orales aumentan el riesgo de ciertos tumores benignos y malignos del hígado.15
Los anticonceptivos hormonales aumentan el riesgo de ataques al corazón y accidents vasculares cerebrales
Las formulaciones anticonceptivas orales de primera y segunda generación se han relacionado con un mayor riesgo de ataques cardíacos (infartos de miocardio) y accidente cereberovascular isquémico.16 Las píldoras anticonceptivas orales de tercera generación son asociadas con un mayor riesgo de accidente cerebrovascular isquémico17. El análisis del 2015 de múltiples estudios mostró que las mujeres que usan píldoras anticonceptivas combinadas tiene 1,6 mayor riesgo de sufrir un ataque cardíaco o un derrame cerebral.18
Los anticonceptivos hormonales tienen efectos nocivos para el matrimonio y la sociedad
Las hormonas para el control de la natalidad fomentan la mentalidad de que los hombres y las mujeres son incapaces del auto-control y por lo tanto no son capaces de abstenerse de tener relaciones sexuales. La introducción de los anticonceptivos hormonales fue el catalizador de la revolución sexual y produjo un incremento dramático del sexo pre-marital, el adulterio, el divorcio, el aborto, y los nacimientos fuera del matrimonio. Los anticonceptivos hormonales han tenido un papel indirecto en el aumento abrumador de padres solteros, madres solteras, pobreza y otros males sociales en los Estados Unidos.19,20
Los métodos de PNF son un medio excelente para planificar la familia
PFN está libre de efectos secundarios perjudiciales para la mujer y para la familia, y cuando se utiliza por motivos serios, y su uso puede sermuy bueno para el matrimonio.21
Referencias
Klipping, C., Duijkers, I., Fortier, M. P., Marr, J., Trummer, D., & Elliesen, J. (2012). Long-term tolerability of ethinylestradiol 20 mug/drospirenone 3 mg in a flexible extended regimen: Results from a randomized, controlled, multicentre study. The Journal of Family Planning and Reproductive Health Care, 38(2), 84-93. doi:10.1136/jfprhc-2011-100214 [doi]
Chowdhury, V., Joshi, U. M., Gopalkrishna, K., Betrabet, S., Mehta, S., & Saxena, B. N. (1980). ‘Escape’ ovulation in women due to the missing of low dose combination oral contraceptive pills. Contraception, 22(3), 241-247. doi:S0010-7824(80)80003-5 [pii]
Baerwald, A. R., Olatunbosun, O. A., & Pierson, R. A. (2006). Effects of oral contraceptives administered at defined stages of ovarian follicular development. Fertility and Sterility, 86(1), 27-35. doi:S0015-0282(06)00573-5 [pii]
Jones, R. K., Darroch, J. E., & Henshaw, S. K. (2002). Contraceptive use among U.S. women having abortions in 2000-2001. Perspectives on Sexual and Reproductive Health, 34(6), 294-303.
Morch, L. S., Skovlund, C. W., Hannaford, P. C., Iversen, L., Fielding, S., & Lidegaard, O. (2017). Contemporary hormonal contraception and the risk of breast cancer. The New England Journal of Medicine, 377(23), 2228-2239. doi:10.1056/NEJMoa1700732 [doi]
Kahlenborn C. Breast Cancer, Its Link to Abortion and the Birth Control Pill. 2000.
Kahlenborn, C., Modugno, F., Potter, D. M., & Severs, W. B. (2006). Oral contraceptive use as a risk factor for premenopausal breast cancer: A meta-analysis. Mayo Clinic Proceedings, 81(10), 1290-1302. doi:S0025-6196(11)61152-X [pii]
van Hylckama Vlieg, A., Helmerhorst, F. M., Vandenbroucke, J. P., Doggen, C. J., & Rosendaal, F. R. (2009). The venous thrombotic risk of oral contraceptives, effects of oestrogen dose and progestogen type: Results of the MEGA case-control study. BMJ (Clinical Research Ed.), 339, b2921. doi:10.1136/bmj.b2921 [doi]
Poulter, N. R. (2000). Risk of fatal pulmonary embolism with oral contraceptives. Lancet (London, England), 355(9221), 2088-6736(00)02369-2. doi:S0140-6736(00)02369-2 [pii]
de Bastos, M., Stegeman, B. H., Rosendaal, F. R., Van Hylckama Vlieg, A., Helmerhorst, F. M., Stijnen, T., & Dekkers, O. M. (2014). Combined oral contraceptives: Venous thrombosis. The Cochrane Database of Systematic Reviews, (3):CD010813. doi(3), CD010813. doi:10.1002/14651858.CD010813.pub2 [doi]
Skovlund, C. W., Morch, L. S., Kessing, L. V., Lange, T., & Lidegaard, O. (2018). Association of hormonal contraception with suicide attempts and suicides. The American Journal of Psychiatry, 175(4), 336-342. doi:10.1176/appi.ajp.2017.17060616 [doi]
Piltonen, T., Puurunen, J., Hedberg, P., Ruokonen, A., Mutt, S. J., Herzig, K. H.,…Tapanainen, J. S. (2012). Oral, transdermal and vaginal combined contraceptives induce an increase in markers of chronic inflammation and impair insulin sensitivity in young healthy normal-weight women: A randomized study. Human Reproduction (Oxford, England), 27(10), 3046-3056.
Wooltorton, E. (2005). Medroxyprogesterone acetate (depo-provera) and bone mineral density loss. CMAJ : Canadian Medical Association Journal = Journal De l’Association Medicale Canadienne, 172(6), 746. doi:cmaj.050158 [pii]
La Vecchia, C., & Boccia, S. (2014). Oral contraceptives, human papillomavirus and cervical cancer. European Journal of Cancer Prevention: The Official Journal of the European Cancer Prevention Organisation (ECP), 23(2), 110-112. doi:10.1097/CEJ.0000000000000000 [doi]
Giannitrapani, L., Soresi, M., La Spada, E., Cervello, M., D’Alessandro, N., & Montalto, G. (2006). Sex hormones and risk of liver tumor. Annals of the New York Academy of Sciences, 1089, 228-236. doi:1089/1/228 [pii]
Tanis, B. C., van den Bosch, M. A., Kemmeren, J. M., Cats, V. M., Helmerhorst, F. M., Algra, A., . . . Rosendaal, F. R. (2001). Oral contraceptives and the risk of myocardial infarction. The New England Journal of Medicine, 345(25), 1787-1793. doi:10.1056/NEJMoa003216 [doi]
Baillargeon, J. P., McClish, D. K., Essah, P. A., & Nestler, J. E. (2005). Association between the current use of low-dose oral contraceptives and cardiovascular arterial disease: A meta-analysis. The Journal of Clinical Endocrinology and Metabolism, 90(7), 3863-3870. doi:jc.2004-1958 [pii]
Roach, R. E., Helmerhorst, F. M., Lijfering, W. M., Stijnen, T., Algra, A., & Dekkers, O. M. (2015). Combined oral contraceptives: The risk of myocardial infarction and ischemic stroke. The Cochrane Database of Systematic Reviews, (8):CD011054. doi(8), CD011054. doi:10.1002/14651858.CD011054.pub2 [doi]
Akerlof, GA, et al. An analysis of out-of-wedlock childbearing in the United States. Q J Econ. 1996 May; 111(2):277-317.
Akerlof, GA. Men without children. Econ J. 1998 Mar; 108(447): 287-309.
Fehring, R. J. (2015). The influence of contraception, abortion, and natural family planning on divorce rates as found in the 2006-2010 national survey of family growth. The Linacre Quarterly, 82(3), 273-282. doi:10.1179/2050854915Y.0000000007 [doi]
November 15, 2013 (Heritage) – Analysts at a recent forum on the downward trends in marriage and religion in the United States agree that the two are not isolated phenomena but, in fact, influence and exacerbate one another.
Brad Wilcox, director of the National Marriage Project, has shown that family dissolution is linked to a further erosion of civil society in which American men are increasingly disconnected from core cultural institutions, including a religious congregation. Likewise, Mary Eberstadt, a senior fellow at the Ethics and Public Policy Center, has found that marriage and family life often engender an impulse for religious engagement and that, as more couples cohabit, divorce, or never marry, religious participation has decreased.
The impact of the downturns in family formation and religious practice have real-world and long-term implications for the lives of Americans—particularly the rising generation.
Children raised by two married, biological parents tend to fare better than peers in other households. Those who grow up in married-parent families are 82 percent less likely to live in poverty, and intact families tend to fare better in a wide range of economic measures. Youth who are raised in an intact family tend to fare better on a range of emotional and psychological outcomes, have higher levels ofacademic achievement and educational attainment, and are less likely to engage in high-risk behaviors such as sexual activity or substance abuse and less likely to exhibit anti-social behavior.
Like family structure, religious affiliation and participation is linked to the well-being of individuals, families, and society. Children whose mothers more frequently participated in religious activities are less likely to exhibit aggressive and delinquent behavior. Religious practice is associated with higher levels of economic well-being and academic performance as well reductions in the incidence of crime, delinquency, drug and alcohol addiction, and problems related to physical and emotional health. Coupled with the association between religiosity, empathy, charity, and volunteerism, the improved prospects of more religious and intact families can have positive ripple effects throughout society.
Given the wide-ranging and mutually supporting benefits of religion and family, it is critical for the public interest to bolster both—and a starting point would be to support policies that promote marriage and strengthen families.
Nov. 28, 2013 (PJSaunders) – A debate at University College London on Monday night allowed the issue of assisted suicide to be addressed.
UCL’s Cruciform Building was the impressive setting for the motion, ‘This House would legalise Assisted Dying.’ I was in the opposition team with Lord Carlile, Baroness Finlay and Robert Preston – leading lights in the think tank Living and Dying Well.
We were given seven minutes each. Here is my talk which focussed on the issue of the ‘slippery slope’.
The four main groups resisting the legalisation of assisted dying in this country – doctors, disabled people, faith groups and parliamentarians – do so primarily because they are anxious about the consequences of licensing of doctors to dispense lethal drugs.
Their concerns are both about how such a system could be regulated and also about the pressure legalization would place on vulnerable people to end their lives for fear of being a financial or emotional burden on others.
This is heightened by the evidence of incremental extension or mission creep in other jurisdictions.
In the Netherlands which legalised assisted suicide and euthanasia in 2002 there has been an increase of 10 to 20% of euthanasia cases per year since 2006 from 1,923 to 4,188. The 2012 figures included 42 with early dementia and 13 with psychiatric conditions.
In addition in 2001 about 5.6% of all deaths in the Netherlands were related to deep-continuous sedation. This rose to 8.2% in 2005 and 12.3% in 2010. A significant proportion of these deaths involve doctors deeply sedating patients and then withholding fluids with the explicit intention that they will die.
Children as young as twelve can already have euthanasia and a 2005 paper in the New England Medical Journal reported on 22 babies with spina bifida and/or hydrocephalus who were killed by lethal injection in the Netherlands over a seven year period. It estimated that there actually 15 to 20 newborns being killed in this way per year – despite this still being illegal. The culture and public conscience have changed.
In Belgium, which legalised euthanasia in 2002, there has been a 500% increase in euthanasia deaths over ten years between 2003 and 2012. High profile cases include Mark and Eddy Verbessem, the 45-year-old deaf identical twins, who were euthanised by the Belgian state, after their eyesight began to fail; then there is Nathan/Nancy Verhelst, whose life was ended in front of TV cameras, after a series of botched sex-change operations. His mother said she hated girls, found her child ‘so ugly’ at birth and did not mourn his death. And then there is Ann G, who had anorexia and who opted to have her life ended after being sexually abused by the psychiatrist who was supposed to be treating her for the life-threatening condition.
Organ donation euthanasia is already practised in Belgium and the Belgian Senate is tomorrow discussing plans to extend the programme to minors and people with dementia (they have since recommended this). Already in parts of Belgium one in three cases of euthanasia is involuntary and half go unreported. And there has been not one prosecution for abuses in the last ten years – perhaps because the one of the lead euthanasia practitioners – Distelmans – chairs the very committee that is meant to regulate his activity.
Switzerland, where assisted suicide is legal, first released assisted suicide statistics in 2009, laying bare a 700% rise in cases (from 43 to 297) from 1998 to 2009. Amongst those travelling from abroad to end their lives at the notorious Dignitas facility have been many people who could not by any stretch be described as terminally ill – and included cases of people who could have lived for decades ending their lives – with arthritis, blindness, spinal injury, diabetes, mental illness – or people who were essentially well but could not bear to live without their spouses.
Dignitas has attracted much criticism in recent years over accounts of discarded cremation urns dumped in Lake Zurich, reports of body bags in residential lifts, suicides being carried out in car parks, the selling of the personal effects of deceased victims and profiteering with fees approaching £8,000 per death.
In the US state of Oregon there has been a 350% increase assisted in suicide deaths since legalisation. I’ll leave it to my colleagues to expand on the details but notable are two people with cancer – Randy Stroup and Barbara Wagner – who were told that the Oregon Health Authority would not pay for their chemotherapy but would happily pay for their assisted suicide – which was of course much cheaper. Is this really the kind of temptation that we wish to put before NHS managers in Britain? Is it any wonder that over 120 attempts to change the law through US state parliaments have failed?
The problem is that any law allowing assisted suicide or euthanasia will carry within it the seeds of its own extension.
And whilst Lord Falconer may claim to have limited objectives – on his coat tails are a host of other UK groups with more radical agendas – FATE, SOARS, the BHA, NSS and EXIT International.
They will not be satisfied with the so-called modest changes he seeks but they are using exactly the same arguments to advance their case – ‘compassion’ and ‘choice’
They are able to use exactly the same arguments because Lord Falconer’s position is at heart both illogical and discriminatory.
If adults can have it why can’t children who are judged to be Gillick competent?
If competent people can have it what about those with dementia who it is argued would have wanted it?
If people who are terminally ill why not the chronically ill or disabled who are suffering unbearably?
If it’s for those with physical suffering why not those with mental suffering?
Or as Exit international asks – why not the elderly bereaved and the troubled teen?
There will inevitably be pressure to extend the boundaries which may well not survive legal challenge once the so-called ‘right’ is available for some.
We will hear – it is only for this group or only for that group – but I tell you – it is only the beginning
Any law allowing assisted suicide or euthanasia in any circumstances at all will be subject to extension – or abuse.
And that it is the other problem – changing the law would give doctors a degree of power over life and death that some will inevitably abuse.
It will be doctors who see the patients, fill out the forms, dispense the lethal drugs. Some of them will push the boundaries. Some will falsify certification. There may be some who, like Harold Shipman, will develop a taste for killing and they will be very difficult to detect.
But many will simply be too busy, too pressured and facing too many demands to make the kind of cool comprehensive objective assessments that this kind of law requires. And very few of them will really know the patients or their families.
We have seen this already with abortion. We began with a very strict law which allowed it only in limited circumstances. Now there are 200,000 cases a year. Most of them fall outside the boundaries of the law. There is illegal pre-signing of forms, abortions for sex selection, abortions on demand for spurious mental health reasons. And only one conviction for illegal abortion in 45 years.
Society is reluctant to touch and question doctors. The police are reluctant to investigate. The DPP hesitates to prosecute. The courts are unwilling to convict. Parliament turns a blind eye. It is simply not safe to give doctors this sort of power because some will abuse it as they have in other countries and it will be very difficult to stop them.
It’s far better not to go there at all.
The best system available is that which we have currently – a law carrying a blanket prohibition on both assisted suicide and euthanasia but with discretion given to both prosecutors and judges to temper justice with mercy in hard cases – the current law has both a stern face and a kind heart.
In other words the penalties that it holds in reserve act as a powerful deterrent to exploitation and abuse of vulnerable people
And it works – there are very few cases observed (just 15-20 per year make the trip to Switzerland) but also very few prosecutions.
VATICAN CITY, November 26, 2013 (LifeSiteNews.com) – In a high level teaching document released this morning, Pope Francis has firmly responded to those who have expressed hope that the Catholic Church may one day change its teachings on abortion, writing, “the Church cannot be expected to change her position on this question.”
“I want to be completely honest in this regard. This is not something subject to alleged reforms or ‘modernizations’,” he added.
Entitled “Evangelii Gaudium” (The Joy of the Gospel), the Apostolic Exhortation – a document which, while important, is of less weight than an encyclical – noted, “Among the vulnerable for whom the Church wishes to care with particular love and concern are unborn children, the most defenceless and innocent among us.”
He lamented that, “Nowadays efforts are made to deny them their human dignity and to do with them whatever one pleases, taking their lives and passing laws preventing anyone from standing in the way of this.”
“Frequently, as a way of ridiculing the Church’s effort to defend their lives, attempts are made to present her position as ideological, obscurantist and conservative. Yet this defence of unborn life is closely linked to the defence of each and every other human right.”
“It involves the conviction that a human being is always sacred and inviolable, in any situation and at every stage of development,” he said. “Human beings are ends in themselves and never a means of resolving other problems. Once this conviction disappears, so do solid and lasting foundations for the defence of human rights, which would always be subject to the passing whims of the powers that be.”
The document marks the pope’s most in-depth discussion of abortion since his election.
The pope added that it is important to do more to more to “accompany women in very difficult situations, where abortion appears as a quick solution to their profound anguish, especially when the life developing within them is the result of rape or a situation of extreme poverty.”
The Holy Father stated that the truth about human life can be discovered with reason alone, but from a faith perspective the gravity of the evil of abortion is manifest.
“Reason alone is sufficient to recognize the inviolable value of each single human life, but if we also look at the issue from the standpoint of faith, ‘every violation of the personal dignity of the human being cries out in vengeance to God and is an offence against the creator of the individual,’” he said, quoting a previous Apostolic Exhortation by Pope John Paul II.
“Every unborn child, though unjustly condemned to be aborted, has the face of the Lord, who even before his birth, and then as soon as he was born, experienced the rejection of the world,” the pope said at the time.
In a recent homily, seen by some Vatican watchers as wake up call to liberal Catholics to abandon hopes of Pope Francis altering Church teaching on abortion and contraception, he warned against the desire to “be like everyone else” and what he called an “adolescent progressivism”. “Lord,” the pope prayed, “give me the discernment to recognize the subtle conspiracies of worldliness that lead us to negotiate our values and our faith.”
Similarly, in Evangelii Gaudium Pope Francis writes, “It is not ‘progressive’ to try to resolve problems by eliminating a human life.”
MOSCOW, November 25, 2013 (LifeSiteNews.com) – The Russian Federation has enacted a new law banning abortion advertising in the ongoing effort to stem the country’s decline in population, according to Russian media.
TR Novosti reports that the abortion ad ban is part of broader changes to Russia’s Federal Law on Advertising that include a ban on advertising campaigns offering free drug samples if these samples contain narcotic or psychotropic substances, and restrictions on the advertising of traditional “folk medicine” practices.
The Duma is considering a number of other proposals that would stop Russia’s demographic death spiral, fueled by an abortion rate of 1,022 per 1,000 births, according to some statistics. The United Nations estimates that the population of Russia, which stood at 143 million in 2008, will shrink to 116 million by 2050.
To combat the abortion epidemic, legislation has been proposed that would ban free abortions at government-run health clinics; require prescriptions for the ‘morning-after’ pill; require parental consent for teenagers and a husband’s consent for married women; and mandate a one-week waiting period before an abortion is performed. Other proposals have included increasing the 2,000 ruble ($70) monthly government subsidy offered to pregnant women.
Steven Mosher, President of the Population Research Institute, pointed out that despite government incentives such as a baby bonus that offers the equivalent of $9,000 upon the birth of every child after the first, and calls from Russian President Vladimir Putin for families to have at least three children, abortion is still occurring in epidemic proportions.
“As long as society fails to recognize the value of human life, and wantonly destroys it in large numbers, it will be difficult to establish a new three-child norm. Abortion must cease being a way of life in Russia if her people are to survive,” Mosher said.
Earlier this month the head of the State Duma Committee for Family and Children said the Russian people must stop tolerating abortion and the recent rise in surrogacy because they threaten to “wipe out the population of Russia.”
Speaking at a history forum dedicated to the 400th anniversary of the Russian royal house of Romanov, MP Elena Mizulina said, “The problems of abortion prevention and the shift in public opinion towards abortion are currently very urgent. Although the number of abortions in Russia is falling, it still exceeds 5 million every year.”
Mizulina added that though the practice of surrogacy was relatively new in Russia, the societal implications are of great concern to her.
“We still can stop the consequences of this practice from happening. It can and must be used only in exceptional cases,” Mizulina explained.
“Humanity will probably understand one day that as we ban nuclear weapons to prevent the death of Mother Earth, so should we ban the technology destroying the natural environment and natural childbirth, the natural way of human reproduction,” the MP said.
She said that she believes the Russian people as a whole are against surrogacy, as they are in favor of “Orthodox Christian spiritual values and the family as the keeper of these values.”
Pro-life legislation aimed at rolling back Russia’s abortion culture has been strongly supported by the Russian Orthodox Church.
Patriarch Kirill of Moscow and All Russia proposed a series of measures on the Moscow Patriarchate’s website, urging the Ministry of Health and Social Development to make “preservation of pregnancy a priority task for the doctor” and discourage incentives for abortion.
The Russian patriarch also advocated state support for pro-motherhood media campaigns, and suggested setting up crisis pregnancy centers in every maternity hospital to help “lonely mothers in difficult life situations.”
In October, a representative of the Russian Orthodox Church blasted the legality of surrogacy in Russia as “mutiny against God.”
Dmitry Smirnov, the head of the Moscow Patriarchy Commission for Family, Motherhood and Childhood, made the comment after Russian media reported in September that a 64-year-old Russian pop star and her 37-year-old husband had two children born through surrogate motherhood.
“I would ban this, of course. We can see that a bad example is contagious,” the senior church representative was quoted to say by Interfax. “This is mutiny against God, this is very happy fascism with a contract, the money and confiscation of a child.”
Pro-abortion advocates have relentlessly denied a link between abortion and breast cancer, but a new study has emerged from China that seems to show that such a link not only exists, but that the risk rises with each abortion a woman has.
Dr. Joel Brind, professor of endocrinology at Baruch College, City University of New York and a director at the Breast Cancer Prevention Institute, called the findings a “real game changer” for deniers of the so-called ABC link.
Incidences of breast cancer in China have increased at an “alarming rate” over the past two decades, corresponding with the rise of the Chinese Communist Party’s one-child policy.
The research was conducted by Yubei Huang et al. from the Department of Epidemiology and Biostatistics in the Tianjin Medical University Cancer Hospital.
The researchers say they were initially puzzled by their findings, stating that Chinese women “historically” have had lower rates of breast cancer compared to women from western countries such as the US.
They found, however, that incidences of breast cancer in China increased at an “alarming rate” over the past two decades, corresponding with the rise of the Chinese Communist Party’s one-child policy.
The one-child policy is strictly enforced, and women who transgress the quota are often forced to abort. Over 336 million babieshave been aborted in China since the 1980s.
“The marked change in breast cancer incidence was parallelled to the one-child-per-family policy,” the researchers stated.
Reggie Littlejohn, President of Women’s Rights Without Frontiers, said the research revals “yet another human rights violation in connection with China’s One Child Policy.”
“So, the women of China have to endure the tremendous trauma of late term forced abortion, taking their babies from them, and then years later, breast cancer, taking their health and even their lives from them,” she told LifeSiteNews.com.
The researchers reached their conclusions after examining 36 studies that investigated the associations between abortion and breast cancer.
The overall risk of developing breast cancer among women having only one abortion increased by 44 percent.
Calling it the “dose-response relationship” researchers also found that the risk of breast cancer increased as the number of abortions increased. Two abortions increased the risk by 76 percent, three by 89 percent.
“In summary, the most important implication of this study is that IA was significantly associated with an increased risk of breast cancer among Chinese females, and the risk of breast cancer increases as the number of IA increases,” concluded the researchers.
The researchers called their findings “consistent” with those of Dr. Brind, who found in a 1996 meta-analysis that women had a 30 percent greater chance of developing breast cancer after aborting their child.
“Not only does [the study] validate the earlier findings from 1996, but its findings are even stronger,” Brind told LifeSiteNews.com.
Brind said that pro-abortion advocates should be “very concerned” about the research since it shows how “millions upon millions” of women in Asia are negatively affected by what abortion’s most vocal proponents call a “safe” procedure.
He lamented, however, that “anything that challenges the ‘safe abortion’ mythology is to be challenged, denied, belittled, discredited, dumped on.”
The Chinese research follows on the heels of two similar studies earlier this year. One studypublished in the IndianJournal of Community Medicine in May found a 6-fold greater risk of breast cancer among Indian women with a history of induced abortion when compared to the women with no such history. A similar study from Bangladesh published in the Journal of the Dhaka Medical College in April found that women with a history of induced abortion had a 20-fold increase in likelihood of developing breast cancer when compared to women with no such history.
In areportlast month, Brind called the findings of the two studies “of the sort of magnitude that has typified the link between cigarettes and lung cancer.”
COLUMBUS, OH, November 22, 2013 (LifeSiteNews.com) – Pro-life activists in the Columbus area are mounting a petition drive to ask Catholic-affiliated Mount Carmel Hospital to sever its relationships with several local abortionists, in deference to church teaching opposing abortion.
According to Right to Life of Greater Columbus, Mount Carmel allows at least two, possibly three, abortionists to maintain admitting privileges at the hospital, despite its Catholic affiliation.
In Ohio, state law requires abortion providers to maintain admitting privileges at a nearby hospital in order to legally perform the procedure. By allowing these abortionists transfer privileges, the hospital is effectively helping them stay in business.
In the past, the group says they have directed questions about Mt. Carmel’s policy on admitting privileges to hospital officials. But after learning that the hospital had begun actively referring patients to doctors and facilities that perform abortions, they decided they had to act.
The group is asking pro-life supporters to sign on to a petition they have composed and will be sending to hospital president Claus von Zychlin, asking him to sever all ties with two known abortionists, along with a third doctor who works out of an abortion facility.
“As members of the local prolife community, we strongly appreciate Mt. Carmel’s commitment and mission to ‘… serve together at Mount Carmel in Trinity Health, in the spirit of the Gospel, to heal body, mind and spirit, to improve the health of our communities, and to steward the resources entrusted to us’ while adhering to a moral ethic that upholds the innate dignity due to every human from the moment of conception until natural death,” the petition reads. “We know you are serious when you say ‘Mount Carmel conducts all of its operations and patient care in a manner that is consistent with our Mission and values.’ We sincerely appreciate that you have placed all medical staff on notice that they are to ‘abide by generally recognized standards of medical and professional ethics including, but not limited to, the Ethical and Religious Directives for Catholic Healthcare.’”
“Recently, it has come to our attention that Mt. Carmel hospital’s online physician referral page refers patients to several physicians and facilities that demonstrably violate our shared respect for human life,” the petition states. “It is our goal to bring these concerns to your attention in the fervent hope that you will use your positions of leadership to make the necessary changes in light of these oversights and implement institutional safeguards to prevent future lapses.”
The petition goes on to name three local doctors connected to abortion: known abortionists Milroy Samuel and Karl Shaeffer, and a third doctor, Patrick Muffley, who has worked at Samuel’s abortion facility in the past.
All three doctors have spotty records when it comes to the safety of their female patients. Investigators at Milroy Samuel’s Complete Health Care for Women abortion clinic found rusted and dirty IV equipment, improperly sterilized surgical tools, expired medications, and lax infection control standards in 2012.
Karl Shaeffer’s Founder’s Women’s Health abortion facility was cited by health inspectors that same year for unsafe operating rooms and dangerous equipment, including patient tables that shocked patients when connected to electricity. Some staff at Shaeffer’s facility had expired surgical licenses, and in some cases, could not even prove they had a valid medical license at all.
Patrick Muffley is facinga 60 day suspension of his medical license for allegedly sending inappropriately sexual text messages to a patient.
Noting that hospital-affiliated abortionists have “greatly profited off the blood of the unborn,” the petitioners request that hospital executives “review the physicians mentioned above and the scope of their practices and take the appropriate action to disassociate Mount Carmel from the bloody abortion industry.”
November 21, 2013 (HLI) – In a very rareeventearlier this year, a pregnant woman in Hungary who was declared “brain dead” was kept alive for three months on life support by doctors until her baby could be safely born.
The 31-year-old expectant mother suffered a stroke and was transported by a helicopter to the Neurological Clinic of Debrecen in Eastern Hungary. While the surgery was initially considered a success, sadly, she was declared brain dead two days later. An ultrasound showed that her 15-week-old preborn child was alive and very active.
“In the first two days we fought to save the mother’s life and it was proven … that circulation and functions stopped,” said Dr. Béla Fülesdi, president of the University of Debrecen Medical and Health Science Centre. “On the second day when [other] examinations were carried out, we found the baby was alive and kicking well in its mother’s body.”
Photo taken in Debrecen, Hungary on June 1 (the Day of Life declared by the UN) when we walked to the Ob-Gyn Clinic of University of Debrecen. The text reads: Peace in the womb! Amnesty for us – amnesty for our children before birth!
Dr. Tamás Szilveszter Kovács, one of the physicians who cared for the mother and child, struggled for a time over the situation, as he was unsure whether helping a baby live when the mother died was in the best interests of the child. But after meeting with the father and grandparents he changed his mind: “They convinced me that the child would mean, paradoxically, a special surviving of the mother for the grieving father and the grandparents. So the child will be reared in a complete family, and we would commit a sin if we would not do everything we could for them that modern science makes possible.”
The father and maternal grandparents of the child together asked doctors to keep the mother alive in an effort to save the child until he could be delivered safely.
Every provision possible was taken to try to give the child the best chance possible at developing naturally and safely. The father and grandparents came three times a week from the countryside to the hospital to talk to the baby and caressed the belly of the mother. A music therapist was even employed to stimulate the baby’s healthy development.
Doctors had to fight numerous infections and, as they would with any patient who was unable to move, would rotate her in order to avoid bedsores. While they were hoping to keep the child in the womb as long as possible, in the 27th week, the mother’s circulation became unstable and so they decided to deliver the baby because the womb was no longer safe. So at 27 weeks, the baby was delivered by cesarean section in July of this year, weighing just 1.4 kilograms (3 pounds, 1.8 ounces). The Hungarian doctors who delivered the baby in July believe the birth is one of only three such cases in history, in which the mother was kept alive medically for an extended period in order to save the child in her womb.
The baby was discharged from the hospital last month but doctors wanted to wait to make the announcement about the delivery until they were sure the baby would survive.
He (the sex of the child is not known) is now developing well at home and doctors say he does not show any illnesses related to premature births although he will be continuously monitored.
The father, grandparents and medical professionals who made this extraordinary situation possible deserve the highest respect for making difficult decisions in a very trying environment.
As pro-life professor Dr. Fülesdi said, “I am happy that this team representing the unit of care and several medical experts was a community as well, which was able to pass this dramatic test of 92 days not just from the point of view of medicine but from the spiritual one as well.”
Further evidence for this kind of spiritual awakening can be seen in Hungary’s “Easter Constitution,” enacted in January 2012 as the first national post-Communist constitution. With this serious move toward national independence and sovereignty, Hungary has begun to reclaim its Christian roots, including respect for life, religious freedom, marriage and family. Its pro-life provisions do not yet have the full effect of law, but we pray that this process may be hastened, especially since Hungary continues to suffer spiritually, economically and demographically from decades of oppression and abortion.
Amidst acknowledging the heroic efforts of the family and doctors that saw to it that this small child was welcomed into life, we also mourn a mother who would not live to meet her child face to face. As tragic as this is, it bodes well for the child that so many in his young life have demonstrated such great love and care for his well-being. Let this serve as an example to all of the great harmony between being open to life, and providing the best care possible for everyone.
Whenever we go out on the streets for a “Face the Truth” Tour, we can always count on someone happening by our display to tell us that by showing the pictures of abortion victims in the public square, we’re doing more harm than good. This is a charge we’ve heard often enough that we address it as one of the most Common Objections we hear.
In our response to this oft-raised argument, we plainly make the observation that throughout modern history, any number of successful social reform movements — from the movement to enact child labor laws to the civil rights movement — have used disturbing images that depict victims of maltreatment and violence, and that public support for the reforms these movements sought could not have been garnered without publicly showing these images.
Putting a Human Face on the Victims
The intent behind displaying graphic abortion pictures is the same, of course, for it puts a human face on the victims of what is, for far too many people, merely a theoretical concept or political issue.
Lewis Hine believed it was necessary to show victims of cruelty of the child labor industry, and Mamie Till believed it was necessary to have an open-casket funeral for her son Emmett after he was brutally murdered by violent racists.
We display pictures of abortion victims for the same reason: because they work. That is, in the eyes of the viewer, the images elicit sympathy for the victims of injustice.
In the case of reform movements that have employed the use of graphic pictures in working to effect social change, it perhaps goes without saying that one commonality these movements share is that it is members of the movements themselves that are the ones who initially seek to disseminate them.
However, a movement closely associated with one of the martyrs whose feast day the Catholic Church celebrates tomorrow provides an exception to this rule.
The Murder of Blessed Miguel Pro, S.J.
During the 1920s, Mexico was ruled by the virulently anti-Catholic President Plutarco Calles, who began what Graham Greene called “the fiercest persecution of religion anywhere since the reign of Elizabeth.” Chief among the many Catholic groups who vigorously opposed Calles were the Cristero rebels, whose story is depicted in the 2012 film For Greater Glory.
One of the most well known Cristeros, Blessed Miguel Pro, S.J., was falsely implicated in an assassination attempt on former Mexican President Álvaro Obregón in November 1927, which provided the Calles regime with the pretext for ordering his death.
Father Pro went to his execution on November 23, 1927. Before the firing squad was ordered to shoot, Fr. Pro raised his arms in cruciform and shouted the cry of the Cristeros, “Viva Cristo Rey!”(“Long live Christ the King!”) After the first shots of the firing squad failed to kill him, a soldier shot him point blank in the head.
Calles, seeking to cow other Cristeros into submission, had the execution photographed, and newspapers throughout Mexico carried pictures of the executed priest on their front page the next day. (As George Weigel has observed, Blessed Miguel Pro was likely the first martyr ever to be photographed at the very moment of his death.)
But Calles’ plan backfired. Instead, the images of Pro’s murder further emboldened the Cristeros to stand up to his oppressive regime.
Graphic Images Work, Regardless of the Intentions of Those Displaying Them
This instance of a public display of graphic images of violence is unique in that the initial act of displaying the images was done by the perpetrators themselves, and not by sympathizers of the victims. Yet the act of displaying these shocking images still played a major role in combating injustices committed by the perpetrators, proving that regardless of the motivations behind displaying graphic images of violence and injustice, their effect is the same.
Pro-Life Action League National Director Joe Scheidler has often remarked that seeing a picture of an aborted baby in the fall of 1972 — just a few months before the Supreme Court’s Roe v. Wadedecision — was the impetus for him to commit himself to full-time pro-life work. Along these same lines, I can’t tell you how many times we’ve heard from passersby at our Face the Truth demonstrations comments along the lines of, “I had no idea what abortion was until I saw your signs.”
Because of the overwhelming evidence that graphic pictures do elicit sympathy for the victims of injustice in the eyes of the public, we can surely be confident of their inestimable value in the fight against abortion.
November 15, 2013 (Heritage) – Analysts at a recent forum on the downward trends in marriage and religion in the United States agree that the two are not isolated phenomena but, in fact, influence and exacerbate one another.
Brad Wilcox, director of the National Marriage Project, has shown that family dissolution is linked to a further erosion of civil society in which American men are increasingly disconnected from core cultural institutions, including a religious congregation. Likewise, Mary Eberstadt, a senior fellow at the Ethics and Public Policy Center, has found that marriage and family life often engender an impulse for religious engagement and that, as more couples cohabit, divorce, or never marry, religious participation has decreased.
The impact of the downturns in family formation and religious practice have real-world and long-term implications for the lives of Americans—particularly the rising generation.
Children raised by two married, biological parents tend to fare better than peers in other households. Those who grow up in married-parent families are 82 percent less likely to live in poverty, and intact families tend to fare better in a wide range of economic measures. Youth who are raised in an intact family tend to fare better on a range of emotional and psychological outcomes, have higher levels ofacademic achievement and educational attainment, and are less likely to engage in high-risk behaviors such as sexual activity or substance abuse and less likely to exhibit anti-social behavior.
Like family structure, religious affiliation and participation is linked to the well-being of individuals, families, and society. Children whose mothers more frequently participated in religious activities are less likely to exhibit aggressive and delinquent behavior. Religious practice is associated with higher levels of economic well-being and academic performance as well reductions in the incidence of crime, delinquency, drug and alcohol addiction, and problems related to physical and emotional health. Coupled with the association between religiosity, empathy, charity, and volunteerism, the improved prospects of more religious and intact families can have positive ripple effects throughout society.
Given the wide-ranging and mutually supporting benefits of religion and family, it is critical for the public interest to bolster both—and a starting point would be to support policies that promote marriage and strengthen families.
Cardinal Dolan thought he heard Barack Obama pledge respect for the Catholic Church’s rights of conscience.
Then came the contraception coverage mandate.
By James Taranto, March 31, 2012, New York
The president of the U.S. Conference of Bishops is careful to show due respect for the president of the United States. “I was deeply honored that he would call me and discuss these things with me,” says the newly elevated Cardinal Timothy Dolan, archbishop of New York. But when Archbishop Dolan tells me his account of their discussions of the ObamaCare birth-control mandate, Barack Obama sounds imperious and deceitful to me.
Mr. Obama knew that the mandate would pose difficulties for the Catholic Church, so he invited Archbishop Dolan to the Oval Office last November, shortly before the bishops’ General Assembly in Baltimore. At the end of their 45-minute discussion, the archbishop summed up what he understood as the president’s message:
“I said, ‘I’ve heard you say, first of all, that you have immense regard for the work of the Catholic Church in the United States in health care, education and charity. . . . I have heard you say that you are not going to let the administration do anything to impede that work and . . . that you take the protection of the rights of conscience with the utmost seriousness. . . . Does that accurately sum up our conversation?’ [Mr. Obama] said, ‘You bet it does.'”
The archbishop asked for permission to relay the message to the other bishops. “You don’t have my permission, you’ve got my request,” the president replied.
“So you can imagine the chagrin,” Archbishop Dolan continues, “when he called me at the end of January to say that the mandates remain in place and that there would be no substantive change, and that the only thing that he could offer me was that we would have until August. . . . I said, ‘Mr. President, I appreciate the call. Are you saying now that we have until August to introduce to you continual concerns that might trigger a substantive mitigation in these mandates?’ He said, ‘No, the mandates remain. We’re more or less giving you this time to find out how you’re going to be able to comply.’ I said, ‘Well, sir, we don’t need the [extra time]. I can tell you now we’re unable to comply.'”
The administration went ahead and announced the mandate. A public backlash ensued, and the archbishop got another call from the president on Feb. 10. “He said, ‘You will be happy to hear religious institutions do not have to pay for this, that the burden will be on insurers.'” Archbishop Dolan asked if the president was seeking his input and was told the modified policy was a fait accompli. The call came at 9:30 a.m. The president announced the purported accommodation at 12:15 p.m.
Editorial board member Joe Rago predicts how the Supreme Court will rule on ObamaCare’s Medicaid expansion and the law’s severability.
Sister Carol Keehan of the pro-ObamaCare Catholic Health Association immediately pronounced herself satisfied with the change, and the bishops felt pressure to say something. “We wanted to avoid two headlines. Headline 1 was ‘Bishops Celebrate . . . Accommodations.’ . . . The other headline we wanted to avoid is ‘Bishops Obstinate.'” They rushed out a “circumspect” statement, which Archbishop Dolan sums up as follows: “We welcome this initiative, we look forward to studying it, we hope that it’s a decent first step, but we still have very weighty questions.”
Within hours, “it dawned on us that there’s not much here, and that’s when we put out the more substantive [statement] by the end of the day, saying, ‘Whoa, now we’ve had time to hear what was said at the announcement and to read the substance of it, and this just doesn’t do it.'”
Having rushed to conciliate, they got the “Bishops Obstinate” headlines anyway. Archbishop Dolan explains that the “accommodation” solves nothing, since most church-affiliated organizations either are self-insured or purchase coverage from Catholic insurance companies like Christian Brothers Services and Catholic Mutual Group, which also see the mandate as “morally toxic.” He argues that the mandate also infringes on the religious liberty of non-ministerial organizations like the Knights of Columbus and Catholic-oriented businesses such as publishing houses, not to mention individuals, Catholic or not, who conscientiously object.
“We’ve grown hoarse saying this is not about contraception, this is about religious freedom,” he says. What rankles him the most is the government’s narrow definition of a religious institution. Your local Catholic parish, for instance, is exempt from the birth-control mandate. Not exempt are institutions such as hospitals, grade schools, universities and soup kitchens that employ or serve significant numbers of people from other faiths and whose main purpose is something other than proselytization.
“We find it completely unswallowable, both as Catholics and mostly as Americans, that a bureau of the American government would take it upon itself to define ‘ministry,'” Archbishop Dolan says. “We would find that to be—we’ve used the words ‘radical,’ ‘unprecedented’ and ‘dramatically intrusive.'”
It also amounts to penalizing the church for not discriminating in its good works: “We don’t ask people for their baptismal certificate, nor do we ask people for their U.S. passport, before we can serve them, OK? . . . We don’t serve people because they’re Catholic, we serve them because weare, and it’s a moral imperative for us to do so.”
To be sure, not all Catholics see it that way. Archbishop Dolan makes an argument—which he prefaces with the admission that “I find this a little uncomfortable”—that federal intrusion bolsters those who are more selfishly inclined: “Some Catholics . . . are now saying, ‘Fine, we’ll get out of all that. It’s dragging us down anyway. Rather than be supporting 50 Catholic schools in the inner city where most of the kids are not Catholic, and using a big chunk of diocesan money to do that, we’ll just use it for the schools that have all Catholics, and it’ll serve us a lot better.’ . . .
“I find that, by the way, to be rather un-Catholic,” he continues. “I don’t know what that would say to the gospel mandate to be ‘light to the world’ and ‘salt of the earth.’ It’s part of our religion to be right out there in the forefront, right there in the nitty-gritty.”
An insular attitude, Archbishop Dolan suggests, plays into the hands of ideologues who favor an ever-more-powerful secular government: “I get this all the time: I would have some people say, ‘Cardinal Dolan, you need to go to Albany and say, “If we don’t get state aid by September, I’m going to close all my schools.”‘ I say to them, ‘You don’t think there’d be somersaults up and down the corridors?'”
Another story comes from the nation’s capital: “The Archdiocese of Washington, in a very courteous way, went to the City Council and said, ‘We just want to be upfront with you. If this goes through that we have to place children up for adoption with same-sex couples, we’ll have to get out of the adoption enterprise, which everybody admits we probably do better than anybody else.’ And one of the City Council members said, ‘Good. We’ve been trying to get you out of it forever. And besides, we’re paying you to do it. So get out!'”
What about the argument that vast numbers of Catholics ignore the church’s teachings about sexuality? Doesn’t the church have a problem conveying its moral principles to its own flock? “Do we ever!” the archbishop replies with a hearty laugh. “I’m not afraid to admit that we have an internal catechetical challenge—a towering one—in convincing our own people of the moral beauty and coherence of what we teach. That’s a biggie.”
For this he faults the church leadership. “We have gotten gun-shy . . . in speaking with any amount of cogency on chastity and sexual morality.” He dates this diffidence to “the mid- and late ’60s, when the whole world seemed to be caving in, and where Catholics in general got the impression that what the Second Vatican Council taught, first and foremost, is that we should be chums with the world, and that the best thing the church can do is become more and more like everybody else.”
The “flash point,” the archbishop says, was “Humanae Vitae,” Pope Paul VI’s 1968 encyclical reasserting the church’s teachings on sex, marriage and reproduction, including its opposition to artificial contraception. It “brought such a tsunami of dissent, departure, disapproval of the church, that I think most of us—and I’m using the first-person plural intentionally, including myself—kind of subconsciously said, ‘Whoa. We’d better never talk about that, because it’s just too hot to handle.’ We forfeited the chance to be a coherent moral voice when it comes to one of the more burning issues of the day.”
Without my having raised the subject, he adds that the church’s sex-abuse scandal “intensified our laryngitis over speaking about issues of chastity and sexual morality, because we almost thought, ‘I’ll blush if I do. . . . After what some priests and some bishops, albeit a tiny minority, have done, how will I have any credibility in speaking on that?'”
Yet the archbishop says he sees a hunger, especially among young adults, for a more authoritative church voice on sexuality. “They will be quick to say, ‘By the way, we want you to know that we might not be able to obey it. . . . But we want to hear it. And in justice, you as our pastors need to tell us, and you need to challenge us.'”
As we talk about sex, Archbishop Dolan makes a point of reiterating that his central objection to the ObamaCare mandate is that it violates religious liberty. In their views on that subject, and their role in politics more generally, American Catholics have in fact become “more like everybody else.” When John F. Kennedy ran for president in 1960, he found it necessary to reassure Protestants that, in the archbishop’s paraphrase, “my Catholic faith will not inspire my decisions in the White House.”
“That’s worrisome,” Archbishop Dolan says. “That’s a severe cleavage between one’s moral convictions and the judgments one is called upon to make. . . . It’s bothersome to us as Catholics, because that’s the kind of apologia that we expect of no other religion.” But times have changed. Today devout Catholic Rick Santorum is running on the promise that his faith will inform his decisions—and his greatest support comes from evangelical Protestants.
The archbishop sees a parallel irony in his dispute with Mr. Obama: “This is a strange turn of the table, that here a Catholic cardinal is defending religious freedom, the great proposition of the American republic, and the president of the United States seems to be saying that this is a less-than-important issue.”
Religious freedom has received a more sympathetic hearing at the U.S. Supreme Court—which, coincidentally, has had a Catholic majority since 2006. In January, inHosanna-Tabor v. EEOC, the court ruled unanimously in favor of an evangelical Lutheran church’s right to classify teachers as ministers and therefore not subject to federal employment law. Archbishop Dolan sums up the decision: “Nowhere, no how, no way can the federal government seek to intrude upon the internal identity of a religion in defining its ministers.”
But whether the government has the authority to define a ministry—excluding, as the ObamaCare mandate does, church-affiliated institutions like hospitals and schools—is a separate legal question, one that may be resolved in litigation over the birth-control mandate.
It’s possible that the Supreme Court or a new president will render the issue moot. After our interview, the archbishop has a question for me: If the high court rules against ObamaCare, will that be the end of the birth-control mandate? Probably not, I tell him—though such an outcome seems much likelier now than it did early in the week when we met. The justices could end up striking a blow for religious liberty without the question even having reached their docket.
Mr. Taranto, a member of the Journal’s editorial board, writes the Best of the Web Today column for OpinionJournal.com.
Albuquerque, NM, Nov. 18, 2013 (OperationRescue) — On the weekend before a municipal election that will determine if Albuquerque, New Mexico, will become the first city in the nation to ban abortions after 20 weeks, a woman has come forward in a new video to tell why, when faced with a prenatal diagnosis of a child with severe fetal anomalies, she heroically rejected pressure to abort her son, Chance.
Calling the bid to end late-term abortion a “humanitarian issue,” Chantel Stuckman told of the heart-wrenching moment when she and her husband were told that her 24 week pre-born son had deformities so severe that he was not expected to live. While her doctors did not demand that she abort, they pressured her to rapidly make a life-or-death decision.
Chantel, who had an abortion as a teen that she deeply regrets, says she knew that this baby must be given a chance at life, however slim.
“Chance was diagnosed with hydrocephaly and other conditions that often lead to abortions out of a misguided concern that the don’t want their child to suffer,” said Tara Shaver, Chairperson of ABQ Voters For Late Term Abortion Ban. “Aborting babies who are sick or disabled isn’t something a compassionate society should do. We should let life take its course, and when we do, sometimes unexpected blessings come from what seems at first like tragedy.”
Chantel agrees, noting that doctors told her that her son would not survive, but he did. They said he would never walk, talk, or read, but he can do all three.
“I think that all children struggle,” said Chantell. “And I don’t think that killing them is ever our first option. I don’t think we look at a child who’s going through drug abuse and say, ‘You know, they’re really struggling. Maybe it would be better if I killed him.’ I don’t think we look at a child who is diagnosed with a terminal illness and say, ‘Well, maybe we should just kill him because their suffering is going to be too much.’ So I don’t see the fact that a child may or may not suffer as a reason to end their life.”
Today, Chance is a happy 14-year old teen who is a joy to all who know him.
Chantel says she supports the Pain Capable Unborn Child Protection Ordinance because she understands more than most the heartbreak of a poor fetal diagnosis – and that abortion is not the answer. In a new video, produced by Shaver and Cheryl Sullenger of Operation Rescue, Chantel urges Albuquerque voters to support the Pain Capable Unborn Child Protection Ordinance for the sake of children like Chance.
Watch this video of Chantel Stuckman describing her experience having a child diagnosed with abnormalities too severe to survive: http://www.youtube.com/watch?feature=player_embedded&v=xhUaaMQaF28
WOODBURN, Indiana, November 8, 2013 (LifeSiteNews.com) – The 17-year-old woman had been terrorized, humiliated and crushed by what had happened to her. She had been raped. Now, to make matters worse, she was pregnant. Her mother had forced her to visit a back alley abortionist, to solve “the problem.” But at the last moment, Sandy decided not to go through with the illegal procedure. The year was 1972.Two weeks later, Sandy’s father suddenly died. Her entire world had now completely come crashing down upon her. All she wanted was her life back. All she could wonder was what was to become of her and the little new life beginning to stir inside her…
Last month something remarkable happened to Monica Kelsey, 40, that confirmed to her that no life, no matter how it came to be, is a mistake: She found a diamond in a field of plowed dirt. Monica had been abandoned by her raped birthmother, Sandy, at a hospital two hours after being born and was soon adopted. She grew up completely unaware of her turbulent beginnings. It was only three years ago that she connected with her birthmother and heard the true account of her life for the first time.
“When I found my birthmother she said to me: ‘It’s amazing how something so beautiful has come out of something so horrible,’” Monica said in an interview with LifeSiteNews.com.
When Sandy unexpectedly passed away this past March, Monica connected with relatives at the funeral who had not even known of her existence. “I prayed for a relationship with my birth family,” Monica said. “When I finally found them, no one knew about me. I was literally the family secret.”
Monica decided to travel from her home in Indiana to Arkansas last month to explore her roots. She wanted to experience for herself the sights and sounds that had been a part of her birthmother’s life.
During her stay, Monica and a few of her newly discovered relatives decided to try their luck treasure hunting at Crater of Diamonds State Park in Arkansas, the only diamond-producing site in the world where the public can find real diamonds and keep them.
Geologists believe that a volcano brought the diamonds to the surface about 100 million years ago. Diamonds form deep in the earth at extremely high temperatures and pressures. Less than one percent of the 150,000 visitors to the park each year find a diamond.
After two hours of poking about the 37 acres of plowed eroded volcanic surface at the park, the group, with wet clothes and dirty shoes, decided to call it a day. But as Monica went to pick up her bucket and join her newfound family, she noticed something on the ground glimmering in the sunlight. Stooping to pick it up, she knew immediately what she had found: a yellow diamond.
“It’s amazing how I found this shining sparkling diamond in a field of dirt,” she said.
Park staff confirmed the find. The diamond, the 400th found that year, weighed just over half a carat (56 points).
For Monica, finding the diamond was filled with the deepest significance. It suddenly dawned on her that she, conceived in the horrible act of rape, was really her birthmother’s “diamond in the rough”.
“I did correlate finding this diamond as a kind of sign that my life [despite its rough beginnings] is still shining, that the sparkle is still there,” she said. “God took my birthmother’s deepest pain and turned it into the most precious of jewels.”
“I just praise God that my birthmother was strong enough to walk out of the abortion clinic,” she said.
Monica, a firefighter and medic who is married with three children, has become a public advocate for children conceived in rape after first learning of her beginnings.
She said that she used to be against abortion “except in the case of rape” – that is, until she “became educated.” Now she will tell anyone who will listen that her life “isn’t any different than your life simply because of the way I was conceived.”
Monica will gently tell people that “abortion has never fixed a rape, it never has and it never will.”
“Abortion just adds more trauma to rape and makes the child a victim as well, but unfortunately by the mother’s own hands,” she said.
Monica believes that women who become pregnant by rape should think about the new life flourishing inside them as their own “diamond in the rough.”
“There is a diamond in this pregnancy that will shine later on, you just have to let it grow,” she said. “Girls today don’t give themselves enough credit about how strong they can be.”
Monica plans to make a necklace with her diamond, leaving it uncut. She will wear it in memory of her birthmother’s sacrifice to give her the greatest gifts of all, life and her adoptive family.
“She is my hero, she truly is.”
Monica says she has nothing but gratitude for the choices her raped mother made.
“Life is sacred. Life is precious. Life is a gift. Thank you, Lord, for my birthmother.”
Follow Monica’s pro-life work on her website and on her Facebook page.
by Steven Ertelt | The Vatican | LifeNews.com | 11/7/13
The praise for Pope Francis since becoming the leader of the Catholic Church has been consistent over the last several months. Catholics and Protestants alike have showered him with praise for not only his pro-life position but his willingness to show extended love and support for the disabled.
Just days after getting international acclaim for letting a teen with Down Syndrome take a spin in the Popemobile, Pope Francis is drawing accolades for showing love to a disabled man covered in boils.The Pope wasted no time in kissing and blessing the man.
Bill Hallowell at The Blaze has more on what happened:
On Wednesday, Pope Francis took the time to do one simple thing that has now captivated the globe: He embraced and prayed with a man who was covered in tumors in St. Peter’s Square.
The encounter between the pontiff and the unnamed individual reportedly unfolded after Pope Francis addressed his general audience and the man approached the Catholic leader and asked to be blessed.
The afflicted individual reportedly suffers from neurofibromatosis, a disease described by the Mayo Clinic as a “genetic disorder that disturbs cell growth in your nervous system, causing tumors to form on nerve tissue.”
While individuals suffering from neurofibromatosis are sometimes shunned as a result of their appearance, Pope Francis wasted no time kissing the man’s face, embracing him and offering up a blessing.
by Steven Ertelt | San Diego, CA | LifeNews.com | 11/7/13
Alexis Clarke weighed just 11 ounces at birth — smaller than a can of soda. That was six months ago, when she was delivered at UCSD Medical Center at just 25 weeks. The smallest baby ever born at the medical center, Alexis is only now finally able to head home.
After months of medical care, Alexis is now bigger and healthier — and her family has supported her each and every day.
The U.S. Senate saw the introduction of a bill today that will protect babies like Aleixs from abortions. It would ban abortions on unborn children starting at 20 weeks – just five weeks ahead of when Alexis was born.
“She was 11 ounces. So, she was 340-grams,” mother Laurie Clarke said, holding up the palm of her hand to describe just how small her little girl was at birth. “[She was] smaller than a can of soda. But when I got to see her, she was just our baby angel.”
Alexis was born three-and-a-half months early. According to her mother, doctors had to deliver Alexis early due to complications stemming from an under-developed placenta.
At Alexis’ small size, Clarke said her baby’s odds of survival were low – less than 25 percent. Given survival, doctors told Alexis’ family that her odds of significant and permanent complications were high.
For the first-time mother, watching her baby spend several months in an incubator meant an almost unbearable wait to just hold her child, and wonder what went wrong with the pregnancy.
“Honestly, it was a lot of, ‘What did I do wrong?’” said Clarke between tears. “Hearing that it wasn’t anything that I did definitely helped.”
According to the National Center for Health Statistics (NCHS), of the Centers for Disease Control and Prevention (CDC), babies born at 28 weeks or later survive 90 percent of the time.
Babies born between 24 and 27 weeks – as in Alexis’ case – survive 80 percent of the time.
Despite the precarious odds, Alexis, her parents and UCSD medical staff fought for her survival. For the first few months, Clarke said the situation was very much touch-and-go. Immediately, the baby was placed in the Neonatal Intensive Care Unit (NICU) at UCSD Medical Center, surrounded by nurses and doctors tending to her 24 hours a day, seven days a week.
If all goes according to plan, Clarke said her little girl will be released from the hospital and headed home for the first time ever by Thanksgiving.
“We have something definitely huge to be thankful for,” said Clarke.
by Steven Ertelt | Washington, DC | LifeNews.com | 11/8/13
Tens of millions of women who have had abortions over the last decades worldwide regret their abortions. Marie Ideson of England is one of them.
Every morning when she wakes up she misses the six-year-old little girl who she named Lillie and planned to give a wonderful life — than is until an amniocenteses discovered Lillie had Down Syndrome.
“Despite any disability, my daughter would have been incredibly well loved. And whatever her future was, I would always have been there for her,” Ideson tells the London Daily Mail newspaper.
But that love will never be given out. Days playing in the rain, carting Lillie off to school, hugs and kisses, applying bandages to scrapped knees. They’re never happen, because Lillie is one of the millions of babies who have been killed by abortion.
Not only did the abortion take Lillie’s life and deprive Ideson of a daughter who could have blessed her life, it tore apart her family. She and her partner had another child but that didn’t save the relationship.
Yet when she was a little over 16 weeks pregnant with Lillie — and having been told by doctors that tests showed her much-wanted daughter had Down’s syndrome — Marie did something that still torments her and which she blames for the breakdown of her marriage: she underwent a termination.
‘Looking back, I was bullied into going ahead with an abortion,’ says Marie, 46, a GP surgery manager. ‘I only wish I could turn the clock back. I think of the daughter I never had every day. I will always regret it.’
‘When I said I wanted to keep the baby, I was told she could be born needing emergency heart surgery and have bowel and muscle tone problems — and that was if she survived.
‘At no time did anyone suggest we might keep our baby. A termination was presented as the only way forward.’
Not only that, but Marie also thinks she was made to feel guilty about wanting to continue with her pregnancy.
‘A nurse said not aborting my baby would cause it to suffer, and she’d only become a burden on society if I went ahead,’ says Marie. ‘She even said: “Ninety-nine per cent of women in your situation wouldn’t want the baby.” ’
About her husband, she says:
She adds: ‘It might sound unreasonable, but I blamed him as well as the doctors for the abortion. He knew I was anti-abortion and that I wanted to keep my baby.
‘I was upset that he had allowed me to take the pill and didn’t just take me home. I believed he’d sided with the consultant. And when Reuben arrived, I also realized nothing was going to bring Lillie back and a new baby couldn’t solve the issues in our marriage.’
By the time Reuben was two, the couple had split. Marie, who never signed a consent form for the abortion, spent thousands of pounds in legal fees in a bid to gain an apology from the hospital — although she was eventually forced to abandon legal action due to the expense.
Of her broken marriage she says: ‘I couldn’t get over what happened — neither of us could come to terms with it. The trauma was always there between Allan and I. The rift it caused just couldn’t be healed.’
She says: ‘My eldest sons are now aged 25. When pregnant with them, I knew of women having Down’s syndrome babies. But when I had Reuben, I heard of no one.
‘Today, I never see mums with Down’s syndrome babies. I can’t help feeling other women must be having abortions they don’t want. I can’t believe that everyone who finds out their baby has Down’s syndrome willingly chooses to abort it.’
by Bobby Schindler | Washington, DC | LifeNews.com | 11/4/13
Former Governor Sarah Palin, whether it was intentional or not, certainly began the discussion on end of life issues when she referred to “death panels” in a 2009 debate about federal health care legislation to cover the uninsured in the US.
Governor Palin was referring to death panels in the context of government officials making life and death decisions if/when the government took over our health care system.
However, what the general public doesn’t seem to realize is that death panels (if you want to use that label) already exist. Perhaps even more alarming, however is the extent that our medical rights have deteriorated due to an unrelenting anti-life agenda that has slowly transformed our laws – and our culture – into accepting the killing of our most medically vulnerable American citizens.
Patients and family members are now seeing health care professionals empowered to make life and death decisions – quality of life assessments – when a person should or should not receive treatment regardless of what the patient wants or what the family wants.
To make things worse, we have the vast majority of the mainstream media, by the manner in which they report on this issue, desensitizing the general public when it comes to how we treat our medically vulnerable. Ironically, each one of us is now in the position to potentially become a victim of this acceptance.
But not only are we seeing physicians having more control over our health care decisions, there has been a fundamental shift when it comes to the mentality of these caretakers, particularly when it comes to treating, or not treating, those with profound cognitive disabilities, Alzheimer’s disease, the elderly, and countless other medically vulnerable persons.
Add to this the laws that have now changed, and you can see the fear of some and the possibility of a euthanasia explosion occurring in our nation’s health care system. Perhaps, as I seem to think, this is already a reality.
No longer, for example, is food and water (via feeding tubes) considered basic and ordinary care. We now define food and water as medical treatment, and as such, depending on the state you live in, can make it rather easy to deny food and water to individuals, even when they have expressed wishes that they want food and water.
In fact, according to a recent report by the Robert Powell Center for Medical Ethics, “the laws of all but twelve states may allow doctors and hospitals to disregard advance directives when they call for treatment, food, or fluids.” So call them what you want, but the reality is that “ethics committees” are now empowered to deny even the most basic care from each and every one of us, if they decide that is what they want to do.
For many years, Bioethicists Wesley J. Smith has been writing about these issues and the ominous direction we are moving as a nation. In particular, pointing out time and time again how the media, for the most part, is helping push the agenda.
Perhaps the only good news is the fact that there has been so much talk about Obamacare and how it relates to end of life issues and “death panels” that some people are now beginning to pay at least some attention to what is happening. Indeed they should, because not only may it affect their end of life care, but any type of medical treatment they may or may not receive, as well.
How is it that all you hear about from those who support euthanasia and assisted suicide is that a patient’s rights must be protected and we must allow the patient to make the decision if they want to take their life. But what happens when it is their choice that they want to live and receive certain treatments? What happens then?
In a recent case involving a hospital in Liverpool, Britain’s highest court ruled in favor of the hospital to withhold treatment from a terminally ill man despite the family’s opposition. Not to mention that in Belgium, they are now considering euthanasia for children, if you can believe that. From the AP, “Belgium considering new euthanasia law for kids.”
Should children have the right to ask for their own deaths? In Belgium, where euthanasia is now legal for people over the age of 18, the government is considering extending it to children — something that no other country has done. The same bill would offer the right to die to adults with early dementia.
All of this is very troubling and we can no longer say this is only happening “across the pond”, so to speak. Every single day, here in the United States, people are being euthanized either by terminal sedation, denial of food and water, or withholding treatment. And I’m sure there are other ways where death is being imposed upon patients.
Sadly, other than some awareness that is being raised, there seems to be no real push back coming from the general public or the organizations equipped to expose this insidious and growing culture of death issue.
Maybe it is due to the fact that we have become a nation so desensitized to the value and dignity of all life that when we see the medically vulnerable, we have convinced ourselves that we are acting out of “compassion” to end their lives, rather than caring for them. Whatever the reasons, and I am sure there are many, as widespread as I believe euthanasia is occurring across our nation’s health care facilities, we are only seeing the tip of the iceberg.
by Steven Ertelt | Washington, DC | LifeNews.com | 11/4/13
A woman with stage four gallbladder cancer is one of the millions of Americans who are losing their health insurance thanks to the rules and regulations that are a part of Obamacare. Edie Littlefield Sundby details her plight in a new article the Wall Street Journal published:
Everyone now is clamoring about Affordable Care Act winners and losers. I am one of the losers.
My grievance is not political; all my energies are directed to enjoying life and staying alive, and I have no time for politics. For almost seven years I have fought and survived stage-4 gallbladder cancer, with a five-year survival rate of less than 2% after diagnosis. I am a determined fighter and extremely lucky. But this luck may have just run out: My affordable, lifesaving medical insurance policy has been canceled effective Dec. 31.
My choice is to get coverage through the government health exchange and lose access to my cancer doctors, or pay much more for insurance outside the exchange (the quotes average 40% to 50% more) for the privilege of starting over with an unfamiliar insurance company and impaired benefits.
Countless hours searching for non-exchange plans have uncovered nothing that compares well with my existing coverage. But the greatest source of frustration is Covered California, the state’s Affordable Care Act health-insurance exchange and, by some reports, one of the best such exchanges in the country. After four weeks of researching plans on the website, talking directly to government exchange counselors, insurance companies and medical providers, my insurance broker and I are as confused as ever. Time is running out and we still don’t have a clue how to best proceed.
Before the Affordable Care Act, health-insurance policies could not be sold across state lines; now policies sold on the Affordable Care Act exchanges may not be offered across county lines.
What happened to the president’s promise, “You can keep your health plan”? Or to the promise that “You can keep your doctor”?
During the 2012 presidential elections, abortion activists and the Obama campaign concocted all sorts of phony “War on Women” stories to make it appear pro-life organizations and pro-life candidates somehow didn’t care about women.
Now that the election is done and Obamacare is in place, the real perpetrator of the War on Women is getting exposed. Exhibit A is Jennifer Harris of California, who is three months pregnant, is losing her current insurance thanks to the Obamacare rules.
by Cheryl Sullenger | Albuquerque, NM | LifeNews.com | 11/4/13
Archbishop Michael Sheehan urged Albuquerque Catholics to cast their votes for the historic Pain Capable Unborn Child Protection Ordinance Sunday, telling them that a vote for the ordinance is the only way a Catholic should vote.
“Let us say ‘yes’ to Jesus, let us say ‘yes’ to the unborn child, and urge others to do the same,” he said during his homily at the Shrine of Bernadette. His message resonated with parishioners, some of which plan to take advantage of early voting which is now open.
Meanwhile ABQ Voters for Late Term Abortion Ban have released a new 1-minute promotional videourging Christians to vote for the Pain Capable Unborn Child Protection Ordinance during an upcoming municipal election on Tuesday, November 19. This video was shown in several churches across Albuquerque yesterday in English and Spanish.
The church-focused “Get Out the Vote” campaign is a strategic one.
“Since launching our campaign last month ABQ Voters For Late Term Abortion Ban has been getting out the vote in local ABQ churches. The Christian churches make up the majority of our voting base and that is where our focus is, and where our votes “FOR” the Pain Capable Unborn Child Protection Ordinance will come from,” stated Tara Shaver, Chair.
“Our campaign volunteers have been warmly welcomed into dozens of local churches who are eager to see this ordinance pass,” shaver continued. “In lieu of a mainstream television commercial, we are proud to launch our latest effort to remind voters within the churches to cast their ballot vote “FOR” the Pain Capable Unborn Child Protection Ordinance. This video is relevant among our base and cuts to the heart of the issue. Will we continue to kill innocent human beings in the womb who can feel pain? That is what’s on the ballot and what ABQ voters will decide.”
A recent ABQ Journal Poll showed that the proposed ordinance, this first of its kind on the Municipal level, enjoys the support of 54% of likely voters.
EWTN Global Catholic Network filed a new lawsuit October 28 in Federal Court against the Department of Health & Human Services, HHS Secretary Kathleen Sebelius, and other federal agencies seeking to stop the government from imposing the HHS contraception mandate as well as asking the court to find that it is unconstitutional. The State of Alabama, through its Attorney General Luther Strange, has joined EWTN as a co-plaintiff in the lawsuit.
“EWTN has no other option but to continue our legal challenge to the mandate,” said EWTN Chairman and CEO Michael P. Warsaw. “The revised rules, published by the government in July, have done nothing to address the serious issues of conscience and religious freedom that EWTN has been raising since the mandate was first published last year. The government has decided that EWTN is apparently not religious enough to be exempt from the rule. It has still placed us in a situation where we are forced to offer contraception, sterilization, and abortion-inducing drugs as part of our employee health plan or to offer our employees and their families no insurance at all. Neither of these options is acceptable. The mission of EWTN is not negotiable.”
EWTN’s original lawsuit opposing the mandate was filed Feb. 9, 2012, but was dismissed by Federal Judge Sharon Lovelace Blackburn on March 25, 2013. In her order dismissing the original suit, Judge Blackburn noted that the government had promised to implement a new rule addressing the issues raised by EWTN. Blackburn’s opinion stated that “common sense weighs in favor of withholding judicial review until new regulations are created and finalized. At that point, if EWTN still has objections, it may then file suit.”
The Department of Health and Human Services issued a new set of rules on July 23, 2013 which Secretary Sebelius claimed addressed the concerns of EWTN and other similar organizations.
“When the government opened up a period for public comment earlier this year in advance of publishing its revised rules, EWTN submitted extensive remarks and an explanation of its moral objections to the mandate,” Warsaw continued. “We sincerely hoped that our concerns would be addressed. Instead, the government ignored our comments entirely and pressed forward with a rule that changed nothing. We are in the same position today as we were when the mandate was first published.
“As an organization that was founded to uphold the teachings of the Catholic Church, we do not believe that contraception, voluntary sterilization, and abortion-inducing drugs constitute health care. We simply cannot facilitate these immoral practices,” said Warsaw.
“Version 2.0 of the mandate is just as bad as version 1.0,” said Lori Windham, Senior Counsel at the Becket Fund, which filed both the original and new lawsuits on EWTN’s behalf. “It would still force the world’s preeminent Catholic network to betray publicly the very teachings it was founded to promote, and which it promotes on a daily basis.”
In 2012, shortly after the first EWTN lawsuit was filed, Alabama Attorney General Luther Strange petitioned the court to join the EWTN complaint. In this new lawsuit, the State of Alabama has joined EWTN as a co-plaintiff from the start.
Commenting on this new lawsuit, Attorney General Strange said, “I am proud to stand with EWTN to oppose this unconscionable mandate. … The freedom of religion, and to believe as one sees fit, is our ‘first freedom’ under the United States Constitution. The people of Alabama have recognized the importance of this freedom and have enshrined it in their Constitution as well. Alabama law does not allow anyone to be forced to offer a product that is against his or her religious beliefs or conscience.”
“EWTN is extremely grateful to Attorney General Strange for his support on this important issue. The Attorney General clearly understands what is at stake here, not just for EWTN, but for all people who feel that government cannot take away the right to religious freedom,” said Warsaw.
EWTN Global Catholic Network, in its 32nd year, is available in over 230 million television households in more than 140 countries and territories. With its direct broadcast satellite television and radio services, AM & FM radio networks, worldwide short-wave radio station, Internet website www.ewtn.com, electronic and print news services, and publishing arm, EWTN is the largest religious media network in the world.
The Becket Fund for Religious Liberty is a non-profit, public-interest law firm dedicated to protecting the free expression of all religious traditions. The Becket Fund has a 17-year history of defending religious liberty for people of all faiths. Its attorneys are recognized as experts in the field of church-state law, and they recently won a 9-0 victory against the federal government at the U.S. Supreme Court in Hosanna-Tabor v. EEOC.
by Shawn Carney | Washington, DC | LifeNews.com | 10/28/13
Are you ready for another serving of Monday morning good news? Here it is! So far during this 40 Days for Life campaign, we now know of 371
babies whose mothers decided to reject abortion! Here are the stories of two of those babies … their parents … and grandparents.
—————————————————–
LITTLE ROCK, ARKANSAS
—————————————————–
On a typical Saturday morning, there are around two dozen people praying outside the abortion center in Little Rock. But the volunteers have a new obstacle now. “Water sprinklers were installed on top of the
privacy fence and constantly spray the sidewalk and driveway,” said Mary in Little Rock. That makes it much harder to talk to women entering the building. “We have suggested the sidewalk counselors wear rain gear now,” she said. The sprinklers can’t stop the prayers. A woman walked through the curtain of water to tell Mary that her 16-year-old daughter would not be getting an abortion. “She hugged the three of us praying and I directed her to the pregnancy care center across the street for help,” Mary said. “Praise God!”
Mary asked the abortion center’s security guard “if he really thought a little water would keep us away. He did not respond.”
—————————————————–
NEWBURGH, NEW YORK
—————————————————–
A young lady arrived at Planned Parenthood along with her boyfriend and sister. “Although her boyfriend and sister did not support her decision to have the abortion,” said Wendy in Newburgh, “her mother was pressuring her.”
The boyfriend was upset over this decision, but felt he had no say in the matter. “He said that she was nine weeks pregnant and she even had an ultrasound picture of the baby,” she said. “He couldn’t bring himself to look at that picture knowing the fate of his baby.”
The prayer volunteers encouraged him to go inside Planned Parenthood and get his girlfriend out. They told him to not give up on that baby because they certainly refused to do so. As he went inside, they
prayed fervently.
Finally, they all came out. “This young man looked like he had the weight of the world lifted off his shoulders,” Wendy said. As he drove off, he smiled and gave a thumbs-up.
“Don’t ever doubt that your prayers and presence make a difference,” said Wendy.
LifeNews.com Note: Shawn Carney is the campaign director for the 40 Days for Life pro-life prayer campaign against abortion
by Steven Ertelt | St. Joseph, MO | LifeNews.com | 10/28/13
A mother in Missouri and her baby are both healthy after a rare and undiscovered ectopic pregnancy. Jonna Snodgrass, 36, delivered
Jatelyn Snodgrass at Heartland Regional Medical Center’s New Beginnings Unit earlier this month.
Doctors discovered the baby girl was ectopic and didn’t implant in the uterus. For more details, go to http://www.newspressnow.com/news/local_news/article_3b429a07-24ab-50c4-9fd6-399fbdc5ee7c.html
From birth weight to length, the decor, affixed to a labor/delivery/recovery/post-partum room in the maternity wing, announced the details of Katelyn Snodgrass’ birth at 11:49 a.m. Monday.
Not included, however, was the fact that she was brought into the world following an unusual gestation. Instead of growing inside her mother’s uterus, her embryo had taken root on an ovary
Katelyn’s mother, St. Joseph resident Jonna Snodgrass, 36, said finding out that fact, after undergoing a C-section delivery, was a bigsurprise.
“I was shocked and I don’t know how we both survived it, but we’re both here,” she said.Ms. Snodgrass said nothing about her pregnancy
seemed out of place. “Really nothing was different, except for the C section,that was totally new to me,” she said. “Everything else was pretty much the same.”
The Snodgrasses noted that Katelyn’s location was undetected by two
sonograms done after the 20-week mark.Dr. Brooke Seevers was Ms. Snodgrass’ obstetrician throughout the pregnancy. Dr.
Seevers said ectopic pregnancies,pregnancies where an embryo implants
outside of the uterus, are uncommon.“It’s a very rare complication to develop fora pregnancy,” she said.Ms. Snodgrass’ case was an even rarerform of ectopic pregnancy in terms ofwhere the embryo implanted. Ovarian ectopic pregnancies account for about half a percent of all ectopic pregnancies, Dr. Seevers said.
Implantation on the fallopian tubes is far more common.
She said typically ectopic pregnancy patients receive the diagnosis after experiencing pain and bleeding early on. In addition to being potentiallylife-threatening to the mother, they also run a high
risk of miscarriage or premature birth.
Sterilization Reversal – A Generous Act of Love is a compilation of 20 stories of couples who were sterilized and then sought sterilization reversal. It is the first book that discusses, from a Roman Catholic perspective, the destructive impact that sterilization has on marriage and the joyous spiritual and marital renewal experienced by couples after reversal. As such, Sterilization Reversal – A Generous Act of Love is a unique resource for clergy, religious educators and laypeople. It is an especially useful tool for the pastoral counseling of persons who have repented their sterilization. It is also a particularly effective means of informing people who are considering sterilization of the emptiness and heartbreak that often follow as well as the NFP alternative that nourishes the marital relationship rather than attacks it. (more…)
DETROIT, Sept. 24, 2013 (LifeSiteNews.com) – Despite strong criticism and a public rebuke from another bishop, Detroit’s Archbishop Allen Vigneron has reaffirmed his insistence that Catholics who support same-sex “marriage” should not receive Holy Communion.
The archbishop was speaking to media at a pro-life vigil in Motor City on Saturday.
“I don’t think they were hurtful,” he said of his comments from April, according to the Detroit Free Press. “I think they were straightforward. There’s nothing hurtful in telling people the truth.”
“And the truth is that… the teaching of the church about marriage is God’s way for us to flourish,” he added. “That’s what I want people to know.”
On April 7th, the archbishop had stressed, in the wake of the Supreme Court’s ruling striking down the Defense of Marriage Act, that a Catholic must be committed to Church teaching if they present themselves for Holy Communion.
“For a Catholic to receive holy Communion and still deny the revelation Christ entrusted to the church is to try to say two contradictory things at once: ‘I believe the church offers the saving truth of Jesus, and I reject what the Church teaches,’” he said. “In effect, they would contradict themselves. This sort of behavior would result in publicly renouncing one’s integrity and logically bring shame for a double-dealing that is not unlike perjury.”
Four days later, Bishop Thomas Gumbleton, a retired auxiliary bishop for the Archdiocese with a strongly liberal reputation who has made a name for himself as an opponent of Church teaching, gave an interview to oppose Vigneron’s stance.
“Don’t stop going to communion. You’re okay,” Gumbleton told Fox News.
The highest authorities of the Church, including Pope Benedict himself, have insisted, however, that the Church’s law not only bars public advocates of abortion and same-sex “marriage” from receiving Communion but, in Canon 915, instructs clergy to deny them Communion if they refuse to recant after receiving instruction.
Canon 915 states that those who are “obstinately persevering in manifest grave sin are not to be admitted to Holy Communion.”
Archbishop Vigneron offered a Mass at Assumption Grotto church for about 200 pro-lifers, and then joined a walk to two abortion facilities where he led a Rosary. The event was organized by the Helpers of God’s Precious Infants.
In his homily, he told the pro-lifers who gathered that they were part of the “field hospital” spoken of by Pope Francis in his widely-publicized interview published last week.
by Steven Ertelt | Washington, DC | LifeNews.com | 10/12/13
With the exchanges of Obamacare activated this month, it has become evident that it is nearly impossible for individuals to try to determine which exchange plans on their state exchange, if any, exclude abortion, said a group of lawmakers at a bipartisan press conference Wednesday.
U.S. Rep. Chris Smith (NJ-04) unveiled his legislation, H.R. 3279, the “Abortion Insurance Full Disclosure Act” —cosponsored by 70 other Members of the House—to ensure full disclosure of abortion coverage, requiring prominent and transparent disclosure of abortion coverage for each plan offered on an exchange. This is crucial information for millions of Americans since the many plans that include elective abortion are required by law to impose a monthly mandatory abortion surcharge. Many Americans object to paying a surcharge into a fund to be used solely for the purpose of aborting unborn babies.
Smith said the inauguration of the Obamacare exchanges reveals that many health insurance plans throughout the nation will include abortion on demand—even late term abortions. Smith recalled that in October 2009, President Obama said in a speech to a joint session of Congress that, “under our plan, no federal dollars will be used to fund abortion… .” A week after the Obamacare rollout, many are now discovering that—contrary to solemn promises made by the President himself—Obamacare violates the Hyde Amendment by funding plans that include abortion.
“The new law requires premium payers to be assessed an abortion surcharge every month to pay for abortions,” said Rep. Smith. “But many pro-life Americans may unwittingly purchase pro-abortion plans because of a marketing secrecy clause embedded in Obamacare which stipulates that the surcharge be minimally disclosed only at the time of enrollment. In other words, bury it in the fine print. This is a Right to Know bill. Americans have a right to know upfront and with full transparency when they are purchasing a plan that subsidizes the killing of unborn children. Even the most ardent advocate of abortion should embrace full disclosure.”
Joining Smith and Dan Lipinksi (D-IL), co-chairs of the Pro-Life Caucus, were Reps. Joe Pitts (PA-16) and Diane Black (TN-06), Vicky Hartzler (MO-04) and Trent Franks (AZ-08).
“Americans buying their insurance through the new healthcare exchanges shouldn’t have to spend hours trying to figure out if the money they pay for premiums will be spent to provide abortions. This bill will give the American people the transparency they need to make informed decisions that are in line with their religious and moral beliefs,” Rep. Dan Lipinski said. “None of this would be a problem if we pass the ‘No Taxpayer Funding for Abortion Act.’ There is a longstanding principle in our country that the federal government does not subsidize abortions. Yet under Obamacare, taxpayer money under the guise of federal subsidies will be paying for insurance that covers elective abortion. This needs to stop.”
“The President tells Americans that they can go online, find the plan that covers what they need, and make a selection,” said Rep. Joe Pitts. “If Obamacare is all about choice, then why is the administration making it so difficult for people to find out about whether a plan pays for abortion? It’s time that we got some truth in advertising.”
“The Obamacare exchange launch has been an unmitigated disaster,” said Congressman Diane Black. “One of the most troubling problems is that many consumers are unclear as to what exactly will be covered by the plans they purchase online. Clearly Americans who are pro-life would object to paying for a health care plan that included abortion coverage and then be forced to pay an abortion surcharge into a fund that is meant to be used solely for the purposes of destroying human life. And this is equally problematic for the millions of Americans who simply don’t believe the federal government should be subsidizing abortions. The Abortion Insurance Full Disclosure Act would simply require that all plans on the exchanges disclose whether or not the plan includes abortion coverage. This is not a partisan issue—this is commonsense.”
I support the legislation that Rep. Chris Smith has put forward, and I adamantly believe that we need to lift the veil of secrecy from Obamacare while ensuring transparent policies,” said Rep. Vicky Hartzler. “I commend every member that has signed on to this bill, and I also encourage members of both parties and the Senate to vote for this common-sense legislation. We must eliminate the “secrecy clauses” and “abortion fees” from current taxpayer subsidized insurance plans and fight to restore individual religious liberty and moral conscience to our medical decisions.”
It happens every day. A couple, excited about their pregnancy and the birth of their child, receive the devastating news of a
prenatal diagnosis.
But even if the diagnosis includes those heartbreaking words – “incompatible with life” – every life deserves to be celebrated, and every baby deserves to be loved. As the friend or family member of someone who has received such a diagnosis, you have the power and the ability to help the couple cope, heal, and find joy.
Listen
Many parents who receive a diagnosis of their unborn children are being told by their doctors that abortion is the best option. Even if the parents don’t want to abort, they may be feeling a lot of pressure to do so. Some may even have doctors and family members telling that keeping their baby is selfish. It’s the hardest time in this couple’s lives, and the last thing they need from you is your unsolicited advice. It is best to listen to them. Let them cry. Let them get angry.
Let them experience the pain that this diagnosis has caused them. In the beginning, they don’t need you to tell them anything. They just need you to listen and hug them. Don’t disappear for fear of upsetting them. Make yourself available whenever your friend needs to talk, and call to check in on her. When the couple is ready to listen to your advice, be kind and non-judgmental. Remember that they want their baby, but they are afraid. Use examples of other families in similar situations to show them that loving a child is not dependent on a child’s health.
Support
Be there to support your friends’ decision to continue with the pregnancy. It’s the right decision, but they may be getting a lot of flak from doctors, friends, and even family about how others think they are doing their child a disservice. Attend doctor appointments with the expectant mom if her partner can’t be there. Be a positive, life-affirming presence in her life. Let her cry when she wants to cry. Let her yell when she wants to yell. Let her know she’s doing the right thing. Make her dinner. Take her to lunch. Help her find resources of support concerning her child’s condition.
Celebrate
Most expectant moms get a baby shower to celebrate their new bundles of joy. But when a couple receives a diagnosis for their unborn child, family and friends often worry about whether or not to throw a baby shower. They often wonder how they can possibly celebrate during such an emotionally devastating time. Before planning a Celebration of Life shower, talk with the couple and make sure they’re okay with it. If they are, help them start a baby registry. Even if they have been told their child won’t survive birth, there is always the hope and the chance that the baby will. The baby may even end up going home after all.
You can ask guests to bring gifts for the mom that include gift cards to restaurants or a spa for a day of pampering. Gifts can also include blankets and quilts with the baby’s name on them. An amazing gift would be a pregnancy photo session. And of course, include the usual gifts such as outfits and baby toys.
Just because a baby has received a prenatal diagnosis does not mean his or her life should go uncelebrated. This child, and his or her parents, need all the love and support they can get, and there’s no better way to do that than by showing how much you care for all of them.
LifeNews Note: Nancy is a work at home mom who writes about parenting, special needs children, and the right to life. She is the lucky mother of two spirited little girls, one who has cystic fibrosis, and she spends any free moment she can find fundraising for a cure for CF. You can read her personal blog atwww.ChronicAdmissions.com. Reprinted fromLive Action News.
Houston, late ’90s. Veronica Arnold, Dorothy Richardson, and Theresa Camara were busy home-schooled kids who spent their time running around the city with their families to take part in every Catholic and/or home-school activity Houston had to offer. All from relatively large families and all raised in a pro-life atmosphere, the girls were eventually destined to cross paths, and they’ve been friends ever since they did. In time, they finished school all left Houston to move on to different colleges. But this particular city has a way of pulling people back in, and, kind of like boomerangs, they again found themselves together in their shared hometown after college.
Each young woman eventually found herself accepting a position at one of three of Houston’s largest pro-life organizations. Each is using her unique talents to contribute to the pro-life enterprise: Dorothy works tirelessly at the Houston Coalition for Life as the programs director, Veronica assists with legislative undertakings at Texas Right to Life (the state affiliate of National Right to Life), and Theresa runs the maternal assistance program at the Foundation for Life. Although they each do vastly different work on a daily basis, the pro-life common denominator ties them together, and their ultimate goal is the same: to see an end to abortion in their lifetime.
When asked why a young person should consider standing up for life, maybe even as a career path, Veronica, Dorothy, and Theresa all spoke from a place of personal experience and conviction. Veronica, who works in legislation, said: To make abortion unthinkable, we need pro-life missionaries. To make abortion illegal, we need pro-life politicians. All too often I hear people say that our government is corrupt, and they won’t have anything to do with politics. Young people won’t even register to vote. But how can we fix the problems if we don’t act? Young people, we need more politicians. We need pro-lifers to run for office, to fight, to win, or even to run and lose – to cut through the muck and forge the pathway for the next pro-lifer to win. We can’t overturn Roe v. Wade without pro-lifers in public office. Whether you work full time in the pro-life movement or not, you can help end abortion by learning the issues, talking about the issues (to everyone!), and voting for the good guys.
Theresa, whose primary job is one-on-one maternal assistance for moms and babies in need, cautioned that the battle won’t end when Roe v. Wade is overturned, pointing out that there will always be mothers and children who need help regardless of the legislative status of abortion: It is important to realize that even if abortion was made illegal tomorrow, there would be a huge number of women who would still be in crisis situations who would need to think about adoption or parenting assistance.
Even if Planned Parenthood was removed from our schools tomorrow, there would be a huge poisoned vacuum which would need to be positively filled and healed. There would be huge legal and social battles to address. We need the young people to stand up and be that true friend for each young pregnant woman… So many young women change their mind simply because their friend or their coworker said, at some point in the conversation, “I think that you will be a great mom!” and “You’re feeling stuck? These people help girls in your situation all the time.” Dorothy, whose day-to-day work is focused on outreach to the community, had a quick answer to the question of why other young people should do pro-life work: “Because it could have been you.” She continued: Because no woman deserves the trauma of abortion. Because no father should miss out on the chance to become a better man. Because no baby deserves to die alone and in horrific pain.
But if somehow that isn’t enough, you should know that this is the ultimate human rights cause, that taking your place on the battle line will bring more graces and more beauty into your life than you can imagine, especially when the fight is hardest. Standing on the sidewalk outside an abortion facility and praying seems so simple but women have changed their minds from abortion to life just because they saw someone standing there (on the sidewalk). Even our smallest pro-life efforts have a tremendous ripple effect.
LifeNews Note: Lauren is a Legislative Associate for Texas Right to Life and a graduate of Ave Maria University. This post originally appeared at Live Action News and is reprinted with permission.
The Bill and Melinda Gates Foundation (GF) has been awarded the most prestigious prize in public health, the “Lasker Award for Public Service”. This award constitutes an important precedent for the Nobel Prize. It honors scientists for pioneering research in the medical field. The GF received the award for taking a novel approach to the way we view the world’s most prominent health problems and improve the lives of millions of vulnerable people in the world, according to the Lasker Foundation.
The award was shared with Richard H. Scheller and Thomas C. Südhof for their discoveries concerning the molecular machinery and regulatory mechanism underlying the rapid release of neurotransmitters, and Graeme M. Clark, of S. Blake Ingeborg Hochmair and Wilson, for development of a modern cochlear implant, a device that gives hearing to profoundly deaf people.
It should be noted that the Gates Foundation funds some meritorious programs, such as sponsoring the research of Dr. William Foege, who discovered the vaccine that eradicated smallpox. However, their primary and almost exclusive efforts are now directed to universal birth control. Their so-called family planning programs really mean abortion, both chemical/medical and surgical. Their goal is one child per woman, especially in the countries of Asia and Africa.
The “Millennium Goals” established by the United Nations in 2002, are a top priority of the GF. These goals have eight human development objectives. Objectives 3 and 4 seek to reduce child mortality and improve maternal health. To meet these two objectives, the Gates Foundation has made very generous donations to flood mainly the countries in Asia and Africa, with contraceptive and abortifacient drugs there are supposed to improve the health of children and women.
GF rhetoric includes the antiquated notion that population growth must stop, “Population growth causes changes in climate, and it can cause huge disaster; we cannot tolerate that the population reaches 9 billion. We need provide better reproductive options to women (… ) but there are women who have children for ideological and religious reasons. ” The GF is also promoting research vaccine use to reduce population.
“Family Planning 2020 Empowering Women Worldwide” is another public health project that is supported by the GF. This is a global partnership to provide 120 million women with access to contraceptive methods by 2020. According to Global News, the GF is collaborating with the Merck and Bayer laboratories, the UN Population Fund (UNFPA ), the Clinton Health Access Initiative, the Children’s Investment Foundation and the governments of Norway Sweden, United Kingdom and United States, to produce contraceptive implants (abortifacients ), Jadelle and Implanon.
The GF will fund Pfizer laboratories for production of injectable contraceptives (abortificients ) for the Department for International Development of the UK, the U.S. Agency for International Development (USAID ) of USA and the Fund for UN Population.
Bill Gates has stated that the “beneficiary” countries will bear half of the costs of the ” Family Planning 2020 ” program, these alleged ” beneficiary countries” will fund early abortions ( by chemical means ) and sterilization of its women and girls. These countries are really been victimized by sterilizing their population, paying for the genocide of their unborn children, and becoming indebted to international organizations.
Public and private organizations thus become partners with the pharmaceutical industries, benefiting from their profits, and allowing the GF to recover some of their alleged donations.
Is public health advanced by flooding women with abortifacient contraceptives that increase the risk of debilitating acute and chronic diseases that are life-threatening?
DETROIT, Sept. 24, 2013 (LifeSiteNews.com) – Despite strong criticism and a public rebuke from another bishop, Detroit’s Archbishop Allen Vigneron has reaffirmed his insistence that Catholics who support same-sex “marriage” should not receive Holy Communion.
September 24, 2013 (PriestsforLife.org) – As the Director of Priests for Life, known worldwide as a ministry within the Catholic Church that urges more preaching, teaching, and action against abortion, I was asked by many alarmed and confused people these past few days about the reported comments of the Pope that the Church should not be “obsessed” with this issue, and that there should be “balance” and “context.
MADISON, WI, September 12, 2013 (LifeSiteNews.com) – Catholic schoolchildren will no longer take field trips to a center that conducts embryonic stem cell research and gives students the opportunity to handle the aborted cells, the Diocese of Madison has announced in a letter.
A teenage contestant in the “Face of Europe” beauty pageant has fought her way back from a debilitating stroke that left her partially blind and in need of daily medication to thin her blood.
The American College of Obstetricians and Gynecologists (ACOG) and the American Society for Reproductive Medicine (ASRM) urged gynecologists to ask for changes in government policies to identify and reduce exposure to toxic environmental agents. The joint committee of ACOG and ASRM warn of toxic chemicals in the environment that lead to infertility, adverse effects in pregnancy, and many other long term health problems. However, these organizations promote the use of hormonal contraceptives such as the pill, which has been classified a Group I carcinogen.
Jeanne A. Conry, MD, PhD, ACOG’s president said: “Legislators should require the Environmental Protection Agency of the United States and industry to define and estimate the risks for pregnant women, infants and children with exposure to chemicals and act to protect the most vulnerable populations.” There is a great concern about chemicals in the environment; however, ACOG promotes the use of long-acting reversible contraception (LARC), IUDs and contraceptive implants with high doses of steroids for women and adolescents girls.
It is known that exposure to toxic environmental agents can cause miscarriage and stillbirth. Similarly, hormonal contraceptives change the uterine lining (endometrium) creating a hostile environment for a newly created human being. The newly conceived baby can’t implant and is aborted.
There is scientific evidence showing that exposure to toxic environmental agents before conception and during pregnancy can have significant and lasting effects on reproductive health. “For example, pesticide exposure in men is associated with poor semen quality, infertility and prostate cancer,” said Linda C. Giudice, MD, PhD, president of the ASRM. Similarly, recent studies have observed the feminization and decreased fertility in aquatic animals due to the presence of estrogenic compounds in the water, some from wastewater contaminated with oral contraceptives. There is a possibility that exposure to oral contraceptives in drinking water contributes to the recent increase in the problems of human reproduction.
“As reproductive health care specialists, we are uniquely positioned to help prevent prenatal exposure to toxic environmental agents and to educate our patients on how to avoid them in the home, in the community and at work,” said Dr Giudice.
We hope these organizations of specialists who know about the health risks with exposure to toxic substances in the environment could realize that hormonal contraceptives are toxic, and doctors prescribe them to women, even teenagers, not only causing effects long and short term, but also doing damage to the environment.
ROME, September 6, 2013 (LifeSiteNews.com)
– Anna Romano, 35, couldn’t believe her ears when she picked up the phone a few days ago. On the other end of the telephone was Pope Francis himself, who called to offer to baptize her baby after she refused to have an abortion.
“I was just so surprised that he had telephoned me. He said that he had read my letter and he wanted to speak to me personally about it and reassure me that someone was worried about me,” Anna, hailing from Arezzo near Florence, told the Daily Mail.
Feeling humiliated, betrayed, and that she had no one else to turn to, Anna wrote to Pope Francis a few months ago about her crisis situation. She revealed that she was pregnant with the child of an already married man who had demanded she abort.
In her letter, Anna told the Pope that she would not have an abortion and that she had told the married man to “get out of my life.”
Anna never dreamed of a reply. Then, when she was on holiday, she received the surprising call. “At the beginning I thought it was a joke, but then he referred to the letter, which only my best friend and my parents knew about,” Anna told Italy’s Corriere della Sera.
“We were only on the phone for a few minutes but my heart was filled with joy, as we spoke I was rubbing my tummy at the same time,” she told the Daily Mail. “I would never have imagined that the Pope would pick up a telephone and call me and speak to me as if I was a dear friend.”
During the call, Pope Francis reassured Anna that a “child was a gift from God, a sign of Divine Providence” and that she would “never be left alone,” Anna remembered.
“He said that as Christians we should never be afraid,” she said. “He told me I had been very brave and strong for my unborn child.”
When Anna told the Pope that she desired baptism for her baby but was afraid that her divorce and her being a single mom would be an obstacle, the Pope said that he would be her “spiritual father” and would baptize the baby himself.
“I’m not sure if he will,” said Anna, who said she can only think back to the call as if it were a dream. “But if he did baptize my baby it would be something else. That telephone call has changed my life.”
Anna said that if the baby the Pope baptizes is a boy, then she will name him Francis.
Every month, we will post a quote about why babies, children, and new lives are a wonderful, beautiful blessing. We hope that, one positive quote at a time, we can change our society’s attitude towards children. If you like the quote, please post it on facebook, tweet it, pin it, or email it to your friends and family. We hope that, one message at a time, we can change peoples’ attitude towards having another child and children in general.
It is giving witness to Christ in our married and family life. It is transmitting the love we experience in our homes. It is an experience which we cannot and should not silence. And I believe many of us feel that need: We experience something so beautiful in our families that we have to proclaim it as Good News. We should proclaim the Gospel of the family, the Good News of Christian marriage, and the profound joy of married and family communion.
That experience we are having in our homes should give us the strength to not only speak, but also to strive that the world be more of a family: that other families are happy…..that there are laws which respect the rights of the family. But these great tasks can be accomplished only if they stem from a lived ideal, from a profound experience. And that experience we have to have with Christ in the Eucharist and –as an experience of human love –in our own home.
We, married couples, should transmit the ideal of family to the world. We have to feel that mission consciousness, because that fire which burns in our homes –if we transmit it well –is a fire which can transform the world. Our families are the basis for the renewal: renewal of the Church, society, and the world.
Man possessed by his mission.
I believe it is impossible to accomplish the objectives of helping to transform the world without a strong awareness of mission consciousness. It is a very large task. The present circumstances are extremely difficult. We, human instruments, are extremely fragile. Often, the awareness of mission consciousness is not enough. We have to be possessed (captivated, thoroughly aware) of the mission because he who is not “possessed” by God –by his mission –will be incapable of overcoming difficulties he has to face in a pluralistic society.
He who does not believe he has a divine mission, will succumb, he will not risk himself for God. I think we all still lack that irresistible push to bring our mission to fruition.
Lacking is the man who knows he is chosen and sent by God and who thus lives and vibrates for his mission. It is necessary to have awareness of mission consciousness in order to intervene in the history of our Church and our country, like the great Prophets and Saints. Are we possessed by our mission?
God calls us to transform the world. If we want to make Him present, we cannot stay tranquilly in our home, living there our Heaven. We have to strive so that our land can become a colony of Heaven. It means promoting a new Christian culture, a civilization of love, a new social order.
Heroism is necessary. It is daily heroism, heroism with daily and ordinary things: to do everything with the greatest love, surrender, and generosity. It is the heroism of married and family life: but not about poor surrender –
complaining and petty –but of a magnanimous surrender, faithful and without excuses, of a constant growth in love. The question is if we really want to escape lukewarmness, mediocrity and heroically journey toward sanctity. It is only our own personal and family decision if we want to gamble with life or if we want to risk life.
The opposite to all of this are the spectators for whom the world situation, society and the Church, are only seen as a commentary –like an external situation –and not like a “battlefield” where we have to shape our complete vision…..spirits on hold –in apathy and indifference –who are not disposed and who do not have the strength to take mortal leaps.
Questions for reflection
1. What do I do so that the world can be more like a family?
2. Am I aware that God entrusted a mission to me?
3. Am I grateful for what God has given me or am I a person who complains?
Translation: Carlos Cantú, Schoenstatt Family
Federation, La Feria, Texas USA 0113 2011
Original article published on Catholic New World
For Dr. Robert Lawler, the decision to conform his obstetrics and gynecology practice to the teachings of the Catholic Church came down to one thing: “I want to get to heaven,” said Lawler.
Lawler and Dr. Anthony Caruso recently opened Downers Grove OB-GYN, 1121 Warren Ave., Ste. 200, in Downers Grove, with Dr. Anthony Caruso, a reproductive endocrinologist who also has forsworn procedures that conflict with church teaching.
Lawler, a parishioner at St. James-Sag Bridge, and Caruso, who attends St. John Cantius, both came to the realization that they needed to bring their professional lives into line with their beliefs after they started practicing medicine.
For Lawler, who went into practice about 15 years ago, the realization came with the help of urging by his wife and others.
“I was finding pamphlets about ‘Humanae Vitae’ (Pope Paul VI’s 1968 encyclical confirming the church’s teaching against artificial contraception) in my golf bag,” he joked.
At first, he thought, not performing or referring patients for abortions was enough. As for prescribing birth control pills, he said, everybody did it, including Catholic doctors that he liked and respected.
“I thought, if they were doing it, it must be OK,” he said. “There’s not many of us who feel it’s important to be Catholic 24/7.”
Then he came to understand that whatever anybody else was doing, it was definitely not OK.
“I had visions of meeting the Lord at Judgment Day and him saying to me, ‘OK, Robert, what part of “intrinsically evil” did you not understand about contraception?'” Lawler said.
At the same time, he said, younger and younger girls were coming in, with their parents, and asking for contraceptives.
“I would no more hand them contraceptives than I would a pack of cigarettes,” he said. “People said they will do it anyway; I said how about a little less birth control and a little more self-control?”
So he stopped prescribing birth control and performing sterilizations, while remaining in a general OB-GYN practice where other doctors provided those services.
In the beginning, he said, it wasn’t easy.
“That first day when I told patients I would no longer be prescribing birth control was a very long day, and it was a very long year,” he said. “People weren’t shy about sharing what they thought of the Catholic Church or this Catholic doctor.”
But his resolve was bolstered by his belief that what he was doing was medically — as well as morally — right. Giving hormone pills to women to induce a state of false pregnancy, indefinitely, with no medical indication that there is anything wrong, makes no sense, he said. And giving them to women and girls to mask symptoms of other problems is even worse.
“Say a young girl comes in with terrible, painful periods,” Lawler said. “If she goes to a regular gynecologist, nine times out of 10, she’s going to leave with a prescription for the pill in her hand. But why does she have painful periods? Does she have endometriosis or is there something else going on? We are going to dig deeper. … I don’t consider oral contraceptives as a treatment for anything. It may suppress the symptoms, but you aren’t treating anything.”
Caruso, whose epiphany came a bit later, was supported by a friendship with Lawler that started when a priest suggested he contact the other doctor. But Caruso — a reproductive endocrinologist whose practice once included assisted reproduction technologies such as in vitro fertilization and artificial insemination — now can offer his expertise in endocrinology as well as general obstetrics and gynecology.
As part of their services, the doctors support women using all forms of natural family planning, but they encourage them to consider that there is no bad time for a baby once a couple is married. Having children earlier is often easier, avoiding fertility problems that increase with age.
On the other hand, they don’t suggest that there’s something wrong with women who conceive and bear children in their 40s.
That’s appreciated by Sue Zabilka, who first met Lawler because her children attended Everest Academy in Lemont with his, and later learned about the nature of his practice and became a patient. Zabilka has three sons, ages 17, 13 and 2, and she suffered two miscarriages.
She began seeing Lawler 10 or 11 years ago, she said, and she loves the new practice.
“I took a whole stack of business cards and I am giving them to everybody,” she said. “It’s such a welcoming, loving feeling.”
When she was pregnant with her youngest, she said, Lawler took the time to reassure her that women in their 40s can and do have healthy pregnancies, using the example of his own mother, who had her youngest child at 46.
“It just gave me such peace of mind,” Zabilka said.
Caruso, who has six children, said that after he was laid off from his university job, he worked as a hospitalist — a doctor who coordinates the care of patients in the hospital — for a few years, while he tried to get the idea of a center similar to the practice he and Lawler started off the ground. His idea was that it would be part of a Catholic hospital. The proposal came closest to fruition at Alexian Brothers hospital in Elk Grove Village, even becoming the topic of an article in the Chicago Tribune.
But when progress on that front snagged, the best course seemed to be to open a freestanding practice with Lawler, he said.
The two hope that it will become a regional center for patients who want care not only in accord with church teaching, but also with those who want to live a life as free of unnecessary chemicals as possible — those who seek out organic food, for example, and avoid other medications where possible.
“I believe that this kind of care is for everyone,” Caruso said. “It doesn’t put poison in female bodies. We try to get to the bottom of what the problem is and fix it at its source.”
Both doctors believe that the stakes for their new practice are higher than their own professional success.
“There are people out there rooting for us, and there are people out there hoping we crash and burn,” Lawler said. “But I think there are also some fence-sitters out there, Catholic doctors who would like to do this, but want so see if it will work.”
(Life action news) Can’t we all just get along? Apparently not in Ohio, where LifeSiteNews reports that the National Right to Life Committee has cut the cord to Cleveland Right to Life because the latter has criticized pro-life Republican Sen. Rob Portman for supporting…same-sex marriage?
In June, CRTL announced that they were expanding their mission to include the defense of marriage, arguing that the move was necessary in order to cultivate an enduring culture of life:
“The prolife movement must recognize that without this inclusion the efforts to protect human life are diminished. If we are to hasten the end of the culture of death in America we must recognize the role of a stable family that has at its core; committed parents.” said Cleveland Right to Life board member, Jerry Cirino. Social and scientific studies continue to support the role of both mother and father in children’s lives. In a recent report by the Census Bureau the negative impact of single parent households on society is enormous and while CRTL affirms their commitment to support for all children in the womb, the organization also recognizes that single gender parenting should be recognized for what it is – a less then perfect situation for the child.
Recently, Cleveland Right to Life announced that it has embraced an advocacy agenda that includes issues beyond the right to life. Moreover, it promptly issued public criticisms of and implicit political threats against a U.S. Senator who has supported the right-to-life position on every vote that has come before the Senate, and who is a sponsor of major NRLC-backed bills – because the chapter disagrees with his position on a non-right-to-life issue.
By these actions, Cleveland Right to Life has violated National Right to Life policy, causing the chapter to disaffiliate itself from NRLC.
We respectfully insist that you remove from your website the claim that you are affiliated with NRLC, and from this point forward, cease and desist from any representation that “Cleveland Right to Life” is affiliated with the National Right to Life Committee.
According to LSN, CRTL “has never had a direct affiliation with NRTL, only a tiered relationship that is maintained through the state organization, Ohio Right to Life,” with whom CRTL remains in good standing.
As a conservative, I happen to strongly agree with CRTL’s thesis that marriage protection is essential to a comprehensive view of a healthy society, and if CRTL wanted to reinvent themselves into a general social conservative organization, more power to them. That groups like Family Research Council and the Heritage Foundation tackle multiple issues doesn’t prevent them from working with pro-lifers.
However, their name remains Cleveland Right to Life, and as much overlap as there is between the pro-life and pro-marriage communities, any issue-based organization’s members and supporters have a right to expect an agenda focused on that issue. Branching out into separate causes carries the potential for distraction, confusion, and roadblocks to building as broad a coalition as possible for unborn rights—an area where our movement could sometimes use some work. You can’t blame NRLC for wanting their affiliates to keep their eye on the ball.
Then again, publicly severing all ties to CRTL seems a little extreme, no? Admittedly, I don’t presume to know what behind-the-scenes communications took place prior to NRLC’s letter, but it certainly doesn’t read like it’s interested in meeting the Cleveland group halfway, or like it was in reaction to further slights by them—it makes pretty clear that CRTL’s marriage advocacy and criticism of Portman were sufficient deal-breakers all on their own.
Stray from right-to-life issues though CRTL did, they’re still dedicated to fighting for the unborn, and even if their criticism of Portman ever expanded to full-blown opposition, it’s not as if they would advocate replacing him with a Senator who’s less pro-life. If working together to end the scourge of abortion requires pro-lifers to set aside their differences on other issues, then such a magnanimous spirit of commitment to the big picture should cut both ways.
A young journalism student has written a candid account revealing that she eventually gave up using birth after after she developed life-threatening blood clots in her legs and lungs after just four months’ use of the birth control pill.
“I started taking birth control pills in January 2011. By May of that year, my doctor discovered that a blood clot had developed in my right leg and spread to my lungs,” wrote Jamie Hergenrader in an article published in the Huffington Post.
“The pain in my hip, the swelling of my entire right leg and the breathing difficulty I experienced should’ve scared me enough to check it out,” she remarked, but she rationalized away her symptoms. “It wasn’t until my mother dragged me into the doctor,” Hergenrader wrote, “that I learned something was really wrong.”
The 19-year-old, studying journalism at the University of Missouri-Columbia, had developed deep vein thrombosis – a blood clot in a vein, usually in the leg, that becomes fatal when it migrates to other parts of the body such as the lungs, a condition known as a pulmonary embolism.
Although the clot took only four months to develop, “Recovery was a seven-month process of ER trips, doctor visits three to four times a week and a few blood-thinning medications consisting of shots injected in my abdomen and a daily pill,” Hergenrader explained. “I became severely anemic and had to go to the ER, where they considered giving me a blood transfusion.”
Hergenrader stated that before she started using the pill she was made aware of the side effects but dismissed them as unlikely to affect her. “Why would I worry? I had been perfectly healthy for 19 years. With the exception of one broken bone and a case of strep throat, sickness and injury were not a part of my past. I had no reason to worry because I had no idea what kind of damage birth control could cause,” she wrote.
Hergenrader said the contraceptive pill she had been taking contained drospirenone, a synthetic version of the female hormone progesterone used in newer generation birth control pills that has a higher risk of producing blood clots than older forms of synthetic progestins.
The Food and Drug Administration (FDA) noted in a 2011 public announcement that it was conducting a safety review of birth control products containing drospirenone, that “all birth control pills pose a risk of blood clots,” but two studies published in the British Medical Journal contended that the contraceptives containing drospirenone posed two to three times a greater risk than other contraceptives containing the older form of progestin called levonorgestrel.
However, users of the older generations of contraceptive pills are also subject to a much higher risk of blood clots than women who don’t use contraception. The dangers of the older generations of contraceptive pills are outlined in the Physicians Desk Reference (PDR), which states that users of birth control are three times more likely to develop superficial venous thrombosis, and have a 4 to 11 times greater risk for deep vein thrombosis or pulmonary embolism than non-users. The risk is even higher for those who are genetically predisposed to blood clots.
The French National Agency for the Safety of Drugs and Health Products (ANSM) found that between 2000 and 2011, contraceptive pills were linked to an average of 2,529 annual cases of venous thromboembolism (blood clots). The health watchdog also found that the newer generation pills caused more than twice as many deaths as the earlier pills. The ANSM’s study estimated that 14 of the 20 annual deaths of French women attributed to birth control pill use were caused by the third and fourth generation pills which contain drospirenone.
The drug is produced and marketed by Bayer Pharmaceuticals under such trade names as Yaz, Beyaz, Yasmin, and Safyral, as well as other brand names such as Ocella, Syeda, Zarah, Gianvi and Loryna.
Hergenrader noted that in the course of her research into the drug that had almost killed her she met other women who had similar experiences. She related that Kaitlin Schroeder of Boulder, Colorado, told her she developed a portal vein thrombosis (the vein that carries blood from the stomach to the liver) as a side-effect of the NuvaRing, a flexible ring inserted once a month, when she was 22.
Jaimie Kuchar, a 22-year-old from Minnesota, told her she also had a deep vein thrombosis in her leg from a three-month estrogen pill, Gilessa. “Talking with other women who shared the same experience really sparked my interest in the dangers of birth control,” Hergenrader recalled.
“Jaimie, Kaitlin, and I are lucky to have caught ours early enough,” Hergenrader wrote. “About half of people who have blood clots show no symptoms, making it much harder to diagnose, and therefore, possibly fatal. Even those who survive might have life-long health problems. Kaitlin must take blood thinners indefinitely. Jaimie suffered from a blood infection.”
“I’m fortunate that my parents forced me to go to the doctor when I thought I had just pulled a muscle,” she wrote.
Today, the young journalism student is happier – and wiser – for having given up birth control. After trying another form of contraception, she gave it up altogether. Hergenrader stated that her experience with birth control pills resulted in a decision to reject birth control, but it has also left her anxious about her future health.
“After overcoming something life-threatening, I’m constantly in fear something can and will go wrong again. Every time I feel a twinge in my leg, I get scared. Every time I feel a shortness of breath, my heart races,” she said.
Family members and medical personnel at a hospital in Lindrina, Brazil, say they are stunned after a baby declared dead apparently came back to life after being placed on the altar in the hospital’s chapel.
According to local news sources, Yasmin Gomes was born premature earlier this month, and almost immediately stopped breathing. Doctors attempted for nearly an hour to revive the girl, who weighed only 2.6 pounds, but after their attempts failed they declared the baby dead and issued a death certificate.
Yasmin’s mother, Jenifer Gomes da Silva, 22, told Brazil’s Tanosite that when she was told her daughter had died, “My world crashed down right then. It was the most desperate moment when all my dreams were snatched away.”
However, Nurse Ana Claudia Oliveira asked that instead of being sent to the morgue, the body of the child be placed in a box and put on the altar in the chapel.
“She’s a little angel, a child. I just couldn’t face the thought of her being sent down to the morgue,” she told Globo G1.
The nurse testified that in every possible way, the baby appeared to be dead.
“I can assure you, the child was dead. Her pupils didn’t respond to light. All her signs pointed to the complete absence of life,” she said.
“I saw it with my own eyes. She was blue all over, completely dead,” she added.
Three hours later, the baby’s grandmother went to fetch the baby with a mortician. But what they saw left them weeping tears of joy, instead of sadness.
When they went to pick up the baby, she kicked.
“At first I couldn’t believe it; we couldn’t accept that it could happen,” said grandmother Elza Silva. “Then we saw she was breathing. We hugged each other and started to shout, ‘She’s alive. She’s alive.’ It was a miracle.”
One of the doctors who fought to save the baby’s life is as stunned as the family.
“In 20 years of medicine, I have never witnessed anything like this,” said Dr. Aurelius Filipak. When asked if the event was a miracle, however, the physician said he would not speculate.
The family, on the other hand, is less circumspect.
“Miracles have no explanation. Everything happens as God wants. If it was God’s will that our daughter left, we would accept [it], but there must be some greater purpose in all this,” said the mother.
Tanosite reports, however, that the baby is still in serious condition in the hospital. The family is asking for continued prayers.
World leaders should unite to end anti-Christian persecution, Vladimir Putin says
By Hilary White, Thu Aug 01, 2013
http://www.lifesitenews.com/news/world-leaders-should-unite-to-end-anti-christian-persecution-vladimir-putin
MOSCOW, August 1, 2013 (LifeSiteNews.com) – Vladimir Putin has urged the world’s political leaders to stop the violent persecutions against Christians that have erupted in many Middle Eastern countries.
Speaking at a meeting with Orthodox Christian leaders in Moscow last week, the Russian President said he noted “with alarm” that “in many of the world’s regions, especially in the Middle East and in North Africa inter-confessional tensions are mounting, and the rights of religious minorities are infringed, including Christians and Orthodox Christians.”
“This pressing problem should be a subject of close attention for the entire international community,” Putin said. “It is especially important today to make efforts to prevent intercultural and interreligious conflicts, which are fraught with the most serious upheavals.”
Putin praised the growth of cooperation between the Orthodox Churches and the Russian state, saying, “We act as genuine partners and colleagues to solve the most pressing domestic and international tasks, to implement joint initiatives for the benefit of our country and people.”
The Russian Federation recently passed legislation making it illegal to promote homosexuality as normal, a move that, while condemned by many European leaders, was strongly supported by the Orthodox Church.
Putin added Thursday that the Church was giving Russians a moral compass when so many were looking for help. “Today when people are once again searching for moral support, millions of our compatriots see it in religion,” he said. “They trust the wise, pastoral word of the Russian Orthodox Church.”
He added that it was the Church that was ultimately responsible for the development and rise of “culture and education” in Russia over the last 1,000 years. “The adoption of Christianity became a turning point in the fate of our fatherland, made it an inseparable part of the Christian civilization and helped it turn into one of the largest world powers,” Putin said.
The head of the Russian Orthodox Church, Patriarch Kirill, said at the same meeting that the attempts to push Christians out of Syria would lead to a “civilization catastrophe.” Kirill and other Orthodox leaders have been critical of the lack of response to the crisis facing Christians in the Middle East by US and other Western leaders.
The meeting was held with the leaders of all 15 Orthodox Churches to commemorate the 1,025th anniversary of the “Baptism of Russia” – the official adoption of Christianity and establishment of the Russian Orthodox Church in Kievan Rus by Prince Vladimir in 988 A.D.
Orthodox leaders at the meeting also condemned the growing secularist suppression of Christian freedoms in non-Muslim countries like Britain, where “gay marriage” has just been created.
Metropolitan Hilarion, the Russian Orthodox Church’s chief ecumenical officer, said “secularization in disguise of democratization” is leading Western nations toward totalitarianism. He spoke of a “powerful energy today [that] strives to finally break with Christianity, which controlled its totalitarian impulses during 17 centuries.”
Metropolitan Hilarion said, “Eventually, it unconsciously strives to set up an absolute dictatorship that demands total control over each member of society. Don’t we move to it when ‘for the sake of security’ we agree to obligatory electronic passports, dactyloscopy [fingerprint identification] for everyone, and photo cameras occurring everywhere?”
He highlighted the attempt to create same-sex “marriage” in France, which he called an attempt to make “immorality normal,” saying, that the French government has “consciously and demonstratively ignored demands of people and used tear gas to disperse them.”
Later, at a reception in Kiev, Putin and Patriarch Kirill took part in a prayer service with Ukrainian leader Viktor Yanukovych. He urged the leaders of Ukraine to turn towards a greater unity with Russia, and away from its overtures to the European Union, citing a natural cultural and spiritual relationship that is not present with the heavily secularist EU.
Patriarch Kirill added that it is the Orthodox religion that creates genuine unity between Slavic peoples. “Our ancestors adopted the Christian faith and, together with it, a system of values and morals…that no historical upheavals were able to destroy,” he said. Russians, Ukrainians, and Belarusians have a shared spiritual foundation that unites them more than their national boundaries divide them.
Patriarch Kirill said of the same-sex “marriage” fad sweeping the Western world, “This is a very dangerous apocalyptic symptom, and we must do everything so that sin is never validated by the laws of the state in the lands of Holy Rus, because this would mean that the people are starting on the path of self-destruction.”
Today, Canadian Foreign Affairs Minister John Baird, blasted the Russian government for its law banning gay propaganda, calling it “hateful.”
Baird said that the Canadian delegation was among those governments that tried to dissuade the Russian leadership not to adopt the law that outlaws all attempts to normalize homosexuality or other forms of non-traditional sexuality, especially to children.
“This mean-spirited and hateful law will affect all Russians 365 days of the year, every year. It is an incitement to intolerance, which breeds hate. And intolerance and hate breed violence,” Baird told the Canadian Press today.
The comments follow an announcement by Russia’s sports minister, Vitaly Mutko, who said the law would be enforced against athletes and visitors to Russia during next year’s winter Olympic games.
La Planificación Natural de la Familia acepta nuestra fertilidad.
La Planificación Natural de la Familia (PNF) es la aceptación completa dentro del matrimonio del don divino de la fertilidad, un método por medio del cual la pareja observa sus síntomas de fertilidad para determinar sus períodos fértiles e infértiles a fin de lograr o posponer el embarazo. No debe de confundirse con el antiguo y significativamente menos efectivo “método del ritmo” que estima y proyecta los períodos fértiles e infértiles de la pareja basándose en la observación de cuando ocurrieron estas fases en los ciclos anteriores.
La PNF tiene fuerte base científica.
La gran efectividad de la PNF se debe a métodos más precisos y sistemáticos por los cuales, dependiendo del método, las parejas observan los cambios en las mucosidades cervicales de la mujer, los cambios de temperatura y/u otras señales para determinar las fases fértiles o infértiles. Puesto que tanto las mucosidades cervicales como la temperatura responden a los cambios químicos/hormonales que regulan la fertilidad, las parejas que usan la PNF pueden determinar con gran certeza cuando están fértiles y cuando no. El anticuado método del ritmo era más que todo una adivinanza educada que se basaba en lo que a menudo era suposición equivocada de que los ciclos de fertilidad son constantes de mes a mes.
Dear friends,
Three women physicians—Donna Harrison, Mary Davenport and Martha Shuping—were invited months ago to give lectures on complications of abortion for the MWIA, the Medical Women’s International in Seoul, South Korea.
Donna Harrison’s presentation demonstrated that nations with laws protective of mothers and unborn babies have excellent [low] maternal mortality statistics. Mary Davenport had a talk about abortion as a risk factor for preterm birth, the cause of 15 million neonatal deaths each year internationally. Martha Shuping had a presentation that included two case reports of women who suffered severe psychological harm from abortion, even though they had obvious risk factors that were not discussed in the informed consent process. These risk factors were actually quoted from an abortion provider textbook endorsed by the National Abortion Federation!
This was valuable information for physicians to hear, especially those from developing nations who are under tremendous pressure to legalize abortion due to the false belief that legalized abortion is a panacea for maternal mortality.
However, our presentations were cancelled at the last minute. This was not a total shock to us, because many physicians and scientists have long been hampered in attempts to inform the scientific community and patient about risks of abortion. Very important information has been suppressed and even lied about. With the cancellation of our talks, our host Anna Choi, head of a group of 680 Korean ob/gyn physicians who stopped doing abortions, had decided to set up a radio and newspaper interview for us during the time that we were supposed to present.
When we got to the “radio” interview that Anna had set up, we found that it was actually a television interview, and the newspaper reporter was there also.
They put the three of us up front like a “panel” discussion, and the reporters started asking us questions about our presentation, allowing us an opportunity to talk about what we came to present. About 20 minutes into the interview, the Secretary General of MIWA, a Canadian, burst into the room (I kid you not…and all of this is on camera), and came up to the table and said “What presentation is this? Donna Harrison said “it’s not a presentation”. So she snarled, “Why are you being interviewed?” At that point, the answers were left to Anna, our host. Anna said that this was a requested interview by the press.
The SecGen then said, “Who gave you permission to interview these people?” And the reporters said, “We are the press, we don’t need anyone’s permission. We have freedom of the press”. And the Sec Gen snarled at Anna and said, “Did you arrange this? Did you talk to the organizing committee?” And Anna said, “I am on the organizing committee. I don’t need to talk to anyone.” And the Sec Gen stood in front of the camera, and refused to move, and said, “The interview is over.” Then the reporters said, “You can’t do this. We have the freedom of the press. You are interfering with the freedom of the press.” But the Sec Gen would not move and said, “The interview is over.”
We exited to the hall, and a Belgian and German woman waiting. They started to make fun of the Korean translator, and to snap pictures in her face. And she said, “You can’t do this. This is my country. I will call the police.” They actually grabbed at her, and then one of the Korean reporters put a huge camera in the Belgian woman’s face and started taking photos of her. A fist fight almost ensued between the women, but another of the Koreans stepped in and kept any contact from happening. All of this was on camera. Then our Korean hosts ushered us down the hall, and down the elevator, along with the reporters and camera crew, and we resumed the interview in the commons area downstairs by the trash cans and the bathroom. We were able to complete the entire interview. Now, instead of our audience being a few women doctors from the conference, we have an audience of probably a few thousand. [We can make it many millions!]
It was an incredible display of arrogance on the part of the Canadian, US and European physicians at the MWIA, who initiated preventing us from speaking. It will be interesting to see what press picks this up. I just wish it would go viral; it’s such a glaring example of exactly what we were saying about suppression of information.
You will be able to access the banned presentations at: www.aaplog.org
July 12, 2013 (The Public Discourse) –
Several events at the end of June call to mind John Paul II’s wordsin Evangelium Vitae describing the elements of a true humanitarian crisis. An act previously and nearly universally condemned, that hurts vulnerable lives, is celebrated as a “right” by people in the best position to protect those lives. How does John Paul II diagnose the cause of such a crisis? He identifies a serious misunderstanding of freedom—one that divorces freedom from solidarity, from reason and truth, and from the inevitability of human suffering. Sadly, his observations fit painfully well the events of the last week of June.
First, legislator Wendy Davis filibustered a bill in the Texas legislature that would ban killing unborn
children in the last twenty weeks of pregnancy and require abortion clinics to meet the medical standards required of other “ambulatory surgical centers.” Had these standards been observed,
they might have saved lives at the charnel house of Philadelphia abortionist and convicted murderer Kermit Gosnell. For her efforts, Davis was lauded by the press as one of the Democratic Party’s “most popular politicians,” and a “hero.” The president of the United States joined the chorus of praise, tweeting “#StandWithWendy.”
Second, on June 26, the Supreme Court issued two same sex marriage opinions. Following upon the Court’s holding in Hollingsworth v. Perry, same-sex couples are already obtaining marriage licenses in California, despite the votes of seven million Californians in favor of ballot initiative Proposition 8. The Court in United States v. Windsor struck down Section Three of the Defense of Marriage Act (DOMA), which defined marriage for purposes of federal law as the union of one man and one woman. The majority opinion authored by Justice Kennedy held that federal legislators (Democrats
and Republicans) and President Clinton passed DOMA strictly for the “purpose” of “impos[ing] a disadvantage… and so a stigma upon all who enter into same-sex marriages made lawful by the unquestioned authority of the States.” According to the majority, lawmakers intended to “demean” and “injure” same-sex couples, and to “humiliate” any children they were raising.
The majority did not devote a single line to the lawmakers’ well-documented interests in assuring a
special regard, nationally, for the wellbeing of children as a class, children for whom natural marriage is simply the only vehicle for tying their fathers to their mothers and to themselves, and indeed for preserving their entire historical and genealogical identity in this world. Not a
line. Instead, the Court declared that—in the opinion of five persons—marriage is rather about conferring a “dignity and status of immense import,” about granting a “far-reaching legal acknowledgment” of “intimate relationships,” and about “protect[ing]” “personhood and dignity.”
As Justice Scalia’s dissent observed, the majority held that to disagree with their understanding of marriage is to be an “enemy of the human race.”
Third, on June 28, the Department of Health and Human Services issued the final iteration of a health insurance mandate concerning contraception, sterilization, and early abortifacients. What did it decide? It decided to force insurers to provide “free” birth control and morning-after pills to the employees (and their family members, including minor daughters) of religious employers, regardless of whatever conscientious objection the employers might have. HHS wrote that its decision
“respect[s] the concerns of non-profit religious organizations that object to contraceptive coverage.”
They did this despite hundreds of thousands of opposing comments and dozens of (mostly successful) lawsuits against the government. They did it despite the fact that the “scientific report” undergirding the mandate has no empirical data proving the oft-repeated claim that free
contraception will prevent women’s illnesses. http://www.lifesitenews.com/news/without-words-to-describe
In sum, according to the powers-that-be, supporting killing unborn human beings is “heroic,” supporting natural familial bonds for children is “demeaning,” and forcing religious employers to insure (and really to pay for) services for their employees that they cannot
in good conscience support is “respecting religious freedom.”
My head is spinning. So is the Merriam-Webster Dictionary. And Americans are not alone in wondering at what moment reasoned discourse on life or marriage or religious freedom became impossible. Similar difficulties beset our neighbors in Ireland and the United Kingdom.
Ireland is soon to vote on legalizing abortion. It would legalize abortion to save the life of the mother (current law requires saving the life of both mother and child). This proposed new law would allow abortion most notably in circumstances wherein it is believed the mother would commit suicide without recourse to abortion. It is easy to see how, in practice, the legislation will open the floodgates to abortion, though the sponsors call the bill “restrictive” and “life-saving.” But there is even
another problem: the best empirical data from Europe also indicate that abortion is likely a cause of female suicide, not a preventive measure.
In the UK, Parliament is considering a bill to grant “marriage” to same-sex couples. Besides ignoring child welfare, the bill undercuts two additional, intrinsic, and perennial features of marriage: it voids the requirement of consummation (lawmakers couldn’t agree how to define it for same-sex partners), and it undermines the norm of fidelity by abolishing the possibility of same-sex adultery.
In other words, if a person granted a same-sex “marriage” has a sexual encounter with another person of the same sex (but not a person of the opposite sex), it is not what people have always thought “cheating” must constitute in the context of a marital relationship, i.e. “adultery.” In short, the UK bill grants marriage rights, while simultaneously voiding longstanding and definitional essentials of marriage.
Defenders of human life, religious freedom, and children’s interests in marriage should excuse themselves these days for sputtering—for having literally no words to offer in response to recent events. It appears words are currently useless. All the words we would ordinarily reach for are taken, and have suddenly been redefined. To add insult to injury, the movers and shakers redefining
the ordinary and natural meanings of things—and thus redefining culture and society, not just law—are beyond our democratic influence. Our hundreds of thousands of comments to HHS about the contraception and early abortifacient mandate command no legal deference. The mind of Justice Kennedy (who effectively controls the Court’s marriage decision-making given the otherwise 4/4
split) is not open to rational arguments from those who disagree with him. President Obama—who, in his days as a state legislator, already indicated how far removed he is from normal sensibilities regarding the value of human life by refusing to use his power to stop the killing of disabled, born alive human infants in Illinois—has proved himself deaf to all our calls, letters, comments, and
lawsuits.
In fact, when the president’s opinions are challenged, he often responds with even more extreme versions of earlier positions. For example, after he refused to defend Section Three of DOMA on the grounds of unconstitutionality, and won in the Supreme Court, he suggested the very next
day that same-sex marriage should be imposed on the fifty states by means of repealing Section Two of DOMA, which presently allows states to make their own decisions about the legal definition of marriage. But of course we have to find our voice again, to insist upon the natural meanings of words, and upon the necessity of logic. In addition, in this age, we need to use images and stories. Once again we have to be willing to be publicly visible—so as to dispel the notion that we do
not exist, or that we have given up the fight to ensure rational discourse, and pursue and disseminate relevant, truthful data. We have to be publicly visible also because that’s the most effective way to dispel the negative, one dimensional portrait of our ranks. We have to be willing
to help organize the currently disenfranchised majority who do possess ordinary humanitarian sensibilities about the good of life over death, the good of natural marriage, and the good of living in integrity with our religious convictions.
Reprinted with permission from The Public Discourse
Helen Alvaré is a Professor of Law at George Mason University School of Law, where she teaches Family Law, Law and Religion, and Property Law. She publishes on matters concerning marriage, parenting, non-marital households, abortion and the First Amendment
Religion clauses
Discovering the Truth about contraception can be one of the most defining moments in a couple’s marriage. But quite often, the joy of this discovery is accompanied by fears, doubts, and many questions. My husband Larry and I experienced all of the above in January, 2002 when, after 13 years of marriage, we finally decided to live our lives according to God’s plan for love and life. We literally threw out the contraception. This was the best decision we ever made, and we have never looked back. It was THE defining moment in our marriage.
Today, we continue to joyfully celebrate our conversion. We celebrate the beginning of a whole new way of life together and a whole new way of loving each other. But we also vividly remember how difficult it was to be in the middle of this conversion process. Our transformation wasn’t so “joyful” when we were actually going through it. To be honest, we were a mess. We stayed up night after night until the wee hours of the morning trying to figure out, “HOW ARE WE GOING TO LIVE THIS???” Discovering the Truth about love wasn’t enough. What to do with this Truth proved to be a far greater challenge.
Perhaps you have struggled with the issue of contraception. Perhaps you have ignored the Church’s teachings in your marriage for many years. Perhaps you or your spouse has been sterilized. But now, for whatever reasons, you find yourself wanting to change, wanting something better, wanting authentic love and unity in your marriage. This longing is the first step on the road to holiness and healing. Do not ignore this longing! The road ahead may be filled with obstacles; it may be frightening and uncertain. But take comfort in Sacred Scripture, set your foot to the path, and take one tiny step forward. I hope the following suggestions will encourage you on your journey and help you take the next step. Be not afraid! Joy awaits you! Authentic love and real freedom await you! Just say “yes” and take one tiny step.
#1 Receive the Sacrament of Reconciliation
No matter how often Larry and I may have rationalized it, using contraception was a sin in our marriage. In order to start anew, we needed the grace of this sacrament. This was the first and most important step for both of us. It was through the Sacrament of Reconciliation that we resolved to “never go back.”
Find a priest who understands the Church’s teaching. Make an appointment if necessary, and do not delay in confessing this sin. Resolve to amend your life. It doesn’t matter what you’ve done, where you’ve gone, or how long you’ve been away—NO sin is too great. Remember, you can just throw out the contraception—or you can throw out the contraception AND experience redemption, mercy, peace, and healing through the Sacrament of Reconciliation. The choice is yours.
#2 Gain Knowledge of the Truth—Read, Read, Read!
Larry and I literally had to re-learn how to love each other. We didn’t know that every sexual union was meant to be a renewal of our marriage vows; we had never heard that real love is free, total, faithful, and fruitful. We didn’t understand why the Church says what it says, and we were still unsure about many issues regarding sex. But when we discovered the Theology of the Body, it was like finding “the pearl of great price” for our marriage. The Theology of the Body is a collection of talks given by Pope John Paul II on the meaning of human sexuality. The truths revealed in the Theology of the Body reflected the deepest desires of our hearts. We immersed ourselves into this teaching in order to understand the language of our bodies and how we communicate. It was only then that we saw the beauty of God’s original plan for our sexuality. This is what we had been searching for! Our hearts were transformed, and to this day, we are still in awe of the Theology of the Body.
You may have many questions that are still unanswered. Perhaps your spouse considers the Church’s teachings to be a burden and is therefore reluctant to change. Pray for faith and reason; search for answers! Gain knowledge and understanding of authentic love—the only love that satisfies. Read books or listen to CDs together. Re-learn the meaning of your marriage, and immerse yourselves in Truth. Go to onemoresoul.com for a wealth of resources. I recommend the following to get you started: Good News About Sex and Marriage by Christopher West, Theology of the Body for Beginners by Christopher West, Contraception: Why Not by Professor Janet E Smith, “Prove It, God!”. . . And He Did by Patty Schneier
#3 Take a Class on Natural Family Planning
Natural Family Planning (NFP) is fertility awareness that is simple, scientific, and reliable. It is basic knowledge that can be used either to achieve a pregnancy or to avoid a pregnancy when there are serious reasons for doing so. Many people don’t realize, however, that there are different methods of NFP—all of which are in harmony with Church teaching. The most widely used methods include the Sympto-Thermal Method, Creighton Model, Ovulation Method, and Marquette Model. Each has different levels of instruction and different physical observations. Find out which method is right for you and sign up for a class. Both spouses should attend together. A National directory of NFP Teachers and NFP Centers is available at onemoresoul.com (800-307-7685). Call your Diocesan Family Life Office or local Catholic hospital for information about classes in your area.
#4 Switch to an NFP-Only Physician
This may sound drastic but, if it is at all possible, find an NFP-only physician. For me, this was a very important step—one that I didn’t want to take, because I “loved” my former Ob-Gyn who had delivered all our children. Soon after our conversion, however, I realized that his practice of prescribing contraception no longer fit with our values. I couldn’t follow his advice, and I didn’t agree with his assumptions. When I found my new physician, I felt as if I had truly come home to an entire practice that understood me and valued my fertility as a gift and a blessing—not a disease or an inconvenience that needed to be “controlled.” Despite a much longer commute to this new practice, it has been well worth it!
An NFP-only physician will affirm your decision, help you make the switch, and lend great support with medical truths and NFP experience. If you have been given hormonal contraceptives for “medical reasons,” an NFP-only physician can evaluate the underlying problem and utilize natural hormones or surgeries to restore proper function of your body. An NFP-only physician may also be able to assist couples who seek sterilization reversal. Because physicians have such a powerful influence on their patients and have a relationship built on trust, it is crucial that you find an NFP-only physician. Go to https://onemoresoul.com/nfp-directory to find your nearest NFP-only physician. If none is available in your area, ask an NFP teacher to recommend an NFP-friendly physician. If switching physicians is not possible, you may need to educate your current physician. Get materials, take them to your physician, and encourage him/her to learn the scientific facts and moral reasoning behind modern methods of NFP. Unfortunately, many physicians remain unaware and uneducated in this area. You can help change that!
#5 Connect with Others
When Larry and I converted to the Church’s teachings, we knew five other couples who did not use contraception. That’s it—five other couples out of our entire parish, list of acquaintances, colleagues, neighbors, and relatives. But these five couples were more than enough. These were the families we had always admired and respected. They soon became our confidants and closest friends. It felt so good to be able to talk with them! We swapped books and CDs; we swapped stories and experiences; we shared laughter and tears. Through it all, we witnessed their joy and learned how beautiful marriage can be. They encouraged us, taught us, and loved us throughout our entire journey. We are forever grateful.
Chances are, you know of at least one other family that practices NFP. You may not know them well, but you probably know who they are. Perhaps their marriage and family life have been an inspiration to you. Seek them out and share your story. The best place to look is within your own parish. These families can be a tremendous support for you. I strongly recommend that men seek out other men who have gone through this journey. Despite the initial awkwardness of discussing these personal issues, it can be most encouraging. You are not alone!
#6 Remain Grounded in Sacred Scripture
There were so many Scripture passages that strengthened me when I was afraid or confused. Two verses in particular were crucial at these times: Mark 1:17 “They dropped their nets and followed him.” I knew that contraception was my “net,” and I needed to drop it in order to follow Jesus. Luke 5:37 spoke to my heart as well: “No one pours new wine into old wineskins.” I wanted “new wine” in my marriage. But in order to get that, I had to get rid of the old wineskins. There was no other way. . . . The truths of these scriptures helped me to stay focused on God. His Word sustained me throughout this journey.
Pray for wisdom, strength, perseverance, and purity. Read the Bible. I recommend reading the following verses over and over again: Romans 12:1-2, Philippians 1:9-11, Ephesians 1:3-4, and Ephesians 3:14-21. Let them sink into your heart and speak to you personally. Know that you can be pure and blameless; know that you can be rooted and grounded in real love; trust that through grace you will be strengthened with power and Truth!
Finally, I share with you the life-changing question that Larry asked me after reading Good News About Sex and Marriage. I was extremely confused, frightened, and in turmoil after discovering the truth about contraception, and I didn’t know what to do. He simply asked, “What do you want for our marriage?” I replied, “I don’t know. . . but I want what’s in that book.” That was it. That’s how we began our journey together—reading, learning, praying, and talking. Then we took one step at a time to build the marriage we had always wanted. With time, our communication, our physical relationship, and our entire lifestyle changed for the better. May you be abundantly blessed as you discover God’s plan for your marriage, and may you be steadfast in your search for Truth. Make the switch. It could be THE defining moment in YOUR marriage.
NFP Contact Information
Sympto-Thermal
Couple to Couple League www.ccli.org 513-471-2000
Northwest Family Services www.nwfs.org 503-215-6377
Ovulation
Family of the Americas Foundation www.familyplanning.net 301-627-3346 Billings Ovulation
Billings Ovulation Method Association www.boma-usa.org 651-699-8139 Creighton
Pope Paul VI Institute www.popepaulvi.com 402-390-6600 Marquette
Marquette U. School of Nursing www.marquette.edu/nursing/NFP 414-288-3854
On Friday, Catholics throughout the United States will begin observing two weeks known as the Fortnight for Freedom. For a second consecutive year, the U.S. Catholic Church has set aside this time leading up to Independence Day to draw attention to the need to resist erosions of religious liberty so that faith can continue to enrich our public life.
How appropriate that the Fortnight should begin with a nationally televised Mass from our own Basilica of the Assumption, the first Catholic cathedral in the United States. Blessed Pope John Paul II once referred to the Basilica as a worldwide symbol of religious freedom. President Thomas Jefferson assisted in the Basilica’s uniquely American design — the brainchild of architect Benjamin Latrobe, who also designed the U.S. Capitol. The Basilica is the embodiment of what it means to be both Catholic and American, the intersection of faith and public life that is at the very heart of the Fortnight for Freedom.
Standing in New York Harbor, the Statue of Liberty is one of our most beloved landmarks, both as New Yorkers and as Americans. So many of our ancestors fondly recalled seeing Lady Liberty, their first vision of a new homeland. Many of them told the story of seeing her for the first time, and not a few of them had to pause in retelling it because of a lump in their throat or a tear in their eye.
Japan’s health ministry issued a nationwide notice that cervical cancer vaccinations should no longer be recommended for girls due to several hundred adverse reactions to the vaccines reported.
One of the problems with vaccinations such as HPV is that they are not preventative, they do compromise safety and physicians will never provide accurate explanations of vaccine risks and benefits because they do not know themselves. Physicians can only rely on the information from vaccine manufacturers and since long-term pharmacokinetic effects which study the bodily absorption, distribution, metabolism and excretion of vaccines and their ingredients are never examined or analyzed, a Physician can never fully inform of patient of any benefits or risks. (more…)
“Not to us, Lord, not to us, but to your name be the glory!” I gratefully accept this prestigious Wilberforce Award, if you agree to certain conditions, okay?
We New Yorkers are tough negotiators, as you know, so, listen carefully to these conditions: Ready?
Condition #1: that receiving this award be an occasion, like every event in life should be, for me to praise God, from whom all blessings flow, and His Son, our Lord and Savior, Jesus Christ, whose Resurrection we radiantly confess this paschaltide. “Not to us, Lord, not to us, but to your name be the glory!” (more…)
After getting the kiddos situation in the kitchen with an art project this morning I set off for the family room to fold clothes. Exciting I know! While folding I turned on the TV and quickly found myself being pulled into a talk show. The topic was unconventional marriages. The host was interviewing a traditional Orthodox Jewish marriage. First I found it ironic that the topic was unconventional marriages and the couple was in a traditional marriage. My second thought was, when did the traditional marriage become unconventional? Then I listen further and found myself mesmerized by the tradition, romance, and respect that this couple shared.
“IRS officials have, of course, confessed that they inappropriately targeted conservative groups — especially those with ‘tea party’ or ‘patriot’ in their names — for extra scrutiny when they sought non-profit status. Allegations of abuse or harassment have since broadened to include groups conducting grassroots projects to ‘make America a better place to live,’ to promote classes about the U.S. Constitution or to raise support for Israel.
“However, it now appears the IRS also challenged some individuals and religious groups that, while defending key elements of their faith traditions, have criticized projects dear to the current White House, such as health-care reform, abortion rights and same-sex marriage.”
Terry Mattingly, director, Washington Journalism Center; weekly column, May 22
Let’s begin this week with a simple statement of fact. America’s Catholic bishops started pressing for adequate health-care coverage for all of our nation’s people decades before the current administration took office. In the Christian tradition, basic medical care is a matter of social justice and human dignity. Even now, even with the financial and structural flaws that critics believe undermine the 2010 Affordable Care Act, the bishops continue to share the goal of real health-care reform and affordable medical care for all Americans.
As lawmakers investigate the IRS harassment of Tea Party, conservative, evangelical, Catholic, and other political organizations, a leading pro-life lawyer told Fox News that he “can't help but think” someone ordered the intense scrutiny his clients have experienced.
Peter Breen, executive director of the Thomas More Society, appeared on Megyn Kelly's program last week to detail how the tax agency began subjecting pro-life groups to an unconstitutional and illegal level of scrutiny during the Obama administration.
A stranger came into the sacristy after Sunday Mass. In an incriminating huff he said, “I have been away from the area for fifteen years; where are the people? And now you are tearing down the school? I went there as a kid.” I put my hands up to quiet him from further talking and I calmly said, “Let me ask you a question: How many kids did you have?” He said, “Two.” Then I said, “So did everyone else. When you only have two kids per family there is no growth.” His demeanor changed, and then he dropped his head and said, “And they aren’t even going to Mass anymore.”
I never thought I would be asking that question, but since I had to close our parish school, I’ve grown bolder and I started to ask that question more often. When I came to my parish five years ago, the school was on its proverbial “last legs.” In its last two years we did everything we could to recruit more students, but eventually I had to face the fact that after 103 years of education the school was no longer viable. In one of the pre-closure brain-storming sessions with teachers, I was asked what to do to get more students. I replied, “Well, I know what to do, but it takes seven years.” The older teachers laughed, but the others needed me to state the obvious to the oblivious, viz. we need more babies. In my January 2010 letter to my bishop asking his permission to close our school, I wrote:
Public Library of Science (PLOS) is a leading journal created in 2003 to rival existing elite journals such as Science and Nature.
In 2012 PLOS reported the increased incidence of a serious neurologic disorder called Narcolepsy.
Annual incidence of narcolepsy by age group and year of diagnosis. doi:10.1371/journal.pone.0033723.g003 (Adapted from PLOS)
As it is depicted in the chart adults were not affected but children were seriously affected. The most injured were the 11-16 y group (in red).
How serious is narcolepsy. A report from Kate Kelland, Health and Science Correspondent from Reuters UK of January of 2013 tells the story of Emelie.
She is one of around 800 children in Sweden and elsewhere in Europe who developed narcolepsy, an incurable sleep disorder, after being immunised with the Pandemrix H1N1 swine flu vaccine made by British drug maker GlaxoSmithKline in 2009.
Emelie is plagued by hallucinations and nightmares. When she wakes up, she’s often paralysed, unable to breathe properly or call for help. During the day she can barely stay awake, and often misses school or having fun with friends. She is only 14, but at times she has wondered if her life is worth living.
Abortion activists love their folklore. Women. Hangers. Millions of deaths. None of it’s true, but it sure sounds scary in a sound bite. Planned Parenthood’s own Medical Director, Dr. Mary Calderone, in a 1959 article decrying the lack of social acceptance of abortion declared: “Abortion is no longer a dangerous procedure…90% of all illegal abortions are presently being done by physicians. Many of these physicians are in good standing in their communities.”
The Radiance Foundation exposes the mythology of “back alley” abortions
In its quarterly examination of the economic outlook for the world’s major economies, the Conference Board of Canada identifies rapidly aging populations coupled with well-below-replacement-level birth rates in the Asia-Pacific region as indicators that the once powerful economies of these countries are headed toward economic collapse.
“Productivity gains and a large, young working-age population have done much to boost Asian economic growth over the past three decades. But Asia’s demographic dividend is quickly coming to an end. Due to fewer births and longer life expectancies, the average age of the population in Asia is increasing rapidly,” says Kip Beckman, principal economist and author of the Conference Board’s World Outlook-Spring 2013. (more…)
From John F. Brehany, Ph.D., S.T.L. Executive Director and Ethicist Catholic Medical Association
The Obama administration is continuing its attacks on conscience rights and religious freedom, and Congress is not hearing from enough American citizens that this is an important issue. It is essential that we step up and make our voices heard TODAY! Today, there is a concerted effort to rally people across the nation to speak out on this issue.
Here is what we ask you to do:
Contact your elected representatives in the House and Senate. Tell them you are concerned about lack of protection for conscience rights and religious freedom — particularly in health care — and ask them to co-sponsor and vote for legislation that will provide effective protections;
Post this Action Alert on your FaceBook page TODAY and send it to all your FaceBook Friends;
Post this Action Alert on Twitter TODAY and forward tweets on the subject. #ConscienceProtection #ReligiousFreedom.
If we do not defend conscience rights and religious freedom, for ourselves and future generations, we will lose them, because there are powerful, determined people who want to take these profound goods away from us. TAKE ACTION NOW, TODAY!
Thank you.
John F. Brehany, Ph.D., S.T.L.
Executive Director and Ethicist
Catholic Medical Association
In Christ,
Source: Roanoke.com BUENA VISTA — With a word of thanks to Southern Virginia University students who pitched in on his presidential campaign, Mitt Romney invited the school’s 145th class to dive wholeheartedly into life to raise families and serve God.
“Hundreds of you gave up vacation time to help a candidate for president, for which I owe you deeply. Thank you so much,” he said.
But he didn’t come to talk politics to the small college where most share his Mormon faith.
In only his second public speech since losing the election, Romney set his theme by quoting a verse from the Gospel of Luke when Jesus advised fishermen who had failed to catch anything to head farther out and launch their boat into deeper waters to set his theme. (more…)
Our news outlets are not known for their squeamish attitude toward violence. On the contrary, reporters are often criticized for fixating on violence, exploiting it as fodder for the 24-hour news cycle.
We rarely see journalists shying away from a gruesome case. Yet, the media has been reluctant to cover the trial of Dr. Kermit Gosnell – a Philadelphia abortionist accused of committing unspeakable crimes at his “Women’s Medical Center.” (more…)
MANILA, April 23, 2013 (LifeSiteNews.com) – With less than three weeks until the May 13 elections in the Philippines, one of the country’s largest Catholic archdioceses has prepared a list of candidates that have publicly taken a stand on the side of church teaching on pro-life and pro-family issues.
Speaking on the Mornings@ANC TV show, Lipa Archbishop Ramon Arguelles said the decision to distribute sample ballots containing names of candidates who are “one with the church on controversial issues,” came in response to requests from Catholics to the archdioceses for guidance.
“The people are asking to be told,” said the archbishop. “The others have made the choice but many want to know who are the right persons, so we make it available. We're starting to do that now.”
He said that the list of acceptable candidates was created after consultations with lay leaders, who ranked candidates according to their stand on abortion, divorce, the new reproductive-health law, and protection of the environment.
DAGUPAN CITY, Philippines, April 17, 2013 (LifeSiteNews.com) – A leading Filipino prelate has issued a pastoral letter encouraging Catholics to support only those candidates in the forthcoming election who “declare a categorical and clear NO to divorce, abortion, euthanasia, total birth control and homosexual marriages”
Most Rev. Socrates B. Villegas, the archbishop of the archdiocese of Lingayen-Dagupan, said that while the Church does not interfere in elections by endorsing candidates, it does offer guidance to voters to examine the candidates “from the viewpoint of faith and with the mind of the Church enlightened by the values of the Gospel.”
The archbishop offered ten concrete moral guidelines to the faithful in the light of which to consider the candidates, with the admonition that “If Jesus would vote, for whom would he vote? Vote like Jesus. If you cannot find Jesus from among the candidates just make sure you do not make Judas or Barabbas win.”
JAMA Pediatrics published a new study today looking at vaccination rates. The results of that study are making headlines throughout the “mainstream” media outlets, but none of them have headlines like ours. Yet, ours is probably the most factual headline representing the true facts of what this study found.
Just as chess requires players to seriously consider every possible consequence of their moves, we need to seriously consider every possible consequence of the push for same-sex marriage, especially for children.
In our sometimes misguided efforts to expand our freedom, selfish adults have systematically dismantled that which is most precious to children as they grow and develop. That’s why I am now speaking out against same-sex marriage.
by Msgr. Charles Pope
Homosexual Marriage Is The Logical Conclusion For A Culture That Celebrates Sterility! Widespread Acceptance of the Homosexual Lifestyle Is God’s Punishment for Sin!
There is, among faithful Catholics, a dismay, and even an understandable anger at the events unfolding at the Supreme Court these past days related to gay unions. And even if the court were to uphold traditional marriage (which does not seem likely), or merely return the matter to the States, it seems quite clear where our culture is going regarding this matter, approving things once, not so long ago, considered unthinkable.
What then to do with our dismay and anger? It is too easy to vent anger, which is not only unproductive, but in the current state of “hyper-tolerance” for all things gay, angry denunciations are counter-productive. (more…)
Emergency contraception (EC) is the use of pills or devices after sex to try to prevent pregnancy.1 EC is promoted when a woman has been raped, when a couple has chosen to have sex without using any form of contraception, or when there is a suspected contraceptive failure. Types of EC may include pills or the insertion of the Copper-T Intrauterine Device (IUD) up to five days after intercourse. The use of other drugs as emergency contraception is under investigation.2
What is the “Morning After Pill”?
The phrase “Morning After Pill” (MAP) describes a set of contraceptive pills taken after a sexual act, to prevent pregnancy. One type of MAP contains only the synthetic progestin levonorgestrel (LNG), which is the main drug in other commercial contraceptives. Commercial names for the MAP include Plan B One Step, Take Action, Next Choice One Dose, My Way, and others.3 The Food and Drug Administration has approved Plan B One Step for sale without age restrictions. A second type of MAP is the anti-progesterone “Ella”, available with prescription in the United States. A third type of MAP is the “off label” use of combined oral contraceptive pills. A fourth type of EC is the abortion pill Mifepristone (RU 486), used outside the USA.
How does the Morning After Pill work?
The new baby (blastocyst) migrates from the fallopian tube to the uterus where it implants 5-7 days after conception.
Conception of a new human being is possible only during a few days in the woman’s cycle. Sperm can survive in the woman’s body 3-5 days, and the ovum dies 12-24 hours after ovulation. Fertilization normally occurs in the fallopian tube after ovulation. The new human being (blastocyst) moves from the fallopian tube to the uterus where it implants 5-7 days after conception. A delicate hormonal balance is necessary for the baby’s survival.
Some studies seem to show that Plan B works by changing the cervical mucus or by attacking sperm. More recent studies, however, show that these effects may happen when the drug is taken regularly (like birth control pills), but NOT after one dose (like EC).4,5
Advocates of EC claim that the active ingredient in Plan B works mainly by stopping or delaying ovulation Available studies show that when Plan B was given to women in the fertile part of their cycle, 80% OR MORE of them ovulated, although NONE of them became obviously pregnant (see diagram below).6,7 If sperm and an egg are present in the woman’s body but no obvious pregnancy develops, then abortion is the most likely cause.8 Some studies also show that Plan B disturbs the hormonal balance needed to maintain pregnancy.9,10
What about other types of emergency contraception?
Copper-T IUDs—Copper ions released from an IUD are toxic for sperm and the ovum, decreasing the probability of fertilization.11 Also, the Copper-T IUD lowers the chances of survival of any embryo that may be formed before it reaches the womb. The Copper-T IUD stops the lining of the womb from accepting a newly formed embryo.12 Thus the Copper-T IUD may have a post-fertilization effect, meaning it destroys a young human embryo.
Ella and Mifepristone (RU-486) change the body’s ability to react to some hormones. They can block the action of the hormone progesterone,13 thereby destroying a new human life through chemical abortion. Ella can also delay or block ovulation if taken before ovulation.14
If conception (fertilization) has already taken place, then the only way the IUD and the morning after pill (MAP) can be effective is by destroying the new life. When a woman takes theses pills or when the IUD is inserted, there is currently no way for her or her doctor to know whether or not she has already conceived. A pregnancy test cannot give this information before implantation. Whenever these pills are taken, or a Copper-T IUD is inserted after sexual activity, there is the risk that a new human life will be destroyed.
Remember that a new life is destroyed when implantation is prevented.
Does this mean that emergency contraception is an abortifacient— that it can cause an abortion?
A new human life begins at conception, also called fertilization. However, in September 1965, the American College of Obstetricians and Gynecologists (ACOG) attempted to redefine “pregnancy” as beginning at the time of implantation, and not at the time of conception. The effectiveness of pills and devices that do not prevent fertilization depends on destruction of a new human life. This should be called an “abortion” in spite of the medical definition from the ACOG.
In a recent study 8 out of 10 women who took the MAP ovulated. This means that if they had sex, some of these 8 women likely became pregnant. None had an obvious pregnancy, so the women who became pregnant probably experienced an early abortion.
How effective is emergency contraception?
The Copper-T IUD prevents 99% of expected pregnancies. Ella and Plan B prevent some of expected pregnancies after unprotected intercourse.15 The effect of EC in reducing unintended pregnancies and induced abortions has not yet been proven. Available studies show that EC may have no effect on unintended pregnancies, it may even increase them.16, 17, 18,19 Women with high body mass may also find that EC has decreased or no effectiveness in preventing pregnancy.20 In addition, providing emergency contraception in advance has the negative effect of increasing risky sexual behavior.21 Overall, the evidence suggests that the Morning After Pill is not effective for preventing unintended pregnancies.
How safe is emergency contraception?
A Morning After Pill that contains LNG can cause heavier or lighter menstrual bleeding, nausea, vomiting, abdominal pain, fatigue, headache, dizziness, breast tenderness, delay of menses (up to 7 days), and diarrhea. The use of LNG also increases the risk of ectopic pregnancy.22 The use of Ella has been connected with headache, abdominal or upper abdominal pain, nausea, dysmenorrhea, fatigue, and dizziness.23 Women who use the Copper-T IUD can experience uterine cramps and other undesirable effects such as ectopic pregnancy, septic abortion, pelvic infection, perforation, embedment, anemia, backache, painful periods, pain during intercourse, vaginal discharges, prolonged menstrual flow, menstrual spotting, cramping, and vaginitis.24
One study reported that women may repeatedly use EC due to an exaggerated perception of its effectiveness.25 Another study found that over-the-counter access to EC leads to increased Sexually Transmitted Infections by approximately 12% for women ages 15-44 due to increased risky sexual behavior.26 More time and research are needed to know the long-term effects of emergency contraception on the health and safety of women.
Are there other options?
If you are single, the surest way to avoid pregnancy or a sexually transmitted infection is abstinence, and it always works. If you are married, the modern methods of Natural Family Planning (NFP) are the safest, healthiest, least toxic, and least expensive means for family planning. Victims of rape or sexual abuse need and deserve the best medical care and human support possible. The additional stress and health risks of emergency contraception add further harm. (Pregnancy due to rape is estimated at 5%).27 For the vast majority of these women, emergency contraceptives impose significant health risks with no benefit. If conception has already occurred, then a very early abortion is the only means for emergency contraception to be effective. Abortion carries with it many serious adverse consequences such as increased rates of breast cancer, depression, anxiety, suicidal behaviors, and substance use disorders.28 A far safer approach is to carry the child to term. Adoption is always an option.
Confidential pregnancy assistance services are available throughout the U.S. and Canada by calling Option Line at 800-395-HELP (4357) and Abortion Pill Reversal Network at 877-558-0333.
REFERENCES:
1. Trussell J, PhD and Raymond, EG, MD, MPH. Emergency contraception: a last chance to prevent unintended pregnancy. Retrieved from: http://ec.princeton.edu/questions/ec-review.pdf, July 28 2015.
2. Jesam C, Salvatierra AM, Schwartz JL, & Croxatto HB. (2010). Suppression of follicular rupture with meloxicam, a cyclooxygenase-2 inhibitor: Potential for emergency contraception. Human Reproduction (Oxford, England), 25(2), 368-373.
3. Emergency Contraception Pills. Retrieved from http://ec.princeton.edu/info/ecp.html, July 28 2015.
4. Nascimento JA, Seppala M, Perdigao A., Espejo-Arce X, Munuce MJ, Hautala L, et al. (2007). In vivo assessment of the human sperm acrosome reaction and the expression of glycodelin-A in human endometrium after levonorgestrel-emergency contraceptive pill administration. Human Reproduction (Oxford, England), 22(8), 2190-2195.
5. Hermanny A, Bahamondes MV, Fazano F, Marchi NM, Ortiz ME, Genghini MH, et al. (2012). In vitro assessment of some sperm function following exposure to levonorgestrel in human fallopian tubes. Reproductive Biology and Endocrinology : RB&E, 10, 8-7827-10-8.
6. Brache V, Cochon L, Deniaud M, Croxatto, HB. Ulipristal acetate prevents ovulation more effectively than levonorgestrel: analysis of pooled data from three randomized trials of emergency contraception regimens. Contraception. Nov 2013; 88(5): 611-618.
7. Noe G, Croxatto HB, Salvatierra AM, Reyes V, Villarroel C, Munoz C, et al. Contraceptive efficacy of emergency contraception with levonorgestrel given before or after ovulation. Contraception. Nov 2011; 84(5): 486-492.
8. Kahlenborn C, Peck R, & Severs WB. (2015). Mechanism of action of levonorgestrel emergency contraception. The Linacre Quarterly, 82(1), 18-33.
9. Croxatto HB, Brache V, Pavez M, Cochon L, Forcelledo ML, Alvarez F, et al. Pituitary-ovarian function following the standard levonorgestrel emergency contraceptive dose or a single 0.75-mg dose given on the days preceding ovulation. Contraception. Dec 2004; 70(6): 442-450.
10. Hapangama D, Glasier AF, Baird DT. The effects of peri-ovulatory administration of levonorgestrel on the menstrual cycle. Contraception. Mar 2001; 63(3): 123-129.
11. Ortiz ME, Croxatto HB. Copper-T intrauterine device and levonorgestrel intrauterine system: biological bases of their mechanism of action. Contraception. Jun 2007; 75(6 Suppl): S16-30.
12. Gemzell-Danielsson K, Berger C & Lalitkumar PGL. (2013). Emergency contraception–mechanisms of action. Contraception, 87(3), 300-308.
13. Keenan JA. Ulipristal acetate: contraceptive or contragestive? Ann Pharmacother. Jun 2011; 45(6): 813-815.
15. Fred F. Ferri M.D., F.A.C.P. (2016). Ferri’s clinical advisor 2016 Elsevier, Inc
16. Rodriguez MI, Curtis KM, Gaffield ML, Jackson E, Kapp N. Advance supply of emergency contraception: a systematic review. Contraception. May 2013; 87(5): 590-601.
17. Raymond EG, Trussell J, Polis CB. Population effect of increased access to emergency contraceptive pills: a systematic review. Obstet Gynecol. January 2007; 109(1): 181-188.
18. Walsh TL, Frezieres RG. Patterns of emergency contraception use by age and ethnicity from a randomized trial comparing advance provision and information only. Contraception. Aug 2006; 74(2): 110-117.
19. Glasier A, Fairhurst K, Wyke S, Ziebland S, Seaman P, Walker J, et al. Advanced provision of emergency contraception does not reduce abortion rates. Contraception. May 2004; 69(5): 361-366.
20. Glasier A, Cameron ST, Blithe D, Scherrer B, Mathe H, Levy D, et al. (2011). Can we identify women at risk of pregnancy despite using emergency contraception? data from randomized trials of ulipristal acetate and levonorgestrel. Contraception, 84(4), 363-367.
21. Belzer M, Sanchez K, Olson J, Jacobs AM, Tucker D. Advance supply of emergency contraception: a randomized trial in adolescent mothers. J Pediatr Adolesc Gynecol. Oct 2005; 18(5): 347-354.
22. Zhang J, Li C, Zhao WH. Xi X, Cao SJ, Ping H, et al. (2015). Association between levonorgestrel emergency contraception and the risk of ectopic pregnancy: A multicenter case-control study. Scientific Reports, 5, 8487.
23. Ulipristal Acetate. http://www.pdr.net/drug-summary/ella?druglabelid=1278 August 10 2015
24. Intrauterine Copper Contraceptive Paragard. Retrieved from http://www.pdr.net/drug-summary/paragard?druglabelid=572 August 10 2015
25. Melton L, Stanford JB, Dewitt MJ. Use of levonorgestrel emergency contraception in Utah: is it more than “plan B”? Perspect Sex Reprod Health. Mar 2012; 44(1): 22-29.
26. Mulligan K. (2015). Access to emergency contraception and its impact on fertility and sexual behavior. Health Economics (Published Online).
27. Holmes MM, Resnick HS, Kilpatrick DG, Best CL. Rape-related pregnancy: estimates and descriptive characteristics from a national sample of women. Am J Obstet Gynecol. August 1996; 175(2): 320-324.
28. Fergusson DM, Horwood LJ, Ridder EM. Abortion in young women and subsequent mental health. J Child Psychol Psych. January 2006; 47(1): 16-24.
“As different as night and day” is an expression we’ve all used. But that distinction has become blurred over generations by ever increasing sources and length of light. As a result, many women do not experience a true nighttime anymore. They are in, or surrounded by, light 24 hours a day.
Since the Fall of 1976, we have consistently observed that the presence of light during the woman’s major sleep period can affect one or more phases of her menstrual cycle. This will be seen in the woman’s charted pattern, and also applies in determining breastfeeding and pre-menopausal Basic Infertile Patterns. (more…)
(National Right to Life News) – A colleague at National Right to Life recently emailed me a photo of an ad that appeared in her local newspaper. It was titled, “Reflections: the Ultimate Prenatal Experience” and was about 3d and 4D ultrasounds.
Truth Booths are unmanned kiosks showing ultrasound images of the developing unborn child in the womb. Millions have already seen them at malls, community fairs, schools and other public and private venues throughout the United States and Canada. (more…)
She is not sick. Stop jacking your wife up on hormones.
Freedom. It is dumb to let a little pill control your wife.
All. Nothing says “I love you” better than actions that say “I desire your complete goodness, fertility included.”
Counter-culture. Planned Parenthood will think you are crazy; this is a good thing.
Adventure. So many pay lots of money for extreme experiences like Tough Mudders or sky diving; natural bio-tracking encourages looking at life as an adventure inside your own home.
Self-control. Tough? Yes. Impossible? No. You are more than the sum of your sexual urges.
Humility. Trust me, when you are fighting the urge to abuse yourself, you realize how weak you may be and how much you need grace.
Common sense. A stomach digests. Lungs help you breath. The tongue tastes and helps you speak. The marital act is designed for unity AND procreation; it is not rocket science to know this.
Fulfilled. Yea, you know that emptiness is-this-all-there-is-to-sex feeling after contracepted un-intercourse? It goes away over time when you re-familiarize yourself with the mystery of the human person and how sex is such a great gift when shared completely and totally free.
Obedience. The Church says it is wrong. Why take advice from some old white guy in Rome? Well, he leans on 2000 years of history, a global mindset, and is the Vicar of Christ. I might ask you, “Why take the advice from some MTV sex symbol that thinks he knows better than 2000 years of tradition?”
This is an amazing story of twin baby girls. One baby was not expected to live.
A hospital nurse fought to put them in the same incubator. The stronger baby wrapped her arm around her sister, and her touch allowed the struggling baby’s heart to stabilize and her temperature to return to normal.
In the UK he is a household name. He has
done a beautiful series of documentaries for BBC on
the world’s wildlife. He was even knighted by the
Queen.
And he is a bona-fide, certified, take-noprisoners
people hater.
The hater in question, Sir David
Attenborough, made the news last week by
comparing the human race (that is, you and me) to a
plague on the planet. Going even further, he
predicted that disaster would befall us within the
next half-century unless something is done to stop
our reckless reproduction. (more…)
Who would have thought President Obama would do a promo for the March for Life and start a revolution.
[youtube=http://www.youtube.com/watch?v=Opl0jnKbn5Y]
Source LifeSiteNews.com JillStanek.com –Scientific American termed the research findings another way: “Scientists discover children’s cells living in mothers’ brains.”
But I wanted to drive home a touching point: Mothers who terminate their pregnancies apparently don’t completely rid themselves of their babies. The cells of murdered children live on inside their mothers to help – or perhaps – hurt them:
Cells may migrate through the placenta between the mother and the fetus, taking up residence in many organs of the body including the lung, thyroid muscle, liver, heart, kidney and skin. These may have a broad range of impacts, from tissue repair and cancer prevention to sparking immune disorders.
By Bryan Kemper
Source:LifeSiteNews.com
Should pro-lifers compare abortion to things like the Connecticut tragedy? To answer this question one must first answer the question: what is abortion?
Abortion is simply a word used to describe the action of killing a human person in one of the early stages of that human person’s development, just as shooting is simply a word to describe how the human persons in that school in Connecticut or the theatre in Colorado were killed. Both words describe a different method used to end the life of human persons who are all in different stages of their life and development.
In the same way, when I compare the Nazi Holocaust and the Abortion Holocaust, I am showing that they are both horrific events that have claimed the lives of millions of innocent human persons. One took place 70 years ago and one is taking place right now.
I could easily show comparisons to many other events in history such as Columbine, slavery, earthquakes and many more tragic events that have claimed so many innocent lives. (more…)
A new photo of a baby reaching out of the womb and holding a doctor’s finger during a Caesarian section delivery has gone viral and is being passed around Facebook by tens of thousands of people.
A Phoenix-area couple took the picture during the delivery of Nevaeh — Heaven spelled backward — and a local news report says even the physician and hospital nursing staff were surprised by what unfolded.
“It was such an amazing photo. [Hospital staff] had possibly heard of it happening but they had never seen a photo of it,” said Alicia Atkins, Nevaeh’s mother.
Few lives will be as well documented as little Nevaeh’s. Her mother is a professional photographer who owns A Classic Pin-Up in Glendale. However, it was her dad, Randy, who snapped the picture.
“The doctor called me over and said, ‘Hey, she’s grabbing my finger.’ So I ran over there and just grabbed the shot and I was just in awe looking at it. It was such an amazing picture,” said Randy Atkins, adding that he was nervous about missing the precious and fleeting moment as he hurried to snap a picture.
Now, the picture has been liked and shared by thousands and the couple has offers to buy the photo, which they never intended to place online for public viewing.
“I can FINALLY share this!!!!” Alicia said on her Facebook page when posting the photo on December 26. “This was 10 weeks ago when I was having my c-section and
Dr. Sawyer broke my water and my daughter reached up out of my stomach and grabbed the Dr.’s finger and my hubby caught this special moment.”
“Truly amazing. I am in awe of this photo. Something to remember forever,” she adds. “Thank you for helping me deliver 3 of the most amazing wonderful gifts I could ever ask for. A Couple of miracle children. You are truly an amazing Dr. and couldn’t ask for a better one. I had this printed for my OBGYN on a canvas.”
Putin Calls for Three-Child Family to Become the Norm
by Steven W. Mosher and Elizabeth Crnkovich
What do you do when your country is dying, one coffin at a time? Well, if you are Russian President Vladimir Putin, you call upon Russian couples to be fruitful and multiply, and have at least three children.
It is hard to exaggerate the demographic straits that Mother Russia finds itself in. According to the projections of the UN Population Division–we are speaking here of the so-called “low variant,” historically the most accurate–the Russian population will shrink by more than 30 million by mid-century if current trends continue. The population will age rapidly, from an average age of 37.9 in 2010 to and average age of 49 by 2050. In other words, most Russians will be beyond their childbearing years, and Russia’s demographic fate will be sealed. (more…)
Who could be a better role model for how to love one’s spouse than the Ultimate Lover, God? But, just how does God love? Having meditated on this question, Pope Paul VI and Pope John Paul II discerned four key characteristics of God’s love. God’s love is always: free, total, faithful and fruitful. Each key is also one of the four essential qualities of authentic married love. This brochure will introduce you to these four very important keys for starting out on, or getting back onto, the road to a great marriage. Through the graces that come from the sacrament of Holy Matrimony, together with prayer and regular reception of the sacraments of Reconciliation and the Eucharist, spouses are given all the strength and power to love each other as Jesus loves His Church: freely, totally, faithfully and fruitfully. These are the four keys to authentic conjugal love. Through the Sacraments and learning more about the four keys to marital love presented in this brochure, couples can open the door to an ever more satisfying and fulfilling marriage.1(more…)
You know a contraceptive drug or device is in trouble when the lawsuits begin to multiply.
A growing number of American women are turning to intrauterine devices (IUDs), reports Lawrence Finer of the Guttmacher Institute. Of all American women using birth control, some 7.5 percent had IUDs implanted by 2009. These numbers were double what they had been a few short years before.
As befits an employee of a population control organization, Finer is pleased that women are choosing “long-acting” contraceptives over “short-acting, less effective methods.” Fertility delayed is fertility denied, as we say in demographic circles.
Most of the increase in IUD use has come from sales of Bayer’s levonorgestrel IUD, a so-called “second generation” contraceptive, which is marketed under the trade name “Mirena.” No surprise here. Since Mirena was approved by the FDA in 2000, Bayer has spent tens of millions of dollars advertising the IUD directly to the consumer.
Dear friends who usually get my homilies: I am sending
along a homily from my friend, young Father Jeffrey Montz.
He was ordained a priest a year ago, and is now the Parochial
Vicar at St. Frances of Assisi [New Orleans]. Perhaps, as
moving as the homily is Fr. Jeff’s note to me which I have
copied and attached to the end of the homily.
Here is Fr. Jeff’s Homily: In the year 2009, I was distributing
communion to the faithful when a young woman approached
and extended her hands to receive the Eucharist. Almost as
soon as I had placed the Host in her hands, she began moving
away and in the process she dropped the host. Standing over the
fallen Host lying on the ground, a slight giggle, shrug of the
shoulders, and re-extended hands, her body language said to
me, “Ooops, I dropped it. Can you give me another one?” (more…)
I want to begin today by thanking those of you who went out on Tuesday and voted for the sacredness of human life. Just as the widow’s deed in our 1st reading will never be forgotten as long as the Scriptures are read, be assured that no righteous deed that we ever undertake will be forgotten by Almighty God.
This past Wednesday, the day after the election, I received a message on my phone at the parish office, from a gentleman who didn’t identify himself by name but who said he was a parishioner. And in this message, this gentleman ranted for several minutes about Tuesday’s election results. And here were the first words out of his mouth, “You lost Father; you lost!” Well, the first thing I want to say about Tuesday night’s election results is that I didn’t lose on Tuesday night our entire country lost! (more…)
2011 was a tumultuous year for Meg Booth, her husband Jeff and their children Hannah (11) and Nathan (5). In August, Meg discovered a lump in her right breast, which she had examined in September. A mammogram with “suspicious” results lead to a biopsy in December.
In the meantime, on October 29, Meg landed in an emergency room thinking she might have a stomach virus. She told her local paper, The Valdosta Daily Times, “After questions and bloodwork, the doctor came in and said, ‘I think congratulations are in order. You’re pregnant.’ I about died.”
Meg and Jeff had faced years of infertility, “so,” explains Meg, “it was a huge, huge surprise to find out I was pregnant.” (more…)
I was sitting on a bean bag in my dorm room when I got the call. It was a friend of mine—let’s call her “Sara”—and she was sobbing so hard it took me a moment to know who it was.
Finally, she pulled herself together enough to speak. With a voice that sounded as weary as if she had aged 100 years since the last time we talked, she said, “I’m pregnant.”
My heart sunk on her behalf. I was completely pro-choice and didn’t find the idea of abortion to be troubling, but I knew that she was not comfortable with it. She had always said that she respected other women’s rights to choose, but that she could never do that. Yet I also knew that she was not entirely thrilled with this guy she was dating, a young man named Rob. He was handsome and charismatic, but he had a serious drinking problem, and didn’t treat her with the respect she deserved. (more…)
The One More Soul “newspaper” response to the HHS mandate.
One More Soul is pleased to offer this “newspaper” response to the HHS mandate as a supplement to the resources already available from the USCCB and other sources. It is an educational piece that draws attention to several “concerns” prompted by the HHS mandate. They are concerns for all of us, whether involved in Catechesis, Bible Study, Faith Sharing, Altar-Rosary, Knights of Columbus, St Vincent De Paul, Catholic Charities and Social Services, Catholic hospitals, high schools, and universities. Please fit this issue into your agenda for as long as required to end the HHS assault on our Constitution and our Church.Our Lord Jesus told us to, “be not afraid”, and “cast out into the deep”. Our God will provide; our God is merciful; our God has a plan.Our Faith is being tested. How shall we respond? (more…)
Please prayerfully considering getting involved in this effort, get a PROTECT RELIGIOUS FREEDOM yard sign for your yard, and forward to all your friends.
We are a group of concerned citizens organizing an effort across midwestern-southwestern Ohio to pray, educate, and witness for the protection of religious liberty. Below are details on our plans and how you can get involved. (more…)
In a recent video interview with Catholic News Service, Archbishop Charles Chaput of Philadelphia said that the position of the Democrat Party on abortion has “gotten worse” over time because Catholics within the party haven’t taken a strong moral stand and shown a willingness to abandon the Democrat Party.
“I think many of the Democrats have [taken] Democrat Catholic votes for granted because they’ll go with them no matter what the party position might be on abortion,” Archbishop Chaput said. “That’s why the position of the Democrat Party has gotten worse, and worse, and worse as time goes on because Catholics haven’t abandoned them as they’ve moved in that direction.” (more…)
A summary of the medical data presented in the Women Speak for Themselves amicus brief
Oral Contraceptives
Heart Attack and Stroke –
According to the New England Journal of Medicine, oral contraceptive pills double the risk of heart attack in women. The risk increases for women with hypertension (5x), who smoked (12x), with diabetes (16x), and with high cholesterol (23x).[REF. 1] The British Journal of Medicine reported that oral contraceptives cause an increased risk of ischemic stroke (3x) as well as an increased incidence of blood clots and pulmonary embolism. [REF. 2] (more…)
Researchers studying the incidence of birth defects in California have found that children conceived by in vitro fertilization have a significantly higher rate of genetic disorders compared to children conceived naturally.
UCLA researchers presented findings from their study, titled, “Congenital Malformations Associated With Assisted Reproductive Technology: A California Statewide Analysis,” on October 20 at the American Academy of Pediatrics National Conference in New Orleans. (more…)
It’s been all over the news lately, particularly in the Catholic and conservative spheres, how Dr. Shinya Yamanaka won the Nobel Prize in medicine for reprogramming adult cells into induced pluripotent stem cells (iPSCs). People praised this research for creating new pluripotent stem cell lines to study without creating or destroying embryos. They claimed that the process doesn’t require any morally tainted source cells. They announced the feat as an achievement of great ethical significance, a beautiful and ethical science. They pointed out that the process does not pose ethical issues because embryos are not manipulated, and that embryonic stem cell research will soon be largely put out of business. What a moral victory!
However, digging into and decoding the scientific methodological explanations reveals that what is being praised is definitely not so praiseworthy. It reveals something quite significant, and it mostly hinges on one word — reprogramming. Did anyone notice that in all the cheering, little was explained about the method itself?(more…)
ESPN airs a weekly show called “E:60.” This investigative hour-long show highlights stories – often personal, touching, and sometimes tragic ones – related to sports. On October 1, ESPN posted a segment of “E:60″ called “Perfect” to YouTube. “Perfect” is nothing less than a gripping, life-changing tale. (more…)
The Women of Grace show on EWTN features a series by Dr. Chris Kahlenborn, MD called The Misogyny of Women’s Health Care – the titles of the programs are listed below. (more…)
Source: Unmaskingchoice.ca
Canadian Centre for Bio-Ethical Reform (CCBR)
by Ruth Shaw
There are a few moments in a woman’s life that are 100 % unforgettable, and one of those includes birthing a child (did I say child? I meant sub-human non-person blob.) Six and a half weeks ago, I had my memorable experience when I gave birth to our little son, William.
In the past few weeks between feeding, changing and cleaning William several times a day, I have had the opportunity to reflect on my birth experience, but more fundamentally, how my experience can help save babies. (more…)
Over four years ago it was obvious to my eye that autism disorder rates changed dramatically in certain specific years. Looking at autism disorder prevalence data from the US Dept of Education it was clear that there were three specific years in which autism prevalence rose dramatically, and Sound Choice Pharmaceutical Institute (SCPI) went on to perform the statistical analysis to show that 1980, 1988 and 1996 were ‘changepoint’ years for autism disorder. In 2010 the EPA published data confirming the 1988 changepoint as a worldwide autism disorder changepoint. As the EPA scientists point out in their publication, identification of ‘changepoints’ such as these tell us that some environmental factor was introduced that triggered such a sudden and dramatic rise in autism. Pasted below are the 3 changepoints Sound Choice identified for autism disorder prevalence in the US. (more…)
Diocese of Springfield Illinois, 23 September 2012
My dear brothers and sisters in Christ:
Much attention was given at the Democratic National Convention held recently in Charlotte, N.C., to the fact that all references to God had been purged from the draft version of the party platform. After outcries of protest from outside as well as within the Democratic Party, the sentence with the same reference to God used in 2008 was restored to read, “We need a government that stands up for the hopes, values and interests of working people, and gives everyone willing to work hard the chance to make the most of their God-given potential.” (more…)
The pre-born babies provide living cells that cross the placenta and live for decades in the mom’s blood (1). These fetal cells remain in the mother blood stream and mobilize themselves where ever injury is occurring in the body. The fetal cells are not attacked by the mother, but rather work as stem cells that transform themselves into new tissue that gives new life to the mother.
That was the case for a mother of five who had hepatitis C (2). During a biopsy the cells were analyzed and it was found that cells from her son had come to the lesion and converted themselves into hepatic cells. The woman became healthy again with the help of her offspring! (more…)
More and more countries are hearing the death knell of low birth rates.
We live in an age unique in human history. Per capita incomes have never been higher, lifespans have never been longer, and people are better fed and educated than ever before. At the same time, birth rates have fallen to historically low levels. In fact, they have fallen to levels so low that they will extinguish whole populations unless something is done.
The developed countries are suffering a severe birth dearth and, as a result, an enormous shift in global power will soon be upon us. Europe will recede demographically, while America will be hard-pressed to hold its own against younger and more populous countries. More and more countries are undertaking programs to raise their birth rates, although none of these policies has as yet made much of a difference.
Let’s take a quick tour around the world, thanks to the research of our own Elizabeth Crnkovich: (more…)
Note: Rebecca Kiessling, who was herself conceived in rape, is the co-founder of Hope After Rape Conception which advocates on behalf of rape survivors and their children. This past week, Congressman Akin was publicly chastised for his comments on abortion in the case of rape, employing the controversial term “legitimate rape.” (more…)
August 22, 2012 (Omaha, NEBRASKA) – According to Thomas W. Hilgers, MD, an obstetrician-gynecologist who directs a reproductive ultrasound center that specializes in the study of naturally-occurring ovulation events at the National Center for Women’s Health in Omaha, Nebraska, “the question of rape always stirs the emotions whenever it is introduced into the abortion debate. Unfortunately, the emotional impact of rape often clouds a legitimate and truthful discussion.” (more…)
Homily by: Father Thomas Dufner.
July 22, 2012
Epiphany Church
Coon Rapids, Minnesota, USA
Outline:
Jeremiah says, “Woe to the Shepherds who mislead and scatter the flock of my pasture.”
In the last few weeks we’ve heard the true role of the prophet to lead and guide the people
There were many false prophets who served only themselves.
Typically, the true prophets faced opposition because their message was unpopular.
From Amos to Ezekiel, and from Jeremia and John the Baptist, they spoke the truths that God wanted them to speak, popular or unpopular, welcome or unwelcome. They served the Lord.
By Francis Cardinal George, OMI, Archbishop of Chicago
Source: Archdiocese of Chicago
Recent comments by those who administer our city seem to assume that the city government can decide for everyone what are the “values” that must be held by citizens of Chicago. I was born and raised here, and my understanding of being a Chicagoan never included submitting my value system to the government for approval. Must those whose personal values do not conform to those of the government of the day move from the city? Is the City Council going to set up a “Council Committee on Un-Chicagoan Activities” and call those of us who are suspect to appear before it? I would have argued a few days ago that I believe such a move is, if I can borrow a phrase, “un-Chicagoan.” (more…)
By Steven W. Mosher and Elizabeth Crnkovich
Source: pop.org.
Social security is about to go belly up, financially speaking. And at the head of this crisis is a demographic disproportion: there are simply too few young people coming into the workforce to support the increasing numbers of elderly baby boomers who are retiring. (more…)
“Your husband isn’t with you?” The doctor looked concerned. Hannah Boland had decided to go alone for her follow-up appointment.
Only a short while before, a pregnancy had ended in a miscarriage. But this pregnancy was different. They were out of the danger zone. The baby was already twenty weeks gestation. Alison and Harry, Hannah’s two toddlers, aged three and two respectively, were going to have another sibling.
“I like having the husband or partner present in these sorts of situations. We detected a problem with your baby’s scan,” the doctor continued. “There seems to be a problem with his brain.” (more…)
Melinda Gates and her partners, including the British government and the world’s largest abortion providers, have launched a $4 billion campaign to push birth control for poor women in Africa, Asia and Latin America. Ms. Gates claims that there is “no controversy” in powerful groups and governments promoting birth control for poor women, but the facts are that contraception IS controversial for a number of reasons. Share the facts today at http://www.FactsforMelindaGates.com.
“We’re 21st century kids. And as such, we’ve had delivered to us a world with sky-high rates of divorce, abortion, and STDs; a world bored with sex and bored with romance; a world in which more and more people are turning to pornography to find sexual satisfaction; a world in which 1 in 5 women report being sexual assaulted, and the human body — the sexiest thing in the universe — is used to sell cars.
After extremely little consideration, we decided we don’t want that. We want awesome relationships and mind-blowing sex lives. We want women and men to be respected and loved for who they are, to the very depths of their being. We want sex free from fear, love free from use, and a world of people who love and respect their own bodies. In short, we want sexy back. In fact, we demand it.
1Flesh.org means just that. One flesh. Total union. No wrapping men in rubber or pumping women with artificial hormones. No interrupting the act of making love. Once the sex act became something in which women were “controlled” and men were “restrained” everything seemed to fall apart. Suddenly “objectification” wasn’t such a hard thing to do. Instead of repeating the mistakes of our parents, we’re trying to spread words of rebellion; that sex should be awesome, that pregnancy can be justly avoided without harmful chemicals, and that love is worth fighting for.”
In an astounding show of solidarity, a diverse group of countries rallied together with the Holy See to successfully remove any mention of reproductive rights or population control from the final outcome document produced during the last round of UN negotiations at the Rio +20 conference this week. (more…)
A groundbreaking study reveals that adult children of homosexual and lesbian parents experience far greater negative social, economic and emotional outcomes than children raised within intact biological families. (more…)
by
Liliana Cote de Bejarano, MD, MPH
About 1.5 million couples in the United States opt for sterilization every year .1 According to the Guttmacher Institute, 9.9% of couples in the US use vasectomy as a contraceptive method, and more than 500,000 vasectomies are performed in the United States every year.2 The medical community and most family planning advocates consider vasectomy safe and simple. This pamphlet provides current research on vasectomy that indicates the procedure has a number of short- and long-term complications and is not a healthy choice.
Here is everything you wanted to tell your married child, and everything you wish your parents had told you about marriage. First Comes Love is a collection of the very best the Church has to offer to help couples have long and very happy marriages. Drawing from Popes John Paul II and Benedict XVI, Christopher West, Emily Sederstrand, Steve Wood, St John Chrysostom, and many others, this publication offers articles, quotes, personal testimonies, graphs, prayers, and recommendations. Subjects include finding the right mate, the blessings of children, the value of Natural Family Planning, how chastity works inside of marriage, and infertility; everything a young couple needs to get their marriage onto a solid foundation.
Welcome to One More Soul’s “Mandate Busting Resources” store. We believe that these resources will help you challenge the government’s mandated coverage of contraception, abortifacients, and sterilization by all “health” insurance plans. (more…)
After months of pro-life protests and opposition, PepsiCo has indicated it will alter its contract with biotech firm Senomyx Inc., which uses cells from a baby killed in an abortion to conduct flavor testing.
The second-largest beverage company in the world contracted with the firm in a $30 million deal in August 2010 and once Debi Vinnedge of the pro-life group Children of God for Life uncovered the connection, numerous pro-life groups, including LifeNews, joined together to promote a boycott of Pepsi until it ends the Senomyx contract.
Vinnedge informed LifeNews today of Pepsi’s decision and hailed it as a major breakthrough and achievement by thousands of concerned consumers who have been writing and boycotting PepsiCo beverages since last May. (more…)
Back in November, the Wall Street Journal featured a prominent article with the following headline: “The Hidden Toll of Traffic Jams; Scientists Increasingly Link Vehicle Exhaust With Brain-Cell Damage, Higher Rates of Autism”. It was careful to point out that current evidence is circumstantial; no one is certain about such a connection between traffic, exhaust, brain-cell damage and autism. After all, vehicles today put out far, far less pollution than those operating decades ago, when autism rates were far, far lower.
Traducido por: Lydia Mendez y Liliana Cote de Bejarano
Grabado en los estudios de SEMACOM Foundation
Voces: Padre Antonio La Roca y Daniel Bejarano
Introducción:
Saludos. Soy el obispo Víctor Galeone de la Diócesis de San Agustín en la Florida. A continuación usted
oirá una presentación maravillosa por Steve Patton, el director de la oficina de Vida Familiar. Steve explica claramente por qué la sabiduría para todos los tiempos de la Iglesia que trata del amor conyugal trae mucha alegría a las parejas casadas y una profunda satisfacción para los sacerdotes que les sirven. Tenga cuidado, sin embargo, este mensaje podría tener un impacto duradero para bien en su vida. Disfrute de la presentación.
With the buzz of OCTOBERBABY fresh in the air, I imagine there will be many new questions posed by children to their parents, “mom (or dad), was I a WANTED child????”
Now that the Affordable Health Care Act is law, we have been talking about the appropriateness of contraception and abortion in health care. The mantra seems to be “make every child a wanted child”. But the pill and the availability of abortion was supposed to solve this dilemma, and we have given it 50 years, yet there are still a lot of unwanted children being born, and aborted. It seems there are many in our secular culture who deem that only those children who are wanted are, in fact, valuable and worth having.
However, what about those children who were not actively planned or initially sought after? OCTOBERBABY attempts to answer that most important question.
I, too, was an unwanted child. I grew up always knowing that I was adopted, and this was a source of much shame for me. My parents told me nothing about the details of my biological mother’s history, but they always told me I was “special”. At the age of 25 years old, I was able to find out nonidentifying information about the circumstances around my adoption. I found out my biological mother was in college on a piano scholarship, but that she had been “date-raped” by my father, who was just about to be shipped out to Vietnam. The year was 1965 and Roe v Wade was not yet legalized. My mother had the courage to interrupt her college, go to a home for unwed mothers, and give me life, even though I was most certainly NOT WANTED.
As an obstetrician and gynecological surgeon, it is my duty to inform women of the risks of any procedure they undergo. Providing honest and accurate medical information to a woman before a procedure is required to live up to the ethical standard of informed consent. The need for such informed consent is especially critical when the procedure being considered is an induced abortion. (more…)
Not too long ago I went to my family doctor for a yearly physical wellness exam. A very friendly nurse measured me, weighed me, and took my temperature. She also asked me the regular series of questions for women, such as, “When was your last menstrual period,” and “Is there any chance that you are pregnant?” To the latter question, I answered no. At that point I was a 21-year-old college student who, by God’s grace, was saving my virginity for marriage, trying to live a chaste life, and feeling very strongly about my convictions in this area. The nurse proceeded to ask me, at this point seemingly deviating from the questions on the form, if I was on any kind of birth control. (more…)
We had negotiated our mid-life passage without the proverbial crises. My wife pierced another hole in her ears for a second set of earrings. I started wearing contact lenses because she told me it made me look younger. That was about it.
The youngest of our six children was then 9 years old. Each milestone he had passed gave us a growing sense of freedom: last one out of diapers, last to tie his shoes, ride a bike, learn to swim, go to school. There was a sense of anticipation. What might we do with the next chapter of our life? After 20 years of marriage, I sensed we were on the verge of a whole new direction in 1996. (more…)
In a Feb. 7, 2012 Wall St. Journal op-ed, you claimed that President Obama’s HHS mandate, which forces everyone, including religious institutions, to pay for abortifacients, oral contraceptives (OCPs), and sterilizations as mandatory benefits in health insurance policies, was a victory for women’s health. As practicing physicians, we can attest that nothing is further from the truth. President Obama’s mandate is bad for women’s health and for the profession of medicine. (more…)
In a shocking decision delivered February 28, President Obama’s Security and Exchange Commission ruled that PepsiCo’s use of aborted fetal remains in its research and development agreement with Senomyx to produce flavor enhancers falls under “ordinary business operations.” (more…)
Anti-abortion activists have been holding prayer vigils outside a Kettering abortion clinic for decades, but on Sunday they plan to up the ante by saying prayers of exorcism.
The Rev. Steve J. Angi, chancellor of the Roman Catholic Archdiocese of Cincinnati, has given permission for priests to say exorcism prayers at a 2 p.m. rally outside the Women’s Med Center, 1401 E. Stroop Road, the Miami Valley’s only abortion clinic. The clinic is closed on Sundays.
Ruth Reddens, an organizer of the 40 Days for Life campaign that plans the vigil, sought Angi’s permission to perform the “exorcism of locality,” designed to drive evil out of a place, rather than out of a person. “Hopefully, the spiritual battle will be won,” she said. (more…)
A video promoting the benefits of Natural Family Planning. The video points out the inconsistency of those who strive to eat a pesticide- and hormone-free diet yet take a hormone-laced contraceptive pill without thinking. Produced by the Catholic Advance, Diocese of Wichita.
Twice in recent weeks, I have written you to express my gratitude for our unity in faith
and action as we move forward to protect our religious freedom from unprecedented intrusion
from a government bureau, the Department of Health and Human Services (HHS). I remain
deeply grateful to you for your determined resolve, to the Chairmen of our committees directly
engaged in these efforts – Cardinal Daniel DiNardo, Cardinal Donald Wuerl, Bishop Stephen
Blaire and Bishop William Lori -who have again shown themselves to be such excellent leaders
during these past weeks, and to all our staff at the USCCB who work so diligently under the
direction of the Conference leadership. (more…)
We are immersed in a culture of images and the external
appearance of things. Too seldom are we asked to contemplate
the inner reality, the inner being of what we see.
In the following meditation, we are asked to reflect on
how Jesus Christ, for whom and in whom all the world is created,
took on both the external appearance and the inner reality of a
developing human person, from the moment he is conceived by
the Holy Spirit to the day of his birth. We are not accustomed
to seeing him thus, because this development is hidden within
the protective womb of Mary. But today’s technology allows us
to pull aside the veil surrounding this early development of the
child. Photography and ultrasound imagery allows us to see the
physical appearance of the child and the science of embryology
and fetology provides us with the intricate and amazing details of
the child’s development.
“The Lord called me from the womb, from the body of my
mother he named my name.” (Isaiah 49:1)
The humility of the Son of God in submitting his
personhood to this development bestows an infinite dignity on
this bodily phenomenon. Every preborn child shares in this
dignity and is called to union with Christ, even to receiving into his
body the Eucharistic Body and Blood of Christ.
Christ’s external appearance is not always attractive to
the eye. There was the time in his life that, “He had no form or
comeliness that we should look at him, and no beauty that we
should desire him.” (Isaiah 53: 2). Yet the inner reality of the
divine-human Person is such a brilliant beauty that our eyes are
not strong enough to behold it. In his condescension, he has
hidden himself in the simplicity of the Eucharistic Host.
Fr. John Hollowell’s truly amazing monologue needs to be spread far and wide. It’s a wake up call, and one of the most encouraging statements I’ve heard in a long time. It’s a Divine battle cry!
The talk heats up after minute 2 where he notes in this talk addressed to Planned Parenthood Pres. Cecile Richards that “we have not doubt” that in the future Planned Parenthood will be seen as the “slave traders, the Nazis, the Communists and all those groups that seek to oppress people.”
He then warns PP and President Obama: “You better knock us out now. You and the President better knock us out right now, because Cecile, I can promise you – Here comes the Catholic Church … you’ve awakened a sleeping giant.”
“Priests and bishops that have in the past been content to remain quiet are no longer so. … The Truth is being rained down everywhere. … Here comes the Catholic Church.”
He notes that PP since its founding “have proclaimed yourselves sworn enemies of the Catholic Church,” but “we’re in the ring now, the gloves are off.” He acknowledges that Cecile has every worldly advantage in her corner – the President of the United States, the media. But Goliath too had every worldly advantage.
The powerful talk ends quoting Tolkein: “The board is set, the pieces are now in motion, at last we come to it – the great battle of our age.”
by Keith Riler “Contraception reduces unintended pregnancies” has joined its fantastic make-believe friends “death with dignity,” the “efficacy” of embryonic stem cells, the “certainty” of man-made global warming, and the “positive” multiplier effect in the leftist vernacular. Hopeful that repetition supplants truth, choirs of liberal faithful are singing:
Dear Friends, I just wanted you to see this thread of a discussion on some points related to the HHS mandate.
Although the religious liberty issue is universally compelling, another crucial point is that birth control is NOT preventative care (see below). The current administration wants this to be about the Catholic Bishops denying women their “women’s health”. This is why I feel our recent research article is so timely and important right now (1). The pill is not a warm little fuzzy harmless object. It causes significant harm and the American people have been deceived for long enough. As a practicing physician, I see the fallout every day—young women with blood clots in their legs, strokes, early breast cancer, HPV, and cervical cancer. This is NOT about women’s health; it is about preventing and killing babies. The present administration will try to pit US Bishops against women and try to portray the bishops as a bunch of old men that don’t want women to have their “women’s health” options, but this has no credibility.
Every day, I, my husband Benjamin, and other doctors like us do TRUE preventative care. We do pap smears looking for cervical cancer, perform breast exams looking for breast cancer, refer for mammograms, order colonoscopies looking for colon cancer, and give immunizations to prevent pneumonia and influenza. These time-tested measures are very different from prescribing a pill to prevent a CHILD. A child is not a disease. Pregnancy and fertility are not disease states; they are normal physiological processes of the human body. (more…)
+ February 10, 2012
Dear Brothers & Sisters in Christ:
As you are most undoubtedly aware, on January 20, 2012, the Department of Health and Human Services announced its decision not to expand the unacceptably narrow “religious employer” exemption to its mandate that virtually all health insurance plans must include, as so-called “preventive services” sterilizations, abortifacients, and contraception. Since that time, the United States Conference of Catholic Bishops and I began immediately preparing to meet this challenge.
The Bishops’ Conference committee on Religious Liberty is actively engaged in planning a nation-wide response on a number of levels. I simply want you to know that the bishops are fully engaged in this process, and a significant, sustainable, and long-term strategy is our goal.
You are invited to visit the USCCB website for continually updated information regarding our efforts to defend freedoms of conscience and religious liberty, and to better inform yourself as to what you can do as individuals. There is already information on this website to assist you in writing your representatives to express your deep concern for the protections of freedom of conscience and religious liberty. (more…)
How about some respect for Catholics and others who object to treating pregnancy as a disease?
Religious freedom is the lifeblood of the American people, the cornerstone of American
government. When the Founding Fathers determined that the innate rights of men
and women should be enshrined in our Constitution, they so esteemed religious
liberty that they made it the first freedom in the Bill of Rights.
In particular, the Founding Fathers fiercely defended the right of conscience.
George Washington himself declared: “The conscientious scruples of all men
should be treated with great delicacy and tenderness; and it is my wish and
desire, that the laws may always be extensively accommodated to them.” James
Madison, a key defender of religious freedom and author of the First Amendment,
said: “Conscience is the most sacred of all property.” (more…)
During my training, I remember dreading those patient visits where I was expected to provide “safe sex” counseling to my patients. It wasn’t necessarily the awkwardness of speaking about such matters to a complete stranger so much as it was the difficult position of trying to meet the expectations of my evaluators without personally contributing to this irrational and flawed set of beliefs held by the “secular” medical establishment. Ironically, the ones promoting biased, false, and misleading information are not the abstinence-based programs, but the condom devotees who arrogantly discredit such abstinence-based programs as failing to provide medically accurate material. (more…)
Let’s be honest.
Media isn’t the best place to get ideas about how to show physical affection or how relationships should start and progress.
If you want real love, you have to build a real friendship. That means not just looking for physical pleasure or emotional comfort.
If you are interested in defending
your relationship against using each other, “how far is too far?”
may not be the question to ask.
These ideas can be a solid place to start
or deepen a relationship. Get beyond what the culture tells you is normal—take time to actually get to know yourself and each other for who you are
and see if you enjoy each other’s company!
“OK, SO WHAT CANWE DO??”
First things first: Examine what is stirring in you. Are you craving contact with another person? Know that the desire to be in relationships is not bad (since we’re made in God’s image, we’re made to love!) but we should not use others to fill us up. The reality is, only God can do that.
If you are asking “how far is too far?” you may have good intentions—but a better question is “how can I really love this person?”
God is the Standard for Love (see back panel) and we are made to love like Him—not to settle for less or to use each other. Know that “rules” are meant to uphold real love and the dignity of every person involved.
If you see people as a means to your own end, you will treat them that way. Purity in action flows from purity of heart and thought. Aim to act as God made us to be from the very beginning: good to the core.
The draw toward physical and emotional expressions of love will very quickly get stronger when you really connect with someone. It’s good to acknowledge that fact and not just push the feelings down—but it’s also not OK to simply indulge. There is a balance to be found.
Rather than being stuck in the two extremes, you can re-focus: pray, thinkandbe creative!
Thank God for the other person and for the good gift of your desire to love!
Ask God to show you how to take all that energy and direct it toward loving like HE loves.
Examine what you have learned about relationships from family, culture, media, etc… you may have some untwist any lies.
Contemplate who, why & how you are choosing to love! Let God guide your heart and don’t brush off internal warnings; pray about them and talk them out!
Commit to speaking the Truth with your body! A sincere embrace or kiss speaks a language: it should bless the other with a message of love and commitment. Real love doesn’t push boundaries that warm you up for sexual intercourse. In Marriage, the body-soul union of spouses is a renewal of their vows.
Definitions to think about:
Friendship are good and needed. Don’t confuse the healthy close, mutual admiration or friendship with sexual attraction. Don’t let it get flirty, just be you.
‘Dating’ has classically meant a guy asking a variety of ladies out over time because in order to get to know them, while keeping the idea of marriage in mind. This same intent can be accomplished by hanging out in small groups at school, work, church, etc. One-on-one time (going out on dates) should be fun and low–key, but don’t get into the ‘friends with benefits’ or ‘hook up’ mentality!
‘Courtship’ is a foreign word to most. Our culture calls exclusive relationships ‘dating’ but usually gives little thought to marriage. A good mindset is to not be wooed into this more serious relationship unless you have already been friends for a while and he or she is the type of person you think you could marry. Courtship is where conversation and knowledge about the other & yourself goes deeper and deeper. Spending a lot of time around family and friends will help you gain perspective about the other person as you start to pray and talk about marriage.
Engagement declares the intent to marry but it’s not just about planning the reception. Go on a marriage preparation retreat before you set the wedding date! Get specific in conversations about daily life expectations, finances and family. Take a NFP (Natural Family Planning) class so you truly know what’s going on. This time of waiting for sexual union will reveal the variety of ways you can deepen your love for each other.
Public vows of Marriageare meant to protect the intimate body-soul bond of love between one man and one woman so that they and their children have a permanentplace to grow in love together! If one of these intentions is missing (to bond permanently or openness to procreating children), the true meaning of marriage is not being upheld. Prior to the vows when a couple declares ‘for better or worse until death do us part’, each says ‘I do’ to the following:
Do you come here freely and without reservation?
Are you prepared to love and honor each other for as long as you both shall live?
Will you accept children lovingly from God?
LOVE is:
A choice to make a gift of yourself to another person.
To want & work toward the best for someone else, even when it is difficult. It goes beyond emotion.
A participation in God’s love…the real thing is:
FREE: not forced or enslaved to urges.
TOTAL/FULL: not conditional. In marriage, it is not partial or holding back any part of a person.
FAITHFUL: steadfast; never abandons. In marriage, vows are permanent, only broken by death.
Shown in different ways to different people! Various ways go giving and receiving love are appropriate between spouses, family members, friends, strangers in need, etc. Though many of us are in this habit, it is not an accurate word to use toward food, animals or objects.
LUST is:
Not seeing the other as a person but as an object.
Sexual desire that distorts God’s love. Sexual desire itself is notthe sin; it is a gift from God that points to a good desire for love, but it can easily be twisted!
Using (in thought or in action) someone (body or soul) for your own benefit. (FYI, Marriage isn’t an outlet for lust!)
[youtube=http://www.youtube.com/watch?v=Djyx2c0V6Bg]
The Irish pro-life organization Youth Defense has created a powerful Christmas video that features stunning imagery of the unborn child in the womb.
“The wonder of life. Part of the Christmas story and every human story since life began,” says a narrator as the camera leaves the womb and shows the child Jesus in the manger. “The gift of life. Protect it. Cherish it.
Source: LifeSiteNews.com
Over sixty leaders of faith-based organizations or who work with faith-based organizations wrote a public letter the Obama administration protesting the very narrow exemption to the health insurance contraceptives mandate. The letter also asked that the administration not adopt in its place a different definition of “religious employer” for the exemption, suggested by some groups, that would still leave out many faith-based organizations. (more…)
Researchers from Canada have found an association between the pill and prostate cancer. The principal investigator Dr. David Mergel is a urologist and fellow in uro-oncology at Princess Margaret Hospital in Toronto. Dr. Margel and his colleague Dr. Neil Fleshner analyzed the pill use and the incidence of prostate cancer on 87 countries. They found a positive association between the pill and prostate cancer. Condoms, Intra Uterine Devices (IUDs) and vaginal barriers were also included in the analysis. These other types of contraception did not have the association with prostate cancer. (more…)
The next topic was generated in response to a recent article published in a pro-abortion religion magazine wherein the author claims that the conscientious objection, by some American physicians, to participate in abortions is somehow endangering the lives of women. (more…)
Recent news reports of responses in persons declared “brain dead” should have alerted everyone that “brain death” is not true death. These observed responses prevented the organ transplantation protocols from going further. Zack Dunlap later reported how he could hear discussions of his death, but he could not respond at that time. Val Thomas had flat brain waves for 17 hours before her response was observed. While these might be of only passing interest to many, it ought to be of grave concern to every citizen of the United States of America, and the rest of the world. (more…)
I ended my article last time with a brief introduction to the concept of lactational ammenorrhea. Again, this is that natural process where the hormones associated with milk production in the nursing mother delay further ovulation for a time. For the vast majority of women (over 98%), this spacing of fertility lasts for at least 6 months if they are exclusively breast-feeding. After 6 months, most babies are starting to eat other foods and the effect on continued breast-feeding varies from woman to woman. (more…)
The Population Research Institute (PRI) just released the fifth episode of their highly popular YouTube cartoon series—just in time for the world’s population to reach 7 billion people, according to UN data. The series, which has to date garnered over 800,000 views, is designed to humorously refute the idea of overpopulation with stick figure animation.
“The fight against the myth of overpopulation does not have to be a bare-knuckled brawl,” says Steven Mosher, PRI’s president. “These videos are funny (more…)
NEW YORK, October 6 (C-FAM) It is commonplace now for UN officials and American law professors to tell foreign governments that they are required by international law to liberalize their abortion laws. Just last month the UN Special Rapporteur on Health issued a report making this claim. The Secretary General endorsed his report. Shortly thereafter the UN High Commission on Human Rights said the same thing.
Pro-life activists have been saying for years that this is a false assertion. (more…)
An 11 year old boy in California has begun the process of “gender reassignment surgery.”
Thomas Lobel, who says he prefers to be called Tammy, is undergoing “controversial hormone blocking treatment” that will “stop him from experiencing puberty.”
And the not so shocking family circumstances of this confused little boy?
He has two mommies.
Yes, “Tammy” Lobel is being raised by lesbian parents, Debra Lobel and Pauline Moreno.
He has no father, no masculine influence, no male role model to bring him up as a man. (more…)
Belief is difficult.
Sometimes we need to see to believe.
Jesus was gentle with Thomas and his doubts.
He allowed him to touch His wounded heart.
Is He doing the same for us now,
in this new millennium?
A statue of Christ mysteriously weeps and bleeds in Cochabamba, Bolivia
In the same city Katya Rivas experiences the wounds of the crucifixion of Christ, the stigmata. Although theologically uneducated she writes profound teachings which she says are dictated by Christ.
In Argentina, a communion host (bread) changes to living flesh.
Are these claims true?
Is it the body and blood of Jesus Christ?
What does Science have to say?
Low rates of breastfeeding add $2.2 billion a year to medical costs. Babies who are fed formula and stop breastfeeding early have higher rates of obesity, diabetes, and respiratory and ear infections, and tend to require more doctor visits, hospitalizations and prescriptions.
Despite the acknowledged benefits of breastfeeding — including protecting against childhood obesity — many U.S. hospitals fare poorly when it comes to providing sufficient support and encouragement, according to a new report sponsored by the Centers for Disease Control and Prevention (CDC). (more…)
Author Emily Sederstrand with husband Tom and son Owen
In 2005, my husband, Tom, and I relocated from Ohio to upstate NY with three young children in tow. God provided for us, and we quickly made wonderful and faith-filled friends. Soon after settling in, I was invited to a “mom’s dinner,” an evening out to get refreshed. There, I was introduced to Joan, who was at the time the mother of nine and newly expecting her tenth. I looked at her in awe, unsure how anyone could have nine children!
“Oh,” she exclaimed, “you’re in the darkest part of motherhood! It’s going to get better!”
Joan was elegant and well-spoken. She turned to me and cheerfully asked, “So, what are the ages of your children?” I answered a bit sheepishly, “4 ½, 2 ½, and 1 ½,” unsure of where the conversation was heading. “Oh,” she exclaimed, “you’re in the darkest part of motherhood! It’s going to get better!” Say what? I was totally surprised, and frankly, relieved. (more…)
Most physicians, family docs and I think OBGYNs, and most researches if you ask them,
“Does the birth control pill increase the risk of breast cancer?” They will go back to a study which was a pooled analysis of all the world studies, done in 1996. It look at 54 studies, 53,000 women, 25 countries and they basically said their conclusion: “Women who are currently using combined oral contraceptives or have used them in the past 10 years are at a slightly increased risk of having breast cancer diagnosed, although the additional cancers tend to be localized to the breast.”
“New Perspectives on Contraception is an excellent
summary of the battle between good and evil in modern times,
where the battlefield has been over the graves of millions of helpless
babies, conceived lovelessly and ruthlessly destroyed, where the casualties
have been marriages and other relationships fragmented by
contraception, where the only answers that could have solved the
problems of these unhappy people were Truth and Love.”
“It is hoped that this book will find a wide distribution. It could be
extremely helpful to priests, marriage counsellors, senior High
School students and young adults contemplating marriage.”
Hormonal contraceptives alter women's local and systemic immunities making HIV infection more likely
Thirty years after the Center for Disease Control (CDC) reported the first US case of Acquired Immune Deficiency Syndrome (AIDS), the disease continues to stretch its shroud of death across the world. This, despite the billions of dollars that have been invested in the development of vaccines, spent on anti-retroviral therapies, and strewn about in condom distribution and sexual education schemes.
But there is a strange and disturbing trend now evident in the new cases of HIV/AIDS being reported, and it concerns women of reproductive age.
According to the most recent report of the Joint United Nations Programme on HIV/AIDS, published in 2009, close to 50% of all newly acquired Human Immunodeficiency Virus (HIV)-1 infections across the globe now occur in women of reproductive age. Only a decade before, in 1998, only roughly 36% of reported cases concerned women of all ages. Why this vast increase? Why, when treatment for HIV has become more accessible and the overall death toll has slowly been decreasing, are more and more women being infected? And why is the increase concentrated in women in their childbearing years?
Heterosexual intercourse is the point of transmission for the majority of these newly infected women. No surprise here. But sex is not just sex these days. Heavily funded population control programs have promoted, and even imposed, powerful, steroid-based contraceptive drugs on tens of millions of Third World women. What they trumpet as “greater global access to family planning methods” has in fact given the HIV virus greater access to women’s bodies by altering women’s local and systemic immunities, cervico-vaginal responses and protective vaginal flora—all in directions that make infection more likely.
Statistics gathered over the past 20 years reveal a parallel between an increase in contraceptive drug use and an increase in HIV-1 infections in women. Several epidemiological studies over the same period also seem to demonstrate a link. These studies were conducted with various cohorts of women from married mothers to single adolescents to “sex workers”, and were carried out, for the most part, among the populations of users of African family planning clinics. A link between the use of contraceptive drugs and HIV-1 disease acquisition and progression seemed evident, although most of the studies—for whatever reason—failed to draw any consistent or strong conclusions about this link. And none suggested that family planning programs ought to be modified or scaled back as a result.
One meta-analysis of 28 studies in 1999 suggested a positive association between oral contraceptives and HIV-1 incidence. A later study, however, carried out in 2006, claimed that there was no overall risk of acquiring HIV-1 as a result of such drug use. Such disparate results enable the promoters of population control programs to continue to rely on such contraceptive drugs, claiming, “the science is not settled.” Many of the organizations involved in such programs are, for obvious reasons, reluctant to offer clarity to women on the correlation between contraceptive use and HIV- disease prevalence in women. Indeed, several studies almost seem designed to deliberately obscure this fact.
Additional evidence of such a link comes from other studies that conclusively demonstrate that hormonal contraceptive use is positively associated with an increased risk of several other sexually transmitted infections (STI’s) such as Chlamydia.
So why are the studies involving HIV-1 transmission so inconclusive? Reasons include poor controls on variables such as age and sexual lifestyle variants, infrequent assessment, lack of follow-up and widely varying contraceptive delivery methods. Attempts at rendering comparative data are difficult, and some of the statistical compilations and some of the meta-analytical efforts, seemed designed to serve population politics.
There are other lacunae as well. Few studies consider the different effects of estrogen and progesterone—and their synthetic steroid-based counterparts–on vaginal and cervical structure and immunity. The studies that have been done broadly compare “hormonal contraceptive” use to HIV-1 acquisition and progression across a diverse range of deliverables–oral, injectible, intra-uteral, etc.—that are lumped together under one generic “hormonal contraceptive” title. The most common such amalgamation, Combined Oral Contraceptives (COC’s), consists of both hormonal (estrogen-like compounds) and steroidal (progestin) agents that work together to prevent ovulation, taken daily as “the pill.”
Other forms of contraceptive delivery include progestogen-only, such as the high-dose injectables Depo-Provera (DMPA) and Noristerat, moderate-dose pills, low-dose subdermal implants and laced intra-uterine devices (IUD’s). These steroidal forms of preventing pregnancy affect the female reproductive system somewhat differently than their estrogen-like counterparts. In low-dose delivery regimens, progestins cause a thickening of cervical mucus inhibiting sperm viability and penetration. In high-dose delivery, cervico-vaginal changes also occur: follicular development is halted along with ovulation and the endometrium is thinned. The progestogen-only effects are clear: they weigh heavily on women’s cervico-vaginal structure and protective flora, hence reducing a woman’s ability to ward off infection. As far back as 1991 abnormal changes in the condition of the cervix was found to be strongly been associated with increased susceptibility to HIV/AIDS acquisition.
The chain of reasoning is straightforward: Women who take drug-based hormonal and steroidal contraceptives are at increased risk of STI’s. HIV/AIDS is an STI. Therefore, women who take powerful steroid-based drugs called “hormonal contraceptives” are at increased risk of contracting the HIV virus.
It’s time that researchers and policy makers faced these facts responsibly, for women’s sake.
New health plan guidelines announced by the Obama Administration would significantly violate the religious liberty of Catholic colleges and universities and the families who entrust students to Catholic education.
“The HHS guidelines would force Catholic colleges to violate the law or violate the Catholic faith,” said Patrick J. Reilly, President of The Cardinal Newman Society. “Neither option is acceptable.
“It appears that Catholic colleges will be forced into the untenable position of helping students as well as employees obtain free contraceptives and sterilization,” Reilly said. “Our religious freedom is under attack.”
Under the new guidelines to be implemented as part of the Affordable Care Act signed into law last year, health plans will be required to cover without co-pay “all Food and Drug Administration approved contraceptive methods, sterilization procedures, and patient education and counseling for all women with reproductive capacity.”
The guidelines include a very narrow religious exemption that applies primarily to churches, but would likely not exempt most Catholic colleges and universities that serve students regardless of their religious beliefs. The guidelines exempt a religious employer that “(1) has the inculcation of religious values as its purpose; (2) primarily employs persons who share its religious tenets; (3) primarily serves persons who share its religious tenets; and (4) is a non-profit organization…” Such language has been used in California and other states to ensure that most religious organizations are not exempted from contraceptive mandates.
“The HHS language is ambiguous and likely to be interpreted with a bias against Catholic agencies,” Reilly said. “For instance, does a college ‘primarily’ serve Catholic students if more than half the students are Catholic? 75 percent? What is the threshold? It’s left to the discretion of federal bureaucrats who have demonstrated repeated disregard for Catholic institutions.”
“Meanwhile, this only increases the importance of Catholic colleges ensuring a strong and consistent Catholic identity, including clear ‘hiring for mission’ policies, so that they can demand First Amendment protection from unfair laws and regulations,” Reilly added.
The Cardinal Newman Society has raised serious concerns about increasing threats to the religious liberty of Catholic colleges and universities. The Equal Employment Opportunity Commission has failed to reply to an appeal from Belmont Abbey College, which was charged with “discrimination” for refusing to include contraceptives in its employee health plan. This year the National Labor Relations Board has twice ignored federal court rulings and asserted jurisdiction over Catholic colleges. An attorney is suing The Catholic University of America for allegedly violating the District of Columbia Human Rights Act by reverting to single-sex dorms.
Sterilization Reversal, A Generous Act of Love contains the touching personal stories of 20 couples who chose sterilization as a solution for family difficulties and then were given the grace to choose healing and wholeness in a radical way. Appendices cover medical aspects of reversing sterilization and pastoral reflections on sterilization and reversal by a bishop and a moral theologian.
You can use the following viewer to read it. There is a full screen option in the right upper corner of the viewer. To buy pdf see below.
Physicians Healed contain the stories of 15 physicians who do not prescribe contraceptives and who promote Natural Family Planning. These are powerful accounts of conversion, courage, and conviction. Learn what moved these doctors to risk losing patients, income, and the respect of their peers. Many physicians have been converted after reading this book.
You can use the following viewer to read it. There is a full screen option in the right upper corner of the viewer. To buy see below.
The book is available for download (file size 2MB. It has been optimized to reduce the file size).
You can also purchase a hard copy for you and your friends. We have quantity discounts 6+ $3.98, see link below.
The Vatican invited 150 bloggers from around the world to a first-ever blogging summit, increasingly aware of the important role faith-based blogging is playing in spreading Catholicism.
“We’re here for a dialogue, a dialogue that from our side means the conviction of the concrete, important and unique role of your presence in the world of communication,” Monsignor Claudio Maria Celli, head of the Vatican’s social communication’s office, told the bloggers.
The Vatican has been seeking to engage more with the online world: For the beatification of Pope John Paul II, the Vatican created a special Facebook page, Twitter account, ran clips of his 27-year pontificate on its YouTube channel and let the faithful send electronic postcards to one another about what they were experiencing via its youth-based news portal.
The blogging summit was another step in that direction.
The Rev. Roderick Vonhogen, a Dutch blogger, said blogging for Catholic priests is a great way to spread the faith to people who aren’t necessarily looking for it. He says it can be even more effective than sitting in his remote parish celebrating Mass for 200 because he can reach 40,000 people around the world.
“If we just do what we do in our churches, behind closed doors, we will have empty buildings by the end of the day,” he said.
The Vatican also unveiled at the meeting a state-of-the-art Vatican news Website. The new site will be found at www.news.va, currently you can submit your email to be informed when the site will be open.
Federal drug regulators are now reviewing studies that say some modern birth control pills may pose a serious risk of clots to women who take them.
The US Food and Drug Administration (FDA) announced Tuesday that they were conducting a safety review of birth control products containing drospirenone, a synthetic female sex hormone or progestin.
German pharmaceutical maker Bayer’s oral contraceptives Yaz, Yasmine, Safyral, Beyaz, and their generics are part of a chemical family of contraceptives containing drospirenone, and are among the oral contraceptives whose effects the FDA intends to review.
Bayer faces 7000 Yaz-related lawsuits from women who say the drug-manufacturer misrepresented the dangers associated with using the birth control pills – side effects including stroke, cardiac arrest, blood clots, and gallbladder problems.
Bayer has marketed heavily its Yaz oral contraceptive products to teenagers and young adult women, saying its products were not just for preventing pregnancy, but also could treat PMS symptoms and acne.
One wrongful death lawsuit involves an 18-year-old New Jersey college student, Michelle Pfleger, who died of cardiac arrest after taking Yaz for acne treatment. A blood clot had lodged in her lungs resulting in her sudden death on her way to classes on September 24, 2010. Her mother Joan Cummins filed suit against Bayer on May 10.
The FDA noted in its public announcement that “[a]ll birth control pills pose a risk of blood clots,” but two studies posed in the British Medical Journal contended that the contraceptives containing drospirenone posed two to three times a greater risk than other contraceptives containing the progestin levonorgestrel.
The FDA said it was going to conduct a study of 800,000 women in order to resolve the conclusions of conflicting studies on drospirenone-containing contraceptives. The results of the study are due sometime in the summer.
Rather than remain neutral in the culture war, The Home Depot has chosen to sponsor and participate in numerous gay pride parades and festivals. Most grievous is The Home Depot’s deliberately exposing small children to lascivious displays of sexual conduct by homosexuals and cross-dressers, which are a common occurrence at these events.
Home Depot is sponsoring “Southern Maine Pride” in Portland, Maine next weekend. Last year, Home Depot set up a Kid’s Workshop booth at the event. Children were exposed to “drag queens,” nudity, and other homosexual activities.
Take Action
1. Post this alert to your Facebook page and encourage others to do the same.
2. Call your local store manager and politely let him know you are boycotting Home Depot. You can find your local store number here (click “store finder”).
3. Forward this alert to all your family and friends.
– Columbus, OH – Sinclair Community College of Dayton, OH met a force of young missionaries on May 17, 2011. Ohio-based Created Equal teamed up with Survivors of the Abortion Holocaust to educate the campus about the injustice of abortion. The six “Survivors,” all under 25 years old, included Dayton in their two-month Campus Life Tour crossing the nation.
Kristina Garza, Campus Outreach Director for Survivors, said, “It’s exciting for us to come across the country and find a like-minded organization. We are excited to partner with Created Equal.”
Outside building 7 and inside building 8, the Survivors and Created Equal stood by signs displaying the grisly reality of abortion. Steve Koob, founder of One More Soul, arrived on site to interview Created Equal’s Director of Training, Seth Drayer, and the Survivors on his Radio Maria program, “The Quest for a Culture of Life in America.”
Seth Drayer commented, “It is encouraging to see youth taking ownership of this battle. The Survivors are on a mission to restore civil rights to all humans, including the preborn. Created Equal is excited to stand along with them.”
“Someone may say that my abortion was justified because of my age, the drugs, and the fire,” she says. “I do not believe anything can justify taking my baby’s life. The action is wrong. I pray that our nation will change its laws so that the lives of innocent unborn babies are protected.”
“Our nation’s young girls, especially those like me, who have experienced trauma and abuse, and are vulnerable to exploitation, should not be used as sexual playthings, scarred by abortions to free their male partners from financial responsibility, and then like their unborn children, tossed aside as an unwanted object.
“Marriage and the family are the building blocks of all virtuous societies. I learned this lesson in a trial by fire that taught me to trust God’s plan no matter what occurs. I pray that our nation may also find its way back to God by respecting the life of unborn children and strengthening the sanctity of marriage.”
With just a click of your mouse, you can cut funding to the United Nations Population Fund (UNFPA).
For those of you who are unfamiliar with the YouCut program, it is an initiative developed by House Majority Leader Eric Cantor, which allows the public to submit ideas for programs they believe should be eliminated. One of the ideas currently on the list? Cut funding to the UNFPA. How it works. Each week, three ideas for programs to cut are posted online. Once they have been posted, anyone can vote for the one that they most want the House of Representatives to consider cutting. Whichever program gets the most votes will be sponsored by the YouCut program, and the public will be able to track its progress on the website as it moves through the legislative process.
Defunding UNFPA could be considered by the House soon, but only if this option gets the most votes on the YouCut website. That’s where you come in. If you think the United States House of Representatives should cut funding to the UNFPA, then vote for that option on the YouCut web site, and urge everyone you know to do the same.
To vote to cut funding to the UNFPA, visit the YouCut program HERE and click “vote” next to the “Terminate U.S. Contributions to the United Nations Population Fund” option.
In a week replete with news of presidential candidates entering and leaving the race, a story brewing in Indiana points the way toward greater political cooperation between pro-life and small government activists – cooperation that could be key for politicians working to build broad coalitions.
In late April, the Hoosier state became the first in the nation to prohibit state officials from entering into contracts with or making grants to any entity (including, notably, Planned Parenthood) that performs abortions or that maintains or operates facilities where abortions are performed when Governor Mitch Daniels signed a law that also bans abortions after the 20th week of pregnancy. The effect of the new law is to deny Planned Parenthood about $3 million in public funds unless they decide that providing common preventive care for women (such as prenatal care, pap tests, and screening for sexually-transmitted diseases) is more important than providing abortions.
Hours after the governor signed the bill into law, Planned Parenthood was in U.S. District Court in Indianapolis requesting a restraining order. U.S. District Judge Tanya Walton Pratt refused to enter a temporary injunction. A full hearing on Planned Parenthood’s request for a permanent injunction against the law is expected in June.
Despite the judge’s initial ruling, Planned Parenthood of Indiana continues to claim that the bill is unconstitutional.
Media analysts have noted that the law defunding Planned Parenthood could improve Gov. Daniels standing among social conservatives as he considers a run for the presidency in 2012. More
Last week, Oklahoma Governor Mary Fallin (at left) signed another pro-life bill into law, HB 1970 — this time prohibiting dangerous, off-label use of the abortion-inducing drug RU 486, also known as mifepristone.
The law was sponsored by Rep. Randy Grau and Sen. Greg Treat. The new legislation requires that abortion-inducing drugs be distributed in accordance with the FDA-approved drug label and does not allow dangerous off-label use by abortion providers seeking to maximize their profits at the expense of women’s health. More
Based on six years of study and a meticulous analysis of hundreds of scientific papers and other sources, Dr. Chris Kahlenborn documents the effect that abortion and hormonal contraception have on breast cancer, as well as uterine, cervical, liver, and other cancers, and even the transmission of AIDS! Hormonal contraceptive use before first full term pregnancy is found to increase risk of breast cancer by at least 40%. The book gives special attention to black women, to various populations of the world, and to effective steps for prevention. This is a very timely and powerful work.
The book is available for download (file size 1MB. It has been optimized to reduce the file size). You can also purchase a hard copy, see link below.
Quantity pricing for the paperback only.Based on six years of study and a meticulous analysis of hundreds of scientific papers and other sources, Dr. Chris Kahlenborn documents the effect that abortion and hormonal contraception have on breast cancer, as well as uterine, cervical, liver, and other cancers, and even the transmission of AIDS! Hormonal contraceptive…
“We need to have the correct attitude toward children. Without this we have no future,”
Russia has experienced a dramatic population decline, going from 148.5 million people in 1995 to 143 million today.
Legislators in Russia’s lower house of parliament have prepared a draft law that they hope will reduce the more than 1 million abortions performed in the country each year.
Source: C-FAM
As the 2012 budget battles began, Clare Coleman, CEO of the National Family Planning and Reproductive Health Association, took to the pages of the Washington Post. In a piece called “Five Myths about Planned Parenthood,” she argued that defunding the organization was an ignoble goal for members of Congress looking to cut the bloated federal budget.
She said she wanted to address “misperceptions” about the abortion-industry giant. She was joined in her goal on the front page of the Washington Post by reporter Sandhya Somashekhar, who painted a picture of Planned Parenthood that minimized the role abortion plays at the organization’s health-care affiliates.
In presenting Planned Parenthood as mainly focused on prevention, Ms. Coleman neglects to mention several statistics, gleaned from the organization’s own annual reports and fact sheets, that illustrate its heavy (and increasing) involvement in abortion, as well as its practices that routinely place women’s health and safety secondary to its own bottom line.
While the Washington Post declined to present an alternative to the Planned Parenthood way of thinking, there are a multitude of other facts to consider. To add to the discussion of whether Planned Parenthood should continue to be funded, let’s consider five truths about an industry that receives more than $360 million in taxpayer subsidies annually.
1. Planned Parenthood is the nation’s largest abortion provider, performing (and profiting from) one out of every four abortions in the United States.
In 2009, abortion was a “service” that Planned Parenthood provided to 12 percent of its patients overall, and to 97.6 percent of its patients who reported themselves pregnant. It performed 332,278 abortions in that one year alone. That is an average of 910 abortions each and every day.
Since the average cost of an early surgical abortion was $451 (according to the Guttmacher Institute, Planned Parenthood’s former “special affiliate”), abortion accounted for approximately 37 percent of Planned Parenthood’s health-care-center income in 2009. And that figure — nearly $150 million in revenue from abortion — is a low estimate, considering that Planned Parenthood also performs later and more expensive abortions.
In terms of time, money, and unduplicated patients — rather than the bloated “services” rhetoric — abortion contributes significantly more than the 3 percent Ms. Coleman implies to Planned Parenthood’s bottom line.
2. Planned Parenthood increases its abortion numbers with each passing year, bucking the nearly 20-year national trend of a decreasing abortion rate.
Today, Planned Parenthood performs nearly double the number of abortions it did in 1999. And over the last twelve years — during which the amount of taxpayer funding Planned Parenthood receives has, coincidentally, also doubled — it has dramatically reduced the other pregnancy-related services it provides. In 2009, Planned Parenthood made referrals for only 997 adoptions, in contrast to the 2,999 referrals it made in 1999. Similarly, Planned Parenthood’s clients for prenatal care dropped from 18,878 to only 7,021.
Abby Johnson, the former director of Planned Parenthood’s clinic in Bryan, Texas, reports that, in 2009, her clinic was given an increased abortion quota in order to raise revenue. (According to Mrs. Johnson, “the assigned budget always included a line for client goals under abortion services.”) Mrs. Johnson has said that her superiors gave her “the clear and distinct understanding that I was to get my priorities straight, that abortion was where my priorities needed to be because that’s where the revenue was.”
The latest annual report for the affiliate Ms. Coleman headed before she assumed her current post, Planned Parenthood of Mid-Hudson Valley (PPMHV), seems to corroborate Mrs. Johnson’s claim that Planned Parenthood is increasing abortion services with an eye toward increased revenue. PPMHV is relocating its consolidated clinics to open larger and more “modern” facilities, which, notably, have “the addition of surgical abortion services.” The PPMHV report “anticipates” that these new centers will lead to “increasing our revenue and sustainability.”
Planned Parenthood’s new use of Skype to dispense abortion-inducing drugs and its mandate that all affiliates provide abortion services by 2013 also indicate that the organization wants its abortion-increasing trend to continue.
3. Planned Parenthood affiliates have failed to be good stewards of taxpayer funds.
In some cases where Planned Parenthood has not been legally allowed a “financial cushion” through a government health-care program, it has felt entitled to build one for itself. For example, a California audit report showed that in one year alone Planned Parenthood of San Diego and Riverside Counties received $5 million more than it should have because of improper billing practices.
And contrary to Ms. Coleman’s claim, Planned Parenthood does have sources of money other than the government dole. In fact, for its fiscal year ending June 30, 2009, Planned Parenthood Federation of America (PPFA) and its affiliates reported receiving $308.2 million in “Private Contributions and Bequests.” It also made $404.9 million in “Health Center Income.” Though individual affiliates have recorded losses, Planned Parenthood overall reported an “excess of revenue over expenses” of $63.4 million in 2009.
4. Planned Parenthood fights reasonable laws to protect women and girls because such laws might undermine its ability to make money.
Planned Parenthood’s consistent and financially motivated opposition to federal and state legislation designed to protect women and girls makes clear that its abortion business trumps its professed concern for these women and girls. Just this spring, a Planned Parenthood affiliate in Illinois fought a bill to make reporting of sex abuse mandatory, because Planned Parenthood allegedly feared that the legislation might overload the responsible agency with too many cases of suspected abuse.
Planned Parenthood’s longstanding efforts across the nation to overturn common-sense laws that safeguard women’s health and safety further underscore the organization’s pattern and practice of refusing to make caring for women a priority. Just a few years ago, Planned Parenthood challenged a Missouri law that required abortion clinics to meet the same standards as the ambulatory-surgery centers in the state. Its reason? Bringing its clinics into compliance with these medically accepted standards would be prohibitively costly.
5. Planned Parenthood partners with those who sexually abuse and exploit women and girls.
Substantial evidence suggests that Planned Parenthood — far from being a defender of women and girls — defends and abets those who sexually abuse and exploit them. Planned Parenthood has shown itself to be a perfect partner to the pimp, sex trafficker, or child abuser. It hides his crimes through its willful failure to report suspected sexual abuse of children to authorities and its refusal to comply with parental-involvement laws. For example, Planned Parenthood of Central and Northern Arizona was found negligent and civilly liable for failing to report the sexual abuse of a young girl who was being raped by her foster brother, and Planned Parenthood Minnesota/North Dakota/South Dakota was fined $50,000 for ignoring Minnesota’s parental-notice law. Planned Parenthood’s failure to intervene in cases of abuse reflects a lack of concern for the women and girls who go to Planned Parenthood seeking trustworthy care and counsel.
One of Ms. Coleman’s five “myths” is the assertion that “People do not really need Planned Parenthood.” The truth is this: People do not need Planned Parenthood to stay in the abortion business (nor to annually increase its stake in it). People do not need Planned Parenthood to protect adult men who prey on and abuse young girls. People do not need Planned Parenthood’s anti-woman, bottom-line-oriented view that pushes abortion at the expense of women’s health and safety. Above all, people do not need Planned Parenthood’s scandal-ridden and abortion-heavy business practices to be subsidized by taxpayer dollars.
Original source HLI
A resolution voted on today by Johnson & Johnson (JNJ) shareholders asked JNJ not to discriminate against a job applicant because of her health status. The resolution, which was opposed by JNJ, was voted down by shareholders.
Offered by Human Life International, the resolution was prompted, in part, by the numerous breast cancer survivors who have gone public with their travails to better educate woman about breast cancer and its prevention. In addition to their physical concerns, these courageous women face possible job discrimination because of potential medical liabilities they may pose to future employers. The resolution asks JNJ not to discriminate against these women or others, like AIDS victims, because of their health status. In a letter to shareholders, JNJ recommended shareholders vote against this policy because “The Board (of JNJ) does not believe it is necessary….”
In addition, the resolution highlighted the connection between breast cancer and oral contraceptives by citing a meta-analysis study by Dr. Chris Kahlenborn, which showed 21 out of 23 studies indicated a link between breast cancer and oral contraceptive use. The International Agency on Cancer Research, a branch of the World Health Organization, classified hormonal contraceptives in 2005 as a group one carcinogen, along with asbestos and radium. JNJ sells hundreds of millions of dollars worth of oral contraceptives every year. Dr. Kahlenborn gave a short presentation: quote
Representing Human Life International’s stockholder resolution
Annual Stockholder’s Meeting, Johnson and Johnson
April 28, 2011
Trenton, NJ
Good Morning. Thank you for the opportunity to address all of you today. Each year, over 200,000 women develop invasive breast cancer in the United States. In regard to Johnson and Johnson, it is good to affirm a resolution that promises not to discriminate against hiring women who have developed breast cancer; but it is not enough. This company has a unique opportunity to be a leader against the fight against breast cancer by working to prevent it.
In October, 2006, four researchers, including myself, published a meta-analysis in the Mayo Clinic Proceedings on the subject of oral contraceptives and pre-menopausal breast cancer (1). After reviewing all of the world’s data, we found that 21 out of 23 studies showed an increased risk of developing invasive premenopausal breast cancer if women took oral contraceptives prior to the birth of their first child, which is when most women take them. These women incurred a 44% increased risk, which rose to 52% if they took them for at least 4 years prior to the birth of their first child. Both of these results were significant at the 99% confidence interval-the highest standard used in research. In addition we noted that the World Health Organization had recently classified oral contraceptives as a Group I carcinogen-the most dangerous type known to humankind (2).
Recently our study was quoted in the Frontiers of Medicine in China (3) whose researchers performed their own meta-analysis and found that women who took oral contraceptives sustained a 112% increased risk in developing breast cancer. In addition, a recent collaborative study co-authored by investigators from the National Cancer Institute, the Hutchinson Cancer Center and the University of Washington cited our meta-analysis and also noted significant breast cancer risk with oral contraceptives (4).
In conclusion, I note that there are three good reasons for you to consider the alternative of ceasing all hormonal contraceptive sales while specifically and publicly citing the breast cancer risk:
1) Limitation of bad press. Instead of picking up Bloomberg Businessweek and cringing you would be a step ahead of the curve and your competitors and would be seen as a leader. People want to see Johnson and Johnson as a company that makes safe products like your shampoo-not products that are becoming controversial, such as oral contraceptives.
2) Limitation of future lawsuits: Suits against the thrombotic potential of oral contraceptives are increasing and the breast cancer link may well be the next frontier.
3) It is the right thing to do. I ask the executives and board members of Johnson and Johnson to simply ask yourselves one question: knowing what you know today, would you be comfortable if your wife or daughter were to take Johnson and Johnson’s hormonal contraceptive pills?
Thank you for your time and attention. I will be available for questions and this presentation and its sources will be posted on the Human Life International website. I have a couple of extra copies for those interested here.
“I took birth control for years, and I have to wonder if it caused my breast cancer. I also have a niece who was on birth control and at 19 had a stroke due to blood clotting aggravated by the pill,” said Bonnie Borel-Donohue, a breast cancer survivor, in response to the vote. “Having profited for years from the sale of carcinogenic and stroke-provoking birth control products, JNJ should see that this resolution is but the smallest step it could have taken to rectify the injustices and harms suffered by unsuspecting users/victims of their birth control products.”
“The way to plan the family is Natural Family Planning, not contraception. In destroying the power of giving life, through contraception, a husband or wife is doing something to self. This turns the attention to self and so destroys the gift of love in him or her. In loving, the husband and wife must turn the attention to each other. Once that living love is destroyed by contraception, abortion follows very easily.”
~ Blessed Mother Teresa (in front of Bill and Hillary Clinton)
H/T to CatholicFire for the quote.
From nfpworksblog.
I want to share what I learned….but I fear not being able to convey it as well as I want.
I will share anyway.
He (Louie) was talking about how inconceivably BIG our God is…how He spoke the universe into being…how He breathes stars out of His mouth that are huge raging balls of fire…etc. etc. Then He went on to speak of how this star-breathing, universe creating God ALSO knitted our human bodies together with amazing detail and wonder. At this point I am LOVING it (fascinating from a medical standpoint, you know.) …..and I was remembering how I was constantly amazed during medical school as I learned more and more about God’s handiwork. I remember so many times thinking….”How can ANYONE deny that a Creator did all of this???”
Louie went on to talk about how we can trust that the God who created all this, also has the power to hold it all together when things seem to be falling apart…how our loving Creator is also our sustainer.
And then I lost my breath.
And it wasn’t because I was running my treadmill, either!!!
It was because he started talking about laminin.
I knew about laminin. Here is how wikipedia describes them :”Laminins are a family of proteins that are an integral part of the structural scaffolding of basement membranes in almost every animal tissue.” You see….laminins are what hold us together….LITERALLY. They are cell adhesion molecules. They are what holds one cell of our bodies to the next cell. Without them, we would literally fall apart. And I knew all this already. But what I didn’t know is what laminin LOOKED LIKE.
But now I do. And I have thought about it a thousand times since (already)….
Here is what the structure of laminin looks like…AND THIS IS NOT a “Christian portrayal” of it….if you look up laminin in any scientific/medical piece of literature, this is what you will see…
Now tell me that our God is not the coolest!!!
Amazing.
The glue that holds us together….ALL of us….is in the shape of the cross.
Immediately Colossians 1:15-17 comes to mind.
“He is the image of the invisible God, the firstborn over all creation.
For by him all things were created; things in heaven and on earth , visible and invisible,
whether thrones or powers or rulers or authorities;
all things were created by him and for him.
He is before all things,
and in him all things HOLD TOGETHER. ”
Colossians 1:15-17
Call me crazy. I just think that is very, very, very cool.
Thousands of years before the world knew anything about laminin, Paul penned those words. And now we see that from a very LITERAL standpoint, we are held together…one cell to another….by the cross.
You would never in a quadrillion years convince me that is anything other than the mark of a Creator who knew EXACTLY what laminin “glue” would look like long before Adam even breathed his first breath!!
Taken from Northern Kentucky Right To Life Newsletter Vol. 40, No. 2 April 2011
U.S. Rep. Nancy Pelosi (D) (Speaker of the U.S. House until her party was overwhelmingly turned out by the voters last November) made an interesting remark in a press briefing at a Catholic Community Conference on Capitol Hill, where she said that her favorite word was “the word, as in the Word made flesh.” She added that people have to give voice to “what that means in terms of public policy that would be in keeping with the values of the Word.”
Her remark led to a very embarrassing question put to her then at a later press briefing by CNS News reporter Jane McGrath: “So, when was the Word made flesh? Was it at the Annunciation, when Jesus was conceived by the power of the Holy Spirit, as the Creator says, or was it at the Nativity when He was born of the Virgin Mary? And when did the Word get the right to life?” Pelosi’s evasive answer to her obvious hypocritical position favoring the destruction of unborn children was that the question just put to her is one that “we talk about in church, and that’s where I’d like to talk about that.”
NEW YORK, 2011 (Zenit.org).- The Holy See’s permanent observer to the United Nations is challenging the erroneous view that human fertility and population growth is something to be feared.
Archbishop Francis Chullikatt stated this Tuesday in an address to the 44th Session of the Commission on Population and Development in a meeting on “Fertility, Reproductive Health and Development.”
He noted, “Unfortunately many discussions in the present day continue to be led by a false notion that, in the context of population growth, the very act of giving life is something to be feared rather than affirmed.”
“Such thinking is based on a radical individualism,” the prelate said, “which sees human reproduction as a commodity that must be regulated and improved in order to encourage greater market efficiency and development.”
He continued: “How can such a view be consistent with the objectives of the United Nations? Put most candidly, it cannot.”
The archbishop asserted that “this flawed understanding leads to the distorted view that population growth, especially among the poor, must be decreased in order to address poverty, illiteracy and malnutrition.”
“It is also based upon the consistently disproven theory that population increase will devastate the environment, lead to global competition and confrontation for resources and undermine the ability of women to interact fully with society,” he said.
Human sexuality
“These apprehensions contribute to the advancement of forms of reproductive technology which denigrate the nature of human sexuality,” Archbishop Chullikatt noted.
He observed that “the combination of these misconceptions have led some national governments to adopt laws and policies which discourage parents from exercising their fundamental and non-derogable right to have children free of coercion and which even make it illegal for mothers to give birth in some cases or for a child to have one’s own brothers and sisters.”
The prelate urged, “Instead of focusing political and financial resources on efforts to reduce the number of poor persons through methods which trivialize marriage and the family and deny the very right to life of unborn children, let us instead focus these resources on providing the promised development assistance to the approximately 920 million people living on less than $1.25 per day.”
He continued: “Let us feed the nearly 1 billion people who are malnourished, and let us provide skilled birth attendants at every birth to reduce the incidents of maternal and child morality.
“Let us achieve our promise of providing primary education to the 69 million children who risk becoming another generation without such basic assistance.”
The archbishop concluded, “These children of today will be the citizens of tomorrow who have much to contribute to the welfare and common good of all.”
April 14, 2011 One More Soul representative Ethel Borel-Donahue recently distributed several copies of OMS pamphlet “Breast Cancer Risk from Abortion” to her classmates at Sinclair Community College in Dayton, Ohio. The college responded by emphasizing its policy that no literature may be distributed in classrooms and other “working areas” of the college. This action and the related policy raise important questions about free speech by students on campus.
UPDATE FROM: WorldNETDaily
Sinclair Community College has ordered a student not to distribute pamphlets highlighting breast cancer’s link to abortion and oral contraceptives, drawing a challenge that cites, among other things, the idea of free speech.
The confrontation began during Breast Cancer Awareness Month in October of 2010 when Ethel Borel-Donohue, a paralegal studies student, shared two sets of roughly 15 pamphlets after a class.
The pamphlets, published by a Catholic organization, asserted overwhelming evidence that abortion and oral contraceptives substantially increase a woman’s risk of developing breast cancer.
But the chairman of the department, Michael Brigner, censored the material from all class areas after a complaint from a fellow student who had had an abortion. And in doing so, he revealed Sinclair’s broad constraints on free speech, which go well beyond the classroom and this particular incident.
From Sinclair’s policy on social and commercial activity:
“Literature may not be distributed in working areas, including: classrooms, laboratories, lecture halls, gymnasiums, libraries, offices, work stations, conference rooms, and corridors leading directly thereto which are an integral part of the work areas.”
“So you can distribute literature, but you just can’t do it anywhere,” jibed Borel-Donohue. “I’ve been to several universities, but Sinclair, it seems, is really totalitarian in their control.”
Ohio College Prohibits Student from Peacefully Distributing Literature on Abortion, Birth Control
Sinclair Community College has banned a student from distributing literature about abortion, birth control, and breast cancer to her classmates after class. The college also bans all distribution of literature on vast areas of campus. Student Ethel Borel-Donohue, who never disrupted class with her literature, came to FIRE for help. Read Full Article
By Most Rev. Michael J. Sheehan Archbishop of Santa Fe
Dear Brothers and Sisters in Christ,
We are all painfully aware that there are many Catholics today who are living in cohabitation. The Church must make it clear to the faithful that these unions are not in accord with the Gospel, and to help Catholics who find themselves in these situations to do whatever they must do to make their lives pleasing to God.
First of all, we ourselves must be firmly rooted in the Gospel teaching that, when it comes to sexual union, there are only two lifestyles acceptable to Jesus Christ for His disciples: a single life of chastity, or the union of man and woman in the Sacrament of Matrimony. There is no “third way” possible for a Christian. The Bible and the Church teaches that marriage is between one man and one woman and opposes same sex unions.
We have three groups of people who are living contrary to the Gospel teaching on marriage: those who cohabit; those who have a merely civil union with no previous marriage; and those who have a civil union who were married before. These people are objectively living in a state of mortal sin and may not receive Holy Communion. They are in great spiritual danger. At the best – and this is, sadly, often the case – they are ignorant of God’s plan for man and woman. At the worst, they are contemptuous of God’s commandments and His sacraments.
Of these three groups, the first two have no real excuse. They should marry in the Church or separate. Often their plea is that they “cannot afford a church wedding” i.e. the external trappings, or that “what difference does a piece of paper make?” – as if a sacramental covenant is nothing more than a piece of paper! Such statements show religious ignorance, or a lack of faith and awareness of the evil of sin.
The third group, those who were married before and married again outside the Church, can seek a marriage annulment and have their marriage blest in the Church. Please remember that divorce still is no reason to refrain from Holy Communion as long as they have not entered into another marriage or sinful relationship. Many Catholics are confused on this point.
Christ our Lord loves all these people and wishes to save them – not by ignoring their sin, or calling evil good, but by repentance and helping them to change their lives in accordance with His teaching. We, as His Church, must do the same. In accord with this, I would remind you of the following:
1. People in the above three situations cannot receive the Sacraments, with the important exception of those who agree to live chastely (“as brother and sister”) until their situation is regularized. Of course, those in danger of death are presumed to be repentant.
2. These people may not be commissioned as Extraordinary Ministers of Holy Communion, not only because of scandal, but even more because one commits the sin of sacrilege by administering a Sacrament in the state of mortal sin.
3. Nor are such people to be admitted to the role of sponsor for Baptism or Confirmation, as is clearly stated on the Archdiocesan Affidavit for a Sponsor. It is critical for the sponsor to be a practicing Catholic – and can anyone be seriously called a practicing Catholic who is not able to receive the sacraments because they are living in sin?
4. When it comes to other parish ministries and organizations, I feel it best to leave these situations to the judgment of the pastor. Prudence is needed, avoiding all occasions of scandal. We must see their involvement in the parish as an opportunity to work urgently to bring such people to repentance and the regularization of their lifestyle.
5. Many of these sins are committed out of ignorance. I ask that our pastors preach on the gravity of sin and its evil consequences, the 6th and 9th Commandments of God, and the sacramental nature and meaning of Christian marriage. Our catechetical programs in our parishes – children, youth, and adult – must clearly and repeatedly teach these truths.
A Church wedding does not require some lavish spectacle and entertainment costing vast sums of money (Indeed, how often we have seen the most costly weddings end in divorce in but a few months or years!). While beauty and joy should surround a Christian wedding, we must remind everyone that it is a sacrament, not a show.
6. Those who are married outside the Church because of a previous union are urged to seek an annulment through our Marriage Tribunal. If it can be found that the first marriage lacked some essential quality for a valid marriage, the Tribunal can grant an annulment. Your pastor can help someone start a marriage case for this purpose. It is important for such couples to continue to pray and get to Mass even though they may not receive Communion, until their marriage can be blest in the Church.
Our popular American culture is often in conflict with the teachings of Jesus and His Church. I urge especially young people to not cohabitate which is sinful, but to marry in the Church and prepare well for it.
I congratulate and thank those thousands of Catholic married couples who role model the Sacrament of Marriage according to the teachings of Jesus and his Church.
Sincerely yours in the Risen Lord,
Most Rev. Michael J. Sheehan
Archbishop of Santa Fe
Por el Reverendísimo Michael J. Sheehan Arzobispo de Santa Fe
Todos somos dolorosamente conscientes de que hay muchos Católicos hoy que viven juntos, en cohabitación. La Iglesia debe dejar claro a los fieles que estas uniones no están de acuerdo con el Evangelio y ha de ayudar a los Católicos que se encuentran en esta situación a hacer lo que deben para que sus vidas sean agradables a Dios.
En primer lugar, debemos enraizarnos con firmeza en la enseñanza del Evangelio que, en lo que se refiere a la unión sexual, muestra solo dos estilos de vida que Jesucristo acepta para sus discípulos: una vida de castidad en soltería, o la unión de un hombre y una mujer en el Sacramento del Matrimonio. Para un cristiano, no hay una “tercera vía” posible. La Biblia y la Iglesia enseñan que el matrimonio es entre un hombre y una mujer y se opone a las uniones del mismo sexo.
Tenemos tres grupos de gente que viven contra la enseñanza del Evangelio sobre el matrimonio: los que cohabitan, los que tienen sólo una unión civil sin matrimonio previo y los que viven en unión civil que se casaron con anterioridad. Esta gente vive objetivamente en un estado de pecado mortal y no pueden recibir la Santa Comunión. Están en gran peligro espiritual. En el mejor de los casos, y tristemente así suele ser, ignoran el plan de Dios para el hombre y la mujer. En el peor, desprecian los mandamientos de Dios y sus sacramentos.
De estos tres grupos, los dos primeros no tienen realmente una excusa. Deberían casarse por la Iglesia o separarse. A menudo aseguran que “no podemos permitirnos una boda por la Iglesia” (es decir, los ropajes externos) o que “¿y en qué cambia el tener un pedazo de papel?”, ¡como si la alianza sacramental fuese nada más que una pedazo de papel! Estas afirmaciones muestran ignorancia religiosa o una falta de fe y de conciencia en la maldad del pecado.
El tercer grupo, los que antes estuvieron casados y se han casado otra vez fuera de la Iglesia, pueden buscar una nulidad matrimonial y hacer que su matrimonio quede bendecido por la Iglesia.
Por favor, recordad que el divorcio no es causa para abstenerse de la Santa Comunión siempre que no se haya entrado en otro matrimonio o en una relación pecaminosa. Muchos católicos se confunden en este detalle.
Cristo Nuestro Señor ama a todas estas personas y desea salvarlas, no ignorando su pecado ni llamando bueno a lo que es malo, sino mediante el arrepentimiento y ayudándoles a cambiar sus vidas de acuerdo con su enseñanza. Nosotros, como su Iglesia, debemos hacer lo mismo. Por eso, os recordaría lo siguiente:
1. Las personas que están en las tres situaciones mencionadas no pueden recibir los sacramentos, con la importante excepción de los que viven castamente (“como hermano y hermana”) hasta que su situación se regularice. Por supuesto, los que estén en peligro de muerte se supone que se arrepienten.
2. Estas personas no pueden ser elegidas como ministros extraordinarios de la Santa Comunión, no solo por el escándalo, sino más aún, porque se comete pecado de sacrilegio al administrar un sacramento en estado de pecado mortal.
3. Ni deben estas personas ser admitidas como padrinos de bautismo o confirmación, como explica claramente el Documento Archidiocesano sobre Padrinos. Es importantísimo que el padrino sea un católico practicante. ¿Y puede llamarse seriamente Católico practicante a quien no es capaz de recibir los sacramentos porque vive en pecado?
4. En lo que se refiere a otros ministerios parroquiales y otras organizaciones, creo que es mejor dejar que discierna el pastor. Se necesita prudencia y evitar toda posibilidad de escándalo. Debemos ver la participación de estas personas en la parroquia como una oportunidad para trabajar con urgencia con ellas para acercarlas al arrepentimiento y la regularización de su estilo de vida.
5. Muchos de estos pecados se cometen por ignorancia. Pido a nuestros pastores que prediquen sobre la gravedad del pecado y sus malignas consecuencias, sobre el 6º y 9º mandamiento de Dios y sobre la naturaleza sacramental y el significado del matrimonio cristiano. Nuestros programas catequéticos parroquiales, para niños, jóvenes y adultos, deben enseñar estas verdades de forma clara y repetida.
Una boda por la Iglesia no requiere espectáculos y entretenimientos que cuesten grandes sumas de dinero. De hecho, ¡cuántas veces hemos visto las bodas más costosas acabar en divorcio al cabo de unos meses o pocos años! Si bien la belleza y el gozo deben rodear una boda cristiana, hay que recordar a todos que es un sacramento, no un espectáculo.
6. A aquellos que se casan fuera de la Iglesia debido a una unión previa les urgimos a buscar una nulidad mediante nuestro tribunal matrimonial. Si se muestra que el primer matrimonio carecía de alguna cualidad esencial para un matrimonio válido, el tribunal puede conceder la nulidad. Tu pastor te puede ayudar a empezar la causa matrimonial con este propósito. Es importante que estas parejas sigan rezando y acudiendo a misa aunque no puedan recibir la comunión hasta que su matrimonio sea bendecido por la Iglesia.
Nuestra cultura popular americana a menudo está en conflicto con las enseñanzas de Jesús y su Iglesia. Animo especialmente a los jóvenes a no cohabitar, que es pecaminoso, sino a casarse por la Iglesia y prepararse bien para ello.
Felicito y doy las gracias a los miles de matrimonios católicos que son un modelo del sacramento del matrimonio según las enseñanzas de Jesús y su Iglesia.
Sinceramente vuestro en el Señor Resucitado,
Reverendísimo Michael J. Sheehan, arzobispo de Santa Fe
(Largo, FL) Children of God for Life is calling for a public boycott of major food companies partnering with Senomyx, a biotech company that produces artificial flavor enhancers using aborted fetal cell lines to test their products.
In 2010, the pro-life organization wrote to Senomyx CEO Kent Snyder, pointing out that moral options for testing their food additives could and should be used. But when Senomyx ignored their letter, they wrote to the companies Senomyx listed on their website as “collaborators” warning them of public backlash and threatened boycott. Food giants Pepsico, Kraft Foods, Campbell Soup, Solae and Nestlé are the primary targets of the boycott.
Senomyx website states: “The company’s key flavor programs focus on the discovery and development of savory, sweet and salt flavor ingredients that are intended to allow for the reduction of MSG, sugar and salt in food and beverage products….Using isolated human taste receptors, we created proprietary taste receptor-based assay systems that provide a biochemical or electronic readout when a flavor ingredient interacts with the receptor.”
Their collaborators provide Senomyx research and development funding plus royalties on sales of products using their flavor ingredients.
“What they don’t tell the public is that they are using HEK 293 – human embryonic kidney cells taken from an electively aborted baby to produce those receptors”, stated Debi Vinnedge, Executive Director for Children of God for Life, a pro-life watch dog group that has monitored the use of aborted fetal material in medical and consumer products for years. Here is their patent (read the abstract …expression methods will use HEK-293 cells…).
“They could have easily chosen animal, insect, or other morally obtained human cells expressing the G protein for taste receptors”, she added.
In writing to their collaborators, it took three letters before Nestlé finally admitted the truth about their relationship with Senomyx, noting the cell line was “well established in scientific research”.
Both Pepsico and Campbell Soup also responded.
Shockingly, Pepsico wrote: “We hope you are reassured to learn that our collaboration with Senomyx is strictly limited to creating lower-calorie, great-tasting beverages for consumers. This will help us achieve our commitment to reduce added sugar per serving by 25% in key brands in key markets over the next decade and ultimately help people live healthier lives.”
Campbell Soup was more sensitive in their response: “Every effort is made to use the finest ingredients and develop the greatest selection of products, all at a great value. With this in mind, it must be said that the trust we have cultivated and developed over the years with our consumers is not worth compromising to cut costs or increase profit margins.”
While Campbell didn’t state they would change their methods, their response, gave Vinnedge hope.
“If enough people voice their outrage and intent to boycott these consumer products, it may convince Senomyx to change their methods”, she noted. “Otherwise, we will be buying Coca-Cola, Lipton soups and Hershey products!”
UPDATE!!! March 29, 2011 11:45AM ( from Children of God for Life)
Within hours of our press release, Children of God for Life received notice from Campbell Soup that they have severed their ties with Senomyx.
Stated Juli Mandel Sloves, Senior Manager of Nutrition & Wellness Communications at Campbell Soup Company, “We are no longer in partnership with Senomyx. This fact was discussed during the Senomyx conference call with its investors earlier this month.”
If you choose to write to Campbell Soup, please thank them for their decision. Mmmm good!
By Chris Slattery,
EMC Frontline Pregnancy Care Monday, February 21st,
2011
My wife Eileen and I mourn the death of our dear friend and mentor,
Dr. Bernard Nathanson. I met Bernie in late 1970s, when I was a young
salesman in the magazine industry. after he’d published his first
book, Aborting America.
I got to know him at talks at Human Life International, before he
released his first, earth-shaking film, The Silent Scream. He
explained the sinister and deceptive way in which abortion had been
legalized by lies and manipulation. I could see how much difference
one man could make. He got me angry, and motivated me to dedicate my
life to this cause.
When Bernie and his partners founded NARAL–the National Association
for the Repeal of Abortion Laws–and set out to legalize abortion,
they were lionized at first by the media. They coddled the press with
lies and exaggerations. In 1972, the year before Roe vs. Wade, the
Centers for Disease Control reported that there were 39 deaths from
illegal abortions. But Bernie simply made up the figure of “5,000 to
10,000 per year,” and the press bought it.
He estimated that through the abortion clinic he and his partners
founded in Manhattan, the Center for Reproductive and Sexual Health
(CRASH), he was responsible for the deaths of 60,000 children. But
with the development of ultrasound in the 1970s, Bernie began to
realize what he had been doing. He changed his mind about abortion and
set out to do whatever he could, by speaking, writing, and making
films, to right the wrong he had done. The same media and opinion-
makers who had praised him now attacked him as an opportunist, a
quack, and an eccentric.
He wouldn’t be stopped. His three books and three films became the
primary tools of many pro-life activists. I can tell you that over the
years, his films alone had a huge impact on expectant mothers, and
saved the lives of tens of thousands of children in our EMC FrontLine
Pregnancy Centers and elsewhere.
He went back to school, getting a degree in bioethics from Vanderbilt
University in 1996. He became an expert witness before legislatures
and juries, using his authoritative voice to teach the uninformed
about the reality of life in the womb and the deceptions of the
abortion industry. He is a featured speaker in the current film about
that industry, Blood Money.
He became a consultant to us when we opened our first pregnancy center
in Manhattan on East 23rd Street and he helped provide pre-natal care
to our moms, and he did a fund-raiser for us in his townhouse in
Chelsea, and spoke for us elsewhere. He also helped with my wife’s own
pre-natal care when Eileen had a difficult pregnancy with our third
child, Brigid.
After he renounced abortion, Bernie was still not a religious man. He
described it as a seminal moment in his awakening when he and I next
to each were among hundreds of pro-lifers dragged away from the
doorways of Planned Parenthood on E 22nd Street, and Second Avenue in
Manhattan. On that cold January morning in 1989, with Operation Rescue
we helped shut down seven abortion mills in New York. Planned
Parenthood, his former ally, sued us and about 6 other rescue leaders
in Federal court.
Bernie carried a very heavy burden of guilt for his crimes. He began
talking with Fr. C. John McCloskey of the Prelature of Opus Dei, and
read a great many excellent spiritual books at his suggestion. Then
the man who in the 1960s had fought to destroy the reputation and
influence of the Church now asked to be baptized a Catholic. He had a
wholehearted conversion, praying for forgiveness and God’s mercy.
In 1996, in the crypt under St. Patrick’s Cathedral in New York, pro-
life heroine Joan Andrews Bell acted as Bernie’s godmother. I was his
Confirmation sponsor. And John Cardinal O’Connor said Mass and
administered First Holy Communion to Bernard Nathanson.
It’s with great sorrow that we lose our movement’s most famous
defector from the abortion industry. Like St. Paul, he struggled
against the Light, but came to his senses a new man and became the
Truth’s champion.
Bernie fought the good fight, and has finished the race.
God bless you, Dr. Nathanson, and may you rest in peace.
Maybe it was because I am a little sleep deprived because three out of four children were finishing up their antibiotics for ear infection and I just got started on antibiotics myself for an ear and sinus infection. Maybe it was because I am four weeks pregnant with child number five and feel so protective during this fragile time. Maybe it was because he weighed in at over 200 pounds with a stature (?) of six plus feet and had an easy time pushing his fairly empty cart. You know those carts of retired people, only filled with a quarter gallon of milk, a small box of cereal, two apples, and one box of Little Debbie Snack Cakes. Well, I felt ill-matched. Weighing in at 117, five foot five inches, carrying my one year old on my hip, sweat dripping down my brow, all the while trying to single handedly maneuver an overflowing Wal-Mart cart with a defective wheel. My cart is bursting with gallons of milk, three cereal boxes, a smorgasbord of fruit and vegetables, cans and cans of food and bags of kitty litter at the bottom of the cart for proper weight distribution. Forget the Little Debbie Snack Cake box because I have my three year old sitting in the cart seat taking up any extra space that would be for sweet treats. My six year old and five year old are at the bow of our immense ship as we try to sail through the sales of Wal-Mart. Little did I know in Wal-Mart I would meet my daily dose of Goliath and I would confront him.
As we politely steered our cart around his, this retired gentleman started the quick jabs at me. “Are these all your kids?” he snidely said. I graciously nodded my head with a smile. Before I could dodge, another punch came my way. “Man, you sure have a lot of them. Bing, bing, bing! They are so close together!” he quipped rudely. “If I were you I would be taking Tylenol and aspirin all day due to headaches from those kids!” He laughed loudly as he played to the single crowd of the Wal-Mart employee who was stocking shelves right by us. I turned the corner of that aisle and could still hear their laughter bellowing at his comments.
I looked at my four little boys and their innocence and I thanked God for the child within my womb. This Goliath wanted to rumble, but this mama on first glance conceded the match. Three aisles and a checkout lane later, we meet again face to face. The six- year- old was unloading the cart and the three and five year old were quietly entertaining themselves, so I knew I was out of ear shot of them. With baby still on hip I turned to him, “Sir, the comments you made previously were rude and hurtful. It was inappropriate for you to make them especially in front of my children. I love my children and they are not headaches. They are blessings!”
I thought by this time he would be tired from sparring, but I was wrong. “Well, you have them bing, bing, bing, so close together. You must have started your family late in life. You really have your hands full.” So now my Goliath is not only commenting on the size and spacing of my family, but he is making remarks about a woman’s age. “I love my children and I wish you would not make such hurtful remarks again,” I firmly restated my position.
He grunted, “I have five children of my own and they have been trouble. If I see you again don’t worry I won’t make those comments to you.” I retorted, “I would appreciate it if you would never make those comments to ANY family.” I could see that my statements regarding the sanctity of life were not affecting him and in shear desperation to make a point I stooped low and went for the jugular by pointing out the blatant rudeness of his comments. “Sir, I love my children and I am sorry that you have had difficulties raising your children. But I must confess, my children don’t cause me headaches, it is just people like you who make comments like those that give me headaches and make me reach for my aspirin.” The uppercut blinded and silenced him.
I turned back to my corner of the ring and saw that my six year old had completely unloaded the whole cart and was already loading it back up again with the bagged groceries. The check-out woman commented what a good helper he was and said that he worked harder than any teenager. My heart was warmed. We headed out of the store and got loaded up into our vehicle. I hugged each of my boys as I loaded them into their car seats. You think I would have rallied at the final last witty knock-out punch I threw at my Goliath that day, but this victory was bitter-sweet.
The sweet part was in realizing what silenced my Goliath. It was my five smooth stones–my five children around me–their being, their smiles, their innocence, their sticky faces, their plethora of questions, their shoelaces that always need tying. Some say that David’s five stones represent the first five books of the Old Testament, which is the Word of God. David defeated Goliath with the Word of God. My children represent God’s word- “Go forth and multiply.”
The bitter part is that this poor man didn’t value his children as blessings; thus, they caused him grief which left him embittered. Unfortunately, I would venture to say that he doesn’t have any grandchildren to share his Little Debbie Snack Cakes with. Looking at my four smooth “stones” strapped in their car seats and patting the one “stone” growing in my womb, I know that today I left this battle with no scars, only the deep need to pray for this gentleman.
We were ill-matched, he was the one who was bitter and lonely and I was the one witnessing to the happiness of life and God’s creation. I threw up a prayer asking God to bring good to the situation, heal his wounded heart, and to make up for all charity that was lacking on my part. “But I also pray, my Eternal Giver, to continue to load my arsenal with as many ‘stones’ as you deem fit.” One should never be empty-handed when in Wal-Mart.
“Before I formed you in the womb I knew you…” Jeremiah 1:5
My young boys and I were coming home one day from a town about an hour and a half from us. About ten miles outside of one small town on our journey, we started seeing homemade signs dotting the sides of the country road. They read: “Happy 50th birthday Cindy”, “Cindy is 50”, “Honk! Cindy is 50”, “We love you Cindy!”. There had to be at least eight or so of them scattered along the road on our drive. The boys and I had fun reading them and pointing them out. They kept asking me who Cindy was- thinking that everyone probably knew this celebrity and they needed to know who this famous person was, too.
Feeling like a mother should say more than, “I don’t know.” I responded, “Cindy is someone very special. God created her nine months before this day and He really loves her. He picked her out before He created the world and God said, ‘I want Cindy to be born.’ God loves Cindy so much just as he loves you and everyone else. We should always remember to celebrate life because God is life—the source of all life.”
So on our way home we stopped at the grocery store and I bought a birthday cake—that is a birthday cake for the infamous Cindy. I was already feeling like I kind of knew her just from passing all those signs. We got home, sang our best rendition of happy birthday to Cindy and thanked God for creating Cindy. We ate Cindy’s birthday cake. I hope Cindy would have preferred white cake with white frosting.
One might think it is strange to celebrate a birthday of someone whom we don’t know. We don’t know Cindy, what value does she have to us? That is not the proper question. The question is what value does she have to God? And the answer to that is infinite value! We, in our self-centered worlds, gage the worth of people by their value to us, but instead we should come into reality and gage the worth of people by their value to God. If we were to do this, we would realize that everyone is infinitely valuable. I wanted my kids to know this and that is why we celebrated a birthday of someone we don’t know. I am sure heaven was sporting similar road signs that day for Cindy. Cindy we love you because God loved you first.
MEDIA ADVISORY, Oct. 18 /Christian Newswire/ — Mike Goss, President and founder of Abstinence America, is challenging parents to recognize the power they have to influence their children and to use that influence to help kids avoid the devastating consequences of early sexual experimentation. Goss has spent the last seven years talking to more than 30,000 young people about character, responsibility, relationship intelligence and smart sexual choices. Now he is speaking to their parents. He is launching a new program called Sex-Ed for Parents.
Goss says, “If we are going to change these numbers, – 900,000 teen pregnancies and six million cases of sexually transmitted disease — parents must be equipped, motivated and ready to engage kids in meaningful dialogue about sex.”
Research demonstrates that when it comes to sex, kids still rely most heavily on the advice of their parents, but unfortunately many parents don’t know where to start, what to say or how to communicate effectively with kids. That’s where Goss comes in. He sees his role as a trusted delegate coming along side to guide and educate, but acknowledging the parents’ role as the primary authority.
Sex-EdforParents.org. is a video web blog that offers parents a free membership where they can receive videos and an e-newsletter with up-to-date news in the world of adolescent sexuality as well as age appropriate resources to help jumpstart the conversation with kids from elementary age through college.
Goss will soon be introducing another revolutionary communications resource . “This is a whole new approach to sexuality education and it surpasses anything that has been done before,” says Goss. Parents who are looking for help will now have an extraordinary resource.”
Mike Goss has talked to more than 30,000 students in the last seven years, teaching them to make smart sexual choices. Abstinence America, a non-profit corporation, has been established as the undisputed leader in the Houston Metropolitan area in character-based sex education. Students have written Mike over 1,000 letters validating the impact of his work.
Omaha, Neb., Oct 15, 2010 / 06:06 am (CNA/EWTN News).- Planned Parenthood and the American Congress of Obstetricians and Gynecologists (ACOG) began a new joint effort this week to lobby the Department of Health and Human Services to make free contraception a part of new federal requirements for all hospitals. In response Dr. Thomas Hilgers, an expert in women’s health and family planning methods, stated that the plan would not help women, nor promote public health as contraception advocates claim.
The United States Conference of Catholic Bishops has already rejected efforts to mandate contraceptive coverage, saying it would violate the religious rights of Catholic hospitals and doctors. On October 14, Dr. Hilgers wrote to CNA from Omaha, Nebraska (where he directs treatment and research at the Pope Paul VI Institute for the Study of Human Reproduction) to explain the plan’s inherent problems from a scientific and medical standpoint.
As part of her effort to convince the HHS to accept her proposal, Planned Parenthood’s president Cecile Richards argued women would not have to “pay $50 for birth control pills anymore” if her idea became law.
But Dr. Hilgers said Richards’ accounting ignores the real price women pay, when fertility is regarded as a sickness needing “preventive care.” He noted that prominent side effects of the pill include circulatory problems, breast cancer, cervical cancer and liver tumors, and warned there were “many others beyond this as well.”
Hilgers also disputed remarks by the ACOG’s Vice President for Practice Activities Hal Lawrence, who claimed that contraceptive care leads to “healthier pregnancies.”
“Nothing could be further from the truth,” Hilgers wrote. “Once a woman discontinues oral contraceptives, the ‘time to pregnancy’ is longer than it would be if they were not on oral contraceptives. This is a form of infertility induced by the birth control pill.”
Hilgers, who is the Clinical Professor of Obstetrics and Gyneconology at Creighton University, said he knew of “no evidence at all that suggests that the birth control pill leads to ‘healthier pregnancies’.”
He also warned that promotion of contraception, particularly by the federal government, cannot be considered a “middle ground in the abortion wars,” as one research consultant to Planned Parenthood has called it.
Most popular methods of contraception, he explained, actually cause the abortion of a new and genetically distinct human life. Hilgers said that consistent advocates of the pro-life position should instead consider recent advances in natural family planning, including his own NaProTechnology.
“The oral contraceptive (pill) has basically three mechanisms of action,” he explained. “It inhibits ovulation, blocks the cervical mucus and renders the lining of the uterus hostile to an early implanting blastocyst. The latter is an abortifacient effect,” he stated, saying that scientists do not yet know how frequently oral contraceptives cause this form of abortion. He went on to mention that “the intrauterine device is associated with early abortions as well.”
Dr. Hilgers additionally observed that the spread of contraception, and the attendant separation of sex from reproduction, had not improved public health or social stability at the national level.
Instead, he said, artificial contraception had been verified by sociologists as “the main ingredient to the increase in the divorce rate” beginning in 1962, and a primary factor behind the current “epidemic of sexually-transmitted diseases.”
NEW YORK, October 18, 2010 (LifeSiteNews.com) – New York’s Catholic Bishops are telling the state’s Catholics this year that the right to life must be their first concern when they step into the voting booth in November, not party loyalty or other issues where good people may differ in opinion or judgment.
The pastoral letter “Our Cherished Right, Our Solemn Duty,” signed by New York Archbishop Timothy Dolan and seven other New York state bishops, says Catholics must be “cautious” when they cast votes this election, so as “not to be guided solely by party loyalty or by self interest.”
While state and national officials will have great influence on issues important to the voting Catholic, such as foreign policy, war and peace, the right to life, education, and “how we treat the poor and the vulnerable,” the bishops emphasize that “not every issue is of equal moral gravity.”
In fact, the bishops make clear that while it is “rare” for a candidate to agree with the Church on all these issues, it is the right to life that has to rank number one in Catholics’ minds at the voting booth.
“The inalienable right to life of every innocent human person outweighs other concerns where Catholics may use prudential judgment, such as how best to meet the needs of the poor or to increase access to health care for all,” they state.
“The right to life is the right through which all others flow. To the extent candidates reject this fundamental right by supporting an objective evil, such as legal abortion, euthanasia or embryonic stem cell research, Catholics should consider them less acceptable for public office,” they continue. “As Faithful Citizenship teaches, ‘Those who knowingly, willingly, and directly support public policies or legislation that undermine fundamental moral principles cooperate with evil.’”
The letter admits that the job of investigating where the candidates stand on the issues is no easy task.
“Yet our state is facing many critical issues which are of vital concern to faithful Catholics,” they emphasize. “Thus it is absolutely necessary for good citizens to take a careful look at every candidate and to vote accordingly for the better candidates.”
The letter also provides a whole list of questions for Catholics to consider in forming their consciences before entering the voting booth, under the following headings: “The Right to Life,” “Parental Rights in Education,” “Protecting Marriage,” “Immigration Reform,” “Access to Health Care,” “Protecting the Poor,” and “Religious Liberty.”
The bishops provide a list of all candidates for elected office at the website for the New York Catholic Conference. www.nyscatholic.org
The letter is signed by Timothy Dolan Archbishop of New York; Howard Hubbard Bishop of Albany; Nicholas DiMarzio, Bishop of Brooklyn; Edward U. Kmiec, Bishop of Buffalo; Terry R. LaValley, Bishop of Ogdensburg; Robert J. Cunningham, Bishop of Syracuse; Matthew H. Clark, Bishop of Rochester, and William F. Murphy, Bishop of Rockville Centre.
BONN, Germany, October 18, 2010 (LifeSiteNews.com) – Scientists announcing their success at achieving a new genetic defect-screening technique have at the same time admitted that many of the two-thirds of IVF embryos that fail to survive do so because of genetic abnormalities.
Luca Gianaroli, chairman of the European Society of Human Reproduction and Embryology (ESHRE), and Cristina Magli, an embryologist from Bologna, Italy, announced their success in a study of a genetic testing procedure called “comparative genomic hybridization (CGH) by microarray,” after two women gave birth to healthy children following screening of the embryos using the technique.
However, Gianaroli said in a statement that, “We have learnt from more than 30 years of IVF that many of the embryos we transfer (into the womb) have chromosome abnormalities,” and went on to explain that two out of every three embryos implanted into a woman’s womb during the IVF procedure fail to develop into a pregnancy, often because of genetic abnormalities.
“The whole world of IVF has been trying to find an effective way of screening for these abnormalities for more than a decade,” Gianaroli said. “Now we have a new technology … and our hopes are that this will finally provide a reliable means of assessing the chromosomal status of the embryos we transfer.”
The admission by the scientists of the high rate of genetic defects inherent in the IVF procedure aligns with the high rate of over-all health problems suffered by IVF children compared to naturally conceived children.
Congenital malformation rates as high as 11% have been reported by some studies of IVF children.
A recent French study found that over 4% of children born through assisted reproductive technology had some form of congenital deformity, compared to the rate of between 2% and 3% for children conceived naturally.
A large-scale study by the National Research and Development Center for Welfare and Health in Helsinki, Finland, found an overall increase in poor health among IVF children, including recurring specific abnormalities such as heart diseases, cerebral palsy, and malformations of the uro-genital system.
A summary of the research published by the European Society of Human Reproduction and Embryology is available here.
by Steven Ertelt
LifeNews.com Editor
October 13, 2010
Babol, Iran (LifeNews.com) — Researchers in Iran have published the results of a new study showing women who have an abortion face a 193% increased risk of breast cancer. On the other hand, women who carry a pregnancy to term find a lowered breast cancer risk compared with women who have never been pregnant.
The study folllows on the heels of new reports indicating Komen for the Cure gave $7.5 million to the Planned Parenthood abortion business in 2009.
The findings were reported in the April 3, 2010 issue of Medical Oncology but are coming to the public’s attention only now.
Hajian-Tilaki K.O. and Kaveh-Ahangar T. from Babol University of Medical Sciences compared 100 cases of women who were newly diagnosed with breast cancer compared with 200 age-matched controls to review several reproductive factors.
The researchers discovered abortion significantly elevated breast cancer risks. Also, having a first pregnancy at an older age increases the breast cancer risk by 310 percent — which has implications for women who have relied on birth control and delayed a first pregnancy until later in life.
The Iranian scientists also confirmed what other studies have found, namely that increasing parity or the number of births reduces the breast cancer risk significantly.
Reporting on the study, the FoodConsumer web site indicated women with parity equal to or greater than 5 reduced their breast cancer risk by 91 percent compared with women who had never been pregnant and not given birth. Each additional birth also reduced the breast cancer risk by 50 percent.
The Iranian study came just before another research study conducted by scientists in Sri Lanka, which found women who had an abortion in the past were 242 percent more likely to contract breast cancer.
That study was published in the journal Cancer Epidemiology and found a 3.42 odds ratio against women having abortions compared with those who kept their baby.
Abortion was the most significant factor in the study on breast cancer risk and researchers found a significantly reduced risk associated with prolonged duration of breastfeeding a newborn.
Malintha De Silva and colleagues from the University of Colombo led the study.
Combined with the Iranian study and others from the U.S., China and Turkey, five studies in the last 18 months have shown abortion elevates breast cancer risk.
In the one from the Unite States, Louise Brinton, a NCI branch chief, served as co-author.
She and her colleagues admitted that “…induced abortion and oral contraceptive use were associated with increased risk of breast cancer.” The authors cited a statistically significant 40% increased risk of breast cancer following an abortion.
“It’s becoming increasingly difficult for the NCI to keep its fingers and toes in the dike,” said Malec, “especially since many researchers in other parts of the world do not depend on the agency for grants.”
Last year, we wrote that a study published in the American Journal of Epidemiology concluded that birth control pill use is linked with an increased risk of breast cancer. Now, Slate is reporting that, also last year, a study of over 50,000 African-American women revealed a 65-percent increase in a specific, and highly aggressive form of breast cancer in women who ever took a birth-control pill, said Slate.
The study was led by Boston University epidemiologist Lynn Rosenberg, who also found that the risk doubled in women who used a birth-control pill in the prior five years and had taken it in excess of 10 years, noted Slate. The pill, said Slate, celebrates its 50th anniversary this year. While commemorative pieces have celebrated the pill’s virtues through the years, including an MSN.com piece in which it stated “taking the pill has no impact on breast cancer risk,” some research disagrees.
Rosenberg chose the African American demographic because of the dearth of research into that group, noting that this group tends to suffer from a significantly higher rate of so-called “triple negative” breast cancer, said Slate. This is a rare strain with genes that appear to be unresponsive to standard treatment, including tamoxifen, and which presents with the highest, quickest mortality rates. Rosenberg’s research linked these virulent cancers to the pill, as did other studies involving women of various races, including research conducted in New England, South Carolina, New York, and Scandinavia.
A prior study used information from the Case-Control Surveillance Study to look at birth control pill use and breast cancer risk in women diagnosed with breast cancer between 1993 and 2007, said Reuters. The study looked at race and tumor hormone receptors and involved over 2600 women, 907 with breast cancer and 1771 without.
The team found that women who had taken oral contraceptives for at least one year experienced a 50 percent greater chance of developing breast cancer over women who took the pills for less time or who had never taken the pills, said Reuters. Also, greater duration, use in the past decade, and being of black ethnicity, all seemed to raise the incidence of breast cancer; hormone receptor status did not affect the link.
Estrogens, said the Denver Wellness Examiner last year, cause cells to multiply and divide, noting that the more a cell divides, the greater the chance for cancer to develop. The National Cancer Institute (NCI) explained that two types of oral contraceptives are available in the United States. The combined pill contains two artificial versions of the natural female hormones estrogen and progesterone, similar to what the ovaries normally produce. The minipill only contains a type of progesterone.
Estrogen stimulates the growth and development of the uterus at puberty, causes the endometrium, or inner uterine lining, to thicken during the first half of the menstrual cycle, and affects breast tissue throughout a woman’s lifetime, specifically from puberty to menopause. Progesterone is produced during the last half of the menstrual cycle; prepares the endometrium to receive the egg; and if an egg is fertilized, continues producing to prevent further egg release. It is because of this that progesterone is called, said the NCI, the “pregnancy-supporting” hormone.
In 2003, an NCI-sponsored study examined risk factors for breast cancer among women ages 20 to 34 versus women ages 35 to 54 and looked at women diagnosed with breast cancer and women’s oral contraceptive use. The study found that breast cancer risk was highest in women who used oral contraceptives within five years prior to diagnosis, with women in the younger group being most susceptible.
NewsInferno.com disclaimer: This article: Birth Control Pill Cancer Link Debated was posted on Tuesday, September 21st, 2010 at 9:34 am at NewsInferno.com and is filed under Health Concerns, Pharmaceuticals.
ROME, September 22, 2010 (LifeSiteNews.com) – Europe will grow more “Islamicized” if Christian Europeans do not start having more children, and going back to Church, a senior Vatican official said this month. Msgr. Piero Gheddo, a famous missionary and an official with the Vatican’s Pontifical Institute for Foreign Missions, told Zenit news service that Europe’s indigenous inhabitants have abandoned Christianity and are becoming “paganized.”
“The fact is that, as a people, we are becoming ever more pagan and the religious vacuum is inevitably filled by other proposals and religious forces,” said Msgr. Gheddo, who founded AsiaNews, the Christian missionary news service. As religious practice diminishes in Christian Europe, “indifference spreads; Christianity and the Church are attacked.”
“If we consider ourselves a Christian country, we should return to the practice of Christian life, which would also solve the problem of empty cradles.”
Msgr. Gheddo pointed to demographic statistics showing that the population of native Italians is decreasing by 120,000 or 130,000 a year “because of abortion and broken families.” At the same time, 200,000 legal immigrants a year are moving into Italy. More than half of these, he said, are Muslims who continue to have the large families that Italians now eschew.
“Newspapers and television programs never speak of this,” he said. “However, an answer must be given above all in the religious and cultural fields and in the area of identity.”
Msgr. Gheddo was responding to the taunts of Libyan leader Moammar Gadhafi, who angered many on a recent official visit to Italy when he said that Europe should convert to Islam. He gave a lecture to 500 young women, who had been paid to attend, in which he urged them to convert and offered to find them Muslim husbands in Libya. The comments were denounced by Archbishop Robert Sarah, secretary of the Vatican Congregation for the Evangelization of Peoples, who called them a “provocation.”
But Msgr. Gheddo warned that the provocation could well have been a mere prediction.
“No newspaper – except Avvenire, the newspaper of the Italian Episcopal Conference – has seriously taken into consideration how to respond to this challenge of Islam, which sooner or later will conquer the majority in Europe,” he said.
Recent surveys conducted in Italy by local Catholic dioceses have found that the much-quoted number of Italians claiming to attend Mass weekly, 30 percent, can be deceptive. In Venice, it was discovered that the number of those actually attending is closer to 18 percent, and the numbers drop dramatically among younger Italians.
Although the Italian birth rate has crept up in recent years, from being the lowest in Europe at 1.2 children per woman, it still sits at only 1.31, a level sometimes referred to by demographers as the “death spiral,” in which a society’s population will inevitably begin to shrink.
Piero Gheddo is the author of over 80 books on the conditions of people in the developing world, with the first being published in 1956.
In a recent blog post, Fr. Gheddo, who refers to himself as a “missionary journalist,” decried the closure of Christian youth facilities and churches and the deterioration of schools and family life due to high Italian divorce rates.
What, he asks, has the “so-called ‘secular morality’ thing” done for young people?
“It replaced the [Church-run youth facilities] with the clubs that many call centers of distribution of alcohol and drugs.” Secularism has created a culture in which teenagers run wild, a new phenomenon in Italy. The culture promoted in these clubs, he said, is one in which “perversion and chaos and spiritual emptiness reign supreme.”
“Drugs, alcohol, free sex and psychedelic music for hours at high volume are some ‘diversions’ that kids seek and find allowed in these places, which are sometimes encouraged and financed by local governments.”
“All this is the fruit of our civilization ever more distant from God and then from the education of young people.”
TODAY show – exposing the dangers of the Birth Control Patch “Ortho Evra” from Johnson & Johnson – lawsuits finally to expose the dangers of the patch…over 2400 women injured and 2 dozen deaths contributed to the patch…and the FDA still allows it on the market! This is a must see video – so important for women to be aware of how women are often used as guinea pigs in the birth control market….$$$ drive the industry over a woman’s dignity
WASHINGTON, D.C., September 20, 2010 (LifeSiteNews.com) – The Department of Health and Human Services (HHS) should not require coverage of contraception or sterilization in group and individual health plans as part of “preventive” services for women, said representatives of the United States Conference of Catholic Bishops (USCCB) this week. The HHS is currently deliberating on a final list of required preventive services under the Patient Protection and Affordable Care Act (PPACA).
“These drugs, devices and procedures prevent not a disease condition, but the healthy condition known as fertility,” said Anthony Picarello, USCCB general counsel, and Michael Moses, associate general counsel, in a September 17 letter to HHS. They added that contraception and sterilization “pose significant risks of their own to women’s life and health; and a federal program to mandate their inclusion would pose an unprecedented threat to rights of conscience.”
The Catholic Medical Association, Southwest Ohio Guild will host a seminar titled “Assisted Reproductive Technologies: Theology and Science.” The presentation, by brothers Fr. Earl K. Fernandes, S. T. D., Dean of Mount St. Mary’s Seminary and Ashley Fernandes, M.D., Ph.D., will be May 19, 2010, at 6:30 p.m. in the Sears Recital Hall at the University of Dayton. This presentation will address fundamental moral issues related to fertility care and will explain methods of treatment that are morally acceptable. This program is free and open to the public. It is intended for medical practitioners and lay people.
Catholic Bishops' Conference of the Philippines HQ
The Catholic Bishops’ Conference of the Philippines (CBCP) has called for a ban on condom advertisements in public places, in print, and broadcast media, saying these commercials “weaken the moral fiber” of the youth.
The “multi-million dollar condom business… heavily targets the adolescent market, at the expense of morality and family life,” the CBCP said in a statement posted on its website on Wednesday.
The announcement came after the Department of Health distributed condoms last month.
“Condom advertisements should be banned on television, radio, movies, newspapers, magazines, and public places, as they desensitize the youth’s delicate conscience and weaken their moral fiber as future parents,” CBCP president Bishop Nereo Odchimar said in the same statement. (more…)
Language that has been used in support of a Bill to legalize euthanasia has almost always been worded so as to appear most humane. Words such as “compassion”, “autonomy”, “dignity”, and expressions like “medical assistance in dying” or “medically recommended course of treatment” often pad the arguments and, unfortunately, deceive the unwary. Consider the expression: “medical assistance in dying”, or “medically recommended course of treatment”. The word “medical” comes from the Latin medicor, which means “to heal”. To make someone die, by lethal injection for example, is not medical at all, despite it being administered by a medical doctor, but is radically anti-medical. There are many linguistic traps like these, which is why we should become familiar with some of the basic principles of Catholic Life Ethics to help us see through some of the arguments of those who belong to the culture of death. (more…)
Since the birth of the first “test tube baby” in 1978, more than three million children have been born with the help of reproductive technology. Most of them are healthy. But as a group they’re at a higher risk for low birth weight, which is associated with obesity, hypertension and type 2 diabetes later in life.
Carmen Sapienza, a geneticist at Temple University School of Medicine in Philadelphia, is studying two groups of children—one comprising those conceived naturally, the other made up of children conceived via assisted reproductive technology—to identify epigenetic (changes in gene expression caused by molecular mechanisms other than mutations in the DNA sequence itself) differences among them. He is particularly interested in a chromosomal modification called “DNA methylation,” research he presented February 22 at the annual meeting of the American Association for the Advancement of Science. “We found that 5 to 10 percent of these chromosome modifications were different in children born through assisted reproduction, and this altered the expression of nearby genes,” Sapienza says. Several of the genes whose expression differed between the two groups have been implicated in chronic metabolic disorders, such as obesity and type 2 diabetes. (more…)
Eugene, OR (LifeNews.com) — A Planned Parenthood affiliate in southwestern Oregon will begin selling the dangerous abortion drug to women that has already claimed the lives of more than 13 women worldwide and injured thousands more. Planned Parenthood of Southwest Oregon will sell the mifepristone drug to women starting next month.
A study last year found 20 percent of women using the abortion drug face medical complications.
Planned Parenthood CEO Cynthia Pappas informed media outlets the abortion business will sell the abortion drug to women whose pregnancies are not yet at the ninth week.
Pappas said the coming retirement of more abortion practitioners makes it so Planned Parenthood needs to look more closely at increasing access to the dangerous abortion drug. She also indicated the decision makes abortion more available to rural women. (more…)
Dr. Kermit Gosnell’s license was temporarily suspended this week after investigators found blood on the floor, fetus parts in jars and a recovery area consisting of recliners.
Gosnell, 69, is named in nearly four dozen lawsuits going back 20 years. Ten are malpractice suits, including one by the family of a young woman who died after a March 2000 abortion at his West Philadelphia clinic.
Semika Shirelle Shaw called the office the day after her abortion because she was bleeding badly but wasn’t told to get checked there or at a hospital, according to court documents. The lawsuit alleged that Shaw, a 22-year-old mother of two, died two days later of a perforated uterus and sepsis. (more…)
WASHINGTON, DC, February 22, 2010 (LifeSiteNews.com) – A new health care bill proposed by President Obama Monday threatens to expand abortion even more drastically than the health care bills stymied in Congress over the past several months, says the National Right to Life Committee.
The White House is threatening to ram the proposal through the Senate on a 51-vote majority using a tactic known as budget reconciliation. The process circumvents the need for a filibuster-proof 60-vote majority by placing the health care overhaul under the heading of a “budget” bill.
“Any member of Congress who votes for the final legislation proposed by President Obama will be voting for direct federal funding of elective abortion through Community Health Centers, and also an array of other pro-abortion federal subsidies and mandates,” said NRLC Legislative Director Douglas Johnson in a statement Monday. (more…)
The "Shop of Horrors". The West Philadelphia abortion center Women's Medical Society run by Kermit Gosnell.
Philadelphia, PA (LifeNews.com) — Officials investigating an abortion business in Philadelphia after a woman died from a botched legal abortion last November have made a grisly discovery. They found dozens of apparently late-term unborn children who were killed in abortions as long as 30 years ago.
The “Shop of Horrors” case involves the West Philadelphia abortion center Women’s Medical Society run by Kermit Gosnell.
Authorities were prompted to investigate Women’s Medical Society after an abortion patient died last November. Massive amounts of drugs found in the victim’s system led authorities to suspect Gosnell was illegally prescribing pain-killers.
Officials also suspected the woman died from the botched abortion in part because she had been treated by unlicensed personnel.
The State Board of Medicine says Gosnell had the unlicensed staff member vaginal exams and administer the drugs Demerol, Promethazine and Diazepam. He was eventually fined $1,000 for the violations. (more…)
NEW YORK, Feb. 23 /Christian Newswire/ — Terri’s Foundation and Priests for Life are happy to announce that Ave Maria University will once again host “The National Mass for Terri’s Day” at the Ave Maria Oratory at Ave Maria University, located near Naples, Florida.
Father Frank Pavone, National Director of Priests for Life, and Father Thomas Euteneuer, President of Human Life International, will be joined by many other priests and faithful for the Mass at 5 PM on Wednesday, March 31.
Priests for Life and Terri’s Foundation established the “International Day of Prayer and Remembrance for Terri Schindler Schiavo, and All of Our Vulnerable Brothers and Sisters” (“Terri’s Day”) two years ago. (more…)
Aukland, New Zealand, Feb 21, 2010 / 06:09 pm (CNA).- Pro-life doctors have gone to court to challenge new medical guidelines that require doctors to advise patients who have doubts about continuing a pregnancy that abortion is one of their options.
One of the doctors challenging the guidelines is believed to be Mary English, who is a General Practitioner from Wellington and the wife of Deputy Prime Minister Bill English. According to The New Zealand Herald, Dr. English is a Catholic whose opposition to abortion is widely known. She and her husband have six children.
The doctors filed an application in the country’s High Court concerning the New Zealand Medical Council guidelines, which are titled “Beliefs and Medical Practice.” (more…)
Washington, DC (LifeNews.com) — The latest 40 Days for Life pro-life prayer campaign is only six days along, but organizers say reports from local pro-life advocates show it has already saved the lives of 45 unborn children from abortions. The campaign has thousands of pro-life advocates helping women at abortion centers nationwide.
“Thus far during this 40 Days for life campaign, 45 lives have already been saved from abortion,” national coordinator David Bereit told LifeNews.com.
He said the news was an excellent way for pro-life advocates to start their week.
Bereit pointed to examples of lives saved locally and noted that pro-life advocates in Louisville, Kentucky helped three women change their minds about abortion. (more…)
Milwaukee, WI (LifeNews.com) — New undercover video footage shows the tenth Planned Parenthood abortion center across the nation engaged in covering up a potential case of sexual abuse of a minor. The video shows staff at a Wisconsin facility counseling a purportedly 14-year-old girl to not divulge how a 31-year-old man impregnated her.
The video also shows Planned Parenthood staff coaching the girl on how to obtain an abortion without her parent’s consent — in violation of Wisconsin state law.
The new video is the latest from Live Action, a group of college students dedicated to exposing illegal and unethical practices at Planned Parenthood abortion centers. Their investigative work has exposed Planned Parenthood facilities in five other states resulting in firing staff, attempts to cut Planned Parenthood government funding, and investigations from the state health department. (more…)
Boise, ID (LifeNews.com) — An Idaho state Senate committee approved a bill today that would create statutory protections for health care professionals in specific areas of medical practice. The Senate State Affairs committee voted 6-3 to send SB 1353 to the Senate floor with a recommendation that the Senate pass it.
The legislation makes it so pro-life health care workers don’t have to fear for their jobs if they decide they don’t want to dispense drugs that could be used to cause abortions or kill patients at the end of their life.
David Ripley, the director of Idaho Chooses Life, talked more about the passage of the pro-life bill.
“Opposition to the bill came largely from the abortion lobby because of their fears that it will create impediments to easy distribution of so-called emergency contraception,” he said. “Much of the morning debate was taken up with a debate of how the drug works.”
“Oddly enough, the debate was settled by the closing testimony of retired abortionist Duane St. Clair, who acknowledged that emergency contraception can sometimes cause the destruction of an embryo by making the uterine wall inhospitable to the new human life,” he added.
Idaho Right to Life and the Catholic Diocese of Boise supported the legislation along with ICL and Dr. Will Rainford, representing Bishop Driscoll, emphasized the spiritual gravity of forcing Christian medical personnel to participate in medical procedures they know to be wrong.
Sen. Chuck Winder, a Republican from Eagle, is the lead sponsor of the measure.
“It really is an issue dealing with the right of an individual to exercise their right of conscience,” he told the panel, according to the Idaho Reporter. “The intent of this legislation is not to restrict or limit, in any way, health care services to women or men in Idaho.”
Senate Minority Leader Kate Kelly, D-Boise, opposed the plan as did Marty Durand with Planned Parenthood of Idaho and Taryn Magrini, public policy director for the Idaho Women’s Network.
The measure receive the votes of six Republicans: Chairman Curt McKenzie, Pro Tem Geddes, Sens. Bart Davis, Russ Fulcher, Monty Pearce and Denton Darrington supported the measure.
Republican Sen. Joe Stegner (R-Lewiston) joined Democrats Kelly and Stennett in opposing the bill.
What does it take to replace ourselves? Are we doing it? These are some questions asked by a website called Over Population is a Myth. It’s becoming more and more evident that the earth is experiencing a demographic crisis, a crisis that, according to the Vatican, the Canadian parliament, and other organizations has dramatically increased the effects of (and perhaps even caused) the global financial crisis. Check out the video:
(via Washington Post) – “Be fruitful and multiply,” God instructed Adam and Eve, and men and women have heeded those words ever since. But over the years, God’s creatures have become sophisticated enough to rewrite the rules of being fruitful, and most of the new rules don’t sit well with leaders of the Roman Catholic Church.
There is “great confusion among lay Catholics regarding the church’s teaching on human reproductive technologies,” Philadelphia’s Cardinal Justin Rigali said at the meeting of U.S. bishops in Baltimore in November. “There is a need to help Catholics understand specific differences between the Catholic understanding and a secular understanding of human life.”
The bishops are sympathetic. When Rigali was archbishop of St. Louis, he celebrated a Mass for infertile couples, and the current St. Louis archbishop, Robert Carlson, did the same recently. But many Catholic couples suffering through the heartache of infertility think that the church contributes to their pain by erecting roadblocks to medically assisted pregnancy. (more…)
Baby Claire is shown above as she appears on 4-D ultrasound imaging. From left, Pam Caylor, Jamie Stout and Marina Cortopassi discuss the events that led up to Stout's daughter's rescue.
Last November, one yet-to-be-born baby with the highest odds stacked against her did, thanks to a couple of never-give-up pro-life people and her courageous mom.
The dramatic intervention to rescue this baby is only part of the story. The far-reaching lesson the story tells is one that many pro-life workers and even doctors aren’t aware of or are reluctant to admit: Some abortions already under way can be reversed to save the baby.
“The execution had been ordered and started.”
So remembers Pam Caylor, executive director of First Choice Pregnancy Services in Las Vegas, about this major rescue of a 20-week-old unborn baby. (more…)
For all those in the Midwest, this looks like a great array of speakers. Check it out!
Diocesean Marriage & Family Conference
Notre Dame Conference Center • Saturday, March 20, 2010
Conference Description
It’s easy to lose sight of the “big picture” in the day-to-day business of raising a family and making a marriage work. This inaugural diocesan conference aims to deepen the understanding of marriage and family life as a vocation from God and encourage an appreciation of its many dimensions. Through a combination of plenary sessions and workshops, this conference will explore the Church’s rich vision of marriage and family life as it relates to topics such as the theology of the body, communication and intimacy, financial stewardship, responsible parenthood, dealing with infertility, and raising teens. A series of workshops also will be presented in Spanish. This conference is for adults of all ages and circumstances; married couples, couples preparing for marriage, single parents, college students, clergy, pastoral ministers and anyone else interested in enriching their understanding of the vocation of marriage and family life.
OTTAWA, February 18, 2010 (LifeSiteNews.com) – One of the first official reports to indicate the disastrous consequences of Canada’s long-term below replacement birth rate was released in Ottawa today by Parliamentary Budget Officer Kevin Page. While pro-life leaders have been warning of the impending disaster for years as abortion and contraception have wreaked demographic havoc, the financial fallout is beginning to strike home to governments worldwide.
Taking into account Canada’s steady 1.5 birth rate, far below the 2.1 replacement rate, along with the accompanying ageing of the population, the report warns that “a major demographic transition is underway.”
“During this time, the ageing of the population will move an increasing share of Canadians out of their prime working- age and into their retirement years,” says the report. “With an older population, spending pressures in areas such as health care and elderly benefits are projected to intensify. At the same time, slower labour force growth is projected to restrain growth in the economy, which will in turn slow the growth of government revenue.” (more…)
(via WashingtonPost.com) Raegan McDonald-Mosley’s complaint [“The right reversal on contraception,” letters, Feb. 11], that pro-life groups exaggerate the abortive effects of emergency contraception, warrants a response. Praising the Pentagon change to allow the morning-after pill, Dr. McDonald-Mosley argued that the pill prevents ovulation and prevents life before it begins. The problem is, when they administer the pill, doctors don’t know whether conception has occurred. Taken after ovulation and before implantation, life would have begun and the pill would kill it.
Dr. McDonald-Mosley asks that we favor science over propaganda. Gladly. Science recognizes that life begins at conception, with sperm-egg fusion resulting in a one-cell embryo, which immediately functions as a highly structured, protein-producing, coordinated organism to promote growth, health and maturation. From its first moment a one-cell embryo is a whole and complete member of the human species with tremendous potential.
The true debate is not about when life begins but about whether and when young humans should be valued and protected. My Hippocratic oath commands me to protect human life at all stages. Ideology can color science, and Dr. McDonald-Mosley should refrain from using ideological talking points as scientific certainty.
The writer, an obstetrician/gynecologist, is founder of the Tepeyac Family Center.
(via her-menutics) A team of researchers at Georgia’s health science university, the Medical College of Georgia (MCG), announced last week that they are conducting a clinical trial using stem cells from umbilical-cord blood as a treatment for cerebral palsy. The trial will build on a successful series of past tests using adult stem cells in regenerative medicine.
“Evidence up to this point has been purely anecdotal,” said James Carroll, chief of pediatric neurology at the MCG and principal investigator on the study. “While a variety of cord blood stem-cell therapies have been used successfully for more than 20 years, this study is breaking new ground in advancing therapies for brain injury.” (more…)
La anticoncepción de emergencia (AE) se refiere al uso de píldoras o la inserción de aparatos para tratar de prevenir el embarazo después del acto sexual.1 La AE es promovida cuando una mujer ha sido violada, cuando una pareja ha escogido tener sexo sin utilizar cualquier forma de anticoncepción, o cuando hay la sospecha de que un anticonceptivo falló. Los tipos de AE incluyen el uso de píldoras y la inserción del dispositivo Intrauterino (DIU-T de cobre). Fuera de los estados unidos la píldora abortiva RU-486 es usada como AE. Otras drogas son actualmente estudiadas para ser usadas como AE.2
¿Qué es “la píldora del día después”?
La frase “píldora del día después” (PDD) se utiliza para describir píldoras que se toman después de un acto sexual, con el propósito de prevenir del embarazo. La PDD actualmente es comercializada en los Estados Unidos bajo más de 25 nombres. Un primer tipo de PDD incluye las píldoras, que al igual que otros anticonceptivos orales, contienen sólo la progestina sintética levonorgestrel (LNG). Nombres comerciales de estas pildoras incluyen: Plan B One Step, Next Choice One Dose, My Way y otros.3 La Federación de Drogas y Alimentos de Los Estados Unidos ha aprobado este tipo de PDD para venta sin fórmula médica sin restricciones de edad. Un segundo tipo de PDD es el fármaco anti-progesterona acetato de ulipristal (Ella), disponible con fórmula medica en los Estados Unidos. El tercer tipo de PDD es el uso “extra oficial” de anticonceptivos orales combinados que contienen estrógeno sintético y progestina.
¿Cómo funciona el Plan B?
La concepción de un nuevo ser humano sólo es posible durante unos pocos días en el ciclo de fertilidad de la mujer. Los espermatozoides pueden sobrevivir en el tracto reproductivo femenino 3-5 días y el óvulo no fecundado muere 12-24 horas después de la ovulación. La fertilización normalmente ocurre en las trompas de Falopio después de la ovulación. El nuevo ser humano (blastocisto) migra desde las trompas de Falopio hasta el útero donde se implanta 6-12 días después de la concepción.4 Un delicado equilibrio hormonal es necesario para la supervivencia del bebé.
Algunos estudios parecen demostrar que Plan B funciona cambiando el moco cervical o atacando a los espermatozoides. Estudios más recientes, sin embargo, muestran que estos efectos pueden ocurrir cuando las píldoras se toman con regularidad (como las píldoras de control de la natalidad), pero no después de una sola dosis (usada en la AE ).5,6
Los defensores de la AE afirman que el ingrediente activo en el Plan B funciona básicamente impidiendo o retrasando la ovulación. Sin embargo recientes estudios mostraron que cuando se le dio el plan B a mujeres en la parte fértil de su ciclo, el 80% o más de ellas ovularon, aunque ninguna de ellas quedo embarazada (ver el diagrama de abajo).7,8 Si el espermatozoide y el óvulo están presentes en el cuerpo de la mujer, y la concepción ocurre y no hay embarazo, se deduce que el aborto ha ocurrido.9 Otros estudios también han demostrado que el plan B altera el equilibrio hormonal necesario para mantener el embarazo.10,11
¿Cómo actúan otros tipos de anticoncepción de emergencia?
DIU-T de cobre: Los iones de cobre liberados por el DIU son tóxicos para los espermatozoides y el óvulo, disminuyendo la probabilidad de fertilización.12 Además, el DIU-T de cobre disminuye las posibilidades de supervivencia de cualquier embrión que puede estar formado, antes de que llegue al útero. El DIU-T de cobre vuelve el revestimiento del útero hostil para aceptar una nueva vida.13 Así, el DIU-T de cobre puede tener un efecto post-fertilización, lo que significa que destruye el nuevo embrión humano.
Ella y mifepristona (RU-486) cambian la capacidad del cuerpo para reaccionar ante algunas hormonas. Pueden bloquear la acción de la hormona progesterona14, alterar el endometrio y así destruir una nueva vida humana a través del aborto químico. Ella también puede retrasar o bloquear la ovulación si se toma antes de que esta ocurra.15
Si la concepción (fecundación) ya ha sucedido, entonces la única manera por la cual el DIU o las PDD pueden ser efectivas es destruyendo la nueva vida. Con la tecnología actualmente disponible, una mujer o su médico no pueden saber, en el momento que ella toma estas píldoras o el DIU es introducido, si ella ya ha concebido o no. Una prueba de embarazo no le puede dar esta información antes de la implantación. Por lo tanto, siempre que estas píldoras son tomadas o un DIU-T de cobre es introducido después del acto sexual, hay el riesgo que una nueva vida humana sea destruida.
¿Esto significa que la anticoncepción de emergencia es un abotivo—que puede causar un aborto?
Una nueva vida humana comienza en la concepción, también llamado fertilización. Embriólogos han encontrado que desde el primer momento de unión entre el ovulo y el espermatozoide, el código genético del nuevo ser humano esta completo, y con un ambiente adecuado en el útero sigue su desarrollo como todo ser humano. Sin embargo, en septiembre de 1965, el Colegio Americano de Obstetras y Ginecólogos (ACOG) intentó redefinir “el embarazo” comenzando el momento de la implantación (que ocurre 6 a 12 días después del momento de la fertilización). La eficacia de píldoras y dispositivos que no impiden la fertilización depende de la destrucción de una nueva vida humana. Esto debe ser llamado un “aborto” a pesar de la definición médica de la ACOG.
¿Cuan efectiva es la anticoncepción de emergencia?
El DIU-T de cobre previene hasta el 99% de los embarazos esperados. Ella y el Plan B previenen algunos de los embarazos si se utilizan antes de la ovulación.16,17 El efecto de la AE en la reducción de los embarazos no deseados y abortos inducidos aún no ha sido demostrado. Los estudios disponibles muestran que la AE puede no tener ningún efecto sobre los embarazos no deseados, y puede incluso aumentarlos.18,19,20,21 La efectividad de la AE para prevenir el embarazo esta disminuida en las mujeres con un índice de masa corporal alto.22 Además, proporcionando la AE por adelantado tiene el efecto negativo aumentando comportamientos sexuales arriesgados.23 En general, la evidencia sugiere que la AE no del todo es eficaz para la prevención de embarazos no deseados.
¿Es segura la anticoncepción de emergencia?
Las PDD que contienen LNG pueden causar sangrado menstrual más fuerte/ ligero, náuseas, vómitos, dolor abdominal, fatiga, dolor de cabeza, mareos, sensibilidad en los senos, retraso de la menstruación (>7 días), y diarrea. El uso del LNG aumenta el riesgo de embarazo ectópico.24
Dolor de cabeza, dolor abdominal, náuseas, dismenorrea, fatiga y mareos son efectos secundarios con el uso de Ella.25 Las mujeres que utilizan el DIU-T de cobre puede experimentar calambres en el útero y otros efectos no deseados, tales como: embarazo ectópico, aborto séptico, infección pélvica, perforación, empotramiento, anemia, dolor de espalda, menstruaciones dolorosas, dolor durante el coito, flujo vaginal, flujo menstrual prolonga–do, sangrado irregular, calambres y vaginitis.26
Un estudio reciente reportó que mujeres usan repetidamente la anticoncepción de emergencia, probablemente debido a una percepción exagerada de su efectividad.27 Otro estudio encontró que la venta sin formula de los anticonceptivos de emergencia conduce a un aumento (aproximadamente de 12%) en las infecciones de transmisión sexual en mujeres entre 15-44 años. Lo anterior debido al incremento en comportamientos sexuales arriesgados.28 Mas tiempo e investigación son necesarios para conocer los efectos a largo plazo de la anticoncepción de emergencia en la seguridad de su uso y los efectos en la salud de las mujeres.
¿Hay otras opciones?
Si usted es soltera, la manera más segura para evitar el embarazo o una infección de transmisión sexual es la abstinencia, siempre funciona. Si usted es casada, los métodos modernos de reconocimiento de la fertilidad son la alternativa más segura, más sana, y menos costosa para planificar la familia.
Las víctimas de violación o del abuso sexual merecen el mejor cuidado médico y soporte humano posible. El estrés y los peligros para la salud adicionales de la anticoncepción de emergencia agregarán daño adicional. El embarazo debido a una violación es estimado en 5.0%.29 Para la inmensa mayoría de estas mujeres, los anticonceptivos de emergencia imponen peligros para la salud significativos sin ningún beneficio. Si la concepción ya ha ocurrido, entonces un aborto muy temprano es el único medio por el cual la anticoncepción de emergencia puede ser efectiva. El aborto lleva consigo muchas consecuencias adversas graves tales como el aumento en el riesgo del cáncer de seno, depresión, ansiedad, conductas suicidas y abuso de sustancias.30 Un enfoque más seguro es darle la oportunidad al bebe de nacer. La adopción es siempre una opción.
Servicios confidenciales de ayuda para las mujeres enfrentando embarazos no deseados están disponibles en los Estados Unidos y Canadá llamando a la línea gratuita 1-866-7OPCION (767-2466) y la red para revertir la píldora abortiva 1-877-558-0333.
Referencias
1. Trussell J, PhD and Raymond, EG, MD, MPH. Emergency contraception: a last chance to prevent unintended pregnancy. Retrieved from: http://ec.princeton.edu/questions/ec-review.pdf March 2016
2. Weiss, E. A., & Gandhi, M. (2016). Preferential cyclooxygenase 2 inhibitors as a nonhormonal method of emergency contraception: A look at the evidence. Journal of Pharmacy Practice, 29(2), 160-164.
3. Emergency Contraception Pills. Retrieved from http://ec.princeton.edu/questions/dose.html#dose April 2016
4. Wilcox, A. J., Baird, D. D., & Weinberg, C. R. (1999). Time of implantation of the conceptus and loss of pregnancy. The New England Journal of Medicine, 340(23), 1796-1799.
5. Nascimento JA, Seppala M, Perdigao A., Espejo-Arce X, Munuce MJ, Hautala L, et al. (2007). In vivo assessment of the human sperm acrosome reaction and the expression of glycodelin-A in human endometrium after levonorgestrel-emergency contraceptive pill administration. Human Reproduction (Oxford, England), 22(8), 2190-2195.
6. Hermanny A, Bahamondes MV, Fazano F, Marchi NM, Ortiz ME, Genghini MH, et al. (2012). In vitro assessment of some sperm function following exposure to levonorgestrel in human fallopian tubes. Reproductive Biology and Endocrinology : RB&E, 10, 8-7827-10-8.
7. Brache V, Cochon L, Deniaud M, Croxatto, HB. Ulipristal acetate prevents ovulation more effectively than levonorgestrel: analysis of pooled data from three randomized trials of emergency contraception regimens. Contraception. Nov 2013; 88(5): 611-618.
8. Noe G, Croxatto HB, Salvatierra AM, Reyes V, Villarroel C, Munoz C, et al. Contraceptive efficacy of emergency contraception with levonorgestrel given before or after ovulation. Contraception. Nov 2011; 84(5): 486-492.
9. Kahlenborn C, Peck R, & Severs WB. (2015). Mechanism of action of levonorgestrel emergency contraception. The Linacre Quarterly, 82(1), 18-33.
10. Croxatto HB, Brache V, Pavez M, Cochon L, Forcelledo ML, Alvarez F, et al. Pituitary-ovarian function following the standard levonorgestrel emergency contraceptive dose or a single 0.75-mg dose given on the days preceding ovulation. Contraception. Dec 2004; 70(6): 442-450.
11. Hapangama D, Glasier AF, Baird DT. The effects of peri-ovulatory administration of levonorgestrel on the menstrual cycle. Contraception. Mar 2001; 63(3): 123-129.
12. Ortiz ME, Croxatto HB. Copper-T intrauterine device and levonorgestrel intrauterine system: biological bases of their mechanism of action. Contraception. Jun 2007; 75(6 Suppl): S16-30.
13. Gemzell-Danielsson K, Berger C & Lalitkumar PGL. (2013). Emergency contraception–mechanisms of action. Contraception, 87(3), 300-308.
14. Keenan JA. Ulipristal acetate: contraceptive or contragestive? Ann Pharmacother. Jun 2011; 45(6): 813-815.
16. Leung, V. W., Soon, J. A., Lynd, L. D., Marra, C. A., & Levine, M. (2016). Population-based evaluation of the effectiveness of two regimens for emergency contraception. International Journal of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics,
17. Li, H. W., Lo, S. S., Ng, E. H., & Ho, P. C. (2016). Efficacy of ulipristal acetate for emergency contraception and its effect on the subsequent bleeding pattern when administered before or after ovulation. Human Reproduction (Oxford, England),
18. Rodriguez MI, Curtis KM, Gaffield ML, Jackson E, Kapp N. Advance supply of emergency contraception: a systematic review. Contraception. May 2013; 87(5): 590-601.
19. Raymond EG, Trussell J, Polis CB. Population effect of increased access to emergency contraceptive pills: a systematic review. Obstet Gynecol. January 2007; 109(1): 181-188.
20. Walsh TL, Frezieres RG. Patterns of emergency contraception use by age and ethnicity from a randomized trial comparing advance provision and information only. Contraception. Aug 2006; 74(2): 110-117.
21. Glasier A, Fairhurst K, Wyke S, Ziebland S, Seaman P, Walker J, et al. Advanced provision of emergency contraception does not reduce abortion rates. Contraception. May 2004; 69(5): 361-366.
22. Glasier A, Cameron ST, Blithe D, Scherrer B, Mathe H, Levy D, et al. (2011). Can we identify women at risk of pregnancy despite using emergency contraception? data from randomized trials of ulipristal acetate and levonorgestrel. Contraception, 84(4), 363-367.
23. Belzer M, Sanchez K, Olson J, Jacobs AM, Tucker D. Advance supply of emergency contraception: a randomized trial in adolescent mothers. J Pediatr Adolesc Gynecol. Oct 2005; 18(5): 347-354.
24. Zhang J, Li C, Zhao WH. Xi X, Cao SJ, Ping H, et al. (2015). Association between levonorgestrel emergency contraception and the risk of ectopic pregnancy: A multicenter case-control study. Scientific Reports, 5, 8487.
25. Ulipristal Acetate. http://www.pdr.net/drug-summary/ella?druglabelid=1278 April 2016
26. Intrauterine Copper Contraceptive Paragard. Retrieved from http://www.pdr.net/drug-summary/paragard?druglabelid=572 April 2016
27. Melton L, Stanford JB, Dewitt MJ. Use of levonorgestrel emergency contraception in Utah: is it more than “plan B”? Perspect Sex Reprod Health. Mar 2012; 44(1): 22-29.
28. Mulligan, K. (2016). Access to emergency contraception and its impact on fertility and sexual behavior. Health Economics, 25(4), 455-469.
29. Holmes MM, Resnick HS, Kilpatrick DG, Best CL. Rape-related pregnancy: estimates and descriptive characteristics from a national sample of women. Am J Obstet Gynecol. August 1996; 175(2): 320-324.
30. Fergusson DM, Horwood LJ, Ridder EM. Abortion in young women and subsequent mental health. J Child Psychol Psych. January 2006; 47(1): 16-24.
New Executive Director Jenn Girioux called on many of her pro-life friends to make an appearance, and we were glad to help. Read more about the event at Pro-Life Action League’s blog.
Back row, from left: Fr. Tom Euteneuer of Human Life International; Brian Gail, author of the book Fatherless; David Bereit of 40 Days for Life, Joe Scheidler of Pro-Life Action League; Bobby Schindler of the Terri Schindler Schiavo Foundation. Front row, from left: Jenn Giroux of One More Soul; Lila Rose of LiveAction.org, Dr. Janet Smith, author of Contraception: Why Not; Jill Stanek
And yes, we danced! I learned the Electric Slide even.On the right side is first a photo of Bobby and Lila, then one of Bobby and me.
Rich and I drove to Cincinnati from Chicago. After we were well on our way, I realized I left my purse – and driver’s license – in the other car. Oh, well. We decided nothing would happen and I drove on. (more…)
Washington D.C., Feb 17, 2010 / 08:08 am (CNA).- Day Gardner of the National Black Pro-Life Union has said that during Black History Month Americans should acknowledge abortion’s disproportionate impact on blacks and should see abortion advocacy as a form of “ethnic cleansing” that targets the black community. “Abortion providers are still being located for the most part in black neighborhoods and are still delivering the same old message,” Gardner said, claiming their message is that black, poor urban children are “not worthy of life” and that America would “be a better place without black people.”
Writing in a Tuesday commentary, she recounted the history of black oppression at the hands of groups like the Ku Klux Klan (KKK).
“The Klan’s aim was to prevent African-Americans from voting, getting an education, competing for jobs and owning property,” she explained.
While the KKK conducted a “lynching war” on blacks in the American South, Gardner charged that Planned Parenthood founder Margaret Sanger and her allies were devising an “evil plan” to enforce what Sanger called “race hygiene.” (more…)
Madrid, Spain, Feb 17, 2010 / 02:59 pm (CNA).- This week, Spanish pro-life organizations delivered more than one million signatures to their country’s government supporting life and opposing Spain’s new law on abortion. The petition predicts that the new law “will only bring more death and suffering to thousands of women.”
A total of 1,067,315 people signed the petition against “all laws allowing abortion.” After government officials Jose Bono and Teresa Cunillera refused to accept the signatures, they were delivered to the Deputy Speakers of Congress, Jorge Fernandez Diaz and Ana Pastor.
The signatures were gathered throughout Spain between April 2009 and January 2010. The petition in part reads:
“Abortion always constitutes the violent death of a human being and a terrible tragedy for the woman who experiences it, forced by their circumstances.
“The Spanish law abandons women in their time of need and pushes them to obtain abortions. All ‘abortion laws’ are a terrible hypocrisy against women, as well as an atrocious injustice to the children they leave unprotected. (more…)
Catholic Bishops' Conference of the Philippines HQ
MANILA, February 16, 2010 (LifeSiteNews.com) – The Catholic Bishops of the Philippines have condemned the government’s initiative to distribute free condoms in its attempt to fight the spread of AIDS in the poorest parts of Manila and other regions of the country.
The distribution of condoms started on 13 February at the initiative of Eric Tayag, head of the Department of Health and Epidemiology of Manila, according to an Asia News report.
Tayag indicated that the government’s condom campaign would proceed despite a halt on debate in Congress of the controversial Reproductive Health Bill, which encourages sterilization and the use of contraceptives, calls for universal sex education of children and pushes for a coercive 2-child family limit. (more…)
Next week the Polish arm of the Center for Bio-Ethical Reform will begin displaying this sign on a huge billboard (74 feet by 32 feet) in a large city in Poland, remaining unnamed for now so as not to jeopardize the plan.
Translation: Abortion for Polish women introduced by Hitler on March 9, 1943
Coincidentally, March 8 is International Women’s Day, a special day for feminists in Poland. Each year to celebrate they organize demonstrations in major cities, including Poznan, to demand abortion without limits.
Obama has allowed the Planned Parenthood abortion business unfettered access to the White House.
Washington, DC (LifeNews.com) — Visitor logs reveal what pro-life advocates suspected would happen once President Barack Obama took over as presdient. He and his administration have allowed the Planned Parenthood abortion business unfettered access to the White House and top staffers.
The visitor logs reveal Planned Parenthood president Cecile Richards has visited the White House and spent time with Obama administration officials on four occasions.
The documents show Obama wasted little time in giving Richards access, with her first visit coming on January 20 — the date of Obama’s inauguration — for a luncheon reception with 299 total people.
Richards’ next visit appears undocumented in the visitor logs. (more…)
Jefferson City, MO (LifeNews.com) — A new bill in the Missouri legislature would provide women considering an abortion information on the pain the unborn baby feels during the procedure. The bill also installs a 24 hour waiting period to allow women a chance to consider positive alternatives.
Republican Sen. Rob Mayer of Dexter is the sponsor of the legislation and he appeared before the Senate Judiciary Committee on Monday to talk about his bill.
According to an AP report, Mayer told the committee the legislation would help women avoid abortions and make better choices.
But AP indicates a Planned Parenthood representative called the bill a burden and said much of the information women would receive is already available. (more…)
(via ABC News Australia) The ABC has learned that Canberra Hospital recommended a late-term abortion for a baby who was later born healthy.
The incident has come to light after nine obstetricians left the hospital during the past 13 months amid claims of bullying by senior staff and a hostile working environment.
There are now fears that Canberra’s biggest hospital will not be able to staff its new maternity unit because some experienced obstetricians are not prepared to work there.
Fiona Vanderhook came close to never knowing her 14-month-old son Diesel.
When she was five weeks pregnant, a trainee doctor told Ms Vanderhook she had lost the baby. (more…)
(via KTVZ.com) In “a difficult decision for all those involved,” the Bend-based Catholic Diocese of Baker announced Monday its intention to dissolve the official sponsorship relationship of St. Charles Medical Center-Bend by the Catholic Church over sterilization procedures performed at the hospital.
Here’s the rest of the statement, provided by the hospital under the letterhead of the office of :
The Sisters of St. Joseph of Tipton, Ind., founded St. Charles Bend 92 years ago with a mission to serve all patients in need in Central Oregon.
Although the hospital became a community nonprofit organization in the 1970s, it has maintained a relationship with the Catholic Church and has continued voluntarily to follow the Catholic Ethical and Religious Directives for Health Care Services.
Recently, hospital administrators and Bishop Robert Vasa of the Diocese of Baker have respectfully disagreed on the meaning of some of those directives.
In particular, St. Charles-Bend offers patients the service of tubal ligations, a form of permanent female reproductive sterilization, which, according to Vasa, goes against the Church’s teachings.
“It is my responsibility to ensure the hospital is following Catholic principles both in name and in fact,” Vasa said. “It would be misleading for me to allow St. Charles Bend to be acknowledged as Catholic in name while I am certain that some important tenets of the Ethical and Religious Directives are no longer being observed.”
Vasa asked St. Charles Bend in 2007 for an audit of the hospital’s compliance with the Ethical and Religious Directives. The hospital has been transparent about its practices and openly provided the Bishop with the information he requested. Since that time, the two parties have had a number of discussions about the future of the hospital as a Catholic institution.
“We are saddened by this decision because of the 92 years of history the St. Charles Bend hospital has had with the Catholic Church,” said James A. Diegel, FACHE, president and CEO of Cascade Health-care Community, the parent company of St. Charles-Bend. “But we have an obligation to provide comprehensive health care services to our patients while remaining true to our values of compassion and caring for all.”
Diegel said the CHC Board of Directors has every intention of continuing to use the Ethical and Religious Directives as they have been historically interpreted by the hospital and will likely adopt its own version of the ethical directives in the near future.
Vasa has encouraged the hospital to stay as close to the Directives as possible in the future.
“St. Charles has gradually moved away from adherence to the requirements of the Church without a clear knowledge that it was doing so,” Vasa said. “Unfortunately, that distance is now too great to sustain a formal sponsorship relationship, but I believe that using the Church’s Directives as a basis for their local ethical guidelines is a good idea.”
Vasa and Diegel agreed that for all practical purposes ,very little will change at St. Charles Bend as a result of this decision. However, Catholic Mass will no longer be celebrated in the hospital’s chapel, and all items considered Catholic will be removed from the hospital and returned to the church.
St. Charles Bend’s name will remain the same, and the cross will remain on top of the hospital building.
“We are not going to abandon who we are,” Diegel said. “The mission of the hospital, to serve all in a spirit of love and compassion, and the Catholic values the hospital was founded on, will continue to guide St. Charles Bend’s leaders and caregivers.”
Washington, DC (16 February 2010 – American Life League) – Over 50 women in Indiana are filing lawsuits against Bayer Pharmaceuticals charging that use of the company’s Yaz and Yasmin hormonal birth control pills caused conditions ranging from gallbladder-related injuries to strokes.
There are now over 25,000 similar reported cases across the United States.
“We’re seeing an increasing awareness of the very real health risks associated with hormonal birth control,” said Marie Hahnenberg, project director of American Life League’s The Pill Kills project. “For years, criticism of birth control has been a sacrosanct topic, but the victims of hormonal birth control are too numerous to ignore any longer.” (more…)
They were the first words God spoke to his creation, and his creation has heeded them ever since. But over the years, God’s creation has become sophisticated enough to rewrite the original rules of being fruitful, and most of the new rules don’t sit well with leaders of the Roman Catholic Church.
There is “great confusion among lay Catholics regarding the church’s teaching on human reproductive technologies,” Philadelphia’s Cardinal Justin Rigali said at the U.S. bishops’ meeting in Baltimore in November. “There is a need to help Catholics understand specific differences between the Catholic understanding and a secular understanding of human life.” (more…)
Washington, DC (LifeNews.com) — The latest 40 Days for Life pro-life campaign is set to begin nationwide on Wednesday with pro-life advocates reaching out to their local communities. The pro-life campaign kicks off in 165 cities across the United States and also cities and towns in Canada, Australia, and Northern Ireland.
Some of the local pro-life campaigns will hold kick off events today and tomorrow while others begin on Wednesday.
David Bereit, the national director of the 40 Days for Life campaign is encouraging pro-life advocates to participate in a national video feed from a live rally on Tuesday evening. (more…)
(via Cassy Fiano) Breaking news: a Birmingham Planned Parenthood clinic has been placed on probation due to Lila Rose’s undercover work with the Mona Lisa project.
A Birmingham abortion clinic that was targeted in an undercover sting by anti-abortion activists has been put on probation by the state.
State health officials tell The Associated Press that the Planned Parenthood clinic has until next week to present its plan to correct violations involving minors receiving abortions.
Investigators with the department said records at the clinic showed several minors aged 13-15 had received abortions without proper verification of parental consent since November 2008.
Activists with “Live Action,” a California-based anti-abortion group, posed as a pregnant 14-year-old girl who needed a secret abortion. In an audio tape from the visit, an employee allegedly suggests that someone other than a parent or legal guardian could give consent.
The group’s claim last year led Alabama health officials to investigate.
COLUMBUS, Ohio, February 10, 2010 (LifeSiteNews.com) – Ohio House Speaker Armond Budish (D-Beechwood) has reversed a decision to disallow the presentation on the House floor of a routine legislative honor to a local pro-life teen, and will make room in the Ohio General Assembly’s schedule for the honor, according to the speaker’s office.
Ohio teen Elizabeth Trisler had been set to be presented on February 3 with an honorary legislative resolution, authored by Rep. John Adams, which recognized her accomplishment as the winner of the 2009 National Right to Life Oratory Contest. However, as LifeSiteNews.com (LSN) reported yesterday, the planned presentation was scuttled by Speaker Budish, apparently because Budish disagreed with Trisler’s pro-life values.
But Keary McCarthy, communications director for Speaker Budish, contacted LSN today to say that “the Speaker has reconsidered the request and will allow for the resolution presentation to occur at the next general assembly session or whenever they can schedule it.” (more…)
(via ChristianTelegraph.com) The Delhi High Court has ruled that an unborn child can be considered equivalent to a minor child and has directed an insurance company to pay compensation of 250,000 rupees (about $5750 Canadian) to a man who lost his pregnant wife in a road accident a year and half ago, reports Thaddeus M. Baklinski, LifeSiteNews.com.
Justice J R Midha allowed an appeal filed by a Mr. Prakash seeking compensation for the death of his unborn child when his plea was ignored by the Motor Accident Claim Tribunal (MACT), which rules on insurance claim disputes in India.
“This court holds that an unborn child — aged five months onwards in the mother’s womb till its birth — is treated as equal to a child … the fetus is another life in a woman and loss of the fetus is actually loss of a child in the offing,” Justice Midha stated. (more…)
The moment I heard that Josie, the Duggars’ 19th child, was born prematurely, weighing only 1 lb. 6 oz., I knew the stars of the TLC reality series 19 Kids and Counting would face some harsh criticism for continuing to have children despite the risks.
But really? This couple was facing some pretty tough criticism already. (more…)
Atlanta, GA (LifeNews.com) — Atlanta drivers will soon see billboards all over the city that educate them about the racist component of abortions — that pro-life advocates point out target black Americans. In a city with a large African-American population, the billboards are already sparking controversy and they’ve not been put up yet.
The Radiance Foundation is sponsoring a campaign of 65 billboards across town and they should be visible starting on February 15.
“We’re aiming for a lot more, but that’s where we’re at,” Ryan Bomberger, co-founder of the group, recently told the Atlanta Journal Constitution. (more…)
Washington, DC (LifeNews.com) — As Valentine’s Day approaches and many youth and young adults decide whether or not have to have sex for the first time, the Day of Purity presents a pro-abstinence response. A project of the Liberty Counsel, the projects asks youth to make an abstinence pledge on February 12.
The Day of Purity marks its seventh year this year with its calls for youth of all ages to remain sexually pure until marriage.
“The Day of Purity gives the youth of our nation an opportunity to stand against cultural expectations shoved on them through the media. We are encouraging youth to respect themselves and their friends,” says Amber Haskew, the Day of Purity national coordinator. (more…)
Archbishop Celestino Migliore, apostolic nuncio and permanent observer of the Holy See to the United Nations, has told a UN commission that population growth, rather than population control, can help societies overcome poverty. Archbishop Migliore made his remarks on February 8 at a meeting of the Commission for Social Development of the UN’s Department of Economic and Social Affairs, which is considering the theme of social integration.
“Focusing on human relations necessarily calls for an openness to life which is a positive contribution to social and economic development,” said Archbishop Migliore. He continued: (more…)
ROME, FEB. 8, 2010 (Zenit.org).- Bankers are not the cause of the global economic crisis, according to the president of the Institute for the Works of Religion. Rather, the cause is ordinary people who do not “believe in the future” and have few or no children.
“The true cause of the crisis is the decline in the birth rate,” Ettore Gotti Tedeschi, said in an interview on Vatican Television’s “Octava Dies.”
He noted the Western world’s population growth rate is at 0% — that is, two children per couple — and this, he said, has led to a profound change in the structure of society.
“Instead of stimulating families and society to again believe in the future and have children […] we have stopped having children and have created a situation, a negative economic context decrease,” Gotti Tedeschi observed. “And decrease means greater austerity.” (more…)
NASHVILLE, Tennessee, February 8, 2010 (LifeSiteNews.com) – A new country music star has been born – and with a pro-life ballad, no less, that is steadily climbing the country music charts.
Matt Kennon’s debut hit single “the Call” has risen to No. 39 on the Billboard 200 list of top country music hits and packs a compelling pro-life, or what some may call a “whole life,” message.
Accompanied by his guitar, Kennon sings about the lives of two individuals that would have ended very differently without the timely intervention of a phone call. The music video for “The Call” – already played on Country Music Television – captures even better the happiness in so many lives that would never have happened without “the call.” (more…)
"Stand and Deliver," a new report by the International Planned Parenthood Federation, advocates that children as young as 10 be given extensive sex education.
(FoxNews.com) A new report by the International Planned Parenthood Federation is advocating that children as young as 10 be given extensive sex education, including an awareness of sex’s pleasures.
The report, “Stand and Deliver,” charges that religious groups, specifically Catholics and Muslims, deny their young access to comprehensive sexual programs and education.
“Young people’s sexuality is still contentious for many religious institutions. Fundamentalist and other religious groups — the Catholic Church and madrasas (Islamic Schools) for example — have imposed tremendous barriers that prevent young people, particularly, from obtaining information and services related to sex and reproduction. Currently, many religious teachings deny the pleasurable and positive aspects of sex.” the report states. (more…)
Miami, FL (LifeNews.com) — When tens of millions of people around the world tune in for the Super Bowl tomorrow, they will finally get a chance to see the commercial celebrating the life of Tim Tebow. But viewers may not know Clyce Christensen, the assistant head coach of the Indianapolis Colts, has his own potential abortion story that changed his life.
Christensen’s mother was an unwed teenager who gave birth to him when she was 15 — an age where many teens have an abortion because their pregnancy is frequently a result of sexual assault.
“I also can’t help but look back and think of how easily my life and thus generations to follow could have been snuffed out before it ever got started,” Christensen shared last year at a site for adopted people.
“I can’t help but think of a 15-year-old, unwed, pregnant teen who made a courageous decision not to abort her child, but instead gave him a chance at life that over 50 million children since have not had. That child was me,” he said. (more…)
Meticulously researched, brilliantly crafted, Fatherless takes the reader on an unforgettable journey inside Fortune 500 boardrooms and Madison Avenue screening rooms, behind one-way mirrors in America’s heartland and two-way screens in church confessionals, to the very peak of Ireland’s highest mountain and inside the papal dining room of John Paul II in Rome.
Hear and learn the inspiration behind the novel readers said they “can’t put down!”
Tune In to Sound Insight on Tuesday February 9th to hear
Dr. Tom Curran’s exclusive interview with Author Brian Gail
8:00 am PST on Sacred Heart Radio
Seattle AM 1050/ Spokane AM 970
(via The Escapist) The study used functional magnetic resonance imaging (fMRI) technology, which provides a picture of brain activity in real time. Patients were asked to think a certain way in response to questions about their life. Using this technique, one study published in the New England Journal of Medicine claimed that it was possible to communicate with 4 patients out of 23 who were diagnosed to be in a vegetative state.
We’ve all heard horrible stories of people in car accidents, or otherwise seriously brain damaged, who enter a coma. They are effectively asleep, and can last that way for several weeks and sometimes years. It’s possible, however, for such a patient to advance to a vegetative state, which is only slightly more awake. Their bodies still function enough to maintain life, but they are completely unresponsive to stimuli because of the severe damage to their brains. (more…)
Washington D.C., Feb 4, 2010 / 06:20 am (CNA).– The Montgomery County Council in Maryland on Tuesday voted to require pregnancy counseling centers to post a disclaimer saying they do not have medical professionals on staff. Pro-life advocates said the centers are being unfairly targeted because they do not provide abortion or contraception.
The county council approved the new regulation by a 7-2 vote. The rule also requires centers to post notices encouraging women to consult a licensed health care provider.
Backers of the proposal said it was intended to address “misleading information from opponents of abortion rights,” the Washington Post reports.
The Archdiocese of Washington, which supports four pregnancy centers in the county, charged that the proposal “unfairly targets” pregnancy resource centers, saying they provide a “valuable safety net” of material support and referrals, but not medical care, for pregnant women in need. (more…)
(via Large Families Today) Having a big family is a little odd, we admit, in this day and age. But we are certainly not alone! Here are 10 sites we love that also talk about having a large family and the day-to-day issues they face.
1.) Large Family Mothering – The thoughts and experiences of a homeschooling mother of 15!
2.) A Baker’s Dozen – Homeschooling mom of 13, blogger and photographer.
3.) Large Family Logistics – 9 Kids and a little perspective…”All of our lives must be surrendered to God. We live for His glory not our own (1 Corinthians 10:31). Say no to yourself, do the hard thing, finish the work, do what you say you are going to do, be timely, organize yourself. ”
4.) Jeub Family – 15 Kids and no stranger to the media. The Jeub Family has books and has been on TV. The Jeubs answer a lot of the “how do you…?” questions on their website.
5.) A Christian Home – A resource to other sites and some great comebacks for when people say “Are they all yours?” (more…)
(ChristianTelegraph) Over 50,000 people have reportedly submitted comments to a website in support of college football star Tim Tebow’s appearance in a pro-life Super Bowl ad, reports Catholic News Agency.
The Susan B. Anthony List set up the site BlockHardForTebow.com to show support for the ad, in which Tebow and his mother Pam discuss how Pam refused to abort Tebow despite a life-threatening infection.
“When someone this prominent is willing to put himself out there with a positive message about Life, we need to defend him,” the site says.
The website, launched Jan. 27, allows visitors to send personal comments of support to Tebow. It also hosts a short ESPN video about Tebow.
The ad, sponsored by Focus on the Family for broadcast on CBS, has drawn protest from the National Organization for Women (NOW) and other pro-abortion women’s groups. (more…)
London, England, Feb 2, 2010 / 08:31 am (CNA).- A new “emergency contraception” pill called Ellaone is being distributed in the U.K. and claims to be effective up to five days after sexual relations. Some pro-life groups have opposed the drug, saying its use could kill a newly conceived human being.
Dr. Donna Harrison, president of the American Association of Pro-Life Obstetricians and Gynecologists, told ABC News that fertilization of egg and sperm can only happen within 24 hours of sexual relations. Any emergency contraception five days after intercourse must work by preventing the fertilized egg from implanting in the uterus.
“To label this as emergency contraception when it’s clearly an abortive action is dishonest,” Harrison charged. “This is a thinly-veiled attempt to get an abortion drug over-the-counter.” (more…)
Washington, DC (LifeNews.com) — A national Christian doctors organization is applauding a new study showing how abstinence education is more effective than either comprehensive sexual education or teaching only about contraception. They say the results coincide with polling data showing parents favor teaching their children abstinence.
Dr. David Stevens, the head of the 16,000-member Christian Medical Association, said he appreciated the new study, published in the Archives of Pediatric & Adolescent Medicine.
Science has finally caught up with logic and what parents have known for centuries by empirically demonstrating that equipping teens to abstain from sexual activity is an effective way to prevent teen pregnancy and sexually transmitted diseases,” he said. (more…)
(Washington Post) Sex education classes that focus on encouraging children to remain abstinent can convince a significant proportion to delay sexual activity, researchers reported Monday in a landmark study that could have major implications for the nation’s embattled efforts to protect young people against unwanted pregnancies and sexually transmitted diseases.
In the first carefully designed study to evaluate the controversial approach to sex ed, researchers found that only about a third of 6th and 7th graders who went through sessions focused on abstinence started having sex in the next two years. In contrast, nearly half of students who got other classes, including those that included information about contraception, became sexually active. (more…)
(Christian Post Reporter) Three additional states have taken up the “personhood” cause in a push to guarantee the constitutional rights of the preborn.
Iowa, Virginia and Kansas are now among more than 30 states pursuing personhood amendments – a move pro-lifers view as their best chance of ending abortion in the U.S.
“Personhood is a revolution of the pro-life movement,” said Keith Mason, co-founder of Personhood USA, in a statement. “It challenges what’s been done in the past, stimulates the movement’s present, and eradicates the need for pro-life efforts in the future. Personhood is the best hope to end abortion in America.”
In Kansas, a new pro-life organization – Personhood Kansas – is currently collecting petition signatures to push the state legislature to pass a personhood amendment. The petition is being passed around and promoted among Christians and other pro-lifers across the state. (more…)
In today’s environmentally conscious society, natural is the way to go — even when it comes to deciding the right time to have a baby.
More couples are turning to natural family planning as a way to achieve or postpone a pregnancy. Whether for religious, health or environmental reasons, these couples are shying away from contraceptives and having the family they always wanted.
“It just made sense,” said Juli Currie, a mother of seven from Chanhassen. “This fits with what we believe.”
Natural family planning has come a long way from the old rhythm model, which chanced conception on the calendar. Today’s methods incorporate scientific-backed research with impressive success rates.
Natural family planning is about understanding a woman’s hormonal balance, said Mary Beth Biese, a natural family planning instructor from Eden Prairie. Unlike men who are always fertile, women go through monthly cycles of fertility and non-fertility determining whether a woman is capable of conceiving. (more…)
Rome, Italy, Jan 28, 2010 / 04:28 am (CNA).- Archbishop Charles J. Chaput of Denver followed his keynote address to the Emmanuel Community of Rome’s conference on “Priests and Laity in the Mission” with a short reflection on the “disappointing times” he is experiencing. He also elaborated on a major theme of his talk—the reality of Satan and the importance of “spiritual combat.”
Just before launching into a question and answer session, Archbishop Chaput gave a reflection on his years as a bishop to stimulate discussion, saying, “I thought that after 20 years more of my life things would change and things would be a lot better but I don’t think they are.
“I think we live in disappointing times, in times of confusion, and in some ways that is the result of our failure to understand that we have an enemy in the Devil, but also we have enemies in the world around us.”
He pointed to a “great talk” from an American Protestant pastor he once heard which was titled “We preach as though we don’t have enemies,” and reflected that this sentiment “is true in the United States… .” (more…)
Dublin, Ireland (LifeNews.com) — Human rights apparently don’t include the right to life — at least according to the pro-abortion group Human Rights Watch. The New York-based organization released a document today entitled “A State of Isolation: Access to Abortion for Women in Ireland” attacking Ireland’s pro-life laws.
Among other things, it claims that Ireland is in breach of its international human rights obligations for not allowing legalised abortion in this country.
“Women in need of abortion services should, as a matter of international law and human decency, be able to count on support from their government as they face a difficult situation,” said Marianne Mollmann, the women’s rights advocacy director at Human Rights Watch. “But in Ireland they are actively stonewalled, stigmatised, and written out.”
Dr Ruth Cullen of the Pro-Life Campaign told LifeNews.com today she is disappointed that a foreign group would attack Ireland’s desire to protect women and children. (more…)
GLENVIEW, IL (January 27, 2010) – Four challenges to marriage were addressed by the U.S. Catholic Bishops in a pastoral letter last November, and the one given the most attention was contraception.
In the letter, “Marriage: Love and Life in the Divine Plan,” the bishops based their teaching on birth control on Pope Paul VI’s 1968 encyclical Humanae Vitae (on Human Life), which states that the unitive and procreative meanings of marriage must not be separated, as they are in contraception.
The letter also discusses Natural family planning (NFP), which can be used both to achieve and to postpone a pregnancy:
“NFP makes use of periodic abstinence from sexual intercourse based upon the observation of the woman’s natural signs of fertility, in order to space births or to limit the number of children when there is a serious reason to do so. NFP methods require that couples learn, accept, and live with the wonders of how God made them. This is essentially different from contraception. (more…)
MOBILE, Alabama, January 26, 2010 (LifeSiteNews.com) – College football superstar Tim Tebow is standing fast behind a pro-life ad developed by Focus on the Family and set to air on CBS on Super Bowl Sunday. Although the ad has not been released, abortion advocacy groups are already demanding that it be scrapped, since it likely features the story of how Tebow’s mother chose life when doctors were urging her abort her now-famous son.
The college football superstar, who just ended his last season quarterbacking for the Florida Gators, has been an anomaly among top-tier athletes. Tebow makes no bones about his Christian faith, his pro-life convictions, and the fact that he wants to save himself for marriage.
But Tebow’s pro-life convictions spring from an unusually personal source: back in 1987, his mother contracted amoebic dysentery while pregnant with him in the Philippines, and doctors recommended abortion. Had Pam Tebow taken that advice, Tebow fans would never have seen the football phenomenon win the Heisman Trophy in 2007 and carry the Gators to victory in two major championships. (more…)
New York, NY (LifeNews.com) — A New York woman has apparently died as a result of a failed abortion done at the A-1 Women’s Care abortion center located in the Jackson Heights section of Queens. Reports indicate emergency officials responded to an emergency call from the A1 Medicine facility at 95-45 Roosevelt on Monday afternoon.
WPIX-TV indicates a woman in her 30s was reportedly undergoing heavy bleeding and was rushed to Elmhurst Hospital Center where she was later pronounced dead.
The television station indicates an investigation into the failed abortion is ongoing and that one question officials are examining is whether the center was licensed to do abortions.
Another local media outlet, 1010 WINS, indicated the abortion practitioner severed an artery during the abortion procedure.
The A-1 Women’s Care abortion business does abortions but advertises gynecology and plastic surgery on the sign located outside the building. (more…)
Researchers have found that half of all urban teenage girls will acquire at least one sexually transmitted infection (STI) within two years of becoming sexually active. It also found that 92 percent of these teens were re-infected within four years of their first infection.
According to an Indiana University (IU) School of Medicine and Regenstrief Institute study, researchers followed 381 girls between the ages of 14 and 17 and found that half of the girls contracted chlamydia, gonorrhea and trichomoniasis within one year of becoming sexually active. They also found that re-infection rates were also high.
“Depending on the organism, within four to six months after treatment of the previous infection, a quarter of the women were re-infected with the same organism,” said Wanzhu Tu, Ph.D., associate professor of medicine at the IU School of Medicine and a Regenstrief Institute investigator. (more…)
Embryos are regularly being destroyed by IVF clinics for minor disorders suffered by individuals as successful as Charles de Gaulle and Pete Sampras.
The Human Fertilisation and Embryology Authority, the government fertility watchdog, has drawn up a list of more than 100 inherited conditions which clinics can screen out without special permission.
While some of the conditions on the list can result on deformity, severe pain and premature death, others are simply minor conditions which do not prevent sufferers leading a happy life.
The exemption list was lambasted by pro-life campaigners who said it was wrong to dispose of a life just because it was not perfect in every way.
David King, director of Human Genetics Alert, said: ‘It contributes to a social climate in which even minor deviations from “normality” are seen as unacceptable.’ (more…)
(via TheInsider.com) In her first interview with Oprah Winfrey, former vice presidential candidate Sarah Palin’s daughter Bristol opened up about her decision to wait until she’s married to have sex.
“I think it’s a goal to have and other women should have that goal,” Bristol said. “It’s a realistic goal for myself.”
Sarah has faith that Bristol, who is the mother to a 13-month-old son, can fulfill that vow.
“I believe her,” she says. “She’s a strong independent woman who can do this. She’s committed to this. ”
But Bristol admits being a single mother is no walk in the park, describing the day she broke down in tears when her son Tripp wouldn’t stop crying.
“I have this big supportive family, but I felt so alone,” she tells Oprah of that day. “Reality sunk in, that I have a kid, this is my life, my full-time job.”
Meanwhile, Sarah also spoke about her new TV gig for FOX news, not denying she might throw her hat back in the political race.
“I’m not closing any door that may be I find opened in the future,” she says. “Thankfully FOX has allowed me to leave that door open.”
(Source) Medicine changed forever in 1960 when the FDA approved the oral contraceptive pill. Society was quick to reap the consequences in the form of ’sexual liberation’ for women. It was, and for many people today still is, the panacea of medical science that a pill could free people from the ‘burden’ of new life.
Jump forward 50 years, what do we have today? We have a society completely obsessed with and addicted to sex, a complete breakdown of marriage, women more ‘enslaved’ than before they were ‘liberated’ and a medical field that has lost the vision of what they are here to do in the first place: heal. Janet Smith, a professor in the USA, gives a wonderful talk about the consequences of contraception titled, ‘Contraception Why Not?’. I would highly recommend you take the time to read and listen if you get the chance. (more…)
Bishop Thomas J. Olmsted of Phoenix has decided to intensify the church's teaching for people planning a Catholic marriage.
With the definition of marriage being challenged nationwide, the Catholic Church in Phoenix has introduced significant changes in its program for couples who want a church wedding, lengthening the preparation time from six to nine months.
Partly in response to efforts promoting gay marriage and a growing trend of unwed couples living together, Bishop Thomas J. Olmsted of Phoenix has decided to intensify the church’s teaching for people planning a Catholic marriage. The new rules for pre-marriage preparation include more time and deeper education.
// The goal is to strengthen marriages and a couple’s Catholic faith at a time when marriage is on the decline in the United States. Few dispute the value of marriage-preparation programs. Studies indicate that a solid course of marriage preparation, particularly one based on developing interpersonal skills, succeeds in reducing divorces. (more…)
Have you ever considered the economic impact of a decision made 37 years ago?
Since 1973, 50.2 million babies have been aborted in the U.S, far exceeding all the Americans killed in all the wars combined since America began. Combine that with the children and grandchildren that will never be born because of generations being wiped out through abortion.
Because there are fewer and fewer workers supporting a growing retiree population, both Social Security and Medicare face future bankruptcy.
Lawmakers can raise taxes or cut benefits, but not make up the economic impact of 50.2 million lives lost to abortion. The loss of lives means not only the loss of their productivity and their taxes, but also new ideas, inventions, cures, industries, jobs and an increased standard of living for all.
Plus many would now be parents of future workers? (more…)
(CNA) In a literary world comprised of the works of Danielle Steele, Stephen King, Nicholas Sparks and J.K. Rowling, many people have forgotten the power or purpose of the novel. What is normally used as an escape or for a bit of entertainment once had the power to change the world. Books like The Jungle, 1984, Fahrenheit 451, and Lord of the Flies both captivated their audiences and caused people to think and sometimes even act.
Brian J. Gail’s book “Fatherless” is a renaissance of the serious novel, and it even creates a new genre: the serious Catholic novel. I have to admit, when I first picked up the book, I thought I was in for a nice, entertaining story about some nice, Catholic people. Creating such a story, however, was not the author’s intent. Gail’s novel delves right into the heart of American Catholicism. His Church is neither the church of the pedophiliac priests which the media tends to overemphasize, nor is it the Church that many young people know today: a Church vibrant with the truth reemphasized by Pope John Paul II, ready to march for life, interested in going to Theology on Tap, and actively reminding Catholics to live their faith in the public square. (more…)
(via WND) In April 2009, seven researchers from organizations highly respected in scientific academia published a study, “Risk factors for triple-negative breast cancer in women under the age of 45 years,” in the prestigious journal Cancer Epidemiology, Biomarkers and Prevention.
The focus of the report was the revelatory finding that “a distinct etiology” exists between oral contraceptive use and triple-negative breast cancer, a particularly virulent form of the disease that typically strikes women under 45, many African-American.
TNBC was only first described in scientific literature in 2007. So for this study the seven researchers re-examined 897 saved cancerous breast tissue specimens from two previous studies to see if they tested positive for TNBC.
This study was funded by the National Institutes of Health.
The seven researchers concluded the risk for TNBC rose an appalling 250 to 420 percent, depending on the length of oral contraceptive use. (more…)
YOUNGSTOWN, OH (LifeSiteNews.com) – After 34 years in the abortion business, the Mahoning Women’s Center in Youngstown, Ohio, permanently closed its doors on January 12, 2010. The owner has retired and the building will be sold. The closure leaves the community of Youngstown abortion-free.
“This is such great news for the people of Ohio and all Americans. It means that lives will be saved,” said Operation Rescue President Troy Newman. “We know from experience that when abortion clinics close, many women who would otherwise have opted for abortion will instead happily keep their babies or release them for adoption.”
The closure follows a well-documented national trend. In 1991, there were nearly 2,200 abortion clinics, but today there are 712. Since 1991 over two-thirds of all abortion clinics have permanently closed. That trend appears to reflect the shifting attitude of Americans toward the pro-life position. (more…)
Fox News reporter Kelly Wright's mother conceived her son following a rape, but decided against having an abortion.
January 19, 2010 (LifeSiteNews.com) – This past Saturday, former Fox & Friends Weekend co-anchor Kelly Wright talked with Mike Huckabee on his Fox News show about his mother’s decision to give birth to him despite having conceived him in rape. Kelly made the appearance to promote his new book, “America’s Hope in Troubled Times.”
In his new book, Wright describes how his mother was raped when she was 16 years old, and how he was the result of that rape.
Calling the way he came into the world “very unique Wright explained that in the summer of 1954 his mother had become close friends with the young wife of a pastor. One day, Wright’s mother went to her friend’s house to go shopping. However, her friend had already left, and when Wright’s mother entered the home of the pastor, he assaulted her.
Wright explained that there was nothing his mother could have done against the pastor because, “It would be her word against a reputable member of the community.” (more…)
St. Petersburg, FL (LifeNews.com) — The family of Terri Schiavo, the disabled woman whose husband killed her by depriving her of food and water, will sponsor a benefit concert to raise funds for its foundation to help other patients like her. The show will feature popular country music recording artists Randy Travis and Collin Raye.
The Terri Schindler Schiavo Foundation is sponsoring the first-annual “Terri Schiavo Life and Hope” concert which will be held at the Murat Theatre in Indianapolis, Indiana on Sunday, April 11.
“The concert comes just days after the fifth anniversary of Terri Schiavo’s death and will benefit the Foundation established by her family,” the Schindler family told LifeNews.com today. (more…)
Hollywood, Calif., Jan 17, 2010 / 07:10 pm (CNA).- Maddy Curtis, a sixteen-year-old from a Virginia family of twelve, is one of the contestants advancing in the American Idol singing contest. Curtis, the ninth child in the family, has an older brother and three adopted brothers with Down’s syndrome.
Speaking on a segment of American Idol, Maddy said being ninth of twelve kids was “a crazy experience, but it’s awesome.”
Describing her disabled brothers, she said “Those four boys bring out the best in every person they meet. They see the world in colors, and we need to see the world that way.”
At the American Idol try-outs in Boston in June 2009, a mildly nervous Maddy delivered a strong performance of Leonard Cohen’s “Hallelujah.” (more…)
PARIS, January 18, 2010 (LifeSiteNews.com) – 25,000 pro-lifers, consisting largely of families and youth, marched peacefully against abortion in Paris on Sunday in the 6th annual Paris “March for Life.” The event brought together 15 French pro-life advocacy groups against abortion on the 35th anniversary of its legalization in the country.
Cécile Edel, president of Choisir La Vie, called upon her countrymen to reflect upon “the disastrous result” of 35 years of legal abortion: the “unspeakable sufferings” of millions of women, and the “blatant injustice” towards millions of their unborn brothers and sisters.
Despite having one of the very highest contraception rates in the world, France today has the second highest abortion rate in Western Europe, second only to Sweden – a situation even the sponsor of France’s 1975 abortion legalization law, Simone Veil, has deemed “distressing.” (more…)
United States (AHN) – Florida Gator Tim Tebow and his mother Pam are going to appear in a Super Bowl ad. They will be in a :30 spot for the pro-life group Focus on the Family.
Tebow, one of the most esteemed college football players ever, has been very vocal about his Christian faith and his love for Jesus Christ.
According to the Orlando Sentinel, the commercial will focus on abortion. The mother and son combo will share a personal story based on the theme “Celebrate Family, Celebrate Life.”
Jim Daly, president and CEO of Focus on the Family, didn’t elaborate on the specifics of the message, but said it’s needed.
“Tim and Pam share our respect for life and our passion for helping families thrive,” Daly said. “They live what we see every day – that the desire for family closeness is written on the hearts of every generation. Focus on the Family is about nurturing that desire and strengthening families by empowering them with the tools they need to live lives rooted in morals and values.”
Tebow’s parents were on a mission trib to the phillippines in the late 80’s while Pam was pregnant with Tim.
Pam became ill with issues connected to her pregancy and doctors advised her to abort the pregnancy.
Of course she didn’t, and Tim was born in 1987 and went on to win a Heisman Trophy and two national championships.
The Swiss Federation of Service to Patients (Patientenstellen der Schweiz) has called for a ban on one type of contraceptive pill after it was linked to the death of a 17-year-old German girl in a Swiss hospital last month. The girl, who died at the University Hospital of Basel, was taking a pill that includes drospirenone, a synthetic progestin compound used in newer brands such as Yaz, Yasmin and Yasminelle.
This was the third grave incident reported in Switzerland this year involving such contraceptives. In each case, the woman suffered a pulmonary embolism.
In May, one victim was left severely disabled after a three-month coma, and in September another woman died. “As no study has proven that the side effects caused by these contraceptives are not worse than in the case of other pills, they should be banned”, demanded Erika Ziltener, President of the Federation. Swissmedic, the country’s medical regulatory body, insists that the product need not be taken off the shelves, but it noted that all contraceptive pills carry dangers.
In the USA, people have filed more than 100 lawsuits against the pills’ maker, Bayer Pharmaceuticals, alleging it overstated the drugs’ benefits, downplayed their side effects, and failed to do proper research before releasing them onto the market. Parenting Freedom/Ennis & Ennis PA/LifeSite. December 24-26.
The Archbishop of San Francisco has responded to remarks made by House Speaker Nancy Pelosi in an interview for NEWSWEEK’s year-end issue. He sharply rebuts Pelosi, who worships in his jurisdiction, for citing the Catholic teaching of free will to support her belief that reproductive choice for women is not at odds with what she was raised to believe as a practicing Catholic. The archbishop slaps her down, saying “Free will cannot be cited as justification for society to allow moral choices that strike at the most fundamental rights of others. Such a choice is abortion, which constitutes the taking of innocent human life, and cannot be justified by any Catholic notion of freedom.” (more…)
Rebecca St. James is adding her voice and national media presence to those speaking out in favor of January’s recognition as “Sanctity of Life Month.”
St. James will be seen tomorrow (15th) on CBN’s flagship “700 Club,” speaking about the heartening acceptance accorded the release of her first starring role on film in “Sarah’s Choice,” a movie with a strong pro life message.
Next week, Rebecca will be in New York for major mainstream media, including a Tuesday (19th) appearance on “Hannity,” on the Fox News Channel. She will later next week be in Colorado Springs for radio tapings with Focus On The Family as well as the presentation of her music and message at their Sanctity of Life chapel gathering on Friday, January 22nd. (more…)
GLENVIEW, Il (MetroCatholic) – Jesse, the mother of a newborn in Bloomfield, NE, began taking the birth control pill Yasmin and never suspected it would cause problems. She had talked to her doctor about its possible side effects and he mentioned only blood clots. But after only a few months on the drug, she suffered severe stomach pains, and a medical exam revealed that she needed gall bladder surgery.
The news illustrates the wisdom of Catholic teaching on birth control.
“I thought you could only get blood clots if you were a smoker, so I wasn’t worried about taking this drug,” Jesse argues on a lawyers’ website. “I guess I trusted doctors and drugs in general…. I wasn’t worried about Yasmin.” (more…)
Concord, NH (LifeNews.com) — The New Hampshire House of Representatives defeat a bill on Wednesday that would have made the state the fourth to legalize assisted suicide. Oregon, Washington and Montana already allow the practice and the New Hampshire bill would have targeted the elderly and terminally ill as well.
The House voted 242-113 against the measure, which would have allowed physicians to dispense lethal drugs to patients to use to kill themselves.
The vote came after a majority of the members of the House Judiciary Committee recommended the state House kill the bill. Some lawmakers wanted to send the legislation back to the panel for more study but a majority decided to defeat the measure.
Alex Schadenberg, the head of the Euthanasia Prevention Coalition, told LifeNews.com today that Margaret Dore and members of the coalition worked hard to defeat the legislation. (more…)
Every so often, the FDA has to slap the wrists of drug companies for … well, pretty much everything. On the naughty list this week were several companies that the FDA didn’t feel presented the whole truth and nothing but the truth. Among them:
– Cephalon received a nasty note for not including risks of taking cancer drug Treanda on its dosing card. According to the FDA letter, these risks include skin reactions, infection and death.
– Amylin and Eli Lilly were called out for misleading statements about the diabetes medication Byetta.
“On June 10, 2009, the Lilly representative claimed that 94% of patients in a study lost 7 to 8 pounds without diet or exercise in 30 days. On June 11, 2009, an Amylin representative claimed that 80% of patients in a study lost about 7 to 8 pounds over 30 weeks.”
Which one’s right, you ask? Neither, says the FDA.
The tease, posted on the magazine’s website today…
Bristol Palin didn’t know what she was in for when she made the life-changing and controversial choice to have a baby at the young age of 18. But after she gave birth to her son, Tripp, in December 2008 – and broke up with her boyfriend, Levi Johnston – the reality of single motherhood quickly set in.
“I remember sitting on a black recliner, just bawling my eyes out,” Bristol tells In Touch. “I was just rocking Tripp to sleep because he had been screaming for so long. I was just like, ‘What am I going to do? This is as bad as it gets.”
Though raising an infant has been challenging, Bristol has the unconditional love and support of her family – especially her mother, Sarah Palin. (more…)
(USAtoday) Being a parent can be stressful, but new research calls into question some long-held beliefs about physical and psychological effects of having kids. A study published today in Annals of Behavioral Medicine finds that parents have better blood pressure readings than childless adults.
“Women were driving the effect,” says co-author Julianne Holt-Lunstad, a psychologist at Brigham Young University in Provo, Utah. “Women with children had the lowest blood pressure, and women without had the highest” of those studied.
Holt-Lunstad, along with researchers from the University of Utah in Salt Lake City and California State University-Long Beach, monitored the blood pressure of 198 adults ages 20-68. Participants wore portable monitors, which took random readings three times an hour, multiple times a day, over 24 hours, including while they slept. (more…)
CALGARY, Alberta, January 12, 2010 (LifeSiteNews.com) – In one of a pair of recent articles by major Canadian media exploring how women are increasingly turning away from hormonal contraception, the executive director for Sexual Health Access Alberta (formerly known as Planned Parenthood Alberta), bemoans the lack of information about natural family planning.
The pill has served for decades as a symbol of the feminist push for “reproductive freedom,” but in the most recent of the two articles, published yesterday in Canwest papers across the country, the SHAA director criticized the medical establishment for its pill-focused approach to contraception.
“What I see in our communities is an absolute failure to move beyond the idea that hormonal birth control is the be-all and end-all,” said Laura Wershler. “What’s happening is we’re not developing support, programs and advocacy for women looking for non-hormonal methods.”
“There’s this lack of knowledge and understanding within my own field,” Wershler continued, referring to natural methods of birth regulation that involve awareness about the woman’s reproductive cycle. “Women are going to sexual-health clinics and being laughed off by the doctors and clinics for looking for alternatives.” (more…)
Teenage girls in Britain appear to be using abortion as a form of contraception. Statistics show teenagers are having repeat abortions, some as many as four by the age of 18. One reported case involved a teen having an eighth abortion.
“It’s just the tip of the iceberg for them because so many of those young women will suffer from what’s called ‘post-abortion stress’ and will have some serious problems emotionally and physically in their future,” says Leslee Unruh, head of the National Abstinence Clearing House.
Some of those problems include later difficulty with becoming pregnant, safely carrying the baby to term, and suffering a higher risk of breast cancer. In addition to that, the suicide rate after one abortion is high.
“These young women are involving themselves emotionally, buying the lie of sex and lust and not love, and not getting a love message,” notes Unruh. “There’s so much more than the physical, and we need to start teaching young men and woman about love versus lust.”
One of the chief criticisms of Planned Parenthood’s “safe-sex” education program is that it encourages children to become intimate, provided it is followed through responsibly. That effort deems abstinence programs ineffective, despite the fact those programs prevent pregnancy and sexually transmitted diseases altogether.
WARSAW, January 11, 2010 (LifeSiteNews.com) – A group of Polish scientists have issued a document demanding that the government legislate a statutory ban on artificial (in vitro) fertilization procedures. The 100 signatories also call for full government funding of NaProTechnology, an ethically acceptable and highly successful method of evaluating and treating infertility.
The demand from the scientists follows on the heels of an open letter delivered to the Polish parliament last September from hundreds of doctors and medical professionals, urging them to vote against legalizing in vitro fertilization (IVF) and opt instead for the more successful, safer, and natural treatment for fertility problems.
Several proposals had been brought forward in the fall session of parliament to deal with the widely available, though officially illegal practice of IVF. Proposals range from taxpayer funding for all IVF treatments without restriction, including for lesbians, to an outright ban of the creation of human embryos outside the mother’s body. (more…)
Beijing, China (LifeNews.com) — A new report indicates the one-child family planning policy in China — which has given way to sex-selection abortions and infanticides of girl babies — has created a nation of bachelors. The report says more than 24 million men may be unable to find a bride by the end of the decade.
The Chinese Academy of Social Sciences, described as the nation’s leading think-tank, issued the report.
It describes the tremendous gender imbalance the pro-abortion policy has created as the most serious demographic problem facing China.
According to a London Times story, the new report describes the bachelors as “bare branches” because they will be unable to complete a family tree beyond themselves. (more…)
The Catholic Diocese of Metuchen will honor pro-life advocate Dr. Angela Lanfranchi, a parishioner of Our Lady of Lourdes Parish in Whitehouse Station, with the 2010 Pro-Vita award at its Annual Respect Life Mass to be held Sunday, Jan. 24, at St. Francis of Assisi Cathedral in Metuchen.
Dr. Lanfranchi, a breast cancer surgeon and co-founder and current president of the Breast Cancer Prevention Institute, is being honored for her work in educating the public about the abortion-breast cancer link. She has co-authored a booklet on breast cancer risks and prevention, and written brochures on reproductive and hormonal risk factors.
She has traveled internationally to speak at medical schools, hospitals, universities, cancer organizations, governmental bodies and the United Nations about breast cancer risks, including its association with induced abortion and hormonal contraceptives. She is collaborating with other breast cancer researchers on projects to determine the genetic changes and reproductive risk factors involved in the etiology of proliferative breast disease and cancer.
All are invited to the Pro-Vita Mass and reception which will follow in the Cathedral Community Room. For more information call the diocesan Respect for Life Office at 732-562-1990, ext. 1629 or visit diometuchen.org.
MEDIA ADVISORY, Jan. 6 /Christian Newswire/ — Less than two months since the U.S. Preventative Services Task Force issued new guidelines recommending against routine mammograms for women in their forties, a second breast cancer scandal involving a U.S. government panel of experts has come to light which has implications for healthcare reform.
An April 2009 study by Jessica Dolle et al. of the Fred Hutchinson Cancer Research Center examining the relationship between oral contraceptives (OCs) and triple-negative breast cancer (TNBC) in women under age 45 contained an admission from U.S. National Cancer Institute (NCI) researcher Louise Brinton and her colleagues (including Janet Daling) that abortion raises breast cancer risk by 40%. [1]
Additionally, Dolle’s team showed that women who start OCs before age 18 multiply their risk of TNBC by 3.7 times and recent users of OCs within the last one to five years multiply their risk by 4.2 times. TNBC is an aggressive form of breast cancer associated with high mortality. (more…)
It is indeed a startling revelation- breast cancer is a more common occurrence than ever before. It tops the list of all cancers and presents a surging number of 182,480 new cases being diagnosed in American women this year- a 26 percent rise in US alone. Breast cancer was the most common malignancy in all GCC countries, ranging from 16.1% of female cancers in Oman to 35.4% in Bahrain. Science earlier claimed that ‘genetically predisposed’ women were are high risk of developing this disease. But today, this is rather questionable, as 85 percent of diagnosed cases have no predefined risks associated with them. There doesn’t seem to be a definitive way to pre-empt the possibility of a healthy women coming down with breast cancer.
Breast cancer, by virtue of its newfound popularity, is very well read and talked about by most women. Unfortunately, one can never muster ample resilience to withstand the emotional whirlwind that a breast cancer diagnosis brings along. Some women cannot do much about their genetic make up that makes them more susceptible to the disease. A few others can definitely bring down their risk by implementing lifestyle changes that are proven to actively contribute to this growing population. Top ten New Year resolutions for breast cancer are: (more…)
Living in the exotic Old City of Yerushalayim, and needing to make ends meet by renting out our guest room, I have hosted many young, accomplished American women travelers as my boarders. Over herb tea in my kitchen, some have wanted to talk about Eastern religions, some about Israeli politics, and some about feminist issues.
One young woman confided in me her shock and dismay at discovering that most religious families have half a dozen children, and some a full dozen! To her, this was a flagrant violation of her most cherished ideal of zero population growth. (more…)
APPLETON (FOX 11)- There are some new ads airing on radio and TV in Northeast Wisconsin that endorse emergency contraception. The problem? They come from a group that claims to be Catholic. It’s members call the ads informative, but other area Catholics say they deliberately mislead.
The spots come from the group Young Catholics for Choice, based in Washington DC. Some local Catholics not only find the ads offensive, they seriously question the name behind them.
“It’s frustrating, it’s sad to see these young girls smiling and doing this commercial saying I’m Catholic and its okay, when it’s not,” Jeanne Griffith of Menasha said.
Griffith is Catholic and says part of being Catholic is following church teaching. The Catholic Church is opposed to all contraceptives, including the so called “Morning After Pill.” (more…)
ScienceDaily (Dec. 22, 2009) — Nearly half of women using depot medroxyprogesterone acetate (DMPA), commonly known as the birth control shot, will experience high bone mineral density (BMD) loss in the hip or lower spine within two years of beginning the contraceptive, according to researchers at the University of Texas Medical Branch at Galveston.
The study, reported in the January 2010 issue of Obstetrics and Gynecology, was the first to show that women on DMPA who smoke, have low levels of calcium intake and never gave birth are at the highest risk for BMD loss. The researchers also found that high risk women continued to experience significant losses in BMD during the third year of DMPA use, especially in the hip — the most common facture site in elderly women.
DMPA is an injected contraceptive administered to patients every three months. According to the American College of Obstetricians and Gynecologists, more than two million American women use DMPA, including approximately 400,000 teens. DMPA is relatively inexpensive compared with some other forms of birth control, has a low failure rate and doesn’t need to be administered daily, which contributes to the contraceptive’s popularity. (more…)
Washington, DC (LifeNews.com) — A new poll shows 72 percent of Americans oppose paying for abortions with their tax dollars under the government-run health care bill in Congress. As the Senate prepares to vote on legislation that contains massive abortion funding, a Quinnipiac University survey released today shows opposition.
American voters mostly disapprove of the pro-abortion health care bill, by a 53-36 percent margin.
They also disapprove of pro-abortion President Barack Obama’s handling of the health care issue by a similar 56-38 percent margin, the new survey showed.
But abortion funding draws strenuous opposition from the American public, regardless of political persuasion, with 72 percent saying they oppose “using any public money in the health care overhaul to pay for abortions” and just 23 percent saying they favor it. (more…)
CHESAPEAKE, Va. (Catholic Online) – In case there’s any doubt, it’s not true that Americans don’t worship. We are indeed still a nation that faithfully goes to the altar to worship and give our lives. We give our money & our time, and we choose our leaders accordingly. Some things are worth protecting and defending, so we make darn sure the important things are kept safe.
What has changed is the object of our worship. No longer is the one we adore holy and all-powerful. No longer is our master a loving and merciful one. We have a new god.
Sex is a new false god. Our society worships at the altar of sex, and by extension, the altar of abortion. Every part of our daily lives seems to glorify and revolve around sex. There is no escaping the pervasive presence of indulgent sex. It has infiltrated every corner of our culture and radically changed the way we view ourselves and the way we treat each other.
Satan has so skillfully enslaved us in a prison of self-centeredness and obsession with sex that he no longer has to convince us to come to this altar – we come running of our own volition. We can’t get enough sex. Bondage tastes like freedom on our tongues and we beg for more. We are addicted to our lethal injection. (more…)
MILWAUKEE, December 15, 2009 (LifeSiteNews.com) – The incoming Archbishop of Milwaukee, Jerome Listecki, has responded to a campaign by “Young Catholics for Choice” to promote use of contraception and abortion among Catholic youth.
Using media advertising the group is, says the Archbishop-Designate, “attempting to convey the message that Catholics can disregard Church teaching regarding contraception, abortion and human sexuality in general and remain Catholics in good standing.” However, “Nothing could be further from the truth.” (more…)
by David Brody, CBN News White House Correspondent
Below is some reaction from Pro-Life leaders on the defeated Nelson-Hatch abortion amendment in the Senate:
Tony Perkins.President of Family Research Council Action
“In rejecting the Nelson-Hatch amendment, pro-abortion Senators have broken the three decade long truce over government funding of abortion and have demonstrated they would rather have mandate federal funding for abortion than enact ‘health care reform.’ (more…)
Pulling from the CDC, Government, and other “official” sources, Brian Gail (author of Fatherless) delivers some shocking statistics concerning marriage, contraception, and abortion.
Too often the discussion of the morality of contraception fragments into a specific treatment of individual devices and methods wherein the overarching theological and philosophical essence of contraception is obfuscated. We lose sight of the forest for the trees. Behind every device and method of contraception is a fundamental breach of God’s design for marital sexuality. Without this perspective, the Church’s condemnation of contraception might appear to be a knee-jerk reaction to modernity or a rejection of science and man’s dominion over the material universe. The more we can recover the root of the Church’s prohibition of contraception, the more consistent and comprehensive will be our objections. (more…)
LONDON, November 24, 2009 (LifeSiteNews.com) – Speaking at the Annual Theos Lecture in London on November 4, Britain’s Chief Rabbi Johnathan Sacks, warned that Europe was bound to meet the same fate as ancient Greece due to its abysmal failure to inspire larger families.
“Parenthood involves massive sacrifice: of money, attention, time and emotional energy,” he said. “Where today, in European culture with its consumerism and its instant gratification ‘because you’re worth it,’ in that culture, where will you find space for the concept of sacrifice for the sake of generations not yet born?” (more…)
(HealthDay News) — Want to be a happy married couple? Consider having kids.
A new study found that having children boosts happiness. And the more, literally, the merrier.
But unmarried couples shouldn’t expect to find greater happiness through child-raising. The study, published in the Oct. 14 online edition of the Journal of Happiness Studies, suggests that having children has little or no effect on boosting happiness among couples who aren’t hitched.
The findings contradict previous research that suggested that having more offspring doesn’t lead to greater happiness and might even make people less satisfied with their lives. One theory behind the conclusion is that parents don’t receive many rewards in return for the hard work of raising children. (more…)
In "Prove it God" Patty Schneier speaks as a Catholic woman and mother in our modern times. She tells her personal story of how God worked in her heart to turn her away from contraception and toward Natural Family Planning.
Patty Schneier's "Prove It, God" ...And He Did is available to listen to for free! Order it!
Stephen Patton M.A., J.D.
Stephen Patton's "Why Contraception Matters" talk is available to listen to for free! Read it!Order it!
La charla de Stephen Patton "Porque Importa la Anticoncepción" esta disponible aqui para que la escuchen gratis! Leela!Ordenala!
 A judge has ruled that the teenager, declared dead in California, may not be dead. From the East Bay Express story:
A judge has ruled that the teenager, declared dead in California, may not be dead. From the East Bay Express story:
 A number of women are having to undergo hysterectomies to remove a sterilisation device used on the NHS, the Victoria Derbyshire show has found.
A number of women are having to undergo hysterectomies to remove a sterilisation device used on the NHS, the Victoria Derbyshire show has found.

 There are the women whose waiting doesn’t matter. And then there are the women whose waiting is especially terrible and reported on at regular intervals.
There are the women whose waiting doesn’t matter. And then there are the women whose waiting is especially terrible and reported on at regular intervals. Nearly every day the news presents yet another article on sexbots, robots that are designed to take the place of women. This is the most obvious “objectification” of women that has followed upon the sexual revolution, the literal creation of an artificial object, a robotic woman, for the sexual pleasure of men degraded enough to prefer a machine to the real thing.
Nearly every day the news presents yet another article on sexbots, robots that are designed to take the place of women. This is the most obvious “objectification” of women that has followed upon the sexual revolution, the literal creation of an artificial object, a robotic woman, for the sexual pleasure of men degraded enough to prefer a machine to the real thing.
 August 24, 2017
August 24, 2017  Recently Pope Francis tells of talking with his predecessor, Pope Benedict, who remarked that we are living in an “epoch of sins against God the Creator.” What did he mean? Evidently, other epochs had sins but they were not directed against the Creator. The sins we were to repent in the Redemption were not primarily directed against the Creator.
Recently Pope Francis tells of talking with his predecessor, Pope Benedict, who remarked that we are living in an “epoch of sins against God the Creator.” What did he mean? Evidently, other epochs had sins but they were not directed against the Creator. The sins we were to repent in the Redemption were not primarily directed against the Creator. MICAIAH BILGER AUG 25, 2017 | 1:21PM WASHINGTON, DC
MICAIAH BILGER AUG 25, 2017 | 1:21PM WASHINGTON, DC
 For the second time in a year, a group of scientists managed to create an artificial womb that one day could save very premature babies’ lives.
For the second time in a year, a group of scientists managed to create an artificial womb that one day could save very premature babies’ lives.
 August 17, 2017
August 17, 2017 
 M
M
 Wesley Smith Aug 11, 2017 | 3:50PM Washington, DC http://www.lifenews.com
Wesley Smith Aug 11, 2017 | 3:50PM Washington, DC http://www.lifenews.com St. Padre Pio was not only a holy man, miracle worker, and mystic, he was also a prophet.
St. Padre Pio was not only a holy man, miracle worker, and mystic, he was also a prophet.

 August 8th, 2017
August 8th, 2017 EDITOR’S NOTE: This article addresses a specific question regarding whether Catholic hospitals should administer Plan B in rape cases based on the scientific evidence regarding how the drug works. The discussion does not in any way imply that contraceptives are or can be morally licit. The Catholic Church teaches that “every action which, whether in anticipation of the conjugal act, or in its accomplishment, or in the development of its natural consequences, proposes, whether as an end or as a means, to render procreation impossible” is intrinsically evil (CCC 2370 quoting Humanae Vitae 14).
EDITOR’S NOTE: This article addresses a specific question regarding whether Catholic hospitals should administer Plan B in rape cases based on the scientific evidence regarding how the drug works. The discussion does not in any way imply that contraceptives are or can be morally licit. The Catholic Church teaches that “every action which, whether in anticipation of the conjugal act, or in its accomplishment, or in the development of its natural consequences, proposes, whether as an end or as a means, to render procreation impossible” is intrinsically evil (CCC 2370 quoting Humanae Vitae 14). Is it possible to talk about the pollution of sexuality in the same way that we can talk about the pollution of the air with sulfur dioxide belched out of smoke stacks or pollution of the water through industrial waste dumped in rivers?
Is it possible to talk about the pollution of sexuality in the same way that we can talk about the pollution of the air with sulfur dioxide belched out of smoke stacks or pollution of the water through industrial waste dumped in rivers?
 After meeting with President Trump in the Oval Office on May 4, I sat in the Rose Garden and listened as the president promised the
After meeting with President Trump in the Oval Office on May 4, I sat in the Rose Garden and listened as the president promised the  NAPA, California, August 1, 2017 (
NAPA, California, August 1, 2017 (


 In a modern-day version of eugenics, inmates in White County, Tennessee are volunteering to receive vasectomies or birth control implants in exchange for credit toward their jail sentence.
In a modern-day version of eugenics, inmates in White County, Tennessee are volunteering to receive vasectomies or birth control implants in exchange for credit toward their jail sentence. https://theguidingstarproject.com
https://theguidingstarproject.com

 July 23 marks the beginning of Natural Family Planning (NFP) Awareness Week in the United States. In this article Gerard Migeon, founder and CEO of
July 23 marks the beginning of Natural Family Planning (NFP) Awareness Week in the United States. In this article Gerard Migeon, founder and CEO of 


 It’s almost NFP Awareness week (July 23)! It’s easy to get swept away in NFP promotion and forget that it’s not always a breezy journey for everyone. So here we have laid out the guide to promoting Natural Family Planning without the rose-colored glasses. The three most important things to keep in mind when sharing your love of Natural Family Planning are sincerity in the struggles you have encountered, joy in the wonderful parts, and flexibility in allowing others to be where they are on their journey.
It’s almost NFP Awareness week (July 23)! It’s easy to get swept away in NFP promotion and forget that it’s not always a breezy journey for everyone. So here we have laid out the guide to promoting Natural Family Planning without the rose-colored glasses. The three most important things to keep in mind when sharing your love of Natural Family Planning are sincerity in the struggles you have encountered, joy in the wonderful parts, and flexibility in allowing others to be where they are on their journey. For many women, the decision to go on birth control is a normal part of womanhood. At well-woman checks and appointments after a baby’s birth doctors say it’s time to talk about birth control, and the general assumption is that you’ll use birth control until it’s the perfect time to have exactly as many kids as you want.
For many women, the decision to go on birth control is a normal part of womanhood. At well-woman checks and appointments after a baby’s birth doctors say it’s time to talk about birth control, and the general assumption is that you’ll use birth control until it’s the perfect time to have exactly as many kids as you want.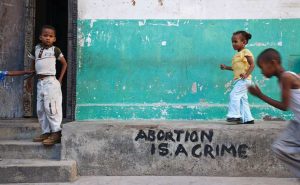 OTTAWA, July 12, 2017 (
OTTAWA, July 12, 2017 (
 July 10, 2017
July 10, 2017 
 When I started nursing school 50 years ago, medical ethics was not a course but rather common sense principles incorporated into our education. There was no controversy about not harming patients, integrity, equality of treatment regardless of status, etc.
When I started nursing school 50 years ago, medical ethics was not a course but rather common sense principles incorporated into our education. There was no controversy about not harming patients, integrity, equality of treatment regardless of status, etc. T
T D
D If you’ve read any of my posts, you know that this is one of the questions that pervades my work. Do we really know what we think we know? More often than not, the answer is no. Upon examination, what we hold true falls short. In the field of pharmaceutical medicine, where money plays an enormous role in determining what is known about a particular drug, finding the real and honest truth about a medication is difficult and sometimes impossible. Hormonal contraception, because it has been on the market for decades and because as women we really want it to be safe and absent negative side effects, is one of those drugs where what we think we know and what we actually know are two entirely different things.
If you’ve read any of my posts, you know that this is one of the questions that pervades my work. Do we really know what we think we know? More often than not, the answer is no. Upon examination, what we hold true falls short. In the field of pharmaceutical medicine, where money plays an enormous role in determining what is known about a particular drug, finding the real and honest truth about a medication is difficult and sometimes impossible. Hormonal contraception, because it has been on the market for decades and because as women we really want it to be safe and absent negative side effects, is one of those drugs where what we think we know and what we actually know are two entirely different things.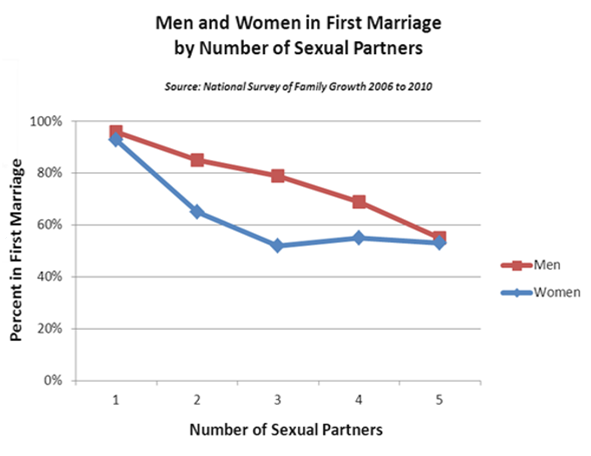

 Fr. Shenan Boquet
Fr. Shenan Boquet DES MOINES, Iowa, June 21, 2016 (
DES MOINES, Iowa, June 21, 2016 (




 CAMBRIDGE, Massachusetts, June 19, 2017 (
CAMBRIDGE, Massachusetts, June 19, 2017 (
 (
( by
by 
 Cardinal Carlo Caffarra, archbishop emeritus of Bologna, Italy, has a key message to deliver: Great efforts must be made in Catholic education and catechesis if the Church is to combat today’s attacks on marriage, life and the family.
Cardinal Carlo Caffarra, archbishop emeritus of Bologna, Italy, has a key message to deliver: Great efforts must be made in Catholic education and catechesis if the Church is to combat today’s attacks on marriage, life and the family. June 12, 2017
June 12, 2017  BISHKEK, Kyrgyzstan, May 31, 2017 (
BISHKEK, Kyrgyzstan, May 31, 2017 ( Robert Cardinal Sarah’s recent book
Robert Cardinal Sarah’s recent book 
 The dedication and legacy of a prodigious pro-life hero
The dedication and legacy of a prodigious pro-life hero June 7, 2017 (
June 7, 2017 (

 The Brazilian priest Alexandre Awi Mello, the National Director of Brazil’s Schönstatt Movement, will serve as the new secretary for the the Dicastery for Laity, Family and Life. He was born Rio de Janeiro in 1971, and was ordained a priest in 2001.
The Brazilian priest Alexandre Awi Mello, the National Director of Brazil’s Schönstatt Movement, will serve as the new secretary for the the Dicastery for Laity, Family and Life. He was born Rio de Janeiro in 1971, and was ordained a priest in 2001. Let’s say he lived in Philadelphia in the 1950s. He came from an Italian American family. He sees his Dad, his uncles, his grandfather. They are working class. They sweat in dangerous jobs to support their large families. They come home to a little house full of kids. Its a good life, but its a hard life.
Let’s say he lived in Philadelphia in the 1950s. He came from an Italian American family. He sees his Dad, his uncles, his grandfather. They are working class. They sweat in dangerous jobs to support their large families. They come home to a little house full of kids. Its a good life, but its a hard life. I am often asked to speak about sex to high school students. Many adults shudder at the thought of talking to kids about sex, but I love it. First, I have a captive audience, and second, I get to talk about two things that I am very passionate about: the dangers of teen sex and the joys of sex in marriage. Many adults worry that kids will be too shy to ask questions but on the contrary, I have found them eager to have ever their questions answered in an honest, upbeat manner.
I am often asked to speak about sex to high school students. Many adults shudder at the thought of talking to kids about sex, but I love it. First, I have a captive audience, and second, I get to talk about two things that I am very passionate about: the dangers of teen sex and the joys of sex in marriage. Many adults worry that kids will be too shy to ask questions but on the contrary, I have found them eager to have ever their questions answered in an honest, upbeat manner.
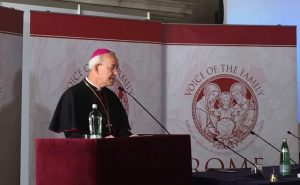 Editor’s note: This address was delivered by His Excellency Bishop Athanasius Schneider, auxiliary bishop of Astana in Kazakhstan, on 19 May 2017 at the fourth annual Rome Life Forum, which is organised by Voice of the Family.
Editor’s note: This address was delivered by His Excellency Bishop Athanasius Schneider, auxiliary bishop of Astana in Kazakhstan, on 19 May 2017 at the fourth annual Rome Life Forum, which is organised by Voice of the Family. In an attempt to continue her desired “transition” from female to male, Evan Michael Minton was scheduled by her surgeon to undergo a hysterectomy at Dignity Health chain’s Catholic Mercy San Juan Medical Center in Carmichael, California last summer. The surgery was denied by the Catholic hospital’s policy. And, although Minton was able to have the surgery at another Dignity Health chain hospital in September, she
In an attempt to continue her desired “transition” from female to male, Evan Michael Minton was scheduled by her surgeon to undergo a hysterectomy at Dignity Health chain’s Catholic Mercy San Juan Medical Center in Carmichael, California last summer. The surgery was denied by the Catholic hospital’s policy. And, although Minton was able to have the surgery at another Dignity Health chain hospital in September, she  March 28, 2017 (LifeSiteNews) — I had always dreamed as a little girl of Prince Charming, castles, and fairytale endings. But what took place exactly one week before my birthday in September 2009 was no childhood dream, but an evil nightmare filled with pain and utter disbelief.
March 28, 2017 (LifeSiteNews) — I had always dreamed as a little girl of Prince Charming, castles, and fairytale endings. But what took place exactly one week before my birthday in September 2009 was no childhood dream, but an evil nightmare filled with pain and utter disbelief. When I get in touch with Rosa Pich by Skype during Holy Week, I discover that she is on holiday with 12 of her children in Torreciudad, a shrine dedicated to Our Lady in northern Spain. “We are trying to return to normal life,” she says, following the death of her husband, Chema, of liver cancer little more than a month earlier. “We have cried a lot, we have prayed a lot, but life continues,” she says. “I have come to see that when God gives you a cross to carry, he always gives you the grace you need to bear it.”
When I get in touch with Rosa Pich by Skype during Holy Week, I discover that she is on holiday with 12 of her children in Torreciudad, a shrine dedicated to Our Lady in northern Spain. “We are trying to return to normal life,” she says, following the death of her husband, Chema, of liver cancer little more than a month earlier. “We have cried a lot, we have prayed a lot, but life continues,” she says. “I have come to see that when God gives you a cross to carry, he always gives you the grace you need to bear it.” http://www.ewtnnews.com/catholic-news/US.php?id=15601
http://www.ewtnnews.com/catholic-news/US.php?id=15601 The message of Fatima is, in its basic nucleus, a call to conversion and repentance, as in the Gospel. This call was uttered at the beginning of the twentieth century, and it was addressed particularly to this present century. … The call to repentance is a motherly one, and at the same time it is strong and decisive. (Pope Saint John Paul II,
The message of Fatima is, in its basic nucleus, a call to conversion and repentance, as in the Gospel. This call was uttered at the beginning of the twentieth century, and it was addressed particularly to this present century. … The call to repentance is a motherly one, and at the same time it is strong and decisive. (Pope Saint John Paul II, 





 May 9, 2017 (
May 9, 2017 (
 When doctors told Chelsea Torres that she was carrying conjoined twins, they warned her that the babies probably would not survive past the first trimester.
When doctors told Chelsea Torres that she was carrying conjoined twins, they warned her that the babies probably would not survive past the first trimester. Baby Dexter was not supposed to be.
Baby Dexter was not supposed to be.
 MICHAEL COOK MAY 2, 2017 | 5:45PM BRUSSELS, BELGIUM
MICHAEL COOK MAY 2, 2017 | 5:45PM BRUSSELS, BELGIUM MANCHESTER, England, April 27, 2016 (
MANCHESTER, England, April 27, 2016 ( In a society where preborn children are treated as disposable property, and disregarded in the name of cold, sterile, euphemisms such as “reproductive rights” and “choice,” it’s rare to find a mother who actually does the opposite of putting herself above her child.
In a society where preborn children are treated as disposable property, and disregarded in the name of cold, sterile, euphemisms such as “reproductive rights” and “choice,” it’s rare to find a mother who actually does the opposite of putting herself above her child.
 Elizabeth Bradley on April 21, 2017
Elizabeth Bradley on April 21, 2017 A new study has reinforced what many women have been
A new study has reinforced what many women have been  NEW YORK, April 24, 2017 (
NEW YORK, April 24, 2017 ( Although many in the media
Although many in the media 
 By Madeline Holcombe, CNN
By Madeline Holcombe, CNN
 Bradley Mattes
Bradley Mattes April 10, 2017 (
April 10, 2017 ( A funny thing happened on the way to our supposed brave new world of assisted suicide.
A funny thing happened on the way to our supposed brave new world of assisted suicide. VATICAN CITY, April 20, 2017 (
VATICAN CITY, April 20, 2017 (
 For the second time in the past three months, Option Line—a 24-7 pregnancy helpline operated by Heartbeat International—is celebrating a high-water mark, having reached 28,414 women with life-affirming help in the month of March.
For the second time in the past three months, Option Line—a 24-7 pregnancy helpline operated by Heartbeat International—is celebrating a high-water mark, having reached 28,414 women with life-affirming help in the month of March.
 New evidence about the Zika virus and the potential link to defects in unborn babies came out this week.
New evidence about the Zika virus and the potential link to defects in unborn babies came out this week.
 BAKER CITY, Oregon, March 31, 2017 (LifeSiteNews) – Matt and Elsa Cunningham thought they’d lost their young son in a drowning accident earlier this month. But 22-month-old Matty made it through the terrible ordeal with no medical complications.
BAKER CITY, Oregon, March 31, 2017 (LifeSiteNews) – Matt and Elsa Cunningham thought they’d lost their young son in a drowning accident earlier this month. But 22-month-old Matty made it through the terrible ordeal with no medical complications.


 With infertility more common than ever and birth rates around the world at a record low, a crucial first step for couples trying to get pregnant is to clearly understand exactly when they are fertile. Yet that is something just 13 per cent of women surveyed were able to identify according to a new study just published in the Australian and New Zealand Journal of Obstetrics and Gynaecology which surveyed over 1000 New Zealand women. That was despite a third of the women reporting that they monitored their ovulation.
With infertility more common than ever and birth rates around the world at a record low, a crucial first step for couples trying to get pregnant is to clearly understand exactly when they are fertile. Yet that is something just 13 per cent of women surveyed were able to identify according to a new study just published in the Australian and New Zealand Journal of Obstetrics and Gynaecology which surveyed over 1000 New Zealand women. That was despite a third of the women reporting that they monitored their ovulation. March 23, 2017 (LiveActionNews) — In a village in the Philippines in 2014, a little girl was born without limbs. At six months old she was placed in an orphanage for children with special needs, where she waited for a family to adopt her.
March 23, 2017 (LiveActionNews) — In a village in the Philippines in 2014, a little girl was born without limbs. At six months old she was placed in an orphanage for children with special needs, where she waited for a family to adopt her.

 March 16, 2017 (
March 16, 2017 ( A Newcastle fertility clinic has been given a license by the Human Fertilization and Embryology Authority (HFEA) to carry out the controversial “three-parent baby” technique.
A Newcastle fertility clinic has been given a license by the Human Fertilization and Embryology Authority (HFEA) to carry out the controversial “three-parent baby” technique.






 The Natural Cycles app Photograph: Danijela Froki/Natural Cycles
The Natural Cycles app Photograph: Danijela Froki/Natural Cycles 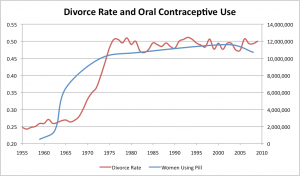


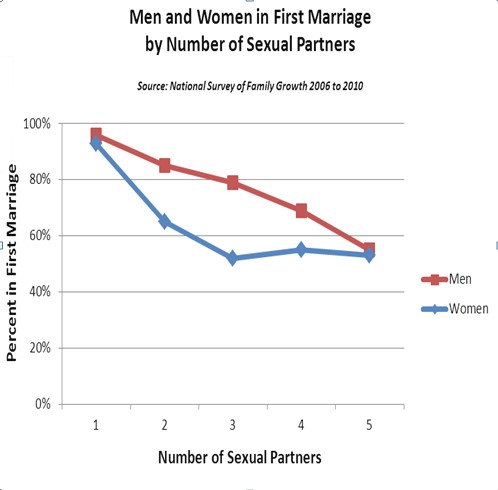





 Doctors suggested that Hayley Lampshire may have to abort one of her unborn sons after they discovered the twins shared an amniotic sac and placenta.
Doctors suggested that Hayley Lampshire may have to abort one of her unborn sons after they discovered the twins shared an amniotic sac and placenta.
 The year 2017 already is bringing strong hopes for future babies in the womb.
The year 2017 already is bringing strong hopes for future babies in the womb. STATE ERIN PARFET JAN 31, 2017 | 2:44PM BATON ROUGE, LOUISIANA
STATE ERIN PARFET JAN 31, 2017 | 2:44PM BATON ROUGE, LOUISIANA Did You Know?
Did You Know?




















 As a labor and delivery nurse, there are countless times I’ve talked with women about
As a labor and delivery nurse, there are countless times I’ve talked with women about 
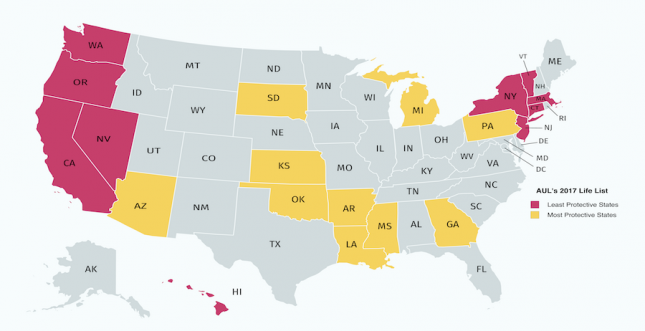

 Then came the answer to prayer. They thought they were watching her breathe her last breaths, and they wept. Instead, after 30 minutes, her oxygen levels were up to 100%, and she was doing it on her own. “It’s just amazing,” said Mrs. Moore-Williams. “It’s like we have won the lottery.”
Then came the answer to prayer. They thought they were watching her breathe her last breaths, and they wept. Instead, after 30 minutes, her oxygen levels were up to 100%, and she was doing it on her own. “It’s just amazing,” said Mrs. Moore-Williams. “It’s like we have won the lottery.”
 Congress approved legislation to defund the Planned Parenthood abortion business last year only to see pro-abortion President Barack Obama veto it. Today, a leading pro-life me member f the House of representatives introduced a bill to yank taxpayer funding from the nation’s biggest abortion company.
Congress approved legislation to defund the Planned Parenthood abortion business last year only to see pro-abortion President Barack Obama veto it. Today, a leading pro-life me member f the House of representatives introduced a bill to yank taxpayer funding from the nation’s biggest abortion company. A newly-born baby boy was rescued by a Catholic church employee on Wednesday shortly before mass at the Cathedral of St. Paul in St. Paul, Minnesota, Fox9 News reports.
A newly-born baby boy was rescued by a Catholic church employee on Wednesday shortly before mass at the Cathedral of St. Paul in St. Paul, Minnesota, Fox9 News reports. Mexico City, Mexico, Dec 31, 2016 / 02:33 pm (
Mexico City, Mexico, Dec 31, 2016 / 02:33 pm (




 The vicious cycle of fatherlessness and poverty
The vicious cycle of fatherlessness and poverty  Rethinking our approach to poverty
Rethinking our approach to poverty  Graph: Marriage Foundation UK
Graph: Marriage Foundation UK

 Rihanna Truman is a young woman who will give birth in just one week to her first child. What makes her unique is not only that she is 16-years-old, but that she is also battling cancer.
Rihanna Truman is a young woman who will give birth in just one week to her first child. What makes her unique is not only that she is 16-years-old, but that she is also battling cancer.




 November 2, 2016 (LifeSiteNews) — In 1979 I arrived, elated yet diffident, in the Chinese village that would be my home for the next year. Within a few months of my arrival, pregnant mothers were being rounded up by local Communist officials and marched off to abortuaries. China’s one-child policy had begun.
November 2, 2016 (LifeSiteNews) — In 1979 I arrived, elated yet diffident, in the Chinese village that would be my home for the next year. Within a few months of my arrival, pregnant mothers were being rounded up by local Communist officials and marched off to abortuaries. China’s one-child policy had begun. Less than a week before Americans cast their votes for president, Catholic bishops are urging their congregants to educate themselves about the candidates’ positions on abortion.
Less than a week before Americans cast their votes for president, Catholic bishops are urging their congregants to educate themselves about the candidates’ positions on abortion.

 Strange things happen in election years. That was clear to me last Monday morning as I opened the newspaper to a full-page ad from an organization called “Catholics for Choice” referring to “Abortion in Good Faith” and misrepresenting Catholic social teaching by claiming that “public funding for abortion is a Catholic social justice value.” This ad, with slight regional variations, appeared in newspapers across the country, and represented the latest in a series of public relations efforts by this organization to promote a pro-abortion agenda by attempting to counter the Church’s consistent and convincing proclamation of the Gospel of life.
Strange things happen in election years. That was clear to me last Monday morning as I opened the newspaper to a full-page ad from an organization called “Catholics for Choice” referring to “Abortion in Good Faith” and misrepresenting Catholic social teaching by claiming that “public funding for abortion is a Catholic social justice value.” This ad, with slight regional variations, appeared in newspapers across the country, and represented the latest in a series of public relations efforts by this organization to promote a pro-abortion agenda by attempting to counter the Church’s consistent and convincing proclamation of the Gospel of life.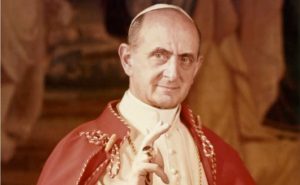 WASHINGTON, D.C., September 21, 2016 (LifeSiteNews) — More than 400 Catholic academics released a statement affirming the Catholic Church’s teaching on contraception and human sexuality in response to recent calls for the Church to change her teaching as the 50th anniversary of Humanae Vitae approaches. Opponents of Catholic teaching presented those calls Tuesday at the United Nations.
WASHINGTON, D.C., September 21, 2016 (LifeSiteNews) — More than 400 Catholic academics released a statement affirming the Catholic Church’s teaching on contraception and human sexuality in response to recent calls for the Church to change her teaching as the 50th anniversary of Humanae Vitae approaches. Opponents of Catholic teaching presented those calls Tuesday at the United Nations.
 It is fitting that this day falls adjacent to September 11, the anniversary of the terrorist attacks in New York and Arlington, Virginia. Though the number of lives taken by abortion is much larger than that taken on that terrible day fifteen years ago, both acts of mass murder rely on the same evil, the denial of the humanity of others.
It is fitting that this day falls adjacent to September 11, the anniversary of the terrorist attacks in New York and Arlington, Virginia. Though the number of lives taken by abortion is much larger than that taken on that terrible day fifteen years ago, both acts of mass murder rely on the same evil, the denial of the humanity of others. In September 2015 the United Nations General Assembly adopted a series of goals and targets in order to eradicate poverty, eliminate inequality, and subdue climate change by 2030. These Sustainable Development Goals (SDGs), comprising 17 goals, 169 targets, and 230 indicators (to measure progress) replaced the eight Millennium Development Goals that had guided UN development policy thinking over the previous 15 years. Secretary-General Ban Ki-moon characterized the SDGs as heralding “an historic turning point for our world”; they will probably be the hallmark of his legacy as he ends his decade-long reign at the helm of the UN in December.
In September 2015 the United Nations General Assembly adopted a series of goals and targets in order to eradicate poverty, eliminate inequality, and subdue climate change by 2030. These Sustainable Development Goals (SDGs), comprising 17 goals, 169 targets, and 230 indicators (to measure progress) replaced the eight Millennium Development Goals that had guided UN development policy thinking over the previous 15 years. Secretary-General Ban Ki-moon characterized the SDGs as heralding “an historic turning point for our world”; they will probably be the hallmark of his legacy as he ends his decade-long reign at the helm of the UN in December. First, a refresher as to exactly what Implanon is: an implantable birth control device, small and thin akin to the size of a toothpick, that’s inserted below the skin in the upper arm and designed to provide birth control protection through the measured release of the progestin etonogestrel for about three years before removal. Various advocates of the device claim that it can last as long as four years – but three years is the recommended window.
First, a refresher as to exactly what Implanon is: an implantable birth control device, small and thin akin to the size of a toothpick, that’s inserted below the skin in the upper arm and designed to provide birth control protection through the measured release of the progestin etonogestrel for about three years before removal. Various advocates of the device claim that it can last as long as four years – but three years is the recommended window.


 Abortion seemed liked a logical answer. After all, in 2014, senior editor of Elle Magazine
Abortion seemed liked a logical answer. After all, in 2014, senior editor of Elle Magazine  ABOUT THE NOVENA FOR OUR NATION
ABOUT THE NOVENA FOR OUR NATION RIO DE JANEIRO, Brazil, August 10, 2016
RIO DE JANEIRO, Brazil, August 10, 2016 
 August 3, 2016 (
August 3, 2016 ( Editor’s note: The following address was given in a catechesis to youth at World Youth Day.
Editor’s note: The following address was given in a catechesis to youth at World Youth Day.
 (NaturalNews) It has been on the U.S. drug market since the early 1990s, and population control organizations like Planned Parenthood continue to push it heavily on black women and other ethnic minorities as a form of contraception. But the injectable contraceptive drug Depo-Provera, manufactured by Pfizer, has an extensive track record of causing serious harm to women, including its tendency to trigger the development of cancer.
(NaturalNews) It has been on the U.S. drug market since the early 1990s, and population control organizations like Planned Parenthood continue to push it heavily on black women and other ethnic minorities as a form of contraception. But the injectable contraceptive drug Depo-Provera, manufactured by Pfizer, has an extensive track record of causing serious harm to women, including its tendency to trigger the development of cancer. July 21, 2016 (
July 21, 2016 ( July 27, 2016
July 27, 2016 According to a 2016 study, the hormones released by oral contraceptives may influence women’s ability to process emotional situations—especially during their “pill-free” days.
According to a 2016 study, the hormones released by oral contraceptives may influence women’s ability to process emotional situations—especially during their “pill-free” days.





































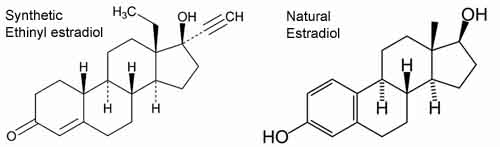


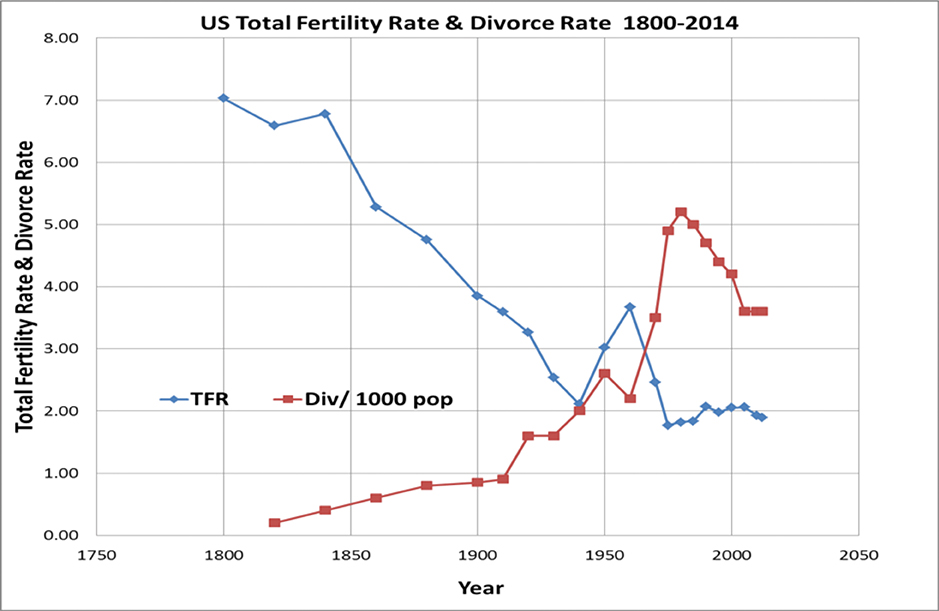












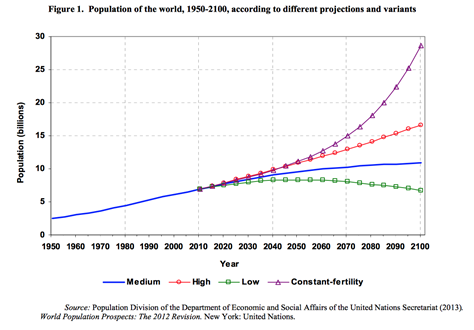



 True freedom is the ability of every human being to seek their own good and potential; it is an expression of their intrinsic worth as made in the image of God and naturally harmonizes with the good for humanity as a whole and therefore does not involve killing or harming the human person. Law naturally recognizes this in the case of adults; we have a prohibition against murder, assault, and even illicit drug use that harms the individual himself and thus the wider social community of which he is an inseparable part.
True freedom is the ability of every human being to seek their own good and potential; it is an expression of their intrinsic worth as made in the image of God and naturally harmonizes with the good for humanity as a whole and therefore does not involve killing or harming the human person. Law naturally recognizes this in the case of adults; we have a prohibition against murder, assault, and even illicit drug use that harms the individual himself and thus the wider social community of which he is an inseparable part. Stephanie Pacheco is a writer, blogger, and speaker in Northern Virginia. She earned a M.A. in Theological Studies, summa cum laude, from Christendom College and holds a B.A. from the University of Virginia in Religious Studies with a minor in Government and Political Theory. She has presented at a conference of the American Catholic Historical Association and for Christian Women in Action. She lives with her husband and two young children.
Stephanie Pacheco is a writer, blogger, and speaker in Northern Virginia. She earned a M.A. in Theological Studies, summa cum laude, from Christendom College and holds a B.A. from the University of Virginia in Religious Studies with a minor in Government and Political Theory. She has presented at a conference of the American Catholic Historical Association and for Christian Women in Action. She lives with her husband and two young children.















 Twenty years ago this month, on the solemnity of the Annunciation, St. John Paul II published Evangelium Vitae (The Gospel of Life). It was the 17th year of his pontificate. He was 75 years old.
Twenty years ago this month, on the solemnity of the Annunciation, St. John Paul II published Evangelium Vitae (The Gospel of Life). It was the 17th year of his pontificate. He was 75 years old. March 4, 2015 (
March 4, 2015 (

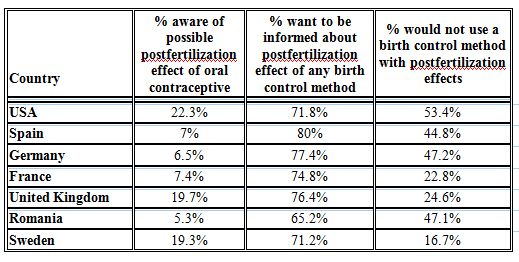













 ill never be a meal where everyone is happy with the food.
ill never be a meal where everyone is happy with the food.











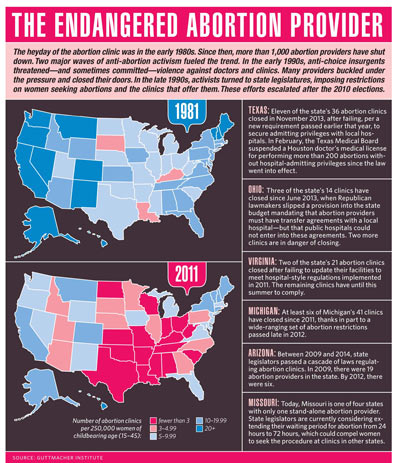
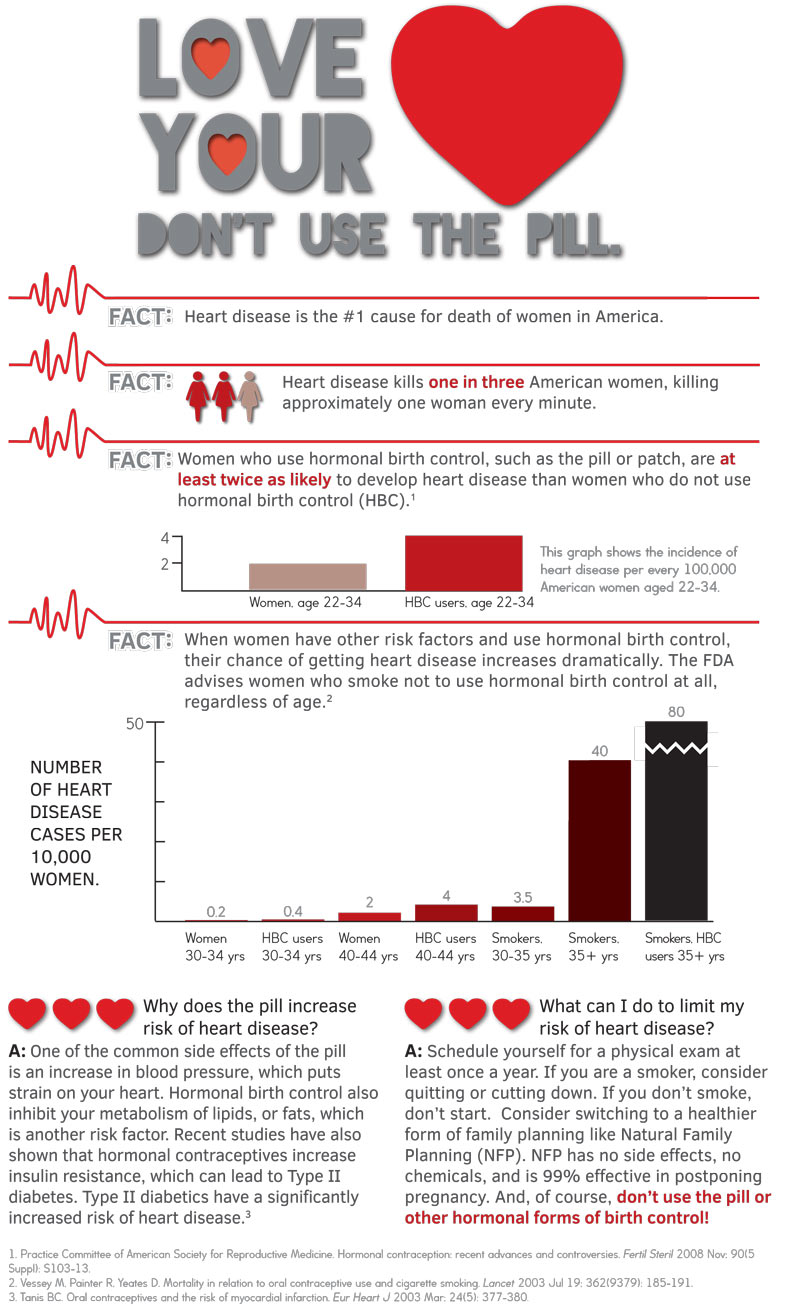















 babies … their parents … and grandparents.
babies … their parents … and grandparents.








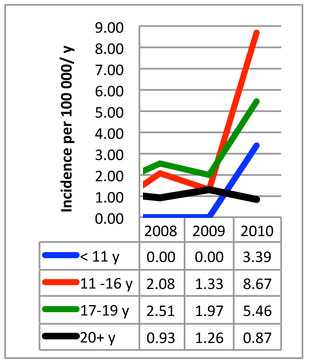








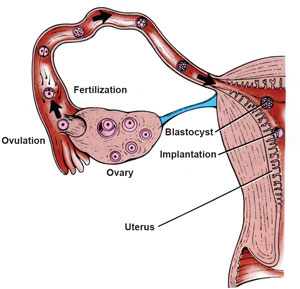




































 Back in November, the Wall Street Journal featured a prominent
Back in November, the Wall Street Journal featured a prominent 
























![Sterilization Reversal - A Generous Act of Love [PDF] 2003 edition](https://onemoresoul.com/files/2024/01/thumbnail_1108_789.gif)









 As the 2012 budget battles began, Clare Coleman, CEO of the National Family Planning and Reproductive Health Association, took to the pages of the Washington Post. In a piece called “Five Myths about Planned Parenthood,” she argued that defunding the organization was an ignoble goal for members of Congress looking to cut the bloated federal budget.
As the 2012 budget battles began, Clare Coleman, CEO of the National Family Planning and Reproductive Health Association, took to the pages of the Washington Post. In a piece called “Five Myths about Planned Parenthood,” she argued that defunding the organization was an ignoble goal for members of Congress looking to cut the bloated federal budget.  Original source
Original source
















 ción.4 Un delicado equilibrio hormonal es necesario para la supervivencia del bebé.
ción.4 Un delicado equilibrio hormonal es necesario para la supervivencia del bebé.





























 Tebow, one of the most esteemed college football players ever, has been very vocal about his Christian faith and his love for Jesus Christ.
Tebow, one of the most esteemed college football players ever, has been very vocal about his Christian faith and his love for Jesus Christ.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
‘Nonexistent’ commission to revise Humanae Vitae given exclusive access to Vatican secret archives
After the story was first reported by Marco Tosatti on May 11 and soon given further confirmation by Maike Hickson at One Peter Five, the Vatican refused to verify or deny it for an entire month, prompting Tosatti to quip that the silence “could in itself be a sign.”
Finally, in mid-June, Italian journalist Roberto de Mattei further confirmed the story and even listed the members of the alleged commission, including its head, Fr. Gilfredo Marengo, a theologian at the Pontifical John Paul II Institute for Studies on Marriage and Family.
This led Archbishop Vincenzo Paglia, the grand chancellor of the institute, to finally break the Vatican’s silence with an ambiguous denial made in an interview with the Catholic News Agency (CNA), in which he claimed that “there is no pontifical commission called to re-read or to reinterpret Humanae vitae” but added that “we should look positively on all those initiatives, such as that of Professor Marengo of the John Paul II Institute, which aim at studying and deepening this document in view of the 50th anniversary of its publication.”
Marengo himself told CNA that stories about such a “commission” were nothing more than an “imaginative report” and assured the agency that “the issue of a conciliation between Amoris Laetitia and Humanae Vitae is not in the agenda.” He described his work as a “historical-critical investigation without any aim other than reconstructing as well as possible the whole process of composing the encyclical.”
Despite such attempts to dismiss reports about Marengo’s Humanae Vitae “commission,” concerns continued to be raised in Catholic media, and on July 25 Fr. Marengo gave an extensive interview to Vatican Radio in an apparent attempt to quell them. However, in the interview Marengo not only confirmed details given by de Mattei about his “commission” — which he calls a “study group” — but also drops a new bombshell, revealing that he has been given what appears to be exclusive access to the Vatican’s secret archives for the purpose of carrying out this Humanae Vitae “study.”
In the interview, published on the Vatican Radio website only in Italian, Marengo acknowledged that his “study group” consists of the same people named more than a month earlier by de Mattei: Pierangelo Sequeri, president of the Pontifical John Paul II Institute; Philippe Chenaux, a professor of Church history at the Pontifical Lateran University; and Angelo Maffeis, president of the Paul VI Institute of Brescia.
“From the point of view of historical-theological research, it will be very useful to reconstruct the process of composing [the encyclical], which developed in distinct phases from June 1966 to its publication, by examining the documentation kept in some archives of the Holy See,” Marengo told Vatican Radio. “Given the approaching date of this 50th anniversary [of publication of Humanae Vitae], I have received permission to begin searching the archives, alongside some prominent scholars, Professors Sequeri, Maffeis and Chenaux.”
The next day, Marengo reaffirmed to the Catholic News Service that, in the words of CNS, “he felt it was important to ask the Vatican to set aside rules that prevent scholars from accessing Vatican archival material for 70 years.” CNS goes on to quote Marengo saying, “The competent Vatican authorities accepted my request, permitting access particularly to the collections of the Vatican Secret Archives and the archive of the Congregation for the Doctrine of the Faith.”
The privilege of accessing the archives of this period is no small matter. The Vatican excludes scholars from virtually all material in the archives dating from the pontificate of Pope Pius XII to the present, and has done so for many years, citing the need to catalog and prepare the material before scholars can be permitted to view it. The Holy See has maintained this position for decades despite much pressure to open the archives arising from controversy over Pope Pius XII’s conduct during World War II.
The Vatican has long claimed that it is simply unable to accommodate requests for such material and continues to tell scholars that all material following the pontificate of Pius XI is unavailable to the public, except for documents relating to Vatican II. Only when the cataloguing process is complete will scholars be permitted to see documents from later periods, officials have repeatedly said, citing the principle that material in the archive should be opened to scholarly access only after 70 years.
Fr. Marengo and his “study group,” however, have been given exclusive access to this restricted section of the archives, something that other historians have been unable to achieve after decades of insistent requests. It is, to put it mildly, an unimaginable privilege for a group of scholars who wish to do nothing more than an historical recounting of the composition of an encyclical, a purely academic walk down memory lane. Such access had to be granted at the highest levels of authority in the Vatican. If this is not a “pontifical commission,” as Archbishop Paglia put it, it has privileges that certainly would seem to rival one.
Fr. Marengo’s curious project
The repeated attempts by Vatican officials to evade questions about this Humanae Vitae non-commission and to deny its significance, despite the unique privileges granted to it, raises an urgent question: What, precisely, does this exclusive Vatican “study group” intend to do?
In his interview with Catholic News Service, Marengo described the group’s activity as a “a work of historical-critical investigation without any aim other than reconstructing as well as possible the whole process of composing the encyclical,” in view of its upcoming 50th anniversary in 2018.
“Historical-critical” methods of textual interpretation are those that seek to understand texts by means of the processes that produced them as well as the social and cultural contexts in which they were written. With regard to the Bible, they have been used in doctrinally orthodox ways but have also been used to justify revisionist forms of interpretation that deny traditional understandings of Scriptural texts. This leads to claims that miracle stories, even those in the New Testament, are nothing more than literary devices, and even bringing into question such articles of the faith as the Virgin Birth of Christ and his resurrection from the dead.
Why, on the anniversary of an encyclical that was published within the living memory of a large percentage of the population, would the Vatican have need of an “historical-critical” analysis of the encyclical?
Although Fr. Marengo and Archbishop Paglia have protested much that no revision of the document is intended, Marengo himself seems already to be in the process of reinterpreting Humanae Vitae in troubling ways, telling Catholic News Service, in their words, that “procreation … was seen by many as the primary purpose of marriage, so Pope Paul’s insistence in ‘Humanae Vitae’ that sex within marriage is both procreative and unitive was something new, as was his declaration ‘without uncertainty that the exercise of responsible parenthood is an objective value for Christian families’ when done using natural methods.’” Marengo made similar statements during his Vatican Radio interview.
Both of these statements are, to put it bluntly, deeply erroneous interpretations of the encyclical. Pope Paul VI was no innovator in such matters; the canon law and moral theology of the Church has long understood the sexual act as the consummation of an absolutely indissoluble sacramental union between the spouses, whether or not it results in procreation. Both the catechisms of the Council of Trent and of Pope Pius X list the unity of the spouses and their mutual support as among the primary ends of marriage, and Pope Pius XI writes at length about the unitive purpose of the sexual act in his encyclical Casti Connubii. Moreover, the Vatican’s Apostolic Penitentiary began to publicly permit periodic abstinence to avoid conception in the late 19th century. In Humanae Vitae, Paul VI never contradicts the Church’s teaching that the primary purpose of the sexual act is procreation.
It’s true that Humanae Vitae lists the unitive purpose before the procreative, but this was nothing new — the Catechism of the Council of Trent, 400 years earlier, had done the same thing, listing the first purpose of marriage as the satisfaction of the urge toward the companionship of the opposite sex, and mutual support in old age, and the second being the desire for begetting and raising children for the purpose of educating them in the faith. This order did not necessarily refer to any ultimate teleological priority but to the temporal sequence of ends sought in marriage.
Marengo has laughed off the idea that he somehow wants to reconcile Humanae Vitae with Pope Francis’ confused apostolic exhortation Amoris Laetitia, but that is exactly what his recent scholarship has sought to do. Only a few months ago, Marengo wrote an article for Vatican Insider called “Humanae Vitae and Amoris Laetitia,” in which he belittles the Church’s condemnation of birth control, asking if “the polemical game – the pill yes – the pill no, like today’s — Communion to the divorced yes – Communion to the divorced no — is only an appearance of discomfort and strain, [which is] much more decisive in the fabric of ecclesial life.”
In the same article, Marengo parrots the reasoning of Amoris Laetitia that seeks to lower Catholic moral dogma to an often unattainable and purely abstract ideal. “Every time the Christian community falls into error and proposes models of life derived from too abstract and artificially constructed theological ideals, it conceives its pastoral action as the schematic application of a doctrinal paradigm,” said Marengo, and cited Amoris Laetitia in asserting, “We have presented a too abstract theological ideal on marriage, almost artificially constructed, far from the concrete situation and the effective possibilities of families as they really are. This excessive idealization, above all when we have reawakened trust in grace, has not made marriage more attractive and desirable, but quite the opposite.”
Archbishop Paglia, Fr. Marengo, and their media sympathizers have labored mightily to convince Catholic journalists to “move along,” because there’s nothing to see here. They accuse them of hatching “conspiracy theories,” and even go so far as to claim that Pope Francis has never hinted at changing Humanae Vitae. In fact, Pope Francis has made statements that contradict Humanae Vitae almost verbatim, claiming that contraception can be justified as a lesser evil (a claim expressly condemned in the same encyclical). His apparently offhanded statement, made to reporters during a flight, was reaffirmed by Vatican spokesman Fr. Federico Lombardi soon after.
Moreover, Pope Francis’ recent conduct with regard to the Church’s perennial doctrines on life and family has given Catholics much cause for suspicion. His administration and its allies engaged in deceptive tactics to manipulate two synods of bishops in order to justify the subversive novelties against the integrity of marriage contained in Amoris Laetitia. Chillingly, Francis has made statements about Humanae Vitae hinting that he has a similar agenda for the document on its 50th anniversary of publication.
In a 2014 interview with the Italian newspaper Corriere della Sera, Francis was specifically asked about “tak[ing] up again the topic of birth control” half a century after the publication of Humanae Vitae. “Your confrere, Cardinal [Carlo Maria] Martini [the late Archbishop of Milan] believed it was now time,” added the interviewer.
“It all depends on how the text of ‘Humanae Vitae’ is interpreted,” responded Francis. “Paul VI himself, towards the end, recommended to confessors much mercy and attention to concrete situations.” Francis then complimented Paul VI, calling him a “prophetic” genius, but added, “The object is not to change the doctrine, but it is a matter of going into the issue in depth and to ensure that the pastoral ministry takes into account the situations of each person and what that person can do.”
The Catholic faithful have heard this language from Pope Francis before – it is the rationale underlying Amoris Laetitia’s apparent acceptance of permitting adulterers to receive Holy Communion, which has become the cause of immense scandal regarding the sacrament of marriage, and the greatest doctrinal controversy connected to a pope for more than six centuries. It’s hardly a cause for optimism regarding Fr. Marengo’s curious non-commission, and its “historical-critical” review of Humanae Vitae.
Posted in News & Commentary | No Comments »